Antimicrobial resistance: a global threat - Biofarmaka IPB
36
E S S E N T I A L D R U G S MONITOR The Essential Drugs Monitor is produced and distributed by the WHO Department of Essential Drugs and Medicines Policy (EDM). It is published in Chinese, Eng- lish, French, Spanish and Russian, and has a global readership of some 300,000 to whom it is free of charge. The Monitor carries news of developments in national drug policies, therapeutic guidelines, cur- rent pharmaceutical issues, educational strategies and operational research. WHO’s Department of Essential Drugs and Medicines Policy seeks to ensure that all people – wherever they may be – are able to obtain the drugs they need at a price that they and their country can afford; that these drugs are safe, effective and of good quality; and that they are prescribed and used rationally. All correspondence should be addressed to: The Editor Essential Drugs Monitor World Health Organization CH-1211 Geneva 27, Switzerland Fax: +41 22-791-4167 e-mail: [email protected] Essential Drugs Monitor E D I T O R I A L DOUBLE ISSUE – N o 28 & 29 (2000) T Newsdesk 2–6 Pregnant women in developing countries face unacceptable health risks New international training course promotes better community drug use Organizations draw up ethical guidelines And much more... Antimicrobial Resistance 7–19 We look at the problem and some possible solutions to one of the world’s greatest health challenges Letters to the Editor 19 National Drugs Policy 20–21 Africa’s essential drug programme managers discuss future WHO’s Director-General speaks out for generics Plus Australia’s National Medicines Policy Access 22–27 Initiatives to create a healthier world NGOs focus on access to drugs Improving drug supply in Dar es Salaam Drug Information 28–31 Pakistan’s Drug Helpline Increasing workload for Tehran’s Drug and Poison Information Centre Research 31 Burkina Faso study shows importance of qualitative monitoring Meetings, Courses & Netscan 32–33 Published Lately 33–34 Traditional Medicine 35 India’s Biodiversity Bill World Trade 35–36 A health-sensitive approach to patent legislation WORLD HEALTH ORGANIZATION I N T H I S I S S U E : Spain USA Mexico Colombia South Africa South Korea Uruguay Brazil Argentina Chile Hong Kong Thailand Philippines singapore/ Malaysia Taiwan, China Spread of resistant pneumococcus first identified in Spain Antimicrobial resistance: a global threat Source: K. Klugmann, South African Institute of Medical Research wenty years ago physicians in industrialised countries believed that infectious diseases were a scourge of the past. With indus- trialisation came improved sani- tation, housing and nutrition, as well as the revolutionary development of disease- fighting antimicrobials. Populations living in those nations were not only enjoying an unprecedented decrease in mortality and morbidity but a corresponding increase in life expectancy. In the developing world – where poverty and ongoing civil distur- bance offset often modest health gains – people could nevertheless look forward to a time when an increased quality of life might one day lead to a relatively disease free future. The tools were there. Confident in the available pharmacopoeia, the major drug manufacturers turned away from intensive antibacterial research and con- centrated their energies on seeking cures for heart disease and other chronic conditions. Since the l980s significant breakthroughs have been largely confined to the develop- ment of antiviral agents targeting the ever-widening HIV epidemic. But tragically, and even before devel- oping countries were able to fully benefit from medical advances, we face a major risk that diseases considered vanquished in industrialised countries, will once again become killers stalking society, bringing an ever present threat of sudden death and dis- ability. The risk that threatens to turn back the clock to a darker age in industrialised countries and to block health progress in the developing world is antimicrobial resistance. As early as half a century ago – just a few years after penicillin was put on the market – scientists began noticing the emergence of a penicillin/resistant strain of Staphylococcus aureus, a common bacte- rium in the human body’s normal bacterial flora. Resistant strains of gonorrhoea, dys- entery-causing shigella (a major cause of premature death in developing countries) and salmonella rapidly followed. From that first case of resistant staphylococcus, the problem of antimicrobial resistance has snowballed to a serious public health con- cern with economic, social and political implications that are global in scope, and cross all environmental and ethnic boun- daries. Multi-drug resistant tuberculosis (MDR/TB) is no longer confined to any one country or to those co-infected with HIV, but has appeared in locations as diverse as Africa, Asia and Eastern Europe, among health care workers and in the general popu- lation. Penicillin resistant pneumococci are likewise spreading rapidly, while resistant malaria is on the rise, disabling and killing millions of children and adults each year. In 1990 almost all cholera isolates in New Delhi, India, were sensitive to the cheap, first-line drugs furazolidone, ampicillin, co-trimoxazole and nalidixic acid. Now, formerly effective drugs are largely useless in the battle to contain cholera epidemics. Although most drugs are still active, the lengthening shadow of resistance means that many of them may not be for long. In the case of tuberculosis, the emergence of multi-drug resistant bacteria means that medication that once cost US$20 must now be replaced with drugs a hundred times more expensive. Pathogens develop resisistance to anti- microbials through a process known as natural selection. When a microbial popu- lation is exposed to an antibiotic, more susceptible organisms will succumb, leaving behind only those resistant to the antimicrobial onslaught. These organisms can then either pass on their resistance genes to their offspring by replication, or to other related bacteria through “conjuga- tion” whereby plasmids carrying the genes “jump” from one organism to another. This process is a natural, unstoppable phenom- enon exacerbated by the abuse, overuse and misuse of antimicrobials in the treatment of human illness and in animal husbandry, aquaculture and agriculture. Disease – and therefore resistance – also thrives in conditions of civil unrest, poverty, mass migration and environmental degradation where large numbers of people are exposed to infectious diseases, with little in the way of the most basic health care. Our challenge is to slow the rate at which resistance develops and spreads. This Monitor examines the growing spread of antimicrobial resistance and its underlying causes. It reports on the actions of WHO and others to raise awareness of the issue and to counteract this serious menace to public health. And it looks at what you, the reader, whether you are a policy-maker, health care professional, health advocate or member of the public, can do to help tackle the problem. ❏
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of Antimicrobial resistance: a global threat - Biofarmaka IPB

E S S E N T I A L D R U G S
M O N I T O RThe Essential Drugs Monitor is producedand distributed by the WHO Departmentof Essential Drugs and Medicines Policy(EDM). It is published in Chinese, Eng-lish, French, Spanish and Russian, andhas a global readership of some 300,000to whom it is free of charge. The Monitorcarries news of developments in nationaldrug policies, therapeutic guidelines, cur-rent pharmaceutical issues, educationalstrategies and operational research.
WHO’s Department of Essential Drugsand Medicines Policy seeks to ensure thatall people – wherever they may be – areable to obtain the drugs they need at a pricethat they and their country can afford; thatthese drugs are safe, effective and of goodquality; and that they are prescribed andused rationally.
All correspondenceshould be addressed to:
The EditorEssential Drugs MonitorWorld Health OrganizationCH-1211 Geneva 27, SwitzerlandFax: +41 22-791-4167e-mail: [email protected]
Essential Drugs Monitor E D I T O R I A L
DOUBLE ISSUE – No 28 & 29 (2000)
T
Newsdesk 2–6Pregnant women in developing
countries face unacceptablehealth risks
New international training coursepromotes better community drug use
Organizations draw up ethicalguidelines
And much more...
Antimicrobial Resistance 7–19We look at the problem and some
possible solutions to one of theworld’s greatest health challenges
Letters to the Editor 19
National Drugs Policy 20–21Africa’s essential drug programme
managers discuss futureWHO’s Director-General speaks out
for genericsPlus Australia’s National Medicines
Policy
Access 22–27Initiatives to create a healthier worldNGOs focus on access to drugsImproving drug supply in Dar es
Salaam
Drug Information 28–31Pakistan’s Drug HelplineIncreasing workload for Tehran’s Drug
and Poison Information Centre
Research 31Burkina Faso study shows importance
of qualitative monitoring
Meetings, Courses & Netscan 32–33
Published Lately 33–34
Traditional Medicine 35India’s Biodiversity Bill
World Trade 35–36A health-sensitive approach to
patent legislation
WORLD HEALTH ORGANIZATION
I N T H I S I S S U E :SpainUSA
Mexico
Colombia
SouthAfrica
SouthKorea
Uruguay
Brazil
Argentina
Chile
Hong KongThailand
Philippinessingapore/Malaysia
Taiwan, China
Spread of resistant pneumococcusfirst identified in Spain
Antimicrobialresistance:a global threat
Source: K. Klugmann, South African Institute of Medical Research
wenty years ago physicians inindustrialised countries believedthat infectious diseases were ascourge of the past. With indus-trialisation came improved sani-
tation, housing and nutrition, as well as therevolutionary development of disease-fighting antimicrobials. Populations livingin those nations were not only enjoying anunprecedented decrease in mortality andmorbidity but a corresponding increase inlife expectancy. In the developing world –where poverty and ongoing civil distur-bance offset often modest health gains –people could nevertheless look forward toa time when an increased quality of lifemight one day lead to a relatively diseasefree future. The tools were there. Confidentin the available pharmacopoeia, the majordrug manufacturers turned away fromintensive antibacterial research and con-centrated their energies on seeking cures forheart disease and other chronic conditions.Since the l980s significant breakthroughshave been largely confined to the develop-ment of antiviral agents targeting theever-widening HIV epidemic.
But tragically, and even before devel-oping countries were able to fully benefitfrom medical advances, we face a majorrisk that diseases considered vanquishedin industrialised countries, will once againbecome killers stalking society, bringing anever present threat of sudden death and dis-ability. The risk that threatens to turn backthe clock to a darker age in industrialisedcountries and to block health progress inthe developing world is antimicrobialresistance.
As early as half a century ago – just afew years after penicillin was put on themarket – scientists began noticing theemergence of a penicillin/resistant strain ofStaphylococcus aureus, a common bacte-rium in the human body’s normal bacterialflora. Resistant strains of gonorrhoea, dys-entery-causing shigella (a major cause ofpremature death in developing countries)and salmonella rapidly followed. From thatfirst case of resistant staphylococcus, theproblem of antimicrobial resistance hassnowballed to a serious public health con-cern with economic, social and politicalimplications that are global in scope, and
cross all environmental and ethnic boun-daries. Multi-drug resistant tuberculosis(MDR/TB) is no longer confined to any onecountry or to those co-infected with HIV,but has appeared in locations as diverse asAfrica, Asia and Eastern Europe, amonghealth care workers and in the general popu-lation. Penicillin resistant pneumococci arelikewise spreading rapidly, while resistantmalaria is on the rise, disabling and killingmillions of children and adults each year.
In 1990 almost all cholera isolates in NewDelhi, India, were sensitive to the cheap,first-line drugs furazolidone, ampicillin,co-trimoxazole and nalidixic acid. Now,formerly effective drugs are largely uselessin the battle to contain cholera epidemics.
Although most drugs are still active, thelengthening shadow of resistance meansthat many of them may not be for long. Inthe case of tuberculosis, the emergence ofmulti-drug resistant bacteria means thatmedication that once cost US$20 must nowbe replaced with drugs a hundred timesmore expensive.
Pathogens develop resisistance to anti-microbials through a process known asnatural selection. When a microbial popu-lation is exposed to an antibiotic, moresusceptible organisms will succumb,
leaving behind only those resistant to theantimicrobial onslaught. These organismscan then either pass on their resistancegenes to their offspring by replication, orto other related bacteria through “conjuga-tion” whereby plasmids carrying the genes“jump” from one organism to another. Thisprocess is a natural, unstoppable phenom-enon exacerbated by the abuse, overuse andmisuse of antimicrobials in the treatmentof human illness and in animal husbandry,aquaculture and agriculture. Disease –and therefore resistance – also thrives inconditions of civil unrest, poverty, massmigration and environmental degradationwhere large numbers of people are exposedto infectious diseases, with little in the wayof the most basic health care. Our challengeis to slow the rate at which resistancedevelops and spreads.
This Monitor examines the growingspread of antimicrobial resistance and itsunderlying causes. It reports on the actionsof WHO and others to raise awareness ofthe issue and to counteract this seriousmenace to public health. And it looks atwhat you, the reader, whether you are apolicy-maker, health care professional,health advocate or member of the public,can do to help tackle the problem. ❏

2 E S S E N T I A L D R U G S M O N I T O R
Issue No. 28 & 29, 2000
A world of difference:grim statistics on maternal healthin developing countries
woman living in Africa has a life-time risk of dying from compli-cations related to pregnancy 200times greater than a woman liv-
ing in a wealthy industrialised country,according to research findings reviewedin the WHO Bulletin*.
WHO data show that of the more than500,000 maternal deaths every year, over99% are in developing countries and lessthan 1% in the industrialised world. Themain causes of these deaths are unsafeabortion, haemorrhage, infections, highblood pressure and obstructed labour. Aquarter to a third of all deaths of women
and reproductive ill-health because theyalso suffer discrimination in access tobasic needs, health services and theexercise of human rights.”
Another Bulletin article reviews datasuggesting that making abortion safercould save the lives of many thousandsof women a year. ❏
* Bulletin of the World Health Organization,May 2000 (available on the Web at: http://www.who.int/bulletin/). For subscriptiondetails contact: World Health Organization,Marketing and Dissemination, CH 1211Geneva 27, Switzerland.
Doctors revise ethicalguidelines on medical research
First conference onconsumer adversereaction reporting
With so many excellent reasons fordirect consumer reporting, why, onemight ask, is it not already established?It is because in most countries, consumerreports are simply not eligible for inclu-sion in the existing physician-basedsystems, and because consumers lackpower and knowledge.
The Conference recommended that,prior to wide-scale implementation, con-sumer reporting on medicines system/sshould be piloted in regions or withpatient groups, and handled by an inde-pendent body at arm’s length fromgovernment and industry. In aggregatedform, reports should be made availableto all interested parties, including themass media. The data would also berelated to the current data from the 59national physician-based schemes in theUppsala Monitoring Centre (a WHO Col-laborating Centre for International DrugMonitoring). Appropriate arrangementsshould be made to enable hospitalisedpatients as well as participants in clinicaldrug trials to file reports.
Expert analysis neededThe principle of the subject’s freedom
to report should be laid down in Guide-lines for Good Clinical Practice acceptedby the European Commission and in clini-cal trial protocols, subject to approval byethics committees and analogous bodies.Confidentiality agreements concludedbetween an industrial sponsor and a clini-cal investigator should never be allowedto impede reporting of adverse effects byparticipants. Provided there is properfeedback and careful expert analysis ofreports, it will not necessarily be moredifficult to eliminate mischievous, mis-leading or ambiguous reports than hasbeen the case in professional-basedsystems.
A system of consumer reporting onmedicines might be supported from pub-lic funds, drug licensing fees or researchorganizations, including the EuropeanUnion. Its value will depend to some parton enlisting support from existing sys-tems, allaying unjustified concerns andcountering possible misunderstandings.
Delegates warned that while develop-ing consumer empowerment, one mustalso seek to counter potentially harmfulinfluences, such as current efforts to ex-tend Direct-to-Consumer-Advertising ofprescription drugs from New Zealand andthe USA to the rest of the world. ❏
* David Finer is a medical writer and wasChairperson of the Conference.
Further Conference information can be foundon the Web at: www.kilen.org
N E W S D E S K
T
A➢ DAVID FINER*
he First International Conferenceon Consumer Reports on Me-dicines was held in Sigtuna,Sweden, from 29 September–
1 October 2000, with some 70 partici-pants from 35 countries. The Conferencesought to call attention to the experiencesof consumers as a crucial, untapped forcein pharmacovigilance, beneficial for drugsafety, but also in terms of consumerempowerment in its own right.
Direct consumer reporting of adversedrug events is indeed credible but alsocontroversial in some camps. Yet it isthe only system based on the end-usersthemselves.
The Conference was organized by theSwedish organization KILEN (ConsumerInstitute for Medicines and Health) incooperation with the Dag HammarskjöldFoundation, Health Action International,People’s Health Assembly 2000, theUppsala Monitoring Centre, the SwedishConsumers’ Association, and the SigtunaFoundation. Participants included expertsfrom the medical and pharmaceuticalprofessions, drug regulatory authorities,the consumer movement and WHO.
Presentations of existing consumerreporting systems/initiatives were madeby representatives from Australia, theNetherlands, Sweden, Switzerland andthe UK.
A consensus report from the Con-ference states that general reasons forconsidering consumer reports on medi-cines relate to the need to promoteprinciples of equity, therapeutic advances,accountability and responsiveness. Also,existing physician-based systems haveserious deficiencies, which might to someextent be compensated for by the estab-lishment of consumer reporting. Foremostamong these limitations are the small pro-portion of practising physicians (oftenless than 5%) who contribute data. Inputfrom existing systems relates primarily tonew drugs, despite the fact that new prob-lems can emerge with older drugs evenafter decades of use.
Consumers give morecomplete picture
Delegates heard that benefits of con-sumer reporting of adverse drug effectsinclude an earlier accumulation of signals,covering a wider spectrum of organ sys-tems and adverse events. Consumersprovide more informative, vivid and com-plete accounts of unwanted experiencesand situations, about which physicians arenot informed and so cannot report, suchas self-treatment with over-the-counterdrugs or herbals.
he World Medical AssociationGeneral Assembly has sent astrong signal to all involved inmedical research that rich
populations should not exploit poorpopulations by testing on them new treat-ments from which they will never benefit.The Assembly held in Edinburgh, Scot-land, in October 2000, approved a revisedDeclaration of Helsinki. Initially drawnup in 1964, the Declaration has since be-come the most widely accepted guidanceworldwide on medical research involv-ing human participants. Commenting onthe changes, Dr Anders Milton, chairmanof the Association, said: “Research shouldnot be carried out in countries in devel-opment just because it is cheaper and thelaws are more lax. The same ethical rulesshould apply wherever research is beingconducted”.
The new Declaration emphasises inmuch clearer terms than ever before theduty that doctors owe to participantsin medical research. It says that freelygiven informed consent, preferably inwriting, should be obtained from allparticipants. People who cannot giveinformed consent should be includedin research only under exceptionalconditions.
Strengtheningparticipants’ rights
The Declaration specifies that doctorsparticipating in research have an obli-gation to declare any financial or otherpotential conflict of interest. Research isjustified only if the populations to be stud-ied stand to benefit. The Declarationstates that every patient entered into astudy should have access to the best treat-ment identified by that study once it iscompleted. Furthermore, testing of anynew treatment should be done against thebest current method, where that exists,and not against a placebo. This wouldmean that people in developing countrieswould at least get access to the best cur-rent treatment if they agree to take part inresearch into new treatments.
The revised Declaration of Helsinkiwill be distributed to WHO, nationalbioethics commissions, patients’ repre-sentatives groups and other relevantstakeholders. The full text is on theWorld Medical Association’s Web site:www.wma.net ❏
Source: BMJ 2000;321:913
T
of reproductive age arethe result of complica-tions of pregnancy orchildbirth.
“The poor fare farworse than the rest of so-ciety on all reproductivehealth outcome indica-tors. But poverty is notan insurmountable bar-rier to health when thereis a high level commit-ment to investing inhealth,” a Bulletin articlestates. “Gender-baseddiscrimination is animportant determinantof poor reproductivehealth. Women suffer themajor burden of sexual
Hopefully a trouble-free pregnancy for this woman in Haiti. Butwomen in the developing world have an unacceptably high riskof dying from pregnancy-related complications
Phot
o: W
HO
/PA
HO
/A
. Waa
k

3E S S E N T I A L D R U G S M O N I T O R
Issue No. 28 & 29, 2000
New course targets bettercommunity drug use
Welcome new HIV/AIDSresource for francophone Africa
new HIV/AIDS information network for Central and West Africa has beenlaunched – the first network of this type in French. Known as SAFCO (SIDAen Afrique du Centre et de l’Ouest), it will encourage discussion and theelectronic exchange of information on HIV/AIDS-related issues. The service
is particularly welcome because there is a scarcity of such information and technicalmaterial in French in Africa, the continent hardest hit by the virus.
As well as information exchange, SAFCO aims to: strengthen advocacy efforts;improve information about current projects; promote prevention measures; reinforceaccess to care and treatment; disseminate the results of international conferences andsupport their implementation.
SAFCO, with over 700 members, is a UNAIDS supported initiative. One of itsmain strengths is that it is a public cross-sectoral and inter-community informationforum. It has input from both the “grassroots” – concerned individuals, governmentrepresentatives, NGOs, educators, investigators, practitioners and others – and fromnational and international institutions. ❏
Joining the SAFCO network is free of charge, just send a message to: [email protected]
APUA’s smallgrants programme
he Alliance for Prudent Use ofAntibiotics (APUA) has initiateda small grants programme, whichprovides chapters with seed
money of US$1,500 for projects designedto curb antibiotic resistance and topromote the rational use of these drugs.
APUA’s national chapters form a glo-bal network of health care practitionersand scientific groups working to controlantimicrobial resistance. They provideinformation and tailor the Alliance’smessage to local customs and medicalpractices, and the small grants programmeis intended to encourage these efforts.Projects submitted for grants are eva-luated according to their objectives,collaborative components and manage-ment plans. To date grants are helping tosupport research and education in sevendeveloping and transitional countries. ❏
For further information contact: The Alliancefor Prudent Use of Antibiotics, P.O. Box 1372,Boston MA 021171372, USA. E-mail:[email protected]
WHO’s EmergencyLibrary Kits
ibrary Kits containing essentialdocuments related to publichealth in emergencies are nowavailable from WHO. Intended
to provide technical guidance to field-operating agencies, the Kit includes 120documents – guidelines and referencemanuals produced by WHO, other UNorganizations and external publishers.The contents will be updated regularly.
Packed in a metal trunk that convertsinto a bookcase, the Emergency LibraryKit costs approximately US$1,320, plustransport charges. ❏
For further information contact: World HealthOrganization, Department of Emergency andHumanitarian Action, 1211 Geneva 27,Switzerland.
WHO list ofcomparatorproducts
ultisource (generic) drugs need tomeet the same quality, safety andefficacy standards as the originalbrand name or innovator product.
WHO has now published a list of globallyrecognised comparator products, to helpregulators identify the product againstwhich bioequivalence and interchange-ability of generic versions can beassessed.
The list includes 147 drugs from theWHO Model List for which a compara-tor product has already been identified.It names the manufacturer who is the in-novator, and the national market wherethat manufacturer considers that the prod-uct meets the best safety, quality, efficacyand labelling standards. A second listgives the remaining essential drugs forwhich a comparator product has yet to beselected. ❏
The information is available in WHO DrugInformation Volume 13, No.3, 1999.
N E W S D E S K
Next Promoting Rational Drug Usein the Community Course
If you would like to know more about the course in Entebbe, Uganda, from 11–24November 2001, please complete and return this form. Alternatively, further detailsand an application form can be printed out directly from the EDM web-page at:http://www.who.int/medicines/organization/par/secondcourse.html. Course feesare US$2,950, which covers tuition, course materials and accommodation. Thedeadline for receipt of applications is 1 October 2001.
Name
Occupation
Full postal address
Tel Fax
Please return to the address below:
University of AmsterdamFaculty of Social and Behavioural SciencesAttn. Dr Ria ReisOudezijds Achterburgwal 1851012 DK AmsterdamThe NetherlandsTel: +31 20 525 4779Fax: +31 20 525 3010E-mail: [email protected]
countries, valued the helpgiven to identify clear objec-tives, based on realisticexpectations of impact onfuture work.
The skills and experi-ences of everyone on thishighly participatory courseproved a major resource.Teaching methods weregroup activities, field work,presentations and discus-sions. Participants spent thefinal two days preparing adetailed plan of action totackle an important commu-nity drug use problem in
L
T
A
M
A
Creating a message that counts – participants working on aposter during the course
their home country. They also took homea set of session materials and a small corecommunications library. But from theircomments it was evident that coursemembers were leaving Thailand withmuch more. As one participant put it, “Irealise that in my professional life I haveonly been looking at half of the picture...”.Another said the course would “help meuse scarce resources to implement themost appropriate/feasible and needed in-terventions.” And for a third it was “agreat experience, well planned and wellorganized”.
After such initial success the courseis set to become a regular event, with thenext one being held in Entebbe, Uganda,from 11–24 November 2001. ❏
Reference
WHO. Public education in rational drug use: a globalsurvey. EDM Research Series No.24. Geneva: WorldHealth Organization; 1997. WHO/DAP/97.5.
Phot
o: S
. San
ders
, Mah
idol
Uni
vers
ity, B
angk
ok
t a time when the majority ofmedicines are purchased directlyby consumers without prescrip-tion, community education is
vital, and a new course is setting out tomeet the needs of those with a critical roleto play in this much neglected area. Justhow neglected was shown by a WHO glo-bal survey on public education in rationaldrug use1, which revealed a shortage ofexpertise, support and funds for this typeof work, in spite of its public health andeconomic benefits.
Developed by WHO’s Department ofEssential Drugs and Medicines Policyand the University of Amsterdam, in col-laboration with experts world wide, thecourse, Promoting Rational Drug Use inthe Community, was held for the first timein October 2000 in Bangkok. Enthusias-tic participants learned how to effectivelyidentify and prioritise community druguse problems; choose and developappropriate intervention strategies andcommunication channels; pretest materi-als; evaluate impact; and fundraise andnetwork for support and sustainability.
Anyone who came looking for “quickfixes” would have been disappointed.Participants learned that interventionsmust take into account the social and eco-nomic context in which health- andmedicine-seeking behaviour take place,and be developed with community input.The course emphasises that change isusually incremental. So programmeobjectives may start with awareness train-ing, move on to knowledge acquisition,and then finally on to behavioural change.
Twenty-five participants, from 14

4 E S S E N T I A L D R U G S M O N I T O R
Issue No. 28 & 29, 2000
Leading organizations’new guidelines on ethics
t a time of increased focus onethical issues in the pharmaceu-tical sector, UNAIDS and theEuropean Medicines Evaluation
Agency are among many organizationsproducing their own guidelines.
UNAIDS and vaccineresearch
In the case of the Joint United NationsProgramme on HIV/AIDS (UNAIDS)the ethical guidelines cover HIV vaccineresearch for those giving trial AIDSvaccines. It is widely thought that devel-oping such a vaccine offers the best hopeof controlling the AIDS epidemic, espe-cially in developing countries. But expertssay it will be a lengthy and complex proc-ess, because of the scientific and ethicalchallenges involved in clinical trialsamong human volunteers.
The guidance document, which
addresses some of these ethical chal-lenges, took over two years to draw up. Itwas based on a series of consultations or-ganized by UNAIDS and which involvedrepresentatives from 33 countries. Themeetings took place in Brazil, Thailandand Uganda (countries that are participat-ing in HIV vaccine trials) as well as inGeneva and Washington. They involvedlawyers, activists, NGOs, people livingwith HIV/AIDS, social scientists, ethi-cists, epidemiologists, health policyspecialists, and agencies and institutionsinvolved in vaccine development.
There was consensus on most, but notall, issues. The most contentious area wasthe level of treatment that should be of-fered to participants in vaccine trials whobecome infected with HIV, not throughthe trials (vaccines cannot cause HIV in-fection) but through eventual behaviouralexposure. According to the UNAIDS
reflecting a number of issues, including:
➤ international ethical responsibility tosupport vaccine trials;
➤ the obligation to provide an effectivevaccine to populations where trials areconducted and to other populations inneed;
➤ the need to strengthen ethical reviewcapacity in developing countries;
➤ the importance of social and behav-ioural aspects of testing, and future useof an HIV vaccine.
Collective responsibilityThe guidelines identify responsibili-
ties for the “sponsors” of vaccine trials.In modern vaccine development pro-grammes, sponsors are not usually asingle pharmaceutical company. Instead,there tend to be multiple sponsors, withone or more corporations, one or morenational governments, and one or moreinternational agencies.
The guidelines highlight the impor-tance of involving communities early inthe design, development, implementationand distribution of results of HIV vaccineresearch. They are designed as a frame-work to enable communities to decidewhat is appropriate for them.
Agency acts to ensureintegrity, independence,transparency
The European Medicines EvaluationAgency is to have a code of conduct giv-ing specific guidance on conflicts ofinterest, gifts and confidentiality.
The Code applies to managementboard, scientific committee and workingparty members, European experts listedby the Agency, all Agency staff andby analogy all visiting staff. Three cat-egories of interest are listed: financialinterests, work carried out for the phar-maceutical industry in the previous fiveyears, and other links, such as grants forstudy or research, or fellowships endowedby industry in the previous five years.
Anyone with direct interests in thepharmaceutical industry has to end themto remain with the Agency. If there areindirect interests they must be neutralised,for example by preventing someone fromtaking part in certain tasks.
In general staff have to discouragegifts of anything more than token valuewhich can be shared openly with col-leagues. Any gifts of a personal naturemust be returned, and staff must not useitems with pharmaceutical companylogos at work.
The Code states that invitations to pre-dominantly leisure events cannot beaccepted, and at meetings or on missionsstaff should normally pay for their ownmeals. Invitations from individual phar-maceutical companies, suppliers, etc.should not be accepted. In addition nopayment may be accepted for speeches,lectures or publications directly related toAgency activities. Permission to speak atconferences will be refused “if network-ing or gaining influence must be assumedto be the major objective of the organ-izer”. Invitations from congresses ormeetings organized by pharmaceuticalcompanies are unacceptable. ❏
Africa’s strategy ontraditional medicine
N E W S D E S K
A
HT
ElectronicHAI-Lights
AI-Lights has become the firstHAI-Europe publication de-signed to be read and used elec-tronically. All of the information
included in the newsletter’s August 2000double issue appears in easy to find linksshown on the cover page. HAI-Europehas been working towards a Web-basedversion of the regional newsletter forsome time, due to members’ demand forfaster information and more accessiblematerial.
It is planned to link the newsletter’scontent to a Web site search function sothat articles on various issues can beretrieved quickly and easily.
Access the August issue of HAI-Lightsat: http://www.haiweb.org/pubs/hailights/aug2000/
The entire newsletter is also availablein a downloadable text format. You canchoose Word for either PC or Mac to reador print out the issue’s complete contentsor a specific section. ❏
document, “Care and treat-ment should be provided,with the ideal being toprovide the best proventherapy, and the minimumto provide the highest levelof care attainable in the hostcountry” under the circum-stances in which the trial isconducted.
With resources in indus-trialised and developingcountries so different, how-ever, not every country canexpect to provide the samelevel of care.
The document contains18 “guidance points”
The AIDS virus. Development of a vaccine is considered to bethe best hope of controlling the AIDS epidemic. Guidelinesare now in place to address the complex ethical issuesinvolved in testing such a vaccine
Phot
o: W
HO
/In
stitu
t Pas
teur
/C
. Dau
get
he Strategy for Traditional Medi-cine for the African Region(2000–2001) is being developedby the WHO Regional Office for
Africa. Its aim is to assist Member Statesto integrate traditional medicine intohealth systems and services, and topromote appropriate and rational use.In December 1999, WHO held a consul-tative meeting on the Strategy, whichbrought together 23 experts from 15 coun-tries for three days of intensive debate inHarare, Zimbabwe.
Combatting priority diseasesParticipants recommended that action
plans be developed to implement theStrategy at regional and national levels,so that by 2020 traditional medicinewill be an integrated component of theminimum health care package in African
countries. Much discussion focusedon ensuring the protection of the intel-lectual property rights of indigenousknowledge in traditional medicine, andthe cultivation and conservation of nativemedicinal plants. Delegates asked WHOto provide technical and financial supportfor developing traditional medicinal prod-ucts to combat priority diseases, such asmalaria, hypertension, diabetes and HIV/AIDS-related conditions.
Closing the meeting the WHO Re-gional Director for Africa, Dr EbrahimSamba, said he wanted to see the contin-ued use of African herbal plants andtraditional medicines to treat diseases. Hehoped that such traditional medicinalproducts would eventually be exported,after clinical trials have proved their effi-cacy and safety. Dr Samba stressed the
economic importance this could have forAfricans.
As a follow-up to the December con-sultative meeting, WHO’s RegionalOffice for Africa organized the AfricanForum on the role of traditional medi-cine in health systems, in Harare inFebruary 2000. Over 100 participantsfrom throughout the region held wideranging discussions, reviewed current andneeded research on these medicines,and identified local production issues.Recommendations from the meetingincluded: ensuring adequate legal andregulatory frameworks to promote tra-ditional medicines; establishing orstrengthening traditional medicine prac-titioners’ associations; and increasingcollaboration among healers, scientistsand doctors. ❏

