List of Essential Medicinal Plants and their Therapeutic ...
Upload
khangminh22Category
view
1download
0
Approaches towards Evaluation of Medicinal Plants prior to
Clinical Trials
Organized By
The Foundation for Medical Research 84-A, R. G. Thadani Marg, Worli, Mumbai – 400018, India
At
Yashwantrao Chavan Academy of Development Administration (YASHADA), Pune, India
November 8, 2006
Proceedings

Acknowledgements
The Foundation for Medical Research gratefully acknowledges the funding
support received for the workshop from the Pirojsha Godrej Foundation, Mumbai,
the Council of Scientific and Industrial Research, Government of India and The
Lotus Trust, Mumbai.
The publication of the workshop proceedings has been made possible through
the funding obtained from the Hinduja Foundation, Mumbai.
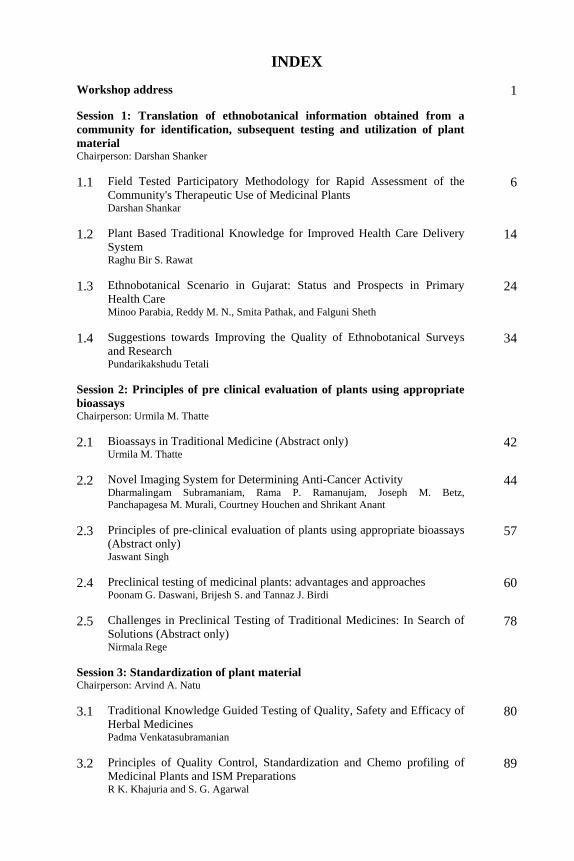
INDEX Workshop address
1
Session 1: Translation of ethnobotanical information obtained from a community for identification, subsequent testing and utilization of plant material Chairperson: Darshan Shanker
1.1 Field Tested Participatory Methodology for Rapid Assessment of the Community's Therapeutic Use of Medicinal Plants Darshan Shankar
6
1.2 Plant Based Traditional Knowledge for Improved Health Care Delivery System Raghu Bir S. Rawat
14
1.3 Ethnobotanical Scenario in Gujarat: Status and Prospects in Primary Health Care Minoo Parabia, Reddy M. N., Smita Pathak, and Falguni Sheth
24
1.4 Suggestions towards Improving the Quality of Ethnobotanical Surveys and Research Pundarikakshudu Tetali
34
Session 2: Principles of pre clinical evaluation of plants using appropriate bioassays Chairperson: Urmila M. Thatte
2.1 Bioassays in Traditional Medicine (Abstract only)
Urmila M. Thatte
42
2.2 Novel Imaging System for Determining Anti-Cancer Activity Dharmalingam Subramaniam, Rama P. Ramanujam, Joseph M. Betz, Panchapagesa M. Murali, Courtney Houchen and Shrikant Anant
44
2.3 Principles of pre-clinical evaluation of plants using appropriate bioassays (Abstract only) Jaswant Singh
57
2.4 Preclinical testing of medicinal plants: advantages and approaches Poonam G. Daswani, Brijesh S. and Tannaz J. Birdi
60
2.5 Challenges in Preclinical Testing of Traditional Medicines: In Search of Solutions (Abstract only)
Nirmala Rege
78
Session 3: Standardization of plant material Chairperson: Arvind A. Natu
3.1 Traditional Knowledge Guided Testing of Quality, Safety and Efficacy of Herbal Medicines Padma Venkatasubramanian
80
3.2 Principles of Quality Control, Standardization and Chemo profiling of Medicinal Plants and ISM Preparations R K. Khajuria and S. G. Agarwal
89

3.3 Approaches to Standardization of Medicinal Plant Preparations Brijesh S., Poonam G. Daswani and Tannaz J. Birdi
102
3.4 Medicinal Plant Compositional Consistency for Reliable Therapeutic Action Profiling: Key Issues and Concerns for Phytotherapeutics Rajender S. Sangwan
119
Abridged overview
129
List of participants
136

Workshop Address
Dr. Antia, ladies and gentlemen,
Good morning and welcome to this historic city of the Peshwas and to this
workshop organized by the Foundation for medical Research, Mumbai.
Established in 1974 as a public trust and an educational institute affiliated to the
University of Mumbai and located in a still beautiful area of Mumbai with a
glorious view of the Arabian Sea, this Foundation is 33 years young and is a
brainchild of Dr. Antia who we are honored to have on this dias with us. My
inheritance of piloting this Foundation, which began in September 2006 on Dr.
Antia’s retirement, is built on his mixed legacy of both innovative thought and
compassion both of which can see the light of day only through hard work and
motivation. I would like to take the opportunity of this occasion to pay tribute to
the originator of this precious inheritance, to my teacher and mentor, who has led
this Foundation for the past 33 years not only on the path of excellent and creative
science but also on a path of useful and compassionate science for the people of
this country.
Though small in size, the Foundation has developed a formidable reputation
in all the fields it has touched viz., the neurology and immunology of leprosy,
epidemiology and evolution of drug resistant tuberculosis and the preclinical
screening of medicinal for infectious diseases. The selection of these areas of the
Foundation’s work was guided firstly by the relevance quotient to the health
problems of the vast majority of this country, the availability of elegant but simple
technology to address these problems and the asking of the right questions that
could provide insights to larger and even universal issues.
To talk about the importance of herbal remedies or medicinal plants to this
audience would be impertinent. Nevertheless the work in the area of medicinal
plants was initiated by my senior colleague and long time friend, Tannaz Birdi, in
the late 90’s in collaboration with Vaidya Antarkar and our sister FRCH. The
initial documentation of herbal remedies for diarrhoeal diseases in children
whetted her appetite to ask more challenging questions. Cautious about jumping
straightaway into clinical trials, FMR chose to look at the fundamental area of
1

preclinical testing of antidiarrhoeal plants. This was a generic choice grounded in
several considerations, viz.,
• Geographical and environmental variation in medicinal plant properties
• Symbiotic and antagonistic interaction between plant constituents
• The identification of novel pathways of plant action that exert their action
through host parasite interaction rather than by direct action on pathogens
which unfortunately forms the bulk of screening assays employed currently.
Whilst the thrust in the work was to devise innovative assays that could
identify plant product actions, a rather major but ill expressed goal included a
desire to contribute to a resurgence of India’s traditional science and healing
heritage. The work initiated was meant to provide Ayurveda and modern science
and medicine articulated eloquently by Prof. RD. Lele in his seminal publication.
Ayurveda considers disease as disequilibria at the molecular level either
through excessive interaction between molecules (atiyoga) absence of interaction
(ayoga)) and erroneous interaction (mithyayoga). Restoration of that equilibrium
is the objective of medicine. The tridosh or the personalized concept is essentially
a concept also of molecular biology, which has expanded our understanding of not
only disease but also health through concepts of cell signaling and
communication, repair enzymes and molecular policemen and quiet cellular death
such as apoptosis.
Based on observation and experiential wisdom, Charaka, Sushruta and
Vagbhat described 700 herbal drugs with their properties and clinical effects.
Based on these they described 50 categories of drugs. It is our belief that by
eschewing the pathway of fishing expeditions that the modern pharmaceutical
industry often emplys, subjecting Ayurvedic drugs to mechanism based screening
will be very rewarding because their choice has already been backed by centuries
of experiential wisdom provided. We also consider the dynamism of evolution and
development in modification of plant properties over the centuries. As the R&D
process is long and demands large investments, research interests are lacking in
both industry and academia. Repeated attempts by the DST to arrange meetings
for arriving at preclinical screening norms had no takers and the meetings had to
be eventually cancelled. Pharmacopoeia standards and volumes on 326 single
drugs are published by the AYUSH department but there are no monographs for
2

extracts that could reduce bulk drug utilization, help develop dosages, aid quality
assurance and reduce microbial / symptom burden.
This Workshop has attempted to devise a holistic programme that
encompasses ethnobotany and post assay downstreaming and standardization
besides biological screening in preclinical activities. The size of the Workshop has
been kept deliberately small so that the invited speakers and participants, all of
whom have been significant contributors in their field, can deliberate with focus
and in depth in the substantial time available after the presentations. The lead
discussants selected with same care as the participants have been pre-prepared
with presentation content so that the issues that they raise are critical. The
essential contributions that can be expected from this one day Workshop are
• Addressing of specific pitfalls that are likely to be encountered in the three
areas of ethnobotanical data collection, assay design and standardization
• Articulation of guiding principles for each of the three areas
• Articulation of inputs that pre-clinical screening can provide to clinical trials
• Building of a database for expertise available for each of the areas
These may please be borne in mind during the discussions so that definite
issues and recommendations are possible as outcomes.
It is not customary to thank in-house hands and heads who have helped in
shaping this Workshop. Nevertheless those who have supported this Workshop
with belief and finances deserve a mention:
• Mr. Jamshyd Godrej and the Pirjshah Godrej Foundation for their long-term
support to both FMR and this workshop
• The Hinduja Foundation for their contribution to the publication of the
Workshop proceedings
• The Council for Scientific and Industrial Research of the Govt. of India
• Dr. Bhushan Patwardhan of the University of Pune who lead us to many of
today’s participants and agreed to have this as a quiet satellite of the World
Ayurvedic Congress starting on 10th November at the University
• Our collaborators including the FRCH, Pune and the field investigators at its
rural project site of Parinche in Purandhar taluka; Dr. Tetali and his student
from The Naoroji Godrej Centre for Plant Research at Shirwal; Drs. Natu and
3

Rojatkar from The National Chemical Labs, Pune; Drs. Minoo Parabia and
Kothari from South Gujarat University, Surat; Dr. Bhate from Analytical
Solutions, Mumbai. Our clinician friends include the late Vaidya Antarkar
and Dr. H.B. Singh, formerly of The Poddar Ayurvedic College Mumbai. We
hope we can make more friends and partners by the end of the day.
• The studies at FMR have been funded by Sir Dorabji Tata and Sir Ratan Tata
Trusts, Department of Science and Technology, Government of India and
now The Indian Council for Medical Research.
• Mrs. Jayalakshmi Iyer, FMR, for her administrative assistance throughout.
• Finally I would like to thank Mrs. Rajam John, Col. Phatak for the transport
team of FRCH for supporting us in their home territory. Also the staff of
Yashada for their extreme helpfulness and in ensuring all arrangements.
If the eminent physician Charaka was here instead of me giving you this
introduction then this is what he may have said;
I had charged you to learn the medical texts, but never to lose sight of reason
in the practice of medicine
Obsession with the written word is the habit of the mediocre; the wise go
beyond and inherit the experience of the world.
I urge you to learn from the sages and the shepherds: both are teachers in
their own way
I am not immutable or an icon. You made me one unaware that other nations
are sailing on.
You have taken to heart that where you proclaimed I was super-intelligent, I
have none; where you found plentiful cures in my texts, you now find none.
Distraught you have replaced me with new icons.
You have enthroned reason to the rejection of all other authority and justified
morality only in terms of reason and knowledge. It has escaped you that by setting
them apart you have enslaved morality to knowledge.
Does it worry you that the tree of knowledge without morality has given you a
harvest of bitter fruits?
4

Do not expect miracles of me. I have left you a heritage which though all-
embracing exists within a world of unknown reserves of knowledge, experience
and faith. It behoves you to explore the trackless land as your forefathers did.
But far from seeking only knowledge, you should celebrate a good mind and
good conduct, free from extreme positions and errors of judgement.
In seeking to know my legacy, you but see the leaves of a universal tree too
vast for your eyes. May your sight grow and your quest never ends.
Thank you for your hearing and above all your presence and participation at
this Workshop.
Nerges Mistry, Ph. D. Director, The Foundation for Medical Research
5

1.1 Field Tested Participatory Methodology for Rapid Assessment of the Community's Therapeutic Use of Medicinal Plants Darshan Shankar Foundation for Revitalisatoin of Local Health Traditions (FRLHT), Bangalore – 560064, India Email: [email protected]
1. Introduction
India has had a rich, vibrant and diverse cultural history. An important component
of this culture and tradition is that of health and healing. Thus there is a large
health and healing related knowledge base present in all ethnic communities
across the diverse ecosystems. However, over the last few centuries, this
knowledge base has been diluted with increased influences from the mainstream
culture, which is derisive of local health traditions. It is important to urgently put
in place effective documentation and assessment programs to revitalize local
health traditions otherwise this great people’s health culture will be irretrievably
lost.
There are two key Sanskrit words that describe the nature of the Indian
knowledge society. These are prakrit & sams-krit. The word prakrit refers to
ecosystem & ethnic community specific knowledge traditions. It is derived from
the term prakriti or nature, which means that dynamic phenomenon (kriti) that has
always existed (pra). The prakrit knowledge therefore refers to such emperical
traditions of knowledge that are directly derived from nature they include prakrit
language, arts, music, weaving, agriculture, architecture, and of course healthcare.
The word sams-krit refers to such dynamic phenomenon (kriti) that has been
refined or modified (samskar – from the prakrit state). This word thus refers in
Indian tradition to the various shastras or sciences like linguistics (vyakaran), the
fine and performing arts (shilpa, sangeet, nritya etc.,), agriculture (krishishastra),
architecture (vastu shastra) and healthcare (ayurveda).
In Indian society the samskrit traditions enjoy a symbiotic relationship with
the prakrit because samskriti (culture: in the broad sense of the term including all
arts and sciences) is derived from prakriti (nature). Thus ayurveda and folk
healthcare (lok swasthya parampar) are related and one should not visualize the
6

future of Ayurevda, without envisaging the future of its prakrit counterpart which
lives amongst common folk in the society in both rural and urban areas.
The folk health traditions or lok swasthya paramparas are embedded in the
lifestyle, diet and health practices of thousands of local communities all over
India.
There are estimated to be around a million folk healers in the country. The
break up of these healers is shown in the chart below:
Carriers of village-based health traditions:
Traditional carrier Subjects Numbers Housewives Home remedies – Food & nutrition Millions Traditional Birth Attendants Normal deliveries 7 lakhs Herbal Healers Common ailments 3 lakhs Bone-setters Orthopaedics 60,000 Visha Vaidyas [Snake, Scorpion, Dog]
Natural poisons 60,000
Specialists Eyes Skin Respiratory Dental Arthritis Mental diseases Liver GIT Wounds Fistula/Piles
1000 in every State in rural communities
Figures based on extrapolations from micro-studies.
Apart from the distinct class of folk healers, there are also several millions of
mostly rural (and to a much lesser extent urban) knowledgeable households who
are also carriers of the community based oral health traditions of India. The
households have knowledge of home remedies about local food and their
nutritional value. The health traditions of households are based on the local eco-
system resources.
In the context of self-reliance of local communities in primary health care, it
is very important to strengthen and revitalize these community based health
traditions. Their revitalization holds the key to health security of the rural and
urban poor, even in the 21st century.
7

1.1 Genesis of the Documentation of LHTs.
In the early nineties, the Foundation for the Revitalisation of Local Health
Traditions (FRLHT), started work with the mission for the revitalization of
India’s health traditions. FRLHT has been involved in Documentation and
Rapid Assessment (DRALHT) of the community's therapeutic use of
medicinal plants. Over the years, FRLHT has been able to consolidate its
work in the form of a fairly standardized documentation and assessment
process.
The DRALHT process consists of the following 3 steps:
• Ethnographic documentation and Identification of important local health
traditions
• Community validation of these identified traditions along with multi-
disciplinary assessment (using a comprehensive Ayurveda, Siddha,
Unani, and Pharmacology data-base) for encouraging the best practices,
adding to the incomplete and discouraging distorted ones.
• Promotion of the use of the validated health traditions at household and
community level.
1.2 Why Assess Local Health Traditions?
Assessment of community's therapeutic use of medicinal plants helps:
• To assess efficacy of local health traditions.
• To assess, differentiate and identify the sound practices from the
unsound.
• To understand the worldviews/ epistemologies of folk practitioners and
household health traditions.
2. The Method
The documentation of local health traditions is aimed at systematic recording of
Local Health Traditions and the resources used in it.
The next step after documentation is Rapid Assessment of Local Health
Traditions (RALHT). RALHT is aimed at selecting the best practices in household
8

health traditions and folk health traditions, for their promotion in primary health
care, by means of a rapid assessment exercise. This form of assessment is termed
‘Rapid’ as it does not involve laboratory or clinical studies.
Community’s own assessment based on empirical data on efficacy
Desk Research consulting databases & Literature References from Ayurveda, Siddha, Unani and modern pharmacology Rapid Assessment of prioritized
Local Health Traditions
Identifications of Effective Remedies
Design of Promotional Programs led by Community Based Organizations and facilitated by NGOs
Community’s Prioritization of Health Conditions for assessment
Comprehensive ethnographic Documentation of Local Health Traditions
2.2 Data Sheets for ISM, Community & Pharmacological assessment
LHT DATA SHEET Local name of the prioritized condition Description (Cause/ stages) of the condition Ingredients name
Botanical Name
Part used Proportion used
Purification/ Remarks
Preparation of the medicine:
Dosage & Administration How much? How many times? How long? Pathya/ Apathya (Food & Regime advice) Any other remarks (contra indications, special precaution etc)
Reports of Successful Community Use Specify the number of people who reported using the remedy OR
Specify the number of villages, the remedy reported from OR
Specify the number of Talukas/ Districts remedy was reported from
9

AYURVEDIC DATA SHEET (For individual resource references)
1 Local Name 2 Scientific Name 3 Rasa 4 Guna 5 Veerya 6 Vipakam 7 Dosha Karma 8 Prabhava 9 Rogagnatha
References from classical texts:
Disease/ Condition & stage
Text Chapter Sthana Mode of Administration
Other ingredients
Remark
SIDDHA DATA SHEET (For individual resource references)
No Plants/ Minerals/ Animal Names 1 Local Names 2 Scientific Name 3 Suvai 4 Gunam 5 Veeriyam 6 Vipakam 7 Others
References from classical texts: Disease Type
Condition Text Chapter Section
Mode of Administration
Other ingredients
Remarks
UNANI DATA SHEET
No Plants/ Minerals/ Animal – Unani Names 1 Local Names 2 Scientific Name & synonyms if any including family:
Part used
3 Mahiyath (Morphology): 4 Mizaj (Temperament):
10

5 Afaal (Actions): 6 Istamal (Uses): 7 Nafaekhas (Specific action): 8 Muzir (Contra Indication): 9 Muslah (Antidote): 10 Badal (Substitute): 11 Meqdar-e-kurak (Dosage):
PHARMACOLOGY DATA SHEET
Resource Name Botanical / Scientific name: (including family name) Part LHT uses Active constituents Biological activity Clinical reports Remarks Reference
2.3 Botanist
Herbarium records of the plants used by the community are sent to competent
local taxonomist for identification.
2.4 Desk Research Report
The report consists of assessment of the local health practices based on the
three Indian systems of medicine and the pharmacology report. An
ethnographically sensitive approach is used to draw correlation of the locally
described health problem with an ISM or modern health condition. This is a
pre-requisite to assess the local remedies. The details of the locally used
formulation such as the ingredients in local name, botanical names, part used,
proportions used, method of preparation, form of medicine and the dosage
used are conveyed to the evaluators.
3. RALHT Workshop
This is an essentially participatory method of assessment, which involves the
community, vaidyas, and medical practitioners from various systems of medicine,
11

pharmacologists, botanists and the facilitators (NGOs, People’s Organisations
etc.)
3.1 Workshop Proceedings
The prioritized list of health conditions/illness and the causes and symptoms
are presented to the panel of practitioners present. The panel discusses with
the community (in the case of RALHT for household remedies) and the folk
healers (in the case of RALHT for folk remedies) and seeks clarifications if
required. The members of the panel then finalise their respective rapid
assessment proformas.
After the panel has filled in their data sheets, the following steps are
undertaken:
• Treatment or practice followed in the community with all the details as
given in the LHT data sheet.
• Presentation about understanding of health conditions and illness in the
community.
• Presentation of the assessment by writing on the blackboard or reading it
out.
• Initiating the discussion between the community members and
practitioners.
During the analysis, the following are noted:
• The total number of formula having consensus from the community and
all the experts of the Indian Systems of Medicine and modern medicine.
• The number of formulae having consensus from the community and one
of the ISM experts.
• Formulae suggested for modification or additions.
• Formulae to be discouraged as per consensus of the participants.
At the end of the exercise an ‘Analysis Chart For Assessment Result’ is
presented as given below:
12
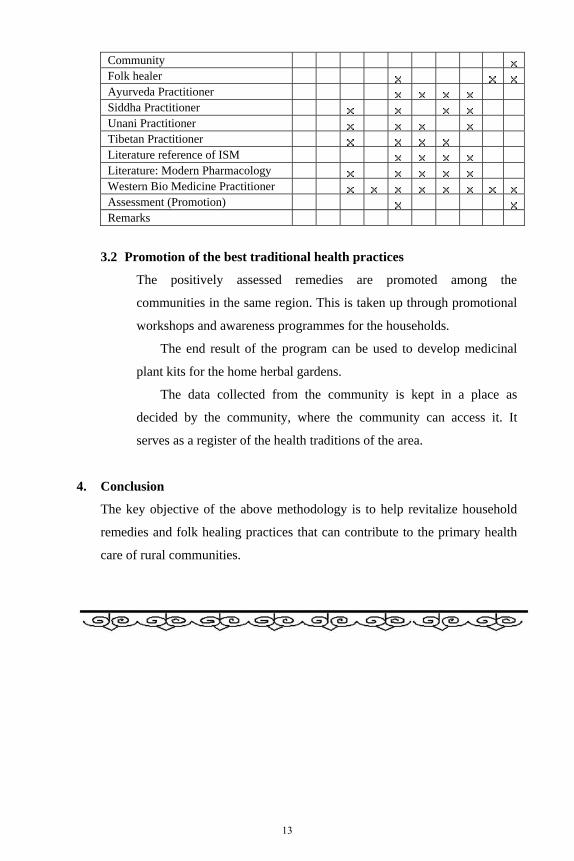
Community Folk healer Ayurveda Practitioner Siddha Practitioner Unani Practitioner Tibetan Practitioner Literature reference of ISM Literature: Modern Pharmacology Western Bio Medicine Practitioner Assessment (Promotion) Remarks
3.2 Promotion of the best traditional health practices
The positively assessed remedies are promoted among the
communities in the same region. This is taken up through promotional
workshops and awareness programmes for the households.
The end result of the program can be used to develop medicinal
plant kits for the home herbal gardens.
The data collected from the community is kept in a place as
decided by the community, where the community can access it. It
serves as a register of the health traditions of the area.
4. Conclusion
The key objective of the above methodology is to help revitalize household
remedies and folk healing practices that can contribute to the primary health
care of rural communities.
13

1.2 Plant Based Traditional Knowledge for Improved Health Care Delivery System Raghu Bir S. Rawat Medicinal and Aromatic Plants Programme in Asia, International Centre for Integrated Mountain Development (ICIMOD), GPO Box 3226, Kathmandu, Nepal Email: [email protected] Introduction:
The identification of plants useful to human beings from natural stands
commenced in prehistoric times. Experiments and trials were the two main ways
through which humans have learnt the various uses of plants. The use of plant
resources for medicinal and other purposes is one of a number of practices
developed by ancient people.
Plant derived medicines are used in all civilizations and cultures and, hence,
plants have always played a key role in health care systems worldwide. In most
developing countries, the indigenous modes of herbal treatment are a part of the
culture and the dominant method of healing therapy. These remedies, with a
considerable extent of effectiveness, are socially accepted, economically viable
and, mostly, are the only available source. Plants used in traditional medicine,
therefore, have a critical role in the maintenance of health all over the world.
Traditional medicine:
Initially all drugs were natural, such as vegetable, animal and mineral products in
their crude forms. Before the emergence of the twentieth century, all medical
practice was what we now call the traditional system. The World Health
Organization (WHO) has defined traditional medicine as “the sum total of all the
knowledge and practices, whether explicable or not, used in diagnosis, prevention
and elimination of physical, mental or social imbalance and relying exclusively on
practical experience and observation handed down from generation to generation,
whether verbally or in writing” (WHO, 1978). Traditional medicine is, therefore,
used mainly to distinguish the ancient and culture-bound health care practices,
which existed before the application of science to health matters in official
modern scientific medicine or allopathy. Some frequently used synonyms are
14

indigenous, unorthodox, alternative, folk, ethno, fringe, and unofficial medicine
and healing.
All traditional medicines have their roots in folk medicines and household
remedies. WHO has listed 20,000 medicinal plants used in different parts of the
world. Other estimates indicate the number to range between 35,000 and 70,000
worldwide (Lewington, 1993; Bhattarai and Karki, 2004). Some of the earliest
remedies and prescriptions became widespread and were subjected to certain
refinements, revisions and improvements through practices by trained or
experienced medicine men and then got incorporated in organized or codified
systems of medicines. These organized or codified traditional medical systems
employ relatively few species, viz. 500-600 in traditional Chinese medicine, 1100
in Tibetan medicine (Sowangpa), 1500 in the Ayurveda, 450 in the Homoeopathy,
342 in the Unani, and 328 in the Siddha systems. Also, the various plants used in
these systems happen to be common both species-wise as well as disease-wise in
most of the cases. However, a major bulk of the plant species used as medicines
remained endemic to certain regions or people. Due to lack of communication,
intermingling and breeding of ideas, and varying ways of life, many of these
earlier remedies survived only by word of mouth from generation to generation.
This category of information and their uses still dominates the healing tradition in
the world.
WHO Concern:
Many countries, especially in Asia, Africa and East European countries, have
officially recognized the use of plant-based traditional medicine in their health
care delivery systems. WHO has estimated that 80% of the world’s populations
rely primarily on traditional medicine (WHO, 1978; Okerele, 1992). Considering
the coverage and effectiveness of various systems of traditional medicine
throughout the world, the Alma-Ata Declaration of the WHO in 1978 proposed
the theme “Health for all by the year 2000”. The examination of drugs used in
traditional medicine in the various parts of the world is, therefore, one of the
priority programs of the WHO (Pasquale, 1984).
15
Characteristics of Traditional Medicines:
In almost every part of the world traditional healers are practicing means of health
care coverage that is culturally acceptable to the local population, dealing more or
less satisfactorily with many of their health problems. Animal sacrifices,
exorcism, religious ceremonies, preaching of supernatural powers and evil spirits,
psychotherapy, cauterization, prevention, surgery, use of animal and mineral
products, etc., are the important parts of most folk therapies. Occasionally, there
may be liberal use of musico-therapy, often associated with tribal dances and with
ritually induced trances or hypnotism. Herbal medicine is, however, the most
popular.
There are common features for herbal medicines:
• Herbal medicines are different from clinically defined medicines in their
character as well as in their medicinal value.
• They are based mostly on herbal products.
• Usually, they are multi-drug formulations including animal and mineral
products as essential components or additives.
• In herbal therapy, data on pre-clinical investigations are often incomplete
although in majority of cases the therapeutic experiences have been
accumulated over centuries.
• Some of them follow practices based on, for example, mistaken beliefs, faulty
experimentation, or inaccurate information that can be dangerous.
• They mostly include empirically defined doses and course of medication.
• The identity of plant species used is often controversial.
• Safety measures are poorly adopted, in most cases.
• Additives are frequently used; many of them also have therapeutic actions.
Use of plants in modern medicine
Many drugs of modern medicine have had their origin in traditional medicine.
Some common examples include the discovery of the alkaloid diosgenin in
Dioscorea deltoidea used as source for the partial synthesis of cortisone and
steroid hormones in the forties, the discovery of the hypotensive alkaloid reserpine
in Rauvolfia serpentina and the analgesic alkaloid aspirin in Filipendula ulmaria
in the fifties, the discovery of anti-asthmatic alkaloid ephedrine in Ephedra sinica
16

and the anti-cancer alkaloid podophyllotoxin in Podophyllum hexandrum in the
sixties, to mention a few (Table 1).
Table 1: Important plant-derived drugs used in modern medicine
Drug Medicinal Use Plant species Family Ajmalicin Antihypertensive,
tranquilizer Apocynaceae
Ajmalin Heart arrhythmia Rauvolfia serpentina Apocynaceae Ajmaline Antihypertensive,
tranquilizer Rauvolfia serpentina Apocynaceae
Asprin Analgesic, anti-inflammation
Filipendula ulmaria Apocynaceae
Artemisine Antimalarial Artemisia annua Asteraceae Atropin Ophthalmology Atropa belladonna Solanaceae Benzoine Oral disinfectant Styrax tonkinensis Styracaceae Caffeine Stimulant Camellia sinensis Theaceae Camphor Rheumatic pain Cinnamomum
camphora Lauraceae
Cascara Purgative Rhamnus purshiana Rhamnaceae Cocaine Ophthalmologic
anaesthetic Erythroxylum coca Erythroxylaceae
Codeine Analgesic, antitussive
Papaver somniferum Papaveraceae
Colchicine Gout Colchicum autumnale Liliaceae Demecolcine Leukemia Colchicum autumnale Liliaceae Deserpidine Hypertension Rauvolfia canescens
Rauvolfia serpentina Apocynaceae Apocynaceae
Dicoumarol Thrombosis Mililotus officinale Fabaceae Digitoxin Atrial fibrillation Digitalis purpurea Scrophulariaceae Digoxin Atrial fibrillation Digitalis purpurea Scrophulariaceae Digoxin Cardiotonic Digitalis lanata Scrophulariaceae Diosgenin Induces
steralization Dioscorea deltoidea Dioscoreaceae
Emetine Antiamoebic Psychotria ipecacuanha Rubiaceae Emetine Amoebic
dysentery Cephaelis ipecachuanha
Rubiaceae
Ephedrine Bronchodilator Ephedra sinica Ephedraceae Eugenol Toothache Syzygium aromaticum Myrtaceae Gallotanins Hemorrhoid
suppository Hamamelis virginiana Hamamelidaceae
Gossypol Male contraceptive Gossypium herbaceum Malvaceae Hyoscyamine Anticholinergic Atropa belladonna
Datura stramonium Hyoscyamus muticus
Solanaceae
Hyoscyamine Anticholinergic Hyoscyamus niger Solanaceae Ipecac Emetic Cephaelis ipecacuanha Rubiaceae Ipratropium Bronchodilator Hyoscyamus niger Solanaceae
17

