Bagali C S.pdf
123
“ CLINICAL STUDY ON APRAJA VANDHYA (PRIMARY INFERTILITY) BY AN INDIGENOUS COMPOUND W.S.R TO OVULATORY DYSFUNCTION” By Dr.Smt.BAGALI.C.S A dissertation submitted to the R R R a a a j j j i i i v v v G G G a a a n n n d d d h h h i i i U U U n n n i i i v v v e e e r r r s s s i i i t t t y y y o o o f f f H H H e e e a a a l l l t t t h h h S S S c c c i i i e e e n n n c c c e e e s s s , , , K K K a a a r r r n n n a a a t t t a a a k k k a a a , , , B B B a a a n n n g g g a a a l l l o o o r r r e e e . In partial fulfillment of the requirements for the degree of AYURVEDA DHANVANTARI- M.S. (AYURVEDA) In PRASUTI TANTRA & STREE ROGA Under the guidance of Dr. Susmita Priyadarshinee Otta M.S (P.T.S.R) POST GRADUATE DEPARTMENT OF PRASUTI TANTRA & STREE ROGA N.K.J. AYURVEDIC MEDICAL COLLEGE & PG CENTRE, BIDAR. 2009
-
Upload
khangminh22 -
Category
Documents
-
view
6 -
download
0
Transcript of Bagali C S.pdf
“ CLINICAL STUDY ON APRAJA VANDHYA (PRIMARY
INFERTILITY) BY AN INDIGENOUS COMPOUND W.S.R TO
OVULATORY DYSFUNCTION”
By Dr.Smt.BAGALI.C.S
A dissertation submitted to the
RRRaaajjjiiivvv GGGaaannndddhhhiii UUUnnniiivvveeerrrsssiiitttyyy ooofff HHHeeeaaalllttthhh SSSccciiieeennnccceeesss,,, KKKaaarrrnnnaaatttaaakkkaaa,,, BBBaaannngggaaalllooorrreee.
In partial fulfillment
of the requirements for the degree of
AYURVEDA DHANVANTARI- M.S.
(AYURVEDA)
In
PRASUTI TANTRA & STREE ROGA
Under the guidance of Dr. Susmita Priyadarshinee Otta
M.S (P.T.S.R)
POST GRADUATE DEPARTMENT OF PRASUTI TANTRA
& STREE ROGA
N.K.J. AYURVEDIC MEDICAL COLLEGE & PG CENTRE, BIDAR. 2009

RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES, KARNATAKA,
BANGALORE
NKJ AYURVEDIC MEDICAL COLLEGE AND PG CENTRE, BIDAR
POST GRADUATE DEPARTMENT
OF PRASUTI TANTRA & STREE ROGA
Certificate by the guide
This is to certify that the dissertation entitled “ Clinical Study on Apraja
Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory
dysfunction” is a bonafide clinical research work done by Dr. Smt Bagali C.S.
in partial fulfillment of the requirement for the degree of M.S. (Ayurveda) in
Prasuti Tantra & Stree Roga.
Signature of the Guide Dr. Susmita Priyadarshinee Otta
MS(P.T.S.R.) Asst.Prof. Dept.of Prasuti Tantra & Stree Roga
NKJ Ayurvedic Medical College & PG Centre Bidar – 585403
Karnataka.
Date : ________ Place : BIDAR
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES, KARNATAKA, BANGALORE.
NKJ AYURVEDIC MEDICAL COLLEGE AND PG CENTRE, BIDAR.
POST GRADUATE DEPARTMENT
OF PRASUTI TANTRA & STREE ROGA
Endorsement by the HOD, Principal/Head of the institution
This is to certify that the dissertation entitled “Clinical Study on Apraja
Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory
dysfunction”” is a bonafide clinical research work done by Dr. Smt Bagali C.S.
under the guidance of Dr. Susmita Priyadrashinee Otta, Asst. Professor, Post
Graduate Department of Prasuti Tantra & Stree Roga, N.K.J Ayurvedic
Medical College & P.G. Centre, Bidar.
Seal and signature of the HOD Prof.Dr.L.V.RATHNAKAR.A
M.D,(K.B)(B.H.U) NKJ Ayurvedic Medical College & PG Centre
Bidar – 585403 Karnataka
Date : _________ Place : BIDAR .
Seal and signature of the Principal/Dean Prof. Dr.K.V.L.N. ACHARYULU M.D (SIDDNTA) NKJ Ayurvedic Medical College & PG Centre
Bidar – 585403 Karnataka Date : _________ Place :BIDAR .

RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES, KARNATAKA,
BANGALORE
NKJ AYURVEDIC MEDICAL COLLEGE AND PG CENTRE, BIDAR
POST GRADUATE DEPARTMENT
OF PRASUTI TANTRA & STREE ROGA
Declaration by the candidate
I here by declare that this dissertation/ thesis entitled “Clinical Study on
Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to
Ovulatory dysfunction”is a bonafide and genuine research work carried out by me
under the guidance of Dr.Susmita Priyadarshinee Otta, M.S. (P.T.S.R) Asst. Prof.
PG Department of Prasuti Tantra & Stree Roga.
Date : _________ Signature of the candidate
Dr. Smt.Bagali C.S. Place : BIDAR

RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES, KARNATAKA, BANGALORE
N.K.J. AYURVEDIC MEDICAL COLLEGE AND PG CENTRE, BIDAR
POST GRADUATE DEPARTMENT
OF PRASUTI TANTRA & STREE ROGA
Copyright
Declaration by the candidate
I here by declare that the Rajiv Gandhi University of Health Sciences,
Karnataka shall declare the rights to preserve, use and disseminate this dissertation/
thesis in print or electronic format for academic/ research purpose.
Date : __________ Signature of the candidate Dr. Smt. Bagali C.S.
Place : BIDAR
DEDICATED TO
My Father and Mother
Late Shri. Siddappa.B.Bagali
and
Smt. Gurubai.S.Bagali
ACKNOWLEDGEMENT
With The blessing of Shri Siddharoodha Mahaswamiji. I wish to record my
gratitude towards the revered President. His Holiness Sri Shivakumar Swamiji for
his mangnanimous support.
I owe a special debt of gratitude to my guide Dr.Susmita Priyadarshinee
Otta M.S (PTSR) Assistant Professor, Post Graduate studies in Prasooti Tantra for
her scientific advice, constructive suggestions, constant encouragement & kind
cooperation throughout my period of research work.
“A good suggestion says the first word of everything.”
I will feel short of my duties if I fail to acknowledge Prof. Dr Prabha
Sharma,M.D,PhD( B.H.U)former H.O.D Dept of Prasooti Tantra ,who helped me in
selecting the topic guided me in clinical work .
I am extremely grateful to my teacher Dr. L.V Rathnakara Professor & Head
of Department of P.G studies in Prasooti & Streerooga & Koumara Bhritya N.K.J
A.M.C. P.G Center Bidar for his timely help.
I wish to external my heartiest thanks to the Principal Prof Dr.
K.V.L.N.Acharyulu & vice Principal Dr. P.V.Savanur N.K.J.Ayurvedic medical
College & P.G Center for providing the necessary facilities in the college for
conducting research work.
I express my thank to Dr. V.S Patil Medical Director of N.K.J.Ayurvedic
medical College & P.G Center for his advise and momentary support.
I humbly express my indebtedness to Dr. Shankar Deputy Medical
Superintendent & staff of Shri Siddharoodha Charitable Hospital for their help.

I am thankful to Dr. Bandeppa.S Head of the Department, Dr. Praveen
Simpi & Asst Mohan Reddy, Channappa of Rasa shastra & Bhaisajya kalpana Dept
N.K.J A.M.C Bidar for their constant guidance in the preparation of medicine for the
clinical study.
Any amount of thankfulness will be in adequate for all the faculty members &
of my Department namely Dr.Sridevi Swamy, Dr.Sheela Halli, & Dr.Manisha
Bhandari for providing all possible guidance & support.
I am very thankful to Dr. T.P.Sahu M.D (Dravya Guna) for his expert
guidance in identifying the plant Shivalingi.
I express my gratitude & regards to Dr. Y.P.Shamarao, Dr.Murthy,
Dr.Kotur, Dr.Mulimani, Dr.Tripathy, Parmeshwar Bhat & Dr.Halli. For their
timely advice.
I am deeply indebted to Sri M.Suranagi Ph.D(Statistics) Asst Prof
Veterinary College Bidar for his valuable help, co-operation & guidance in data
processing.
In addition to this I am also very grateful to my batch mates or Dr.Vivek,
Dr.Pradeep, Dr.Mahesh, Dr.Gourish & Junior Dr.Joyti. H& Departmental Seniors
& Juniors for their mental support which enabled me to complete the dissertation.
My special thanks to my friends Dr.Jayasheela Goni, Dr.Vandana
Galiyawar & Dr.Anita Murki for their support.
I extend my gratefulness to library staff of N.K.J AMC Mr. Kadam,
Mr. Rajkumar &Smt. Saku Bai for their help & co-opration during my research
work.

I offer my sincere thanks to all the staff member of N.K.J AMC College Sri
Bagali, Sri Ramesh, Sri Kaddi, Sri Chandrakant, Sri Reddy, and Sri Gururaj.
For their help & co-operation on during my study.
I cannot forget my brother Sri Bhimashankar Bagali & Nephew Kr.Sagar
& Sri Ravikant Bagali and sisters Smt. Sharada, Smt Shobha, Smt Manjula for
their incessant love and who always act & a source of energy to me in this world of
uncertainty.
I express my deep sense of love & gratitude to my husband Dr. Anil. K
Bagalkoti & my beloved son Chi. Prateek & others family members who efficiently
shouldered my responsibilities for fulfilling the dissertation work.
Last but not least. I express all sense of gratitude to my well wishers and
patients who helped me directly or indirectly throughout the study.
Place :- BIDAR.
Date: - Dr.Smt. Bagali.C.S

LIST OF ABBREVIATIONS
RV - Rigveda
AV - Atharvaveda
AH - Ashtang Hrudaya
AS - Ashtang Sangraha
BP - Bhava Prakash
B.R - Bhaishajya Ratnavali
BRN - Bhava Prakash Nighantu
Cha. S. - Charaka Shareer sthana
Cha.Chi - Charaka Chikitsa sthana
D.N. - Dhanvantri Nighantu
Ha.S - Harita Samhita
Kas.S - Kashyapa Samhita
kalp kalpasthan
Kas.S - Kashyapa Samhita
Siddhi Siddhisthana
M.N. - Madhava Nidhana
N.A - Nighantu Adarsha
RN - Raja Nighantu
Sha. S. - Sharangdhar Samhita
Su. S . - Sushruta Samhita
Su.Sha - Sushruta Sharisrsthana
Su.Su - Sushruta Sutrasthana
Su.Utt - Sushruta Uttarsthana
YR. - Yoga Ratnakara
LIST OF ABBREVIATIONS
FSH = Follicular Stimulating Hormone
LH = Luteinizing Hormone
GnRH = Gonadotropin Releasing Hormone
CRH = Corticotrophin Releasing Hormone
TSH = Thyroid Stimulating Hormone
IGF-II = Insulin like Growth Factor-II
IUCD = Intra Uterine Contraceptive Devices
PID = Pelvic Inflammatory Disease
SCMCT = Sperm Cervical Mucus Contact Test
hMG = Human Menopausal Gonadotrophin
PCR = Polymerase Chain Reaction
USG = Ultra Sonography
HSG = Hystero Salpingo Graphy
HCG = Human Chorionic Gonadotrophin
LUF = Luteal Unrupturad Follicle
Mg = Milligram
Mm = Millimeter
Ng = Nanogram
ABSTRACT
Primary Infertility with a correlation to Apraja vandhya is one of the common
gynecological problem faced in daily practice.
The most common cause of infertility is ovulatory disorder characterized by
anovulation or by infrequent & / or irregular ovulation. Menstrual disorder like
oligomenorrhoea or complete amenorrhoea usually indicates ovulatory disorders.
30 patients being diagnosed as primary Infertility according to inclusion &
exclusion criteria where divided in to two groups of 15 each.
Group A where treated with Indigenous Compound Ghanasatwa.
Group B where treated with placebo drug.
The entire patients were assessed clinically, pathologically & sonographically
at the end of each cycle & finally the results were analyzed statistically before
treatment & after each cycle & at the end of three cycles.
Finally the effectiveness of the trial drug was assessed 84.85% in the
Infertility. During the treatment no side effect was observed.
KEY WORDS
Infertility, anovulation, apraja vandhya, shivalingi, putramjivaka.

TABLE OF CONTENTS
PAGE No.
1) INTRODUCTION 1-3
2) OBJECTIVES 3
3) REVIEW OF LITERATURE
a. Historical Review 4-6
b. Ayurvedic Review 7-23
c. Modern Review 24-
56
d. Drug Review 57-76
4) CLINICAL STUDY
a. Material & Method 77-81
b. Observation 82-110
5) DISCUSSION 111-117
6) CONCLUSION 118
7) SUMMARY 119-120
8) BIBLIOGRAPHY 121-123
9) REFERENCES 124-128
10) ANNEXURE
a. Research Case Performa


LIST OF TABELS
Table No. Name of the Table Page
No.
Table No. 1 Showing method day of cycle observation 35
Table No. 2 Showing 30 Patients According to Age. 83
Table No. 3 Showing 30 Patients According to Marital Status. 84
Table No. 4 Showing 30 Patients According to Occupation. 85
Table No. 5 Showing 30 Patients According to Socio Economic Status. 86
Table No. 6 Showing 30 Patients According to Educational Status. 87
Table No. 7 Showing 30 Patients According to Infertility Duration. 88
Table No. 8 Showing 30 Patients According to Menstrual History. 89
Table No. 9 Showing 30 Patients According to Bleeding Duration 90
Table No.10 Showing 30 Patients According to Interval Period. 91
Table No.11 Showing 30 Patients According to Character of Bleeding. 92
Table No.12 Showing 30 Patients According to Dysmenorrhoea. 93
Table No.13 Showing 30 Patients According to Oligomenorrhoea. 94
Table No.14 Showing 30 Patients According to Uterurine Position 95
Table No.15 Showing 30 Patients According to Fornix 96

Table No. Name of the Table Page
No.
Table No.16 Showing 30 Patients According to Vaginal Discharge 97
Table No.17 Statistical Analysis of Dysmenorrhoea in Group-A 98
Table No.18 Statistical Analysis of Dysmenorrhoea in Group-B 98
Table No.19 Comparison between Dysmenorrhoea of two groups. 99
Table No.20 Statistical Analysis of Oligomenorrhoea in Group-A 99
Table No.21 Statistical Analysis of Oligomenorrhoea in Group-B 100
Table No.22 Comparison between Oligomenorrhoea of two groups 100
Table No.23 Statistical Analysis of Bleeding Duration in Group-A 101
Table No.24 Statistical Analysis of Bleeding Duration in Group-B 101
Table No.25 Comparison between Bleeding Duration of two groups 102
Table No.26 Statistical Analysis of Interval duration in Group-A 102
Table No.27 Statistical Analysis of Interval duration in Group-B 103
Table No.28 Comparison between Interval Duration of two groups. 103
Table No.29 Statistical Analysis of Cervical mucus Viscosity in Group-A 104
Table No.30 Statistical Analysis of Cervical mucus Viscosity in Group B 104
Table No. Name of the Table Page
No.
Table No.31 Comparisons between Cervical mucus viscosity Duration of
two groups
105
Table No.32 Statistical Analysis of Cervical mucus Ferning in Group-A 105
Table No.33 Statistical Analysis of Cervical mucus Ferning in Group-B 106
Table No.34 Comparisons between Cervical mucus Ferning of two
groups.
106
Table No.35 Statistical Analysis of Cervical mucus Spin Barkeit in
Group-A
107
Table No.36 Statistical Analysis of Cervical mucus Spin Barkeit in
Group-B
107
Table No.37 Comparisons between Cervical mucus Spin Barkeit of two
groups
108
Table No.38 Statistical Analysis of Follicular study in Group-A 108
Table No.39 Statistical Analysis of Follicular study in Group-B 109
Table No.40 Comparisons between Follicular study of two groups. 109
Table No 41 Overall Effect of Result 110

LIST OF FIGURES
Figure No. Name of the Figures Page No.
Figure No. 1 Internal Structure of ovary 24
Figure No. 2 Musali 74
Figure No. 3 Daruharidra 74
Figure No. 4 Bala 74
Figure No. 5 Palasha 74
Figure No. 6 Dhataki 75
Figure No. 7 Shivalingi 75
Figure No. 8 Misreya 75
Figure No. 9 Putranjeevaka 75
Figure No.10 Prepared trial drug powder 76
Figure No.11 Capsules of Ghansatwa 76

LIST OF GRAPHS
Graph No. Name of the Graphs Page No.
Graph No. 1 Distribution of patients according to Age 83
Graph No. 2 Distribution of patients according to Marital Status 84
Graph No. 3 Distribution of patients according to Socio-economic status 85
Graph No. 4 Distribution of patients according to Education 86
Graph No. 5 Distribution of patients according to Infertility duration 87
Graph No. 6 Distribution of patients according to Menstrual history 88
Graph No. 7 Distribution of patients according to Occupation 89
Graph No. 8 Distribution of patients according to Bleeding duration 90
Graph No. 9 Distribution of patients according to Interval period 91
Graph No.10 Distribution of patients according to Character of bleeding 92
Graph No.11 Distribution of patients according to Dysmenorrhoea 93
Graph No.12 Distribution of patients according to Uterus position 94
Graph No13 Distribution of patients according to Fornix 95
Graph No14 Distribution of patients according to Oligomenorrhoea 96
Graph No 15 Distribution of patients according to Vaginal discharge 97
Graph No 16 Over all Result of Group A 110
Graph No. Name of the Graphs Page No.
Graph No 17 Over all Result of Group B 110