5E S S E N T I A L D R U G S M O N I T O R
Issue No. 28 & 29, 2000
A World Health Reportwith a difference
Celebrating the Chinese version ofthe Monitor
French set to curbdrug spending
Indian training course highlightspharmacists’ evolving role
group of community and hospital pharmacists and pharmacy students fromthe Bengal area benefited from a break in routine when in September 1999they spent two days looking at broader issues affecting their profession. Twenty-six participants held wide-ranging discussions on subjects including their
changing role, the structure of the country’s pharmaceutical industry and thepatent situation. Run jointly by the Community Development Medicinal Unit, Cal-cutta, and the Indian Pharmaceutical Association, Bengal Branch, the training course,Good Community Pharmacy Practice, was so successful that it is planned to repeat itevery year.
Upgrading knowledge and skillsIn the varied programme, a session on formulations marketed in India although
banned by the Government generated animated debate. So too did the topic of clinicalwaste management – an area new to many of the participants. The second day beganwith a discussion on how best to respond to symptoms of common ailments, followedby tips on improving drug dispensing, and medical stores management.
Although maybe not of immediate relevance to the job description of mostparticipants, two sessions provided plenty of food for thought. One was on the
he World Health Report 2000 –Health Systems: ImprovingPerformance1 is an expert analy-sis of the increasingly important
influence of health systems in people’sdaily lives. In recent decades, health sys-
system to carry out four main functions:service provision, resource generation,financing and stewardship. Chaptersdevoted to each function offer new con-ceptual insights and practical advice onhow to assess performance and achieve
he French Government haswarned that the rate of growth ofpharmaceutical spending is stillfar too high, and that it is decid-
ing which products will have price orreimbursement cuts, or be removed fromthe list of reimbursable products.
Speaking at a press conference in May2000, Labour and Solidarity Minister,Martine Aubry, said that health careexpenditure was still rising strongly, par-ticularly in the pharmaceutical sector,which increased by 6.3% in 1999. Whileprojections for 2000 are for a cut of 0.7%this is far higher than the target set byGovernment of 2%. Addressing theSocial Security Accounts Commissionshortly before her press conference, MsAubry said that it was “absolutely neces-sary” to bring pharmaceutical expenditureinto line with Government targets.
She singled out “unjustifiable pre-scribing”, saying that some products werequickly capturing a sizeable share of themarket more because of what she termed“aggressive commercial policies towardsdoctors than because they are advancesin public health”. “Information arrives indoctors’ surgeries from pharmaceuticalcompanies and only from them” she con-tinued. “ I am not criticising the industry.It does its job, which is to sell and selleven more. But she said that she did notwant doctors to be “left alone to face theindustry”. The Government intends tosupply doctors with independent infor-mation on the correct use of medicines.While encouraged by increasing genericsubstitution, Ms Aubry said that shewanted to see more generic products onthe market soon.
The French pharmaceutical industry
N E W S D E S K
T
A
T Ttems have contributed enor-mously to better health formost of the global population.But they have the potential toachieve further improvements,especially for the poor. As DrBrundtland, WHO’s Director-General, comments in herintroduction to the Report,“The poor are treated with lessrespect, given less choice ofservice providers and offeredlower-quality amenities. In trying to buyhealth from their own pockets, they payand become poorer.”
To date very little has been done tounravel the complex factors that explaingood or bad performance by individualhealth systems. Given equal resources,why do some succeed where others fail?Is performance simply driven by the lawsof supply and demand, or does anotherlogic apply? Why is dissatisfaction withservices so widespread, even in wealthycountries offering the latest interven-tions? If systems need improvement, whattools exist to measure performance andoutcomes?
These are some of the questions thatthe Report addresses, as it presents theresults of the first ever analysis of theworld’s health systems. It provides anindex of performance based on threefundamental goals: improving the leveland distribution of health, enhancing theresponsiveness of the system to the le-gitimate expectations of the population,and assuring fair financial contributions.
As the Report argues, good perform-ance depends critically on the delivery ofhigh-quality services. But health sys-tems must also protect citizens from thefinancial risks of illness and meet theirexpectations with dignified care. The pub-lication shows how the achievement ofthese goals depends on the ability of each
improvements with availableresources.
The analysis revealed anumber of problems commonto many countries. Amongthem are that:➤ many health ministries
focus on the public sectorand often disregard thefrequently much largerprivate sector health care;
➤ in many countries, some ifnot most physicians work simultane-ously for the public sector and inprivate practice. This means that thepublic sector ends up subsidisingunofficial private practice;
➤ many governments fail to prevent a“black market” in health, where wide-spread corruption, bribery, “moon-lighting” and other illegal practicesflourish. The black markets, whichthemselves are caused by mal-functioning health systems, andhealth workers’ low incomes, furtherundermine those systems;
➤ many health ministries fail to enforceregulations that they themselves havecreated or are supposed to implementin the public interest.
The Report aims to stimulate debateabout better ways of measuring healthsystem performance and overcomingsuch problems. By shedding new light onwhat makes systems behave in certainways, WHO also hopes to help policy-makers understand the many complexissues involved, weigh their options andmake wise choices. ❏
Reference1. WHO. The world health report 2000 – health systems:
improving performance. Geneva: World HealthOrganization; 2000. Available from: Marketing and Dis-semination, World Health Organization, 1211 Geneva 27,Switzerland. Price: Sw.fr.15/US$13.50, and in develop-ing countries Sw.fr.10.50. The full report is available onthe Web at: http://www.who.int/home/reports.html
An elderly patient in France, where the Government isacting to reduce rising pharmaceutical expenditure
association, SNIP, has criticisedthe Government’s target of a2% increase in pharmaceuticalspending in 2000. The Govern-ment cost-containment ini-tiatives (prescribing guidelines,computerization of doctors’ sur-geries, the encouragement ofgenerics and reimbursementreview) were necessary, SNIPstated, but had failed to bringspending into line with the 2%limit. ❏
Source: Scrip, No.2543, 26 May2000.
scientific principles of pharmaceutical in-ventory management. The other coveredthe structure of the pharmaceutical indus-try in India, recent changes in nationaldrug policy and the Indian patentsscenario. ❏
For further information contact: CommunityDevelopment Medicinal Unit, 47/1B GarchaRoad, Calcutta-700 019, West Bengal,India, or see: http://education.vsnl.com/cdmudocu/CDMUHome.htm
Participants engrossed by a demonstration ofspecial dosage forms
Phot
o: W
HO
/E.
Sch
wab
Phot
o: C
DM
U/
IPA
he Essential Drugs Division ofChina’s State Drug Adminis-tration has seen its hard workrewarded as the first two issues
of the Monitor in Chinese have rolled offthe printing presses, to an enthusiasticreception.
Ten thousand copies of each issuehave been printed and distributed, freeof charge, to Government departments,medical institutes and experts in thepharmaceutical sector. While these firstissues contain a selection of key articlesfrom recent editions, future copies willreproduce the text of the most recentMonitor. ❏

6 E S S E N T I A L D R U G S M O N I T O R
Issue No. 28 & 29, 2000
Oxfam campaigns to lowerdrug prices
Update on drug donationsDrug donations problemin Venezuela
staff and increase working hours simplyto classify what has been received.
Dr Francisco Griffin, Director-General of the Production Service, saidhe thought some companies had deliber-ately sent expired products, considered astoxic waste, to evade the cost of havingto deal with them themselves. In 1996WHO published interagency guidelineson drug donations1 in response to increas-ing reports of such problems being causedby inappropriate donations.
However, Dr Griffin accepted thatthe Service had not anticipated such amassive international response to thelandslides. When the disorganized natureof the donations and the “titanic work”required to sort through them becameclear, advertisements were belatedlyposted on the Web sites of internationalorganizations asking only for specificallyrequested products.* ❏
Source: BMJ 2000;320:1491.
➤ While nurses were the most likelyhealth workers to be in charge of phar-macies and of selecting, prescribingand dispensing drugs, donors usuallydecided the quantity of each drug tosend.Researchers concluded that:
➤ Donated drugs are more appropriatewhen the recipient, not the donor,decides which drugs are sent.
➤ As nurses play a central role in drugdonations they must understand theprinciples of good donation practices.
➤ There is still a need to promote theessential drugs concept and use of es-sential drugs lists by both donors andrecipients. ❏
For further information on the study contact:Dr Eva Ombaka, The Pharmaceutical Pro-gramme, World Council of Churches/Community Initiatives Support Services Inter-national, P.O. Box 73860, Nairobi, Kenya.
Source: Practical Pharmacy, No. 14, 1999.
New public health channel piloted in AfricaorldSpace Foundation andSATELLIFE have announced anew health service that will pro-vide a steady stream of material
to assist medical professionals in Africain the diagnosis, prevention and treatmentof prevalent diseases. The service, calledthe Public Health Channel, aims to over-come the barriers of poverty, geographyand unreliable communications infra-structures, to help stop the rise of diseasessuch as malaria, tuberculosis and HIV/AIDS.
“The ability to widely disseminateinformation about the treatment and pre-vention of HIV/AIDS and other diseasesis the reason the WorldSpace systemwas created,” says Gracia Hillman,WorldSpace Foundation President.
“The goal of SATELLIFE’s informa-tion services is to connect the healthpractitioner in the developing worldwith a range of high-quality informationresources in a cost-effective manner,
by making use of the most affordable,efficient and appropriate technology”,states SATELLIFE Executive Director,Holly Ladd. “The Public Health Chan-nel will employ the technology of theWorldSpace system to exponentially in-crease the amount of information healthpractitioners throughout Africa canaccess – information that most healthpractitioners in the United States andEurope take for granted.”
The Public Health Channel will belaunched in four countries: Ethiopia,Kenya, Uganda and Zimbabwe. After aninitial test period, the project will expandto other African countries, as fundingbecomes available. WorldSpace receiverswill be placed in hospitals, medicalschools, medical libraries, health clinics,health ministries and research settings.
WorldSpace receivers provide crystalclear digital audio channels, and can alsoserve as a modem, downloading text-based material and dynamic images from
the AfriStar satellite directly to comput-ers. TheWorldSpace system transcendsthe difficulties of unreliable telephonesystems at a fraction of the cost of mostInternet-based projects.
N E W S D E S K
WorldSpace Foundation works withNGOs and other humanitarian groups tobring life-saving information to peoplewho are disadvantaged by poverty, rurallocation and the digital divide. ❏
SATELLIFE is an international not-for-profit humanitarian organization. Its mission is toimprove health by improving connections between professionals in the field, throughelectronic communications and information exchange in the areas of public health,medicine and the environment. Particular emphasis is on areas of the world wherepoor communications, economic conditions or natural disasters limit access.
SATELLIFE produces two e-mail publications, HealthNet News and HealthNet News–AIDS, which feature materials from 21 journals, including the British Medical Journal,Lancet and East African Medical Journal.
SATELLIFE also operates and maintains several global electronic discussion groupson subjects relevant to developing countries. (See Netscan page 32 for moreinformation on SATELLIFE’s services).
WorldSpace Foundation is a non profit organization created in 1997. Based inWashington DC, USA, its work encompasses Africa, Asia-Pacific, Latin America andthe Caribbean. It has 5% of the channel capacity of the three WorldSpaceCorporation satellites for non commercial social development and distance learningprogramming.
W
study carried out by CommunityInitiatives Support Services Inter-national has investigated thebenefits and problems of donated
drugs at 24 mission health facilities inKenya and Tanzania between 1997 and1998. It found that:➤ On average health facilities received
four deliveries of donated drugs peryear.
➤ Approximately a quarter of all do-nated drugs had a shelf-life of less thanone year.
➤ A quarter of donated drugs wereantibiotics.
➤ Three-quarters of the health facilitieshad sent a list of drugs required to thedonor, but only half received drugsfrom that list.
➤ When donated drugs were not re-quested by the health facility it wasmore likely that good drug donationpractices were not adhered to.
Aonths after devastating floods andlandslides left up to 30,000 peo-ple dead or missing and 200,000homeless, the Bolivarian Repub-
lic of Venezuela was being inundatedagain by a flood of unusable medical aid.Harrowing television pictures of the dis-aster in December 1999 in the coastalstates of Vargas and Falcon, near Cara-cas, sparked a massive humanitarianresponse, and tonnes of medicines arrivedfrom around the world.
However, health workers helping thevictims say that huge quantities of medi-cal aid remain stockpiled in warehouses,and up to 70% will have to be inciner-ated. A report by the Government’sPharmacological Production Service saysmany products cannot be used becausethey are out of date, unnecessary, havebeen partially used, or have no Spanishlabelling. As a result, the Government hasalready had to spend at least 10m bolivars(approximately US$16,000) to hire extra
M
Calm waters on Lake Maracaibo for this auxiliary healthworker doing her rounds, but floods in Venezuela in 1999caused massive devastation
* There are signs that coun-tries are beginning to speakout, to avoid receiving un-necessary drugs when facedwith disasters. For example,Mozambique required alldonations to be consistentwith WHO’s Interagencyguidelines when areas of thecountry were flooded inFebruary and March 2000.
Reference
1. WHO. Interagency guidelines fordrug donations. Geneva: WorldHealth Organization; 1996.(Second edition published 1999).
Phot
o: W
HO
/P.
Alm
say
Oxfam, the international development agency, is launching a campaign onaccess to medicines, with a focus on the issue of affordability. Oxfam hasdrawn on its programme experience and local research to produce a number ofreports looking at the determinants of drug prices, and at policies that can
bring them down. It is paying particular attention to the influence of World TradeOrganization intellectual property rules and to the policies of the pharmaceuticalindustry, and makes policy recommendations to the main actors.
The British-based organization is seeking to raise public awareness on the issuesas part of a broader international campaign to make the world trading system workmore to the advantage of poor communities and poor countries. Oxfam has humanitar-ian and development programmes in over 70 low-income countries. It is also aprominent NGO advocate on international economic development issues, includingtrade and debt. ❏
For more information visit Oxfam’s Web site at: www.oxfam.org.uk or e-mail: <[email protected]>. Alternatively, write to George Tarvit, Campaign Department, Oxfam, 274Banbury Road, Oxford, OX2 7DZ, UK.

7E S S E N T I A L D R U G S M O N I T O R
Issue No. 28 & 29, 2000
A N T I M I C R O B I A L R E S I S T A N C E
ver the past decade, there has been a dramatic upsurge world widein the spread of drug-resistant microbes. Major infectious diseasessuch as tuberculosis, pneumonia and malaria are becoming increas-ingly difficult and expensive to treat, as microbes develop resist-
ance to many of the medicines available. How widespread is the problem?How does drug resistance develop? And what is WHO doing to containthis threat? Rosamund Williams, Coordinator, Anti-infective Drug Resistanceand Containment at WHO explains.
a year in the United States alone, are al-most always caused by drug-resistantmicrobes. Foodborne infections are alsoon the increase – promoting growing con-cern about drug resistance in pathogenssuch as Salmonella and Campylobacter.Meanwhile, tropical diseases, such asleishmaniasis (see box p.8) and Africantrypanosomiasis, which haunt the poorand marginalised communities of theworld, are becoming increasingly diffi-cult to treat among people also infectedwith HIV. Treatment with the usual(and sometimes only) drug is increasinglyineffective.
How widespreadis the problem?
Drug resistance is a global problem –affecting both developing and developedcountries. Its spread is helped by the enor-mous increase in global travel and trade.
transmission) or through acquisition fromother bacteria of resistance genes (hori-zontal transmission). This dual means ofacquiring resistance explains why theresistance trait can spread rapidly andreplace a previously drug-susceptiblepopulation of bacteria.
Are antimicrobial drugsto blame?
No. Antimicrobial drugs do not causeresistance. But the process is acceleratedwhen antimicrobials are misused. What
be killed and the infection resolvedbefore resistance has time to emerge.However, in the treatment of chronicinfections such as TB and HIV/AIDS –especially if treatment compliance ispoor – drug-resistant mutants have timeto emerge and multiply and replacethe drug-susceptible population ofmicrobes. Under these circumstances, itis likely that the treatment outcome willbe poor.
So why is it that the microbes in-volved in acute infections have alsobecome resistant to many of the first-line
Antimicrobial resistance: the facts
Antimicrobial resistance is on the in-crease – threatening our ability to treatsome of the infectious diseases that causemost deaths. Diseases such as tuberculo-sis (TB), which was once thought to beunder control, are becoming increasinglydifficult to treat as medicines become lesseffective – steadily depleting the arsenalof drugs available.
Infectious diseases still account for45% of deaths in low-income countriesand for almost one in two prematuredeaths worldwide. And most of thesedeaths (about 90%) are due to no morethan six diseases: acute respiratory infec-tions (mainly pneumonia), diarrhoealdisease, HIV/AIDS, TB, malaria andmeasles. Antimicrobial resistance istoday challenging our ability to treateffectively at least four of these infec-tions: acute respiratory infections,diarrhoeal disease, malaria and TB.
O
DECLINING RESPONSE TOANTIMALARIAL DRUGS
1976 1980 1988 1992
100%
80
60
40
20
0
Mefloquine
Quinine
Sulfadoxine-Pyrimethine
Chloroquine
1984
Chloroquine, for example – once thefirst-line treatment for malaria – is nolonger effective in 81 of the 92 countrieswhere the disease is a public health prob-lem. In some regions, over half of all casesof streptococcal pneumonia are resis-tant to penicillin. And over 20% of newTB cases are now multidrug-resistant.
To make matters worse, resistanceis already emerging to anti-HIV drugs.There are reports of resistance to allcurrently marketed antiretroviral drugs.And resistance is also widespread amongsexually-transmitted infections, such asgonorrhoea, that enhance the spread ofHIV.
But the problem does not end there.Hospital-acquired (nosocomial) infec-tions, which account for 40,000 deaths
Documented examples include:
➤ cases of drug-resistant gon-orrhoea acquired by touristsvisiting South-East Asia andtransmitted among commu-nities in Australia;
➤ outbreaks of multidrug-resistant TB in Western Eu-rope traced back to EasternEuropean countries whereTB control is poor;
➤ two outbreaks of MRSA(methicillin-resistant Sta-phylococcus aureus) hospitalinfection in Canada involv-ing patients who acquired thestrain in India.
In addition, cases of drug-resistant malaria occur amongtravellers returning to developedcountries from malaria-endemic
drugs available? The problem is thatantimicrobial drugs not only kill themicrobe being targeted, they also “treat”other normally harmless microbes(“normal flora”) in the body as well.For example, Streptococcus pneumoniae,as well as causing otitis, pneumoniaand meningitis, is also carried by manypeople, especially children, as part oftheir normal throat flora, without caus-ing any symptoms. So every time theytake an antimicrobial – for whateverreason – their streptococci are exposed.If a mutant emerges, it will have a selec-tive advantage and can spread to otherpeople. A similar process occurs whensalmonella bacteria are exposed toantimicrobials incorporated into ani-mal feed. While these bacteria maynot cause the animal any harm, they canbe spread to humans through the foodchain.
What is multidrug-resistance?
There are many different classesof antimicrobials, and microbes havedevised ways to resist the action ofeach and every one. In addition, a singlemicrobial cell can carry resistancegenes to a whole series of totallyunrelated antimicrobial drugs. Over
PENICILLIN-RESISTANTPNEUMOCOCCI IN THE 1990s
Israel
80
70
60
50
40
30
20
10
0
% in hospital patients
South Korea
Saudi Arabia
EgyptBulgariaKenyaSingaporeHong KongM
exicoCzech Republic
happens is that natural selection– a natural biological process –favours the survival of microbesthat develop resistance genesby chance when exposed toantimicrobials. All uses ofantimicrobials – both appro-priate and inappropriate – applya selective pressure on micro-bial populations. However, themore antimicrobials are used,the greater this pressure willbe. Thus it is critical to gainmaximum benefit from the cura-tive effects of antimicrobials –especially in developing coun-tries, where they are not onlymisused, but often under-useddue to financial constraints. Atthe same time, it is also essen-tial to minimise the opportunitiesfor resistance to emerge. Inpractice this means usingantimicrobials both widelyand wisely – neither too little,nor too much, and never inap-propropiately. Inappropriateprescribing practices – includingthe wrong choice of drug and incorrectdosage or length of treatment – poorcompliance with treatment, and the useof low quality (sometimes counterfeit)drugs all contribute to the emergence ofdrug-resistant microbes.
How does resistancedevelop?
If a person develops an acute infec-tion such as pneumonia with a drug-susceptible strain of Streptococcuspneumoniae, for example, and is treatedpromptly with penicillin, the bacteria will
...cont’d on page 8 ➠
THE PARADOX OF CONTROLLINGDRUG RESISTANCE
Antibiotics tooreadily available
Undertreatment and inadequateaccess to antibiotics
Encouragesresistance
Resistant infectionsnot properly treated
sistance is high. These drug-resistant infections will notspread in developed countriesprovided there are no mosquitovectors. But global warmingcould change all that.
What is antimicrobialresistance?
When antimicrobial resist-ance occurs, it is the microbe(bacterium, virus, fungus or pro-tozoan) that is resistant; not thedrug, nor the patient. Species ofbacteria that are normally resist-ant to penicillin, for example, candevelop resistance to these drugseither through mutation (vertical
Source: The Southeast Journal of Tropical Medicine andPublic Health, Mekong Malaria, Volume 30, Supplement 4,p 68, 1999
Source: World Health Organization/CDS
countries where re-
Source: Collected from published data

8 E S S E N T I A L D R U G S M O N I T O R
Issue No. 28 & 29, 2000
A N T I M I C R O B I A L R E S I S T A N C E
The example of leishmaniasisLeishmaniasis is an insect-borne disease that is showing resistance to the highlytoxic, heavy metal-based antimonials at rates of 64% in some developing nations.Currently, visceral leishmaniasis – otherwise known as Kala-azar – afflicts 500,000people each year in 61 countries in East Africa, India and the Mediterranean basin.The sandfly-transmitted parasite attacks the spleen, liver and bone marrow and ischaracterised by fever, severe weight loss and anaemia. Left untreated, the diseaseis fatal. Drug-resistant leishmaniasis results when treatment courses are too short,interrupted, or consist of poor-quality or counterfeit drugs. Once infected, victimsremain vulnerable to potentially fatal flare-ups throughout their life. As with mostinfectious diseases, resistant strains flourish in areas where poverty is high, surveil-lance is low and treatment frequently inconsistent due to limited medical access,inadequate diagnosis, the availability of parallel-market drugs, and political discord.Active monitoring procedures that could reveal the true extent of the disease arehindered by lack of available funds and civil unrest. In one study, WHO researchersconducting a house-to-house search discovered that the actual rate of infection was48 times that which had been initially reported.
In the State of Bihar in north-western India, up to 70% of cases are non-responsive tocurrent treatments, while in Bangladesh, Brazil – and particularly Sudan (where 90%of all cases originate), resistance continues to grow. In developed Mediterraneannations, drug-resistant leishmaniasis is spreading as the number of patients co-infected with HIV increases. Those infected with HIV or who are immuno-suppressedin any way (as a result of cancer treatments or organ transplants) are likewisevulnerable. Any kind of immuno-suppression can potentially increase the number ofparasites in the blood, thereby giving rise to the likelihood of transmission throughthe bite of the sandfly. This cycle facilitates a destructive spiral of greater resistance,higher parasitic levels and increased infection-producing potential.
War, globalisation, increased travel and climatic change places this parasiticinfection solidly in the category of emerging diseases with rapidly-evolvingresistance.
time, the dysentery-causing bacteriumShigella, for example, has becomeresistant to each successive classof antimicrobials used in treatment. Asa result, it has a string of genes, each
Antimicrobial resistance...cont’d from pg. 7
TACKLING THE PROBLEM
Can antimicrobialresistance be halted?
No. But it can be contained. Antimi-crobial resistance is a natural biologicalphenomenon – the response of microbessubjected to the selective pressure of an-timicrobial drug use. The main priority
RESISTANCE CAN BEEFFECTIVELY TREATED
Ideal drug usage involves:• The correct drug• Administered by the best route• In the right amount• At optimum intervals• For the appropriate period• After an accurate diagnosis
Problems occur in both developed and developingcountries when antimicrobials are:• Not equitably available• Used by too many people• To treat the wrong disease• In the wrong dosage• For the wrong period of time• Not in the correct formulation or strength
Antimicrobial resistance is not a new or surprisingphenomenon. All micro-organisms have the abilityto evolve various ways of protecting themselvesfrom attack BUT over the last decade or so:• Antimicrobial resistance has increased• The pace of development for new and replacementantimicrobials has decreased
RESISTANCE MEANS THAT:• People can’t be effectively treated• People are ill for longer• People are at greater risk of dying• Epidemics are prolonged• Others are at greater risk of infection
coding for resistance to a different anti-microbial. To make matters worse, thisstring of genes can be transmitted fromone bacterial cell to another. Thus apreviously susceptible Shigella can, inone fell swoop, acquire five or sixresistance genes.
Why is antimicrobialresistance spreadingso fast?
Although mutations are rare events(about one in a million bacteria mayshow a mutation which might leadto resistance), microbes multiplyvery rapidly – thereby enabling a singlemutant to rapidly become dominant.Microbes also spread readily fromperson to person. Thus one patient in-fected with a resistant strain may be animportant source of spread, not only ofthe infection, but of a resistant infec-tion. This is demonstrated in hospitals,where one patient infected with MRSA,for example, is often the source fromwhich many others become infected orcolonised.
Thus in taking action to containresistance, both the emergence of resist-ance and the spread of resistant strainsneed to be considered.
should be to prevent infection in thefirst place. After that, containmentof the problem is the best we canaim for. And since it is antimicro-bial use that drives resistance, thefocus of any containment strategyshould be on minimising anyunnecessary, inappropriate or irra-tional use of antimicrobial drugs.Many groups of people play a rolein determining how and whereantimicrobials are used:
➤ patients and the general public;
➤ all groups of prescribers anddispensers;
➤ hospital managers and healthcare professionals;
➤ users of antimicrobials inagriculture;
➤ national governments;
➤ pharmaceutical, diagnostic and“surveillance” industries;
➤ international agencies, NGOs,professional societies.
Source: World Health Organization/CDS
All of these groups need to be engagedin developing and implementing a resistancecontainment action plan.
What is WHO doing?
WHO has taken the lead in developing aGlobal Strategy for the Containment of Antimi-crobial Resistance. The strategy is designed toreduce the emergence of resistance and slow thespread of resistant infections, in an effort to re-duce the mortality, morbidity, and high costs
Source: World Health Organization/CDS
associated with antimicrobial resistance. The strategy is based on pub-lished evidence, expert opinion, and the deliberations of other expert bodies.It includes a review of the factors responsible for the emergence and spreadof resistance and of the interventions that have been tested or proposed toaddress the problem. The strategy provides a framework of interventionsfor implementation. It also highlights the gaps in current knowledge andthe many outstanding research needs. Foremost among these is the need todevelop new drugs to combat drug-resistant infections, and to develop anew environment of incentives and public-private partnerships to addressthe challenges of antimicrobial resistance. ❏
For further details contact: Dr Rosamund Williams, Communicable Diseases Clus-ter, Anti-infective Drug Resistance and Containment, World Health Organization,1211 Geneva 27, Switzerland.
Source: WHO. Overcoming antimicrobial resistance. Geneva: World Health Organization; 2000.
A female patientwith Leishmaniaaethiopicainfection
Phot
o: W
HO
/TD
R

9E S S E N T I A L D R U G S M O N I T O R
Issue No. 28 & 29, 2000
Who contributes tomisuse of antimicrobials?
information, leading to uncertaintyabout the diagnosis and the mostappropriate drug(s), and fear of poorpatient outcome
➤ patient demand➤ earning a living through selling
medicines.
the time), they are stillgreatly influenced by pa-tients’ demands. Many tra-ditional practitioners are nowprescribing allopathic me-dicines instead of herbal orother kinds of medicines be-cause this is what patientswant. In Tanzania 60% ofhealth workers admitted toprescribing inappropriatedrugs demanded by sociallyinfluential patients, to avoidbeing labelled “difficult”.6
Many people in India believein ‘tonics’ and will not returnto a doctor unless he or sheprescribes according to theirwishes. Even though doctorsmay know that ‘tonics’ are
A
of antibiotic purchases were for 10 orfewer capsules, which in most circum-stances would be less than a full course.
In conclusion, antibiotics are oftenprescribed irrationally (over-prescriptionand inappropriate prescription) andthis contributes to the development ofantimicrobial resistance. However, pre-scribers may have very rational reasonsfor prescribing irrationally and it is notjust a question of lack of knowledge. Onlyby understanding the reasons underlyinginappropriate prescribing can one designeffective interventions to change suchbehaviour. ❏
* Dr Kathleen Holloway is a Medical Of-ficer in the Department of Essential Drugsand Medicines Policy at the World HealthOrganization.
References1. Gilson L, Jaffar S, Mwankusye S, Teuscher T. Assessing
prescribing practice: a Tanzanian example. InternationalJournal of Health Planning and Management 1993;8:37–58.
2. Uppal R, Sarkar U, Giriyappanavar Cr, Kacker V. Anti-microbial drug use in primary health care. Journal ofClinical Epidemiology 1993;46(7):671–673.
3. Hui L, Li X.S, Zeng X.J, Dai Y.H, Foy H.M. Patternsand determinants of use of antibiotics for acute respira-tory tract infection in children in China. PaediatricInfectious Disease Journal 1997;16(6):560–564.
4. Bosu W.K, Afori-Adjei D. Survey of antibiotic prescrib-ing patterns in government health facilities of the WassaWest District of Ghana. East African Medical Journal1997;74(3):138–142.
5. Nizami S, Khan I, Bhutta Z. Drug prescribing practicesof general practitioners and paediatricians for childhooddiarrhoea in Karachi, Pakistan. Social Science andMedicine 1996;42(8):1133–1139.
6. Mnyika K.S, Killewo J.Z.J. Irrational drug use in Tanza-nia. Health Policy and Planning 1991;6(2):180–184.
7. Nichter M, Pharmaceuticals, health commodificationand social relations: ramifications for primary healthcare, Anthropology and International Health, South AsianCase Studies 1989; Section 3, No.9:233–277. (KluwerAcademic Publishers).
8. Branthwaite A, Pechere J-C. Pan-European survey ofpatients’ attitudes to antibiotics and antibiotic use. Jour-nal of International Medical Research 1996;24(3):229–238.
9. Britten N, Ukoumunne O. The influence of patients’hopes of receiving a prescription on doctors’ perceptionsand the decision to prescribe: a questionnaire survey.British Medical Journal 1997;315:1506–1510.
10. Paredes P, de la Pena M, Flores-Guerra E, Diaz J, TrostleJ. Factors influencing physicians’ prescribing behaviourin the treatment of childhood diarrhoea: knowledgemay not be the clue. Social Science and Medicine1996;42(8):1141–1153.
11. Trap B, Hansen E.H, Hogerzeil H.V. Prescribing by dis-pensing and non-dispensing doctors in Zimbabwe.Copenhagen: Royal Danish School of Pharmacy; 2000.(Unpublished study).
12. Shao-Kang Z, Sheng-Ian T, You-de G, Bloom G. Drugprescribing in rural health facilities in China: implica-tions for service quality and cost. Tropical Doctor1998;28:42–48.
Table 1Inappropriate use of antibiotics inteaching hospitals
Country Inappropriate Type/departmentuse (%)
Canada 1977 42% Surgical ward – injections, antibiotics
50% Gynaecology ward12% Medical ward
USA 1978 41% All patientsAustralia 1979 86–91% ProphylaxisCanada 1980 30% Paediatric medical cases
63% Paediatric surgical casesAustralia 1983 48% All departmentsKuwait 1988 39% Paediatric inpatientsAustralia 1990 64% Patients on vancomycinThailand 1990 91% All departmentsSouth Africa 1991 54% Gynaecology inpatients
22–100% Unrestricted antibioticsThailand 1991 41% All departments
79.7% Surgical prophylaxis40.2% Documented infection
Source: Hogerzeil HV. British Journal of ClinicalPharmacology 1995;39:1–6.
PrescribersThere is a wide variation in the pre-
scribing of antimicrobials and otherdrugs. In primary health care 30–60% ofpatients receive antibiotics (see Figure 1),perhaps twice what is clinically needed.Misuse is common and may take the form
➢ KATHLEEN HOLLOWAY*
ntimicrobial resistance is a natural consequence of antimicrobial use,which kills the sensitive organisms leaving the resistant ones to surviveand multiply (selection of resistance). Overuse and misuse of antimicrobialsdo not help patients, they merely add to the problem of resistance
and waste resources.
Figure 1Percentage of primary health care patientsreceiving antibiotics
of incorrect dosage or inappropriate pre-scription. In Tanzania, 91% of antibioticswere prescribed with incorrect dosage1
and in India over 90% of prescriptionsdid not have dose specifications.2 Inap-propriate prescription of antibiotics has
Many prescribers in de-veloping countries havelittle access to good qualityinformation about diagnosisand drugs. Standard treat-ment guidelines are oftenunavailable and healthworkers are often unsup-ported and unsupervised.Frequently, drug companyrepresentatives are doctors’only source of information.Such information may wellbe biased, particularly withregard to how effective theircompany’s drug is com-pared to rival drugs of thesame class. Uncertainty ofthe diagnosis, fear of poorpatient outcome, (and in in-dustrialised countries, fearof litigation), lead to over-presciption of antibiotics. Inmany developing countries,the diagnostic process isoften inadequate to arrive at
a diagnosis with any certainty (Figure 2).
Patient demand orprescriber perception?
Even if prescribers are certain of theirdiagnoses (and none of them will be all
Figure 2Adequacy of diagnostic process
Sources: Thaver et al, Social Science and Medicine 1998. Guyonet al, WHO Bulletin 1994. Krause et al, Tropical Medicine andInternational Health 1998. Bitran, Health Policy and Planning1995. Bjork et al, Health Policy and Planning 1992, Kanji et al,Health Policy and Planning 1995.
ineffective, they prescribe them becausethey are dependent on the patient return-ing for their livelihood.7 In Europe, over50% of mothers interviewed in a studyexpected to receive antibiotics for mostrespiratory infections.8
Prescribers citing patient demand asa cause of irrational prescribing has beenreported in many countries. And patientdemand for specific drugs has beenwidely observed by researchers. How-ever, the degree to which prescribers areinfluenced by their patients is unknownand probably varies according to the skillsand confidence of the prescriber. Thereis some evidence that it is a prescriber’sperception of patient demand, ratherthan actual patient demand, during theconsultation process that may affect theprescribing decision.9,10
Effects ofdispensing doctors
Many prescribers, as well as drugretailers, earn their living by sellingmedicines and not by charging a consul-tation fee. It has been shown in manycountries that prescribers who earnmoney from dispensing medicinesconsistently prescribe more drugs thanthose who do not make money fromdispensing. In a study in Zimbabwe11
dispensing doctors prescribed antibioticsto 58% of their patients compared tonon-dispensing doctors who prescribedantibiotics to 48% of their patients.In China, after the ‘socialist marketeconomy’ reforms of the late 1970s, drugsales became an important source ofincome for providers, including healthworker salary supplements. Once drugsales formed part of health worker sala-ries, greater polypharmacy was observed,and the average prescription was foundto cost two to six times the average percapita daily income.12 Selling high costitems, such as antibiotics, may earndispensing prescribers more profit, butunfortunately many patients cannot affordsuch drugs and may buy incompletecourses. In a study in the Philippines 90%
0% 10%
% of PHC patients receiving antibiotics
20% 30% 40% 50% 60% 70%
Sudan
Swaziland
Cameroon
Ghana
Tanzania
Zimbabwe
Indonesia
Nepal
Bangladesh
Eastern Caribbean
El Salvador
Jamaica
Guatemala
AFRICA
LATIN AMERICA & CARIBBEAN
ASIA
Pakistan
Bangladesh
Burkina Faso
Senegal
Angola
Tanzania
0 10 20 30 40 50 60
% observed consultations where the diagnostic process was adequate
been reported to occur for vi-ral respiratory tract infectionsin 97% of cases in China3 and81% of cases in Ghana.4 In-appropriate prescription ofantibiotics for childhood di-arrhoea commonly occurs, asreported in Pakistan. Here pri-vate general practitioners werefound to prescribe significantlymore antibiotics (41% of pae-diatric cases) than paedia-tricians (36% of paediatriccases) in the public hospitals.5
Hospital prescribers are of-ten the role models for primaryhealth care prescribers. Unfor-tunately, antimicrobials aremisused just as much in hospi-tals as in primary health care,as shown in Table 1.
Why do providers prescribeantimicrobials too often andunnecessarily? There are manycauses including:➤ lack of knowledge or
A N T I M I C R O B I A L R E S I S T A N C E
Source: Managing Drug Supply, 2nd ed. Quick JD, Rankin JR,Laing RO, O’Connor RW, Hogerzeil HV, Dukes MN, Garnett A,eds. Hartford CT: Kumarian Press; 1997.

