ANGANWADI WORKER ANGANWADI WORKER
131
A Doctor’s Tribute A Doctor’s Tribute A Doctor’s Tribute A Doctor’s Tribute 2013 ANGANWADI WORKER ANGANWADI WORKER ANGANWADI WORKER ANGANWADI WORKER INDIA’S PREVENTIVE CARDIOLOGIST INDIA’S PREVENTIVE CARDIOLOGIST INDIA’S PREVENTIVE CARDIOLOGIST INDIA’S PREVENTIVE CARDIOLOGIST Dr Kunda Silimkhan, M.D
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of ANGANWADI WORKER ANGANWADI WORKER
A Doctor’s TributeA Doctor’s TributeA Doctor’s TributeA Doctor’s Tribute
2013
ANGANWADI WORKERANGANWADI WORKERANGANWADI WORKERANGANWADI WORKER INDIA’S PREVENTIVE CARDIOLOGISTINDIA’S PREVENTIVE CARDIOLOGISTINDIA’S PREVENTIVE CARDIOLOGISTINDIA’S PREVENTIVE CARDIOLOGIST
Dr Kunda Silimkhan, M.D
ANGANWADI WORKER
India’s Preventive Cardiologist
A Doctor’s Tribute
Dr Kunda Silimkhan, M.D.
Self Published e-book
©Author
Panaji- Goa
Version 2013
Please send your suggestions at:
Sitara Building , Ground floor
C-6/3 Portais ,Panaji-Goa
403001
Preface
India has seen a rapid rise in lifestyle diseases in recent years. To combat the
problem, the Goa Lifestyle Project was introduced which took us to different
segments of society.
After studying the whole picture, I feel that an Aaganwadi based intervention
could be most cost effectivein dealing with lifestyle diseases. At the grass
roots, the Aanganwadi worker has a pivotal role in both communication and
networking especially in the rural areas. An empowered worker can reap huge
dividends for the country. This book is an attempt to highlight the possible role
of the aaganwadi worker in India’s preventive and promotive health program.
Beside the role of aaganwadi workers, I have addressed here the complete
strategy to tackle the problem of lifestyle diseases to put things in the right
perspective.
We will know for sure only when we draw a specific program and implement
it. Sometimes, we lose time trying to prove some facts or collect data. It is
easier to extrapolate from existing data. If we rope in volunteers, we will need
to spend very little from Government funds.
A doctor who treats heart attacks is well paid but the one who prevents
hundreds of heart attacks every year is overlooked and receives a pittance in
compensation. What better tribute could be there to this silent worker but a
book in her name?
This book may motivate the aaganwadi workers themselves to chalk out the
right course of action. They know the ground realities best.
Although this book is written with the people of Goa in mind since I am more
familiar with the aanganwadi functioning here, it applies to the whole of India.
As the program gets implemented, more states could join in. Many such books
may be written in the different languages of India.

This book is not a scholastic endeavor nor is it a research paper. While reading
this book people will be taken from the farm to boardroom, from the
Panchayat to Parliament, nutrition to social health, pre-independence to
current times to the next millennium because that is how the complex web is.
Simplifying it has been the cause of many of our troubles.This is an attempt to
give practical tips to the aaganwadi workers and some members of the public
who dream of a healthier India for the future generation.
To realize this vision of healthier India, the country must consolidate action
with the help of communities, health care professionals, voluntary and
professional organizations, the private sector, Governmental agencies, and
academic institutions.
Contents
The Background ....................................................................................................................................... 8
CHAPTER 1 ............................................................................................................................................. 11
THE PROBLEMS ...................................................................................................................................... 11
CHAPTER 2 ............................................................................................................................................. 15
THE SOLUTION ....................................................................................................................................... 15
WHERE TO START .................................................................................................................................. 29
CHAPTER 3 ............................................................................................................................................. 32
THE MESSENGER ................................................................................................................................... 32
CHAPTER 4 ............................................................................................................................................. 34
THE MESSAGE ........................................................................................................................................ 34
CHAPTER 5 ............................................................................................................................................. 72
EMPOWERING THE MESSENGER: .......................................................................................................... 72
CHAPTER 6 ............................................................................................................................................. 79
THE METHODS ....................................................................................................................................... 79
CHAPTER 7 ............................................................................................................................................. 85
UNDERSTANDING CONNECTEDNESS .................................................................................................... 85
CHAPTER 8 ........................................................................................................................................... 100
INTERVENTIONS .................................................................................................................................. 100
CHAPTER 9 ........................................................................................................................................... 103
HARD DECISIONS FOR THE COMMUNITY ............................................................................................ 103
CHAPTER10 .......................................................................................................................................... 109
FUNDING AND VOLUNTEERS:.............................................................................................................. 109
CHAPTER 11 ......................................................................................................................................... 113
SUMMARY: .......................................................................................................................................... 113
APPENDIX ............................................................................................................................................ 119
About the Author ................................................................................................................................ 129


The Background
How did this idea of this book come about?
I have been interested in heart disease for a long time. My dissertation for M.D
was on heart attacks. I had been treating heart disease for over two decades
when somewhere along the way the concept of primordial prevention was
introduced.
Primordial prevention refers to decreasing the risk factors that cause heart
disease and smoking, as a singular cause being the most amenable to
correction.
At the hospital I worked in, we were doing piecemeal prevention, working here
and there whenever an opportunity provided itself. Since no funds were ear–
marked for preventive or promotive measures, getting a comprehensive
preventive program implemented was far out of our reach.
But providence willed otherwise. I happened to attend an International
Preventive Cardiology Conference along with a friend who works for a CSIR lab.
A few days after the conference, I was invited to address some staff members
and scientists at the CSIR lab.
Knowing that scientists like to grill speakers, I was determined to be doubly
prepared. A colleague lent me a publication of the Cardiology Society of India
which provided useful references.
The year was 2003 and I had no ready access to a good library locally. Even the
internet did not provide as much information as is available now. All the same,
I managed to gather a lot of useful data.
Of all the wonderful studies I read, one particular study resonated well with
the topic called ‘The North Karelia Project of Finland’, which is a community
based program aimed at preventing heart attack deaths.
Subsequently, ‘The Goa Lifestyle Project’ was born and I went from pillar to
post to find a way to start the pilot project in Goa to be imitated by the rest of
India.
The project did not click as was intended. Nevertheless, along with friends,
well-wishers and opposition we managed to get some messages across.
I offered my services to the DHS which were rejected because preventive
cardiology did not fit into their requirements then. Looking back, it was a
blessing in disguise because I could work independent of the DHS closer to
ground zero.
Whatever has been done so far is at the micro level and very subtle. At times,
nobody knows where the work has been initiated but it gnaws at the very
foundation of obsolete rigidity in which the old system is mired.
As I was struggling along with the program, I faced new challenges. My initial
intention was addressing the main risk factors, smoking, diet and exercise.
Transferring the information was easy but motivating people to change was
difficult. We needed numbers to build a visible success story. So, we started
addressing people’s minds.
Anyone in the hospital who was interested was invited to join hands. Nurses
volunteered and took on extra responsibilities of counseling and motivating
patients for no extra remuneration. The usual definition of Government staff
was shattered. We learnt that people are intrinsically motivated to motivate
others.
Management was cooperative most of the times except for a few bottlenecks
who knew no better than to create hurdles. After all the ridicule and
disappointments, I did find moments of satisfaction at an occasional positive
story.
We also introduced a yoga program at the hospital to deal with stress but in
spite of a holistic and systems approach we were not doing as well as we had
envisioned. Being ISO certified we were checking ourselves regularly.
That was the time I realized that we had to move more backwards ..to the
community … to early childhood… perhaps even to the antenatal period… or
right up to the adolescent girl child and for that, a hospital program would not
suffice.
So, I tried garnering support from the community. At most places, I was told
that a preventive program was not practical.
But at one meeting in 2005, a participant suggested that I should use the
services of the Aanganwadi workers to gather data. Having worked at the grass
roots while doing my nutrition course at NIN, I was aware that the Aanganwadi
worker was already overloaded and underpaid. Asking her to gather more data
would mean adding one more register to her existing 14 and decrease the
quality of her work.
I brushed aside the idea but returned back to it a few years later. I realized that
with the introduction of NRHM and RCH programs, the aaganwadi worker was
already doing the work but was not getting any recognition. It was time to
highlight her seminal role in India’s health care infrastructure.
There are good people working in the right direction all over India. It is only a
matter of time before the drops become an ocean. The seeds have been sown,
some have sprouted and in the course of time many more ideas will blossom.
I invite all the readers to keep adding to this beautiful garden to make our land
healthier and happier. Money, in spite of its promises can make a man neither
happy nor healthy. There have to be better ways and these need to be
discovered.
CHAPTER 1
THE PROBLEMS
Financial Implications:
The Global Scenario:
We don’t have very authentic statistical financial data from India. So, I will give
foreign figures. In a global village, all the winds of change that start in America
finally land at the Indian sub continent…. from computers .. to neutral families
…..to divorces. It is intelligence to learn from one’s own mistake. It takes
wisdom to learn from another’s.
If it is not health and well being but money which motivates the policy makers,
then I think it is fair that I address the finances first. My knowledge of financial
matters is poor but I could still make an attempt.
Everybody is so concerned about the GDP, CAD and the economic crisis. If I
could explain to people the dollar or pound equivalent of every pound or
penny or cent saved, it will make economic cents (sense) to their rupee –tuned
ears.
A few ears will definitely pause to listen. So, here is my weak attempt. The well
trained statisticians of our country can provide the financial software as we
course along. But for starters, this could do.
United States,
In 2006, the United States spent $7,000 per person on health which was more
than twice the average of 29 other developed countries.
And this expenditure is growing at a fast pace having tripled over a twenty year
period from 1990.
However, this increased expenditure has not reflected either in life expectancy
or healthy life years.
Ironically, more than 75% of this money is spent on chronic diseases which are
essentially preventable conditions. Moreover, 70% of deaths in the US are due
to chronic diseases.
We first allow these chronic diseases to flourish and then spend billions
treating them.
The Double Burden of Disease in India:
In contrast, India is plagued with the double burden of disease, the
communicable, infectious diseases and malnutrition related problems on one
hand and over nutrition and lifestyle related diseases on the other hand.
We have been gifted with some of the world’s best scientists in the field of
health but inadequate policies and siphoning of funds has led to a sorry state
of affairs.
To top all this, we have a HIV problem and worse, some unscrupulous people
are trying to make money at the cost of people’s plight.
The tuberculosis problem has re-surfaced, malaria is replaced by Dengue and
Chikungunya, leprosy is silently creeping beneath the surface.
On the other side, we have the monsters of diabetes, cardiovascular disease
and arthritis leading to disease and debility.
Today, you don’t see a plain pneumonia but a nosocomial (hospital acquired)
pneumonia in a diabetic HIV patient. Getting ill is a very costly ordeal.
The drug interactions and doctor-doctor interactions are mind -boggling. When
I see and analyze the situations from outside the system, I wonder whether we
are doing the patient more harm than good.
This is not a whimsical statement. I have taken a serious look at 20- year
records in a hospital. After all the analysis, when I sought to take corrective
action, I realized that prevention is the only solution.
All countries the world over are now turning in the direction of prevention but
the main bottleneck everywhere is the food and health industry with its
intricate ramifications which are difficult to comprehend and nearly impossible
to tackle.
But some attempt has to be made somewhere and if we begin today we may
see the results in 20 or 50 years time.

The Price Tag on Chronic Disease
United States
Cardiovascular Disease and Stroke-$313.8 billion in 2009
Cancer-$89.0 billion in 2007
Smoking-$96 billion in 2004
Diabetes-$116 billion in 2007
Arthritis-$80.8 billion in 2003
Obesity-$61 billion in 2000
United Kingdom:
In the UK, four out of five deaths of people <75 years are estimated to be
preventable, with a total annual cost of £187 billion (19% of total GDP)
Above, I have listed the cost burden of chronic diseases on the US and UK
exchequer.
With India’s burgeoning population, we can imagine the financial burden of
disease. India’s health expenditure both in publicly funded institutions and
private institutions is increasing every year.
More and more money is being spent on costly machinery having a limited life-
span. And percentage- wise, less is being spent on preventive aspects.
If US spent $7000 per person in 2006, assuming that they are spending the
same amount today, India would ideally need to spend Rs 4,20,000 per person.
We are not spending even one tenth the amount on a poor Indian.
CHAPTER 2
THE SOLUTION
Life – cycle approach in the management of lifestyle diseases:
Chronic diseases are the leading cause of mortality in the world, representing
60% of all deaths. It has been well documented that lifestyle and other risk
factors have a significant impact on health, leading to chronic illness and
premature death.
At least 80% of premature heart disease, stroke and type 2 diabetes can be
prevented through healthy diet, regular physical activity and avoidance of
tobacco products.
Chronic diseases and the increased mortality associated with them are not
distributed evenly across social groups. Earlier these were considered diseases
of affluence but trends have changed. The most disadvantaged socioeconomic
group shows the highest mortality.
Lifestyles play an important role in determining chronic diseases and unhealthy
lifestyle changes are likely to be responsible for a significant proportion of their
increase over time.
Changing behaviors in adults is difficult and the effort does not pay off well.
Hence, it is important to start good habits in childhood.
Secondly, lifestyle diseases are epigenetic diseases, i.e. the gene and
environment interacting to produce disease.
The course of lifestyle disease begins right with the adolescent girl-child or the
future mother.
If the mother is healthy, she will give birth to a healthy baby who is at a lower
risk of disease. Coupled with healthy nurturing, the risk will decrease even
further.
Adolescent Girl Child-
The key person in life course management is the adolescent girl child.
Improving her health would change the course of health in the future
generation. It would be a good idea to build the nutrition status of the
adolescent girl child .She should be nutritionally and mentally equipped for
pregnancy.
One of the chief problems of the young mothers- to -be of India is iron
deficiency anemia. To counteract the problem, the RCH program advocates
supplementing with iron tablets. These cause constipation and many mothers
do not take the tablets and throw them out. Both iron and calcium stores need
to be built up during adolescence. Healthy bone mass during adolescence can
decrease fractures in old age.
Many malnutrition problems in the well-to-do states of India are not due to
lack of food but because of a deficiency of health education. We have blanket
programs across the country without considering local needs. Community
participatory programs will definitely help here.
One very important research in the field of nutrition is that food preferences
develop in utero. If a mother- to -be makes a conscious attempt to eat healthy
foods, the child will prefer healthy foods. This is a converse of the pica concept.
Dysmenorrhoea is a common problem with the adolescent girl child
Belly dancing and ṇadishuddhi pranayam are very useful exercises to decrease
dysmenorrheal in the adolescent girl child. They regulate the swadhisthan
chakra and so help control hormones and emotions.

