Associations between Cigarette Smoking and Each of 21 Types of Cancer: A Multi-Site Case-Control...
11
international Journal of Epidemiology Vol. 24. No. 3 international Epidemiological Associalion 1995 Printed in Great Bfiiair Associations between Cigarette Smoking and Each of 21 Types of Cancer: A Multi-Site Case- Control Study JACK SIEMIATYCKI,'" DANIEL KREWSKI, U EDUABDO FRANCO*" AND MURRAY KAISERMAN* Siemiatycki J (Epidemiology and Biostatistics Unit, Institui Armand-Frappier, University du Quebec, Laval-des-Rapides, Quebec H7V 187, Canada), Krewski D, Franco E and Kaisemnan M. Associations between cigarette smoking and each of 21 types of cancer. A multi-site case-control study. IntemationatJoumalotEpidemiology 1995; 24; 504—514. Background. Although the effects of cigarette smoking on cancer risk have been well documented, there remain several outstanding issues to be clarified, including the determination of which types of cancer are associated with smoking and estimation of the magnitude of the effect of smoking on different types of cancer. A further issue is whether the effects seen elsewhere can be demonstrated in Canada, where tobacco products differ somewhat from those in other countries. Methods. A case-control study was undertaken in Montreal to investigate the associations between a large number of environmental and occupational exposures on the one hand, and several types of cancer on the other. Between 1979 and 1985, interviews were canned out with incident male cases of 21 types of cancer, including 15 anatomical sites and six histological subtypes. The interview was designed to obtain detailed information on smoking histories, job histories, and other potential confounders. Altogether. 3730 cancer patients and 533 population controls were interviewed. For each type of cancer analysed, two control groups were used: population controls and cancer controls (selected from among other cancer patients). The purpose of the present analysis is to estimate the relative risk of each of 21 types of cancer in relation to smoking and to estimate the percentage of cancer cases attributable to cigarette smoking. Results. Separate analyses conducted with the two control groups produced similar results. Of the many sites of cancer examined, the following were not associated with cigarette smoking: colon, rectum, liver, prostate, kidney and skin (melanoma). Within the lymphoreticular system, there was no excess risk of Hodgkin's lymphoma, although the results for non-Hodgkin's lymphoma were weakly suggestive of an association with smoking. The following sites were clearly associated with smoking: lung (odds ratio {OR] =12.1), bladder (OR = 2.4). oesophagus (OR = 2.4), stomach (OR = 1.7), and pancreas {OR = 1.6). Population attributable risk percentages due to smoking were 90% for lung, 53% for bladder, 54% for oesophagus, 35% for stomach, and 33% for pancreas. Conclusions. Of the 21 types of cancer examined, the following were associated with smoking among men in Montreal: lung (including all major histotogicaJ subtypes), bladder (and its main histological subtypes), oesophagus, stomach and pancreas. Smoking likely accounts for a large proportion of cancers occurring at these sites. Cigarette smoking is the best known, best documented, and in public health terms, the most important risk factor for cancer. 1 " 3 Since 1950, a large number of epidemi- ological studies have been published on the cancer risks among cigarette smokers. There have been at least eight prospective cohort studies, in five different countries, in which the mortality experience of large numbers of * Epidemiology and Biosutistici Unit, Institut Annand-Frappier. University du Quebec, Laval-d«-Rapidcs, Quebec H7V IB7, Canada. ** Department of Epidemiology and Biostaiisuci, McGUI University, Montreal, Quebec H3A ] A2. Canada. 'Health Protection Branch, Healib Canada, Oitawa. Ontario K1A 0L2. Canada. * Department of Mathematics and Statistics, Carl too University, Ottawa, Ontario K1S 5B6, Canada. subjects have been monitored for periods ranging from 4 to 20 years- 4 There have also been a large number of case-control studies, with each one focused on a par- ticular cancer site. 12 The evidence to date indicates that cigarette smoking increases the risk of cancer at a number of anatomical sites, including the buccal cavity, pharynx, larynx; oesophagus, pancreas, lung, bladder, kidney, uterine cervix and possibly stomach and liver. 12 All of the main histological types of lung cancer are associated with smoking. The population attributable risk per cent (PARP), due to smoking has been estimated to be 10 the range 80-95% for lung cancer and 25-60% for bladder cancer; 13 " 14 the attributable risk for other sites is less certain. There have been scattered reports linking 504
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Associations between Cigarette Smoking and Each of 21 Types of Cancer: A Multi-Site Case-Control...

international Journal of Epidemiology Vol. 24. No. 3 international Epidemiological Associalion 1995 Printed in Great Bfiiair
Associations between Cigarette Smoking and Each of 21 Types of Cancer: A Multi-Site Case-Control Study
JACK SIEMIATYCKI,'" DANIEL KREWSKI,U EDUABDO FRANCO*" AND MURRAY KAISERMAN*
Siemiatycki J (Epidemiology and Biostatistics Unit, Institui Armand-Frappier, University du Quebec, Laval-des-Rapides, Quebec H7V 187, Canada), Krewski D, Franco E and Kaisemnan M. Associations between cigarette smoking and each of 21 types of cancer. A multi-site case-control study. IntemationatJoumalotEpidemiology 1995; 24; 504—514. Background. Although the effects of cigarette smoking on cancer risk have been well documented, there remain several outstanding issues to be clarified, including the determination of which types of cancer are associated with smoking and estimation of the magnitude of the effect of smoking on different types of cancer. A further issue is whether the effects seen elsewhere can be demonstrated in Canada, where tobacco products differ somewhat from those in other countries. Methods. A case-control study was undertaken in Montreal to investigate the associations between a large number of environmental and occupational exposures on the one hand, and several types of cancer on the other. Between 1979 and 1985, interviews were canned out with incident male cases of 21 types of cancer, including 15 anatomical sites and six histological subtypes. The interview was designed to obtain detailed information on smoking histories, job histories, and other potential confounders. Altogether. 3730 cancer patients and 533 population controls were interviewed. For each type of cancer analysed, two control groups were used: population controls and cancer controls (selected from among other cancer patients). The purpose of the present analysis is to estimate the relative risk of each of 21 types of cancer in relation to smoking and to estimate the percentage of cancer cases attributable to cigarette smoking. Results. Separate analyses conducted with the two control groups produced similar results. Of the many sites of cancer examined, the following were not associated with cigarette smoking: colon, rectum, liver, prostate, kidney and skin (melanoma). Within the lymphoreticular system, there was no excess risk of Hodgkin's lymphoma, although the results for non-Hodgkin's lymphoma were weakly suggestive of an association with smoking. The following sites were clearly associated with smoking: lung (odds ratio {OR] =12.1), bladder (OR = 2.4). oesophagus (OR = 2.4), stomach (OR = 1.7), and pancreas {OR = 1.6). Population attributable risk percentages due to smoking were 90% for lung, 53% for bladder, 54% for oesophagus, 35% for stomach, and 33% for pancreas. Conclusions. Of the 21 types of cancer examined, the following were associated with smoking among men in Montreal: lung (including all major histotogicaJ subtypes), bladder (and its main histological subtypes), oesophagus, stomach and pancreas. Smoking likely accounts for a large proportion of cancers occurring at these sites.