10 E S S E N T I A L D R U G S M O N I T O R
Issue No. 28 & 29, 2000
Problems from antimicrobialuse in farming
➢ KLAUS STÖHR*
ollowing their success in human medicine, antimicrobials have beenincreasingly used to treat disease in animals, fish and plants. They alsobecame an important element of intense animal husbandry because oftheir observed growth enhancing effect, when added in sub-therapeutic
doses to animal feed. Some growth promoters belong to groups of antimicrobials(for example, glycopeptides and streptogramins), which are essential drugsin human medicine for the treatment of serious, potentially life-threateningbacterial diseases. These include Staphylococcus or Enterococcus infections.
Scale of use
The total amount of antimicrobialsused in food animals is not preciselyknown, although it is estimated that abouthalf of the antimicrobials produced glo-bally are used in farming, particularly inpig and poultry production.
In Europe, all classes of antimicrobiallicensed for disease therapy in humans arealso registered for use in animals, a situ-ation comparable with other regions in theworld, although comprehensive regis-tration data are much more difficult toobtain. National statistics on the amountand pattern of antimicrobial use, in hu-man medicine or anything else, exist inonly a few countries.
An average of 100 milligrams ofantimicrobials are used in animals in Eu-rope to produce one kilogram of meat forhuman consumption. Statistics from otherregions are scarce, but increased meatproduction in many developing countriesis mainly due to intensified farming,which is often coupled with greater anti-microbial use for both disease therapy andgrowth promotion.
Factors contributingto overuse➤ Education on antimicrobial resistance
and prudent antimicrobial use islacking amongst dispensers and pre-scribers of antimicrobials, and in
many countries, people who are inad-equately trained dispense them. Onestudy reported that more than 90% ofthe drugs used in animals in the UnitedStates in 1987 were administeredwithout professional veterinary con-sultation. Inappropriate doses andcombinations of drugs are frequentlyused in animals. And antimicrobialsadministered to animal flocks andherds in their feed causes problems ofinaccurate dosing, and the inevitabletreatment of all animals irrespectiveof health status.
➤ Empiric treatment predominatesbecause of the widespread lack ofdiagnostic services, particularly in de-veloping countries. In many places,it is uncommon to submit clinicalspecimens and samples from sick ani-mals, due to the costs involved, timerestrictions and the limited number oflaboratories.
➤ Drug sales constitute a significant por-tion of veterinarians’ income in somecountries and may lead to unnecessaryprescribing.
➤ In many countries, including severaldeveloped ones, antimicrobials areavailable over-the-counter and may bepurchased without prescription.
➤ Inefficient regulatory mechanismsor poor enforcement, with lack ofquality assurance and marketing ofsubstandard drugs, are importantcontributory factors. Discrepanciesbetween regulatory requirements andprescribing/dispensing realities areoften wider than in human medicine.
➤ Antimicrobial growth promoters arenot considered drugs and are licensed,if at all, as feed additives.
➤ As in human medicine, pharma-ceutical industry marketing ofantimicrobials influences veteri-narians’ and farmers’ prescribingbehaviour and use patterns. There arecurrently few countries with industrycodes or government rules for over-seeing advertising practices forantimicrobials for non human use.
➤ There is a significant increase inintensive animal production, particu-larly in countries with economies intransition where all the factors listedhere are present. When animal pro-duction appears to benefit from the useof antimicrobials, economic incen-tives may take precedence over thepossible transfer of resistance to hu-mans, and the potential negativeimpact on human health.
Examples of theconsequences of overuse
◆ Shortly after the licensing and useof fluoroquinolone, a powerfulnew class of antimicrobials, inpoultry, fluoroquinolone-resistantSalmonella and Campylobacterisolations from animals, and soonafterward from humans, becamemore common. Community andfamily outbreaks, as well asindividual cases, of Salmonellosisand Campylobacteriosis resistantto treatment with fluoroquinoloneshave since been reported fromseveral countries.
◆ With the emergence of vancomy-cin-resistant strains of Staphylo-coccus and Enterococcus bacteriain many hospitals around theworld, the question arose if theuse of those antimicrobial agentsin agriculture could have com-pounded the worsening problem.Vancomycin-resistant Enterococciwere isolated in animals, foodand non-treated volunteers incountries where vancomycins werealso used as growth promoters inanimals. By 1997 all Europeancountries had banned vancomy-cin, and after this the prevalenceof resistant Enterococci in animalsand food, particularly in poultrymeat, fell sharply.
How to tacklethe problem
WHO, the UN Food and AgricultureOrganization, the Office Internationaldes Epizooties and 14 other internationalgovernmental and nongovernmental or-ganizations and professional societieshave developed a framework of recom-mendations to reduce the overuse andmisuse of antimicrobials in food animalsfor the protection of human health.(For further information see: http://www.who.int/emc/diseases/zoo/who_global_principles.html).
What the various stakeholdersneed to doResponsibilities of regulatoryand other relevant authorities
All antimicrobials used in food ani-mals should be reassessed in relation totheir propensity to cause antimicrobialresistance in bacteria which can be trans-mitted to humans. Priority should begiven to those products considered mostimportant in human medicine.
After the licensing of veterinaryantimicrobials, surveillance of resistanceto antimicrobials belonging to classesconsidered important in human medicineshould be conducted. In this way emer-gence of antimicrobial resistance willbe detected in time to allow corrective
The widespread use of antimicrobialsin farming is of serious concern as someof the newly emerging resistant bacteriain animals are transmitted to humans,mainly from food of animal origin orthrough direct contact with farm animals.Treating disease caused by these resist-ant bacteria in humans is more difficultand costly and, in some cases, availableantimicrobials are no longer effective.The best-known examples are diseasescaused by the foodborne pathogenic bac-teria Salmonella and Campylobacter andthe commensal (harmless in healthypersons and animals) bacteria Enterococ-cus. Research has shown that resistancein these bacteria is often a consequenceof using certain antimicrobials inagriculture.
More studies are needed, however, asthe impact of the widespread distributionof non-metabolised antimicrobialsthrough manure and other effluents intothe environment is still unknown. Andinformation is also scarce on the type andamount of antimicrobials used in the ex-panding aquaculture sector. Based on thelessons learned from species living onland, there is an urgent need to reviewcurrent practices to identify potential haz-ards. This also applies to other uses ofantimicrobials, in plant protection and inindustry, for example.
F
A butcher’s stall in the Dominican Republic. There is increasing evidence of the problems causedby feeding antimicrobials to farm animals
Phot
o: W
HO
/PA
HO
/A
. Waa
k
A N T I M I C R O B I A L R E S I S T A N C E

11E S S E N T I A L D R U G S M O N I T O R
Issue No. 28 & 29, 2000
Promoting resistance?➢ JOEL LEXCHIN*
he Autumn 1996 issue of Health Horizons, the magazine of the Interna-tional Federation of Pharmaceutical Manufacturers Associations, ran atwo-page feature entitled “International Mobilization Against New andResistant Diseases.” This article highlighted the efforts being made by
international organizations and the pharmaceutical industry to deal with thethreat of increasing antibiotic resistance. What the article didn’t mention wasthat some in the industry can also play a role in promoting bacterial resistanceto currently available medications.
that otitis media, at least in children olderthan two years, should not be treatedwith antibiotics unless the child fails toimprove after 48 hours.
What these advertisements do is topromote, as first line choices, the use ofantibiotics that should be kept in reserve,and promote the use of antibiotics forconditions that will probably resolvewithout any intervention. Both situationsrepresent inappropriate use of antibioticsand clearly have the potential to lead toincreased resistance.
The other common feature of theseadvertisements is that they are for new,expensive antibiotics; drugs that can gen-erate large profits for companies, if salesvolumes are large. What doctors do notsee is advertising for older, less expen-sive antibiotics, even though these drugsare the ones that are the most appropri-ate. When was the last time there was anad for penicillin for streptococcal phar-yngitis or for trimethoprim for a urinarytract infection?
This scenario is not limited to Canada,the situation is, if anything, worse in otherparts of the world. The Medical Lobbyfor Appropriate Marketing (MaLAM)has received a number of examples ofinappropriate antibiotic promotion in de-veloping countries. Advertisements in1994 and 1995 in the Philippines advo-cated the use of lincomycin for tonsillitis/pharyngitis and clindamycin in upper res-piratory tract infections. The most likelycause of any of these conditions is a viralinfection where antibiotics are useless.Once again, antibiotics are being adver-tised for conditions that do not requirethem.
1997 advertising claims in Indiafor clarithromycin used the words “pae-diatric suspension . . . speed, . . . strength,. . . spectrum, . . . safety” without anyqualification. In MaLAM’s opinion itwould have been reasonable for readers
of this ad to interpret those words tomean that clarithromycin has clinicallyimportant advantages over alternativeantimicrobials and thus was a first lineantibiotic for common childhood in-fections. As MaLAM pointed out, autho-ritative sources did not recommendclarithromycin as the treatment of choicefor paediatric otitis media, pharyngitisor sinusitis. The parallels with the Cana-dian example of the advertisement forciprofloxacin are clear; the advertise-ments are encouraging the overuse ofsecond-line drugs.
A couple of American studies, span-ning almost a quarter of a century, makethe point that the concern about promo-tion leading to the misuse of antibioticsis more than just a theoretical problem.The first of these, published in the early1970s, showed that more appropriate useof the antibiotic chloramphenicol wasrelated to infrequent use of journal ads tolearn about usefulness of new drugs, anddisapproval of detailers as sources of pre-scribing information for new drugs.1
The second study came out in 1996. Inthis case, researchers presented a groupof primary care doctors with three casescenarios, two of which involved infec-tious diseases, and asked them to choosebetween four treatment options of equalefficacy but with widely varying costs.The more credibility that doctors attachedto information coming from sales repre-sentatives the higher the physician’s costof prescribing.2
In many cases in developing countriesdoctors lack sources of objective infor-mation about antibiotics. These doctorsare totally reliant on promotional mate-rial from companies, with all of the biasesthat this material entails. In the mid 1980sphysicians practicing in a peripheralhealth centre in Sri Lanka where poly-pharmacy, multiple antibiotic therapy andthe use of mixtures of unproven efficacywere common, were totally dependent on,and positive towards, drug informationfrom drug companies.3
Drug companies are now racing tobring out new, more powerful antibioticsto combat drug resistance, and we shouldwelcome these medications. But if theindustry is sincere about wanting todo something about resistance then itshould start by monitoring its promotionalpractices more closely. ❏
* Dr Joel Lexchin is an emergency physicianin Toronto, Canada, and the Secretary-Treasurer of the Medical Lobby for Appropri-ate Marketing. He is also a co-author of Drugsof Choice: A Formulary for General Practice.
References
1. Becker MH, Stolley PD, Lasagna L, McEvilla JD, SloaneLM. Differential education concerning therapeuticsand resultant physician prescribing patterns. Journal ofMedical Education 1972;47:118–27.
2. Caudill TS, Johnson MS, Rich EC, McKinney WP. Phy-sicians, pharmaceutical sales representatives, and thecost of prescribing. Archives of Family Medicine1996;5:201–6.
3. Tomson G, Angunawela I. Patients, doctors and theirdrugs: a study at four levels of health care in an area ofSri Lanka. European Journal of Clinical Pharmacology1990;39:463–7.
According to one company, cipro-floxacin is “an appropriate choice for your[doctors’] patients at risk.” This was themessage in an advertisement that ap-peared in the 3rd October 2000 issue ofthe Canadian Medical Association Jour-nal. “Appropriate” for whom? To answerthat question readers had to notice asmall asterisk after the word “risk” andthen look down to the bottom of thepage, where in small print they foundthe definition. “Appropriate” for what?Once again in small type was the an-swer; ciprofloxacin should be used in“challenging” respiratory tract infections.Challenging was never defined. In thesame advertisement the company claimedthat it supports the appropriate use ofantibiotics.
Advertisements that do not give clearinformation or that give it in print that re-quires the use of a magnifying glass arenot supportive of appropriate use of me-dications. The message in the ad forciprofloxacin is that doctors should feelfree to use this medication as a first lineagent any time they are worried abouttheir patients, or think that there is some-thing unusual going on. Ciprofloxacin isa good first choice for a limited numberof problems but not for most respiratorytract infections. The Australian Scheduleof Pharmaceutical Benefits restricts theuse of this antibiotic in these situationsand the same is true in some Canadianprovinces.
Another recent Canadian journal ad-vertisement, this time for azithromycin,had a young baseball pitcher, his facedetermined, ready to release the ball withthe message “tough on acute otitis me-dia, easy on kids.” The message in thiscase was that doctors and their youngpatients need a powerful medicationto deal with otitis media and thatazithromycin fits the bill. However, thisdoes not reflect the growing consensus
T
Farming... cont’d from pg. 10
A N T I M I C R O B I A L R E S I S T A N C E
strategies to be implemented as part ofan efficient post-licensing review.
Authorities should ensure that allantimicrobials for disease control in ani-mals are classified as prescription-onlymedicines.
Distribution/sales/marketingEnforcement policies should be
designed to ensure compliance withlaws and regulations on the authori-sation, distribution and sale, and useof antimicrobials. They should aim atpreventing the illicit manufacture,importation, and sale of antimicro-bials, and at controlling their distributionand use.
Special attention should be paid tothe distribution and sale of counterfeit,sub-potent and misbranded veterinaryantimicrobials. Enforcement actionshould be taken to stop such distribu-tion and sale by relevant authorities, incoordination with the exporting country,if appropriate.
Antimicrobial growth promotersUse of antimicrobial growth promot-
ers that belong to classes of antimicrobialagents used (or submitted for approval)in humans and animals should be termi-nated or rapidly phased-out in the absenceof risk-based evaluations.
Surveillance ofantimicrobial resistance
Programmes to monitor antimicro-bial resistance in animal pathogens,zoonotic agents (for example, Salmonellaspp. and Campylobacter spp.), and bac-teria known to be indicators of anti-microbial resistance (for example, Es-cherichia coli and Enterococcus faecium)should be implemented on bacteria fromanimals, food of animal origin andhumans.
Surveillance of antimicrobial useInformation on the amounts of anti-
microbials given to food animals shouldbe made publicly available at regularintervals, be compared to data from sur-veillance programmes on antimicrobialresistance, and be structured to permitfurther epidemiological analyses.
Prophylactic use of antimicrobialsUse of antimicrobials for prevention
of disease can only be justified where itcan be shown that a particular disease ispresent or is likely to occur. The routineprophylactic use of antimicrobials shouldnever be a substitute for good animalhealth management.
Prophylactic use of antimicrobials incontrol programmes should be regularlyassessed for effectiveness and whetheruse can be reduced or stopped. Efforts toprevent disease should continuously bein place, aimed at reducing the need forthe prophylactic use of antimicrobials.
Education and trainingVeterinary undergraduate, postgra-
duate and continuing education shouldbe evaluated to ensure that preventivemedicine, prudent antimicrobial use andantimicrobial resistance are given highpriority. The effectiveness of this train-ing should be continuously monitored.
Education strategies emphasising the
importance and benefits of prudent useprinciples must be developed and imple-mented to provide relevant informationon antimicrobial resistance for producersand stakeholders. Emphasis must also begiven to the importance of optimisinganimal health through implementation ofdisease prevention programmes and goodmanagement practices.
The public should be informed ofthe human health aspects of antimicro-bial use in food animals, so that they cansupport efforts to control antimicrobialresistance.
ResearchStakeholders should identify research
priorities to address public health issuesof antimicrobial resistance from anti-microbial use in farming. Governments,universities, research foundations andindustry should give high priority tosupporting research in these areas. ❏
* Dr Klaus Stöhr is a Scientist at the WorldHealth Organization, Communicable Dis-eases Cluster, Animal and Food-RelatedPublic Health Risks, Department of Commu-nicable Disease Surveillance and Response.

12 E S S E N T I A L D R U G S M O N I T O R
Issue No. 28 & 29, 2000
Antibiotic use and bacterial resistance toantibiotics in children in a Vietnamesecommunity
n 1999 a household survey was conducted in one agricultural districtin sub-tropical north Viet Nam. This district has 32 community healthstations, one district hospital, three licensed private pharmacies, a fewprivate practitioners, about 16 drug outlets and 362 villages. The re-
searchers randomly selected 200 children, aged 1–5 years, within 166households, from the 225 households in five villages (out of 67 villages wherethere is a surveillance programme). Nasopharygeal and throat specimens werecollected from each child, and their carers were interviewed to obtain drug useinformation. Researchers explained the purpose of the study to each householdand obtained permission to collect the specimens.
species identification and susceptibilitytesting.
Ignoring treatmentguidelines
It was found that 82% of the childrenhad at least one symptom of acute respi-ratory infection during the four weeksprior to interview, and that of thesechildren 91% had been treated withantibiotics. Thus, 75% of all the children(both with and without symptoms) had
been treated with antibiotics. On averageantibiotics were given for 3.9 days andampicillin was the commonest choice;this is contrary to the national treat-ment guidelines, which recommendcotrimoxazole for acute respiratoryinfection.
When deciding which antibiotic touse, 67% of carers used a pharmacy, 11%decided themselves, and 22% followeda doctor’s prescription. The carers wereasked what drug information they paidattention to when treating their children,and replied as below:
daily dosage 87%how to take the drug 52% (e.g. with water)total dosage 12%contraindictions 8%expiry date 3%antibiotic resistance 1 person
Eighty percent of the antibiotics werepurchased from small shops and pedlars,18% from community health stations and2% from a national hospital pharmacy.
A disturbing levelof resistance
One hundred and sixty-three isolatesfrom 145 children were susceptibilitytested. The carrier rate for S.pneumoniaewas 50%, for H.influenzae 39%, and forM.catarrhalis 17%. In 74% of the 145
A standardised questionnaire wasdeveloped, piloted and then used by fourexperienced local interviewers. Theyasked questions about the types of anti-biotics which had been used, how longfor, where they were purchased, andwhat they knew about them. At the sametime, microbiologists from Hanoi Uni-versity collected nasopharygeal (pos-terior nares) and throat (tonsillar) swabs.The swabs were immediately placedin charcoal transport medium, and trans-ported to the laboratory for culture,
ISymptom(s) of ARI 4 weeks preceding thestudy and treated with antibiotics 75%
Symptom(s) of ARI 4 weekspreceding the study. Nottreated with antibiotics 7%
No symptoms/Not treated withantibiotics 18%
Penicillin 12%
Amoxicillin 11%
Erythromycin 5%Tetracycline 4%Other 3%
Don’t know 11%Ampicillin 74%
Eighty-two percent of the 200 children had symptoms of ARI four weeks preceding the study (left pie chart)and seventy-five percent of these children had used antibiotics within this four week period (right piechart). As some antibiotics were used in combination, the percentages total more than 100%.
Figure 1Antibiotic consumption amongst children
Table 1Prevalence of antibiotic resistant (R) and intermediate susceptible (I)strain of H. influenzae, S. pneumoniae and M. catarrhalis
H. influenzae S. pneumoniae M. catarrhalisn = 74 n = 62 n = 27
Antibiotics R I R I R I
Ampicillin 18% 6% – – 19% 30%Chloramphenicol 24% 0% 25% 3% 15% 4%Ciprofloxacin 6% 6% 0% 80% 0% 19%Erythromycin 4% 49% 23% 3% – –Gentamicin 0% 2% 3% 95% 0% 0%Loracarbef 2% 0% – – 0% 4%Penicillin V 24% 60% 6% 5% 54% 31%Tetracycline 32% 32% 88% 2% 13% 0%Trimethoprim/ 44% 3% 32% 12% 59% 19% SulphonamideVancomycin – – 2% 2% – –
Number of susceptibility tested strains susceptibility tested (n). Antibiotic not tested (–).
children resistant pathogens were found.Resistance to one or more antibiotics wasshown in 68% (50/74) of H.influenzaeisolates, 90% (56/62) of S.pneumoniaeisolates, and 74% (20/27) of M.catarr-halis isolates. The prior consumption ofampicillin or pencillin was associatedwith a significantly greater ampicillinor penicillin resistance, odds ratio 2.3(p<0.05). Multi-drug resistance to a com-bination of trimethoprim/sulphonamide,tetracycline, chloramphenicol, penicillinV and ampicillin was found in 26% ofH.influenzae isolates. Multi-drug resist-ance was found in 31% of S.pneumoniaeisolates. Almost all S.pneumoniae isolateswere resistant to both tetracycline andtrimethoprim/sulphonamide and abouthalf were resistant to chloramphenicoland/or erythromycin.
The authors conclude that there isa serious public health problem in theVietnamese community. A majority ofchildren will suffer acute respiratory in-fection symptoms within any one month.They will be treated inappropriatelywith antibiotics, which are contributingto significant levels of resistance. ❏
Source: Larsson M, et al. Antibiotic medica-tion and bacterial resistance to antibiotics: asurvey of children in a Vietnamese commu-nity. Tropical Medicine and InternationalHealth 2000;5(20):711–721.
Working to decrease costsof anti-TB drugs➢ MARCOS ESPINAL, RAJESH GUPTA,
MARIO RAVIGLIONE*
mong infectious diseases tuber-culosis (TB) remains a leadingcause of adult mortality.1 Over thelast decade, the rising spectre of
multidrug-resistant TB (MDR-TB) began
to threaten global TB control efforts.MDR-TB is defined as disease caused byMycobacterium tuberculosis resistant toat least isoniazid and rifampicin, the twomost powerful anti-TB drugs. There isevidence that short-course chemotherapywith first-line anti-TB drugs used to treatdrug-susceptible cases is not as effective
to cure MDR-TB cases.2 In some areasof the world (especially countries of theformer Soviet Union and eastern Europe),rates of MDR-TB among new and pre-viously-treated cases are so high thatthey are considered “internationalpublic health emergencies” given thepossibility of international spread.3,4
To respond to the challenge, WHO andseveral partners have launched pilotprojects to manage MDR-TB within pro-gramme conditions in settings of limitedresources. However, one of the greatestobstacles to providing treatment topatients infected with MDR-TB has beenthe high cost of the second-line anti-TB
A
A N T I M I C R O B I A L R E S I S T A N C E

13E S S E N T I A L D R U G S M O N I T O R
Issue No. 28 & 29, 2000
drugs needed for the management ofMDR-TB.5 Over the last three years,open market prices for these second-lineanti-TB drugs have been as high asUS$15,000 for an 18-month treatmentregimen. In contrast, the first-line anti-TB drugs needed for management ofdrug-susceptible TB cost as little asUS$11 for a six-month treatment regi-men.6 In order to decrease the cost of thesedrugs, the WHO Working Group (spe-cially created to deal with MDR-TB) hasnegotiated with both the research-basedand generic pharmaceutical industry. Ne-gotiations have resulted in a preferentialprice decrease in the cost of treatmentregimens of up to 90% in comparison tothe open market price. These preferentialprices were partially achieved throughglobal procurement of drugs. Consolidat-ing the market into a single-demandsource not only allowed for some marketforces to arise, but also for industry mem-bers to conduct more accurate demandforecasts that, previously, had been verydifficult.
At the same time, in order to protectagainst the misuse of drugs and creationof resistance to these drugs (the last lineof chemotherapeutic defence against TB),these preferentially priced drugs are onlyreleased to those projects adhering tostandard scientific guidelines as deter-mined by an independent body called the
Green Light Committee.7
This Committee, housedin WHO, is currently com-prised of six institutions:Centres for Disease Controland Prevention, HarvardMedical School, MédecinsSans Frontières, the Na-tional TB Programme –Peru, Royal NetherlandsTB Association and WHO(serving as a permanentmember and secretariat).Most of the work conductedby the Green Light Com-mittee is performed viavideoconference, telecon-ference and e-mail. Alldecisions are made byconsensus.8
Overall, the process hasworked well due to the jointefforts of all institutionsinvolved. Pilot projectshave benefited from theprocurement process andthe negotiations, which, byvirtue of the mechanism
References
1. Raviglione MC, Snider DEJr, Kochi A. Global epide-miology of tuberculosis.Morbidity and mortalityof a worldwide epide-mic. JAMA 1995;273(3):220–26.
2. Espinal MA, et al. Standardshort-course chemotherapyfor drug-resistant tuberculo-sis: treatment outcome in sixcountries. JAMA 2000;283(19):2537–2545.
3. WHO, International UnionAgainst Tuberculosis andLung Disease. Anti-tuber-culosis drug resistancein the world: the WHO/IUATLD Global Projecton Anti-tuberculosis DrugResistance Surveillance,Report No. 2. Geneva:World Health Organiza-tion; 2000. WHO/TB/2000.278.
4. Harvard Medical Schooland Open Society Institute.The global impact ofdrug-resistant tuberculosis.Programme in InfectiousDisease and Social Change.1999.
5. WHO. Procurement of sec-ond-line anti-tuberculosisdrugs for DOTS-Plus PilotProjects. Proceedings of a
described, guarantee that high-quality anti-TB drugs provided at preferential pricesare used in the best possible, controlled manner. This method of procurement helps toensure the scientific integrity of the pilot projects and should be explored for use inother infectious diseases, including HIV/AIDS. ❏
* The authors work for the World Health Organization, Communicable Diseases Cluster, inStrategy Development and Monitoring for Endemic Bacterial and Viral Diseases, Communi-cable Disease Control, Prevention and Eradication.
meeting. Gupta R, Brenner JG, Henry CL, et al, eds.Geneva: World Health Organization; 2000. WHO/CDS/TB/2000.276.
6. Khatri. Personal Communication. 2000.
7. WHO. Guidelines for establishing DOTS-Plus PilotProjects for the management of multi-drug-resistant tu-berculosis. Geneva: World Health Organization; 2000.WHO/CDS/TB/2000.279.
8. WHO. DOTS-Plus and the Green Light Committee. Ge-neva: World Health Organization, 2000. WHO/CDS/TB/2000.283.
A patient in Tanzania suffering from TB, a disease which is becoming increasinglycommon and increasingly resistant to drug treatments
Phot
o: W
HO
/O
. Har
rer
How Chile tackled overuseof antimicrobials
I
Committee on Health of the NationalCongress. Professional organizations ofphysicians and chemists, and the NationalDepartment of Consumer Affairs werealso consulted, with a view to informingthe general public before adoptingany potentially unpopular measures.This was necessary because peoplewere accustomed to purchasing anti-biotics without a prescription, and even
individual tablets in Chile’s pharmacies.
Hitting the headlinesAt the end of September 1999, after
this consultative process, the Ministryof Health acted to control antibiotics, bymaking them available only throughchemists and on prescription. Compliancewith the measure was encouraged by dis-tributing leaflets in private chemists,
displaying posters and by extensivecoverage on radio and television newsprogrammes. In addition, the attentionof the pharmaceutical chemists respon-sible for the technical management ofpharmacists was drawn to the increase inantibiotic consumption over the previous10 years.
Table 1Percentage increases in consumption of selectedantibiotics and groups of antibiotics, 1988–1997
Antimicrobial 1988 1997 VariationDDD/1000 DDD/1000 % increasepop. per day* pop. per day
cloxacillin 0.39 0.417 7ampicillin 0.54 0.613 14amoxicillin 0.87 5.204 498clavul. amoxicillin 0.0025 0.414 16460cotrimoxazole 0.965 1.163 20cephalosporins 0.064 0.262 309fluoroquinolones 0.049 0.281 473
* Defined Daily Dose per 1,000 population per dayThese children playing happily in Chile stand to benefit from thecountry’s actions to minimise antimicrobial resistance
Phot
o: W
HO
/PA
HO
/C
. Gag
gero
A N T I M I C R O B I A L R E S I S T A N C E
Anti-TB drugs...cont’d from pg. 12
➢ LUIS BAVESTRELLO
AND ANGELA CABELLO*
n 1998, the Pan American Infec-tious Diseases Society and thePan-American Health Organiza-tion carried out a study in Chile
on trends in antimicrobials use during theprevious 10 years.1 The study revealed asignificant increase in antibiotic con-sumption, expressed in terms of DDD(defined daily dose) per 1,000 populationper day over the 10 years, based on an-nual sales data for antibiotics in terms ofboth grams consumed and units of sale.2
Noteworthy findings included increasesin sales of amoxicillin (+ 498%), oralcephalosporins (+ 309%) and oral fluoro-quinolones (+ 473%) between 1988 and1997. The only antibiotic with decliningconsumption was chloramphenicol(-18%). See Tables 1 and 2.
These findings were submitted to theChilean Ministry of Health, and meetingsarranged to study what to do about theproblem. Health Ministry staff met withscientific associations, the body regulat-ing drug manufacture and prescribing,the Institute of Public Health and the ...cont’d on page 14 ➠

14 E S S E N T I A L D R U G S M O N I T O R
Issue No. 28 & 29, 2000
Nepal: an economic strategyto improve prescribing
pre-post with control study wasconducted in 33 health facilities(10–12 per district) in three dis-tricts in Eastern Nepal1. In 1992
all three districts charged the same flatfee per prescription, covering all drugs inwhatever amounts. In 1995 the controldistrict charged the same fee, but the othertwo districts had instituted new fee sys-tems. One district charged a single fee perdrug item (1-band item fee), whateverthe drug, but covering a full course of thedrug. A second district charged a higherfee per expensive item (e.g. antibioticsand injections) and a lower fee per cheapitem (e.g. vitamins), each fee covering afull course of the drug. All the fees werepriced so as to cost patients about 25% ofaverage daily household income for twodrug items. Prescribing was monitored inall health facilities before and after the
fee systems were changed.Table 1 shows that both item fees were
associated with significantly better pre-scribing quality than the prescription fee.The percentage of patients receiving an-tibiotics decreased and the proportion ofprescriptions conforming to standardtreatment guidelines increased in bothitem fee districts as compared to the pre-scription fee district. The 1-band fee wasassociated with a greater reduction incheap vitamins and tonics, and the 2-bandfee with a greater reduction in expensiveinjections. ❏
Reference1. Holloway KA, Gautam BR. The effects of different
charging mechanisms on rational drug use in eastern ru-ral Nepal. Paper presented at the First InternationalConference on Improving Use of Medicines; 1997 April1 to 4; Chiang Mai, Thailand. Available on the Web at:www.who.int/dap-icium/posters/4e2_Text.html
ATable 1The effects of different kinds of user fee on prescribing qualityin Nepal
Fees system Control flat fee / Px 1-band fee / drug item 2-band fee / drug itemn=12 n=10 n=11
Av. no. 2.9 ➜ 2.9 (0%) 2.9 ➜ 2.0 (-31%) 2.8 ➜ 2.2 (-21%)items/Px
% Px with 66.7 ➜ 67.5 (+0.8%) 63.5 ➜ 54.8 (-8.7%) 60.7 ➜ 54.3 (-6.4%)antibiotics
% Px with 23.4 ➜ 20.0 (-3.4%) 19.8 ➜ 16.1 (-3.7%) 21.8 ➜ 14.9 (-6.9%)injections
% Px with 27.0 ➜ 22.1 (-4.9%) 26.5 ➜ 8.4 (-18.1%) 23.5 ➜ 15.8 (-7.8%)vitamins or tonics
% Px conforming 23.5 ➜ 26.3 (+2.8%) 31.5 ➜ 45.0 (+13.5%) 31.2 ➜ 47.7 (+16.5%)to STGs
Av. cost / 24.3 ➜ 33.0 (+35.8%) 27.7 ➜ 28.0 (+1.1%) 25.6 ➜ 24.0 (-6.3%)Px (NRs)
Px = prescription
Table 2Annual sales of packs of antimicrobials in private pharmacies in Chile, by antimicrobial group, 1988–1997
Year Macrolides Penicillin: broad Penicillin: Cephalo- Cotrimox- Tetra- Chloram- Fluoro-spectrum M-R Spectrum sporin azole cycline phenicol quinolone
1988 765,800 3,199,000 3,488,600 ..... 1,409,800 836,500 392,600 ....1989 798,400 3,373,700 3,797,800 185,200 1,457,000 851,400 457,100 ....1990 989,235 3,633,271 3,379,425 214,084 1,478,396 870,288 398,428 ....1991 1,053,390 4,104,949 3,354,194 221,457 1,717,625 1,028,031 402,170 ....1992 1,118,807 4,368,913 3,240,031 247,261 1,578,412 914,297 278,566 ....1993 1,435,275 5,151,850 3,289,910 322,135 1,752,653 883,301 298,809 240,1671994 1,400,078 5,090,712 3,250,074 367,539 1,543,922 844,178 276,392 269,4521995 1,615,879 6,213,139 3,548,893 505,036 1,532,223 1,016,890 320,594 307,3761996 1,818,824 6,858,590 3,676,448 537,154 1,550,226 979,917 341,639 335,7281997 2,076,073 7,799,949 4,035,888 563,902 1,692,889 1,055,055 330,348 414,625
… = No data available Source: International Marketing System
Table 4Dollar sales of groups of antimicrobials by private pharmacies inChile, 1998–1999
Group of 1998 1999 Difference(US$)antimicrobials
macrolides 14,763,740 12,448,627 2,315,113broad spectrum penicillins 13,747,242 11,227,954 2,519,288oral cephalosporin 4,488,543 4,193,849 294,694fluoroquinolone 4,075,818 4,115,261 -39,443med.-nar. spect. penicillin 4,121,100 3,275,517 845,583cotrimoxazole 2,316,260 1,767,612 548,648
Total 43,512,703 37,028,820 6,483,883
Source: International Marketing System
Table 3Changes in consumption by DDD/1000 pop./per day between the lastquarter of 1998 and the same quarter of 1999 (immediately afterthe introduction of the Ministry of Health regulation)
Antimicrobials 4th quarter 1998 4th quarter 1999 Variation (%)
clarithromycin 0.366 0.446 21.8azithromycin 0.342 0.353 3.2erythromycin 0.536 0.370 -30.9amoxicillin 4.639 2.943 -36.5ampicillin 0.391 0.182 -53.4clavulanic amoxicillin 0.459 0.443 -3.5cloxacillin 0.424 0.338 -20.3phenoxymethylpenicillin 0.184 0.111 -39.7cotrimoxazol 0.913 0.633 -30.7tetracycline 0.499 0.340 -31.8ciprofloxacin 0.317 0.386 21.8
A N T I M I C R O B I A L R E S I S T A N C E
Three months after the Ministry’saction an evaluation study showed adownturn in consumption. This furtherstudy, entitled “Preliminary evaluation ofthe impact of the measures to regulate out-patient consumption of antimicrobials inChile”, involved a comparison betweenthe same two quarters of two years, oneimmediately before the introduction of themeasure, the other immediately after. Thestudy showed a decline in consumptionof 36% in amoxicillin, 56% in ampicillinand 30% in erythromycin between the lastquarter of 1998 and the same quarter of1999.
Expenditure dropped byUS$6,483,883 between 1998 and 1999,representing a saving for the populationas shown in Table 4.
Studies reveal that the Ministry ofHealth’s control measures introducedafter consultation with scientific, profes-sional and consumer associations, andwith Parliament, had a clear impact on
the sale and consumption of antibioticsin Chile. As a result, in Chile antibioticsmay now only be purchased by prescrip-tion. This has reduced self-medicationand the concomitant threat of microbialresistance.
This Chilean example shows thatgiven political will, determination, con-sultation and public education, effectivemeasures that save lives – by promotingrational use of antibiotics – and moneyare possible. ❏
* Dr Luis Bavestrello is a clinical pharma-cologist and Head of the Infectious DiseasesDepartment, Dr Gustavo Fricke Hospital, and
Angela Cabello is a pharmaceutical chemistin the Pharmaceutical Unit, Dr Gustavo FrickeHospital, Alvarez 1532, Viña del Mar, Chile.Tel/fax: + 56 32 652450.
References1. PAHO. Resistencia antimicrobiana en las Américas:
Magnitud del problema y su contención. EditoresSalavtierra-González R, Benguigui Y. OPS/HCP/HCT/163/2000 pp.234–240.
2. Bavestrello L, Cabello A. Estudio del consumo deantimicrobianos en la comunidad. Chile, diez añosdespués. Rev Chil Infect (1999);16(3):185–190.
Chile... cont’d from pg. 13

