Ayurveda interventions for Gout: A systematic review
13
Page 1/13 Ayurveda interventions for Gout: A systematic review Aswani PS ( [email protected] ) National Ayurveda research Institute for Panchakarma, Cheruthuruthy, Thrissur, Kerala Pratibha P Nair National Ayurveda research Institute for Panchakarma, Cheruthuruthy, Thrissur, Kerala Sreedeepthi G N National Ayurveda research Institute for Panchakarma, Cheruthuruthy, Thrissur, Kerala Azeem Ahemmed Central Council for Research in Ayurvedic Sciences (CCRAS), New Delhi B.C.S. Rao Central Council for Research in Ayurvedic Sciences (CCRAS), New Delhi D Sudhakar National Ayurveda research Institute for Panchakarma, Cheruthuruthy, Thrissur, Kerala N Srikanth Central Council for Research in Ayurvedic Sciences (CCRAS), New Delhi Systematic Review Keywords: Ayurveda, Systematic review, Gout, Vatarakta, Vatashonita Posted Date: March 30th, 2022 DOI: https://doi.org/10.21203/rs.3.rs-1504922/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Ayurveda interventions for Gout: A systematic review

Page 1/13
Ayurveda interventions for Gout: A systematic review
Aswani PS ( [email protected] )National Ayurveda research Institute for Panchakarma, Cheruthuruthy, Thrissur, Kerala
Pratibha P Nair National Ayurveda research Institute for Panchakarma, Cheruthuruthy, Thrissur, Kerala
Sreedeepthi G N National Ayurveda research Institute for Panchakarma, Cheruthuruthy, Thrissur, Kerala
Azeem Ahemmed Central Council for Research in Ayurvedic Sciences (CCRAS), New Delhi
B.C.S. Rao Central Council for Research in Ayurvedic Sciences (CCRAS), New Delhi
D Sudhakar National Ayurveda research Institute for Panchakarma, Cheruthuruthy, Thrissur, Kerala
N Srikanth Central Council for Research in Ayurvedic Sciences (CCRAS), New Delhi
Systematic Review
Keywords: Ayurveda, Systematic review, Gout, Vatarakta, Vatashonita
Posted Date: March 30th, 2022
DOI: https://doi.org/10.21203/rs.3.rs-1504922/v1
License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License

Page 2/13
AbstractBackground
Patients with gout frequently use complementary and alternative medicines including Ayurveda medications and treatment procedures and hence it isimportant to determine their safety and e�cacy.
Objectives
A systematic review of the published clinical data in view of safety and effectiveness of Ayurvedic treatment protocols in gout viz-a-viz vatarakta.
Methods
We searched the PubMed, Cochrane Library (Cochrane Central Register of Controlled Trials: Issue 6 of 12, June 2018), Google Scholar, AYUSH Research Portal(Govt. of India), DHARA, Ancient Science of Life, Shodhganga@INFLIBNET, Online clinical trial registers and grey literature available from GovernmentAyurveda College, Trivandrum (Manual search) IPGT & RA, Gujrat Ayurveda UniversityPRISMA (preferred reporting items for systematic review and meta-analysis) guided systematic literature review was performed. We excluded abstract only publications. We were unable to do meta-analysis due tounavailability of suitable studies. Study eligibility criteria: Cases diagnosed as gout by laboratory �ndings and/or clinical symptoms, who underwentAyurvedic treatment/Cases clinically diagnosed as Vatarakta, who underwent Ayurvedic treatment. Participants and interventions and controls: We includedcases of either sex diagnosed as gout by laboratory �ndings and/or clinical symptoms, who underwent Ayurvedic treatment/Cases clinically diagnosed asVatarakta or gout, who underwent Ayurvedic treatment either Randomized controlled trials (RCTs), Quasi-Experimental Trials, Single group clinical trials,Comparative Clinical Trials (CCTs) and Pragmatic trials
Results
A total of 398 potentially relevant studies were found and 21 studies met the inclusion criteria among which 10 studies were pre-post studies, 7 studies wereincluded among Randomized Comparative Clinical Trials, and 4 were among Comparative clinical trials.
Conclusions and implications of key �ndings
Even though Ayurveda physicians are pragmatically treating/rehabilitating Vatarakta/gout cases and reported satisfactory results in term of both safety ande�cacy, this review is unable to produce strong valid evidence to prove the e�cacy and safety of Ayurveda over Non-Ayurveda interventions or Placebo due tolack of quality and unavailability of published works. So the authors propose well-organized and methodologically sound quality research works in this regard.
Systematic review registration number- PROSPERO (CRD42019131198)
1. IntroductionAyurveda the science of life gives a holistic approach to the physical, mental and social health of an individual. It is the Indian traditional system of medicine,which gives utmost importance to the preventive aspect along with the curative aspects. Vatashonita (VS) or Vatarakta (VR) in Ayurvedic parlance has thesame features as that of gout. Etiology, Pathology, and clinical features are common under both these headings (1).
Gout is a metabolic disorder, which causes in�ammation of the joints. Due to the excessive buildup of uric acid crystals in the body, tiny needle-shapedcrystals of uric acid accumulate over joints which, in turn, trigger in�ammation. (2). According to available data the worldwide prevalence of gout ranges from0.1% to approximately 10%, and the incidence ranges from 0.3 to 6 cases per 1,000 persons. Genetic and environmental factors play a major role incontributing the disease. Other major risk factors for gout include hyperuricemia, dietary factors, medications, co morbidities and exposure to lead (3).Mortality is higher in individuals with cardiovascular co morbidity. Tophi, joint deformity, osteoarthritis, bone loss and ocular complications like conjunctivitis,uveitis, or scleritis are very common in patients of gout. Major complications like urate nephropathy and nephrolithisis are not uncommon. Increasedprevalence of gout among individuals with chronic diseases such as hypertension, chronic kidney disease, diabetes, obese, congestive heart failure,myocardial infarction etc. increases the disease burden and risk of death (4) (5) (6) (7).
Patients usually present with acute joint pain. The pain is usually of sudden onset waking the patient from sleep or it may have developed gradually overhour’s reaching the maximum intensity in 24 hours (8). The pain will be of excruciating nature. Gout �are-ups are often presented as local in�ammation whichpresents as erythematous, swollen and a warm joint. Systemic features of the joint in�ammation may include fever, fatigue and general malaise (9).Eventhough conventional treatment for gout is good for the management of symptoms, side effects, long-term effects on vital organs and interactions with theirother medications are of great concern (10).
As already mentioned, gout can be considered as Vatarakta in Ayurvedic parlance, where the vitiation of Vata and Rakta causes manifestation of the diseasein joints. Vatarakta is characterized by Ruk (severe pain), Swayathu (Swelling), Daha (burning sensation), Stabdha Sandhi (joint stiffness), ShyavaRaktaVarnata (blackish-red color), and Sparsasahatwa (severe tenderness and hyperesthesia) in the affected joint. The characteristic feature of this disease isthat it begins at the Hasta or Pada Moolam (small joints of hands and foot) and spreads quickly like rat poison or Akhuvisha(11).
Research works on Ayurvedic treatment for gout is not yet compiled and analyzed. A systemic review on Ayurveda interventions is of utmost importance toprovide knowledge in detail regarding the safety and e�cacy of Ayurveda interventions concerned in this regard. Systematic review is de�ned as ‘acomprehensive review of literature which differs from a traditional literature review in that it is conducted in a methodical (or systematic) manner, according to

Page 3/13
a pre-speci�ed protocol to minimize bias, with the aim of synthesizing the retrieved information’ (12). Assessments of the validity of the �ndings were carriedout in detail to assess the safety and e�cacy of Ayurveda interventions for the management of gout. In this study published data and gray literature onAyurveda management of gout viz-à-viz Vatarakta to establish its safety and clinical effectiveness were thoroughly reviewed. This study shall provide moreprecise estimates of various Ayurveda interventions’ effects in the management of gout either as stand-alone or as an add-on to conventional management.
2. MethodsThe protocol for this review was published in a peer reviewed journal (13).
2.1. Search strategy
For electronic searches we used PubMed, Cochrane Library (Cochrane Central Register of Controlled Trials: Issue 6 of 12, June 2018), Google Scholar, AYUSHResearch Portal (Govt. of India), DHARA, Ancient Science of Life, Shodhganga@INFLIBNET and Online clinical trial registers for identi�cation of trials. We havedone Manual search in Central and departmental libraries of Govt. Ayurveda College, Trivandrum; IPGT & RA, GAU, Jamnagar with due permissions andAyurveda Research Database from authorities. There were no language restrictions. Studies published till date (November 2020) were sought. We repeated thesearches just before the �nal analyses and further studies retrieved for inclusion.
2.2 Inclusion criteria
Types of interventions
We included clinical trials with following intervention and control groups.
i. Intervention - Ayurvedic treatment protocol (Shamana or/and Shodhana) with different dosage forms, type, schedule, drug, treatment procedures, with orwithout Pathayapathya (Lifestyle modi�cations and or speci�c diet charts).
ii. Control - Ayurvedic treatment protocol (Shamana or/and Shodhana) with different dosage forms, type, schedule, drug, treatment procedures, with orwithout Pathayapathya (Lifestyle modi�cations and or speci�c diet charts) were the comparative group to intervention(s)/ exposure(s).Placebo and/orsham therapy and/or Shamana therapy were also considered.
2.3 Data extraction and quality assessment
i. Selection of studies – To determine the studies to be assessed further, 3 authors (APS, PPN and SGN) independently scanned the abstract, title, or bothsections
ii. Three investigators independently screened all citations and abstracts identi�ed by a primary comprehensive search and sorted out potentially eligibletrials. Full articles of potentially eligible trials were obtained and independently evaluated for inclusion in the review based on types of participants(inclusion criteria). Data extraction forms for individual study were prepared. Which included 1) Methods used in the study (Randomization/ allocationconcealment/blinding/ sampling and sample size calculation/length of follow up) 2) Participant characteristics of individual studies (along with diseasecharacteristics/ Number of participants randomized/ Number of participants completing follow up/ reasons for withdrawal from the study) 3)Interventions (Treatment protocol administered/ Formulations used/ SOP’s administered/ Adverse events while the protocol) 4) Outcomes (in terms ofsafety/effectiveness/e�cacy/ Improvement in QoL). For each outcome measured from individual studies, efforts were taken to discuss the risk of bias,consistency, precision and reporting bias. When disagreement happened or in case of ambiguity in data extraction clari�cations were obtained directlyfrom authors/co-authors as much as possible. PRISMA �ow chart (Fig 1) (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) (14)(Liberati 2009) (15).
iii. Data extraction and managementFor studies that ful�lled inclusion criteria, three authors independently extracted the data using standard extraction tables for data (for details seedescription of studies). Disparities were resolved by discussion. We �xed any changes in data extraction by accord and by referring back to originalarticle. When needed, data was sought from authors of the studies.
iv. Dealing with duplicate publicationsIn the case of identical publications and companion papers of a principal study, we tried to maximize the yield of information by simultaneous evaluationof all available data. In cases of doubt, the original publication (usually the oldest version) was given priority.
v. Assessment of risk of bias in included studiesTwo authors (APS and SGN) independently assessed each trial separately. We resolved any disagreements by consensus, or with consultation with thirdauthor (PPN). We assessed risk of bias by using Cochrane RoB tool (Fig 2 and 3) (Sterne JAC 2019). We used the following criteria- Was the randomization process being adequate?- Was there is concealment of allocation sequence until participants were enrolled and allocated to interventions?- Whether there any deviations from intended interventions?- Whether there any missing of outcome data?- The measurement of outcome was appropriate?- Were the reports of the study being free of selective reporting?- Was the study free of other problems that could put it in a high risk of bias?
vi. Measures of treatment effect- the treatment effect were measured by using data available in the individual studies.

Page 4/13
vii. Unit of analysis issues- the levels at which randomization were done and what was the effect of interventions in comparative clinical trials and in pre poststudies.Dealing with missing data we obtained relevant missing data if needed from the authors itself and cautiously made the assessment such as screened,randomized patients as well as ITT (Intention to treat), PP (Treated and per protocol) population. We investigated drop outs, losses to follow up, ADR/AE(Adverse Drug Reaction or Adverse Events).
2.4 Data presentation
We presented the characteristics of each study with type of study, sample size, outcome measures, �ndings and adverse events so that the readers can easilyaccess the risk and bene�ts of each study.
3. ResultsAs shown in �g.1, we found 398 potentially relevant studies after searching electronic databases and grey literature. After perusal of the titles and abstracts,we exclude 377 trials because they didn’t meet the inclusion criteria. 21 studies were included in this review, among which 10 studies were pre post studies, 7studies were included among Randomized Comparative Clinical Trials and 4 among Comparative clinical trials – (Table 1) (16-36)
Risk of bias in included studies
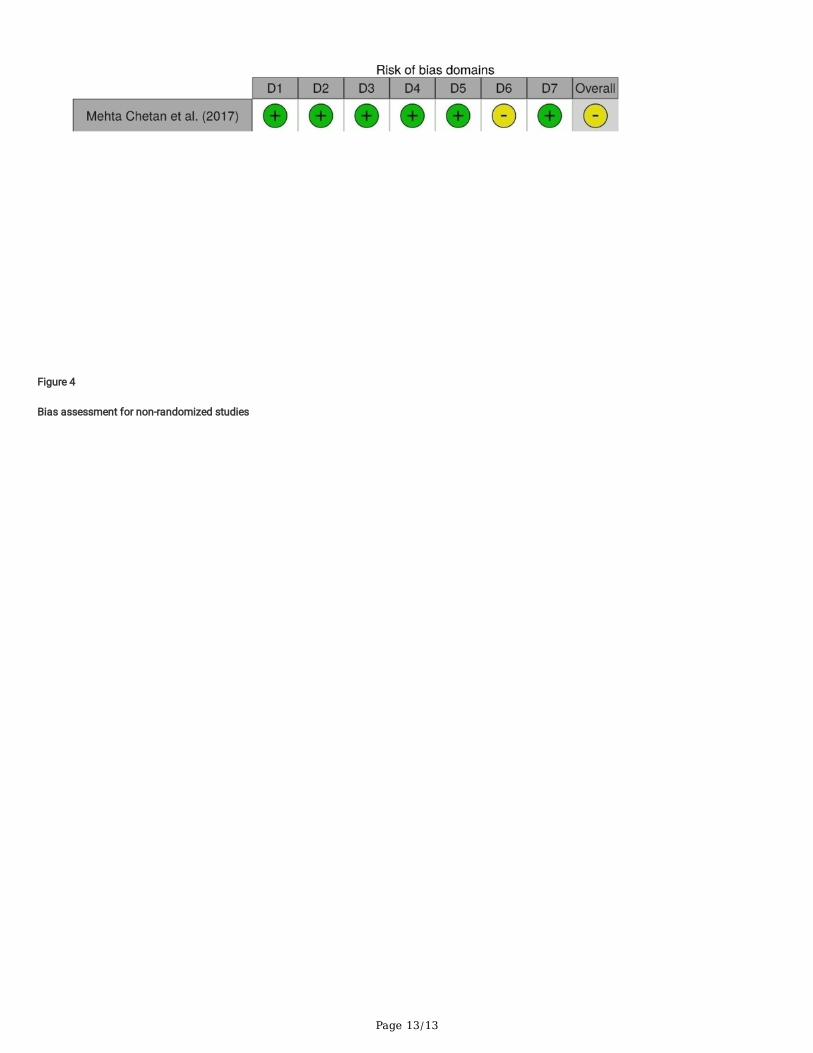
Out of 7 RCTs selected for the review, only two studies had blinding (single blinding) in the procedure (2 studies conducted by by Kuvettu H et al., 2016) and allremaining others were open trials. Two of them were three arm trials (Afshan Begam et al., 2019; Vishwajeet Manjhi et al., 2015) and remaining studies hadonly two arms (Aditya Acharya K et al., 2013; Deepika Gupta et al., 2019; Sharma parvesh et al., 2019; Kuvettu H et al., 2016 (2)).The risk of bias assessmentsis summarized in �gure 2 and 3. The bias assessment of Non-randomized-comparative parallel design is summarized in �gure 4.
Effect of Ayurvedic herbal preparations/ Ayurvedic procedures
No study reported or was designed to investigate complications, hospitalizations, death from any cause and economic data.
Adverse Effects-Adverse effects were not reported in any of the study.
4. DiscussionThis review included trials on Vatrakta or gout. While searching electronic databases and grey literature it was found that there are discrepancies indiagnosing cases as gouty arthritis to Vatarakta by some authors and some authors considered RA, ischemic conditions, psoriatic arthritis, SLE, peripheralischemia etc. to Vatarakta. This was the major problem faced while screening and selecting trials. We included cases diagnoses as Vatarkta/gout based onsigns and symptoms of Vatarakta and serum uric acid levels and excluded cases diagnosed as RA, SLE, psoriatic arthritis etc. Few studies were used onlypure Ayurveda diagnostic criteria’s. Out of 7 RCTs selected for the review, only two studies had blinding (single blinding) in the procedure and all remainingothers were open trials. Two of them were three arm trials and remaining studies had only two arms Subgroup analyses were performed in one study, but theywere done only for participant variables such as Prakruti and Agni, and not for assessment parameters. A total of 1,073 participants from these 07 studiesdiagnosed with Gout were randomly allocated into study and comparison groups. The sample size varies from 462 to 30 in RCTs. The method of samplingwas mentioned only in one study). Six studies used classical symptoms of Vatarakta as per Ayurvedic sciences along with elevated serum uric levels as thediagnostic parameter for Gout whereas one study used only the classical symptoms of Vatarakta as the diagnostic feature.Out of the 7 RCTs, the interventionin 3 studies were only internal medications. In the remaining four studies, three studies had procedures such as Basti treatment in one group while the thirdone had Pradeha (local applicants) in one. Similar comparator was found in only one group.
There were four non-randomized comparative parallel designs as per the inclusion criteria. Amongst these, three studies clearly described about theinterventions given in each and one study had not mentioned this vividly. The assessment criteria were purely based on signs and symptoms of Vataraktha inone study; Ayurvedic parameters like Sandhi shula, Sandhi shotha, Raga, Tvaka vaivarnya, Sparsashyata, Vidaha,Stabdhata, Shithilata along with modernparameters in another study and in the third study, they used American College of Rheumatology 1980 classi�cation criteria. There was no clarity in theassessment parameter, age speci�city and procedure adopted in the fourth study.
Out of ten non-comparative before after trials, �ve trials were about the effect of simple formulations or single drugs). Four trials comprised of interventionswith internal medication along with some procedures and one trial was about the effect of Leech therapy
The signi�cant change in e�cacy between groups of each study was slight as there was slight difference in interventions adopted in study and comparators.It is understandable that the chances of confounders could de�nitely not be excluded as there was no proper randomization in most of the studies. In singlegroup before after trials, only the effect of the individual intervention/Panchakarma procedure as part of a treatment protocol can be assessed. The rationalvalue of such interventions can’t be understood unless an RCT is conducted.
Thus the following drawbacks exist while systematic review of all these studies.
Method of randomization was not proper in most of the trials. Hence, studies with correct method of randomization and blinding will give more unbiasedresults.
Few trials are a combination of procedures and medications. Hence, the protocol for black box or Pragmatic trials will be more suitable for them ratherthan strict RCTs.
Page 5/13
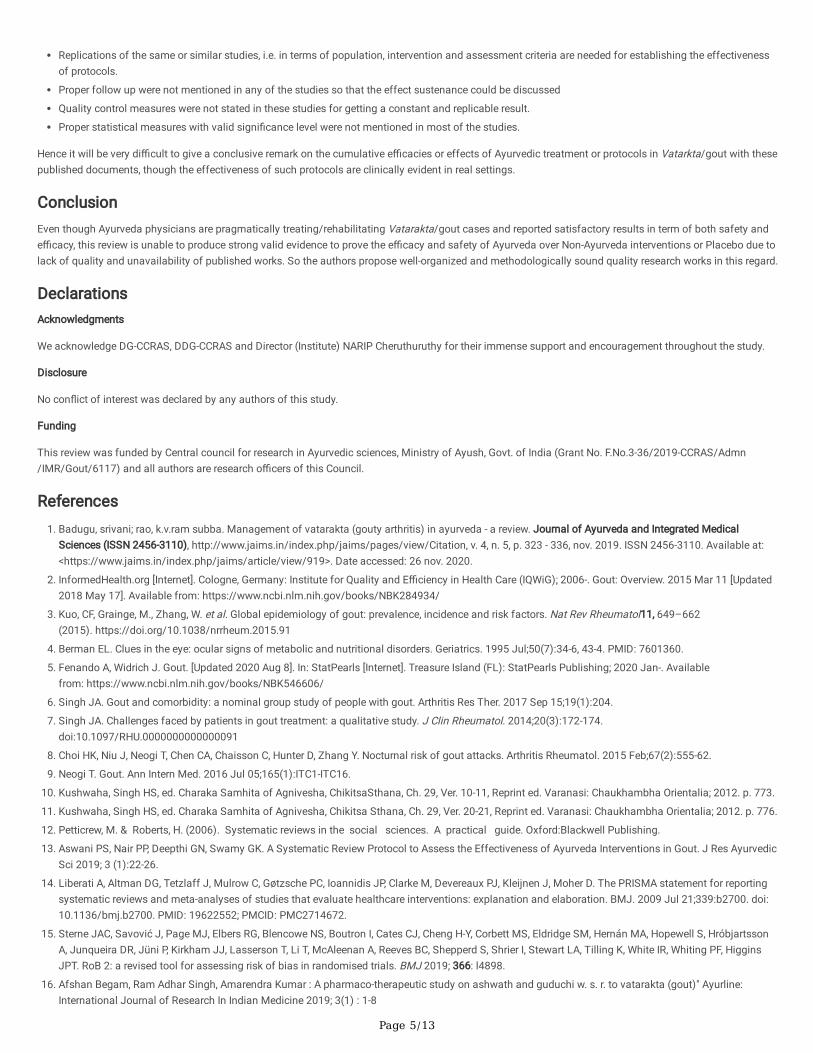
Replications of the same or similar studies, i.e. in terms of population, intervention and assessment criteria are needed for establishing the effectivenessof protocols.
Proper follow up were not mentioned in any of the studies so that the effect sustenance could be discussed
Quality control measures were not stated in these studies for getting a constant and replicable result.
Proper statistical measures with valid signi�cance level were not mentioned in most of the studies.
Hence it will be very di�cult to give a conclusive remark on the cumulative e�cacies or effects of Ayurvedic treatment or protocols in Vatarkta/gout with thesepublished documents, though the effectiveness of such protocols are clinically evident in real settings.
ConclusionEven though Ayurveda physicians are pragmatically treating/rehabilitating Vatarakta/gout cases and reported satisfactory results in term of both safety ande�cacy, this review is unable to produce strong valid evidence to prove the e�cacy and safety of Ayurveda over Non-Ayurveda interventions or Placebo due tolack of quality and unavailability of published works. So the authors propose well-organized and methodologically sound quality research works in this regard.
DeclarationsAcknowledgments
We acknowledge DG-CCRAS, DDG-CCRAS and Director (Institute) NARIP Cheruthuruthy for their immense support and encouragement throughout the study.
Disclosure
No con�ict of interest was declared by any authors of this study.
Funding
This review was funded by Central council for research in Ayurvedic sciences, Ministry of Ayush, Govt. of India (Grant No. F.No.3-36/2019-CCRAS/Admn/IMR/Gout/6117) and all authors are research o�cers of this Council.
References1. Badugu, srivani; rao, k.v.ram subba. Management of vatarakta (gouty arthritis) in ayurveda - a review. Journal of Ayurveda and Integrated Medical
Sciences (ISSN 2456-3110), http://www.jaims.in/index.php/jaims/pages/view/Citation, v. 4, n. 5, p. 323 - 336, nov. 2019. ISSN 2456-3110. Available at:<https://www.jaims.in/index.php/jaims/article/view/919>. Date accessed: 26 nov. 2020.
2. InformedHealth.org [Internet]. Cologne, Germany: Institute for Quality and E�ciency in Health Care (IQWiG); 2006-. Gout: Overview. 2015 Mar 11 [Updated2018 May 17]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK284934/
3. Kuo, CF, Grainge, M., Zhang, W. et al. Global epidemiology of gout: prevalence, incidence and risk factors. Nat Rev Rheumatol11, 649–662(2015). https://doi.org/10.1038/nrrheum.2015.91
4. Berman EL. Clues in the eye: ocular signs of metabolic and nutritional disorders. Geriatrics. 1995 Jul;50(7):34-6, 43-4. PMID: 7601360.
5. Fenando A, Widrich J. Gout. [Updated 2020 Aug 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Availablefrom: https://www.ncbi.nlm.nih.gov/books/NBK546606/
�. Singh JA. Gout and comorbidity: a nominal group study of people with gout. Arthritis Res Ther. 2017 Sep 15;19(1):204.
7. Singh JA. Challenges faced by patients in gout treatment: a qualitative study. J Clin Rheumatol. 2014;20(3):172-174.doi:10.1097/RHU.0000000000000091
�. Choi HK, Niu J, Neogi T, Chen CA, Chaisson C, Hunter D, Zhang Y. Nocturnal risk of gout attacks. Arthritis Rheumatol. 2015 Feb;67(2):555-62.
9. Neogi T. Gout. Ann Intern Med. 2016 Jul 05;165(1):ITC1-ITC16.
10. Kushwaha, Singh HS, ed. Charaka Samhita of Agnivesha, ChikitsaSthana, Ch. 29, Ver. 10-11, Reprint ed. Varanasi: Chaukhambha Orientalia; 2012. p. 773.
11. Kushwaha, Singh HS, ed. Charaka Samhita of Agnivesha, Chikitsa Sthana, Ch. 29, Ver. 20-21, Reprint ed. Varanasi: Chaukhambha Orientalia; 2012. p. 776.
12. Petticrew, M. & Roberts, H. (2006). Systematic reviews in the social sciences. A practical guide. Oxford:Blackwell Publishing.
13. Aswani PS, Nair PP, Deepthi GN, Swamy GK. A Systematic Review Protocol to Assess the Effectiveness of Ayurveda Interventions in Gout. J Res AyurvedicSci 2019; 3 (1):22-26.
14. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, Clarke M, Devereaux PJ, Kleijnen J, Moher D. The PRISMA statement for reportingsystematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009 Jul 21;339:b2700. doi:10.1136/bmj.b2700. PMID: 19622552; PMCID: PMC2714672.
15. Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, Cates CJ, Cheng H-Y, Corbett MS, Eldridge SM, Hernán MA, Hopewell S, HróbjartssonA, Junqueira DR, Jüni P, Kirkham JJ, Lasserson T, Li T, McAleenan A, Reeves BC, Shepperd S, Shrier I, Stewart LA, Tilling K, White IR, Whiting PF, HigginsJPT. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 2019; 366: l4898.
1�. Afshan Begam, Ram Adhar Singh, Amarendra Kumar : A pharmaco-therapeutic study on ashwath and guduchi w. s. r. to vatarakta (gout)" Ayurline:International Journal of Research In Indian Medicine 2019; 3(1) : 1-8

Page 6/13
17. Adithya Acharya K, Ahalya Sharma : Evaluation of the e�cacy of Siravyadha and Guduchi Siddha Yoga Basti in the management of Vatarakta withspecial reference to Gout. IJRAP_International Journal of Research in Ayurveda and Pharmacy May-June 2013.
1�. VishwajeetManjhi et.al :A Clinical Study Of Amritadi Kashayaand Ardhamatrika Basti In The Management Ofvata-Raktaw.S.R. Gout..International JournalOf Medical Science And Clinical Inventions Volume 2 issue 06 2015 page no. 994-1009
19. Dr. Deepika Gupta, Dr. Kamal Sachdev, Dr. Richa Garg : A clinical study to evaluate the e�cacy of Patoladi Kwath (SU. CH.) with or without RasnadiPradeh (CH. SU.) in cases of Vatarakta (W.S.R. to Gouty Arthritis). Journal of Drug Delivery and Therapeutics
20. Dr. Sharma Parvesh : A Comparative Study of Bodhitawak Churan in The Management of Vata-Rakta w.s.r Anupana Madhu and Jala. World Journal ofPharmaceutical and Life Sciences
21. H Kuvettu, S Acharya, AN Nagappa : Clinical Evaluation of Amritha Guggulu in the Management of Gout :Open Archive.DOI: https://doi.org/10.1016/j.jval.2016.08.116
22. H Kuvettu1, A Jyothy, S Acharya, AN Nagappa: Clinical Evaluation of Guduchi Sadhita Sneha in the Management of Gout: Open Archive. DOI:https://doi.org/10.1016/j.jval.2016.03.1169
23. Mehta Chetan1, Bhardwaj Anil ,Bhatia Yogesh , Tripathy B. P : A Comparative Study of Siravyadha and Kokilakshadi Kshayama in Vaatarakta W.S.R toGOUT Research and Reviews: A Journal of Ayurvedic Science, Yoga and Naturopathy ISSN: 2395-6682 (Online) Volume 4, Issue 3 www.stmjournals.com
24. Dr. Vikas Rana, Dr. Anjana Mishra, Prof. B. L. Mehra : Effect of punarnavamrita guggulu with amritadi kvath in the management of vata rakta w.s.r. to gout– a clinical trial. World Journal of Pharmaceutical Research Vol 6, Issue 8, 2017
25. Ashok Kumar Panda et. Al : Effectiveness of Leech Therapy in Gambhira Vata-Rakta (Acute Gout): APilot Study. J Homeop Ayurv Med 2012, 1:2http://dx.doi.org/10.4172/2167-1206.1000108
2�. Dr V Balendu Krishnan, Dr Prashanth A S , Dr S G Chavan: Pre test and post test design study to evaluate the e�cacy of vasti and virechana in goutyarthritis. Pparveshana international journal of ayurvedic research pijar[/july-august-2018/volume-2/issue-6
27. Harbans Singh et al : An Open Label E�cacy Study of Amrita Guggulu and Pinda Taila in the Management of Hyperuricemia in Gout (Vatarakta)Patients.Journal of Research in Ayurvedic Sciences, January-March 2017;1(1):25-3325JRASJRAS10.5005/jp-journals-10064-
2�. Shashank Jha, 2.Londhe PD ROLE OF LEECH APPLICATION IN VATARAKTA: A PILOT STUDY international Journal of Ayurvedic Medicine | Year : 2014 |Volume : 5 | Issue : 1 | Page : 129-132
29. Dr. G.P.Upadhyay, Dr. Anurag Girdhar Vatrakt- A Clinical Study .Journal of Ayurveda Vo\.2 No.2 Apr-Jun 2008
30. L.Prasanna Kumar ROLE OF GUDOOCHYADI KSHEERA VASTIN VATA RAKTA : International Journal of Research in Ayurveda and Pharmacy | Year : 2011 |Volume : 2 | Issue : 1 | Page : 44-46
31. Dr. Harsh Sehgal*1, Dr. Bhavna Singh2 and Dr. Sanandan Thapliyal3Role of Kalmegha (Andrographis paniculata (Burm.F.) Wall. Ex Nees) in treatingVatarakta (Gout) Available online on 15.11.2018 at http://jddtonline.info Journal of Drug Delivery and Therapeutics Open Access to Pharmaceutical andMedical Research
32. Alok Kumar et al. Role of Amrita Gugguluin the management of Vata-rakta -A Clinical Trial International Journal of Pharmaceutical & Biological Archives2014; 5(4): 45 -51
33. Usha Sharma, Krishna Kumar Sharma, Maksudan Singh, Alok Kumar Srivastava, Gyanendra Datta Shukla Mohita Bohra : ROLE OF PUNARNAVA AMRITAGUGGULU IN THE MANAGEMENT OF VATARAKTA – A CLINICAL TRIAL Ayurpharm Int J Ayur Alli Sci., Vol. 4, No. 1 (2015) Pages 1 – 9
34. Yogita Deepak Khore, Subodh Patil : EFFICACY OF DRAKSHA KASHAYA ERAND TAIL VIRACHANA IN VATRAKTA (W.S.R. GOUT) INTERNATIONALAYURVEDIC MEDICAL JOURNAL IAMJ: Volume 8, Issue 1, January - 2020 (www.iamj.in)
35. Shivaprasad Huded, 2. Sonia V Gummadi, 3. Kuber Sankh, 2. H.N. Asha, 2. H.S. Ashwini, 2. K. Lingadore : EVALUATION OFGUDUCHIYOGA IN THEMANAGEMENT OF VATARAKTA (GOUTY ARTHRITIS): A CLINICAL STUDY International Journal of Research in Ayurveda and Pharmacy | Year : 2013 |Volume : 4 | Issue : 5 | Page : 688-692
3�. Pundpal Amitkumar B A CLINICAL STUDY TO EVALUATE THE THERAPEUTIC EFFECT OF VATARAKTANTAK RASA AND LEKHANA BASTI IN VATARAKTAInternational Ayurvedic Medical Journal ISSN:2320 5091 IAMJ: Volume 4; Issue 04; March- 2016.
Table 1

Page 7/13
CHARACTERISTICS OF STUDIES
Reference
Studydesign
N; mean age(years)
Disease Intervention (name; dosageor frequency; duration)
Outcome measures Findings andcomments
Afshan Begamet al.
ComparativeClinical Trial
6811 to 70years
Signs andsymptoms ofVatarakta
Group 1-Aswath KasayaDosage-40 ml bd Duration-90 daysGroup 2-Guduchi Kashaya Dosage-40 ml bd Duration-90 daysGroup 3-Combined group –Aswath Guduchi KashayaDosage-40 ml bd Duration-90 days
Subjective Criteria-PainindexObjective criteria-Serum uric acid
Group 3 is moreeffective
AdithyaAcharya K et al.
ComparativeClinical Trial
40 20-65 years
Hyperuricemia,less than 10year’s chronicity,withoutmanifestation oftophi and jointdestruction.
Group A-Siravyadha/bloodletting twice with aninterval of 11 days.Follow up on 24 th dayGroup B-Guduchi siddhayogabasti in 8 daysFollow up on 24 th day
Subjective parameters-Pricking pain (Sandhitoda), Tenderness(Sparshasahyata),Redness (Raga),Swelling(Sandhishotha),Sandhi Supti(Numbness of joints), Objective parametersSerum Uric acid
Subjectiveparameters- InGroup A Prickingpain (Sandhi toda)relieved rapidly, butin group B gradualrelieved .Tenderness(Sparshasahyata)-highly signi�cantresult in group B,Redness (Raga)-Early relief observedin Group A thangroup B, Swelling(Sandhishotha)Early relief observedin Group A thangroup B, SandhiSupti (Numbness ofjoints) Early reliefobserved in Group Athan group B, Overall responsewas marked inGroup A (35%) thanGroup B (0 %)ObjectiveparametersSerum Uric acid Group B (21 %)showed morereduction in serumuric acid comparedto group A(13.33%).
VishwajeetManjhi et al.
Randomisedopencomparativeclinical trial
4520-60 years
Elevated serumuric acid level >6.8 mg/dl,Vatarakta
Group A – Amritadi Kashaya80 ml bd in empty stomachwith 10 ml castor oil for 16days.Group B- Ardhamatrika bastias per Kalabasti schedule (16days)Group C- combined group for16 days.
Subjective criteria-Signs and symptomsof Vatarakta withscoring pattern. Objective parameter-Serum Uric acid
Group A- 26.75 %were moderatelyimproved, 46.75 %got mildimprovement and26.75 % showed noimprovement.Group B-46.75 % gotmoderateimprovement, 53.33% showed mildimprovement and 0% was inunimprovedcategory. Group C- 73.33 %showed moderateimprovement, 26.75% showed mildimprovwmt. No patient showedcomplete cure in anygroups. Objective criteria-Group A showedsigni�cantimprovement inserum uric acid level,Group B and Cshowed highlysigni�cantimprovement.
Deeika Gupta etal.
Phase-2rational
5621-60 years
Vatarkata(Gouty arthritis)
Group A-Patoladi kwath 40ml bd after food for 90 days
Subjective criteria-Sandhishu ruk-pain in
Group A-48% gotcomplete relief, 28%

Page 8/13
randomized(sequentialpattern)parallelgroup study.
y ( y )Having Seumuric acid > 7mg/dl in malesand >5.7 mg/dlin females
yGroup B-Patoladi kwath 40ml bd & Rasnadi pradeha(local application) During evening for 90 days.
paffected joint,Sandhishu Raga -Redness , Sandhishuswayathu- Swelling,Sparshasahyata –Tenderness, sandhishukathinya-decreased /restricted movements, ,skin discoloration ofaffected area, itchingon affected part,burning sensationObjective parameter-Serum uric acid, ESR,Hb, TLC, DLC, KFT, LFT,FBS, PPBSassessmentdone on every fortnightafter administration oftrial drugs.
pmoderately relievedand 20 % got mildimprovement and 4% not responded totreatment. In Group B-76 % gotcomplete relief, 16 %got moderateimprovement, 8 %showed mildimprovement and nocase recorded asunchanged.
Dr SharmaParvesh et al.
30 20-60 years
Randomisedopen clinicaltrial.
Vatarakta,serum uric acidlevel 5.5-10mg/dl.
Group A-Bodhivriksha twakchurn with madhu 3 gm bdGroup B-Bodhivriksha twakchurn with jala 3 gm bdDuration-45 days
Pain, tenderness,swelling, stiffness,burning sensation injoints, Hb, serum Uricacid, Serum creatinine,X-Ray, Urine RE andMicroscopicexamination.
The study washighly signi�cant(P<0.001) for allsubjectiveparameters, serumuric acid and wasinsigni�cant(P>0.05)for Haemoglobinand serumcreatinine in groupA. In group B,swelling, stiffness,joint pain and serumuric acid showedhighly signi�cantresults. Fortenderness andburning sensationthe p value was<0.05 and forhaemoglobin andserum creatinine theresult wasinsigni�cant(P>0.005) in groupB.
H Kuvettu et.al Arandomizedsingle blindclinical studywith pretestand posttestdesign
37820-60 years
Gouty arthritis Group A - 190 patients wereadministered Amritaguggulu500 mg 2 tablets thrice dailyfor 30 days. Group B - 188 patients wereadministered Kaisoraguggulu500 mg 2 tablets thrice dailyfor 30 days. During thestudy, special diet wasfollowed
Subjective parameter-The signs andsymptoms of gout-burning sensation,pain, swelling,stiffness, mobility,deformity of joints.were assessed.Objective parameters -haemoglobinpercentage, ESR andserum uric acid.
Markedimprovement wasfound for 68% ofpatients in group A,whereas in group Bit was only 42%. Thestudy showedstatistically highlysigni�cant resultsfor all subjective andobjective parametersin both the groups.The study concludedthat Amritagugguluwas more effectivethanKaisoragugguluinthe management ofgouty arthritis.
H Kuvettu et.al Arandomizedsingle blindclinical studywith pre-testand post-testdesign
46220-60 years
Gouty arthritis Group A -234 patients wereadministered KarmaBastiprepared with for 30days. Group B - 228 patientswereadministered Kaisoraguggulu500 mg 2 tablets thrice dailyfor 30 days. .
The signs andsymptoms of gout-burning sensation,pain, swelling,stiffness, mobility,deformity of jointswere assessed undersymptom gradeparameter. Objectiveparameters included,haemoglobinpercentage, ESR andserum uric acid.
Markedimprovement wasfound for 56% ofpatients in group A,whereas in group Bit was only 33%. Thestudy showedstatistically highlysigni�cant resultsfor all subjective andobjective parametersin both the groups.The study concludedthat GuduchiSadhita Grithawasmore effective thanKaisoraguggulu inthe management ofgouty arthritis.
Mehta Chetan Comparative 60 Vatarakta. Group A-Kokilakshadi Ks Subjective parameter- In both groups 33.33

Page 9/13
et.al study 16 & 70years
with Pippali Churna Group B - Siravyadha (on thedorsum of hand/foot, 2Angula(Fingers-approx. 4cm) abovethe Kshipramarma)
The signs andsymptoms ofvatarakta, VAS, Hb, TC,DC, FBS, Uric acid
% patients did notget any relief. Ingroup A 30% gotmild relief and ingroup B 56.66 % gotmild relief. 33.33 5got moderate reliefin group a and 10 %got moderate reliefin group B. In groupA 1 patient gotcomplete relief andnone got completerelief in group B.
Dr Vikas Ranaet.al(2017)
Non-randomized-comparativeparallelgroup design
3020-70 years
Vatarakta. Group 1- 15 patients wereadministered with SadyaMrudu Sneha VirechanaofErand Taila10-50 ml withKsheerafor 3-5 days forKoshtasuddhi followed byadministration of 2 tablets ofPunarnnava AmaritaGuggulu500 mg withAmrithadi Kvath 24 gas Anupanafor 8 weeks. Group 2 - 15 patients weregiven only 2 tablets ofPunarnnava AmaritaGuggulu500 mg withAmrithadi Kvath24 gas Anupanafor 8 weeks.
The subjective criteriasassessed were sandhisoola, sandhi shotha,sparshasahyata, raga,vidaha, twak vaivarnya,stabdata, shithilta,hritspanadanand sandhi vikriti. Theobjective parameterwas serum uric acid.
In group 1, 80 % gotmoderateimprovement and 20% got mildimprovement. Ingroup B, 20% gotmarkedimprovement, 53.3%got moderateimprovement and26.6% got mildimprovement. Thestudy found, group 1and group 2 wereequally effective insymptoms likesparshasahyata,raga and shithilta.Sandhi shotha, ragaand vidaha wereimproved to greaterextent in group 1,whereas sandhisoola, twakvaivarnyaand stabdata werebetter controlled ingroup 2.
Asok KumarPanda et.al
nonrandomizedcontrolledpilot study
22Mean age47
GambheeraVata-Raktadiagnosedas acute gout.
Study group-12 were treatedwith leech for 7 days with 4weeks follow upControl group-10 patientswho were not willing toparticipate in leechapplication were given localdiclofenac application for 7days
Pain, joint swelling,joint tenderness, jointerythema, patient’sglobal assessment toresponse to therapyand investigator’sglobal assessment toresponse to therapy.
leech application iseffective in reducingpain, joint swelling,joint tenderness andjoint erythema.
Dr V BalenduKrishnan et.al(2018)
Comparativeclinical trialwth Pre-testand post-testdesign
4018-60 years
Gouty arthritis Group A-amapachana withSunti churna, Kalavasti withvasaguluchyadi kashaya andguluchyadi gritha(anuvasana), Moorchita tilataila for abhyanga withmrudu swedana followed byshaman oushadis-punarnnavadi guggulu 2 bidwith kokilakshakam kashaya(30-45 ml).Gropu B- amapachana withSunti churna , snehapanawith guduchyadi grithafollowed by virechanawithNimbamrutadi erandataila and Moorchita tila tailafor abhyanga with mrudusweda followed by shamanoushadis-rasnaguggulu 2 bidwith manjishtadi kashaya(30-45 ml)Follow up-48 days for GroupA, 30 days for group B.
Sandhigraha, SandhiShoola, Sandhi Shotha,jointcolour, Sparshasahatvaand serum uric acid
Both groups werehighly signi�cant inreducing thesubjective andobjective criteria’s. Ingroup A, thepercentage of reliefwas 77.74% and ingroup B, it was56.50%. The studyconcluded that boththe groups werehaving signi�cantrole in goutyarthritis, but Vastihas morecontributory effectcompared toVirechana. Thestatistical analysiswas also unclear inthis study too.
Harbans Singhet al2017
Prospectiveopen-labelmulticentrestudy withpre-postdesign
10025-60 years
Primary goutyarthritis
Amrita guggulu tab 2 Tab of500 mg twice daily with lukewarm water for 12 weeks andPinda taila externalapplication on affectedjoint(s)
Serum uric acid, QOL,using SF-36, HealthSurvey Questionnaire,Patient’s GlobalAssessment scale,Physician’s globalassessment scale,VAS,LFT, KFT
Statisticallysigni�cant result ofSerum uric acid, VASscore, QOL, Patient’sGlobal AssessmentScale, Physician’sglobal assessmentscale. LFT and KFTwere performed atbaseline and at theend of the treatment.

Page 10/13
Though somechanges wereobserved, they werewithin the normalrange.
Shashank Jhaet.al 2014
Non-comparativetrials withpre-postdesign
1020-65 years
signs andsymptomsof Vatarakta andserum uric acidlevel
Leech therapy -3 times atintervals of 3 weeks.Treatment schedule:
Sandhishoola,Sandhishopha, Sandhivaivarna Sandhidaha,Serumuric acid
Statisticallysigni�cant result.
Upadhyaya GPet.al.,2010
Non-comparativetrials withpre-postdesign
35Notmentioned
signs andsymptomsof Vatarakta andserum uric acidlevel
Punarnnava Guggulu tab -2tab (500 mg each) aftermeals with water for 45 daysand follow-up were done for15 days.
Subjective criteria-signs and symptomsof VataraktaObjective criteria-Serum uric acid, ESR,TLC, DLC, Urine routine,and microscopicexamination.
Statisticallysigni�cant result.Maximum effectwas observed inkandu(itching),Sparsasahatva(tenderness). Castsand epithelial cellswere found reducedsigni�cantly fromurine.
LPrasannakumaret.al
Non-comparativetrials withpre-postdesign
516-70 years
signs andsymptomsof Vatarakta andserum uric acidlevel
Guduchyadi ksheera vasthias yoga vasthi
Pain, burningsensation, malaise,sleep, tenderness,oedema, walkingability
For four patients,uric acid came tonormal. No patientgot complete relieffrom symptoms. 20% remainedunchanged.
Harsh Segal etal., 2018
Non-comparativetrials withpre-postdesign
3120-60 years
signs andsymptoms ofVatarakta (Gout), Serumuric acid level5.5 to 10.0mg/dl
Two grams of powder ofAndrographis paniculatathrice daily with water.
Subjective criteria-Oedema, stiffness,in�ammation, itching,heaviness, numbness,piercing pain, fatigue,pallor, thirst,indigestionObjective criteria-serumuric acid
Except symptompallor, the p valuewas either <0.05 or<0.01.
Sharma Usha etal., 2014
Non-comparativesingle blindtrials withpre-postdesign
3020-60 years
signs andsymptomsof Vatarakta andserum uric acidlevel
Tablet Amrita Guggulu 500mg thrice daily with anupanaof amritadi Kashaya 72 ml.
Subjective criteriaSandhi shola (pain injoints), Sandhi shotha(swelling in joints),Raga (Redness), Kandu(Pruritis), Vidaha, Twakvaivarnyata,Sparsasahishnuta(tenderness)Objective criteria-Serum uric acid, Hb,TLC, DLC, ESR, RAfactor
Statisticallysigni�cant result.
Sharma Usha etal.
Non-comparativesingle blindtrials withpre-postdesign
3020-60 years
signs andsymptomsof Vatarakta andserum uric acidlevel(>6 mg/dl)
Tablet Punarnnava amritaGuggulu 500 mg thrice dailywith anupana of amritadiKashaya 72 ml.
Subjective criteriaSandhi shola (pain injoints), Sandhi shotha(swelling in joints),Raga (Redness), Kandu(Pruritis), Vidaha, Twakvaivarnyata,Sparsasahishnuta(tenderness)Objective criteria-Serum uric acid, Hb,TLC, DLC, ESR, RAfactor
Statisticallysigni�cant result.
Yogita DeepakKhore et.al.
Pre-postdesign
1020-60 years
signs andsymptomsof Vatarakta andserum uric acidlevel(>6 mg/dl)
Virechana with drakshakashaya (40 ml) and erandataila (40 ml)
Subjective criteria-Shotha, shola,aaraktata, kathinya,sparshasahatva, dahaObjective criteria-Serum uric acid
60 % relief instiffness &tenderness, 50 %relief in swelling andpain, uric acid leveldecreased slightly.
SivaprasadHuded et.al
Randomizedsingle blindstudy withpre-test post-test design
2018-60 years
Vatarakta, acutegouty arthritis-Hyperuricemia
Guduchi yoga (aqueousextract of Guduchi andTrapusha) 2 g bid with lukewarm water after food for 12weeks .
Subjective parameter-Sandhishula, daham,sandhisotha,sparshasahatwam,twaklohitaObjective parameter-serum uric acid
Statisticallysigni�cant resultsalong withattainmaent ofnormal serum uricacid andimprovement ingeneral well being ofthe patients.
PundapalAmitkumar B
Single blindtrials with
2016-70 years
Vatarakta Lekhana basti as Kalabastiprotocol-16 days
Pain, burningsensation, malaise,
Statisticallysigni�cant results

Page 11/13
et.al pre-postdesign
Vataraktantaka Rasa-250 mgtds for 30 days.
disturbance of sleep,tenderness, walkingability, peripheral pulse,lipid pro�le.
Figures
Figure 1
PRISMA 2009 Flow Diagram

Page 12/13
Figure 2
Risk of bias graph
Figure 3
Risk of bias summary
Page 13/13
Figure 4
Bias assessment for non-randomized studies