Cigarette smoking is the best known, best documented, and in public health terms, the most important risk factor for cancer.1"3 Since 1950, a large number of epidemi-ological studies have been published on the cancer risks among cigarette smokers. There have been at least eight prospective cohort studies, in five different countries, in which the mortality experience of large numbers of
* Epidemiology and Biosutistici Unit, Institut Annand-Frappier. University du Quebec, Laval-d«-Rapidcs, Quebec H7V IB7, Canada. ** Department of Epidemiology and Biostaiisuci, McGUI University, Montreal, Quebec H3A ] A2. Canada. 'Health Protection Branch, Healib Canada, Oitawa. Ontario K1A 0L2. Canada. * Department of Mathematics and Statistics, Carl too University, Ottawa, Ontario K1S 5B6, Canada.
subjects have been monitored for periods ranging from 4 to 20 years-4 There have also been a large number of case-control studies, with each one focused on a par-ticular cancer site.12
The evidence to date indicates that cigarette smoking increases the risk of cancer at a number of anatomical sites, including the buccal cavity, pharynx, larynx; oesophagus, pancreas, lung, bladder, kidney, uterine cervix and possibly stomach and liver.12 All of the main histological types of lung cancer are associated with smoking. The population attributable risk per cent (PARP), due to smoking has been estimated to be 10 the range 80-95% for lung cancer and 25-60% for bladder cancer;13"14 the attributable risk for other sites is less certain. There have been scattered reports linking
504

CANCER RISKS AMONG SMOKERS 505
smoking with other types of cancer such as leukaemia and prostate cancer. The range of sites affected by smoking is of more than academic interest. Accurate estimates of the risks of different lypes of cancer are needed to elucidate the aetiopathology of cancer and to fully appreciate the potential benefits of smoking cessation.
The present report, based on an analysis of cigarette smoking and many types of cancer from a population-based multi-site case-control study in Montreal, ad-dresses the following issues: a) which sites of cancer are affected by cigarette smoking; b) what are the relative risks for different target sites; and c) what is the population attributable risk of each type of cancer due to cigarette smoking? This study offers several advant-ages in addressing these issues. Many, though not all, sites of cancer were investigated using a common proto-col and standardized data collection procedures, assur-ing comparability of results among sites. Whereas most cohort studies have depended on death certificate information for disease ascertainment, case ascertain-ment in the present study entailed high quality diag-nostic confirmation. In contrast with cohort studies in which smoking information was collected at the time the cohort was established and not during the sub-sequent period of mortality follow-up, our smoking data were collected retrospectively at the time of diag-nosis, thereby providing lifetime smoking histories up to the time of disease onset. For most sites, sufficient numbers of cases have been assembled to ensure that the statistical power for detecting elevated risks com- yes favourably with that in previous studies. Another -avantage of the present population-based study is
the opportunity to estimate the PARP due to cigar-ette smoking for each type of cancer associated with
smoking. A further motivation for examining the carcinogenic
effects of cigarette smoking in this population is that Canadian cigarettes differ from both American and Euro-pean brands. Cigarettes manufactured in Canada are made with Virginia flue-cured tobacco, which is grown primarily in southern Ontario.15 American cigarettes, on the other hand, are made with mixtures of bright, burley and oriental tobaccos.16 These differences have implications for the chemical composition of the tobacco smoke. Specifically, the concentration of nico-tine and the distribution of nicotine in vapour and paniculate phases of tobacco smoke differ among different types of tobacco. Both N'-nitrosonornicotine (NNN)and 4-(raethyinitrosamino)-l-(3-pyridyl)-I-bu-tanone (NNK) are important constituents of tobacco smoke, which have been shown to be lung carcino-gens in animals.16'17 On average, Canadian cigarettes
can deliver approximately two-thirds less NNN and one-quarter less NNK than American cigarettes, and about one-quarter more of both NNN and NNK than British cigarettes.18
SUBJECTS AND METHODS In 1979 we undertook a study to determine the relation-ships between specific occupational and environmental exposures and many types of cancer. The design has been detailed elsewhere,19'21 and will be summarized only briefly here.
Case Groups The target population consisted of males, aged 35-70, resident in the Montreal metropolitan area who were initially diagnosed (i.e. incident cases) between September 1979 and June 1985 with a histologically confirmed cancerous lesion of one of the following sites: oeso-phagus, stomach, small intestine, colon, rectum, liver, gallbladder, pancreas, peritoneum (mesothelioma only), . lung, pleura (mesothelioma only), skin (melanoma only), prostate, penis, testis, bladder, kidney, eye (melanoma only), lymphoid tissue (both Hodgkin's and non-Hodgkin's), and multiple myeloma. Because of limited resources, there were some periods during which case recruitment for some cancer sites was interrupted. All major hospitals in the area participated, thus assuring virtually complete ascertainment of cases occurring in the target population. Altogether, 4576 eligible cases were identified. Completed interviews or questionnaires were obtained for 3730 subjects, of which 82% were with the subject himself and the rest with a next-of-kin. Reasons for non-response were: unable to contact the patient or next-of-kin (9.7%) and refusal (8.1%).
For each case, information was available on the topology and histology of the tumour. For purposes of statistical analysis we used the first three digits of the International Classification of Diseases22 topography axis to define case series. The 78 cases which were diagnosed with primary tumours at two different sites have been included in both relevant site series. Where numbers permitted we analysed as case series, major histologicaJ subcategories of certain sites, notably, lung, bladder and kidney.