15E S S E N T I A L D R U G S M O N I T O R
Issue No. 28 & 29, 2000
Containing drug resistancethrough hospital infection control
➢ NIZAM DAMANI*
ospitals are a crucial componentof the antimicrobial resistanceproblem world wide, becausehighly vulnerable patients often
require prolonged antibiotic therapy, andthe problem of cross infection arises.
Every hospital should make con-tainment and control of multi-resistantmicro-organisms a high priority, and it re-quires a team approach. The first step isto establish an active and effective infec-tion control committee with responsibilityfor formulating, implementing and audit-ing an infection control programmethroughout the hospital.
The microbiologylaboratory’s role
A good diagnostic microbiology labo-ratory service is essential. Laboratoriesshould use internationally recognisedprotocols to identify organisms andantibiotic sensitivity, and their range ofdiagnostic facilities should cover nonbacterial and unusual infections. Closeliaison with clinicians, the infectioncontrol team and the drug and therapeu-tics committee is essential. Laboratoriesshould serve as an important source oflocal surveillance data both for thehospital and the community.
Antibiotic prescribing:a crucial element
Hospital drug and therapeuticscommittees should be responsible forthe promotion of rational prescribing,drug use monitoring and cost con-tainment. They must regularly reviewantibiotic use, conduct audits and givedoctors feedback to influence prescribinghabits. Committees should also approvethe use of newer antimicrobial agents,which should be restricted to agreedclinical conditions.
Doctors must be trained to take re-sponsibility for rational prescribing andto justify their antimicrobial use. Theirprescribing policy must be evidence-based and should reflect local antibioticresistance surveillance data. This can beachieved by having a written hospital for-mulary, and an antibiotic policy that isregularly updated and has broad input andconsensus among all involved.
Infection control measuresBarrier precautions are vital to pre-
vent the spread of multi-resistant micro-organisms in hospitals. These includeisolating patients with multi-resistantorganisms, and ensuring that staff ad-heres to hand hygiene procedures anduse of appropriate personal protectiveequipment. It is important for infectioncontrol measures to be based on thelocal epidemiology and be tailored to
suit individual needs.Hospitals should have a written dis-
infectant policy with procedures to ensureadequate decontamination of equipmentand the environment. Internationallyrecommended sterility checks must becarried out on a regular basis. As multi-resistant organisms can survive in theenvironment for prolonged periods, andmay act as a reservoir for infection, thehospital environment should be keptclean, dry and dust free.
Therapeutic devices, such as urinaryand intravenous catheters, are not onlyresponsible for the majority of hospital-acquired (nosocomial) bacteraemias, butalso for cross infection/outbreaks of
catheter-associated and intravenous lineinfection is not recommended.
A universal challenge
The control and containment of multi-resistant micro-organisms represents auniversal challenge requiring nationaland international efforts, as ease of longdistance travel no longer limits spread.Every hospital should devote ade-quate resources to an infection controlprogramme or health and health careresources could suffer. ❏
* Dr Nizam Damani is Clinical Director andConsultant Microbiologist, Craigavon Area
HHospital, 68 Lurgan Road, Portadown, Co.Armagh BT63 5QQ, Northern Ireland, UK.Tel: + 44 128 38 33 4444 ext. 2654, fax:+ 44 128 38 33 4582.
References
1. WHO. Recommendations for the control of meticillin-resistant Staphylococcus aureus (MRSA). Geneva: WorldHealth Organization; 1996. WHO/EMC/LTS/96.1.
2. The Hospital Infection Control Practices Advisory Com-mittee. Recommendations for preventing the spread ofVancomycin resistance. Morbidity and Mortality WeeklyReport 1995;44:1–13.
3. Global consensus conference on infection control issuesrelated to antimicrobial resistance: Final recommenda-tions. American Journal of Infection Control 1999;27:503–513.
Changing prescriber behaviourTRAINING AND TREATMENTGUIDELINES IMPROVEPRESCRIBING IN UGANDA
randomised controlled trial to testthe impact of standard treatmentguidelines (STGs) plus trainingand supervision on rational pre-
scribing was carried out in 127 healthunits in Uganda. Prescribing was moni-tored in all facilities both before and afterthe interventions. In a control group of42 health units, no intervention was in-troduced. In a second group of 42 healthunits, the national standard treatmentguidelines were disseminated but notraining or supervision was conducted.In a third group of 29 health units, thenational standard treatment guidelineswere introduced and on-site training ontherapeutic problems conducted. In afourth group of 14 health units, the samewas done as for the third group but, inaddition, four supervisory visits wereconducted over a six-month period.
Table 1 shows how prescribingchanged in the different groups. Prescrib-ing quality, (as judged by the percentage
of prescriptions conforming to standardtreatment guidelines) did not improvewhen only guidelines were disseminated,but greatly improved if dissemination wasaccompanied by training and supervision.The intervention used was not only di-rected at antibiotic prescribing, but otheraspects of prescribing also. This mayaccount for why the changes in prescrib-ing quality (percentage of prescriptions
conforming to treatment guidelines) weremuch greater than for antibiotic use alone(percentage of prescriptions containingantibiotics). ❏
Reference
Kafuko J.M, Zirabumuzaale C, Bagenda D. Rational druguse in rural health units of Uganda: effect of nationalstandard treatment guidelines on rational drug use. Finalreport. Kampala: UNICEF, Uganda; 1996.
Table 1Randomised controlled trial in Uganda
Randomised group n % prescriptions % prescriptionscontaining antibiotics conforming to STG
Control group 42 53.0 ➜ 58.0% +5.0% 24.8 ➜ 29.9% +5.1%
Dissemination of STG 42 51.6 ➜ 57.8% +6.2% 24.8 ➜ 32.3% +7.5%
STG + on-site training 29 51.7 ➜ 50.7% -1% 24.0 ➜ 52.0% +28.0%in therapeutic problems
STG + on-site training 14 54.3 ➜ 54.3% 0% 21.4 ➜ 55.2% +33.8%in therapeutic problems+ 4 supervisory visitsin 6 months
A
No one is more vulnerable to multi-drug resistance than peopleadmitted to hospital wards
4. The Hospital Infection Control Practices Ad-visory Committee. Guidelines for isolationprecautions in hospitals. American Journal ofInfection Control 1996;24:24–52.
5. Shlaes DM, Gerding DN, John JF, et al. Soci-ety of Healthcare Epidemiology of Americaand Infectious Diseases Society of AmericaJoint Committee on the Prevention of Antimi-crobial Resistance: Guidelines for preventionof antimicrobial resistance in hospitals. Infec-tion Control and Hospital Epidemiology1997;18:279–291.
6. Goldman DA, et al. Strategies to prevent andcontrol the emergence and spread of antimi-crobial-resistant micro-organisms in hospitals.Journal of American Medical Association1996; 275:234–240.
■ ■ ■
multi-resistant organisms. Urinarycatheters should be inserted onlywhen necessary and removed whenno longer required. All hygieneprecautions must be followed.The use of antibiotics should berestricted to patients who showclinical signs of infection.
The majority of primary bloodstream infections are associatedwith the use of intravascular de-vices. Again the best prevention isto insert an intravascular line onlyif necessary and to keep it in placefor a minimum period. The rou-tine use of antibiotics to prevent
Phot
o: W
HO
/PA
HO
/A
. Waa
k
A N T I M I C R O B I A L R E S I S T A N C E

16 E S S E N T I A L D R U G S M O N I T O R
Issue No. 28 & 29, 2000
Prioritising interventions tocontain antimicrobial resistance
➢ KATHLEEN HOLLOWAY*
ust as there are many actors and activities that contribute towards anti-microbial resistance, so there are many potential strategies to containthe growth and spread of resistance. The WHO Global Strategy to con-tain resistance, (which will be published in 2001 and will be available
on the Web via http://www.who.int/emc/amr), identifies 64 interventions intotal. Of these, 44 interventions are aimed at improving the use of antimicrobialdrugs in humans at the national level or below, (i.e. excluding interventionsconcerning animal use, new vaccine and drug development and internationalmeasures).
described. The first method was used intwo WHO Regional Offices and onecountry, whilst the Global Strategy wasbeing developed. From the problems en-countered using the first method, a secondmethod was developed and used at WHOHeadquarters in finalising the presentdraft of the Global Strategy.
THE REGIONS’PRIORITISATION PROCESS
Step one: deciding whoparticipates in the process
A list of participants was agreed lo-cally. In the Regional Office for the
Eastern Mediterranean (EMRO) and theRegional Office for South-East Asia(SEARO), participants were WHO staffmembers. In Nepal they were from theMinistry of Health, academic institutionsand local NGOs. All health disciplinesconcerned with antimicrobial use and/orresistance were invited, including allthose concerned with communicable dis-eases, health systems, essential drugs andprimary health care.
Step two: developing a listof interventions
EMRO participants developed a listof interventions starting from thoserecommended in the WHO draft GlobalStrategy. SEARO and Nepali parti-cipants also agreed to use this list (seeTable 1).
Step three: voting on theproposed interventions
Each intervention was scored accord-ing to:
(1) the importance or relevance of anyimpact it might have, and
(2) the feasibility of implementation.
It was agreed that “relevance” wouldtake into account whether an interventionwould impact on the diseases of particu-lar concern locally, and that “feasibility”would take into consideration both costof implementation and the political con-text. The scoring was as follows:
0 = not feasible or no relevant impact1 = medium feasibility or medium
relevant effect2 = good feasibility or very relevant
effect
Step four: collating the voting dataAll the participants’ scores for likely
relevant impact and feasibility for eachintervention were added up and then plot-ted on a matrix. Interventions that werelikely to have the greatest impact and befeasible appeared in the top right-hand
corner of the chart and were judged to beof highest priority. Those interventionsthat appeared in the bottom left-handcorner of the chart were judged less fea-sible and relevant. For example, in agroup of 11 people, the maximum scorean intervention could receive for eitherimportance or feasibility was 22 (11 par-ticipants awarding a maximum of twopoints). The points plotted on the matrixwould therefore be 22 for importance and22 for feasibility.
Diverse viewsThe graphs below (figures 1–3) in-
dicate the priority given to differentinterventions. Comparison shows how thevarious regions agreed and disagreed onwhich interventions should have highestpriority. The reasons for differences in thepriorities between these three groups mayhave been due to different priorities indifferent areas, but were also in large partdue to the different expertise of partici-pants in the different groups. For example,in SEARO there was no one specialisingin health systems or drug regulation, inNepal microbiologists were poorly rep-resented, as were agriculturalists in bothEMRO and SEARO.
The most feasible and important inter-ventions agreed by everyone included:
➤ training of prescribers and dispensers,and the use of guidelines and formu-laries;
➤ establishing infection control commit-tees, guidelines for antimicrobial use,and surveillance of antimicrobial usein hospitals;
➤ developing national drug policies,essential drugs lists and standardtreatment guidelines;
➤ ensuring undergraduate and post-graduate training on antimicrobialresistance;
Critical decisionsNo country in the world is imple-
menting all of these recommendedinterventions and most would find it im-possible to do so. Therefore, all countrieswill need to prioritise the interventionsand choose which ones to implement firstand which to implement later. Develop-ing countries in particular will need toprioritise and choose only those interven-tions that, in their local contexts, are bothfeasible and likely to have the greatestimpact. This article discusses the prob-lem of how to choose which interventionswill be both feasible and have a signifi-cantly large impact. Two methods are
J
Table 1Agreed list of interventions to contain antimicrobial resistance
Target group Recommended interventions
A 1. Education on appropriate usePatients and 2. Education on hygienethe public 3. Discourage self-medication
B 1. TrainingPrescribers and 2. Guidelines and formulariesdispensers 3. Monitoring and supervision
4. Regulation of professionals5. Educate prescribers about promotion
C 1. Therapeutic committeesHealth systems 2. Infection control committees
3. Guidelines for antimicrobial use4. Antimicrobial use surveillance5. Laboratory network and epidemiological
resistance surveillance
D 1. National AMR task force with budgetGovernment 2. Drug policies e.g. essential drugs list, standardpolicies, strategies treatment guidelinesand regulations 3. Registration of all drug outlets
4. Antimicrobials by prescription-only5. Dispensing of antimiocrobials by licensed staff only6. Quality assurance system7. Drug licensing to include resistance data8. Undergraduate and postgraduate training on AMR9. Access to evidence-based drug information10. Cut perverse rational drug use economic incentives11. Monitor and supervise drug promotion12. Monitor and link AMR and drug use data
E 1. Incentives for industry to do research and developmentPharmaceutical 2. Monitor and supervise drug promotionindustry 3. Production according to Good Manufacturing
Practice standards
F 1. Surveillance of resistance and useNon-human 2. Phase-out growth promotersantimicrobial use 3. Educate farmers and vets
A N T I M I C R O B I A L R E S I S T A N C E
A pharmacy in Colombia. Ensuring good dispensing practices is seen as a high priority in thefight against antimicrobial resistance
Phot
o: W
HO
/PA
HO
/A
.Waa
k

17E S S E N T I A L D R U G S M O N I T O R
Issue No. 28 & 29, 2000
Figure 1Prioritisation of interventions by the 11 membersof EMRO antimicrobial resistance task force
Figure 2Prioritisation of interventions by 15 health officials in Nepal
Figure 3Prioritisation of interventions by 7 staff members of SEARO
Priorities in the WHO Global Strategyfor Containment of Antimicrobial Resistance
Although all interventions were classi-fied into fundamental, high, mediumand low, only the first two categoriesare shown below. Within the twopriority groupings shown here,interventions are not ranked.
Fundamental interventionsMake containment of antimicrobialresistance a national priorityincluding:◆ creating a national task force;◆ allocating resources to implement
interventions to contain antimicrobialresistance;
◆ developing indicators to monitorand evaluate the impact of anantimicrobial resistance strategy;
◆ designating or developing referencemicrobiology laboratory facilities.These would coordinate effective,epidemiologically-sound, surveillanceof antimicrobial resistance amongcommon pathogens in the community,hospitals and other health carefacilities.
High priority interventions1. Patient education on:◆ the importance of measures to
prevent infection such as immuniza-tion, vector control, use of bed-nets;
◆ simple measures that may reducetransmission of infection in thehousehold and community, such ashand washing, food hygiene.
2. Prescriber and dispenser (includingdrug seller) education on:
◆ the importance of appropriateantimicrobial use and containmentof antimicrobial resistance;
◆ disease prevention (includingimmunization) and infection controlissues.
3. Targeted undergraduate and post-graduate education programmesfor all prescribers, dispensers andother health care workers, andveterinarians, on accurate diagnosisand management of commoninfections.
4. Development, updating and use ofstandard treatment guidelines andtreatment algorithms to fosterappropriate use of antimicrobials.
5. Infection control programmes withresponsibility for effective manage-ment of antimicrobial resistance inhospitals.
6. Diagnostic laboratories that provide:◆ microbiology laboratory services
which are appropriately matchedto the level of the hospital (e.g.secondary, tertiary);
◆ appropriate diagnostic tests, bacte-rial identification, antimicrobialsusceptibility tests of key pathogens,with adequate quality assurance,and timely, relevant reporting ofresults.
7. Limiting the availability ofantimicrobials to prescription-onlystatus, except in special circum-stances where they may bedispensed on the advice of atrained health care professional.
8. Ensuring that only antimicrobialsmeeting international standards ofquality, safety and efficacy aregranted marketing authorisation.
The figures should be viewed in conjunction with Table 1, as the different shapes and colours on thethree graphs each represent one of the six target groups (A–F) listed in the Table. For example, agreen circle signifies D – interventions involving government policies, strategies and regulations.The numbers within each shape correspond to the different recommended interventions in each ofthe target groups. So there are 12 green circles on the map numbered 1 to 12, corresponding to thenumbered list of interventions under D in Table 1. Their position on the graph is dependent on thescores participants awarded them. For example, D10 – cutting perverse rational drug use economicincentives – appears in the bottom left-hand corner of the graph, showing that it received the lowestscores for both importance and feasibility.
The dotted green cross lines signify where the average score (1 point for both importance andfeasibility awarded by each person in the group) would appear.
4
Impo
rtanc
e
25
20
15
10
5
0 5 10 15 20 25Feasibility
Not feasible or relevant
Feasible and relevant
interventions targeting patients, families, communitiesinterventions targeting prescribers and dispensersinterventions targeting health systemsinterventions involving government policies, strategies, regulationsinterventions targeting the pharmaceutical industryinterventions targeting non-human antimicrobial use
1
2
13
3
2
5
1
33
5
2
11
2
0F
E
C
B
A
D
82
3923
65
4
12
7
11
10
14
1
1
Impo
rtanc
e
25
20
15
0 10 15 20 25Feasibility
Not feasible or relevant
Feasible and relevant
0
interventions targeting patients, families, communitiesinterventions targeting prescribers and dispensersinterventions targeting health systemsinterventions involving government policies, strategies, regulationsinterventions targeting the pharmaceutical industryinterventions targeting non-human antimicrobial use
1
2
3
3
2
5
1
4
3
2
3
35
2
1
2
4
5
4
10 12
7
1 6
11 13
9
3
28
F
E
C
B
A
D
Impo
rtanc
e
15
10
5
00 5 10 15
Feasibility
Not feasible or relevant
Feasible and relevant
F
E
C
B
A
D
4
1
2
1 3 3
2 5
1
3 3
5
21 1
2
8
23
9
23
6
5
4
12
7
11
10
4
interventions targeting patients, families, communitiesinterventions targeting prescribers and dispensersinterventions targeting health systemsinterventions involving government policies, strategies, regulationsinterventions targeting the pharmaceutical industryinterventions targeting non-human antimicrobial use
1
A N T I M I C R O B I A L R E S I S T A N C E
➤ ensuring drugs are produced accord-ing to Good Manufacturing Practicestandards.
The least feasible and important inter-ventions agreed by everyone included:
➤ ensuring that antimicrobials are dis-pensed by licensed staff and only witha prescription;
➤ cutting perverse economic incentivesto prescribe antibiotics – for examplethe problem of dispensing prescribersearning more money from sellingantibiotics than from other drugs;
➤ monitoring and linking data concern-ing antimicrobial resistance andantimicrobial use;
➤ monitoring and supervising drug pro-motion both for human and animaluse;
➤ phasing out growth promoters inanimal use.
PRIORITISINGINTERVENTIONS FOR THE
WHO GLOBAL STRATEGY
As a result of the diverse views ob-tained from the regions, a differentprocess of prioritisation was conductedfor the draft Global Strategy, in order toproduce some concrete practical advicefor Member States.
Experts in the fields of drug use,
clinical microbiology and other relateddisciplines from all over the world wereinvited to a workshop in Geneva. Parti-cipants were divided into three workinggroups, with each considering inter-ventions aimed at a particular targetaudience:
Group 1: Prescribers and dispensers
Group 2: Hospitals
Group 3: Health systems
For each target audience, the interven-tions were prioritised according to theirrelative merits and ranked according tosequence and importance of implemen-tation. This complex task requiredconsideration of multiple factors relatingto each intervention including:
➤ overall importance of the interven-tion to improving the appropriate useof antimicrobials and containingantimicrobial resistance;
➤ likely impact, allowing for the ex-pected cost of implementation;
➤ complexity of implementation, con-sidering the capacity of various healthcare systems and political realities;
➤ time required for implementationand the expected lag period beforeoutcomes could be expected;
➤ the accuracy with which most healthcare systems could assess the efficacyof each intervention;
...cont’d on page 18 ➠
➤ the interrelationship between variousinterventions, including the need toundertake some interventions in alogical sequence.
As a result of this process, interven-tions were ranked as high, medium and
low, and consideration was given towhether the ranking would vary accord-ing to a national health system’s level ofdevelopment.
Once interventions for each target

18 E S S E N T I A L D R U G S M O N I T O R
Issue No. 28 & 29, 2000
Useful websites on antimicrobial resistance
A N T I M I C R O B I A L R E S I S T A N C E
audience were ranked, the interventionswere then ranked according to their over-all importance and timing (sequence) ofimplementation, without consideration oftheir target audience. This was done byall the participants in a plenary session(see box). It was recognised that somepriorities might vary depending on thehealth care system in which they wouldbe implemented. However, this did notimpact to any significant extent on thepriority given to the majority of very highpriority interventions.
Although it was not planned to addressissues relating to consumers and drugpromotion at this workshop, in fact theywere also considered. This was becauseparticipants, particularly in Group 1,felt that prescribers and dispenserscould not be considered separately fromconsumers.
INTERVENTIONS FORMAXIMUM IMPACT
Comparison of the priorities identifiedat country, regional and internationallevels shows many similarities. The in-terventions agreed by everyone to be bothhigh priority and feasible are:
1. training prescribers and dispensers,and using guidelines and formularies;
2. establishing infection control commit-tees and guidelines for antimicrobialuse;
3. developing national drug policies,essential drugs lists and standard treat-ment guidelines;
4. ensuring undergraduate and post-graduate training on antimicrobialresistance;
5. ensuring that drugs are produced ac-cording to good manufacturingpractice standards and are of adequatequality.
Dep
artm
ent o
f Hea
lth, U
K
A leaflet from the UK’s public educationcampaign on the correct use of antibiotics
APUA-Alliance for the Prudent Use of Antibioticshttp://www.antibiotic.org (see also EDM No.24 p.20)
AR InfoBank-WHO Antimicrobial Resistance Information Bankhttp://oms2.b3e.jussieu.fr/arinfobank
BUBL Catalogue of Internet Resources – Infectious Diseaseshttp://bubl.ac.uk/link/i/infectiousdiseases.htm
Center for Adaptation Genetics and Drug Resistancehttp://www.healthsci.tufts.edu/labs/Sblevy/home.html
Center for Complex Infectious Diseaseshttp://www.ccid.org/
Centers for Disease Control, Drug Resistance Homepagehttp://www.cdc.gov/drugresistance/
CIA. The global infectious disease threat and its implicationsfor the United States. 1999http://www.odci.gov/cia/publications/nie/report/nie99-17d.html
EARSS-European antimicrobial resistance surveillance systemhttp://EARSS.rivm.nl
Eurosurveillancehttp://eurosurv.org/
Global Polio Eradication Initiativehttp://www.polioeradication.org
Infectious Disease Newshttp://www.slackinc.com/general/idn/idnhome.htm
International Society for Infectious Diseaseshttp://isid.organize-it.com/
Johns Hopkins University – Infectious Diseaseshttp://www.hopkins-id.edu/index_id_links.html
Karolinska Institute, Swedenhttp://micf.mic.ki.se/Diseases/
National Foundation for Infectious Diseases, USAhttp://www.nfid.org/
Project Icare: Intensive Care Antimicrobial ResistanceEpidemiologyhttp://www.sph.emory.edu/ICARE/
Roll Back Malariahttp://www.rbm.who.int/
Stop TB Initiativehttp://www.stoptb.org
The Hot Zone: Emerging Infectious Diseases Reportsand Web Siteshttp://www.qis.net/~edwardmc/eid.htm
UK Public Health Laboratoryhttp://www.phls.co.uk/
US National Center for Infectious Diseaseshttp://www.cdc.gov/ncidod/eidtopics.htm
Washington University Infectious Disease Division, USAhttp://www.id.wustl.edu/
WHO Communicable Diseases Home Pagehttp://www.who.int/health-topics/idindex.htm
WHO/TDR (Special Programme for Tropical Diseaseand Research)http://www.who.int/tdr
Selected references
Coast J, Smith RD, Millar MR. An economic perspective onpolicy to reduce antimicrobial resistance. Soc Sci Med1998;46:29–38.
Fidler DP. Legal issues associated with antimicrobial drugresistance. Emerg Infect Dis 1998;4:169–77.
Finch RG, Williams RJ. Eds. Antibiotic resistance. Clin InfectDis 1999;5(2).
Goldmann DA, Huskins WC. Control of nosocomial anti-microbial-resistant bacteria: a strategic priority for hospitalsworldwide. Clin Infect Dis 1997;24 (Supplement 1):S139–45.
Hart CA, Kariuki S. Antimicrobial resistance in developingcountries. BMJ 1998;317:647–650.
Institute of Medicine. Antimicrobial resistance: issues andoptions. Workshop report. Washington D.C.: National AcademyPress; 1998. http://books.nap.edu/books/0309060842/html/R1.html#pagetop
Pittet D et al. Effectiveness of a hospital-wide programme toimprove compliance with hand hygiene. Lancet 2000;356:1307–1312.
Polk HC Jr, Christmas AB. Prophylactic antibiotics in surgeryand surgical wound infections. Am Surg 2000;66:105–11.
UK Standing Medical Advisory Committee Sub-Group onAntimicrobial Resistance. The path of least resistance. London:Department of Health; 1998.http://www.open.gov.uk/doh/smac.htm
WHO. World Health Assembly 1998. Emerging and othercommunicable diseases: antimicrobial resistance. WHA51.17,agenda item 21.3.http://www.who.int/emc/
WHO. Anti-tuberculosis drug resistance in the world. TheWHO/International Union Against Tuberculosis and LungDisease global report on anti-tuberculosis drug resistancesurveillance 1994–97. Geneva: World Health Organization;1997. WHO/TB/97.229.
WHO. Guidelines for the management of drug-resistanttuberculosis. Geneva: World Health Organization; 1997. WHO/TB/96.210.
WHO. Integrated management of childhood illnesses: A WHO/UNICEF initiative. WHO Bulletin 1997;75 (Supplement 1).
WHO. The medical impact of the use of antimicrobials in foodanimals: Report and proceedings of a WHO meeting, Berlin,Germany, 13–17 October 1997. Geneva: World HealthOrganization; 1997. WHO/EMC/ZOO/97.4.
WHO. Treatment of tuberculosis: guidelines for nationalprogrammes; 2nd ed. Geneva: World Health Organization;1997. WHO/TB/97.220.
WHO. Use of quinolones in food animals and potential impacton human health. Report and proceedings of a WHO meeting,Geneva, Switzerland, 2–5 June 1998. Geneva: World HealthOrganization; 1998. WHO/EMC/ZDI/98.12.
WHO. Basis for the development of an evidence-basedcase-management strategy for MDR-TB within the WHO’sDOTS Strategy. Geneva: World Health Organization; 1999.WHO/TB/99.269.
WHO. Containing antimicrobial resistance. Review of theliterature and report of a WHO workshop on the development ofa global strategy for the containment of antimicrobial resistance.Geneva, Switzerland, 4–5 February 1999. Geneva: WorldHealth Organization; 1999. WHO/CDS/CSR/DRS/99.2.www.who.int/emc/WHO_docs/general.htm
WHO. WHO report on infectious diseases. Removing obstaclesto healthy development. Geneva: World Health Organization;1999. WHO/CDS/99.1.http://www.who.int/infectious-disease-report/
WHO. Anti-tuberculosis drug resistance in the world. Reportno. 2. Prevalence and trends. The WHO/International UnionAgainst Tuberculosis and Lung Disease global report on anti-tuberculosis drug resistance surveillance. Geneva: World HealthOrganization; 2000. WHO/CDS/TB/2000.278.
WHO. Global tuberculosis control: WHO Report 2000. Geneva:World Health Organization; 2000. WHO/CDS/TB/2000.275.
WHO. Guidelines for establishing DOTS-Plus pilot projects forthe management of multidrug-resistant tuberculosis (MDR-TB).Geneva: World Health Organization; 2000. WHO/CDS/TB/2000.279.
WHO. Management of the child with a serious infection orsevere malnutrition: guidelines for care at the first-referral levelin developing countries. Geneva: World Health Organization;2000. WHO/FCH/00.1.
WHO. World Health Organization report on infectious diseases2000. Overcoming antimicrobial resistance. Geneva: WorldHealth Organization; 2000. WHO/CDS/2000.2.http://www.who.int/infectious-disease-report-2000
WHO. Surveillance standards for antimicrobial resistance.Geneva: World Health Organization; 2000. CDS/CSR/DRS2000.2 (in preparation).
Interestingly, regional staff felt thatsurveillance of antimicrobial use in hos-pitals was feasible and important, andgave it higher priority than the expertsinvited to Geneva did. On the other hand,while the Geneva group felt that restrict-ing antimicrobials to prescription-onlystatus was very important, regional stafffelt that it was not feasible.
There is no hard evidence as to whichinterventions are most important and havethe greatest impact, and expert opinionvaries. Nevertheless the two differentprocesses of prioritisation identified thefive interventions listed above. Everyoneagreed that these interventions were fea-sible and would have the greatest impacton antimicrobial resistance if adequatelyimplemented. ❏
* Dr Kathleen Holloway is a Medical Of-ficer in the Department of Essential Drugsand Medicines Policy at the World HealthOrganization.
Prioritising interventions...cont’d from pg. 17

