Antihypertensive Dmg Treatment - Oxford Academic
28
POSTERS: Antihypertensive Dmg Treatment Ft HYPOTENSIVE EFFECT AND CARDIAC WORKLOAD CHANGES INDUCED BY METOCLOPRAMIDE IN HYPERTENSIVE PATIENTS. Blanco M,Vasquez M,Vargas R,Trias Y,Palomo D,Rodriguez Mand Velasco M*. Clinical Pharmacology Unit, Vargas Medica! School,Central University of Venezuela Caracas, Venezuela,S.A. Metoclopramide(MTC)a DA2 doparninergic blocker reduces blood pressure both in normotensive and hypertensive subjects during cold pressor test(Blanco M,Amer.J.Therap.in press, 1995), exercise treadmill test (Blanco et al,submitted for publication, 1995).1n the present study we are reporting the hypotensive effect induced by intraveneus MTC in hypertensive patients without changes in cardiac workload. Eleven( 11) hypertensive subjects were studied After an hour resting period, subjects were submilled to the following protocol:Two placebo periods 5% glucose solution infusion i.v. during 30 min were administered before and after a drug treatment period of MTC at the rate of7.5uglkglmin for 30min period.At the end ofeach period and during MTC infusion(every five minutes) blood pressure and heart rate measurements were done.Cardiac work load was calculated by the product of systolic blood pressure and heart rate. MTC lowered blood pressure from 146±3.52/90±4.27 mmHg to 138±6.26/84±4.09 mmHg at 30 min period (p<0.03; p<0.001for systolic/diastolic values, respectively) However,diastolic blood pressure lowered at IOmin until 30 min period(p<O.OOI) and heart rate was increased at 20 min until 30 min period(p<0.01).2) MTC did nol alter cardiac workload at any time period. The hypotensive effect of MTC in hypertensive patients is in agreement with previous report from our Iaberatory in which we found the same hypotensive effect in untrained,trained normotensive subjects. We have also shown that MTC caused a decrease in blood pressure and cardiac workload during cold pressor test and exercise treadmill test both in normotensive and hypertensive subjects.2)MTC induces this hypotensive effect by cardiac and peripheral actions and possible through CNS actions.3)Controlled trials should be done in patients with hypertension,hypertensive crisis and in pregnancy- induced hypertension. Key Words: hypertension,metoclopramide,cardiac workload, hypotensive effect. F3 A TTENUATED METOCLOPRAMIDE-INDUCED V ASCULAR HYPERREACTIVITY TO COLD PRESSOK STRESS IN ATHLETIC SUBJECTS. Velasco M*.Jelambi l,Perez G,Franco T,Hurtado N and M.Bianco. Clinical Pharmacology Unit,Vargas Medica( School,Central University ofVenezuela,Caracas Venezuela,S.A Cold exposure(CPT) increases blood pressure in normotensive and hypertensive subjects.Metocloprarnide(MTC) A known DA2 dopaminergic blocker, induces vascular hyperreactivity in normotensive untrained subjects. We have performed this work to evaluate the MTC-induced vascular reactivity in trained subjects to know a probable dopaminergic influence. Twenty(20)untrained normotensive subjects and thirty two(32)trained normotensive subjects(football players and runners)were studied.Subjects received two 5%glucose solutions periods before and after an intraveneus MTC infusion at the dose of 7 .5ug!Kglmin period duration.At the end of each period blood pressure and heart rate were measured. Normotensive untrained subjects responded with increase in blood pressure after CPT (17.2 vs 21.4 mmHg systolic,and 17.9 vs 24.lmmHg diastolic)before and after MTC administration.Football players responded with increase in blood pressure after CPT, however systolic blood pressure response was rather minor.Runners responded with increase in blood pressure after CPT(I7.8 vs 18.7mmHg systolic,and 15.8 vs 13.9mmHg diastolic)before and after MTC administration.Heart rate only increased in trained subjects prior to MTC. Conclusions: 1 )Metoclopramide-induced vascular hyperreactivity was nol evident in trained. subjects,2)Cardiovascular responses to CPT are attenuated in athletic subjects as compared to those in untrained subjects,and 3)This may meao a probable dopaminergic system adaptation during exercise. Key Words: cold pressor test,metoclopramide,athletic subjects AJH 1996; 9:140A-167A F2 VERAPAMIL SR 180 MG, TAANDOLAPRIL 2 MG AND THE FIXED COMBINATION THEREOF FOR THE TREATMENT OF MODERATE ESSENTIAL HYPERTENSION. JR Viskoper'; R Dies"; P Zilles". •sarzilai Medica! Centre, Ashkelon, Israel; •• Knoll AG, Ludwigshafen, Germany A multicentre, double-blind, randomized, parallel group comparison was performed to evaluate !he superiority of the fixed combination verapamil SR!trandolapril 180/2 mg (VT) over both monocompounds verapamil SR 180 mg and Irandolapril 2 mg. Alter a 4 week placebo run-in period 310 patients with moderate hypertension (diast.BP 100 to 109 mmHg) were treated with either Irandolapril 2 mg o.d. (Tran) or verapamil SR 180 mg o.d. (VSR) or !he combination verapamil SR/trandolapril 180/2 mg o.d. (VT) lor eight weeks. Sitting office blood pressure was measured conventionally in the morning (trough) and additionally in a subgroup of patients (n=90) 24h-ABPM was performed. The treatment groups were well matehad lor demographic data as well as lor baseline blood pressure values. Mean conventionally measured sitting blood pressure was reduced under VSR by 10.319.6 mmHg, Tran 12.5/10.9 mmHg and VT 17.6/13.2 mmHg. The fixed combination VT was highly significant (p = 0.0109, Snapinn's Tal superior over bolh monocompounds. 24h total time mean blood pressure was decreased under VSR by 2.6/3.8 mmHg, Tran 10.0/5.2 mmHg and VT 16.8/11.1 mmHg. The p value lor superiority of VT over both monocompounds was 0.0021 (Snappin's Tal· All three traalment regimes were welltolerated. The incidence of adverse events was 23 to 25 % in all treatment groups. The most frequent adverse events were constipation (7, 1, 6 pis. VSR, Tran, VT), cough (2, 7, 5 pts.) and asthenia (2, 4, 3 pis.) So there was no evidence of an increase of adverse effects lor !he combination. Alllhree active treatments employed in lhis study reduced blood pressure with clear superiority of VT. Adverse even! rates were low and similar in alltreatment groups. Key Words: Trandolapril, verapamil, combination treatment, 24h-ABPM F4 ARE ANTIHYPERTENSIVE AGENTS SIMILAR IN AFFECTING CIRCADIAN VARlATION OF BLOOD PRESSURE? Y Mochizuki, M Okutani, H lwasaki, I Kohno, H lshii, H ljiri*, S Komori,and K Tamura• Dept. of Med., Yamanashi Med. University, Yamanashi, Japan We evaluated different effect of antihypertensive agents on circadian variation of blood pressure (BP) in hypertension. 78 pts. with essential hyperlension (WHO 1-11) were examined with ambulatory BP monitorings ,which were repeated befare and after the treatment to monitor BP and heart rate (HR) for 48 hr. every 30 min. Bunazosin (1mg, t.i.d.) was administered to 9 pts. (a group), nipradilol (3-6mg, b.i.d.) or metoprol {40mg, t.i.d.) to 19 pts. { group), nicardipine-retard {20-40mg, b.i.d. ) or nilvadipine {4 mg, b.i.d.) to 24 pts. {N group), diltiazem {30-60 mg, t.i.d.) to 12 pts. {D group), captopril-retard {18.75mg, b.i.d.) to 14 pts. {C group) for at least 4 wks. The following parameters were assessed 1) Nocturnal reduction rate {NRR {%)= {Daytime mean - Nighttime mean) I Daytime mean X 1 00) 2) Prevalenee of "Non-dippers {NRR of Systolic and/or Diastolic BP < 10% )" befare and/or after treatment. Reductioi'IRale("lo).ITIMII±SD Noctumal Reduction Aate (%), mean±SD Prevalenee of S lic . stolic BP S !olie BP Diaslolic BP "Non-di r" % a 8.1+3 . .9 8.5+4.2 n.3±7.1 3.0±7.5/10.6±7.9 42 5112 /42 5112 + + 13.6±6.4/12.9±4.8 16.0±6.2/15.9±4. 32 7/22 /27 6122 8.6+4.7 8.9±5.5 5.1 ±5.7 113.7±5.6 29 7/24 /54 13124 D 10.3+4.7 11.1+6.1 11.0±9.4/10.0±9.1 3.2±9.2/11.5±8.662 8113 /54 7/13 7.2 5.8 13.0±7.1/14.9±6.3 4.3±6.3/16.0±6.6 33 5/15 /33 5/15) be!Ofe Tx.l after Tx. All drugs, except for dihydropyridine derivatives, did notaffect the circadian variation of BP. Treatment with dihydropyridine derivatives increased the prevalenee of "Non-dipper". Key Words: antihypertensive agents, circadian variation, ambulatory blood pressure, noctumal reduction rate Downloaded from https://academic.oup.com/ajh/article/9/4/140A/2462180 by guest on 05 July 2022
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Antihypertensive Dmg Treatment - Oxford Academic

POSTERS: Antihypertensive Dmg Treatment
Ft HYPOTENSIVE EFFECT AND CARDIAC WORKLOAD
CHANGES INDUCED BY METOCLOPRAMIDE IN
HYPERTENSIVE PATIENTS. Blanco M,Vasquez M,Vargas R,Trias Y,Palomo D,Rodriguez Mand
Velasco M*. Clinical Pharmacology Unit, Vargas Medica! School,Central
University of Venezuela Caracas, Venezuela,S.A.
Metoclopramide(MTC)a DA2 doparninergic blocker reduces blood
pressure both in normotensive and hypertensive subjects during cold
pressor test(Blanco M,Amer.J.Therap.in press, 1995), exercise
treadmill test (Blanco et al,submitted for publication, 1995).1n the
present study we are reporting the hypotensive effect induced by
intraveneus MTC in hypertensive patients without changes in cardiac
workload. Eleven( 11) hypertensive subjects were studied After an hour resting
period, subjects were submilled to the following protocol:Two
placebo periods 5% glucose solution infusion i.v. during 30 min
were administered before and after a drug treatment period of MTC at
the rate of7.5uglkglmin for 30min period.At the end ofeach period
and during MTC infusion(every five minutes) blood pressure and
heart rate measurements were done.Cardiac work load was calculated
by the product of systolic blood pressure and heart rate.
MTC lowered blood pressure from 146±3.52/90±4.27 mmHg to
138±6.26/84±4.09 mmHg at 30 min period (p<0.03; p<0.001for
systolic/diastolic values, respectively) However,diastolic blood
pressure lowered at IOmin until 30 min period(p<O.OOI) and heart rate
was increased at 20 min until 30 min period(p<0.01).2) MTC did nol
alter cardiac workload at any time period.
The hypotensive effect of MTC in hypertensive patients is in
agreement with previous report from our Iaberatory in which we
found the same hypotensive effect in untrained,trained normotensive
subjects. We have also shown that MTC caused a decrease in blood
pressure and cardiac workload during cold pressor test and exercise
treadmill test both in normotensive and hypertensive subjects.2)MTC
induces this hypotensive effect by cardiac and peripheral actions and
possible through CNS actions.3)Controlled trials should be done in
patients with hypertension,hypertensive crisis and in pregnancy
induced hypertension. Key Words: hypertension,metoclopramide,cardiac workload,
hypotensive effect.
F3 A TTENUATED METOCLOPRAMIDE-INDUCED V ASCULAR
HYPERREACTIVITY TO COLD PRESSOK STRESS IN
ATHLETIC SUBJECTS. Velasco M*.Jelambi l,Perez G,Franco T,Hurtado N and M.Bianco.
Clinical Pharmacology Unit,Vargas Medica( School,Central
University ofVenezuela,Caracas Venezuela,S.A Cold exposure(CPT) increases blood pressure in normotensive and
hypertensive subjects.Metocloprarnide(MTC) A known DA2
dopaminergic blocker, induces vascular hyperreactivity in
normotensive untrained subjects. We have performed this work to
evaluate the MTC-induced vascular reactivity in trained subjects to
know a probable dopaminergic influence. Twenty(20)untrained normotensive subjects and thirty two(32)trained
normotensive subjects(football players and runners)were
studied.Subjects received two 5%glucose solutions periods before and
after an intraveneus MTC infusion at the dose of 7 .5ug!Kglmin period
duration.At the end of each period blood pressure and heart rate were
measured. Normotensive untrained subjects responded with increase in blood
pressure after CPT (17.2 vs 21.4 mmHg systolic,and 17.9 vs
24.lmmHg diastolic)before and after MTC administration.Football
players responded with increase in blood pressure after CPT, however
systolic blood pressure response was rather minor.Runners responded
with increase in blood pressure after CPT(I7.8 vs 18.7mmHg
systolic,and 15.8 vs 13.9mmHg diastolic)before and after MTC
administration.Heart rate only increased in trained subjects prior to
MTC. Conclusions: 1 )Metoclopramide-induced vascular hyperreactivity was
nol evident in trained. subjects,2)Cardiovascular responses to CPT
are attenuated in athletic subjects as compared to those in untrained
subjects,and 3)This may meao a probable dopaminergic system
adaptation during exercise.
Key Words: cold pressor test,metoclopramide,athletic subjects
AJH 1996; 9:140A-167A
F2 VERAPAMIL SR 180 MG, TAANDOLAPRIL 2 MG AND THE
FIXED COMBINATION THEREOF FOR THE TREATMENT OF
MODERATE ESSENTIAL HYPERTENSION. JR Viskoper'; R
Dies"; P Zilles". •sarzilai Medica! Centre, Ashkelon, Israel; ••
Knoll AG, Ludwigshafen, Germany
A multicentre, double-blind, randomized, parallel group
comparison was performed to evaluate !he superiority of the
fixed combination verapamil SR!trandolapril 180/2 mg (VT) over
both monocompounds verapamil SR 180 mg and Irandolapril 2
mg. Alter a 4 week placebo run-in period 310 patients with
moderate hypertension (diast.BP 100 to 109 mmHg) were
treated with either Irandolapril 2 mg o.d. (Tran) or verapamil SR
180 mg o.d. (VSR) or !he combination verapamil SR/trandolapril
180/2 mg o.d. (VT) lor eight weeks. Sitting office blood pressure
was measured conventionally in the morning (trough) and
additionally in a subgroup of patients (n=90) 24h-ABPM was
performed. The treatment groups were well matehad lor
demographic data as well as lor baseline blood pressure values.
Mean conventionally measured sitting blood pressure was
reduced under VSR by 10.319.6 mmHg, Tran 12.5/10.9 mmHg
and VT 17.6/13.2 mmHg. The fixed combination VT was highly
significant (p = 0.0109, Snapinn's Tal superior over bolh
monocompounds. 24h total time mean blood pressure was
decreased under VSR by 2.6/3.8 mmHg, Tran 10.0/5.2 mmHg
and VT 16.8/11.1 mmHg. The p value lor superiority of VT over
both monocompounds was 0.0021 (Snappin's Tal· All three
traalment regimes were welltolerated. The incidence of adverse
events was 23 to 25 % in all treatment groups. The most
frequent adverse events were constipation (7, 1, 6 pis. VSR,
Tran, VT), cough (2, 7, 5 pts.) and asthenia (2, 4, 3 pis.) So
there was no evidence of an increase of adverse effects lor !he
combination. Alllhree active treatments employed in lhis study reduced blood
pressure with clear superiority of VT. Adverse even! rates were
low and similar in alltreatment groups.
Key Words:
Trandolapril, verapamil, combination treatment, 24h-ABPM
F4 ARE ANTIHYPERTENSIVE AGENTS SIMILAR IN AFFECTING CIRCADIAN VARlATION OF BLOOD PRESSURE? Y Mochizuki, M Okutani, H lwasaki, I Kohno, H lshii, H ljiri*, S Komori,and K Tamura• Dept. of Med., Yamanashi Med. University, Yamanashi, Japan
We evaluated different effect of antihypertensive agents on circadian variation of blood pressure (BP) in hypertension. 78 pts. with essential hyperlension (WHO 1-11) were examined with ambulatory BP monitorings ,which were repeated befare and after the treatment to monitor BP and heart rate (HR) for 48 hr. every 30 min. Bunazosin (1mg, t.i.d.) was
administered to 9 pts. (a group), nipradilol (3-6mg,
b.i.d.) or metoprol {40mg, t.i.d.) to 19 pts. { ~ group), nicardipine-retard {20-40mg, b.i.d. ) or nilvadipine {4 mg, b.i.d.) to 24 pts. {N group), diltiazem {30-60 mg, t.i.d.) to 12 pts. {D group), captopril-retard {18.75mg, b.i.d.) to 14 pts. {C group) for at least 4 wks. The following parameters were assessed 1) Nocturnal reduction rate {NRR {%)= {Daytime mean - Nighttime mean) I Daytime mean X 1 00) 2) Prevalenee of "Non-dippers {NRR of Systolic and/or Diastolic BP < 10% )" befare and/or after treatment.
Reductioi'IRale("lo).ITIMII±SD Noctumal Reduction Aate (%), mean±SD Prevalenee of
S lic . stolic BP S !olie BP Diaslolic BP "Non-di r" %
a 8.1+3 . .9 8.5+4.2 n.3±7.1 10.~7.5 3.0±7.5/10.6±7.9 42 5112 /42 5112
+ + 13.6±6.4/12.9±4.8 16.0±6.2/15.9±4. 32 7/22 /27 6122
8.6+4.7 8.9±5.5 12.5±_5~9/10_._5±6,8 5.1 ±5.7 113.7±5.6 29 7/24 /54 13124
D 10.3+4.7 11.1+6.1 11.0±9.4/10.0±9.1 3.2±9.2/11.5±8.662 8113 /54 7/13 7.2 5.8 13.0±7.1/14.9±6.3 4.3±6.3/16.0±6.6 33 5/15 /33 5/15)
be!Ofe Tx.l after Tx.
All drugs, except for dihydropyridine derivatives, did notaffect the circadian variation of BP. Treatment with dihydropyridine derivatives increased the prevalenee of "Non-dipper".
Key Words: antihypertensive agents, circadian variation, ambulatory blood pressure, noctumal reduction rate
Dow
nloaded from https://academ
ic.oup.com/ajh/article/9/4/140A/2462180 by guest on 05 July 2022

AfH-APRIL 1996-VOL. 9, NO. 4, PART 2
F5 NORMOHEMODYNAMIC GOAL-ORIENTED ANTIHYPERTENSIVE THERAPY IMPROVES THE OUTCOME. BB Sramek*, JA Tichy, M Hojerova, and V Cervenka. Hemo Sapiens. lrvine. CA. and Institule lor Prevenlive Care. Prague. Czech Republic.
Normohemodynamic state involves a simultaneous normoteosion and normadynamie circulation. A noninvasive meesurement of cardiac output and the hemadynamie management chart, which identifies the causes of ob normal hemodynamics (the percentage deviations in volume. inotropy, vasoactivity and chronotropy trom their normal levels). were added to the noninvasive armamant tor treatment of hyperlension and implemenled info a computerized system. used in the study. Inslead of· a conventional selection of antihypertensive drugs by trial-anderror. we were a bie to identify and ad minister such antihypertensive drug(s). which were optima! and specific tor each patient:
383 randomly selected hypertensive pa tienis (230 men and 153 wamen). previously treated by a conventional therapy of at least 2 antihypertensive drugs between 2 and 42 years (mean 12.5 years), were used in the study. During the initia! noninvasive hemadynamie assessment. 61 patients (15.9%) had their blood pressure wifhin !he normotensive range (MAP< 105 Torr) and were excluded trom turfher porticipation in !he study. (This percentage is consistent with the 5th Report of JNC on Detection. Evaluation & Treatmenl of Hypertension. 1993. NIH.) The remaining 322 patients covered mild, moderate and severe hyperlension categories. 51 of these (15. 9%) were hypodynemie hypertensives. 210 (65.2%) were normadynamie hypertensives and 61 (18.9%) were hyperdynemie hypertensives. All these 322 hypertensives were then prescribed antihypertensive drugs, which generic categories were suggested by the Syslem. as to aim tor both normolension and normadynamie state. All patients were measured again in approximately 3 weeks. Though normolension could nol be achieved previously by a conventional antihypertensive therapy in any of these 322 patients. the normohemodynamic goa1-oriented therapy produced normolension in 203 of !hem (63%). In addition. 242 patients (75%) became normodynamic. This profound hemadynamie impravement look place in the first therapeutic iteration.
Key Words:
F7
Outcome. hemodynamics, normohemodynamic goal
REN AL HEMODYNAMICS, SODIUM EXCRETION, URINARY KALLICREIN AND MICROALBUMINURIA FOLLOWING TREATMENT WITH SPIRAPRIL, ISRADIPINE AND THE ASSOCIATION OF ISRADIPINE AND SPIRAPRIL. E.R. Maccaricllo, V.G.A. Fagundes•, A.G. Rocha, E.A. Francischetti*. Hy11ertcnsion Clinic, Laboratory of Clinical and Experimental Patho11hysiology, Rio de Janeiro State U niversity, Brazil.
In this crossovcr, double-blind study we evaluated the effects of lsradipinc (IS-SR0)-5mg, Spirapril (SP)-6 mg and the association of JS-5m~ + SP-6mg on glomcrular fiJtration rate (""'T' DTPA), effecti,·e renal plasma flow('" 1-Hippuran), urinary sodium excretion (U,,V), urinary kallicrein excretion (UKal) and urinary albumin excretion (UAE) in 12 essendal hypertensive patients with moderate renal dysfunction. The drugs were admini•1ered during 12 weeks (A) preceded by a 4 weeks placebo phase (B).
MBP B
IS 127,75 SP 126,83 IS+SP 129,45
A B
106,58* 71,08 111,92* 72,67 104,55* 70,82
GFR A
70,83 73,42 71,91
ERPF B
472,83 454,17 466,91
A
450,02 444~'10
460,00
IS - Isradipine; SP - Spirapril; MBP - meao blood pressure; GFR -glomerularfiltration rate: ERPF -effective renal plasma flow: *p<O.OOI.
Despite a significant blood pressure reduction, renal hemodynamics was mainteined stabie in all therapeutic periods. The u •• V increased significantly with IS and the association of IS and SP (0,16 vs 0,25 mEq/min, p< .05; 0,21 vs 0,29 mEq/min, p< .05, respectively).UEA remained unchanged during the three drug protocols. The UKal increased significantly during IS (0,30 vs 0,49 mU/min, p< .05). In conclusion, the drugs were effective in controlling blood pressure while maintaining stabie renal function. However, only the association of IS and SP increased renal sodium excretion which may be a hetter alternative than SP alone in patients with renal failure. Key Words: renal hemodynamics, urinary kallicrein,
urinary albumin excrelion, isradipine, spirapril.
POSTERS: Antihypertensive Drug Treatment 141A
F6 DOUBLE-BLIND COMPARISON OF ENALAPRIL (E), DIL TIAZEM ER (DJ AND THEIR COMBINATION (EID) IN STAGE 1-3 ESSENTIAL HYPERTENSION. WC Cushman*, JO Cohen, RP Jonas, TC Marbury•, RB Rhoades. LK Smith. VA Medica! Center, Memphis, TN.
11 is frequenUy necessary to employ more than one drug to effectively control el evaled blood pressure. A combination product of !wo pharmacologically different agents often improves both blood pressure control and drug compliance. In a mutticenter. randomized, double-blind, placebo-controlled, parallel group study, compansons were made betweenES mg, D 120 mg, D 180 mg, ES/0120, ES/0180 and placebo. Patients (N=891) with baseline sitting diaslotic blood pressures (SiDBP) between 95 and 11S mmHg were randomly assigned to the six treatment groups. Medicatiens were taken once daily and BP was obtained at 24±2 hrs postdose. After the 12-week double-blind phase, 562 of 891 patients enrolled in the 36-week open-label phase. Data were analyzed using the intent-totreat approach. The six treatment groups were comparable at baseline.
MEAN CHANGE FROM BASELINE IN SiDBP (12-Week and 36-Week Extension Phase)
ADJ. MEAN STAT. TREATMENT N BASELINE ENDSTUDY CHANGE SIG." 12-Weeks Placebo 147 101.7 98.2 -3.3 ES 140 101.6 95.8 -S.7 a 0120 146 101.7 96.3 -S.1 a 0180 147 102.2 95.9 -6.0 a ES/0120 146 101.3 93.7 -7.6 abc ES/0180 141 1 01.S 93.0 -6.3 abcd 36-Weeks Mean Change ES/0120 161 98.S 86.S -12.0 ES/0180 106 100.1 87.1 -13.1 E10/D360 136 101.8 88.0 -13.8 E10/D360/H2S 1SO 105.3 89.6 -1S.7 (*Stat. Sig. (p<0.05): a, vs placebo; b, vs ES; c, vs 0120; d, vs 0180)
The most common drug-retated adverse events in both study phases were headache, edema/swelling, dizziness, asthenialfatigue and cough.The fixed-combinations of E1D were effective and generally well-toterated.
Key Words:
enalapril, diltiazem ER, combination product
FS ACE INHIBITORS GIVEN AT NIGHT GIVE BETIER CONTROL OF EARL Y MORNING BLOOD PRESSURE. A Anderson and TO Morgan*. Hypertension Unit, Austin and Repatriation Medica! Centre, Heidelberg, Victoria, Australia.
Once daity medication usually given in the morning may not prevent the early morning rise in blood pressure which is associated with increased mortality from myocardial infarction and sudden death. Perindopril (P) 4 mg was given at 9:00 or 2 I :00 h in a randomised crossover study for 4 weeks to 22 patients with essential hypertension. Clinic blood pressure was taken between 7:30 and 9:00 and an ambulatory BP monitor (Spacelabs) was applied at 9:00am. Compared with placebo, clinic BP, 24h mean, daytime mean and nightime mean were significantly reduced 10 a similar extent by both regimes. The peak morning blood pressure on placebo was 173/108 mmHg. Th is feil significantly 10 153/95 (p < 0.001) with the 9:00h drug dose and 10 148/91 (p <0.001) with the 21:00h dose. The value on the 21 :OOh dose was lower (p < 0.05) than on the 9:00h dose.
In a separate but similar study enalapril 20 mg was given to 12 hypertensive patients. Daytime, nightime and 24h mean pressure were reduced significantly compared to placebo. The peak morning pressure on placebo was 169/106 mmHg which feil on the 9:00h drug dose to 156/96 (p < 0.01) and on the 21:00h dose to 149/90 (p <0.001). This later value was lower (p < 0.01) than the 9:00h drug dose value.
Perindopril 4 mg and enalapril 20 mg both had an effect that lasted for 24h. However when the drugs were given at night the earl y morning rise in blood pressure was less than with the morning dose.
Key Words: Chronotherapy, perindopril, enalapril, ACE inhibitors, ABPM
Dow
nloaded from https://academ
ic.oup.com/ajh/article/9/4/140A/2462180 by guest on 05 July 2022

142A ASH XI ABSTRACTS
F9 EFFECTS OF SEMOTIADIL FUMARATE (SD-3211), A NOVEL BENZOTHIAZINE CALCIUM CHANNEL BLOCKER, ON LEFf VENTRICULAR HYPERTROPHY AND FUNCI'ION IN PATIENTS WlTI:I ESSENTIAL HYPERTENSION T Sumimoto*, K Hiwada*, T Ito, T Ochi, H Hashimoto, and H Kukita. Ehime University School of Medicine, Ehime, Japan
Semotiadil fumarate (SD-3211) is a nondihydropyridine calcium channel blocker, which bas a structure quite different from those of diltiazem and velapamil. We examined the effects of a long-term treatment with semotiadil fumarate on cardiac hypertrophy and function. Fifteen uncomplicated essential hypertensive patients with left ventricular hypertrophy, aged 58±8 years, were treated with semotiadil fumarate alone for 6 months. All patients underwent M-mode and Doppier echocardiography to assess cardiac structure and function before and after the treatment. We measured left ventricular mass index, ejection fraction, fractional shortening, isovolurnic relaxation time and peak early to peak atrial velocity (E/A) ratio of left ventricular inflow. After the treatment, blood pressure was decreased significantly from 171±12/98±6 to 152±18/84±10 mmHg (each, P<O.Ol), whereas heart rate did notchange (66±13 versus 67±11 beats/min). The left ventricular mass index was decreased significantly from 132±31 to 118±30 g!m2 (P<O.Ol). Isovolurnic relaxation time decreased significantly after the treatment. No significant changes occurred in the ejection fraction, fractional shortening and E/A ratio. Although there was no significant relationship between changes of blood pressure and changes of E/ A ratio, a significant inverse relationship was observed between changes ofE/A ratio and changes of left ventricular mass index (r=-0.58, P<0.05). It is concluded that semotiadil fumarate regressed left ventricular hypertrophy and improved left ventricular diastolic function in hypertensive patients with left ventricular hypertrophy.
Key Words:
Fll
calcium channel blocker, left ventricular hypertrophy, cardiac function
TROUGH/PEAKRATIO AND BLOOD PRESSURE V ARIABIUTY AFI'ER TREATMENT WITH DILTIAZEM EXTENDED-RELEASE 240 mg GIVEN ONCE·DAILY IN ESSENTIAL HYPERTENSION Coca A*, Sobrino J, Soler J, Módol J, Patos MA, Mingnez A, Esqué J, Plana J, Cases M, Oosas J, V ergés J, De la Sierra A*. Hypertension Research Foundation ofthe Catalan Community Hospitals,
Barcelona, SPAIN.
The aim of tbe study was to delermine the trough/peak ratio (f /P) and the effect of Diltiazem-ER 240 mg (DL1) given once-daily on circadian blood pressure profile and BP variability, in mild-to-moderate essential hypertensive patients. After a 4 week wasb-out period, 30 patients (17m,13f) aged 25 to 76 years sbowing a mean daytime-DBP higher than 90 mmHg were treated with DLT 240 mg for 8 weeksin a multicenter, open study. Twenty-four hour ABPM was perforrned at the end of the 4 drug-free baseline period and during the last week of treatment. A significant rednetion of the mean valnes of clinic blood pressure (161.6±16.2 to 151.2±15.6 mmHg; p<0.01 for SBP and 101.1±4.8 to 93.3±9.2 mmHg; p< 0.001 for DBP) was observed at the end of treatment in the complete group of 30 patients, with no significant changes in heart ra te. Likewise, mean valnes of SBP, DBP, SBP-load and DBP-load obtained by ABPM were significantly reduced. Twenty one (70%) patients were responders (lowering of 24h-DBP > 5 mmHg). The mean peak BP lowering was -17.5±._11.1 mmHg for SBP and -14.3±7.0 mmHg for DBP. The trough effect was -10.4±9.8 and -7.2±6.1 mmHg respectively. The TIP ratio was estimated as 0.59 for SBP and 0.51 for DBP. Long-term variability estimated as the mean hourly standard deviation of BP for the 24-hour period was reduced in responders (16.2±4.3 to 14.6±2.7 mmHg; p=0.0395 for SBP and 12.1±2.7 to 10.7±2.5 mmHg; p=0.0019 for DBP), withno changes in HR variability. No patients discontinued the study due to treatrnent-related adverse effects. We coneinde that Diltiazem-ER 240 mg given once-daily was effective and well tolerated. Blood pressure was controlled over the entire
period of 24 hour preserving the circadian profile and improving longterm variability in responders, what may have important implirations
regarding end-organ damage proteetion in essential hypertension.
Key Words: Calcium channel blockers, Diltiazem-ER, Blood
pressure variability, Trougb/Peak ratio, treatment.
AfH-APRIL 1996-VOL. 9, NO. 4, PART 2
FlO lilTlAL PllSI OF nPI!RTDSIOI: DICI IS BmD A BITA OR A CALCIOI CIAIRL BLOCIIll?. A LOIG-flllll STODY. f....AUW,FJ lruda,l L6pe1-lovales,JL Pizarro,l Frutos. lyperteasioa Unit, Geaeral Hospita!. Spail, llilaqa.
Ai.a;. Betablockers have been considered as the best choice to treat initia! phase of essential HBP. We hypothetized that a CCB vith negative chronotropie effect {Verapamil) is a better choice lor this kind of hypertensives. Desip and aethods :We compared 2 groups of recently diagnosed essential hypertensives {EH) treated during 20 aonths either vith 50-100 mg OD Atenoio I {AT) {n-29/12-41,41 vomen, Hean age:36. 7!3) or 240 mg OD Verapamil SR{VRSR) {n-31/13-41,91 vomen, Mean age: 39,3±4) We measured BP, HR, BMI and tolerance, and a!so determined lipids, insulin and glucose toleranee test, as vel! as 24.h. Natu and m.icroalbuminuria at 0, 6, 12, 18 aonths follov-up. We also considered the need for more antihypertensives alonq the follov-up. Resu!ts:Aiong the study there vere not dillerences in mean BMI and BP reductions;although 48,11EH vith AT needed to add ether drugs te control HBP instead of 16, 71EH vith VRSR. Af IR IDL·ck Glucose(aqdl) Insulia la+u
Iontbs (b/nn) {aq/dl) 0 120 Basal{ID/al) {aol/24hl 0 87!10 49!10 94,3±17 ll6±34 13,2±7 148±46
(x) (x) (xx) (xx) (x)
DAK (aq24h) 3,3±35
18 YIISR
0
71!6 38±11 106±21 138,2±48 21,3±10 157±59 18,2±47
84±12 44±12 96,8±12 127,2±39 15.6±7 159±53 16, 9±36 (X)
18 73±8 46,8±12 95,1±42 124,7±42 17,3±7 173±71 12,4±35 (x) p<O.OOI(xxl p<0.05. Rest biochemica! parameters:No differences. Clinical side effects (and Withdrawals)(I);Atenolol: 34,5(13,8) ;VRSR:22, 6(3, 23). Coaclusion:VRSR may be preierred to AT tor long-term treatment of initia! essential HBP due to its hiqher therapeutic efficacy and toleranee.
Key Words: Essential Hypertension. Betablockers.
Calcium Chànnel Blockers.
F12 NIFEDIPINE AND FEWDIPIN IN SLOW RELEASE FORMULATIONS- EFFICACY AND ADVERSE EVENTS IN HYPERTENSIVE PATIENTS. Thulin T, Katzman Pand Nilsson P. Dept of!ntemal Medicine, University Hospita!, Lund; Dept of Medicine, Helsingborg
Hospita( and Dept of Community Health Science, University of
Lund, Sweden. Introduction: Nifedipine (N) in a new slow-release
formulation OROS may show advantages in camparisen with
older fonnulations regarding the blood pressure (BP) control as
wellas actverse events (EA). The aim ofthe study was to
campare the effects of the new N formulation OROS with that
of an established calcium antagonist felodipine ER (F) in
patients with mild to moderate hypertension.
Subjects and methods: After an initia( placebo period, 65
patients were treated during four weeks with N and F in a
randomized, double-blind, cross-over study with at least four
weeks wash-out between the two active regimens. Office BP
and heart rate were recorded in the sitting position. After the
initia( placebo and after the two periods on active treatment
they also went through ambulatory blood pressure monitoring
(ABPM) during 24h for evalutation oftrough-to-peak ratios.
AE were registrated after each treatment period.
Results: Out of 65 patients 48 were evaluable. Thus 17 patients
were excluded due to either technica( problems or violatien to
the protocol. N and F were equally effective in decreasing BP.
Heart rate did not change. During the 24h ABPM there were no
ditTerences recorded between N and F during the day, night or
early morning hours. Th is was also shown for trough-to-peak
ratios. EA did not differ between the two drugs.
Conclusion: The new formulation of nifedipine (OROS) seems
to have the same BP lowering effect as felodipine ER at office
and during 24h ABPM recordings. The drugs were also equally
tolerable. Key Words:
ABPM, calcium antagonist, felodipine ER, nifedipine, OROS
Dow
nloaded from https://academ
ic.oup.com/ajh/article/9/4/140A/2462180 by guest on 05 July 2022