Controls A population control group of 740 males was selected from electoral lists in the Montreal area, age-stratified to match the age distribution of the cancer patients. Among these subjects, 533 (72%) consented to be inter-viewed. Because the response rate among population controls was substantially lower than among cases, it is
506 INTERNATIONAL JOURNAL OF EPIDEMIOLOGY
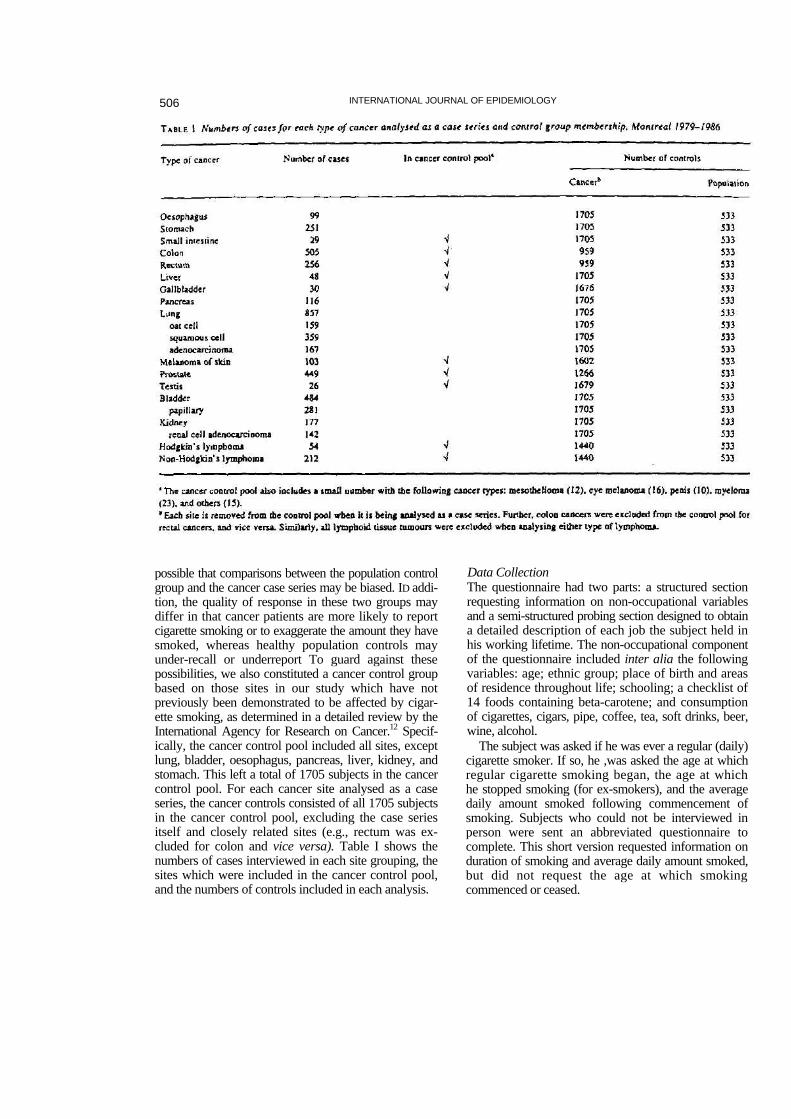
possible that comparisons between the population control group and the cancer case series may be biased. ID addi-tion, the quality of response in these two groups may differ in that cancer patients are more likely to report cigarette smoking or to exaggerate the amount they have smoked, whereas healthy population controls may under-recall or underreport To guard against these possibilities, we also constituted a cancer control group based on those sites in our study which have not previously been demonstrated to be affected by cigar-ette smoking, as determined in a detailed review by the International Agency for Research on Cancer.12 Specif-ically, the cancer control pool included all sites, except lung, bladder, oesophagus, pancreas, liver, kidney, and stomach. This left a total of 1705 subjects in the cancer control pool. For each cancer site analysed as a case series, the cancer controls consisted of all 1705 subjects in the cancer control pool, excluding the case series itself and closely related sites (e.g., rectum was ex-cluded for colon and vice versa). Table I shows the numbers of cases interviewed in each site grouping, the sites which were included in the cancer control pool, and the numbers of controls included in each analysis.
Data Collection The questionnaire had two parts: a structured section requesting information on non-occupational variables and a semi-structured probing section designed to obtain a detailed description of each job the subject held in his working lifetime. The non-occupational component of the questionnaire included inter alia the following variables: age; ethnic group; place of birth and areas of residence throughout life; schooling; a checklist of 14 foods containing beta-carotene; and consumption of cigarettes, cigars, pipe, coffee, tea, soft drinks, beer, wine, alcohol.
The subject was asked if he was ever a regular (daily) cigarette smoker. If so, he ,was asked the age at which regular cigarette smoking began, the age at which he stopped smoking (for ex-smokers), and the average daily amount smoked following commencement of smoking. Subjects who could not be interviewed in person were sent an abbreviated questionnaire to complete. This short version requested information on duration of smoking and average daily amount smoked, but did not request the age at which smoking commenced or ceased.

CANCER RISKS AMONG SMOKERS 507
A team of chemisis and hygienists examined each ompleted questionnaire and translated each job into a ist of potential exposures.l9-23 This was done using a hecklist which included some 300 of the most common iccupational exposures in Montreal. In addition to ttributing individual exposures to each subject, we Iso derived a composite index of the 'dirtiness' of each ubject's working environments over the course of his working lifetime. This last variable represents an ttempt to distinguish 'clean' work histories from 'dirty' nes, or white-collar jobs from blue-collar ones. This was based on an evaluation of the 'dirtiness' of the ob corresponding to each four-digit category in the anadiao occupational classification system. For each ear of the subject's career, we derived a score associ-ted with the job title held. The overall dirtiness score /as an average of these annual scores over the subject's /orking lifetime.
M'ethods of Analysis or each type of cancer listed in Table I, separate lalyses were carried out with each control group ;ancer controls and population controls) based on gistic regression models using the SPSS logistic
gressioo modelling program.24,25
A composite cigarette smoking exposure variable as defined as the product of the average number of garettes smoked per day and the duration of smoking years, and will be referred to as cumulative cigarette- ars of smoking. (We preferred to use 'cigarette-years' the more commonly reported 'pack-years' because i size of packs has changed over time and different ck sizes are now available.) This variable was cat- orized into four approximately equal subgroups for dysis. For case series with over 50 subjects, we in- idcd the following variables as covariates in the alyses: age, ethnic group, socioeconomic status (SES) measured by self-reported income, the blue-coljar/ ite-collar dirtiness score, a coffee consumption re, a composite alcohol consumption score, and a aposite beta-carotene consumption score. Ethnicity i entered as a categorical variable; the remaining itinuous covariates were entered as linear terms in regression models. We have shown elsewhere2* that n for the two sites which are considered to be among
most important target organs for occupational :inogens, lung and bladder, extensive control for upational exposures had virtually no effect on the mates of the smoking-cancer associations. Con- jently, we did not adjust for individual occupa- al exposures in the present analysis. The dirtiness x serves as an aggregate adjustment for any funding that might occur, even though i i i s
probably unnecessary to include any occupational variables if SES and ethnicity are already in the model. For case series with fewer than 50 subjects, only age, ethnicity and SES were included as confounders.
For each site for which subgroups based on cigarette-years were analysed, we also carried out a test for trend across the four subgroups, using a likelihood ratio test with the four subgroups numbered I to 4, compared to a model in which there were no dose-related subgroups.
Attributable Risk For each site which was associated with cigarette smok-ing in our data set, we estimated the population attributable risk per cent (PARP) adjusted for all con-founders in the model, using the method described by Bruzzi et at.27 A 95% confidence interval for the PARP was derived by using the 95% confidence limits of the odds ratio (OR), treating the prevalence of exposure as a known constant.