The Cost of Prevention:
Lifestyle diseases are preventable and will incur no costs to minimal costs
provided we decide to spend enough on health education and motivation. And
have enough legislation to curb the disease causing or promoting factors.
What is an acceptable level of cost effectiveness?
This determines how much a country is saving by preventing these diseases
compared to the costs of treatment. This differs from country to country. The
developed countries are ready to spend more and more to prevent a single
DALY.
Take a look,
Acceptable amount per DALY saved
UK Less than £20,000-£30,000
US Less than US$50,000
Australia A$50,000
Europe €20,000
DALY- DISABILITY ADJUSTED LIFE YEARS
As unhealthy industries find it difficult to sustain themselves in these countries
they start moving to India. And if necessary, have no scruples about greasing
palms. Sometimes the funds go to NGOs as Corporate Social Responsibility
(CSR), the NGO indirectly belonging to the politicians or bureaucrats.
Otherwise, it would be difficult to bring the dangerous food stuff into the
country.

Cost saving: benefits outweigh costs, i.e. pays for itself.
A rich country like UK spends only 4% of its medical budget on prevention and
health promotion
The health benefits and economic value of prevention are greatest when
prevention is implemented at the earliest opportunity. .
For example,
Walking for 30 minutes five days of the week caused a loss of 10-15 pounds of
weight and decreased diabetes by 58%. For the US, it translates roughly as a
savings of 50 billion dollars. This has to be compared to the amount spent in
motivating people to walk.
Thirty minutes of added activity was estimated to save €815 million per year in
costs linked to cardiovascular heart disease, stroke, type 2 diabetes, breast
cancer, colon cancer, depression and falls.
This equals 17% of the total health costs linked with the medical conditions.
For every 1% improvement in health outcomes from preventive programmes,
-there would be a reduction in public expenditure by £190 million,
-a reduction in family/societal spending of £700m
-lowering of employer costs by £110m,
Plus the reduction in premature death and disability
(National Social Marketing Centre, 2010).
In the ‘Toward No Tobacco program’, it was found that for every dollar
invested in the school program, $20 was saved in future medical care costs.
The right time to instil the healthy behaviour software is before the age of 6
years. At teenage, children are likely to be rebellious and default but they will
soon return to the initial program if they were well trained in early childhood.
Investing in the anganwadi makes great economic sense in terms of holistic
health of the future Indian. I cannot but emphasize enough the role of the
anganwadi worker in this regard.
If we visit any school in and around a city in Goa at the school interval time, we
will see children eating samosas ,patties , batatawadas, chips and drinking soft
drinks. Some of these children come from poor families but they pressurize
their parents to give them ten rupees every day.
Since the mothers go to work even before the children leave for school, they
have no time to pack their tiffins.
Parents and teachers tell me that the children don’t listen. There is no one to
own responsibility.
If we had a ceiling on the amount TFA and saturated fat in products sold to
children, these unhealthy items would not qualify for sale. Or we could
incentivize healthy products sold at school food counters.
My own school canteen sold samosas and bhajjis but only the teachers would
buy them. The children carried their tiffins or ate raw mangoes, cucumbers or
guavas from a shop near the school.
PRIMORDIAL PREVENTION:
Chronic diseases are major drivers of health care costs, as well as associated
economic losses. The rising burden of chronic disease is due mainly to lifestyle
factors. Many chronic conditions such as cardiovascular disease, adult-onset
diabetes and hypertension are amenable to prevention.
A shift from costly hospital based interventions towards primary care and
population- based interventions can deliver a reduction in chronic diseases and
an increase in the health of the population.
Let us now take a look of the main risk factors
SEDENTARY LIFESTYLE:
In the US, the cost linked with inactivity and obesity was 9.4% of the National
health expenditure in 1995.
Each dollar invested in physical activity (time and equipment) is estimated to
produce medical cost savings of over three dollars.
United Kingdom:
The annual economic cost of obesity in Ireland is about €2.7 billion.
Canada:
In Canada physical inactivity results in about 6% of total health care costs
(WHO, 2003).
SMOKING
The true cost of smoking
Scotland : 2008-2009 ,
Profits through tobacco duty - £940 million.
Direct costs to the Scottish Health Services due to smoking have been
estimated at £2.7 billion
The costs of
-Treating smoking attributable disease -£271 million
-Productivity losses due to excess absenteeism, smoking breaks and lost output
due to premature death cost £692 million
-Premature deaths due to second-hand smoke exposure in the home cost £60
million in lost productivity
Clearing smoking-related litter
-Clearing smoking-related litter from the streets costs £34 million
-Fires caused by smoking in commercial properties cost £12 million.
US:
The annual direct costs > $298 billion,
Workplace productivity losses- $67.5 billion,
Premature death losses - $117 billion,
Direct medical expenditures of - $116 billion.
Cost of cigarette $5.51 per pack
Cost after adjustment for losses would work out to be - $18.05 per pack
If Government increases cost by applying a health tax, the consumption will
decrease.

Quit Smoking Programs:
Counselling can be seen to benefit cessation.
It is never too late to quit but it always better never to start
Comprehensive programmes which have integrated components like
education, counter-marketing, community partnerships and law enforcement
produced a decline in adult and youth smoking prevalence.
Passive Smoking
If mothers of aanganwadi children tell their brothers or fathers about passive
smoking and its impact on children, they may listen but telling the husband or
father in law to quit smoking increases tensions in the family.
Peer Pressure
Teaching children to say ‘No’ is important.
Nowadays, if we visit metro cities we see young IT professionals just out of
their teens at tea stalls puffing away to misery.
Political Will
If all political parties get together on this issue, we could eradicate tobacco
cultivation in ten years time.
Meanwhile, we could import cigarettes or use nicotine gums to help those
already addicted.
Mental Health
The disability costs due to depression are considered one of the fastest
growing costs for employers.
Ireland 2010,
Ireland spent 5.2% of health budget on mental health.
21 million of 466 million were affected by depression in 28 countries
No comparative figures are available for India but by extrapolating from
here, even a very conservative estimate of the financial burden is colossal.
India spends very little on prevention and most of it goes to the immunization
program. Money which is spent on prevention is usually consumed by NGOs as
in the case of HIV. Many of which are off-shoots of the Government system
giving very little to the net user.
When I meet NGO workers who are doing genuine work in the health sector, I
find them always hard pressed for funds while some others have funds for
seminars in 5 star hotels.
The social benefits of a preventive holistic health program: How long does it
take to see results?
The ECD Program:
A preventive program in childhood is very costly and time-consuming. It takes
17 years for the net effects would turn positive and 25 years for the financial
benefits to exceed the investment costs.
In addition to health and economic benefits, there were social benefits with
decreased need for services and others like,
It raised the GDP by 0.5% in 45 years- $107 billion
Decreased crime rates saving $155 billion
In 1994, the US Public Health Service checked the effectiveness of
community based strategies in 6 areas, viz. heart disease, stroke ,
occupational injuries, road traffic accidents, low birth weight and
gunshot wounds.
Spending on community interventions in these six areas was
estimated to result in a saving of $ 69 billion by 2000 or six years
amounting to 11% of medical spending in these areas.
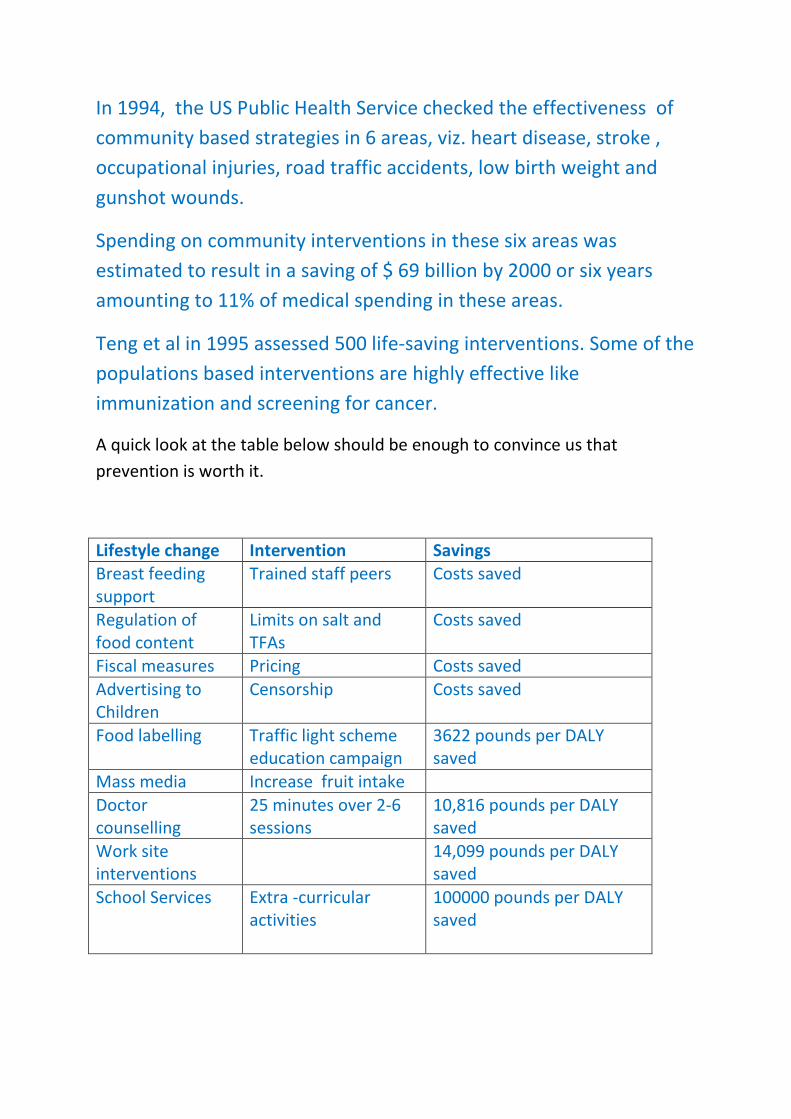
Teng et al in 1995 assessed 500 life-saving interventions. Some of the
populations based interventions are highly effective like
immunization and screening for cancer.
A quick look at the table below should be enough to convince us that
prevention is worth it.
Lifestyle change Intervention Savings
Breast feeding
support
Trained staff peers Costs saved
Regulation of
food content
Limits on salt and
TFAs
Costs saved
Fiscal measures Pricing Costs saved
Advertising to
Children
Censorship Costs saved
Food labelling Traffic light scheme
education campaign
3622 pounds per DALY
saved
Mass media Increase fruit intake
Doctor
counselling
25 minutes over 2-6
sessions
10,816 pounds per DALY
saved
Work site
interventions
14,099 pounds per DALY
saved
School Services
Extra -curricular
activities
100000 pounds per DALY
saved
What does this table say?
The earlier in life cycle you intervene, the more you save. Now, you will
understand why I call the aaganwadi workers preventive cardiologists.
It is not just about saving money. As a doctor that should be my last concern.
Giving health should be primary. But I have to prove this to people who make
the interventional policies. And also to the fraternity who think promoting
prevention is a waste of effort.
Every education class I have taken in the country, has fetched the country
economic and health returns, whether I was paid for the class or not.
Sitting in my clinic, I could not have achieved even 1/10th
of what I could
achieve in the community although I might have earned a 100 times more.
India’s attempt at corrective action:
Our greatest challenge at present is keeping the healthy rural people healthy
and not letting the wave of non- communicable disease grip the rural poor. If
this happens, the villagers will lose their earning capacity as they ill afford the
costly treatments.
Since there is some power in the law of attraction, we should prevent more
private cardiothoracic units from proliferating. All heart care should be
provided at the Government hospitals. People may go to a private hospital out
of choice but not compulsion.
Since independence, India has made many attempts at drawing a good health
policy. After successful programs directed at nutrition and communicable
diseases, we are now looking at more comprehensive programs, NRHM,
NUHM, MGNREGA , Immunization program, and the Food Security Bill.
Some are successful and some not so successful. I will attempt to highlight a
few aspects of some of the programs.
CHD Mortality in India
In 2004, CHD was the leading cause of death in India, leading to:
1.46 million deaths (14% out of a total of 10.3 million deaths)
130.7 deaths per 100,000
207.7 age-standardized deaths per 100,000
15,588,000 DALYs
1,931 age-adjusted DALYs per 100,000
(WHO, 2004; WHO, 2009)
In 2009, The Government of India (GOI) launched the National Program for
Prevention and Control of Diabetes, CVD and Stroke (NPDCS), an Integrated
Diseases Surveillance Project (IDSP) at multiple sites, and a CVD risk factor
surveillance project. The largest research project to carry out these and other
programs are based in New Delhi and Bangalore.
Block-level surveillance data is being collected through the Integrated Disease
Surveillance Project (IDSP) in collaboration with the ICMR, while the
interventions are school-, work-, and community-based programs. In addition,
there is a weekly CVD/stroke specialty clinic in each district.
NPDCS:
This pilot program has begun in ten districts in ten states (Assam, Punjab,
Rajasthan, Karnataka, Tamil Nadu, Kerala, Andhra Pradesh, Madhya Pradesh,
Sikkim, and Gujarat) with a budget of Rs 4,91,60,000 per state(Government of
India, 2009).
The program is continuing but I could not get the surveillance figures as of
2013.
I had written to the local Government in 2003 and again in 2005 to start a pilot
project in Goa and in 2005 to the Central Ministry. Goa, being a small state
with high Coronary artery disease (CAD) and faulty lifestyles could be an
excellent place to start a project.
Even if Goa received 1/10th
of the funds due to its small size we could get Rs
50,00,000/- which would break even in five years.
I can say this confidently with my experience. Just adding one nurse at the
OPD for counseling, in a Government sector hospital decreased the bed
occupancy from forty/forty to fifteen/forty.
Food Security Bill: drawbacks and implications.
Of the different programs directly or indirectly related to health, the Food
Security Bill has drawn the greatest flak. One reason is that it is being mooted
in a hurry. Participatory notes of experts gathered by various opposition
parties are ignored to expedite the bill. We may create more problems in the
long run to address short -term solutions.
The discussions in this space are written with respect to health of the rural and
urban poor. I have no intentions of criticizing any Government policy or have
any political agenda. If anyone thinks of using these arguments as a political
weapon it is in severe bad taste.
The opposition parties could launch a successful health model in the states
ruled by them or even in municipalities under their sway and show the country
a new direction in health care.
The politicization of health issues is to be strongly condemned. Living with
diabetes, heart disease or arthritis is not easy. We should not make a road
show or mockery of people’s plight.
There are interrelated issues like production, procurement, storage and
distribution and siphoning of food linked with the bill. The poor farmer does
not need the PDS grains. He needs water and power supply. If local unpolished
rice could be procured and given through the PDS, health will be protected and
it will boost local agriculture. Using polished rice and then Rice bran oil does
not make economic sense.