Khellin Vascodilator Ammi visnaga Apiaceae L-DOPA Antiparkinsonian Mucuna pruriens Papilionaceae Marsilin Sedative,
anticonvulsant Marsilea minuta Marsileaceae
Morphine Analgesic Papaver somniferum Papaveraceae Noscapine Antitussive Papaver somniferum Papaveraceae Papain Attenuates mucus Carica papaya Caricaceae Papaverine Antispasmodic Papaver somniferum Papaveraceae Physotigmine Glaucoma Physostigma
venenosum Fabaceae
Picrotixon Barbiturate antidote
Anamirta cocculus Menispermaceae
Pilocarpine Glaucoma Pilocarpus jaborandi Rutaceae Podophyllotoxin Vermifuge, Cancer Podophyllum
hexandrum Podophyllum peltatum
Berberidaceae Berberidaceae
Proscillaridin Cardiac malfunction
Drimia maritime Liliaceae
Protoveratrine Hypertension Veratrum album Liliaceae Pseudoephedrine Central nervous
system stimulant Ephedra sinica Ephedraceae
Pseudoephedrine Rhinitis Ephedra sinica Ephedraceae Psoralen Vitiligo Psoralea corylifolia Fabaceae Quinidine Cardiac arrhythmia Cinchona pubescens Rubiaceae Quinine Malaria
prophylaxis Cinchona pubescens Rubiaceae
Rescinnamine Hypertension Rauvolfia canescens Rauvolfia serpentina
Apocynaceae Apocynaceae
Reserpine Hypertension Rauvolfia canescens Rauvolfia serpentina
Apocynaceae Apocynaceae
Rutine Decreases capillary fragility
Ruta graveolens Rutaceae
Sennoside-A Laxative Cassia angustifolia Caesalpiniaceae Sennoside-B Laxative Cassia angustifolia Caesalpiniaceae Scopolamine Motion sickness Datura stramonium Solanaceae Stigmasterol Steroidal precursor Physostigma
venenosum Fabaceae
Strophanthin Congestive heart failure
Strophanthus gratus Apocynaceae
Taxol Overian cancer, Breast cancer
Taxus brevifolia Taxus wallichiana
Taxaceae Taxaceae
Teniposide Bladder neoplasms Podophyllum hexandrum Podophyllum peltatum
Berberidaceae Berberidaceae
THC Antiemetic Cannabis sativa Cannabinaceae Theobromine Diuretic,
myocardial stimulant, vasodilator
Camellia sinensis Theaceae
Theophylline Cardiac stimulant, Camellia sinensis Theaceae
18

vasodilator, smooth muscle relaxant
Theophylline Diuretic, asthma Camellia sinensis Theaceae Toxiferine Surgery, relaxant Strychnos guianensis Loganiaceae Tubocurarine Muscle relaxant Chondrodendron
tomentosum Menispermaceae
Vinblastine Hodgkin’s disease Catharanthus roseus Apocynaceae Vincristine Pediatric leukemia Catharanthus roseus Apocynaceae Xanthotoxin Vitiligo Ammi majus Apiaceae
Today, there are 121 pure chemical substances extracted from about 130
species of higher plants used in the modern pharmacopoeias throughout the world.
Out of these, 89 plant derived drugs, currently used in modern medicine, were
originally discovered through the study of traditional cures and folk knowledge of
indigenous people (Choudhary and Atta-ur-Rahman, 2002; Bhattarai and Karki,
2004). In many countries modern medicines have replaced plants with many
synthetic products but almost 30% pharmaceutical preparations are still obtained
directly or indirectly from plants, majority of them based on ethnobotanical
information (Marino-Bettolo, 1980). There are 121 drugs in current use in the
USA derived from plant, with 95 species acting as sources, more than one drug
being obtained from some species. Approximately 25% of all prescriptions
dispensed in the United States contain plant extracts or active ingredients obtained
from, or patterned after, plant materials (Anonymous, 1994). Likewise, about 25%
of all prescription drugs in the Organization for Economic Cooperation and
Development (OECD) countries, and up to 60% of those in Eastern Europe,
consist of unmodified or slightly altered higher plant products (The Lancet, 1994).
Preference of herbal drugs in modern societies
Recent years have witnessed a renewed interest in plants as pharmaceuticals in the
western world. In the global context, herbal medicines flourish as the method of
therapy of choice in many parts of the world. In recent years, the increasing
demand for herbal medicines is being fueled by a growing consumer interest in
natural products. Now it is finding new popularity as an alternative conventional
medicine even in the industrialized countries and the adoption of crude extracts of
plants for self-medication by the general public is in the increase.
19

The landmark survey by Eisenberg et al. (1993) demonstrated a great demand
for alternative medical services in the United States. McPortland and Soons
(1997) reported that one-third of Americans used alternative medicine, and
approximately 10% of the Americans visited an alternative practitioner in the
calendar year 1990.
Safe and Efficacious Herbal Drugs
The overall goal in drug development is quality, safety and efficacy. All measures
in drug development are directed to this goal. The requirements of health
authorities on quality, safety and efficacy are standardized on a high level based
on the development procedure for the herbal as well as synthetic drugs. Health
authorities are reluctant to accept traditional drug preparations from other cultural
areas without well-documented data on quality, safety and efficacy. In many
developing countries, appropriate utilization of local resources to cover drug
needs is dependent on preliminary scientific study to determine the efficacy and
safety of the preparations based on plant drugs that are used on an empirical basis
in traditional medicine.
Despite many shortcomings, the number of users of herbal drugs is increasing
in the developing as well as the industrialized world. Traditional herbal medicines,
although currently serving the health care needs of majority of the world’s
population, can be further increased in coverage and broadened in terms of safety
and efficacy provided that some basic principles of drug preparation, evaluation
and uses are brought into practice.
The message is clear that phytotherapy acts as a bridge between traditional
medicine and modern medicine. The development of plant derive drugs have
always been a multi-step procedure starting with a crude extract followed by the
standardized extract and ending up with isolated constituents. Quite often
sufficient quality control and drug standardization is lacking for traditional
recipes. Ethnopharmacological leads have resulted in the introduction of new
single molecule drugs but have a greater role to play if crude extracts are accepted
for clinical use in the West.
20

Conclusions
Considering the status and trend of herbal medicine, and also considering the
shortcomings in the herbal mode of treatments, it is high time to suggest the
following measures:
• The herbal samples and raw materials should be genuine, well-identified and
harvested from the wild or organically cultivated sources and their subsequent
handling following the internationally recognized practices like those
suggested by WHO (2002, 2003) and other international bodies
(WHO/EDM/TRM, 2002; WHO/IUCN/WWF/TRAFFIC, 2004; Leaman and
Salvador, 2005).
• Herbal medicine for laboratory and clinical trials should be considered
together with its different components including substitutes and additives.
• The overall pharmaceutical practice including methods of drug preparation,
preparation of dosage forms, dose and course and route of drug
administration should be fully considered while conducting the laboratory and
clinical trials.
• Clinical trials and detailed case studies should be documented and well-
disseminated.
It has been realized that many of the modern tools used for the cure of
diseases are blunt, brutal, cumbersome and costly. What is needed is one that is
safe, effective and less expensive. Billions of people on earth depend mainly on
herbal medicines that have been significantly contributing to their primary health
care needs. Therefore, the role of medicinal plants in providing effective health
care services in most rural parts of the world is likely to continue far beyond the
recently emerged 21st century.
In the present state of rapidly expanding population, the rural health-related
challenges are enormous. The timely question, of course, is how the health
authorities are going to face these challenges. The most acceptable solution
would be to bring health care services to the rural people by helping them to apply
what are available in their environment and what is traditionally known to them.
But, otherwise, for the rural scenario to get better with more equality and evenly
shared health care facilities, the struggle ahead is sure to be long and difficult.
21

References
1. Anonymous, 1994. Interest increases in plant as medicine. Industrial
Uses/IUS 4: 17-19.
2. Bhattarai N, Karki, M. 2004. Medicinal and aromatic plants - Ethnobotany
and conservation status. In: J. Burley, J. Evans and J. Youngquist (Eds.).
Encyclopedia of Forest Sciences. Academic Press, London, UK. pp. 523-532.
3. Choudhary MI, Atta-ur-Rahman. 2002. Recent trends in medicinal plant
research. In: N. Bhattarai and M. Karki (Eds.). Sharing local and national
experience in conservation of medicinal and aromatic plants in South Asia.
Ministry of Forests and Soil Conservation, HMG/Nepal and International
Development Research Centre, SARO, New Delhi, India. pp. 62-66.
4. Eisenberg DM, Kessler RC, Foster C, Norlock FE, Calkins DR, Delbanco TL.
1993. Unconventional medicine in the United States – Prevalence, costs, and
patterns of use. N Engl J Med. 328: 245-252.
5. Leaman DJ, Salvador S. 2005. An international standard for sustainable wild
collection of medicinal and aromatic plants (ISSC-MAP): Principles, criteria,
indicators, and means of verification. Draft 2, April 2005. Steering group for
the development of practice standards and performance criteria for the
sustainable wild collection of medicinal and aromatic plants. 52p.
6. Lewington A. 1993. Medicinal plants and plant extracts: A review of their
importation into Europe. Traffic International, Cambridge, UK.
7. Marino-Bettolo, GB. 1980. Present aspect of the use of plants in traditional
medicine. J Ethnopharmacol. 2: 5-7.
8. McPartland JM, Soons KR. 1997. Alternative medicine in Vermont – A
census of practitioners: prevalence, patterns of use, and national projections.
The Journal of Alternative and Complementary Medicine 3(4): 337-342.
9. Okerele O. 1992. WHO Guidelines for the Assessment of Herbal Medicines.
Fitoterapia 63 (2): 99-110.
10. Pasquale AD. 1984. Pharmacognosy: The oldest modern science. J
Ethnopharmacol. 11: 1-16.
11. The Lancet, 1994. Pharmaceuticals from plants: great potential, few funds.
The Lancet 343: 1513-1515.
22
12. WHO. 1978. The Promotion and Development of Traditional Medicine.
WHO Technical Report Series, No. 622:8, Geneva, Switzerland.
13. WHO. 2002. WHO Traditional Medicine Strategy 2002-2005. World Health
Organization, Geneva, Switzerland. pp. 61.
14. WHO. 2003. WHO Guidelines on Good Agricultural and Collection Practices
(GACP) for Medicinal Plants. World Health Organization, Geneva,
Switzerland. pp. 72.
15. WHO/EDM/TRM. 2002. WHO Guideline on Good Sourcing Practices (GSP)
for Medicinal plants. World Health Organization, Geneva, Switzerland,
16. WHO/IUCN/WWF/TRAFFIC. 2004. Guidelines on the Conservation of
Medicinal Plants. World Health Organization, Geneva, Switzerland.
23

1.3 Ethnobotanical Scenario in Gujarat: Status and Prospects in Primary Health Care Minoo H. Parabia*, M. N. Reddy, Smita Pathak, and Falguni Sheth Shri Bapalal Vaidya Botanical Research Centre, Department of Biosciences, Veer Narmad South Gujarat University, Udhna-Magdalla Road, Surat – 395007, India Email: [email protected] * Corresponding Author Abstract
The state of Gujarat harbours approximately 2000 species of flowering plants. Out
of them about 1275 species are identified as medicinally useful. Different workers
at ten Universities of the state and few major institutions (Governmental and non
Governmental) are presently engaged in the studies. The ethnobotanical studies
began as gathering of supplementary information on the uses of plants. Gradually
the casual approach turned into a methodical and devoted study on ethnobotany.
The State has a document prepared by the concerted efforts of the workers of the
State and the support of the Government of Gujarat.
The article gives comprehensive results of the plants used for different
ailments hither to known as incurable by a modern medicine. The ailments
prevailing amongst tribes and their herbal treatments are suggested. Institutional
efforts for the revival of knowledge system are elucidated.
Introduction:
Ethnobotanical explorations in Gujarat dates back to early fifties. The important
ethnobotanical contributions are those of Bedi (1969), Bhatt (1975), Bhatt (1987),
Bhatt and Mitaliya (1999), Bhatt and Sabnis (1987), Chavan et al. (1963), Chavda
(2006), Chohan and Shah (1969), Gopal (1983), Gopal and Shah (1989), Hamir
(2001), Inamdar (1968), Jadeja (2006), Joshi et al. (1980), Joshi (1988), Karatela
(1974), Mitaliya (1998), More (1972), Murthy (1957), Nagar (2000), Oza (1961),
Oza (1991), Padte (1973), Patel (1971), Patel (2001), Patel (2002), Prajapati
(2002), Punjani (1997), Rao (1970), Shah (2006), Shah & Vyas (1973), Shah and
Yadav (1979), Suryanarayana (1968), Umadevi (1988), Umadevi et al. (1989).
24

The contributions could be classified into pre Shah (1978) and post Shah
(1978) publications. In addition to publications the sizeable amount of data is
buried in the Ph.D. thesis covering floristics of Gujarat. It just began as the
additional information on the economic uses of the components of flora of the
area.
With the advent of Jain’s series of publications viz. Medicinal Plants (1968),
Contribution to Indian Ethno botany (1981), Dictionary of Indian Folk Medicine
and Ethnobotany (1991), and with the establishment of Ethnobotanical Society in
1989, the ethnobotanical studies received the momentum. There was quite a good
flow of publications from the different corners of the state. Still, the publications
dealt only with the name of the taxa and the mention of their importance.
The monumental work than was created by Umadevi (1988), followed by a
comprehensive publication, by Umadevi et al. (1989).
In 2001 Gujarat Ecological Education and Research (GEER) Foundation
launched a state level coordinated project on the status of medicinal plants in
Gujarat. The sole purpose was to survey the identification, distribution and
relative abundance of medicinal plants in Gujarat. The project culminated in to the
publication of a document viz. Medicinal Plants of Gujarat (Pandey et al., 2005).
Shah (2006) carried out another survey viz. “Status of Ethnomedicine and
Grandma’s prescription in Valsad district (Gujarat), where data on 223 disorders
and 318 species were detailed out with recipes and posology.
In the mean time Shri Bapalal Vaidya Botanical Research Centre (BVBRC)
of Veer Narmad South Gujarat University took up work on the Primary Validation
of ethnic claims; such work is also underway at SRISTI, Ahmedabad as far as the
ethnoveterinary claims are concerned. The document viz. Ethnovet Heritage,
encompassing the details on the ethnoveterinary plants was prepared by Anjaria et
al. (2002)
The preliminary validation – a pilot studies - have so far been carried out for
the hypertension, oral disorders, dental hygiene, spondylosis, bronchial disorders,
osteoporosis and malaria at BVBRC, Surat.
BVBRC has also identified some simple recipes which could be taught to the
different tribes, underprivileged groups to help them in maintaining their primary
health. The recipes selected were aimed to help in dental care, burns, dandruff,
25

earache, constipation, cough-cold, general debility, cardio tonic, uterine fibroid,
asthma, diarrhoea, dysentery, menorrhagia, hyperacidity, malaria, joint pains, skin
ailments, iron deficiency etc.
Bird’s eye view of the ethno botanical research in Gujarat
The survey revealed that the numbers of papers published on Ethno botany of
Gujarat are about 49, the major floristic theses including notes on ethno botany are
32 and the theses devoted to the Ethno botany are 11.
The Universities/Institutions engaged in the ethnobotanical studies are Veer
Narmad South Gujarat University, Surat; The M.S. University, Baroda; Gujarat
University, Ahemedabad; H. North Gujarat University, Patan; S.P. University,
Vallabh Vidyanagar; Anand Agriculture University; Junagadh Agriculture
University; Bhavnagar Univeristy; Saurashtra University, Rajkot and Gujarat
Ayurved Univeristy, Jamnagar.
Most of the institutions are concentrating at the collection of data for the
purpose of documenting the information prevailing amongst tribes and the rural
communities. V.N.S.G.U. has also ventured into collecting recipes prevailing
amongst people at large in urban and rural communities. This has yielded a
beautiful work comprising information on 318 species used for 223 recipes (Shah,
2006). V.N.S.G.U. is also attempting to carryout validation of tribal claims. Pilot
studies completed so far covers ailments like Spondylosis, Psoriasis, Malaria,
hypertension, and dental hygiene.
V.N.S.G.U. and S.P.U. are presently handling collaborative D.S.T. funded
major research project entitled “Development and Standardization of herbal
antimalarial drug.”
Shri Bapalal Vaidya Botanical Research Centre of V.N.S.G.U. is solely
devoted to the studies in Medicinal Plants. The centre is presently holding leads
on diseases like Gangrene, Leukaemia, Neuralgia, Lupus nephritis, Spondylosis,
Panrcreatic tumor, Rabies, Pimples – acne, Obesity and Amoebiosis. It is hoped to
put them to critical scientific appraisal.
The tribes were consulted not only for obtaining information from them on
the medicinal cures but also to study their life style and the sufferings.
26

The major ailments noted are dental care, burns, dandruff, earache,
constipation, cough-cold, general debility, cardic disorders, iron deficiency,
diarrhoea, uterine fibroid, asthma, leucorrhoea, menorrhagia, hyperacidity, joint
pains, skin ailments, liver dysfunction, malaria etc.
It was also noted that the knowledge of medicine is not common for all the
tribesmen. Knowledge is largely scattered, each one having specialization in one
or few of the ailments. At times a wise man having knowledge would protect it
being highly reticent.
Authors, therefore, decided to disseminate the knowledge by way of
arranging training workshops.
The training workshops are normally arranged for 3 days. The first day, fore
noon will be reserved for introducing the plants growing around the camp area.
The participants were also being encouraged to bring more fresh samples for
discussions.
The participants were also told about the basic principles of hygiene and the
symptoms to identify the ailments. About 19 recipes were selected. They were
trained in the actual preparation of medicines. The prepared medicines were
distributed among the participants, so as they can carry the medicine home for
their personal use.
The recipes selected are given below.
• Burns & Dandruff: Creamy emulsion is prepared by emulsifying oils of
Azadirachta indica A. Juss. and Derris pinnata Lour. Oils were emulsified
with Ral (Shorea robusta Gaertn. f. resin). This is used as hair cream.
• Cardio tonic & Bone fractures: Powdered bark of Terminalia arjuna
(Roxb.) W. & A. is given orally, 5g twice a day either with water or as a
Kshir Pak to enhance the fracture healing. The Kshir Pak is prepared by
boiling 5g. of churna with 150 ml of water and 150 ml of milk, till the 150 ml
of water burns out. This is allowed to cool and given to drink.
• Joint pains: Make a paste of 100g Calotropis procera (Ait.) R. Br. leaves,
100g of Vitex negundo L. leaves, 100g of Tinospora cordifolia (Willd.)Miers
stem and boil with 250g of Sesame oil till water evaporates. Strain and store
the oil. Administer 5ml orally, twice a day.
27

• General Debility: Rasayan Churna (Tinospora cordifolia (Willd.) Miers,
Tribulus terrestris L., Emblica officinale Gaertn.) 5g twice a day with water.
• Cough – cold: Trikatu (Zingiber officinale Rosc., Piper nigrum Linn., P.
longum Linn.) 5g twice a day with water or milk.
• Constipation: Mix Harde (Terminalia chebula Retz.) and Sonamukhi
(Cassia angustifolia Vahl) in equal proportion. Give 5g at night with water.
• Diarrhoea: Roast a spoonful of Poppy (Papaver somniferum L.) seeds and
two fruits of Cardamom. Crush and give with a pinch of sugar. This recipe is
good for kids too.
• Hyperacidity: Poha (Rice flakes) and Saunf (Foeniculum vulgare Mill.) are
mixed in equal proportion and reduced to powder. 30g of this powder is
soaked in a litre of water overnight. Next day this liquid is to be taken during
the day whenever thirsty.
• Iron deficiency: Mix 5g of Trifala churna [Harde (Terminalia chebula
Retz.), Amla (Emblica officinale Gaertn), Baheda (T. bellirica (Gaertn.)
Roxb.)] with spoonful of jaggery and little water. Smear the mixture on the
wall of a small iron vessel at night. Next day in the morning add little warm
water and drink daily for about three weeks. The haemoglobin content is
usually restored, if not, continue for two more weeks.
• Earache: Crush 10g each of leaves of Annona squamosa L., Azadirachta
indica A. Juss., Ocimum basilicum L. and cloves of garlic (Allium sativum
L.). Boil with 100g of sesame oil till all water evaporates. Filter and store. Put
two – three drops twice a day in ears.
• Asthma Make a powder of following dried material:
Plant Species Part Used Qty. (g)
Justicia adhatoda L. leaves 500
Solanum surattense Burm. f. whole plant 500
Zizyphus jujuba Lam. bark 100
Terminalia bellirica (Gaertn.) Roxb. fruit rind 200
Datura metel Linn. leaves 50
Calotropis procera (Ait. )R..Br. leaves 50
Clerodendron serratum (Linn.) Moon wood & bark 50
28

Piper longum Linn. fruits 50
Cinnamomum zeylanica Breyn. bark 50
Glycirrhiza glabra Linn. roots 200
Mix them well and store. Give 5g four times a day. Patients are advised to
drink warm water only.
• Leucorrhoea & Menorrhagia: Soak 5g of gum of Sterculia urens Roxb. in
200ml of water or milk in the morning. The content will become a gel. Add
sugar and elaichi (Cardemon seeds) to taste and consume after lunch.
Continue till cured.
• Malaria: Make a powder of following material:
Plant Species Part Used Qty. (g)
Alstonia scholaris R.Br. bark 50
Calotropis procera (Ait.) R.Br. young apical bud 100
Enicostemma littorale Blume whole plant 100
Mix all and store. Take two gram thrice a day with warm water.
• Skin ailments: Paste of fresh rhizome of Curcuma domestica Valeton and
mature fresh leaves of Calotropis procera (Ait.) R. Br. is boiled in oil of
Brassica juncea (L.) Czern and Coss. till water part is evaporated. This
medicated oil is applied on affected part twice a day.
• Dental Care: Calcium powder is mixed with juice of fresh leaves of
Mimusops elengi L. to make a paste. Mix crystals of Menthol, Thymol and
Camphor. They will deliquesce. Add few drops of this mixture and bottle the
content after mixing thoroughly. Apply twice a day on teeth.
• Dysentery: Mix Belgarbha (Aegle marmelos (L.) Corr.), Indrajav
[Holarrhena antidysenterica (Heyne ex Roth) Wall.], Kutaj [Wrightia
tinctoria R. Br. (bark)] in equal proportion. Powder the mixture and store.
One spoonful three times a day is given with water.
• Uterine fibroid: Dried flowers of Woodfordia floribunda Salisb (Dhataki),
Cuminum cyminum L.(Jeera), Symplocos racemosa Roxb. (Lodra), in equal
proportion is taken and powdered. These powders are mixed with jaggery or
crushed raisins. Bolus are prepared. One bolus twice a day is prescribed.
• Liver Dysfunction (Jaundice): Swallow 10g of Aloe vera (L.) Webb. &
Berth. gel with water twice a day for two weeks.
29

• Aloe Health Drink: Scoop off the gel from the sheared leaves of Aloe. Mix
equal quantity of water. Add sugar (900g / L) and boil to attain a syrup of
good consistency. Add in a pack of flavours and preservative of a sherbet
maker available in the market. Filter and fill up the bottle. Daily dose
recommended is 30 ml with water.
Discussion:
There is a dire need of preparing comprehensive database on the ethnomedicinal
information. Each should have online database, inviting contribution from all
concerned. This must be a continuous process.
To re-establish the importance of local herbal resources the tribal training
programmes have shown some encouraging signs.
The follow up of tribal training programmes revealed that a very small
percentage of trainees took this up seriously and started using the knowledge for
monitoring their health. Some enterprising persons even sold their preparations.
We propose to develop a cadre of primary health workers trained in herbology. A
nation wide move in this regard could bring better results.
References:
1. Anjaria J, Parabia MH, Dwivedi S. (ed.) 2002. Ethnovet Heritage. Indian
Ethnoveterinary Medicine: An overview, 1st edn. Pathik Enterprise,
Ahmedabad.
2. Bedi SJ. 1969. Flora of Ratanmahal hills in Panchmahals, Ph.D. thesis, M.S.
University of Baroda, Vol. I & II.
3. Bhatt RG. 1975. Contribution to the floristics and phytosociology of
Panchmahals district in Gujarat State, Ph.D. thesis, S.P. University, Vallabh
Vidyanagar.
4. Bhatt DC, Mitaliya KD. 1999. Ethnomedicinal Plants of Victoria Park
(Reserve forest) near Bhavnagar, Ethnobotany Vol. II.
5. Bhatt MP. 1987. A contribution to the flora of Navsari area with reference to
Ethnobotany, Ph.D. thesis, South Gujarat University, Surat.
6. Bhatt RP, Sabnis SD. 1987. Contribution to the Ethnobotany of Khedbrahma
region of North Gujarat. J Econ Tax Bot. 9(1): 139-145.
30

7. Chavan AR, Bedi SJ, Sabnis SD. 1963. On useful plants of Devgadh Baria
hills, Gujarat State. Bull Soc Coll Sci Nagpur. 6: 8-12.
8. Chavda GK. 2006. Floristic and Ethnobotanical study of angiosperms of
Keshod, Mendarda and Vanthly talukas of Junagadh district, Gujarat, Ph.D.
thesis, Bhavnagar University, Bhavnagar.
9. Chohan JG, Shah GL. 1969. Some more plants from Pavagadh. Ibid. 66 (2):
405 – 409.
10. Gopal GV. 1983. Ethnobotanical studies in the forest areas of some parts of
Gujarat. Ph.D. thesis, S.P.University, Vallabh Vidyanagar.
11. Gopal GV, Shah GL. 1989. Ethnobotanical – Lore of Gujarat State. In:
Proceedings of All India Symposium on the Biology and Utility of Wild
Plants. Prof.G.L. Shah Commemoration Volume. Pp. 89 – 96.
12. Hamir AM. 2001. Ethnobotanical studies of angiosperms of Arawally hills,
Dist – Banaskantha, Gujarat, Ph. D. thesis, North Gujarat University, Patan.
13. Inamdar JA. 1968. A preliminary survey of the flora of Dharampur forests in
Gujarat. Bull Bot Surv India. 10: 126-132.
14. Jadeja BA. 2006. Ethnobotanical Study of Angiosperms of Barda Hills,
Gujarat, India. Ph.D. thesis, Bhavnagar University, Bhavnagar.
15. Jain SK. Medicinal Plants. 1968. National Book Trust, India, New Delhi.
16. Jain SK. 1981. Glimpses of Indian Ethnobotany. Oxford and IBH Publishing
Co. New Delhi, Bombay, Calcutta, India.
17. Jain SK. 1991. Dictionary of Indian Folk Medicine and Ethnobotany, Deep
Publications, New Delhi.
18. Joshi MC. 1988. Pharmaceutically important medicinal plants of Gujarat
Forests. Bull Medico-Ethno Bot Res. 10(4): 372-373.
19. Joshi MC, Patel MB, Mehta PJ. 1980. Some folk medicines of Dangs,
Gujarat State. Bull Med Ethnobot Res. 1: 8-24.
20. Karatela YY. 1974. A contribution to the floristics and phytosociology of the
Chhotaudepur forest divisions in Gujarat State. Ph.D. thesis, S. P. University,
Vallabh Vidyanagar.
21. Mitaliya KD. 1998. Ethnomedicinal study of angiosperms of Bhavnagar.
Ph.D. thesis, Bhavnagar University, Bhavnagar.
31

22. More PG. 1972. A contribution to the flora of Parnera hills, Pardi and
Udwada areas in South Gujarat. Ph.D. thesis, S. P. Uiversity, Vallabh
Vidyanagar.
23. Murthy MHS. 1957. The vegetation of Bhavnagar and its biological
spectrum. F Guj Univ. 1: 42-46.
24. Nagar PS. 2000. Biodiversity of the Barda Hills. Ph.D. thesis, Saurashtra
University, Rajkot.
25. Oza GM. 1961. Flora of Pavagadh, Ph.D. thesis, The M.S. University,
Baroda.
26. Oza JD. 1991. Taxonomical and Ecological Studies of the flora of and around
Bhavnagar.
27. Padte SN. 1973. Studies on the flora and vegetation of Savli Taluka, Ph.D.
thesis, The M.S. University, Baroda.
28. Pandey CN, Raval BR, Mali S, Salvi H. 2005. Medicinal plants of Gujarat
(compilated). Gujarat Ecological Education and Research (GEER)
Foundation, Gandhinagar.
29. Patel RM. 1971. The flora of Bulsar and its environs. Ph.D. thesis, Sardar
Patel University, Vallabh Vidyanagar, Part I & II.
30. Patel KC. 2002. Floristic and Ethnobotanical studies on Danta forest of North
Gujarat, Ph.D. thesis, Sardar Patel University, Vallabh Vidyanagar.
31. Patel NK. 2001. Study of angiospermic plants with relation to
phytosociological and ethnobotanical study of Danta taluka, district
Banaskantha, Ph.D. thesis, North Gujarat University, Patan.
32. Prajapati MM. 2002. Study of plant community and study of ethnobotanical
aspects of Shamlaji forests, hills and hillocks, Ph.D. thesis, North Gujarat
University, Patan.
33. Punjani BL. 1997. An ethnobotanical study of tribal areas of district
Sabarkantha (North Gujarat). Ph.D. thesis, North Gujarat University, Patan.
34. Rao RS. 1970. Studies on the flora of Kutch, Gujarat State (India) and their
utility in the economic development of the semi-arid region. Ann Arid Zone.
9(2): 125-142.
35. Shah GL. 1978. Flora of Gujarat State. Published by Sardar Patel University,
Vallabh Vidyanagar. Part I & II
32