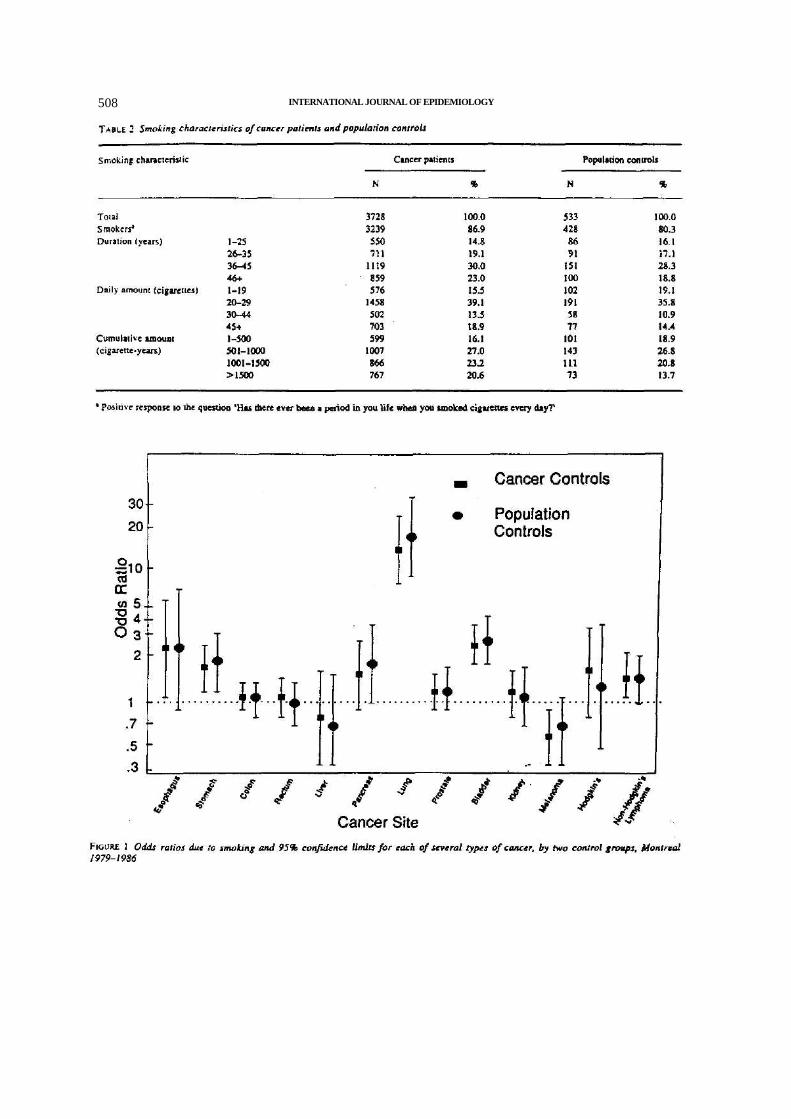
RESULTS Smoking characteristics of cancer patients (all sites combined) and population controls are shown in Table 2. Non-smokers represented a small minority of study subjects. Relatively few subjects smoked for less than 20 years or smoked less than one pack per day. Among smokers, the mean daily consumption was 30.5 cigar-ettes per day in the cancer patient group as compared to 27.6 cigarettes per day in the population controls. On average, cancer patients and population controls bad smoked for 37.2 and 36.2 years respectively.
Figure 1 shows the OR for ever versus never smok-ing, for each of 13 sites, for both the population and cancer controls. The OR tended to be slightly higher with population controls than with cancer controls, and, because of smaller numbers of population controls, the confidence intervals were wider. However, the differ-ences in OR estimates between the two control groups were of little practical consequence. In the remaining Tables, we present only one set of results, those based on population controls.
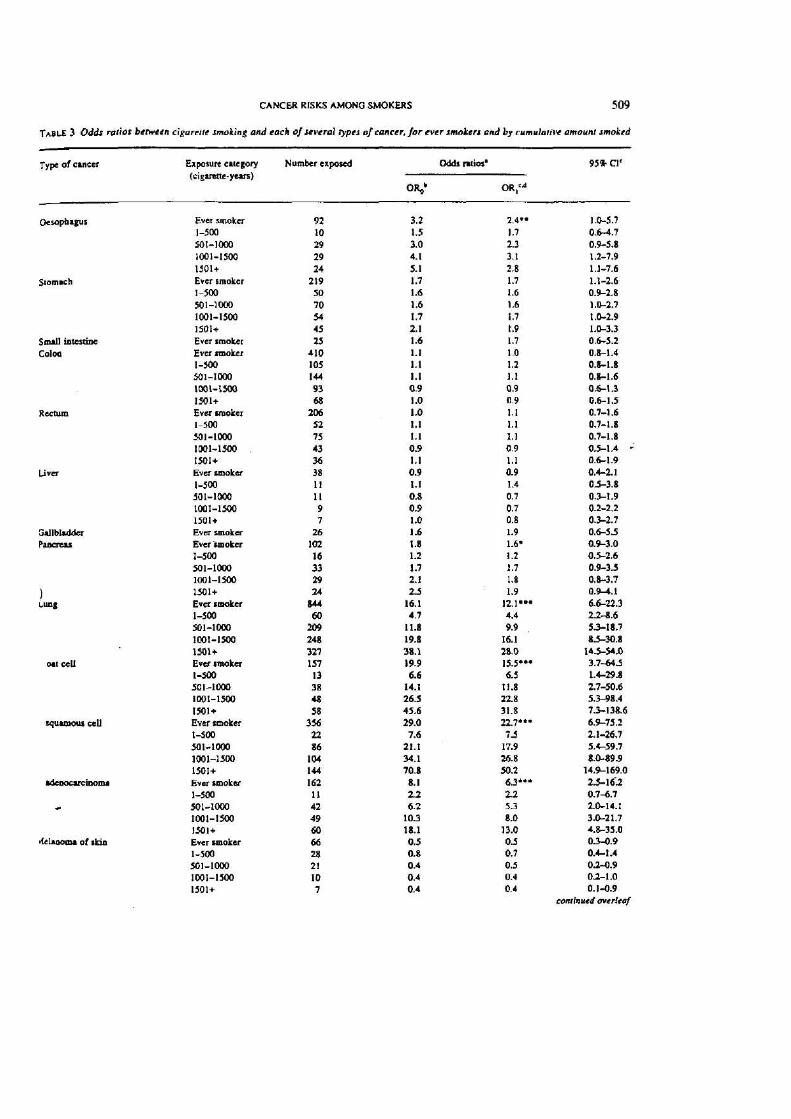
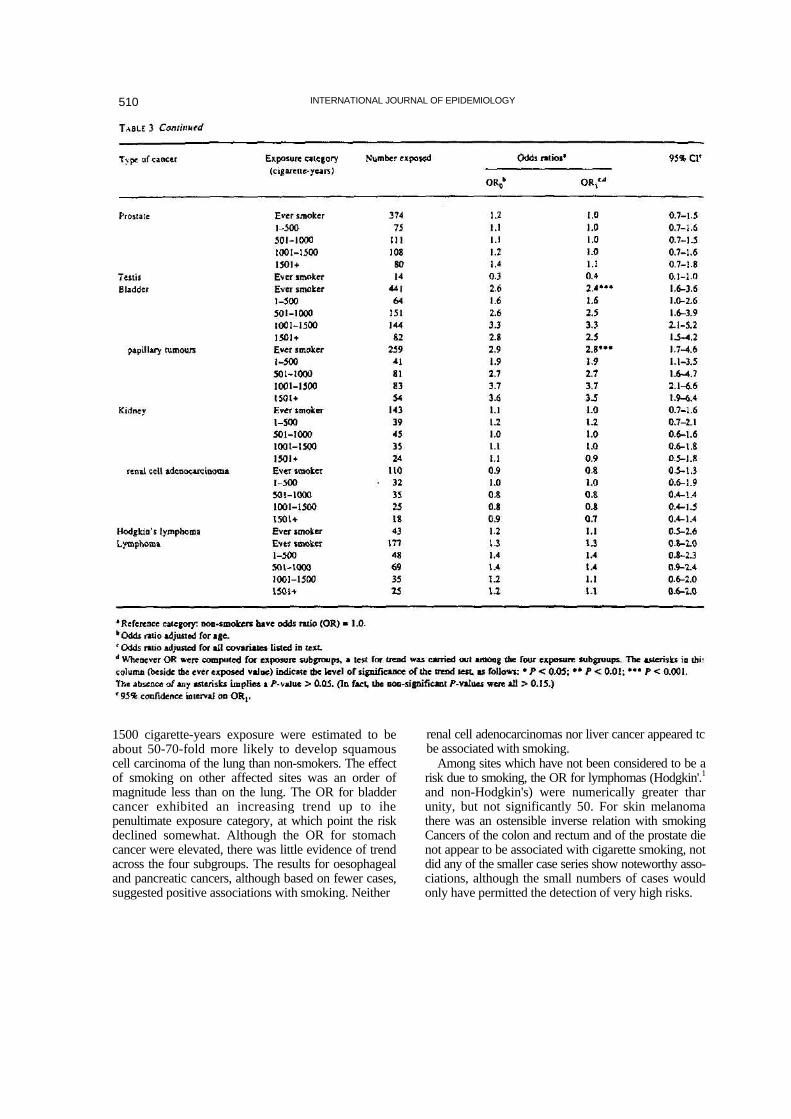
Table 3 shows the OR due to smoking, for ever smokers and for subcategories defined by the cumulat-ive amount smoked, for 21 types of cancer. Results by cumulative amount smoked are not presented for case series with fewer than 40 subjects. As expected, the risk of lung cancer was significantly elevated as a con-sequence of cigarette smoking, with increases evident for all three histological subgroups examined here. The strongest dose-response relationship is with squa-mous cell tumours, followed by oat cell tumours, and adenocarcinoma of the lung. Subjects with over
508 INTERNATIONAL JOURNAL OF EPIDEMIOLOGY
510 INTERNATIONAL JOURNAL OF EPIDEMIOLOGY