AfH-APRIL 1996-VOL. 9, NO. 4, PART 2
F13 ANGIOTENSIN CONVERTING ENZYME INHIBITOR MIGHT NORMALIZE ABNORMAL CIRCADIAN RHYTHM OF TOTAL VASCULAR TONE IN ESSENTIAL HYPERTENSION. H.Mori•, Y.Hoshi, Y. Yokono, N.Fujiwara and H.Toyamori. Aomori Prefectural Central Hospital,Aomori,Japan.
We studied the effect of long acting Angiotensin converting enzyme inhibitor (imidapril 10 mg once a day) on the circadian rhythm of the total vascular tone (TVT) index (TVTI,calculated as total vascular resistance).The subjects were 34 patients with essential bypertension (EH) according to WHO's classification and 21 healthy individuals used as a control group. Noninvasive ambulatory blood pressure (BP) monitors and noninvasive continuous cardiac output (CO) monitors were simultaneously attached over 24-hour period. BP,heart rate,CO and TVTI measured immediately prior to ,and 4 weeks following the administration of the agent. TVT was calculated as follows:(mean BP/ cardiac index) X 1,332 dyne/sec/cm- 5 •
TVTI was measured based on the value at 2:00a.m. as follows: [(each hourly value - value at 2:00a.m.) /value at 2:00a.m. 1 x 100. Twenty-four hour period were divided into waking (W) hours and sleeping (S) hours. The TVTI before administration of the agent were significantly larger than those of the control. The TVTI after the administration of the agent in both W and S changed the TVTI to the level of the control group. It suggests that EH causes abnormal circadian rhythm of TVT, but long acting Angiotensin converting enzyme inhibitor might normalize the abnormal circadian rhythm of TVT in patients with EH.
Key Words: circadian rhythm, total vascular tone, Angiotensin converting enzyme inhibitor
F15 AIILODIPIU YERSDS THAIDOLAPRIL 11 TYPE 2 DIABETIC ESSEITIAL mERTDSIYES: A LOIC-TERI COIIPARISOI STOOT. ~- lJ.Araada. K. lrutos. E. L6pu Rovales. lyperteasion Dait.lephroloiJJ. S. lospital Regional. lilaga. Spaia.
In an open, randomised, ambulatory study, we compared the lonq·term antihypertensive, metabolic and renal effects of Trandolapril IT.) versus Alllodipine IA.). We included 36 121-58,31 vomen) type 2 diabetics vith mild-moderate IOBP 90-lll llllll!q) essential HBP treated either with T. ln-18112-66,71 wonen). Hean aqe: 56,3±9, BliJ: 27,8!3,2. BP: l73±16/104,2!5,51111ll!q) or vith A. ln-1819· 501 vomen). Mean aqe 58,1±8, BIII:28,1±3, BP:l71,8±6 llllll!q). We measured casual BP, HR, and BK! and clinical side-effects monthly and also determined !asten levels of qlucose, HGA!c• lipids, uric acid, creatinine, x+ and 24 h. Na+u and microalbuminuria at 0,3,6 and 12 months of the follov-up - A 24 h. ABPH recordinq vas performed at 0 and 12 months. All patients received Glybenclamide 12,5-15 mq/day) and started either vitb T. 2 mq 00 or A. 5 mq 00. After I month, those with a OBP > 90 lllll!q double the initia! dose; and in case of uncontrol of BP, then both qroups added Ooxazosin 2 to 4 aq 00 every month later. Results: Mean 24 h ABPimmHq) Microalbuminuria Ha+
systolic Oiastolic lmmHq/24 hl lmq 24 hl T. A. T. A. T. A. T. A.
Initia!: 142,1 140,8 92,2 91,6 124,8 149,1 151 4,18
x+ lmmol/1) T. A.
149 4,28
l'l l'l l'l l'l l'l l'l Ins) Ins) l"l Ins) I year: 132,3 121,6 19,8 81,1 51,6 68,8 162 168 4,51 4,31 l*)p<0,001 l")p<0,05 BK!, HR, HbA1c, and rest of the biochemica! parienters: no significant chanqes. With monotherapy ve controlled 61, I pts vith T. and 66,11 vith A. Doxazosin increased the control to 83,31 vith both druqs. Clinical side·effects: 22,2 vith T. and 21,81 vith A. In Conclusion: Both druqs shoved a siailar antihypertensive efficacy, metabolic and clinical toleranee in the type 2 diabetic essentia1 hypertensives.
Key Words: Type 2 Diabetes. Essential Hypertension Amlodipine. Trandolapril.
POSTERS: Antihypertensive Drug Treatment 143A
F14 RESPONSE OF BLOOD GLUCOSE TO THE DIURETIC TORASEMIDE IN HEALTHY SUBJECTS. WP Leary, AJ Reyes*, and K van der Byl. University College, Cork, Ireland,
The objective of this study was to evaluate the response of blood glucose to the loop diuretic torasemide (T), Single oral doses of 2.5 and 5 mg T do not raise and raise mildly, respectively, 24-h natriuresis in healthy subjects; however, both are effective antihypertensives when used as once-daily monopharmacotherapy. Sixteen healthy subjects received oncedaily oral doses of placebo (P), and of T 2. 5, 5 and 10 mg, during four conveniently separated single-treatment periods of 7 days each. An individually randomized, crossover and double-blind design was followed,
mg Day Mean serum glucose (mmol.l- 1 ) Hours after dosing at hour 08.00
0 1.5 6 24 p 1 4.5 4.1 4.1 4.4 p 7 4.4 4.0 4.4 4.5 T 2.5 1 4.6 4.1 4.3 3.4 T 2.5 7 4,3 4,1 4.3 4.4 T 5 1 4.4 3,9 4.0 4,4 T 5 7 4,3 3.8 4.2 4,4 T 10 1 4.5 4.3 4.2 4.4 T 10 7 4.3 4.1 4,6 4.4 None of the T mean values differed significantly from its P mean, nor did any of the day-7 means differ from its day-1 mean. Dose-effect relationships of diuretics differ for different variables. Torasemide 2.5 and 5 mg behave as low doses with respect to blood glucose, as they do with respect to 24-h natriuresis.
Key Words: blood glucose, diuretics, torasemide.
F16 TAANDOLAPRIL IN COMBINATION WITH VERAPAMIL SR IN PATIENTS WITH SEVERE ESSENTIAL HYPERTENSION. HA Punzi*. BA Novrit, and the Trandolapril Study Group, Trinity Hypertension Research Center, CarroiHon, TX. This open label trial was designed to evaluate a muHiple drug regimen consisting of Trandolapril (Tran), Verapamil (Ver), and Hydrochlorathiazide (HCTZ) in patients wHh severe hyperlension (Stage 111-IV). The study design consisled of a single-blind placebo run-in period of 3-14 days alter which patients were randomized to active therapy H dia BP 2,115 or ~135 mmHg. Ninety patients, mean age 51±11.1 years (63M, 27F), were enrolled at 11 study sHes. Fifty·eight were whHe and thirty-two were black. Mean body weight was 210.5±45.41bs. The average sup. sysVdia BP at baseline was 182.3/119.8 mmHg. Open label medications were titrated up to BP response defined as dia BP ~90 mmHg. Caucasians were starled on 2mg Tran and titrated up to 4mg. African Americans were starled on 4mg and tHrated up to 8mg. 11 BP response was nol achieved, Ver was added foliowed by HCTZ (12.5-25mg). The following table gives the mean supine sysVdia BP lor 87 analyzable patients:
ALL PATIENTS
TAAN ~ 87 Sysi/Dia BP* ·5.31·9.0 mmHg Clinical Resp. Rata" 44.8%
TRAN+VER -N~--- 75 Sysi/Dia BP" ·14.61·13.9 mmHg Clinical Resp. Rata" 56.0%
TRAN+VEA+HCTZ N= 72 Sysi/Dia BP* ·27.01·19.0 mmHg Clinical Resp. Rata" n.7%
epresems cnange rom oaseune 'Reduction in Dia BP of .?,1 0 mmHg ar <90 mmHg
Key Words: SEVERE ESSENTIAL HYPERTENSION TRANDOLAPRIL VERAPAMIL HYDROCHLORATHIAZIDE
Dow
nloaded from https://academ
ic.oup.com/ajh/article/9/4/140A/2462180 by guest on 05 July 2022

144A ASH XI ABSTRACTS
F17 LONG ACTING NISOLDIPINE CORE-COA T (CC) IN SEVERE
BLACK HYPERTENSJVES. EFFECTS ON AMBULATORY
BLOOD PRESSURE PROFILES AND LEFT VENTRICULAR
MASS. L Radevski, D. Skudicky, S. Sathekge, P. Sareli*.
Baragwanath Hospita!, Johannesburg, South Africa
Nisoldipine, a new vascular selective dihydropyridine in a slow
release formulation (cc), was tested in black severe hypertensives
(24 hour DBP :::._ 110 nunHg). Sixty pts (26 males, mean age
43±15 years) were enrolled. Nisoldipine was initiated at a dose of
10 mg daily, and was uptitrated to 20, 40 and 60 mg in a 4 week
period if blood pressure was not controlled (DBP < 95nunHg on
conventional measurement). All pts required 60mg at the end of the
titration pcriod. Results of 24 hour ABPM after 4 months of
treatment are as follows:
24 Hour SBP (nunHg) Baseline 180±13 119±7
4 Months 144±14
p <0.001
Day
DBP (nunHg) HR (beats/min) 78±10 SBP (nunHg) 184±12
94±9 81±8 147±15
<0.001
<0.001
DBP (nunHg) 123±7 98±10 <0.001
Night SBP (nunHg) 176±16 139±15 <0.001
DBP (nunHg) 113±8 89±5 <0.001
Mean 24 hour DBP < 90nunHg and < 95nunHg was achieved at 4
months in 30% and 53% of pts respectively. A reduction of the
mean 24 hour DBP :ê: 20nunHg was noted in 72% ofpts. The mean
DBP and SBP drop for the first 18 hours vs the last 6 hours was 23
vs 26nunHg and 39 vs 37nunHg respectively. Left ventricular
mass index measured on echocardiography regressed from
148±4lgrfm2 to 127±34grfm2 (n=44, p=O.Ol), without any
deleterious effect on LV systolic performance. No serious actverse
effects or biochemica! abnormalities were noted. In condusion
Nisoldipine cc has shown a profound and sustained antihypertensive
effect in severe black hypertensives associated with significant
regression of LV hypertrophy and no serious side effects.
Key Words: Nisoldipine, ambulatory blood pressure monitoring,
severe hypettcnsion
F19 SUBCUTANEDUS TISSUE PRESSURE AS A METHOD
TO EVALUATE THE OEDEMATIGENOUS POTENTlAL OF AMLODIPINE VERSUS VERAPAMIL GD Ma!amanj*
P. Preti, S. Mariotti, S.Savino, P.Lusardi. A.Zoppi*. R. Fogari*.
Department of Internal Medicine and Therapeutics.
University of Pavia; Pavia, IT AL Y. Aim of the study was to evaluate whether the pretibial
subcutaneous tissue pressure (PSTP) can be used as an index
to quantify the calcium channel blockers (CCB) oedematigenous effect.
Thirty-five hypertensive patients aged 38-73 yr were studied. Their PSTP and their ankle circumference (AC) were
evaluated in basal condition and after 12 weeks of antihypertensive treatment with 2 different CCB: 17 patients were randomized to Amlodipine (A) 10 mg o.d., 18 paticnts
to Verapamil SR (V) 240 mg o.d.; PSTP was evaluated through
a system consisting in a graduate capillary tube ending in a
needie and full of saline solution; when the needie is
threated into the subcutaneous prctibial tissue the system
become closed: then the system is connectcd to a water
manometer where, after saline solution balancing. the PSTP
is read. Amlodipine chronic administration induced a mean
increase in PSTP of 4,5± I ,9 cm H20 (p<O,O I) and an iocrcase
of AC of 1,65±0,41 cm (p<0,05). No significant correlation
was found between PSTP and AC changes. After Verapamil
chronic treatment PSTP increase was of 0, 9±0,5 cm H20 and
AC incrcase was 0,4±0,2 cm (NS). Our data show that in hypcrtensive patients chronically
treated with CCB monotherapy A cause a great increase in
PSTP as well as in ankle enlargement while V does not significantly modify ncither PSTP and AC. This agree with
the well known clinical report that anklc ocdcma is
particulary complained with dihydropyridines. On tbc whole
our results suggcst that PSTP can be proposcd as a metbod to
quantify the ocdematigenous effect of CCB.
Key Words: subcutaneous tissue pressure; amlodipine; verapamil; ankle oedema.
AfH-APRIL 1996-VOL. 9, NO. 4, PART 2
F18 EVALUATION OF RESERPINE AND CLOPAMID ALONE OR IN COMBINATION FOR FIRST-LlNE TREATMENT OF HYPERTENSION O.B. Pittrow', B. Krönig', W. Kirch3 , and G. Weidinger'. 'Clinical Research, Sandoz AG, Nürnberg; 2Ev. Elisabeth Hospita!. Trier; 'Dept. of Clinical Pharmacology, University of Dresden, Germany.
Low-dose combination therapy has been proposed to be a rational first-line approach to hyperlension treatment. However, respective data trom controlled studies are sparse. We compared the efficacy and tolerability of the fixed combination of reserpine 0,1 mg plus the thiazide di uretic clopamid 5mg with its single componentsas wellas the calcium-antagonist nitrendipine 20mg. In 18 centers throughout Germany, 273 hypertensive patients (100 ,;DBP,;114 mmHg) were randomised in this double-blind. parallel-group study. Blood pressure (BP) was measured with a semi-autornaled cuff-oscillometric device ('boso-Oscillomat'). The 4 groups did nol ditter regarding baseline characteristics (mean age 58y; 51% ma les; mean BP after a 2-week placebo run-in period 158-160/103-104mmHg). After 6 weeks of treatment with one capsule medication daily, mean reductions trom baseline in silting BP 24h after dosing in the reserpine-clopamid'combination (R/C), reserpine 0 1 mg (R), clopamid 5mg (C) and nitrendipine 20mg (N) groupwere -23.0/-17.1,-14.0/-11.7,-13.6/-11.9, -11.6/-123mmHg [2p<0.01]. The corresponding normalisation rates (DBP < 90 mmHg) were 55% (R/C), 40% (R), 36% (C) and 33% (N). All patients whose BP had nol been normalised at this time point received a double dose of the respective medication o.a.d. trom week 7 to 12. At the end of the study, mean BP reductions we re -25.7/-18.1 (R/C), -14.6/-12.2 (R), -17.7/-13.4 (C) and -14.9/-15.3
mmHg (N) [2p<0.01]. The respective normalisation rates were 70% (R/C), 37% (R), 42% (C) and 46% (N) [2p<0.001]. Concerning tolerability, adverse events (AE) were observed in 27% (R/C), 28% (R), 29% (C) and 48% (N) [2p<0.05]. The rates of premature discontinuations due to AE were 3% (R/C). 3% (R), 7% (C) and 13% (N) [2p=0.06].
The low-dose combination of reserpine and clopamid lowers BP significantly more than either of its components alone and than nitrendipine. Moreover, the combination is toleraled as well as its components and significantly better than nitrendipine. Key Words:
Combination therapy, first-line treatment, reserpine, clopamid, nitrendipine.
F20 LONG-TERM EFFECTS OF DILTIAZEM EXTENDED-RELEASE IN AGED HYPERTENSIVES. Feraco E, Grandinetti 0, Cosentino G, Tomaselli C,
Department of Cardiology, I.N.R.C.A. (ltalian Natienat Research
Centre on Aging), Cosenza, Italy Objective: to compare, by means of ambulatory blood pressure
monitoring (ABPM) and 24-h ambulatory ECG monitoring (AEM), the efficacy and the safety of Diltiazem hydrachloride ( DTZ HCI) in
aged patients (pts) with mild-to-moderate systemic hypertension showing echocardiographic evidence of left ventricular hypertrophy ( LVH). Design and Methods: after a two-week wash-out period, 21 pts
(9M,12F; mean age 73±4.6y) with DBP 95 to 114 mmHg were assigned, not randomly and 41% previously untreated, to a 3-month treatement period with DTZ 120 mg bid and then, after a new two-week wash-out period, to a 3-month treatment period with DTZ od extended-release formulation (300mg). BP was measured manually in the morning prior to dosing. 24-h ABPM
and 2 4-h AEM were performed at the onset and at the end of both
active treatment periods. Echocardiographic left ventricular mass
(LVM) index was calculated using the cube formula; LVH was
considered to be present when the LVM index exceeded 130 g/m 2
Results: the therapeutic goal (target DBP<95mmllg or a 10% DBP reduction) was achieved with DTZ bid in 13 cases (SBP from
152.8±9.4 to 138.8±6.7 mmHg; p<0.001; DBP from 90.4±6.7 to 79.5±5.3; p<0.001) and with DTZ od in 15 (SBP from 153.3±8.2 to 136.5±7.9 mmHg; p<0.001; DBP from 91.3±6.5 to 77.9±5.7;p<0.001). The adjusted mean change from baseline SBPIDBP was -12/8 and -13/8
mmHg, respectively. LVM index decreased significantly after treatment ( 149± 12.5 to 131.8± 14.4; p<0.001) and E/ A ratio
increased (0. 73±0.13 to 0. 90±0.09; p<0.001 ). Sino-atrial block
cx::curred in four pts (three while taking DTZ bid and one DTZ od); transient 1 st grade A-V block was observed in two pts taking DTZ
bid. The average maximum change in HR was -6 b/m' for both
doses of DTZ. Only one pt withdrew during DTZ bid treatment (headache). There was no particular pattern of changes in
Iabaratory values. Conclusions: results indicate that DTZ at doses of 240 and 300
mg/day was equally effective in reducing elevated BP in 62% to
71% of aged pts, throughout the day and night, and especially
during the early morning; moreover both therapeutic regimens
were safe and well-tolerated and were associatcd with a significant
reduction in L\/11.
Key Words: Diltiazem, Systemic Hypertension,
Left Ventricular Hypertrophy, Elderly
Dow
nloaded from https://academ
ic.oup.com/ajh/article/9/4/140A/2462180 by guest on 05 July 2022
AfH-APRIL 1996-VOL. 9, NO. 4, PART 2
F21 ORGAN DAMAGE IN TREA TED HYPERTENSIVES COMPARED TO NORMOTENSIVES. I Burtscher, IE Enstrom, JAI Eskilsson, EK Holm, SL Holtäs, POT Thulin, KM Pennert•, Kavlinge Health Centre, Kavlinge, Lund Univarsity Hospita!, Lund and Zeneca As•, Göteborg, Sweden. The purpose of the study was to find out whether organ damage in the heart, brain and eyeground dittered between treated hypertensives {HT) and nonnotensives {NT).The subjects were randomly selected trom a blood pressure screened population. Out of 40, {20 men) treated HTwith mean age 54.7 {41-64) years and 40 NT {20 men) with mean age 51.4 {44-64) years, echocardiography was perfonned in all 80 subjects, brain magnetic resonance imaging {MRI) in 70 and eyeground-photographing in 74. All 80 subjects had previously perfonned non-invasive ambulatory blood pressure monitoring twice during 24 hours. Office blood pressure was measured in the supine position when the ambulatory equipment was attached and removed. Lef! ventricular mass {LVM) dittered significantly between HT 104 {29) glm2
and NT 87 {25) glm2 {p<0.01). More women {10~ than men {4) had LVM above nonnal range 110 and 134 g/m , respectively. Left atrium {LA) also showed significant ditterenee {p<0.01) between HT 21{4) mm/m2 and NT 19 {2) mmtm2, while diastolic lef! ventricular tunetion {EA-quotient) did not ditter. MRI changes did not ditter significantly {p=0.07) between the 36 HT{periventricular or deep matter changes in 18 and grey matter changes in 8 patients) and the 34 NT {white matter changes in 8 and grey matter changes in 4 subjects). Eyeground changes did not ditter between the HT and NT. Keith-Wagener 11 and IV was not found in any patient, grade lil in only 5% of HT and 2.5% in the NT and grade I in 43% of HTand 49% of NT. Office blood pressure and 24-hour blood pressure systolic/diastolic was 141/86 {1317) mm Hg and 129/81{11/6) mm Hg in HTand 125/78 {10/8) mm Hg and 118n 4 {8/5) mm Hg in NT. Although both office and ambulatory blood pressure seemed to be acceptable, HT had significantly increased LVM and LA and a trend towards more white and grey matter changes in the brain compared to NT. We can only speculate if ear1ier trestment or further blood pressure reduction could have eliminaled these ditterences.
Key Words: Hypertension, organ damage, heart, brain, eyeground.
F23 HYPERTENSIVE PATIENTS CONSIDERED BAVING NORHAL BLOOD PRESSURE ON DISCHARGE ARE NOT CONTROLLED. *S. Zoneraich, A.K. Lodha, J.L. Mollura. Flushing Hospital Medical Center (F.H.M.C.) -Albert Einstein College of Medicine, New York.
Most of the patients (pts) admitted to the hospital for treatment of hypertension are discharged as soon as the B.P. is considered normal befare discharge. Objective: We assessed the B.P. in pts. adrnitted for treatment to F.H.M.C., and dischared as soon as they attained normal values~l40/90. We assessed normal B.P. values on admission campared to 24 hour Ambulatory B.P. Monitoring(A.B.P.M) befare discharge (average 2.9 days). Material & Methods: The study includes 30 hypertensive pts. admitted with B.P.~140/90. There were 21 females mean age 59.47 years, 9 rnales 61.22 years. On admission all, but 2 pts. were treated with antihypertensive medications (beta blockers, 12, calcium blockers 18, ACE Inhibitors 7, diurectics 8, alfa blockers, 3, and vasodilators 9). Ten pts received a single drug, 18 received 2 ar more, and 2 pts. none. On admission, 17 pts. were found to have uncontrolled B.P. New drugs were given to uncontrolled pts. On discharge, the last 2 pts. who were on no medicatien were also placed on treatment. The 24 hr. A.B.P.M. of all pts were evaluated with SpaceLab. Model 90207. Results: On discharge, 24 hour A.B.P.M. indicated, uncontrolled B.P. in 13 pts (40.31%) and controlled in 17 pts (59.69%). In 5 pts(38.46%) B.P. was normal befare discharge, but uncontrolled by 24 hr. A.B.P.M. Conclusion:This initial pilot study cleary demonstrates that 1) 38.46% of the hypertensive pts considered to be controlled during the hospital stay were not controlled.2) 24 hour A.B.P.M. is an adjuvant in treating hypertension befare discharge
Key Words: Ambulatory B.P., Treatment, Uncontrolled B.P.
POSTERS: Antihypertensive Drug Treatment 145A
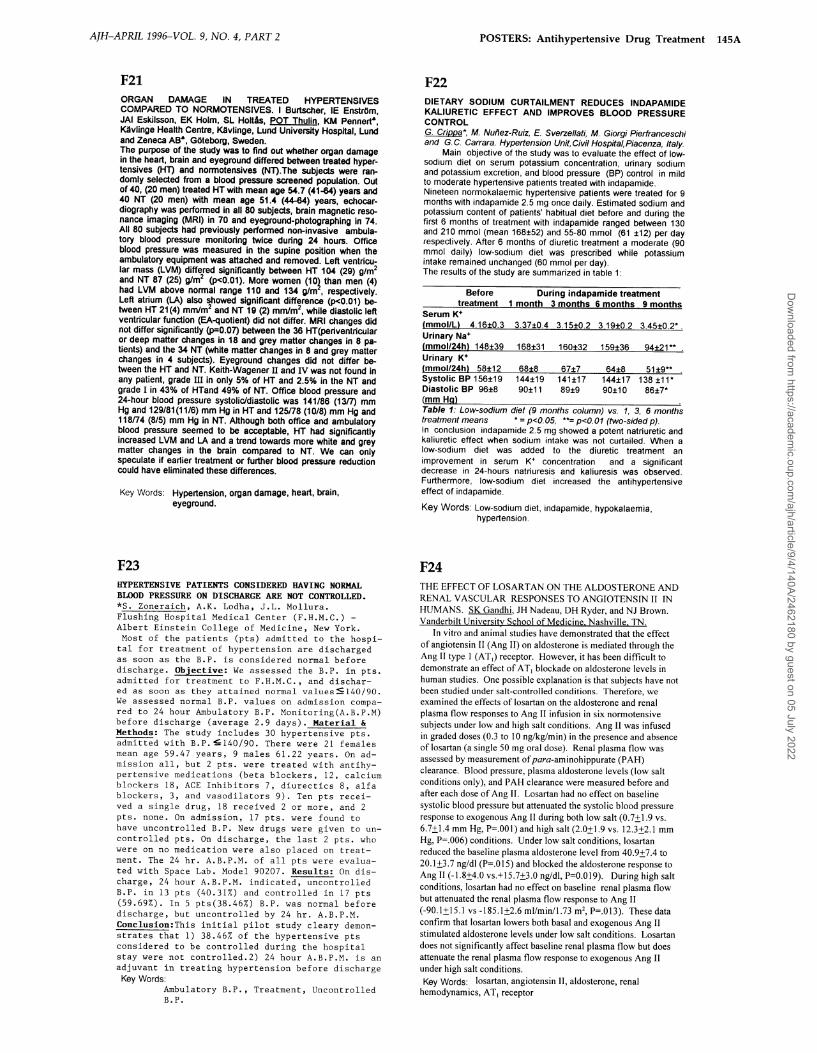
F22 DIETARY SODIUM CURTAILMENT REDUCES INDAPAMIDE KALIURETIC EFFECT AND IMPROVES BLOOD PRESSURE CONTROL G. Crippa*, M. Nuilez-Ruiz, E. Sverzellati, M. Giorgi Pierfranceschi and G.C. Carrara. Hypertension Unit,Civil Hospitai,Piacenza, ltaly
Ma in objective of the study was to evaluate the effect of lowsodium die! on serum potassium concentration, urinary sodium and potassium excretion, and blood pressure (BP) control in mild to moderate hypertensive patients treated with indapamide. Nineteen normokalaemic hypertensive patients were treated for 9 months with indapamide 2.5 mg once daily. Estimated sodium and potassium content of patients' habitual diet before and during the first 6 months of treatment with indapamide ranged between 130 and 210 mmol (mean 168±52) and 55-80 mmol (61 ±12) per day respectively. After 6 months of diuretic treatment a moderate (90 mmol daily) low-sodium diet was prescribed while potassium intake remained unchanged (60 mmol per day). The results of the study are summarized in table 1:
Before During indapamide treatment treatment 1 month 3 months 6 months 9 months
Serum K• (mmoi/Ll 4.16±0.3 3.37±0.4 3.15±02 3.19±0.2 3.45±02*. Urinary Na• (mmol/24hl 148±39 168±31 160±32 159±36 94±21** Urinary K• !mmol/24hl 58±12 68±8 67±7 Systolic BP 156±19 144±19 141±17 Oiastolic BP 96±8 (mmHgl
90±11 89±9
64±8 51±9** 144±17 138±11* 90±10 86±7*
Tab/e 1: Low-sodium dief (9 months column) vs. 1, 3, 6 months treatment means • = p<O.OS, ••= p<O.Ot (two-sided p). In conclusion indapamide 2.5 mg showed a potent natriuretic and kaliuretic effect when sodium intake was nol curtailed. When a low-sodium diet was added to !he diuretic treatment an impravement in serum K• concentratien and a significant decrease in 24-hours natriuresis and kaliuresis was observed. Furthermore, low-sodium diet increased the antihypertensive effect of indapamide.
Key Words: Low-sodium diet, indapamide, hypokalaemia, hypertension.
F24 THE EFFECT OF LOSARTAN ON THE ALDOSTERONE AND REN AL V ASCULAR RESPONSES TO ANGIOTENSIN 11 IN HUMANS. SK Gandhi, JH Nadeau, DH Ryder, and NJ Brown. Vanderbilt University School ofMedicine Nashville TN.
In vitro and animal studies have demonstraled that the effect of angiotensin !I (Ang !I) on aldosterone is medialed through the Ang 11 type I (AT,) receptor. However, it has been difficult to demonsirale an effect of A T1 blockade on aldosterone levels in human studies. One possible explanation is that subjects have not been studied under sali-eontrolled conditions. Therefore, we examined the effects of losartan on the aldosterone and renal plasma flow responses to Ang 11 in fusion in six nonnotensive subjects under low and high salt conditions. Ang !I was infused in graded doses (0.3 to I 0 ng/kglmin) in the presence and absence of losartan (a single 50 mg oral dose). Renal plasma flow was assessed by measurement of para-aminohippurate (PAH) clearance. Blood pressure, plasma aldosterone levels (low salt conditions only), and PAH clearance were measured befare and aftereach do se of Ang 11. Losartan had na effect on baseline systolic blood pressure but attenuated the systolic blood pressure response to exogenous Ang 11 during bath low salt (0.7±1.9 vs. 6.7±1.4 mm Hg, P=.OOl) and high salt (2.0±1.9 vs. 12.3±2.1 mm Hg, P=.006) conditions. Under low salt conditions, losartan reduced the baseline plasma aldosterone level from 40.9±7.4 to 20.1 ±3.7 ng/dl (P=.O 15) and blocked the aldosterone response to Ang li (-1.8±4.0 vs.+l5.7±3.0 ngldl, P=O.Ol9). During high salt conditions, losartan had na effect on baseline renal plasma flow but attenuated the renal plasma flow response to Ang 11 (-90.1±15.1 vs -185.1±2.6 ml/min/1.73 m2, P=.Ol3). These data confinn that losartan lowers bath basal and exogenous Ang !I stimulated aldosterone levels under low salt conditions. Losartan does not significantly affect baseline renal plasma flow but does attenuate the renal plasma flow response to exogenous Ang 11 under high salt conditions. Key Words: losartan, angiotensin 11, aldosterone, renal
hemodynamics, AT 1 receptor
Dow
nloaded from https://academ
ic.oup.com/ajh/article/9/4/140A/2462180 by guest on 05 July 2022