Introduction
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 1
INTRODUCTION
Existence of the human race revolves around the women to whom is also
assigned the name “Janani” because of her power to bring a new life in the universe.
Women are the makers of the home, the nation and world. It is indeed the woman who
shapes the generation.
Women is placed in a high position in society since the time immortal , but
when a lady never conceives for some period it is a curse for her. She looses all her
name, fame, faith & belief from family for being barren. This makes a gap in the
relation.
Motherhood is a great dream for a woman in her life, but when a couple is
unable to initiate the reproduction after one year marital relations, they are said to be
Infertile.
Infertility is a major problem in our society. Now a days the rate of infertility
is steadily increasing, because of change of life style of human begins.
People wants to lead luxurious life for that they are running behind the money
& thus people get more stressed & tensed out at work.
Delayed marriage, higher education & high ambitions are the cause for
infertility.
Today’s life is very fast, the food habits are also changed, the intake of fast
food, junk food & adulterated food also impacts fertility.
Infertility does not cause any serious effect on the body; the psychoneurotic
upset resulting from infertility affects her physical as well as mental health. The
Introduction
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 2
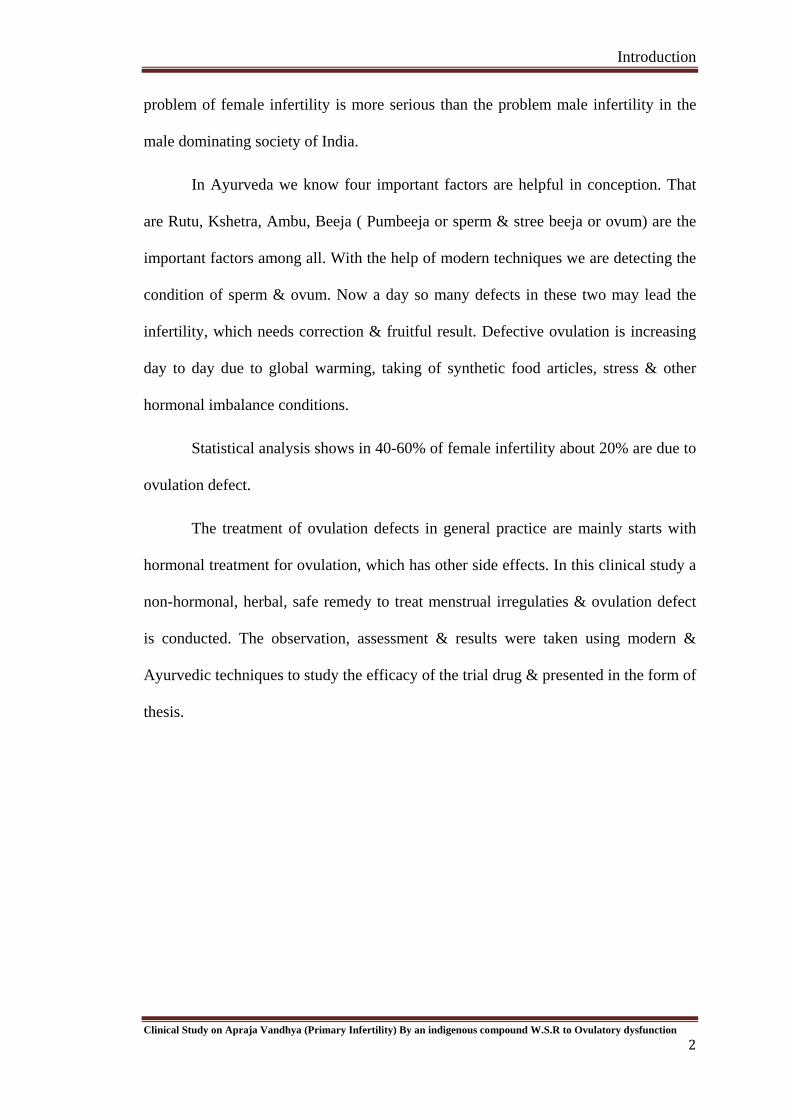
problem of female infertility is more serious than the problem male infertility in the
male dominating society of India.
In Ayurveda we know four important factors are helpful in conception. That
are Rutu, Kshetra, Ambu, Beeja ( Pumbeeja or sperm & stree beeja or ovum) are the
important factors among all. With the help of modern techniques we are detecting the
condition of sperm & ovum. Now a day so many defects in these two may lead the
infertility, which needs correction & fruitful result. Defective ovulation is increasing
day to day due to global warming, taking of synthetic food articles, stress & other
hormonal imbalance conditions.
Statistical analysis shows in 40-60% of female infertility about 20% are due to
ovulation defect.
The treatment of ovulation defects in general practice are mainly starts with
hormonal treatment for ovulation, which has other side effects. In this clinical study a
non-hormonal, herbal, safe remedy to treat menstrual irregulaties & ovulation defect
is conducted. The observation, assessment & results were taken using modern &
Ayurvedic techniques to study the efficacy of the trial drug & presented in the form of
thesis.

Objective of the study
OBJECTIVE OF THE STUDY
1. To assess the efficacy of Ayurvedic remedy in the management of infertility
2. To conduct conceptual study of female infertility and to establish the
correlation with Apraja vandhya (Primary infertility)
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
3

Review of Literature
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 4
AAYYUURRVVEEDDIICC RREEVVIIEEWW
HISTORICAL REVIEW :
History of any particular subject enables us to understand the origin, progress
and other aspects of that subject. Vandhyatva has been a long standing problem of
human community right from ancient period up to this modern era.
If we think the antiquity of the Vandhyatva, we can see the praise of the
women having children and slander of the barren women and the solutions to her
barrenness are also mentioned in the Vedas, Upanishadas and Puranas.
VEDA KALA
The Vedas are considered as most ancient literature available in the world.
There are four vedas Rig-veda, Yajur-veda, Sama-veda, and Atharva-veda. Ayurveda
is considered as the Upaveda of Atharva-veda.
We find the references of Vandhyatva & its treatment even in Vedas, Puranas
& Upanishadas. The oldest epic Rig-veda describes about the miraculous work of
Ashwinee kumars, the divinely physicians, as it is written that Ashwinee kumar's
treated infertile Badh-rimatee & she was blessed with a son named Hiranya Hasta1.
In Atharva-veda 'Purandhriyosha' is mentioned which means that when a man
enters into Grihasthashrama he prays to God, & he wishes that his wife should be
"Purandhriyosha"( pregnant). In this we find descriptions regarding conception by
enchanting mantra.2&3. Mantras are also advocated to cure the Garbha dosha 4.
Emphasis has been put on the herb Apamarga to procedure a male child 5

Review of Literature
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 5
PURANA KALA.
In Padma Purana it is mentioned that a woman having one child is called as
"Kaka Vandhya"6.
In Brahma Purana, while explaining the importance of "Sri Krishna Durga
Strotra", it is said that a woman who as a Vandhya, Kakavandhya, Mrtavatsa or
Durbhaga can conceive by reciting this strotra, within one year6.
SAMHITA KALA
Caraka and Vagbhata, have referred Vandhya due to abnormality of Bijamsa
and mentioned as the Upadrava of Yoni Vyapada.7&8
In Sushruta Samhita, Vandhyatva has been described under the title of
Vandhya Yonivyapada, which is included amongst twenty gynaecological disorders
(Yoni vyapada) 9
In Kasyapa Samhita under the description of Jataharinis, he has mentioned
one Puspaghni having useless Puspa and certain others characterised with repeated
expulsion of foetus of different gestational periods 10
In Harita Samhita, Harita has described Vandhyatva as a disease, in eighty
VatajaVyadhi. He has defined Vandhyatva as a failure to achieve a child rather than
pregnancy, because he has included Garbhasravi, Mritavatsa also under the
classification11
In Madhava Nidana, the types of Vandhyatva have been described12 In
Sarangadhara Samhita, Rasaratna Saumuccaya, Yoga Ratnakara and Bhaisajya
Ratnavali etc. have described some therapeutics of Vandhyatva.
Review of Literature
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 6
VANDHYATVA AS A DISEASE :
We does not find unequivocal description of Vandhyatva in any of the
Ayurvedic classics except Harita Samhita. But in Harita Samhita also, he has given
classification only, no specific etiology or pathogenesis was explained. Vandhyatva
as a disease is only given by Harita while describing eighty Vataja Vyadhi. While
other Acharyas has not considered it as a independent disease, rather a cardinal
feature of so many diseases.
Apart from this they have not used word Vandhyatva, but it is the only
symptom i.e.failure to achieve pregnancy, has been referred under various conditions
like coitus with old, young or diseased woman; coitus in abnormal posture, woman
having diseased yoni or abnormality of Artava etc.
In Kasyapa Samhita he mentioned that, the couple having number of children
with proper growth and development due to effect of nature (Savbhavat) or their own
deads (Svakarmaparinamat) are fortunate, otherwise should be treated, i.e. it will be a
disease condition which needs Chikista.
Acarya Harita in classification of Vandhyatva includes Garbhasravi, Mrtavatsa
etc. From above references we can consider Vandhyatva as a disease. Vandhyatva
may be defined as the inability of a couple to achieve child rather than pregnancy by
their Svabhava and Svakarma.
Review of Literature
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 7
DISEASE REVIEW(AYURVEDIC)
VYUTPATTI:
Vandhya:
The word "Vandhya" is derived from the root "Vandha" with 'Yak' suffix
which means barren, unproductive, fruitless and useless.
NIRUKTI: rÉxrÉÉ aÉpÉïkÉÉUhÉ qÉÉaÉïÂmÉ oÉlkÉlÉÇ xÉÇmrÉÌiÉ xÉ
uÉlkrÉÉ | ( zÉ.Mü.SìÓqÉ 395)
The woman in whom there is hindrance of any kind to the normal process of
conception is Vandhya
DEFINITION:
A woman whose Artava is perished is called Vandhya9
SYNONYMES:
Vasa VIphala
Nisphala Aprajashv
Aparyasunyago Avatoka
Avakesi Sravatgarbha
Aphala
CLASSIFICATION:
Vandhyatva has been classified in the following ways according to different
Acarayas.
Caraka Samhita: In Caraka Samhita, classification is not given but considering the
references together it can be as follows:

Review of Literature
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 8
(1) Vandhya - Vandhya refers to incurable congenital or acquired abnormalities
resulting into absolute sterlity.
(2) Apraja : Infertility in which woman conceives after treatment13
(3) Sapraja : Sapraja is a condition in which woman in her active reproductive age
does not conceive, after giving birth to one or more children.
Harita : Harita has described six types of Vandhya11
(1) Garbhakosabhanga - During childhood in case there is Garbhakosabhanga
(injury to the uterus) and loss of Dhatus, woman never conceive.
(2) Kakavandhya - one child infertility.
(3) Anapatya - No child
(4) Garbhasravi - Repeated abortion
(5) Mritavatsa - Repeated still births
(6) Balaksaya - Infertility due to loss of Bala.
Rasaratna - Samuchaya : He classified Vandhyatva in nine types14
(1) Adivandhyatva (2) Vataja
(3) Pittaja (4) Kaphaja
(5) Sannipataj (6) Bhutaja
(7) Daivaja (8) Raktaja
(9) Abhicaraja
MADHAVA NIDANA:
Madhavakara has described nine types of vandhya12.
(1) Adivandhya (2) Raktaja

Review of Literature
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 9
(3) Vataja (4) Pitaja
(5) Kaphaja (6) Tridoshaja
(7) Bhutaja (8) Daivaja
(9) Abhicharaja.
Avandhya--The word Avandhya suggest a childless woman, but capacity to
conceive with quite delay ( Chakrapani).
Kasyapa samhita The available portion of kashyapa samhita presents an
unique chapter in its kalpa sthana as “Revati Kalpadhyaya". In this chapter thirty
different types of Revaties inflicting various disorders to females are described.
NIDANA OF VANDHYATA
In classics specific causitive factors of Vandhyatva are not given. To get the
complete picture of Nidana, the subject matter from all related places are recapulated
here. First of all we will see the factors responsible for fertility / conception.
Acarya Susruta15 equating germination of seed with achievement of
conception quoted that if Ritu (period near ovulation i.e. Rtukala), bija (ovum and
sperms), Ksetra (female reproductive system) and Ambu (nourishment) assemble
together the conception will definitely occurs.
While Caraka16 quoted that when both male and female after observing the
advocated dietetic regimen and other mode of life and perform coitus and ejaculated
unvitiated sukra, passing through healthy yoni, reaches healthy garbhasaya and gets
mixed with disease free sonita, then conception is definite.
Vagbhata has given importance to Ksetra and Bija. while Vagbhata II17 has
emphasize that besides healthy Garbhashaya, Marga, Rakta (ovum), Sukra, properly
Review of Literature
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 10
functioning Vayu and normal psychological status (happy mood) are also essential.
Summarizing the above description it can be said that for achievement of
conception,
(1) Healthy and properly functioning female reproductive system (Yoni). i.e
includes ovary, fallopian tubes, uterus, cervix, vagina.
(2) Healthy sperms and ovum
(3) Proper functioning Vayu
(4) Normal psychology
(5) Healthy partners
(6) Proper nursing factor
(7) Proper coitus
(8) Healthy Diet
When these factors are in favorable condition cause conception, but the diseased
condition of any one or many of these factors cause Vandhyatva.18
NIDANA OF VANDHYATVA W.S.R. TO ANOVULATION:
Failure of the ovary to produce a matured ovum is anovulation. Menstrual cycle
without having a mature ovum is called as anovulatory cycle, and is the main cause of
infertility. Some conditions with their Nidanas, are available in classics, which seems
to be related with anovulation causing vandhyatva are being mentioned here:
(1) Revati Jatharini (Puspaghni):10
Under the description of jatharinies Kasyapa has mentioned one Puspaghni, the
woman affected menstruates in regular interval, but is unable to conceive. The other
symptoms given are, she has corpulent and hairy cheeks.

Review of Literature
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 11
(2) Astartava Dusti:
Acharyas have mentioned that Astartava Dusti if remains untreated or not
properly treated then it causes Abijata i.e. it is unable for Prajotpadana19.
Susruta, just after describing eight disorders of Sukra, has enumerated eight
disorders of Artava.
Dalhana has clarified that the clinical features of Artava are identical to those
for Sukra. Both the Vagbhatas have expressed similar views20.
Disorders of Artava have been classified by Susruta on the basis of
predominance of Dosas and disorders of Sukra on the basis of main clinical feature.
Actually there is no difference in both these, at one place (in Artava), the causative
factor has been given the importance and at other, the clinical features.
Since all the classics have mentioned that Artava also exhibits similar clinical
features of Sukra disorders of Artava are being given on the basis of description of
disorders of Sukra.
Classification of Artava Dusti:
(1) On the basis of Causative Dosa
(a) Vataja (b) Pittaja (c) Slesmaja (d) Raktaja (e) Vata Pittaja
(f) Pitta Kaphaja (g) Vata Kaphaja (h) Tridosaja
(2) On the basis of specific clinical features
(a) Vataja (b) Pittaja (c) Kaphaja (d) Kunapa Gandhi
(e) Granthi - Bhuta (h) Putipuya (i) Kshina and (j) Mutrapurisa Tulya or
Malatulya
Review of Literature
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 12
Clinical features21:
(1) Vataja Artava Dusti: The Artava Vitiated by Vata is Red, black or dark violet in
colour. Thin dry, frothy and scattered. It is excreted slowly and with pain specially
perforating or piercing type pain.
(2) Pittaja Artava Dusti:
The Artava vitiated by Pitta is –
Yellowish or bluish in color. It is free from unctuousness, smells like pus, fungus
blood or has putrid smell. At the time of excretion is hot, associated with severe
burning and feeling of heat.
(3) Kaphaja Artava Dusti : The Artava vitiated by Kapha is -
Whitish or slightly yellowish in colour mixed with Majja. It is too much thick,
slippery or lubricous, unctuous and settles down if put in the water.
(4) Kunapa Gandhi Artava Dusti : The Artava vitiated by Rakta -
It smells like a dead body. Artava discharged more and red like fresh blood. It
is also associated with heat and burning etc. features of Pitta.
(5) Granthibhuta Artava Dusti : The Artava vitiated by Vata and Slesma -
It has clotted appearance associated features are of both the dosas (pain due to
Vata and unctuousness due to Kapha etc.
(6) Putipuya or Puya Artava Dusti: The Artava vitiated by Pittakapha-
Putipuya means it is putrid and purulent. It is characterised with other features
of Pitta and Kapha (burning, fever, heat due to Pitta and heaviness etc. due to Kapha).
(7) Ksina Artava Dusti: The Artava vitiated by Pitta and Vayu -
It is scanty, less in quantity and delayed. Associated with pain in Vagina and

Review of Literature
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 13
also the features of Vata and Pitta Dosas.
(8) Mutra Purisa Gandhi Artava Dusti : The Artava vitiated by Tridosa-
It smells like urine and feces.
Nidana of Artavadusti 22
Authors have not described any specific etiology of these Astartava dusti. But
as it is similar to that of Sukra Dusti. We can correlate Sukradusti Nidana with its
causative factor in some extent.
(1) Viharajanya - Excessive sexual indulgence, untimely sexual congress,
sexual abstinence, sexual congress with an unresponsive woman, supression of the
natural urges.
(2) Aharajanya - Habitual use of unwholesome diet, habitual use of dry bitter,
astringent very saltish, acid or hot articles.
(3) Other - Owing to old age, worry grief or lack of mutual confidence, injury
by weapons, caustics or fire, owing to fear, angry, black magic, emaciation due to
disease, vitiation of body elements. Due to this Nidanasevana, the Dosas get provoked
either sinlgy or collectively and reaching the (Retovaha Sira) Rajovahi sira, soon they
vitiate the (semen) Artava excessively.
In classics Sudhaartava has been told as one of the essential factor for the
conception, complete growth and development of the foetus along with its normal full
term birth. In the quotation as given in the vitiated Artava has been mentioned as one
of the main cause of infertility. This means that if the Artava (Bahipuspa,
menstruating blood) is vitiated by the Dosas then there will be no production of Bija
(Antapuspa, ovum).

Review of Literature
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 14
In Sushruta Samhita, the Garbhotpatti has been compared with the Ankur
Utpatti and it has been mentioned clearly that the Artava of a woman vitiated by the
deranged Vata, Pitta, Kapha or Rakta either singly or in combination of two or more
Dosas, should be likewise considered as unfit for the purpose of fecundation.
In modern science the menstrual phenomenon and the ovulation are correlated.
In many ovarian dysfunctions the menstrual pattern get disturbed.
In Kasayapa Samhita some Nidanas are given for Artava Dusti.23
(1) Use of Nasya during menstruation.
(2) Consumption of excessive not eatables and drinks.
(3) Use of excessive medicines for Sodhana purpose to the woman of Mrdu Kostha
having received Snehana and Svedana.
Avarana24
In the concept of Artavanasa both Susruta and Vagbhata has described that
both Vata and Kapha when aggravated, obstruct the path, thus Artava is destroyed.
Though Artava is not finished completely however it is not discharged monthly.
Acarya Kasyapa has defined clearly the bad effect of Tiksna Virecana in a
person having Mrdukostha. According to him, due to this, Vata is aggravated and
causes Svasa, Kasa etc. along with Bijopaghata in case of female. Vata mainly Apana
Vata responsible for all type of abnormalities25
Artava Vaha Srotasa Viddhata 26
According to Acarya Susruta the trauma on the Artava Vaha Srotasa cause
anovulation and is the cause of infertility.