1500 cigarette-years exposure were estimated to be about 50-70-fold more likely to develop squamous cell carcinoma of the lung than non-smokers. The effect of smoking on other affected sites was an order of magnitude less than on the lung. The OR for bladder cancer exhibited an increasing trend up to ihe penultimate exposure category, at which point the risk declined somewhat. Although the OR for stomach cancer were elevated, there was little evidence of trend across the four subgroups. The results for oesophageal and pancreatic cancers, although based on fewer cases, suggested positive associations with smoking. Neither
renal cell adenocarcinomas nor liver cancer appeared tc be associated with smoking.
Among sites which have not been considered to be a risk due to smoking, the OR for lymphomas (Hodgkin'.1
and non-Hodgkin's) were numerically greater thar unity, but not significantly 50. For skin melanoma there was an ostensible inverse relation with smoking Cancers of the colon and rectum and of the prostate die not appear to be associated with cigarette smoking, not did any of the smaller case series show noteworthy asso-ciations, although the small numbers of cases would only have permitted the detection of very high risks.
CANCER RISKS AMONG SMOKERS 511
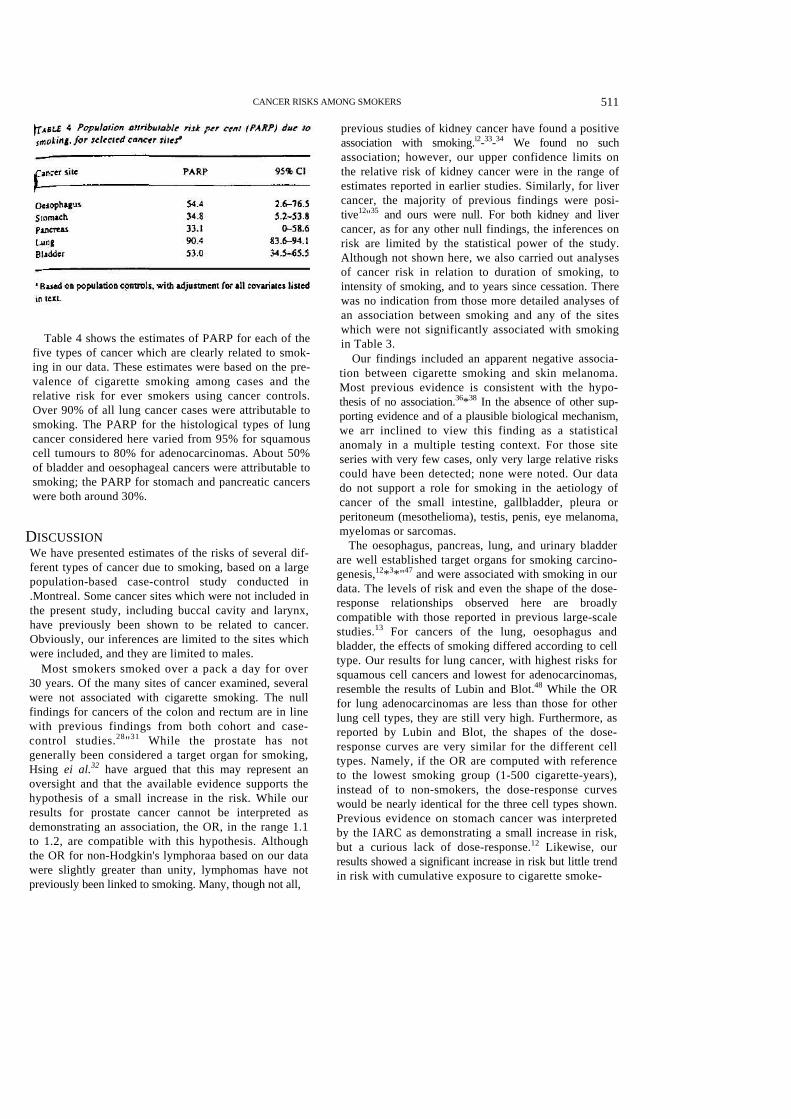
Table 4 shows the estimates of PARP for each of the five types of cancer which are clearly related to smok-ing in our data. These estimates were based on the pre-valence of cigarette smoking among cases and the relative risk for ever smokers using cancer controls. Over 90% of all lung cancer cases were attributable to smoking. The PARP for the histological types of lung cancer considered here varied from 95% for squamous cell tumours to 80% for adenocarcinomas. About 50% of bladder and oesophageal cancers were attributable to smoking; the PARP for stomach and pancreatic cancers were both around 30%.