19E S S E N T I A L D R U G S M O N I T O R
Issue No. 28 & 29, 2000
Private sector prescribing
Editor,When I worked as a pharmacist in the
public sector I found it relatively easy topromote rational use of drugs throughadherence to the essential drugs list,standard treatment guidelines and formu-laries. However, now employed in theprivate sector, I find these tools difficultto use because of prescribers’ resistanceto what they see as restrictions upon them.
Obviously the forces driving the pri-vate sector are unlike those in the publicsector. For example, cost containment isnot a priority, as the consumer (generallythose dissatisfied with the public healthcare system) pays for services, mainlythrough some form of health insurance.My question is, in the private sector is itreally possible to rationalise medicines’use and still have a good income? I wouldbe interested to hear readers’ views.
—Dr Atieno Ojoo, P.O. Box 13576, Nairobi,Kenya.
✍ ✍ ✍
A simple solution to outpatientrecord keeping?
Editor,In developing countries the idea of
keeping medical records in hospital
offices is impractical, and often impossi-ble to implement. Here in Tanzania’sDodoma region the Out Patient Servicehas adopted my suggestion of patientskeeping a “health booklet”. The bookletis in fact a primary school exercise book,widely available and priced at aroundUS$0.06. As the booklet is the patient’sproperty, a sense of ownership means itis usually well kept and made availablewhenever requested.
The system’s advantages are that it canprovide a full patient history, particularlyuseful in cases such as hypertension, dia-betes, asthma or allergy. Also data arerecorded chronologically, whereas beforewe often had to sort through numerouspieces of paper and put them in date or-der. When there is a shortage of hospitalcards and files, the booklet can also beused as an in patient file or as a growthchart for the under-fives. As senior doc-tors can comment on and change previousdiagnoses and treatments, the system canhelp in improving junior colleagues’ skillsand prescribing practices.
Lack of supplies and of motivated staffshould convince hospital managements torely more on user commitment, and letpatients document their own medicalhistories.
—Dr Massimo Serventi, Paediatrician,Dodoma General Hospital, Box 1498,Dodoma, Tanzania.
✍ ✍ ✍
L E T T E R S T O T H E E D I T O R
Substandard chloroquinein Ghana
Editor,Countries in tropical Africa account
for more than 90% of total malaria inci-dence and the great majority of malariadeaths, with children the most vulnerableto the disease. Cloroquine is one of themost frequently used drugs in preventionand treatment. But in recent years in someendemic areas certain strains of plasmo-dium falciparum, one of the parasitesresponsible for malaria, has become re-sistant to chloroquine. Among the reasonscited for this is the manufacture, sale anduse of substandard chloroquine formula-tions. In Ghana we have completed aneight-year study to discover the scale ofthe problem, and it has reinforced con-cerns about the quality of chloroquineavailable here.
Thirty-eight samples of chloroquinephosphate tablets and 57 samples of syr-ups, manufactured locally by differentfirms, were tested in the Ghana StandardsBoard’s laboratories between 1992 and1999. All the samples were analysed ac-cording to British Pharmacopoiea assaymethods. The Pharmacopoiea’s specifi-cation for the content of chloroquinephosphate in tablets ranges between92.5% and 107% of the label claim. InGhanaian produced tablets 250 mg ofchloroquine is the norm and for syrup the
Paul Ehrlich, 1854–1915
A German medical scientist renownedfor his pioneering work in haematol-ogy, immunology and chemotherapy,Ehrlich won the 1908 Nobel Prize forhis discovery of the first effectivetreatment for syphilis. As well as hisresearch into early chemotherapy,Ehrlich also developed “side chain
theory” a hypothesis that provided the first plausibledescription of the body’s own immunological responseto destructive pathogens.
Louis Pasteur, 1822–1895
Considered one of the greatest Frenchbiologists of the nineteenth century,Pasteur devoted his life to solvingpractical problems in industry, agri-culture and medicine. Pasteur wasthe first to discover that fermentationand putrefaction only took place in thepresence of living organisms. With
further research he developed the technique of pasteuri-zation that not only revolutionized the dairy industry,but food processing as well.
A N T I M I C R O B I A L R E S I S T A N C E
Pioneers ofantimicrobial resistance
acceptable level is between 118.75 and131.25 per 5ml.
Of the 38 tablet samples analysed, fourcontained levels of chloroquine phosphatebelow the minimum requirement, withone sample at 38.9%. Of the 57 samplesof syrup 10 contained levels of active in-gredient below the minimum required.
We conclude that during the eight-yearstudy period some malaria sufferers wereexposed to significant amounts of sub-standard chloroquine phosphate in bothtablets and syrups. However, lessons havebeen learned, and steps taken to improvematters. One local manufacturer had towithdraw affected batches of drugs andhad his factory closed until an effectivequality assurance scheme was in place.Local manufacturers supplying the Min-istry of Health must now have theirproducts tested and certified by the na-tional quality control laboratory. TheFood and Drugs Board is implementingmeasures to assure drug quality in manu-facture, supply and distribution. Andduring 1999 an association of drug manu-facturers was formed, pledging to complywith WHO Good ManufacturingPractices.
—Charlotte Ohene-Manu and JonathanMartey, Ghana Standards Board, Drugsand Cosmetics Department, P.O. Box MB,245, Accra, Ghana.
✍ ✍ ✍
Selman Waksman, 1888–1973
A Ukrainian-born biochemist, SelmanWaksman played a major role in initi-ating a calculated, systematic search forantibiotics among microbes. His dis-covery of streptomycin – effective inthe treatment of tuberculosis – garneredhim the Nobel Prize in 1952.
Sir Alexander Fleming, 1881–1955
Honoured with a Nobel Prize for hisdiscovery of penicillin, Flemingtransformed medical science withthe development of the world’s firstantibiotic. While working with Sta-phylococcus bacteria in 1928, theScottish bacteriologist noticed abacteria-free circle around a mould
growth contaminating a culture of staphylococci. Uponfurther investigation he discovered a substance thatprevented bacterial replication even when diluted800 times. In 1943 he was elected fellow of the RoyalSociety and knighted in 1944.
Robert Koch, 1843–1910
A 1905 Nobel Prize honoree, Koch wasthe first scientist to identify the organ-ism that causes tuberculosis, Koch isconsidered the founder of modernbacteriology because he successfullyisolated several disease-causing bacte-ria and discovered the animal vectorsof a number of major diseases includ-
ing anthrax. Through his many experiments, Kochdiscovered how to obtain microorganisms from animals,and how to culture those same samples. It was Kochwho discovered that cholera is primarily a water-bornedisease.
John Enders, 1897–1985
American microbiologist and Nobellaureate John Enders led a researchteam which developed a technique forgrowing viruses in cultured cells. Heshowed that poliomyelitis viruses grewin both brain and cultured tissues andin this way caused cell destruction.
John Enders went on to demonstrate the safety of cul-tured viruses in producing immunity, and proved thatmeasles could be prevented through vaccination.◆ ◆ ◆

20 E S S E N T I A L D R U G S M O N I T O R
Issue No. 28 & 29, 2000
Brazil: WHO’s Director-Generalspeaks out for generics
r Gro Harlem Brundtland,WHO’s Director-General, hasmade a major speech in Brazilstrongly supportive of generic
drug strategies. Testifying before thecountry’s Parliamentary Commission onInvestigation of Medicines in April 2000,she discussed national drug policies,essential drugs and the importance ofgenerics in promoting affordability ofmedicines.
Saying that there are no “simplisticsolutions and no magic bullets”, DrBrundtland explored how people livingin poverty might get sustainable accessto drugs at affordable prices. She spoke
of pharmaceutical companies’ moral ob-ligation to contribute to the solution, butalso said that protective tariff barriers anddistribution margins for drugs shouldcome down. Dr Brundtland highlightedthe need for political acceptance of theconcept of “equity pricing”, especially fornewer essential drugs of vital publichealth importance. Equity pricing meansthat the poor would not have to pay thesame price for life-saving drugs as thosewho are better off. She urged govern-ments of industrialised countries to leadin its establishment. While developingcountry governments must facilitateaccess by “improving financing, impor-
cost, increasing choice and helping torationalise both the selection and use ofpharmaceuticals.
Relevance for theprivate sector
Dr Brundtland told Commissionmembers that policies advocating gener-ics – which are frequently only associatedwith the public sector – can be just asbeneficial in the private sector, becausethey promote efficiency within pharma-ceutical markets. She stressed theimportance of this in developing coun-tries, where up to 90% of drug con-sumption is through the private sector.She added that generic strategies in-volve much more than legal mandates;“they need support and enforcement, mustrespond to the concerns of involved par-ties and provide adequate economicincentives”.
More countries adoptthe strategy
Dr Brundtland spoke of the progressmade to date. In Latin America, severalcountries have already enacted legislationrelevant to generic strategies, but in mostcases implementation is limited. Overall,however, the results indicate that lowerprices have resulted where solid and
transparent legislation exists. The Direc-tor-General pointed out that in the USAgeneric drugs represent half of the mar-ket in volume. One of the EuropeanUnion’s three major policy regulations onpharmaceutical pricing and reimburse-ment is to enhance competition by makingthe market more transparent and encour-aging generics. And many hospitals indeveloped countries have lists of ap-proved drugs which identify products bygeneric name.
In conclusion, Dr Brundtland saidthat WHO has, for a long time, been en-couraging drug policies based on thepromotion of generic drugs of assuredquality – a cost-effective strategy incontaining drug expenditure. She toldCommission Members that WHO is,therefore, in favour of so called “earlyworkings” of patented drugs for genericmanufacturers, to encourage competitionand give impetus to research for improvedproducts. This includes the use of pat-ented drugs for research and testing,which necessitates prompt registrationand early production of generic drugs, theDirector-General said. Countries withvariations of early workings provisionsinclude Argentina, Australia, Canada,Hungary, Israel and the USA. ❏
■ ■ ■A young patient in Brazil, where generic drugs are rapidlyincreasing their share of the pharmaceutical market
tation, purchasing anddistribution systems formedicines, vaccines andmedical equipment”, DrBrundtland continued.
Brazil’s National DrugPolicy highlights genericdrug prescribing and use,and stipulates mandatoryadoption of generic namesin all public purchases.The Director-General saidthat promoting genericscan help meet the ob-jectives of health sectorreforms by improvingaffordability, reducing
D
Phot
o: W
HO
/PA
HO
/C
. Gag
gero
Meetings give impetus to Africa’sessential drugs programmes
ssential drugs programme manag-ers in Africa have met to debate arange of pharmaceutical issuesand move forward their agenda to
ensure access to essential medicines. Attwo critical meetings they endorsed theIntensified Essential Drugs Programmefor the African Region, and madenumerous policy recommendations.
The first meeting, in South Africa inMarch 2000, brought together managersfrom 16 anglophone countries. Theycalled on health authorities to adoptgood procurement practices for essentialdrugs. Authorities should capitaliseon economies of scale, and make pricinginformation available to prescribers,dispensers, consumers and health insur-ance companies, to enable them to makeinformed decisions. Participants also pro-posed that governments should encouragelocal production of essential drugs, andremove taxes on both the drugs and theirraw materials.
The managers endorsed the idea ofjoint bulk purchasing of drugs for prior-ity health problems, and urged WHO toprovide more information to MemberStates on the benefits and limitations ofsuch schemes. However, they insisted
that local industries should not be put atan undue disadvantage in the biddingprocess.
Delegates emphasised that easy accessto reliable information on pharmaceu-tical suppliers and pricing was vital toachieve optimal quality at affordableprices. A Web site should be established,coordinated by WHO, to make such in-formation freely available and keep itupdated.
Participants also wanted informationdisseminated on the concept and benefits
and efficiency.Rational use of drugs was high on the
agenda. Participants recommendedthat Member States develop strategiesand incorporate rational use principles inhealth workers’ training curricula. Phar-macotherapeutics committees were seenas a way to improve rational use by pre-scribers and dispensers, and should beintroduced at all levels of care.
Acknowledging the role of traditionalmedicines in African health care, pro-gramme managers urged WHO to
N A T I O N A L D R U G P O L I C Y
inspection services; and the legislationand regulations necessary to ensure drugquality. As in South Africa there wasmuch discussion on improved pricingpolicy. Participants called for com-plementarity between the public andprivate sectors, the creation of autono-mous central medical stores, promotionof local production, and state and com-munity co-financing to improve drugsupply and access. They also discussedintegrating drug policy programmes inhealth development plans, creating ra-tional drug use strategies, and improvingstaff training.
At both meetings WHO requestedcountries to specify the activities theywould carry out to implement the Inten-sified Essential Drugs Programme, so thatthe Organization can make detailed plansfor supporting them. But important workis already underway. The WHO RegionalOffice for Africa is running training ingood manufacturing practices, and theAFRO Essential Drugs Price Indicatorhas been launched. Countries continue toreceive support in implementing nationaldrug policies, assessing drug regula-tory capacity in Member States andreviewing pharmaceutical legislation. ❏
E
of harmonisation of drugregulatory activities, andthe promotion of commonminimum standards. Thiswould generate confi-dence in the quality ofservices. Public healthneeds rather than commer-cial interests should drivethe harmonisation pro-cess, delegates stressed. Inaddition, Member Statesshould strengthen the ca-pacity of drug regulatoryagencies and grant themsome degree of autonomy,to ensure effectiveness
The AFRO Essential Drugs PriceIndicator – one of the welcomeinitiatives introduced by theAFRO Intensified EssentialDrugs Programme
give support to countriesin deciding how best touse them within healthsystems.
In August 2000 it wasthe turn of 38 essentialdrugs programme manag-ers from 20 francophonecountries to spend timereflecting on their workand planning ahead. Meet-ing in Lomé, Togo, theyrecommended: the crea-tion of Directorates ofPharmacy and Medicines;quality control labora-tories; pharmaceutical

21E S S E N T I A L D R U G S M O N I T O R
Issue No. 28 & 29, 2000
Progress on drug policyin FYR Macedonia
he Former Yugoslav Republic of Macedonia launched its National Drug Policydevelopment process in February 2000, with the support of WHO/EURO andWHO Humanitarian Assistance Office, Skopje.
Five working groups were created to develop different elements of policy:legislation and regulations; drug selection; drug information; rational drug use; supplyand economic strategies; and human resource development. By October the groupswere ready to move to the next phase of the process – combining the different draftsto produce one comprehensive document. Macedonia is now deciding on futureactivities and a time frame for policy implementation. ❏
Launch of the AustralianNational Medicines Policy
➢ ANTHONY SMITH*
ustralia has gained a reputation asan innovative country for its workon the quality of use of medicines,and for its recently established
National Prescribing Service. It maytherefore come as a surprise to learn that,until recently, Australia had no formal,comprehensive, endorsed National Me-dicines Policy. The reasons are historicrather than political.
For more than 50 years, acceptablequality, safety and efficacy of medicineshave been assured through the work ofthe Therapeutic Goods Administration.
Equity of access to medicines is pro-vided through the PharmaceuticalBenefits Scheme which, by a system ofgraduated co-payments, allows access tomedicines for all including the poorestmembers of society – in the extreme atno cost to the consumer. This Scheme hasoperated for half a century.
While the pharmaceutical industrymay have some ambivalence about its re-lationships with government, financialincentives have been provided to enhanceindustry’s viability, both in Australiaand as a presence in the South-EastAsia/Western Pacific region.
In line with the prototype policyelaborated by WHO, rational use (or qual-ity use, as we chose to call it) of medicinesbecame the fourth component of Austra-lian policy in 1992. Therefore, ourMedicines Policy evolved over a longperiod in contrast to that of many coun-tries who have devised theirs over aperiod as short as a few months.
At last, and primarily through thework of the Australian PharmaceuticalAdvisory Council (APAC), all this activ-ity has come together in the NationalMedicines Policy which was formallylaunched by the Joint ParliamentarySecretary for Health, Senator GrantTambling, on 10 December 1999.
APAC was a good vehicle for the de-velopment of the Policy document as itsmembership reflects the partnership ap-proach which has become central,particularly, to the Quality Use of Me-dicines Programme in Australia. Con-sumers, the pharmaceutical industry,government and health professionals areall represented on APAC. The documentreflects all of their views including, mostrecently, those relating to the communityrole of complementary medicines (Aus-tralia has a Federal Government Officefor Complementary Medicines and a
World Health Assembly 2000:drug debates focus on HIV/AIDS
comprehensive resolution onHIV/AIDS was among the high-lights of the World Health Assem-bly, held in Geneva in May 2000.
Ninety-five percent of the 34 millionpeople living with HIV/AIDS are indeveloping countries. And it was thesecountries’ representatives who success-fully campaigned for WHO to increaseits role in advising on the best treatmentoptions, and how to overcome drugpricing and access problems. Duringdiscussions on the Revised Drug Strat-egy delegates also stressed the need forWHO to support broader approaches todrug financing, and to address the grow-ing dangers of unregulated sale ofmedicines on the Internet and counterfeitdrugs.
Among its provisions resolutionWHA53.14 on confronting the HIV/AIDS epidemic requests the Director-General to: support the implementationof drug price monitoring systems in Mem-ber States, to promote equitable access tocare, including essential drugs; promoterational use of drugs by strengtheningMember States’ capacity to implementdrug monitoring systems; and continue todevelop methods and support for moni-toring the pharmaceutical and publichealth implications of trade agreements.
Numerous delegates stressed the needfor WHO to retain its independent voicewhen advising countries on the com-plex subject of health-related aspects oftrade.
At one of the many side meetings dur-ing the Assembly, public health advocatesfrom Health Action International, Mé-decins Sans Frontières and ConsumerProject on Technology held a joint brief-ing for Member States on improvingaccess to essential drugs. And they added
their voices to support for WHO’s role inproviding global pricing information onquality medicines for people living withHIV/AIDS.
Tackling counterfeit drugsA well-attended technical briefing on
drug quality at the Assembly focused oncounterfeits. The presence of senior healthofficials, and representatives from Inter-pol, the pharmaceutical industry andNGOs reflected the multi-faceted nature
N A T I O N A L D R U G P O L I C Y
N E W S D E S K
A
A
separate evaluation committee for theseproducts).
As a country we have been veryfortunate that several of the essentialingredients of a National MedicinesPolicy have been in existence for so long.
Bridging the digital divide
Nevertheless, our comprehensive policyhas finally won the endorsement of Gov-ernment and with this endorsement goesthe expectation that continuing resourceswill be made available to ensure that wecan implement strategies in the many ar-eas which are currently less than ideal. Itwould have been good to have had thispolicy and its endorsement a long whileago!
The Australian Medicines Policydocument may be accessed and down-loaded from: http://www.health.gov.au:80/haf/docs/nmp2000.htm ❏
* Anthony Smith is Professor of Clinical Phar-macology, Newcastle University MaterMisericordiae Hospital, Waratah NSW2298, Australia.
of the problem. The audience was told ofhighly sophisticated operations in whichcriminals take advantage of cross-borderloopholes. Supplies, production, shippingre-labelling, financing and distribution ofthese drugs are often handled in differentcountries.
The meeting called for closer coop-eration between law-enforcing agencies,legislative bodies and the pharmaceuti-cal industry. Saying that there was “anurgent need for action”, Dr YasuhiroSuzuki, Executive Director of WHO’sHealth Technology and PharmaceuticalsCluster, referred to the “deadly combina-tion of demand for cheap drugs and fatprofit margins” that makes counterfeitingdrugs so attractive to criminals and sucha threat to society. ❏
T
Aborigines in Kalgoorlie, Australia. Adoptionof the National Drug Policy has formalisedthe country’s efforts to provide qualitymedicines for all
nly a small fraction of globalhealth research expenditure goesto research into diseases andhealth issues that affect the
poor, such as malaria, killer childhooddiseases and nutrition. One step towardschanging this is to facilitate researchin the countries that have first-handexperience of these problems. NowWHO and the Open Society Institute(part of the Soros Foundation network)have teamed up with information provid-ers ISIO and SilverPlatter, and otherpartners to do just that. They will provide
medical and health research institutionsin Africa, Central Asia and Eastern Eu-rope with Internet access to qualityscientific information from around theworld.
The project’s first year pilot phasewill enable scientists at leading researchinstitutions in Armenia, Ghana, Mali,Mozambique, Mongolia, Uganda, Tanza-nia and Uzbekistan to access informationin digital format. In this way integrationof the world scientific communitythrough electronic communication willadvance. WHO will be among those
negotiating with service providers in theeight initial countries to provide high-speed connection to the Internet. Researchstaff in the countries will receive com-prehensive training to ensure maximumbenefit from the project. It is anticipatedthat by the end of its second year between30 and 40 countries will have joinedthe project, which is part of the widerUnited Nations programme “HealthInterNetwork”. This aims to improve pub-lic health world wide by facilitating theflow of health information using Internettechnologies. ❏
O
Phot
o: W
HO
: H. A
nend
en

22 E S S E N T I A L D R U G S M O N I T O R
Issue No. 28 & 29, 2000
WHO and partners – taking theinitiative to make a healthier world
Opening a meeting of 200 health andadvocacy experts from 70 countries inWinterthur, Switzerland, Dr Brundtlandsaid that although the world had longknown that illness and poverty are closelylinked, recent data show a much moredevastating economic impact on devel-oping country economies by a fewinfectious diseases, particularly malaria,HIV/AIDS and tuberculosis. But anumber of effective health interventionsexist that dramatically reduce mortalityof these killers, she emphasised. “Quitesimply, if we can take these interven-tions to scale – and by that I mean to aglobal scale – we have in our hands aconcrete, result-oriented and measurableway of starting to reduce poverty.” DrBrundtland said that a concerted globaleffort was needed that would involve aprocess, a road to follow, a framework forthinking and a set of values to underpinit all.
The forum followed recent announce-ments by the G8 leading industrial nationsof targets to reduce the burden of malariaand tuberculosis by 50% within 10 years,and to reduce the spread of HIV/AIDSby 25% within the same time period. Italso comes after the creation of a newpolicy framework by the European Com-mission intended to focus the EuropeanUnion’s aid effort on reaching thosetargets.
ACCESSING VACCINES
Every year, nearly three million chil-dren die from diseases that could beprevented with currently availablevaccines. The Global Alliance forVaccines and Immunization (GAVI),formed in 1999, is a coalition of interna-tional organizations, with a mission toensure that every child is protected againstvaccine-preventable diseases. It wantsto close the growing gap in the numberof vaccines available to children inindustrialised and developing countries.GAVI is working to:
➤ improve access to sustainable immu-nization services;
➤ expand the use of all existing cost-effective vaccines;
➤ accelerate the development and intro-duction of new vaccines;
➤ accelerate research and developmentefforts for vaccines and related prod-ucts specifically needed by developingcountries;
➤ make immunization coverage anintegral part of the design and
assessment of health systems andinternational development efforts.
Since its inception the Alliance hasreceived a great deal of interest from de-veloping countries wanting to benefitfrom its work. On 20th September 2000the Global Vaccine Fund, one of thefinancial tools used by the initiative, an-nounced that it will be giving more thanUS$150 million worth of vaccines andfunding over five years to improve im-munization rates in Africa, Asia and LatinAmerica. According to estimates morethan 100,000 lives will be saved everyyear due to initial grants to 13 countries.
For further information check:www.who.int/vaccines/aboutus/gavi.htm
ROLLING BACK MALARIA
When she became WHO’s Director-General in 1998, Dr Gro HarlemBrundtland decided that malaria would beone of the Organization’s top priori-ties. She instigated Roll Back Malaria,a partnership involving a wide rangeof organizations at country, regionaland global levels. The initiative’s goalsinclude:
➤ support to endemic countries in devel-oping their national health systemsas a major strategy for controllingmalaria;
➤ efforts to develop the broader healthsector – all providers of health care tothe community. This includes the pub-
intensive final phase in order to mop upthe final pockets of the virus.
In September 2000, a broad spectrumof leaders from business, governments,UN agencies and humanitarian groups,met at the United Nations in New Yorkto galvanise the necessary financial re-sources and political will for the Initiativeto ensure it meets the 2005 deadline. Over250 participants pledged to help over-come the challenges: poliovirus was stillcirculating in up to 20 countries at the endof 2000, and US$450 million in new fund-ing is needed to conquer the disease inthose places. The 20 high-risk countriesalso present some of the most difficultlogistical challenges to polio eradication,including populations that are geogra-phically isolated and, in a handful ofcountries, living in the midst of severecivil conflict. Emphasising the urgencyof the task, UN Secretary-General, KofiAnnan, said that “our race to reach thelast child is a race against time. If we donot seize the chance now, the virus willregain its grip and the opportunity willelude us forever”.
A recent milestoneThe WHO Western Pacific Region
was certified polio-free on 29 October2000 by an independent panel of interna-tional public health experts. The Regionincludes 37 countries and areas rangingfrom tiny islands to China with a popula-tion of 1.2 billion people. The RegionalCertification Commission on Poliomyeli-tis Eradication confirmed that no newcases of indigenous polio have been de-tected in the Western Pacific in the lastthree years, despite excellent surveillancefor the virus – the major benchmark forcertification.
For more news on the Polio Eradi-cation Initiative check: www.who.int/vaccines-polio/
STOPPING TBTuberculosis (TB) remains the larg-
est killer of young people and adults inthe world, and the problem is growingwith the spread of HIV/AIDS and drugresistant strains of the disease. Stop TBis a global movement to accelerate socialand political action to stop the unneces-sary spread of TB around the world. Itsmission is to ensure that every person withTB has all the necessary informationand access to treatment and cure. StopTB is a partnership working with publicand private organizations from the localto the global level. Donors, research in-stitutions, industry, international agencies,governments and NGOs are all playinga role in:
➤ linking TB control to health sectordevelopment;
➤ linking TB control to poverty allevia-tion;
➤ linking TB control to relevant aspectsof socioeconomic development;
➤ promoting a more client-centeredapproach for wider coverage andcompliance by partnering withcommunity-based groups and others.
For further information check:www.stoptb.org/stop.tb.initiative/index.html#StopTB
One of Stop TB’s partners is the Glo-bal Alliance for TB Drug Development,a not-for-profit venture that is accelerat-ing the discovery and development of newdrugs to fight the disease by drawing uponbest practice and resources from the pub-lic and private sectors (see page 19). TheAlliance aims to fill a gap in TB drugdevelopment by using a lean research anddevelopment operating model thatoutsources projects to public or privatepartners. It will survey all TB drug de-velopment and selectively intervene whenits actions will help move a drug candi-date towards registration and use intherapy. In this way the Global Alliancewill build a portfolio of projects withvarying levels of funding, managementand ownership.
Further information is available at:www.tballiance.org/home.cfm
IMPROVING INJECTIONPRACTICES
Injections are predominantly neededfor the treatment of severe diseases,mostly in hospital settings. Nevertheless,they are overused to administer medica-tions in many countries because of aningrained preference for injections amonghealth workers and patients. In develop-ing countries up to 50% of injectionsare administered with re-used syringesand needles. Such unsafe practices havebeen linked to the transmission of many
A C C E S S
T
A sight that will soon disappear? A polio victimlearns to walk with callipers
Phot
o: W
HO
/PA
HO
/C
. Gag
gero
here are several important and new international health initiatives involv-ing WHO in global partnerships that are addressing some of the mostpressing health problems of our time. Here we focus on some of them,beginning with WHO Director-General Gro Harlem Brundtland’s call for
a concerted global effort to tackle diseases of poverty, made in October 2000.
lic sector health system, civil so-ciety, NGOs and private healthproviders (including drug ven-dors and traditional healers) andothers;
➤ encouragement to obtain thenecessary human and financialinvestments for health systemdevelopment.
In recent months Roll Back Ma-laria has received a major boost fromthe African summit meeting, whichset the agenda for the continent’sefforts to beat the disease (see reporton page 23).
Find out more at: www.rbm.who.int
ERADICATING POLIO
The Polio Eradication Initiativeis on track to certify global eradica-tion of the disease in 2005, with morethan 190 countries and territorieswhich will have interrupted polio-virus transmission by the end of theyear 2000. This is an initiative thatbegan in 1988, but it is entering an

23E S S E N T I A L D R U G S M O N I T O R
Issue No. 28 & 29, 2000
pathogens between patients, including thehepatitis, HIV, Ebola and dengue feverviruses, and the malaria parasite.
The Safe Injection Global Network(SIGN) is a coalition of several publicand private partners, including WHO,UNICEF, UNAIDS, NGOs, govern-ments, universities, health workers andindustry. Formed in Geneva in October1999, it aims to unite the partners’strengths and skills to work together oninjection safety. Because there have beenfew integrated programmes that link com-munity and health systems to promotesafe injection use, SIGN is coordinatingthe launch of pilot projects in five coun-tries. Results of the pilot projects’evaluation should be available by 2002,and will enable the Network to identifyand adopt successful strategies tocounter unsafe injections.
Positive developmentsSIGN’s annual meeting, held in Cairo
in October 2000, showed that there hasalready been progress. For example, Pa-kistan has set up a national “SIGN” group,Tanzania has launched an education cam-paign for the public and health workers,and Burkina Faso has made significantimprovements in injection safety recently.Participants reviewed the previous year’sactivities, exchanged information andcoordinated their advocacy and publicawareness activities.
New technical guidelines on prevent-ing infection from injections are beingprepared, and a provisional documentopen for comments from the public willbe available on the SIGN Web site:www.injectionsafety.org ❏
New drugs needed to fight TB
alaria, a disease that is prevent-able, treatable and curable, killsone million people a year inAfrica, with nine out of 10 cases
occurring in the sub-Saharan region.Now, the first summit of African headsof state to focus on the disease has com-mitted to intensive efforts to halve malariamortality by 2010. Held in Abuja, Nigeria,in May 2000, the summit was attendedby representatives of forty-four of the fiftymalaria-affected countries in Africa. Alsopresent were officials from United Na-tions agencies and major internationaldonors. The meeting culminated in thesigning of the Abuja Declaration and thePlan of Action in which the leaders re-solved to initiate sustainable actions tostrengthen health systems, so that by2005:
➤ at least 60% of those suffering frommalaria have prompt access to, and areable to correctly use, affordable andappropriate treatment within 24 hoursof the onset of symptoms;
➤ at least 60% of those at risk of ma-laria, particularly children under five
years of age and pregnant women,benefit from the most suitable combi-nation of personal and communityprotective measures. These include in-secticide treated mosquito nets andother accessible and affordable inter-ventions, to prevent infection andsuffering;
➤ at least 60% of all pregnant womenwho are at risk of malaria, especiallythose in their first pregnancies, haveaccess to chemoprophylaxis or pre-sumptive intermittent treatment.
Commitment, targetsand resources
The Heads of State called upon allcountries to undertake and continue healthsystems reforms that will promote com-munity participation in rolling backmalaria, and so increase sustainability.Diagnosis and treatment of malariashould be available as peripherally aspossible (including home treatment), andaccessible to the poorest.
Amongst other things the signatoriesto the Declaration pledged to: prevent
re-emergence of malaria;provide reliable informationon the disease to decision-makers at all levels; and toreduce or waive taxes andtariffs for mosquito nets,insecticides, anti-malarialdrugs, and other goods andservices needed for malariacontrol strategies.
Hidden costsreinforce urgency
The summit’s impor-tance was reinforced bysimultaneous publicationof a report showing that thecost of malaria is substan-
A C C E S S
M
M
The world’s biggest bednet was erected at Abuja as a symbolof the 225 African children who die every two and a halfhours from malaria
tially greater than economists previouslyestimated. According to the report,1 thedisease results in a loss of economicgrowth of more than one percentage pointper year.
Previous estimates have looked onlyat immediate short-term financialimplications, such as the loss of labourand the costs of treatment and prevention.
Beating malaria:leaders pledge action at historic summit
Phot
o: W
HO
/RB
M
But the longer-term costs are even moredevastating to the country, the reportargues. ❏
Reference1. Gallup JL, Sachs JD. Economics of malaria. Centre for
International Development, Harvard University and theLondon School of Hygiene and Tropical Medicine.(Forthcoming). Executive summary available on the Webat: http://www.malaria.org/jdsachseconomic.html
Cre
dit:
WH
O
ore than 120 tuberculosis (TB)and public health experts, govern-ment and industry representa-tives, researchers and donors
discussed TB drug development at a two-day workshop in Cape Town, SouthAfrica, in February 2000. They met be-cause of the urgent need for new drugs toensure shorter TB treatments and to fightthe increasing resistance to existing drugs.Basic TB drugs are already 20–30 yearsold, and few new drugs have beenmarketed in recent years.
TB experts, including WHO repre-sentatives, described the need for new TBdrugs, researchers presented promisingstate-of-the-art research methods andfindings, and drug companies explainedthe difficulties of drug development.
Mixed panels discussed the pharmaco-economics of the TB drug market, whichis predicted to be US$700 million fortreating 10,000,000 TB patients world-wide by 2008. The general opinion wasthat the size of this market should enablethe development of at least one or twonew drugs.
But some participants argued thatthere was a reluctance to develop drugsfor a market where most of the people arepoor, and where developing countries,institutional buyers and agencies work-ing on TB demand low prices. Aguaranteed off-take or market would bea strong incentive for manufacturers.There was a view that “corporate aware-ness” of the problem is increasing. Somecompanies have specific TB projects, oth-
ers are considering “donating” thelicensing rights of economicallyless viable second-line TB drugsto public bodies.
Not only money…Many participants warned that
low cost drugs or even donationsare no guarantee of solving the TBproblem, as managerial problemsin many countries with mid leveleconomies have meant that theyhave only achieved 50–60% curerates. Poor patient adherenceafter the first two months of a six-month treatment period increasesthe risk of drug resistance.
The meeting discussed acceleratingthe development of new TB drugs to im-prove prevention and treatment of thedisease. It also decided to develop a de-dicated Global Alliance for TB DrugDevelopment, with partners from aca-demia, industry, major agencies, NGOsand donors worldwide.
From vision to fruition…By October 2000 the participants’
push for a Global Alliance for TB DrugDevelopment became a reality with itslaunch by WHO’s Director-General, DrGro Harlem Brundtland, at a meeting inBangkok. And in February 2001 the Alli-ance opened its head office in Cape Town,South Africa, to coordinate and fundresearch in tuberculosis in developingcountries.
The main aim is to find a major newtreatment for TB by 2010, specifically adrug that is more effective so that it needsto be used for a shorter time, reducing thetreatment period by at least 50 per cent,and so increasing adherence.
The Alliance will not to set up its ownresearch institutions but will support ex-isting projects, particularly in developingcountries, and coordinate their findings.The first funding allocations will be madein April 2001. ❏
For further information on the Global Alliancefor TB Drug Development see page 22.