Review of Literature
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 15
Beejadusti 27
During antenatal period if mother takes Vata Prakopaka Ahara and Vihara, the
Vata get aggravated and spoil the Beeja or Beejabhaga or Beejabhagavayava in
female child and that in turn results in the congenital abnormality of female genital
organs which is termed as Vandhya in Caraka Samhita Sarira Sthana and Sandhi Yoni
in Cikistasthana by all acharyas.
Dietic habit23
Due to Ati Usna Annapana, Virya, Artava, Beeja become Upachita. Use of
excess hot water & diet accumulation (maturation / formation) of retas( semen) asrk
(ovum) & egg ( implantation) get vitiated.
Yonivyapada :
Acarya Caraka mentioned that Yoni (reproductive system) of woman when
afflicted with Dosas or diseases, causes, Apatyavighata, does not retain Sukra and
Garbha, i.e. become infertile. Also causes Upadravas like Gulma, Arsa, Pradara and
other Vata disorders, Stambha and Sula28&29
Some specific Yonivyapada related to Vandhyatva. W.S.R. to Anovulation.
Acharana yonivyapada30&31
Dalhana mentioned that in this disease the woman is hyperexcited during
coitus than the man or she feels excessive itching and therefore fertilization also not
occurs.
Madhava Nidana, Bhavaprakasa and Yogaratnakara also mentioned the same
description.

Review of Literature
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 16
Aticharana 32&33
Susruta explained that Aticharana yonivyapada is cause due to excessive
sexual act and she doesnot retain the Beeja. While commenting Dalhana quotes that is
woman does not achieve conception.
Putraghni / Jatagni 34&35
The aggravated Vata due to predominance of Ruksa property, repeatedly
destroy the foetus. Dusta Sonita is also a causative factor which was given by Susruta
also in different manner as "Raktasansravat".
Suska 36
Only Adhamalla has mentioned Nasta Artava as the onlysymptom of Suska
Yonivyapada.
Vamini 37
All Acharyas mentioned that the disorder, in which Sukra (sperm) only or
admixed with Raja, is expelled with or without pain within six to seven days of its
entry into uterus is termed as Vamini.
Vandhya 9
Susruta defined the Vandhya Yonivyapada with the absence of Artava.
Sandhi yonivyapada :
It is explained in Bijadustijanya Nidana.
Asrja or Apraja38
Acharya Caraka, only explain that due to aggrevation of Rakta and Pitta, there
is bleeding even after achievement of conception. Chakrapani in addition comments
that excessive bleeding leads to abortion, thus the woman remains without progency

Review of Literature
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 17
(Praja) hence; it is also termed as Apraja.
Summarizing all those references, it can be stated that the Nidana of
Yonivyapada given by Acharyas can be taken as the Nidana of Vandyatva and also
for the anovulation causing Vandhyatva
(1) Aharaja Nidana - Mithyaahara, Dustabhojana
(2) Viharaja Nidana - Mithyavihara Coitus with Ruksa, Durbala, Bala, Excessive
coitus, Use of foreign bodies for sexual organisms
(3) Pradusta Artava -
(4) Beeja Dosa i.e,. Abnormalities of sperm or ovum
(5) Daiva - unknown or idiopathic factor39
Thus etiologies of Vandhyatva can be boldly categorized under 4 headings as
specified by the classics. Though we find number of reasons for Anovulation they go
no,where beyond these four Vyapaka Nidana.
SAMPRAPTI 40
The Vyadhijanaka, Vyapara is called as Samprapti. In detail, the manner in
which the vitiated dosa diffuses in the body to liberate the disease is known as
Samprapti. It is also called Jati and Agati41. Susruta, while explaining Vyadhi
formation specify the "Kha Vaigunya" "Kha" means the Akasa or Avakasa and the
Avakasayukta Bhava (organ) of Sarira are Srotasa42
Srotasas play very important role because no substance in the body can grow
and develop or waste and atrophy independent of Srotasa.
The general causes of Srotodusti given by Charaka are related to Dosa and
Dhatu43. Also the general Srotodusti Laksanas are Atipravrtti Sanga. Siragranthi,
Review of Literature
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 18
Vimargagamana, among these Sanga may be explained by three ways,
(1) The substance to be produce is less.
(2) The production is normal but the channel is small
3) Or the channel may be obstructed.
Vagbhata stated the importance of Agni in Roganirmana. The Agni and Ama
are interrelated. Also the normal or vitiated state of Dosa depends on Agni. The
Samprapti of Vandhyatva W.S.R. to Anovulation begins with the various factors
explained under Nidana and ends up with Anovulation which is the main cause for the
symptomatology of Vandhyatva.
SAMPRAPTI GHATAKA:
Dosa - Tridosa with predominant Vata
Dhatu - Rasa, Rakta
Upadhatu – Artava
Srotasa - Artavavaha
Srotodusti - Sanga
Udbhavasthana - Pakvasaya (Mulasthana of Vata)
Adhisthana - Yoni & Garbhasaya
Marga - Abhyantara (Garbhasaya as Kosthanga)
The specific etiological factors mentioned previously cause provocation of
vata, pitta and kapha. Vata the main dosa vitiates with its own causative factors also.
vata on account of its quality of subtleness (suksmatvata) is really the impeller of
other two humours. Vitiated vata agitates the other two humors and throw them in the
Review of Literature
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 19
place having kha vaigunya. Here the khavaigunya is in artavavaha Srotasa specially in
the beejagranthi.
Due to nidana sevana, dosa and agni get vitiated, mandagni is the main cause
of ama formation. The ama formed executes hazardous effects, it adhers to srotasa
and forms avarodhatmaka dusti. Ama spreads throughout the body, propelled by the
vitiated vata along the rasavaha srotasa and in modern physiology, a variety of
transforming and transmitting substances present in the body like enzymes, hormones,
catalyst etc. When these are unable to function properly entirely different metabolites
are formed which the body is not acquainted to process. These accumulated in the
body in different systems affecting the normal mechanism of that particular system.
These may be formed as ama.
Due to hypo functioning of jatharagni, dhatvagni mandya also occurs. Due to
mandagni and nidanasevana, rasa, rakta dhatu get vitiated. Also the dhatvagnimandya
causes the ksayatmaka effect on the artava i.e. the production of artava, upadhatu of
rasadhatu or raktadhatu becomes less. Thus it is the Upadhatvatmaka dusti.
Visvamitra has clarified that hair thin vessels fill the uterus for whole month
to receive bija and due to rasadusti posanatmaka dusti can cause Anovulation.
The vitiated apanavayu and kapha when get mix can cause avaranatmaka dusti
causing Anovulation. The vitiated Vata along with Pitta causes the artavaksaya i.e.
ksayatmaka dusti causing Anovulation.
Line of treatment:
1. Treatment of specific causes responsible for infertility such as treatment of all the
Gynecological disorders including injury to the uterus or its prolapsed, diseases of

Review of Literature
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 20
shukra & artava & yonyarsha etc to be done. The acharyas have mentioned
unequivocally that pregnancy occurs only in case of healthy reproductive organs.
2. For saking of different etiological factors such as abnormal diet and mode of life,
coitus before or after ritukala, psychological trouble etc.
3. Use of strength producing and brumhana articles to compensate the loss of bala
and dhatus.
4. After using oleation, sudation, emesis, purgation, astapana & anuvasana basti in
consecutive order, the man should be given milk and grita medicated with sweet
drug and oil & masha to the women according to the opinion of some authors.
Kashyapa said that after using cleansing measures ie panchakarma both the
partners should be prescribed congenial diet.
5. Infertile woman should be prescribed with emesis, purgation & astapana basti,
with the help of these procedures the woman conceives positively and delivers
normally.
6. The use of basti in infertility due to diseases of vata is highly beneficial. By the
use of basti the yoni becomes healthy & even a sterile woman would conceive.
The basti is beneficial to the woman having repeated abortions, short lived &
weak children who are delicate & indulge daily in coitus.
7. The drugs prescribed for pumsavana karma can also be used.
Specific treatment:
The drugs prescribed for gynecological disorders to be used to eradicate the
causes of infertility, but there are certain recipes were described by our ancient rishis
which are indicated for achievement of conception by an infertile woman. They were
advocated in various forms. Some of them are used externally& some internally. The
Review of Literature
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 21
externally applied drugs are in the form of nasya, abhyanga & basti. Whereas
medicines to be taken orally is numerous.
• Nasya(nasal instillation):-
1. Lakshmana triaturated with cow’s milk.
2. Amulet of root of lankakara lakshamana tied round the neck & nasya of
lakshamana triaturated with cow’s ghrita.
3. Narayana taila.
4. Shatapushpa taila.
• Abhyanga (massage)
1. Narayana taila.
2. Shatapushpa taila.
• Basti (enema)
Narayana taila. Shatapushpa taila.
Lasuna taila. Shatapaka taila.
Trivrita sneha. Bala taila.
Shatavaryadi anuvasana. Guduchyadi Rasayana.
Sahacharyadi yapana. Mustadi yapana.
Shatavryadi Rasayana. Jeevantyadi anuvasana.
• Drugs for oral use:
Kalka:
1. Paste of chandana, ushira, manjista,girikarni & sugar candy mixed with cow’s
milks.

Review of Literature
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 22
2. Paste of sweta-girikarni, sweta-gunja, sweta-punarnava with cow’s milks.
3. Paste of roots of swetarka in milk or Paste of sweta-girikarni or sweta-agrikarni in
milk.
4. Paste of triphala, girikarni, aragvadha, vatsaka, payasa in cow’s milk.
Churnas:
1. Baladhy churna, chandanadya churna, drakshadya churna, khandakadya churna,
& punarnavadya churna.
2. Shatapushpa kalpa
Swarasa or juices:
1. 8 leaf buds of vata, lakshmana & cow’s milk.
2. Bala, sharkara, atibala, madhuka, leaf buds of vata, gajakeshara mixed with
honey, milk & ghee.
3. Root of lakshmana (taken in pushya nakshatra) & pounded with milk by a virgin.
4. Root of kuranta flowers of dhataki leaf buds of vata & neelotpala triturated with
milk.
5. Parswa pippala with jeeraka & white visikha punkha.
Kwath (Decoction)
1. Maharasnadi Kwatha
2. A woman having taken bath after menstruation, if uses milk medicated with
decoction of Ashwagandha in the morning hours, definitely conceives.
Pana
1. Lakshamana with milk
Review of Literature
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 23
2. Tila taila, milk, phanita, curd and ghee churned and mixed.
3. Entire seeds of one matulunga pounded with milk.
Gutika (Tablets)
1. Yogaraj Guggulu
Taila (Oils)
Narayana Taila Shatavari taila
Baladya taila Satapusphpa taila
Ghritas
Laghuphala ghruta Phala ghruta
Kamadeva ghruta Paniya kalyanaka ghruta
Seetakalyanaka ghruta Brihat shatavari or Shatavari ghruta
Kashmaryadi ghruta Jeevaniya Ghana siddha gruta
Shatavaryadi ghruta Lasuna ghruta
Aristas
1. Dashamoola Arista
Rasa aushaddhi
1. Khandakadya Louha
Paka
1. Puga paka
Review of Literature
MODERM REVIEW
FUNCTIONAL ANATOMY OF OVARY
OVARY:
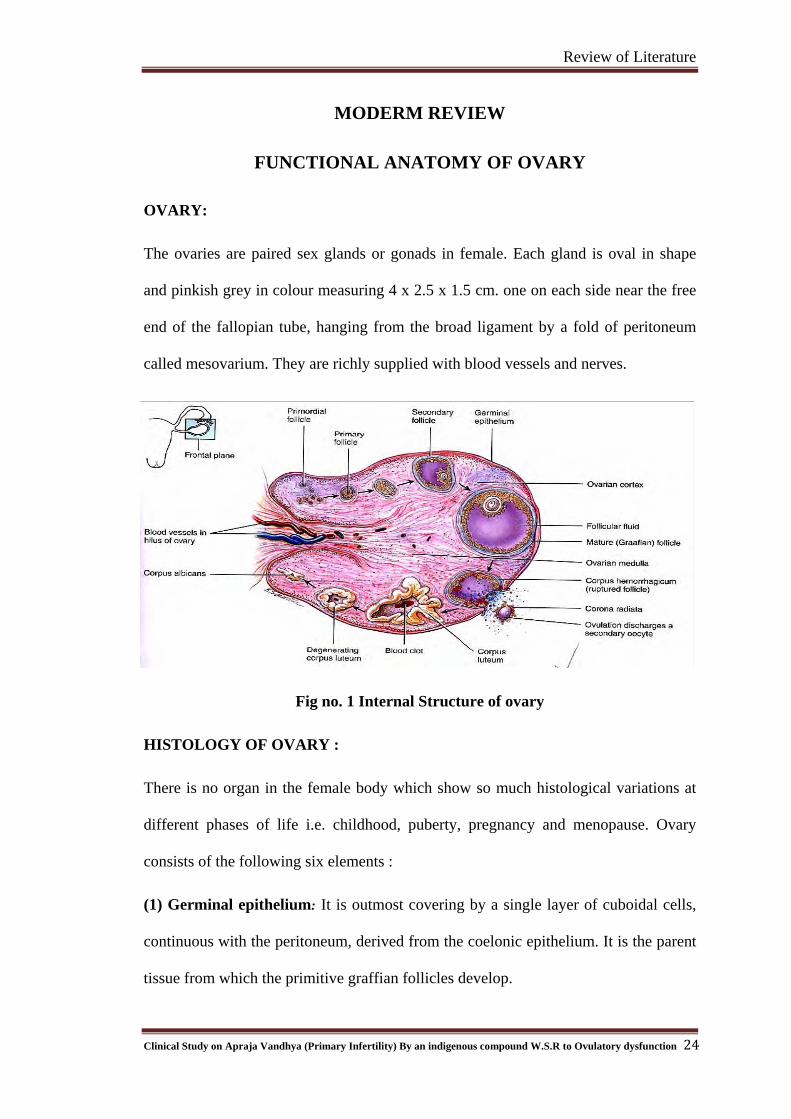
The ovaries are paired sex glands or gonads in female. Each gland is oval in shape
and pinkish grey in colour measuring 4 x 2.5 x 1.5 cm. one on each side near the free
end of the fallopian tube, hanging from the broad ligament by a fold of peritoneum
called mesovarium. They are richly supplied with blood vessels and nerves.
Fig no. 1 Internal Structure of ovary
HISTOLOGY OF OVARY :
There is no organ in the female body which show so much histological variations at
different phases of life i.e. childhood, puberty, pregnancy and menopause. Ovary
consists of the following six elements :
(1) Germinal epithelium: It is outmost covering by a single layer of cuboidal cells,
continuous with the peritoneum, derived from the coelonic epithelium. It is the parent
tissue from which the primitive graffian follicles develop.
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
24

Review of Literature
(2) Tunica albuginia : This layer of eosinophilic collagenous connective tissue of
low cellularity under germinal epithelium.
(3) Stroma: It is a connective tissue network continuous with the tunica albuginia and
containing spindle shaped cells with a few involuntary muscle fibers. It supports the
essential ovarian tissues and carries blood vessels, lymphatics and nerves.
(4) Vesicular follicles or Graffian follicle : Small Islands of cells in various stages of
development are scattered mostly at the peripheral part of the ovary. These immature
ones are called as the primordial follicles. The central cell is the ovum. The remaining
cells surround the ovum in a single layer forming a sort of capsule.
(5) Corpus luteum : When the graffian follicle ruptures corpus luteum develops on
the remnants of the ruptured follicle.
(6) Interstitial cells : Groups of polyhedral cells containing lipid granules
representing stored active principle. They develop the stroma cells or from the cells of
the unruptured follicles.
FUNCTIONS OF OVARY :
The ovaries have two functions, Exocrine function i.e. the production of ova
(ovulation) and Endocrine function i.e. the production of hormones.
The latter is secondary to the former and is present to a limited extent for a
few years before regular ovulation is established and for some time after ovulation.
Both these functions are controlled through the hypothalamic - pituitary
ovarian axis by endocrine, paracrine and autocrine pathways.
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
25
Review of Literature
ESTABLISHMENT OF OVULATION:
The ovary probably first sheds an ovum (ovulation) about the time of the onset
of menstruation, but ovulation is not usually established as a regular phenomenon
until 2-3 years after the menarche. It than continues until the age of 45-50 years,
although it may get less frequent and less regular after the age of 40 years.
Ovulation occasionally precedes the establishment of menstruation and
sometimes occurs even after the cessation of menstrual period. This accounts for the
rare cases of pregnancy reported to have occurred before the menarche and after the
menopause.
'Lipshutz Law of follicular constancy', according to the law the ovulation is
maintained every month even if one ovary is removed.
THE NUMBER OF OVA IN OVARY :
In embryonic life period, in yolk sac, primordial germ cells originate in the
endoderm and ovary is formed by genital ridge.
Oogenesis begins in ovary - 6-8 weeks gestation
Formation of oogonia - 16 to 20 weeks gestation
Transformation of oogonia to oocyte - 11 to 12 weeks gestation. Here the
oocyte enter the 1st meitotic phase and arrest in prophase.
The primary oocyte at birth in both ovary - 2 millions
The primary oocyte in both ovary at puberty - 3,00,000 to 5,00,000 From this
number of primary oocyte, not more than 500 are destined to mature during
the individuals lifetime and the remainder will be lost by some form of
generative process.
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
26