36. Shah GL, Vyas KJ. 1973. Some interesting plants of Gujarat State. F Bombay
Nat Hist Soc. 69: 684-686.
37. Shah GL, Yadav SS. 1979. A contribution to the flora of Dangs forest in
Gujarat. Floristic composition, Floristic elements and Biological Spectrum.
Indian Journal of Forestry. 2(1): 13-19.
38. Shah BK. 2006. Status of Ethnomedicine and Grandma’s prescription in
Valsad district (Gujarat), Ph.D. thesis, Veer Narmad South Gujarat
University, Surat.
39. Suryanarayana B. 1968. A contribution to the flora of dang forest, Gujarat.
Ph.D. thesis, Sardar Patel University, Vallabh Vidyanagar.
40. Umadevi AJ. 1988. Identification and status survey of medicinal plants of
Gujarat. Ph.D. thesis, South Gujarat University, Surat.
41. Umadevi AJ, Parabia MH, Reddy MN. Medicinal plants of Gujarat. 1989. A
survey. In: Proceedings of All Indian Symposium on the Biology and Utility
of Wild plants. Prof. G.L. Shah Commemoration Volume. Department of
Biosciences, South Gujarat University, Surat.
33
1.4 Suggestions towards Improving the Quality of Ethnobotanical Surveys and Research Pundarikakshudu Tetali Naoroji Godrej Centre for Plant Research, Gat No. 431, Shindewadi, Shirwal – 421801, Dist. Satara, Maharashtra, India Email: [email protected] “I am tired of sending rejection letters to authors of Ethnobotanical research.” – McClatchey (2006).
Abstract
Design and development of appropriate health care delivery system is one of the
most critical factors that determine the success of health related programmes all
over the world. The role of ethnobotany in health care and health care delivery
systems is vital, particularly for traditional societies who are not accessible to
modern health care facilities. The World Health Organization (WHO) and the
United Nations Educational, Scientific & Cultural Organization (UNESCO) have
rightly recognised the importance of Traditional botanical knowledge, its
utilization and practice as a heritage. This heritage needs to be properly
documented, protected and sustained. Documentation of plants that are used by
traditional societies for health purpose is an important branch of ethnobotany,
which is multidisciplinary and needs expertise in plant taxonomy, pharmacology
and medicine. Mc Clatchey recognized clear cut pattern of problems that cause
poor quality ethnobotany manuscripts i.e two categories – a) poor quality
presentation of science and b) poor quality science. We on the other side believe
that the problem lies more in the training and curriculum since documentation of
ethnobotanical information is generally carried out by plant taxonomists who are
not generally familiar with the terminology and science of pharmacology and
medicine. As a result, the documented and deciphered information becomes either
diluted to process further or filled with misleading terms. In either case the
research is useless. We therefore, feel the need to integrate the science of
ethnobotany with other subjects such as pharmacology and medicine. This is
possible through the introduction of integrated syllabus/ courses or preparation of
34

special work-manuals to train ethno botanists. This would help to create a more
meaningful and technically appropriate database that can be scientifically
screened, tested, utilized and finally can be integrated into health care delivery
systems.
Introduction
Health systems designed by nations all over the world aim to improve, maintain or
restore citizen’s health. Nations, therefore, design and implement their own
appropriate health care systems that suit to the needs of people. India, like many
other biodiversity rich countries rightly opted to promote the so-called traditional
or alternate systems of medicine. Among these, Ethno medicine is one such
branch of science which tries to decipher hitherto unknown traditional medicinal
knowledge that was transmitted orally from generation to generation is gained
considerable importance in recent years. Ethno medical information when
properly documented, evaluated and analyzed can help to attain the highest
possible level of health to millions of people. Moreover, sustenance and
revitalization of this system is crucial for the survival of many traditional societies
who are not generally accessible to modern systems of medicine.
On the other hand, as a nation we boast about a great heritage of well
established anicent medical systems. India is a Centre sub-centre of origin for
many traditional systems of medicine such as Ayurveda, Unani, Siddha, Tibetian
yoga etc. In addition, we are number one interims of documented ethnomedical
information. The published data is enormous. About 40% of the known 17,500
flowering plants are recorded to have some or other medicinal use. It is claimed
that Jeevaka an ancient Ayurvedic specialist in cranial surgery, who also reputed
to have cured Buddha, claimed to have said that "He found no plant that is not
medicinal". Despite all the positive points and support of our systems of medicine,
there is an increasing feeling among people that our public health care systems are
very poorly organized to cater the needs of the people. Child deaths due to
epidemics and other diseases are still very high. The available statistics casts
shadow on our claims. We know now that it is not just economic success alone
that puts us in the list of developed nations but the general health of citizens which
35

is a determining factor that decides the successful and developed nations. If it is
so, then are we in the right direction? What is the role of alternate systems of
medicines and how far they are really successful in delivering at least primary
health care to the people? Why is it that we are still a small player in global
medical plant business? Where did we fail to convert our ethnomedical knowledge
into producing competitive formulations? How far we are successful to integrate
ethnomedicines of our systems into modern systems of medicine? There are many
such questions which I don't want to dwell. Never the less I have deliberately
highlighted these questions before the respectable scientific community so as to
show that they are somewhat linked to the type of ethnomedical research
information that we are generating.
McClatchey identified two types of basic problems in ethnobotanical research
– a) Poor quality presentation of science and b) Poor quality science. I am not
tired but worried in a different context. My worries are concerned with ethno
medical surveys and conversion of the published data into useful products.
If we are able to see things in a proper perspective, we can recognize that
hypothesis, accuracy of information and proper interpretation are important points
that decide the quality of a research paper. In case of ethnomedical research
communications tactful questioning, careful interpretation of answers, deciphering
of oral communication and giving clues to other researchers to explore the
problem further becomes the hall mark. Such research based knowledge will help
other researchers to analyze further and come out with better products/
medicines/solutions. In the present paper, I would like to discuss some of these
points that cripple processing of ethno medical research. These can be broadly
classified as 1) Vague data 2) Insufficient data, 3) Ignorance in other related fields
of science, and 4) Wrong deciphering of information.
Methodology
Ethno medical information presented in each example is collected from journals
and books published in India. References have been deliberately not cited so as to
avoid controversies.
1. Vague data
E.g. 1: Parts sold: Leaves
36

Botanical name: Andrographis paniculata Nees.
Vernacular name: Nilavaembu
Family: Acanthaceae
Properties/cures: Antidote
• Antidote is a noun, means a medicine etc. taken or given to counteract
poison. Here, recording just “antidote” does not signify anything.
• The author should specify clearly for what poison it is used as an
antidote.
E.g. 2: Saussurea albescens (DC) Sch. (Asteraceae). ‘Pushkar’ 950. Powder
of dried roots mixed with mustard oil on skin diseases.
• Skin is the largest organ of the body.
• Although many skin diseases are isolated, some are manifestations of
internal disease. Wikipedia, the free encyclopedia lists about 93 diseases
of skin. Ranging from simple Acne to Skin cancer
(http://en.wikipedia.org/w/index.php, List of skin diseases = 119633219).
• Some skin diseases are occupational in nature.
• It is imperative to discuss, finalize and publish such information with a
professional Dermatologist (Skin specialist).
E.g. 3: Scabiosa speciosa Royle (Dipsacaceae). ‘Munik, 775’. Extract of
leaves for abdominal pain.
• Abdomen is the part of the body containing the stomach, bowels,
reproductive organs, etc. The information is impossible to interpret. The
pain could be from any above mentioned parts.
2. Insufficient data
E.g. 1: Albizzia amara Boiv. (Mimosaceae) Narlangi- Leaf paste in goat’s
milk is applied externally over fractures 4-5 times for fast healing.
Leaf paste: Leaves could be fresh or dried; young or mature.
Goat’s milk: Milk could be fresh or boiled/ hot or cold
Fractures: Specific location, Fracture/ hair split/ injury
4-5 times: Per day/ per week/ during the whole healing process.
How is it applied? ; Is it possible to apply the paste when fractured portion is
bandaged?
37

• Authors in the present case have collected insufficient information.
• A few more questions during the interview would have served the
purpose better.
• Giving details about mode of application and time of application is also
necessary.
E.g. 2: Salvia campanulata Wall. (Lamiaceae) ‘Kokai’, ‘Sholar’ 1089.
Infusion of herb applied to scalp supposed to darken hair and stimulate their
growth. Decoction of tender herb in water for tooth ache.
• Infusion: To extract the content in liquid
• The information needs to be elaborated further by adding preparation,
dosage & application procedures.
3. Where knowledge from other fields of science is necessary
Ex: 1: Plumbago zeylanica Linn. (Plumbaginaceae) Chitramulam – The root
paste is applied over Snake bite and Scorpion sting for relief.
• Snakes are classified as poisonous and non poisonous.
• Venom is a poisonous fluid secreted by snakes and scorpions.
• There are around 2,700 snake species. India has about 261 species of
snakes. Most of them are non poisonous. Snake venom is classified into
two types – 1) Neurotoxic - affects the nervous system (Cobra, Krait &
Sea snakes) 2) Haemotoxic – affects the cardiac system (Russel’s viper,
Saw scaled viper) (Khaire, 1996).
• All scorpions possess venomous sting. However, majority of the
scorpions are harmless but the sting is extremely painful and requires
treatment. Globally about 20-25 species of scorpions are known to be
dangerous and their sting can cause death. About 84 species of scorpions
are reported from India. The sting of Buthus tamulus can be fatal.
Scorpions’ venomos are a mixture of neurotoxins.
• While presenting ethnomedical information about antidotes to snake bites
and scorpion stings it is important to present some data relevant to the
Zoological or vernacular names of snakes or scorpions of the study area.
38

If it is not possible, mention at least poisonous or non poisonous snakes
by asking more relevant questions.
• Relief from pain or poison or from both.
E.g. 2: Cardioprotective medicinal plants; Antiplatelet plants.
Name of plant & its family: Zingiber officinale
Vernacular name: Ginger, Adrak
Part used: Rhizome
Active constituents: 6-gingerol; 6, 10-Dehydrogi-mgerdione and 6, 10-
gingerdione
• The medical information related to usage and active constituents
provided by the authors might not be original, but appears to be copied
from other literature (No reference is given). Its usage described is
accurate but with many typing and other errors.
• The author is not familiar with the rules of botanical nomenclature. He
has not mentioned the family name as well as the authority of the taxon.
• The author is also not familiar with agricultural knowledge. Zinger is a
cultivated species. A number of cultivars and varieties are available in its
centres of origin and distribution. The author would have bothered to
check and incorporate the vernacular name of the cultivars that have been
tested for the purpose.
• Cardiac drugs are different from other drugs as they work directly on
heart. Also cardiac drugs are in general are alkaloids they are potent in
dosage. It is therefore essential for the authors to mention the dosage
regime. Otherwise it can lead to dangerous complications.
E.g. 3: List of Trees and Climbers that can be promoted for Primary Health
Care.
Emblica officinalis: Gooseberry, Amla (Hindi); Eyes, promotes growth of
hair (fruit juice).
• Information provided is insufficient.
• The Indian Gooseberry or Anola is indigenous to Tropical South East
Asia. The author must know that the tree is found in wild as well as
cultivated conditions. More than 5 named cultivars are grown
commercially (Banarsi, Chakaiya, Francis etc.) in different parts of India.
39

• The author must specify in the first case whether he is talking about wild
or cultivated varieties. Secondly if they are cultivated they should
disclose the name of varieties or cultivars. The help of Agriculture
botanists is essential in such situations.
4. Misinterpretation of oral information
E.g. 2: Ricinus communis Linn. (Euphorbiaceae) V: Arandi; Andaua. Seeds
are used as purgative, scorpion sting and in impotency.
• The Castor plant is native to North-east Africa and Middle East. It is
cultivated in many parts of the world. India A number of varieties are
available all over the world and
• The author made a dangerous misinterpretation. It is the seed oil that is
used as purgative not the seeds.
• The seeds of castor contain a powerful cytotoxin called ricin and RCA
(Ricinus communis agglutinin). Ricin is a protein and causes weak
agglutination of Red Blood Cells (RBC), while RCA is a powerful
hemagglutinin. It is said that Ricin content of just one seed is toxic
enough to kill a child. Poisioning in humans is only due to ricin ( Knight,
1979; www.ansci.cornell.edu/plants/toxicagents/ricin.html
The research data cited above did not include common minimum details
such as formulation preparation, dosage regiment, contraindications,
frequency of quotes etc. Without which the data becomes obsolete.
Discussion
Designing and implementation of appropriate health system is one of the critical
indicators that determine the progress and development of a nation. Common man
recognizes only two types of medical systems – the one that works for him and the
one that don’t work. . It is therefore necessary for planners to understand some of
the ground realities and to adopt the health systems. Ethnomedical research is
believed to offer new vistas for planning and implementing appropriate health
care systems in India. Nonetheless, lot of money is already pumped into this
discipline to recognize and identify some solutions to some of the health problems
of our country. Despite the generation of a huge ethnomedical database, we have
40

failed to take the knowledge a few steps further and convert it into useful
medicines for the society. It is suggested here that it is not just poor quality
presentation of science or poor science as McClatchey highlighted in his editorial,
but the abilities and training of the surveyor in a) questioning, b) collecting
complete information, c) its interpretation, d) knowledge in other disciplines
accounts to the quality and usefulness of data. Hence, the author suggests that
ethno botanists must be trained in other related fields of science such as medicine,
pharmacy, agriculture, intellectual prosperity rights etc. or make it mandatory to
form research teams with specialists from different disciplines to generate
authentic and useful ethnomedical information. The other option, may be little
difficult to implement, but essential keeping the intellectual prosperity rights in
mind that is to create a platform for tribals to train and document their own
information with the coordinated efforts of ethnobotanists and other experts. The
research information generated through such organized efforts will help other
researchers to evaluate and convert into useful formulations/drugs. This can
ultimately help to design and develop appropriate health care systems.
Acknowledgements: The author thanks Mr. V.M. Crishna, Director, Naoroji
Godrej Centre for Plant Research, for encouragement and Mr. Ravindra Ghule for
useful discussions.
References
1. Khaire N. 1996. Indian snakes. Indian Herpetological Society, Usant, Pune.
2. Knight B. 1979. Ricin – a potential homicidal poison. Br Med J. 278. 350-
351.
3. McClatchey. 2006. Improving quality of international ethnobotany research
and publications. www.ethnobotanyjournal.org/vol3/i1547-3465-04-001.pdf
41

2.1 Bioassays in Traditional Medicine Urmila Thatte Department of Clinical Pharmacology, TN Medical College & BYL Nair Charitable Hospital, Mumbai – 400008, India. Email: [email protected], [email protected] Abstract
Drug development poses great challenges in traditional medicine. From the choice
and standardisation of test material to the choice of which bioassay to use, the
path is long and treacherous – perhaps more so than when working with new
chemical entities. This paper examines some of these challenges.
In vitro assays are very useful to identify putative drug actions while working
with pure compounds. However, with herbal materials several issues come up. For
example, what dose to use, what extract to use and what cut-offs to use? Doing
viability assays (using Trypan Blue exclusion or MTT assays) help in deciding
upper cut-offs, however, it is not fail-safe to lead to potentially active
concentrations. Many herbal extracts are not water soluble and therefore a solvent
that is not toxic to cells have to be selected and this has to be used as a control.
Extrapolation from an in vivo dose helps in identifying the possibly effective dose
– but with crude extracts acceptable cut-offs must be predetermined. If the extract
is coloured, then interpretation of results when being estimated colourimetrically
has to be done cautiously. Incorporation of appropriate controls is also essential
to confirm robustness of the assay system. If the substance is not soluble and we
use suspensions, this can seriously interfere with assays e.g. when we use herbo-
mineral preparations. Bioassays are expensive and need sophisticated
instrumentation and expert personnel. Additionally, de-differentiation and
instability of cell lines adds to some uncertainties. Additional variables that affect
analysis include variability in media composition, temperature, viscosity,
osmolarity, and buffering. Naturally, therefore, in vitro bioassays cannot totally
replace in vivo studies
However, the advantages of in vitro studies are many. Thus, we can study cell
interactions, cell-environment interactions, intracellular activity, cell products, site
and mechanism of action and genetic studies with the herbal medicines are
42
possible. The technology to use stem cells has opened new vistas. Apart from the
convenience, the lack of ethical dilemmas (unlike in human or animal studies), a
control of the experimental environment, the ability to characterize the sample and
maintenance of homogeneity in the procedure are other advantages. Up-scaling
and mechanization are also major advantages, allowing high-throughput screens.
It must be emphasized here that in vivo bioassays are also a powerful tool used in
pharmacology for studying the effects of medicines, and are also of some use in
herbal drug development. Dose relationships and mechanistic studies are some of
the classical examples. However, the challenges with in vivo animal studies are
also many, including what dose, route and for how long? Extrapolation of data
from animals to humans and vice versa is difficult.
Using examples of research from our group, these issues will be discussed to
map out a path for drug development in traditional medicine.
Full text not received
43

2.2 Novel Imaging System for Determining Anti-Cancer Activity Dharmalingam Subramaniam1, Rama P. Ramanujam2, Joseph M. Betz3, Panchapagesa M. Murali4, Courtney Houchen1 and Shrikant Anant1, 5,*
1Department of Medicine, Digestive Diseases and Nutrition, and 5Department of Cell Biology, University of Oklahoma Health Sciences Center, 920 Stanton L. Young Blvd WP1360, Oklahoma City, OK 73190, USA 2Swaasth, Inc., 800 Research Pkwy Ste 350, Oklahoma City, OK 73104, USA 3Dietary Supplement Methods and Reference Materials Program, Office of Dietary Supplements, National Institutes of Health, 6100 Executive Blvd, Bethesda, MD 20892, USA 4Dalmia Centre for Research and Development, B-133, Siruvani Main Rd, Kalampalayam, Coimbatore 641010, India
* Corresponding Author
Abstract
The lack of effectiveness with modern medicines combined with increased
consumer desire for better health has resulted in a dramatic increase in the use of
dietary supplements to improve ones general health by reducing pain and
inflammation, improving mental alertness and enhancing energy levels. Our
studies and those of others have indicated that dietary curcumin, an active
ingredient in the spice turmeric, potently inhibits intestinal tumorigenesis and
inflammation. We have now characterized the mechanisms by which curcumin
modulates this function. Curcumin and turmeric have been used extensively in
the Ayurvedic system of medicine for treatment of many disorders including
inflammation and cardiovascular disease. Inflammation is a common consequence
to injury in general. In particular, diet-induced injury to gastrointestinal tract can
occur due to varying constituents in the ingested materials, resulting in a robust
inflammatory response. The ubiquitous transcription factor nuclear factor kappa B
(NF-κB) differentially regulates cyclooxygenase-2 (COX-2) expression in colon
cancer cells. NF-κB directs high-level transcription of many cytokines, adhesion
molecules, and other pro-inflammatory genes in tissue cultures; however, the
extent to which NF-κB controls specific biological processes in vivo is unknown.
NF-κB is regulated at the posttranscriptional level by ubiquitination-mediated
proteosomal degradation of the inhibitor I-κB protein. My presentation will
highlight some of our recent studies on developing a rapid high throughput system
44

using the IkappaB degradation activity for identifying anti-cancer medicinal
activity.
Background and Aims: Dietary supplements are being increasingly consumed by
the local population in United States of America. However, there is no specific
assay available to determine batch-to-batch variations and between those of
different companies of any given product. This study aimed to develop a high
throughput assay to identify the activity of dietary supplements. Methods: We
generated an HCT-116 colon cancer cell line stably expressing a chimeric I-κB-
luciferase fusion protein. In vitro assay was performed to demonstrate that
curcumin and turmeric extracts inhibit the proliferation of these cells in the
presence and absence of prostaglandin E2 (PGE2). Western blot was performed to
demonstrate the phosphorylation and degradation of endogenous I-κB. Luciferase
activity measurements were performed to determine the levels of the I-κB-
luciferase fusion protein. Results: HCT-116 cells proliferation was significantly
inhibited by both curcumin and turmeric extracts in a dose dependent manner even
in the presence of a PGE2, a potent apoptotic inhibitor. Western blot analyses
demonstrated that TNF-α induced degradation of I-κB in the cells, which was
inhibited by turmeric extracts. Luciferase assay measurements also demonstrated
that curcumin and turmeric extracts inhibited TNF-α-mediated degradation of I-
κB-luciferase fusion protein in the cells. Conclusion: This assay may be utilized
to demonstrate the level of activity in turmeric extracts based on its ability to
inhibit TNF-α-mediated degradation of the I-κB-luciferase fusion protein.
Introduction
In recent years, due to the increasing dissatisfaction with modern medicines and
increased consumer desire in healthy living, there has been a dramatic increase in
the consumption of natural foods and the use of dietary supplements. However,
although some natural products have been reported to have clinically proven
health benefits, they have been used in all cultures from ancient times without any
functional quality-assurance testing. In addition, it is evident that many natural
foods may contain potentially toxic substances and cause adverse interactions with
45

modern drugs. This problem is apparent with functional foods such as fruits,
vegetables and nuts containing beneficial amounts of polyphenols and flavanoids
(Halsted, 2003).
The major issues for the use of natural products for public benefits or risks,
relate to the content of active constituents and bioavailability of such active
ingredients Currently, High Pressure Liquid Chromatography (HPLC) appear to
detect the presence of chemical constituents in foods and dietary supplements
(Reddy, et al., 1982, Robins, 1994). But, there is a serious lack of adequate
scientific tools and techniques to analyze the bioavailability of active ingredients
in ingested foods and dietary supplements.
Epidemiologic studies and laboratory tests of animals have indicated that
consumption of spices, fruits, vegetables and whole grains can reduce the risk of
cancer and inflammation (Corpet and Tache, 2002; Reddy, 1992, Slaga and
Gimenez-Conti, 1992). However, traditional dietary recommendations lack
physiological specification to determine the appropriate beneficial dietary dosage
to be consumed from spices, fruits and vegetables. Accordingly, in this report, we
demonstrate a gene expression measurement (GEMTM) assay using the
degradation of I-κB to measure activity of antiproliferative and anti-inflammatory
compounds. As a proof-of-principle, we have used extracts of turmeric (Curcuma
longa Linn), a commonly used spice that is used worldwide as a seasoning and is
an essential ingredient of curry. In addition, we have tested the effects of
curcumin, an active ingredient in turmeric (Aggarwal et al., 2003; Sharma et al.,
2005, Sinha et al., 2003). In the Indian subcontinent and in Southeast Asia,
curcumin has been traditionally used in the treatment of throat ulcers,
inflammation, skin wounds and cancer (Sinha et al., 2003).
Materials and Methods
Preparation of turmeric extracts and chemical reagents: The turmeric rhizome
was obtained from a farm in South India. Hard-dry turmeric rhizomes were
pulverized to a fine powder with the aid of a kitchen mixer, and ethanolic extracts
were prepared. Curcumin was purchased from LKT Laboratories, Inc, St. Paul,
Minnesota, USA. All routine molecular biology reagents were purchased from
Sigma-Aldrich, St. Louis, MO, USA.
46

Cell culture: HCT-116 human colon cancer cells were grown in Dulbecco’s
modified Eagle medium (DMEM) containing 10% heat inactivated fetal bovine
serum (Sigma Chemical Co, St. Louis, MO), standard antibiotics in a carbon
dioxide incubator with 5% CO2 at 37 0 C. The cells were stably transfected with
PGL3- I-κB firefly luciferase (I-κB FLuc) plasmid as previously described (Gross
and Piwnica-Worms, 2005).
Proliferation assay: HCT116 cells were seeded on a 96 well plates at a density of
1x 103 cells/ well and allowed to adhere and grow overnight. The cells were then
treated with increasing concentration (0-50 µg/ml) curcumin or turmeric extracts
in DMEM-10% FBS. Where indicated, the cells were also treated with
Prostaglandin E2 (1 μM). Proliferation activity was determined by enzymatic assay
as previously described (Landegren, 1984). Results were further confirmed by
manual cell counts.
Western Blot Analysis: HCT 116 cells were treated with curcumin (10 µg/ml) or
turmeric extracts (10 µg/ml) for 90 min, followed by PGE2 (1 µM) or TNF-α (10
ng/ml) for 30 min. Cell lysates were prepared and subjected to polyacrylamide gel
electrophoresis and blotted onto Immobilon polyvinylidene difluoride membranes
(Millipore, Bedford, MA). Antibodies were purchased from Santa Cruz
Biotechnology (Santa Cruz, CA). Specific proteins were detected by the enhanced
chemiluminescence system (Amersham Pharmacia Biotech, Piscataway, NJ).
Determination of the effect of turmeric extracts on I-kappaB-luciferase
expression: Briefly, HCT-116 cells stably expressing I-κB-FLuciferase were
plated in a 6-well dishes at a concentration of 5 x 105 cell/well and allowed and
grow for 24 h. The cells were treated with increasing concentrations of curcumin
or turmeric extracts (0-10 μg/ml) for 90 min, followed by TNF-α (10 ng/ml final
concentration) for 20 min. The cells were lyzed with a lysis buffer (Promega,
Madison, USA), and luminescence was measured by using a luciferase assay
reagent (Promega, Madison, USA) in the Synergy-HT 96 well plate reader
(BioTek, USA).
47

Results and Discussion
Curcumin and turmeric extracts inhibit HCT-116 cell proliferation. Curcumin is
an active ingredient in turmeric, and the amount of curcumin varies depending on
the source of turmeric. Hence, the first step in the evaluation of the turmeric
activity to determine the level of curcumin. Fresh turmeric was obtained from
Erode in Tamil Nadu, and an ethanolic extract was prepared and subject to HPLC
analysis. The curcumin content in the extract was determined to be 2.2% (data not
shown). As a comparison for the subsequent studies, curcumin was commercially
obtained and determined to be 98% pure using a HPLC assay (data not shown).
Minor amounts of bisdemethoxycurcumin and demethoxycurcumin were present
in the preparation.
Previous studies have demonstrated that curcumin is a potent inhibitor of
colon cancer cell proliferation (Aggarwal et al., 2003). To determine whether the
turmeric extract that we generated is also active in inhibiting proliferation of colon
cancer cells, we performed an in vitro proliferation assay. Cells were treated with
increasing concentrations of pure curcumin or the turmeric extract for 24 h and its
effect on cell proliferation was determined. Both curcumin and turmeric inhibited
the proliferation of HCT-116 cells in a dose dependent manner (Fig 1). PGE2 has
been shown to stimulate colon cancer cell growth through its heterotrimeric
guanine nucleotide-binding protein (G protein)-coupled receptor, EP2 (Castellone
et al., 2005). To determine whether curcumin and turmeric can inhibit colon
cancer cell proliferation in the presence of PGE2, we performed the experiments in
the presence of exogenous PGE2. Both, curcumin and turmeric extract inhibited
proliferation of the cells even in the presence of PGE2 (Fig 1), suggesting that
curcumin and turmeric were able to override the PGE2-mediated growth induction
activity.
48

Fig. 1: Curcumin and turmeric inhibits the proliferation of HCT 116 Cells. HCT 116 cells treated with increasing doses of curcumin or turmeric (0-50 µg/ml) and presence or absence of PGE2 (1 µM) for 24 h were analyzed for proliferation based using a hexosaminidase enzyme activity. Curcumin (Panel A) and turmeric (Panel B) treatment resulted in dose dependant decrease in cell number in HCT116 cells. The presence of PGE2 did naffect the proliferation inhibition activity of either curcumin or the turmeric extracts.
ot
Curcumin and turmeric extracts were further investigated at various
concentrations to determine their inhibition Concentration (IC50) values for the
inhibition of proliferation. Curcumin and turmeric extracts, a 50% reduction in
proliferation was observed at a dose of 5 and 6 µg/ml, respectively (Fig 2). Based
on the molecular weight (368), the calculated concentration of curcumin that
demonstrated a 50% inhibition was 1.5 µM. Since, turmeric only contains 2.2%
curcumin, the concentration of curcumin in the turmeric extracts was calculated to
be 132 nM. These data suggest that additional active ingredients are present in the
extract, which either act by themselves or enhance curcumin function.
49
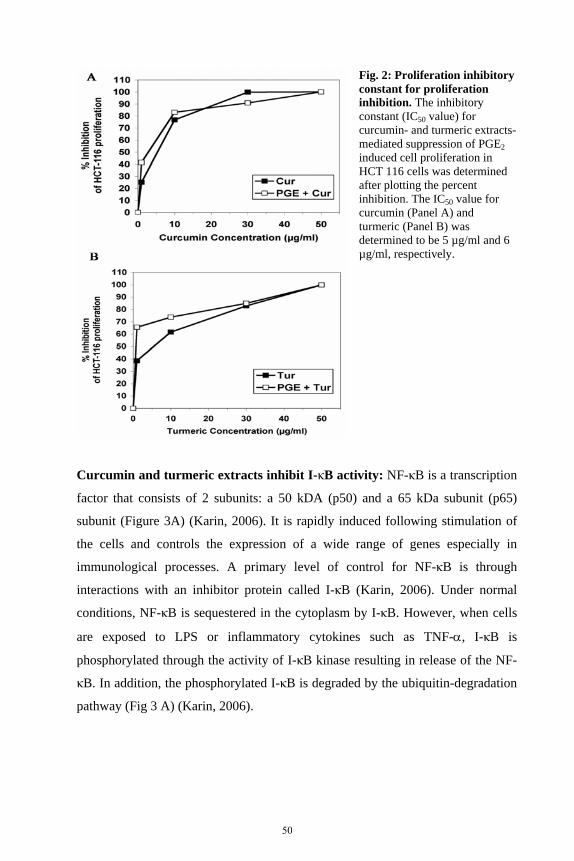
Fig. 2: Proliferation inhibitory constant for proliferation inhibition. The inhibitory constant (IC50 value) for curcumin- and turmeric emediated suppression of PGE
xtracts-
on in 2
induced cell proliferatiHCT 116 cells was determined after plotting the percent inhibition. The IC50 value for curcumin (Panel A) and turmeric (Panel B) was determined to be 5 µg/ml and 6 µg/ml, respectively.
Curcumin and turmeric extracts inhibit I-κB activity: NF-κB is a transcription
factor that consists of 2 subunits: a 50 kDA (p50) and a 65 kDa subunit (p65)
subunit (Figure 3A) (Karin, 2006). It is rapidly induced following stimulation of
the cells and controls the expression of a wide range of genes especially in
immunological processes. A primary level of control for NF-κB is through
interactions with an inhibitor protein called I-κB (Karin, 2006). Under normal
conditions, NF-κB is sequestered in the cytoplasm by I-κB. However, when cells
are exposed to LPS or inflammatory cytokines such as TNF-α, I-κB is
phosphorylated through the activity of I-κB kinase resulting in release of the NF-
κB. In addition, the phosphorylated I-κB is degraded by the ubiquitin-degradation
pathway (Fig 3 A) (Karin, 2006).
50