24 E S S E N T I A L D R U G S M O N I T O R
Issue No. 28 & 29, 2000
NGO meetings on drug accessollowing their successful confer-ence on compulsory licensingheld in Geneva in March 1999(see EDM-27), Médecins Sans
Frontières, Health Action Internationaland the Consumer Project on Technologyhave organized two more meetings on oneof today’s most topical issues. A con-ference entitled Increasing Access toEssential Drugs in a Globalised Economy– Working Towards Solutions, broughttogether 350 people from 50 countries inAmsterdam in November 1999. Healthadvocates and public health profes-sionals from developing countries,
The presentation of a new study show-ing that East Africans pay more thanEuropeans for life-saving drugs1 was oneof the conference highlights. Amongthe many examples cited in the studyis that of the antibiotic, ciprofloxacin,which was found to be twice as expen-sive in Uganda as in Norway. Anotherexample is fluconazole, a treatment forAIDS-related meningitis. In Thailand,where generic competition has loweredprices, fluconazole costs only US$0.30.However, the same drug costs US$18.00in Kenya, where it is patent protected.
Participants argued that the reasons
Trade and access:Ugandan groups push for progress
A C C E S S
F
he title of a workshop held inKampala, Uganda, in February2000, certainly conveyed thespirit of the event and the breadth
of subjects addressed. “Advocacy andCampaign for Better Trade, Access toEssential Medicine and PromotingRational Drug Use in Uganda ” was theresult of collaboration between Uganda’sConsumers Protection Association,Action Aid Uganda, Health ActionInternational and Médecins SansFrontières.
Participants left this lively meeting inFebruary 2000 determined to push forbetter trade policy, improved health serv-ices and increased consumer awarenessof pharmaceutical issues. They agreedthat access to drugs is a crosscutting is-sue, and that to be more effective they
need to network and to create awareness of key issues using various media. Discus-sions also highlighted the importance of involvement in legislation review andformulation (particularly the draft bill on intellectual property rights), and participa-
This ambulance may be stuck in the mud in Uganda, butthe description could not apply to campaigners pushingfor improvements in the pharmaceutical sector
Phot
o: E
. Pat
erso
n
tion in Uganda’s National DrugPolicy review. Delegates wereurged to campaign for improvedinfrastructure. Only when this isin place can important develop-ments get underway, such asoffering incentives to open drugoutlets in poor rural areas. ❏
For further information contact:R. Mutambi, Health and GenderOfficer, Uganda ConsumersProtection Association, DesaiHouse, Plot 4, Parliament Avenue,PO Box 23783, Kampala,Uganda. Tel: + 256 41 234 002,Fax: + 234003, e-mail: [email protected]
T
Five key messages from WHO ontrade agreements and pharmaceuticals
◆ ◆ ◆
“First, patent protection is a necessary and effective incentive for research anddevelopment for needed new drugs. Essential drugs are a public good and notsimply just another commodity. Patents must therefore be managed in an impartialway to benefit both the patent holders and the public.
Protectionism has never benefited public health. WHO supports governments to enactnational legislation which can draw advantage from more open trade and a betterregulated international system. And we support governments in incorporating thesafeguards that have been built into the WTO TRIPS Agreement to protect the rightsof the public.
Second, priority-setting for research and development in the pharmaceutical marketis imperfect. There are also striking market failures when there is such desperatedemand for products that are available – but not within reach of those in need.
WHO has initiated, with other partners, innovative mechanisms to stimulate researchand development in areas of high public health need, such as malaria and tuber-culosis. Through its Medicines for Malaria Venture (MMV), the Global Alliance forVaccines and Immunization (GAVI) and other initiatives, WHO is actively encourag-ing public sector financing for critical public health problems and neglected tropicaldiseases.
Third, WHO strongly supports development of mechanisms for preferential lowprices for essential drugs in lower-income countries. Lower-income countries simplycannot be expected to pay the same price for essential drugs as the wealthiercountries.
For governments, industry, and other stakeholders, there is a range of measureswhich might be used to achieve preferential pricing. But where there is an abuse ofpatent rights, where patented essential drugs are unavailable or where a nationalemergency exists, recourse to compulsory licensing is a legitimate measure consistentwith the TRIPS Agreement.
Fourth, WHO supports implementation of the TRIPS Agreement to ensure promptavailability of generic drugs upon patent expiration. WHO has long promoted useof generic drugs of assured quality. Experience from countries with “generic-friendly”policies clearly demonstrates that the market competition created by these policiesincreases affordability of medicines, stimulates true innovation within the research-based industry, and encourages increased production efficiency by the genericindustry.
Finally, trade agreements should not create barriers to trade. An important WTOprinciple is that technical regulations, standards and assessment procedures shouldbe based on international standards, guides and recommendations. In the area ofpharmaceuticals, WHO norms, standards and guidelines represent such internationalconsensus. So we will actively promote these guidelines”.
representatives from domestic and inter-national NGOs, the pharmaceuticalindustry, international organizations, na-tional governments and academics allcontributed their ideas on how to achieveaccess to essential medicines. After twodays intensive work, the Conference cul-minated in the drawing up of theAmsterdam Statement, which includes arecommendation for the World TradeOrganization to create a Standing Work-ing Group on Access to Medicines. TheGroup would work within the WTO toconsider the impact of trade policies onpeople in developing and least developedcountries. It would provide a public healthframework for the interpretation of keyfeatures of WTO agreements, and WHOand other international organiza-tions would support the activities of theWorking Group.
Among the many thought-provokingspeeches, Dr Gro Harlem Brundtland,WHO’s Director-General, told delegatesthat “Making a difference requires theoften painful work to build consensusamong stakeholders that can move thingsin the right direction. Health productsand health services are tradable. Healthproducts such as pharmaceuticals are pro-duced, marketed and sold across the globe– benefiting some but failing to reach toomany. So the rules that regulate this tradeare key”, she told delegates.
The Director-General listed WHO’sfive key public health messages oninternational trade agreements andpharmaceuticals (see box).
Moving on to AfricaThe NGO campaign on access to es-
sential drugs gathered further momentumin Nairobi in June 2000. The Kenyancapital was the venue for the East AfricaAccess to Drugs Conference, where rep-resentatives from 21 countries met todevise a regional strategy.
medicines are expensive in EastAfrica include high tariffs, taxes andlack of generic competition as wellas strong patent protection. Discus-sion focused on strategies to enactlegal safeguards to remedy the cur-rent situation. Delegates heard that,within existing international traderules, such safeguards include par-allel importing (the right to shoparound for the best prices of brandedproducts) and compulsory licensing(granting limited production rightsto generic producers).
Another report presented at the meet-ing on patent protection and medicinesin Kenya and Uganda2, calls on govern-ments to ensure these safeguards, and toinclude Ministry of Health representativesand health professionals when negotiat-ing and adopting trade agreements. ❏
References
1. Myhr K. Pharmaceutical pricing: law of the jungle.Amsterdam: Health Action International; 2000.
2. Boulet P. Patent protection of medicines in Kenya andUganda. Geneva: Médecins Sans Frontières; 2000.
Further information on this series of meetingson access to essential drugs can be foundat: www.haiweb.org
Intense concentration on the faces of delegates at theNairobi meeting, which tackled complex andcontroversial issues
Phot
o: M
édec
ins
Sans
Fro
ntiè
res

25E S S E N T I A L D R U G S M O N I T O R
Issue No. 28 & 29, 2000
Transforming drugsupply in Dar es Salaam
➢ KARIN WIEDENMAYER,DEO MTASIWA*
n 1990 the inadequacy of the pharmaceutical supply system in Dar esSalaam, commercial capital of the United Republic of Tanzania, wasevident. There was chronic shortage of drugs at health facilities, supplywas erratic as was Government funding, drug supply management was
poor and use of drugs irrational. Despite a national policy to provide drugs freeof charge, unofficially patients often had to pay for them. Drugs were purchasedfrom the national Central Medical Stores, which was seen as inefficient, unreli-able and poorly stocked. Drug quality was questionable and pharmacy premiseswere often unsuitable – hot, humid and cluttered with piles of drugs, some ofthem expired. Pharmacists tended to have low professional visibility and not tobe involved in hospital committees. At a time when studies showed that patientsequated availability of drugs with good quality of care1, a survey of user pat-terns in Dar es Salaam in 1990 reported that “the majority of patients complainedthat usually health facilities do not have drugs at all”.
as well as irrational use.In 1984, the Government created the
Essential Drugs Programme to provideessential drugs to health facilities. TheProgramme introduced a prepacked drugkit system, which partially improved thesituation for health centres and dispensa-ries, but not for the hospital sector. Andthe foreign financed and operated (byWHO, the Danish International Develop-ment Agency and the United NationsChildren’s Fund) drug kit system did nothelp to improve management of the drugsector’s infrastructure.
In the early 1990s, when the Dar esSalaam Urban Health Project began, Tan-zania started to restructure the economytowards a market-oriented environment.In the health sector this translated into theappearance of the private profit orientedsector and the introduction of userfees. In 1991, Tanzania formulated theNational Drug Policy, which aimed toimprove the whole pharmaceuticalsector, and ensure a regular supply andrational use of essential drugs through-out the country. Later, the Health SectorReform Action Plan 1996–1999 covereddecentralised district-based drug supplyand management, liberalised drugprocurement, quality assurance, and eq-uitable access and affordability of drugs.Here we highlight the main elements ofthe Health Project’s work and how againstthis background, it has transformed drugsupply in the region.
BUYING DRUGS: WHICH,HOW MUCH AND WHERE?
Drug need quantification was initiallydone by morbidity and later by the con-sumption method. Drug selection wasbased on the National Essential Drug List.Drug kits for the Dar es Salaam HealthProject were procured through restrictedinternational tender. The kit system wascentrally and externally organized, donorfunded, supplied and imported fromoverseas, with little or no involvement or
commitment from the recipient side. Theproject bypassed the national procure-ment system, the former Central MedicalStores being unreliable and inefficient.Later the organization was restructuredand became an autonomous departmentwithin the Ministry of Health, under theresponsibility of an external managementteam. In 1996, the new Medical StoresDepartment was operating efficiently, andit was considered appropriate to start us-ing the existing local drug procurementinfrastructure. The Department’s per-formance has been good overall, with anadequate product range, appropriatepricing, good quality and service, andsufficient provision for emergency situa-tions. The Medical Stores Departmenthas become the backbone of the Project’ssupply system.
Drug kits are a good but not optimalsolution. Because of their predeterminedcontents (selection and quantity) certainitems were regularly out of stock, otherswere piling up and some even expiredbefore redistribution. Quantificationwas therefore introduced at the healthfacilities and ordering is now done bydecentralised requisition, i.e. the indentsystem has gradually replaced the pushsystem with prepacked kits. A recentstudy on quality of care showed a signifi-cant improvement in drug availability. Forexample, the level of availability of fourkey drugs rose to 95% in 1998 comparedwith 64% in 1992.
DISTRIBUTION AND STORAGE
Initially drug kits were deliveredmonthly to the three district hospitalpharmacies. From there, subsequentdistribution to the hospitals, healthcentres and dispensaries was the res-ponsibility of the district pharmacist,who supervised all peripheral distributionand monitoring. Delivery of drugs fromthe district stores to the hospital posedno problems as they were on the samepremises. From the district hospitals thekits were distributed by vehicle to healthcentres and dispensaries on a monthlybasis. Logistics were more problematicand deliveries were often delayed due to
inventory management was donehaphazardly and did not follow goodpractice. Bin cards were unavailable,drug flow monitoring was difficult anddocumentation was poor.
By 2000, full decentralisation to thedistricts was complete, on structural,administrative and operational levels.Pharmacy premises have been reorgan-ized, and hospital and district pharmacieshave been physically separated. The sepa-ration of these premises considerablyfacilitates storage and inventory practice,as well as drug flow monitoring, whichhave consequently improved. Districtpharmacies are located within the newlyconstructed district medical offices, at adistance from the district hospitals.
KEEPING TRACK OF DRUGS:MONITORING ANDDOCUMENTATION SYSTEM
The Project implemented a diseaseand drug monitoring system. Forms weredeveloped for data collection on morbid-ity, drug consumption and kit distribution.However these were not used routinely,little evaluation was done, and little at-tempt made to give health facilitiesfeedback on the data. Follow-up of drugconsumption, distribution and perform-ance monitoring was almost impossible.Drug flow could not be traced andaccountability was difficult to enforce.
To improve this situation, a PharmacyPlan of Operations and a Monitoring/Supervision Form were drawn up withall pharmacists. Operational objectives/activities, implementors, a timeframe,reporting channels and evaluation out-puts were defined. Several documents andforms have been standardised, incorpo-rated in the documentation system andused in all health facilities. Today, phar-macy management tools are availableand are to varying degrees integrated intodistrict and hospital operational plans.Documentation and monitoring of drugflow have improved.
Security of drugs has always been a
A C C E S S
Ten years on and the picture is verydifferent. Dar es Salaam has a decentral-ised supply system with drug requisitionat district level and local procurementfrom a newly restructured Medical StoresDepartment, financed by cost-sharingschemes and Government contributions,and based on the National Drug Policy.How was this achieved?
The structural and functional rehabili-tation of Dar es Salaam’s Governmenthealth facilities, based on primary healthcare principles, started in 1990 with anintergovernmental agreement betweenSwitzerland and Tanzania, with the SwissTropical Institute as the executing agency.The overall goal of the Dar es SalaamUrban Health Project, created at this time,was, and remains, to improve the healthstatus of people in the Dar es Salaam re-gion. As regards drug supply, the mainaim was to improve resource adminis-tration at all levels of care, to create areliable, efficient and sustainable drugmanagement system, addressing both ef-fective supply and rational use of essentialdrugs.
The Project serves three districts eachwith one district hospital, one or twohealth centres and a total of about 60dispensaries in urban and semi-ruralareas. In 1990 the population of Dar esSalaam was estimated at 1.5 million andthe current population is approximately2.5 million.
THE BACKGROUND: DRUG SUPPLYHISTORY IN DAR ES SALAAM
During the late 1960’s the number ofhealth units in Tanzania increased con-siderably. This increase and the economiccrisis of the late 1970’s led to a drug cri-sis in the public health sector. The lack ofdrugs was caused by: the acute shortageof foreign currency; an increase in accessto health units; people’s greater aware-ness of modern medicines; and wastageof drugs due to poor planning, procure-ment, storage, distribution and transport,
I
Delivering drug kits to a dispensary in Dar es Salaam
Phot
o: K
. Wie
denm
ayer
lack of transport, distanceand road conditions. Healthworkers inspected the kitson arrival and documentedreceipt. All reorganized fa-cilities had adequate andsecure drug storage areas.Functioning cold chainequipment was also avail-able, however, storage con-ditions in district stores wereinadequate, with high tem-peratures and humidityaffecting drug quality. Pile-ups and expired drugs thatwere not disposed of took upvaluable space. Storage and
...cont’d on page 26 ➠

26 E S S E N T I A L D R U G S M O N I T O R
Issue No. 28 & 29, 2000
➔ ➔➔
major concern. Not all drugs used to reachthe intended patient. Pilferage and mis-appropriation was a significant problemthat is hard to quantify. Despite there be-ing sufficient drugs, some patients stillcomplained about not receiving drugs orof occasionally being forced to pay. In-ternal monitoring also indicated thatdrugs, particularly antibiotics, were usedby health staff for their own and theirfamilies’ treatment. However, increasedsupervision, professional ownership andaccountability are improving the situa-tion. Good inventory practice and drugmonitoring have helped reduce pilferage.Each health facility has a Health Board,so involving the concerned community,which has also helped to reduce theproblem.
QUALITY OF DRUGS
The main mechanism used for qual-ity assurance of drugs is supplier selectionand contract conditions with the MedicalStores Department. However, there is noformal reporting system for drug qualityproblems. Pharmacists and patients haveto learn that they have a right and a dutyto complain and follow-up on substand-ard drugs. Since 1997, operations andmanagement at the National PharmacyBoard have been restructured in order toenforce drug regulation and quality as-surance. More recently a new qualitycontrol laboratory has begun operating.
BEING IN CHARGE OF DRUGS:HUMAN RESOURCES AND TRAINING
At the beginning, the Project’s phar-macists generally had limited manage-ment skills – a major reason why the drugsupply system functioned poorly. Today,each district has a district pharmacist op-erationally responsible for supervision ofdistrict health facilities, including districthospitals. Hospital pharmacists are moreinvolved in the usual drug supply man-agement activities, such as quantification,procurement, storage and distribution ofdrugs, as well as in some clinical activi-ties within hospital committees and indrug information. However, pharmaceu-tical management capacity, particularly atdistrict level, remains weak and shouldbe strengthened. Decentralisation needsto be founded on capacity-building atlocal level.
With the focus on general districtmanagement in the Project’s early years,training for pharmacists did not receivethe necessary attention. Human resourceswere neglected. Only much later werethe district pharmacists and pharmacytechnicians consulted, and invited to dis-cussions and activities aimed to improvethe drug supply system. Pharmacists havetherefore mainly been responders tochange rather than reformers themselves,even though policy implementationand operational planning in part dependon them.
Ten years later pharmacists are moreinvolved, visible and in control. Theyhave gained some self-confidence and a
voice. Pharmacists are part of the hospi-tal and district health management team.One pharmacist received training in theUK and all pharmacy staff participatedin the training programme on rationalprescribing (see below).
PROMOTING RATIONAL USE
All efforts put into a well functioningdrug supply system can be futile if notfollowed by rational use of drugs by pre-scribers, dispensers and patients. From itsinception, the Project has emphasised theimportance of promoting rational druguse. In 1994, a programme was started toimprove prescribing. A general quantita-tive drug use indicator study clarified thedrug use situation. A concurrent qualita-tive study investigated motivations andunderlying causes of prescribing habitsand constraints within the system. Prob-lems identified were overprescribing ofantibiotics and injections, low availabil-ity of the national Standard TreatmentGuidelines and incorrect prescribingaccording to norms. Based on these find-ings, interventions were selected andimplemented to improve prescribingand quality of care. They include newStandard Treatment Guidelines, a DrugInformation Manual, concurrent training,continuing education and supervision.
Since printed material alone hasshown very little effect on prescribingpractices, continuing education and su-pervision are necessary tools to assuresustained impact. Training sessions wereconducted in all districts. Within fivemonths a total of 328 Project prescribers(80%) in the three districts’ health facili-ties were trained. Unfortunately, despitethe existence of approved tools and anagreed schedule, planned activities forcontinuing education and supervision arenot yet conducted in a systematic way.
PAYING FOR DRUGS
After liberalisation of the health sec-tor, a 1995 study identified that about 35%of the population used public health fa-cilities as first contact. It was estimatedthat drug expenditure for essentialdrugs to all public health facilities ofthe City Council amounted to betweenUS$0.7million and US$1.1million a year.This represents a yearly per capita drugexpenditure of about US$1 to 1.5, whichis in line with the generally accepted fig-ure for essential drugs coverage in Africa3.A recent study concluded that drugs ac-count for 40% of the total governmentaland external health expenditures at Dares Salaam level.
From 1992 until 1996, the City Coun-cil health facilities were supplied withessential drugs financed by an untied non-reimbursable allocation from the SwissGovernment. In 1993, the Tanzanian Par-liament allowed health services to becharged for. Cost sharing was introducedin Dar es Salaam public hospitals as inthe rest of the country. A pilot Bamako-type project successfully implementedfull cost-recovery of drugs in a few Dares Salaam public dispensaries. The do-nor contribution gradually decreased andended in 2000 with that phase of the
Project. The budget gap has been filledby Tanzanian Government contributionsand cost-sharing schemes.
Currently, all dispensaries and healthcentres operate a Bamako-type model ofa drug revolving fund. Hospitals haveintroduced 50% to 80% cost-sharingand are supported with donor and, un-fortunately irregular, Government con-tributions. User fees allowed donorcontributions to gradually decrease. Gov-ernment funding is still essential forhospitals, cost-sharing exemptions, staffcosts etc., and needs to continue to com-plement user fees or future insuranceschemes. The system is no longer depend-ent on donor funds. Long-term sus-tainability will require continued politi-cal will and Government funding,together with further improvements indrug supply management and accounting.
REVIEW OF EXPERIENCE
The objective of drug availability hasbeen achieved with large investments andis one of the Project’s recognised accom-plishments: visible, appreciated by pa-tients and health workers, and valuablefor the health care system. This has con-tributed greatly to the credibility of Dares Salaam’s health care delivery systemand the willingness of patients to sharethe cost of services.
Professionally defined quality of carerelating to drugs (availability, prescribingpractice, drug quality) has improved,whereas community perceived quality ofservices (dispensing practice, patient care,affordability) is less enthusiastic.
Achievements➤ The Project has a functional drug
supply system in place that assurescontinued availability of essentialdrugs at Dar es Salaam public healthfacilities. The drug supply system isdecentralised and integrated as partof the general district managementstructure within a reformed healthorganization in the framework ofhealth sector reform. Pharmacistshave gained a voice, are moreinvolved, better informed, more inter-ested in their work and more presentin the system.
➤ A purchase agreement with the Medi-cal Stores Department constitutes thebasis for local procurement of drugs.Drugs are of good quality since mostare bought from a reputable non profitinternational procurement agency.Storage and inventory practice hasimproved. Monitoring and documen-tation tools are available and partiallyused. The indent system (drug requi-sition) has been introduced and kitsare gradually being phased out.
➤ Drugs are financed by full drug cost-recovery at dispensaries and healthcentres, and by cost sharing at hospi-tals. Attendance rates have changedlittle, and exemption policies are inplace. The budget gap is filled withGovernment and donor contribu-tions. Financial sustainability seemspossible provided there is continued
political support, and improvementsin management and accounting.
➤ A programme to promote rationaldrug use has been implemented,with Standard Treatment Guidelinesand training of all prescribers in thedistricts.
Shortcomings➤ Management capacity is still insuffi-
cient (storage, inventory management,documentation, monitoring of drugflow) particularly at district hos-pital level. Supervision needs to bestrengthened and accountabilityreinforced.
➤ The human resource potential of phar-macy staff should be strengthenedfurther (knowledge, skills, motivationand involvement). Quality of care interms of attitude and patient careneeds improvement.
➤ Rational drug use needs further pro-motion to improve prescribingbehaviour (continuing training and su-pervision). Dispensing of drugs needsattention (training of drug dispen-sers). There is a great need to educatepatients about drug use.
➤ Dialogue with the private sector isminimal.
Summary of development andachievements of Dar es SalaamUrban Health Project drug supply
Drug related 1990 2000activities
Selection Appropriate
Procurement Foreign kit import
Distribution Deficient
Storage Poor
Monitoring and Poor documentation
Quality assurance Poor & security
Promotion of Irrational use rational drug use
Management Poor
Training None
Financing Donor dependent
Indicators 1990 2000
Availability Poor
Affordability Free *
Quality Poor
Rational use Poor
Sustainability No
Quality of care Poor
significant improvement
some improvement* Cost-sharing/full cost recovery with little
change in attendance rates, exemptionpolicy
LESSONS LEARNT
The Dar es Salaam Urban HealthProject’s drug supply experience wasand is a learning process. An efficient,
A C C E S S
...cont’d on page 27 ➠
➔➔
➔➔
➔➔
➔ ➔➔ ➔
➔➔
➔➔
➔➔
➔ ➔➔ ➔
➔
Dar es Salaam...cont’d from pg. 25
➔
(kits being phased out)
(reduction in dependence)

27E S S E N T I A L D R U G S M O N I T O R
Issue No. 28 & 29, 2000
reliable and sustainable drug supply sys-tem depends on a variety of internal andexternal factors, and many componentsand actors determine its success. In ret-rospect we learnt the following lessons:
➤ Initially there was mainly an externalmaterials injection, i.e. provision ofdrugs, which increased their short-term availability. Human resources,infrastructure such as pharmacypremises, and drug supply manage-ment skills were neglected. Theprovision of drugs was important, as
a visible symbol of development, togain people’s confidence and satisfypoliticians, but it was not sustainableby itself.
➤ There was insufficient effort to in-volve, train, empower and motivatepharmacy staff. To have had phar-macy staff proficient in drug supplymanagement from the beginningwould have been extremely importantfor improving allegiance and coopera-tion, including early capacity-buildingand training. Emphasis needed to beplaced on improving skills, increas-ing motivation and changing attitudes.Supportive supervision and monitor-ing as well as continued education areimportant tools.
➤ In order to follow-up, monitor andevaluate the quantitative and quali-tative outcome of a high invest-ment drug supply system over 10years, a detailed baseline assessmentwith structure, process and outcomeindicators should have been con-ducted at the beginning of the pro-ject. However only some ratherrandomly and informally collectedinformation was available, which
A C C E S S
makes evidence-derived outcomemeasurement difficult.
➤ An efficient national Medical StoresDepartment has proven to be one ofthe main pillars for the drug supplysystem, providing drugs of goodquality at affordable prices. Thus ex-ternally organized tendering andimport from overseas could be re-placed by local and professional bulkpurchasing, clearing, distribution andstorage of essential drugs.
➤ The Tanzanian National Drug Policyhas been an important tool and frame-work for the development of a moreefficient, equitable and sustainabledrug supply system for the Dar esSalaam Project.
A TENTATIVE OUTLOOK
A drug supply system cannot be man-aged in an isolated way but needs to beconsidered as part of a larger socio-cultural, political and economic contextand environment. It is also part of an or-ganization, the supporting health sys-tem, from which it cannot be isolated.Each sub-system, such as drug supply, is
a resource for and in interrelation withother sub-systems that have to be coordi-nated. For the new drug supply system,which developed over nearly 10 years, tobe sustainable active consolidation isnecessary. New structures and processesneed to be kept alive, to be to imple-mented and to become established, toavoid falling back into old patterns. Ac-tive consolidation involves strengtheningas well as internal and external support.This translates into careful monitoring,supportive supervision and continuingeducation. A key assumption is a stableand supportive political environment. ❏
* Dr Karin Wiedenmayer is a pharmacist atthe Swiss Tropical Institute, Socinstrasse 57,CH-4002, Basle, Switzerland, and DrDeo Mtasiwa is the City Medical Officer ofHealth, Dar es Salaam, United Republic ofTanzania.
References
1. Kanji N, Kilima PM, Munishi GM. Quality of primarycurative care in Dar es Salaam. Dar es Salaam: Dar esSalaam Urban Health Project; 1992.
2. Wyss K, Whiting D, Kilima P, Mc Larty DG, MtasiwaD, Tanner M, Lorenz N. Utilisation of Government andprivate health services in Dar es Salaam. East AfricanMedical Journal 1996; 73:357.
3. World Bank. Better health in Africa. Experiences andlessons learnt. Washington D.C.: World Bank; 1994.
Dar es Salaam...cont’d from pg. 26
Training prescribers in rational use of drugs
Phot
o: K
. Wie
denm
ayer
Ratio oflowest tohighest price
Why do the poor pay more?Survey reveals disparity in drug prices
hat effect is an increasinglyglobalised economy with tighterintellectual property systemshaving on developing countries’
efforts to make essential drugs availableand affordable? A Consumers Interna-tional and HAI survey in 1999 addressedthis crucial question. The survey exam-ined retail prices of 16 drugs in 36countries – 10 advanced economies and25 developing ones in Africa, Asia andLatin America, plus one from theCommonwealth of Independent States.
For the study the drugs were groupedinto three categories according to theirpatent status: those still under patent insome countries; drugs whose patents willexpire soon or have recently expired;and multisource drugs with severalcompanies’ products available in allthe countries. The drugs are all widelyprescribed.
HAI partners and Consumers Inter-national members visited leading retailpharmacies in the 36 capital citiesseeking information on the:
➤ availability and retail prices of the pro-prietary or brand name product of the16 drugs;
➤ total number of products which in-clude the originator’s brand, brandedgenerics and generics of each of the16 drugs available in the pharmacy;
➤ retail prices of the originator’s brandand the package size. Where severalproducts of the drug were available,the prices of the next two best-sellingproducts in addition to the proprietarybrand or top-selling brand.
➤ prices of each package size in the na-tional currency and then converted toUS dollars.In line with the results of other stud-
ies reported at the Nairobi Conference(see page 20), the survey found a verywide variation in retail prices in the coun-tries surveyed. Among its most strikingfindings were that:➤ in some developing countries retail
prices were higher than in developedcountries. This was the case for 15 outof 18 dosage forms of 11 drugs (thosefor which comparable data exist);
➤ proprietary brand forms of several ofthe multisource drugs surveyed are theonly products available in many of theAfrican countries. This is even thoughlow priced generic equivalents areavailable in the world market, in coun-tries not offering patent protection topharmaceuticals;
➤ survey differences in the retail pricesof proprietary drugs are much wider(range 1:16–1:59), than those forprices of generic equivalents (range1:7–1:18);
➤ variations in the retail prices ofmultisource drugs in developing coun-tries are much wider than thevariations in the developed countries.While the study did not analyse the
sources of price variations, researcherssuggest that the small difference in pricesin the industrialised countries may in partbe due to co-marketing arrangements bymanufacturers, parallel importing, refer-ence pricing and drug pricing policies.Other studies have shown that producer/
importer prices vary between countries.And that import duties and distributioncosts, pharmacy margins and local taxesalso vary greatly between countries, butparticularly from one developing coun-try to another, so contributing to pricedifferentials.
This wide range in proprietary drugprices in developing countries (1:4–1:59)is shown in the Table, with India havingthe lowest prices for six out of nine dos-age forms. Consumers International andHAI argue that the Indian situation provesthat competition is possible in the phar-maceuticals market and that it bringsprices down. They say that India under-scores the need for national policies onintellectual property systems with provi-sions to enable national firms to beginproduction of new drugs as quickly aspossible. Indian firms could do this by
reverse engineering (a practice for discov-ering the manufacturing process of aproduct starting from the finished prod-uct), as the country’s legislation did notprovide patent protection for products, theauthors state.
The report advocates that provisionsfor compulsory licensing and parallelimports should be in all national legisla-tion on intellectual property rights aspermitted by TRIPS. It states that this willhelp developing countries ensure regularaccess to good quality essential drugs ataffordable prices. ❏
For further information contact: ConsumersInternational, 5th Floor Wisma WIM, 7 JalanAbang Haji Openg, Taman Tun Dr. Ismail,60000 Kuala Lumpur, Malaysia. Fax: + 603 772 61599, e-mail: [email protected]
W
Price comparison of 8 proprietary brand drugsin developing countries in the study
Generic name Retail price of 100 units in US$Country Price Country Price
Lowest Highest
Acyclovir 200mg Togo 50 Indonesia 371 1:7Acyclovir 800mg1 India 94 South Africa 790 1:8Atenolol 25mg India 03 Cameroon 53 1:18Ciprofloxacin 500mg India 15 Mozambique 740 1:49Diclofenac 50mg India 02 Argentina 118 1:59Nifedipine 20mg India 03 Peru 96 1:32Omeprazole 20mg Zambia 30 Brazil 477 1:11Ranitidine 150 mg India 02 South Africa 116 1:58Zidovudine 100mg Pakistan 81 Argentina 316 1:4
28 E S S E N T I A L D R U G S M O N I T O R
Issue No. 28 & 29, 2000
D R U G I N F O R M A T I O N
Introducing Pakistan’s first DrugHelpline for professionals and patients
➢ AYESHA AHMED*
roviding independent drug information to health professionals andconsumers through specially designated drug information centres is arelatively new concept in Pakistan. Although many countries automati-cally incorporate such centres in hospitals, in Pakistan they are rare.
Those that exist, such as at the Aga Khan Medical University Hospital andJinnah Post-Graduate Hospital, Karachi, and Lahore’s Children’s Hospital, areonly for use by health professionals. But recently The Network-Association forRational Use of Medication in Pakistan has established a Drug InformationHelpline, the first of its kind in the country. Catering to the needs of doctorsand patients, it is not hospital based but is run from The Network’s office inIslamabad.
Meeting a need
As elsewhere, the available sources ofdrug information for Pakistan’s healthprofessionals, apart from pharmaceuticalcompanies, are the standard pharmacol-ogy textbooks, and local and internationalcompendia. These are not only cumber-some but soon become outdated. Busyphysicians have little time to go throughthese sources and may relymostly on industry infor-mation about medicines.
Although patientinformation leafletssupplied by the manu-facturer accompanyeach medicine, theconsumers’ sources ofinformation about drugsare mainly their pre-scriber and word ofmouth. But prescribershave little or no time totell people about possible ad-verse/side-effects, precautions or druginteractions, as there are usually otherpatients waiting. They may also be una-ware of some details if the drug companydoes not provide complete information.Sales representative may minimise theimportance of side-effects and precau-tions, for example. This creates a situationwhere there is insufficient information forthe doctor and even less for the consumer.In the vast majority of cases people dis-cuss their medicines with others showingsimilar symptoms, leading to abuse ofmedicines and the use of completelyinappropriate drugs.
The Network’s efforts
Since it became involved in the healthsector nine years ago, The Network, anot-for-profit organization, has been com-mitted to protecting consumers fromharmful effects of medicines caused bylack of knowledge and misinformation.Through its publications, especially theDrug Bulletin, The Network has beencatering to the information needs of healthprofessionals and consumers, but on anindividual level there was no system todeal with specific requests. The Helplinehas filled this gap. Started with initial
support from WHO, it aims to giveadequate, objective and up-to-dateinformation on request.
A comprehensive service
A pharmacist, trained at the WHOCollaborating Centre for Drug Informa-tion, The National Poison Centre inPenang, Malaysia, runs the Helpline.
Consumers and health professionalsaccess the service by phone, fax,
mail and e-mail. Working hoursare quite short, 9am–5pm
Monday to Friday, main-ly due to financial andstaffing constraints.
The Helpline providesinformation on drug dos-
age, formulations, effectsand adverse reactions, andprobable drug interactions
with food and with otherallopathic medicines used to-
gether. The service does not offer anyhelp with disease diagnosis or with pre-scribing medication to consumers, nordoes it provide information on herbal orhomeopathic medicines.
Requests from health professionalsand consumers are dealt with in differentways. Consumers have to supply addi-tional information about their prescribersand their prescriptions. Requests aredocumented on a standard form (seeright) and scheduled on the basis of theirurgency and the available resources – allare answered as quickly as possible. Dif-ferent queries about the same drug bythe same person are recorded as one.For example: if a request comes in formisoprostol and the doctor has askedfor its availability, drug interactions,contraindications, precautions and side-effects, staff complete only one form andthe various categories are marked on it.
Our resources
The Centre uses the latest version ofMICROMEDEX, the standard updateddatabase. It has the Drug Index and thepoisoning information database, PoisonIndex. In addition, the Australian Pre-scriber, Prescrire International, Drug andTherapeutics Bulletin, Worst Pills Best
Pills, American Hospital FormularyService, Physician’s Desk Reference, USPDrug Information, WHO Drug Informa-tion, British National Formulary andEllenhorne’s Medical Toxicology areavailable. Information is also gatheredfrom the electronic discussion groupsEssential Drug (E-Drug) and InternationalNetwork of Drug Information Centres(INDICES).
Much in demand
Although it is early to assess its con-tribution to rational drug use, the ser-vice is catering to the needs of elevenhospitals, both Government- and nonGovernment-run. Analysis after 12
Ref No.
The Network’s Drug Information Helpline
Administrative Record:Requestor (Name): Date:Profession (Please tick the right option): Time:❏ Doctor ❏ Pharmacist ❏ Nurse Status: ❏ New ❏ Follow up❏ Paramedic ❏ Medical/ Pharmacy students Method of communication:❏ Public ❏ Verbal ❏ Written
Address of the requestor:Tel:Patient Information:Age: Diagnosis:Sex: Allergies:Weight: Medication being used:Occupation:Marital Status: Laboratory values:Additional Information:
Request:Drug Information:❏ General product information ❏ Drug interaction (unknown/drug/
laboratory/disease/food)❏ Pharmacokinetics/Pharmacology ❏ Side effects/Adverse effects/
Contraindication❏ Therapy Evaluation/Drug of choice ❏ Teratogenecity/Genetic effects❏ Dosage/Regimen recommendation ❏ Poisoning/Toxicology❏ Pharmaceutical (formulation) ❏ Pregnancy/Lactation/Infant risks❏ Others ❏ Compatibility/Stability/Administration
(rate/method)
Search Conducted (Source and utility, record specific data):
Findings/ Evaluation:
Response:
Responder: Method of response: Verbal, WrittenDate: Time: Time spent:
Follow Up: Additional Comment:❏ Effective❏ Required additional help❏ Unsatisfactory
Pmonths in operation showed that 47% ofusers were health professionals includingdoctors, pharmacists and paramedic staff,and 53% consumers. The most frequentlyasked questions concern side-effects,availability and cost of medicines, fol-lowed by drug dosage regimen, drugsof choice, drug interactions and drug useduring pregnancy. Approximately 95%of questions are answered by telephone,and the rest receive written replies.
Spreading the word
The Helpline has printed separate pub-licity brochures in English and Urdu andposters in the local Urdu language. Eachhospital in Islamabad and Rawalpindi was
The
Net
wor
k’s D
rug
Bulle
tin

