BHARATHIAR UNIVERSITY
168
1 DEVELOPMENTAL BIOLOGY AND HUMAN WELFARE M.Sc Zoology II YEAR BHARATHIAR UNIVERSITY COIMBATORE – 641046 SCHOOL OF DISTANCE EDUCATION
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of BHARATHIAR UNIVERSITY

1
DEVELOPMENTAL BIOLOGY
AND
HUMAN WELFARE
M.Sc Zoology
II YEAR
BHARATHIAR UNIVERSITY
COIMBATORE – 641046
SCHOOL OF DISTANCE EDUCATION

2

3
DEVELOPMENTAL BIOLOGY
AND
HUMAN WELFARE TABLE OF CONTENTS
UNIT TITLE PAGES
I GAMETOGENESIS 4
II FERTILIZATION PROCESS 30
III EMBRYOGENESIS 43
IV EMBRYONIC INDUCTION 73
V HUMAN WELFARE 105

4
UNIT I
GAMETOGENESIS Sexual reproduction involves the formation of male and female gametes and the
mechanisms necessary for the gametes to come together and fuse to form one cell that
represents the beginning of a new individual with a distinct genetic identity.
Preparation for pregnancy involves two main programs of events: The process of
formation of the male and female gametes occurs in the gonads (ovary or testis).
SPERMATOGENESIS 1.0 INTRODUCTION
1.1 STRUCTURE OF THE GERMINAL EPITHELIUM
1.2 DEVELOPMENTAL STAGES OF SPERMATOGENESIS
1.3 THE TEMPORAL COURSE OF SPERMATOGENESIS
1.4 SPERMATOCYTOGENESIS
1.5 LOCAL COURSE OF SPERMATOGENESIS - THE SPERMATOGENESIS WAVE
1.6 SPERMIOGENESIS (SPERMATOHISTOGENESIS) AND STRUCTURE OF THE
SPERM CELL
1.7 LEYDIG'S INTERSTITIAL CELLS AND HORMONAL REGULATION
1.0 INTRODUCTION Spermatogenesis is initiated in the male testis with the beginning of puberty.
This comprises the entire development of the spermatogonia (former primordial germ
cells) up to sperm cells. The gonadal cords that are solid up till then in the juvenile testis
develop a lumen with the start of puberty. They then gradually transform themselves
into spermatic canals. They are termed convoluted seminiferous tubules (Tubuli
seminiferi contorti) and are so numerous and thin that in an adult male testicle. They
are coated by a germinal epithelium that exhibits two differing cell populations: some
are sustentacular cells (= Sertoli's cells) and the great majority of the germ cells in
various division and differentiation.

5
Fig. Convoluted seminiferous tubules. For an optimal sperm cell production a certain
milieu is needed. By transferring the testicles into the scrotum a testicular temperature
2-3 ºC lower than body temperature is attained. In addition, a slightly elevated pressure
from the surroundings is necessary. This is why when the taut tunica albuginea is slit
open, the testicular parenchyma bulges out by itself. Evidently, both elevated pressure
and lowered temperature are necessary for producing sperm cells.
Fig. Histological transverse section of a portion of convoluted seminiferous tubules in
an adult. Outside its basal lamina a layer of myofibroblasts and fibrocytes surround the
tubule. The germinal epithelium lies on the tubule wall. One can recognize the
spermatogonia sitting on the basal lamina. The nuclei of the Sertoli's sustentacular cells
1. Basal lamina (membrane) (not recognizable) 2. Myofibroblast 3. Fibrocyte 4. Sertoli's cell 5. Spermatogonia 6. Various stages of the germ cells during spermatogenesis 7. Spermatozoon 8. Lumen

6
have a rarified chromatin and the nuclei with clear nucleolus that are often oriented
perpendicular to the basal lamina. The overall picture, though, is dominated by the cells
occupied with spermatogenesis.
The development of the germ cells begins with the spermatogonia at the
periphery of the seminal canal and advances towards the lumen over spermatocytes I
(primary spermatocytes), spermatocytes II (secondary spermatocytes), spermatids and
finally to mature sperm cells.
1.1 STRUCTURE OF GERMINAL EPITHELIUM The epithelium consists of Sertoli's sustentacular cells and the spermatogenic
cells. The Sertoli's cells form a single-layered lamina and extend from the basal lamina
to the tubule lumen. With their labyrinthine cellular processes they surround the
individual types of germ cells more or less completely. Spermatogenesis is thus
accomplished in close contact with the Sertoli's cells, which not only have supportive
and nourishing functions, but also secrete hormones and phagocytize cell fragments.
Somewhat above the basal lamina they are bound to each other through complicated
occluding junctional complexes (tight junctions), so that 2 separated compartments are
present in the epithelium: a basal one, in which the spermatogonia are lined up, and a
luminal one, in which all the other stages of spermatogenesis are found.
1. Peritubular cells, 2. Basal membrane, 3. Spermatogonia, 4. Tight junction, 5. Spermatocyte I, 6. Spermatocyte II, 7a. Spermatids, 7b. Spermatids, 8.Acrosome, 9. Residual bodies, 10. Spermatozoas, 11. Cell nucleus of sustentacular cells (Sertoli), A. Basal zone, B. Adluminal zone

7
Fig. Germinal epithelium. Schema of the germinal epithelium: The supportive (Sertoli)
cells sit on the basal membrane. Towards the lumen of the spermatogonia (lowest row
of cells) the Sertoli cells are connected with each other by the occluding junctional
complexes (tight junctions). This seal gives rise to the blood-testicle barrier. The
cytoplasm of these supportive cells gets formed into complicated processes because
they surround all of the cells involved with spermatogenesi.
Through the occluding junctional complexes of the Sertoli's cells a
"blood/testicle" barrier is created in the tubule. This means that outside this barrier, in
the tubular periphery, cells, substances and hormones from the blood have unhindered
access.
On the other hand, the inner compartment of the tubule is protected by the
barrier, which is selectively permeable and serves as an entry check. This is of practical
importance because haploid cells in the inner part of the tubule exhibit surface antigenic
properties, different from all other body cells. They must thus be kept secluded from
the immune system of the organism by the "blood/testicle" barrier.
1.2 DEVELOPMENTAL STAGES OF SPERMATOGENESIS In the course of spermatogenesis the germ cells move towards the lumen as they
mature. The following developmental stages are thereby passed through:
• A-spermatogonium
• B-spermatogonium
• Primary spermatocyte (= spermatocyte order I)
• Secondary spermatocyte (= spermatocyte order II)
• Spermatid
• Sperm cell (= spermatozoon)
The spermatogenesis can be subdivided into two successive sections:
The first comprises the cells from the spermatogonium up to and including the
secondary spermatocyte and is termed spermatocytogenesis.

8
The second one comprises the differentiation/maturation of the sperm cell, starting
with the spermatid phase and is termed spermiogenesis (or spermiohistogenesis).
Fig. The spermatogenesis generations. The stem cell population of the germinal cells
lies on the basal lamina of the convoluted seminiferous tubules. These are Type A
spermatogonia. These cells undergo mitosis: one of the daughter cells renew the stock
of type A spermatogonia, the other becomes a type B spermatogonia. These divide and
their daughter cells migrate towards the lumen. In roughly 64 days they differentiate
themselves thereby into sperm cells up to the outer surface of the epithelium (one
should note that in these cellular divisions, the separation of the cytoplasm is not
complete. Whole networks of connected cells arise. So, for example in the last
generation, the spermatids, far more cells are bound to each other than as shown here).
1.3 THE TEMPORAL COURSE OF SPERMATOGENESIS The approximate 64 day cycle of the spermatogenesis can be subdivided into
four phases that last differing lengths of time:

9
Mitosis of the
spermatogonia
16 days Up to the primary spermatocytes
First meiosis 24 days For the division of the primary
spermatocytes to form secondary
spermatocytes
Second meiosis A few hours For engendering the spermatids
Spermiogenesis 24 days Up to the completed sperm cells
1.4 SPERMATOCYTOGENESIS Among the spermatogonia (all in all, over 1 billion in both testicles) that form the
basal layer of the germinal epithelium, several types can be distinguished: certain type
A cells are seen as spermatogonia that divide mitotically and reproduce themselves
(homonymous division), whereby the spermatogonia population is maintained.
The beginning of spermatogenesis is introduced through the so-called
heteronymous division, in which the daughter cells (second group of type A cells)
remain bound together by thin bridges of cytoplasm. Through the preservation of these
cytoplasmic connections, spermatogonia are inducted into the spermatogenesis process.
After a further mitotic division type B spermatogonia are engendered that also
divide themselves mitotically into primary spermatocytes (I).
The freshly created primary spermatocytes (I) now enter into the first meiosis.
They then go immediately into the S phase (that is, into the preleptotene meiosis),
double their internal DNA, leave the basal compartment and reach the special milieu of
the luminal compartment. Following the S phase, these cells attain the complex stage of
the prophase of the meiosis and become thereby noticeably visible with a light
microscope. This prophase, which lasts 24 days, can be divided into five sections:
Leptotene , Zygotene, Pachytene, Diplotene and Diakinesis.
In the prophase in every germ cell a new combination of maternal and paternal
genetic material occurs. After the long prophase follow the metaphase, anaphase and

10
telophase that take much less time. One primary spermatocyte yields two secondary
spermatocytes.
In the heteronymous division the cytoplasmic division is not completed; the
daughter cells stay bound together through thin cytoplasmic bridges. Also in the
subsequent meiosis the cytoplasmic division is incomplete, so that from one
spermatogonium a network of daughter cells arises that doubles in size in each
generation. The forming of such networks assures that all of the processes in each
generation occur in step with each other.
The secondary spermatocytes go directly into the second meiosis, out of which
the spermatids emerge. Since in the secondary spermatocytes neither DNA
reduplication nor a recombination of the genetic material occurs, the second meiosis can
take place quickly. It lasts only around five hours and for that reason secondary
spermatocytes are rather seldom seen in a histological section. Through the division of
the chromatids of a secondary spermatocyte, two haploid spermatids arise that contain
only half the original DNA content.
Besides the sperm cells the spermatids are the smallest cells of the germinal
epithelium. In a process lasting several weeks (so-called spermiogenesis or
spermiohistogenesis) they are transformed into sperm cells with the active assistance of
the Sertoli's cells.
1.5 LOCAL COURSE OF SPERMATOGENESIS - THE SPERMATOGENESIS WAVE In examining a cross-section of a convoluted seminiferous tubule one notices that
cells appear in groups having the same maturation stages. However, not all the
spermatogenesis stages are found in a cross-section.

11
Fig. Various developmental stages in a light microscope cross-section through a
convoluted seminiferous tubule.
On the one hand, the reason for this appearance lies in the fact that the daughter
cells, generated by each meiotic step, remain bound together by thin cytoplasmic
bridges. Thus with each meiotic step the following generation is twice as large, until the
cells have formed a relatively complex network. The result is that cells of the same
development stages are seen there in groups. On the other hand, in addition, other
spermatogenesis generations are wound around each other in spirals along the
seminiferous tubule. This is why one meets with groupings of various generations in a
tubule cross-section. Thus, it is highly improbable that all of the development stages
will be seen in a single section at the same time.
1. Leptotene/zygotene of the spermatocytes typ I
2. Pachytene of the spermatocytes typ I
3. Young spermatids 4. Older spermatids (sperm
cells heads can be recognized)
5. Sertoli's cells 6. Spermatogonia

12
1.6 SPERMIOGENESIS (SPERMATOHISTOGENESIS) AND STRUCTURE OF THE SPERM CELL
The differentiation of the spermatids into sperm cells is called spermiogenesis. It
corresponds to the final part of spermatogenesis and comprises the following
individual processes that partially proceed at the same time:
• Nuclear condensation: thickening and reduction of the nuclear size,
condensation of the nuclear contents into the smallest space.
• Acrosome formation: Forming a cap (acrosome) containing enzymes that play an
important role in the penetration through the pellucid zone of the oocyte.
• Flagellum formation: generation of the sperm cell tail.
• Cytoplasme reduction: elimination of all unnecessary cytoplasm.
Fig. Three differing stages of spermiogenesis: on the left a fresh spermatid, on the right
an immature sperm cell, and in the middle an in-between stage. A rotation of the
nucleus causes a repositioning of the acrosomal vesicle to occur. This inverts itself like a
1. Axonemal structure, first flagellar primordium, 2. Golgi complex, 3. Acrosomal vesicle, 4. Pair of centrioles (distal and proximal), 5. Mitochondrion, 6. Nucleus, 7. Flagellar primordium, 8. Microtubules, 9. Sperm cells tail, 10. Acrosomal cap

13
cap over the nucleus that continues to be condensed (dotted line). The cytoplasm cell
components that are no longer needed are discarded and phagocytized by Sertoli's cells.
The mitochondria are packed thickly (tightly) together around the beginning part of the
flagellum (mid-piece). As a sign of its immaturity, the sperm cell (on the right) that has
issued into the lumen still has a bit of cytoplasm around its neck.
NUCLEAR CONDENSATION
The nucleus becomes smaller, denser and takes on a characteristic, flattened
form. Seen from above, the nucleus is oval and, from the narrow side, is pear-shaped.
The acrosome lies over the tip. Nucleus and acrosome form the sperm cell's head that is
bound to the mid-piece by a short neck.
ACROSOME FORMATION
The Golgi complex engender the vesicles, which then merge into a larger
formation that settles close to the cell nucleus and finally inverts itself like a cap over
the largest part of the nucleus. The acrosome corresponds functionally to a lysosome
and thus contains lysosomal enzymes (hyaluronidase among others).
DEVELOPMENT OF THE FLAGELLUM
The future axonemal structure grows out of one centriole (distal). This consists of
a bundle of nine peripheral double microtubules and two single ones in the center.
During its development, through the rotation of the nucleus and acrosomal vesicle, the
flagellum primordium comes to lie on the opposite side of the acrosome.
Four parts of the finished flagellum can be distinguished:
• The neck contains the two centrioles (proximal and distal) among other things.
• The mid piece consists of a sheath of ring-shaped mitochondria grouped around
the axoneme to provide the energy for the flagellar movement.
• The principle piece has a sheath of ring fibers around the axoneme.
• The tail consists of only the 9+2 structure of the axoneme

14
The mature sperm cell is approximately 60 µm long and completely enveloped
by the plasma membrane.
Fig. The mature sperm cell. The mature sperm cell is slender; in the middle part, the
mitochondria are thick and ring-shaped. The DNA in the nucleus is maximally
condensed.
CYTOPLASMIC REDUCTION
The cytoplasm of the spermatids that is no longer needed is phagocytized by
Sertoli's cells or is disposed of in the lumen of the tubules. A clump of cytoplasm, though,
can remain hanging on the neck and mid piece of the sperm cell for a little while.
During sperm cell production considerable individual variations exist that are
also partially influenced by psychological factors. Per day roughly 100 million sperm
cells are produced. It is said that in each ejaculate an average number of 50-200 million
sperm cells are present (WHO standard value: over 40 million).
1.7 LEYDIG'S INTERSTITIAL CELLS AND HORMONAL REGULATION Between the seminal canals lie Leydig's interstitial cells. These are endocrine cells
that mainly produce testosterone, the male sexual hormone, and release it into the
blood and into the neighboring tissues. An initial active stage of these cells occurs
1. Plasma membrane, 2. Outer acrosomal membrane, 3. Acrosome, 4. Inner acrosomal membrane,5. Nucleus, 6. Proximal centriole, 7. Rest of the distal centriole, 8. Thick outer longitudinal fibers, Mitochondrion, 10. Axoneme, 11. Anulus, 12. Ring fibers A). Head, B). Neck, C). Mid piece, D). Principal piece, E). Endpiece

15
during the embryonic development of the testis. Later in juvenile life, due to the
influence of the LH (luteinizing hormone) secreted by the anterior hypophysis
(pituitary gland), Leydig's interstitial cells enter a second, long lasting stage of activity.
Together with the hormones secreted by the adrenal cortex, testosterone initiates
puberty and thus the maturation of the sperm cells.
Fig. Leydig's interstitial cells. Group of large cells in the interstice between tubules.
Leydig's interstitial cells characteristically contain large protein crystals (crystalloids of
Reinke), the importance of which is unknown. The crystals are uncolored and stand out
as light structures against the red cytoplasm of Leydig's interstitial cells.
Testosterone production is directed by LH (luteinizing hormone), secreted by the
anterior lobe of the hypophysis. Pronounced cycles in hormone production, as are
present in women, do not exist. The second hormone secreted by the anterior
hypophysis, FSH (follicle-stimulating hormone) affects Sertoli's cells, in that it triggers
the formation of a testosterone-binding protein. Thereby testosterone can be
transported by Sertoli's cells into the luminal compartment and there be concentrated.
Testosterone is decisive for spermatogenesis. Testosterone is also carried away via
blood and lymph fluid. Testosterone has effects on all tissues, especially also on the
brain during development as well as on the sexual organs.
1. Leydig's interstitial cells, 2. Crystalloids of Reinke

16
OOGENESIS I. DEVELOPMENT OF THE GERM CELLS IN THE OVARY
II. STRUCTURE OF THE OVARY
III. THE FOLLICLE STAGES FROM PRIMORDIAL FOLLICLE TO TERTIARY
FOLLICLE
a. PRIMORDIAL FOLLICLE
b. PRIMARY FOLLICLE
c. SECONDARY FOLLICLE
d. TERTIARY FOLLICLE
e. GRAAFIAN FOLLICLE
IV. TEMPORAL COURSE OF THE NUMBER OF GERM CELLS / FOLLICLES
a. ATRESIA -- THE CUSTOMARY FATE OF A FOLLICLE
V. THE OVARIAN CYCLE
a. THE HORMONAL CYCLE
The most interesting in connection with oogenesis is the development of the
different follicle stages. The complex processes that are connected with it are treated in
the fertilization module.
I. DEVELOPMENT OF THE GERM CELLS IN THE OVARY Following the immigration of the primordial germ cells into the gonadal ridge,
they proliferate, are enveloped by coelomic epithelial cells, and form germinal cords
that , though, keep their connection with the coelom epithelium. Now a cortical zone
(cortex ovarii) and a medulla can be distinguished, whereby it should be mentioned
that in females the germinal cords never penetrate into the medullary zone. In the
genital primordium the following processes then take place:
• A wave of proliferation begins that lasts from the 15th week to the 7th month:
primary germ cells arise in the cortical zone via mitosis of oogonia clones, bound
together in cellular bridges, that happens in rapid succession. The cell bridges are
necessary for a synchronous onset of the subsequent meiosis.
17
• With the onset of the meiosis (earliest onset in the prophase in the 12th week) the
designation of the germ cells changes. They are now called primary oocytes. The
primary oocytes become arrested in the diplotene stage of prophase I (the
prophase of the first meiotic division). Shortly before birth, all the fetal oocytes in
the female ovary have attained this stage. The meiotic resting phase that then
begins is called the dictyotene and it lasts till puberty, during which each month
(and in each month thereafter until menopause) a pair of primary oocytes
complete the first meiosis. Only a few oocytes (secondary oocytes plus one polar
body), though, reach the second meiosis and the subsequent ovulation. The
remaining oocytes that mature each month become atretic. The primary oocytes
that remain in the ovaries can stay in the dictyotene stage up to menopause, in
the extreme case, without ever maturing during a menstrual cycle.
• While the oogonia transform into primary oocytes, they become restructured so
that at the end of prophase I (the time of the dictyotene) each one gets enveloped
by a single layer of flat, follicular epithelial cells (descendents of the coelomic
epithelium). (oocyte + follicular epithelium = primordial follicle).
From birth there are thus two different structures to be distinguished that, at
least conceptually, do not develop further synchronously:
• On the one hand, the female germ cell that at birth is called the primary oocyte,
and which can develop further only during (and after) puberty (hormonal cycle
is necessary).
• On the other hand, the follicular epithelium that can develop further from the
primordial follicle via several follicle stages while oocytes remain in their
primary state.
The developmental sequence of the female germ cells is as follows:

18
Primordial germ cell - oogonium - primary oocyte - primary oocyte in the
dictyotene
Birth: The continuation of the development / maturation of the oocyte begins
again only a few days before ovulation (fertilization module).
The developmental sequence of a follicle goes through various follicle stages:
Primordial follicle - primary follicle - secondary follicle - tertiary follicle (graafian
follicle). Since a follicle can die at any moment in its development (= atresia), not all
reach the tertiary follicle stage.
II. STRUCTURE OF THE OVERY An ovary is subdivided into cortical (ovarian cortex) and medullary
compartments (ovarian medulla). Both blood and lymph vessels are found in the loose
connective tissue of the ovarian medulla.
In the cortical compartment the oocytes are present within the various follicle
stages.
The sex hormones influence the primordial follicles to grow and a restructuring
to take place. From the primordial follicles the primary follicles, secondary follicles, and
tertiary follicles develop in turn. Only a small percentage of the primordial follicles
reach the tertiary follicle stage - the great majority meet their end beforehand in the
various maturation stages. Large follicles leave scars behind in the cortical compartment
and the small ones disappear without a trace. The tertiary follicles get to be the largest
and, shortly before ovulation, can attain a diameter up to 2.5 mm through a special
spurt of growth. They are then termed graafian follicles.

19
Fig. Follicle stage in the ovary: The follicles in various stages are shown in the ovarian
cortical compartment. This very schematic drawing shows the relationships shortly
before ovulation. In reality the primordial follicles are the most prevalent numerically.
III. THE FOLLICLE STAGES FROM PRIMORDIAL FOLLICLE TO TERTIARY FOLLICLE
A. PRIMORDIAL FOLLICLE
At the time of birth all the surviving primary oocytes are surrounded by thin,
single layers of so-called follicular epithelial cells. These are delimited from the rest of
the ovarian stroma by a thin basal lamina. Follicular epithelial cells are former coelomic
epithelial cells. The primordial follicles always form the majority of the follicles in the
ovary.
Under the influence of the sex hormones some of them are able to develop
further to one or more of the subsequent stages in the following 50 years. Although this
further development can already take place sporadically in the time before birth and up
to puberty, the main part occurs as soon as a regular hormonal cycle is established.
Particularly the last phase of the maturation of a tertiary follicle to become a
largefollicle, ready to rupture, remains reserved for the time of regular cycles.
1. Primordial follicle 2. Primary follicle 3. Secondary follicle 4. Tertiary follicle 5. Antrum folliculi 6. Cumulus oophorus

20
B. PRIMARY FOLLICLE
Primory follicle In the transition of the primordial follicles into primary follicles
the follicular epithelium that surrounds the oocyte becomes iso- to highly prismatic.
Fig. Scheme of the development from primordial follicle to primary follicle.
C. SECONDARY FOLLICLE
When primary follicles survive, secondary follicles with follicular epitheliums
encompassing multiple rows are engendered. This is now called the stratum
granulosum. In the secondary follicles a glycoprotein layer, the pellucid zone, between
the oocyte and follicular epithelium becomes visible. Cytoplasmic processes of the
granulosa cells that lie upon it reach the oocyte through the pellucid zone and thereby
assure their maintenance function. Outside the basal lamina the stroma ovarii organizes
itself to become theca folliculi cells.
Fig. Scheme of a secondary follicle:in the transition from primary to secondary follicle
the stratum granulosum is engendered from the cells of the follicular epithelium. The
stroma ovarii organizes itself around the secondary follicle to become the theca folliculi
(interna and externa).
A. Primordial follicle B. Primary follicle
1. Oocyte 2. Follicular
1. Oocyte, 2. Pellucid zone, 3. Stratum granulosum, 4. Theca folliculi cells

21
D. TERTIARY FOLLICLE
If the secondary follicles survive, tertiary follicles are engendered. Their
identifying characteristic is a fluid-filled cavity, the antral follicle. The oocyte lies at the
edge in a mound made of granulosa epithelial cells, the cumulus oophorus. In the
meantime it has grown so large that its cellular nucleus has attained the size of a whole
primordial follicle. The connective tissue around the follicle has already clearly
differentiated itself into a theca interna, well supplied with capillaries, out of large,
lipid-rich cells (hormone production) and a theca externa, which forms a transition to
the stroma ovarii and contains larger vessels.
Fig. In a tertiary follicle the theca can be subdivided into an interna (hormone
production) and an externa (transition to the ovarian stroma).
Decisive for a successful follicle growth is a well-developed net of capillaries in
the theca interna. The precise steering mechanism that leads to the selection of a follicle
and its subsequent maturation to become a graafian follicle is still unknown. Before
ovulation a growth spurt of the tertiary follicles takes place.
E. GRAAFIAN FOLLICLE
This corresponds to an especially large tertiary follicle that can be expected to
suffice for ovulation.
1. Oocyte 2. Pellucid zone 3. Stratum granulosum 4. Theca interna 5. Theca externa 6. Antral follicle 7. Cumulus oophorus (Granulosa
cells, together with the oocyte) 8. Basal lamina between theca and
stratum granulosum

22
IV. TEMPORAL COURSE OF THE NUMBER OF GERM CELLS / FOLLICLES During the fetal period, the count of germ cells in the female organism is subject
to large variations. These arise due to the fact that the phases of proliferation and
decomposition of oocytes described below take place partially stepwise and partially in
parallel.
Phase A: Primordial germ cells grow, proliferate and become sheathed with
coelomic epithelial cells. Gonadal cords arise; 6th to 8th week.
Phase B: Spurt of growth: cellular clones of the oogonia are formed, whereby the
cells remain connected with each other through cellular bridges; 9th to the 22nd week.
Phase C: The oogonia become primary oocytes that enter the prophase of the first
meiosis; 12th to the 25th week.
Phase D: The primary oocytes become arrested in the dictyotene stage of the
prophase: the primordial follicles are engendered; 16th to the 29th week.
Phase E: At around the 14th week a quantitatively increased decline in the
number of germ cells commences as well as atresia in all of the follicle stages.
Up to the 22nd week of pregnancy, the primordial germ cells multiply along
with the resulting oogonia by mitosis. The maximum number of germ cells (7 million),
found in an ovary, is reached already in the 20th week due to the concomitant massive
degeneration of germ cells that begins in the 14th week. At the time of birth only about
2 million germ cells are still present in the ovary. The very first primary oocytes enter
the prophase in the 12th week. The passage through the various stages, up to the
arresting of further development, takes approximately 4 weeks and is accompanied by a
restructuring of the epithelial covering (coelomic epithelium --> follicular epithelium),
so that the first primordial follicle with the primary oocyte, arrested in the dictyotene
stage, appears roughly 4 weeks later in the 16th week. Today it is assumed that the
generation of the primordial follicles is complete by the time of birth. The result of these
processes on the count of germ cells is portrayed in the following diagram.

23
Fig. Development of the germ cell count in the various phases
Development of the germ cell count in the various phases.
The upper plot shows the time span in which specific processes operate on the
germ cells.The lower plot shows the age-dependent changes of the total number of
oogonia (or oocytes) and follicles in a single ovary.
ATRESIA - THE CUSTOMARY FATE OF A FOLLICLE
The normal, common fate of a follicle or female germ cell is known as atresia -
ovulation represents an exceptional destiny.
The above plot shows clearly how the number of germ cells decreases from the
20th week in order that they are all gone by about 50 years of age. Even though the
decrease actually proceeds continuously, three moments in the life of a woman are
apparent in which this takes place more rapidly. The largest decrease occurs in the 20th
week after the maximum number of 7 million germ cells (per ovary) is reached, thus
still in the fetal period. Immediately following birth a further, short period of
accelerated decline happens. The third, temporally longest period, of increased decline
takes place during puberty.
One terms the decline or the regression of follicles of each stage at every time in
the life of a woman follicular atresia. These follicles do not ovulate and the name is
derived from that fact. Follicle atresia occurs more intensely, though, at certain
moments (fetal period, early postnatal, begin of the menarche).

24
V. THE OVARIAN CYCLE: Of the roughly 500'000 follicles that are present in the two ovaries at the
beginning of sexual maturity, only around 480 reach the graafian follicle stage and are
thus able to release oocytes (ovulation). This number is simply derived by multiplying
the number of cycles per year (12) and the number of years in which a woman is fertile
(40).
OVULATION REPRESENTS AN EXCEPTIONAL FATE OF A FOLLICLE
A. THE HORMONAL CYCLE:
Cyclic changes in the hormone household (hormonal cycle), governed by the
hypothalamic-pituitary system, are responsible for the periodicity of the ovulation. In a
woman, the rhythmic hormonal influence leads to the following cyclic events:
1. the ovarian cycle (follicle maturation) that peaks in the ovulation and the
subsequent luteinization of the granulose cells
2. cyclic alterations of the endometrium that prepare the uterine mucosa so
fertilized oocytes can "nest" there. In the absence of implantation, the mucosa
will be eliminated (menstrual bleeding).
In the center of this hormonal control is the hypothalamamics-hypophysial
(pituitary gland) system with the two hypophysial gonadotropins FSH and LH. The
pulsating liberation of GnRH by the hypothalamus is the fundamental precondition for
a normal control of the cyclic ovarian function. This cyclic activity releases FSH and LH,
both of which stimulate the maturation of the follicles in the ovary and trigger
ovulation. During the ovarian cycle, estrogen is produced by the theca interna and
follicular cells (in the so-called follicle phase) and progesterone by the corpus luteum
(so-called luteal phase). GnRH: Gonadotropin- releasing hormone, FSH: Follicle-
stimulating hormone, LH: Luteinizing hormone.
The control circuit of the hormonal cycle has two essential control elements:
1. The pulsatile liberation of GnRH, as well as FSH and LH

25
2. The long-loop feedback-effect of estrogen and progesterone on the
hypothalamic-hypophysial-system (these two hormones are synthesized in the
[ready to rupture] follicle and so originate in the ovary, thus the name "long
loop").
As a rule, the ovarian cycle lasts 28 days. It is subdivided into two phases:
1. Follicle phase: recruitment of a so-called follicle cohort and, within this, the
selection of the mature follicle. This phase ends with ovulation. Estradiol is the
steering hormone. Normally, it lasts 14 days, but this can vary considerably.
2. Luteal phase: progesteron production by the "yellow body" (= corpus luteum)
and lasts 14 days (relatively constant).
Recruitment of the so-called follicle cohort: In the recruiting a certain number of
primordial follicles are stimulated to mature and to go through the following follicle
stages.
Fig. Course of the hormonal concentrations within the ovarian cycle.
A, Follicle phase, B, Luteal phase, C, Primary follicle, D, Secondary follicle,
E, Tertiary follicle, F, Graafian follicle, E2, Estradiol, Pr, Progesterone,
LH, Luteinizing hormone, FSH, Follicle stimulating hormone

26
TYPES OF ANIMAL EGGS
The animal eggs are classified on the basis of (1) amount of yolk (2) distribution
of yolk (3) presence or absence of shell and (4) Types of development.
1. AMOUNT OF YOLK
(i) Alecithal : When the egg contains no yolk it is called Alecithal egg. Eg. Eggs of
eutherian mammals.
(ii) Microlecithal : When the egg contains a small or negligible amount of yolk, Eg.
Amphioxus.
(iii) Macrolecithal : When the egg contains enormous amount of yolk. Yolk interferes
with cleavage Eg. Birds.