Fig. 3: Curcumin and turmeric extracts inhibit I-κB degradation. A. Schematic representation of NF-κB pathway. The diagram shows the signaling cascade that flows from the signaling complex to the activation of NF-κB. Both curcumin and turmeric extracts inhibit the I-κB phosphorylation. B. Turmeric extracts protect endogenous I-κB from TNF-α-mediated degradation. Total lysates from HCT-116 cells were subjected to western blot analyses for phosphorylated I-κB. Cells were pretreated with either curcumin or turmeric (10 µg/ml) followed by treatment with PGE2 or TNF-α Turmeric inhibited both the phosphorylation and degradation of I-κB *p<0.001.
Curcumin has been previously shown to inhibit NF-κB activation by
inhibiting the degradation of I-κB (Aggarwal and Shishodia, 2006). To confirm
that curcumin, and determine whether the turmeric extracts that we prepared also
inhibited I-κB degradation, we performed a western blot analysis. We incubated
cells with TNF-α, a cytokine that binds to one of to surface membrane receptors,
tumor necrosis factor receptor (TNFR) 1 and 2, and triggers a signal cascade that
results in the activation of I-κB kinase (Fig 3 A) (Clark, et al., 2005). Treatment of
cells with TNF-α resulted in significant decrease in total I-κB levels in cells (Fig 3
B). Furthermore, pretreatment of the cells with 10 µg/ml curcumin did not affect
the levels of total I-κB in the TNF-α treated cells. On the other hand, pretreatment
of the cells with 10 µg/ml turmeric significantly increased the levels of total I-κB
in the cells suggesting that it inhibited the TNF-α-mediated degradation of I-κB
51
(Fig 3 B). When the cells were treated with PGE2, no such effect was observed in
the time frame of the experiment. However, incubation of the cells for longer
times with PGE2 resulted in a similar degradation activity (data not shown). Since
degradation requires the initial step of phosphorylation, we also determined the
effect of the extracts on TNF-α-mediated I-κB phosphorylation. Increased
phosphorylation over baseline was not observed following TNF-α treatment (Fig
3B). However, we believe this is because the protein is rapidly shunted to the
ubiquitin-proteosome degradation pathway following when it is phosphorylated.
Hence the steady state levels of phosphorylated I-κB may not be significantly
changed. On the other pretreatment of the cells with turmeric significantly
suppressed the phosphorylation of I-κB at baseline in the TNF-α-treated cells.
Again, curcumin at the dose used did not demonstrate this activity, but also
significantly suppressed I-κB phosphorylation when used at higher levels (data not
shown). Taken together, these data suggests that the extracts inhibit I-κB
degradation in the cells and hence was used to develop a rapid in vitro assay
presented below.
Development of an in vitro assay using I-kB degradation activity. As a first
step in the development of a high throughput detection mechanism for I-κB in
colon cancer cells, we generated HCT-116 cells that were stably transfected with a
plasmid that encodes I-κB as a fusion protein with the firefly luciferase under of
the cytomegalovirus immediate early gene promoter-enhancer. Presence of I-κB
was monitored by luminescence activity. As a first step, we determined if the
fusion protein is subject to similar levels of degradation in response to a TNF-α
similar to that observed above with the native I-κB. Total cell lysates from TNF-α
treated cells demonstrated significant decrease in the luciferase levels, suggesting
that the protein underwent TNF-alpha-mediated degradation (Fig 4 A). To
determine whether curcumin and turmeric extracts protected the protein from
TNF-α induced degradation, the cells were pretreated with the compounds. Both
curcumin and turmeric extracts suppressed TNF-α-mediated degradation of the I-
κB-luciferase fusion protein (Fig 4 B). We have performed similar studies is a
second cell line, HeLa cells, a cervical carcinoma cell line and obtained similar
results (data not shown). These data demonstrate that the I-κB-luciferase fusion
52

protein responds to external stimuli in manner similar to that observed with
endogenous I-κB.
NF-
ed
e
1
. The
-10
ic
Fig. 4: Curcumin and turmeric extracts protect I-κB from Tinduced degradation. A. TNF-α induces degradation. HCT-116 cells stably expressing the I-κB-Fluc fusion protein were treatwith TNF-α. Total cell lysates were prepared and the luciferasactivity was measured. TNF-α induced the degradation of the IκB-luciferase protein. *P<0.0B. Curcumin and turmeric extracts protect I-κB-Fluc fromTNF-α-induced degradationcells were pretreated with increasing concentrations (0mg/ml) of curcumin or turmeric extracts for 90 min, followed by the treatment with 10 ng/ml TNF-α. Both curcumin and turmerextracts demonstrated a dose dependent protection against TNF-α induced I-κB degradation. *P<0.01
We further determined the inhibitory constant for curcumin and the turmeric
extracts in inhibting the TNF-α-mediated degradation of the I-κB-luciferase by
plotting the percent inhibtion of the degradation against the amount of the
compound/mixture used (Fig 5 B). The calculated IC50 value for curcumin was
0.4µg/ml and 0.25 µg/ml for curcumin and turmeric respectively. For curcumin,
the IC50 value was further calculated to be 75 nM. In addition, based on the
amount of curcumin that is present in the turmeric extract, it is apparent that other
ingredients in the extract, which could include other curcuminoids, also have
activity in inhibiting the degradation of the protein. This is further proof that the
purified molecule in the extract is not better than the whole extract in regulating
anti-inflammatory function through inhibiting I-κB degradation.
53

Fig. 5: Inhibitory constant value for I-κB degradation. The inhibitory constant (IC50 value) for curcumin- and turmeric extracts-mediated suppression of TNF-α-mediated I-κB degradation in the HCT-116-I-κB-FLuc cells was determined after plotting the percent inhibition. The IC50 value for curcumin (Panel A) and turmeric (Panel B) was determined to be 0.4 µg/ml and 0.25 µg/ml, respectively.
Finally, these data demonstrate the feasibility of using this approach to
determine the activity of phytochemical compounds that regulate NF-κB activity
in cells. The utility of this system is in the development of a high throughput assay
to determine the activity of the various turmeric extracts including different lots of
the same material or different mixtures. Collectively, these observations suggest
that turmeric and curcumin may qualify for use as anti-proliferation and anti-
inflammatory compound(s) for in vitro studies and the development of high
throughput IC50 unit measurement system to quality assure turmeric and other
phytochemicals as chemo-preventive agents.
Acknowledgements
This work is partly funded by NIH grant CA109269 (to SA) and a NIH-ODS MD-
611266 (to RPR). We gratefully acknowledge the gift of the luciferase plasmid
from Dr. David Piwnica-Worms of Washington School of Medicine.
54

References
1. Aggarwal BB, Kumar A, Bharti AC. 2003. Anticancer potential of curcumin:
preclinical and clinical studies. Anticancer Res. 23: 363-98.
2. Aggarwal BB, Shishodia S. 2006. Molecular targets of dietary agents for
prevention and therapy of cancer. Biochem Pharmacol. 71: 1397-421.
3. Castellone MD, Teramoto H, Williams BO, Druey KM, Gutkind JS. 2005.
Prostaglandin E2 promotes colon cancer cell growth through a Gs-axin-beta-
catenin signaling axis. Science 310:1504-10.
4. Clark J, Vagenas P, Panesar M, Cope AP. 2005. What does tumour necrosis
factor excess do to the immune system long term? Ann Rheum Dis. 64 (S4):
70-6.
5. Corpet DE, Tache S. 2002. Most effective colon cancer chemopreventive
agents in rats: a systematic review of aberrant crypt foci and tumor data,
ranked by potency. Nutr Cancer. 43:1-21.
6. Gross S, Piwnica-Worms D. 2005. Real-time imaging of ligand-induced IKK
activation in intact cells and in living mice. Nat Methods. 2:607-14.
7. Halsted CH. 2003. Dietary supplements and functional foods: 2 sides of a
coin? Am J Clin Nutr. 77:1001S-7S.
8. Karin M. 2006. Nuclear factor-kappaB in cancer development and
progression. Nature. 441:431-6.
9. Landegren U. 1984. Measurement of cell numbers by means of the
endogenous enzyme hexosaminidase. Applications to detection of
lymphokines and cell surface antigens. J Immunol Methods. 67:379-88.
10. Reddy BS. 1992. Dietary fat and colon cancer: animal model studies. Lipids.
27: 807-13.
11. Reddy NR, Pierson MD, Sathe SK, Salunkhe DK. 1982. Legume-based
fermented foods: their preparation and nutritional quality. Crit Rev Food Sci
Nutr. 17: 335-70.
12. Robins SP. 1994. Biochemical markers for assessing skeletal growth. Eur J
Clin Nutr. 48 (S1):S199-209.
13. Sharma RA, Gescher AJ, Steward WP. 2005. Curcumin: the story so far. Eur
J Cancer. 41: 1955-68.
55

14. Sinha R, Anderson DE, McDonald SS, Greenwald P. 2003. Cancer risk and
diet in India. J Postgrad Med. 49: 222-8.
15. Slaga TJ, Gimenez-Conti IB. 1992. An animal model for oral cancer. J Natl
Cancer Inst Monogr. 13: 55-60.
56

2.3 Principles of pre-clinical evaluation of plants using appropriate bioassays Jaswant Singh Division of Pharmacology, Indian Institute of Integrative Medicine (formerly Regional Research Laboratory), Canal Road, Jammu-Tawi – 180001, India Email: [email protected] Abstract
The molecular and cellular mechanisms that underlie the pathophysiology of
various diseases vary in proportions to the changes in their genes expression and
therefore of phenotypes of the cells. Understanding of the molecular basis of the
disease is therefore important for rational approach to drug design and
development. Newer knowledge in every distinct disease adds to the existing
information to define and refine molecular targets so as to develop active leads to
convert into safer therapeutics. In some cases a single molecular target may be
important for disease modification and presumably its prevention, but to manage a
disease process effectively and provide a quality life, several targets nevertheless
are to be considered. This undoubtedly asks for a battery of bioassays to apply in
screening herbal products against disease phenomena. Ancient knowledge in the
traditional use of herbal plants has provided us a treasure, which continues to
bolster therapeutics, leads and template molecules to be developed into new
chemical entities and investigative new drugs. A brief discussion shall highlight
some current emerging targets with respect to diabetes, liver dysfunctions, drug
bioavailability enhancement, inflammation/ arthritis neurodegenerative diseases,
etc. while our current efforts into the development of therapeutic leads from plants
shall be discussed in detail.
It is of paramount importance first to standardize plant extract to establish a
chemical profile using modern chemical instrumentation. The extract is subjected
to fractionation for which again chemical signature is established. Pure molecules
are isolated from bioactivity-guided fractions while bioactivity depends upon the
bioassay employed. Several types of in vitro and in vivo systems are employed to
screen and validate the bioactivity of the test extract/fraction/molecules. Use of
mammalian cell cultures mimicking in vivo functions is important for rapid
57

screening of large number of plant extracts /isolates. This would minimize
dependency on indiscriminate killing of large number of animals. With known 3D
structures of proteins as molecular targets, drug like molecules can be designed
using in silico biology approaches to get the best Hits to be taken for in vivo
validation.
My group is actively engaged in the pre-clinical development of anticancer
plant leads employing mechanism driven approaches using human cancer cell
lines. We know that dysregulation of apoptosis (programmed cell death) is the
hall-mark of many cancer cells. It plays an essential role in the control of cell
number while apoptosis is impaired in many human tumors suggesting that
disruption of apoptosis contributes substantially in the transformation of normal
cell into tumor cell. Thus, induction of apoptosis in cancer cells provides
pragmatic means to develop early anti-cancer therapeutic leads. Thus apoptosis
has become a focal point in chemotherapy-induced tumor cell killing. Apoptosis is
a complex phenomenon where the switching on and off of apoptosis is
determined by the ratio of pro-apoptotic and anti-apoptotic proteins. Therefore
many plant products may induce apoptosis by triggering the core components of
the cell death machinery, which involves chromatin condensation, cell blebbing
and DNA fragmentation into apoptotic bodies. More than 50 % of anti-cancer
drugs in clinical practice have come from plants, which are also rich source of
simple to complex molecules. We treat human cancer cell lines with the test
compounds and measure the extent of apoptosis employing several end-points
assays using flow cytometry, agarose gel electrophoresis, fluorescence
microscopy; the bioassays offer rapid screening of plant products as pro-apoptotic
agents. In cancer cell several genes are mutated and the next interest would be to
find the cell signaling pathways involved in cancer cell death by the test plant
material and that how the test material induces apoptosis.
Once the plant products produce apoptosis in cancer cells, other studies into
the mechanism of action would help in optimizing leads in suitable in vitro and in
vivo tumor models. Moreover, such leads may also form important adjuncts in
traditional chemotherapy besides protecting normal human cells from the
chemotherapeutic drugs. Thus investigations into the inter-relationship between
pro-apoptotic compounds and anti-cancer activity will be a promising field to
58
understand and elucidate the possible mechanisms for the functionality of
medicinal plants for cancer prevention and treatment. The lead molecules are
subjected to PK studies, acute and sub-acute toxicity as a part of pre-clinical
profile. Some highlights of our current studies shall be discussed.
Full text not received
59

2.4
Preclinical testing of medicinal plants: advantages and approaches Poonam G. Daswani, Brijesh S. and Tannaz J. Birdi*
The Foundation for Medical Research, 84A, RG Thadani Marg, Worli, Mumbai - 400018, Maharashtra, India. Email: [email protected] * Corresponding Author Abstract
According to WHO, 80% of the population of developing countries rely on
traditional medicines, mostly plant drugs, for their primary health care needs.
Also, modern pharmacopoeias still contain at least 25% drugs derived from plants.
With the growing importance and popularity of plants, several attempts are being
made to provide validation to the use of medicinal plants. Approaches towards
validation include both preclinical and clinical testing. However in view of the
limitations of directly utilizing clinical trials on the basis of information obtained
from databases, cited literature and/or ethnobotanical studies, preclinical testing
becomes an important prerequisite.
The paper will underline the various advantages of preclinical testing of medicinal
plants justifying its niche. Shortcomings of some of the commonly used
preclinical assays especially with respect to screening for antimicrobial activity
and generalized immunological parameters will also be discussed. The various
approaches to preclinical testing with emphasis on using bioassays representative
of disease process as exemplified by data obtained at FMR on plants with
antidiarrhoeal activity will also be discussed.
Introduction
There is no doubt that modern medicine offers tremendous advantages and its
application is wide spread. Despite this, traditional medicine has maintained its
popularity all over the developing world and its use is rapidly spreading. The
history of usage of plants is probably as ancient as the human civilization; modern
pharmacopoeias contain at least 25% drugs derived from plants. Even today it is
60

estimated that 80% of the population of developing countries relies on traditional
medicines, mostly plant drugs, for their primary health care needs. However use
of these medicines is mainly in raw and semi-standardized form and often based
on empirical evidence. The lack of pharmacological and clinical data on the
majority of herbal medicinal products is a major impediment to the integration of
herbal medicines into conventional medical practice. The present paper will
discuss some of the relevant issues associated with the preclinical testing of plants
related to the approaches, the advantages and the limitations.
Before covering the pre clinical testing, the various approaches to plant
selection and some issues related to adverse effect profile, clinical testing of
medicinal plants are briefly discussed.
Approaches to Medicinal Plant Selection
Several reviews have described approaches that can be used for selecting plants of
potential therapeutic interest (Verpoorte, 2000; Phillipson and Anderson, 1989;
Kinghorn, 1994; Vlietinck and Vanden Berghe, 1991; Farnsworth, 1996;
Farnsworth and Bingel, 1977).
The search can follow three main routes: random, ethno (including
ethnobotanical, ethnomedical and ethnopharmacological) and ecological search
(Fabricant and Farnsworth, 2001). The ethnobotanical and ethnopharmacological
approach uses information obtained from traditional medical practitioners and
other people such as village elders and local women who are traditional users of
medicinal plants. Ethnomedical information is available from ancient texts of
different systems of medicines such as Ayurveda, Unani, Kampo, and traditional
Chinese medicine. Plants with medicinal properties can also be selected using the
ecological approach. The absence of predation in areas infested with herbivores,
for example, can indicate the presence of toxic compounds. Selection can also be
based on an approach called zoopharmacognosy, a variation to the ecological
approach, which proposes the selection of plant species regularly ingested by
animals, mostly primates for reducing pain, microbial or worm infestations (Berry
et al., 1995).
61

Evaluation of Medicinal Plants
Artuso (1997) has outlined the entire process which include formulating an
appropriate strategy, obtaining biologic extracts, screening those extracts,
isolating active compounds, conducting preclinical tests and chemical
modification, etc. This approach is very demanding since there is an estimated
250,000 species of higher plants present on this earth (Ayensu and DeFilipps,
1978). Of the 6% plants that have been screened for biologic activity, only 15%
have been evaluated phytochemically (Verpoorte, 2000). However, this scenario
would change due to use of the advanced screening methods that are available
today. Reverse pharmacology based on the documented therapeutic effects of
plants in ancient texts can prove to be a more productive and cost effective
approach in development of safe, effective and acceptable therapeutic agents
(Vaidya, 2006).
Before a plant can be used and popularized, depending on the intended usage,
it is necessary to establish its efficacy through biological assays and obtain its
adverse effect profile through literature or from toxicological studies (both short
term and long term) followed by controlled clinical trials.
Clinical Studies:
Well-established, randomized controlled clinical studies lead to the better
acceptance of herbal medicines. Clinical studies are necessary to confirm the
pharmacological effects of medicinal plants before they can be integrated into
conventional medical practice. This would be especially true in case of some
unrelated effects of therapy contributing to efficacy that may be difficult to
measure pre-clinically. Well recorded case reports can contribute towards useful
information at such times and put forward new hypothesis and stimulate further
study (Morris, 1989). However, double blind clinical trials may not be required
when an extensive and detailed database of case studies is available. Such a
database is especially important when a particular treatment is individualized.
The methods and guidelines used for clinical validation of modern medicines
must be applied to herbal products even though the latter has a holistic approach
to treatment. However, conventional concepts of clinical research design may be
difficult to apply when using clinical research to evaluate various systems and
62

practices of traditional medicine (WHO, 2000). This could be due to the fact that
herbal remedies are individualized (each person has certain predispositions to
disease and susceptible to factors like environment, genetics, dietary and lifestyle)
therapies.
The number of patients required for undertaking clinical trial of medicinal
plants is large not only since the study design needs to be adequate and
statistically appropriate but also to cater to the control, confounders and placebo
groups to provide sufficient evidence for judging efficacy of the plant under study.
The increase in patient number also increases the time commitment and the
expenses involved. Moreover, it may not always be possible to include all the
groups in a single study for e.g., use of a placebo may not be possible when the
plant preparation has a strong smell or taste as is the case of certain essential oils.
In addition, patients who have been treated previously with the herbal medicine
under investigation that has a characteristic organoleptic property cannot be
randomized into control groups (WHO, 2000).
Therefore only a limited number of plants can be subjected to clinical
trials. Hence, it is essential to undertake appropriate preclinical testing to
short list plants for clinical evaluation. The main goals of the preclinical
studies are to determine a drugs pharmacodynamics, pharmacokinetics and
toxicity through animal studies. This data allows researchers to estimate a
safe starting dose of drug for clinical trials in humans.
Preclinical testing
Preclinical testing is an integral part of the modern drug discovery process which
helps in collection of important efficacy and safety data before clinical trials can
be carried out. It is a vital step towards sources of new, effective and safe drugs.
The preclinical evaluation of medicinal plants involves documentation and
testing of their biological efficacy, studies of toxicology and chemical profiling.
These have been covered in the subsequent sections.
Phytochemical studies:
Medicinal plant preparations are chemically complex and may contain one or
many structurally related active compounds that produce a combined effect.
63
Phytochemical studies help in standardizing the herbal preparations so as to get
the optimal concentrations of these active constituents, as well as in preserving
their activities. The aim of phytochemical studies is to identify the bioactive
constituents in the plants, devise suitable methods for their extraction, help in
standardization and quality control. For a detailed discussion see (Brijesh et al.,
this issue).
Toxicity studies:
Toxicological studies include acute, subchronic and special toxicology such as
immunotoxicity, genotoxicity, carcinogenicity and reproductive toxicity (Remirez,
2006). These test help in the identification of possible target organs involved and
the toxic symptoms. Studies of special toxicology such as carcinogenesis are very
important if the plants contain compounds with known mutagenic or carcinogenic
activities (Chanabra et al., 2003). It is recommended that a minimum of 2 or 3
mammalian species be used for the in vivo screen. Rodents like mice, rats, or
guinea pigs are used in the initial screen to be used later in combination with other
species such as dogs and monkeys.
Adverse effect profile: It is often argued that prolonged and apparently uneventful
use usually is testimony of safety of medicinal plants. However, a history of
traditional usage is not always a reliable guarantee of safety since it is difficult for
traditional practitioners to detect or monitor delayed effects (e.g. mutagenicity),
rare adverse effects, and adverse effects arising from long-term use (Ernst, 1998),
such as for food supplements and nutraceuticals. Absence of any such
documentation does not automatically rule out the possibility of toxicity. It is
possible that that the plant preparation taken up for clinical trial may lead to some
unanticipated / unknown / unrelated side effect that may vary from person to
person.
The use of herbal preparations may also lead to hypersensitivity reactions
ranging from transient dermatitis to anaphylactic shock (Ernst, 1998). Many
widely used medicinal plants have been implicated as possible causes of long-
term disease manifestations such as liver and kidney diseases. The widespread use
of Scenecio, Crotalaria and Cynoglossum has been implicated in the occurrence
64

of liver lesions and tumours, lung and kidney diseases in certain areas of Ethiopia
(Addae-Mensah, 1992). Another example is of Psoralea corylifolia Linn. which is
used for treating conditions like psoriasis, leucoderma, and non-healing ulcers and
wounds is known to cause hepatosplenomegaly in experimental animals
(CHEMEXCIL, 1992).
There is increasing information available on adverse side effect such as
undesirable outcome on excessive or prolonged usage e.g., Glycyrrhiza glabra
which is used for conditions like bronchitis and peptic ulcers causes not only
hypertension, weight gain and hypokalaemia but also lower levels of aldosterone
and anti diuretic hormone on excessive or prolonged usage (Newall et al., 1996;
toxic effects, e.g., Kava-kava, a well-established hypnotic drug, was reported to
show hepatotoxicity and had to be eventually banned in most countries worldwide
(Wheatley, 2005); allergic reactions, e.g., allergic reactions such as
rhinoconjunctivitis and contact dermatitis have been reported with Allium cepa
(Valdivieso et al., 1994)., interactions with drugs and other herbs, e.g., it has
been advised not to use Silybum marianum with a protease inhibitor during
antiretroviral therapy (Rogers, 2004).
Hence it becomes necessary to carry out toxicological studies, both short
term and long term before initiation of clinical trials, and the risk-benefit
ratio of the herbal drugs also need to be evaluated (Seth and Sharma, 2004).
Biological testing:
Biological screening is a necessary approach to provide a scientific basis for the
continued use of the plants, thereby validating their traditional utilization. It is
necessary not only to establish the therapeutic potential of medicinal plants but
also for identifying and comparing various plant preparations for potency.
Additionally, these studies aid to correlate the activity with some component in
the plant. Thus biological screening along with chemical profiling aids in
standardization of plant material.
Biological screening involves
1. In Vitro Screening: wherein isolated cells, tissues and organs provide an in
vitro model system to initially determine the biological activity of the drug.
65

2. In Vivo Screening: wherein the in vitro biological activity is assessed in
suitable animal models. Animals are also used when a suitable in vitro model
is not available for a particular condition. Besides testing of plant in powder
form or products active on in vivo breakdown, which cannot be tested in vitro
system, have to be tested in animals. Animal testing lays the foundation for
the later clinical trials by aiding in determining several important parameters
like – route of administration, dosage, duration of treatment, fate of the drug
within the host, etc.
Designing of screening assays: The design of a screening assay is an array of
multiple choices, all of which have significant impacts on the outcome of the
overall drug discovery process. The selected assay should be able to mimic the in
vivo dynamics as far as possible with high sensitivity and specificity in examining
the target activity. The basis for designing a screening assay is the identification of
valid target. An estimated 30-40% of experimental drugs fail due to an
inappropriate target (Butcher, 2003) and hence it is important to develop new
screening assays with newer and more appropriate targets. It is crucial to establish
the role of the target in question in the cause or symptoms of a disease (Williams,
2003). Pharmacological manipulation of the target should consistently lead to
desired phenotypic changes. The desired changes must also be reproducible in at
least one relevant animal model (Drews, 2003). To meet these demands, a great
deal of research is required in areas such as target selection and in the
development of improved methodologies for detection and cell based screens.
Emphasis has to be placed on assessment of assay quality and validation of the
parameters being used.
Assay formats employed in screening can be either cell-based or biochemical.
Though the logistics of cell-based assays are more challenging than with
biochemical assays due to requirement of significant investments in cell culture
infrastructure (Moore and Rees, 2001), the current trend in drug discovery is
clearly shifting towards cell-based assays. Cell-based screening has multiple
advantages. It can provide biologically more relevant information on the nature of
the activity (Moore and Rees, 2001; Johnston and Johnston, 2002). In addition,
66

information regarding cellular membrane permeability and cytotoxicity can also
be obtained.
Several researchers have worked on medicinal plants with activity against
different ailments. However, a large proportion of medicinal plant research is
focused on nutraceuticals, chronic and metabolic disorders (diabetes,
cardiovascular etc.) and other diseases like HIV/AIDS, malaria etc. Common
infectious diseases, especially in resource poor communities, such as diarrhoeal
diseases and acute respiratory tract infections are often not addressed or testing is
limited to microbicidal assays.
The general approaches that are commonly used for studying the
pharmacological effects of medicinal plants are: use of single bioassay for
screening multiple plants and use of multiple bioassays for studying single plant.
The latter approach has been used widely for metabolic diseases; bioassays often
represent different steps of a disease cascade with individual bioassay representing
one or more steps in the disease process e.g screening of Magnifera indica for
inhibitory effect on tumor necrosis factor (TNF) and nitric oxide (NO)
representing antioxidative activity (Remirez, 2006).
Unfortunately when screening plants for infectious diseases the assay system
is often limited to testing for antimicrobial activity. However this approach is not
always appropriate. Plants can exhibit their efficacy against infectious diseases by
mechanisms other than antimicrobial activity. When screening plants for immuno-
enhancing properties, often synthetic antigens and immunological assays are used
which do not have any biological relevance to disease(s) in question. The
importance of using relevant and where necessary multiple bioassays for
screening medicinal plants for infectious diseases is highlighted in the studies
conducted by Foundation for Medical Research on antidiarrhoeal (infectious
diarrhoea) medicinal plants. In these studies, medicinal plants were studied for
their effect on different stages of diarrhoeal pathogenesis and not restricted to
antimicrobial profile / gastrointestinal motility as reported by others (Akah et al.,
1999; Kambu et al., 1990; Tona et al., 1999). To the best of our knowledge the
effect of medicinal plants on infectious diarrhoeal pathogenesis has not been
studied.
67

Based on the pathogenesis, adherence & invasion (as markers of colonization)
to HEp-2 epithelial cells and production & action of bacterial enterotoxins [E. coli
heat labile toxin (LT) and cholera toxin (CT); and E. coli heat stable toxin (ST)] in
addition to the antimicrobial activity were used at FMR to test the efficacy of
medicinal plant for antidiarrhoeal activity and thus define the possible
mechanism(s) of action in infectious diarrhoea. The decoctions of two plants viz.
Cyperus rotundus (unpublished data) and Pongamia pinnata (Brijesh et al., 2006)
tested using the multiple bioassays have been used in this paper as examples.
C. rotundus decoction had no antibacterial to six strains of bacteria (Fig. 1a)
or antirotaviral activity (data not shown), but had a static action against G. lamblia
(Fig. 2a). It inhibited production of CT but not its action (Fig. 3a). On the other
hand it inhibited action of LT but not its production (Fig. 4a). It had no effect on
ST (Fig. 5a). The decoction reduced the bacterial adherence to and invasion of
HEp-2 cells (Fig. 6a and 7a respectively). In comparison, P. pinnata had no
antimicrobial activity (Fig. 1b and 2b); reduced only production of CT (Fig. 3b)
and bacterial invasion (Fig. 7b). It did not reduce bacterial adherence (Fig. 6b) and
had no effect on action of CT (Fig. 3b) or production & action of LT (Fig. 4b) and
ST (Fig. 5b).
A B
Fig. 1: Antibacterial Activity: (A) Cyperus rotundus; (B) Pongamia pinnata.
68
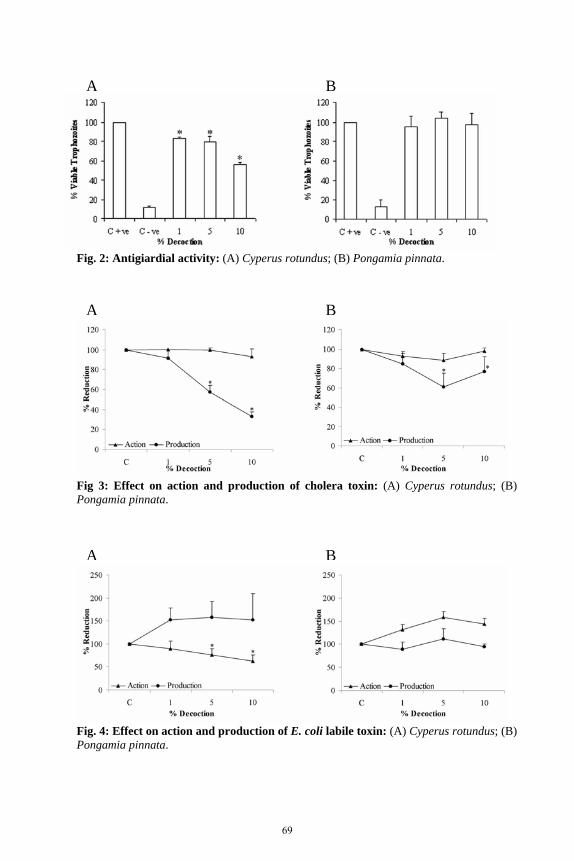
Fig. 2: Antigiardial activity: (A) Cyperus rotundus; (B) Pongamia pinnata.
A B
Fig 3: Effect on action and production of cholera toxin: (A) Cyperus rotundus; (B)
A B
Pongamia pinnata.
A B
Fig. 4: Effect on action and production of E. coli labile toxin: (A) Cyperus rotundus; (B) Pongamia pinnata.
69