Review of Literature
OVULATION :
Ovulation is the process by which an ovum, in the form of secondary oocyte,
is discharged from the ovary to become a gamete.
PROCESS :
In the ovarian cycle, which occupies approximately 28 days, ovulation takes
place at the midphase, having follicular and luteal phase before and after the
ovulation. The two phases are separated by ovulation.
Changes during follicular phase : In this phase the ovum is prepared for ovulation
by follicle ripening, primordial follicle grows to graffian follicle. The commencement
of ripening of a follicle is heralded by an increase in size of the ovum and of its
nucleus.
The surrounding granulose cells become cuboidal and multiply quickly to
become many layered. At the same time, they begin to secrete liquor follicule, which
form small pools separating groups of cells. These pools later run together to form a
single lake and the system becomes a graffian follicle. This cystic structure is lined by
several layers of granulosa cells which are collectively called the membrane
granulosa. The ovum is surround by a palestaining non-cellular porous area of
glycoproteins the zona pellucida. Between the ovum and zona pellucida is the
periviteline space. The granulosa cells immediately around the ovum constitute the
corona radiata outside the membrane granulosa, the layer of stromal cells, theca
interna and outside this again theca extrena.
27
During the process of ripening, the graffain follicle, by asymmetrical
development seen particularly in the form of a cone shaped theca interna, makes its
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction

Review of Literature
way to the surface of the ovary, easily piearcing the tunica albaginea. It thus arranges
itself so that the discuss proligerous with the ovum lies on the side of the follicle
adjacent to the peritoneal cavity. Thus in this stage the ovum is awaiting for release
from ovary in the form of a primary oocyte surrounded by granulosa cells.
Follicular ripening does not take place at an even ratio throughout the earlier
14 days and the major histological changes only appear within the last few hours or
days. An immature follicle is only 0.03 mm in diameter. A ripe follicle is 16-24 mm
diameter immediately before rupture, so it is visible to the necked eye.
Maturation of the ovum :
All the primary occyte in the ovary of a newborn baby are already in the early
stages of the meiotic division. The process becomes arrested in the late prophase stage
and remains dormant until follicular ripening is established.
In the midcycle, due to preovulatory LH surge, meiosis is resumed and is
completed within the 35-45 hours prior to the ovulation. This first maturation
division, during which the number of chromosomes in the nucleus is halved, results in
the formation of a secondary oocyte and a polar body. The latter comes to lie in the
perivitelline space of the oocyte. The second division, which results in the oocyte
casting off another polar body and the 1st polar body dividing into two, only occurs
after the ovum is liberated and probably only after it is fertilized.
During maturation, the ovum increases in a diameter from 0.2 to 0.1 mm and
at the end its nucleus is off centre and displays a prominent nucleolus.
Rupture of the follicle - ovulation :
28
The word rupture implies an explosive or dramatic occurrence, but the
discharge of the ovum from the follicle is a comparatively gradual process occupying
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
Review of Literature
many seconds if not minutes during which the ovum, still surrounded by a corona
radiata of variable thickness, oozes out. The follicular fluid escapes with the ovum
and occasionally slight bleeding takes place from the site of rupture.
Ovulation usually occurs from 13th to 17th day (day 14th) of 28 day menstrual
cycle. It occurs 14 days before onset of next menses irrespective of length of
menstrual cycle (Knaus, 1934).
Life time :
Unless fertilized, the ovum survives only 12-24 hours and then disintegrates in
the tube without leaving any trace. Nevertheless ova have been recovered from the
fimbria and from the lumen of the tube 2-4 days after ovulation, and from the uterus
4-5 days after ovulation. Such if not already fertilized is probably degenerate or
certainly incapable of being fertilized.
Causes of ovulation :
(1) Ovulation occurs as a result of thinning and degeneration of the cyst wall, this
being associated with the production of proteolytic enzymes. The activity is enhanced
by progesterone.
(2) The progesterone induced mid-cycle rise in FSH also serves to free the oocyte
from its follicular attachments.
(3) Plasminogen activators activate plasmin which generates active collagenase
leading to degeneration of the collagen in the cell wall, especially at the follicular
apex or stigma.
29
(4) Exit of the ovum may possible be encouraged by contraction of micromuscle cells
present in the theca externa and the stroma. These being activated by prostaglandins
which are said to be essential to follicle rupture and the ovarian content of which is
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
Review of Literature
increased by the action of LH.
Changes during Luteal phase : Just after the ovulation profound changes takes place
in the wall of follicle. The cyst collapses and the lining cells undergo leuteinization, a
process in which they enlarge by limbering fluid. Their bloatedness causes them to
become closely packed and makes their nuclei look relatively small. Luteinization,
which is brought about by enzyme action, affects both the granulosa layer (granulosa
lutein cells) and the theca interna (theca lutein cells), the latter being more prominent
in the early stages and former in the later stages.
The corpus luteum is 1-2 cm in diameter and projects from the surface of the
ovary. Some of the expansion is taken up by the layers of cells folding into the old
cavity and this gives the corpus luteum its characteristic crehatel shape on section.
The mature structure has a yellow colour on naked eye examination because of the
presence of lipoids. In its early stages, the corpus luteum is grey or greyish yellow.
Within 2-3 days of ovulation, the corpus luteum becomes supplied with blood vessels
which grow down the core of each invagination from the theca interna. During this
process there is often a little bleeding into the cavity where the blood mixes and
makes the appearance red or orange, the corpus haemorrhagicum.
The development is completed in 5 days during which time, it is already
functioning. Its activity is at a maximum during following 3-4 days, but when there
after as degenerative changes commence 4-6 days before the near menstrual period.
30
Degeneration is 1st made evident by the cells becoming vacuolated, there after
they lose their staining capacity, colloid degeneration and fatty changes are described.
But these are followed by hyalinization so that ultimately the corpus luteum is
converted into hyaline tissues, known as a corpus albicans. It is absorbed over the
course of 6-12 months.
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
Review of Literature
Hormonal control :
The cyclical production of FSH and LH in the adult woman is itself largely
controlled by the ovarian cycle. This is by way of a feedback mechanism, which
operates through the hypothalamus and which can be explained in a simplified form
as follows. The discharge of FSH and a little LH from the pituitary, initiated by the
hypothalamus, causes follicle in the ovary to ripen and secrete estrogen. It resulting
high level of estrogen in circulation increases GnRH receptor concentration. A surge
in GnRH accompanies the LH surge. A high level of LH induced ovulation and
corpus luteum formation with a consequent increase in the secretion of progesterone.
Control of ovulation (pituitary ovarian relations) :
The neurohormonal connections are again illustrated by the control of
ovulation in certain animals such as rabit. In those follicular ripening proceeds
spontaneously but ovulation only occurs as a result of coitus. This act by mechanical
stimulation of the cervix. From the cervix, nerve impulses travel through the spinal
cord to the hypothalamic pituitary system which liberates LH to cause ovulation 18
hours after the initial stimulus. In woman, ovulation ordinarily occurs independent of
coitus and is spontaneous but this does not excludes the possibility that it may
sometimes be determined by outside influence.
Correlation of endometrial and ovarian cycles :
By the end of, if not just before the onset of a menstrual period, a new follicle
is beginning to ripen in the ovary; endometrial proliferation therefore occurs during
the follicular phase in the ovary and is the direct result of a mounting estrogen
influence. Ovulation marks the change over from the proliferative to the secretary
phase in the endometrium. Secretary activity and decidual reaction are manifestations
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
31

Review of Literature
of the luteal phase in the ovary and are brought about by progesterone acting in the
absence of estrogens.
The Shrinkage of the endometrium menstrually coincides with commencing
failure of corpus luteum activity and is the direct result of the withdrawal, of the
supporting effect of estrogen and progesterone. For the practical purpose, in mature
women regular menstruation means regular ovulation.
Post menstrually the endometrium is only 1 mm thick where as at the end of
proliferative phase (i.e. 10 days after the end of menstruation the fourteenth day of the
cycle), it measures 2-3 mm. In the periovulatory period it appears sonographically as
a triple layer in the long axis of the uterus and is usually about 10-12 mm in diameter.
In luteal phase endometrium loses both the hyperechogenicity and the triple layered
appearance.
CHANGES DURING OVULATION :
(1) Myometrial changes: The activity of uterine muscle increases with the estrogen
stimulus of approaching ovulation, which is i.e. contractions are small and frequent
and having limited response to oxytocis in the follicular phase.
(2) Tubal changes : The muscles of the fallopian tube behaves like myometrium in
that it shows increased movement about the time of ovulation. This is an estrogen
effect as is the increased cilial activity at that time. These changes are timed to propel
the ovum towards the uterus.
(3) Cervical changes : At the time of ovulation the secretion is so profuse that it may
be noticeable as a vaginal discharge the 'ovulation cascade'. Under the influence of
estrogen, actively secreted mucus shows some characteristic features. The mucus will
stretch into threads measuring more than 6.5 cm, and even 10-15 cm, at the time of
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
32
Review of Literature
ovulation. This property is known us spinnbarkeit. The mucus absorbs water and salts
and when allowed to dry, deposits crystals of sodium chloride and potassium chloride
in a characteristic pattern which suggest the fronds of fern.
All these special characters at this time make for its easy penetration by
spermatozoa. With comparison to luteal phase i.e. after ovulation the position of
cervical spincter which is due to tone of muscles of the isthmus and internal os, is less
tighter and competent during (ovulation) follicular phase which is due to
progesterone.
(4) Vaginal changes : It show histological changes in the vaginal epithelium, but they
are not clearly defined in tissue sections.
DIAGNOSIS OF OVULATION :
The following methods are available for diagnosis.
(A) Analysis of symptoms during ovulation :
(a) Cyclical bleeding : The occurrence of regular normal menstrual losses is strong
presumptive of monthly ovulation.
(b) Ovulation pain (Mittelschmerz) : Many women feel some discomfort in the
hypogastrium or in one or other iliac fossa for 12-24 hours just before or just after
ovulation.
(c) Ovulation bleeding or discharge (Mittelblut) : Some women experience a slight
loss of blood or of mucus tinged with blood at the time of ovulation. This may be
associated with ovulation pain although each can occur independently.
33
(d) Premenstrual mastalgia : Premenstrual pain and tenderness in the breasts is in
some way related to corpus luteum action. So its occurrence is fairly reliable evidence
that ovulation has occurred during that particular cycle.
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
Review of Literature
(B) Temperature changes : The body temperature shows variations during follicular
phase, luteal phase, pregnancy also. For this test to be of value it is essential for the
temperature to be recorded daily under standard conditions, before rising from bed in
the morning and before eating or drinking.
The biphasic curve in the chart is evidence of ovulation as opposed to
anovular menstruation and the thermal shift is a fairly accurate indication of the time
of ovulation.
(C) Endometrial changes : By histological changes in the endometrium can diagnose
evidence of ovulation not the time of ovulation.
(D) Changes in cervical mucus: The different effects of estrogen and progesterone
on the physicochemical properties of cervical mucus are utilized in the fern test. A
failure to demonstrate ferning during the premenstrual week, denote dominant
progesterone influence and suggest that ovulation has occurred. Also the amount and
nature of cervical mucus shows the changes in preovulatory and ovulation stage.
(E) Hormone assay : Ovulation can be reliably confirmed by an estimation of the
mid luteal phase plasma progesterone level i.e. 5-8 days after ovulation. A minimum
of 6.5 ng/ml is taken to indicate ovulation.
(F) Ultrasound : It has been used to describe ovarian and follicular characteristics
throughout the cycle.
(G) Direct observation : Recent ovulation can be diagnosed by the finding of an
active corpus luteum on inspecting the ovary during laparoscopy or laparotomy.
OVULATION DETECTION METHODS
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
34

Review of Literature
Table. No 1: Showing Method Day of cycle Observations
Method Day of cycle Observation
B.B.T Throughout cycle Secretary Endometrium
Cervical mucus
Nature
Spin barkeit
Fern pattern
12-14 & 21-23
12-14days 21-23days
Clear watery, thick viscid
+ -
+ -
Vaginal Cytology 12-14 & 21-23days
12-14 21-23
Discreade cells Folded edges
pyknotic nuclei inclumps.
Background clear Background dirty
Serum progesterone
8 & 21
On 8th < 1 ng/ml 21st > 6 ng/ml
Serial USG
12-14
Follicular measurements
approaching 20 mm
Laparoscopy
Secretary phase
Recent corpus luteum seen
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
35

Review of Literature
ANOVULATION
Anovulation is a very common problem that present in a variety of clinical
manifestations including amenorrhea, irregular menses and hirsutism. serious
consequences of chronic anovulation are infertility & a greater risk for developing
carcinoma of the endometrium and perhaps the breast. The clinician must recognize
the clinical impact of anovulation and undertake therapeutic management of all
anovulatory patients to avoid these unwanted consequences.
Normal ovulation requires co-ordination of the menstrual system at all levels :
a) central hypothalamic – pituitary axis,
b) The feedback signals, and
c) Local responses within the ovary.
The loss of ovulation can be due to any one of assortment of factors operating
at each of these levels. the end result is a dysfunctional state, anovulation and
polycystic ovary.
CENTRAL DEFFECTS
The hypothalamic pituitary axis may be unable to respond, even if given
adequate and appropriately timed feedback signals. Normal pituitary ovulatory
response to the follicles steroid signals requires the presence of gonadotropin
releasing hormone (GnRH) pulsatile secretion within a critical range. Increasing
intensity of GnRH suppression is associated with increasing dysfunction and a
changing clinical presentation.
36
A variety of problems such as stress and anxiety, borderline anorexia nervosa
and acute weight loss after a crash diet, is associated with an inhibition of normal
GnRH pulsatile secretion, the mechanism for this suppression of GnRH is excessive
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
Review of Literature
hypothalamic activity of corticotrophin - releasing hormone(CRH), a response to
stress. these patients present more commonly with amenorrhea. However if GnRH is
only partially suppressed homeostatic pituitary – ovarian function is maintained, and
the patients will be anovulatory.
Anovulation and polycystic ovaries have been reported to be more prevalent
in women with epilepsy. This is another example of how any disruption of normal
ovulation.
Specific clinical syndrome of central anovulatory dysfunction has been
recognized hyper-prolactinemia. Increasing levels of prolactin can cause a woman to
progress through a spectum, beginning with an inadequate luteal phase to anovulation
to the amenorrhea associated with complete GnRH suppression. A search for
galactorrhea and measurement of the prolactin level are important screening
procedures for all women who are not ovulating normally.
ABNORMAL FEEDBACK SIGNALS:
LOSS OF FSH STIMULATION :
In order to achieve recycling a nadir in blood sex steroid level must occur so
that the initial event in the cycle, the rise in FSH, can take place. Sustained estrogen at
such a key movement would not permit FSH stimulation of follicular growth and
maturation and recycling would be threatened.
PERSISTENT ESTROGEN SECRETION :
37
The most common clinical example of anovulation associated with continued
secretion of sex steroids is pregnancy. Persistent and elevated secretion of estrogen
can be encountered rarely with an ovarian or adrenal tumor. In such a case
anovulation or amenorrhea may be present.
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction

Review of Literature
ABNORMAL ESTROGEN CLEARANCE AND METABOLISM :
The clearance and metabolism of estrogen can be impaired by other
pathologic condition, such as thyroid or hepatic disease. Both hyper-thyroidism and
hypo-thyroidism can cause persistent anovulation by altering not only metabolic
clearance but also the peripheral conversion rates among the various steroids. When
hypo-thyroidism associated with elevated prolactin levels, demands screening of an
ovulatory and amenorrheic women with a thyroid stimulating hormone(TSH)
measurement.
EXTRAGLANDULAR ESTROGEN PRODUCTION :
Extra glandular contribution to the blood estrogen level can reach significant
proportions. This is accomplished by the extragonadal peripheral conversion of C-19
androgenic precursors, mainly androstenedione to estrogen. Psychological or physical
stress may increase the adrenal contribution of estrogenic precursor. Adipose tissue is
capable of converting andostenedione to estrogen: hence the percent conversion
increases with increasing body weight.
LOSS OF LH STIMULATION:
A failure in gonadal production of estrogen need not be absolute, obviously,
the patient with gonadal dysgenesis and ovarian failure will present with amenorrhea
and infertility because of total lack of estrogen secretion. The failure to achieve a
critical midcycle level of estradiol necessary to trigger the gonadotropin surge may be
due to a relative deficiency in steroid production.
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
38

Review of Literature
LOCAL OVARIAN CONDITIONS :
A follicle can fail to grow and ovulate because of inadequate expression or
impaired function of any of the following local ovarian activities.
1. Selection of the dominant follicle is established during days 5-7 and consequently
peripheral levels of estradiol begins to rise significantly by cycle day 7.
2. Derived from the dominant follicle , etradiol levels increase steadily and through
negative feedback effect, exert a progressively greater suppressive influence on
FSH release.
3. Insulin like growth factor Ⅱ (IGF-II) is produced in theca cells in response to
gonadotropin stimulation, and this response is enhanced by estradiol and growth
hormone. In an autocrine action IGF-II increases LH stimulation of androgen
production in theca cells.
4. IGF-II stimulates granulose cell proliferation aromatizes activity, and
progesterone synthesis.
5. FSH inhibits IGF binding protein synthesis and thus maximizes growth factor
availability.
6. FSH stimulates inhibin and activin production by granulose cells.
7. Activin, augments FSH activities :FSH receptor expression aromatization, inhibin
/activin production, and LH receptor expression.
8. Inhibin enhances LH stimulation of androgen synthesis in the theca to provide
substrate for aromatization to estrogen in the granulose.
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
39
Review of Literature
9. While directing a decline in FSH levels, the mid-follicular rise in estradiol exerts a
positive feedback influence on LH secretion. LH level rises steadily during the
late follicular phase, stimulating androgen production in the theca.
10. The positive action of estrogen also includes modification of the gonadotropin
molecule, increasing the quality (the bioactivity) and the quantity of LH at mid-
cycle.
11. Inhibin and less importantly, follistain, secreted by the granulose cells in response
to FSH : directly suppress pituitary FSH secreation.
12. FSH includes the appearance of LH receptors on granulosa cells, and the final
maturation of the follicle requires LH support.
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
40
Review of Literature
DISEASE REVIEW (MODERN)
INFERTILITY
Infertility:- in + fer + til + i + ti ( lack of ability to reproduce).
Synonym:-
Absolute: - Due to removal of genital organs like hysterectomy, radiation or
oopherectomy, impossible to conceive.
Partially: - Due to ill health conception does not occur till she achieve good health.
Definition: - Infertility is defined as the inability of a couple to achieve conception
after one year of unprotected coitus.
1) Sterility : Implies that inability to conceive. It is an absolute term.
2) Infertility : Implies that failure to conceive. Infertility is again divided into two
types i.e.
a) Primary Infertility : Infertility where conception has not occurred.
b) Secondary Infertility : The conception has failed to occur after a period of
fertility.
Incidence:- 10 to 15% of marriages prove to be childless.
Fertility also varies from time to time in the same individual. In the male these
are not obvious except during childhood and less absolutely in old age, but in the
female physiological infertility is seen.
• Before puberty
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
41
Review of Literature
• After puberty & before maturation. ( fertility is low until the age of 16-17
years) because anovular cycle.
• During pregnancy when ovulation is suppressed.
• During lactation
• Before the menopause
• After the menopause.
Conception rates also depend on many factors such as
• The tendency for smaller families.
• Elderly age at marriage.
• Use of contraceptions for 1 or 2 years for carrier benefit
• Changing life styles like DINK, SINK.
Causes of Infertility
The main etiological factor is found in Female 40%, Male 35%, Combined 10 to
20%, Unexplained --05%.
Female
1) Ovarian factor (5%)
In women menstruating regularly is a cause operating in about 15% of cases of
infertility. Regular anovulation in menstruating women can be a feature of
hypothalamic anovulation, hyperprolactinaemia; other causes of anovulation include
pituitary adenoma or primary hypothyroidism, polycystic ovaries, subclinical adrenal
failure and diabetes mellitus. Luteinized unruptured follicles & luteal phase
deficiency are two other clinical entities where infertility is seen.
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
42

