
aal@ home: a New Home Care Wireless Biosignal Monitoring Tool for Ambient Assisted Living
Upload
khangminh22Category
view
0download
0
Assisted Living Resource Guide
Florida Senior Living Association 2292 Wednesday Street, Suite 1
Tallahassee, FL 32308 (850) 708-4972
[email protected] www.floridaseniorliving.org
Current as of October 1, 2019


[email protected] 2292 Wednesday Street, Suite 1 www.floridaseniorliving.org Tallahassee, FL 32308
Assisted Living Resource Guide Table of Contents
About Florida Senior Living Association (FSLA)
Meet FSLA’s ALF Core Trainer
Department of Elder Affairs (DOEA) ALF Core Curriculum Outline
SECTION TAB
AHCA Regulations
Chapter 408, Part II, F.S (Health Care Licensing: General Provisions). . . . . . . . . . . . . . . . . . . . 1
Rule Chapter 59A-35, F.A.C. (Health Care Licensing Procedures). . . . . . . . . . . . . . . . . . . . . . . .2
Chapter 419, F.S. (Community Residential Homes) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3
Chapter 435, F.S. (Background Screening). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
Chapter 429, Part I, F.S. (Assisted Living Facilities) and
Section 429.905, F.S. (Adult Day Care Center Exemptions) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Assisted Living Rule Transfer Table,
Rule Chapter 59A-36, F.A.C. (Assisted Living Facility Effective July 1, 2019), and
Rule Chapter 58A-5, F.A.C. (Original Assisted Living Rule transferred to 59A-36). . . . . . . . . . 6
DOH Regulations
Rule Chapter 64E-11, F.A.C. (Food Hygiene). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .7
Rule Chapter 64E-12, F.A.C. (Community Based Residential Facilities). . . . . . . . . . . . . . . . . . . 8
Rule Chapter 64E-16, F.A.C. (Biomedical Waste). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Chapter 464, F.S. (Nursing). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
DCF Regulations
Chapter 415, F.S (Adult Protective Services). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
Florida Building Code
Rule Chapter 61G20-1, FBC (Florida Building Code Adopted) and
Chapter 4, Section 464, FBC (Assisted Living Facilities) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
Fire Marshal or Local Authority Having Jurisdiction
Uniform Fire Safety Standards for Assisted Living Facilities (Rule Chapter 69A-40, F.A.C.) .13
Appendix. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14

[This space intentionally left blank.]

[email protected] 2292 Wednesday Street, Suite 1 www.floridaseniorliving.org Tallahassee, FL 32308
Dear Colleague,
Florida Senior Living Association (FSLA) is the preeminent statewide association that represents more than 400 professionally managed senior assisted living, independent, and memory care communities. Our expert staff provides members with current regulatory information and consistent communications to keep you and your staff up to date with the latest changes. Moreover, our national affiliate partner, Argentum, provides resources at the federal level.
FSLA’s Assisted Living Resource Guide is a resource that we offer assisted living community (ALF) operators. The Guide will be your go-to reference tool. It contains the most up-to-date regulatory information including statutes and rules necessary to operate an ALF in Florida. It also contains sample forms and links necessary for the day-to-day operation of an ALF.
In addition to regulatory assistance, FSLA offers professional education courses. We provide both the required core training for individuals interested in becoming assisted living administrators as well as professional development courses for continuing education. These courses meet the education requirements under 429.52, F.S., and offered both online and in person. If you choose to participate in FSLA’s Core Training Program, the Guide will be referenced throughout the course to help you become more familiar with Florida’s regulations. Studying the Guide and becoming familiar with the laws and rules will help you prepare for the core training state exam and can be used as a resource once you pass the exam and become an administrator. Remember to check our website on a regular basis for any updates that may be available for download to replace any outdated laws and rules. If you aren’t already a member, we hope that you will consider having your community join the association. For more information or if you have any questions, please contact us at: [email protected] and visit our website at floridaseniorliving.org. Sincerely,
Gail Matillo President/CEO

Meet Florida Senior Living Association’s ALF Core Trainer
Monica Wilson, MS, President, ICE Bridge Consulting
Monica Wilson has extensive experience as a consultative trainer and educator with more than
15 years’ experience supporting those who serve older adults. Monica provides consultation on
issues related to compliance, team building and service delivery with a focus on supporting
independence and quality of life for older adults who are experiencing physical and cognitive
changes correlated with advanced age. She has held management positions in senior living
companies, and with the Florida Department of Elder Affairs. She has consulted for other states
on policy issues and led local advocacy efforts in support of policies that support aging in place.
Monica has a Master of Science in Gerontology from the School of Business and
Entrepreneurship at Nova Southeastern University and is currently an Adjunct Professor at Palm
Beach State College.

DO
EA A
LF Core
Curriculum
Outline






1. Chapter 408, Part II, F.S


1 – 1
CHAPTER 408
PART II
HEALTH CARE LICENSING: GENERAL PROVISIONS
(ss. 408.801-408.832) 408.801 Short title; purpose.
408.802 Applicability.
408.803 Definitions.
408.804 License required; display.
408.805 Fees required; adjustments.
408.806 License application process.
408.8065 Additional licensure requirements for home health agencies, home medical equipment providers, and
health care clinics.
408.807 Change of ownership.
408.808 License categories.
408.809 Background screening; prohibited offenses.
408.810 Minimum licensure requirements.
408.811 Right of inspection; copies; inspection reports; plan for correction of deficiencies.
408.812 Unlicensed activity.
408.813 Administrative fines; violations.
408.814 Moratorium; emergency suspension.
408.815 License or application denial; revocation.
408.816 Injunctions.
408.817 Administrative proceedings.
408.818 Health Care Trust Fund.
408.819 Rules.
408.820 Exemptions.
408.821 Emergency management planning; emergency operations; inactive license.
408.831 Denial, suspension, or revocation of a license, registration, certificate, or application.
408.832 Conflicts.
408.801 Short title; purpose.—
(1) This part may be cited as the “Health Care Licensing Procedures Act.”
(2) The Legislature finds that there is unnecessary duplication and variation in the requirements for licensure by
the agency. It is the intent of the Legislature to provide a streamlined and consistent set of basic licensing
requirements for all such providers in order to minimize confusion, standardize terminology, and include issues that
are otherwise not adequately addressed in the Florida Statutes pertaining to specific providers.
History.—s. 5, ch. 2006-192.

1 – 2
408.802 Applicability.—The provisions of this part apply to the provision of services that require licensure as
defined in this part and to the following entities licensed, registered, or certified by the agency, as described in
chapters 112, 383, 390, 394, 395, 400, 429, 440, 483, and 765:
(1) Laboratories authorized to perform testing under the Drug-Free Workplace Act, as provided under ss.
112.0455 and 440.102.
(2) Birth centers, as provided under chapter 383.
(3) Abortion clinics, as provided under chapter 390.
(4) Crisis stabilization units, as provided under parts I and IV of chapter 394.
(5) Short-term residential treatment facilities, as provided under parts I and IV of chapter 394.
(6) Residential treatment facilities, as provided under part IV of chapter 394.
(7) Residential treatment centers for children and adolescents, as provided under part IV of chapter 394.
(8) Hospitals, as provided under part I of chapter 395.
(9) Ambulatory surgical centers, as provided under part I of chapter 395.
(10) Nursing homes, as provided under part II of chapter 400.
(11) Assisted living facilities, as provided under part I of chapter 429.
(12) Home health agencies, as provided under part III of chapter 400.
(13) Nurse registries, as provided under part III of chapter 400.
(14) Companion services or homemaker services providers, as provided under part III of chapter 400.
(15) Adult day care centers, as provided under part III of chapter 429.
(16) Hospices, as provided under part IV of chapter 400. 1(17) Adult family-care homes, as provided under part II of chapter 429.
(18) Homes for special services, as provided under part V of chapter 400.
(19) Transitional living facilities, as provided under part XI of chapter 400.
(20) Prescribed pediatric extended care centers, as provided under part VI of chapter 400.
(21) Home medical equipment providers, as provided under part VII of chapter 400.
(22) Intermediate care facilities for persons with developmental disabilities, as provided under part VIII of
chapter 400.
(23) Health care services pools, as provided under part IX of chapter 400.
(24) Health care clinics, as provided under part X of chapter 400.
(25) Multiphasic health testing centers, as provided under 2part I of chapter 483. 1(26) Organ, tissue, and eye procurement organizations, as provided under part V of chapter 765.
History.—s. 5, ch. 2006-192; s. 89, ch. 2007-5; s. 132, ch. 2007-230; s. 19, ch. 2009-218; s. 23, ch. 2012-160; s.
9, ch. 2015-25; s. 68, ch. 2018-24. 1Note.—Section 11, ch. 2006-192, provides that “[a]ll provisions that apply to the entities specified in s. 408.802,
Florida Statutes, as created by this act, in effect on October 1, 2006, that provide for annual licensure fees are hereby
adjusted to provide for biennial licensure fees with a corresponding doubling of the amount.” 2Note.—Redesignated as part I of chapter 483 to conform to the repeal of former part I of that chapter by s. 97,
ch. 2018-24.

1 – 3
408.803 Definitions.—As used in this part, the term:
(1) “Agency” means the Agency for Health Care Administration, which is the licensing agency under this part.
(2) “Applicant” means an individual, corporation, partnership, firm, association, or governmental entity that
submits an application for a license to the agency.
(3) “Authorizing statute” means the statute authorizing the licensed operation of a provider listed in s. 408.802
and includes chapters 112, 383, 390, 394, 395, 400, 429, 440, 483, and 765.
(4) “Certification” means certification as a Medicare or Medicaid provider of the services that require licensure,
or certification pursuant to the federal Clinical Laboratory Improvement Amendment (CLIA).
(5) “Change of ownership” means:
(a) An event in which the licensee sells or otherwise transfers its ownership to a different individual or entity as
evidenced by a change in federal employer identification number or taxpayer identification number; or
(b) An event in which 51 percent or more of the ownership, shares, membership, or controlling interest of a
licensee is in any manner transferred or otherwise assigned. This paragraph does not apply to a licensee that is
publicly traded on a recognized stock exchange.
A change solely in the management company or board of directors is not a change of ownership.
(6) “Client” means any person receiving services from a provider listed in s. 408.802.
(7) “Controlling interest” means:
(a) The applicant or licensee;
(b) A person or entity that serves as an officer of, is on the board of directors of, or has a 5-percent or greater
ownership interest in the applicant or licensee; or
(c) A person or entity that serves as an officer of, is on the board of directors of, or has a 5-percent or greater
ownership interest in the management company or other entity, related or unrelated, with which the applicant or
licensee contracts to manage the provider.
The term does not include a voluntary board member.
(8) “License” means any permit, registration, certificate, or license issued by the agency.
(9) “Licensee” means an individual, corporation, partnership, firm, association, governmental entity, or other
entity that is issued a permit, registration, certificate, or license by the agency. The licensee is legally responsible for
all aspects of the provider operation.
(10) “Moratorium” means a prohibition on the acceptance of new clients.
(11) “Provider” means any activity, service, agency, or facility regulated by the agency and listed in s. 408.802.
(12) “Relative” means an individual who is the father, mother, stepfather, stepmother, son, daughter, brother,
sister, grandmother, grandfather, great-grandmother, great-grandfather, grandson, granddaughter, uncle, aunt, first
cousin, nephew, niece, husband, wife, father-in-law, mother-in-law, son-in-law, daughter-in-law, brother-in-law,
sister-in-law, stepson, stepdaughter, stepbrother, stepsister, half-brother, or half-sister of a patient or client.
(13) “Services that require licensure” means those services, including residential services, that require a valid
license before those services may be provided in accordance with authorizing statutes and agency rules.
(14) “Voluntary board member” means a board member or officer of a not-for-profit corporation or
organization who serves solely in a voluntary capacity, does not receive any remuneration for his or her services on
the board of directors, and has no financial interest in the corporation or organization.
History.—s. 5, ch. 2006-192; s. 90, ch. 2007-5; s. 47, ch. 2009-223; s. 69, ch. 2018-24.

1 – 4
408.804 License required; display.—
(1) It is unlawful to provide services that require licensure, or operate or maintain a provider that offers or
provides services that require licensure, without first obtaining from the agency a license authorizing the provision
of such services or the operation or maintenance of such provider.
(2) A license must be displayed in a conspicuous place readily visible to clients who enter at the address that
appears on the license and is valid only in the hands of the licensee to whom it is issued and may not be sold,
assigned, or otherwise transferred, voluntarily or involuntarily. The license is valid only for the licensee, provider,
and location for which the license is issued.
(3) Any person who knowingly alters, defaces, or falsifies a license certificate issued by the agency, or causes
or procures any person to commit such an offense, commits a misdemeanor of the second degree, punishable as
provided in s. 775.082 or s. 775.083. Any licensee or provider who displays an altered, defaced, or falsified license
certificate is subject to the penalties set forth in s. 408.815 and an administrative fine of $1,000 for each day of
illegal display.
History.—s. 5, ch. 2006-192; s. 24, ch. 2012-160.
408.805 Fees required; adjustments.—Unless otherwise limited by authorizing statutes, license fees must be
reasonably calculated by the agency to cover its costs in carrying out its responsibilities under this part, authorizing
statutes, and applicable rules, including the cost of licensure, inspection, and regulation of providers.
(1) Licensure fees shall be adjusted to provide for biennial licensure under agency rules.
(2) The agency shall annually adjust licensure fees, including fees paid per bed, by not more than the change in
the Consumer Price Index based on the 12 months immediately preceding the increase.
(3) An inspection fee must be paid as required in authorizing statutes.
(4) Fees are nonrefundable.
(5) When a change is reported that requires issuance of a license, a fee may be assessed. The fee must be based
on the actual cost of processing and issuing the license.
(6) A fee may be charged to a licensee requesting a duplicate license. The fee may not exceed the actual cost of
duplication and postage.
(7) Total fees collected may not exceed the cost of administering this part, authorizing statutes, and applicable
rules.
History.—s. 5, ch. 2006-192.
408.806 License application process.—
(1) An application for licensure must be made to the agency on forms furnished by the agency, submitted under
oath or attestation, and accompanied by the appropriate fee in order to be accepted and considered timely. The
application must contain information required by authorizing statutes and applicable rules and must include:
(a) The name, address, and social security number, or individual taxpayer identification number if a social
security number cannot legally be obtained, of:
1. The applicant;
2. The administrator or a similarly titled person who is responsible for the day-to-day operation of the provider;
3. The financial officer or similarly titled person who is responsible for the financial operation of the licensee or
provider; and
4. Each controlling interest if the applicant or controlling interest is an individual.

1 – 5
(b) The name, address, and federal employer identification number or taxpayer identification number of the
applicant and each controlling interest if the applicant or controlling interest is not an individual.
(c) The name by which the provider is to be known.
(d) The total number of beds or capacity requested, as applicable.
(e) The name of the person or persons under whose management or supervision the provider will operate and
the name of the administrator, if required.
(f) If the applicant offers continuing care agreements as defined in chapter 651, proof shall be furnished that the
applicant has obtained a certificate of authority as required for operation under chapter 651.
(g) Other information, including satisfactory inspection results, that the agency finds necessary to determine the
ability of the applicant to carry out its responsibilities under this part, authorizing statutes, and applicable rules.
(h) An attestation, under penalty of perjury, as required in s. 435.05(3), stating compliance with the provisions
of this section and chapter 435.
(2)(a) The applicant for a renewal license must submit an application that must be received by the agency at
least 60 days but no more than 120 days before the expiration of the current license. An application received more
than 120 days before the expiration of the current license shall be returned to the applicant. If the renewal
application and fee are received prior to the license expiration date, the license shall not be deemed to have expired
if the license expiration date occurs during the agency’s review of the renewal application.
(b) The applicant for initial licensure due to a change of ownership must submit an application that must be
received by the agency at least 60 days prior to the date of change of ownership.
(c) For any other application or request, the applicant must submit an application or request that must be
received by the agency at least 60 days but no more than 120 days before the requested effective date, unless
otherwise specified in authorizing statutes or applicable rules. An application received more than 120 days before
the requested effective date shall be returned to the applicant.
(d) The licensee’s failure to timely file a renewal application and license application fee with the agency shall
result in a $50 per day late fee charged to the licensee by the agency; however, the aggregate amount of the late fee
may not exceed 50 percent of the licensure fee or $500, whichever is less. The agency shall provide a courtesy
notice to the licensee by United States mail, electronically, or by any other manner at its address of record or mailing
address, if provided, at least 90 days before the expiration of a license. This courtesy notice must inform the licensee
of the expiration of the license. If the agency does not provide the courtesy notice or the licensee does not receive
the courtesy notice, the licensee continues to be legally obligated to timely file the renewal application and license
application fee with the agency and is not excused from the payment of a late fee. If an application is received after
the required filing date and exhibits a hand-canceled postmark obtained from a United States post office dated on or
before the required filing date, no fine will be levied.
(e) The applicant must pay the late fee before a late application is considered complete and failure to pay the
late fee is considered an omission from the application for licensure pursuant to paragraph (3)(b).
(3)(a) Upon receipt of an application for a license, the agency shall examine the application and, within 30 days
after receipt, notify the applicant in writing of any apparent errors or omissions and request any additional
information required.
(b) Requested information omitted from an application for licensure, license renewal, or change of ownership,
other than an inspection, must be filed with the agency within 21 days after the agency’s request for omitted

1 – 6
information or the application shall be deemed incomplete and shall be withdrawn from further consideration and
the fees shall be forfeited.
(c) Within 60 days after the receipt of a complete application, the agency shall approve or deny the application.
(4)(a) Licensees subject to the provisions of this part shall be issued biennial licenses unless conditions of the
license category specify a shorter license period.
(b) Each license issued shall indicate the name of the licensee, the type of provider or service that the licensee is
required or authorized to operate or offer, the date the license is effective, the expiration date of the license, the
maximum capacity of the licensed premises, if applicable, and any other information required or deemed necessary
by the agency.
(5) In accordance with authorizing statutes and applicable rules, proof of compliance with s. 408.810 must be
submitted with an application for licensure.
(6) The agency may not issue an initial license to a health care provider subject to the certificate-of-need
provisions in part I of this chapter if the licensee has not been issued a certificate of need or certificate-of-need
exemption, when applicable. Failure to apply for the renewal of a license prior to the expiration date renders the
license void.
(7)(a) An applicant must demonstrate compliance with the requirements in this part, authorizing statutes, and
applicable rules during an inspection pursuant to s. 408.811, as required by authorizing statutes.
(b) An initial inspection is not required for companion services or homemaker services providers, as provided
under part III of chapter 400, or for health care services pools, as provided under part IX of chapter 400.
(c) If an inspection is required by the authorizing statute for a license application other than an initial
application, the inspection must be unannounced. This paragraph does not apply to inspections required pursuant to
ss. 383.324, 395.0161(4), and 429.67(6).
(d) If a provider is not available when an inspection is attempted, the application shall be denied.
(8) The agency may establish procedures for the electronic notification and submission of required information,
including, but not limited to:
(a) Licensure applications.
(b) Required signatures.
(c) Payment of fees.
(d) Notarization or attestation of applications.
Requirements for electronic submission of any documents required by this part or authorizing statutes may be
established by rule. As an alternative to sending documents as required by authorizing statutes, the agency may provide
electronic access to information or documents.
(9) A licensee that holds a license for multiple providers licensed by the agency may request that all related
license expiration dates be aligned. Upon such request, the agency may issue a license for an abbreviated licensure
period with a prorated licensure fee.
History.—s. 5, ch. 2006-192; s. 91, ch. 2007-5; s. 48, ch. 2009-223; s. 19, ch. 2010-114; s. 25, ch. 2012-160; s. 2,
ch. 2014-84; s. 70, ch. 2018-24.

1 – 7
408.8065 Additional licensure requirements for home health agencies, home medical equipment
providers, and health care clinics.—
(1) An applicant for initial licensure, or initial licensure due to a change of ownership, as a home health agency,
home medical equipment provider, or health care clinic shall:
(a) Demonstrate financial ability to operate, as required under s. 408.810(8) and this section. If the applicant’s
assets, credit, and projected revenues meet or exceed projected liabilities and expenses, and the applicant provides
independent evidence that the funds necessary for startup costs, working capital, and contingency financing exist
and will be available as needed, the applicant has demonstrated the financial ability to operate.
(b) Submit projected financial statements, including a balance sheet, income and expense statement, and a
statement of cash flows for the first 2 years of operation which provide evidence that the applicant has sufficient
assets, credit, and projected revenues to cover liabilities and expenses.
(c) Submit a statement of the applicant’s estimated startup costs and sources of funds through the break-even
point in operations demonstrating that the applicant has the ability to fund all startup costs, working capital costs,
and contingency financing requirements. The statement must show that the applicant has at a minimum 3 months of
average projected expenses to cover startup costs, working capital costs, and contingency financing requirements.
The minimum amount for contingency funding may not be less than 1 month of average projected expenses.
All documents required under this subsection must be prepared in accordance with generally accepted accounting
principles and may be in a compilation form. The financial statements must be signed by a certified public accountant.
(2) For initial, renewal, or change of ownership licenses for a home health agency, a home medical equipment
provider, or a health care clinic, applicants and controlling interests who are nonimmigrant aliens, as described in 8
U.S.C. s. 1101, must file a surety bond of at least $500,000, payable to the agency, which guarantees that the home
health agency, home medical equipment provider, or health care clinic will act in full conformity with all legal
requirements for operation.
(3) In addition to the requirements of s. 408.812, any person who offers services that require licensure under
part VII or part X of chapter 400, or who offers skilled services that require licensure under part III of chapter 400,
without obtaining a valid license; any person who knowingly files a false or misleading license or license renewal
application or who submits false or misleading information related to such application, and any person who violates
or conspires to violate this section, commits a felony of the third degree, punishable as provided in s. 775.082, s.
775.083, or s. 775.084.
History.—s. 4, ch. 2009-193; s. 8, ch. 2009-223; s. 26, ch. 2012-160.
408.807 Change of ownership.—Whenever a change of ownership occurs:
(1) The transferor shall notify the agency in writing at least 60 days before the anticipated date of the change of
ownership.
(2) The transferee shall make application to the agency for a license within the timeframes required in s.
408.806.
(3) The transferor shall be responsible and liable for:
(a) The lawful operation of the provider and the welfare of the clients served until the date the transferee is
licensed by the agency.
(b) Any and all penalties imposed against the transferor for violations occurring before the date of change of
ownership.

1 – 8
(4) Any restriction on licensure, including a conditional license existing at the time of a change of ownership,
shall remain in effect until the agency determines that the grounds for the restriction are corrected.
(5) The transferee shall maintain records of the transferor as required in this part, authorizing statutes, and
applicable rules, including:
(a) All client records.
(b) Inspection reports.
(c) All records required to be maintained pursuant to s. 409.913, if applicable.
History.—s. 5, ch. 2006-192.
408.808 License categories.—
(1) STANDARD LICENSE.—A standard license may be issued to an applicant at the time of initial licensure,
license renewal, or change of ownership. A standard license shall be issued when the applicant is in compliance with
all statutory requirements and agency rules. Unless sooner revoked, a standard license expires 2 years after the date
of issue.
(2) PROVISIONAL LICENSE.—An applicant against whom a proceeding denying or revoking a license is
pending at the time of license renewal may be issued a provisional license effective until final action not subject to
further appeal. A provisional license may also be issued to an applicant applying for a change of ownership. A
provisional license must be limited in duration to a specific period of time, up to 12 months, as determined by the
agency.
(3) INACTIVE LICENSE.—An inactive license may be issued to a health care provider subject to the
certificate-of-need provisions in part I of this chapter when the provider is currently licensed, does not have a
provisional license, and will be temporarily unable to provide services but is reasonably expected to resume services
within 12 months. Such designation may be made for a period not to exceed 12 months but may be renewed by the
agency for up to 12 additional months upon demonstration by the licensee of the provider’s progress toward
reopening. However, if after 20 months in an inactive license status, a statutory rural hospital, as defined in s.
395.602, has demonstrated progress toward reopening, but may not be able to reopen prior to the inactive license
expiration date, the inactive designation may be renewed again by the agency for up to 12 additional months. For
purposes of such a second renewal, if construction or renovation is required, the licensee must have had plans
approved by the agency and construction must have already commenced pursuant to s. 408.032(4); however, if
construction or renovation is not required, the licensee must provide proof of having made an enforceable capital
expenditure greater than 25 percent of the total costs associated with the hiring of staff and the purchase of
equipment and supplies needed to operate the facility upon opening. A request by a licensee for an inactive license
or to extend the previously approved inactive period must be submitted to the agency and must include a written
justification for the inactive license with the beginning and ending dates of inactivity specified, a plan for the
transfer of any clients to other providers, and the appropriate licensure fees. The agency may not accept a request
that is submitted after initiating closure, after any suspension of service, or after notifying clients of closure or
suspension of service, unless the action is a result of a disaster at the licensed premises. For the purposes of this
section, the term “disaster” means a sudden emergency occurrence beyond the control of the licensee, whether
natural, technological, or manmade, which renders the provider inoperable at the premises. Upon agency approval,
the provider shall notify clients of any necessary discharge or transfer as required by authorizing statutes or
applicable rules. The beginning of the inactive license period is the date the provider ceases operations. The end of

1 – 9
the inactive license period shall become the license expiration date. All licensure fees must be current, must be paid
in full, and may be prorated. Reactivation of an inactive license requires the approval of a renewal application,
including payment of licensure fees and agency inspections indicating compliance with all requirements of this part,
authorizing statutes, and applicable rules.
(4) OTHER LICENSES.—Other types of license categories may be issued pursuant to authorizing statutes or
applicable rules.
History.—s. 5, ch. 2006-192; s. 2, ch. 2009-45; s. 49, ch. 2009-223; s. 20, ch. 2010-114.
408.809 Background screening; prohibited offenses.—
(1) Level 2 background screening pursuant to chapter 435 must be conducted through the agency on each of the
following persons, who are considered employees for the purposes of conducting screening under chapter 435:
(a) The licensee, if an individual.
(b) The administrator or a similarly titled person who is responsible for the day-to-day operation of the
provider.
(c) The financial officer or similarly titled individual who is responsible for the financial operation of the
licensee or provider.
(d) Any person who is a controlling interest.
(e) Any person, as required by authorizing statutes, seeking employment with a licensee or provider who is
expected to, or whose responsibilities may require him or her to, provide personal care or services directly to clients
or have access to client funds, personal property, or living areas; and any person, as required by authorizing statutes,
contracting with a licensee or provider whose responsibilities require him or her to provide personal care or personal
services directly to clients, or contracting with a licensee or provider to work 20 hours a week or more who will
have access to client funds, personal property, or living areas. Evidence of contractor screening may be retained by
the contractor’s employer or the licensee.
(2) Every 5 years following his or her licensure, employment, or entry into a contract in a capacity that under
subsection (1) would require level 2 background screening under chapter 435, each such person must submit to level
2 background rescreening as a condition of retaining such license or continuing in such employment or contractual
status. For any such rescreening, the agency shall request the Department of Law Enforcement to forward the
person’s fingerprints to the Federal Bureau of Investigation for a national criminal history record check unless the
person’s fingerprints are enrolled in the Federal Bureau of Investigation’s national retained print arrest notification
program. If the fingerprints of such a person are not retained by the Department of Law Enforcement under s.
943.05(2)(g) and (h), the person must submit fingerprints electronically to the Department of Law Enforcement for
state processing, and the Department of Law Enforcement shall forward the fingerprints to the Federal Bureau of
Investigation for a national criminal history record check. The fingerprints shall be retained by the Department of
Law Enforcement under s. 943.05(2)(g) and (h) and enrolled in the national retained print arrest notification
program when the Department of Law Enforcement begins participation in the program. The cost of the state and
national criminal history records checks required by level 2 screening may be borne by the licensee or the person
fingerprinted. Until a specified agency is fully implemented in the clearinghouse created under s. 435.12, the agency
may accept as satisfying the requirements of this section proof of compliance with level 2 screening standards
submitted within the previous 5 years to meet any provider or professional licensure requirements of the agency, the
Department of Health, the Department of Elderly Affairs, the Agency for Persons with Disabilities, the Department
1 – 10
of Children and Families, or the Department of Financial Services for an applicant for a certificate of authority or
provisional certificate of authority to operate a continuing care retirement community under chapter 651, provided
that:
(a) The screening standards and disqualifying offenses for the prior screening are equivalent to those specified
in s. 435.04 and this section;
(b) The person subject to screening has not had a break in service from a position that requires level 2 screening
for more than 90 days; and
(c) Such proof is accompanied, under penalty of perjury, by an attestation of compliance with chapter 435 and
this section using forms provided by the agency.
(3) All fingerprints must be provided in electronic format. Screening results shall be reviewed by the agency
with respect to the offenses specified in s. 435.04 and this section, and the qualifying or disqualifying status of the
person named in the request shall be maintained in a database. The qualifying or disqualifying status of the person
named in the request shall be posted on a secure website for retrieval by the licensee or designated agent on the
licensee’s behalf.
(4) In addition to the offenses listed in s. 435.04, all persons required to undergo background screening
pursuant to this part or authorizing statutes must not have an arrest awaiting final disposition for, must not have been
found guilty of, regardless of adjudication, or entered a plea of nolo contendere or guilty to, and must not have been
adjudicated delinquent and the record not have been sealed or expunged for any of the following offenses or any
similar offense of another jurisdiction:
(a) Any authorizing statutes, if the offense was a felony.
(b) This chapter, if the offense was a felony.
(c) Section 409.920, relating to Medicaid provider fraud.
(d) Section 409.9201, relating to Medicaid fraud.
(e) Section 741.28, relating to domestic violence.
(f) Section 777.04, relating to attempts, solicitation, and conspiracy to commit an offense listed in this
subsection.
(g) Section 817.034, relating to fraudulent acts through mail, wire, radio, electromagnetic, photoelectronic, or
photooptical systems.
(h) Section 817.234, relating to false and fraudulent insurance claims.
(i) Section 817.481, relating to obtaining goods by using a false or expired credit card or other credit device, if
the offense was a felony.
(j) Section 817.50, relating to fraudulently obtaining goods or services from a health care provider.
(k) Section 817.505, relating to patient brokering.
(l) Section 817.568, relating to criminal use of personal identification information.
(m) Section 817.60, relating to obtaining a credit card through fraudulent means.
(n) Section 817.61, relating to fraudulent use of credit cards, if the offense was a felony.
(o) Section 831.01, relating to forgery.
(p) Section 831.02, relating to uttering forged instruments.
(q) Section 831.07, relating to forging bank bills, checks, drafts, or promissory notes.
(r) Section 831.09, relating to uttering forged bank bills, checks, drafts, or promissory notes.

1 – 11
(s) Section 831.30, relating to fraud in obtaining medicinal drugs.
(t) Section 831.31, relating to the sale, manufacture, delivery, or possession with the intent to sell, manufacture,
or deliver any counterfeit controlled substance, if the offense was a felony.
(u) Section 895.03, relating to racketeering and collection of unlawful debts.
(v) Section 896.101, relating to the Florida Money Laundering Act.
If, upon rescreening, a person who is currently employed or contracted with a licensee as of June 30, 2014, and was
screened and qualified under ss. 435.03 and 435.04, has a disqualifying offense that was not a disqualifying offense
at the time of the last screening, but is a current disqualifying offense and was committed before the last screening, he
or she may apply for an exemption from the appropriate licensing agency and, if agreed to by the employer, may
continue to perform his or her duties until the licensing agency renders a decision on the application for exemption if
the person is eligible to apply for an exemption and the exemption request is received by the agency no later than 30
days after receipt of the rescreening results by the person.
(5) A person who serves as a controlling interest of, is employed by, or contracts with a licensee on July 31,
2010, who has been screened and qualified according to standards specified in s. 435.03 or s. 435.04 must be
rescreened by July 31, 2015, in compliance with the following schedule. If, upon rescreening, such person has a
disqualifying offense that was not a disqualifying offense at the time of the last screening, but is a current
disqualifying offense and was committed before the last screening, he or she may apply for an exemption from the
appropriate licensing agency and, if agreed to by the employer, may continue to perform his or her duties until the
licensing agency renders a decision on the application for exemption if the person is eligible to apply for an
exemption and the exemption request is received by the agency within 30 days after receipt of the rescreening
results by the person. The rescreening schedule shall be:
(a) Individuals for whom the last screening was conducted on or before December 31, 2004, must be rescreened
by July 31, 2013.
(b) Individuals for whom the last screening conducted was between January 1, 2005, and December 31, 2008,
must be rescreened by July 31, 2014.
(c) Individuals for whom the last screening conducted was between January 1, 2009, through July 31, 2011,
must be rescreened by July 31, 2015.
(6) The costs associated with obtaining the required screening must be borne by the licensee or the person
subject to screening. Licensees may reimburse persons for these costs. The Department of Law Enforcement shall
charge the agency for screening pursuant to s. 943.053(3). The agency shall establish a schedule of fees to cover the
costs of screening.
(7)(a) As provided in chapter 435, the agency may grant an exemption from disqualification to a person who is
subject to this section and who:
1. Does not have an active professional license or certification from the Department of Health; or
2. Has an active professional license or certification from the Department of Health but is not providing a
service within the scope of that license or certification.
(b) As provided in chapter 435, the appropriate regulatory board within the Department of Health, or the
department itself if there is no board, may grant an exemption from disqualification to a person who is subject to this
section and who has received a professional license or certification from the Department of Health or a regulatory
1 – 12
board within that department and that person is providing a service within the scope of his or her licensed or
certified practice.
(8) The agency and the Department of Health may adopt rules pursuant to ss. 120.536(1) and 120.54 to
implement this section, chapter 435, and authorizing statutes requiring background screening and to implement and
adopt criteria relating to retaining fingerprints pursuant to s. 943.05(2).
(9) There is no reemployment assistance or other monetary liability on the part of, and no cause of action for
damages arising against, an employer that, upon notice of a disqualifying offense listed under chapter 435 or this
section, terminates the person against whom the report was issued, whether or not that person has filed for an
exemption with the Department of Health or the agency.
History.—s. 5, ch. 2006-192; s. 50, ch. 2009-223; s. 21, ch. 2010-114; s. 61, ch. 2012-30; s. 2, ch. 2012-73; s.
166, ch. 2014-19; s. 3, ch. 2014-84; s. 7, ch. 2016-78; s. 71, ch. 2018-24.
408.810 Minimum licensure requirements.—In addition to the licensure requirements specified in this part,
authorizing statutes, and applicable rules, each applicant and licensee must comply with the requirements of this
section in order to obtain and maintain a license.
(1) An applicant for licensure must comply with the background screening requirements of s. 408.809.
(2) An applicant for licensure must provide a description and explanation of any exclusions, suspensions, or
terminations of the applicant from the Medicare, Medicaid, or federal Clinical Laboratory Improvement Amendment
(CLIA) programs.
(3) Unless otherwise specified in this part, authorizing statutes, or applicable rules, any information required to
be reported to the agency must be submitted within 21 calendar days after the report period or effective date of the
information, whichever is earlier, including, but not limited to, any change of:
(a) Information contained in the most recent application for licensure.
(b) Required insurance or bonds.
(4) Whenever a licensee discontinues operation of a provider:
(a) The licensee must inform the agency not less than 30 days prior to the discontinuance of operation and
inform clients of such discontinuance as required by authorizing statutes. Immediately upon discontinuance of
operation by a provider, the licensee shall surrender the license to the agency and the license shall be canceled.
(b) The licensee shall remain responsible for retaining and appropriately distributing all records within the
timeframes prescribed in authorizing statutes and applicable rules. In addition, the licensee or, in the event of death
or dissolution of a licensee, the estate or agent of the licensee shall:
1. Make arrangements to forward records for each client to one of the following, based upon the client’s choice:
the client or the client’s legal representative, the client’s attending physician, or the health care provider where the
client currently receives services; or
2. Cause a notice to be published in the newspaper of greatest general circulation in the county in which the
provider was located that advises clients of the discontinuance of the provider operation. The notice must inform
clients that they may obtain copies of their records and specify the name, address, and telephone number of the
person from whom the copies of records may be obtained. The notice must appear at least once a week for 4
consecutive weeks.
(5)(a) On or before the first day services are provided to a client, a licensee must inform the client and his or her
immediate family or representative, if appropriate, of the right to report:

1 – 13
1. Complaints. The statewide toll-free telephone number for reporting complaints to the agency must be
provided to clients in a manner that is clearly legible and must include the words: “To report a complaint regarding
the services you receive, please call toll-free (phone number).”
2. Abusive, neglectful, or exploitative practices. The statewide toll-free telephone number for the central abuse
hotline must be provided to clients in a manner that is clearly legible and must include the words: “To report abuse,
neglect, or exploitation, please call toll-free (phone number).”
3. Medicaid fraud. An agency-written description of Medicaid fraud and the statewide toll-free telephone
number for the central Medicaid fraud hotline must be provided to clients in a manner that is clearly legible and
must include the words: “To report suspected Medicaid fraud, please call toll-free (phone number).”
The agency shall publish a minimum of a 90-day advance notice of a change in the toll-free telephone numbers.
(b) Each licensee shall establish appropriate policies and procedures for providing such notice to clients.
(6) An applicant must provide the agency with proof of the applicant’s legal right to occupy the property before
a license may be issued. Proof may include, but need not be limited to, copies of warranty deeds, lease or rental
agreements, contracts for deeds, quitclaim deeds, or other such documentation.
(7) If proof of insurance is required by the authorizing statute, that insurance must be in compliance with
chapter 624, chapter 626, chapter 627, or chapter 628 and with agency rules.
(8) Upon application for initial licensure or change of ownership licensure, the applicant shall furnish
satisfactory proof of the applicant’s financial ability to operate in accordance with the requirements of this part,
authorizing statutes, and applicable rules. The agency shall establish standards for this purpose, including
information concerning the applicant’s controlling interests. The agency shall also establish documentation
requirements, to be completed by each applicant, that show anticipated provider revenues and expenditures, the
basis for financing the anticipated cash-flow requirements of the provider, and an applicant’s access to contingency
financing. A current certificate of authority, pursuant to chapter 651, may be provided as proof of financial ability to
operate. The agency may require a licensee to provide proof of financial ability to operate at any time if there is
evidence of financial instability, including, but not limited to, unpaid expenses necessary for the basic operations of
the provider. An applicant applying for change of ownership licensure is exempt from furnishing proof of financial
ability to operate if the provider has been licensed for at least 5 years, and:
(a) The ownership change is a result of a corporate reorganization under which the controlling interest is
unchanged and the applicant submits organizational charts that represent the current and proposed structure of the
reorganized corporation; or
(b) The ownership change is due solely to the death of a person holding a controlling interest, and the surviving
controlling interests continue to hold at least 51 percent of ownership after the change of ownership.
(9) A controlling interest may not withhold from the agency any evidence of financial instability, including, but
not limited to, checks returned due to insufficient funds, delinquent accounts, nonpayment of withholding taxes,
unpaid utility expenses, nonpayment for essential services, or adverse court action concerning the financial viability
of the provider or any other provider licensed under this part that is under the control of the controlling interest. A
controlling interest shall notify the agency within 10 days after a court action to initiate bankruptcy, foreclosure, or
eviction proceedings concerning the provider in which the controlling interest is a petitioner or defendant. Any
person who violates this subsection commits a misdemeanor of the second degree, punishable as provided in s.
775.082 or s. 775.083. Each day of continuing violation is a separate offense.

1 – 14
(10) The agency may not issue a license to a health care provider subject to the certificate-of-need provisions in
part I of this chapter if the health care provider has not been issued a certificate of need or an exemption. Upon
initial licensure of any such provider, the authorization contained in the certificate of need shall be considered fully
implemented and merged into the license and shall have no force and effect upon termination of the license for any
reason.
(11) The agency may adopt rules that govern the circumstances under which a controlling interest, an
administrator, an employee, or a contractor, or a representative thereof, who is not a relative of the client may act as
an agent of the client in authorizing consent for medical treatment, assignment of benefits, and release of
information. Such rules may include requirements related to disclosure, bonding, restrictions, and client protections.
(12) The licensee shall ensure that no person holds any ownership interest, either directly or indirectly,
regardless of ownership structure, who:
(a) Has a disqualifying offense pursuant to s. 408.809; or
(b) Holds or has held any ownership interest, either directly or indirectly, regardless of ownership structure, in a
provider that had a license revoked or an application denied pursuant to s. 408.815.
(13) If the licensee is a publicly traded corporation or is wholly owned, directly or indirectly, by a publicly
traded corporation, subsection (12) does not apply to those persons whose sole relationship with the corporation is as
a shareholder of publicly traded shares. As used in this subsection, a “publicly traded corporation” is a corporation
that issues securities traded on an exchange registered with the United States Securities and Exchange Commission
as a national securities exchange.
History.—s. 5, ch. 2006-192; s. 9, ch. 2009-223; s. 27, ch. 2012-160; s. 72, ch. 2018-24.
408.811 Right of inspection; copies; inspection reports; plan for correction of deficiencies.—
(1) An authorized officer or employee of the agency may make or cause to be made any inspection or
investigation deemed necessary by the agency to determine the state of compliance with this part, authorizing
statutes, and applicable rules. The right of inspection extends to any business that the agency has reason to believe is
being operated as a provider without a license, but inspection of any business suspected of being operated without
the appropriate license may not be made without the permission of the owner or person in charge unless a warrant is
first obtained from a circuit court. Any application for a license issued under this part, authorizing statutes, or
applicable rules constitutes permission for an appropriate inspection to verify the information submitted on or in
connection with the application.
(a) All inspections shall be unannounced, except as specified in s. 408.806.
(b) Inspections for relicensure shall be conducted biennially unless otherwise specified by authorizing statutes
or applicable rules.
(2) Inspections conducted in conjunction with certification, comparable licensure requirements, or a recognized
or approved accreditation organization may be accepted in lieu of a complete licensure inspection. However, a
licensure inspection may also be conducted to review any licensure requirements that are not also requirements for
certification.
(3) The agency shall have access to and the licensee shall provide, or if requested send, copies of all provider
records required during an inspection or other review at no cost to the agency, including records requested during an
offsite review.

1 – 15
(4) A deficiency must be corrected within 30 calendar days after the provider is notified of inspection results
unless an alternative timeframe is required or approved by the agency.
(5) The agency may require an applicant or licensee to submit a plan of correction for deficiencies. If required,
the plan of correction must be filed with the agency within 10 calendar days after notification unless an alternative
timeframe is required.
(6)(a) Each licensee shall maintain as public information, available upon request, records of all inspection
reports pertaining to that provider that have been filed by the agency unless those reports are exempt from or contain
information that is exempt from s. 119.07(1) and s. 24(a), Art. I of the State Constitution or is otherwise made
confidential by law. Copies of such reports shall be retained in the records of the provider for at least 3 years
following the date the reports are filed and issued, regardless of a change of ownership.
(b) A licensee shall, upon the request of any person who has completed a written application with intent to be
admitted by such provider, any person who is a client of such provider, or any relative, spouse, or guardian of any
such person, furnish to the requester a copy of the last inspection report pertaining to the licensed provider that was
issued by the agency or by an accrediting organization if such report is used in lieu of a licensure inspection.
History.—s. 5, ch. 2006-192; s. 51, ch. 2009-223; s. 51, ch. 2018-110.
408.812 Unlicensed activity.—
(1) A person or entity may not offer or advertise services that require licensure as defined by this part,
authorizing statutes, or applicable rules to the public without obtaining a valid license from the agency. A
licenseholder may not advertise or hold out to the public that he or she holds a license for other than that for which
he or she actually holds the license.
(2) The operation or maintenance of an unlicensed provider or the performance of any services that require
licensure without proper licensure is a violation of this part and authorizing statutes. Unlicensed activity constitutes
harm that materially affects the health, safety, and welfare of clients, and constitutes abuse and neglect, as defined in
s. 415.102. The agency or any state attorney may, in addition to other remedies provided in this part, bring an action
for an injunction to restrain such violation, or to enjoin the future operation or maintenance of the unlicensed
provider or the performance of any services in violation of this part and authorizing statutes, until compliance with
this part, authorizing statutes, and agency rules has been demonstrated to the satisfaction of the agency.
(3) It is unlawful for any person or entity to own, operate, or maintain an unlicensed provider. If after receiving
notification from the agency, such person or entity fails to cease operation, the person or entity is subject to penalties
as prescribed by authorizing statutes and applicable rules. Each day of operation is a separate offense.
(4) Any person or entity that fails to cease operation after agency notification may be fined $1,000 for each day
of noncompliance.
(5) When a controlling interest or licensee has an interest in more than one provider and fails to license a
provider rendering services that require licensure, the agency may revoke all licenses, impose actions under s.
408.814, and regardless of correction, impose a fine of $1,000 per day, unless otherwise specified by authorizing
statutes, against each licensee until such time as the appropriate license is obtained or the unlicensed activity ceases.
(6) In addition to granting injunctive relief pursuant to subsection (2), if the agency determines that a person or
entity is operating or maintaining a provider without obtaining a license and determines that a condition exists that
poses a threat to the health, safety, or welfare of a client of the provider, the person or entity is subject to the same
actions and fines imposed against a licensee as specified in this part, authorizing statutes, and agency rules.

1 – 16
(7) Any person aware of the operation of an unlicensed provider must report that provider to the agency.
History.—s. 5, ch. 2006-192; s. 73, ch. 2018-24.
408.813 Administrative fines; violations.—As a penalty for any violation of this part, authorizing statutes, or
applicable rules, the agency may impose an administrative fine.
(1) Unless the amount or aggregate limitation of the fine is prescribed by authorizing statutes or applicable
rules, the agency may establish criteria by rule for the amount or aggregate limitation of administrative fines
applicable to this part, authorizing statutes, and applicable rules. Each day of violation constitutes a separate
violation and is subject to a separate fine. For fines imposed by final order of the agency and not subject to further
appeal, the violator shall pay the fine plus interest at the rate specified in s. 55.03 for each day beyond the date set by
the agency for payment of the fine.
(2) Violations of this part, authorizing statutes, or applicable rules shall be classified according to the nature of
the violation and the gravity of its probable effect on clients. The scope of a violation may be cited as an isolated,
patterned, or widespread deficiency. An isolated deficiency is a deficiency affecting one or a very limited number of
clients, or involving one or a very limited number of staff, or a situation that occurred only occasionally or in a very
limited number of locations. A patterned deficiency is a deficiency in which more than a very limited number of
clients are affected, or more than a very limited number of staff are involved, or the situation has occurred in several
locations, or the same client or clients have been affected by repeated occurrences of the same deficient practice but
the effect of the deficient practice is not found to be pervasive throughout the provider. A widespread deficiency is a
deficiency in which the problems causing the deficiency are pervasive in the provider or represent systemic failure
that has affected or has the potential to affect a large portion of the provider’s clients. This subsection does not affect
the legislative determination of the amount of a fine imposed under authorizing statutes. Violations shall be
classified on the written notice as follows:
(a) Class “I” violations are those conditions or occurrences related to the operation and maintenance of a
provider or to the care of clients which the agency determines present an imminent danger to the clients of the
provider or a substantial probability that death or serious physical or emotional harm would result therefrom. The
condition or practice constituting a class I violation shall be abated or eliminated within 24 hours, unless a fixed
period, as determined by the agency, is required for correction. The agency shall impose an administrative fine as
provided by law for a cited class I violation. A fine shall be levied notwithstanding the correction of the violation.
(b) Class “II” violations are those conditions or occurrences related to the operation and maintenance of a
provider or to the care of clients which the agency determines directly threaten the physical or emotional health,
safety, or security of the clients, other than class I violations. The agency shall impose an administrative fine as
provided by law for a cited class II violation. A fine shall be levied notwithstanding the correction of the violation.
(c) Class “III” violations are those conditions or occurrences related to the operation and maintenance of a
provider or to the care of clients which the agency determines indirectly or potentially threaten the physical or
emotional health, safety, or security of clients, other than class I or class II violations. The agency shall impose an
administrative fine as provided in this section for a cited class III violation. A citation for a class III violation must
specify the time within which the violation is required to be corrected. If a class III violation is corrected within the
time specified, a fine may not be imposed.
(d) Class “IV” violations are those conditions or occurrences related to the operation and maintenance of a
provider or to required reports, forms, or documents that do not have the potential of negatively affecting clients.

1 – 17
These violations are of a type that the agency determines do not threaten the health, safety, or security of clients. The
agency shall impose an administrative fine as provided in this section for a cited class IV violation. A citation for a
class IV violation must specify the time within which the violation is required to be corrected. If a class IV violation
is corrected within the time specified, a fine may not be imposed.
(3) The agency may impose an administrative fine for a violation that is not designated as a class I, class II,
class III, or class IV violation. Unless otherwise specified by law, the amount of the fine may not exceed $500 for
each violation. Unclassified violations include:
(a) Violating any term or condition of a license.
(b) Violating any provision of this part, authorizing statutes, or applicable rules.
(c) Exceeding licensed capacity.
(d) Providing services beyond the scope of the license.
(e) Violating a moratorium imposed pursuant to s. 408.814.
History.—s. 5, ch. 2006-192; s. 52, ch. 2009-223; s. 28, ch. 2012-160.
408.814 Moratorium; emergency suspension.—
(1) The agency may impose an immediate moratorium or emergency suspension as defined in s. 120.60 on any
provider if the agency determines that any condition related to the provider or licensee presents a threat to the health,
safety, or welfare of a client.
(2) A provider or licensee, the license of which is denied or revoked, may be subject to immediate imposition of
a moratorium or emergency suspension to run concurrently with licensure denial, revocation, or injunction.
(3) A moratorium or emergency suspension remains in effect after a change of ownership, unless the agency
has determined that the conditions that created the moratorium, emergency suspension, or denial of licensure have
been corrected.
(4) When a moratorium or emergency suspension is placed on a provider or licensee, notice of the action shall
be posted and visible to the public at the location of the provider until the action is lifted.
History.—s. 5, ch. 2006-192.
408.815 License or application denial; revocation.—
(1) In addition to the grounds provided in authorizing statutes, grounds that may be used by the agency for
denying and revoking a license or change of ownership application include any of the following actions by a
controlling interest:
(a) False representation of a material fact in the license application or omission of any material fact from the
application.
(b) An intentional or negligent act materially affecting the health or safety of a client of the provider.
(c) A violation of this part, authorizing statutes, or applicable rules.
(d) A demonstrated pattern of deficient performance.
(e) The applicant, licensee, or controlling interest has been or is currently excluded, suspended, or terminated
from participation in the state Medicaid program, the Medicaid program of any other state, or the Medicare program.
(2) If a licensee lawfully continues to operate while a denial or revocation is pending in litigation, the licensee
must continue to meet all other requirements of this part, authorizing statutes, and applicable rules and file
subsequent renewal applications for licensure and pay all licensure fees. The provisions of ss. 120.60(1) and

1 – 18
408.806(3)(c) do not apply to renewal applications filed during the time period in which the litigation of the denial
or revocation is pending until that litigation is final.
(3) An action under s. 408.814 or denial of the license of the transferor may be grounds for denial of a change
of ownership application of the transferee.
(4) Unless an applicant is determined by the agency to satisfy the provisions of subsection (5) for the action in
question, the agency shall deny an application for a license or license renewal based upon any of the following
actions of an applicant, a controlling interest of the applicant, or any entity in which a controlling interest of the
applicant was an owner or officer when the following actions occurred:
(a) A conviction or a plea of guilty or nolo contendere to, regardless of adjudication, a felony under chapter
409, chapter 817, chapter 893, 21 U.S.C. ss. 801-970, or 42 U.S.C. ss. 1395-1396, Medicaid fraud, Medicare fraud,
or insurance fraud, unless the sentence and any subsequent period of probation for such convictions or plea ended
more than 15 years before the date of the application; or
(b) Termination for cause from the Medicare program or a state Medicaid program, unless the applicant has
been in good standing with the Medicare program or a state Medicaid program for the most recent 5 years and the
termination occurred at least 20 years before the date of the application.
(5) For any application subject to denial under subsection (4), the agency may consider mitigating
circumstances as applicable, including, but not limited to:
(a) Completion or lawful release from confinement, supervision, or sanction, including the terms of probation,
and full restitution;
(b) Execution of a compliance plan with the agency;
(c) Compliance with an integrity agreement or compliance plan with another government agency;
(d) Determination by any state Medicaid program or the Medicare program that the controlling interest or entity
in which the controlling interest was an owner or officer is currently allowed to participate in the state Medicaid
program or the Medicare program, directly as a provider or indirectly as an owner or officer of a provider entity;
(e) Continuation of licensure by the controlling interest or entity in which the controlling interest was an owner
or officer, directly as a licensee or indirectly as an owner or officer of a licensed entity in the state where the action
occurred;
(f) Overall impact upon the public health, safety, or welfare; or
(g) Determination that a license denial is not commensurate with the prior action taken by the Medicare or state
Medicaid program.
After considering the circumstances set forth in this subsection, the agency shall grant the license, with or without
conditions, grant a provisional license for a period of no more than the licensure cycle, with or without conditions, or
deny the license.
(6) In order to ensure the health, safety, and welfare of clients when a license has been denied, revoked, or is set
to terminate, the agency may extend the license expiration date for up to 30 days for the sole purpose of allowing the
safe and orderly discharge of clients. The agency may impose conditions on the extension, including, but not limited
to, prohibiting or limiting admissions, expedited discharge planning, required status reports, and mandatory
monitoring by the agency or third parties. When imposing these conditions, the agency shall consider the nature and
number of clients, the availability and location of acceptable alternative placements, and the ability of the licensee to
continue providing care to the clients. The agency may terminate the extension or modify the conditions at any time.

1 – 19
This authority is in addition to any other authority granted to the agency under chapter 120, this part, and authorizing
statutes but creates no right or entitlement to an extension of a license expiration date.
History.—s. 5, ch. 2006-192; s. 10, ch. 2009-223; s. 2, ch. 2011-61.
408.816 Injunctions.—
(1) In addition to the other powers provided by this part, authorizing statutes, and applicable rules, the agency
may institute injunction proceedings in a court of competent jurisdiction to:
(a) Restrain or prevent the establishment or operation of a provider that does not have a license or is in violation
of any provision of this part, authorizing statutes, or applicable rules. The agency may also institute injunction
proceedings in a court of competent jurisdiction when a violation of this part, authorizing statutes, or applicable
rules constitutes an emergency affecting the immediate health and safety of a client.
(b) Enforce the provisions of this part, authorizing statutes, or any minimum standard, rule, or order issued or
entered into pursuant thereto when the attempt by the agency to correct a violation through administrative sanctions
has failed or when the violation materially affects the health, safety, or welfare of clients or involves any operation
of an unlicensed provider.
(c) Terminate the operation of a provider when a violation of any provision of this part, authorizing statutes, or
any standard or rule adopted pursuant thereto exists that materially affects the health, safety, or welfare of a client.
Such injunctive relief may be temporary or permanent.
(2) If action is necessary to protect clients of providers from immediate, life-threatening situations, the court
may allow a temporary injunction without bond upon proper proofs being made. If it appears by competent evidence
or a sworn, substantiated affidavit that a temporary injunction should be issued, the court, pending the determination
on final hearing, shall enjoin the operation of the provider.
History.—s. 5, ch. 2006-192.
408.817 Administrative proceedings.—Administrative proceedings challenging agency licensure enforcement
action shall be reviewed on the basis of the facts and conditions that resulted in the agency action.
History.—s. 5, ch. 2006-192.
408.818 Health Care Trust Fund.—Unless otherwise prescribed by authorizing statutes, all fees and fines
collected under this part, authorizing statutes, and applicable rules shall be deposited into the Health Care Trust
Fund, created in s. 408.16, and used to pay the costs of the agency in administering the provider program paying the
fees or fines.
History.—s. 5, ch. 2006-192.
408.819 Rules.—The agency is authorized to adopt rules as necessary to administer this part. Any licensed
provider that is in operation at the time of adoption of any applicable rule under this part or authorizing statutes shall
be given a reasonable time under the particular circumstances, not to exceed 6 months after the date of such
adoption, within which to comply with such rule, unless otherwise specified by rule.
History.—s. 5, ch. 2006-192.
408.820 Exemptions.—Except as prescribed in authorizing statutes, the following exemptions shall apply to
specified requirements of this part:
(1) Laboratories authorized to perform testing under the Drug-Free Workplace Act, as provided under ss.
112.0455 and 440.102, are exempt from s. 408.810(5)-(10).
(2) Birth centers, as provided under chapter 383, are exempt from s. 408.810(7)-(10).

1 – 20
(3) Abortion clinics, as provided under chapter 390, are exempt from s. 408.810(7)-(10).
(4) Crisis stabilization units, as provided under parts I and IV of chapter 394, are exempt from s. 408.810(8)-
(10).
(5) Short-term residential treatment facilities, as provided under parts I and IV of chapter 394, are exempt from
s. 408.810(8)-(10).
(6) Residential treatment facilities, as provided under part IV of chapter 394, are exempt from s. 408.810(8)-
(10).
(7) Residential treatment centers for children and adolescents, as provided under part IV of chapter 394, are
exempt from s. 408.810(8)-(10).
(8) Hospitals, as provided under part I of chapter 395, are exempt from s. 408.810(7)-(9).
(9) Ambulatory surgical centers, as provided under part I of chapter 395, are exempt from s. 408.810(7)-(10).
(10) Nursing homes, as provided under part II of chapter 400, are exempt from ss. 408.810(7) and 408.813(2).
(11) Assisted living facilities, as provided under part I of chapter 429, are exempt from s. 408.810(10).
(12) Home health agencies, as provided under part III of chapter 400, are exempt from s. 408.810(10).
(13) Nurse registries, as provided under part III of chapter 400, are exempt from s. 408.810(6) and (10).
(14) Companion services or homemaker services providers, as provided under part III of chapter 400, are
exempt from s. 408.810(6)-(10).
(15) Adult day care centers, as provided under part III of chapter 429, are exempt from s. 408.810(10).
(16) Adult family-care homes, as provided under part II of chapter 429, are exempt from s. 408.810(7)-(10).
(17) Homes for special services, as provided under part V of chapter 400, are exempt from s. 408.810(7)-(10).
(18) Transitional living facilities, as provided under part XI of chapter 400, are exempt from s. 408.810(10).
(19) Prescribed pediatric extended care centers, as provided under part VI of chapter 400, are exempt from s.
408.810(10).
(20) Home medical equipment providers, as provided under part VII of chapter 400, are exempt from s.
408.810(10).
(21) Intermediate care facilities for persons with developmental disabilities, as provided under part VIII of
chapter 400, are exempt from s. 408.810(7).
(22) Health care services pools, as provided under part IX of chapter 400, are exempt from s. 408.810(6)-(10).
(23) Health care clinics, as provided under part X of chapter 400, are exempt from s. 408.810(6), (7), and (10).
(24) Multiphasic health testing centers, as provided under 1part I of chapter 483, are exempt from s. 408.810(5)-
(10).
(25) Organ, tissue, and eye procurement organizations, as provided under part V of chapter 765, are exempt
from s. 408.810(5)-(10).
History.—s. 5, ch. 2006-192; s. 92, ch. 2007-5; s. 20, ch. 2009-218; s. 53, ch. 2009-223; s. 90, ch. 2010-5; s. 10,
ch. 2015-25; s. 74, ch. 2018-24. 1Note.—Redesignated as part I of chapter 483 to conform to the repeal of former part I of that chapter by s. 97,
ch. 2018-24.

1 – 21
408.821 Emergency management planning; emergency operations; inactive license.—
(1) A licensee required by authorizing statutes to have an emergency operations plan must designate a safety
liaison to serve as the primary contact for emergency operations.
(2) An entity subject to this part may temporarily exceed its licensed capacity to act as a receiving provider in
accordance with an approved emergency operations plan for up to 15 days. While in an overcapacity status, each
provider must furnish or arrange for appropriate care and services to all clients. In addition, the agency may approve
requests for overcapacity in excess of 15 days, which approvals may be based upon satisfactory justification and
need as provided by the receiving and sending providers.
(3)(a) An inactive license may be issued to a licensee subject to this section when the provider is located in a
geographic area in which a state of emergency was declared by the Governor if the provider:
1. Suffered damage to its operation during the state of emergency.
2. Is currently licensed.
3. Does not have a provisional license.
4. Will be temporarily unable to provide services but is reasonably expected to resume services within 12
months.
(b) An inactive license may be issued for a period not to exceed 12 months but may be renewed by the agency
for up to 12 additional months upon demonstration to the agency of progress toward reopening. A request by a
licensee for an inactive license or to extend the previously approved inactive period must be submitted in writing to
the agency, accompanied by written justification for the inactive license, which states the beginning and ending
dates of inactivity and includes a plan for the transfer of any clients to other providers and appropriate licensure fees.
Upon agency approval, the licensee shall notify clients of any necessary discharge or transfer as required by
authorizing statutes or applicable rules. The beginning of the inactive licensure period shall be the date the provider
ceases operations. The end of the inactive period shall become the license expiration date, and all licensure fees
must be current, must be paid in full, and may be prorated. Reactivation of an inactive license requires the prior
approval by the agency of a renewal application, including payment of licensure fees and agency inspections
indicating compliance with all requirements of this part and applicable rules and statutes.
(4) The agency may adopt rules relating to emergency management planning, communications, and operations.
Licensees providing residential or inpatient services must utilize an online database approved by the agency to
report information to the agency regarding the provider’s emergency status, planning, or operations.
History.—s. 54, ch. 2009-223.
408.831 Denial, suspension, or revocation of a license, registration, certificate, or application.—
(1) In addition to any other remedies provided by law, the agency may deny each application or suspend or
revoke each license, registration, or certificate of entities regulated or licensed by it:
(a) If the applicant, licensee, or a licensee subject to this part which shares a common controlling interest with
the applicant has failed to pay all outstanding fines, liens, or overpayments assessed by final order of the agency or
final order of the Centers for Medicare and Medicaid Services, not subject to further appeal, unless a repayment plan
is approved by the agency; or
(b) For failure to comply with any repayment plan.
(2) In reviewing any application requesting a change of ownership or change of the licensee, registrant, or
certificateholder, the transferor shall, prior to agency approval of the change, repay or make arrangements to repay

1 – 22
any amounts owed to the agency. Should the transferor fail to repay or make arrangements to repay the amounts
owed to the agency, the issuance of a license, registration, or certificate to the transferee shall be delayed until
repayment or until arrangements for repayment are made.
(3) This section provides standards of enforcement applicable to all entities licensed or regulated by the Agency
for Health Care Administration. This section controls over any conflicting provisions of chapters 39, 383, 390, 391,
394, 395, 400, 408, 429, 468, 483, and 765 or rules adopted pursuant to those chapters.
History.—s. 12, ch. 2002-400; s. 32, ch. 2003-57; s. 28, ch. 2006-71; s. 9, ch. 2006-192; s. 78, ch. 2006-197; s.
55, ch. 2009-223.
408.832 Conflicts.—In case of conflict between the provisions of this part and the authorizing statutes
governing the licensure of health care providers by the Agency for Health Care Administration found in s. 112.0455
and chapters 383, 390, 394, 395, 400, 429, 440, 483, and 765, the provisions of this part shall prevail.
History.—s. 10, ch. 2006-192; s. 93, ch. 2007-5; s. 133, ch. 2007-230.
Notes ______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
_____________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________

2. Rule Chapter 59A
-35, F.A.C
.


2 – 1
CHAPTER 59A-35
HEALTH CARE LICENSING PROCEDURES 59A-35.020 Applicability
59A-35.030 Definitions
59A-35.040 License Required; Display
59A-35.050 Fees Required; Adjustments
59A-35.060 Licensure Application Process.
59A-35.062 Proof of Financial Ability to Operate
59A-35.070 Change of Ownership
59A-35.080 License Categories
59A-35.090 Background Screening; Prohibited Offenses
59A-35.100 Minimum License Requirements
59A-35.110 Reporting Requirements; Electronic Submission
59A-35.120 Right of Inspection; Copies; Inspection Reports
59A-35.150 Moratorium; Emergency Suspension
59A-35.020 Applicability. Rulemaking Authority 408.819 FS. Law Implemented 408.802 FS. History–New 7-14-10, Repealed 1-4-16.
59A-35.030 Definitions.
(1) “Address of record” means the location that is printed on the license and is the address at which the provider
is licensed to operate. In the event a license displays multiple locations including branch offices, satellite offices, or
off-site locations, the address of record is the main or principle office address.
(2) “Agency notification” or “Agency request” means the Agency sends notification by:
(a) Mail or personal delivery to the address of record for a licensee or applicant;
(b) Mail to an alternative mailing address if requested by the licensee or applicant; or
(c) Electronic mail if an electronic mail address has been provided.
(3) “Days” means calendar days.
(4) “Management company” means an entity retained by a licensee to administer or direct the operation of a
provider. This does not include an entity that serves solely as a lender or lien holder.
Rulemaking Authority 408.819 FS. Law Implemented 408.803 FS. History–New 7-14-10.
59A-35.040 License Required; Display.
(1) A license is valid only for the licensee, provider, and location for which the license is issued as it appears on
the license.
(2) Any request to amend a license must be received by the Agency in advance of the requested effective date as
detailed below. Requests to amend a license are not authorized until the license is issued.
(a) Requests to change the address of record must be received by the Agency 60 to 120 days in advance of the
requested effective date for the following provider types:
1. Birth Centers, as provided under Chapter 383, F.S.;
2. Abortion Clinics, as provided under Chapter 390, F.S.;
3. Crisis Stabilization Units, as provided under Chapter 394, Parts I and IV, F.S.;
4. Short Term Residential Treatment Units, as provided under Chapter 394, Parts I and IV, F.S.;
5. Residential Treatment Facilities, as provided under Chapter 394, Part IV, F.S.;
2 – 2
6. Residential Treatment Centers for Children and Adolescents, as provided under Chapter 394, Part IV, F.S.;
7. Hospitals, as provided under Chapter 395, Part I, F.S.;
8. Ambulatory Surgical Centers, as provided under Chapter 395, Part I, F.S.;
9. Nursing Homes, as provided under Chapter 400, Part II, F.S.;
10. Hospices, as provided under Chapter 400, Part IV, F.S.;
11. Homes for Special Services as provided under Chapter 400, Part V, F.S.;
12. Transitional Living Facilities, as provided under Chapter 400, Part V, F.S.;
13. Prescribed Pediatric Extended Care Centers, as provided under Chapter 400, Part VI, F.S.;
14. Intermediate Care Facilities for the Developmentally Disabled, as provided under Chapter 400, Part VIII,
F.S.;
15. Assisted Living Facilities, as provided under Chapter 429, Part I, F.S.;
16. Adult Family-Care Homes, as provided under Chapter 429, Part II, F.S.; and,
17. Adult Day Care Centers, as provided under Chapter 429, Part III, F.S.
(b) Requests to change the address of record must be received by the Agency 21 to 120 days in advance of the
requested effective date for the following provider types:
1. Drug Free Workplace Laboratories as provided under Sections 112.0455 and 440.102, F.S.;
2. Mobile Surgical Facilities, as provided under Chapter 395, Part I, F.S.;
3. Health Care Risk Managers, as provided under Chapter 395, Part I, F.S.;
4. Home Health Agencies, as provided under Chapter 400, Part III, F.S.;
5. Nurse Registries, as provided under Chapter 400, Part III, F.S.;
6. Companion Services or Homemaker Services Providers, as provided under Chapter 400, Part III, F.S.;
7. Home Medical Equipment Providers, as provided under Chapter 400, Part VII, F.S.;
8. Health Care Services Pools, as provided under Chapter 400, Part IX, F.S.;
9. Health Care Clinics, as provided under Chapter 400, Part X, F.S., including certificate of exemption;
10. Clinical Laboratories, as provided under Chapter 483, Part I, F.S.;
11. Multiphasic Health Testing Centers, as provided under Chapter 483, Part II, F.S.; and,
12. Organ and Tissue Procurement Agencies, as provided under Chapter 381, F.S.
(c) All other requests to amend a license including but not limited to services, licensed capacity, and other
specifications which are required to be displayed on the license by authorizing statutes or applicable rules must be
received by the Agency 60 to 120 days in advance of the requested effective date. This deadline does not apply to a
request to amend hospital emergency services defined in Section 395.1041(2), F.S.
(3) Failure to submit a timely request shall result in a $500 fine.
(4) A licensee is not authorized to operate in a new location until a license is obtained which specifies the new
location. Failure to amend a license prior to a change of the address of record constitutes unlicensed activity.
(5) The licensee shall return the license certificate to the Agency upon the rendition of a final order revoking,
cancelling or denying a license, and upon the voluntary discontinuance of operation.
Rulemaking Authority 408.819 FS. Law Implemented 408.804, 408.810, 408.813 FS. History–New 7-14-10.
59A-35.050 Fees Required; Adjustments.
(1) Licensure fees, as defined by authorizing statute or rule, are non-refundable once submitted to the Agency.
An applicant may submit a request for refund if monies in excess of required fees are submitted to the Agency. Such

2 – 3
requests must be made using State of Florida Department of Financial Services, Application for Refund form
number DFS-AA-4, Rev. 0207, incorporated herein by reference, available online at:
http://myfloridacfo.com/aadir/refund_application.htm and submitted to the appropriate licensing unit. The following
are examples of excess fee payments that are eligible for refund:
(a) Fees in excess of the required fee amount;
(b) A renewal reminder letter indicates an error in the required fee amount;
(c) An inspection fee is submitted when no inspection fee is required;
(d) An excess fee is submitted as an accredited provider when the licensee or applicant is not accredited; or
(e) An application is returned due to early submission.
(2) When payment for licensure fees has been dishonored, the licensee has 10 days from the date of notification
to remit to the Agency the licensure fee plus any applicable fees as provided by law in the form of a money order or
cashier’s check. In the event that the licensure fee is not paid, the license may be subject to revocation or suspension.
(3) A request for a replacement license must be accompanied by a $25 fee.
(4) In addition to required application, per-bed, and inspection fees, a request to amend a license must be
accompanied by a $25 fee.
Rulemaking Authority 408.819 FS. Law Implemented 408.805 FS. History–New 7-14-10.
59A-35.060 Licensure Application Process.
(1) The applicant must apply for licensure using the program specific forms listed below and the Health Care
Licensing Application Addendum, AHCA Form 3110-1024, October 2009, available at
http://www.flrules.org/Gateway/reference.asp?No=Ref-05363. All forms are incorporated by reference and available
online at: http://ahca.myflorida.com/HQAlicensureforms.
(a) Drug Free Workplace Laboratories as provided under Sections 112.0455 and 440.102, F.S.; AHCA Form
3170-5001, Rev. July 2009.
(b) Crisis Stabilization Units, as provided under Parts I and IV of Chapter 394, F.S.; AHCA Form 3180-5003,
Rev. July 2009.
(c) Short Term Residential Treatment Units, as provided under Parts I and IV of Chapter 394, F.S.; AHCA
Form 3180-5003, Rev. July 2009.
(d) Residential Treatment Facilities, as provided under Chapter 394, Part IV, F.S.; AHCA Form 3180-5003,
Rev. July 2009.
(e) Residential Treatment Centers for Children and Adolescents, as provided under Chapter 394, Part IV, F.S.;
AHCA Form 3180-5004, Rev. July 2009.
(f) Health Care Risk Managers, as provided under Chapter 395, Part I, F.S.; AHCA Form RM-001, Rev. July
2009.
(g) Nursing Homes, as provided under Chapter 400, Part II, F.S.; AHCA Form 3110-6001, Rev. July 2009.
(h) Home Health Agencies, as provided under Chapter 400, Part III, F.S.; AHCA Form 3110-1011, Rev. July
2009.
(i) Nurse Registries, as provided under Chapter 400, Part III, F.S.; AHCA Form 3110-7004, Rev. July 2009.
(j) Companion Services or Homemaker Services, as provided under Chapter 400, Part III, F.S.; AHCA Form
3110-1003, Rev. July 2009.
(k) Hospices, as provided under Chapter 400, Part IV, F.S.; AHCA Form 3110-4001, Rev. July 2009.

2 – 4
(l) Home for Special Services as provided under Chapter 400, Part V, F.S.; AHCA Form 3110-3001, July 2014,
and available at http://www.flrules.org/Gateway/reference.asp?No=Ref-05202.
(m) Home Medical Equipment Providers, as provided under Chapter 400, Part VII, F.S.; AHCA Form 3110-
1005, Rev. July 2009.
(n) Intermediate Care Facilities for the Developmentally Disabled, as provided under Chapter 400, Part VIII,
F.S.; AHCA Form 3110-5003, Rev. July 2009.
(o) Assisted Living Facilities, as provided under Chapter 429, Part I, F.S.; AHCA Form 3110-1008, Rev. July
2009.
(p) Adult Family-Care Homes, as provided under Chapter 429, Part II, F.S.; AHCA Form 3180-1022, Rev. July
2009.
(q) Adult Day Care Centers, as provided under Chapter 429, Part III, F.S.; AHCA Form 3180-1004, Rev. July
2009.
(r) Clinical Laboratories, as provided under Chapter 483, Part I, F.S.; AHCA Form 3170-2004 (renewal), B
(initial) or C (change of ownership), Rev. July 2009 or AHCA Form 3170-2004D, September 2009 (addition of
specialty, or subspecialty or change in specialty).
(s) Organ and Tissue Procurement Agencies, as provided under Chapter 381, F.S.; AHCA Form 3140-2001,
July 2009.
(2) The licensure fee must be included with any application. Applications will be returned to the applicant
unprocessed if the fee does not accompany the application. Applications from state agencies must include a copy of
the posted journal transactions by State Wide Document Number (SWDN) within benefiting Operating Level
Organization (OLO) and site.
(3) Applications received more than 120 days prior to the date of license expiration or the effective date will be
returned to the applicant unprocessed.
(4) If an applicant, licensee, or controlling interest is required to register or file with the Florida Secretary of
State, Division of Corporations, the principal, fictitious name and mailing addresses submitted with the licensure
application for the applicant, licensee and controlling interests must be the same as the information registered with
the Division of Corporations.
(5) Unresponsive applicant. If certified mail sent to the provider’s address of record, or mailing address if
applicable, is returned as unclaimed or undeliverable, the Agency will send a copy of the letter by regular mail to the
provider’s address of record, or mailing address if applicable, with a copy to the applicant’s address if different from
the provider. The applicant must respond to the request within 21 days of the date of the letter sent by regular mail.
If timely response is not received, the application will be subject to withdrawal or denial.
(6) An application is considered complete upon receipt of:
(a) All required documents and information and appropriate fee;
(b) All required background screening results; and,
(c) Completion of a satisfactory inspection if required by authorizing statutes or rules. Satisfactory inspection
means no regulatory violations exist, or all prior violations found have been determined by the Agency to be
corrected.
(7) A licensure inspection will not be authorized until paragraphs (6)(a) and (6)(b) of this section have been
satisfied.

2 – 5
(8) An application for license renewal may only be filed by the licensee.
Rulemaking Authority 408.819 FS. Law Implemented 400.801, 408.805, 408.806, 408.809, 408.810, 408.811 FS.
History–New 7-14-10, Amended 5-4-15.
59A-35.062 Proof of Financial Ability to Operate.
(1) Proof of financial ability to operate must be demonstrated for initial licensure and change of ownership
applications, by submitting AHCA Form 3100-0009, July 2009, Proof of Financial Ability to Operate, incorporated
herein by reference, and available online at: http://www.ahca.myflorida.com/Publications/Forms/HQA.shtml, as
provided under Section 408.810(8), F.S., for the following provider types:
(a) Nursing Home Facilities, as specified in Chapter 400, Part II, F.S.;
(b) Assisted Living Facilities, as specified in Chapter 429, Part I, F.S.;
(c) Home Health Agencies, as specified in Chapter 400, Part III, F.S.;
(d) Hospices, as specified in Chapter 400, Part IV, F.S.;
(e) Adult Day Care Centers, as specified in Chapter 429, Part III, F.S.;
(f) Prescribed Pediatric Extended Care Centers, as specified in Chapter 400, Part VI, F.S.;
(g) Home Medical Equipment Providers, as specified in Chapter 400, Part VII, F.S.;
(h) Intermediate Care Facilities for the Developmentally Disabled, as specified in Chapter 400, Part VIII, F.S.;
(i) Health Care Clinics, as specified in Chapter 400, Part X, F.S.; and,
(2) Proof of financial ability must be demonstrated for initial licensure and change of ownership applications for
Nurse Registries, as specified in Chapter 400, Part III, F.S., by submitting AHCA Form 3110-7004A, September
2009, Nurse Registry Proof of Financial Ability to Operate, incorporated herein by reference, and available online
at: http://www.ahca.myflorida.com/Publications/Forms/HQA.shtml.
(3) Definitions. The following definitions apply to this section for proof of financial ability to operate.
(a) “Assumptions” means the basis and rationale used in the financial projections to estimate the number and
type of patients, the method of acquiring patients, the amount of resources needed to serve patients, the method by
which these resources will be acquired, the method of recruiting and maintaining staff, the method of collecting
revenue and paying expenses, and the basis for anticipated salaries and employee benefits.
(b) “Charity care” means the term as defined in Section 409.911, F.S.
(c) “Contingency funding” means a source of funding available to the licensee or applicant to cover the cost of
events not considered in the financial projections, including, but not limited to, a drop in patient volume, a delay in
Medicare and/or Medicaid certification, major repairs, purchase of capital equipment. The contingency fund will be
a minimum of one month’s average operating expense over the first year of operations.
(d) “Contractual adjustments” means the difference in the established charges or rates of the provider and the
rates negotiated by Medicare, Medicaid, HMO/PPOs, and Insurers.
(e) ”Financial instability” means the provider cannot meet its financial obligations. Evidence such as the
issuance of bad checks, an accumulation of delinquent bills, or inability to meet current payroll needs shall
constitute prima facie evidence that the ownership of the provider lacks the financial ability to operate. Evidence
shall also include the Medicare or Medicaid program’s indications or determination of financial instability or
fraudulent handling of government funds by the provider.
(f) “Financial projections” means the expected operating results of the applicant as presented on AHCA Form
3100-0009, July 2009.

2 – 6
(g) “Full time equivalent” or “FTE” means a measure of full-time employment of 40 hours per week (1FTE =
40 hours per week or 2,080 hours annually).
(h) “Generally Accepted Accounting Principles” or “GAAP” means the term as defined in Rule 61H1-20.007,
F.A.C., Department of Business and Professional Regulation, Board of Accountancy.
(i) “Liquid assets” means assets of the licensee or applicant that can easily and quickly be converted to cash
such as publicly traded stocks, bonds, certificates of deposit, and money market accounts.
(j) “Net patient service revenue” means patient service revenue minus deductions from revenue. Deductions
from revenue include contractual adjustments and charity care.
(k) “Operating expense” means total expenses incurred through the normal course of business.
(l) “Operating margin” means a measure of profitability and is calculated as follows: ([Net Patient Service
Revenue - Operating Expenses] ÷ Net Patient Service Revenue) = Operating Margin.
(m) “Patient service revenue” means the total charge for a service provided.
(n) “Pre-opening costs” means the costs necessary to begin operations including advertising, equipment
purchases, legal fees, accounting fees, consulting fees, pre-paid insurance, pre-paid rent, licensure fees, deposits
(rent, utilities), requirement, staffing, and training.
(o) “Working capital” means the cash needed to sustain operations until a positive cash flow is achieved.
(Largest cumulative cash need from Schedule 7 Line 21 of AHCA Form 3100-0009, July 2009).
(4) All documents required under this section must be prepared in accordance with generally accepted
accounting principles. All documents required under this section for Home Health Agencies, Home Medical
Equipment Providers and Health Care Clinics must be compiled and signed by a certified public accountant.
(5) A pro forma balance sheet, a pro forma cash flow statement and a pro forma income and expense statement
for the first 2 years of operation which provide evidence of having sufficient assets, credit, and projected revenues to
cover liabilities and expenses must be included. An application for change of ownership may elect not to complete
the 2nd year of operations on AHCA Form 3100-0009, July 2009, if all of the following apply:
(a) As of the date of the application, the entity subject to the change of ownership has been licensed for at least
5 consecutive years;
(b) The applicant’s assets, credit, and projected revenues meet or exceed projected liabilities and expenses by
the end of the first year;
(c) The largest cumulative cash need on Schedule 7, Line 21 on AHCA Form 3100-0009, July 2009 occurs prior
to month 12.
(6) The applicant shall have demonstrated financial ability to operate if the applicant’s assets, credit, and
projected revenues meet or exceed projected liabilities and expenses.
(7) An applicant for renewal of a license shall not be required to provide proof of financial ability to operate,
unless the licensee or applicant has demonstrated financial instability. If an applicant or licensee has shown signs of
financial instability, as provided in Section 408.810(9), F.S., at any time, the Agency may require the applicant or
licensee to provide proof of financial ability to operate by submission of:
(a) AHCA Form 3100-0009, July 2009, Proof of Financial Ability Form, that includes a balance sheet and
income and expense statement for the next 2 years of operation which provide evidence of having sufficient assets,
credit, and projected revenues to cover liabilities and expenses; and

2 – 7
(b) Documentation of correction of the financial instability, including but not limited to, evidence of the
payment of any bad checks, delinquent bills or liens. If complete payment cannot be made, evidence must be
submitted of partial payment along with a plan for payment of any liens or delinquent bills. If the lien is with a
government agency or repayment is ordered by a federal or state court, an accepted plan of repayment must be
provided.
Rulemaking Authority 408.819 FS. Law Implemented 408.806, 408.810 FS. History–New 7-14-10.
59A-35.070 Change of Ownership.
(1) Effective dates of change of ownership.
(a) A change of ownership application must include the effective date of the change of ownership.
(b) The change of ownership effective date cannot be prior to the date the application is received by the Agency.
Failure to submit an application for licensure prior to the effective date of a change of ownership to a different legal
entity constitutes unlicensed activity.
(c) The effective date of the change of ownership shall not be extended more than 60 days from the effective
date reported on the application; written notification of a change in the effective date must be received by the
Agency prior to the originally reported effective date. The Agency will deem the application withdrawn if the
change of ownership does not occur within 60 days of the reported effective date.
(2) All required application documents and information must be received with the application or within 21 days
of the request by the Agency with the exception of the transferee’s proof of right to occupy if required, which must
be received by the Agency within 10 days after the effective date.
(3) When a change of ownership application is submitted during the review of a renewal licensure application,
the pending renewal will be administratively withdrawn from review if the change of ownership application is
approved with an effective date prior to the expiration of the license.
(4) Expiration of a license prior to the approval of the change of ownership application, when no renewal
application has been submitted, will result in the denial of a change of ownership application.
(5) If the applicant has not been issued the license on the effective date of the change of ownership,
documentation must be submitted that provides for continuation of operation of the licensee for those days between
the date of the change of ownership and the date the applicant is licensed by the Agency.
Rulemaking Authority 408.819 FS. Law Implemented 408.803(3), 408.803(5), 408.806, 408.807, 408.810, 408.813
FS. History–New 7-14-10.
59A-35.080 License Categories.
(1) Provisional License. If a license expires while an action to deny or revoke the license is pending and renewal
applications are filed, the Agency may issue a provisional license. The provisional license shall identify the pending
action. The provisional license will expire when the Agency action is final or one year after issuance, whichever
occurs first. The provisional license does not affect the revocation or denial action or constitute a defense on behalf
of the licensee or applicant.
(2) Inactive License. An inactive license may be issued, as provided in Sections 408.808(3), F.S.
(a) Requests for an inactive license must be submitted to the Agency as a written request that includes:
1. The reason that the provider will become inactive;
2. The proposed plan for transferring or discharging clients;
3. A plan for resuming services;

2 – 8
4. The date by which services are expected to resume; and
5. Evidence of a State of Emergency or disaster if applicable.
(b) The inactive license will not be issued until all clients have been properly transferred or discharged. The
expiration date of the inactive license will be issued for a period not to exceed 12 months. An application to extend
the inactive period for an additional 12 months must be submitted 30 days prior to the expiration of the inactive
license.
(c) Notification to reactivate the license and a complete licensure renewal application must be submitted to the
Agency at least 90 days prior to the requested reactivation date. An onsite inspection may be required prior to
reactivation. Licensure fees will be prorated based on the provider’s standard fee divided by the number of months
remaining in the licensure cycle.
Rulemaking Authority 408.819 FS. Law Implemented 408.808(2), (3), FS. History–New 7-14-10.
59A-35.090 Background Screening.
(1) Definitions:
(a) “Arrest Report” means the detailed narrative written by the arresting law enforcement officer explaining the
circumstances of the arrest.
(b) “Disposition” means the sentencing or other final settlement of a criminal case which shall include,
regardless of adjudication, a plea of nolo contendere or guilty, or a conviction by a judge or jury.
(c) “Disqualifying Offense” means any criminal offense prohibited in section 435.04 or 408.809(4), F.S.
(d) “Exemption from Disqualification” means an exemption granted by the Agency following a review of the
Background Screening Application for Exemption, AHCA Form 3110-0019, January 2017, hereby incorporated by
reference, and available at http://www.flrules.org/Gateway/reference.asp?No=Ref-09105, and an informal
teleconference, during which the individual must present clear and convincing evidence to support a reasonable
belief that he or she has been rehabilitated and does not present a danger to the health, safety, and welfare of the
patient or individual as described in section 435.07, F.S.
(e) “FBI” means the Federal Bureau of Investigation.
(f) “FDLE” means the Florida Department of Law Enforcement.
(g) “Level 2 Screening” means an assessment of the criminal history record obtained through a fingerprint
search through the FDLE and FBI to determine whether screened individuals have any disqualifying offenses
pursuant to section 435.04 or 408.809(4), F.S. An analysis and review of court dispositions and arrest reports may be
required to make a final determination.
(h) “Livescan Service Provider” means an entity that scans fingerprints electronically and submits them to
FDLE.
(2) Processing Screening Requests, Required Documents and Fees.
(a) Providers subject to the screening standards outlined in section 408.809, F.S., must follow the requirements
specified in section 435.12, F.S. Care Provider Background Screening Clearinghouse and must register and initiate
all criminal history checks through the Care Provider Background Screening Clearinghouse before referring an
employee or potential employee for electronic fingerprint submission to the Department of Law Enforcement.
Providers can access the Care Provider Background Screening Clearinghouse at:
http://ahca.myflorida.com/MCHQ/Central_Services/Background_Screening/index.shtml.

2 – 9
(b) Persons required to undergo Level 2 background screening must submit fingerprints electronically through a
Livescan Service Provider(s) contracted through the Agency or approved through the Florida Department of Law
Enforcement. Payment for screening services must be made to the Livescan Service Provider at the time of services
or through a payment arrangement with the Livescan Service Provider.
(c) If the individual’s fingerprints are rejected by the FBI due to illegible prints, the requesting provider will be
notified through the Agency’s secure website. The individual must return to the same Livescan Service Provider and
submit a second set of fingerprints in accordance with the guidelines established by the FBI. If the fingerprints are
not resubmitted within 14 days, the individual will be notified by letter from the Agency. The second set of prints
must be submitted within 21 days of the Agency’s request or the screening request will be considered withdrawn. If
withdrawn, the individual must submit a new set of electronic fingerprints through a Livescan Service Provider
accompanied by the required fee.
(d) An Attestation of Compliance with Background Screening Requirements, AHCA Form 3100-0008, January
2017, herein incorporated by reference, available at http://www.flrules.org/Gateway/reference.asp?No=Ref-09106,
and available from the Agency for Health Care Administration at:
http://ahca.myflorida.com/MCHQ/Central_Services/Background_Screening/Regulations_Forms.shtml. This form
must be completed by the individual and retained by the provider upon hire to attest that they meet the requirements
for qualifying for employment, they have not been unemployed for more than 90 days from a position that requires
Level 2 screening, and they agree to inform the employer immediately if arrested for any disqualifying offense.
(e) An administrator or chief financial officer must be screened and qualified prior to appointment to the
position.
(3) Results of Screening and Notification.
(a) Final results of background screening requests will be provided through the Agency’s secure website that
may be accessed by all health care providers applying for or actively licensed through the Agency that are registered
with the Care Provider Background Screening Clearinghouse. The secure website is located at:
apps.ahca.myflorida.com/SingleSignOnPortal.
(b) If a Level 2 criminal history is incomplete, a certified letter will be sent to the individual being screened
requesting the arrest report and court disposition information. If the letter is returned unclaimed, a copy of the letter
will be sent by regular mail. Pursuant to section 435.05(1)(d), F.S., the missing information must be filed with the
Agency within 30 days of the Agency’s request or the individual is subject to disqualification in accordance with
section 435.06(3), F.S.
(c) The eligibility results of employee screening and the signed Attestation referenced in subsection 59A-
35.090(2), F.A.C., must be in the employee’s personnel file, maintained by the provider.
(4) Exemption from Disqualification.
(a) Requests for an exemption from disqualification shall be submitted in writing to the Agency using the
Background Screening Application for Exemption, AHCA Form 3110-0019, January 2017.
(b) Individuals that are licensed or certified in a profession under the jurisdiction of the Department of Health
must apply for an exemption to the appropriate licensing or certifying board at the Department of Health unless the
individual will be working in a position other than for which they are licensed or certified.
(c) The individual shall bear the burden of setting forth clear and convincing evidence of rehabilitation which
includes any information indicating the individual presents no danger to the safety or well being of others. The

2 – 10
individual must present such evidence as arrest reports, court dispositions, parole/probation information, and
reference letters from employers, and/or personal references. Other documents that may be included are records of
successful participation in a rehabilitation program, further education or training, community or church involvement,
special awards or recognition or testimony by self or others.
(d) An “Application for Exemption” will not be reviewed until all required documents are obtained. If the
application is deemed incomplete after 30 days of receipt by the Agency, the application will be closed.
(e) In deciding whether to grant or deny an exemption request, the Agency shall consider factors such as the
facts and circumstances surrounding the disqualifying offense(s), the nature of the harm to the victim, whether the
individual is on probation or parole, whether restitution has been made, other offenses on the criminal history record
and the length of time since the last offense, the history of the person since the disqualifying offense(s), work
experience, personal references, performance evaluations, probation or parole violations, education, other evidence
of rehabilitation, and the honesty and candor of the disqualified individual.
(f) Any exemption granted by the Agency is limited to the information provided at the time of application and
the disqualifying offense or offenses committed prior to the date of the request for exemption.
(g) The Agency shall void any exemption granted to an individual when there is evidence that information
which would adversely affect the decision was not made available at the time of the determination or there is an
arrest or disposition of a new disqualifying offense since the date the exemption was granted.
(5) Unless otherwise specified, information requested pursuant to this section must be filed with the Agency
within 21 days of the Agency’s request.
Rulemaking Authority 408.809, 408.819, 435.01 FS. Law Implemented 408.809, 408.810, 435.07 FS. History–New
7-14-10, Amended 12-16-13, 6-15-15, 2-13-18.
59A-35.100 Minimum Licensure Requirements.
Provider location. A licensee must maintain proper authority for operation of the provider at the address of record. If
such authority is denied, revoked or otherwise terminated by the local zoning or code enforcement authority, the
Agency may deny or revoke an application or license, or impose sanctions.
Rulemaking Authority 408.819 FS. Law Implemented 408.810 FS. History–New 7-14-10, Amended 3-12-12.
59A-35.110 Reporting Requirements; Electronic Submission.
(1) During the two year licensure period, any change or expiration of any information that is required to be
reported under chapter 408, part II, F.S., or authorizing statutes for the provider type as specified in section 408.803(3),
F.S., during the license application process must be reported to the Agency within 21 days of occurrence of the change,
including:
(a) Insurance coverage renewal;
(b) Bond renewal;
(c) Change of administrator or the similarly titled person who is responsible for the day-to-day operation of the
provider;
(d) Annual sanitation inspections;
(e) Fire inspections; and,
(f) Approval of revisions to emergency management plans.
(2) Electronic submission of information.

2 – 11
(a) The following required information must be submitted electronically through the Agency’s Single Sign On
Portal located at https://apps.ahca.myflorida.com/SingleSignOnPortal:
1. Nursing homes:
Adverse incident reports must be submitted electronically to the Agency within 15 calendar days after the occurrence
of the incident as required in section 400.147, F.S. on Nursing Home Adverse Incident, AHCA Form 3110-0010 OL,
April 2017, which is hereby incorporated by reference and availiable at:
https://www.flrules.org/Gateway/reference.asp?No=Ref-08777, and through the Agency’s adverse incident reporting
system which can only be accessed through the Agency’s Single Sign On Portal located at:
https://apps.ahca.myflorida.com/SingleSignOnPortal.
2. Assisted living facilities:
a. Adverse incident reports must be submitted electronically to the Agency within 1 business day after the
occurrence of the incident, and within 15 days after the occurrence of the incident as required in section 429.23, F.S.,
on Assisted Living Facility Adverse Incident, AHCA Form 3180-1025 OL, April 2017, which is hereby incorporated
by reference and availiable at: https://www.flrules.org/Gateway/reference.asp?No=Ref-08778, and through the
Agency’s adverse incident reporting system which can only be accessed through the Agency’s Single Sign On Portal
located at: https://apps.ahca.myflorida.com/SingleSignOnPortal.
b. Liability claim reports required pursuant to section 429.23(5), F.S., and rule 58A-5.0242, F.A.C.
3. Hospitals:
Adverse incident reports must be submitted electronically to the Agency within 15 calendar days after the occurrence
of the incident as required in Section 395.0197, F.S., on Hospital Adverse Incident, AHCA Form 3140-5001 OL, April
2017, which is hereby incorporated by reference and availiable at:
https://www.flrules.org/Gateway/reference.asp?No=Ref-08779, and through the Agency’s adverse incident reporting
system which can only be accessed through the Agency’s Single Sign On Portal located at:
https://apps.ahca.myflorida.com/SingleSignOnPortal.
4. Ambulatory Surgical Centers:
Adverse incident reports must be submitted electronically to the Agency within 15 calendar days after the occurrence
of the incident as required in section 395.0197, F.S., on Ambulatory Surgical Center Adverse Incident, AHCA Form
3140-5004 OL, April 2017, which is hereby incorporated by reference and availiable at:
https://www.flrules.org/Gateway/reference.asp?No=Ref-08780, and through the Agency’s adverse incident reporting
system which can only be accessed through the Agency’s Single Sign On Portal located at:
https://apps.ahca.myflorida.com/SingleSignOnPortal.
(b) The licensee must retain a copy of all documentation generated at time of reporting as confirmation of
successful electronic submission.
(c) If the Agency’s Single Sign On Portal or the online adverse incident reporting system is temporarily out of
service the licensee may contact the Agency directly at 1(888)419-3456 for assistance. Reporting will resume as soon
as online access is restored.
Rulemaking Authority 408.806, 408.819 FS. Law Implemented 408.806, 408.810 FS. History–New 7-14-10, Amended
11-13-17.

2 – 12
59A-35.120 Inspections.
(1) When regulatory violations are identified by the Agency:
(a) Deficiencies must be corrected within 30 days of the date the Agency sends the deficiency notice to the
provider, unless an alternative timeframe is required or approved by the Agency.
(b) The Agency may conduct an unannounced follow-up inspection or off-site review to verify correction of
deficiencies at any time.
(2) If an inspection is completed through off-site record review, any records requested by the Agency in
conjunction with the review, must be received within 7 days of request and provided at no cost to the Agency. Each
licensee shall maintain the records including medical and treatment records of a client and provide access to the
Agency.
(3) Providers that are exempt from Agency inspections due to accreditation oversight as prescribed in
authorizing statutes must provide:
(a) Documentation from the accrediting agency including the name of the accrediting agency, the beginning and
expiration dates of the provider’s accreditation, accreditation status and type must be submitted at the time of license
application, or within 21 days of accreditation.
(b) Documentation of each accreditation inspection including the accreditation organization’s report of findings,
the provider’s response and the final determination must be submitted within 21 days of final determination or the
provider is no longer exempt from Agency inspection.
Rulemaking Authority 408.819 FS. Law Implemented 408.811 FS. History–New 7-14-10.
59A-35.150 Moratorium; Emergency Suspension.
In addition to other remedies permitted by law, violation of a moratorium issued by the Agency is considered a
Class I violation and subject to a fine of $500 per day until the violation is corrected.
Rulemaking Authority 408.819 FS. Law Implemented 408.813, 408.814 FS. History–New 7-14-10.
Notes ______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________ ______________________________________________________________________________
______________________________________________________________________________

3. Chapter 419, F.S.


3 – 1
CHAPTER 419
COMMUNITY RESIDENTIAL HOMES 419.001 Site selection of community residential homes.
419.001 Site selection of community residential homes.—
(1) For the purposes of this section, the term:
(a) “Community residential home” means a dwelling unit licensed to serve residents who are clients of the
Department of Elderly Affairs, the Agency for Persons with Disabilities, the Department of Juvenile Justice, or the
Department of Children and Families or licensed by the Agency for Health Care Administration which provides a
living environment for 7 to 14 unrelated residents who operate as the functional equivalent of a family, including
such supervision and care by supportive staff as may be necessary to meet the physical, emotional, and social needs
of the residents.
(b) “Licensing entity” or “licensing entities” means the Department of Elderly Affairs, the Agency for Persons
with Disabilities, the Department of Juvenile Justice, the Department of Children and Families, or the Agency for
Health Care Administration, all of which are authorized to license a community residential home to serve residents.
(c) “Local government” means a county as set forth in chapter 7 or a municipality incorporated under the
provisions of chapter 165.
(d) “Planned residential community” means a local government-approved, planned unit development that is
under unified control, is planned and developed as a whole, has a minimum gross lot area of 8 acres, and has
amenities that are designed to serve residents with a developmental disability as defined in s. 393.063 but that shall
also provide housing options for other individuals. The community shall provide choices with regard to housing
arrangements, support providers, and activities. The residents’ freedom of movement within and outside the
community may not be restricted. For the purposes of this paragraph, local government approval must be based on
criteria that include, but are not limited to, compliance with appropriate land use, zoning, and building codes. A
planned residential community may contain two or more community residential homes that are contiguous to one
another. A planned residential community may not be located within a 10-mile radius of any other planned
residential community.
(e) “Resident” means any of the following: a frail elder as defined in s. 429.65; a person who has a handicap as
defined in s. 760.22(7)(a); a person who has a developmental disability as defined in s. 393.063; a nondangerous
person who has a mental illness as defined in s. 394.455; or a child who is found to be dependent as defined in s.
39.01 or s. 984.03, or a child in need of services as defined in s. 984.03 or s. 985.03.
(f) “Sponsoring agency” means an agency or unit of government, a profit or nonprofit agency, or any other
person or organization which intends to establish or operate a community residential home.
(2) Homes of six or fewer residents which otherwise meet the definition of a community residential home shall
be deemed a single-family unit and a noncommercial, residential use for the purpose of local laws and ordinances.
Homes of six or fewer residents which otherwise meet the definition of a community residential home shall be
allowed in single-family or multifamily zoning without approval by the local government, provided that such homes
are not located within a radius of 1,000 feet of another existing such home with six or fewer residents or within a
radius of 1,200 feet of another existing community residential home. Such homes with six or fewer residents are not
required to comply with the notification provisions of this section; provided that, before licensure, the sponsoring
agency provides the local government with the most recently published data compiled from the licensing entities

3 – 2
that identifies all community residential homes within the jurisdictional limits of the local government in which the
proposed site is to be located in order to show that there is not a home of six or fewer residents which otherwise
meets the definition of a community residential home within a radius of 1,000 feet and not a community residential
home within a radius of 1,200 feet of the proposed home. At the time of home occupancy, the sponsoring agency
must notify the local government that the home is licensed by the licensing entity. For purposes of local land use and
zoning determinations, this subsection does not affect the legal nonconforming use status of any community
residential home lawfully permitted and operating as of July 1, 2016.
(3)(a) When a site for a community residential home has been selected by a sponsoring agency in an area zoned
for multifamily, the agency shall notify the chief executive officer of the local government in writing and include in
such notice the specific address of the site, the residential licensing category, the number of residents, and the
community support requirements of the program. Such notice shall also contain a statement from the licensing entity
indicating the licensing status of the proposed community residential home and specifying how the home meets
applicable licensing criteria for the safe care and supervision of the clients in the home. The sponsoring agency shall
also provide to the local government the most recently published data compiled from the licensing entities that
identifies all community residential homes within the jurisdictional limits of the local government in which the
proposed site is to be located. The local government shall review the notification of the sponsoring agency in
accordance with the zoning ordinance of the jurisdiction.
(b) Pursuant to such review, the local government may:
1. Determine that the siting of the community residential home is in accordance with local zoning and approve
the siting. If the siting is approved, the sponsoring agency may establish the home at the site selected.
2. Fail to respond within 60 days. If the local government fails to respond within such time, the sponsoring
agency may establish the home at the site selected.
3. Deny the siting of the home.
(c) The local government shall not deny the siting of a community residential home unless the local government
establishes that the siting of the home at the site selected:
1. Does not otherwise conform to existing zoning regulations applicable to other multifamily uses in the area.
2. Does not meet applicable licensing criteria established and determined by the licensing entity, including
requirements that the home be located to assure the safe care and supervision of all clients in the home.
3. Would result in such a concentration of community residential homes in the area in proximity to the site
selected, or would result in a combination of such homes with other residences in the community, such that the
nature and character of the area would be substantially altered. A home that is located within a radius of 1,200 feet
of another existing community residential home in a multifamily zone shall be an overconcentration of such homes
that substantially alters the nature and character of the area. A home that is located within a radius of 500 feet of an
area of single-family zoning substantially alters the nature and character of the area.
(4) Community residential homes, including homes of six or fewer residents which would otherwise meet the
definition of a community residential home, which are located within a planned residential community are not
subject to the proximity requirements of this section and may be contiguous to each other. A planned residential
community must comply with the applicable local government’s land development code and other local ordinances.
A local government may not impose proximity limitations between homes within a planned residential community if
such limitations are based solely on the types of residents anticipated to be living in the community.

3 – 3
(5) All distance requirements in this section shall be measured from the nearest point of the existing home or
area of single-family zoning to the nearest point of the proposed home.
(6) If agreed to by both the local government and the sponsoring agency, a conflict may be resolved through
informal mediation. The local government shall arrange for the services of an independent mediator. Mediation shall
be concluded within 45 days of a request therefor. The resolution of any issue through the mediation process shall
not alter any person’s right to a judicial determination of any issue if that person is entitled to such a determination
under statutory or common law.
(7) The licensing entity shall not issue a license to a sponsoring agency for operation of a community
residential home if the sponsoring agency does not notify the local government of its intention to establish a
program, as required by subsection (3). A license issued without compliance with the provisions of this section shall
be considered null and void, and continued operation of the home may be enjoined.
(8) A dwelling unit housing a community residential home established pursuant to this section shall be subject
to the same local laws and ordinances applicable to other noncommercial, residential family units in the area in
which it is established.
(9) Nothing in this section shall be deemed to affect the authority of any community residential home lawfully
established prior to October 1, 1989, to continue to operate.
(10) Nothing in this section shall permit persons to occupy a community residential home who would constitute
a direct threat to the health and safety of other persons or whose residency would result in substantial physical
damage to the property of others.
(11) The siting of community residential homes in areas zoned for single family shall be governed by local
zoning ordinances. Nothing in this section prohibits a local government from authorizing the development of
community residential homes in areas zoned for single family.
(12) Nothing in this section requires any local government to adopt a new ordinance if it has in place an
ordinance governing the placement of community residential homes that meet the criteria of this section. State law
on community residential homes controls over local ordinances, but nothing in this section prohibits a local
government from adopting more liberal standards for siting such homes.
History.—s. 1, ch. 89-372; s. 1, ch. 90-192; s. 4, ch. 91-429; s. 36, ch. 93-206; s. 6, ch. 95-152; s. 42, ch. 96-169;
s. 222, ch. 97-101; s. 46, ch. 98-280; s. 14, ch. 98-338; s. 53, ch. 99-193; s. 23, ch. 99-284; s. 7, ch. 2000-135; s. 93,
ch. 2004-267; s. 34, ch. 2006-86; s. 110, ch. 2006-120; s. 1, ch. 2006-177; s. 99, ch. 2007-5; s. 30, ch. 2008-245; s.
3, ch. 2010-193; s. 237, ch. 2014-19; s. 29, ch. 2015-30; s. 1, ch. 2016-74.

3 – 4
Notes ______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________

4. Chapter 435, F.S.


4 – 1
CHAPTER 435
EMPLOYMENT SCREENING
435.01 Applicability of this chapter; statutory references; rulemaking.
435.02 Definitions.
435.03 Level 1 screening standards.
435.04 Level 2 screening standards.
435.05 Requirements for covered employees and employers.
435.06 Exclusion from employment.
435.07 Exemptions from disqualification.
435.08 Payment for processing of fingerprints and state criminal records checks.
435.09 Confidentiality of personnel background check information.
435.10 Sharing of personnel information among employers.
435.11 Penalties.
435.12 Care Provider Background Screening Clearinghouse.
435.01 Applicability of this chapter; statutory references; rulemaking.—
(1)(a) Unless otherwise provided by law, whenever a background screening for employment or a background
security check is required by law to be conducted pursuant to this chapter, the provisions of this chapter apply.
(b) Unless expressly provided otherwise, a reference in any section of the Florida Statutes to chapter 435 or to
any section or sections or portion of a section of chapter 435 includes all subsequent amendments to chapter 435 or
to the referenced section or sections or portions of a section. The purpose of this chapter is to facilitate uniform
background screening and, to this end, a reference to this chapter, or to any section or subdivision within this
chapter, constitutes a general reference under the doctrine of incorporation by reference.
(2) Agencies may adopt rules to administer this chapter.
History.—s. 47, ch. 95-228; s. 35, ch. 2010-114.
435.02 Definitions.—For the purposes of this chapter, the term:
(1) “Agency” means any state, county, or municipal agency that grants licenses or registration permitting the
operation of an employer or is itself an employer or that otherwise facilitates the screening of employees pursuant to
this chapter. If there is no state agency or the municipal or county agency chooses not to conduct employment
screening, “agency” means the Department of Children and Families.
(2) “Employee” means any person required by law to be screened pursuant to this chapter, including, but not
limited to, persons who are contractors, licensees, or volunteers.
(3) “Employer” means any person or entity required by law to conduct screening of employees pursuant to this
chapter.
(4) “Employment” means any activity or service sought to be performed by an employee which requires the
employee to be screened pursuant to this chapter.
(5) “Specified agency” means the Department of Health, the Department of Children and Families, the Division
of Vocational Rehabilitation within the Department of Education, the Agency for Health Care Administration, the
Department of Elderly Affairs, the Department of Juvenile Justice, the Agency for Persons with Disabilities, and
local licensing agencies approved pursuant to s. 402.307, when these agencies are conducting state and national
criminal history background screening on persons who work with children or persons who are elderly or disabled.

4 – 2
(6) “Vulnerable person” means a minor as defined in s. 1.01 or a vulnerable adult as defined in s. 415.102.
History.—s. 47, ch. 95-228; s. 207, ch. 99-8; s. 36, ch. 2010-114; s. 9, ch. 2012-73; s. 257, ch. 2014-19; s. 10, ch.
2015-79.
435.03 Level 1 screening standards.—
(1) All employees required by law to be screened pursuant to this section must undergo background screening
as a condition of employment and continued employment which includes, but need not be limited to, employment
history checks and statewide criminal correspondence checks through the Department of Law Enforcement, and a
check of the Dru Sjodin National Sex Offender Public Website, and may include local criminal records checks
through local law enforcement agencies.
(2) Any person required by law to be screened pursuant to this section must not have an arrest awaiting final
disposition, must not have been found guilty of, regardless of adjudication, or entered a plea of nolo contendere or
guilty to, and must not have been adjudicated delinquent and the record has not been sealed or expunged for, any
offense prohibited under s. 435.04(2) or similar law of another jurisdiction.
(3) The security background investigations under this section must ensure that no person subject to this section
has been found guilty of, regardless of adjudication, or entered a plea of nolo contendere or guilty to, any offense
that constitutes domestic violence as defined in s. 741.28, whether such act was committed in this state or in another
jurisdiction.
History.—s. 47, ch. 95-228; s. 15, ch. 96-268; s. 21, ch. 96-322; s. 3, ch. 98-417; s. 87, ch. 2000-153; s. 45, ch.
2000-349; s. 62, ch. 2001-62; s. 50, ch. 2003-1; s. 4, ch. 2004-267; s. 3, ch. 2005-119; s. 89, ch. 2006-197; s. 61, ch.
2006-227; s. 109, ch. 2007-5; s. 16, ch. 2008-244; s. 37, ch. 2010-114; s. 34, ch. 2011-4.
435.04 Level 2 screening standards.—
(1)(a) All employees required by law to be screened pursuant to this section must undergo security background
investigations as a condition of employment and continued employment which includes, but need not be limited to,
fingerprinting for statewide criminal history records checks through the Department of Law Enforcement, and
national criminal history records checks through the Federal Bureau of Investigation, and may include local criminal
records checks through local law enforcement agencies.
(b) Fingerprints submitted pursuant to this section on or after July 1, 2012, must be submitted electronically to
the Department of Law Enforcement.
(c) An agency may contract with one or more vendors to perform all or part of the electronic fingerprinting
pursuant to this section. Such contracts must ensure that the owners and personnel of the vendor performing the
electronic fingerprinting are qualified and will ensure the integrity and security of all personal information.
(d) An agency may require by rule that fingerprints submitted pursuant to this section must be submitted
electronically to the Department of Law Enforcement on a date earlier than July 1, 2012.
(e) Vendors who submit fingerprints on behalf of employers must:
1. Meet the requirements of s. 943.053; and
2. Have the ability to communicate electronically with the state agency accepting screening results from the
Department of Law Enforcement and provide the applicant’s full first name, middle initial, and last name; social
security number or individual taxpayer identification number; date of birth; mailing address; sex; and race.
(2) The security background investigations under this section must ensure that no persons subject to the
provisions of this section have been arrested for and are awaiting final disposition of, have been found guilty of,

4 – 3
regardless of adjudication, or entered a plea of nolo contendere or guilty to, or have been adjudicated delinquent and
the record has not been sealed or expunged for, any offense prohibited under any of the following provisions of state
law or similar law of another jurisdiction:
(a) Section 393.135, relating to sexual misconduct with certain developmentally disabled clients and reporting
of such sexual misconduct.
(b) Section 394.4593, relating to sexual misconduct with certain mental health patients and reporting of such
sexual misconduct.
(c) Section 415.111, relating to adult abuse, neglect, or exploitation of aged persons or disabled adults.
(d) Section 777.04, relating to attempts, solicitation, and conspiracy to commit an offense listed in this
subsection.
(e) Section 782.04, relating to murder.
(f) Section 782.07, relating to manslaughter, aggravated manslaughter of an elderly person or disabled adult, or
aggravated manslaughter of a child.
(g) Section 782.071, relating to vehicular homicide.
(h) Section 782.09, relating to killing of an unborn child by injury to the mother.
(i) Chapter 784, relating to assault, battery, and culpable negligence, if the offense was a felony.
(j) Section 784.011, relating to assault, if the victim of the offense was a minor.
(k) Section 784.03, relating to battery, if the victim of the offense was a minor.
(l) Section 787.01, relating to kidnapping.
(m) Section 787.02, relating to false imprisonment.
(n) Section 787.025, relating to luring or enticing a child.
(o) Section 787.04(2), relating to taking, enticing, or removing a child beyond the state limits with criminal
intent pending custody proceedings.
(p) Section 787.04(3), relating to carrying a child beyond the state lines with criminal intent to avoid producing
a child at a custody hearing or delivering the child to the designated person.
(q) Section 790.115(1), relating to exhibiting firearms or weapons within 1,000 feet of a school.
(r) Section 790.115(2)(b), relating to possessing an electric weapon or device, destructive device, or other
weapon on school property.
(s) Section 794.011, relating to sexual battery.
(t) Former s. 794.041, relating to prohibited acts of persons in familial or custodial authority.
(u) Section 794.05, relating to unlawful sexual activity with certain minors.
(v) Chapter 796, relating to prostitution.
(w) Section 798.02, relating to lewd and lascivious behavior.
(x) Chapter 800, relating to lewdness and indecent exposure.
(y) Section 806.01, relating to arson.
(z) Section 810.02, relating to burglary.
(aa) Section 810.14, relating to voyeurism, if the offense is a felony.
(bb) Section 810.145, relating to video voyeurism, if the offense is a felony.
(cc) Chapter 812, relating to theft, robbery, and related crimes, if the offense is a felony.
(dd) Section 817.563, relating to fraudulent sale of controlled substances, only if the offense was a felony.

4 – 4
(ee) Section 825.102, relating to abuse, aggravated abuse, or neglect of an elderly person or disabled adult.
(ff) Section 825.1025, relating to lewd or lascivious offenses committed upon or in the presence of an elderly
person or disabled adult.
(gg) Section 825.103, relating to exploitation of an elderly person or disabled adult, if the offense was a felony.
(hh) Section 826.04, relating to incest.
(ii) Section 827.03, relating to child abuse, aggravated child abuse, or neglect of a child.
(jj) Section 827.04, relating to contributing to the delinquency or dependency of a child.
(kk) Former s. 827.05, relating to negligent treatment of children.
(ll) Section 827.071, relating to sexual performance by a child.
(mm) Section 843.01, relating to resisting arrest with violence.
(nn) Section 843.025, relating to depriving a law enforcement, correctional, or correctional probation officer
means of protection or communication.
(oo) Section 843.12, relating to aiding in an escape.
(pp) Section 843.13, relating to aiding in the escape of juvenile inmates in correctional institutions.
(qq) Chapter 847, relating to obscene literature.
(rr) Section 874.05, relating to encouraging or recruiting another to join a criminal gang.
(ss) Chapter 893, relating to drug abuse prevention and control, only if the offense was a felony or if any other
person involved in the offense was a minor.
(tt) Section 916.1075, relating to sexual misconduct with certain forensic clients and reporting of such sexual
misconduct.
(uu) Section 944.35(3), relating to inflicting cruel or inhuman treatment on an inmate resulting in great bodily
harm.
(vv) Section 944.40, relating to escape.
(ww) Section 944.46, relating to harboring, concealing, or aiding an escaped prisoner.
(xx) Section 944.47, relating to introduction of contraband into a correctional facility.
(yy) Section 985.701, relating to sexual misconduct in juvenile justice programs.
(zz) Section 985.711, relating to contraband introduced into detention facilities.
(3) The security background investigations under this section must ensure that no person subject to this section
has been arrested for and is awaiting final disposition of, been found guilty of, regardless of adjudication, or entered
a plea of nolo contendere or guilty to, any offense that constitutes domestic violence as defined in s. 741.28, whether
such act was committed in this state or in another jurisdiction.
(4) For the purpose of screening applicability to participate in the Medicaid program, the security background
investigations under this section must ensure that a person subject to screening under this section has not been
arrested for and is not awaiting final disposition of; has not been found guilty of, regardless of adjudication, or
entered a plea of nolo contendere or guilty to; and has not been adjudicated delinquent and the record sealed or
expunged for, any of the following offenses:
(a) Violation of a federal law or a law in any state which creates a criminal offense relating to:
1. The delivery of any goods or services under Medicaid or Medicare or any other public or private health care
or health insurance program, including the performance of management or administrative services relating to the
delivery of goods or services under any such program;

4 – 5
2. Neglect or abuse of a patient in connection with the delivery of any health care good or service;
3. Unlawful manufacture, distribution, prescription, or dispensing of a controlled substance;
4. Fraud, theft, embezzlement, breach of fiduciary responsibility, or other financial misconduct;
5. Moral turpitude, if punishable by imprisonment of a year or more; or
6. Interference with or obstruction of an investigation into any criminal offense identified in this subsection.
(b) Violation of the following state laws or laws of another jurisdiction:
1. Section 817.569, criminal use of a public record or information contained in a public record;
2. Section 838.016, unlawful compensation or reward for official behavior;
3. Section 838.021, corruption by threat against a public servant;
4. Section 838.022, official misconduct;
5. Section 838.22, bid tampering;
6. Section 839.13, falsifying records; or
7. Section 839.26, misuse of confidential information.
(c) Violation of a federal or state law, rule, or regulation governing the Florida Medicaid program or any other
state Medicaid program, the Medicare program, or any other publicly funded federal or state health care or health
insurance program.
History.—s. 47, ch. 95-228; s. 16, ch. 96-268; s. 22, ch. 96-322; s. 4, ch. 98-417; s. 5, ch. 99-284; s. 88, ch. 2000-
153; s. 7, ch. 2001-125; s. 5, ch. 2004-267; s. 4, ch. 2005-119; s. 111, ch. 2006-120; s. 90, ch. 2006-197; s. 110, ch.
2007-5; s. 3, ch. 2007-112; s. 66, ch. 2009-223; s. 6, ch. 2010-31; s. 38, ch. 2010-114; s. 10, ch. 2012-73; s. 4, ch.
2013-80; s. 6, ch. 2014-84; s. 4, ch. 2014-194; s. 3, ch. 2016-162; s. 19, ch. 2017-37; s. 89, ch. 2018-24.
435.05 Requirements for covered employees and employers.—Except as otherwise provided by law, the
following requirements apply to covered employees and employers:
(1)(a) Every person required by law to be screened pursuant to this chapter must submit a complete set of
information necessary to conduct a screening under this chapter.
(b) For level 1 screening, the employer must submit the information necessary for screening to the Department
of Law Enforcement within 5 working days after receiving it. The Department of Law Enforcement shall conduct a
search of its records and respond to the employer or agency. The employer must inform the employee whether
screening has revealed any disqualifying information.
(c) For level 2 screening, the employer or agency must submit the information necessary for screening to the
Department of Law Enforcement within 5 working days after receiving it. The Department of Law Enforcement
shall perform a criminal history record check of its records and request that the Federal Bureau of Investigation
perform a national criminal history record check of its records for each employee for whom the request is made. The
Department of Law Enforcement shall respond to the employer or agency, and the employer or agency must inform
the employee whether screening has revealed disqualifying information.
(d) The person whose background is being checked must supply any missing criminal or other necessary
information upon request to the requesting employer or agency within 30 days after receiving the request for the
information.
(2) Every employee must attest, subject to penalty of perjury, to meeting the requirements for qualifying for
employment pursuant to this chapter and agreeing to inform the employer immediately if arrested for any of the
disqualifying offenses while employed by the employer.

4 – 6
(3) Each employer licensed or registered with an agency must conduct level 2 background screening and must
submit to the agency annually or at the time of license renewal, under penalty of perjury, a signed attestation
attesting to compliance with the provisions of this chapter.
History.—s. 47, ch. 95-228; s. 208, ch. 99-8; s. 46, ch. 2000-349; s. 63, ch. 2001-62; s. 21, ch. 2004-267; s. 67,
ch. 2009-223; s. 39, ch. 2010-114; s. 7, ch. 2014-84.
435.06 Exclusion from employment.—
(1) If an employer or agency has reasonable cause to believe that grounds exist for the denial or termination of
employment of any employee as a result of background screening, it shall notify the employee in writing, stating the
specific record that indicates noncompliance with the standards in this chapter. It is the responsibility of the affected
employee to contest his or her disqualification or to request exemption from disqualification. The only basis for
contesting the disqualification is proof of mistaken identity.
(2)(a) An employer may not hire, select, or otherwise allow an employee to have contact with any vulnerable
person that would place the employee in a role that requires background screening until the screening process is
completed and demonstrates the absence of any grounds for the denial or termination of employment. If the
screening process shows any grounds for the denial or termination of employment, the employer may not hire,
select, or otherwise allow the employee to have contact with any vulnerable person that would place the employee in
a role that requires background screening unless the employee is granted an exemption for the disqualification by the
agency as provided under s. 435.07.
(b) If an employer becomes aware that an employee has been arrested for a disqualifying offense, the employer
must remove the employee from contact with any vulnerable person that places the employee in a role that requires
background screening until the arrest is resolved in a way that the employer determines that the employee is still
eligible for employment under this chapter.
(c) The employer must terminate the employment of any of its personnel found to be in noncompliance with the
minimum standards of this chapter or place the employee in a position for which background screening is not
required unless the employee is granted an exemption from disqualification pursuant to s. 435.07.
(d) An employer may hire an employee to a position that requires background screening before the employee
completes the screening process for training and orientation purposes. However, the employee may not have direct
contact with vulnerable persons until the screening process is completed and the employee demonstrates that he or
she exhibits no behaviors that warrant the denial or termination of employment.
(3) Any employee who refuses to cooperate in such screening or refuses to timely submit the information
necessary to complete the screening, including fingerprints if required, must be disqualified for employment in such
position or, if employed, must be dismissed.
(4) There is no reemployment assistance or other monetary liability on the part of, and no cause of action for
damages against, an employer that, upon notice of a conviction or arrest for a disqualifying offense listed under this
chapter, terminates the person against whom the report was issued or who was arrested, regardless of whether or not
that person has filed for an exemption pursuant to this chapter.
History.—s. 47, ch. 95-228; s. 40, ch. 2010-114; s. 65, ch. 2012-30; s. 11, ch. 2012-73.
435.07 Exemptions from disqualification.—Unless otherwise provided by law, the provisions of this section
apply to exemptions from disqualification for disqualifying offenses revealed pursuant to background screenings

4 – 7
required under this chapter, regardless of whether those disqualifying offenses are listed in this chapter or other
laws.
(1)(a) The head of the appropriate agency may grant to any employee otherwise disqualified from employment
an exemption from disqualification for:
1. Felonies for which at least 3 years have elapsed since the applicant for the exemption has completed or been
lawfully released from confinement, supervision, or nonmonetary condition imposed by the court for the
disqualifying felony;
2. Misdemeanors prohibited under any of the statutes cited in this chapter or under similar statutes of other
jurisdictions for which the applicant for the exemption has completed or been lawfully released from confinement,
supervision, or nonmonetary condition imposed by the court;
3. Offenses that were felonies when committed but that are now misdemeanors and for which the applicant for
the exemption has completed or been lawfully released from confinement, supervision, or nonmonetary condition
imposed by the court; or
4. Findings of delinquency. For offenses that would be felonies if committed by an adult and the record has not
been sealed or expunged, the exemption may not be granted until at least 3 years have elapsed since the applicant for
the exemption has completed or been lawfully released from confinement, supervision, or nonmonetary condition
imposed by the court for the disqualifying offense.
(b) A person applying for an exemption who was ordered to pay any amount for any fee, fine, fund, lien, civil
judgment, application, costs of prosecution, trust, or restitution as part of the judgment and sentence for any
disqualifying felony or misdemeanor must pay the court-ordered amount in full before he or she is eligible for the
exemption.
For the purposes of this subsection, the term “felonies” means both felonies prohibited under any of the statutes cited
in this chapter or under similar statutes of other jurisdictions.
(2) Persons employed, or applicants for employment, by treatment providers who treat adolescents 13 years of
age and older who are disqualified from employment solely because of crimes under s. 796.07(2)(e), s. 810.02(4), s.
812.014(2)(c), s. 817.563, s. 831.01, s. 831.02, s. 893.13, or s. 893.147, or any related criminal attempt, solicitation,
or conspiracy under s. 777.04, may be exempted from disqualification from employment pursuant to this chapter
without application of the waiting period in subparagraph (1)(a)1.
(3)(a) In order for the head of an agency to grant an exemption to any employee, the employee must
demonstrate by clear and convincing evidence that the employee should not be disqualified from employment.
Employees seeking an exemption have the burden of setting forth clear and convincing evidence of rehabilitation,
including, but not limited to, the circumstances surrounding the criminal incident for which an exemption is sought,
the time period that has elapsed since the incident, the nature of the harm caused to the victim, and the history of the
employee since the incident, or any other evidence or circumstances indicating that the employee will not present a
danger if employment or continued employment is allowed.
(b) The agency may consider as part of its deliberations of the employee’s rehabilitation the fact that the
employee has, subsequent to the conviction for the disqualifying offense for which the exemption is being sought,
been arrested for or convicted of another crime, even if that crime is not a disqualifying offense.