Fig. 5: Effect on production and action of E. coli stable toxin: (A) Cyperus rotundus; (B) Pongamia pinnata.
A B
A B
Fig. 6: Effect on adherence of E. coli B170 to HEp-2 cells: (A) Cyperus rotundus; (B) Pongamia pinnata.
A B
Fig. 7: Effect on invasiveness of E. coli E134 and Shigella flexneri to HEp-2 cells: (A) Cyperus rotundus; (B) Pongamia pinnata.
70

In summary, C. rotundus has a wider efficacy and would be effective in most
forms of diarrhoea as compared to P. pinnata which has limited efficacy and
would be effective only against invading organisms (and hence bloody diarrhoea)
and V. cholerae. Thus though both the plants did not have marked antimicrobial
action; they are effective antidiarrhoeal agents with different mechanism(s) of
action. Had the study included only screening for antimicrobial activity, both C.
rotundus and P. pinnata would have been considered not to be efficacious. Thus
the study highlighted the necessity of looking at different parameters and not just
concentrating on singular assays like antimicrobial activity for determining the
biological efficacy of plants. In addition based on the results one can arrive at a
rational plant combination for combating different forms of diarrhoea. Ingredients
of this combination can be used to formulate an appropriate ‘herbal package’ for
diarrhoea, which could be effective against all or most of diarrhoeal agents. Such
a package can then be popularized in rural communities where it is difficult for the
people to differentiate between causative agents. This can then lead to generation
of self-help at grassroots.
Another approach used especially when plants are screened for their
immunomodulatory is studying their effects using general immunological
parameters to defined antigens such as lymphoproliferation, nitric oxide
production, antibody production, monocyte phagocytosis etc. However this
approach is not always appropriate as generalized immunological assays can give
misleading results. For example lymphoproliferation can sometimes measure
DTH, or antibodies may not always be protective against a disease, or increase in
phagocytic activity can lead to paralysis of phagocytes.
1. The studies lead to the determining of the therapeutic effect of the plant in
question and also elucidate the efficacy and / or the mechanism of action of
medicinal plants including cell interactions, cell-environment interactions,
intracellular activity, and genetic studies. Plants with novel and / or multiple
mechanism(s) of action can be identified.
2. One of the major advantages of preclinical studies is that one can easily study
and compare the efficacy of different plants in a cost effective manner in a
71

short period of time. The identification of the most efficacious plant part and
the type of extract to be used can also be achieved simultaneously.
3. Development of a rational drug combination can be achieved. This includes
using multiple bioassays designed on the disease process and / or screening
for activity against a spectra of microorganisms (in case of infectious
diseases) to get an insight of varied and diverse mechanism(s) of action of a
plant under study. An example of this has already been discussed dealing with
FMR data on antidiarrhoeal medicinal plants.
4. Isolation of phytoconstituents in the crude extract will be time consuming and
costly. Bioassay guided fractionization can lead to the identification of active
principles and reduces an overwhelming task to isolate all major compounds
from a crude extract.
5. Important information pertaining to the rate and extent to which the
therapeutic moiety is absorbed; is made available to the site of drug action
and the kinetics of drug absorption, its distribution and elimination can be
achieved through studies on bioavailability and pharmacokinetics of the plant
in question.
6. Shelf life of plant material is usually ignored due to the general belief that the
plant materials do not have an expiry date. However this is not always true.
Biological screening can help monitor the degradation of plant material and
decide the appropriate storage period.
7. Preclinical pharmacological safety data obtained from both in vitro (cell-
based or biochemical) and in vivo studies on animals can be used as indicators
of potential toxicity.
8. Unlike the clinical trials, the burden of ethics in the preclinical testing is
minimal.
Limitations of Preclinical testing:
1. Suitable pharmacological models have not yet been developed for many
common diseases with unknown, or multifactorial origins (Hamburger and
Hostettmann, 1991)
2. The lack of a positive result in a screening assay does not always mean the
absence of bioactive constituents. This may occur under two circumstances-
72

a) the active principle (s) may be present in insufficient quantities in the crude
extracts to show activity in the dose levels employed, b) the assay system
employed may not be the appropriate one. Alternatively, if the active
principle is present in high enough quantities, there could be other
constituents exerting antagonistic effects or negating the positive effects of
the active principles during the assay (Farnsworth, 1993).
3. The in vitro bioassays used for preclinical testing often have certain
limitations for e.g. Phenols can affect enzyme-based targets while saponins
may disrupt membranes in cellular targets or dislodge substrates absorbed
onto assay wells (Taylor et al., 2001). Another limitation would be the
interference of pigments in colorimetric or quenched assays (Taylor et al.,
2001).
4. In vitro assays cannot screen for active principles that are generated as
metabolized products in vivo (Farnsworth, 1993)
5. The pharmacological investigation of drug interactions in multi /compound
preparations is difficult due to the presence of constituents from several plants
where some plants may show less specific activity and some plants may have
been added to reduce the toxicity of the more therapeutically effective plants
(Taylor et al., 2001).
6. In case of bioassay-guided fractionation, there is a possibility of loss of
activity as the compound in question may be sensitive to temperature, light,
acidity, basicity or the extracting solvent and consequently it is progressively
degraded during fractionation. Alternatively, some compounds are inactive in
situ but act synergistically with other constituents of the extract. Separation
into different fractions during purification will thus result in a decrease or
total loss in activity in all the fractions e.g. loss of activity of Cirriformia
tentaculata upon its hexane fractionization (Kicklighter et al., 2003).
7. All human ailments do not have animal models.
8. Some of the most common side effects are difficult to recognize in animal
models e.g. nausea, nervousness, lethargy, heartburn, headache, depression,
stiffness, etc.
9. Extrapolation of in vitro dose to in vivo animal models and humans is
difficult.
73

10. Difficult to test organic extracts and dry powders not soluble in water in vitro.
Conclusions:
The area of medicinal plant research is fast developing. Both pre clinical and
clinical testing are integral components of medicinal plant research. Preclinical
testing of plants for medicinal properties is of vital importance, not only to
provide a scientific basis for their usage but also validate their historical utilization
by traditional healers and herbalists, and thus provides the society with sources of
new, effective and safe drugs. With the opening of newer vistas in the field of
medicine including the modern molecular biology tools, high output automated
bioassays and newer technologies for rapid structure determination in the area of
medicinal plant research, the field of preclinical testing seems to have a bright
future. Despite the limitations, the various advantages the pre clinical testing
offers, justify it as an essential prerequisite of a drug discovery process. It is
possible that with the advancement of technology, current tests could prove
successful where negative results may have been obtained 20 years ago (Prance,
1994). Thus preclinical testing can serve as an important link between a plant
selection and its subsequent mass usage following proper clinical testing.
Acknowledgements
The financial assistance of Sir Dorabji Tata Trust, Sir Ratan Tata Trust and
Department of Science and Technology, Ministry of Science and Technology,
Government of India (grant number 91283) is acknowledged.
References
1. Addae-Mensah I. 1992. Towards a Rational Scientific Basis for Herbal
Medicine – a Phytochemist’s Two-Decade Contribution.Accra: Ghana
Universities Press.
2. Akah PA, Aguwa CN, Agu RU. 1999. Studies on the antidiarrhoeal properties
of Pentaclethra macrophylla leaf extracts. Phytother Res.13:292-5.
3. Artuso A. 1997. Drugs of Natural Origin: Economic and policy aspects of
discovery, development, and marketing. Pharmaceutical Products Press, New
York.
74

4. Ayensu ES, DeFilipps RA. 1978. Endangered and Threatened Plants of the
United States. Smithsonian Institution, Washington DC.
5. Berry JP, McFerren MA, Rodriguez E. 1995. Zoopharmacognosy: A
“biorational” strategy for phytochemical prospecting. In: Gustine DL, Flores
H. (eds.), Phytochemicals and Health, ASPP, Rockville, Pp. 165-178.
6. Brijesh S, Daswani PG, Tetali P, Rojatkar SR, Antia NH, Birdi TJ. 2006.
Studies on Pongamia pinnata (L.) Pierre leaves: Understanding the
mechanism(s) of action in infectious diarrhea. J Zhejiang Univ. SCIENCE B.
7: 665-674.
7. Butcher SP. 2003. Target discovery and validation in the postgenomic era.
Neurochem Res. 28: 367-371.
8. Chanabra RS, Bucher M, Wolfe abd Portier C. 2003. Toxicity
Characterization of environmental chemicals by US National Toxicology
Program: an Overview Int J Hyg Environ Health. 206:437-445.
9. CHEMEXCIL. 1992. Selected Medicinal Plants of India, Bhartiya Vidya
Bhavan's Swami Prakashanand Ayurveda Research Centre, Bombay.
10. Drews J. 2003. Strategic trends in the drug industry. Drug Discov Today. 8:
411-420.
11. Ernst E.1998. Harmless herbs? A review of the recent literature. Am J Med.
104: 170–178.
12. Fabricant D, Farnsworth NR. 2001. The value of plants used in traditional
medicine for drug discovery. Environmental Health Perspectives, 109: 63-75.
13. Farnsworth NR. 1993. Biological approaches to the screening and evaluation
of natural products. In: Rasoanaivo P, Ratsimamanga-Urverg S. (eds.)
Biological Evaluation of Plants with Reference to the Malagasy Flora,
Monograph from the IFS-NAPRECA Workshop on Bioassays. Madagascar,
Pp 35– 43.
14. Farnsworth NR. 1996. Biological and phytochemical screening of plants. J
Pharm Sci. 55: 225-276.
15. Farnsworth NR, Bingel AS. 1977. Problems and prospects of discovering new
drugs from higher plants by pharmacological screening. In: Wagner H, Wolff
P. (eds.), New Natural Products and Plant Drugs with Pharmacological,
Biological or Therapeutical Activity. Springer, Berlin, Germany. Pp: 1-22.
75

16. Hamburger M, Hostettmann K. 1991. Bioactivity in plants: The link between
phytochemistry and medicine. Phytochem. 30: 3864–3874.
17. Johnston PA, Johnston PA. 2002. Cellular platforms for HTS: Three case
studies. Drug Discov Today. 7: 353-363.
18. Kambu K, Tona L, Luki N, Cimanga K, Uvoya A. 1990. Antibacterial
activity of extracts from plants used in preparations as antidiarrheal at
Kinshasa, Zaire. Ann Pharm Fr. 48:255-63.
19. Kicklighter CE, Kubanek J, Barsby T, Hay ME. 2003. Palatability and
defense of some tropical infaunal worms: alkylpyrrole sulfamates as
deterrents to fish feeding. Mar Ecol Prog Ser. 263: 299-306.
20. Kinghorn AD. 1994. The discovery of drugs from higher plants.
Biotechnology. 26:81-108.
21. Miranda D, Pereira L, Sirsat SM, Antarkar DS, Vaidya AB. 1993. In vitro
action of Dadima (Punica granatum Linn.) against microorganisms involved
in human gastrointestinal infections – isolation and identification of tannins.
Journal of Research in Ayurveda and Siddha. 14:154-64.
22. Moore K, Rees S. 2001. Cell-based versus isolated target screening: How
lucky do you feel? J Biomol Screen. 6: 69-74.
23. Morris BA. 1989. Importance of case reports. Can Med Assoc J. 141: 875-
876.
24. Newall CA, Anderson LA, Phillipsen DJ. 1996. Herbal Medicines: A Guide
for Health Care Professionals, The Pharmaceutical Press, London, Pp. 296.
25. Phillipson JD, Anderson LA. 1989. Ethnopharmacology and Western
medicine. J Ethnopharmacol. 25: 61-72.
26. Prance GT. 1994. Introduction. In: Ethnobotany and the Search for New
Drugs. Ciba Foundation Symposium 185. Chichester: John Wiley & Sons, p
1–3.
27. Remirez DC. 2006. Update in Pre-Clinical Regulatory Requirements for
Phytomedicines in Latin America. J Compl Int Med. 3(1): Article 3.
28. Rogers T. 2004. CATIE Fact sheet: Herb drug interaction. p1-6
29. Seth SD, Sharma B. 2004. Medicinal plants in India. Indian J Med Res. 120:
9-11.
76

30. Taylor JLS, Rabe T, McGaw LJ, Jäger AK, van Staden J. 2001. Towards the
scientific validation of traditional medicinal plants. Plant Growth Regulation.
34: 23–37.
31. Tona L, Kambu K, Mesia K, Cimanga K, Apers S, DeBruyne T, et al. 1999.
Biological screening of traditional preparations from some medicinal plants
used as antidiarrhoeal in Kinshasa, Congo. Phytomedicine. 6:59-66.
32. Valdivieso R, Subiza J, Varela-Losada S, Subiza JL, Narganes MJ, Martinez-
ocera C, Cabrera M. 1994. Bronchial asthma, rhinoconjunctivitis, and contact
dermatitis caused by onion. J Allergy Clin Immunol. 94(5):928-30.
33. Vaidya ADB. 2006. Reverse pharmacological correlates of ayurvedic drug
actions. Indian J Pharmacol. 38:311-315.
34. Verpoorte R. 2000. Pharmacognosy in the new millennium: lead finding and
biotechnology. J Pharm Pharmacol. 52: 253-262.
35. Vlietinck AJ, Vanden Berghe DA. 1991. Can ethnopharmacology contribute
to the development of antiviral drugs? J Ethnopharmacol. 32: 141-153.
36. Williams M. 2003. Target validation. Curr Opin Pharmacol. 3: 571-577.
37. Wheatley D. 2005. Medicinal plants for insomnia: a review of their
pharmacology, efficacy and tolerability. J Psychopharmacol. 19(4):414-21.
38. WHO. 2000. General guidelines for methodologies on research and
evaluation of traditional medicine. World Health Organization, Geneva.
77

2.5 Challenges in Preclinical Testing of Traditional Medicines: In Search of Solutions Nirmala Rege Department of Pharmacology and Therapeutics, Seth GS Medical College &KEM Hospital, Mumbai - 400012, India. Email: [email protected] Abstract
There is no doubt that pre-clinical development of plant drugs from traditional
systems of medicines should be based on scientific principles. However, while
working with drugs from traditional medicines several problems are posed
pertaining to agent itself, assay methods and analysis of data. These are discussed
by the speakers of this session giving examples of various assays they have used
in their laboratories.
What is additionally important is the review of literature, both from
traditional system of medicine and modern science. Critical appraisal and
interpretation of the text of traditional system helps one to select appropriate
extraction and fractionation procedure and also provide guidance for selection of
relevant model.
Ideal conditions for pre-clinical testing are described in the literature and it is
necessary for the researcher to use standardized plant material for the study and
adhere to the GLP. At the same time, to meet these ideal criteria may not always
be possible. It is therefore essential to define bare minimum or acceptable limits.
Selection of appropriate concentration for in vitro assay and its correlation to the
dose for in vivo model remains the problem for traditional drugs. However, it is
essential to clarify whether the concentrations/doses are expressed in terms of
extract concentration or crude drug concentration. In case of former, percentage
yield from the crude drug needs to be mentioned. Without proper clarification, if a
cut-off for concentration is decided then, a clinically used drug may get rejected in
bioassay. In vitro effects may not correlate with in vivo effects and it is essential to
use at least 2-3 in vivo models to confirm the results.
The combined results of in vitro and in vitro models assist in extrapolating the
findings to human in better way.
78

Some other points which need to be discussed are unique mode of action of a
plant drug, especially herbo-mineral formulation which may be totally different
from the known drugs in that therapeutic area; widely used screening models may
not be suitable for detecting therapeutically relevant pharmacological properties of
plant drug; and in conventional in vitro models effect of metabolites are not
detected.
The discussion of the present session will focus on addressing these
challenges and deriving the best possible solutions.
Full text not received
79

3.1 Traditional Knowledge Guided Testing of Quality, Safety and Efficacy of Herbal Medicines Padma Venkatasubramanian Joint Director, Foundation for Revitalization of Local Health Traditions (FRLHT), B74/2, Jarakbande Kaval, Post Attur, Via Yelahanka, Bangalore – 560064, India. Email: [email protected] Abstract
The world is witnessing an unprecedented growth in the usage of herbal products
at national as well as international levels. The issue of quality is becoming more
and more pertinent since the herbal medicines available in a country may have its
origins in an alien country/culture, thereby making regulation and quality control
that much more difficult. Unlike in olden times where traditional physicians
prepared and tested the quality of herbal medicines, the problems faced today are
those of economics of industrial scale production, shelf-life, and distribution to
long distances. These have necessitated development of modern and objective
standards for evaluating the quality, safety and efficacy of these medicines. The
current standards, parameters and protocols available to test the quality of herbal
medicines were originally developed for allopathic drugs and can at best
authenticate the identity of plant materials (maybe purity to some extent) not their
safety or efficacy.
Herbal medicines are natural products and their phytoconstitutents vary
depending on time and region, processing and storage. Variations in the
collection, processing or storage of an herb could impact its efficacy profile. Since
prior knowledge regarding appropriate collection and usage of most medicinal
plants exists in tradition, it can be used as a guide to quality standardisation. The
parameters of testing of the quality of materials (dravya) in traditional medicines,
such as rasa (taste), guna (properties), virya (potency), vipaka (post-digestion
effect) and karma (action), are very different from the western methods. These
traditional parameters reflect not only the quality but also efficacy. Having said
which, there are no direct written protocols available in traditional medicine either
for collection or for testing the action. The methods of testing are lost today and
need revivification.
80

The issues for deliberation in the present paper would be:
1. medicinal plant quality and factors affecting the same
2. the relevance of western & traditional parameters used to identify the quality
of a herbal product
3. R & D efforts at FRLHT, Bangalore
The objective of research at FRLHT is two-fold with respect to quality
standardization of medicinal plants: (i) development of modern scientific
standards for medicinal plants taking into consideration the traditional advice on
medicinal plant identity, collection, processing and storage and (ii) development
of contemporary scientific methods to test traditional parameters such as rasa.
The strategy adopted has been to firstly document the advice and protocols on
medicinal plants usage from texts and from living traditions of medical
practitioners, conduct preliminary laboratory tests and then to identify the unique
chemical/biological markers. The laboratory techniques such as phytochemistry,
chromatography (HPLC, HPTLC), molecular biology and bioassays are used to
study the quality. Biological activities are subsequently verified through
appropriate animal testing.
In a pioneering attempt, modern sensory evaluation has been used in a
systematic manner, as one of the quality testing tools for evaluation of quality of
herbal medicines. Sensory evaluation methods and standards are being developed
for herbal medicines.
Why do we need new strategies?
The standards used for checking the quality of medicinal plants are broadly based
on modern botanic description (macroscopy), anatomy, chemistry and
microbiology. On scrutiny (Table 1) one can understand that the values indicated
in a modern Certificate of Analysis (CoA) for any raw drug either reflects its
identity, purity or strength but not its biological activity, when the whole purpose
of using the raw drug is for its medicinal properties. The specific conditions
(time/ region) of collection of the plant are also not specified. These are precisely
the drawbacks in the current approaches to standardization of medicinal plants.
81
Table 1: Modern Certificate of Analysis for Ginger (Mukherjee, 2002)
Botanical Name: Zingiber officinale Roscos Part Used: Rhizome Organoleptic characters: Yellowish brown, in colour, aromatic, pungent
Test Limits Protocol used Foreign Organic Matter <1 % Sand & silica Absent WHO Insects Nil Rodents Nil Ash Content <8 % w/w Acid Insoluble Ash <1.0 % w/w Moisture Content <12 % w/w WHO Volatile Oil Content 1-2.6 % w/w Water Soluble Extractive >14% w/w Alcohol soluble extractive >6% w/w Markers/Active Gingerol, Shogaol Phytoconstituents TLC Fingerprint HPLC Fingerprint
Traditional Indian Medicine such as Ayurveda has a different way of
classification of quality of medicinal plants which combines at once the
pharmcognosy (properties) and pharmacology (action). The parameters of quality
in Ayurveda (Table 2) are rasa (taste), guna (properties), virya (potency), vipaka
(post-digestive effect) and karma (action).
Table 2: Ayurvedic standards of ginger (Anonymous, 2001)
Parameter Standard Rasa (Taste) Katu (pungent) Guna (Properties) Laghu (light), Snigdha (unctuous) Virya (Potency) Usna (hot) Vipaka (Post-digestive effect)
Madhura (sweet)
Karma (Action) Deepaka (stimulates digestive), Pachana (digestive), Hrdya (good for heart), Anulomana (creates movement) etc.
It can be noted that the pharmacognosy and pharmacology of the raw drug are
inseparably evaluated in Ayurveda. This was done by trained scholars called
aptas, through human perception. As to know when these qualities are fully
expressed there were general (Table 3) as well as specific recommendations either
available in texts or are well known to the traditional healers and physicians.
82

Table 3: Ayurvedic recommendations for collection of medicinal plant parts
Plant Part Collection Season Branches & leaves Rainy & Spring Roots Summer & Late winter Bark, Rhizome, Sap Autumn Heartwood Early winter Flowers & Fruits As per season
However, the major hurdle in this is the access to information and protocols
of assessment of Ayurvedic properties. It is not methodically documented and
available as a ready reckoner. Significant proportion of the information may also
be lost over the centuries. Due to this, modern parameters and standards are being
used to screen/test Ayurvedic medicines, which do not truly reflect its safety or
efficacy. These include phytochemical, anatomical or molecular standards.
Unlike in Ayurveda, which used human body and perception to study the
properties and action of a drug, there is no single instrument in modern S & T that
can check at once the pharmacognosy and pharmacology of the drug. Human
sensory evaluation is of particular value in the Food & Beverage industry (such as
wine and tea) but not in the modern pharma sector. Sensory evaluation is still
used by the traditional Ayurvedic drug industries for raw drug identification and
preparation of formulations, but protocols are not documented and therefore
appear subjective. With the onset of industrialisation of Ayurvedic products, finer
details such as best time and place of collection etc are being ignored.
The team at FRLHT has taken a traditional knowledge guided approach to
standardize the quality of medicinal plants. It is two-pronged approach: (i) the
method of reverse pharmacognosy is being employed, where, the plant material
taken for standardization is according to traditional knowledge, (ii) Traditional
Quality Parameters, such as rasa are being researched both from Ayurvedic view
point as well as through modern scientific tools.
Strategy
The following strategy has been adopted for research into Traditional Quality
Standards (TQS) at FRLHT:
83
1. Documentation: Since there are no ready-reckoners available in traditional
knowledge on quality standards, advice on collection etc. of medicinal plants,
it is important to firstly document the same from traditional texts such as
Caraka Samhita as well as from living traditions. Through a limited study
funded by National Geographic Society, over 20000 verses pertaining to
quality aspects of 2000 medicinal plant names have been compiled from
12 classical Ayurvedic texts by FRLHT (Venkatasubramanian and
Geeta, 2004). Important information on traditional methods of processing
and purification of 10 toxic plants such as Strychnos nux-vomica, Croton
tiglium, and Abrus precatorius were also documented from traditional elderly,
but practicing physicians during this study.
2. Informatics: In order to store, retrieve and analyse the wealth of information
compiled, a prototype CD, has been developed with information on the
purification methods on 10 toxic plants. This contains facility to query, save,
print and browse not only text but also crucial images and video-clippings
collected during the documentation (FRLHT, 2004).
3. Prioritisation of Specific Recommendations: A prioritized list of 30
recommendations was prepared based on the specificity and practicality of
the traditional advice. A few examples are provided in Table 4. These
recommendations were taken up for conducting further studies.
Table 4: Examples of specific traditional advice on medicinal plants
Identity Vidanga seeds (Embelia ribes) are also called chitra tandula (patterns on the seeds) and resemble Kapala (bowl shaped structure)
White Seeds of Abrus precatorius are better than red ones for medicine preparation
Collection Mature vidari (Ipomea mauritiana) should be used in formulations Haridra (Curcuma longa) is best collected at night
Bhallataka (Semecarpus anacardium) fruits should be collected when it resembles ripened ‘Jamboo’ (Syzygium cumini) fruits
Processing Pippali (Piper longum) should be prepared as a milk decoction Commiphora mukul (guggul) should only be used after shodhana (purifiction)
Vidanga (Embelia ribes) seeds should be used after storing for one year
Storage
84

4. Inter-cultural studies: Understanding the context and purpose of traditional
advice requires an inter-cultural approach that in turn requires a dialogue
between different disciplines such as trade and distribution information on the
raw drug, Ayurvedic information from text and practice, collection of
botanically correct specimens for testing and standardization using modern
phytochemistry/biological methods.
Study 1: Inter-cultural study on Vidanga
FRLHT has conducted an inter-cultural study to identify the authentic species
that can be called as vidanga as per Ayurveda. Vidanga is one of the 10 most
traded plants in volume and there are at least 3-4 botanical species being
traded as Vidanga. Prior correlations have indicated that Embelia ribes to be
the authentic species. However, our market and distribution study pointed out
that > 95% of the traded species are E. tsjeriam-cottam. There were also other
Myrsinacea members such as Myrsine africana, My. capitellata and Maesa
indica that were being used as vidanga. On analysis of Ayurvedic
terminologies pertaining to vidanga, such as chitratandula (patterns on
seeds), kapaala (bowl-shaped structure), kshudra tandula (small seeds), some
of the candidates such as M. indica and My.africana were eliminated. The
closest matches were E. ribes and E. tsjeriam-cottam (Fig 1).
Fig. 1: Characteristics of vidanga seed.
Bowl shaped
Patterns on seed
Upon learning that both E. ribes and E. tsjeriam-cottam are good
candidates for vidanga as per Ayurveda, further work on microscopy, HPTLC
and HPLC were used to distinguish the authentic from the adulterants.
85

Molecular tools such as RAPD-PCR have been used to distinguish between
the species at the DNA level (Fig 2).
Fig 2: Distinction of species traded as vidanga RAPD-PCR technique.
Study 2: Traditional knowledge guided Quality standards for Ipomea
mauritiana tubers
Tuber of Vidari (I. mauritiana) is a galactagogue and an immunomodulator as
per Ayurveda. However, the immature tubers are discarded while selecting
the mature ones during preparation of medicine. The main parameter based
on which the distinction is made by physicians is through the size. Mature
ones are larger than the immature ones (Fig 3).
Our aim was to (i) determine if the traditional ways of culling had a
bearing on the activity of the raw drug (ii) identify the chemicals that would
reflect its activity not just the identity. The culling of the tubers was done by
a qualified and experienced physician on which grading was noted as per size
and categorized as totally immature and totally mature. The bioactivities of
the extracts of the tubers were compared to reflect their overall difference
through Brine Shrimp Bioassay (Meyer et al., 1982). The bioactivities of the
mature tubers were twice as active as that of the immature ones. The HPLC
profiles of the tubers indicated that the ratio of peaks at ~11 min and 15 min
increased significantly with maturity (Fig 4). Fig. 3: Morphology of mature and immature tubers of I. mauritiana.
86

Preliminary studies on immunomodulatory effect on rats (Indian ink,
oral) have shown that the phagocytic index of mature extracts is twice that of
immature. The compounds of interest appear to be β-sitosterol as studied
through LC-MS. Further investigations are ongoing to identify maturity and
bioactivity related marker.
Minutes0.0 2.5 5.0 7.5 10.0 12.5 15.0 17.5 20.0 22.5 25.0 27.5 30.0
Vol
ts
0.000
0.025
0.050
0.075
0.100
0.125
0.150
0.175
Vol
ts
0.000
0.025
0.050
0.075
0.100
0.125
0.150
0.175
2.90
8
3.72
54.
267
4.83
3
6.15
06.
483
6.75
07.
008
7.60
8
9.02
5
10.2
17
11.2
5011
.975
13.3
75
15.0
92
16.3
58 16.8
7517
.508
20.7
42 29.8
58
Detector A - 1 (254nm)L0512009 3stage (2.5 mgpml)L0512008 3stage (2mg-1ull)
Detector A - 1 (254nm)L0512016 10 stage (2.5 mgpml)L0512016 10 stage (2mg-1ul)
Retention Time -- Mature Fig 4: Comparative HPLC of mature and immature tubers of Ipomea mauritiana.
-- Immature
Study 3: Sensory Evaluation as a Quality Control tool
Even today, sensory evaluation is used by the managers in traditional
medicine industry (especially small scale manufacturing units) to check the
quality of raw ingredients as well of end products. It also is an effective on-
line process control tool. Sensory evaluation is an accepted scientific quality
control tool in the food and beverage industry as well as the perfume industry.
It requires rigorous protocol development for each product, testing by trained
panel and statistical analysis. At FRLHT, protocols have been developed
(combining traditional and modern sensory parameters) for 3 products and 10
raw drugs including trikatu choorna, nisha amlaki and bala taila. Easy-to-use
formats and instructions have been developed for use by the SSUs.
Conclusion
Standards for medicinal plants have to reflect not only the identity but also their
efficacy and safety. Working out the safety and efficacy profiles through animal
studies and clinical trials for the enormous number of plants would not only be
expensive but also time-consuming. Traditional knowledge about collection and
usage of medicinal plants has the advantage of experience that can be tapped. Just
87

as these days, reverse pharmacology is being used to identify bioactive molecules
from sound formulations of traditional medicine, reverse pharmacognosy can be
employed to identify quality determining standards as per traditional knowledge.
The paper has illustrated with examples the strategy that needs to be followed in a
traditional knowledge guided approach to build relevant standards.
The hurdles that need to be crossed are of various kinds, such as:
• Policy and fund allocation for research in Traditional Medicine
• Mind set of modern scientists & journals in accepting the importance of
cross-cultural research
• Documentation of TQS from texts and living traditions
• Access of plants and information to researchers
• Identification of appropriate scientific tools to study the TQS
• Networking and sharing of research findings/standards within and outside the
country, especially the users such as small scale manufacturing units,
physicians, farmers.
References
1. Anonymous. 2001. The Ayurvedic Pharmacopoeia of India, Vol 1 Part 1
(First Edition), pp 103
2. FRLHT’s Traditional Quality Standards—Purification of 10 Toxic Plants. A
Prototype CD. 2004, FRLHT, Bangalore.
3. Meyer BN, Ferrigni NR, Putnam JE, Jacobsen LB, Nichols DE, McLaughlin
JL. 1982. Brine Shrimp: A Convenient General Bioassay for Active Plant
Constituents. Planta Medica 45: 31-34.
4. Mukherjee P. 2002. Quality Control of Herbal Drugs, Pharmaceutical
Publishers.
5. Venkatasubramanian P, Geeta UG. 2004. Documentation of traditional Indian
Methods of Medicinal Plants Collection, Processing and Storage- A Report
submitted to National Geographic Society, FRLHT, Bangalore.
88