Review of Literature
Generally, failure to ovulate is associated with amenorrhea or
oligomenorrhoea and has the same causes. These include sex chromosome
disturbances premature ovarian failure due to premature menopause or resistant ovary
syndrome is also seen. Anovulation is also a feature of luteal phase deficiency and the
luteinized enraptured follicle.
Luteal phase defect can be short or long, but is more often the latter. There is
decreased hormone production by the corpus luteum as well as decreased levels of
follicle stimulating hormone (FSH) and luteinizing hormone (LH). Some women have
hyperprolactinaemia and hypothyroidism; others have unexplained infertility with
normal cycles, or habitual aborters.
2) Peritoneal Factors:-
1. Pelvic adhesions:-
2. Defective ovum pickup: - May operate by preventing the tube performing its
"octopus" function at the time of ovulation or by creating a mechanical barrier
between the ovary & the tubal ostium. They result from pelvic peritonitis of
any kind but especially that seen in association with appendicitis, and post
abortal or puerperal infections.
3. Endometriosis:- Is seen in at least 15% of women investigated for infertility, if
all grades are Considered.
3) Tubal Factors
Obstruction –
43
(a) Complete - peritoneal & tubal factors may account for up to 35% of all
cases of infertility. Partial or complete bilateral tubal obstruction results from
previous salpingitis. Most commonly this is post abortal, puerperal, gonococcal,
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction

Review of Literature
chlamydial or tuberculoses in nature
(b) Partial - loss of cilliary function.
4) Uterine Factors
• Uterine absence, congenital anomalies, septatet uterus, bicorn uterus,
atrophy or hypoplasia at a degree sufficient to bar the ascent of
spermatozoa causes amenorrhea as well as infertility.
• Tubercular endometritis.
• Intrauterine adhesions (Asherman's syndrome) due to previous overzealous
curettage or previous surgery on the uterus
• Submucous polyp, endometrial polyp
• Uterine leiomyomas unresponsive endometrium, hypoplasia, devoid of
secretary gland.
5) Cervical Factors
• Thick-impenetrable cervical mucus or poorly penetrable mucus
• Presence of local sperm antibodies
• To low PH of the mucus at mid cycle.
• Loss of mucus due to amputation of the cervix, cone biopsies or
overenthusiastic cervical diathermy.
• Faculty direction of the cervix such as is found in retroversion or severe
prolapse
• Chronic cervicities.
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
44
Review of Literature
6) Vaginal Factors
Purulent discharge - This is doutful cause of infertility because spermatozoa
can thrive in pus under in vitro conditions.
COITAL ERRORS
Apareunia & dyspareunia
1-2% of couple found not to have consummated their marriage due to fear of
pain during sexual act
Frequency & timing of coitus
Some couple never know the fertile period 72 hrs during ovulation is the
period when conception takes place but due to lack of proper knowledge they missed
to do coitus has to take place every 48 hours during the fertile period to offer the
optimum chance of conception
Lubricants
For easy sex act in dry vagina, or less lubricated vagina many couples use
lubricants without realizing that these have a contraceptive action. [Proprietary jellies
are often acidic & therefore spermicidal]
OTHER FACTORS
Orgasm
It is unnecessary for the woman to experience orgasm in order to conceive if it
were otherwise pregnancy would never result from rape.
Effluvium Seminis
45
Immediately after coitus most of the semen escapes from the vagina is known
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
Review of Literature
as effluvium seminis, which is normal & is never be a cause for infertility but it
accounts a wrong idea about.
Anxiety & Depresion
It is commonly believed that a nervous temperament, particularly extreme
anxiety to conceive lowers fertility.
Occupation & Environment
Fertility rate is higher in rural population because they have no planning.
Diet
• Deficient or unbalanced diet may interfere with ovarian function
• Deficiency of zinc & folate are implicated in decreased
spermatogenesis possibly through defective DNA & RNA synthesis.
• Deficiency of dietary antioxidant micronutrients e.g., beta- carotene,
lycopene, retinol and Alpha-tocopherol may decrease genital tract
secretions in men, leading to infertility especially through
immunological mechanisms.
Contraception
Hormonal contraceptive (oral) may hamper ovulation while intrauterine
devices (IUCD) can cause salpingitis & tubal blockage.
INVESTIGATION
Detailed general & reproductive history has importance in investigating the
infertile couple.
• Age & Occupation
Age over 35 years & sedentary habit favors infertility.
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
46

Review of Literature
• Associated illness
Any other ailments apart from infertility, like menstrual disorders, white
discharge, obesity, dyspareunia urinary trouble to be noted.
Previous illness
Of mumps, gonorrhea, syphilis, hypothyroidism, appendicitis, tuberculosis,
diabetes mellitus any abdominal or vaginal operations to be carefully recorded.
• Family History
Fertility in the family twining, history of tuberculosis, diabetes are to be
enquired.
• Personal History
Mode of life on various aspects like family means domestic work, job stress,
worry , dietary, habit, intake of alcohol, tobacco , smoking habit is to be enquired.
• Menstrual History
This should be interrogated in the routinely
Age at menarche
Duration of cycle
Amount of loss
Dysmenorrhoea
Last menstrual period
Delayed menarche
Scanty and irregular menses
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
47

Review of Literature
Amenorrhea is often associated with infertility.
• Marital & Sexual History
Age at marriage
Marital life duration
Frequency & nature of intercourse
Use of fertile period ,
Dyspareunia,
Contraceptive measures
Period of noncontraceptive intercourse to be enquired.
• Obstetrical History :-This is necessary in secondary infertility.
• Psychological History: - marital disharmony plays a role in it well socially
adjusted couples also takes time for psychosexual coordination,
• General examination:-
Obesity / Extreme lean and thin Special emphasis given to obesity or
marked reduction in weight in recent years.
Hirsuitsm abnormal distribution of hair
Under development of secondary sex characters
• Systemic examination :-
Hypertension
Organic heart disease
Chronic renal lesion
Endocrinopathies
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
48

Review of Literature
Tuberculosis primary & secondary
• Gynecological Examination to be done to note the following
P/V Vaganitis
Chronic cevictits/erosion
Congenital elongated cervix
Hypoplastic uterus
Presence of Adenexal mass
P.I.D
P/S Visible thick & purulent cervical discharge
Pin hole cervix
Cervical erosion
New growth i.e., polyps
Ectropion/Entropion
CLINICAL EVIDENCE OF OVULATION
• Diagnosis of ovulation
1. Indirect 2.Direct 3.Conclusion
• Indirect method
Very regular 28 days menstrual cycle.
Ovulation anticipated by rise of body temperature & mild in pain in abdomen
with in 11th to 13th days
Thin cervical discharge during mid cycle
49
• B B T Method :- The body temperature is recorded in a special chart paper during
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
Review of Literature
whole month at the morning time ovulatory BBT is a biphasic drop of 0.50 F of
temperature followed by sustained rise by 10 F during luteal phase . In anovulatory
cycle Monophasic B B T is seen i.e., no rise during second half of cycle.
• Cervical & vaginal mucus study:-
Fern pattern Test:-
Alteration of the physical chemical properties of the cervical mucus occurs due
to the effect of estrogen & progesterone. Disappearance of fern pattern beyond 22nd
day of the cycle which was present in the midcycle is suggestive of ovulation.
Persistence of fern pattern even beyond 22nd day suggest anovulation. Progesterone
causes dissolution of the sodium chloride crystals.
Spinbarkeit test:-
There is loss of stretchability (spinbarket) which was present in the midcycle
due to high estrogen level during this period.
Sperm cervical mucus contact test:-
Equal quality of semen & mucus is mixed, so there is no interface. In presence
of antibodies more than 25% sperms show jerky or shaky movements by 30 minutes.
The cross check with the donor semen will indicate the source of antibodies. Whether
it is cervical or seminal antibodies.
Post coital test:-
Sperm cervical mucus interaction is detected in this test. mucus is removed
from the cervix with a nasal polyp forceps, a pipette or a tuberculin syringe and
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
50
Review of Literature
examined at various times after coitus with in 8 hr (sim's test huhner's test) to see if
the mucus is invaded by spermatozoa & whether they retain their activity.
The test must be carried out at the time of ovulation because at other times the
cervical mucus is normally unreceptive Examinations are advised within 2-8 hrs of
coitus normally 15 spermatozoa are found in each high power field & that these show
progressive, not rotatory activity. this suggests presence antisperm antibodies in
cervical mucus.
ASSESSMENT OF FEMALE INFERTILITY
Ultrasonography:-
• For follicular growth
• Endometrium thickness
• Luteinized enraptured follicle
USG is commonly used to track follicle development and is better observed
with transvaginal probe than with abdominal ultrasound. The follicle size at ovulation
is very variable but usually the dominated follicle is 14-16mm in diameter. Follicles
are larger in stimulated cycles, being 18-20mm in diameter and larger with
clomiphene than with human menopausal gonadotrophin ( hMG).
The endometrium increases in thickness from a thin broken line in the early
follicular phase to double its size, in the peri-ovulatory period it appears
sonographically as a triple layer in the, long axis of the uterus and is usually about 10-
12 mm in diameter. The luteal endometrium loses both the hyperechogenicity & the
triple layered appearance.
The diagnosis at luteinized unruptured follicle is made on ultrasound when the
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
51

Review of Literature
follicle does not rupture, although serum progesterone raises to follicular study
postovulatory levels.
Hormone Assays:-
• Serum Progesterone
Serum progesterone level measured during the midluteal phase is the most
reliable method of confirming ovulation.The minimum level being 6.5 ng /ml
& preferably over 10 ng / ml. Low progesterone level detected once
insufficient to judge the adequacy at the luteal phase.
• Serum LH
Detection of the preovulatory LH surge has also been used to predict
ovulation. Urinary LH lcits and salivary progesterone also have been used for the
same FHS:LH
• Thyroid hormones
Other hormones which may need to be assessed are free T3, T4 &TSH, Serum
FSH & LH in the immediate post menstrual phase.
• Serum Prolactin- Normal level is 5 -20 ng/ml
Endometrial Biopsy:-
Endometrial aspiration or biopsy taken in the premenstrual phase can be
histological dated. The procedure is still one of the initial outpatient investigations in
developing countries where genital tuberculosis is a significant problem.
Alternatively, it can be carried out in conjunction with laparoscopy under general
anesthesia. If the endometrium in the second half of the menstrual cycle is found to be
in a secretary phase, it can be presumed that during that cycle at least, the woman
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
52
Review of Literature
ovulated.
A diagnosis of luteal phase defect can be made if the endometrium is 2-3 days
out of phase from the day of cycle on repeated biopsy but this is not always accurate.
Curetted material is also sent for bacteriological evaluation for acid fast
bacilli.Polymerase chain reaction (PCR) for m.tuberculosis can be done in selected
cases depending on the clinical profile.
Tubal Patency Test
These are best carried out between the 7th to 10th day of the cycle. At that time
there is practically no risk of disturbing a fertilized ovum. The risk of embolism & of
retrograde dissemination of infection & endometriosis makes it imperative not to
carry out the tests while any uterine bleeding is taking place & for 2 days afterwards.
a) Hystero salpingo graphy(HSG)
b) Hystero contrast sonography ( HyCoSy)
TREATMENT
Couple instruction
• Reassurance
The infertile couple remains psychologically disturbed right from the
beginning more so as the investigation progress. In all cases optimism should be the
keynote, tempered with realism, even when the investigations suggest that the
prospects for pregnancy are poor.
• Correction of coital difficulties
Some couples require instruction on the difficulties of coitus on its timing &
spacing they should not be advised to try to time coitus to coincide with ovulation &
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
53
Review of Literature
to conserve their energies at other times. Conception is most likely between the 10th
to 18th days of a 28 day cycle at which time coitus should be practiced at 48 hour
intervals. Change in coital position can be tried in case of mechanical difficulty.
Immediately after coitus the wife should rest quietly for 10 minutes to ensure that
some semen remains in contact with the cervix.
• Correction of general ill health
Attention to matters such as overwork anxiety, obesity & intemperance in
smoking & drinking. A long care free holiday may sometimes be the answer.
Medical Treatment Of Female Infertility
• The only clear indication for hormone therapy is a proven failure of
ovulation.
• In practice this generally means infertility which is associated with
amenorrhea or Oligomenorrhoea.
• Even in such cases ovulation can never be induced unless the ovaries
contain ova capable of being stimulated.
• To facilitate effective folliculogenesis & ovulation the following drugs may
be helpful.
1) Clomiphene citrate
• ovulation should be induced with clomiphene citrate (CC) with a dose of
50 mg/day starting from day 2 to day 6 of the cycle.
• ovulation is monitored by serial ultrasound monitoring of follicular size
and occurrence of ovulation.
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
54
Review of Literature
2) If C.C fails then FSH & HCG therapy.
3) In hypothalamic disorder: GnRH is given to stimulate the pituitary FSH & LH and
folliculogenesis monitored.
4) Combination of CC+hMG (PCOD). CC 50 to 100 mg/day from 2 to 6 days.
Inj hMG 75 units’ intramuscularly on day 3, 5, 7 & more if so required.
5) Prednisolone: women with anovulation & increased androstenedione. 5.0 mg
prednisolone at night + 2.5 mg every morning until spontaneous
ovulation.
6) Hyperprolactinaemia: bromocriptine 1.25 mg at bedtime daily for 7 days.
7) Laparoscopic ovarian drilling: In PCOD medical line of treatment fails,
laparoscopic ovarian drilling of follicles with monopolar cautery/ laser.
8) Corpus luteal phase defect: Treated with intramuscular progesterone 100mg or
micronized 300-600 mg vaginal tablet daily.
9) For with LUF Luteal phase insufficiency treatment with micronized progesterone
or hCG.
Surgical Treatment:-
1) Wedge resection to induce ovulation in case of failure in response to clomiphene
citrate.
2) Surgery to ovarian tumor
3) Tuboplasty or microsurgery in case of peritubal adhesions, inflammatory
endosalpingeal damage & tubal occlusion by infection. Tuboplasty can be done in the
following methods:-
a) adhesiolysis -- separation or division at adhesion
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
55
Review of Literature
b) Fimbriolysis -- separation of the fimbrae to open up the abdominal ostium.
c) salpingotomy -- to create a new opening in the occluded tube.
d) Tubo tubal anastomosis .
e) Tubo corneal anastomosis.
f) Gilliam's type of operation for retroverted uterus
g) Myomectomy-- specially in sub mucous fibroid.
h) metroplasty
i) Apart from cauterization amputation of the cervix may have to be done for
congenital elongation of the cervix.
j) Enlargement of the vaginal introitus (Fenton’s operation) or removal of
vaginal septum causing dyspareunia.
Assisted Reproductive Technology
ATH -- Artificial insemination Husband
TTH -- Therapeutic, Insemination Husband
AID -- Artificial Insemination of Donor
TID -- Therapeutic Insemination of Donor
IUI -- Intra Uterine Insemination
IVF-ET -- In Vitro Fertilization & Embryo Transfer
GIFT -- Gamete Intra Fallopian Transfer
ZIFT -- Zygote Intra Fallopian Transfer
MIST -- Micro Insemination Sperm Transfer
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
56