4 – 8
(c) The decision of the head of an agency regarding an exemption may be contested through the hearing
procedures set forth in chapter 120. The standard of review by the administrative law judge is whether the agency’s
intended action is an abuse of discretion.
(4)(a) Disqualification from employment under this chapter may not be removed from, nor may an exemption
be granted to, any personnel who is found guilty of, regardless of adjudication, or who has entered a plea of nolo
contendere or guilty to, any felony covered by s. 435.03 or s. 435.04 solely by reason of any pardon, executive
clemency, or restoration of civil rights.
(b) Disqualification from employment under this chapter may not be removed from, nor may an exemption be
granted to, any person who is a:
1. Sexual predator as designated pursuant to s. 775.21;
2. Career offender pursuant to s. 775.261; or
3. Sexual offender pursuant to s. 943.0435, unless the requirement to register as a sexual offender has been
removed pursuant to s. 943.04354.
(c) Disqualification from employment under this chapter may not be removed from, and an exemption may not
be granted to, any current or prospective child care personnel, as defined in s. 402.302(3), and such a person is
disqualified from employment as child care personnel, regardless of any previous exemptions from disqualification,
if the person has been registered as a sex offender as described in 42 U.S.C. s. 9858f(c)(1)(C) or has been arrested
for and is awaiting final disposition of, has been convicted or found guilty of, or entered a plea of guilty or nolo
contendere to, regardless of adjudication, or has been adjudicated delinquent and the record has not been sealed or
expunged for, any offense prohibited under any of the following provisions of state law or a similar law of another
jurisdiction:
1. A felony offense prohibited under any of the following statutes:
a. Chapter 741, relating to domestic violence.
b. Section 782.04, relating to murder.
c. Section 782.07, relating to manslaughter, aggravated manslaughter of an elderly person or disabled adult,
aggravated manslaughter of a child, or aggravated manslaughter of an officer, a firefighter, an emergency medical
technician, or a paramedic.
d. Section 784.021, relating to aggravated assault.
e. Section 784.045, relating to aggravated battery.
f. Section 787.01, relating to kidnapping.
g. Section 787.025, relating to luring or enticing a child.
h. Section 787.04(2), relating to leading, taking, enticing, or removing a minor beyond the state limits, or
concealing the location of a minor, with criminal intent pending custody proceedings.
i. Section 787.04(3), relating to leading, taking, enticing, or removing a minor beyond the state limits, or
concealing the location of a minor, with criminal intent pending dependency proceedings or proceedings concerning
alleged abuse or neglect of a minor.
j. Section 794.011, relating to sexual battery.
k. Former s. 794.041, relating to sexual activity with or solicitation of a child by a person in familial or
custodial authority.
l. Section 794.05, relating to unlawful sexual activity with certain minors.

4 – 9
m. Section 794.08, relating to female genital mutilation.
n. Section 806.01, relating to arson.
o. Section 826.04, relating to incest.
p. Section 827.03, relating to child abuse, aggravated child abuse, or neglect of a child.
q. Section 827.04, relating to contributing to the delinquency or dependency of a child.
r. Section 827.071, relating to sexual performance by a child.
s. Chapter 847, relating to child pornography.
t. Chapter 893, relating to a drug abuse prevention and control offense, if that offense was committed in the
preceding 5 years.
u. Section 985.701, relating to sexual misconduct in juvenile justice programs.
2. A misdemeanor offense prohibited under any of the following statutes:
a. Section 784.03, relating to battery, if the victim of the offense was a minor.
b. Section 787.025, relating to luring or enticing a child.
c. Chapter 847, relating to child pornography.
3. A criminal act committed in another state or under federal law which, if committed in this state, constitutes
an offense prohibited under any statute listed in subparagraph 1. or subparagraph 2.
(5) Exemptions granted by one agency shall be considered by subsequent agencies, but are not binding on the
subsequent agency.
History.—s. 47, ch. 95-228; s. 47, ch. 2000-349; s. 64, ch. 2001-62; s. 29, ch. 2004-267; s. 9, ch. 2005-128; s. 41,
ch. 2010-114; s. 8, ch. 2014-84; ss. 1, 3, ch. 2016-98; s. 26, ch. 2016-104; s. 37, ch. 2016-105; s. 15, ch. 2016-238;
s. 20, ch. 2017-37; s. 26, ch. 2018-103.
435.08 Payment for processing of fingerprints and state criminal records checks.—The employer or the
employee is responsible for paying the costs of screening. Payment shall be submitted to the Department of Law
Enforcement with the request for screening. The appropriate agency is responsible for collecting and paying any fee
related to fingerprints retained on its behalf to the Department of Law Enforcement for costs resulting from the
fingerprint information retention services. The amount of the annual fee and procedures for the submission and
retention of fingerprint information and for the dissemination of search results shall be established by rule of the
Department of Law Enforcement.
History.—s. 47, ch. 95-228; s. 209, ch. 99-8; s. 48, ch. 2000-349; s. 42, ch. 2010-114.
435.09 Confidentiality of personnel background check information.—No criminal or juvenile information
obtained under this section may be used for any purpose other than determining whether persons meet the minimum
standards for employment or for an owner or director of a covered service provider. The criminal records and
juvenile records obtained by the department or by an employer are exempt from s. 119.07(1).
History.—s. 47, ch. 95-228; s. 282, ch. 96-406; s. 49, ch. 2000-349.
435.10 Sharing of personnel information among employers.—Every employer of employees covered by this
chapter shall furnish copies of personnel records for employees or former employees to any other employer
requesting this information pursuant to this section. Information contained in the records may include, but is not
limited to, disciplinary matters and any reason for termination. Any employer releasing such records pursuant to this
chapter shall be considered to be acting in good faith and may not be held liable for information contained in such
records, absent a showing that the employer maliciously falsified such records.

4 – 10
History.—s. 47, ch. 95-228.
435.11 Penalties.—
(1) It is a misdemeanor of the first degree, punishable as provided in s. 775.082 or s. 775.083, for any person
willfully, knowingly, or intentionally to:
(a) Fail, by false statement, misrepresentation, impersonation, or other fraudulent means, to disclose in any
application for voluntary or paid employment a material fact used in making a determination as to such person’s
qualifications for a position of special trust.
(b) Use records information for purposes other than screening for employment or release records information to
other persons for purposes other than screening for employment.
(2) It is a felony of the third degree, punishable as provided in s. 775.082, s. 775.083, or s. 775.084, for any
person willfully, knowingly, or intentionally to use juvenile records information for any purposes other than
specified in this section or to release such information to other persons for purposes other than specified in this
section.
History.—s. 47, ch. 95-228; s. 283, ch. 96-406.
435.12 Care Provider Background Screening Clearinghouse.—
(1) The Agency for Health Care Administration in consultation with the Department of Law Enforcement shall
create a secure web-based system, which shall be known as the “Care Provider Background Screening
Clearinghouse” or “clearinghouse,” and which shall be implemented to the full extent practicable no later than
September 30, 2013, subject to the specified agencies being funded and equipped to participate in such program.
The clearinghouse shall allow the results of criminal history checks provided to the specified agencies for screening
of persons qualified as care providers under s. 943.0542 to be shared among the specified agencies when a person
has applied to volunteer, be employed, be licensed, or enter into a contract that requires a state and national
fingerprint-based criminal history check. The Agency for Health Care Administration and the Department of Law
Enforcement may adopt rules to create forms or implement procedures needed to carry out this section.
(2)(a) To ensure that the information in the clearinghouse is current, the fingerprints of an employee required to
be screened by a specified agency and included in the clearinghouse must be:
1. Retained by the Department of Law Enforcement pursuant to s. 943.05(2)(g) and (h) and (3), and the
Department of Law Enforcement must report the results of searching those fingerprints against state incoming arrest
fingerprint submissions to the Agency for Health Care Administration for inclusion in the clearinghouse.
2. Retained by the Federal Bureau of Investigation in the national retained print arrest notification program as
soon as the Department of Law Enforcement begins participation in such program. Arrest prints will be searched
against retained prints at the Federal Bureau of Investigation and notification of arrests will be forwarded to the
Florida Department of Law Enforcement and reported to the Agency for Health Care Administration for inclusion in
the clearinghouse.
3. Resubmitted for a Federal Bureau of Investigation national criminal history check every 5 years until such
time as the fingerprints are retained by the Federal Bureau of Investigation.
4. Subject to retention on a 5-year renewal basis with fees collected at the time of initial submission or
resubmission of fingerprints.
5. Submitted with a photograph of the person taken at the time the fingerprints are submitted.

4 – 11
(b) Until such time as the fingerprints are enrolled in the national retained print arrest notification program at
the Federal Bureau of Investigation, an employee with a break in service of more than 90 days from a position that
requires screening by a specified agency must submit to a national screening if the person returns to a position that
requires screening by a specified agency.
(c) An employer of persons subject to screening by a specified agency must register with the clearinghouse and
maintain the employment status of all employees within the clearinghouse. Initial employment status and any
changes in status must be reported within 10 business days.
(d) An employer must register with and initiate all criminal history checks through the clearinghouse before
referring an employee or potential employee for electronic fingerprint submission to the Department of Law
Enforcement. The registration must include the employee’s full first name, middle initial, and last name; social
security number; date of birth; mailing address; sex; and race. Individuals, persons, applicants, and controlling
interests that cannot legally obtain a social security number must provide an individual taxpayer identification
number.
(3) An employee who has undergone a fingerprint-based criminal history check by a specified agency before
the clearinghouse is operational is not required to be checked again solely for the purpose of entry in the
clearinghouse. Every employee who is or will become subject to fingerprint-based criminal history checks to be
eligible to be licensed, have their license renewed, or meet screening or rescreening requirements by a specified
agency once the specified agency participates in the clearinghouse shall be subject to the requirements of this section
with respect to entry of records in the clearinghouse and retention of fingerprints for reporting the results of
searching against state incoming arrest fingerprint submissions.
History.—s. 12, ch. 2012-73; s. 9, ch. 2014-84.

4 – 12
Notes
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________

5. Chapter 429, Part I,
& Section 429.905, F.S.


5 – 1
CHAPTER 429
ASSISTED CARE COMMUNITIES
PART I
ASSISTED LIVING FACILITIES
(ss. 429.01-429.55)
&
PART III
ADULT DAY CARE CENTERS
(s. 429.905)
429.01 Short title; purpose.
429.02 Definitions.
429.04 Facilities to be licensed; exemptions.
429.07 License required; fee.
429.075 Limited mental health license.
429.08 Unlicensed facilities; referral of person for residency to unlicensed facility; penalties.
429.11 Initial application for license; provisional license.
429.12 Sale or transfer of ownership of a facility.
429.14 Administrative penalties.
429.17 Expiration of license; renewal; conditional license.
429.174 Background screening.
429.176 Notice of change of administrator.
429.177 Patients with Alzheimer’s disease or other related disorders; certain disclosures.
429.178 Special care for persons with Alzheimer’s disease or other related disorders.
429.18 Disposition of fees and administrative fines.
429.19 Violations; imposition of administrative fines; grounds.
429.195 Rebates prohibited; penalties.
429.20 Certain solicitation prohibited; third-party supplementation.
429.22 Receivership proceedings.
429.23 Internal risk management and quality assurance program; adverse incidents and reporting requirements.
429.24 Contracts.
429.255 Use of personnel; emergency care.
429.256 Assistance with self-administration of medication.
429.26 Appropriateness of placements; examinations of residents.
429.27 Property and personal affairs of residents.
429.275 Business practice; personnel records; liability insurance.
429.28 Resident bill of rights.

5 – 2
429.29 Civil actions to enforce rights.
429.293 Presuit notice; investigation; notification of violation of residents’ rights or alleged negligence; claims
evaluation procedure; informal discovery; review; settlement offer; mediation.
429.294 Availability of facility records for investigation of resident’s rights violations and defenses; penalty.
429.295 Certain provisions not applicable to actions under this part.
429.296 Statute of limitations.
429.297 Punitive damages; pleading; burden of proof.
429.298 Punitive damages; limitation.
429.31 Closing of facility; notice; penalty.
429.34 Right of entry and inspection.
429.35 Maintenance of records; reports.
429.41 Rules establishing standards.
429.42 Pharmacy and dietary services.
429.44 Construction and renovation; requirements.
429.445 Compliance with local zoning requirements.
429.47 Prohibited acts; penalties for violation.
429.49 Resident records; penalties for alteration.
429.52 Staff training and educational programs; core educational requirement.
429.53 Consultation by the agency.
429.54 Collection of information; local subsidy.
429.55 Consumer information website.
429.01 Short title; purpose.—
(1) This act may be cited as the “Assisted Living Facilities Act.”
(2) The purpose of this act is to promote the availability of appropriate services for elderly persons and adults
with disabilities in the least restrictive and most homelike environment, to encourage the development of facilities
that promote the dignity, individuality, privacy, and decisionmaking ability of such persons, to provide for the
health, safety, and welfare of residents of assisted living facilities in the state, to promote continued improvement of
such facilities, to encourage the development of innovative and affordable facilities particularly for persons with low
to moderate incomes, to ensure that all agencies of the state cooperate in the protection of such residents, and to
ensure that needed economic, social, mental health, health, and leisure services are made available to residents of
such facilities through the efforts of the Agency for Health Care Administration, the Department of Elderly Affairs,
the Department of Children and Families, the Department of Health, assisted living facilities, and other community
agencies. To the maximum extent possible, appropriate community-based programs must be available to state-
supported residents to augment the services provided in assisted living facilities. The Legislature recognizes that
assisted living facilities are an important part of the continuum of long-term care in the state. In support of the goal
of aging in place, the Legislature further recognizes that assisted living facilities should be operated and regulated as
residential environments with supportive services and not as medical or nursing facilities. The services available in
these facilities, either directly or through contract or agreement, are intended to help residents remain as independent

5 – 3
as possible. Regulations governing these facilities must be sufficiently flexible to allow facilities to adopt policies
that enable residents to age in place when resources are available to meet their needs and accommodate their
preferences.
(3) The principle that a license issued under this part is a public trust and a privilege and is not an entitlement
should guide the finder of fact or trier of law at any administrative proceeding or in a court action initiated by the
Agency for Health Care Administration to enforce this part.
History.—ss. 1, 2, ch. 75-233; ss. 12, 13, ch. 80-198; s. 2, ch. 81-318; ss. 79, 83, ch. 83-181; s. 2, ch. 87-371; s.
2, ch. 91-263; s. 28, ch. 92-33; ss. 1, 38, 39, ch. 93-216; s. 6, ch. 95-210; s. 46, ch. 95-418; s. 122, ch. 99-8; s. 2, ch.
2006-197; s. 243, ch. 2014-19.
Note.—Former s. 400.401.
429.02 Definitions.—When used in this part, the term:
(1) “Activities of daily living” means functions and tasks for self-care, including ambulation, bathing, dressing,
eating, grooming, and toileting, and other similar tasks.
(2) “Administrator” means an individual at least 21 years of age who is responsible for the operation and
maintenance of an assisted living facility.
(3) “Agency” means the Agency for Health Care Administration.
(4) “Aging in place” or “age in place” means the process of providing increased or adjusted services to a person
to compensate for the physical or mental decline that may occur with the aging process, in order to maximize the
person’s dignity and independence and permit them to remain in a familiar, noninstitutional, residential environment
for as long as possible. Such services may be provided by facility staff, volunteers, family, or friends, or through
contractual arrangements with a third party.
(5) “Assisted living facility” means any building or buildings, section or distinct part of a building, private
home, boarding home, home for the aged, or other residential facility, regardless of whether operated for profit,
which through its ownership or management provides housing, meals, and one or more personal services for a
period exceeding 24 hours to one or more adults who are not relatives of the owner or administrator.
(6) “Chemical restraint” means a pharmacologic drug that physically limits, restricts, or deprives an individual
of movement or mobility, and is used for discipline or convenience and not required for the treatment of medical
symptoms.
(7) “Community living support plan” means a written document prepared by a mental health resident and the
resident’s mental health case manager in consultation with the administrator of an assisted living facility with a
limited mental health license or the administrator’s designee. A copy must be provided to the administrator. The
plan must include information about the supports, services, and special needs of the resident which enable the
resident to live in the assisted living facility and a method by which facility staff can recognize and respond to the
signs and symptoms particular to that resident which indicate the need for professional services.
(8) “Cooperative agreement” means a written statement of understanding between a mental health care provider
and the administrator of the assisted living facility with a limited mental health license in which a mental health
resident is living. The agreement must specify directions for accessing emergency and after-hours care for the

5 – 4
mental health resident. A single cooperative agreement may service all mental health residents who are clients of the
same mental health care provider.
(9) “Department” means the Department of Elderly Affairs.
(10) “Emergency” means a situation, physical condition, or method of operation which presents imminent
danger of death or serious physical or mental harm to facility residents.
(11) “Extended congregate care” means acts beyond those authorized in subsection (17) that may be performed
pursuant to part I of chapter 464 by persons licensed thereunder while carrying out their professional duties, and
other supportive services which may be specified by rule. The purpose of such services is to enable residents to age
in place in a residential environment despite mental or physical limitations that might otherwise disqualify them
from residency in a facility licensed under this part.
(12) “Guardian” means a person to whom the law has entrusted the custody and control of the person or
property, or both, of a person who has been legally adjudged incapacitated.
(13) “Limited nursing services” means acts that may be performed by a person licensed under part I of chapter
464. Limited nursing services shall be for persons who meet the admission criteria established by the agency for
assisted living facilities but are not complex enough to require 24-hour nursing supervision and may include such
services as the application and care of routine dressings and care of casts, braces, and splints.
(14) “Managed risk” means the process by which the facility staff discuss the service plan and the needs of the
resident with the resident and, if applicable, the resident’s representative or designee or the resident’s surrogate,
guardian, or attorney in fact, in such a way that the consequences of a decision, including any inherent risk, are
explained to all parties and reviewed periodically in conjunction with the service plan, taking into account changes
in the resident’s status and the ability of the facility to respond accordingly.
(15) “Mental health resident” means an individual who receives social security disability income due to a
mental disorder as determined by the Social Security Administration or receives supplemental security income due
to a mental disorder as determined by the Social Security Administration and receives optional state
supplementation.
(16) “Office” has the same meaning as in s. 400.0060.
(17) “Personal services” means direct physical assistance with or supervision of the activities of daily living,
the self-administration of medication, or other similar services that the agency may define by rule. The term may not
be construed to mean the provision of medical, nursing, dental, or mental health services.
(18) “Physical restraint” means a device which physically limits, restricts, or deprives an individual of
movement or mobility, including, but not limited to, a half-bed rail, a full-bed rail, a geriatric chair, and a posey
restraint. The term “physical restraint” shall also include any device which was not specifically manufactured as a
restraint but which has been altered, arranged, or otherwise used for this purpose. The term shall not include
bandage material used for the purpose of binding a wound or injury.
(19) “Relative” means an individual who is the father, mother, stepfather, stepmother, son, daughter, brother,
sister, grandmother, grandfather, great-grandmother, great-grandfather, grandson, granddaughter, uncle, aunt, first
cousin, nephew, niece, husband, wife, father-in-law, mother-in-law, son-in-law, daughter-in-law, brother-in-law,
sister-in-law, stepson, stepdaughter, stepbrother, stepsister, half brother, or half sister of an owner or administrator.
5 – 5
(20) “Resident” means a person 18 years of age or older, residing in and receiving care from a facility.
(21) “Resident’s representative or designee” means a person other than the owner, or an agent or employee of
the facility, designated in writing by the resident, if legally competent, to receive notice of changes in the contract
executed pursuant to s. 429.24; to receive notice of and to participate in meetings between the resident and the
facility owner, administrator, or staff concerning the rights of the resident; to assist the resident in contacting the
State Long-Term Care Ombudsman Program or local ombudsman council if the resident has a complaint against the
facility; or to bring legal action on behalf of the resident pursuant to s. 429.29.
(22) “Service plan” means a written plan, developed and agreed upon by the resident and, if applicable, the
resident’s representative or designee or the resident’s surrogate, guardian, or attorney in fact, if any, and the
administrator or designee representing the facility, which addresses the unique physical and psychosocial needs,
abilities, and personal preferences of each resident receiving extended congregate care services. The plan shall
include a brief written description, in easily understood language, of what services shall be provided, who shall
provide the services, when the services shall be rendered, and the purposes and benefits of the services.
(23) “Shared responsibility” means exploring the options available to a resident within a facility and the risks
involved with each option when making decisions pertaining to the resident’s abilities, preferences, and service
needs, thereby enabling the resident and, if applicable, the resident’s representative or designee, or the resident’s
surrogate, guardian, or attorney in fact, and the facility to develop a service plan which best meets the resident’s
needs and seeks to improve the resident’s quality of life.
(24) “Supervision” means reminding residents to engage in activities of daily living and the self-administration
of medication, and, when necessary, observing or providing verbal cuing to residents while they perform these
activities.
(25) “Supplemental security income,” Title XVI of the Social Security Act, means a program through which the
Federal Government guarantees a minimum monthly income to every person who is age 65 or older, or disabled, or
blind and meets the income and asset requirements.
(26) “Supportive services” means services designed to encourage and assist aged persons or adults with
disabilities to remain in the least restrictive living environment and to maintain their independence as long as
possible.
(27) “Twenty-four-hour nursing supervision” means services that are ordered by a physician for a resident
whose condition requires the supervision of a physician and continued monitoring of vital signs and physical status.
Such services shall be: medically complex enough to require constant supervision, assessment, planning, or
intervention by a nurse; required to be performed by or under the direct supervision of licensed nursing personnel or
other professional personnel for safe and effective performance; required on a daily basis; and consistent with the
nature and severity of the resident’s condition or the disease state or stage.
History.—s. 3, ch. 75-233; ss. 12, 14, ch. 80-198; s. 2, ch. 81-318; ss. 6, 19, ch. 82-148; ss. 41, 79, 83, ch. 83-
181; s. 4, ch. 85-145; s. 3, ch. 87-371; s. 10, ch. 89-294; s. 3, ch. 91-263; s. 1, ch. 93-209; ss. 2, 38, 39, ch. 93-216; s.
7, ch. 95-210; ss. 1, 22, 47, ch. 95-418; s. 2, ch. 97-82; s. 1, ch. 98-80; s. 98, ch. 2000-318; ss. 2, 29, ch. 2006-197; s.
138, ch. 2007-230; s. 34, ch. 2015-31; s. 5, ch. 2015-126; s. 79, ch. 2018-24; s. 8, ch. 2019-11.
Note.—Former s. 400.402.

5 – 6
429.04 Facilities to be licensed; exemptions.—
(1) For the administration of this part, facilities to be licensed by the agency shall include all assisted living
facilities as defined in this part.
(2) The following are exempt from licensure under this part:
(a) Any facility, institution, or other place operated by the Federal Government or any agency of the Federal
Government.
(b) Any facility or part of a facility licensed by the Agency for Persons with Disabilities under chapter 393, a
mental health facility licensed under chapter 394, a hospital licensed under chapter 395, a nursing home licensed
under part II of chapter 400, an inpatient hospice licensed under part IV of chapter 400, a home for special services
licensed under part V of chapter 400, an intermediate care facility licensed under part VIII of chapter 400, or a
transitional living facility licensed under part XI of chapter 400.
(c) Any facility licensed as an adult family-care home under part II.
(d) Any person who provides housing, meals, and one or more personal services on a 24-hour basis in the
person’s own home to not more than two adults who do not receive optional state supplementation. The person who
provides the housing, meals, and personal services must own or rent the home and must have established the home
as his or her permanent residence. For purposes of this paragraph, any person holding a homestead exemption at an
address other than that at which the person asserts this exemption is presumed to not have established permanent
residence. This exemption does not apply to a person or entity that previously held a license issued by the agency
which was revoked or for which renewal was denied by final order of the agency, or when the person or entity
voluntarily relinquished the license during agency enforcement proceedings.
(e) Any home or facility approved by the United States Department of Veterans Affairs as a residential care
home wherein care is provided exclusively to three or fewer veterans.
(f) Any facility that has been incorporated in this state for 50 years or more on or before July 1, 1983, and the
board of directors of which is nominated or elected by the residents, until the facility is sold or its ownership is
transferred; or any facility, with improvements or additions thereto, which has existed and operated continuously in
this state for 60 years or more on or before July 1, 1989, is directly or indirectly owned and operated by a nationally
recognized fraternal organization, is not open to the public, and accepts only its own members and their spouses as
residents.
(g) Any facility certified under chapter 651, or a retirement community, may provide services authorized under
this part or part III of chapter 400 to its residents who live in single-family homes, duplexes, quadruplexes, or
apartments located on the campus without obtaining a license to operate an assisted living facility if residential units
within such buildings are used by residents who do not require staff supervision for that portion of the day when
personal services are not being delivered and the owner obtains a home health license to provide such services.
However, any building or distinct part of a building on the campus that is designated for persons who receive
personal services and require supervision beyond that which is available while such services are being rendered
must be licensed in accordance with this part. If a facility provides personal services to residents who do not
otherwise require supervision and the owner is not licensed as a home health agency, the buildings or distinct parts
of buildings where such services are rendered must be licensed under this part. A resident of a facility that obtains a

5 – 7
home health license may contract with a home health agency of his or her choice, provided that the home health
agency provides liability insurance and workers’ compensation coverage for its employees. Facilities covered by this
exemption may establish policies that give residents the option of contracting for services and care beyond that
which is provided by the facility to enable them to age in place. For purposes of this section, a retirement
community consists of a facility licensed under this part or under part II of chapter 400, and apartments designed for
independent living located on the same campus.
(h) Any residential unit for independent living which is located within a facility certified under chapter 651, or
any residential unit which is colocated with a nursing home licensed under part II of chapter 400 or colocated with a
facility licensed under this part in which services are provided through an outpatient clinic or a nursing home on an
outpatient basis.
(3) Upon agency investigation of unlicensed activity, any person or entity that claims that it is exempt under
this section must provide documentation substantiating entitlement to the exemption.
History.—ss. 4, 5, ch. 75-233; ss. 12, 15, ch. 80-198; s. 2, ch. 81-318; ss. 42, 79, 83, ch. 83-181; s. 4, ch. 87-371;
s. 4, ch. 91-263; ss. 3, 38, 39, ch. 93-216; s. 19, ch. 93-268; s. 2, ch. 94-206; s. 1055, ch. 95-148; s. 8, ch. 95-210; s.
2, ch. 98-80; s. 1, ch. 98-148; ss. 2, 30, ch. 2006-197; s. 80, ch. 2018-24.
Note.—Former s. 400.404.
429.07 License required; fee.—
(1) The requirements of part II of chapter 408 apply to the provision of services that require licensure pursuant
to this part and part II of chapter 408 and to entities licensed by or applying for such licensure from the agency
pursuant to this part. A license issued by the agency is required in order to operate an assisted living facility in this
state.
(2) Separate licenses shall be required for facilities maintained in separate premises, even though operated
under the same management. A separate license shall not be required for separate buildings on the same grounds.
(3) In addition to the requirements of s. 408.806, each license granted by the agency must state the type of care
for which the license is granted. Licenses shall be issued for one or more of the following categories of care:
standard, extended congregate care, limited nursing services, or limited mental health.
(a) A standard license shall be issued to facilities providing one or more of the personal services identified in s.
429.02. Such facilities may also employ or contract with a person licensed under part I of chapter 464 to administer
medications and perform other tasks as specified in s. 429.255.
(b) An extended congregate care license shall be issued to each facility that has been licensed as an assisted
living facility for 2 or more years and that provides services, directly or through contract, beyond those authorized in
paragraph (a), including services performed by persons licensed under part I of chapter 464 and supportive services,
as defined by rule, to persons who would otherwise be disqualified from continued residence in a facility licensed
under this part. An extended congregate care license may be issued to a facility that has a provisional extended
congregate care license and meets the requirements for licensure under subparagraph 2. The primary purpose of
extended congregate care services is to allow residents the option of remaining in a familiar setting from which they
would otherwise be disqualified for continued residency as they become more impaired. A facility licensed to
provide extended congregate care services may also admit an individual who exceeds the admission criteria for a

5 – 8
facility with a standard license, if he or she is determined appropriate for admission to the extended congregate care
facility.
1. In order for extended congregate care services to be provided, the agency must first determine that all
requirements established in law and rule are met and must specifically designate, on the facility’s license, that such
services may be provided and whether the designation applies to all or part of the facility. This designation may be
made at the time of initial licensure or relicensure, or upon request in writing by a licensee under this part and part II
of chapter 408. The notification of approval or the denial of the request shall be made in accordance with part II of
chapter 408. Each existing facility that qualifies to provide extended congregate care services must have maintained
a standard license and may not have been subject to administrative sanctions during the previous 2 years, or since
initial licensure if the facility has been licensed for less than 2 years, for any of the following reasons:
a. A class I or class II violation;
b. Three or more repeat or recurring class III violations of identical or similar resident care standards from
which a pattern of noncompliance is found by the agency;
c. Three or more class III violations that were not corrected in accordance with the corrective action plan
approved by the agency;
d. Violation of resident care standards which results in requiring the facility to employ the services of a
consultant pharmacist or consultant dietitian;
e. Denial, suspension, or revocation of a license for another facility licensed under this part in which the
applicant for an extended congregate care license has at least 25 percent ownership interest; or
f. Imposition of a moratorium pursuant to this part or part II of chapter 408 or initiation of injunctive
proceedings.
The agency may deny or revoke a facility’s extended congregate care license for not meeting the criteria for an
extended congregate care license as provided in this subparagraph.
2. If an assisted living facility has been licensed for less than 2 years, the initial extended congregate care
license must be provisional and may not exceed 6 months. The licensee shall notify the agency, in writing, when it
has admitted at least one extended congregate care resident, after which an unannounced inspection shall be made to
determine compliance with the requirements of an extended congregate care license. A licensee with a provisional
extended congregate care license that demonstrates compliance with all the requirements of an extended congregate
care license during the inspection shall be issued an extended congregate care license. In addition to sanctions
authorized under this part, if violations are found during the inspection and the licensee fails to demonstrate
compliance with all assisted living facility requirements during a followup inspection, the licensee shall immediately
suspend extended congregate care services, and the provisional extended congregate care license expires. The
agency may extend the provisional license for not more than 1 month in order to complete a followup visit.
3. A facility that is licensed to provide extended congregate care services shall maintain a written progress
report on each person who receives services which describes the type, amount, duration, scope, and outcome of
services that are rendered and the general status of the resident’s health. A registered nurse, or appropriate designee,
representing the agency shall visit the facility at least twice a year to monitor residents who are receiving extended
congregate care services and to determine if the facility is in compliance with this part, part II of chapter 408, and

5 – 9
relevant rules. One of the visits may be in conjunction with the regular survey. The monitoring visits may be
provided through contractual arrangements with appropriate community agencies. A registered nurse shall serve as
part of the team that inspects the facility. The agency may waive one of the required yearly monitoring visits for a
facility that has:
a. Held an extended congregate care license for at least 24 months;
b. No class I or class II violations and no uncorrected class III violations; and
c. No ombudsman council complaints that resulted in a citation for licensure.
4. A facility that is licensed to provide extended congregate care services must:
a. Demonstrate the capability to meet unanticipated resident service needs.
b. Offer a physical environment that promotes a homelike setting, provides for resident privacy, promotes
resident independence, and allows sufficient congregate space as defined by rule.
c. Have sufficient staff available, taking into account the physical plant and firesafety features of the building,
to assist with the evacuation of residents in an emergency.
d. Adopt and follow policies and procedures that maximize resident independence, dignity, choice, and
decisionmaking to permit residents to age in place, so that moves due to changes in functional status are minimized
or avoided.
e. Allow residents or, if applicable, a resident’s representative, designee, surrogate, guardian, or attorney in fact
to make a variety of personal choices, participate in developing service plans, and share responsibility in
decisionmaking.
f. Implement the concept of managed risk.
g. Provide, directly or through contract, the services of a person licensed under part I of chapter 464.
h. In addition to the training mandated in s. 429.52, provide specialized training as defined by rule for facility
staff.
5. A facility that is licensed to provide extended congregate care services is exempt from the criteria for
continued residency set forth in rules adopted under s. 429.41. A licensed facility must adopt its own requirements
within guidelines for continued residency set forth by rule. However, the facility may not serve residents who
require 24-hour nursing supervision. A licensed facility that provides extended congregate care services must also
provide each resident with a written copy of facility policies governing admission and retention.
6. Before the admission of an individual to a facility licensed to provide extended congregate care services, the
individual must undergo a medical examination as provided in s. 429.26(4) and the facility must develop a
preliminary service plan for the individual.
7. If a facility can no longer provide or arrange for services in accordance with the resident’s service plan and
needs and the facility’s policy, the facility must make arrangements for relocating the person in accordance with s.
429.28(1)(k).
(c) A limited nursing services license shall be issued to a facility that provides services beyond those authorized
in paragraph (a) and as specified in this paragraph.
1. In order for limited nursing services to be provided in a facility licensed under this part, the agency must first
determine that all requirements established in law and rule are met and must specifically designate, on the facility’s

5 – 10
license, that such services may be provided. This designation may be made at the time of initial licensure or
licensure renewal, or upon request in writing by a licensee under this part and part II of chapter 408. Notification of
approval or denial of such request shall be made in accordance with part II of chapter 408. An existing facility that
qualifies to provide limited nursing services must have maintained a standard license and may not have been subject
to administrative sanctions that affect the health, safety, and welfare of residents for the previous 2 years or since
initial licensure if the facility has been licensed for less than 2 years.
2. A facility that is licensed to provide limited nursing services shall maintain a written progress report on each
person who receives such nursing services. The report must describe the type, amount, duration, scope, and outcome
of services that are rendered and the general status of the resident’s health. A registered nurse representing the
agency shall visit the facility at least annually to monitor residents who are receiving limited nursing services and to
determine if the facility is in compliance with applicable provisions of this part, part II of chapter 408, and related
rules. The monitoring visits may be provided through contractual arrangements with appropriate community
agencies. A registered nurse shall also serve as part of the team that inspects such facility. Visits may be in
conjunction with other agency inspections. The agency may waive the required yearly monitoring visit for a facility
that has:
a. Had a limited nursing services license for at least 24 months;
b. No class I or class II violations and no uncorrected class III violations; and
c. No ombudsman council complaints that resulted in a citation for licensure.
3. A person who receives limited nursing services under this part must meet the admission criteria established
by the agency for assisted living facilities. When a resident no longer meets the admission criteria for a facility
licensed under this part, arrangements for relocating the person shall be made in accordance with s. 429.28(1)(k),
unless the facility is licensed to provide extended congregate care services.
(4) In accordance with s. 408.805, an applicant or licensee shall pay a fee for each license application submitted
under this part, part II of chapter 408, and applicable rules. The amount of the fee shall be established by rule.
(a) The biennial license fee required of a facility is $300 per license, with an additional fee of $50 per resident
based on the total licensed resident capacity of the facility, except that no additional fee will be assessed for beds
designated for recipients of optional state supplementation payments provided for in s. 409.212. The total fee may
not exceed $10,000.
(b) In addition to the total fee assessed under paragraph (a), the agency shall require facilities that are licensed
to provide extended congregate care services under this part to pay an additional fee per licensed facility. The
amount of the biennial fee shall be $400 per license, with an additional fee of $10 per resident based on the total
licensed resident capacity of the facility.
(c) In addition to the total fee assessed under paragraph (a), the agency shall require facilities that are licensed
to provide limited nursing services under this part to pay an additional fee per licensed facility. The amount of the
biennial fee shall be $250 per license, with an additional fee of $10 per resident based on the total licensed resident
capacity of the facility.
(5) Counties or municipalities applying for licenses under this part are exempt from the payment of license fees.

5 – 11
History.—s. 6, ch. 75-233; s. 8, ch. 79-12; ss. 12, 16, ch. 80-198; s. 2, ch. 81-318; ss. 43, 79, 83, ch. 83-181; s. 2,
ch. 86-104; s. 5, ch. 87-371; s. 11, ch. 89-294; s. 5, ch. 91-263; s. 10, ch. 91-282; s. 22, ch. 93-177; ss. 4, 38, 39, ch.
93-216; s. 20, ch. 95-146; s. 9, ch. 95-210; ss. 2, 18, 23, ch. 95-418; s. 3, ch. 97-82; s. 18, ch. 97-96; s. 3, ch. 98-80;
s. 99, ch. 2000-318; s. 33, ch. 2001-45; ss. 2, 31, ch. 2006-197; s. 101, ch. 2007-5; s. 139, ch. 2007-230; s. 141, ch.
2010-102; s. 6, ch. 2015-126.
Note.—Former s. 400.407.
429.075 Limited mental health license.—An assisted living facility that serves one or more mental health
residents must obtain a limited mental health license.
(1) To obtain a limited mental health license, a facility must hold a standard license as an assisted living
facility, must not have any current uncorrected violations, and must ensure that, within 6 months after receiving a
limited mental health license, the facility administrator and the staff of the facility who are in direct contact with
mental health residents must complete training of no less than 6 hours related to their duties. This designation may
be made at the time of initial licensure or relicensure or upon request in writing by a licensee under this part and part
II of chapter 408. Notification of approval or denial of such request shall be made in accordance with this part, part
II of chapter 408, and applicable rules. This training must be provided by or approved by the Department of
Children and Families.
(2) A facility that is licensed to provide services to mental health residents must provide appropriate
supervision and staffing to provide for the health, safety, and welfare of such residents.
(3) A facility that has a limited mental health license must:
(a) Have a copy of each mental health resident’s community living support plan and the cooperative agreement
with the mental health care services provider or provide written evidence that a request for the community living
support plan and the cooperative agreement was sent to the Medicaid managed care plan or managing entity under
contract with the Department of Children and Families within 72 hours after admission. The support plan and the
agreement may be combined.
(b) Have documentation provided by the department that each mental health resident has been assessed and
determined to be able to live in the community in an assisted living facility that has a limited mental health license
or provide written evidence that a request for documentation was sent to the department within 72 hours after
admission.
(c) Make the community living support plan available for inspection by the resident, the resident’s legal
guardian or health care surrogate, and other individuals who have a lawful basis for reviewing this document.
(d) Assist the mental health resident in carrying out the activities identified in the resident’s community living
support plan.
(4) A facility that has a limited mental health license may enter into a cooperative agreement with a private
mental health provider. For purposes of the limited mental health license, the private mental health provider may act
as the case manager.
History.—s. 3, ch. 95-418; s. 37, ch. 96-169; s. 4, ch. 97-82; s. 66, ch. 97-100; s. 4, ch. 98-80; s. 2, ch. 2006-197;
s. 140, ch. 2007-230; s. 244, ch. 2014-19; s. 7, ch. 2015-126.
Note.—Former s. 400.4075.

5 – 12
429.08 Unlicensed facilities; referral of person for residency to unlicensed facility; penalties.—
(1)(a) This section applies to the unlicensed operation of an assisted living facility in addition to the
requirements of part II of chapter 408.
(b) Any person who owns, rents, or otherwise maintains a building or property used as an unlicensed assisted
living facility commits a felony of the third degree, punishable as provided in s. 775.082, s. 775.083, or s. 775.084.
Each day of continued operation is a separate offense.
(c) Any person found guilty of violating paragraph (a) a second or subsequent time commits a felony of the
second degree, punishable as provided under s. 775.082, s. 775.083, or s. 775.084. Each day of continued operation
is a separate offense.
(d) In addition to the requirements of s. 408.812, any person who owns, operates, or maintains an unlicensed
assisted living facility after receiving notice from the agency commits a felony of the third degree, punishable as
provided in s. 775.082, s. 775.083, or s. 775.084. Each day of continued operation is a separate offense.
(e) The agency shall publish a list, by county, of licensed assisted living facilities. This information may be
provided electronically or through the agency’s Internet site.
(2) It is unlawful to knowingly refer a person for residency to an unlicensed assisted living facility; to an
assisted living facility the license of which is under denial or has been suspended or revoked; or to an assisted living
facility that has a moratorium pursuant to part II of chapter 408.
(a) Any health care practitioner, as defined in s. 456.001, who is aware of the operation of an unlicensed facility
shall report that facility to the agency. Failure to report a facility that the practitioner knows or has reasonable cause
to suspect is unlicensed shall be reported to the practitioner’s licensing board.
(b) Any provider as defined in s. 408.803 which knowingly discharges a patient or client to an unlicensed
facility is subject to sanction by the agency.
(c) Any employee of the agency or department, or the Department of Children and Families, who knowingly
refers a person for residency to an unlicensed facility; to a facility the license of which is under denial or has been
suspended or revoked; or to a facility that has a moratorium pursuant to part II of chapter 408 is subject to
disciplinary action by the agency or department, or the Department of Children and Families.
(d) The employer of any person who is under contract with the agency or department, or the Department of
Children and Families, and who knowingly refers a person for residency to an unlicensed facility; to a facility the
license of which is under denial or has been suspended or revoked; or to a facility that has a moratorium pursuant to
part II of chapter 408 shall be fined and required to prepare a corrective action plan designed to prevent such
referrals.
History.—s. 17, ch. 88-350; s. 6, ch. 91-263; s. 29, ch. 92-33; ss. 5, 39, ch. 93-216; s. 10, ch. 95-210; ss. 4, 48,
ch. 95-418; s. 5, ch. 98-80; s. 1, ch. 99-179; s. 1, ch. 2000-318; s. 36, ch. 2001-62; s. 2, ch. 2004-344; ss. 2, 33, ch.
2006-197; s. 141, ch. 2007-230; s. 60, ch. 2009-223; s. 245, ch. 2014-19; s. 81, ch. 2018-24.
Note.—Former s. 400.408.
429.11 Initial application for license; provisional license.—
(1) Each applicant for licensure must comply with all provisions of part II of chapter 408 and must:

5 – 13
(a) Identify all other homes or facilities, including the addresses and the license or licenses under which they
operate, if applicable, which are currently operated by the applicant or administrator and which provide housing,
meals, and personal services to residents.
(b) Provide the location of the facility for which a license is sought and documentation, signed by the
appropriate local government official, which states that the applicant has met local zoning requirements.
(c) Provide the name, address, date of birth, social security number, education, and experience of the
administrator, if different from the applicant.
(2) The applicant shall provide proof of liability insurance as defined in s. 624.605.
(3) If the applicant is a community residential home, the applicant must provide proof that it has met the
requirements specified in chapter 419.
(4) The applicant must furnish proof that the facility has received a satisfactory firesafety inspection. The local
authority having jurisdiction or the State Fire Marshal must conduct the inspection within 30 days after written
request by the applicant.
(5) The applicant must furnish documentation of a satisfactory sanitation inspection of the facility by the county
health department.
(6) In addition to the license categories available in s. 408.808, a provisional license may be issued to an
applicant making initial application for licensure or making application for a change of ownership. A provisional
license shall be limited in duration to a specific period of time not to exceed 6 months, as determined by the agency.
(7) A county or municipality may not issue an occupational license that is being obtained for the purpose of
operating a facility regulated under this part without first ascertaining that the applicant has been licensed to operate
such facility at the specified location or locations by the agency. The agency shall furnish to local agencies
responsible for issuing occupational licenses sufficient instruction for making such determinations.
History.—s. 7, ch. 75-233; s. 3, ch. 77-323; ss. 12, 17, ch. 80-198; s. 2, ch. 81-318; ss. 7, 19, ch. 82-148; ss. 44,
47, 79, 83, ch. 83-181; s. 5, ch. 85-145; s. 1, ch. 85-251; s. 6, ch. 87-371; s. 12, ch. 89-294; s. 7, ch. 91-263; ss. 6,
38, 39, ch. 93-216; s. 5, ch. 95-418; s. 6, ch. 98-80; s. 42, ch. 98-171; ss. 2, 34, ch. 2006-197; s. 142, ch. 2007-230.
Note.—Former s. 400.411.
429.12 Sale or transfer of ownership of a facility.—It is the intent of the Legislature to protect the rights of
the residents of an assisted living facility when the facility is sold or the ownership thereof is transferred. Therefore,
in addition to the requirements of part II of chapter 408, whenever a facility is sold or the ownership thereof is
transferred, including leasing:
(1) The transferee shall notify the residents, in writing, of the change of ownership within 7 days after receipt of
the new license.
(2) The transferor of a facility the license of which is denied pending an administrative hearing shall, as a part
of the written change-of-ownership contract, advise the transferee that a plan of correction must be submitted by the
transferee and approved by the agency at least 7 days before the change of ownership and that failure to correct the
condition which resulted in the moratorium pursuant to part II of chapter 408 or denial of licensure is grounds for
denial of the transferee’s license.

5 – 14
History.—ss. 45, 83, ch. 83-181; s. 7, ch. 87-371; s. 8, ch. 91-263; ss. 7, 38, 39, ch. 93-216; s. 772, ch. 95-148; s.
11, ch. 95-210; s. 6, ch. 95-418; ss. 2, 35, ch. 2006-197; s. 143, ch. 2007-230.
Note.—Former s. 400.412.
429.14 Administrative penalties.—
(1) In addition to the requirements of part II of chapter 408, the agency may deny, revoke, and suspend any
license issued under this part and impose an administrative fine in the manner provided in chapter 120 against a
licensee for a violation of any provision of this part, part II of chapter 408, or applicable rules, or for any of the
following actions by a licensee, any person subject to level 2 background screening under s. 408.809, or any facility
staff:
(a) An intentional or negligent act seriously affecting the health, safety, or welfare of a resident of the facility.
(b) A determination by the agency that the owner lacks the financial ability to provide continuing adequate care
to residents.
(c) Misappropriation or conversion of the property of a resident of the facility.
(d) Failure to follow the criteria and procedures provided under part I of chapter 394 relating to the
transportation, voluntary admission, and involuntary examination of a facility resident.
(e) A citation for any of the following violations as specified in s. 429.19:
1. One or more cited class I violations.
2. Three or more cited class II violations.
3. Five or more cited class III violations that have been cited on a single survey and have not been corrected
within the times specified.
(f) Failure to comply with the background screening standards of this part, s. 408.809(1), or chapter 435.
(g) Violation of a moratorium.
(h) Failure of the license applicant, the licensee during relicensure, or a licensee that holds a provisional license
to meet the minimum license requirements of this part, or related rules, at the time of license application or renewal.
(i) An intentional or negligent life-threatening act in violation of the uniform firesafety standards for assisted
living facilities or other firesafety standards which threatens the health, safety, or welfare of a resident of a facility,
as communicated to the agency by the local authority having jurisdiction or the State Fire Marshal.
(j) Knowingly operating any unlicensed facility or providing without a license any service that must be licensed
under this chapter or chapter 400.
(k) Any act constituting a ground upon which application for a license may be denied.
(2) Upon notification by the local authority having jurisdiction or by the State Fire Marshal, the agency may
deny or revoke the license of an assisted living facility that fails to correct cited fire code violations that affect or
threaten the health, safety, or welfare of a resident of a facility.
(3) The agency may deny a license of an applicant or a controlling interest as defined in part II of chapter 408
which has or had a 25 percent or greater financial or ownership interest in any other facility that is licensed under
this part, or in any entity licensed by this state or another state to provide health or residential care, if that facility or
entity during the 5 years prior to the application for a license closed due to financial inability to operate; had a

5 – 15
receiver appointed or a license denied, suspended, or revoked; was subject to a moratorium; or had an injunctive
proceeding initiated against it.
(4) The agency shall deny or revoke the license of an assisted living facility if:
(a) There are two moratoria, issued pursuant to this part or part II of chapter 408, within a 2-year period which
are imposed by final order;
(b) The facility is cited for two or more class I violations arising from unrelated circumstances during the same
survey or investigation; or
(c) The facility is cited for two or more class I violations arising from separate surveys or investigations within
a 2-year period.
(5) An action taken by the agency to suspend, deny, or revoke a facility’s license under this part or part II of
chapter 408, in which the agency claims that the facility owner or an employee of the facility has threatened the
health, safety, or welfare of a resident of the facility, shall be heard by the Division of Administrative Hearings of
the Department of Management Services within 120 days after receipt of the facility’s request for a hearing, unless
that time limitation is waived by both parties. The administrative law judge shall render a decision within 30 days
after receipt of a proposed recommended order.
(6) As provided under s. 408.814, the agency shall impose an immediate moratorium on an assisted living
facility that fails to provide the agency with access to the facility or prohibits the agency from conducting a
regulatory inspection. The licensee may not restrict agency staff from accessing and copying records at the agency’s
expense or from conducting confidential interviews with facility staff or any individual who receives services from
the facility.
(7) Agency notification of a license suspension or revocation, or denial of a license renewal, shall be posted and
visible to the public at the facility.
(8) If a facility is required to relocate some or all of its residents due to agency action, that facility is exempt
from the 45-day notice requirement imposed under s. 429.28(1)(k). This subsection does not exempt the facility
from any deadlines for corrective action set by the agency.
History.—s. 8, ch. 75-233; ss. 12, 18, ch. 80-198; s. 2, ch. 81-318; ss. 46, 79, 83, ch. 83-181; s. 8, ch. 87-371; s.
13, ch. 89-294; s. 30, ch. 91-71; s. 46, ch. 92-58; ss. 8, 38, 39, ch. 93-216; s. 50, ch. 94-218; s. 39, ch. 95-228; s. 7,
ch. 95-418; s. 38, ch. 96-169; s. 126, ch. 96-410; s. 7, ch. 98-80; s. 43, ch. 98-171; s. 73, ch. 2000-349; s. 34, ch.
2001-45; s. 19, ch. 2003-57; s. 13, ch. 2004-267; ss. 2, 36, ch. 2006-197; s. 144, ch. 2007-230; s. 61, ch. 2009-223;
s. 28, ch. 2010-114; s. 108, ch. 2014-17; s. 8, ch. 2015-126.
Note.—Former s. 400.414.
429.17 Expiration of license; renewal; conditional license.—
(1) Limited nursing, extended congregate care, and limited mental health licenses shall expire at the same time
as the facility’s standard license, regardless of when issued.
(2) A license shall be renewed in accordance with part II of chapter 408 and the provision of satisfactory proof
of ability to operate and conduct the facility in accordance with the requirements of this part and adopted rules,
including proof that the facility has received a satisfactory firesafety inspection, conducted by the local authority
having jurisdiction or the State Fire Marshal, within the preceding 12 months.

5 – 16
(3) In addition to the requirements of part II of chapter 408, each facility must report to the agency any adverse
court action concerning the facility’s financial viability, within 7 days after its occurrence. The agency shall have
access to books, records, and any other financial documents maintained by the facility to the extent necessary to
determine the facility’s financial stability.
(4) In addition to the license categories available in s. 408.808, a conditional license may be issued to an
applicant for license renewal if the applicant fails to meet all standards and requirements for licensure. A conditional
license issued under this subsection shall be limited in duration to a specific period of time not to exceed 6 months,
as determined by the agency, and shall be accompanied by an agency-approved plan of correction.
(5) When an extended care or limited nursing license is requested during a facility’s biennial license period, the
fee shall be prorated in order to permit the additional license to expire at the end of the biennial license period. The
fee shall be calculated as of the date the additional license application is received by the agency.
(6) The agency may by rule establish renewal procedures, identify forms, and specify documentation necessary
to administer this section and may adopt rules to administer part II of chapter 408.
History.—s. 9, ch. 75-233; ss. 12, 19, ch. 80-198; s. 2, ch. 81-318; ss. 9, 19, ch. 82-148; ss. 47, 79, 83, ch. 83-
181; s. 2, ch. 88-350; s. 14, ch. 89-294; s. 9, ch. 91-263; s. 23, ch. 93-177; ss. 10, 38, 39, ch. 93-216; s. 9, ch. 95-
418; s. 9, ch. 98-80; s. 44, ch. 98-171; s. 212, ch. 99-13; s. 20, ch. 2003-57; ss. 2, 38, ch. 2006-197; s. 146, ch. 2007-
230; s. 9, ch. 2019-11.
Note.—Former s. 400.417.
429.174 Background screening.—The agency shall require level 2 background screening for personnel as
required in s. 408.809(1)(e) pursuant to chapter 435 and s. 408.809.
History.—ss. 15, 25, ch. 89-294; ss. 11, 38, 39, ch. 93-216; s. 10, ch. 98-80; ss. 45, 71, ch. 98-171; s. 142, ch. 98-
403; s. 213, ch. 99-13; s. 74, ch. 2000-349; s. 25, ch. 2001-53; s. 2, ch. 2001-67; s. 148, ch. 2001-277; s. 418, ch.
2003-261; s. 14, ch. 2004-267; ss. 2, 39, ch. 2006-197; s. 147, ch. 2007-230; s. 29, ch. 2010-114.
Note.—Former s. 400.4174.
429.176 Notice of change of administrator.—If, during the period for which a license is issued, the owner
changes administrators, the owner must notify the agency of the change within 10 days and provide documentation
within 90 days that the new administrator has completed the applicable core educational requirements under s.
429.52. A facility may not be operated for more than 120 consecutive days without an administrator who has
completed the core educational requirements.
History.—ss. 44, 83, ch. 83-181; s. 10, ch. 91-263; ss. 12, 38, 39, ch. 93-216; ss. 10, 24, ch. 95-418; s. 11, ch. 98-
80; s. 46, ch. 98-171; ss. 2, 40, ch. 2006-197; s. 148, ch. 2007-230; s. 82, ch. 2018-24.
Note.—Former s. 400.4176.
429.177 Patients with Alzheimer’s disease or other related disorders; certain disclosures.—A facility
licensed under this part which claims that it provides special care for persons who have Alzheimer’s disease or other
related disorders must disclose in its advertisements or in a separate document those services that distinguish the
care as being especially applicable to, or suitable for, such persons. The facility must give a copy of all such
advertisements or a copy of the document to each person who requests information about programs and services for
persons with Alzheimer’s disease or other related disorders offered by the facility and must maintain a copy of all

5 – 17
such advertisements and documents in its records. The agency shall examine all such advertisements and documents
in the facility’s records as part of the license renewal procedure.
History.—s. 2, ch. 93-105; s. 2, ch. 2006-197.
Note.—Former s. 400.4177.
429.178 Special care for persons with Alzheimer’s disease or other related disorders.—
(1) A facility which advertises that it provides special care for persons with Alzheimer’s disease or other related
disorders must meet the following standards of operation:
(a)1. If the facility has 17 or more residents, have an awake staff member on duty at all hours of the day and
night; or
2. If the facility has fewer than 17 residents, have an awake staff member on duty at all hours of the day and
night or have mechanisms in place to monitor and ensure the safety of the facility’s residents.
(b) Offer activities specifically designed for persons who are cognitively impaired.
(c) Have a physical environment that provides for the safety and welfare of the facility’s residents.
(d) Employ staff who have completed the training and continuing education required in subsection (2).
(2)(a) An individual who is employed by a facility that provides special care for residents who have
Alzheimer’s disease or other related disorders, and who has regular contact with such residents, must complete up to
4 hours of initial dementia-specific training developed or approved by the department. The training must be
completed within 3 months after beginning employment and satisfy the core training requirements of s.
429.52(3)(g).
(b) A direct caregiver who is employed by a facility that provides special care for residents who have
Alzheimer’s disease or other related disorders and provides direct care to such residents must complete the required
initial training and 4 additional hours of training developed or approved by the department. The training must be
completed within 9 months after beginning employment and satisfy the core training requirements of s.
429.52(3)(g).
(c) An individual who is employed by a facility that provides special care for residents with Alzheimer’s
disease or other related disorders, but who only has incidental contact with such residents, must be given, at a
minimum, general information on interacting with individuals with Alzheimer’s disease or other related disorders,
within 3 months after beginning employment.
(3) In addition to the training required under subsection (2), a direct caregiver must participate in a minimum of
4 contact hours of continuing education each calendar year. The continuing education must include one or more
topics included in the dementia-specific training developed or approved by the department, in which the caregiver
has not received previous training.
(4) Upon completing any training listed in subsection (2), the employee or direct caregiver shall be issued a
certificate that includes the name of the training provider, the topic covered, and the date and signature of the
training provider. The certificate is evidence of completion of training in the identified topic, and the employee or
direct caregiver is not required to repeat training in that topic if the employee or direct caregiver changes
employment to a different facility. The employee or direct caregiver must comply with other applicable continuing
education requirements.

5 – 18
(5) The department, or its designee, shall approve the initial and continuing education courses and providers.
(6) The department shall keep a current list of providers who are approved to provide initial and continuing
education for staff of facilities that provide special care for persons with Alzheimer’s disease or other related
disorders.
(7) Any facility more than 90 percent of whose residents receive monthly optional supplementation payments is
not required to pay for the training and education programs required under this section. A facility that has one or
more such residents shall pay a reduced fee that is proportional to the percentage of such residents in the facility. A
facility that does not have any residents who receive monthly optional supplementation payments must pay a
reasonable fee, as established by the department, for such training and education programs.
(8) The department shall adopt rules to establish standards for trainers and training and to implement this
section.
History.—s. 15, ch. 97-82; ss. 2, 41, ch. 2006-197; s. 9, ch. 2015-126.
Note.—Former s. 400.4178.
429.18 Disposition of fees and administrative fines.—Income from fees and fines collected under this part
shall be directed to and used by the agency for the following purposes:
(1) Up to 50 percent of the trust funds accrued each fiscal year under this part may be used to offset the
expenses of receivership, pursuant to s. 429.22, if the court determines that the income and assets of the facility are
insufficient to provide for adequate management and operation.
(2) An amount of $5,000 of the trust funds accrued each year under this part shall be allocated to pay for
inspection-related physical and mental health examinations requested by the agency pursuant to s. 429.26 for
residents who are either recipients of supplemental security income or have monthly incomes not in excess of the
maximum combined federal and state cash subsidies available to supplemental security income recipients, as
provided for in s. 409.212. Such funds shall only be used where the resident is ineligible for Medicaid.
(3) Any trust funds accrued each year under this part and not used for the purposes specified in subsections (1)
and (2) shall be used to offset the costs of the licensure program, verifying information submitted, defraying the
costs of processing the names of applicants, and conducting inspections and monitoring visits pursuant to this part
and part II of chapter 408.
History.—ss. 12, 20, ch. 80-198; s. 2, ch. 81-318; ss. 8, 19, ch. 82-148; ss. 48, 75, 79, 83, ch. 83-181; s. 53, ch.
83-218; s. 16, ch. 89-294; s. 11, ch. 91-263; s. 11, ch. 91-282; ss. 13, 38, 39, ch. 93-216; s. 19, ch. 95-418; s. 12, ch.
98-80; ss. 2, 42, ch. 2006-197; s. 149, ch. 2007-230.
Note.—Former s. 400.418.
429.19 Violations; imposition of administrative fines; grounds.—
(1) In addition to the requirements of part II of chapter 408, the agency shall impose an administrative fine in
the manner provided in chapter 120 for the violation of any provision of this part, part II of chapter 408, and
applicable rules by an assisted living facility, for the actions of any person subject to level 2 background screening
under s. 408.809, for the actions of any facility employee, or for an intentional or negligent act seriously affecting
the health, safety, or welfare of a resident of the facility.

5 – 19
(2) Each violation of this part and adopted rules shall be classified according to the nature of the violation and
the gravity of its probable effect on facility residents. The agency shall indicate the classification on the written
notice of the violation as follows:
(a) Class “I” violations are defined in s. 408.813. The agency shall impose an administrative fine for a cited
class I violation in an amount not less than $5,000 and not exceeding $10,000 for each violation.
(b) Class “II” violations are defined in s. 408.813. The agency shall impose an administrative fine for a cited
class II violation in an amount not less than $1,000 and not exceeding $5,000 for each violation.
(c) Class “III” violations are defined in s. 408.813. The agency shall impose an administrative fine for a cited
class III violation in an amount not less than $500 and not exceeding $1,000 for each violation.
(d) Class “IV” violations are defined in s. 408.813. The agency shall impose an administrative fine for a cited
class IV violation in an amount not less than $100 and not exceeding $200 for each violation.
(e) Regardless of the class of violation cited, instead of the fine amounts listed in paragraphs (a)-(d), the agency
shall impose an administrative fine of $500 if a facility is found not to be in compliance with the background
screening requirements as provided in s. 408.809.
(3) For purposes of this section, in determining if a penalty is to be imposed and in fixing the amount of the
fine, the agency shall consider the following factors:
(a) The gravity of the violation, including the probability that death or serious physical or emotional harm to a
resident will result or has resulted, the severity of the action or potential harm, and the extent to which the provisions
of the applicable laws or rules were violated.
(b) Actions taken by the owner or administrator to correct violations.
(c) Any previous violations.
(d) The financial benefit to the facility of committing or continuing the violation.
(e) The licensed capacity of the facility.
(4) Each day of continuing violation after the date fixed for termination of the violation, as ordered by the
agency, constitutes an additional, separate, and distinct violation.
(5) Any action taken to correct a violation shall be documented in writing by the owner or administrator of the
facility and verified through followup visits by agency personnel. The agency may impose a fine and, in the case of
an owner-operated facility, revoke or deny a facility’s license when a facility administrator fraudulently
misrepresents action taken to correct a violation.
(6) Any facility whose owner fails to apply for a change-of-ownership license in accordance with part II of
chapter 408 and operates the facility under the new ownership is subject to a fine of $5,000.
(7) In addition to any administrative fines imposed, the agency may assess a survey fee, equal to the lesser of
one half of the facility’s biennial license and bed fee or $500, to cover the cost of conducting initial complaint
investigations that result in the finding of a violation that was the subject of the complaint or monitoring visits
conducted to verify the correction of the violations.
(8) During an inspection, the agency shall make a reasonable attempt to discuss each violation with the owner
or administrator of the facility, prior to written notification.

5 – 20
(9) The agency shall develop and disseminate an annual list of all facilities sanctioned or fined for violations of
state standards, the number and class of violations involved, the penalties imposed, and the current status of cases.
The list shall be disseminated, at no charge, to the Department of Elderly Affairs, the Department of Health, the
Department of Children and Families, the Agency for Persons with Disabilities, the area agencies on aging, the
Florida Statewide Advocacy Council, the State Long-Term Care Ombudsman Program, and state and local
ombudsman councils. The Department of Children and Families shall disseminate the list to service providers under
contract to the department who are responsible for referring persons to a facility for residency. The agency may
charge a fee commensurate with the cost of printing and postage to other interested parties requesting a copy of this
list. This information may be provided electronically or through the agency’s Internet site.
History.—ss. 12, 21, ch. 80-198; s. 254, ch. 81-259; s. 2, ch. 81-318; ss. 49, 75, 79, 83, ch. 83-181; s. 53, ch. 83-
218; s. 17, ch. 89-294; s. 12, ch. 91-263; ss. 14, 38, 39, ch. 93-216; s. 13, ch. 98-80; s. 2, ch. 99-179; s. 19, ch. 2000-
263; s. 142, ch. 2000-349; s. 62, ch. 2000-367; s. 35, ch. 2001-45; s. 21, ch. 2003-57; ss. 2, 43, ch. 2006-197; s. 41,
ch. 2006-227; s. 150, ch. 2007-230; s. 62, ch. 2009-223; s. 246, ch. 2014-19; s. 35, ch. 2015-31; s. 10, ch. 2015-126;
s. 83, ch. 2018-24.
Note.—Former s. 400.419.
429.195 Rebates prohibited; penalties.—
(1) An assisted living facility licensed under this part may not contract or promise to pay or receive any
commission, bonus, kickback, or rebate or engage in any split-fee arrangement in any form whatsoever with any
person, health care provider, or health care facility as provided under s. 817.505.
(2) This section does not apply to:
(a) An individual employed by the assisted living facility, or with whom the facility contracts to provide
marketing services for the facility, if the individual clearly indicates that he or she works with or for the facility.
(b) Payments by an assisted living facility to a referral service that provides information, consultation, or
referrals to consumers to assist them in finding appropriate care or housing options for seniors or disabled adults if
the referred consumers are not Medicaid recipients.
(c) A resident of an assisted living facility who refers a friend, family members, or other individuals with whom
the resident has a personal relationship to the assisted living facility, in which case the assisted living facility may
provide a monetary reward to the resident for making such referral.
(3) A violation of this section is patient brokering and is punishable as provided in s. 817.505.
History.—ss. 18, 25, ch. 89-294; s. 13, ch. 91-263; ss. 15, 38, 39, ch. 93-216; s. 773, ch. 95-148; s. 12, ch. 95-
210; s. 14, ch. 98-80; s. 2, ch. 2006-197; s. 29, ch. 2012-160.
Note.—Former s. 400.4195.
429.20 Certain solicitation prohibited; third-party supplementation.—
(1) A person may not, in connection with the solicitation of contributions by or on behalf of an assisted living
facility or facilities, misrepresent or mislead any person, by any manner, means, practice, or device whatsoever, to
believe that the receipts of such solicitation will be used for charitable purposes, if that is not the fact.
(2) Solicitation of contributions of any kind in a threatening, coercive, or unduly forceful manner by or on
behalf of an assisted living facility or facilities by any agent, employee, owner, or representative of any assisted

5 – 21
living facility or facilities is grounds for denial, suspension, or revocation of the license of the assisted living facility
or facilities by or on behalf of which such contributions were solicited.
(3) The admission or maintenance of assisted living facility residents whose care is supported, in whole or in
part, by state funds may not be conditioned upon the receipt of any manner of contribution or donation from any
person. The solicitation or receipt of contributions in violation of this subsection is grounds for denial, suspension,
or revocation of license, as provided in s. 429.14, for any assisted living facility by or on behalf of which such
contributions were solicited.
(4) An assisted living facility may accept additional supplementation from third parties on behalf of residents
receiving optional state supplementation in accordance with s. 409.212.
History.—ss. 50, 83, ch. 83-181; ss. 16, 38, 39, ch. 93-216; s. 13, ch. 95-210; ss. 2, 44, ch. 2006-197.
Note.—Former s. 400.42.
429.22 Receivership proceedings.—
(1) As an alternative to or in conjunction with an injunctive proceeding, the agency may petition a court of
competent jurisdiction for the appointment of a receiver, if suitable alternate placements are not available, when any
of the following conditions exist:
(a) The facility is operating without a license and refuses to make application for a license as required by ss.
429.07 and 429.08.
(b) The facility is closing or has informed the agency that it intends to close and adequate arrangements have
not been made for relocation of the residents within 7 days, exclusive of weekends and holidays, of the closing of
the facility.
(c) The agency determines there exist in the facility conditions which present an imminent danger to the health,
safety, or welfare of the residents of the facility or a substantial probability that death or serious physical harm
would result therefrom.
(d) The facility cannot meet its financial obligation for providing food, shelter, care, and utilities.
(2) Petitions for receivership shall take precedence over other court business unless the court determines that
some other pending proceeding, having similar statutory precedence, shall have priority. A hearing shall be
conducted within 5 days of the filing of the petition, at which time all interested parties shall have the opportunity to
present evidence pertaining to the petition. The agency shall notify, by certified mail, the owner or administrator of
the facility named in the petition and the facility resident or, if applicable, the resident’s representative or designee,
or the resident’s surrogate, guardian, or attorney in fact, of its filing, the substance of the violation, and the date and
place set for the hearing. The court shall grant the petition only upon finding that the health, safety, or welfare of
facility residents would be threatened if a condition existing at the time the petition was filed is permitted to
continue. A receiver shall not be appointed ex parte unless the court determines that one or more of the conditions in
subsection (1) exist; that the facility owner or administrator cannot be found; that all reasonable means of locating
the owner or administrator and notifying him or her of the petition and hearing have been exhausted; or that the
owner or administrator after notification of the hearing chooses not to attend. After such findings, the court may
appoint any qualified person as a receiver, except it may not appoint any owner or affiliate of the facility which is in
receivership. The receiver may be selected from a list of persons qualified to act as receivers developed by the

5 – 22
agency and presented to the court with each petition for receivership. Under no circumstances may the agency or
designated agency employee be appointed as a receiver for more than 60 days; however, the receiver may petition
the court, one time only, for a 30-day extension. The court shall grant the extension upon a showing of good cause.
(3) The receiver must make provisions for the continued health, safety, and welfare of all residents of the
facility and:
(a) Shall exercise those powers and perform those duties set out by the court.
(b) Shall operate the facility in such a manner as to assure safety and adequate health care for the residents.
(c) Shall take such action as is reasonably necessary to protect or conserve the assets or property of the facility
for which the receiver is appointed, or the proceeds from any transfer thereof, and may use them only in the
performance of the powers and duties set forth in this section and by order of the court.
(d) May use the building, fixtures, furnishings, and any accompanying consumable goods in the provision of
care and services to residents and to any other persons receiving services from the facility at the time the petition for
receivership was filed. The receiver shall collect payments for all goods and services provided to residents or others
during the period of the receivership at the same rate of payment charged by the owners at the time the petition for
receivership was filed, or at a fair and reasonable rate otherwise approved by the court.
(e) May correct or eliminate any deficiency in the structure or furnishings of the facility which endangers the
safety or health of residents while they remain in the facility, if the total cost of correction does not exceed $10,000.
The court may order expenditures for this purpose in excess of $10,000 on application from the receiver after notice
to the owner and a hearing.
(f) May let contracts and hire agents and employees to carry out the powers and duties of the receiver.
(g) Shall honor all leases, mortgages, and secured transactions governing the building in which the facility is
located and all goods and fixtures in the building of which the receiver has taken possession, but only to the extent
of payments which, in the case of a rental agreement, are for the use of the property during the period of the
receivership, or which, in the case of a purchase agreement, become due during the period of the receivership.
(h) Shall have full power to direct and manage and to discharge employees of the facility, subject to any
contract rights they may have. The receiver shall pay employees at the rate of compensation, including benefits,
approved by the court. A receivership does not relieve the owner of any obligation to employees made prior to the
appointment of a receiver and not carried out by the receiver.
(i) Shall be entitled to and take possession of all property or assets of residents which are in the possession of a
facility or its owner. The receiver shall preserve all property, assets, and records of residents of which the receiver
takes possession and shall provide for the prompt transfer of the property, assets, and records to the new placement
of any transferred resident. An inventory list certified by the owner and receiver shall be made immediately at the
time the receiver takes possession of the facility.
(4)(a) A person who is served with notice of an order of the court appointing a receiver and of the receiver’s
name and address shall be liable to pay the receiver for any goods or services provided by the receiver after the date
of the order if the person would have been liable for the goods or services as supplied by the owner. The receiver
shall give a receipt for each payment and shall keep a copy of each receipt on file. The receiver shall deposit
accounts received in a separate account and shall use this account for all disbursements.

5 – 23
(b) The receiver may bring an action to enforce the liability created by paragraph (a).
(c) A payment to the receiver of any sum owing to the facility or its owner shall discharge any obligation to the
facility to the extent of the payment.
(5)(a) A receiver may petition the court that he or she not be required to honor any lease, mortgage, secured
transaction, or other wholly or partially executory contract entered into by the owner of the facility if the rent, price,
or rate of interest required to be paid under the agreement was substantially in excess of a reasonable rent, price, or
rate of interest at the time the contract was entered into, or if any material provision of the agreement was
unreasonable, when compared to contracts negotiated under similar conditions. Any relief in this form provided by
the court shall be limited to the life of the receivership, unless otherwise determined by the court.
(b) If the receiver is in possession of real estate or goods subject to a lease, mortgage, or security interest which
the receiver has obtained a court order to avoid under paragraph (a), and if the real estate or goods are necessary for
the continued operation of the facility under this section, the receiver may apply to the court to set a reasonable
rental, price, or rate of interest to be paid by the receiver during the duration of the receivership. The court shall hold
a hearing on the application within 15 days. The receiver shall send notice of the application to any known persons
who own the property involved at least 10 days prior to the hearing. Payment by the receiver of the amount
determined by the court to be reasonable is a defense to any action against the receiver for payment or for possession
of the goods or real estate subject to the lease, security interest, or mortgage involved by any person who received
such notice, but the payment does not relieve the owner of the facility of any liability for the difference between the
amount paid by the receiver and the amount due under the original lease, security interest, or mortgage involved.
(6) The court shall set the compensation of the receiver, which will be considered a necessary expense of a
receivership.
(7) A receiver may be held liable in a personal capacity only for the receiver’s own gross negligence,
intentional acts, or breach of fiduciary duty.
(8) The court may require a receiver to post a bond.
(9) The court may direct the agency to allocate funds from the Health Care Trust Fund to the receiver, subject
to the provisions of s. 429.18.
(10) The court may terminate a receivership when:
(a) The court determines that the receivership is no longer necessary because the conditions which gave rise to
the receivership no longer exist or the agency grants the facility a new license; or
(b) All of the residents in the facility have been transferred or discharged.
(11) Within 30 days after termination, the receiver shall give the court a complete accounting of all property of
which the receiver has taken possession, of all funds collected, and of the expenses of the receivership.
(12) Nothing in this section shall be deemed to relieve any owner, administrator, or employee of a facility
placed in receivership of any civil or criminal liability incurred, or any duty imposed by law, by reason of acts or
omissions of the owner, administrator, or employee prior to the appointment of a receiver; nor shall anything
contained in this section be construed to suspend during the receivership any obligation of the owner, administrator,
or employee for payment of taxes or other operating and maintenance expenses of the facility or of the owner,

5 – 24
administrator, employee, or any other person for the payment of mortgages or liens. The owner shall retain the right
to sell or mortgage any facility under receivership, subject to approval of the court which ordered the receivership.
History.—ss. 12, 22, ch. 80-198; s. 255, ch. 81-259; s. 2, ch. 81-318; ss. 51, 75, 79, 83, ch. 83-181; s. 53, ch. 83-
218; s. 14, ch. 91-263; ss. 18, 38, 39, ch. 93-216; s. 774, ch. 95-148; s. 15, ch. 98-80; ss. 2, 45, ch. 2006-197; s. 152,
ch. 2007-230.
Note.—Former s. 400.422.
429.23 Internal risk management and quality assurance program; adverse incidents and reporting
requirements.—
(1) Every facility licensed under this part may, as part of its administrative functions, voluntarily establish a risk
management and quality assurance program, the purpose of which is to assess resident care practices, facility
incident reports, deficiencies cited by the agency, adverse incident reports, and resident grievances and develop
plans of action to correct and respond quickly to identify quality differences.
(2) Every facility licensed under this part is required to maintain adverse incident reports. For purposes of this
section, the term, “adverse incident” means:
(a) An event over which facility personnel could exercise control rather than as a result of the resident’s
condition and results in:
1. Death;
2. Brain or spinal damage;
3. Permanent disfigurement;
4. Fracture or dislocation of bones or joints;
5. Any condition that required medical attention to which the resident has not given his or her consent,
including failure to honor advanced directives;
6. Any condition that requires the transfer of the resident from the facility to a unit providing more acute care
due to the incident rather than the resident’s condition before the incident; or
7. An event that is reported to law enforcement or its personnel for investigation; or
(b) Resident elopement, if the elopement places the resident at risk of harm or injury.
(3) Licensed facilities shall provide within 1 business day after the occurrence of an adverse incident, by
electronic mail, facsimile, or United States mail, a preliminary report to the agency on all adverse incidents specified
under this section. The report must include information regarding the identity of the affected resident, the type of
adverse incident, and the status of the facility’s investigation of the incident.
(4) Licensed facilities shall provide within 15 days, by electronic mail, facsimile, or United States mail, a full
report to the agency on all adverse incidents specified in this section. The report must include the results of the
facility’s investigation into the adverse incident.
(5) Each facility shall report monthly to the agency any liability claim filed against it. The report must include
the name of the resident, the dates of the incident leading to the claim, if applicable, and the type of injury or
violation of rights alleged to have occurred. This report is not discoverable in any civil or administrative action,
except in such actions brought by the agency to enforce the provisions of this part.

5 – 25
(6) Abuse, neglect, or exploitation must be reported to the Department of Children and Families as required
under chapter 415.
(7) The information reported to the agency pursuant to subsection (3) which relates to persons licensed under
chapter 458, chapter 459, chapter 461, chapter 464, or chapter 465 shall be reviewed by the agency. The agency
shall determine whether any of the incidents potentially involved conduct by a health care professional who is
subject to disciplinary action, in which case the provisions of s. 456.073 apply. The agency may investigate, as it
deems appropriate, any such incident and prescribe measures that must or may be taken in response to the incident.
The agency shall review each incident and determine whether it potentially involved conduct by a health care
professional who is subject to disciplinary action, in which case the provisions of s. 456.073 apply.
(8) If the agency, through its receipt of the adverse incident reports prescribed in this part or through any
investigation, has reasonable belief that conduct by a staff member or employee of a licensed facility is grounds for
disciplinary action by the appropriate board, the agency shall report this fact to such regulatory board.
(9) The adverse incident reports and preliminary adverse incident reports required under this section are
confidential as provided by law and are not discoverable or admissible in any civil or administrative action, except
in disciplinary proceedings by the agency or appropriate regulatory board.
(10) The agency may adopt rules necessary to administer this section.
History.—s. 36, ch. 2001-45; s. 2, ch. 2006-197; s. 63, ch. 2009-223; s. 247, ch. 2014-19; s. 10, ch. 2019-11.
Note.—Former s. 400.423.
429.24 Contracts.—
(1) The presence of each resident in a facility shall be covered by a contract, executed at the time of admission
or prior thereto, between the licensee and the resident or his or her designee or legal representative. Each party to the
contract shall be provided with a duplicate original thereof, and the licensee shall keep on file in the facility all such
contracts. The licensee may not destroy or otherwise dispose of any such contract until 5 years after its expiration.
(2) Each contract must contain express provisions specifically setting forth the services and accommodations to
be provided by the facility; the rates or charges; provision for at least 30 days’ written notice of a rate increase; the
rights, duties, and obligations of the residents, other than those specified in s. 429.28; and other matters that the
parties deem appropriate. A new service or accommodation added to, or implemented in, a resident’s contract for
which the resident was not previously charged does not require a 30-day written notice of a rate increase. Whenever
money is deposited or advanced by a resident in a contract as security for performance of the contract agreement or
as advance rent for other than the next immediate rental period:
(a) Such funds shall be deposited in a banking institution in this state that is located, if possible, in the same
community in which the facility is located; shall be kept separate from the funds and property of the facility; may
not be represented as part of the assets of the facility on financial statements; and shall be used, or otherwise
expended, only for the account of the resident.
(b) The licensee shall, within 30 days of receipt of advance rent or a security deposit, notify the resident or
residents in writing of the manner in which the licensee is holding the advance rent or security deposit and state the

5 – 26
name and address of the depository where the moneys are being held. The licensee shall notify residents of the
facility’s policy on advance deposits.
(3)(a) The contract shall include a refund policy to be implemented at the time of a resident’s transfer,
discharge, or death. The refund policy shall provide that the resident or responsible party is entitled to a prorated
refund based on the daily rate for any unused portion of payment beyond the termination date after all charges,
including the cost of damages to the residential unit resulting from circumstances other than normal use, have been
paid to the licensee. For the purpose of this paragraph, the termination date shall be the date the unit is vacated by
the resident and cleared of all personal belongings. If the amount of belongings does not preclude renting the unit,
the facility may clear the unit and charge the resident or his or her estate for moving and storing the items at a rate
equal to the actual cost to the facility, not to exceed 20 percent of the regular rate for the unit, provided that 14 days’
advance written notification is given. If the resident’s possessions are not claimed within 45 days after notification,
the facility may dispose of them. The contract shall also specify any other conditions under which claims will be
made against the refund due the resident. Except in the case of death or a discharge due to medical reasons, the
refunds shall be computed in accordance with the notice of relocation requirements specified in the contract.
However, a resident may not be required to provide the licensee with more than 30 days’ notice of termination. If
after a contract is terminated, the facility intends to make a claim against a refund due the resident, the facility shall
notify the resident or responsible party in writing of the claim and shall provide said party with a reasonable time
period of no less than 14 calendar days to respond. The facility shall provide a refund to the resident or responsible
party within 45 days after the transfer, discharge, or death of the resident. The agency shall impose a fine upon a
facility that fails to comply with the refund provisions of the paragraph, which fine shall be equal to three times the
amount due to the resident. One-half of the fine shall be remitted to the resident or his or her estate, and the other
half to the Health Care Trust Fund to be used for the purpose specified in s. 429.18.
(b) If a licensee agrees to reserve a bed for a resident who is admitted to a medical facility, including, but not
limited to, a nursing home, health care facility, or psychiatric facility, the resident or his or her responsible party
shall notify the licensee of any change in status that would prevent the resident from returning to the facility. Until
such notice is received, the agreed-upon daily rate may be charged by the licensee.
(c) The purpose of any advance payment and a refund policy for such payment, including any advance payment
for housing, meals, or personal services, shall be covered in the contract.
(4) The contract shall state whether or not the facility is affiliated with any religious organization and, if so,
which organization and its general responsibility to the facility.
(5) Neither the contract nor any provision thereof relieves any licensee of any requirement or obligation
imposed upon it by this part or rules adopted under this part.
(6) In lieu of the provisions of this section, facilities certified under chapter 651 shall comply with the
requirements of s. 651.055.
(7) Notwithstanding the provisions of this section, facilities which consist of 60 or more apartments may
require refund policies and termination notices in accordance with the provisions of part II of chapter 83, provided
that the lease is terminated automatically without financial penalty in the event of a resident’s death or relocation
due to psychiatric hospitalization or to medical reasons which necessitate services or care beyond which the facility

5 – 27
is licensed to provide. The date of termination in such instances shall be the date the unit is fully vacated. A lease
may be substituted for the contract if it meets the disclosure requirements of this section. For the purpose of this
section, the term “apartment” means a room or set of rooms with a kitchen or kitchenette and lavatory located within
one or more buildings containing other similar or like residential units.
(8) The agency may by rule clarify terms, establish procedures, clarify refund policies and contract provisions,
and specify documentation as necessary to administer this section.
History.—s. 11, ch. 75-233; ss. 12, 23, ch. 80-198; s. 2, ch. 81-318; ss. 52, 79, 83, ch. 83-181; s. 10, ch. 87-371;
s. 1, ch. 88-364; s. 15, ch. 91-263; ss. 19, 38, 39, ch. 93-216; s. 775, ch. 95-148; s. 2, ch. 98-148; ss. 2, 46, ch. 2006-
197; s. 84, ch. 2018-24; s. 11, ch. 2019-11.
Note.—Former s. 400.424.
429.255 Use of personnel; emergency care.—
(1)(a) Persons under contract to the facility, facility staff, or volunteers, who are licensed according to part I of
chapter 464, or those persons exempt under s. 464.022(1), and others as defined by rule, may administer medications
to residents, take residents’ vital signs, manage individual weekly pill organizers for residents who self-administer
medication, give prepackaged enemas ordered by a physician, observe residents, document observations on the
appropriate resident’s record, report observations to the resident’s physician, and contract or allow residents or a
resident’s representative, designee, surrogate, guardian, or attorney in fact to contract with a third party, provided
residents meet the criteria for appropriate placement as defined in s. 429.26. Nursing assistants certified pursuant to
part II of chapter 464 may take residents’ vital signs as directed by a licensed nurse or physician.
(b) All staff in facilities licensed under this part shall exercise their professional responsibility to observe
residents, to document observations on the appropriate resident’s record, and to report the observations to the
resident’s physician. However, the owner or administrator of the facility shall be responsible for determining that the
resident receiving services is appropriate for residence in the facility.
(c) In an emergency situation, licensed personnel may carry out their professional duties pursuant to part I of
chapter 464 until emergency medical personnel assume responsibility for care.
(2) In facilities licensed to provide extended congregate care, persons under contract to the facility, facility
staff, or volunteers, who are licensed according to part I of chapter 464, or those persons exempt under s.
464.022(1), or those persons certified as nursing assistants pursuant to part II of chapter 464, may also perform all
duties within the scope of their license or certification, as approved by the facility administrator and pursuant to this
part.
(3)(a) An assisted living facility licensed under this part with 17 or more beds shall have on the premises at all
times a functioning automated external defibrillator as defined in s. 768.1325(2)(b).
(b) The facility is encouraged to register the location of each automated external defibrillator with a local
emergency medical services medical director.
(c) The provisions of ss. 768.13 and 768.1325 apply to automated external defibrillators within the facility.
(4) Facility staff may withhold or withdraw cardiopulmonary resuscitation or the use of an automated external
defibrillator if presented with an order not to resuscitate executed pursuant to s. 401.45. The agency shall adopt rules
providing for the implementation of such orders. Facility staff and facilities may not be subject to criminal

5 – 28
prosecution or civil liability, nor be considered to have engaged in negligent or unprofessional conduct, for
withholding or withdrawing cardiopulmonary resuscitation or use of an automated external defibrillator pursuant to
such an order and rules adopted by the agency. The absence of an order to resuscitate executed pursuant to s. 401.45
does not preclude a physician from withholding or withdrawing cardiopulmonary resuscitation or use of an
automated external defibrillator as otherwise permitted by law.
(5) The agency may adopt rules to implement the provisions of this section relating to use of an automated
external defibrillator.
History.—ss. 16, 38, ch. 91-263; ss. 20, 38, 39, ch. 93-216; s. 4, ch. 99-331; s. 3, ch. 2000-295; s. 100, ch. 2000-
318; ss. 2, 47, ch. 2006-197; s. 1, ch. 2010-200; s. 12, ch. 2019-11.
Note.—Former s. 400.4255.
429.256 Assistance with self-administration of medication.—
(1) For the purposes of this section, the term:
(a) “Informed consent” means advising the resident, or the resident’s surrogate, guardian, or attorney in fact,
that an assisted living facility is not required to have a licensed nurse on staff, that the resident may be receiving
assistance with self-administration of medication from an unlicensed person, and that such assistance, if provided by
an unlicensed person, will or will not be overseen by a licensed nurse.
(b) “Unlicensed person” means an individual not currently licensed to practice nursing or medicine who is
employed by or under contract to an assisted living facility and who has received training with respect to assisting
with the self-administration of medication in an assisted living facility as provided under s. 429.52 prior to providing
such assistance as described in this section.
(2) Residents who are capable of self-administering their own medications without assistance shall be
encouraged and allowed to do so. However, an unlicensed person may, consistent with a dispensed prescription’s
label or the package directions of an over-the-counter medication, assist a resident whose condition is medically
stable with the self-administration of routine, regularly scheduled medications that are intended to be self-
administered. Assistance with self-medication by an unlicensed person may occur only upon a documented request
by, and the written informed consent of, a resident or the resident’s surrogate, guardian, or attorney in fact. For the
purposes of this section, self-administered medications include both legend and over-the-counter oral dosage forms,
topical dosage forms and topical ophthalmic, otic, and nasal dosage forms including solutions, suspensions, sprays,
and inhalers.
(3) Assistance with self-administration of medication includes:
(a) Taking the medication, in its previously dispensed, properly labeled container, including an insulin syringe
that is prefilled with the proper dosage by a pharmacist and an insulin pen that is prefilled by the manufacturer, from
where it is stored, and bringing it to the resident.
(b) In the presence of the resident, reading the label, opening the container, removing a prescribed amount of
medication from the container, and closing the container.
(c) Placing an oral dosage in the resident’s hand or placing the dosage in another container and helping the
resident by lifting the container to his or her mouth.
(d) Applying topical medications.

5 – 29
(e) Returning the medication container to proper storage.
(f) Keeping a record of when a resident receives assistance with self-administration under this section.
(g) Assisting with the use of a nebulizer, including removing the cap of a nebulizer, opening the unit dose of
nebulizer solution, and pouring the prescribed premeasured dose of medication into the dispensing cup of the
nebulizer.
(h) Using a glucometer to perform blood-glucose level checks.
(i) Assisting with putting on and taking off antiembolism stockings.
(j) Assisting with applying and removing an oxygen cannula but not with titrating the prescribed oxygen
settings.
(k) Assisting with the use of a continuous positive airway pressure device but not with titrating the prescribed
setting of the device.
(l) Assisting with measuring vital signs.
(m) Assisting with colostomy bags.
(4) Assistance with self-administration does not include:
(a) Mixing, compounding, converting, or calculating medication doses, except for measuring a prescribed
amount of liquid medication or breaking a scored tablet or crushing a tablet as prescribed.
(b) The preparation of syringes for injection or the administration of medications by any injectable route.
(c) Administration of medications by way of a tube inserted in a cavity of the body.
(d) Administration of parenteral preparations.
(e) Irrigations or debriding agents used in the treatment of a skin condition.
(f) Rectal, urethral, or vaginal preparations.
(g) Medications ordered by the physician or health care professional with prescriptive authority to be given “as
needed,” unless the order is written with specific parameters that preclude independent judgment on the part of the
unlicensed person, and at the request of a competent resident.
(h) Medications for which the time of administration, the amount, the strength of dosage, the method of
administration, or the reason for administration requires judgment or discretion on the part of the unlicensed person.
(5) Assistance with the self-administration of medication by an unlicensed person as described in this section
shall not be considered administration as defined in s. 465.003.
(6) The agency may by rule establish facility procedures and interpret terms as necessary to implement this
section.
History.—s. 16, ch. 98-80; s. 214, ch. 99-13; ss. 2, 48, ch. 2006-197; s. 11, ch. 2015-126; s. 13, ch. 2019-11.
Note.—Former s. 400.4256.
429.26 Appropriateness of placements; examinations of residents.—
(1) The owner or administrator of a facility is responsible for determining the appropriateness of admission of
an individual to the facility and for determining the continued appropriateness of residence of an individual in the
facility. A determination shall be based upon an assessment of the strengths, needs, and preferences of the resident,
the care and services offered or arranged for by the facility in accordance with facility policy, and any limitations in
law or rule related to admission criteria or continued residency for the type of license held by the facility under this

5 – 30
part. A resident may not be moved from one facility to another without consultation with and agreement from the
resident or, if applicable, the resident’s representative or designee or the resident’s family, guardian, surrogate, or
attorney in fact. In the case of a resident who has been placed by the department or the Department of Children and
Families, the administrator must notify the appropriate contact person in the applicable department.
(2) A physician, physician assistant, or nurse practitioner who is employed by an assisted living facility to
provide an initial examination for admission purposes may not have financial interest in the facility.
(3) Persons licensed under part I of chapter 464 who are employed by or under contract with a facility shall, on
a routine basis or at least monthly, perform a nursing assessment of the residents for whom they are providing
nursing services ordered by a physician, except administration of medication, and shall document such assessment,
including any substantial changes in a resident’s status which may necessitate relocation to a nursing home, hospital,
or specialized health care facility. Such records shall be maintained in the facility for inspection by the agency and
shall be forwarded to the resident’s case manager, if applicable.
(4) If possible, each resident shall have been examined by a licensed physician, a licensed physician assistant,
or a licensed nurse practitioner within 60 days before admission to the facility. The signed and completed medical
examination report shall be submitted to the owner or administrator of the facility who shall use the information
contained therein to assist in the determination of the appropriateness of the resident’s admission and continued stay
in the facility. The medical examination report shall become a permanent part of the record of the resident at the
facility and shall be made available to the agency during inspection or upon request. An assessment that has been
completed through the Comprehensive Assessment and Review for Long-Term Care Services (CARES) Program
fulfills the requirements for a medical examination under this subsection and s. 429.07(3)(b)6.
(5) Except as provided in s. 429.07, if a medical examination has not been completed within 60 days before the
admission of the resident to the facility, a licensed physician, licensed physician assistant, or licensed nurse
practitioner shall examine the resident and complete a medical examination form provided by the agency within 30
days following the admission to the facility to enable the facility owner or administrator to determine the
appropriateness of the admission. The medical examination form shall become a permanent part of the record of the
resident at the facility and shall be made available to the agency during inspection by the agency or upon request.
(6) Any resident accepted in a facility and placed by the department or the Department of Children and
Families shall have been examined by medical personnel within 30 days before placement in the facility. The
examination shall include an assessment of the appropriateness of placement in a facility. The findings of this
examination shall be recorded on the examination form provided by the agency. The completed form shall
accompany the resident and shall be submitted to the facility owner or administrator. Additionally, in the case of a
mental health resident, the Department of Children and Families must provide documentation that the individual has
been assessed by a psychiatrist, clinical psychologist, clinical social worker, or psychiatric nurse, or an individual
who is supervised by one of these professionals, and determined to be appropriate to reside in an assisted living
facility. The documentation must be in the facility within 30 days after the mental health resident has been admitted
to the facility. An evaluation completed upon discharge from a state mental hospital meets the requirements of this
subsection related to appropriateness for placement as a mental health resident providing it was completed within 90
days prior to admission to the facility. The applicable department shall provide to the facility administrator any

5 – 31
information about the resident that would help the administrator meet his or her responsibilities under subsection (1).
Further, department personnel shall explain to the facility operator any special needs of the resident and advise the
operator whom to call should problems arise. The applicable department shall advise and assist the facility
administrator where the special needs of residents who are recipients of optional state supplementation require such
assistance.
(7) The facility must notify a licensed physician when a resident exhibits signs of dementia or cognitive
impairment or has a change of condition in order to rule out the presence of an underlying physiological condition
that may be contributing to such dementia or impairment. The notification must occur within 30 days after the
acknowledgment of such signs by facility staff. If an underlying condition is determined to exist, the facility shall
arrange, with the appropriate health care provider, the necessary care and services to treat the condition.
(8) The Department of Children and Families may require an examination for supplemental security income
and optional state supplementation recipients residing in facilities at any time and shall provide the examination
whenever a resident’s condition requires it. Any facility administrator; personnel of the agency, the department, or
the Department of Children and Families; or a representative of the State Long-Term Care Ombudsman Program
who believes a resident needs to be evaluated shall notify the resident’s case manager, who shall take appropriate
action. A report of the examination findings shall be provided to the resident’s case manager and the facility
administrator to help the administrator meet his or her responsibilities under subsection (1).
(9) A terminally ill resident who no longer meets the criteria for continued residency may remain in the facility
if the arrangement is mutually agreeable to the resident and the facility; additional care is rendered through a
licensed hospice, and the resident is under the care of a physician who agrees that the physical needs of the resident
are being met.
(10) Facilities licensed to provide extended congregate care services shall promote aging in place by
determining appropriateness of continued residency based on a comprehensive review of the resident’s physical and
functional status; the ability of the facility, family members, friends, or any other pertinent individuals or agencies to
provide the care and services required; and documentation that a written service plan consistent with facility policy
has been developed and implemented to ensure that the resident’s needs and preferences are addressed.
(11) No resident who requires 24-hour nursing supervision, except for a resident who is an enrolled hospice
patient pursuant to part IV of chapter 400, shall be retained in a facility licensed under this part.
History.—ss. 12, 30, ch. 80-198; s. 2, ch. 81-318; ss. 53, 75, 79, 83, ch. 83-181; s. 53, ch. 83-218; s. 6, ch. 85-
145; s. 11, ch. 87-371; s. 19, ch. 89-294; s. 17, ch. 91-263; ss. 21, 38, 39, ch. 93-216; s. 776, ch. 95-148; s. 15, ch.
95-210; ss. 25, 49, ch. 95-418; s. 39, ch. 96-169; s. 5, ch. 97-82; s. 215, ch. 99-13; s. 101, ch. 2000-318; s. 75, ch.
2000-349; s. 37, ch. 2001-45; s. 61, ch. 2002-1; ss. 2, 49, ch. 2006-197; s. 153, ch. 2007-230; s. 64, ch. 2009-223; s.
248, ch. 2014-19; s. 36, ch. 2015-31.
Note.—Former s. 400.426.
429.27 Property and personal affairs of residents.—
(1)(a) A resident shall be given the option of using his or her own belongings, as space permits; choosing his or
her roommate; and, whenever possible, unless the resident is adjudicated incompetent or incapacitated under state
law, managing his or her own affairs.

5 – 32
(b) The admission of a resident to a facility and his or her presence therein shall not confer on the facility or its
owner, administrator, employees, or representatives any authority to manage, use, or dispose of any property of the
resident; nor shall such admission or presence confer on any of such persons any authority or responsibility for the
personal affairs of the resident, except that which may be necessary for the safe management of the facility or for the
safety of the resident.
(2) A facility, or an owner, administrator, employee, or representative thereof, may not act as the guardian,
trustee, or conservator for any resident of the assisted living facility or any of such resident’s property. An owner,
administrator, or staff member, or representative thereof, may not act as a competent resident’s payee for social
security, veteran’s, or railroad benefits without the consent of the resident. Any facility whose owner, administrator,
or staff, or representative thereof, serves as representative payee for any resident of the facility shall file a surety
bond with the agency in an amount equal to twice the average monthly aggregate income or personal funds due to
residents, or expendable for their account, which are received by a facility. Any facility whose owner, administrator,
or staff, or a representative thereof, is granted power of attorney for any resident of the facility shall file a surety
bond with the agency for each resident for whom such power of attorney is granted. The surety bond shall be in an
amount equal to twice the average monthly income of the resident, plus the value of any resident’s property under
the control of the attorney in fact. The bond shall be executed by the facility as principal and a licensed surety
company. The bond shall be conditioned upon the faithful compliance of the facility with this section and shall run
to the agency for the benefit of any resident who suffers a financial loss as a result of the misuse or misappropriation
by a facility of funds held pursuant to this subsection. Any surety company that cancels or does not renew the bond
of any licensee shall notify the agency in writing not less than 30 days in advance of such action, giving the reason
for the cancellation or nonrenewal. Any facility owner, administrator, or staff, or representative thereof, who is
granted power of attorney for any resident of the facility shall, on a monthly basis, be required to provide the
resident a written statement of any transaction made on behalf of the resident pursuant to this subsection, and a copy
of such statement given to the resident shall be retained in each resident’s file and available for agency inspection.
(3) A facility, upon mutual consent with the resident, shall provide for the safekeeping in the facility of
personal effects not in excess of $500 and funds of the resident not in excess of $500 cash, and shall keep complete
and accurate records of all such funds and personal effects received. If a resident is absent from a facility for 24
hours or more, the facility may provide for the safekeeping of the resident’s personal effects in excess of $500.
(4) Any funds or other property belonging to or due to a resident, or expendable for his or her account, which is
received by a facility shall be trust funds which shall be kept separate from the funds and property of the facility and
other residents or shall be specifically credited to such resident. Such trust funds shall be used or otherwise
expended only for the account of the resident. At least once every 3 months, unless upon order of a court of
competent jurisdiction, the facility shall furnish the resident and his or her guardian, trustee, or conservator, if any, a
complete and verified statement of all funds and other property to which this subsection applies, detailing the
amount and items received, together with their sources and disposition. In any event, the facility shall furnish such
statement annually and upon the discharge or transfer of a resident. Any governmental agency or private charitable
agency contributing funds or other property to the account of a resident shall also be entitled to receive such
statement annually and upon the discharge or transfer of the resident.

5 – 33
(5) Any personal funds available to facility residents may be used by residents as they choose to obtain
clothing, personal items, leisure activities, and other supplies and services for their personal use. A facility may not
demand, require, or contract for payment of all or any part of the personal funds in satisfaction of the facility rate for
supplies and services beyond that amount agreed to in writing and may not levy an additional charge to the
individual or the account for any supplies or services that the facility has agreed by contract to provide as part of the
standard monthly rate. Any service or supplies provided by the facility which are charged separately to the
individual or the account may be provided only with the specific written consent of the individual, who shall be
furnished in advance of the provision of the services or supplies with an itemized written statement to be attached to
the contract setting forth the charges for the services or supplies.
(6)(a) In addition to any damages or civil penalties to which a person is subject, any person who:
1. Intentionally withholds a resident’s personal funds, personal property, or personal needs allowance, or who
demands, beneficially receives, or contracts for payment of all or any part of a resident’s personal property or
personal needs allowance in satisfaction of the facility rate for supplies and services; or
2. Borrows from or pledges any personal funds of a resident, other than the amount agreed to by written
contract under s. 429.24,
commits a misdemeanor of the first degree, punishable as provided in s. 775.082 or s. 775.083.
(b) Any facility owner, administrator, or staff, or representative thereof, who is granted power of attorney for
any resident of the facility and who misuses or misappropriates funds obtained through this power commits a felony
of the third degree, punishable as provided in s. 775.082, s. 775.083, or s. 775.084.
(7) In the event of the death of a resident, a licensee shall return all refunds, funds, and property held in trust to
the resident’s personal representative, if one has been appointed at the time the facility disburses such funds, and, if
not, to the resident’s spouse or adult next of kin named in a beneficiary designation form provided by the facility to
the resident. If the resident has no spouse or adult next of kin or such person cannot be located, funds due the
resident shall be placed in an interest-bearing account, and all property held in trust by the facility shall be
safeguarded until such time as the funds and property are disbursed pursuant to the Florida Probate Code. Such
funds shall be kept separate from the funds and property of the facility and other residents of the facility. If the funds
of the deceased resident are not disbursed pursuant to the Florida Probate Code within 2 years after the resident’s
death, the funds shall be deposited in the Health Care Trust Fund administered by the agency.
(8) The agency may by rule clarify terms and specify procedures and documentation necessary to administer
the provisions of this section relating to the proper management of residents’ funds and personal property and the
execution of surety bonds.
History.—s. 12, ch. 75-233; ss. 12, 24, ch. 80-198; s. 2, ch. 81-152; s. 2, ch. 81-318; ss. 4, 19, ch. 82-148; ss. 54,
79, 83, ch. 83-181; s. 3, ch. 86-104; s. 12, ch. 87-371; s. 72, ch. 91-224; s. 18, ch. 91-263; ss. 22, 38, 39, ch. 93-216;
s. 777, ch. 95-148; s. 3, ch. 98-148; s. 216, ch. 99-13; ss. 2, 50, ch. 2006-197; s. 12, ch. 2015-126; s. 14, ch. 2019-11.
Note.—Former s. 400.427.
429.275 Business practice; personnel records; liability insurance.—The assisted living facility shall be
administered on a sound financial basis that is consistent with good business practices.

5 – 34
(1) The administrator or owner of a facility shall maintain accurate business records that identify, summarize,
and classify funds received and expenses disbursed and shall use written accounting procedures and a recognized
accounting system.
(2) The administrator or owner of a facility shall maintain personnel records for each staff member which
contain, at a minimum, documentation of background screening, if applicable, documentation of compliance with all
training requirements of this part or applicable rule, and a copy of all licenses or certification held by each staff who
performs services for which licensure or certification is required under this part or rule.
(3) The administrator or owner of a facility shall maintain liability insurance coverage that is in force at all
times.
(4) The agency may by rule clarify terms, establish requirements for financial records, accounting procedures,
personnel procedures, insurance coverage, and reporting procedures, and specify documentation as necessary to
implement this section.
History.—s. 4, ch. 98-148; s. 2, ch. 2006-197; s. 15, ch. 2019-11.
Note.—Former s. 400.4275.
429.28 Resident bill of rights.—
(1) No resident of a facility shall be deprived of any civil or legal rights, benefits, or privileges guaranteed by
law, the Constitution of the State of Florida, or the Constitution of the United States as a resident of a facility. Every
resident of a facility shall have the right to:
(a) Live in a safe and decent living environment, free from abuse and neglect.
(b) Be treated with consideration and respect and with due recognition of personal dignity, individuality, and
the need for privacy.
(c) Retain and use his or her own clothes and other personal property in his or her immediate living quarters, so
as to maintain individuality and personal dignity, except when the facility can demonstrate that such would be
unsafe, impractical, or an infringement upon the rights of other residents.
(d) Unrestricted private communication, including receiving and sending unopened correspondence, access to a
telephone, and visiting with any person of his or her choice, at any time between the hours of 9 a.m. and 9 p.m. at a
minimum. Upon request, the facility shall make provisions to extend visiting hours for caregivers and out-of-town
guests, and in other similar situations.
(e) Freedom to participate in and benefit from community services and activities and to pursue the highest
possible level of independence, autonomy, and interaction within the community.
(f) Manage his or her financial affairs unless the resident or, if applicable, the resident’s representative,
designee, surrogate, guardian, or attorney in fact authorizes the administrator of the facility to provide safekeeping
for funds as provided in s. 429.27.
(g) Share a room with his or her spouse if both are residents of the facility.
(h) Reasonable opportunity for regular exercise several times a week and to be outdoors at regular and frequent
intervals except when prevented by inclement weather.
(i) Exercise civil and religious liberties, including the right to independent personal decisions. No religious
beliefs or practices, nor any attendance at religious services, shall be imposed upon any resident.

5 – 35
(j) Assistance with obtaining access to adequate and appropriate health care. For purposes of this paragraph, the
term “adequate and appropriate health care” means the management of medications, assistance in making
appointments for health care services, the provision of or arrangement of transportation to health care appointments,
and the performance of health care services in accordance with s. 429.255 which are consistent with established and
recognized standards within the community.
(k) At least 45 days’ notice of relocation or termination of residency from the facility unless, for medical
reasons, the resident is certified by a physician to require an emergency relocation to a facility providing a more
skilled level of care or the resident engages in a pattern of conduct that is harmful or offensive to other residents. In
the case of a resident who has been adjudicated mentally incapacitated, the guardian shall be given at least 45 days’
notice of a nonemergency relocation or residency termination. Reasons for relocation shall be set forth in writing. In
order for a facility to terminate the residency of an individual without notice as provided herein, the facility shall
show good cause in a court of competent jurisdiction.
(l) Present grievances and recommend changes in policies, procedures, and services to the staff of the facility,
governing officials, or any other person without restraint, interference, coercion, discrimination, or reprisal. Each
facility shall establish a grievance procedure to facilitate the residents’ exercise of this right. This right includes
access to ombudsman volunteers and advocates and the right to be a member of, to be active in, and to associate
with advocacy or special interest groups.
(2) The administrator of a facility shall ensure that a written notice of the rights, obligations, and prohibitions
set forth in this part is posted in a prominent place in each facility and read or explained to residents who cannot
read. The notice must include the statewide toll-free telephone number and e-mail address of the State Long-Term
Care Ombudsman Program and the telephone number of the local ombudsman council, the Elder Abuse Hotline
operated by the Department of Children and Families, and, if applicable, Disability Rights Florida, where complaints
may be lodged. The notice must state that a complaint made to the Office of State Long-Term Care Ombudsman or a
local long-term care ombudsman council, the names and identities of the residents involved in the complaint, and the
identity of complainants are kept confidential pursuant to s. 400.0077 and that retaliatory action cannot be taken
against a resident for presenting grievances or for exercising any other resident right. The facility must ensure a
resident’s access to a telephone to call the State Long-Term Care Ombudsman Program or local ombudsman
council, the Elder Abuse Hotline operated by the Department of Children and Families, and Disability Rights
Florida.
(3)(a) The agency shall conduct a survey to determine general compliance with facility standards and
compliance with residents’ rights as a prerequisite to initial licensure or licensure renewal. The agency shall adopt
rules for uniform standards and criteria that will be used to determine compliance with facility standards and
compliance with residents’ rights.
(b) In order to determine whether the facility is adequately protecting residents’ rights, the biennial survey shall
include private informal conversations with a sample of residents and consultation with the ombudsman council in
the district in which the facility is located to discuss residents’ experiences within the facility.
(4) The facility shall not hamper or prevent residents from exercising their rights as specified in this section.
5 – 36
(5) A facility or employee of a facility may not serve notice upon a resident to leave the premises or take any
other retaliatory action against any person who:
(a) Exercises any right set forth in this section.
(b) Appears as a witness in any hearing, inside or outside the facility.
(c) Files a civil action alleging a violation of the provisions of this part or notifies a state attorney or the
Attorney General of a possible violation of such provisions.
(6) A facility that terminates the residency of an individual who participated in activities specified in subsection
(5) must show good cause in a court of competent jurisdiction. If good cause is not shown, the agency shall impose a
fine of $2,500 in addition to any other penalty assessed against the facility.
(7) Any person who submits or reports a complaint concerning a suspected violation of the provisions of this
part or concerning services and conditions in facilities, or who testifies in any administrative or judicial proceeding
arising from such a complaint, shall have immunity from any civil or criminal liability therefor, unless such person
has acted in bad faith or with malicious purpose or the court finds that there was a complete absence of a justiciable
issue of either law or fact raised by the losing party.
History.—ss. 12, 31, ch. 80-198; s. 2, ch. 81-318; ss. 55, 75, 79, 83, ch. 83-181; s. 53, ch. 83-218; s. 65, ch. 91-
221; s. 19, ch. 91-263; ss. 23, 38, 39, ch. 93-216; s. 778, ch. 95-148; s. 11, ch. 95-418; s. 17, ch. 98-80; s. 20, ch.
2000-263; ss. 76, 143, ch. 2000-349; s. 63, ch. 2000-367; s. 38, ch. 2001-45; ss. 2, 51, ch. 2006-197; s. 37, ch. 2015-
31; s. 13, ch. 2015-126; s. 85, ch. 2018-24.
Note.—Former s. 400.428.
429.29 Civil actions to enforce rights.—
(1) Any person or resident whose rights as specified in this part are violated shall have a cause of action. The
action may be brought by the resident or his or her guardian, or by a person or organization acting on behalf of a
resident with the consent of the resident or his or her guardian, or by the personal representative of the estate of a
deceased resident regardless of the cause of death. If the action alleges a claim for the resident’s rights or for
negligence that caused the death of the resident, the claimant shall be required to elect either survival damages
pursuant to s. 46.021 or wrongful death damages pursuant to s. 768.21. If the action alleges a claim for the resident’s
rights or for negligence that did not cause the death of the resident, the personal representative of the estate may
recover damages for the negligence that caused injury to the resident. The action may be brought in any court of
competent jurisdiction to enforce such rights and to recover actual damages, and punitive damages for violation of
the rights of a resident or negligence. Any resident who prevails in seeking injunctive relief or a claim for an
administrative remedy is entitled to recover the costs of the action and a reasonable attorney’s fee assessed against
the defendant not to exceed $25,000. Fees shall be awarded solely for the injunctive or administrative relief and not
for any claim or action for damages whether such claim or action is brought together with a request for an injunction
or administrative relief or as a separate action, except as provided under s. 768.79 or the Florida Rules of Civil
Procedure. Sections 429.29-429.298 provide the exclusive remedy for a cause of action for recovery of damages for
the personal injury or death of a resident arising out of negligence or a violation of rights specified in s. 429.28. This
section does not preclude theories of recovery not arising out of negligence or s. 429.28 which are available to a
5 – 37
resident or to the agency. The provisions of chapter 766 do not apply to any cause of action brought under ss.
429.29-429.298.
(2) In any claim brought pursuant to this part alleging a violation of resident’s rights or negligence causing
injury to or the death of a resident, the claimant shall have the burden of proving, by a preponderance of the
evidence, that:
(a) The defendant owed a duty to the resident;
(b) The defendant breached the duty to the resident;
(c) The breach of the duty is a legal cause of loss, injury, death, or damage to the resident; and
(d) The resident sustained loss, injury, death, or damage as a result of the breach.
Nothing in this part shall be interpreted to create strict liability. A violation of the rights set forth in s. 429.28 or in any
other standard or guidelines specified in this part or in any applicable administrative standard or guidelines of this
state or a federal regulatory agency shall be evidence of negligence but shall not be considered negligence per se.
(3) In any claim brought pursuant to this section, a licensee, person, or entity shall have a duty to exercise
reasonable care. Reasonable care is that degree of care which a reasonably careful licensee, person, or entity would
use under like circumstances.
(4) In any claim for resident’s rights violation or negligence by a nurse licensed under part I of chapter 464,
such nurse shall have the duty to exercise care consistent with the prevailing professional standard of care for a
nurse. The prevailing professional standard of care for a nurse shall be that level of care, skill, and treatment which,
in light of all relevant surrounding circumstances, is recognized as acceptable and appropriate by reasonably prudent
similar nurses.
(5) Discovery of financial information for the purpose of determining the value of punitive damages may not be
had unless the plaintiff shows the court by proffer or evidence in the record that a reasonable basis exists to support
a claim for punitive damages.
(6) In addition to any other standards for punitive damages, any award of punitive damages must be reasonable
in light of the actual harm suffered by the resident and the egregiousness of the conduct that caused the actual harm
to the resident.
(7) The resident or the resident’s legal representative shall serve a copy of any complaint alleging in whole or in
part a violation of any rights specified in this part to the Agency for Health Care Administration at the time of filing
the initial complaint with the clerk of the court for the county in which the action is pursued. The requirement of
providing a copy of the complaint to the agency does not impair the resident’s legal rights or ability to seek relief for
his or her claim.
History.—ss. 12, 32, ch. 80-198; s. 2, ch. 81-318; ss. 56, 75, 79, 83, ch. 83-181; s. 53, ch. 83-218; ss. 24, 38, 39,
ch. 93-216; s. 779, ch. 95-148; s. 31, ch. 99-225; s. 39, ch. 2001-45; ss. 2, 52, ch. 2006-197.
Note.—Former s. 400.429.
429.293 Presuit notice; investigation; notification of violation of residents’ rights or alleged negligence;
claims evaluation procedure; informal discovery; review; settlement offer; mediation.—
(1) As used in this section, the term:

5 – 38
(a) “Claim for residents’ rights violation or negligence” means a negligence claim alleging injury to or the
death of a resident arising out of an asserted violation of the rights of a resident under s. 429.28 or an asserted
deviation from the applicable standard of care.
(b) “Insurer” means any self-insurer authorized under s. 627.357, liability insurance carrier, joint underwriting
association, or uninsured prospective defendant.
(2) Prior to filing a claim for a violation of a resident’s rights or a claim for negligence, a claimant alleging
injury to or the death of a resident shall notify each prospective defendant by certified mail, return receipt requested,
of an asserted violation of a resident’s rights provided in s. 429.28 or deviation from the standard of care. Such
notification shall include an identification of the rights the prospective defendant has violated and the negligence
alleged to have caused the incident or incidents and a brief description of the injuries sustained by the resident which
are reasonably identifiable at the time of notice. The notice shall contain a certificate of counsel that counsel’s
reasonable investigation gave rise to a good faith belief that grounds exist for an action against each prospective
defendant.
(3)(a) No suit may be filed for a period of 75 days after notice is mailed to any prospective defendant. During
the 75-day period, the prospective defendants or their insurers shall conduct an evaluation of the claim to determine
the liability of each defendant and to evaluate the damages of the claimants. Each defendant or insurer of the
defendant shall have a procedure for the prompt evaluation of claims during the 75-day period. The procedure shall
include one or more of the following:
1. Internal review by a duly qualified facility risk manager or claims adjuster;
2. Internal review by counsel for each prospective defendant;
3. A quality assurance committee authorized under any applicable state or federal statutes or regulations; or
4. Any other similar procedure that fairly and promptly evaluates the claims.
Each defendant or insurer of the defendant shall evaluate the claim in good faith.
(b) At or before the end of the 75 days, the defendant or insurer of the defendant shall provide the claimant with
a written response:
1. Rejecting the claim; or
2. Making a settlement offer.
(c) The response shall be delivered to the claimant if not represented by counsel or to the claimant’s attorney,
by certified mail, return receipt requested. Failure of the prospective defendant or insurer of the defendant to reply to
the notice within 75 days after receipt shall be deemed a rejection of the claim for purposes of this section.
(4) The notification of a violation of a resident’s rights or alleged negligence shall be served within the
applicable statute of limitations period; however, during the 75-day period, the statute of limitations is tolled as to all
prospective defendants. Upon stipulation by the parties, the 75-day period may be extended and the statute of
limitations is tolled during any such extension. Upon receiving written notice by certified mail, return receipt
requested, of termination of negotiations in an extended period, the claimant shall have 60 days or the remainder of
the period of the statute of limitations, whichever is greater, within which to file suit.
(5) No statement, discussion, written document, report, or other work product generated by presuit claims
evaluation procedures under this section is discoverable or admissible in any civil action for any purpose by the
5 – 39
opposing party. All participants, including, but not limited to, physicians, investigators, witnesses, and employees or
associates of the defendant, are immune from civil liability arising from participation in the presuit claims evaluation
procedure. Any licensed physician or registered nurse may be retained by either party to provide an opinion
regarding the reasonable basis of the claim. The presuit opinions of the expert are not discoverable or admissible in
any civil action for any purpose by the opposing party.
(6) Upon receipt by a prospective defendant of a notice of claim, the parties shall make discoverable
information available without formal discovery as provided in subsection (7).
(7) Informal discovery may be used by a party to obtain unsworn statements and the production of documents
or things, as follows:
(a) Unsworn statements.—Any party may require other parties to appear for the taking of an unsworn
statement. Such statements may be used only for the purpose of claims evaluation and are not discoverable or
admissible in any civil action for any purpose by any party. A party seeking to take the unsworn statement of any
party must give reasonable notice in writing to all parties. The notice must state the time and place for taking the
statement and the name and address of the party to be examined. Unless otherwise impractical, the examination of
any party must be done at the same time by all other parties. Any party may be represented by counsel at the taking
of an unsworn statement. An unsworn statement may be recorded electronically, stenographically, or on videotape.
The taking of unsworn statements is subject to the provisions of the Florida Rules of Civil Procedure and may be
terminated for abuses.
(b) Documents or things.—Any party may request discovery of relevant documents or things. The documents
or things must be produced, at the expense of the requesting party, within 20 days after the date of receipt of the
request. A party is required to produce relevant and discoverable documents or things within that party’s possession
or control, if in good faith it can reasonably be done within the timeframe of the claims evaluation process.
(8) Each request for and notice concerning informal discovery pursuant to this section must be in writing, and a
copy thereof must be sent to all parties. Such a request or notice must bear a certificate of service identifying the
name and address of the person to whom the request or notice is served, the date of the request or notice, and the
manner of service thereof.
(9) If a prospective defendant makes a written settlement offer, the claimant shall have 15 days from the date of
receipt to accept the offer. An offer shall be deemed rejected unless accepted by delivery of a written notice of
acceptance.
(10) To the extent not inconsistent with this part, the provisions of the Florida Mediation Code, Florida Rules of
Civil Procedure, shall be applicable to such proceedings.
(11) Within 30 days after the claimant’s receipt of defendant’s response to the claim, the parties or their
designated representatives shall meet in mediation to discuss the issues of liability and damages in accordance with
the mediation rules of practice and procedures adopted by the Supreme Court. Upon stipulation of the parties, this
30-day period may be extended and the statute of limitations is tolled during the mediation and any such extension.
At the conclusion of mediation, the claimant shall have 60 days or the remainder of the period of the statute of
limitations, whichever is greater, within which to file suit.
History.—s. 40, ch. 2001-45; ss. 2, 53, ch. 2006-197.