3.2 Principles of Quality Control, Standardization and Chemo profiling of Medicinal Plants and ISM Preparations Ravi K. Khajuria* and S. G. Agarwal Indian Institute of Integrative Medicine (formerly Regional Research Laboratory), Canal Road, Jammu Tawi – 180001, India * Corresponding Autior Overview:
The recent years have witnessed resurgence of interest in herbal medicines as
more and more people throughout world are turning to use medicinal plant
products in healthcare system. The sales for herbal medicine products have
plateaued to such an extent that these products have become available to
consumers as positive healthcare just like vitamins. They are now found in
supermarkets, pharmacies and numerous other main stream retail outlets as over-
the-counter drug products.
Botanical medicines, similar to all pharmacologically active substances have
the potential to contribute positively, neutrally, or negatively to the health status of
the people. World wide need of alternative medicine has resulted in growth of
natural product markets and interest in traditional systems of medicine. The use of
plants for health or medicinal purposes has been a part of every culture or region
but now this science of herbal drugs is passing through the age of renaissance.
Through out the world, the major problem that hinders the prospects of herbal
products in becoming the main stay of any treatment modality is the difficulty in
standardizing a formulation. System of Ayurveda is well respected globally and
many of the herbals used in Ayurveda, are covered in WHO monographs on
selected medicinal plants, thus confirming the efficacy of the Ayurvedic, Siddha
and Unani (ASU) System.
There are about 10,000 plant species which are being used in Indian System
of Medicines (ISM) /traditional medicines in Indian subcontinent. Out of these,
450-500 species are mostly utilized in over 85% of the Ayurvedic, Unani and
Siddha formulations and about 40 plant species are used in modern drugs. Twenty
five of these are cultivated while other plant species are collected by
89

proper/destructive harvesting. Important parameters for collection of the plant
materials are proper botanical identification, proper chemo-type/ecotype, desired
state of maturity, post-harvest processing technology and proper storage
conditions. These herbals account for a large chunk of global drug market,
therefore assurance of their quality, safety and efficacy needs additional attention.
Safety Parameters:
Standardization of herbal drugs is gaining momentum in India and as a result, it is
also proposed to include the safety parameters as per International norms. So far
as drugs are concerned one must remember that “Safety comes first and quality
afterwards”. Therefore, In addition to proper botanical identification and physico-
chemical parameters, test for heavy metals (Mercury, Lead, Cadmium, Arsenic),
microbial contaminants (Total viable aerobic count, Total Enterobacteriaceae,
Total fungal count), specific pathogens (E. coli, Salmonella spp., S. aureus,
Pseudomonas aeruginosa), pesticide residue (organochlorine, organophosphorus,
pyrethroids & others), aflatoxin (B1, B2, G1, G2) should also be an important part
of any Quality control protocol. State-of-art facilities have been installed at
Quality Control Laboratory of RRL, Jammu to test such parameters.
Botanical concerns: (Identification of true ASU herbal drugs, Taxonomic
characterization, Collection, Post-Harvest Processing and Storage)
Many a time similar names have been very frequently used for several related
umbelliferous fruits, mint leaves and various other plant materials and thus,
different plant species are sold in the market under the same name in different
parts of Indian sub-continent. We would like to mention a few to draw attention.
“Ajamoda” (Trachspermum roxbrghianum), a reputed drug of the Ayurvedic and
Unani systems of medicine but in the market Apium graveolens, Apium
leptophyllum, Trachspermum roxbrghianum and T. ammi are sold under one trade
name i.e. Ajamoda (Table1) in different regions (Dutt, 1974). The major chemical
constituents of all these four-plant spp. are different and can easily be
characterized on the basis of chemical markers (S. G. Agarwal, unpublished data).
Many species of Mentha such as M. spicata, M. virides, M. longifolia, M.
piperita, M. arvensis, M. aquaicta and M. pulegium are sold under one name i.e.
90

Pudina in various parts of the country but all the spp. contain different
monoterpenes. In some cases constituting monoterpenes are same; they are
present in different amounts in different species (Agnihotri et al., 2005). Three
plant species such as Carum carvi, Bunium persicum and Bunium cylindricum are
sold under one name i.e. Kalazeera and all the three contain entirely different
constituents. Fruit of another plant i.e. Cuminum cyminum is sold under the name
of Safed zeera has constituents similar to one of Kalazeera i.e. Bunium persicum
[Thappa et al., 1991; Agarwal et al., 1974; Agarwal et al., 1979 (Table 3)].
Similarly different ecotypes yield different constituents with various proportions
(Table 4)
On the other hand, many a time different plant species contain similar
chemical markers and same is true with Mucuna puriens, M. utilis and M.
cochchinensis, which all contain L-dopa as marker compound, although these are
very much different in size and appearance. Our own studies (Ahmed et al.,
2006) on three Tinospora spp which are sold in the market under the name of
“Guduchi” have revealed that there is lot of variation in the chemical constituents
of three spp of the plant i.e. Tinospora cordifolia, T. malabarica and T. crispa.
Further, chemical composition of many plant species is directly related to the
phenological stages of plant growth and changes with season. The best example is
commonly used vasaka (Adhatoda vasica) for cough & cold. At vegetative stage,
the total alkaloid content are highest with vasicine (90%) and vasicinone (5%); but
at full bloom stage alkaloid content falls with simultaneous variations in
quantitative composition with vasicine (45%) and of vasicinone (25%) of the
total alkaloids along with several other water soluble glycosylated, oxides and
other derivatives of vasicine/ vasicinone (Pandita et al., 1993). The post harvest
processing of Crocus sativus stigma by traditional methods which takes 3-5 days,
the amount of total crocins content is 7-9% and if the same stigma is processed at
45oC ± 5oC with tray load of 1M3 which requires 6-7 hours of drying, the amount
of crocins (Table 5) from the plant increases to more than 14% (Raina et al.,
1996).
Thus, there is a need to remove ambiguities related to proper herbals to be
used in ASU System of medicine followed by proper taxonomical identification,
harvesting time, post-harvest processing, storage conditions etc. as these are of
91

utmost importance in maintaining the quality of an herbal product. Therefore,
“Standard Operating Procedures” should be adopted for collection, processing
storage and sampling of herbs and herbal products. Further, ASU drugs should be
categorized separately, from the EU Herbal drugs, as these have evidence based
documented records and are widely used in Indian sub-continent for centuries.
Additionally, ASU drugs belong to organized system of healthcare and practiced
by experts in the field.
Chemical Standardization and Chemo-profiling of ASU drugs:
There are always chances of wide variations with respect of their chemical
contents in crude drugs/ raw materials of plant origin due to varied reasons such as
climatic conditions, geographical distribution, source and season of collection and
lack of scientific methods of post-harvest processing, storage and preservation.
Keeping these facts in view for acceptance or rejection criteria, minimum-
maximum limits for marker compounds, based on chemical analysis of large
number of samples for each drug/ herbal collected from different agro-climatic
zones with passport data has to be worked out, to have reproducible results.
Therefore, the only solution to place ASU System of medicines on global
market, is to chromatographically standardize the herbal products and wherever
possible quantitate them for active/or phytochemical marker(s). Thin Layer
chromatography is a powerful and simple analytical tool, used for this purpose;
there were situations where this tool of analysis did not give satisfactory results
because of its own limitations (Singh et al., 2003). Quantitative and qualitative
HPLC, HPLC/MS, HPLC/MS/MS, GC, GC/MS, GC/MS/MS, HPLC-UV–DAD
and HPTLC are well-suited analytical methods of choice to control the quality of
phyto-pharmaceuticals.
In modern times the issues of quality, safety and efficacy of medicines are
interrelated. The quality of drug is of paramount importance as it can affect the
issues of efficacy and safety. Long history of use and better patient tolerance as
well as acceptance, renewable source, cultivation and processing, environmental
friendly, local availability especially in the third world and several important
recent break-through are the major factors responsible for the resurgence of
interest in plant based drugs. The people all over the world have realized that vast
92

plant wealth has much to offer in the shape of new remedies which are
efficacious, safe and accessible to masses. By laying guidelines for the assessment
of herbal medicines under the programme on traditional medicines, WHO has
recognized the role of traditional system of medicines in healthcare programmers
all over the world. We in India therefore, have to gear up to the challenge
especially when we possess wealth of natural drugs second to none in the world.
According to world statistics developing one new drug needs screening of
10,000 molecules with 10-15 years of time and an expenditure of more than $ 900
million. But if we screen plant drugs from known natural sources with assured
therapeutic efficacy, the percentage of hits be increased, thus saving time and
money. WHO currently encourages, recommends and promotes traditional herbal
remedies in national healthcare programmes because such drugs are available at
reasonable price, comparatively safe and people have faith in such remedies. At
the same time, WHO in its number of resolutions have emphasized the need to
ensure quality.
In the present global market scenario related to traditional and herbal drugs,
People Republic of China is leading with 50% market share followed by Japan
(20%) and Russia (16%).Unfortunately India’s share is only 2.5% although the
internal market has crossed over Rs.4000 crore per year. The reason is very simple
and to ensure fair share in world market the quality control and scientific
evaluation data for Indian products has to be generated / presented to global
community. Development of ASU drugs with proper efficacy has been undertaken
by Department of Ayush, ICMR and CSIR through Golden Triangle Programme
utilizing traditional knowledge, latest safety, chemo-profiling and reverse
pharmacology route to arrive at standardized formulation (preferably with 3 to 5
ingredients) with IPR, for placing at global market.
Why standardization?
Reproducible assays of the plant preparation generate confidence in the mind of
the user and prescriber. To ensure consistent quality of the preparation, the
qualitative and quantitative chromatographic fingerprint on the basis of
characteristic substance(s) for raw materials and finished products should be
provided. Thus, the standardization of the herbal drugs and preparation thereof is
93

not just an analytical operation that ends with the identification and assay of an
active principle; rather it embodies total information (passport data of raw
material, quality parameters, process control) and controls that are necessary to
guarantee consistency of composition. The question of quality acquires greater
relevance today than ever before. Regulatory agencies and consumer groups on
one hand and increasingly stringent quality norms for global positioning of the
products on the other hand, demand that new materials and herbal products there
from, used for medicinal, nutritional and cosmetic purposes should be of
consistent reproducibility; scientifically (chemically and biologically) validated
and supplemented by data on documented evidence of efficacy and safety through
limited human clinical trials.
However, with rapid advancement in the field of instrumentation where limits
of detection (LOD) and limits of quantification (LOQ) have routinely been
upgraded to femto & atto levels, the chemical standardization of herbal products
by hyphenated techniques (HPTLC, HPLC, LC/MS and LC/MS, GC/MS) has
become more credible than biological evaluation of data.
Although liquid and gas chromatography are powerful tools for chemical
profiling of the herbals, but these in combination with mass spectrometric
detection has become more effective and convenient. The techniques are very
useful for the characterization and quantification of the individual constituents in
the plant extracts. LC/MS and GC/MS based multi component hyphenated
methods allow the determination of the components in the mixture. These
techniques are sensitive, selective, fast with inexpensive clean up for sample
preparation; where simultaneous separation as well as identification of the
components in a mixture is possible. LC/GC perform the function of separation
whereas MS performs the function of identification of the components in the
mixture on the basis of molecular mass and fragmentation pattern. It gives us two
dimensional information, the information from the UV/VIS or diode array
detector in LC and FID/ECD/NPD detectors in GC is the a first dimensional
information in the form of retention time whereas the second dimension of
information comes from the mass detector in the form of molecular mass and
fragmentation pattern. Techniques are very sensitive, selective and specific and
allow the detection of the compounds even in picogram amounts.
94

LC/MS has been playing a more significant role in plant medicine research
(Caig et al., 2002) because the technique is capable of characterizing active
components ranging from small molecules to macromolecules and recent
scientific results and publications show that application of LC/MS has been
rapidly expanding into the area of structure elucidation and characterization of
active components, in addition to valuable quantitative analysis. The LC/GC-MS
instruments are of two types, Ion trap and linear quadrupoles. Linear quadrupole
instruments are very sensitive and are used for quantitative analysis whereas Ion
trap technology is multi step fragmentation technology and the instruments based
on this technology are used for characterization of the molecule. Under CSIR’s
NMITLI Project, our studies on quantification of four chemical markers in
different cultivars (cultivated/ wild accessions) of Withania somnifera (Khajuria et
al., 2004) have provided us a very valuable and significant data. These studies
have revealed that an accession cultivated at Regional Research Laboratory
(CSIR), Jammu and coded, as AGB002 can be the best source for withaferin-A.
The PCR based RAPD and AFLP studies on this accession have revealed that this
accession has entirely different DNA sequence when compared with other
accessions. Gradual improvements in the LC/MS methods led to the development
of methods for quantification on the basis of five (Fig.1), seven (Fig.2) and finally
eight withanolides and withanosides (Fig.3).
LC/MS methods are very useful in determining active components and their
metabolites in pre-clinical studies. Studies on the metabolites of piperine, an
alkaloid constituent of Piper nigrum and Piper longum led to the characterization
(Bajad et al., 2003; Bajad et al., 2003) of two metabolites in rat urine. These
metabolites were characterized on the basis of LC/MS/MS and LC/NMR/MS/MS
data.
95

Fig. 1: HPLC Chromatogram of five markers of Withania somnifera
Fig. 2: HPLC Chromatogram of seven markers of Withania somnifera
Fig. 3: HPLC Chromatogram of eight markers of Withania somnifera
Over recent decade, a number of lead compounds and new natural products
derived from medicinal herbs have been successfully isolated and identified.
96
Chemical analysis plays a central role in development and modernization of
herbal or herbal-based medicines and mass spectrometry coupled to LC is
emerging as the technique of choice in the identification of active ingredients,
compositional analysis and chemical finger printing studies. Tandem mass
spectrometry (MS/MS) is a powerful technique for detecting a target compound in
complex matrices, including plant extracts and herbal drugs. The strength of this
technique lays in the selectivity, high sensitivity and fast screening capabilities
compared with many other separation and identification techniques. We have
developed a rapid LC/MS/MS screening method for detection of camptothecin in
an endophytic fungus Entrophosphere infrquens, which resides in the plant
Nothapodytes foetida (Touseef et al., 2006). For preparation of marker grade
hyperforin from Hypericum perforatum a preparative HPLC method (Anand et al.,
2003) has been developed by our group and similarly a very sensitive LC-MS
method was developed to check the purity and stability of the same. LC/MS
methods for the detection of different compounds like ß, ß-dimethylacrylshikonin
in tissue cultures of Onosoma echiodes etc. have been developed (Lattoo et al.,
2005). These methods are also used to detect the same compounds in the plant
extracts.
Conclusions
Proper botanical identification, proper chemo type/ecotype, proper/desired stage
of maturity, post harvest processing, storage, isolation of marker compounds
(preferably the therapeutic ones), validated analytical (GC, GCMS, LC, LC-MS
and LC-MS/MS) methodologies for the quantification of the extracts/fractions
are the important milestones in the herbal drug standardization. Ever increasing
discovery costs and increased failures at the end of the discovery line makes
medicines unaffordable to the developing countries. This makes new approaches
such as system biology and reverse pharmacology more attractive that provide
innovation opportunities that are based on experiential wisdom and holistic view
point of ‘Traditional Medicine’. It is known to all of us that drug discovery
pipeline in modern drug discovery is getting dry and modern world is looking
towards the herbal world with great expectations.
97

Table 1: Different plants sold under the name Ajmoda
Ajmoda Species constituent Volatile Oil Important 1. Apium graveolens
(Celery) 1-2% Limonene (~85%), pentyl benzene, 3-
n-butyl phthalide & other phthalides 2. Apium leptophyllum 1-2% Monoterpenes, coumarins 3. T. roxberghianum 4-5% Limonene (~15%), Cadinener (~ 24%),
β-cyclolavandulala/ acid is 15-25%, Seselin (~12-15%)
4. T. ammi 2-5% p-cymene, γ-terpinene, thymol Table 2 Different species of Mentha sold under the same name as Pudina
Pudina Species Volatile Oil
O
O
O
OH
O
O
Important constituents M. spicata l-limonene, l-carvone
M. virides Piperitenone oxide
M. longifolia l-limonene, l-carvone
M. piperita l-menthol (~ 50%), isomenthone others
M. arvensis l-menthol (~75%), menthone, others
M. aquatica Isopinocamphone O
O
M. pulegium Pulegone (~80%), piperitone, menthone
98

Table 3 : Different plants sold under the name Kalazeera and Safed Zeera
Zeera Species Volatile Oil Important constituents Kala Zeera Carum Carvi 2.5-4% d-limonene, d-carvone Bunium persicum 4-12% p-cymene, γ-terpinene, cuminaldehyde, p-
mentha-1,3-dienals, p-mentha-1,4-dienals Bunium cylindricum 1-2% Myristicin, Dillapiole, elemenes Nigella sativa - Carvone, limonene, p-cymene, thymol,
nigellone Safed Zeera Cumin cyminum 1.5-3% p-cymene, γ-terpinene, Cuminaldehyde, p-
mentha-1,3-dienals, p- mentha-1,4-dienals Table 4: Different ecotypes giving different constituents in different ratios
Ecotype Ajwain (Trachyspermum ammi)
Oil Thymol p-cymene + γ-terpinene
Moti Ajwain 1-3% 85-90% 10-15 % Choti Black 3-5% 35-45% 40-60% Khus (Vetiveria zizaniodes)
North Indian oil l -Vetiverol 63-78%
South Indian oil d-Khusinol (major) Table 5: Yields of crocins by using different drying techniques Crocus sativus
Post Harvest Processing Crocins pigment content Traditional processing 3-5 days 7-9% Processing at 45oC + 5oC (6 hrs drying) 14-17%
References
1. Agarwal SG, Thappa RK, Dhar KL, Atal CK. 1979. Essential oils of the
seeds of Bunium bulbocastanum Linn. Carum gracile Lindle and Cuminum
cyminum Linn. Indian Perfumer. 23: 34-37.
2. Agarwal SG, Vashist VN, Thappa RK, Singh K, Ghosh SC, Atal CK. 1974.
Terpenes and other components from Bunium cylindricum seeds.
Phytochemistry, 13: 2024-2025.
3. Agnihotri VK, Agarwal SG, Dhar PL, Thappa RK, Meena B, Kapahi BK,
Saxena RK, Qazi GN. 2005. Essential oil composition of Mentha pulegium L.
Flavour& Fragrance Journal. 20: 607-610.
99

4. Ahmed SM, Manhas LR, Verma V, Khajuria RK. 2006. Quantitative
Determination of four Constituents of Tinospora sps. by Reverse Phase
HPLC- UV(DAD) method: Broad based studies revealing variation in content
of four secondary metabolites in the plant in different eco-geographical
regions in Indian J Chromatographic Sci. 44: 504.
5. Anand A, Puri SC, Verma N, Handa G, Khajuria RK, Gupta VK, Suri OP,
Qazi, GN. 2003. A simple and reliable semi preparative HPLC technique for
the isolation of marker grade hyperforin from Hypericum Perforatum L. J
Chromatographic Sci. 41(8): 444-446.
6. Bajad S, Coumar M, Khajuria RK, Bedi KL, Suri OP. 2003. Characterization
of a new major metabolite 3,4-methylenedioxy phenyl-2E.4E-pentadienoic
acid - N-(3yl-propionic acid) amide of piperine , an ominipresent food
component by LC-NMR- Positive ESI-MS. European J Pharmaceutical Sci.
19(5): 413-421.
7. Bajad S, Khajuria RK, Bedi KL, Suri OP, Singla AK. 2003. Characterisation
of a new minor urinary metabolite by LC-MS/MS. J Separation Sci. 26 (9-
10): 943-946.
8. Caig Z, Lee FSC, Wang XR, Yu WJ. 2002. A capsule review of recent
studies on the application of mass spectrometry in the analysis of Chinese
medicinal herbs. J Mass Spectrometry. 37: 1013-1024.
9. Dutt AK. 1974. The Botanical Identity of Ajmoda. J Res Ind Med. 9: 96-98.
10. Lattoo, SK, Kaul S, Dhar MK, Khajuria, RK, Gupta DK, Qazi GN. 2005.
Production of β-dimethylacryl shikonin in callus cultures of Onosoma
hispidum, Var. hispidum. J Plant Biochem Biotechnol. 14: 193-196.
11. Khajuria RK, Suri KA, Gupta RK, Satti NK, Amina M, Suri OP, Qazi GN.
2004. Separation, identification, and quantification of selected withanolides in
plant extracts of Withania somnifera by HPLC-UV (DAD) - Positive ion
electrospray ionisation-mass spectrometry. J Separation Sci. 27(7-8): 541-
546.
12. Pandita K, Bhatia MS, Thappa RK, Agarwal SG, Dhar KL, Atal CK. 1983.
Seasonal variation of the alkaloids of Adhatoda vasica and the detection of
glycosides and N-oxides of vasicine and vasicinone. Planta Medica. 48: 81-
82.
100

13. Raina BL, Agarwal SG, Bhatia AK, Gaur GS. 1996. Changes in pigments
and volatiles of saffron (Crocus sativus L) during processing and storage. J
Sci Food Agric.71: 27-32.
14. Singh S, Pandey SC, Srivastava S, Gupta VS, Paetro B, Ghosh AC. 2003.
Chemistry and medicinal properties of Tinospora cordifolia (GUDUCHI)
Indian J Pharmacol. 35: 83-91.
15. Thappa RK, Agarwal SG, Singh K, Ghosh S. 1991. Comparative studies on
the major volatiles of Kalazira (Bunium persicum Seed) of wild and cultivated
sources. Food Chemistry. 41: 129-134.
16. Touseef A, Khajuria RK, Puri SC, Verma V, Qazi GN. 2006. Determination
and quantification of camptothecin in an endophytic fungus by liquid
chromatography - Positive mode electrospray ionisation tandem mass
spectrometry. Curr Sci. 91(2): 208-212.
101

3.3 Approaches to Standardization of Medicinal Plant Preparations Brijesh S., Poonam G. Daswani and Tannaz J. Birdi*
The Foundation for Medical Research, 84A, RG Thadani Marg, Worli, Mumbai - 400018, Maharashtra, India. Email: [email protected] * Corresponding Author Introduction
In the not too distant past disease treatment was entirely managed by traditional
forms of medicine, what is now considered in the developed world as alternative
medicine, especially of herbal origin. The interest in traditional medicine started
declining in late 19th century after the discoveries of antibiotics and other medical
technologies. However, currently it is estimated that about 80% of the world
population residing in the vast rural areas of the developing and under developed
countries still rely mainly on medicinal plants since it is the only affordable and
accessible source of primary health care especially in the absence of access to
modern medical facilities (WHO, 2002). Herbal medicinal preparations are
becoming popular in some developed countries also such as Germany, France,
Italy and the United States (Calixto, 2000). Significant economic gains have been
attained by the global and national markets as the demand for herbal medicines
have increased rapidly over the last two decades. According to the Secretariat of
the Convention on Biological Diversity, global sales of herbal products were an
estimated US $ 60000 million in 2000.
The increased use of herbal medicines in developed countries is mainly due to
the failure of modern medicine in providing effective treatment for chronic
diseases and emergence of multi-drug resistant bacteria and parasites. These
include various new diseases such as cancer, HIV/AIDS, diabetes, hepatitis,
allergies and mental disorders. The adverse effects of chemical drugs, questioning
of the approaches and assumptions of allopathic medicine, their increasing costs
and greater public access to information on safety and efficacy of medicinal plants
has also led to an increased interest in medicinal plants (WHO, 2002).
102

With the tremendous increase in their global use there have been several
concerns regarding the safety and quality of the herbal medicines from health
authorities and the public alike (WHO, 2002). There have been reports of
adverse/suboptimal effects of herbal medicines which have been attributed to
several factors such as inadvertent use of the wrong plant species, adulteration,
contamination, over dosage, inappropriate use by health-care providers or
consumers, and interaction with other medicines, resulting in an adverse drug
interaction.
The poor quality of herbal medicines can be attributed to the use of
substandard raw medicinal plant materials. The factors that can affect the safety
and quality of the raw medicinal plant materials and finished products can be
either intrinsic e.g. genetic or extrinsic such as environment, collection methods,
cultivation, harvest, post-harvest processing, transport and storage practices.
Microbial or chemical contamination during processing can also compromise the
safety and quality. Mistakes in proper identification of the plant species,
accidental contamination or intentional adulteration by other species or plant parts
can also lead to poor quality of the end product.
It is necessary to standardize the safety and quality assurance measures so as
to ensure a steady, affordable and sustainable supply of medicinal plant materials
of good quality. The pharmaceutical industry has shown interest in development
of standardized plant preparations with proven safety and efficacy. However, their
focus has been on isolating newer active principles from plants unlike the rural
communities that use fresh/dried plant material or their crude extracts. Moreover,
it is generally believed that standardization of the plant material is not required
when used by rural communities for their primary health care. But, regardless of
whether the medicinal plant is to be used by local communities or by
industry, a systematic approach is required for the validation of efficacy and
safety of the medicinal plants.
To ensure safety and quality of the medicinal plants it is necessary to focus on
all aspects of the medicinal plant research: from ethno-pharmacology, utilization,
isolation and identification of active constituents to efficacy evaluation, safety,
formulation and clinical evaluation. Quality control of the medicinal plants starts
right at the source of the plant material. The phytochemical composition of the
103

plant material and the resulting quality can vary due to several factors including a
number of environmental factors such as geographical location, soil quality,
temperature and rainfall etc. Taxonomy, the time of collection, method of
collection, cultivation, harvesting, drying and storage conditions, preparation and
other processing methods can also affect composition. Contamination by
microbes, chemical agents such as pesticides and heavy metals, as well as by
insects and animals during any of these stages can also lead to poor quality of the
finished product. Standardization of all these factors is necessary to meet the
current standards of quality, safety, and efficacy.
Source of Plant Material
Wild harvesting is still the prominent mode of obtaining medicinal plants and
most of the requirement of medicinal plants for the industries is still met through
wild collection (Lange, 1998). Though many medicinal plants are commonly
available in the wild and can be freely harvested, collection and sale of large
quantities of plant material from the forest can lead to destruction of many forest
plants especially the endemic species that have a restricted geographical
distribution. For example, medicinal plants like Curcuma caesia, Rauwolfia
serpentina were reported to occur abundantly (IUCN, 1994) in central India.
However, due to their growing economic importance and rampant harvesting,
these plants have now been categorized as critically endangered (Prasad and
Patnaik, 1998). The present deteriorating condition of medicinal plants in forests
needs immediate attention not only for conservation but also for propagation.
Countries can protect their biodiversity in medicinal plants by working with
industry towards monitoring and maintaining controlled non-destructive
harvesting with habitat management.
Cultivation of medicinal plants would seem as a commercially attractive
option to companies because they have greater control over supply of the plant
material and it is easier to control post-harvest treatment. Moreover, cultivation
can reduce the dependence on collection of plants from wild and thus have the
potential to save wild populations and conserve their genetic diversity.
The feasibility of such an approach would, however, depend on a number of
factors such as the ability of the species to thrive under mono culturing, while its
104

economic viability will depend on the demand and market prices. Moreover,
cultivation of medicinal plants requires intensive care and management and the
conditions and duration required can vary depending on the quality of the
medicinal plant material required. Risks of contamination from pollution by
hazardous chemicals should be avoided. Introduction of non-indigenous plant
species into cultivation can lead to detrimental consequences on the ecological
balance of the region (Sharma et al., 2005). However, collection from the wild
may be unavoidable for those medicinal plants that grow slowly, are difficult to
domesticate or for which only small quantities are needed.
A point that needs specific consideration is that cultivated plants are
sometimes considered qualitatively inferior to the wild collections. The medicinal
properties in plants are due to the combinations of secondary products. Different
plants often have taxonomically distinct combinations of these secondary
metabolites resulting in unique medicinal properties in individual plants (Wink,
1999). Secondary metabolites that are generally produced for defense against
predators, pathogens or competitors or for protection/adaptation to environmental
stress related to changes in soil conditions, temperature, water status, light levels,
UV exposure, and mineral nutrients in their natural habitats; and are responsible
for most of the biological activities, perhaps would not be expressed when
cultivated under optimum conditions to obtain better vegetative yields. For
example, the wild ginseng roots are 5-10 times more valuable than cultivated roots
because the cultivated roots lack the characteristic shape of wild roots (Robbins,
1998.). These beliefs were also reflected in the conclusion reached through
research on Arnica montana by the herbal company Weleda (Ellenberger, 1998).
Analysis of the biochemical properties of the cultivated plants showed differences
when compared with wild plants that grow in poor meadows with acidic soils in
mountainous areas of Europe. The rhizomes of the cultivated stocks had lost much
of Arnica’s characteristics, reducing its commercial potential.
Selection of Plants
As per WHO guidelines (WHO, 2003), the plant selected for collection should be
taxonomically same as recommended by the national pharmacopoeia or other
related documents. If a new plant is being selected for collection then it should be
105
properly identified and documented. The voucher specimens of the plant material
should be submitted to regional or national herbaria for authentication. Complete
taxonomical identification including varieties of the medicinal plants is an
important factor during selection as taxonomy of the plant species can play an
important role in their biological activity. This was observed in our study with two
varieties of Zingiber officinale wherein one variety showed immune enhancing
properties while the other did not (unpublished data).
Several reviews have described approaches that can be used for selecting
plants of potential therapeutic interest (Verpoorte, 2000; Phillipson and Anderson,
1989; Kinghorn, 1994; Vlietinck and Vanden Berghe, 1991; Farnsworth, 1996;
Farnsworth and Bingel, 1977). In general, the search for the medicinal plants can
follow three main routes: random, ecological (Fabricant and Farnsworth, 2001)
and ethno (including ethnobotanical, ethnomedical and ethnopharmacological)
based search. Random search is extremely laborious and the success rate could be
very low (Basso et al., 2005). The ecological approach uses information such as
absence of predation in a particular area infested with herbivores, which would
indicate the presence of toxic compounds.
The ethnobotanical, ethnomedical or ethnopharmacological approach is based
on information obtained from ethnobotanical survey. Undertaking of the survey
should be by a team of local botanists, traditional healers and medical
practitioners. While the traditional healers would identify medicinal plants for
treatment of different diseases, the botanist can carry out appropriate taxonomical
and botanical characterization of these medicinal plants, whereas the medical
practitioners would help in proper identification of the disease conditions (e.g.
differentiate between muscle pain and pain due to arthritis) and help in
understanding whether a treatment is curative or is alleviating the symptoms only
or whether it is a placebo effect.
It has to be specifically understood that there are certain differences in
approaches when selecting plants for an industrial or a rural application. The rural
community requires medicinal plants for their primary health care and hence
focuses more on selection of plants for treatment of common diseases such as
diarrhoea, malaria, pneumonia, wound infections etc. On the other hand
pharmaceutical industry requires medicinal plants for formulation of herbal drugs
106