DISCUSSION We have presented estimates of the risks of several dif-ferent types of cancer due to smoking, based on a large population-based case-control study conducted in .Montreal. Some cancer sites which were not included in the present study, including buccal cavity and larynx, have previously been shown to be related to cancer. Obviously, our inferences are limited to the sites which were included, and they are limited to males.
Most smokers smoked over a pack a day for over 30 years. Of the many sites of cancer examined, several were not associated with cigarette smoking. The null findings for cancers of the colon and rectum are in line with previous findings from both cohort and case-control studies.28"31 While the prostate has not generally been considered a target organ for smoking, Hsing ei al.32 have argued that this may represent an oversight and that the available evidence supports the hypothesis of a small increase in the risk. While our results for prostate cancer cannot be interpreted as demonstrating an association, the OR, in the range 1.1 to 1.2, are compatible with this hypothesis. Although the OR for non-Hodgkin's lymphoraa based on our data were slightly greater than unity, lymphomas have not previously been linked to smoking. Many, though not all,
previous studies of kidney cancer have found a positive association with smoking.i2-33-34 We found no such association; however, our upper confidence limits on the relative risk of kidney cancer were in the range of estimates reported in earlier studies. Similarly, for liver cancer, the majority of previous findings were posi-tive12"35 and ours were null. For both kidney and liver cancer, as for any other null findings, the inferences on risk are limited by the statistical power of the study. Although not shown here, we also carried out analyses of cancer risk in relation to duration of smoking, to intensity of smoking, and to years since cessation. There was no indication from those more detailed analyses of an association between smoking and any of the sites which were not significantly associated with smoking in Table 3.
Our findings included an apparent negative associa-tion between cigarette smoking and skin melanoma. Most previous evidence is consistent with the hypo-thesis of no association.36*38 In the absence of other sup-porting evidence and of a plausible biological mechanism, we arr inclined to view this finding as a statistical anomaly in a multiple testing context. For those site series with very few cases, only very large relative risks could have been detected; none were noted. Our data do not support a role for smoking in the aetiology of cancer of the small intestine, gallbladder, pleura or peritoneum (mesothelioma), testis, penis, eye melanoma, myelomas or sarcomas.
The oesophagus, pancreas, lung, and urinary bladder are well established target organs for smoking carcino-genesis,12*3*"47 and were associated with smoking in our data. The levels of risk and even the shape of the dose-response relationships observed here are broadly compatible with those reported in previous large-scale studies.13 For cancers of the lung, oesophagus and bladder, the effects of smoking differed according to cell type. Our results for lung cancer, with highest risks for squamous cell cancers and lowest for adenocarcinomas, resemble the results of Lubin and Blot.48 While the OR for lung adenocarcinomas are less than those for other lung cell types, they are still very high. Furthermore, as reported by Lubin and Blot, the shapes of the dose-response curves are very similar for the different cell types. Namely, if the OR are computed with reference to the lowest smoking group (1-500 cigarette-years), instead of to non-smokers, the dose-response curves would be nearly identical for the three cell types shown. Previous evidence on stomach cancer was interpreted by the IARC as demonstrating a small increase in risk, but a curious lack of dose-response.12 Likewise, our results showed a significant increase in risk but little trend in risk with cumulative exposure to cigarette smoke-
512 INTERNATIONAL JOURNAL OF EPIDEMIOLOGY
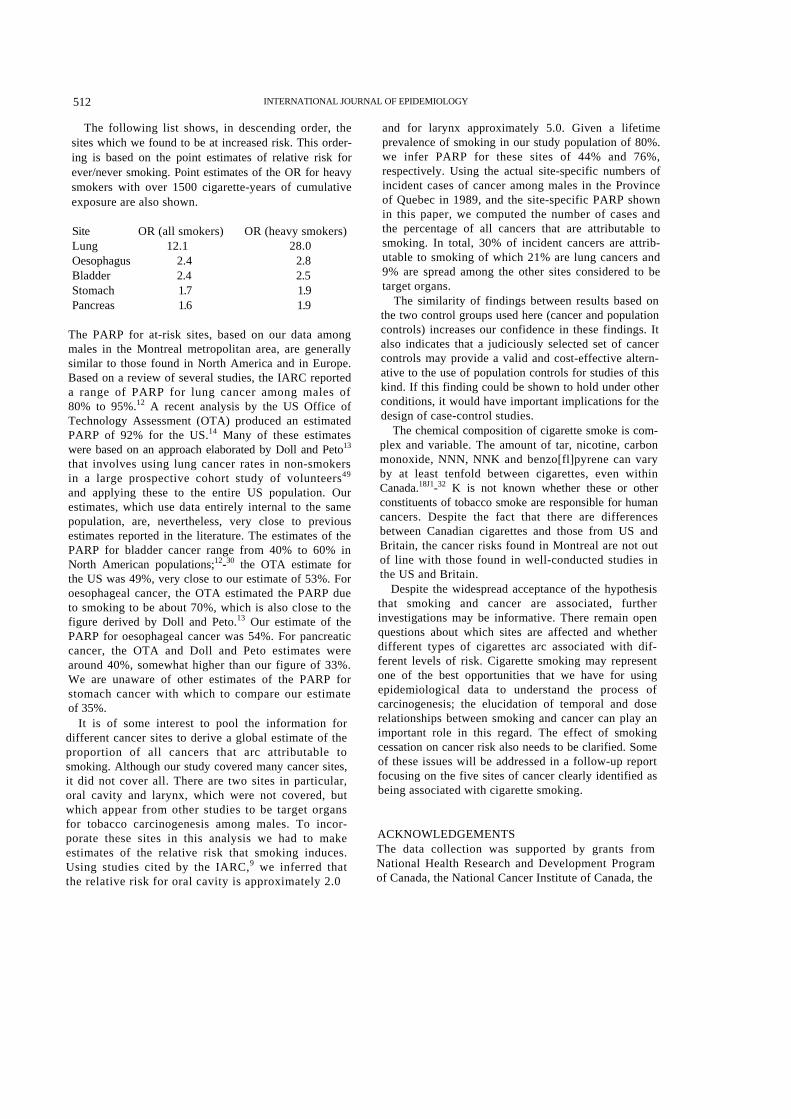
The following list shows, in descending order, the sites which we found to be at increased risk. This order-ing is based on the point estimates of relative risk for ever/never smoking. Point estimates of the OR for heavy smokers with over 1500 cigarette-years of cumulative exposure are also shown.