5 – 40
Note.—Former s. 400.4293.
429.294 Availability of facility records for investigation of resident’s rights violations and defenses;
penalty.—
(1) Failure to provide complete copies of a resident’s records, including, but not limited to, all medical records
and the resident’s chart, within the control or possession of the facility in accordance with s. 400.145, shall
constitute evidence of failure of that party to comply with good faith discovery requirements and shall waive the
good faith certificate and presuit notice requirements under this part by the requesting party.
(2) No facility shall be held liable for any civil damages as a result of complying with this section.
History.—s. 41, ch. 2001-45; s. 2, ch. 2006-197; s. 86, ch. 2018-24.
Note.—Former s. 400.4294.
429.295 Certain provisions not applicable to actions under this part.—An action under this part for a
violation of rights or negligence recognized herein is not a claim for medical malpractice, and the provisions of s.
768.21(8) do not apply to a claim alleging death of the resident.
History.—s. 42, ch. 2001-45; s. 2, ch. 2006-197.
Note.—Former s. 400.4295.
429.296 Statute of limitations.—
(1) Any action for damages brought under this part shall be commenced within 2 years from the time the
incident giving rise to the action occurred or within 2 years from the time the incident is discovered, or should have
been discovered with the exercise of due diligence; however, in no event shall the action be commenced later than 4
years from the date of the incident or occurrence out of which the cause of action accrued.
(2) In those actions covered by this subsection in which it can be shown that fraudulent concealment or
intentional misrepresentation of fact prevented the discovery of the injury, the period of limitations is extended
forward 2 years from the time that the injury is discovered with the exercise of due diligence, but in no event not
more than 6 years from the date the incident giving rise to the injury occurred.
(3) This section shall apply to causes of action that have accrued prior to the effective date of this section;
however, any such cause of action that would not have been barred under prior law may be brought within the time
allowed by prior law or within 2 years after the effective date of this section, whichever is earlier, and will be barred
thereafter. In actions where it can be shown that fraudulent concealment or intentional misrepresentation of fact
prevented the discovery of the injury, the period of limitations is extended forward 2 years from the time that the
injury is discovered with the exercise of due diligence, but in no event more than 4 years from the effective date of
this section.
History.—s. 43, ch. 2001-45; s. 2, ch. 2006-197.
Note.—Former s. 400.4296.
429.297 Punitive damages; pleading; burden of proof.—
(1) In any action for damages brought under this part, no claim for punitive damages shall be permitted unless
there is a reasonable showing by evidence in the record or proffered by the claimant which would provide a
reasonable basis for recovery of such damages. The claimant may move to amend her or his complaint to assert a
claim for punitive damages as allowed by the rules of civil procedure. The rules of civil procedure shall be liberally

5 – 41
construed so as to allow the claimant discovery of evidence which appears reasonably calculated to lead to
admissible evidence on the issue of punitive damages. No discovery of financial worth shall proceed until after the
pleading concerning punitive damages is permitted.
(2) A defendant may be held liable for punitive damages only if the trier of fact, based on clear and convincing
evidence, finds that the defendant was personally guilty of intentional misconduct or gross negligence. As used in
this section, the term:
(a) “Intentional misconduct” means that the defendant had actual knowledge of the wrongfulness of the conduct
and the high probability that injury or damage to the claimant would result and, despite that knowledge, intentionally
pursued that course of conduct, resulting in injury or damage.
(b) “Gross negligence” means that the defendant’s conduct was so reckless or wanting in care that it constituted
a conscious disregard or indifference to the life, safety, or rights of persons exposed to such conduct.
(3) In the case of an employer, principal, corporation, or other legal entity, punitive damages may be imposed
for the conduct of an employee or agent only if the conduct of the employee or agent meets the criteria specified in
subsection (2) and:
(a) The employer, principal, corporation, or other legal entity actively and knowingly participated in such
conduct;
(b) The officers, directors, or managers of the employer, principal, corporation, or other legal entity condoned,
ratified, or consented to such conduct; or
(c) The employer, principal, corporation, or other legal entity engaged in conduct that constituted gross
negligence and that contributed to the loss, damages, or injury suffered by the claimant.
(4) The plaintiff must establish at trial, by clear and convincing evidence, its entitlement to an award of punitive
damages. The “greater weight of the evidence” burden of proof applies to a determination of the amount of
damages.
(5) This section is remedial in nature and shall take effect upon becoming a law.
History.—s. 44, ch. 2001-45; s. 2, ch. 2006-197.
Note.—Former s. 400.4297.
429.298 Punitive damages; limitation.—
(1)(a) Except as provided in paragraphs (b) and (c), an award of punitive damages may not exceed the greater
of:
1. Three times the amount of compensatory damages awarded to each claimant entitled thereto, consistent with
the remaining provisions of this section; or
2. The sum of $1 million.
(b) Where the fact finder determines that the wrongful conduct proven under this section was motivated
primarily by unreasonable financial gain and determines that the unreasonably dangerous nature of the conduct,
together with the high likelihood of injury resulting from the conduct, was actually known by the managing agent,
director, officer, or other person responsible for making policy decisions on behalf of the defendant, it may award an
amount of punitive damages not to exceed the greater of:

5 – 42
1. Four times the amount of compensatory damages awarded to each claimant entitled thereto, consistent with
the remaining provisions of this section; or
2. The sum of $4 million.
(c) Where the fact finder determines that at the time of injury the defendant had a specific intent to harm the
claimant and determines that the defendant’s conduct did in fact harm the claimant, there shall be no cap on punitive
damages.
(d) This subsection is not intended to prohibit an appropriate court from exercising its jurisdiction under s.
768.74 in determining the reasonableness of an award of punitive damages that is less than three times the amount of
compensatory damages.
(e) In any case in which the findings of fact support an award of punitive damages pursuant to paragraph (b) or
paragraph (c), the clerk of the court shall refer the case to the appropriate law enforcement agencies, to the state
attorney in the circuit where the long-term care facility that is the subject of the underlying civil cause of action is
located, and, for multijurisdictional facility owners, to the Office of the Statewide Prosecutor; and such agencies,
state attorney, or Office of the Statewide Prosecutor shall initiate a criminal investigation into the conduct giving
rise to the award of punitive damages. All findings by the trier of fact which support an award of punitive damages
under this paragraph shall be admissible as evidence in any subsequent civil or criminal proceeding relating to the
acts giving rise to the award of punitive damages under this paragraph.
(2) The claimant’s attorney’s fees, if payable from the judgment, are, to the extent that the fees are based on the
punitive damages, calculated based on the final judgment for punitive damages. This subsection does not limit the
payment of attorney’s fees based upon an award of damages other than punitive damages.
(3) The jury may neither be instructed nor informed as to the provisions of this section.
(4) Notwithstanding any other law to the contrary, the amount of punitive damages awarded pursuant to this
section shall be equally divided between the claimant and the Quality of Long-Term Care Facility Improvement
Trust Fund, in accordance with the following provisions:
(a) The clerk of the court shall transmit a copy of the jury verdict to the Chief Financial Officer by certified
mail. In the final judgment, the court shall order the percentages of the award, payable as provided herein.
(b) A settlement agreement entered into between the original parties to the action after a verdict has been
returned must provide a proportionate share payable to the Quality of Long-Term Care Facility Improvement Trust
Fund specified herein. For purposes of this paragraph, a proportionate share is a 50-percent share of that percentage
of the settlement amount which the punitive damages portion of the verdict bore to the total of the compensatory and
punitive damages in the verdict.
(c) The Department of Financial Services shall collect or cause to be collected all payments due the state under
this section. Such payments are made to the Chief Financial Officer and deposited in the appropriate fund specified
in this subsection.
(d) If the full amount of punitive damages awarded cannot be collected, the claimant and the other recipient
designated pursuant to this subsection are each entitled to a proportionate share of the punitive damages collected.
(5) This section is remedial in nature and shall take effect upon becoming a law.
History.—s. 45, ch. 2001-45; s. 419, ch. 2003-261; s. 2, ch. 2006-197.

5 – 43
Note.—Former s. 400.4298.
429.31 Closing of facility; notice; penalty.—
(1) In addition to the requirements of part II of chapter 408, the facility shall inform each resident or the next of
kin, legal representative, or agency acting on each resident’s behalf, of the fact and the proposed time of
discontinuance of operation, following the notification requirements provided in s. 429.28(1)(k). In the event a
resident has no person to represent him or her, the facility shall be responsible for referral to an appropriate social
service agency for placement.
(2) Immediately upon the notice by the agency of the voluntary or involuntary termination of such operation,
the agency shall monitor the transfer of residents to other facilities and ensure that residents’ rights are being
protected. The agency, in consultation with the Department of Children and Families, shall specify procedures for
ensuring that all residents who receive services are appropriately relocated.
(3) All charges shall be prorated as of the date on which the facility discontinues operation, and if any payments
have been made in advance, the payments for services not received shall be refunded to the resident or the resident’s
guardian within 10 working days of voluntary or involuntary closure of the facility, whether or not such refund is
requested by the resident or guardian.
(4) The agency may levy a fine in an amount no greater than $5,000 upon each person or business entity that
owns any interest in a facility that terminates operation without providing notice to the agency and the residents of
the facility at least 30 days before operation ceases. This fine shall not be levied against any facility involuntarily
closed at the initiation of the agency. The agency shall use the proceeds of the fines to operate the facility until all
residents of the facility are relocated.
History.—s. 13, ch. 75-233; ss. 12, 25, ch. 80-198; s. 2, ch. 81-318; ss. 57, 79, 83, ch. 83-181; s. 20, ch. 91-263;
ss. 25, 38, 39, ch. 93-216; s. 780, ch. 95-148; s. 50, ch. 95-418; s. 123, ch. 99-8; ss. 2, 54, ch. 2006-197; s. 154, ch.
2007-230; s. 249, ch. 2014-19; s. 16, ch. 2019-11.
Note.—Former s. 400.431.
429.34 Right of entry and inspection.—
(1) In addition to the requirements of s. 408.811, a duly designated officer or employee of the agency, of the
Department of Children and Families, of the Medicaid Fraud Control Unit of the Office of the Attorney General, or
of the state or local fire marshal, or a representative of the State Long-Term Care Ombudsman Program or a member
of the state or local long-term care ombudsman council has the right to enter unannounced upon and into the
premises of any facility licensed under this part in order to determine the state of compliance with this part, part II of
chapter 408, and applicable rules. Data collected by the State Long-Term Care Ombudsman Program, local long-
term care ombudsman councils, or the state or local advocacy councils may be used by the agency in investigations
involving violations of regulatory standards. A person specified in this section who knows or has reasonable cause
to suspect that a vulnerable adult has been or is being abused, neglected, or exploited shall immediately report such
knowledge or suspicion to the central abuse hotline pursuant to chapter 415.
(2)(a) In addition to the requirements of s. 408.811, the agency may inspect and investigate facilities as
necessary to determine compliance with this part, part II of chapter 408, and rules adopted thereunder. If an assisted
living facility is cited for a class I violation or three or more class II violations arising from separate surveys within a

5 – 44
60-day period or due to unrelated circumstances during the same survey, the agency must conduct an additional
licensure inspection within 6 months.
(b) During any calendar year in which a survey is not conducted, the agency may conduct monitoring visits of
each facility cited in the previous year for a class I or class II violation or for more than three uncorrected class III
violations.
History.—s. 14, ch. 75-233; s. 1, ch. 77-174; ss. 12, 26, ch. 80-198; s. 2, ch. 81-318; ss. 10, 18, 19, ch. 82-148;
ss. 58, 79, 83, ch. 83-181; s. 1, ch. 88-350; s. 24, ch. 93-177; ss. 26, 38, 39, ch. 93-216; s. 51, ch. 95-418; s. 124, ch.
99-8; s. 144, ch. 2000-349; s. 64, ch. 2000-367; s. 46, ch. 2001-45; s. 3, ch. 2004-344; s. 2, ch. 2006-197; s. 155, ch.
2007-230; s. 250, ch. 2014-19; s. 38, ch. 2015-31; s. 14, ch. 2015-126; s. 87, ch. 2018-24; s. 17, ch. 2019-11.
Note.—Former s. 400.434.
429.35 Maintenance of records; reports.—
(1) Every facility shall maintain, as public information available for public inspection under such conditions as
the agency shall prescribe, records containing copies of all inspection reports pertaining to the facility that have been
issued by the agency to the facility. Copies of inspection reports shall be retained in the records for 5 years from the
date the reports are filed or issued.
(2) Within 60 days after the date of the biennial inspection visit required under s. 408.811 or within 30 days
after the date of any interim visit, the agency shall forward the results of the inspection to the local ombudsman
council in the district where the facility is located; to at least one public library or, in the absence of a public library,
the county seat in the county in which the inspected assisted living facility is located; and, when appropriate, to the
district Adult Services and Mental Health Program Offices.
(3) Every facility shall post a copy of the last inspection report of the agency for that facility in a prominent
location within the facility so as to be accessible to all residents and to the public. Upon request, the facility shall
also provide a copy of the report to any resident of the facility or to an applicant for admission to the facility.
History.—ss. 12, 27, ch. 80-198; s. 2, ch. 81-318; ss. 75, 79, 83, ch. 83-181; s. 53, ch. 83-218; s. 1, ch. 88-145; s.
19, ch. 90-347; s. 21, ch. 91-263; ss. 27, 38, 39, ch. 93-216; s. 16, ch. 95-210; s. 57, ch. 2000-139; s. 145, ch. 2000-
349; s. 65, ch. 2000-367; s. 2, ch. 2006-197; s. 102, ch. 2007-5; s. 156, ch. 2007-230; s. 118, ch. 2008-4; s. 39, ch.
2015-31.
Note.—Former s. 400.435.
429.41 Rules establishing standards.—
(1) It is the intent of the Legislature that rules published and enforced pursuant to this section shall include
criteria by which a reasonable and consistent quality of resident care and quality of life may be ensured and the
results of such resident care may be demonstrated. Such rules shall also ensure a safe and sanitary environment that
is residential and noninstitutional in design or nature. It is further intended that reasonable efforts be made to
accommodate the needs and preferences of residents to enhance the quality of life in a facility. Uniform firesafety
standards for assisted living facilities shall be established by the State Fire Marshal pursuant to s. 633.206. The
agency may adopt rules to administer part II of chapter 408. In order to provide safe and sanitary facilities and the
highest quality of resident care accommodating the needs and preferences of residents, the agency, in consultation

5 – 45
with the Department of Children and Families and the Department of Health, shall adopt rules, policies, and
procedures to administer this part, which must include reasonable and fair minimum standards in relation to:
(a) The requirements for and maintenance of facilities, not in conflict with chapter 553, relating to plumbing,
heating, cooling, lighting, ventilation, living space, and other housing conditions, which will ensure the health,
safety, and comfort of residents suitable to the size of the structure.
1. Firesafety evacuation capability determination.—An evacuation capability evaluation for initial licensure
shall be conducted within 6 months after the date of licensure.
2. Firesafety requirements.—
a. The National Fire Protection Association, Life Safety Code, NFPA 101 and 101A, current editions, shall be
used in determining the uniform firesafety code adopted by the State Fire Marshal for assisted living facilities,
pursuant to s. 633.206.
b. A local government or a utility may charge fees only in an amount not to exceed the actual expenses incurred
by the local government or the utility relating to the installation and maintenance of an automatic fire sprinkler
system in a licensed assisted living facility structure.
c. All licensed facilities must have an annual fire inspection conducted by the local fire marshal or authority
having jurisdiction.
d. An assisted living facility that is issued a building permit or certificate of occupancy before July 1, 2016,
may at its option and after notifying the authority having jurisdiction, remain under the provisions of the 1994 and
1995 editions of the National Fire Protection Association, Life Safety Code, NFPA 101, and NFPA 101A. The
facility opting to remain under such provisions may make repairs, modernizations, renovations, or additions to, or
rehabilitate, the facility in compliance with NFPA 101, 1994 edition, and may utilize the alternative approaches to
life safety in compliance with NFPA 101A, 1995 edition. However, a facility for which a building permit or
certificate of occupancy is issued before July 1, 2016, that undergoes Level III building alteration or rehabilitation,
as defined in the Florida Building Code, or seeks to utilize features not authorized under the 1994 or 1995 editions
of the Life Safety Code must thereafter comply with all aspects of the uniform firesafety standards established under
s. 633.206, and the Florida Fire Prevention Code, in effect for assisted living facilities as adopted by the State Fire
Marshal.
3. Resident elopement requirements.—Facilities are required to conduct a minimum of two resident elopement
prevention and response drills per year. All administrators and direct care staff must participate in the drills, which
shall include a review of procedures to address resident elopement. Facilities must document the implementation of
the drills and ensure that the drills are conducted in a manner consistent with the facility’s resident elopement
policies and procedures.
(b) The preparation and annual update of a comprehensive emergency management plan. Such standards must
be included in the rules adopted by the agency after consultation with the Division of Emergency Management. At a
minimum, the rules must provide for plan components that address emergency evacuation transportation; adequate
sheltering arrangements; postdisaster activities, including provision of emergency power, food, and water;
postdisaster transportation; supplies; staffing; emergency equipment; individual identification of residents and
transfer of records; communication with families; and responses to family inquiries. The comprehensive emergency

5 – 46
management plan is subject to review and approval by the local emergency management agency. During its review,
the local emergency management agency shall ensure that the following agencies, at a minimum, are given the
opportunity to review the plan: the Department of Health, the Agency for Health Care Administration, and the
Division of Emergency Management. Also, appropriate volunteer organizations must be given the opportunity to
review the plan. The local emergency management agency shall complete its review within 60 days and either
approve the plan or advise the facility of necessary revisions.
(c) The number, training, and qualifications of all personnel having responsibility for the care of residents. The
rules must require adequate staff to provide for the safety of all residents. Facilities licensed for 17 or more residents
are required to maintain an alert staff for 24 hours per day.
(d) All sanitary conditions within the facility and its surroundings which will ensure the health and comfort of
residents. The rules must clearly delineate the responsibilities of the agency’s licensure and survey staff, the county
health departments, and the local authority having jurisdiction over firesafety and ensure that inspections are not
duplicative. The agency may collect fees for food service inspections conducted by the county health departments
and transfer such fees to the Department of Health.
(e) License application and license renewal, transfer of ownership, proper management of resident funds and
personal property, surety bonds, resident contracts, refund policies, financial ability to operate, and facility and staff
records.
(f) Inspections, complaint investigations, moratoriums, classification of deficiencies, levying and enforcement
of penalties, and use of income from fees and fines.
(g) The enforcement of the resident bill of rights specified in s. 429.28.
(h) The care and maintenance of residents, which must include, but is not limited to:
1. The supervision of residents;
2. The provision of personal services;
3. The provision of, or arrangement for, social and leisure activities;
4. The arrangement for appointments and transportation to appropriate medical, dental, nursing, or mental
health services, as needed by residents;
5. The management of medication;
6. The nutritional needs of residents;
7. Resident records; and
8. Internal risk management and quality assurance.
(i) Facilities holding a limited nursing, extended congregate care, or limited mental health license.
(j) The establishment of specific criteria to define appropriateness of resident admission and continued
residency in a facility holding a standard, limited nursing, extended congregate care, and limited mental health
license.
(k) The use of physical or chemical restraints. The use of physical restraints is limited to half-bed rails as
prescribed and documented by the resident’s physician with the consent of the resident or, if applicable, the
resident’s representative or designee or the resident’s surrogate, guardian, or attorney in fact. The use of chemical
restraints is limited to prescribed dosages of medications authorized by the resident’s physician and must be

5 – 47
consistent with the resident’s diagnosis. Residents who are receiving medications that can serve as chemical
restraints must be evaluated by their physician at least annually to assess:
1. The continued need for the medication.
2. The level of the medication in the resident’s blood.
3. The need for adjustments in the prescription.
(l) The establishment of specific policies and procedures on resident elopement. Facilities shall conduct a
minimum of two resident elopement drills each year. All administrators and direct care staff shall participate in the
drills. Facilities shall document the drills.
(2) In adopting any rules pursuant to this part, the agency shall make distinct standards for facilities based upon
facility size; the types of care provided; the physical and mental capabilities and needs of residents; the type,
frequency, and amount of services and care offered; and the staffing characteristics of the facility. Rules developed
pursuant to this section may not restrict the use of shared staffing and shared programming in facilities that are part
of retirement communities that provide multiple levels of care and otherwise meet the requirements of law and rule.
If a continuing care facility licensed under chapter 651 or a retirement community offering multiple levels of care
licenses a building or part of a building designated for independent living for assisted living, staffing requirements
established in rule apply only to residents who receive personal, limited nursing, or extended congregate care
services under this part. Such facilities shall retain a log listing the names and unit number for residents receiving
these services. The log must be available to surveyors upon request. Except for uniform firesafety standards, the
agency shall adopt by rule separate and distinct standards for facilities with 16 or fewer beds and for facilities with
17 or more beds. The standards for facilities with 16 or fewer beds must be appropriate for a noninstitutional
residential environment; however, the structure may not be more than two stories in height and all persons who
cannot exit the facility unassisted in an emergency must reside on the first floor. The agency may make other
distinctions among types of facilities as necessary to enforce this part. Where appropriate, the agency shall offer
alternate solutions for complying with established standards, based on distinctions made by the agency relative to
the physical characteristics of facilities and the types of care offered.
(3) Rules adopted by the agency shall encourage the development of homelike facilities that promote the
dignity, individuality, personal strengths, and decisionmaking ability of residents.
(4) The agency may waive rules adopted under this part to demonstrate and evaluate innovative or cost-
effective congregate care alternatives that enable individuals to age in place. Such waivers may be granted only in
instances where there is reasonable assurance that the health, safety, or welfare of residents will not be endangered.
To apply for a waiver, the licensee shall submit to the agency a written description of the concept to be
demonstrated, including goals, objectives, and anticipated benefits; the number and types of residents who will be
affected, if applicable; a brief description of how the demonstration will be evaluated; and any other information
deemed appropriate by the agency. Any facility granted a waiver shall submit a report of findings to the agency
within 12 months. At such time, the agency may renew or revoke the waiver or pursue any regulatory or statutory
changes necessary to allow other facilities to adopt the same practices. The agency may by rule clarify terms and
establish waiver application procedures, criteria for reviewing waiver proposals, and procedures for reporting
findings, as necessary to implement this subsection.

5 – 48
(5) The agency may use an abbreviated biennial standard licensure inspection that consists of a review of key
quality-of-care standards in lieu of a full inspection in a facility that has a good record of past performance.
However, a full inspection must be conducted in a facility that has a history of class I or class II violations,
uncorrected class III violations, confirmed ombudsman council complaints, or confirmed licensure complaints
within the previous licensure period immediately preceding the inspection or if a potentially serious problem is
identified during the abbreviated inspection. The agency shall develop the key quality-of-care standards with input
from the State Long-Term Care Ombudsman Council and representatives of provider groups for incorporation into
its rules.
History.—s. 16, ch. 75-233; ss. 12, 29, ch. 80-198; s. 2, ch. 81-318; ss. 59, 79, 83, ch. 83-181; s. 7, ch. 85-145; s.
1, ch. 86-87; s. 13, ch. 87-371; s. 20, ch. 89-294; s. 22, ch. 91-263; s. 25, ch. 93-177; s. 26, ch. 93-211; ss. 28, 38,
39, ch. 93-216; ss. 12, 20, 52, ch. 95-418; s. 27, ch. 97-100; s. 99, ch. 97-101; s. 5, ch. 98-148; s. 15, ch. 99-332; s.
47, ch. 2001-45; s. 7, ch. 2004-298; s. 2, ch. 2004-386; ss. 2, 55, ch. 2006-197; s. 157, ch. 2007-230; s. 142, ch.
2010-102; s. 343, ch. 2011-142; s. 137, ch. 2013-183; s. 251, ch. 2014-19; s. 15, ch. 2015-126; s. 1, ch. 2016-92; s.
18, ch. 2019-11.
Note.—Former s. 400.441.
429.42 Pharmacy and dietary services.—
(1) Any assisted living facility in which the agency has documented a class I or class II deficiency or
uncorrected class III deficiencies regarding medicinal drugs or over-the-counter preparations, including their
storage, use, delivery, or administration, or dietary services, or both, during a biennial survey or a monitoring visit or
an investigation in response to a complaint, shall, in addition to or as an alternative to any penalties imposed under s.
429.19, be required to employ the consultant services of a licensed pharmacist, a licensed registered nurse, or a
registered or licensed dietitian, as applicable. The consultant shall, at a minimum, provide onsite quarterly
consultation until the inspection team from the agency determines that such consultation services are no longer
required.
(2) A corrective action plan for deficiencies related to assistance with the self-administration of medication or
the administration of medication must be developed and implemented by the facility within 48 hours after
notification of such deficiency, or sooner if the deficiency is determined by the agency to be life-threatening.
(3) The agency shall employ at least two pharmacists licensed pursuant to chapter 465 among its personnel who
biennially inspect assisted living facilities licensed under this part, to participate in biennial inspections or consult
with the agency regarding deficiencies relating to medicinal drugs or over-the-counter preparations.
(4) The agency may by rule establish procedures and specify documentation as necessary to implement this
section.
History.—s. 1, ch. 89-218; s. 1, ch. 90-192; s. 23, ch. 91-263; ss. 29, 38, 39, ch. 93-216; s. 17, ch. 95-210; s. 18,
ch. 98-80; s. 6, ch. 98-148; ss. 2, 56, ch. 2006-197; s. 19, ch. 2019-11.
Note.—Former s. 400.442.
429.44 Construction and renovation; requirements.—
(1) The requirements for the construction and renovation of a facility shall comply with chapter 553 which
pertains to building construction standards, including plumbing, electrical code, glass, manufactured buildings,

5 – 49
accessibility for persons with disabilities, and the state minimum building code and with s. 633.206, which pertains
to uniform firesafety standards.
(2) Upon notification by the local authority having jurisdiction over life-threatening violations which seriously
threaten the health, safety, or welfare of a resident of a facility, the agency shall take action as specified in s. 429.14.
History.—s. 17, ch. 75-233; s. 3, ch. 79-152; s. 2, ch. 81-318; ss. 79, 83, ch. 83-181; ss. 30, 38, 39, ch. 93-216; s.
14, ch. 95-418; s. 7, ch. 98-148; ss. 2, 57, ch. 2006-197; s. 138, ch. 2013-183; s. 34, ch. 2015-4.
Note.—Former s. 400.444.
429.445 Compliance with local zoning requirements.—No facility licensed under this part may commence
any construction which will expand the size of the existing structure unless the licensee first submits to the agency
proof that such construction will be in compliance with applicable local zoning requirements. Facilities with a
licensed capacity of less than 15 persons shall comply with the provisions of chapter 419.
History.—s. 2, ch. 85-251; s. 24, ch. 91-263; ss. 31, 39, ch. 93-216; s. 2, ch. 2006-197.
Note.—Former s. 400.4445.
429.47 Prohibited acts; penalties for violation.—
(1) While a facility is under construction, the owner may advertise to the public prior to obtaining a license.
Facilities that are certified under chapter 651 shall comply with the advertising provisions of s. 651.095 rather than
those provided for in this subsection.
(2) A freestanding facility shall not advertise or imply that any part of it is a nursing home. For the purpose of
this subsection, “freestanding facility” means a facility that is not operated in conjunction with a nursing home to
which residents of the facility are given priority when nursing care is required. A person who violates this subsection
is subject to fine as specified in s. 429.19.
(3) Any facility which is affiliated with any religious organization or which has a name implying religious
affiliation shall include in its advertising whether or not it is affiliated with any religious organization and, if so,
which organization.
(4) A facility licensed under this part which is not part of a facility authorized under chapter 651 shall include
the facility’s license number as given by the agency in all advertising. A company or person owning more than one
facility shall include at least one license number per advertisement. All advertising shall include the term “assisted
living facility” before the license number.
History.—s. 18, ch. 75-233; s. 2, ch. 81-318; ss. 79, 83, ch. 83-181; s. 14, ch. 87-371; s. 25, ch. 91-263; ss. 32,
38, 39, ch. 93-216; s. 18, ch. 95-210; s. 217, ch. 99-13; ss. 2, 58, ch. 2006-197; s. 158, ch. 2007-230.
Note.—Former s. 400.447.
429.49 Resident records; penalties for alteration.—
(1) Any person who fraudulently alters, defaces, or falsifies any medical or other record of an assisted living
facility, or causes or procures any such offense to be committed, commits a misdemeanor of the second degree,
punishable as provided in s. 775.082 or s. 775.083.
(2) A conviction under subsection (1) is also grounds for restriction, suspension, or termination of license
privileges.
History.—s. 48, ch. 2001-45; s. 2, ch. 2006-197.

5 – 50
Note.—Former s. 400.449.
429.52 Staff training and educational programs; core educational requirement.—
(1) Effective October 1, 2015, each new assisted living facility employee who has not previously completed
core training must attend a preservice orientation provided by the facility before interacting with residents. The
preservice orientation must be at least 2 hours in duration and cover topics that help the employee provide
responsible care and respond to the needs of facility residents. Upon completion, the employee and the administrator
of the facility must sign a statement that the employee completed the required preservice orientation. The facility
must keep the signed statement in the employee’s personnel record.
(2) Administrators and other assisted living facility staff must meet minimum training and education
requirements established by the agency by rule. This training and education is intended to assist facilities to
appropriately respond to the needs of residents, to maintain resident care and facility standards, and to meet
licensure requirements.
(3) The agency, in conjunction with providers, shall develop a competency test and a minimum required score
to indicate successful completion of the training and educational requirements. The required training and education
must cover at least the following topics:
(a) State law and rules relating to assisted living facilities.
(b) Resident rights and identifying and reporting abuse, neglect, and exploitation.
(c) Special needs of elderly persons, persons with mental illness, and persons with developmental disabilities
and how to meet those needs.
(d) Nutrition and food service, including acceptable sanitation practices for preparing, storing, and serving
food.
(e) Medication management, recordkeeping, and proper techniques for assisting residents with self-
administered medication.
(f) Firesafety requirements, including fire evacuation drill procedures and other emergency procedures.
(g) Care of persons with Alzheimer’s disease and related disorders.
(4) A new facility administrator must complete the required training and education, including the competency
test, within 90 days after date of employment as an administrator. Failure to do so is a violation of this part and
subjects the violator to an administrative fine as prescribed in s. 429.19. Administrators licensed in accordance with
part II of chapter 468 are exempt from this requirement. Other licensed professionals may be exempted, as
determined by the agency by rule.
(5) Administrators are required to participate in continuing education for a minimum of 12 contact hours every
2 years.
(6) Staff involved with the management of medications and assisting with the self-administration of
medications under s. 429.256 must complete a minimum of 6 additional hours of training provided by a registered
nurse, a licensed pharmacist, or agency staff. The agency shall establish by rule the minimum requirements of this
additional training.
(7) Other facility staff shall participate in training relevant to their job duties as specified by rule of the agency.

5 – 51
(8) If the agency determines that there are problems in a facility which could be reduced through specific staff
training or education beyond that already required under this section, the agency may require, and provide, or cause
to be provided, the training or education of any personal care staff in the facility.
(9) The agency shall adopt rules related to these training requirements, the competency test, necessary
procedures, and competency test fees and shall adopt or contract with another entity to develop a curriculum, which
shall be used as the minimum core training requirements. The agency shall consult with representatives of
stakeholder associations and agencies in the development of the curriculum.
(10) The training required by this section other than the preservice orientation must be conducted by persons
registered with the agency as having the requisite experience and credentials to conduct the training. A person
seeking to register as a trainer must provide the agency with proof of completion of the minimum core training
education requirements, successful passage of the competency test established under this section, and proof of
compliance with the continuing education requirement in subsection (5).
(11) A person seeking to register as a trainer must also:
(a) Provide proof of completion of a 4-year degree from an accredited college or university and must have
worked in a management position in an assisted living facility for 3 years after being core certified;
(b) Have worked in a management position in an assisted living facility for 5 years after being core certified
and have 1 year of teaching experience as an educator or staff trainer for persons who work in assisted living
facilities or other long-term care settings;
(c) Have been previously employed as a core trainer for the agency or department; or
(d) Meet other qualification criteria as defined in rule, which the agency is authorized to adopt.
(12) The agency shall adopt rules to establish trainer registration requirements.
History.—ss. 12, 34, ch. 80-198; s. 2, ch. 81-318; ss. 60, 75, 79, 83, ch. 83-181; s. 53, ch. 83-218; s. 3, ch. 85-
251; s. 21, ch. 89-294; s. 27, ch. 91-263; ss. 33, 38, 39, ch. 93-216; s. 19, ch. 95-210; ss. 15, 26, 53, ch. 95-418; s.
16, ch. 97-82; s. 29, ch. 97-100; s. 19, ch. 98-80; s. 25, ch. 2003-57; s. 3, ch. 2003-405; ss. 2, 59, ch. 2006-197; s. 1,
ch. 2007-219; s. 16, ch. 2015-126; s. 88, ch. 2018-24; s. 57, ch. 2018-110; s. 20, ch. 2019-11.
Note.—Former s. 400.452.
429.53 Consultation by the agency.—
(1) The area offices of licensure and certification of the agency shall provide consultation to the following upon
request:
(a) A licensee of a facility.
(b) A person interested in obtaining a license to operate a facility under this part.
(2) As used in this section, “consultation” includes:
(a) An explanation of the requirements of this part and rules adopted pursuant thereto;
(b) An explanation of the license application and renewal procedures;
(c) The provision of a checklist of general local and state approvals required prior to constructing or developing
a facility and a listing of the types of agencies responsible for such approvals;
(d) An explanation of benefits and financial assistance available to a recipient of supplemental security income
residing in a facility;

5 – 52
(e) Any other information which the agency deems necessary to promote compliance with the requirements of
this part; and
(f) A preconstruction review of a facility to ensure compliance with agency rules and this part.
(3) The agency may charge a fee commensurate with the cost of providing consultation under this section.
History.—ss. 15, 19, ch. 87-371; s. 22, ch. 89-294; ss. 34, 38, 39, ch. 93-216; s. 2, ch. 2006-197.
Note.—Former s. 400.453.
429.54 Collection of information; local subsidy.—
(1) To enable the agency to collect the information requested by the Legislature regarding the actual cost of
providing room, board, and personal care in facilities, the agency is authorized to conduct field visits and audits of
facilities as necessary. The owners of randomly sampled facilities shall submit such reports, audits, and accountings
of cost as the agency may require by rule; provided that such reports, audits, and accountings shall be the minimum
necessary to implement this section. Any facility selected to participate in the study shall cooperate with the agency
by providing cost of operation information to interviewers.
(2) Local governments or organizations may contribute to the cost of care of local facility residents by further
subsidizing the rate of state-authorized payment to such facilities. Implementation of local subsidy requires agency
approval and may not result in reductions in the state supplement.
History.—ss. 12, 35, ch. 80-198; s. 2, ch. 81-318; ss. 75, 79, 83, ch. 83-181; s. 53, ch. 83-218; ss. 38, 39, ch. 93-
216; s. 2, ch. 2006-197; s. 21, ch. 2019-11.
Note.—Former s. 400.454.
429.55 Consumer information website.—The Legislature finds that consumers need additional information
on the quality of care and service in assisted living facilities in order to select the best facility for themselves or their
loved ones. Therefore, the Agency for Health Care Administration shall create content that is easily accessible
through the home page of the agency’s website either directly or indirectly through links to one or more other
established websites of the agency’s choosing. The website must be searchable by facility name, license type, city,
or zip code. By November 1, 2015, the agency shall include all content in its possession on the website and add
content when received from facilities. At a minimum, the content must include:
(1) Information on each licensed assisted living facility, including, but not limited to:
(a) The name and address of the facility.
(b) The name of the owner or operator of the facility.
(c) The number and type of licensed beds in the facility.
(d) The types of licenses held by the facility.
(e) The facility’s license expiration date and status.
(f) The total number of clients that the facility is licensed to serve and the most recently available occupancy
levels.
(g) The number of private and semiprivate rooms offered.
(h) The bed-hold policy.
(i) The religious affiliation, if any, of the assisted living facility.
(j) The languages spoken by the staff.

5 – 53
(k) Availability of nurses.
(l) Forms of payment accepted, including, but not limited to, Medicaid, Medicaid long-term managed care,
private insurance, health maintenance organization, United States Department of Veterans Affairs, CHAMPUS
program, or workers’ compensation coverage.
(m) Indication if the licensee is operating under bankruptcy protection.
(n) Recreational and other programs available.
(o) Special care units or programs offered.
(p) Whether the facility is a part of a retirement community that offers other services pursuant to this part or
part III of this chapter, part II or part III of chapter 400, or chapter 651.
(q) Links to the State Long-Term Care Ombudsman Program website and the program’s statewide toll-free
telephone number.
(r) Links to the websites of the providers.
(s) Other relevant information that the agency currently collects.
(2) Survey and violation information for the facility, including a list of the facility’s violations committed
during the previous 60 months, which on July 1, 2015, may include violations committed on or after July 1, 2010.
The list shall be updated monthly and include for each violation:
(a) A summary of the violation, including all licensure, revisit, and complaint survey information, presented in
a manner understandable by the general public.
(b) Any sanctions imposed by final order.
(c) The date the corrective action was confirmed by the agency.
(3) Links to inspection reports that the agency has on file.
(4) The agency may adopt rules to administer this section.
History.—s. 17, ch. 2015-126.

5 – 54
CHAPTER 429 ASSISTED CARE COMMUNITIES
PART III ADULT DAY CARE CENTERS
(s. 429.905)
429.905 Exemptions; monitoring of adult day care center programs colocated with assisted living
facilities or licensed nursing home facilities.—
(1) The following are exempt from this part:
(a) Any facility, institution, or other place that is operated by the Federal Government or any agency thereof.
(b) Any freestanding inpatient hospice facility that is licensed by the state and which provides day care services
to hospice patients only.
(2) A licensed assisted living facility, a licensed hospital, or a licensed nursing home facility may provide
services during the day which include, but are not limited to, social, health, therapeutic, recreational, nutritional, and
respite services, to adults who are not residents. Such a facility need not be licensed as an adult day care center;
however, the agency must monitor the facility during the regular inspection and at least biennially to ensure
adequate space and sufficient staff. If an assisted living facility, a hospital, or a nursing home holds itself out to the
public as an adult day care center, it must be licensed as such and meet all standards prescribed by statute and rule.
For the purpose of this subsection, the term “day” means any portion of a 24-hour day.
History.—s. 4, ch. 78-336; s. 2, ch. 81-318; ss. 79, 83, ch. 83-181; s. 6, ch. 88-235; ss. 4, 17, ch. 93-215; s. 20,
ch. 95-210; s. 4, ch. 2006-197; s. 30, ch. 2012-160.
Note.—Former s. 400.553.

6 – 1
Assisted Living Rule Transfer Table
The rules and the rulemaking function for assisted living communities was transferred from the
Department of Elder Affairs to the Agency for Health Care Administration during the past legislative
session (Chapter 2019-11, Laws of Florida), effective July 1, 2019. The following is a crosswalk of the
transfer of each rule in Chapter 58A-5 (assisted living operations) and Chapter 58T-1 (assisted living core
trainer requirements) to Chapter 59A-36, Florida Administrative Code.
Transferred from DOEA Rule Chapter 58A-5
Transferred to AHCA Rule Chapter 59A-36
58A-5.0131 59A-36.002 58A-5.014 59A-36.003 58A-5.016 59A-36.004 58A-5.0161 59A-36.005 58A-5.0181 59A-36.006 58A-5.0182 59A-36.007 58A-5.0185 59A-36.008 58A-5.0186 59A-36.009 58A-5.019 59A-36.010 58A-5.0191 59A-36.011 58A-5.020 59A-36.012 58A-5.021 59A-36.013 58A-5.023 59A-36.014 58A-5.024 59A-36.015 58A-5.0241 59A-36.016 58A-5.0242 59A-36.017 58A-5.025 59A-36.018 58A-5.026 59A-36.019 58A-5.029 59A-36.020 58A-5.030 59A-36.021 58A-5.031 59A-36.022 58A-5.033 59A-36.023 58A-5.035 59A-36.024 58A-5.036 59A-36.025 58T-1.203 59A-36.027 58T-1.205 59A-36.028 58T-1.207 59A-36.029 58T-1.209 59A-36.030 58T-1.211 59A-36.031

6 – 2
[This space intentionally left blank.]

Effective July 1, 2019 6A – 1
CHAPTER 59A-36
ASSISTED LIVING FACILITY 59A-36.001 Standards and Criteria for Determining Compliance with Facility Standards and Resident Rights
59A-36.002 Definitions
59A-36.003 Licensing and Change of Ownership
59A-36.004 License Requirements
59A-36.005 Inspection Responsibilities
59A-36.006 Admission Procedures, Appropriateness of Placement and Continued Residency Criteria
59A-36.007 Resident Care Standards
59A-36.008 Medication Practices
59A-36.009 Do Not Resuscitate Orders (DNROs)
59A-36.010 Staffing Standards
59A-36.011 Staff Training Requirements and Competency Test
59A-36.012 Food Service Standards
59A-36.013 Fiscal Standards
59A-36.014 Physical Plant Standards
59A-36.015 Records
59A-36.016 Adverse Incident Report
59A-36.017 Liability Claim Report
59A-36.018 Resident Contracts
59A-36.019 Emergency Management
59A-36.020 Limited Mental Health
59A-36.021 Extended Congregate Care Services
59A-36.022 Limited Nursing Services
59A-36.023 Administrative Enforcement
59A-36.024 Waivers
59A-36.025 Emergency Environmental Control for Assisted Living Facilities
59A-36.027 ALF Core Training Provider Qualifications
59A-36.028 ALF Minimum Core Training Curriculum Requirements
59A-36.029 ALF Core Training Provider Initial Registration Process
59A-36.030 Process for Maintaining ALF Core Training Provider Registration
59A-36.031 Registered ALF Core Training Provider Responsibilities
59A-36.001 Standards and Criteria for Determining Compliance with Facility Standards and Resident
Rights.
(1) DEFINITIONS.
In addition to the terms defined in section 429.02, F.S., and rule 59A-36.002, F.A.C., the following definitions are
applicable in this rule chapter.
(a) “Core Survey Task” means tasks conducted by Agency survey staff that focus on core areas of regulations.
(b) “Timely Manner” means as soon as possible, but not to exceed 24 hours of Agency staff having requested
materials.

Effective July 1, 2019 6A – 2
(2) SURVEY PROCESS FOR RESIDENT RIGHTS.
The following core survey tasks shall be utilized during survey activities in order to determine the facility’s
compliance with resident rights pursuant to section 429.28, F.S., and rule 59A-36.007, F.A.C.
(a) The surveyor(s) conducts a tour of the facility to determine if the residents’ health, safety, and welfare are
maintained. The tour includes observations and assessments of the following:
1. Resident behavior and demeanor;
2. Adherence to facility abuse prohibition policy and procedure;
3. Adherence to infection control policy and procedure;
4. General physical plant standards in accordance with rule 59A-36.014, F.A.C.;
5. Overall appearance of residents and observations of any special care needs;
6. Posting of Resident Bill of Rights and required phone numbers in accordance with rule 59A-36.007, F.A.C.;
7. Resident access to phones and unrestricted private communication;
8. Resident opportunity to exercise;
9. Staff availability and responsiveness to resident care needs;
10. Medication storage and security;
11. Chemical and physical restraint use;
12. Positioning/transferring processes utilized by staff;
13. Any specialized care provided by the facility with a specialty license;
14. Any license conditions or restrictions as a result of Agency action.
(b) The surveyor(s) conducts interviews with residents, family members/representatives, staff, and any other
persons the surveyor(s) deems relevant to the survey.
1. The facility may not restrict Agency staff from conducting confidential interviews pursuant to section
429.14(6), F.S.
2. Interviews may be conducted both in person and telephonically.
(c) The surveyor(s) reviews facility records to determine compliance with:
1. Licensure requirements in accordance with rule 59A-36.004, F.A.C.;
2. Inspection responsibilities in accordance with rule 59A-36.005, F.A.C.;
3. Admissions procedures and appropriateness of placement and continued residency criteria in accordance with
rule 59A-36.007, F.A.C.;
4. Resident care standards in accordance with rule 59A-36.007, F.A.C.;
5. Medication practices in accordance with rule 59A-36.008, F.A.C.;
6. Do not resuscitate orders (DNROs) in accordance with rule 59A-36.009, F.A.C.;
7. Staffing standards in accordance with rule 59A-36.010, F.A.C.;
8. Staff training requirements and competency training in accordance with rule 59A-36.011, F.A.C.;
9. Alzheimer’s Disease or Related Disorders training provider and curriculum approval in accordance with rule
58A-5.0194, F.A.C.;
10. Food service standards in accordance with rule 59A-36.012, F.A.C.;
11. Fiscal standards in accordance with rule 59A-36.013, F.A.C.;
12. Physical plant standards in accordance with rule 59A-36.014, F.A.C.;
13. Records in accordance with rule 59A-36.015, F.A.C.;

Effective July 1, 2019 6A – 3
14. Resident contracts in accordance with rule 59A-36.018, F.A.C.;
15. Emergency management in accordance with rule 59A-36.019, F.A.C.
(d) The facility must provide agency staff with requested documents in a timely manner and allow the agency
staff to obtain copies.
(e) Surveyor(s) conducts specific and general observations throughout the survey to determine compliance with:
dietary standards, medication standards, infection control standards, resident activities, assistance with activities of
daily living, facility practices, and resident daily routines.
(f) For facilities licensed to provide specialty services such as Limited Mental Health, Extended Congregate
Care, and Limited Nursing Services: the surveyor(s) reviews the required components in accordance with rules 59A-
36.020, 59A-36.021, and 59A-36.021, F.A.C.
Rulemaking Authority 429.28(3)(a) FS. Law Implemented 429.28 FS. History–New 11-28-16.
59A-36.002 Definitions.
In addition to the terms defined in section 429.02, F.S., the following definitions are applicable in this rule chapter:
(1) “Advertise” means any written, printed, oral, visual, or electronic promotion, statement of availability,
qualifications, services offered, or other similar communication appearing in or on television, radio, the Internet,
billboards, newspapers, magazines, business cards, flyers, brochures or other medium for the purpose of attracting
potential residents to an assisted living facility. A complimentary listing of a licensed facility’s name, address, and
telephone number in the telephone directory is not considered advertising.
(2) “Agency Central Office” means the Agency for Health Care Administration Assisted Living Unit (ALU),
located at 2727 Mahan Drive, Mail Stop 30, Tallahassee, FL 32308-5403. The ALU telephone number and website
address are (850)412-4304, and
http://ahca.myflorida.com/MCHQ/Health_Facility_Regulation/Assisted_Living/alf.shtml.
(3) “Agency Field Office” means the Agency for Health Care Administration’s Office in a particular geographic
area. Information regarding local offices is available online at: http://ahca.myflorida.com/mchq/index.shtml#six.
(4) “Apartment” means a self-contained dwelling unit with a bathroom, kitchen area, and living and sleeping
space that is contracted for use as a residence by one or more persons who maintain a common household.
(5) “Anti-Embolism Stockings and Hosiery” means prescribed close-fitting elastic-type coverings for
therapeutic treatment of the legs. They may be knee high or thigh high length and have transparent, open-toe, or
similar foot design.
(6) “Assistance with Activities of Daily Living” means individual assistance with the following:
(a) Ambulation – Providing physical support to enable the resident to move about within or outside the facility.
Physical support includes supporting or holding the resident’s hand, elbow, or arm; holding on to a support belt
worn by the resident to assist in providing stability or direction while the resident ambulates; or pushing the
resident’s wheelchair. The term does not include assistance with transfer.
(b) Bathing – Assembling towels, soaps, or other necessary supplies; helping the resident in and out of the
bathtub or shower; turning the water on and off; adjusting water temperatures; washing and drying portions of the
body that are difficult for the resident to reach; or being available while the resident is bathing.
(c) Dressing – Helping residents to choose, put on, and remove clothing.
(d) Eating – Helping residents with or by cutting food, pouring beverages, or feeding residents who are unable
to feed themselves.

Effective July 1, 2019 6A – 4
(e) Grooming – Helping residents with shaving, oral care, care of the hair, or nail care.
(f) Toileting – Assisting the resident to the bathroom, helping the resident to undress, positioning the resident on
the commode, and helping the resident with related personal hygiene including assistance with changing an adult
brief and assistance with the routine emptying of a catheter or ostomy bag.
(7) “Assistance With Transfer” means providing verbal and physical cuing or physical assistance or both while
the resident moves between bed and a standing position or between bed and chair or wheelchair. The term does not
include total physical assistance with transfer provided by staff to residents.
(8) “Bedridden” means confined to bed because of inability to ambulate or transfer to a wheelchair even with
assistance, or to sit safely in a chair or wheelchair without personal assistance or physical restraint.
(9) “Capacity” means the number of residents for which a facility has been licensed to provide residential care.
(10) “Case Manager” means an individual employed by or under contract with any agency or organization,
public or private, who has the responsibility for assessing resident needs; planning services for the resident;
coordinating and assisting residents with gaining access to needed medical, mental health, social, housing,
educational or other services; monitoring service delivery; and evaluating the effects of service delivery.
(11) “Certified Nursing Assistant (CNA)” means an individual certified under chapter 464, part II, F.S.
(12) “Day Care Participant” means an individual who receives services at a facility for less than 24 hours per
day.
(13) “Deficiency” means an instance of non-compliance with the requirements of part II of chapter 408, F.S.,
part I of chapter 429, F.S., rule chapter 59A-35, F.A.C., and this rule chapter.
(14) “Direct Care Staff” means Staff in Regular Contact or Staff in Direct Contact with residents who provide
personal or nursing services to residents, including administrators and managers providing such services.
(15) “Distinct Part” means designated bedrooms or apartments, bathrooms and a living area; or a separately
identified wing, floor, or building that includes bedrooms or apartments, bathrooms and a living area. The distinct
part may include a separate dining area, or meals may be served in another part of the facility.
(16) “Elopement” means an occurrence in which a resident leaves a facility without following facility policy
and procedures.
(17) “Food Service” means the storage, preparation, service, and clean up of food intended for consumption in a
facility either by facility staff or through a formal agreement that meals will be regularly catered by a third party.
(18) “Glucose Meter” or “glucometer” means a medical device that determines the approximate concentration
of glucose in the blood.
(19) “Health Care Provider” means a physician or physician’s assistant licensed under chapter 458 or 459, F.S.,
or advanced registered nurse practitioner licensed under chapter 464, F.S.
(20) “Licensed Dietitian or Nutritionist” means a dietitian or nutritionist licensed under chapter 468, part X, F.S.
(21) “Local fire safety authority” means the authority having jurisdiction as defined in rule chapter 69A-40,
F.A.C.
(22) “Long-term Care Ombudsman Program (LTCOP)” means the long-term care ombudsman program
established under chapter 400, Part I, F.S.

Effective July 1, 2019 6A – 5
(23) “Manager” means an individual who is authorized to perform the same functions as a facility administrator,
and is responsible for the operation and maintenance of an assisted living facility while under the supervision of the
administrator of that facility. A manager does not include staff authorized to perform limited administrative
functions during an administrator’s temporary absence.
(24) “Mental Disorder” for the purposes of identifying a mental health resident, means schizophrenia and other
psychotic disorders; affective disorders; anxiety related disorders; and personality and dissociative disorders.
However, mental disorder does not include residents with a primary diagnosis of Alzheimer’s disease, other
dementias, or mental retardation.
(25) “Mental Health Care Provider” means an individual, agency, or organization providing mental health
services to clients of the Department of Children and Families; an individual licensed by the state to provide mental
health services; or an entity employing or contracting with individuals licensed by the state to provide mental health
services.
(26) “Mental Health Case Manager” means a case manager employed by or under contract to a mental health
care provider to assist mental health residents residing in a facility holding a limited mental health license.
(27) “Nurse” means a licensed practical nurse (LPN), registered nurse (RN), or advanced registered nurse
practitioner (ARNP) licensed under chapter 464, F.S.
(28) “Nursing Assessment” means a written review of information collected from observation and interaction
with a resident, including the resident’s record and any other relevant sources of information, the analysis of the
information, and recommendations for modification of the resident’s care, if warranted. The assessment must
contain the signature and credential initials of the person who conducted the assessment.
(29) “Nursing Progress Notes” or “Progress Report” means a written record of nursing services, other than
medication administration or the taking of vital signs, provided to each resident who receives such services in a
facility with a limited nursing or extended congregate care license. The progress notes must be completed by the
nurse who delivered the service; must describe the date, type, scope, amount, duration, and outcome of services that
are rendered; must describe the general status of the resident’s health; must describe any deviations in the residents
health; must describe any contact with the resident’s physician; and must contain the signature and credential initials
of the person rendering the service.
(30) “Optional State Supplementation (OSS)” means the state program providing monthly payments to eligible
residents pursuant to section 409.212, F.S., and rule chapter 65A-2, F.A.C.
(31) “Owner” means a person, partnership, association, limited liability company, or corporation, that owns or
leases the facility that is licensed by the agency. The term does not include a person, partnership, association, limited
liability company, or corporation that contracts only to manage or operate the facility.
(32) “Physician” means an individual licensed under chapter 458 or 459, F.S.
(33) “Pill organizer” means a container that is designed to hold solid doses of medication and is divided
according to day or time increments.
(34) “Registered Dietitian” means an individual registered with the Commission on Dietetic Registration, the
accrediting body of the Academy of Nutrition and Dietetics.
(35) “Respite Care” means facility-based supervision of an impaired adult for the purpose of relieving the
primary caregiver.

Effective July 1, 2019 6A – 6
(36) “Significant Change” means either a sudden or major shift in the behavior or mood of a resident that is
inconsistent with the resident’s diagnosis, or a deterioration in the resident’s health status such as unplanned weight
change, stroke, heart condition, enrollment in hospice, or stage 2, 3 or 4 pressure sore. Ordinary day-to-day
fluctuations in a resident’s functioning and behavior, short-term illnesses such as colds, or the gradual deterioration
in the resident’s ability to carry out the activities of daily living that accompanies the aging process are not
considered significant changes.
(37) “Staff” means any individual employed by a facility, contracting with a facility to provide direct or indirect
services to residents, or employed by a firm under contract with a facility to provide direct or indirect services to
residents when present in the facility. The term includes volunteers performing any service that counts toward
meeting any staffing requirement of this rule chapter.
(38) “Staff in Regular Contact” or “Staff in Direct Contact” mean all staff whose duties may require them to
interact with residents on a daily basis.
(39) “Third Party” means any individual or business entity providing services to residents in a facility that is not
staff of the facility.
(40) “Universal Precautions” are a set of precautions designed to prevent transmission of human
immunodeficiency virus (HIV), hepatitis B virus (HBV), and other bloodborne pathogens when providing first aid
or health care. Universal precautions require that the blood and certain body fluids of all residents be considered
potentially infectious for HIV, HBV, and other bloodborne pathogens.
(41) “Unscheduled Service Need” means a need for a personal service, nursing service, or mental health
intervention that cannot be predicted in advance and that must be met promptly to ensure that the health, safety, and
welfare of residents is preserved.
Rulemaking Authority 429.41, 429.929 FS. Law Implemented 429.07, 429.075, 429.11, 429.14, 429.19, 429.41,
429.47, 429.52, 429.905 FS. History–New 9-30-92, Formerly 10A-5.0131, Amended 10-30-95, 6-2-96, 4-20-98, 11-
2-98, 10-17-99, 1-9-02, 7-30-06, 4-15-10, 4-17-14, 5-10-18, Formerly 58A-5.0131, 7-1-19.
59A-36.003 Licensing and Change of Ownership.
(1) LICENSE APPLICATION. An applicant for a standard assisted living facility license, a limited mental
health license, an extended congregate care license, or a limited nursing services license may apply for licensure
pursuant to the requirements of chapters 408, part II, 429, part I, F.S., and rule chapter 59A-35, F.A.C.
(2) CHANGE OF OWNERSHIP. In addition to the requirements for a change of ownership contained in
chapter 408, part II, F.S., section 429.12, F.S., and rule chapter 59A-35, F.A.C., the following provisions relating to
resident funds apply pursuant to section 429.27, F.S.:
(a) At the time of transfer of ownership, all resident funds on deposit, advance payments of resident rents,
resident security deposits, and resident trust funds held by the current licensee must be transferred to the applicant.
Proof of such transfer must be provided to the agency at the time of the agency survey and before the issuance of a
standard license. This provision does not apply to entrance fees paid to a continuing care facility subject to the
acquisition provisions in section 651.024, F.S.
(b) The transferor must provide to each resident a statement detailing the amount and type of funds held by the
facility and credited to the resident.

Effective July 1, 2019 6A – 7
(c) The transferee must notify each resident in writing of the manner in which the transferee is holding the
resident’s funds and state the name and address of the depository where the funds are being held, the amount held,
and type of funds credited.
(3) CONDITIONAL LICENSE. Except as provided in section 429.14, F.S., the agency may issue a conditional
license to a facility if, at the time of license renewal the facility is found to have uncorrected violations that the
facility has had an opportunity to correct. The issuance of a conditional license does not change the biennial license
expiration date.
(4) OSS RESIDENT DETERMINATION. With respect to the fee per bed required for a standard license, the
number of OSS recipients claimed shall be the average number per month residing in the facility during the previous
license period. An additional per bed charge shall be added to the bed fee for facilities whose average number of
OSS residents per month was less than the number of beds designated for OSS recipients during the previous license
period.
Rulemaking Authority 429.17, 429.27, 429.41 FS. Law Implemented 429.04, 429.07, 429.075, 429.11, 429.12,
429.17, 429.27, 429.41 FS. History–New 5-14-81, Amended 1-6-82, 5-19-83, 9-17-84, Formerly 10A-5.14, Amended
10-20-86, 6-21-88, 8-15-90, 9-30-92, Formerly 10A-5.014, Amended 10-30-95, 4-20-98, 10-17-99, 7-30-06, 4-17-
14, 5-10-18, Formerly 58A-5.014, 7-1-19.
59A-36.004 License Requirements.
(1) SERVICE PROHIBITION. An assisted living facility may not represent that it provides any service other
than a service for which it is licensed to provide.
(2) CHANGE IN USE OF SPACE REQUIRING AGENCY CENTRAL OFFICE APPROVAL. A change in the
use of space that increases or decreases a facility’s capacity must not be made without prior approval from the
Agency Central Office. Approval must be based on the compliance with the physical plant standards provided in
rule 59A-36.014, F.A.C., as well as documentation of compliance with applicable fire safety and sanitation
inspection requirements referenced in rule 59A-36.005, F.A.C.
(3) CHANGE IN USE OF SPACE REQUIRING AGENCY FIELD OFFICE APPROVAL. A change in the use
of space that involves converting an area to resident use, which has not previously been inspected for such use, must
not be made without prior approval from the Agency Field Office. Approval must be based on compliance with the
physical plant standards provided in rule 59A-36.014, F.A.C., as well as documentation of compliance with
applicable fire safety and sanitation inspection standards referenced in rule 59A-36.005, F.A.C.
(4) CONTIGUOUS PROPERTY. If a facility consists of more than one building, all buildings included under a
single license must be on contiguous property. “Contiguous property” means property under the same ownership
separated by no more than a two-lane street that traverses the property. A licensed location may be expanded to
include additional contiguous property with the approval of the agency to ensure continued compliance with the
requirements and standards of chapters 408, Part II, 429, Part I, F.S. and rule chapter 59A-35, F.A.C., and this rule
chapter.
(5) PROOF OF INSPECTIONS. A copy of the annual fire safety and sanitation inspections described in rule
59A-36.005, F.A.C., must be submitted annually to the Agency Central Office. The annual inspections must be
submitted no later than 30 calendar days after the inspections. Failure to comply with this requirement may result in
administrative action pursuant to chapter 408, part II, and section 429.14, F.S., and rule chapter 59A-35, F.A.C.

Effective July 1, 2019 6A – 8
(6) RESIDENTS RECEIVING STATE-FUNDED SERVICES. Upon request, the facility administrator or
designee must identify residents receiving state-funded services to the agency and the department for monitoring
purposes authorized by state and federal laws.
Rulemaking Authority 429.41 FS. Law Implemented 429.41, 429.44 FS. History–New 5-15-81, Amended 1-6-82, 9-
17-84, Formerly 10A-5.16, Amended 6-21-88, 9-30-92, Formerly 10A-5.016, Amended 10-30-95, 10-17-99, 7-30-06,
4-15-10, 4-17-14, Formerly 58A-5.016, 7-1-19.
59A-36.005 Inspection Responsibilities.
(1) County health departments are responsible for inspecting all license applicants and licensed facilities in
matters regulated by:
(a) Rule 64E-12.004, F.A.C., and rule chapter 64E-11, F.A.C., relating to food hygiene.
(b) Chapter 64E-12, F.A.C., relating to sanitary practices in community-based residential facilities.
(c) Chapter 64E-16, F.A.C., relating to biomedical waste.
(2) The local authority having jurisdiction over fire safety or State Fire Marshal is responsible for inspecting all
license applicants and licensed facilities in matters regulated by section 429.41, F.S., relating to uniform fire safety
standards and chapter 69A-40, F.A.C., Uniform Fire Safety Standards for Assisted Living Facilities.
(3) The agency is responsible for inspecting all license applicants and licensed facilities in all other matters
regulated by this rule chapter.
Rulemaking Authority 429.41 FS. Law Implemented 429.41 FS. History–New 8-15-90, Formerly 10A-5.0161,
Amended 10-30-95, 10-17-99, 3-13-14, Formerly 58A-5.0161, 7-1-19.
59A-36.006 Admission Procedures, Appropriateness of Placement and Continued Residency Criteria.
(1) ADMISSION CRITERIA.
(a) An individual must meet the following minimum criteria in order to be admitted to a facility holding a
standard, limited nursing services, or limited mental health license:
1. Be at least 18 years of age.
2. Be free from signs and symptoms of any communicable disease that is likely to be transmitted to other
residents or staff. An individual who has human immunodeficiency virus (HIV) infection may be admitted to a
facility, provided that the individual would otherwise be eligible for admission according to this rule.
3. Be able to perform the activities of daily living, with supervision or assistance if necessary.
4. Be able to transfer, with assistance if necessary. The assistance of more than one person is permitted.
5. Be capable of taking medication, by either self-administration, assistance with self-administration, or
administration of medication.
a. If the resident needs assistance with self-administration of medication, the facility must inform the resident of
the professional qualifications of facility staff who will be providing this assistance. If unlicensed staff will be
providing assistance with self-administration of medication, the facility must obtain written informed consent from
the resident or the resident’s surrogate, guardian, or attorney-in-fact.
b. The facility may accept a resident who requires the administration of medication if the facility employs a
nurse who will provide this service or the resident, or the resident’s legal representative, designee, surrogate,
guardian, or attorney-in-fact, contracts with a third party licensed to provide this service to the resident.
6. Not have any special dietary needs that cannot be met by the facility.

Effective July 1, 2019 6A – 9
7. Not be a danger to self or others as determined by a physician, or mental health practitioner licensed under
chapter 490 or 491, F.S.
8. Not require 24-hour licensed professional mental health treatment.
9. Not be bedridden.
10. Not have any stage 3 or 4 pressure sores. A resident requiring care of a stage 2 pressure sore may be
admitted provided that:
a. The resident either:
(I) Resides in a standard or limited nursing services licensed facility and contracts directly with a licensed home
health agency or a nurse to provide care; or
(II) Resides in a limited nursing services licensed facility and care is provided by the facility pursuant to a plan
of care issued by a health care provider;
b. The condition is documented in the resident’s record and admission and discharge logs; and,
c. If the resident’s condition fails to improve within 30 days as documented by a health care provider, the
resident must be discharged from the facility.
11. Residents admitted to standard, limited nursing services, or limited mental health licensed facilities may not
require any of the following nursing services:
a. Artificial airway management of any kind, except that of continuous positive airway pressure may be
provided through the use of a CPAP or bipap machine;
b. Assistance with tube feeding,
c. Monitoring of blood gases,
d. Management of post-surgical drainage tubes and wound vacuum devices;
e. The administration of blood products in the facility; or
f. Treatment of surgical incisions or wounds, unless the surgical incision or wound and the underlying condition
have been stabilized and a plan of care has been developed. The plan of care must be maintained in the resident’s
record.
12. In addition to the nursing services listed above, residents admitted to facilities holding only standard and/or
limited mental health licenses may not require any of the following nursing services:
a. Hemodialysis and peritoneal dialysis performed in the facility;
b. Intravenous therapy performed in the facility.
13. Not require 24-hour nursing supervision.
14. Not require skilled rehabilitative services as described in rule 59G-4.290, F.A.C.
15. Be appropriate for admission to the facility as determined by the facility administrator. The administrator
must base the determination on:
a. An assessment of the strengths, needs, and preferences of the individual;
b. The medical examination report required by section 429.26, F.S., and subsection (2) of this rule, if available;
c. The facility’s admission policy and the services the facility is prepared to provide or arrange in order to meet
resident needs. Such services may not exceed the scope of the facility’s license unless specified elsewhere in this
rule; and,
d. The ability of the facility to meet the uniform fire safety standards for assisted living facilities established in
rule chapter 69A-40, F.A.C.
Effective July 1, 2019 6A – 10
(b) A resident who otherwise meets the admission criteria for residency in a standard licensed facility, but who
requires assistance with the administration and regulation of portable oxygen or assistance with routine colostomy
care of stoma site flange placement, may be admitted to a facility with a standard license as long as the facility has a
nurse on staff or under contract to provide the assistance or to provide training to the resident on how to perform
these functions themselves.
(c) Nursing staff may not provide training to unlicensed persons, as defined in section 429.256(1)(b), F.S., to
perform skilled nursing services, and may not delegate the nursing services described in this section to certified
nursing assistants or unlicensed persons. This provision does not restrict a resident or a resident’s representative
from contracting with a licensed third party to provide the assistance if the facility is agreeable to such an
arrangement and the resident otherwise meets the criteria for admission and continued residency in a facility with a
standard license.
(d) An individual enrolled in and receiving hospice services may be admitted to an assisted living facility as
long as the individual otherwise meets resident admission criteria.
(e) Resident admission criteria for facilities holding an extended congregate care license are described in rule
59A-36.021, F.A.C.
(2) HEALTH ASSESSMENT. As part of the admission criteria, an individual must undergo a face-to-face
medical examination completed by a health care provider as specified in either paragraph (a) or (b) of this
subsection.
(a) A medical examination completed within 60 calendar days before the individual’s admission to a facility
pursuant to section 429.26(4), F.S. The examination must address the following:
1. The physical and mental status of the resident, including the identification of any health-related problems and
functional limitations,
2. An evaluation of whether the individual will require supervision or assistance with the activities of daily
living,
3. Any nursing or therapy services required by the individual,
4. Any special diet required by the individual,
5. A list of current medications prescribed, and whether the individual will require any assistance with the
administration of medication,
6. Whether the individual has signs or symptoms of Tuberculosis, Methicillin Resistant Staphylococcus Aureus,
Scabies or any other communicable disease, which are likely to be transmitted to other residents or staff,
7. A statement on the day of the examination that, in the opinion of the examining health care provider, the
individual’s needs can be met in an assisted living facility; and,
8. The date of the examination, and the name, signature, address, telephone number, and license number of the
examining health care provider. The medical examination may be conducted by a health care provider licensed
under chapter 458, 459 or 464, F.S.
(b) A medical examination completed after the resident’s admission to the facility within 30 calendar days of
the admission date. The examination must be recorded on AHCA Form 1823, Resident Health Assessment for
Assisted Living Facilities, March 2017, which is incorporated by reference and available online at:
http://www.flrules.org/Gateway/reference.asp?No=Ref-09170. Faxed or electronic copies of the completed form are
acceptable. The form must be completed as instructed.

Effective July 1, 2019 6A – 11
1. Items on the form that have been omitted by the health care provider during the examination may be obtained
by the facility either orally or in writing from the health care provider.
2. Omitted information must be documented in the resident’s record. Information received orally must include
the name of the health care provider, the name of the facility staff recording the information, and the date the
information was provided.
3. Electronic documentation may be used in place of completing the section on AHCA Form 1823 referencing
Services Offered or Arranged by the Facility for the Resident. The electronic documentation must include all of the
elements described in this section of AHCA Form 1823.
(c) Any information required by paragraph (a), that is not contained in the medical examination report
conducted before the individual’s admission to the facility must be obtained by the administrator using AHCA Form
1823 within 30 days after admission.
(d) Medical examinations of residents placed by the department, by the Department of Children and Families, or
by an agency under contract with either department must be conducted within 30 days before placement in the
facility and recorded on AHCA Form 1823 described in paragraph (b).
(e) An assessment that has been conducted through the Comprehensive, Assessment, Review and Evaluation for
Long-Term Care Services (CARES) program may be substituted for the medical examination requirements of
section 429.26, F.S. and this rule.
(f) Any orders issued by the health care provider conducting the medical examination for medications, nursing,
therapeutic diets, or other services to be provided or supervised by the facility may be attached to the health
assessment. A health care provider may attach a DH Form 1896, Florida Do Not Resuscitate Order Form, for
residents who do not wish cardiopulmonary resuscitation to be administered in the case of cardiac or respiratory
arrest.
(g) A resident placed in a facility on a temporary emergency basis by the Department of Children and Families
pursuant to section 415.105 or 415.1051, F.S., is exempt from the examination requirements of this subsection for
up to 30 days. However, a resident accepted for temporary emergency placement must be entered on the facility’s
admission and discharge log and counted in the facility census. A facility may not exceed its licensed capacity in
order to accept such a resident. A medical examination must be conducted on any temporary emergency placement
resident accepted for regular admission.
(3) ADMISSION PACKAGE.
(a) The facility must make available to potential residents a written statement(s) that includes the following
information listed below. Providing a copy of the facility resident contract or facility brochure containing all the
required information meets this requirement.
1. The facility’s admission and continued residency criteria;
2. The daily, weekly or monthly charge to reside in the facility and the services, supplies, and accommodations
provided by the facility for that rate;
3. Personal care services that the facility is prepared to provide to residents and additional costs to the resident,
if any;
4. Nursing services that the facility is prepared to provide to residents and additional costs to the resident, if
any;
5. Food service and the ability of the facility to accommodate special diets;

Effective July 1, 2019 6A – 12
6. The availability of transportation and additional costs to the resident, if any;
7. Any other special services that are provided by the facility and additional cost if any;
8. Social and leisure activities generally offered by the facility;
9. Any services that the facility does not provide but will arrange for the resident and additional cost, if any;
10. The facility rules and regulations that residents must follow as described in rule 59A-36.007, F.A.C.;
11. The facility policy concerning Do Not Resuscitate Orders pursuant to section 429.255, F.S., and rule 59A-
36.009, F.A.C., and Advance Directives pursuant to chapter 765, F.S.;
12. If the facility is licensed to provide extended congregate care, the facility’s residency criteria for residents
receiving extended congregate care services. The facility must also provide a description of the additional personal,
supportive, and nursing services provided by the facility including additional costs and any limitations on where
extended congregate care residents may reside based on the policies and procedures described in rule 59A-36.021,
F.A.C.;
13. If the facility advertises that it provides special care for individuals with Alzheimer’s disease and related
disorders, a written description of those special services as required in section 429.177, F.S.; and,
14. The facility’s resident elopement response policies and procedures.
(b) Before or at the time of admission, the resident, or the resident’s responsible party, guardian, or attorney-in-
fact, if applicable, must be provided with the following:
1. A copy of the resident’s contract that meets the requirements of rule 59A-36.018, F.A.C.,
2. A copy of the facility statement described in paragraph (a) of this subsection, if one has not already been
provided,
3. A copy of the resident’s bill of rights as required by rule 59A-36.007, F.A.C.; and,
4. A Long-Term Care Ombudsman Program brochure that includes the telephone number and address of the
district office.
(c) Documents required by this subsection must be in English. If the resident is not able to read, or does not
understand English and translated documents are not available, the facility must explain its policies to a family
member or friend of the resident or another individual who can communicate the information to the resident.
(4) CONTINUED RESIDENCY. Except as follows in paragraphs (a) through (c) of this subsection, criteria for
continued residency in any licensed facility must be the same as the criteria for admission. As part of the continued
residency criteria, a resident must have a face-to-face medical examination by a health care provider at least every 3
years after the initial assessment, or after a significant change, whichever comes first. A significant change is
defined in rule 59A-36.002, F.A.C. The results of the examination must be recorded on AHCA Form 1823, which is
incorporated by reference in paragraph (2)(b) of this rule and must be completed in accordance with that paragraph.
Exceptions to the requirement to meet the criteria for continued residency are:
(a) The resident may be bedridden for no more than 7 consecutive days.
(b) A resident requiring care of a stage 2 pressure sore may be retained provided that:
1. The resident contracts directly with a licensed home health agency or a nurse to provide care, or the facility
has a limited nursing services license and services are provided pursuant to a plan of care issued by a health care
provider,
2. The condition is documented in the resident’s record; and,

Effective July 1, 2019 6A – 13
3. If the resident’s condition fails to improve within 30 days, as documented by a health care provider, the
resident must be discharged from the facility.
(c) A terminally ill resident who no longer meets the criteria for continued residency may continue to reside in
the facility if the following conditions are met:
1. The resident qualifies for, is admitted to, and consents to receive services from a licensed hospice that
coordinates and ensures the provision of any additional care and services that the resident may need;
2. Both the resident, or the resident’s legal representative if applicable, and the facility agree to continued
residency;
3. A licensed hospice, in consultation with the facility, develops and implements a interdisciplinary care plan
that specifies the services being provided by hospice and those being provided by the facility; and,
4. Documentation of the requirements of this paragraph is maintained in the resident’s file.
(d) The facility administrator is responsible for monitoring the continued appropriateness of placement of a
resident in the facility at all times.
(e) A hospice resident that meets the qualifications of continued residency pursuant to this subsection may only
receive services from the assisted living facility’s staff which are within the scope of the facility’s license.
(f) Assisted living facility staff may provide any nursing service permitted under the facility’s license and total
help with the activities of daily living for residents admitted to hospice; however, staff may not exceed the scope of
their professional licensure or training.
(g) Continued residency criteria for facilities holding an extended congregate care license are described in rule
59A-36.021, F.A.C.
(5) DISCHARGE. If the resident no longer meets the criteria for continued residency, or the facility is unable to
meet the resident’s needs, as determined by the facility administrator or health care provider, the resident must be
discharged in accordance with section 429.28, F.S.
Rulemaking Authority 429.07, 429.41 FS. Law Implemented 429.07, 429.26, 429.28, 429.41 FS. History–New 9-17-
84, Formerly 10A-5.181, Amended 10-20-86, 6-21-88, 8-15-90, 9-30-92, Formerly 10A-5.0181, Amended 10-30-95,
6-2-96, 10-17-99, 7-30-06, 10-9-06, 4-15-10, 10-14-10, 4-17-14, 5-10-18, Formerly 58A-5.0181, 7-1-19.
59A-36.007 Resident Care Standards.
An assisted living facility must provide care and services appropriate to the needs of residents accepted for
admission to the facility.
(1) SUPERVISION. Facilities must offer personal supervision as appropriate for each resident, including the
following:
(a) Monitoring of the quantity and quality of resident diets in accordance with rule 59A-36.012, F.A.C.
(b) Daily observation by designated staff of the activities of the resident while on the premises, and awareness
of the general health, safety, and physical and emotional well-being of the resident.
(c) Maintaining a general awareness of the resident’s whereabouts. The resident may travel independently in the
community.
(d) Contacting the resident’s health care provider and other appropriate party such as the resident’s family,
guardian, health care surrogate, or case manager if the resident exhibits a significant change.
(e) Contacting the resident’s family, guardian, health care surrogate, or case manager if the resident is
discharged or moves out.

Effective July 1, 2019 6A – 14
(f) Maintaining a written record, updated as needed, of any significant changes, any illnesses that resulted in
medical attention, changes in the method of medication administration, or other changes that resulted in the
provision of additional services.
(2) SOCIAL AND LEISURE ACTIVITIES. Residents shall be encouraged to participate in social, recreational,
educational and other activities within the facility and the community.
(a) The facility must provide an ongoing activities program. The program must provide diversified individual
and group activities in keeping with each resident’s needs, abilities, and interests.
(b) The facility must consult with the residents in selecting, planning, and scheduling activities. The facility
must demonstrate residents’ participation through one or more of the following methods: resident meetings,
committees, a resident council, a monitored suggestion box, group discussions, questionnaires, or any other form of
communication appropriate to the size of the facility.
(c) Scheduled activities must be available at least 6 days a week for a total of not less than 12 hours per week.
Watching television is not an activity for the purpose of meeting the 12 hours per week of scheduled activities unless
the television program is a special one-time event of special interest to residents of the facility. A facility whose
residents choose to attend day programs conducted at adult day care centers, senior centers, mental health centers, or
other day programs may count those attendance hours towards the required 12 hours per week of scheduled
activities. An activities calendar must be posted in common areas where residents normally congregate.
(d) If residents assist in planning a special activity such as an outing, seasonal festivity, or an excursion, up to 3
hours may be counted toward the required activity time.
(3) ARRANGEMENT FOR HEALTH CARE. In order to facilitate resident access to health care as needed, the
facility must:
(a) Assist residents in making appointments and remind residents about scheduled appointments for medical,
dental, nursing, or mental health services.
(b) Provide transportation to needed medical, dental, nursing or mental health services, or arrange for
transportation through family and friends, volunteers, taxi cabs, public buses, and agencies providing transportation.
(c) The facility may not require residents to receive services from a particular health care provider.
(4) ACTIVITIES OF DAILY LIVING. Facilities must offer supervision of or assistance with activities of daily
living as needed by each resident. Residents should be encouraged to be as independent as possible in performing
activities of daily living.
(5) NURSING SERVICES.
(a) Pursuant to section 429.255, F.S., the facility may employ or contract with a nurse to:
1. Take or supervise the taking of vital signs,
2. Manage pill-organizers and administer medications as described in rule 59A-36.008, F.A.C.,
3. Give prepackaged enemas pursuant to a physician’s order; and,
4. Maintain nursing progress notes.
(b) Pursuant to section 429.255(2), F.S., the nursing services listed in paragraph (a), may also be delivered in
the facility by family members or friends of the resident provided the family member or friend does not receive
compensation for such services.
(6) RESIDENT RIGHTS AND FACILITY PROCEDURES.
(a) A copy of the Resident Bill of Rights as described in section 429.28, F.S., or a summary provided by the

Effective July 1, 2019 6A – 15
Long-Term Care Ombudsman Program must be posted in full view in a freely accessible resident area, and included
in the admission package provided pursuant to rule 59A-36.006, F.A.C.
(b) In accordance with section 429.28, F.S., the facility must have a written grievance procedure for receiving
and responding to resident complaints and a written procedure to allow residents to recommend changes to facility
policies and procedures. The facility must be able to demonstrate that such procedure is implemented upon receipt
of a complaint.
(c) The telephone number for lodging complaints against a facility or facility staff must be posted in full view in
a common area accessible to all residents. The telephone numbers are: the Long-Term Care Ombudsman Program,
1(888)831-0404; Disability Rights Florida, 1(800)342-0823; the Agency Consumer Hotline 1(888)419-3456, and
the statewide toll-free telephone number of the Florida Abuse Hotline, 1(800)96-ABUSE or 1(800)962-2873. The
telephone numbers must be posted in close proximity to a telephone accessible by residents and the text must be a
minimum of 14-point font.
(d) The facility must have a written statement of its house rules and procedures that must be included in the
admission package provided pursuant to rule 59A-36.006, F.A.C. The rules and procedures must at a minimum
address the facility’s policies regarding:
1. Resident responsibilities;
2. Alcohol and tobacco use;
3. Medication storage;
4. Resident elopement;
5. Reporting resident abuse, neglect, and exploitation;
6. Administrative and housekeeping schedules and requirements;
7. Infection control, sanitation, and universal precautions; and,
8. The requirements for coordinating the delivery of services to residents by third party providers.
(e) Residents may not be required to perform any work in the facility without compensation. Residents may be
required to clean their own sleeping areas or apartments if the facility rules or the facility contract includes such a
requirement. If a resident is employed by the facility, the resident must be compensated in compliance with state and
federal wage laws.
(f) The facility must provide residents with convenient access to a telephone to facilitate the resident’s right to
unrestricted and private communication, pursuant to section 429.28(1)(d), F.S. The facility must allow unidentified
telephone calls to residents. For facilities with a licensed capacity of 17 or more residents in which residents do not
have private telephones, there must be, at a minimum, a readily accessible telephone on each floor of each building
where residents reside.
(g) In addition to the requirements of section 429.41(1)(k), F.S., the use of physical restraints by a facility on a
resident must be reviewed by the resident’s physician annually. Any device, including half-bed rails, which the
resident chooses to use and can remove or avoid without assistance, is not considered a physical restraint.
(7) THIRD PARTY SERVICES.
(a) Nothing in this rule chapter is intended to prohibit a resident or the resident’s representative from
independently arranging, contracting, and paying for services provided by a third party of the resident’s choice,
including a licensed home health agency or private nurse, or receiving services through an out-patient clinic,
provided the resident meets the criteria for admission and continued residency and the resident complies with the

Effective July 1, 2019 6A – 16
facility’s policy relating to the delivery of services in the facility by third parties. The facility’s policies must require
the third party to coordinate with the facility regarding the resident’s condition and the services being provided.
(b) When residents require or arrange for services from a third party provider, the facility administrator or
designee must allow for the receipt of those services, provided that the resident meets the criteria for admission and
continued residency. The facility, when requested by residents or representatives, must coordinate with the provider
to facilitate the receipt of care and services provided to meet the particular resident’s needs.
(c) If residents accept assistance from the facility in arranging and coordinating third party services, the
facility’s assistance does not represent a guarantee that third party services will be received. If the facility’s efforts to
make arrangements for third party services are unsuccessful or declined by residents, the facility must include
documentation in the residents’ record explaining why its efforts were unsuccessful. This documentation will serve
to demonstrate its compliance with this subsection.
(8) ELOPEMENT STANDARDS.
(a) Residents Assessed at Risk for Elopement. All residents assessed at risk for elopement or with any history of
elopement must be identified so staff can be alerted to their needs for support and supervision. All residents must be
assessed for risk of elopement by a health care provider or a mental health care provider within 30 calendar days of
being admitted to a facility. If the resident has had a health assessment performed prior to admission pursuant to
paragraph 59A-36.006(2)(a), F.A.C., this requirement is satisfied. A resident placed in a facility on a temporary
emergency basis by the Department of Children and Families pursuant to section 415.105 or 415.1051, F.S., is
exempt from this requirement for up to 30 days.
1. As part of its resident elopement response policies and procedures, the facility must make, at a minimum, a
daily effort to determine that at risk residents have identification on their persons that includes their name and the
facility’s name, address, and telephone number. Staff trained pursuant to paragraph 59A-36.011(10)(a) or (c),
F.A.C., must be generally aware of the location of all residents assessed at high risk for elopement at all times.
2. The facility must have a photo identification of at risk residents on file that is accessible to all facility staff
and law enforcement as necessary. The facility’s file must contain the resident’s photo identification upon admission
or upon being assessed at risk for elopement subsequent to admission. The photo identification may be provided by
the facility, the resident, or the resident’s representative.
(b) Facility Resident Elopement Response Policies and Procedures. The facility must develop detailed written
policies and procedures for responding to a resident elopement. At a minimum, the policies and procedures must
provide for:
1. An immediate search of the facility and premises,
2. The identification of staff responsible for implementing each part of the elopement response policies and
procedures, including specific duties and responsibilities,
3. The identification of staff responsible for contacting law enforcement, the resident’s family, guardian, health
care surrogate, and case manager if the resident is not located pursuant to subparagraph (8)(b)1.; and,
4. The continued care of all residents within the facility in the event of an elopement.
(c) Facility Resident Elopement Drills. The facility must conduct and document resident elopement drills
pursuant to sections 429.41(1)(a)3. and 429.41(1)(l), F.S.
(9) OTHER STANDARDS. Additional care standards for residents residing in a facility holding a limited
mental health, extended congregate care or limited nursing services license are provided in rules 59A-36.020, 59A-

Effective July 1, 2019 6A – 17
36.021 and 59A-36.022, F.A.C., respectively.
Rulemaking Authority 429.41 FS. Law Implemented 429.255, 429.26, 429.28, 429.41 FS. History–New 9-17-84,
Formerly 10A-5.182, Amended 10-20-86, 6-21-88, 8-15-90, 9-30-92, Formerly 10A-5.0182, Amended 10-30-95, 4-
20-98, 11-2-98, 10-17-99, 7-30-06, 10-9-06, 4-15-10, 4-17-14, 5-10-18, Formerly 58A-5.0182, 7-1-19.
59A-36.008 Medication Practices.
Pursuant to sections 429.255 and 429.256, F.S., and this rule, licensed facilities may assist with the self-
administration or administration of medications to residents in a facility. A resident may not be compelled to take
medications but may be counseled in accordance with this rule.
(1) SELF ADMINISTERED MEDICATIONS.
(a) Residents who are capable of self-administering their medications without assistance must be encouraged
and allowed to do so.
(b) If facility staff observes health changes that could reasonably be attributed to the improper self-
administration of medication, staff must consult with the resident concerning any problems the resident may be
experiencing in self-administering the medications. The consultation should describe the services offered by the
facility that aid the resident with medication administration through the use of a pill organizer, through providing
assistance with self-administration of medications, or through administering medications. The facility must contact
the resident’s health care provider when observable health changes occur that may be attributed to the resident’s
medications. The facility must document such contacts in the resident’s records.
(2) PILL ORGANIZERS.
(a) Only a resident who self-administers medications may maintain a pill organizer.
(b) Unlicensed staff may not provide assistance with the contents of pill organizers.
(c) A nurse may manage a pill organizer to be used only by residents who self-administer medications. The
nurse is responsible for instructing the resident in the proper use of the pill organizer. The nurse must manage the
pill organizer in the following manner:
1. Obtain the labeled medication container from the storage area or the resident,
2. Transfer the medication from the original container into a pill organizer, labeled with the resident’s name,
according to the day and time increments as prescribed,
3. Return the medication container to the storage area or resident; and,
4. Document the date and time the pill organizer was filled in the resident’s record.
(d) If there is a determination that the resident is not taking medications as prescribed after the medicinal
benefits are explained, it must be noted in the resident’s record and the facility must consult with the resident
concerning providing assistance with self-administration or the administration of medications if such services are
offered by the facility. The facility must contact the resident’s health care provider regarding questions, concerns, or
observations relating to the resident’s medications. Such communication must be documented in the resident’s
record.
(3) ASSISTANCE WITH SELF-ADMINISTRATION.
(a) Any unlicensed person providing assistance with self-administration of medication must be 18 years of age
or older, trained to assist with self administered medication pursuant to the training requirements of rule 59A-
36.011, F.A.C., and must be available to assist residents with self-administered medications in accordance with
procedures described in section 429.256, F.S. and this rule.

Effective July 1, 2019 6A – 18
(b) In addition to the specifications of section 429.256(3), F.S., assistance with self-administration of
medication includes, in the presence of the resident, reading the medication label aloud and verbally prompting a
resident to take medications as prescribed.
(c) In order to facilitate assistance with self-administration, trained staff may prepare and make available such
items as water, juice, cups, and spoons. Trained staff may also return unused doses to the medication container.
Medication, which appears to have been contaminated, must not be returned to the container.
(d) Trained staff must observe the resident take the medication. Any concerns about the resident’s reaction to
the medication or suspected noncompliance must be reported to the resident’s health care provider and documented
in the resident’s record.
(e) When a resident who receives assistance with medication is away from the facility and from facility staff,
the following options are available to enable the resident to take medication as prescribed:
1. The health care provider may prescribe a medication schedule that coincides with the resident’s presence in
the facility,
2. The medication container may be given to the resident, a friend, or family member upon leaving the facility,
with this fact noted in the resident’s medication record,
3. The medication may be transferred to a pill organizer pursuant to the requirements of subsection (2), and
given to the resident, a friend, or family member upon leaving the facility, with this fact noted in the resident’s
medication record, or
4. Medications may be separately prescribed and dispensed in an easier to use form, such as unit dose
packaging.
(f) Assistance with self-administration of medication does not include the activities detailed in section
429.256(4), F.S.
1. As used in section 429.256(4)(g), F.S., the term “competent resident” means that the resident is cognizant of
when a medication is required and understands the purpose for taking the medication.
2. As used in section 429.256(4)(h), F.S., the terms “judgment” and “discretion” mean interpreting vital signs
and evaluating or assessing a resident’s condition.
(g) All trained staff must adhere to the facility’s infection control policy and procedures when assisting with the
self-administration of medication.
(4) MEDICATION ADMINISTRATION.
(a) For facilities that provide medication administration, a staff member licensed to administer medications
must be available to administer medications in accordance with a health care provider’s order or prescription label.
(b) Unusual reactions to the medication or a significant change in the resident’s health or behavior that may be
caused by the medication must be documented in the resident’s record and reported immediately to the resident’s
health care provider. The contact with the health care provider must also be documented in the resident’s record.
(c) Medication administration includes conducting any examination or other procedure necessary for the proper
administration of medication that the resident cannot conduct personally and that can be performed by licensed staff.
(d) A facility that performs clinical laboratory tests for residents, including blood glucose testing, must be in
compliance with the federal Clinical Laboratory Improvement Amendments of 1988 (CLIA) and chapter 483, part I,
F.S. A valid copy of the State Clinical Laboratory License, if required, and the federal CLIA Certificate must be
maintained in the facility. A state license or federal CLIA certificate is not required if residents perform the test

Effective July 1, 2019 6A – 19
themselves or if a third party assists residents in performing the test. The facility is not required to maintain a State
Clinical Laboratory License or a federal CLIA Certificate if facility staff assist residents in performing clinical
laboratory testing with the residents’ equipment. Information about the State Clinical Laboratory License and federal
CLIA Certificate is available from the Laboratory Unit, Agency for Health Care Administration, 2727 Mahan Drive,
Mail Stop 32, Tallahassee, FL 32308; telephone (850)412-4500.
(5) MEDICATION RECORDS.
(a) For residents who use a pill organizer managed in subsection (2), the facility must keep either the original
labeled medication container; or a medication listing with the prescription number, the name and address of the
issuing pharmacy, the health care provider’s name, the resident’s name, the date dispensed, the name and strength of
the drug, and the directions for use.
(b) The facility must maintain a daily medication observation record for each resident who receives assistance
with self-administration of medications or medication administration. A medication observation record must be
immediately updated each time the medication is offered or administered and include:
1. The name of the resident and any known allergies the resident may have;
2. The name of the resident’s health care provider and the health care provider’s telephone number;
3. The name, strength, and directions for use of each medication; and,
4. A chart for recording each time the medication is taken, any missed dosages, refusals to take medication as
prescribed, or medication errors.
(c) For medications that serve as chemical restraints, the facility must, pursuant to section 429.41, F.S., maintain
a record of the prescribing physician’s annual evaluation of the use of the medication.
(6) MEDICATION STORAGE AND DISPOSAL.
(a) In order to accommodate the needs and preferences of residents and to encourage residents to remain as
independent as possible, residents may keep their medications, both prescription and over-the-counter, in their
possession both on or off the facility premises. Residents may also store their medication in their rooms or
apartments if either the room is kept locked when residents are absent or the medication is stored in a secure place
that is out of sight of other residents.
(b) Both prescription and over-the-counter medications for residents must be centrally stored if:
1. The facility administers the medication;
2. The resident requests central storage. The facility must maintain a list of all medications being stored
pursuant to such a request;
3. The medication is determined and documented by the health care provider to be hazardous if kept in the
personal possession of the person for whom it is prescribed;
4. The resident fails to maintain the medication in a safe manner as described in this paragraph;
5. The facility determines that, because of physical arrangements and the conditions or habits of residents, the
personal possession of medication by a resident poses a safety hazard to other residents, or
6. The facility’s rules and regulations require central storage of medication and that policy has been provided to
the resident before admission as required in rule 59A-36.006, F.A.C.
(c) Centrally stored medications must be:
1. Kept in a locked cabinet; locked cart; or other locked storage receptacle, room, or area at all times;

Effective July 1, 2019 6A – 20
2. Located in an area free of dampness and abnormal temperature, except that a medication requiring
refrigeration must be kept refrigerated. Refrigerated medications must be secured by being kept in a locked
container within the refrigerator, by keeping the refrigerator locked, or by keeping the area in which the refrigerator
is located locked;
3. Accessible to staff responsible for filling pill-organizers, assisting with self-administration of medication, or
administering medication. Such staff must have ready access to keys or codes to the medication storage areas at all
times; and,
4. Kept separately from the medications of other residents and properly closed or sealed.
(d) Medication that has been discontinued but has not expired must be returned to the resident or the resident’s
representative, as appropriate, or may be centrally stored by the facility for future use by the resident at the
resident’s request. If centrally stored by the facility, the discontinued medication must be stored separately from
medication in current use, and the area in which it is stored must be marked “discontinued medication.” Such
medication may be reused if prescribed by the resident’s health care provider.
(e) When a resident’s stay in the facility has ended, the administrator must return all medications to the resident,
the resident’s family, or the resident’s guardian unless otherwise prohibited by law. If, after notification and waiting
at least 15 days, the resident’s medications are still at the facility, the medications are considered abandoned and
may disposed of in accordance with paragraph (f).
(f) Medications that have been abandoned or have expired must be disposed of within 30 days of being
determined abandoned or expired and the disposal must be documented in the resident’s record. The medication may
be taken to a pharmacist for disposal or may be destroyed by the administrator or designee with one witness.
(g) Facilities that hold a Special-ALF permit issued by the Board of Pharmacy may return dispensed medicinal
drugs to the dispensing pharmacy pursuant to rule 64B16-28.870, F.A.C.
(7) MEDICATION LABELING AND ORDERS.
(a) The facility may not store prescription drugs for self-administration, assistance with self-administration, or
administration unless they are properly labeled and dispensed in accordance with chapters 465 and 499, F.S., and
rule 64B16-28.108, F.A.C. If a customized patient medication package is prepared for a resident, and separated into
individual medicinal drug containers, then the following information must be recorded on each individual container:
1. The resident’s name; and,
2. The identification of each medicinal drug in the container.
(b) Except with respect to the use of pill organizers as described in subsection (2), no individual other than a
pharmacist may transfer medications from one storage container to another.
(c) If the directions for use are “as needed” or “as directed,” the health care provider must be contacted and
requested to provide revised instructions. For an “as needed” prescription, the circumstances under which it would
be appropriate for the resident to request the medication and any limitations must be specified; for example, “as
needed for pain, not to exceed 4 tablets per day.” The revised instructions, including the date they were obtained
from the health care provider and the signature of the staff who obtained them, must be noted in the medication
record, or a revised label must be obtained from the pharmacist.
(d) Any change in directions for use of a medication that the facility is administering or providing assistance
with self-administration must be accompanied by a written, faxes, or electronic copy of a medication order issued
and signed by the resident’s health care provider. The new directions must promptly be recorded in the resident’s

Effective July 1, 2019 6A – 21
medication observation record. The facility may then obtain a revised label from the pharmacist or place an “alert”
label on the medication container that directs staff to examine the revised directions for use in the medication
observation record.
(e) A nurse may take a medication order by telephone. Such order must be promptly documented in the
resident’s medication observation record. The facility must obtain a written medication order from the health care
provider within 10 working days. A faxed or electronic copy of a signed order is acceptable.
(f) The facility must make every reasonable effort to ensure that prescriptions for residents who receive
assistance with self-administration of medication or medication administration are filled or refilled in a timely
manner.
(g) Pursuant to section 465.0276(5), F.S., and rule 61N-1.006, F.A.C., sample or complimentary prescription
drugs that are dispensed by a health care provider, must be kept in their original manufacturer’s packaging, which
must include the practitioner’s name, the resident’s name for whom they were dispensed, and the date they were
dispensed. If the sample or complimentary prescription drugs are not dispensed in the manufacturer’s labeled
package, they must be kept in a container that bears a label containing the following:
1. Practitioner’s name,
2. Resident’s name,
3. Date dispensed,
4. Name and strength of the drug,
5. Directions for use; and,
6. Expiration date.
(h) Pursuant to section 465.0276(2)(c), F.S., before dispensing any sample or complimentary prescription drug,
the resident’s health care provider must provide the resident with a written prescription, or a faxed or electronic copy
of such order.
(8) OVER THE COUNTER (OTC) PRODUCTS. For purposes of this subsection, the term over the counter
includes, but is not limited to, over the counter medications, vitamins, nutritional supplements and nutraceuticals,
hereafter referred to as OTC products, that can be sold without a prescription.
(a) A facility may keep a stock supply of OTC products for multiple resident use. When providing any OTC
product that is kept by the facility as a stock supply to a resident, the staff member providing the medication must
record the name and amount of the OTC product provided in the resident’s medication observation record. All OTC
products kept as a stock supply must be stored in a locked container or secure room in a central location within the
facility and must be labeled with the medication’s name, the date of purchase, and with a notice that the medication
is part of the facility’s stock supply.
(b) OTC products, including those prescribed by a health care provider but excluding those kept as a stock
supply by the facility, must be labeled with the resident’s name and the manufacturer’s label with directions for use,
or the health care provider’s directions for use. No other labeling requirements are required.
(c) Residents or their representatives may purchase OTC products from an establishment of their choice.

Effective July 1, 2019 6A – 22
(d) A health care provider’s order is required when a nurse provides assistance with self-administration or
administration of OTC products. When an order for an OTC product exists, the order must meet the requirements of
paragraphs (b) and (c) of this subsection. A health care provider’s order for OTC products is not required when a
resident self-administers his or her medications, or when unlicensed staff provides assistance with self-
administration of medications.
Rulemaking Authority 429.256, 429.41 FS. Law Implemented 429.255, 429.256, 429.41 FS. History–New 10-17-99,
Amended 7-30-06, 4-15-10, 10-14-10, 3-13-14, 5-10-18, Formerly 58A-5.0185, 7-1-19.
59A-36.009 Do Not Resuscitate Orders (DNROs).
(1) POLICIES AND PROCEDURES.
(a) Each assisted living facility must have written policies and procedures that explain its implementation of
state laws and rules relative to Do Not Resuscitate Orders (DNROs). An assisted living facility may not require
execution of a DNRO as a condition of admission or treatment. The assisted living facility must provide the
following to each resident, or resident’s representative, at the time of admission:
1. Form SCHS-4-2006, “Health Care Advance Directives – The Patient’s Right to Decide,” April 2006, or with
a copy of some other substantially similar document, which incorporates information regarding advance directives
included in chapter 765, F.S. Form SCHS-4-2006 is available from the Agency for Health Care Administration,
2727 Mahan Drive, Mail Stop 34, Tallahassee, FL 32308 or the agency’s website at:
http://ahca.myflorida.com/MCHQ/Health_Facility_Regulation/HC_Advance_Directives/docs/adv_dir.pdf; and,
2. DH Form 1896, Florida Do Not Resuscitate Order Form, December, 2004, which is hereby incorporated by
reference. This form may be obtained by calling the Department of Health’s toll free number 1(800)226-1911,
extension 2780 or online at: http://www.flrules.org/Gateway/reference.asp?No=Ref-04005.
(b) There must be documentation in the resident’s record indicating whether a DH Form 1896 has been
executed. If a DH Form 1896 has been executed, a yellow copy of that document must be made a part of the
resident’s record. If the assisted living facility does not receive a copy of a resident’s executed DH Form 1896, the
assisted living facility must document in the resident’s record that it has requested a copy.
(c) The executed DH Form 1896 must be readily available to medical staff in the event of an emergency.
(2) LICENSE REVOCATION. An assisted living facility’s license is subject to revocation pursuant to section
408.815, F.S., if, as a condition of treatment or admission, the facility requires an individual to execute or waive DH
Form 1896.
(3) DNRO PROCEDURES. Pursuant to section 429.255, F.S., an assisted living facility must honor a properly
executed DH Form 1896 as follows:
(a) In the event a resident experiences cardiac or pulmonary arrest, staff trained in cardiopulmonary
resuscitation (CPR) or a health care provider present in the facility, may withhold cardiopulmonary resuscitation
(artificial ventilation, cardiac compression, endotracheal intubation and defibrillation).
(b) In the event a resident is receiving hospice services and experiences cardiac or pulmonary arrest, facility
staff must immediately contact hospice staff. The hospice procedures take precedence over those of the assisted
living facility.
Rulemaking Authority 429.255 FS. Law Implemented 429.255 FS. History–New 4-15-10, Amended 4-17-14,
Formerly 58A-5.0186, 7-1-19.
Effective July 1, 2019 6A – 23
59A-36.010 Staffing Standards.
(1) ADMINISTRATORS. Every facility must be under the supervision of an administrator who is responsible
for the operation and maintenance of the facility including the management of all staff and the provision of
appropriate care to all residents as required by chapters 408, part II, 429, part I, F.S., and rule chapter 59A-35,
F.A.C., and this rule chapter.
(a) An administrator must:
1. Be at least 21 years of age;
2. If employed on or after October 30, 1995, have, at a minimum, a high school diploma or G.E.D.;
3. Be in compliance with Level 2 background screening requirements pursuant to sections 408.809 and 429.174,
F.S.;
4. Complete the core training and core competency test requirements pursuant to rule 59A-36.011, F.A.C., no
later than 90 days after becoming employed as a facility administrator. Administrators who attended core training
prior to July 1, 1997, are not required to take the competency test unless specified elsewhere in this rule; and,
5. Satisfy the continuing education requirements pursuant to rule 59A-36.011, F.A.C. Administrators who are
not in compliance with these requirements must retake the core training and core competency test requirements in
effect on the date the non-compliance is discovered by the agency or the department.
(b) In the event of extenuating circumstances, such as the death of a facility administrator, the agency may
permit an individual who otherwise has not satisfied the training requirements of subparagraph (1)(a)4. of this rule,
to temporarily serve as the facility administrator for a period not to exceed 90 days. During the 90 day period, the
individual temporarily serving as facility administrator must:
1. Complete the core training and core competency test requirements pursuant to rule 59A-36.011, F.A.C.; and,
2. Complete all additional training requirements if the facility maintains licensure as an extended congregate
care or limited mental health facility.
(c) Administrators may supervise a maximum of either three assisted living facilities or a group of facilities on a
single campus providing housing and health care Administrators who supervise more than one facility must appoint
in writing a separate manager for each facility. However, an administrator supervising a maximum of three assisted
living facilities, each licensed for 16 or fewer beds and all within a 15 mile radius of each other, is only required to
appoint two managers to assist in the operation and maintenance of those facilities.
(d) An individual serving as a manager must satisfy the same qualifications, background screening, core
training and competency test requirements, and continuing education requirements as an administrator pursuant to
paragraph (1)(a) of this rule. Managers who attended the core training program prior to April 20, 1998, are not
required to take the competency test unless specified elsewhere in this rule. In addition, a manager may not serve as
a manager of more than a single facility, except as provided in paragraph (1)(c) of this rule, and may not
simultaneously serve as an administrator of any other facility.
(e) Pursuant to section 429.176, F.S., facility owners must notify the Agency Central Office within 10 days of a
change in facility administrator on the Notification of Change of Administrator form, AHCA Form 3180-1006, June
2016, which is incorporated by reference and available online at:
http://www.flrules.org/Gateway/reference.asp?No=Ref-09393.
(2) STAFF.
(a) Within 30 days after beginning employment, newly hired staff must submit a written statement from a health

Effective July 1, 2019 6A – 24
care provider documenting that the individual does not have any signs or symptoms of communicable disease. The
examination performed by the health care provider must have been conducted no earlier than 6 months before
submission of the statement. Newly hired staff does not include an employee transferring without a break in service
from one facility to another when the facility is under the same management or ownership.
1. Evidence of a negative tuberculosis examination must be documented on an annual basis. Documentation
provided by the Florida Department of Health or a licensed health care provider certifying that there is a shortage of
tuberculosis testing materials satisfies the annual tuberculosis examination requirement. An individual with a
positive tuberculosis test must submit a health care provider’s statement that the individual does not constitute a risk
of communicating tuberculosis.
2. If any staff member has, or is suspected of having, a communicable disease, such individual must be
immediately removed from duties until a written statement is submitted from a health care provider indicating that
the individual does not constitute a risk of transmitting a communicable disease.
(b) Staff must be qualified to perform their assigned duties consistent with their level of education, training,
preparation, and experience. Staff providing services requiring licensing or certification must be appropriately
licensed or certified. All staff must exercise their responsibilities, consistent with their qualifications, to observe
residents, to document observations on the appropriate resident’s record, and to report the observations to the
resident’s health care provider in accordance with this rule chapter.
(c) All staff must comply with the training requirements of rule 59A-36.011, F.A.C.
(d) An assisted living facility contracting to provide services to residents must ensure that individuals providing
services are qualified to perform their assigned duties in accordance with this rule chapter. The contract between the
facility and the staffing agency or contractor must specifically describe the services the staffing agency or contractor
will provide to residents.
(e) For facilities with a licensed capacity of 17 or more residents, the facility must:
1. Develop a written job description for each staff position and provide a copy of the job description to each
staff member; and,
2. Maintain time sheets for all staff.
(f) Level 2 background screening must be conducted for staff, including staff contracted by the facility to
provide services to residents, pursuant to sections 408.809 and 429.174, F.S.

Effective July 1, 2019 6A – 25
(3) STAFFING STANDARDS.
(a) Minimum staffing:
1. Facilities must maintain the following minimum staff hours per week:
Number of Residents, Day Care Participants, and Respite Care Residents Staff Hours/Week
0-5 168
6-15 212
16- 25 253
26-35 294
36-45 335
46-55 375
56- 65 416
66-75 457
76-85 498
86-95 539
For every 20 total combined residents, day care participants, and respite care residents over 95 add 42 staff hours per
week.
2. Independent living residents, as referenced in subsection 59A-36.015(3), F.A.C., who occupy beds included
within the licensed capacity of an assisted living facility but do not receive personal, limited nursing, or extended
congregate care services, are not counted as residents for purposes of computing minimum staff hours.
3. At least one staff member who has access to facility and resident records in case of an emergency must be in
the facility at all times when residents are in the facility. Residents serving as paid or volunteer staff may not be left
solely in charge of other residents while the facility administrator, manager or other staff are absent from the facility.
4. In facilities with 17 or more residents, there must be at least one staff member awake at all hours of the day
and night.
5. A staff member who has completed courses in First Aid and Cardiopulmonary Resuscitation (CPR) and holds
a currently valid card documenting completion of such courses must be in the facility at all times.
a. Documentation of attendance at First Aid or CPR courses pursuant to subsection 59A-36.011(5), F.A.C.,
satisfies this requirement.
b. A nurse is considered as having met the course requirements for First Aid. An emergency medical technician
or paramedic currently certified under chapter 401, part III, F.S., is considered as having met the course
requirements for both First Aid and CPR.
6. During periods of temporary absence of the administrator or manager of more than 48 hours when residents
are on the premises, a staff member who is at least 21 years of age must be physically present and designated in
writing to be in charge of the facility. No staff member shall be in charge of a facility for a consecutive period of 21
days or more, or for a total of 60 days within a calendar year, without being an administrator or manager.
7. Staff whose duties are exclusively building or grounds maintenance, clerical, or food preparation do not
count towards meeting the minimum staffing hours requirement.

Effective July 1, 2019 6A – 26
8. The administrator or manager’s time may be counted for the purpose of meeting the required staffing hours,
provided the administrator or manager is actively involved in the day-to-day operation of the facility, including
making decisions and providing supervision for all aspects of resident care, and is listed on the facility’s staffing
schedule.
9. Only on-the-job staff may be counted in meeting the minimum staffing hours. Vacant positions or absent
staff may not be counted.
(b) Notwithstanding the minimum staffing requirements specified in paragraph (a), all facilities, including those
composed of apartments, must have enough qualified staff to provide resident supervision, and to provide or arrange
for resident services in accordance with the residents’ scheduled and unscheduled service needs, resident contracts,
and resident care standards as described in rule 59A-36.007, F.A.C.
(c) The facility must maintain a written work schedule that reflects its 24-hour staffing pattern for a given time
period. Upon request, the facility must make the daily work schedules of direct care staff available to residents or
their representatives.
(d) The facility must provide staff immediately when the agency determines that the requirements of paragraph
(a) are not met. The facility must immediately increase staff above the minimum levels established in paragraph (a),
if the agency determines that adequate supervision and care are not being provided to residents, resident care
standards described in rule 59A-36.007, F.A.C., are not being met, or that the facility is failing to meet the terms of
residents’ contracts. The agency will consult with the facility administrator and residents regarding any
determination that additional staff is required. Based on the recommendations of the local fire safety authority, the
agency may require additional staff when the facility fails to meet the fire safety standards described in rule chapter
69A-40, F.A.C., until such time as the local fire safety authority informs the agency that fire safety requirements are
being met.
1. When additional staff is required above the minimum, the agency will require the submission of a corrective
action plan within the time specified in the notification indicating how the increased staffing is to be achieved to
meet resident service needs. The plan will be reviewed by the agency to determine if it sufficiently increases the
staffing levels to meet resident needs.
2. When the facility can demonstrate to the agency that resident needs are being met, or that resident needs can
be met without increased staffing, the agency may modify staffing requirements for the facility and the facility will
no longer be required to maintain a plan with the agency.
(e) Facilities that are co-located with a nursing home may use shared staffing provided that staff hours are only
counted once for the purpose of meeting either assisted living facility or nursing home minimum staffing ratios.
(f) Facilities holding a limited mental health, extended congregate care, or limited nursing services license must
also comply with the staffing requirements of rules 59A-36.020, 59A-36.021 or 59A-36.022, F.A.C., respectively.
Rulemaking Authority 429.41, 429.52, 429.929 FS. Law Implemented 429.174, 429.176, 429.41, 429.52, 429.905
FS. History–New 5-14-81, Amended 1-6-82, 9-17-84, Formerly 10A-5.19, Amended 10-20-86, 6-21-88, 8-15-90, 9-
30-92, Formerly 10A-5.019, Amended 10-30-95, 4-20-98, 11-2-98, 10-17-99, 7-30-06, 4-15-10, 4-17-14, 5-10-18,
Formerly 58A-5.019, 7-1-19.
59A-36.011 Staff Training Requirements and Competency Test.
(1) ASSISTED LIVING FACILITY CORE TRAINING REQUIREMENTS AND COMPETENCY TEST.

Effective July 1, 2019 6A – 27
(a) The assisted living facility core training requirements established by the department pursuant to section
429.52, F.S., shall consist of a minimum of 26 hours of training plus a competency test.
(b) Administrators and managers must successfully complete the assisted living facility core training
requirements within 3 months from the date of becoming a facility administrator or manager. Successful completion
of the core training requirements includes passing the competency test. The minimum passing score for the
competency test is 75%. Administrators who have attended core training prior to July 1, 1997, and managers who
attended the core training program prior to April 20, 1998, shall not be required to take the competency test.
Administrators licensed as nursing home administrators in accordance with chapter 468, part II, F.S., are exempt
from this requirement.
(c) Administrators and managers shall participate in 12 hours of continuing education in topics related to
assisted living every 2 years.
(d) A newly hired administrator or manager who has successfully completed the assisted living facility core
training and continuing education requirements, shall not be required to retake the core training. An administrator or
manager who has successfully completed the core training but has not maintained the continuing education
requirements will be considered a new administrator or manager for the purposes of the core training requirements
and must:
1. Retake the assisted living facility core training; and,
2. Retake and pass the competency test.
(e) The fees for the competency test shall not exceed $200.00. The payment for the competency test fee shall be
remitted to the entity administering the test. A new fee is due each time the test is taken.
(2) STAFF PRESERVICE ORIENTATION.
(a) Facilities must provide a preservice orientation of at least 2 hours to all new assisted living facility
employees who have not previously completed core training as detailed in subsection (1).
(b) New staff must complete the preservice orientation prior to interacting with residents.
(c) Once complete, the employee and the facility administrator must sign a statement that the employee
completed the preservice orientation which must be kept in the employee’s personnel record.
(d) In addition to topics that may be chosen by the facility administrator, the preservice orientation must cover:
1. Resident’s rights; and,
2. The facility’s license type and services offered by the facility.
(3) STAFF IN-SERVICE TRAINING. Facility administrators or managers shall provide or arrange for the
following in-service training to facility staff:
(a) Staff who provide direct care to residents, other than nurses, certified nursing assistants, or home health
aides trained in accordance with rule 59A-8.0095, F.A.C., must receive a minimum of 1 hour in-service training in
infection control, including universal precautions and facility sanitation procedures, before providing personal care
to residents. The facility must use its infection control policies and procedures when offering this training.
Documentation of compliance with the staff training requirements of 29 CFR 1910.1030, relating to blood borne
pathogens, may be used to meet this requirement.

Effective July 1, 2019 6A – 28
(b) Staff who provide direct care to residents must receive a minimum of 1 hour in-service training within 30
days of employment that covers the following subjects:
1. Reporting adverse incidents.
2. Facility emergency procedures including chain-of-command and staff roles relating to emergency evacuation.
(c) Staff who provide direct care to residents, who have not taken the core training program, shall receive a
minimum of 1 hour in-service training within 30 days of employment that covers the following subjects:
1. Resident rights in an assisted living facility.
2. Recognizing and reporting resident abuse, neglect, and exploitation. The facility must use its abuse
prevention policies and procedures when offering this training.
(d) Staff who provide direct care to residents, other than nurses, CNAs, or home health aides trained in
accordance with rule 59A-8.0095, F.A.C., must receive 3 hours of in-service training within 30 days of employment
that covers the following subjects:
1. Resident behavior and needs.
2. Providing assistance with the activities of daily living.
(e) Staff who prepare or serve food, who have not taken the assisted living facility core training must receive a
minimum of 1-hour-in-service training within 30 days of employment in safe food handling practices.
(f) All facility staff shall receive in-service training regarding the facility’s resident elopement response policies
and procedures within thirty (30) days of employment.
1. All facility staff shall be provided with a copy of the facility’s resident elopement response policies and
procedures.
2. All facility staff shall demonstrate an understanding and competency in the implementation of the elopement
response policies and procedures.
(4) HUMAN IMMUNODEFICIENCY VIRUS/ACQUIRED IMMUNE DEFICIENCY SYNDROME
(HIV/AIDS). Pursuant to section 381.0035, F.S., all facility employees, with the exception of employees subject to
the requirements of section 456.033, F.S., must complete a one-time education course on HIV and AIDS, including
the topics prescribed in the section 381.0035, F.S. New facility staff must obtain the training within 30 days of
employment. Documentation of compliance must be maintained in accordance with subsection (12), of this rule.
(5) FIRST AID AND CARDIOPULMONARY RESUSCITATION (CPR). A staff member who has completed
courses in First Aid and CPR and holds a currently valid card documenting completion of such courses must be in
the facility at all times.
(a) Documentation that the staff member possess current CPR certification that requires the student to
demonstrate, in person, that he or she is able to perform CPR and which is issued by an instructor or training
provider that is approved to provide CPR training by the American Red Cross, the American Heart Association, the
National Safety Council, or an organization whose training is accredited by the Commission on Accreditation for
Pre-Hospital Continuing Education satisfies this requirement.
(b) A nurse shall be considered as having met the training requirement for First Aid. An emergency medical
technician or paramedic currently certified under chapter 401, Part III, F.S., shall be considered as having met the
training requirements for both First Aid and C.P.R.
(6) ASSISTANCE WITH THE SELF-ADMINISTRATION OF MEDICATION AND MEDICATION
MANAGEMENT. Unlicensed persons who will be providing assistance with the self-administration of medications

Effective July 1, 2019 6A – 29
as described in rule 59A-36.008, F.A.C., must meet the training requirements pursuant to section 429.52(6), F.S.,
prior to assuming this responsibility. Courses provided in fulfilment of this requirement must meet the following
criteria:
(a) Training must cover state law and rule requirements with respect to the supervision, assistance,
administration, and management of medications in assisted living facilities; procedures and techniques for assisting
the resident with self-administration of medication including how to read a prescription label; providing the right
medications to the right resident; common medications; the importance of taking medications as prescribed;
recognition of side effects and adverse reactions and procedures to follow when residents appear to be experiencing
side effects and adverse reactions; documentation and record keeping; and medication storage and disposal. Training
shall include demonstrations of proper techniques, including techniques for infection control, and ensure unlicensed
staff have adequately demonstrated that they have acquired the skills necessary to provide such assistance.
(b) The training must be provided by a registered nurse or licensed pharmacist who shall issue a training
certificate to a trainee who demonstrates, in person and both physically and verbally, the ability to:
1. Read and understand a prescription label;
2. Provide assistance with self-administration in accordance with section 429.256, F.S., and rule 59A-36.008,
F.A.C., including:
a. Assist with oral dosage forms, topical dosage forms, and topical ophthalmic, otic and nasal dosage forms;
b. Measure liquid medications, break scored tablets, and crush tablets in accordance with prescription
directions;
c. Recognize the need to obtain clarification of an “as needed” prescription order;
d. Recognize a medication order which requires judgment or discretion, and to advise the resident, resident’s
health care provider or facility employer of inability to assist in the administration of such orders;
e. Complete a medication observation record;
f. Retrieve and store medication;
g. Recognize the general signs of adverse reactions to medications and report such reactions;
h. Assist residents with insulin syringes that are prefilled with the proper dosage by a pharmacist and insulin
pens that are prefilled by the manufacturer by taking the medication, in its previously dispensed, properly labeled
container, from where it is stored, and bringing it to the resident for self-injection;
i. Assist with nebulizers;
j. Use a glucometer to perform blood glucose testing;
k. Assist residents with oxygen nasal cannulas and continuous positive airway pressure (CPAP) devices,
excluding the titration of the oxygen levels;
l. Apply and remove anti-embolism stockings and hosiery;
m. Placement and removal of colostomy bags, excluding the removal of the flange or manipulation of the stoma
site; and,
n. Measurement of blood pressure, heart rate, temperature, and respiratory rate.
(c) Unlicensed persons, as defined in section 429.256(1)(b), F.S., who provide assistance with self-administered
medications and have successfully completed the initial 6 hour training, must obtain, annually, a minimum of 2
hours of continuing education training on providing assistance with self-administered medications and safe

Effective July 1, 2019 6A – 30
medication practices in an assisted living facility. The 2 hours of continuing education training may be provided
online.
(d) Trained unlicensed staff who, prior to the effective date of this rule, assist with the self-administration of
medication and have successfully completed 4 hours of assistance with self-administration of medication training
must complete an additional 2 hours of training that focuses on the topics listed in sub-subparagraphs (6)(b)2.h.-n. of
this section, before assisting with the self-administration of medication procedures listed in sub-subparagraphs
(6)(b)2.h.-n.
(7) NUTRITION AND FOOD SERVICE. The administrator or person designated by the administrator as
responsible for the facility’s food service and the day-to-day supervision of food service staff must obtain, annually,
a minimum of 2 hours continuing education in topics pertinent to nutrition and food service in an assisted living
facility. This requirement does not apply to administrators and designees who are exempt from training requirements
under paragraph 59A-36.012(1)(b). A certified food manager, licensed dietician, registered dietary technician or
health department sanitarian is qualified to train assisted living facility staff in nutrition and food service.
(8) EXTENDED CONGREGATE CARE (ECC) TRAINING.
(a) The administrator and ECC supervisor, if different from the administrator, must complete core training and 4
hours of initial training in extended congregate care prior to the facility receiving its ECC license or within 3 months
of beginning employment in a currently licensed ECC facility as an administrator or ECC supervisor. Successful
completion of the assisted living facility core training shall be a prerequisite for this training. ECC supervisors who
attended the assisted living facility core training prior to April 20, 1998, shall not be required to take the assisted
living facility core training competency test.
(b) The administrator and the ECC supervisor, if different from the administrator, must complete a minimum of
4 hours of continuing education every two years in topics relating to the physical, psychological, or social needs of
frail elderly and disabled persons, or persons with Alzheimer’s disease or related disorders.
(c) All direct care staff providing care to residents in an ECC program must complete at least 2 hours of in-
service training, provided by the facility administrator or ECC supervisor, within 6 months of beginning
employment in the facility. The training must address ECC concepts and requirements, including statutory and rule
requirements, and the delivery of personal care and supportive services in an ECC facility.
(9) LIMITED MENTAL HEALTH TRAINING.
(a) Pursuant to section 429.075, F.S., the administrator, managers and staff, who have direct contact with mental
health residents in a licensed limited mental health facility, must receive the following training:
1. A minimum of 6 hours of specialized training in working with individuals with mental health diagnoses.
a. The training must be provided or approved by the Department of Children and Families and must be taken
within 6 months of the facility’s receiving a limited mental health license or within 6 months of employment in a
limited mental health facility.
b. Training received under this subparagraph may count once for 6 of the 12 hours of continuing education
required for administrators and managers pursuant to section 429.52(5), F.S., and subsection (1) of this rule.
2. A minimum of 3 hours of continuing education, which may be provided by the ALF administrator, online, or
through distance learning, biennially thereafter in subjects dealing with one or more of the following topics:
a. Mental health diagnoses; and,
b. Mental health treatment such as:

Effective July 1, 2019 6A – 31
(I) Mental health needs, services, behaviors and appropriate interventions;
(II) Resident progress in achieving treatment goals;
(III) How to recognize changes in the resident’s status or condition that may affect other services received or
may require intervention; and,
(IV) Crisis services and the Baker Act procedures.
3. For administrators and managers, the continuing education requirement under this subsection will satisfy 3 of
the 12 hours of continuing education required biennially pursuant to section 429.52(5), F.S., and subsection (1) of
this rule.
4. Administrators, managers and direct contact staff affected by the continuing education requirement under this
subsection shall have up to 6 months after the effective date of this rule to meet the training requirement.
(b) Administrators, managers and staff do not have to repeat the initial training should they change employers
provided they present a copy of their training certificate to the current employer for retention in the facility’s
personnel files. They must also ensure that copies of the continuing education training certificates, pursuant to
subparagraph (a)2. of this subsection, are retained in their personnel files.
(10) ALZHEIMER’S DISEASE AND RELATED DISORDERS (“ADRD”) TRAINING REQUIREMENTS.
Facilities which advertise that they provide special care for persons with ADRD, or who maintain secured areas as
described in Chapter 4, Section 464.4.6 of the Florida Building Code, as adopted in rule 61G20-1.001, F.A.C.,
Florida Building Code Adopted, must ensure that facility staff receive the following training.
(a) Facility staff who interact on a daily basis with residents with ADRD but do not provide direct care to such
residents and staff who provide direct care to residents with ADRD, shall obtain 4 hours of initial training within 3
months of employment. Completion of the core training program between April 20, 1998 and July 1, 2003 shall
satisfy this requirement. Facility staff who meet the requirements for ADRD training providers under paragraph (g)
of this subsection, will be considered as having met this requirement. Initial training, entitled “Alzheimer’s Disease
and Related Disorders Level I Training,” must address the following subject areas:
1. Understanding Alzheimer’s disease and related disorders;
2. Characteristics of Alzheimer’s disease;
3. Communicating with residents with Alzheimer’s disease;
4. Family issues;
5. Resident environment; and,
6. Ethical issues.
(b) Staff who have successfully completed both the initial one hour and continuing three hours of ADRD
training pursuant to sections 400.1755, 429.917 and 400.6045(1), F.S., shall be considered to have met the initial
assisted living facility Alzheimer’s Disease and Related Disorders Level I Training.
(c) Facility staff who provide direct care to residents with ADRD must obtain an additional 4 hours of training,
entitled “Alzheimer’s Disease and Related Disorders Level II Training,” within 9 months of employment. Facility
staff who meet the requirements for ADRD training providers under paragraph (g) of this subsection, will be
considered as having met this requirement. Alzheimer’s Disease and Related Disorders Level II Training must
address the following subject areas as they apply to these disorders:
1. Behavior management,
2. Assistance with ADLs,

Effective July 1, 2019 6A – 32
3. Activities for residents,
4. Stress management for the care giver; and,
5. Medical information.
(d) A detailed description of the subject areas that must be included in an ADRD curriculum which meets the
requirements of paragraphs (a) and (b) of this subsection, can be found in the document “Training Guidelines for the
Special Care of Persons with Alzheimer’s Disease and Related Disorders,” dated March 1999, incorporated by
reference, available from the Department of Elder Affairs, 4040 Esplanade Way, Tallahassee, Florida 32399-7000.
(e) Direct care staff shall participate in 4 hours of continuing education annually as required under section
429.178, F.S. Continuing education received under this paragraph may be used to meet 3 of the 12 hours of
continuing education required by section 429.52, F.S., and subsection (1) of this rule, or 3 of the 6 hours of
continuing education for extended congregate care required by subsection (7) of this rule.
(f) Facility staff who have only incidental contact with residents with ADRD must receive general written
information provided by the facility on interacting with such residents, as required under section 429.178, F.S.,
within three (3) months of employment. “Incidental contact” means all staff who neither provide direct care nor are
in regular contact with such residents.
(g) Persons who seek to provide ADRD training in accordance with this subsection must provide the department
or its designee with documentation that they hold a Bachelor’s degree from an accredited college or university or
hold a license as a registered nurse, and:
1. Have 1 year teaching experience as an educator of caregivers for persons with Alzheimer’s disease or related
disorders, or
2. Three years of practical experience in a program providing care to persons with Alzheimer’s disease or
related disorders, or
3. Completed a specialized training program in the subject matter of this program and have a minimum of two
years of practical experience in a program providing care to persons with Alzheimer’s disease or related disorders.
(h) With reference to requirements in paragraph (g), a Master’s degree from an accredited college or university
in a subject related to the content of this training program can substitute for the teaching experience. Years of
teaching experience related to the subject matter of this training program may substitute on a year-by-year basis for
the required Bachelor’s degree referenced in paragraph (g).
(11) DO NOT RESUSCITATE ORDERS TRAINING.
(a) Currently employed facility administrators, managers, direct care staff and staff involved in resident
admissions must receive at least one hour of training in the facility’s policies and procedures regarding Do Not
Resuscitate Orders.
(b) Newly hired facility administrators, managers, direct care staff and staff involved in resident admissions
must receive at least one hour of training in the facility’s policy and procedures regarding DNROs within 30 days
after employment.
(c) Training shall consist of the information included in rule 59A-36.009, F.A.C.