Review of Literature
DRUG REVIEW
DHATAKI
Synonyms:
Dhataki, vahnipushpi, tamrapushpi, dahani, parvati, kumuda, guchhapushpa, madani,
pramadani, bahupushpi, vahnijwala, dhatupushpi, kunjara, subhiksa, madhyavasini.
Eng : Downy grislea or fire flame bush. Hindi : dhaya.
Kan : dhataki Marathi :Dhalasa
Lat : woodfordia floribunda kurz (salisb). Family : Lytheraceae.
Kula : Madayantika kula (dhayati kula).
Varga:Chandanadi - (Dha.Ni), Pippalyadi – (Ra.Ni)
Gana : purishasangrhaniya, Mutravirajaneeya, sandhaniya,- (Charaka )
Priyangvadi, Ambashthadi –(Sushruta)
Habitat : all over India , mainly at hilly regions.
Properties :
Guna- Laghu, Ruksha .Rasa – kashaya, katu.
Virya – sheeta. Vipaka – katu.
Karma : grahi, Garbhastapana, vishaghna, krimighna, sandhaniya.
Dosha : kapha-pitta nashaka Dhatu : rakta(hemostat), majja(narcotic).
Botanical description: A shrub with many branches, Leaves – sessile, resemble
pompgranate leaves, 5-10 cm long, stalkless, the leaf is hairy from beneath because at
which it looks wheatish. Flowers – shiny, red coloured,Seed – is grey and slimy, The
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
57
Review of Literature
plant bears flowers in winter and fruits in rainy season, leaves and new branches have
black spots on them.
Parts used : Flowers, Leaves. Dose: 1 -3gm
Chemical composition : Flower contains 2% tannin & glucosidellagic acid, β-
sitosterol, polystachoside, octacosanol, myricetin-3-galactoside, cyanidind-3, 5-
diglucoside, pelargonidin-3, chrysophanol-8-0-B-D-glucopyranoside.
USES :
External uses :Being refrigerant, haemostatic, wound healer, powdered flower is
sprinkled externally over bleeds and wounds, powder flower is rubbed over gums to
prevent teething problems & the juice is used for massage in headache induced by
pitta.
Internal uses :
Reproductive system: useful in per vaginal discharges. In menorrhagia or
leucorrhoea it is given either with rice water or honey.
Therapeutic uses:
1. Swetapradara: Dhathaki powder shall be given with honey
2. Prajasthapana: Nilotpala & dhathaki flower are mixed & taken with honey in the
morning during the rutukala(Ga.Ni)47
Important formulations:
1. Dhatakyadi taila, 4. Dhatakyadi churna,
2. Pushyanuga churna, 5. Aravindasava,
3. Brahat gangadhara churna,
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
58
Review of Literature
DARUHARIDRA
Synonyms – Daru haridra, dravi, pitadra, pitika, kaleyak, peetadaru, sthiraraga,
kamini, katankaderi, pajranya, pitadarunisha, kaliyaka, kamavati, darupita,
pachampcha, karkatakic.
Eng: Indian Berbery Hindi : Daru haldi
Kan : Maradarishina Marathi : Daru haldar
Lat: Berberis aristata. Family: Berberidaceae.
Kula : Daruharidra Kula.
Varga : Pippalyadi , prabhadi, daruharidradi, gudduchadi varga
Gana : Arshogna, kandughna, lekhaniya – (Caraka)
Haridradi, musthadi, lakshadi –( Susrutha)
Habitat : Himalaya from chota Bengal to Nepal.
Properties :
Guna- Laghu , Ruksha Rasa – Tikta Kasay
Virya – Ushna Vipaka –Katu
Karma : Kapha pittahara chedana, sthanya shodhana, sthanya doshahara,dosha
Pachana
Dosha : Reduce kapha Dhatu :Meda, Rasayana, raktagami
Mala – Mutra- purisha , sweda Organs – Eye, liver, spleen and skin.
Botanical description: Evergreen shrub having height 1.25 to 3 meters Leaves – are
strong with fine whorled venation. Strength, but with dentate or corrugated margin,
dark green above pale beneath.
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
59

Review of Literature
Inflorescence – 5 to 8 cms long, with large yellow color flowers. Fruits – Bluish,
purple and small. Flowers – Bloom in the spring and fruits in the winter.
Different varieties:
Berberis aristata Berberis chitra
Berberis lyceum
Part used – Root , stem. Fruit, extract
Chemical composition : karachine (a protoberberine alkaloid), taxilamine, berberine,
palmatine, jatrorrhizine, oxycanthine. Stem & root contain the alkaloid berberine.
Dose : Juice of root 10 – 20ml Kwath – 5-10ml Ghanasatwa- 500mg – 1 gm.
Indications:- Prameha, kustha, netraroga, swetapradara, kamala, varuna, visarpa.
Therapeutic / Internal Uses:
Reproductive system – Useful in uterine inflammations and vaginal discharges.
Sweta pradara – Decoction of daruharidra given with honey
Mutra krccha – Daru haridra kwatha and amalaki with honey
Pradara – Daryadi kwathaa
Important formulations :
1. Ashwagandha arista 4 Bhrangaraja Taila
2. Khadiradi gutika 5 Khadira arista
3. Jatyadi taila 6 Triphala gratha
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
60

Review of Literature
BALA
Synonyms: Bala, odanika, bhadra, samanga, baladhya, vatika, sanasa, maha
samanga, kharayahtika, sheetapaki, veeryabala.
Eng : Country mallow Hindi : Variyara
Kan :Hettuti Marathi :Chikana
Lat : Sida cardifolia linn. Family: malvacea
Kula : karpasa kula.
Varga : Karpasadi varga –( Nighantu adarsha)
Shatavyadhi varga –( Raj Nighantu)
Gana : Balya, Brumhaniya, Prajasthapana
Madhuskandha – (Charaka)
Vatasamshamana –( Susrutha)
Habitat :All over the India
Properties :
Guna- Guru, snigdha, picchila Rasa – Madhur
Virya – Seeta Vipaka –madhura
Dosha : Tridosha Dhatu:Rakta,Mamsa,Shukra,Oja
Karma : Vrishya, balya, tridoshanashaka, oja, vriddikara Mala: -Purisha
Botanical description: A small shrub of height 5-10cm .Root and trunk are stronge
hence it is called as bala. Leaves : -Alternate 2.5 – 5 cm long 5 cm broad,
ciliate,round having 7-9 veins on it and serrated margin.Flowers : -yellow in color
and originate from the angel of the leaf stalk. Flowers have five petals and five
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
61

Review of Literature
sepals.Fruits – like a moonga divided into five partsSeeds: -Small, dusky are called
as beeja bandha.The plants bears flowers and fruits at the end of rainy season.
Different varieties:
a. Bala c Atibala
b. Mahabala d Nagbala
Part used:- moola, patra, beeja, panchanga
Chemical composition:- Measures components of seeds are alkaloids mainly
ephedrine. It is also contains fatty acids, musin, potassium nitrate and resin
Dose :Churna 1-3 gm Swarasa 10-20ml
Uses :
External uses: Paste is analgesic alleviates edema it is locally applied over
inflammation and eye disorders.
Internal uses :
1. Being neural tonic and vata shamaka used in paralysis, facial palsy.
2. Emollient, deflatulent and astringent useful in flatulence, sprue
3. Cardiac tonic and alleviates hemorrhagic disorders
Reproductive System: Aphrodisiacs & useful in spermatirrhoea, 46
Diuretic so useful in dysuria being tonic it is helpful in
general debility tuberculosis & undernourishment
Important formulations :
1. Baladi kwatha 3. Baladhya ghrita
2. Baladhyaarista 4. Chandana bala lakshadi taila
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
62

Review of Literature
PALASHA
Synonyms – palasha, kimshuka, raktapushpaka, ksharashrestha, brahmavruksha,
samidwara, tripana, vakrapushpa, trivrunta, parna, yagniya, vatahara.
Eng : Downy branch Butea or Bastered peak Hindi : Dak, palasha.tesu
Kan :Muttuga Marathi :Palasa
Lat : Butea monosperma (linn) kuntz Family: Leguminoceae or pappilonaceae
Kula : Simbi kula Upakula – Aparajita kula
Varga : Vatadi varga –(Bha. Ni) Karaviradi varga – (Ra Ni)
Gana :Rodradi , mushakadi, ambasthadi Nyagrodadhi –(Susrutha)
Habitat :Entire India
Properties :
Guna- laghu, snigdha, sara Rasa – Katu, tikta, kasaya
Virya –Seeta Vipaka –Katu
Dosha : kaphavata shamaka
Karma :Agni deepana, saraka, vrsya, sandhaniya, grahi, kusthaghna, rakta stambana
Botanical description: Tree grows 13-16m high stem is crooked with torn bark,
Leaves --10-15 cm long. Flowers – Beautiful red colored, grow in spring. It has pale
yellow trek from which dark saffron color is deribed legume 12-20 cm long 2cm
broad and contains flattened, round, reddish black seeds, gum oozes from the cracked
bark which is known as Butea gum or Bengal kino.Flower bloom in spring and then
tree bears fruits. In summer the blossomed tree is very attractive saffron color of the
is used for ranga panchami which is known as kimshuka.
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
63
Review of Literature
Different varieties:
1. Rakta pushpa 3. Peetapushpa
2. Sitapushp 4. Neelapushpa
Part used – bark, flowers, leaf , gum and seeds
Chemical composition: Bark and gum contains kino and tannic acid. 50% gallic acid,
seeds contain 18 %, Stable oil which is called as kino oil.
Dose : Flowers powder 10 – 30gms, Kwatha – 5-10tola, Puspa – 1 – 1 ½ mashi
Uses :
Internal uses : Krimi, raktabhishyanda, raktapitta, jwara, daha, sharkara- Susrutha
Twak roga, arsha, atisara mutrakricha - Caraka
Reproductive system
Gum is aphrodisiac, seed is stimulant and flowers are astringent, Gum is given
orally in sperm debility.
Decoction of flower is useful in vaginal discharges.
For pumsavana karma leaf of palasha is used.(Y.R)45
For garbhinee paricharya in 1st month it has been indicated,
Important formulations :
1. Kumkumadi taila 4. Palasha kshara
2. Vanga bhasma 5. Palasha beejadi churna
3. Palsha pushpasava 6. Krimimudga rasa
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
64
Review of Literature
PUTRANJEEVAK
Synonyms: Putranjiva, pavitra, garbhad, sutajivaka, kutajiva, apathyajiva, siddhid,
arthasadhaka, garbhakara, kumarbeeja, akstaphala.
Eng : Child-life tree. Hindi : Jeeyapota, pittojeeya, pitijeeya.
Kan : Putrajiva, Putrajivaka. Marathi : Putrajivaka vruksha.
Lat : Putranjiva roxburghii Roxb. Family : Euphorbeaceae.
Kula : Eranda kula. Gana:Arkadigana
Varga : Prabhadradi varga (Ra.Ni), Vatadi varga ( Bha. Ni), Amalakyadi –( Ni .Ad)
Habitat: Tropical territory of India
Properties:
Guna- Guru, ruksha. Rasa – madhura, lavana, katu.
Virya – sheeta. Vipaka – katu.
Dosha : Vatakapha nashaka Dhatu : Shukra, Artava.
Botanical description: leafy medium sized or large trees up to 15-18 m height.
Leave :obliquely elliptic oblong to ovate, coriacoaus, dark green above, glaucous
Beneath.
Different verities: Putranjiva eylanica, Muell. Arg(In shrilanka).
Parts used: Leaves, fruits, seed.
Chemical composition : seed contains fatty oil those are oleic, linoleic, palmitic,
stearic and arachidic. Fruit pulp contains large proportion of manitol and small
quantities of a saponin glycoside and unidentified alkaloids.
Dose : seeds powder 3-6gm ,leaves juice 10-20 ml
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
65

Review of Literature
Uses :
External uses : Its paste is useful as analgesic in headache, inflammation and abscess
Internal uses : Aphrodisiac and beneficial to foetus.
Decoction of leaves and fruits is given in fever and common cold
Also used for to obtained male child.
Root of putrjiva, visnukanta and shivlingi are recommended for eight days
during pregnancy 44
Specially the seeds of putranjivaka are given in sterility in order to promote
conception and also checks miscarriage
Susrutha – Sleepad Vangasena – Urograha
Bhava prakasha- VIsphota Nighantus – Garbhakara
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
66
Review of Literature
MUSHALI
Synonyms: Muusali, talamilli, sulvaha, talumulika, godapadi,hemapuspi, bhutali,
deerga Kaundika.
Eng : Asparagus. Hindi : Musali .
Kan :Nelatod. Marathi :kali and pandhari musali.
Lat : Asparagus adseenedenus Roxb. Family : Liliaceae.
Gana: Sukrajanana
Varga :Mulakadi varga (R.N),Mulsali kand varga (Ni.Ad), Guduchyadi varga (B.P)
Types:- Sweta and Krishna musali
Habitat: North India
Properties:
Guna-Guru snigdha Rasa –Madhura
Virya –sheeta ,ushna(Bhavamisra) Vipaka –Madhura
Karma : Shukrajana, Vrushya, Bala,Rasayana
Dosha :Vatapitta shamaka,Kapha vardhaka
Botanical description:
A thorny shrub like Asparagus racemosus stem long tall round and oily.
Branches greenish, hallow and ascending it is full of thick and straight throns
measuring 1-1.5 cm Leaves- stalk in long, hairy round, measuring 1.5-4cm and
bearing 6-20 foliates in racemose form. Roots- oblong.
Parts used: Root
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
67

Review of Literature
Chemical composition : Major chemical constituent. Two stigmastoid ,Glucosides,
saponin sars apogenin, Resin, Tanin, mucilar and starch and ash containing oxalate
and calcium.
Dose :3-6 gm powder
Uses: Bitter aromatic, tonic and demulicent, used in general debility in afflictions of
the urino genitor system as importance , also in asthama, piles, dysuriea, diarrhea.
Menorrhoea and gonorrhea. As a tonic it is generally mixed with aromatic
bitters and aphrodsiac, medications (R.N)
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
68

Review of Literature
MISHREYA
Synonyms: Chatra, madhurika, misi, salina, saleya. Talaparni, talapatra, sitashiva,
vanaja, avakapuspi, sanhita puspika, supushpa, suraja nad vanya.
Eng : Fennel seed Hindi : Saunf
Kan : Dodda sampu Marathi :Badi saunf
Lat : Feeniculum vulgarcea Family : Umbelliferacea
Kula : Shatapuspa kula
Varga : Hareethakyadi varga – B.P
Shatavarhadi varga –R.N
Habitat :All over India
Properties :
Guna- laghu, ruksha Rasa – madhura, katu , tikta
Virya –sheeta Vipaka –madhura
Karma :Deepana, hrudya, balya, anulomana, ama dosha hara.
Dosha : Vatapitta shamaka
Botanical description: Perennial plant, but usually of short duration with erect,
branched stem 0.5-1 m height. Leave – 3-4 times pinnate with very narrow Linear
and subulate segments. Flower: in white umbels 15-20 rays more or less glucose
Fruit :6 mm long the vittae very conspiluous .
Parts used : Beeja and mula.
Different varieties: Vanya , Gramya
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
69

Review of Literature
Chemical composition :Ascorbic acid, niacien, riboflavin, tocopherts, choline,
trigonelline, anethols, anisaldehyde, comphene, estrogole, fenchone, foeniculin,
methylchaviol, cynavin, columbianetin, marmesin, ostenenol, B-sitosterol, triterpenes,
umbelliferone. Fennel fruit contain oil. Fruit contains iodine, Vit. A, thiamine, traces
of albumin barium,cithinium, copper, manganese, silicon and titanium have been
reported.
Dose :beeja churna 3-6 gm.
Uses : Artava janana.,Stanya jana.
In kastartava and sutika streeJwara, adhmana, shoola, raktavikara, stanyalpata,
mutrakraccha, pravahika and shukra khsya
Important formulations :
1. Misreya arka
2. Mishrakadi churna
3. Dhanyakadi hima
4. Dhanyaka panchaka kasaya
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
70

Review of Literature
SHIVALIGNI
Synonyms: Lingini, Shivaligni, Chitra, phala, Lingini, Pahupatra, Iswanri,
Shaivamallika, Swayambhu, Linga Sambhuta, Lingi, Amrutra, Pandoli, Lingaja devi
chanda, Apastambini, Shivaja & Shivavalli.
Eng:- Bryony Kan:-Shivalingi
Hindi:- Shivaligni, Marathi :Kavale che dole, Analgesic.
Lat : Bryonia lacinosa. Family : Cucurbitaceae
Varga : kushmandadi Varga
Guduchyadi
Habitat :Southern part of Indian in konkar region
Properties :
Guna- laghu, ruksha Rasa – Katu, Ruksa
Virya –Ushna Vipaka –Kata
Karma:- Rasayana vrishya.
71
Botanical description:-Annual slender herbs, glabrous, spreading climbers. Leaves
deeply palmately 5-lobed, 8-12 cm in diameter , 5 cabrous above, smooth, beneath,
margin denticulate undulate. Penduncle(in male flowers ) 5-15mm long, calyxtube
2-4*3-6mm, lobes spreading 1mm long, corolla greenish-yellow, shortly papillose 4-
10mm, broad lobes ovate, acute filaments 1-15mm long, anothers ca 2mm long,
female flower fasciculate, ovary globose. Flowers monoeicious, often male & female
clastered togethers. Calyx companule, lobes Subulate corolla campanulate, 5 partite,
segments often refleved pendicels shorter in male flowers. Fruits berries sphevicle
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction

Review of Literature
yellowish green 6 strippe, 12-17mm thick up to 2cm across seeds avoid with
thickened corrugated margins seed cal 5*3 mm grey flowering & furting during the
period from august to December.
Parts used: Seeds
Dose: 3-5 grams.
Internal Use
For pumsavana karma seeds are given with milk 48
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
72

Review of Literature
PERPARATION OF GANASATWA
Indigenous drugs( Putra mjivaka, Shivalingi, Palasha, Dhataki, Daruharidra,
Bala, Mishrey, Musali) are collected from herbal garden under the supervisation of
experts of Dravyaguna Department and dried well in ventilated room. Then Yavakuta
Churna of Indigenous drugs are prepared in udukhala yantra and placed in vessels.
Then added 48 liters of water and subjected to Mandagni. Throughout the procedure,
mandagni is maintained until the quantity is reduced to ¼ (marked on a stick and
dipped into the liquid content). The vessel is removed from gas and kashaya is filtered
in separate vessel. Kashaya obtained by this process is = 11 liters.
b) Preparation of Ghansatwa
Apparatus : Vessel, Gas stove etc.,
Drugs : Kashay of Indigenous drugs.
Quantity : 11 liters.
Procedure
Kashaya of Indigenous drugs is placed in vessels, and subjected to Mandagni
and stirred well. After 10 – 11 hours, the kashaya become semisolid then mild heat is
given and stirred more carefully. After a period of 2 hours, it was dried and then
removed from the gas stove. Then it is dried in to shade and the obtained churna
(dried powder of decoction) and it is about 1.75 kg. It is filled into capsule sheath of
500mg.
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
73

Review of Literature
Fig No. 2 Musali Fig no. 3 Daruharidra
Fig. no. 4 Bala Fig No. 5 Palasha
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
74

Review of Literature
Fig No. 6 Dhataki Fig No. 7 Shivalingi
Fig No. 8 Misreya Fig. No. 9 Putranjeevaka
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
75
Review of Literature
Fig No. 10 PREPARED TRIAL DRUG GHANASATWA
Fig No. 11 Capsules of Ghanasatwa
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction
76
Materials & Methods
A Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 77
MATERIALS AND METHODS
The present “Clinical study on Apraja vandhya (primary infertility) by an
indigenous compound WSR to ovulatory dysfunction” was carried out on 30 infertile
women attending the OPD of prasooti tantra and stree roga department, N.K.J.
Ayurvedic Medical College and P.G Centre attached Sri Siddharoodha charitable
hospitals. The study included primary infertility cases of varying age and duration of
infertility.
Criteria for selection of cases
Inclusion criteria
1. Married women of age group between 20-35 yrs.
2. Patients having symptoms of Apraja vandhya ( Primary infertility)
3. Scanty, Irregular period with anovulation
Exclusion Criteria
1. Patient suffering from STD,HIV, and Hepatitis B
2. Patient suffering from any systemic diseases like DM,TB
3. Hyper and Hypothyroidism
4. Patients with severe anemia
5. Secondary infertility
6. Nephritis
Subjective Parameters
1. Irregular and scanty menstrual history
2. Primary infertility