27
2. DISTRIBUTION OF YOLK
(i) Isolecithal: An even distribution of yolk throughout the cytoplasm. Eg. Amphioxus.
(ii) Telolecithal : Yolk concentrated at one pole, most vertebrate eggs are telolecithal.
The presence of yolk at one end of the egg imposes polarity on the egg. The pole with
the yolk is the vegetal pole, opposite hemisphere has the nucleus but little yolk and is
the animal hemisphere eg. Frog.
(iii) Centrolecithal : Yolk is concentrated at the center of the egg. Cytoplasm forms a
superficial cortex around the surface. Eg. Arthropods.
3.PRESENCE OR ABSENCE OF SHELL
Cleidoic eggs: Fully laden with yolk and surrounded by albumen and a water proof
shell, made up of calcium eg. Reptiles and Birds.
Non cleidoic eggs: Non cleidoic eggs are not protected by shells
4. BASIS OF DEVELOPMENT
Determinate or Mosaic eggs : Definite fate of every part of egg is predetermined. If a
particular portion of the egg is removed the developing embryo will be lacking in a
particular organ. Eg. Annelids and Arthropods.
Indeterminate or Regulative eggs : In majority of animals, there is no pre-
determination. If a particular portion of the egg is removed it can develop into a normal
embryo without any defect. This type of egg is called regulative egg. Eg. Amphioxus.
BIOCHEMICAL CHANGES DURING OOGENESIS
The generation of ova or eggs, the female gametes. Primordial germ cells, once
they have populated the gonads, proliferate and differentiate into sperm (in the testis)
or ova (in the ovary). The decision to produce either spermatocytes or oocytes is based
primarily on the genotype of the embryo. In rare cases, this decision can be reversed by
the hormonal environment of the embryo, so that the sexual phenotype may differ from
the genotype. Formation of the ovum most often involves substantial increases in cell
volume as well as the acquisition of organellar structures that adapt the egg for

28
reception of the sperm nucleus, and support of the early embryo. In histological
sections, the structure of the oocyte often appears random but as the understanding of
its chemical and structural organization increases, an order begins to emerge.
Among lower vertebrates and invertebrates, mitotic divisions of the precursor
cells, the oogonia, continue throughout the reproductive life of the adult; thus
extremely large numbers of ova are produced. In the fetal ovary of mammals, the
oogonia undergo mitotic divisions until the birth of the fetus, but a process involving
the destruction of the majority of the developing ova by the seventh month of gestation
reduces the number of oocytes from millions to a few hundred. Around the time of
birth, the mitotic divisions cease altogether, and the infant female ovary contains its full
complement of potential ova. At puberty, the pituitary hormones, follicle stimulating
hormone (FSH), and luteinizing hormone (LH) stimulate the growth and differentiation
of the ova and surrounding cells (see illustration).
One important feature of oocyte differentiation is the reduction of the chromosome
complement from the diploid state of the somatic cells to the haploid state of gametes.
Fusion with the haploid genome of the sperm will restore the normal diploid number of
chromosomes to the zygote. The meiotic divisions which reduce the chromosome content of
the oocyte occur after the structural differentiation of the oocyte is complete, often only
after fertilization. Unlike the formation of sperm, in which the two divisions of meiosis
produce four equivalent daughter cells, the cytoplasm of the oocyte is divided unequally, so
that three polar bodies with reduced cytoplasm and one oocyte are the final products.
Generally, each fertilized oocyte produces a single embryo, but there are exceptions.
Identical twins, for example, arise from the same fertilized egg.
The provision of nutrients for the embryo is a major function of the egg, and this is
accomplished by the storage of yolk in the cytoplasm. Yolk consists of complex mixtures of
proteins (vitellins), lipids, and carbohydrates in platelets, which are membrane-surrounded
packets dispersed throughout the egg cytoplasm (ooplasm). The amount of yolk in an egg
correlates with the nutritional needs of the embryo. Although the eggs of mammals are

29
extremely small as compared to the fetus, the bulk of the nutrition is supplied by the
placenta; yolk is required only until implantation in the uterine wall.
Egg cytoplasm also contains large stores of ribonucleic acid (RNA) in the form of
ribosomal, messenger, and transfer RNA. These RNAs direct the synthesis of proteins in
the early embryo, and may have a decisive influence on the course of development. The
mechanism by which the RNA is supplied to the egg is the basis for a major
classification of ovary types. Panoistic ovaries, in which the egg nucleus is responsible
for the production of all the stored RNA in the ooplasm, are typical of vertebrates,
primitive insects, and a number of invertebrates. The amounts of RNA produced during
the meiotic prophase in such ovaries are much larger than those produced by a somatic
cell, and thus special mechanisms seem to be involved in the synthetic process.
Fig. Three-dimensional view of the cyclic changes in the mammalian ovary

30
UNIT II
FERTILIZATION PROCESS 2.0 INTRODUCTION
2.1 GAMETOGENESIS – AN OVERVIEW
2.2 GAMET INTERACTIONS
2.3 SPERM-EGG FUSION
2.4 EGG ACTIVATION AND PRONUCLEI FORMATION
2.4.1 SPERM ENTRY AND ACROSOME REACTION ON SEA URCHIN CELL
2.4.2 POLYSPERMY IN MAMMAL
2.4.3 ACTIVATION OF EGG METABOLISM
2.0 INTRODUCTION The sperm and the ovum are highly specialized haploid cells, that are formed
through a complex set of cell divisions, differentiation and maturation steps called
gametogenesis. In mammals, the life history of germ cells begins during embryonic life
with the extragonadal appearance of primordial germ cells and the colonization of the
genital ridges, where germ cells associate with somatic cells; it continues with their
multiplication, growth and maturation, and ends at fertilization. The oocyte undergoes
a tremendous growth and stockpiles a large amount of macromolecules. In contrast, the
spermatozoon is an extremely streamlined, highly polarized cell, containing only
elements for essential functions such as motility and a few critical enzymes to ensure
efficient transmission of the paternal genome to the oocyte at fertilization. The union of
sperm and egg is an extraordinary cell fusion event that gives rise to an original
individual and triggers a very sophisticated developmental program.
2.1 GAMETOGENESIS At the stage of spermatogonia and oogonia, germ cells multiply by mitosis,
subsequently, they undergo meiosis to become the fully matured gametes. Meiosis
involves two consecutive divisions with only one DNA replication cycle and results in
the production of haploid gametes. The pairing of homologous chromosomes is unique

31
to meiosis. The first meiotic division enhances genetic variability by independent
assortment (random distribution) of the different maternal and paternal homologs and
by crossing-over between homologous non sister chromatids. The second meiotic
division resembles a normal mitosis without DNA replication. Meiosis is dominated by
prophase of the first meiotic division, that occupies a long period and is divided into 5
sequential stages—leptotene, zygotene, pachytene, diplotene and diakinesis—defined
by morphological criteria.
DEVELOPMENT OF THE SPERM
Spermatogonia develop from primordial germ cells that migrate into the
undifferentiated gonad early in embryogenesis. In the wall of the forming seminiferous
tubules two different kinds of cells are already clearly distinguishable at this stage: the
supporting Sertoli cells, thought to derive from the surface epithelium of the genital
ridge, and the spermatogonia, derived from primordial germ cells. During the fetal
period, spermatogonia enter a dormant or arrested phase of development, and the
Sertoli cells constitute most of the seminiferous epithelium. At sexual maturity,
spermatogonia begin to increase in number. It is at this time that spermatogenesis really
starts since this term usually refers to the sequence of events by which spermatogonia
are transformed into spermatozoa. Spermatogenesis includes three main phases:
spermatogonial multiplication, meiosis, and spermiogenesis. The cells at these different
stages are called spermatogonia, spermatocytes and spermatids, respectively. In men
spermatogonial multiplication occurs through regular intervals of 16 days.
Spermatogonia can be divided in two main types, the noncycling ones (Ao), and those
that will differentiate into spermatocytes after six mitotic divisions. Type (Ao)
spermatogonia are able to repopulate the seminiferous epithelium when cycling
spermatogonia decrease in number. The cycling spermatogonia provide the stem cell
population for meiosis, which begins when preleptotene spermatocytes start DNA
replication. Each primary spermatocyte, actually the largest germ cell in the tubules,

32
undergoes the first meiotic division, forming two secondary spermatocytes that are
about half the size of the primary spermatocyte. Subsequently, these two secondary
spermatocytes undergo the second meiotic division, forming four haploid spermatids
that are about half the size of secondary spermatocytes. The spermatids are gradually
transformed into mature sperm by an extensive process of differentiation known as
spermiogenesis; finally the differentiated sperm is released from the seminiferous
epithelium and becomes a free spermatozoon, a process called spermiation. In human
the process of spermatogenesis extends over a period of about 60 days.
An intriguing and unique feature of spermatogenesis is that the developing male
germ cells fail to complete cytoplasmic division during mitosis and meiosis, so that all
the daughter cells, except for the least differentiated spermatogonia remain connected
by cytoplasmic bridges. These bridges persist until the very end of sperm
differentiation. It has indeed been shown that sperm nuclei are haploid but sperm cell
differentiation is directed by the diploid genome.
The sperm cell consists of two morphologically and functionally distinct regions.
A head containing an unusually highly condensed haploid nucleus and a tail propelling
the sperm to the egg helping to enter through the egg coat. The DNA in the nucleus is
inactive and extremely tightly packed as a result of its association with highly positively
charged proteins, the protamines, instead of histones, which have been displaced
during spermiogenesis. The head also contains a membrane-limited organelle, the
acrosome, whose contents are thought to have a function in the penetration of the
spermatozoon into the ovum. A variety of enzymes, including proteinases,
glycosidases, phosphatases, arylsulfatases and phospholipases are present in the
acrosome and in the preacrosomal membrane.
Sperm released from the seminiferous epithelium are not capable of fertilization.
The long series of changes that the spermatozoa endure between casting off from the
Sertoli cells, and fusing with the egg, i. e. till the fully functional state of the

33
spermatozoa, is referred to as sperm maturation. Throughout their journey from testis
to the proximity of the ovum, sperm cells are suspended in transudations and secretions
of the male and female genital tracts. The chemical and physical nature of this medium
progressively changes and the spermatozoa also change structurally, chemically and
behaviourally. Several proteins from testicular and epididymal environment have been
shown to bind to specific regions of the sperm surface that are involved in sperm
maturation and in part of the gamete recognition process. Biochemical modifications of
some sperm surface components are also involved, as well as an increase in
interchromatin disulfide bonds for chromatin condensation during this travel which
lasts several days. Sperm cells develop gradual motility and ability to bind and
penetrate eggs as they progress from the caput to the cauda epididymidis.
Ejaculates contain complex secretions from the accessory glands—the Cowper’s
gland, prostate, and seminal vesicles—which, contain a variety of energy substrates,
hormones, nonenzymatic and enzymatic proteins and various ions. The last step of
sperm cell maturation is called capacitation, which is a functional term used to indicate
the changes in mammalian spermatozoa that must occur in the female genital tract, or
during in vitro incubations, as preparation for the acrosome reaction. Capacitation is a
reversible reaction which does not involve morphological changes; it is accompanied by
a hyperactivation of sperm motility: the flagellar beat pattern changes from a low
amplitude favoring progressive motility to a high amplitude with little progression.
Capacitation includes a lowering of the cholesterol/phospholipid ratio in the sperm
membrane, a loss of sperm surface coating components (loss of the antifertility factor
from human seminal plasma) probably involved with the acquisition of zona pellucida
binding activity, and the phosphorylation of some plasma membrane proteins.
DEVELOPMENT OF THE EGG
The unfertilized egg is the end product of a discontinuous course called
oogenesis, that begins during fetal development and ends in the sexually mature adult.

34
Oogonia develop from primordial germ cells in the ovary, and multiply by mitosis only
during the fetal life. By the 5th month of gestation in women, all germ cells stop
proliferation and enter meiosis but pause at the prophase of the first meiotic division;
arrest may last from 12 to 50 years. The spherical dictyate oocytes become enclosed
within a few squamous somatic cells to form what is called primordial follicles; the
oocytes are then called primordial oocytes. It is in this period of life that the ovary
contains the highest number of oocytes—about one to two millions—since many of
them will degenerate before puberty and through the reproductive life of a woman. At
puberty only about 300’000 primary oocytes remain. They represent a stockpile from
which a few are selected at any given time for development towards preovulatory
follicles containing fully grown oocytes. The oocyte and its surrounding follicle grow
coordinately, rather than simultaneously. Indeed, the oocyte completes its growth
before the formation of the follicular antrum, i.e., the major part of follicular growth
occurs after the oocyte has stopped growing. The oocyte growth results in the formation
of one of the largest cells in the body. During this period its volume increases more than
300-fold; from a diameter of about 20 µm at the primordial stage, the oocyte reaches a
maximal diameter of about 120 µm. Completion of growth takes approximately 2.5-3
months. The nucleus of the growing oocyte, called the germinal vesicle, is particularly
apparent and contains a very refractile nucleolus. During oocyte growth an extracellular
coat develops around the plasma membrane. This acellular layer, called the zona
pellucida (ZP), is constituted by three major glycoproteins (ZP1, ZP2 and ZP3) that are
assembled into long, interconnected filaments to form a relatively porous coat about 5
µm thick.
From the time of puberty, one developing follicle is stimulated each month to
mature to complete development and to ovulate. This means that during the
approximately 40 years of a woman’s reproductive life, only 400 to 500 eggs will have
been released. All the rest will have degenerated. The LH surge released by the

35
pituitary will, each month, activate one antral follicle to mature. Fully grown primary
oocytes enclosed in Graafian follicles resume meiosis just prior to ovulation. This phase
is called meiotic maturation. The first macroscopically observable event of meiotic
maturation is the dissolution of the nuclear membrane; this process is referred to as
germinal vesicle breakdown or GVBD. The oocyte then progresses through metaphase,
anaphase, and telophase of the first division, emits the first polar body, and, without
stopping, enters the second division up to metaphase. It is around this time that
ovulation occurs, by rupture of the follicle wall at the surface of the ovary. In the
oviduct, the oocyte remains at metaphase II until it is triggered by fertilization to
complete the second meiotic division.
2.2 GAMETE INTERACTION In comparison to the large number of spermatozoa laid down in the vagina at
coitus, only very few sperm cells reach the ampulla and are found in the proximity of
the egg. Although sperm attraction to follicular factor(s) has been claimed, sperm
chemotaxis in mammalian fertilization has not been demonstrated. The leading role in
the sperm-egg encounter is played by the molecular organization of their surfaces, and
abundant evidence suggests that the species-specific gamete recognition and binding is
mediated by receptor molecules at the gamete surface.
Initial contact between gametes occurs when the sperm attach to the unfertilized
extracellular coat or zona pellucida. Capacitated, acrosome-intact sperm are capable of
binding to the zona pellucida via the plasma membrane of the sperm head. Binding is
an important prerequisite step for zona penetration because it initiates events that
culminate in induction of the acrosome reaction.
One of the components of the zona pellucida (ZP3) representing the primary
sperm receptor, is responsible for both the sperm-binding activity and the ability to
induce a complete acrosome reaction. Acrosome-intact sperm bind to ZP3 in a relatively
species specific manner, this gamete recognition and binding is mediated by

36
carbohydrates and not by the polypeptide chain. Many sperm are released from the
zona pellucida after undergoing the acrosome reaction, yet maintenance of sperm
binding is achieved by interaction of acrosome-reacted sperm with ZP2; thus, ZP2
serves as a secondary receptor.
Putative ZP-binding-glycoproteins of spermatozoa have been recognized in
various species. Several egg-binding proteins are envisaged on the sperm membrane
that impart species specificity. The postulated candidates are the following: a 95kDa
protein (p95SPERM) showing a tyrosine kinase activity that is stimulated on binding
and whose activation requires aggregation, a 56kDa protein (p56) of unknown function,
an antigen designated p200/220 (whose monoclonal antibody is named M42) necessary
for zona-induced acrosomal reaction, another related antigen the SAA-1 antigen
detected on all mammalian sperm acrosomes, a ß-1,4-galactosyl-transferase mediating
fertilization by binding oligosaccharide residues on zona pellucida glycoprotein. Many
evidence suggest also the possible involvement of protease inhibitor sites and
mannosidase sites or of other molecules called spermadhesins showing features of
serine proteases having lectin-like activity.
Proteolytic enzymes appear to participate in multiple phases of mammalian
fertilization, including acrosome reaction, sperm binding to zona pellucida (ZP), ZP
penetration and zona reaction, however, the enzymes involved have not been
completely identified. A role for sperm proacrosin and acrosin, the best characterized
sperm protease, in ZP binding and penetration has been postulated. Several
observations suggest that the plasminogen activator/plasmin system might play a role
in mammalian fertilization. First, both mouse gametes express plasminogen-dependent
proteolytic activities: ovulated eggs contain and secrete tissue-type PA (t-PA) and
ejaculated spermatozoa exhibit urokinase-type PA (uPA). Second, t-PA is significantly
higher in follicular fluids and granulosa cells from follicles containing oocytes that can
be fertilized in vitro compared to follicles containing oocytes that fail to fertilize. Third,

37
the addition of plasminogen to the fertilization medium increases the frequency of eggs
fertilized in vitro.
Sperm cells must undergo the acrosome reaction before they can penetrate the
zona pellucida and fuse with the egg plasma membrane. Acrosome reaction progresses
from multiple fusion-points between the plasma and outer acrosomal membranes,
which expose the inner acrosomal membrane and the acrosomal contents (enzymes), to
complete vesiculation and loss of the integrity of the acrosome. The acrosome reaction
bears a strong resemblance to ligand-mediated exocytotic reactions in somatic cells
proceeding through an intracellular signal transduction system, it involves the
participation of a Gi protein, of phospholipase C and of protein kinase C. In addition, an
increase in intracellular calcium is concomitant with the induction of acrosomal loss.
Acrosome reaction can be induced by biological agents such as follicular fluid
(progesterone), cumulus cells or zonae pellucidae or by physiochemical agents such as
calcium ionophores, lysophosphatidylcholine and electropermeabilization or by the
aggregation of zona binding sites on the sperm heads.
2.3 SPERM-EGG FUSION After sperm entry into the perivitelline space, the final stages of sperm-egg
interaction include the binding and fusion of the sperm and egg plasma membranes,
and entry of the sperm into the egg. Sperm binding to the egg surface occurs on the
lateral face of the head, with the firm point of attachment between the sperm and egg
plasma membranes occurring at the equatorial segment. Little is known concerning the
sperm and egg surface complementary molecules (binding sites) that participate in
gamete plasma membranes fusion in mammals. It has been recently shown that a sperm
surface protein (PH-30, a guinea-pig sperm antigen), known to be involved in sperm-
egg fusion, shares biochemical characteristics with viral fusion proteins and contains an
integrin ligand domain. These results suggest that an integrin-mediated adhesion event
takes place and leads to fusion.

38
Fusion of a single sperm sets in motion a series of egg reactions to prevent
additional sperm entry, thus avoiding the lethal consequences of polyspermy. Egg
cortical reaction takes place soon after fusion, causing the zona pellucida to become "
hardened " and refractory to both binding and penetration of supernumerary sperm.
Zona binding is prevented by the inactivation of the sperm primary receptor (and
acrosome inducer) ZP3 and zona penetration is stopped through modification of the
sperm secondary receptor ZP2. The cortical reaction involves the exocytosis of cortical
granules and the release of their enzymatic content into the perivitelline space. The
oligosaccharides of ZP3 responsible for gamete recognition and adhesion are modified
by cortical granule glycosidase(s) and the glycoprotein ZP2 undergoes limited
proteolysis making the zona pellucida more insoluble and " hardened ", preventing the
maintenance of binding of acrosome-reacted sperm to the zona pellucida. It has been
suggested that the oocyte plasminogen activator may participate in this proteolytic
process although the evidence is poor.
2.4 EGG ACTIVATION AND PRONUCLEI FORMATION Gamete fusion triggers responses within the egg that culminate in the activation
of the embryonic developmental program. Activation may also be induced
parthenogenetically under various physical or chemical stimuli, in all cases, calcium is
an obligatory mediator. In mammals, sperm may cause both a persistent production of
inositol trisphosphate (InsP3) and an increase in calcium permeability of the plasma
membrane to maintain internal calcium oscillations. The early calcium increase induces
cortical granule exocytosis (cortical reaction), which involves a signal transduction
system that is similar to that of somatic cells, and that leads to the hardening of the zona
pellucida. Activation leads to the resumption of the cell cycle: the second meiotic
division is achieved, by the extrusion of the second polar body and the egg enters into
interphase with formation of pronuclei. Pronuclear formation takes place a few hours
after fertilization, and requires a calcium increase and a cytoplasmic alcalinization of

39
the zygote. Following anaphase II, the egg chromosomes remaining in the cytoplasm
disperse and the female pronucleus forms. Similarly, after cell fusion, the sperm nucleus
is decondensed and transformed into a male pronucleus. The biochemical transitions
responsible for the remodelling of the sperm nucleus consist of changes in the majority
of sperm specific chromatin proteins and the acquisition of chromosomal proteins
which induce a chromatin conformation compatible with fusion of male and female
pronuclei. Maternal chromatin and sperm pronuclear development are regulated by
common egg cytoplasmic factors involved in the regulation of the cell cycle and
dependent on oocyte maturation. The pronuclear development in fertilized eggs is
known to proceed through a series of transformations, which restore the transcriptional
competence of the inactive gamete chromatin and re-establish the functional diploid
genome of the embryo. Two stages of decondensation are observed: i) a very rapid
chromatin expansion dependent on egg nucleoplasmin, and ii) a slow membrane-
dependent decondensation involving protein migration into the nucleus reliant on
nuclear envelope formation recruited from maternal pool.
The two pronuclei move towards the egg center, and spermaster increases in size
during their migration. The end result of the migration of the pronuclei is their
juxtaposition, following pronuclear envelope breakdown, giving rise to a group of
chromosomes for the ensuing division. The spatial organization of microtubule arrays
in a cell is largely dependent on organizing centers, the centrosomes. The proximal
centriole of the sperm and its centrosomal material between apposed pronuclei are
involved in the fertilization events. Human centrioles as those of other animals except
the mouse are paternally derived. Eventually, there is an intermixing of the maternally
and paternally derived chromosomes to establish the genome of the embryo and hence
the process of fertilization can be considered as concluded.

40
2.4.1 SPERM ENTRY AND ACROSOMAL REACTION The acrosome is the tip of the sperm head. The acrosomal reaction is a change in
the sperm that is common to many animals. Its function is best understood in the sea
urchin.
1. Receptor proteins in the sperm plasma membrane contact the sea urchin jelly
coat (vitelline layer). This contact between receptor proteins and the jelly coat
(vitelline layer) causes the acrosomal membrane to dissolve, releasing acrosomal
enzymes.
2. In the egg, Na+ channels open in the plasma membrane (BELOW the jelly
coat/vitelline layer.) Normally, Na+ concentration is higher outside the cell than
inside. So Na+ ions flow down their gradient into the egg and the plasma
membrane depolarizes (positive charges neutralize the more negative charge
inside the egg cytoplasm.) This depolarization causes the fast block to
polyspermy.
3. The depolarization (neutralization of charge difference) causes voltage-sensitive
Ca2+ channels to open in the egg endoplasmic reticulum (ER).
4. Digestive enzymes from the acrosomal vesicle digest the jelly coat and vitelline
membrane. Ca2+ also activates a Na+:H+ ion exchanger, which pumps H+ out of
the cell, increasing intracellular pH. This pH change causes the polymerization of
actin subunits into microfilament cables that thrust acrosomal processes toward
the egg plasma membrane. Bindin released from the acrosomal vesicle coats the
acrosomal process.
5. The increase in intracellular calcium causes water to enter the cell, increasing
hydrostatic pressure. This aids in the extension of the acrosomal process. At last
the acrosome fuses with the egg's plasma membrane (beneath the vitelline layer).
The sperm head now has access to the cytoplasm.

41
6. The Ca2+ moves in a wave across the cell. This Ca++ results in the fusion of
cortical vesicles with the egg plasma membrane, releasing their contents into the
space surrounding the egg, called the perivitelline space. This raises the vitelline
membrane, and inactivates bindin receptors on the vitelline membrane. Thus,
any additional sperm are released from the vitelline membrane and no more
bind. This is known as the slow block to polyspermy.
7. The sperm head now enters the cytoplasm, where it forms a male pronucleus.
The pronucleus fuses with the egg nucleus, regenerating 2N chromosomes.
Mitosis (first cleavage) then occurs. Fertilization is complete.
Fig. Acrosome reaction
After making its way through the jelly coat, the sperm makes contact with the
vitelline envelope. Species-specific bindin receptors on the vitelline envelope are only
able to recognize bindin molecules from the same species. This "lock and key"
mechanism ensures that eggs are fertilized only by sperm of the same species. After
making its way through the vitteline envelope, the sperm and egg plasma membranes
fuse, and the sperm nucleus enters the cytoplasm of the egg.
42
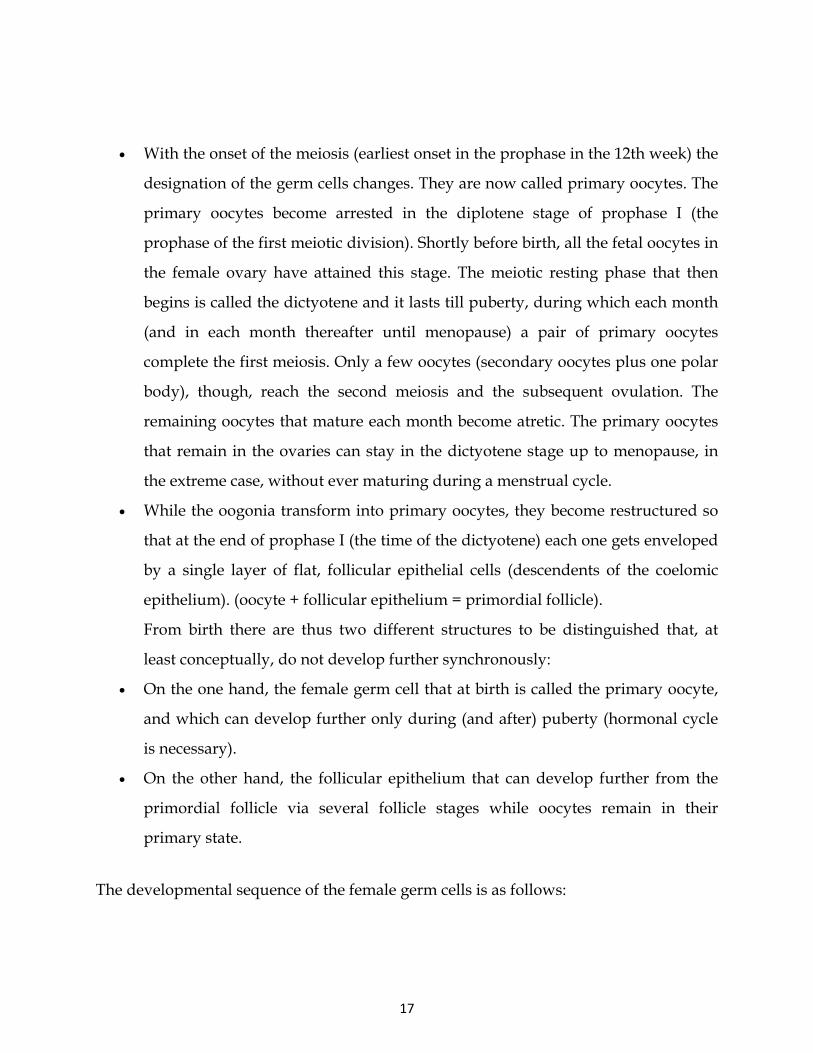
Fig. Acrosome reaction and formation of fertilization membrane
2.4.2 PREVENTING POLYSPERMY Although many sperm attach to the coats surrounding the egg, it is important
that only one sperm fuses with the egg plasma membrane and delivers its nucleus into
the egg. Two mechanisms are used by animals to ensure that only one sperm fertilizes a
given egg: the fast block to polyspermy and the slow block to polyspermy.
2.4.3 FAST BLOCK TO POLYSPERMY In marine invertebrates, including the sea urchin, a fast block to polyspermy
occurs within a tenth of a second of fusion. The fast block to polyspermy involves the
opening of Na+ channels in the egg plasma membrane. Na+ flows into the egg cell,
depolarizing the membrane. This depolarization prevents additional sperm from fusing
to the egg plasma membrane. The egg plasma membrane is restored to its normal -
70mV potential within minutes of fusion as the Na+ channels close, other + ions flow
out of the cell, and Na+ is pumped out. If depolarization is prevented, polyspermy
occurs - but how depolarization blocks polyspermy is not yet understood.