146A ASH XI ABSTRACTS
F25 ANGIOTENSIN U MAY MODULATE THE OXIDATIVE STRESS
IN HYPERTENSIVE ARTERIES RC Sham1a, AB Shil, M Lai, A Sevanian Vascular Research, Cardiology, University of Southem Califomia Los
Angeles, CA Increased lipid peroxidation in the hypertensive arterial wall may play a
major role in the pathogenesis of accelerated atherosclerosis. Locally
synthesized angiotensin Ilmay be involved in the increased oxidation
LDL in the hypertensive arteries. Treatment with vasoselective ACE
inhibitor ramipril, therefore, may suppress lipid peroxidation in the
arteries. Forty standard chow-fed, normocholesterolemic NZW rabbits
were divided as 01-10 nonnotensive, 30 animals were rendered
hypertensive by aartic coarctation and were randomly subdivided as
02-10 hypertensive 8 weeks, 03-10 hypertensive 16 weeks, 04-10
hypertensive 8 weeks +8 weeks ramipril (.lmg/kg/PO). Ramipril
treatmenl nonnalized the elevated blood pressure in 04 animals while in
03 the hyperlension was sustained for 16 weeks. At aulopsy, total
cholesterol (C) and C-oxides content of the thoracic aorta was
detemlined by using gas chromatography and mass spectrometry. The
following ox-ysterols : cholest-5-ene-3 beta; 7 alpha-diol; 7-ketocholesterol; 5,6 alpha-epoxy-5 alpha cholestane-3 alpha-al and 5
alpha-cholestane-3 beta,5,6, beta triallevels were significantly increased
in 02 ( 3.5 fold) and 03 (6.5 fold) groups as compared toOI. Treatment
with ramipril significantly reduced the elevated conjugated diene levels (p>0.05). The following is the data summary:
Final BP + Total C Total C-Oxide 26-0H Cholesterol
nun Hg Mean±SEM: ug/g (wet tissue) 01 81/56 3187± 124 6 07± 1.5 0 ± 0 02 108/74. 517.3 ± 171* 21.4±3.3* 0.2 ± 0.04 03 131/89 •• 1763.4 ± 346** 39.9 ± 4.3** 0.57± 0.09 04 83/56*# 796.3 ± 170 7.1 ±0.7# 0± 0 + =Systolic/diastolic; *p<0.05(01 vs 02; **p< 0.05(01 vs 03;
#p=not significant 0 I vs 04 Conclusion: Angiotensin U may be involved in the formation oflipid
peroxidation produels in the hypertensive arteries . Treatment with ACE
inhibitor ramipril nat only effectively reversed the elevated blood
pressure but also reduced the arterial oxidative stress.
Key Words: Hypertension, Oxidative stress, Cholesterol oxide,
Angiotensin I!, Ramipril, Rabbits
F27 INTOLERANCE RISK FACTORS TO THE ACE-INHIBITOR
TRANDOLAPRIL: LARGE SCALE ANALYSIS. I.aurent Yaur. Natbalie Genès1, Claire Dutrey-Dupagne1, AIUle Pochoy1,
Francais Elkik1, Alain Rauss2·
1Laboratoires Roussel. medical department. Paris. 2Roussei-Uclaf. Corporale Drug Safe()' and Epidemiology Depanment, Romainville, France.
~ To investigate the incidence of adverse events (AE) and the prognostic value of various intolerance risk factors in a large population of unselected hypertensives treated with the ACE·(inhibitor ACE-I) Irandolapril (T).
Mnlmdi Data was colleeled during a retrospective post-marketing study. Each investigator had to report information on the first five consulting patients previously treated with T whether or nat the drug was discontinued for AE. The following parameters, considered as potential risk factors for AE occurrence (RF), were collected: age, sex, body mass index, smoking habits, alcohol consumption, renal impairment, renal artery stenosis, prior intalerance to ACE-I or to other antihypertensive agents, combination with
diuretics, P-blockers, calcium channel blockers, centrally acting antihypertensives, NSAIDS, antidiabetic agents, hypolipemie agents ar non
antihypertensive drug. Univariate analysis was perfonned to pre-identify RF: all variables for which the p-value was less than 0.2 were incorporated in a multivariate analysis using a stepwise logistic regression model.
Rl:sulls:. 30072 hypertensive patients aged 61±12, treated by T (2mg/d in 96% of cases) for 7±6 weeks (range 1-100 weeks) entered the study. 2289 AE accured in 1813 patients (6.0%). The most frequentABwere coughing (944 pts-3.1 %), dizziness (0.7%), headache (0.6%) and asthenia (0.5%). Main RF, listed according to their rank in the final model of the multivariate analysis, are: prior intolerance to ACE-I ( Odds Ratio: 4.19, p<O.OOOOI), female gender (OR: 1.46, p<O.OOOOI), prior intalerance to other antihypertensive drug (OR: 1.27, p<O.OOOOI), smoker (OR: 0.76, p<O.OOOOI) and combination with IJ-blocker (OR: 1.31, p=0.0008). At-risk patient profiles have been determined from these individual RF.For example, a non-smoking woman having a prior intolerance to ACE-I has a 6. I -fold increased risk of AE occurrence as compared toa patient having oone of these risk-factors.
Conc!usjon·This study allowed (I) the categorisation of T-related AE risk factors, and (2) the quantification of the risk increase due to each factor, either alone or in combination.
Key Words: ACE-inhibitor, adverse event, risk factors
AJH-APRIL 1996-VOL. 9, NO. 4, PART 2
F26 ROLE OF OBESITY AND GENDER IN REGULATlNG RESPONSIVENESS TO lRBESARTAN, CAPTOPRIL AND ANGlOTENSlN ll IN A HYPERTENSlVE RAT MODEL (SHHF/Mcc.fa"'). BJ Holycross, SA McCune, T Hoepf, J Carraway, and MJ Radin . The Ohio State University,
Columbus, OH. These studies were designed to determine: 1) the
antihypertensive effect of chronic therapy with the ACE inhibitor, captopril (Cap)(1 00 mg/kg bw/day). and the angiotensin type 1 receptor antagonist, irbesartan (lrb) (SR 47436) (50 mg/kg bw/day), in lean male and obese temale ~pontaneously J:!ypertensive, J:!eart Eailure (SHHF) rats; and 2) possible mechanisms accounting for
the lack of depressor effect of Cap and lrb in obese SHHF temale rats. Drugs were administered in drinking water for 3 months. Systolic blood pressure (SBP) was measured by tail cuff (n =4·5/group). SBP in lean male rats was lowered significantly by 1 wk, and was maintained throughout 3 mo therapy (Cap= 96 ± 2, lrb = 106 ± 2, Control = 155 ± 2 mmHg). Obese temales showed no depressor response to Cap or lrb after 1 wk or 3 mo therapy (Cap= 162 ± 4, lrb = 149 ± 2, Control = 1 60 ± 5 mmHg). Lean and obese temale rats (n = 5/ group) were anesthetized with pentobarbital, the left carotid artery and jugular vein we re cannulated, and presser responses to bolus injections of angiotensin 11 (Angll) were measured. Obese temale rats were significantly more sensitive to Angll than lean temale rats (ED50 obese = 1 .9 ng [3. 7 ng/kg] vs ED50 lean = 14.3 ng [73. 1 ng/kg]). Presser responses to 1 pg Ang 11 in obese temale SHHF were not blocked by 1 .2 mg/kg lrb, whereas lrb inhibited Angll presser response by 47% in lean temale SHHF. These data suggest that obese temale SHHF are resistant to the antihypertensive actions of drugs which antagonize the renin-angiotensin system. Enhanced receptor sensitivity to Angll in obese animals may contribute to the lack of drug response. (This study was supported by a grant from Bristol-Myers Squibb and Sanofi-Winthrop). Key Words: Angiotensin 11, Captopril, lrbesartan,
Obesity
F28 DEMONSTRATION OF DIFFERENCES IN ACE INHIDITORS DURATJON OF ACTION BY SELF BLOOD PRESSURE MEASUREMENT C Dutrey-DupaKoe1, G. Bobrie1, L. Vaur2, I. Dubroca 2, N. Genès2, F. Elkik? 1 Service de néphrologie et d'HTA, Vannes, 2 Lab. Roussel, Paris, France
The blood pressure lowering effects of the recommanded daily morning doses of traDdolapril 2 mg <n and perindopril 4 mg (P) were compared 12 and 24 hours after drug intake by home self blood pressure measurement (SBPM) in a double-blind randomised study. After a 2-week placebo run-in period, 152 patients whose office DBP was in the range 95-119 mmHg and home DBP over 85 mmHg. were treated for 28 days. Drugs were packaged in electrooie pill-boxes. One week of SBPM (A&D UA751), was planned at the end of bath the run-in and the treatment period. Three consecutive measurements were requested in the moming before drug intake (8 am) and in the evening (8 pm). Only evening measurements occuring 12 ± 4 hours and morning measurements occuring 24 ± 4 hours after last drug intake were taken into account. Patients with less than 6 moming or 6 evening measures we re excluded. Average of all available measurements was used to define each patient's SBPM level in the morning and in the evening. 128 patients were evaluable for antihypertensive efficacy (8 excluded for
protocol deviations and 16 for bad perfonnance of SBPM). For placebo and treatment periods, 94% and 90% of the expected measurements were respectively available. During the run-in period, meao home systolic and
diastolic blood pressure levels for the 128 patients were: 148 ± 16/97 ± 8 mmHg in the moming and 151 ± 15/97 ± 8 mmHg in the evening. They were camparabie in T and P groups. SBPM decreases between placebo and treatment periods are presented in the following table:
!J.SBP(mmHg) !J. DBP (mmHg)· Evening Moming Evening Moming
TraDdolapril 13.4 ± 13 9.5 ± 12 7.6± 8 6.2± 8 Perindopril 11.7±10 5.8 ± 9 7.0 ± 7 3.9 ± 5
p* ns 0.04 ns 0.06 * Student' s pa i red t test between T and P
For cesponders patients (evening DBP decrease > 6mmHg) DBP moming decrease over DBP evening decrease was calculated individually (M/E ratio). Meao of individual MiE ratios were 0. 73 ± 0.6 for T group and 0.53 ± 0.4 for P group (p< 0.10). In conclusion, despite similar BP decreases 12 hours after dosage, a difference between treatments was observed at trough. Home SBPM was able to show a difference between duration of action of ACE inhibitors. Key Words: ACE inhibitors, Self- Blood Pressure Measurement
Dow
nloaded from https://academ
ic.oup.com/ajh/article/9/4/140A/2462180 by guest on 05 July 2022

AfH-APRIL 1996-VOL. 9, NO. 4, PART 2
F29 TIIE CALCIUM ANTAGONIST MffiEFRADIL INCREASES SURVIVAL IN A RAT MODEL OF CHRONIC HEART FAILURE. P. Mulder V. Richard, J.P. Henry, J.P. Clozel, F. Lallemand, B. Macé, C. Thuillez. Dept of Phannacology (V ACOMED, IFRMP n° 23), Rouen Univ. Med. School, France.
The use of calcium antagonists in chronic heart failure (CHF) may be limited by their negative inotropic effects. Mibefradil (Mib; Ro 40 5967) is a new calcium antagonist which blocks both Land T -type calcium channels and displays potent anti-ischemie effects despite only moderate negative inotropic properties. We investigated the effects of a 9 month treatment with Mib (15 mg/kg/day in chow) in a rat model of CHF (coronary artery ligation; n=60 per group ), and compared these effects to those of the angiotensin converting enzyme inhibitor cilazapril (Cil, I 0 mg/kglday). After 9 months, systolic blood pressure (SBP, mm Hg) and heart rate (HR, bts/min) were measured in conscious rats, and left ventrienlar dP/dt (LV dP/dt, IO'mm Hglsec) was measured in anesthetized animals. Mib decreased SBP (control 119±2; Mib 91±2; p<.05), although toa lesser extent than Cil (82±1; p<.05 vs Mib). Neither Mib nor Cil affected HR (control 394±10; Mib 392±9; Cil408±9) or LV dP/dt (contro16.7±0.4; Mib 5.6±0.3; Cil 5.8±0.4). Mib and Cil decreased heart weight (control 1.83±0.05; Mib 1.67±0.03; Cil 1.44±0.04g; both p<.05 vs control) and LV collagen density ( control 3.3±0.2; Mib 2.3±0.1; Cil 2.2±0.1 %; both p<.05 vs control). Figure shows survival (*:p<.05 vs control).
1 ()() Titus, in this rat model
~
ê 80
of CHF, Mib improved survival to the same
-..,--...._-.,.• extent as Cil, and decreased caniiac pre
-- control _...._ Cilazapril
* and afterload and LV hypertrophy and fibrosis. These results suggest that Mibefradil
---v-Mi befradii 40
0 3 6 9 might be beneficia) in
Key Words: Time (Months) CHF.
Calcium Antagonists, Experimental Heart Failure
F31 24-HOUR NON-INVASIVE BLOOD PRESSURE MONITORING OF FELOD!PINE-METOPROLOL EXTENDED RELEASE TABLET A.H. Watt on behalf of the Scottish Lngimax'" Group
This study was perfonned in 23 hypertensive pa tienis (13 M and 10 F) aged 60-77 years, mean 69 years with a diastolic blood pressure (BP), between 95-114 mmHg aftera 2-4 weeks' placebo run-in. Felndipine ER 5 mg and metoprolol CR 50 mg given nnce daily as fixed nr free combination and placebo were compared in tenns of (BP) response measured by ambulatory BP monitoring at the end of each treatment period. The study was a doubleblind, randombed 3 way cro~.s-over design, each treatment period lasting for 4 weeks. A generallinear model (ANOV A), including sequence, period and treatment as fixed effects and subjectsas a random effect, was used to analyse AUC for BP resp(mst•. RESULTS Mean treatment differences for diastolic BP (mmHg) over 24 hrs b ABPM
Tn·atment Estimated 95% confidence p-value di Herences limits
PI acebo-free 10.2 7.H -12.6 < 0.0001 Placebo-fixl•d 10.3 7.9-12.6 < 0.0001 Free-fixed 0.1 -2.3- 2.5 0.9356
Mean treatrnent differences for diastolic BP(mmHg) during night-time by ABPM Treatment Estimated 95% confidence p-value
differences limits Placeb• >-free 7.0 2.6-11.4 < 0.0026 Placebo-fixed 6.6 2.2-10.9 < 0.003H Frel•-fixed -0.4 -4.9-4.1 O.H55Y
The results indicate that the pharmacodynamic action of felodipine ER 5 mg and metoprolol CR 50 mg are similar whether they are given in fix~-d or free combination. Both were significantly more effl"'tiw than placebo over the whole dosing interval in ad dition to producing a uniform BP con trol. Key Words: felodipine, metoprolol, fixed combination,
hypt•rtension, ABPM
POSTERS: Antihypertensive Drug Treatment 147 A
F30 EFFECTS OF DIFFERENT ANTIHYPERTENSIVE DRUGS ON
DAIL Y BLOOD PRESSURE PROFILE F.Rabbia, F.Veglio, R.Melchio, B.Gagliardi, MP Sibona. R. Conterno. AG De Micheli, L.Chiandussi. Dept. of Internat
Medicine. University of Turin. llaly The purpose of this study to analyze the effects of different
classes of antihypertensive drugs on diurnal BP profile and variability in mild moderate essential hypertensives. Methods: 87 patients were studied. Alter 2 weeks placebo run-in period, they were randomly assigned to 1 of the following drugs: ll-Biock (Atenolol), äB-Biock (carvedilol), CEBs (lacidipine isradipine). ACE I (fosinopril). central ä-agonists (transdermal clonidine). All drugs, but clonidine were given O.O. at 8 a.m. 24-h ABPM was performed befere and 12 weeks alter therapy (Spacelabs 90207). Runs test was used to deleet the presence of a circadian BP rhythm. Truncated Fourier series with 4 harmonies were applied to evaluate overall amplitude (AMP). acrophase (AP) and mesor (M) of BP and HR. Moreover. nocturnal BP dip. day/night BP and HR
difference (DND). and R2 (%of varianee explained by !he model) were calculated. Before therapy, 86% of pts had BP rhythm, 80% were dippers. and R2 values were 60%±1 0. The response rate to drugs was 90%. All drugs preserved BP circadian rhythm; all. but clonidine reduced BP variability (represented by AMP reduction). ll and äB blockers showed similar patterns: significantly reduced DND (from 16±6 to 6±4) and increased the% of non dippers. CEBs significantly reduced M, and shilted AP trom morning to alternoon hours (11 a.m. to 4 p.m.) didn't change DND and BP dip ACE I were effective in BP M reduction. and gived the higher increase of R2 (>10%) didn't modify nocturnal BP dip. Clonidine. only reduced BP M. but didn't show ether modifications of BP and HA parameters. In conclusion. the statistica! approach. we used revealed peculiar differences of effect of antihyprtensive drugs on daily BP profile. !hal may be important lor the evaluation of !heir effectiveness in cardiovascular risk reduction.
Antihypertensive drugs. ambulatory BP ~i!llRf\lfcircadian rhythm
F32 DOSE-DEPENDENT HEMODYNAMIC AND RENAL EFFECTS OF FENOLDOP AM DURING PROLONGED INFUSIONS IN HYPERTENSIVE PATIENTS. AA TIIYlor*, R Mangoo-Karim, R Luther, KD Ballard and JL Pool*, Baylor College ofMedicine, Houston, TX and Neurex Inc, Menlo Park, CA
The dopamine-I receptor agonist, fenoldoparn (Fen), was infused iv for 48 hr into 18 moderately hypertensive patients at doses ranging from 0.04 to 1.6 J.lg/kg/min. Active drug infusion was preceeded and foliowed by 24 hr of saline placebo infusion. Blood pressure (BP) and heart rate (HR) were monitored every 15 min during the 4-day hospitalization and urine collected every 12 hr for calculations of the clearancesof creatinine (Cr), Na+, K+, er, Ca++, P04-- and
uric acid (UA). Plasma Fen was deterrnined every 6 hr. Blood pressure was reduced and heart rate increased during 48-hr Fen infusion; these effects were close-dependent and most pronounced during the first 12 hr of infusion. The time
to peak effect of Fen on blood pressure was 2-4 hr afterstart
of infusion whereas the HR response occurred within min. Despite dose-dependent BP rednetion there was maintenance of creatinine clearance (CrCI) during Fen infusion. Fractional
clearances of sodium (NaCI/CrCI) and of chloride (CIC!/ CrCI) were reduced during Fen infusion whereas those ofK+, Ca++, P04-- and UA remained unchanged. We coneinde that
the antihypertensive effect of Fen is maintained over 48 hr of infusion, is maximum during the first 2-4 hr of infusion, is predicted by Fen pharrnacokinetics, and is associated with preservalion of glomerular tiltration and renal tubular adaptation to BP reduction.
Key Words: dopamine agonist, fenoldoparn, hypotension, tachycardia, pharrnacokinetics, renal function, glomerular tiltration
Dow
nloaded from https://academ
ic.oup.com/ajh/article/9/4/140A/2462180 by guest on 05 July 2022

148A ASH XI ABSTRACI'S
F33 DOXAZOSIN (DZN) PREVENTS ALBUMINURIA AND LUWERS GLYCATED HbA1 IN DIABETIC RATS. GN Jyothirmayi, Indira Alluru, and AS Reddi. UMDNJ-NJ Medica! School, Newark, NJ.
We previously demonstrated a decrease in glomerular synthesis of heparan sulfate (HS)associated with significant albuminuria in long-term diabetic rats. HS confers a negative charge to the glomerular basement membrane and participates in charge-selective properties of the membrane. ACE-inhibitors and eertaio calcium antagoniste were found to reduce albuminuria by preventing glomerular loss of HS. We now present data that DZN, an a 1-adrenergic blocker, would similarly prevent renal loss of HS and albumin in diabetic rats. Diabetes was induced in male Wistar rats by streptozotocin. One week after persistent hyperglycemia, the rats were given DZN (75mg/L) in drinking water for 20 weeks. The effects of DZN were compared with these of diabetic rats whose glucose was controlled by insulin. DZN significantly lowered SBP in diabetic rats. However, it had na effect either in normal ar diabetic rats with good glycemia. Glomerular heparan sulfate synthesis was significantly lower and urinary albumin excretion higher in diabetic than in normal rats. Bath DZN treatment and good glycemia normalized these abnormalities in diabetic rats. Plasma glucose and glycated HbA1
concentrations were normalized by insulin. However, these were also significantly lowered by chronic treatment of DZN in diabetic rats. Plasma cholesterol, triglyceride, very low density lipoprotein and low density lipoproteincholesterol were elevated and high density lipoprotein-cholesterol decreased in diabetic compared with normal rats. These abnormalities in plasma lipids were normalized by good glycemia and favorably improved by DZN treatment. These results indicate that DZN prevents albuminuria, preserves glomerular synthesis of HS and favorably impraves plasma glucose and lipid levels in diabetic rats. The effects of DZN are thus comparable to those of ACE-inhibitors and certain calcium antagoniste. However, DZN has an additional effect of improving glycated HbA1 in diabetic rats. Key Words:
F35
Doxazosin, a 1-blocker, albuminuria, glycated HbA1 , lipoprotein, streptozotocin-diabetic rats.
EFFECTS OF LONG TERM ANTIHYPERTENSIVE TIIERAPY ON LEFf VENTRICULAR REMODELING: TIIE lREATMENT OF MILD HYPERTENSION STUDY.SB Dianzumba*. PR Liebson*, G Grandits, RJ Prineas,RH Grimm,Jr*.,J Stamler, for the TOMHS Research Group. MCP-Hahnemann University, Allegheny Campus, Pittsburgh, PA.
We previously have shown that all 5 classes of antihypertensive agents used in TOMHS produce similar levels of L VH regression in participants(pts) with stage I hypertension.This report analyzes the effectiveness of these agents in reducing left vennicular(L V) remodeling in stage I hypertension (mean BP 140/91). Of the 902 participantsin TOMHS, 844 had adequate 2-D guided M-mode echocardiograms for LV mass (LVM) and re1ative wall thickness (RWT) estimation at baseline and during a 48-month follow-up. All underwent intense, lifestyle modification. Of the 625 pts randomized todrug therapy, 58.7% had normal geometry(normal LVM and RWT) vs 55.3% in placebo(N=219, p=NS) at baseline. Normal LV geometry rose to 72.8% in the active group vs 66.4% in placebo group(p=0.074) at 3 mantbs and 74.3% vs 63.3%(p=0.035) at 12 months. Both groups were equal at 48 months(80.7% vs 77.3%, p=NS). When individual drugs are analyzed, amlodipine( calcium channel blocker) significantly reduced RWT at 12 months(p=0.016), 36(p=0.049) and 48 months(p=0.019), while acebutolol( beta-blocker) was borderline at 3 moths(p=0.060), significant at 12 moths(p=0.020) and 24 months(p=0.038) compared to placebo, but sirnilar to placebo at 36 and 48 months (p=NS). In contrast, there was no difference between placebo and chlorthalidone(diuretic), enalapril( ACE inhibitor) or doxazosin(alpha-1 inhibitor) throughout the study. In conclusion, amlodipine and acebutolol are more effective than placebo in normalizing LV geometry in stage I hypertension, with amlodipine showing more sustained long term effects. Key Words: LV remodeling, hypertension,
antihypertensive therapy
AfH-APRIL 1996-VOL. 9, NO. 4, PART 2
F34 RACIAL DIFFERENCES IN PHARMACODYNAMIC (PD)- RESPONSE TO HYDROCHWROTBIAZIDE (HCTZ) ARE NOT EXPLAINED BY PHARMACOKINETIC DIFFERENCES (PK) EBD R!p!ey*. K KIDg. TWB Gebr, D Ska*, Medlall Collep ofV!rpnla, Rlcbmoad, VA, USA
Tbe PK lUid PD of HCTZ were emUIIted ID !I blad< (B) (2M(TF, 46:!_7.6 yrs, !ll::!:I!IAq) lUid !I whlte (W) (7.M(1F, 4l:!:SA yrs, 811::!:18Aq) byperteaslw Jllldenls (eltber cm medleallon or BP ~ 14Uj!IO). After a 4 week wasbout period, lUid a 7 day controlled dlet (ISOmEq Na•/llllmEq K") Jlllllenls .-lved 25 m1 HCTZ wltb oerlal blood lUid urine oolleciiCHlo Oftr lbo - 36 bn. Urlnary (U), HCTZ, oodlum, potasslum, ud lldooterone (ALDO) eKredCHl (e:a:) were IDOIISured. Mean arterlll pressure (MAP) was measured suplne lUid upri&hl 111 0 lUid 24 bours pool dooe. Data Is reporled as mean±SD for BfW. On dlel, lbore were DO dllferOD<es In bllseiiDe Na• (ll2::!:42/117::!:20 ml!qf24bn) or K• (45::!:20/57::!:!1 ml!qf24 bn) exc. Tbere were DO dllfennces In PK as assessed by U e:a: parometen (mulmum e:a: rate of HCTZ .... 46.3;:!:12{46.11::!:18 mcrfmln, TIDIU< 4::!:2/2.11!1 bn, 'I dooe recowred In 36 bn 4!1;tlfil55::!:!1'1 ). Suplne MAP al 0 bour was slmDar In B lUid W patlellis (103::!:!111'6::!:8 mmHJ). Al 24 bn, snplne MAP slplfk:anlly lell oody ID B Jlllllenls (96!.!1J116!.7 mmHJ). Uprigbl MAP was slmDar In bolb poups 111 0 bour (106:!:.11/97::!:6 mmHg) lUid remalned ucbaJIIed 111 24 boiD"I (102:t!l/102:t6 mmHg).
.. 12... ~... _ ... U Na• EK (mEq) BtW :103+44/203:1:31 6l+17/5l+17 ~3413~17 Ult"Ex(JDI!q)II/W G+Ïitl6l+f" z.t~ÏO ~ u ALDO (acg) BtW 6.5!3~ s-4!217~• 15!4/13.8!6 Wllb-..! aiifttciD, "1>!0.115 B .. W, Op!9.0S W 12-24 .. 11-12 lln.
Na• e:a: slgnlllcandy IDcreased aller HCTZ, wltb DO dllfereDCe belween lbo ponpo. Total K" e:a: ,.. bighor In W, wllh lbo prlmary dlll'ereDce durÜIJI lbo llrsl 12 bn. U ALDO e:a: slpiii<IIDIIy decre-d In W belween 12-14 bn as COIIIJNired to lbo &.12 br period. B bad Jower U ALDO e:a: durlJII lbo llrsl 12 bn OODIJNII"ed to W. U ALDO e:a: remalned amstanl In lbo B c1urtJ11 eKb of lbo 12 bour perlods.
B byperlenslw Jlllllenls baw dasleaUy beea reprded as uqulsltely dluredc SOllillive ID lbo lreatmeDI of lbolr bypertensiOD. Tbe meebanlom for lbo eiDciOD<y of medleaiiCHlo llb HCTZ bas 1101 been runy elucldaled. Tbls study shows !bal PK lUid Na" PD are slmDar 1D B and W byperleDslves. H01111C111111, BP lUid biluretic dllferOD<es In Ibis sludy may have rellected ...-lalloou In counterTegnlatory aud/or clrcadlaa mecbanlsms.
Key Words: Race, Hypertension, Diuretic
F36 NIFEDIPINE SR REPLACING NIFEDIPINE GITS: 24 HOUR AMBULATORY BLOOD PRESSURE ASSESSMENT OF EFFICACY. C Rahima-Maoz, E Grossman•, N Nussinovitch, A Katz and T Boseothal•. Chortey Hypertension Unit, Chaim Sheba Medica! Center, Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, lsrael
N~edipine SB 30-40 mg/day (twice daily ingestion) was replaced by n~edipine GITS 30 mg (one daily dose) in 38 patients. Concomitant therapy with B-blocking agents was nol changed. 15 subjects underwent 24 h ambulatory blood pressure monitoring (ABPM) on both treatments.
In the 23 subjects who did nol undergo monitoring, trough blood pressure on nifedipine SR was 171±98 mmHg, and went down to 148±88 mmHg (p<0.01) on nifedipine GITS. The resuHs on the ABPM group are summarized in the table.
Mean systolic blood pressure SBP!mmHgl ~ 2400 · 0600 night 129.20±21.93 0600-2400 day 128.05±15.65 Mean diastolic blood pressure DBP !mmHgl .aB...2Qmg 2400 ·0600 night 77.18±13.15 0600- 2400 day 80.32±1 0.88 Mean heart rate .l:iB...(bsmJl 2400 · 0600 night 0600 - 2400 day
~ 59.87±8.39
68.75±11.60
ma 126.60±17.92 125.4513.75
ma 74.23±7.33 76.88±9.15
ma 60.01±6.44
68.65±12. 71
..ll. 0.309 0.091
..ll. 0.204 0.003
..ll. 0.972 0.851
lt is concluded that a once daily dose of n~edipine GITS was advantageous over twice daily treatment with nifedipine SR.
Key Words: nifedipine SR, n~edipine GITS, 24 h blood pressure monitoring
Dow
nloaded from https://academ
ic.oup.com/ajh/article/9/4/140A/2462180 by guest on 05 July 2022

AfH-APRIL 1996-VOL. 9, NO. 4, PART 2
F37 EFFECT OF BENIDIPINE, A SECOND GENERATION CALCIUM ANTAGONIST, ON DIURNAL CHANGE OF BLOOD PRESSURE AND PRESSOR RESPONSE TO MENTAL STRESS Muneta S 1 l, Kohara K* 2), Watanabe S 1 l, ltoh T 3),
Hiwada K* 2). 1) Matsuyama Red-Cross Hospita!, 2) 2nd Department of Internat Medicine, Ehime University, 3) lmabari Hospita!, Ehime, Japan.
Ob)ectlve: The effect of benidipine, secend generation of calcium channel blocker, on diurnal change of blood pressure and presser response to mental stress were investigated in essential hypertensive patients.
Method: Nine essential hypertensive patients (M/F=8/1), were treated with benidipine 4 mg once a day tor 12 weeks. Twenty-four-hour blood pressure as well as presser response to mental arithmetic test were evaluated befere and atter the treatment.
Results: Befere After
n ~ ~ 24h SBP/ DBP (mmHg) 142:t11/88:t7 129±10**/81:!::7** daytime SBP/ DBP 145±12/90:!:8 130±10**/83±7** nighttime SBP/ DBP 131±10/79:!:6 124±13/ 78:!:9 Presser Response 26:!:11/10:!:5 19+-21*/10:!:8
Values are mean±SD. * p<O.OS, ** p<0.01 vs Betere. Benidlpine had no effects on heart rate.
Conclustons: Once a day administration of secend generation Ca antagonist showed mild but significant reduction in blood pressure with little effect on noctumal levels of blood pressure. Impravement of presser responses to mental stress also benefited the treatment of hypertension.
Key Words:
24-hour blood pressure, mental stress, calcium antagonist.
F39 LAcK OF EFFECT OF NSAIQ:; ON BP CONTROL IN HYPERTENSNE SUBJECTS ON FOSINOPRIL AND HCTZ. Tha!rur V". Cook ME•, Andersm MC, Wallin JO". Dept. of Medicine. LSU Sdtool of Medicine, New Orleans, IA
NSAIDs are frequently reported to interfere with blood pressure lowering actions of various antihypertensive medicatims. We studied 17 wamen with arthritis and hyperlension who were receiving fosinopril and hydrochlorothiazide, and we administered sequentially in random order ibuprofen (1), sulindac (S), and nabumetone (N) for 1 month, with an intervening 2-week washout period between each treatment period. During the washout period the subjects received acetaminophen. Blood pressure at the end of 2 weeks of acetaminophen was compared with BP following administratim of NSAID for a month. Twenty-four-hour urine was collected at the beginning of eadl phase of the study to detect any manges in sodium excretim. The following table summarizes the data m BP rontrol an d odi f . . (Na/C ) s urn excretim per gram o !l'eatmme r.
Nabumetone Sulindac lbuprofen (n=17) (n=l7) (n=17)
Time Pre* Post Pre* Post Pre* Post MAP 108± 107± 108± 108± 108± 107±
7 9 9 9 8 9 Na/Cr lUl± 132± 111± 134± 121± HT7±
24 39 31 34 32 32
• Washout eriod p There was no increase in MAP or significant
deaease in urinary Na/Creat ratio. We conclude that the antihypertensive effect of the combinatim of fosinopril and HCTZ may not he prostaglandindependent.
Key Words: NSAIDs, ACEis, Diuretia;, Hypertensim
POSTERS: Antihypertensive Drug Treatment 149A
F38 EFFICACY OF COMBINATION THERAPY OF TRANDOLAPRIL AND VERAPAMIL SR IN PRIMARY HYPERTENSION: A MUL TI FACTORIAL TRIAL. V DeOuattro* and D Lee. USC School of Medicine, Los Angeles, CA.
To evaluate the efficacy and safety of combination (Co) therapy (Rx) of trandolapril (T) - an ACE inhibitor, wi th verapamil SR (V) - a sustained release calcium antagonist, in a 4 by 4 factorial trial: 3 oral doses of T (0.5, 2, 8 mgjday), V (120, 180, and 240 mgjday) and in Co were given to 726 primary hypertensives (PH) in 39 centers, double-blind, randomized, parallel, and with placebo (Pl) control. After 4 week single-blind Pl run-in period, 456 males, 270 females, age 55 ± 11 (24-83), 83% white, 13% black, received either T or V mono Rx or Co Rx of TjV or Pl each morning (7-9 am) for 6 weeks. At peak sitting (Sit) diastolic blood pressures (DBP) were reduced withall Rxs except T 0.5 and V 120 compared to Pl (p<.Ol). Co Rxs of T2jV180, T2jV240 and T8jV240 had greatest reduction in Sit DBP (p<Ol, 05, 05) at trough compared to each mono Rx component (corrected by Pl). T2, TB and Co Rx reduced supine, Sit, and standing systolic BPs at trough. BP response to all Rx' s was similar: between white vs. black, age <60 vs. 2:60. Co Rx of T2jV240 achieved highest percentage of responders (DBP <90 or a rednetion of 2:10 mmHg from baseline) at trough (62.8%) compared to Pl (3.8%). There was no difference in the incidence of adverse reactions between Ht with any Rx and Pl. Rx's with T or V or Co of TjV were well tolerared in PH. Co Rx of T2jV180, T2jV240 and T8jV240 yielded best BP control and all reductions were improved over T or V mono Rx.
Key Words:
F40
Trandolapril, combination therapy, blood pressure reduction
MUSCLE SYMPATHETIC NERVE ACTIVITY RESPONSE TO CHRONIC FELODIPINE THERAPY. DA Calhoun*, Vascular Biology and Hypertension Program, University of Alabama at Birmingham, Binningharn, AL.
Recently publisheel retrospective studies suggest that use of short-acting calcium channel antagonists may increase long-tenn mortality, compared to other classes of antihypertensive agents. It is hypothesized that the short-acting dihydropyridines increase risk of myocardial infarction secondary to reflexive increases in sympathetic activity. Sustained increases in sympathetic activity have been shown to induce left ventricular hypertrophy, smooth muscle cell hyperplasia, and ventricular arrhythmias and is hypothesized to increase the risk of atherosclerotic plaque rupture. Not known is the effect of the newer, longer-acting dihydropyridines on sympathetic activity. Using microneurography to measure muscle sympathetic nerve activity (MSNA) from the peroneal nerve, the present study was designed to
detennine this effect. Thirteen hypertensive subjects were withdrawn from all antihypertensive therapy for a minimum of 2-wks prior to
study. Seven of the subjects were randomized to felodipine 5 mg once a day and 6 were randomized to placebo once a day in single blind fashion. Subjects were studied at baseline and after 4-wks of therapy at trough drug levels (24-hrs post-dosing). Values were compared by
ANOV A. The felodipine (6 males, I female) and the placebo groups (3 males, 3 females) were of similar age and weight (57±3 vs. 57±3 years and 84±4 vs. 87±7 kg; felodipine vs. placebo) Mean arterial pressure (MAP), heart rate (HR), and MSNA values were:
baseline after 4-wks of theraov MAP HR MSNA MAP HR MSNA
(mmHg) (bpm) (burstslm) (mmHg) (bpm) (bursts/m)
felodipine 121±5 64±3 31±5 110±4* 65±2 30±5 placebo 115±4 69±3 22±7 113±2 71±4 21±4 bpm, beats/min; bursts/m, burstslmin; • different from baseline, p<0.05.
The above data demonstrate that peripheral sympathetic nervous system activity is not increased by trough levels offelodipine, suggesting that chronic use of a long-acting dihydropyridine does not induce sustained increases in sympathetic activity.
Key Words: microneurography, hypertension, felodipine (The project was supported by the HOT International Study).
Dow
nloaded from https://academ
ic.oup.com/ajh/article/9/4/140A/2462180 by guest on 05 July 2022