Effective July 1, 2019 6A – 33
(12) TRAINING DOCUMENTATION AND MONITORING.
(a) Except as otherwise noted, certificates, or copies of certificates, of any training required by this rule must be
documented in the facility’s personnel files. The documentation must include the following:
1. The title of the training program,
2. The subject matter of the training program,
3. The training program agenda,
4. The number of hours of the training program,
5. The trainee’s name, dates of participation, and location of the training program,
6. The training provider’s name, dated signature and credentials, and professional license number, if applicable.
(b) Upon successful completion of training pursuant to this rule, the training provider must issue a certificate to
the trainee as specified in this rule.
(c) The facility must provide the Department of Elder Affairs and the Agency for Health Care Administration
with training documentation and training certificates for review, as requested. The department and agency reserve
the right to attend and monitor all facility in-service training, which is intended to meet regulatory requirements.
Rulemaking Authority 429.178, 429.41, 429.52 FS. Law Implemented 429.07, 429.075, 429.178, 429.41, 429.52 FS.
History–New 9-30-92, Formerly 10A-5.0191, Amended 10-30-95, 6-2-96, 4-20-98, 11-2-98, 10-17-99, 7-5-05, 7-30-
06, 10-9-06, 7-1-08, 4-15-10, 5-10-18, Formerly 58A-5.0191, 7-1-19.
59A-36.012 Food Service Standards.
(1) GENERAL RESPONSIBILITIES. When food service is provided by the facility, the administrator, or an
individual designated in writing by the administrator, must be responsible for total food services and the day-to-day
supervision of food services staff. In addition, the following requirements apply:
(a) If the designee is an individual who has not completed an approved assisted living facility core training
course, such individual must complete the food and nutrition services module of the core training course before
assuming responsibility for the facility’s food service. The designee is not subject to the 1 hour in-service training in
safe food handling practices.
(b) If the designee is a certified food manager, certified dietary manager, registered or licensed dietitian, dietetic
registered technician, or health department sanitarian, the designee is exempt from the requirement to complete the
food and nutrition services module of the core training course before assuming responsibility for the facility’s food
service as required in paragraph (1)(a) of this rule.
(c) An administrator or designee must perform his or her duties in a safe and sanitary manner.
(d) An administrator or designee must provide regular meals that meet the nutritional needs of residents, and
therapeutic diets as ordered by the resident’s health care provider for residents who require special diets.
(e) An administrator or designee must comply with the food service continuing education requirements
specified in rule 59A-36.011, F.A.C.
(2) DIETARY STANDARDS.
(a) The meals provided by the assisted living facility must be planned based on the current USDA Dietary
Guidelines for Americans, 2010, which are incorporated by reference and available for review at:
http://www.flrules.org/Gateway/reference.asp?No=Ref-04003, and the current summary of Dietary Reference
Intakes established by the Food and Nutrition Board of the Institute of Medicine of the National Academies, 2010,
which are incorporated by reference and available for review at:

Effective July 1, 2019 6A – 34
http://iom.edu/Activities/Nutrition/SummaryDRIs/~/media/Files/Activity%20Files/Nutrition/DRIs/New%20Materia
l/5DRI%20Values%20SummaryTables%2014.pdf. Therapeutic diets must meet these nutritional standards to the
extent possible.
(b) The residents’ nutritional needs must be met by offering a variety of meals adapted to the food habits,
preferences, and physical abilities of the residents, and must be prepared through the use of standardized recipes. For
facilities with a licensed capacity of 16 or fewer residents, standardized recipes are not required. Unless a resident
chooses to eat less, the facility must serve the standard minimum portions of food according to the Dietary
Reference Intakes.
(c) All regular and therapeutic menus to be used by the facility must be reviewed annually by a licensed or
registered dietitian, a licensed nutritionist, or a registered dietetic technician supervised by a licensed or registered
dietitian, or a licensed nutritionist to ensure the meals meet the nutritional standards established in this rule. The
annual review must be documented in the facility files and include the original signature of the reviewer, registration
or license number, and date reviewed. Portion sizes must be indicated on the menus or on a separate sheet.
1. Daily food servings may be divided among three or more meals per day, including snacks, as necessary to
accommodate resident needs and preferences.
2. Menu items may be substituted with items of comparable nutritional value based on the seasonal availability
of fresh produce or the preferences of the residents.
(d) Menus must be dated and planned at least 1 week in advance for both regular and therapeutic diets.
Residents must be encouraged to participate in menu planning. Planned menus must be conspicuously posted or
easily available to residents. Regular and therapeutic menus as served, with substitutions noted before or when the
meal is served, must be kept on file in the facility for 6 months.
(e) Therapeutic diets must be prepared and served as ordered by the health care provider.
1. Facilities that offer residents a variety of food choices through a select menu, buffet style dining, or family
style dining are not required to document what is eaten unless a health care provider’s order indicates that such
monitoring is necessary. However, the food items that enable residents to comply with the therapeutic diet must be
identified on the menus developed for use in the facility.
2. The facility must document a resident’s refusal to comply with a therapeutic diet and provide notification to
the resident’s health care provider of such refusal.
(f) For facilities serving three or more meals a day, no more than 14 hours must elapse between the end of an
evening meal containing a protein food and the beginning of a morning meal. Intervals between meals must be
evenly distributed throughout the day with not less than 2 hours nor more than 6 hours between the end of one meal
and the beginning of the next. For residents without access to kitchen facilities, snacks must be offered at least once
per day. Snacks are not considered to be meals for the purposes of calculating the time between meals.
(g) Food must be served attractively at safe and palatable temperatures. All residents must be encouraged to eat
at tables in the dining areas. A supply of eating ware sufficient for all residents, including adaptive equipment if
needed by any resident, must be on hand.
(h) A 3-day supply of nonperishable food, based on the number of weekly meals the facility has contracted with
residents to serve, must be on hand at all times. The quantity must be based on the resident census and not on
licensed capacity. The supply must consist of foods that can be stored safely without refrigeration. Water sufficient

Effective July 1, 2019 6A – 35
for drinking and food preparation must also be stored, or the facility must have a plan for obtaining water in an
emergency, with the plan coordinated with and reviewed by the local disaster preparedness authority.
(3) FOOD HYGIENE. Copies of inspection reports issued by the county health department for the last 2 years
pursuant to rule 64E-12.004, or chapter 64E-11, F.A.C., as applicable, depending on the licensed capacity of the
assisted living facility, must be on file in the facility.
(4) CONTRACTED FOOD SERVICE. When food service is contracted by the facility, the facility must ensure
that the contracted food service meets all dietary standards imposed by this rule and is adequately protected upon
delivery to the facility pursuant to subsection 64E-12.004(4), F.A.C. The facility must maintain:
(a) A copy of the current contract between the facility and the food service contractor.
(b) A copy of the annually issued certificate or license authorizing the operation of the food service contractor
issued by the applicable regulating agency. The license or certificate must provide documentation of the food service
contractor’s compliance with food service regulatory requirements.
Rulemaking Authority 429.41 FS. Law Implemented 429.41, 429.52 FS. History–New 5-14-81, Amended 1-6-82, 5-
19-83, 9-17-84, Formerly 10A-5.20, Amended 10-20-86, 6-21-88, 8-15-90, 9-30-92, Formerly 10A-5.020, Amended
10-30-95, 6-2-96, 10-17-99, 4-17-14, Formerly 58A-5.020, 7-1-19.
59A-36.013 Fiscal Standards.
(1) FINANCIAL STABILITY. The facility must be administered on a sound financial basis in order to ensure
adequate resources to meet resident needs pursuant to the requirements of chapter 408, part II, part I, F.S., and rule
chapter 59A-35, F.A.C., and this rule chapter.
(2) RESIDENT TRUST FUNDS. Funds or other property received by the facility belonging to or due a
resident, including personal funds, must be held as trust funds and expended only for the resident’s account.
Resident funds or property may be held in one bank account if a separate written accounting for each resident is
maintained. A separate bank account is required for facility funds; co-mingling resident funds with facility funds is
prohibited. Written accounting procedures for resident trust funds must include income and expense records of the
trust fund, including the source and disposition of the funds.
(3) SURETY BONDS. Pursuant to the requirements of section 429.27(2), F.S.:
(a) For entities that own more than one facility in the state, one surety bond may be purchased to cover the
needs of all residents served by the entities.
(b) The following additional bonding requirements apply to facilities serving residents receiving OSS:
1. If serving as representative payee for a resident receiving OSS, the minimum bond proceeds must equal twice
the value of the resident’s monthly aggregate income, which must include any supplemental security income or
social security disability income plus the OSS payments, including the personal needs allowance.
2. If holding a power of attorney for a resident receiving OSS, the minimum bond proceeds must equal twice
the value of the resident’s monthly aggregate income, which must include any supplemental security income or
social security disability income; the OSS payments, including the personal allowance; plus the value of any
property belonging to a resident held at the facility.
(c) Upon the annual issuance of a new bond or continuation bond, the facility must file a copy of the bond with
the Agency Central Office.
(4) LIABILITY INSURANCE. Pursuant to section 429.275, F.S., facilities must maintain liability insurance
coverage, as defined in section 624.605, F.S., that remains in force at all times. On the renewal date of the facility’s

Effective July 1, 2019 6A – 36
policy or whenever a facility changes policies, the facility must file documentation of continued coverage with the
Agency Central Office. Such documentation must be issued by the insurance company and must include the name
and street address of the facility, a reference that the facility is an assisted living facility, the facility’s licensed
capacity, and the dates of coverage.
Rulemaking Authority 429.24, 429.27, 429.275, 429.41 FS. Law Implemented 429.27, 429.275 FS. History–New 5-
14-81, Amended 1-6-82, 9-17-84, Formerly 10A-5.21, Amended 6-21-88, 8-15-90, 9-30-92, Formerly 10A-5.021,
Amended 10-30-95, 6-2-96, 10-17-99, 4-17-14, Formerly 58A-5.021, 7-1-19.
59A-36.014 Physical Plant Standards.
(1) NEW FACILITIES. Newly constructed facilities to be licensed as assisted living facilities, and existing
structures, not previously licensed as assisted living facilities, to be converted to assisted living facilities, as well as
any subsequent additions, modifications, alterations, renovations or refurbishing of such facilities, are required by
governmental entities other than the Department of Elder Affairs to adhere to certain building code and fire safety
standards. Such standards may be found in:
(a) Chapter 4, Section 464, of the Florida Building Code as adopted in rule 61G20-1.001, F.A.C.;
(b) Section 633.022, F.S., Uniform Firesafety Standards and rule chapter 69A-40, F.A.C. The Uniform Fire
Safety Standards for Assisted Living Facilities; and,
(c) The National Fire Protection Association codes described in section 429.41, F.S.
(2) EXISTING FACILITIES.
(a) An assisted living facility must comply with the rule or building code in effect at the time of initial licensure,
as well as the rule or building code in effect at the time of any additions, modifications, alterations, refurbishment,
renovations or reconstruction. Determination of the installation of a fire sprinkler system in an existing facility must
comply with the requirements described in section 429.41, F.S.
(b) A facility undergoing change of ownership is considered an existing facility for purposes of this rule.
(3) OTHER REQUIREMENTS.
(a) All facilities must:
1. Provide a safe living environment pursuant to section 429.28(1)(a), F.S.;
2. Be maintained free of hazards; and,
3. Ensure that all existing architectural, mechanical, electrical and structural systems, and appurtenances are
maintained in good working order.
(b) Pursuant to section 429.27, F.S., residents must be given the option of using their own belongings as space
permits. When the facility supplies the furnishings, each resident bedroom or sleeping area must have at least the
following furnishings:
1. A clean, comfortable bed with a mattress no less than 36 inches wide and 72 inches long, with the top surface
of the mattress at a comfortable height to ensure easy access by the resident,
2. A closet or wardrobe space for hanging clothes,
3. A dresser, chest or other furniture designed for storage of clothing or personal effects,
4. A table or nightstand, bedside lamp or floor lamp, and waste basket; and,
5. A comfortable chair, if requested.
(c) The facility must maintain master or duplicate keys to resident bedrooms to be used in the event of an
emergency.

Effective July 1, 2019 6A – 37
(d) Residents who use portable bedside commodes must be provided with privacy during use.
(e) Facilities must make available linens and personal laundry services for residents who require such services.
Linens provided by a facility must be free of tears, stains and must not be threadbare.
Rulemaking Authority 429.41 FS. Law Implemented 429.27, 429.28, 429.41 FS. History–New 5-14-81, Amended 1-
6-82, 5-19-83, 9-17-84, Formerly 10A-5.23, Amended 10-20-86, 6-21-88, 8-15-90, 9-30-92, Formerly 10A-5.023,
Amended 10-30-95, 6-2-96, 10-17-99, 7-30-06, 4-15-10, 4-17-14, Formerly 58A-5.023, 7-1-19.
59A-36.015 Records.
The facility must maintain required records in a manner that makes such records readily available at the licensee’s
physical address for review by a legally authorized entity. If records are maintained in an electronic format, facility
staff must be readily available to access the data and produce the requested information. For purposes of this section,
“readily available” means the ability to immediately produce documents, records, or other such data, either in
electronic or paper format, upon request.
(1) FACILITY RECORDS. Facility records must include:
(a) The facility’s license displayed in a conspicuous and public place within the facility.
(b) An up-to-date admission and discharge log listing the names of all residents and each resident’s:
1. Date of admission, the facility or place from which the resident was admitted, and if applicable, a notation
indicating that the resident was admitted with a stage 2 pressure sore; and,
2. Date of discharge, reason for discharge, and identification of the facility or home address to which the
resident was discharged. Readmission of a resident to the facility after discharge requires a new entry in the log.
Discharge of a resident is not required if the facility is holding a bed for a resident who is out of the facility but
intending to return pursuant to rule 59A-36.018, F.A.C. If the resident dies while in the care of the facility, the log
must indicate the date of death.
(c) A log listing the names of all temporary emergency placement and respite care residents if not included on
the log described in paragraph (b).
(d) The facility’s emergency management plan, with documentation of review and approval by the county
emergency management agency, as described in rule 59A-36.019, F.A.C., that must be readily available by facility
staff.
(e) The facility’s liability insurance policy required in rule 59A-36.013, F.A.C.
(f) For facilities that have a surety bond, a copy of the surety bond currently in effect as required by rule 59A-
36.013, F.A.C.
(g) The admission package presented to new or prospective residents (less the resident’s contract) described in
rule 59A-36.006, F.A.C.
(h) If the facility advertises that it provides special care for persons with Alzheimer’s disease or related
disorders, a copy of all such facility advertisements as required by section 429.177, F.S.
(i) A grievance procedure for receiving and responding to resident complaints and recommendations as
described in rule 59A-36.007, F.A.C.
(j) All food service records required in rule 59A-36.012, F.A.C., including menus planned and served and
county health department inspection reports. Facilities that contract for food services, must include a copy of the
contract for food services and the food service contractor’s license or certificate to operate.

Effective July 1, 2019 6A – 38
(k) All fire safety inspection reports issued by the local authority or the State Fire Marshal pursuant to section
429.41, F.S., and rule chapter 69A-40, F.A.C., issued within the last 2 years.
(l) All sanitation inspection reports issued by the county health department pursuant to section 381.031, F.S.,
and chapter 64E-12, F.A.C., issued within the last 2 years.
(m) Pursuant to section 429.35, F.S., all completed survey, inspection and complaint investigation reports, and
notices of sanctions and moratoriums issued by the agency within the last 5 years.
(n) The facility’s resident elopement response policies and procedures.
(o) The facility’s documented resident elopement response drills.
(p) For facilities licensed as limited mental health, extended congregate care, or limited nursing services,
records required as stated in rules 59A-36.020, 59A-36.021 and 59A-36.022, F.A.C., respectively.
(2) STAFF RECORDS.
(a) Personnel records for each staff member must contain, at a minimum, a copy of the employment application,
with references furnished, and documentation verifying freedom from signs or symptoms of communicable disease.
In addition, records must contain the following, as applicable:
1. Documentation of compliance with all staff training and continuing education required by rule 59A-36.011,
F.A.C.,
2. Copies of all licenses or certifications for all staff providing services that require licensing or certification,
3. Documentation of compliance with level 2 background screening for all staff subject to screening
requirements as specified in section 429.174, F.S., and rule 59A-36.010, F.A.C.,
4. For facilities with a licensed capacity of 17 or more residents, a copy of the job description given to each staff
member pursuant to rule 59A-36.010, F.A.C.,
5. Documentation verifying direct care staff and administrator participation in resident elopement drills pursuant
to paragraph 59A-36.007(8)(c), F.A.C.
(b) The facility is not required to maintain personnel records for staff provided by a licensed staffing agency or
staff employed by an entity contracting to provide direct or indirect services to residents and the facility. However,
the facility must maintain a copy of the contract between the facility and the staffing agency or contractor as
described in rule 59A-36.010, F.A.C.
(c) The facility must maintain the written work schedules and staff time sheets for the most current 6 months as
required by rule 59A-36.010, F.A.C.
(3) RESIDENT RECORDS. Resident records must be maintained on the premises and include:
(a) Resident demographic data as follows:
1. Name,
2. Sex,
3. Race,
4. Date of birth,
5. Place of birth, if known,
6. Social security number,
7. Medicaid and/or Medicare number, or name of other health insurance carrier,
8. Name, address, and telephone number of next of kin, legal representative, or individual designated by the
resident for notification in case of an emergency; and,

Effective July 1, 2019 6A – 39
9. Name, address, and telephone number of the health care provider and case manager, if applicable.
(b) A copy of the Resident Health Assessment form, AHCA Form 1823 described in rule 59A-36.006, F.A.C.
(c) Any orders for medications, nursing services, therapeutic diets, do not resuscitate orders, or other services to
be provided, supervised, or implemented by the facility that require a health care provider’s order.
(d) Documentation of a resident’s refusal of a therapeutic diet pursuant to rule 59A-36.012, F.A.C., if
applicable.
(e) The resident care record described in paragraph 59A-36.007(1)(e), F.A.C.
(f) A weight record that is initiated on admission. Information may be taken from AHCA Form 1823 or the
resident’s health assessment. Residents receiving assistance with the activities of daily living must have their weight
recorded semi-annually.
(g) For facilities that will have unlicensed staff assisting the resident with the self-administration of medication,
a copy of the written informed consent described in rule 59A-36.006, F.A.C., if such consent is not included in the
resident’s contract.
(h) For facilities that manage a pill organizer, assist with self-administration of medications or administer
medications for a resident, copies of the required medication records maintained pursuant to rule 59A-36.008,
F.A.C.
(i) A copy of the resident’s contract with the facility, including any addendums to the contract as described in
rule 59A-36.018, F.A.C.
(j) For a facility whose owner, administrator, staff, or representative thereof, serves as an attorney in fact for a
resident, a copy of the monthly written statement of any transaction made on behalf of the resident as required in
section 429.27, F.S.
(k) For any facility that maintains a separate trust fund to receive funds or other property belonging to or due a
resident, a copy of the quarterly written statement of funds or other property disbursed as required in section 429.27,
F.S.
(l) If the resident is an OSS recipient, a copy of the Department of Children and Families form Alternate Care
Certification for Optional State Supplementation (OSS), CF-ES 1006, October 2005, which is hereby incorporated
by reference and available for review at: http://www.flrules.org/Gateway/reference.asp?No=Ref-04004. The absence
of this form will not be the basis for administrative action against a facility if the facility can demonstrate that it has
made a good faith effort to obtain the required documentation from the Department of Children and Families.
(m) Documentation of the appointment of a health care surrogate, health care proxy, guardian, or the existence
of a power of attorney, where applicable.
(n) For hospice patients, the interdisciplinary care plan and other documentation that the resident is a hospice
patient as required in rule 59A-36.006, F.A.C.
(o) The resident’s Do Not Resuscitate Order, DH Form 1896, if applicable.
(p) For independent living residents who receive meals and occupy beds included within the licensed capacity
of an assisted living facility, but who are not receiving any personal, limited nursing, or extended congregate care
services, record keeping may be limited to the following at the discretion of the facility:
1. A log listing the names of residents participating in this arrangement,
2. The resident demographic data required in this paragraph,
3. The health assessment described in rule 59A-36.006, F.A.C.,

Effective July 1, 2019 6A – 40
4. The resident’s contract described in rule 59A-36.018, F.A.C.; and,
5. A health care provider’s order for a therapeutic diet if such diet is prescribed and the resident participates in
the meal plan offered by the facility.
(q) Except for resident contracts, which must be retained for 5 years, all resident records must be retained for 2
years following the departure of a resident from the facility unless it is required by contract to retain the records for a
longer period of time. Upon request, residents must be provided with a copy of their records upon departure from the
facility.
(r) Additional resident records requirements for facilities holding a limited mental health, extended congregate
care, or limited nursing services license are provided in rules 59A-36.020, 59A-36.021 and 59A-36.022, F.A.C.,
respectively.
(4) RECORD INSPECTION.
(a) The resident’s records must be available to the resident; the resident’s legal representative, designee,
surrogate, guardian, attorney in fact, or case manager; or the resident’s estate, and such additional parties as
authorized in writing or by law.
(b) Pursuant to section 429.35, F.S., agency reports that pertain to any agency survey, inspection, or monitoring
visit must be available to the residents and the public. In facilities that are co-located with a licensed nursing home,
the inspection of record for all common areas is the nursing home inspection report.
Rulemaking Authority 429.41, 429.275 FS. Law Implemented 429.24, 429.255, 429.256, 429.26, 429.27, 429.275,
429.35, 429.41, 429.52 FS. History–New 5-14-81, Amended 1-6-82, 5-19-83, 9-17-84, Formerly 10A-5.24, Amended
10-20-86, 6-21-88, 8-15-90, 9-30-92, Formerly 10A-5.024, Amended 10-30-95, 4-20-98, 11-2-98, 10-17-99, 7-30-
06, 10-9-06, 4-17-14, Formerly 58A-5.024, 7-1-19.
59A-36.016 Adverse Incident Report.
(1) INITIAL ADVERSE INCIDENT REPORT. The preliminary adverse incident report required by section
429.23(3), F.S., must be submitted within 1 business day after the incident pursuant to rule 59A-35.110, F.A.C.,
which requires online reporting.
(2) FULL ADVERSE INCIDENT REPORT. For each adverse incident reported in subsection (1), above, the
facility must submit a full report within 15 days of the incident. The full report must be submitted pursuant to rule
59A-35.110, F.A.C., which requires online reporting.
Rulemaking Authority 429.23 FS. Law Implemented 429.23 FS. History–New 1-9-02, Amended 7-30-06, 4-17-14,
Formerly 58A-5.0241, 7-1-19.
59A-36.017 Liability Claim Report.
(1) MONTHLY LIABILITY CLAIM REPORT. Each assisted living facility must report monthly any liability
claim filed against the facility pursuant to rule 59A-35.110, F.A.C., which requires online reporting. Each facility
must comply with the reporting time frames and transmission requirements specified in section 429.23(5), F.S.
(2) If a liability claim has not been filed against the facility in a given month, no report is required.
Rulemaking Authority 429.23 FS. Law Implemented 429.23 FS. History–New 1-9-02, Amended 3-13-14, Formerly
58A-5.0242, 7-1-19.

Effective July 1, 2019 6A – 41
59A-36.018 Resident Contracts.
(1) Pursuant to section 429.24, F.S., the facility must offer a contract for execution by the resident or the
resident’s legal representative before or at the time of admission. The contract must contain the following
provisions:
(a) A list of the specific services, supplies and accommodations to be provided by the facility to the resident,
including limited nursing and extended congregate care services that the resident elects to receive;
(b) The daily, weekly, or monthly rate;
(c) A list of any additional services and charges to be provided that are not included in the daily, weekly, or
monthly rates, or a reference to a separate fee schedule that must be attached to the contract;
(d) A provision stating that at least 30 days written notice will be given before any rate increase;
(e) Any rights, duties, or obligations of residents, other than those specified in section 429.28, F.S.;
(f) The purpose of any advance payments or deposit payments, and the refund policy for such advance or
deposit payments;
(g) A refund policy that must conform to section 429.24(3), F.S.;
(h) A written bed hold policy and provisions for terminating a bed hold agreement if a facility agrees in writing
to reserve a bed for a resident who is admitted to a nursing home, health care facility, or psychiatric facility. The
resident or responsible party must notify the facility in writing of any change in status that would prevent the
resident from returning to the facility. Until such written notice is received, the agreed upon daily, weekly, or
monthly rate may be charged by the facility unless the resident’s medical condition prevents the resident from giving
written notification, such as when a resident is comatose, and the resident does not have a responsible party to act on
the resident’s behalf;
(i) A provision stating whether the facility is affiliated with any religious organization and, if so, which
organization and its relationship to the facility;
(j) A provision that, upon determination by the administrator or health care provider that the resident needs
services beyond those that the facility is licensed to provide, the resident or the resident’s representative, or agency
acting on the resident’s behalf, must be notified in writing that the resident must make arrangements for transfer to a
care setting that is able to provide services needed by the resident. In the event the resident has no one to represent
him or her, the facility must refer the resident to the social service agency for placement. If there is disagreement
regarding the appropriateness of placement, provisions outlined in section 429.26(8), F.S., will take effect;
(k) A provision that residents must be assessed upon admission pursuant to subsection 59A-36.006(2), F.A.C.,
and every 3 years thereafter, or after a significant change, pursuant to subsection (4), of that rule;
(l) The facility’s policies and procedures for self-administration, assistance with self-administration, and
administration of medications, if applicable, pursuant to rule 59A-36.008, F.A.C. This also includes provisions
regarding over-the-counter (OTC) products pursuant to subsection (8) of that rule; and,
(m) The facility’s policies and procedures related to a properly executed DH Form 1896, Do Not Resuscitate
Order.
(2) The resident, or the resident’s representative, must be provided with a copy of the executed contract.
(3) The facility may not levy an additional charge for any supplies, services, or accommodations that the facility
has agreed by contract to provide as part of the standard daily, weekly, or monthly rate. The resident or resident’s
representative must be furnished in advance with an itemized written statement setting forth additional charges for

Effective July 1, 2019 6A – 42
any services, supplies, or accommodations available to residents not covered under the contract. An addendum must
be added to the resident contract to reflect the additional services, supplies, or accommodations not provided under
the original agreement. Such addendum must be dated and signed by the facility and the resident or resident’s legal
representative and a copy given to the resident or resident’s representative.
Rulemaking Authority 429.24, 429.41 FS. Law Implemented 429.24, 429.41 FS. History–New 10-17-99, Amended 7-
30-06, 4-15-10, 3-13-14, Formerly 58A-5.025, 7-1-19.
59A-36.019 Emergency Management.
(1) EMERGENCY PLAN COMPONENTS. Pursuant to section 429.41, F.S., each facility must prepare a
written comprehensive emergency management plan in accordance with the “Emergency Management Criteria for
Assisted Living Facilities,” dated October 1995, which is incorporated by reference and available at
http://www.flrules.org/Gateway/reference.asp?No=Ref-04010. This document is available from the local emergency
management agency. The emergency management plan must, at a minimum, address the following:
(a) Provision for all hazards;
(b) Provision for the care of residents remaining in the facility during an emergency, including pre-disaster or
emergency preparation; protecting the facility; supplies; emergency power; food and water; staffing; and emergency
equipment;
(c) Provision for the care of residents who must be evacuated from the facility during an emergency including
identification of such residents and transfer of resident records; evacuation transportation; sheltering arrangements;
supplies; staffing; emergency equipment; and medications;
(d) Provision for the care of additional residents who may be evacuated to the facility during an emergency
including the identification of such residents, staffing, and supplies;
(e) Identification of residents with Alzheimer’s disease or related disorders, and residents with mobility
limitations who may need specialized assistance either at the facility or in case of evacuation;
(f) Identification of and coordination with the local emergency management agency;
(g) Arrangement for post-disaster activities including responding to family inquiries, obtaining medical
intervention for residents, transportation, and reporting to the local emergency management agency the number of
residents who have been relocated, and the place of relocation; and,
(h) The identification of staff responsible for implementing each part of the plan.
(2) EMERGENCY PLAN APPROVAL. The plan must be submitted for review and approval to the local
emergency management agency.
(a) If the local emergency management agency requires revisions to the emergency management plan, such
revisions must be made and the plan resubmitted to the local office within 30 days of receiving notification that the
plan must be revised.
(b) A new facility as described in rule 59A-36.014, F.A.C., and facilities whose ownership has been transferred,
must submit an emergency management plan within 30 days after obtaining a license.
(c) The facility must review its emergency management plan on an annual basis. Any substantive changes must
be submitted to the local emergency agency for review and approval.
1. Changes in the name, address, telephone number, or position of staff listed in the plan are not considered
substantive revisions for the purposes of this rule.

Effective July 1, 2019 6A – 43
2. Changes in the identification of specific staff must be submitted to the local emergency management agency
annually as a signed and dated addendum that is not subject to review and approval.
(d) The local emergency management agency is the final administrative authority for emergency management
plans prepared by assisted living facilities.
(e) Any plan approved by the local emergency management agency is considered to have met all the criteria and
conditions established in this rule.
(3) PLAN IMPLEMENTATION.
(a) All staff must be trained in their duties and are responsible for implementing the emergency management
plan.
(b) If telephone service is not available during an emergency, the facility must request assistance from local law
enforcement or emergency management personnel in maintaining communication.
(4) FACILITY EVACUATION. The facility must evacuate the premises during or after an emergency if so
directed by the local emergency management agency.
(a) The facility must report the evacuation to the local office of emergency management or designee and to the
agency within 6 hours of the evacuation order. If the evacuation takes more than 6 hours, the facility must report
when the evacuation is completed.
(b) The facility must not be re-occupied until the area is cleared for reentry by the local emergency management
agency or its designee and the facility can meet the immediate needs of the residents.
(c) A facility with significant structural damage must relocate residents until the facility can be safely re-
occupied.
(d) The facility is responsible for knowing the location of all residents until the residents have been relocated to
another facility.
(e) The facility must provide the agency with the name of a contact person who must be available by telephone
24 hours a day, seven days a week, until the facility is re-occupied.
(f) The facility must assist in the relocation of residents, and must cooperate with outreach teams established by
the Department of Health or emergency management agency to assist in relocation efforts. Resident needs and
preferences must be considered to the extent possible in any relocation decision.
(5) EMERGENCY SHELTER. In the event a state of emergency has been declared and the facility is not
required to evacuate the premises, the facility may provide emergency shelter above the facility’s licensed capacity
provided the following conditions are met:
(a) Life safety will not be jeopardized for any individual;
(b) The immediate needs of residents and other individuals sheltered at the facility can be met by the facility;
(c) The facility reports the number of individuals over its licensed capacity and the conditions causing it to the
Agency Field Office within 48 hours or as soon as practical. As an alternative, the facility may report to the Agency
Central Office at (850)412-4304. If the facility will continue to be over capacity after the declared emergency ends,
the agency will review requests for excess capacity on a case-by-case basis; and,
(d) The facility maintains a log of the additional individuals being housed in the facility. The log must include
the individual’s name, usual address, and the dates of arrival and departure. The log must be available for review by
representatives of the agency, the department, the local emergency management agency or its designee. The

Effective July 1, 2019 6A – 44
admissions and discharge log maintained by the facility may be used for this purpose provided the information is
maintained in a manner that is easily accessible.
Rulemaking Authority 429.41 FS. Law Implemented 429.41 FS. History–New 10-17-99, Amended 7-30-06, 4-17-14,
Formerly 58A-5.026, 7-1-19.
59A-36.020 Limited Mental Health.
(1) LICENSE APPLICATION.
(a) Any facility intending to admit one or more mental health residents must obtain a limited mental health
license from the agency before accepting the mental health resident.
(b) Facilities applying for a limited mental health license that have uncorrected deficiencies or violations found
during the facility’s last survey, complaint investigation, or monitoring visit will be surveyed before the issuance of
a limited mental health license to determine if such deficiencies or violations have been corrected.
(2) RECORDS.
(a) A facility with a limited mental health license must maintain an up-to-date admission and discharge log
containing the names and dates of admission and discharge for all mental health residents. The admission and
discharge log required in rule 59A-36.015, F.A.C., satisfies this condition provided that all mental health residents
are clearly identified.
(b) Staff records must contain documentation that designated staff have completed limited mental health
training as required by rule 59A-36.011, F.A.C.
(c) Resident records must include:
1. Documentation, provided by a mental health care provider within 30 days of the resident’s admission to the
facility, that the resident is a mental health resident as defined in section 394.4574, F.S., and that the resident is
receiving social security disability or supplemental security income and optional state supplementation as follows:
a. An affirmative statement on the Alternate Care Certification for Optional State Supplementation (OSS) form,
CF-ES 1006, October 2005, which is hereby incorporated by reference and available for review at:
http://www.flrules.org/Gateway/reference.asp?No=Ref-03988, that the resident is receiving SSI or SSDI due to a
mental disorder,
b. Written verification provided by the Social Security Administration that the resident is receiving SSI or SSDI
for a mental disorder. Such verification may be acquired from the Social Security Administration upon obtaining a
release from the resident permitting the Social Security Administration to provide such information, or
c. A written statement from the resident’s case manager or other mental health care provider that the resident is
an adult with severe and persistent mental disorder. The case manager or other mental health care provider must
consider the following minimum criteria in making that determination:
(I) The resident is eligible for, is receiving, or has received mental health services within the last 5 years, or
(II) The resident has been diagnosed as having a severe or persistent mental disorder.
2. An appropriate placement assessment provided by the resident’s mental health care provider within 30 days
of admission to the facility that the resident has been assessed and found appropriate for residence in an assisted
living facility. Such assessment must be conducted by a psychiatrist, clinical psychologist, clinical social worker,
psychiatric nurse, or an individual supervised by one of these professionals.
a. Any of the following documentation that contains the name of the resident and the name, signature, date, and
license number, if applicable, of the person making the assessment, meets this requirement:

Effective July 1, 2019 6A – 45
(I) Completed Alternate Care Certification for Optional State Supplementation (OSS) form, CF-ES Form 1006,
(II) Discharge Statement from a state mental hospital completed no more than 90 days before admission to the
assisted living facility provided it contains a statement that the individual is appropriate to live in an assisted living
facility, or
(III) Other signed statement that the resident has been assessed and found appropriate for residency in an
assisted living facility.
b. A mental health resident returning to a facility from treatment in a hopsital or crisis stabilization unit will not
be considered a new admission and will not require a new assessment. However, a break in a resident’s residency
that requires the facility to execute a new resident contract or admission agreement will be considered a new
admission and the resident’s mental health care provider must provide a new assessment.
3. A Community Living Support Plan. Each mental health resident and the resident’s mental health case
manager must, in consultation with the facility administrator, prepare a plan within 30 days of the resident’s
admission to the facility or within 30 days after receiving the appropriate placement assessment in paragraph (2)(c),
whichever is later, that:
a. Includes the specific needs of the resident that must be met in order to enable the resident to live in the
assisted living facility and the community,
b. Includes the clinical mental health services to be provided by the mental health care provider to help meet the
resident’s needs, and the frequency and duration of such services,
c. Includes any other services and activities to be provided by or arranged for by the mental health care provider
or mental health case manager to meet the resident’s needs, and the frequency and duration of such services and
activities,
d. Includes the obligations of the facility to facilitate and assist the resident in attending appointments and
arranging transportation to appointments for the services and activities identified in the plan that have been provided
or arranged for by the resident’s mental health care provider or case manager,
e. Includes a description of other services to be provided or arranged by the facility,
f. Includes a list of factors pertinent to the care, safety, and welfare of the mental health resident and a
description of the signs and symptoms particular to the resident that indicate the immediate need for professional
mental health services,
g. Is in writing and signed by the mental health resident, the resident’s mental health case manager, and the
assisted living facility administrator or manager and a copy placed in the resident’s file. If the resident refuses to
sign the plan, the resident’s mental health case manager must add a statement that the resident was asked but refused
to sign the plan,
h. Is updated at least annually or if there is a significant change in the resident’s behavioral health,
i. May include the Cooperative Agreement described in subparagraph (2)(c)4. If included, the mental health
care provider must also sign the plan; and,
j. Must be available for inspection to those who have legal authority to review the document.
4. Cooperative Agreement. The mental health care provider for each mental health resident and the facility
administrator or designee must prepare a written statement, within 30 days of the resident’s admission to the facility
or receipt of the resident’s appropriate placement assessment, whichever is later. The statement:

Effective July 1, 2019 6A – 46
a. Provides procedures and directions for accessing emergency and after-hours care for the mental health
resident. The provider must furnish the resident and the facility with the provider’s 24-hour emergency crisis
telephone number;
b. Must be signed by the administrator or designee and the mental health care provider, or by a designated
representative of a Medicaid prepaid health plan if the resident is on a plan and the plan provides behavioral health
services in section 409.912, F.S.;
c. May cover all mental health residents of the facility who are clients of the same provider; and,
d. May be included in the Community Living Support Plan described in subparagraph (2)(c)3.
5. Missing documentation will not be the basis for administrative action against a facility if the facility can
demonstrate that it has made a good faith effort to obtain the required documentation from the appropriate party. A
documented request for such missing documentation made by the facility administrator within 72 hours of the
resident’s admission will be considered a good faith effort. The documented request must include the name, title,
and phone number of the person to whom the request was made and must be kept in the resident’s file.
(3) RESPONSIBILITIES OF FACILITY. In addition to the staffing and care standards of this rule chapter to
provide for the welfare of residents in an assisted living facility, a facility holding a limited mental health license
must:
(a) Meet the facility’s obligation to assist the resident in carrying out the activities identified in the Community
Living Support Plan;
(b) Provide an opportunity for private face-to-face contact between the mental health resident and the resident’s
mental health case manager or other treatment personnel of the resident’s mental health care provider;
(c) Observe resident behavior and functioning in the facility, and record and communicate observations to the
resident’s mental health case manager or mental health care provider regarding any significant behavioral or
situational changes that may signify the need for a change in the resident’s professional mental health services,
supports, and services described in the community living support plan, or that the resident is no longer appropriate
for residency in the facility;
(d) If the facility initiates an involuntary mental health examination pursuant to section 394.463, F.S., the
facility must document the circumstances leading to the initiation of the examination;
(e) Ensure that designated staff have completed limited mental health training as required by rule 59A-36.011,
F.A.C.; and,
(f) Maintain facility, staff, and resident records in accordance with the requirements of this rule chapter.
Rulemaking Authority 429.41 FS. Law Implemented 429.075, 429.26, 429.41 FS. History–New 8-15-90, Amended 9-
30-92, Formerly 10A-5.029, Repromulgated 10-30-95, Amended 6-2-96, 11-2-98, 7-30-06, Amended 4-17-14, 5-10-
18, Formerly 58A-5.029, 7-1-19.
59A-36.021 Extended Congregate Care Services.
(1) LICENSING.
(a) Any facility intending to establish extended congregate care services must obtain a license from the agency
before accepting residents needing extended congregate care services.
(b) Only the portion of a facility that meets the physical requirements of subsection (3), and is staffed in
accordance with subsection (4), is considered licensed to provide extended congregate care services to residents who
meet the admission and continued residency requirements of this rule.

Effective July 1, 2019 6A – 47
(2) EXTENDED CONGREGATE CARE POLICIES. Policies and procedures established through extended
congregate care services must promote resident independence, dignity, choice, and decision-making. The facility
must develop and implement specific written policies and procedures that address:
(a) Aging in place;
(b) The facility’s residency criteria developed in accordance with the admission and discharge requirements
described in subsection (5), and extended congregate care services listed in subsection (8);
(c) The personal and supportive services the facility intends to provide, how the services will be provided, and
the identification of staff positions to provide the services including their relationship to the facility;
(d) The nursing services the facility intends to provide, identification of staff positions to provide nursing
services, and the license status, duties, general working hours, and supervision of such staff;
(e) Identifying potential unscheduled resident service needs and mechanisms for meeting those needs including
the identification of resources to meet those needs;
(f) A process for mediating conflicts among residents regarding choice of room or apartment and roommate;
and,
(g) How to involve residents in decisions concerning the resident. The services must provide opportunities and
encouragement for the resident to make personal choices and decisions. If a resident needs assistance to make
choices or decisions, a family member or other resident representative must be consulted. Choices must include at a
minimum whether:
1. To participate in the process of developing, implementing, reviewing, and revising the resident’s service plan,
2. To remain in the same room in the facility, except that a current resident transferring into an extended
congregate care services may be required to move to the part of the facility licensed for extended congregate care, if
only part of the facility is so licensed,
3. To select among social and leisure activities,
4. To participate in activities in the community. At a minimum the facility must arrange transportation to such
activities if requested by the resident; and,
5. To provide input with respect to the adoption and amendment of facility policies and procedures.
(3) STAFFING REQUIREMENTS. The following staffing requirements apply for extended congregate care
services:
(a) Supervision by an administrator who has a minimum of two years of managerial, nursing, social work,
therapeutic recreation, or counseling experience in a residential, long-term care, or acute care setting or agency
serving elderly or disabled persons. If an administrator appoints a manager as the supervisor of an extended
congregate care facility, both the administrator and manager must satisfy the requirements of subsection 59A-
36.010(1), F.A.C.
1. A baccalaureate degree may be substituted for one year of the required experience.
2. A nursing home administrator licensed under chapter 468, F.S., is qualified under this paragraph.
(b) Provide staff or contract the services of a nurse who must be available to provide nursing services,
participate in the development of resident service plans, and perform monthly nursing assessments for extended
congregate care residents.
(c) Provide enough qualified staff to meet the needs of extended congregate care residents in accordance with
rule 59A-36.010, F.A.C., and to provide the services established in each resident’s service plan.

Effective July 1, 2019 6A – 48
(d) Ensure that adequate staff is awake during all hours to meet the scheduled and unscheduled needs of
residents.
(e) Immediately provide additional or appropriately qualified staff, when the agency determines that service
plans are not being followed or that residents’ needs are not being met because insufficient staffing, in accordance
with the staffing standards established in rule 59A-36.010, F.A.C.
(f) Ensure and document that staff receive extended congregate care training as required in rule 59A-36.011,
F.A.C.
(4) ADMISSION AND CONTINUED RESIDENCY.
(a) An individual must meet the following minimum criteria in order to receive extended congregate care
services:
1. Be at least 18 years of age;
2. Be free from signs and symptoms of a communicable disease that is likely to be transmitted to other residents
or staff; however, an individual who has human immunodeficiency virus (HIV) infection may be admitted to a
facility, provided that he or she would otherwise be eligible for admission according to this rule;
3. Be able to transfer, with assistance if necessary. The assistance of more than one individual is permitted;
4. Not be a danger to self or others as determined by a health care provider or mental health practitioner
licensed under chapter 490 or 491, F.S.;
5. Not be bedridden;
6. Not have any stage 3 or 4 pressure sores;
7. Not require any of the following nursing services:
a. Artificial airway management of any kind except that of continuous positive airway pressure may be
provided through the use of a CPAP or bipap machine,
b. Nasogastric tube feeding,
c. Monitoring of blood gases,
d. Management of post-surgical drainage tubes or wound vacuums,
e. Skilled rehabilitative services as described in rule 59G-4.290, F.A.C., or
f. Treatment of a surgical incision, unless the surgical incision and the condition that caused it have been
stabilized and a plan of care developed. The plan of care must be maintained in the resident’s record at the facility.
8. Not require 24-hour nursing supervision; and,
9. Have been determined to be appropriate for admission to the facility by the facility administrator or manager.
The administrator or manager must base his or her decision on:
a. An assessment of the strengths, needs, and preferences of the individual, the health assessment required by
subsection (6) of this rule, and the preliminary service plan developed in subsection (7),
b. The facility’s residency criteria, and services offered or arranged for by the facility to meet resident needs;
and,
c. The ability of the facility to meet the uniform fire safety standards for assisted living facilities established in
rule chapter 69A-40, F.A.C.
(b) Criteria for continued residency in an extended congregate care services must be the same as the criteria for
admission, except as specified below.
1. A resident may be bedridden for up to 14 consecutive days.

Effective July 1, 2019 6A – 49
2. A terminally ill resident who no longer meets the criteria for continued residency may continue to reside in
the facility if the following conditions are met:
a. The resident qualifies for, is admitted to, and consents to the services of a licensed hospice that coordinates
and ensures the provision of any additional care and services that may be needed,
b. Continued residency is agreeable to the resident and the facility,
c. An interdisciplinary care plan, which specifies the services being provided by hospice and those being
provided by the facility, is developed and implemented by a licensed hospice in consultation with the facility; and,
d. Documentation of the requirements of subparagraph (5)(b)2., is maintained in the resident’s file.
3. The extended congregate care administrator or manager is responsible for monitoring the appropriateness of
continued residency of a resident in extended congregate care services at all times.
4. A hospice resident that meets the qualifications of continued residency pursuant to this rule may only receive
services from the assisted living facility’s staff within the scope of the facility’s license.
5. Staff may provide any nursing service permitted under the facility’s license and total help with the activities
of daily living for residents admitted to hospice. Staff may not exceed the scope of their professional licensure or
training in any licensed assisted living facility.
(5) HEALTH ASSESSMENT. Before receiving extended congregate care services, all persons. including
residents transferring within the same facility to that portion of the facility licensed to provide extended congregate
care services, must be examined by a health care provider pursuant to rule 59A-36.006, F.A.C. A health assessment
conducted no more than 60 days before receiving extended congregate care services meets this requirement. Once
receiving services, a new health assessment must be obtained at least annually.
(6) SERVICE PLANS.
(a) Before receiving services, the extended congregate care administrator or manager must develop a
preliminary service plan that includes an assessment of whether the resident meets the facility’s residency criteria,
an appraisal of the resident’s unique physical, psychological and social needs and preferences, and an evaluation of
the facility’s ability to meet the resident’s needs.
(b) Within 14 days of receiving services, the extended congregate care administrator or manager must
coordinate the development of a written service plan that takes into account the resident’s health assessment
obtained pursuant to subsection (6); the resident’s unique physical, psychological and social needs and preferences;
and how the facility will meet the resident’s needs including the following if required:
1. Health monitoring,
2. Assistance with personal care services,
3. Nursing services,
4. Supervision,
5. Special diets,
6. Ancillary services,
7. The provision of other services such as transportation and supportive services; and,
8. The manner of service provision, and identification of service providers, including family and friends, in
keeping with resident preferences.
(c) Pursuant to the definitions of “shared responsibility” and “managed risk” as provided in section 429.02, F.S.,
the service plan must be developed and agreed upon by the resident or the resident’s representative or designee,

Effective July 1, 2019 6A – 50
surrogate, guardian, or attorney-in-fact, and must reflect the responsibility and right of the resident to consider
options and assume risks when making choices pertaining to the resident’s service needs and preferences.
(d) The service plan must be reviewed and updated quarterly to reflect any changes in the manner of service
provision, accommodate any changes in the resident’s physical or mental status, or pursuant to recommendations for
modifications in the resident’s care as documented in the nursing assessment.
(7) EXTENDED CONGREGATE CARE SERVICES. All services must be provided in the least restrictive
environment, and in a manner that respects the resident’s independence, privacy, and dignity.
(a) A facility providing extended congregate care services may provide supportive services including social
service needs, counseling, emotional support, networking, assistance with securing social and leisure services,
shopping service, escort service, companionship, family support, information and referral, assistance in developing
and implementing self-directed activities, and volunteer services. Family or friends must be encouraged to provide
supportive services for residents. The facility must provide training for family or friends to enable them to provide
supportive services in accordance with the resident’s service plan.
(b) A facility providing extended congregate care services must make available the following additional
services if required by the resident’s service plan:
1. Total help with bathing, dressing, grooming and toileting,
2. Nursing assessments conducted more frequently than monthly,
3. Measurement and recording of basic vital functions and weight,
4. Dietary management including provision of special diets, monitoring nutrition, and observing the resident’s
food and fluid intake and output,
5. Assistance with self-administered medications, or the administration of medications and treatments pursuant
to a health care provider’s order. If the individual needs assistance with self-administration the facility must inform
the resident of the qualifications of staff who will be providing this assistance, and if unlicensed persons will be
providing such assistance, obtain the resident’s or the resident’s surrogate, guardian, or attorney-in-fact’s informed
written consent to provide such assistance as required in section 429.256, F.S.,
6. Supervision of residents with dementia and cognitive impairments,
7. Health education and counseling and the implementation of health-promoting programs and preventive
regimes,
8. Provision or arrangement for rehabilitative services; and,
9. Provision of escort services to health-related appointments.
(c) Nursing staff providing extended congregate care services may provide any nursing service permitted within
the scope of their license consistent with the residency requirements of this rule and the facility’s written policies
and procedures, provided the nursing services are:
1. Authorized by a health care provider’s order and pursuant to a plan of care,
2. Medically necessary and appropriate for treatment of the resident’s condition,
3. In accordance with the prevailing standard of practice in the nursing community,
4. A service that can be safely, effectively, and efficiently provided in the facility,
5. Recorded in nursing progress notes; and,
6. In accordance with the resident’s service plan.

Effective July 1, 2019 6A – 51
(d) At least monthly, or more frequently if required by the resident’s service plan, a nursing assessment of the
resident must be conducted.
(8) RECORDS. In addition to the records required in rule 59A-36.015, F.A.C., a facility providing extended
congregate care services must maintain the following:
(a) The service plans for each resident receiving extended congregate care services;
(b) The nursing progress notes for each resident receiving nursing services;
(c) Nursing assessments; and,
(d) The facility’s extended congregate care policies and procedures.
(9) DISCHARGE. If the facility and the resident are unable to agree on a service plan, the facility is unable to
meet the resident’s needs as identified in the service plan, or the resident no longer meets the criteria for continued
residency, the resident must be discharged or relocated in accordance with sections 429.26 and 429.28, F.S.
Rulemaking Authority 429.07, 429.41 FS. Law Implemented 429.07, 429.255, 429.26, 429.28, 429.41 FS. History–
New 9-30-92, Formerly 10A-5.030, Amended 10-30-95, 6-2-96, 4-20-98, 11-2-98, 10-17-99, 7-30-06, 4-17-14, 5-10-
18, Formerly 58A-5.030, 7-1-19.
59A-36.022 Limited Nursing Services.
Any facility intending to provide limited nursing services must obtain a license from the agency.
(1) NURSING SERVICES. In addition to any nursing service permitted under a standard license pursuant to
section 429.255, F.S., a facility with a limited nursing services license may provide nursing care to residents who do
not require 24-hour nursing supervision and to residents who do require 24-hour nursing care and are enrolled in
hospice.
(2) RESIDENT CARE STANDARDS.
(a) A resident receiving limited nursing services in a facility holding only a standard and limited nursing
services license must meet the admission and continued residency criteria specified in rule 59A-36.006, F.A.C.
(b) In accordance with rule 59A-36.010, F.A.C., the facility must employ sufficient and qualified staff to meet
the needs of residents requiring limited nursing services based on the number of such residents and the type of
nursing service to be provided.
(c) Limited nursing services may only be provided as authorized by a health care provider’s order, a copy of
which must be maintained in the resident’s file.
(d) Facilities licensed to provide limited nursing services must employ or contract with a nurse(s) who must be
available to provide such services as needed by residents. The facility’s employed or contracted nurse must
coordinate with third party nursing services providers to ensure resident care is provided in a safe and consistent
manner. The facility must maintain documentation of the qualifications of nurses providing limited nursing services
in the facility’s personnel files.
(e) The facility must ensure that nursing services are conducted and supervised in accordance with chapter 464,
F.S., and the prevailing standard of practice in the nursing community.
(3) RECORDS.
(a) A record of all residents receiving limited nursing services and the type of services provided must be
maintained at the facility.
(b) Nursing progress notes must be maintained for each resident who receives limited nursing services.

Effective July 1, 2019 6A – 52
(c) A nursing assessment conducted at least monthly must be maintained on each resident who receives a
limited nursing service.
Rulemaking Authority 429.41 FS. Law Implemented 429.07, 429.255, 429.26, 429.41 FS. History–New 9-30-92,
Formerly 10A-5.031, Amended 10-30-95, 10-17-99, 7-30-06, 3-13-14, 5-10-18, Formerly 58A-5.031, 7-1-19.
59A-36.023 Administrative Enforcement.
Facility staff shall cooperate with Agency personnel during surveys, complaint investigations, monitoring visits,
implementation of correction plans, license application and renewal procedures and other activities necessary to
ensure compliance with part I of chapter 429, F.S., and this rule chapter.
(1) INSPECTIONS.
(a) Pursuant to section 429.34, F.S., the agency shall conduct a survey, investigation, or appraisal of a facility:
1. Prior to issuance of a license;
2. Prior to biennial renewal of a license;
3. When there is a change of ownership;
4. To monitor facilities licensed to provide limited nursing or extended congregate care services, or who were
cited in the previous year for a Class I or Class II, or 4 or more uncorrected Class III violations;
5. Upon receipt of an oral or written complaint of practices that threaten the health, safety, or welfare of
residents;
6. If the agency has reason to believe a facility is violating a provision of part III of chapter 429, F.S., or this
rule chapter;
7. To determine if cited deficiencies have been corrected; and
8. To determine if a facility is operating without a license.
(b) The inspection shall consist of full access to and examination of the facility’s physical premises and facility
records and accounts, and staff and resident records.
(c) Agency personnel shall interview facility staff and residents in order to determine whether the facility is
respecting resident rights and to determine compliance with resident care standards. Interviews shall be conducted
privately.
(d) Agency personnel shall respect the private possessions of residents and staff while conducting facility
inspections.
(2) ABBREVIATED SURVEY.
(a) An applicant for license renewal who does not have any class I or class II violations or uncorrected class III
violations, confirmed long-term care ombudsman council complaints reported to the agency by the LTCOC, or
confirmed licensing complaints within the two licensing periods immediately preceding the current renewal date
shall be eligible for an abbreviated biennial survey by the agency. Facilities that do not have two survey reports on
file with the agency under current ownership are not eligible for an abbreviated inspection. Upon arrival at the
facility, the agency shall inform the facility that it is eligible for and that an abbreviated survey will be conducted.
(b) Compliance with key quality of care standards described in the following statutes and rules will be used by
the agency during its abbreviated survey of eligible facilities:
1. Section 429.26, F.S., and rule 59A-36.006, F.A.C., relating to residency criteria;
2. Section 429.27, F.S., and rule 59A-36.013, F.A.C., relating to proper management of resident funds and
property;

Effective July 1, 2019 6A – 53
3. Section 429.28, F.S., and rule 59A-36.007, F.A.C., relating to respect for resident rights;
4. Section 429.41, F.S., and rule 59A-36.007, F.A.C., relating to the provision of supervision, assistance with
ADLs, and arrangement for appointments and transportation to appointments;
5. Section 429.256, F.S., and rule 59A-36.008, F.A.C., relating to assistance with or administration of
medications;
6. Section 429.41, F.S., and rule 59A-36.010, F.A.C., relating to the provision of sufficient staffing to meet
resident needs;
7. Section 429.41, F.S., and rule 59A-36.011, F.A.C., relating to minimum dietary requirements and proper food
hygiene;
8. Section 429.075,.F.S., and rule 59A-36.020, F.A.C., relating to mental health residents’ community support
living plan;
9. Section 429.07, F.S., and rule 59A-36.021, F.A.C., relating to meeting the environmental standards and
residency criteria in a facility with an extended congregate care license; and
10. Section 429.07, F.S., and rule 59A-36.022, F.A.C., relating to the provision of care and staffing in a facility
with a limited nursing license.
(c) The agency will expand the abbreviated survey or conduct a full survey if violations which threaten or
potentially threaten the health, safety, or security of residents are identified during the abbreviated survey. The
facility shall be informed that a full survey will be conducted. If one or more of the following serious problems are
identified during an abbreviated survey, a full biennial survey will be immediately conducted:
1. Violations of rule chapter 69A-40, F.A.C., relating to firesafety, that threaten the life or safety of a resident;
2. Violations relating to staffing standards or resident care standards that adversely affect the health or safety of
a resident;
3. Violations relating to facility staff rendering services for which the facility is not licensed; or
4. Violations relating to facility medication practices that are a threat to the health or safety of a resident.
(3) SURVEY DEFICIENCY.
(a) Prior to or in conjunction with a notice of violation issued pursuant to section 429.19 and chapter 120, F.S.,
the agency shall issue a statement of deficiency for Class I, II, III, and IV violations which are observed by Agency
personnel during any inspection of the facility. The deficiency statement shall be issued within ten (10) working
days of the Agency’s inspection and shall include:
1. A description of the deficiency;
2. A citation to the statute or rule violated;
3. A time frame for the correction of the deficiency;
4. A request for a plan of correction which shall include time frame for correction of the deficiency; and
5. A description of the administrative sanction that may be imposed if the facility fails to correct the deficiency
within the established time frame.
(b) Additional time may be granted to correct specific deficiencies if a written request is received by the agency
prior to the time frame included in the agency’s statement.
(c) The facility’s plan of correction must be received by the agency within 10 working days of receipt of the
deficiency statement and is subject to approval by the agency.

Effective July 1, 2019 6A – 54
(4) EMPLOYMENT OF A CONSULTANT.
(a) Medication Deficiencies.
1. If a Class I, Class II, or uncorrected Class III deficiency directly relating to facility medication practices as
established in rule 59A-36.008, F.A.C., is documented by agency personnel pursuant to an inspection of the facility,
the agency shall notify the facility in writing that the facility must employ, on staff or by contract, the services of a
pharmacist licensed pursuant to section 465.0125, F.S., or registered nurse, as determined by the agency.
2. The initial on-site consultant visit shall take place within 7 working days of the identification of a Class I or
Class II deficiency and within 14 working days of the identification of an uncorrected Class III deficiency. The
facility shall have available for review by the agency a copy of the pharmacist’s or registered nurse’s license and a
signed and dated recommended corrective action plan no later than 10 working days subsequent to the initial on-site
consultant visit.
3. The facility shall provide the agency with, at a minimum, quarterly onsite corrective action plan updates until
the agency determines after written notification by the consultant and facility administrator that deficiencies are
corrected and staff has been trained to ensure that proper medication standards are followed and that such consultant
services are no longer required. The agency shall provide the facility with written notification of such determination.
(b) Dietary Deficiencies.
1. If a Class I, Class II, or uncorrected Class III deficiency directly related to dietary standards as established in
rule 59A-36.012, F.A.C., is documented by agency personnel pursuant to an inspection of the facility, the agency
shall notify the facility in writing that the facility must employ, on staff or by contract, the services of a registered
dietitian or licensed dietitian/nutritionist.
2. The initial on-site consultant visit shall take place within 7 working days of the identification of a Class I or
Class II deficiency and within 14 working days of the identification of an uncorrected Class III deficiency. The
facility shall have available for review by the agency a copy of the dietitian’s license or registration card and a
signed and dated dietary consultant’s recommended corrective action plan no later than 10 working days subsequent
to the initial on-site consultant visit.
3. The facility shall provide the agency with, at a minimum, quarterly on-site corrective action plan updates
until the agency determines after written notification by the dietary consultant and facility administrator that
deficiencies are corrected and staff has been trained to ensure that proper dietary standards are followed and that
such consultant services are no longer required. The agency shall provide the facility with written notification of
such determination.
(5) ADMINISTRATIVE SANCTIONS. Administrative fines shall be imposed for Class I and Class II
violations, or Class III or IV violations which are not corrected within the time frame set by the Agency, and for
repeat Class III violations, as set forth in section 429.19, F.S.
(a) The Agency shall notify facilities of the imposition of sanctions, their right to appeal the sanctions, the
remedies available, and the time limit for requesting such remedies as provided under chapter 120, F.S., and part II
of chapter 59-1, F.A.C.
(b) When an administrative fine payment is returned from the applicant’s bank for whatever reason, the agency
shall add to the amount due a service fee of $20 or 5 percent of the face amount of the check, whichever is greater,
up to a maximum charge of $200. Proceeds from this fee shall be deposited in the same agency account as the fine.
Rulemaking Authority 429.41, 429.42 FS. Law Implemented 429.07, 429.08, 429.11, 429.12, 429.14, 429.17,

Effective July 1, 2019 6A – 55
429.19, 429.256, 429.26, 429.27, 429.28, 429.34, 429.41, 429.42 FS. History–New 9-30-92, Formerly 10A-5.033,
Amended 10-30-95, 10-17-99, 1-9-02, 7-30-06, 4-15-10, 3-13-14, Formerly 58A-5.033, 7-1-19.
59A-36.024 Waivers.
The agency, in consultation with the department, may waive rules promulgated pursuant to part I, chapter 429, F.S.,
if the waiver request meets the conditions set forth in section 429.41(4), F.S., and demonstrates and evaluates
innovative or cost-effective congregate care alternatives which will enable individuals to age in place.
(1) Application Process.
(a) Licensed assisted living facilities proposing a waiver under this statute must submit the request in writing.
All requests must include the facility name and address, license number, administrator’s name and contact
information for the requestor, or its attorney. Petitions for waiver of rules other than for the objectives detailed in
section 429.41(4), F.S., including emergency waivers, will not be considered under this section but should follow
the petition for waiver provisions of section 120.542, F.S., and rule chapter 28-104, Variance or Waiver, F.A.C.
(b) The written request must address the elements required in section 429.41(4), F.S. In addition, the following
information must be included in order to demonstrate how a waiver of the stated rule will permit development of a
concept that will achieve the purpose of the underlying statute:
1. The rule or rules for which the waiver is requested.
2. The licensee’s anticipated date or dates for implementation of the concept.
3. If applying based on cost-effectiveness or cost-savings, a cost-benefit analysis of the proposed alternative to
both residents or potential residents as well as facility operations.
4. An analysis of the impact the alternative will have on the relevant local community, including any barriers
such as zoning or use issues, which may need resolution prior to implementation.
5. Specific performance measures with an annual projection of objectives and goals to be achieved broken into
quarterly increments or an annual projection of outcome measures, if the concept will be implemented in less than
90 days.
6. If applying based on cost-effectiveness or cost-savings, an annual budget projection for the proposed
alternative broken into quarterly increments.
(c) A waiver can be requested at the time of the initial license application, relicensure, or any time during the
licensure period.
(d) Waiver requests must be submitted to the Agency for Health Care Administration, Assisted Living Unit,
2727 Mahan Drive, Mail Stop 30, Tallahassee, Florida 32308-5403.
(2) In accordance with section 120.542(6), F.S., the agency shall post notice of the request within fifteen (15)
days of receipt of the request. The agency shall make any requests for additional information within 30 days of
receipt of the request. If additional information is provided, the agency may request clarification of only that
information no later than 30 days following receipt of the information. The agency shall process the waiver request
pursuant to the time frame referenced in section 120.542(8), F.S.
(3) The agency, in consultation with the department, will evaluate all requests in light of the likelihood the
concept, as described in detail, will achieve the underlying statutory objectives of innovative or cost effective
congregate care alternatives to enable individuals to age in place, as provided in section 429.41(4), F.S. Waivers
may be granted only so long as there is reasonable assurance that the health, safety or welfare of residents will not
be endangered by the waiver.

Effective July 1, 2019 6A – 56
(4) The agency shall grant or deny the request for waiver and enter an order summarizing the facts it relied on
and reasons supporting its decision. The agency must provide notice of its order as described in section 120.542(8),
F.S. The requestor shall be advised that a denial of the request may be reviewed as provided in subsection (5) of this
rule.
(5) Report of Findings. A facility that has been granted a waiver must submit an annual report within 12 months
of the order granting the waiver as specified in section 429.41(4), F.S. If the report is not submitted as required, the
agency may revoke the waiver.
(a) The agency will review the report of findings to determine whether the waiver shall be renewed or revoked.
The agency shall make the determination based on whether the facility has met the requirements outlined in
subparagraph (1)(b) of this rule. The agency shall enter an order providing the general basis for making its decision
and notify the licensee of its opportunity to seek review of a revocation in accordance with sections 120.569 and
120.57, F.S. and rule 28-106.111, F.A.C.
(b) The agency may also consider other material which is available relative to this review.
(c) A waiver is effective unless revoked by the agency or superseded by statutory or regulatory change.
(d) In reviewing the report of findings, the agency, in consultation with the department, shall assess whether
statutory or regulatory changes should be pursued to enable other facilities to adopt the same practices.
Rulemaking Authority 429.41 FS. Law Implemented 120.542, 429.41 FS. History–New 9-30-92, Formerly 10A-
5.035, Amended 10-30-95, 7-1-08, 4-17-14, Formerly 59A-36.024, 7-1-19.
59A-36.025 Emergency Environmental Control for Assisted Living Facilities.
(1) DETAILED EMERGENCY ENVIRONMENTAL CONTROL PLAN. Each assisted living facility shall
prepare a detailed plan (“plan”) to serve as a supplement to its Comprehensive Emergency Management Plan, to
address emergency environmental control in the event of the loss of primary electrical power in that assisted living
facility which includes the following information:
(a) The acquisition of a sufficient alternate power source such as a generator(s), maintained at the assisted living
facility, to ensure that current licensees of assisted living facilities will be equipped to ensure ambient air
temperatures will be maintained at or below 81 degrees Fahrenheit for a minimum of ninety-six (96) hours in the
event of the loss of primary electrical power.
1. The required temperature must be maintained in an area or areas, determined by the assisted living facility, of
sufficient size to maintain residents safely at all times and that is appropriate for resident care needs and life safety
requirements. For planning purposes, no less than twenty (20) net square feet per resident must be provided. The
assisted living facility may use eighty percent (80%) of its licensed bed capacity as the number of residents to be
used in the calculation to determine the required square footage. This may include areas that are less than the entire
assisted living facility if the assisted living facility’s comprehensive emergency management plan includes allowing
a resident to congregate when he or she desires in portions of the building where temperatures will be maintained
and includes procedures for monitoring residents for signs of heat related injury as required by this rule. This rule
does not prohibit a facility from acting as a receiving provider for evacuees when the conditions stated in section
408.821, F.S. and subsection 59A-36.019(5), F.A.C., are met. The plan shall include information regarding the
area(s) within the assisted living facility where the required temperature will be maintained.
2. The alternate power source and fuel supply shall be located in an area(s) in accordance with local zoning and
the Florida Building Code.

Effective July 1, 2019 6A – 57
3. Each assisted living facility is unique in size; the types of care provided; the physical and mental capabilities
and needs of residents; the type, frequency, and amount of services and care offered; and staffing characteristics.
Accordingly, this rule does not limit the types of systems or equipment that may be used to achieve ambient
temperatures at or below 81 degrees Fahrenheit for a minimum of ninety-six (96) hours in the event of the loss of
primary electrical power. The plan shall include information regarding the systems and equipment that will be used
by the assisted living facility and the fuel required to operate the systems and equipment.
a. An assisted living facility in an evacuation zone pursuant to chapter 252, F, S. must maintain an alternative
power source and fuel as required by this subsection at all times when the assisted living facility is occupied but is
permitted to utilize a mobile generator(s) to enable portability if evacuation is necessary.
b. Assisted living facilities located on a single campus with other facilities under common ownership, may share
fuel, alternative power resources, and resident space available on the campus if such resources are sufficient to
support the requirements of each facility’s residents, as specified in this rule. Details regarding how resources will
be shared and any necessary movement of residents must be clearly described in the emergency power plan.
c. A multistory facility, whose comprehensive emergency management plan is to move residents to a higher
floor during a flood or surge event, must place its alternative power source and all necessary additional equipment so
it can safely operate in a location protected from flooding or storm surge damage.
(b) The acquisition of sufficient fuel, and safe maintenance of that fuel at the facility, to ensure that in the event
of the loss of primary electrical power there is sufficient fuel available for the alternate power source to maintain
ambient temperatures at or below 81 degrees Fahrenheit for a minimum of ninety-six (96) hours after the loss of
primary electrical power during a declared state of emergency. The plan must include information regarding fuel
source and fuel storage.
1. Facilities must store minimum amounts of fuel onsite as follows:
a. A facility with a licensed capacity of 16 beds or less must store 48 hours of fuel onsite.
b. A facility with a licensed capacity of 17 or more beds must store 72 hours of fuel onsite.
2. An assisted living facility located in an area in a declared state of emergency area pursuant to section 252.36,
F.S. that may impact primary power delivery must secure ninety-six (96) hours of fuel. The assisted living facility
may utilize portable fuel storage containers for the remaining fuel necessary for ninety-six (96) hours during the
period of a declared state of emergency.
3. Piped natural gas is an allowable fuel source and meets the onsite fuel supply requirements under this rule.
4. If local ordinances or other regulations limit the amount of onsite fuel storage for the assisted living facility’s
location, then the assisted living facility must develop a plan that includes maximum onsite fuel storage allowable
by the ordinance or regulation and a reliable method to obtain the maximum additional fuel at least 24 hours prior to
depletion of onsite fuel.
(c) The acquisition of services necessary to maintain, and test the equipment and its functions to ensure the safe
and sufficient operation of the alternate power source maintained at the assisted living facility.
(d) The acquisition and maintenance of a carbon monoxide alarm.
(2) SUBMISSION OF THE PLAN.
(a) Each assisted living facility licensed prior to the effective date of this rule shall submit its plan to the local
emergency management agency for review within 30 days of the effective date of this rule. Assisted living facility

Effective July 1, 2019 6A – 58
plans previously submitted and approved pursuant to emergency rule 58AER17-1 will require resubmission only if
changes are made to the plan.
(b) Each new assisted living facility shall submit the plan required under this rule prior to obtaining a license.
(c) Each existing assisted living facility that undergoes any additions, modifications, alterations, refurbishment,
renovations or reconstruction that require modification of its systems or equipment affecting the facility’s
compliance with this rule shall amend its plan and submit it to the local emergency management agency for review
and approval.
(3) APPROVED PLANS.
(a) Each assisted living facility must maintain a copy of its approved plan in a manner that makes the plan
readily available at the licensee’s physical address for review by a legally authorized entity. If the plan is maintained
in an electronic format, assisted living facility staff must be readily available to access and produce the plan. For
purposes of this section, “readily available” means the ability to immediately produce the plan, either in electronic or
paper format, upon request.
(b) Within two (2) business days of the approval of the plan from the local emergency management agency, the
assisted living facility shall submit in writing proof of the approval to the Agency for Health Care Administration.
(c) The assisted living facility shall submit a consumer-friendly summary of the emergency power plan to the
Agency. The Agency shall post the summary and notice of the approval and implementation of the assisted living
facility emergency power plans on its website within ten (10) business days of the plan's approval by the local
emergency management agency and update within ten (10) business days of implementation.
(4) IMPLEMENTATION OF THE PLAN.
(a) Each assisted living facility licensed prior to the effective date of this rule shall, no later than June 1, 2018,
have implemented the plan required under this rule.
(b) The Agency shall allow an extension up to January 1, 2019 to providers in compliance with paragraph (c)
below and who can show delays caused by necessary construction, delivery of ordered equipment, zoning or other
regulatory approval processes. Assisted living facilities shall notify the Agency that they will utilize the extension
and keep the Agency apprised of progress on a quarterly basis to ensure there are no unnecessary delays. If an
assisted living facility can show in its quarterly progress reports that unavoidable delays caused by necessary
construction, delivery of ordered equipment, zoning or other regulatory approval processes will occur beyond the
initial extension date, the assisted living facility may request a waiver pursuant to section 120.542, F.S.
(c) During the extension period, an assisted living facility must make arrangements pending full implementation
of its plan that provides the residents with an area or areas to congregate that meets the safe indoor air temperature
requirements of subsection (1) (a) for a minimum of ninety-six (96) hours.
1. An assisted living facility not located in an evacuation zone must either have an alternative power source
onsite or have a contract in place for delivery of an alternative power source and fuel when requested. Within
twenty-four (24) hours of the issuance of a state of emergency for an event that may impact primary power delivery
for the area of the assisted living facility, it must have the alternative power source and no less than ninety-six (96)
hours of fuel stored onsite.
2. An assisted living facility located in an evacuation zone pursuant to chapter 252, F.S. must either:
a. Fully and safely evacuate its residents prior to the arrival of the event; or

Effective July 1, 2019 6A – 59
b. Have an alternative power source and no less than ninety-six (96) hours of fuel stored onsite, within twenty-
four (24) hours of the issuance of a state of emergency for the area of the assisted living facility.
(d) Each new assisted living facility shall implement the plan required under this rule prior to obtaining a
license.
(e) Existing assisted living facilities that undergo any additions, modifications, alterations, refurbishment,
renovations or reconstruction that require modification of the systems or equipment affecting the assisted living
facility’s compliance with this rule shall implement its amended plan concurrent with any such additions,
modifications, alterations, refurbishment, renovations or reconstruction.
(f) The Agency for Health Care Administration may request cooperation from the State Fire Marshal to conduct
inspections to ensure implementation of the plan in compliance with this rule.
(5) POLICIES AND PROCEDURES.
(a) Each assisted living facility shall develop and implement written policies and procedures to ensure that the
assisted living facility can effectively and immediately activate, operate and maintain the alternate power source and
any fuel required for the operation of the alternate power source. The procedures shall ensure that residents do not
experience complications from fluctuations in ambient air temperatures inside the facility. Procedures must address
the care of residents occupying the facility during a declared state of emergency, specifically, a description of the
methods to be used to mitigate the potential for heat related injury including:
1. The use of cooling devices and equipment;
2. The use of refrigeration and freezers to produce ice and appropriate temperatures for the maintenance of
medicines requiring refrigeration;
3. Wellness checks by assisted living facility staff to monitor for signs of dehydration and heat injury; and
4. A provision for obtaining medical intervention from emergency services for residents whose life safety is in
jeopardy.
(b) Each assisted living facility shall maintain the written policies and procedures in a manner that makes them
readily available at the licensee’s physical address for review by a legally authorized entity. If the policies and
procedures are maintained in an electronic format, assisted living facility staff must be readily available to access the
policies and procedures and produce the requested information. For purposes of this section, “readily available”
means the ability to immediately produce the policies and procedures, either in electronic or paper format, upon
request.
(c) The written policies and procedures must be readily available for inspection by each resident; each resident’s
legal representative, designee, surrogate, guardian, attorney in fact, or case manager; each resident’s estate; and such
additional parties as authorized in writing or by law.
(6) REVOCATION OF LICENSE, FINES OR SANCTIONS. For a violation of any part of this rule, the
Agency for Health Care Administration may seek any remedy authorized by chapter 429, part I, or chapter 408, part
II, F.S., including, but not limited to, license revocation, license suspension, and the imposition of administrative
fines.
(7) COMPREHENSIVE EMERGENCY MANAGEMENT PLAN.
(a) Assisted living facilities whose comprehensive emergency management plan is to evacuate must comply
with this rule.

Effective July 1, 2019 6A – 60
(b) Each facility whose plan has been approved shall submit the plan as an addendum with any future
submissions for approval of its comprehensive emergency management plan.
(8) NOTIFICATION.
(a) Within five (5) business days, each assisted living facility must notify in writing, unless permission for
electronic communication has been granted, each resident and the resident’s legal representative:
1. Upon submission of the plan to the local emergency management agency that the plan has been submitted for
review and approval;
2. Upon final implementation of the plan by the assisted living facility.
(b) Each assisted living facility must maintain a copy of each notification set forth in paragraph (a) above in a
manner that makes each notification readily available at the licensee’s physical address for review by a legally
authorized entity. If the notifications are maintained in an electronic format, facility staff must be readily available to
access and produce the notifications. For purposes of this section, “readily available” means the ability to
immediately produce the notifications, either in electronic or paper format, upon request.
Rulemaking Authority 429.41, FS. Law Implemented 429.19, 429.41, FS. History–New 3-26-18, Formerly 58A-
5.036, 7-1-19.
59A-36.027 ALF Core Training Provider Qualifications.
(1) PRIMARY REQUIREMENTS. In order to register as an assisted living facility core training provider
(hereafter referred to as “core training provider,” “training provider,” or “provider”), all applicants must meet the
requirements outlined in section 429.52(10), F.S. The requirements are as follows:
(a) Completion of the minimum core training requirements developed by the department pursuant to section
429.52(9), F.S., and rule 59A-36.028, F.A.C.;
(b) Successful passage of the competency test, which requires a minimum score of 75%; and,
(c) Compliance with the minimum of 12 contact hours of continuing education in topics related to assisted
living every 2 years pursuant to section 429.52(5), F.S., and paragraph 58A-5.0191(1)(c), F.A.C.
(2) ADDITIONAL REQUIREMENTS. In addition to meeting the 3 primary requirements set forth in
subsection (1), of this rule, applicants must meet one of the requirements outlined in section 429.52(11), F.S., or one
of the requirements established in this subsection. The requirements are as follows:
(a) A minimum of 5 years of employment with the Agency for Health Care Administration (AHCA), or
formerly the Department of Health and Rehabilitative Services, as a surveyor of assisted living facilities; or
(b) A minimum of 5 years of employment in a professional position in the AHCA Assisted Living Unit; or
(c) A minimum of 5 years of employment as an educator or staff trainer for persons working in an ALF or other
long-term care (LTC) settings; or
(d) A minimum of 5 years of employment as an assisted living facility core trainer, which was not directly
associated with the department; or
(e) A minimum of a 4-year degree from an accredited college or university in areas of healthcare, gerontology,
social work, education or human services; and a minimum of 3 years experience as an educator or staff trainer for
persons working in an ALF or other LTC settings after core certification.
Rulemaking Authority 429.52 FS. Law Implemented 429.52 FS. History–New 6-15-09, Formerly 58T-1.203, 7-1-19.

Effective July 1, 2019 6A – 61
59A-36.028 ALF Minimum Core Training Curriculum Requirements.
(1) CURRICULUM REQUIREMENTS. An approved core training provider must conduct core training using
the curriculum outlined in DOEA Form ALFCT-001, Assisted Living Facility Minimum Core Training Curriculum,
June, 2009, which is incorporated by reference in this rule. The curriculum is available from the Department of
Elder Affairs, Elder Housing Unit, 4040 Esplanade Way, Tallahassee, Florida 32399-7000 or the department’s
website at: http://elderaffairs.state.fl.us/english/ruleforms/ALFCT-001.doc.
(2) MONITORING. The department reserves the right to do the following:
(a) Attend and monitor core training courses;
(b) Review provider records and course materials pursuant to this rule; and,
(c) Conduct on-site monitoring, follow-up monitoring, and require implementation of a corrective action plan if
the provider does not adhere to the approved curriculum.
Rulemaking Authority 429.52 FS. Law Implemented 429.52 FS. History–New 6-15-09, Formerly 58T-1.205, 7-1-19.
59A-36.029 ALF Core Training Provider Initial Registration Process.
(1) REGISTRATION PROCESS.
(a) Before core training can be conducted, an applicant must meet the training provider qualifications outlined
in section 429.52(10), F.S., and rule 59A-36.027, F.A.C. Additionally, an applicant must register with, and obtain
from, the department a unique provider registration number as set forth in this subsection.
(b) An applicant must complete DOEA Form ALFCT-002, Application for Assisted Living Facility (ALF) Core
Training Provider Registration, June, 2009. The form is hereby incorporated by reference and may be obtained from
the Department of Elder Affairs, Elder Housing Unit, 4040 Esplanade Way, Tallahassee, Florida 32399-7000 or the
department’s website at: http://elderaffairs.state.fl.us/english/ruleforms/ALFCT-002.doc.
(2) APPROVAL PROCESS. Within 30 calendar days after receiving a core training provider application, the
department must submit written notification approving or denying the application, or requesting supplemental
information or clarification.
(a) If the application is approved, the department must include a unique provider registration number in the
notice.
(b) If the application is denied, the department must provide the reason or reasons for denial in the notice.
(c) If the application is determined to require supplemental information or clarification, the department must
state the supplemental information or clarification that is being requested.
1. If the department does not receive the requested information within 30 calendar days of the request, the
application will be deemed incomplete and closed.
2. If the department receives the requested information within 30 calendar days of the request, the department
must process the training provider application within 30 calendar days after all required information is received.
Rulemaking Authority 429.52 FS. Law Implemented 429.52 FS. History–New 6-15-09, Formerly 58T-1.207, 7-1-19.
59A-36.030 Process for Maintaining ALF Core Training Provider Registration.
(1) MAINTAINING ALF CORE TRAINING PROVIDER REGISTRATION.
(a) After receiving the initial core training provider registration, the approved provider must re-register with the
department every 2 years by submitting documentation of his or her compliance with the continuing education
requirement as specified in section 429.52(5), F.S., and this rule.

Effective July 1, 2019 6A – 62
(b) The provider must submit the documentation to the address referenced on DOEA Form ALFCT-001. It must
be submitted no later than 30 calendar days after each two-year continuing education cycle. The 2-year cycle begins
on the date of the initial training provider registration. Documentation must include the following:
1. Title of the training program;
2. Subject matter of the training program;
3. The training program agenda including topics discussed;
4. The core training provider’s name and registration number;
5. Date(s) of participation;
6. Number of hours of the training program; and
7. The continuing education training provider’s name, signature, credentials, and professional license number, if
applicable.
(2) APPROVAL PROCESS.
(a) Within 30 calendar days after receiving the required continuing education documentation, the department
must notify the provider in writing that the continuing education requirement:
1. Has been met; or
2. Has not been met and the reasons why; or
3. Has omissions or additional information is requested.
a. If the department does not receive the omitted or additional information within 30 calendar days of the
request, the provider’s registration shall be cancelled. The department must provide written notification of its
decision, including the reason for the cancellation, no later than 30 calendar days after the deadline for the request
for the omitted or additional information.
b. If the department receives the omitted or additional information as requested within the 30 calendar day time
period, the department must process the core training provider’s registration within 30 calendar days after all
required information is received. The department must provide written notification to the provider of its decision.
(b) Failure to submit proof of the continuing education requirement as specified in this rule shall result in
cancellation of the core training provider’s registration. The department must provide written notification of such
action no later than 30 calendar days after the information was due.
(c) If the provider’s registration is cancelled under paragraphs (a) and (b) of this subsection, and the provider
subsequently meets the continuing education requirement, he or she may re-apply for registration as specified in rule
59A-36.029, F.A.C., and include documentation that the continuing education requirement has been met pursuant to
this rule.
Rulemaking Authority 429.52 FS. Law Implemented 429.52 FS. History–New 6-15-09, Formerly 58T-1.209, 7-1-19.
59A-36.031 Registered ALF Core Training Provider Responsibilities.
The following are the responsibilities of a registered core training provider:
(1) USE OF MINIMUM CORE TRAINING CURRICULUM. A registered core training provider is responsible
for the following:
(a) Conducting core training using the minimum core training curriculum required by rule 59A-36.028, F.A.C.;
and
(b) Ensuring that all changes in ALF statutes and rules are immediately incorporated into the contents of his or
her core training curriculum.

Effective July 1, 2019 6A – 63
(2) CERTIFICATES. After a trainee successfully completes core training, the approved training provider must
issue a certificate to him or her. In addition to the provider’s unique registration number, the certificate must include
the information referenced in paragraph 58A-5.0191(12)(a), F.A.C. The provider’s signature and registration
number shall serve as documentation that the trainee has completed the required training.
(3) RECORDS. Approved providers must maintain records of each course taught for a minimum of 5 years.
Course records must include the following information:
(a) The title of the training program;
(b) The agenda;
(c) The curriculum and any accompanying documentation and training aids;
(d) The training provider’s name and registration number;
(e) The trainees’ names, dates of participation and training location; and
(f) Training evaluations and roster signed by trainees.
(4) COMPETENCY EXAM.
(a) Approved training providers must submit the names of trainees completing core training to the testing
authority within 10 calendar days after completion of the course. Names must be submitted to the following address:
ALF Certification Testing, University of South Florida, 4202 E. Fowler Avenue, EDU105, Tampa, Florida 33620.
Names may be alternately submitted via email to [email protected].
(b) The testing authority shall not process any requests for the competency exam, nor sit any individual for the
exam, unless proper notice is submitted by an approved training provider pursuant to paragraph (a), of this
subsection.
(5) GUEST SPEAKERS. If a core training provider uses guest trainers to teach or participate in specific training
modules covered in the minimum core training curriculum referenced in rule 59A-36.028, F.A.C., the core trainer is
responsible to ensure that the guest speaker meets the following minimum conditions:
(a) Has expertise in the specific subject matter; and
(b) Covers all components of the subject matter if he or she provides the module or portion of the module
instruction.
Rulemaking Authority 429.52 FS. Law Implemented 429.52 FS. History–New 6-15-09, Formerly 58T-1.211, 7-1-19.

Effective July 1, 2019 6A – 64
Notes
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________

6. Rule Chapter 59A
-36, F.A
.C., and C
rosswalk


CHAPTER 59A-36 ASSISTED LIVING FACILITY
59A-36.001 Standards and Criteria for Determining Compliance with Facility Standards and Resident Rights 59A-36.002 Definitions 59A-36.003 Licensing and Change of Ownership 59A-36.004 License Requirements 59A-36.005 Inspection Responsibilities 59A-36.006 Admission Procedures, Appropriateness of Placement and Continued Residency Criteria 59A-36.007 Resident Care Standards 59A-36.008 Medication Practices 59A-36.009 Do Not Resuscitate Orders (DNROs) 59A-36.010 Staffing Standards 59A-36.011 Staff Training Requirements and Competency Test 59A-36.012 Food Service Standards 59A-36.013 Fiscal Standards 59A-36.014 Physical Plant Standards 59A-36.015 Records 59A-36.016 Adverse Incident Report 59A-36.017 Liability Claim Report 59A-36.018 Resident Contracts 59A-36.019 Emergency Management 59A-36.020 Limited Mental Health 59A-36.021 Extended Congregate Care Services 59A-36.022 Limited Nursing Services 59A-36.023 Administrative Enforcement 59A-36.024 Waivers 59A-36.025 Emergency Environmental Control for Assisted Living Facilities 59A-36.027 ALF Core Training Provider Qualifications 59A-36.028 ALF Minimum Core Training Curriculum Requirements 59A-36.029 ALF Core Training Provider Initial Registration Process 59A-36.030 Process for Maintaining ALF Core Training Provider Registration 59A-36.031 Registered ALF Core Training Provider Responsibilities
59A-36.001 Standards and Criteria for Determining Compliance with Facility Standards and Resident Rights. (1) DEFINITIONS.
In addition to the terms defined in section 429.02, F.S., and rule 59A-36.002, F.A.C., the following definitions are applicable in this rule chapter.
(a) “Core Survey Task” means tasks conducted by Agency survey staff that focus on core areas of regulations. (b) “Timely Manner” means as soon as possible, but not to exceed 24 hours of Agency staff having requested materials. (2) SURVEY PROCESS FOR RESIDENT RIGHTS.
The following core survey tasks shall be utilized during survey activities in order to determine the facility’s compliance with resident rights pursuant to section 429.28, F.S., and rule 59A-36.007, F.A.C.
(a) The surveyor(s) conducts a tour of the facility to determine if the residents’ health, safety, and welfare are maintained. The tour includes observations and assessments of the following:
1. Resident behavior and demeanor; 2. Adherence to facility abuse prohibition policy and procedure; 3. Adherence to infection control policy and procedure; 4. General physical plant standards in accordance with rule 59A-36.014, F.A.C.; 5. Overall appearance of residents and observations of any special care needs;

6. Posting of Resident Bill of Rights and required phone numbers in accordance with rule 59A-36.007, F.A.C.; 7. Resident access to phones and unrestricted private communication; 8. Resident opportunity to exercise; 9. Staff availability and responsiveness to resident care needs; 10. Medication storage and security; 11. Chemical and physical restraint use; 12. Positioning/transferring processes utilized by staff; 13. Any specialized care provided by the facility with a specialty license; 14. Any license conditions or restrictions as a result of Agency action. (b) The surveyor(s) conducts interviews with residents, family members/representatives, staff, and any other persons the
surveyor(s) deems relevant to the survey. 1. The facility may not restrict Agency staff from conducting confidential interviews pursuant to section 429.14(6), F.S. 2. Interviews may be conducted both in person and telephonically. (c) The surveyor(s) reviews facility records to determine compliance with: 1. Licensure requirements in accordance with rule 59A-36.004, F.A.C.; 2. Inspection responsibilities in accordance with rule 59A-36.005, F.A.C.; 3. Admissions procedures and appropriateness of placement and continued residency criteria in accordance with rule 59A-
36.007, F.A.C.; 4. Resident care standards in accordance with rule 59A-36.007, F.A.C.; 5. Medication practices in accordance with rule 59A-36.008, F.A.C.; 6. Do not resuscitate orders (DNROs) in accordance with rule 59A-36.009, F.A.C.; 7. Staffing standards in accordance with rule 59A-36.010, F.A.C.; 8. Staff training requirements and competency training in accordance with rule 59A-36.011, F.A.C.; 9. Alzheimer’s Disease or Related Disorders training provider and curriculum approval in accordance with rule 58A-5.0194,
F.A.C.; 10. Food service standards in accordance with rule 59A-36.012, F.A.C.; 11. Fiscal standards in accordance with rule 59A-36.013, F.A.C.; 12. Physical plant standards in accordance with rule 59A-36.014, F.A.C.; 13. Records in accordance with rule 59A-36.015, F.A.C.; 14. Resident contracts in accordance with rule 59A-36.018, F.A.C.; 15. Emergency management in accordance with rule 59A-36.019, F.A.C. (d) The facility must provide agency staff with requested documents in a timely manner and allow the agency staff to obtain
copies. (e) Surveyor(s) conducts specific and general observations throughout the survey to determine compliance with: dietary
standards, medication standards, infection control standards, resident activities, assistance with activities of daily living, facility practices, and resident daily routines.
(f) For facilities licensed to provide specialty services such as Limited Mental Health, Extended Congregate Care, and Limited Nursing Services: the surveyor(s) reviews the required components in accordance with rules 59A-36.020, 59A-36.021, and 59A-36.021, F.A.C.
Rulemaking Authority 429.28(3)(a) FS. Law Implemented 429.28 FS. History–New 11-28-16.
59A-36.002 Definitions. In addition to the terms defined in section 429.02, F.S., the following definitions are applicable in this rule chapter:
(1) “Advertise” means any written, printed, oral, visual, or electronic promotion, statement of availability, qualifications, services offered, or other similar communication appearing in or on television, radio, the Internet, billboards, newspapers, magazines, business cards, flyers, brochures or other medium for the purpose of attracting potential residents to an assisted living facility. A complimentary listing of a licensed facility’s name, address, and telephone number in the telephone directory is not considered advertising.
(2) “Agency Central Office” means the Agency for Health Care Administration Assisted Living Unit (ALU), located at 2727

Mahan Drive, Mail Stop 30, Tallahassee, FL 32308-5403. The ALU telephone number and website address are (850)412-4304, and http://ahca.myflorida.com/MCHQ/Health_Facility_Regulation/Assisted_Living/alf.shtml.
(3) “Agency Field Office” means the Agency for Health Care Administration’s Office in a particular geographic area. Information regarding local offices is available online at: http://ahca.myflorida.com/mchq/index.shtml#six.
(4) “Apartment” means a self-contained dwelling unit with a bathroom, kitchen area, and living and sleeping space that is contracted for use as a residence by one or more persons who maintain a common household.
(5) “Anti-Embolism Stockings and Hosiery” means prescribed close-fitting elastic-type coverings for therapeutic treatment of the legs. They may be knee high or thigh high length and have transparent, open-toe, or similar foot design.
(6) “Assistance with Activities of Daily Living” means individual assistance with the following: (a) Ambulation – Providing physical support to enable the resident to move about within or outside the facility. Physical support
includes supporting or holding the resident’s hand, elbow, or arm; holding on to a support belt worn by the resident to assist in providing stability or direction while the resident ambulates; or pushing the resident’s wheelchair. The term does not include assistance with transfer.
(b) Bathing – Assembling towels, soaps, or other necessary supplies; helping the resident in and out of the bathtub or shower; turning the water on and off; adjusting water temperatures; washing and drying portions of the body that are difficult for the resident to reach; or being available while the resident is bathing.
(c) Dressing – Helping residents to choose, put on, and remove clothing. (d) Eating – Helping residents with or by cutting food, pouring beverages, or feeding residents who are unable to feed
themselves. (e) Grooming – Helping residents with shaving, oral care, care of the hair, or nail care. (f) Toileting – Assisting the resident to the bathroom, helping the resident to undress, positioning the resident on the commode,
and helping the resident with related personal hygiene including assistance with changing an adult brief and assistance with the routine emptying of a catheter or ostomy bag.
(7) “Assistance With Transfer” means providing verbal and physical cuing or physical assistance or both while the resident moves between bed and a standing position or between bed and chair or wheelchair. The term does not include total physical assistance with transfer provided by staff to residents.
(8) “Bedridden” means confined to bed because of inability to ambulate or transfer to a wheelchair even with assistance, or to sit safely in a chair or wheelchair without personal assistance or physical restraint.
(9) “Capacity” means the number of residents for which a facility has been licensed to provide residential care. (10) “Case Manager” means an individual employed by or under contract with any agency or organization, public or private,
who has the responsibility for assessing resident needs; planning services for the resident; coordinating and assisting residents with gaining access to needed medical, mental health, social, housing, educational or other services; monitoring service delivery; and evaluating the effects of service delivery.
(11) “Certified Nursing Assistant (CNA)” means an individual certified under chapter 464, part II, F.S. (12) “Day Care Participant” means an individual who receives services at a facility for less than 24 hours per day. (13) “Deficiency” means an instance of non-compliance with the requirements of part II of chapter 408, F.S., part I of chapter
429, F.S., rule chapter 59A-35, F.A.C., and this rule chapter. (14) “Direct Care Staff” means Staff in Regular Contact or Staff in Direct Contact with residents who provide personal or
nursing services to residents, including administrators and managers providing such services. (15) “Distinct Part” means designated bedrooms or apartments, bathrooms and a living area; or a separately identified wing,
floor, or building that includes bedrooms or apartments, bathrooms and a living area. The distinct part may include a separate dining area, or meals may be served in another part of the facility.
(16) “Elopement” means an occurrence in which a resident leaves a facility without following facility policy and procedures. (17) “Food Service” means the storage, preparation, service, and clean up of food intended for consumption in a facility either
by facility staff or through a formal agreement that meals will be regularly catered by a third party. (18) “Glucose Meter” or “glucometer” means a medical device that determines the approximate concentration of glucose in the
blood. (19) “Health Care Provider” means a physician or physician’s assistant licensed under chapter 458 or 459, F.S., or advanced
registered nurse practitioner licensed under chapter 464, F.S.

(20) “Licensed Dietitian or Nutritionist” means a dietitian or nutritionist licensed under chapter 468, part X, F.S. (21) “Local fire safety authority” means the authority having jurisdiction as defined in rule chapter 69A-40, F.A.C. (22) “Long-term Care Ombudsman Program (LTCOP)” means the long-term care ombudsman program established under
chapter 400, Part I, F.S. (23) “Manager” means an individual who is authorized to perform the same functions as a facility administrator, and is
responsible for the operation and maintenance of an assisted living facility while under the supervision of the administrator of that facility. A manager does not include staff authorized to perform limited administrative functions during an administrator’s temporary absence.
(24) “Mental Disorder” for the purposes of identifying a mental health resident, means schizophrenia and other psychotic disorders; affective disorders; anxiety related disorders; and personality and dissociative disorders. However, mental disorder does not include residents with a primary diagnosis of Alzheimer’s disease, other dementias, or mental retardation.
(25) “Mental Health Care Provider” means an individual, agency, or organization providing mental health services to clients of the Department of Children and Families; an individual licensed by the state to provide mental health services; or an entity employing or contracting with individuals licensed by the state to provide mental health services.
(26) “Mental Health Case Manager” means a case manager employed by or under contract to a mental health care provider to assist mental health residents residing in a facility holding a limited mental health license.
(27) “Nurse” means a licensed practical nurse (LPN), registered nurse (RN), or advanced registered nurse practitioner (ARNP) licensed under chapter 464, F.S.
(28) “Nursing Assessment” means a written review of information collected from observation and interaction with a resident, including the resident’s record and any other relevant sources of information, the analysis of the information, and recommendations for modification of the resident’s care, if warranted. The assessment must contain the signature and credential initials of the person who conducted the assessment.
(29) “Nursing Progress Notes” or “Progress Report” means a written record of nursing services, other than medication administration or the taking of vital signs, provided to each resident who receives such services in a facility with a limited nursing or extended congregate care license. The progress notes must be completed by the nurse who delivered the service; must describe the date, type, scope, amount, duration, and outcome of services that are rendered; must describe the general status of the resident’s health; must describe any deviations in the residents health; must describe any contact with the resident’s physician; and must contain the signature and credential initials of the person rendering the service.
(30) “Optional State Supplementation (OSS)” means the state program providing monthly payments to eligible residents pursuant to section 409.212, F.S., and rule chapter 65A-2, F.A.C.
(31) “Owner” means a person, partnership, association, limited liability company, or corporation, that owns or leases the facility that is licensed by the agency. The term does not include a person, partnership, association, limited liability company, or corporation that contracts only to manage or operate the facility.
(32) “Physician” means an individual licensed under chapter 458 or 459, F.S. (33) “Pill organizer” means a container that is designed to hold solid doses of medication and is divided according to day or
time increments. (34) “Registered Dietitian” means an individual registered with the Commission on Dietetic Registration, the accrediting body
of the Academy of Nutrition and Dietetics. (35) “Respite Care” means facility-based supervision of an impaired adult for the purpose of relieving the primary caregiver. (36) “Significant Change” means either a sudden or major shift in the behavior or mood of a resident that is inconsistent with
the resident’s diagnosis, or a deterioration in the resident’s health status such as unplanned weight change, stroke, heart condition, enrollment in hospice, or stage 2, 3 or 4 pressure sore. Ordinary day-to-day fluctuations in a resident’s functioning and behavior, short-term illnesses such as colds, or the gradual deterioration in the resident’s ability to carry out the activities of daily living that accompanies the aging process are not considered significant changes.
(37) “Staff” means any individual employed by a facility, contracting with a facility to provide direct or indirect services to residents, or employed by a firm under contract with a facility to provide direct or indirect services to residents when present in the facility. The term includes volunteers performing any service that counts toward meeting any staffing requirement of this rule chapter.
(38) “Staff in Regular Contact” or “Staff in Direct Contact” mean all staff whose duties may require them to interact with
residents on a daily basis. (39) “Third Party” means any individual or business entity providing services to residents in a facility that is not staff of the
facility. (40) “Universal Precautions” are a set of precautions designed to prevent transmission of human immunodeficiency virus (HIV),
hepatitis B virus (HBV), and other bloodborne pathogens when providing first aid or health care. Universal precautions require that the blood and certain body fluids of all residents be considered potentially infectious for HIV, HBV, and other bloodborne pathogens.
(41) “Unscheduled Service Need” means a need for a personal service, nursing service, or mental health intervention that cannot be predicted in advance and that must be met promptly to ensure that the health, safety, and welfare of residents is preserved.
Rulemaking Authority 429.41, 429.929 FS. Law Implemented 429.07, 429.075, 429.11, 429.14, 429.19, 429.41, 429.47, 429.52, 429.905 FS. History–New 9-30-92, Formerly 10A-5.0131, Amended 10-30-95, 6-2-96, 4-20-98, 11-2-98, 10-17-99, 1-9-02, 7-30-06, 4-15-10, 4-17-14, 5-10-18, Formerly 58A-5.0131, 7-1-19.
59A-36.003 Licensing and Change of Ownership. (1) LICENSE APPLICATION. An applicant for a standard assisted living facility license, a limited mental health license, an
extended congregate care license, or a limited nursing services license may apply for licensure pursuant to the requirements of chapters 408, part II, 429, part I, F.S., and rule chapter 59A-35, F.A.C.
(2) CHANGE OF OWNERSHIP. In addition to the requirements for a change of ownership contained in chapter 408, part II, F.S., section 429.12, F.S., and rule chapter 59A-35, F.A.C., the following provisions relating to resident funds apply pursuant to section 429.27, F.S.:
(a) At the time of transfer of ownership, all resident funds on deposit, advance payments of resident rents, resident security deposits, and resident trust funds held by the current licensee must be transferred to the applicant. Proof of such transfer must be provided to the agency at the time of the agency survey and before the issuance of a standard license. This provision does not apply to entrance fees paid to a continuing care facility subject to the acquisition provisions in section 651.024, F.S.
(b) The transferor must provide to each resident a statement detailing the amount and type of funds held by the facility and credited to the resident.
(c) The transferee must notify each resident in writing of the manner in which the transferee is holding the resident’s funds and state the name and address of the depository where the funds are being held, the amount held, and type of funds credited.
(3) CONDITIONAL LICENSE. Except as provided in section 429.14, F.S., the agency may issue a conditional license to a facility if, at the time of license renewal the facility is found to have uncorrected violations that the facility has had an opportunity to correct. The issuance of a conditional license does not change the biennial license expiration date.
(4) OSS RESIDENT DETERMINATION. With respect to the fee per bed required for a standard license, the number of OSS recipients claimed shall be the average number per month residing in the facility during the previous license period. An additional per bed charge shall be added to the bed fee for facilities whose average number of OSS residents per month was less than the number of beds designated for OSS recipients during the previous license period.
Rulemaking Authority 429.17, 429.27, 429.41 FS. Law Implemented 429.04, 429.07, 429.075, 429.11, 429.12, 429.17, 429.27, 429.41 FS. History–New 5-14-81, Amended 1-6-82, 5-19-83, 9-17-84, Formerly 10A-5.14, Amended 10-20-86, 6-21-88, 8-15-90, 9-30-92, Formerly 10A-5.014, Amended 10-30-95, 4-20-98, 10-17-99, 7-30-06, 4-17-14, 5-10-18, Formerly 58A-5.014, 7-1-19.
59A-36.004 License Requirements. (1) SERVICE PROHIBITION. An assisted living facility may not represent that it provides any service other than a service for
which it is licensed to provide. (2) CHANGE IN USE OF SPACE REQUIRING AGENCY CENTRAL OFFICE APPROVAL. A change in the use of space
that increases or decreases a facility’s capacity must not be made without prior approval from the Agency Central Office. Approval must be based on the compliance with the physical plant standards provided in rule 59A-36.014, F.A.C., as well as documentation of compliance with applicable fire safety and sanitation inspection requirements referenced in rule 59A-36.005, F.A.C.
(3) CHANGE IN USE OF SPACE REQUIRING AGENCY FIELD OFFICE APPROVAL. A change in the use of space that involves converting an area to resident use, which has not previously been inspected for such use, must not be made without prior approval from the Agency Field Office. Approval must be based on compliance with the physical plant standards provided in rule

59A-36.014, F.A.C., as well as documentation of compliance with applicable fire safety and sanitation inspection standards referenced in rule 59A-36.005, F.A.C.
(4) CONTIGUOUS PROPERTY. If a facility consists of more than one building, all buildings included under a single license must be on contiguous property. “Contiguous property” means property under the same ownership separated by no more than a two-lane street that traverses the property. A licensed location may be expanded to include additional contiguous property with the approval of the agency to ensure continued compliance with the requirements and standards of chapters 408, Part II, 429, Part I, F.S. and rule chapter 59A-35, F.A.C., and this rule chapter.
(5) PROOF OF INSPECTIONS. A copy of the annual fire safety and sanitation inspections described in rule 59A-36.005, F.A.C., must be submitted annually to the Agency Central Office. The annual inspections must be submitted no later than 30 calendar days after the inspections. Failure to comply with this requirement may result in administrative action pursuant to chapter 408, part II, and section 429.14, F.S., and rule chapter 59A-35, F.A.C.
(6) RESIDENTS RECEIVING STATE-FUNDED SERVICES. Upon request, the facility administrator or designee must identify residents receiving state-funded services to the agency and the department for monitoring purposes authorized by state and federal laws.
Rulemaking Authority 429.41 FS. Law Implemented 429.41, 429.44 FS. History–New 5-15-81, Amended 1-6-82, 9-17-84, Formerly 10A-5.16, Amended 6-21-88, 9-30-92, Formerly 10A-5.016, Amended 10-30-95, 10-17-99, 7-30-06, 4-15-10, 4-17-14, Formerly 58A-5.016, 7-1-19.
59A-36.005 Inspection Responsibilities. (1) County health departments are responsible for inspecting all license applicants and licensed facilities in matters regulated by: (a) Rule 64E-12.004, F.A.C., and rule chapter 64E-11, F.A.C., relating to food hygiene. (b) Chapter 64E-12, F.A.C., relating to sanitary practices in community-based residential facilities. (c) Chapter 64E-16, F.A.C., relating to biomedical waste. (2) The local authority having jurisdiction over fire safety or State Fire Marshal is responsible for inspecting all license
applicants and licensed facilities in matters regulated by section 429.41, F.S., relating to uniform fire safety standards and chapter 69A-40, F.A.C., Uniform Fire Safety Standards for Assisted Living Facilities.
(3) The agency is responsible for inspecting all license applicants and licensed facilities in all other matters regulated by this rule chapter.
Rulemaking Authority 429.41 FS. Law Implemented 429.41 FS. History–New 8-15-90, Formerly 10A-5.0161, Amended 10-30-95, 10-17-99, 3-13-14, Formerly 58A-5.0161, 7-1-19.
59A-36.006 Admission Procedures, Appropriateness of Placement and Continued Residency Criteria. (1) ADMISSION CRITERIA. (a) An individual must meet the following minimum criteria in order to be admitted to a facility holding a standard, limited
nursing services, or limited mental health license: 1. Be at least 18 years of age. 2. Be free from signs and symptoms of any communicable disease that is likely to be transmitted to other residents or staff. An
individual who has human immunodeficiency virus (HIV) infection may be admitted to a facility, provided that the individual would otherwise be eligible for admission according to this rule.
3. Be able to perform the activities of daily living, with supervision or assistance if necessary. 4. Be able to transfer, with assistance if necessary. The assistance of more than one person is permitted. 5. Be capable of taking medication, by either self-administration, assistance with self-administration, or administration of
medication. a. If the resident needs assistance with self-administration of medication, the facility must inform the resident of the professional
qualifications of facility staff who will be providing this assistance. If unlicensed staff will be providing assistance with self-administration of medication, the facility must obtain written informed consent from the resident or the resident’s surrogate, guardian, or attorney-in-fact.
b. The facility may accept a resident who requires the administration of medication if the facility employs a nurse who will provide this service or the resident, or the resident’s legal representative, designee, surrogate, guardian, or attorney-in-fact, contracts with a third party licensed to provide this service to the resident.
6. Not have any special dietary needs that cannot be met by the facility. 7. Not be a danger to self or others as determined by a physician, or mental health practitioner licensed under chapter 490 or
491, F.S. 8. Not require 24-hour licensed professional mental health treatment. 9. Not be bedridden. 10. Not have any stage 3 or 4 pressure sores. A resident requiring care of a stage 2 pressure sore may be admitted provided that: a. The resident either: (I) Resides in a standard or limited nursing services licensed facility and contracts directly with a licensed home health agency
or a nurse to provide care; or (II) Resides in a limited nursing services licensed facility and care is provided by the facility pursuant to a plan of care issued by
a health care provider; b. The condition is documented in the resident’s record and admission and discharge logs; and, c. If the resident’s condition fails to improve within 30 days as documented by a health care provider, the resident must be
discharged from the facility. 11. Residents admitted to standard, limited nursing services, or limited mental health licensed facilities may not require any of
the following nursing services: a. Artificial airway management of any kind, except that of continuous positive airway pressure may be provided through the
use of a CPAP or bipap machine; b. Assistance with tube feeding, c. Monitoring of blood gases, d. Management of post-surgical drainage tubes and wound vacuum devices; e. The administration of blood products in the facility; or f. Treatment of surgical incisions or wounds, unless the surgical incision or wound and the underlying condition have been
stabilized and a plan of care has been developed. The plan of care must be maintained in the resident’s record. 12. In addition to the nursing services listed above, residents admitted to facilities holding only standard and/or limited mental
health licenses may not require any of the following nursing services: a. Hemodialysis and peritoneal dialysis performed in the facility; b. Intravenous therapy performed in the facility. 13. Not require 24-hour nursing supervision. 14. Not require skilled rehabilitative services as described in rule 59G-4.290, F.A.C. 15. Be appropriate for admission to the facility as determined by the facility administrator. The administrator must base the
determination on: a. An assessment of the strengths, needs, and preferences of the individual; b. The medical examination report required by section 429.26, F.S., and subsection (2) of this rule, if available; c. The facility’s admission policy and the services the facility is prepared to provide or arrange in order to meet resident needs.
Such services may not exceed the scope of the facility’s license unless specified elsewhere in this rule; and, d. The ability of the facility to meet the uniform fire safety standards for assisted living facilities established in rule chapter
69A-40, F.A.C. (b) A resident who otherwise meets the admission criteria for residency in a standard licensed facility, but who requires
assistance with the administration and regulation of portable oxygen or assistance with routine colostomy care of stoma site flange placement, may be admitted to a facility with a standard license as long as the facility has a nurse on staff or under contract to provide the assistance or to provide training to the resident on how to perform these functions themselves.
(c) Nursing staff may not provide training to unlicensed persons, as defined in section 429.256(1)(b), F.S., to perform skilled nursing services, and may not delegate the nursing services described in this section to certified nursing assistants or unlicensed persons. This provision does not restrict a resident or a resident’s representative from contracting with a licensed third party to provide the assistance if the facility is agreeable to such an arrangement and the resident otherwise meets the criteria for admission and continued residency in a facility with a standard license.
(d) An individual enrolled in and receiving hospice services may be admitted to an assisted living facility as long as the individual otherwise meets resident admission criteria.

(e) Resident admission criteria for facilities holding an extended congregate care license are described in rule 59A-36.021, F.A.C.
(2) HEALTH ASSESSMENT. As part of the admission criteria, an individual must undergo a face-to-face medical examination completed by a health care provider as specified in either paragraph (a) or (b) of this subsection.
(a) A medical examination completed within 60 calendar days before the individual’s admission to a facility pursuant to section 429.26(4), F.S. The examination must address the following:
1. The physical and mental status of the resident, including the identification of any health-related problems and functional limitations,
2. An evaluation of whether the individual will require supervision or assistance with the activities of daily living, 3. Any nursing or therapy services required by the individual, 4. Any special diet required by the individual, 5. A list of current medications prescribed, and whether the individual will require any assistance with the administration of
medication, 6. Whether the individual has signs or symptoms of Tuberculosis, Methicillin Resistant Staphylococcus Aureus, Scabies or any
other communicable disease, which are likely to be transmitted to other residents or staff, 7. A statement on the day of the examination that, in the opinion of the examining health care provider, the individual’s needs
can be met in an assisted living facility; and, 8. The date of the examination, and the name, signature, address, telephone number, and license number of the examining health
care provider. The medical examination may be conducted by a health care provider licensed under chapter 458, 459 or 464, F.S. (b) A medical examination completed after the resident’s admission to the facility within 30 calendar days of the admission
date. The examination must be recorded on AHCA Form 1823, Resident Health Assessment for Assisted Living Facilities, March 2017, which is incorporated by reference and available online at: http://www.flrules.org/Gateway/reference.asp?No=Ref-09170. Faxed or electronic copies of the completed form are acceptable. The form must be completed as instructed.
1. Items on the form that have been omitted by the health care provider during the examination may be obtained by the facility either orally or in writing from the health care provider.
2. Omitted information must be documented in the resident’s record. Information received orally must include the name of the health care provider, the name of the facility staff recording the information, and the date the information was provided.
3. Electronic documentation may be used in place of completing the section on AHCA Form 1823 referencing Services Offered or Arranged by the Facility for the Resident. The electronic documentation must include all of the elements described in this section of AHCA Form 1823.
(c) Any information required by paragraph (a), that is not contained in the medical examination report conducted before the individual’s admission to the facility must be obtained by the administrator using AHCA Form 1823 within 30 days after admission.
(d) Medical examinations of residents placed by the department, by the Department of Children and Families, or by an agency under contract with either department must be conducted within 30 days before placement in the facility and recorded on AHCA Form 1823 described in paragraph (b).
(e) An assessment that has been conducted through the Comprehensive, Assessment, Review and Evaluation for Long-Term Care Services (CARES) program may be substituted for the medical examination requirements of section 429.26, F.S. and this rule.
(f) Any orders issued by the health care provider conducting the medical examination for medications, nursing, therapeutic diets, or other services to be provided or supervised by the facility may be attached to the health assessment. A health care provider may attach a DH Form 1896, Florida Do Not Resuscitate Order Form, for residents who do not wish cardiopulmonary resuscitation to be administered in the case of cardiac or respiratory arrest.
(g) A resident placed in a facility on a temporary emergency basis by the Department of Children and Families pursuant to section 415.105 or 415.1051, F.S., is exempt from the examination requirements of this subsection for up to 30 days. However, a resident accepted for temporary emergency placement must be entered on the facility’s admission and discharge log and counted in the facility census. A facility may not exceed its licensed capacity in order to accept such a resident. A medical examination must be conducted on any temporary emergency placement resident accepted for regular admission.
(3) ADMISSION PACKAGE. (a) The facility must make available to potential residents a written statement(s) that includes the following information listed
below. Providing a copy of the facility resident contract or facility brochure containing all the required information meets this

requirement. 1. The facility’s admission and continued residency criteria; 2. The daily, weekly or monthly charge to reside in the facility and the services, supplies, and accommodations provided by the
facility for that rate; 3. Personal care services that the facility is prepared to provide to residents and additional costs to the resident, if any; 4. Nursing services that the facility is prepared to provide to residents and additional costs to the resident, if any; 5. Food service and the ability of the facility to accommodate special diets; 6. The availability of transportation and additional costs to the resident, if any; 7. Any other special services that are provided by the facility and additional cost if any; 8. Social and leisure activities generally offered by the facility; 9. Any services that the facility does not provide but will arrange for the resident and additional cost, if any; 10. The facility rules and regulations that residents must follow as described in rule 59A-36.007, F.A.C.; 11. The facility policy concerning Do Not Resuscitate Orders pursuant to section 429.255, F.S., and rule 59A-36.009, F.A.C.,
and Advance Directives pursuant to chapter 765, F.S.; 12. If the facility is licensed to provide extended congregate care, the facility’s residency criteria for residents receiving
extended congregate care services. The facility must also provide a description of the additional personal, supportive, and nursing services provided by the facility including additional costs and any limitations on where extended congregate care residents may reside based on the policies and procedures described in rule 59A-36.021, F.A.C.;
13. If the facility advertises that it provides special care for individuals with Alzheimer’s disease and related disorders, a written description of those special services as required in section 429.177, F.S.; and,
14. The facility’s resident elopement response policies and procedures. (b) Before or at the time of admission, the resident, or the resident’s responsible party, guardian, or attorney-in-fact, if
applicable, must be provided with the following: 1. A copy of the resident’s contract that meets the requirements of rule 59A-36.018, F.A.C., 2. A copy of the facility statement described in paragraph (a) of this subsection, if one has not already been provided, 3. A copy of the resident’s bill of rights as required by rule 59A-36.007, F.A.C.; and, 4. A Long-Term Care Ombudsman Program brochure that includes the telephone number and address of the district office. (c) Documents required by this subsection must be in English. If the resident is not able to read, or does not understand English
and translated documents are not available, the facility must explain its policies to a family member or friend of the resident or another individual who can communicate the information to the resident.
(4) CONTINUED RESIDENCY. Except as follows in paragraphs (a) through (c) of this subsection, criteria for continued residency in any licensed facility must be the same as the criteria for admission. As part of the continued residency criteria, a resident must have a face-to-face medical examination by a health care provider at least every 3 years after the initial assessment, or after a significant change, whichever comes first. A significant change is defined in rule 59A-36.002, F.A.C. The results of the examination must be recorded on AHCA Form 1823, which is incorporated by reference in paragraph (2)(b) of this rule and must be completed in accordance with that paragraph. Exceptions to the requirement to meet the criteria for continued residency are:
(a) The resident may be bedridden for no more than 7 consecutive days. (b) A resident requiring care of a stage 2 pressure sore may be retained provided that: 1. The resident contracts directly with a licensed home health agency or a nurse to provide care, or the facility has a limited
nursing services license and services are provided pursuant to a plan of care issued by a health care provider, 2. The condition is documented in the resident’s record; and, 3. If the resident’s condition fails to improve within 30 days, as documented by a health care provider, the resident must be
discharged from the facility. (c) A terminally ill resident who no longer meets the criteria for continued residency may continue to reside in the facility if the
following conditions are met: 1. The resident qualifies for, is admitted to, and consents to receive services from a licensed hospice that coordinates and
ensures the provision of any additional care and services that the resident may need; 2. Both the resident, or the resident’s legal representative if applicable, and the facility agree to continued residency; 3. A licensed hospice, in consultation with the facility, develops and implements a interdisciplinary care plan that specifies the
services being provided by hospice and those being provided by the facility; and, 4. Documentation of the requirements of this paragraph is maintained in the resident’s file. (d) The facility administrator is responsible for monitoring the continued appropriateness of placement of a resident in the
facility at all times. (e) A hospice resident that meets the qualifications of continued residency pursuant to this subsection may only receive services
from the assisted living facility’s staff which are within the scope of the facility’s license. (f) Assisted living facility staff may provide any nursing service permitted under the facility’s license and total help with the
activities of daily living for residents admitted to hospice; however, staff may not exceed the scope of their professional licensure or training.
(g) Continued residency criteria for facilities holding an extended congregate care license are described in rule 59A-36.021, F.A.C.
(5) DISCHARGE. If the resident no longer meets the criteria for continued residency, or the facility is unable to meet the resident’s needs, as determined by the facility administrator or health care provider, the resident must be discharged in accordance with section 429.28, F.S.
Rulemaking Authority 429.07, 429.41 FS. Law Implemented 429.07, 429.26, 429.28, 429.41 FS. History–New 9-17-84, Formerly 10A-5.181, Amended 10-20-86, 6-21-88, 8-15-90, 9-30-92, Formerly 10A-5.0181, Amended 10-30-95, 6-2-96, 10-17-99, 7-30-06, 10-9-06, 4-15-10, 10-14-10, 4-17-14, 5-10-18, Formerly 58A-5.0181, 7-1-19.
59A-36.007 Resident Care Standards. An assisted living facility must provide care and services appropriate to the needs of residents accepted for admission to the facility.
(1) SUPERVISION. Facilities must offer personal supervision as appropriate for each resident, including the following: (a) Monitoring of the quantity and quality of resident diets in accordance with rule 59A-36.012, F.A.C. (b) Daily observation by designated staff of the activities of the resident while on the premises, and awareness of the general
health, safety, and physical and emotional well-being of the resident. (c) Maintaining a general awareness of the resident’s whereabouts. The resident may travel independently in the community. (d) Contacting the resident’s health care provider and other appropriate party such as the resident’s family, guardian, health care
surrogate, or case manager if the resident exhibits a significant change. (e) Contacting the resident’s family, guardian, health care surrogate, or case manager if the resident is discharged or moves out. (f) Maintaining a written record, updated as needed, of any significant changes, any illnesses that resulted in medical attention,
changes in the method of medication administration, or other changes that resulted in the provision of additional services. (2) SOCIAL AND LEISURE ACTIVITIES. Residents shall be encouraged to participate in social, recreational, educational and
other activities within the facility and the community. (a) The facility must provide an ongoing activities program. The program must provide diversified individual and group
activities in keeping with each resident’s needs, abilities, and interests. (b) The facility must consult with the residents in selecting, planning, and scheduling activities. The facility must demonstrate
residents’ participation through one or more of the following methods: resident meetings, committees, a resident council, a monitored suggestion box, group discussions, questionnaires, or any other form of communication appropriate to the size of the facility.
(c) Scheduled activities must be available at least 6 days a week for a total of not less than 12 hours per week. Watching television is not an activity for the purpose of meeting the 12 hours per week of scheduled activities unless the television program is a special one-time event of special interest to residents of the facility. A facility whose residents choose to attend day programs conducted at adult day care centers, senior centers, mental health centers, or other day programs may count those attendance hours towards the required 12 hours per week of scheduled activities. An activities calendar must be posted in common areas where residents normally congregate.
(d) If residents assist in planning a special activity such as an outing, seasonal festivity, or an excursion, up to 3 hours may be counted toward the required activity time.
(3) ARRANGEMENT FOR HEALTH CARE. In order to facilitate resident access to health care as needed, the facility must: (a) Assist residents in making appointments and remind residents about scheduled appointments for medical, dental, nursing, or
mental health services.
(b) Provide transportation to needed medical, dental, nursing or mental health services, or arrange for transportation through family and friends, volunteers, taxi cabs, public buses, and agencies providing transportation.
(c) The facility may not require residents to receive services from a particular health care provider. (4) ACTIVITIES OF DAILY LIVING. Facilities must offer supervision of or assistance with activities of daily living as needed
by each resident. Residents should be encouraged to be as independent as possible in performing activities of daily living. (5) NURSING SERVICES. (a) Pursuant to section 429.255, F.S., the facility may employ or contract with a nurse to: 1. Take or supervise the taking of vital signs, 2. Manage pill-organizers and administer medications as described in rule 59A-36.008, F.A.C., 3. Give prepackaged enemas pursuant to a physician’s order; and, 4. Maintain nursing progress notes. (b) Pursuant to section 429.255(2), F.S., the nursing services listed in paragraph (a), may also be delivered in the facility by
family members or friends of the resident provided the family member or friend does not receive compensation for such services. (6) RESIDENT RIGHTS AND FACILITY PROCEDURES. (a) A copy of the Resident Bill of Rights as described in section 429.28, F.S., or a summary provided by the Long-Term Care
Ombudsman Program must be posted in full view in a freely accessible resident area, and included in the admission package provided pursuant to rule 59A-36.006, F.A.C.
(b) In accordance with section 429.28, F.S., the facility must have a written grievance procedure for receiving and responding to resident complaints and a written procedure to allow residents to recommend changes to facility policies and procedures. The facility must be able to demonstrate that such procedure is implemented upon receipt of a complaint.
(c) The telephone number for lodging complaints against a facility or facility staff must be posted in full view in a common area accessible to all residents. The telephone numbers are: the Long-Term Care Ombudsman Program, 1(888)831-0404; Disability Rights Florida, 1(800)342-0823; the Agency Consumer Hotline 1(888)419-3456, and the statewide toll-free telephone number of the Florida Abuse Hotline, 1(800)96-ABUSE or 1(800)962-2873. The telephone numbers must be posted in close proximity to a telephone accessible by residents and the text must be a minimum of 14-point font.
(d) The facility must have a written statement of its house rules and procedures that must be included in the admission package provided pursuant to rule 59A-36.006, F.A.C. The rules and procedures must at a minimum address the facility’s policies regarding:
1. Resident responsibilities; 2. Alcohol and tobacco use; 3. Medication storage; 4. Resident elopement; 5. Reporting resident abuse, neglect, and exploitation; 6. Administrative and housekeeping schedules and requirements; 7. Infection control, sanitation, and universal precautions; and, 8. The requirements for coordinating the delivery of services to residents by third party providers. (e) Residents may not be required to perform any work in the facility without compensation. Residents may be required to clean
their own sleeping areas or apartments if the facility rules or the facility contract includes such a requirement. If a resident is employed by the facility, the resident must be compensated in compliance with state and federal wage laws.
(f) The facility must provide residents with convenient access to a telephone to facilitate the resident’s right to unrestricted and private communication, pursuant to section 429.28(1)(d), F.S. The facility must allow unidentified telephone calls to residents. For facilities with a licensed capacity of 17 or more residents in which residents do not have private telephones, there must be, at a minimum, a readily accessible telephone on each floor of each building where residents reside.
(g) In addition to the requirements of section 429.41(1)(k), F.S., the use of physical restraints by a facility on a resident must be reviewed by the resident’s physician annually. Any device, including half-bed rails, which the resident chooses to use and can remove or avoid without assistance, is not considered a physical restraint.
(7) THIRD PARTY SERVICES. (a) Nothing in this rule chapter is intended to prohibit a resident or the resident’s representative from independently arranging,
contracting, and paying for services provided by a third party of the resident’s choice, including a licensed home health agency or private nurse, or receiving services through an out-patient clinic, provided the resident meets the criteria for admission and continued

residency and the resident complies with the facility’s policy relating to the delivery of services in the facility by third parties. The facility’s policies must require the third party to coordinate with the facility regarding the resident’s condition and the services being provided.
(b) When residents require or arrange for services from a third party provider, the facility administrator or designee must allow for the receipt of those services, provided that the resident meets the criteria for admission and continued residency. The facility, when requested by residents or representatives, must coordinate with the provider to facilitate the receipt of care and services provided to meet the particular resident’s needs.
(c) If residents accept assistance from the facility in arranging and coordinating third party services, the facility’s assistance does not represent a guarantee that third party services will be received. If the facility’s efforts to make arrangements for third party services are unsuccessful or declined by residents, the facility must include documentation in the residents’ record explaining why its efforts were unsuccessful. This documentation will serve to demonstrate its compliance with this subsection.
(8) ELOPEMENT STANDARDS. (a) Residents Assessed at Risk for Elopement. All residents assessed at risk for elopement or with any history of elopement
must be identified so staff can be alerted to their needs for support and supervision. All residents must be assessed for risk of elopement by a health care provider or a mental health care provider within 30 calendar days of being admitted to a facility. If the resident has had a health assessment performed prior to admission pursuant to paragraph 59A-36.006(2)(a), F.A.C., this requirement is satisfied. A resident placed in a facility on a temporary emergency basis by the Department of Children and Families pursuant to section 415.105 or 415.1051, F.S., is exempt from this requirement for up to 30 days.
1. As part of its resident elopement response policies and procedures, the facility must make, at a minimum, a daily effort to determine that at risk residents have identification on their persons that includes their name and the facility’s name, address, and telephone number. Staff trained pursuant to paragraph 59A-36.011(10)(a) or (c), F.A.C., must be generally aware of the location of all residents assessed at high risk for elopement at all times.
2. The facility must have a photo identification of at risk residents on file that is accessible to all facility staff and law enforcement as necessary. The facility’s file must contain the resident’s photo identification upon admission or upon being assessed at risk for elopement subsequent to admission. The photo identification may be provided by the facility, the resident, or the resident’s representative.
(b) Facility Resident Elopement Response Policies and Procedures. The facility must develop detailed written policies and procedures for responding to a resident elopement. At a minimum, the policies and procedures must provide for:
1. An immediate search of the facility and premises, 2. The identification of staff responsible for implementing each part of the elopement response policies and procedures,
including specific duties and responsibilities, 3. The identification of staff responsible for contacting law enforcement, the resident’s family, guardian, health care surrogate,
and case manager if the resident is not located pursuant to subparagraph (8)(b)1.; and, 4. The continued care of all residents within the facility in the event of an elopement. (c) Facility Resident Elopement Drills. The facility must conduct and document resident elopement drills pursuant to sections
429.41(1)(a)3. and 429.41(1)(l), F.S. (9) OTHER STANDARDS. Additional care standards for residents residing in a facility holding a limited mental health,
extended congregate care or limited nursing services license are provided in rules 59A-36.020, 59A-36.021 and 59A-36.022, F.A.C., respectively.
Rulemaking Authority 429.41 FS. Law Implemented 429.255, 429.26, 429.28, 429.41 FS. History–New 9-17-84, Formerly 10A-5.182, Amended 10-20-86, 6-21-88, 8-15-90, 9-30-92, Formerly 10A-5.0182, Amended 10-30-95, 4-20-98, 11-2-98, 10-17-99, 7-30-06, 10-9-06, 4-15-10, 4-17-14, 5-10-18, Formerly 58A-5.0182, 7-1-19.
59A-36.008 Medication Practices. Pursuant to sections 429.255 and 429.256, F.S., and this rule, licensed facilities may assist with the self-administration or administration of medications to residents in a facility. A resident may not be compelled to take medications but may be counseled in accordance with this rule.
(1) SELF ADMINISTERED MEDICATIONS. (a) Residents who are capable of self-administering their medications without assistance must be encouraged and allowed to do

so. (b) If facility staff observes health changes that could reasonably be attributed to the improper self-administration of medication,
staff must consult with the resident concerning any problems the resident may be experiencing in self-administering the medications. The consultation should describe the services offered by the facility that aid the resident with medication administration through the use of a pill organizer, through providing assistance with self-administration of medications, or through administering medications. The facility must contact the resident’s health care provider when observable health changes occur that may be attributed to the resident’s medications. The facility must document such contacts in the resident’s records.
(2) PILL ORGANIZERS. (a) Only a resident who self-administers medications may maintain a pill organizer. (b) Unlicensed staff may not provide assistance with the contents of pill organizers. (c) A nurse may manage a pill organizer to be used only by residents who self-administer medications. The nurse is responsible
for instructing the resident in the proper use of the pill organizer. The nurse must manage the pill organizer in the following manner: 1. Obtain the labeled medication container from the storage area or the resident, 2. Transfer the medication from the original container into a pill organizer, labeled with the resident’s name, according to the
day and time increments as prescribed, 3. Return the medication container to the storage area or resident; and, 4. Document the date and time the pill organizer was filled in the resident’s record. (d) If there is a determination that the resident is not taking medications as prescribed after the medicinal benefits are explained,
it must be noted in the resident’s record and the facility must consult with the resident concerning providing assistance with self-administration or the administration of medications if such services are offered by the facility. The facility must contact the resident’s health care provider regarding questions, concerns, or observations relating to the resident’s medications. Such communication must be documented in the resident’s record.
(3) ASSISTANCE WITH SELF-ADMINISTRATION. (a) Any unlicensed person providing assistance with self-administration of medication must be 18 years of age or older, trained
to assist with self administered medication pursuant to the training requirements of rule 59A-36.011, F.A.C., and must be available to assist residents with self-administered medications in accordance with procedures described in section 429.256, F.S. and this rule.
(b) In addition to the specifications of section 429.256(3), F.S., assistance with self-administration of medication includes, in the presence of the resident, reading the medication label aloud and verbally prompting a resident to take medications as prescribed.
(c) In order to facilitate assistance with self-administration, trained staff may prepare and make available such items as water, juice, cups, and spoons. Trained staff may also return unused doses to the medication container. Medication, which appears to have been contaminated, must not be returned to the container.
(d) Trained staff must observe the resident take the medication. Any concerns about the resident’s reaction to the medication or suspected noncompliance must be reported to the resident’s health care provider and documented in the resident’s record.
(e) When a resident who receives assistance with medication is away from the facility and from facility staff, the following options are available to enable the resident to take medication as prescribed:
1. The health care provider may prescribe a medication schedule that coincides with the resident’s presence in the facility, 2. The medication container may be given to the resident, a friend, or family member upon leaving the facility, with this fact
noted in the resident’s medication record, 3. The medication may be transferred to a pill organizer pursuant to the requirements of subsection (2), and given to the
resident, a friend, or family member upon leaving the facility, with this fact noted in the resident’s medication record, or 4. Medications may be separately prescribed and dispensed in an easier to use form, such as unit dose packaging. (f) Assistance with self-administration of medication does not include the activities detailed in section 429.256(4), F.S. 1. As used in section 429.256(4)(g), F.S., the term “competent resident” means that the resident is cognizant of when a
medication is required and understands the purpose for taking the medication. 2. As used in section 429.256(4)(h), F.S., the terms “judgment” and “discretion” mean interpreting vital signs and evaluating or
assessing a resident’s condition. (g) All trained staff must adhere to the facility’s infection control policy and procedures when assisting with the self-
administration of medication. (4) MEDICATION ADMINISTRATION.

(a) For facilities that provide medication administration, a staff member licensed to administer medications must be available to administer medications in accordance with a health care provider’s order or prescription label.
(b) Unusual reactions to the medication or a significant change in the resident’s health or behavior that may be caused by the medication must be documented in the resident’s record and reported immediately to the resident’s health care provider. The contact with the health care provider must also be documented in the resident’s record.
(c) Medication administration includes conducting any examination or other procedure necessary for the proper administration of medication that the resident cannot conduct personally and that can be performed by licensed staff.
(d) A facility that performs clinical laboratory tests for residents, including blood glucose testing, must be in compliance with the federal Clinical Laboratory Improvement Amendments of 1988 (CLIA) and chapter 483, part I, F.S. A valid copy of the State Clinical Laboratory License, if required, and the federal CLIA Certificate must be maintained in the facility. A state license or federal CLIA certificate is not required if residents perform the test themselves or if a third party assists residents in performing the test. The facility is not required to maintain a State Clinical Laboratory License or a federal CLIA Certificate if facility staff assist residents in performing clinical laboratory testing with the residents’ equipment. Information about the State Clinical Laboratory License and federal CLIA Certificate is available from the Laboratory Unit, Agency for Health Care Administration, 2727 Mahan Drive, Mail Stop 32, Tallahassee, FL 32308; telephone (850)412-4500.
(5) MEDICATION RECORDS. (a) For residents who use a pill organizer managed in subsection (2), the facility must keep either the original labeled
medication container; or a medication listing with the prescription number, the name and address of the issuing pharmacy, the health care provider’s name, the resident’s name, the date dispensed, the name and strength of the drug, and the directions for use.
(b) The facility must maintain a daily medication observation record for each resident who receives assistance with self-administration of medications or medication administration. A medication observation record must be immediately updated each time the medication is offered or administered and include:
1. The name of the resident and any known allergies the resident may have; 2. The name of the resident’s health care provider and the health care provider’s telephone number; 3. The name, strength, and directions for use of each medication; and, 4. A chart for recording each time the medication is taken, any missed dosages, refusals to take medication as prescribed, or
medication errors. (c) For medications that serve as chemical restraints, the facility must, pursuant to section 429.41, F.S., maintain a record of the
prescribing physician’s annual evaluation of the use of the medication. (6) MEDICATION STORAGE AND DISPOSAL. (a) In order to accommodate the needs and preferences of residents and to encourage residents to remain as independent as
possible, residents may keep their medications, both prescription and over-the-counter, in their possession both on or off the facility premises. Residents may also store their medication in their rooms or apartments if either the room is kept locked when residents are absent or the medication is stored in a secure place that is out of sight of other residents.
(b) Both prescription and over-the-counter medications for residents must be centrally stored if: 1. The facility administers the medication; 2. The resident requests central storage. The facility must maintain a list of all medications being stored pursuant to such a
request; 3. The medication is determined and documented by the health care provider to be hazardous if kept in the personal possession
of the person for whom it is prescribed; 4. The resident fails to maintain the medication in a safe manner as described in this paragraph; 5. The facility determines that, because of physical arrangements and the conditions or habits of residents, the personal
possession of medication by a resident poses a safety hazard to other residents, or 6. The facility’s rules and regulations require central storage of medication and that policy has been provided to the resident
before admission as required in rule 59A-36.006, F.A.C. (c) Centrally stored medications must be: 1. Kept in a locked cabinet; locked cart; or other locked storage receptacle, room, or area at all times; 2. Located in an area free of dampness and abnormal temperature, except that a medication requiring refrigeration must be kept
refrigerated. Refrigerated medications must be secured by being kept in a locked container within the refrigerator, by keeping the

refrigerator locked, or by keeping the area in which the refrigerator is located locked; 3. Accessible to staff responsible for filling pill-organizers, assisting with self-administration of medication, or administering
medication. Such staff must have ready access to keys or codes to the medication storage areas at all times; and, 4. Kept separately from the medications of other residents and properly closed or sealed. (d) Medication that has been discontinued but has not expired must be returned to the resident or the resident’s representative, as
appropriate, or may be centrally stored by the facility for future use by the resident at the resident’s request. If centrally stored by the facility, the discontinued medication must be stored separately from medication in current use, and the area in which it is stored must be marked “discontinued medication.” Such medication may be reused if prescribed by the resident’s health care provider.
(e) When a resident’s stay in the facility has ended, the administrator must return all medications to the resident, the resident’s family, or the resident’s guardian unless otherwise prohibited by law. If, after notification and waiting at least 15 days, the resident’s medications are still at the facility, the medications are considered abandoned and may disposed of in accordance with paragraph (f).
(f) Medications that have been abandoned or have expired must be disposed of within 30 days of being determined abandoned or expired and the disposal must be documented in the resident’s record. The medication may be taken to a pharmacist for disposal or may be destroyed by the administrator or designee with one witness.
(g) Facilities that hold a Special-ALF permit issued by the Board of Pharmacy may return dispensed medicinal drugs to the dispensing pharmacy pursuant to rule 64B16-28.870, F.A.C.
(7) MEDICATION LABELING AND ORDERS. (a) The facility may not store prescription drugs for self-administration, assistance with self-administration, or administration
unless they are properly labeled and dispensed in accordance with chapters 465 and 499, F.S., and rule 64B16-28.108, F.A.C. If a customized patient medication package is prepared for a resident, and separated into individual medicinal drug containers, then the following information must be recorded on each individual container:
1. The resident’s name; and, 2. The identification of each medicinal drug in the container. (b) Except with respect to the use of pill organizers as described in subsection (2), no individual other than a pharmacist may
transfer medications from one storage container to another. (c) If the directions for use are “as needed” or “as directed,” the health care provider must be contacted and requested to provide
revised instructions. For an “as needed” prescription, the circumstances under which it would be appropriate for the resident to request the medication and any limitations must be specified; for example, “as needed for pain, not to exceed 4 tablets per day.” The revised instructions, including the date they were obtained from the health care provider and the signature of the staff who obtained them, must be noted in the medication record, or a revised label must be obtained from the pharmacist.
(d) Any change in directions for use of a medication that the facility is administering or providing assistance with self-administration must be accompanied by a written, faxes, or electronic copy of a medication order issued and signed by the resident’s health care provider. The new directions must promptly be recorded in the resident’s medication observation record. The facility may then obtain a revised label from the pharmacist or place an “alert” label on the medication container that directs staff to examine the revised directions for use in the medication observation record.
(e) A nurse may take a medication order by telephone. Such order must be promptly documented in the resident’s medication observation record. The facility must obtain a written medication order from the health care provider within 10 working days. A faxed or electronic copy of a signed order is acceptable.
(f) The facility must make every reasonable effort to ensure that prescriptions for residents who receive assistance with self-administration of medication or medication administration are filled or refilled in a timely manner.
(g) Pursuant to section 465.0276(5), F.S., and rule 61N-1.006, F.A.C., sample or complimentary prescription drugs that are dispensed by a health care provider, must be kept in their original manufacturer’s packaging, which must include the practitioner’s name, the resident’s name for whom they were dispensed, and the date they were dispensed. If the sample or complimentary prescription drugs are not dispensed in the manufacturer’s labeled package, they must be kept in a container that bears a label containing the following:
1. Practitioner’s name, 2. Resident’s name, 3. Date dispensed, 4. Name and strength of the drug,

5. Directions for use; and, 6. Expiration date. (h) Pursuant to section 465.0276(2)(c), F.S., before dispensing any sample or complimentary prescription drug, the resident’s
health care provider must provide the resident with a written prescription, or a faxed or electronic copy of such order. (8) OVER THE COUNTER (OTC) PRODUCTS. For purposes of this subsection, the term over the counter includes, but is not
limited to, over the counter medications, vitamins, nutritional supplements and nutraceuticals, hereafter referred to as OTC products, that can be sold without a prescription.
(a) A facility may keep a stock supply of OTC products for multiple resident use. When providing any OTC product that is kept by the facility as a stock supply to a resident, the staff member providing the medication must record the name and amount of the OTC product provided in the resident’s medication observation record. All OTC products kept as a stock supply must be stored in a locked container or secure room in a central location within the facility and must be labeled with the medication’s name, the date of purchase, and with a notice that the medication is part of the facility’s stock supply.
(b) OTC products, including those prescribed by a health care provider but excluding those kept as a stock supply by the facility, must be labeled with the resident’s name and the manufacturer’s label with directions for use, or the health care provider’s directions for use. No other labeling requirements are required.
(c) Residents or their representatives may purchase OTC products from an establishment of their choice. (d) A health care provider’s order is required when a nurse provides assistance with self-administration or administration of
OTC products. When an order for an OTC product exists, the order must meet the requirements of paragraphs (b) and (c) of this subsection. A health care provider’s order for OTC products is not required when a resident self-administers his or her medications, or when unlicensed staff provides assistance with self-administration of medications.
Rulemaking Authority 429.256, 429.41 FS. Law Implemented 429.255, 429.256, 429.41 FS. History–New 10-17-99, Amended 7-30-06, 4-15-10, 10-14-10, 3-13-14, 5-10-18, Formerly 58A-5.0185, 7-1-19.
59A-36.009 Do Not Resuscitate Orders (DNROs). (1) POLICIES AND PROCEDURES. (a) Each assisted living facility must have written policies and procedures that explain its implementation of state laws and rules
relative to Do Not Resuscitate Orders (DNROs). An assisted living facility may not require execution of a DNRO as a condition of admission or treatment. The assisted living facility must provide the following to each resident, or resident’s representative, at the time of admission:
1. Form SCHS-4-2006, “Health Care Advance Directives – The Patient’s Right to Decide,” April 2006, or with a copy of some other substantially similar document, which incorporates information regarding advance directives included in chapter 765, F.S. Form SCHS-4-2006 is available from the Agency for Health Care Administration, 2727 Mahan Drive, Mail Stop 34, Tallahassee, FL 32308 or the agency’s website at: http://ahca.myflorida.com/MCHQ/Health_Facility_Regulation/HC_Advance_Directives/docs/adv_dir.pdf; and,
2. DH Form 1896, Florida Do Not Resuscitate Order Form, December, 2004, which is hereby incorporated by reference. This form may be obtained by calling the Department of Health’s toll free number 1(800)226-1911, extension 2780 or online at: http://www.flrules.org/Gateway/reference.asp?No=Ref-04005.
(b) There must be documentation in the resident’s record indicating whether a DH Form 1896 has been executed. If a DH Form 1896 has been executed, a yellow copy of that document must be made a part of the resident’s record. If the assisted living facility does not receive a copy of a resident’s executed DH Form 1896, the assisted living facility must document in the resident’s record that it has requested a copy.
(c) The executed DH Form 1896 must be readily available to medical staff in the event of an emergency. (2) LICENSE REVOCATION. An assisted living facility’s license is subject to revocation pursuant to section 408.815, F.S., if,
as a condition of treatment or admission, the facility requires an individual to execute or waive DH Form 1896. (3) DNRO PROCEDURES. Pursuant to section 429.255, F.S., an assisted living facility must honor a properly executed DH
Form 1896 as follows: (a) In the event a resident experiences cardiac or pulmonary arrest, staff trained in cardiopulmonary resuscitation (CPR) or a
health care provider present in the facility, may withhold cardiopulmonary resuscitation (artificial ventilation, cardiac compression, endotracheal intubation and defibrillation).

(b) In the event a resident is receiving hospice services and experiences cardiac or pulmonary arrest, facility staff must immediately contact hospice staff. The hospice procedures take precedence over those of the assisted living facility.
Rulemaking Authority 429.255 FS. Law Implemented 429.255 FS. History–New 4-15-10, Amended 4-17-14, Formerly 58A-5.0186, 7-1-19.
59A-36.010 Staffing Standards. (1) ADMINISTRATORS. Every facility must be under the supervision of an administrator who is responsible for the operation
and maintenance of the facility including the management of all staff and the provision of appropriate care to all residents as required by chapters 408, part II, 429, part I, F.S., and rule chapter 59A-35, F.A.C., and this rule chapter.
(a) An administrator must: 1. Be at least 21 years of age; 2. If employed on or after October 30, 1995, have, at a minimum, a high school diploma or G.E.D.; 3. Be in compliance with Level 2 background screening requirements pursuant to sections 408.809 and 429.174, F.S.; 4. Complete the core training and core competency test requirements pursuant to rule 59A-36.011, F.A.C., no later than 90 days
after becoming employed as a facility administrator. Administrators who attended core training prior to July 1, 1997, are not required to take the competency test unless specified elsewhere in this rule; and,
5. Satisfy the continuing education requirements pursuant to rule 59A-36.011, F.A.C. Administrators who are not in compliance with these requirements must retake the core training and core competency test requirements in effect on the date the non-compliance is discovered by the agency or the department.
(b) In the event of extenuating circumstances, such as the death of a facility administrator, the agency may permit an individual who otherwise has not satisfied the training requirements of subparagraph (1)(a)4. of this rule, to temporarily serve as the facility administrator for a period not to exceed 90 days. During the 90 day period, the individual temporarily serving as facility administrator must:
1. Complete the core training and core competency test requirements pursuant to rule 59A-36.011, F.A.C.; and, 2. Complete all additional training requirements if the facility maintains licensure as an extended congregate care or limited
mental health facility. (c) Administrators may supervise a maximum of either three assisted living facilities or a group of facilities on a single campus
providing housing and health care Administrators who supervise more than one facility must appoint in writing a separate manager for each facility. However, an administrator supervising a maximum of three assisted living facilities, each licensed for 16 or fewer beds and all within a 15 mile radius of each other, is only required to appoint two managers to assist in the operation and maintenance of those facilities.
(d) An individual serving as a manager must satisfy the same qualifications, background screening, core training and competency test requirements, and continuing education requirements as an administrator pursuant to paragraph (1)(a) of this rule. Managers who attended the core training program prior to April 20, 1998, are not required to take the competency test unless specified elsewhere in this rule. In addition, a manager may not serve as a manager of more than a single facility, except as provided in paragraph (1)(c) of this rule, and may not simultaneously serve as an administrator of any other facility.
(e) Pursuant to section 429.176, F.S., facility owners must notify the Agency Central Office within 10 days of a change in facility administrator on the Notification of Change of Administrator form, AHCA Form 3180-1006, June 2016, which is incorporated by reference and available online at: http://www.flrules.org/Gateway/reference.asp?No=Ref-09393.
(2) STAFF. (a) Within 30 days after beginning employment, newly hired staff must submit a written statement from a health care provider
documenting that the individual does not have any signs or symptoms of communicable disease. The examination performed by the health care provider must have been conducted no earlier than 6 months before submission of the statement. Newly hired staff does not include an employee transferring without a break in service from one facility to another when the facility is under the same management or ownership.
1. Evidence of a negative tuberculosis examination must be documented on an annual basis. Documentation provided by the Florida Department of Health or a licensed health care provider certifying that there is a shortage of tuberculosis testing materials satisfies the annual tuberculosis examination requirement. An individual with a positive tuberculosis test must submit a health care provider’s statement that the individual does not constitute a risk of communicating tuberculosis.
2. If any staff member has, or is suspected of having, a communicable disease, such individual must be immediately removed

from duties until a written statement is submitted from a health care provider indicating that the individual does not constitute a risk of transmitting a communicable disease.
(b) Staff must be qualified to perform their assigned duties consistent with their level of education, training, preparation, and experience. Staff providing services requiring licensing or certification must be appropriately licensed or certified. All staff must exercise their responsibilities, consistent with their qualifications, to observe residents, to document observations on the appropriate resident’s record, and to report the observations to the resident’s health care provider in accordance with this rule chapter.
(c) All staff must comply with the training requirements of rule 59A-36.011, F.A.C. (d) An assisted living facility contracting to provide services to residents must ensure that individuals providing services are
qualified to perform their assigned duties in accordance with this rule chapter. The contract between the facility and the staffing agency or contractor must specifically describe the services the staffing agency or contractor will provide to residents.
(e) For facilities with a licensed capacity of 17 or more residents, the facility must: 1. Develop a written job description for each staff position and provide a copy of the job description to each staff member; and, 2. Maintain time sheets for all staff. (f) Level 2 background screening must be conducted for staff, including staff contracted by the facility to provide services to
residents, pursuant to sections 408.809 and 429.174, F.S. (3) STAFFING STANDARDS. (a) Minimum staffing: 1. Facilities must maintain the following minimum staff hours per week:
Number of Residents, Day Care Participants, and Respite Care Residents Staff Hours/Week 0-5 168 6-15 212
16- 25 253 26-35 294 36-45 335 46-55 375 56- 65 416 66-75 457 76-85 498 86-95 539
For every 20 total combined residents, day care participants, and respite care residents over 95 add 42 staff hours per week. 2. Independent living residents, as referenced in subsection 59A-36.015(3), F.A.C., who occupy beds included within the
licensed capacity of an assisted living facility but do not receive personal, limited nursing, or extended congregate care services, are not counted as residents for purposes of computing minimum staff hours.
3. At least one staff member who has access to facility and resident records in case of an emergency must be in the facility at all times when residents are in the facility. Residents serving as paid or volunteer staff may not be left solely in charge of other residents while the facility administrator, manager or other staff are absent from the facility.
4. In facilities with 17 or more residents, there must be at least one staff member awake at all hours of the day and night. 5. A staff member who has completed courses in First Aid and Cardiopulmonary Resuscitation (CPR) and holds a currently
valid card documenting completion of such courses must be in the facility at all times. a. Documentation of attendance at First Aid or CPR courses pursuant to subsection 59A-36.011(5), F.A.C., satisfies this
requirement. b. A nurse is considered as having met the course requirements for First Aid. An emergency medical technician or paramedic
currently certified under chapter 401, part III, F.S., is considered as having met the course requirements for both First Aid and CPR. 6. During periods of temporary absence of the administrator or manager of more than 48 hours when residents are on the
premises, a staff member who is at least 21 years of age must be physically present and designated in writing to be in charge of the facility. No staff member shall be in charge of a facility for a consecutive period of 21 days or more, or for a total of 60 days within a calendar year, without being an administrator or manager.
7. Staff whose duties are exclusively building or grounds maintenance, clerical, or food preparation do not count towards
meeting the minimum staffing hours requirement. 8. The administrator or manager’s time may be counted for the purpose of meeting the required staffing hours, provided the
administrator or manager is actively involved in the day-to-day operation of the facility, including making decisions and providing supervision for all aspects of resident care, and is listed on the facility’s staffing schedule.
9. Only on-the-job staff may be counted in meeting the minimum staffing hours. Vacant positions or absent staff may not be counted.
(b) Notwithstanding the minimum staffing requirements specified in paragraph (a), all facilities, including those composed of apartments, must have enough qualified staff to provide resident supervision, and to provide or arrange for resident services in accordance with the residents’ scheduled and unscheduled service needs, resident contracts, and resident care standards as described in rule 59A-36.007, F.A.C.
(c) The facility must maintain a written work schedule that reflects its 24-hour staffing pattern for a given time period. Upon request, the facility must make the daily work schedules of direct care staff available to residents or their representatives.
(d) The facility must provide staff immediately when the agency determines that the requirements of paragraph (a) are not met. The facility must immediately increase staff above the minimum levels established in paragraph (a), if the agency determines that adequate supervision and care are not being provided to residents, resident care standards described in rule 59A-36.007, F.A.C., are not being met, or that the facility is failing to meet the terms of residents’ contracts. The agency will consult with the facility administrator and residents regarding any determination that additional staff is required. Based on the recommendations of the local fire safety authority, the agency may require additional staff when the facility fails to meet the fire safety standards described in rule chapter 69A-40, F.A.C., until such time as the local fire safety authority informs the agency that fire safety requirements are being met.
1. When additional staff is required above the minimum, the agency will require the submission of a corrective action plan within the time specified in the notification indicating how the increased staffing is to be achieved to meet resident service needs. The plan will be reviewed by the agency to determine if it sufficiently increases the staffing levels to meet resident needs.
2. When the facility can demonstrate to the agency that resident needs are being met, or that resident needs can be met without increased staffing, the agency may modify staffing requirements for the facility and the facility will no longer be required to maintain a plan with the agency.
(e) Facilities that are co-located with a nursing home may use shared staffing provided that staff hours are only counted once for the purpose of meeting either assisted living facility or nursing home minimum staffing ratios.
(f) Facilities holding a limited mental health, extended congregate care, or limited nursing services license must also comply with the staffing requirements of rules 59A-36.020, 59A-36.021 or 59A-36.022, F.A.C., respectively.
Rulemaking Authority 429.41, 429.52, 429.929 FS. Law Implemented 429.174, 429.176, 429.41, 429.52, 429.905 FS. History–New 5-14-81, Amended 1-6-82, 9-17-84, Formerly 10A-5.19, Amended 10-20-86, 6-21-88, 8-15-90, 9-30-92, Formerly 10A-5.019, Amended 10-30-95, 4-20-98, 11-2-98, 10-17-99, 7-30-06, 4-15-10, 4-17-14, 5-10-18, Formerly 58A-5.019, 7-1-19.
59A-36.011 Staff Training Requirements and Competency Test. (1) ASSISTED LIVING FACILITY CORE TRAINING REQUIREMENTS AND COMPETENCY TEST. (a) The assisted living facility core training requirements established by the department pursuant to section 429.52, F.S., shall
consist of a minimum of 26 hours of training plus a competency test. (b) Administrators and managers must successfully complete the assisted living facility core training requirements within 3
months from the date of becoming a facility administrator or manager. Successful completion of the core training requirements includes passing the competency test. The minimum passing score for the competency test is 75%. Administrators who have attended core training prior to July 1, 1997, and managers who attended the core training program prior to April 20, 1998, shall not be required to take the competency test. Administrators licensed as nursing home administrators in accordance with chapter 468, part II, F.S., are exempt from this requirement.
(c) Administrators and managers shall participate in 12 hours of continuing education in topics related to assisted living every 2 years.
(d) A newly hired administrator or manager who has successfully completed the assisted living facility core training and continuing education requirements, shall not be required to retake the core training. An administrator or manager who has successfully completed the core training but has not maintained the continuing education requirements will be considered a new

administrator or manager for the purposes of the core training requirements and must: 1. Retake the assisted living facility core training; and, 2. Retake and pass the competency test. (e) The fees for the competency test shall not exceed $200.00. The payment for the competency test fee shall be remitted to the
entity administering the test. A new fee is due each time the test is taken. (2) STAFF PRESERVICE ORIENTATION. (a) Facilities must provide a preservice orientation of at least 2 hours to all new assisted living facility employees who have not
previously completed core training as detailed in subsection (1). (b) New staff must complete the preservice orientation prior to interacting with residents. (c) Once complete, the employee and the facility administrator must sign a statement that the employee completed the
preservice orientation which must be kept in the employee’s personnel record. (d) In addition to topics that may be chosen by the facility administrator, the preservice orientation must cover: 1. Resident’s rights; and, 2. The facility’s license type and services offered by the facility. (3) STAFF IN-SERVICE TRAINING. Facility administrators or managers shall provide or arrange for the following in-service
training to facility staff: (a) Staff who provide direct care to residents, other than nurses, certified nursing assistants, or home health aides trained in
accordance with rule 59A-8.0095, F.A.C., must receive a minimum of 1 hour in-service training in infection control, including universal precautions and facility sanitation procedures, before providing personal care to residents. The facility must use its infection control policies and procedures when offering this training. Documentation of compliance with the staff training requirements of 29 CFR 1910.1030, relating to blood borne pathogens, may be used to meet this requirement.
(b) Staff who provide direct care to residents must receive a minimum of 1 hour in-service training within 30 days of employment that covers the following subjects:
1. Reporting adverse incidents. 2. Facility emergency procedures including chain-of-command and staff roles relating to emergency evacuation. (c) Staff who provide direct care to residents, who have not taken the core training program, shall receive a minimum of 1 hour
in-service training within 30 days of employment that covers the following subjects: 1. Resident rights in an assisted living facility. 2. Recognizing and reporting resident abuse, neglect, and exploitation. The facility must use its abuse prevention policies and
procedures when offering this training. (d) Staff who provide direct care to residents, other than nurses, CNAs, or home health aides trained in accordance with rule
59A-8.0095, F.A.C., must receive 3 hours of in-service training within 30 days of employment that covers the following subjects: 1. Resident behavior and needs. 2. Providing assistance with the activities of daily living. (e) Staff who prepare or serve food, who have not taken the assisted living facility core training must receive a minimum of 1-
hour-in-service training within 30 days of employment in safe food handling practices. (f) All facility staff shall receive in-service training regarding the facility’s resident elopement response policies and procedures
within thirty (30) days of employment. 1. All facility staff shall be provided with a copy of the facility’s resident elopement response policies and procedures. 2. All facility staff shall demonstrate an understanding and competency in the implementation of the elopement response
policies and procedures. (4) HUMAN IMMUNODEFICIENCY VIRUS/ACQUIRED IMMUNE DEFICIENCY SYNDROME (HIV/AIDS). Pursuant to
section 381.0035, F.S., all facility employees, with the exception of employees subject to the requirements of section 456.033, F.S., must complete a one-time education course on HIV and AIDS, including the topics prescribed in the section 381.0035, F.S. New facility staff must obtain the training within 30 days of employment. Documentation of compliance must be maintained in accordance with subsection (12), of this rule.
(5) FIRST AID AND CARDIOPULMONARY RESUSCITATION (CPR). A staff member who has completed courses in First Aid and CPR and holds a currently valid card documenting completion of such courses must be in the facility at all times.
(a) Documentation that the staff member possess current CPR certification that requires the student to demonstrate, in person,

that he or she is able to perform CPR and which is issued by an instructor or training provider that is approved to provide CPR training by the American Red Cross, the American Heart Association, the National Safety Council, or an organization whose training is accredited by the Commission on Accreditation for Pre-Hospital Continuing Education satisfies this requirement.
(b) A nurse shall be considered as having met the training requirement for First Aid. An emergency medical technician or paramedic currently certified under chapter 401, Part III, F.S., shall be considered as having met the training requirements for both First Aid and C.P.R.
(6) ASSISTANCE WITH THE SELF-ADMINISTRATION OF MEDICATION AND MEDICATION MANAGEMENT. Unlicensed persons who will be providing assistance with the self-administration of medications as described in rule 59A-36.008, F.A.C., must meet the training requirements pursuant to section 429.52(6), F.S., prior to assuming this responsibility. Courses provided in fulfilment of this requirement must meet the following criteria:
(a) Training must cover state law and rule requirements with respect to the supervision, assistance, administration, and management of medications in assisted living facilities; procedures and techniques for assisting the resident with self-administration of medication including how to read a prescription label; providing the right medications to the right resident; common medications; the importance of taking medications as prescribed; recognition of side effects and adverse reactions and procedures to follow when residents appear to be experiencing side effects and adverse reactions; documentation and record keeping; and medication storage and disposal. Training shall include demonstrations of proper techniques, including techniques for infection control, and ensure unlicensed staff have adequately demonstrated that they have acquired the skills necessary to provide such assistance.
(b) The training must be provided by a registered nurse or licensed pharmacist who shall issue a training certificate to a trainee who demonstrates, in person and both physically and verbally, the ability to:
1. Read and understand a prescription label; 2. Provide assistance with self-administration in accordance with section 429.256, F.S., and rule 59A-36.008, F.A.C., including: a. Assist with oral dosage forms, topical dosage forms, and topical ophthalmic, otic and nasal dosage forms; b. Measure liquid medications, break scored tablets, and crush tablets in accordance with prescription directions; c. Recognize the need to obtain clarification of an “as needed” prescription order; d. Recognize a medication order which requires judgment or discretion, and to advise the resident, resident’s health care
provider or facility employer of inability to assist in the administration of such orders; e. Complete a medication observation record; f. Retrieve and store medication; g. Recognize the general signs of adverse reactions to medications and report such reactions; h. Assist residents with insulin syringes that are prefilled with the proper dosage by a pharmacist and insulin pens that are
prefilled by the manufacturer by taking the medication, in its previously dispensed, properly labeled container, from where it is stored, and bringing it to the resident for self-injection;
i. Assist with nebulizers; j. Use a glucometer to perform blood glucose testing; k. Assist residents with oxygen nasal cannulas and continuous positive airway pressure (CPAP) devices, excluding the titration
of the oxygen levels; l. Apply and remove anti-embolism stockings and hosiery; m. Placement and removal of colostomy bags, excluding the removal of the flange or manipulation of the stoma site; and, n. Measurement of blood pressure, heart rate, temperature, and respiratory rate. (c) Unlicensed persons, as defined in section 429.256(1)(b), F.S., who provide assistance with self-administered medications
and have successfully completed the initial 6 hour training, must obtain, annually, a minimum of 2 hours of continuing education training on providing assistance with self-administered medications and safe medication practices in an assisted living facility. The 2 hours of continuing education training may be provided online.
(d) Trained unlicensed staff who, prior to the effective date of this rule, assist with the self-administration of medication and have successfully completed 4 hours of assistance with self-administration of medication training must complete an additional 2 hours of training that focuses on the topics listed in sub-subparagraphs (6)(b)2.h.-n. of this section, before assisting with the self-administration of medication procedures listed in sub-subparagraphs (6)(b)2.h.-n.
(7) NUTRITION AND FOOD SERVICE. The administrator or person designated by the administrator as responsible for the facility’s food service and the day-to-day supervision of food service staff must obtain, annually, a minimum of 2 hours continuing

education in topics pertinent to nutrition and food service in an assisted living facility. This requirement does not apply to administrators and designees who are exempt from training requirements under paragraph 59A-36.012(1)(b). A certified food manager, licensed dietician, registered dietary technician or health department sanitarian is qualified to train assisted living facility staff in nutrition and food service.
(8) EXTENDED CONGREGATE CARE (ECC) TRAINING. (a) The administrator and ECC supervisor, if different from the administrator, must complete core training and 4 hours of initial
training in extended congregate care prior to the facility receiving its ECC license or within 3 months of beginning employment in a currently licensed ECC facility as an administrator or ECC supervisor. Successful completion of the assisted living facility core training shall be a prerequisite for this training. ECC supervisors who attended the assisted living facility core training prior to April 20, 1998, shall not be required to take the assisted living facility core training competency test.
(b) The administrator and the ECC supervisor, if different from the administrator, must complete a minimum of 4 hours of continuing education every two years in topics relating to the physical, psychological, or social needs of frail elderly and disabled persons, or persons with Alzheimer’s disease or related disorders.
(c) All direct care staff providing care to residents in an ECC program must complete at least 2 hours of in-service training, provided by the facility administrator or ECC supervisor, within 6 months of beginning employment in the facility. The training must address ECC concepts and requirements, including statutory and rule requirements, and the delivery of personal care and supportive services in an ECC facility.
(9) LIMITED MENTAL HEALTH TRAINING. (a) Pursuant to section 429.075, F.S., the administrator, managers and staff, who have direct contact with mental health residents
in a licensed limited mental health facility, must receive the following training: 1. A minimum of 6 hours of specialized training in working with individuals with mental health diagnoses. a. The training must be provided or approved by the Department of Children and Families and must be taken within 6 months of
the facility’s receiving a limited mental health license or within 6 months of employment in a limited mental health facility. b. Training received under this subparagraph may count once for 6 of the 12 hours of continuing education required for
administrators and managers pursuant to section 429.52(5), F.S., and subsection (1) of this rule. 2. A minimum of 3 hours of continuing education, which may be provided by the ALF administrator, online, or through
distance learning, biennially thereafter in subjects dealing with one or more of the following topics: a. Mental health diagnoses; and, b. Mental health treatment such as: (I) Mental health needs, services, behaviors and appropriate interventions; (II) Resident progress in achieving treatment goals; (III) How to recognize changes in the resident’s status or condition that may affect other services received or may require
intervention; and, (IV) Crisis services and the Baker Act procedures. 3. For administrators and managers, the continuing education requirement under this subsection will satisfy 3 of the 12 hours of
continuing education required biennially pursuant to section 429.52(5), F.S., and subsection (1) of this rule. 4. Administrators, managers and direct contact staff affected by the continuing education requirement under this subsection
shall have up to 6 months after the effective date of this rule to meet the training requirement. (b) Administrators, managers and staff do not have to repeat the initial training should they change employers provided they
present a copy of their training certificate to the current employer for retention in the facility’s personnel files. They must also ensure that copies of the continuing education training certificates, pursuant to subparagraph (a)2. of this subsection, are retained in their personnel files.
(10) ALZHEIMER’S DISEASE AND RELATED DISORDERS (“ADRD”) TRAINING REQUIREMENTS. Facilities which advertise that they provide special care for persons with ADRD, or who maintain secured areas as described in Chapter 4, Section 464.4.6 of the Florida Building Code, as adopted in rule 61G20-1.001, F.A.C., Florida Building Code Adopted, must ensure that facility staff receive the following training.
(a) Facility staff who interact on a daily basis with residents with ADRD but do not provide direct care to such residents and staff who provide direct care to residents with ADRD, shall obtain 4 hours of initial training within 3 months of employment. Completion of the core training program between April 20, 1998 and July 1, 2003 shall satisfy this requirement. Facility staff who

meet the requirements for ADRD training providers under paragraph (g) of this subsection, will be considered as having met this requirement. Initial training, entitled “Alzheimer’s Disease and Related Disorders Level I Training,” must address the following subject areas:
1. Understanding Alzheimer’s disease and related disorders; 2. Characteristics of Alzheimer’s disease; 3. Communicating with residents with Alzheimer’s disease; 4. Family issues; 5. Resident environment; and, 6. Ethical issues. (b) Staff who have successfully completed both the initial one hour and continuing three hours of ADRD training pursuant to
sections 400.1755, 429.917 and 400.6045(1), F.S., shall be considered to have met the initial assisted living facility Alzheimer’s Disease and Related Disorders Level I Training.
(c) Facility staff who provide direct care to residents with ADRD must obtain an additional 4 hours of training, entitled “Alzheimer’s Disease and Related Disorders Level II Training,” within 9 months of employment. Facility staff who meet the requirements for ADRD training providers under paragraph (g) of this subsection, will be considered as having met this requirement. Alzheimer’s Disease and Related Disorders Level II Training must address the following subject areas as they apply to these disorders:
1. Behavior management, 2. Assistance with ADLs, 3. Activities for residents, 4. Stress management for the care giver; and, 5. Medical information. (d) A detailed description of the subject areas that must be included in an ADRD curriculum which meets the requirements of
paragraphs (a) and (b) of this subsection, can be found in the document “Training Guidelines for the Special Care of Persons with Alzheimer’s Disease and Related Disorders,” dated March 1999, incorporated by reference, available from the Department of Elder Affairs, 4040 Esplanade Way, Tallahassee, Florida 32399-7000.
(e) Direct care staff shall participate in 4 hours of continuing education annually as required under section 429.178, F.S. Continuing education received under this paragraph may be used to meet 3 of the 12 hours of continuing education required by section 429.52, F.S., and subsection (1) of this rule, or 3 of the 6 hours of continuing education for extended congregate care required by subsection (7) of this rule.
(f) Facility staff who have only incidental contact with residents with ADRD must receive general written information provided by the facility on interacting with such residents, as required under section 429.178, F.S., within three (3) months of employment. “Incidental contact” means all staff who neither provide direct care nor are in regular contact with such residents.
(g) Persons who seek to provide ADRD training in accordance with this subsection must provide the department or its designee with documentation that they hold a Bachelor’s degree from an accredited college or university or hold a license as a registered nurse, and:
1. Have 1 year teaching experience as an educator of caregivers for persons with Alzheimer’s disease or related disorders, or 2. Three years of practical experience in a program providing care to persons with Alzheimer’s disease or related disorders, or 3. Completed a specialized training program in the subject matter of this program and have a minimum of two years of practical
experience in a program providing care to persons with Alzheimer’s disease or related disorders. (h) With reference to requirements in paragraph (g), a Master’s degree from an accredited college or university in a subject
related to the content of this training program can substitute for the teaching experience. Years of teaching experience related to the subject matter of this training program may substitute on a year-by-year basis for the required Bachelor’s degree referenced in paragraph (g).
(11) DO NOT RESUSCITATE ORDERS TRAINING. (a) Currently employed facility administrators, managers, direct care staff and staff involved in resident admissions must receive
at least one hour of training in the facility’s policies and procedures regarding Do Not Resuscitate Orders. (b) Newly hired facility administrators, managers, direct care staff and staff involved in resident admissions must receive at
least one hour of training in the facility’s policy and procedures regarding DNROs within 30 days after employment.

(c) Training shall consist of the information included in rule 59A-36.009, F.A.C. (12) TRAINING DOCUMENTATION AND MONITORING. (a) Except as otherwise noted, certificates, or copies of certificates, of any training required by this rule must be documented in
the facility’s personnel files. The documentation must include the following: 1. The title of the training program, 2. The subject matter of the training program, 3. The training program agenda, 4. The number of hours of the training program, 5. The trainee’s name, dates of participation, and location of the training program, 6. The training provider’s name, dated signature and credentials, and professional license number, if applicable. (b) Upon successful completion of training pursuant to this rule, the training provider must issue a certificate to the trainee as
specified in this rule. (c) The facility must provide the Department of Elder Affairs and the Agency for Health Care Administration with training
documentation and training certificates for review, as requested. The department and agency reserve the right to attend and monitor all facility in-service training, which is intended to meet regulatory requirements.
Rulemaking Authority 429.178, 429.41, 429.52 FS. Law Implemented 429.07, 429.075, 429.178, 429.41, 429.52 FS. History–New 9-30-92, Formerly 10A-5.0191, Amended 10-30-95, 6-2-96, 4-20-98, 11-2-98, 10-17-99, 7-5-05, 7-30-06, 10-9-06, 7-1-08, 4-15-10, 5-10-18, Formerly 58A-5.0191, 7-1-19.
59A-36.012 Food Service Standards. (1) GENERAL RESPONSIBILITIES. When food service is provided by the facility, the administrator, or an individual
designated in writing by the administrator, must be responsible for total food services and the day-to-day supervision of food services staff. In addition, the following requirements apply:
(a) If the designee is an individual who has not completed an approved assisted living facility core training course, such individual must complete the food and nutrition services module of the core training course before assuming responsibility for the facility’s food service. The designee is not subject to the 1 hour in-service training in safe food handling practices.
(b) If the designee is a certified food manager, certified dietary manager, registered or licensed dietitian, dietetic registered technician, or health department sanitarian, the designee is exempt from the requirement to complete the food and nutrition services module of the core training course before assuming responsibility for the facility’s food service as required in paragraph (1)(a) of this rule.
(c) An administrator or designee must perform his or her duties in a safe and sanitary manner. (d) An administrator or designee must provide regular meals that meet the nutritional needs of residents, and therapeutic diets as
ordered by the resident’s health care provider for residents who require special diets. (e) An administrator or designee must comply with the food service continuing education requirements specified in rule 59A-
36.011, F.A.C. (2) DIETARY STANDARDS. (a) The meals provided by the assisted living facility must be planned based on the current USDA Dietary Guidelines for
Americans, 2010, which are incorporated by reference and available for review at: http://www.flrules.org/Gateway/reference.asp?No=Ref-04003, and the current summary of Dietary Reference Intakes established by the Food and Nutrition Board of the Institute of Medicine of the National Academies, 2010, which are incorporated by reference and available for review at: http://iom.edu/Activities/Nutrition/SummaryDRIs/~/media/Files/Activity%20Files/Nutrition/DRIs/New%20Material/5DRI%20Values%20SummaryTables%2014.pdf. Therapeutic diets must meet these nutritional standards to the extent possible.
(b) The residents’ nutritional needs must be met by offering a variety of meals adapted to the food habits, preferences, and physical abilities of the residents, and must be prepared through the use of standardized recipes. For facilities with a licensed capacity of 16 or fewer residents, standardized recipes are not required. Unless a resident chooses to eat less, the facility must serve the standard minimum portions of food according to the Dietary Reference Intakes.
(c) All regular and therapeutic menus to be used by the facility must be reviewed annually by a licensed or registered dietitian, a licensed nutritionist, or a registered dietetic technician supervised by a licensed or registered dietitian, or a licensed nutritionist to

ensure the meals meet the nutritional standards established in this rule. The annual review must be documented in the facility files and include the original signature of the reviewer, registration or license number, and date reviewed. Portion sizes must be indicated on the menus or on a separate sheet.
1. Daily food servings may be divided among three or more meals per day, including snacks, as necessary to accommodate resident needs and preferences.
2. Menu items may be substituted with items of comparable nutritional value based on the seasonal availability of fresh produce or the preferences of the residents.
(d) Menus must be dated and planned at least 1 week in advance for both regular and therapeutic diets. Residents must be encouraged to participate in menu planning. Planned menus must be conspicuously posted or easily available to residents. Regular and therapeutic menus as served, with substitutions noted before or when the meal is served, must be kept on file in the facility for 6 months.
(e) Therapeutic diets must be prepared and served as ordered by the health care provider. 1. Facilities that offer residents a variety of food choices through a select menu, buffet style dining, or family style dining are
not required to document what is eaten unless a health care provider’s order indicates that such monitoring is necessary. However, the food items that enable residents to comply with the therapeutic diet must be identified on the menus developed for use in the facility.
2. The facility must document a resident’s refusal to comply with a therapeutic diet and provide notification to the resident’s health care provider of such refusal.
(f) For facilities serving three or more meals a day, no more than 14 hours must elapse between the end of an evening meal containing a protein food and the beginning of a morning meal. Intervals between meals must be evenly distributed throughout the day with not less than 2 hours nor more than 6 hours between the end of one meal and the beginning of the next. For residents without access to kitchen facilities, snacks must be offered at least once per day. Snacks are not considered to be meals for the purposes of calculating the time between meals.
(g) Food must be served attractively at safe and palatable temperatures. All residents must be encouraged to eat at tables in the dining areas. A supply of eating ware sufficient for all residents, including adaptive equipment if needed by any resident, must be on hand.
(h) A 3-day supply of nonperishable food, based on the number of weekly meals the facility has contracted with residents to serve, must be on hand at all times. The quantity must be based on the resident census and not on licensed capacity. The supply must consist of foods that can be stored safely without refrigeration. Water sufficient for drinking and food preparation must also be stored, or the facility must have a plan for obtaining water in an emergency, with the plan coordinated with and reviewed by the local disaster preparedness authority.
(3) FOOD HYGIENE. Copies of inspection reports issued by the county health department for the last 2 years pursuant to rule 64E-12.004, or chapter 64E-11, F.A.C., as applicable, depending on the licensed capacity of the assisted living facility, must be on file in the facility.
(4) CONTRACTED FOOD SERVICE. When food service is contracted by the facility, the facility must ensure that the contracted food service meets all dietary standards imposed by this rule and is adequately protected upon delivery to the facility pursuant to subsection 64E-12.004(4), F.A.C. The facility must maintain:
(a) A copy of the current contract between the facility and the food service contractor. (b) A copy of the annually issued certificate or license authorizing the operation of the food service contractor issued by the
applicable regulating agency. The license or certificate must provide documentation of the food service contractor’s compliance with food service regulatory requirements.
Rulemaking Authority 429.41 FS. Law Implemented 429.41, 429.52 FS. History–New 5-14-81, Amended 1-6-82, 5-19-83, 9-17-84, Formerly 10A-5.20, Amended 10-20-86, 6-21-88, 8-15-90, 9-30-92, Formerly 10A-5.020, Amended 10-30-95, 6-2-96, 10-17-99, 4-17-14, Formerly 58A-5.020, 7-1-19.
59A-36.013 Fiscal Standards. (1) FINANCIAL STABILITY. The facility must be administered on a sound financial basis in order to ensure adequate
resources to meet resident needs pursuant to the requirements of chapter 408, part II, part I, F.S., and rule chapter 59A-35, F.A.C., and this rule chapter.

(2) RESIDENT TRUST FUNDS. Funds or other property received by the facility belonging to or due a resident, including personal funds, must be held as trust funds and expended only for the resident’s account. Resident funds or property may be held in one bank account if a separate written accounting for each resident is maintained. A separate bank account is required for facility funds; co-mingling resident funds with facility funds is prohibited. Written accounting procedures for resident trust funds must include income and expense records of the trust fund, including the source and disposition of the funds.
(3) SURETY BONDS. Pursuant to the requirements of section 429.27(2), F.S.: (a) For entities that own more than one facility in the state, one surety bond may be purchased to cover the needs of all residents
served by the entities. (b) The following additional bonding requirements apply to facilities serving residents receiving OSS: 1. If serving as representative payee for a resident receiving OSS, the minimum bond proceeds must equal twice the value of the
resident’s monthly aggregate income, which must include any supplemental security income or social security disability income plus the OSS payments, including the personal needs allowance.
2. If holding a power of attorney for a resident receiving OSS, the minimum bond proceeds must equal twice the value of the resident’s monthly aggregate income, which must include any supplemental security income or social security disability income; the OSS payments, including the personal allowance; plus the value of any property belonging to a resident held at the facility.
(c) Upon the annual issuance of a new bond or continuation bond, the facility must file a copy of the bond with the Agency Central Office.
(4) LIABILITY INSURANCE. Pursuant to section 429.275, F.S., facilities must maintain liability insurance coverage, as defined in section 624.605, F.S., that remains in force at all times. On the renewal date of the facility’s policy or whenever a facility changes policies, the facility must file documentation of continued coverage with the Agency Central Office. Such documentation must be issued by the insurance company and must include the name and street address of the facility, a reference that the facility is an assisted living facility, the facility’s licensed capacity, and the dates of coverage.
Rulemaking Authority 429.24, 429.27, 429.275, 429.41 FS. Law Implemented 429.27, 429.275 FS. History–New 5-14-81, Amended 1-6-82, 9-17-84, Formerly 10A-5.21, Amended 6-21-88, 8-15-90, 9-30-92, Formerly 10A-5.021, Amended 10-30-95, 6-2-96, 10-17-99, 4-17-14, Formerly 58A-5.021, 7-1-19.
59A-36.014 Physical Plant Standards. (1) NEW FACILITIES. Newly constructed facilities to be licensed as assisted living facilities, and existing structures, not
previously licensed as assisted living facilities, to be converted to assisted living facilities, as well as any subsequent additions, modifications, alterations, renovations or refurbishing of such facilities, are required by governmental entities other than the Department of Elder Affairs to adhere to certain building code and fire safety standards. Such standards may be found in:
(a) Chapter 4, Section 464, of the Florida Building Code as adopted in rule 61G20-1.001, F.A.C.; (b) Section 633.022, F.S., Uniform Firesafety Standards and rule chapter 69A-40, F.A.C. The Uniform Fire Safety Standards for
Assisted Living Facilities; and, (c) The National Fire Protection Association codes described in section 429.41, F.S. (2) EXISTING FACILITIES. (a) An assisted living facility must comply with the rule or building code in effect at the time of initial licensure, as well as the
rule or building code in effect at the time of any additions, modifications, alterations, refurbishment, renovations or reconstruction. Determination of the installation of a fire sprinkler system in an existing facility must comply with the requirements described in section 429.41, F.S.
(b) A facility undergoing change of ownership is considered an existing facility for purposes of this rule. (3) OTHER REQUIREMENTS. (a) All facilities must: 1. Provide a safe living environment pursuant to section 429.28(1)(a), F.S.; 2. Be maintained free of hazards; and, 3. Ensure that all existing architectural, mechanical, electrical and structural systems, and appurtenances are maintained in good
working order. (b) Pursuant to section 429.27, F.S., residents must be given the option of using their own belongings as space permits. When
the facility supplies the furnishings, each resident bedroom or sleeping area must have at least the following furnishings:

1. A clean, comfortable bed with a mattress no less than 36 inches wide and 72 inches long, with the top surface of the mattress at a comfortable height to ensure easy access by the resident,
2. A closet or wardrobe space for hanging clothes, 3. A dresser, chest or other furniture designed for storage of clothing or personal effects, 4. A table or nightstand, bedside lamp or floor lamp, and waste basket; and, 5. A comfortable chair, if requested. (c) The facility must maintain master or duplicate keys to resident bedrooms to be used in the event of an emergency. (d) Residents who use portable bedside commodes must be provided with privacy during use. (e) Facilities must make available linens and personal laundry services for residents who require such services. Linens provided
by a facility must be free of tears, stains and must not be threadbare.
Rulemaking Authority 429.41 FS. Law Implemented 429.27, 429.28, 429.41 FS. History–New 5-14-81, Amended 1-6-82, 5-19-83, 9-17-84, Formerly 10A-5.23, Amended 10-20-86, 6-21-88, 8-15-90, 9-30-92, Formerly 10A-5.023, Amended 10-30-95, 6-2-96, 10-17-99, 7-30-06, 4-15-10, 4-17-14, Formerly 58A-5.023, 7-1-19.
59A-36.015 Records. The facility must maintain required records in a manner that makes such records readily available at the licensee’s physical address for review by a legally authorized entity. If records are maintained in an electronic format, facility staff must be readily available to access the data and produce the requested information. For purposes of this section, “readily available” means the ability to immediately produce documents, records, or other such data, either in electronic or paper format, upon request.
(1) FACILITY RECORDS. Facility records must include: (a) The facility’s license displayed in a conspicuous and public place within the facility. (b) An up-to-date admission and discharge log listing the names of all residents and each resident’s: 1. Date of admission, the facility or place from which the resident was admitted, and if applicable, a notation indicating that the
resident was admitted with a stage 2 pressure sore; and, 2. Date of discharge, reason for discharge, and identification of the facility or home address to which the resident was
discharged. Readmission of a resident to the facility after discharge requires a new entry in the log. Discharge of a resident is not required if the facility is holding a bed for a resident who is out of the facility but intending to return pursuant to rule 59A-36.018, F.A.C. If the resident dies while in the care of the facility, the log must indicate the date of death.
(c) A log listing the names of all temporary emergency placement and respite care residents if not included on the log described in paragraph (b).
(d) The facility’s emergency management plan, with documentation of review and approval by the county emergency management agency, as described in rule 59A-36.019, F.A.C., that must be readily available by facility staff.
(e) The facility’s liability insurance policy required in rule 59A-36.013, F.A.C. (f) For facilities that have a surety bond, a copy of the surety bond currently in effect as required by rule 59A-36.013, F.A.C. (g) The admission package presented to new or prospective residents (less the resident’s contract) described in rule 59A-36.006,
F.A.C. (h) If the facility advertises that it provides special care for persons with Alzheimer’s disease or related disorders, a copy of all
such facility advertisements as required by section 429.177, F.S. (i) A grievance procedure for receiving and responding to resident complaints and recommendations as described in rule 59A-
36.007, F.A.C. (j) All food service records required in rule 59A-36.012, F.A.C., including menus planned and served and county health
department inspection reports. Facilities that contract for food services, must include a copy of the contract for food services and the food service contractor’s license or certificate to operate.
(k) All fire safety inspection reports issued by the local authority or the State Fire Marshal pursuant to section 429.41, F.S., and rule chapter 69A-40, F.A.C., issued within the last 2 years.
(l) All sanitation inspection reports issued by the county health department pursuant to section 381.031, F.S., and chapter 64E-12, F.A.C., issued within the last 2 years.
(m) Pursuant to section 429.35, F.S., all completed survey, inspection and complaint investigation reports, and notices of sanctions and moratoriums issued by the agency within the last 5 years.

(n) The facility’s resident elopement response policies and procedures. (o) The facility’s documented resident elopement response drills. (p) For facilities licensed as limited mental health, extended congregate care, or limited nursing services, records required as
stated in rules 59A-36.020, 59A-36.021 and 59A-36.022, F.A.C., respectively. (2) STAFF RECORDS. (a) Personnel records for each staff member must contain, at a minimum, a copy of the employment application, with references
furnished, and documentation verifying freedom from signs or symptoms of communicable disease. In addition, records must contain the following, as applicable:
1. Documentation of compliance with all staff training and continuing education required by rule 59A-36.011, F.A.C., 2. Copies of all licenses or certifications for all staff providing services that require licensing or certification, 3. Documentation of compliance with level 2 background screening for all staff subject to screening requirements as specified in
section 429.174, F.S., and rule 59A-36.010, F.A.C., 4. For facilities with a licensed capacity of 17 or more residents, a copy of the job description given to each staff member
pursuant to rule 59A-36.010, F.A.C., 5. Documentation verifying direct care staff and administrator participation in resident elopement drills pursuant to paragraph
59A-36.007(8)(c), F.A.C. (b) The facility is not required to maintain personnel records for staff provided by a licensed staffing agency or staff employed
by an entity contracting to provide direct or indirect services to residents and the facility. However, the facility must maintain a copy of the contract between the facility and the staffing agency or contractor as described in rule 59A-36.010, F.A.C.
(c) The facility must maintain the written work schedules and staff time sheets for the most current 6 months as required by rule 59A-36.010, F.A.C.
(3) RESIDENT RECORDS. Resident records must be maintained on the premises and include: (a) Resident demographic data as follows: 1. Name, 2. Sex, 3. Race, 4. Date of birth, 5. Place of birth, if known, 6. Social security number, 7. Medicaid and/or Medicare number, or name of other health insurance carrier, 8. Name, address, and telephone number of next of kin, legal representative, or individual designated by the resident for
notification in case of an emergency; and, 9. Name, address, and telephone number of the health care provider and case manager, if applicable. (b) A copy of the Resident Health Assessment form, AHCA Form 1823 described in rule 59A-36.006, F.A.C. (c) Any orders for medications, nursing services, therapeutic diets, do not resuscitate orders, or other services to be provided,
supervised, or implemented by the facility that require a health care provider’s order. (d) Documentation of a resident’s refusal of a therapeutic diet pursuant to rule 59A-36.012, F.A.C., if applicable. (e) The resident care record described in paragraph 59A-36.007(1)(e), F.A.C. (f) A weight record that is initiated on admission. Information may be taken from AHCA Form 1823 or the resident’s health
assessment. Residents receiving assistance with the activities of daily living must have their weight recorded semi-annually. (g) For facilities that will have unlicensed staff assisting the resident with the self-administration of medication, a copy of the
written informed consent described in rule 59A-36.006, F.A.C., if such consent is not included in the resident’s contract. (h) For facilities that manage a pill organizer, assist with self-administration of medications or administer medications for a
resident, copies of the required medication records maintained pursuant to rule 59A-36.008, F.A.C. (i) A copy of the resident’s contract with the facility, including any addendums to the contract as described in rule 59A-36.018,
F.A.C. (j) For a facility whose owner, administrator, staff, or representative thereof, serves as an attorney in fact for a resident, a copy
of the monthly written statement of any transaction made on behalf of the resident as required in section 429.27, F.S. (k) For any facility that maintains a separate trust fund to receive funds or other property belonging to or due a resident, a copy

of the quarterly written statement of funds or other property disbursed as required in section 429.27, F.S. (l) If the resident is an OSS recipient, a copy of the Department of Children and Families form Alternate Care Certification for
Optional State Supplementation (OSS), CF-ES 1006, October 2005, which is hereby incorporated by reference and available for review at: http://www.flrules.org/Gateway/reference.asp?No=Ref-04004. The absence of this form will not be the basis for administrative action against a facility if the facility can demonstrate that it has made a good faith effort to obtain the required documentation from the Department of Children and Families.
(m) Documentation of the appointment of a health care surrogate, health care proxy, guardian, or the existence of a power of attorney, where applicable.
(n) For hospice patients, the interdisciplinary care plan and other documentation that the resident is a hospice patient as required in rule 59A-36.006, F.A.C.
(o) The resident’s Do Not Resuscitate Order, DH Form 1896, if applicable. (p) For independent living residents who receive meals and occupy beds included within the licensed capacity of an assisted
living facility, but who are not receiving any personal, limited nursing, or extended congregate care services, record keeping may be limited to the following at the discretion of the facility:
1. A log listing the names of residents participating in this arrangement, 2. The resident demographic data required in this paragraph, 3. The health assessment described in rule 59A-36.006, F.A.C., 4. The resident’s contract described in rule 59A-36.018, F.A.C.; and, 5. A health care provider’s order for a therapeutic diet if such diet is prescribed and the resident participates in the meal plan
offered by the facility. (q) Except for resident contracts, which must be retained for 5 years, all resident records must be retained for 2 years following
the departure of a resident from the facility unless it is required by contract to retain the records for a longer period of time. Upon request, residents must be provided with a copy of their records upon departure from the facility.
(r) Additional resident records requirements for facilities holding a limited mental health, extended congregate care, or limited nursing services license are provided in rules 59A-36.020, 59A-36.021 and 59A-36.022, F.A.C., respectively.
(4) RECORD INSPECTION. (a) The resident’s records must be available to the resident; the resident’s legal representative, designee, surrogate, guardian,
attorney in fact, or case manager; or the resident’s estate, and such additional parties as authorized in writing or by law. (b) Pursuant to section 429.35, F.S., agency reports that pertain to any agency survey, inspection, or monitoring visit must be
available to the residents and the public. In facilities that are co-located with a licensed nursing home, the inspection of record for all common areas is the nursing home inspection report.
Rulemaking Authority 429.41, 429.275 FS. Law Implemented 429.24, 429.255, 429.256, 429.26, 429.27, 429.275, 429.35, 429.41, 429.52 FS. History–New 5-14-81, Amended 1-6-82, 5-19-83, 9-17-84, Formerly 10A-5.24, Amended 10-20-86, 6-21-88, 8-15-90, 9-30-92, Formerly 10A-5.024, Amended 10-30-95, 4-20-98, 11-2-98, 10-17-99, 7-30-06, 10-9-06, 4-17-14, Formerly 58A-5.024, 7-1-19.
59A-36.016 Adverse Incident Report. (1) INITIAL ADVERSE INCIDENT REPORT. The preliminary adverse incident report required by section 429.23(3), F.S.,
must be submitted within 1 business day after the incident pursuant to rule 59A-35.110, F.A.C., which requires online reporting. (2) FULL ADVERSE INCIDENT REPORT. For each adverse incident reported in subsection (1), above, the facility must
submit a full report within 15 days of the incident. The full report must be submitted pursuant to rule 59A-35.110, F.A.C., which requires online reporting.
Rulemaking Authority 429.23 FS. Law Implemented 429.23 FS. History–New 1-9-02, Amended 7-30-06, 4-17-14, Formerly 58A-5.0241, 7-1-19.
59A-36.017 Liability Claim Report. (1) MONTHLY LIABILITY CLAIM REPORT. Each assisted living facility must report monthly any liability claim filed
against the facility pursuant to rule 59A-35.110, F.A.C., which requires online reporting. Each facility must comply with the reporting time frames and transmission requirements specified in section 429.23(5), F.S.
(2) If a liability claim has not been filed against the facility in a given month, no report is required.

Rulemaking Authority 429.23 FS. Law Implemented 429.23 FS. History–New 1-9-02, Amended 3-13-14, Formerly 58A-5.0242, 7-1-19.
59A-36.018 Resident Contracts. (1) Pursuant to section 429.24, F.S., the facility must offer a contract for execution by the resident or the resident’s legal
representative before or at the time of admission. The contract must contain the following provisions: (a) A list of the specific services, supplies and accommodations to be provided by the facility to the resident, including limited
nursing and extended congregate care services that the resident elects to receive; (b) The daily, weekly, or monthly rate; (c) A list of any additional services and charges to be provided that are not included in the daily, weekly, or monthly rates, or a
reference to a separate fee schedule that must be attached to the contract; (d) A provision stating that at least 30 days written notice will be given before any rate increase; (e) Any rights, duties, or obligations of residents, other than those specified in section 429.28, F.S.; (f) The purpose of any advance payments or deposit payments, and the refund policy for such advance or deposit payments; (g) A refund policy that must conform to section 429.24(3), F.S.; (h) A written bed hold policy and provisions for terminating a bed hold agreement if a facility agrees in writing to reserve a bed
for a resident who is admitted to a nursing home, health care facility, or psychiatric facility. The resident or responsible party must notify the facility in writing of any change in status that would prevent the resident from returning to the facility. Until such written notice is received, the agreed upon daily, weekly, or monthly rate may be charged by the facility unless the resident’s medical condition prevents the resident from giving written notification, such as when a resident is comatose, and the resident does not have a responsible party to act on the resident’s behalf;
(i) A provision stating whether the facility is affiliated with any religious organization and, if so, which organization and its relationship to the facility;
(j) A provision that, upon determination by the administrator or health care provider that the resident needs services beyond those that the facility is licensed to provide, the resident or the resident’s representative, or agency acting on the resident’s behalf, must be notified in writing that the resident must make arrangements for transfer to a care setting that is able to provide services needed by the resident. In the event the resident has no one to represent him or her, the facility must refer the resident to the social service agency for placement. If there is disagreement regarding the appropriateness of placement, provisions outlined in section 429.26(8), F.S., will take effect;
(k) A provision that residents must be assessed upon admission pursuant to subsection 59A-36.006(2), F.A.C., and every 3 years thereafter, or after a significant change, pursuant to subsection (4), of that rule;
(l) The facility’s policies and procedures for self-administration, assistance with self-administration, and administration of medications, if applicable, pursuant to rule 59A-36.008, F.A.C. This also includes provisions regarding over-the-counter (OTC) products pursuant to subsection (8) of that rule; and,
(m) The facility’s policies and procedures related to a properly executed DH Form 1896, Do Not Resuscitate Order. (2) The resident, or the resident’s representative, must be provided with a copy of the executed contract. (3) The facility may not levy an additional charge for any supplies, services, or accommodations that the facility has agreed by
contract to provide as part of the standard daily, weekly, or monthly rate. The resident or resident’s representative must be furnished in advance with an itemized written statement setting forth additional charges for any services, supplies, or accommodations available to residents not covered under the contract. An addendum must be added to the resident contract to reflect the additional services, supplies, or accommodations not provided under the original agreement. Such addendum must be dated and signed by the facility and the resident or resident’s legal representative and a copy given to the resident or resident’s representative.
Rulemaking Authority 429.24, 429.41 FS. Law Implemented 429.24, 429.41 FS. History–New 10-17-99, Amended 7-30-06, 4-15-10, 3-13-14, Formerly 58A-5.025, 7-1-19.
59A-36.019 Emergency Management. (1) EMERGENCY PLAN COMPONENTS. Pursuant to section 429.41, F.S., each facility must prepare a written
comprehensive emergency management plan in accordance with the “Emergency Management Criteria for Assisted Living Facilities,” dated October 1995, which is incorporated by reference and available at http://www.flrules.org/Gateway/reference.asp?No=Ref-04010. This document is available from the local emergency management

agency. The emergency management plan must, at a minimum, address the following: (a) Provision for all hazards; (b) Provision for the care of residents remaining in the facility during an emergency, including pre-disaster or emergency
preparation; protecting the facility; supplies; emergency power; food and water; staffing; and emergency equipment; (c) Provision for the care of residents who must be evacuated from the facility during an emergency including identification of
such residents and transfer of resident records; evacuation transportation; sheltering arrangements; supplies; staffing; emergency equipment; and medications;
(d) Provision for the care of additional residents who may be evacuated to the facility during an emergency including the identification of such residents, staffing, and supplies;
(e) Identification of residents with Alzheimer’s disease or related disorders, and residents with mobility limitations who may need specialized assistance either at the facility or in case of evacuation;
(f) Identification of and coordination with the local emergency management agency; (g) Arrangement for post-disaster activities including responding to family inquiries, obtaining medical intervention for
residents, transportation, and reporting to the local emergency management agency the number of residents who have been relocated, and the place of relocation; and,
(h) The identification of staff responsible for implementing each part of the plan. (2) EMERGENCY PLAN APPROVAL. The plan must be submitted for review and approval to the local emergency
management agency. (a) If the local emergency management agency requires revisions to the emergency management plan, such revisions must be
made and the plan resubmitted to the local office within 30 days of receiving notification that the plan must be revised. (b) A new facility as described in rule 59A-36.014, F.A.C., and facilities whose ownership has been transferred, must submit an
emergency management plan within 30 days after obtaining a license. (c) The facility must review its emergency management plan on an annual basis. Any substantive changes must be submitted to
the local emergency agency for review and approval. 1. Changes in the name, address, telephone number, or position of staff listed in the plan are not considered substantive
revisions for the purposes of this rule. 2. Changes in the identification of specific staff must be submitted to the local emergency management agency annually as a
signed and dated addendum that is not subject to review and approval. (d) The local emergency management agency is the final administrative authority for emergency management plans prepared by
assisted living facilities. (e) Any plan approved by the local emergency management agency is considered to have met all the criteria and conditions
established in this rule. (3) PLAN IMPLEMENTATION. (a) All staff must be trained in their duties and are responsible for implementing the emergency management plan. (b) If telephone service is not available during an emergency, the facility must request assistance from local law enforcement or
emergency management personnel in maintaining communication. (4) FACILITY EVACUATION. The facility must evacuate the premises during or after an emergency if so directed by the local
emergency management agency. (a) The facility must report the evacuation to the local office of emergency management or designee and to the agency within 6
hours of the evacuation order. If the evacuation takes more than 6 hours, the facility must report when the evacuation is completed. (b) The facility must not be re-occupied until the area is cleared for reentry by the local emergency management agency or its
designee and the facility can meet the immediate needs of the residents. (c) A facility with significant structural damage must relocate residents until the facility can be safely re-occupied. (d) The facility is responsible for knowing the location of all residents until the residents have been relocated to another facility. (e) The facility must provide the agency with the name of a contact person who must be available by telephone 24 hours a day,
seven days a week, until the facility is re-occupied. (f) The facility must assist in the relocation of residents, and must cooperate with outreach teams established by the Department
of Health or emergency management agency to assist in relocation efforts. Resident needs and preferences must be considered to the extent possible in any relocation decision.

(5) EMERGENCY SHELTER. In the event a state of emergency has been declared and the facility is not required to evacuate the premises, the facility may provide emergency shelter above the facility’s licensed capacity provided the following conditions are met:
(a) Life safety will not be jeopardized for any individual; (b) The immediate needs of residents and other individuals sheltered at the facility can be met by the facility; (c) The facility reports the number of individuals over its licensed capacity and the conditions causing it to the Agency Field
Office within 48 hours or as soon as practical. As an alternative, the facility may report to the Agency Central Office at (850)412-4304. If the facility will continue to be over capacity after the declared emergency ends, the agency will review requests for excess capacity on a case-by-case basis; and,
(d) The facility maintains a log of the additional individuals being housed in the facility. The log must include the individual’s name, usual address, and the dates of arrival and departure. The log must be available for review by representatives of the agency, the department, the local emergency management agency or its designee. The admissions and discharge log maintained by the facility may be used for this purpose provided the information is maintained in a manner that is easily accessible.
Rulemaking Authority 429.41 FS. Law Implemented 429.41 FS. History–New 10-17-99, Amended 7-30-06, 4-17-14, Formerly 58A-5.026, 7-1-19.
59A-36.020 Limited Mental Health. (1) LICENSE APPLICATION. (a) Any facility intending to admit one or more mental health residents must obtain a limited mental health license from the
agency before accepting the mental health resident. (b) Facilities applying for a limited mental health license that have uncorrected deficiencies or violations found during the
facility’s last survey, complaint investigation, or monitoring visit will be surveyed before the issuance of a limited mental health license to determine if such deficiencies or violations have been corrected.
(2) RECORDS. (a) A facility with a limited mental health license must maintain an up-to-date admission and discharge log containing the
names and dates of admission and discharge for all mental health residents. The admission and discharge log required in rule 59A-36.015, F.A.C., satisfies this condition provided that all mental health residents are clearly identified.
(b) Staff records must contain documentation that designated staff have completed limited mental health training as required by rule 59A-36.011, F.A.C.
(c) Resident records must include: 1. Documentation, provided by a mental health care provider within 30 days of the resident’s admission to the facility, that the
resident is a mental health resident as defined in section 394.4574, F.S., and that the resident is receiving social security disability or supplemental security income and optional state supplementation as follows:
a. An affirmative statement on the Alternate Care Certification for Optional State Supplementation (OSS) form, CF-ES 1006, October 2005, which is hereby incorporated by reference and available for review at: http://www.flrules.org/Gateway/reference.asp?No=Ref-03988, that the resident is receiving SSI or SSDI due to a mental disorder,
b. Written verification provided by the Social Security Administration that the resident is receiving SSI or SSDI for a mental disorder. Such verification may be acquired from the Social Security Administration upon obtaining a release from the resident permitting the Social Security Administration to provide such information, or
c. A written statement from the resident’s case manager or other mental health care provider that the resident is an adult with severe and persistent mental disorder. The case manager or other mental health care provider must consider the following minimum criteria in making that determination:
(I) The resident is eligible for, is receiving, or has received mental health services within the last 5 years, or (II) The resident has been diagnosed as having a severe or persistent mental disorder. 2. An appropriate placement assessment provided by the resident’s mental health care provider within 30 days of admission to
the facility that the resident has been assessed and found appropriate for residence in an assisted living facility. Such assessment must be conducted by a psychiatrist, clinical psychologist, clinical social worker, psychiatric nurse, or an individual supervised by one of these professionals.
a. Any of the following documentation that contains the name of the resident and the name, signature, date, and license number, if applicable, of the person making the assessment, meets this requirement:

(I) Completed Alternate Care Certification for Optional State Supplementation (OSS) form, CF-ES Form 1006, (II) Discharge Statement from a state mental hospital completed no more than 90 days before admission to the assisted living
facility provided it contains a statement that the individual is appropriate to live in an assisted living facility, or (III) Other signed statement that the resident has been assessed and found appropriate for residency in an assisted living facility. b. A mental health resident returning to a facility from treatment in a hopsital or crisis stabilization unit will not be considered a
new admission and will not require a new assessment. However, a break in a resident’s residency that requires the facility to execute a new resident contract or admission agreement will be considered a new admission and the resident’s mental health care provider must provide a new assessment.
3. A Community Living Support Plan. Each mental health resident and the resident’s mental health case manager must, in consultation with the facility administrator, prepare a plan within 30 days of the resident’s admission to the facility or within 30 days after receiving the appropriate placement assessment in paragraph (2)(c), whichever is later, that:
a. Includes the specific needs of the resident that must be met in order to enable the resident to live in the assisted living facility and the community,
b. Includes the clinical mental health services to be provided by the mental health care provider to help meet the resident’s needs, and the frequency and duration of such services,
c. Includes any other services and activities to be provided by or arranged for by the mental health care provider or mental health case manager to meet the resident’s needs, and the frequency and duration of such services and activities,
d. Includes the obligations of the facility to facilitate and assist the resident in attending appointments and arranging transportation to appointments for the services and activities identified in the plan that have been provided or arranged for by the resident’s mental health care provider or case manager,
e. Includes a description of other services to be provided or arranged by the facility, f. Includes a list of factors pertinent to the care, safety, and welfare of the mental health resident and a description of the signs
and symptoms particular to the resident that indicate the immediate need for professional mental health services, g. Is in writing and signed by the mental health resident, the resident’s mental health case manager, and the assisted living
facility administrator or manager and a copy placed in the resident’s file. If the resident refuses to sign the plan, the resident’s mental health case manager must add a statement that the resident was asked but refused to sign the plan,
h. Is updated at least annually or if there is a significant change in the resident’s behavioral health, i. May include the Cooperative Agreement described in subparagraph (2)(c)4. If included, the mental health care provider must
also sign the plan; and, j. Must be available for inspection to those who have legal authority to review the document. 4. Cooperative Agreement. The mental health care provider for each mental health resident and the facility administrator or
designee must prepare a written statement, within 30 days of the resident’s admission to the facility or receipt of the resident’s appropriate placement assessment, whichever is later. The statement:
a. Provides procedures and directions for accessing emergency and after-hours care for the mental health resident. The provider must furnish the resident and the facility with the provider’s 24-hour emergency crisis telephone number;
b. Must be signed by the administrator or designee and the mental health care provider, or by a designated representative of a Medicaid prepaid health plan if the resident is on a plan and the plan provides behavioral health services in section 409.912, F.S.;
c. May cover all mental health residents of the facility who are clients of the same provider; and, d. May be included in the Community Living Support Plan described in subparagraph (2)(c)3. 5. Missing documentation will not be the basis for administrative action against a facility if the facility can demonstrate that it
has made a good faith effort to obtain the required documentation from the appropriate party. A documented request for such missing documentation made by the facility administrator within 72 hours of the resident’s admission will be considered a good faith effort. The documented request must include the name, title, and phone number of the person to whom the request was made and must be kept in the resident’s file.
(3) RESPONSIBILITIES OF FACILITY. In addition to the staffing and care standards of this rule chapter to provide for the welfare of residents in an assisted living facility, a facility holding a limited mental health license must:
(a) Meet the facility’s obligation to assist the resident in carrying out the activities identified in the Community Living Support Plan;
(b) Provide an opportunity for private face-to-face contact between the mental health resident and the resident’s mental health

case manager or other treatment personnel of the resident’s mental health care provider; (c) Observe resident behavior and functioning in the facility, and record and communicate observations to the resident’s mental
health case manager or mental health care provider regarding any significant behavioral or situational changes that may signify the need for a change in the resident’s professional mental health services, supports, and services described in the community living support plan, or that the resident is no longer appropriate for residency in the facility;
(d) If the facility initiates an involuntary mental health examination pursuant to section 394.463, F.S., the facility must document the circumstances leading to the initiation of the examination;
(e) Ensure that designated staff have completed limited mental health training as required by rule 59A-36.011, F.A.C.; and, (f) Maintain facility, staff, and resident records in accordance with the requirements of this rule chapter.
Rulemaking Authority 429.41 FS. Law Implemented 429.075, 429.26, 429.41 FS. History–New 8-15-90, Amended 9-30-92, Formerly 10A-5.029, Repromulgated 10-30-95, Amended 6-2-96, 11-2-98, 7-30-06, Amended 4-17-14, 5-10-18, Formerly 58A-5.029, 7-1-19.
59A-36.021 Extended Congregate Care Services. (1) LICENSING. (a) Any facility intending to establish extended congregate care services must obtain a license from the agency before accepting
residents needing extended congregate care services. (b) Only the portion of a facility that meets the physical requirements of subsection (3), and is staffed in accordance with
subsection (4), is considered licensed to provide extended congregate care services to residents who meet the admission and continued residency requirements of this rule.
(2) EXTENDED CONGREGATE CARE POLICIES. Policies and procedures established through extended congregate care services must promote resident independence, dignity, choice, and decision-making. The facility must develop and implement specific written policies and procedures that address:
(a) Aging in place; (b) The facility’s residency criteria developed in accordance with the admission and discharge requirements described in
subsection (5), and extended congregate care services listed in subsection (8); (c) The personal and supportive services the facility intends to provide, how the services will be provided, and the identification
of staff positions to provide the services including their relationship to the facility; (d) The nursing services the facility intends to provide, identification of staff positions to provide nursing services, and the
license status, duties, general working hours, and supervision of such staff; (e) Identifying potential unscheduled resident service needs and mechanisms for meeting those needs including the
identification of resources to meet those needs; (f) A process for mediating conflicts among residents regarding choice of room or apartment and roommate; and, (g) How to involve residents in decisions concerning the resident. The services must provide opportunities and encouragement
for the resident to make personal choices and decisions. If a resident needs assistance to make choices or decisions, a family member or other resident representative must be consulted. Choices must include at a minimum whether:
1. To participate in the process of developing, implementing, reviewing, and revising the resident’s service plan, 2. To remain in the same room in the facility, except that a current resident transferring into an extended congregate care
services may be required to move to the part of the facility licensed for extended congregate care, if only part of the facility is so licensed,
3. To select among social and leisure activities, 4. To participate in activities in the community. At a minimum the facility must arrange transportation to such activities if
requested by the resident; and, 5. To provide input with respect to the adoption and amendment of facility policies and procedures. (3) STAFFING REQUIREMENTS. The following staffing requirements apply for extended congregate care services: (a) Supervision by an administrator who has a minimum of two years of managerial, nursing, social work, therapeutic
recreation, or counseling experience in a residential, long-term care, or acute care setting or agency serving elderly or disabled persons. If an administrator appoints a manager as the supervisor of an extended congregate care facility, both the administrator and manager must satisfy the requirements of subsection 59A-36.010(1), F.A.C.
1. A baccalaureate degree may be substituted for one year of the required experience.

2. A nursing home administrator licensed under chapter 468, F.S., is qualified under this paragraph. (b) Provide staff or contract the services of a nurse who must be available to provide nursing services, participate in the
development of resident service plans, and perform monthly nursing assessments for extended congregate care residents. (c) Provide enough qualified staff to meet the needs of extended congregate care residents in accordance with rule 59A-36.010,
F.A.C., and to provide the services established in each resident’s service plan. (d) Ensure that adequate staff is awake during all hours to meet the scheduled and unscheduled needs of residents. (e) Immediately provide additional or appropriately qualified staff, when the agency determines that service plans are not being
followed or that residents’ needs are not being met because insufficient staffing, in accordance with the staffing standards established in rule 59A-36.010, F.A.C.
(f) Ensure and document that staff receive extended congregate care training as required in rule 59A-36.011, F.A.C. (4) ADMISSION AND CONTINUED RESIDENCY. (a) An individual must meet the following minimum criteria in order to receive extended congregate care services: 1. Be at least 18 years of age; 2. Be free from signs and symptoms of a communicable disease that is likely to be transmitted to other residents or staff;
however, an individual who has human immunodeficiency virus (HIV) infection may be admitted to a facility, provided that he or she would otherwise be eligible for admission according to this rule;
3. Be able to transfer, with assistance if necessary. The assistance of more than one individual is permitted; 4. Not be a danger to self or others as determined by a health care provider or mental health practitioner licensed under chapter
490 or 491, F.S.; 5. Not be bedridden; 6. Not have any stage 3 or 4 pressure sores; 7. Not require any of the following nursing services: a. Artificial airway management of any kind except that of continuous positive airway pressure may be provided through the use
of a CPAP or bipap machine, b. Nasogastric tube feeding, c. Monitoring of blood gases, d. Management of post-surgical drainage tubes or wound vacuums, e. Skilled rehabilitative services as described in rule 59G-4.290, F.A.C., or f. Treatment of a surgical incision, unless the surgical incision and the condition that caused it have been stabilized and a plan of
care developed. The plan of care must be maintained in the resident’s record at the facility. 8. Not require 24-hour nursing supervision; and, 9. Have been determined to be appropriate for admission to the facility by the facility administrator or manager. The
administrator or manager must base his or her decision on: a. An assessment of the strengths, needs, and preferences of the individual, the health assessment required by subsection (6) of
this rule, and the preliminary service plan developed in subsection (7), b. The facility’s residency criteria, and services offered or arranged for by the facility to meet resident needs; and, c. The ability of the facility to meet the uniform fire safety standards for assisted living facilities established in rule chapter
69A-40, F.A.C. (b) Criteria for continued residency in an extended congregate care services must be the same as the criteria for admission,
except as specified below. 1. A resident may be bedridden for up to 14 consecutive days. 2. A terminally ill resident who no longer meets the criteria for continued residency may continue to reside in the facility if the
following conditions are met: a. The resident qualifies for, is admitted to, and consents to the services of a licensed hospice that coordinates and ensures the
provision of any additional care and services that may be needed, b. Continued residency is agreeable to the resident and the facility, c. An interdisciplinary care plan, which specifies the services being provided by hospice and those being provided by the
facility, is developed and implemented by a licensed hospice in consultation with the facility; and, d. Documentation of the requirements of subparagraph (5)(b)2., is maintained in the resident’s file.

3. The extended congregate care administrator or manager is responsible for monitoring the appropriateness of continued residency of a resident in extended congregate care services at all times.
4. A hospice resident that meets the qualifications of continued residency pursuant to this rule may only receive services from the assisted living facility’s staff within the scope of the facility’s license.
5. Staff may provide any nursing service permitted under the facility’s license and total help with the activities of daily living for residents admitted to hospice. Staff may not exceed the scope of their professional licensure or training in any licensed assisted living facility.
(5) HEALTH ASSESSMENT. Before receiving extended congregate care services, all persons. including residents transferring within the same facility to that portion of the facility licensed to provide extended congregate care services, must be examined by a health care provider pursuant to rule 59A-36.006, F.A.C. A health assessment conducted no more than 60 days before receiving extended congregate care services meets this requirement. Once receiving services, a new health assessment must be obtained at least annually.
(6) SERVICE PLANS. (a) Before receiving services, the extended congregate care administrator or manager must develop a preliminary service plan
that includes an assessment of whether the resident meets the facility’s residency criteria, an appraisal of the resident’s unique physical, psychological and social needs and preferences, and an evaluation of the facility’s ability to meet the resident’s needs.
(b) Within 14 days of receiving services, the extended congregate care administrator or manager must coordinate the development of a written service plan that takes into account the resident’s health assessment obtained pursuant to subsection (6); the resident’s unique physical, psychological and social needs and preferences; and how the facility will meet the resident’s needs including the following if required:
1. Health monitoring, 2. Assistance with personal care services, 3. Nursing services, 4. Supervision, 5. Special diets, 6. Ancillary services, 7. The provision of other services such as transportation and supportive services; and, 8. The manner of service provision, and identification of service providers, including family and friends, in keeping with
resident preferences. (c) Pursuant to the definitions of “shared responsibility” and “managed risk” as provided in section 429.02, F.S., the service
plan must be developed and agreed upon by the resident or the resident’s representative or designee, surrogate, guardian, or attorney-in-fact, and must reflect the responsibility and right of the resident to consider options and assume risks when making choices pertaining to the resident’s service needs and preferences.
(d) The service plan must be reviewed and updated quarterly to reflect any changes in the manner of service provision, accommodate any changes in the resident’s physical or mental status, or pursuant to recommendations for modifications in the resident’s care as documented in the nursing assessment.
(7) EXTENDED CONGREGATE CARE SERVICES. All services must be provided in the least restrictive environment, and in a manner that respects the resident’s independence, privacy, and dignity.
(a) A facility providing extended congregate care services may provide supportive services including social service needs, counseling, emotional support, networking, assistance with securing social and leisure services, shopping service, escort service, companionship, family support, information and referral, assistance in developing and implementing self-directed activities, and volunteer services. Family or friends must be encouraged to provide supportive services for residents. The facility must provide training for family or friends to enable them to provide supportive services in accordance with the resident’s service plan.
(b) A facility providing extended congregate care services must make available the following additional services if required by the resident’s service plan:
1. Total help with bathing, dressing, grooming and toileting, 2. Nursing assessments conducted more frequently than monthly, 3. Measurement and recording of basic vital functions and weight, 4. Dietary management including provision of special diets, monitoring nutrition, and observing the resident’s food and fluid

intake and output, 5. Assistance with self-administered medications, or the administration of medications and treatments pursuant to a health care
provider’s order. If the individual needs assistance with self-administration the facility must inform the resident of the qualifications of staff who will be providing this assistance, and if unlicensed persons will be providing such assistance, obtain the resident’s or the resident’s surrogate, guardian, or attorney-in-fact’s informed written consent to provide such assistance as required in section 429.256, F.S.,
6. Supervision of residents with dementia and cognitive impairments, 7. Health education and counseling and the implementation of health-promoting programs and preventive regimes, 8. Provision or arrangement for rehabilitative services; and, 9. Provision of escort services to health-related appointments. (c) Nursing staff providing extended congregate care services may provide any nursing service permitted within the scope of
their license consistent with the residency requirements of this rule and the facility’s written policies and procedures, provided the nursing services are:
1. Authorized by a health care provider’s order and pursuant to a plan of care, 2. Medically necessary and appropriate for treatment of the resident’s condition, 3. In accordance with the prevailing standard of practice in the nursing community, 4. A service that can be safely, effectively, and efficiently provided in the facility, 5. Recorded in nursing progress notes; and, 6. In accordance with the resident’s service plan. (d) At least monthly, or more frequently if required by the resident’s service plan, a nursing assessment of the resident must be
conducted. (8) RECORDS. In addition to the records required in rule 59A-36.015, F.A.C., a facility providing extended congregate care
services must maintain the following: (a) The service plans for each resident receiving extended congregate care services; (b) The nursing progress notes for each resident receiving nursing services; (c) Nursing assessments; and, (d) The facility’s extended congregate care policies and procedures. (9) DISCHARGE. If the facility and the resident are unable to agree on a service plan, the facility is unable to meet the
resident’s needs as identified in the service plan, or the resident no longer meets the criteria for continued residency, the resident must be discharged or relocated in accordance with sections 429.26 and 429.28, F.S.
Rulemaking Authority 429.07, 429.41 FS. Law Implemented 429.07, 429.255, 429.26, 429.28, 429.41 FS. History–New 9-30-92, Formerly 10A-5.030, Amended 10-30-95, 6-2-96, 4-20-98, 11-2-98, 10-17-99, 7-30-06, 4-17-14, 5-10-18, Formerly 58A-5.030, 7-1-19.
59A-36.022 Limited Nursing Services. Any facility intending to provide limited nursing services must obtain a license from the agency.
(1) NURSING SERVICES. In addition to any nursing service permitted under a standard license pursuant to section 429.255, F.S., a facility with a limited nursing services license may provide nursing care to residents who do not require 24-hour nursing supervision and to residents who do require 24-hour nursing care and are enrolled in hospice.
(2) RESIDENT CARE STANDARDS. (a) A resident receiving limited nursing services in a facility holding only a standard and limited nursing services license must
meet the admission and continued residency criteria specified in rule 59A-36.006, F.A.C. (b) In accordance with rule 59A-36.010, F.A.C., the facility must employ sufficient and qualified staff to meet the needs of
residents requiring limited nursing services based on the number of such residents and the type of nursing service to be provided. (c) Limited nursing services may only be provided as authorized by a health care provider’s order, a copy of which must be
maintained in the resident’s file. (d) Facilities licensed to provide limited nursing services must employ or contract with a nurse(s) who must be available to
provide such services as needed by residents. The facility’s employed or contracted nurse must coordinate with third party nursing services providers to ensure resident care is provided in a safe and consistent manner. The facility must maintain documentation of the qualifications of nurses providing limited nursing services in the facility’s personnel files.

(e) The facility must ensure that nursing services are conducted and supervised in accordance with chapter 464, F.S., and the prevailing standard of practice in the nursing community.
(3) RECORDS. (a) A record of all residents receiving limited nursing services and the type of services provided must be maintained at the
facility. (b) Nursing progress notes must be maintained for each resident who receives limited nursing services. (c) A nursing assessment conducted at least monthly must be maintained on each resident who receives a limited nursing
service.
Rulemaking Authority 429.41 FS. Law Implemented 429.07, 429.255, 429.26, 429.41 FS. History–New 9-30-92, Formerly 10A-5.031, Amended 10-30-95, 10-17-99, 7-30-06, 3-13-14, 5-10-18, Formerly 58A-5.031, 7-1-19.
59A-36.023 Administrative Enforcement. Facility staff must cooperate with agency personnel during surveys, complaint investigations, monitoring visits, license application and renewal procedures and other activities necessary to ensure compliance with Part II, Chapter 408, F.S., Part I, Chapter 429, F.S., Rule Chapter 59A-35, F.A.C., and this rule chapter.
(1) Abbreviated Survey. (a) An applicant for license renewal who does not have any class I or class II violations or uncorrected class III violations,
confirmed long-term care ombudsman program complaints, or confirmed licensing complaints within the two licensing periods immediately preceding the current renewal date, is eligible for an abbreviated biennial survey by the agency. For the purpose of this rule, a confirmed long-term care ombudsman program complaint is a complaint that is verified and referred to a regulatory agency for further action. Facilities that do not have two survey reports on file with the agency under current ownership are not eligible for an abbreviated inspection. Upon arrival at the facility, the agency must inform the facility that it is eligible for an abbreviated survey, and that an abbreviated survey will be conducted.
(b) Compliance with key quality of care standards described in the following statutes and rules will be used by the agency during its abbreviated survey of eligible facilities:
1. Section 429.26, F.S., and Rule 58A-5.0181, F.A.C., relating to residency criteria; 2. Section 429.27, F.S., and Rule 58A-5.021, F.A.C., relating to proper management of resident funds and property; 3. Section 429.28, F.S., and Rule 58A-5.0182, F.A.C., relating to respect for resident rights; 4. Section 429.41, F.S., and Rule 58A-5.0182, F.A.C., relating to the provision of supervision, assistance with the activities of
daily living, and arrangement for appointments and transportation to appointments; 5. Section 429.256, F.S., and Rule 58A-5.0185, F.A.C., relating to assistance with or administration of medications; 6. Section 429.41, F.S., and Rule 58A-5.019, F.A.C., relating to the provision of sufficient staffing to meet resident needs; 7. Section 429.41, F.S., and Rule 58A-5.020, F.A.C., relating to minimum dietary requirements and proper food hygiene; 8. Section 429.075, F.S., and Rule 58A-5.029, F.A.C., relating to mental health residents’ community support living plan; 9. Section 429.07, F.S., and Rule 58A-5.030, F.A.C., relating to meeting the environmental standards and residency criteria in a
facility with an extended congregate care license; and 10. Section 429.07, F.S., and Rule 58A-5.031, F.A.C., relating to the provision of care and staffing in a facility with a limited
nursing services license. (c) The agency will expand the abbreviated survey or conduct a full survey if violations which threaten or potentially threaten
the health, safety, or welfare of residents are identified during the abbreviated survey. The facility must be informed when a full survey will be conducted. If one or more of the following serious problems are identified during an abbreviated survey, a full biennial survey will be immediately conducted:
1. Violations of Rule Chapter 69A-40, F.A.C., relating to firesafety, that threaten the life or safety of a resident; 2. Violations relating to staffing standards or resident care standards that adversely affect the health, safety, or welfare of a
resident; 3. Violations relating to facility staff rendering services for which the facility is not licensed; or 4. Violations relating to facility medication practices that are a threat to the health, safety, or welfare of a resident. (2) Survey Deficiency. (a) Before or in conjunction with a notice of violation issued pursuant to Part II, Chapter 408, F.S., and Section 429.19, F.S., the

agency shall issue a statement of deficiency for class I, II, III, and IV violations which are observed by agency personnel during any inspection of the facility. The deficiency statement must be issued within 10 working days of the agency’s inspection and must include:
1. A description of the deficiency; 2. A citation to the statute or rule violated; and 3. A time frame for the correction of the deficiency. (b) Additional time may be granted to correct specific deficiencies if a written request is received by the agency before the
expiration of the time frame included in the agency’s statement. (3) Employment of A Consultant. (a) Medication Deficiencies. 1. If a class I, class II, or uncorrected class III deficiency directly relating to facility medication practices as established in Rule
58A-5.0185, F.A.C., is documented by agency personnel pursuant to an inspection of the facility, the agency must notify the facility in writing that the facility must employ or contract the services of a pharmacist licensed pursuant to Section 465.0125, F.S., or registered nurse as determined by the agency.
2. After developing and imprementing a corrective action plan in compliance with Section 429.42(2), F.S., the initial on-site consultant visit must take place within 7 working days of the notice of a class I or class II deficiency and within 14 working days of the notice of an uncorrected class III deficiency. The facility must have available for review by the agency a copy of the license of the consultant pharmacist or registered nurse and the consultant’s signed and dated review of the corrective action plan no later than 10 working days subsequent to the initial on-site consultant visit.
3. The facility must provide the agency with, at a minimum, quarterly on-site corrective action plan updates until the agency determines after written notification by the consultant and facility administrator that deficiencies are corrected and staff has been trained to ensure that proper medication standards are followed and that such consultant services are no longer required. The agency must provide the facility with written notification of such determination.
(b) Dietary Deficiencies. 1. If a class I, class II, or uncorrected class III deficiency directly related to dietary standards as established in Rule 58A-5.020,
F.A.C., is documented by agency pursuant to an inspection of the facility, the agency must notify the facility in writing that the facility must employ or contract the services of a registered or licensed dietitian, or a licensed nutritionist.
2. The initial on-site consultant visit must take place within seven working days of the notice of a class I or II deficiency or within 14 working days of the notice of an uncorrected class III deficiency. The facility must have available for review by the agency a copy of the license or registration of the consultant dietitian or nutritionist and the consultant’s signed and dated review of the facility’s corrective action plan, if a plan is required by the agency, no later than 10 working days after the initial on-site consultant visit.
3. If a corrective action plan is required, the facility must provide the agency with, at a minimum, quarterly on-site corrective action plan updates until the agency determines after written notification by the dietary consultant and facility administrator, that deficiencies are corrected and staff has been trained to ensure that proper dietary standards are followed and consultant services are no longer required. The agency must provide the facility with written notification of such determination.
Rulemaking Authority 429.41, 429.42 FS. Law Implemented 429.19, 429.34, 429.41, 429.42 FS. History–New 9-30-92, Formerly 10A-5.033, Amended 10-30-95, 10-17-99, 1-9-02, 7-30-06, 4-15-10, 3-13-14, Formerly 58A-5.033, 7-1-19.
59A-36.024 Waivers. The agency, in consultation with the department, may waive rules promulgated pursuant to part I, chapter 429, F.S., if the waiver request meets the conditions set forth in section 429.41(4), F.S., and demonstrates and evaluates innovative or cost-effective congregate care alternatives which will enable individuals to age in place.
(1) Application Process. (a) Licensed assisted living facilities proposing a waiver under this statute must submit the request in writing. All requests must
include the facility name and address, license number, administrator’s name and contact information for the requestor, or its attorney. Petitions for waiver of rules other than for the objectives detailed in section 429.41(4), F.S., including emergency waivers, will not be considered under this section but should follow the petition for waiver provisions of section 120.542, F.S., and rule chapter 28-104, Variance or Waiver, F.A.C.

(b) The written request must address the elements required in section 429.41(4), F.S. In addition, the following information must be included in order to demonstrate how a waiver of the stated rule will permit development of a concept that will achieve the purpose of the underlying statute:
1. The rule or rules for which the waiver is requested. 2. The licensee’s anticipated date or dates for implementation of the concept. 3. If applying based on cost-effectiveness or cost-savings, a cost-benefit analysis of the proposed alternative to both residents or
potential residents as well as facility operations. 4. An analysis of the impact the alternative will have on the relevant local community, including any barriers such as zoning or
use issues, which may need resolution prior to implementation. 5. Specific performance measures with an annual projection of objectives and goals to be achieved broken into quarterly
increments or an annual projection of outcome measures, if the concept will be implemented in less than 90 days. 6. If applying based on cost-effectiveness or cost-savings, an annual budget projection for the proposed alternative broken into
quarterly increments. (c) A waiver can be requested at the time of the initial license application, relicensure, or any time during the licensure period. (d) Waiver requests must be submitted to the Agency for Health Care Administration, Assisted Living Unit, 2727 Mahan Drive,
Mail Stop 30, Tallahassee, Florida 32308-5403. (2) In accordance with section 120.542(6), F.S., the agency shall post notice of the request within fifteen (15) days of receipt of
the request. The agency shall make any requests for additional information within 30 days of receipt of the request. If additional information is provided, the agency may request clarification of only that information no later than 30 days following receipt of the information. The agency shall process the waiver request pursuant to the time frame referenced in section 120.542(8), F.S.
(3) The agency, in consultation with the department, will evaluate all requests in light of the likelihood the concept, as described in detail, will achieve the underlying statutory objectives of innovative or cost effective congregate care alternatives to enable individuals to age in place, as provided in section 429.41(4), F.S. Waivers may be granted only so long as there is reasonable assurance that the health, safety or welfare of residents will not be endangered by the waiver.
(4) The agency shall grant or deny the request for waiver and enter an order summarizing the facts it relied on and reasons supporting its decision. The agency must provide notice of its order as described in section 120.542(8), F.S. The requestor shall be advised that a denial of the request may be reviewed as provided in subsection (5) of this rule.
(5) Report of Findings. A facility that has been granted a waiver must submit an annual report within 12 months of the order granting the waiver as specified in section 429.41(4), F.S. If the report is not submitted as required, the agency may revoke the waiver.
(a) The agency will review the report of findings to determine whether the waiver shall be renewed or revoked. The agency shall make the determination based on whether the facility has met the requirements outlined in subparagraph (1)(b) of this rule. The agency shall enter an order providing the general basis for making its decision and notify the licensee of its opportunity to seek review of a revocation in accordance with sections 120.569 and 120.57, F.S. and rule 28-106.111, F.A.C.
(b) The agency may also consider other material which is available relative to this review. (c) A waiver is effective unless revoked by the agency or superseded by statutory or regulatory change. (d) In reviewing the report of findings, the agency, in consultation with the department, shall assess whether statutory or
regulatory changes should be pursued to enable other facilities to adopt the same practices.
Rulemaking Authority 429.41 FS. Law Implemented 120.542, 429.41 FS. History–New 9-30-92, Formerly 10A-5.035, Amended 10-30-95, 7-1-08, 4-17-14, Formerly 58A-5.035, 7-1-19.
59A-36.025 Emergency Environmental Control for Assisted Living Facilities. (1) DETAILED EMERGENCY ENVIRONMENTAL CONTROL PLAN. Each assisted living facility shall prepare a detailed
plan (“plan”) to serve as a supplement to its Comprehensive Emergency Management Plan, to address emergency environmental control in the event of the loss of primary electrical power in that assisted living facility which includes the following information:
(a) The acquisition of a sufficient alternate power source such as a generator(s), maintained at the assisted living facility, to ensure that current licensees of assisted living facilities will be equipped to ensure ambient air temperatures will be maintained at or below 81 degrees Fahrenheit for a minimum of ninety-six (96) hours in the event of the loss of primary electrical power.
1. The required temperature must be maintained in an area or areas, determined by the assisted living facility, of sufficient size

to maintain residents safely at all times and that is appropriate for resident care needs and life safety requirements. For planning purposes, no less than twenty (20) net square feet per resident must be provided. The assisted living facility may use eighty percent (80%) of its licensed bed capacity as the number of residents to be used in the calculation to determine the required square footage. This may include areas that are less than the entire assisted living facility if the assisted living facility’s comprehensive emergency management plan includes allowing a resident to congregate when he or she desires in portions of the building where temperatures will be maintained and includes procedures for monitoring residents for signs of heat related injury as required by this rule. This rule does not prohibit a facility from acting as a receiving provider for evacuees when the conditions stated in section 408.821, F.S. and subsection 59A-36.019(5), F.A.C., are met. The plan shall include information regarding the area(s) within the assisted living facility where the required temperature will be maintained.
2. The alternate power source and fuel supply shall be located in an area(s) in accordance with local zoning and the Florida Building Code.
3. Each assisted living facility is unique in size; the types of care provided; the physical and mental capabilities and needs of residents; the type, frequency, and amount of services and care offered; and staffing characteristics. Accordingly, this rule does not limit the types of systems or equipment that may be used to achieve ambient temperatures at or below 81 degrees Fahrenheit for a minimum of ninety-six (96) hours in the event of the loss of primary electrical power. The plan shall include information regarding the systems and equipment that will be used by the assisted living facility and the fuel required to operate the systems and equipment.
a. An assisted living facility in an evacuation zone pursuant to chapter 252, F, S. must maintain an alternative power source and fuel as required by this subsection at all times when the assisted living facility is occupied but is permitted to utilize a mobile generator(s) to enable portability if evacuation is necessary.
b. Assisted living facilities located on a single campus with other facilities under common ownership, may share fuel, alternative power resources, and resident space available on the campus if such resources are sufficient to support the requirements of each facility’s residents, as specified in this rule. Details regarding how resources will be shared and any necessary movement of residents must be clearly described in the emergency power plan.
c. A multistory facility, whose comprehensive emergency management plan is to move residents to a higher floor during a flood or surge event, must place its alternative power source and all necessary additional equipment so it can safely operate in a location protected from flooding or storm surge damage.
(b) The acquisition of sufficient fuel, and safe maintenance of that fuel at the facility, to ensure that in the event of the loss of primary electrical power there is sufficient fuel available for the alternate power source to maintain ambient temperatures at or below 81 degrees Fahrenheit for a minimum of ninety-six (96) hours after the loss of primary electrical power during a declared state of emergency. The plan must include information regarding fuel source and fuel storage.
1. Facilities must store minimum amounts of fuel onsite as follows: a. A facility with a licensed capacity of 16 beds or less must store 48 hours of fuel onsite. b. A facility with a licensed capacity of 17 or more beds must store 72 hours of fuel onsite. 2. An assisted living facility located in an area in a declared state of emergency area pursuant to section 252.36, F.S. that may
impact primary power delivery must secure ninety-six (96) hours of fuel. The assisted living facility may utilize portable fuel storage containers for the remaining fuel necessary for ninety-six (96) hours during the period of a declared state of emergency.
3. Piped natural gas is an allowable fuel source and meets the onsite fuel supply requirements under this rule. 4. If local ordinances or other regulations limit the amount of onsite fuel storage for the assisted living facility’s location, then
the assisted living facility must develop a plan that includes maximum onsite fuel storage allowable by the ordinance or regulation and a reliable method to obtain the maximum additional fuel at least 24 hours prior to depletion of onsite fuel.
(c) The acquisition of services necessary to maintain, and test the equipment and its functions to ensure the safe and sufficient operation of the alternate power source maintained at the assisted living facility.
(d) The acquisition and maintenance of a carbon monoxide alarm. (2) SUBMISSION OF THE PLAN. (a) Each assisted living facility licensed prior to the effective date of this rule shall submit its plan to the local emergency
management agency for review within 30 days of the effective date of this rule. Assisted living facility plans previously submitted and approved pursuant to emergency rule 58AER17-1 will require resubmission only if changes are made to the plan.
(b) Each new assisted living facility shall submit the plan required under this rule prior to obtaining a license.

(c) Each existing assisted living facility that undergoes any additions, modifications, alterations, refurbishment, renovations or reconstruction that require modification of its systems or equipment affecting the facility’s compliance with this rule shall amend its plan and submit it to the local emergency management agency for review and approval.
(3) APPROVED PLANS. (a) Each assisted living facility must maintain a copy of its approved plan in a manner that makes the plan readily available at
the licensee’s physical address for review by a legally authorized entity. If the plan is maintained in an electronic format, assisted living facility staff must be readily available to access and produce the plan. For purposes of this section, “readily available” means the ability to immediately produce the plan, either in electronic or paper format, upon request.
(b) Within two (2) business days of the approval of the plan from the local emergency management agency, the assisted living facility shall submit in writing proof of the approval to the Agency for Health Care Administration.
(c) The assisted living facility shall submit a consumer-friendly summary of the emergency power plan to the Agency. The Agency shall post the summary and notice of the approval and implementation of the assisted living facility emergency power plans on its website within ten (10) business days of the plan's approval by the local emergency management agency and update within ten (10) business days of implementation.
(4) IMPLEMENTATION OF THE PLAN. (a) Each assisted living facility licensed prior to the effective date of this rule shall, no later than June 1, 2018, have
implemented the plan required under this rule. (b) The Agency shall allow an extension up to January 1, 2019 to providers in compliance with paragraph (c) below and who
can show delays caused by necessary construction, delivery of ordered equipment, zoning or other regulatory approval processes. Assisted living facilities shall notify the Agency that they will utilize the extension and keep the Agency apprised of progress on a quarterly basis to ensure there are no unnecessary delays. If an assisted living facility can show in its quarterly progress reports that unavoidable delays caused by necessary construction, delivery of ordered equipment, zoning or other regulatory approval processes will occur beyond the initial extension date, the assisted living facility may request a waiver pursuant to section 120.542, F.S.
(c) During the extension period, an assisted living facility must make arrangements pending full implementation of its plan that provides the residents with an area or areas to congregate that meets the safe indoor air temperature requirements of subsection (1) (a) for a minimum of ninety-six (96) hours.
1. An assisted living facility not located in an evacuation zone must either have an alternative power source onsite or have a contract in place for delivery of an alternative power source and fuel when requested. Within twenty-four (24) hours of the issuance of a state of emergency for an event that may impact primary power delivery for the area of the assisted living facility, it must have the alternative power source and no less than ninety-six (96) hours of fuel stored onsite.
2. An assisted living facility located in an evacuation zone pursuant to chapter 252, F.S. must either: a. Fully and safely evacuate its residents prior to the arrival of the event; or b. Have an alternative power source and no less than ninety-six (96) hours of fuel stored onsite, within twenty-four (24) hours of
the issuance of a state of emergency for the area of the assisted living facility. (d) Each new assisted living facility shall implement the plan required under this rule prior to obtaining a license. (e) Existing assisted living facilities that undergo any additions, modifications, alterations, refurbishment, renovations or
reconstruction that require modification of the systems or equipment affecting the assisted living facility’s compliance with this rule shall implement its amended plan concurrent with any such additions, modifications, alterations, refurbishment, renovations or reconstruction.
(f) The Agency for Health Care Administration may request cooperation from the State Fire Marshal to conduct inspections to ensure implementation of the plan in compliance with this rule.
(5) POLICIES AND PROCEDURES. (a) Each assisted living facility shall develop and implement written policies and procedures to ensure that the assisted living
facility can effectively and immediately activate, operate and maintain the alternate power source and any fuel required for the operation of the alternate power source. The procedures shall ensure that residents do not experience complications from fluctuations in ambient air temperatures inside the facility. Procedures must address the care of residents occupying the facility during a declared state of emergency, specifically, a description of the methods to be used to mitigate the potential for heat related injury including:
1. The use of cooling devices and equipment; 2. The use of refrigeration and freezers to produce ice and appropriate temperatures for the maintenance of medicines requiring

refrigeration; 3. Wellness checks by assisted living facility staff to monitor for signs of dehydration and heat injury; and 4. A provision for obtaining medical intervention from emergency services for residents whose life safety is in jeopardy. (b) Each assisted living facility shall maintain the written policies and procedures in a manner that makes them readily available
at the licensee’s physical address for review by a legally authorized entity. If the policies and procedures are maintained in an electronic format, assisted living facility staff must be readily available to access the policies and procedures and produce the requested information. For purposes of this section, “readily available” means the ability to immediately produce the policies and procedures, either in electronic or paper format, upon request.
(c) The written policies and procedures must be readily available for inspection by each resident; each resident’s legal representative, designee, surrogate, guardian, attorney in fact, or case manager; each resident’s estate; and such additional parties as authorized in writing or by law.
(6) REVOCATION OF LICENSE, FINES OR SANCTIONS. For a violation of any part of this rule, the Agency for Health Care Administration may seek any remedy authorized by chapter 429, part I, or chapter 408, part II, F.S., including, but not limited to, license revocation, license suspension, and the imposition of administrative fines.
(7) COMPREHENSIVE EMERGENCY MANAGEMENT PLAN. (a) Assisted living facilities whose comprehensive emergency management plan is to evacuate must comply with this rule. (b) Each facility whose plan has been approved shall submit the plan as an addendum with any future submissions for approval
of its comprehensive emergency management plan. (8) NOTIFICATION. (a) Within five (5) business days, each assisted living facility must notify in writing, unless permission for electronic
communication has been granted, each resident and the resident’s legal representative: 1. Upon submission of the plan to the local emergency management agency that the plan has been submitted for review and
approval; 2. Upon final implementation of the plan by the assisted living facility. (b) Each assisted living facility must maintain a copy of each notification set forth in paragraph (a) above in a manner that
makes each notification readily available at the licensee’s physical address for review by a legally authorized entity. If the notifications are maintained in an electronic format, facility staff must be readily available to access and produce the notifications. For purposes of this section, “readily available” means the ability to immediately produce the notifications, either in electronic or paper format, upon request.
Rulemaking Authority 429.41, FS. Law Implemented 429.19, 429.41, FS. History–New 3-26-18, Formerly 58A-5.036, 7-1-19.
59A-36.027 ALF Core Training Provider Qualifications. (1) PRIMARY REQUIREMENTS. In order to register as an assisted living facility core training provider (hereafter referred to
as “core training provider,” “training provider,” or “provider”), all applicants must meet the requirements outlined in section 429.52(10), F.S. The requirements are as follows:
(a) Completion of the minimum core training requirements developed by the department pursuant to section 429.52(9), F.S., and rule 59A-36.028, F.A.C.;
(b) Successful passage of the competency test, which requires a minimum score of 75%; and, (c) Compliance with the minimum of 12 contact hours of continuing education in topics related to assisted living every 2 years
pursuant to section 429.52(5), F.S., and paragraph 58A-5.0191(1)(c), F.A.C. (2) ADDITIONAL REQUIREMENTS. In addition to meeting the 3 primary requirements set forth in subsection (1), of this
rule, applicants must meet one of the requirements outlined in section 429.52(11), F.S., or one of the requirements established in this subsection. The requirements are as follows:
(a) A minimum of 5 years of employment with the Agency for Health Care Administration (AHCA), or formerly the Department of Health and Rehabilitative Services, as a surveyor of assisted living facilities; or
(b) A minimum of 5 years of employment in a professional position in the AHCA Assisted Living Unit; or (c) A minimum of 5 years of employment as an educator or staff trainer for persons working in an ALF or other long-term care
(LTC) settings; or (d) A minimum of 5 years of employment as an assisted living facility core trainer, which was not directly associated with the

department; or (e) A minimum of a 4-year degree from an accredited college or university in areas of healthcare, gerontology, social work,
education or human services; and a minimum of 3 years experience as an educator or staff trainer for persons working in an ALF or other LTC settings after core certification.
Rulemaking Authority 429.52 FS. Law Implemented 429.52 FS. History–New 6-15-09, Formerly 58T-1.203, 7-1-19.
59A-36.028 ALF Minimum Core Training Curriculum Requirements. (1) CURRICULUM REQUIREMENTS. An approved core training provider must conduct core training using the curriculum
outlined in DOEA Form ALFCT-001, Assisted Living Facility Minimum Core Training Curriculum, June, 2009, which is incorporated by reference in this rule. The curriculum is available from the Department of Elder Affairs, Elder Housing Unit, 4040 Esplanade Way, Tallahassee, Florida 32399-7000 or the department’s website at: http://elderaffairs.state.fl.us/english/ruleforms/ALFCT-001.doc.
(2) MONITORING. The department reserves the right to do the following: (a) Attend and monitor core training courses; (b) Review provider records and course materials pursuant to this rule; and, (c) Conduct on-site monitoring, follow-up monitoring, and require implementation of a corrective action plan if the provider
does not adhere to the approved curriculum.
Rulemaking Authority 429.52 FS. Law Implemented 429.52 FS. History–New 6-15-09, Formerly 58T-1.205, 7-1-19.
59A-36.029 ALF Core Training Provider Initial Registration Process. (1) REGISTRATION PROCESS. (a) Before core training can be conducted, an applicant must meet the training provider qualifications outlined in section
429.52(10), F.S., and rule 59A-36.027, F.A.C. Additionally, an applicant must register with, and obtain from, the department a unique provider registration number as set forth in this subsection.
(b) An applicant must complete DOEA Form ALFCT-002, Application for Assisted Living Facility (ALF) Core Training Provider Registration, June, 2009. The form is hereby incorporated by reference and may be obtained from the Department of Elder Affairs, Elder Housing Unit, 4040 Esplanade Way, Tallahassee, Florida 32399-7000 or the department’s website at: http://elderaffairs.state.fl.us/english/ruleforms/ALFCT-002.doc.
(2) APPROVAL PROCESS. Within 30 calendar days after receiving a core training provider application, the department must submit written notification approving or denying the application, or requesting supplemental information or clarification.
(a) If the application is approved, the department must include a unique provider registration number in the notice. (b) If the application is denied, the department must provide the reason or reasons for denial in the notice. (c) If the application is determined to require supplemental information or clarification, the department must state the
supplemental information or clarification that is being requested. 1. If the department does not receive the requested information within 30 calendar days of the request, the application will be
deemed incomplete and closed. 2. If the department receives the requested information within 30 calendar days of the request, the department must process the
training provider application within 30 calendar days after all required information is received.
Rulemaking Authority 429.52 FS. Law Implemented 429.52 FS. History–New 6-15-09, Formerly 58T-1.207, 7-1-19.
59A-36.030 Process for Maintaining ALF Core Training Provider Registration. (1) MAINTAINING ALF CORE TRAINING PROVIDER REGISTRATION. (a) After receiving the initial core training provider registration, the approved provider must re-register with the department
every 2 years by submitting documentation of his or her compliance with the continuing education requirement as specified in section 429.52(5), F.S., and this rule.
(b) The provider must submit the documentation to the address referenced on DOEA Form ALFCT-001. It must be submitted no later than 30 calendar days after each two-year continuing education cycle. The 2-year cycle begins on the date of the initial training provider registration. Documentation must include the following:

1. Title of the training program; 2. Subject matter of the training program; 3. The training program agenda including topics discussed; 4. The core training provider’s name and registration number; 5. Date(s) of participation; 6. Number of hours of the training program; and 7. The continuing education training provider’s name, signature, credentials, and professional license number, if applicable. (2) APPROVAL PROCESS. (a) Within 30 calendar days after receiving the required continuing education documentation, the department must notify the
provider in writing that the continuing education requirement: 1. Has been met; or 2. Has not been met and the reasons why; or 3. Has omissions or additional information is requested. a. If the department does not receive the omitted or additional information within 30 calendar days of the request, the provider’s
registration shall be cancelled. The department must provide written notification of its decision, including the reason for the cancellation, no later than 30 calendar days after the deadline for the request for the omitted or additional information.
b. If the department receives the omitted or additional information as requested within the 30 calendar day time period, the department must process the core training provider’s registration within 30 calendar days after all required information is received. The department must provide written notification to the provider of its decision.
(b) Failure to submit proof of the continuing education requirement as specified in this rule shall result in cancellation of the core training provider’s registration. The department must provide written notification of such action no later than 30 calendar days after the information was due.
(c) If the provider’s registration is cancelled under paragraphs (a) and (b) of this subsection, and the provider subsequently meets the continuing education requirement, he or she may re-apply for registration as specified in rule 59A-36.029, F.A.C., and include documentation that the continuing education requirement has been met pursuant to this rule.
Rulemaking Authority 429.52 FS. Law Implemented 429.52 FS. History–New 6-15-09, Formerly 58T-1.209, 7-1-19.
59A-36.031 Registered ALF Core Training Provider Responsibilities. The following are the responsibilities of a registered core training provider:
(1) USE OF MINIMUM CORE TRAINING CURRICULUM. A registered core training provider is responsible for the following:
(a) Conducting core training using the minimum core training curriculum required by rule 59A-36.028, F.A.C.; and (b) Ensuring that all changes in ALF statutes and rules are immediately incorporated into the contents of his or her core training
curriculum. (2) CERTIFICATES. After a trainee successfully completes core training, the approved training provider must issue a
certificate to him or her. In addition to the provider’s unique registration number, the certificate must include the information referenced in paragraph 58A-5.0191(12)(a), F.A.C. The provider’s signature and registration number shall serve as documentation that the trainee has completed the required training.
(3) RECORDS. Approved providers must maintain records of each course taught for a minimum of 5 years. Course records must include the following information:
(a) The title of the training program; (b) The agenda; (c) The curriculum and any accompanying documentation and training aids; (d) The training provider’s name and registration number; (e) The trainees’ names, dates of participation and training location; and (f) Training evaluations and roster signed by trainees. (4) COMPETENCY EXAM. (a) Approved training providers must submit the names of trainees completing core training to the testing authority within 10
calendar days after completion of the course. Names must be submitted to the following address: ALF Certification Testing,

University of South Florida, 4202 E. Fowler Avenue, EDU105, Tampa, Florida 33620. Names may be alternately submitted via email to [email protected].
(b) The testing authority shall not process any requests for the competency exam, nor sit any individual for the exam, unless proper notice is submitted by an approved training provider pursuant to paragraph (a), of this subsection.
(5) GUEST SPEAKERS. If a core training provider uses guest trainers to teach or participate in specific training modules covered in the minimum core training curriculum referenced in rule 59A-36.028, F.A.C., the core trainer is responsible to ensure that the guest speaker meets the following minimum conditions:
(a) Has expertise in the specific subject matter; and (b) Covers all components of the subject matter if he or she provides the module or portion of the module instruction.
Rulemaking Authority 429.52 FS. Law Implemented 429.52 FS. History–New 6-15-09, Formerly 58T-1.211, 7-1-19.

7. Rule Chapter
64E-11, F.A.C
.


Transferred to 59A-36 6B – 61
CHAPTER 64E-11
FOOD HYGIENE 64E-11.001 Food Hygiene General (Repealed)
64E-11.002 Definitions
64E-11.003 Food Hygiene Standards Supplies
64E-11.004 Food Protection (Repealed)
64E-11.005 Personnel (Repealed)
64E-11.006 Food Equipment and Utensils (Repealed)
64E-11.007 Sanitary Facilities and Controls (Repealed)
64E-11.008 Other Facilities and Operations (Repealed)
64E-11.009 Temporary Food Service Events (Repealed)
64E-11.010 Vending Machines (Repealed)
64E-11.011 Procedure When Infection Is Suspected
64E-11.012 Manager Certification
64E-11.013 Sanitation Certificates and Fees
64E-11.014 Mobile Food Units
64E-11.015 Afterschool Meal Program
64E-11.001 Food Hygiene General.
Rulemaking Authority 381.0072 FS. Law Implemented 381.0072 FS. History–New 1-1-77, Formerly 10D-13.21,
Amended 2-21-91, Retained here and Transferred to 7C-4.008, Amended 6-1-93, 8-28-96, Formerly 10D-13.021,
Repealed 12-29-16.
64E-11.002 Definitions.
Unless defined below, terms and phrases have the same definition provided in paragraph 1-201.10(B), Food Code,
2013 Recommendations of the United States Public Health Service, Food and Drug Administration, NTISP PB2013-
110462 (“Food Code”). The Food Code is incorporated by reference and available at
https://www.flrules.org/Gateway/reference.asp?No=Ref-09894.
(1) “Adulterated” – Food shall be considered to be adulterated:
(a) If it bears or contains any poisonous or deleterious substance which may render it injurious to health; but in
case the substance is not an added substance such food shall not be considered adulterated under this clause if the
quantity of such substance in such food does not ordinarily render it injurious to health, or
(b) If it bears or contains any added poisonous or added deleterious substance, other than one which is a pesticide
chemical in or on a raw agricultural commodity, which in or on the raw agricultural commodity has been removed to
the extent possible in good manufacturing practice, and the concentration of such residue in the processed food when
ready to eat, is not greater than the tolerance prescribed for the raw agricultural commodity, or
(c) If it consists in whole or in part of a diseased, contaminated, filthy, putrid, or decomposed substance, which
renders it unfit for consumption, or
(d) If it has been produced, prepared, packed or held under insanitary conditions whereby it may become
contaminated with filth, or whereby it may have been rendered diseased, unwholesome, or injurious to health, or
(e) If it is the product of a diseased animal, an animal which has died otherwise than by slaughter, or an animal
that has been fed the uncooked offal from a slaughter house, or from other food establishments, or

Transferred to 59A-36 6B – 62
(f) If its container is composed, in whole or in part, of any poisonous or deleterious substance which may render
the contents injurious to health.
(2) “Air gap” – The unobstructed vertical distance, through the free atmosphere, between the lowest opening from
any pipe or faucet supplying water to a tank, plumbing fixture, or other device and the flood-level rim of the receptacle,
or the lowest opening from any waste outlet pipe and the flood-level rim of the receptacle.
(3) “Air Curtain” – A mechanical device which produces a controlled plane of moving air at a minimum velocity
of 500 feet per minute across the opening protected and directed so as to prevent the entrance of flying insects and
other airborne contaminants.
(4) Approved Source – Food originated from an establishment that is under the regulatory authority of a state or
federal agency.
(5) Bars and Lounges – A facility which possesses a consumption on premises alcoholic beverage license from
the Division of Alcoholic Beverages & Tobacco; where food service is limited to:
(a) The preparation of drinks; or
(b) The service of snack foods (such as, chips, popcorn and pretzels); or
(c) The service of time/temperature control for safety foods and no preparation of time/temperature control for
safety food occurs.
(6) Catering Operation – A food service establishment operation that prepares food at one location for delivery to
and individual portion service at another location.
(7) Civic – Any organization, excluding Division of Blind Services, who offers food service to the public; and,
(a) Possesses tax exempt status under 26 U.S.C. section 501(c)(4), or
(b) Is incorporated and operates primarily to further the common good and general welfare of the people of the
community, whether for profit or not.
(8) “Commissary” – A food service establishment or any other commercial establishment where food, containers,
or supplies are stored, prepared, or packaged, or where utensils are sanitized for transit to, and sale or service at, other
locations.
(9) Community Based Residential Facility – A facility as defined in rule 64E-12.002, of the Florida Adminstrative
Code.
(10) Extensively Remodeled – Structural changes to an existing establishment which costs in excess of 50 percent
of the establishment’s assessed value, as indicated by the county property appraiser.
(11) “Fixed food establishment” – A food service establishment which operates at a specific location and is
connected to electrical, water, and sewage disposal systems.
(12) “Food preparation” – The manipulation of foods intended for human consumption by such means as washing,
slicing, peeling, chipping, shucking, scooping, and/or portioning. The term also includes those activities involving
temperature changes, combining ingredients, opening ready-to-eat food packages, or any other activity causing
physical or chemical alterations in the food.
(13) Fraternal – An organization primarily operating for social, intellectual, educational, charitable, benevolent,
moral, patriotic, or religious purposes for the benefit of its members, that offers food service to its members or the
public at their facility and possesses a charter.
(14) Frankfurter – As defined in 9 C.F.R. §319.180 (01-01-2018) herein incorporated by reference and available
at https://www.flrules.org/Gateway/reference.asp?No=Ref-09895.

Transferred to 59A-36 6B – 63
(15) “Garbage” – Food waste generated on premises that is not disposed of through the sewage disposal system.
The term also includes solid waste such as discarded containers or wrappers that are contaminated with food waste.
(16) Highly Susceptible Population – A group of persons who are more likely than other populations to experience
foodborne disease because they are immunocompromised, institutionalized older adults, preschool age children in
custodial care, or elementary school age children.
(17) Hot Water – A minimum water temperature of 100 degrees Fahrenheit or above.
(18) “Indirect waste connection” – An indirect waste connection is a liquid waste pipe that is connected with the
sewerage system through an air gap or air break.
(19) Limited Food Service Operation – Any establishment with a food service operation, so limited by the type
and quantity of foods prepared and the equipment utilized, that it poses a lesser degree of risk to the public’s health,
and, for the purpose of fees, requires less time to monitor. The term includes small seasonally operated concessions
stands at schools, regardless of the level of food preparation, provided the concession stand is only operated in
conjunction with sporting events, festivals, or similar activites, as well as satellite kitchens that dispense catered meals
and similar facilities.
(20) “Manager” – An individual who has direct authority, control or supervision over employees engaged in the
storage, preparation, display and serving of food to the public.
(21) “Misbranded” – Food shall be considered to be misbranded:
(a) If in packaged form it lacks a label containing the name and place of business of the manufacturer, packer, or
distributor; or an accurate statement of the contents, or
(b) If it is offered for sale under the name of another food, or
(c) If it purports to be or is represented as a food for which a definition and standard of identity has been prescribed
and it is not.
(22) “Mobile food unit” – Any food service unit which is self-propelled or otherwise moveable from place to
place and is self-sufficient for utilities, such as gas, water, electricity and liquid waste disposal, whose commissary is
a DOH regulated food service establishment.
(23) Perishable Food – Any food of such type or in such condition as may spoil. Food contained in hermetically
sealed containers processed by heat or other means to prevent spoilage and properly packaged, dehydrated, dried or
powdered foods so low in moisture content as to retard development of microorganisms are not considered readily
perishable.
(24) “Plumbing authority” – The local governing body, such as a county or city building inspection department
which has adopted a plumbing code and has authority to interpret, inspect, and provide enforcement of plumbing
standards.
(25) Premises – The physical food service establishment and the contiguous land or property under the control of
the manager, operator or owner of the establishment.
(26) “Product thermometer” – A thermometer, thermocouple, thermistor or other device that when inserted into
food indicates the temperature of the food. This term does not include non-product ambient temperature sensing
devices.
(27) “Reconstitute” – The recombination of dehydrated food products with potable water or other suitable liquids.
(28) “Sanitation Certificate” – A license issued by the department to operate a food service establishment.
(29) Safe Temperature – 135 degrees Fahrenheit or above or 41 degrees Fahrenheit or below.

Transferred to 59A-36 6B – 64
(30) Snack – A commercially pre-packaged, non-time/temperature control for safety ready-to-eat-food item that
is wrapped for individual consumption.
(31) “Temporary food service event” – Any event offering food service on the premises of a food service
establishment approved by the department. These events are at a fixed location for a temporary period of time not to
exceed any combination of 18 days within a calendar year and in conjunction with a single event or celebration.
(32) Theater – A facility that shows motion pictures and offers food, such as popcorn, hot dogs, soft drinks, nachos
and cheese, and pre-packaged snack items, for consumption by the admittees of such theaters.
(33) “Wholesome” – Food which is in sound condition, clean, free from adulteration and otherwise suitable for
human consumption.
Rulemaking Authority 381.0072 FS. Law Implemented 381.0072 FS. History–New 1-1-77, Amended 1-6-81, Formerly
10D-13.22, Amended 2-21-91, 5-12-92, Retained here and Transferred to 7C-4.009, Amended 6-1-93, 11-30-93, 8-
28-96, Formerly 10D-13.022, Amended 3-15-98, 7-14-03, 4-1-09, 9-26-18.
64E-11.003 Food Hygiene Standards.
(1) Food Supplies – Except as specifically provided in this subsection, the standards for food supplies are
governed by Part 3-2 of the Food Code, as incorporated by reference in rule 64E-11.002, F.A.C.
(a) Food received or used in food service establishments must be from sources approved or considered satisfactory
by the department and must be clean, wholesome, free from spoilage, adulteration and misbranding, and safe for
human consumption. Food must have been prepared, processed, handled, packaged, transported and stored in a
sanitary manner so as to be protected from contamination and spoilage.
(b) Meat and meat products received or used in a food service establishment shall be identified as having been
officially inspected for wholesomeness and sanitation by a federal or state regulatory program.
(c) Food prepared in a private home shall not be used, sold, or offered to the public by a food service establishment
or theater.
(2) Food Protection – Except as specifically provided in this subsection, the standards for food protection are
governed by Parts 3-3 through 3-8 of the Food Code, as incorporated by reference in rule 64E-11.002, F.A.C.
(a) Food while being transported, stored, prepared, displayed, served or sold at a food service establishment must
be protected from dust, flies, rodents or other vermin, toxic materials, unclean equipment and utensils, unnecessary
handling, coughs and sneezes, flooding by sewage, overhead leakage and all other sources of contamination.
(b) In the event of an emergency occurrence such as a fire, flood, power outage or similar event that might result
in the contamination of food, or that might prevent potentially hazardous food from being held at a safe temperature,
the person in charge must immediately notify the department.
(3) Personnel – Except as specifically provided in this subsection, the standards for personnel are governed by
Parts 2-2 through 2-5 of the Food Code, as incorporated by reference in rule 64E-11.002, F.A.C.
(a) No person while affected with any disease in a communicable form or while a carrier of such disease or while
afflicted with boils, infected wounds, sores, or an acute respiratory infection, can work in any area of a food service
establishment in any capacity in which there is a likelihood of such person contaminating food or food-contact surfaces
with pathogenic organisms, or transmitting disease to other individuals, and no person known or suspected of being
affected with any such disease or condition can be employed in such an area or capacity. If the management of the
food service establishment has reason to suspect that an employee has contracted any disease in a communicable form
or has become a carrier of such disease that can be transmitted by normal food service operation, the department must

Transferred to 59A-36 6B – 65
be notified immediately. Both management and employee are responsible for compliance with the requirements of
this section.
(b) Infants and children under 14 years of age are not permitted in food preparation areas. Only authorized
individuals, necessary for the operation of the food service establishment, or as part of an organized educational event,
are allowed in the food preparation or utensil washing areas.
(4) Food Equipment and Utensils – Except as specifically provided in this subsection, the standards for food
equipment and utensils are governed by Chapter 4 of the Food Code, as incorporated by reference in rule 64E-11.002,
F.A.C. Every food service establishment must have equipment and utensils so designed, constructed, located, installed,
maintained and operated as to permit full compliance with the provisions of this chapter. Only equipment necessary
for the proper operation of the activities of the food service establishment is required.
(5) Sanitary Facilities and Controls – except as specifically provided in this subsection, the standards for sanitary
facilities and controls are governed by Chapter 5 of the Food Code, as incorporated by reference in rule 64E-11.002,
F.A.C.
(a) Water Supply – The water supply must be adequate, of safe sanitary quality and from an approved source in
accordance with provisions of chapters 62-550 and 62-555, F.A.C., or chapter 64E-8, F.A.C. Chapters 62-550 and 62-
555, F.A.C. (07/2018) are incorporated by reference and available at
https://www.flrules.org/Gateway/reference.asp?No=Ref-09896 and at
https://www.flrules.org/Gateway/reference.asp?No=Ref-09897. Hot and cold running water under pressure must be
provided in all areas where food is prepared and where equipment and multi-use utensils are washed.
(b) Sewage Disposal – Sewage must be disposed of in a public sewerage system or other approved sewerage
system in accordance with provisions of chapter 64E-6 or chapter 62-600, F.A.C., whichever is applicable. Chapter
62-600, F.A.C. (07/2018) is incorporated by reference and available at
https://www.flrules.org/Gateway/reference.asp?No=Ref-09898. Grease interceptors must be readily accessible for
cleaning. Grease interceptors must be designed and installed in accordance with provisions of chapter 64E-6, F.A.C.,
or the applicable plumbing authority.
(c) Plumbing – Plumbing must be sized, installed, and maintained in accordance with provisions of the applicable
plumbing authority. The plumbing must provide adequate quantities of potable water to required locations throughout
the establishment; prevent contamination of the water supply; properly convey sewage and liquid wastes from the
establishment to the sewerage system; and must not constitute a source of contamination of food, equipment or utensils
or create an unsanitary condition or nuisance. An indirect waste connection is required between the sewerage system
and any drains originating from equipment in which food, portable equipment, or utensils are placed.
(d) Handwashing Facilities – Lavoratories must be located in or immediately adjacent to all toilet rooms. At least
one employee handwashing facility must be located within each food preparation area, within 20 feet of the duty
station, visible and accessible through an unobstructed area.
1. For school concession stands existing and operating prior to January 2010, an employee handwashing facility
is not required in an outdoor cooking area, provided that the outdoor cooking area is adjacent to a concession stand
building that meets the employee handwashing facility requirements.
2. Where only prepackaged food items are served and workers do not open prepackaged items or otherwise come
into contact with exposed food, a handwashing sink must be within 100 feet and on the same floor where food items
are distributed.

Transferred to 59A-36 6B – 66
(e) Garbage and Rubbish Disposal – All garbage and rubbish must be removed from the food establishment
premises with sufficient frequency to prevent nuisance conditions and must be disposed of in accordance with
provisions of chapter 62-701, F.A.C. (07/2018), which is incorporated by reference and available at
https://www.flrules.org/Gateway/reference.asp?No=Ref-09899.
(f) Vermin Control – Insecticides or pesticides, when used, must be used in full compliance with chapter 5E-14,
F.A.C. (07/2018), which is incorporated by reference and available at
https://www.flrules.org/Gateway/reference.asp?No=Ref-09900.
(6) Other Facilities and Operations – Except as specifically provided in this subsection, the standards for other
facilities and operations are governed by Chapters 6-7 of the Food Code, as incorporated by reference in rule 64E-
11.002, F.A.C.
(a) Ventilation – All rooms in which food is stored, prepared or served, utensils are washed, toilet, dressing and
locker rooms and garbage storage areas must be well ventilated. Filters, where used, must be readily removable for
cleaning unless designed to be cleaned in place. Ventilation systems must comply with applicable fire prevention
requirements and must discharge in such a manner as not to create a nuisance. Intake and exhaust air ducts must be
maintained to prevent the entrance of dust, dirt, and other contaminating materials.
(b) At least one utility sink or curbed cleaning facility with a floor drain must be provided and used for the cleaning
of mops or similar wet floor cleaning tools and for the disposal of mop water or similar liquid wastes. The use of
lavatories, utensil washing or equipment washing, or food preparation sinks for this purpose is prohibited.
1. Each utility sink or curbed cleaning facility must be supplied with hot and cold water under pressure.
2. School concession stands that operate only in conjunction with sporting events, festivals, or similar actvities
are exempt from this requirement when a self-contained mopping apparatus is used in accordance with the
manufacturer’s instructions and is available for use at all times and
a. The school concession stand was existing and operating prior to January 1, 2010, or
b. The school concession stand was constructed and operating on or after January 1, 2010, and the food operation
is restricted to the service of prepackaged food items.
(c) Live Birds and Animals – No live birds or animals, excluding crustacea, shellfish, and fish in aquariums, are
allowed in a food service establishment, in vehicles used for transporting food, or in any other area or facility used to
conduct food service operations, except as provided under section 413.08, F.S.
(7) Temporary Food Service Events – Food service operations at temporary food service events must comply
with all applicable sanitary requirements of this rule, unless otherwise exempted in this subsection.
(a) Notification – Temporary food service event sponsors or vendors must complete form DH8004-DCHP-
02/2018, Temporary Food Service Event Application, 02/18, which is incorporated by reference and available at
https://www.flrules.org/Gateway/reference.asp?No=Ref-09901.
(b) Facilitites – Specific requirements for the physical facility where the food service operation is to be conducted
are based on the type food that is to be prepared or served, the length of the event, and the amount of food preparation
that is to be conducted at the temporary facility.
1. If the food service operation is intended for the sale of only packaged, non-time/temperature control for safety
(non-TCS) food or drink, the food packages must be protected from dust, dirt, and other sources of contamination
during storage and serving.

Transferred to 59A-36 6B – 67
2. Overhead protection must be provided at all food service operations when food is prepared or portioned on
premises.
3. When time/temperature control for safety (TCS) food is prepared at temporary food service events of more
than 3 days, the physical structure where the food preparation occurs must be protected from the entrance of flying
insects and other vermin.
(c) All food and beverages served at temporary food service events must be from approved sources in accordance
with provisions of this chapter or prepared on premises.
(d) All food served at temporary food service events must be protected in accordance with provisions of this
chapter.
(e) Food and food-contact surfaces must be protected from contamination by customers and dust. Where
necessary, effective shields or covers must be provided.
(f) Ice which will be consumed or which will come into contact with food must be obtained from an approved
source. The ice must be held in a way that protects it from contamination until dispensed.
(g) Storage of packaged food in contact with water or undrained ice is prohibited. Beverage containers may be
stored in direct contact with ice when:
a. The storage facility is equipped with adequate drains which preclude the accumulation of water during use;
b. The melt water is disposed of so as not to create a nuisance; and
c. The storage facility is kept clean.
(h) When all necessary washing and sanitizing of utensils and equipment are conducted at an approved
commissary or food service establishment, a utensil washing sink is not required, provided that an adequate supply of
spare preparation and serving utensils are maintained in the establishment and used to replace those that become
soiled. A sanitizer solution in a bucket or spray bottle to adequately sanitize the food preparation surfaces must be
available at all times.
(i) All food service operations which prepare food on premises must provide an adequate supply of potable water
for cleaning and employee handwashing. An adequate supply may be provided in clean, portable containers equipped
with on/off valves. Soap and single-service towels must be available for handwashing and hand drying.
(j) Equipment must be installed in such a manner that the establishment can be kept clean and the food will not
become contaminated.
(k) Liquid waste which is not discharged into a sewerage system must be disposed of in a manner that will not
create a public health hazard or a sanitary nuisance.
(l) Floor construction in establishments which prepare food on premises must be of durable material. Dirt or
gravel subflooring can be used when graded to drain, and covered with platforms, duckboards, plastic film, wood
chips, shavings, or similar suitable material such as a sufficient cover of grass or turf to control dust.
(m) Walls and ceilings, when required, must be constructed to minimize the entrance of flies and dust. Ceilings
may be of wood, canvas, or other materials which protect the interior of the establishment from the elements and walls
may be of such materials or of 16 mesh screening or equivalent. Doors to food preparation areas, when required, must
be solid or screened and shall be self-closing. Counter service openings, for facilities with wall enclosures, must not
be larger than necessary for the particular operation conducted and must be kept closed at all times, except when food
is actually being served.

Transferred to 59A-36 6B – 68
(n) All food service operations at temporary food service events without effective facilities for cleaning and
sanitizing tableware must provide only single-service articles for use by the consumer.
(8) Vending Machines – Except as specifically provided in this subsection, the standards for vending machines
are governed by Section 4-204.12 – Section 4-204.111 of the Food Code, as incorporated by reference in rule 64E-
11.002, F.A.C.
(a) Food Supplies – All foods, beverages, and ingredients offered for sale through vending machines offering
time/temperature control for safety foods, which are located at food service establishments regulated under this
chapter, must be from approved sources in accordance with provisions of subsection (1); must be manufactured,
processed, and prepared in an approved food service establishment or food processing plant; and must be delivered to
the vending machine from an approved commissary or other approved food establishment.
(b) Food Protection – All food must be protected in accordance with provisions of subsection (2). A thermometer
accurate to plus or minus 3 degrees Fahrenheit must be provided to indicate the air temperature of food storage
compartments used for time/temperature control for safety foods.
(c) Cleaning – All food-contact surfaces of vending machines must be thoroughly cleaned and subjected to
effective bactericidal treatment at scheduled intervals, based upon the type of product being dispensed, as approved
by the department in accordance with provisions of subsection (4). A record of such cleaning and sanitizing operations
must be maintained in each machine and must be current for at least the past 30 days. The cavities and door edges of
microwave ovens and similar equipment, used in conjunction with the beverages or food from a vending machine,
must be cleaned at least once a day and must be kept free of encrusted grease deposits and other accumulated soil.
Food-contact surfaces of all equipment and utensils must be protected from contamination at all times, including while
being transported from the commissary to the vending location.
(d) Single-Service Containers – All single-service containers which receive food or beverage from machines
dispensing products in bulk must be purchased in sanitary cartons or packages, which protect the containers from
contamination; must be stored in a clean dry place in the original carton or package until introduced into the container
magazine or dispenser of the vending machine; and must be handled in a sanitary manner. Single-service containers
stored within the vending machine must be protected from manual contact, leakage, dust, insects, rodents and other
contamination.
(e) Equipment Location – Vending machines, ovens, and other equipment associated with the use of beverages
or food from a vending machine, must be located in a room, area or space which can be maintained in a clean condition
and which is protected from overhead leakage from drains, piping and other sources.
1. Each machine must be so located that the space around and under the machine can be readily cleaned and so
that insect and rodent harborage is not created. The immediate area must be well lighted and ventilated. The floor area
upon which vending machines are placed must be of such construction as to be easily cleaned and must be kept clean
and in good repair.
2. Adequate handwashing facilities, including hot and cold running water, soap and individual, single-service
towels must be located within 50 feet of machine locations where employees service bulk food machines.
Handwashing facilities must be within 20 feet of machine locations where employees handle unpackaged or exposed
foods.
(f) Interior Construction and Maintenance – All interior surfaces and component parts of vending machines must
be so designed and constructed as to permit easy cleaning and shall be kept clean.

Transferred to 59A-36 6B – 69
1. All food-contact surfaces of vending machines must be smooth, in good repair, and free of breaks, corrosion,
open seams, cracks, and chipped places. The design of such surfaces must be such as to preclude routine contact
between food and V-type threaded surfaces, except that in equipment where such contact is unavoidable, such as ice
makers, such threads must be minimized. All joints and welds in food-contact surfaces must be smooth; and all internal
angles and corners of such surfaces must be rounded to facilitate cleaning. If solder is used, it must be composed of
safe materials and be corrosion resistant. All food-contact surfaces of vending machines, including containers, pipes,
valves and fittings, must be constructed of non-toxic, corrosion resistant, and nonabsorbent materials and must be kept
clean. All containers, valves, fittings, chutes and faucets which are in contact with food must be easily disassembled
and when disassembled, all surfaces must be visible for inspection and cleaning. In machines of such a design that
pipes or tubing are in contact with food but are not readily removable, in-place cleaning of such pipes and pipe fittings
may be permitted; provided:
a. They are so arranged that cleaning and bactericidal solutions can be circulated throughout the fixed system;
b. Such solutions will contact all interior surfaces;
c. The system is self-draining or otherwise capable of being completely evacuated; and
d. The cleaning procedures result in thorough cleaning of the equipment.
2. The openings into all nonpressurized containers used for the storage of vendable foods and ingredients
including water must be provided with covers which prevent contamination from reaching the interior of the
containers. Such covers must be designed to provide a flange which overlaps the opening and must be sloped to
provide drainage from the cover surface wherever the collection of condensation, moisture or splash is possible.
Concave covers or cover areas are prohibited. Any port opening through the cover must be flanged upward at least
three sixteenth inch and must be provided with an overlapping cover flanged downward. Condensation or drip
deflecting aprons must be provided on all piping, thermometers, equipment, rotary shafts and other functional parts
extending into the container, unless a watertight joint is provided. Such aprons must be considered as satisfactory
covers for those openings which are in continuous use. Gaskets, if used, must be of a material which is nontoxic,
stable, and nonabsorbent and must have a smooth surface. All gasket retaining grooves must be easily cleanable.
3. The delivery tube or chute and orifice of all bulk food vending machines must be protected from normal manual
contact, dust, insects, rodents and other contamination. Design must be such as to divert condensation or other moisture
from the normal filling position of the container receiving the food or beverage. The vending stage of such machines
must be provided with a tight fitting, self-closing door or cover which is kept closed, except when food is being
removed.
4. The food storage compartment and other compartments in refrigerated vending machines which are subject to
condensation or cooling water retention must be so constructed as to be self-draining or must be provided with a drain
outlet which permits complete draining of the compartment. In vending machines designed to store cartoned
beverages, diversion devices and retention pans or drains for leakage must be provided. All such drains, devices and
retention pans must be easily cleanable.
5. Opening devices which come into contact with the food or the food-contact surface of the containers must be
constructed of smooth, nontoxic, corrosion resistant and nonabsorbent materials. Unless the opening device is of a
single-service type, it must be readily removable for cleaning and must be kept clean. Parts of multi-use opening
devices which come into contact with the food or food-contact surface of containers must be protected from manual
contact, dust, insects, rodents and other contamination and such parts must be readily removable for cleaning and must

Transferred to 59A-36 6B – 70
be kept clean.
(g) Delivery of Foods, Equipment, and Supplies – Food, single-service containers, and food-contact surfaces of
equipment, containers, and devices must be protected from the elements, dirt, dust, insects, rodents, and other
contaminants while in transit to vending machine locations. Time/temperature control for safety foods must be
maintained at safe temperatures while in transit.
(h) Personnel – Individuals servicing or replenshing these machines must comply with all applicable provisions
of subsection (3), rule 64E-11.012, and rule 64E-11.013, F.A.C.
Rulemaking Authority 381.006, 381.0072 FS. Law Implemented 381.006, 381.0072 FS. History–New 1-1-77,
Amended 1-6-81, Formerly 10D-13.23, Amended 2-21-91, Retained here and Transferred to 7C-4.010, Amended 6-
1-93, 8-28-96, Formerly 10D-13.023, Amended 3-15-98, 7-14-03, 9-26-18.
64E-11.004 Food Protection.
Rulemaking Authority 381.0072 FS. Law Implemented 120.542, 381.0072 FS. History–New 1-1-77, Amended 1-6-81,
Formerly 10D-13.24, Amended 2-21-91, 5-12-92, Retained here and Transferred to 7C-4.011, Amended 6-1-93, 8-
28-96, Formerly 10D-13.024, Amended 3-15-98, 7-14-03, Repealed 9-26-18.
64E-11.005 Personnel.
Rulemaking Authority 381.0072 FS. Law Implemented 381.0072 FS. History–New 1-1-77, Amended 1-6-81, Formerly
10D-13.25, Amended 2-21-91, 5-12-92, Retained here and Transferred to 7C-4.012, Amended 6-1-93, Formerly 10D-
13.025, Amended 3-15-98, 7-14-03, Repealed 9-26-18.
64E-11.006 Food Equipment and Utensils.
Rulemaking Authority 381.0072 FS. Law Implemented 381.0072 FS. History–New 1-1-77, Amended 1-6-81, Formerly
10D-13.26, Amended 2-21-91, 5-12-92, Retained here and Transferred to 7C-4.013, Amended 6-1-93, 8-28-96,
Formerly 10D-13.026, Amended 3-15-98, 7-14-03, Repealed 9-26-18.
64E-11.007 Sanitary Facilities and Controls.
Rulemaking Authority 381.006, 381.0072 FS. Law Implemented 381.006, 381.0072 FS. History–New 1-1-77,
Amended 1-6-81, Formerly 10D-13.27, Amended 2-21-91, 5-12-92, Retained here and Transferred to 7C-4.014,
Formerly 10D-13.027, Amended 3-15-98, 7-14-03, Repealed 9-26-18.
64E-11.008 Other Facilities and Operations.
Rulemaking Authority 381.006, 381.0072 FS. Law Implemented 381.006, 381.0072 FS. History–New 1-1-77,
Amended 1-6-81, Formerly 10D-13.28, Amended 2-21-91, 5-12-92, Retained here and Transferred to 7C-4.015,
Amended 8-28-96, Formerly 10D-13.028, Amended 3-15-98, Repealed 9-26-18.
64E-11.009 Temporary Food Service Events.
Rulemaking Authority 381.0072 FS. Law Implemented 381.0072 FS. History–New 6-1-93, Formerly 10D-13.0292,
Amended 3-15-98, Repealed 9-26-18.
64E-11.010 Vending Machines.
Rulemaking Authority 381.0072 FS. Law Implemented 381.0072 FS. History–New 6-1-93, Formerly 10D-13.0331,
Amended 3-15-98, Repealed 9-26-18.
64E-11.011 Procedure When Infection Is Suspected.
When the department has reasonable cause to suspect possibility of disease transmission from any food service
establishment employee, the department shall secure a morbidity history of the suspected employee, or make other
such investigation as may be indicated and take appropriate action. The department may require any or all of the

Transferred to 59A-36 6B – 71
following measures:
(1) Immediate exclusion of the employee from all food service establishments.
(2) Immediate closure of the food service establishment concerned until, in the opinion of the department, no
further danger of disease outbreak exists.
(3) Restriction of the employee’s service to some area of the establishment where there would be no danger of
transmitting the disease.
(4) Adequate medical and laboratory examination of the employee or other employees.
Rulemaking Authority 381.006, 381.0072(2) FS. Law Implemented 381.006, 381.0072(2) FS. History–New 1-1-77,
Amended 1-6-81, Formerly 10D-13.36, Amended 2-21-91, Retained here and Transferred to 7C-4.022, Formerly 10D-
13.036.
64E-11.012 Manager Certification.
(1) All managers who are responsible for the storage, preparation, display, and serving of foods to the public must
have passed a written certification test which complies with section 509.039, Florida Statutes, within 30 days after the
effective date of employment. Those managers who successfully pass the certification examination will be issued a
certificate which is valid for a period of five years from the date of issuance.
(2) All establishments must designate in writing the food service manager or managers for each location.
Establishments that serve highly susceptible populations, or have three or more employees at one time engaged in the
storage, preparation, display, or serving of food must have at least one certified manager present at all times when said
activities are taking place. All other establishments must have a certified manager or managers responsible for all
periods of operation, but said manager or managers need not be present at all times.
(3) It is the responsibility of the certified manager or person in charge to train or ensure the training of all
employees under their supervision and control who engage in the storage, preparation, or serving of food, or cleaning
of equipment, utensils, or food contact and non-food contact surfaces, and to do so in accordance with acceptable
sanitary practices as described in this chapter. The trainings must be annual and provided to employees by March 31
of each year. Employees hired after the annual training has been provided for that calendar year must receive training
within 30 days of being hired. The certified manager or person in charge must also maintain a copy of the
establishment’s most recent regular food service inspection form provided by the department. Employees shall present
this inspection form to guests or patrons for their review upon request.
(4) If a food service establishment, which possesses a santitation certificate and initially met the requirements of
this section, becomes noncompliant with subsection (2), above, the food service establishment will have a period of
30 days to become compliant with subsection (2), above.
(5) The food service employee training must inform the employee regarding basic public health food protection
practices, as specified in this chapter and which relates to their assigned duties. Employees who prepare foods must
be knowledgeable about safe methods of thawing, cooking, cooling, handling, holding, and storing foods. Service
personnel must be knowledgeable about safe methods of food service. Employees who clean equipment and facilities
must be knowledgeable about proper cleaning and sanitization methods. Employees responsible for maintaining the
premises must be knowledgeable about proper insect and vermin control methods. Managers must obtain and maintain
an attendance roster of all employees present during training. Both the training curriculum and attendance roster must
be maintained for three years and available upon request by the department. Establishments that are not compliant
with the employee training requirements and record retention of this section must schedule a training and testing with

Transferred to 59A-36 6B – 72
the department and pay any applicable fees. In lieu of the department providing training and testing, the establishment
may schedule training and testing with an outside course provider, who in addition to providing employee-level
training, is also an approved manager certification test provider. The training and testing for employees must be
completed within 60 days of the violation, or prior to the renewal of the sanitation certificate, whichever comes first.
(6) Persons are considered certified under these rules when a written examination is a requirement for licensure
by the Department of Health, Division of Medical Quality Assurance in a dietary field and when these persons have
acquired and maintained an active license, provided that they comply with subsection (2), above. The following
establishments are exempt from the manager certification requirements of this section, however, the establishment
must have a person in charge:
(a) Any theater, if the primary use is as a theater and patron service is limited to food items customarily served to
admittees of theaters such as popcorn, hot dogs, soft drinks, nachos and cheese, and pre-packaged snack foods;
(b) Establishments listed in section 381.0072, F.S., as being exempt from this certification;
(c) Food service establishments that limit their food service operation to non-time/temperature control for safety
prepackaged food items;
(d) Culinary arts and similar food programs, which do not offer, sale, or serve food beyond the program’s
instructors and participants.
Rulemaking Authority 381.0072 FS. Law Implemented 381.0072 FS. History–New 2-21-91, Amended 5-12-92,
Retained here and Transferred to 7C-4.023, Amended 6-1-93, 8-28-96, Formerly 10D-13.037, Amended 3-15-98, 7-
14-03, 9-26-18.
64E-11.013 Sanitation Certificates and Fees.
(1) Sanitation Certificate Required.
(a) All food service establishment sanitation certificates expire on September 30. Initial sanitation certificates
issued for a period less than a calendar year will be prorated on a quarterly basis, in accordance with section
381.0072(4), F.S.
(b) Food service establishments containing multiple food operations housed in the same building, at the same
location, under the same ownership and operation or concession stands operating on the premise of K-12 schools,
must function according to either one of the following:
1. Each food operation must operate under the umbrella of the sanitation certificate issued to the main food service
operation, in which case the sanitation certificate must be posted in a conspicuous location at the main food service
establishment, or
2. Each food operation must be issued its own individual sanitation certificate, in which case each food service
establishment must post their own sanitation certificate in a conspicuous location in their establishment. The owner
or operator of the food service establishment must decide which of the sanitation certificate processes listed above,
will be followed.
(c) Food service establishments where multiple food operations are located in different buildings at the same
location regardless of ownership must each be issued their own individual sanitation certificate, in which case each
such food operation must post their own sanitation certificate in a conspicuous location in their food service operation.
School concession stands under the same ownership, may elect to comply with the provisions of subparagraph (b)1.
Regardless of location, provided that the school concession stands are located on the same premises and there are no
more than four concession stand operations.

Transferred to 59A-36 6B – 73
(2) Application and Renewal of Sanitation Certificates.
(a) Each person who plans to construct, purchase, reopen, or operate a food service establishment or an
establishment subject to the requirements of this chapter, must apply for and receive a sanitation certificate from the
department prior to the commencement of operation. Applications for certificates must be made to the department on
DH 4086, Application for Sanitation Certificate, 02/18, incorporated herein by reference and available at
https://www.flrules.org/Gateway/reference.asp?No=Ref-09902.
(b) Applications for sanitation certificates must be submitted with the facility plans as described in paragraph (c),
below, the annual fee and any other applicable fee that is required in subsection (3).
(c) Prior to the renovation of a food service establishment, notification must be provided to the department. This
notification must include construction schedules and details of the work to be completed. Prior to the construction or
extensive remodeling of a food service establishment, or the conversion of a structure for use as a food service
establishment, or remodeling which includes the addition or relocation of major equipment, plans of the facility and
its operation must be submitted to and approved by the department. Plans may be submitted by the owner, prospective
operator or their designated representative. All plans must comply with the requirements of this chapter. Plans must
be drawn to scale, describe the layout, construction, and general operation of the facility, equipment design and
installation, the intended menu, and similar aspects of the facility’s operation that relate to the requirements of this
chapter, and be accompanied by DH8003-DCHP-02/2018, Food Service Establishment Plan Review Application,
02/18, incorporated by reference and available at https://www.flrules.org/Gateway/reference.asp?No=Ref-09903.
(d) Before a sanitation certificate is issued to a newly constructed or extensively remodeled food service
establishment, an inspection must be made by a representative of the department for the determination of compliance
with the requirements of this chapter, and section 381.0072, F.S.
(3) Fees.
(a) Fees must be submitted to the department for sanitation certificates, as well as the provision of other required
public health services at food service establishments. Sanitation certificates must be renewed annually and the fee will
not be prorated. Fees for all other sanitation certificates, such as change of ownership, reinstatement after revocation
of a sanitation certificate, or new establishments, after the first quarter will be prorated on a quarterly basis. Proration
will be based on the quarter the department receives an application for a Sanitation Certificate to operate a food service
establishment. Upon request of the applicant, the initial fee for school concession stands may be prorated on a quarterly
basis regardless of the date of application, provided that it does not operate for more than one quarter, the conditions
of subparagraph (1)(b)1., do not apply, and the annual fee used to determine the prorated amount is prescribed by sub-
subparagraph (b)5.b., below
Transferred to 59A-36 6B – 74
(b) Except for establishments specifically exempted from fees in subsection (4), all food service establishments
must pay an annual or prorated fee to the department according to the following schedule:
ANNUAL SANITATION CERTIFICATE FEE OR INSPECTION FEE SCHEDULE
Total
1. Detention Facility $250.00
2. Bar/Lounge $190.00
3. Fraternal/Civic Organization $190.00
4. Movie Theater Inspection $190.00
5. School Cafeteria
a. Cafeteria requiring 3 routine inspections per year $170.00
b. Cafeteria requiring 4 routine inspections per year $200.00
c. Concession Stand $100.00
6. Community Based Residential Facility $135.00
7. Afterschool Meal Program $170.00
8. Prescribed Pediatric Extended Care Center $110.00
9. Limited Food Service Operation $110.00
10. Caterering Operation $180.00
11. Mobile Food Unit $180.00
12.Vending Machine Dispensing Time/Temperature Control for Safety Food $ 85.00
(c) Food service establishments with multiple food operations, as described in subparagraph (1)(b)1., above, will
be assessed a single annual fee of $300. That fee will be assessed on the main food service establishment, and it will
cover the other food service facilities operating in that same building under the umbrella of the main food service
establishment. This fee provision also applies to school concession stands that elect to comply with the provisions of
paragraph (1)(b).
(d) Food service establishments with multiple food operations, as described in paragraph (1)(c), above, will be
assessed separate annual fees for each food operation based on the category of establishments listed in paragraph
(3)(b), above.
(e) Except for school concession stands that elect to comply with the provisions of subparagraph (1)(b)1. above,
food service establishments as described in paragraph (1)(c), will be assessed separate annual fees for each food
operation based on the category of establishments listed in paragraph (3)(b), above.
(f) Vending machines dispensing time/temperature control for safety food, catering operations and mobile food
units that are located at or operated from an establishment listed in section 381.0072, F.S., will be charged the fees
listed in paragraph (3)(b), above, when they are not operating under an existing Sanitation Certificate that has already
been issued for the main food service establishment where they are located.

Transferred to 59A-36 6B – 75
(g) The following schedule of fees is established for plan reviews, food service worker training and testing,
alcoholic beverage establishment sanitation inspections, reinspections, late renewals:
1. Plan review per hour.
Public schools, colleges, and vocational teaching facilities are exempt from this fee.
$40.00
2. Food establishment worker training course (per person). $10.00
3. Sanitation inspection.
a. Alcoholic beverage inspection approval. $30.00
b. Requests for inspection. $40.00
4. Reinspection
(for each reinspection after the first).
$75.00
5. Late renewal of certificate. $25.00
6. Temporary event food service establishment.
a. Sponsor without an existing sanitation certificate. $100.00
b. Vendor or booth at an establishment or location without an existing sanitation certificate. $50.00
(h) All fees submitted to the department are nonrefundable, once review has started on the application.
(4) Exemptions. The following limited food service establishments are exempt from the fee requirements of this
section:
(a) Food service establishments that only serve catered meals which have been prepared in an approved food
establishment and where no warewashing, and no storage, reheating, or re-service of the catered food takes place on-
site; such as satellite kitchens at schools and other institutions, and similar operations.
(b) Food service establishments that serve only snacks which are not kept overnight, or that require individuals
in attendance to bring their own meals to the facility, which do not require any food preparation.
Rulemaking Authority 381.0072, 154.06 FS. Law Implemented 381.0072(2), 154.06 FS. History–New 2-21-91,
Amended 5-12-92, Retained here and Transferred to 7C-4.024, Amended 6-1-93, 11-30-93, 8-28-96, Formerly 10D-
13.038, Amended 3-15-98, 7-14-03, 4-1-09, 9-26-18.
64E-11.014 Mobile Food Units.
All mobile food units required to have vehicle identification numbers must submit their vehicle identification number
to the department on the application for licensure. The license decal must be affixed to the mobile food unit. Mobile
food units must comply with rules 64E-11.001 through 64E-11.003, and 64E-11.011 through 64E-11.013, F.A.C.,
except that such mobile food units are not required to have employee/patron toilet facilities or mop sinks. No license
will be granted to a mobile food unit until the following additional requirements have been met:
(1) A potable water supply system of sufficient capacity (minimum 5 gallons) to furnish an adequate quantity of
hot and cold water for food preparation, cleaning, and handwashing purposes must be provided during all periods of
operation. The water inlet must be located so that it will not be contaminated by waste discharge, road dust, oil or
grease, and it must be kept capped unless being filled. It must be provided with a transition connection of a size or
type that will prevent its use for any other service.
(2) A suitable liquid waste system, including a waste tank having a capacity at least 15 percent greater than the
water supply system, shall be provided. All connections on the unit for servicing mobile food unit waste disposal
facilities shall be of a different size or type than those used for supplying potable water to the mobile food units. The
waste tank shall be capable of being completely drained and flushed.

Transferred to 59A-36 6B – 76
(3) Serving openings shall not be larger than necessary for the particular operation conducted and shall be kept
closed at all times except when food is actually being served. Mobile food units shall provide only single-service
articles for use by the consumer.
(4) Waste containers shall be provided for the deposit of food scraps, food wrappings, cups, napkins and discarded
single-service articles.
(5) Mobile food units must operate from an approved commissary that meets all applicable requirements of this
rule. The commissary must be provided with potable water and adequate facilities for disposal of liquid and solid
waste. The mobile food unit must report to the commissary to store or replenish supplies, clean utensils, and equipment
or dispose of liquid and solid waste. Mobile food units which are self-sufficient for equipment, storage, and utilities
must report to the commissary at least once weekly or as often as needed to replenish supplies, clean the interior of
the unit, or dispose of liquid or solid wastes. A letter from the commissary must be submitted as part of the application
confirming the arrangements above. A mobile food unit which is self-sufficient includes a three compartment sink for
washing, rinsing, and sanitizing of equipment and utensils, a separate handwash sink, adequate refrigeration and
storage capacity, full provision of power utilities including electrical, LP gas, or a portable power generation unit, and
a liquid waste disposal system, and potable water holding tank in accordance with subsections (1) and (2). Mobile
food units which are not self-sufficient must report to their commissary at least once daily. The exterior of the unit
may be washed in any location, provided the waste water does not create a sanitary nuisance.
(6) When a service area is provided at the commissary for cleaning and servicing mobile food units, the service
area must include at least overhead protection for any supplying, cleaning or servicing operation. Such area must be
physically separated from other food operations; must be equipped to furnish approved potable water in accordance
with applicable provisions of chapters 62-550 and 62-555 or chapter 64E-8, F.A.C.; and must provide facilities for the
drainage and disposal of liquid wastes in accordance with applicable provisions of chapter 64E-6 or 62-600, F.A.C.,
and the plumbing authority. The surface of the servicing area must be constructed of a smooth, nonabsorbent material
such as concrete or machine laid asphalt and must be maintained in good repair, kept clean and be graded to drain.
Chapters 62-550, 62-555, and 62-600, F.A.C. (07/2018) are incorporated by reference and available at
https://www.flrules.org/Gateway/reference.asp?No=Ref-09929,
https://www.flrules.org/Gateway/reference.asp?No=Ref-09930, and
https://www.flrules.org/Gateway/reference.asp?No=Ref-09931.
(7) Mobile food units which are limited to the sale of non-time/temperature control for safety food only are exempt
from:
(a) The requirements of employee hand washing sink, provided that only pre-packaged items are offered; and,
(b) The requirements of a utensil washing sink when all necessary washing and sanitizing of utensils and
equipment are conducted at a designated approved commissary or fixed food establishment. An adequate supply of
spare preparation or serving utensils must be maintained in the unit and used to replace any utensils that become
contaminated.
(8) Mobile food units may temporarily connect to an approved utility system for a time period not to exceed one
day’s operation, provided the utility system is adequate to meet the needs of the unit, sanitary facilities are made
available for employees and patrons in accordance with the applicable plumbing authority, and the unit returns to its
base commissary in accordance with subsection (5).

Transferred to 59A-36 6B – 77
(9) Mobile food units which limit the preparation of food to frankfurters only, must comply with all applicable
requirements of this section, except that subsection (3) does not apply when adequate precautions are utilized to
prevent contamination of the frankfurters during cooking operations. Potentially hazardous time/temperature control
for safety foods such as chili, cooked onions and peppers, cheese, and cheese sauce may only be served in individually
portioned and packaged or pre-packaged containers which are maintained at proper temperatures on the unit. Non-
time/temperature control for safety foods such as relish, raw onions and peppers, and other such condiments may be
served directly from the unit. Bulk beverages from approved sources may be dispensed from covered urns or other
protected containers.
Rulemaking Authority 381.0072 FS. Law Implemented 381.0072 FS. History–New 3-15-98, Amended 7-14-03, 9-26-
18.
64E-11.015 Afterschool Meal Program.
(1) Facilities participating in the United States Department of Agriculture (USDA) Afterschool Meal Program,
which are not used for any other food service operation or for multiple USDA Afterschool Meal Programs, shall
comply with all applicable sanitary requirements of this chapter when minimum standards are not specified in this
section.
(2) Food preparation sink – The sanitizing compartment of a two or three compartment sink may be used as a
food preparation sink provided that the Afterschool Meal Program entity has a written procedure of use, which has
been approved by the Department prior to the implementation of the procedure. At minimum, the written procedures
shall:
(a) Ensure the third compartment is clean to the sight and touch and sanitized, prior to and after use as a food
preparation sink;
(b) Ensure no other sink compartment(s) is used for any other purpose while the sink is in use as a food preparation
sink;
(c) Ensure only workers, who have been trained on the procedure, use the sink for food preparation; and,
(d) Ensure the approved procedure is posted at the sink.
(3) Hot and Cold Holding Equipment – In order to comply with holding temperature requirements, electronic hot
and cold holding equipment shall be used for food storage; however, controls for the adjustment of temperature are
not required.
(4) Cleaning facilities – Food operations restricted to the receipt of pre-portioned catered meals or service of
prepackaged food items may use a self-contained mopping apparatus, provided it is used in accordance with the
manufacturer’s instructions and always available for use.
(5) Manual washing, rinsing and sanitizing – Sinks, drainboards and dishtables must be cleaned prior to use. A
two-compartment sink may be used when warewashing is limited to a batch operation in which cleaning of
kitchenware and tableware is suspended until the end of the service period. For batch cleaning, the following process
applies:
(a) Prior to using this process, Department approval shall be obtained;
(b) Prior to washing, multi-use tableware and kitchenware must be pre-flushed or pre-scraped and, when
necessary, pre-soaked to remove gross food particles and soil;
(c) Immediately before use, prepare the cleaning and sanitizing solutions in sinks, which are free of debris and
residue and clean to the sight and touch;

Transferred to 59A-36 6B – 78
(d) In the first compartment use a detergent-sanitizer product, which is a detergent that contains a sanitizer, and
apply the detergent-sanitizer in accordance with the manufacturer’s instructions;
(e) In the second compartment use a sanitization method in accordance with rule 64E-11.006, F.A.C. If using a
chemical sanitizer, the sanitizing agent must be the same chemical agent contained in the detergent-sanitizer; and,
(f) Immediately after use, drain sinks.
(6) Drains – For an existing building with an existing food service operation, all drainage connections are
considered acceptable if in good working order and capable of being maintained in a sanitary condition. Replacement
materials and repairs must meet the requirements specified in rule 64E-11.007, F.A.C.
(7) Handwashing Facilities – For sites that receive pre-portioned catered meals or only serve prepackaged food
items and employees do not open prepackaged items or otherwise come into contact with exposed food, a designated
lavatory, equipped with hand cleansing soap or detergent and individual single use sanitary towels or a heated-air hand
drying device is required but need not be in the same room. However, where food is served, dispensed, or otherwise
unpackaged, a designated handwashing lavatory, equipped with hand cleansing soap or detergent and individual single
use sanitary towels or a heated-air hand drying device, shall be located in the same room and within 20 feet of the area
where food is served or dispensed.
(8) Hot Water – Food operations restricted to the receipt of proportioned catered meals or service of prepackaged
food items and do not require ware washing are not required to have hot water.
(9) Manager Certification – manager certification standards in accordance with Rule 64E-11.012, F.A.C., shall
be required for the following Afterschool Meal Program sites:
(a) Those sites routinely inspected three times or four times per year and which result in three consecutive routine
inspections each containing violations involving three of the four foodborne illness risk factors listed in paragraph (c),
below.
(b) Those sites routinely inspected one time or two times per year and which result in two out of three consecutive
routine inspections each containing violations involving three of the four foodborne illness risk factors listed in
paragraph (c), below.
(c) Risk Factors are significant contributors to foodborne illness and are identified as:
1. Employee health and hygiene, such as improper handwashing and the presence of ill food workers in
accordance with rule 64E-11.005, F.A.C.,
2. Holding temperatures (Hot and cold holding and cooling),
3. Inadequate cooking or reheating; and,
4. Food from unapproved sources.
(10) Time as a public health control – Time may be used in lieu of the holding temperature requirements of
subsection 64E-11.003(2), F.A.C., provided that time/temperature control for safety foods are cooked or reheated in
accordance with subsection 64E-11.003(2), F.A.C.; the Department is notified at least 14 days prior to the
implementation of time as a public health control; and the Afterschool Meal Program:
(a) Provides the Department a copy of the written procedures, which at a minimum indicates the meal service
times and the following:
1. The specific location where the time/temperature control for safety foods proposed for use under time as a
public health control are prepared;

Transferred to 59A-36 6B – 79
2. The proposed delivery schedule, if time/temperature control for safety foods are received from an outside
approved source; and,
3. The names of the food workers who have been trained regarding these written procedures.
(b) Maintains a daily log for time/temperature control for safety foods cooked or reheated on-site, which indicates
the date, name of the time/temperature control for safety foods, final cooking temperature, and the time that the final
cooking temperature was reached. In addition, each time/temperature control for safety food product or the container
holding the product must be labeled with an expiration time, which must not exceed 4 hours from the time that the
product reached the final cooking temperature. Time/temperature control for safety food products must be discarded
upon reaching the expiration time or if no expiration time is indicated.
(c) Maintains a valid copy of the caterer’s license, if a catering operation is used, and documents the name of food
suppliers, for ready-to-eat time/temperature control for safety food products that are not cooked or reheated on-site.
In addition, a daily product log must be maintained that documents the following: the date, name, and quantity of the
time/temperature control for safety food products that are obtained or received; the time and temperature of
time/temperature control for safety food products received or obtained by the Afterschool Meal Program; the
expiration time, which must not exceed 4 hours from the time that the Afterschool Meal Program takes possession of
the time/temperature control for safety food product; and the name and quantity of time/temperature control for safety
food products discarded.
(d) Provides and documents training for food workers regarding the Afterschool Meal Program site’s use of time
as a public health control, including written procedures and this section. Only trained employees shall complete the
daily logs and document expiration times.
(e) Maintains all documentation, including logs and licenses, for one year on site and makes them available to the
Department upon request.
(11) During transport between food service establishments or while being transported from a food service
establishment to another location, all food must be in covered containers or otherwise wrapped or packaged to ensure
protection from contamination. Time/temperature control for safety food products must be kept at safe temperatures
during all periods of transportation and delivery. Food utensils must be completely wrapped or packaged to protect
them from contamination. Any time/temperature control for safety food product that does not meet these requirements
must not be accepted or served by the Afterschool Meal Program Site.
Rulemaking Authority 381.0072 FS. Law Implemented 381.0072 FS. History New 2-18-14, Amended 9-26-18.

Transferred to 59A-36 6B – 80
Notes ______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________

8. Rule Chapter
64E-12, F.A.C
.


8 – 1
CHAPTER 64E-12
COMMUNITY BASED RESIDENTIAL FACILITIES 64E-12.001 General
64E-12.002 Definitions
64E-12.003 Water Supply
64E-12.004 Food Service: Tiers and Catering.
64E-12.005 Housing
64E-12.006 Vector and Vermin Control
64E-12.007 Bedding, Towels, Clothing and Personal Items
64E-12.008 Laundry
64E-12.009 Medications, Alcohol, Poisonous or Toxic Substances
64E-12.010 Garbage and Rubbish
64E-12.011 Recreational Areas
64E-12.012 Radon Testing (Repealed)
64E-12.013 Animal Health and Safety
64E-12.001 General.
(1) This rule chapter prescribes sanitary practices relating to construction, operation and maintenance of
community based residential facilities. If a requirement in this rule chapter conflicts with a specific requirement in
any other Florida state licensing agency’s rule, then that agency’s standards shall prevail and will be addressed by
that agency’s officials.
(2) Base camps of wilderness programs shall be exempt from subsections (6) and (7) of Rule 64E-12.005,
F.A.C., of this chapter, and the mobile components of wilderness programs shall be exempt from all sections of this
rule.
(3) Personal services may be provided to the residents through coordinated outsourcing by the community based
residential facility or by a contract provider.
Specific Authority 381.006, 381.006(16) FS. Law Implemented 381.006(16), 386 FS. History–New 6-18-87,
Formerly 10D-23.001, Amended 1-20-08.
64E-12.002 Definitions.
For the purpose of this chapter, the following words and phrases shall have the meaning indicated:
(1) Approved – means acceptable by law.
(2) Community Based Residential Facilities – means group care facilities as established under Section
381.006(16), F.S., used as a primary domicile by the resident and located in any building or buildings, section of a
building, or distinct part of a building or other place, whether operated for profit or not, which undertakes, through
its ownership or management, to provide for a period exceeding 24 hours, housing, food service, and one or more
personal services for persons not related to the owner or administrator by blood or marriage, who require such
services. This term does not include family foster homes as defined in Section 409.175(2)(e), F.S., or foster care
facilities as defined in Section 393.063(15), F.S., and correctional facilities, such as detention centers, jails or
prisons.
(3) Department – means the Florida Department of Health and county health departments.

8 – 2
(4) Food Preparation – means the manipulation of foods intended for human consumption by such means as
washing, slicing, peeling, chipping, shucking, scooping, and or portioning. The term also includes those activities
involving temperature changes, combining ingredients, opening ready-to-eat food packages, or any other activity
causing physical or chemical alterations in the food.
(5) Hot Water – means water heated to a minimum temperature of 100 degrees Fahrenheit (°F).
(6) Law – means applicable statutes, rules, codes, or ordinances adopted by local, state, and federal agencies
that have regulatory oversight or inspection authority.
(7) Minor – means any person under the age of 18 years old.
(8) Open Water Hazard – means any body of water such as canals, creeks, holding ponds, rivers, lakes, or
swamps which are unrestricted by a barrier at least 4 feet in height, on or abutting the property of a community
based residential facility. This term does not include pools or spas and small ornamental fish ponds, or above ground
fountains which are less than 24 inches deep and have less than 200 square feet of surface area.
(9) Personal Services – means providing supervision, custodial care, or assisting a resident with the tasks or
functions in their daily living activities, such as bathing, dressing, laundry, eating, ambulation, grooming, toileting,
or monitoring medications.
(10) Potentially Hazardous Food – means any perishable food which consists in whole or in part of milk or milk
products, eggs, meat, poultry, fish, shellfish, edible crustacea, or other ingredients, including synthetic ingredients,
in a form capable of supporting:
(a) Rapid and progressive growth of infectious or toxigenic microorganisms; or
(b) The slower growth of Clostridium botulinum.
The term “potentially hazardous food” does not include foods which have a pH level of 4.6 or below, or a water
activity (Aw) value of 0.85 or less, or air-cooled hard-boiled eggs with the shell intact.
(11) Renovation – means any structural or equipment changes in the food storage, service, preparation, or dining
area. This does not include replacing existing equipment with like equipment. Substantial renovation includes
structural changes to an existing establishment which costs in excess of 33 percent of the assessed value of the
facility as determined by the county property appraiser.
(12) Resident – means a person living in and receiving personal services from a community based residential
facility, or personal services through coordinated outsourcing, typically due to a specific emotional, social, or health
related condition.
(13) Vector – means an organism that transmits a pathogen. This term includes, but is not limited to insects,
rodents and bats.
(14) Wading Pool – means a temporary and portable pool that holds water, is less than 24 inches in depth, and
without motors. It may also be known as a kiddy pool.
Specific Authority 381.006(16) FS. Law Implemented 381.006(16) FS. History–New 6-18-87, Amended 8-7-96,
Formerly 10D-23.002, Amended 1-20-08.

8 – 3
64E-12.003 Water Supply.
(1) Water supplies shall be adequate to serve the demands of the facility and shall be constructed, operated and
maintained in accordance with requirements of Chapters 62-550 and 62-555 or Chapter 64E-8, Florida
Administrative Code (F.A.C.).
(a) Routine Testing. Facilities served by a drinking water system not regulated by Chapter 64E-8 or 62-550,
F.A.C., shall test the water and submit bacteriological water test results to the local county health department
(CHD):
1. Before opening the facility,
2. At least every 12 months,
3. Upon relocation,
4. Before having the well placed in service after construction, repair, or modification or,
5. After an emergency situation, such as a flood, that may introduce contaminants to the system.
(b) Test results must be negative for bacteriological contamination.
(c) Positive test results require the facility to temporarily provide potable water from a source approved by law
for the purpose of drinking, cooking, and oral contact until test results are negative. In addition, wells that test
positive shall be disinfected, flushed, and tested for bacterial contamination.
(d) Laboratory test results must be submitted to the local county health department in writing by the testing
laboratory.
(e) Testing can be obtained through the local county health department or a certified independent laboratory.
(2) Drinking water shall be accessible to all residents. When drinking fountains are available, they shall be
designed in compliance with the applicable plumbing provisions of the State Building Code, as adopted in Rule 9B-
3.047, F.A.C. When no approved drinking fountains are available, residents shall be provided with single service
cups or clean drinking utensils which shall be stored and dispensed in a manner to prevent contamination. Common
drinking cups are prohibited.
(3) Hot and cold running water under pressure and at safe temperatures, not to exceed 120° Fahrenheit at the
faucet to prevent scalding, shall be provided to all restroom lavatories and bathing areas.
Specific Authority 381.006, 381.006(16) FS. Law Implemented 381.006(16) FS. History–New 6-18-87, Amended 8-
7-96, Formerly 10D-23.003, Amended 1-20-08.
64E-12.004 Food Service: Tiers and Catering.
There are three tiers of food service, each with different minimal requirements based on facility type or the number
of residents in care. Only one tier of service as listed in subsections (1)-(3) below will be applied to any facility.
Facilities receiving or providing catered food must meet applicable standards as described in subsection (4) below.
(1) Tier 1. Facilities meeting the definition of “adult family-care home” regardless of the number of residents as
defined in Section 429.65(2), F.S., and other community based residential facilities with a maximum capacity to
house up to 5 residents, shall comply with the following requirements:
(a) Food used in the facility shall be clean, wholesome, free from spoilage and safe for human consumption.
Home canned food shall not be used. Canned food shall be from sources that are approved by law.
(b) The facility shall protect the food from dust, flies, rodents and other vermin, toxic materials, unclean
equipment and utensils, unnecessary handling, coughs and sneezes, flooding by sewage, overhead leakage and all

8 – 4
other sources of contamination at all times during storage, food preparation, transportation both on and off premises,
and service.
(c) Food storage equipment shall be provided to keep all potentially hazardous foods at safe temperatures, 41°
Fahrenheit or below or 140° Fahrenheit or above, except during necessary periods of preparation and service.
Potentially hazardous food shall not have been out of temperature more than 4 cumulative hours during the course of
thawing, preparation, service and cooling.
(d) At least one sink with hot and cold potable water under pressure shall be provided in the food preparation
area.
(e) Refrigeration units and hot food storage units used for the storage of potentially hazardous foods shall be
provided with a numerically scaled indicating thermometer accurate to plus or minus 3°F. The thermometer shall be
located in the warmest or coldest part of the units as may be applicable and of such type and so situated that the
temperature can be easily and readily observed.
(f) Labeling and Dating. Food containers shall be labeled with their contents and labels shall correctly identify
the contents of the container. Potentially hazardous foods and potentially hazardous foods that are in a form which is
edible without washing, cooking, or additional preparation, including previously cooked foods such as leftovers,
must be stored in accordance with the date marking and disposition requirements of subsections 64E-11.004(14) and
(15), F.A.C.
(2) Tier II. Except as described in subsection (1) above, if food service is provided in a facility with a maximum
capacity to house from 6 to 10 residents, the facility shall comply with the following requirements:
(a) In Chapter 64E-11, F.A.C.:
1. 64E-11.002, Definitions;
2. 64E-11.003, Food Supplies;
3. 64E-11.004, Food Protection;
4. 64E-11.005(1), (2)(b), (c), (e), (f), (3), (4), (5), Personnel;
5. 64E-11.013(3)(c), 1., 2., 4.
(b) Facilities opening, initially licensed by the licensing agency, or renovating on or after January 1, 2008 shall,
prior to construction or renovation of a food service operation or prior to substantial facility renovation, notify the
department and provide plans of the proposed construction or renovation, for review and approval at least 90 days
prior to the start of the project. Plans shall be submitted by the owner, prospective operator, or their designated
representative. All plans shall be in compliance with this section, shall be drawn to scale, describe the layout,
construction, finish schedule, general operation of the facility, equipment design and installation, and similar aspects
of the facility’s food service operation. A copy of the intended menu shall be provided to the department as part of
the plan review.
(c) The floor surfaces in kitchens, all the rooms and areas in which food is stored or prepared and in which
utensils are washed or stored, shall be of smooth, nonabsorbent material and constructed so they can be easily
cleaned and shall be kept clean and in good repair.
(d) The walls and shelving of all food preparation areas, food storage areas, utensil washing and handwashing
rooms or areas shall have smooth, easily cleanable surfaces. Walls shall be washable up to the highest level reached
by splash or spray.

8 – 5
(e) Hot and cold running water under pressure shall be easily accessible where food is prepared and where
utensils are washed.
(f) A handwashing sink, provided with hot and cold running water under pressure, shall be located within the
food preparation area. A sign must be posted clearly designating the sink for handwashing purposes. A handwashing
sink shall not be used for any other purpose. Facilities inspected and approved by the department prior to January 1,
2008, are exempt from this requirement until such time as kitchen renovation will occur or substantial renovation
will occur at the facility.
(g) In addition to the designated one compartment handwashing sink in paragraph (f) above, a two compartment
sink or one compartment sink and a residential use dishwasher shall be provided for warewashing. Notwithstanding
the provisions in subsection (f) above, if a facility has a two compartment sink and a residential dishwasher, one
compartment of the two compartment sink can be designated as a handwashing sink when labeled and used
exclusively as such. Existing facilities shall have until December 31, 2008, to comply with this requirement.
(h) Multi-use equipment and utensils shall be constructed and repaired with materials that are non-toxic,
corrosion resistant and nonabsorbent; and shall be smooth, easily cleanable and durable under conditions of normal
use; and shall not impart odors, color or taste nor contribute to the contamination of food.
(i) All multi-use eating and drinking utensils shall be thoroughly cleaned with hot water and an effective
detergent, then shall be rinsed free of such solution.
(j) Refrigeration units and hot food storage units used for the storage of potentially hazardous foods shall be
provided with a numerically scaled indicating thermometer accurate to plus or minus 3° Fahrenheit. The
thermometer shall be located in the warmest or coldest part of the units as may be applicable and of such type and so
situated that the temperature can be easily and readily observed.
(k) Potentially hazardous foods and potentially hazardous foods that are in a form which is edible without
washing, cooking, or additional preparation, including previously cooked foods such as leftovers, must be stored in
accordance with the date marking and disposition requirements of subsections 64E-11.004(14) and (15), F.A.C.
(l) The facility shall protect food and food equipment from all sources of contamination at all times during
storage, food preparation, service, and transportation both on and off premises.
(m) Live animals and pets living in or visiting a community based residential facility shall not enter the kitchen
or any food preparation areas when food is being prepared or served. Preventing pets and animals from entering the
kitchen or food preparation areas must be effective and may consist of passive restraint through obedience training,
use of physical barriers such as a gate, physical restraint such as limiting the animal to a room outside of the kitchen
or food preparation area, or any other effective means. Animals and pets shall not be fed, watered, bedded, kept, or
caged in the kitchen, food preparation, food storage, or dining area. Animal care supplies shall not be kept in the
kitchen or other food storage areas. If live animals have access to kitchen and dining areas during non-food
preparation and service times, then the facility shall effectively sanitize the dining tables, kitchen counter top
surfaces, food preparation surfaces, and other similar surfaces immediately before the next meal service or food
preparation begins. Persons handling or having direct physical contact with an animal must wash their hands
immediately prior to preparing or serving food.
(n) As part of an organized activity, residents may participate in food preparation under direct supervision of the
designated staff person in charge of food service activities, who is knowledgeable in food hygiene safety.

8 – 6
(o) Labeling. Food containers shall be labeled with their contents and labels shall correctly identify the contents
of the container.
(3) Tier III. If food service is provided in a hospice facility, or a facility with a maximum capacity of 11 or more
residents, it shall comply with Chapter 64E-11, F.A.C. Existing facilities shall have until December 31, 2008, to
comply with the requirements of Chapter 64E-11, F.A.C., except for item paragraph (b) below.
(a) Any organized food preparation activity in which residents may participate in food preparation as part of the
organized activity must be under the direct supervision of a trained food service employee, per Rule 64E-11.012,
F.A.C. This does not apply to specific designated therapeutic classes with activities for an individual or a group of
individuals provided by a licensed occupational or physical therapist as part of their occupational, physical, or
rehabilitation therapy activities to regain basic self sufficiency skills.
(b) Facilities with capacities of 11-24 residents that have been in continuous operation since initial regulation or
licensing by the department prior to January 1, 2008, are exempt from subsection 64E-11.008(7), F.A.C., until the
facility remodels the kitchen or dining area, or substantially remodels the facility.
(4) Catering. If food is catered from outside sources, the caterer shall be licensed or regulated by a state or
federal regulatory food program. If a community based residential facility caters additionally to outside sources, it
must meet all Chapter 64E-11, F.A.C., licensing standards.
(a) When catering is provided as the primary means of food supply, a copy of a current catering agreement shall
be provided to the local county health department at least annually and when a change in the agreement occurs. The
agreement shall minimally include the designated delivery times, method of hot and cold holding once food is
delivered, whether bulk or individually portioned food will be provided, and a designated responsible party for
cleaning and sanitizing any multi-use equipment and utensils.
(b) Upon delivery of catered food to a community based residential facility, catered food must be adequately
protected from contamination. The facility shall maintain a daily log indicating the date and time of delivery, name
or type of potentially hazardous food(s), and using an accurate food thermometer measure and log the food
temperatures upon arrival. Entries in the log shall be made at the time of delivery. These temperature logs shall be
maintained and retained at the facility for a period not less than 6 months. The records required by this section must
be made available for review by the department upon department request.
(c) If outside catering is not the primary means of food supply to the facility, and the facility only partakes in
the occasional carry-out or delivery of items such as, pizza, wings, sub-sandwiches, fried chicken, or barbequed
food, the catering requirements listed in paragraphs (a) and (b) above, do not apply.
Specific Authority 381.006(16), 381.0072(2)(a) FS. Law Implemented 381.006(16), 381.0072(2)(a), (b), (c) FS.
History–New 6-18-87, Formerly 10D-23.006, Amended 1-20-08.
64E-12.005 Housing.
(1) The facility shall provide safe and sanitary housing free from objects, materials, and conditions of an
environmental origin that constitute a danger to the residents.
(2) Floors, walls, ceilings, windows, doors and all appurtenances of the structures shall be of sound
construction, properly maintained, easily cleanable and shall be kept clean.

8 – 7
(a) Floor surfaces shall be of non-slip type and maintained free of loose or broken tiles and boards, holes,
uneven projections, protruding nails, tears, splinters, water spillage and other tripping hazards. Bathtubs and showers
shall contain slip-resistent strips, slip-resistent rubber bath mats, or slip-resistent surfaces.
(b) Wall surfaces shall be maintained free of hazardous projections, splinters, loose moldings, and broken
plaster.
(c) Overhead surfaces shall be free of water damage, loose, missing or broken tiles, plaster, lath, or loose
hanging fixtures, pipes and electric wiring.
(d) All external windows designed to open shall be accessible and operable.
(3) All housing facilities shall be kept free of offensive odors by adequate cleanliness and proper ventilation.
(4) All areas of the facility shall be well lighted. Dormitories, bedrooms, toilets, bathing rooms, shower rooms,
and dayrooms shall have light fixtures that provide at least 20 foot candles of illumination in all areas of the room,
measured at a distance 30 inches from the floor, to permit observation, cleaning and maintenance. Light fixtures
shall be maintained to work as designed and kept clean.
(5) All areas of the facility occupied by residents, including sleeping rooms, common areas, hallways,
bathrooms, and dining areas shall have natural or mechanical ventilation.
(a) If natural ventilation is utilized, the opened window area for ventilation purposes should be equal to one-
tenth of the floor space.
(b) When mechanical ventilation systems are employed, the systems shall be maintained to operate as designed
and kept clean. Intake air ducts shall be designed and installed so that dust or filters can be readily removed. In
resident occupied areas mechanical ventilation systems shall provide a minimum of 10 cubic feet of fresh or filtered
recirculated air per minute for each resident occupying the area.
(c) All toilet rooms shall be provided with direct openings to the outside or provided with mechanical
ventilation to the outside.
(6) Adequate heating facilities shall be provided to maintain a minimum temperature of 68° Fahrenheit, 20
inches above the floor in all resident occupied rooms.
(7) Mechanical cooling devices shall be used and in working condition in those areas of buildings occupied by
residents when inside temperatures exceed 85° Fahrenheit. Exceptions are made when the resident is capable and in
control of the thermostat or cooling devices in their personal area and chooses for it to exceed 85° Fahrenheit.
(8) All heating and cooling systems shall be consistent with current building and fire code rules applicable to
the area where the facility is located, as determined by building and fire officials.
(9) All furniture and furnishings must be in good repair and kept clean.
(10) Plumbing shall be maintained in compliance with the requirements of the applicable plumbing provisions
of the State Building Code, as adopted in Rule 9B-3.047, F.A.C., and Section 553.06, F.S.
(11) Sanitary facilities shall comply with the requirements of Chapter 64E-10, F.A.C.
(12) Sewage and liquid waste shall be disposed of in accordance with Chapter 62-601 or Chapter 64E-6, F.A.C.,
whichever is applicable.
Specific Authority 381.006, 381.006(16) FS. Law Implemented 381.006, 381.006(6), (16) FS. History–New 6-18-87,
Amended 8-7-96, Formerly 10D-23.009, Amended 1-20-08.

8 – 8
64E-12.006 Vector and Vermin Control.
(1) Effective control measures shall be utilized to minimize the presence of rodents, flies, cockroaches and other
vectors and vermin on the premises. The primary means of pest control shall be the use of integrated pest
management (IPM) systems and tools. IPM tools, such as “Integrated Pest Management for Schools: How-to
Manual” dated May 2, 2006, which are recognized by the United States Environmental Protection Agency, are
approved practices for the control of pests throughout a residential facility. The manual is available at
http://www.epa.gov/pesticides/ipm/schoolipm/index.html or by writing for a free copy to EPA Pesticides Section,
U.S. EPA Region 9, 75 Hawthorne Street (CMD-5), San Francisco, CA 94105. Use of IPM systems and tools does
not restrict the use of licensed pest control companies or individuals.
(2) The creation, maintenance or causing of any condition capable of propagating vectors and vermin will not
be permitted. All building shall be effectively maintained rodent-proofed and rodent free. All outside openings shall
be effectively sealed or screened with 16 mesh screening or equivalent, to prevent entry of insects, rodents, or other
vectors and vermin, except in wilderness programs when mosquito netting is provided to each resident.
Specific Authority 381.006, 381.006(16) FS. Law Implemented 381.006, 381.006(16) FS. History–New 6-18-87,
Amended 8-7-96, Formelry 10D-23.010, Amended 1-20-08.
64E-12.007 Bedding, Towels, Clothing and Personal Items.
Beds, mattresses and bedding shall be provided and kept in good repair and shall be cleaned regularly. Mattresses
and pillows shall have cleanable covers which shall be cleaned between uses by different residents. Sheets, towels
and personal clothing shall be washed at least weekly. Blankets shall be washed or dry cleaned as necessary and
between uses by different residents. Blankets, sheets, towels and clean clothing shall be stored in a clean, dry place
between laundering and use. Separate, individually assigned spaces shall be provided for storage of personal items
and toiletries. The use of common towels is prohibited.
Specific Authority 381.006(16) FS. Law Implemented 381.006(6), (16) FS. History–New 6-18-87, Formerly 10D-
23.011.
64E-12.008 Laundry.
(1) Where laundry facilities are provided, they shall be adequate to ensure an ample quantity of clean clothing,
bed linens and towels. Laundry facilities shall be of sound construction and shall be kept clean and in good repair.
Adequate space shall be provided for the complete separation of clean and soiled clothing, linen and towels.
(2) Laundry rooms shall have fixtures that provide at least 30 foot-candles of illumination, be kept clean and
free of lint build-up, and be properly ventilated as specified in the applicable building provisions of the State
Building Code, as adopted in Rule 9B-3.047, F.A.C. Lighting will be measured 30 inches above the floor. Clothes
dryers shall be vented to the exterior. Carts used for transporting dirty clothes, linens and towels shall not be used
for transporting clean articles unless they have been thoroughly cleaned and sanitized.
Specific Authority 381.006, 381.006(16) FS. Law Implemented 381.006, 381.006(16) FS. History–New 6-18-87,
Formerly 10D-23.012, Amended 1-20-08.
8 – 9
64E-12.009 Medications, Alcohol, Poisonous or Toxic Substances.
(1) Poisonous or toxic substances are to be stored apart from food and other areas that would constitute a hazard
to the residents. All containers containing poisonous or toxic substances must be clearly labled to indicate their
contents.
(2) All toxic, poisonous, and alcoholic substances shall be kept in locked areas, such as a locked office, locked
cabinet, or locked cupboard at all times when not in use. This does not apply to alcoholic beverages. Alcoholic
beverages shall be kept out of a child’s reach.
(3) Medications shall be kept in locked areas, such as a locked office, locked cabinet, or locked box at all times
when not in use. This is in addition to a childproof medicine bottle cap, lid, or other packaging. Exceptions are
extended to adults capable of self medication, life saving medications such as epinephrine pens, insulin, nitro
glycerin, or asthma inhalers that may be needed by the resident who is capable of self-medication in an emergency
due to illness or disease. Medicine containers or packaging must be clearly labeled indicating the prescribed
individual’s name and its contents. Medications requiring refrigeration or which are stored in a food service or food
storage area, shall be stored in such a manner that they do not pose a contamination hazard to food.
Specific Authority 381.006, 381.006(16) FS. Law Implemented 381.006, 381.006(6), (16) FS. History–New 6-18-87,
Formerly 10D-23.013, Amended 1-20-08.
64E-12.010 Garbage and Rubbish.
(1) All garbage, trash and rubbish shall be collected daily and placed in storage facilities. Garbage shall be
removed from storage facilities frequently enough to prevent a sanitary nuisance, as defined in Chapter 386, F.S.
Wet garbage shall be collected and stored in impermeable, leak proof, fly tight containers pending disposal. All
containers, storage areas and surrounding premises shall be kept clean and free of vermin.
(2) The method of disposal shall not create sanitary nuisance conditions and shall comply with provisions of
Chapter 62-701, F.A.C.
Specific Authority 381.006(16) FS. Law Implemented 381.006(6), (16) FS. History–New 6-18-87, Amended 8-7-96,
Formerly 10D-23.014.
64E-12.011 Recreational Areas.
(1) The recreational area shall be safe and free from hazardous conditions. Recreational equipment shall have
no jagged or sharp projections or other hazardous construction, and shall be maintained in a structurally sound
condition.
(2) Outdoor recreational areas shall be well drained and kept free of litter and trash.
(3) If swimming pools, spas, or open water hazards are located on the property of a community based residential
facility, the facility shall provide direct supervision by an adult employee when in use or when the area is occupied
by minors and other residents that cannot swim. The individual responsible for supervision during water activites or
near water hazards must have successfully completed the community water safety course specified in paragraph (b)
below.
(a) A wading or kiddy pool is not allowed.
(b) All community based residential facilities with swimming pools, spas, or open water hazards must have a
person on staff who has completed a community water safety course administered by the American Red Cross,
YMCA, or any aquatic training program granted approval under paragraph 64E-9.008(1)(d), F.A.C.

8 – 10
(c) A community based residential facility with a pool or spa not currently regulated by Chapter 64E-9, F.A.C.,
shall minimally, regardless of construction date, meet the barrier requirements in one of the following references:
Section 424.2.17 through 424.2.17.3 of the 2004 Florida State Building Code for private swimming pools or Section
515.29, F.S.
(d) Water safety devices shall be provided for residential pools. A shepherd’s hook shall be provided securely
attached to a one piece pole not less than 16 feet in length, and at least one 18 inch diameter lifesaving ring with
sufficient rope attached to reach all parts of the pool from the pool deck. Safety equipment shall be mounted in a
conspicuous place and be readily available for use. Residential spas and hot tubs are exempt from this requirement.
Specific Authority 381.006, 381.006(16) FS. Law Implemented 381.006, 381.006(16) FS. History–New 6-18-87,
Amended 8-7-96, Formerly 10D-23.015, Amended 1-20-08.
64E-12.012 Radon Testing.
Rulemaking Authority 404.056(4), (6), 381.006 FS. Law Implemented 404.056(4), 381.006(16) FS. History–
New 1-20-08, Repealed 12-29-16.
64E-12.013 Animal Health and Safety.
(1) Animals requiring rabies vaccination under Section 828.30, F.S., must be vaccinated for rabies and their
vaccinations must be current at the time of inspection. Proof of rabies vaccination or veterinary certification of
vaccination exemption shall be kept on the premises at all times.
(2) All animals must be kept in good health and free from disease or under treatment by a licensed veterinarian.
Indoor animals frequenting the outside must have an annual screening for internal parasites by a licensed
veterinarian. Any animal positive for internal parasites must be treated appropriately by the licensed veterinarian.
Animals being kept or having access to the indoors must be treated for flea control throughout the year to prevent
infestations.
(3) Aggressive, venomous, or potentially dangerous animals must be restricted from access by the residents at
all times and kept in such a manner so as not to be able to become free roaming and cause or inflict harm to the
residents, visitors, or employees. These animals may not be housed in the residents’ sleeping quarters.
Specific Authority 381.006(6), (16) FS. Law Implemented 381.006(6), (16) FS. History–New 1-20-08.

9. Rule Chapter
64E-16, F.A.C
.


9 – 1
CHAPTER 64E-16
BIOMEDICAL WASTE 64E-16.001 General
64E-16.002 Definitions
64E-16.003 Facility Policies and Procedures
64E-16.004 Storage and Containment
64E-16.005 Labeling
64E-16.006 Generator Requirements
64E-16.007 Treatment
64E-16.008 Biomedical Waste Transport
64E-16.009 Registration of Biomedical Waste Transporters
64E-16.010 Inspections
64E-16.011 Permits
64E-16.012 Fees
64E-16.013 Enforcement and Penalties (Repealed)
64E-16.001 General.
(1) This chapter prescribes minimum sanitary practices relating to the management of biomedical waste,
including segregation, handling, labeling, storage, transport, and treatment. This chapter applies to all facilities that
generate, transport, store, or treat biomedical waste to ensure that the waste is properly handled to protect public
health. Further, this chapter prescribes minimum standards for permitting biomedical waste generators, storage
facilities and treatment facilities, and for registering biomedical waste transporters.
(2) This chapter does not apply to biomedical waste incinerators. This chapter does not apply to linen
incinerators. This chapter does not apply to linen that is to be laundered and re-used. Further, this chapter does not
apply to dead bodies that are disposed of by a person licensed under the provisions of Chapter 470, F.S., or to the
transport of bodies, parts of bodies, or tissue specimens in furtherance of lawful examination, investigation, or
autopsy conducted pursuant to Section 406.11, F.S. Specimens or samples collected for laboratory testing or use in
medical research or teaching are not considered biomedical waste until such time as the material is discarded.
(3) The Department of Health shall regulate the packaging, transport, storage, and treatment of biomedical
waste. The Department of Environmental Protection shall regulate biomedical waste incineration and biomedical
waste disposal.
(4) Health care providers shall inform their home user clients verbally and in writing of the recommended
method for handling biomedical waste generated in the home setting. Health care providers who deliver in-home
medical services shall remove or have removed by a registered biomedical waste transporter all biomedical waste
generated during the performance of these services.
(5) Home users should segregate and package their biomedical waste in a manner that reduces the chance of
exposure to the public.
(6) Inspections, permitting and enforcement of emergency medical services that generate biomedical waste shall
be performed by the Bureau of Emergency Medical Services.
Rulemaking Authority 381.006, 381.0098 FS. Law Implemented 381.006, 381.0098 FS. History–New 6-19-89,
Amended 12-14-92, 1-23-94, 6-3-97, Formerly 10D-104.001.

9 – 2
64E-16.002 Definitions.
For the purpose of this chapter, the following words and phrases shall have the meanings indicated:
(1) American Society for Testing Materials, also referred to as ASTM – A technical society with headquarters
located at 100 Barr Harbor Drive, West Conshohocken, Pennsylvania, 19428-2959, which publishes national
standards for the testing and quality assurance of materials.
(2) Biomedical waste – Any solid or liquid waste which may present a threat of infection to humans, including
nonliquid tissue, body parts, blood, blood products, and body fluids from humans and other primates; laboratory and
veterinary wastes which contain human disease-causing agents; and discarded sharps. The following are also
included:
(a) Used, absorbent materials saturated with blood, blood products, body fluids, or excretions or secretions
contaminated with visible blood; and absorbent materials saturated with blood or blood products that have dried.
(b) Non-absorbent, disposable devices that have been contaminated with blood, body fluids or, secretions or
excretions visibly contaminated with blood, but have not been treated by an approved method.
(3) Biomedical waste generator – A facility or person that produces biomedical waste. The term includes
hospitals, skilled nursing or convalescent hospitals, intermediate care facilities, clinics, dialysis clinics, dental
offices, health maintenance organizations, surgical clinics, medical buildings, physicians' offices, laboratories,
veterinary clinics and funeral homes.
(a) Mobile health care units, such as bloodmobiles, that are part of a stationary biomedical waste generator, are
not considered individual biomedical waste generators.
(b) Funeral homes that do not practice embalming are not considered biomedical waste generators.
(4) Body fluids – Those fluids which have the potential to harbor pathogens, such as human immunodeficiency
virus and hepatitis B virus and include blood, blood products, lymph, semen, vaginal secretions, cerebrospinal,
synovial, pleural, peritoneal, pericardial and amniotic fluids. In instances where identification of the fluid cannot be
made, it shall be considered to be a regulated body fluid. Body excretions such as feces and secretions such as nasal
discharges, saliva, sputum, sweat, tears, urine, and vomitus shall not be considered biomedical waste unless visibly
contaminated with blood.
(5) Contaminated – Soiled by any biomedical waste.
(6) Decontamination – The process of removing pathogenic microorganisms from objects or surfaces, thereby
rendering them safe for handling.
(7) Department – The Department of Health or its representative county health department.
(8) Disinfection – A process which results in a minimum Log 6 kill against the vegetative organisms listed in
Table 1, and a minimum Log 4 kill against Bacillus stearothermophilus spores utilizing steam or a minimum Log 4
kill against Bacillus Subtilis spores utilizing dry heat, chemicals, or microwave shredding.
(9) Facility – All contiguous land, structures, and other appurtenances which are owned, operated, and licensed
as a single entity which may consist of several generating, treatment, or storage units.
(10) Hazardous waste – Those materials defined in Chapter 62-730, F.A.C.
(11) Health Care Provider – Any person who provides medical care or personal services, as that term is defined
in Section 400.402, F.S., to another individual.
(12) Home User – An individual who generates biomedical waste as a result of self-care or care by a family
member or other non health care provider.

9 – 3
(13) Leak resistant – Prevents liquid from escaping to the environment in the upright position.
(14) Outer container – Any rigid type container used to enclose packages of biomedical waste.
(15) Packages – Any material that completely envelops biomedical waste. This includes red bags, sharps
containers and outer containers.
(16) Person – Any individual, partnership, corporation, association, or public body engaged in the generation,
storage, transport, or treatment of biomedical waste.
(17) Point of origin – The room or area where the biomedical waste is generated.
(18) Public sharps collection program – A cooperative program designed as a non-profit community service to
assist the home user in the safe disposal of discarded sharps.
(19) Puncture resistant – Able to withstand punctures from contained sharps during normal usage and handling.
(20) Restricted – The use of any measure, such as a lock, sign, or location, to prevent unauthorized entry.
(21) Saturated – Soaked to capacity.
(22) Sealed – Free from openings that allow the passage of liquids.
(23) Sharps – Objects capable of puncturing, lacerating, or otherwise penetrating the skin.
(24) Sharps container – A rigid, leak and puncture resistant container, designed primarily for the containment of
sharps, clearly labeled with the phrase and international biological hazard symbol as described in Section 64E-
16.004(2)(a), F.A.C., and manufactured with dyes meeting the requirements for incidental metals as described in
Section 64E-16.004(2)(b)1.b., F.A.C.
(25) Sterilization – A process which results in a minimum Log 6 kill against Bacillus stearothermophilus spores
utilizing steam or a minimum Log 6 kill against Bacillus Subtilis spores utilizing dry heat, chemicals, or microwave
shredding.
(26) Storage – The holding of packaged biomedical waste for a period longer than three days at a facility or in a
transport vehicle.
(27) Transfer – The movement of biomedical waste within a facility.
(28) Transport – The movement of biomedical waste away from a facility.
(29) Transport vehicle – A motor vehicle, as defined in Section 320.01, F.S., a rail car, watercraft or aircraft,
used for the transportation of biomedical waste.
(30) Treatment – Any process, including steam, chemicals, microwave shredding, or incineration, which
changes the character or composition of biomedical waste to render it noninfectious by disinfection or sterilization.
Rulemaking Authority 381.006, 381.0098 FS. Law Implemented 381.006, 381.0098, 395.002(13), 395.1011 FS.
History–New 6-19-89, Amended 4-2-90, 12-14-92, 1-23-94, 8-20-95, 6-3-97, Formerly 10D-104.002.
64E-16.003 Facility Policies and Procedures.
(1) All biomedical waste facilities shall comply with the following:
(a) Biomedical waste mixed with hazardous waste, as defined in Chapter 62-730, F.A.C., Hazardous Waste,
shall be managed as hazardous waste.
(b) Biomedical waste mixed with radioactive waste shall be managed in a manner that does not violate the
provisions of Chapter 64E-5, F.A.C. The biomedical waste shall be managed in accordance with the provisions of
Chapter 64E-16, F.A.C., after the radioactive component has decayed in storage as provided for in Chapter 64E-5,
F.A.C., or is otherwise not regulated under Chapter 64E-5, F.A.C. The packaging requirements of Chapter 64E-5,
F.A.C., shall be followed, unless the requirements of Chapter 64E-16, F.A.C., are more restrictive.

9 – 4
(c) Any other solid waste or liquid, which is neither hazardous nor radioactive in character, combined with
untreated biomedical waste, shall be managed as untreated biomedical waste.
(d) All surfaces contaminated with spilled or leaked biomedical waste shall be decontaminated as part of the
cleaning process.
(2) Each biomedical waste facility shall implement a written operating plan to manage biomedical waste, in
accordance with this chapter. This plan shall be available for review by the department and facility personnel. The
plan shall include the following: a description of training for personnel; procedures for segregating, labeling,
packaging, transporting, storing, and treating, biomedical waste; procedures for decontaminating biomedical waste
spills; and a contingency plan for emergencies. Facilities which have multiple specialty services shall include
procedures specific to each specialty if procedures vary. Plans shall be updated when regulations, facility policies, or
procedures change.
(a) Each facility or their designee shall train new personnel who handle biomedical waste as part of their work
responsibilities. This training shall be provided prior to commencement of duties related to biomedical waste
handling. Refresher training shall be completed annually by all personnel who handle biomedical waste. Training
shall detail compliance with the facility's operating plan and Chapter 64E-16, F.A.C., and shall be maintained as a
part of the operating plan.
(b) All biomedical waste management records shall be maintained for 3 years and shall be available for review
by the department.
Rulemaking Authority 381.006, 381.0098 FS. Law Implemented 381.006, 381.0098, 395.002(13), 395.1011 FS.
History–New 6-19-89, Amended 4-2-90, 12-14-92, 1-23-94, 8-20-95, 6-3-97, Formerly 10D-104.003.
64E-16.004 Storage and Containment.
(1) Storage.
(a) Storage of biomedical waste at the generating facility shall not exceed 30 days. The 30 day period shall
commence when the first non-sharps item of biomedical waste is placed into a red bag or sharps container, or when
a sharps container containing only sharps is sealed.
(b) Storage of biomedical waste in a place other than at the generating facility shall not exceed 30 days. The 30
day storage period shall begin on the day the waste is collected from the generator.
(c) Indoor storage areas shall have restricted access and be designated in the written operating plan. They shall
be located away from pedestrian traffic, be vermin and insect free, and shall be maintained in a sanitary condition.
They shall be constructed of smooth, easily cleanable materials that are impervious to liquids.
(d) Outdoor storage areas, including containers and trailers, shall, in addition to the above criteria, be
conspicuously marked with the international biological hazard symbol as described in paragraph 64E-16.004(2)(b),
F.A.C., and shall be secured against vandalism and unauthorized entry. The international biological hazard symbol
on an outdoor storage area shall be a minimum of six inches in diameter.
(2) Containment.
(a) Packages of biomedical waste shall remain sealed until treatment, except when compacted in accordance
with the requirements of this chapter as stated in Section 64E-16.006(2), F.A.C. Ruptured or leaking packages of
biomedical waste shall be placed into larger packaging without disturbing the original seal.

9 – 5
(b) All packages containing biomedical waste shall be visibly identifiable with the international biological
hazard symbol and one of the following phrases: “BIOMEDICAL WASTE”, “BIOHAZARDOUS WASTE”,
“BIOHAZARD”, “INFECTIOUS WASTE”, or “INFECTIOUS SUBSTANCE”. The symbol shall be red, orange, or
black and the background color shall contrast with that of the symbol or comply with the requirements cited in
subpart Z of 29 C.F.R. subparagraph 1910.1030(g)(1)(C), Occupational Exposure to Bloodborne Pathogen Standard.
(c) Bags.
1. Biomedical waste, except sharps, shall be packaged and sealed at the point of origin in impermeable, red
plastic bags or, at the discretion of the generator, into sharps containers. The international biological hazard symbol
shall be at least six inches in diameter on bags 19'' × 14'' or larger, and at least one inch in diameter on bags smaller
than 19'' × 14''. Each plastic bag shall meet the following physical properties:
a. Impact resistance of 165 grams and tearing resistance of 480 grams in both the parallel and perpendicular
planes with respect to the length of the bag. Impact resistance shall be determined using ASTM D-1709-91, and
tearing resistance shall be determined using ASTM D-1922-89.
b. Incidental sum concentrations of lead, mercury, hexavalent chromium and cadmium shall be no greater than
100 ppm for dyes used in the coloration of bags.
(d) Sharps containers.
1. Sharps shall be discarded at the point of origin into single use or reusable sharps containers. Needles and
scalpel blades shall not be placed directly into double-walled corrugated containers. Sharps containers must be
sealed when full. A sharps container is considered full when materials placed into it reach the designated fill line, or,
if a fill line is not indicated, when additional materials cannot be placed into the container without cramming or
when no additional materials are to be placed in the container.
2. Permanently mounted sharps container holders shall bear the phrase and the international biological hazard
symbol described in paragraph 64E-16.004(2)(a), F.A.C., if this information on the sharps container is concealed by
the sharps container holder.
3. Reusable sharps containers shall only be emptied into a treatment cart or directly into a treatment unit. They
shall be constructed of smooth, easily cleanable materials, and shall be decontaminated after each use.
4. The international biological hazard symbol shall be at least one inch in diameter on sharps containers.
(e) All outer containers shall be rigid, leak-resistant and puncture-resistant. Reusable outer containers shall be
constructed of smooth, easily cleanable materials and shall be decontaminated after each use.
(f) The international biological hazard symbol shall be at least six inches in diameter on outer containers 19'' ×
14'' or larger, and at least one inch in diameter on outer containers less than 19'' × 14''.
Rulemaking Authority 381.006, 381.0098 FS. Law Implemented 381.006, 381.0098, 395.002(13), 395.1011 FS.
History–New 6-19-89, Amended 4-2-90, 12-14-92, 1-23-94, 8-20-95, 6-4-97, Formerly 10D-104.004.

9 – 6
64E-16.005 Labeling.
(1) Biomedical waste bags and sharps containers shall be labeled with the generator’s name and address unless
treatment occurs at the generating facility.
(a) If a bag or sharps container is placed into a larger bag prior to transport, the label for the exterior bag shall
comply with subsection 64E-16.005(1), F.A.C. Inner bags and inner sharps containers are exempt from the labeling
requirements of subsection 64E-16.005(1), F.A.C.
(b) Outer containers shall be labeled with the transporter’s name, address, registration number, and 24-hour
telephone number prior to transport.
(2) The transporter may provide labels for bags or sharps containers that are generator-specific, such as bar
codes or specific container numbers. Use of these generator-specific labels satisfies the requirements of paragraph
64E-16.005(1)(a), F.A.C.
Rulemaking Authority 381.006, 381.0098 FS. Law Implemented 381.006, 381.0098, 395.002(13), 395.1011 FS.
History–New 6-19-89, Amended 4-2-90, 12-14-92, 1-23-94, 8-20-95, 6-3-97, Formerly 10D-104.005.
64E-16.006 Generator Requirements.
(1) A biomedical waste generator shall not negotiate for the transport of biomedical waste with a person who is
not registered with the department as a biomedical waste transporter.
(2) Compacting packages of biomedical waste within the generating facility, except recognizable human tissue,
bulk liquids, or sharps, is acceptable provided the following conditions are met:
(a) Packages of biomedical waste shall not be compacted to a density greater than 22 pounds per cubic foot.
(b) Compacted packages of biomedical waste shall not be subjected to further compacting.
(c) Any residual or incidental liquid shall be contained within the inner bag or outer container. Should the inner
bag or outer container rupture during compaction, residual or incidental liquids shall be disposed of directly into the
sanitary sewer, an on-site sewage treatment and disposal system, or other system approved to receive such wastes by
the Department of Environmental Protection or the department;
(d) Discharge of noxious air shall be kept to a minimum through use of HEPA filters having a pore size of 2
microns or less, negative pressure rooms, or other safety methods;
(e) Compacted packages of biomedical waste shall be treated by incineration or other approved treatment
process. Treatment processes, such as steam, chemical, gas, dry heat, or microwaving, shall be considered by the
department upon written request and microbiological evidence that the proposed process provides the same degree
of treatment for compacted waste as for uncompacted waste. Steam treatment systems shall be tested against
Bacillus stearothermophilus spores, as described in subsection 64E-16.007(2), F.A.C. Other proposed treatment
processes shall demonstrate efficacy using subsection 64E-16.007(4), F.A.C.
Rulemaking Authority 381.006, 381.0098 FS. Law Implemented 381.006, 381.0098, 395.002(13), 395.1011 FS.
History–New 6-19-89, Amended 4-2-90, 12-14-92, 1-23-94, 8-20-95, 6-3-97, Formerly 10D-104.006.

9 – 7
64E-16.007 Treatment.
(1) Biomedical waste shall be treated by steam, incineration, or an alternative process approved by the
department as described in subsection 64E-16.007(4), F.A.C., prior to disposal. Treatment shall occur within 30
days of collection from the generator.
(2) Steam treatment units shall subject loads of biomedical waste to sufficient temperature, pressure, and time to
demonstrate a minimum Log 4 kill of Bacillus stearothermophilus spores placed at the center of the waste load, and
shall be operated in accordance with the following:
(a) Before placing a steam treatment unit into service, operating parameters such as temperature, pressure, and
treatment time shall be determined according to the following:
1. Test loads of biomedical waste which consist of the maximum weight and density of biomedical waste to be
treated shall be prepared. Separate loads of red bags, sharps containers, boxes, and compacted waste shall be
prepared if they are to be treated separately.
2. Prior to treatment, Bacillus stearothermophilus spores shall be placed at the bottom and top of each treatment
container, at the front of each treatment container at a depth of approximately one-half of the distance between the
top and bottom of the load, in the approximate center of each treatment container, and in the rear of each treatment
container at a depth of approximately one-half of the distance between the top and bottom of the load.
3. If the operating parameters used during the treatment of the test loads demonstrate a minimum Log 4 kill of
Bacillus stearothermophilus spores at all locations, the steam treatment unit shall operate under those parameters
when placed into service. If the operating parameters fail to provide a minimum Log 4 kill of Bacillus
stearothermophilus spores at all locations, treatment time, temperature, or pressure shall be increased and the tests
must be repeated until a minimum Log 4 kill of Bacillus stearothermophilus spores is demonstrated at all locations.
The steam treatment unit shall be operated under those parameters when placed into service. Tests shall be repeated
and new parameters established if the type of biomedical waste to be treated is changed.
(b) When operating parameters have been established and documented using the criteria in paragraph 64E-
16.007(2)(a), F.A.C., the steam treatment unit may be placed into service.
(c) The steam treatment unit shall be serviced for preventive maintenance in accordance with the manufacturer's
specifications. Records of maintenance shall be onsite and available for review.
(d) Unless a steam treatment unit is equipped to continuously monitor and record temperature and pressure
during the entire length of each treatment cycle, each package of biomedical waste to be treated will have a
temperature tape or equivalent test material such as a chemical indicator placed on a non-heat conducting probe at
the center of each treatment container in the load that will indicate if the treatment temperature and pressure have
been reached. Waste shall not be considered treated if the tape or equivalent indicator fails to show that a
temperature of at least 250 degrees F (121 degrees C) was reached during the process.
(e) Each steam treatment unit shall be evaluated for effectiveness with spores of Bacillus stearothermophilus at
least once each 7 days for permitted treatment facilities, or once each 40 hours of operation for generators who treat
their own biomedical waste. The spores shall be placed at the center of the waste load. Evaluation results shall be
maintained onsite and available for review.
(f) A written log shall be maintained for each steam treatment unit. The following shall be recorded for each
usage:
1. The date, time, and operator name;

9 – 8
2. The type and approximate amount of waste treated;
3. The post-treatment confirmation results by either
a. recording the temperature, pressure, and length of time the waste was treated, or
b. the temperature and pressure monitoring indicator;
(g) A current written operating procedure shall specify, at a minimum, the following:
1. Parameters, determined from testing, that provide consistent treatment, such as exposure time, temperature,
and pressure.
2. Identification of standard treatment containers and placement of the load in the steam treatment unit.
(3) Incineration of biomedical waste shall be achieved in a biological waste incinerator permitted by the
Department of Environmental Protection.
(4) An alternative treatment process, such as chemical, gas, dry heat, or microwave shredding, shall be
considered by the department upon receipt of a written request. The written request shall be directed to the State
Health Officer and shall include:
(a) The specific treatment process and type of facility for which acceptance is sought;
(b) The reason for the request;
(c) Microbiological evidence, using the organisms listed in Table 1, that the proposed process provides
sterilization or a satisfactory level of disinfection. Using the protocol described in subsection 64E-16.007(4), F.A.C.,
alternative treatment systems must show either:
1. For disinfection, a minimum Log 6 kill for the vegetative organisms listed in Table 1 and a minimum Log 4
kill against Bacillus stearothermophilus spores utilizing steam or a minimum Log 4 kill against Bacillus Subtilis
spores utilizing dry heat, chemicals, or microwave shredding, or
2. For sterilization, a minimum Log 6 kill against Bacillus stearothermophilus spores utilizing steam or a
minimum Log 6 kill against Bacillus Subtilis spores utilizing dry heat, chemicals, or microwave shredding.
Table 1
1. Bacteria
a. Bacillus spores – mandatory, species determined by treatment process
Any two
b. Enterococcus faecalis
c. Pseudomonas aeruginosa
d. Staphylococcus aureus
e. Nocardia species
2. Mycobacteria species – any one
a. Mycobacterium bovis
b. Mycobacterium fortuitum
3. Fungus – any one
a. Candida albicans
b. Aspergillus fumigatus
4. Protozoa – Giardia intestinalis or similar
5. Virus – Poliovirus or similar.

9 – 9
(d) Each step of the efficacy testing must be thoroughly described in the application for approval. A detailed
description of the treatment process, preparation of organisms, preparation of test loads, recovery of organisms, and
raw data must be provided.
(e) To begin the efficacy testing, two challenge loads must be sterilized. These loads must be composed of
materials commonly found in biomedical waste (tissues, sharps, plastics, glass, woven materials, blood and blood
products, etc.), and must be of adequate quantity to equal the maximum capacity of the treatment system. The test
load must be fully described (weight, moisture content, composition, etc.).
(f) The purity of all organisms and spores must be certified by a clinical or commercial laboratory. Each
organism must be processed separately and placed in the test load in the most difficult location to treat. Before each
test run, the total number of viable test organisms must be determined and documented. Treatment of the test load
must take place within thirty minutes of inoculating the load with the test organism.
(g) The test load containing the test organism must be processed without the agent (e.g., chemical, microwaves,
etc.) used to kill the test organisms. If this agent is a liquid, it must be replaced with an equal amount of sterile saline
solution or tapwater. After the test load has completed one cycle in the treatment device, a minimum of three grab
samples must be taken from the test load and the number of test organisms present determined. If the number of
organisms recovered after the test run is less than Log 6, the number of organisms originally introduced into the
device must be increased, and the run must be performed again, until at least Log 6 organisms are recovered. If the
number of organisms recovered from the test run is Log 6 or greater, there is an adequate number of organisms
being introduced into the device, and the inoculum size should be equal to this number.
(h) Using the inoculum size determined in the above procedure, the second sterilized test load must be
inoculated separately. During these test runs, the chemical or physical agent used to treat the waste must be used.
(i) After each test run is completed, the log kill for that particular organism or spore must be calculated. The
number of organisms that were not recovered from the initial (non-treating) test run must be subtracted from the
number of organisms that were introduced into the second (treatment) run. The number of organisms that survive the
treatment process must be subtracted from the first calculation. The resulting figure is the log kill provided by the
treatment process.
(j) Approved alternative treatment processes, except single-use, shall meet the requirements of paragraph 64E-
16.007(2)(e), F.A.C.
(5) Biomedical waste may be disposed into a sanitary sewer system, an onsite sewage treatment and disposal
system, or other system approved to receive such waste by The Department of Environmental Protection or the
department, if it is in a liquid or semi-solid form and aerosol formation is minimal.
(6) Body tissues that have been histologically fixed are considered treated biomedical waste. Tissues prepared
by frozen sectioning only are not considered treated.
(7) Acute care hospitals, licensed under Chapter 395, F.S., which utilize a certified onsite treatment process
involving grinding and treatment, may dispose of such treated biomedical waste in the normal municipal solid waste
stream upon notifying the local government responsible for solid waste collection and disposal under the following
conditions:
(a) For the purposes of this chapter, certified shall mean that the treatment process is steam treatment, or has
been approved as an alternative biomedical waste treatment process under subsection 64E-16.007(4), F.A.C.
(b) For the purposes of this chapter, grinding shall also mean shredding or hammermilling.

9 – 10
(c) If grinding takes place prior to treatment, procedures that minimize the chance of exposure to waste handlers
must be developed and implemented should the grinder fail or become jammed.
(d) Individuals operating the treatment unit must be trained in all aspects of its operation, including contingency
procedures.
(e) Acute care hospitals must inform the department in writing of the installation of the unit at least 30 days
prior to placing the unit into service.
(f) Inspection of the unit, including treatment and maintenance records, will occur during the annual inspection
for the hospital's biomedical waste permit.
Rulemaking Authority 381.006, 381.0098 FS. Law Implemented 381.006, 381.0098, 395.002(13), 395.1011 FS.
History–New 6-19-89, Amended 12-14-92, 1-23-94, 8-20-95, 6-3-97, Formerly 10D-104.007.
64E-16.008 Biomedical Waste Transport.
(1) No registered transporter may knowingly accept biomedical waste for transport unless it has been properly
segregated, packaged, and labeled.
(2) Each registered transporter shall provide the generator with a receipt of pick-up.
(3) During transport, no registered transporter shall compact biomedical waste or allow it to leak into the
environment.
(4) Transfer of biomedical waste from one transport vehicle to another is not allowed unless the transfer occurs
at a permitted storage or treatment facility, except as provided in paragraph 64E-16.008(10)(a), F.A.C. Intermodal
transfers of biomedical waste are allowed provided transport shipping seals remain intact.
(5) Any registered transporter who unknowingly fails to comply with subsections (3) or (4) of this section
because such biomedical waste has not been properly segregated or separated from other solid wastes by the
generating facility is not guilty of a violation under this rule.
(6) No registered transporter shall knowingly deliver biomedical waste for storage or treatment to a facility
which does not have a valid permit issued by the department.
(7) All transport vehicles containing biomedical waste shall be visibly identified with the business name,
registration number, a 24 hour telephone number, and placards showing the phrase and the international biological
hazard symbol as described in paragraph 64E-16.004(2)(a), F.A.C. The symbol shall be at least six inches in
diameter.
(8) All transport vehicles containing biomedical waste shall be fully enclosed and secured when unattended.
(9) Registered transporters shall notify the department within one working day by telephone and shall submit a
follow-up report to the department within 10 days, in writing, if there is an accident that results in a spill of
biomedical waste.
(10) In case of an emergency situation, including mechanical failure, the following is allowed:
(a) If the emergency occurs during transport, biomedical waste may be transferred to another transport vehicle,
including a rental vehicle, without being at a storage or treatment facility.
(b) If a rental vehicle is used, the department shall be notified of its use on the first working day after the
emergency. A copy of the written authorization from the rental agency stating awareness of the intended use of the
vehicle shall be submitted to the department within seven days.
(c) Biomedical waste shall be removed and transported to a permitted storage or treatment facility within 24
hours of the emergency.

9 – 11
(d) Before return to the rental agency, the vehicle shall be decontaminated.
Rulemaking Authority 381.0098 FS. Law Implemented 381.0098 FS. History–New 6-3-97, Formerly 10D-104.0073.
64E-16.009 Registration of Biomedical Waste Transporters.
(1) Biomedical waste transporters shall be registered with the department. Biomedical waste generators
transporting less than 25 pounds of their own biomedical waste, in their own transport vehicle, on any single
occasion, are exempt from transporter registration, fee, and placarding requirements of this chapter.
(2) Each owner or operator of a transport vehicle shall submit to the department a completed application for
registration on form DH 4106, herein incorporated by reference.
(3) Biomedical waste transporter registrations shall expire on September 30 each year. Renewal applications
will not be considered complete without the submission of an annual report on form DH 4109, herein incorporated
by reference. Biomedical waste transporters with valid registrations, on the effective date of this chapter, shall renew
their registration by September 30 following the expiration date of their existing registration.
(4) Registered transporters shall notify the department in writing within 30 days of any changes made to their
registration form currently on file with the department.
(5) Any registered biomedical waste transporter is subject to having their biomedical waste transporter
registration denied, suspended, or revoked, pursuant to Section 381.0098, F.S., and in accordance with the
procedural requirements of Section 120.60, F.S., upon a finding by the department that the transporter:
(a) Has submitted false or inaccurate information in the application or annual report;
(b) Has violated the provisions of any statute or rule which the department is authorized to enforce;
(c) Has refused to allow inspection of records or equipment by department personnel.
Rulemaking Authority 381.0098 FS. Law Implemented 381.0098 FS. History–New 6-3-97, Formerly 10D-104.0074.
64E-16.010 Inspections.
(1) Department personnel shall inspect registered transport vehicles, permitted generators, storage, and
treatment facilities at least once a year. Those facilities exempted from the registration and fee requirements under
Section 381.0098(4), F.S., shall be inspected at least once every three years. Reinspections may be conducted when
a facility is found to be in non-compliance with this chapter. Results of each inspection shall be recorded on a form
provided by the department.
(2) To provide consistency of inspections throughout the state, all department personnel who inspect biomedical
waste facilities shall attend training annually, which shall be approved by the Bureau of Environmental Health
Programs.
Rulemaking Authority 381.006, 381.0098 FS. Law Implemented 381.006, 381.0098 FS. History–New 12-14-92,
Amended 1-23-94, 8-20-95, 6-3-97, Formerly 10D-104.0075.
64E-16.011 Permits.
(1) All biomedical waste facilities, except those facilities operating under a Department of Environmental
Protection permit, shall obtain a permit from the department annually. Application forms and annual report forms
used by the public may be obtained from the environmental health section of the county health department in the
county of their location or from the Department of Health, Bureau of Facility Programs, 4052 Bald Cypress Way,
Bin #A08, Tallahassee, Florida 32399-1710. All forms listed in this section are incorporated by reference.
(a) A biomedical waste generator, who produces or treats less than 25 pounds of biomedical waste in each 30
day period, shall be exempt from all permit and fee requirements of this chapter.

9 – 12
(b) Application for an initial biomedical waste generator permit or exemption from permitting shall be
submitted to the department on form DH 4089, Application for Biomedical Waste Generator Permit/Exemption,
8/98. Biomedical waste treatment facilities which were constructed prior to December 31, 1995, or for which an
operation permit was submitted to the Department of Environmental Protection prior to December 31, 1995, shall
meet the requirements of this chapter at the time of renewal of their existing permit.
(c) Application for an initial biomedical waste storage facility permit shall be submitted to the department on
form DH 4107, Application for Biomedical Waste Storage Permit, 8/98.
(d) Application for an initial biomedical waste treatment facility permit shall be submitted to the department on
form DH 4111, Application for a Biomedical Waste Treatment Permit, 8/01. Renewals will not be considered
complete without the submission of an annual report submitted on form DH 4110, Biomedical Waste Treatment
Facility Annual Report, 8/01.
(e) Application for an initial biomedical waste sharps collection program permit shall be submitted to the
department on form DH 4108, Application for Biomedical Waste Sharps Collection Program Permit, 8/98.
(f) Permits shall not be transferable from one person to another. In the event of an address or name change, an
amended application for permit shall be submitted to the department. A permitted generator may work at a branch
office for no more than six hours in any seven day period without applying for an additional permit. These
generators must notify the local county health department biomedical waste coordinator of the existence and
operating hours of the branch office.
1. In the event of a change of ownership of the facility or a newly constructed facility, an application for an
initial permit shall be submitted to the department within 30 days of the commencement of business.
2. When a facility is leased by the owner to a second party for operation, the second party shall apply to the
department for an initial permit within 30 days of the commencement of business. The second party shall be held
responsible for the operation and maintenance of the facility.
(g) Permits shall expire on September 30 each year. The permit, or a copy thereof, shall be maintained within
the facility and shall be made available for review by department personnel.
(2) Persons engaged in a sharps collection program with single or multiple facility locations may operate under
a single permit provided:
(a) The sharps collection program is open to the general public;
(b) A list identifying the location of each facility is attached to the application; and
(c) Each facility meets the applicable permit requirements.
Rulemaking Authority 381.006, 381.0098 FS. Law Implemented 381.006, 381.0098 FS. History–New 12-14-92,
Amended 1-23-94, 6-3-97, Formerly 10D-104.0076, Amended 11-5-02.
64E-16.012 Fees.
(1) State-owned and operated biomedical waste facilities are exempt from the permit fee.
(2) Fee schedule.
Generator Permit:
(application received by October 1) $ 85.00
(application received after October 1) $105.00
Treatment Permit:
(application received by October 1) $ 85.00

9 – 13
(application received after October 1) $105.00
Storage Permit:
(application received by October 1) $ 85.00
(application received after October 1) $105.00
Transporter Registration (one vehicle):
(application received by October 1) $ 85.00
(application received after October 1) $105.00
Additional Vehicle $ 10.00
No fee or combination of fees shall exceed the maximum amount established by the statute.
(3) All fees collected pursuant to this section shall be placed in a specially designated account within the individual
county health department trust fund to be used to meet the cost of administering the biomedical waste program
described in this chapter.
Rulemaking Authority 381.006, 381.0098(4) FS. Law Implemented 381.006, 381.0098 FS. History–New 12-14-92,
Amended 1-23-94, 6-3-97, Formerly 10D-104.0078, Amended 1-12-09.
64E-16.013 Enforcement and Penalties.
Rulemaking Authority 381.006, 381.0098(5) FS. Law Implemented 381.0012, 381.002(13), 381.0025, 381.006,
381.0061, 381.0098, 395.1011, 775.082, 775.083 FS. History–New 6-19-89, Amended 12-14-92, 1-23-94, 6-3-97.
Formerly 10D-104.008, Amended 11-5-02, Repealed 12-2-15.
Notes ______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________

9 – 14
Notes ______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________

10. Chapter 464, F.S.


10 – 1
CHAPTER 464
PART I
NURSE PRACTICE ACT
464.001 Short title.
464.002 Purpose.
464.003 Definitions.
464.004 Board of Nursing; membership; appointment; terms.
464.005 Board headquarters.
464.006 Rulemaking authority.
464.008 Licensure by examination.
464.009 Licensure by endorsement.
464.0095 Nurse Licensure Compact.
464.0096 Nurse Licensure Compact; public records and meetings exemptions.
464.012 Licensure of advanced practice registered nurses; fees; controlled substance prescribing.
464.013 Renewal of license or certificate.
464.014 Inactive status.
464.015 Titles and abbreviations; restrictions; penalty.
464.016 Violations and penalties.
464.017 Sexual misconduct in the practice of nursing.
464.018 Disciplinary actions.
464.019 Approval of nursing education programs.
464.0195 Florida Center for Nursing; goals.
464.0196 Florida Center for Nursing; board of directors.
464.0205 Retired volunteer nurse certificate.
464.022 Exceptions.
464.027 Registered nurse first assistant.
464.001 Short title.—This part may be cited as the “Nurse Practice Act.”
History.—ss. 1, 6, ch. 79-225; ss. 2, 3, ch. 81-318; ss. 1, 17, 18, ch. 86-284; s. 58, ch. 91-137; s. 5, ch. 91-156; s.
4, ch. 91-429; s. 119, ch. 2000-318.
464.002 Purpose.—The sole legislative purpose in enacting this part is to ensure that every nurse practicing in
this state meets minimum requirements for safe practice. It is the legislative intent that nurses who fall below
minimum competency or who otherwise present a danger to the public shall be prohibited from practicing in this
state.
History.—ss. 1, 6, ch. 79-225; ss. 2, 3, ch. 81-318; ss. 2, 17, 18, ch. 86-284; s. 58, ch. 91-137; s. 5, ch. 91-156; s.
4, ch. 91-429; s. 120, ch. 2000-318.
10 – 2
464.003 Definitions.—As used in this part, the term:
(1) “Accredited program” means a program for the prelicensure education of professional or practical nurses
that is conducted in the United States at an educational institution, whether in this state, another state, or the District
of Columbia, and that is accredited by a specialized nursing accrediting agency that is nationally recognized by the
United States Secretary of Education to accredit nursing education programs.
(2) “Advanced or specialized nursing practice” means, in addition to the practice of professional nursing, the
performance of advanced-level nursing acts approved by the board which, by virtue of postbasic specialized
education, training, and experience, are appropriately performed by an advanced practice registered nurse. Within
the context of advanced or specialized nursing practice, the advanced practice registered nurse may perform acts of
nursing diagnosis and nursing treatment of alterations of the health status. The advanced practice registered nurse
may also perform acts of medical diagnosis and treatment, prescription, and operation as authorized within the
framework of an established supervisory protocol. The department may, by rule, require that a copy of the protocol
be filed with the department along with the notice required by s. 458.348.
(3) “Advanced practice registered nurse” means any person licensed in this state to practice professional
nursing and who is licensed in an advanced nursing practice, including certified nurse midwives, certified nurse
practitioners, certified registered nurse anesthetists, clinical nurse specialists, and psychiatric nurses.
(4) “Approved program” means a program for the prelicensure education of professional or practical nurses that
is conducted in the state at an educational institution and that is approved under s. 464.019. The term includes such a
program placed on probationary status.
(5) “Board” means the Board of Nursing.
(6) “Clinical preceptor” means a registered nurse or licensed practical nurse who is employed by a clinical
training facility to serve as a role model and clinical resource person for a specified period to students enrolled in an
approved program.
(7) “Clinical simulation” means a strategy used to replicate clinical practice as closely as possible to teach
theory, assessment, technology, pharmacology, and skills.
(8) “Clinical training” means direct nursing care experiences with patients or clients, or clinical simulation of
such experiences, which offer the student the opportunity to integrate, apply, and refine specific skills and abilities
based on theoretical concepts and scientific principles.
(9) “Community-based clinical experience” means activities consistent with the curriculum and involving
individuals, families, and groups with the intent of promoting wellness, maintaining health, and preventing illness.
(10) “Curriculum” means a planned sequence of course offerings and learning experiences that comprise a
nursing education program.
(11) “Department” means the Department of Health.
(12) “Educational institution” means a school, college, or university.
(13) “Graduate passage rate” means the percentage of a program’s graduates who, as first-time test takers, pass
the National Council of State Boards of Nursing Licensing Examination during a calendar year, as calculated by the
contract testing service of the National Council of State Boards of Nursing.
(14) “Licensed practical nurse” means any person licensed in this state or holding an active multistate license
under s. 464.0095 to practice practical nursing.

10 – 3
(15) “Nursing diagnosis” means the observation and evaluation of physical or mental conditions, behaviors,
signs and symptoms of illness, and reactions to treatment and the determination as to whether such conditions, signs,
symptoms, and reactions represent a deviation from normal.
(16) “Nursing treatment” means the establishment and implementation of a nursing regimen for the care and
comfort of individuals, the prevention of illness, and the education, restoration, and maintenance of health.
(17) “Practice of practical nursing” means the performance of selected acts, including the administration of
treatments and medications, in the care of the ill, injured, or infirm; the promotion of wellness, maintenance of
health, and prevention of illness of others under the direction of a registered nurse, a licensed physician, a licensed
osteopathic physician, a licensed podiatric physician, or a licensed dentist; and the teaching of general principles of
health and wellness to the public and to students other than nursing students. A practical nurse is responsible and
accountable for making decisions that are based upon the individual’s educational preparation and experience in
nursing.
(18) “Practice of professional nursing” means the performance of those acts requiring substantial specialized
knowledge, judgment, and nursing skill based upon applied principles of psychological, biological, physical, and
social sciences which shall include, but not be limited to:
(a) The observation, assessment, nursing diagnosis, planning, intervention, and evaluation of care; health
teaching and counseling of the ill, injured, or infirm; and the promotion of wellness, maintenance of health, and
prevention of illness of others.
(b) The administration of medications and treatments as prescribed or authorized by a duly licensed practitioner
authorized by the laws of this state to prescribe such medications and treatments.
(c) The supervision and teaching of other personnel in the theory and performance of any of the acts described
in this subsection.
A professional nurse is responsible and accountable for making decisions that are based upon the individual’s
educational preparation and experience in nursing.
(19) “Probationary status” means the status of an approved program that is placed on such status pursuant to s.
464.019.
(20) “Registered nurse” means any person licensed in this state or holding an active multistate license under s.
464.0095 to practice professional nursing.
(21) “Required passage rate” means the graduate passage rate required for an approved program pursuant to s.
464.019(5)(a).
History.—ss. 1, 6, ch. 79-225; ss. 2, 3, ch. 81-318; ss. 3, 4, ch. 82-32; ss. 3, 17, 18, ch. 86-284; s. 18, ch. 88-392;
s. 58, ch. 91-137; s. 5, ch. 91-156; s. 4, ch. 91-429; s. 121, ch. 94-218; s. 1, ch. 96-274; s. 76, ch. 97-264; s. 210, ch.
98-166; s. 121, ch. 2000-318; s. 1, ch. 2007-167; s. 82, ch. 2008-6; s. 1, ch. 2009-168; s. 2, ch. 2010-37; s. 1, ch.
2014-92; s. 3, ch. 2016-139; s. 11, ch. 2016-224; ss. 1, 55, ch. 2018-106.
464.004 Board of Nursing; membership; appointment; terms.—
(1) The Board of Nursing is created within the department and shall consist of 13 members to be appointed by
the Governor and confirmed by the Senate.
(2) Seven members of the board must be registered nurses who are residents of this state and who have been
engaged in the practice of professional nursing for at least 4 years, including at least one advanced practice
registered nurse, one nurse educator member of an approved program, and one nurse executive. These seven board

10 – 4
members should be representative of the diverse areas of practice within the nursing profession. In addition, three
members of the board must be licensed practical nurses who are residents of this state and who have been actively
engaged in the practice of practical nursing for at least 4 years prior to their appointment. The remaining three
members must be residents of the state who have never been licensed as nurses and who are in no way connected
with the practice of nursing. No person may be appointed as a lay member who is in any way connected with, or has
any financial interest in, any health care facility, agency, or insurer. At least one member of the board must be 60
years of age or older.
(3) As the terms of the members expire, the Governor shall appoint successors for terms of 4 years, and such
members shall serve until their successors are appointed.
(4) All provisions of chapter 456 relating to activities of the board shall apply.
(5) The executive director of the board appointed pursuant to s. 456.004(2) or his or her designee shall serve as
the state administrator of the Nurse Licensure Compact as required under s. 464.0095.
History.—ss. 1, 6, ch. 79-225; ss. 2, 3, ch. 81-318; ss. 4, 17, 18, ch. 86-284; s. 15, ch. 87-172; ss. 12, 58, ch. 91-
137; s. 5, ch. 91-156; s. 4, ch. 91-429; s. 122, ch. 94-218; s. 3, ch. 96-274; s. 77, ch. 97-264; s. 66, ch. 98-166; s.
123, ch. 2000-160; s. 4, ch. 2016-139; s. 56, ch. 2018-106.
464.005 Board headquarters.—The board shall maintain its official headquarters in Tallahassee.
History.—ss. 1, 6, ch. 79-225; ss. 2, 3, ch. 81-318; ss. 17, 18, ch. 86-284; s. 58, ch. 91-137; s. 5, ch. 91-156; s. 4,
ch. 91-429; s. 94, ch. 2001-277.
464.006 Rulemaking authority.—The board has authority to adopt rules pursuant to ss. 120.536(1) and 120.54
to implement the provisions of this part conferring duties upon it.
History.—ss. 1, 6, ch. 79-225; ss. 2, 3, ch. 81-318; ss. 5, 17, 18, ch. 86-284; s. 58, ch. 91-137; s. 5, ch. 91-156; s.
4, ch. 91-429; s. 125, ch. 98-200; s. 122, ch. 2000-318.
464.008 Licensure by examination.—
(1) Any person desiring to be licensed as a registered nurse or licensed practical nurse shall apply to the
department to take the licensure examination. The department shall examine each applicant who:
(a) Has completed the application form and remitted a fee set by the board not to exceed $150 and has remitted
an examination fee set by the board not to exceed $75 plus the actual per applicant cost to the department for
purchase of the examination from the National Council of State Boards of Nursing or a similar national
organization.
(b) Has provided sufficient information on or after October 1, 1989, which must be submitted by the
department for a statewide criminal records correspondence check through the Department of Law Enforcement.
(c) Is in good mental and physical health, is a recipient of a high school diploma or the equivalent, and has
completed the requirements for:
1. Graduation from an approved program;
2. Graduation from a prelicensure nursing education program that the board determines is equivalent to an
approved program;
3. Graduation on or after July 1, 2009, from an accredited program; or
4. Graduation before July 1, 2009, from a prelicensure nursing education program whose graduates at that time
were eligible for examination.

10 – 5
Courses successfully completed in a professional nursing education program that are at least equivalent to a practical
nursing education program may be used to satisfy the education requirements for licensure as a licensed practical
nurse.
(d) Has the ability to communicate in the English language, which may be determined by an examination given
by the department.
(2)(a) Each applicant who passes the examination and provides proof of meeting the educational requirements
specified in subsection (1) shall, unless denied pursuant to s. 464.018, be entitled to licensure as a registered
professional nurse or a licensed practical nurse, whichever is applicable.
(b) An applicant who resides in this state, meets the licensure requirements of this section, and meets the
criteria for multistate licensure under s. 464.0095 may request the issuance of a multistate license from the
department.
(c) A nurse who holds a single-state license in this state and applies to the department for a multistate license
must meet the eligibility criteria for a multistate license under s. 464.0095 and must pay an application and licensure
fee to change the licensure status.
(d) The department shall conspicuously distinguish a multistate license from a single-state license.
(3) Any applicant who fails the examination three consecutive times, regardless of the jurisdiction in which the
examination is taken, shall be required to complete a board-approved remedial course before the applicant will be
approved for reexamination. After taking the remedial course, the applicant may be approved to retake the
examination up to three additional times before the applicant is required to retake remediation. The applicant shall
apply for reexamination within 6 months after completion of remediation. The board shall by rule establish
guidelines for remedial courses.
(4) If an applicant who graduates from an approved program does not take the licensure examination within 6
months after graduation, he or she must enroll in and successfully complete a board-approved licensure examination
preparatory course. The applicant is responsible for all costs associated with the course and may not use state or
federal financial aid for such costs. The board shall by rule establish guidelines for licensure examination
preparatory courses.
(5) A person holding an active multistate license in another state pursuant to s. 464.0095 is exempt from the
licensure requirements of this section.
History.—ss. 1, 6, ch. 79-225; ss. 2, 3, ch. 81-318; ss. 6, 17, 18, ch. 86-284; s. 12, ch. 88-205; s. 10, ch. 88-219;
s. 34, ch. 89-162; s. 58, ch. 91-137; s. 5, ch. 91-156; s. 4, ch. 91-429; s. 94, ch. 92-149; s. 5, ch. 96-274; s. 78, ch.
97-264; s. 116, ch. 99-397; s. 95, ch. 2001-277; s. 3, ch. 2010-37; s. 2, ch. 2014-92; s. 5, ch. 2016-139; s. 28, ch.
2016-224.
464.009 Licensure by endorsement.—
(1) The department shall issue the appropriate license by endorsement to practice professional or practical
nursing to an applicant who, upon applying to the department and remitting a fee set by the board not to exceed
$100, demonstrates to the board that he or she:
(a) Holds a valid license to practice professional or practical nursing in another state or territory of the United
States, provided that, when the applicant secured his or her original license, the requirements for licensure were
substantially equivalent to or more stringent than those existing in Florida at that time;

10 – 6
(b) Meets the qualifications for licensure in s. 464.008 and has successfully completed a state, regional, or
national examination which is substantially equivalent to or more stringent than the examination given by the
department; or
(c) Has actively practiced nursing in another state, jurisdiction, or territory of the United States for 2 of the
preceding 3 years without having his or her license acted against by the licensing authority of any jurisdiction.
Applicants who become licensed pursuant to this paragraph must complete within 6 months after licensure a Florida
laws and rules course that is approved by the board. Once the department has received the results of the national
criminal history check and has determined that the applicant has no criminal history, the appropriate license by
endorsement shall be issued to the applicant.
(2) Such examinations and requirements from other states and territories of the United States shall be presumed
to be substantially equivalent to or more stringent than those in this state. Such presumption shall not arise until
January 1, 1980. However, the board may, by rule, specify states and territories the examinations and requirements
of which shall not be presumed to be substantially equivalent to those of this state.
(3) An applicant for licensure by endorsement who is relocating to this state pursuant to his or her military-
connected spouse’s official military orders and who is licensed in another state that is a member of the Nurse
Licensure Compact shall be deemed to have satisfied the requirements of subsection (1) and shall be issued a license
by endorsement upon submission of the appropriate application and fees and completion of the criminal background
check required under subsection (4).
(4) The applicant must submit to the department a set of fingerprints on a form and under procedures specified
by the department, along with a payment in an amount equal to the costs incurred by the Department of Health for
the criminal background check of the applicant. The Department of Health shall submit the fingerprints provided by
the applicant to the Florida Department of Law Enforcement for a statewide criminal history check, and the Florida
Department of Law Enforcement shall forward the fingerprints to the Federal Bureau of Investigation for a national
criminal history check of the applicant. The Department of Health shall review the results of the criminal history
check, issue a license to an applicant who has met all of the other requirements for licensure and has no criminal
history, and shall refer all applicants with criminal histories back to the board for determination as to whether a
license should be issued and under what conditions.
(5) The department shall not issue a license by endorsement to any applicant who is under investigation in
another state, jurisdiction, or territory of the United States for an act which would constitute a violation of this part
or chapter 456 until such time as the investigation is complete, at which time the provisions of s. 464.018 shall
apply.
(6) The department shall develop an electronic applicant notification process and provide electronic notification
when the application has been received and when background screenings have been completed, and shall issue a
license within 30 days after completion of all required data collection and verification. This 30-day period to issue a
license shall be tolled if the applicant must appear before the board due to information provided on the application or
obtained through screening and data collection and verification procedures.
(7) A person holding an active multistate license in another state pursuant to s. 464.0095 is exempt from the
requirements for licensure by endorsement in this section.

10 – 7
History.—ss. 1, 6, ch. 79-225; ss. 2, 3, ch. 81-318; ss. 7, 17, 18, ch. 86-284; s. 1, ch. 87-240; s. 58, ch. 91-137; s.
5, ch. 91-156; s. 4, ch. 91-429; s. 6, ch. 96-274; s. 1104, ch. 97-103; s. 79, ch. 97-264; s. 123, ch. 2000-318; s. 96,
ch. 2001-277; s. 5, ch. 2002-230; s. 9, ch. 2004-230; s. 6, ch. 2016-139; s. 28, ch. 2016-224.
464.0095 Nurse Licensure Compact.—The Nurse Licensure Compact is hereby enacted into law and entered
into by this state with all other jurisdictions legally joining therein in the form substantially as follows:
ARTICLE I
FINDINGS AND DECLARATION OF PURPOSE
(1) The party states find that:
(a) The health and safety of the public are affected by the degree of compliance with and the effectiveness of
enforcement activities related to state nurse licensure laws.
(b) Violations of nurse licensure and other laws regulating the practice of nursing may result in injury or harm to
the public.
(c) The expanded mobility of nurses and the use of advanced communication technologies as part of the nation’s
health care delivery system require greater coordination and cooperation among states in the areas of nurse licensure
and regulation.
(d) New practice modalities and technology make compliance with individual state nurse licensure laws difficult
and complex.
(e) The current system of duplicative licensure for nurses practicing in multiple states is cumbersome and
redundant for both nurses and states.
(f) Uniformity of nurse licensure requirements throughout the states promotes public safety and public health
benefits.
(2) The general purposes of this compact are to:
(a) Facilitate the states’ responsibility to protect the public’s health and safety.
(b) Ensure and encourage the cooperation of party states in the areas of nurse licensure and regulation.
(c) Facilitate the exchange of information among party states in the areas of nurse regulation, investigation, and
adverse actions.
(d) Promote compliance with the laws governing the practice of nursing in each jurisdiction.
(e) Invest all party states with the authority to hold a nurse accountable for meeting all state practice laws in the
state in which the patient is located at the time care is rendered through the mutual recognition of party state licenses.
(f) Decrease redundancies in the consideration and issuance of nurse licenses.
(g) Provide opportunities for interstate practice by nurses who meet uniform licensure requirements.
ARTICLE II
DEFINITIONS
As used in this compact, the term:
(1) “Adverse action” means any administrative, civil, equitable, or criminal action permitted by a state’s laws
which is imposed by a licensing board or other authority against a nurse, including actions against an individual’s
license or multistate licensure privilege, such as revocation, suspension, probation, monitoring of the licensee,
limitation on the licensee’s practice, or any other encumbrance on licensure affecting a nurse’s authorization to
practice, including issuance of a cease and desist action.
(2) “Alternative program” means a nondisciplinary monitoring program approved by a licensing board.

10 – 8
(3) “Commission” means the Interstate Commission of Nurse Licensure Compact Administrators established by
this compact.
(4) “Compact” means the Nurse Licensure Compact recognized, established, and entered into by the state under
this compact.
(5) “Coordinated licensure information system” means an integrated process for collecting, storing, and sharing
information on nurse licensure and enforcement activities related to nurse licensure laws which is administered by a
nonprofit organization composed of and controlled by licensing boards.
(6) “Current significant investigative information” means:
(a) Investigative information that a licensing board, after a preliminary inquiry that includes notification and an
opportunity for the nurse to respond, if required by state law, has reason to believe is not groundless and, if proved
true, would indicate more than a minor infraction; or
(b) Investigative information that indicates that the nurse represents an immediate threat to public health and
safety regardless of whether the nurse has been notified and had an opportunity to respond.
(7) “Encumbrance” means a revocation or suspension of, or any limitation on, the full and unrestricted practice
of nursing imposed by a licensing board.
(8) “Home state” means the party state that is the nurse’s primary state of residence.
(9) “Licensing board” means a party state’s regulatory body responsible for issuing nurse licenses.
(10) “Multistate license” means a license to practice as a registered nurse (RN) or a licensed practical/vocational
nurse (LPN/VN) issued by a home state licensing board which authorizes the licensed nurse to practice in all party
states under a multistate licensure privilege.
(11) “Multistate licensure privilege” means a legal authorization associated with a multistate license permitting
the practice of nursing as either an RN or an LPN/VN in a remote state.
(12) “Nurse” means an RN or LPN/VN, as those terms are defined by each party state’s practice laws.
(13) “Party state” means any state that has adopted this compact.
(14) “Remote state” means a party state other than the home state.
(15) “Single-state license” means a nurse license issued by a party state which authorizes practice only within the
issuing state and does not include a multistate licensure privilege to practice in any other party state.
(16) “State” means a state, territory, or possession of the United States, or the District of Columbia.
(17) “State practice laws” means a party state’s laws, rules, and regulations that govern the practice of nursing,
define the scope of nursing practice, and create the methods and grounds for imposing discipline. The term “state
practice laws” does not include requirements necessary to obtain and retain a license, except for qualifications or
requirements of the home state.
ARTICLE III
GENERAL PROVISIONS AND JURISDICTION
(1) A multistate license to practice registered or licensed practical/vocational nursing issued by a home state to a
resident in that state shall be recognized by each party state as authorizing a nurse to practice as an RN or as an
LPN/VN under a multistate licensure privilege in each party state.
(2) Each party state must implement procedures for considering the criminal history records of applicants for
initial multistate licensure or licensure by endorsement. Such procedures shall include the submission of fingerprints
or other biometric-based information by applicants for the purpose of obtaining an applicant’s criminal history record

10 – 9
information from the Federal Bureau of Investigation and the agency responsible for retaining that state’s criminal
records.
(3) In order for an applicant to obtain or retain a multistate license in the home state, each party state shall require
that the applicant fulfills the following criteria:
(a) Meets the home state’s qualifications for licensure or renewal of licensure, as well as all other applicable state
laws.
(b)1. Has graduated or is eligible to graduate from a licensing board-approved RN or LPN/VN prelicensure
education program; or
2. Has graduated from a foreign RN or LPN/VN prelicensure education program that has been approved by the
authorized accrediting body in the applicable country and has been verified by a licensing board-approved independent
credentials review agency to be comparable to a licensing board-approved prelicensure education program.
(c) If the applicant is a graduate of a foreign prelicensure education program not taught in English, or if English
is not the applicant’s native language, has successfully passed a licensing board-approved English proficiency
examination that includes the components of reading, speaking, writing, and listening.
(d) Has successfully passed an NCLEX-RN or NCLEX-PN Examination or recognized predecessor, as
applicable.
(e) Is eligible for or holds an active, unencumbered license.
(f) Has submitted, in connection with an application for initial licensure or licensure by endorsement, fingerprints
or other biometric data for the purpose of obtaining criminal history record information from the Federal Bureau of
Investigation and the agency responsible for retaining that state’s criminal records.
(g) Has not been convicted or found guilty, or has entered into an agreed disposition other than a disposition that
results in nolle prosequi, of a felony offense under applicable state or federal criminal law.
(h) Has not been convicted or found guilty, or has entered into an agreed disposition other than a disposition that
results in nolle prosequi, of a misdemeanor offense related to the practice of nursing as determined on a case-by-case
basis.
(i) Is not currently enrolled in an alternative program.
(j) Is subject to self-disclosure requirements regarding current participation in an alternative program.
(k) Has a valid United States social security number.
(4) All party states may, in accordance with existing state due process law, take adverse action against a nurse’s
multistate licensure privilege, such as revocation, suspension, probation, or any other action that affects the nurse’s
authorization to practice under a multistate licensure privilege, including cease and desist actions. If a party state takes
such action, it shall promptly notify the administrator of the coordinated licensure information system. The
administrator of the coordinated licensure information system shall promptly notify the home state of any such actions
by remote states.
(5) A nurse practicing in a party state must comply with the state practice laws of the state in which the patient is
located at the time service is provided. The practice of nursing is not limited to patient care but shall include all nursing
practice as defined by the state practice laws of the party state in which the patient is located. The practice of nursing
in a party state under a multistate licensure privilege subjects a nurse to the jurisdiction of the licensing board, the
courts, and the laws of the party state in which the patient is located at the time service is provided.

10 – 10
(6) A person not residing in a party state shall continue to be able to apply for a party state’s single-state license
as provided under the laws of each party state. The single-state license granted to such a person does not grant the
privilege to practice nursing in any other party state. This compact does not affect the requirements established by a
party state for the issuance of a single-state license.
(7) A nurse holding a home state multistate license, on the effective date of this compact, may retain and renew
the multistate license issued by the nurse’s then-current home state, provided that:
(a) A nurse who changes his or her primary state of residence after the effective date must meet all applicable
requirements under subsection (3) to obtain a multistate license from a new home state.
(b) A nurse who fails to satisfy the multistate licensure requirements under subsection (3) due to a disqualifying
event occurring after the effective date is ineligible to retain or renew a multistate license, and the nurse’s multistate
license shall be revoked or deactivated in accordance with applicable rules adopted by the commission.
ARTICLE IV
APPLICATIONS FOR LICENSURE
IN A PARTY STATE
(1) Upon application for a multistate license, the licensing board in the issuing party state shall ascertain, through
the coordinated licensure information system, whether the applicant has ever held, or is the holder of, a license issued
by any other state, whether there are any encumbrances on any license or multistate licensure privilege held by the
applicant, whether any adverse action has been taken against any license or multistate licensure privilege held by the
applicant, and whether the applicant is currently participating in an alternative program.
(2) A nurse may hold a multistate license, issued by the home state, in only one party state at a time.
(3) If a nurse changes his or her primary state of residence by moving from one party state to another party state,
the nurse must apply for licensure in the new home state, and the multistate license issued by the prior home state
shall be deactivated in accordance with applicable rules adopted by the commission.
(a) The nurse may apply for licensure in advance of a change in his or her primary state of residence.
(b) A multistate license may not be issued by the new home state until the nurse provides satisfactory evidence
of a change in his or her primary state of residence to the new home state and satisfies all applicable requirements to
obtain a multistate license from the new home state.
(4) If a nurse changes his or her primary state of residence by moving from a party state to a nonparty state, the
multistate license issued by the prior home state shall convert to a single-state license valid only in the former home
state.
ARTICLE V
ADDITIONAL AUTHORITY VESTED IN
PARTY STATE LICENSING BOARDS
(1) In addition to the other powers conferred by state law, a licensing board or state agency may:
(a) Take adverse action against a nurse’s multistate licensure privilege to practice within that party state.
1. Only the home state has the power to take adverse action against a nurse’s license issued by the home state.
2. For purposes of taking adverse action, the home state licensing board or state agency shall give the same
priority and effect to conduct reported by a remote state as it would if such conduct had occurred within the home
state. In so doing, the home state shall apply its own state laws to determine appropriate action.

10 – 11
(b) Issue cease and desist orders or impose an encumbrance on a nurse’s authority to practice within that party
state.
(c) Complete any pending investigation of a nurse who changes his or her primary state of residence during the
course of such investigation. The licensing board or state agency may also take appropriate action and shall promptly
report the conclusions of such investigation to the administrator of the coordinated licensure information system. The
administrator of the coordinated licensure information system shall promptly notify the new home state of any such
action.
(d) Issue subpoenas for both hearings and investigations that require the attendance and testimony of witnesses
or the production of evidence. Subpoenas issued by a licensing board or state agency in a party state for the attendance
and testimony of witnesses or the production of evidence from another party state shall be enforced in the latter state
by any court of competent jurisdiction according to the practice and procedure of that court applicable to subpoenas
issued in proceedings pending before it. The issuing authority shall pay any witness fees, travel expenses, and mileage
and other fees required by the service statutes of the state in which the witnesses or evidence is located.
(e) Obtain and submit, for each nurse licensure applicant, fingerprint or other biometric-based information to the
Federal Bureau of Investigation for criminal background checks, receive the results of the Federal Bureau of
Investigation record search on criminal background checks, and use the results in making licensure decisions.
(f) If otherwise permitted by state law, recover from the affected nurse the costs of investigations and disposition
of cases resulting from any adverse action taken against that nurse.
(g) Take adverse action based on the factual findings of the remote state, provided that the licensing board or
state agency follows its own procedures for taking such adverse action.
(2) If adverse action is taken by the home state against a nurse’s multistate license, the nurse’s multistate licensure
privilege to practice in all other party states shall be deactivated until all encumbrances are removed from the multistate
license. All home state disciplinary orders that impose adverse action against a nurse’s multistate license shall include
a statement that the nurse’s multistate licensure privilege is deactivated in all party states during the pendency of the
order.
(3) This compact does not override a party state’s decision that participation in an alternative program may be
used in lieu of adverse action. The home state licensing board shall deactivate the multistate licensure privilege under
the multistate license of any nurse for the duration of the nurse’s participation in an alternative program.
ARTICLE VI
COORDINATED LICENSURE
INFORMATION SYSTEM
AND EXCHANGE INFORMATION
(1) All party states shall participate in a coordinated licensure information system relating to all licensed RNs
and LPNs/VNs. This system shall include information on the licensure and disciplinary history of each nurse, as
submitted by party states, to assist in the coordination of nurse licensure and enforcement efforts.
(2) The commission, in consultation with the administrator of the coordinated licensure information system, shall
formulate necessary and proper procedures for the identification, collection, and exchange of information under this
compact.
(3) All licensing boards shall promptly report to the coordinated licensure information system any adverse action,
any current significant investigative information, denials of applications, the reasons for application denials, and nurse

10 – 12
participation in alternative programs known to the licensing board regardless of whether such participation is deemed
nonpublic or confidential under state law.
(4) Current significant investigative information and participation in nonpublic or confidential alternative
programs shall be transmitted through the coordinated licensure information system only to party state licensing
boards.
(5) Notwithstanding any other provision of law, all party state licensing boards contributing information to the
coordinated licensure information system may designate information that may not be shared with nonparty states or
disclosed to other entities or individuals without the express permission of the contributing state.
(6) Any personal identifying information obtained from the coordinated licensure information system by a party
state licensing board may not be shared with nonparty states or disclosed to other entities or individuals except to the
extent permitted by the laws of the party state contributing the information.
(7) Any information contributed to the coordinated licensure information system which is subsequently required
to be expunged by the laws of the party state contributing that information shall also be expunged from the coordinated
licensure information system.
(8) The compact administrator of each party state shall furnish a uniform data set to the compact administrator of
each other party state, which shall include, at a minimum:
(a) Identifying information.
(b) Licensure data.
(c) Information related to alternative program participation.
(d) Other information that may facilitate the administration of this compact, as determined by commission rules.
(9) The compact administrator of a party state shall provide all investigative documents and information
requested by another party state.
ARTICLE VII
ESTABLISHMENT OF THE
INTERSTATE COMMISSION OF
NURSE LICENSURE COMPACT ADMINISTRATORS
(1) The party states hereby create and establish a joint public entity known as the Interstate Commission of Nurse
Licensure Compact Administrators.
(a) The commission is an instrumentality of the party states.
(b) Venue is proper, and judicial proceedings by or against the commission shall be brought solely and
exclusively, in a court of competent jurisdiction where the commission’s principal office is located. The commission
may waive venue and jurisdictional defenses to the extent it adopts or consents to participate in alternative dispute
resolution proceedings.
(c) This compact does not waive sovereign immunity except to the extent sovereign immunity is waived in the
party states.
(2)(a) Each party state shall have and be limited to one administrator. The executive director of the state licensing
board or his or her designee shall be the administrator of this compact for each party state. Any administrator may be
removed or suspended from office as provided by the law of the state from which the administrator is appointed. Any
vacancy occurring on the commission shall be filled in accordance with the laws of the party state in which the vacancy
exists.

10 – 13
(b) Each administrator is entitled to one vote with regard to the adoption of rules and the creation of bylaws and
shall otherwise have an opportunity to participate in the business and affairs of the commission. An administrator shall
vote in person or by such other means as provided in the bylaws. The bylaws may provide for an administrator’s
participation in meetings by telephone or other means of communication.
(c) The commission shall meet at least once during each calendar year. Additional meetings shall be held as set
forth in the commission’s bylaws or rules.
(d) All meetings shall be open to the public, and public notice of meetings shall be given in the same manner as
required under Article VIII of this compact.
(e) The commission may convene in a closed, nonpublic meeting if the commission must discuss:
1. Failure of a party state to comply with its obligations under this compact;
2. The employment, compensation, discipline, or other personnel matters, practices, or procedures related to
specific employees or other matters related to the commission’s internal personnel practices and procedures;
3. Current, threatened, or reasonably anticipated litigation;
4. Negotiation of contracts for the purchase or sale of goods, services, or real estate;
5. Accusing any person of a crime or formally censuring any person;
6. Disclosure of trade secrets or commercial or financial information that is privileged or confidential;
7. Disclosure of information of a personal nature where disclosure would constitute a clearly unwarranted
invasion of personal privacy;
8. Disclosure of investigatory records compiled for law enforcement purposes;
9. Disclosure of information related to any reports prepared by or on behalf of the commission for the purpose of
investigation of compliance with this compact; or
10. Matters specifically exempted from disclosure by federal or state statute.
(f) If a meeting, or portion of a meeting, is closed pursuant to this subsection, the commission’s legal counsel or
designee shall certify that the meeting, or portion of the meeting, is closed and shall reference each relevant exempting
provision. The commission shall keep minutes that fully and clearly describe all matters discussed in a meeting and
shall provide a full and accurate summary of actions taken, and the reasons therefor, including a description of the
views expressed. All documents considered in connection with an action shall be identified in such minutes. All
minutes and documents of a closed meeting shall remain under seal, subject to release by a majority vote of the
commission or order of a court of competent jurisdiction.
(3) The commission shall, by a majority vote of the administrators, prescribe bylaws or rules to govern its conduct
as may be necessary or appropriate to carry out the purposes and exercise the powers of this compact, including, but
not limited to:
(a) Establishing the commission’s fiscal year.
(b) Providing reasonable standards and procedures:
1. For the establishment and meetings of other committees.
2. Governing any general or specific delegation of any authority or function of the commission.
(c) Providing reasonable procedures for calling and conducting meetings of the commission, ensuring reasonable
advance notice of all meetings, and providing an opportunity for attendance of such meetings by interested parties,
with enumerated exceptions designed to protect the public’s interest, the privacy of individuals, and proprietary
information, including trade secrets. The commission may meet in closed session only after a majority of the

10 – 14
administrators vote to close a meeting in whole or in part. As soon as practicable, the commission must make public
a copy of the vote to close the meeting revealing the vote of each administrator, with no proxy votes allowed.
(d) Establishing the titles, duties and authority, and reasonable procedures for the election of the commission’s
officers.
(e) Providing reasonable standards and procedures for the establishment of the commission’s personnel policies
and programs. Notwithstanding any civil service or other similar laws of any party state, the bylaws shall exclusively
govern the commission’s personnel policies and programs.
(f) Providing a mechanism for winding up the commission’s operations and the equitable disposition of any
surplus funds that may exist after the termination of this compact after the payment or reserving of all of its debts and
obligations.
(4) The commission shall publish its bylaws and rules, and any amendments thereto, in a convenient form on the
commission’s website.
(5) The commission shall maintain its financial records in accordance with the bylaws.
(6) The commission shall meet and take such actions as are consistent with this compact and the bylaws.
(7) The commission has the power to:
(a) Adopt uniform rules to facilitate and coordinate implementation and administration of this compact. The rules
shall have the force and effect of law and are binding in all party states.
(b) Bring and prosecute legal proceedings or actions in the name of the commission, provided that the standing
of any licensing board to sue or be sued under applicable law is not affected.
(c) Purchase and maintain insurance and bonds.
(d) Borrow, accept, or contract for services of personnel, including employees of a party state or nonprofit
organizations.
(e) Cooperate with other organizations that administer state compacts related to the regulation of nursing,
including sharing administrative or staff expenses, office space, or other resources.
(f) Hire employees, elect or appoint officers, fix compensation, define duties, grant such individuals appropriate
authority to carry out the purposes of this compact, and establish the commission’s personnel policies and programs
relating to conflicts of interest, qualifications of personnel, and other related personnel matters.
(g) Accept any and all appropriate donations, grants, and gifts of money, equipment, supplies, materials, and
services and receive, use, and dispose of the same, provided that, at all times, the commission shall avoid any
appearance of impropriety or conflict of interest.
(h) Lease, purchase, accept appropriate gifts or donations of, or otherwise own, hold, improve, or use any
property, whether real, personal, or mixed, provided that, at all times, the commission shall avoid any appearance of
impropriety.
(i) Sell, convey, mortgage, pledge, lease, exchange, abandon, or otherwise dispose of any property, whether real,
personal, or mixed.
(j) Establish a budget and make expenditures.
(k) Borrow money.
(l) Appoint committees, including advisory committees comprised of administrators, state nursing regulators,
state legislators or their representatives, consumer representatives, and other interested persons.
(m) Provide information to, receive information from, and cooperate with law enforcement agencies.

10 – 15
(n) Adopt and use an official seal.
(o) Perform such other functions as may be necessary or appropriate to achieve the purposes of this compact
consistent with the state regulation of nurse licensure and practice.
(8) Relating to the financing of the commission, the commission:
(a) Shall pay, or provide for the payment of, the reasonable expenses of its establishment, organization, and
ongoing activities.
(b) May also levy and collect an annual assessment from each party state to cover the cost of its operations,
activities, and staff in its annual budget as approved each year. The aggregate annual assessment amount, if any, shall
be allocated based on a formula to be determined by the commission, which shall adopt a rule that is binding on all
party states.
(c) May not incur obligations of any kind before securing the funds adequate to meet the same; and the
commission may not pledge the credit of any of the party states, except by and with the authority of such party state.
(d) Shall keep accurate accounts of all receipts and disbursements. The commission’s receipts and disbursements
are subject to the audit and accounting procedures established under its bylaws. However, all receipts and
disbursements of funds handled by the commission shall be audited yearly by a certified or licensed public accountant,
and the report of the audit shall be included in, and become part of, the commission’s annual report.
(9) Relating to the sovereign immunity, defense, and indemnification of the commission:
(a) The administrators, officers, executive director, employees, and representatives of the commission are
immune from suit and liability, either personally or in their official capacity, for any claim for damage to or loss of
property or personal injury or other civil liability caused by or arising out of any actual or alleged act, error, or omission
that occurred, or that the person against whom the claim is made had a reasonable basis for believing occurred, within
the scope of commission employment, duties, or responsibilities. This paragraph does not protect any such person
from suit or liability for any damage, loss, injury, or liability caused by the intentional, willful, or wanton misconduct
of that person.
(b) The commission shall defend any administrator, officer, executive director, employee, or representative of
the commission in any civil action seeking to impose liability arising out of any actual or alleged act, error, or omission
that occurred within the scope of commission employment, duties, or responsibilities or that the person against whom
the claim is made had a reasonable basis for believing occurred within the scope of commission employment, duties,
or responsibilities, provided that the actual or alleged act, error, or omission did not result from that person’s
intentional, willful, or wanton misconduct. This paragraph does not prohibit that person from retaining his or her own
counsel.
(c) The commission shall indemnify and hold harmless any administrator, officer, executive director, employee,
or representative of the commission for the amount of any settlement or judgment obtained against that person arising
out of any actual or alleged act, error, or omission that occurred within the scope of commission employment, duties,
or responsibilities or that such person had a reasonable basis for believing occurred within the scope of commission
employment, duties, or responsibilities, provided that the actual or alleged act, error, or omission did not result from
the intentional, willful, or wanton misconduct of that person.

10 – 16
ARTICLE VIII
RULEMAKING
(1) The commission shall exercise its rulemaking powers pursuant to the criteria set forth in this article and the
rules adopted thereunder. Rules and amendments become binding as of the date specified in each rule or amendment
and have the same force and effect as provisions of this compact.
(2) Rules or amendments to the rules shall be adopted at a regular or special meeting of the commission.
(3) Before adoption of a final rule or final rules by the commission, and at least 60 days before the meeting at
which the rule will be considered and voted upon, the commission shall file a notice of proposed rulemaking:
(a) On the commission’s website.
(b) On the website of each licensing board or the publication in which each state would otherwise publish
proposed rules.
(4) The notice of proposed rulemaking shall include:
(a) The proposed time, date, and location of the meeting in which the rule will be considered and voted upon.
(b) The text of the proposed rule or amendment and the reason for the proposed rule.
(c) A request for comments on the proposed rule from any interested person.
(d) The manner in which an interested person may submit notice to the commission of his or her intention to
attend the public hearing and any written comments.
(5) Before adoption of a proposed rule, the commission shall allow persons to submit written data, facts, opinions,
and arguments, which shall be made available to the public.
(6) The commission shall grant an opportunity for a public hearing before it adopts a rule or amendment.
(7) The commission shall publish the place, time, and date of the scheduled public hearing.
(a) Hearings shall be conducted in a manner providing each person who wishes to comment a fair and reasonable
opportunity to comment orally or in writing. All hearings will be recorded, and a copy will be made available upon
request.
(b) This article does not require a separate hearing on each rule. Rules may be grouped for the convenience of
the commission at hearings required by this article.
(8) If no interested person appears at the public hearing, the commission may proceed with adoption of the
proposed rule.
(9) Following the scheduled hearing date, or by the close of business on the scheduled hearing date if the hearing
is not held, the commission shall consider all written and oral comments received.
(10) The commission shall, by majority vote of all administrators, take final action on the proposed rule and shall
determine the effective date of the rule, if any, based on the rulemaking record and the full text of the rule.
(11) Upon determination that an emergency exists, the commission may consider and adopt an emergency rule
without prior notice, opportunity for comment, or hearing, provided that the usual rulemaking procedures provided in
this compact and in this article shall be applied retroactively to the rule as soon as reasonably possible within 90 days
after the effective date of the rule. For the purposes of this subsection, an emergency rule is one that must be adopted
immediately in order to:
(a) Meet an imminent threat to public health, safety, or welfare;
(b) Prevent a loss of commission or party state funds; or
(c) Meet a deadline for the adoption of an administrative rule that is required by federal law or rule.

10 – 17
(12) The commission may direct revisions to a previously adopted rule or amendment for purposes of correcting
typographical errors, errors in format, errors in consistency, or grammatical errors. Public notice of any revisions shall
be posted on the commission’s website. The revision is subject to challenge by any person for 30 days after posting.
The revision may be challenged only on grounds that the revision results in a material change to a rule. A challenge
must be made in writing and delivered to the commission before the end of the notice period. If no challenge is made,
the revision shall take effect without further action. If the revision is challenged, the revision may not take effect
without the commission’s approval.
ARTICLE IX
OVERSIGHT, DISPUTE RESOLUTION,
AND ENFORCEMENT
(1) Oversight of this compact shall be accomplished by:
(a) Each party state, which shall enforce this compact and take all actions necessary and appropriate to effectuate
this compact’s purposes and intent.
(b) The commission, which is entitled to receive service of process in any proceeding that may affect the powers,
responsibilities, or actions of the commission and has standing to intervene in such a proceeding for all purposes.
Failure to provide service of process in such proceeding to the commission renders a judgment or order void as to the
commission, this compact, or adopted rules.
(2) When the commission determines that a party state has defaulted in the performance of its obligations or
responsibilities under this compact or the adopted rules, the commission shall:
(a) Provide written notice to the defaulting state and other party states of the nature of the default, the proposed
means of curing the default, or any other action to be taken by the commission.
(b) Provide remedial training and specific technical assistance regarding the default.
(3) If a state in default fails to cure the default, the defaulting state’s membership in this compact may be
terminated upon an affirmative vote of a majority of the administrators, and all rights, privileges, and benefits
conferred by this compact may be terminated on the effective date of termination. A cure of the default does not relieve
the offending state of obligations or liabilities incurred during the period of default.
(4) Termination of membership in this compact shall be imposed only after all other means of securing
compliance have been exhausted. Notice of intent to suspend or terminate shall be given by the commission to the
governor of the defaulting state, to the executive officer of the defaulting state’s licensing board, and each of the party
states.
(5) A state whose membership in this compact is terminated is responsible for all assessments, obligations, and
liabilities incurred through the effective date of termination, including obligations that extend beyond the effective
date of termination.
(6) The commission shall not bear any costs related to a state that is found to be in default or whose membership
in this compact is terminated unless agreed upon in writing between the commission and the defaulting state.
(7) The defaulting state may appeal the action of the commission by petitioning the United States District Court
for the District of Columbia or the federal district in which the commission has its principal offices. The prevailing
party shall be awarded all costs of such litigation, including reasonable attorney fees.
(8) Dispute resolution may be used by the commission in the following manner:

10 – 18
(a) Upon request by a party state, the commission shall attempt to resolve disputes related to the compact that
arise among party states and between party and nonparty states.
(b) The commission shall adopt a rule providing for both mediation and binding dispute resolution for disputes,
as appropriate.
(c) In the event the commission cannot resolve disputes among party states arising under this compact:
1. The party states may submit the issues in dispute to an arbitration panel, which will be comprised of individuals
appointed by the compact administrator in each of the affected party states and an individual mutually agreed upon by
the compact administrators of all the party states involved in the dispute.
2. The decision of a majority of the arbitrators is final and binding.
(9)(a) The commission shall, in the reasonable exercise of its discretion, enforce the provisions and rules of this
compact.
(b) By majority vote, the commission may initiate legal action in the United States District Court for the District
of Columbia or the federal district in which the commission has its principal offices against a party state that is in
default to enforce compliance with this compact and its adopted rules and bylaws. The relief sought may include both
injunctive relief and damages. In the event judicial enforcement is necessary, the prevailing party shall be awarded all
costs of such litigation, including reasonable attorney fees.
(c) The remedies provided in this subsection are not the exclusive remedies of the commission. The commission
may pursue any other remedies available under federal or state law.
ARTICLE X
EFFECTIVE DATE, WITHDRAWAL,
AND AMENDMENT
(1) This compact becomes effective and binding on the date of legislative enactment of this compact into law by
no fewer than 26 states or on December 31, 2018, whichever occurs first. All party states to this compact which were
also parties to the prior Nurse Licensure Compact (“prior compact”), superseded by this compact, are deemed to have
withdrawn from the prior compact within 6 months after the effective date of this compact.
(2) Each party state to this compact shall continue to recognize a nurse’s multistate licensure privilege to practice
in that party state issued under the prior compact until such party state is withdrawn from the prior compact.
(3) Any party state may withdraw from this compact by enacting a statute repealing the compact. A party state’s
withdrawal does not take effect until 6 months after enactment of the repealing statute.
(4) A party state’s withdrawal or termination does not affect the continuing requirement of the withdrawing or
terminated state’s licensing board to report adverse actions and significant investigations occurring before the effective
date of such withdrawal or termination.
(5) This compact does not invalidate or prevent any nurse licensure agreement or other cooperative arrangement
between a party state and a nonparty state that is made in accordance with the other provisions of this compact.
(6) This compact may be amended by the party states. An amendment to this compact does not become effective
and binding upon the party states unless and until it is enacted into the laws of all party states.
(7) Representatives of nonparty states to this compact shall be invited to participate in the activities of the
commission, on a nonvoting basis, before the adoption of this compact by all party states.

10 – 19
ARTICLE XI
CONSTRUCTION AND SEVERABILITY
This compact shall be liberally construed so as to effectuate the purposes thereof. The provisions of this compact
are severable, and if any phrase, clause, sentence, or provision of this compact is declared to be contrary to the
constitution of any party state or of the United States, or if the applicability thereof to any government, agency, person,
or circumstance is held invalid, the validity of the remainder of this compact and the applicability thereof to any
government, agency, person, or circumstance is not affected thereby. If this compact is declared to be contrary to the
constitution of any party state, the compact shall remain in full force and effect as to the remaining party states and in
full force and effect as to the party state affected as to all severable matters.
History.—s. 7, ch. 2016-139.
464.0096 Nurse Licensure Compact; public records and meetings exemptions.—
(1) A nurse’s personal identifying information, other than the nurse’s name, licensure status, or licensure
number, obtained from the coordinated licensure information system, as defined in s. 464.0095, and held by the
department or the board is exempt from s. 119.07(1) and s. 24(a), Art. I of the State Constitution unless the state that
originally reported the information to the coordinated licensure information system authorizes the disclosure of such
information by law. Under such circumstances, the information may only be disclosed to the extent permitted by the
reporting state’s law.
(2)(a) A meeting or portion of a meeting of the Interstate Commission of Nurse Licensure Compact
Administrators established under s. 464.0095 at which matters specifically exempted from disclosure by federal or
state statute are discussed is exempt from s. 286.011 and s. 24(b), Art. I of the State Constitution.
(b) Recordings, minutes, and records generated during an exempt meeting are exempt from s. 119.07(1) and s.
24(a), Art. I of the State Constitution.
(3) This section is subject to the Open Government Sunset Review Act in accordance with s. 119.15 and shall
stand repealed on October 2, 2021, unless reviewed and saved from repeal through reenactment by the Legislature.
History.—s. 1, ch. 2016-97.
464.012 Licensure of advanced practice registered nurses; fees; controlled substance prescribing.—
(1) Any nurse desiring to be licensed as an advanced practice registered nurse must apply to the department and
submit proof that he or she holds a current license to practice professional nursing or holds an active multistate
license to practice professional nursing pursuant to s. 464.0095 and that he or she meets one or more of the
following requirements as determined by the board:
(a) Certification by an appropriate specialty board. Such certification is required for initial state licensure and
any licensure renewal as a certified nurse midwife, certified nurse practitioner, certified registered nurse anesthetist,
clinical nurse specialist, or psychiatric nurse. The board may by rule provide for provisional state licensure of
certified registered nurse anesthetists, clinical nurse specialists, certified nurse practitioners, psychiatric nurses, and
certified nurse midwives for a period of time determined to be appropriate for preparing for and passing the national
certification examination.
(b) Graduation from a program leading to a master’s degree in a nursing clinical specialty area with preparation
in specialized practitioner skills. For applicants graduating on or after October 1, 1998, graduation from a master’s
degree program is required for initial licensure as a certified nurse practitioner under paragraph (4)(a).

10 – 20
1. For applicants graduating on or after October 1, 2001, graduation from a master’s degree program is required
for initial licensure as a certified registered nurse anesthetist who may perform the acts listed in paragraph (4)(b).
2. For applicants graduating on or after October 1, 1998, graduation from a master’s degree program is required
for initial licensure as a certified nurse midwife who may perform the acts listed in paragraph (4)(c).
3. For applicants graduating on or after July 1, 2007, graduation from a master’s degree program is required for
initial licensure as a clinical nurse specialist who may perform the acts listed in paragraph (4)(d).
(2) The board shall provide by rule the appropriate requirements for advanced practice registered nurses for the
advanced nursing practices of certified nurse midwives, certified nurse practitioners, certified registered nurse
anesthetists, clinical nurse specialists, and psychiatric nurses.
(3) An advanced practice registered nurse shall perform those functions authorized in this section within the
framework of an established protocol that must be maintained on site at the location or locations at which an
advanced practice registered nurse practices. In the case of multiple supervising physicians in the same group, an
advanced practice registered nurse must enter into a supervisory protocol with at least one physician within the
physician group practice. A practitioner currently licensed under chapter 458, chapter 459, or chapter 466 shall
maintain supervision for directing the specific course of medical treatment. Within the established framework, an
advanced practice registered nurse may:
(a) Prescribe, dispense, administer, or order any drug; however, an advanced practice registered nurse may
prescribe or dispense a controlled substance as defined in s. 893.03 only if the advanced practice registered nurse
has graduated from a program leading to a master’s or doctoral degree in a clinical nursing specialty area with
training in specialized practitioner skills.
(b) Initiate appropriate therapies for certain conditions.
(c) Perform additional functions as may be determined by rule in accordance with s. 464.003(2).
(d) Order diagnostic tests and physical and occupational therapy.
(e) Order any medication for administration to a patient in a facility licensed under chapter 395 or part II of
chapter 400, notwithstanding any provisions in chapter 465 or chapter 893.
(4) In addition to the general functions specified in subsection (3), an advanced practice registered nurse may
perform the following acts within his or her specialty:
(a) The certified nurse practitioner may perform any or all of the following acts within the framework of
established protocol:
1. Manage selected medical problems.
2. Order physical and occupational therapy.
3. Initiate, monitor, or alter therapies for certain uncomplicated acute illnesses.
4. Monitor and manage patients with stable chronic diseases.
5. Establish behavioral problems and diagnosis and make treatment recommendations.
(b) The certified registered nurse anesthetist may, to the extent authorized by established protocol approved by
the medical staff of the facility in which the anesthetic service is performed, perform any or all of the following:
1. Determine the health status of the patient as it relates to the risk factors and to the anesthetic management of
the patient through the performance of the general functions.
2. Based on history, physical assessment, and supplemental laboratory results, determine, with the consent of
the responsible physician, the appropriate type of anesthesia within the framework of the protocol.

10 – 21
3. Order under the protocol preanesthetic medication.
4. Perform under the protocol procedures commonly used to render the patient insensible to pain during the
performance of surgical, obstetrical, therapeutic, or diagnostic clinical procedures. These procedures include
ordering and administering regional, spinal, and general anesthesia; inhalation agents and techniques; intravenous
agents and techniques; and techniques of hypnosis.
5. Order or perform monitoring procedures indicated as pertinent to the anesthetic health care management of
the patient.
6. Support life functions during anesthesia health care, including induction and intubation procedures, the use
of appropriate mechanical supportive devices, and the management of fluid, electrolyte, and blood component
balances.
7. Recognize and take appropriate corrective action for abnormal patient responses to anesthesia, adjunctive
medication, or other forms of therapy.
8. Recognize and treat a cardiac arrhythmia while the patient is under anesthetic care.
9. Participate in management of the patient while in the postanesthesia recovery area, including ordering the
administration of fluids and drugs.
10. Place special peripheral and central venous and arterial lines for blood sampling and monitoring as
appropriate.
(c) The certified nurse midwife may, to the extent authorized by an established protocol which has been
approved by the medical staff of the health care facility in which the midwifery services are performed, or approved
by the nurse midwife’s physician backup when the delivery is performed in a patient’s home, perform any or all of
the following:
1. Perform superficial minor surgical procedures.
2. Manage the patient during labor and delivery to include amniotomy, episiotomy, and repair.
3. Order, initiate, and perform appropriate anesthetic procedures.
4. Perform postpartum examination.
5. Order appropriate medications.
6. Provide family-planning services and well-woman care.
7. Manage the medical care of the normal obstetrical patient and the initial care of a newborn patient.
(d) The clinical nurse specialist may perform any or all of the following acts within the framework of
established protocol:
1. Assess the health status of individuals and families using methods appropriate to the population and area of
practice.
2. Diagnose human responses to actual or potential health problems.
3. Plan for health promotion, disease prevention, and therapeutic intervention in collaboration with the patient
or client.
4. Implement therapeutic interventions based on the nurse specialist’s area of expertise and within the scope of
advanced nursing practice, including, but not limited to, direct nursing care, counseling, teaching, and collaboration
with other licensed health care providers.
5. Coordinate health care as necessary and appropriate and evaluate with the patient or client the effectiveness
of care.

10 – 22
(e) A psychiatric nurse, who meets the requirements in s. 394.455(35), within the framework of an established
protocol with a psychiatrist, may prescribe psychotropic controlled substances for the treatment of mental disorders.
(5) The board shall approve for licensure, and the department shall issue a license to, any nurse meeting the
qualifications in this section. The board shall establish an application fee not to exceed $100 and a biennial renewal
fee not to exceed $50. The board is authorized to adopt such other rules as are necessary to implement the provisions
of this section.
(6)(a) The board shall establish a committee to recommend a formulary of controlled substances that an
advanced practice registered nurse may not prescribe or may prescribe only for specific uses or in limited quantities.
The committee must consist of three advanced practice registered nurses licensed under this section, recommended
by the board; three physicians licensed under chapter 458 or chapter 459 who have work experience with advanced
practice registered nurses, recommended by the Board of Medicine; and a pharmacist licensed under chapter 465
who is a doctor of pharmacy, recommended by the Board of Pharmacy. The committee may recommend an
evidence-based formulary applicable to all advanced practice registered nurses which is limited by specialty
certification, is limited to approved uses of controlled substances, or is subject to other similar restrictions the
committee finds are necessary to protect the health, safety, and welfare of the public. The formulary must restrict the
prescribing of psychiatric mental health controlled substances for children younger than 18 years of age to advanced
practice registered nurses who also are psychiatric nurses as defined in s. 394.455. The formulary must also limit the
prescribing of Schedule II controlled substances as listed in s. 893.03 to a 7-day supply, except that such restriction
does not apply to controlled substances that are psychiatric medications prescribed by psychiatric nurses as defined
in s. 394.455.
(b) The board shall adopt by rule the recommended formulary and any revision to the formulary which it finds
is supported by evidence-based clinical findings presented by the Board of Medicine, the Board of Osteopathic
Medicine, or the Board of Dentistry.
(c) The formulary required under this subsection does not apply to a controlled substance that is dispensed for
administration pursuant to an order, including an order for medication authorized by subparagraph (4)(b)3.,
subparagraph (4)(b)4., or subparagraph (4)(b)9.
(d) The board shall adopt the committee’s initial recommendation no later than October 31, 2016.
(7) This section shall be known as “The Barbara Lumpkin Prescribing Act.”
(8) The department and board shall establish a transition timeline and process for practitioners certified as of
September 30, 2018, as advanced registered nurse practitioners or clinical nurse specialists, to convert a certificate in
good standing to a license that becomes effective on October 1, 2018, to practice as an advanced practice registered
nurse. An advanced registered nurse practitioner or a clinical nurse specialist holding a certificate to practice in good
standing on September 30, 2018, may continue to practice with all rights, authorizations, and responsibilities under
this section for licensure as an advanced practice registered nurse and may use the applicable title under s. 464.015
after the effective date of this act while the department and board complete the transition from certification to
licensure, as established under this act. This subsection may not be construed to limit or restrict the department’s or
board’s disciplinary authority or enforcement responsibilities for safe nursing practice. This subsection expires on
October 1, 2020.
History.—ss. 1, 6, ch. 79-225; ss. 2, 3, ch. 81-318; s. 4, ch. 84-268; ss. 8, 17, 18, ch. 86-284; s. 58, ch. 91-137; s.
5, ch. 91-156; s. 4, ch. 91-429; s. 7, ch. 96-274; s. 1105, ch. 97-103; s. 80, ch. 97-264; s. 8, ch. 2006-251; s. 3, ch.

10 – 23
2007-167; s. 9, ch. 2010-37; s. 8, ch. 2016-139; s. 4, ch. 2016-145; ss. 12, 13, 25, ch. 2016-224; s. 7, ch. 2016-231;
ss. 2, 3, ch. 2017-134; s. 3, ch. 2018-106.
464.013 Renewal of license or certificate.—
(1) The department shall renew a license upon receipt of the renewal application and fee.
(2) The department shall adopt rules establishing a procedure for the biennial renewal of licenses.
(3) The board shall by rule prescribe up to 30 hours of continuing education biennially as a condition for
renewal of a license or certificate.
(a) A nurse who is certified by a health care specialty program accredited by the National Commission for
Certifying Agencies or the Accreditation Board for Specialty Nursing Certification is exempt from continuing
education requirements. The criteria for programs must be approved by the board.
(b) Notwithstanding the exemption in paragraph (a), as part of the maximum 30 hours of continuing education
hours required under this subsection, advanced practice registered nurses licensed under s. 464.012 must complete at
least 3 hours of continuing education on the safe and effective prescription of controlled substances. Such continuing
education courses must be offered by a statewide professional association of physicians in this state accredited to
provide educational activities designated for the American Medical Association Physician’s Recognition Award
Category 1 credit, the American Nurses Credentialing Center, the American Association of Nurse Anesthetists, or
the American Association of Nurse Practitioners and may be offered in a distance learning format.
(c) Notwithstanding the exemption in paragraph (a), as part of the maximum biennial continuing education
hours required under this subsection, the board shall require each person licensed or certified under this chapter to
complete a 2-hour continuing education course on human trafficking, as defined in s. 787.06(2). The continuing
education course must consist of data and information on the types of human trafficking, such as labor and sex, and
the extent of human trafficking; factors that place a person at greater risk of being a victim of human trafficking;
public and private social services available for rescue, food, clothing, and shelter referrals; hotlines for reporting
human trafficking which are maintained by the National Human Trafficking Resource Center and the United States
Department of Homeland Security; validated assessment tools for identifying a human trafficking victim and general
indicators that a person may be a victim of human trafficking; procedures for sharing information related to human
trafficking with a patient; and referral options for legal and social services. All licensees must complete this course
for every biennial licensure renewal on or after January 1, 2019.
History.—ss. 1, 6, ch. 79-225; ss. 2, 3, ch. 81-318; ss. 9, 17, 18, ch. 86-284; s. 11, ch. 88-219; s. 1, ch. 89-170; s.
58, ch. 91-137; s. 5, ch. 91-156; s. 4, ch. 91-429; s. 176, ch. 94-119; s. 8, ch. 96-274; s. 81, ch. 97-264; s. 3, ch.
2014-92; s. 14, ch. 2016-224; s. 6, ch. 2017-23; s. 57, ch. 2018-106.
464.014 Inactive status.—
(1) The board shall adopt rules relating to application procedures for inactive status, to the biennial renewal of
inactive licenses, and to the reactivation of licenses. The board shall prescribe by rule an application fee for inactive
status, a renewal fee for inactive status, a delinquency fee, and a fee for the reactivation of a license. None of these
fees may exceed the biennial renewal fee established by the board for biennial renewal of an active license.
(2) The department may not reactivate a license unless the inactive or delinquent licensee has paid any
applicable biennial renewal or delinquency fee, or both, and a reactivation fee.

10 – 24
History.—ss. 1, 6, ch. 79-225; s. 319, ch. 81-259; ss. 2, 3, ch. 81-318; ss. 11, 17, 18, ch. 86-284; s. 12, ch. 88-
219; s. 35, ch. 89-162; s. 2, ch. 89-170; s. 58, ch. 91-137; s. 5, ch. 91-156; s. 4, ch. 91-429; s. 177, ch. 94-119; s. 9,
ch. 96-274; s. 82, ch. 97-264.
464.015 Titles and abbreviations; restrictions; penalty.—
(1) Only a person who holds a license in this state or a multistate license pursuant to s. 464.0095 to practice
professional nursing or who performs nursing services pursuant to the exception set forth in s. 464.022(8) may use
the title “Registered Nurse” and the abbreviation “R.N.”
(2) Only a person who holds a license in this state or a multistate license pursuant to s. 464.0095 to practice as a
licensed practical nurse or who performs practical nursing services pursuant to the exception set forth in s.
464.022(8) may use the title “Licensed Practical Nurse” and the abbreviation “L.P.N.”
(3) Only persons who are graduates of prelicensure nursing education programs listed in s. 464.008(1)(c) may
use the term “Graduate Nurse” and the abbreviation “G.N.,” pending the results of the first licensure examination for
which they are eligible.
(4) Only persons who are graduates of prelicensure nursing education programs listed in s. 464.008(1)(c) may
use the term “Graduate Practical Nurse” and the abbreviation “G.P.N.,” pending the results of the first licensure
examination for which they are eligible.
(5) Only persons who hold valid licenses to practice as clinical nurse specialists in this state may use the title
“Clinical Nurse Specialist” and the abbreviation “C.N.S.”
(6) Only persons who hold valid certificates to practice as certified registered nurse anesthetists in this state
may use the title “Certified Registered Nurse Anesthetist” and the abbreviations “C.R.N.A.” or “nurse anesthetist.”
(7) Only persons who hold valid certificates to practice as certified nurse midwives in this state may use the
title “Certified Nurse Midwife” and the abbreviations “C.N.M.” or “nurse midwife.”
(8) Only persons who hold valid licenses to practice as advanced practice registered nurses in this state may use
the title “Advanced Practice Registered Nurse” and the abbreviation “A.P.R.N.”
(9) A person may not practice or advertise as, or assume the title of, registered nurse, licensed practical nurse,
clinical nurse specialist, certified registered nurse anesthetist, certified nurse midwife, certified nurse practitioner, or
advanced practice registered nurse or use the abbreviation “R.N.,” “L.P.N.,” “C.N.S.,” “C.R.N.A.,” “C.N.M.,”
“C.N.P.,” or “A.P.R.N.” or take any other action that would lead the public to believe that person was authorized by
law to practice as such or is performing nursing services pursuant to the exception set forth in s. 464.022(8) unless
that person is licensed, certified, or authorized pursuant to s. 464.0095 to practice as such.
(10) A violation of this section is a misdemeanor of the first degree, punishable as provided in s. 775.082 or s.
775.083.
History.—ss. 1, 6, ch. 79-225; ss. 2, 3, ch. 81-318; ss. 12, 17, 18, ch. 86-284; s. 58, ch. 91-137; s. 5, ch. 91-156;
s. 4, ch. 91-429; s. 4, ch. 2007-167; s. 4, ch. 2010-37; s. 9, ch. 2016-139; ss. 58, 59, ch. 2018-106.
464.016 Violations and penalties.—
(1) Each of the following acts constitutes a felony of the third degree, punishable as provided in s. 775.082, s.
775.083, or s. 775.084:
(a) Practicing advanced or specialized, professional, or practical nursing, as defined in this part, unless holding
an active license or certificate to do so.
(b) Using or attempting to use a license or certificate which has been suspended or revoked.

10 – 25
(c) Knowingly employing unlicensed persons in the practice of nursing.
(d) Obtaining or attempting to obtain a license or certificate under this part by misleading statements or
knowing misrepresentation.
(2) Each of the following acts constitutes a misdemeanor of the first degree, punishable as provided in s.
775.082 or s. 775.083:
(a) Using the name or title “Nurse,” “Registered Nurse,” “Licensed Practical Nurse,” “Clinical Nurse
Specialist,” “Certified Registered Nurse Anesthetist,” “Certified Nurse Practitioner,” “Certified Nurse Midwife,”
“Advanced Practice Registered Nurse,” or any other name or title which implies that a person was licensed or
certified as same, unless such person is duly licensed or certified.
(b) Knowingly concealing information relating to violations of this part.
History.—ss. 1, 6, ch. 79-225; ss. 2, 3, ch. 81-318; ss. 13, 17, 18, ch. 86-284; s. 58, ch. 91-137; s. 5, ch. 91-156;
s. 90, ch. 91-224; s. 4, ch. 91-429; s. 183, ch. 99-397; ss. 54, 124, ch. 2000-318; s. 5, ch. 2007-167; s. 60, ch. 2018-
106.
464.017 Sexual misconduct in the practice of nursing.—The nurse-patient relationship is founded on mutual
trust. Sexual misconduct in the practice of nursing means violation of the nurse-patient relationship through which
the nurse uses said relationship to induce or attempt to induce the patient to engage, or to engage or attempt to
engage the patient, in sexual activity outside the scope of the practice or the scope of generally accepted examination
or treatment of the patient. Sexual misconduct in the practice of nursing is prohibited.
History.—ss. 1, 6, ch. 79-225; s. 320, ch. 81-259; ss. 2, 3, ch. 81-318; ss. 17, 18, ch. 86-284; s. 58, ch. 91-137; s.
5, ch. 91-156; s. 4, ch. 91-429.
464.018 Disciplinary actions.—
(1) The following acts constitute grounds for denial of a license or disciplinary action, as specified in ss.
456.072(2) and 464.0095:
(a) Procuring, attempting to procure, or renewing a license to practice nursing or the authority to practice
practical or professional nursing pursuant to s. 464.0095 by bribery, by knowing misrepresentations, or through an
error of the department or the board.
(b) Having a license to practice nursing revoked, suspended, or otherwise acted against, including the denial of
licensure, by the licensing authority of another state, territory, or country.
(c) Being convicted or found guilty of, or entering a plea of guilty or nolo contendere to, regardless of
adjudication, a crime in any jurisdiction which directly relates to the practice of nursing or to the ability to practice
nursing.
(d) Being convicted or found guilty of, or entering a plea of guilty or nolo contendere to, regardless of
adjudication, any of the following offenses:
1. A forcible felony as defined in chapter 776.
2. A violation of chapter 812, relating to theft, robbery, and related crimes.
3. A violation of chapter 817, relating to fraudulent practices.
4. A violation of chapter 800, relating to lewdness and indecent exposure.
5. A violation of chapter 784, relating to assault, battery, and culpable negligence.
6. A violation of chapter 827, relating to child abuse.
7. A violation of chapter 415, relating to protection from abuse, neglect, and exploitation.

10 – 26
8. A violation of chapter 39, relating to child abuse, abandonment, and neglect.
9. For an applicant for a multistate license or for a multistate licenseholder under s. 464.0095, a felony offense
under Florida law or federal criminal law.
(e) Having been found guilty of, regardless of adjudication, or entered a plea of nolo contendere or guilty to,
any offense prohibited under s. 435.04 or similar statute of another jurisdiction; or having committed an act which
constitutes domestic violence as defined in s. 741.28.
(f) Making or filing a false report or record, which the nurse knows to be false, intentionally or negligently
failing to file a report or record required by state or federal law, willfully impeding or obstructing such filing or
inducing another person to do so. Such reports or records shall include only those which are signed in the nurse’s
capacity as a licensed nurse.
(g) False, misleading, or deceptive advertising.
(h) Unprofessional conduct, as defined by board rule.
(i) Engaging or attempting to engage in the possession, sale, or distribution of controlled substances as set forth
in chapter 893, for any other than legitimate purposes authorized by this part.
(j) Being unable to practice nursing with reasonable skill and safety to patients by reason of illness or use of
alcohol, drugs, narcotics, or chemicals or any other type of material or as a result of any mental or physical
condition. In enforcing this paragraph, the department shall have, upon a finding of the State Surgeon General or the
State Surgeon General’s designee that probable cause exists to believe that the nurse is unable to practice nursing
because of the reasons stated in this paragraph, the authority to issue an order to compel a nurse to submit to a
mental or physical examination by physicians designated by the department. If the nurse refuses to comply with
such order, the department’s order directing such examination may be enforced by filing a petition for enforcement
in the circuit court where the nurse resides or does business. The nurse against whom the petition is filed shall not be
named or identified by initials in any public court records or documents, and the proceedings shall be closed to the
public. The department shall be entitled to the summary procedure provided in s. 51.011. A nurse affected by this
paragraph shall at reasonable intervals be afforded an opportunity to demonstrate that she or he can resume the
competent practice of nursing with reasonable skill and safety to patients.
(k) Failing to report to the department any person who the nurse knows is in violation of this part or of the rules
of the department or the board. However, a person who the licensee knows is unable to practice nursing with
reasonable skill and safety to patients by reason of illness or use of alcohol, drugs, narcotics, chemicals, or any other
type of material, or as a result of a mental or physical condition, may be reported to a consultant operating an
impaired practitioner program as described in s. 456.076 rather than to the department.
(l) Knowingly violating any provision of this part, a rule of the board or the department, or a lawful order of the
board or department previously entered in a disciplinary proceeding or failing to comply with a lawfully issued
subpoena of the department.
(m) Failing to report to the department any licensee under chapter 458 or under chapter 459 who the nurse
knows has violated the grounds for disciplinary action set out in the law under which that person is licensed and who
provides health care services in a facility licensed under chapter 395, or a health maintenance organization
certificated under part I of chapter 641, in which the nurse also provides services.
(n) Failing to meet minimal standards of acceptable and prevailing nursing practice, including engaging in acts
for which the nurse is not qualified by training or experience.

10 – 27
(o) Violating any provision of this chapter or chapter 456, or any rules adopted pursuant thereto.
(p) For an advanced practice registered nurse:
1. Presigning blank prescription forms.
2. Prescribing for office use any medicinal drug appearing on Schedule II in chapter 893.
3. Prescribing, ordering, dispensing, administering, supplying, selling, or giving a drug that is an amphetamine,
a sympathomimetic amine drug, or a compound designated in s. 893.03(2) as a Schedule II controlled substance, to
or for any person except for:
a. The treatment of narcolepsy; hyperkinesis; behavioral syndrome in children characterized by the
developmentally inappropriate symptoms of moderate to severe distractibility, short attention span, hyperactivity,
emotional lability, and impulsivity; or drug-induced brain dysfunction.
b. The differential diagnostic psychiatric evaluation of depression or the treatment of depression shown to be
refractory to other therapeutic modalities.
c. The clinical investigation of the effects of such drugs or compounds when an investigative protocol is
submitted to, reviewed by, and approved by the department before such investigation is begun.
4. Prescribing, ordering, dispensing, administering, supplying, selling, or giving growth hormones, testosterone
or its analogs, human chorionic gonadotropin (HCG), or other hormones for the purpose of muscle building or to
enhance athletic performance. As used in this subparagraph, the term “muscle building” does not include the
treatment of injured muscle. A prescription written for the drug products identified in this subparagraph may be
dispensed by a pharmacist with the presumption that the prescription is for legitimate medical use.
5. Promoting or advertising on any prescription form a community pharmacy unless the form also states: “This
prescription may be filled at any pharmacy of your choice.”
6. Prescribing, dispensing, administering, mixing, or otherwise preparing a legend drug, including a controlled
substance, other than in the course of his or her professional practice. For the purposes of this subparagraph, it is
legally presumed that prescribing, dispensing, administering, mixing, or otherwise preparing legend drugs, including
all controlled substances, inappropriately or in excessive or inappropriate quantities is not in the best interest of the
patient and is not in the course of the advanced practice registered nurse’s professional practice, without regard to
his or her intent.
7. Prescribing, dispensing, or administering a medicinal drug appearing on any schedule set forth in chapter 893
to himself or herself, except a drug prescribed, dispensed, or administered to the advanced practice registered nurse
by another practitioner authorized to prescribe, dispense, or administer medicinal drugs.
8. Prescribing, ordering, dispensing, administering, supplying, selling, or giving amygdalin (laetrile) to any
person.
9. Dispensing a substance designated in s. 893.03(2) or (3) as a substance controlled in Schedule II or Schedule
III, respectively, in violation of s. 465.0276.
10. Promoting or advertising through any communication medium the use, sale, or dispensing of a substance
designated in s. 893.03 as a controlled substance.
(q) For a psychiatric nurse:
1. Presigning blank prescription forms.
2. Prescribing for office use any medicinal drug appearing in Schedule II of s. 893.03.

10 – 28
3. Prescribing, ordering, dispensing, administering, supplying, selling, or giving a drug that is an amphetamine,
a sympathomimetic amine drug, or a compound designated in s. 893.03(2) as a Schedule II controlled substance, to
or for any person except for:
a. The treatment of narcolepsy; hyperkinesis; behavioral syndrome in children characterized by the
developmentally inappropriate symptoms of moderate to severe distractibility, short attention span, hyperactivity,
emotional lability, and impulsivity; or drug-induced brain dysfunction.
b. The differential diagnostic psychiatric evaluation of depression or the treatment of depression shown to be
refractory to other therapeutic modalities.
c. The clinical investigation of the effects of such drugs or compounds when an investigative protocol is
submitted to, reviewed by, and approved by the department before such investigation is begun.
4. Prescribing, ordering, dispensing, administering, supplying, selling, or giving growth hormones, testosterone
or its analogs, human chorionic gonadotropin (HCG), or other hormones for the purpose of muscle building or to
enhance athletic performance. As used in this subparagraph, the term “muscle building” does not include the
treatment of injured muscle. A prescription written for the drug products identified in this subparagraph may be
dispensed by a pharmacist with the presumption that the prescription is for legitimate medical use.
5. Promoting or advertising on any prescription form a community pharmacy unless the form also states: “This
prescription may be filled at any pharmacy of your choice.”
6. Prescribing, dispensing, administering, mixing, or otherwise preparing a legend drug, including a controlled
substance, other than in the course of his or her professional practice. For the purposes of this subparagraph, it is
legally presumed that prescribing, dispensing, administering, mixing, or otherwise preparing legend drugs, including
all controlled substances, inappropriately or in excessive or inappropriate quantities is not in the best interest of the
patient and is not in the course of the advanced practice registered nurse’s professional practice, without regard to
his or her intent.
7. Prescribing, dispensing, or administering a medicinal drug appearing on any schedule set forth in chapter 893
to himself or herself, except a drug prescribed, dispensed, or administered to the psychiatric nurse by another
practitioner authorized to prescribe, dispense, or administer medicinal drugs.
8. Prescribing, ordering, dispensing, administering, supplying, selling, or giving amygdalin (laetrile) to any
person.
9. Dispensing a substance designated in s. 893.03(2) or (3) as a substance controlled in Schedule II or Schedule
III, respectively, in violation of s. 465.0276.
10. Promoting or advertising through any communication medium the use, sale, or dispensing of a substance
designated in s. 893.03 as a controlled substance.
(2)(a) The board may enter an order denying licensure or imposing any of the penalties in s. 456.072(2) against
any applicant for licensure or nurse who is found guilty of violating subsection (1) or s. 456.072(1).
(b) The board may take adverse action against a nurse’s multistate licensure privilege and impose any of the
penalties in s. 456.072(2) when the nurse is found guilty of violating subsection (1) or s. 456.072(1).
(3) The board shall not reinstate the license of a nurse, or cause a license to be issued to a person it has deemed
unqualified, until such time as it is satisfied that such person has complied with all the terms and conditions set forth
in the final order and that such person is capable of safely engaging in the practice of nursing.

10 – 29
(4) The board shall not reinstate the license of a nurse who has been found guilty by the board on three separate
occasions of violations of this part relating to the use of drugs or narcotics, which offenses involved the diversion of
drugs or narcotics from patients to personal use or sale.
(5) The board shall by rule establish guidelines for the disposition of disciplinary cases involving specific types
of violations. Such guidelines may include minimum and maximum fines, periods of supervision or probation, or
conditions of probation or reissuance of a license.
History.—ss. 1, 6, ch. 79-225; s. 321, ch. 81-259; ss. 2, 3, ch. 81-318; s. 1, ch. 83-27; s. 27, ch. 83-329; ss. 14,
17, 18, ch. 86-284; s. 40, ch. 88-1; s. 13, ch. 88-219; s. 19, ch. 88-277; s. 19, ch. 88-392; s. 3, ch. 89-170; s. 33, ch.
91-57; s. 58, ch. 91-137; s. 5, ch. 91-156; s. 4, ch. 91-429; s. 44, ch. 92-149; s. 24, ch. 94-134; s. 24, ch. 94-135; s.
20, ch. 95-152; s. 48, ch. 95-228; s. 136, ch. 95-418; s. 10, ch. 96-274; s. 1106, ch. 97-103; s. 83, ch. 97-264; s. 155,
ch. 98-403; s. 2, ch. 99-335; s. 125, ch. 2000-318; s. 103, ch. 2000-349; s. 31, ch. 2001-277; s. 6, ch. 2002-230; s.
30, ch. 2004-267; s. 9, ch. 2005-240; s. 83, ch. 2008-6; s. 51, ch. 2010-114; s. 10, ch. 2016-139; s. 15, ch. 2016-224;
s. 8, ch. 2016-231; s. 14, ch. 2017-41; s. 61, ch. 2018-106.
464.019 Approval of nursing education programs.—
(1) PROGRAM APPLICATION.—An educational institution that wishes to conduct a program in this state for
the prelicensure education of professional or practical nurses must submit to the department a program application
and review fee of $1,000 for each prelicensure nursing education program to be offered at the institution’s main
campus, branch campus, or other instructional site. The program application must include the legal name of the
educational institution, the legal name of the nursing education program, and, if such institution is accredited, the
name of the accrediting agency. The application must also document that:
(a)1. For a professional nursing education program, the program director and at least 50 percent of the
program’s faculty members are registered nurses who have a master’s or higher degree in nursing or a bachelor’s
degree in nursing and a master’s or higher degree in a field related to nursing.
2. For a practical nursing education program, the program director and at least 50 percent of the program’s
faculty members are registered nurses who have a bachelor’s or higher degree in nursing.
The educational degree requirements of this paragraph may be documented by an official transcript or by a written
statement from the educational institution verifying that the institution conferred the degree.
(b) The program’s nursing major curriculum consists of at least:
1. Fifty percent clinical training in the United States, the District of Columbia, or a possession or territory of the
United States for a practical nursing education program, an associate degree professional nursing education
program, or a professional diploma nursing education program.
2. Forty percent clinical training in the United States, the District of Columbia, or a possession or territory of
the United States for a bachelor’s degree professional nursing education program.
(c) No more than 50 percent of the program’s clinical training consists of clinical simulation.
(d) The program has signed agreements with each agency, facility, and organization included in the curriculum
plan as clinical training sites and community-based clinical experience sites.
(e) The program has written policies for faculty which include provisions for direct or indirect supervision by
program faculty or clinical preceptors for students in clinical training consistent with the following standards:
1. The number of program faculty members equals at least one faculty member directly supervising every 12
students unless the written agreement between the program and the agency, facility, or organization providing

10 – 30
clinical training sites allows more students, not to exceed 18 students, to be directly supervised by one program
faculty member.
2. For a hospital setting, indirect supervision may occur only if there is direct supervision by an assigned
clinical preceptor, a supervising program faculty member is available by telephone, and such arrangement is
approved by the clinical facility.
3. For community-based clinical experiences that involve student participation in invasive or complex nursing
activities, students must be directly supervised by a program faculty member or clinical preceptor and such
arrangement must be approved by the community-based clinical facility.
4. For community-based clinical experiences not subject to subparagraph 3., indirect supervision may occur
only when a supervising program faculty member is available to the student by telephone.
A program’s policies established under this paragraph must require that a clinical preceptor who is supervising
students in a professional nursing education program be a registered nurse or, if supervising students in a practical
nursing education program, be a registered nurse or licensed practical nurse.
(f) The professional or practical nursing curriculum plan documents clinical experience and theoretical
instruction in medical, surgical, obstetric, pediatric, and geriatric nursing. A professional nursing curriculum plan
shall also document clinical experience and theoretical instruction in psychiatric nursing. Each curriculum plan must
document clinical training experience in appropriate settings that include, but are not limited to, acute care, long-
term care, and community settings.
(g) The professional or practical nursing education program provides theoretical instruction and clinical
application in personal, family, and community health concepts; nutrition; human growth and development
throughout the life span; body structure and function; interpersonal relationship skills; mental health concepts;
pharmacology and administration of medications; and legal aspects of practice. A professional nursing education
program must also provide theoretical instruction and clinical application in interpersonal relationships and
leadership skills; professional role and function; and health teaching and counseling skills.
(2) PROGRAM APPROVAL.—
(a) Upon receipt of a program application and review fee, the department shall examine the application to
determine if it is complete. If the application is not complete, the department shall notify the educational institution
in writing of any errors or omissions within 30 days after the department’s receipt of the application. A program
application is deemed complete upon the department’s receipt of:
1. The initial application, if the department does not notify the educational institution of any errors or omissions
within the 30-day period; or
2. A revised application that corrects each error and omission of which the department notifies the educational
institution within the 30-day period.
(b) Following the department’s receipt of a complete program application, the board may conduct an onsite
evaluation if necessary to document the applicant’s compliance with subsection (1). Within 90 days after the
department’s receipt of a complete program application, the board shall:
1. Approve the application if it documents compliance with subsection (1); or
2. Provide the educational institution with a notice of intent to deny the application if it does not document
compliance with subsection (1). The notice must specify written reasons for the board’s denial of the application.
The board may not deny a program application because of an educational institution’s failure to correct an error or

10 – 31
omission that the department failed to provide notice of to the institution within the 30-day notice period under
paragraph (a). The educational institution may request a hearing on the notice of intent to deny the program
application pursuant to chapter 120.
(c) A program application is deemed approved if the board does not act within the 90-day review period
provided under paragraph (b).
(d) Upon the board’s approval of a program application, the program becomes an approved program.
(3) ANNUAL REPORT.—By November 1 of each year, each approved program shall submit to the board an
annual report comprised of an affidavit certifying continued compliance with subsection (1), a summary description
of the program’s compliance with subsection (1), and documentation for the previous academic year that, to the
extent applicable, describes:
(a) The number of student applications received, qualified applicants, applicants accepted, accepted applicants
who enroll in the program, students enrolled in the program, and program graduates.
(b) The program’s retention rates for students tracked from program entry to graduation.
(c) The program’s accreditation status, including identification of the accrediting agency.
(4) INTERNET WEBSITE.—The board shall publish the following information on its Internet website:
(a) A list of each accredited program conducted in the state and the program’s graduate passage rates for the
most recent 2 calendar years, which the department shall determine through the following sources:
1. For a program’s accreditation status, the specialized accrediting agencies that are nationally recognized by
the United States Secretary of Education to accredit nursing education programs.
2. For a program’s graduate passage rates, the contract testing service of the National Council of State Boards
of Nursing.
(b) The following data for each approved program, which includes, to the extent applicable:
1. All documentation provided by the program in its program application if submitted on or after July 1, 2009.
2. The summary description of the program’s compliance submitted under subsection (3).
3. The program’s accreditation status, including identification of the accrediting agency.
4. The program’s probationary status.
5. The program’s graduate passage rates for the most recent 2 calendar years.
6. Each program’s retention rates for students tracked from program entry to graduation.
(c) The average passage rates for United States educated, first-time test takers on the National Council of State
Boards of Nursing Licensing Examination for the most recent 2 calendar years, as calculated by the contract testing
service of the National Council of State Boards of Nursing. The average passage rates shall be published separately
for each type of comparable degree program listed in subparagraph (5)(a)1.
The information required to be published under this subsection shall be made available in a manner that allows
interactive searches and comparisons of individual programs selected by the website user. The board shall update the
Internet website at least quarterly with the available information.
(5) ACCOUNTABILITY.—
(a)1. An approved program must achieve a graduate passage rate for first-time test takers which is not more
than 10 percentage points lower than the average passage rate during the same calendar year for graduates of
comparable degree programs who are United States educated, first-time test takers on the National Council of State
Boards of Nursing Licensing Examination, as calculated by the contract testing service of the National Council of

10 – 32
State Boards of Nursing. For purposes of this subparagraph, an approved program is comparable to all degree
programs of the same program type from among the following program types:
a. Professional nursing education programs that terminate in a bachelor’s degree.
b. Professional nursing education programs that terminate in an associate degree.
c. Professional nursing education programs that terminate in a diploma.
d. Practical nursing education programs.
2. Beginning with graduate passage rates for calendar year 2010, if an approved program’s graduate passage
rates do not equal or exceed the required passage rates for 2 consecutive calendar years, the board shall place the
program on probationary status pursuant to chapter 120 and the program director shall appear before the board to
present a plan for remediation, which shall include specific benchmarks to identify progress toward a graduate
passage rate goal. The program must remain on probationary status until it achieves a graduate passage rate that
equals or exceeds the required passage rate for any 1 calendar year. The board shall deny a program application for a
new prelicensure nursing education program submitted by an educational institution if the institution has an existing
program that is already on probationary status.
3. Upon the program’s achievement of a graduate passage rate that equals or exceeds the required passage rate,
the board, at its next regularly scheduled meeting following release of the program’s graduate passage rate by the
National Council of State Boards of Nursing, shall remove the program’s probationary status. If the program, during
the 2 calendar years following its placement on probationary status, does not achieve the required passage rate for
any 1 calendar year, the board may extend the program’s probationary status for 1 additional year, provided the
program has demonstrated adequate progress toward the graduate passage rate goal by meeting a majority of the
benchmarks established in the remediation plan. If the program is not granted the 1-year extension or fails to achieve
the required passage rate by the end of such extension, the board shall terminate the program pursuant to chapter
120.
(b) If an approved program fails to submit the annual report required in subsection (3), the board shall notify
the program director and president or chief executive officer of the educational institution in writing within 15 days
after the due date of the annual report. The program director shall appear before the board at the board’s next
regularly scheduled meeting to explain the reason for the delay. The board shall terminate the program pursuant to
chapter 120 if the program director fails to appear before the board, as required under this paragraph, or if the
program does not submit the annual report within 6 months after the due date.
(c) A nursing education program, whether accredited or nonaccredited, which has been placed on probationary
status shall disclose its probationary status in writing to the program’s students and applicants. The notification must
include an explanation of the implications of the program’s probationary status on the students or applicants.
(d) If students from a program that is terminated pursuant to this subsection transfer to an approved or an
accredited program under the direction of the Commission for Independent Education, the board shall recalculate the
passage rates of the programs receiving the transferring students, excluding the test scores of those students
transferring more than 12 credits.
(6) DISCLOSURE OF GRADUATE PASSAGE RATE DATA.—
(a) For each graduate of the program included in the calculation of the program’s graduate passage rate, the
department shall disclose to the program director, upon his or her written request, the name, examination date, and
determination of whether each graduate passed or failed the National Council of State Boards of Nursing Licensing

10 – 33
Examination, if such information is provided to the department by the contract testing service of the National
Council of State Boards of Nursing. The written request must specify the calendar years for which the information is
requested.
(b) A program director to whom confidential information exempt from public disclosure pursuant to s. 456.014
is disclosed under this subsection must maintain the confidentiality of the information and is subject to the same
penalties provided in s. 456.082 for department employees who unlawfully disclose confidential information.
(7) PROGRAM CLOSURE.—
(a) An educational institution conducting an approved program or accredited program in this state, at least 30
days before voluntarily closing the program, shall notify the board in writing of the institution’s reason for closing
the program, the intended closure date, the institution’s plan to provide for or assist in the completion of training by
the program’s students, and the arrangements for storage of the program’s permanent records.
(b) An educational institution conducting a nursing education program that is terminated under subsection (5)
or closed under subparagraph (9)(b)3.:
1. May not accept or enroll new students.
2. Shall submit to the board within 30 days after the program is terminated or closed a written description of
how the institution will assist in completing the training of the program’s students and the institution’s arrangements
for storage of the program’s permanent records.
(c) If an educational institution does not comply with paragraph (a) or paragraph (b), the board shall provide a
written notice explaining the institution’s noncompliance to the following persons and entities:
1. The president or chief executive officer of the educational institution.
2. The Board of Governors, if the program is conducted by a state university.
3. The district school board, if the program is conducted by an educational institution operated by a school
district.
4. The Commission for Independent Education, if the program is conducted by an educational institution
licensed under chapter 1005.
5. The State Board of Education, if the program is conducted by an educational institution in the Florida
College System or by an educational institution that is not subject to subparagraphs 2.-4.
(d) A program that is terminated or closed under this section may not seek program approval under its original
name or a new program name for a minimum of 3 years after the date of termination or closing. An institutional
name change or the creation of a new educational institution with the same ownership does not reduce the waiting
period for reapplication.
(8) RULEMAKING.—The board does not have rulemaking authority to administer this section, except that the
board shall adopt rules that prescribe the format for submitting program applications under subsection (1) and
annual reports under subsection (3), and to administer the documentation of the accreditation of nursing education
programs under subsection (11). The board may adopt rules relating to the nursing curriculum, including rules
relating to the uses and limitations of simulation technology. The board may not impose any condition or
requirement on an educational institution submitting a program application, an approved program, or an accredited
program, except as expressly provided in this section.

10 – 34
(9) APPLICABILITY TO ACCREDITED PROGRAMS.—
(a) Subsections (1)-(3), paragraph (4)(b), and paragraph (5)(b) do not apply to an accredited program.
(b) If an accredited program ceases to be accredited, the educational institution conducting the program:
1. Within 10 business days after the program ceases to be accredited, must provide written notice of the date
that the program ceased to be accredited to the board, the program’s students and applicants, and each entity
providing clinical training sites or community-based clinical experience sites for the program. The educational
institution must continue to provide the written notice to new students, applicants, and entities providing clinical
training sites or community-based clinical experience sites for the program until the program becomes an approved
program or is closed under subparagraph 3.
2. Within 30 days after the program ceases to be accredited, must submit an affidavit to the board, signed by the
educational institution’s president or chief executive officer, which certifies the institution’s compliance with
subparagraph 1. The board shall notify the persons and applicable entities listed in paragraph (7)(c) if an educational
institution does not submit the affidavit required by this subparagraph.
3. May apply to become an approved program under this section. If the educational institution:
a. Within 30 days after the program ceases to be accredited, submits a program application and review fee to
the department under subsection (1) and the affidavit required under subparagraph 2., the program shall be deemed
an approved program from the date that the program ceased to be accredited until the date that the board approves or
denies the program application. The program application must be denied by the board pursuant to chapter 120 if it
does not contain the affidavit. If the board denies the program application under subsection (2) or if the program
application does not contain the affidavit, the program shall be closed and the educational institution conducting the
program must comply with paragraph (7)(b).
b. Does not apply to become an approved program pursuant to sub-subparagraph a., the program shall be
deemed an approved program from the date the program ceased to be accredited until the 31st day after that date. On
the 31st day after the program ceased to be accredited, the program shall be closed and the educational institution
conducting the program must comply with paragraph (7)(b).
(10) IMPLEMENTATION STUDY.—The Florida Center for Nursing shall study the administration of this
section and submit reports to the Governor, the President of the Senate, and the Speaker of the House of
Representatives annually by January 30, through January 30, 2020. The annual reports shall address the previous
academic year; provide data on the measures specified in paragraphs (a) and (b), as such data becomes available;
and include an evaluation of such data for purposes of determining whether this section is increasing the availability
of nursing education programs and the production of quality nurses. The department and each approved program or
accredited program shall comply with requests for data from the Florida Center for Nursing.
(a) The Florida Center for Nursing shall evaluate program-specific data for each approved program and
accredited program conducted in the state, including, but not limited to:
1. The number of programs and student slots available.
2. The number of student applications submitted, the number of qualified applicants, and the number of
students accepted.
3. The number of program graduates.
4. Program retention rates of students tracked from program entry to graduation.
5. Graduate passage rates on the National Council of State Boards of Nursing Licensing Examination.

10 – 35
6. The number of graduates who become employed as practical or professional nurses in the state.
(b) The Florida Center for Nursing shall evaluate the board’s implementation of the:
1. Program application approval process, including, but not limited to, the number of program applications
submitted under subsection (1); the number of program applications approved and denied by the board under
subsection (2); the number of denials of program applications reviewed under chapter 120; and a description of the
outcomes of those reviews.
2. Accountability processes, including, but not limited to, the number of programs on probationary status, the
number of approved programs for which the program director is required to appear before the board under
subsection (5), the number of approved programs terminated by the board, the number of terminations reviewed
under chapter 120, and a description of the outcomes of those reviews.
(c) The Florida Center for Nursing shall complete an annual assessment of compliance by programs with the
accreditation requirements of subsection (11), include in the assessment a determination of the accreditation process
status for each program, and submit the assessment as part of the reports required by this subsection.
(11) ACCREDITATION REQUIRED.—
(a) A nursing education program that prepares students for the practice of professional nursing, that was
approved under this section before July 1, 2014, and that enrolled students before July 1, 2014, must become an
accredited program by July 1, 2019.
(b) A nursing education program that prepares students for the practice of professional nursing and that was
approved under this section before July 1, 2014, but did not enroll students before that date, must become an
accredited program within 5 years after the date of enrolling the program’s first students.
(c) A nursing education program that prepares students for the practice of professional nursing and that is
approved under this section after June 30, 2014, must become an accredited program within 5 years after the date of
enrolling the program’s first students.
(d) This subsection does not apply to a nursing education program provided by an institution that is exempt
from licensure by the Commission for Independent Education under s. 1005.06(1)(e).
(e) A nursing education program that fails to meet the accreditation requirements shall be terminated and is
ineligible for reapproval under its original name or a new program name for a minimum of 3 years after the date of
termination. An institutional name change or the creation of a new educational institution with the same ownership
does not reduce the waiting period for reapplication.
History.—ss. 1, 6, ch. 79-225; ss. 2, 3, ch. 81-318; ss. 17, 18, ch. 86-284; s. 58, ch. 91-137; s. 5, ch. 91-156; s. 4,
ch. 91-429; s. 11, ch. 96-274; s. 84, ch. 97-264; s. 126, ch. 2000-318; s. 7, ch. 2002-230; s. 2, ch. 2009-168; s. 5, ch.
2010-37; s. 98, ch. 2012-184; s. 4, ch. 2014-92; s. 4, ch. 2017-134.
464.0195 Florida Center for Nursing; goals.—
(1) There is established the Florida Center for Nursing to address issues of supply and demand for nursing,
including issues of recruitment, retention, and utilization of nurse workforce resources. The Legislature finds that
the center will repay the state’s investment by providing an ongoing strategy for the allocation of the state’s
resources directed towards nursing.
(2) The primary goals for the center shall be to:
(a) Develop a strategic statewide plan for nursing manpower in this state by:

10 – 36
1. Establishing and maintaining a database on nursing supply and demand in the state, to include current supply
and demand;
2. Analyzing the current supply and demand in the state and making future projections of such, including
assessing the impact of this state’s participation in the Nurse Licensure Compact under s. 464.0095; and
3. Selecting from the plan priorities to be addressed.
(b) Convene various groups representative of nurses, other health care providers, business and industry,
consumers, legislators, and educators to:
1. Review and comment on data analysis prepared for the center;
2. Recommend systemic changes, including strategies for implementation of recommended changes; and
3. Evaluate and report the results of these efforts to the Legislature and others.
(c) Enhance and promote recognition, reward, and renewal activities for nurses in the state by:
1. Promoting nursing excellence programs such as magnet recognition by the American Nurses Credentialing
Center;
2. Proposing and creating additional reward, recognition, and renewal activities for nurses; and
3. Promoting media and positive image-building efforts for nursing.
(3) The Board of Nursing shall include on its initial and renewal application forms a question asking each nurse
to voluntarily contribute to funding the Florida Center for Nursing in addition to paying the fees imposed at the time
of licensure and licensure renewal. Revenues collected from nurses over and above the required fees shall be
transferred from the Medical Quality Assurance Trust Fund to the Grants and Donations Trust Fund within the
Department of Health and shall be used solely to support and maintain the goals and functions of the center. Before
giving a nurse the opportunity to contribute to funding the center at the time of licensure renewal, the Board of
Nursing shall provide the nurse with a summary of the center’s work, a link to the center’s Internet website, and the
following statement: “The Florida Center for Nursing’s operating revenues are derived in part from your donation.
In order for the Florida Center for Nursing to continue its work on behalf of nurses, please donate.”
(4) The center may request from the board, and the board must provide to the center upon its request, any
information held by the board regarding nurses licensed in this state or holding a multistate license pursuant to s.
464.0095 or information reported to the board by employers of such nurses, other than personal identifying
information.
History.—s. 97, ch. 2001-277; s. 1, ch. 2002-229; s. 6, ch. 2004-245; s. 5, ch. 2008-19; s. 1, ch. 2009-145; s. 11,
ch. 2016-139.
464.0196 Florida Center for Nursing; board of directors.—
(1) The Florida Center for Nursing shall be governed by a policy-setting board of directors. The board shall
consist of 16 members, with a simple majority of the board being nurses representative of various practice areas.
Other members shall include representatives of other health care professions, business and industry, health care
providers, and consumers. The members of the board shall be appointed by the Governor as follows:
(a) Four members recommended by the President of the Senate, at least one of whom shall be a registered nurse
recommended by the Florida Organization of Nurse Executives and at least one other representative of the hospital
industry recommended by the Florida Hospital Association;

10 – 37
(b) Four members recommended by the Speaker of the House of Representatives, at least one of whom shall be
a registered nurse recommended by the Florida Nurses Association and at least one other representative of the long-
term care industry;
(c) Four members recommended by the Governor, two of whom shall be registered nurses;
(d) One nurse educator recommended by the Board of Governors who is a dean of a College of Nursing at a
state university; and
(e) Three nurse educators recommended by the State Board of Education, one of whom must be a director of a
nursing program at a Florida College System institution.
(2) The initial terms of the members shall be as follows:
(a) Of the members appointed pursuant to paragraph (1)(a), two shall be appointed for terms expiring June 30,
2005, one for a term expiring June 30, 2004, and one for a term expiring June 30, 2003.
(b) Of the members appointed pursuant to paragraph (1)(b), one shall be appointed for a term expiring June 30,
2005, two for terms expiring June 30, 2004, and one for a term expiring June 20, 2003.
(c) Of the members appointed pursuant to paragraph (1)(c), one shall be appointed for a term expiring June 30,
2005, one for a term expiring June 30, 2004, and two for terms expiring June 30, 2003.
(d) Of the members appointed pursuant to paragraph (1)(d), the terms of two members recommended by the
State Board of Education shall expire June 30, 2005; the term of the member who is a dean of a College of Nursing
at a state university shall expire June 30, 2004; and the term of the member who is a director of a state community
college nursing program shall expire June 30, 2003.
After the initial appointments expire, the terms of all the members shall be for 3 years, with no member serving more
than two consecutive terms.
(3) The board shall have the following powers and duties:
(a) To employ an executive director.
(b) To determine operational policy.
(c) To elect a chair and officers, to serve 2-year terms. The chair and officers may not succeed themselves.
(d) To establish committees of the board as needed.
(e) To appoint a multidisciplinary advisory council for input and advice on policy matters.
(f) To implement the major functions of the center as established in the goals set out in s. 464.0195.
(g) To seek and accept nonstate funds for sustaining the center and carrying out center policy.
(4) The members of the board are entitled to receive per diem and allowances prescribed by law for state boards
and commissions.
History.—s. 98, ch. 2001-277; s. 55, ch. 2007-217; s. 119, ch. 2014-17.
464.0205 Retired volunteer nurse certificate.—
(1) Any retired practical or registered nurse desiring to serve indigent, underserved, or critical need populations
in this state may apply to the department for a retired volunteer nurse certificate by providing:
(a) A complete application.
(b) Verification that the applicant had been licensed to practice nursing in any jurisdiction in the United States
for at least 10 years, had retired or plans to retire, intends to practice nursing only pursuant to the limitations
provided by the retired volunteer nurse certificate, and has not committed any act that would constitute a violation
under s. 464.018(1).

10 – 38
(c) Proof that the applicant meets the requirements for licensure under s. 464.008 or s. 464.009.
(2) All related administrative costs shall be borne by the applicant.
(3) The board may deny a retired volunteer nurse certificate to any applicant who has committed, or who is
under investigation or prosecution for, any act that would constitute a ground for disciplinary action under s.
464.018.
(4) A retired volunteer nurse receiving certification from the board shall:
(a) Work under the direct supervision of the director of a county health department, a physician working under
a limited license issued pursuant to s. 458.317 or s. 459.0075, a physician licensed under chapter 458 or chapter 459,
an advanced practice registered nurse licensed under s. 464.012, or a registered nurse licensed under s. 464.008 or s.
464.009.
(b) Comply with the minimum standards of practice for nurses and be subject to disciplinary action for
violations of s. 464.018, except that the scope of practice for certified volunteers shall be limited to primary and
preventive health care, or as further defined by board rule.
(c) Work only in a setting for which there are provisions for professional liability coverage for acts or
omissions of the retired volunteer nurse.
(d) Provide services under the certificate only in settings whose sponsors have been approved by the board.
(5) A retired volunteer nurse receiving certification from the board shall not:
(a) Administer controlled substances.
(b) Supervise other nurses.
(c) Receive monetary compensation.
(6) A retired volunteer nurse certified under this section may practice only in board-approved settings in public
agencies or institutions or in nonprofit agencies or institutions meeting the requirements of s. 501(c)(3) of the
Internal Revenue Code, which agencies or institutions are located in areas of critical nursing need as determined by
the board. Determination of underserved areas shall be made by the board after consultation with the Department of
Health, the Department of Children and Families, the Agency for Health Care Administration, and the Department
of Elderly Affairs; however, such determination shall include, but not be limited to, health manpower shortage areas
designated by the United States Department of Health and Human Services. The sponsoring agencies desiring to use
certified retired volunteer nurses shall submit to the board verification of their status under s. 501(c)(3) of the
Internal Revenue Code, the sites at which such volunteer nurses would work, the duties and scope of practice
intended for such volunteer nurses, and the training or skills validation for such volunteer nurses.
(7) The retired volunteer nurse certificate shall be valid for 2 years, and a certificateholder may reapply for a
certificate so long as the certificateholder continues to meet the eligibility requirements of this section. Any
legislatively mandated continuing education on specific topics must be completed by the certificateholder prior to
renewal; otherwise, the provisions of s. 464.013 do not apply.
History.—s. 85, ch. 97-264; s. 101, ch. 2001-277; s. 269, ch. 2014-19; ss. 27, 28, ch. 2016-224; s. 62, ch. 2018-
106.
464.022 Exceptions.—No provision of this part shall be construed to prohibit:
(1) The care of the sick by friends or members of the family without compensation, the incidental care of the
sick by domestic servants, or the incidental care of noninstitutionalized persons by a surrogate family.
(2) Assistance by anyone in the case of an emergency.

10 – 39
(3) The practice of nursing by students enrolled in approved schools of nursing.
(4) The practice of nursing by graduates of prelicensure nursing education programs listed in s. 464.008(1)(c),
pending the result of the first licensing examination for which they are eligible following graduation, provided they
practice under direct supervision of a registered professional nurse. The board shall by rule define what constitutes
direct supervision.
(5) The rendering of services by nursing assistants acting under the direct supervision of a registered
professional nurse.
(6) Any nurse practicing in accordance with the practices and principles of the body known as the Church of
Christ Scientist; nor shall any rule of the board apply to any sanitarium, nursing home, or rest home operated in
accordance with the practices and principles of the body known as the Church of Christ Scientist.
(7) The practice of any legally qualified nurse or licensed attendant of another state who is employed by the
United States Government, or any bureau, division, or agency thereof, while in the discharge of official duties.
(8) Any nurse currently licensed in another state or territory of the United States from performing nursing
services in this state for a period of 60 days after furnishing to the employer satisfactory evidence of current
licensure in another state or territory and having submitted proper application and fees to the board for licensure
prior to employment. If the nurse licensed in another state or territory is relocating to this state pursuant to his or her
military-connected spouse’s official military orders, this period shall be 120 days after furnishing to the employer
satisfactory evidence of current licensure in another state or territory and having submitted proper application and
fees to the board for licensure prior to employment. The board may extend this time for administrative purposes
when necessary.
(9) The rendering of nursing services on a fee-for-service basis, or the reimbursement for nursing services
directly to a nurse rendering such services by any government program, commercial insurance company, hospital or
medical services plan, or any other third-party payor.
(10) The establishment of an independent practice by one or more nurses for the purpose of rendering to
patients nursing services within the scope of the nursing license.
(11) The furnishing of hemodialysis treatments in a patient’s home, using an assistant chosen by the patient,
provided that the assistant is properly trained, as defined by the board by rule, and has immediate telephonic access
to a registered nurse who is licensed pursuant to this part and who has dialysis training and experience.
(12) The practice of nursing by any legally qualified nurse of another state whose employment requires the
nurse to accompany and care for a patient temporarily residing in this state for not more than 30 consecutive days,
provided the patient is not in an inpatient setting, the board is notified prior to arrival of the patient and nurse, the
nurse has the standing physician orders and current medical status of the patient available, and prearrangements with
the appropriate licensed health care providers in this state have been made in case the patient needs placement in an
inpatient setting.
(13) The practice of nursing by individuals enrolled in board-approved remedial courses.
History.—ss. 1, 6, ch. 79-225; ss. 2, 3, ch. 81-318; ss. 15, 17, 18, ch. 86-284; s. 1, ch. 88-270; s. 58, ch. 91-137;
s. 5, ch. 91-156; s. 4, ch. 91-429; s. 86, ch. 97-264; s. 117, ch. 99-397; s. 127, ch. 2000-318; s. 8, ch. 2002-230; s.
10, ch. 2004-230; s. 6, ch. 2010-37.

10 – 40
464.027 Registered nurse first assistant.—
(1) LEGISLATIVE INTENT.—The purposes of this section are to:
(a) Encourage the use of registered nurse first assistants who meet the qualifications of this section as
“assistants at surgery” by physicians and hospitals to provide quality, cost-effective surgical intervention to health
care recipients in the state.
(b) Provide for reimbursement for the registered nurse first assistant from managed health care agencies, state
agencies, workers’ compensation carriers, and private insurance companies.
(2) DEFINITIONS.—As used in this section, the term:
(a) “Perioperative nursing” means a practice of nursing in which the nurse provides preoperative,
intraoperative, and postoperative nursing care to surgical patients.
(b) “Recognized program” means a program that:
1. Addresses all content of the Association of Operating Room Nurses, Inc. Core Curriculum for the Registered
Nurse First Assistant, and
2. Includes 1 academic year, defined as 45 hours of didactic instruction and 120 hours of clinical internship or
its equivalent of 2 college semesters.
(c) “Registered nurse first assistant” means a person who meets the qualifications listed in this section.
(3) QUALIFICATIONS.—A registered nurse first assistant is any person who:
(a) Is licensed as a registered nurse under this part;
(b) Is certified in perioperative nursing; and
(c) Holds a certificate from, and has successfully completed, a recognized program.
(4) INSTITUTIONAL POWERS.—Each health care institution must establish specific procedures for the
appointment and reappointment of registered nurse first assistant staff members and for granting, renewing, and
revising their clinical privileges.
History.—s. 4, ch. 94-96; s. 129, ch. 2000-318.

10 – 41
PART II
CERTIFIED NURSING ASSISTANTS
464.201 Definitions.
464.202 Duties and powers of the board.
464.203 Certified nursing assistants; certification requirement.
464.204 Denial, suspension, or revocation of certification; disciplinary actions.
464.205 Availability of disciplinary records and proceedings.
464.206 Exemption from liability.
464.207 Penalties.
464.208 Background screening information; rulemaking authority.
464.201 Definitions.—As used in this part, the term:
(1) “Approved training program” means:
(a) A course of training conducted by a public sector or private sector educational center licensed by the
Department of Education to implement the basic curriculum for nursing assistants which is approved by the
Department of Education. Beginning October 1, 2000, the board shall assume responsibility for approval of training
programs under this paragraph.
(b) A training program operated under s. 400.141.
(2) “Board” means the Board of Nursing.
(3) “Certified nursing assistant” means a person who meets the qualifications specified in this part and who is
certified by the board as a certified nursing assistant.
(4) “Department” means the Department of Health.
(5) “Practice of a certified nursing assistant” means providing care and assisting persons with tasks relating to
the activities of daily living. Such tasks are those associated with personal care, maintaining mobility, nutrition and
hydration, toileting and elimination, assistive devices, safety and cleanliness, data gathering, reporting abnormal
signs and symptoms, postmortem care, patient socialization and reality orientation, end-of-life care,
cardiopulmonary resuscitation and emergency care, residents’ or patients’ rights, documentation of nursing-assistant
services, and other tasks that a certified nurse assistant may perform after training beyond that required for initial
certification and upon validation of competence in that skill by a registered nurse. This subsection does not restrict
the ability of any person who is otherwise trained and educated from performing such tasks.
(6) “Registry” means the listing of certified nursing assistants maintained by the board.
History.—s. 204, ch. 99-397; s. 79, ch. 2000-318; s. 4, ch. 2005-62.
Note.—Former s. 468.821.
464.202 Duties and powers of the board.—The board shall maintain, or contract with or approve another
entity to maintain, a state registry of certified nursing assistants. The registry must consist of the name of each
certified nursing assistant in this state; other identifying information defined by board rule; certification status; the
effective date of certification; other information required by state or federal law; information regarding any crime or
any abuse, neglect, or exploitation as provided under chapter 435; and any disciplinary action taken against the
certified nursing assistant. The registry shall be accessible to the public, the certificateholder, employers, and other
state agencies. The board shall adopt by rule testing procedures for use in certifying nursing assistants and shall
adopt rules regulating the practice of certified nursing assistants and specifying the scope of practice authorized and

10 – 42
the level of supervision required for the practice of certified nursing assistants. The board may contract with or
approve another entity or organization to provide the examination services, including the development and
administration of examinations. The board shall require that the contract provider offer certified nursing assistant
applications via the Internet, and may require the contract provider to accept certified nursing assistant applications
for processing via the Internet. The board shall require the contract provider to provide the preliminary results of the
certified nursing examination on the date the test is administered. The provider shall pay all reasonable costs and
expenses incurred by the board in evaluating the provider’s application and performance during the delivery of
services, including examination services and procedures for maintaining the certified nursing assistant registry.
History.—s. 204, ch. 99-397; s. 79, ch. 2000-318; s. 5, ch. 2005-62.
Note.—Former s. 468.822.
464.203 Certified nursing assistants; certification requirement.—
(1) The board shall issue a certificate to practice as a certified nursing assistant to any person who demonstrates
a minimum competency to read and write and successfully passes the required background screening pursuant to s.
400.215. If the person has successfully passed the required background screening pursuant to s. 400.215 or s.
408.809 within 90 days before applying for a certificate to practice and the person’s background screening results
are not retained in the clearinghouse created under s. 435.12, the board shall waive the requirement that the applicant
successfully pass an additional background screening pursuant to s. 400.215. The person must also meet one of the
following requirements:
(a) Has successfully completed an approved training program and achieved a minimum score, established by
rule of the board, on the nursing assistant competency examination, which consists of a written portion and skills-
demonstration portion approved by the board and administered at a site and by personnel approved by the
department.
(b) Has achieved a minimum score, established by rule of the board, on the nursing assistant competency
examination, which consists of a written portion and skills-demonstration portion, approved by the board and
administered at a site and by personnel approved by the department and:
1. Has a high school diploma, or its equivalent; or
2. Is at least 18 years of age.
(c) Is currently certified in another state; is listed on that state’s certified nursing assistant registry; and has not
been found to have committed abuse, neglect, or exploitation in that state.
(d) Has completed the curriculum developed under the Enterprise Florida Jobs and Education Partnership Grant
and achieved a minimum score, established by rule of the board, on the nursing assistant competency examination,
which consists of a written portion and skills-demonstration portion, approved by the board and administered at a
site and by personnel approved by the department.
(2) If an applicant fails to pass the nursing assistant competency examination in three attempts, the applicant is
not eligible for reexamination unless the applicant completes an approved training program.
(3) An oral examination shall be administered as a substitute for the written portion of the examination upon
request. The oral examination shall be administered at a site and by personnel approved by the department.
(4) The board shall adopt rules to provide for the initial certification of certified nursing assistants.
(5) Certification as a nursing assistant, in accordance with this part, may be renewed until such time as the
nursing assistant allows a period of 24 consecutive months to pass during which period the nursing assistant fails to

10 – 43
perform any nursing-related services for monetary compensation. When a nursing assistant fails to perform any
nursing-related services for monetary compensation for a period of 24 consecutive months, the nursing assistant
must complete a new training and competency evaluation program or a new competency evaluation program.
(6) A certified nursing assistant shall maintain a current address with the board in accordance with s. 456.035.
(7) A certified nursing assistant shall complete 24 hours of inservice training during each biennium. The
certified nursing assistant shall maintain documentation demonstrating compliance with this subsection.
(8) The department shall renew a certificate upon receipt of the renewal application and imposition of a fee of
not less than $20 and not more than $50 biennially. The department shall adopt rules establishing a procedure for the
biennial renewal of certificates. Any certificate that is not renewed by July 1, 2006, is void.
History.—s. 204, ch. 99-397; s. 164, ch. 2000-160; s. 79, ch. 2000-318; s. 50, ch. 2001-45; s. 77, ch. 2002-1; s. 6,
ch. 2005-62; s. 43, ch. 2010-114; s. 28, ch. 2011-213; s. 14, ch. 2012-73; s. 100, ch. 2012-184; s. 21, ch. 2016-230.
Note.—Former s. 468.823.
464.204 Denial, suspension, or revocation of certification; disciplinary actions.—
(1) The following acts constitute grounds for which the board may impose disciplinary sanctions as specified in
subsection (2):
(a) Obtaining or attempting to obtain certification or an exemption, or possessing or attempting to possess
certification or a letter of exemption, by bribery, misrepresentation, deceit, or through an error of the board.
(b) Intentionally violating any provision of this chapter, chapter 456, or the rules adopted by the board.
(2) When the board finds any person guilty of any of the grounds set forth in subsection (1), it may enter an
order imposing one or more of the following penalties:
(a) Denial, suspension, or revocation of certification.
(b) Imposition of an administrative fine not to exceed $150 for each count or separate offense.
(c) Imposition of probation or restriction of certification, including conditions such as corrective actions as
retraining or compliance with the department’s impaired practitioner program operated by a consultant as described
in s. 456.076.
(3) The board may, upon the request of a certificateholder, exempt the certificateholder from disqualification of
employment in accordance with chapter 435 and issue a letter of exemption. The board must notify an applicant
seeking an exemption from disqualification from certification or employment of its decision to approve or deny the
request within 30 days after the date the board receives all required documentation.
History.—s. 204, ch. 99-397; s. 165, ch. 2000-160; s. 79, ch. 2000-318; s. 15, ch. 2017-41.
Note.—Former s. 468.824.
464.205 Availability of disciplinary records and proceedings.—Pursuant to s. 456.073, any complaint or
record maintained by the department pursuant to the discipline of a certified nursing assistant and any proceeding
held by the board to discipline a certified nursing assistant shall remain open and available to the public.
History.—s. 204, ch. 99-397; s. 166, ch. 2000-160; s. 79, ch. 2000-318.
Note.—Former s. 468.825.
464.206 Exemption from liability.—If an employer terminates or denies employment to a certified nursing
assistant whose certification is inactive as shown on the certified nursing assistant registry or whose name appears
on a criminal screening report of the Department of Law Enforcement, the employer is not civilly liable for such
termination and a cause of action may not be brought against the employer for damages, regardless of whether the

10 – 44
employee has filed for an exemption from the board under s. 464.204(3). There may not be any monetary liability on
the part of, and a cause of action for damages may not arise against, any licensed facility, its governing board or
members thereof, medical staff, disciplinary board, agents, investigators, witnesses, employees, or any other person
for any action taken in good faith without intentional fraud in carrying out this section.
History.—s. 204, ch. 99-397; s. 79, ch. 2000-318; s. 105, ch. 2000-349.
Note.—Former s. 468.826.
464.207 Penalties.—It is a misdemeanor of the first degree, punishable as provided under s. 775.082 or s.
775.083, for any person, knowingly or intentionally, to fail to disclose, by false statement, misrepresentation,
impersonation, or other fraudulent means, in any application for voluntary or paid employment or certification
regulated under this part, a material fact used in making a determination as to such person’s qualifications to be an
employee or certificateholder.
History.—s. 204, ch. 99-397; s. 79, ch. 2000-318.
Note.—Former s. 468.827.
464.208 Background screening information; rulemaking authority.—
(1) The Agency for Health Care Administration shall allow the board to electronically access its background
screening database and records.
(2) An employer, or an agent thereof, may not use criminal records or juvenile records relating to vulnerable
adults for any purpose other than determining if the person meets the requirements of this part. Such records and
information obtained by the board shall remain confidential and exempt from s. 119.07(1).
(3) If the requirements of the Omnibus Budget Reconciliation Act of 1987, as amended, for the certification of
nursing assistants are in conflict with this part, the federal requirements shall prevail for those facilities certified to
provide care under Title XVIII (Medicare) or Title XIX (Medicaid) of the Social Security Act.
History.—s. 204, ch. 99-397; s. 129, ch. 2000-153; s. 79, ch. 2000-318; s. 106, ch. 2000-349; s. 101, ch. 2012-
184.
Note.—Former s. 468.828.

11. Chapter 415, F.S.


11 – 1
CHAPTER 415
ADULT PROTECTIVE SERVICES 415.101 Adult Protective Services Act; legislative intent.
415.102 Definitions of terms used in ss. 415.101-415.113.
415.103 Central abuse hotline.
415.1034 Mandatory reporting of abuse, neglect, or exploitation of vulnerable adults; mandatory reports of death.
415.1035 Facility’s duty to inform residents of their right to report abusive, neglectful, or exploitive practices.
415.1036 Immunity.
415.104 Protective investigations of cases of abuse, neglect, or exploitation of vulnerable adults; transmittal of
records to state attorney.
415.1045 Photographs, videotapes, and medical examinations; abrogation of privileged communications;
confidential records and documents.
415.105 Provision of protective services with consent; withdrawal of consent; interference.
415.1051 Protective services interventions when capacity to consent is lacking; nonemergencies; emergencies;
orders; limitations.
415.1052 Interference with investigation or with the provision of protective services.
415.1055 Notification to administrative entities.
415.106 Cooperation by the department and criminal justice and other agencies.
415.107 Confidentiality of reports and records.
415.1071 Release of confidential information.
415.1099 Court and witness fees not allowed.
415.1102 Adult protection teams.
415.1105 Training programs.
415.111 Criminal penalties.
415.1111 Civil actions.
415.1113 Administrative fines for false report of abuse, neglect, or exploitation of a vulnerable adult.
415.1115 Civil actions involving elderly parties; speedy trial.
415.113 Statutory construction; treatment by spiritual means.
415.101 Adult Protective Services Act; legislative intent.—
(1) Sections 415.101-415.113 may be cited as the “Adult Protective Services Act.”
(2) The Legislature recognizes that there are many persons in this state who, because of age or disability, are in
need of protective services. Such services should allow such an individual the same rights as other citizens and, at
the same time, protect the individual from abuse, neglect, and exploitation. It is the intent of the Legislature to
provide for the detection and correction of abuse, neglect, and exploitation through social services and criminal
investigations and to establish a program of protective services for all vulnerable adults in need of them. It is
intended that the mandatory reporting of such cases will cause the protective services of the state to be brought to
bear in an effort to prevent further abuse, neglect, and exploitation of vulnerable adults. In taking this action, the
Legislature intends to place the fewest possible restrictions on personal liberty and the exercise of constitutional
rights, consistent with due process and protection from abuse, neglect, and exploitation. Further, the Legislature
intends to encourage the constructive involvement of families in the care and protection of vulnerable adults.

11 – 2
History.—ss. 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, ch. 73-176; s. 1, ch. 77-174; ss. 3, 5, ch. 79-287; s. 15, ch. 79-298; s.
1, ch. 80-293; s. 1, ch. 83-82; s. 61, ch. 85-81; s. 27, ch. 86-220; s. 93, ch. 95-418; s. 1, ch. 2010-31.
415.102 Definitions of terms used in ss. 415.101-415.113.—As used in ss. 415.101-415.113, the term:
(1) “Abuse” means any willful act or threatened act by a relative, caregiver, or household member which causes
or is likely to cause significant impairment to a vulnerable adult’s physical, mental, or emotional health. Abuse
includes acts and omissions.
(2) “Activities of daily living” means functions and tasks for self-care, including ambulation, bathing, dressing,
eating, grooming, toileting, and other similar tasks.
(3) “Alleged perpetrator” means a person who has been named by a reporter as the person responsible for
abusing, neglecting, or exploiting a vulnerable adult.
(4) “Capacity to consent” means that a vulnerable adult has sufficient understanding to make and communicate
responsible decisions regarding the vulnerable adult’s person or property, including whether or not to accept
protective services offered by the department.
(5) “Caregiver” means a person who has been entrusted with or has assumed the responsibility for frequent and
regular care of or services to a vulnerable adult on a temporary or permanent basis and who has a commitment,
agreement, or understanding with that person or that person’s guardian that a caregiver role exists. “Caregiver”
includes, but is not limited to, relatives, household members, guardians, neighbors, and employees and volunteers of
facilities as defined in subsection (9). For the purpose of departmental investigative jurisdiction, the term
“caregiver” does not include law enforcement officers or employees of municipal or county detention facilities or
the Department of Corrections while acting in an official capacity.
(6) “Deception” means a misrepresentation or concealment of a material fact relating to services rendered,
disposition of property, or the use of property intended to benefit a vulnerable adult.
(7) “Department” means the Department of Children and Families.
(8)(a) “Exploitation” means a person who:
1. Stands in a position of trust and confidence with a vulnerable adult and knowingly, by deception or
intimidation, obtains or uses, or endeavors to obtain or use, a vulnerable adult’s funds, assets, or property with the
intent to temporarily or permanently deprive a vulnerable adult of the use, benefit, or possession of the funds, assets,
or property for the benefit of someone other than the vulnerable adult; or
2. Knows or should know that the vulnerable adult lacks the capacity to consent, and obtains or uses, or
endeavors to obtain or use, the vulnerable adult’s funds, assets, or property with the intent to temporarily or
permanently deprive the vulnerable adult of the use, benefit, or possession of the funds, assets, or property for the
benefit of someone other than the vulnerable adult.
(b) “Exploitation” may include, but is not limited to:
1. Breaches of fiduciary relationships, such as the misuse of a power of attorney or the abuse of guardianship
duties, resulting in the unauthorized appropriation, sale, or transfer of property;
2. Unauthorized taking of personal assets;
3. Misappropriation, misuse, or transfer of moneys belonging to a vulnerable adult from a personal or joint
account; or
4. Intentional or negligent failure to effectively use a vulnerable adult’s income and assets for the necessities
required for that person’s support and maintenance.

11 – 3
(9) “Facility” means any location providing day or residential care or treatment for vulnerable adults. The term
“facility” may include, but is not limited to, any hospital, state institution, nursing home, assisted living facility,
adult family-care home, adult day care center, residential facility licensed under chapter 393, adult day training
center, or mental health treatment center.
(10) “False report” means a report of abuse, neglect, or exploitation of a vulnerable adult to the central abuse
hotline which is not true and is maliciously made for the purpose of:
(a) Harassing, embarrassing, or harming another person;
(b) Personal financial gain for the reporting person;
(c) Acquiring custody of a vulnerable adult; or
(d) Personal benefit for the reporting person in any other private dispute involving a vulnerable adult.
The term “false report” does not include a report of abuse, neglect, or exploitation of a vulnerable adult which is made
in good faith to the central abuse hotline.
(11) “Fiduciary relationship” means a relationship based upon the trust and confidence of the vulnerable adult
in the caregiver, relative, household member, or other person entrusted with the use or management of the property
or assets of the vulnerable adult. The relationship exists where there is a special confidence reposed in one who in
equity and good conscience is bound to act in good faith and with due regard to the interests of the vulnerable adult.
For the purposes of this part, a fiduciary relationship may be formed by an informal agreement between the
vulnerable adult and the other person and does not require a formal declaration or court order for its existence. A
fiduciary relationship includes, but is not limited to, court-appointed or voluntary guardians, trustees, attorneys, or
conservators of a vulnerable adult’s assets or property.
(12) “Guardian” means a person who has been appointed by a court to act on behalf of a person; a preneed
guardian, as provided in chapter 744; or a health care surrogate expressly designated as provided in chapter 765.
(13) “In-home services” means the provision of nursing, personal care, supervision, or other services to
vulnerable adults in their own homes.
(14) “Intimidation” means the communication by word or act to a vulnerable adult that that person will be
deprived of food, nutrition, clothing, shelter, supervision, medicine, medical services, money, or financial support or
will suffer physical violence.
(15) “Lacks capacity to consent” means a mental impairment that causes a vulnerable adult to lack sufficient
understanding or capacity to make or communicate responsible decisions concerning person or property, including
whether or not to accept protective services.
(16) “Neglect” means the failure or omission on the part of the caregiver or vulnerable adult to provide the care,
supervision, and services necessary to maintain the physical and mental health of the vulnerable adult, including, but
not limited to, food, clothing, medicine, shelter, supervision, and medical services, which a prudent person would
consider essential for the well-being of a vulnerable adult. The term “neglect” also means the failure of a caregiver
or vulnerable adult to make a reasonable effort to protect a vulnerable adult from abuse, neglect, or exploitation by
others. “Neglect” is repeated conduct or a single incident of carelessness which produces or could reasonably be
expected to result in serious physical or psychological injury or a substantial risk of death.
(17) “Obtains or uses” means any manner of:
(a) Taking or exercising control over property;
(b) Making any use, disposition, or transfer of property;

11 – 4
(c) Obtaining property by fraud, willful misrepresentation of a future act, or false promise; or
(d)1. Conduct otherwise known as stealing; larceny; purloining; abstracting; embezzlement; misapplication;
misappropriation; conversion; or obtaining money or property by false pretenses, fraud, or deception; or
2. Other conduct similar in nature.
(18) “Office” has the same meaning as in s. 400.0060.
(19) “Position of trust and confidence” with respect to a vulnerable adult means the position of a person who:
(a) Is a parent, spouse, adult child, or other relative by blood or marriage;
(b) Is a joint tenant or tenant in common;
(c) Has a legal or fiduciary relationship, including, but not limited to, a court-appointed or voluntary guardian,
trustee, attorney, or conservator; or
(d) Is a caregiver or any other person who has been entrusted with or has assumed responsibility for the use or
management of the vulnerable adult’s funds, assets, or property.
(20) “Protective investigation” means acceptance of a report from the central abuse hotline alleging abuse,
neglect, or exploitation as defined in this section; investigation of the report; determination as to whether action by
the court is warranted; and referral of the vulnerable adult to another public or private agency when appropriate.
(21) “Protective investigator” means an authorized agent of the department who receives and investigates
reports of abuse, neglect, or exploitation of vulnerable adults.
(22) “Protective services” means services to protect a vulnerable adult from further occurrences of abuse,
neglect, or exploitation. Such services may include, but are not limited to, protective supervision, placement, and in-
home and community-based services.
(23) “Protective supervision” means those services arranged for or implemented by the department to protect
vulnerable adults from further occurrences of abuse, neglect, or exploitation.
(24) “Psychological injury” means an injury to the intellectual functioning or emotional state of a vulnerable
adult as evidenced by an observable or measurable reduction in the vulnerable adult’s ability to function within that
person’s customary range of performance and that person’s behavior.
(25) “Records” means all documents, papers, letters, maps, books, tapes, photographs, films, sound recordings,
videotapes, or other material, regardless of physical form or characteristics, made or received pursuant to a
protective investigation.
(26) “Sexual abuse” means acts of a sexual nature committed in the presence of a vulnerable adult without that
person’s informed consent. “Sexual abuse” includes, but is not limited to, the acts defined in s. 794.011(1)(h),
fondling, exposure of a vulnerable adult’s sexual organs, or the use of a vulnerable adult to solicit for or engage in
prostitution or sexual performance. “Sexual abuse” does not include any act intended for a valid medical purpose or
any act that may reasonably be construed to be normal caregiving action or appropriate display of affection.
(27) “Victim” means any vulnerable adult named in a report of abuse, neglect, or exploitation.
(28) “Vulnerable adult” means a person 18 years of age or older whose ability to perform the normal activities
of daily living or to provide for his or her own care or protection is impaired due to a mental, emotional, sensory,
long-term physical, or developmental disability or dysfunction, or brain damage, or the infirmities of aging.
(29) “Vulnerable adult in need of services” means a vulnerable adult who has been determined by a protective
investigator to be suffering from the ill effects of neglect not caused by a second party perpetrator and is in need of
protective services or other services to prevent further harm.

11 – 5
History.—ss. 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, ch. 73-176; s. 1, ch. 77-174; ss. 3, 5, ch. 79-287; s. 15, ch. 79-298; s.
1, ch. 80-293; s. 1, ch. 83-82; s. 28, ch. 86-220; s. 29, ch. 87-238; s. 26, ch. 89-294; s. 1, ch. 90-50; s. 44, ch. 90-306;
s. 1, ch. 91-57; s. 35, ch. 95-210; s. 94, ch. 95-418; s. 9, ch. 97-98; s. 127, ch. 97-101; s. 41, ch. 97-264; s. 1, ch. 98-
182; s. 68, ch. 2000-153; s. 26, ch. 2000-349; s. 4, ch. 2003-57; s. 1, ch. 2006-131; s. 57, ch. 2006-227; s. 2, ch.
2010-31; s. 234, ch. 2014-19; s. 28, ch. 2015-31.
415.103 Central abuse hotline.—
(1) The department shall establish and maintain a central abuse hotline that receives all reports made pursuant
to s. 415.1034 in writing or through a single statewide toll-free telephone number. Any person may use the statewide
toll-free telephone number to report known or suspected abuse, neglect, or exploitation of a vulnerable adult at any
hour of the day or night, any day of the week. The central abuse hotline must be operated in such a manner as to
enable the department to:
(a) Accept reports for investigation when there is a reasonable cause to suspect that a vulnerable adult has been
or is being abused, neglected, or exploited.
(b) Determine whether the allegations made by the reporter require an immediate, 24-hour, or next-working-
day response priority.
(c) When appropriate, refer calls that do not allege the abuse, neglect, or exploitation of a vulnerable adult to
other organizations that might better resolve the reporter’s concerns.
(d) Immediately identify and locate prior reports of abuse, neglect, or exploitation through the central abuse
hotline.
(e) Track critical steps in the investigative process to ensure compliance with all requirements for all reports.
(f) Maintain data to facilitate the production of aggregate statistical reports for monitoring patterns of abuse,
neglect, or exploitation.
(g) Serve as a resource for the evaluation, management, and planning of preventive and remedial services for
vulnerable adults who have been subject to abuse, neglect, or exploitation.
(2) Upon receiving an oral or written report of known or suspected abuse, neglect, or exploitation of a
vulnerable adult, the central abuse hotline must determine if the report requires an immediate onsite protective
investigation. For reports requiring an immediate onsite protective investigation, the central abuse hotline must
immediately notify the department’s designated protective investigative district staff responsible for protective
investigations to ensure prompt initiation of an onsite investigation. For reports not requiring an immediate onsite
protective investigation, the central abuse hotline must notify the department’s designated protective investigative
district staff responsible for protective investigations in sufficient time to allow for an investigation to be
commenced within 24 hours. At the time of notification of district staff with respect to the report, the central abuse
hotline must also provide any known information on any previous report concerning a subject of the present report
or any pertinent information relative to the present report or any noted earlier reports. If the report is of known or
suspected abuse of a vulnerable adult by someone other than a relative, caregiver, or household member, the report
shall be immediately transferred to the appropriate county sheriff’s office.
(3) The department shall set standards, priorities, and policies to maximize the efficiency and effectiveness of
the central abuse hotline.

11 – 6
History.—ss. 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, ch. 73-176; s. 1, ch. 77-174; ss. 3, 5, ch. 79-287; s. 15, ch. 79-298; s.
1, ch. 80-293; s. 1, ch. 83-82; s. 67, ch. 86-163; s. 29, ch. 86-220; s. 30, ch. 87-238; s. 16, ch. 88-337; s. 27, ch. 89-
294; s. 2, ch. 90-50; s. 45, ch. 90-306; s. 2, ch. 91-57; s. 14, ch. 91-71; s. 36, ch. 95-210; s. 95, ch. 95-418; s. 27, ch.
2000-349; s. 3, ch. 2010-31.
415.1034 Mandatory reporting of abuse, neglect, or exploitation of vulnerable adults; mandatory reports
of death.—
(1) MANDATORY REPORTING.—
(a) Any person, including, but not limited to, any:
1. Physician, osteopathic physician, medical examiner, chiropractic physician, nurse, paramedic, emergency
medical technician, or hospital personnel engaged in the admission, examination, care, or treatment of vulnerable
adults;
2. Health professional or mental health professional other than one listed in subparagraph 1.;
3. Practitioner who relies solely on spiritual means for healing;
4. Nursing home staff; assisted living facility staff; adult day care center staff; adult family-care home staff;
social worker; or other professional adult care, residential, or institutional staff;
5. State, county, or municipal criminal justice employee or law enforcement officer;
6. Employee of the Department of Business and Professional Regulation conducting inspections of public
lodging establishments under s. 509.032;
7. Florida advocacy council or Disability Rights Florida member or a representative of the State Long-Term
Care Ombudsman Program; or
8. Bank, savings and loan, or credit union officer, trustee, or employee,
who knows, or has reasonable cause to suspect, that a vulnerable adult has been or is being abused, neglected, or
exploited shall immediately report such knowledge or suspicion to the central abuse hotline.
(b) To the extent possible, a report made pursuant to paragraph (a) must contain, but need not be limited to, the
following information:
1. Name, age, race, sex, physical description, and location of each victim alleged to have been abused,
neglected, or exploited.
2. Names, addresses, and telephone numbers of the victim’s family members.
3. Name, address, and telephone number of each alleged perpetrator.
4. Name, address, and telephone number of the caregiver of the victim, if different from the alleged perpetrator.
5. Name, address, and telephone number of the person reporting the alleged abuse, neglect, or exploitation.
6. Description of the physical or psychological injuries sustained.
7. Actions taken by the reporter, if any, such as notification of the criminal justice agency.
8. Any other information available to the reporting person which may establish the cause of abuse, neglect, or
exploitation that occurred or is occurring.
(2) MANDATORY REPORTS OF DEATH.—Any person who is required to investigate reports of abuse,
neglect, or exploitation and who has reasonable cause to suspect that a vulnerable adult died as a result of abuse,
neglect, or exploitation shall immediately report the suspicion to the appropriate medical examiner, to the
appropriate criminal justice agency, and to the department, notwithstanding the existence of a death certificate
signed by a practicing physician. The medical examiner shall accept the report for investigation pursuant to s.

11 – 7
406.11 and shall report the findings of the investigation, in writing, to the appropriate local criminal justice agency,
the appropriate state attorney, and the department. Autopsy reports maintained by the medical examiner are not
subject to the confidentiality requirements provided for in s. 415.107.
History.—s. 96, ch. 95-418; s. 10, ch. 97-98; s. 42, ch. 97-264; s. 256, ch. 98-166; s. 21, ch. 2000-263; s. 2, ch.
2000-318; s. 28, ch. 2000-349; s. 29, ch. 2015-31.
415.1035 Facility’s duty to inform residents of their right to report abusive, neglectful, or exploitive
practices.—The department shall work cooperatively with the Agency for Health Care Administration, the Agency
for Persons with Disabilities, and the Department of Elderly Affairs to ensure that every facility that serves
vulnerable adults informs residents of their right to report abusive, neglectful, or exploitive practices. Each facility
must establish appropriate policies and procedures to facilitate such reporting.
History.—s. 97, ch. 95-418; s. 29, ch. 2000-349; s. 58, ch. 2006-227.
415.1036 Immunity.—
(1) Any person who participates in making a report under s. 415.1034 or participates in a judicial proceeding
resulting therefrom is presumed to be acting in good faith and, unless lack of good faith is shown by clear and
convincing evidence, is immune from any liability, civil or criminal, that otherwise might be incurred or imposed.
This section does not grant immunity, civil or criminal, to any person who is suspected of having abused, neglected,
or exploited, or committed any illegal act upon or against, a vulnerable adult. Further, a resident or employee of a
facility that serves vulnerable adults may not be subjected to reprisal or discharge because of the resident’s or
employee’s actions in reporting abuse, neglect, or exploitation pursuant to s. 415.1034.
(2) Any person who makes a report under s. 415.1034 has a civil cause of action for appropriate compensatory
and punitive damages against any person who causes detrimental changes in the employment status of the reporting
party by reason of the reporting party’s making the report. Any detrimental change made in the residency or
employment status of such a person, such as, but not limited to, discharge, termination, demotion, transfer, or
reduction in pay or benefits or work privileges, or negative evaluations, within 120 days after the report is made
establishes a rebuttable presumption that the detrimental action was retaliatory.
History.—s. 98, ch. 95-418; s. 30, ch. 2000-349.
415.104 Protective investigations of cases of abuse, neglect, or exploitation of vulnerable adults;
transmittal of records to state attorney.—
(1) The department shall, upon receipt of a report alleging abuse, neglect, or exploitation of a vulnerable adult,
begin within 24 hours a protective investigation of the facts alleged therein. If a caregiver refuses to allow the
department to begin a protective investigation or interferes with the conduct of such an investigation, the appropriate
law enforcement agency shall be contacted for assistance. If, during the course of the investigation, the department
has reason to believe that the abuse, neglect, or exploitation is perpetrated by a second party, the appropriate law
enforcement agency and state attorney shall be orally notified. The department and the law enforcement agency shall
cooperate to allow the criminal investigation to proceed concurrently with, and not be hindered by, the protective
investigation. The department shall make a preliminary written report to the law enforcement agencies within 5
working days after the oral report. The department shall, within 24 hours after receipt of the report, notify the
appropriate Florida local advocacy council, or the State Long-Term Care Ombudsman Program, when appropriate,
that an alleged abuse, neglect, or exploitation perpetrated by a second party has occurred. Notice to the Florida local
advocacy council or the State Long-Term Care Ombudsman Program may be accomplished orally or in writing and

11 – 8
shall include the name and location of the vulnerable adult alleged to have been abused, neglected, or exploited and
the nature of the report.
(2) Upon commencing an investigation, the protective investigator shall inform all of the vulnerable adults and
alleged perpetrators named in the report of the following:
(a) The names of the investigators and identifying credentials from the department.
(b) The purpose of the investigation.
(c) That the victim, the victim’s guardian, the victim’s caregiver, and the alleged perpetrator, and legal counsel
for any of those persons, have a right to a copy of the report at the conclusion of the investigation.
(d) The name and telephone number of the protective investigator’s supervisor available to answer questions.
(e) That each person has the right to obtain his or her own attorney.
Any person being interviewed by a protective investigator may be represented by an attorney, at the person’s own
expense, or may choose to have another person present. The other person present may not be an alleged perpetrator in
any report currently under investigation. Before participating in such interview, the other person present shall execute
an agreement to comply with the confidentiality requirements of ss. 415.101-415.113. The absence of an attorney or
other person does not prevent the department from proceeding with other aspects of the investigation, including
interviews with other persons. In an investigative interview with a vulnerable adult, the protective investigator may
conduct the interview with no other person present.
(3) For each report it receives, the department shall perform an onsite investigation to:
(a) Determine that the person is a vulnerable adult as defined in s. 415.102.
(b) Determine whether the person is a vulnerable adult in need of services, as defined in s. 415.102.
(c) Determine the composition of the family or household, including the name, address, date of birth, social
security number, sex, and race of each person in the household.
(d) Determine whether there is an indication that a vulnerable adult is abused, neglected, or exploited.
(e) Determine the nature and extent of present or prior injuries, abuse, or neglect, and any evidence thereof.
(f) Determine, if possible, the person or persons apparently responsible for the abuse, neglect, or exploitation,
including name, address, date of birth, social security number, sex, and race.
(g) Determine the immediate and long-term risk to each vulnerable adult through utilization of standardized risk
assessment instruments.
(h) Determine the protective, treatment, and ameliorative services necessary to safeguard and ensure the
vulnerable adult’s well-being and cause the delivery of those services.
(4) No later than 60 days after receiving the initial report, the designated protective investigative staff of the
department shall complete the investigation and notify the guardian of the vulnerable adult, the vulnerable adult, and
the caregiver of any recommendations of services to be provided to ameliorate the causes or effects of abuse,
neglect, or exploitation.
(5) Whenever the law enforcement agency and the department have conducted independent investigations, the
law enforcement agency shall, within 5 working days after concluding its investigation, report its findings to the
state attorney and to the department.
(6) Upon receipt of a report which alleges that an employee or agent of the department acting in an official
capacity has committed an act of abuse, neglect, or exploitation, the department shall commence, or cause to be

11 – 9
commenced, a protective investigation and shall notify the state attorney in whose circuit the alleged abuse, neglect,
or exploitation occurred.
(7) With respect to any case of reported abuse, neglect, or exploitation of a vulnerable adult, the department,
when appropriate, shall transmit all relevant reports to the state attorney of the circuit where the incident occurred.
(8) Within 15 days after completion of the state attorney’s investigation of a case reported to him or her
pursuant to this section, the state attorney shall report his or her findings to the department and shall include a
determination of whether or not prosecution is justified and appropriate in view of the circumstances of the specific
case.
(9) The department shall not use a warning, reprimand, or disciplinary action against an employee, found in that
employee’s personnel records, as the sole basis for a finding of abuse, neglect, or exploitation.
History.—ss. 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, ch. 73-176; s. 1, ch. 77-174; ss. 3, 5, ch. 79-287; s. 15, ch. 79-298; s.
1, ch. 80-293; s. 1, ch. 83-82; s. 5, ch. 84-226; s. 2, ch. 85-143; s. 30, ch. 86-220; s. 31, ch. 87-238; s. 17, ch. 88-337;
s. 28, ch. 89-294; s. 3, ch. 90-50; s. 46, ch. 90-306; s. 3, ch. 91-57; s. 64, ch. 97-103; s. 200, ch. 99-8; s. 22, ch.
2000-263; s. 31, ch. 2000-349; s. 30, ch. 2015-31.
415.1045 Photographs, videotapes, and medical examinations; abrogation of privileged communications;
confidential records and documents.—
(1) PHOTOGRAPHS AND VIDEOTAPES.—
(a) The protective investigator, while investigating a report of abuse, neglect, or exploitation, may take or cause
to be taken photographs and videotapes of the vulnerable adult, and of his or her environment, which are relevant to
the investigation. All photographs and videotapes taken during the course of the protective investigation are
confidential and exempt from public disclosure as provided in s. 415.107.
(b) Any photographs or videotapes made pursuant to this subsection, or copies thereof, must be sent to the
department as soon as possible.
(2) MEDICAL EXAMINATIONS.—
(a) With the consent of the vulnerable adult who has the capacity to consent or the vulnerable adult’s guardian,
or pursuant to s. 415.1051, the department may cause the vulnerable adult to be referred to a licensed physician or
any emergency department in a hospital or health care facility for medical examination, diagnosis, or treatment if
any of the following circumstances exist:
1. The areas of trauma visible on the vulnerable adult indicate a need for medical examination;
2. The vulnerable adult verbally complains or otherwise exhibits signs or symptoms indicating a need for
medical attention as a consequence of suspected abuse, neglect, or exploitation; or
3. The vulnerable adult is alleged to have been sexually abused.
(b) Upon admission to a hospital or health care facility, with the consent of the vulnerable adult who has
capacity to consent or that person’s guardian, or pursuant to s. 415.1051, the medical staff of the facility may
examine, diagnose, or treat the vulnerable adult. If a person who has legal authority to give consent for the provision
of medical treatment to a vulnerable adult has not given or has refused to give such consent, examination and
treatment must be limited to reasonable examination of the patient to determine the medical condition of the patient
and treatment reasonably necessary to alleviate the medical condition or to stabilize the patient pending a
determination by the court of the department’s petition authorizing protective services. Any person may seek an

11 – 10
expedited judicial intervention under rule 5.900 of the Florida Probate Rules concerning medical treatment
procedures.
(c) Medical examination, diagnosis, and treatment provided under this subsection must be paid for by third-
party reimbursement, if available, or by the vulnerable adult, if he or she is able to pay; or, if he or she is unable to
pay, the department shall pay the costs within available emergency services funds.
(d) Reports of examination, diagnosis, and treatment made under this subsection, or copies thereof, must be
sent to the department as soon as possible.
(e) This subsection does not obligate the department to pay for any treatment other than that necessary to
alleviate the immediate presenting problems.
(3) ABROGATION OF PRIVILEGED COMMUNICATIONS.—The privileged quality of communication
between husband and wife and between any professional and the professional’s patient or client, and any other
privileged communication except that between attorney and client or clergy and person, as such communication
relates to both the competency of the witness and to the exclusion of confidential communications, does not apply to
any situation involving known or suspected abuse, neglect, or exploitation of a vulnerable adult and does not
constitute grounds for failure to report as required by s. 415.1034, for failure to cooperate with law enforcement or
the department in its activities under ss. 415.101-415.113, or for failure to give evidence in any judicial or
administrative proceeding relating to abuse, neglect, or exploitation of a vulnerable adult.
(4) MEDICAL, SOCIAL, OR FINANCIAL RECORDS OR DOCUMENTS.—
(a) The protective investigator, while investigating a report of abuse, neglect, or exploitation, must have access
to, inspect, and copy all medical, social, or financial records or documents in the possession of any person,
caregiver, guardian, or facility which are relevant to the allegations under investigation, unless specifically
prohibited by the vulnerable adult who has capacity to consent.
(b) The confidentiality of any medical, social, or financial record or document that is confidential under state
law does not constitute grounds for failure to:
1. Report as required by s. 415.1034;
2. Cooperate with the department in its activities under ss. 415.101-415.113;
3. Give access to such records or documents; or
4. Give evidence in any judicial or administrative proceeding relating to abuse, neglect, or exploitation of a
vulnerable adult.
(5) ACCESS TO RECORDS AND DOCUMENTS.—If any person refuses to allow a law enforcement officer
or the protective investigator to have access to, inspect, or copy any medical, social, or financial record or document
in the possession of any person, caregiver, guardian, or facility which is relevant to the allegations under
investigation, the department may petition the court for an order requiring the person to allow access to the record or
document. The petition must allege specific facts sufficient to show that the record or document is relevant to the
allegations under investigation and that the person refuses to allow access to such record or document. If the court
finds by a preponderance of the evidence that the record or document is relevant to the allegations under
investigation, the court may order the person to allow access to and permit the inspection or copying of the medical,
social, or financial record or document.
(6) WORKING AGREEMENTS.— The department shall enter into working agreements with the
jurisdictionally responsible county sheriff’s office or local police department that will be the lead agency for

11 – 11
conducting any criminal investigation arising from an allegation of abuse, neglect, or exploitation of a vulnerable
adult. The working agreement must specify how the requirements of this chapter will be met. For the purposes of
such agreement, the jurisdictionally responsible law enforcement entity may share Florida criminal history and local
criminal history information that is not otherwise exempt from s. 119.07(1) with the district personnel. A law
enforcement entity entering into such agreement must comply with s. 943.0525. Criminal justice information
provided by the law enforcement entity may be used only for the purposes specified in the agreement and shall be
provided at no charge. Notwithstanding any other provision of law, the Department of Law Enforcement shall
provide to the department electronic access to Florida criminal justice information that is lawfully available and not
exempt from s. 119.07(1), only for the purpose of protective investigations and emergency placement. As a
condition of access to the information, the department shall execute an appropriate user agreement addressing the
access, use, dissemination, and destruction of such information and comply with all applicable laws and rules of the
Department of Law Enforcement.
History.—s. 99, ch. 95-418; s. 2, ch. 98-182; s. 32, ch. 2000-349; s. 4, ch. 2002-174; s. 1, ch. 2003-262; s. 136,
ch. 2010-102.
415.105 Provision of protective services with consent; withdrawal of consent; interference.—
(1) PROTECTIVE SERVICES WITH CONSENT.—If the department determines through its investigation that
a vulnerable adult demonstrates a need for protective services or protective supervision, the department shall
immediately provide, or arrange for the provision of, protective services or protective supervision, including in-
home services, provided that the vulnerable adult consents. A vulnerable adult in need of services as defined in s.
415.102 shall be referred to the community care for disabled adults program, or to the community care for the
elderly program administered by the Department of Elderly Affairs.
(2) WITHDRAWAL OF CONSENT.—If the vulnerable adult withdraws consent to the receipt of protective
services or protective supervision, the services may not be provided, except pursuant to s. 415.1051.
(3) INTERFERENCE WITH THE PROVISION OF PROTECTIVE SERVICES.—When any person refuses to
allow the provision of protective services to a vulnerable adult who has the capacity to consent to services, the
department shall petition the court for an order enjoining the person from interfering with the provision of protective
services. The petition must allege specific facts sufficient to show that the vulnerable adult is in need of protective
services and that the person refuses to allow the provision of such services. If the court finds by clear and convincing
evidence that the vulnerable adult is in need of protective services and that the person refuses to allow the provision
of such services, the court may issue an order enjoining the person from interfering with the provision of protective
services to the vulnerable adult.
History.—ss. 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, ch. 73-176; s. 1, ch. 77-174; ss. 3, 5, ch. 79-287; s. 15, ch. 79-298; s.
1, ch. 80-293; s. 1, ch. 83-82; s. 31, ch. 86-220; s. 29, ch. 89-294; s. 21, ch. 95-144; s. 37, ch. 95-210; s. 100, ch. 95-
418; s. 3, ch. 98-182; s. 33, ch. 2000-349.
415.1051 Protective services interventions when capacity to consent is lacking; nonemergencies;
emergencies; orders; limitations.—
(1) NONEMERGENCY PROTECTIVE SERVICES INTERVENTIONS.—If the department has reasonable
cause to believe that a vulnerable adult or a vulnerable adult in need of services is being abused, neglected, or
exploited and is in need of protective services but lacks the capacity to consent to protective services, the department
shall petition the court for an order authorizing the provision of protective services.

11 – 12
(a) Nonemergency protective services petition.—The petition must state the name, age, and address of the
vulnerable adult, allege specific facts sufficient to show that the vulnerable adult is in need of protective services and
lacks the capacity to consent to them, and indicate the services needed.
(b) Notice.—Notice of the filing of the petition and a copy of the petition must be given to the vulnerable adult,
to that person’s spouse, guardian, and legal counsel, and, when known, to the adult children or next of kin of the
vulnerable adult. Such notice must be given at least 5 days before the hearing.
(c) Hearing.—
1. The court shall set the case for hearing within 14 days after the filing of the petition. The vulnerable adult
and any person given notice of the filing of the petition have the right to be present at the hearing. The department
must make reasonable efforts to ensure the presence of the vulnerable adult at the hearing.
2. The vulnerable adult has the right to be represented by legal counsel at the hearing. The court shall appoint
legal counsel to represent a vulnerable adult who is without legal representation.
3. The court shall determine whether:
a. Protective services, including in-home services, are necessary.
b. The vulnerable adult lacks the capacity to consent to the provision of such services.
(d) Hearing findings.—If at the hearing the court finds by clear and convincing evidence that the vulnerable
adult is in need of protective services and lacks the capacity to consent, the court may issue an order authorizing the
provision of protective services. If an order for protective services is issued, it must include a statement of the
services to be provided and designate an individual or agency to be responsible for performing or obtaining the
essential services on behalf of the vulnerable adult or otherwise consenting to protective services on behalf of the
vulnerable adult.
(e) Continued protective services.—
1. No more than 60 days after the date of the order authorizing the provision of protective services, the
department shall petition the court to determine whether:
a. Protective services will be continued with the consent of the vulnerable adult pursuant to this subsection;
b. Protective services will be continued for the vulnerable adult who lacks capacity;
c. Protective services will be discontinued; or
d. A petition for guardianship should be filed pursuant to chapter 744.
2. If the court determines that a petition for guardianship should be filed pursuant to chapter 744, the court, for
good cause shown, may order continued protective services until it makes a determination regarding capacity.
3. If the department has a good faith belief that the vulnerable adult lacks the capacity to consent to protective
services, the petition to determine incapacity under s. 744.3201 may be filed by the department. Once the petition is
filed, the department may not be appointed guardian and may not provide legal counsel for the guardian.
(f) Costs.—The costs of services ordered under this section must be paid by the perpetrator if the perpetrator is
financially able to do so; or by third-party reimbursement, if available. If the vulnerable adult is unable to pay for
guardianship, application may be made to the public guardian for public guardianship services, if available.
(2) EMERGENCY PROTECTIVE SERVICES INTERVENTION.—If the department has reasonable cause to
believe that a vulnerable adult is suffering from abuse or neglect that presents a risk of death or serious physical
injury to the vulnerable adult and that the vulnerable adult lacks the capacity to consent to emergency protective
11 – 13
services, the department may take action under this subsection. If the vulnerable adult has the capacity to consent
and refuses consent to emergency protective services, emergency protective services may not be provided.
(a) Emergency entry of premises.—If, upon arrival at the scene of the incident, consent is not obtained for
access to the alleged victim for purposes of conducting a protective investigation under this subsection and the
department has reason to believe that the situation presents a risk of death or serious physical injury, a representative
of the department and a law enforcement officer may forcibly enter the premises. If, after obtaining access to the
alleged victim, it is determined through a personal assessment of the situation that no emergency exists and there is
no basis for emergency protective services intervention under this subsection, the department shall terminate the
emergency entry.
(b) Emergency removal from premises.—If it appears that the vulnerable adult lacks the capacity to consent to
emergency protective services and that the vulnerable adult, from the personal observations of the representative of
the department and specified medical personnel or law enforcement officers, is likely to incur a risk of death or
serious physical injury if such person is not immediately removed from the premises, then the representative of the
department shall transport or arrange for the transportation of the vulnerable adult to an appropriate medical or
protective services facility in order to provide emergency protective services. Law enforcement personnel have a
duty to transport when medical transportation is not available or needed and the vulnerable adult presents a threat of
injury to self or others. If the vulnerable adult’s caregiver or guardian is present, the protective investigator must
seek the caregiver’s or guardian’s consent pursuant to subsection (4) before the vulnerable adult may be removed
from the premises, unless the protective investigator suspects that the vulnerable adult’s caregiver or guardian has
caused the abuse, neglect, or exploitation. The department shall, within 24 hours after providing or arranging for
emergency removal of the vulnerable adult, excluding Saturdays, Sundays, and legal holidays, petition the court for
an order authorizing emergency protective services.
(c) Emergency medical treatment.—If, upon admission to a medical facility, it is the opinion of the medical
staff that immediate medical treatment is necessary to prevent serious physical injury or death, and that such
treatment does not violate a known health care advance directive prepared by the vulnerable adult, the medical
facility may proceed with treatment to the vulnerable adult. If a person with legal authority to give consent for the
provision of medical treatment to a vulnerable adult has not given or has refused to give such consent, examination
and treatment must be limited to reasonable examination of the patient to determine the medical condition of the
patient and treatment reasonably necessary to alleviate the emergency medical condition or to stabilize the patient
pending court determination of the department’s petition authorizing emergency protective services. Any person
may seek an expedited judicial intervention under rule 5.900 of the Florida Probate Rules concerning medical
treatment procedures.
(d) Emergency protective services petition.—A petition filed under this subsection must state the name, age,
and address of the vulnerable adult and allege the facts constituting the emergency protective services intervention
and subsequent removal of the vulnerable adult or provision of in-home services, the facts relating to the capacity of
the vulnerable adult to consent to services, the efforts of the department to obtain consent, and the services needed or
delivered.
(e) Notice.—Notice of the filing of the emergency protective services petition and a copy of the petition must
be given to the vulnerable adult, to that person’s spouse, to that person’s guardian, if any, to legal counsel

11 – 14
representing the vulnerable adult, and, when known, to adult children or next of kin of the vulnerable adult. Such
notice must be given at least 24 hours before any hearing on the petition for emergency protective services.
(f) Hearing.—When emergency removal has occurred under this subsection, a hearing must be held within 4
days after the filing of the emergency protective services petition, excluding Saturday, Sunday, and legal holidays,
to establish reasonable cause for grounds to continue emergency protective services.
1. The court shall determine, by clear and convincing evidence, whether an emergency existed which justified
the emergency protective services intervention, whether the vulnerable adult is in need of emergency protective
services, whether the vulnerable adult lacks the capacity to consent to emergency protective services, and whether:
a. Emergency protective services will continue with the consent of the vulnerable adult;
b. Emergency protective services will continue without the consent of the vulnerable adult; or
c. Emergency protective services will be discontinued.
2. The vulnerable adult has the right to be represented by legal counsel at the hearing. The court shall appoint
legal counsel to represent a vulnerable adult who is without legal representation.
3. The department must make reasonable efforts to ensure the presence of the vulnerable adult at the hearing.
4. If an order to continue emergency protective services is issued, it must state the services to be provided and
designate an individual or agency to be responsible for performing or obtaining the essential services, or otherwise
consenting to protective services on behalf of the vulnerable adult.
(g) Continued emergency protective services.—
1. Not more than 60 days after the date of the order authorizing the provision of emergency protective services,
the department shall petition the court to determine whether:
a. Emergency protective services will be continued with the consent of the vulnerable adult;
b. Emergency protective services will be continued for the vulnerable adult who lacks capacity;
c. Emergency protective services will be discontinued; or
d. A petition should be filed under chapter 744.
2. If it is decided to file a petition under chapter 744, for good cause shown, the court may order continued
emergency protective services until a determination is made by the court.
3. If the department has a good faith belief that the vulnerable adult lacks the capacity to consent to protective
services, the petition to determine incapacity under s. 744.3201 may be filed by the department. Once the petition is
filed, the department may not be appointed guardian and may not provide legal counsel for the guardian.
(h) Costs.—The costs of services ordered under this section must be paid by the perpetrator if the perpetrator is
financially able to do so, or by third-party reimbursement, if available.
(3) PROTECTIVE SERVICES ORDER.—In ordering any protective services under this section, the court shall
adhere to the following limitations:
(a) Only such protective services as are necessary to ameliorate the conditions creating the abuse, neglect, or
exploitation may be ordered, and the court shall specifically designate the approved services in the order of the
court.
(b) Protective services ordered may not include a change of residence, unless the court specifically finds such
action is necessary to ameliorate the conditions creating the abuse, neglect, or exploitation and the court gives
specific approval for such action in the order. Placement may be made to such facilities as adult family-care homes,

11 – 15
assisted living facilities, or nursing homes, or to other appropriate facilities. Placement may not be made to facilities
for the acutely mentally ill, except as provided in chapter 394.
(c) If an order to continue emergency protective services is issued, it must include the designation of an
individual or agency to be responsible for performing or obtaining the essential services on behalf of the vulnerable
adult or otherwise consenting to protective services on behalf of the vulnerable adult.
(4) PROTECTIVE SERVICES INTERVENTIONS WITH CAREGIVER OR GUARDIAN PRESENT.—
(a) When a vulnerable adult who lacks the capacity to consent has been identified as the victim, the protective
investigator must first request consent from the caregiver or guardian, if present, before providing protective
services or protective supervision, unless the protective investigator suspects that the caregiver or guardian has
caused the abuse, neglect, or exploitation.
(b) If the caregiver or guardian agrees to engage or provide services designed to prevent further abuse, neglect,
or exploitation, the department may provide protective supervision.
(c) If the caregiver or guardian refuses to give consent or later withdraws consent to agreed-upon services, or
otherwise fails to provide needed care and supervision, the department may provide emergency protective services
as provided in subsection (2). If emergency protective services are so provided, the department must then petition
the court for an order to provide emergency protective services under subsection (3).
(5) INTERFERENCE WITH COURT-ORDERED PROTECTIVE SERVICES.—When a court order exists
authorizing protective services for a vulnerable adult who lacks capacity to consent and any person interferes with
the provision of such court-ordered protective services, the appropriate law enforcement agency shall enforce the
order of the court.
(6) LIMITATIONS.—This section does not limit in any way the authority of the court or a criminal justice
officer, or any other duly appointed official, to intervene in emergency circumstances under existing statutes. This
section does not limit the authority of any person to file a petition for guardianship under chapter 744.
History.—s. 101, ch. 95-418; s. 11, ch. 97-98; s. 34, ch. 2000-349; s. 2, ch. 2006-131; s. 4, ch. 2010-31.
415.1052 Interference with investigation or with the provision of protective services.—
(1) If, upon arrival of the protective investigator, any person refuses to allow the department to begin a
protective investigation, interferes with the department’s ability to conduct such an investigation, or refuses to give
access to the vulnerable adult, the appropriate law enforcement agency must be contacted to assist the department in
commencing the protective investigation.
(2) When any person refuses to allow the provision of protective services to the vulnerable adult who has the
capacity to consent to services, the department shall petition the court for an order enjoining the person from
interfering with the provision of protective services. The petition must allege specific facts sufficient to show that
the vulnerable adult is in need of protective services and that the person refuses to allow the provision of such
services. If the court finds by clear and convincing evidence that the vulnerable adult is in need of protective
services and that the person refuses to allow the provision of such services, the court may issue an order enjoining
the person from interfering with the provision of protective services to the vulnerable adult.
History.—s. 102, ch. 95-418; s. 35, ch. 2000-349.
415.1055 Notification to administrative entities.—
(1) Upon receipt of a report that alleges that an employee or agent of the department, the Agency for Persons
with Disabilities, or the Department of Elderly Affairs, acting in an official capacity, has committed an act of abuse,

11 – 16
neglect, or exploitation, the department shall notify the state attorney in whose circuit the abuse, neglect, or
exploitation occurred. This notification may be oral or written.
(2) If at any time during a protective investigation the department has reasonable cause to believe that a
vulnerable adult has been abused, neglected, or exploited by another person, the state attorney having jurisdiction in
the county in which the abuse, neglect, or exploitation occurred shall be notified immediately, either orally or in
writing.
(3) If at any time during a protective investigation the department has reasonable cause to believe that a
vulnerable adult has been abused, neglected, or exploited by another person, the appropriate law enforcement
agency shall be immediately notified. Such agency may begin a criminal investigation concurrent with or
independent of the protective investigation of the department. This notification may be oral or written.
(4) If at any time during a protective investigation the department has reasonable cause to believe that abuse,
neglect, or exploitation of a vulnerable adult has occurred within a facility that receives Medicaid funds, the
department shall notify the Medicaid Fraud Control Unit within the Department of Legal Affairs, Office of the
Attorney General, in order that it may begin an investigation concurrent with the protective investigation of the
department. This notification may be oral or written.
(5) If at any time during a protective investigation the department has reasonable cause to believe that an
employee of a facility, as defined in s. 415.102, is the alleged perpetrator of abuse, neglect, or exploitation of a
vulnerable adult, the department shall notify the Agency for Health Care Administration, Division of Health Quality
Assurance, in writing.
(6) If at any time during a protective investigation the department has reasonable cause to believe that
professional licensure violations have occurred, the department shall notify the Division of Medical Quality
Assurance within the Department of Health. This notification must be in writing.
(7) The department shall notify the state attorney having jurisdiction in the county in which the abuse, neglect,
or exploitation occurred if evidence indicates that further criminal investigation is warranted. This notification must
be in writing.
(8) At the conclusion of a protective investigation at a facility, the department shall notify either the Florida
local advocacy council or the State Long-Term Care Ombudsman Program or the long-term care ombudsman
council of the results of the investigation. This notification must be in writing.
(9) When a report involving a guardian of the person or property, or both, is received, the department shall
notify the probate court having jurisdiction over the guardianship, in writing.
(10) When a report has been received and the department has reason to believe that a vulnerable adult resident
of a facility licensed by the Agency for Health Care Administration or the Agency for Persons with Disabilities has
been the victim of abuse, neglect, or exploitation, the department shall provide a copy of its investigation to the
appropriate agency. If the investigation determines that a health professional licensed or certified under the
Department of Health may have abused, neglected, or exploited a vulnerable adult, the department shall also provide
a copy to the Department of Health.
History.—s. 103, ch. 95-418; s. 12, ch. 97-98; s. 30, ch. 98-166; s. 4, ch. 98-182; s. 69, ch. 2000-153; s. 23, ch.
2000-263; s. 36, ch. 2000-349; s. 59, ch. 2006-227; s. 31, ch. 2015-31.

11 – 17
415.106 Cooperation by the department and criminal justice and other agencies.—
(1) All criminal justice agencies have a duty and responsibility to cooperate fully with the department so as to
enable the department to fulfill its responsibilities under ss. 415.101-415.113. Such duties include, but are not
limited to, forced entry, emergency removal, emergency transportation, and the enforcement of court orders
obtained under ss. 415.101-415.113.
(2) To ensure coordination, communication, and cooperation with the investigation of abuse, neglect, or
exploitation of vulnerable adults, the department shall develop and maintain interprogram agreements or operational
procedures among appropriate departmental programs and the State Long-Term Care Ombudsman Program, the
Florida Statewide Advocacy Council, and other agencies that provide services to vulnerable adults. These
agreements or procedures must cover such subjects as the appropriate roles and responsibilities of the department in
identifying and responding to reports of abuse, neglect, or exploitation of vulnerable adults; the provision of
services; and related coordinated activities.
(3) To the fullest extent possible, the department shall cooperate with and seek cooperation from all appropriate
public and private agencies, including health agencies, educational agencies, social service agencies, courts,
organizations, or programs providing or concerned with human services related to the prevention, identification, or
treatment of abuse, neglect, or exploitation of vulnerable adults.
History.—ss. 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, ch. 73-176; s. 1, ch. 77-174; ss. 3, 5, ch. 79-287; s. 15, ch. 79-298; s.
1, ch. 80-293; s. 1, ch. 83-82; s. 32, ch. 86-220; s. 27, ch. 93-177; s. 104, ch. 95-418; s. 24, ch. 2000-263; s. 37, ch.
2000-349; s. 32, ch. 2015-31.
415.107 Confidentiality of reports and records.—
(1) In order to protect the rights of the individual or other persons responsible for the welfare of a vulnerable
adult, all records concerning reports of abuse, neglect, or exploitation of the vulnerable adult, including reports made
to the central abuse hotline, and all records generated as a result of such reports shall be confidential and exempt
from s. 119.07(1) and may not be disclosed except as specifically authorized by ss. 415.101-415.113.
(2) Upon the request of the committee chairperson, access to all records shall be granted to staff of the
legislative committees with jurisdiction over issues and services related to vulnerable adults, or over the department.
All confidentiality provisions that apply to the Department of Children and Families continue to apply to the records
made available to legislative staff under this subsection.
(3) Access to all records, excluding the name of the reporter which shall be released only as provided in
subsection (6), shall be granted only to the following persons, officials, and agencies:
(a) Employees or agents of the department, the Agency for Persons with Disabilities, the Agency for Health
Care Administration, or the Department of Elderly Affairs who are responsible for carrying out protective
investigations, ongoing protective services, or licensure or approval of nursing homes, assisted living facilities, adult
day care centers, adult family-care homes, home care for the elderly, hospices, residential facilities licensed under
chapter 393, or other facilities used for the placement of vulnerable adults.
(b) A criminal justice agency investigating a report of known or suspected abuse, neglect, or exploitation of a
vulnerable adult.
(c) The state attorney of the judicial circuit in which the vulnerable adult resides or in which the alleged abuse,
neglect, or exploitation occurred.

11 – 18
(d) Any victim, the victim’s guardian, caregiver, or legal counsel, and any person who the department has
determined might be abusing, neglecting, or exploiting the victim.
(e) A court, pursuant to s. 825.1035(4)9h); by subpoena, upon its finding that access to such records may be
necessary for the determination of an issue before the court; however, such access must be limited to inspection in
camera, unless the court determines that public disclosure of the information contained in such records is necessary
for the resolution of an issue then pending before it.
(f) A grand jury, by subpoena, upon its determination that access to such records is necessary in the conduct of
its official business.
(g) Any appropriate official of the Florida advocacy council, State Long-Term Care Ombudsman Program, or
long-term care ombudsman council investigating a report of known or suspected abuse, neglect, or exploitation of a
vulnerable adult.
(h) Any appropriate official of the department, the Agency for Persons with Disabilities, the Agency for Health
Care Administration, or the Department of Elderly Affairs who is responsible for:
1. Administration or supervision of the programs for the prevention, investigation, or treatment of abuse,
neglect, or exploitation of vulnerable adults when carrying out an official function; or
2. Taking appropriate administrative action concerning an employee alleged to have perpetrated abuse, neglect,
or exploitation of a vulnerable adult in an institution.
(i) Any person engaged in bona fide research or auditing. However, information identifying the subjects of the
report must not be made available to the researcher.
(j) Employees or agents of an agency of another state that has jurisdiction comparable to the jurisdiction
described in paragraph (a).
(k) The Public Employees Relations Commission for the sole purpose of obtaining evidence for appeals filed
pursuant to s. 447.207. Records may be released only after deletion of all information that specifically identifies
persons other than the employee.
(l) Any person in the event of the death of a vulnerable adult determined to be a result of abuse, neglect, or
exploitation. Information identifying the person reporting abuse, neglect, or exploitation shall not be released. Any
information otherwise made confidential or exempt by law shall not be released pursuant to this paragraph.
(4) The Department of Health, the Department of Business and Professional Regulation, and the Agency for
Health Care Administration may have access to a report, excluding the name of the reporter, when considering
disciplinary action against a licensee or certified nursing assistant pursuant to allegations of abuse, neglect, or
exploitation.
(5) The department may release to any professional person such information as is necessary for the diagnosis
and treatment of, and service delivery to, a vulnerable adult or the person perpetrating the abuse, neglect, or
exploitation.
(6) The identity of any person reporting abuse, neglect, or exploitation of a vulnerable adult may not be
released, without that person’s written consent, to any person other than employees of the department responsible
for protective services, the central abuse hotline, or the appropriate state attorney or law enforcement agency. This
subsection grants protection only for the person who reported the abuse, neglect, or exploitation and protects only
the fact that the person is the reporter. This subsection does not prohibit the subpoena of a person reporting the

11 – 19
abuse, neglect, or exploitation when deemed necessary by the state attorney or the department to protect a vulnerable
adult who is the subject of a report, if the fact that the person made the report is not disclosed.
(7) For the purposes of this section, the term “access” means a visual inspection or copy of the hard-copy
record maintained in the district.
(8) Information in the central abuse hotline may not be used for employment screening.
History.—ss. 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, ch. 73-176; s. 1, ch. 77-174; ss. 3, 5, ch. 79-287; s. 15, ch. 79-298; s.
1, ch. 80-293; s. 1, ch. 83-82; s. 33, ch. 86-220; s. 32, ch. 87-238; s. 7, ch. 88-219; s. 18, ch. 88-337; s. 4, ch. 89-170;
s. 30, ch. 89-294; s. 4, ch. 90-50; s. 7, ch. 90-208; s. 47, ch. 90-306; s. 4, ch. 91-57; s. 15, ch. 91-71; ss. 43, 47, ch.
92-58; s. 31, ch. 93-39; s. 15, ch. 93-214; s. 57, ch. 94-218; s. 38, ch. 95-210; s. 106, ch. 95-418; s. 267, ch. 96-406;
s. 1, ch. 98-111; s. 9, ch. 98-182; s. 2, ch. 98-255; s. 41, ch. 98-280; s. 70, ch. 2000-153; s. 25, ch. 2000-263; s. 38,
ch. 2000-349; s. 3, ch. 2006-131; s. 60, ch. 2006-227; s. 235, ch. 2014-19; s. 33, ch. 2015-31.
415.1071 Release of confidential information.—
(1) Any person or organization, including the Department of Children and Families, may petition the court for
an order making public the records of the Department of Children and Families which pertain to investigations of
alleged abuse, neglect, or exploitation of a vulnerable adult. The court shall determine whether good cause exists for
public access to the records sought or a portion thereof. In making this determination, the court shall balance the best
interests of the vulnerable adult who is the focus of the investigation together with the privacy right of other persons
identified in the reports against the public interest. The public interest in access to such records is reflected in s.
119.01(1), and includes the need for citizens to know of and adequately evaluate the actions of the Department of
Children and Families and the court system in providing vulnerable adults of this state with the protections
enumerated in s. 415.101. However, this subsection does not contravene s. 415.107, which protects the name of any
person reporting the abuse, neglect, or exploitation of a vulnerable adult.
(2) In cases involving serious bodily injury to a vulnerable adult, the Department of Children and Families may
petition the court for an order for the immediate public release of records of the department which pertain to the
protective investigation. The petition must be personally served upon the vulnerable adult, the vulnerable adult’s
legal guardian, if any, and any person named as an alleged perpetrator in the report of abuse, neglect, or exploitation.
The court must determine whether good cause exists for the public release of the records sought no later than 24
hours, excluding Saturdays, Sundays, and legal holidays, after the date the department filed the petition with the
court. If the court does not grant or deny the petition within the 24-hour time period, the department may release to
the public summary information including:
(a) A confirmation that an investigation has been conducted concerning the alleged victim.
(b) The dates and brief description of procedural activities undertaken during the department’s investigation.
(c) The date of each judicial proceeding, a summary of each participant’s recommendations made at the judicial
proceeding, and the ruling of the court.
The summary information shall not include the name of, or other identifying information with respect to, any person
identified in any investigation. In making a determination to release confidential information, the court shall balance
the best interests of the vulnerable adult who is the focus of the investigation together with the privacy rights of other
persons identified in the reports against the public interest for access to public records. However, this subsection does
not contravene s. 415.107, which protects the name of any person reporting abuse, neglect, or exploitation of a
vulnerable adult.

11 – 20
(3) When the court determines that good cause for public access exists, the court shall direct that the department
redact the name of and other identifying information with respect to any person identified in any protective
investigation report until such time as the court finds that there is probable cause to believe that the person identified
committed an act of alleged abuse, neglect, or exploitation.
History.—s. 18, ch. 2004-335; s. 236, ch. 2014-19.
415.1099 Court and witness fees not allowed.—In all proceedings under ss. 415.101-415.113, court fees must
not be charged to the department; to any party to a petition; to any legal custodian of records, documents, or persons;
or to any adult named in a summons. In a proceeding under ss. 415.101-415.113, witness fees are not allowed to the
department; to any party to a petition; to any legal custodian of records, documents, or persons; or to any adult
named in a summons.
History.—s. 108, ch. 95-418.
415.1102 Adult protection teams.—
(1) Subject to an appropriation, the department may develop, maintain, and coordinate the services of one or
more multidisciplinary adult protection teams in each of the districts of the department. As used in this section, the
term “multidisciplinary adult protection team” means a team of two or more persons who are trained in the
prevention, identification, and treatment of abuse of elderly persons, as defined in s. 430.602, or of dependent
persons and who are qualified to provide a broad range of services related to abuse of elderly or dependent persons.
(2) Such teams may be composed of, but need not be limited to:
(a) Psychiatrists, psychologists, or other trained counseling personnel;
(b) Police officers or other law enforcement officers;
(c) Medical personnel who have sufficient training to provide health services;
(d) Social workers who have experience or training in preventing the abuse of elderly or dependent persons;
and
(e) Public and professional guardians as described in part II of chapter 744.
(3) The department shall utilize and convene the teams to supplement the protective services activities of the
protective services program of the department.
(4) This section does not prevent a person from reporting under s. 415.1034 all suspected or known cases of
abuse, neglect, or exploitation of a vulnerable adult. The role of the teams is to support activities of the protective
services program and to provide services deemed by the teams to be necessary and appropriate to abused, neglected,
and exploited vulnerable adults upon referral. Services must be provided with the consent of the vulnerable adult or
that person’s guardian, or through court order.
(5) If an adult protection team is providing certain services to abused, neglected, or exploited vulnerable adults,
other offices and units of the department shall avoid duplicating those services.
History.—s. 32, ch. 89-294; s. 48, ch. 90-306; s. 109, ch. 95-418; s. 6, ch. 98-182; s. 71, ch. 2000-153; s. 39, ch.
2000-349; s. 2, ch. 2003-262; s. 35, ch. 2016-40.
415 .1105 Training programs.—
(1) The department shall, within available resources, provide appropriate preservice and inservice training for
adult protective investigation staff.
(2) Within available resources, the department shall cooperate with other appropriate agencies in developing
and providing preservice and inservice training programs for those persons specified in s. 415.1034(1)(a).
11 – 21
History.—s. 110, ch. 95-418; s. 65, ch. 2013-18.
415.111 Criminal penalties.—
(1) A person who knowingly and willfully fails to report a case of known or suspected abuse, neglect, or
exploitation of a vulnerable adult, or who knowingly and willfully prevents another person from doing so, commits a
misdemeanor of the second degree, punishable as provided in s. 775.082 or s. 775.083.
(2) A person who knowingly and willfully makes public or discloses any confidential information contained in
the central abuse hotline, or in other computer systems, or in the records of any case of abuse, neglect, or
exploitation of a vulnerable adult, except as provided in ss. 415.101-415.113, commits a misdemeanor of the second
degree, punishable as provided in s. 775.082 or s. 775.083.
(3) A person who has custody of records and documents the confidentiality of which is abrogated under s.
415.1045(3) and who refuses to grant access to such records commits a misdemeanor of the second degree,
punishable as provided in s. 775.082 or s. 775.083.
(4) If the department or its authorized agent has determined after its investigation that a report is false, the
department shall, with the consent of the alleged perpetrator, refer the reports to the local law enforcement agency
having jurisdiction for an investigation to determine whether sufficient evidence exists to refer the case for
prosecution for filing a false report as defined in s. 415.102. During the pendency of the investigation by the local
law enforcement agency, the department must notify the local law enforcement agency of, and the local law
enforcement agency must respond to, all subsequent reports concerning the same vulnerable adult in accordance
with s. 415.104 or s. 415.1045. If the law enforcement agency believes that there are indicators of abuse, neglect, or
exploitation, it must immediately notify the department, which must assure the safety of the vulnerable adult. If the
law enforcement agency finds sufficient evidence for prosecution for filing a false report, it must refer the case to
the appropriate state attorney for prosecution.
(5) A person who knowingly and willfully makes a false report of abuse, neglect, or exploitation of a vulnerable
adult, or a person who advises another to make a false report, commits a felony of the third degree, punishable as
provided in s. 775.082 or s. 775.083.
(a) The department shall establish procedures for determining whether a false report of abuse, neglect, or
exploitation of a vulnerable adult has been made and for submitting all identifying information relating to such a
false report to the local law enforcement agency as provided in this subsection and shall report annually to the
Legislature the number of reports referred.
(b) Anyone making a report who is acting in good faith is immune from any liability under this subsection.
History.—ss. 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, ch. 73-176; s. 1, ch. 77-174; ss. 3, 5, ch. 79-287; s. 15, ch. 79-298; s.
1, ch. 80-293; s. 1, ch. 83-82; s. 36, ch. 86-220; s. 19, ch. 88-337; s. 1, ch. 89-322; s. 49, ch. 90-306; s. 5, ch. 91-57;
s. 16, ch. 91-71; s. 250, ch. 91-224; s. 1, ch. 91-258; s. 4, ch. 95-140; s. 20, ch. 95-158; s. 111, ch. 95-418; s. 7, ch.
96-293; s. 2, ch. 98-111; s. 10, ch. 98-182; s. 40, ch. 2000-349; s. 4, ch. 2002-70.
415.1111 Civil actions.—A vulnerable adult who has been abused, neglected, or exploited as specified in this
chapter has a cause of action against any perpetrator and may recover actual and punitive damages for such abuse,
neglect, or exploitation. The action may be brought by the vulnerable adult, or that person’s guardian, by a person or
organization acting on behalf of the vulnerable adult with the consent of that person or that person’s guardian, or by
the personal representative of the estate of a deceased victim without regard to whether the cause of death resulted
from the abuse, neglect, or exploitation. The action may be brought in any court of competent jurisdiction to enforce

11 – 22
such action and to recover actual and punitive damages for any deprivation of or infringement on the rights of a
vulnerable adult. A party who prevails in any such action may be entitled to recover reasonable attorney’s fees, costs
of the action, and damages. The remedies provided in this section are in addition to and cumulative with other legal
and administrative remedies available to a vulnerable adult. Notwithstanding the foregoing, any civil action for
damages against any licensee or entity who establishes, controls, conducts, manages, or operates a facility licensed
under part II of chapter 400 relating to its operation of the licensed facility shall be brought pursuant to s. 400.023,
or against any licensee or entity who establishes, controls, conducts, manages, or operates a facility licensed under
part I of chapter 429 relating to its operation of the licensed facility shall be brought pursuant to s. 429.29. Such
licensee or entity shall not be vicariously liable for the acts or omissions of its employees or agents or any other third
party in an action brought under this section.
History.—s. 112, ch. 95-418; s. 23, ch. 96-418; s. 41, ch. 2000-349; s. 12, ch. 2001-45; s. 86, ch. 2006-197.
415.1113 Administrative fines for false report of abuse, neglect, or exploitation of a vulnerable adult.—
(1) In addition to any other penalty authorized by this section, chapter 120, or other law, the department may
impose a fine, not to exceed $10,000 for each violation, upon a person who knowingly and willfully makes a false
report of abuse, neglect, or exploitation of a vulnerable adult, or a person who counsels another to make a false
report.
(2) If the department alleges that a person has knowingly and willfully filed a false report with the central abuse
hotline, the department must file a notice of intent that alleges the name, age, and address of the individual; the facts
constituting the allegation that the individual made a false report; and the administrative fine that the department
proposes to impose on the person. Each time that a false report is made constitutes a separate violation.
(3) The notice of intent to impose the administrative fine must be served by certified mail, return receipt
requested, upon the person alleged to have filed the false report and upon the person’s legal counsel, if any.
(4) Any person alleged to have filed the false report is entitled to an administrative hearing under chapter 120
before the imposition of the fine becomes final. The person must request an administrative hearing within 60 days
after receipt of the notice of intent by filing a request with the department. Failure to request an administrative
hearing within 60 days after receipt of the notice of intent constitutes a waiver of the right to a hearing, making the
administrative fine final.
(5) At the hearing, the department must prove by clear and convincing evidence that the person knowingly and
willfully filed a false report with the central abuse hotline. The person has the right to be represented by legal
counsel at the hearing.
(6) In determining the amount of fine to be imposed, if any, the following factors must be considered:
(a) The gravity of the violation, including the probability that serious physical or emotional harm to any person
will result or has resulted, the severity of the actual or potential harm, and the nature of the false allegation.
(b) Actions taken by the false reporter to retract the false report as an element of mitigation, or, in contrast, to
encourage an investigation on the basis of false information.
(c) Any previous false reports filed by the same individual.
(7) A decision by the department, following the administrative hearing, to impose an administrative fine for
filing a false report constitutes final agency action within the meaning of chapter 120. Notice of the imposition of
the administrative fine must be served upon the person and upon the person’s legal counsel, by certified mail, return
receipt requested, and must state that the person may seek judicial review of the administrative fine under s. 120.68.

11 – 23
(8) All amounts collected under this section must be deposited into the Operations and Maintenance Trust Fund
within the Adult Services Program of the department.
(9) A person who is determined to have filed a false report of abuse or neglect is not entitled to confidentiality.
Subsequent to the conclusion of all administrative or other judicial proceedings concerning the filing of a false
report, the name of the false reporter and the nature of the false report must be made public, pursuant to s. 119.01(1).
Such information is admissible in any civil or criminal proceeding.
(10) Any person who makes a report and acts in good faith is immune from any liability under this section and
continues to be entitled to have the confidentiality of his or her identity maintained.
History.—s. 113, ch. 95-418; s. 68, ch. 97-103; s. 3, ch. 98-111; s. 11, ch. 98-182; s. 201, ch. 99-8; s. 42, ch.
2000-349.
415.1115 Civil actions involving elderly parties; speedy trial.—In a civil action in which a person over the
age of 65 is a party, such party may move the court to advance the trial on the docket. The presiding judge, after
consideration of the age and health of the party, may advance the trial on the docket. The motion may be filed and
served with the initial complaint or at any time thereafter.
History.—s. 1, ch. 91-251; s. 115, ch. 95-418.
Note.—Former s. 415.114.
415.113 Statutory construction; treatment by spiritual means.—Nothing in ss. 415.101-415.1115 shall be
construed to mean a person is abused, neglected, or in need of emergency or protective services for the sole reason
that the person relies upon and is, therefore, being furnished treatment by spiritual means through prayer alone in
accordance with the tenets and practices of a well-recognized church or religious denomination or organization; nor
shall anything in such sections be construed to authorize, permit, or require any medical care or treatment in
contravention of the stated or implied objection of such person. Such construction does not:
(1) Eliminate the requirement that such a case be reported to the department;
(2) Prevent the department from investigating such a case; or
(3) Preclude a court from ordering, when the health of the individual requires it, the provision of medical
services by a licensed physician or treatment by a duly accredited practitioner who relies solely on spiritual means
for healing in accordance with the tenets and practices of a well-recognized church or religious denomination or
organization.
History.—s. 1, ch. 85-143; s. 114, ch. 95-418; s. 43, ch. 2000-349; s. 53, ch. 2016-10.

11 – 24
Notes
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________

12. Florida Building C
ode Adopted


12 – 1
RULE CHAPTER 61G20-1
FLORIDA BUILDING CODE ADOPTED 61G20-1.001 State Building Code Adopted
61G20-1.002 Alternative Design Method for Screen Enclosure (Repealed)
61G20-1.001 Florida Building Code Adopted.
(1) The Florida Building Code, 5th Edition (2014), as updated by the Florida Building Commission on
November 13, 2014, incorporated herein by reference is hereby adopted as the building code for the State of Florida.
(2) The material incorporated and adopted in subsection (1) is copyrighted material that is available for public
inspection and examination at the Department of State, Administrative Code and Register Section, Room 701, The
Capitol, Tallahassee, Florida 32399-0250, and at the Office of Codes and Standards, 1940 North Monroe Street,
Room 90, Tallahassee, Florida 32399-0772.
(3) Modifications and Amendments. All proposed modifications to the selected base codes and amendments to
the Florida Building Code shall be submitted on the form adopted by reference in subsection 61G20-2.002(4),
F.A.C., that must be completed in full prior to submittal. The text of the proposed modification or amendment must
be provided in legislative format, with underlining indicating where new language is added to the existing provisions
and strikeout indicating where existing language is deleted. Copies of the form may be obtained by writing to the
Office of Codes and Standards, 1940 North Monroe Street, Room 90, Tallahassee, Florida 32399-0772.
Rulemaking Authority 553.73(1), (7) FS. Law Implemented 553.37(1), 553.72, 553.73 FS., Sections 32, 33, 34, 36,
44, 46, 48, Chapter 2005-147, Laws of Florida, Section 1, Chapter 2006-65, Laws of Florida, Section 10, Chapter
2007-1, Laws of Florida. History–New 7-18-90, Amended 3-30-93, 10-17-93, 8-28-95, 9-24-96, 12-26-96, 4-27-97,
10-5-97, 10-14-97, 9-7-00, 11-28-00, 2-7-01, 12-16-01, 6-30-03, 4-3-05, 12-11-05, 12-8-06, 5-21-07, 10-1-08, 2-17-
09, 10-1-09, Formerly 9B-3.047, Amended 11-10-11, Formerly 9N-1.001, Amended 4-25-13, 6-30-15.
61G20-1.002 Alternative Design Method for Screen Enclosure.
Rulemaking Authority Chapter 2012-13, Section 19, Laws of Florida, 553.76, 553.77 FS. Law Implemented Chapter
2012-13, Section 19, Laws of Florida, 553.76, 553.77 FS. History New 4-25-13, Repealed 2-9-16.

12 – 2
FLORIDA BUILDING CODE
SECTION 464 ASSISTED LIVING FACILITIES 464.1 Scope.
Assisted living facilities shall comply with the following design and construction standards as described herein.
Note: Other administrative and programmatic provisions may apply. See Agency of Health Care Administration
(AHCA) Rule 58A-5, Florida Administrative Code and Chapter 400 Part III, Florida Statutes.
464.2 Definitions.
AGENCY. The Agency for Health Care Administration.
AHCA CENTERAL OFFICE. The Assisted Living Unit, Agency for Health Care Administration.
ASSISTED LIVING FACILITY. Any building or buildings, section or distinct part of a building, private home,
boarding home, home for the aged or other residential facility, whether operated for profit or not, which undertakes
through its ownership or management to provide housing, meals and one or more personal services for a period
exceeding 24 hours to one or more adults who are not relatives of the owner or administrator. The following are
exempted from this definition.
1. Any facility, institution, or other place operated by the federal government or any agency of the federal
government.
2. Any facility or part of a facility licensed under Chapter 393, Florida Statutes, or Chapter 394, Florida Statutes.
3. Any facility licensed as an adult family care home under Part VII Chapter 400, Florida Statutes.
4. Any person who provides housing, meals and one or more personal services on a 24-hour basis in the person’s
own home to not more than two adults who do not receive optional state supplementation. The person who provides
the housing, meals, and personal services must own or rent the home and reside therein.
5. Any home or facility approved by the United States Department of Veterans Affairs as a residential care home
wherein care is provided exclusively to three or fewer veterans.
6. Any facility that has been incorporated in this state for 50 years or more on or before July 1, 1983, and the board
of directors of which is nominated or elected by the residents, until the facility is sold or its ownership is transferred;
or any facility, with improvements or additions thereto, which has existed and operated continuously in this state for
60 years or more on or before July 1, 1989, is directly or indirectly owned and operated by a nationally recognized
fraternal organization, is not open to the public, and accepts only its own members and their spouses as residents.
7. Any facility certified under Chapter 651, Florida Statutes, or a retirement community, may provide services
authorized under this section or Part IV of Chapter 400, Florida Statutes to its residents who live in single-family
homes, duplexes, quadruplexes, or apartments located on the campus without obtaining a license to operate an
assisted living facility if residential units within such buildings are used by residents who do not require staff
supervision for that portion of the day when personal services are not being delivered and the owner obtains a home
health license to provide such services. However, any building or distinct part of a building on the campus that is
designated for persons who receive personal services and require supervision beyond that which is available while
such services are being rendered must be licensed in accordance with this section. If a facility provides personal
services to residents who do not otherwise require supervision and the owner is not licensed as a home health
agency, the buildings or distinct parts of buildings where such services are rendered must be licensed under this
section. A resident of a facility that obtains a home health license may contract with a home health agency of his or
her choice, provided that the home health agency provides liability insurance and workers’ compensation coverage

12 – 3
for its employees. Facilities covered by this exemption may establish policies that give residents the option of
contracting for services and care beyond that which is provided by the facility to enable them to age in place. For
purposes of this section, a retirement community consists of a facility licensed under this section or under Part II of
Chapter 400, Florida Statutes, and apartments designed for independent living located on the same campus.
8. Any residential unit for independent living which is located within a facility certified under Chapter 651, Florida
Statutes, or any residential unit which is colocated with a nursing home licensed under Part II of Chapter
400,Florida Statutes, or colocated with a facility licensed under this section in which services are provided through
an outpatient clinic or a nursing home on an outpatient basis.
CAPACITY. The number of residents for which a facility has been licensed to provide residential care.
DEPARTMENT. The Department of Elderly Affairs.
DISTINCT PART. Designated bedrooms or apartments, bathrooms and a living area; or a separately identified
wing, floor or building which includes bedrooms or apartments, bathrooms and a living area. The distinct part may
include a separate dining area, or meals may be served in another part of the facility.
DOEA ASSISTED LIVING PROGRAM. The Assisted Living Program, Department of Elder Affairs.
EXTENDED CONGREGATE CARE. Acts beyond those authorized in subsection (5) that may be performed
pursuant to Part I of Chapter 464, Florida Statutes by persons licensed thereunder while carrying out their
professional duties. The purpose of such services is to enable residents to age in place in a residential environment
despite mental or physical limitations that might otherwise disqualify them from residency in a facility licensed
under this part.
FOOD SERVICE. The storage, preparation, serving and cleaning up of food intended for consumption in a facility
or a formal agreement that meals will be regularly catered by a third party.
PERSONAL SERVICES. Direct physical assistance with or supervision of the activities of daily living and the
self-administration of medication and other similar services which the department may define by rule. Personal
services shall not be construed to mean the provision of medical, nursing, dental or mental health services.
RELATIVE. An individual who is the father, mother, stepfather, stepmother, son, daughter, brother, sister,
grandmother, grandfather, great-grandmother, great-grandfather, grandson, granddaughter, uncle, aunt, first cousin,
nephew, niece, husband, wife, father-in-law, mother-in-law, son-in-law, daughter-in-law, brother-in-law, sister-in-
law, stepson, stepdaughter, stepbrother, stepsister, half brother or half sister of an owner or administrator.
RENOVATION. Additions, repairs, restorations or other improvements to the physical plant of the facility within a
five-year period that costs in excess of 50 percent of the value of the building as reported on the tax rolls, excluding
land, before the renovation.
RESIDENT. A person 18 years of age or older, residing in and receiving care from a facility.
RESIDENT’S REPRESENTATIVE OR DESIGNEE. A person other than the owner, or an agent or employee of
the facility, designated in writing by the resident, if legally competent, to receive notice of changes in the contract
executed pursuant to Section 400.424, Florida Statutes; to receive notice of and to participate in meetings between
the resident and the facility owner, administrator or staff concerning the rights of the resident; to assist the resident
in contacting the ombudsman council if the resident has a complaint against the facility; or to bring legal action on
behalf of the resident pursuant to Section 400.429, Florida Statutes.
464.3 Codes and standards for the design and construction of assisted living facilities.
Except as modified and required by this section of the code, Chapter 58A-5, Florida Administrative Code or Chapter

12 – 4
429 Part III, Florida Statutes, all new assisted living facilities and all additions, alterations, or renovations to
existing assisted living facilities with more than 16 licensed beds shall also be in compliance with The Guidelines
for the Design and Construction of Health Care Facilities (The Guidelines) Part I General, and Section 4.1.4
Requirements for Assisted Living of Part 4, Residential Health Care Facilities, incorporated by reference.
464.4 Additional physical plant requirements for assisted living facilities.
In addition to the codes and standards referenced in Section 464.3 of the code, the following minimum essential
facilities shall apply to all new assisted living facilities.
464.4.1
Indoor radon testing as mandated by Section 404.056(5), Florida Statutes, shall be completed by all facilities.
464.4.2 Heating and cooling.
464.4.2.1
When outside temperatures are 65°F (18°C) or below, an indoor temperature of at least 72°F (22°C) shall be
maintained in all areas used by residents during hours when residents are normally awake. During night hours when
residents are asleep, an indoor temperature of at least 68°F (20°C) shall be maintained.
464.4.2.2
During hours when residents are normally awake, mechanical cooling devices, such as electric fans, must be used in
those as are of buildings used by residents when inside temperatures exceed 85°F (29°C) provided outside
temperatures remain below 90°F (32°C). No residents shall be in any inside area that exceeds 90°F (32°C).
However, during daytime hours when outside temperatures exceed 90°F (32°C), and at night, an indoor temperature
of no more than 81°F (27°C) must be maintained in all areas used by residents.
464.4.2.3
Residents who have individually controlled thermostats in their bedrooms or apartments shall be permitted to control
temperatures in those areas.
464.4.3 Common areas.
464.4.3.1
A minimum of 35 square feet (3 m2) of living and dining space per resident, live-in staff and live-in family member
shall be provided except in facilities comprised of apartments. This space shall include living, dining, recreational or
other space designated accessible to all residents, and shall not include bathrooms, corridors, storage space or
screened porches which cannot be adapted for year round use. Facilities with apartments may count the apartment’s
living space square footage as part of the 35-square-footage (3 m2) living and dining space requirement.
Those facilities also serving as adult day care centers must provide an additional 35 square feet (3 m2) of living and
dining space per adult day care client. Excess floor space in residents’ bedrooms or apartments cannot be counted
toward meeting the requirement of 35 square feet (3 m2) of living and dining space requirements for adult day care
participants. Day care participants may not use residents’ bedrooms for resting unless the room is currently vacant.
464.4.3.2
A room, separate from resident bedrooms, shall be provided where residents may read, engage in socialization or
other leisure time activities. Comfortable chairs or sofas shall be provided in this communal area.
464.4.3.3
The dining area shall be furnished to accommodate communal dining.
464.4.4 Bedrooms.

12 – 5
464.4.4.1
Resident sleeping rooms designated for single occupancy shall provide a minimum inside measurement of 80 square
feet (7 m2) of usable floor space. Usable floor space does not include closet space or bathrooms.
464.4.4.2
Resident bedrooms designated for multiple occupancy shall provide a minimum inside measurement of 60 square
feet (6 m2) of usable floor space per room occupant.
464.4.4.3
Resident bedrooms designated for multiple occupancy in facilities newly licensed or renovated six months after
October 17, 1999, shall have a maximum occupancy of two persons.
464.4.4.4
All resident bedrooms shall open directly into a corridor, common use area or to the outside. A resident must be able
to exit his bedroom without having to pass through another bedroom unless the two rooms have been licensed as one
bedroom.
464.4.4.5
All resident bedrooms shall be for the exclusive use of residents. Live-in staff and their family members shall be
provided with sleeping space separate from the sleeping and congregate space required for residents.
464.4.5 Bathrooms.
464.4.5.1
There shall be at least one bathroom with one toilet and sink per six persons, and one bathtub or shower per eight
persons. All residents, all live-in staff and family members, and respite care participants must be included when
calculating the required number of toilets, sinks, bathtubs and showers. All adult day care participants shall be
included when calculating the required number of toilets and sinks.
464.4.5.2
Each bathroom shall have a door in working order to assure privacy. The entry door to bathrooms with a single toilet
shall have a lock which is operable from the inside by the resident with no key needed. A nonlocking door shall be
permitted if the resident’s safety would otherwise be jeopardized.
464.4.5.3
There shall be nonslip safety devices such as bath mats or peel off stickers in the showers and bathtubs of all
facilities. Showers and bathtubs with a nonskid surface require a separate nonskid device only if the surface is worn.
Grab bars shall be required in showers and bathtubs. Grab bars, whether portable or permanent, must be securely
affixed to the floor or adjoining walls. Facilities newly licensed or renovated six months after October 17, 1999 must
have grab bars next to the commode.
464.4.5.4
Sole access to a toilet or bathtub or shower shall not be through another resident’s bedroom, except in apartments
within a facility.
464.4.6 Security.
External boundaries of a facility or a distinct part of a facility, including outside areas, may be secured using egress
control or perimeter control devices if the following conditions are met.
464.4.6.1
The use of the device complies with all lifesafety requirements.

12 – 6
464.4.6.2
Residents residing within a secured area are able to move freely throughout the area, including the resident’s
bedroom or apartment, bathrooms and all common areas, and have access to outdoor areas on a regular basis and as
requested by each resident.
464.4.6.3
Residents capable of entering and exiting without supervision have keys, codes or other mechanisms to exit the
secured area without requiring staff assistance.
464.4.6.4
Staff who provide direct care or who have regular contact with residents residing in secured areas complete Level 1
Alzheimer’s training as described in Rule 58A-5.0191.
464.4.6.5
Pursuant to Section 400.441, Florida Statutes, facilities with 16 or fewer residents shall not be required to maintain
an accessible telephone in each building where residents reside, maintain written staff job descriptions, have awake
night staff or maintain standardized recipes as provided in Rules 58A-5.0182(6)(g), 58A-5.019(2)(e), 58A-
5.019(4)(a) and 58A-5.020(2)(b), respectively.
464.5 Extended congregate care.
464.5.1 Physical site requirements.
Each extended congregate care facility shall provide a homelike physical environment which promotes resident
privacy and independence, including:
464.5.1.1
A private room or apartment, or a semiprivate room or apartment shared with a roommate of the resident’s choice.
The entry door to the room or apartment shall have a lock which is operable from the inside by the resident with no
key needed. The resident shall be provided with a key to the entry door on request. The resident’s service plan may
allow for a nonlocking entry door if the resident’s safety would otherwise be jeopardized.
464.5.1.2
A bathroom, with a toilet, sink and bathtub or shower, which is shared by a maximum of four residents. A centrally
located hydromassage bathtub may substitute for the bathtub or shower in two of the bath rooms. The entry door to
the bathroom shall have a lock which is operable from the inside by the resident with no key needed. The resident’s
service plan may allow for a nonlocking bathroom door if the resident’s safety would otherwise be jeopardized.
13. Rule Chapter
69A-40, F.A
.C.


13 – 1
CHAPTER 69A-40
UNIFORM FIRE SAFETY STANDARDS FOR ASSISTED LIVING FACILITIES 69A-40.022 Title
69A-40.023 Purpose
69A-40.024 Scope
69A-40.027 Definitions
69A-40.028 Standards of the National Fire Protection Association Adopted
69A-40.029 Evacuation Capability Evaluation
69A-40.031 Automatic Fire Sprinkler Systems
69A-40.033 Heating, Ventilating, and Air Conditioning Equipment
69A-40.035 Code Conflict Resolution
69A-40.036 Fire Exit Drills
69A-40.037 Intergenerational Respite Care Assisted Living Facility
69A-40.022 Title.
These rules, comprising Rule Chapter 69A-40, F.A.C., shall be known as “The Uniform Fire Safety Standards for
Assisted Living Facilities.” Rulemaking Authority 633.104, 633.206 FS. Law Implemented 429.11, 633.206 FS. History–New 11-29-89, Amended 1-7-97,
Formerly 4A-40.022.
69A-40.023 Purpose.
The purpose of this rule chapter is to establish uniform requirements to provide a reasonable degree of safety from
fire in buildings and structures used as assisted living facilities. These rules try to avoid requirements which might
result in unreasonable hardship, or unnecessary inconvenience or interference with the normal use and occupancy of
a building, but at the same time insist upon compliance with uniform standards for fire safety consistent with the
public interest, even though a financial hardship may result in some individual cases. Rulemaking Authority 633.104, 633.206 FS. Law Implemented 429.11, 633.206 FS. History–New 11-29-89, Amended 1-7-97,
Formerly 4A-40.023.
69A-40.024 Scope.
(1) These rules apply to any institution, building, or buildings, residence, private home, boarding home, home
for the aged, or any other place, whether operated for profit or not, which is an assisted living facility under the
definitions of Chapter 429, F.S., and of Chapter 58A-5, F.A.C., and include the intergenerational respite care
assisted living facility created pursuant to Section 429.071, F.S. These rules do not apply to transient rentals, as
defined in Section 212.03, F.S.
(2) These rules are concerned with life safety during fires and similar emergencies. They address particular
matters of construction, protection and occupancy of buildings to try to minimize danger to life from fire, smoke,
fumes, or panic before buildings are vacated. Rulemaking Authority 633.104, 633.206 FS. Law Implemented 429.41, 633.206 FS. History–New 11-29-89, Amended 1-7-97,
Formerly 4A-40.024, Amended 1-15-07.

13 – 2
69A-40.027 Definitions.
(1) “Administrator” shall mean an individual who has general administrative charge of an assisted living
facility.
(2) “Assisted Living Facility” (ALF) shall be as defined in Section 429.02(5), F.S. The definition does not apply
to transient rentals as defined in Section 509.013(11), F.S. For firesafety purposes, the size of the facility is
determined by the license as issued by the Agency for Health Care Administration.
(3) “Authority having jurisdiction” shall mean the governmental entity, organization, office, or individual
responsible by law or ordinance to conduct and enforce uniform fire safety requirements in accordance with Section
633.206(2)(b), F.S.
(4) “Existing” shall refer to any assisted living facility that has been licensed prior to January 1, 1996.
(5) “Final Administrative Interpreting Authority” shall mean the State Fire Marshal.
(6) “Intergenerational Respite Care Assisted Living Facility” means a facility licensed pursuant to a 5 year pilot
program established by the Agency for Health Care Administration to provide temporary personal, respite, and
custodial care to minors and adults with disabilities and elderly persons with special needs who do not require 24-
hour nursing services, and that provides respite care services for minors and adults with disabilities and elderly
persons with special needs for a period of at least 24 hours but not more than 14 consecutive days, in which minors
and adults reside in distinct and separate living units, with a maximum of 48 beds located in Miami-Dade County,
and is operated as a not-for-profit entity.
(7) “NFPA” is the abbreviation for the National Fire Protection Association.
(8) “Owner” shall refer to the person, partnership, association, or corporation that owns the assisted living
facilities enterprise, whether licensed or not. In the event a facility is operated by a person that leases the physical
plant which is owned by another person, “owner” means the person that operates the facility. When the person that
owns the physical plant is an affiliate of the person that operates the facility and has significant control over the day-
to-day operation for the facility, he is considered an owner of the facility.
(9) “Point of Safety” shall be as defined in Chapter 22 and 23, NFPA 101, Life Safety Code, incorporated by
reference in subsection 69A-40.028(1), F.A.C.
(10)(a) “Satisfactory Firesafety Inspection” shall mean there are no uncorrected firesafety deficiencies in the
facility associated with fire alarm systems, installed fire sprinkler systems, or means of egress/escape components.
For purposes of this definition, firesafety deficiencies associated with maintenance items, such as “an exit light
burned out” or “an electrical wall outlet cover plate missing”, would not be considered as items for an unsatisfactory
firesafety inspection.
(b) Facilities shall be granted a period of time to correct firesafety deficiencies that are determined by the
firesafety authority having jurisdiction citing the deficiencies. The time periods granted shall be based on the risk to
life and property created by the violation and the ease of correction. Those existing facilities that are required to
install fire sprinkler systems shall be granted the time frames specified in Section 429.41(1)(a)2.i., F.S.
(c) During these time frames, the lack of a required fire sprinkler system shall not be grounds for denial of a
“Satisfactory Firesafety Inspection.” Rulemaking Authority 633.104, 633.206 FS. Law Implemented 429.41, 633.206 FS. History–New 11-29-89, Amended 1-7-97,
Formerly 4A-40.027, Amended 1-15-07.

13 – 3
69A-40.028 Standards of the National Fire Protection Association Adopted.
(1) Assisted living facilities shall comply with Chapter 22 or 23, of the “Life Safety Code”, NFPA 101, 1994
Edition, adopted and incorporated herein by reference, except as modified by Chapter 429, F.S.
(2)(a) When Chapters 22 and 23 of NFPA 101 Life Safety Code, 1994 edition, refer to other chapters or
sections of the Code or other NFPA standards, the referenced standard shall be as stated in chapter 32, NFPA 101,
Life Safety Code, 1994 edition, as is adopted and incorporated in subsection (1) above. Those standards are adopted
and incorporated by reference and are as follows:
NFPA 10-1990, Standard for Portable Fire Extinguishers
NFPA 13-1994, Standard for the Installation of Sprinkler Systems
NFPA 13D-1994, Standard for the Installation of Sprinkler Systems in One- and Two-Family Dwellings and
Manufactured Homes
NFPA 13R-1994, Standard for the Installation of Sprinkler Systems in Residential Occupancies up to and including
Four Stories in Height
NFPA 14-1993, Standard for the Installation of Standpipe and Hose Systems
NFPA 25-1992, Standard for the Inspection, Testing, and Maintenance of Water-Based Fire Protection Systems
NFPA 30-1993, Flammable and Combustible Liquids Code
NFPA 31-1992, Standard for the Installation of Oil Burning Equipment
NFPA 40-1988, Standard for the Storage and Handling of Cellulose Nitrate Motion Picture Film
NFPA 45-1991, Standard on Fire Protection for Laboratories Using Chemicals
NFPA 54-1992, National Fuel Gas Code
NFPA 58-1992, Standard for Storage and Handling of Liquefied Petroleum Gases
NFPA 70-1993, National Electrical Code
NFPA 72-1993, National Fire Alarm Code
NFPA 80-1992, Standard for Fire Doors and Fire Windows
NFPA 82-1994, Standard on Incinerators and Waste and Linen Handling Systems and Equipment
NFPA 88A-1991, Standard for Parking Structures
NFPA 90A-1993, Standard for the Installation of Air Conditioning and Ventilating Systems
NFPA 90B-1993, Standard for the Installation of Warm Air Heating and Air Conditioning Systems
NFPA 91-1992, Standard for Exhaust Systems for Air Conveying of Materials
NFPA 96-1994, Standard for Ventilation Control and Fire Prevention of Commercial Cooking Operations
NFPA 99-1993, Standard for Health Care Facilities
NFPA 102-1992, Standard for Assembly Seating, Tents, and Membrane Structures
NFPA 110-1993, Standard for Emergency and Standby Power Systems
NFPA 111-1993, Standard on Stored Electrical Energy Emergency and Standby Power Systems
NFPA 211-1992, Standard for Chimneys, Fireplaces, Vents and Solid Fuel Burning Appliances
NFPA 220-1992, Standard on Types of Building Construction
NFPA 241-1993, Standard for Safeguarding Construction, Alteration, and Demolition Operations
NFPA 251-1990, Standard Methods of Fire Tests of Building Construction and Materials
NFPA 252-1990, Standard Methods of Fire Tests of Door Assemblies

13 – 4
NFPA 253-1990, Standard Methods of Test for Critical Radiant Flux of Floor Covering Systems Using a Radiant
Heat Energy Source
NFPA 255-1990, Standard Method of Test of Surface Burning Characteristics of Building Materials
NFPA 256-1993, Standard Methods of Fire Tests of Roof Coverings
NFPA 257-1990, Standard for Fire Tests of Window Assemblies
NFPA 260-1994, Standard Methods of Tests and Classification Systems for Cigarette Ignition Resistance of
Components of Upholstered Furniture
NFPA 261-1994, Standard Method of Test for Determining Resistance of Mock-Up Upholstered Furniture Material
Assemblies to Ignition by Smoldering Cigarettes
NFPA 265-1994, Standard Methods of Fire Tests for Evaluating Room Fire Growth Contribution of Textile Wall
Coverings
NFPA 701-1989, Standard Methods of Fire Tests for Flame-Resistant Textiles and Films
NFPA 703-1992, Standard for Fire Retardant Impregnated Wood and Fire Retardant Coatings for Building Materials
NFPA 1126-1992, Standard for the Use of Pyrotechnics before a Proximate Audience
(b) The codes and standards published by the National Fire Protection Association may be obtained by writing to the
NFPA at: 1 Batterymarch Park, Quincy, Massachusetts 02269. All standards incorporated by reference in this rule
are also available for public inspection during regular business hours at the Division of Fire Marshal, Larson
Building, 200 East Gaines Street, Tallahassee, Florida.
(3) The Evacuation Capability Evaluation shall be in accordance with chapter 5, NFPA 101A, Guide on
Alternative Approaches to Life Safety, 1995 edition, which is adopted and incorporated herein by reference. Rulemaking Authority 633.104, 633.206 FS. Law Implemented 429.11, 633.206 FS. History–New 11-29-89, Amended 1-7-97,
Formerly 4A-40.028.
69A-40.029 Evacuation Capability Evaluation.
(1) The assisted living facility administrator shall conduct an “Evacuation Capability Evaluation” and the local
authority having jurisdiction shall validate the evacuation capability evaluation as required in Section 429.41(1)(a),
F.S. For purposes of this section, “validate” shall mean that the evacuation capability evaluation forms are reviewed
by the local authority having jurisdiction to insure completeness in accordance with Chapter 5, NFPA 101A, Guide
on Alternative Approaches to Life Safety, 1995 edition, as incorporated in subsection 69A-40.028(3), F.A.C.
(2) Existing, licensed, sprinklered ALF’s are not required to conduct an evacuation capability evaluation. The
State Fire Marshal’s office does recommend that evacuation capability be determined using a method acceptable to
the local authority having jurisdiction over fire safety.
(3) Residents shall be permitted to relocate to a “Point of Safety” as defined in subsection 69A-40.027(9),
F.A.C., and as specified in Section 429.41(1)(a)1.a., F.S. Rulemaking Authority 633.104, 633.206 FS. Law Implemented 429.11, 429.41(1)(a), 633.206 FS. History–New 11-29-89,
Amended 1-7-97, Formerly 4A-40.029.
69A-40.031 Automatic Fire Sprinkler Systems.
All requirements relating to automatic fire sprinkler systems for assisted living facilities are identified in Section
429.41(1)(a), F.S. Rulemaking Authority 633.104, 633.206 FS. Law Implemented 429.11, 429.41(1)(a), 633.206 FS. History–New 11-29-89,
Amended 1-7-97, Formerly 4A-40.031.
13 – 5
69A-40.033 Heating, Ventilating, and Air Conditioning Equipment.
In accordance with the applicable sections of Chapters 22 and 23, NFPA 101, Life Safety Code, 1994 edition, small
facilities (16 or fewer residents) are not required to comply with NFPA 96, Standard on Ventilation Control and Fire
Protection of Commerical Cooking Operations. Large facilities shall comply with NFPA 96. Rulemaking Authority 633.104, 633.206 FS. Law Implemented 429.11, 633.206 FS. History–New 11-29-89, Amended 1-7-97,
Formerly 4A-40.033.
69A-40.035 Code Conflict Resolution.
(1) Code enforcement conflict resolution of code issues cited by local government shall be resolved by the local
governmental agency and city and/or county enforcement boards which have been established and identified in
Section 553.73, F.S.
(2) Code enforcement conflict resolution of code issues cited by the Agency for Health Care Administration
(AHCA) should be resolved between the Agency for Health Care Administration and the authority having
jurisdiction.
(3) The State Fire Marshal’s Office is the final administrative interpreting authority and as such will render
interpretations and explanations of the codes. Rulemaking Authority 633.104, 633.206 FS. Law Implemented 429.11, 633.206 FS. History–New 11-29-89, Amended 1-7-97,
Formerly 4A-40.035.
69A-40.036 Fire Exit Drills.
(1) An existing, unsprinklered ALF shall conduct fire exit drills monthly and at least twelve fire drills shall have
been conducted during the previous year (four times per year on each new shift). New facilities with eight or fewer
residents and a “Prompt” evacuation capability evaluation shall follow the above guidelines. If a facility has been in
operation less than one year, it shall be permitted to have conducted a fire drill for each month of its operation.
(2) A new or existing sprinklered ALF shall conduct at least six fire drills per year, one every two months, with
a minimum of two drills conducted during the night when residents are sleeping.
(3) Facilities that are fully sprinklered and in compliance with other firesafety standards are not required to
conduct more than one of the required fire drills between the hours of 11 p.m. and 7 a.m. per year.
(4) Residents shall be permitted to relocate to a “Point of Safety” as defined in subsection 69A-40.027(8),
F.A.C., and as specified in Section 429.41(1)(a), F.S. Rulemaking Authority 633.104, 622.206 FS. Law Implemented 429.11, 633.206 FS. History–New 1-7-97, Formerly 4A-40.036.
69A-40.037 Intergenerational Respite Care Assisted Living Facility.
(1) The living area for any minor, including the available means of egress, shall be on the level of exit
discharge.
(2) Each living area or portion of living area for personal use, comprised of bathrooms, bathing areas, and
sleeping areas serving minors, shall be served by exits separate from those serving other intergenerational respite
care residents.
(3) Any exit designed to serve both minors and adults in any area other than the living area or portion of the
living area for personal use referred to in subsection (2), such as living rooms and dining areas, shall be increased in
size to 1.5 times the minimum required egress width. Rulemaking Authority 633.104, 633.206 FS. Law Implemented, 429.41, 633.206 FS. History–New 1-15-07.

13 – 6
Notes ______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________

14. Appendix


Appendix Table of Contents
SECTION APPENDIX
Links to Documents Incorporated in Rule and Resource Websites. . . . . . . . . . . . . . . . . . . . . . . . . . . A
Resident Health Assessment for ALFs – AHCA 1823 Form (March 2017) . . . . . . . . . . . . . . . . . . . . .B
Attestation of Compliance with Background Screening Requirements. . . . . . . . . . . . . . . . . . . . . . . . C
AHCA Consumer Friendly Summary of the Emergency Environmental Control Plan . . . . . . . . . . D
Community Residential Homes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . E
Community Living Support Plan and Cooperative Agreement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . F
Health Care Advance Directives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .G
Do Not Resuscitate Order . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . H
U.S. FDA Food Code 2013 (specific sections referenced in 64E-11).. . . . . . . . . . . . . . . . . . . . . . . . . . . I
Department of Health Physical Plant Standards Important Notice . . . . . . . . . . . . . . . . . . . . . . . . . . . J
Department of Health Physical Plant Standard Forms. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .K
ALF Staff Training Requirements Table . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .L

[This space intentionally left blank.]

A– 1
Appendix A – Documents Incorporated in Rule and Resource Websites
Documents & Links Incorporated in Rule • AHCA Assisted Living Unit (licensing documents and requirements)
www.ahca.myflorida.com/MCHQ/Health_Facility_Regulation/Assisted_Living/alf.shtml
• AHCA Hotline Poster (scroll down to Nursing Home Links and click on “Hotline Poster”)
ahca.myflorida.com/publications/Publications.shtml
• Long-Term Care Ombudsman Residents’ Rights Poster (towards bottom of webpage)
ombudsman.myflorida.com/Publications.php
• Choose My Plate – www.choosemyplate.gov
• Food Code – U.S. Public Health Service https://www.fda.gov/Food/GuidanceRegulation/RetailFoodProtection/FoodCode/default.htm
• Food Service Establishment Plan Review Form DH8003-DCHP-02/2018
https://www.flrules.org/Gateway/reference.asp?No=Ref-09903
• USDA Dietary Guidelines for Americans, 2010
• https://www.flrules.org/gateway/readRefFile.asp?refId=4003&filename=Rule%205.020%202a%20Dietary%20
Guidelines.pdf
• Application for Sanitation Certificate Form DH 4086 02/18 – can be found at
https://www.flrules.org/Gateway/reference.asp?No=Ref-09902
• Do Not Resuscitate Orders (Must be printed on YELLOW paper) – can be found at http://www.floridahealth.gov/about-the-department-of-health/about-us/patient-rights-and-safety/do-not-
resuscitate/index.html
Useful Resources
• Florida Senior Living Association Website – www.floridaseniorliving.org
• Agency for Health Care Administration (main website) – www.ahca.myflorida.com
• AHCA ALF Aspen State Regulation Set (select assisted living facility)
https://ahca.myflorida.com/MCHQ/Field_Ops/Regulations/Current_Regs.shtml
• AHCA Top Ten Deficiencies (click on report name for the most current year under Facility Surveys
– Most Frequently Cited Health and Life Safety Deficiencies) https://ahca.myflorida.com/Publications/Publications.shtml
• Background Screening Webpage (access the Background Screening Clearinghouse Portal)
ahca.myflorida.com/MCHQ/Central_Services/Background_Screening/index.shtml
• FloridaHealthFinder.gov – http://floridahealthfinder.gov/index.html
• USF ALF Test Registration Link – www.alf.usf.edu

[This space intentionally left blank.]

B – 1
Appendix B – Resident Health Assessment for ALFS – AHCA 1823 Form (March 2017)
Form can be found at https://www.flrules.org/Gateway/reference.asp?No=Ref-09170

B – 2

B – 3

B – 4
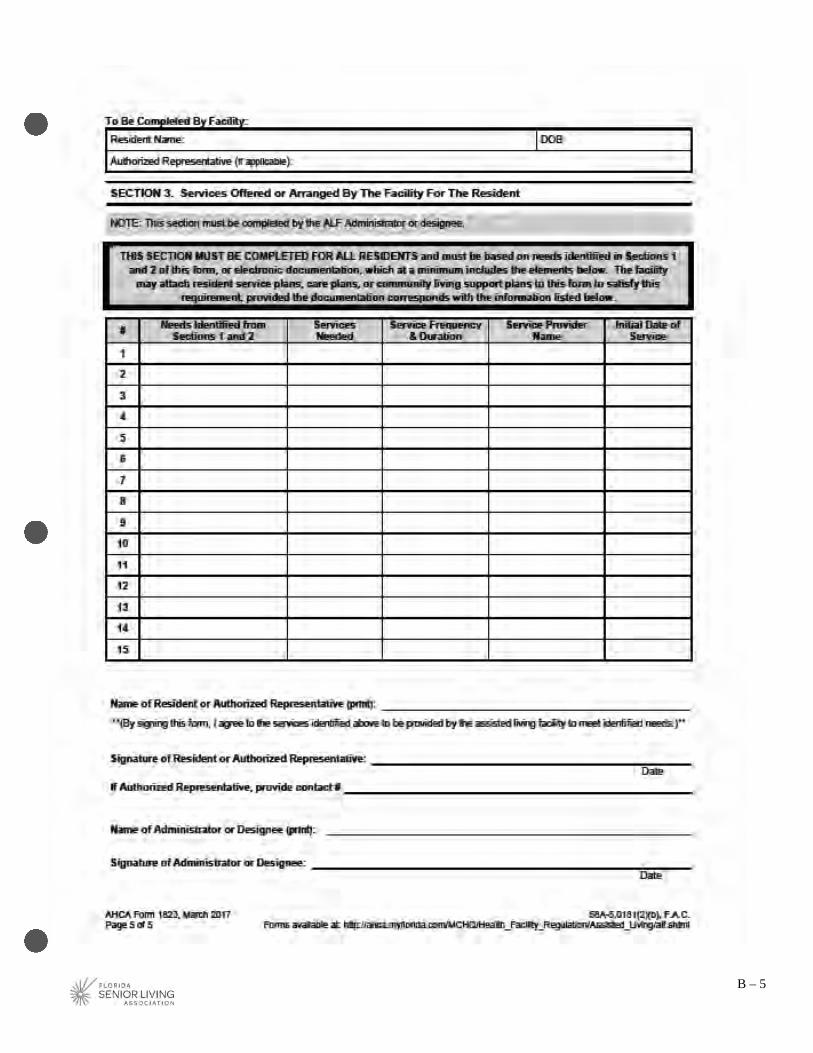
B – 5

[This space intentionally left blank.]

C– 1
Appendix C – Attestation of Compliance with Background Screening
Attestation and additional forms can be found on AHCA’s Background Screening webpage at
https://ahca.myflorida.com/MCHQ/Central_Services/Background_Screening/Regulations_Forms.shtml

C– 2

C– 3

C– 4

D– 1
Appendix D – AHCA Consumer-Friendly Summary of the Emergency
Environmental Control Plan - It can be found at
http://www.ahca.myflorida.com/MCHQ/Health_Facility_Regulation/Assisted_Living/alf.shtml
D– 2
[This space intentionally left blank.]

E – 1
Appendix E – Community Residential Homes
Chapter 419, F.S., Community Residential Homes, requires that applicants meeting certain size and location
criteria comply with notice to the local zoning authority. Facilities can complete the Community Residential Home
Affidavit of Compliance with Chapter 419, Florida Statutes form on the following page once the information has
been verified and obtained from the following agencies.
Verify this information by contacting the following entities.
• Homes licensed by the Agency for Health Care Administration--visit the AHCA website
at http://www.floridahealthfinder.gov*
• Homes licensed by the Department of Children and Families--visit the DCF website
at http://www.dcf.state.fl.us/regions/ to locate the Community Residential Home licensing staff in the
appropriate district.
• Homes licensed by the Agency for Persons with Disabilities--visit the APD website
at http://www.flddresources.org/html/contact_us.htm to locate the APD staff in the appropriate district.
* (Please do not use as the sole source of information for determining distance between community
residential homes.)

E – 2
Community Residential Home Affidavit of Compliance Recommended Form – can be found at
http://ahca.myflorida.com/MCHQ/Health_Facility_Regulation/Hospital_Outpatient/forms/CommResHome
_AffidavitofComplianceWithCh419.pdf

F – 1
Appendix F – Community Living Support Plan and Cooperative Agreement Found at http://ahca.myflorida.com/MCHQ/Health_Facility_Regulation/Assisted_Living/alf.shtml under resources
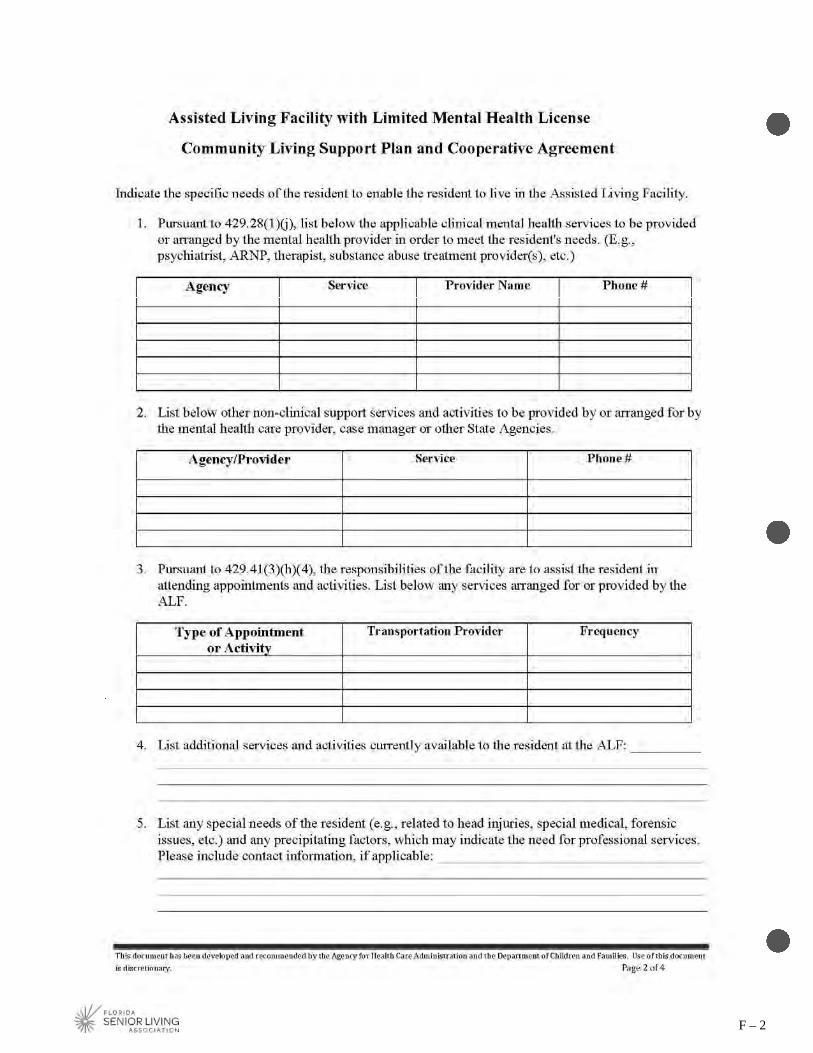
F – 2

F – 3
F – 4

G – 1
Appendix G – Health Care Advance Directives The Patient’s Right to Decide Every competent adult has the right to make decisions concerning his or her own health, including the right to choose or refuse
medical treatment.
When a person becomes unable to make decisions due to a physical or mental change, such as being in a coma or developing dementia
(like Alzheimer’s disease), they are considered incapacitated. Only your primary physician can determine if you are incapacitated. To
make sure that an incapacitated person’s decisions about health care will still be respected, the Florida legislature enacted legislation
pertaining to health care advance directives (Chapter 765, Florida Statutes). The law recognizes the right of a competent adult to
make an advance directive instructing his or her physician to provide, withhold, or withdraw life-prolonging procedures; to designate
another individual to make treatment decisions if the person becomes unable to make his or her own decisions; and/or to indicate the
desire to make an anatomical donation after death. Additionally, the law states that you do not have to be incapacitated to elect a
health care surrogate to make your decisions.
By law hospitals, nursing homes, home health agencies, hospices, and health maintenance organizations (HMOs) are required to
provide their patients with written information, such as this pamphlet, concerning health care advance directives. The state rules that
require this include 58A-2.0232, 59A-3.254, 59A-4.106, 59A-8.0245, and 59A-12.013, Florida Administrative Code.
Questions About Health Care Advance Directives
What is an advance directive?
It is a written or oral statement about how you want medical decisions made should you not be able to make them yourself and/or
it can express your wish to make an anatomical donation after death. Some people make advance directives when they are
diagnosed with a life-threatening illness. Others put their wishes into writing while they are healthy, often as part of their estate
planning.
Three types of advance directives are:
• A Living Will
• A Health Care Surrogate Designation
• An Anatomical Donation
You might choose to complete one, two, or all three of these forms. This pamphlet provides information to help you decide what will
best serve your needs.
What is a living will?
It is a written or oral statement of the kind of medical care you want or do not want if you become unable to make your own
decisions. It is called a living will because it takes effect while you are still living. You may wish to speak to your health care
provider or attorney to be certain you have completed the living will in a way that your wishes will be understood.
What is a health care surrogate designation?
It is a document naming another person as your representative to make medical decisions for you if you are unable to make them
yourself. You can include instructions about any treatment you want or do not want, similar to a living will. You can also
designate an alternate surrogate.
Which is best?
Depending on your individual needs you may wish to complete any one or a combination of the three types of advance directives.
What is an anatomical donation?
It is a document that indicates your wish to donate, at death, all or part of your body. This can be an organ and tissue donation to
persons in need, or donation of your body for training of health care workers. You can indicate your choice to be an organ donor

G – 2
by designating it on your driver’s license or state identification card (at your nearest driver’s license office), signing a uniform
donor form (seen elsewhere in this pamphlet), or expressing your wish in a living will.
Am I required to have an advance directive under Florida law?
No, there is no legal requirement to complete an advance directive. However, if you have not made an advance directive,
decisions about your health care or an anatomical donation may be made for you by a court-appointed guardian, your wife or
husband, your adult child, your parent, your adult sibling, an adult relative, or a close friend.
The person making decisions for you may or may not be aware of your wishes. When you make an advance directive, and
discuss it with the significant people in your life, it will better assure that your wishes will be carried out the way you want.
Must an attorney prepare the advance directive?
No, the procedures are simple and do not require an attorney, though you may choose to consult one.
However, an advance directive, whether it is a written document or an oral statement, needs to be witnessed by two
individuals. At least one of the witnesses cannot be a spouse or a blood relative.
Where can I find advance directive forms?
Florida law provides a sample of each of the following forms: a living will, a health care surrogate, and an anatomical
donation. Elsewhere in this pamphlet we have included sample forms as well as resources where you can find more information
and other types of advance directive forms.
Can I change my mind after I write an advance directive?
Yes, you may change or cancel an advance directive at any time. Any changes should be written, signed and dated. However, you
can also change an advance directive by oral statement; physical destruction of the advance directive; or by writing a new
advance directive.
If your driver’s license or state identification card indicates you are an organ donor, but you no longer want this designation, contact
the nearest driver’s license office to cancel the donor designation and a new license or card will be issued to you.
What if I have filled out an advance directive in another state and need treatment in Florida?
An advance directive completed in another state, as described in that state's law, can be honored in Florida.
What should I do with my advance directive if I choose to have one?
• If you designate a health care surrogate and an alternate surrogate be sure to ask them if they agree to take this responsibility,
discuss how you would like matters handled, and give them a copy of the document.
• Make sure that your health care provider, attorney, and the significant persons in your life know that you have an advance
directive and where it is located. You also may want to give them a copy.
• Set up a file where you can keep a copy of your advance directive (and other important paperwork). Some people keep original
papers in a bank safety deposit box. If you do, you may want to keep copies at your house or information concerning the
location of your safety deposit box.
• Keep a card or note in your purse or wallet that states that you have an advance directive and where it is located.
• If you change your advance directive, make sure your health care provider, attorney and the significant persons in your life have
the latest copy.
If you have questions about your advance directive you may want to discuss these with your health care provider, attorney, or the
significant persons in your life.
More Information On Health Care Advance Directives
Before making a decision about advance directives you might want to consider additional options and other sources of information,
including the following:

G – 3
• As an alternative to a health care surrogate, or in addition to, you might want to designate a durable power of attorney. Through
a written document you can name another person to act on your behalf. It is similar to a health care surrogate, but the person
can be designated to perform a variety of activities (financial, legal, medical, etc.). You can consult an attorney for further
information or read Chapter 709, Florida Statutes.
If you choose someone as your durable power of attorney be sure to ask the person if he or she will agree to take this
responsibility, discuss how you would like matters handled, and give the person a copy of the document.
• If you are terminally ill (or if you have a loved one who is in a persistent vegetative state) you may want to consider having a
pre-hospital Do Not Resuscitate Order (DNRO). A DNRO identifies people who do not wish to be resuscitated from
respiratory or cardiac arrest. The pre-hospital DNRO is a specific yellow form available from the Florida Department of Health
(DOH). Your attorney, health care provider, or an ambulance service may also have copies available for your use. You, or
your legal representative, and your physician sign the DNRO form. More information is available on the DOH website
or www.MyFlorida.com (type DNRO in these website search engines) or call (850) 245-4440.
When you are admitted to a hospital the pre-hospital DNRO may be used during your hospital stay or the hospital may have its
own form and procedure for documenting a Do Not Resuscitate Order.
• If a person chooses to donate, after death, his or her body for medical training and research the donation will be coordinated by
the Anatomical Board of the State of Florida. You, or your survivors, must arrange with a local funeral home, and pay, for a
preliminary embalming and transportation of the body to the Anatomical Board located in Gainesville, Florida. After being
used for medical education or research, the body will ordinarily be cremated. The cremains will be returned to the loved ones,
if requested at the time of donation, or the Anatomical Board will spread the cremains over the Gulf of Mexico. For further
information contact the Anatomical Board of the State of Florida at (800) 628-2594 or www.med.ufl.edu/anatbd.
• If you would like to learn more on organ and tissue donation, please visit the Joshua Abbott Organ and Tissue Donor Registry
at www.DonateLifeFlorida.org where you can become organ, tissue and eye donors online. If you have further questions about
organ and tissue donation you may want to talk to your health care provider.
• Various organizations also make advance directive forms available. One such document is “Five Wishes” that includes a living
will and a health care surrogate designation. “Five Wishes” gives you the opportunity to specify if you want tube feeding,
assistance with breathing, pain medication, and other details that might bring you comfort such as what kind of music you
might like to hear, among other things. You can find out more at:
Aging with Dignity
www.AgingWithDignity.org
(888) 594-7437
Other resources include:
American Association of Retired Persons (AARP)
www.aarp.org (Type “advance directives” in the website’s search engine)
Your local hospital, nursing home, hospice, home health agency, and your attorney or health care provider may be able to assist
you with forms or further information.
Brochure: End of Life Issues
www.FloridaHealthFinder.gov
(888) 419-3456

G – 4
Sample Living Will – can be found at
https://fhfstore.blob.core.windows.net/documents/reports-guides/documents/LivingWill.pdf

G – 5

G – 6
Sample Designation of Health Care Surrogate – can be found at https://fhfstore.blob.core.windows.net/documents/reports-guides/documents/DesignationofHealthCareSurrogate.pdf

G – 7
Sample Designation of Health Care Surrogate – can be found at https://fhfstore.blob.core.windows.net/documents/reports-guides/documents/DesignationofHealthCareSurrogate.pdf

G – 8
Sample Designation of Health Care Surrogate – can be found at https://fhfstore.blob.core.windows.net/documents/reports-guides/documents/DesignationofHealthCareSurrogate.pdf
The card below may be used as a convenient method to inform others of your health care advance directives. Complete
the card and cut it out. Place in your wallet or purse. You can also make copies and place another one on your
refrigerator, in your car glove compartment or other easy to find place.
Produced and distributed by the Florida Agency for Health Care Administration. This publication can be copied for public use. To
view or print other publications from the Agency for Health Care Administration please visit www.FloridaHealthFinder.gov.

H – 1
Appendix H – Do Not Resuscitate Orders (Must be printed on YELLOW paper) Found at http://www.floridahealth.gov/about-the-department-of-health/about-us/patient-rights-and-safety/do-not-
resuscitate/index.html

H – 2

I– 1
Appendix I – 64E-11 Specific U.S. FDA Food Code 2013 Food Service Establishment Plan Review Form DH8003-DCHP-02/2018 – can be found at
https://www.fda.gov/Food/GuidanceRegulation/RetailFoodProtection/FoodCode/default.htm
(click on current food code adopted in rule to download entire code)
Applicable sections of the Food Code 2013 referenced in 64E-11, F.A.C.:
Chapter 1
Chapter 2, Sections 2-2 through 2-5
Chapter 3, Section 3-2 through 3-8
Chapter 4
Chapter 5
Chapter 6
Chapter 7

I– 2

I– 3
Food Code 2013 – Chapter 1

I– 4

I– 5

I– 6

I– 7

I– 8

I– 9

I– 10

I– 11

I– 12

I– 13

I– 14

I– 15

I– 16

I– 17

I– 18

I– 19

I– 20

I– 21

I– 22

I– 23

I– 24

I– 25

I– 26

I– 27
Food Code 2013 – Chapter 2, Sections 2-2 Through 2-5

I– 28

I– 29

I– 30

I– 31

I– 32

I– 33
I– 34

I– 35

I– 36

I– 37

I– 38

I– 39

I– 40
I– 41

I– 42

I– 43

I– 44

I– 45

I– 46

I– 47

I– 48
Food Code 2013 – Chapter 3, Section 3-2

I– 49

I– 50

I– 51

I– 52

I– 53

I– 54

I– 55

I– 56

I– 57

I– 58

I– 59
Food Code 2013 – Chapter 3, Sections 3-3 Through 3-8

I– 60

I– 61

I– 62

I– 63

I– 64

I– 65

I– 66

I– 67

I– 68

I– 69

I– 70

I– 71

I– 72

I– 73

I– 74

I– 75

I– 76

I– 77

I– 78

I– 79

I– 80

I– 81

I– 82

I– 83

I– 84

I– 85

I– 86

I– 87

I– 88

I– 89

I– 90

I– 91

I– 92

I– 93

I– 94

I– 95

I– 96

I– 97

I– 98

I– 99

I– 100

I– 101

I– 102

I– 103
Food Code 2013 – Chapter 4

I– 104

I– 105

I– 106

I– 107

I– 108

I– 109

I– 110

I– 111
I– 112

I– 113

I– 114

I– 115

I– 116

I– 117

I– 118

I– 119

I– 120

I– 121

I– 122

I– 123

I– 124

I– 125

I– 126
I– 127

I– 128

I– 129

I– 130

I– 131

I– 132

I– 133

I– 134
I– 135

I– 136

I– 137

I– 138

I– 139
I– 140

I– 141

I– 142

I– 143

I– 144

I– 145
I– 146
Food Code 2013 – Chapter 5

I– 147

I– 148

I– 149

I– 150

I– 151

I– 152

I– 153

I– 154

I– 155
I– 156

I– 157

I– 158

I– 159

I– 160

I– 161

I– 162

I– 163

I– 164

I– 165

I– 166
Food Code 2013 – Chapters 6 & 7

I– 167

I– 168

I– 169

I– 170

I– 171

I– 172

I– 173

I– 174

I– 175

I– 176

I– 177

I– 178

I– 179
I– 180

I– 181

I– 182

I– 183

I– 184

I– 185

I– 186

I– 187

I– 188

I– 189

I– 190
[This space intentionally left blank.] [This space intentionally left blank.]


J – 1
Appendix J – DOH Physical Plant Standards Important Notice Found at http://ahca.myflorida.com/MCHQ/Health_Facility_Regulation/Assisted_Living/alf.shtml under resources
[This space intentionally left blank.]

K – 1
Appendix K – DOH Physical Plant Standards Forms Food Service Establishment Plan Review Form DH8003-DCHP-02/2018 – can be found at
https://www.flrules.org/Gateway/reference.asp?No=Ref-09903 (click on the pdf to download)

K – 2
Application for Sanitation Certificate Form DH 4086 02/18 – can be found at
https://www.flrules.org/Gateway/reference.asp?No=Ref-09902 (click on the pdf to download)

L – 1
Appendix L – ALF Staff Training Requirements Table

L – 2

L – 3

L – 4

L – 5

M– 1
This page left intentionally blank.
Copyright © 2022 FDOKUMEN




