Others like the Land Acquisition Bill will interfere with employment, food
security and nutrition. There will be a lot of manipulation to transfer land to
the land sharks. Poor farmers and farm laborers will be rendered jobless and
without grain. The employment generated will be negligible. Even after ten
generations, the farmers may not be able to acquire cultivable land.
Destruction of green land is a crime rather a sin against all living beings not just
humans.
I have seen the manipulations and effects of these acquisitions first hand that I
dare to make such toxic remarks. I always tell people to use all means to keep
their land and don’t look at the money they get. Money is only paper and
nothing beyond.
If forced to give land, they should ask for land as replacement instead of
money, may be away from the same area
Look at what mining has done to Goa. Pre-mining era we had 100% local food
security. Now, it is less than 10% and is declining every year. Other states
should learn from Goa’s mistakes.
The Singur Project , the aftermath of which in a way pushed the Land
Acquisition Bill, was to ensure a small and affordable car to every Indian.
But did we plan the roads to accommodate the traffic congestion? A person
addicted to a car cannot walk or go by bus. And a small car makes you aspire
for a big car, so more environmental burden.
What about the import of petrol, increasing CAD and collapse of rupee?
Today, the Prime Minister wants people to decrease the consumption of
petroleum, while passing the LAB, yet another irony.
Fifty years down the line, our children will have a concrete jungle all around
and no food to eat. The industrialists and politicians have enough dough to
settle in a plush orchard abroad.
For those who dream of riding cars, we could build some car rental agencies
which could give everyone a chance to ride a car for a penny and incentivize
bicycle production for normal times.
WHERE TO START
When the problem is big, we always wonder where to start. Let’s get to basics.
Basic needs and the rights of every Indian citizen:
What every Indian needs
1.Potable water
2.A staple cereal and millet-rice, wheat, maize, bajra ,ragi etc.
3.Plenty of fruits and vegetables grown locally
4. A protein source- dal and beans
Mung and masoor can easily be cultivated I most places
5. An oilseed source- groundnut and coconut
Cashewnuts and almonds wherever possible to cultivate
6. Spices: turmeric(haldi), chillie , coriander, cumin (jeera), cloves, cinnamon,
nutmeg, pepper, fenugreek, mustard and saunf, ginger, garlic, tamarind. All of
these can be easily cultivated locally all over India.
7. Herbal medicines: tulsi , lemon grass, aloe vera, castor etc.
8.Soap, tooth paste, tooth brush, matchboxes combs, cotton clothes ,few
woollens, shoes ,umbrellas, brooms--can be manufactured small scale
industries
9. Safe and clean house with clean surrounding
10.Sanitation
11.Schooling
12.Water for irrigation
13 Power supply to pump water in fields
14.Access to information
15.Land for cultivation for the landless labourers
16.Health care especially immunization and antenatal services.
17.Participatory entertainment like folk dances
THINK!
None of these need great technology, or FDI or FII.
The needs and wants of 70-80% of India’s content population can be easily met
provided we nip those forces in the bud which are seeking to sow discontent in
people’s mind.
We talk of a big CA AAAA…..R but where are BROAD roads?
Think!
Do we need a HYDEL project today and a flood tomorrow?
A small dam can regulate water management for the farmers across states. A
hydel is a live water bomb.
Do we need a nuclear power plant today and a holocaust tomorrow?
Very little of technology is humanistic, if we consider a 1000 year period.
Our myopic vision does not allow us to see beyond our own lifespan?
Some things like mobile, television and computers may have a role in
educating people say over the next 5-25 year period.
But when better systems are put in place we will have to rid ourselves of these
harmful technologies too.
Science has a useful role. But it is important for us to remember that we
cannot know the whole truth. Even doctors make mistakes on health advice.
A doctor’s mistake can prove very costly.

Two examples
1. Discontinuing breast feeding early and staring weaning feeds.
And the doctors did it with a confidence of all -knowing.
The ‘bonny baby’ syndrome was all driven by infant formula foods.
There was no clear evidence, yet most doctors just followed their teachers
without looking at the issue afresh.
2.Sex determination tests on ultrasound. There are many more but these two
will suffice.
Now, no one is held accountable for these mistakes.
In this book, I have raised many issues. I want the readers to study the
recommendations with an open mind, read more before adopting any change.
The idea is not to give advice but to raise awareness and encourage
participation in the decision making process.
It is public health so, everyone has a right to have a say in health matters.
CHAPTER 3
THE MESSENGER
Why aaganwadi sevika?
The success of the aaganwadi sevikas so far:
The aaganwadi workers have contributed substantially to health programs, be
it the immunization program, rural sanitation, personal hygiene, breast
feeding, family planning, institutional deliveries or mid-day meals.
society
students
anganwadi

The amount of work they do:
The aanganwadi sevika cares for the children under five years, pregnant and
lactating mothers.
The following are the duties of an aaganwadi sevika through the ICDS.
1. Survey and records on under- fives, pregnant and lactating mothers
2.Non-formal education
3. Supplement nutrition and weighment of food and child to record growth.
4. Liaison with other departments in mother and child related schemes.. e.g.
Health services- immunization, breast feeding, antenatal care etc.
5. Maintenance of records.
In Goa, the aaganwadi workers have to fill in 14 registers. In other states, they
have some 34 registers to fill in.
Sabala scheme /adolescent girl child also comes under the aanganwadi.

CHAPTER 4
THE MESSAGE
The food guide pyramid or the plate model evolved in the west may have to be
adapted for Indian conditions. We are largely subsisting on cereals.
Other major nutrients are missing from our diets and in recent years, most of
the micronutrients have also been excluded.
We need to give clear messages to the children and mothers in the following
areas
1.Physical health
2.Mental health
3. Social health
4. Spiritual health
Under physical healt , we need to address nutrition and exercise
Under mental health we talk about inner child healing and resilience
Under social health we discuss social support, group empowerment,
motivation and change ,sustainable development and environmental
protection.
Under spiritual health, we explore values, taboos, belief systems ethics,
consumptive consumerism and soul agenda

Physical Health:
EXERCISE
Exercise is slowly disappearing from children’s lives. Children are now glued to
the idiot box. It would be a good idea to introduce surya namaskars and
dancing at the aaganwadi.
Exercise is essential for the body as much as running the car is necessary to
keep it in road shape. If we don’t exercise our muscles, they lose power. They
lose muscle fibers and gain fat. Fat in the muscle makes you fatter. This is
common knowledge.
In spite of knowing the benefits, we do not exercise. The reasons are manifold.
Motivation is one the chief reasons. Second to follow are our priorities. Health
is not a priority with Indians. Most Indians have been exercising by default till
now.
Since there was always a scarcity of macronutrients, people were not overfed.
Today, our people are overfed with macronutrients and are deprived of
micronutrients. The damage is serious.
We see more diabetes and heart disease in the poor and rural population
where treatment is not available, accessible or affordable. We are killing them
slowly and doubly, first, with physical disease and then with financial dis-ease.
All this can be prevented though it will take a lot of effort. The foundation for a
good exercise program has to be set in childhood. The collective numbers are
needed.

We need to see the connectivity even in exercise. As long as we hero- worship
people who own big cars we will not think of exercising. Our media has to
show us the ordinary people exercising and keeping healthy.
We know that actor X goes to a big gym in a big car. We wait for the big car
and the big gym both of which never come. So, we land one day at the
Government hospital.
Heart disease is happening at a younger age and in larger numbers. Many
people are dying before they reach the hospital. We like to turn a blind eye to
facts.
This is not to say that we are not doing anything. We are ….but we are not
doing enough. Time is running out for us. There were visionaries who saw this
trend coming and had warned us but money and greed over ruled reason.
(Tagore’s poem was ignored- ‘Where the clear stream of reason has not lost its
way in the dreary desert sand of dead habit’)
But we still cannot give up. There are ways to mend the situation and every
effort counts.
Actions speak louder than words:
When I was promoting exercise at MPT, Goa, I could not have done it
successfully if the then Chairman, Dr Jose Paul did not walk every morning on
the specially constructed road overlooking the sea. My pushing people to walk
and the Chairman’s pulling people to walk made a big difference.
Since I walked to work, many people would stop by to give me a lift. After I
refused a few times, they got even more convinced about the importance of
walking.
There was a patient in his thirties with hypertension. I met him ten years later
and failed to recognize him. He looked much younger and stress-free.
He told me that he had rid himself of his hypertension.
“How?” I asked.

“I walked it away” was the amusing reply.
A few years back when I used to say ‘belly dance or tango to health’ people
would laugh.
Today, when I address women and talk about belly dance, I get claps.
‘The Dancing Super Moms’ have done my work a lot easier.
There are many who follow me after class and ask “Will you teach me belly
dancing?”
Young India is growing well. All we need to give it, is a little direction.
NUTRITION
The second aspect of health is nutrition. I have discussed nutrition in detail in
my other books. Here, I am highlighting what messages an aaganwadi sevika
could give to the public.
WATER
Today, in the Indian villages you will get bottled water, soft drinks but no
potable and safe drinking water.
Water Sapping
If ground water is tapped to fill bottles and manufacture soft drinks or growing
sugarcane in drought areas, in the absence of adequate rainfall and water
harvesting procedures, the ground water table is bound to go down .
Fluoride:
A low flouride level in water causes cavities in teeth. Community water
fluoridation resulted in fewer cavities among community members.
In one study of communities with at least 20,000 residents, every $1 invested
in community water fluoridation yielded about $38 in savings from fewer
cavities treated.
Flourosis:
Tube walls are dug in South India to manage water scarcity. The drawback is
that the fluoride content of this water is very high. This gives rise to flourosis, a
condition which affects the bones and teeth. Tamarind precipitates flouride
and decreases its absorption. Shifting from tomatoes to tamarind can decrease
flourosis.
Safety of Water
The question is how do we make water safe for consumption?
Boiling is a good option but LPG prices are going up.
We need to preserve our forest and decrease other fuels like saw dust or dung
cakes to avoid air pollution.
Solar heating is the best option.
Bio-gas has been successfully used in some districts of Tamil Nadu.
With LPG prices going up, water -guards have flooded the market and every
celebrity seems to be endorsing one brand.
There are no long term safety studies on water- guard purified water. Using
microwaves or RO or infrared rays to purify water is not a solution. We like the
easy way out. You will have plenty of people selling water guards but their
after -sales service is next to nil.
Some years back, when there was a Hepatitis E outbreak in the State, I had a
discussion with the Professor of Microbiology to know the water purification
options. He told me that he uses a water guard but checks the microbial count
of his water regularly and boils his microwaved water for double protection.
Few of us could afford this luxury, so we could still stick to boiling. At least till
we find better options. Using a porcelain water filter could also be considered.

Chlorination is not totally safe as believed and in the village if you have your
own well far away from sewage drainage you could use potassium
permanganate to clean regularly.
Soft Drinks:
These are unnecessary health hazards. The main health problems caused by
soft drinks are weak bones, weak teeth, obesity, hypertension and indirectly
heart disease.
Besides these, the main concern is the ground water depletion they cause. Any
‘well connected’ soft drink company can get enough water supply for its plant
even when the wells and taps outside its campus are running dry.
And lowering of the water table fosters flourosis as I have discussed.
And what was sickest about the whole thing was… the NDTV -Coca Cola School
Campaign.
Should such a campaign be allowed at all?
It raises larger questions like whether we will allow a cigarette company to
sponsor a school quiz program.
NDTV was believed to have a socialistic leaning but this time around it got
sucked into the capitalistic hose.
If this was not enough, they roped in a celebrity cricketer, now a Rajya Sabha
member to do the ads while the censors and Public Health Officials turned a
blind eye and deaf ear.
As a people’s representative, does not one hold any moral responsibility not to
accept an advertisement if it anti-health? Do ends justify the means?
Could not NDTV do it with the Government or some Basmati rice or tea?
Cola drinks are supposed to contain caramel which is cancer causing.
FDA has asked the companies to label it. The companies are slated to replace it
with a chemical soon.

How can we link a poison with a school programs?
It defies all sane logic.
Who is responsible?
On one hand, we have people who are trying to promote health and decrease
obesity by decreasing soft drink consumption which is soon counter foiled by
the soft drinks companies by using all strategies. This will leave young children
confused. This is one place where public health authorities and well known
doctors should come in the open and assert as to what is permissible and what
is not permissible.
Religious leaders can also play a defining role because this area does not need
scientific information (which we have plenty) but ethics.
Sweet Security: the Sugar –love link
In Goa, when a child falls someone will come rushing, lift the child and apply
sugar to its lips forming an association between sugar, love and security.
So, when we become adults, sweets become our greatest solace. Plus the ads
tell us that to show love we need to give chocolates.
I mean …..they tell us that love is as cheap as chocolates… wrapped in some
brightly colored paper with a golden lining and we get sucked in.
Obesity has its root cause in this association.
If we would give the child a piece of banana or just plain water, we would have
a healthy association.
Feeling low …..drink water
Feeling unloved …eat bananas
Teeth

Processed food prevents children from biting and chewing.
The result is that their jaws are not well developed and permanent teeth have
no place to erupt giving rise to crooked teeth.
Sucrose which is a part of processed food is the most cariogenic (caries
causing) of all the sugars.
MILK
Is Milk essential?
Sadguru Jaggi Vasudev of ISHA foundation calls milk an emergency food. SSY
people teach that milk is not essential for health. PETA people are dead against
milk. They have very nice posters that give startling facts.
I personally believe in the freedom of choice and would not like to mind-wash
anyone. Give people enough information from both sides and let them decide.
But the poor mothers really have no choice. They cannot afford milk.
The quality of milk in India s sub-standard. According to a TV investigation, 73
% of milk in India is contaminated. The hormones and antibiotics injected in
the imported hybrid cattle do not auger well for India’s health. More hormone
exposure is not good for the girl child’s or woman’s health.
Many a mother will give a sigh of relief when they learn that milk is not
needed. Rather, that there are better substitutes for milk. Hence, I do not
mind recommending the elimination of milk from the diet. It will save money
for other healthier food.
It is said that if we need to rely on milk as the chief or only source of calcium
than we need to give 700 ml of milk per person per day. For a family of six, that
works out to be 4.2 liters at the cost of Rs160 per day.
How many Indians can really afford this?
Even if we are taking 50% of our calcium from milk, then it works out to be 2
litres per day at Rs 80/- , still very high.