150A ASH XI ABSTRACTS
F41 The Effect of Adding Doxazosin to Current Therapy in Refractory Hypertensives
HR Black, JS Soliins and JL Garafalo, Rush-PresbyterianSt. Lukes Medica! Center, Chicago, IL, USA
Though unusual, refractory hypertension (failure to reach goal BP with adequate doses of two or more antihypertensives) is a persistent problem in rnanaging hypertensives. We randomized 29 patients with refractory hypertension to receive doxazosin (D) or placebo (P) in addition to their current therapy. Dor matching P was begun at 1 mg and titrated if needed to 16 mg/day. Those at goal (sitting DBP ~89 mm Hg or a decrease of~ 10 mm Hg) we re continued on treatment tor 4 weeks of maintenance. 14 patients (6 men and 8 women) received D and 15 P (12 men and 3 women). The groups were otherwise well matched with an avg BP at enrollment of 156.5/100.7 forD and 158.21100.3 tor P. At the end of titration those receiving D had a fall in BP of 25/15 mm Hg (to 132/85 mm Hg) compared toa drop of 6/5 mm Hg (to 152/95 mm Hg) in the P group (p<0.002). Ten (71%) of the D patients were at goal compared to 3 (20%) of the P group (p<0.001 ). The avg dose of D was 8.8 mg (range 2-16 mg). All but 1 patient on D was still at goal after maintenance. 5 patients on D had an adverse reaction (3 fatigue and 2 dizziness) and 2 on P had headache. One only patient stopped medication (on P for rash). Those randomized toD had a drop of 26.3 mg/dl in total cholesterol (TC) and 18.7 mg/dl in LDL-C. Forthoseon P, TC fell11.2 mg/dl and LDL-C rose 7.5 mg/dl (p <0.05 tor TC and <0.0001 for LDL-C) compared to those on D. Changes in TG and HDL-C were not statistically significantly different. Conclusion: We conclude that D is an effective and well toleraled agent for hypertensives with refractory hypertension and offers the added advantage of inducing a favorable lipid profile as it does when used as monotherapy. Key Words:
Alpha bloc kers, Refractory hypertension
F43 BENEFITS OF LONG-TERM ANTIHYPERTENSIVE TREATMENT ON PROGNOSIS IN DIABETIC NEPHROPATHY H-H Parving P Jacobsen, K Rossing, U Smid!, and P. Rossing Steno Diabetes Center, Copenhagen, Denmark.
Our aim was to asses the effect of long term antihypertensive treatment on the prognosis of diabetic nephropathy as compared to the reported prognosis during the natura! history of this complication. We performed a prospective study of all lOOM patients aged under 50 with onset of diabetes befare the age of 31 who developed diabetic nephropathy between 1974 and 1978 at Steno Diabetes Center, a tertiary referral center. 45 patients (20 wamen) with a mean age of 30 (SD 7) years and a mean duration of diabetes of 18 (7) years at onset of persistent proteinuria were foliowed until death or tor at least 16 years (1994). Conventional antihypertensive treatment was starled 3 (0-13) years (median (range)) alter onset of diabetic nephropathy. Two patients (4%) recieved no treatment, and 7 (16%), 16 (36%), 20 (44%) were treated with one, two, or three ar more drugs, respectively. The median follow up was 16 (4-21) years. Mean arterial blood pressure at start of antihypertensive treatment was 148/96 (SD 12/10) mmHg and 143/86 (16/6) mmHg during antihypertensive treatment (p<0,01). The cumuialive death rate was 45% (95% C.l. 38-52) 16 years alter onset of diabetic nephropathy, in contrast to previous reports of 88% and 94% 12 and 16 years alter onset of diabetic nephropathy, respectively. The median survival time in our study exceeded 16 years as compared to 5 and 7 years in the past. As in previous studies, uraemia was the ma in ca u se of death ( 12 patients; 55%). The cumuialive incidence of end stage renal disease was 31% (95%C.I. 23-39) and the cumuialive incidence of dubling of serum-creatinine (>177 ~moi/L) was 44% (95%C.I. 27-61) 16 years alter onset of diabetic nephropathy. In 1994 serum-creatinine was 116 (7 4-311) ~moi/L in the 23 surviving patients
In condusion the preservalion of kidney tunetion and the prognosis of diabetic nephropathy has improved during the past two decades mainly because of effective antihypertensive treatment.
Key Words: Diabetic nephropathy, kidney function, antihypertensive treatment, insulindependent diabetes mellitus
AfH-APRIL 1996-VOL. 9, NO. 4, PART 2
F42 REVERSAL OF ERYTHROPOIETIN (EPO) INDUCED HYPERTENSION (HTN) AND THE ASSOCIATED RISE IN CYTOSOLJC [Ca••], BY FELODIPINE IN RATS WITH CHRONIC RENAL FAILURE (CRF). K Wang, Z Ni, and ND Vaziri* Div. ofNephrology, Univ. ofCalifornia, lrvine, CA.
In previous studies, we have shown that regular EPO administration in CRF rats results in a hematocrit-independent HTN marked by elevation of [Ca++],. The present study was designed to test the hypothesis that EPO-induced HTN can be abrogated by preventing the rise in [Ca++], using a calcium channel blocker. Sprague Dawley rats were randomized into the following groups: CRF (5/6 nephrectomy), EPO-CRF (CRF animals given lP injections of EPO, 150 U/kg, twice weekly for 6 wecks), F-EPO-CRF (CRF animals treated with EPO and felodipine delivered by osmotic pump) and normal controts (recciving sham operatien and placebo therapies). Tail arterial blood pressure (BP) was manilored regularly, and platelet [Ca++], was measured by spectrofluorometry using Fura-2AM. Compared to the control group, the CRF group showed significant rises in BP (148±0.8 mmHg vs 130±1.0 mmHg, p <0.01) and [Ca++], (90.7±4.4 nM vs 72.5±1.5 nM, p <0.05). EPO therapy compoundcd the CRF-associated HTN ( 169± 1.0 mmHg, p <0.01 vs CRF) and further elevated [Ca•], (101±2.6 nM, p <0.05 vs CRF). Concomitant therapy with felodipine abrogated EPOinduced IITN (143±4 mmHg, p=NS vs CRF group) and normalized the (Ca++], (68± 1.5 nM, p=NS vs control group).
Thus. association of EPO-induced HTN with elevated [Ca•], and its rcversal with normalization of[ ca·], points to the primary role of increased [Ca++], as mediator of EPO-induced HTN and cfficacy of calcium channel blocker as the therapy of choice in this condition.
Key Words:
F44
Hypertension, erythropoietin, felodipine, calcium channel blocker, cytosolic calcium
COMPARISON OF NIFEDIPINE ALONE AND IN COMBINATION WITH DIL TIAZEM AND VERAPAMIL IN HYPERTENSION. J.J. Saseen,B.L. Carter,T.E. Brown, W.J. Elliott,* H.R. Black.* University of Colorado, Denver, CO; Health Sciences Center, Winnipeg, MB; and RushPresbyterian-St.Luke's Medica! Center, Chicago, IL.
Th is study compared blood pressure reductions using the combinations of sustained-release nifedipine/diltiazem and nifedipine/verapamil to nifedipine alone, and determined whether combinations alter nifedipine pharmacokinetics. Sixteen patients with essential hypertension (12 rnales and 4 females, mean age 48 years) were evaluated. After baseline supine blood pressure measurements, subjects received open-label nifedipine 30 mg/day for two weeks. lf still hypertensive, they were randomized (double-blind) to receive additional diltiazem 180 mg/day or verapamil 180 mg/day for two weeks, then crossed-over for the final two weeks. All medications were sustained-release, once-daily fomulations. During the final day of each treatment, blood pressures, and nifedipine concentrations were measured. Both combination therapies resulted in lower mean systolic and diastolic blood pressure compared to nifedipine alone (p<0.05, ANOVA). Mean diastolic blood pressures were significantly lower at 8 hr (77.6 vs 84.6 mmHg; p<0.05, ANOVA), and 12 hr (81.5 vs 87.1 mmHg; p<0.05, ANOVA) with nifedipine/diltiazem than nifedipine/verapamil. Mean nifedipine concentrations were inversely correlated with mean blood pressures. Mean nifedipine area under the curve values were higher with diltiazem than verapamil (1393 vs. 1132 ng*hr/ml; p=0.036, paird I-test), with both higher than nifedipine alone (995 ng*hr/ml; p<0.05, ANOVA). Nifedipine/diltiazem causes a greater antihypertensive effect than nifedipine/verapamil. Diltiazem caused greater increases in nifedipine concentrations than verapamil, which further reduce blood pressure. These data suggest combination calcium channel blockers result in additive antihypertensive effects. Key Words: hypertension, calcium channel blockers, combination therapy
Dow
nloaded from https://academ
ic.oup.com/ajh/article/9/4/140A/2462180 by guest on 05 July 2022

AfH-APRIL 1996-VOL. 9, NO. 4, PART 2
F45 NIFEDIPINE-RETARD(N) IMPROVES REDUCED INSULIN(INS) SENSITIVITY IN BOTH YOUNG AND ELDERLY HYPERTENSIVES K. Masuo*, H. Mikami*, T. Ogihara*, M.L. Tuck*. Dept. of Geriatrie Med., Osaka University Medical School, Osaka, Japan, and Sepulveda VA Medical Center and UCLA School of Medicine, Los Angeles,CA
To clarify the ameliorative effects of N on reduced INS sensitivity or hyperinsulinemia and impaired sympathetic nerve responsiveness, we conducted this study. In 12 young normotensive(NT;45+6(SD)yrs,23.0 +1.1kg/m2, 109/65mmHg), 25 young hypertensive(HT; 46+6, 22.9+1.1, 177/98), 12 elderly NT(78+7, 22.9+ 1.3, 109/64) and 24 elderly HT(78+6, 23.0+1.2, 174/ 102), BP, blood glucose, plasma INS and n;repinephrine(NE) levels were measured every 30min for 2hrs after 75g oral glucose ingestion in supine position without any medications. And the same parameters were measured after 1yr-treatment(Tx) by N. None changed their BMI for 1yr. Fasting BG and changes in BG after 1yr in young and elderly NT didn't differ from those in entry period, while those in young & elderly HT decreased after 1yr-Tx compared to those in pre-Tx. Basal and changes in INS in elderly NT & HT were significantly greater than those in young subjects(NT;F=10.51,P=0.001, HT;F= 15.45,P=0.001), and those in HT were also greater than in NT(young;F=10.70,P=0.001, elderly;F=17.76, P=0.001). However, basal and changes in INS decreased significantly after 1yr-Tx by N in both young & elderly HT, and became to similar to those in NT( young HT after 1yr-Tx vs young NT;F=1.71,P=0.192, elderly HT;F=3.43,P=0.087). In addition, basal and changes in plasma NE in young & elderly HT after 1yr-Tx were similar to those in NT, despite plasma NE in HT in pre-Tx were significantly greater than those in NT. These results demonstrated that longterm Tx by N improved the reduced INS sensitivity a~y~,Jf.ed sympathetic nerve responsiveness.
Hyperinsulinemia, Calcium channel blocker, Sympathetic nerve activity, Long-term treatment
F47 LONG TERM EFFECTS OF RAMIPRIL AND NITRENDIPINE ON ALBUMINURIA IN DIABETIC HYPERTENSIVE PATIENTS WITH IMPAIRED RENAL FUNCTION. L Corradi*, R Fogari*, A Zoppi*, P Lusardi*, P Preti. P Lazzari and RM Pesce. Department of Intemal Medicine and Therapeutics - University of Pavia - Pavia, Italy.
Aim: To campare the effects of chronic treatment with Ramipril or Nitrendipine on urinary albumin excretion (UAE) in hypertensive patients with non insulin dependent diabetes mellitus (NIDDM) and impaired renal function. Methods: Forty-one patients with mild hypertension. NIDDM and persistent albuminuria (> 300 mg/24 h) were studied. After a 3-week placebo period patients were randomly treated with Ramipril 5 mg o.d. or Nitrendipine 20 mg o.d. for 1 year according to a double blind design. Blood pressure, UAE, Creatinine Clearance (Cr. CL) and glucosilated haemoglobin (Gl. H.) were evaluated at the end of the placebo period and after 3, 6 and 12 months of active treatment. Results:The main results are as follows:
RAMIPRll. NITRENDIPINE p 3m 6m 12m P 3 m 6 m 12 m
SBPmmHg 166 147' 145' 144' 165 147' 148' 149' DBPmmHg 102 88' 86' 87' !OI 99' 88' 89' UAE mg/24h 779 629* 560' 519' 760 680 696 625* CrCI ml/min 42 41 41 40 41 43 44 45 GI.H% 7.7 7.5 7.6 7.6 7.6 7.7 7.6 7.7
*p<0,05 'p<O,Ol
Conclusion: Antiproteinuria effect of Nitrendipine is evident only after 1 year of treatment. On the opposite despite equivalent BP control Ramipril causes an earlier and greater reduction in UAE. thus suggesting that antiproteinuria effect of Ramipril is at least partially independent of its antihypertensive effect.
Key Words:
Albuminuria, Ramipril, Nitrendipine.
POSTERS: Antihypertensive Drug Treatment 151A
F46 EFFECT OF NEBIVOLOL AND ATENOLOL ON BLOOD PRESSURE AND INSULIN SENSITIVITY IN HYPERTENSIVE PATIENTS WITH DIABETES MELLITUS. A Zoppi*, P Lazzari, A Mugellini, P Lusardi*, L Poletti, RM Pesce and R Fogari*. Department of Intemal Medicine and Therapeutics - University of Pavia - Pavia, Italy.
The aim of this study was to campare the effects of Nebivolol and Atenolol on Insulin Sensitivity in hypertensive patients with non insulin dependent diabetes mellitus. Methods: Thirty patients were enrolled in a double blind parallel group design trial. After a 4-week placebo period patients eligible for entry were randomized to receive Nebivolol 5 mg o.d. or Atenolol 50 mg o.d. for 6 months. At the end of the placebo and of the treatment period BP was measured, urinary c peptide (U-cp) was evaluated and an euglicaemic hyperinsulinaemic damp was performed; glucose infusion rate (GlR) during the last 60 min of clamp and total glucose requirement (TGR) were evaluated. Results:The main results are as follows:
Placebo Nebivolol Placebo Atenolol
SBPmmHg 164,9±2t 139,2±15* 165,9±20 137,2±17* DBPmmHg 103,2±12 85,3±10* 103,3±13 84,5±9* GIR mg/min/k8 4,8±04 4,8±0,5 5,5±0,4 5,7±0,5 TGRg 20,4±3,3 19,9±3,8 21,1±4,1 21,2±4,4 Ucp ng/ml 27,5±5 26,9±4 29;1±6 29,3±5
• p < 0,01 Conclusion: Nebivolol 5 mg o.d. has comparable efficacy to Atenolol 50 mg o.d. at lowering BP. Neither beta-blocker appeared to have any significant effect on carboidrate metabolism, in terms of insulin sensitivity, whole body glucose utilisation and C peptide 24 h urinary excretion. These results suggest that both Nebivolol and Atenolol do not interfere with the diabetes in hypertensive-diabetic patients.
KeyWords:
Insulin sensitivity. Anetolol, NebivoloL
F48 SEXUAL ACTIVJTY IN HYPERTENSIVE MALES TREATED WITH LISINOPRIL OR A TENOLOL: A CROSS-OVER STUDY. ~. L Corradi*, L Poletti, A Zoppi*, P Lusardi* and GD Malamani*. Department of Intemal Medicine and Therapeutics -University of Pavia- Pa via, Italy.
Aim: to evaluate the effect of antihypertensive treatment with Lisinopril or with Atenolol on the sexual activity in hypertensive rnales never treated for hypertension. Methods: we studied 89 newly diagnosed never treated hypertensive rnales (DBP ~ 95 mmHg) aged 40-49 yr., all married and without any previous sexual disfunction, nol diabetic and nol taking any drug. After a 4-week placebo (P) period they were mndomized to receive Atenolol (Al) 100 mg o.d. or Lisinopril (Lis) 20 mg o.d. for 16 wecks; thcn aftcr a new 4-wcck P period a cross-over was pcrformcd between the 2 treatmcnts and the patients were treated for other 16 weeks. At the screening visit, at the end of cach P period, and aller 4 and 16 wecksof each trcatmcnt pcriod BP was evaluated and patients wcre intcrviewed by a questionnaire about their sexual activity. Results: BP significanlly decreased wilh both treatments with a 51% of normalisation with Lis. and 47% with At. Mean frequency of sexual activity per weck for the 2 treatmcnt sequcnces was as follows: Screening P At. 4w At. l6w P Lis. 4w Lis 16w 2.1 1.89 t,l 1,0 1,7 t.3 1,9 Screening P Lis 4w Lis 16w P At. 4w At. l6w 2.2 1.8 t,2 2,0 2,1 1.2 1,1 Sexual disfunctions (decreased libido, erectile disfunction) were spontaneously complained by 15 paticnts with At and by 3 patients with Lis. Conclusion: Male sexual activity deercases during the first month of antihypertensive treatment both with Lis and with At; it could be due to the BP lowering itself or to pharmacological mechanisms. Ongoing with the treatment the sexual activity tends to recovery only in the patients treated with Lis. These data suggest that ~blockers induce a chronic worsening of sexual activity while Aceinhibitors induce only a temporary sexual activity decrease.
Key Words:
Sexual activity, Hypertension, Lisinopril, Atenolol.
Dow
nloaded from https://academ
ic.oup.com/ajh/article/9/4/140A/2462180 by guest on 05 July 2022

152A ASH XI ABSTRACTS
F49 EFFECTS OF LIS IN OPRIL AND LOSART AN ON INSULIN SENSITIVITY IN NON DIABETIC HYPERTENSIVE PATIENTS. R..E!u:ari*. P Lusardi *, L Corradi*, A Zoppi*, P Lazzari, P Preti and L Poletti. Department of Internal Medicine and Therapeutics -University of Pa via - Pavia, Italy.
The aim of this study was to compare the effects of Lisinopril vs Losartan on insulin sensitivity in non diabetic hypertensive patients. Methods: Twelve non diabetic mild to moderate hypertensive patients (7 F, 5 M aged 44-62 yr) after a 4-week placebo (P) period were randomized to receive Lisinopril (Lis) 20 mg o.d. or Losartan (Los) 50 mg o.d. for 6 weeks; then after a new 4-week P period a cross over was perfomled between the two treatments and the patients were treated for other 6 weeks. The last day of the P period and of each treatment period BP was measured and insulin sensitivity was assessed by the euglycaemic hyperinsulinemie clamp technique. Glucose Infusion Rate (GIR) during the last 30' of clamp and Total Glucose Requirement (TGR) were evaluated. Results:The main results are as follows:
Placebo
SBP (mmHg) 165 ± 20 DBP (mmHg) 102 ± 13 GIR (mg/min/Kg) 5,72 ± 0,40 TGR (g) 32.5 ± 3.2
• p < 0,05
Losartan Lisinopril
147 ±17** 145 ± 16** 89 ± 11.. 87 ± 10••
6.28 ± 0,42 7.94 ± 0.39* 3.8 ± 3.3 39.8 + 3.6•
** p < 0,01
Conclusion: Both Lisinopril and Losartan significantly reduce BP without any difference between the two treatments. However only Lisinopril improved insulin sensitivity while Losartan did not affect it. These data suggest that the improvement in insulin sensitivity produced by ACE-inhibitors is not dependent on Angiotensin 11 blockade but rather on other mechanisms, probably on the Kinin system.
Key Words:
Insulin sensitivity, Lisinopril, Losanan.
F51 THE ANTIHYPERTENSIVE EFFECTS OF IRBESARTAN IN PATIENTS WITH MILD-TC-MODERATE HYPERTENSION. JL Poot•, Baylor College of Medicine, Houston, TX, RM Guthrie•, Ohio State Univ, Columbus, OH, T Littlejohn•, Winston-Salem, NC, P Raskin•, Univ Texas, Dallas, TX, AMM Shepherd•, Univ of Texas, San Antonio, TX, MA Weber", SUNY, NV, MR Weir", U Maryland, MD, TW Wilson, U Saskatchewan, Saskatoon, Saskatchewan, Canada, JM Wright, UBC, Vancouver, BC, Canada and H. deRuyter and RA Reeves•, Bristoi-Myers Squibb, Princeton, NJ.
Jrbesarum (IRBE, SR 47436; BMS-186295; BMS/Sanofi Wintbrop) is a highly selective angiotensin 11 receptor (ATt) antagonist. Primary objectives in two sirnilar multicenter studies were to assess IRBE in patients with seated diastolic BP (SeDBP) of 95-110 rnmHg regarding: I) the reduction in BP following 8 wks of trestment and 2) safety and tolerability.
The dose-ranging studies were conducted in a total of 889 patients with parallel groups (;;; 80 patients/gp) given doses over a range of I to 300mg IRBE in a double-blind placebo (PBO)-controlled design. Doses were: Study I, I, 5, 10, 25, 50, or IOOmg IRBE once daily; Study 2, 100, 200, or 300mg IRBE once daily. Baseline and demograpbic cbaracteristics were sirnilar: Study I, 67"/o male, 16% Black, age 54±10yr, 16o/~5 yr; Study 2, 69% male, 13% Black, age 53 yr, 12% > 65 yr. Mean SeDBP in both studies was 101 rnmHg.
At wk 8, mean trougb seated BP reductions (rnmHg) from baseline were:
The % therapeutic response (SeDBP $ 90rnmHg or a Ll I 0 rnmHg from baseline) with 50mg was 32%, which increased progressively by dose to reach 68% with 300mg. Adverse events (including cough) and labomtory safety parameters were sirnilar among all groups, including placebo.
Jrbesarum 50 to 300mg once-daily significantly reduced BP in a doserelated manoer in patients with hypertension, while all doses were equally well tolerated.
Key Words: irbesartan, angiotensin 11 receptor antagonist, dose response
AfH-APRIL 1996-VOL. 9, NO. 4, PART 2
FSO ENALAPRIL IN FORMULATION WITH A VERY LOW DOSE OF HYDROCHLOROTHIAZIDE IS EFFICACIOUS AND WELL TOLERATED IN MILD TO MODERATE HYPERTENSIVES I. Os, T. Hotnes , C.E. Mogensen. Department of Nephrology, Ulleväl sykehus, Oslo, Medica! Centre, T"nsberg, Norway and Department of Medicine. Árhus Hospita!, Denmark
In a double-blind, parallel, randomised multicenter study performed in Denmark, Finland and Norway , enalapril (El 20 mg in lormulation with 6 mg hydrochlorothiazide (HCTZ) was compared with respect to efficacy and tolerabilily wilh atenolol (A) 50 mg in 396 Caucasian patients (mean age 51.4..:!: 9.5 yeers) with mild la moderate hyperlension for 12 weeks aller a 4-week placebo period.
Filly-seven (57) % of lhe palients were previously unlreated. Baseline sitting (si) BP was 159.1! 15.51102.7! 5.5 (E+HCTZ) and 159.9! 14.91102.4! 4.9 mmHg (A). Both E+HCTZ and A reduced si systolic (S)(17.3 vs 13.4 mmHg,p=0.02) and D BP ( 11.8 vs 10.9 mmHg, NS) efficiently. There were slighlly more responders (D BP < 90 mmHg) with E+HCTZ than with A, 46.4 vs 35.8% (p=0.05). A similar number of patients reached S BP below 140 mmHg alter 12 weeks, 49.7 vs 43.3 (A)% (NS) in bath groups. No dilterences were reported in standing BP. Insuffoeient response caused withdrawal in 1.6%. while 7.2% (27 patients) discontinued due to clinical adverse experiences, 8.1% in E+HCTZ- and 6.4% in the A-group.
A similar number of adverse experiences (AE) was reported in both groups. 48.9 versus 47.9%, with probable or possibly drugreisled AE being slighlly higher in lhe E+HCTZ lhan in A-group (30.6 versus 21.8%. p=O.OS). The most common reported AE (>4%) in eilher E+HCTZ or A were cough (8.6 vs 4.3%), asthenia (5.4 v• 7.4%), dizziness (5.4 vs 1.6%) and headache (4.3 vs 1.6%). ûne case of angioneurotic oedema and 1 with hypolension was seen in E+HCTZ, and 2 cases of myocardial infarction, and 1 case of cerebrovascular accidents in A-group. Overall tolerability was evaluated by lhe doctors as good or very good lor 88% of the patients in bath lreatment modalities. The palients' own assessment with respect to how they lelt alter treatmenl was nol significanlly different in the two trestment modalities: 47% with E+HCTZ lelt better or much better as compared to 45% with A, whereas 5% with E+HCTZ feit worse ar much worse compared to 8% wilh A
In conclusion, although both drug rnadalities are efficacious, the tormulation with E and a very smal! dose of HCTZ has a more pronounced effect on siS BP than A. Bath modalities were well tolerated, however, more cough and dizziness were reported with the combined E+HCTZ.
Key Words:
Atenolol, efficacy, enalapnl, hypertenston. thtaz1ae
F52 EFFECTS OF AMLODIPINE VS FOSINOPRIL ON MICROALBUMINURIA IN ELDERLY HYPERTENSIVE PATIENTS WITH TYPE 11 DIABETES. !.....!:l!n:ill*. P Lusardi*, C Pasolli, A Zoppi*, P Pre ti, P Lazzari and R Fogari*. Department of Internal Medicine and Therapeutics- University of Pa via- Pavia, Haly.
The aim of the study was to campare the effects on urinary albumin excrelion (UAE) of Amlodipine and Fosinopril in elderly hypertensive patients with type 2 diabetes. Methods: We studied 49 elderly (60-75 yrs) hypertensive patients (DBP > 90 mmHg) with concomitant well controlled NIDDM. After a 4-week antihypcrtensive placebo period they were randomized to receive Amlodipine 5 to 10 mg o.d. (24 pts) or Fosinopril 10 to 20 mg o.d. (25 pts) for I year. The patients non responders to monotherapy were discominued after 4 weeks. At the end of the placebo period and after 3 and 12 mantbs of treatment blood pressure, UAE and creatinine clear:mce (CtO) were evaluatcd. Results:The main results were as follows (mean ± SEM):
SBPnunllg DBPmmllg UAE mg/2-lh C1GmVmin
AMLODIPINE (11=24) P 3 m 12 m
162±1.8 141±2° 14-l±2,5° 102±0,8 89±F 90±1° 9t±6 88±7 70±5.5' 89±2,5 91±2 98±1.9 *p<0.05
FOSINOPRIL (n=25) P 3m l2m
161±1,9 144±1.6~ 1-16±1,9° 101±0,7 92±1° 91±1,3° 94±7 70±6* 60±6,5• 90±2.1 88±2,1 88±1.8
0 p <0.01
Bolh Amlodipine and Fosinopril significantly reduced BP without aiTccting glucose homoeostasis. At 3 months UAE was significantly rcduccd only in the Fosinopril group. but at 12 momhs it dccreased significantly with both drugs. UAE% deercase was significantly corrclatcd with SBP% deercase in both trcatmcnl groups. Cr. Cl. was unaiTcctcd by Fosinopril whercas it was signilïcantly increased by Amlodipine. Conclusions: Long term trcatment with both Amlodipine cmd Fosinopril was effective in reducing UAE in eldcrly hypertensive paticnts with NIDDM and microalbuminuria. Our data also suggest !hal thc association of these 2 drugs could lead to a further improvcmenl of the kidney function in this type of paticnts.
Key Words:
Microalbuminuria. Amlodipine. Fosinopril.
Dow
nloaded from https://academ
ic.oup.com/ajh/article/9/4/140A/2462180 by guest on 05 July 2022