Materials & Methods
A Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 78
Objective Parameters
1. B.B.T
2. Cervical mucus study
3. Sonography (Follicular study)
A detailed history of all the cases was recorded in a specially prepared
proforma. The general examination and pelvic examination including per speculum
and bimanual examination were performed and noted in the case paper.Labrotary
investigations were carried out as per necessity
1. Blood – Hb %
W.B.C (TLC and DLC)
E.S.R
2. Urine - Albumin
Sugar
Microscopic
3 Cervical mucus study (on 14th day) to check the
Nature
Viscosity
Fern pattern
Thread ability or Spin barkiet
MATERIAL

Materials & Methods
A Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 79
Individual drugs Viz. (Putramjivaka,Shivlingi, Palasha, Dhataki, Daruharidra,
Bala, Mishrey, Musali) are collected from market under the supervision of dravya
guna specialist. Ghana satva of these drugs are prepared at Rasa shala according to
standard method mentioned in the Ayurvedic text under the supervision of Rasa
shastra department.
This Ghanasatwa (capsules) is administered orally in the dose of two capsules
TID with warm milk as anupana for 20 days (from 5th day of menses up to 25th day)
for 3 consecutive cycles, assessment done after each cycle.
METHODS
Patients fulfilling above criteria were assigned into two groups.
GROUP A – 15 patients will be given trial drug Ghanasatva in a capsule form
GROUP B – 15 patients will be given placebo.
Follow up – Evaluation of symptoms will be done before treatment after 1st
cycle, 2nd cycle and 3rd cycle.
ASSESMENT CRITERIA
The clinical assessment was made depending upon the changes in the
subjective and objective features as mentioned in assessment scale.
1. Fertility or Amenorrhea along with positive response in velocit kit.
2. Ovulation positive by follicular study ( ovulatory study)
3. Regulation and relief of associated symptoms of menstruation
4. Relief from sexual problems
5. Relief from other associated symptoms
ASSESSMENT SCALE

Materials & Methods
A Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 80
Fertility will be assessed by absence of menstruation or amenorrhea followed
by positive U.P.T
Ovulation will be assessed by follicular study.
a. Ovulated G0 0
b. > 20 mm ( non ovulation ) G1 1
c. 12 – 20 mm follicular size G2 2
d. < 12 mm follicular size G3 3
Dysmenorrhoea
a. No dysmenorrhoea G0 0
b. Mild dysmenorrhoea G1 1
c. Moderate – dysmenorrhoea G2 2
d. Severe dysmenorrhoea G3 3
Oligomenorrhoea
a. 3 days G0 0
25 – 30 days
b. 2 days G1 1
30 – 35 days
c. 1 day G2 2
35 – 40 days
d. 1 day G3 3
40 -45 days
Bleeding Duration

Materials & Methods
A Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 81
a. 4-5 days – G0 0
b. 3-4 days – G1 1
c. 2-3 days – G2 2
d. 1-2 days - G3 3
Interval duration
a. 28-30 days G0 0
b. 30-35 days G1 1
c. 35- 40 days G2 2
d. more than 40 G3 3
Cervical mucus Viscosity
a. Thin viscous (Normal) G0 0
b. Mildly viscous G1 1
c. Intermediate G2 2
d. Thick viscous G3 3
Ferning
a. Tertiary Ferning G0 0
b. Primary /secondary G1 1
c. Atypical Ferning G2 2
d. No fern G3 3
Spin Barkeit
a. > 9 cm G0 0

Materials & Methods
A Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 82
b. 5 to 8 cm G1 1
c. 1 to 4 cm G2 2
d. < 1 cm G3 3

Discussion
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 111
DISCUSSION
It is a clinical study to evaluate the efficiency of indigenous compound in
vandhyatva.
Vandhyatva has been a long standing problem of human community right
from ancient period up to this modern era.
If we think the antiquity of the vandhyatva, we can see the praise of the
women having children & slander of the barren women & the solutions to her
barrenness are also mentioned in the Vedas, Upanishadas & Puranas.
In samhita kala charaka has explained types of vandhyatva as apraja, sapraja
& vandhyatva.Harita has described vandhyatva as a disease, in eighty vataja vyadhi.
He has defined vandhyatva as a failure to achieve a child rather than pregnancy
because he has included Garbhasravi, Mritavasta, Garbhakostha Bhanga, Balaksaya,
Kakavandhya, Anapatya.
Sashruta described the causative factor for vandhya is artavavaha srotovighata.
Vandhyatva is described by our Acharyas in a very wide sense including the
nidana & chikista, but the etiological factors held responsible for infertility according
to modern science can not be correlated with nidana mentioned in ayurveda, similarly
is the case with treatment so many formulations has been given in our texts for
achieving a conception, but at which type of infertility or on which factors like Ritu,
Kshetra, Beeja, Ambu it will act it is not mentioned clearly.
Now in these days of research in Ayurveda in modern era of science it is the
need of time that we should evaluate all these things separately.

Discussion
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 112
30 patients were taken for the present study after proper clinical & laboratory
investigations according to inclusion criteria are divided in two groups.
Group A:-15 patients treated by trial drug i.e.,indigeneous compound of
(Putramjivaka,Shivalingi,Palasha,Dhataki,Daruharidra,Bala,Mishery,Musali)ghanasat
wa filled in capsule at a dose of 500mg trice with milk for 3 cycles.
Group B: - 15 patients treated by placebo at a dose 3 gm BD with milk for 3
cycles.
After each cycles assessment was done using selected parameters to know the
improvement.
Probable mode of Action of the Drugs
In this compound eight drugs mainly Putramjeevaka, Shivalingi, Palasha,
Dhataki, Daruharidra, Bala, Mishery, Musali are prepared,
1. Putramjeevaka (Putramjiva roxburghii)-Having the properties of guru, ruksha
guna, madhur, katu, lavana rasa katu vipak & sheeta veerya having the action
of vata kapha shamak & it has specific impact on the Garbha to form the male
in the contemporary science. But in modern science it has anti-inflammatory
& analagesic action.
2. Shivalingi (Bryonia Lacinios): Having the properties of guru, ruksha guna,
katu, tikta rasa ushana virya katu vipak & action has Rejuvenator,
Aphrodisiac, & promotes the body constituents, Since Medieval period it has
been used treat the infertile women’s to achieve conception. Where the recent
research shows it has Anti-tumor, Antioxidant action & also acts as a uterine
tonic with non-hormonal, Anti-inflammatory, Antispasmodic & Analgesic
action are used to treat DUB & PCOD.

Discussion
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 113
3. Palasha (Butea monosperma): Having the properties of laghu, snigdha, Sara
guna, katu, tikta, kasaya rasa, katu vipak & sheeta veerya acts as katha vata
shamak it has actions to increase the Agni, Binds the body tissue works as
Haemostatic agent, Purifies blood & acts as Aphrodisiac. The specific action
for to achieve the conception & in first month Grabhinee Parcharya has been
given imphasiase in the ancient text, as per the recent research it has non-
hormonal Anti inflammatory action.
4. Dhataki (Woodfordia fruticosa): Having the properties of guru, ruksha guna,
kashaya, katu rasa, katu vipak, sheeta veerya action as Kapha Pitta Shamak &
special action as haemostatic, body tissue binding & helps for fertilization &
fetal growth as per the recent research Anti-inflammatory action.
5. Daruharidra (Berberis aristata D C): Having the properties of laghu, ruksha
guna, tikta, kasaya rasa ushana virya, katu vipaka& action as kapha nashaka &
it works as Rejuvenator, Aphrodisiac, blood purifies & special used in uterine
inflammation & vaginal discharges & in the urinary tract infection it is used as
diuretic as per the modern science it is used as Antispasmodic &
Immenagogue action.
6. Bala (Sida cardifolia): Having the properties of guru, snigdha, pichila, guna
madhura rasa, madhura vipak, and sheeta veerya & tridosha nashaka. Special
action as Rejuvenator, Aphrodisiac, nutritive & increases the oja. Where the
recent research it has Antioxidant action & having progesterone like substance
which helps for proper conception & normal growth of fetus.
7. Mishreya ( Feeniculum vulgare, apiacae) : Having the properties of guru,
ruksha guna, madhura, katu, tikta rasa ,sheeta veerya, madhura vipak, action

Discussion
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 114
as kapha, vata nashaka, increases agni, Immenagogue, Galactogogue, purifies
blood as per the recent research act as Estrogenic action, Antioxidant, Anti-
inflammatory & Analgesic action.
8. Musali (Asparagus adscendens Roxb); Having the properties of guru,
snigdha,guna madhura rasa, sheeeta veerya, vata, pitta, shamaka & has a
action of Rejuvenator, Aphrodisiac, mainly used in UTI, & as per the modern
research it’s action is Stimulate Insulin, increase sexual desire, prostaglandin
release & Antispasmodic action.
OBSERVATIONS
Age: - For assessment of infertility we have selected the patients among age
group of 20-35 yrs .which is divided in to 3 groups. In that 20-25yrs age group are
40% and 26-30yrs having 46.66%, and 31-35yrs having 13.33%. In the 26-30yrs, age
group fertility problems detected and now a day the marriage age is increased. So we
get more number of patients in this age group.
Marital Life:-In present clinical trial patients belonging to 1-5yrs period of
marital life are 46.66% and 6-10yrs having 50% and 11-15yrs No patients and 15-
20yrs 3.33%. In the modern era life style has been changed. Couples don’t want child
very fast. The carrier conscion couple postpones the fertility for 2to3yrs. Then they
think about & so delayed fertility is turned in to problematic fertility.
Socio –Economic Status:-In this clinical study majority of patients are taken
from lower middle class i.e., 46.66% & upper middle class 36.66% & poor are
16.66%. Because of deficient nutritive diet and neglected irregular periods became
troublesome after marriage and contributes to infertility.
Discussion
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 115
Education Status:-In this clinical trial patients belongs into primary school
33.33% and high school women are 33.33% and graduates are 30% and uneducated
women are 3.33%.
Infertility Duration :-In present clinical trial patient belonging to 1-5yrs
periods infertility duration are 60.00% and 6-10yrs period 36.66% and 11-15yrs
period 3.33%.
Occupation: - In present clinical trial patient belonging to 53.33% house wife,
10.00% Government job, 26.66% Private Job & 10.00% are labors.
Menstrual History:-In this study majority of patient belong to irregular
menstrual cycles are 53.33% and 46.66% are having regular cycles.
Bleeding Duration:-In present clinical trial patient from 1-2 days, which is
having 16.66% and 2-3days are 23.33% and 3-4 days are 36.66% and 4-5 days are
23.33%.
Interval Period:-In this clinical trial 28-30 days period are 46.66% and 30-35
days period are 13.33% 35-40 days period are 33.33% and more than 40 days are
10.00%
Character of Menstrual Bleeding:-In this clinical trial character of menstrual
bleeding with normal flow are 66.66%, with cloth are 30.00% and with heavy
bleeding are 3.33%.
Uterine Position: The above study shows that 83.33% of patients are having
normal AV/AF uterus and 16.66% of patients are having RV/RT uterus.
Vaginal Discharge:-The above clinical study shows that the normal vaginal
discharge is present i.e., 46.66% and vaginal discharge is absent i.e.,53.33% out of 30

Discussion
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 116
cases.Becouse vaginal discharge decreases the cervical hostility which results the
ifflusium semenis and infertility.
B.B.T:-BBT chart was given to all patients to mark the temperature at
morning time, but some patients did not follow the instruction. Due to inconvenience
we exclude this observation .We had another parameters for detection of ovulation
like follicular study and cervical mucous study for confirmation of ovulation.
Effect of Treatment:-
Effect of treatment was accessed both clinically as well as by lab investigation
included. Cx-mucus study & ultrasonography for follicular study in very cycle.
Observation of 30 patients have been presented with the data are recorded in
previous pages. The critical & descriptive note on the data as follows.
Effect on Dysmenorrhoea: -
When the Dysmenorrhoea is considered then 80.00% got cured in group-A
and 45.16% got cured in group-B. This shows group-A is more effective than
group-B.
Oligomenorrhoea: -
When the Oligomenorrhoea is considered then 80.00% got cured in group-A
and 46.88% got cured in group-B. This shows group-A is more effective than
group-B.
Bleeding Duration: -
When the bleeding duration is considered then 83.87% got cured in group-A
and 52.78% got cured in group-B. This shows that group-A is more effective than
group-B.
Discussion
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 117
Interval of Bleeding: -
When the bleeding duration is considered then 84.85% got cured in group-A
and 52.78% got cured in group-B. This shows that group-A is more effective than
group-B.
Cervical Mucus Study:-
Viscosity: -
When the viscosity considered than 81.82% got cured in group-A and 35.48%
got cured in group-B. This shows that group-A is more effective than group-B.
Ferning: -
When the Ferning considered than 80.65% got cured in group-A and 34.38%
got cured in group-B. This shows that group-A drug is more effective than group-B
drug.
Spin Barkeit: -
When the Spin Barkeit considered than 80.65% got cured in group-A and
34.48% got cured in group-B. This shows that group-A is more effective than
group-B.
Follicular Study: -
When the Follicular Study considered than 82.86% got cured in group-A and
57.14% got cured in group-B. This shows that group-A drug is more effective than
group-B drug.
Special Observations: -
During the clinical study in Group-A out of 15 patients only 3 patients
conceived and Group-B out of 15 patients No patients are conceived.

Conclusion
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 118
CONCLUSION
1) Primary Infertility is a condition where the couple never conceives after one
or more years of regular & unprotected intercourse.
2) Though the defect in process of fertilization lies in both partners the female is
responsible to 40-60% of cases.
3) Commonly the lacuna in female reflects as irregular & scanty menstruation
which suggestive of defective ovulation, thus contributes 20% cases.
4) Primary Infertility correlated with Apraja vandhya or Adi vandhya, Anapathya
advised to be treated with a fruitful result by herbal medicines.
5) Patients with ovulatory dysfunction charecterised by menstrual abnormalities
were selected & treated with indigenous compound ghanasatwa.
6) The idigenous medicine(ghanasatwa) was prepared (Shivalingi, Putramjivaka,
Palasha, Dhataki, Daruharidra, Bala, Mishery, Musali) as per classical
preparation method.
7) Based on their individual action like Anti-inflammatory, Analgesic,
Antioxidant, Estrogenic, Progesteranic on female reproductive system, they
were found to be effective & normalizing & regularizing the menstrual
abnormalities & ovarian dysfunction.
8) However the present clinical study shows effectiveness of Shivalingi,
Putramjivaka, Palasha, Dhataki, Daruharidra, Bala, Mishery, Musali upon
ovarian dysfunction & menstrual problems. Probable action of drug may fully
established with a large sample size in further research.

Summary
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 119
SUMMARY
This study entitled ‘A Clinical study on Apraja Vandhya(Primary Infertility) by an
indigenous compound W.S.R to ovulatory dysfunction was designed under 5 parts.
Part - I : Conceptual study
Part - II : Drug review
Part - III : Clinical study
Part - IV : Discussion
Part - V : Conclusion
Part - I : Conceptual study
It comprises the following sections.
Section -1
Historical Review:
This section comprises historical aspect, which is related to disease.
Section -2
Ayurvedic Review:
The general description of vandhyatva like vyutpatti, nirukti, paribhasha, synonyms,
samanya nidana, bheda, samprapti and chikitsa is explained.
Section -3
Modern Review :
In this functional anatomy of ovary, An ovulation & Infertility definition, incidence,
synonyms,causes,clinical,manifestation,pathogenesis,pathology,pathophysiology,
classification, symptoms, investigations, and principle of management.

Summary
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 120
Part – 2 : Drug Review
A general introduction regarding the importance of drug and treatment approach.
The description of trial drug regarding its guna, karma, etc & preparation of drug.
Part – 3 : Clinical Study
In this part aim and objectives, material and methods, selection criteria of patients,
drug dose duration, criteria for assessment of result, scoring pattern, general observation and
effect of therapy in different headings along with total effect of therapy.
Part – 4 : Discussion
Here total report of descriptive discussion based on conceptual study and clinical
study are included. Mode of action of drug is also focused here.
Part – 5 : Conclusion
Conclusion drawn at the end of study.
Bibliography
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 121
BIBLIOGRAPHY
1. Pandit Ramagovind Trivedi, Rigveda samhita, Vol. Ist , Varanasi,
Chaoukhambha Vidhyabhavana. PP: 888
2. Pandit Ramaswaroopa Sharma Goud, Atharavana Veda samhita, Vol- III,
varanasi Chaoukhambha Vidhyabhavana. PP:149, 481.
3. Pandit Ramaswaroopa Sharma Goud, Atharavana Veda samhita, Vol- IV,
varanasi Chaoukhambha Vidhyabhavana. PP:583,587.
4. Dr. Bramhanand Tripathi, Charaka Samhita, Vol-I, Re-printed, Varanasi,
chaoukhambha Surabharti Prakashan, 2004 : PP:888, 938,448.
5. Sri narsimha Kavacha http://www.hknet.org Google.com
6. Pandit Kashinath Shastri, Charaka Samhita of Agnivesha, Part II, Eight
Edition,Varanasi, Chaoukhambha Sanskrit Sansthana, 2004: PP: 756,770,755
7. Kaviraj Dr. Ambika Datta Shastri, Susrutha samhita of Susrutha, uttaratantra,
(Part II), 17th Edition, Varanasi, Chaoukhambha Sanskrit Sansthana,
2003:PP:157
8. Porf. (KM) Tewari,P.V, Kasyapa Samhita,Re-Printed, Varanasi,
Chaoukhambha Visvabharati, 2002:PP:357,381,282.
9. Pandit Hariprasad Tripathi, Haritha Samhita, Ist Edition, Varanasi,
chaoukhambha, Krishnadas Academy,2005:PP:448.
10. Prof. Yadunandana Upadhyaya, Madhava Nidanam, Part II, Re-Printed,
Varanasi, Chaoukhambha Prakashan,2009: PP:593,594, 424
Bibliography
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 122
11. Raja Radhakanta Dev, The Sabda Kalpadruma, Vol-III, Re-Print, Delhi, Nag
Publishers,1987:PP:395.
12. Vaidhya Jadavaji Trikamji Acharya, Charaka Samhita of Chakrapani Tika, 5th
Edition, Varanasi, Chaoukhambha Sanskrit Sansthana, 2001:PP:302.
13. Kaviraj Shri. Ambika Datta Shastri, Rasaratna Samuchaya, 8th Edition,
Varanasi, Chaoukhambha Amarabharati Parakashan, 1988:PP:449
14. Kaviraj Shri. Ambika Datta Shastri, Susrutha Samhita of Maharashi
Susrutha,Part I, 14th Edition, Varanasi, Chaoukhambha Sanskrit
Sansthana,2003:PP:55,9,13,72.
15. Kaviraj Atrideva Gupta, Astanga Hrudayam of Vagbhata, 10th Edition,
Varanasi, Chaoukhambha Sanskrit Sansthana,1987:PP:170
16. Professor K.R.Srikanta Murthy, Astanga Sangraha of Vagbhata, Vol-II, 5th
Edition, Varanasi, Chaoukhambha, Orientialia,2005: PP:6,7.
17. Shri Pandit Lalachandra Vaidya, Astanga Sangraha, Vol-II, Ist Edition,
Nagapur Sri Baidhyanath Ayurveda Bhavana Prvt Limited, 1989,PP:11,15.
18. Professor K.R.Srikanta Murthy, Bhava Praksa of Bhavamisra, Vol-II, 3rd
Edition Varanasi, Chaoukhambha, Krishnadas Academy, 2005 PP:779
19. Pandit Shri Brahma Sankara Misra, , Bhava Praksa of Shri Bhavamisra, Part-
2, 9th Edition, Varanasi, Chaoukhambha, Sanskrit Sansthana,2005 PP:781.
20. Vaidhy Shri Laxmipati Shatri, Yogaratnakar, 8th Edition , Varanasi,
Chaoukhambha, Sanskrit Sansthana, 2004 PP:406.
21. Dr. Indra Dev Tripati, Raj Nighantu, 3rd Edition, Varanasi, Chaoukhambha,
Krishnadas Academy, 2003 PP:175,64,93,36,37.