43
UNIT III
EMBRYOGENESIS 3.0 INTRODUCTION
3.1 CLEAVAGE
3.1.1 MECHANISM
3.1.2 TYPES OF CLEAVAGE
A) DETERMINATE
B)INDETERMINATE
C) HOLOBLASTIC
(i) BILATERAL
(ii) RADIAL
(iii) ROTATIONAL
(iv) SPIRAL
(D) MEROBLASTIC
(i) DISCOIDAL
(ii) SUPERFICIAL
(E) MAMMALS
3.2 BLASTRULATION
3.3 GASTRULATION
3.4 FATE MAPE
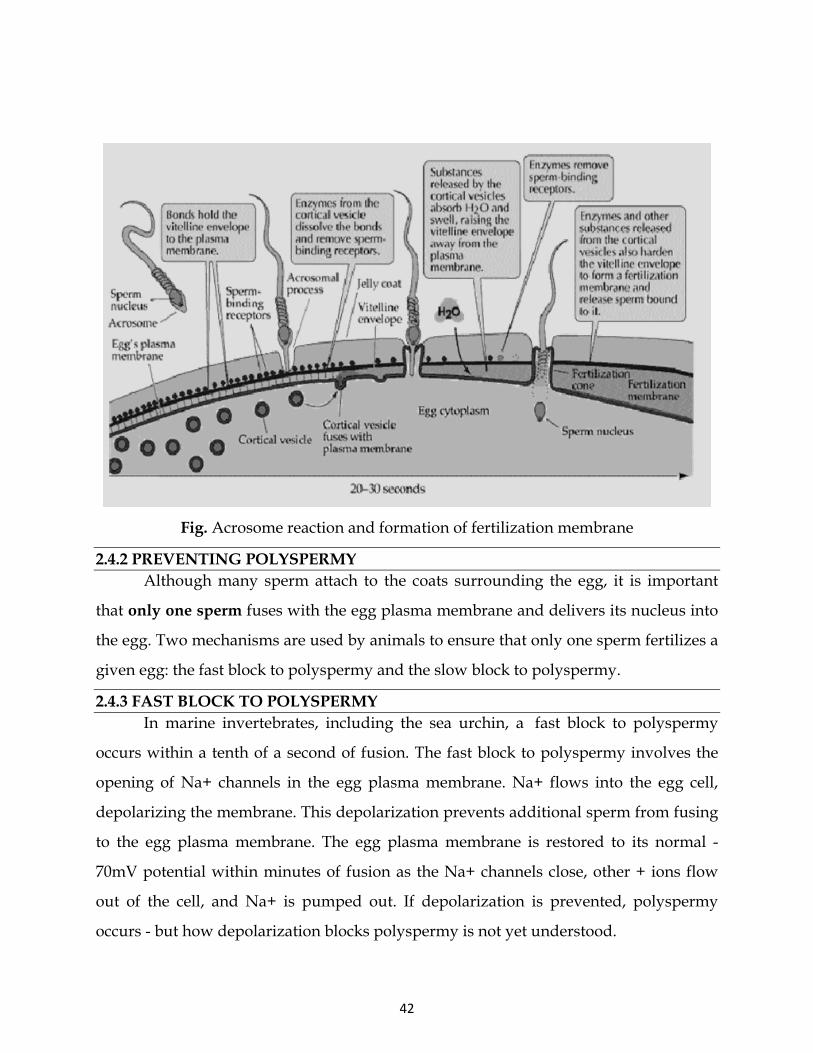
3.0 INTRODUCTION The zygotes of many species undergo rapid cell cycles with no significant
growth, producing a cluster of cells the same size as the original zygote, the early
embryo.
3.1 CLEAVAGE In embryology, the division of cells in the early embryo is termed as cleavage.
The different cells derived from cleavage are called blastomeres and form a compact
mass called the morula. Cleavage ends with the formation of the blastula.

44
Depending mostly on the amount of yolk in the egg, the cleavage can be
holoblastic (total or entire cleavage) or meroblastic (partial cleavage). The pole of the
egg with the highest concentration of yolk is referred to as the vegetal pole while the
opposite is referred to as the animal pole.
The rapid cell cycles are facilitated by maintaining high levels of proteins that
control cell cycle progression such as the cyclins and their associated cyclin-dependent
kinases (cdk). The complex CyclinB/cdc2 a.k.a. MPF (maturation promoting factor)
promotes entry into mitosis.
3.1.1 MECHANISM The processes of karyokinesis (mitosis) and cytokinesis work together to result in
cleavage. The mitotic apparatus is made up of a central spindle and polar asters made
up of polymers of tubulin protein called microtubules. The asters are nucleated by
centrosomes and the centrosomes are organized by centrioles brought into the egg by
the sperm as basal bodies. Cytokinesis is mediated by the contractile ring made up of
polymers of actin protein called microfilaments. Karyokinesis and cytokinesis are
independent but spatially and temporally coordinated processes. While mitosis can
occur in the absence of cytokinesis, cytokinesis requires the mitotic apparatus.
The end of cleavage coincides with the beginning of zygotic transcription. This
point is referred to as the midblastula transition and appears to be controlled by the
nuclear: cytoplasmic ratio (about 1/6).
3.1.2 TYPES OF CLEAVAGE
(A) DETERMINATE Determinate is the form of cleavage in most protostomes. It results in the
developmental fate of the cells being set early in the embryo development. Each cell
produced by early embryonic cleavage does not have the capacity to develop into a
complete embryo.

45
(B) INDETERMINATE A cell can only be indeterminate if it has a complete set of undisturbed animal/
vegetal cytoarchitectural features. It is a characteristic of deuterostomes - when the
original cell in a deuterostome embryo divides, the two resulting cells can be separated,
and each one can individually develop into a whole organism.
CLEAVAGE PATTERNS FOLLOWED BY HOLOBLASTIC AND MEROBLASTIC
EGGS
In 1923, embryologist E. B. Wilson reflected on how little we knew about
cleavage: “To our limited intelligence, it would seem a simple task to divide a nucleus
into equal parts. The cell, manifestly, entertains a very different opinion.” Indeed,
different organisms undergo cleavage in distinctly different ways. The pattern of
embryonic cleavage particular to a species is determined by two major parameters: the
amount and distribution of yolk protein within the cytoplasm, and factors in the egg
cytoplasm that influence the angle of the mitotic spindle and the timing of its formation.
Holoblastic Meroblastic
Bilateral (tunicates, amphibians)
Radial (sea urchin, amphioxus)
Rotational (mammals)
Spiral (annelids, mollusks)
Discoidal (fish, birds, reptiles)
Superficial (insects)
(C) HOLOBLASTIC In the absence of a large concentration of yolk, four major cleavage types can be
observed in isolecithal cells (cells with a small even distribution of yolk) or in
mesolecithal cells (moderate amount of yolk in a gradient) - bilateral holoblastic, radial
holoblastic, rotational holoblastic, and spiral holoblastic, cleavage. These holoblastic
cleavage planes pass all the way through isolecithal zygotes during the process of
cytokinesis. Coeloblastula is the next stage of development for eggs that undergo these

46
radial cleavaging. In holoblastic eggs the first cleavage always occurs along the vegetal-
animal axis of the egg, the second cleavage is perpendicular to the first. From here the
spatial arrangement of blastomeres can follow various patterns, due to different planes
of cleavage, in various organisms.
(i) BILATERAL The first cleavage results in bisection of the zygote into left and right halves. The
following cleavage planes are centered on this axis and result in the two halves being
mirror images of one another. In bilateral holoblastic cleavage, the divisions of the
blastomeres are complete and separate; compared with bilateral meroblastic cleavage,
in which the blastomeres stay partially connected.
(ii) RADIAL Radial cleavage is characteristic of the deuterostomes, which include some
vertebrates and echinoderms, in which the spindle axes are parallel or at right angles to
the polar axis of the oocyte.
(iii) ROTATIONAL Mammals display rotational cleavage, and an isolecithal distribution of yolk
(sparsely and evenly distributed). Because the cells have only a small amount of yolk,
they require immediate implantation onto the uterine wall in order to receive nutrients.
Rotational cleavage involves a normal first division along the meridional axis,
giving rise to two daughter cells. The way in which this cleavage differs is that one of
the daughter cells divides meridionally, whilst the other divides equatorially.
(iv) SPIRAL Spiral cleavage is conserved between many members of the lophotrochozoan
taxa, referred to as Spiralia. This group includes annelids, molluscs, and sipuncula.
Spiral cleavage can vary between species, but generally the first two cell divisions result
in four macromeres, also called blastomeres, (A, B, C, D) each representing one
quadrant of the embryo. These first two cleavages are oriented in planes that occur at
right angles parallel to the animal-vegetal axis of the zygote. At the 4-cell stage, the A

47
and C macromeres meet at the animal pole, creating the animal cross-furrow, while the
B and D macromeres meet at the vegetal pole, creating the vegetal cross-furrow. With
each successive cleavage cycle, the macromeres give rise to quartets of smaller
micromeres at the animal pole. The divisions that produce these quartets occur at an
oblique angle, an angle that is not a multiple of 90o, to the animal-vegetal axis. Each
quartet of micromeres is rotated relative to their parent macromere, and the chirality of
this rotation differs between odd and even numbered quartets, meaning that there is
alternating symmetry between the odd and even quartets. In other words, the
orientation of divisions that produces each quartet alternates between being clockwise
and counterclockwise with respect to the animal pole. The alternating cleavage pattern
that occurs as the quartets are generated produces quartets of micromeres that reside in
the cleavage furrows of the four macromeres. When viewed from the animal pole, this
arrangement of cells displays a spiral pattern.
Fig. D quadrant specification through equal and unequal cleavage mechanisms. At the
4-cell stage of equal cleavage, the D macromere has not been specified yet. It will be
specified after the formation of the third quartet of micromeres. Unequal cleavage
occurs in two ways: asymmetric positioning of the mitotic spindle, or through the
formation of a polar lobe (PL).
Equal cleavage Unequal cleavage Asymmetric Positioning of mitotic spindle Formation of polar lobe

48
Specification of the D macromere and is an important aspect of spiralian
development. Although the primary axis, animal-vegetal, is determined during
oogenesis, the secondary axis, dorsal-ventral, is determined by the specification of the D
quadrant. The D macromere facilitates cell divisions that differ from those produced by
the other three macromeres. Cells of the D quadrant give rise to dorsal and posterior
structures of the spiralian. Two known mechanisms exist to specify the D quadrant.
These mechanisms include equal cleavage and unequal cleavage.
In equal cleavage, the first two cell divisions produce four macromeres that are
indistinguishable from one another. Each macromere has the potential of becoming the
D macromere. After the formation of the third quartet, one of the macromeres initiates
maximum contact with the overlying micromeres in the animal pole of the embryo. This
contact is required to distinguish one macromere as the official D quadrant blastomere.
In equally cleaving spiral embryos, the D quadrant is not specified until after the
formation of the third quartet, when contact with the micromeres dictates one cell to
become the future D blastomere. Once specified, the D blastomere signals to
surrounding micromeres to lay out their cell fates.
In unequal cleavage, the first two cell divisions are unequal producing four cells
in which one cell is bigger than the other three. This larger cell is specified as the D
macromere. Unlike equally cleaving spiralians, the D macromere is specified at the
four-cell stage during unequal cleavage. Unequal cleavage can occur in two ways. One
method involves asymmetric positioning of the cleavage spindle. This occurs when the
aster at one pole attaches to the cell membrane, causing it to be much smaller than the
aster at the other pole. This results in an unequal cytokinesis, in which both macromeres
inherit part of the animal region of the egg, but only the bigger macromere inherits the
vegetal region. The second mechanism of unequal cleavage involves the production of
an enucleate, membrane bound, cytoplasmic protrusion, called a polar lobe. This polar
lobe forms at the vegetal pole during cleavage, and then gets shunted to the D

49
blastomere. The polar lobe contains vegetal cytoplasm, which becomes inherited by the
future D macromere.
Fig. Spiral cleavage in marine snail of the genus Trochus.
(D) MEROBLASTIC In the presence of a large amount of yolk in the fertilized egg cell, the cell can
undergo partial, or meroblastic, cleavage. Two major types of meroblastic cleavage are
discoidal and superficial.
(i) DISCOIDAL In discoidal cleavage, the cleavage furrows do not penetrate the yolk. The
embryo forms a disc of cells, called a blastodisc, on top of the yolk. Discoidal cleavage is
commonly found in birds, reptiles, and fish which have telolecithal egg cells (egg cells
with the yolk concentrated at one end).
(ii) SUPERFICIAL In superficial cleavage, mitosis occurs but not cytokinesis, resulting in a
polynuclear cell. With the yolk positioned in the center of the egg cell, the nuclei
migrate to the periphery of the egg, and the plasma membrane grows inward,
partitioning the nuclei into individual cells. Superficial cleavage occurs in arthropods
which have centrolecithal egg cells (egg cells with the yolk located in the center of the
cell).
(E) MAMMALS
50
Fig. The initial stages of human embryogenesis.
There are several differences between the cleavage in mammals and the cleavage
in other animals. Mammals have a slow rate of division that is between 12 and 24 hours.
These cellular divisions are asynchronous. Zygotic transcription starts at the two, four,
or eight-cell stage. Cleavage is holoblastic and rotational.
At the eight-cell stage, the embryo goes through some changes. Most of the
blastomeres in this stage become polarized and develop tight junctions with the other
blastomeres. This process leads to the development of two different populations of cells:
polar cells on the outside and apolar cells on the inside. The outer cells, called the
trophoblast cells, pump sodium in from the outside which automatically brings water
in with it to the basal (inner) surface to form a blastocoel cavity in a process called
compaction. The embryo is now called a blastula or early blastocyst. The trophoblast
cells will eventually give rise to the embryonic contribution to the placenta called the
chorion. The inner cells are pushed to one side of the cavity (because the embryo isn't
getting any bigger) to form the inner cell mass (ICM) and will give rise to the embryo
and some extraembryonic membranes. At this stage, the embryo is called a blastocyst.

51
Fig. Summary of the main patterns of cleavage
The amount and distribution of yolk determines where cleavage can occur and
the relative size of the blastomeres. When one pole of the egg is relatively yolk-free, the
cellular divisions occur there at a faster rate than at the opposite pole. The yolk-rich
pole is referred to as the vegetal pole; the yolk concentration in the animal pole is
relatively low. The zygote nucleus is frequently displaced toward the animal pole. In
general, yolk inhibits cleavage. At one extreme are the eggs of sea urchins, mammals,
and snails. These eggs have sparse, equally spaced yolk and are thus isolecithal (Greek,

52
“equal yolk”). In these species, cleavage is holoblastic (Greek holos, “complete”).
meaning that the cleavage furrow extends through the entire egg. These embryos must
have some other way of obtaining food. Most will generate a voracious larval form,
while mammals get their nutrition from the placenta.
At the other extreme are the eggs of insects, fishes, reptiles, and birds. Most of their
cell volumes are made up of yolk. The yolk must be sufficient to nourish these animals.
Zygotes containing large accumulations of yolk undergo meroblastic cleavage, wherein
only a portion of the cytoplasm is cleaved. The cleavage furrow does not penetrate into the
yolky portion of the cytoplasm. The eggs of insects have their yolk in the center (i.e., they
are centrolecithal), and the divisions of the cytoplasm occur only in the rim of cytoplasm
around the periphery of the cell (i.e., superficial cleavage). The eggs of birds and fishes have
only one small area of the egg that is free of yolk (telolecithal eggs), and therefore, the cell
divisions occur only in this small disc of cytoplasm, giving rise to the discoidal pattern of
cleavage. These are general rules, however, and closely related species can evolve different
patterns of cleavage in a different environment.
However, the yolk is just one factor influencing a species' pattern of cleavage.
There are also inherited patterns of cell division that are superimposed upon the
constraints of the yolk. This can readily be seen in isolecithal eggs, in which very little
yolk is present. In the absence of a large concentration of yolk, four major cleavage
types can be observed: radial holoblastic, spiral holoblastic, bilateral holoblastic, and
rotational holoblastic cleavage. We will see examples of these cleavage patterns below
when we take a more detailed look at the early development of four different
invertebrate groups.
3.2 BLASTULATION The blastula (from Greek blastos, meaning "sprout") is a solid sphere of cells formed
during an early stage of embryonic development in animals. The blastula is created when
the zygote undergoes the cell division process known as cleavage. The blastula is preceded
by the morula and precedes the gastrula in the developmental sequence. A common feature

53
of a vertebrate blastula is that it consists of a layer of blastomeres, known as the blastoderm,
which surrounds an interior central cavity known as the blastocoel. In mammals,
blastulation leads to the formation of the blastocyst, which must not be confused with the
blastula. The blastocyst contains an embryoblast, which is homologous to the blastula.
However, it also includes the trophoblast, which goes on to form the extraembryonic
tissues.
Fig. Blastulation: A - morula, B – blastula (day-4 of fertilization)
BLASTOCYST OF MAMMAL
Blastulation is the formation of a blastula from a morula. The morula is an
embryo filled evenly with cells (blastomeres), but the blastula contains a fluid cavity
called blastocoel. In mammals, the blastula is called a blastocyst which consists of inner
cell mass, trophoblast and blastocoels.
Fig. Blastocyst
During blastulation, cells continue to divide and begin to differentiate. The outer
cells of the morula are polarized. That is, one side of the cell differs from the other side.
The outer, polar cells give rise to trophoblast and the inner, apolar cells become the
inner cell mass. The watery fluid of the blastocoel is secreted by trophoblast cells and
transported in from the exterior. For the human, the blastocyst is formed by days 5 to 6

54
after fertilization. At this time, the blastocyst has reached the uterus, but has not yet
implanted into the uterine wall. The day 5, preimplantation human embryo contains
200 to 250 cells, only 30 to 34 of which are inner cell mass cells. In subsequent
development, the cells of the inner cell mass will give rise to all tissues of the embryo's
body. The embryonic stem cells are derived from the inner cell mass.
3.3 GASTRULATION Gastrulation is a phase early in the development of most animal embryos, during
which the morphology of the embryo is reorganized to form the three germ layers:
ectoderm, mesoderm, and endoderm. The molecular mechanism and timing of
gastrulation is different in different organisms. Gastrulation is followed by
organogenesis, when individual organs develop within the newly formed germ layers
Fig. Gastrulation of a diploblast: The formation of germ
layers from a blastula to agastrula. Some of the
ectoderm cells move inward forming the endoderm .

55
Fig. Typical organization of late gastrula
DEVELOPMENT
Gastrulation creates the three embryonic germ layers: the ectoderm, mesoderm, and
endoderm. Each layer gives rise to specific tissues and organs in the developing
embryo.
• The ectoderm gives rise to:
o epidermis structures such as the skin, nails, and hair
o neural crest and neural tissues, which give rise to the nervous system
• The mesoderm is found between the ectoderm and the endoderm and gives rise
to:
o somites, which form muscle, the cartilage of the ribs and vertebrae, and
the dermis
o notochord
o blood and blood vessels

56
o bone and connective tissue
• The endoderm gives rise to:
o epithelium of the digestive system and respiratory system
o organs associated with the digestive system, such as the liver and
pancreas
The embryo must have the correct amount of each germ layer, which must be
properly oriented within the embryo for the organs to develop correctly. Thus,
gastrulation must be tightly regulated for proper embryo development.
LOSS OF SYMMETRY
In preparation for gastrulation, the embryo must become asymmetric along both
the proximal-distal axis and the anterior-posterior axis. The proximal-distal axis is
formed when the cells of the embryo form the “egg cylinder,” which consists of the
extraembryonic tissues, which give rise to structures like the placenta, at the proximal
end and the epiblast at the distal end. Many signaling pathways contribute to this
reorganization, including BMP, FGF, nodal, and Wnt. Visceral endoderm surrounds the
epiblast. The distal visceral endoderm (DVE) migrates to the anterior portion of the
embryo, forming the “anterior visceral endoderm” (AVE). This breaks anterior-
posterior symmetry and is regulated by nodal signaling.
Fig. Epithelial to Mesenchmyal Cell Transition – loss of cell adhesion leads to
constriction and extrusion of newly mesenchymal cell.

57
FORMATION OF THE PRIMITIVE STREAK
The primitive streak is formed at the beginning of gastrulation and is found at
the junction between the extraembryonic tissue and the epiblast on the posterior side of
the embryo and the site of ingression. Formation of the primitive streak is reliant upon
nodal signaling within the cells contributing to the primitive streak and BMP4
signaling from the extraembryonic tissue. Furthermore, Cer1 and Lefty1 restrict the
primitive streak to the appropriate location by antagonizing nodal signaling. The region
defined as the primitive streak continues to grow towards the distal tip.
EPITHELIAL TO MESENCHYMAL TRANSITION AND INGRESSION
In order for the cells to move from the epithelium of the epiblast through the
primitive streak to form a new layer, the cells must undergo an epithelial to
mesenchymal transition (EMT) to lose their epithelial characteristics, such as cell-cell
adhesion. FGF signaling is necessary for proper EMT. FGFR1 is needed for the up
regulation of Snai1, which down regulates E-cadherin, causing a loss of cell adhesion.
Following the EMT, the cells ingress through the primitive streak and spread out to
form a new layer of cells or join existing layers. FGF8 is implicated in the process of this
dispersal from the primitive streak.
GASTRULATION IN AMPHIBIANS
During cleavage in amphibians, a higher density of yolk in the vegetal half of the
embryo results in the blastocoel cavity being placed asymmetrically in the animal half
of the embryo. Unlike in sea urchins, the cells surrounding the blastocoel are thicker
than a monolayer. The blastocoel cavity prevents signaling between the animal cap and
provides a space for involuting cells during gastrulation.
There are four kinds of tissue movements that drive gastrulation in Xenopus:
invagination, involution, convergent extension and epiboly. At the vegetal edge of the
dorsal marginal zone, cells change from a columnar shape to become a bottle cell and
drive invagination. At this invagination, cells begin to involute into the embryo. This

58
initial site of involution is called the dorsal lip. The involuting cells migrate along the
inside of the blastocoel toward the animal cap. This migration is mediated by
fibronectin of the extracellular matrix (ECM) assembled by the blastocoel roof.
Eventually, cells from the lateral and ventral sides begin to involute to form a ring of
involuting cells surrounding the yolk plug. These involuting cells will eventually form
the archenteron which displaces and eventually replaces the blastocoel. Cells from the
lateral marginal zone intercalate with cells closer to the dorsal midline. Directed cell
intercalation within the dorsal mesoderm drives convergent extension. The dorsal cells
become the first to migrate along the roof of the blastocoel cavity and form the
anterior/posterior axis of the embryo. Both prior to and during the involution, the
animal cap undergoes epiboly and spread toward the vegetal pole.
Fig. Gastrulation in a frog embryo. In the frog blastula, the blastocoel is displaced
toward the animal pole and is surrounded by a wall several cells thick. The cell

59
movements that begin gastrulation occur on the dorsal side of the blastula, where the
gray crescent was located in the zygote. Although still visible as gastrulation begins, the
gray crescent is not shown here.
1. Gastrulation begins when a small indented crease, the dorsal lip of the
blastopore, appears on one side of the blastula. The crease is formed by cells
changing shape and pushing inward from the surface (invagination). Additional
cells then roll inward over the dorsal lip (involution) and move into the interior,
where they will form endoderm and mesoderm. Meanwhile, cells of the animal
pole, the future ectoderm, change shape and begin spreading over the outer
surface.
2. The blastopore lip grows on both sides of the embryo, as more cells invaginate.
When the sides of the lip meet, the blastopore forms a circle that becomes smaller
as ectoderm spreads downward over the surface. Internally, continued
involution expands the endoderm and mesoderm, and the archenteron begins to
form; as a result, the blastocoel becomes smaller.
3. Late in gastrulation, the endoderm-lined archenteron has completely replaced
the blastocoel and the three germ layers are in place. The circular blastopore
surrounds a plug of yolk-filled cells.

60
FISH
At the time of mid-blastula transition, the zebrafish embryo is composed of three
distinct cell layers: the enveloping layer (EVL), deep cells, and the yolk syncytial layer
(YSL) formed from the fusion of cells adjacent to the yolk cells.
The first stage of gastrulation begins with the epiboly of the EVL and the deep
cells over the YSL. This epiboly is driven by the migration of nuclei and cytoplasm in
the YSL and attachments between the YSL and the EVL. Intercalation of the deep cells
with the EVL help drive this movement. At about 50% of epiboly, a fate map similar to
that of the Xenopus can be derived. The EVL develops into an extraembryonic
membrane and does not contribute to the embryo.
The second stage of gastrulation occurs when the leading edge of the epibolizing
blastoderm thickens. The dorsal side forms a larger thickening and is known as the
embryonic shield. The deep cells in the embryonic shield form two layers. The epiblast
forms near the surface and will give rise to the ectoderm. The hypoblast forms next to
the YSL and will form a mixture of endoderm and mesoderm. The hypoblast is formed
through involution and/or ingression. The movement of cells in the hypoblast are
similar to the involuting mesoderm of amphibians. The end result of gastrulation is an
asymmetric involution of cells that form the dorsal structures of the embryo.
BIRDS
After cleavage, the blastoderm of chick embryos that sits above the yolk secretes
fluid basally into the space between the yolk and the blastoderm called the subgerminal
space. The region of the blastoderm above the subgerminal space is called the area
pellucida. The region of the blastoderm above the yolk is the area opaca. The region
where these two zones meet is called the marginal zone. At the posterior marginal zone
(PMZ), there is a condensation of cells that is important in gastrulation. Within the
PMZ, there is another thickening of cells called the Koller's sickle. Before gastrulation
begins, the blastoderm forms two layers: the epiblast and the hypoblast. The epiblast

61
gives rise to the embryo and some of the extraembryonic structures while the hypoblast
contributes entirely to the extraembryonic membranes. The hypoblast comes from the
primary hypoblast which delaminate out of the epiblast. This structure is equivalent to
the organizer in amphibians and the embryonic shield in fish. Cells ingress through the
primitive groove into the blastocoel cavity, migrate anteriorly through Hensen's node
and then laterally through the rest of the groove. Cells that are fated to become the
endoderm migrate to the bottom of the cavity and replace the hypoblast cells. Cells that
are fated to become mesoderm remain in between the future endoderm cells and the
epiblast and the epiblast cells remain to become ectodermal cells. The ectoderm,
however, is undergoing epiboly to surround the yolk mass. The cells at the edge of the
area opaca send out long filopida that attach to fibronectin in the vitelline membrane
surrounding the embryo and yolk mass and pull the ectodermal cells toward the
vegetal pole.
As gastrulation proceeds, the primitive streak regresses posteriorly with
pharyngeal endoderm, the head process, and the notochord being laid down as it
recedes. This results in a temporal gradient of development with the anterior forming
organs while the posterior is still going through gastrulation.
INVERTEBRATES
SEA URCHINS
The following description concerns gastrulation in echinoderms, representative
of the triploblasts, or animals with three embryonic germ layers. Sea urchins deviate
from simple cleavage at the fourth cleavage. The four vegetal blastomeres divide
unequally to produce four micromeres at the vegetal pole and four macromeres in the
middle of the embryo. The animal cells divide meridionally and produce mesomeres.
At the beginning of vertebrate gastrulation, the embryo is a hollow ball of cells
known as the blastula, with an animal pole and a vegetal pole. The vegetal pole begins
to flatten to form the vegetal plate. Some of the cells of the vegetal pole detach and

62
through ingression become primary mesenchyme cells. The mesenchyme cells divide
rapidly and migrate along the extracellular matrix (basal lamina) to different parts of
the blastocoel. The migration is believed to be dependent upon sulfated proteoglycans
on the surface of the cells and molecules on the basal lamina such as fibronectin. The
cells move by forming filopodia that identify the specific target location. These filopodia
then organize into syncytial cables that deposit the calcium carbonate that makes up the
spicules (the skeleton of the pluteus larva).
During the second phase of gastrulation, the vegetal plate invaginates into the
interior, replacing the blastocoelic cavity and thereby forming a new cavity, the
archenteron (literally: primitive gut), the opening into which is the blastopore. The
arechenteron is elongated by three mechanisms. First, the initial invagination is caused
by a differential expansion of the inner layer made of fibropellins and outer layer made
of hyalin to cause the layers to bend inward. Second, the archenteron is formed through
convergent extension. Convergent extension results when cells intercalate to narrow the
tissue and move it forward. Third, secondary mesenchyme pull the tip of the
archenteron towards the animal pole. Secondary mesenchyme are formed from cells
that ingress from, but remain attached to, the roof of the archenteron. These cells extend
filopodia that use guidance cues to find the future mouth region. Upon reaching the
target site, the cells contract to pull the archenteron to fuse with the ectoderm. Once the
archenteron reaches the animal pole, a perforation forms, and the archenteron becomes
a digestive tract passing all the way through the embryo. The three embryonic germ
layers have now formed. The endoderm, consisting of the archenteron, will develop
into the digestive tract. The ectoderm, consisting of the cells on the outside of the
gastrula that played little part in gastrulation, will develop into the skin and the central
nervous system. The mesoderm, consisting of the mesenchyme cells that have
proliferated in the blastocoel, will become all the other internal organs.

63
3.4 FATE MAP A map of an embryo showing areas that are destined to develop into specific
adult tissues and organs. A map of the developmental fate of a zygote or early embryo
showing the adult organs that will develop from material at a given position on the
zygote or early embryo.
A fate map is a representation of the developmental history of each cell in the
body of an adult organism. Thus, a fate map traces the products of each mitosis from
the single-celled zygote to the multi-celled adult. The process of fate mapping was
developed by Walter Vogt.
Fate mapping is a technique that is used to show how a cell or tissue moves and
what it will become during normal development. Fate mapping was developed by
Walter Vogt as a means by which to trace the development of specific regions of the
early embryo. To do this, Vogt used agar chips impregnated with vital dyes.
The fate map of vulval development in C. elegans has been completely
characterized at a molecular level. In an adult C. elegans, the vulva is the egg-laying
organ that consists of only 22 cells. The differentiation and division of these Px.p cells is
dictated by the anchor cell through a morphogen gradient of LIN-3. Mapping each cell's
fate was accomplished by studying mutants and through tissue grafts.