29E S S E N T I A L D R U G S M O N I T O R
Issue No. 28 & 29, 2000
contacted separately, with a letter and pro-motional materials sent to the MedicalSuperintendent or Executive Director.Doctors and other health staff receivedpublicity materials at seminars about theservice, which were held at all hospitals.The Drug Bulletin and our Urdu publica-tion featured articles, as did the nationaldaily English and Urdu newspapers whenthe Helpline was launched.
Educational activitiesThe drug information Helpline has
regular input in The Network’s Drug Bul-letin and the Urdu publication SarfeenAur Sehat. As well as providing articleson specific drugs, the service also passeson the information it has on drug usetrends, who is accessing the Helpline andthe types of requests it is receiving.
Transparency in US drug approval system –a lesson for others?
t is common practice for manu-facturers to selectively makeclinical trial results of new drugsavailable only as abstracts or in
meeting presentations, rather than pub-lishing full length journal articles. Thiscreates a problem for those wantingcomplete information. However, it is thecompanies’ data, and the release of someresults may have a negative impact onsales. But even when manufacturers dogive a more complete report, the bounda-ries may be blurred between what isscience – publication of peer reviewedjournal articles – and what is basicallydrug promotion. An independent assess-ment of the drug becomes impossible.
A partial solution can be found in thetransparency of the US drug approvalprocess, at least for drugs approved there.The Freedom of Information Act givespublic access to Food and Drug Admin-istration (FDA) reviews of the clinicaltrials and other data submitted by manu-facturers as part of a new drug application.
These reviews are referred to as approvalpackages and are available for manydrugs approved since 1997 on the FDA’sweb site at http://www.fda.gov/cder/foi/nda/index.htm Approval packages typi-cally contain pharmacology/toxicology,biopharmaceutics and pharmacokinetics,and statistical reviews of the data submit-ted in a new drug application. The FDAMedical Officer also writes an overallassessment of a drug’s safety and efficacy,based on the reviews and the clinicaltrials submitted in the application.
Transcripts of FDA Advisory Com-mittees are also valuable in that they canreveal members’ concerns about a drug’ssafety and efficacy. Committee membersare outside experts who make recommen-dations to the Agency about a drug’sapproval that are not always followed.Meetings are conducted under the Fed-eral Advisory Committee Act to ensurethat the public has access to the workingsof the government. Transcripts are foundat http://www.fda.gov/foi/electrr.htm on
the FDA’s web site, although not all drugsgo before FDA Advisory Committees.
Copies of approval packages and Ad-visory Committee transcripts for drugsapproved prior to 1997 can be obtainedfrom the FDA through a request underthe Freedom of Information Act. Accessto these documents is not limited to UScitizens and US non-profit organizationsare granted a fee waiver when the re-quested information is shared with thepublic. Procedures for making a Free-dom of Information Act request can befound at http://www.fda.gov/opacom/backgrounders/foiahand.html on theAgency’s web site.
Since January 2000, FDA reviews ofnew drugs are available on the FDA’s website at least one day before Advisory Com-mittee meetings. About 30% of the drugsapproved by the FDA go before an Advi-sory Committee. Legal hearings havebeen taking place to decide if safety andefficacy data can be considered confi-dential commercial information that is
exempt from public disclosure under theFreedom of Information Act until a drugis approved.
The selective publication of clinicaltrials by manufacturers can influence theperception of a new drug’s therapeuticvalue by only making available evidencethat is most favorable to the drug. It nowappears necessary to wait until a drug’sapproval package is publicly availablefrom the FDA before independent recom-mendations or formulary decisions can bemade about new drugs. Controlled accessto published clinical trial results by manu-facturers and the lack of transparencyin the drug approval process in othercountries remain problems. ❏
Source: E-Drug electronic discussion groupmessage from Larry D. Sasich, ResearchAnalyst, Public Citizen Health ResearchGroup, 1600 20th Street, NW, Washing-ton DC, 20009, USA. Fax: + 1 202-588-7796, e-mail: [email protected], Web Site:www.citizen.org/hrg
Iowa Drug Information Service too.Currently our dedicated phone-line
is sufficient for people calling from withinIslamabad and Rawalpindi. But it is in-convenient for people calling fromoutside the cities, mainly because it is ex-pensive to call during the peak daytimehours. A separate toll free telephone linewould solve this problem.
Proving our value
Since the Helpline started as a smallpilot project in Islamabad in November1999, it has proved popular with doctorsand consumers. Now it is facilitatingseveral hospitals, including majorGovernment-run ones. We now believethat if information services are basedwithin hospitals, doctors and patientscould access them quicker. It could also
D R U G I N F O R M A T I O N
I
boost the profile of hospital pharmacistsand give them an opportunity to becomea more integral part of the health team.
Independent and objective drug infor-mation is essential for achieving rationaldrug use. If it is to be effective, this in-formation has to be tailored to the leveland specific needs of the enquirer. But thisis a complex process. By starting small,with what we had, we have shown thatHelplines can be successful. We intend
One of the posters produced by the Service as part ofits publicity campaign
UK’s new bulletin fillspatient information gap
or many years the UK’s Con-sumers’ Association has beenproviding professionals andconsumers with impartial in-
formation about health. Now, as morepatients want to be involved in the in-creasingly complex decisions regardingtheir health care, the Association is intro-ducing a new information service. It willreinterpret the information it gives todoctors and pharmacists in its Drugand Therapeutics Bulletin in a new bul-letin for health care consumers. Thedoctor- or pharmacist-supplied leafletwill be accurate, concise, easy to readand up-to-date.
The Association acted because al-though there is a plethora of health andmedical information available, especiallyon the Internet, many patients do not haveaccess to it or cannot find the right infor-mation when they need it. Also, it wasfelt that the quality of Internet informa-tion is mixed and can be heavily biasedtowards commercial sources. The
Consumers Association decided therewas still a dearth of high-quality, impar-tial information about drugs and medi-cal treatments designed expressly forpatients.
The new information bulletin willcover one topic per leaflet, for example,antibiotic resistance or weight loss. It willgive background information for thenewly diagnosed patient, and advice andrecommendations that match the “parent”Drug and Therapeutics Bulletin. Pilot is-sues were tested with patients and healthprofessionals. The Association hopes lo-cal health authorities will purchase thebulletin and make it available, free ofcharge, in doctors’ surgeries and commu-nity pharmacies. An electronic versionshould follow soon. ❏
For further information contact: Philip Taylor,Consumer’s Association: Drug and Therapeu-tics Bulletin, 2 Marylebone Road, LondonNW1 4DF, UK. Tel: + 44 20 71 830 7608,fax: + 44 20 71 830 7664, e-mail: [email protected]
FMoney matters
The service’s major constraint islack of finance. Eventually, we wantto create a national service, but forthis we need more staff. At presentanswering queries and promotingour service are the major activities,and one person is sufficient to runthe Centre. But we need to publi-cise our work in other cities; weneed money to travel to them, andmore staff to handle the increasednumber of queries. We want to openat least 12 hours a day or even be-come a round-the-clock service.Resources and equipment alsoneed to be updated. At present wehave older editions of the coretitles and our subscription toMICROMEDEX, one of our majorinformation sources, must be re-newed in 2001. Moreover, we wantto improve the service by using the
to form a network of such services, basedwithin hospitals, and once we have shownour value nationally, we hope to attractthe funding to ensure sustainability. ❏
* Ayesha Ahmed is the pharmacist in chargeof the Helpline. For further information con-tact: The Network For Consumer Protection,40-A, Ramzan Plaza, G-9 Markaz,Islamabad, Pakistan. Tel: + 92 51 2296802,fax: + 92 51 2291552, e-mail: [email protected]
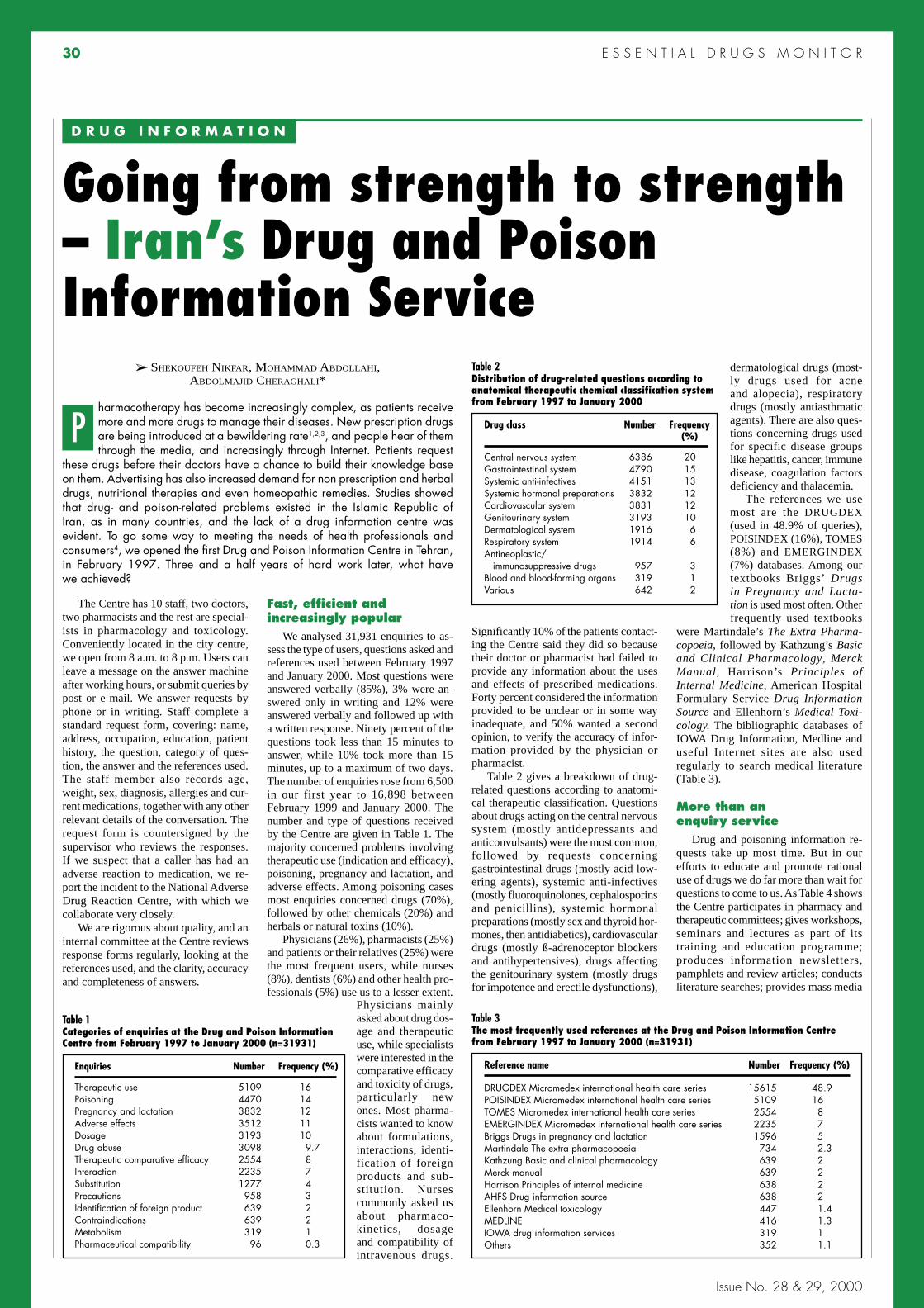
30 E S S E N T I A L D R U G S M O N I T O R
Issue No. 28 & 29, 2000
Going from strength to strength– Iran’s Drug and PoisonInformation Service
➢ SHEKOUFEH NIKFAR, MOHAMMAD ABDOLLAHI,ABDOLMAJID CHERAGHALI*
harmacotherapy has become increasingly complex, as patients receivemore and more drugs to manage their diseases. New prescription drugsare being introduced at a bewildering rate1,2,3, and people hear of themthrough the media, and increasingly through Internet. Patients request
these drugs before their doctors have a chance to build their knowledge baseon them. Advertising has also increased demand for non prescription and herbaldrugs, nutritional therapies and even homeopathic remedies. Studies showedthat drug- and poison-related problems existed in the Islamic Republic ofIran, as in many countries, and the lack of a drug information centre wasevident. To go some way to meeting the needs of health professionals andconsumers4, we opened the first Drug and Poison Information Centre in Tehran,in February 1997. Three and a half years of hard work later, what havewe achieved?
The Centre has 10 staff, two doctors,two pharmacists and the rest are special-ists in pharmacology and toxicology.Conveniently located in the city centre,we open from 8 a.m. to 8 p.m. Users canleave a message on the answer machineafter working hours, or submit queries bypost or e-mail. We answer requests byphone or in writing. Staff complete astandard request form, covering: name,address, occupation, education, patienthistory, the question, category of ques-tion, the answer and the references used.The staff member also records age,weight, sex, diagnosis, allergies and cur-rent medications, together with any otherrelevant details of the conversation. Therequest form is countersigned by thesupervisor who reviews the responses.If we suspect that a caller has had anadverse reaction to medication, we re-port the incident to the National AdverseDrug Reaction Centre, with which wecollaborate very closely.
We are rigorous about quality, and aninternal committee at the Centre reviewsresponse forms regularly, looking at thereferences used, and the clarity, accuracyand completeness of answers.
Fast, efficient andincreasingly popular
We analysed 31,931 enquiries to as-sess the type of users, questions asked andreferences used between February 1997and January 2000. Most questions wereanswered verbally (85%), 3% were an-swered only in writing and 12% wereanswered verbally and followed up witha written response. Ninety percent of thequestions took less than 15 minutes toanswer, while 10% took more than 15minutes, up to a maximum of two days.The number of enquiries rose from 6,500in our first year to 16,898 betweenFebruary 1999 and January 2000. Thenumber and type of questions receivedby the Centre are given in Table 1. Themajority concerned problems involvingtherapeutic use (indication and efficacy),poisoning, pregnancy and lactation, andadverse effects. Among poisoning casesmost enquiries concerned drugs (70%),followed by other chemicals (20%) andherbals or natural toxins (10%).
Physicians (26%), pharmacists (25%)and patients or their relatives (25%) werethe most frequent users, while nurses(8%), dentists (6%) and other health pro-fessionals (5%) use us to a lesser extent.
Significantly 10% of the patients contact-ing the Centre said they did so becausetheir doctor or pharmacist had failed toprovide any information about the usesand effects of prescribed medications.Forty percent considered the informationprovided to be unclear or in some wayinadequate, and 50% wanted a secondopinion, to verify the accuracy of infor-mation provided by the physician orpharmacist.
Table 2 gives a breakdown of drug-related questions according to anatomi-cal therapeutic classification. Questionsabout drugs acting on the central nervoussystem (mostly antidepressants andanticonvulsants) were the most common,followed by requests concerninggastrointestinal drugs (mostly acid low-ering agents), systemic anti-infectives(mostly fluoroquinolones, cephalosporinsand penicillins), systemic hormonalpreparations (mostly sex and thyroid hor-mones, then antidiabetics), cardiovasculardrugs (mostly ß-adrenoceptor blockersand antihypertensives), drugs affectingthe genitourinary system (mostly drugsfor impotence and erectile dysfunctions),
dermatological drugs (most-ly drugs used for acneand alopecia), respiratorydrugs (mostly antiasthmaticagents). There are also ques-tions concerning drugs usedfor specific disease groupslike hepatitis, cancer, immunedisease, coagulation factorsdeficiency and thalacemia.
The references we usemost are the DRUGDEX(used in 48.9% of queries),POISINDEX (16%), TOMES(8%) and EMERGINDEX(7%) databases. Among ourtextbooks Briggs’ Drugsin Pregnancy and Lacta-tion is used most often. Otherfrequently used textbooks
D R U G I N F O R M A T I O N
P
Table 1Categories of enquiries at the Drug and Poison InformationCentre from February 1997 to January 2000 (n=31931)
Enquiries Number Frequency (%)
Therapeutic use 5109 16Poisoning 4470 14Pregnancy and lactation 3832 12Adverse effects 3512 11Dosage 3193 10Drug abuse 3098 9.7Therapeutic comparative efficacy 2554 8Interaction 2235 7Substitution 1277 4Precautions 958 3Identification of foreign product 639 2Contraindications 639 2Metabolism 319 1Pharmaceutical compatibility 96 0.3
Physicians mainlyasked about drug dos-age and therapeuticuse, while specialistswere interested in thecomparative efficacyand toxicity of drugs,particularly newones. Most pharma-cists wanted to knowabout formulations,interactions, identi-fication of foreignproducts and sub-stitution. Nursescommonly asked usabout pharmaco-kinetics, dosageand compatibility ofintravenous drugs.
Table 2Distribution of drug-related questions according toanatomical therapeutic chemical classification systemfrom February 1997 to January 2000
Drug class Number Frequency(%)
Central nervous system 6386 20Gastrointestinal system 4790 15Systemic anti-infectives 4151 13Systemic hormonal preparations 3832 12Cardiovascular system 3831 12Genitourinary system 3193 10Dermatological system 1916 6Respiratory system 1914 6Antineoplastic/ immunosuppressive drugs 957 3Blood and blood-forming organs 319 1Various 642 2
Table 3The most frequently used references at the Drug and Poison Information Centrefrom February 1997 to January 2000 (n=31931)
Reference name Number Frequency (%)
DRUGDEX Micromedex international health care series 15615 48.9POISINDEX Micromedex international health care series 5109 16TOMES Micromedex international health care series 2554 8EMERGINDEX Micromedex international health care series 2235 7Briggs Drugs in pregnancy and lactation 1596 5Martindale The extra pharmacopoeia 734 2.3Kathzung Basic and clinical pharmacology 639 2Merck manual 639 2Harrison Principles of internal medicine 638 2AHFS Drug information source 638 2Ellenhorn Medical toxicology 447 1.4MEDLINE 416 1.3IOWA drug information services 319 1Others 352 1.1
were Martindale’s The Extra Pharma-copoeia, followed by Kathzung’s Basicand Clinical Pharmacology, MerckManual, Harrison’s Principles ofInternal Medicine, American HospitalFormulary Service Drug InformationSource and Ellenhorn’s Medical Toxi-cology. The bibliographic databases ofIOWA Drug Information, Medline anduseful Internet sites are also usedregularly to search medical literature(Table 3).
More than anenquiry service
Drug and poisoning information re-quests take up most time. But in ourefforts to educate and promote rationaluse of drugs we do far more than wait forquestions to come to us. As Table 4 showsthe Centre participates in pharmacy andtherapeutic committees; gives workshops,seminars and lectures as part of itstraining and education programme;produces information newsletters,pamphlets and review articles; conductsliterature searches; provides mass media

31E S S E N T I A L D R U G S M O N I T O R
Issue No. 28 & 29, 2000
Table 4Percentage of time spent on Drug and Poison InformationCentre activities from February 1997 to January 2000
Activity Frequency (%)
Providing drug and poisoning information 30Producing newsletters and pamphlets 14Providing seminars and giving lectures 10Reporting to the Adverse Drug Reaction Centre 10Preparing review articles 9Providing workshops, training and education 8Establishing new drug and poison information centres 7Participating in pharmacy and therapeutic committees 5Conducting literature searches 4Providing mass media information 3
D R U G I N F O R M A T I O N
As our drug and poisoninformation pamphlets are sopopular, the Centre has cre-ated a subscription service,which includes over 20,000health professionals. Theyregularly receive literaturepromoting rational drug use,often based on our mostinteresting queries.
We want as many Irani-ans as possible to haveaccess to drug information,not only those living in thecapital. So we have estab-lished new drug and poisoninformation centres – morethan 15 to date – all withaccess to a computer andreferences (see map). TheTehran Centre supports them
information to help increase rational useof drugs; and reports to the Adverse DrugReaction Centre. As the Service’s popu-larity has grown so too has the variety oforganizations we assist.
The Centre tries to ensure that the lit-erature it produces meets the needs ofusers. So, when we do quality checks onour responses we also assess the need foreducation materials on particular topics.For example, we were receiving questionsfrom young men about the effects of ana-bolic drugs that might be used for bodybuilding. We immediately increased ourdissemination of information on this sub-ject in seminars, the mass media and ournewsletters.
Burkina Faso: study shows value ofqualitative monitoring
hile prescribing practices havebeen studied in various develop-ing countries, most research haslimited evaluation to numerical
analysis, such as the number of drugs pre-scribed or the percentage of prescriptionscontaining an antibiotic. But a studycarried out in Burkina Faso1 used bothqualitative and quantitative indicators toinvestigate the rationality of drug pre-scriptions at outpatient consultations. Thestudy results demonstrate the importanceof a multifaceted research approach, andadd to the evidence that greater effortsmust be made to improve prescribingpractices globally.
Specially trained medical students andnurses observed a total of 313 outpatientconsultations in nine health centres inthree rural districts. Data on 2,815 drugprescriptions were also analysed. Thesehad been copied from patient registerstwo months before observation began, inorder to compare prescribing habits inobserved and unobserved consultations.
During the two-week study period 366prescriptions for 793 drugs were givenout and an average of 2.3 drugs wasprescribed per visit. A total of 33.1% ofprescriptions contained antibiotics and24.6% contained injections. Of the drugsprescribed, 88.0% were on the essential
drugs list, but only 59.3% of prescriptionsconformed to standard treatment guide-lines. In all other prescriptions at least onedrug was not indicated or the dosage waswrong. Errors in dosage occurred signifi-cantly more often in children under theage of five, mostly in terms of dangerousoverdosing. Seven out of 21 pregnantwomen received drugs contraindicated inpregnancy. In two-thirds of all cases the
patients received no information on howlong a prescribed drug had to be taken.Prescribing was similar in both the ob-served and the unobserved consultations.
The study concludes that a significantproportion of patients probably receivedineffective or even harmful prescriptions,although the interpretation of quantitativeindicators alone would have led to a posi-tive evaluation of prescribing practices.
R E S E A R C H
New drug and poison information centres are being set upthroughout Iran
by providing reference materials andfunds.
After our first assessment of the Cen-tre we are optimistic about its future.Questionnaires distributed to health pro-fessionals during seminars showed thatthey thought our service has an impacton prescribing practice, and in most casesusers were satisfied with their consulta-tion. The increased rate of enquiries andusers are other positive indicators.
Now we want to build on success.The Centre is preparing more referencematerials for health professionals andexpanding its e-mailing of informa-tion on specific diseases to patients. Weare doing more evaluation of Internet
sources for patients. We are also consid-ering having a computer-based systemto assist in analysing information, anddocumenting the Centre’s activities andeffectiveness.
Staff believe they could be even moreeffective if health professionals’ trainingand continuing education covered the roleand use of drug information centres. Wealso want to see more training in appliedtoxicology, to reduce the large number ofpoisoning queries we receive.
Our work with the public is very im-portant, particularly given our findings onthe lack of information patients receiveabout their prescribed medicines, andpeople’s increased exposure to advertise-ments and media-provided information.Correct, unbiased and practical drug andpoison information is one of the best waysto neutralise the effect of drug promotionand reduce drug-related adverse effects.
Our analysis of queries has shown thattoo little of this exists in Iran and under-lines the Centre’s crucial role in the healthcare system and the community. ❏
* Dr Shekoufeh Nikfar, is Director of the Drugand Poison Information Centre, Tehran, DrMohammad Abdollahi, is Associate Profes-sor of Pharmacology and Toxicology, Facultyof Pharmacy, Tehran University of MedicalSciences, and Scientific Consultant to theDrug and Poison Information Centre, Tehran,and Dr Abdolmajid Cheraghali is AssociateProfessor of Pharmacology and Toxicology,Faculty of Medicine, Baghiyatallah Univer-sity of Medical Sciences, and ScientificConsultant to the Drug and Poison Informa-tion Centre, Tehran, Iran. For furtherinformation contact: Drug and Poison Infor-mation Centre, 2nd floor, Under-Secretary ofFood and Drugs, Ministry of Health, Fakhr-E-Razi Street, Engheleb Avenue, Tehran-Iran.
References1. Johnson JA, Bootman JL.
Drug-related morbidity andmortality. Arch Intern Med1995;155:1949–1956.
2. Fontanarosa PB, LundbergGD. Alternative medicinemeets science. JAMA 1998;20:1615–22.
3. Rodriguez C, Arnau JM, VidalX, Laporte JR. Therapeuticconsultation: a necessary ad-junct to independent druginformation. Br J Clin Pharma-col 1993;l 35:46–50.
4. Hemminki E, Herxheimer A.Should drug information be anintegral part of health care? JR Coll Physicians Lond 1996;30:104–6.
Science shopping in the Netherlands
Only by correlating prescriptions to pa-tients’ diagnoses was it possible to detectproblems of false dosage and contra-indications, and to identify certain riskgroups. So while quantitative drug useindicators have proved very useful for arapid and economic assessment of gen-eral drug use habits, in-depth studiesmay be necessary from time to time. Ad-ditionally this methodology allowed theidentification of special risk issues andrisk groups, so helping to determine thefocus of further interventions. ❏
Reference1. Krause G et al. Rationality of drug prescriptions in rural
health centres in Burkina Faso. Health Policy andPlanning 1999;14(3):291-298.
move to bring science out of the“ivory tower” and into the serv-ice of a wider public has beenproving very successful in the
Netherlands. The idea for Science Shopsoriginated in the 1970s, and today thereare more than 30 such research informa-tion centres, affiliated with 11 universitiesand covering a wide field – from healthto literature. Financed by the universi-ties, the Shops may work free of chargefor non profit social organizations need-ing help with community-based research.One of them is the Science Shop forMedicines attached to Utrecht Uni-versity’s Faculty of Pharmacy, which
receives many of its research questionsfrom patients’ associations, consumerorganizations and women’s groups.
When a question comes in, the Sci-ence Shop looks for a staff member in thePharmacy Faculty whose work ties in tothe topic, which generally concerns phar-macotherapy or pharmacoepidemiology.Then, under supervision, a student doesa literature review and receives studypoints for the work. The study is usuallywritten up as a short report or brochure,available from the Shop for a nominalcharge. While a literature review is usu-ally what is required, other types ofresearch, such as surveys, interviews and
drug analyses are also possible. In recentyears many questions have been askedabout the use of drugs for psychiatric dis-orders and about women’s health issues.
As well as collaborating with the otherresearch information centres at UtrechtUniversity, the Science Shop for Medi-cines often works with GroningenUniversity’s Medicines Shop and thecountry’s seven Health Shops. ❏
For further information contact: Science Shopfor Medicines, Sorbonnelaan 16, Postbus80082, 3508 TB Utrecht, the Netherlands.Tel: + 31 30 253 7309, fax: + 31 30 2539166, e-mail: [email protected]
W
A
Dru
g an
d Po
ison
Info
rmat
ion
Cen
tre, T
ehra
n
Drug and Poison Information Centres

32 E S S E N T I A L D R U G S M O N I T O R
Issue No. 28 & 29, 2000
Catch up on theAustralian Prescriber
For the first time the Internet version ofthe journal Australian Prescriber is avail-able in PDF format, with Acrobat readersoftware provided. Back issues of thejournal (from 1994) are also availableon the Web site at http://www.australianprescriber.com
◆ ◆ ◆
Read INRUD Newson the Web
INRUD News, the twice-yearly journalof the International Network for RationalUse of Drugs (INRUD) is now available onthe Web. Published twice a year, over3,000 copies of the journal are distributedfree of charge worldwide. Contents includeupdates on INRUD global activities, newsfrom country and support groups, meet-ing and workshop reports, research briefs,and references to articles on rational useof drugs.
You can subscribe to INRUD News, and readcurrent and previous issues by clicking on thenewsletter icon at http://www.msh.org/inrud
◆ ◆ ◆
Lancet’s electronic researcharchive
The Lancet has launched an experimen-tal electronic research archive (ERA) ininternational health. This self-archive willbe owned by authors and administered bythe Lancet. Access will be unrestrictedthrough the ERA Web site: http://www.thelancet.com/newlancet/eprint
The objective is to create a searchableelectronic public library of research ininternational health. It is hoped to coverall issues relevant to medicine in the
developing world, and the Lancet is ap-pealing for support in its effort to makeknowledge accessible to all members ofthe international health community.
◆ ◆ ◆
SATELLIFE InformationServices’ new automaticresponse
There is a new and easy way tolearn about the free information servicesthat SATELLIFE makes available tohealth professionals, particularly thosein the developing world. Send a requestto <[email protected]> insert-ing no text in the body of your messageand leaving the subject line blank. Youwill soon receive details of SATELLIFE’sservices.
For further information see page 6. You can alsovisit SATELLIFE on the Web at: http://www.healthnet.org
◆ ◆ ◆
Drug Price Indicator Guideupdated
The International Drug Price IndicatorGuide, available on Management Sci-ences for Health Manager’s ElectronicResource Centre Web site at: http//erc.msh.org has been updated. Datafor the 1996, 1998, 1999 and 2000 edi-tions are on line. Search capabilities havealso been improved, and new featuresadded.
To obtain a print version of the 1999 Guide con-tact: the MSH Bookstore. Fax: + 1 617-524-2825,e-mail: [email protected]
◆ ◆ ◆
Children and medicinesThe United States Pharmacopoeia has
posted “References for Children andMedicines” with abstracts on its Web site:www.usp.org This is a 47-page documentwith references primarily relating to be-haviour, ethics and rates of use. Sendsuggestions for additions to Patricia J. Bush,e-mail: [email protected]
◆ ◆ ◆
Ordering WHO books onpharmaceuticals?
Check out WHO priced publicationson pharmaceuticals at: http://www.who.int/dsa/cat98/phar8htm
◆ ◆ ◆
No Free LunchNo Free Lunch, which is dedicated to
evidence-based health care, has createda listserve, called nofreelunchserve. Thelist is intended to serve as a forum for theexchange of ideas and information.
Subscribe at: http://[email protected]
◆ ◆ ◆
International Digest ofHealth Legislation on-linedatabase
The International Digest of Health Leg-islation contains a selection of national andinternational health legislation, mainly of-ficial publications and other documentsforwarded by WHO Member States. Sometexts are summarised, while only the titlesare given for others, but where possible
links are provided to other Web sitescontaining full texts of the legislation.
You can query a database by selecting a country,a subject, a volume, and by looking for a specifickeyword. Check out the site at: http://www.who.int/idhl
◆ ◆ ◆
HIF-net at WHOHIF-net at WHO is an e-mail discus-
sion list for people who want to improveaccess to reliable information for healthworkers in developing and transitionalcountries.
To join, send an email message tothe list moderator at: [email protected]
In the body of the message, say youwant to participate in HIF-net at WHO andadd a few lines about your professionalinterest in health information. This will beused as your HIF Participant Profile. Yourname will be added to the list and theWHO server will automatically send youa welcome message with details on howto participate.
For an information sheet on HIF-net atWHO, send an e-mail to: [email protected] leave the subject line blank, andin the message-box type: info hif-net
Messages to the whole list should besent to [email protected]
Health Information Forum (HIF) is runas an activity of the INASP-Health Pro-gramme, a cooperative network of partnerswhich aims to improve global access toinformation and knowledge.
Contact: Dr Neil Pakenham-Walsh, ProgrammeManager, INASP-Health, 27 Park End Street,Oxford OX1 1HU, UK. E-mail: [email protected]
Web site: http://www.inasp.org.uk
◆ ◆ ◆
C O U R S E S & M E E T I N G S
Lebanon hostsdrug policy seminar
The many issues surrounding drug pro-curement, production, regulation and use,and how best to develop, implement andevaluate a national drug policy were hotlydebated at a seminar held in Lebanon inOctober 2000. The event was organizedby Boston University’s Centre for Interna-tional Health and the Inter-MinisterialCouncil for Health Reform in Lebanon, incollaboration with WHO.
The seminar’s workshop format com-bined lectures, in-depth discussion of casestudies and small-group exercises, plusseveral field visits to health facilities andcommunity pharmacies. The meeting at-tracted policy-makers and senior managersresponsible for pharmaceutical systemsin developing and transitional countries,and senior officials of funding agenciesthroughout the region.
Previous seminars have been heldsuccessfully in Africa, India and the USA.
For information on future seminars contact: DrRichard Laing, Associate Professor of Interna-tional Health, Boston University School of PublicHealth, 715 Albany St, T4W, Boston MA 02118,USA. Tel: + 617 414-1444, fax: + 617 638-4476,e-mail: [email protected]
◆ ◆ ◆
N E T S C A N
Diploma in DrugEvaluation andPharmaceutical Sciences
Today’s potent drugs, combinedwith the complex issues of their produc-tion and use, have created a growingneed for evaluation of their safety andefficacy.
For such evaluation wide-ranging ex-pertise is required in the areas of chemistry,pharmaceutics, pharmacology and toxi-cology, clinical medicine, and legal andethical considerations.
The new Graduate Diploma inDrug Evaluation and PharmaceuticalSciences offered by the University ofMelbourne, Australia, offers a systematicoverview of these areas and how theyaffect drug evaluation. The course isaimed at pharmacists, research nurses,scientists and those involved in regulatoryaffairs.
For further information contact: Mrs Nicola Cash,Drug Evaluation Unit, Austin and RepatriationMedical Centre, Studley Road, HeidelbergVic 3084, Australia. Tel: + 61 3 9496 3420,fax: + 61 3 9459 3510, e-mail: [email protected]
◆ ◆ ◆
Zimbabwe hosts rational use courseThe next INRUD/MSH/EDM course on Promoting Rational Drug Use will be held at
Victoria Falls, Zimbabwe, from 26 August – 8 September 2001. Topics will includeidentifying drug use problems, developing and evaluating interventions and developingpublic and prescriber educational materials and campaigns. This highly participatorycourse is intended for physicians, pharmacists, health programme managers, policy-makers, researchers and others interested in improving the use of drugs.
For further information contact: PRDU course, NDTPAC, Directorate of Pharmacy Services, Ministry ofHealth and Child Welfare, Box CY924, Harare, Zimbabwe. Tel: + 263 4 730970 or + 263 4 795353,e-mail: [email protected]
◆ ◆ ◆
Community-based health education and healthpromotion course
A 10-week course to update managers, project and field staff on new developmentsin health education and health promotion will run from 30th April 2001 at Leeds Metro-politan University, UK. The course provides skills in research, planning, managementand evaluation of programme’s education and promotion components. Its flexible struc-ture allows participants to follow a topic of particular interest, and the chance to applytheir new skills to a problem from their own work-setting.
Applicants should have field experience/training in a subject area relevant to healthpromotion and a good working knowledge of English. The fee for academic tuition,course materials and field visits is £3600. In addition students will have to pay travel,subsistence and accommodation expenses.
For further information contact: Overseas Admissions Tutor, Health Education, Queens Square House,Leeds Metropolitan University, Calverley Street, Leeds, LS1 3HE, UK. Tel: + 44 113 2831915, fax: + 44113 2831916, e-mail: [email protected] or [email protected]
◆ ◆ ◆