Also, if 50% calcium is coming from other sources then why not get all of it
from other sources?
If this message could be taken to the masses, we will not need hybrid cows and
hormone rich and antibiotic enriched milk.
Plus milk could be used only in tea. There is no need to drink whole glasses of
milk. The milk producers could plan from now to invest their money in some
other healthy business. So, there are no financial losses or loss of jobs.
If we eliminate milk and ghee based sweets like peda and barfi from the Indian
market then much of the contaminated milk will leave the place. For this
religious leaders will have to play a big role. The ‘bhog’ in North India is a
health hazard. People eat in the name of God.
Traditionally, in most of South India and Maharashtra, you take either a
coconut or a few bananas to the temple. That too, the smaller varieties of
bananas. No other fruits are taken. Even a rich man takes the same number of
bananas as the poor man. There is no competition in a temple.
Tea
Once milk is eliminated from diet, we need to tackle the tea issue. Shifting
from black tea to green tea; sugared tea to tea without sugar can be
promoted. Lemon teas, herbal teas etc. are other options. Once a tea plant is
grown it will last for a hundred years. Many areas in India are suited for tea
plantations. The highlanders can grow their own tea plants for family
consumption.
Though milk is not essential in tea, many in the present generation are used to
drinking tea with milk. Strong tea which is actually of an inferior quality is a
means of social exchange. Everything happens in India over a cup of tea.
Fortunately, concepts of lemon tea, iced tea are slowly making its presence
felt.
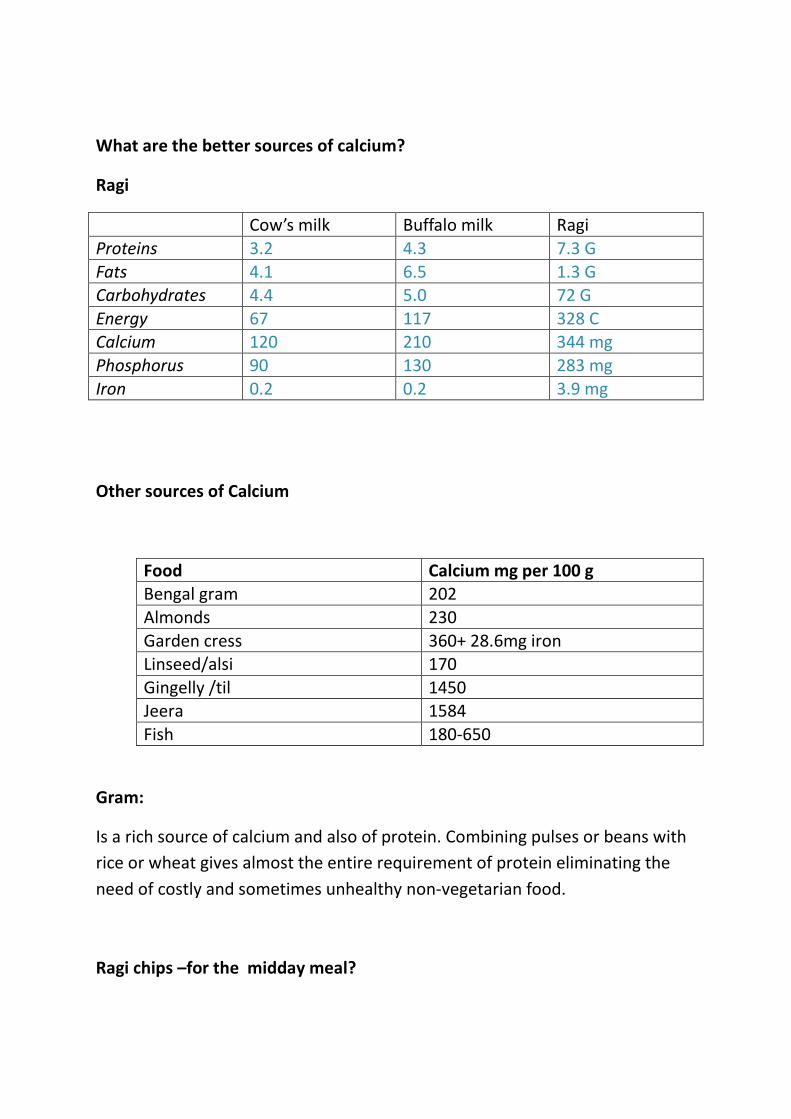
What are the better sources of calcium?
Ragi
Cow’s milk Buffalo milk Ragi
Proteins 3.2 4.3 7.3 G
Fats 4.1 6.5 1.3 G
Carbohydrates 4.4 5.0 72 G
Energy 67 117 328 C
Calcium 120 210 344 mg
Phosphorus 90 130 283 mg
Iron 0.2 0.2 3.9 mg
Other sources of Calcium
Food Calcium mg per 100 g
Bengal gram 202
Almonds 230
Garden cress 360+ 28.6mg iron
Linseed/alsi 170
Gingelly /til 1450
Jeera 1584
Fish 180-650
Gram:
Is a rich source of calcium and also of protein. Combining pulses or beans with
rice or wheat gives almost the entire requirement of protein eliminating the
need of costly and sometimes unhealthy non-vegetarian food.
Ragi chips –for the midday meal?

I recently discovered that that a famous eatery in Panaji -Goa sells fried ragi
chips. If these same chips could be baked, then they would be an excellent
midday snack for aanganwadi children. The local college of Home Science
could develop such a technique. I am also trying to develop one.
It is better than the laddoos made from TFA or Dalda . Even if we could ensure
that the chips are fried in fresh oil, we could give them to children.
Coimbatore has started millet joints where millet dosas and other dishes are
served. We need to replace the pizza culture with some ethnic ware which is
doubly attractive to children.
Increasing Ragi Cultivation:
When I was trying to motivate people in Goa to increase ragi production as a
rabi crop , I talked to some farmers. The common belief in Goa is that people
don’t want to labour and hence the fields are lying barren.
True, there many farmers whose children have migrated or are in Government
jobs or in IT. But there are still enough farmers who don’t have land to
cultivate. The practicing farmers are at present taking three paddy crops in a
year and have no additional land to cultivate ragi. Paddy pays double to triple
returns compared to ragi.
Ragi can be grown on hill-slopes and less irrigated areas. But the tenancy law
makes it difficult for people to give or get land. When I studied the problem in
other parts of the country, there were different options.
For example,
In Orissa, there is a provision for contract farming. The elderly farmer contracts
his field to another farmer annually till a time when his son after completing
his education returns home to take over. The fields are generally not allowed
to lie barren. Real estate sharks have not yet taken over.
In the North-West, consolidating of farms by the rich farmers is common. Large
tracts of land , mechanization, marketing and exporting have taken over. Rice
which requires a lot of water is cultivated in spite of poor rainfall because it
fetches a price.
In South India, farmers are more aware. There is a genuine problem of water
shortage which is solvable but for the fact that it makes political capital. All the
rivers could be interconnected.
In Maharashtra, monocultures like sunflower, hybrid seeds, sugarcane has
completely destroyed the soil culture and ground water tables.
When I talked to a lady from Maharashtra living in Goa but cultivating
sugarcane at a border district of Maharashtra, this is what I understood.
Sugarcane has to be planted every four years. The sugar mill people send their
men and they have to be paid around 2000- 4000/- per harvest.
The gains are less but investment is also less with least risk of crop loss.
It is very good short term solution but if we don’t see into the future, India will
be inundated-by more Vidarbhas.
What our ancestors took ages to build is going to be destroyed over the next
50 years only because of greed and poor planning.
Molasses:
Traditionall , Goan farmers produced molasses and then jaggery from it in an
organic process. This molasses (kaakai) can last at room temperature for more
than 10 years without bacterial contamination. It is made from a special
variety of sugarcane with a red coat and thicker girth.
Kakai can be used in cooking thus decreasing the need for chemically treated
castor sugar. It will decrease the water and power needs of the community and
bring power back to the farmer. Solar kilns are the best option for heating the
juice. A locally -manufactured mechanical stirrer can eliminate the hard labour.
Increasing Fibre Intakes
Whole Wheat Bread
In rural Goa, we say Good morning with Chaou and Pao ….black tea almost a
glass full and a bread loaf.
If pao (bread) is such a essential item for people we should make it healthy.
Generally, it is made from maida or refined flour.
The best bread loaves of the world are made in Scandinavian countries and
they are made from whole wheat. Their art of bread –making is as old as their
wine- making.
Whole wheat bread is rich in bran and healthier. But it is costlier to
manufacture whole wheat bread. The process takes more time and is labour
intensive. Moreover, maida is subsidized by the Government while whole
wheat is not.
A single change from maida to whole wheat can increase the fiber intake of a
meal. On one hand, we have to motivate the people to demand whole grain
breads and on the other negotiate with the bakers, bridging the demand-
supply gap.
Wheat Allergy
In the villages of Goa there are many people who report being allergic to
chapattis. This is probably due to gluten allergy. To such people we could give
ragi bread or rice idlis.
Whole Grain Rice:
If locally available parboiled rice and whole grain raw rice could be procured
for the PDS, it would boost local farming. The poor rice growing farmer does

not need the rice supplied by PDS and may not wish to eat wheat. So, he could
be given pulses instead to boost his nutrition.
Increasing Micronutrients and Anti_Oxidants
Fruits And Vegetables:
It is recommended by World Health Organization (WHO) that people consume
local fruits and seasonally available vegetables, at least 400g per day.
Today, the fruits we get in the market are hardly healthy.
To obtain many banana saplings from one plant, tissue culture is used. These
tissue- cultured bananas look good from outside but have stone like
formations inside.
We also do not know their effects on our genes. Furthermore, fruits are dipped
in carbide to ripen them. Water melons are sweetened by injecting saccharin.
This problem would be eliminated if could get the fruits directly from the
fields. Going local is beneficial.
Increasing consumption of fruits and vegetables:
To increase the consumption of fruits and vegetables, we tried a novel
method.
The members of TNAI of MPT Hospital, Vasco –Goa made posters on the
benefit of fruit & vegetable consumption and distributed them in the vegetable
market. The material for the posters had all came from waste.
Some of the vendors did put up the posters. I was convinced about its
usefulness when my patient’s daughter reported having seen the posters. She
believed that it was a selling gimmick but when she learnt that it was our
hospital initiative, she understood its implications and agreed to join hands
with us.
In the capital city of Panaji, we had children of a large colony do paintings for
the vendors. Some of the vendors did not like the posters so they made their
own flexiboards of fruits and put it up in their stalls. The visual effects were
quite strong and the children learn de-facto.
Moreover, the intention effect was so powerful that within a year, there were
fruit stalls at every corner of Panaji… the law of attraction.
I strongly believe in the power of thought and use it to full advantage. A few
more strong minded thinkers joining their thoughts with me will help India
prevent the undesirable monster of lifestyle disease.
The Power of Thought:
Some of you reading the foregoing statement may feel that I am being
unscientific. So, I will give you some more information and you can decide for
yourself.
The Robotics and Research team of A-Set has developed a robot that can play
football and can read your thoughts and carry out your orders. These are
neither miracles, nor superstitions nor great wonders.
Thoughts are a form of energy. In the universe, something that is not matter is
energy and both are interconvertible. The robot exchanges energy with human
mind.
If mind can direct a robot’s action, it will also be able change another person
with a mind (soft- ware). I have measured this in many people with my RFITM
machine. However, much more research would be needed to make these
things universally applicable.
I am working on how mind can be used to change biology.
If a human mind can affect the robot’s software, could a robot be made to
affect the human mind?
Now, even if someone develops a full-proof technology to change another’s
mind, it would be dangerous to share the knowledge with people. The research
on scalar electro-magnetic waves had to be called off.
So, it is better we use only positive thinking and not some machine. The mind
in the body has some higher level control from the intellect or discretionary
power. The robot and operator may go awry. Worse, the operator may lose
control on the robot.
Hurdles in Fruit Production and Consumption:
Consumption of Fruits
In a survey conducted in 2007 in the US, only 24% of U.S. adults ate 5 or more
servings of fruits and vegetables per day.
Less than 22% of high school students report eating fruits and vegetables 5 or
more times daily.
In the Nurses’ Health Study it was seen that only 9% of participants consumed
the recommended fruit intake.
What does this suggest?
There is affordability yet low consumption of fruits (Americans got enough
dole in 2007).
There is availability. US can force Latin America to grow oranges for them.
There is accessibility. All supermarkets which stock the pastries, cookies ,
chocolate- bars and ice-creams, also stock fruits and vegetables but people
swarm like bees to the dangerous stuff thanks to the ever innovative
advertisement industry.
In India, the problem is quite the opposite. In the yester years, the poor
children in the villages were always seen munching into some wild berries even
while missing school (till the Forest Department became very strict).
You could smuggle sandalwood or teak but not touch the berries. People’s
ancestral orchards were replaced with hotels and real estates. The Tenancy Act
neither helped the tenant, landowner nor landless laborer but served a rich
meal to the land sharks. Thirty percent of land is converted from the green belt
setting the stage for acute food shortages in future.
Recently, I visited a Goan village called Casaulim.
I was in awe of the great trouble the villagers have taken to maintain
sustainable development.
With a little Government help, many such model villages could be built up in
India. Greed and not need is the root cause of trouble.
Empowerment:
Everything is connected and we need to see this connectivity if we need to get
lasting solutions to health problems.
So, the problem is just not information, education, availability, affordability or
accessibility. It is motivation to choose right and we need to install this
program right in childhood along with an antivirus software called ‘Caution’
which flashes in the backdrop of our mind, “Beware of Ads”.
Every time an ad for chips or chocolates flashes in front of us, we will
automatically activate this program and
I accept / exit, will flash in our mind.
I can think of no better agency than the aaganwadi sevika to install this
program.
How to convince people:
To convince diabetic patients that they could and should eat all fruits we would
distribute fruits or other healthy dishes before starting the diabetes education
class every week. The fruits etc. were sponsored by volunteers.
We also had a best diabetic dish contest. Financially, we invested little but the
short term gains were soon visible, in terms of better controlled sugars and
decreased admissions.
Doing this small exercise gave the following messages…NLP style
Nutrition is important otherwise they would not bother to bring the dishes for
us.
These people care for us …we are important to them.. that is why they are
spending from their pockets. Let us listen to them and hear what they have to
say. Let us take care for ourselves.
Let me also contribute because it feels good to contribute.
The education classes soon became social get-togethers. Though there was
resistance from some people as is to be expected while doing anything good,
most people took the opportunity to learn.
Before the participatory approach, we were talking to the walls.
Later we had to sit and listen.
One empowered patient talking to the others.
Another empowered person from the audience adding something and so on….
A similar method can be used in the aaganwadi.
Government could provide for the fruits.
Most Government hospital staff do care for their patients but this care is not
communicated.
The Traditional Fruit Produces:
Everywhere I go, I tell people about the need to consume fruits and
vegetables.
I am faced with three questions about accessibility, affordability and quality.
“But from where to get the good stuff?”
‘All the markets have only this rotten stuff’ is a usual complaint.
It time we had our say and build our own local network.
Tissue Cultures of Bananas:
My grandmother grew bananas for 50 years plus. Never did she require to get
newer saplings. She was a master gardener and knew exactly when to replant a
new shoot. I don’t see why we need to make saplings by tissue culture.
What was special about her bananas?
My grandmother’s bananas were nearly 10 inches long and 1-1/2 to 2 inches
in diameter.
I could not ever eat a full banana. No fertilizers and pesticides were used. They
were nurtured with the kitchen waste. They were never watered. All kitchen
water was systematically routed there. They were ripened naturally.
I have never ever seen a rotted banana from my grandmother’s plants. I am
sure you are going to go into nostalgic moments about your own grandmother.
A friend of mine, Mrs Helen still cultivates choice bananas at Aagshi.
Hers are the only bananas that seem to match my grandmothers’.
Today, you buy a banana and though appearing clean from outside, half of it
will be hard and unpalatable.
The quality of some of these cultured variety is not worthy for human
consumption. We have the technology and knowledge but lack the wisdom
which our grandmothers possessed. In tissue cultures, you get 1000 new
shoots from one banana plant. But where is the place to plant these thousand?
Tomatoes:
Another easily available fruit (though called vegetable) is the tomato. It is very
rich in anti-oxidants. Eat one tomato per day and you will not have to look for
antioxidants in your tooth paste.
Any antioxidant put in a tablet or paste will start getting oxidized the minute it
is put on the shelf and very little will reach your body.
When I was working in Kolar, I witnessed the tomato strikes. Every harvest
time, tons of tomatoes would be strewn along the road side because the
Government would not give them a good minimum support price. The animals
would not eat them because they were sprayed with poison.
When I checked the requirement of tomatoes in the market, I learnt that
tomatoes used in making sauce in India was imported from China as a tomato
pulp by the sauce making multinational companies .
Many times, carrots or any yellow-orange fruit was used for thickening.
Red colour is used to make the ketchup appear nourishing.
There is no guarantee of what the Chinese will put in the pulp.
It is better to encourage children to eat tomatoes directly or set up a pulp
factory at Kolar. I gave my patients a ketchup recipe so that they could make it
at home .I have appended it in this book
A Small Pearl:
In Goa, grandmothers used to add a sour fruit like hog plum or raw mango to
prawn and other curries. In Kerala, fish is marinated in tamarind before frying,
North India used Aamchoor or mango powder and lime.
Did our ancestors intuitively understand that they needed to balance the
oxidants in the curry with anti-oxidants?
Fish:
Fish is a good source of omega 3 fatty acids or the DHA which is so much
advertised today.
But the amount of fish we need for brain growth is as little as 100-200 g per
week provided we do not load our system with extra omega 6 from sunflower
oil or corn oil. Fish in industrialized coastal areas is found to be contaminated
with Mercury so a regular check on Mercury content has to be carried out by
the Health Services along with the Fisheries Department.
TFA: Gift Wrapped Poison
Go to any store in the village. Hanging from the rafters of the shop or on hooks
you will see loads and loads of cheap chips. They are sold very cheap. The
actual cost of a Rs 5/- chip packet costs the country may be Rs 100/- in terms
of health, I don’t even dare speculate because the implications are limitless.
These chips are fried in trans fatty acids or partially hydrogenated fat to
increase the shelf life. To mind-wash people it is often labeled as partially
hydrogenated fat which is equally dangerous.
According to Dr Katan, TFAs are responsible for 35,000 deaths annually in the
US.
It is beyond my imagination to understand how anyone can manufacture, sell
or work in a factory which manufactures such killers, the Government allow it,
we elect such a Government and the last but not the least ,eat them.
The people in India always ate fried chips. Coconut chips in Kerala, sweet
potato and Karande chips in Goa and potato chips in most parts of the country
. But there was a limit on consumption because they were made at home or
bought at the local fair. We could see them being manufactured right in front
of our eyes.
People in those times wanted to run their lives with their business and not
make quick and easy money at the cost of people’s health. A strong belief in
after-life either in the form of re-birth or a purgatory was a deterrent to
malpractices. Now, we don’t see beyond this year. Forget about next life.