for commercial gain and hence focuses more on urban problems such as metabolic
disorders, chronic diseases, and multi-drug resistance among infectious pathogens.
Whether for rural community or for industrial application the selection of plant
should be based on its therapeutic efficacy in terms of its effect on the causative
agent or on the host. From the rural perspective, since the understanding of
disease in terms of causative agents is not possible in the community, it is
important that the plant formulation should address the common causative agents
resulting in a given symptom e.g. diarrhea which is caused by various infectious
agents including bacteria, viruses and protozoa. The plants selected for utilization
by rural communities should be able to control the respective diseases or else at
least act as a stop gap until further medical aid becomes available. Moreover,
these plants should be easily available so that the users of these medications can
become self reliant.
Collection of Medicinal Plants
Good collection practices are necessary for the long term survival of wild
populations and their habitats. WHO guidelines (WHO, 2003) can be followed
while collecting medicinal plant materials. Prior to initiating collection, essential
information regarding the target plant species should be obtained. The botanical
identity, scientific name including genus, species, subspecies or variety and family
of the plant should be recorded. If available, the local name should also be
verified. Information regarding environmental conditions, such as topography,
geology, soil, climate and vegetation at the collection site, should be obtained.
Information such as the geographical distribution of the plant, its abundance,
whether it is threatened or endangered, shrub/fast growing tree etc should also be
obtained. It is of immense importance that a voucher specimen be deposited in a
national or regional herbarium for identification and further consultation by other
researchers.
Medicinal plant materials should be collected in the proper season so as to
ensure the best possible quality of both the starting material as well as the finished
product. Seasonal variations can affect the chemical composition of the plants and
thus its biological activity. This was demonstrated in one of our studies where the
decoctions of Psidium guajava leaves collected in two different seasons showed
107

variable antibacterial activity against six bacterial strains, the November collection
being more active than the March collection (data unpublished). In most cases,
maximum accumulation of chemical constituents occurs at the time of flowering
which then declines at the beginning of the fruiting stage (Mendonca-Filho, 2006).
The time of harvest should also depend on the plant part to be used since it is well
known that depending on the plant species the level of biologically active
constituents can vary in different parts at different stages of the plant growth and
development. For example, Kursar et al. (1999) found that younger leaves of
tropical rainforest plants contained secondary metabolites that were either present
in very little quantities or totally absent in matured leaves. The extracts from these
younger leaves showed better biological activity when tested for anticancer
activity or activity against Bacillus subtilis and Artemia salina (brine shrimp). It
also applies to other components in the plant material such as the toxic
components. Climatic conditions, e.g. light, rainfall, and temperature (including
daytime and nighttime temperature differences) also influence the physical,
chemical and biological qualities of medicinal plants. The water and temperature
stress related increase in the content of active constituents such as the total
phenolic compunds was shown by Nacif de Abreu and Mazzafera (2005) in
Hypericum brasilience. Hence the best time of collection should be determined
according to the levels of the biologically active constituents rather than the
vegetative yield.
Information such as the correct plant parts that are used (roots, leaves, fruits
etc.) and whether these parts are seasonal or replenishable should be obtained. The
collection levels and the collection practices should also be known before
initiating collection. It is necessary that the collection practices employed should
be non-destructive. For example, while collecting roots, the main root should not
be cut or dug up or while collecting bark, the tree should not be girdled or
completed stripped of its bark. Parts that are not required or are decomposed and
any foreign matter such as soil or toxic weeds should be removed during
collection.
Collection of medicinal plants should not be done from places that are prone
to or close to sources of contamination such as areas where high levels of
pesticides or other possible contaminants are used or found e.g. roadsides,
108

drainages, mine tailings, garbage dumps and industrial facilities which may
produce toxic chemicals or active pastures that may lead to microbial
contamination. Quality control ensures that the plant material is not contaminated
with microbes, pesticides, heavy metals or other toxic agents (Mendonça-Filho,
2006) and that the final product is of consistent high standard.
Rapid and safe transportation of the collected plant materials should be
arranged in advance. Handling of the plant material such as cleaning, drying and
storage, should be carried out by trained personnel.
Processing of Plant Materials and their Preparation
Preliminary processing of the plant material that can be done include elimination
of undesirable materials and contaminants, washing to remove soil, sorting and
cutting. It would be advisable to dry the plant materials prior to transportation if
the processing facilities are located away from the collection sites. Cross
contamination of the different collected plants or plant parts should be avoided
during transportation. The plant materials should be protected from conditions that
may cause deterioration such as rain, moistures etc during or after transportation
till the processing begins. The plant materials that need to be used fresh should be
delivered as quickly as possible to the processing facility to prevent microbial
fermentation or thermal degradation.
Specific processing methods are often required, to reduce drying time, to
detoxify the inherent toxic constituents, to reduce side effects or to enhance
therapeutic effects. For example, the methods and temperatures used for drying
may have a considerable impact on the quality of the resulting medicinal plant
materials. Shade drying is the preferred method for drying plant material since it
can maintain or minimize loss of color of leaves and flowers; and the lower
temperatures can prevent the loss of volatile substances in the plant materials
(Ibanez et al., 2003; Bartram, 1995). However, plants can be dried in a number of
other ways: in drying ovens/rooms and solar dryers; by indirect fire; baking;
lyophilization; microwave; or infrared devices. Pre-selection, peeling the skins of
roots and rhizomes, boiling in water, steaming, soaking, pickling, distillation,
fumigation, roasting, natural fermentation, treatment with lime and chopping are
some of the common processing practices. All processed medicinal plant materials
109

should be protected from contamination and decomposition as well as from
insects, rodents, birds and other pests, and from livestock and domestic animals.
Medicinal plant preparations can be prepared in several ways that usually
vary based upon the plant being used, and sometimes, the condition for which it is
being used. These preparations can be in the form of infusions, decoctions,
tinctures, macerations, fresh juices etc. Some other methods include hot baths,
powdered plants, steam inhalation and even aromatherapy. Adherence to the
method of preparation as mentioned in the ancient texts or by traditional
practitioner is necessary depending on the form of preparation or the plant used as
they may hold important information for obtaining an effective herbal preparation.
A juice of a plant may be recommended instead of decoction/powder if the active
ingredients are volatile or thermo labile e.g. fresh leaf juice of Adhatoda vasica is
used for reducing blood glucose level of diabetic patients (Ahmad, 2007).
Sometimes, it is possible that due to the difficulty in preparation of the extracts
and the time required, whole fresh material (e.g. leaves) or dried powder is used
instead of the required extract for treatment. This may lead to potential toxicity
which would otherwise not be observed due to the elimination of the toxic
constituent during extraction. In this context, an example that can be cited from
our study is the extraction of negligible amounts of the toxic component karanjin
from the leaves of Pongamia pinnata in the aqueous decoction (Brijesh et al.,
2006).
The medicinal property of plants is closely related to the different classes of
phytoconstituents (such as essential oils, alkaloids, acids, steroids, tannins,
saponins etc.) present in the plant, each of which would have a preferred effective
method of extraction, facilitating maximum yield in preparation. E.g. preparing a
decoction might extract a group of anti-inflammatory plant steroids to treat
arthritis and yet when the same plant is prepared in alcohol different antibacterial
alkaloids are extracted instead (http://www.rain-tree.com/prepmethod.htm)
Storage
Storage can also influence the physical appearance and chemical quality of plant
materials and hence it is necessary to maintain appropriate storage conditions so
as to increase their shelf life. It is customary to store the plant material in dried
110

form since preparations like decoctions/infusions can only be stored for a few
days. Dried plant materials can be stored in whole, crushed or powdered forms in
storage conditions that include use of cloth bags, clear glass bottles and plastic.
Plant materials that are used fresh should be stored under refrigeration, in jars or
sandboxes, or using enzymatic or other appropriate conservation methods.
However, they should be used as quickly as possible to avoid microbial
contamination. Shelf life of plant material is usually ignored due to the general
belief that the plant materials do not have an expiry date, however, dried plant
materials usually retain their activity for about six months only. It is observed that
the powdered plant material degrades faster than the whole or crushed plant
material (unpublished data). Different types of plastics can be used which prevent
absorption of moisture and oxidation of the plant material by preventing the
exchange of gasses to increase the shelf life of the plant material.
Phytochemical Studies
Medicinal plant preparations are chemically complex and may contain one or
many structurally related active compounds that produce a combined effect.
Phytochemical studies help in standardizing the herbal preparations so as to get
the optimal concentrations of these active constituents, as well as in preserving
their activities. The aim of phytochemical studies is to identify the bioactive
constituents in the plants, devise best methods for their extraction, understand
their side effects and calculate appropriate dosages.
Standardization can be carried out by obtaining a chemical fingerprint/profile
or through bioactivity guided fractionation. Chemical fingerprints through
chromatographic techniques are more commonly used for standardization and are
obtained in terms of one or more marker compounds. It would be ideal to use the
active constituent in the plant as the marker compound, however in cases where
active constituents are not known, the marker compound can be independent of
the therapeutic activity. Furthermore, the plant extracts can also be standardized to
class of compounds e.g. ginsenosides in ginseng, kava lactones in kava, or
oxindole alkaloids in cat’s claw. Such an approach would be suited to situations
where though the active constituents are not known but are expected to belong to a
particular class of compounds.
111

According to European Medicines Agency guidelines (EMEA, 2005),
quantification of substances with known therapeutic activity or markers is
obligatory. As per the European Pharmacopoeia, marker compounds should be
characteristic or unique for the herbal material or herbal preparation; have an
established chemical structure; be present in the starting material as well as the
finished product in sufficient amounts; be accessible to quantification with
common analytical methods such as high-performance liquid chromatography
(HPLC) or high-performance thin layer chromatography (HPTLC); be sufficiently
stable; and be commercially available or able to be isolated by the company in its
own laboratory.
Thin layer chromatography (TLC) and HPLC are the most commonly used
methods for obtaining chemical fingerprints and identification of the crude plant
extracts. However, there are several possibilities that may arise while using these
techniques for standardizing the crude extracts. It is possible that the plant
materials collected from the same plant in two different seasons can show
different phytochemical fingerprint and therefore different biological activity or
two plants with identical taxonomy collected under same environmental
conditions can show different phytochemical fingerprint but similar biological
activity. In such situations comparisons of the phytochemical profiles as an
indicator of important constituents can act as a shortcut for identifying
biologically active constituents. Another possibility that may arise is when two
different plants showing similar phytochemical fingerprints show different
biological activity. In such situations bioassay guided fractionation or any other
suitable method is the only option in identifying the biologically active
constituents.
DNA fingerprinting is another technique, which though still in its early years,
seems to be of immense potential in identification of medicinal plants, particularly
when profiling the genotypic differences (Vasudevan, 2004). Apart from
identifying these genetic variations, it can also aid in identification of germplasms
of important or endangered plants for future cultivation or conservation.
Use of isolated compounds can result in better biological activity due to
higher concentrations, but it can also lead to potential side effects e.g. the active
constituent conessine isolated from Holarrhena antidysenterica, a plant
112

commonly used by Ayurvedic practitioners in treatment of diarrhea, was found to
be toxic to the central nervous system (CHEMEXCIL, 1992). More recent studies
have also indicated at reduced biological activity with isolated active constituents
compared to crude extracts (Kicklighter et al., 2003).
When using crude extract, a factor that can affect the outcome in terms of the
biological activity, as observed above, is the synergism between the different
active constituents that may be present in the extract. Synergism can lead to better
activity as well as decrease in potential toxicity of some individual constituents.
Synergism can be due to the individual action of different constituents present in
the extract at multiple target sites/parameters. This was observed in a study
conducted by FMR on the antidiarrhoeal activity of P. guajava (unpublished
data). It was observed that the decoction of the dried leaves of P. guajava showed
antidiarrhoeal activity by showing antimicrobial activity against five out of the six
bacterial strains tested, Giardia lamblia and rotavirus. It inhibited adherence to
and invasion of the bacterial pathogens to the epithelial cells. It also inhibited
production and action of enterotoxins such as Escherichia coli labile toxin and
cholera toxin. These results suggested that the different constituents present in the
decoction could be individually responsible for the different activities observed
against these parameters. Another mechanism by which these constituents can
show synergism is by having an additive effect against a single target
site/parameter. It was observed that the decoction of P. guajava leaves were
consistently more active at a dilution of 1% than at 5% against bacterial adherence
to epithelial cells. This effect could be due to the fact that the ratio of constituents
achieved at 1% was more optimal for activity than at 5%.
The modern analytical and isolation methods that are used for screening and
isolation of plant constituents are the chromatographic and spectroscopic
techniques such as TLC, thin layer electrophoresis, HPLC, nuclear magnetic
resonance, HPTLC etc. These techniques have proved very useful in isolation
and proper identification of the active constituents in the plant extracts.
These techniques, however, are not applicable at the grassroots, as they
cannot be used by the community. Hence it is necessary to devise simple
techniques for standardization that can be used by the community for identifying
113
plants with good biological activity. Use of a class of compounds, as mentioned
earlier, as a surrogate marker is a potential approach to identifying plants with
good biological activity at the grassroots. For example, instead of a single
polyphenol, tannins can be used as surrogate marker, which the schoolchildren
can estimate easily in their laboratories. This approach has been attempted by us
in collaboration with the Foundation for Research in Community Health, in their
field project at Parinche, Maharashtra.. We estimated levels of tannins in
decoctions (prepared as per standard Ayurvedic texts) of five different
collections of P. guajava leaves and compared them with their respective
activities against action of cholera toxin (data unpublished). It was observed that
the decoctions with >10.5 mg/ml tannins showed good activity with no
significant difference in their activities. However, below this level the activity
was significantly poorer. Hence, 10.5mg/ml tannin level may be taken as a cut-
off value for differentiating a P. guajava plant with good activity from that with
poor activity.
Biological Screening
Biological screening along with phytochemical standardization forms an integral
part of preclinical studies that is essential for generating important efficacy and
safety data to validate the claimed therapeutic potential of the plant before it is
tested in clinical trials. It is helpful in understanding various factors affecting the
biological activity of a plant right from the selection to the formulation of the
herbal drug and their standardization. This point, however, will not be discussed
in detail in this paper.
Conclusions
With the tremendous increase in the global use of medicinal plants, several
concerns regarding the safety and quality of the herbal medicines have also been
observed. Hence it has become necessary to standardize the safety and quality
assurance measures so as to ensure supply of medicinal plant materials of good
quality. Though the pharmaceutical industry has been focusing on standardization
of plant materials when manufacturing herbal drugs, it is generally believed that
114

standardization is not required when used by rural community for their primary
health care. However, irrespective of whether the plant is being used by the
industry or by the rural community standardization of plant material is required.
The difference comes when using isolated active constituents that are required by
the pharmaceutical industry for manufacturing herbal drugs whereas rural
communities may use standardized extracts. The decision on whether to collect
plants from the wild or to cultivate it would depend on the feasibility of the
approach for that particular species. After proper botanical identification, WHO
guidelines should be followed for collecting plant material in terms of proper
season and climatic conditions, correct plant part, practices that are non-
destructive and would prevent contamination from soil, toxic weeds or microbes.
Post collection, appropriate processing and storage conditions are required to
reduce drying time, detoxification to reduce side effects and to enhance
therapeutic value of the plant material and to improve its shelf life. Phytochemical
standardization for identification of the plant material can be carried out by
obtaining chemical fingerprint through chromatographic techniques in terms of a
known marker compound or through bioassay guided fractionation and/or DNA
fingerprinting techniques. Chromatographic and spectroscopic techniques have
proved very useful in isolation and proper identification of active constituents in
the plant extracts. Biological screening plays a vital role in generating important
efficacy and safety data to validate the claimed therapeutic potential of the plant
before clinical trials are carried out. Hence, ‘standardization’ involves the quality
control of various factors affecting the therapeutic activity of a plant right from
selection of the plant species to the formulation of the herbal drug so that it
minimized batch-to-batch variation and meets standards of quality, safety, and
efficacy.
Acknowledgements The financial assistance of Sir Dorabji Tata Trust, Sir Ratan Tata Trust and
Department of Science and Technology, Ministry of Science and Technology,
Government of India (grant number 91283) is acknowledged.
115

References
1. Ahmad M, Khan MA, Zafar M, Sultana S. 2007. Treatment of common
ailments by plant-based remedies among the people of district attock (Punjab)
of northern Pakistan. Afr J Trad CAM. 4 (1): 112 –120.
2. Bartram T. 1995. Encyclopaedia of Herbal Medicine. Grace: Dorset.
3. Basso LA, Pereira da Silva LH, Fett-Neto AG, Filgueira de Azevedo Junior
W, de Souza Moreira Í, Palma MS, Calixto JB, Filho SA, Ribeiro dos Santos
R, Soares MBP, Santos DS. 2005. The use of biodiversity as source of new
chemical entities against defined molecular targets for treatment of malaria,
tuberculosis, and T-cell mediated diseases – A Review. Mem Inst Oswaldo
Cruz, Rio de Janeiro. 100(6): 575-606.
4. Brijesh S, Daswani PG, Tetali P, Rojatkar SR, Antia NH, Birdi TJ. 2006.
Studies on Pongamia pinnata (L.) Pierre leaves: Understanding the
mechanism(s) of action in infectious diarrhea. J Zhejiang Univ SCIENCE B.
7: 665-674.
5. Calixto JB. 2000. Efficacy, safety, quality control, marketing and regulatory
guidelines for herbal medicines (phytotherapeutic agents). Braz J Med Biol
Res. 33:179-189.
6. CHEMEXCIL. 1992. Selected Medicinal Plants of India, Bhartiya Vidya
Bhavan's Swami Prakashanand Ayurveda Research Centre, Bombay,
7. Ellenberger A. 1998. Assuming responsibility for a protected plant: Weleda’s
endeavour to secure the firm’s supply of Arnica montana. In: First
international symposium on the conservation of medicinal plants in trade in
Europe, TRAFFIC Europe, Kew, UK. Pp. 127-130.
8. EMEA. 2005. Guideline on specifications: Test procedures and acceptance
criteria for herbal substances, herbal preparations and herbal medicinal
products / traditional herbal medicinal products. European Medicines Agency
(EMEA) Committee for Medicinal Products for Human Use (CHMP)
Committee for Medicinal Products for Veterinary Use (CVMP), London, UK.
9. Fabricant D, Farnsworth NR. 2001. The value of plants used in traditional
medicine for drug discovery. Environmental Health Perspectives. 109: 63-75
10. Farnsworth NR. 1996. Biological and phytochemical screening of plants. J
Pharm Sci. 55:225–276.
116
11. Farnsworth NR, Bingel AS. 1977. Problems and prospects of discovering new
drugs from higher plants by pharmacological screening. In: Wagner H, Wolff
P. (eds.), New Natural Products and Plant Drugs with Pharmacological,
Biological or Therapeutical Activity. Springer, Berlin, Germany. Pp: 1-22.
12. I.U.C.N. 1994. Guidelines on the conservation of medicinal plants.
International Union for Conservation of Nature (IUCN), Gland. Pp: 50.
13. Ibanez E, Kubatova A, Senorans FJ, Cavero S, Reglero G, Hawthorne SB.
2003. Subcritical water extraction of antioxidant compounds from rosemary
plants. J Agric Food Chem. 51: 375–382.
14. Kicklighter CE, Kubanek J, Barsby T, Hay ME. 2003. Palatability and
defense of some tropical infaunal worms: alkylpyrrole sulfamates as
deterrents to fish feeding. Mar Ecol Prog Ser. 263: 299–306
15. Kinghorn AD. 1994. The discovery of drugs from higher plants.
Biotechnology. 26:81–108.
16. Kursar TA, Capson TL, Coley PD, Corley DG, Gupta MB, Harrison LA,
Ortega-Barría E, Windsor DM. 1999. Ecologically guided bioprospecting in
Panama. Pharmaceutical Biol. 37: S114–S126.
17. Lange D. 1998. Europe’s medicinal and aromatic plants: their use, trade and
conservation. Traffic Europe/International, Cambridge UK.
18. Mendonça-Filho RR. 2006. Bioactive Phytocompounds: New Approaches in
the Phytosciences. In: Ahmad I, Aqil F, Owais M (eds). Modern
Phytomedicine: Turning Medicinal Plants into Drugs. WILEY-VCH Verlag
GmbH & Co. KGaA, Weinheim.
19. Nacif de Abreu I and Mazzafera P. 2005. Effect of water and temperature
stress on the content of active constituents of Hypericum brasiliense Choisy.
Plant Physiology and Biochemistry. 43:241-248.
20. Phillipson JD, Anderson LA. 1989. Ethnopharmacology and Western
medicine. J Ethnopharmacol. 25:61–72.
21. Prasad R and Patnaik S. 1998. Conservation Assessment and Management
Planning (CAMP) workshop for Non Timber Forest products in MP. CAMP
workshop briefing book. IIFM, Bhopal (MP), India.
22. Robbins CS. 1998. American ginseng. The root of North America's medicinal
herb trade. TRAFFIC North America, Washington DC, USA.
117

23. Sharma GP, Singh JS, Raghubanshi AS. 2005. Plant invasions: Emerging
trends and future implications. Current Science. 88(5): 726-734
24. Vasudevan H. 2004. DNA fingerprinting in the standardization of herbs and
nutraceuticals. The Science Creative Quaterly.
(http://www.scq.ubc.ca/?p=286).
25. Vlietinck AJ, Vanden Berghe DA. 1991. Can ethnopharmacology contribute
to the development of antiviral drugs? J Ethnopharmacol. 32:141–153.
26. Verpoorte R. 2000. Pharmacognosy in the new millennium: lead finding and
biotechnology. J Pharm Pharmacol. 52:253–262.
27. Wink M. 1999. Introduction: Biochemistry, role and biotechnology of
secondary products. In: Wink M. (ed.), Biochemistry of Secondary Product
Metabolism. CRC Press, Boca Raton, FL, USA. Pp 1-16
28. WHO. 2002. WHO Traditional Medicine Strategy 2002-2005. World Health
Organization, Geneva.
29. WHO. 2003. WHO guidelines on good agricultural and collection practices
(GACP) for medicinal plants. World Health organization, Geneva.
118

3.4 Medicinal Plant Compositional Consistency for Reliable Therapeutic Action Profiling: Key Issues and Concerns for Phytotherapeutics Rajender S. Sangwan Central Institute of Medicinal and Aromatic Plants, PO CIMAP, Lucknow-226 015, India Email: [email protected] The putative efficacy of medicinal herbs relies on empirical or anecdotal data and
on traditions of use that frequently fail to satisfy the requirements of evidence
based medicine. Consequently, establishing sound pharmacological basis of
therapeutic action remains a constant challenge and that necessitates consistency
of the quality of the test herbal material or therapeutic product thereof. The quality
of a phytomedicine is defined by several parameters in sequence like quality of
herbal resource and herb, manufacturing of the drug preparations from the herb,
properties of the finished product etc., thus, demanding special quality attention
on each individual herbal species in accordance with Good Manufacturing
Practice (GMP) standards at each step.
The new era of popularity with medicinal plants stems from at least two
distinct fields of activism: (i) current-model discovery of therapeutic activity
associated with one or more phytochemicals isolated from the herbs, (ii)
increasing trust in ancient systems of medicines to deal with new era ailments like
stress, geriatric and oxidative damages, focus on ageing healthily, aspirations of
longer life span etc. The former began either as an inspiration from traditional
pharmacies (like Ayurveda, TCM, Unani, Kampo etc.) or as an ab initio
pharmacological research driven on novel/characteristic phytochemical isolates to
scientifically evolve out the individual plant molecule or its derivative (e.g.
artemisinin, taxol, podophyllotoxin, morphanes, ergot alkaloids, vinblatine,
vincristine etc.) as drugs with molecular mechanisms of action. However, the later
is largely a trendy holistic phytotherapy approach primarily based on beliefs on
ancient knowledge insufficiently reinforced with consistent
clinical/epidemiological data (e.g. Echinacea, Kava Kava, Sal Palmetto,
Hypericum etc.). Thus, for convenience of addressing the issues, the applicable
quality pointers in the former case may be called as Type-One Quality Standards
119

(TOQS) while those for the later case may be referred to as Type-Two Quality
Standards (TTQS).
The type one quality parameters applicable to the pure phyto-molecules with
established, validated drug action and cleared full sequence of clinical trails
(clinical action, bioavailability, toxicology, contra-indications etc.) are more or
less similar to those relevant to their synthetic counterparts in allopathic
medicines. Nevertheless, specifically stating they include important aspects like
herbal resources of minimized variation in phytochemical composition as any
significant deviation would result in hurdles in assurance of pure phytochemical
molecules during the manufacturing process, disease-free herbal phyto-resources
as use of diseased botanical parts of the plant may entail contamination of
microbial toxins, some of which could be fatal at even at levels of contamination
usually considered insignificant for the other contaminant so the drug.
The type two quality parameters applicable for the herbs or herbal preparation
(except the pure phyto-molecules isolated there from) bear issues and concerns
that are a brand different and need stringent and special attention, if their case in
clinics is to be advanced. Facets of their standardization are far more diverse and
complicated due to several reasons. Some of the concerns that need to be a priori
considered are while focusing on the applicable quality parameters needed to be
recruited and assessed:
• although, some of the plants of the herbs under group-II (TTQS) are well
documented for their unique secondary metabolome but scientifically strong
correspondence between the phytocemicals and clinical affects is yet be
established, thus, phytochemical markers to be applicable and tested can not
be unambiguously selected.
• clinical action, if any, residing with chemical(s) contained, the phytochemical
data need to be more comprehensive to promote their status from botanical
markers to therapeutic markers.
• data from different laboratories/research groups on a herb, formulation of the
herb and even on different batches of the same formulation can not be
compared unless the existing huge compositional variability in the herb
(mainly due to its random resourcing or wild crafting) is minimized.
120