AfH-APRIL 1996-VOL. 9, NO. 4, PART 2
F53 EFFECT OF NIFEDIPINE GITS ON LEFT VENTRICULAR MASS AND HEART RATE VARIABILITY IN HYPERTENSIVES WITH VENTRICULAR HYPERTROPHY. ~. L Corradi*, A Zoppi*, A Mugellini, P Pre ti, S Savino and R. Fogari*. Department of Internal Medicine and Therapeutics -University of Pavia- Pavia, Italy.
The aim of this study was to assess the effect of Nifedipine GITS antihypertensive monotherapy on Left Ventricular Mass Index (LVMI) and Heart Rate Variability (HRV) in hypertensive patients with left ventricular hypertrophy. Methods: Twenty-three hypertensive patients (DBP ;" 95 and,;; II4 mmHg) aftera 4-week placebo period were treated with 30 to 60 mg of Nifedipine GITS o.d. for 6 months. At the end of the placebo and of the treatment period all subjects underwent an echocardiographic examination and a HRV evaluation. LVMI, Ejection Fraction (EF) and Peak Filling Rate (PFR) wcre asscssed. The short term analysis of R-R interval provided a frequcncy domain mcasure of R-R variability expressed as Total Power (TP), Low Frequcncy (LF) and High Frcquency (HF). Results:The main results are as follows (meao ± SEM):
Placebo Nifcdipine GITS SBP (mmHg) 161 ± 3 133 ± 2•• DBP (mmHg) 103 ± 2 87 ± 1**
LVMI (g/m2) 182 ± 8 145 ± 6** EF(%) 62 ± 2 67 ± 2 PFR (vol/sec) 2.29 ± 0.2 2.66 ± 0.2
TP (mscc2) 684 ± 134 1148 ± 162*
LF (mscc2) 342 ± 101 497 ± 114
HF (mscc2) 251 ± 91 392 ± 123 • p < 0.05 •• p < 0.01 Changes in LVMI did not significantly COlTelale with SBP or DBP changes. Conclusion: Nifedipine G lTS decreased BP and L VMI, and increased HRV in patients with essential hypcrtension. Regression of LVMI improved systolic and diastolic venu·icular function; the increasing of HR V is to be considered a positive outcome, as a decreased HR V associated with L VH re present an increasing risk of sudden cardiac dcath.
Key Words:
Ventricular hypertrophy, heart rate variability, nifedipine.
F55 AN1DI\"PERTENSIVE EfJIECJS OF AMLODIPINE 48-HOURS AFJER LAST DOSE: AN
AMBULATOilYBLOODPRBSUilEYONliOIUNGSnJDY. ~CCcaho.
A Am1aDo, L E Bmera. S ~ M A Pldrlclo IIDd C E GoDzaJez. Nuewo llolpir.l avD. Guadalljara.Mrào. 'lbe c:um~~tstudymalymd lhe Mltihypcl'teniMetiec:&sclamlodipillc (AML)
with 24 h mbul.atory blood paAU8 (ABP) lllDilitoriDa; after fint dosap. 10 weeb ei u.tmcat with S-10 mg po q.d. aad 48 h pollilall dole. 1hirty C~Mntial hyper1eDaive puienD (25 'liCIIDNl,
Smett)apl :KJ.6S,_s.(mnD.52.9}.~ l·lor3 (INC·V)MRiludied.. A24-b.ABPmcaitoriq
.,. doae ftr :z-weet liqlc bliDd. plaocbo. cluriq the fint 00.,. day, IIIIer lCDweebal AML
treatmeut, aDd 48 h alter miMbJs a cbe. ABP .. IIIHIIIIed, wilh 81lll11tomaled. DOD-inwlive oac:illomotric dewk:ll (Pube 'lmld Rlllmed.) Blood preiiURI (BP) waa regilhd auromarlcally every 15minduriaalhedaytimemd.,.,..,.:zomioduriagthealgbrt.ila. 'Ihemw•aaligb.t ~
ol BP aad beart rUe (BR) in 6nt 24 h cl tmltmBDt (p> ~ the delta N8Ultl on 24h
.ABPmDaitori!agllllheendof.:tiw bellm0Dtaad48h afterllliMIDsadolearefiUIIDbUized in the
tilde, RB. - llt tbe ead al 'IIICtÎ9C tmabneot 1111111 48 h palt 1.-t cbe+o..8 lllld .().4 bcalllmin
-(p>D.Q5).
............. lll'i.it ...... (~-·with AML trealallat aad 48-b .&er lilt dale
24bperiod
IJ, SliP 6 DBP A SBP 4 DBP 4 SBP 6 DBP
AML 48-b AML 48-h AML 48-h AML 48-h AML 48-h AML 48-
-U.6 ·11.1 ~7 -4.9 -16.7 ·10.7 -4.9 -5.3 -IQ.8 .U ·6.9 -3.3 .. .. SBP- SJ11D1ic BP, DBP- Dplfolic BP "P<Q05. A P>O.OS.
CltdJ aae pmint JR110Dted BP< IXVS> mmJJa duribS Diabt-dme ABP moailmillg lfler ac:1:iw t!811tmmlB-~ 1WopadeDIIp!WC!Itedllll.>90~mlncluriDgthcfbst24h
eX AliL treat:ment Ollly clurlDs daJ time. Al t.be ead r:L aclive treiiDDDDt two palieDtl pRKD.b
Jlll>90 bealrl min (91-97) ûo dudq day time.lD coac:luioa: AIIL t. a.qht effed: cm 2o4 h
SBPIDdDBPiflerftntcklllpwid!.oom-.eiD HR;afterlO-a~nduoed24h
SBPmd.DBP,bochdurlDgdllyaad.ai&hl48h lflerlllrdclc: ••effoct:MOIII:ydurmgday-time., ---" ... ___ m"bto<lmo.
Key Words: ---·----
POSTERS: Antihypertensive Drug Treatment 153A
F54 ANTIHYPERTENSIVE EFFICACY OF LISINOPRIL AS ASSESSED BY 36-HOUR AMBULATORY BLOOD PRESSURE MONITORING IN ESSENTIAL HYPERTENSION. A Zoppi*, P Lusardi*, P Preti, A Mugellini, GD Ma1amani*, R Fogari* and RM Pesce. Department of Internar Medicine and Therapeutics -University of Pa via - Pavia, Ita1y.
The aim of this study was to test the duration of the antihypertensive efficacy of Lisinopril administered once a day on outpatients with essentia! hypertension. Methods: After a 2-week placebo period 16 mild to moderate hypertensive patients (DBP ~ 95 and ~ I 14 mmHg) were treated with Lisinopril 20 mg o.d. (to be taken between 8:00- and 9:00 a.m.) for 4 weeks. At the end of the placebo and of the treatment periact a 36 hour ambulatory blood pressure monitoring was perforrned with a Spacelabs 90207 device set up to measure blood pressure every 15 minutes. The recording started between 8:00 a.m. and 10:00 a.m. and stopped between 8:00 p.m. and 10:00 p.m. of the following day. Results:The main results are as follows (mean SBP/DBP values ± SEM).
How-s
09:00-21:00 21:00-09:00 09:00-21.00
Placebo SBP DBP
154±1,6 139±6 152±1,5**
93±1,2 80±1,0 92±1,2
• p < 0,05
Lisinopril SBP DBP
137±1,4** 126±4** 141±1,3**
80±1,0** 70±0,9** 85±1,1.
•• p < 0,001
Conclusion: The antihypertensive effect of Lisinopril 1asts considerably Jonger than 24 hours and is still evident 36 ho~rs after the last drug administration. This may be of advantage in patients with a non perfect compliance to treatment.
Key Words:
Lisinopril, Blood Pressure, ABPM.
F56 EFFECTS OF TBE ONCE-A-DA Y AMLODIPINE AND TRANDOLAPRIL ON 24-HOUR AMBULATORY BLOOD PRESSURE AND lTS SHORT-TERM V ARIABll..ITY.
Winnicki M", Sobiczewski W, Bartlomiejczyk-Majcbrowicz K", Rynkiewicz A, Krupa-Wojciechowska B". Department of
Hypertension and Diabetology", I Department of Cardio1ogy Medical University of Gdallsk, Poland. The object of the study was to evaluate the effects of once-a-day amlodipine (5-!0 mg) and Irandolapril (2-4 mg) on 24-hour blood pressure and its short-term variability in patients with mild-tamoderate essential hypertension. In two groups of 20 patients (12 women, 28 men), taking amlodipine (A) or trandolapril (T), 24-hour ambulatocy blood pressure monitoring (ABPM) was performed (Spacelabs 90207 or Oxford Medilog) after 4-week wash out and after 8-week active treatment. Standard deviation of daytime (8.00-22.00), nighttime (0.00-ó.OO) and 24-hour systolic (SBP) and eliastolie (DBP) ABP was taken as an index of short-term variability (v). Both amlodipine and trandolapril reduced effectively 24-hour SBP (A-144,7±9,7 vs. 136,2±6,6 mmHg, p<0,01; T-139,3±11,7 vs.
13!,2±!4,0mmHg, p<0,05) and DBP (A-98,5±7,5 vs.
92,2±4,8mmHg, p<0,01; T-85,6±8,0 vs. 80,0±7,7mmHg, p<0,05) as
wellas daytime SBP (A-152,8±8,7 vs.144,3±9,3mmHg, p<0,01; T-
144,6±11,9 vs. 13S,1±l4,6mmHg, p<0,05) and DBP (A-103,0±5,9
vs. 98,7±6,3mmHg, p<0,05; T-89,8±7,6 vs. 83,3±8,lmmHg, p<0,05). Only amlodipine was able to reduce effectively nightime
DBP (A-88,1±9,9 vs. 79,1±6,3mmHg, p<0,005). Both drugs failed to
reduce nightime SBP. 24-hour SBPv (A-17,8±5,7 vs. 16,8±3,8
mmHg, NS; T-15,2±4,0 vs. 14,8±3,9mmHg, NS) and DBPv (A-
12,2±3,6 vs. !5,3±8,8mmHg, NS; T-11,6±3,1 vs. 11,8±3,0mmHg,
NS), daytime SBPv (A-14,5±5,0 vs. 12,7±3,5mmHg, NS; T-II,8
±3,2 vs. 12,1±3,3mmHg, NS) and DBPv (A-10,2±3,4 vs.
13,0±12,4mmHg, NS; T-8,7±2,7 vs. !0,0±2,9mmHg, NS), nightime
SBPv (A-9,4±5,3 vs. 10,7±6,9mmHg, NS; T-!0,4±3,1 vs. 10,2±
4,1mmHg, NS) and DBPv (A-7,6±3,7 vs. 8,6±4,3mmHg, NS; T-
7,7±2,7 vs. 8,5±4,0mmHg, NS) was not affected by neither amlodipine nor trandolapril. We concluded that amlodipine and Irandolapril reduce 24-hour and daytime SBP and DBP. Our results indicate that only amlodipine effectively reduce nightime DBP. Both drugs do notaffect blood pressure variability. Key words: amlodipine, trandolapril, ambulatory monitoring.
Dow
nloaded from https://academ
ic.oup.com/ajh/article/9/4/140A/2462180 by guest on 05 July 2022

154A ASH XI ABSTRACTS
F57 DISPARATE HEMODYNAMIC RESPONSE TO STRESS UNDER TREATMENT WITH ALPHA- AND BETA-RECEPTOR BLOCKERSRESULTS OF A DOUBLE-BLIND RANDOMIZED STUDY. CD Ga!zka, HP Schobel, RE Schmieder*. Dept. of Medicine IV, Univarsity of Erlangen-Nuremberg, Germany. Uttle is known about lhe effects of a- and P-receptor blocking agents on cardiac hemodynamics under sympathetic stimulation. We investigated 43 hypertensive patients (29 men, 14 women) in a double-blind, randomized study after 6 months of therapy with either the alphablocker bunazosin (6-12 mg o.d.) or the betablocker metoprolol (100-200 mg o.d.). We measured cardiac hemodynamics by impedance cardiography before and after a 5 minute mental stress test ((3-sympathetic stimulation) and during isometrie exereise (handgrip, a- and P-stimulation): After therapy alphabloeker betabloeker p At BP (mmHg) 140±21/82±12 145±25/84±6 n.s. rest HR (bpm) 73±14 53±7 p<0,001
CO (I/min) 5,3±1,1 4,0±0,9 p<0,01 TPR (U) 23,5±6,4 28,1±9,1 p<0,01
Mental BP (mmHg) +12±8/+6±5 +15±121+6±5 n.s. stress HR (bpm) +8±5 +5±4 p<0,05
CO (I/min) +0,8±0,8 +0,4±0,4 p<0,05 TPR (U) -1,0±2,2 -0,4±2,2 n.s.
Hand- BP (mmHg) +22±121+14±8 +35±17/+20±8 p<0,05 grip HR (bpm) +20±7 + 7±4 p<0,01
CO (I/min) +0,8±1,1 +0,4±0,3 p<0,05 TPR (U) +0,4±3,0 +4,1±3,8 p<0,01
At similar levels of blood pressure (BP), both heart rate (HR) and eardiac output (CO) at rest were signifieantly lower in the betabloeker group, even alter six months of treatment. In addition, heart rate and cardiae output increased less in response to mental stress and isometrie exereise. BP and total peripheral resistanee (TPR) increased more in the betabloeker group under isometrie exereise as eompared to the alphablocker group. We eonclude that antihypertensive treatment with the alphabloeker maintained the hemadynamie response to mental stress and attenuated the BP response to isometrie exercise. In contrast, the betabloeker redueed eardiac output at rest and caused an unphysiologieal peripheral vasoconstrietion at rest, which inereased during isometrie exereise.
Key Words: hemodynamics, sympatholyties, stress, isometrie exereise
F59 PERSISTENCE OF ANTIHYPERTENSIVE EFFECT OF TRANSDERMAL CLONIDINE AFTER TREATMENT WITHDRAWAL: A 48-HOUR ABPM STUDY. P Lusardi*, A Mugellini, P Pre ti, GD Malamani*, A Zoppi*, S Savino and R Fogari*. Department of Internal Medicine and Therapeutics -University of Pavia- Pavia. Italy.
Aim: to evaluate the blood pressure during the 24 hours following treatment withdrawal in hypertensive patients chronically treated with transdermal Clonidine monotherapy. Methods: Following a 3-week run-in period 19 mild hypertensive patients (DBP 2: 95, ,;; 105 mmHg) were treated with transdermal Clonidine 0,1 mg/24 h (TTS 1) for 8 weeks. The last 2 days of runin period the patients underwent a 48-hour ABPM and at the end of the treatment period a 2nd 48-hour ABPM was performed. The latter covered the last 24-hours of the treatment period and the first 24-hours of the treatment withdrawal, after patch delachment and its replacement with a placebo patch. ABPM was performed by a Spacelabs 90207 device; the monitoring starled in the morning and BP readings were obtained every 15 minutes. Results: Befare treatment the average of the first 24 hours was 146±12/83±6 mmHg (mean ± SD) and this values were signifcantly reduced by transdermal Clonidine (15±12/8±6 mmHg). This BP rcduction was almast entirely maintaincd in the 2nd 24-hour period. Thc main BP changes in comparison to run-in period are as follows:
SBP DBP
1 st day (treatment) 8-20 20-8
-16±13** -12±10** - 9± 5** - 8± 6**
** p < 0,001
2nd day (withdrawal) 8-20 20-8
-13±12** -9±8** - 7± 6** -6±6*
* p < 0,05
Conclusion: Transdermal Clonidine is cffectively antihypertensive over the 24 hours and its effect is long lasting also after patch detachment. This may be of advalllage in patients with a non perfect compliance to trcatment.
K~o;;{~[,~;,: Blood Pressure, ABPM.
AfH-APRIL 1996-VOL. 9, NO. 4, PART 2
F58 EFFECTS OF ONCE WEEKLY TRANSDERMAL CLONIDINE ON 24-HOUR BP PROFILE IN MILD-MODERATE HYPERTENSION. L Savi*, MR Montebelli, L Fazzari, M Mettimano, A Migneco, F Pichetti, A Giuliani, G Folli Patologia Medica, Centro Ipertensione Universita' Cattolica, Roma, Italy Efficacy and tolerability of transdermal clonidine (TTB-Cl were evaluated in 36 patients with mildmoderate essential hypertension ever a one-year treatment period. 24-hour BP was measured at 15 min intervals~ using a noninvasive automatic (jevice (Spacelabs 90207), following a two-week placebo run in and after 6 month of active treatment. Office clinostatic, orthostatic and sitting BP were measured every month. Transdermal clonidine administration was started at the lewest dose (TTS .1) in ever·y pa tien t; i.n 18 of them, the dose was doubled (TTB 2) after 1 m~1th of treatment, due to poor BP control-7 out of 36 patients had to quit the study because of skin reactions~ 2 because of ether side effects. 5 patients did not achieve BP control after two months of active treatment and were excluded from the continuatien of study. Both systolic and diastolic BP were significantly lowered by TTS-C. No significant alterations in circadian rhythm were observed-
Key Words: Tr··ansdermal clonidine, ABPM
F60 RENOPROTECTION OF CALCIUM ANTAGONIST : EFFECT OF MANIDIPINE ON URINARY MICROALBUMIN EXCRETION AND LIPID PEROXIDATION_ M Yamakado~ H Shimomura, and E Maehata. Department of Health Care, Mitsui Memorial Hospital, Chiyoda-ku, Tokyo, Japan_
The effect of calcium antaginist on hypertensive renal damage is still controversial. To clarify the mechanism of calcium antagonist on renal protective action, the effect of manidipine , a dihydropyridine calcium antagonist on urinary microalbumin excretion ( U-Alb ), and lipid peroxides ( LPO ) formation which may participate in the pathogenesis of hypertensive renal damage were determined in patients with essential hypertension ( EHT ). Before, 12 weeks, and 54 weeks after the treatment of manidipine, U-Alb, and plasma LPO were determined in 19 patients with EHT. U-Alb was measured by TIA method, and plasma LPO was by fluorametrie assay method by Yagi, respectively. Manidipine significantly reduced blood pressure from 165 ± 102 mmHg to 144 ± 88 12 weeks, and to 148 ± 88 54 weeks after the treatment. Manidipine significantly decreased U-Alb from 34 ± 7 mg/g creatinine to 18 ± 4, and 17 ± 5. Also, manidipine significantly decreased plasma LPO from 3_9 ± 0.7 nmol/ml to 1.9 ± 0.2, and to 1.4 ± 0.2, respectively. There was a relationship between changes in U-Alb and plasma LPO to manidipine. In conclusion, manidipine significantly decreased U-Alb associated with decreasing LPO formation. These results suggest that manidipine might have renal protective action through its effect of antioxidant property.
Key Words: ca 1 c1 urn antagom st, renoproteet 10n, microalbum1n, l1p1d peroX1dat1on, ant1ox1dant
Dow
nloaded from https://academ
ic.oup.com/ajh/article/9/4/140A/2462180 by guest on 05 July 2022

AfH-APRIL 1996-VOL. 9, NO. 4, PART 2
F61 EFFECT OF LACIDIPINE ON ENDOTHELIAL FUNCTION IN HYPERTENSIVE PATIENTS. L Ghiadoni, S Taddei*, A Magagna, A Virdis, S Uleri, A Salvetti*. I Clinica Medica, University of Pisa, Pisa, Italy .
Essential hypertensive patients (EH) are characterized by impaired endothelium (END)-dependent vasodilation (VD). This study was
designed to test whether the antihypertensive treatment with the Ca channel blocker lacidipine (LAC) can imprave END-dependent VD in HT. In 12 EH (46.1± 5.4 yrs, BP: 152.2±11.2/100.6±6.2 mmHg) we tested the effect of acute (intraarterial infusion at 0.03 ng/100 mi /min for 20 min) and prolonged (2 manthes oral treatment 6 mg!die p.o.) LAC on forearm blood flow (FBF, strain-gauge plethysmography) modifications induced by the intrabrachial infusion of acetylcholine
(ACH: 0.15, 0.45,1.5,4.5,15 f'g/100 mi/min) and bradykinin (BDK: 5, 15,50 ng/1 00 mi/min), two endothelium-dependentvasodilators, acting thraugh different receptars and signa! transduetion pathways, and sodium
nitroprusside (SNP: 1,2,4 f'g/100 mi/min), an en dothelium independent vasodilator. As compared to normotensive controls (n~IO, NT, age
45.8±4.6 yrs, BP 119±7.6178.3±4.9 mmHg), EH showed a significantly (p<O.O I) blunted response to BDK (%FBF increase above basal;x±SEM; NT: 215±28,332±32,543±49; EH:95± 16, 197±24, 278±41 %) and to ACH
(%FBF: NT:l5±4,52±8,264±32,473±59, 611±58%; EH:7±2, 38± 12, 109±16,211±27,296±37%) while the response to SNP was similar in the two graups (%FBF: NT: 183± 19, 267±35,370±40; EH:
175±20,246±30,349±38). Acute LAC infusion failed to increase VD to Ach(% FBF: 12±5,52±15, 125±19,224±32, 328±41), orto BOK(% FBF: 99±11, 186±19,271±34)andto SNP(I41±22,219±25,300±36). In contrast
two month LAC treatment significantly (p< 0.001) decreased BP (I 40.1± 11.2/89.3±6.4 mmHg) and increased (*p<.05, #p<.O I) VD to the
highest dose of ACH (%FBF:9±3,44±11,137±15,288±33,407±54*) and to BDK (%FBF: 135±22#,267±35*,345±45#), while it did nat alter the response to SNP (135±17,267±34,345±38). In EH pro1onged (two monthes) oral treatment with LAC increases endothelium-dependent vasodilation to ACh and BDK, suggesting that this drug can imprave endothelial function in EH.
Key Words: endothelium, vasodilation, lacidipine
F63 INDUCTION OF NOCTURN AL BLOOD PRESSURE (BP) FALL BY ISRADIPINE (ISRAD) RX IN HYPERTENSION (HTN) AFTER LIVER TRANSPLANTATION (LTx). SC Textor*, L Schwartz, SJ Taler*, VJ Canzanello*, R Wiesner, M Porayko, R Krom, Mayo Clinic, Rochester, MN.
HTN develops soon after LTx using cyclosporine plus steroid-based immunosuppression. The normal noctumal BP fall is lost, although restored partially over years. We examined the day-night BP variations during monotherapy with a short-acting dihydropyridine calcium channel blocker, isradipine (ISRAD average daily dose 4.1 mg b.i.d.) for 3 months in 16 LTx recipients early after Tx. ABPM recordings (SpaceLabs) were divided into awake and noctumal5-hour time bleeks, excluding a 2-hour sleep transition. BP rose from Pre-Tx {110±2/64±2 to 151±4/ 90±3 mmHg one month after LTx P<.01). Pre-Rx CSA dose was 662±59 mg/d and Prednisone dose was 33± mg/d. Pre-ISRAD: A wake 5-hr Nocturnal5-hr
SBP (mmHg) 147±4 143±5 DBP (mmHg) 94±2 91±2 HR (bpm) 86±3 75±3
ISRADRx: SBP (mmHg) 129±3 120±3 DBP (mmHg) 83±2 75±3 HR (mmHg) 86±3 73±3
Mean±SEM, *p<.05 vs awake, tp<.05 vs Pre-Rx
NS NS
t* t* *
During ISRAD Rx the fraction having a noctumal fa!! ~10% rose from 0% to 68% (p<.01). Analysis of ABPM records demonstraled a transient rise in HR and fa!! in BP after the noctumal IS RAD dose, suggesting a pharmacologic effect on BP. These data demonstrate restoration of noctumal BP fa!! during Rx with a short-acting CCB, which was not observed in previous studies with extended release nifedipine. Our results indicate that post-Tx noctumal BP pattemscan be altered favorably, potentially avoiding the adverse target effects of noctumal HTN.
Key Words: ABPM, cyclosporine, transplantation, steroids, circadian rhythm, hyperlension
POSTERS: Antihypertensive Drug Treatment 155A
F62 Acute and long-term adaptation of central hemodynamics and renal physiology in hypertensive patients on Logimax, a metoprolol/felodipine fixed dose combination . by Ove K Anderssen M.D., Ph.D., Marian Wysocki M.D., Peter Friberg M.D.Ph.D. Departmanis of lnternal Medicine, Hyperten
sion Unit, and Clinical Physiology;Sahlgrenska Univarsity Hesp.,
Gothenburg; Sweden. Aftera 4-w placebo period,central hemodynamics and renal
tunetion was menilored during baseline and during tour hours
following !he first dose of a metoprolol/ felodipine fixed dose combination in 11 hypertensive patients (WHO 11). BP was measured i. a and cardiac output by dye-dilution and in !he samesetting GFR by Cr-EDTA, and renal blood flow by PAHclearence. These measurements were !hen repeated after 12
weeksof chronic therapy(24 hours post-dose=chronic trough and then 4 hours post-dose=chronic peak). Results(conf.int) Baseline Chronic through Chronic peak
MAP (mmHg) 129 110 (-25, -13) 105 (-29,-19) CO (I/min) 6.5 6.2(-0,96,0.39) 5.7(-1.55,-0.04)
TPR (units) 21 18 (-4.7,-0.3) 19 (-4.2,0.7) HR (b/min) 70 63(-12,7,-2.3) 59(-15.6,-6.0)
GFR (mi/min) 376 420(-41,131) 453(-17,173) RBF (mi/min) 97 94(-22,16) 98(-13,14)
FF 1%) 26 221-8 -1) 22(-8 1) MAP=mean arterial pressure;CO=cardiac output;TPR=total peri
pheral resistance;HR=heart rate;GFR=glomerular filtratien rate;
RBF=renal blood flow;FF=filtration fraction. Conclusion:Chronic traalment with Logimax effectively lewers BP
mainly by vasodilation but also a beta-adrenoceptor inhibititory
effect is evident since heart-rate was significantly reduced as was cardiac output at peak-effect during chronic treatment. No significant change in renal blood flow or filtratien was noticed
while filtratien fraction tended te normalize. The through/peak ratio
for the change in MAP was 79 % (conf.int.58.2,99.0).
Hemodynamics,renal function,calcium antagonist,felodipin,
metoprolol,logimax.
F64 PERSISTENT ANTIHYPERTENSIVE EFFECT OF AMLODIPINE 3 DAYS
AFTER DISCONTINUATION 0~ THERAPY: A PROSPECTIVE DOUBLE BLIND RANDOMISED STUDY_. Biston P*, Mélot C'. Oegaute JP', Clement 0 '*, Quoidbach A*** Hypertension Units, Erasme Hospitai-Brussels*, Univarsity of Ghent** and
Höpital Civil Ju met••• Ta assess the residual antihypertensive effect of amlodipine (A) 3 days
alter discontinuatio11 of therapy, a multicenter double-blind study was performed in 33 patients with mild to moderate primary hyperlens ion. Alter ene month wash-out (V1), all patients received A 5 mg a.d.lor 8 weeks (V2). Alter this, patients were given double-blind either placebo (14 patients) or A (19 patients) lor 3 more days IV3). Office (OBP) and the 24-h ambulatory blood pressure (ABPM) were measured at V1. V2, V3. Because of technica! difficulties, high quality ABPM was available only in 9 patients receiving placebo and 15 patients receiving A Results (mmHg ± S D ) are given in the table
BP V1 V2 V3
AM OBP(mmHg) 168±19/101 ±7 148±11/68±5 152±14/90±8 !.
daytlme BP 156±19195±12 145± 10/88±9 144±11/88±10 (mmHg) nightime 137±17/80±11 129±11/76±10 128±11/74±11 BP(mmHg) 24-hour 148±19/88±11 139±9/ 83±9 138±11/82±10 BP(mmHg)
f!. OBP(mmHg) 172±141101±5 144± 12/85±6 146± 14/85± 9 daytime BP 152±15194±8 143±13188±8 144±13/89±8 (mmHg) nightime 129±24176± 14 121 ± 161 71 ± 121 ±18/72±13 BP(mmHg) 12 24-hour 145±17/87±8 136± 41 81 ± 8 137±14/84± 8 BP(mmHg)
The 2 groups were camparabie tor thetr mam demographtc data as well as their BP va lues at baseline (V1) and after 6 weeks of A (V2), p> 0.05. Replacement of A by placebo did not cause any increase of BP even at 3 days alter cessation of administration
Thus, !he antihypertensive effect of A is well maintained far beyond !he 24-hour span when administered in a 5 mg once daily dosage. This property could imprave pallent's therapeutic coverage ( in partly compliant patients). and incidentally, would open possibilities for low frequency dosage form.
KeyWords: "no..ol)a;>.'\lo." 1 ~Oi!>-'~ottrcc~-y ~L<'<-J)
i"llr"u~r: 1\lf/nwfl.l\ C"'Wr, , l.!cn ~"'' t~Vt..-fl'
Dow
nloaded from https://academ
ic.oup.com/ajh/article/9/4/140A/2462180 by guest on 05 July 2022

156A ASH XI ABSTRACTS
F65 COMPARATIVE EFFECTS OF THE NOVEL CALCIUM ANTAGONIST, MIBEFRADIL, AND NIFEDIPINE GITS IN PATIENTS WITH MODERATE TO SEVERE ESSENTIAL HYPERTENSION. Y Lacourcière*, L Poirier, J Lefebvre, F Archambault, S Dalle Ave+, E Lindberg+. Hypertension Unit, Research Center, Le Centre Hospitalier de I'Université Lava!, Quebec, Canada and Hoffmann-LaRoche+, Base!, Switzerland. Previous studies suggest that mibefradil (Mb), a navel long-acting tetraline derivative (CA) that blocks L and T -type calcium channels, reduces peripheral vascular resistance without reflex tachycardia and negative inttopic effect. This study was conducted to campare its antihypertensive efficacy with that of nifedipine GITS (Nt) in moderate to severe hypertensives with ambulatory hypertension. Seventy-one patients were randomised in a double-blind, parallel group, forced-titration study. At the end of a I to 4-week placebo period, patients in whom clinic sitting diastolic BP was 110-125 mm Hg and mean daytime ambulatory diastolic BP was >90 mm Hg were eligible for active treatrnents. They were then randomized to 50, 100 and 150 mg of Mb (n=35, 31M/4F, mean age 53 years) or 30,60 and 90 mg ofNf(n=36, 28H/8F, mean age 52 years) with a forced tilration every 2 weeks. Clinic and ambulatory BPs were assessed at the end of the placebo period as well as after 2, 4 and 6 weeks of active treatrnent. After 6 weeks of treatrnent, clinic and ambulatory systolic and diastolic BPs were significantly reduced by bath study drugs with a significantly greater reduction (p<0.05) in patients treared with Mb for diastolic BP (p<0.05) in the clinic (-3.7 mm Hg) as well as during the mean 24-hour (-4.8 mm Hg), daytime (-4.4 mm Hg), nighttime (-3.7 mm Hg) and early moming ( -3.3 mm Hg) periods. Baseline heart rate (70 beats/min) was modified significantly by Mb ( -10.1 beats/min) but nol by Nf ( +3.1 beats/min). No patients experienced clinically significant atrioventricular conduction abnormalities. All in all, bath drugs were generally well toleraled The administration of the navel calcium antagonist Mb produced similar reductions in clinic and ambulatory systolic BP but significantly greater reductions in diastolic BP than Nf. Moreover, the significant decrease in heart rate induced by Mb was nol associated with clinically significant atrioventricular conduction defects.
Key Words: Mibefradil Calcium antagonist
F67
Arobuiatory blood pressure monitoring Moderate-to-severe hyperlension
TROUGH PEAK RATIO IN THE ASSESSMENT OF THE HYPOTENSIVE EFFECT OF ACEBUTOLOL. K.Kawccka-Jaszcz. B.Bacior. J.Kochman. J.Grodccki. K.Szymura. J.Oicksiak. M.Walc~.ak. J.Bury I Cardiac Dpt.and Dpt.of Pharmacokinetics Jagicllonian Univcrsity Coll. Mcd. Kraków. PL
Tbc aim of tbc study was to asscss hypotcnsivc effect of acebutolol cxpresscd as trough: peak ratio with respect to its scrum concentration. Tbc study includcd 20 patients, aged 58-63 years (x= 59.4± 2.8) with mild hypertension. randomized to 4-week acebutolol treatment 2x200 mg daily or placebu. lnitially and at 4 week ABPM (SpaceLabs 90207) was performed and serum concentration of acebutolol (AC) and diacetolol (oe) was determined by HPLC. Changes in 24-hr mean systolic (SBP) and diastolic (OBP) blood pressure were analyscd from 30 min recordings at two intervals : 06.00 - 22.00 and 22.00 - 06.00. Mean SBP and DBP for each hour and the trough:peak (tip) ratio were also calculated. AC and oe concentrations were measured before and at hourly intervals for 8 hrs after the morning dose. Results:
hours 06.00- 22.00 22.00- 06.00
BP xSBP xDBP xSBP xDBP Initiallv 1365 84,8 1247 741 Placebo 133 8 83 5 1219 727 Acebutoio I 1290* 790* 121 2 714
* p< 0,05 The tip ratio for SBP and DBP in the daytime was 91,7% and 86,8%, respectively (no significant nocturnal blood pressure fall was observed). Mean half-life for AC and oe was 3,8 and 15,1 hrs, respectively. Conclusions: I. Acebutolol 2 x 200 mg daily produced a significant hypotensive effect which was associated with high tip ratio, thus confirming its choice in the treatment of arterial hypertension. 2. A sustained hypotensive effect may be related to the presence of slowly eliminating active metabolite.
Key Words: acebutolol, trough:peak ratio, hyperlension
AfH-APRIL 1996-VOL. 9, NO. 4, PART 2
F66 ANTIOXIDANT PROPERTIES OF INDAPAMIDE, 5-0H
INDAPAMIDE AND HYDROCHLOROTIDAZIDE EV ALUATED BY OXYGEN-RADICAL ABSORBANCE CAPACITY AND EPR
M.K. Walker, C. Vergely, M. Zeiler, J.R. Radernakers, V. Maupoil, P. Schiavi*1, D. Guez*1 and L. Roebette
L.P.P.C.E. Facultés de Médecine et de Phannacie, 21000 Dijon, and 1 I.R.I.S., 92415 Courbevoie FRANCE
Jndapamide (IND) an antihypertensive diuretic and 5-0H Jndapamide (5-0H IND), one of its principal metabolites, were tested to assess !heir antioxidant properties compared to the effects of the diuretic hydrochlorothiazide (KfZ). Superoxide scavenging properties of these diuretics were measured by Electronic Paramagnetic Resonance (EPR), and the Oxygen-Radical Absorbing Capacity (ORAC) by fluorescence.
I) EPR: Superoxide (02 ") radicals were genersled by a xanthine/xanthine oxidase system, with spin trapping by DMPO and spectra obtained aller 60 sec. DMSO used as a solvent at a final concentration of I % had no elfeet under our experimental conditions. HIZ (0.2 mglml reaction mixture) demonstraled no scavenging effect, whereas IND inhibiled DMPQ.OOH fannation by 20% and 5-0H IND by 60% at the same concentration. The concentration of scavenger required to inhibit spin adduct formation by 50% (IC50) was 0.045 mg/ml ( -100 I!M) for 5-0H JND. These results showed that the 5-0H metabolite of IND was the most potent superoxide scavenger compared to IND and HTZ.
2) In the second part of these studies, allophycocyanin was used as an indicator of free radical medialed protein damage. In the assay, 2,2'azobis(2-amidinopropane) hydrochloride (AAPH) was used as a peroxyl radical generator, and the loss of fluorescence was monitored. Antioxidant effects of the diuretics were expressed in ORAC onits, where I ORAC onit equals the net proteetion produced by li!M trolox. HTZ showed no proteetion up to I 00 I!M fmal concentration. IND and 5-0H JND showed linear correlations with respect to concentration when expressed in ORAC onits, with 5-0H IND giving the greatest proteetion against peroxyl radicals than IND. Expressed upon a rnalar basis, the relative peroxyl radical absorbance capacity of trolox, IND and 5-0H IND is I : 0.95: 1.48.
The observations above show that IND and 5-0H IND are elfective radical scavengers with the metabolite 5-0H IND having a higher potency than IND under our espcrimental conditions. By contrast, HTZ had no effect. These radical scavenging properties of IND may be of clinical interest for vascular and myocardial protection.
Key Words: lndapamide, Free Radicals, EPR, Fluorescence.
F68 INTEGRA TED EFFECTS OF THE COMBINATION OF THE ACE-INHIBITOR TRANDOLAPRIL WITH THE CACHANNEL-ANTAGONIST VERAPAMIL IN PHYSICALL Y ACTIVE PATIENTS WITH ESSENTIAL HYPERTENSION. HG Predel, T Schramm, C Robden , F Roveda, U Zanger, U Prinz, R Rost. Institute of Cardiology and Sport Medicine, Gerrnan Sport University, Cologne, Gerrnany
Few data are available concerning the integrated effects of various antihypertensive medications on systemic haemodynamics, carbohydrate and lipid metabolism, oxygen uptake (V02) and physical performance in patients with essential hyperlension (EH). The present double-blind, placebo-controlled prospeklive study included 44 physically active patients with EH: Age: 52± I! yearsbody mass index 24.9±2,7- RR: 154±9/96±5. Aftera wash-out period a bicycle spiroergometry until exhaustion (WHO) was performed foliowed by a 30-min. submaximal exercise test on the 2mmol/llactate-level 48 h later. Blood samples were taken before, during and after exercise. Subsequently, patients were randomly assigned to one of the following treatment regimens: A: ACEInhibitor-Monotherapy (Trandolapril 2mg); !l ACE-Inhibitor+ Ca-Antagonist (Trandolapril I mg/ Verapamil 180mg); Ç: Di uretic + Betablocker-combination (Atenolo150mg/Chlortalidon 12,5mg); Q: Placebo. Significant reduction in blood-pressure (BP) with AQ. Work capacity, V02max, heart rate (HR) and exercise-induced increase in BP remained unaltered with A, B. D. Work capacity at 2 mmmol/ blood-lactat moderately increased with A,..!! and was reduced with Ç. V02max, total-, LDL- and HDL- cholesterol, triglycerides, glycerol, insulin, cortisol and human growth hormone (hGH) remained unaltered. During exercise glucose and FF A were reduced with Ç. Physical capacity, energy metabolism and substrate flow remained unetfected with A, B, D, whereas it was moderally suppressed with.,Ç. ACE-Monotherapy (A) and the combination ACE-Inhibitor+ Ca-Antagonist (.!!) are especially suitable in physically active patients with mild to moderate EH.
Key Words: essential hypertension, antihypertension medication, physical capacity, energy metabolism
Dow
nloaded from https://academ
ic.oup.com/ajh/article/9/4/140A/2462180 by guest on 05 July 2022

AfH-APRIL 1996-VOL. 9, NO. 4, PART 2
F69 MALONDIALDEHYDE PRODUCTION AND PLATELET
AGGREGATION IN HYPERTENSIVE PATIENTS ON AMWDIPINE OR ENALAPRIL
R Hemández-Hemández 111 , MC Armas-Padilla, MJ Armas-Hernández, AR Carvajal, J Guerrero--Pajuelo and B Pacheco
Clinktd Pllrunuu:o/ogy Unit, School of Medicine. UniversU/tUl CenJro
Occirknlal Lis1111dro Alwuado. Bruqllisimeto. Venezuela.
Witb tbe aim to compared tbe effects of amlodlpine and enalapril on platelet aggregation and platelet malondialdebyde (MDA) production was carrled out a study in 30 patlento with mild to moderate hypertension. Fifteen patients in eacb group received amlodipine or enalapril in a double blind parallel fasbion. Patlento received placebo initially (4 weeks) then amlodipine (5 mgldally) or enalapril (20 mgldaily) at 7am for 12 weeks. Dosage was doubled after 4 weeks when DBP > 90 mmHg for both agents. At the end of placebo and active phases was carried out, platelet aggregation test (Bom Method), using adenosine dipbosphate (10
.,M), collagen (l!'g/ml) and adrenaline (2"M) and platelet production of MDA either in basal conditions (MDA-B) and after the stimulation of araebidooie acid pathway by adding ethylmaleimide (MDA-A). Enalapril paticnts received and average of JO. 7 mgldaily meanwhile amlodipine patient.s received and average of 7.3 mgldaily to control their blood pressure. Office placebo sitting BP, taken 23 ± 1 bours after last dose, was 165.5
(4.7)/104.5(1.1) mmHg (S.E. in brackets) in enalapril group and 169.2(3.3)/105.9(1.0) mmHg in amlodipine group (NS); at the end of activo phase, enalapril group had 138.5(2.9)/89.3(1.2) mmHg (p< 0.001) and patients from amlodipine group had blood pressure values of 134.7(3.1)/84.3 (1.9) mmHg (p< 0.001). Pistelet aggregation was reduced by amlodipine in 15.24°/• for ADP, 15.29°/o for collagen and 13.52°/e for adrenaline (p<0.005); meanwhile enalapril increased platelet aggregation by 2.23°/o, 7.13°/e and 0.09°/o for the three agents respectively (p: > 0.05). MDA was reduced by amlodipine by 21.4% for MDA-Basal; 3.85% by MDA~activated and the MDA~Basai/MDA~activated ratio in 25.9°/o
(p<0.05). Enalapril increased MDA~Basal in 21.8°/o; MDA~activated in 2.31% and reduced MDA ratio in 1.5% (p > 0.05). In conclusion, both drugs reduced blood pressure but only amlodipine was able to reduced platelet aggregation and platelet malondialdehyde production, indicating its action on the arachidonic acid pathway at platelet level in hypertensive patients.
Key Words: Amlodipine, Enalapril, P1atelet Aggregation, Malondia1dehyde
F71 RENALIIEMODYNAMICS, SODIUM EXCRETION, URINARY KALLIKREIN AND MICROALBUMINURIA FOLLOWING
TREATMENT WITH SPIRAPRIL, ISRADIPINE AND THE
ASSOCIATION OF ISRADIPINE AND SPIRAPRIL. !,R. Maccariello. V.G.A. Fagwades*, A.G. Rocba, E.A. Franeilehetti*.
Hyperteasion CHnic, Laberatory of Clinical aad Espenmental
Pathophysiology, Rio de Janeiro State Univenity, BraziL
In tlais cniiSOftr, doable-blind stndy we ewluated tlae effects
oflsradipiae (IS-SRO)-Smg, Spirapril (SP)-6 mg aad the usodation of IS-!!mg + SP-6mg on glomeralar liltration rate (."-" DTPA),
effecli\'C reul plasma flow ("'1-Hlpparan), urinary sodium u:cretion
(U,., V), III'ÎIIary kallikrem euretion (UKal) and lll'inary albnmin
exretioll (UAE) ia 12essencial hyperteillive patleniS wlth moderate
reaal dysfimdion. Tlle drngs were administered dlll'iDg 12 weeks
(A) preceded by a 4 weeks placebo phase (B).
MBP GFR ERPF
8 A B A B A
IS 127,75 106,58* 71,08 70,83 472,83 450,02
SP 126,83 111,92* 72,67 73,42 4!14,17 444,50
IS+SP 129,45 104,55* 70,82 71,91 466,91 460,00
IS - Isradipine; SP - Spirapril; MBP - mean blood pressure; GFR -glomerular tiltration rate; ERPF- effective renal plasma flow; "p< 0.001.
Despite a signifil:ant blood pressnre reduction, reaal hemodynamics
was maintailled stabie in au therapeutic period& The u,.. V increased
significaatly with IS allll the assodation of IS and SP (0,16 w 0,25
mEq/min, p< .0!!; 0,21 w 0,29 mEq/miD, p< .05, respecli\'Ciy).UEA
remained unchanged dlll'iDg the tilree drng protocols. Tlle UKal
increased significantly daring IS (0,30 w 0,49 mU/min, p< .0!!). In
conclusion, the drngs were effective iD coatrolling blood pressnre
wllile maintaiDing stabie renal function. However, only IS and tlle
a!ISCK:iation of IS aad SP increased renal sodium exretion whic:h
may he a hetter altenative tban SP alone In patients wlth renal
failure. Key Words: reaal hemodyuamics, nriDary kallikrein,
urlaary albamiD u:cretion, isradipine, spirapriL
POSTERS: Antihypertensive Drug Treatment 157 A
F70 ANTlliYPERTENSIVE EFFECT OF TWO COMBINATIONS OF NIFEDIPINE WITH ATENOLOL IN MILD HYPERTENSION. K.S. Kraft*, S. SchieBI, and H. Vetter. Medizinische Poliklinik Bonn, Germany.
The control of blood pressure (BP) by a combination of a betablocker and a dihydropyridine derivative is very efficient and has a low rate of side effects. Studies in which the optirnal doses are evaluated, are rare. In a double-blind randomised placebo-contraled study 36 patients (mlf: 18/18; age: 37-80, mean 57.8) with mild hyperlension were included. After a 14 days' placebo period they were treated with a combination of 20 mg retarded nifedipine and 25 or 50 mg atenolol (AT) for 6 weeks each. Group A starled with 25 mg, group B with 50 mg AT. Casual sitting BP was measured automatically (Dinamap 1486) every 2nd week, routine Iabaratory parameters and side effects were evaluated at the end of the placebo and the verurn phases. Placebo BP of the groups was camparabie and was reduced by 31.6/14.7 mm Hg (group A) or 29.9/15.8 mm Hg (group B) (p< 0.001 vs. placebo) after 6 weeks. BP was not furlher reduced in the second treatment phase. The response rate was 92% for both combinations, neither age- nor sex-related differences could be found. Laberatory parameters were nor altered by treatment. The rate and severeness of side effects was equal in both groups. It is concluded that in patients with mild uncomplicated hyperlension a combination of 20 mg nifedipine with 25 mg AT is as efficient and safe as with 50 mg AT.
Key Words: Atenolol, nifedipine, mild hyperlension, safety, efficiency
F72 ANTIHYPERTENSIVE EFFICACY OF HALF DOSE FIXED COMBINATION CAPTOPRIL + HYDROCHLOROTHIAZIDE MEASURED BY 24-HOUR AMBULATORY BLOOD PRESSURE MONITORING ~.X. de Pompignan1• La Tirnone Hospita!, Marseille, 1Bellon, Neuilly sur Seine, France. Long~term treatment with the fixed-dose combination therapy captopril SOmg + hydrochlorothiazide (HCTZ) 25mg has proven to be effectivo throughout the nycthemeral in essential hypertensive patients. However, in some cases (elderly
patients) semi-dosage may be sufficient. The aim of this single-center,
prospective, open study was to evaluate the efficacy and safety of half dose
regimen of this combination therapy by ambulatory blood pressure monitoring
(ABPM) and the number of responders. After a 2-week placebo run-in period, allowing withdrawal ofprevious antihypertensive therapy, 47 patients (31 men, 16
women) meao age 60 ± 12,1 (SD) years, BMI (24,02 ± 2,35 kglm2) with mild to moderate hyperlension (95:::; casual (C) diastolic (D) BP:::; 114 mmHg and 24h
mean systolic (S) ABP > 137 mmHg and/or 24h mean DABP > 87 mmHg] were
included to receive captopril25 mg + HCTZ 12,5 mg once daily, for 60 days. All
CBP were measured supine and resulted from the average of 3 consecutive
evaluations. ABP measurements were taken every 15mn for 24 h on Day 0 and
Day 60 (SpaceLabs 90207). The primary efficacy criteria was the change in the 24h-DABP (from DO to 060). Patients were classified as ABPM responders if a
DABP decrease of more than 5 mmHg was recorded during the first 6 hours ofthe
day. At baseline (DO), the mean casual SBP and DBP was 166 ± 16,7 mmHg and
lOl ± 5,2 mmHg respectively. The mean 24 h SABP and DABP were 148 ± 15,7
mmHg and 91 + 12,5 mmHg, respectively. -All patlenis (mmHg) Responders (mmHg)
àSBP/A DBP àSBP/àDBP CBP Supine -22+ 16"/-16+9' -23+ 17/-16+9
24h -12+ 10'/-8+6" -14+8/-9+5 ABPM Daytime -14+10'/-8+1" -17+ 10/-10+6
Night-time -10+ 12*/-7+9' -12+ 10/-8+8 Last 3 hours -10+ 14*/-5+ 12* -12+ 14/-6+ 13
('p <0.05) Analysis of efficacy on an intent-to-treat basis, showed a significant deeresse in
casual SBP and DBP as well as in SABP and DABP measured during the 24 h, last
3 hours, daytime (7:00 am-IO:OOpm) and night-time (10:00pm-7:00am)of monitoring (•p <0.05). Of the 47 patients, 35 were classified as ABP responders
(74,5%). BP circadian variability and meao hearl rate were not atfected. There
were no serious adverse event or discontinuation of treatment. In conclusion, the results of this study indicate that the semi-dosage combination
therapy of captopril 25 mg + HCTZ 12,5 mg (I) is effectivo and well-to1erated in the treatment of mild to moderate essential hyperlension (2) allows BP control
over 24 hours with a high number of responders. Key Words:
captopril - hydrochlorothiazide- hyperlension- ambulatory blood pressure
monitoring - ABPM responder
Dow
nloaded from https://academ
ic.oup.com/ajh/article/9/4/140A/2462180 by guest on 05 July 2022

158A ASH XI ABSTRACTS
F73 THE IMPACT OF LACIDIPINE ON CARBOHYDRATE AND LIPID METABOLISM. C Spieker*, M Barenbrock, W Zidek. Med. Univ.-Poliklinik Münster, Germany
In an open multicenter study the ca2+ antagonist, lacidipine was tested for efficacy and safety, especially with respect te lipid and carbohydrate metabolism. The study was performed in 2127 patients with essential hypertension. The patients were treated with lacidipine orally in a dosage of 2 · 6 mg daily for 48 weeks. Whereas lacidipine decreased blood pressure significantly by 20 .± 17 (systolic) and 14 .± 10 (diastolic, bath p<0.0001), there were no adverse effects on lipid and carbohydrate metabolism, neither in the total group nor in a subset of diabetic er hyperlipidemie patients. lt is concluded that lacidipine is a safe and effective drug in the long-term antihypertensive treatment of patients with essential hyperlension and with concomitant metabolic disorders such as diabetes mellitus er dyslipidemia.
Key Words:
F75
Antihypertensive Treatment -Lipid and Glucose - Metabolism
SIMILAR EFFECTS OF 3 MONTHS TREA TMENT WITH LOSARTAN AND ENALAPRIL ON ALBUMINURIA, BLOOD GLUCOSE AND LIPlOS IN PATIENTS WITH ESSENTIAL HYPERTENSION. Seren Nielsen, Jens Dollerup aod Carl Erik Mogensen". Medica) Department M, Aarbus Kommunehospital, Aarbus & Merck Research Laboratories, Copenbagen, Denmark.
In a double-blind, raodomized, double-dummy, comparative, 12 weeks study we evaluated tbe effects on Enalapril (E) 20 mg daily (n=46) versus the aogiotensin 11 receptorblocker Losartan (L) 50 mg daily (n =47) on blood pressure, albuminuria, aod blood glucose aod lipids in 93 patients witb essential hyperlension (57 males, 36 females, age 53 (9) years (meao (SD)), BMI 27.5 (4.1) kg/m2), normal serum creatinine aod without proteinuria ( urinary albumin/creatinine ratio (Ualb/cr) < 20 mg/mmol). Blood pressure was similarly reduced by botb treatments (E: from 157/103 (16/5) (meao (SD) to 144/94 (1717) mm Hg; L: from 158/103 (16/6) to 147/94 (19/9) mm Hg, botb p <0.001). Ualb/cr was significaotly reduced during L (from 1.05 (x/+ 2.39) (geometrie meao (x/+antilog SD) to 0.74 (x/+ 1.89) mg/mmol, p<O.OOI), as well as during E (from 1.03 (x/+2.55) to 0.79 (x/+2.52) mg/mmol, both p<O.OOI). The effect on albuminuria was especially evident in patients (33%) witb microalbuminuria (Ualb/cr 2-20 mg/mmol). The difference between the two treatments was not statistically significant. Fasting blood glucose, total cholesterol, HOLcholesterol and triglycerides were oot unchanged during L, whereas minor reductions were found in all lipids during E. No difference was observed between the groups. Conclusion: Enalapril 20 mg daily and Losartan 50 mg daily reduce blood pressure equally in essential hypertensive patients. No adverse effects were seen on glucose and lipid concentrations. Moreover, Losartan treatment reduces albuminuria at least as effectively as Enalapril, suggesting that tbe level of glomerular leakage of albumin is profoundly affected by tbe effects angiotensin 11. Key Words:
Essential hypertension, Urinary albumin excretion, Lipids
AJH-APRIL 1996-VOL. 9, NO. 4, PART 2
F74 SODIUM NITROPRUSSIDE VERSUS URAPIDIL IN THE TREATMENT OF HYPERTENSIVE CRISES. MM Hirschl*, M Binder, A Bur, H Herkner, A Wagner, AN Laggner. Department of Emergency Medicine, Univarsity of Vienna, Austria, Europa.
Whereas urapidil, a peripheral alpha-blockar and a central serotonin-agonist, is !he drug of choice in !he traalment of hypertensive crises in Europa, sodium nitroprusside is the preterred drug in !he states. As urapidil is still an investigational drug in !he States, studies camparing safety and efficacy of both drugs in patients with hypertensive crises are rare. 80 patients with hypertensive emergencies (diastolic blood pressure > 11 OmmHg and evidence of end-organ damage) were randomized to the study protocol. Response to treatment was defined as a reduction of diastolic blood pressure < 90 mmHg and release of symptoms within 90 minutes alter start of treatment. 12.5 mg urapidil was applicated intravenously every 15 minutes until goal of treatment was achieved (maximum dose: 75 mg). lnfusion of sodium nitroprusside starled with 0.5 IJg/kg/min and was increased ervery 15 minutes by 0.5 11g until blood pressure reduction was sufficient (maximum dose: 6 IJg/kg/min). Severe side-effects were defined as discontinuatien of the drug due to severe hypolension (systolic blood pressure <1 OOmmHg), clinical signs of carebral or coronary h rfusion or volume substitution.
Camparing both drugs a significant higher response rate has been observed in patients receiving nitroprusside. However, the use of sodium nitroprusside is associated with a considerable percentage of severe side-effects. Therefore, in patients with ischemie stroke, especially elderly people, nitroprusside should be used cautiously. In contrast, urapidil is a safe and highly effective drug, which can be used in all kinds of hypertensive emergencies. Key Words:
urapidil, sodium nitroprusside, hypertensive crisis
F76 ENALAPRILIHCTZ 20/6 MG REDUCES ALBUMINURIA IN PATIENTS WITH ESSENTIAL HYPERTENSION. AN ATENOLOL CONTROLLED 3 MONTHS STUDY. Soren Nielsen, Jens Dollerup and Carl Erik Mogensen'. Medica! Department M, Aarbus Kommunehospital, Aarbus & Merck Research Laboratories, Copenbagen, Denmark.
Elevated urinary albumin excretion (UAE), a common feature of essential hypertension, may be reduced by ACE inbibition through independent reductions of systemic and/or intraglomerular hyperlension. We enrolled 175 patients witb essential hyperlension (aged 51 (9) years (meao (SD)), BMI 27.7 (4.0) kg/m2) with normal serum creatinine and without proteinuria (urinary albumin/creatinine ratio (Ualb/cr)<20 mg/mmol) in a doubleblind, randomized, double-dummy, comparative, 12 weeks study camparing tbe effect of Synerprii~(S) (Enalaprii!HCTZ 20/6 mg) daily (n=84) and Atenolol (A) 50 mg daily (n=91) on blood pressure and UAE. Blood pressure was similarly reduced by botb treatments (S: from 159/104 (18/6) (meao (SD) to 141/92 (16/8) mm Hg; A: from 159/103 (13/5) to 145/91 (18/8) mm Hg, botb p<O.OOI). Ualb/cr was significantly reduced during S (from 0.67 (x/+2.38) (geometrie meao (x/+antilog SD) to 0.54 (x/+ 1.93) mg/mmol, p<O.Ol), but was unchanged during A (from 0.62 (x/+2.11) to 0.62 (x/+2.04) mg/mmol, NS). The difference between tbe two treatments was statistically significant (p =0.015, repeated measures ANOVA), and was also evident when normoalbuminuric (Ualb/cr <2 mg/mmol) patients (91 %) were evaluated alone (p =0.034). Conclusion: Synerpril~ 20/6 mg daily and Atenolol 50 mg daily possess equal antihypertensive potency in patients with essential hypertension. Altbough reduction of abnormal albuminuria can be achieved by reducing systemic blood pressure, our Atenoio I controlled study of Synerpril~ indicate, that reduction of intraglomerular blood pressure through ACE inbibition is a significant determinant of albuminuria in patients with urinary albumin excretion in tbe normal range. Key Words:
Essential hyperlension, Urinary albumin excretion
Dow
nloaded from https://academ
ic.oup.com/ajh/article/9/4/140A/2462180 by guest on 05 July 2022

AfH-APRIL 1996-VOL. 9, NO. 4, PART 2
F77 LOW-DOSE COMBINATION OF MOEXIPRIL AND HCTZ: AN OPTION IN ANTIHYPERTENSIVE TREATMENT B. Koch, M. Stimpel*, Dept. of Clinical Research, Schwarz Pharma, Monheim, Germany
Low-dose antihypertensive drug combinations are supposed to achieve significant blood pressure reductions and to minimize adverse events (AE) by reducing the risk of close-dependent side effects. The aim of this placebo-controlled study was to evaluate the efficacy and safety of a low-dose combination of moexipril plus hydrochlorothiazide (HCTZ) in patients with mild to moderate hyperlension At the end of a 4 week single-blind placebo period 223 hypertensive outpatients with a sitting diastolic blood pressure between 95 and 114 mmHg were randomized to receive placebo or moexipril 3.75mg plus HCTZ 6.25mg for the 12 week double-blind period. At biweekly visits blood pressure (BP) and pulse measurements were done and the occurrence of AEs was documented. At 12 week study endpoint low-dose combination therapy with moexipril 3.75mg plus HCTZ 6.25mg caused a significantly higher decrease in sitting diastolic BP compared to placebo (-7.6mmHg vs. -3.9mmHg, p<O.OOI). The difference in systolic BP rednetion was also statistically significant in favor of the moexiprii/HCTZ combination group over the placebo group at all trough time points. Adjusted mean changes in sitting systolic BP at study endpoint were -7. 7mmHg and +0.2mmHg in the combination and placebo groups, respectively (p<O.OOI). The percentages ofpatients having one or more AEs in the combination and placebo groups were 58% and 66%, respectively. lncreased cough and headache which are the most frequently reported A Es associated with ACE inhibitors were reported by 6% and I 0% of patients in the active treatment group and 5% and 18% of patients having received placebo. This study indicates that the low-dose combination ofmoexipril 3.75mg plus HCTZ 6.25mg given once daily was significantly more effective and as safe as placebo. Prescrihing of low-dose combination of moexiprii/HCTZ may be considered in cases when blood pressure is adequately controlled on higher doses of monotherapy but patients are suffering from dose-related side-effects.
Key Words:
F79
Moexipril - Hydrochlorothiazide -Low-Dose Combination
DO PATIENTS WITII MODERATE IIYPERTENSION PROFIT FROM A COMBINATION TIIERAPY WITII MOEXIPRII. PLUS IICTZ? B. Koch, M. Stimpel*, Dept. of Clinical Research, Schwarz Pharma, Monheim, Germany
The combination of thiazide therapy with an angiotensin converting enzyme (ACE) inhibitor has proved to be a good alternative in the treatment of hyperlension when monotherapy fails. The purpose of this study was to evaluate the efficacy and safety of two dose combinations of moexipril (Moex) - an orally active, long-acting, nonsulfhydryl-containing, nonpeptide ACE inhibitor- and hydrochlorothiazide (HCTZ) in comparison to the individual components in patients with moderate essential hypertension. Aller an up to 4 week single-blind placebo period 272 hypertensive patients with a sitting diastol ie blood pressure between 100 and 114mmHg, inclusive, were randomized to receive Moex 15mg, 30mg, HCTZ 25mg, 50mg, Moex 15mg plus HCTZ 25mg or Moex 30mg plus HCTZ 50mg for an 8 week double-blind treatment period. At biweekly visits blood pressure (BP) and pul se measurements were done. The occurrence of adverse events (AE) was doeurnenled as wel I. At endpoint significantly more patients responded to combination therapy (74-83% vs. 30-59%, p,;0.005) which also caused significantly larger reductions from baseline in sitting BP than each individual component alone. Doubling the dosage of Moex 15mg plus HCTZ 25mg to Moex 30mg plus HCTZ 50mg did nol cause any significant increase in BP response. Adjusted mean changes from baseline in systolic/diastolic BP (mmHg) are shown in the following table:
OmgHCTZ 25mg HCTZ 50mgHCTZ
-8.4/-8.1 -14.0/-11.0
15mg Moex -6.4/-8.0
-19.7/-16.0
30mg Moex -12.2/-9.7
-24.2/-17.9
Moex and HCTZ were generally well tolerated. The incidence of cough and headache which are the most frequent A Es associated with ACE inhibitors was similar in all treatment groups. Combination treatment had a tendency to neutralize the potassium loss seen in the HCTZ groups. This study indicates that Moex and HCTZ show additive antihypertensive effects and constitute a clinical valuable combination in the treatment of moderate hypertension. By reasoos of efficacy and safety Moex 15mg plus HCTZ 25mg is the most favorable dosage in these patients.
Key Words: Moexipril- HydrochlorothiazideCombination therapy - Hypertension
POSTERS: Antihypertensive Drug Treatment 159A
F78 EFFICACY AND SAFETY OF MOEXIPRILIHCTZ VERSUS METOPROLOLIHCTZ IN PATIENTS WITH MILD TO MODERATE HYPERTENSION B. Koch, M. Stimpel*, Dept. of Clinical Research, Schwarz Pharma, Monheim, Germany
Combination therapy with the new ACE inhibitor moexipril plus hydrochlorothiazide (HCTZ) results in significant blood pressure reductions. Is this combination as effective and safe as other well established standard combinations in the treatment of hype11ension? This study compares the efficacy and safety of moexipril 7.5mg plus HCTZ 12.5mg and metoprolol I OOmg plus HCTZ 12.5mg in patients with mild to moderate hypertension. Aller a I month placebo run-in period 140 hypertensive patients whose sitting diastolic blood pressure averaged 95-114mmllg were randomized to receive either once daily moexipril 7.5mg!HCTZ 12.5mg or metoprolol I 00 mg!HCTZ 12.5mg for the following 12 week doubleblind treatment period. At biweekly visits blood pressure (BP) was controlled sphygmomanometrically and the occurrence of adverse events (AE) was documented. At study endpoint adjusted mean reductions in sitting systolic/diastolic BP seen with both combinations were -17.6mmHg/-12.7nunHg and -17.2mmHg/-13.9mmllg in the moexiprii/HCTZ and metoproloi/HCTZ groups, respectively. The response rate to both kinds of combinations were very similar - 79% and 82% in the moexiprii/HCTZ and metoproloi/HCTZ groups, respectively -. Both combination therapies were generally well tolerated. The percentage of patients which experienced one or more AEs were 46% in the moexiprii/HCTZ and 61% in the metoproloi/HCTZ group. Headache and cough which are the most frequently reported A Es aller treatment with ACE inhibitors were seen in 9% and I 0% of the patients in the moexiprii/HCTZ group compared to I 0% and 4% in the metoproloi/IICTZ group. This study indicates that the combination of moexipril 7.5mg plus HCTZ 12.5mg is as efficacious as metoprolol I OOmg plus HCTZ 12.5mg in the treatment of mild to moderate hyperlension while showinga slightly favorable safety profile.
Key Words:
FBO
Moexipril- Metoprolol - HydrochlorothiazideHypertension
COUGH, ACE-I AND THROMBOXANE ANTAGONISM Malini PL , Strocchi E, Zanardi M, Lisi L, Ambrosioni E. Clinica Medica III, S.Orsola University Hospita!, Bologna, Italy.
Cyclooxygenase (CO) inhibition leads to attenuation of ACE-I induced cough suggesting that an increased PG activity may result in the side effect; we investigated a possible role for Thromboxane A2 (TXA), another endoperoxyde downstream of CO. On the basis of the results of a pilot single blind-stndy, nine mild essenrial hypenensive pts (5 F; 4 M) with past hystory of ACE-I induced cough were evaluated for cough frequency while untreated (baseline) by a 10-cm visual analog scale (V AS), secred by unassisted pts immediately before medical visits. Pts were then rechallenged with Enalapril 20 mg/d (EN) and 5-7 days after the recurrence of cough, while continuing the ACE-I, in a double-blind cross-over study were assigned to concomitantly receive either Placebo (P) or Picotamide (PICO, a platelet antiaggregant which inhibits TXA synthesis and receptors, but does oot interfere with CO activity) -600 mg bid- for two wks; treatments were then crossed-over and continued for two funher wks. Cough was assessed at the end of EN alone and of each cross-over period by V AS. Interim analysis in five completed pts shows : V AS score was 0.5±0.3 at baseline, 4.9±1.2 at the end of EN alone, was reduced to 1.5± 1.7 on PICO and was 5.2± 1.3 on P. Cough suppression reached the maximum within 48-72 h of treatment start and continued constant throughout PICO adruinistration. In 3 pts dry cough disappeared. These data are highly suggestive for a role of TXA in the pathogenesis of ACE-I induced cough. Lab evaluation of PG/TXA metabolites urinary excretion in ACE-I non-eaughers and at different time points in this study is currently being cartied out to verify a relationship between cough and endoperoxyde production and between clinical and biochemica! effects of PICO.
KeyWords:
ACE-I, cough, thromboxane, side-effects
Dow
nloaded from https://academ
ic.oup.com/ajh/article/9/4/140A/2462180 by guest on 05 July 2022

160A ASH XI ABSTRACTS
F81 V AGAL ACTIVITY, BP V ARIABILITY AND ACE-I IN HYPERTENSIVE TYPE 11 DIABETIC PATIENTS. E Strocchi, M Zanardi , L Lisi, A Ciavarella, P Vannini , PL Malini, E Ambrosioni. Clinica Medica III aod Centro Antidiabetico, S.Orsola University Hospita!, Bologna, Italy.
Tbe purpose was to evaluate the relationship between vagal activity (VA) and BP variability (var.) in diabetics (often with depressed V A) and to assess the effect of ACE-I (known to increase VA in Essential HBP- EH-). Eighteen pts with EH, stage I WHO, and 28 HBP diabetics (DIA) with no evidence of target orgao darnage aod no orthostalie hypolension were enrolled. After 3 wks of Placebo (P) and of Enalapril (10 mg bid -EN-) vagal function was assessed by calculation of SD of R-R intervals during deep breath for one min (SDRR); BP aod HR var. was assessed by SD of 24h ABPM values (Spacelab). All reponed comparisons aod changes are statistically significaot. BP values on P were similar in EH aod DIA. SDRR was lower in DIA vs EH (49 vs 67 msec), indicating V A impainnent, aod for a superimposable decrease of BP (both casual aod at ABPM) after EN, it increased to 79 msec in EH (increase in 95% of pts) while in DIA increased non-significaotly to 56 msec due to a more variabie behaviour (increase in 60% of pts only). ABPM showed that DIA as compared to EH, had a higher HR (82 vs 72 bpm) with lower var. (12.4 vs 14.2%); Systolic BP (SBP) var. was greater in DIA than in EH in the 24 hrs (15.4 vs 13.5 mmHg) aod particularly during nighttime, when fewer confaunding influences are present (11.1 vs 8. 9 mmHg). Similar results were obtained when SBP var. was calculated as percentage. An highly significaot negative correlation was found between SDRR and SBP var. (highest for night-time period : -0.65 in DIA aod -0.58 in EH). After ACE-I, in DIA SBP var. decreased (8. 5 to 7.4 %) while HR var. increased to 14.4%. In EH a similar behaviour was observed. No between-groups differences were observed for Diastolic BP var. which was unrelated to SDRR aod was not modified by EN. It is concluded that a relationship exists between V A and BP/HR variability; ACE-I deercases BP var. in EH and DIA: the modulation of V A might be involved in this effect.
Key Words:
ACE-I, BP variability, Diabetes, vagal activity.
F83 IN FAWN-HOODED (FHH) RATS THE EFFICACY OF ACEINHIBITION IS AGE-DEPENDENT. AP Provoost, GH Verscput, and Koumans HA, Brasmus Univcrsity Rotterdam and University Hospita!, Utrecht, Tbc Netherlands
Littlc is known about tbc effects of angiotcnsin convcrting enzymc-inhibition (ACE-i) when starled in advanced stages of cxpcrimcntal rcnal discasc. Male inbred FHH-rats, dcvelop spontancous systcmic and glomcrular hypertension, progressive proteinuria (UpV) and glomerulosclcrosis rcsulting in terminal rcnal f ai! ure. Tbcy wcrc uscd to study tbc cff ects of lisinopril (LIS; 50 mg/1 drinking water) on systolic blood prcssurc (SBP) and UpV. LIS was starled at 7, 22, 36, or 50 wecksof agc. In surviving animals tbc experiment was stopped at 72 wceks of agc. Median survival time of all untrcatcd FHH rats (n~58) was 52 wccks. LIS starled at 7 wceks of age (n ~ 10), complctely prevenled tbc iocrcase in SBP and tbc developmcnt of Up V, and all rats survivcd tbc 72 weck follow-up pcriod. Ten rats trcatcd from weck 22, initia! SBP 166±6 mm Hg (mcan±sd), initia! Up V 216±55 mg/day, normalizcd SBP and Up V aftcr 4 wccks of LIS. SBP rcmaincd normotcnsivc during follow-up, but from weck 40 most rats sbowcd a moderate to markcd iocrcase in Up V. Aftcr 3 wccks of LIS, startingat 36 wccks of age (n ~ 12), SBP feil from 163±13 to 1Hl±12 mm Hg, and UpV from 427±120 to 149±99 mg/day. Tbc Up V response was quitc variablc, mainly de pending on tbc level of UpV beforc LIS and not on tbc fall in SBP. During follow-up, 6 rats (witb tbc highest UpV on LIS) dicd prcmaturely from rcnal failurc. A similar outcomc was notcd whcn treatmcnt was starled at 50 wccks of agc (n~9). SBP feil from 161±9 to 1Hl±16 mm Hg, UpV from 392±111 tu 173±124 mg/day aftcr 3 wccks of LIS. Fivc rats, again with tbc highest Up V after LIS, dicd bcforc tbc end of follow-up.
Wc concludc tbat in FHH rats an carly start of ACE-i is esscntial f or complete rcnal protcction. Starting later in lifc ACE-i normalizes SBP and rcduccs UpV, but irrcvcrsiblc glomcrular damagc sccms present, limiting tbc thcrapcutic efficacy. Howcver, with a late start ACE-i is still ablc to rcduce tbc rate of progression and prolong survival time.
Key Words: ACE-inhibition, hypcrtension, protcinuria, renal
failurc, fawn-hoodcd rat
AfH-APRIL 1996-VOL. 9, NO. 4, PART 2
F82 THE EFFICACY OF CLONIDINE IN THE PREVENTION AND TREATMENT OF RENAL DAMAGE IN THE FAWNHOODED (FHH) RAT. AP Provoost, GH Vcrscput, RPE van Dokkum, and HA Koomans, Brasmus Univcrsity Rotterdam, and Univcrsity Hospita!, Utrecht, Tbc Nctherlands.
Littlc is known about tbc cfficacy of anti-hypcrtcnsivcs othcr than ACE-inhibitors in progrcssivc rcnal damagc. Pilot studies in FHH rats, a model of spontancous hypcrtcnsion-associatcd f ucal glomcrulosclcrosis (FGS), indicatcd that clonidinc (C) might bc cffcctivc in prcvcnting rcnal damagc. Wc studicd tbc effects of C in a dosc of I (C-l), 2 (C-2),or 3 (C-3) mg/1 drinking fluid on tail cuff systulic blood prcssurc (SBP), protcinuria (UpV), and tbc incidcncc of FGS. Tbc rcsults wcrc comparcd with untrcatcd controls (CON) and rats trcatcd with tbc ACE-inhibitor lisinopril (LIS, 50 mg/1). Trcatmcnt was starled al 6 or 26 wccks of agc. At tbc end of tbc 13 weck f ollow-up pcriod starled at 6 wccks of a ge (n~6), mcan levels of SBP, UpV, and FGS wcre:
CON C-1 C-2 C-3 LIS SBP (mm Hg) 165 I.W 138 137 100 lJpV (mgfday) 197 29 22 19 6 HlS(% glom) 17.1 1.8 0.7 O.X 0.4 C attcnuatcd tbc incrca;c in SBP and Up V, albcit les; than LIS. FGS wa> almosl absent in hoth C and LIS trcatcd rats. At start of trcatmcnt, tbc 26 wcck-old FHH rats alrcady had stabie hyperlension and progrcssivc lJpV (circa 250-300 mg/day). Thc mcan levels of SBP, lJpV, and FGS at thc end of tbc 13 weck follow-up pcriod in these oldcr rats (n ~6) wcrc:
CON C-l C-2 C-3 LIS SBP (mm Hg) 164 146 14'! 116 100 UpV (mg/day) 411! 247 194 157 22 FGS ('i{ glom) 49 34 44 34 24 Thus C causcd some rcduction in SBP and Up V, albcit much less than ohservcd witb LIS. Tbc incidcncc of FGS af ter C was only numcrically less than CON, and higher than LIS treated rats.
Tbc findings indicatc tbat in FHH rats, C bas ;ome rcnoprotcctivc..: cff eet which i:, more prunounccd with carly on !loet of trcalmcnl. At both agc>, howcvcr, Cis lc;s cffcctivc than LIS.
Key Words: clonidinc, ACE-inhihition,
prulcinuria, rcnal failurc, fawn-hoodcd rat
F84
bypcrtension,
RENAL FUNCTION AND ANTIHYPERTENSIVE THERAPY. A TEN YEAR STUDYIN ESSE!'ITL-\L HYPERTENSION. L Serena, A Gebbin, A Fontebasso, R V alle, C Simonella. A Monari, A Semplicini*, A C Pessina. Instilute of Clinical Medicine - Cniversity of Padova Me<tical School , Padova, Italy All\l: To evaluate long term renal timetion changes according to drug treatment in patients "'ith essenti?J hyperlension (EH). METHODS: Patients were retrospectively selecteà form the Outpatient Ciinic Data Base if they had EH, normal renal fimction at baseline, and, at least, I) ten year follow-up. 2) one physician evaluation evexy year, 3) four creatinine rneasnrements. the tirst and the last ten years apart. They were dassified into tOur groups according to the presence of ACE inhibitors (ACE!), caicium entry blockers (CEB). !heir combination (ACEI,CEB) or difl"erent dmgs (ELSE) dUJing more than 50% follow-up. RESl'LTS: 64 patients (35 male, aged 48:_11) fitllfilled the selection ctiteria. After 11:':1 year follow-up semm creatinine (sCr) increased only from 88:>:20 to 92:::19 ~moLL but the change was significantly lower in ACE!, CEB and ACEI+CEB thart in ELSE group. despite
sirnihil ba~eline JTe~ll~cîT-ru,_n.e ~ti~e~e~i~~~lr-i'i~~Jr~ l=----c---;;c--- (n~20) (n~I q_ J3 (n~23] __ l.f!"'!QL BasehnesCr 86+17 89•25 91:::21 1 79"17 Al/Cr% I year 0 3 + I 2 0 2 + I 9 0 ]";']011.7 _; 1.1•
Baseline SBP f--~=~:~- ~94c2_6*if-j§_7:l9 Hml<Be "H' ''""'' ~t'"" ' ·'·""." BaselineDEP ll0~9 105+6 113:':14 106:-:6 l Final DBP 89+5 87+9 88-:;:<) gg-:]j-10 }T mean DBP 90 + 3 Tio ~ 9 ~·- - '.J! ;_-8 j__]}Q~_c
*p<0.05,A."iOVAand TukeyTest, BP~mmHg,sCt=~moLL CONCLUSIONS: ACE! and CEB have a renoprotective etlèct in essential hypenensives which is indipendent from the antihypertensive action.
Key Words: hypertension, drug-therapy, renal function
Dow
nloaded from https://academ
ic.oup.com/ajh/article/9/4/140A/2462180 by guest on 05 July 2022

AfH-APRIL 1996-VOL. 9, NO. 4, PART 2
F85 EFFICACY AND SAFETY OF LOSARTAN IN HUMAN RENOVASCULAR HYPERTENSION LM Ruilope•, JM Alcázar, C Campo, J Wallin, A Dominiczak, R Cavanillas, R Segal, S Shahinfar. Madrid, Spain; Glasgow, UK; New Orleans, USA & Merck Research Laboratories, West Point, Pennsylvania, USA.
Blockade of renin-angiotensin system can induce the development of renal insufficiency in human renovascular hypertension. This is especially the case in the presence of a bilateral renal artery stenosis or a single kidney with estenosis. The aim of the presence study was to investigate the efficacy and tolerability in human renovascular hypertension due to unilateral renal artery stenosis in an open-label study. A group of 6 patients (4m, 2f, aged 41-68 years) entered the study. They were diagnosed as having atherosclerotic unilateral renal artery stenosis. After a 2-week placebo washout period losartan 25 mg was initiated. The dose was titrated if needed to 50 and 100 mg. At week 6, hydrochlorothiazide and/or labetalol was added if SiDBP was > 90 mmHg. Blood pressure control was attained in every patient; in three with losartan alone. Serum creatinine, creatinine clearance and serum potassium did net exhibit any significant change during the 8 weeks of fellow-up. Plasma renin activity exhibited a significant increase (p<0.051 after 4 and 8 weeksof fellow-up. The results of this small study suggest losartan to be efficacious, generally safe and well tolerated in patients with renovascular hypertension due to unilateral renal artery stenosis.
Losartan, renovascular hypertension, renin-Key Words: angiotensin system.
F87 PREFERENTlAL ANTAGONISM BY AMLODIPINE (AMLO) OF THE LOCAL SYMPATHETIC REFLEX REGULATION OF SKIN BLOOD FLOW IN ESSENTIAL HYPERTENSIVES (EH) labichella M. L., Catapano G. Deii'Omo G, Melillo E',Pedrinelli R Clinica Medica I, Medicina lnterna', Azienda Ospedaliera Pisana & Universita' di Pisa, Haly Locally-evoked sympathetic mechanisms (veno-arteriolar reflex. VAR) autoregulate skin blood flow and avoid !luid extravasation by preventing gravitational increases in capillary pressure through artericlar vasoconstriction. Thus, int erferenee with V AR tunetion might explain why dihydropiridine (DHP)s therapy causes subcutaneous edema, a frequent side-effect of calcium entry blockar (CEB)s in EH. Studies were conducted in n;7 unirealed mild-moderate uncomplicated EH (2 F, age: 43±5 yrs). Drugs were administered tor two weeks, preceded and foliowed by !woweek washouts. The experimental design was a cross-over. sequence-randomized cernparisen of amlodipine (AMLO, 10 mg od), a DHP CEB, with doxazosin (DOXA, 4 mg od), a selective a-
1 antagonist vasodilator. Supine BP (indirect method. mmhg). skin flow at the first right metatarsal space (laser doppier flowmetry, LDF, perfusion units) and leg blood flow (LBF, strain gauge piethysmography, mV100mVmin) were the evaluation variables. VAR (elicited by right leg dangling lor 10 minutes) was quantified as the % LDF reduction from supine to dependent position. AMLO (115±8 to 103±5, p<.01) and DOXA (115.±11 to 110.±9, p<.02) decreased MBP; both increased supine LDF (AMLO: 6.9±3 to 10.7±4; DOXA: 6.3+3.1 to 13.6±6, p<.01) and LBF (2.8±.6 to 3.4±.9, DOXA: 2.3±.5 to 3.2±.9, p<.05). However, AMLO blunted postural cutaneous vasoconstriction (51.3±18% to 3.±44., p<.001) while DOXA (47.±14.3 to 45.4±11.3 %) did nol. Thus, AMLO antagonized VAR independentiy from hypolension and local vasodilation. Possibly, cutaneous vasoconstrictor reilexes utilize preferenzially u-2 medialed mechanisms since DOXA, an u-1 blocker, was ineffective. VAR antagonism might potentially explain dependent edema during DHP treatment, although further studies are needed to evaluate the relevanee of this hypothesis in the clinical setting.
Kev Words: Calcium Channel Blockers, a, Antagonists, Vene-Artericlar Reflex, Subcutaneous Edema
POSTERS: Antihypertensive Drug Treatment 161A
F86 IJ!.'TA-ll.üKI:-:Rf; VERSI-S CAJ.CH.IM AN'l'!GJHISI'S IN 'lHERAPV OF PATJr:IITS WITH AII'J'folUAL. HYPER'lNISIOII, loKl HAD Pk'<Xii&:SSI VE AJ«ilHA 1. 1..\lKYdQOVa. vu. sumlKO. o. SY(:hev. H. I:l ShchUPaK. Institute of cardioJogy
we stUdled the wnuence Of dlfferent variantes of antihYPertensive drugs on deVeloPJrent in Patients (Plsl with arterial h'l'Pel'tenslon <AH> after PJ'Oflresslve amllna <PAl of maior card.Lo-vascular events (CVE): JDYocardiac mfarct.Lon. cardiac deatb and s~.
Hl<! Pts wlth AH after PA were stUdled dur'Ulll 30 IIDllths :tollow-UP. All Pts were seJ>arated on tbree groups ltrr. l : 1st Iw i tb Pls, wo were treated bY onlY reta-llloKers>. 2nd lwlth Pls. wo received beta-bloKers and calci\111 antagonistsl and 3rd twith Pls, wo were cured bY onlY caiCl\111 antasonlsts - nlfedlPlnel. Rates of CVE were calculated bY KaPian-Meiers Jrethod.
Hain resultes are Present in the table: = R Gro\JP: H= (PlS) Rate Of CVEIY.l R = n u R I 1st 20 10 0.27 n n 2nd 33 GT 1. 19 11
I 3rd li9 28 1 • .116 u
In conclusion: UPls with AH after PA had best resultes dilrillil terapy onlY beta-bloJWrs: 2l we not can to reearendate tberaPY of nlfediPine for 101111 cure of Péltients with bieb ischemie beart disease ri~ as 10000-tberaPY and so as J>art of druil callllnatlon.
Key Words: arterial tm>errtension. drug tberaPY
F88 PERINOOPRIL VS. TRANDOLAPRIL - FIRST OOSE EFEECT ON BLOOD PRESSURE PROFILE IN ACUTE MYOCARDlAL INFARCTION. W Sobiczewski, L Mierzejewski , J Jagoda, T Nylk, D Cieéwierz, M Gruchala, A Rynkiewicz. I Dep. ofCardiology, Medica! University of Gdalisk, Gdailsk, Poland. We have estimated the hypotensive effects of early treatment with ACE inhibitors: perindopril and Irandolapril in patients with acute myocardial infarction. 26 J)atients (4 female. 22 male. age 60±11 y., EF 51±9 %) with acute myocardial infarction \\ere included in this study (TP). On the third day of acute myocardial infarction 16 patients received 2 mg. of Irandolapril and I 0 patients 2 mg. of perindopril per os. Control group (C) consisled of 11 patients with acute myocardial infarction (mean age 55±11 y., EF 54±9%). Noninvasive 24-h ambulatory blood pressure monitoring was performed by means of Spacelabs 90207 monitor. Patients \\ere in the roeurnbent position for 24 hour. The monitor was programmed to measure blood pressure every 20 min. during a day and every 30 min. at night. Plasma ACE activity was estimated at 0, 4, and 24 hours after thirst dose of ACE inhibitor by spectrophotometric metbod utilizing tripeptide F APGG. Mean 24-h systolic blood pressure (SBP) in TP group was significantly lo\\er than in C (TP:IIO±I5, C:I22+15 mmHg, p<0.04). Mean 24-h diastolic blood pressure (DBP) was similar in both groups (TP: 70± I 0, C: 72±9). The 24-h heart rate ( TP:, C:79±13). Day-night difference in SBP in TP was 3 mmHg and in C: 5 mmHg ( non significant). Daynight difference in DBP in TP was 3 mmHg, in C: I mmHg. There \\ere no significant differences in blood pressure and heart rate responses benwen perindopril and IrandolapriL Plasma ACE activity in Irandolapril group decreased by 68% after 4h and by 53% after 24h, in perindopril group decreased to 50% after 4h and to 46% after 24h. We conclude that early trestment with ACE inhibitors 72-h after acute myocardial infarction is safe and did not produce exacerbated hypotension.
Key Words: ACE inhibitors, acute myocardial infarction,
Dow
nloaded from https://academ
ic.oup.com/ajh/article/9/4/140A/2462180 by guest on 05 July 2022

162A ASH XI ABSTRACTS
F89 A DOUBLE-BLIND COMPARISON OF PERINOOPRIL and ENALAPRIL ON 24-H CONTROL OF BLOOD PRESSURE IN HYPERTENSIVE PATIENTS. ~·. M Pego, J Calaça, A Felizardo, A Santos, I Colaço, J Martins Correia. Un. F. Clinica, Fac. Med Pono, Serviços Cardiologia HU Caimbra, H Pulido Valente Usboa, Ponugal.
This multicentric, randomized, double-blind, parallel, controlled trial compared the antihypertensive efficacy and safety of perindopril (PER, 4-8mgld) and enalapril (EN, 10-20mgld) administered (after 3 weeks on placebo) once daily for 8 weeks in patients with mild to moderate hypertension. Patients were included if on placebo, diastolic blood pressure (BP) was between 95-114 mmHg. PER 8mgld orEN 20mgld were used if after I month on the lower doses, DBP was still > 95mmHg. After 2 months 17 patients completed treatment with PER (7 on 4mgld and 9 on 8mgld) and 13 with EN (5 on IOmgld and 8 on 20mgld). There was no difference in age (53±7 v 50±9yrs) or in any demograpbic data within both groups. Arobuiatory BP monitoring for 24h (ABPM) was performed on placebo (VO) and at the end of treatments (112). Results (table) are mean (SEM).
EN-VO EN-1'2 PER • VO PER - 1'2 24h ABPM 146/95 (6/3) 1351/87# (713) 145/92 (3n) 131*185• (4/3)
daytime nighttime
154/95 (6/3) 1421/92# (1/4) 150/97 (3/2) 138*/90• (4/3) 126/80 (6/4) 119/ 76 (5/4) 132/80 (5/3) 118*173' (4/2)
V2 v VO: § P<O.OS, # P<0.02; * P<O.Ol.
Trough-to-peak (TIP) ratios (corrected for placebo) of both drugs were measured for systolic BP by two different methods: Adirectly from curves that averaged all individual hourly 24h ABPM (TP of EN=0.54 and TP of PER=0.53) and B-averaging all individual TIP ratios after ABPM data were averaged for 3h intervals (TIP of EN=0.38±0.08 and TIP of PER=0.51±0.06, P=0.056). Five patients on each group reported mild side effects. We conclude that PER and EN have similar short term antihypertensive activity, although for the doses used PER is lik el Y. to show a better T lP ratio. Key Words: Perindopril, enalapril, efficacy, safety, trough-
peak ratio.
F91 EFFICACY OF · LOSARTAN AS AN ANTIBYPERTENSIVE DRUG ASSESSED BY AMBULATORY BLOOD PRESSURE MONITORING, HAND GRIP TEST AND ECHOCARDIOGRAPHIC STUDY. Maiorano G Bartolomucci F, Contursi V and Minenna F.S. Hypertension Group - Intemal Medicine - University of Bari (lT AL Y) The effects of LOSART AN (!..), an orally active angiotensin 11 antagonist, on blood pressure monitoring, on the response to isometrie stress and on the left ventricular diastolic function, were studied in a group of 15 patients (mean 49 ± SD ± 10.2) with mild to moderate essential hypertension. The patients enrolled and admitted to the study should have received no previous antihypertensive treatrnent. Alter 3-week of observation period, L was administered once daily (50 mg) for a 8 week treatrnent period. Clinic and 24-hour ambulatory blood pressure (Spacelabs 90207 device), hand-grip exercise (Asimow Dynamometer, LA, CA) and echocardiographic study (Esaote AU3) according to the American Society of Echocardiography, were performed at the end of each period. The differences between pre-treatrnent and post-treatment periods were assesed by the Student't-test for paired observations. Compared to the pre-treatrnent period, both systolic (SBP) and diastolic (DBP) blood pressure were significantly less at rest (rispectively p<O.Ol, p<0.05) durlog the administration of therapy. Arobuiatory blood pressure data, showed a significalive rednetion on 24-hour average of SBP and heart rate (HR) (p<0.05), but no differences were noted on DBP values. Blood pressure response to isometrie exercise showed no significalive differences between pre and post-treatrnent period. All the patients refered no side effects durlog the treatrnent. Doppler-<:eho data showed no significalive differences of interventricular septurn thickness, fractional shortening, systolic stress and sistemie vascular resistences. Our data indicates that Losartan 50 mg/day was effective in lowering blood pressure values at rest, whilst it does oot demonsirale the same efficacy to reduce DBP in 24-hour monitoring. The response to isometrie exercise with hand-grip test, was oot improved durlog treatment, prohabily implying an inefficacy of the drug in stress conditions. Losartan also caused a slight but significant rednetion in HR both durlog day and night time because it produced inhibition of the vasoconstriction indoeed by angiotensin I e 11 as ACE-inhibitors but without significantly influencing the bradykinin-induced vasodilation. This effect should be regarded as a favourable feature because of HR has been found to be a risk factor for cardiovascular disease and death. Key Words: 24-hour blood pressure,Echocardiography.Hand Grip Test,Losartan.
AfH-APRIL 1996-VOL. 9, NO. 4, PART 2
F90 A COMPARATIVE AMBULATORY STUDY OF CIL.AZAPRIL COMBINED WITH EITHER ISRADIPINE, HYDROCHLOROTHIAZIDE OR BISOPROLOL. B Vaïsse, D Herpin, S Boutelant, V Gressin, R Asmar. HOpital de la Timone, Marseille, France.
The purpose of lhis study was to assess wilh ambulatory blood pressure (ABP) monitoring, !he efficacy of combination lherapy in !he 162 out of 407 patients (43%) with essential mild to moderate hyperlension which level of 24-hour ABP (Novacor or Spacelabs, 96 measures/24 hr) was high (> 139 or 87 mmHg, Staessen 1991) afler a 6-week open treatmenl wilh cilazapril 2.5 mg/day OD (C). In this multicenter study, these non-rasponders patients were randomized to a double-blind lreatment with C combined with eilher isradipine 2.5 mg/day OD (1), hydrochlorothiazide 12.5 mg/day OD (H) or bisoprolol 5 mg/day OD (B) tor 6 additional weeks. ABP was assessed again at !he end of this treatment phase (day 84). Casual BP C +I (n = 61) C + H (n =46) C + B (n = 54) Day42 SBP 162± 10" 160±15'" 158± 15"'
DBP 97± 10' 98± 10' 95± 9'" Day84 SBP 153±19'" 152±17'" 152±16'
DBP 92±9"' 92± 11'" 91 ± 10" àday SBP 8± 14"' 8±12'" 6± 17' 42·84 DBP 5± 19"' 6±10'" 5±11" 24-hr ABP C +I (n = 61) C + H (n =46) C + B(n = 54) Day42 SBP 148± 15 147± 11 148±13
DBP 92 ± 9 92±9 93±8 Day 84 SBP 142±13'" 141 ±14'" 137 ± 14'"
DBP 88±9'" 89± 10'" 84± 8'" àday SBP 5±10'" 6±12'" 11±11"' 42·84 DBP 5±7*** 4±8" 8±7'"
Intent to treat analys1s. p < 0.05" p < 0.01 '"0.001 day 42 vs 84 ; àSABP : p < 0.01 C + I vs C + B, p < 0.05 C + H vs C + B ; àDABP : p < 0.01 C + I and C+HvsC+B
We conclude !hal, although casual BP is nol different, ABP data indicate !hal the combination of cilazapril and bisoprolol is more effective than that with isradipine or hydrochlorolhiazide.
Key words : ambulatory blood pressure, combination therapy, bela·blockers, angiotensin converting enzyme inhibitors
F92 A NEJf SEIECTIVE l\NIWDIIST CF THE CUIB1UN PRESSeR EFFEX:T. P Ftgrari H. Ferrarxii., L. Duzzi, G. Padoani, E. Mi.notti, P. Malloni. PrassiS-Si9'1" Tau, Settime M. se, Milan, Italy
Increased levels of encbgenous ooabain-like factor (CXF) have been demoostratecl in experimental an:i genetic animal hypertensim an:i in aroun::l 30% of essential hypertensive patients. Olronic infusioo. of Qlabain (aJ) causes hypertensian in rats. Tlrus, OIF an:i Ql could be phazmacological targets for new antihypertensi ve drugs. we have synthetized a new CCI!p)ll(XI (PST 2238) which di.splaoes aJ fran the Na!IATPase and it is devoid of inotrcpic activity an:i affinity for adrenez:gic, Ca channel, Angio II and ho>:m:>nal steroid reoeptors. 'llle antihypertensive activity of PST 2238 was assayed in rats w:i.th both experinental, irdloed by aJ infusicn (50 y/Kg/di.e x 4 weeks; OS rats) , an:i g:metic hypertension sustained by inc>:eased levels of erx:logenous OIF (MIS rats). PST 2238 was gi.ven to OS rats at 1, 10 and 100 y/"Eq os for 4 weeles and to young prehypertensive MilS at 0.1, 3 an:i 90 y/Kg os for 5 weeks. Systolic blood pressure (SBP) and beart rate (HR) were reeordered weekly. Kidooy neclulla (K) , left ventricle (LV) an:i hypothalamic (Hy) Na!IATPase activity were neasured at tbe end of treat:nent onl y in OS rats. PST 2238 reduced SBP in os rats at all doses ( -20 mnHg, p<O. 01) . K an:i LV NaKase activity increased in OS ctr. (K = 2.55 ±.1; LV = 0.23±.01 jlm::ll/min/ng, p<0.01) as canpared to sham salire-infused rats (K=l.47±.15; LV=0.159±.01 )JII\01/min/ng). PST 2238 at 100 Yf"Eq restored the NaKase activity at the sham' s levels in both tissues (K=l. 7±.11, LV~.l51±.01 jlm::ll/min/ng). In Hy the a3-isofom NaKase activity was dec>:eased in OS ctr. (1.44± .1 jlm::ll/min/ng,p<0.01) as catpared to sham rats (2.01±.36 )JII\01/min/ng), and returned towarcl the sham' s levels by PST 2238 both at 1 (1. 92 ± 0.01 jlm::ll/min/ng) and 100 y/"Eq (1. 79 ± 0 .1 jlm::ll/min/ng) . In MiS PST 2238 reduoed in a dose-depen:lent way the develCl!Jl"'rlt of hypertension (-5, -12*, -16* mnllg, *p< 0.01). In conclusion PST 2238 is a prototype of a new class of antihypertensive drtgs which at very low doses select i vel y antagonizes the presser effect of aJ or CXF by interterring at the level of the NaK ATPase.
ûuabain, ouabain-like factor, ouabain ~~~à't_, hypertensian, antihypertensive CCI!p)ll(XI
Dow
nloaded from https://academ
ic.oup.com/ajh/article/9/4/140A/2462180 by guest on 05 July 2022

AfH-APRIL 1996-VOL. 9, NO. 4, PART 2
F93 INSULIN SENSITIVITY PREDICTS THE RESPONSE TO ANTIHYPERTENSIVE THERAPY: A SUBSTUDY TO CAPPP. J Östergren1, H Isaksson2 and T Kahan3. Karolinska institutet, Depts of lnternal Medicine, 1Karolinska Hospita!, 2Söder Hospita! and 3Danderyd Hospita!, Stockholm, Sweden.
In cross-sectional studies obesity and/or an elevated insulin response to glucose have been associated to a poor response to antihypertensive therapy. This prospective study examines the relationship between insulin sensitivity and therapy response. 50 previously untreated non-diabctic patients (29 men, mean age 51±8 ys) with mild to moderate primary hyperlension taking part in the Captopril Prevenlive Project (CAPPP) were randomized to 50 mg metoprolol or 50 mg captopril daily. All were examined befare therapy and at 6 and 12 months. Doses were adjusted every 1-2 months to achieve a BP of <140/90 mmHg. If 100 mg of captopril or metoprol al daily proved insufficient a low dose thiazide or felodipine was added. Daily defined doses (DDD) were chosen as effect variabie to allow for individual dose titration. Insulin sensitivity index (MI) was calculated as the ratio between glucose uptake (euglucemic insulin clamp, 40 mU/m2 BSA for 120 min) and mean serum insulin level. 24 h ABPM was performed by Spacelabs 90207 equipment. At 12 months BP was reduced by 18/13 mmHg. Pretreatment MI was predielive of the DDD at 6 and 12 months, independent of BMI (P <.05 adjusted for initia! BP). Day-to-night systolic BP variation was related toMI, serum insulin and BMI (r= .34, -.41 and -.36, respectively; P <.05), with si mi lar results for diastolic BP. MI decreased (P <.05) and serum insulin increased (P <.01) in patients requiring higher doses. Thus, an impaired insulin sensitivity seems to reduce the response to antihypertensi ve drugs. Th is may establish a vicious ei rele and further jeopardize the conditions in these patients, in particular if drugs with negative intlucnee on glucose metabolism are added or given in higher doses, in order to overcome therapy resistance.
Key Words: Antihypertensive drug therapy, insulin resistance, ambulatory blood pressure monitoring
F95 EFFICACY AND SAFETY OF 1WO DIFFERENT DOSAGE OF FELODIPINE IN THE TREATMENT OF HYPERTENSION.
G. Ft:rlllino, C . .As~ioti, A Rt:ndla.
Cardiology Service and Coronary Care Unit. Hospita/ of Lamezia Terme ( Italy ).
Aim of the present study has been that to evalute the efficacy and safety of a long-tenn trea1rnent With Felodipine: 5 and I 0 mg once a day in the trea1rnent of moderate hypertension.
64 Patients (Ptz), with Diastolic Blood Pressure (DBP) between 100 and 115 mmllg, after a run-in period of 2 weeks with placebo were enrolled in the study. Ptz with Acute Myocardiallnfarction and Ictus during the last 6 months before the run-in period were excluded. All enrolled ptz, after the Placebo period, begon a trea1rnent with Felodipine (5mg/daily) for 4 weeks. After this period, all ptz with a DBP >90 mmHg were treated with Felodipine (I Omgldaily) and for a further period of 16 weeks.
We have obtained the following results Feloclipine .~mg!claily: 24164 pl7. (37..~%) hacl a ORP s; 90mmHg afler 4 weeks period of trea1rnent. Felodipine lOmg/daily: 40/64 ptz (62.5%) bad a DBP :S 90nunHg after a further 16 weeks period of trea1rnent.
In partjeular we have verified the trend of following parameters: Systolic Blood Pressure (SBP), DBP and Hearte Rate (HR).
Felodipine 5mg(24ptz)
Felodipine JOmg (38plz)
Baoeline 4 Weeks 16 Weeks SBP 16.5±16 136±!0 140±11 DDP10315 8416 8315 HR 71±4 70±5 69±4 SBP 16.5±16 146±10 137±7 DBP 103±5 101±4 83±5 HR 71+4 73+3 71+3
Only 2 ptz (3.2%) did not have an adequate response to the treatment with Felodipine and were successively treated with other therapy. No important side-etlècts (pretibilll oedemn only in 4 ptz) wt:re noll:d dwing all period of iJ·•Klm•nl.
In conclusion, our data demonstrate a very good efficacy and safety ofFelodipine in the trea1rnent of moderate hypertension. Key Words:
Fclodipinc, Moderate Hypertension
POSTERS: Antihypertensive Drug Treatment 163A
F94 COMPARISON OF INCIDENCE OF SIDE-EFFECTS IN THE TRF.ATMF.NT OF HYPF.RTF.NSION WITH VA RIOIJS C:AI.C:IlJM ANTAGONISTS
G. Ferlaino, C. Ascioti and A. Renelia
Cardiology Service and Coronary Care Unit, Hospita! of Larnezia Terme (ltaly).
Aim of the present study has been that to compare the mcidence of side-etTects in 3 ditTerent groups of patients with moderate hypertension (Diastolic Blood Pressure between I 00 and 115 mmHg) and trcatcd, aftcr a placebo run-in pcriod of 2 wccks with Fclodipinc (10 mg), Amlodipine (10 mg) and Nifedipine (30 mg) once a day and tor a period of 12 weeks.
89 patients were enrolled in this study and divided in 3 groups as fellow:
Felodipine Amlodipine Nifedioine
24 22 23
Age
58:!:Ï 61±5 57+9
Sex 13M; IIF llM; llF lOM· 13F
We have obtained the following results:
Amlodipine Felodipine Nifedipine p Oedema I I 2 NS Headeache 2 2 2 NS Dizziness 0 I 0 NS Astherria 0 1 0 NS Vomitus 0 0 0 NS Flushing I I 2 NS
In conclwilm~ uw· W.la dt:tiiOIIlSilllll: lhal ll•• ii••id•nc• of sid• effects in the trea1rnent of hyperlension with calcium antagonists as Felodipine, Amlodipine and Nifedipine is very low. No statistically difference in the incidence of side- effects was noted between these drugs.
Key Words: Side-effects; Calcium-antagonists.
F96 VERAPAMIL (V), TRANDOLAPRIL (T) AND THEIR FIXED COMBINATION (VIT) IN HYPERTENSION:THE VERATRAN STUDY G Mancia on behalf of the VeraTran Study lnvestigators lnternal Medicine Department,S.Gerardo Hospitai,Monza,Ciinical Physiology and Hypertension lnstitute,University of Milan, ltaly The aim of the study was the evaluation of the antihypertensive efficacy and safety of V, T and their fixed combination V fT over the 24 h. Afler a 4-week placebo (PL) run-in, 272 hypertensive patients (age 49.2±8.9 years, BP 158.5±13.5/1 03.8±3.4 mmHg,means±SD) received randomly V 180 mg SR, T 1 mg,the combination V and T 1 mg or PL od for 8 weeks, in a double blind parallel group study.Ciinic (C), semiautomatic (SA) and ambulatory (A) BP were measured at the end of run-in and afler 8 weeks of treatment. ABP was recorded also at 1 st day of treatment.Standard safety (laboratory tests and adverse events) was also assessed during the study. 234 patients were included in efficacy analysis, while 38 patients excluded for drop-out or poor ABP data quality. PL treatment slightly reduced C but not SA BP. Both C and semiautomatic BP were significantly reduced by V, T and, to a greater extent, V!T (p<0.01 for all vs baseline).At 1st day of treatment, average 24 h and day-time systolic (S) and diastolic (D)BP feil significantly in V and T groups, but the fall was even greater in V fT group (p<0.01 for all vs baseline and V!T vs others).Afler 8 weeks of treatmeni, average 24 h, day and night BP fall was significant in V and T group but again more marked in V fT group (8/6, 10/7 and 14/11 mmHg, p<0.01 tor all vs baseline and p<0.05 V!T vs others).Similar data were obtained for peak (P)(greatest BP fall between 2nd and Bth h trom drug intake) and trough (T)(Iast 2 h from drug intake) BP falls {p<0.01 tor all).The T/Pratios were better tor V fT than tor V and T alone (0.5 vs 0.2 and 0.2 tor SBP, 0.9 vs 0.7 and 0.4 tor DBP). 24h, day and night HR feil slightly in V and V!T groups only.ABP and HR were not affected by PL. Adverse events were 25.9% forT, 21.0% tor V, 16.7% tor V!T and 19.4% tor PL. Thus, antihypertensive treatment with fixed combination V fT is more effective and balanced over 24 h than with V and T alone.
Key Words: Verapamil, trandolapril, combination therapy, 24 hour BP, trough-to-peak ratio
Dow
nloaded from https://academ
ic.oup.com/ajh/article/9/4/140A/2462180 by guest on 05 July 2022

164A ASH XI ABSTRAerS
F97 OPEN DOSE TITRATION SAFETY STUDY OF IMIDAPRIL IN MILD TO MODERATE ESSENTIAL HYPERTENSION. IM Dews, MJ VandenBurg, P Lièvre. IBRD ROSTRUM Ltd., Romford, Essex, Uniled Kingdom
lmidapril is a new ACE inhibitor shown to have antihypertensive efficacy in short-term double-blind studies. 354 patients (18- 80 years) with sitting diastolic blood pressure (DBP) 95- 115 mmHg after 2 weeks' placebo run-in were treated with imidapril b mg daily !hen titrated at 4 week intervals through 10 mg and 20 mg. lf uncontrolled (sitting DBP > 90 mmHg) at 20 mg, furosemide 20 mg was added. Treatment was continued up to 1 year. There was a sustl'lined and significant fall in mean sitting DBP from 102.3 to 87.9 mmHg at the final visit. 85% of patients responded (sitting DBP ~ 90 mmHg or feil by ~10 mmHg). Most frequent adverse events were cough (13%), headache (9%) and bronchitis (7%). 2 deaths, considered unrelated to treatment, occurred. We conclude that imidapril appears to be a clinically valuable and well toleraled long-term antihypertensive agent.
Key Words: imidapril, hypertension, open
F99 REDUCTION BY (-) CICLETANINE OF VASCULAR REACTIVITY TO ANGIOTENSIN 11 IN THE RAT M Alvarez-Guerra, 0 Alda, E Morin, M Allard, RP Garay. INSERM U400, Fac.Médecine, Créteil, and IPSEN, Paris, France
Cicletanine (particularly its (-) enantiomer) inhibits calcium/calmodulin cyclic GMP phosphodiesterase in vascular smooth muscle and potentiales the vasorelaxant actions of the guanylate cyclase activators sodium nitroprusside and atriopeptin 11, but the relevanee for vasopressor stimuli is unknown. Here, racemie (+/-) cicletanine was tested for its ability to modify the vascular responses to several vasocontractant agents in pitbed rats. The most significant results were obtained with angiotensin 11. Hence, the dose of angiotensin 11 increasing by 50 mmHg the carotid artery blood pressure was twice as large in cicletanine (50 mg/Kg p.o.) than in vehicle given animals (ED50 = 0.48 ± 0.012 vs. 0.25 ± 0.007 !lglkg, p < 0.05). The displacement by cicletanine represented 47.2 % of that obtained with losartan. (-) Cicletanine (20 mg/kg, p.o.) produced a significant 3-fold rightwards shift of the dose-pressor response curve to angiotensin 11 as compared to the vehicle curve (ED50 = 0.56 ± 0.06 vs. 0.19 ± 0.02 !lglkg, p < 0.05). By contrast, in rats dosed orally with ( +) cicletanine (20 mglkg) the dose-response curve to angiotensin 11 was virtually coïncident with the vehicle curve. Similar results were obtained after intravenous administration of cicletanine enantiomers. In isolated rat aorta, the contraction by angiotensin 11 was reduced by (-) cicletanine in non-competitive manner (the % reduction was independent of· the angiotensin 11 concentration). In conclusion, (-) cicletanine may reduce non-competitively the vascular reactivity to angiotensin 11 which plays a substantial pathological role in several forrns of hypertension. These findings are compatible with an action of (-) cicletanine at any of the numerous steps which couple the occupation of angiotensin 11 receptors to the final response, such as calcium/calmodulin cyclic GMP phosphodiesterase.
Key Words : Cicletanine - Yesseis - Angiotensin 11
AfH-APRIL 1996-VOL. 9, NO. 4, PART 2
F98 CELIPROLOL: AGONIST AND ANTAGONIST EFFECTS AT CARDIAC BJ·ADRENOCEPTORS AND VASCULAR fhADRENOCEPTORS IN THE RAT. RP Garay, M AlvarezGuerra, C Sauzeau, and B Crozatier. INSERM U400, Faculté de Médecine, Créteil, and Lab. BELLON, Paris, France.
Celiprolol is a B-adrenoceptor antagonist which has desirabie ancillary properties since it is cardioselective and produces direct vasodilator and bronchodilator effects. This investigation aims to unveil and quantify the agonist and antagonist effects of celiprolol at the level of cardiac 81- and vascular 82-adrenoceptors under in vivo conditions. All experiments were carried out in catecholamine-depleted (syrosingopine) rats to exclude the participation of endogenous norepinephrine.
Celiprolol (30 11glkg to 3 mg/kg i.v.) produced dose-related increases in heart rate and decreases in mean carotid artery blood pressure of Jonger duration than isoprenaline and salbutamol respectively. Maximal increase in heart rate (110±4 beats/min, n=7) was 50% lower than that of isoprenaline. Furtherrnore, active doses of isoprenaline were 800-fold higher than those of celiprolol. Betaxolol (0.1-1 mg/kg i.v.) a BJadrenoceptor antagonist, strongly inhibited tachycardie effects of celiprolol. By contrast, hypotensive effects of celiprolol were markedly antagonized by ICI 118,551, a selective B2-adrenoceptor antagonist. In rats pretrealed with celiprolol (0.1 and I mg/kg i.v.) the heart rate dose-response curves to isoprenaline were shifted to the right of those in control animals. In this respect, celiprolol exhibited a cardiac BJadrenoceptor blocking potency slightly greater than betaxolol. Furtherrnore, celiprolol antagonized hypotensive effects of salbutamol with 70-fold less potency than ICI 118,551.
In conclusion, celiprolol has the ability of stimulating and blocking nol only cardiac B1-adrenoceptors but also B2-adrenoceptors. However, the potency of celiprolol as an antagonist of cardiac BJ-adrenoceptors is many fold higher than the agonist potency at these receptors as well as an agonist and antagonist of vascular B2-adrenoceptors. This pharmacological profile implies that celiprolol may function as a modulator of cardiac and vascular B-adrenoceptors.
Key Words: B-adrenoceptor antagonists - vessels - heart
FlOO OBSERVATION ON HORMONAL AND HEMODYNAMIC VARIABLES DURINO 45-DEGREES PASSIVE HEAD-UP TILT IN THE ELDERL Y MALES WITH SYSTOLIC HYPERTENSION (SHTN) BEFORE AND AITER WNG TERM HYDROCHLOROTHIAZIDE (HCTZ) THERAPY (Rx).
Suman Vardan•, Nonna E. Hili, Kisban G. Mchmtra, Saktipada Mookhc:ajee and Harold S.Wiyan. V A Mecti.al and SUNY Health Science Centers and Syracusc Univenity, Syracusc, NewYèrk.
During supine and at I 5 IJIIJlUies (min) of 45" possive-boacJ.up-incliDc oo a mecbani<:al tih table 14eldatypalicnls(pls.) between 60 and 75 years with SHTN clefined as systolic (S) blooei prosoure (BP) > 160 mmllg and distolic (D) BPs 90 mmllg. aDel wRbout prior billory of orlhoolalic8)111l0p)'<rdiabelaimollitus were otudied. We..........S plalma Rllin adivity (PRA),
- (ALDO), nor-<pinqimne (NE), aod atrialllllrimdic peptide (ANP) levds oloog with SBP, DBP,Uirate (HR), canliac ou1pU1 (CO) and oyatemic vuculat ............ (SVR) in bodt pooitioiB. Tbe BP was oloo ..........S immediately aller the IISIIUillJitioo ofthe tiltod pooitioo. All -.....-."""'apin dotamineclafter 1..-11 (mo) aod I yeor (yr) ofHCTZ diuretic Rx to control their SIITN. Tbe reaults are as fotlotw:
No. Before Rx No. I mooth Rx lyr of SupiDc 0-min I 5 min of Supine 0-Min IS Min I
Pis Tih Tih Pis Tih Tih SBPmmHg 14 191±18 177±20 190±19 13 169±21 160±26 170±26 U DPBmmllg 14 76±12 82±11 76±10 13 69± 8 73±9 69±7 N HRbeats/min 14 69±14 75±17 13 68±14 7S±I7 C CO llmin 14 5.7±1.0 4.6±1.2 13 5.3±1.0 4.1±.9 H SVRdynes s cnf'l4 1681±381 2213±550 13 164S±377 2166±538 A PRAnglmlnr 13 .48±.50 .51±.37 11 1.6±1.4 1.8±1.5 N ALDOD&'dl 11 15.1±9.5 17.5±13.2 10 16.2±8.6 15.4±8.3 G NE PWmJ 11 242±96 366±203 9 29S±ll0 481±240 E ANPPWmJ 10 66.5±82.0 45.3±45.9 8 40.2±37.1 42.1±37.2 D
M<Rthan IOomllgmb:lianinthe SBP at 0 min 45' tih suggested 1hat ..-atic !11resB bas been adJieved. Maidainonce ofthe tiltod pooitioo f<r I 5 min ....ulted in hemodnamic ponlllOiers reverting baclt toward the volues at the boseline supine position. Tbe moasured hc<monal variabloo did oot show statisticallysignificant change at 15 min. in thetiltod pooitiro However, !bere appean>dto be slighiWII in the levels of these variables in the ._me directinc. Aller I mo aDel I yr oftherapy wbicb ....,ltod in s.-ined control oftheir SHTN, the hemodynamic and honnonal profile showed similat reoponoeo during the ideoti.al repoat prooe<luns of poslive tihstudy.
The above observations may suggest an increased seusitivity to these bonnoDes in tbe ...,..vaüoo ofbemodynamic homeostasis in the elderly with SHTN. Loog 1enn HCTZ diurotic therapy did oot seem to alfeet the....,..,.. to orthostatic,..... at 45-degree head-up-tih.
Key Words: Systolic Hypertensioo, ~ Stress, bonnonal profile, Thiazide diuretic
Dow
nloaded from https://academ
ic.oup.com/ajh/article/9/4/140A/2462180 by guest on 05 July 2022

AfH-APRIL 1996-VOL. 9, NO. 4, PART 2
F101 EFFECTS OF LONG-TERM ISRADIPINE TREATMENT ON ENOOTHELIAL VASODILATION IN HYPERTENSIVES. F Perticone, R Ceravolo, R Maio, C Cosco, F Pugliese, PL Mattioli. Dpt of Medicina Sperimentale e Clinica at Catanzaro, Univarsity of Reggio Calabria, ltaly.
In systemic hyperlension the endothelium depedent vascular relaxation is abnormal. This study was designed to determine whether antihypertensive treatment with calcium channels blocker isradipine (ISR) can rastora the impaired
11 •pco.OSnH endothelium
dependent :::::: vasodilatation
__ , Acht Ac:h3
in hypertensives. By using a strain gauge plethysmography (Hokanson EC SR), the vascu
lar responses to acetylcholine [7.5 (Ach1), 15 (Ach2), and 30 (Ach3) 11g/min] and sodium ni-troprusside (N) (0.8, 1.2 and 3.2 j1g/min) were examined in 8 hypertensives before (group H) and after 2 and 6 mounths of ISR treatment (5 mg/day). The middle- and long-term ISR treatment significanUy improved endothelium function; however, no significant differences were observed after 2 and 6 months ISR treatment (figure). On the contrary, no ditterences were found in the responses to N. After ISR vascular resistance were significantly reduced from 16::!:7 U to 9::!:4 U (2 months) and to 9::!:2 U (6 months). In conclusion, our data show that the middle-term ISR treatment improves impaired endothelium.dependent foraarm vasodilation in hypertensives and its effect persists fora long time.
Key Words:
F103
hypertension, endothelium tunetion calcium channels blockers.
REST AND EFFORT HEMODYNAMIC (HD) RESPONSES DURING PROLONGED TREATMENT WITH FELODIPINE (F), ABPMAND ECHOCARDIOGRAPIDC CHANGES. R. Zimlichman*, R Tuvar. Wolfson Medica! Center, Holon, Sackler School ofMedicine, Tel Aviv University, Israel. 16 patients with essential hyperlension were treated with 5 mg F- OD for three months with dosage tilration up to lO mg if BP response was insufficient. Hemadynamie (liD) indices were assessed, (impedance cardiography), at rest and during isometrie elfort (IE) at 0, 3-7, 30, 60, 90 days of treatment. ABPM and eehocardiography were performed before and after 3 months of treatment. All patients had their BP normalized, 5 mg in 7 and l 0 mg in 9 patients. Rest systolic diastolic and mean BP decreased during the study (P<O.Ol). The deercase in BP was significant on day 3-7 oftreatment (P<O.Ol) and deereased further with continuation of treatment. Heart rate (HR) at rest did oot change throughout the study. ABPM showed lower systolic, diastolic and MAP after treatment with F . Mean HR during ABPM did oot differ before and after 3 months of treatment. When ABPM was divided to day-time (6 am to midnight), and night-time (midnight to 06 am), a significant deercase during day hours was found after 3 months of treatment (P<O.Ol), while sleep measurements showed a deerease that was of borderline significanee (P<0.054). Although BP levels deereased after treatment, the circadian rhythm of blood pressure fluctuations did oot change and rernained stable. LV maximal and minimal dimensions during diastole and systole did oot change during treatment. IVS and PW thickness tended to deerease but the deerease was of borderline significanee as were L VM, L VMIBSA and L VMJ height. HD measurements performed at rest, at peak elfort of IE and l-2 minutes post elfort showed no difference in VET, HR and Cl. However rest SVR and MAP decreased significantly during treatment.
Key Words: Felodipine, Hemodynamics, Blood pressure, ABPM.
POSTERS: Antihypertensive Drug Treatment 165A
F102 BEVOND TROUGH:PEAK RATIO: A NEW INDEX OF THE SMOOTHNESS OF THE ANTIHYPERTENSIVE EFFECT OF A DRUG D. Rizzoni ', E. Agabiti-Rosei '. Chair of Semeiotica and Metodologia Medica, Dept. of Medical Sciences, Univarsity of Brescia, ltaly. Background and objective: The trough:peak ratio (T /P) is considered an important parameter lor !he assessment of !he clinical effects of a drug. However, it is charged by many limitations, since it takes into account only two "spots" (peak and through effect) of !he antihypertensive action. Since TIP may be calculated trom data obtained with non-invasive ambulatory blood pressure monitoring (ABPM) (peak: 2-6 hour post dosing), it seems te be reasanabie te use more than only two data in !he evaluation of !he smoothness of the antihypertensive effect of a drug. Therefore, we consider worthwile to test another index, !he inverse ratio of !he varlation coefficent of !he hou~y
dillerences between ABPM perfonned in basal conditions and during therapy (smoothness index, SI). Melhods: We have created with the help of a personal computer live dillerent pattems of hourly dillerences between ABPM perfonned during placebo and during antihypertensive therapy, in which !he smoothness of the blood pressure control throughout !he 24 hours was progressively worse (trom !he 1•' to the 5• pattern) (dosing: 8.00 A.M.). Then, we applied tothese pattems the calculation ofthe PIT and ofthe SI. Results: The values obtained lor PIT were 100%, 85%, 55%, 59%, 105% (trom 1" to 5• pattern). while !he values obtained trom SI were, respectively 20, 7.3, 5.38, 4.12, 1.29). Therefore, The SI correctly ranked the five pattems trom the best to !he worst, while the PIT could nol correctly allocate in the rank !he last 2 of !he 5 pattems. Expecially !he simuiatien of the worst smoothness of blood pressure control (see figure, 5• pattem), was wrongly allocated by the PIT in 1•• place (105%) inslead of at !he 5•place.
Conclusions: SI seems to have some advantage over the PIT in the evaluation of !he smoothness of !he blood pressure control, even i! it is necessary to ~~-ical application belore drawing any conclusion.
Trough/peak ratio, ABPM, drug therapy
F104 PROTECTION AGAINST ISCHEMIC STRESS IN ERYTHROCYTES: ROLE OF INTRACELLOLAR FREE MAGNESIUM. M.Barbagallo, L.M.Resnick*,Div. Endoc/Hypertension, Wayne State U Med Ctr, Detroit, MI.
To study mechanism(s) underlying the myocardial protective effects of sulfhydryl agents and SH-containing converting enzyme inhibitors, 31 P-NMR spectroscopie measurements of phosphorylate roetabelites and intracellular magnesium (Mg1 ) were obtained in erythrocytes during 6 hours of anaerobic incubation with and without captopril, enalapril, and the sulhydryl reagents, MPG, N-acetyl cysteine, and penicillamine (1-300 ~M).
Captopril, as well as the ether SHcompounds, but not enalapril, significantly elevated Mg1 levels (p<O.OOl). At 4 and 6 h , captopril, compared to control, retarded the rise in P1 (p<0.008/p<O.D25), and the fall in ATP and 2,3 DPG content (p<0.035/p<0.038). The higher the initia! Mg1 , and the greater the captopril-induced rise in Mg1 , the greater the protective effect (r=0.768, p<0.05).
We conclude i) captopril and ether sulfhydryl compounds exert directy retard roetabelite depletion following oxygen deprivation; and ii) this protective effect may be due to its ability to stimulate and maintain Mg1
content. Key Words:
ACE-inhibitors, ischemia, NMR, magnesium
Dow
nloaded from https://academ
ic.oup.com/ajh/article/9/4/140A/2462180 by guest on 05 July 2022

166A ASH XI ABSTRACTS
FlOS THERAPEUTICAL APPROACH WITH ENDOMYOCARDIAL BIOPSY PROVED MICROVASCULAR HEART DISEASE IN PATIENTS WITH HYPERTENSION OF LONG-YEAR DURATION D Bene R Jung, M Obradovic, D Zivkov-Saponja, A Stojsic, M Bikicki. J Mi/in, D Vuckovic, D Stojsic lnstitute ofCVD, lnstîtute ofTuberculosis and Lung Diseases, Sremska Kamenica, Instîtute ofHistology, Novi Sad, Yugoslavia
In the period from 1986-1994, 93 patients with long-year arterial hyperlension (mean age 38.5±7 .9), 94.11% female, were investigated. They all had chest pain, ECG changes and positive stress-test. Dipyridamol test was positive in 62 patients (75%). All patients underwent heart catheterisation with normal coronary angiography finding. Endomyocardial biopsy (EMB) was also performed in all of them. Specimens were sent to light-, electron-microscopy and histoenzymatic analysis. Patients were divided according to dominant histologie features in two groups.
In group 1, degeneralive changes were dominant, while in the group 11 reactive changes. Histologie parameters were dominant in the group 1: I. thickening of intramural arterioles due to muscle proliferation;2.interstitium with enlargement of theelastic fibres (Weigert);3.traffic-pinocytotic vesicle indicate a pathway of macromolecules through degenerative endothelial cells; 4 decreased number of metarterioles.
In group 11, the most common pathohistologic findings were: I. rich revascularisation with evident hypofunctional hyperemy without traflic vesicles;2.arterioles were thickened due to proliferation ofthe muscular layer; tunica media of the arteriola may be splitled into layers; arterioles without any histomorphological changes indicated the discontinuity ofthis process; 3. narrowed lumen ofarterioles; 4.endothel with normal appearance; swollen endothelial cells indicated progressive structural alteration ofarterioles; 5. narrowed capillary and metacapillary lumen with visible tortourosity; 6. arterioles and venules tilled with eritrocytes which is a blood stasis indicator.
Patients were divided in two groups according to the treatment. Group A was treated with ACE inhibitors Ramipril, beta-blockers and nitrates. Group B was treated with ACE inhibitors, beta-blockers and Molsidomin. After 6 months treatment, a significant impravement was noticed in group B, with fewer angina! attacks and better ECG finding on stress-test.
CONCLUSION: lt is recommmended that patients with pathohistologic changes on distal and intramural coronary vessels and long-year hypertension, should be treated with Molsidamin as well, for decrease of angina! attacks.
Key Words:
F107
endomyocardial biopsy, microvascular heart disease, hypertension
MINOXIDIL SULFATE STIMULATES ENDOTHELIAL PROSTACYCLIN FORMATION AND INHIBITS PLATELET THROMBOXANE FORMATION
H.-J. Kruse, E.V. Negrescu, P.C. Weber, and W. Siess Institut für Prophylaxe und Epidemiologie der Kreislaufkrankheiten, University of Munieh, Germany
The vasodilating effect of the potent antihypertensive drug minoxidil sulfate (MS) is medialed by opening of K+ channcls of smooth muscle cclls thaileads to hyperpolari;-~tion and thus relaxation of the cells. We have investigated the inl1uence of MS on the receptor-operaled Ca2+ in11ux and on prost.anoid synthesis of cultivated human endothelial cells (HUVEC), and on the stimulated aggregation of human platelets.
In unstimulatcd HUVEC, MS did neither affect basal intracellular ea2+ coneentration (measured spectro11uorometrically with fura-2), nor basal levels of prostacyclin (PG12), but augmenled both Ca2+ inl1ux and synthesis of PG!z stimulated by thrombin. In contrast, MS inhibited thromboxane Bz (TXBz) formation and platelet aggregation induced by rollagen, arachictonic acid, epinephrine and the thrombin receptor-activating peptide (TRAP).
We conclude that in endothelial cells, opening of K+ channels by MS enhances thrombin-stimulated synthesis of prostacyclin. This occurs most likely through hyperpolarization of the cell membrane, that leads to inllux of extracellular ea2+_ In contrast, MS inhibits platelet aggregation through inhibition of cyclooxygenase, and reduced synthesis of TXBz. Thus, increased endothelial production of vaso-dilatory PGiz and reduced formation of vasoconstrictory TXBz may enhance the direct vasorelaxant effect of MS on vascular smooth muscle cells.
Key Words: endothelial cells, prostacyclin, platelet aggregation, potassium channel opener
AfH-APRIL 1996-VOL 9, NO. 4, PART 2
F106 EFFECTS OF ONCE-DAILY FELODIPINE IN HYPERTENSIVE SUBJECTS EVALUATED BY AMBULATORY BLOOD PRESSURE MONITORING. M.M.Cangelosi,M.P.PoPto,G.Baccifava,A.SaponaPo, F.Leggio. INRCA-CaPdiology DepaPtment-Rome-Italy.
In ouP PeseaPch we evaluated the effects of Long-tePm tPeatment with dihydPopyPidine calcium antagonist Felodipine in essential hypePtension. 40 hypePtensive subjects,mean age 55t6, (22 f- 18 m ), with mild to modePate essential hypePtension, office blood wessuPe (OBPJ ~160/95 mmHg, without diabetes meZLitus and Penal OP caPdiac diseases, wePe enPoLZed afteP 1-week placebo Pun-in. The patients wePe tPeated with Felodipine (sustained peLease foPmulation 5-10 mg once-a-daily) foP 1 year, 24-h blood pPessuPe monitoPing was pePfoPmed by d~ vice Takeda 2420 at baseline and again at 3 months and 1 yeaP: Peadings wePe pPogPammed at 15-m inte~ vals daily (? am-10 pm) and 30-m nightly(10 pm- ? am). AfteP 3 months of thePapy, 24-h mean systolic and diastaZie BP (SBP-DBPJ decPeased fPom 151z8 to 133z11 mmHg and fPom 94±? to 80±9 Pespectively lp = 0.001); mean SBP day and night-time decPeased fPom 156~6 to 13?±9 and fPom 132±5 to 123±? Pespectively (p = 0.001). Mean DEP day and night-time decPeased fPom 9?±? to 85±6 and fPom 84±4 to ?5±3 Pespectively!p=0.001J.No significant changes of BP values WePe obsePved afteP 1 yeaP of tPeatment. GuP Pesults indicate that Zong-tePm anti-hypePtensive tPeatment with Felodipine once-a-day can significantly Peduce BP with na change in 24-h mean heaPt-Pate. Key Words: HypePtension, Felodipine calcium antago
nist, 24-h blood pPessuPe monitoPing
FlOS THE BENEFITlAL EFFECT OF L<YäRTAN af ANGICYrENSnlCCKVERT:mG ENZIME :mHIBITCIIS (ACE) COOOH;
Jo I&aJcy-1 Mo .Angela, L. Grandin, Jo Godoy Internal Medioine Departmant National Univarsity o:r ~o Mandoza A.rgentilla o:r the varions side-e:ffects of ACE inhibitors sane serious and saille not, oough bas EIJlerged as one o:r the most trouhl.esane and oamon whioh may lead to drug witdrawalo In acme centers, the incidance o:r cough is thought to be as high as 1 0% to 15% or more. Increased formatien of b~ and prostaglandine u.y- p.1a.y a role.
Saveral studies suggest reliet of cough by added nonsteroidal. anti.ini'lamatory drugs with the downsiele o:r dilllinished ant~rtansive ei'i'ects.
Logically, a change to an Angiotensin II reoept;or inhibitor (lozartan) should consistantl.y benei'it.In our bypertensive clinic all patiants en ACE inhibitors with ncn prod.uctive dry cough and in absence of other causa of cough persistent during therapey- and repa1ae o:r deohal.enger i1' ACE inhibitor was stoppedo Were cl!ange to lozartan.Total. o:r 17 patients, 11 :t:emales(64,7%)6 mal.es(35,2%) age 6CZ 20 and recei:vini112 pat.Ene.lapril. (70,5%) 3 pat. Lisinopril. (1717J) 2 pa.t.~pr:ll ( 11,7%)
Ware changet to Lozartan 50 mg begi.nin atter 48 h of staping the ACE.
We found that the oough dissapear in all these ~tiants and the control. of the blood pressure lB· P.) did not change significant ai't.er 21 da.ya of lozartan tberapey-.B.P. at end et ACE therapey- 137,94/111. 11 B.P. at 21 th da.y ot Lozartan thera~ 141,05/88.11.
This prellminary report will be :t:ollov in year time to aval.uate the evol.uticn of these patiants, and all others that can be incl.uded.
As tor as we kn011 Lozartan should be the Key Words: drugs ofchoice in bypertansive pa
tiants with cough due to ACE inhibitors. LOZARTAN 1 COOOH
Dow
nloaded from https://academ
ic.oup.com/ajh/article/9/4/140A/2462180 by guest on 05 July 2022

AfH-APRIL 1996-VOL. 9, NO. 4, PART 2
F109 NIGHT AND MORNING BLOOD PRESSURE IS BETTER CONTROllED BY AMLODIPINE THAN FELODIPINE JB Östergren, H. Isaksson, U. Brodin for the study group. Dept of Medicine, Karolinska sjukhuset, Stockholm, Sweden Objective: Amlodipine (A) and felodipine (F) are both dihydropyridines but A has a long tl/2 (35-40 h.) and F in an extended release form has a shorter duration of action. We compared the blood pressure (bp) lowering effects of A and F by 24 h ambulatory bp monitoring (ABPM). Design and methods: 216 patients with essentien hypertension (bp 95-115 mm Hg) were randomised to receive A or F after a 4 week run-in period in a singleblind multicenter study. The starting doses were 5 mg. 1f the target office bp ( 90 mm Hg) had not been achieved after 4 weeks the dose was increased to 10 mg. 24-h ABPM was performed on placebo medicatien befere randomisation and after 4 and 8 weeks on active treatment. Spacelabs equipment was used. Bp was also measured by conventional technique in the office 24 h post drug intake. Results: Significantly more patients responded after 4 weeks treatment with A (50%) as compared with F (33%), (p=0.013). After 8 weeks 83% achieved the target pressure with A and 69% with F, (A vs F, p=0.023). Diastolic office bp measured 24 h post dose was more reduced by A (8.9 mm Hg) compared to F (6.9 mm Hg), (p=0.02). ABPM during daytime (07-23) was similar on both treatments but night bp was more effectively reduced by A (syst;p=0.026:diast;p=0.019). Conclusions: A seems to be more effective than F when the drugs are compared in the same dose both as regards bp 24 h post dose and during the night. The longer duration of amlodipine as compared to felodipine is the probable reason for this finding.
Key Words: Ambulatory blood pressure, calcium antagonists, drug therapy
Flll DISSOCIATION OF LEFT VENTRICULAR HYPERTROPHY AND BLOOD PRESSURE IN HYPERTENSIVE PATIENTS TREATED WITH ACE INHIBITORS. LC Martin,IF Velasco,M Marchioli,B Bojikian-Matsubara,K Okoshi,F Haberrnmam,RC Athanazio-Heliodoro,PJF Tucci,RJS Franco, Nephrology Division, Dept. Medicine, Botucatu Medical School, Botucatu, Säo Paulo, Brasil.
To evaluate the correlation of LVH and MAP in hypertensive patients treated with ACE inhibitors.After 4 weeks of placebo, 53 patients (56±9 years, 22 male) were treated either with enalapril ( 31) or U sinopril ( 13) or captopril ( 9) . Similar doses of each drug were used. Mode M-ECHO was performed to measure LV mass index (LVMi;g/m') prior and after 6 months treatment. Patients were divided as folows: group I (AMAP;,;20mmHg, n=26); group II (AMAP<20mmHg, n=27) and group III (AMAP<10mmHg, n=11). There was no difference amon9 the groups I and II for LVMi. Camparisans of LVM1 among the groups I and II and in the same III were done. No correlation of ALVMi and AMAP was found. Results as (Mean±SD) see the table '
Groups LVMi LVMi ALVMi AMAP(mmHg) prior post
I 116±29 105±29' 12±15 34±12 2
II 123+37 111 +31' 11+18 10+8
III 135+37 114±381 18±18 4±6
1 P<O.OS r~or vs p p est; 2 p<U.U~ I vs rr. In conclusion LVH regression was nat correlated to blood pressure reduction, independent of the ACE inhibitor used.
Key Words· angiotensin converting enzyme inhibi ti ars lert ventdcular hypertrophy, captopril, enalapril, lisinopril.
POSTERS: Antihypertensive Drug Treatment 167 A
FllO ORGAN DAMAGE IN TREATED HYPERTENSIVES IS NOT RELATED TO THE EXTENT OF NOCTURNAL BLOOD PRESSURE DECLINE. SA Rodriguez, HLL Beckers, PN Van Es, MME Krekels, PW De Leeuw·. Dept. of Medicine, Univarsity Hospital Maastricht, The Netherlands.
Ta investigate whether the prevalenee of hypertensive complications is related to the degree of nocturnal blood preesure (BP) decline in treated hypertensives, we measured 24-hour ambulatory BP (Spacelabs) in 54 patients on stable antihypertensive treatment and obtained information concerning hypertensive complications (cerebrovascular accident, left ventricular hypertrophy, myocardlal infarction, retinopathy, peripheral vascular disease and renal function). Nocturnal decline of BP was calculated from the average of the two lewest BP at night (A) and average day BP (B) as: (B-A)/8 xlOO%. Based on this decline the population was divided into tertiles. Tertile I displayed an average fall in nocturnal BP of 14±5 %, whereas in tertile II and III BP fell by 23±4% and 33±4% respectively. Average daytime BP levels were similar in all tertiles, whereas lewest nocturnal BP levels were 101±16 mm Hg (I), 86±9 mm Hg (II) and 74±14 mm Hg (III) respectively. No significant relation was apparent between age, body mass index, BP during the day and the % of nocturnal BP decline. Creatinine levels, however, were significantly lower in tertile III (69±24 ~mol/) than in tertile I (96±30 ~mol/1). In tertile II creatinine averaged 89±20pmol/l. There was na difference in the prevalenee of hypertensive complications between the tertiles (!:66%, !!:77%, III:72%). Moreover, there were na differences between the tertiles as far as the type of organ damage was concerned. These data suggest that the nocturnal decline of BP bears na relationship to the frequency of hypertensive cornplications in genera!. The association between plasma creatinine and nocturnal BP fall remains to be elucidated.
Key Words: 24-hour ambulatory blood pressure-
hypertension-cardiovascular complications
Dow
nloaded from https://academ
ic.oup.com/ajh/article/9/4/140A/2462180 by guest on 05 July 2022