Iodized Salt
Post independence, goiter, hypothyroidism and related mental deficiency in
children were frequent especially in the hilly areas.
To counteract the problem of hypothyroidism in India, universal iodization of
salt was introduced.
Even in places where there was adequate iodine in food and water, people
were asked to switch to iodized salt.
The iodized salt definitely decreased hypothyroidism related illnesses but gave
rise to new concerns.
One of which is infertility due to decreased sperm count and the second is
autoimmune thyroiditis in adult men probably secondary to the silica in the
iodized salt.
In the villages, people still use local salt. One way of seeing whether they are
getting enough salt is to do the urine spot test for iodine.

MENTAL HEALTH
The First Six Years of Life
The first six years of life are the most crucial years. The blueprint for adult
development is set in these few years.
The saying, ‘Give me your child for the first six years and I will you a man’ rings
very true.
If we have installed the right mind programs, we can expect to have a healthy
and mentally strong adult who will not sway to the tune of the public opinion
or malefic influences.
Developing Assertiveness:
A child’s self-identity develops around the age of 3 years.
The child at this time learns to distinguish between ‘I’ and ‘not I’.
If a child’s individuality is suppressed at this stage by parents or teachers, the
child becomes passive and later may develop a passive aggressive personality.
Most parents and teachers feel comfortable with a toddler who is very docile
and obedient.
I get worried stiff about such children. Children at 3-5 years are generally
expected to say “no” first.
The parent or teacher should allow this ‘no’. Convince the child and let it come
to an agreement about yes.
A child who cannot say ‘no’ to his mother will not be able to say ‘no’ to his
peers, when it comes to cigarette, alcohol, sex, pornography ,drugs or bribery.

Imagine what power it is to say ‘no’ to a ‘SIGNIFICANT ELDER’
This suppression of ‘no’ constricts the Manipur chakra and is responsible for
the increasing central obesity and diabetes in Indians.
Many of today’s psychosomatic illnesses have a remote origin in the first six
years of life, in the womb or in an earlier lifetime.
People who are in counseling will agree with me on how difficult it is to heal a
damaged inner child. Even if the counsellor himself has a damaged inner
software program, it is very difficult to develop to one’s full potential.
This is one area where the aaganwadi workers score over the kindergarten
teachers.
When I travel by bus, I meet young adult women who went to aaganwadis.
They might have studied 7th
or 8th
class but they have an air about them .Each
one thinks that she is as important as anyone else in the bus. The healthy inner
child in the woman (or man) is empowered. Some of these women are so
confident though there is no external reason for them to be proud about.
On the other hand, I meet graduate workers or even highly educated and well
placed scientists. Always inwardly feeling that something is missing in them
and are trying to make it up with external aids.
There are women who cannot say ‘no’ to their boss for work or other favours
asked, aspiring actresses who cannot say ‘no’ to the casting couch, young girls
who say yes because the boy-friend threatens to leave them.
The man or woman with a damaged inner child finds herself at the mercy of
the so called public.
‘What will people say?’ dictates all their decisions.
If the aaganwadi sevika gets even a one -day training on the inner child
functioning, she can change a lot in this area of mental health and foster the
growth of resilient empowered assertive adults.
There will be no need for us to take assertive training, anger management or
even stress management in businesses houses.
Soon, big industries will be asking of their prospective employee’s resumé,
‘Please attach a certificate of your aaganwadi attendance’.
In Goa, every school has a counselor. If the school counselor spends one or two
days in a year at the aaganwadi from where her/his future students will come ,
she will have less problems to tackle in future. This could be done on a
volunteer basis.
Kindergarten vs Aanganwadi:
Let me make it clear that I have nothing against kindergarten. I went to a
kindergarten school. My first school used the Cambridge model and if I
remember correctly, imported books. I learnt the Queen’s language before I
could speak my mother tongue.
But here I am looking at equitable distribution of health and wealth. Since the
mother is going to save on school fees and travel she can buy a papaya every
day. Aanganwadi is more cost-effective and health-effective than kindergarten.
Secondly, it terms of child development the aanganwadi is in no way inferior
compared to kindergarten as I have seen across India. That is, when I have
seen the children at age 18 or 19 in the Medical College they are on par with
others except for spoken English which is easily remediable. By the time they
finish PG and are ready to go the US, they are fluent.
Their written English and grasp of subject is better than the Public School
students. This is perhaps because they translate the material into their mother
tongue first. The time spent on a particular topic is increased and the depth of
reading is better.
This is to reassure parents who choose the aaganwadi. The people who choose
kindergarten may have their own reasons for doing so. I am not interested in
raising controversies but want to allay the fears of some parents that their
children may lag behind.
Graphotherapy:
It is the aaganwadi sevika who teaches the first alphabet to the child.
When I was in school, I had made a resolve to teach the first alphabet to every
child of my village. When the child would start crawling, I would request the
mother to allow me to teach her child the first letter either Shree or A as per
the mother’s wishes and most mothers would oblige.
At that time, I did not know how much influence handwriting had on an
individual’s personality. Later as a teacher in a medical college, I realized that
handwriting could make a difference to passing or failing.
I coaxed some of my medical students to change their hand writing.
I even got them copywriting books and together we worked out winning
strategies.
Graphotherapy is a very efficient tool in changing personality but learning to
write well in the first place itself lays the foundation for a strong and balanced
personality.
If the aaganwadi workers know about this, I am sure they will give more
importance to the first letters.
Graphotherapy in local languages is difficult since we do not have trained
people but the basics remain the same.
Gayatri Mantra and mental health:
Some time back I read that the some schools in UK are using the Gayatri
mantra to increase performance.
Some scientists are studying brain wave activity of Tamilian brahminṣ in the
Ṣilicon Valley.
A Principal of a school for special children confirmed that Sanskrit chanting had
improved mental abilities.
Even passing this message to the parents will help. Ṭhe parents can get
cassettes or send their children to bal sanskar vargas run by spiritual groups. At
least 70% of Indians will have no objection to chanting Sanskrit Mantras if it is
going to improve performance as long we don’t try to impose these on people.
Brahmari:
Brahmari pranayam is shown to increase the gamma waves in the
electroencephalogram according to a Japanese researcher. Gamma waves are
generated during peak experiences and deep meditations. A simple technique
like this can be used to increase the performance of school children.
Increasing Memory:
Brahmi
This small herb is used to make hair oil. A leaf a day is supposed to improve
memory.
Suryanamaskars:
It is difficult to learn suryanamaskers in old age. But if one has learnt them as a
child, one can do them even at 90 years.
Suryanamaskers help in physical, mental and spiritual development. This
science was known to Indians but when Macaulay introduced the classroom
model of education in India ,the holistic aspects of education went out.
Vrikshasana: or tree posture to increase the concentration power and
confidence.

Modernization of Education:
The British replaced the indigenous system of education in India with western
model. The Macaulay’s model of education (1835) had marginal benefits in
some areas but there were no miracles.
In spite of modernization , we don’t see any C V Ramans, Swami Vivekanandas,
Visweshwaraiyyas , Ramanujans or Tagores. Quantity has replaced quality.
My maternal grandfather was wheel chair bound two-thirds of his life but kept
a rich collection of books. Whenever he was happy with us, he allowed us
access to the books and we could take some of them.
Today, when I read the essays of the 1940s or 1950s in whichever language
they may be , I am appalled by the literary, scientific and technical genius of
these writers. A Marathi poet could write a scholastic essay on education in
the English language.
Today, we have mass education but the quality of education is very poor.
My grandparents were educated in very mundane settings. But their
knowledge of language, history , culture or mathematics was far superior.
Their spirit of inquiry, even when reading a newspaper was commendable.
Of all the people in our family, only my maternal uncle inherited some of this
inquiry but just about 50% and I will not reach 50% of my uncle. So, there is an
exponential decline over generations.
My kindergarten and first standard teacher was just SSC. My other mentors
who did free mentoring for me were intermediate pass. All these people were
very knowledgeable.
What school gave my grandparents was not information but how to think. Only
one sum was taught and they could do all the sums because the first sum was
taught well. One could choose not to go to school and help at the farm or shop
or kitchen. One went to school because you wished to. And that was why one
learnt well.
And the mental strength school gave was tremendous. Being in a wheel chair
required tremendous enduring power both for the person and spouse. I don’t
think a classroom type of education would make my grand -parents strong
enough to sustain the rigors for all those years.
The Emergence of the Kindergarten School:
In Goa, the Aaganwadi system is slowly dying out. Parents are sending their
children to Kindergarten School. There is a prestige or class effect. If you visit
an aaganwadi and kindergarten in the same area, you will see class differences.
The kindergarten has a kind of externally imposed culture. You wear a fancy
colourful uniform. You are cramped into a miniature table and chair and you
are supposed to obey. You learn discipline at the cost of assertive behavior.
I went through a kindergarten type education myself but since we had classes
in the afternoon I spent the morning hours visiting balwadis or vernacular
schools.
The balwadi teacher was more like a loving aunt. You didn’t have to show a
false respect. You just loved her any way. It is difficult for today’s children to
get the best of both worlds as I did.
But parents need to decide whether this sudden shift of culture is good for a
growing brain. It is not about learning a new language. I was brought up in a
chawl where there was Marathi, Haranyvi, Gujarati, Konkani , Hindi and later,
Tamil, Telugu Malayalam, Kannada ,Bengali . So, I learnt to respect all
languages.
I don’t remember any class differences. Whether you were rich or poor, you
went to the same school because the school was closer to your house or the
teachers were good.
Today, parents worry about their children getting spoilt in bad company in the
local village aaganwadi . So, every day at 8 o’clock they leave the house with
the child to travel 4-6 km to drop their child at kindergarten. Some mothers
wait outside the schools for 3 hours and bring their child home. Every trip costs
them Rs 20-Rs 40.
When I ask them why they do it they reply that the parents of other children
are doing shady business. It is okay for their child to share space with a
kindergarten child whose father is the top- most corrupt government official.
So much for our values!
I have talked to many aaganwadi workers and children. They have stronger
positive values than we care to believe.
SOCIAL AND ENVIRONMENTAL HEALTH
Gender Equality
There is nothing like the Aanganwadi to teach children about gender equality.
If the children are taught well, we will not have to deal with crime against
women as a class or even against men (which is sure to follow as a
repercussion).
I appreciate my own school in this regard. The girls were pushed on to the
football field and the boys were forced to learn needle work.
In class seventh, I was given the task of teaching the boys macramé bags. I
realized that they were better than the girls and made neater knots.
Social Inclusiveness:
Although not seen in Goa, I have seen discrimination in other parts of India.
You have seen a caste or religion based divide in aaganwadis. In Goa, a class
divide is emerging with kindergarten versus aaganwadi but there is no religion
and caste divide in education. It was not there even in the pre- liberation era
from what my grandmother told me. The Portuguese allowed people of all
castes and religions to school together.
Rurbanization:

A major challenge in preventing chronic diseases is keeping the innocent rural
people out of the claws of gluttonous corporate houses first and then the
corporate hospitals. The rural people are best off in the village.
But unfortunately, the sharks have reached the villages. It may not be possible
to buy a mango or get clean drinking water in the village but cookies, chips and
soft drinks have flooded the local ‘kirana’shop.
Inner city populations in the burgeoning urban slums and rural to urban
migrations are other problems.
Free Health camps are no community outreach programs. They are pick-ups
for future patients which is called disease-mongering.
The Problem of The Migrant Workers:
The State of Goa is economically strong and one of the best governed states.
But even when mining industry was at its acme and real estate and tourism
were blooming we did not have 100% coverage in immunization. The children
of the migrant workers were left out.
We like to ape America in consumerism. It would be better to borrow its
respect of all work and dignity for labour. Abraham Lincoln would log wood in
his holidays, George Washington could fell a tree with an axe. Our rich and
famous are very delicate. They can hardly move a spoon.
While we bask in the glory of our quick wealth, showing it off and stacking
some in banks abroad, we care little for souls who are at the receiving ends.
Their parents toil for us under sun and dust but they are far removed from
basic education or health programs like immunization.
The older children are taken care of by the ‘Hamara School’ in some cities but
the under- fives have nowhere to go. They cannot be admitted to regular
aaganwadis since they keep moving. The aaganwadi people cannot get them
even for immunization.
Once when I pointed out the poor immunization rates to a pediatric resident
doctor she replied that it was difficult to trace the migrants. The PSM resident

said that it was the responsibility of DHS to get the numbers. The DHS passed
on the buck to the auxiliary workers. The local population will come anyway.
They are aware. It is the migrants who determine the success of the
immunization program. The Amitabh Bacchan and Aamir Khan ads are great.
But these workers do not have access to television.
Even in the Malaria Control Program, The blood tests cards were collected by
the contractors and got stamped with the help of an insider.
The return on real estate investment is tremendous. Don’t these actual
workers deserve something substantial at least in terms of food, health and
education for leaving their villages and serving in places where local labour is
near extinct?
We will have to tackle these problems with our hearts. The brain cannot reach
out to these people. We have to take responsibility. Something like a mobile
aaganwadi should be on the cards for immediate future.
McDonaldization:
The markets are flooded with fast foods in the form of take- away pizzas and
burgers which offer incentives and are targeting young children. People are
discarding traditional food for the fast food, a phenomenon which is referred
to as McDonaldization.
Impact of Advertisements
Children are brainwashed by the advertising industry. We cannot really
counter these advertisers because they are like borers in wood. They work on
the subliminal mind. A weak mind with a low self esteem is very easy to
capture.
Whenever I get to work with children, I teach them a few ground rules.
• Never buy anything if it says ‘20% extra, or buy one get one free or10%
discount.’
• If someone is giving something free it means that the product is not
selling or the advertiser is trying to capture your mind.
• Wait till the discount sale is over. Then, if you really want it, buy.
• I will not lease my mind to save a few rupees, will you?
• Never buy a product if a celebrity is endorsing it. The company will pay
15 crores to the celebrity and recover it from your pocket.
• Watching television advertisements along with children, I teach them
how to dissect the ad. Children have immense talent. You will be amazed
at their innate creativity.
In the ‘Iss Bandar ko kya dun? Ad , I ask them, “Koun Bandar?” and they
promptly reply, “Doctor Bandar!”
You get micronutrients in fruits, antioxidants in fruits and vegetables, DHA in
fish and vitamin D in sunlight.
But…. not in the Ads.
Subliminal Teaching:
In the aanganwadi and kindergarten, we could hang posters to promote
consumption of fruits and vegetables
A healthy child in a banana or papaya orchard, especially a foreigner will leave
a mark.
‘A thin emaciated child eating chips from a packet’. You don’t have to tell
anymore. The child will never forget the message in his life-time.
Both my grandmothers grew special varieties of bananas and papayas. So
much so that anyone who remembers my maternal grandmother now also
remembers her special bananas. I cannot but admire bananas and papayas
because I loved and admired my grandmothers.
How to make children eat vegetables and healthy snacks?
Parents tell me that they find it very difficult to make their children eat healthy
food and want me to talk to their children.
The last thing we should do is to sermonise children on healthy food.
It sure will drive them away from the good stuff.
Here are some useful techniques I use with young children.
Grate carrots in front of them and tell them not to eat and save it for a carrot
cake.
Make carrot juliennes, sit and eat in front of television without offering it to
them .Slowly, small hands will reach out for them.
Eat boiled gram, groundnuts or corn in front of them .They will soon demand
their share.
Other useful messages
Aluminum Vessels:
Aluminum vessels are suspected to increase kidney diseases.
Wherever possible, it is advisable to stick to earthenware or use stainless steel
vessels.
Teflon:
Teflon cookware is heavily promoted and every household uses it .When the
Teflon coating is breached, the chemical reaches the environment.
The fumes are known to kill birds.
We do not know what harm it will do to human beings especially young
children.
It is very difficult to sell Teflon in developed countries with an EPA ban.
Microwave Ovens:
Eating in a hotel or fast food joint is exposing yourself to microwaved food.
Microwaved food is potentially cancer causing.
Induction Cookers:
Another recent concern is the use of induction cookers in cooking which has
radiation hazards.
Mobiles:
Mobiles and mobile towers have reached every nook and corner of India. It is
one of the cheapest and popular medium of communication.
But it is being misused. Young children who are at the greatest risk of brain
tumours are seen to used them freely
Dangers of EM waves:
Although we are aware of the EM Radiations of mobiles and computers it is
impossible to give these up.
The benefits far outweigh the risks. We will have to develop better quality
instruments.
Garbage Disposal:
Safe disposal of garbage and home composting can be taught at the aaganwadi
itself.
A class Xth
school student from Vasco gave a brilliant project in the ‘Best
garbage disposal project’ competition.
Solar lighting; rainwater harvesting; green housing:
Solar lighting of aaganwadis and Schools, rainwater harvesting can been shown
practically at the aaganwadi itself.
Spiritual Health:
TEACHING CHILDREN VALUES
Life beyond Life:
The greatest lie ever told by scientists is that there is no life other than this.
Hard core physicists and chiselled psychiatrists have concurred that we do not
know much about both the universe and the human soul or mind. Only the
half- baked scientists, copycats of some borrowed ideas assert vehemently
that there is no after life and call it superstition. Ask them, “Have you heard
about parallel universes or about the 26 dimensions of physics?” and they will
stare at you as though they have seen a ghost.
Today, western trained psychiatrists like Drs Bruce Goldberg , Brian Weiss and
Ian Stevenson have provided ample evidence about the recycling of the soul.
Yet, if people are adamant at ignoring such evidence nothing much can be
done about it.
The Eastern religions believed in Karma and the semitic religions believed in
the Judgement day. Both beliefs were spiritual deterrents against social crimes.
I will not even try to disprove such beliefs in the name of science. A science
,which prides itself on discovering nuclear energy and distances itself from the
holocaust has no place in my heart or brain.
The recent case of hoarding of onions is a case in point. Any person who
believes in spiritual accountability will dare not do such crimes even in the
name of business.
There are people who vouch for ahimsa and will not kill an unfertilised egg but
they don’t flinch when they amass huge profits at the stock exchange scams
driving others to suicide. This is Himsa camouflaged. It is time to readdress
these social issues.
But what is the role of the aaganwadi?
Understanding the Child’s Soul Agenda:
It is a well known fact amongst yogis and transpersonal psychologists that the
broad script for this life on Earth is laid even before we think of taking a body.
When the child is just born and up to the age of three years, the crown chakra
or Sahasrar chakra is open. And… as young children less than three years, we
remember our past lives and our scripts.
At this time, the child can be asked about its soul agenda. This will help the
child choose a career and find fulfillment in later life. Just this little bit of
information can go a long way in changing the mental health of a person.
One of the problems faced by successful people today is disillusionment with
life which makes people run from one spiritual retreat to another. It also
creates a lot of psychosomatic ailments.
Children see elemental or bodiless spirits and even converse with them.
But modernized people with an element of ‘I know everything mentality’ not
only deny such facts but are audacious enough to call them whims or even
hallucinations.
There are British children who speak Chinese or American children who
understand Hindustani Classical without ever having learnt these.
When the aaganwadi sevika understands the research in this area, she will not
invalidate the child’s experience or memory as his doctor. She can help him
discover his soul’s agenda.
A child who then keeps recollecting his past birth will definitely want to create
better future births and not indulge in cheap businesses like onion hoarding or
narcotics trade.
The soul knows the truth. All we need to do is to stop killing our conscience.
We need to stop brain-washing our children saying that this is all the life we
have. We can choose to suffer ourselves but we have no right to make our
children suffer.
Ramanujan and Kountilya Sharma: Two great brains of India
One from the South and other from the North; one had excellent analytical
skills and the other has a magnificent memory. Both have come from humble
backgrounds. While Ramanujan did his early schooling in his mother tongue,
Kountilya learns in an English medium school and has instructions in Hindi and
Sanskrit at home. So, the myth that medium of instruction or the fame of a
school determining performance is shattered.
According to Kountilya’s grandfather , a retired Vice –Principal , Kountilya is an
ordinary child with a keen interest. He believes that other children can be
trained likewise.
Both are not fish-eaters. So, I am beginning to doubt whether DHA is really
very important in memory or whether enough is obtained in vegetarian fare.
Most important, Kountilya eats only home –made food and not processed
food from outside.
All children should watch the documentary on Ramanujan produced by
Doordarshan and Kountilya interviews.
Moral of the story: medium of instruction, language spoken at home etc has not much place in early
learning. A child under five is capable of learning many languages if adequately exposed. Some
natural tendencies will be determined by what was acquired in previous births. Life continues so it is
never too late to learn.
I request the retiring employees to learn at least one new language and one musical instrument
after retirement.

CHAPTER 5
EMPOWERING THE MESSENGER:
Bottom- up approach:
Once the aaganwadi workers are empowered, the policy makers and doctors
will learn from the aanganwadi workers as to what is cost effective. Just like
Prince Charles wanted to learn from the dabbawaalas of Mumbai.
The Work Force:
There are roughly one crore workers in the ancillary health sectors that
includes aaganwadi workers ,helpers and Asha volunteers.
In Goa, there are around 1200 aaganwadis with as many sevikas and helpers.
The ASHA scheme is a good case of palming off responsibility with no adequate
compensation. The responsibility of identifying a pregnant lady, taking her to
term and getting an institutional delivery lies on the Asha for which she is paid
a pittance.
While a medical officer in the DHS who paid fulltime and working part time
gets paid Rs 30,000 to 90,000/- feels no responsibility of getting the ladies to
the hospital or increasing the immunization numbers.
The Asha volunteer should get at least 5,000/- per pregnant patient or
alternately a salary of 5,000/-per month
Many Government doctors are busy with their promotion , files related to
transfer etc.. etc
I was waiting outside the Health Ministers cabin for two hours one day to
present a project on promotive health. I learnt that I had to wait in spite of my
appointment because some doctor from DHS had come to lobby for a top post.
Fortunately, he did not get it. I wish he had come to the Health Minister to
improve immunization numbers or better sanitation or garbage disposal. This
mad race and consumerism has taken us far away from the nobility of the
profession. Less than 50% time of DHS doctors is spent in actual patient care.
There is so much paperwork to do.
Economic and Financial aspects
A doctor, cardiologist or cardiothoracic surgeon in a medical college is allowed
to work till seventy longer in private practice. …till his fingers tremble and his
brain becomes hoary
Why ask the aaganwadi worker to retire at sixty if she can continue longer?
If she retires, pension should start at sixty years. At present, she draws a one-
time retirement benefit of 2 lakhs, if she has had 20 years of service.
The aaganwadi worker is high on the Maslow’s pyramid. Akka, tayee, didi ,ben
,ma’am ,sister as she is variously called, she is self- contented.Sometimes, even
a little altruistic. She is very enthusiastic and she wants to learn. Society should
take the trouble to compensate her. If we increase pay, more money- minded
people will come and quality will suffer.
Even in this respect, the law of intention worked. One year back, I
contemplated writing a book on the aanganwadi worker. As a matter of habit ,
I typed the title and outline in a file.
One key aspect was compensation as per service. Now, I am informed that Goa
Government has sanctioned a very attractive and sound renumeration scheme
for them. This should keep the ‘working for money ‘people out and intrinsically
motivated people in. Other states can learn from Goa.
Starting remuneration of Rs 7000/-
Rupees Three thousand from the centre and four thousand from state
>5-10 years 8,000/-
>10-15 years -9000/-
>15-20 years- 11,000/-
>20-25 years-13,000/-
>25 years-15,000/-
Coupled with a good pension scheme, we can keep the workforce happy.
The staggered structure will prevent attrition and people will not use the
aaganwadi as stop-gap or stepping stone. Only really dedicated workers will
join.
Pension Fund:
Consider,
We have 2,39,582 Village Panchayats, at least one aanganwadi worker per
village. Each aaaganwadi worker saving 3 premature heart attacks. Cost saved
is at least 10 lakhs per aangadwadi worker. It is very easy to build a pension
fund for them.
Every year, a certain percentage of the country’s and state health budget
should be ear-marked for the preventive program and if we have built a good
data base, in two year’s time this budget could go directly to the aaganwadis
without much leakage for administrative purposes on the way.
A certain percentage again should be reserved for training and updating which
can come in the form of CDs or online files. Rest could be used to give them
pension.
The Cost effectiveness of the promotive program:
To maintain a cardiothoracic unit will cost a few crore rupees per year even by
conservative estimates.
It includes the pay of one cardiothoracic surgeon, one general surgeon one
cardiologist, one physician, one cardiothoracic anaesthetist , general
anaesthetist anaesthetic assistant, perfusionist, 2 nurses and ICU support.
Such one unit will suffice for the state of Goa given the current heart disease
rates. If nothing is done, the rates will triple in 20 years and we will need three
such units.
The promotive program costs very little. It is one of the most intelligent
investments a community could make.
I have talked about cardiology but all diseases are going to decrease in the long
run.
Training of the Aaganwadi Worker:
Lakhs of rupees are spent on these trainings but the sevikas are not very keen
to attend. The training funds are allotted to the Directorate of Women and
Child Welfare. The training modules of the aaganwadi workers are fixed
centrally. Since many of the workers are there for a long time there are bound
to be repetition of topics. They lose interest in the training.
Since 70-80% training is information mainly about National programs and
administrative aspects, all these could be digitally transferred to them in
future.
The future trainings will have to be based on local needs which are diverse.
When I have looked at these programs as an external observer, the main focus
has been ‘the training’ and not the application or outcomes.
So much energy goes into commutation, food and attendance that the main
purpose of training gets side-tracked.
When I have met the sevikas outside of the sessions, they have confessed that
the training is burdensome to them for various reasons.
If we teach them what they want to learn, perhaps they would be more
interested. What they want should be coupled with what is needed.
The workers sought more training in learning spoken and written English,
Hindi, operating computers, learning art and craft , dance, music etc.
Even training one sevika well and then deputing her to visit each aaganwadi by
rotation will serve a greater purpose.
Her presence at the aaganwadi, where she will interact with the beneficiaries
will boost the image of the aaganwadi.
Since they get leave for a few days in a year, they do not wish to attend any
training during this period. At other times, there will be only one sevika in the
aaganwadi and her taking leave to attend a program disturbs the functioning
of the aaganwadi.
The costs of commuting for the program and the compensation do not match.
In future, this could to a certain extent be eliminated by having an online
training program. Most of the information can be transferred through the net.
All the aaganwadi workers in India will be connected.
A computer may be provided at the aanganwadi and she may be given loan to
buy a tablet or laptop.
Knowledge of Computers
The computer training of the aaganwadi workers could be done by the
hardware companies which are supplying the modems, laptops or tablets by
recruiting volunteers.
We have so many volunteers coming from Europe and US to work in the
villages. In places like Goa, Karnataka, Gujarat or Rajasthan we can easily find
the required number of student volunteers to teach computers to these
workers.
A group of ladies in Rajasthan are working from their homes and provided call
centre services to local farmers. It is run by a NGO, which has set up a data
base of farmers and services.
It will not be very difficult for the aanganwadi workers to learn computers or
even work part-time at call-centres to give health related information.
Making an aaganwadi sevika computer literate will change the picture of rural
India and that of women empowerment.
Spoken English:
Wherever possible, basic spoken and written English should also be taught, so
that they may find a global presence.
If we want to connect people, we need a common language. Within India,
Hindi will do. But if we have to go International, English as of today becomes a
better option.
People should keep learning new languages. Every place I have worked in, has
given me an opportunity to learn the local language free of cost in return for
Hindi and English.
When I try talking health, people will ask, “Why don’t you teach us to speak
English or Hindi?”
They don’t mind paying me for the English lessons but are reluctant to learn
healthy habits for free. And this is true the world over.
A friend of mine residing in Germany conducts free yoga classes and paid
Hindi classes. The Hindi classes run full. People want to understand bollywood
movies and songs!
Some years back a medical student, committed suicide because she could not
handle the ridicule meted out to her as a so-called ‘vernac’.
Recently, I heard an interview of a girl child from Kamathipura. She was
educated in the Marathi language till tenth but went to the US to share stage
with Mallala , the Pakistani inspiration to the world.
This young lady from Mumbai had such a command over English that she could
embarrass all the ‘nose in the air’ public school students.
Is it not great feeling if you can read write and speak your mother tongue ,
National language, English, one more Indian language and another foreign
language?
Through the SALT technique it takes just six months to learn a new language.

And with digitization, we can reach large numbers.
The aaganwadi alumni will be proud to call themselves ‘vernacs’ if they are
taught spoken English along with the regional language. And their inspiration
will come from the aaganwadi sevika.
Transport:
The aaganwadi workers should travel by bicycle. This will maintain their health
and save time. They will inspire their wards.
Hero Cycles have come with a full Aluminum frame light weight version. A high
end bike with gears could also be provided in mountainous areas. Solar
powered bicycles are also a good option.
Qualifications:
The present qualification for an aaganwadi worker is Standard Xth pass. A
graduate mother finds it difficult to send her child to the aaganwadi. With
better pay, even graduates are joining the force. As the educational level of
society improves, more qualified people will come.
Along with qualifications, the Emotional Quotient (EQ) and Spiritual
quotient(SQ) will have to be assessed .When we employ software engineers,
we grill them in various ways.
What about the one who writes the software of our child’s mind?
CHAPTER 6
THE METHODS
The best way to deliver the message is through community participation. I
have written about community participation in another book but here I shall
give a broad outline.
Community Participation
Communities should have the capacity to deliver prevention and self-
management programs through public health professionals and trained
peers/lay workers.
The Strategies
-Create awareness to generate demand for health and health promotion
services
-Create access- economic and material
-Create attitudinal change and acceptance
All three are interlinked. Whatever change we wish to introduce has to
become a need of the community. Only then it will sustain itself.
For example, if the community prefers whole wheat bread, there will be at
least one baker ready to supply or one self help group who will try to cash the
need through chapattis. All the bakers will then switch to whole wheat bread
and will demand subsidized wheat flour from the Government.
Consulting the Stakeholders:
When any change introduced, opposition is to be expected. Hence, we should
consult and negotiate with all the stake holders beforehand. Rolling back a
policy because of opposition weakens the moral stance of the administration
and decreases the motivation of the people concerned.
For example, if we have ban tobacco cultivation, we should start from bottom
up.
Stakes and stake holders:
1.The tobacco companies or cigarette/beedi makers give money to political
parties for electioneering- this is the main bottleneck. At some places, they
may be directly present in politics
2. Administration: Some loss of revenue as duties- this may be tackled by
diverting funds from health to administration as a pledge.
3.The pharma companies
4.The shopkeepers who sell cigarettes
5.The tobacco cultivators
6.The farm labourers
Most of the growers and leaf pickers are landless labourers. If we give them
better employment opportunities or land to grow a millet crop, their income
will not suffer. We will also have to convince the labourers that their labour in
growing tobacco is causing ill-health.
The options to shift from tobacco to another crop are many. Depending on soil
conditions, any of the medicinal plants can be grown.
This will simultaneously tackle the pharma losses.
The shopkeeper who was allowed to stock the cigarette should be allowed to
stock some other new product which is harmless.

For example, to stock cigarettes not much licensing is needed. But if one has to
open a fruit and vegetable shop in a residential area you have to do a few
rounds of the horticulture department.
The situation should have been otherwise. The government should invite
people to open more fruit and vegetable shops closer to people’s homes.
Quality check should be done periodically later.
Your neighborhood shopkeeper is unlikely to sell you contaminated or
chemically sprayed stuff because he has to survive in that same area.
Lastly, the cigarette manufactures will have to be addressed.
At any point of time, around 3 year stock of tobacco is pending. So, we can give
three years time to shift or make nicotine gum.
The smokers can use nicotine gum or use imported cigarettes.
For some years, this will give rise to an underhand trade. But as the newer
generation emerges from aaganwadis, we will be sufficiently empowered.
Many spiritual leaders are also doing great work in this area.
Participatory Learning:
If we can reach out to all the aanganwadi workers, time we will have a huge
force and a great wealth of information in five years. Of course, there will be
counter forces that will prevent this from happening. But once the boulder
gets rolling, there will be hardly any capable power that can change.
I visualize a team of 6-10 lakhs, net- savvy aanganwadi workers who are not
just well informed but have been trained into ‘learning to learn’.It is not easy
to brain wash empowered women.
Today, the developing world especially the African countries have successfully
implemented the participatory learning model in different areas of
development.
DIFFERENT PROJECTS IN LIFE- COURSE MANAGEMENT
“Saath Chale”
How to take the community with us
A Few Tips
1.All messages should be in the local language
2.The message SHOULD APPEAR NEW
Sonakshi Sinha and Akshay Kumar telling about flavanoids, it appears that
flavanoids were discovered yesterday. People like novelty.
3.It should be need based. Unfortunately, people in India today have no need
for health till it is deranged. Their needs are linked to acquisition of material
goods almost bordering on obsession. But as always there are some loop holes.
If I tell people that Aloe Vera or papaya is good for health they are unwilling to
listen. But when I tell them that these are good for their complexion, they are
all ears.
Then I slowly add, “Fresh Aloe Vera is better than the packed one, do you have
a plant?”
4. Use a Bottom To Top Approach
5. The message should have visual component
6. Use posters or stories
In my childhood there was a story told about sharing and carrying called
peruchi fod - a slice of guava
Besides the sharing component it spread a love for guava.
If you love your mother give her your slice of guava.
Thirdly, it taught mathematics.
Fourthly, it used rhyme’ peruchi fod, laagte god’ to reinforce the message.
Hats off to this story teller educator!
I heard this story while eaves- dropping at the balwadi window. I was officially
not admitted.
I have included this story in the appendix and have loads of such stories
collected from my grandmothers and great grandmother.
• Using television SERIALS. Ladies in India are almost addicted to
Television serial. A friend of mine calls it vicarious living. People live lives
in the fantasy world through these serials. But I see an advantage. Any
social message can be given through serials. I note down all the positive
messages in the serials and reinforce them in class. They listen to me
because I talk about their favourite serial or film hero.
People should write to the directors to decrease the cost of production
and make the actors look more authentic. This will decrease
consumptive consumerism.
• Using PUPPETS. In Maharashtra, traditionally the social messages were
given through puppets and the art is revived.
7.RHYMES: The rhyme ‘ Iss bayee, iss dodka kiss’ is an ode to the ridged
gourd.
8.GAMES –a game of snakes and ladders is used to teach values.
You eat fruit and you climb a ladder.
You eat a pizza and you fall down through a snake
9.SKIT- NUKKADS or street plays
Children dressing as different fruits and vegetables in fancy dress
The options are endless.
‘Tell your neighbour’ program
Human beings like to share. They are always sharing information ..at the PDS
counter, bus queues, Aadhar counter ,buses, outside the school etc.
If we give some information to any person which he or she has to pass on to
one neighbor within 2-3 months the information will be circulated and re-
circulated till it reaches the aaganwadi worker as , “You know what………..”
Schools:
Schools can play a major role in ensuring that addictive substances don’t reach
children. The main problem is the supplier-politician nexus with law enforcing
agencies playing a bystander role. The money stakes are high and hence health
concerns get a back seat.
At one prevent tobacco program , I had invited every school in Mormugao
taluka to send two students. Most of the schools obliged. In fact, one teacher
took it upon himself to attend.
The whole hall was decorated with cartoon pictures on smoking.
Very few facts were given verbally and material was flashed visually.
The children had to write a slogan. The name of the best slogan was later
announced in the local newspapers.
The main emphasis of the program was however about ‘doing’. The children
enacted an ex-tempo skit on the emotions linked with of smoking. The
enthusiasm, innovation and sense of involvement was indeed noteworthy.
Another project that has clicked is the ‘hand washing’ project in Northern India, significantly bring
down diarrhea rates.
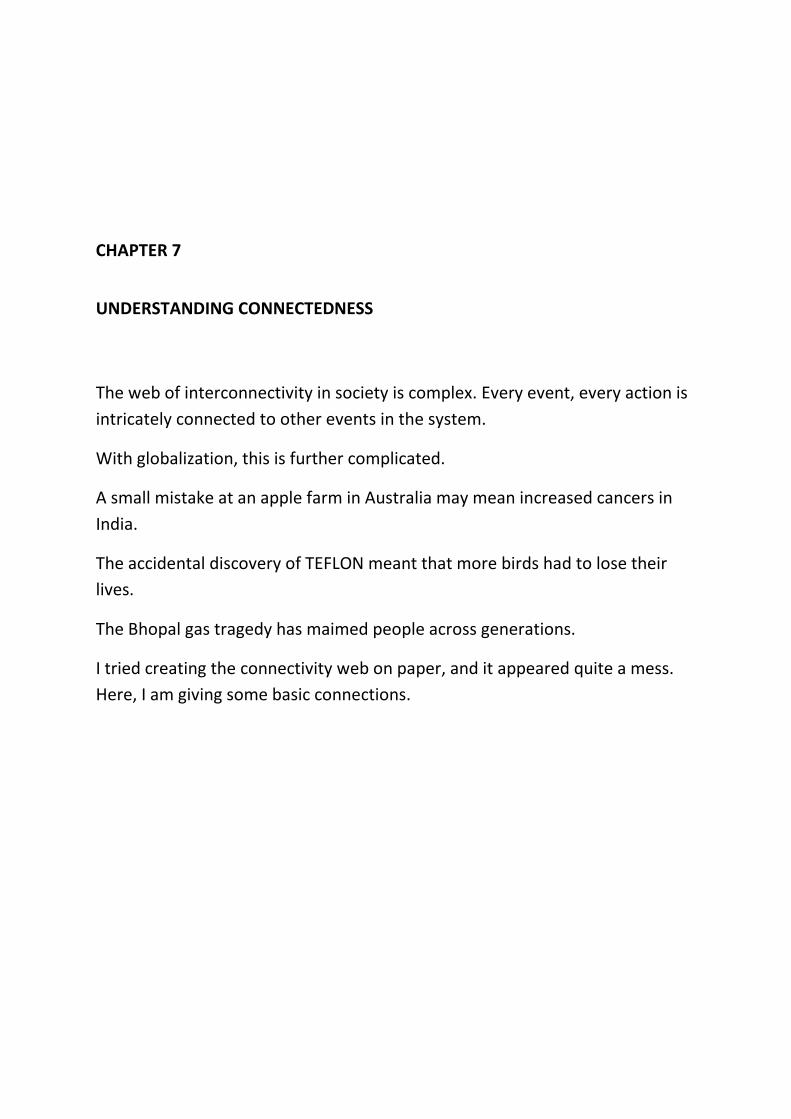
CHAPTER 7
UNDERSTANDING CONNECTEDNESS
The web of interconnectivity in society is complex. Every event, every action is
intricately connected to other events in the system.
With globalization, this is further complicated.
A small mistake at an apple farm in Australia may mean increased cancers in
India.
The accidental discovery of TEFLON meant that more birds had to lose their
lives.
The Bhopal gas tragedy has maimed people across generations.
I tried creating the connectivity web on paper, and it appeared quite a mess.
Here, I am giving some basic connections.
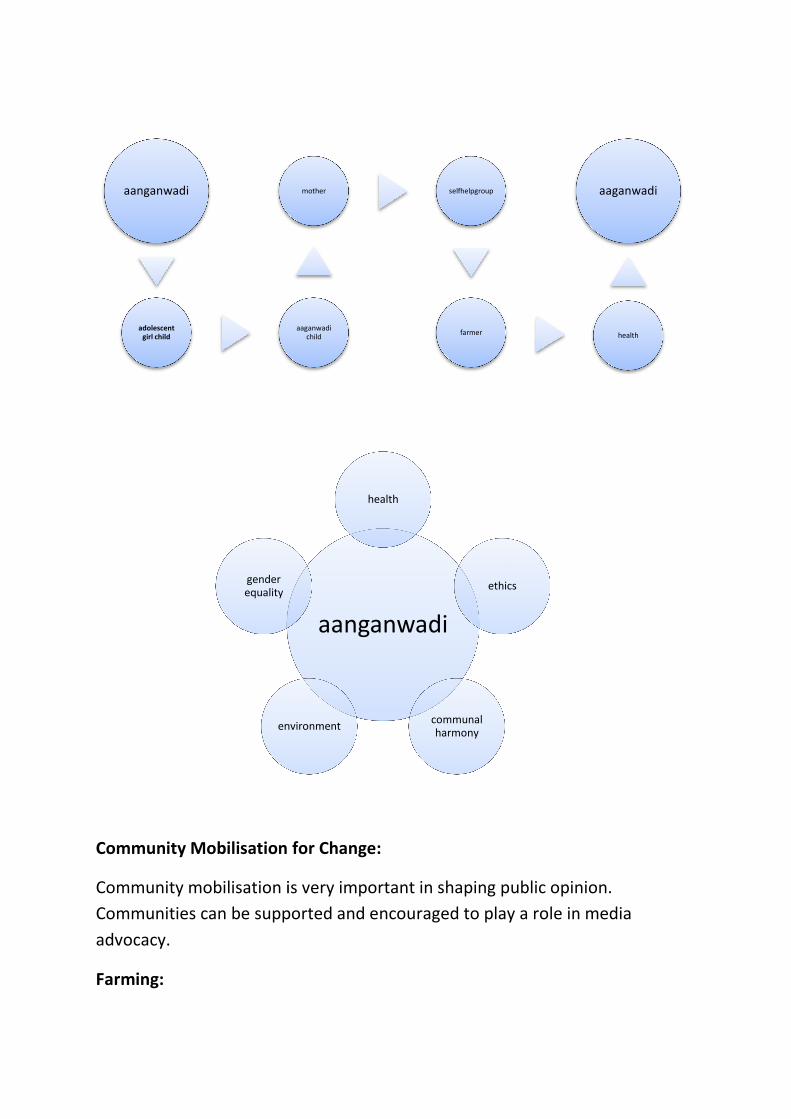
Community Mobilisation for C
Community mobilisation is very important in shaping public opinion.
Communities can be supported and encouraged to play a role in media
advocacy.
Farming:
aanganwadi
adolescent girl child
environment
gender equality
Community Mobilisation for Change:
Community mobilisation is very important in shaping public opinion.
Communities can be supported and encouraged to play a role in media
aaganwadi child
mother selfhelpgroup
farmer
aanganwadi
health
ethics
communal harmony
environment
Community mobilisation is very important in shaping public opinion.
Communities can be supported and encouraged to play a role in media
health
aaganwadi
Europeans may not have PhDs in literature as we Indians are fond of obtaining
but an average man or woman in a Scandinavian country will be very aware of
environmental issues.
Farming is considered a respectable occupation.
In India, if you are a doctor you are great. If you are an IT man you are super
great.
Doctors are needed only if we fall sick. Man has lived millions of years without
IT. We can survive without music, cricket and Bollywood. All these professions
are respected but the most important occupation in our life,farming, is looked
down upon.
We cannot live without food. With the demon of food shortages almost at our
door step, the most important man in India today is the ‘practicing farmer’…
..the man or woman who actually goes to field.
Every year, we should give at least one Padmashri award to a small or marginal
farmer (owning an acre or less) who has changed the landscape of his fields in
spite of all odds with his innovative brain. Giving Krishi Awards is not enough.
I specifically assert that it should be small farmers because we may find a bee-
line of non-practicing politician farmers or Bollywood farmers who after
gaining tax benefits on agricultural lands are now ready for awards too.
Local Food Security:
Nutritionists the world over are talking about local food security but the
Governments do not seem to understand.
Some aaganwadi workers come from farming communities. They are closely
related to Farmers’ clubs. So, we already have a network in place.
It has to be impressed upon people that we need to meet our food security
locally.
Anything which is local is best.
‘An apple a day keeps the doctor away’ has to replaced by papaya and
bananas. Even raw papaya will do.