• some recent revelations in this regard on specific cases like Ashwagandha
(Sangwan et al., 2004), Echinacea, Kava Kava (Krochmal et al., 2004) etc.
bring to light the issue of quality standards in herbals vis-à-vis therapeutic
affects fluctuating between avowal and denial.
• recognition of confounding factors of compositional heterogeneity calls for
generating method and protocols to ensure consistency for useful
therapeutical data.
• even in absence of enough association between the botanical markers and
therapeutic actions of the plant, former can serve at least as ‘surrogate
markers’ to ensure reproducibility and quality of the preparatory process.
• the general premise that traditional use of these medicinal products for
generations establishes their safety does not necessarily attest to their safety
and efficacy. Indeed,
• adverse effects of long-term herbal use, adulteration with toxic compounds
and contamination by toxicogenic microbes or natural toxins like mycotoxins
have been sometimes reported for herbal products and medicinal plants due to
lack of proper quality pre-screens of the herbs traded or tested for the clinical
action.
• herbal multi-component (polyherbal) preparation used in multi-target
therapy, pharmaceutical prerequisites have to be ensured for all components
and for their combinations.
Besides the intensified application of regulatory issues, certain developmental
elements are essential for better perception of their therapeutics in modern
settings. The recent developments in sensitive and high resolution analytical
technologies in combination with advances in disease development and pre-
clinical/clinical research have led to several paths for creating strong knowledge
base via Good Agricultural Practices (GAP) of cultivation, monitoring
composition, ensuring consistency across preparations/samples and on generating
data-based pharmacological inferences on a specific herb. Characteristic
compounds of the extracts/herbs need to be identified and different analytical
methods such as HPTLC, HPLC, CE etc. with low coefficients of variation should
be developed to analyze each of the standardized extracts and the finished
product. Detailed understanding of the constituents and their chemical behavior in
121

the extracts in case of multi-component products is essential as also identification
of phytochemical components co-responsible for efficacy (co-effectors) or as
matrices creators.
The issue of quality standards in herbal medicines fulfilling requirements of
current clinical studies is too vast to be stated briefly. However, thematically, it
may be attempted to be addressed as Seven Phase Process (SPP), each having
several facets of research and application as below:
Selection: The selection of the herb should be made more herb action
information-centric after their critical analyses and each herb need to be defined in
terms of chemotaxonomic status and clustering with other congeners of the
phytomolecules per se or as class/variants. The selection of herbs for exploratory
therapeutics should focus on those health needs that are unmet and appear to be
important to be dealt.
Structure: Anything apart, identification of active and/or characteristic secondary
metabolites or other phytochemical constituents of the herb is necessary not only
to from a firm knowledge to the herb and its action but also for the drug
development in the foreseeable future. The drugs from such phytochemcial and
pharmacological studies in tune with traditional knowledge are highly
motivational like artemisinin from Artemiasia annua, quinine from Cinchona,
camptothecin from Camptotheca, vinblastine and vincristine fron Catharanthus
roseus etc. At the same time, the cohort studies in this line can lead to the
development of herb-specific phytochemical marker library as well as
identification or development of specific chemotypes for the herbs. Such a
development forms the grit to the development of high resolution, sensitive and
validated analytical methods that could serve as standard operating protocols
(SOPs) for the quality evaluations of the herbs proposed to be subjected to the
clinical trials.
Source: The source of the medicinal herb is not merely the authentic identity of
the herb but includes comprehension of its chemotaxonomy and phytochemical
analysis of the larger number of individuals from the populations from diverse
122
geographic locations to discern the different chemotypes. The source of the
therapeutic herb might begin with the taxonomically identification but it never
ends before its specific description as a chemotype and its chemotypic position
within the family of chemotypes known/existing for the plant within the
geographically region sampled but elsewhere. While the present world of
intellectual property rights restricts the movement of live herbs or cultivable part
thereof, globalized and free trade options of the day assure unrestricted movement
of herbs across the glob for manufacturing. Since a good account of chemotypic
position of different herbs in different countries is lacking, it need to be developed
through intense research. Keeping the extens of variability within a chemotype, it
is important to shift the herbal trade description from authenticity of identification
of the herb to its next level, the chemotype. Thus, extending focus from
chemotaxonomy to chemotypes to ensure better quality in terms of compositional
uniformity across generations and regions, development of good agricultural
practices (GAPs), mathematically better defined compositional variation in multi-
agri-environments, standard operating procedures for post harvest management
and processing chemical technologies.
Standardization: Standardization of herbal drugs is most critical parameter for
assurance of quality and compositional consistency but also as a diagnostic tool. A
fully characteristic profile for each herb is not feasible due to the lack of complete
information about the complete composition of the secondary metabolome of each
herb. Nevertheless, several approaches have been proposed to reach a significant
level of reliability of the phytochemical diagnostics for the herbs. These include
marker approach, multi-component approach, pattern approach and multi-pattern
approach chemical fingerprinting, development of chemometric databases, fractal
fingerprints and wavelet analysis, PTR-MS, pharmacological profiling.
The marker approach and multi-component approach both are component
based approaches (Xie et al., 2006). These approaches explicitly focus on content
and concentrations of the specified chemical components present to characterize
the herb, extract or preparation. This system relies on identification through one or
two markers or active compounds and is the simplest kind of marker system.
However, this marker system is far from adequate as the dimensions of variations
123

and chemo-variants of medicinal herbs are much more than the test dimensions in
the system. Therefore, multi-component approaches are being increasingly applied
for the better quality control in herbals. This is a natural extension of the marker
approach and uses quantitative parameters of the all analytes (known or unknown)
in the sample/chromatogram in terms of relative concentration (peak area).
The concept of pattern approach is basically considering whole spectrum as
the feature. Though, seemingly there may be no discernible relationship between
the pattern and chemical composition but under identical conditions the pattern
has its origin in the chemical composition. Such patterns are generated using any
of the spectroscopic techniques like Fourier Transform-Infrared spectroscopy (FT-
IR), Near Infrared Reflectance (NIR), Nuclear magnetic Resonance (NMR), Mass
Spectrometry (MS) etc. Using conceptually such an approach, Wang et al. (2003)
have used both objective and robust NMR-based metabolomics combining high
resolution 1H-NMR spectroscopy with chemometric analysis in chamomile.
Recently, an objective method for the determination of a herb extract’s quality
based headspace measurements by proton-transfer-reaction mass spectrometry
(PTR-MS) that enabled excellent quality assurance and product source diagnosis
of herbals (Jaksch et al., 2004). The advantage of the chromatogram as a whole
rather than peak-centric approach is that it better covers the components of the
herb. Such an approach when used with hyphenated instrumentation, couples the
power of separation with the power of identification. Thus, when the identities of
the components present are not fully known and chromatogram peaks can not be
precisely labeled, similarity of the chromatogram is used as an index of identity
and comparison of herbs. Such component fingerprints for quality verification of
herbs are acceptable in several countries like USA, China, Britain and India and
form part of even World Health Organization guidelines for manufacture of herbal
medicinal products (Mok and Chau, 2006).
Thus, instead of fingerprints constructed from a single chromatogram,
multiple chromatographic fingerprinting (consisting of more than one
chromatographic fingerprinting) is much more adequate to profile the composition
of complex botanicals like multi-herb drug products as the later represents nearly
whole characteristics of chemical composition of complex medicines. Amongst
them binary chromatographic fingerprinting are more common and are
124

significantly more reliable than their single chromatogram counterparts (Fan et al.,
2006). The pattern approach fingerprints are quite often used by the
pharmaceutical industry to examine the source of the drug substance and the
method of chemical preparation. Even such a system can be advanced to provide a
“phytochemcal logo” by augmentation by qualified chemical pattern from safe
and edible herb in the product. However, this approach similar to the component
approaches still bears the limitation of revealing only one set of patterns displayed
by single technique and thus may exclude several other patterns pertaining to
secondary metabolites of other classes. In other words, TLC, HPLC or GC alone
may not be sufficient to reflect all that is contained in the herb. Thus, use of multi-
dimensional data patterns derived from different techniques of resolution form
multi-patterns and use of different detectors along with could add value to such
multi-patterns. Chemometrics assisted application of mathematical and statistical
techniques can greatly improve the quality of the fingerprints (Alonso-Salces et
al., 2004). A major problem with the direct use of chromatograms for comparison
is that retention times on the basis which the comparisons are made often shift
from run to run. Such shifts can be large in HPLC due to gradual degradation of
the stationary phase, environmental fluctuations (temperature, instrumental
reproducibility of the experimental conditions including flow rates, composition
of mobiles phase and gradient elution, shifts in detector responses and interaction
of analytes. Of course, several retention alignment algorithms are available to
estimate the shifts and align chromatograms and these methods work fine for
samples with reasonably closed chemical compositions but less to herbals where
the variations in chemical compositions could be large.
Surveillance: Surveillance of the phytochemical resources that is scheduled to be
procured for the manufacturing processes is essential although the crop cultivation
process to ensure compliance of standard agronomic practices including post
harvest handling, pre-processing storage, residue monitoring, microbial load
assessment, chemical process contamination, pharmaco-surveillance with respect
to use, efficacy, toxicity/ secondary effect(s). The augmentation of the supply
through wild crafted herb (for any reason) is one of the most common practice
and most predominant factor contributing to the variations in the herbal drugs. An
125

appropriate and real-time statistics of cultivated source of herb production and
herbal drug production would provide an estimate of such augmentations in the
industry and trade as a whole. In legal perspectives, it should be mandatory to
codify the phyt-resource of the manufactured drug that could be traceable in the
manufacturing premises although from procurement to processing in quantifiable
terms.
Safety: Doubts on safety of the herbal drugs is one of the most convenient weapon
that comes into play in any event of fall out of ill effects of the herbal drugs, even
when it could be due to misuse or unauthorized use/prescription. Citation of
historical or traditional use is often cited as the basis of safety. However, in
modern perspectives such a reference can only be of collateral corroboration and
appears to lack any significance standalone. Rationally, the safety aspects have
been less rigorously attended and emphasized in the literature. The therapeutic
references on the herb have over-shadowed any effect as the therapeutic action
appears to be the key focus and toxicity appears to have gone barley beyond
tolerating (via co-administration of another herb) or specific linkage of the herb
with food or drinks. Thus, a growing library of the epidemiological, toxicity data,
co-effects, secondary effects etc. need to be appended to the information on
historical/traditional use of the herb. Also, such growing database information
would keep the potential consumers well educated and informed about the herb
and forms an important platform for academic and investigative discussion.
Particularly, sharing, documentation and publication of the negative (adverse
effect) or null data is most important for rational conclusions to be drawn for the
therapeutic action of the herbs. Similarly, a good placebo system needs to be
evolved for herbs and herbal products for corroboration of the claimed benefits. In
my opinion, use of another herb (preferably of the same family or species of the
same genus) that lacks (or has little of) the potential drug action raison de etre
phytochemicals could serve as most convincing secondary controls.
Substantiation: Substantiation of the all claims on analysis, processing and
therapeutic action need to be dynamically substantiated in a diversified and non-
end fashion. Frequent reviewing of the pre-existing data including methodology
126

(as one can not get right data with wrong method), assessment of the cohortness
and robustness of study parameters, sample size, full-scale multi-parallel controls
are key not only to keep the importance of the drug imply but to develop a
knowledge force to drive its importance upstream, en route diminuting the pitfalls.
All these parameters need to be defined for each phytomedicine by SOPs and
all notions need to be subjected to full-scale tests through upstream science to
facilitate creation of a strong, trustable and sustainable herbal medicine regime
sans current caveat emptor. Research into new analytical methods for stricter
standardization of phytomedicines would continue to be a necessity to improve
the accuracy and consistency of phytomedicine preparations. Such a thrust is also
believed to continue from regulatory authorities for speedy and innovative
developments in the area. Very recently, Obradovic et al. (2007) have developed a
new method for the authentication of plant samples by analyzing fingerprint
chromatograms. Instead of conventional procedure of integrating the
chromatograms and using peak heights or areas of several peaks in a supervised
pattern recognition method to confirm the authenticity of the product, these
workers have proposed a section approach of analyzing chromatograms wherein
(i) the chromatograms are split into sections (ii) each section is described by four
variables (number of peaks in the section, average retention time of the peaks in
the section, total area of peaks in the section and average area of peaks in the
section, (iii) these variables have then been used in the statistical analysis. The
approach has been proposed to be especially useful when the peaks on the
chromatogram are not well separated and linking and corresponding peaks across
chromatograms is not easy. The more objective results and ease of interpretation
of data from the approach have been shown for the chromatograms of willow-herb
extracts resolved through capillary electrophoresis. The correct combination of
variables is crucial for such discriminate analysis.
Acknowledgements
I am thankful to The Foundation for Medical Research (FMR) and Dr. Tannaz J.
Birdi and Dr. Nerges Mistry, the Organizers of the conference “Approaches
Towards Evaluation of Medicinal Plants Prior to Clinical Trails” for giving me an
127
opportunity to deliver a lecture at the conference. This paper is the full review of
the subject matter thematically presented and discussed at the conference.
References
1. Alonso-Salces RM, Guyot S, Herrero C, Berrueta LA, Drilleau JF, Gallo B,
Vicente F. 2004. Chemometric characterization of Basque and French ciders
according to their polyphenolic profiles. Anal Bioanal Chem. 379: 464-475.
2. Fan XH, Cheng YY, Ye ZL, Lin RC, Qian ZZ. 2006. Multiple
chromatographic fingerprinting and its application to the quality control of
herbal medicines. Analytica Chemica Acta 555: 217-224.
3. Jaksch D, Hartungen E, Mikoviny T, Abel G, Mark TD. 2004. Quality control
of herbal extracts using PTR-MS. Int J Mass Spectrom. 239: 203-207.
4. Krochmal R, Hardy M, Bowerman S, Lu QY, Wang HJ, Elashoff R, Heber D.
2004. Phytochemical Assays of Commercial Botanical Dietary Supplements.
Evid Based Complement Alternat Med. 1(3):305-313
5. Mok DKW, Chau FT. 2006. Chemical information of Chinese medicines: A
challenge to chemist. Chemometrics and Intelligent Laboratory Systems. 82:
210-217.
6. Obradovic M, Krajsek SS, Dermastia M, Creft S. 2007. A new method for the
authentication of plant samples by analyzing fingerprint chromatograms.
Phytochem Anal. 18: 123-132.
7. Sangwan RS, Chaurasiya ND, Misra LN, Lal P, Uniyal GC, Sharma R,
Sangwan NS, Suri KA, Qazi GN, Tuli R. 2004. Phytochemical variability in
commercial herbal products and preparations of Withania somnifera
(Ashwagandha). Curr Sci. 86: 461-465.
8. Wang Y, Tang H, Nicholson JK, Hylands PJ, Sampson J, Whitecombe I,
Stewaryt CG, Caiger S, Oru I, Holmes E. 2003. Metabolomic strategy for the
classification and quality control of phytomedicine: A case study of
chamomile flower (Matricaria recutita L.). Planta Medica 70: 250-255.
9. Xie P, Chen S, Liang YZ, Wang X, Tian R, Upton R. 2006.
Chromatographic fingerprint analysis- a rational approach for quality
assessment of traditional Chinese herbal medicine. J Chromatogr A. 1112:
171-180.
128

An Abridged Overview
It is estimated that about 80% of the world population of the developing and
under developed countries still rely mainly on medicinal plants. It has become
clear that the use of medicinal plants is not only a valuable resource and a
necessity but also provides an affordable and accessible alternative for primary
health care. Thus medicinal plants have begun to get the attention they deserve.
Conventionally, however, understanding the mode of plant action is often
trivialized with overt emphasis on clinical trials; the pre-clinical testing of
medicinal plants being often neglected. The Foundation for Medical Research
being involved in the medicinal plant research for over a decade, felt a necessity
to have a comprehensive discussion for various approaches towards the preclinical
evaluation of medicinal plants. With this aim, the Foundation organized a one day
workshop with the following three themes:
Translation of ethnobotanical information obtained from a community for
identification, subsequent testing and utilization of plant material.
Principles of pre-clinical evaluation of plants using appropriate bioassays.
Standardization of plant material
Session I:
Session I focused on the importance of ethnobotanical surveys and the
documentation of the information obtained as well as collection, processing of
plant material, that need to be considered prior to validation. The presentations
and the following discussion emphasized that the information obtained would help
in not only preserving and popularizing the local health traditions but also
following of standard protocols for collection and processing would ensure quality
of the medicinal plant preparation.
It was noted that there is an urgent need for effective documentation and
assessment of local health traditions (LHT). Dr. Darshan Shankar pointed out that
the once rich and diverse cultural & traditional heritages of India are getting
diluted due to the increased influences from the mainstream culture. He discussed
129

the work undertaken by FRLHT in the past towards the revitalization of health
traditions and demonstrated the methodology towards revitalizing household
remedies and folk healing practices that can contribute to primary health care of
rural communities. He emphasized that apart from documentation and
identification of important LHT, community validation of these traditions and
their promotion at household and community levels is necessary.
Information obtained through the ethnobotanical survey and previously
documented data can help in development of safe, effective and acceptable
therapeutic agents. WHO guidelines should be followed for sustainable cultivation
and collection of medicinal plant materials to ensure safety and quality. The
necessity of good collection practices for the long term survival of wild plant
populations and their habitats was emphasized by Dr. RS. Rawat. He also
emphasized on the continuous need for finding sensitive and selective analytical
methods towards assessing the safety and quality of not only the raw plant
material but also the finished products.
The importance of ethnobotanical studies was reemphasized by Dr. M.
Parabia and Dr. P. Tetali. Dr. Parabia presented the studies undertaken by Shri
Bapalal Vaidya Botanical research Centre (BVBRC) of Veer Narmad South
Gujarat University, Surat, towards the development of simple recipes for common
ailments that could be taught to tribals and underprivileged groups for their
primary health care. He also gave a brief historic description of several
ethnobotanical surveys in Gujarat and described the work of BVBRC on the
preliminary validation of these ethnic claims.
Dr. Tetali added that one of the main issues was the need to integrate the
science of ethnobotany with other subjects such as pharmacology and medicine.
He opined that the undertaking of ethnobotanical surveys should be by a team
consisting of a local botanist, traditional healer and medical practitioner and
suggested the introduction of an integrated syllabus/ courses or preparation of
special work-manuals to train ethnobotanists to help create a more meaningful and
technically appropriate database that can be scientifically screened, tested, utilized
and finally integrated into health care delivery systems.
As demand for medicinal plants is growing, the necessity for cultivation of
medicinal plants was discussed. In this context, issues related to pesticide residue
130

were highlighted and organic farming suggested. Alternatively, cultivation using
tissue culture could be considered. With respect to the usage, especially within a
community, the need for protection of flora, traditional rights and IPR were
stressed. From the taxonomical point of view, the possibility of developing and
using of molecular tools for classification was suggested. Participation of industry
was highlighted with respect to emphasis on quality of plant material and its
processing. There was an active discussion on whether validation is really
required or can plants directly undergo a Phase III clinical trial which was the
subject matter for the next session.
Session II:
Session II focused on the importance of conducting preclinical screening
assays. It was emphasized that preclinical studies are necessary for validation of
medicinal plants and preparation of rational polyherbals. Each speaker in this
session talked extensively on the principles, the advantages, limitations and the
approaches of conducting preclinical studies on medicinal plants. These included
testing of plants for their pharmacological efficacy in vitro and in vivo systems
and studies of toxicology, specificity, biopharmaceutical properties and drug
interactions.
A number of participants stressed the need for toxicity testing of plants, both
short and long term, depending on the intended usage. It is possible that the plant
treatment taken up for the clinical trials may lead to some
unanticipated/unknown/unrelated side effects. Dr. S. Anant commented upon the
easy purchase on herbal products without a proper prescription and raised the need
to regularize how the traditional medicines are prescribed.
Clinical trials though required for the ultimate validation of medicinal plants,
have several limitations in terms of the number of patients required, the time
commitment and the expenses involved. Several advantages that the preclinical
testing offers, justifies it as an important prerequisite for short listing plants that
can be subjected to clinical trials.
The importance of preclinical testing was reemphasized by Dr. N. Rege who
said that the testing of traditional medicines should be based on scientific
principles. Towards this both the national and international guidelines need to be
131

followed. She opined that research on medicinal plants should be of a
collaborative nature with active participation of academicians, students,
researchers and industry.
Dr. U. Thatte and Dr. Anant stressed on the importance of selecting
appropriate bioassays for studying the pharmacological efficacy of medicinal
plants. Dr. Thatte used the example of Tinospora cordifloria to illustrate this. She
also stated that T. cordifloria when tested for antimicrobial activity failed to show
efficacy but when tested for immunomodulatory activity proved to be an excellent
immunomodulator.
Dr. Anant, on the other hand, discussed high through-put assays. He
elaborated that the basis for designing a high through-put screening assay is the
identification of a valid target; choosing an appropriate testing model and the right
type of extract. He demonstrated their utilization giving the example from his own
laboratory where the high through-put system was used to screen the anti-cancer
activity of curcumin.
The other speakers in this session also stressed on the need for selecting
appropriate bioassays. It was pointed out by Ms. P. Daswani that since the disease
process involves multiple steps several targets need to be considered which
undoubtedly would require a battery of bioassays which may include both in vitro
and in vivo systems. She mentioned that unfortunately when screening plants for
infectious diseases the assay system is often limited to testing for antimicrobial
activity. However plants can exhibit their efficacy against infectious diseases by
mechanisms other than antimicrobial activity. Ms. Daswani highlighted this
approach by presenting data of her work carried out at FMR on antidiarrhoeal
medicinal plants.
Dr. J. Singh mentioned that the use of mammalian cell cultures which mimic
in vivo functions can not only minimize dependency on large number of animals
but also allow for rapid screening of large number of plant extracts/isolates. He
added that modern approaches like silico biology can be used to shortlist best hits
to be taken for in vivo validation.
Dr. Thatte, Dr. Rege and Ms. Daswani all drew attention to the limitations of
the preclinical testing. It was pointed out that the extrapolation of dosage from in
vitro studies to in vivo systems may not always be possible. Secondly some
132

extracts may only show in vivo activity due to the metabolism of inactive
compounds into active forms or conversely, some compounds which show good
activity in vitro may be metabolized in vivo into inactive forms. Besides these, Dr.
Rege pointed out that availability of standard plant material, limited infrastructure
especially in academic institutes and difficulty in obtaining standard markers for
fingerprinting pose a challenge.
In her concluding remarks, Dr. Thatte said, that in order to get Ayurveda
accepted, we need right attitude, motivation, passion and curiosity especially from
young medical students.
Session III:
Session III focused on importance of phytochemical standardization of the
plant preparations. Various aspects and issues regarding standardization of plant
material were discussed. It was noted that stringent norms for standardization of
efficacy and safety measures is necessary to ensure consistent supply of medicinal
plant materials with good quality. All speakers in the session gave a brief
description of procedures that can be followed for standardization.
Dr. R. Sangwan stated that issues related to standardization did not exist
earlier, since herbal healers collected the plants by themselves. However, in the
current scenario of self medication and / or reliance on plant material suppliers
there is an urgent need for standardization. Using Withania somnifera as an
example, he demonstrated the need for standard plant material. With respect to
quality, Dr. Sangwan emphasized on a “seven phase quality process” which
included selection of herbs, structural features of phytochemicals, source of raw
materials, standardization for pre process quality assurance, surveillance of
variability factors, safety assurance and substantiation of effects through stringent
controls.
Dr. P. Venkatasubramanian pointed out that the parameters of testing the
quality of materials (dravya) in traditional medicines, such as rasa (taste), guna
(properties), virya (potency), vipaka (post-digestion effect) and karma (action),
reflect not only the quality but also efficacy. However, as there are no ready,
documented protocols available in traditional medicine either for collection or for
testing the action, there is a need for reviving and verifying these traditional
133
protocols. Towards this, she discussed the two-fold objective of research at
FRLHT with respect to quality standardization of medicinal plants: (i) the method
of reverse pharmacognosy is being employed, where, the plant material taken for
standardization is according to traditional knowledge, (ii) Traditional Quality
Parameters, such as rasa are being researched both from Ayurvedic view point as
well as through modern scientific tools.
Mr. Brijesh reemphasized the need for standardization. In addition he
discussed several factors including collection, processing, storage, that can affect
phytochemical profiles and stressed on the approaches for correlating these to
biological assays. He presented examples from his own studies with antidiarrhoeal
medicinal plants to substantiate this.
Dr. R. Khajuria emphasized on the need for stringent quality norms for global
positioning of herbal products. He discussed some of the procedures that are used
for standardization of medicinal plants and described in detail the rapid strides that
have been made in the field of instrumentation and their applications in isolation
of marker compounds necessary for chemical profiling.
It was suggested that a suitable mode of administration for the plant
formulations like chewing gum / tablet may be considered which would not only
meet the demand of the industries but also be acceptable to the masses.
It was agreed by the participants during the course of discussion that the
standardization of herbal preparation is not just an analytical assay of an active
principle; rather it embodies total information and controls that are necessary to
guarantee consistency of composition. Hence, a systematic approach is required
for a plant identified from traditional medicine, as is followed in modern
medicine.
Citing the example of the variations in W. somnifera as demonstrated by Dr.
Sangwan, Dr. Singh lamented upon “the mess we are in” due to large variations in
plant material. He said that we need to change our present attitude to bring
Ayurveda into international scenario. According to him, instead of tackling
variations, we should concentrate on one plant variety based on traditional
knowledge, apply all the modern tools towards appropriate biological and
phytochemical standardization, and bring out an efficacious formulation in the
134

market. This approach would lead to a “national plant” with clear cut efficacy
based on our rich heritage.
In conclusion, the workshop comprehensively touched on all aspects of
preclinical medicinal plant research, from selection to formulation. Besides re-
emphasizing the importance of medicinal plants, the workshop stressed on
participation/partnership amongst academicians, researchers and the industry to
integrate utilization of medicinal plants into modern medicine.
135

List of Participants
Name Address Anant S.
Associate Professor of Medicine and Cell Biology & Director of Gastroenterology Research, University of Oklahoma Health Sciences Centre, 920 Stanton L. Young Boulevard, WP 1360, Oklahoma City, OK 73190, USA.
Tel: 001-1-405-271-2175, ext. 3, Fax: 001-1-405-271-5450
Email: [email protected]
Antia N. H. Trustee, Foundation for Medical Research & Foundation for Research in Community Health, 6, Koregaon Park, Pune – 411001, India.
Tel: 020-26121875
Email: [email protected]
Bhate V. R.
Director, Analytical Solutions, Plot no. R-610, TTC, MIDC, Rabale, Navi Mumbai – 400701, India.
Tel: 022-27601122, Fax: 022-27602483
Email: [email protected]
Birdi T. J.
Deputy Director, Foundation for Medical Research, 84A, RG Thadani Marg, Worli, Mumbai – 4000018, India.
Tel: 022-24934989 / 24938601, Fax:022-24932876
Email: [email protected]
Brijesh S. Research Student, Foundation for Medical Research, 84A, RG Thadani Marg, Worli, Mumbai – 4000018, India.
Tel: 022-24934989 / 24938601, Fax: 022-24932876
Email: [email protected]
Chaturvedi S. Junior Research Officer, Foundation for Research in Community Health, 3&4, Trimiti B Apts., 85, Anand Park, Aundh - Pune 411007, Maharashtra, India.
Tel: 020-25887020, Fax: 020-25881308
Email: [email protected]
Charegaonkar D. Managing Director, Anchrom Enterprises (I) Pvt. Ltd, 101, Shree Aniket Apartments, Navghar Road, Mulund (E), Mumbai – 400081. India.
Tel: +919870326638
Email: [email protected]
Darshan Shankar
Executive Director, Foundation for Revitalisation of Local Health Traditions (FRLHT), 74/2, Jarakbande Kaval, Post Attur, Via Yelahanka, Bangalore – 560064, India.
Tel: 080 28565708, Fax: 080 28567926
Email: [email protected]
136

Daswani P. G.
Research Assistant, Foundation for Medical Research, 84A, RG Thadani Marg, Worli, Mumbai – 4000018, India.
Tel: 022-24934989 / 24938601, Fax: 022-24932876
Email: [email protected]
Joshi S. P. Division of Organic Chemistry: Technology, National Chemical Laboratory, Homi Bhabha Road, Pune- 411008, India.
Tel: 020-25902327, Fax: 020-25893614
Email: [email protected]
Khajuria R. K.
Head, LC-MS Lab and Bioanalytical Division, Indian Institute of Integrative Medicine (formerly Regional Research Laboratory), Canal Road, Jammu Tawi – 180001, India.
Tel: (0191) 2569000, Fax: (0191) 2569333
Email: [email protected]
Kulkarni D. K.
Senior Scientist, Department of Botany, Agarkar Research Institute, G.G.Agarkar Road, Pune – 411004, India.
Tel: 020-25654357, Fax: 020- 25651542
Email: [email protected]
Mistry N. F.
Director, Foundation for Medical Research, 84A, RG Thadani Marg, Worli, Mumbai – 400018, India.
Tel: 022-24934989 / 24938601, Fax: 022-24932876
Email: [email protected]
Natu A. A.
Indian Institute of Science Education and Research, Near National Chemical Laboratory, Homi Bhabha Road, Pune- 411008, India.
Tel: 020-25536212
Email: [email protected]
Parabia M. H. Professor of Biosciences, Veer Narmad South Gujarat University, Udhna –Magadalla Road, Surat – 395007, India.
Tel: +9198251-34422 (M)
Email: [email protected]
Pendse N. M.
Professor, Kayachikitsa & Panchkarma, Tilak Ayurveda Mahavidyalaya, Deenanath Mangeshwar Hospital, Mahalaxmi Nagar, Bibwewadi, Pune – 411037, India.
Tel: 020-2420 4103/ 020-2432-9353
Email: [email protected]
Ranadive B. Junior Research Officer, The Foundation for Research in Community Health, 3&4, Trimiti B Apts., 85, Anand Park, Aundh - Pune 411007, Maharashtra, India.
Tel: 020-25887020, Fax: 020-25881308
Email: [email protected]
137

Rawat R. B.
Regional Program Co-ordinator, Medicinal and Aromatic Plants Programme in Asia (MAPPA), International Centre for Integrated Mountain Development (ICIMOD), Dhapakel, Lalitpur, PO Box 3226, Kathmandu, Nepal.
Tel: 977-1-5525313, Fax: 977-1-5524509
Email: [email protected]
Rege N. N.
Associate Professor, Pharmacology & Therapeutics, Seth GS College & KEM Hospital, Parel, Mumbai – 400012, India.
Tel: 022-24181744, Fax: 022- 24121711
Email: [email protected], [email protected]
Samathanam G.J. Director, Department of Science & Technology, Ministry of Science & Technology, Technology Bhavan, New Mehrauli Road, New Delhi - 11 0016. India.
Tel: 011-26862512 (telefax)
Email: [email protected]
Sangwan R. S.
Senior Scientist, Department of Biochemistry, Central Institute of Medicinal and Aromatic Plants (CSIR), PO CIMAP, Lucknow – 226016, India.
Tel: 0522-2717434, +919451246764
Email: [email protected], [email protected]
Sharma P. P.
Lecturer, Post Graduate Department of Botany, Deogiri College, Station Road, Aurangabad – 431005, India.
Tel: +919422519569, 0240/2334577, Fax: 0240/2334577
Email: [email protected]
Sharma S. Ayurvedic Physician, C/O, Jan Swasthya Sahyog, Village and PO Ganiyari, Bilaspur – 495112, Chhattisgarh, India.
Tel: 07753-244819, 244819, Fax: 07752 - 247966
Email: [email protected], [email protected]
Singh J.
Deputy Director, Division of Pharmacology, Indian Institute of Integrative Medicine (formerly Regional Research Laboratory), Canal Road, Jammu Tawi – 180001, India.
Tel: 0191-2572002, 2549051, Fax: 0191-2547850
Email: [email protected]
Tetali P. Senior Scientist, Naoroji Godrej Centre for Plant Research, Lawkin Ltd. Campus, Shindewadi, Shirwal, Satara – 412801, India.
Tel: 02169-244401
Email: [email protected]
Thatte U.
Professor & Head, Department of Clinical Pharmacology, T N Medical College and BYL Nair Charitable Hospital, Mumbai Central, Mumbai – 4000008, India.
Tel: 022-23014713, Fax: 022-23050347
Email: [email protected]
138

Venkatasubramanian P.
Joint Director, Foundation for Revitalisation of Local Health Traditions (FRLHT), 74/2, Jarakbande Kaval, Post Attur, Via Yelahanka, Bangalore – 560064, India.
Tel: 080-28565618/080 28568000 ext. 142, Fax: 080-28567926
Email: [email protected]
Wele A. A.
Professor and Head, Dept of Rasashastra and Bhaishajyakalpanavigyan (Ayurveda Pharmacology), BVDU College of Ayurveda, Dhankawadi Campus, Pune – 411043, India.
Tel: +919823059970
Email: [email protected]
139
Copyright © 2022 FDOKUMEN