33E S S E N T I A L D R U G S M O N I T O R
Issue No. 28 & 29, 2000
Now HIV/AIDS informationin French
The SAFCO (SIDA en Afrique duCentre et de l’Ouest) network has beenset up to encourage discussion and theelectronic exchange of information on is-sues related to HIV or AIDS in francophoneAfrica. To subscribe send a messageto: [email protected] (see page 3 for moredetails).
◆ ◆ ◆
What’s new onEDM’s homepage?
The Department of Essential Drugs andMedicines Policy’s homepage is continu-ing to expand and become more userfriendly. As well as introducing the essen-tial drugs concept, national drug policies,and the work of WHO and EDM, manymore of the Department’s documents can
be viewed and downloaded.Among recent highlights are the
addition of Operational Principles forGood Pharmaceutical Procurement (seebelow) and Quality Assurance of Pharma-ceuticals. A Compendium of Guidelinesand Related Materials. Volume 2. GoodManufacturing Practices and Inspection.The WHO Medicines Strategy: Frame-work for Action in Essential Drugs andMedicines Policy 2000–2003 is nowavailable electronically, as is the docu-ment Essential Drugs used in the Care ofPeople Living with HIV: Sources and Prices.Some documents in EDM’s Health Econom-ics and Research Series can also bedownloaded.
The complete English, French andSpanish versions of the Monitor (fromnumber 23 onwards) can be found inPDF format.
Check us out at: http://www.who.int/medicines
◆ ◆ ◆
P U B L I S H E D L A T E L Y
ImportantThe Department of Essential Drugs and MedicinesPolicy cannot supply the publications reviewed onthese pages unless stated otherwise.
Please write to the address given at the end ofeach item.
HIV Testing: A Practical Approach, Healthlink Worldwide, 1999, 48 p.
Intellectual Property Rights, the WTO and Developing Countries. TheTRIPS Agreement and Policy Options, C.M. Correa, 2000, 254 p.
Operational Principles for GoodPharmaceutical Procurement,Interagency Guidelines, WorldHealth Organization, WHO/EDM/PAR/99.5, 2000, 24 p.
Pharmaceutical procurement is a complexprocess and problems are common. This docu-ment from the Interagency PharmaceuticalProcurement Group sets out four strategic ob-jectives and 12 operational principles for goodprocurement. These will be reproduced in fullin EDM-30.
Handbook on AntimicrobialTherapy, (revised edition), TheMedical Letter on Drugs andTherapeutics, 1998, 205 p.
This comprehensive handbook onantibacterials, antifungal and antiviral drugsincludes first-choice and alternative drugs forevery indication, doses and adverse effects.In addition there are chapters on the safety ofantimicrobial drugs in pregnancy, advice fortravellers and drugs for HIV infections. Thenon profit publication also includes price listsfor commonly used oral antibacterial drugs.
Available from: The Medical Letter onDrugs and Therapeutics, 1000 Main Street,New Rochelle, N.Y. 10801-7537, USA. Fax:+ 1 914 632 1733. Price 1–9 copies US$14each, 10–99 copies US$11.20 each, 100+copies US$8.40 each. Special rates are avail-able for subscribers to the journal, TheMedical Letter on Drugs and Therapeutics.
Référentiel pour l’harmonisation des procédures d’enregistrement desmédicaments essentiels génériques dans les pays de la zone franc etpays associés, (Pharmaceutical Sector Collaboration between CFA andAssociated Countries), World Health Organization, WHO/EDM/DAP/99.2, 1999, 25 p.
This guide on harmonization of registration procedures is intended to facilitate the intro-duction of essential drugs on to the markets of Communauté financière africaine (CFA) andassociated countries, and thus improve the availability and affordability of pharmaceuticals.The guidelines, adopted at a seminar in Ouagadougou in February 1999, cover generic drugregistration and marketing authorisation.
Available, free of charge, from: Department of Essential Drugs and Medicines Policy, WorldHealth Organization, 1211 Geneva 27, Switzerland.
Counterfeit and Substandard Drugs in Myanmar and Viet Nam, WorldHealth Organization, EDM Research Series No. 29, WHO/EDM/QSM/99.3, 1999, 55 p.
This report presents the results of two studies, done in Myanmar and Viet Nam, to obtainindependent information on the counterfeit drugs problem, and so help to develop measuresagainst counterfeiting. The research study involved collecting background information on thestatus of drug regulation and also samples of 500 products, which were subjected to laboratoryquality testing. Two hundred and fourteen of these were selected for investigation, with a por-tion of each sent to the drug regulatory authorities in the manufacturing country for analysis.
The report shows that the prevalence of substandard drugs is generally a much greaterproblem than counterfeit drugs in both countries. Products which had passed laboratory testswere sometimes found to be counterfeit (deliberately mislabelled products, for example). Thereport concludes that laboratory tests alone are insufficient to determine whether a product iscounterfeit. Any investigation requires adequate resources, planning, and undercover work,and must be undertaken in collaboration with drug regulatory authorities and manufacturers.
Available, free of charge, from: Department of Essential Drugs and Medicines Policy, WorldHealth Organization, 1211 Geneva 27, Switzerland.
Pharm-policye-discussion group
Discussions in this group cover phar-maceutical policies, particularly thoseinvolving intellectual property, technologytransfer and pricing. Anything significantgets on this discussion group within 24hours: http://lists.essential.org/mailman/listinfo/pharm-policy
◆ ◆ ◆
New Medline search toolBioMail periodically does a user-
customised Medline search and sends allmatching articles recently added toMedline to the users’ e-mail address. Medi-cal researchers and biologists wantingregular updates from journal articles willbenefit from the service, which is free ofcharge. It will be particularly useful forcountries where access to the Internet is
not yet widely available. If people have apermanent e-mail address, but only spo-radic access to the World Wide Web, theyonly need to fill out a BioMail form onceand they will receive new references fromMedline continually.
Find out more at: http://biomail.sourceforge.net/biomail/
Links to other free alert sites:Pubcrawler is another Medline alert
service, available through the Departmentof Genetics, Trinity College, Dublin,Ireland: http://www.pubcrawler.ie
PubMed Query tool: BiotechnologyComputing Facility, Arizona ResearchLaboratories, USA, at: http://bcf.arl.arizona.edu/query/add.html
JADE: also a Medline alert service, TheNational Center for Emergency MedicineInformatics in the USA: http://biodigital.org/jade/
◆ ◆ ◆
N E T S C A N
The structure of international trade isbeing fundamentally altered by the variousagreements which the World Trade Organi-zation polices. This book cuts through thesometimes daunting technicalities of one ofthe most important of these agreements, thatdealing with intellectual property rights. Thepublication clearly explains what the Agree-ment on Trade-Related Aspects of IntellectualProperty Rights (TRIPS) is about and its mainprovisions.
The author is particularly concerned toexplore the Agreement’s implications fordeveloping countries. These relate to thefuture of local research and development, ac-cess to advanced technology, commercial
exploitation of their natural resources andwelfare effects. The book uses Latin Ameri-can and Caribbean experience to illustrate theproblems that have arisen with implementingTRIPS.
Throughout, Correa indicates concreteoptions available at national level to imple-ment the TRIPS Agreement’s provisions in amanner consistent with development objec-tives and public policy concerns. (See alsopage 36).
Available from: Zed Books, 7 Cynthia Street,London N1 9JF, UK. Price: £16.95, plus £2.50postage and packing.
Available, free ofcharge, from: Depart-ment of EssentialDrugs and MedicinesPolicy, World HealthOrganization, 1211Geneva 27, Switzer-land.
HIV testing is an essential part of all HIVprevention and care programmes, to ensuresafe blood supplies and determine HIV sta-tus. And appropriate counselling, education,care and follow-up support are an essentialpart of any HIV testing programme.
HIV testing: a practical approach pro-vides clear information for policy-makers,planners, and health personnel involved incounselling and HIV testing. An update of the1994 publication, Practical issues in HIV test-ing, it reflects recent developments, andlessons learned over the last six years. Topicscovered include: considerations before be-ginning an HIV testing programme; tech-nical aspects of testing, testing individuals
and surveillance; and implementing bloodscreening programmes.
In addition, the publication provides ex-amples of programmes in Africa, Asia andLatin America, and experiences from peoplewho have had HIV tests. A useful resourcelist and detailed technical information on thecharacteristics of some of the most commonlyused tests are also given.
Available from: Healthlink Worldwide,Cityside, 40 Adler Street, London E1 1EE, UK.E-mail: [email protected]: £7.50/US$15. Single copies are freeof charge to indigenous organizations indeveloping countries.

34 E S S E N T I A L D R U G S M O N I T O R
Issue No. 28 & 29, 2000
Globalization, Patents and Drugs: An Annotated Bibliography, 2nd ed.,World Health Organization, Health Economics and Drugs, EDM SeriesNo.10, EDM/PAR/01.1, 2001, 52 p.
Guidelines for the Regulatory Assessment of Medicinal Products for Usein Self-Medication, World Health Organization, WHO/EDM/QSM/00.1,2000, 32 p.
Reclassification of medicinal products from sale on prescription only to non prescription(over-the-counter) sale is increasingly common. Drug regulatory and health authorities have toconsider the types of medicinal products for which reclassification is appropriate, safe andrational in the interest of public health.
The Guidelines suggest criteria and methods which drug regulatory agencies can use todetermine the suitability of medicinal products for use in self-medication. They are also in-tended for marketing authorisation holders applying for the classification of a prescriptionproduct to be changed to non prescription sale. Guidance is given on documentation for newactive substances, never marketed as prescription medicines, to accompany applications forself-medication marketing authorisation.
Available from: World Health Organization, Marketing and Dissemination, 1211 Geneva 27,Switzerland. Price: Sw.fr.10, US$9, and in developing countries Sw.fr.7.
Beyond Our Means? The Cost of Treating HIV/AIDS in the DevelopingWorld, The Panos Institute, 2000, 59 p.
Narcotic and Psychotropic Drugs. Achieving Balance in NationalOpioids Control Policy. Guidelines for Assessment, World HealthOrganization, WHO/EDM/QSM/2000.4, 2000, 37 p.
WHO estimates that by the year 2020 approximately 70% of the annual 20 million newcancer cases will occur in developing countries, where most patients are diagnosed in the latestages of the disease. It is at this time that pain is most prevalent. But cancer pain is frequentlyuntreated and, even when it is, relief is often inadequate. While health worker training andincreased access to palliative care services can help, the publication focuses on solving theproblem of inadequate availability and use of pain medications, particularly opioid analgesics,in developing countries.
The authors state that opioid analgesics, such as codeine and morphine are “absolutelynecessary” for the management of cancer pain and that for moderate to severe pain there is nosubstitute for opioids in the therapeutic group of morphine. But, because of their potential forabuse, opioids are classified as narcotic drugs.
The International Narcotics Control Board, WHO and national governments report thatopioids are not sufficiently available for medical purposes. Reasons for this include the lowpriority of pain care in health systems, greatly exaggerated fears of addiction, overly restrictivenational drug control policies and problems in procurement, manufacture and distribution ofopioids. The publication presents guidelines for governments to determine whether their na-tional drug control policies have the legal and administrative framework to ensure medicalavailability of opioid analgesics, as recommended by the International Narcotics Control Board.
Available, free of charge from: Department of Essential Drugs and Medicines Policy, WorldHealth Organization, 1211 Geneva 27, Switzerland.
Integrating Public Health Concerns into Patent Legislation in DevelopingCountries, C. Correa, South Centre, 2000, 124 p.
The Department of Essential Drugs and Medicines Policy produces a global index offormularies, therapeutic guides and essential drugs lists, which is available free of charge.(Please note that we are unable to supply copies of the publications themselves. Requestsshould be addressed direct to the countries concerned). Some recent additions are:
◆ India, Himachal Pradesh: List of Essential Drugs. 1999. Department of Health andFamily Welfare, Government of Himachal Pradesh. Drugs by generic name, dividedinto 29 therapeutic groups.
◆ Médecins Sans Frontières: Essential Drugs: Practical Guidelines. New editions ofthis useful manual for doctors, pharmacists, nurses and medical auxiliaries are avail-able. A first edition in Portuguese, and second editions in English and Spanish, willsoon be followed by a second edition in Arabic.
◆ Nepal: Standard Treatment Schedules for Health Posts and Sub-Health Posts,3rd ed., 1999. Ministry of Health. Now available in English and Nepali. Includesprinciples of appropriate prescribing and dispensing, and advice for patients.
◆ Russia: Formulary 2000 (Russian Formulary System). 2000. Health of Men Founda-tion, Moscow. Guidelines for doctors on drug use. Approved and recommended bythe Russian Federation Ministry of Health. In Russian.
◆ South Africa: Treatment Guidelines from South Africa’s Department of Healthinclude:– National Guideline on Management and Control of Asthma in Children at Primary
Level. 1999.– National Guideline on Primary Prevention and Prophylaxis of Rheumatic Fever
and Rheumatic Heart for Health Professionals at Primary Level. 1999.– Hypertension: National Programme for Control and Management at Primary Level.
1998.– Diabetes: National Programme for Control and Management of Diabetes Type 2
at Primary Level. 1998.◆ South-East Asia: Essential Drugs for Primary Health Care, 3rd edition. 2000. WHO
Regional Office for South-East Asia. The manual provides community healthworkers and auxiliary health personnel with guidelines on the use of 34 essentialdrugs. It also advises on treatment and referral requirements for 22 common medicalproblems.
◆ Zimbabwe: EDLIZ. 4th Essential Drugs List and Standard Treatment Guidelines.2000. Ministry of Health and Child Welfare. Fewer drugs on the list (from 600 downto 250) and updated advice for Zimbabwe’s health workers.
Drug bulletins and newsletters◆ Introducing Essential Drugs in Brief. Anyone involved in national drug policy im-
plementation who wants a quick update on the latest WHO activities carried out withand for countries should subscribe to the bulletin, Essential Drugs in Brief. The bul-letin, which will be published twice a year, shares information on the latest countrysupport provided or coordinated by EDM’s extended Drug Action Programme teamthrough country, regional and Headquarters’ offices.
◆ And a new look for the WHO Pharmaceuticals Newsletter, which has been rede-signed and has had some content changes. Articles will be restricted to subjects moredirectly related to drug quality assurance and safety. Some more general information,such as new developments, guidelines, and regulations of a general nature, will bepublished only in the quarterly journal WHO Drug Information. The WHO Collabo-rating Centre is now providing the Safety of Medicines section for International DrugMonitoring. The Centre’s Adverse Reactions Newsletter is being discontinued.
◆ With WHO support the Delhi Society for the Promotion of Rational Use of Drugs(DSPRUD) launched its Medical Newsletter in July 1999, to help health care profes-sionals update existing knowledge about drug therapy. Distributed free of charge todoctors, the Newsletter contains a digest of various published articles, which includedrug reactions, news and review articles.
Updates on new formularies, treatment guidelines,essential drugs lists, drug bulletins and newsletters
The impact of globalisation and tradeagreements on access to drugs is an increas-ingly important issue. This annotatedbibliography is intended for those in the healthsector with no particular legal background,who want an overview of the issues and argu-ments involved. It directs readers to keyreports, books and articles from technical andscientific journals, subdivided into general
articles and country specific studies. Thedocument concludes with a section on usefulWeb sites.
Available, free of charge, from: Departmentof Essential Drugs and Medicines Policy,World Health Organization, 1211 Geneva 27,Switzerland.
◆ WHO/EDM is also supporting Spectrum, India-WHO Es-sential Drugs Programme Newsletter, which covers theactivities of the Delhi Society for the Promotion of RationalDrug Use and the Essential Drugs Programme.
◆ Practical Pharmacy packs. Complete sets of Practical Phar-macy are now available to developing countries, free ofcharge, while stocks last. This newsletter for health work-ers of all levels includes easy-to-read information on basicaspects and skills of pharmacy work. Contact: Echo Inter-national Health Services Ltd, Ullswater Crescent, Coulsdon,Surrey CR5 2HR, UK. Tel: + 44 20 8660 2220, fax: + 44 208668 0751.
This report looks at the controversial andcomplex issues surrounding access to HIV/AIDS treatments in developing countries. Itstates that at least 12 million people in thedeveloping world are in urgent need of theantiretroviral drugs which can suppress HIVand indefinitely postpone symptoms of AIDS.But the vast majority of these people live inthe world’s poorest countries, and while pro-viding such treatment is theoretically possible,it is highly improbable in the foreseeablefuture, according to the authors.
A number of factors lie behind this fail-ure to provide full treatment to those in need.These vary from country to country, but, ac-cording to the publication, include lack ofpolitical will, unhelpful economic policies(such as taxing medical products), lack of rel-evant information and lack of appropriatedistribution mechanisms. The authors believetwo other factors are critical. The first is weak
health care systems – poor infrastructures,inadequate facilities, including lack of hospi-tal beds, laboratories and trained staff. Thesecond factor is a combination of the high costof antiretroviral and other drugs, and disputesover patenting and licensing rights for theseproducts.
The publication provides an overview ofthe issues surrounding access to treatment forAIDS, in order to encourage informed debate,further research and considered action. It isintended primarily for policy-makers, AIDSorganizations and medical personnel.
Available from: The Panos AIDS Programme,9 White Lion Street, London N1 9PD, UK.Tel: + 44 20 7278 1111, fax: 44 20 7278 0345.Available on the Panos Web site: www.panos.org.uk Price: £5/US$10. Copies areavailable, free of charge, to resource-poorNGOs in developing countries.
This publication presents options forthe design and implementation of public-health sensitive patent policies in developingcountries. It is particularly concerned withthe TRIPS Agreement (Trade-Related Aspectsof Intellectual Property Rights) which coversprotection of pharmaceutical products andprocesses. World Trade Organization mem-ber countries are obliged to comply with theminimum standards of the Agreement. But,the author points out, they also have con-siderable room to develop their own patentand other intellectual property laws in re-sponse to the characteristics of their legalsystems and development needs. Topics
covered include patentability requirements,special cases in pharmaceuticals, disclosure,exceptions to exclusive rights and compulsorylicensing.
The publication is primarily intended forpolicy-makers, particularly ministries ofhealth and government lawyers responsiblefor drafting TRIPS compliant nationallegislation. For further details see page 36.
Available, free of charge, from: South Cen-tre, Case Postale 228, 1211 Geneva 19,Switzerland. Also available on the SouthCentre Web site at: www.southcentre.org/publications/publichealth/toc.htm
P U B L I S H E D L A T E L Y

35E S S E N T I A L D R U G S M O N I T O R
Issue No. 28 & 29, 2000
W
Delhi Declarationon trade issues
Fears over new regional patentagreement
Research focuses ontraditional antimalarials
India: protectingits heritage ofmedicinal plants
he Indian Government is settingup a programme to protect andpromote its rich tradition in her-bal medicines. One of the main
aims is to prepare standardised formula-tions of traditional medicines that willundergo the same regulatory procedures,including clinical trials, as modernpharmaceuticals.
A new Department for Indian Systemsof Medicines and Homeopathy has been
by a non profit NGO assisted by an ad-visory panel of international experts,and it is hoped that other internationalorganizations will become involved.
Drawing on localknowledge
One of the programme’s key elementsis the involvement of local people, whowill be employed to identify, document
W O R L D T R A D E
T R A D I T I O N A L M E D I C I N E
balancing of rights and obligations under the TRIPS Agreement was one ofthe main demands of the Delhi Declaration released at the end of a two-day workshop on trade issues held in New Delhi in October 1999. In ahard-hitting statement the 65 delegates called for strong, clearly defined
compulsory licensing provisions; protection of traditional knowledge from all formsof patenting; and strengthening of existing anti-monopoly practices by developingcountries.
Participants argued that as international trade agreements contribute to widen-ing the socioeconomic and technological gap between developed and developingcountries, it is necessary to have an alternative framework, incorporating greaterself-reliance.
As well as the TRIPS (Trade-related Aspects of Intellectual Property Rights)Agreement the national and international experts present also addressed issuessuch as food security, competition policies and electronic commerce.
The International Brainstorming Workshop on World Trade OrganizationAgreements and People’s Concerns was organized by the Centre for Study ofGlobal Trade System and Development and the National Working Group onPatent Laws. ❏
Copies of the Delhi Declaration are available from: Centre for Study of Global TradeSystem and Development, A-388, Sarita Vihar, New Delhi 110 044, India. Tel/fax: + 91 11694 7403, e-mail: [email protected]
AA
T
ith modern pharmaceuticalsoften unavailable and unafford-able in the areas most affectedby malaria, and drug resistance
increasing, the use of herbal anti-malarials is very common. But therehas been almost no research into theirclinical effectiveness.
Developing a strategy for moreevidence-based use of traditionalmedicines against malaria, has ledWHO’s Special Programme for Re-search and Training in Tropical Medi-cine to team up with the UK’s GlobalInitiative for Traditional Systems ofHealth. They have formed a ResearchInitiative on Traditional Antimalarials,and in November 1999 the two groupsco-sponsored a meeting in Moshi,
Tanzania, to move the process forward.Delegates included biological and
social scientists, doctors, traditionalhealers and policy-makers from Africa,Asia, Europe and the Americas. Theydeveloped four specialist groups toimplement a research strategy whichwill contribute to malaria control pro-grammes. The topics covered by thegroups are: policy, advocacy andfunding; pre-clinical studies; clinicaldevelopment; and repellance andvector control.
Future plans include updating theResearch Initiative’s database of tradi-tional treatments for malaria, andregulatory guidelines for traditionalmedicines and natural products, casestudies of their use, clinical efficacy,
Research intoherbal antimalarialsaims to improve theplight of sufferers,such as this patientin Congo
safety, screen-ing and clinicalevaluation. ❏
Source: TDR News,June 2000.
Phot
o: W
HO
/H
. Ane
nden
set up and a Biodiversity Bill is go-ing through Parliament. This willestablish a National BiodiversityBoard to oversee access to and use ofmedicinal plants, as well as applyingfor patents when appropriate.
Clinical trialsA pilot project will begin in the
Western Ghats region, where expertswill study and document medicinalplants. A small formulations unit willprocess plants into medicines, whichwill then undergo clinical trials to in-ternational standards. This work will formpart of a digital database of India’s tradi-tional knowledge, which will be includedin the World Intellectual Property Organi-zation’s patent classification system, andmade available to patent offices worldwide. The Government hopes the movewill help to prevent patents being grantedon traditional Indian plants and remedies.
The pilot programme will be run
and cultivate the plants, and participatein running the formulations unit andtherapeutic centre. There are plans to in-volve local schools, and to set up a homefor the elderly who will be encouraged topass on their knowledge of local plantsand their uses. ❏
Source: Scrip No.2547, 9 June 2000.
Crushing and storing medicinal plants at aprocessing plant in Kanzicode, India
Phot
o: W
HO
/A
. Koc
har
new agreement on patent protec-tion for medicines could endangerpeople’s health in some of Africa’spoorest nations, according to
Médecins Sans Frontières. The organizationhas urged countries not to ratify the BanguiAccord, created last year by 15 French-speaking African nations. In these countries,patents are granted through the African In-tellectual Property Organization (OAPI),which acts as a patent office for all its Mem-ber States. Patents are granted and regulatedaccording to the Bangui Agreement (signedin 1977), which was recently revised tocomply with WTO rules, increasing patentprotection from 10 to 20 years.
A report1 issued jointly by WHO,UNAIDS and MSF says the new treaty,which has not yet come into force, couldlead to increased prices for medicines. Thisis because the new Bangui Agreement ismore stringent than the TRIPS Agreementand provides little come back in case ofpatent abuse, the report states. Compulsorylicences are only available provided thatthe patented drug can be manufacturedlocally, yet there is little manufacturingcapacity in the region. Parallel imports are
only possible between OAPI Member Stateswhereas lower prices might be found inother parts of the world.
OAPI counters that in revising the Ban-gui Accord Member States have affirmedtheir conviction that bringing intellectualproperty rights into line with the TRIPSAgreement will attract investors and stimu-late technology transfer. In an InformationMemo* the Organization says that its crit-ics need to look elsewhere for the reasonswhy many Africans lack access to essentialdrugs.
Under WTO rules, the so-called “least-developed countries” – 10 of which arecovered by the Bangui Accord – have untilJanuary 2006 to change their patent sys-tems. But if the Accord is ratified by at least10 members, countries will find themselvesforced to change their systems immediately.So far eight nations have ratified. ❏
Reference1. MSF/WHO. Revue of the pharmaceutical policy in
Cameroon – Medicine patents in francophone Africa.Joint Mission MSF-WHO-UNAIDS. Geneva: MédecinsSans Frontières and World Health Organization; 2000.(Available in English and French).
* The Information Memo is available on the web at:http://www.oapi.wipo.net/

36 E S S E N T I A L D R U G S M O N I T O R
Issue No. 28 & 29, 2000
Patents from a publichealth perspective
➢ CARLOS CORREA*
he Agreement on Trade-RelatedAspects of Intellectual PropertyRights (TRIPS) requires all WTOMember Countries to adapt their
laws to the minimum standards set forthby the Agreement, within establishedtransitional periods. Developing countriesface a special challenge in conformingto international trade obligations, par-ticularly the TRIPS Agreement whichcovers intellectual property rights ofpharmaceutical products and processes.
The way in which countries reformtheir legislation may have a significantimpact on public health policies, and par-ticularly on access to drugs. Any propertyrights system must strike a balance be-tween creating incentives for innovation,and people’s need for availability andaffordability of protected goods. So whenthey draw up their own intellectualproperty rights rules, it is important thatdeveloping countries realise the scopethey have – within the framework of in-ternational treaties – to produce their ownpatent laws.
The TRIPS Agreement does not es-tablish a uniform international law oreven uniform legal requirements. WorldTrade Organization Member Countriesmust comply with the Agreement’s mini-mum standards. But countries maylegitimately adopt regulations that ensurea balance between the minimum stand-ards of intellectual property protectionand the public good. Moreover, they canadopt measures which are conducive tosocial and economic welfare (Article 7of the Agreement). These include stepsnecessary to protect public health, nutri-tion and the public interest in sectors ofvital importance for socio-economic andtechnological development. Countriescan also adopt measures to prevent theabuse of intellectual property rights(Article 8.1 and 8.2).
In those countries that are bound tointroduce patent protection for pharma-ceuticals as a result of TRIPS, patents willonly be available for products for whicha patent application was filed after 1 Janu-ary 1995. This means that other products(including those already applied for orpatented in other countries, or marketedbefore that date) will remain in the pub-lic domain. The exception is where thenational law permits retroactive protec-tion of the so-called “pipeline” products,as is the case in Brazil.
Scope for nationaldifferences
Given diverse national objectives, itis not surprising that different countries’patent systems diverge, in some casessignificantly. There is no single “patentsystem”. Moreover the solutions adoptedin particular countries have changed overtime. They treat specific patent issues –
including eligibility requirements, scopeof protection, exceptions to exclusiverights and compulsory licences – in quitedifferent ways. In drawing up their ownintellectual property rights rules, policy-and law-makers in developing countriesneed to be aware of this. They will bemost successful in meeting their ownneeds if they can draw on the experiencesof national systems worldwide.
Some countries – particularly devel-oped countries – have opted for legalsystems that confer strong patent rights.They have done so in order to protect rev-enues from their already establishedtechnological base and to promote in-vestment in technological innovation.Considerable debate exists in such coun-tries, however, on the level and scope ofprotection which are optimal to foster in-novation without unduly restricting thefree circulation of ideas and stifling com-petition. A growing concern is voiced insome countries on the shortcomings ofthe examination process and the prolif-eration of low quality patents. Moreover,the economics of patent law is still an un-certain area, for which a robust theoreticalframework and empirical evidence arelacking.
Checks and balances
Countries with less advanced tech-nologies may prefer to promote thetransfer of those technologies needed fordevelopment, and to preserve and en-hance competition. They do so in orderto secure access to goods, services andtechnologies on the most favourablemarket conditions. Even in countries withthe strongest intellectual property rightsprotection, national laws provide forchecks and balances, to protect againstpossible abuse of the powers conferredby protection.
Policy-makers should consider cross-cutting issues when they design a nationalpatent system, for example: protection ofpublic health and the environment; pro-motion of competition and technologytransfer; protection of consumers; andsupport for small local inventors. Coun-tries should also respect inventors’ rightsto a reward for contributions to technicalprogress. Other regulatory measuresaffecting public health, such as thoserelating to medicines’ registration, mustbe carefully considered, so that there is aconsistent legal framework that improvesaccess to medicines.
Health-sensitiveapproach
A health-sensitive approach to patentlegislation might address short-termemergencies that justify different tempo-rary measures (for instance, medicines’supply in cases of epidemics or naturaldisasters). Or the approach may be part
more than 880 million people lack accessto health care. Of the more than 33 mil-lion HIV-positive people in the world,95% live in developing countries, andmost of them cannot afford requireddrugs. To deal with this dramatic situa-tion, an integrated approach to the deeplyinter-related issues of national healthpolicy, pharmaceutical policy and patentpolicy is required. None of these poli-cies can be framed or implemented inisolation.
If developing countries are not to bedisadvantaged by new trade rules, they
Tof an integrated medium- or long-termpatent policy. In some cases, a countrymay – within limits permitted by itsinternational obligations – opt for differ-ent levels of protection in different areasof intellectual property. The level woulddepend on its competitive position and theexpected role of national and foreign in-vestors and technology suppliers. It may,for instance, be possible to emphasiseprotection for information technologies,through high levels of copyright pro-tection for computer programmes anddatabases. At the same time lower levels
of protection may be given in areas wherelocal industrial and technological ca-pabilities are low, and unlikely to besignificantly improved through a highstandard of patent protection.
The way in which such options areimplemented should be consistent withthe country’s level of development, par-ticularly its research and manufacturingcapabilities in the pharmaceutical sector.The options followed by a large develop-ing country with significant capabilitiesmay differ from those preferred by a smalleconomy which is totally or substantiallydependent on foreign supplies of pharma-ceuticals. Likewise, patent laws mayevolve as a country develops. It shouldbe remembered, however, that problemsof access to drugs caused by povertyand low income are common to mostdeveloping countries.
Consideringoptions
The protection of public health is oneof the most pressing issues in developingcountries. A large part of the global popu-lation still lacks access to essential drugs.In the poorest parts of Africa, for instance,over 50% of the population lack that ac-cess. An estimated 1,5 billion people arenot expected to survive to age 60, and
must look at options for designing andimplementing public-health-sensitivepatent policies. There must be a balancebetween the public and private interestsinvolved, including the rights of states,patients and suppliers of health-relatedgoods and services. ❏
* Carlos Correa is Director of the MastersProgramme on Science and TechnologyPolicy and Management at the University ofBuenos Aires, Argentina. He is a specialistin global intellectual property law, and wasinvolved in the negotiations on TRIPS duringthe Uruguay Round of trade negotiations. Fur-ther information on legal options for drawingup TRIPS-compatible national legislation canbe found in Professor Correa’s new books,Integrating public health concerns into pat-ent legislation in developing countries, andIntellectual property rights, the WTO and de-veloping countries. (See Published Latelypages 33 and 34).
Other useful documents include Globaliza-tion and access to drugs. Perspectives on theWTO/TRIPS Agreement. Health Economicsand Drugs, EDM Series No. 7, and Globali-zation, patents and drugs: an annotatedbibliography, Second edition. Health Eco-nomics and Drugs, EDM Series No. 10. Bothdocuments are available, free of charge,from: Department of Essential Drugs andMedicines Policy, World Health Organiza-tion, 1211 Geneva 27, Switzerland.
Phot
o: W
HO
/PA
HO
/C
. Gag
gero
W O R L D T R A D E
Taking the medicine in Guatemala. International trade agreements don’t just affect people in therich industrialised nations