Site OR (all smokers) OR (heavy smokers) Lung 12.1 28.0 Oesophagus 2.4 2.8 Bladder 2.4 2.5 Stomach 1.7 1.9 Pancreas 1.6 1.9
The PARP for at-risk sites, based on our data among males in the Montreal metropolitan area, are generally similar to those found in North America and in Europe. Based on a review of several studies, the IARC reported a range of PARP for lung cancer among males of 80% to 95%.12 A recent analysis by the US Office of Technology Assessment (OTA) produced an estimated PARP of 92% for the US.14 Many of these estimates were based on an approach elaborated by Doll and Peto13
that involves using lung cancer rates in non-smokers in a large prospective cohort study of volunteers49
and applying these to the entire US population. Our estimates, which use data entirely internal to the same population, are, nevertheless, very close to previous estimates reported in the literature. The estimates of the PARP for bladder cancer range from 40% to 60% in North American populations;12-30 the OTA estimate for the US was 49%, very close to our estimate of 53%. For oesophageal cancer, the OTA estimated the PARP due to smoking to be about 70%, which is also close to the figure derived by Doll and Peto.13 Our estimate of the PARP for oesophageal cancer was 54%. For pancreatic cancer, the OTA and Doll and Peto estimates were around 40%, somewhat higher than our figure of 33%. We are unaware of other estimates of the PARP for stomach cancer with which to compare our estimate of 35%.
It is of some interest to pool the information for different cancer sites to derive a global estimate of the proportion of all cancers that arc attributable to smoking. Although our study covered many cancer sites, it did not cover all. There are two sites in particular, oral cavity and larynx, which were not covered, but which appear from other studies to be target organs for tobacco carcinogenesis among males. To incor-porate these sites in this analysis we had to make estimates of the relative risk that smoking induces. Using studies cited by the IARC,9 we inferred that the relative risk for oral cavity is approximately 2.0
and for larynx approximately 5.0. Given a lifetime prevalence of smoking in our study population of 80%. we infer PARP for these sites of 44% and 76%, respectively. Using the actual site-specific numbers of incident cases of cancer among males in the Province of Quebec in 1989, and the site-specific PARP shown in this paper, we computed the number of cases and the percentage of all cancers that are attributable to smoking. In total, 30% of incident cancers are attrib-utable to smoking of which 21% are lung cancers and 9% are spread among the other sites considered to be target organs.
The similarity of findings between results based on the two control groups used here (cancer and population controls) increases our confidence in these findings. It also indicates that a judiciously selected set of cancer controls may provide a valid and cost-effective altern-ative to the use of population controls for studies of this kind. If this finding could be shown to hold under other conditions, it would have important implications for the design of case-control studies.
The chemical composition of cigarette smoke is com-plex and variable. The amount of tar, nicotine, carbon monoxide, NNN, NNK and benzo[fl]pyrene can vary by at least tenfold between cigarettes, even within Canada.18J1-32 K is not known whether these or other constituents of tobacco smoke are responsible for human cancers. Despite the fact that there are differences between Canadian cigarettes and those from US and Britain, the cancer risks found in Montreal are not out of line with those found in well-conducted studies in the US and Britain.
Despite the widespread acceptance of the hypothesis that smoking and cancer are associated, further investigations may be informative. There remain open questions about which sites are affected and whether different types of cigarettes arc associated with dif-ferent levels of risk. Cigarette smoking may represent one of the best opportunities that we have for using epidemiological data to understand the process of carcinogenesis; the elucidation of temporal and dose relationships between smoking and cancer can play an important role in this regard. The effect of smoking cessation on cancer risk also needs to be clarified. Some of these issues will be addressed in a follow-up report focusing on the five sites of cancer clearly identified as being associated with cigarette smoking.
ACKNOWLEDGEMENTS The data collection was supported by grants from National Health Research and Development Program of Canada, the National Cancer Institute of Canada, the
CANCER RISKS AMONG SMOKERS 513
stitut de recherche en santé et sécurité du travail de u6bcc. The present analysis was supported in part by e Fonds de recherche en santé du Québec. The fieldwork for this project was supervised by ;sley Richardson, and analyses were carried out by jnald Dewar.
REFERENCES Parkin D M, Sasco A J. Lung cancer: worldwide variation in
occurrence and proportion attributable to tobacco use. Lung Cancer 1993; 9: UI6.
Pcto R, Lopez A D, Boreham J, Thun M. Heath C J. Mortality from tobacco in developed countries: indirect estimation from national vital statistics. Lancet 1992; 339: 1268-78.
Collishaw M F. Leahy K. Mortality attributable to tobacco use in Canada 1989. Chronic Dis Can 1991; 12: 46-49.
Best EWR, Josie G H, Walker C B. A Canadian study of mortality in relation to smoking habits. A preliminary report. Can J Public Health 1961; 52: 99-106.
Cederlof R, Fribcrg L, Hrubec Z, Lorich U. The Relationship of Smoking and Some Social Covariables to Mortality and Cancer Morbidity. A Ten Year Follow-Up in a Probability Sample of 55 000 Swedish Subjects. Age 18-69, Pan I and Pan 2. Stockholm: Department of Environmental Hygiene. The Karolinska Institute. 1975.
Doll R, Pcto R. Mortality in relation to smoking: 20 years' observations on male British doctors. Br Med J 1976; 2: 525-36. lond E C, Horn D. Smoking and death rates—report on irorty-four months of follow-up of 187 783 men. II. Death rates by cause. J Am MedAssoc 1958; 166: 1294-308.
Hammond E C, Seidman H. Smoking and cancer in the United Slates. Prev Med 1980; 9: 169-73.
Hirayama T. A cohort study on cancer in Japan. In: Blot W J, Hirayama T, Joel D G (eds). Statistical Methods in Cancer Epidemiology. Hiroshima: Radiation Effects Research Foundation. 1985.
Rogot E, Murray J L. Smoking and causes of death among US veterans: 16 years of observation. Public Health Rep 19S0; 95: 213-22.
Weir J M, Dunn D E Jr. Smoking and mortality: A prospective study. Cancer 1970; 25: 105-12.
International Agency for Research on Cancer. IARC Monographs on the Evaluation of the Carcinogenic Risk of Chem-icals to Humans, Vol. 38. Tobacco Smoking. Lyon: IARC, 1986.
Doll R, Peto R. The Causes of Cancer. Oxford: Oxford University Press. 1981.
Kronebusch K. Smoking: human and economic costs. Cancer Invest 1989; 7: 463-77.
Rickert W S, Kaiserman M J. Levels of lead, cadmium and mercury in Canadian cigarette tobacco as indicators of environmental change: results from a 21-year study (1968-1988). Environ Sci Technol 1994; 28: 924-27.
US Department of Health and Human Services. Reducing the Health Consequences of Smoking: 25 Years of Progress. A Report of the Surgeon General. (DHHS Publication No. (CDC) 89-8411. Rockville: US Department of Health and Human Services, Public Health Service, Centers for Disease Control, Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 1989.
Hecht S S, Hoffman D. Tobacco-specific niirosamines, an import-am group of carcinogens in tobacco and tobacco smoke. Carcinogenesis 1988; 9: 875-84.
18 Fischer S, Castonguay A, Kaiserman M. Spiegclhaldcr B, Preussmann R. Tobacco-specific nitrosamines in Canadian cigarettes. J Cancer Res Clin Oncol 1990; 116: 563-68.
19 Siemiatycki J. Risk Factors for Cancer in the Workplace. Boca Raton: CRC Press, 1991.
MSiemiatycki J, Day N E, Fabry J, Cooper J A. Discovering car-cinogens in the occupational environment: a novel epidem-iological approach. J Natl Cancer Inst 1981; 66: 217-25.
21 Siemiaiycki J, Wacholder S, Richardson L, Dcwar R, Genn M. Discovering carcinogens in the occupational environment: methods of data collection and analysts of a large case-referent monitoring system. Scand J Work Environ Health 1987; 13: 486-92.
22 WHO {World Health Organization}. Manual of the International Statistical Classification of Diseases, Injuries, and Causes of Death (1CD). (9th can.) Geneva: WHO, 1977.
"Girin M, Siemiatycki J, Ketnper H, Begin D. Obtaining occupational exposure histories in cpidemiologic case-control studies. J Occup Mtd 1985; 27: 420-26.
14 Breslow N E, Day N E. Statistical Methods in Cancer Research. Volume 1—The Analysis of Case-Control Studies. Lyon: International Agency for Research on Cancer, 1980.
23 SPSS Advanced Statistics User's Guide. Chicago: SPSS Inc., 1990.
M Sicmiarycki J, Dewar R, Krewski D, Desy M. Richardson L,' Franco E. Are the apparent effects of cigarette smoking on lung and bladder cancers due to uncontrolled con-founding by occupational exposures? Epidemiology 1994; 5: 57-65. 27 Bruzzi P, Green S B, Byar D P, Brinton L A, Schairer C. Estimating the population attributable risk for multiple risk factors using case-control data. Am J Epidemiol 1985; 122: 904-14.
34 Hactttzel W, Berg J W, Segi M ei al. Large-bowel cancer in Hawaiian Japanese. J Natl Cancer Inst 1973; 51: 1765-79.
29 Ha mmond E C . S m ok ing in r e l a t i on t o t he dea th r a t e s o f one million men and women. Natl Cancer Inst Monogr 1966; 19: 127-204.
30 Sandier R S, Sandier D P, Comstock G W. Hclsing K J, Shore D L. Cigare t t e smoking and the r isk of co lo recta l cancer in women. J Nat l Cancer Ins t 1988; 80: 1329-33.
31 W i l l i a m s R R , H o r m J W . A s s o c i a t i o n o f c a n c e r s i t e s w i t h tobacco and alcohol consumption and socioeconotnic status of patients: interview itudy from the Third National Cancer Survey. J Natl Cancer Inst 1977; 58: 525-47.
M Hsing A W, McLaughlin J K, Hrubec Z, Blot W J, Fraumeni J F, Jr. Tobacco use and prostate cancer. 26-year follow-up of US veterans. Am J Epidemiol 1991; 133: 437-41.
3 3 Brownson RCA case-control s tudy of renal cel l carcinoma in relation to occupation, smoking, and alcohol consumption. Arch Environ Heal th 1988; 43: 238-41.
34 La Vecchia C, Negri E, D'Avanzo B, Franceschi S. Smoking and renal cel l carcinoma. Cancer Res 1990; 50: 5231-33.
35 Bosch F X, Munoz N. Prospects for epidemiologies] s tudies on bepalocellular cancer as a model for assessing viral and chem-ical interactions. In: Bartsch H, Hemminki K, O'Neill I K (cds). Methods for Detecting DNA Damaging Agents in Humans: Applications in Cancer Epidemiology and Preven-Hon. Lyon: IARC, 1988.
3 6 GallagherRP, Elwood J M.Gil l G B. Risk factors for cutaneous ma l ignan t me lanoma : t he Wes te rn Canada Me lanoma Study. Recent Resul ts Cancer Res 1986; 102: 38-55.
514 INTERNATIONAL JOURNAL OF EPIDEMIOLOGY
37 Green A. Bain C. McLennan R. Siskind V. Risk factors for cutaneous malanoma in Queensland. Recent Results Cancer Rex 1986; 102: 76-97.
38 Holman C D J, Armstrong B K. Hcenan P J ei al. The causes of malignant melanoma: results from the West Australian Lions Melanoma Research Project. Recent Results Cancer Res 1986; 102: 18-37.
39 Brownson R C. Chang J C, Davis J R. Gender and histotogic type variations in smoking-related risk of lung cancer. Epidemiology 1992; 3: 61-64.
40 Bueno de Mesquita H B, Maisonneuvc P, Moerman C J. Runia S. Boyle P. Life-time history of smoking and exocrine carcinoma of the pancreas: a population-based case-control study in the Netherlands. Im J Cancer 1991; 49: 816-22.
41 Clavel J. Cordier S. Boccon-Gibod L, Himon D. Tobacco and bladder cancer in males: increased risk for inhalers and smokers of black tobacco. Im J Cancer 1989; 44: 605-10.
42Falk RT. Wil l iams Pickle L, Fontham ET. Correa P, Fraumeni J F, Jr. Life-style risk factors for pancreatic cancer in Louisiana: a case-control study. Am J Epidemiol 1988: 128: 324-36.
43Ghadirian P. Simard A, Baillargeon J. Tobacco, alcohol and coffee and cancer of the pancreas: a population based, case-control study in Quebec, Canada. Cancer 1991; 67: 2664-70.
44 Hartge P. Silverman D, Hoover R el al. Changing cigarette habits and bladder cancer risk: a case control study. J Natl Cancer Inst 1987; 78: 1119-25-
45 lscovich J, Castelleto R, Esteve J el al. Tobacco smoking, occupational exposure and bladder cancer in Argentina. IntJCancer 1987; 40: 734^*0.
46 "Mack TM, Yu M C, Hanisch R, Henderson BE. Pancreas cancer and smoking, beverage consumption, and past medical history. J Nail Cancer Inst 1986; 76: 49-60.
47Norell S E. Ahlbom A, Erwald R ei al. Diet and pancreatic cancer a case-control study. Am J Epidemiol 1986; 124: 894-902.
48Lubin J H, Blot W J. Assessment of lung cancer risk factors by histologic category. J Nail Cancer Inst 1984; 73: 383-89.
49GarfinkeI L. Cancer mortality in nonsmokers: prospective study by the American Cancer Society. J Natl Cancer Inst 1980; «5: 1169-73.
50 Burns P B. Swajison C M- Risk of urinary bladder cancer among blacks and whites—the role of cigarette use and occupa-tion. Cancer Causes Control 1991; 2: 371-79.
51 Kaiserman M J. Rickert W S. Carcinogens in tobacco smoke— benio[ojpyrcnc from Canadian cigarettes and cigarette tobacco. Am J Public Health 1992; 82: 1023-26.
52 Rickert W S. 'Less hazardous' cigarettes: fact or fiction? NY State . SMcrf 1983; tt: 1269-72.
(Revised version received November 1994)'