Bibliography
Clinical Study on Apraja Vandhya (Primary Infertility) By an indigenous compound W.S.R to Ovulatory dysfunction 123
22. Bapalal.G.Vaidhya, Nighantu Adarsa,Vol-I, 1st Edition, Varanasi,
Chaoukhambha Baharti Academy, 1968 PP:49,355,600,152,686,687,657.
23. Dr. Zarkhanda Oja, Dhanvantari Nighantu, 2nd Edition, Varanasi,
Chaoukhambha, Sanskrit Pratistana, 1996 PP:29,87,94,95,144.
24. Vishwanth Drivedi Shastri, Bhavaprakash Nighantu, Re-Print, Delhi, Motilal,
Banarasi Das, 2002 PP:66,71,217,349,352.
25. Dr. J.L.N Sastry, Dravy Guna Vijnana, Vol-I, 2nd Edition, Varanasi,
Chaukhambha, Orientatia, 2005.
26. Professor P.V.Sharma, Dravyagunna Vijnana, Vol-II, Re-prient, Varanasi,
Chaoukhambha Baharti Academy,2005
27. Dr. Gyanendra Pande, Dravy Guna Vijnana, Part –III, Re-print, Varanasi,
Chaoukhambha, Krishnadas Academy, 2004.
28. Professor (Kum) Premvati Tewari, Ayurvediya Prasutitantra Evam Striroga,
Part-II, 2nd Edition, Varanasi, Chaukhambha, Orientatia, 2000.PP 273 to303
29. Neeraja Bhatia, Jeffcoates, Principales of Gynaecology, 5th Edition, Revised,
2001, A member of the Hodder Healdline Group, London.pp 633 to 660
30. D.C.Dutta, Text Book of Gynaecology,3rd Edition, Culcatta, New Central
Book Agency Pvt Ltd, 2001 PP:212 to 239.
31. Dr C.C.Chatterjee,Human Physiology Vol II Reprint 2004 Kolkata Kalyani
Mukharjee PP 231 to 241

RESEARCH PROFORMA
N.K.J.AYURVEDIC MEDICAL COLLEGE AND PG CENTRE.
Post-Graduate Dept of Prasooti-tantra & Stri-roga
2007-2010.
“CLINICAL STUDY ON APRAJA VANDHYA (PRIMARY INFERTILITY) BY AN
INDIGENOUS COMPOUND W.S.R. TO OVULATORY DYSFUNCTION.” Guide Name: Dr. Susmita Priyadarshinee Otta PG Scholar :Dr. Smt. Bagali.C.S
Name of the Patient: Case No. :
Address: OPD No. :
Age; IPD No.:
Sex: Diagnosis:
Occupation: Duration:
Socio Economic status: Date:
Married since:
SOCIAL HISTORY: a) Marital History
1) Married for Yrs.
2) Staying with the husband for Yrs.
b) Education
1) Wife
2) Husband
c) Occupation
1) Wife
2) Husband
d) Monthly Family Income
e) Socio Economic Status-Poor/Lower middle class/ Upper middle class/Rich

CHIEF COMPLAINTS :
1) Duration of Vandhyatwa / Infertility (Primary) for Yrs.
ASSOCIATED COMLAINTS :
1) Sexual Dysfunction
a)Dyspareunia : Yes / No
b) Apareunia :
c) Orgasmic Failure :
2) Purulent Vaginal Discharge : Yes / No
3) Burning Micturation : Yes / No
4) Pain in Lower abdomen : Yes / No
5) Tenderness in Lower Abdomen: Yes / No
6) Backache : Yes / No
HISTORY OF PRESENT ILLNESS ;
Medical History (Past and Present)
a) Record of any previous illness.
b) Use of prolonged cortico-steroid therapy
c) H/o Trauma to lower abdomen
d) Gynecological infection (P.I.D)
MENSTRUAL HISTORY:
a) Age of menarche :
b) Duration of menstrual period : Regular / Irregular
c) Interval of menstruation :
d) Amount of bleeding : Scanty / Average / Heavy
e) Character of bleeding : Normal / With clots / Foul smelling
f) Inter-menstrual bleeding : Yes / No
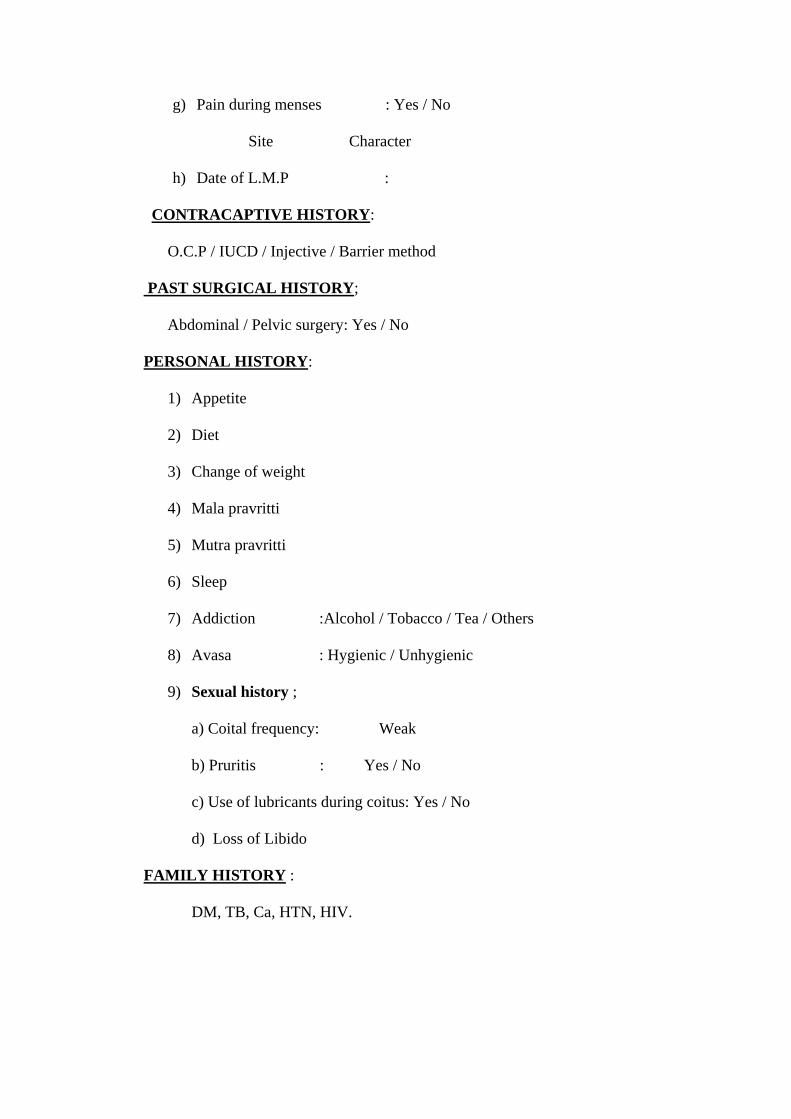
g) Pain during menses : Yes / No
Site Character
h) Date of L.M.P :
CONTRACAPTIVE HISTORY:
O.C.P / IUCD / Injective / Barrier method
PAST SURGICAL HISTORY;
Abdominal / Pelvic surgery: Yes / No
PERSONAL HISTORY:
1) Appetite
2) Diet
3) Change of weight
4) Mala pravritti
5) Mutra pravritti
6) Sleep
7) Addiction :Alcohol / Tobacco / Tea / Others
8) Avasa : Hygienic / Unhygienic
9) Sexual history ;
a) Coital frequency: Weak
b) Pruritis : Yes / No
c) Use of lubricants during coitus: Yes / No
d) Loss of Libido
FAMILY HISTORY :
DM, TB, Ca, HTN, HIV.

GENERAL EXAMINATIONS :
1) Physical ;
a) Height :
b) Weight :
c) Abnormal distribution of hair
d) Height / Weight relation – Thin / Average / Over weight
2) Head & Neck ;
a) Pallor (Anaemia)
b) Irctus (Jaundice)
c) Teeth & Gum
3) Throats ;
a) Thyroid
b) Cervical Lymph glands
4) Superior Extremity ;
a) Pulse
b) Blood pressure
5) Chest ;
a) Under development of secondary sexual characters : Yes / No
Breast : Well developed / Ill developed
Nipple : Retracted / Normal
Development of axillary hairs: Absent / Normal / Abnormal
Galactorrohea : Yes / No
6) Heart (CVS)
7) Lungs (RS)
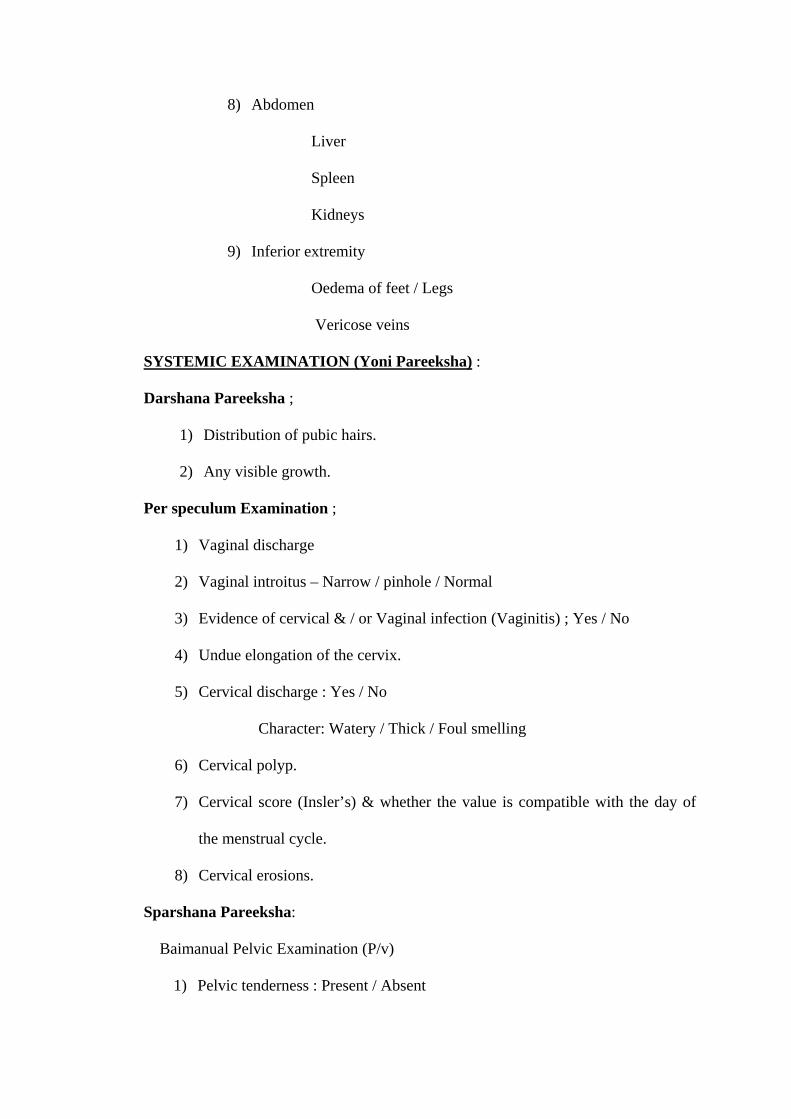
8) Abdomen
Liver
Spleen
Kidneys
9) Inferior extremity
Oedema of feet / Legs
Vericose veins
SYSTEMIC EXAMINATION (Yoni Pareeksha) :
Darshana Pareeksha ;
1) Distribution of pubic hairs.
2) Any visible growth.
Per speculum Examination ;
1) Vaginal discharge
2) Vaginal introitus – Narrow / pinhole / Normal
3) Evidence of cervical & / or Vaginal infection (Vaginitis) ; Yes / No
4) Undue elongation of the cervix.
5) Cervical discharge : Yes / No
Character: Watery / Thick / Foul smelling
6) Cervical polyp.
7) Cervical score (Insler’s) & whether the value is compatible with the day of
the menstrual cycle.
8) Cervical erosions.
Sparshana Pareeksha:
Baimanual Pelvic Examination (P/v)
1) Pelvic tenderness : Present / Absent

2) Undue elongation of cervix.
3) Uterus ;
Size : Normal / Abnormal
Position: Rv / Rf/Av/Af.
Mobility: Mobile / Fix.
4) Presence of adnexal masses : Fixed / Mobile / With or without
Tenderness.
5) Tender & fullness in the pouch of Douglas.
INVESTIGATIONS :
Husband’s seminogram: Normal / Abnormal
For female partner;
a) Urine : Albumin
Sugar
Microscopic
b) Blood : Hb%
R.B.S
V.D.R.L
c) Ultrasonography (USG).
d) Follicular study chart:
e) Hysterosalpingography (HSG).
Management :
1) Drug administration:
2) Date of visit:
3) Dosage:
4) Duration of treatment:
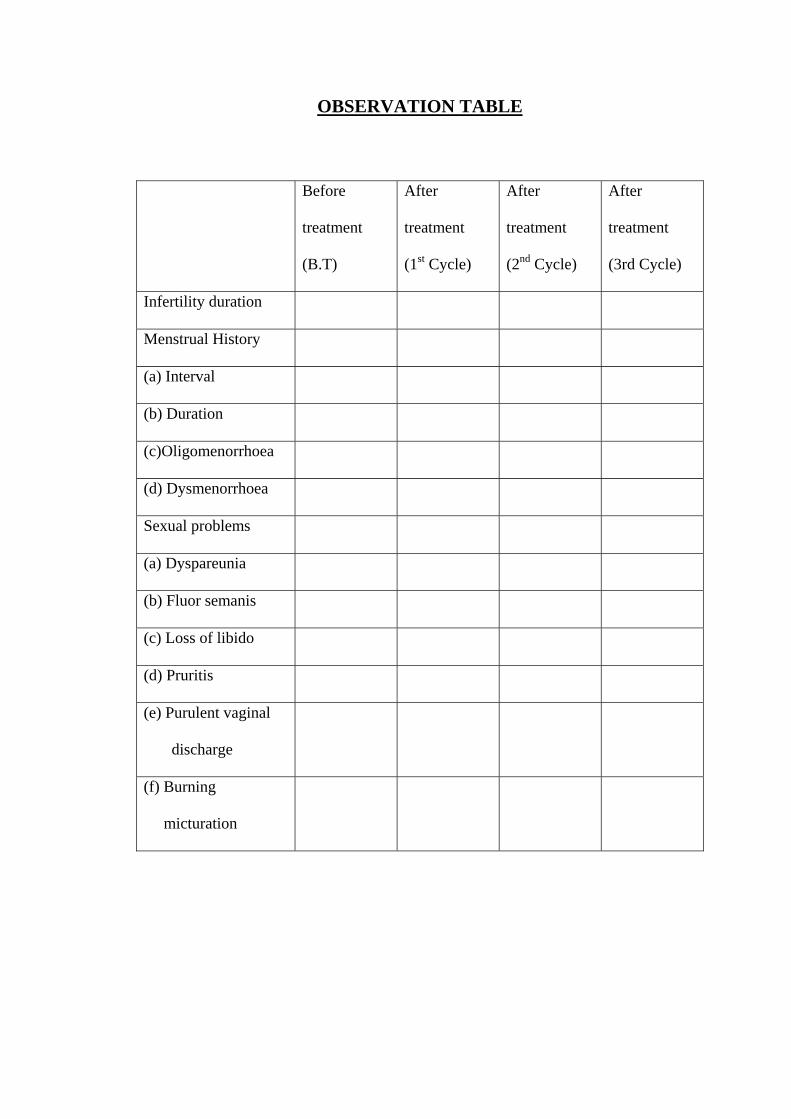
OBSERVATION TABLE
Before
treatment
(B.T)
After
treatment
(1st Cycle)
After
treatment
(2nd Cycle)
After
treatment
(3rd Cycle)
Infertility duration
Menstrual History
(a) Interval
(b) Duration
(c)Oligomenorrhoea
(d) Dysmenorrhoea
Sexual problems
(a) Dyspareunia
(b) Fluor semanis
(c) Loss of libido
(d) Pruritis
(e) Purulent vaginal
discharge
(f) Burning
micturation

Ovulation study :
Before treatment:
After treatment:
RESULT :
1) Conceived during treatment.
2) Relieved some symptoms.
3) Symptoms unchanged.
CONCLUSION :
Signature of Guide: Signature of PG Scholar: