Ayushman Bharat "Niramayam"
49
Ayushman Bharat "Niramayam" Government of Madhya Pradesh GUIDELINES FOR THE EMPANELMENT OF NON NABH S I NG LE lMU LTISPECIALITY /SUPERSPECIALITY HOSPITALS Deen Dayal Swasthya Suraksha Parishad IEC Bureau, JP Hospital Campus, Bhopal, M.P 462003 Phone Number: 07 55-27 62582 Helpline Number: 18002332085, 14555 Emai I : ayushman .bhar at@mp. gov. in Webs ite : r,vt'rv. *).'u sh{n *nhha rat. n:::. €l*rv. i l:r
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Ayushman Bharat "Niramayam"

Ayushman Bharat "Niramayam"Government of Madhya Pradesh
GUIDELINES FOR THE EMPANELMENT OF NON
NABH S I NG LE lMU LTISPECIALITY
/SUPERSPECIALITY HOSPITALS
Deen Dayal Swasthya Suraksha ParishadIEC Bureau, JP Hospital Campus, Bhopal, M.P 462003
Phone Number: 07 55-27 62582Helpline Number: 18002332085, 14555
Emai I : ayushman .bhar at@mp. gov. inWebs ite : r,vt'rv. *).'u sh{n *nhha rat. n:::. €l*rv. i l:r

o,ffi)rw
1 lPage
\
GUIDELINES FOR THE EMPANELMENT OF NON NABH
SINGLE /MULTISPECIALITY /SUPERSPECIALITY HOSPITALS
l.l. Basic Principles:
For providing the benefits envisaged under the Mission, the State Health Agency (SHA)through State Empanelment Committee (SEC) will empanel or cause to empanelNonNABH private health care service providers and facilities as per these guidelines.
1.2. Inclusions:
Sin gle/Nlulti s peciality/ S up er Specialities
General Surgery, ENT, Opthalmology,Obstetrics& Gynaecology, Orthopaedics,CardioThoracic Surgery, Paediatric surgery, Genitourinary Surgery (Urology), Neuro Surgery,
Surgical Oncology, Medical Oncology, Radiation Oncology, Burns,Plastic& reconstructiveSurgery, Polytrauma, Dental Surgery, Paediatric Cancer, Cricital Care, General Medicine,Paediatrics, Neonatology, Cardiology, Nephrology, Neurology, Chest diseases and
respiratory medicine(Pulmonology).
Super Specialities Centres:
Super Speciality centres are the centres which reflect requirement of DMAvICH/DNB orequivalentqualifi ed personnel.
1.3. Process of Empanelment for Non NABH SingleilVlulti speciality/ SuperSpecialitiesprivate health care ssrvice providers:
A. Hospitals can apply for the empanelment throughthe portal only, as a first step forgetting empanelled in the programmehttps:ii.!:or:ililglSd:gli+y-.9*v.i:r .
B. Hospital should have ROHINI provided by Insurance Information Bureau (IIB).C. Hospital need to fulfiI the criteria for various types of specialties catered by the hospitals
(Annexure 1).
D. All the required information and documents will need to be uploaded and submitted bythe hospital through the web portal.
E. Hospitalsneed to attain quality milestones by having at least NABII pre-entry levelaccreditation to be attained within I year with 2 extensions af one year each.
F. Criteria for empanelment has been divided into two broad categories as given below.
,d\.s$:
"d'*
3'f")ffi*t$".*$'btu*st$t;&y-{- swa sthya s uri t<sh a Pa ri s h ad
s\s'. ''

GUIDELINES FOR THE EMPANELMENT OF NON NABH
SINGLE /MULTISPECIALITY /SUPERSPECIALITY HOSPITALS
process for empanelment after 3 year to determine
application30 days of
shouldreceipt
beof
Physical verification team :-
The mode of verification of empanelment application, conducting the physical verificationwill be done by through a team with two members of State Healthlg.n.y(SHA)nominatedby CEO, Ayushman Bharat "Niramayam"lthree member team from District including onemember nominated by CMHO (Should be from CMHO office, Minimum qualification isMBBS)' one member from DQAC&District Epidemiologist, under the broid mandate ofthe instructions provided in these guidelines.The State Government may also require theInsurance Company to mandatorily provide a medical representative to assist the SEC in itsactivities.
Alternatively, the SHA may continue with any existing institution under the respective stateschemes that may be vested with the powers and responsibilities of SEC u, p., theseguidelines.
The Physical verification team will be responsible for:
o Getting the field verification done along with the submission of the verification reportsto the SEC.
o The Team will physically inspect the premises of the hospital and verify the physicalpresence of the details entered in the empanelment application, including but noi limitedto equipment, human resources, service standards and quality and submit a report in asaid format through real time monitoring using an Appby geotagging the phoiographs
2lPage Deen Dayat Swasthya iuraksha parishad

GUIDELINES FOR THE EMPANELMENT OF NON NABH
SINGLE /MULTISPECIALITY /SUPERSPECIALITY HOSPITALS
through the portal along with supporting pictures/videos/document scans which shall beexamined by the officers at the State Health Agency.
o The Physical verification team will also be responsible for recommending, ifapplicable, any relaxation in empanelment criteria that may be required to ensure thatsufficient number of empanelled facilities are available in the district.
o Final approval of relaxation will lie with SEC.o The SEC will consider, among other things, the reports submitted by the physical
verification team and recommendation approve or deny or return to the hospital theempanelment request.
The SHAs through state Empanelment committee (sEC) shall ensure:
. Empanelment within the stipulated timeline.
. The empanelled provider meets the minimum criteria as defined by the guidelines fornon NABH multispecialty private health care service providers;
. Time-bound processing of all applications; and
. Time-bound escalation of appeals.
. In case of refusal, the SEC will record in writing the reasons for refusal and either directthe hospital to remedy the deficiencies, or in case of egregious emissions from theempanelment request, either based on documentary or physical verification, direct thehospital to submit a fresh request for empanelment on the online portal.
. In case the hospital chooses to withdraw from the scheme, it will only be permitted to e-enter/get re-empanelled under the scheme after a period of 6 months.
1.4. Awareness Generation and Facilitation:
The SHA shall ensure that maximum number of eligible hospitals participate in the scheme,and this need to be achieved through IEC campaigns, collaboration with and district,subdistrict and block level workshops.
The state and district administration should strive to encourage all eligible hospitals in theirrespective jurisdictions to apply for empanelment under Ayushman Bharat 'Niramayam'.The SHA shall organize a district workshop to discuss the details of the Mission (includingempanelment criteria, packages and processes) with the hospitals and address any querythat they may have about the mission.
Annexure 1: Detailed Empanelment Criteria
Minimum Criteria:

GUIDELINES FOR THE EMPANELMENT OF NON NABH
SINGLE /MULTISPECIALITY /SUPERSPECIALITY HOSPITALS
A Hospital would be empanelled as a network private hospital with the approval of therespective State Health Authorityl if it adheres with the following minimum criteria:
1. In order to facilitate the effective implementation of PMRSSM, State Govemments shallset up the State Health Authority (SHA) or designate this function under any existingagencyl trust designated for this pu{pose, such as the state nodal agency or a trust set upfor the state insurance program.
2. Qualified doctor is a MBBS approved as per the Clinical Establishment AcV Stategovernment rules & regulations as applicable from time to time.
3. Qualified nurse per unit per shift shall be available as per requirement laid down by theNursing Councili Clinical Establishment Act/ State government rules & regulations asapplicable from time to time.
4. Should have at least 50 inpatient beds at district level and 30 inpatient beds atsubdivision level with adequate infrastructure, spacing and supporting staff as pernonns.
o Exemption may be given for the hospitals in Aspirational districts/ Tribal districts,for non-profitable trust hospitals and single-specialty hospitalsexcept whereMedical College Hospitals are situated.
Aspirational districts Tribal districtsDamoh AlirajpurBarwani AnuppurVidisha Barwani
Singrauli BetulKhandwa Dhar
Chhatarpur DindoriGuna Jhabua
Rajgarh KhargoneMandlaUmaria
5. It should havephysically in
adequate andcharge round
qualified medical andthe clock; (necessary
nursing staff (doctors2 & nurses3),certificates to be produced during
Parishad

GUIDELINES FOR THE EMPANELMENT OF NON NABH
SINGLE /MULTISPECIALITY /SUPERSPECIALITY HOSPITALS
6. Fully equipped and engaged in providing Medical and Surgical services, commensurateto the scope of service/ available specialities and number of beds.o Round-the-clock availability (or on-call) of a Surgeon and Anaesthetist where
surgical services/ day care treatments are offered.o Round-the-clock availability of specialists (or on-call) in the concerned specialties
having sufficient experience where such services are offered.
7. Hospital should have adequate arrangements for round-the-clock support systemsrequired for the above services like Pharmacy, Blood Bank, Laboratory, Dialysis unit,Endoscopy investigation support, Post op ICU care with ventilator support (mandatoryfor providing surgical packages), X-ray facility etc., either 'In-House' or with'Outsourcing arrangements' with appropriate agreements and in nearby vicinity.
8. Round-the-clock Ambulance facilities (own or tie-up).
9. 24 hours emergency services managed by technically qualified staff whereveremergency services are offered.
l0.Casualty should be equipped with Monitors, Defibrillator, Nebulizer with accessories,Crash Cart, Resuscitation equipment, Oxygen cylinders with flow meter/tubing/catheter/face mask/nasal prongs, Suction apparatus etc. and with attached toiletfacility.
ll.Mandatory for hospitals wherever surgical procedures are offered:. Fully equipped Operation Theatre of its own with qualified nursing staff under its
employment round the clock.o Post-op ward with ventilator and other required facilities.
l2.Wherever intensive care services are offered it is mandatory to be equipped with anIntensive Care Unit (For medicaVsurgical ICUAIDU) with requisite staffo The unit is to be situated in close proximity of operation theatre, acute care medical
and surgical ward units.o Suction, oxygen supply and compressed air should be provided for each bed.o Further High Dependency Unit (HDU) - where such packages are mandated should
have the following equipment:1) Piped gases2) Multi-signMonitoringequipment3) Infusion of ionotropic support4) Equipment for maintenance of body temperature

GUIDELINES FOR THE EMPANELMENT OF NON NABH
SINGLT /MULTISPECIALITY /SUPERSPECIALITY HOSPITALS
6. Fully equipped and engaged in providing Medical and Surgical services, commensurate
to the sCope of seryice/ available specialities and number of beds.
o Round-the-clock availability (or on-call) of a Surgeon and Anaesthetist where
surgical services/ day care treatments are offered'. Round-the-clock availability of specialists (or on-call) in the concerned specialties
having sufficient experience where such services are offered.
Z. Hospital should have adequate arrangements for round-the-clock support systems
required for the above serviies like Pharmacy, Blood.Bank, Laboratory, Dialysis unit,
Endoscopy investigation support, Post op ICU care with ventilator support (mandatory
for ptouiOing suigical paikages), X-ray facility etc., either 'In-House' or with.Outsourcing-arrangements' with appropriate agreements and in nearby vicinity.
8. Round-the-clock Ambulance facilities (own or tie-up).
g, 24 hours emergency services managed by technically qualified staff wherever
emergency services are offered.
L0.Casualty should be equipped with Monitors, Defibrillator, Nebulizer with accessories,
Crash Cart, Resusiitation equipment, Oxygen cylinders with flow meter/
tubing/cath eterlface mask/nasal prongs, Suction apparatus etc. and with attached toilet
facility.
ll.Mandatory for hospitals wherever surgical procedures are offered:
o Fully equipped Operation Theatre of its own with qualified nursing staff under its
employment round the clock.o Post-op ward with ventilator and other required facilities.
L2.Wherever intensive care services are offered it is mandatory to be equipped with an
Intensive Care Unit (For medical/surgical ICU/HDU) with requisite staff. The unit is to be situated in close proximity of operation theatre, acute care medical
and surgical ward units.o Suction, oxygen supply and compressed air should be provided for each bed.
o Further High Dependency Unit (HDU) - where such packages are mandated should
have the following equiPment:1) Piped gases
2) Multi-signMonitoringequipment3) Infusion of ionotroPic suPPort
4) Equipment for maintenance of body temperature
W/ $.or:F*E;t+."
- rrf

GUIDELINES FOR THE EMPANELMENT OF NON NABH
SINGLE /MULTISPECIALITY /SUPERSPECIALITY HOSPITALS
5) Weighing scale6) Manpower for 24x7 monitoring
o ICU should also be equipped with all the equipment and manpower as per HDUnoffns, plus paediatric ventilator(s).
l3.Records Maintenanoe: Maintain complete records as required on day-to-day basis and isable to provide necessary records of hospital I patients to the Society/Insurer or hisrepresentative as and when required.. Wherever automated systems are used it should comply with NHA EHR guidelines
(as and when they are enforced and updated)o All Ayushman Bharat cases must have complete records maintained.
l.4.Legalrequirements as applicable by the local/state health authority.
l5.Adherence to Standard treatment guidelines/ Clinical Pathways for procedures as
mandated by NHA from time to time.
l6.Registration with the Income Tax Department.
l7.NEFT enabled bank account
l8.Telephone/Fax
I 9. Safe drinking water facilities.
20.Unintemrpted (24 hour) supply of electricity and generator facility with requiredcapacity suitable to the bed strength of the hospital.
2l.Waste management support services (General and Bio Medical) - in compliance withthe biomedical waste management act.
22, Appr opri ate fi re-s afety measures.
23.Provide space for a separate kiosk for Ayushman Bharat beneficiary management at thehospital reception.
24.[insure a dedicated medical officer to work as a medical co-ordinator towards Ayushmanllharat beneficiary management (including records for follow-up care as prescribed)
Parishad
GUIDELINES FOR THE EMPANELMENT OF NON NABH
SINGLE /MULTISPECIALITY /SUPERSPECIALITY HOSPITALS
25.Ensure appropriate promotion of Ayushman Bharat in and around the hospital (display
bannerso btorhur.r .tr.; to*utds effective publicity of the scheme in co-ordination with
the SHA team.
26,IT Hardware requirements (desktopilaptop with internet, printer, webcam, scanner/ fax,
biometric device etc.) as mandated by the NHA.
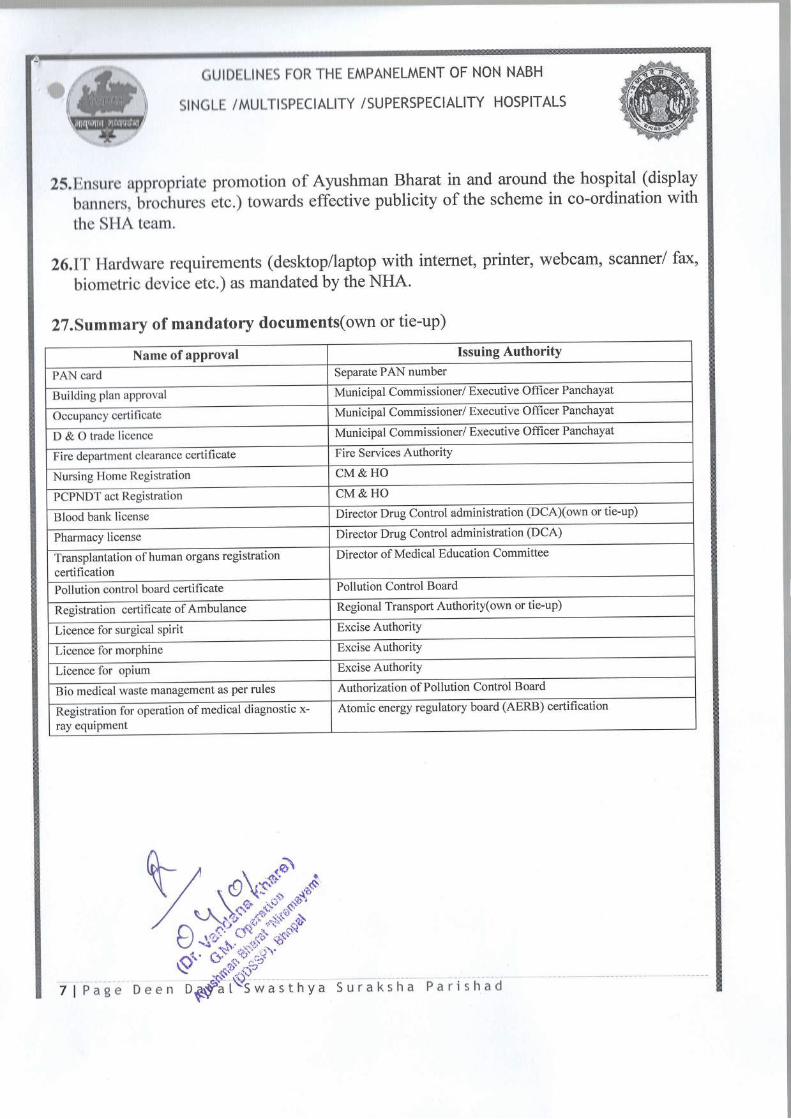
27.Summary of mandatory documents(own or tie-up)
Name of approval Issuing Authority
PAN card Separate PAN number
Building plan approval Municipal Commissioner/ Executive Officer Panchayat
Occupancy certificate Municipal Commissioner/ Executive Offi cer Panchayat
D&Otradelicence Municipal Commissioner/ Executive Offi cer Panchayat
Fire department clearance certificate Fire Services Authority
Nursing Home Registration CM&HO
PCPNDT act Registration CM&HO
Blood bank license Director Drug Control administration (DCA)(own or tie-up)
Pharmacy license Director Drug Control administration (DCA)
Transplantation of human organs registration
certification
Director of Medical Education Committee
Pollution control board certifi cate Pollution Control Board
Registration certificate of Ambulance Regional Transport Authority(own or tie-up)
Licence for surgical sPirit Excise Authority
Licence for morphine Excise Authority
Licence for opium Excise Authority
Bio medical waste management as per rules Authorization of Pollution Control Board
Registration for operation of medical diagnostic x-ray equipment
Atomic energy regulatory board (AERB) certification
7l
h,, .o\d*s\/
/g;'{'"}S{$aQ- d.-*t'ti;t=
Page Deen tE;S*tAlwasitrvi suraksha Parishad

oAmlg[urs]
Criteria for Non-NABH Super Specialtv Hospital Assessment Sheet
| 1 | Keylnputs | 10 | 40 I
o Each checkpoint is accompanied by means of verification in next column.
r The process of assessment will take place in three steps-
1. Under all the categories, there are mandatory requirements which are to be fulfilled compulsorily
2, Means of verifications which require to be assessed on basis of the scoring system as mentioned below
as mlnlmum quality standards.
Scorlnr.for Qualltv Standards -
Followlng general principles may be given following numerical score.
Full Compliance-lf the information gathered gives the impression that all the requirements ofCheckpoints and means of verification are being met, full compliance i.e. Marks-2 should be
provided for that check point.
Partial Compliance- For providing partial compliance at least 5O% or more requirements should be met. For
partial compliance a score of 1 mark should be given
Non-Compliance- Non-compliance is assigned to when facility fails to meet at least 50% of the requirementgiven in a checkpoints and corresponding means of verification. ln this case score 0 is given
Total Score Score Achieved Percentage
t72
3. Based on the super specialty service for which the facility has to be empanelled, the minimum criteria
for respective super speciality have to be fulfilled by the facility.
A Focility should fulfill all the mandatory criterio ond the criterio for super speciolty for which they hove applied ond should at least score
more thon 70% under qualitystondord criterio to be eligible for emponelment under Ayushman Bhorot "Niramoyom"
1 | State Health Agency, Ayushman Bharat "Niramayam"-l\
"01
a\ax,sr^*

O Criteria 1- Key Inputs
This section of key inputs broadly covers the structural part of the hospital.
The certification criteria given in this category take into consideration the -o facilityinfrastructureo human resources requirements and trainingo appropriate space in hospital for patient movement
. proper lighting facility in the hospitalr medical instruments and equipment requirements and maintenance
o fire-fightingequipmento Basic amenities like drinking water, waiting area, canteen, suitable toilets for men and
women etc.
Mandatorv Criteria -
Code Criteria Intemretation Means of Verification YAI
KI 1
Physical facility ofthe building andhospitalenvironment shallbe developed andmaintained for thesafety of Patients,visitors. and staff
This standard guides theprovision ofsafe andsecure environmentforpatients, visitors andstaff.To ensure this, thehospital premises musthmto haci n oc c enli nl ili o c
There should be no cattle or strav animals within theoremisesThe facility should have a guard avulable 24*7
The hospital boundary should be intact and notbrokenHospital (Building(s)) should be well maintained i.e.walls are well plastered (no cracks or seepage) andpainted
of infrastructure andshqll have annualmaintenance planforinfrastructuredevelopment. Thisincludes appearance ofthefacility, cleaningpr o c es s es, infr as tructur em aint enanc e an d c ontr o Iof stray animals at the
facility.
Windows and doors are intact and have erill/ wiremeshworkThe facility should have an annual maintenance planfor its infrastructureNon-structural components such as cupboards,cabinets and other heavy equipment or hangingobiects should be properly fastened and securedHospital building should not have wire hanginglooselyThere should be no stains, grease, cobwebs and birdnest on walls and roofs of the hospitalThere should be a closed drainage system with nodirect contact with the environment
Code Criteria Interpretation Means of Verification YAI
KI2Hospital should haveadequate space forambulance and patientmovement
This standard requires thatfacility should ensureadequate space for smbulancemovement and parking. Theaccess to the emergency/receiving area should besmooth and spaciousfor theease of patient movement andsafe handling.
Ambulance should have direct access tothe emergency/ receiving/ triage areaand access road to emergency should bewide enough to streamline themovement of the patient till theemergency/ receiving areaNo vehicle should be parked on the wayor in front ofthe emergency entrance
Dedicated parking area for theambulance
2 | State Health Agency, Ayushman Bharat "Niramayam"-t ^\
3;#W,\tr)" u'-*1'lr?t'- .$il.sd.'

oCode Criteria Intemretation Means of Verification YAI
KI3
Access to the hospitalshould be providedwithout any physicalbarrier and friendly topeople with disabilities
Prwisions should beav ailabl e for phys icallychal I enge d/ vulner abl eperson to make the entranceaccessible with ramps andgrab bars. Thefocility shouldh n e facil ity of wheelchair,stretcher and trolleys withs afety b elts for immediatesuDDort ofthe natient.
Availability of wheelchair,stretcher for emergency with strapsto protect the patient from fallingThe wheelchair, stretcher andtrolleys should be clean,operational and their wheelsshould be properly alienedAvailability of ramps with railingsat the entrance of the facilitv
Code Criteria Intemretation Means of Verification YA{
KI4
Basic amenitiesshould be providedfor all patients,hospital staff andvisitors
The hospital must hove anappropriate w aiting are a withs e ating arr qngemen| drinkingwater, clean toilets sensitive togender and plrysically challengedvisitors and staf personnel shouldbe present within the premises.
Availability of seating arrangementin the waiting area(s) within thehospital premises for attendantsAvailability of potable drinkingwater on each floor (functionalRO/filters)There should be a provision ofcanteen facility for visitors & staffinside the premises
Every floor should have at least onetoilet for hospital staffand visitorsAvailability of clean and functionaltoilets with no foul smell in andaround the toilet along withfunctional water tapsThe toilets floor should be dry andno drain should be overflowinsAvailability of disabled friendlytoilet with bars or railings and isaccessible throueh a rampAvailability of24*7 workingtelephone help line in hospital foreffective communication
Code Criteria Interpretation Means of Verification YA{
KI5
The hospital shouldensure that all medicalstaff is adequatelycredentialed as per the
The organization shall ensurethat the medical professionalswho have requiredqual i/i c ation, tr aining,exp er i en c e and cons onanc ewith the law are permitted toprovide the seryices and suchinformation should beappr opr i at ely v er iJi e d.
Also, the facility shouldmaintain an adequate numberand mix of staf to meet the
Doctor/ Nurse/ Paramedic StafflAdmin & Support Staff along withthe current designation, educationalqualification, registration council ofname and the associated registrationnumber along with the date ofj oining and arealworkingdeoartrnent
statutorv nonns Organization should plan humanresource with adequate number andwith mix and credentials of staffasper the statutory norms
3 | St.t. Health AgencvAushman Bharat "Niramayam"
,fr'{9W

t care. treqtment and servicesneeds ofpatients.
Hospital has dedicated staff(3members) foTAYUSHMANBHARAT "NIRAMAYAM"
Code Criteria lntemretation Means of Verification YAT
KI6
Hospital shouldhave fire detectionand fire-fightingequipmentinstalled as per firesafety nonns alongwith staff training
The facility should have plan andprovisions for early detection,abatement and containment offire
suah snh
Check if fire extinguisher,fnelsmoke detectors are installed inpatient care areas with firepanel
fire exit plan and trained sta/f,. Theperiodic training shall includeinformation, demonstration to use Jireextinguisher and mock drills
Check for date of expiry on fireextinguisher which should be thebeyond current date
The organization has a documentedsafe exit plan in case of fire andnon-fire emergenciesPeriodic training with mock drill isprovided for using fireextinguishers
Oualitv Stundnrds Criteria -Code Criteria lntemretation Means of Verification Score
KI 7
'fhe indoor andoutdoor areas ofthefacility should bewell-lit
In order to provide safe,secure and comfortableenvironment to patients andstaffthe hospital should haveprwis ion of comfort abl eenvironment in terms ofillumination either thr oughelectric bulbs andtubes qt allthe places, accompanied bynatural source of light. Also,thefront, entry and exit areasshould also be well lit.
There should be proper lighting inthe indoor areas through natural lightand by using sufficient electric bulbs
The facility's front, entry gate andaccess road are well illuminated
Codc Criteria lnternretation Means of Verification Score
KI 8
The facility has
functional equipmentand instruments as perscope ofservices
The hospital must have all theequipment and instrumentsaccording to the scope of servicesthey are offering. Basic functionaldiagnostic equipment should alsobe readv available.
Availability for examination andmonitoring of patients - BP apparatus,Multiparameter Torch, hammer, aninstrument to measure height, weightand Blood Pressure (BP) to conduct ageneral examination
Codc Criteria Intemretation Means of Verification Score
KI9Staff involved in
direct patient careshall be trained in
The organization shall provideregular training to the sta/fproviding direct patient care. Ifthefacility has a CPR team (e.g. code
Training Records for Basic LifeSupport (BLS)
Health Agency, Ayushman Bharat "Niramayam"
j:Ssffia( c'-:e;&$

, Cardio PulmonaryResuscitation (CPR)and Basic LifeSupport (BLS) alongwith a display of thesame in all criticalcare areas
blue team) it shall ensure that it istrained in advancedc ardi opulmonary r e s us c it ati on(adult, pediatric and neonatal) and
There should be a code blue protocolin the organization
,D yrctvr,a att ut, tra,Jtt. 1,t a
and nurses working in ICU/ HDUs h ould unde r go appr opr iat etraining and display the CPRalg.orithm at all the critical areas
Check the display of CPR algorithmin or near ICU, Clinical area andEmergency areas.
Check the records for CPR events &CPR Mock drill along with thecorrective & Preventive measurestaken
Code Criteria Intemretation Means of Verification Score
KI 10
Annual Training Planshould be prepared forall staff covering alltraining needs
The hospital should docamentplan and prepare a trainingcalendar to ensure staffis ableto identify the patient's rightsand r e sp ons i biliti es, p ot enti alhaz ar ds, m aint ain r equir e dqualtty and take appropriateactions during any disaster
Facility prepares training calendar as
per training need assessment, trainingfeedback records - Training onDisaster Management, Patient safetyand rights, facility level QualityAssurance
AYUSHMANBHARAT"NIRAMAYAM" specifi c training(e.g. BIS, TMS, mM & SupportPortal, etc) to all concerned staff.
Criteria 2 - Clinical Services
These are the processes that determine the outcome of services and quality of care.
These standards include processes such as -
q, I State Health Agency, Ayushman Bharat "Niramayam"-l
^\r.@flca
to-
f*.+;$-ffi.c('' sl'.s.].+si'
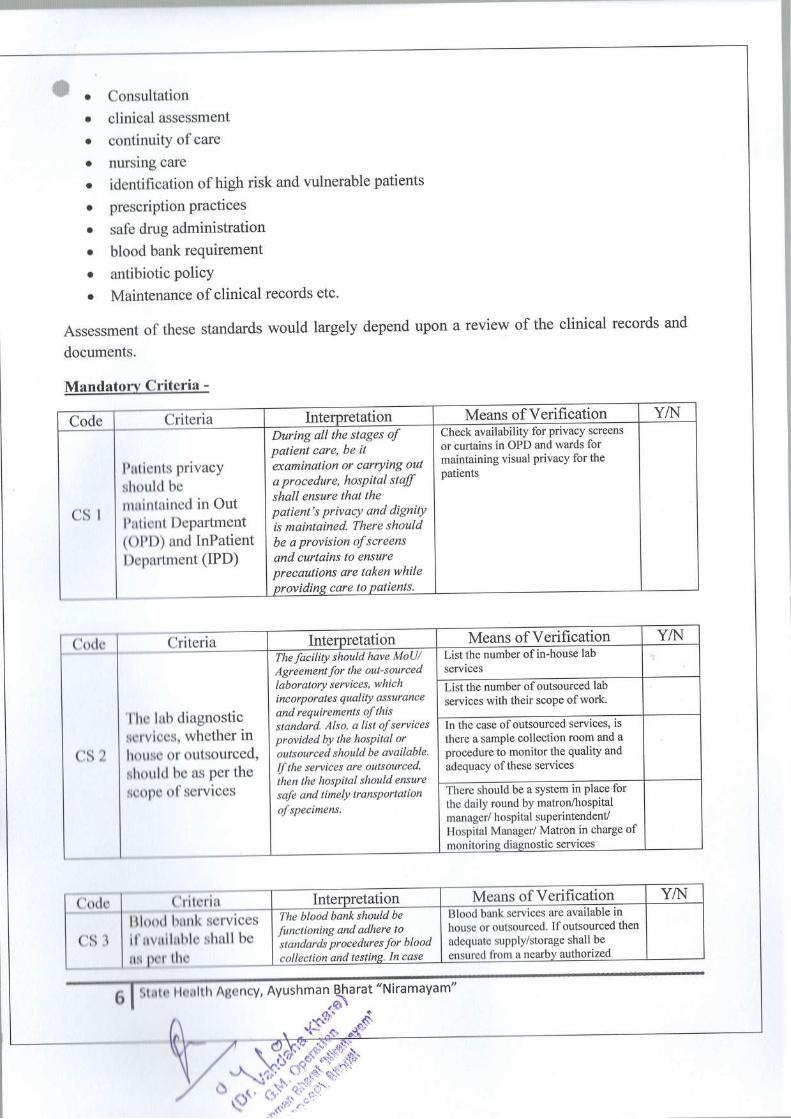
' o Consultation
o clinical assessment
o continuity of care
o nursing care
o identification of high risk and vulnerable patients
o prescriptionPractices
o safe drug administration
o blood bank requirement
o antibiotic PolicYo Maintenance of clinical records etc'
Assessment of these standards would largely depend upon a review of the clinical records and
documents.
Mandatorv Criteria -
'l'lro lubserviccshottso tlshoulcl t
lrOopc o
(lritcrilllood hnnkil'uvnlluhlcnr por thc
Code Criteria Intemretation Means of Verification YA{
csl
l)uticnts privacYshoulcl b0
nruitttuincd in Outl'nticnt DePartment(Olf l)) and InPatientl)cpartment (IPD)
During all the stages oJ
patient care, be itexamination or carrying out
a procedure, hosPital staffshqll ensure that thepatient's privacY and dignitYis maintained. There shouldbe a provision ofscreensand curtains to ensureprecautions are taken whileproviding care to Pqtients'
Check availability for privacy screens
or curtains in OPD and wards formaintaining visual privacy for thepatients
Criteria
b diagnosticls. whether inttr outsourced,I br: as per theol'scrvices
Intemretation Means of Verification YAIThe facility should have MoU/Agreernent for the out-sourcedlaboratory services, which
i nc or p or ate s qual itY as suranc e
and requirements of thisstandard. Also, a list of sewicesprovided by the hosPital oroutsourced should be available.Ifthe services are outsourced,
ihen the hospital should ensure
safe and timely transqortation
ofspecimens,
List the number of in-house lab
services
List the number of outsourced lab
services with their scoPe of work.
In the case ofoutsourced services, is
there a sample collection room and a
procedure to monitor the quality and
adequacy of these services
There should be a system in place forthe daily round by matron/trospitalmanager/ hospital superintendent/Hospital Manager/ Matron in charge ofmonitoring diagnostic services
!q_scrvicesshull be
Interpretation Means of Verification YAIThe blood bank should be
functioning and adhere to
standards procedures for bloodcollection and testing. In case
Blood bank services are available inhouse or outsourced. Ifoutsourced then
adequate supPlY/storage shall be
ensured from a nearby authorized
-Strto Hoalth Agency, Ayushman B-lrarat "Niramayam"
'6\6

Tnotpitot doesn't have the
blood bank it shall have a
MoU with the blood bank or the
organization having a blood
binkwhich has a valid license'
IEC materialfor blooddonation should also be
displaYed at all strategic
locations.
statutory/regulatoryBlood bink has a talid license under
Rule 122(G) Drug and cosmetic act
Btoodian-;;facttttYof blood
collection and storage along with
lEGffitatls dGptaYed in blood
bank and nearbY area to Provideinformation and Promote blood
efr6l for availabilitY of adequate
functional equiPment for bloodproducts - Biood bags refrigerator with
ihermograph and alarm device,
insutatJa ianier boxes with ice packs'
Blood bag weighing machine and deep
M"rtts of Verification YA{Interpretation
Code Critena Cleafito ,es, aprons and masks are
available at the Point of useffiAAW /bodYParts of staff
and patlenis, attendants should
be adhered to bY usingprotective devices and
equiPment, alongwith ^
orecautions as Per law Jor'radiation
safetY. The facilitYshould also ensure standard
I practices, usage andsuPPlY ofI' P ers onal P r otective EquiPment
I rnnt
cs4
The hosPital should
adherc to the
radiation safetyprocautions as per
tho rogulatorYroquircments
TLD b"dg.t-thould be Provided to
each staffmember in the radiation
roomLil aprons, thfoid shields and other
radiation proteition devices should be
provided ior the staff in the radiation
held. These should be tested once in 2
vears as Per AERB r!qm--i;Ai;6i6;rm services
of ve4fig4gq-InterPretatto> Scoretu
M-eu"-t of Verification YA{T6+ar6raf qflrln
Codo I ul!!gll3
I O1'comPlex should
cs5 li;.';ilil[,f0"I roquircmcnts
v P.p"il.#Ald;'the following
areas: Protective zone, clean zone'
sterileione and disposal zone . -
The organization shall ensure
that the oPeration theater has
facilities for demarcated areas'
seDarote changing rooms Jormales and females along with
pr oper illumination and
fumPerature
AGililitffifi ignage stating that the
entry to OT is restricted
Fr€{perative and post-operative area
should be well-lit
efranse t"omt *" a"tlable for male
*i fJ*uf. staff; entry in OT should be
allowed only after change in attire
ffip-erature and humiditY are
mainiained and record of same is kept
ffiGneahn AgencY, AYushm an B\arat "N
f.$s*-:-*

o
CS6
Intensive Care unit(ICU) servicesshould be availableas per the scope ofservices along withthe requiredinfrastructure andmanpower
The ICU should beequippedwith necessqrymonitoring equipment al ongwith the suitably manned bytrained staff. The hospitalshould provide proper andsafe ercvironment to theinfected patients andnecessqry proceduress houl d b e follow e d for thesame.
Flooring ofthe ICU should be non-slipperv and smoothWindows/ air vents if any should beintact and sealedComfortable temperature & humidityshould be maintainedAvailability of general duty doctor,nursing staff, paramedic and securitystaff as Der requirementsCritical care equipment is availableand maintained- Refrigerator, CrashcartlDrug trolley, instrument trolley,dressing trolley, Ventilator, Infusionpump, C-PAP, tray, monitors,Electrical panel with a bed, bedheadpanel with an outlet for Oxygen andvacuum, X-ray view box. defibrillatorAvailability of isolated area forinfectious oatientIsolation and banier nursingprocedures are followed for septicczNes
Code Criteria Intemretation Means of Verification Score
CS7
Look-alike andsound-alikemedicines need to beidentified and storedseparately to avoidany dispensing andadministrationeffors.
The drug store should arrangethe stock in alphabetic/unifu r m/ s t andardiz e d orde rand storage requirement ofthedrugs should be adhered to.The overall cleanliness andtemperature ofthe storage area
Product of similar name and differentstrength (look alike and sound alikedrugs) should be stored separately.Medicine storage shall be in a clean,well lit, and in a safe environment inaccordance with the applicable lawsand regulations
should be maintained. One lookalilre should be stored apartfron its other look alilee
Stock is ananged neatly in alphabeticorder with the name facing the frontand labels must have drug name,strength and frequency
Drug store has inventory managementsoftware
Code Criteria Intemretation Means of Verification Score
CS8
Policies andprocedures foridentification, safedispensing andadministration of allhigh-risk medicinesshould bedocumented andimplemented
Clear policies to be laid down
for dispensing of high-riskmedicines and the list of suchmedicines should be availableat the drug store. The narcoticsdrugs should be stored insecure manner
Documented procedure incorporatingstorage, prescription and dispensing ofmedicationsNarcotic medicines are kept in doublelock
Pharmacy has a list of high-risk drugsavailable with it
Code Criteria Intemretation Means of Verification Score
I I State Health Agency, Ayushman Bharat "Niramayam"' n .$.9\t+
)fr};;fffi-f*+{".r

o
CS9
The facility has
defined andestablished antibioticpolicy
The Hospital must have ane st ab I is he d ant ib i ot i c p o li cyensuring rational use ofantibiotic/drug.
Facility should ensure the rationalusage of antibioticV drugs and policyfor the same is in place andimplemented.
Code Criteria Intemretation Means of Verification Score
CS l0
Pre-operative, Intra-operative andpostoperativeassessment shouldbe done anddocumented byappropriatelyqualified staff instandardized format
All the patients undergoingsurgery should be assessed pre-operative, intra-operative andpost-operative by the trainedstafr, which should bedocumented in a standardized
format. Also, a documentedprocedure should be available
for preventing adverse likewrong site, wrong patient andwrong surgery
There is a procedure for pre-operativeand intra-operative assessment -Physical examination, result of labinvestigation, diagnosis and proposedsurserv (3 samoles)Patient reports with post-operativenotes that should contain vital sigrs,pain control, urine and gastrointestinalfluid output, other medications andLaboratory investigations (3 samples)Documented procedure to address theprevention ofadverse events likewrong site, wrong patient and wrongsurgery.
Code Criteria Intemretation Means of Verification Score
CS 11
Pre-Anesthesiaassessments, type ofAnesthesia and PostAnesthesia statusshould beDocumented
The pre-anesthesia, poslanesthesia and type of
Department has documented procedurefor pre-operative anesthesia checkup
anestnesta snould oe monrtore'and documented in astandardized format. Also thepatient records must containregular and periodicmonitoring records of patients
Anesthesia plan is documented beforeentering into OT
Post anesthesia status is monitored andrecorded
who are under obseryation PostOper ative /Ane s t he s i a for thepurpose of tadng correctiveand preve ntive act i ons.
Post-Operative/Anesthesia monitoringincludes regular and periodic recordingofheart rate, cardiac rhythm,respiratory rate, blood pressure,
oxygen saturation, airway security andDatencv
Criteria 3- Support Services
Support services are fundamental foundation of every healthcare
departrnents things run smoothly.
It includes paftrmeters to evaluate -o Cleanliness
o Sterilizationo infection control practices
o security and facility management
o water and power supply
facility and help other
g I
State Health Agency, Ayushman Bhar$"Niramayam"
|\^. d" .o-t{irw

wo Dietary services and laundry.
These standards also cover some of the administrative processes like legal and statutorycompliances, contract management, Bio-Medical waste disposal etc.
Mandatorv Criteria -
Code Criteria Interpretation Means of Verification YAJ
SS1
The hospital shouldhave arrangement ofwater storage andshould be testedperiodically as perrequirement
The hospital shall ensure thatthere is sfficient water supplyto meet the requirements at allpoint ofuse round the clock.Alternate source of water
At least 200 liters of water per bed perday is available on a daily 24x7 basis.Adequate backup for continuous watersupply should be available (checkaltemate sources also)
should be available as backup
for anyfailure or shortage andsame should be tested onregular basis. The results ofthetests should be documented
Water is available at all points of usefor hand washing, OT, Labor room,wards, Patients toilet & bathroom.All water tanks are kept tightly closedto ensure safety
Check the records for periodic tests ofthe quality of water from the source(municipal supply, borewell, etc.) forbacterial and chemical content as perthe zuidelines
Code Criteria Intemretation Means of Verification YAI
SS2
The hospital shouldhave24 hourssupply of electricityeither through direcisupply or from othersources
Hospital should haveavailability of power back up inthe form ofemergency lights,DG sets, solar energt, UPS,
noiseless generators or anyother suitable source. The staffinvolyed in maintenance ofelectricity must have rubbermats, gloves and bootsfor safeworking and prevention fromanv mis- haooenins.
Check the availability of power backup, availability of UPS, emergencylights or noiseless generators
Rubber mats are available in theelectrical room below the panels andrubber gloves, boots and safety gearsare provided to the electrical staff
Code Criteria Intemretation Means of Verification YAI
SS3
Medical gases andvacuum shall bemade available all thetime and storedsafely. Compressedair should be madeavailable as per thescope of services
Maniftld room should beaccessible and have adequateback up of orygen cylinders.Availability of central orygenand vacuum supply shouldespecially be assessed incritical area like OT and ICUwith standardized colourcoding ofcylinders andpipelines. A promptreplacement procedure andalarm system should beavailable to indicate any
The manifold room should be locatedon the ground floor and entry to theroom is prohibited for theunauthorized people.
The manifold room should have atleast 3 days ofoxygen and othermedical gases stoclg that is chainedaoorooriatelvColor of the gas pipeline (ifapplicable) and the gas cylinder has tobe as per the standardsThe alarm system should beoperational to indicate any abnormalpressure chanse
the room. The instructions foroperating dffirent equipment'sin manifuld room should bedisplayed clearly.
Adequate back-up of B-type cylindersin critical areas like ICU, OT and forpatient transfer DumoseThe procedure being followed forprompt replacement of empty
1n I State Health Agency, Ayushman Bharat "Niramayam"-- I n .',F\.|fi# {i
;ttffi t$,"' 'r\dt,
rt\1' r\' '
".$' ':*;l''
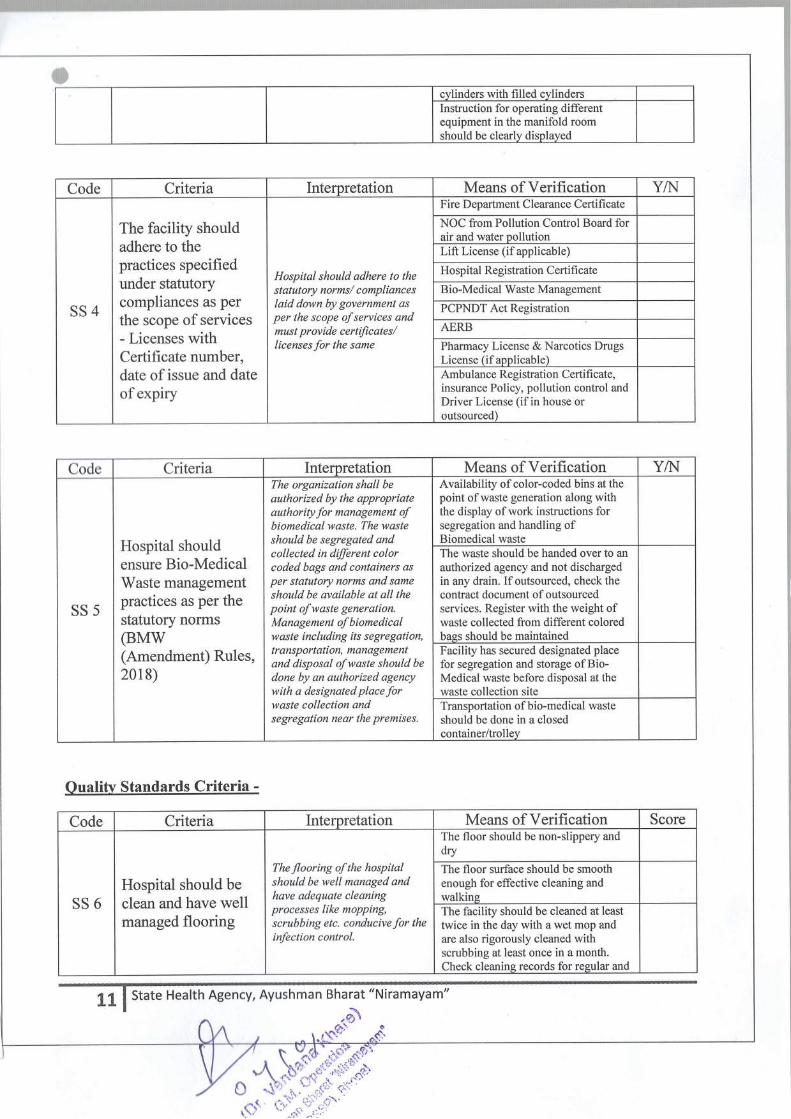
ficvlinders with filled cvlindersInstruction for operating differentequipment in the manifold roomshould be clearlv displayed
Code Criteria Interpretation Means of Verification YAI
SS4
The facility shouldadhere to thepractices specifiedunder statutorycompliances as perthe scope ofservices- Licenses withCertificate number,date of issue and dateof expiry
Hospital should adhere to the
Fire Department Clearance Certificate
NOC from Pollution Control Board forair and water nollutionLift License (if applicable)
Hospital Registration Certifi cate
s tatutory norms / c omp lianceslaid down by government asper the scope of services andmust provide certificates/licenses for the same
Bio-Medical Waste Management
PCPNDT Act Reeistration
AERB
Pharmacy License & Narcotics DrugsLicense (if applicable)Ambulance Registration Certifi cate,insurance Policy, pollution control andDriver License (if in house oroutsourced)
Code Criteria Interoretation Means of Verification YA{
SS5
Hospital shouldensure Bio-MedicalWaste managementpractices as per thestatutory noffns(BMW(Amendment) Rules,2018)
The organization shall be
authorized by the appropriateauthority for management ofbiomedical waste. The wasteshould be segregated andcollected in dffirent colorcoded bags and containers asper statutory norms and sameshould be available at all thepoint of waste generation.Manage m e nt of b i o me di c a Iwaste including its segregation,
Availability of color-coded bins at thepoint of waste generation along withthe display of work instructions forsegregation and handling ofBiomedical wasteThe waste should be handed over to an
authorized agency and not dischargedin any drain. Ifoutsourced, check thecontract document of outsourcedservices. Register with the weight ofwaste collected from different coloredbass should be maintainec
tr a nsp or t at t on, manageme ntand disposal ofwaste should be
done by an authorized agencywith a designated place forwaste collection andsegregation near the premises.
Facility has secured designated placefor segregation and storage ofBio-Medical waste before disposal at thewaste collection site
Transportation of bio-medical waste
should be done in a closedcontainer/trollev
Oualitv Standards Criteria -
Code Criteria Intemretation Means of Verification Score
SS6Hospital should beclean and have wellmanaged flooring
The flooring of the hospitalshould be well managed andhave adequate cleaningprocesses like mopping,scrubbing etc. conducive for theinfection control.
The floor should be non-slippery anddry
The floor surface should be smoothenough for effective cleaning andwalkineThe facility should be cleaned at leasttwice in the day with a wet mop andare also rigorously cleaned withscrubbing at least once in a month.Check cleanins records for resular and
I 1 | State Health Agency, Ayushman Bharat "Niramayam"*- | n -.g.)
'"t,t\
"t: "'

ofrequency ofcleaning
Code Criteria Intemretation Means of Verification Score
SS7
Temperature controland ventilationshould bemaintained in patientcare and nursingarea
Ar r ange me nt for c omfort ab I e
work environment in terms oftemperature control should beavailable in patient care areasand work stations.
Availability of fans/ air conditioning/heating/ exhaust/ air vents as per therequirement and weather condition.
Code Criteria Intemretation Means of Verification Score
12 | state Health Agency, Ayushman Bhara(Niramayam"
{}\".Js"'.
Code Criteria Intemretation Means of Verification Score
SS8
The hospital shouldensure thatappropriate infectioncontrol practices ilebeing followed alongwith hand hygienepractices
The hospital infection controland prevention process should
Availability of wash basin near thepoint of use along with antiseptic soapwith soap dish/ liquid antiseptic withdispenserAvailability of alcohol-based hand rub
Availability of disinfectant/cleaningaeent as ner reouirement
be documented which aims atpreventing and reducing risk ofhealthcare associatedinfe c t i on. The organiz at i onshall also adhere to handhygie ne, cle aning, dis infecti onand s terilization guide line s.
Check if infection control manualshowing periodic update andsurveillance activities available/monitoring takes place
The facility should follow standardpractices and materials for disinfectionand sterilization of instruments/equipmentStaff should be trained for all infectioncontrol practices, hand hygieneguideline, occupational risk and itsorevention.
Code Criteria lntemretation Means of Verification Score
SS9
Hospital shouldensure that servicesi.e. (Laundry,Housekeeping,Dietary, security,Ambulance,Mortuary, CentralSterile SupplyDepartment (CSSD)etc. are available (in-house oroutsourced).
The services lilce laundry,houselreeping, dietary, security,mortuary, ambulance CSSDetc. should be available in-house or out-sourced. Thehospital shall ensure that theyestablish adequate controls byhaving a policy to ntonitor/audit these semices. If these
services are outsourced, thenthey should have MoU/agreement for the same.
Checklist for Desktop Assessment -Availability YesA.lo & If outsourced,MoU should be available for the same.
Intemal audits of the services to beconducted on regular intervals
6is:il'.fl:Ir$$qi;-u'

a
SS 10
Sexual harassmentand grievancehandling procedureshould be available
There should be disciplinaryand grievance handlingprocedures in place with ade dic at e d c omnit t e e /t e an
Committee against sexual harassmentis constituted at the facility
against sexual harassment andvarious other prievances.
Documented disciplinary andgrievance handling procedure
Criteria 4- Patient Care
Giving quality patient care have a positive effect on patient outcomes and recovery experience.
Patients' rights are also an integral part of patient caxe. The important patient rights include
informed consent, confidentiality of medical records, legible prescription etc.
Standards to be assessed are-
o uniform user-friendly signage
o IEC for educating patients
o patient-friendly admission and referral process
o consent policies
o retaining of medical recordo Education of patients
Mandatorv Criteria -Code Criteria Intemretation Means of Verification YAI
13 | State Health Agency, Ayushman Bharat "Niramayam"
^ .S\&tt
Sn-q.ffi$ot* qq*F

PCl
User charges aredisplayed andcommunicated topatients effectivelyat the time ofregistration,admission to theward and in case of achanee in medical
The list ofuser charges must bedisplayed at strategic places(Reception, waiting areas,lobby) in the hospital premises
for better communication topatients and to maintaintransparency. The list must beupdated in case ofany changein medical and surgical plan.
Facility prepares a comprehensive listofuser charges and display at strategicpoints in the hospital
AYUSHMANBHARAT"NIRAMAYAM" benefi ciaries areprovided cashless services
Code Criteria Interpretation Means of Verification YAI
PC2
Medical recordsshould be retained as
per the policies ofHospital based onnational and locallaw
Hospital must abide by thenational and local laws forretaining medical records foreach category ofrecords: Out-patient, in-patient and MLC.The retention and destructionprocess should be included inthe process to maintainconfidentiality and security ofboth manual and electronicrecords system. Also, thereshould be a documentedprocessfor medical records ofAB PMJAY schemebeneficiaries.
Hospital has a policy of retentionperiod with respect to different kindsofrecords and their disposal
Confi dentiality of patient recordsshould be maintained by keeping themproperly in the record room or digitallysaved on a secure network
Hospital has process documentation forAYUSHMAN BHARAT'NIRAMAYAM" scheme
Ouality Standard Criteria-
14 | State Health Agency, Ayushman Bharat "Niramayam"-'I
o@\
:$s-
Code Criteria Interpretation Means of Verification Score
PC3
Hospital should haveuniform and user-friendly signagesystem in Englishand in the locallanguage understoodby Patient I familyand community
Adequate signage should bedisplayed at all strategiclocations which are permanentin nature. The semices,depart me ntal and directionalsignage, and list ofdepartments should beprominently displayed at allstrategic locations in a uniformcolor scheme, Also theessential information lilee list ofemergency c ontact numbers,list ofdoctors, patient rightsand responsibilities etc. shouldbe displayed within thehospital premises. It ispreferable that the signage isdisplayed in bilinguallanguage for the ease andu nde rs t andi ng of patie nt s.
Name of the hospital and entry-exitshould be clearly displayed outside thehospital. Entry to the emergencydepartment should also be defined anddisolaved stratesicallvHospital has directional signage with auniform color scheme.List ofdepartments (as pet scope ofservices) should be displayed inbilingual language (INCLUDINGLOCAL LANGUAGE)The scope ofservices should bedisplayed in the waiting area/ OPD/Emergency/ Reception in bilinguallanguage(INCLUDING LOCALLANGUAGE)All the services registered underAYUSHMAN BHARAT"NIRAMAYAM" are clearly defined& displayed in prominent places inunderstandable language.Display offloor layout at each floor
4u-ffii$.*o$**

Display of patients' rights and
responsibility & other related IECmaterial (outdated and tornposters/wallpapers etc. should not beput on display)Hospital has IEC specific toAYUSHMANBHARAT.NIRAMAYAM".
List ofdoctors (as per scope ofservices) with their departments and
availabilitvNo smoking signage to be Presentwithin the hospital premises
Display of hand washing instruction at
the point of use (5 moments and 7
steps ofhand hygiene)Display of emergency numbersincluding ambulance, blood bank,police and referral centers
Code Criteria lnterpretation Means of Verification Score
PC4
All Signage's those
are required bY lawshould be displayed
at all strategiclocation
All such signage which are
compulsory by law forhospitals to display such as
PC&PNDT Act, AERB andradian hazard, Bio hazardsignage and Fire exit signageshould be displayed in the
hospitals at all strategiclocations
Fire exit signage to be displayed at exitroute plan along with the do's and
don'ts in case of firePC&PNDT Act Signage board to be
displayed at the waiting room and
receotion area
AERB and Radiation hazard signage
Bio-hazard signage to be present
Code Criteria Interpretation Means of Verification Score
PC5
Contact informationof key medical staffand specialist shouldbe readily availablein the emergencydepartrnent
The hospital must have
accessible and readilyavailable contact details ofdoctors and staf members.Also, a nurse call facility and atleast one medical fficer shouldbe available at all times in the
hospital in case of emergencies.
Check ifthe contact details (telephone
or residence address) of doctors/staffare readily availableNurse call facility should be availableto address any patient emergency.
At least one medical officer and a
nurse should be available all the timefor the emergency cases.
Code Criteria lntemretation Means of Verification Score
PC6
Service counters forthe enquiry are
available as per thepatient load and are
duly managed byhospital staff for theregistration of
There should be a dedicatedarea for enquiry as per the
number of patients that visitsthe hospital and dedicatedkioskfor AB PMJAY mannedround the clock Hospital must
malce sure that every Patient is
given a unique identificationnumber at the time ofresistration of the first
Check availability ofa dedicatedenquiry area or reception
Unique identification number is given
to each patient during the process ofregistration while also recordingpatient details such as name, age, sex,
address and chief comPlaint etc.
,}';$*I$::;u*-i]ii.;io-'-
Siite Health Agency, Ayushman Bharat "Niramayam"
.frd#'
15

apatients interaction if the patient with
the organisation. To ensurecontinuity of care these
numbers shall be linked to theuniaue number.
Hospital has AYUSHMAII BHAIL{T'NIRAMAYAM" Kiosk manned 24* 7
Code Criteria Interpretation Means of Verification Score
PC7
Hospital should haveestablishedprocedure foradmission ofpatients
There should be documentedprocedures for registerin( and
Admission is done by written order ofa oualified doctor
admitting the patient. Allpatients assessed in hospitalshall be registered and alladmissions must be authorizedby a doctor. The policy shouldbe defined with respect tod o cwne ntat i on and int imat i onto police in case of MedicoLegal Cases (MLC) as perstatutory requirement
There is an established criterion foradmission through the emergencydepartment
There is established procedure foradmission of Medico-Legal Cases(MLC) as per prevalent laws andprocedure to inform the police.Records for such patients are alsomaintained.
Code Criteria lnterpretation Means of Verification Score
PC8
The patient shouldbe referred to
another facilityalong with the
documented clinicalinformation, in case
of non-availabilityofservices and/or
beds.
The documented procedureaddressing the managing
patients in case ofnonavail ab i I i ty of beds.
P at ie nt s ne e di ng t ransferincluding those who have cometo the emergency but needs to
be transferred after basic first-aid, the hospital shall havedocume nted procedure for
managing patients. Thet r o n.r fe rrin s /re fe r rinq natie nt s
There is an established procedure formanaging patients in case beds are notavailable at the facility
Patient should be referred whileissuing a referral slip and should be bi-directional referral system. The recordof the same should be maintained
Adequate emergency facilities shouldbe available to provide basic first aidbefore transfer/referral
to another focility should bedone through issuing referral
slips.
AYUSHMAN BHARAT*NIRAMAYAM" Benefi ces referredto AYUSHMAN BHARAT"NIRAMAYAM"empanelledHosoitals
Code Criteria Intemretation Means of Verification Score
PC9
General Consent andInformed Consentshould be takenduring the admissionand before anyprocedures /surgeryand anesthesia/sedation
Patients and family rightsinclude that hospital shall takeinformed consent; preferably inbi-lingual and language theycan understand, signed byp at i e nt/r e I at iv e s /c a r e t alee r atthe time of admission andbefore undergoing any surgeryor procedure which discussabout all the risl<s and benefits.The informed consents shouldbe talcn at all specific steps pfpatient care involved withresnonslbilllv.
Consent forms available in bilinguallanguage (LOCAL LANGUAGETHAT IS I-INDERSTOOD BY THEPATIENT) should be signed by thepatients or any caretaker duringadmission and before surgery (separateforms)All risks, benefits and alternativesabout anesthesia should be discussedand mentioned as part ofthe consentform signed by the patients or theircaretaker.
."i'i:iifil-{i;;e'n*'*St"6t

Code Criteria Intemretation Means of Verification Score
PC 10
Patient should beproperly educated onadditional care as
deemed required andall the vitalinformation shouldbe recorded forcontinuity of care
Patient should be educatedforadditional care in respect tousage and efect ofmedication,diet and nutrition which can bedone with the help of dischargesummary and growth summaryrespectively. All the vitalinformation must be recorded
for reas s e s s ment of patientsundergoing observation in thelanguage the patient/ familymembers can understand.
Patients should be educated for usageand effect of medication, diet andnutrition, immunizations and toprevent infections (as deemedappropriate)Discharge summary should contain a
diagnosis, history, physicalexamination, investigation details,treatment provided and instructionsthereof in easy to understand manner(Check 3 samoles)There should be a fixed schedule forreassessment of patient underobservation based on clinical need
Code Criteria Intemretation Means of Verification Score
PC 11
Hospitals shouldensure that allmedications andassociatedinstructions arewritten in theprescription
The organization shall ensurethat the at the minimum theprescription shall have thename of the patient, uniquepatient number, name ofmedicine with thefrequency ofadministration, name andsignature of the doctor. Allhand written prescriptionshould be legible, clear andunderstandable by the patient/family member i.e. preferablyin capital letters.
Prescription should be legible, clearand be explained in the languageunderstood by the patients and iscomprehendible by the clinical staff
Every medical advice and procedure isaccompanied with date, time andsignature, unique patient number.
Criteria 5- Health Outcomes
The importance of measuring and reporting the healthcare outcomes is to improve patient
experience of care and fosters improvement and adoption of best practices, thus further
improving outcomes.
The standards to be assessed under this criteria are-
. OPD and IPD census
. mortality rate
o average length ofstayo Surgical Site Infectiono Urinary Tract Infectiono Blood Stream Infectiono Ventilator Associated (VAP) Infection / Hospital Acquired Pneumonia
o Transfusion reactiono Bedoccupancyo Patient and employee satisfaction
1I I State Health Agency, Ayushman Bharat "Niramayam"

oo reporting of adverse events
o Theft and securitv related events etc.
Mandatory Documents-
Code Criteria Intemretation Means of Verification YAI
HOI
Monthly Out-Patient Department(OPD) and In-Patient Department(IPD) census
A monthly Out-PatientDepartment (OPD) and In-Patient Department (IPD)census data can help to monitorhow nuch OPD patients areconverting into IPD, how nanypatients visited the OPD andIPD and track the trend ofOPD to IPD conversion. Therate is generally affected bypoor patient satisfaction, highcost of IPD or low motivationof doctors to admit OPDpatient.
Out Patient Department (OPD) censusfor last 6 months
In-Patient Department (IPD) census forlast 6 months
AYUSHMANBHARAT'NIRAMAYAM" In-PatientDepartment (IPD) census for last 6months
Code Criteria Intemretation Means of Verification Y/I{
HO2Mortality Rate andAverage Length ofStay (ALS)
MortaliA stufistics provide avaluable measure for assessingcommunity health status. Theimp or tanc e of m ort alitystatistics derives bothfrom thesigniJicance ofdeath in anindividual's life as well as theirpotential to improve thepublic's health when used tosystematically assess andmonitor the health status of awhole community. ALS is averyc o mm on perfornanc e ne asurewhich is used not onlyimportantfor hospitalperformance but als o forclinical quality and infectioncontrol.
Mortality Rate (from the data of last 6months): Number of Patient died/Total number of patient admitted *100
Average
Length ofStay (from the data offorlast 6 months): Sum ofdays spend byeach patient/ Total number of patientadmitted
Code Criteria Intemretation Means of Verification YAI
HO3 Infection Rates
An infection rate is theprobability or risk ofinfectionin a population. It is used totneasure the frequency ofoccurrence ofnew instances of
Surgical Site Infection (from the dataof for last 6 months) = Number ofsurgical site infections/ Number ofpatients operated *100
18 | State Health Agency, Ayushman Bharat "Niramayam"
D
d\

o
Code Criteria Interpretation Means ofVerification Y/NI
HO6Reporting ofAdverse events
Adverse events are usually .
deJined as an unintended injuryor complication resulting inprolonged hospital stay,disability at the time ofdischarge or death caused byhealthcare management ratherthan by the patient's underlyingdisease. A substantial part ofthese events are avoidable andit is important to report them inorder to prevent such events infuture.
Data for last 6 months
19 | State Health Agency, Ayushman eharat,siramayam"
$ \\A.ql;*'P"
i nfe c ti on w it hin a p opu lationduring a speci/ic time period. Itwill help to identifu if anyrecurrent infections persist andimprove infection control in thehospital.
Urinary Tract Infection (from the dataof for last 6 months) = Sum of UrinaryTract Infection Complaints/ TotalNumber of patients admitted *100
Blood Stream Infection (BSI) (fromthe data of for last 6 months) :Number of Catheter related BSI/Number of patients on IV line * 100
Ventilator Associated Pneumonia(VAP/ Hospital Acquired Pneumonia(HAP) (from the data of last 6 months): Sum of Ventilator AssociatedPneumonia/ Number of patients onventilator *100
Code Criteria Interpretation Means of Verification YA{
HO4Reporting ofTransfusionReaction
They are responsible forcompleting blood request
forms, administering blood,m o nit or i ng transfus i ons andbeing vigilant for the signs andsymptoms of adverse reactions.These guidelines are intendedto enhance the inplementationof s t andar d c I inic al tr ansfus ionpractices for inproved patientsafety.
Number of Transfusion Reactions inlast 6 months
Code Criteria Intemretation Means of Verification YAI
HO5 Bed occupancy
A good hospital managementincludes an effectiveallocativeplanningfor beds in ahospital. Bedoccupancy ratesand length ofstay are themeasures that reflect thefunctional abilitv ofa hosoital.
Bed Occupancy: Inpatient days ofcare/ Total number ofbeds available* 100
r$iy,*"},:' s$'iii+Jol'S'*:.--l-$tF'

HO7Reporting of Thefts/ Security relatedincidents
Thefts of medical equipment ormedical records is a majorconcern in hospitals. Healthrecords are being digitized andhence there is the danger ofhe a I th inform ati on be c o mingcompromised or stolenoutright. It is impoftant todecrease the number ofsuchincidents by enhancing securityin the facilin.
Data for last 6 months
Code Criteria Intemretation Means ofVerification YAJ
HO8Reporting of needlestick injuriesInterpretation
Needle stick injury is defined asa penetrating wound typicallyinduced by a needle point orother sharp instrument orobject which could be infectedwith another person's secretion.These injuries can lead totransmis s ion of bl ood-borneviral infections. A continuous
follow-up and reporting ofneedle stick injuries insurgeons is important toprevent future events of needlestick injuries for higher patientsafetv.
Data for last 6 months
Standard Criteria-
Code Criteria Interpretation Means of Verification Score
HO9 Percentage ofPatient satisfaction
Patient satisfaction is animportant and commonly usedindicator for measuring thequality in health care. Aneasure of care quality, patientsatisfaction gives providersinsights into various aspects ofme dic i ne, inc luding t heeffectiveness of their care andtheir level of empathy.
Copy ofthe filled feedback formclearly showing the questions asked (atleast 5 samples)
Patient Satisfaction : Number ofpatients responding extremelysatisfied/ Total number of patientssurveyed *100
Code Criteria Interpretation Means ofVerification Score
HO r0Percentage ofEmployeesatisfaction
Strong employee satisfaction islinlre d w i t h s i gni/ic antirnprovements in patient careand satisfaction therefore itbecomes crucial to study the
Copy ofthe filled feedback formclearly showing the questions asked (atleast 5 samples)
20 | State Health Agency, Ayushman Bharat "Niramayam"
tl\

per c ent age of emPl oY e e s w ho
are satisfied and Perform to
their best ofefforts in the
hospital
Ernployee Satisfaction = Number ofemployees resPonding extremelY
satisfied/ Total number of employees
surveyed *100
Interpretation Means ofVerification ScoreCode Criteria
Delay in discharge ofthepatient increases the Pressureon beds ofthe hosPital and
delay in discharge is badforboth hosPitals and the Patients.Thus it becomes imPortant to
calculate the waiting time in the
hospital in order to decrease
the waiting time and increase
patient safety bY Providingprompt semices
Out-patient Oepartment Waiting Time: Sum oftime from when the Patiententered the outpatient clinic to the time
the patient actually leaves the OPD/
Total Number of OutPatients
HO 1l
Waiting time - OutPatient DePartment(OPD) andDischarge
Oischarge Waiting Time: (Total time
taken for medical record to reach the
billing department from the ward +
Total time taken in the billingdepartment)iTotal Number ofTnnatients
2L State Health Agency, Ayushman Bharat "Niramayam"

N F
il#RIE IEx lil lil
tEI*lgI I tqllls| | tr| | l(D| | toI I lojI I 14
I I lfi
lllFI I lElllllllilllilll'lllIt
als l;=l l9o I too-l loI lt+I loql Esl tEF I l.!'gt
I'll,€l I'ol I''ll
tlot I: <l Iiat IrKl Iilli<l I) (rl Irll/ll
\-it I') =t I?dt I+-l Iilol Ii'e.t Iuol I-rllDllLEI
Ifrt Iol I9t I
El Izt Icel I
l-{lill=lolqlElo.l
lslolo.lol|,tc)lrDlalolo)l?lloF3
I
I
I
I
I
I
I
I
I
tplcl0)I -trlolo-lC,
lelslzl@l-lc,)lo
rlolololqq, t.<t-
I
I
I
I
I
I
I
I
I
I
I
| (')tolliICLlolo
l-
:l
'l
I
1
I
I
I
I
F
o.
Fl
ID
4(D
(D
HU)
.AFd(DEt+.aCA'oo()
io'o(Dg
4of6
o
(D
tlH
sl\H
El\e
BI\:
il[
\\
lr
K.L
IG':" t,, n:;)
:.i, I'iS' '8."
\'"ri-
.ffiri,l,,'i,r"
*lol|/tl
5ggol5'loal6lcl@l(DlcLlul
oE(D
=-lolo)t-Ir+
qllr+(Do,n(D
oo
3q)at
==(De.+
r)t<
oo)tn
3.€(D
==(Dltr
lc
IEod
=(D3
l6'l3lo)loItItto
>lat-rl<lol(,)
3'(D
lc)lr+l<to,| .-tlolo
od.o=J3o
oo)c+
o,ctc5d
PotrroCLVlq):tCLq)ET
Po
(rl=oco-ctoao=lo,
lErlo
(/tl5loCCL
EToosl
lorIttto
(tl IJIoc
o-
st
lg,tul6-
:;.vp

u)ts
uto NIN(oto N{ NC'!
NININrJr | 5 ll^,
NINNIP No F(o Fo F{ PIPorlgr|lF P(ll P
NPP
tso lo
d tic l:I lr(D lt\l:o l.:t l(tn l-o l.E l(; trP li! liol lr.+l5 l,olol(tq l.
FI0Jlol6'lo-Icml\.
1cLl6'[email protected]
Iolol.+l
rlgl+lE Eli
IEIElc ellilg lg I € l,ile lel E lr
*lslB l 3liilE ltl s lifl3l8 | B l.
ilHlFl E I
al+n sl9l | | el3l | | +l| | | 6'l| | | €l| | | €l| | | =lI I I ;l| | | olI | | s. lttlElll(Dlll"IllIll
m l.€ liE I;cL lizt;o11:l{Tr l'6 tlc l,B- lio- t,t llzlcl.3lcrl(Dl;l-t! |
B-lol|/rl
I
I
I
I
I
I
I
I
I
IFF\*\*\FF\A\*\*
1\\\\\\\\\\
a
oco-croo)
g.dcto
ll5o
Ecroooq)go
Vl
oCCL
cr(D
o,
g_,
o,go
t,5ogo-ctooJ
IOJgo
an
oco-croo)
9.dgo
an
oco-ct(D
o,
g.o)E(D
(
oco-ET(D
o)
oJ
o)ET
l6-I
II
I
a
oco-uoog.ilc'l'I
II
I
t
ocCL
CFooooJgo
L
I
I
II
II
a
oco-5oo)
g.6-cr(D
ntc
doo)
o)
o,cr6-
FcroCLVlo5CL
ctoocro-oVr
(D
oc.+o{rtso
It
ocCL
6ooJ
g.ilg(D
a
=ocEcroo,
o,
o)cro
vr
oCo-6(D
oJ
g-oJg(D
atl
ocEcrooOJ
olctlro-I
II
I
II
t
oCo-u(D
oJ
g.OJg(D
tn
ocdct(D
o)
o)
o,CFo
ttoco-E(D
o,
g-o,g(D
tn
oco-cr(D
o)
gq)go
I
I
l
oco-doOJ
g.dgo
t
ogo-cr(D
0,
o,
o)go
l
oco-doogoJgo
ltI4aq.lirt I-lsl+l>lBIflc)l.<l
>l.<tCIvri=3o,5@5It-o,d
=-OJ
3u)
o,3

lsH
F
l-lq)lo-loJl.'+lolrlrnI o.,| -+rl(D
l<tol+tolol-rl<l(nlolTtl5t.<tlntol(,l+Il0€'6-3q,
:7o.,o-o,if.of.E'
t(')vr
lapl5 olo =lir 6'I{.: O-IIE'IJt.<tlAlo| .-tIJlo
;E'6'
cpT'{
!
a)oco-crooc.+anoCooCL
=;toanEIoo.€:t
lel€lc]t8I t'+lolalslo| .-ilo,l6
l<l@l@
tJ1
lc) !?
It Elo) -l- dlvr vllcolm18FI f 1r'l
lol+tlTtItt.<l(,l6'l6'lr
I6'(DffD
9r3(DCLo5'(D
0z@
6)oJoo)
.Dlo-I6'l3lol
<ltll I
tplclo,I -rrl(Dlo-lol:ll8lolsat(,l.+
t<la)t'rlolJlcllo
ancgoo3I3o=atooqa
39.vo)a-o-t(D
o,E']"<l
lol3lc)loIOlqllt.<
0,mfo4at7o1
o5o,
=(1o5o)E.lga
2.
EJoo
ooqoo.+oa
voa-o,
6':tE-o.+oo=.oftJroc+C
(fot
o6-
(D-qJE,Jlo,+co
cpao,(')t
5(D-o,E(t,o.+cE
o,33o
oqao)E5
o-{(/,clo,f
og6-xI
vo,
cf
c)o5(D
=d.o5o,
x7q,
cf
Fq,CLo,13.o=o5.loo0e
tvoco-cro0,
g.o,
1^
oCo-5oo)
o,
ogo
l
ocdcroo,qJ.
o.lgo
an
oco-uotu
oogo
t
ocdcroo,
o.o,go
an
oCo-u(D
OJ
o,
OJct6-
ltr
oCo-cr(D
o,
oJ
o,go
t
ogo-croog.o,g(D
tll
oco-croo)
o,
o)cr(D
t
oco-croOJ
or.
o.,g(D
an5oco-EoOJ
o,
o,crlD
tJl.+o)eoIoo
@o:to
qr
3OJ5(p=o)ao,
zo.l
3o,
o,3

o,@fIovotot
LO)l5tc)lol3loJlgq
lcrct-t<ljl-II
I
I
I
I
II
I
II
I
I
I
I
I
I
II
II
I
ilffi\g\a\'\E\a- 16'l- l" I I l- l-<r'r | | | | l5lpl I I I I l=
\t\\\\\l||l\\\\\\\\II\\\\\\\\Ill||
zl!dtTI lrno toq, lo,-15ol5lololotql
s lslE> l- lg; I 16I l=I loI l8I t-
I loI lFI I laI I l-llleI I t=| | l-
lllsl
\\fItIt\\\
llr
,5o
slolclo-cro0,q)
o,go
Vl
oCodoo.,
o,
0,uo
vloCo-croo)
o)
0,go
trto
dEToo)
g.ogo
t
ocCL
EToog.o,,go
to
dcr(D
o)
g-o,go
Vl
oCCLgoo)
go,go
nto-dcroo)
gq,go
tJr
oCo-croo)
g.o)qo
vrtoCo-ct(D
o)
g-og(D
vr
oCo-cr(D
o,
t=og(D
a,
oco-cr(D
0)
o,
OJct(D
ato
dEoo)
go)g(D
n5o
ddoog-0)g(D
t
oCo-ctoo)
g.o)go
tJl
oco-cro0,
g.o)go
t,.l,,.. tii.l''Jxt;
oCo-rlotol
l*ItWt
vr
ocCL
croq,
ttfIt
JcdcroOJ
t,r
Vl
oco-croo0,3loETd
htcdcroo,
OJ
=oro
vl
oCo-croo,
60,ET.D
n=o=foOJ
OJ
o,qo
l
ogo-trro0)
o,
0,cro
vr
=odtrro0)
o,
olcro
'{l,*/
EIblql5l
ilclvrltl
=lorla@ilg
iz;3o,
i
\l(r\r,>
tr.'g
,, jlo*
" i,"
,it'( :)'

F
AP50,o,
==/\(D:-2 0_t,
9.or+(D
q)Ettl.+
G'T'
T'
r)ocdcr(D
oCc+tioco(Do-+rvloa
E'(D
Q.-ii
5'
0cnIoc).+o-tIog.atr
cpcp(n
(trCEEo,+ano-ct(Dv,oEoo-o,a+
=.9.o,
=3Igr")-IzEP
pco,
=oCL
zoc-oI
rca
oaoof
(1T
zocaotJlc-gao-
zocoltlc!ao
G'o:to
oao€+-o,JvlEo):]-t-tro,g
T'rrt
llrooJ
7q,t,dac)
oocto,
tn
oco-croo,
OJ
ocr6-
vltocECFoo)
o)
o)cro
Vl
ocCL
cto0,
g.6-go
vl
oco-croog_
aJg(D
NCN
,Jlao)do-(Do,
gtIof(')sc6J3o)J@
OJ
o,i
4ao.l
3o,OJ
3
!Caoox3ooa
v1
=.=crlloEc3E'tt
C
o'0)o,
of
oavl
go=?cr=.dt+oa
6-otttooEo
c)I
3
o0,o(D
=.c+
oo)o-
9-o5'
cn{ro)3(D
o-v,(Dto
o(D
3o)
=?(D
o-a
o)cn
o)oao-oC
o,6-ffr-haOJ
3o
€(D
s.oooo.+5(Do,-l-o
zoo-+rct(Do-Vl
a)cz6c
It
oCdcto0J
oog(D
tntoC,
o-d(D
o,
oOJcro
t
oco-croOJ
0).
dgo
vl
oco-uoOJ
oo)grD
l
=ocdCFoog.6-g(D
a
oco-ct(D
o,
o)
o)go
FouoCLvlOJJCLoFoo
t^
oco-uooo
t
ocdcro0)
g.6-cr(D
I

N@
N{ |9('r NUT
NF
N(1,
NN Nll
No Fr(o F6
ts{ Fro l.rUI
FF Frl4l
FN FF |lo
o,
o,g
o_t,N'AJoc-tll6)(D:Jo-o)f-toauo)o-IgEU)oa
o(Dt
or.
o.tg
o-trN5oga
v(D
9.o-of.+0oo.+oVl
q5oJ-+dqaJ(D6' -.9tg
(Do9=
a)-oi O.+ O-6'pfo,1
gogqsvo)o-o6-(ttl
o-o,
(t(l5oln3.at-ho,9.
4.o-l
zcd.=(cI
aq)*o=
oofo.
6'5.Tl0)a.
oa0,@
=og)
==.m3o
(Eofo
oo-0:3o@
CJ)co5'f-n0)g
ox(oo5'T1A)a.
z9ol1o€oTDoa@
3oc@oo-t
=g3u(D
o_t,g(Do-an
zca.3(aCJ)+q)do5
oo=o-
6'5-Tl
og
o-q,@
=oq)
€
m3o(aofo
oo-0:Jo@
@co6'=t.Tl!)o.
ox(oo=11og
z9o'T1o€o-TDoo.@
zr')cu(Do-Vl
:tc3croao6oo-vl
T'ovlIo
E
=.Ft
o:t
=odo-OJfottoo-o.la+
=.c!aovlctn9..+oo-hoc.
fc9.o=T'C3
tJl
ocdct(D
ooJ.
o.,E(D
vl
ocdcroog.OJu6-
Vl
ocEcroooJ.
o)u(D
t
oc
t
oc
vl
oc
a
oC
1
ocEcroo,
oJ
tn
oco-u(D
o,
o)
tscroo-3n
OJfo-
cr oJOcFo-Oq
ooC.+oHo
a
oCdcroo,
o.o,do
th
oco-croo)
g.o,uo
1
oco-ctoog.o)g(D
1
ocdcrooo)
o,cr(D
l,t)
ocd(toOJ
g.o.tcr6-
(n
oC,
o-Eoo.r
g.OJgo
tscroo-UIo)5o-
cro)Ocrqoq
ooc,+o_fi
Po
Vr
oco-croo)gr,
o,go
a
oco_uoq,
o,qJgo
CLgo0,
o
o-ctoo,
o,
o-crooo
o-crooq.!
o)g(D
oE6-
o(to
o)u(D
ogo
oJgo
tno,r+ooo)t:tqtl(Dfo
;c6t3o,
=@:to,1o)i
zo)3o)
o)3
"{6.L -/
"*$n

P
olcl.-t I<lIooc+oan
0oa+g.a
3tr,@U'
ttlcoftof,t(D
ct(Dvlo{roo5(D
o,
trlc-m(D
lol:lt<ltnI
I
II
I
I
acoEo.+t(D
3.at(DlnoE'oCLo,.+=.9.q,f
letgl\lc,la)l-t\l(flzlcPl-II
pcgl
6'o-3OJVrn.otcqqoof
o
!lq)lgtl.+l6'lutltrlmlol.<i
t/, I.+lo)l.+lolI
-l(Dlo.r In
(trl(DJosPcl53o)J(p5o,ao)d
=ao,3o)
o,3
Lfrc.foCr-t,+o.lIt
€(D
To-oc
zoo+r5oo-l
=(1cz6c
zc)ccr(DCLtt5c3cr(D
o-irtrr(DCLan
T'oVra+
IoEE.r-t
o=oJa+oo,JoEogo)
=.o-(Dv,cVlc.4o)a+oo)g
oE'(D
o)t.=ga
tadfoo-li
3'gt|
o)o
='o
3ocGIoo-Vr
fC3croo{rd(Do-tn
o)
og
oN55ocItvolndo
l5l/fl9lotol.+l9tut
=I
octo
oCr+a^ocatoqT'o)d
o6-
(trl
vo)g9-ooa
*o)ga
=owi.o+ro)9-4
PocroCLto,5EL0,go
t
ocdET(D
o)
o,
0,go
t
oco-croo,
9.ogo
1
oco-ctoo,q,
OJcro
PET(Do-vlo)
=CLo,croooco
ocroo-llr
Vl
ogo-croo,
0)
=o)crfD
IttoCo-croo)
o,=o,go
v,
oCEuo0,
g.OJgo
Fcroo-vlofCLo,ctoooco
ocroo-t
tn5oco-croo,
g.o)cro

g-OJq
o+rN5ogvl6)o:toOJr+ocrotox
Ig
(o
l)ovl
vr
oco-ctoo,
oo,lgo
F
pC9l6'o-o9.o(D
ooIA
@E{
T'
o(Df(Da9taC-@(Do:'
tJl
oo=o-olJ1ca
cno-
opl+51o +l
olo-lol=lfot,(Do-a)(coa(Dof
tt,I
of,oE]Io-ogzG'
oa.t
o!toCL.!1ggl|(D
>5q, o)
=Er&Eozo
t
-E=ogr630,o
vr
pc9L
a=rf!0,no
oo.t
=lfto)
o
.v38
N
zvP3=co='2ct
-tqBE
Ed'c='oO-!
==oofEd&ooE(D
dt1t
tnJood
o,of
oa
{
.o9.
0,c30,
D>5o, ql
=ct&EoZo
1
-E+oE'.l
=0,oVl
ptr9r: -=ial0,*,o
ato
tASoq,
o
770=ollvcL
tJr Idloldlol-l(Dlo,t+-5
ctQ(D
=o
;ctt53o,:t@to,1o)t
zo,3o)
o)
3
s { Or gl F w N l..r
o.o,g
o+rNFoc-avo2.oo=a0oofro
l(/)
ETI9P
=TIT'
r)I
F
zIxIv
m-ocEoo-6c5oo-1n
.ttvrooc,a+o=o
l=t(Dl-lolvrlltlolfI ttllo
€qTo-oCEEoo!otna
IoEo,g
5.a
=o5g.ilr+o(acioEof,
€gI
(D
-oc€'t,oo-€OJIta+(D
-oo3
=qio-oc€'Eoo-
ogcfao{
lol-lolfl*lvl(DlEloJ| (')l(Dl3l(Dlfl'+ltalclfrlol-I(D| (./tI
I
III
I
z))-lrtDf-D
=J]1j'a-CFoCLtJ7
l
oCddo0)
g.OJ
d6-
v,
oCE5ooJ
o.o.tg(D
Vr
oCEuooo.Fg(D
tn
ocEuoo,
g.dgfD
atoCo-croo,
oo)uo
ltr
ocdu(D
og.trqo
tn:tocE5(D
oJ
g.dg(D
tsodoCLlno=oo)cto(D
L\T*"
a',"i\'";"r is, :,'1.. -
,11 ,'1,:.'r:,1,,,.,*
l+ ?.{r.":a
.,:4
)
i:!
.,S
\J,,\\t\{z*. l-Jtr, rt\'r." "&"L
,lr,f*o;i i

ru
zoFl
t'e
Fl
rq
{rt)(D
ttlto)froIoOJ
@o=(')s
UIt3o)Jwo,ao)+
=ao,3o,o,3
C'\ |
t).e'J ---
\ {dfJ (h"
?j '*r:i r*r t"+"i ^
\4L 'r':I;j:;,."'i!; {}'+ ''-i! dG*
{1, !,il{b .t'w --.e,
o4o
F|l
Flo (0
(D T'Ftaloo ==oa =o-3€*-tr95'B_ I
5qger*9=''q
3'
BHE'g 1E0'B fd==i
6-P{Eli -.6'o.<= 5a8-rcEH.=o
oocoYoxga=j'(5o9.oo-oOE:rEI9(D9o-
:t
oCvloT'
2.o.+ooEoa
I(D
cE
=.6
g.ogr+
oN'soo{olc
]A
ogdcr(D
OJ
0).
ilgo
1
ocdcroo,
g.o,go
l
oCo-uoOJ
o,
o)u6-
Ic.-t
Cfoodo-VlIfDt+g.vr
G'rt[J1
lacItEoFN
tos.crotn
o_tr
6)(D5(D
9rttlcI
oqoo=
Llr
oJJo-
6)ofogr
!
9.c..o,J
0
oo-()
='o
opZCtp917a'€o-=Za€o=eaorof@o- 6'
=o=o-ga (-S6I .8"
=l2gR3x\.;'3='o(D
=.K+EJ=
8aH.8o.<qgg. o-f
fra5'8
=ottooUq
OJa+
(Do,t.+N
?
{ Or gr F ul N P
o.OJ
=G
o-lrN)5oqVl6)o=o-o,ouo,o7rIc
Eti(D-c)oVl
o,
o)g
o+rN'5oca1
v(D
9.o-ofr+Iocta+oav,
t./lm€.+
o
=.ttltr
o-oc€'3o5
T'oUta+oo6coo,ao
=..+
ofao)GoatiCIfc,o
m:o-otJ7c')oE
=otnt.gqot-ofvlgE!to-a+
€oTo-ctc€'T'(Do-(+
oo,.+oo,a.
=.a
r)I
-3
Io)
2.ttc=
1
oco-5oo,
g.{ud(D
1
5ogEcrooJ
g_
OJgo
oT'f.ofo)
a
oco-Eooo)
t^
oco-crooo)
t
ocdcroOJ
o
Vr
oCo-uoo)
oouo
OJgo
ogo
odo

5'I
ocv,o
ocdltrocooo-!o
oo
(tQ
s7OJgoo
(trl
o-o.t
gaJotd.oo)
_gG
t:toco-croo)
g.OJgo
ts
0c.+Ioc).+ottgo.+g.vr
G'@v,
tJ1cEEo-.+t(D-s.c)(Dtho-trEoo-OJ
=.9.o)
=
IIoC'z@
?pqa o,o--:so\o-9lcz,aG' O-vO)
=.otc-gq(Dof
oIT'(Do-o,
=.o
'rtoCLor
--.al(C0llo
(
ulF
lt1.+o.'.+o-oo,
oqoJc)sc6
=30,
@5OJIo,n
zao)3o,o,3
rt .l
l:t ,:ir;'! '.r..t> .:l
49l,ri1'1r,,,, "' tt,'ttll, ", r,rl ,i
t t.
tC-
Po (o s { ol gr F ul N P
IT'lcltl(Dlotxl.<l3loldlol-
I
I
I
I
I
otrEr
'bn
g
€'OJ-oof
oaVl
:Jc2.o5T'c3Et
vo,o-
!oo-
0o=cr=.OJ.+oa
z(Do5o).+ourdOJgNo)1Lofcf
!olnaIo
T'E.
=of=.o,.+oOJfo-Eoo-o,
=.ooVlcta..+o,doa-+io)g
€g(D
-og.EE(Do-d
oOJd(D
zoocroo-vl
=fggvl?'oo-lrzr)c
=c')c
oJf
€o)
3(D-1
oJ.+=.o
ofao-o1^
5ocEr
v
oco-
r
:tocCL
rocCL
rI#
t
ocCL
trtt*
EocCL
rtF
t^
oco-rIOJllq'|
F
tr,
ocCL
rog,rro
PocroCLvr0,
o-ql
s(D

N(rr N5 N(1,
NN NF No F(0 Fo H{ Por
Fgl F5 Fr(^, FrN Fr
P
t>t<loloJItrl-tl<tol+rINtsI
l=lolsl(,l6)lolold-io-uoc)xIc
Etn(D-o(Dvl
l>I<lo)lolcrtdt.<Ilol-lN)5tocVtnovrdof.+goc),+oIJ'
To='!oo-o,.+=.c,vl
I>t<lo,loIUIr+t.<lol+ll3lol.tlflol-lr)Jf,loIlr)llljld
oovl-ho
-g.gq
I o=t.=15618."'l.+(Dlo\loiOloc| =dt€9 L
lad^-(D5o-o_ TtrO)6+=lOo
(tllsnOJo-o'6-@
3codlvrla!lolEItnlol?latloltl
I
flol-.lo-l
Iflo(rl+I
lzlct;t-.l=loaI lJ1l4loJlFt
lolf
!oo-o,
=.()
o5
=o.+o-
'o(Do-o)e+
=.a)v(Dacvloon.o=T1o)9.
3(-)c(DfDo-tJl
:tc3u(D
octoo-vl
lzlcllnlflsqI t4,| .-tlo)l-floIf
I
t>l-lr)lol5lo-lFt
lol:flTrlo)lol.+t.<
€q)l
oo)
lalclc)| .-tlolfIl'Tllo)lo| .-1.
l<I
I
oxgt|of'Tlo)g.
zr.)cuoo-a
:tc35oo-+rcroo-Vl
an
=.fgtlo!c3E'Vr
1)1
ocdcroOJ
o,
o,cro
an
ocdcroa)
g.OJgo
(n
ocdcroo)
OJ
oJgo
an
ogdEoOJ
g.6-go
th
ocdcroOJ
OJ
ogo
tt1
oco-u(D
o)
g.dE(D
t
oqdE(D
oo.OJuo
tsctoo_Vlo=o-
Uo,(Du+ovtoocfroPc)
at
oco-ooo,
g.dgo
1
oqdctoo,
g.OJgo
a^
ocdcr(D
og.o,cr(D
att
oCdcroo)
o,
OJcr(D
1
oco-uoo)
o,
o56-
tsgoo-tOJ5o-
cr o,@cr+oq
ooca+o{rFo
In
oCdcrooJ
o)
oJgo
,J'l
o)do-oo,
toqoJo
V,53o):t@5o,Io)d
=aID3o,
o)3

l5
IF
ts
I(Df.9.of
oJr)o,
ooq,rf.ofOJ
c)og5anq6-
oJc)o
Ig
Ioo.+o
G'(p(n
Ic
Ioooa
I0o-
oEr+
o,
aooE.t.+o5atg
g.5oCLE'o,o3oo-rr1
pco,
-ir6'CL
I
0IzG'
Cf,c)-
!o,oCL0,
.l0,
=
lJlr Fro (o @ { or ul F w N ts
x0J5gllo,
oo3o(DaoOJ-octo,
t
l+lol=ltlElotaldl=o
C,crq).+ot
lotxI.<tmlolflutc!tE.<-
v(DtcooJ3.ofottc.E'3oJ
=-lrc9.of!c3Evl
€ooa
=foqlato.l
6-
lElclanlololxl='t(Dlo
3occro)
o
7oo-o.l
=d€o,a3(D
z(Do5o.+o(trogNoJ!3.o:Jcf
lzloo
{lEoo-2z6c@(Do-a
t
oco-uoo,
o.o,glD
t
ocdcrooq,
t
oco-uoo,
o
t
ocdcroo,
oo,cr6-
anJoco-ct(D
oor.
dg(D
ai
ocdcr(D
o)
o.o,cr6-
atltocCL
ct(D
o,
g.o)E(D
at
ocdcroo,
g.o)cro
atl
oco-ct(D
o,
g.o,g(D
1
ogo-croo,
o)
o)gfD
tsoct(Do-1
0,:tCLouoo
ocr6-
o,go
ltro,o:Eoo,
@o:ta)
ct
3o.tf@
=rOJao)d
zo)3o,o)3
I
ffi{

tso F{ FlC'r
Frtr PA Pu)
liN
tD5c)=r-=:
occ-tt (D
oct+vlocc)oo-Eo*9_ogq:<7OJo-oo-
oa
o-OJ
cnrfoa4
f1
an
ocdcroo,
g.OJgo
=3o(D-
1
ocdcroo)
g.o)go
lT,IJlol.'+lotdl5loldIEl<lcJ
d
lat;IT'
(D
=sf.o,.+o-
l5l=l='lo)| -+rlol€uo5a)
T'-os.tJ'l
o'5-lroaoo)-ofr+o-o)
5c=.6'f
v,
ocdcr(D
ooJ.
dcro
ti
oco-do0)
o,
an
oco-5(D
oJ
o)
o,cro
vl
oco-5ooo
an
oco-oo0,
oo)go
oct6-
o)go
E
F
-{oJ.
foo-ttao)3oo-a)vl
pzPdsgo=1o(D=a_qoOJ E'
6+o-6='f38I t/lV.+3?
r tJl
-:ooE.1J!:o)ol9ng\
o)fo-!oo-OJr+
=.oooa
oJ
Tootrl5oo3.ofo
ln ott
0J-
3otoo!,(!CL
ooPe
5o-oo
o!to
oooooEo
€e-o.cIcEItoCL
3oCLco,a
:'(Do,t+a(D
-iro)g
3o{o,g
zoo{rcroot
Poeroo-VlotJo-o,Foo
t
oco-cro0)
g.o,go
an
ocCL
croo,
OJ
=o',go
t,:toco.
ro6.ojcro
tntoco-
r0r
E6,gfb
ttloooo
0ao5q
cJ3o,f@JoaOJfr
zo,3o)
o.)
3:
h"-
\ffill_,'-r;ii:{'}
,s i .;;.'ii. : ':'^l
h,r l'l-'

,Jl-oc='a+vlofr
mfcctoo!tofanod
m5d
oE.oftJ1od
oo,coo3oltl(Da+
oofro,ao,cttaod
cf
oEoo)4.f@
()oat,ooE(D
l::lcLt(Dlol6IEl=c+
=o)
3ov,ooE(D
OJ
=oq,
6)ofo'UIooE(D
oOJao3(D
o
ct9_o=qJ
=.of+o:Jo3ofroI
ta
d3
vo*.Jotc)o
oE't+tOJ
3otooE(D
o()
Etrl.+
lzl(Dlo)
q.'.o:tct
o).+
=.d
o-+oI(Dfd
o,:f,
gaco)
oaovl
-{g.an(D.+
=.d
{r0)3o
tJrfo6-:(')OJ
.+oaI-q3
7ot.fo.,
ro)Vr(Da
T'othdo=.oavr(D
cnr
3of.+sd
oc)o3tJl
thfro3
!ot.+(D
=.oatt(D
(trl
3oJ.+(D
=.fgal,.rr
t(D
3
qogOJ
(D
-(Dt,OJ
f!o
DT'c=.=(D5'o-{
T1cJo-c1n
=caothoq.f
5q9.o
gqao)E
q)1
(D-oJo-
Itnoo:eoq,
IlJloq)
=
soa)o3
='t
c3ofttJl
1:'ocdctoo)
g.o)go
Vl
ocdctooo.o.lct(D
t
ogEuoooJ.
(l,go
vr
oCdcroo)
g.o)uo
tJoco-uooJ
o).
ttEo
Vr
oCo-cr(D
o,
or.
OJct(D
t
ogo-Eoo)
o).
tug(D
v,
ocdcroOJ
or.
OJoo
t
ogo-ooo)
o).
ilcr(D
at
ocdd(D
o)
oJ.
OJuo
t
oCo_EoooJ.
o.,cro
Vl5oco-uooo).
o,go
t11
ocdu(D
o,
oJ.
OJoo
tt
oCo_ct(D
oJ
o).
o,Eo
Vl
=oco-Eoo,
g.oJgo
vl
ocdctoq)
o.OJgo
v,
oCo-Eoo.,
o,
ocr(D
tlt
ogdCoo,
g.o,go
vl
ocdctoq,
oJ.
o,ct6-
t
oCdFooo)
0)cr6-
v,
oco-uoo)
o.OJgo
Vl5oco-u(D
o,
g.OJg(D
an:toqdct(D
og.o,go
v,
ocdcroOJ
oo)cro
tn
oco-cr(D
OJ
g_
o)go
t
oCo-6oog.ogo
th
oco-cro0J
OJ
q,go
a
OJt+oIoot+
@oJcl
;c6
3o,J(pJOJa0)d
\
=ao,3It
o)3
tn
oco-croo)q,
dgo

(1,ro
ll,s (A,{ (A,or
(^)(rr
l5tllolclvrlo\octioc-ooCLT'o.ld
oo
qqs7o)a-6'oqq
o-o)oqJotni.o-troa.
t>t<lolo,l5tdl<loNF
octn
oof(D
o)..+o-cro,a)-IcEtos.a,oan
loIt,tdlol3loldl<tTrlo,c)
a
l<l6'laltlclfrlol'<m.ctc€'3offr
lol-lldl(l)lul6-loJfCL
o-{E
ga
ai
an
ocduoOJ
g.OJgo
]A
oco-crooo.o,cro
an
oco-croo)
oo,go
ttl
ocdcroOJ
g.o,go
Vl
oco-croo,
g.dgo
tllGo)-oroo,
@ofo
cvl=3o)fw=rt1JaOJ+
Iz-o,3OJ
o,3
zo)v,oE
=o
zOJanoJ
|,rrooc)c-3
Io().+
o)
rooo-n.+
-oa
oooil4.J(o
ooU'oo
€oo-oE.ttE'oo-c+JoOJfr-o-fro,o.
zoo'TlG'mIv,
(n
ocdcrooo).
{Dgo
1
ogduooo.r,
o,go
vl
oCo-croOJ
g.OJu6-
a
ocd(t(D
ooo,go
Vr
ogo-uo0)
o.OJuo
6
ocdct(D
oo.o)go
an
ogdu(D
o)
o,OJg(D
vl
oCo-croo,
or.
OJu|D
tsocr(Do-Vro)fo-ocroo
C-oJ
lttEor.)c-3
Vl
ogo-EoOJ
o.o)cro

-{o3Eo-oJ
t-oJu3a!-oVlooo(D
3Itoo-ofooo)co-o3o.+o-
!caoo:togo-6'3(D.+o-
CDaoJc)
otnc)oE
tJ1(Di+
ltto,ooo-(D()t+o
o)(n
oo-(Do.+o3lnot
o,fop_o)t
a
rDt+
(1-oIo(')d
oJ
f
tt,od
TImv1(tto
ao)o(DoVlFio3tJ)od
5r+ovlfro3ttlo.+
lJ)(DfrUI-lroa
=oJvloJ
crof(D
-ao)ocao
-{o59.6-c)do
o)Jo-oo-(D5od(Do.+o3vloatr
tt1(D
ov,ooE(D
G'! ftt,
c3oJo)
tt,.+(D
=.No
mz-{(Dxo
=.=o)*.o:tr)o,
(DoJo-o,3E
G'cttt-OJ
3!t
odovlooEI(D
+cfJ
oclT1o-
('/1oq(Dtv1
ttlcc)f.ofoJE'T'oq)i+CVl
z0)lnoaco!f;.o=
mo)
VIca)3.of
a
ocdcroo)
o.,
o,go
tJl5oco-CFoOJ
oOJgo
vl
ocdcroo)
0r.
o)cr6-
1
=ogo_uoo)
g.o,go
(
ocd6oq)
g.dcr6-
(5oco_5oo,
oJ.
o.,uo
t
ocdooOJ
o.dg(D
v1
oco-qoo)
o.o.l6o
vl
ocdctoo,
oJ
og(D
t115ocdctooo.o.loo
vl
ocdo(D
o,
o.o,g(D
t
oco-uooo.o.lcr6-
tJoco-croo)
o)
ogo
to
ocdcoo)
oo)g(D
tt,
=ogo_uoo)
o).
o,cr(D
]n
oco-ct(D
oo,
o,cto
|J)
oco-u(DqJ
oJ.
Fcr6-
Vl5ogo_coo,
g.o,c'.o
tJl
ocduoo,
o,
o5o
Vr
oco-croo,
g.6-cr6-
V,
=oco_croo)
g.o,go
t
ocdF(D
o)
o,
o)go
UI
odctoq)
g.o,d6-
t
oco_croo)
ooJcro
v)
oco_croo,
or.
o,cro
an
ocduoo)
o,
oEo
vt
oco-cto0J
o,
oJcto
ln
oco_CFoOJ
o).
o,cr6-
VtdOJdo-oo,
qqo=o
;c653o,f@to,aOJ
=10,3OJ
o,3:

H
So=Io)fo
co)
lrlolclot?IElot-IClct-lv,lolol-lot-trlot:
Icd
ooofroa
G'@v,
oEt4
o)
3oo-E.1'r+ofc)
;g=oa
o)ao)3ooaltJ1
plFgl8.#tEal=.+16\-, I O,<lr\.
1<lol\.1glzlGrl*l
I
I
lltl
/l
ffi
ffi
5N FIF!'lP(1,(o
=o:o)ootc)oEo
mJo-o5ofa)
=(},eao,thofo-
lmlflo-lolvllololElo'lol!lclEl3lolflfr
o)an.+9.o-tofro)f,o-3c,ao3ooa
€.d
=o-=.
oE11.ofo)
ot,.+o':to,
]iJocdF(D
o)
g.dgo
VI
ocdctaoor,
o,go
ado)
oIo0,
gqo(-)
:<
tn
3OJ
wOJ;lFl
-l2l-. 1dlII(Ul.<lorl3l
:l

P lFr{ lor l-l(tr PF F IFTul lN Frts glololv gl (,rr
+lFl{l$l$lFlf;- lp lR l= l; lH lr5F E l; lglsFuFl l;l-lt.lsl"l I I lil I
oE'o=oo,aoc5v,
IV,t.<t-lflsIT'lcl3lEl.n
I
I
I
I
I
I
_n t# tqo l(D luf, la lf.
dlSlFq 16'lsl- |xl I€t I
an
oco-ctoog.o,go
Vl
ocdEooq,.
o)go
ttt
ocdcroo,
g_
It)go
an
oco--cr(D
OJ
ooCFo
1
oco-crooo.o,cro
trl
oca-croqJ
g.OJgo
t
oco-u(D
o,
o)
ogo
vl
oco--E(D
og.o)cto
Vl
ocd(too)
OJ
og(D
vl
oco-uoog.o,Eo
tn
oco_croo,
o)
OJgo
.A
oco-ct(D
o,
or.
o,E6-
an
oco-coo0)
o,go
{aoJ
3oo-t,oo,3oo-a)Vl
lsqIoct.+o-?@G't,/l
E,Oo-ilE=s;"tr. o--oJcl6<-E
(Jcltt -(D5o)Olna5o
ogq
I{r')-{\<lololJI(Dl(^ldlolJlo-lvl(DlJtr IT'IaloJl.-i Iol-t<lsl(rl(Dtolatt I(DlatI\rlalzl@la.) |flolthldl
f.)totn
!tln!!.o,3
tJlto)do-oo,
@oJo
UI53o)J@5o,-Itfr
IZ)ai(UlIIori.<lorl1l

*Nur
Nl\l
N Nct ts(o ts@
Fr{ Por
Frur
tsA ts(rI tsNT
FFr
tso(o 6 { o ur F w N P
It
0oo(t=.6-doa
!Ctt1(D
ox3oo-
c_g.EOJ-o,
of
oln
r)o,atl
oo)-d
=.d
m3o
cnro5c)
oo-o
='(D
al)g.-o3on-
G'-ofc)
othooE
-{5o-o,oo.J'ooE'(D
lmlflo-lolctlalolflol5l6't-lcfr-o,Vlocfo-
t./l
=.foqo!q3EtJl
lf,t-hlclv,l6'l5l!lcl3loI tJl
of=.(Ue+o-an
lmlc)to,Jlcc'tg.of'Tto)a..+
lotxt.<loalrDlf,IlrlloJlot-.t.<
=grl
oc3oo)fa-o_"+rcu,6'=()oEo)o
q,
=o_E6-oo-gao)atl
3o)a'):t5'(D
!'Tl-l3oc)
='oVr
=.fr+ro,9.
+ro-tttp.To3(Dfr-
vItr:o-u-o5oo1
cloEo
lT1l5oo
15!f.c)ctaofc)
olnc)oEo
!cltloox3odo-ttr
l!l6-lc-o)
FoEttr
Jo(Do-6-(t1
oc-o)c.
z(D5cNo-(J1
IT'lolo)l-l+rlol€l=lotdloI tJl
tn
ocEgoOJ
oJ.
ocr6-
tntodu(D
o)(l).
OJqo
vl
ocdcr(D
o,(U
OJ
CFo
1
5ocd6oOJ
o.OJ
ct6-
a
oo--croo,
o)
o)uo
In5ocdooo)
o)
tn
oCdcroo)
o)
o)u(D
oE!tofo)
t^
ocdcroo)
g.iluo
th
oCo_do
g.o,cr(D
lJl
ocdcto
o
uo
vr
ocdcrooo)
OJc(D
t
=ocduoOJ
o.o.,6o
UI
oco--c'(D
oo).
o,uo
tn
oE5oo)
=:oJ(t(D
an
ocduoo.
oo
1
oCdcr(D
o
=:OJ
5o
l,t1
oco_croOJ
g.o)cto
TA5ocduoo)
o).
o,go
UI
ocdu(D
o)
o.o)co
vr
ocdc'-(D
o)
o)
OJuo
t^
oco_cooJ
=qJ
d(D
6Joco-cro0,
o)
o,o(D
o,66-
lt1OJ+o-oOJ
oaof(')
3o)
@
o)1o.)d
=1o,3o.)
o,3
\"'- f -'r \
-r
(
",L,'t1.,
, l 'i), f,..
'.1 ,
\.t\ ';' t,il.,tr r, (),
l'. -'r'