64
Gastrulation includes a series of morphogenetic movements that re-arrange the
animal embryo and result in the establishment of the primary "germ layers" from
which tissues will develop and differentiate.
Ex. Gastrulation in Xenopus laevis: This animation begins with a fate map of the
surface of a Xenopus embryo (dorsal side to left), showing the animal cap (green); non-
involuting marginal zone (NIMZ; blue); involuting marginal zone (IMZ; yellow);
presumptive bottle cells (orange); and yolky vegetal base (light orange). The blue dotted
line indicates the limit of the prospective neural plate cells. It then cuts away to a sagital
view depicting the movements of cell layers during gastrulation.
FATE MAPPING AXOLOTL EMBRYOS IN EARLY GASTRULATION
BACKGROUND
Since different amphibians execute gastrulation in different ways, the study of
amphibian gastrulation has been complex. A popular method used to examine and
explore gastrulation and determine the future fate of cells in amphibian embryos is the
visualization of cell movement by application of a vital (non-toxic) dye to the region of
interest on the amphibian embryo. This process of observing morphogenetic cell
movements with vital dye and correlating wuth developmental fate is known as fate
mapping (Gilbert, 2000 and Hamburger 1960).
Animal cap: green NIMZ-S: superficial layer of the non-involuting marginal zone NIMZ-D: deep layer of the non-involuting marginal zone IMZ-S: superficial layer of the involuting marginal zone IMZ-D: deep layer of the involuting marginal zone

65
In 1929, Walter Vogt, an embryologist, used vital dyes to construct fate maps of
amphibian embryos. He spread and dried dye and agar on a microscope plate and cut
the ends of the dyed agar to apply to desired regions of the embryo. He placed the
small vital dye chips on the surface of amphibian embryos at various stages of
development to study the movements and fates of various regions of the embryo. Vogt's
fate mapping studies at the gastrula stage introduced embryologists to a very useful
method of determining which portions of the embryo become which larval or adult
Cells of the amphibian blastula have different fates depending on the position of the
cells (dorsal-ventral, anterior-posterior, left-right) and how deep they are in the layers of the
embryo (Gilbert, 2000), We will observe the movement of a population of cells to see what
thieir developmental fate is by dying the embryos superficial regions at two different
positions with respect to the blastopore lip (figure 1).
Assuming that none of my readers are perfectly spherical, you all possess notable
asymmetries—your top half is different from your bottom half, and your front or
ventral half is different from you back or dorsal half. You left and right halves are
probably superficially somewhat similar, but internally your organs are arranged in
lopsided ways. Even so, the asymmetries are relatively specific: you aren't quite like
that Volvox to the right, a ball of cells with specializations scattered randomly within.

66
People predictably have heads on top, eyes in front, arms and legs in useful locations.
This is a key feature of development, one so familiar that we take it for granted.
I'd go so far as to suggest that one of the most important events in our
evolutionary history was the basic one of taking a symmetrical ball of cells and
imposing on it a coordinate system, creating positional information that allowed cells to
have specific identities in particular places in the embryo. When the first multicellular
colony of identical cells set aside a particular patch of cells to carry out a particular
function, say putting one small subset in charge of reproduction, that asymmetry
became an anchor point for establishing polarity. If cells could then determine how far
away they were from that primitive gonad, evolution could start shaping function by
position—maybe cells far away from the gonad could be dedicated to feeding, cells in
between to transport, etc., and a specialized multicellular organism could emerge.
Those patterns are determined by interactions between genes, and we can try to unravel
the evolutionary history of asymmetry with comparative studies of regulatory
molecules in early development.
In developmental biology, those who study early events are often looking at the
formation of these asymmetries. One way to think of development at these stages is as a
process that establishes fields of interacting cells, each field with a general expected role
to play in the embryo, and each with its own different patterns of gene expression. The
distribution of the fields, these fundamental asymmetries, are set up early in
development, and we can map them out. Here, for instance, is a fate map of an early frog
embryo, at a time when it looks like little more than a ball of cells.

67
The embryo itself looks nothing like this, but is just a ball of cells with some
orienting features: there's more pigment at the top (the "Animal" side), and at this early
gastrula stage, there's a little pucker called the dorsal lip, indicated by the short green
line on the right side of the image. What scientists do is mark individual cells—in the
old days, they might use particles of chalk or carbon, pressed up against the surface of
the cells, but nowadays we more commonly inject the cells with a fluorescent dye—and
then let the animal develop and ask where the marker ends up. Mark cells just above
the dorsal lip, for instance, and then look a few days later at the tadpole, and you
discover that only the notochord is fluorescing, and nothing else. Mark cells a little
further towards the animal pole, and only cells in the nervous system are lit up. Do
thousands of experiments like that, and you end up with a map like the one above,
where you've got a good idea of what each cell will do in the embryo. You've also
exposed otherwise invisible asymmetries in the animal.
Way, way back in my grad school days, this kind of work was central to my
Ph.D. thesis project. Others in the Kimmel lab at the University of Oregon were working
to build a fate map of the zebrafish, and I was taking advantage of their work to look at
the developing nervous system. They told me where the cells in the early embryo were
fated to become the nervous system, and Judith Eisen and I would inject single cells in

68
that region, let the embryo grow up to a stage we were interested in, and then we'd
have animals where subsets of neural cells were glowing green, making them easy to
watch.
Fate maps give an idea of prospective changes in the formation of tissues and
organs, but what we ultimately want to examine is the pattern of gene expression in
these cells. For that, we use another tool: the in situ stain. In this procedure, if you know
the sequence of a gene, you can make a probe that complements the sequence of the
mRNA it produces, and tag it with a colored marker. Soak the embryo in your probe, it
sticks to RNA in any cells that are expressing the gene of interest, and can be washed
out of cells that don't have any complementary RNA. The image to the right is of some
other old work I did with Scott Stachel and David Grunwald on zebrafish. Those
spherical balls are early embryos around the time of gastrulation, and we labeled them
with a probe to the gene goosecoid (gsc). That gene is turned on in cells that will become
the notochord, and we could use it as a marker for an early asymmetry—at a time when
the animal was a ball of cells, we could detect that blue lozenge of cells, which were the
population about to become a specific tissue.
Again, after many experiments by many people, we can determine what genes
are turned on where and when in setting up these asymmetries, and here is a partial
map of important genes superimposed on a frog fate map.

69
Fig. Diagram of a fate map for an amphibian embryo indicating the positions of
ectodermal (including the CNS), mesodermal, and endodermal germ layers and some of
the signaling molecules located on the ventral and dorsal (Spemann Organizer) sides
involved in D-V polarity formation.
This is a tiny snippet of what we know—these are just some of the genes involved
in setting up one plane of asymmetry, the dorsal/ventral distinction. BMP4, for
instance, is a ventralizing gene that specifies cells to become part of your front half,
while Chordin/Noggin/Gsc are genes that suppress BMP4 or specify dorsal fates,
contributing to the formation of your notochord and nervous system. These are old, old
genes. We share them with other animals, like insects, so they arose and acquired their
functions in generating asymmetries before our lineages separated, sometime way back
in the pre-Cambrian. They are part of our makeup as members of the Bilaterian
superphylum, the animals with bilateral symmetry, and, we thought, distinguish us
from the Radiata (diploblasts with radial symmetry) and Parazoa (multicellular animals
with no discrete tissues or organs. They seem to be older than we thought, though.
Recent work by Matus et al. has delved into the developmental molecular biology of the
starlet anemone, Nematostella vectensis, specifically plumbing the sequenced anemone
genome for the same genes used in frogs and flies and people to define our dorso-

70
ventral axis, and they're there. What's more, they are expressed asymmetrically, and the
anemone contains a huge amount of hidden complexity in its organization. Here's a
picture of the planula larva of Nematostella—it's really not much of an animal, little more
than a hollow ball with an opening at one end and a tuft of cilia at the other.
Asymmetry along one axis from blastopore to apical tuft is obvious, but anything
equivalent to the dorso-ventral axis isn't; it seems to be radially symmetrical about that
axis.
Fig. Body plan of the anemone N. vectensis. (A and B) Micrographs of a lateral view of a
planula-stage N. vectensis embryo. (A) Differential interference contrast micrograph.
(B) Confocal micrograph with F-actin (green) and nuclei (red) stained with BODIPY-
phalloidin and propidium iodide. The asterisk marks the blastopore and site of the
future mouth. at, apical tuft; b.end, body wall endoderm; b.ect, body wall ectoderm;
pha, pharynx; p.end, pharyngeal endoderm; p.ect, pharyngeal ectoderm.
Not so fast, though—a cross section reveals some subtleties. Look at the
pharyngeal structure in the center, which is flattened along one plane. The authors don't
want to call it a dorso-ventral axis, reasonably enough since it isn't quite the same, and
call it the "directive axis" instead. It is a plane of symmetry that gives a bilateral aspect
to this member of the Radiata.

71
Fig. Cross-sectional diagram of the N. vectensis body plan
showing the different germ layers.
Fig. Gsc is asymmetrically expressed along the directive axis during development.
NvGoosecoid (gsc) is expressed initially in body wall endoderm (b.end) (A) and
pharyngeal endoderm (p.end) and ectoderm (p.ect).
SURFACE FATE MAP
The pictures below provides an overview of the changes in position of various
tissues on the embryo's surface during gastrulation in Xenopus. These pictures are
adapted directly from pictures hand-drawn by Dr. Ray Keller, Univ. of Virginia, and are
based on his fate maps of superficial cells in Xenopus. Note the dramatic spreading of
the light blue material (presumptive epidermis), and the convergence and extension of
the dark blue material (presumptive neural ectoderm) as gastrulation proceeds. Also
note that the yellow material (endoderm) becomes completely covered by ectodermal
tissue by the end of gastrulation. The green material is material that will form part of

72
the archenteron. The dorsal non-involuting marginal zone, which gives rise to the tissue
of the neural plate during neurulation, undergoes convergence and extension,
converging towards the dorsal side of the embryo (on the left here) and extending along
the forming anterior-posterior axis.

73
UNIT IV
EMBRYONIC INDUCTION 4.0 INTRODUCTION
4.1 ORGANIZER
4.1.1 SPEMANN’S PRIMARY EMBRYONIC INDUCTION
4.2 ORGANOGENESIS
4.3 EMBRYONIC ADAPTATION
4.4 POST EMBRYONIC INDUCTION
4.4.1 METAMORPHOSIS
4.4.2 REGENERATION
4.0 INTRODUCTION In 1903, W. HEN and Warren Lewis discovered that the lens of the frog embryo
will develop in flank ectoderm which has been transplanted over the eye cup, he
revealed the phenomenon of embryonic induction, an enigma which has received
considerable attention during the past 50 years. Briefly, embryonic induction can be
defined as the process by which one tissue calls forth specific morphogenetic
development in an adjacent tissue. In the case of the amphibian lens, the optic vesicle
induces the overlying ectoderm, with which it is in contact, to differentiate into a lens.
The mechanisms involved in the process of induction are little understood despite the
accumulation of considerable information from laboratories all over the world.
In the years following the original discoveries of Lewis, Spemann and others, it
was learned that the phenomenon of induction is not limited to lens formation, but in
fact is a general process involved in the development of almost every tissue and organ.
'Our fullest realization of the universal importance of induction came about with the
discovery of the amphibian "organizer" by Hans Spemann and his pupil, Hilde
Mangold. In 1924, Mangold and Spemann carried out a series of insertion ("einsteck")
experiments in which the dorsal lip of the blastopore of an early gastrula was implanted
into the blastocoel of a second embryo. As the events of gastrulation neared completion,

74
the implanted dorsal lip piece was now displaced to the ventral part of the host embryo,
and there, in contact with ventral ectoderm, a second embryo was induced. This
secondary embryo, so induced by the dorsal lip implant, contained neural tube,
notochord, somites, and gut. The character of this induction was completely organized;
thus the grafted dorsal lip was responsible for the orderly differentiation of the host
tissues rather than for a chaotic organization of reacting tissue. With this outstanding
discovery, numerous investigators began to search for an agent or agents which are
contained, presumably, in the "dorsal lip" and which were responsible for the organized
induction observed by Mangold and Spemann and subsequently, by others. Attempts
to obtain and to characterize the inductor-substances proved difficult; however, many
new facts of the inductive process were revealed. Relative to the "organizer", it was soon
learned that this center is not single in nature, but rather is divided subtly into lesser
organizers specific for head, trunk, and tail regions. Although much emphasis was
placed on the element of induction, it was revealed that inductors can only affect tissues
which are competent to respond to inductive stimuli. For instance, if presumptive
epidermis of an early gastrula is transplanted to a prospective neural area of second
gastrula, the transplant will differentiate into neural tissue because in its new
environment it is exposed to a neural induction system to which it is competent to react.
However, if epidermal ectoderm of a tail bud or a larval stage is similarly transplanted
to the prospective neural area of a gastrula, it will not develop into neural tissue
because it is no longer competent to respond to a neural inductor system. Although this
ectoderm has lost its competence for neural induction, it has gained new competences
and can react to inductors for lens, cornea, balancer, ear vesicle, etc. These observations
indicate that there is a "time course" to competence. A similar "time course" exists for
some inductive tissues. In an elegant study of the development of the ear, Yntema has
shown that normal development occurs only with the synchronization of the

75
competence of ectoderm with the sequentially acting inductors, mesoderm and
prospective hindbrain.
As a result of specificities that result from changes in competence and induction
during morphogenesis, chains of induction become important to the neural
development of the organism. For instance, the forebrain and optic vesicles are induced
by the underlying roof of the archenteron. The optic vesicle in turn induces the
formation of the lens which is subsequently active in the induction of the cornea.
4.1 ORGANIZER One of the first major "breakthroughs" in the quest for the identification of the
"organizer" and its inducing substances was derived from Holtfreter's observations that
the "organizer" capacity of dorsal lip material could be modified after heat coagulation,
and that some differentiated tissues of various animal forms possess strong inductive
capacities which are either neural or mesodermal. The latter discovery was taken up
largely by Chuang and by Toivonen and his followers, who showed that the inductive
action of adult tissues is not of a random nature, but that various tissues have a specific
action. The specificity is based upon the ability of various extracts to induce
archencephalic (forebrain, eye, nose), deuterencephalic (midbrain, hindbrain) and
spinocaudal (spinalchord, tail) structures. Such tissues as liver, blood, and kidneys of
some animals possess archencephalic inductive tendencies while kidney of other
animals and bone marrow act as deuterencephalic and spinocaudal inductors.
Generally, deuterencephalic and spinocaudal inductors are thermolabile; on the other
hand, archencephalic inductions are still obtained after heating the inductor tissues.
Toivonen and Saxen have indicated that deuterencephalic structures are a result of
interplay between neuralizing and mesodermalizing inductive substances. The
mesodermalizing substance is prevalent in normal bone marrow such as that of the rat.
It is interesting to note, how- ever, that bone marrow of leukemic rats is practically void
of inductive action.

76
Recently such tissues as bone marrow, liver, and spleen have been extracted and
treated in various ways in an effort to associate specific components with specific
inductive tendencies. The results are still somewhat nebulous; however, it is suggested
that many of these inductor effects are due to a protein or ribonucleoprotein and that
there is relatively little induction attributable to RNA alone.
Of possible relationship to the inductor substances present in various tissues is a
substance promoting nerve growth which has been isolated from sarcomas, snake
venom, and salivary glands. Levi-Montalcini and Cohen (see McElroy and Glass) have
extended the original observations of Bueker and have shown that two types of mouse
sarcomas, snake venom, and mouse salivary gland extract stimulate a tremendous
growth of sensory and sympathetic ganglia of the chick embryo, both in vivo and in
vitro. Their growth which involves both hyperplasia and hypertrophy is so extensive
that some nerve fibers even invade the lumina of blood vessels. Cohen has indicated
that the active substances from these three different sources are protein in nature and
possess similar properties. Although one would hesitate to classify this nerve growth
promoting substance as an inductor, it is reminiscent of the above-mentioned
archencephalic, deuterencephalic, and spinocaudal inductors which are also obtained
from unusual sources.
Although the many experiments utilizing induction by unusual adult tissues
have proven interesting, they must be interpreted with extreme caution. We are
interested, after all, in the inductive substance operating in normal development and as
yet, there is no real indication that inductors taken from adult sources are the same as
those operating during normal morphogenesis.
Attempts to study the chemical nature of inductors from embryonic tissues led to
rather interesting results which were sometimes very encouraging. Very early, it was
found that alcohol or ether extracts of amphibian embryos were inductive. The
inductive capacity was traced to fatty acids. Simultaneously it was discovered that the

77
unsaponifiable fraction of ether extracts of such embryos could also induce neural
differentiation in competent ectoderm. This observation, plus the fact that certain
carcinogenic polycyclic hydrocarbons were active in induction, led some investigators
to believe that embryonic inductors were steroids. Gradually the list of pos- sible
inductors grew to include a variety of unrelated substances. It would not seem feasible
that all of these substances operate as inductors in the normal embryo. Rather, one
might be led to speculate that these sub- stances are operating indirectly through some
mechanism inherent to the embryonic tissue itself. Strong evidence for the latter was
obtained from some important experiments of Holtfreter who showed that if competent
gastrula ectoderm is treated at a high or a low pH for a sufficient time to allow sub
lethal cytolysis, the cytolytic process would release factors from the ectoderm itself
which could cause neural induction. In retrospect, it is reasonable to assume that many
of the inductive effects attributed to various agents could actually be a result of sub
lethal cytolysis caused by the agent being tested.
Over the years, it has generally been assumed that embryonic inductors are
diffusible agents. There is evidence, however, which has led some investigators to
consider induction to be a surface phenomenon which implies an intimate contact
between inductor and reactor. In support of this point, it has been demonstrated that in
the induction of the lens in the chick embryo, the optic vesicle and the prospective lens
epithelium must maintain an intimate union. Apparently this is not really the case for,
recently, Mc Keehan has obtained lens induction in the chick embryo, through a fine
permeable membrane.
One of the more elegant demonstrations of induction in a system in which the
inductor and reactor are separated has been performed by Grobstein. Using an in vitro
system in which the ventral spinal chord induces metanephric mesenchyme to form
kidney tubules, he separated the inductive and reacting tissues by membranes of
known porosity and known thickness. The inductive stimulus readily passes through

78
coarser filters, but does not do so if the filter is made too thick or if the pore size is too
small. Electron microscope examinations of some of the filters, through which induction
occurred, failed to reveal protoplasmic connections between the spinal chord tissue and
the reacting mesenchyme. It seems safe to conclude that in this system, kidney tubule
induction proceeds without the benefit of cytoplasmic contact. Another striking
experiment in which inductors are shown to be diffusible was carried out by Niu and
Twitty. These investigators "conditioned" physiological salt solution by culturing
mesoderm in it for a given period of time. When competent gastrula ectoderm was
cultured in the "conditioned" medium, it was induced to differentiate largely into
neural structures, while similar ectoderm, maintained in unconditioned medium as a
control, developed into typical epithelium. Apparently, the inductor substances of the
mesoderm diffused into the medium and were responsible for the induction which
occurred. Additional proof for the actual presence of active inducing substances in the
conditioned medium was obtained from a series of dilution experiments in which a
direct relationship between the concentration of the medium and the frequency of
induction was observed.
Ultraviolet absorption spectra of the conditioned medium were typical for those
of nucleoproteins; thus it seems possible that compounds of this type are the active
agents in the conditioned medium. In the last few years, Niu has investigated the
possibility that RNA or RNA proteins are embryonic inductors and has found that RNA
and RNA proteins from various sources are active neural inductors. 'Moreover, the
character of neural differentiation is specific for the source of the RNA material. The fact
that treatment of the RNA substances with RNAase is capable of reducing inductive
capacities implies strongly the RNA nature of the inductor substances.
The suggestion that RNA is involved in induction phenomena is not a new one.
On the basis of the distribution of basophilic substances (presumably RNA) in eggs and
embryos of various forms, Brachet has long championed the role of RNA in

79
developmental phenomenon. Specific association of RNA basophilia with an induction
system was demonstrated by Mc Keehan who observed the accumulation of basophilic
substances at the optic vesicle-lens epithelium interface in the chick embryo. The
basophilia was removed after treatment with RNAase.
As one looks back at the literature which has accumulated on the phenomenon of
embryonic induction, it is impressive to note the great number of papers which have
appeared since the time of Spemann. Notwithstanding the efforts of so many
investigators, we are still relatively un- informed with respect to many aspects of
induction. It seems fairly clear that induction frequently involves the passage of
inductive substances from, one tissue to another. The identity of these substances,
however, is still unknown. On fairly solid grounds, we suspect that some of the
embryonic inductors are RNA, protein, or a combination of the two. Even if we are
correct in suggesting that such compounds are the natural inductors, this would only be
the beginning. Large molecules such as these are so variable in structure that it would
be a difficult problem indeed, to determine which specific molecular configurations are
responsible- for which specific inductive events. The multitude of problems which
shroud this mysterious phenomenon must not be faced with pessimism; instead, the
fully motivated investigator or potential investigator must look to the tools which are
being provided daily by colleagues in related fields such as physics and biochemistry.
With these tools and with tempered optimism and perseverance, future investigations
are bound to clarify many of the enigmas of embryonic induction.
4.1.1 PRIMARY EMBRYONIC INDUCTION OR SPEMANN’S PRIMARY ORGANIZER
The most spectacular transplantation experiments were published by Hans
Spemann and Hilde Mangold in 1924. They showed that, of all the tissues in the early
gastrula, only one has its fate determined. This self-differentiating tissue is the dorsal lip
of the blastopore, the tissue derived from the gray crescent cytoplasm. When this dorsal
lip tissue was transplanted into the presumptive belly skin region of another gastrula, it

80
not only continued to be blastopore lip, but also initiated gastrulation and
embryogenesis in the surrounding tissue (Figure). Two conjoined embryos were formed
instead of one!
In these experiments, Spemann and Mangold used differently pigmented
embryos from two new species: the darkly pigmented Triturus taeniatus and the
nonpigmented Triturus cristatus. So when Spemann and Mangold prepared these
transplants, they were able to readily identify host and donor tissues on the basis of
color. When the dorsal lip of an early T. taeniatus gastrula was removed and implanted
into the region of an early T. cristatus gastrula fated to become ventral epidermis (belly
skin), the dorsal lip tissue invaginated just as it would normally have done (showing
self-determination), and disappeared beneath the vegetal cells. The pigmented donor
tissue then continued to self-differentiate into the chordamesoderm (notochord) and
other mesodermal structures that normally form from the dorsal lip. As the new donor-
derived mesodermal cells moved forward, host cells began to participate in the
production of the new embryo, becoming organs that normally they never would have
formed. In this secondary embryo, a somite could be seen containing both pigmented
(donor) and unpigmented (host) tissue. Even more spectacularly, the dorsal lip cells
were able to interact with the host tissues to form a complete neural plate from host
ectoderm. Eventually, a secondary embryo formed, face to face with its host. These
technically difficult experiments have been repeated using nuclear markers, and the
results of Spemann and Mangold have been confirmed (Smith and Slack 1983;
Recanzone and Harris 1985).

81
Figure: Organization of a secondary axis by dorsal blastopore lip tissue. (A) Dorsal lip
tissue from an early gastrula is transplanted into another early gastrula in the region
that normally becomes ventral epidermis. (B) The donor tissue invaginates and forms a
second archenteron, and then a second embryonic axis. Both donor and host tissues are
seen in the new neural tube, notochord, and somites. (C) Eventually, a second embryo
forms that is joined to the host. (D) Structure of the dorsal blastopore lip region in an

82
early Xenopus gastrula. (A-C after Hamburger 1988; D after Winklbauer and Schurfeld
1999 and Arendt and Nübler-Jung 1999).
Spemann (1938) referred to the dorsal lip cells and their derivatives (notochord,
prechordal mesoderm) as the organizer because (1) they induced the host's ventral
tissues to change their fates to form a neural tube and dorsal mesodermal tissue (such
as somites), and (2) they organized host and donor tissues into a secondary embryo
with clear anterior-posterior and dorsal-ventral axes. He proposed that during normal
development, these cells organize the dorsal ectoderm into a neural tube and transform
the flanking mesoderm into the anterior-posterior body axis. It is now known (thanks
largely to Spemann and his students) that the interaction of the chordamesoderm and
ectoderm is not sufficient to “organize” the entire embryo. Rather, it initiates a series of
sequential inductive events. As the process by which one embryonic region interacts
with a second region to influence that second region's differentiation or behavior is
called induction. Because there are numerous inductions during embryonic
development, this key induction wherein the progeny of dorsal lip cells induce the
dorsal axis and the neural tube is traditionally called primary embryonic induction or
Spemann’s primary organizer.
SPEMANN’S PRIMARY ORGANIZER
In Xenopus, the Nieuwkoop Center is the dorsal- and vegetal-most region. It
gives rise to the Primary Organizer (aka Spemann Organizer or Spemann-Mangold
Organizer), which is the region known as the dorsal lip of the blastopore (DLB).
Spemann and Mangold’s experiments found that the DLB dorsalizes surrounding
tissue, thus forming (along with the SEP) the dorsal-ventral axis. In addition to
dorsalizing surrounding tissue, the Primary Organizer: fates overlying ectoderm as
neural plate tissue; and is determined to be notochord tissue. Dorsalized tissue gives
rise to somites and pronephric tubules.
1. A transplanted vegetal dorsal cell (from the DLB) induces a new axis.

83
2. A transplanted vegetal dorsal cell does not itself give rise to new dorsal tissues.
3. A transplanted vegetal dorsal cell restores other cells to correct fates.
The DLB uses induction (interaction with adjacent cells) via secreted diffusible
signals. A cell that can be induced is competent; embryonic tissues are only competent
during gastrulation. The use of diffusible substances was proven when dorsal lip tissue
and ectoderm were cultured together, but separated by a filter with a 0.5µm pore; the
ectoderm was induced into neural tissue, despite no cell processes seen to pass through
the filter. Dr. DeRobertis identified genes expressed only in the organizer via
differential screening of Xenopus dorsal lips. Direct purification was ineffective because
the hypersensitive ectoderm overlying the chordamesoderm was induced by even
unnatural substances. Organizer-specific gene products are divided into two groups:
Transcription factor: Three homeodomain proteins: Lim1, Gooseceoid and Xnot. Also,
HNF3β.
Secreted factor: The noggin, follistatin, chordin and frzb gene products induce the neural
plate by antagonizing the ventralizing and mesodermalizing properties of BMP-4 and
Wnt-8. These genes can induce a second axis when their mRNA is injected into an early
embryo.
Fig. The primary organizer arises in the dorsal marginal zone via induction by the
Nieuwkoop center. The Nieuwkoop center arises in the dorsal vegetal zone due to a

84
gradient of nodal-related proteins (for frogs, Xenopus nodal-related or Xnr). The marginal
zone involutes at the DLB during gastrulation to give rise to the mesoderm.
Fig. Notice that this figure (multi-cellular) differs from the one immediately above
(single-cell) in that the dorsal-ventral axis is now horizontal.
THREE-SIGNAL MODEL
According to this model, ventral mesoderm (which gives rise to blood forming
cells) is induced by underlying vegetal cells (signal 1), the primary organizer (the most
dorsal mesoderm, which gives rise to notochord and somites) is induced by the dorsal-
most vegetal blastomeres (Nieuwkoop center) (signal 2) and the dorsal-most marginal
cells then interact with the adjacent marginal cells (signal 3) and cause them to become
lateral mesoderm (which forms kidney and lateral muscle).

85
The organizer secrets Chordin and Frizbee, diffusible antagonizers of BMP4 and
Wnt-8, to establish a gradient of activity (not concentration) of BMP-4 and Wnt8 activity
in the mesoderm. In response to this gradient, zygotic genes are transcribed in a
gradient: dorsally near the organizer are goosecoid, pintallavis, HNF-3β, Xnot, Xlim-1;
ventrally is Brachyury. Different types of mesoderm form along the dorsal-ventral axis.
1st Signal: Veg1
The first signal (Veg1) is a vegetal-localized maternal mRNA that encodes a TGF-
β. Injection of Veg1 mRNA rescues irradiated embryos, and at high levels induces
dorsal mesoderm. VegT is another vegetal-localized Xenopus mRNA. VegT encodes a T
domain protein required for endoderm formation and transcription of mesoderm-
inducing signals. VegT-ablated embryos form mesoderm and ectoderm but not
endoderm, and cannot induce animal caps to form mesoderm.
2nd Signal: β-catenin
The second signal (β-catenin) differentiates the dorsal region from the ventral
region at an early stage. β-catenin was identified when cortical rotation was noted to
cause a high concentration of β-catenin to appear near the Nieuwkoop Center. When
activated by Wnt signaling, β-catenin links E-cadherin to the actin cytoskeleton and is a
transcription factor. As a result, the Nieuwkoop Center contains higher levels of Veg1,
VegT and β-catenin to produce a signal inducing dorsal mesoderm.
Xenopus Nodal-Related Proteins
Xenopus nodal related molecules (Xnr) are five TGF-β-like signals with
overlapping and similar function. VegT and TCF/LEF (requiring β-catenin as a
cofactor) overlap, establishing a Xnr gradient along the D/V axis. High [Xnr] induces
dorsal mesoderm, while low [Xnr] induces ventral mesoderm. Ablating and increasing
Xnr activity (using Cerberus, a head inducer and Xnr inhibitor) indicates that Xnr is
necessary and sufficient for inducing dorsal and ventral mesoderm at the blastula stage.
Overview So Far

86
The maternal mRNAs VegT and Veg1 are vegetal-localized. β-catenin
accumulates dorsally via cortical rotation. This causes a perfect storm at the vegetal-
and dorsal-most position of Veg1, VegT, TCR/LEF and the cofactor β-catenin. From this
vegetal- and dorsal-most position arises a dorsal to ventral gradient of Xnr activity. The
Xnr gradient is encoded by the zygotic genome. High [Xnr] induce dorsal mesoderm,
and low [Xnr] induce ventral mesoderm.
3rd Signal: Noggin, Chordin & Follistatin
The Spemann Organizer emits the third signal to dorsalize adjacent mesoderm.
This signal consists of: Noggin, Chordin and Follistatin, which bind and inhibit the
ventralizing growth factors BMP-4 and Frzb. Frzb antagonizes Wnt-8. Noggin was
identified when injection of Noggin mRNA dorsalized and partially rescued irradiated
embryos. Chordin and Frzb were identified during a differential screen for genes
expressed only in the DLB. Injection of either Noggin or Chordin mRNA into a four cell
stage embryo induces a second axis. The Spemann Organizer exclusively encodes
transcriptional activators for BMP-4 and Wnt-8 antagonists, including: three homeobox
genes, Goosecoid, Lim1 and Xnot; the fork head protein, HNF3-β.
Xenopus and Drosophila Homologs
This is similar to the the Drosophila Dpp (BMP-4 homolog) activity morphogen
gradient, which is highest at the dorsal region and lowest at the ventral region where
Sog (Chordin homolog) binds and inactivates Dpp to allow Dorsal protein expression.
BMP-4 is a Dpp homolog and Chordin is a Sog homolog. These Xenopus genes can be
interchanged with their Drosophila homologs. However, since the dorsal-ventral axis
(as well as the heart location) was inverted in an ancestor of vertebrates, Dpp promotes
dorsal formation in Drosophila and its homolog BMP-4 promotes ventral formation in
Xenopus (accordingly, the opposite goes for Chordin and Sog). Wnt-8 is a homolog of
Drosophila’s Wingless.
Notable Experiments

87
Methods to identify genes for early Xenopus embryo D/V and A/P patterning
include: differential screening (aka subtractive hybridization) to identify genes expressed at
specific times and places, as with the egg vegetal pole and early gastrula organizer
tissue; testing Xenopus homologs of mammalian cell signaling genes for ability to
induce mesoderm in isolated animal caps; and testing cloned mRNAs for ability, when
injected, to induce a new axis. After identifying relevant genes, their role was assessed
by injecting into the one- or two-cell embryo the corresponding mRNA, antisense DNA
olignucloetides, RNAi or dominant negative or active DNA construct of the gene. After
this injection, the embryo is examined whether it does or does not form an axis
(dorsalize).
Step 1 Niuewkoop found that marginal zone cells from an early blastula (before
64 cell stage) did not form mesoderm when isolated and cultured.
However, marginal zone cells from a blastula after the 64 cell stage did
form mesoderm.
Step 2 Nieuwkoop removed the marginal zone and recombined dye-marked
animal and vegetal caps. Dorsal mesoderm arose from animal cap cells
nearest the vegetal cap, and from vegetal cells opposite the SEP.
Step 3 Other biologists combined the animal cap with different vegetal
blastomere cells. Dorsal vegetal blastomere cells induced dorsal
mesoderm; ventral vegetal blastomere cells induced ventral mesoderm.
Also, dorsal mesoderm induced ventral mesoderm to become lateral
mesoderm. Thus, signaling must be involved in dorsal and central cell
fates.

88
Step 4 Gimlich and Gerhart found that fertilized eggs did not form a D/V axis
when irradiated at the vegetal pole, but could be restored by a single dyed
vegetal- and dorsal-most cell (though this cell was not itself dorsal
mesoderm). Thus, this vegetal- and dorsal-most structure must induce
other regions to become dorsal mesoderm. This vegetal-most and dorsal-
most region first induces the primary organizer (which then induces other
tissues) and was called the Nieuwkoop center.
Step 5 To determine which part of the embryo acts to organize the mesoderm
into dorsal structure and to induce neural tube formation, Spemann and
Mangold transplanted the dorsal lip of the blastopore of an early gastrula
from a light-colored newt into an early gastrula of a dark-colored newt.
The donor tissue formed a second embryonic axis. The notochord of this
second embronic axis was composed entirely of graft (donor) tissue, while
the neural tube and somites were composed only partly of graft (donor)
tissue and the kidney tubules and gut of the new axis were composed
entirely of host tissue. Spemann and Mangold concluded that the graft
tissue induced a new embryonic axis. This structure is named Primary
organizer.
4.2 ORGANOGENESIS In animal development, organogenesis (organo-genesis, compound of the Greek
words όργανον "that with which one works", and γένεσις "origin, creation, generation") is
the process by which the ectoderm, endoderm, and mesoderm develop into the internal
organs of the organism. Internal organs initiate development in humans within the 3rd
to 8th weeks in utero. The germ layers in organogenesis differ by three processes: folds,
splits, and condensation. Developing early during this stage in chordate animals are the
neural tube and notochord. Vertebrate animals all differentiate from the gastrula the

89
same way. Vertebrates develop a neural crest that differentiates into many structures,
including some bones, muscles, and components of the peripheral nervous system. The
coelom of the body forms from a split of the mesoderm along the somite axis.
PRODUCTION
The endoderm produces tissue within the lungs, thyroid, and pancreas. The
mesoderm aids in the production of cardiac muscle, skeletal muscle, smooth muscle,
tissues within the kidneys, and red blood cells. The ectoderm produces tissues within
the epidermis and aids in the formation of neurons within the brain, and melanocytes.
Fig. Organs derived from each germ layer.

90
The proceeding graph represents the products produced by the three germ layers.
GERM LAYER
CATEGORY PRODUCT
Endoderm General[3] Gastrointestinal tract Endoderm General Respiratory tract Endoderm General Endocrine glands and organs (liver and
pancreas) Mesoderm General Bones Mesoderm General Most of the circulatory system Mesoderm General Connective tissues of the gut and integuments Mesoderm General Excretory tract Mesoderm General Mesenchyme Mesoderm General Mesothelium Mesoderm General Muscles Mesoderm General Peritoneum Mesoderm General Reproductive system Mesoderm General Urinary system Mesoderm Vertebrate Chordamesoderm Mesoderm Vertebrate Intermediate mesoderm Mesoderm Vertebrate Lateral plate mesoderm Ectoderm General Nervous system Ectoderm General Outer part of integument Ectoderm Vertebrate Skin (along with glands, hair, nails) Ectoderm Vertebrate Epithelium of the mouth and nasal cavity Ectoderm Vertebrate Lens and cornea of the eye Ectoderm Vertebrate Melanocytes Ectoderm Vertebrate Peripheral nervous system Ectoderm Vertebrate Facial cartilage Ectoderm Vertebrate Dentin (in teeth) Ectoderm Vertebrate Brain (rhombencephalon, mesencephalon and
prosencephalon) Ectoderm Vertebrate Spinal cord and motor neurons Ectoderm Vertebrate Retina Ectoderm Vertebrate Posterior pituitary
4.3 EMBRYONIC ADAPTATION Ocenogenesis, the adaptation of embryos or larvae in the course of evolution to
the environmental conditions in which they develop. Embryo adaptations, arising and

91
ending in the process of embryonic or larval development, are not preserved in the
adult organism.
The term “embryo adaptation” was proposed in 1937 by B. S. Matveev as a
substitute for “cenogenesis” because the latter term was applied by various authors to
any disturbance of palingenesis (that is, the repetition of the stages of phylogenesis in
the process of embryogenesis) as well as to embryo adaptation proper. The two terms
are used interchangeably in the modern literature. Some examples of embryo
adaptation are the placenta in mammals, the fin fold in amphibian larvae, and the fat
drop in the pelagic eggs of certain fishes.
EXTRA EMBRYONIC MEMBRANE STRUCTURE IN REPTILES AND BIRDS
Fig: Extra embryonic Membranes
The embryos of reptiles, birds, and mammals produce 4 extraembryonic
membranes, the amnion yolk sac, chorion, and allantois.
In birds and most reptiles, the embryo with its extraembryonic membranes
develops within a shelled egg.
The amnion protects the embryo in a sac filled with amniotic fluid.
The yolk sac contains yolk — the sole source of food until hatching. Yolk is a
mixture of proteins and lipoproteins.

92
The chorion lines the inner surface of the shell (which is permeable to gases) and
participates in the exchange of O2 and CO2 between the embryo and the outside air.
The allantois stores metabolic wastes (chiefly uric acid) of the embryo and, as it
grows larger, also participates in gas exchange.
With these four membranes, the developing embryo is able to carry on essential
metabolism while sealed within the egg. Surrounded by amniotic fluid, the embryo is
kept as moist as a fish embryo in a pond.
Although (most) mammals do not make a shelled egg, they do also enclose their
embryo in an amnion. For this reason, the reptiles, birds, and mammals are collectively
referred to as the amniota.
Mammals fall into three groups that differ in the way they use the amniotic egg.
MONOTREMES
These primitive mammals produce a shelled egg like their reptilian ancestors. Only
four species exist today: three species of spiny anteater (echidna) and the duckbill platypus.
MARSUPIALS
Marsupials do not produce a shelled egg. The egg, which is poorly supplied with
yolk, is retained for a time within the reproductive tract of the mother. The embryo
penetrates the wall of the uterus. The yolk sac provides a rudimentary connection to the
mother's blood supply from which it receives food, oxygen, and other essentials.
However, this interface between the tissues of the uterus and the extraembryonic
membranes never becomes elaborately developed, and the young are born in a very
immature state.
Fig. The photo (courtesy of Dr. Carl G. Hartman) shows 18
newborn baby opossums fitting easily into a teaspoon.

93
Despite their tiny size, they are able to crawl into a pouch on the mother's
abdomen, attach themselves to nipples, and drink milk from her mammary glands.
Marsupials are still abundant in Australia, but only the opossum is found in North
America.
PLACENTAL MAMMALS
In placental mammals, the extraembryonic membranes form a placenta and
umbilical cord, which connect the embryo to the mother's uterus in a more elaborate
and efficient way. The blood supply of the developing fetus is continuous with that of
the placenta. The placenta extracts food and oxygen from the uterus. Carbon dioxide
and other wastes (e.g., urea) are transferred to the mother for disposal by her excretory
organs.
EGGSHELL
An eggshell is the outer covering of a hard-shelled egg and of some forms of
eggs with soft outer coats. The generalized eggshell structure, which varies widely
among species, is a protein matrix lined with mineral crystals, usually of a calcium
compound such as calcium carbonate. It is calcium build-up and is not made of cells.
Harder eggs are more mineralized than softer eggs.
INSECT EGGS
Insects and other arthropods lay a variety of styles and shapes of eggs. Some
have gelatinous or skin-like coverings, others have hard eggshells. Softer shells are
mostly protein. It may be fibrous or quite liquid. Some arthropod eggs do not actually
have shells, rather, their outer covering is actually the outermost extraembryonic
membrane, the chorion, which serves to protect inner layers. The dog chorion itself can
be a complex structure, and it may have different layers within it. It may have an
outermost layer called an exochorion. Eggs which must survive in dry conditions usually
have hard eggshells, made mostly of dehydrated or mineralized proteins with pore

94
systems to allow respiration. Arthropod eggs can have extensive ornamentation on
their outer surfaces.
FISH, AMPHIBIAN AND REPTILE EGGS
Fish and amphibians generally lay eggs which are surrounded by the
extraembryonic membranes but do not develop a shell, hard or soft, around these
membranes. Some fish and amphibian eggs have thick, leathery coats, especially if they
must withstand physical force or desiccation. These type of eggs can also be very small
and fragile.
While many reptiles lay eggs with flexible, calcified, eggshells, there are some
that lay hard eggs. Eggs laid by snakes generally have leathery shells which often
adhere to one another. Depending on the species, turtles and tortoises lay hard or soft
eggs. Several species lay eggs which are nearly indistinguishable from bird eggs.
Hatching reptiles, like most birds, have egg-teeth with which they slit or peck an
opening into the shell to help them emerge.
BIRD EGGS
Birds are known for their hard-shelled eggs. The eggshell is approximately 95%
calcium carbonate crystals, which are stabilized by a protein matrix. Without the
protein, the crystal structure would be too brittle to keep its form. The standard bird
eggshell is a porous structure, covered on its outer surface with a cuticle (called the
bloom if it is around a chicken egg), which helps the egg retain its water and keep out
bacteria. As an egg develops within a bird's reproductive system, the shell is laid down
as a liquid mineral layer around the already-formed extraembryonic membranes. This
takes place in a part of the bird's oviduct which is called the uterus and serves a very
different purpose from the uterus of a mammal. The shell is laid down by shell glands. In
an average laying hen, the process of shell formation takes around 20 hours.
Pigmentation is added to the shell by papillae lining the oviduct, coloring it any of a
variety of colors and patterns depending on species. Since eggs are usually laid blunt

95
end first, that end is subjected to most pressure during its passage and consequently
shows the most color. The waxy cuticle is deposited on the shell in the bird's oviduct.
The chick has an egg-tooth which it uses to start a hole in the hard eggshell to allow it to
hatch.
MAMMAL EGGS
Monotremes, egg-laying mammals, lay soft-shelled eggs similar to those of
reptiles. The shell is deposited on the egg in layers within the uterus. The egg can take
up fluids and grow in size during this process, and the final, most rigid layer is not
added until the egg is full-size.
4.4 POST EMBRYONIC INDUCTION In the early development of many tissues and organs of complex, multicellular
organisms, the action of one group of cells on another that leads to the establishment of
the developmental pathway in the responding tissue. The groups of cells which
influence the responding cells are termed the inducing tissue. Since specific inducing
tissues cannot act on all types of cells, those cells which can respond are referred to as
competent to react to the action of a specific inducer stimulus.
Embryonic induction is considered to play an important role in the development
of tissues and organs in most animal embryos, from the lower chordates to the higher
vertebrates.
Perhaps the first major induction phenomenon occurs during the final stages of
gastrulation of most animal embryos. Following fertilization, the egg divides to form a
multicellular blastula-stage embryo. The cells of the blastula then undergo a series of
movements which generate a more complex embryo, the gastrula, which contains three
major groups of cells: ectoderm, mesoderm, and endoderm. The mesoderm actually
arises as cells move from the surface of the embryo to the inside. Once inside, they
induce the cells which reside over them, the surface ectoderm cells, to develop into the
neural tube. The neural tube eventually forms the central nervous system. The first

96
induction event of early embryogenesis is called primary embryonic induction. The
migratory cells which invaginate from the surface and induce the development of the
neural tube are termed the embryonic organizer. The first step in the sequence of events
termed primary embryonic induction is the acquisition by the mesoderm of neural
inducing activity. Proteins such as fibro blast growth factor and activin, which belong to
a category of so-called peptide growth factors, play key roles in programming the
mesoderm cells to induce overlying ectoderm to differentiate into neural structures.
The development of a large number of tissues and organs is influenced by
embryonic inductions. Various eye structures (lens, optic cup, and so on), internal ear
structures, as well as several tissues (for example, vertebral cartilage) emerge from cells
which were acted upon by inducer tissues.
Limbs, kidney, nasal structures, salivary glands, pancreas, teeth, feathers, and
hair are organs which require inductive stimuli. It is not known whether a single
common mechanism underlies each of those inductions. Many scientists believe that
inductive interactions are mediated by cell-cell contacts; that is, the developmental
information which is transferred from the inducing tissue is thought to reside at the cell
surface of that tissue. Perhaps the surface of the responding tissue recognizes the signal
molecules present on the surface of the inducing tissue. In other instances, a secreted
protein might move among various cells or tissues and exert its effects on competent
cells.
The principles of animal development also apply to plants. A greater role is,
however, usually played by the diffusion of small-molecular-weight signal molecules
rather than cell-cell contacts or protein growth factors. The earliest stages of plant
embryo development involve groups of cells acquiring the competence to respond to
inductive signals. Later in development, inductive signaling also becomes important.
For example, in flowering plants the distance between nodes along the stem elongates,
and lateral buds form below the shoot apex. The buds are believed to develop in

97
response to a concentration gradient of signal molecules which exists along the stem.
Thus, a process which is analogous to embryonic limb bud formation in animals is
played out, and both plant and animal inductions can be conceptualized in similar
terms.
4.4.1 METAMORPHOSIS Metamorphosis is a biological process by which an animal physically develops
after birth or hatching, involving a conspicuous and relatively abrupt change in the
animal's form or structure through cell growth and differentiation. Some insects,
amphibians, molluscs, crustaceans, cnidarians, echinoderms and tunicates undergo
metamorphosis, which is usually (but not always) accompanied by a change of habitat
or behaviour.
Scientific usage of the term is exclusive, and is not applied to general aspects of
cell growth, including rapid growth spurts. References to "metamorphosis" in mammals
are imprecise and only colloquial.
METAMORPHOSIS (INSECTS AND AMPHIBIANS)
Metamorphosis is a biological process by which an animal physically develops
after birth or hatching, involving a conspicuous and relatively abrupt change in the
animal's body structure through cell growth and differentiation. Some insects,
amphibians, mollusks, crustaceans, Cnidarians, echinoderms and tunicates undergo
metamorphosis, which is usually accompanied by a change of habitat or behavior.
Insect metamorphosis
Metamorphosis usually proceeds in distinct stages, starting with larva or nymph,
optionally passing through pupa, and ending as adult or imago. There are two main
types of metamorphosis in insects, hemimetabolism and holometabolism.
Incomplete metamorphosis in the grasshopper with different instar nymphs.
The immature stages of a species that metamorphosises are usually called larvae,
and in these stages may grow quite quickly. But in the complex metamorphosis of many

98
insect species, only the first stage is called a larva and sometimes even that bears a
different name; the distinction depends on the nature of the metamorphosis.
In hemimetabolism, the development of larva often proceeds in repeated stages
of growth and ecdysis (moulting); these stages are called instars. The juvenile forms
closely resemble adults, but are smaller and, if the adult has wings, lack wings. This
process is also known as "simple", "gradual" or "incomplete" metamorphosis. The
differences between juveniles in different instars are small, often just differences in
body proportions and the number of segments.
In holometabolism, the larvae differ markedly from the adults. Insects which
undergo holometabolism pass through a larval stage, then enter an inactive state called
pupa, or chrysalis, and finally emerge as adults. Holometabolism is also known as
"complete" and "complex" metamorphosis. Whilst inside the pupa, the insect will
excrete digestive juices, to destroy much of the larva's body, leaving a few cells intact.
Some of the remaining cells will begin the growth of the adult, using the nutrients from
the broken down larva. This process of cell death is called histolysis, and cell regrowth
histogenesis.
According to latest researches, adult Manduca sexta is able to retain the
behaviour learned as a caterpillar.
Whether the insect spends more time in its adult stage or in its juvenile form
depends on the species. Notable examples are the mayfly, whose non-eating, adult
stage lives for one day, and the cicada, whose juvenile stage live underground for 13 or
17 years. These species have incomplete metamorphosis. Typically, though not
exclusively, species in which the adult form outlives the juvenile form undergo complex
metamorphosis.
Many observations have indicated that programmed cell death plays a considerable role
during physiological processes of multicellular organisms, particularly during
embryogenesis and metamorphosis.

99
HORMONAL CONTROL
Insect growth and metamorphosis are controlled by hormones synthesized by
endocrine glands near the front of the body.
Neurosecretory cells of an insect's brain secrete a hormone, the
prothoracicotropic hormone that activates prothoracic glands, which secrete a second
hormone, usually Ecdysone (a steroid), that induces metamorphosis.
Moreover, the corpora allata, a retrocerebral organ produces the juvenile
hormone, whose effect is to prevent the development of adult characteristics while
allowing ecdysis. Therefore, the insect is subject to a series of molting, controlled by
Ecdysone, until the production of juvenile hormone ceases and metamorphosis occurs.
Amphibian metamorphosis
In typical amphibian development, eggs are laid in water and larvae are adapted
to an aquatic lifestyle. Frogs, toads, and newts all hatch from the egg as larvae with
external gills. Afterwards, newt larvae start a predatory lifestyle, while tadpoles mostly
scrape food off surfaces with their horny tooth ridges.
Metamorphosis in amphibians is regulated by thyroxin concentration in the
blood, which stimulates metamorphosis, and prolactin, which counteracts its effect.
Specific events are dependent on threshold values for different tissues. Because most
embryonic development is outside the parental body, development is subject to many
adaptations due to specific ecological circumstances. For this reason tadpoles can have
horny ridges for teeth, whiskers, and fins. They also make use of the lateral line organ.
After metamorphosis, these organs become redundant and will be resorbed by
controlled cell death, called apoptosis. The amount of adaptation to specific ecological
circumstances is remarkable, with many discoveries still being made.
FROGS AND TOADS
With frogs and toads, the external gills of the newly hatched tadpole are covered
with a gill sac after a few days, and lungs are quickly formed. Front legs are formed

100
under the gill sac, and hindlegs are visible a few days later. Following that there is
usually a longer stage during which the tadpole lives off a vegetarian diet. Tadpoles use
a relatively long, spiral‐shaped gut to digest that diet.
Rapid changes in the body can then be observed as the lifestyle of the frog changes
completely. The spiral‐shaped mouth with horny tooth ridges is resorbed together with the
spiral gut. The animal develops a big jaw, and its gills disappear along with its gill sac.
Eyes and legs grow quickly, a tongue is formed, and all this is accompanied by
associated changes in the neural networks (development of stereoscopic vision, loss of
the lateral line system, etc.) All this can happen in about a day, so it is truly a
metamorphosis. It isn't until a few days later that the tail is reabsorbed, due to the
higher thyroxin concentrations required for tail resorption.
NEWTS
Fig. The large external gills of the crested newt
In newts, there is no true metamorphosis because newt larvae already feed as
predators and continue doing so as adults. Newts' gills are never covered by a gill sac
and will be resorbed only just before the animal leaves the water. Just as in tadpoles,
their lungs are functional early, but newts don't make as much use of them as tadpoles
do. Newts often have an aquatic phase in spring and summer, and a land phase in
winter. For adaptation to a water phase, prolactin is the required hormone, and for
adaptation to the land phase, thyroxin. External gills do not return in subsequent

101
aquatic phases because these are completely absorbed upon leaving the water for the
first time.
METAMORPHOSIS IN FISH AND INVERTEBRATE AQUATIC ANIMALS
Little known is that also fish, i.e. bony fish, undergo metamorphosis. Fish
metamorphosis is typically under strong control by thyroid hormone. Examples include
the agnatha, salmon, and lamprey, which must change from a freshwater to saltwater
lifestyle (diadromous). Additionally, the flatfish begins its life bilaterally symmetrical,
and one eye must move to join the other side of the fish in its adult form.
4.4.2 REGENERATION In biology, an organism is said to regenerate a lost part, if a substitute for the loss
grows from the rest of the organism, and the substitute is a copy or almost a copy of the
old lost part.
Regeneration of a lost limb occurs in two major steps, first de-differentiation of
adult cells into a stem cell state similar to embryonic cells and second, development of
these cells into new tissue more or less the same way it developed the first time . Some
animals like planarians instead keep clusters of non-differentiated cells within their
bodies, which migrate to the parts of the body that need healing.
REGENERATION IN VARIOUS ANIMALS
The growth of new tissue or organs to replace those lost or damaged through
injury. All animals and plants are capable of regeneration to some extent but, as a
general rule, the more highly evolved an animal is, the less are its powers of
regeneration. Humans, for example, are able to regenerate skin and bone tissue to mend
wounds and fractures, but are unable to regrow even a finger if one should be lost.
Some internal organs can be regenerated if a large enough part remains as a starting
point. The liver is an example; so, too, are the adrenal glands. The replacement of worn-
out tissues is a form of regeneration and goes on throughout life. The most obvious is
the replacement of skin from below as the outer layers rub off.

102
Some animals are able to regenerate new limbs – in fact lizards may actually
shed their tails themselves to confuse enemies and later grow knew ones. Crabs, too,
can throw off a limb to escape from an enemy. The most striking cases of regeneration,
however, are found among the lower animals – the cnidarians and the flatworms.
Flatworms are built up of three layers: an external ectoderm, an endoderm lining
the gut, and a mesoderm occupying the space between the two. Planarians are
flatworms with great powers of regeneration. As long as all three types of tissue are
present, a complete new worm can grow from a tiny portion.
When a planarian is cut in half, both halves can form new animals. The cells of
the damaged region lose their individuality and all become alike. They grow and divide
and the growing mass takes on the correct shape – be it of a head or a tail. Gradually the
cells become specialized again and begin their normal functions. The head region is the
coordinating region and, if missing, is always the first formed structure in a
regenerating body. Not until there is a head, can the other organs be reformed.
Regeneration in Planaria
A fragment of a flatworm can regenerate into a new individual as long as there is
sufficient food reserve in the tissue. The fragment has no mouth and feeding organs and
so cannot get any food from outside. The cells at the cut surface (sometimes all the cells
in the fragment) become alike and multiply. Because food is used up during this

103
process, the fragment gets smaller, but if sufficient cells can be formed, a tiny planarian
will develop. Any original organs remaining in the fragment will be partly absorbed so
that they conform in size to the rest of the new animal. A new head is formed before the
rest of the body develops.
Any fragment of a planarian that regenerates naturally will produce a head at the
original front end. Although the cells are completely reorganized they never lose their
polarity. Regeneration in jellyfish is very similar, but in higher animals, the head cannot
be regenerated. New limbs and bodies can form under the influence of the head but not
vice-versa.
Earthworms are able to regenerate new bodies as long as the front part
containing the vital organs is present. The tail region of a worm, if removed, cannot
continue its existence. Crabs, lobsters, and crayfish are able to break off their limbs at
will – a process called autonomy. More important, they are able to regenerate the lost
parts. At the base of each limb is a special muscle which bends it until it breaks at a
specially weakened place, the breaking point. At first only a miniature replacement limb
is formed, but when the animal next sheds its skin the limb grows rapidly to almost the
size of the original limb.
Insects, too, possess the power of regeneration, when young. Missing legs and
antennae can be regenerated but do not develop fully until after at least one molt. A pad
of regeneration tissue develops at the wound and forms the missing limb. Many
abnormalities of regeneration are known among insects – a mantis has, for example,
been known to grow a leg where an antenna had been lost.
One frequently sees starfish with one or more arms missing. The mouth and part
of the digestive organs are in the central disk of the animal and thus it can continue to
feed even when all the arms are lost. Its powers of regeneration are such that the
starfish can develop new arms from the central disk alone.

104
Regeneration in vertebrates is much more limited. Lizards can regenerate lost
tails but rarely is the new one full sized. Newts have been known to regenerate limbs
and tails, so too have young frogs. In the higher animals, the powers of regeneration are
confined to the mending of broken bones and connective tissues and the re-growth of
some damaged internal organs.
UNIT V

105
HUMAN WELFARE 5.0 INTRODUCTION
5.1 BIRTH CONTROL
5.2 INFERTILITY
5.3 ARTIFICIAL INSEMINATION
5.4 TEST TUBE BABIES
5.5 HUMAN CLONING
5.6 EMBRYO TRANSPLANTATION
5.7 RH FACTOR
5.8 CONGENITAL ANOMALIES
5.9 DISTURBANCES OF GROWTH
5.10 CANCER
5.0 INTRODUCTION Welfare is the sate of doing well or and in the form of money or necessaries for those in
need. Human welfare applies this idea to people.
5.1 BIRTH CONTROL Birth control is a regimen of one or more actions, devices, sexual practices, or
medications followed in order to deliberately prevent or reduce the likelihood of
pregnancy or childbirth. There are three main routes to preventing or ending pregnancy
before birth: the prevention of fertilization of the ovum by sperm cells ("contraception"),
the prevention of implantation of the blastocyst ("contragestion"), and the chemical or
surgical induction or abortion of the developing embryo or, later, fetus. In common
usage, term "contraception" is often used for both contraception and contragestion. The
history of birth control began with the discovery of the connection between coitus and
pregnancy. The oldest forms of birth control included coitus interruptus, pessaries, and
the ingestion of herbs that were believed to be contraceptive or abortifacient. The
earliest record of birth control use is an ancient Egyptian set of instructions on creating
a contraceptive pessary. Different methods of birth control have varying characteristics.

106
Condoms, for example, are the only methods that provide significant protection from
sexually transmitted diseases. Cultural and religious attitudes on birth control vary
significantly.
1. HISTORY OF THE CONCEPT
The words "birth control" entered the English language in 1914 with the American
reformer Margaret Sanger. In 1914 she launched The Woman Rebel, an eight page monthly
newsletter promoting contraception, with the slogan "No Gods and No Masters", and
coining this term. Effective contraception for the masses has been around only since the
1960s, with the development and mass production of the pill and intrauterine devices. This
development also stirred new debates on the topic. The development of modern methods of
artificial contraception met with condemnation from the Roman Catholic Church, which
teaches that every sexual act must remain open to life. Saint Augustine set the tone in his
"Marriage and Concupiscence," in which he condemned any attempt to avoid procreation.
By that he was expressing a comparatively liberal view against Gnostic preaching that all
sex was evil, even within marriage. His views were taken largely from Roman Stoic
teaching that procreation was the rational aim of marriage.
2. METHODS
A. PHYSICAL METHODS
Physical methods may work in a variety of ways, among them: physically
preventing sperm from entering the female reproductive tract; hormonally preventing
ovulation from occurring; making the woman's reproductive tract inhospitable to
sperm; or surgically altering the male or female reproductive tract to induce sterility.
Some methods use more than one mechanism. Physical methods vary in simplicity,
convenience and efficacy.
BARRIER METHODS
Barrier methods place a physical impediment to the movement of sperm into the
female reproductive tract. The most popular barrier method is the male condom, a latex
or polyurethane sheath placed over the penis. The condom is also available in a female

107
version, which is made of polyurethane. The female condom has a flexible ring at each
end — one secures behind the pubic bone to hold the condom in place, while the other
ring stays outside the vagina.
Cervical barriers are devices that are contained completely within the vagina.
The contraceptive sponge has a depression to hold it in place over the cervix. The
cervical cap is the smallest cervical barrier. Depending on the type of cap, it stays in
place by suction to the cervix or to the vaginal walls. The diaphragm fits into place
behind the woman's pubic bone and has a firm but flexible ring, which helps it press
against the vaginal walls.
Spermicide may be placed in the vagina before intercourse and creates a
chemical barrier. Spermicide may be used alone, or in combination with a physical
barrier.
HORMONAL METHODS
Eg. Ortho Tri-cyclen, a brand of oral contraceptive
There are various delivery methods for hormonal contraception. Forms of
synthetic oestrogens and progestins (synthetic progestogens) combinations commonly
used include the combined oral contraceptive pill ("The Pill"), the Patch, and the
contraceptive vaginal ring ("NuvaRing"). A monthly injectable form, Lunelle, is also
available.
Other methods contain only a progestin (a synthetic progestogen). These include
the progesterone only pill (the POP or 'minipill'), the injectables Depo Provera (a depot
formulation of medroxyprogesterone acetate given as an intramuscular injection every
three months) and Noristerat (Norethindrone acetate given as an intramuscular
injection every 8 weeks), and contraceptive implants. The progestin-only pill must be
taken at more precisely remembered times each day than combined pills. The first
contraceptive implant, Norplant, is available in many countries. A single-rod implant

108
called Implanon is approved in the United States. The various progestin-only methods
may cause irregular bleeding during use.
ORMELOXIFENE (CENTCHROMAN)
Ormeloxifene (Centchroman) is a selective estrogen receptor modulator, or
SERM. It causes ovulation to occur asynchronously with the formation of the uterine
lining, preventing implantation of a zygote. It has been widely available as a birth
control method in India since the early 1990s, marketed under the trade name Saheli.
Centchroman is legally available only in Emergency contraception
Some combined pills and POPs may be taken in high doses to prevent pregnancy
after a birth control failure (such as a condom breaking) or after unprotected sex.
Hormonal emergency contraception is also known as the "morning after pill," although
it is licensed for use up to three days after intercourse.
Copper intrauterine devices may also be used as emergency contraception. For
this use, they must be inserted within five days of the birth control failure or
unprotected intercourse.
Emergency contraception appears to work by suppressing ovulation. However,
because it might prevent a fertilized egg from implanting, some people consider it a
form of abortion.
INTRAUTERINE METHODS
(INTRAUTERINE DEVICES (IUDS) OR INTRAUTERINE CONTRACEPTIVE
DEVICES (IUCDS) OR INTRA-UTERINE SYSTEM (IUS)
These are contraceptive devices which are placed inside the uterus. They are
usually shaped like a "T" — the arms of the T help hold the device in place. There are
also frameless IUD's, which are less likely to cause complications; an example would be
GyneFix. There are two main types of intrauterine contraceptives: those that contain
copper (which has a spermicidal effect), and those that release a progestin (a synthetic
progestogen).

109
STERILIZATION
Surgical sterilization is available in the form of tubal ligation for women and
vasectomy for men. Sterilization should be considered permanent. In women, the
process may be referred to as "tying the tubes," but the Fallopian tubes may be tied, cut,
clamped, or blocked. This serves to prevent sperm from joining the unfertilized egg.
The non-surgical sterilization procedure, Essure, is an example of a procedure that
blocks the tubes, wherein micro-inserts are placed into the fallopian tubes by a catheter
passed from the vagina through the cervix and uterus. Although sterilization should be
considered a permanent procedure, it is possible to attempt a tubal ligation reversal to
reconnect the Fallopian tubes in females, or a vasovasostomy by which vasectomies are
reversed in males. The rate of success depends on the type of sterilization that was
originally performed and damage done to the tubes as well as the patient's age.
B. BEHAVIORAL METHODS
Behavioral methods involve regulating the timing or methods of intercourse to
prevent the introduction of sperm into the female reproductive tract, either altogether
or when an egg may be present.
LACTATIONAL
From ancient times women tried to extend breastfeeding in order to avoid a new
pregnancy. The lactational amenorrhea method, or LAM, gives guidelines for
determining the length of a woman's period of breastfeeding infertility.
FERTILITY AWARENESS (NATURAL FAMILY PLANNING (NFP)
Symptoms-based methods of fertility awareness involve a woman's observation
and charting of her body's fertility signs, to determine the fertile and infertile phases of
her cycle. Charting may be done by hand or with the assistance of software. Most
methods track one or more of the three primary fertility signs: changes in basal body
temperature, in cervical mucus, and in cervical position. If a woman tracks both basal

110
body temperature and another primary sign, the method is referred to as symptothermal.
Other bodily cues such as mittelschmerz are considered secondary indicators.
COITUS INTERRUPTUS
Coitus interruptus (literally "interrupted sexual intercourse"), also known as the
withdrawal or pull-out method, is the practice of ending sexual intercourse ("pulling
out") before ejaculation. The main risk of coitus interruptus is that the man may not
perform the maneuver correctly, or may not perform the maneuver in a timely manner.
Although concern has been raised about the risk of pregnancy from sperm in pre-
ejaculate, several small studies have failed to find any viable sperm in the fluid.
AVOIDING SEMEN NEAR VAGINA
There is no risk of pregnancy from non-penetrative sex except for Intercrural sex
and other forms of penis-near-vagina sex (genital rubbing, and the penis exiting from
anal intercourse) where semen can be deposited near the entrance to the vagina and can
itself travel along the vagina's lubricating fluids.
TOTAL ABSTINENCE
Different groups define the term sexual abstinence in different ways. When used
in discussions of birth control, usually the avoidance of all sexual activity—total sexual
abstinence—is the intended meaning. Sometimes people choose to be sexually abstinent
to reduce their risk of pregnancy, and abstinence may be included in lists of birth
control methods. Those who are sexually abstinent do not have unplanned pregnancies.
Other sources instead classify abstinence as not being a form of birth control.
Abstinence is 100% effective in preventing pregnancy; however, not everyone who
intends to be abstinent refrains from all sexual activity, and in many populations there
is a significant risk of pregnancy from nonconsensual sex.
C. INDUCED ABORTION METHOD
In some areas, women use abortion as a primary means to control birth. Abortion
is subject to ethical debate. Surgical abortion methods include suction-aspiration

111
abortion (used in the first trimester) or dilation and evacuation (used in the second
trimester). Medical abortion methods involve the use of medication which is swallowed
or inserted vaginally to induce abortion. Medical abortion can be used if the length of
gestation has not exceeded 8 weeks.
Some herbs are considered abortifacient, and some animal studies have found
various herbs to be effective in inducing abortion in non-human animal species.
Humans generally do not use herbs when other methods are available, due to the
unknown efficacy and due to risks of toxicity.
3. MISCONCEPTIONS
Modern misconceptions and urban legends have given rise to a great many false
claims:
The suggestion that douching with any substance immediately following
intercourse works as a contraceptive is untrue. While it may seem like a sensible
idea to try to wash the ejaculate out of the vagina, it is not likely to be effective.
Due to the nature of the fluids and the structure of the female reproductive tract,
douching most likely actually spreads semen further towards the uterus. Some
slight spermicidal effect may occur if the douche solution is particularly acidic,
but overall it is not scientifically observed to be a reliably effective method.
Douching is neither a contraceptive nor a preventative measure against STDs or
other infections.
It is untrue that a female cannot become pregnant as a result of the first time she
engages in sexual intercourse.
While women are usually less fertile for the first few days of menstruation, it is a
myth that a woman absolutely cannot get pregnant if she has sex during her
period.
Having sex in a hot tub does not prevent pregnancy, but may contribute to
vaginal infections.

112
Although some sex positions may encourage pregnancy, no sexual positions
prevent pregnancy. Having sex while standing up or with a woman on top will
not keep the sperm from entering the uterus. The force of ejaculation, the
contractions of the uterus caused by prostaglandins in the semen, as well as
ability of the sperm to swim overrides gravity.
Urinating after sex does not prevent pregnancy and is not a form of birth control,
although it is often advised anyway to help prevent urinary tract infections.
Toothpaste cannot be used as an effective contraceptive.
Intrauterine devices (IUDs) are popular in many parts of the world and are
extremely safe and effective.
4. EFFECTIVENESS
Effectiveness is generally measured by how many women became pregnant
using a particular birth control method in the first year of use. Thus, if 100 women use a
method that has a ‘0’ percent first-year failure rate, then ‘0’ of the women should
become pregnant during the first year of use. Sometimes the effectiveness is given in
lifetime failure rate, more commonly among methods with high effectiveness, such as
vasectomy after the appropriate negative semen analysis. The most effective methods in
typical use are those that do not depend upon regular user action. Surgical sterilization,
Depo-Provera, implants, and intrauterine devices (IUDs) all have first-year failure rates
of less than one percent for perfect use.
Condoms and cervical barriers such as the diaphragm have similar typical use
first-year failure rates (14 and 20 percent, respectively), but perfect usage of the condom
is more effective (three percent first-year failure vs six percent) and condoms have the
additional feature of helping to prevent the spread of sexually transmitted diseases such
as the HIV virus. Combining two birth control methods, can increase their effectiveness
to 95% or more for less effective methods.[60] Using condoms with another birth control
method is also one of the recommended methods of reducing risk of getting sexually

113
transmitted infections, including HIV. This approach is one of the Dual Protection
Strategies.
Birth control education
Many teenagers, most commonly in developed countries, receive some form of
sex education in school. What information should be provided in such programs is
hotly contested, especially in the United States and United Kingdom. Topics include
reproductive anatomy, human sexual behavior, information on sexually transmitted
diseases (STDs), social aspects of sexual interaction, negotiating skills intended to help
teens follow through with a decision to remain abstinent or to use birth control during
sex, and information on birth control methods. One type of sex education program used
in some more conservative areas of the United States is called abstinence-only
education, and it generally promotes complete sexual abstinence until marriage.
5.2 INFERTILITY Infertility primarily refers to the biological inability of a person to contribute to
conception. Infertility may also refer to the state of a woman who is unable to carry a
pregnancy to full term. There are many biological causes of infertility, some which may
be bypassed with medical intervention. Women who are fertile experience a natural
period of fertility before and during ovulation, and they are naturally infertile during
the rest of the menstrual cycle. Fertility awareness methods are used to discern when
these changes occur by tracking changes in cervical mucus or basal body temperature.
1. DEFINITION
There are strict definitions of infertility used by many doctors. However, there
are also similar terms, e.g. subfertility for a more benign condition and fecundity for the
natural improbability to conceive. Infertility in a couple can be due to either the woman
or the man, not necessarily both.
Reproductive endocrinologists consider a couple to be infertile if:

114
The couple has not conceived after 12 months of contraceptive-free intercourse if
the female is under the age of 34. 12 months is the lower reference limit for Time to
Pregnancy (TTP) by the World Health Organization.
The couple has not conceived after 6 months of contraceptive-free intercourse if
the female is over the age of 35 (declining egg quality of females over the age of 35
accounts for the age-based discrepancy as when to seek medical intervention).
Alternatively, infertility can be defined as failure to conceive after regular
unprotected sexual intercourse for 2 years in the absence of known reproductive
pathology.
Subfertility: A couple that has tried unsuccessfully to have a child for a year or
more is said to be subfertile meaning less fertile than a typical couple. The couple's
fecundability rate is approximately 3-5%. Many of its causes are the same as those of
infertility. Such causes could be endometriosis or polycystic ovarian syndrome.
Primary vs. secondary infertility: Couples with primary infertility have never been
able to conceive, while, on the other hand, secondary infertility is difficulty conceiving after
already having conceived (and either carried the pregnancy to term or had a miscarriage).
Technically, secondary infertility is not present if there has been a change of partners.
2. PREVALENCE
• Generally, worldwide it is estimated that one in seven couples have problems
conceiving, with the incidence similar in most countries independent of the level
of the country's development.
• Fertility problems affect one in seven couples in the UK. Most couples (about
84 out of every 100) who have regular sexual intercourse (that is, every 2 to 3
days) and who do not use contraception will get pregnant within a year. About
92 out of 100 couples who are trying to get pregnant do so within 2 years.
• Women become less fertile as they get older. For women aged 35, about 94
out of every 100 who have regular unprotected sexual intercourse will get

115
pregnant after 3 years of trying. For women aged 38, however, only 77 out of
every 100 will do so. The effect of age upon men’s fertility is less clear.
• In people going forward for IVF in the UK, roughly half of fertility problems
with a diagnosed cause are due to problems with the man, and about half due to
problems with the woman. However, about one in five cases of infertility have
no clear diagnosed cause.
• In Britain, male factor infertility accounts for 25% of infertile couples, while
25% remain unexplained. 50% are female causes with 25% being due to
anovulation and 25% tubal problems/other.
3. CAUSES
CAUSES IN EITHER SEX
Factors that can cause male as well as female infertility are:
• Genetic Factors
o A Robertsonian translocation in either partner may cause recurrent spontaneous
abortions or complete infertility.
• General factors
o Diabetes mellitus, thyroid disorders, adrenal disease
• Hypothalamic-pituitary factors
o Kallmann syndrome
o Hyperprolactinemia
o Hypopituitarism
• Environmental Factors
o Toxins such as glues, volatile organic solvents or silicones, physical agents,
chemical dusts, and pesticides. Tobacco smokers are 60% more likely to be
infertile than non-smokers. Smoking reduces the chances of IVF producing a live
birth by 34% and increases the risk of an IVF pregnancy miscarrying by 30%.

116
German scientists have reported that a virus called Adeno-associated virus might
have a role in male infertility. Though, it is otherwise not harmful. Mutation that alters
human DNA adversely can cause infertility, the human body thus preventing the
tainted DNA from being passed on. This could explain why some radiation victims
from Chernobyl incident
SPECIFIC FEMALE CAUSES
The following causes of infertility may only be found in females.
For a woman to conceive, certain things have to happen: intercourse must take
place around the time when an egg is released from her ovary; the systems that produce
eggs and sperm have to be working at optimum levels; and her hormones must be
balanced.
Some women are infertile because their ovaries do not mature and release eggs. In this
case synthetic FSH by injection or Clomid (Clomiphene citrate) via a pill can be given to
stimulate follicles to mature in the ovaries.
Problems affecting women include endometriosis or damage to the fallopian
tubes (which may have been caused by infections such as chlamydia).
Other factors that can affect a woman's chances of conceiving include being over- or
underweight for her age - female fertility declines sharply after the age of 35. Sometimes
it can be a combination of factors, and sometimes a clear cause is never established.
Common causes of infertility of females include:
• ovulation problems
• tubal blockage
• age-related factors
• uterine problems
• previous tubal ligation

117
COMBINED INFERTILITY
In some cases, both the man and woman may be infertile or sub-fertile, and the
couple's infertility arises from the combination of these conditions. In other cases, the
cause is suspected to be immunological or genetic; it may be that each partner is
independently fertile but the couple cannot conceive together without assistance.
UNEXPLAINED INFERTILITY
Up to 26% of infertile couples have unexplained infertility. In these cases
abnormalities are likely to be present but not detected by current methods. Possible
problems could be that the egg is not released at the optimum time for fertilization, that
it may not enter the fallopian tube, sperm may not be able to reach the egg, fertilization
may fail to occur, transport of the zygote may be disturbed, or implantation fails. It is
increasingly recognized that egg quality is of critical importance and women of
advanced maternal age have eggs of reduced capacity for normal and successful
fertilization. Also, polymorphisms in folate pathway genes could be one reason for
fertility complications in some women with unexplained infertility.
5.3 ARTIFICIAL INSEMINATION Artificial insemination, is the process by which sperm is placed into the
reproductive tract of a female for the purpose of impregnating the female by using
means other than sexual intercourse. In humans, it is used as assisted reproductive
technology, using either sperm from the woman's male partner or sperm from a sperm
donor (donor sperm) in cases where the male partner produces no sperm or the woman
has no male partner (i.e., single women and lesbians). In cases where donor sperm is
used the woman is the gestational and genetic mother of the child produced, and the
sperm donor is the genetic or biological father of the child.
Artificial insemination is widely used for livestock breeding, especially for dairy
cattle and pigs. Techniques developed for livestock have been adapted for use in
humans. Specifically, freshly ejaculated sperm, or sperm which has been frozen and

118
thawed, is placed in the cervix (intracervical insemination – ICI) or, after washing, into
the female's uterus (intrauterine insemination – IUI) by artificial means.
In humans, artificial insemination was originally developed as a means of
helping couples to conceive where there were 'male factor' problems of a physical or
psychological nature affecting the male partner which prevented or impeded
conception. Today, the process is also and more commonly used in the case of choice
mothers, where a woman has no male partner and the sperm is provided by or on
behalf of a sperm donor.
1. PREPARATIONS
A sperm sample will be provided by the male partner of the woman undergoing
artificial insemination, but sperm provided through sperm donation by a sperm donor
may be used if, for example, the woman's partner produces too few motile sperm, if he
carries a genetic disorder, or if the woman has no male partner. Sperm is usually
obtained through masturbation or the use of an electrical stimulator, although a special
condom, known as a collection condom, may be used to collect the semen during
intercourse.
The man providing the sperm is usually advised not to ejaculate for two to three
days before providing the sample in order to increase the sperm count. A woman's
menstrual cycle is closely observed, by tracking basal body temperature (BBT) and
changes in vaginal mucus, or using ovulation kits, ultrasounds or blood tests. When
using intrauterine insemination (IUI), the sperm must have been “washed” in a
laboratory and concentrated in Hams F10 media without L-glutamine, warmed to 37oC.
The process of “washing” the sperm increases the chances of fertilization and removes
any mucus and non-motile sperm in the semen. Pre and post concentration of motile
sperm is counted.
If sperm is provided by a sperm donor through a sperm bank, it will be frozen
and quarantined for a particular period and the donor will be tested before and after

119
production of the sample to ensure that he does not carry a transmissible disease.
Sperm samples donated in this way are produced through masturbation by the sperm
donor at the sperm bank. A chemical known as a cryoprotectant is added to the sperm
to aid the freezing and thawing process. Further chemicals may be added which
separate the most active sperm in the sample as well as extending or diluting the
sample so that vials for a number of inseminations are produced. For fresh shipping, a
semen extender is used.
2. PROCEDURE
When an ovum is released, semen provided by the woman's male partner, or by
a sperm donor, is inserted into the woman's vagina or uterus. The semen may be fresh
or it may be frozen semen which has been thawed. Where donor sperm is supplied by a
sperm bank, it will always be quarantined and frozen and will need to be thawed before
use. Specially designed equipment is available for carrying out artificial inseminations.
In the case of vaginal artificial insemination, semen is usually placed in the vagina by
way of a needleless syringe. A longer tube, known as a 'tom cat' may be attached to the
end of the syringe to facilitate deposit of the semen deeper into the vagina. The woman
is generally advised to lie still for a half hour or so after the insemination to prevent
seepage and to allow fertilization to take place.
A more efficient method of artificial insemination is to insert semen directly into
the woman's uterus. Where this method is employed it is important that only 'washed'
semen be used and this is inserted into the uterus by means of a catheter. Sperm banks
and fertility clinics usually offer 'washed' semen for this purpose, but if partner sperm is
used it must also be 'washed' by a medical practitioner to eliminate the risk of
cramping. Semen is occasionally inserted twice within a 'treatment cycle'. A double
intrauterine insemination has been theorized to increase pregnancy rates by decreasing
the risk of missing the fertile window during ovulation. However, a randomized trial of

120
insemination after ovarian hyperstimulation found no difference in live birth rate
between single and double intrauterine insemination.
An alternative method to the use of a needless syringe or a catheter involves the
placing of partner or donor sperm in the woman's vagina by means of a specially
designed cervical cap, a conception device or conception cap. This holds the semen in
place near to the entrance to the cervix for a period of time, usually for several hours, to
allow fertilization to take place. Using this method, a woman may go about her usual
activities while the cervical cap holds the semen in the vagina. One advantage with the
conception device is that fresh, non-liquified semen may be used.
If the procedure is successful, the woman will conceive and carry to term a baby.
A pregnancy resulting from artificial insemination will be no different from a
pregnancy achieved by sexual intercourse. However, there may be a slight increased
likelihood of multiple births if drugs are used by the woman for a 'stimulated' cycle.
3. DONOR VARIATIONS
Either sperm provided by the woman's husband or partner (artificial
insemination by husband, AIH) or sperm provided by a known or anonymous sperm
donor (artificial insemination by donor, AID or DI) can be used.
4. TECHNIQUES
Intrauterine insemination, Intravaginal insemination, Intracervical insemination,
and Intrabtubal insemination.
A. INTRACERVICAL INSEMINATION (ICI)
ICI is the easiest way to inseminate. This involves the deposit of raw fresh or
frozen semen (which has been thawed) by injecting it high into the cervix with a needle-
less syringe. This process closely replicates the way in which fresh semen is directly
deposited on to the neck of the cervix by the penis during vaginal intercourse. When the
male ejaculates, sperm deposited this way will quickly swim into the cervix and toward
the fallopian tubes where an ovum recently released by the ovary(s) hopefully awaits

121
fertilization. It is the simplest method of artificial insemination and 'unwashed' or raw
semen is normally used. It is probably therefore, the most popular method and is used
in most home, self and practitioner insemination procedures.
B. INTRAUTERINE INSEMINATION(IUI)
'Washed sperm', that is, spermatozoa which have been removed from most other
components of the seminal fluids, can be injected directly into a woman's uterus in a
process called intrauterine insemination (IUI). If the semen is not washed it may elicit
uterine cramping, expelling the semen and causing pain, due to content of
prostaglandins. (Prostaglandins are also the compounds responsible for causing the
myometrium to contract and expel the menses from the uterus, during menstruation.)
The woman should rest on the table for 15 minutes after an IUI to optimize the
pregnancy rate. To have optimal chances with IUI, the female should be under 30 years
of age, and the man should have a TMS of more than 5 million per ml. In practice,
donor sperm will satisfy these criteria. A promising cycle is one that offers two follicles
measuring more than 16 mm, and estrogen of more than 500 pg/mL on the day of hCG
administration. A short period of ejaculatory abstinence before intrauterine
insemination is associated with higher pregnancy rates. However, GnRH agonist
administration at the time of implantation does not improve pregnancy outcome in
intrauterine insemination cycles according to a randomized controlled trial.
C. INTRAUTERINE TUBOPERITONEAL INSEMINATION(IUTPI)
Intrauterine tuboperitoneal insemination (IUTPI) is insemination where both the
uterus and fallopian tubes are filled with insemination fluid. The cervix is clamped to
prevent leakage to the vagina, best achieved with the specially designed Double Nut
Bivalve (DNB) speculum. The sperm is mixed to create a volume of 10 ml, sufficient
enough to fill the uterine cavity, pass through the interstitial part of the tubes and the
ampulla, finally reaching the peritoneal cavity and the Pouch of Douglas where it
would be mixed with the peritoneal and follicular fluid. IUTPI can be useful in

122
unexplained infertility, mild or moderate male infertility, and mild or moderate
endometriosis.
D. INTRATUBAL INSEMINATION(ITI)
IUI can furthermore be combined with intratubal insemination (ITI), into the
Fallopian tube although this procedure is no longer generally regarded as having any
beneficial effect compared with IUI. ITI however, should not be confused with gamete
intrafallopian transfer, where both eggs and sperm are mixed outside the woman's
body and then immediately inserted into the Fallopian tube where fertilization takes
place.
5.4 INVITRO FERTILIZATION OR TEST TUBE BABY In Vitro Fertilisation (IVF) is a process by which egg cells are fertilised by sperm
outside the womb, in vitro. IVF is a major treatment in infertility when other methods of
assisted reproductive technology have failed. The process involves hormonally
controlling the ovulatory process, removing ova (eggs) from the woman's ovaries and
letting sperm fertilise them in a fluid medium. The fertilised egg (zygote) is then
transferred to the patient's uterus with the intent to establish a successful pregnancy.
The first successful birth of a "test tube baby", Louise Brown, occurred in 1978. Before
that, there was a transient biochemical pregnancy reported by Australian Foxton School
researchers in 1973 and an ectopic pregnancy reported by Steptoe and Edwards in 1976.
The term in vitro, from the Latin root meaning within the glass, is used, because
early biological experiments involving cultivation of tissues outside the living organism
from which they came, were carried out in glass containers such as beakers, test tubes, or
petri dishes. Today, the term in vitro is used to refer to any biological procedure that is
performed outside the organism it would normally be occurring in, to distinguish it
from an in vivo procedure, where the tissue remains inside the living organism within
which it is normally found. A colloquial term for babies conceived as the result of IVF,
test tube babies, refers to the tube-shaped containers of glass or plastic resin, called test

123
tubes, that are commonly used in chemistry labs and biology labs. However, in vitro
fertilisation is usually performed in the shallower containers called Petri dishes. (Petri
dishes may also be made of plastic resins.) However, the IVF method of Autologous
Endometrial Coculture is actually performed on organic material, but is yet called in
vitro. This is used when parents are having infertility problems or they want to have
multiple births.
1. INDICATIONS
IVF may be used to overcome female infertility in the woman due to problems of
the fallopian tube, making fertilisation in vivo difficult. It may also assist in male
infertility, where there is defect sperm quality, and in such cases intracytoplasmic
sperm injection (ICSI) may be used, where a sperm cell is injected directly into the egg
cell. This is used when sperm have difficulty penetrating the egg, and in these cases the
partner's or a donor's sperm may be used. ICSI is also used when sperm numbers are
very low. ICSI results in success rates equal to those of IVF fertilisation.
For IVF to be successful it may be easier to say that it requires healthy ova, sperm
that can fertilise, and a uterus that can maintain a pregnancy. Due to the costs of the
procedure, IVF is generally attempted only after less expensive options have failed. This
also avails for egg donation or surrogacy where the woman providing the egg isn't the
same who will carry the pregnancy to term. This means that IVF can be used for females
who have already gone through menopause. The donated oocyte can be fertilised in a
crucible. If the fertilisation is successful, the zygote will be transferred into the uterus,
within which it will develop into an embryo.
IVF can also be combined with preimplantation genetic diagnosis (PGD) to rule
out presence of genetic disorders. A similar but more general test has been developed
called Preimplantation Genetic Haplotyping (PGH).

124
2. METHOD
OVARIAN HYPERSTIMULATION
Treatment cycles are typically started on the 3rd day of menstruation and consist
of a regimen of fertility medications to stimulate the development of multiple follicles of
the ovaries. In most patients injectable gonadotropins (usually FSH analogues) are used
under close monitoring. Such monitoring frequently checks the estradiol level and, by
means of gynecologic ultrasonography, follicular growth. Typically approximately 10
days of injections will be necessary. Spontaneous ovulation during the cycle is typically
prevented by the use of GnRH agonists that are started prior or at the time of
stimulation or GnRH antagonists that are used just during the last days of stimulation;
both agents block the natural surge of luteinising hormone (LH) and allow the
physician to initiate the ovulation process by using medication, usually injectable
human chorionic gonadotropins.
EGG RETRIEVAL (TRANSVAGINAL OOCYTE RETRIEVAL)
When follicular maturation is judged to be adequate, human chorionic
gonadotropin (hCG) is given. This agent, which acts as an analogue of luteinising
hormone, makes the follicles perform their final maturation, and would cause ovulation
about 42 hours after injection, but a retrieval procedure takes place just prior to that, in
order to recover the egg cells from the ovary. The eggs are retrieved from the patient
using a transvaginal technique involving an ultrasound-guided needle piercing the
vaginal wall to reach the ovaries. Through this needle follicles can be aspirated, and the
follicular fluid is handed to the IVF laboratory to identify ova. It is common to remove
between ten and thirty eggs. The retrieval procedure takes about 20 minutes and is
usually done under conscious sedation or general anaesthesia.
EGG AND SPERM PREPARATION
In the laboratory, the identified eggs are stripped of surrounding cells and
prepared for fertilisation. An oocyte selection may be performed prior to fertilization to

125
select eggs with optimial chances of successful pregnancy. In the meantime, semen is
prepared for fertilisation by removing inactive cells and seminal fluid in a process
called sperm washing. If semen is being provided by a sperm donor, it will usually have
been prepared for treatment before being frozen and quarantined, and it will be thawed
ready for use.
FERTILIZATION
The sperm and the egg are incubated together at a ratio of about 75,000:1 in the
culture media for about 18 hours. In most cases, the egg will be fertilised by that time
and the fertilised egg will show two pronuclei. In certain situations, such as low sperm
count or motility, a single sperm may be injected directly into the egg using
intracytoplasmic sperm injection (ICSI). The fertilised egg is passed to a special growth
medium and left for about 48 hours until the egg consists of six to eight cells.
In gamete intrafallopian transfer, eggs are removed from the woman and placed
in one of the fallopian tubes, along with the man's sperm. This allows fertilisation to
take place inside the woman's body. Therefore, this variation is actually an in vivo
fertilisation, not an in vitro fertilisation.
EMBRYO CULTURE
Typically, embryos are cultured until having reached the 6–8 cell stage three
days after retrieval. Embryos are placed into an extended culture system with a transfer
done at the blastocyst stage at around five days after retrieval, especially if many good-
quality embryos are still available on day 3. Blastocyst stage transfers have been shown
to result in higher pregnancy rates. Transfers after 2 days are also common.
Culture of embryos can either be performed in an artificial culture medium or in
an autologous endometrial coculture (on top of a layer of cells from the woman's own
uterine lining). With artificial culture medium, there can either be the same culture
medium throughout the period, or a sequential system can be used, in which the embryo
is sequentially placed in different media. For example, when culturing to the blastocyst

126
stage, one medium may be used for culture to day 3, and a second medium is used for
culture thereafter. Single or sequential medium are equally effective for the culture of
human embryos to the blastocyst stage. Artificial embryo culture media basically
contain glucose, pyruvate, and energy-providing components, but addition of amino
acids, nucleotides, vitamins, and cholesterol improve the performance of embryonic
growth and development.
EMBRYO SELECTION
Laboratories have developed grading methods to judge oocyte and embryo
quality. In order to optimise pregnancy rates, there is significant evidence that a
morphological scoring system is the best strategy for the selection of embryos.
However, presence of soluble HLA-G might be considered as a second parameter if a
choice has to be made between embryos of morphologically equal quality. Also, two-
pronuclear zygotes (2PN) transitioning through 1PN or 3PN states tend to develop into
poorer-quality embryos than those who constantly remain 2PN. In addition to tests that
optimise pregnancy chances, Preimplantation Genetic Diagnosis (PGD) or screening
may be performed prior to transfer in order to avoid inheritable diseases.
EMBRYO TRANSFER
Embryos are graded by the embryologist based on the number of cells, evenness of
growth and degree of fragmentation. The number to be transferred depends on the number
available, the age of the woman and other health and diagnostic factors. A maximum of two
embryos are transferred except in unusual circumstances. According to HFEA regulations,
a woman over 40 may have up to three embryos transferred, whereas, younger women may
have many embryos transferred based on individual fertility diagnosis. Most clinics and
country regulatory bodies seek to minimise the risk of pregnancies carrying multiples. The
embryos judged to be the "best" are transferred to the patient's uterus through a thin, plastic
catheter, which goes through her vagina and cervix. Several embryos may be passed into
the uterus to improve chances of implantation and pregnancy.

127
SUCCESS OR FAILURE FACTORS
Potential factors that may influence pregnancy (and live birth) rates in IVF
include stress, acupuncture, level of DNA fragmentation as measured e.g. by Comet
assay, advanced maternal age and semen quality.
STRESS:
In a 2005 Swedish study, 166 women were monitored starting one month before
their IVF cycles, and the results showed no significant correlation between
psychological stress and IVF outcome. The study concluded with the recommendation
to clinics that it might be possible to reduce the stress experienced by IVF patients
during the treatment procedure by informing them of those findings. While
psychological stress experienced during a cycle might not influence an IVF outcome, it
is possible that the experience of IVF can result in stress that leads to depression. The
financial consequences alone of IVF can influence anxiety and become overwhelming.
However, for many couples, the alternative is infertility, and the experience of infertility
itself can also cause extreme stress and depression.
ACUPUNCTURE:
An increasing number of fertility specialists and centers offer acupuncture as a
part of their IVF protocol. Limited but supportive evidence from clinical trials and case
series suggests that acupuncture may improve the success rate of IVF and the quality of
life of patients undergoing IVF and that it is a safe adjunct therapy.
ACUPUNCTURE MECHANISMS:
Four mechanisms by which it has been suggested that acupuncture may improve
IVF outcomes are
• Neuroendocrinological modulations
• Increased blood flow to uterus and ovaries
• Modulation in cytokines
• Reduction of stress, anxiety, and depression

128
ELECTRO-ACUPUNCTURE IN OOCYTE RETRIEVAL FOR IVF:
Electro-acupuncture has been found to be a good alternative to conventional
medical analgesia, it results in shorter hospitalisation times and lower costs.
OTHER FACTORS:
Other determinants of outcome of IVF include:
• Tobacco smoking reduces the chances of IVF producing a live birth by 34%
and increases the risk of an IVF pregnancy miscarrying by 30%.
• A body mass index (BMI) over 27 causes a 33% decrease in likelihood to have
a live birth after the first cycle of IVF, compared to those with a BMI between 20
and 27.
• Also, pregnant women who are obese have higher rates of congenital
abnormality, miscarriage, gestational diabetes, hypertension, thromboembolism
and problems during delivery. Ideal body mass index is 19–30.
• Salpingectomy before IVF treatment increases chances for women with
hydrosalpinges
• Optimal woman’s age is 23–39 years at time of treatment .
• Success with previous pregnancy and/or live birth increases chances.
• Low alcohol/caffeine intake increases success rate.
1. COMPLICATIONS
The major complication of IVF is the risk of multiple births. This is directly
related to the practice of transferring multiple embryos at embryo transfer. Multiple
births are related to increased risk of pregnancy loss, obstetrical complications,
prematurity, and neonatal morbidity with the potential for long term damage. Strict
limits on the number of embryos that may be transferred have been enacted in some
countries (e.g. England) to reduce the risk of high-order multiples (triplets or more), but
are not universally followed or accepted. Spontaneous splitting of embryos in the
womb after transfer can occur, but this is rare and would lead to identical twins. A

129
double blind, randomised study followed IVF pregnancies that resulted in 73 infants (33
boys and 40 girls) and reported that 8.7% of singleton infants and 54.2% of twins had a
birth weight of < 2500 g. However recent evidence suggests that singleton offspring
after IVF is at higher risk for lower birth weight for unknown reasons.
Another risk of ovarian stimulation is the development of ovarian
hyperstimulation syndrome, particularly if hCG is used to "trigger ovulation".
If the underlying infertility is related to abnormalities in spermatogenesis, it is
plausible, but too early to examine that male offspring is at higher risk for sperm
abnormalities.
Behavior and socioemotional functioning of children conceived by IVF is normal
overall, according to studies on 9–18-year-old IVF children.
A negative pregnancy test after IVF is associated with an increased risk for
depression in women, but not with any increased risk of developing anxiety disorders.
Pregnancy test results do not seem to be a risk factor for depression or anxiety among
men.
BIRTH DEFECTS
The issue of birth defects has been a controversial topic in IVF. Many studies do
not show a significant increase after use of IVF, and some studies suggest higher rates
for ICSI, whereas others do not support this finding. In 2008, an analysis of the data of
the National Birth Defects Study in the US found that certain birth defects were
significantly more common in infants conceived with IVF, notably septal heart defects,
cleft lip with or without cleft palate, esophageal atresia, and anorectal atresia; the
mechanism of causality is unclear.
A 2002 study, reviewing "the birth records of all the IVF babies" in Western Australia
"has found IVF kids are twice as likely to have birth defects as normal births". The study
allowed for the effects of multiple births and the mother's age. The higher incidence of birth
defects "up to one year of age" found include: heart defects, "chromosomal abnormalities

130
like Down Syndrome, spina bifida, gastro-intestinal abnormalities, musculo-skeletal,
dislocated hips", and club feet. The IVF children also were found to have a higher incidence
of lower birth weights, pre-term births, and cerebral palsy.
2. PREIMPLANTATION GENETIC DIAGNOSIS (PGD)
Preimplantation genetic diagnosis used in conjunction with IVF treatments
appeared in the early 1990s, and since then hundreds of normal, healthy babies have
been born using this advanced reproductive technology. PGD technology improves the
likelihood of a successful pregnancy and birth for two distinctly different groups of
patients. Couples with infertility related to recurrent miscarriage or unsuccessful IVF
cycles and couples who are at risk for passing on inherited genetic disease to their
offspring. Patients who also can benefit from PGD include:
• Couples who have a family history of inherited disease
• Couples who want to use gender selection to prevent a gender-linked disease
• Women who have had repeated failures with IVF
• Women with a history of unexplained miscarriage
• Women who are more than 39 years old
PGD screens for chromosomal abnormalities. It screens individual cells from a pre-
embryo during the IVF process. Before the transfer of a pre-embryo back to a woman's
uterus, one or two cells are removed from the pre-embryos. These cells are then evaluated
for normalcy. Typically within one to two days, following completion of the evaluation,
only the normal pre-embryos are transferred back to the woman's uterus. In addition, PGD
can reduce the risk of multiple pregnancies because fewer embryos are needed for
implantation.
3. CRYOPRESERVATION
The first ever pregnancy derived from a frozen human embryo was reported by
Alan Trounson & Linda Mohr in 1983 (although the fetus aborted spontaneously at
about 20 weeks of gestation); the first term pregnancies derived from frozen human
frozen freezing process was born in 1984. Since then and up to 2008 it is estimated that

131
between 350,000 and half a million IVF babies have been born from embryos controlled
rate frozen and then stored in liquid nitrogen; additionally a few hundred births have
been born from vitrified oocytes but firm figures are hard to come by.
On the safety of embryo cryopreservation, a 2008 study reported at the European
Society of Human Reproduction and Embryology discovered that children born from
frozen embryos “did better and had a higher birth weight” than children born from a
fresh transfer. The study was conducted out of Copenhagen and evaluated babies born
during the years 1995–2006. 1267 children born after Frozen Embryo Replacement
(FER), via controlled-rate freezers and storage in liquid nitrogen, were studied and
categorised into three groups. 878 of them were born using frozen embryos that were
created using standard in vitro fertilisation in which the sperm were placed into a dish
close to the egg but had to penetrate the egg on their own. 310 children were born with
frozen embryos created using ICSI in which a single sperm was injected into a single
egg, and 79 were born where the method of creation of the embryos was not known.
17,857 babies born after a normal IVF/ICSI with fresh embryos were also studied
and used as a control group or reference group. Data on all of the children’s outcomes
were taken regarding birth defects, birth weights, and length of pregnancy. The results
of the study showed that the children who came from frozen embryos had higher birth
weights, gave longer pregnancies and produced fewer “pre-term” births. There was no
difference in the rate of birth defects whether the children came from frozen embryos or
fresh embryos. In the FER group, the birth defect rate was 7.7% compared to the fresh
transfer group which was slightly higher at 8.8%. The scientists also found that the risk
for multiple pregnancies was increased in the fresh embryo transfers.
OOCYTE CRYOPRESERVATION
Cryopreservation of unfertilised mature oocytes has been successfully
accomplished, e.g. in women who are likely to lose their ovarian reserve due to
undergoing chemotherapy.

132
Fig. Oocyte with surrounding granulosa cells Fig. "Naked" Egg
Fig. Early embryo development following fertilisation
5.5 HUMAN CLONING Human cloning is the creation of a genetically identical copy of a human (not
usually referring to monozygotic multiple births), human cell, or human tissue. The
ethics of cloning is an extremely controversial issue. The term is generally used to refer
to artificial human cloning; human clones in the form of identical twins are
commonplace, with their cloning occurring during the natural process of reproduction.
There are two commonly discussed types of human cloning: therapeutic cloning and
reproductive cloning. Therapeutic cloning involves cloning cells from an adult for use
in medicine and is an active area of research, while reproductive cloning would involve

133
making cloned humans. Such reproductive cloning has not been performed and is
illegal in many countries. A third type of cloning called replacement cloning is a
theoretical possibility, and would be a combination of therapeutic and reproductive
cloning. Replacement cloning would entail the replacement of an extensively damaged,
failed, or failing body through cloning followed by whole or partial brain transplant.
1. HISTORY
Although the possibility of cloning humans has been the subject of speculation
for much of the twentieth century, scientists and policy makers began to take the
prospect seriously in the 1960s. Nobel Prize winning geneticist Joshua Lederberg
advocated for cloning and genetic engineering in a seminal article in the American
Naturalist in 1966 and again, the following year, in the Washington Post. He sparked a
debate with conservative bioethicist Leon Kass, who wrote at the time that "the
programmed reproduction of man will, in fact, dehumanize him." Another Nobel

134
Laureate, James D. Watson, publicized the potential and the perils of cloning in his
Atlantic Monthly essay, "Moving Toward the Clonal Man", in 1971.
The technology of cloning mammals, although far from reliable, has reached the
point where many scientists are knowledgeable, the literature is readily available, and
the implementation of the technology is not very expensive compared to many other
scientific processes. For that reason Lewis D. Eigen has argued that human cloning
attempts will be made in the next few years and may well have been already begun.
The ethical and moral issues cannot wait and should be discussed, debated and
guidelines and laws be developed now.
"By waiting until the first clone is among us or about to be born, we complicate the problem
immensely and guarantee that we will not be able to have the national and international
conversation and debate to arrive at particularly good decisions."
NOTABLE CLONING ATTEMPTS AND CLAIMS
• Hwang Woo-suk, a South Korean scientist, claimed in 2004 to have cloned
human embryonic stem cells. The scientist in 2006 admitted faking his findings,
after questions of impropriety had emerged.
• Dr. Panayiotis Zavos, an American fertility doctor, revealed on 17 January
2004 at a London press conference that he had transferred a freshly-cloned
embryo into the 35-year-old woman. On 04 February 2004, it emerged that the
attempt had not worked and the woman did not become pregnant.
2. ETHICAL IMPLICATIONS
Advocates of human therapeutic cloning believe the practice could provide
genetically identical cells for inter-regenerative medicine, and tissues and organs for
transplantation. Such cells, tissues and organs would neither trigger an immune
response nor require the use of Immunosuppressive drugs. Both basic research and
therapeutic development for serious diseases such as cancer, heart disease and diabetes,
as well as improvements in burn treatment and reconstructive and cosmetic surgery,

135
are areas that might benefit from such new technology. New York University bioethicist
Jacob M. Appel has argued that "children cloned for therapeutic purposes" such as "to
donate bone marrow to a sibling with leukemia" might someday be viewed as heroes.
Proponents claim that human reproductive cloning also would produce benefits.
Severino Antinori and Panayiotis Zavos hope to create a fertility treatment that allows
parents who are both infertile to have children with at least some of their DNA in their
offspring.
Some scientists, including Dr. Richard Seed, suggest that human cloning might
obviate the human aging process. Dr. Preston Estep has suggested the terms
"replacement cloning" to describe the generation of a clone of a previously living
person, and "persistence cloning" to describe the production of a cloned body for the
purpose of obviating aging, although he maintains that such procedures currently
should be considered science fiction and current cloning techniques risk producing a
prematurely aged child.
In Aubrey de Grey's proposed SENS (Strategies for Engineered Negligible
Senescence), one of the considered options to repair the cell depletion related to cellular
senescence is to grow replacement tissues from stem cells harvested from a cloned
embryo.
3. CURRENT LAW
UNITED NATIONS
On December 12, 2001, the United Nations General Assembly began elaborating
an international convention against the reproductive cloning of humans. A broad
coalition of States, including Spain, Italy, Philippines, the United States, Costa Rica and
the Holy See sought to extend the debate to ban all forms of human cloning, noting that,
in their view, therapeutic human cloning violates human dignity. Costa Rica proposed
the adoption of an international convention to ban all forms of Human Cloning. Unable
to reach a consensus on a binding convention, in March 2005 a non-binding United

136
Nations Declaration on Human Cloning calling for the ban of all forms of Human Cloning
contrary to human dignity, was finally adopted.[15]
UNITED STATES
In 1998, 2001, 2004 and 2007, the United States House of Representatives voted
whether to ban all human cloning, both reproductive and therapeutic. Each time,
divisions in the Senate over therapeutic cloning prevented either competing proposal (a
ban on both forms or reproductive cloning only) from passing. Some American states
ban both forms of cloning, while some others outlaw only reproductive cloning.
Current regulations prohibit federal funding for research into human cloning,
which effectively prevents such research from occurring in public institutions and
private institutions such as universities which receive federal funding. However, there
are currently no federal laws in the United States which ban cloning completely, and
any such laws would raise difficult Constitutional questions similar to the issues raised
by abortion.
UNITED KINGDOM
On January 14, 2001 the British government passed The Human Fertilisation and
Embryology (Research Purposes) Regulations 2001to amend the Human Fertilisation and
Embryology Act 1990 by extending allowable reasons for embryo research to permit
research around stem cells and cell nuclear replacement, thus allowing therapeutic cloning.
However, on 15 November 2001, a pro-life group won a High Court legal challenge, which
struck down the regulation and effectively left all forms of cloning unregulated in the UK.
Their hope was that Parliament would fill this gap by passing prohibitive legislation.
Parliament was quick to pass Human Reproductive Cloning Act 2001 which explicitly
prohibited reproductive cloning. The remaining gap with regard to therapeutic cloning was
closed when the appeals courts reversed the previous decision of the High Court.
The first licence was granted on August 11, 2004 to researchers at the University of
Newcastle to allow them to investigate treatments for diabetes, Parkinson's disease and
Alzheimer's disease. The Human Fertilisation and Embryology Act 2008, a major review of

137
fertility legislation, repealed the 2001 Cloning Act by making amendments of similar effect
to the 1990 Act. The 2008 Act also allows experiments on hybrid human-animal embryos.
4. RELIGIOUS OBJECTIONS
The Roman Catholic Church, under the papacy of Benedict XVI, has condemned
the practice of human cloning, in the magisterial instruction Dignitas Personae, stating
that it represents a "grave offense to the dignity of that person as well as to the
fundamental equality of all people".
Sunni Muslims consider human cloning to be forbidden by Islam. The Islamic
Fiqh Academy, in its Tenth Conference proceedings, which was convened in Jeddah,
Saudi Arabia in the period from June 28, 1997 to July 3, 1997, issued a Fatwā stating that
human cloning is haraam (prohibited by the faith).
How to Clone a Human?
This procedure is based upon the Sheep cloning procedure. The mouse cloning
procedure seems to have worked better.
MATERIALS
• Human Tissue: Pure human cells of one tissue type, from the individual who will
be cloned.
• Human Tissue Culture Media: Media in which these human cells will grow and
divide.
• Minimal Human Tissue Culture Media: Media in which cells will stop dividing,
and enter a state of "quiescence" without dying.
• Laboratory supplies: Incubator, Sterile Hood, petri dishes, microscopes, and tools
capable of removing and implanting cellular organelles, such as the nucleus,
from one cell to another.
• Unfertilized human egg cells.
• Human Egg Cell growth media: Media where fertilized eggs will grow and divide.

138
PROCEDURES
1. Grow the human cells to be cloned until you have a good supply.
2. Transfer the cells to minimal media. [For now, The Sheep Cloning Paper is a
good reference for exactly how long.] This should allow the cells to live, but they
should stop dividing and enter quiescence. This is likely the step in which the
cells lose their differentiation, and revert to a more totipotent state.
3. When the cultured cells are in the quiescent state, get an unfertilized human egg
cell. Remove the nucleus from this egg cell. Try to minimize damage done to this
cell and discard the nucleus.
4. Take one of the quiescent cells in it's entirely, and implant it inside the coat
around the egg (known as the zona pellucida) next to the egg itself.
5. Electroshock the egg. [For now, The Sheep Cloning Paper is probably a good
reference for how much and how long to electroshock.] The electroshock induces
the fusion of the two cells, so you should be able to tell when you've
electroshocked enough just by looking at the cells. The rebooting of the human
genetic program is believed to be initiated by the replacement of donor cell
protien signals by egg cell protien signals, but the electroshock might assist in
moving those protien signals across the nuclear membrane as well.
Electroporation is a common technique for moving DNA molecules through a
cellular membrane.
6. Repeat the last three steps as necessary until you have enough clones. Expect a
lot of them not to survive because of cellular damage and other mishaps. Allow
the embryos to grow and divide a few times in Human Egg Cell growth media.
7. Implant the embryos in human mothers where they will can be carried to term,
and born normally.

139

140
5.6 EMBRYO TRANSFER Embryo transfer refers to a step in the process of in vitro fertilization (IVF)
whereby one or several embryos are placed into the uterus of the female with the intent
to establish a pregnancy. 8-cell embryo for transfer 3 days after fertilization.
1. FRESH VERSUS FROZEN
Embryos can be either “fresh” from fertilized egg cells of the same menstrual
cycle, or “frozen”, that is they have been generated in a preceding cycle, cryopreserved,
and are thawed just prior to the transfer. Babies born from frozen IVF embryos are less
likely to be born prematurely or underweight than are those conceived during fresh
treatment cycles, three independent teams of scientists have found. One of the studies
also recorded lower rates of stillbirth and early death among frozen-embryo babies. The
results, from researchers based in the United States, Australia and Finland, suggest that
far from being riskier than conventional IVF, as is generally thought, cycles using frozen
embryos may actually be safer, Mark Henderson of the Times London reported in
November 2008.
2. UTERINE PREPARATION
In the human, the uterine lining (endometrium) needs to be appropriately
prepared so that the embryo(s) can implant. In a natural or stimulated cycle, the embryo
transfer takes place in the luteal phase at a time where the lining is appropriately
undeveloped in relation to the status of the present Luteinizing Hormone. In a cycle
where a "frozen" embryo is transferred, the recipient woman could be given first
estrogen preparations (about 2 weeks), then a combination of oestrogen and
progesterone so that the lining becomes receptive for the embryo. The time of
receptivity is the implantation window. Limited evidence also supports removal of
cervical mucus before transfer.

141
3. TIMING
In stimulated cycles in human IVF, embryos are typically transferred 3 days after
fertilization and may then be at the eight-cell stage, or they are transferred 2 to 3 days
later when they have reached the blastocyst stage. Embryos who reach the day 3 cell
stage can be tested for chromosal or specific genetic defects prior to possible transfer by
preimplantation genetic diagnosis (PGD).
Monozygotic twinning is not increased after blastocyst transfer compared with
cleavage-stage embryo transfer.
4. PROCEDURE
The embryo transfer procedure starts by placing a speculum in the vagina to
visualize the cervix, which is cleansed with saline solution or culture media. A soft
transfer catheter is loaded with the embryos and handed to the clinician after
confirmation of the patient’s identity. The catheter is inserted through the cervical canal
and advanced into the uterine cavity.
There is good and consistent evidence of benefit in ultrasound guidance, that is,
making an abdominal ultrasound to ensure correct placement, which is 1–2 cm from the
uterine fundus. Anesthesia is generally not required. Single embryo transfers in
particular require accuracy and precision in placement within the uterine cavity. The
optimal target for embryo placement, known as the maximal implantation potential
(MIP) point, is identified using 3D/4D ultrasound. However, there is limited evidence
that supports deposition of embryos in the midportion of the uterus.
After insertion of the catheter, the contents are expelled and the embryos are
deposited. Limited evidence supports making trial transfers before performing the
procedure with embryos. After expulsion, the duration that the catheter remains inside
the uterus has no effect on pregnancy rates. Limited evidence suggests avoiding
negative pressure from the catheter after expulsion. After withdrawal, the catheter is
handed to the embryologist, who inspects it for retained embryos.

142
In the process of zygote intrafallopian transfer (ZIFT), eggs are removed from the
woman, fertilised, and then placed in the woman's fallopian tubes rather than the
uterus.
5. EMBRYO NUMBER
A major issue is how many embryos should be transferred. Placement of
multiple embryos carries the risk of multiple pregnancy. In the past, physicians have
often placed too many embryos in the hope to establish a pregnancy. However, the rise
in multiple pregnancies has led to a reassessment of this approach. Professional
societies and in many countries, the legislature, have issued guidelines or laws to curtail
a practice of placing too many embryos in an attempt to reduce multiple pregnancies.
e-SET
The technique of selecting only one embryo to transfer to the woman is called
elective-Single Embryo Transfer (e-SET) or, when embryos are at the blastocyst stage, it
can also be called elective single blastocyst transfer (eSBT). It lowers the risk of multiple
pregnancies, compared with e.g. Double Embryo Transfer (DET) or double blastocyst
transfer (2BT), with a twinning rate of approximately 3.5% in eSET compared with
approximately 38% in DET, or 2% in eSBT compared with approximately 25% in 2BT.
At the same time, pregnancy rates is not significantly less with eSBT than with 2BT.
Furthermore, SET has better outcomes in terms of mean gestational age at delivery,
mode of delivery, birthweight, and risk of neonatal intensive care unit necessity than
DET. e-SET of embryos at the cleavage stage reduces the likelihood of live birth by 38%
and multiple birth by 94%. Evidence from randomized, controlled trials suggests that
increasing the number of e-SET attempts (fresh and/or frozen) results in a cumulative
live birth rate similar to that of DET.
6. FOLLOW-UP
Patients usually start progesterone medication after egg (also called oocyte)
retrieval. While daily intramuscular injections of progesterone-in-oil (PIO) have been

143
the standard route of administration, PIO injections are not FDA-approved for use in
pregnancy. A recent meta-analysis showed that the intravaginal route with an
appropriate dose and dosing frequency is equivalent to daily intramuscular injections.
In addition, a recent case-matched study comparing vaginal progesterone with PIO
injections showed that live birth rates were nearly identical with both methods. A
duration of progesterone administration of 11 days results in almost the same birth
rates as longer durations.
Patients are also given estrogen medication in some cases after the embryo
transfer. Pregnancy testing is done typically two weeks after egg retrieval.
7. THIRD-PARTY REPRODUCTION
It is not necessary that the embryo transfer be performed on the female who
provided the eggs. Thus another female whose uterus is appropriately prepared can
receive the embryo and become pregnant. Embryo transfer may be used where a
woman who has eggs but no uterus and wants to have a biological baby; she would
require the help of a gestational carrier or surrogate to carry the pregnancy. Also, a
woman who has no eggs but a uterus may resort to egg donor IVF, in which case
another woman would provide eggs for fertilization and the resulting embryos are
placed into the uterus of the patient. Fertilization may be performed using the woman's
partner's sperm or by using donor sperm. 'Spare' embryos which are created for another
couple undergoing IVF treatment but which are then surplus to that couple's needs may
also be transferred. Embryos may be specifically created by using eggs and sperm from
donors and these can then be transferred into the uterus of another woman. A surrogate
may carry a baby produced by embryo transfer for another couple, even though neither
she nor the 'commissioning' couple is biologically related to the child. Third party
reproduction is controversial and regulated in many countries. Persons entering
gestational surrogacy arrangements must make sense of an entirely new type of
relationship that does not fit any of the traditional scripts we use to categorize relations

144
as kinship, friendship, romantic partnership or market relations. Surrogates have the
experience of carrying a baby that they conceptualize as not of their own kin, while
intended mothers have the experience of waiting through nine months of pregnancy
and transitioning to motherhood from outside of the pregnant body. This can lead to
new conceptualizations of body and self.
8. EMBRYO TRANSFER IN LIVESTOCK
Embryo transfer techniques allow top quality female livestock to have a greater
influence on the genetic advancement of a herd or flock in much the same way that
artificial insemination has allowed greater use of superior sires. ET also allows the
continued use of animals such as competition mares to continue training and showing,
while producing foals. The general epidemiological aspects of embryo transfer indicates
that the transfer of embryos provides the opportunity to introduce genetic material into
populations of livestock while greatly reducing the risk for transmission of infectious
diseases. Recent developments in the sexing of embryos before transfer and implanting
has great potential in the dairy and other livestock industries.
5.7 Rh BLOOD GROUP SYSTEM The Rh blood group system (including the Rh factor) is one of the currently 30 human
blood group systems. It is clinically the most important blood group system after ABO.
The Rh blood group system currently consists of 50 defined blood-group antigens,
among which the 5 antigens D, C, c, E, and e are the most important ones. The
commonly-used terms Rh factor, Rh positive and Rh negative refer to the D antigen only.
Besides its role in blood transfusion, the Rh blood group system, in particular the
strongest D antigen, is a relevant cause of the hemolytic disease of the newborn for
which prevention is key.

145
1. Rh FACTOR
Individuals either have, or do not have, the "Rh factor" on the surface of their red
blood cells. This term strictly refers only to the most immunogenic D antigen of the Rh
blood group system. The status is usually indicated by Rh positive (Rh+, does have the D
antigen) or Rh negative (Rh-, does not have the D antigen) suffix to the ABO blood type.
However, other antigens of this blood group system are also clinically relevant. These
antigens are listed separately (Rh nomenclature). In contrast to the ABO blood group,
immunization against Rh can generally only occur through blood transfusion or
placental exposure during pregnancy.
2. HISTORY OF DISCOVERIES
In 1939, Drs. Philip Levine and Rufus Stetson published in a first case report the
clinical consequences of non-recognized Rh factor, hemolytic transfusion reaction and
hemolytic disease of the newborn in its most severe form.[1] It was recognized that the
serum of the reported woman agglutinated with red blood cells of about 80% of the
people although the then known blood groups, in particular ABO were matched. No
name was given to this then for the first time described agglutinin. In 1940, Drs. Karl
Landsteiner and Alexander S. Wiener reported a serum that also reacted with about
85% of different human red blood cells. This serum was produced by immunizing
rabbits with red blood cells from Rhesus macaque. The antigen that induced this
immunization was designated by them as Rh factor "to indicate that rhesus blood had
been used for the production of the serum."
Based on the serologic similarities Rh factor was later also used for antigens, and
anti-Rh for antibodies, found in humans such as the previously described by Levine and
Stetson. Although differences between these two sera were shown already in 1942 and
clearly demonstrated in 1963, the already widely used term "Rh" was kept for the
clinically described human antibodies which are different from the ones related to the
Rhesus ape. This real factor found in Rhesus macaque was classified in the Landsteiner-

146
Wiener antigen system (antigen LW, antibody anti-LW) in honor to the discoverers. It
was recognized that the Rh factor was just one in a system of various antigens. Based on
different models of genetic inheritance, two different terminologies were developed;
both of them are still in use.
The clinical significance of this highly immunizing D antigen (i.e. Rh factor) was
soon realized. Some keystones were to recognize its importance for blood transfusion
including reliable diagnostic tests, and hemolytic disease of the newborn including
exchange transfusion and very importantly the prevention of it by screening and
prophylaxis.
3. Rh NOMENCLATURE
The Rh blood group system has two sets of nomenclatures: one developed by
Fisher and Race, the other by Wiener. Both systems reflected alternative theories of
inheritance. The Fisher-Race system, which is more commonly in use today, uses the
CDE nomenclature. This system was based on the theory that controls the product of
the corresponding antigen (e.g., a "D gene" produces D antigen, and so on). However,
the d gene was hypothetical, not actual.
The Wiener system used the Rh-Hr nomenclature. This system was based on the
theory that there was one gene at a single locus on each chromosome of the pair which
controls production of multiple antigens. In this theory, a gene R is supposed to give
rise to the “blood factors” Rho, rh’, and hr” and the gene r to produce rh’ and hr”.
Notations of the two theories are used interchangeably in blood banking (e.g.,
Rho (D)). Wiener's notation is more complex and cumbersome for routine use. Because
it is simpler to explain, the Fisher-Race theory has become more widely used.
DNA testing has shown that both theories are partially correct. There are in fact
two linked genes (RHCE and RHD), one with multiple specificities and one with a
single specificity. Thus, Wiener's postulate that a gene could have multiple specificities
(something many did not give credence to originally) has been proven correct. On the

147
other hand, Wiener's theory that there is only one gene has proven incorrect, as has the
Fischer-Race theory that there are three genes, rather than the 2.
4. Rh SYSTEM ANTIGENS
The proteins which carry the Rh antigens are transmembrane proteins, whose structure
suggest that they are ion channels.[6] The main antigens are D, C, E, c and e, which are
encoded by two adjacent gene loci, the RHD gene which encodes the RhD protein with the
D antigen (and variants)[7] and the RHCE gene which encodes the RhCE protein with the C,
E, c and e antigens (and variants).[8] There is no d antigen. Lowercase "d" indicates the
absence of the D antigen (the gene is usually deleted or otherwise nonfunctional).
Rhesus genotypes
Genotype symbol Rh (D) status
cde/cde rr Negative
CDe/cde R1 r Positive
CDe/CDe R1R1 Positive
cDE/cde R2 r Positive
CDe/cDE R1R2 Positive
cDE/cDE R2R2 Positive
Rh Phenotypes in Patients and Donors
Rh Phenotype CDE Patients (%) Donors (%)
R1r CcDe 37.4 33.0
R1R2 CcDEe 35.7 30.5
R1R1 CDe 5.7 21.8
rr ce 10.3 11.6
R2r cDEe 6.6 10.4

148
R0R0 cDe 2.8 2.7
R2R2 cDE 2.8 2.4
rr’’ cEe – 0.98
RZRZ CDE – 0.03
rr’ Cce 0.8 –
1. HEMOLYTIC DISEASE OF THE NEWBORN
The hemolytic condition occurs when there is an incompatibility between the
blood types of the mother and the fetus. These terms do not indicate which specific
antigen-antibody incompatibility is implicated. The disorder in the fetus due to Rh D
incompatibility is known as erythroblastosis fetalis.
• Hemolytic comes from two words: "hemo" (blood) and "lysis" (destruction) or
breaking down of red blood cells
• Erythroblastosis refers to the making of immature red blood cells
• Fetalis refers to the fetus.
When the condition is caused by the Rh D antigen-antibody incompatibility, it is
called Rh D Hemolytic disease of the newborn (often called Rhesus disease or Rh
disease for brevity). Here, sensitization to Rh D antigens (usually by feto-maternal
transfusion during pregnancy) may lead to the production of maternal IgG anti-D
antibodies which can pass through the placenta. This is of particular importance to D
negative females at or below childbearing age, because any subsequent pregnancy may
be affected by the Rhesus D hemolytic disease of the newborn if the baby is D positive.
The vast majority of Rh disease is preventable in modern antenatal care by injections of
IgG anti-D antibodies (Rho(D) Immune Globulin). The incidence of Rhesus disease is
mathematically related to the frequency of D negative individuals in a population, so
Rhesus disease is rare in East Asians, South Americans, and Africans, but more
common in Caucasians.

149
• SYMPTOMS AND SIGNS IN THE FETUS:
o Enlarged liver, spleen, or heart and fluid buildup in the fetus' abdomen
seen via ultrasound.
• SYMPTOMS AND SIGNS IN THE NEWBORN:
o Anemia that creates the newborn's pallor (pale appearance).
o Jaundice or yellow discoloration of the newborn's skin, sclera or mucous
membrane. This may be evident right after birth or after 24–48 hours after
birth. This is caused by bilirubin (one of the end products of red blood cell
destruction).
o Enlargement of the newborn's liver and spleen.
o The newborn may have severe edema of the entire body.
o Dyspnea or difficulty breathing.

150
2. POPULATION DATA
The frequency of Rh factor blood types and the RhD neg allele gene differs in
various populations.
Population data for the Rh D factor and the RhD neg allele
Population Rh(D) Neg Rh(D) Pos
Rh(D) Neg alleles
European Basque approx 35% 65% approx 60%
other Europeans 16% 84% 40%
African American approx 7% 93% approx 26%
Native Americans approx 1% 99% approx 10%
African descent less 1% over 99% 3%
Asian less 1% over 99% 1%
INHERITANCE
The D antigen is inherited as one gene (RHD) (on the short arm of the first
chromosome, p36.13-p34.3) with various alleles. As very much simplified, one can think
of alleles that are positive or negative for the D antigen. The gene codes for the RhD
protein on the red cell membrane. D-individuals who lack a functional RHD gene do
not produce the D antigen, and may be immunized by D+ blood.
The epitopes for the next 4 most common Rh antigens, C, c, E and e are
expressed on the highly similar RhCE protein that is genetically encoded in the RHCE
gene. It has been shown that the RHD gene arose by duplication of the RHCE gene
during primate evolution. Mice have just one RH gene.

151
1. FUNCTION
The structure homology data suggest that the product of RHD gene, the RhD
protein, acts as an ion pump of uncertain specificity (CO2 or NH3) and unknown
physiological role. Three recent studies have reported a protective effect of the RhD-
positive phenotype, especially RhD heterozygosity, against the negative effect of latent
toxoplasmosis on psychomotor performance in infected subjects. RhD-negative
compared to RhD-positive subjects without anamnestic titres of anti-Toxoplasma
antibodies have shorter reaction times in tests of simple reaction times. And conversely,
RhD-negative subjects with anamnestic titres (i.e. with latent toxoplasmosis) exhibited
much longer reaction times than their RhD-positive counterparts. The published data
suggested that only the protection of RhD-positive heterozygotes was long term in
nature; the protection of RhD-positive homozygotes decreased with duration of the
infection while the performance of RhD-negative homozygotes decreased immediately
after the infection.
2. ORIGIN OF RhD POLYMORPHISM
For a long time, the origin of RHD polymorphism was an evolutionary enigma.
Before the advent of modern medicine, the carriers of the rarer allele (e.g. RhD-negative
women in a population of RhD positives or RhD-positive men in a population of RhD
negatives) were at a disadvantage as some of their children (RhD-positive children born
to preimmunised RhD-negative mothers) were at a higher risk of fetal or newborn
death or health impairment from hemolytic disease. It was suggested that higher
tolerance of RhD-positive heterozygotes against Toxoplasma-induced impairment of
reaction time and Toxoplasma-induced increase of risk of traffic accident could
counterbalance the disadvantage of the rarer allele and could be responsible both for
the initial spread of the RhD allele among the RhD-negative population and for a stable
RhD polymorphism in most human populations. It was also suggested that differences
in the prevalence of Toxoplasma infection between geographical regions (0–95%) could

152
also explain the striking variation in the frequency of RhD-negative alleles between
populations. According to some parasitologists it is possible that the better
psychomotor performance of RhD-negative subjects in the Toxoplasma-free population
could be the reason for spreading of the “d allele” (deletion) in the European
population. In contrast to the situation in Africa and certain (but not all) regions of Asia,
the abundance of wild cats (definitive hosts of Toxoplasma gondii) in the European
territory was very low before the advent of the domestic cat.
3. WEAK D In serologic testing, D positive blood is easily identified. Units which are D
negative are often retested to rule out a weaker reaction. This was previously referred to
as Du, which has been replaced. In some cases, this phenotype occurs because of an
altered surface protein that is more common in people of African descent. The testing is
difficult, since using different anti-D reagents, especially the older polyclonal reagents,
may give different results.
The practical implication of this is that people with this sub-phenotype will have
a product labeled as "D positive" when donating blood. When receiving blood, they are
sometimes typed as a "D negative", though this is the subject of some debate. Most
"Weak D" patients can receive "D positive" blood without complications. However, it is
important to correctly identify the ones that have to considere D+ or D-. This is
important, since most blood banks have a limited supply of "D negative" blood and the
correct transfusion is clinically relevant. In this respect, genotyping of blood groups has
much simplified this detection of the various variants in the Rh blood group system.
4. OTHER Rh GROUP ANTIGENS Currently, 50 antigens have been described in the Rh group system, among
described D, C, c, E and e antigens are the most important ones. The others are much
less frequently encountered or are rarely clinically significant. Each is given a number,
though the highest assigned number (CEST or RH57 according to the ISBT terminology)

153
is not an accurate reflection of the antigens encountered since many (e.g. Rh38) have
been combined, reassigned to other groups, or otherwise removed.
5.8 CONGENITAL ANOMALY 1. CLASSIFICATION
a. PRIMARILY STRUCTURAL
b. OTHER
2. ANTIBIOTICS
a. PETROLEUM
b. EPIDEMIOLOGY
Congenital disorder or anomaly involves defects in or damage to a developing
fetus. It may be the result of genetic abnormalities, the intrauterine (uterus)
environment, errors of morphogenesis, infection, or a chromosomal abnormality. The
outcome of the disorder will further depend on complex interactions between the pre-
natal deficit and the post-natal environment. Animal studies indicate that the mother's
(and possibly the father's) diet, vitamin intake, and glucose levels prior to ovulation and
conception have long-term effects on fetal growth and adolescent and adult disease.
Congenital disorders vary widely in causation and abnormalities. Any substance that
causes birth defects is known as a teratogen. The older term congenital disorder does not
necessarily refer to a genetic disorder despite the similarity of the words. Some disorders
can be detected before birth through prenatal diagnosis (screening).
1. CLASSIFICATION
Much of the language used for describing congenital conditions predates
genomic mapping, and structural conditions are often considered separately from other
congenital conditions. It is now known that many metabolic conditions may have subtle
structural expression, and structural conditions often have genetic links. Still, congenital
conditions are often classified in a structural basis, organized when possible by primary
organ system affected.

154
a) PRIMARILY STRUCTURAL
Several terms are used to describe congenital abnormalities. (Some of these are
also used to describe noncongenital conditions, and more than one term may apply in
an individual condition.)
• A congenital physical anomaly is an abnormality of the structure of a body part.
An anomaly may or may not be perceived as a problem condition. Many, if not
most, people have one or more minor physical anomalies if examined carefully.
Examples of minor anomalies can include curvature of the 5th finger
(clinodactyly), a third nipple, tiny indentations of the skin near the ears
(preauricular pits), shortness of the 4th metacarpal or metatarsal bones, or
dimples over the lower spine (sacral dimples). Some minor anomalies may be
clues to more significant internal abnormalities.
• Birth defect is a widely-used term for a congenital malformation, i.e. a
congenital, physical anomaly which is recognizable at birth, and which is
significant enough to be considered a problem. According to the CDC most birth
defects are believed to be caused by a complex mix of factors including genetics,
environment, and behaviors, though many birth defects have no known cause.
• A congenital malformation is a congenital physical anomaly that is deleterious,
i.e. a structural defect perceived as a problem. A typical combination of
malformations affecting more than one body part is referred to as a malformation
syndrome.
• Some conditions are due to abnormal tissue development:
o A malformation is associated with a disorder of tissue development.
Malformations often occur in the first trimester.
o A dysplasia is a disorder at the organ level that is due to problems with tissue
development.
• It is also possible for conditions to arise after tissue is formed:

155
o A deformation is a condition arising from mechanical stress to normal tissue.
Deformations often occur in the second or third semester, and can be due to
oligohydramnios.
• A disruption involves breakdown of normal tissues.
• When multiple effects occur in a specified order, it is known as a sequence. When
the order is not known, it is a syndrome.
b) OTHER
• Genetic disorders or diseases are all congenital, though they may not be
expressed or recognized until later in life. Genetic diseases may be divided into
single-gene defects, multiple-gene disorders, or chromosomal defects. Single-
gene defects may arise from abnormalities of both copies of an autosomal gene (a
recessive disorder) or of only one of the two copies (a dominant disorder). Some
conditions result from deletions or abnormalities of a few genes located
contiguously on a chromosome. Chromosomal disorders involve the loss or
duplication of larger portions of a chromosome (or an entire chromosome)
containing hundreds of genes. Large chromosomal abnormalities always
produce effects on many different body parts and organ systems.
• A congenital metabolic disease is also referred to as an inborn error of
metabolism. Most of these are single gene defects, usually heritable. Many affect
the structure of body parts but some simply affect the function.
• Other well defined genetic conditions may affect the production of hormones,
receptors, structural proteins, and ion channels.
2. ANTIBIOTICS
Use of antibiotics around the time of conception, particularly sulfonamides and
nitrofurantoin are associated with major birth defects. Whether or not this association is
causal has not been determined.

156
a) PETROLEUM
Petroleum (oil) and petroleum distillates cause birth defects.
b). EPIDEMIOLOGY
Cell division errors can be due to a lack of nutrients or availability of atomic
building blocks, or the presence of toxins that impede normal growth. Division errors
which occur very early in the development of a multicellular organism can result in
large scale structural and functional differences in the organism's final shape. For
example it is now understood that a lack of folic acid in the diet of a mother can cause
cellular neural tube deformities that result in Spina Bifida.
External physical shocks or constrainment due to growth in a restricted space,
may result in unintended deformation or separation of cellular structures resulting in
an abnormal final shape or damaged structures unable to function as expected.
For multicellular organisms that develop in a womb, the physical interference or
presence of other similarly developing organisms such as twins can result in the two
cellular masses being integrated into a larger whole, with the combined cells attempting
to continue to develop in a matter that satisfies the intended growth patterns of both
cell masses. The two cellular masses can compete with each other, and may either
duplicate or merge various structures. This results in conditions such as conjoined
twins, and the resulting merged organism may die at birth when it must leave the life-
sustaining environment of the womb and must attempt to sustain its biological
processes independently.
Fig. Birth defects.

157
5.9 GROWTH DISTURBANCES What are growth disturbances?
If the growth of your child appears to be stagnant then you should see a doctor.
A growth disturbance is defined as a departure from the normal growth pattern
for children. It is important to remember that because no two children are exactly alike,
the notion of what 'normal' growth is has very broad limits.
Before birth, the growth of the embryo is monitored by midwives and doctors.
After birth, infants should gain between 150 and 200g per week from their second week
to the age of three months. By the age of five months, their birth weight should have
doubled.
Since children differ in size genetically, normal growth cannot be based on just
one examination. For this reason, it is important to follow the child's development over
a period of time using special measurement systems. This way, it is not size as such that
is monitored, instead it is the growth and weight gain of the child.
How is a growth disturbance discovered? It doesn't matter if the child is slighter, taller, or shorter than the established
measurements as long as the general pattern is normal. The problem arises if the child
suddenly deviates sharply from the growth pattern they have been following. If this
happens, you should consult your doctor.
The weight of healthy children can vary substantially. Many infants gain a lot of
weight during their first six months, then less between 10 and 18 months.
Children with short parents will often grow at the same rate as those with tall
parents until around one year old. Then they simply follow a slower growth curve.
After an illness, it is normal for children to rapidly regain any lost weight and
then revert to their original rate of growth. Babies who have grown too slowly in the
womb grow proportionally more than other children after birth. Then they start to
follow the correct growth curve.

158
Babies born prematurely are often measured against a different growth chart.
This is calculated by subtracting the number of weeks premature the baby was from
their current age. This correction can be applied until the child reaches two years of age.
A child's rate of growth and onset of puberty is partly dependent on hereditary
factors. For instance, sometimes a father and his son are both short in early puberty, but
taller in late puberty. Likewise, a mother and her daughter might both be tall at the age
of 12 and get their first period before other girls in their class.
Why do some children have a growth disturbance? A child's growth is mainly determined by a combination of genetics and
environmental factors, especially diet and exercise. However, a number of diseases may
also affect growth including:
o deficiency of growth hormone
o deficiency of thyroid hormone
o nutritional problems.
What can I do myself?
Everybody can measure and weigh their children. However, a professional
growth examination should be carried out regularly by health visitors and doctors.
These often take place at school, or during routine medical check-ups.
How does the doctor diagnose a growth disturbance?
The doctor measures and weighs the child and draws growth curves. The
parents' height and weight as adults, at puberty and as infants will be taken into
consideration.
The doctor will ask questions about the child's diet, appetite, exercise habits,
pattern of defecation and any social problems.
The patient is then examined for signs of disease and, possibly, puberty and/or
tooth development. In addition, an X-ray of the left hand and wrist is sometimes taken
so that the development of the bones may be examined. The so-called 'bone age' may be
ahead or behind in relation to the child's age.
159
If there seems to be a problem, the doctor will probably recommend a
consultation at a paediatric unit in order to determine its cause and the best medical
treatment.
What is the probable outcome and how is the growth disturbance treated?
This depends entirely upon the type of growth disturbance and the cause of the
growth abnormality (Based on a text by Dr Henrik Thybo Christesen, Paediatrician).
5.10. CANCER What is Cancer? What Causes Cancer?
Cancer is a class of diseases characterized by out-of-control cell growth. There are over
100 different types of cancer, and each is classified by the type of cell that is initially
affected. Cancer harms the body when damaged cells divide uncontrollably to form
lumps or masses of tissue called tumors (except in the case of leukemia where cancer
prohibits normal blood function by abnormal cell division in the blood stream). Tumors
can grow and interfere with the digestive, nervous, and circulatory systems and they
can release hormones that alter body function. Tumors that stay in one spot and
demonstrate limited growth are generally considered to be benign.
Fig. Tumor
More dangerous, or malignant, tumors form when two things occur:
1. A cancerous cell manages to move throughout the body using the blood or
lymph systems, destroying healthy tissue in a process called invasion
160
2. that cell manages to divide and grow, making new blood vessels to feed itself
in a process called angiogenesis.
When a tumor successfully spreads to other parts of the body and grows,
invading and destroying other healthy tissues, it is said to have metastasized. This
process itself is called metastasis, and the result is a serious condition that is very
difficult to treat. In 2007, cancer claimed the lives of about 7.6 million people in the
world. Physicians and researchers who specialize in the study, diagnosis, treatment,
and prevention of cancer are called oncologists.
What causes cancer?
Cancer is ultimately the result of cells that uncontrollably grow and do not die.
Normal cells in the body follow an orderly path of growth, division, and death.
Programmed cell death is called apoptosis, and when this process breaks down, cancer
begins to form. Unlike regular cells, cancer cells do not experience programmatic death
and instead continue to grow and divide. This leads to a mass of abnormal cells that
grows out of control.
Genes - the DNA type
Cells can experience uncontrolled growth if there are damages or mutations to
DNA, and therefore, damage to the genes involved in cell division. Four key types of
gene are responsible for the cell division process: oncogenes tell cells when to divide,
tumor suppressor genes tell cells when not to divide, suicide genes control apoptosis
and tell the cell to kill itself if something goes wrong, and DNA-repair genes instruct a
cell to repair damaged
DNA. Cancer occurs when a cell's gene mutations make the cell unable to correct
DNA damage and unable to commit suicide. Similarly, cancer is a result of mutations
that inhibit oncogene and tumor suppressor gene function, leading to uncontrollable
cell growth.

161
Carcinogens
Carcinogens are a class of substances that are directly responsible for damaging
DNA, promoting or aiding cancer. Tobacco, asbestos, arsenic, radiation such as gamma
and x-rays, the sun, and compounds in car exhaust fumes are all examples of
carcinogens. When our bodies are exposed to carcinogens, free radicals are formed that
try to steal electrons from other molecules in the body. Theses free radicals damage cells
and affect their ability to function normally.
Genes - the family type
Cancer can be the result of a genetic predisposition that is inherited from family
members. It is possible to be born with certain genetic mutations or a fault in a gene that
makes one statistically more likely to develop cancer later in life.
Other medical factors
As we age, there is an increase in the number of possible cancer-causing mutations in
our DNA. This makes age an important risk factor for cancer. Several viruses have also
been linked to cancer such as: human papillomavirus (a cause of cervical cancer),
hepatitis B and C (causes of liver cancer), and Epstein-Barr virus (a cause of some
childhood cancers).
Human immunodeficiency virus (HIV) - and anything else that suppresses or weakens
the immune system - inhibits the body's ability to fight infections and increases the
chance of developing cancer.
What are the symptoms of cancer?
Cancer symptoms are quite varied and depend on where the cancer is located, where it
has spread, and how big the tumor is. Some cancers can be felt or seen through the skin
a lump on the breast or testicle can be an indicator of cancer in those locations. Skin
cancer (melanoma) is often noted by a change in a wart or mole on the skin. Some oral
cancers present white patches inside the mouth or white spots on the tongue. Other

162
cancers have symptoms that are less physically apparent. Some brain tumors tend to
present symptoms early in the disease as they affect important cognitive functions.
Pancreas cancers are usually too small to cause symptoms until they cause pain
by pushing against nearby nerves or interfere with liver function to cause a yellowing
of the skin and eyes called jaundice. Symptoms also can be created as a tumor grows
and pushes against organs and blood vessels. For example, colon cancers lead to
symptoms such as constipation, diarrhea, and changes in stool size. Bladder or prostate
cancers cause changes in bladder function such as more frequent or infrequent
urination.
As cancer cells use the body's energy and interfere with normal hormone
function, it is possible to present symptoms such as fever, fatigue, excessive sweating,
anemia, and unexplained weight loss. However, these symptoms are common in
several other maladies as well. For example, coughing and hoarseness can point to lung
or throat cancer as well as several other conditions.
When cancer spreads, or metastasizes, additional symptoms can present
themselves in the newly affected area. Swollen or enlarged lymph nodes are common
and likely to be present early. If cancer spreads to the brain, patients may experience
vertigo, headaches, or seizures. Spreading to the lungs may cause coughing and
shortness of breath. In addition, the liver may become enlarged and cause jaundice and
bones can become painful, brittle, and break easily. Symptoms of metastasis ultimately
depend on the location to which the cancer has spread.
How is cancer classified?
There are five broad groups that are used to classify cancer.
1. Carcinomas are characterized by cells that cover internal and external parts of
the body such as lung, breast, and colon cancer.
2. Sarcomas are characterized by cells that are located in bone, cartilage, fat,
connective tissue, muscle, and other supportive tissues.

163
3. Lymphomas are cancers that begin in the lymph nodes and immune system
tissues.
4.Leukemias are cancers that begin in the bone marrow and often accumulate in
the bloodstream.
5.Adenomas are cancers that arise in the thyroid, the pituitary gland, the adrenal
gland, and other glandular tissues.
Cancers are often referred to by terms that contain a prefix related to the cell type in
which the cancer originated and a suffix such as -sarcoma, -carcinoma, or just -oma.
Common prefixes include:
Adeno- = gland
Chondro- = cartilage
Erythro- = red blood cell
Hemangio- = blood vessels
Hepato- = liver
Lipo- = fat
Lympho- = white blood cell
Melano- = pigment cell
Myelo- = bone marrow
Myo- = muscle
Osteo- = bone
Uro- = bladder
Retino- = eye
Neuro- = brain

164
How is cancer diagnosed and staged?
Early detection of cancer can greatly improve the odds of successful treatment and
survival. Physicians use information from symptoms and several other procedures to
diagnose cancer. Imaging techniques such as X-rays, CT scans, MRI scans, PET scans,
and ultrasound scans are used regularly in order to detect where a tumor is located and
what organs may be affected by it. Doctors may also conduct an endoscopy, which is a
procedure that uses a thin tube with a camera and light at one end, to look for
abnormalities inside the body.
Extracting cancer cells and looking at them under a microscope is the only
absolute way to diagnose cancer. This procedure is called a biopsy. Other types of
molecular diagnostic tests are frequently employed as well. Physicians will analyze
your body's sugars, fats, proteins, and DNA at the molecular level. For example,
cancerous prostate cells release a higher level of a chemical called PSA (prostate-specific
antigen) into the bloodstream that can be detected by a blood test. Molecular
diagnostics, biopsies, and imaging techniques are all used together to diagnose cancer.
After a diagnosis is made, doctors find out how far the cancer has spread and
determine the stage of the cancer. The stage determines which choices will be available
for treatment and informs prognoses. The most common cancer staging method is
called the TNM system. T (1-4) indicates the size and direct extent of the primary tumor,
N (0- 3) indicates the degree to which the cancer has spread to nearby lymph nodes, and
M (0-1) indicates whether the cancer has metastasized to other organs in the body. A
small tumor that has not spread to lymph nodes or distant organs may be staged as (T1,
N0, M0), for example.
TNM descriptions then lead to a simpler categorization of stages, from 0 to 4,
where lower numbers indicate that the cancer has spread less. While most Stage 1
tumors are curable, most Stage 4 tumors are inoperable or untreatable.

165
How is cancer treated?
Cancer treatment depends on the type of cancer, the stage of the cancer (how
much it has spread), age, health status, and additional personal characteristics. There is
no single treatment for cancer, and patients often receive a combination of therapies and
palliative care. Treatments usually fall into one of the following categories: surgery,
radiation, chemotherapy, immunotherapy, hormone therapy, or gene therapy.
Surgery
Surgery is the oldest known treatment for cancer. If a cancer has not
metastasized, it is possible to completely cure a patient by surgically removing the
cancer from the body. This is often seen in the removal of the prostate or a breast or
testicle. After the disease has spread, however, it is nearly impossible to remove all of
the cancer cells. Surgery may also be instrumental in helping to control symptoms such
as bowel obstruction or spinal cord compression.
Radiation
Radiation treatment, also known as radiotherapy, destroys cancer by focusing
high- energy rays on the cancer cells. This causes damage to the molecules that make up
the cancer cells and leads them to commit suicide. Radiotherapy utilizes high-energy
gamma-rays that are emitted from metals such as radium or high-energy x-rays that are
created in a special machine. Early radiation treatments caused severe side-effects
because the energy beams would damage normal, healthy tissue, but technologies have
improved so that beams can be more accurately targeted. Radiotherapy is used as a
standalone treatment to shrink a tumor or destroy cancer cells (including those
associated with leukemia and lymphoma), and it is also used in combination with other
cancer treatments.
Chemotherapy
Chemotherapy utilizes chemicals that interfere with the cell division process -
damaging proteins or DNA - so that cancer cells will commit suicide. These treatments

166
target any rapidly dividing cells (not necessarily just cancer cells), but normal cells
usually can recover from any chemical-induced damage while cancer cells cannot.
Chemotherapy is generally used to treat cancer that has spread or metastasized because
the medicines travel throughout the entire body. It is a necessary treatment for some
forms of leukemia and lymphoma. Chemotherapy treatment occurs in cycles so the
body has time to heal between doses. However, there are still common side effects such
as hair loss, nausea, fatigue, and vomiting. Combination therapies often include
multiple types of chemotherapy or chemotherapy combined with other treatment
options.
Immunotherapy
Immunotherapy aims to get the body's immune system to fight the tumor. Local
immunotherapy injects a treatment into an affected area, for example, to cause
inflammation that causes a tumor to shrink. Systemic immunotherapy treats the whole
body by administering an agent such as the protein interferon alpha that can shrink
tumors. Immunotherapy can also be considered non-specific if it improves cancer-
fighting abilities by stimulating the entire immune system, and it can be considered
targeted if the treatment specifically tells the immune system to destroy cancer cells.
These therapies are relatively young, but researchers have had success with treatments
that introduce antibodies to the body that inhibit the growth of breast cancer cells. Bone
marrow transplantation (hematopoetic stem cell transplantation) can also be considered
immunotherapy because the donor's immune cells will often attack the tumor or cancer
cells that are present in the host.
Hormone therapy
Several cancers have been linked to some types of hormones, most notably breast and
prostate cancer. Hormone therapy is designed to alter hormone production in the body
so that cancer cells stop growing or are killed completely. Breast cancer hormone
therapies often focus on reducing estrogen levels (a common drug for this is tamoxifen)

167
and prostate cancer hormone therapies often focus on reducing testosterone levels. In
addition, some leukemia and lymphoma cases can be treated with the hormone
cortisone.
Gene therapy
The goal of gene therapy is to replace damaged genes with ones that work to addressa
root cause of cancer: damage to DNA. For example, researchers are trying to replace the
damaged gene that signals cells to stop dividing (the p53 gene) with a copy of a
working gene. Other gene-based therapies focus on further damaging cancer cell DNA
to the point where the cell commits suicide. Gene therapy is a very young field and has
not yet resulted in any successful treatments.
How can cancer be prevented?
Cancers that are closely linked to certain behaviors are the easiest to prevent. For
example, choosing not to smoke tobacco or drink alcohol significantly lower the risk of
several types of cancer - most notably lung, throat, mouth, and liver cancer. Even if you
are a current tobacco user, quitting can still greatly reduce your chances of getting
cancer. Skin cancer can be prevented by staying in the shade, protecting yourself with a
hat and shirt when in the sun, and using sunscreen. Diet is also an important part of
cancer prevention since what we eat has been linked to the disease. Physicians
recommend diets that are low in fat and rich in fresh fruits and vegetables and whole
grains. Certain vaccinations have been associated with the prevention of some cancers.
For example, many women receive a vaccination for the human papillomavirus because
of the virus's relationship with cervical cancer. Hepatitis B vaccines prevent the
hepatitis B virus, which can cause liver cancer. Some cancer prevention is based on
systematic screening in order to detect small irregularities or tumors as early as possible
even if there are no clear symptoms present. Breast self-examination, mammograms,
testicular self-examination, and Pap smears are common screening methods for various
cancers.

168
Reference books:
1. Dunbar, B.S., and O’Rand, M.G. (1991): A Comparative Overview of Mammalian
Fertilization. Plenum Press, New York.
2. Metz, C.B., and Monroy, A., editors (1985): Biology of Fertilization, Vol. 1: Model
Systems and Oogenesis. Academic Press, Orlando Florida.
3. Metz, C.B., and Monroy, A., editors (1985): Biology of Fertilization, Vol. 2:
Biology of the Sperm. Academic Press, Orlando Florida.
4. Metz, C.B., and Monroy, A., editors (1985): Biology of Fertilization, Vol. 3: The
Fertilization Response of the Egg. Academic Press, Orlando Florida.
5. Wassarman, P.M. (1987): Science, 235:553-560.
6. Wilt, F. & Hake, S. (2004). Principles of Developmental Biology.
7. Scott F. Gilbert (2003). Developmental Biology.
8. Lombardi, Julian (1998). "Embryogenesis". Springer.
9. Hall, Brian Keith (1998). Evolutionary developmental biology. Birkhäuser.
10. McGeady, Thomas A., ed (2006). "Gastrulation". Veterinary embryology. Wiley-
Blackwell.
11. Scott Gilberet: Developmental Biology.
12. Evers, Christine A., Lisa Starr. Biology:Concepts and Applications. 6th ed. United
States: Thomson, 2006.
13. Balinsky, B.I. An Introduction to Embryology. Holt-Saunders Intl. Edn.