The importance of local food security will be easier to understand from the
current onion problem. This problem is artificially created.
Middlemen are hoarding onions. If the crop is lost, the farmer suffers. The
middleman always gains… rain or shine.
There are many ways to tackle this problem
The first step is to get your food stuff locally.
Prices of local onion in Goa (They are more like shallots) was Rs 80 a kg
compared to Rs 15 or Rs 20 for outside onions. It is important to note that
outside onions may be gamma irradiated and harmful whereas the local onions
are safer.
At least people like Government employees who can afford should buy the
local stuff.
This will collapse the hoarders -adulterers nexus and local farming will get a
boost.
Go to the farm and pick your ware as they do it on Masterchef Australia.
Introducing Agnihotra farming to improve yield has been tried in Europe. We
need to replicate the process in India.
Kitchen Gardens:
The credit for popularizing kitchen gardens in rural Andhra Pradesh may be
given to Dr Bamji. She successfully implemented the kitchen garden model to
ensure, micronutrients,vitamins , minerals plus anti-oxidants to the rural poor.
The slogan, ‘YELLOW -ORANGE FRUITS AND DARK GREEN LEAVES’ works very
well.
There are some really resilient garden crops which are pest resistant too.
The two prize winners are the bachile plant (valchi bhaji) or Indian Spinach
which can be grown in any balcony and drumsticks.
Another creeper, the tendli ( Coccinia Cordifolia) grows very well on your
garden fence. The Kerala tendlis are larger and a few of these could suffice to
meet your daily needs.
Raw papaya is a great vegetable. The ripe could be consumed too. Bananas can
be grown wherever there is a good water supply.
Harvesting kitchen water to meet the garden requirements is also a good
option. You don’t have to use manure. Garbage problem is also eliminated
with the kitchen garden concept.
Bread fruit, curry leaves, other local pest resistant plant like colocasia,
amaranth etc. can all be grown.
I have practiced this for seven years so please don’t think I am talking through
the hat. The amount of garden vegetable and especially saplings in a kitchen
garden nursery is surprising.
I did it in my Government quarters, so if you have even a tiny strip of land, use
it.
Food Miles:
The more food travels on the road, the more unsafe it is as it increases the
environmental burden. The apples you get from Australia come to you gamma
irradiated. Onions and potatoes are also irradiated. Hence, we need to use as
much local food as possible.
It is difficult to change mindsets as adults. If we can collect the mothers
together and make a collective decision to inculcate healthy eating habits in
under- fives, it is easy.
But the greatest challenge is to address the monster called the food industry
and now even the agriculture industry.
In this regard, the effort of an NGO from Chennai , CIKS is indeed laudable.
They have managed to preserve 80 varieties of traditional paddy seeds which
are suited for different soil and climatic conditions. And now, they are
promoting SRI to increase the yield of rice.

A little reflection on this issue will highlight sustainable development.
Years back, we had the Green Revolution where high yielding variety of hybrid
seeds was promoted. The crops were then fed with chemical fertilizers ,
sprayed with chemical pesticides and weedicides and the farmers had to buy
the seeds every year. Traditional seeds were pushed out of the fields because
all subsidies were linked to this technical endeavor called Green Revolution.
In the bargain, the soil was degraded, the ground water sapped by the water
logged newer varieties, driving the farmer into debt and suicide.
Besides, these high yielding crops were far less nutritious gram per gram
Additionally, many had anti -nutrients like lectins.
Did no one see into the future?
Many farmers and quite a number of scientists saw through the game.
In fact, the farmers were resistant to switch over. But these sane voices soon
died out.
I remember the Agriculture Department having meetings in Goan villages
asking people to switch over and offering incentives. An agro chemical
company was also involved in all this agricultural business both directly and
indirectly.
Some well connected scientist trying to get a new hybrid, ruled the roost.
...Yield or perish. The same is presently happening with GM foods.
(GM=genetically modified)
Working alongside Farmers’ Clubs
The aanganwadi workers can work along with the farmer’s clubs to get the
best food on the plate. In many places in India, Farmers’ clubs are very active.
We have the rich farmers who own huge tracts of land, use mechanized
farming and grow Basmati rice or other food for export.

Simla apples, Ratnagiri Alfonso mangoes, Goa cashews are grown for export.
Since Indians need and deserve all these products, it is time we demand from
the Governments that all these should be subsidized in the local market.
If we give sops to exporters let us give bigger sops to people who are human
enough to sell it to locals.
There is co-operative organic farmers group in Chorao, Goa selling their prize
Mangurad Mangoes directly to the consumers at an annual fair.
The Government does not even provide the organic farmers with space. They
have to go after the officials asking for space. It should have been the opposite.
The officials should have approached them, given wide publicity, given subsidy
and invited them to open a fair in every city.
These people are protecting public health. Cricketers and Film stars who
contribute little to the poor man’s welfare are given awards and Rajya Sabha
seats and these genuine farmers are ignored. It is high time we took a re-look
at our priorities.
Linking small businesses with health:
Since land is scarce we need to balance agriculture and horticulture.
No cultivable land (not just cultivated land) should be allowed to be converted
from the green belt.
A common practice in Goa is to abandon land so that is considered non-
cultivable and then you sell it to the builders. The Land Acquisition Bill is the
biggest thorn on the path of food security.
In the short run we benefit but we will have long term irreversible
repercussions.
There is a tendency to value -add food by the food processing market. But
most of the time what we get is not food or nutrition but packed poison.
Whatever processing or preserving is done, it should be done locally.
Traditionally, chillies were dried, powdered and preserved for one year.

In a packet of chillie powder, chemicals may be added or vacuum packing may
be done to keep it from getting spoilt but within few weeks the powder starts
getting fungus.
If you have smelt local chillie powder after one year of preservation compared
to packets, you will know the difference.
Green Farming Methods:
We can use the services of self -help groups in manufacturing organic
pesticides and fertilizers. Azulla cultivation, neem-based pesticides are other
options.
Farmers’ training and establishing gardens and trees are part of the
networking.
Why Organic?
I was a witness to hundreds of pesticide poisonings and a few dozen organo-
phosphorus deaths. The farmers of Kolar find organo-phosphorus compounds
very handy to commit suicide.
With new technology, a total ban on chemical pesticides is possible today. The
OP factory owners can be helped to start new factories of neem cakes or bio-
pesticides with Government partly funding the project.
Neem and Ash:
Many of the aaganwadi workers are farmers themselves. When I asked the
aaganwadi workers of Goa who are also part-time farmers they told me that
they spray their vegetables with ash. In Maharashtra, neem based bio-
pesticdes are used. See appendix
Genetic Modification:
The agriculture researchers in Australia are looking into plant genomics and
trying getting biopesticides to prevent resistant crops. Either you manipulate
the pest genome or the plant genome , but by default you manipulate the
human epigenome, if I may allowed to use the term. You set in motion
something at the genetic level and it is irreversible.

You get away with it because this change takes time and you are not held
accountable.
We should not have a global village but keep our traditional villages intact
with all their indigenous methods.
People who want to experiment can gather together on an island and gamble
with their genes.
Working with the Forest Department
The Forest Department has a big role to play in public health. Local berries like
jamun, ber, and other varieties are great antioxidant suppliers.
I am especially fascinated by a local Goan berry called bhelsan. It grows on
shrubs. As children, we used to consume about half to 1 kg of bhelsan per day
during the rainy season.
Each locality will have its specialty. Local mangoes, for example. All these
should find their way into the mid-day meal.
Every year, on World Environment Day or Vanamahotsava , a symbolic tree is
planted and sapling distributed for at least 30-35 years now. I doubt any of this
grow into trees or we would be living in a forest.
Why not give bhelsan or other shrubs instead?
Some visionary people can do wonders. One powerful man with a strong far
vision can change a landscape. An Ex- Chairman of MPT, planted and nurtured
so many trees that the barren land actually called ‘Sada’ was transformed.
The garden of Chairman’s bungalow now has chickoo trees, mango trees and
many herbs.
Another person is Ex Union Minister Mr R L Jalappa. He had nurtured a
beautiful hibiscus and rose garden which had to be replaced by a building. But
the neem trees he planted in Kolar are still standing tall.
Working with the Self Help Groups
A strong collective force which is emerging in the rural villages is the women’s
self help groups. There are officially 22 lakh SHGs in India and 3 crore thirty
lakh members. The only drawback is that politicians try to influence these
groups or start their own groups. If women don’t want to be manipulated, they
should keep their groups and commerce away from politicians.
I mean politicians and not politics. Politics is essential for women. Being half
the population, they should drive the policy making. Policies should be made
to protect women, her child, their health, her land, her house, her inheritance,
her environment.
What they need to keep out is manipulation on basis of caste, creed, religion,
race, region. Women can be inclusive and synthetic. Men have evolved to be
analytical. It will take another four generations if they have to come on par
with the woman.
So strength of conviction and flexibility of acceptance is what the empowered
man and woman of tomorrow’s India will be. And all this is going to be
delivered by the Aanganwadi sevika very very subtly.
Not a revolution… but a renaissance …an evolution…..
No wars .. no strikes .. no bunds.. no bus burning.. no tear gas.. no water hose.
What is the purpose of these self help groups?
They gather themselves together.
They save together
They are each other’s social support.
They conduct an enterprise together
What do the self help groups manufacture?
In Goa and Maharashtra , they manufacture food items. But unfortunately,
these are not really healthy items.
Helping them to shift from manufacturing unhealthy items to healthy items
while giving them a greater income is a challenge.
Some of the aaganwadi workers are themselves members of a SHG or have
family members who are in the group or some of the beneficiaries who form
part of a group.
So, we train an aaganwadi worker and she passes on the knowledge or
information to one member of a group.
Let us say we want to teach them a certain handicraft. The income generated
should be more than that obtained from making food stuff. And there should
be a ready market.
Making crochet, macramé and knit things in Goa finds a ready market in the
Tourism sector but the readymade business has usurped the local market.
Tourists from Gujarat carry take home souvenirs that were originally made in
Gujarat.
Coir and coconut which has huge potential has not been tapped by the SHGs in
Goa.
Promoting Folk Art:
We need to make products which are ethnic to a place. The emphasis should
be on quality and not mass production. When fewer numbers are made the
value of the product increases.
For example, the Portuguese left a legacy of delicate laces like the pillow lace
but due to lack of promotion, the art has disappeared. There may be hardly a
dozen lace makers in Goa today.
The European lace items had a classy feel about it. What we get in the market
now is machine -made Chinese replications which are one tenth the price of an
original handcrafted design. So, the art will soon die.
Instead of machines we should go more manual. We also get free exercise!

If food is what they want to manufacture, then idli -sambhar, chapattis etc. can
be promoted instead of fried stuff, seviyan instead of ready-made noodles.
Tourism: tourism is a double edged sword. It destroys more than it delivers.
Seeing through the artificialness of the import export racket:
The import- export racket is harming people’s health.
We are exporting food that is essential for our health only to decrease trade
deficit. We are importing third grade Chinese umbrellas to improve bilateral
trade.
As you can see, 90% of Indians do not have access to or really need this
imported stuff. If we could manufacture our computers and mobiles (which are
going to stay anyway), the rest of imported things are optional.
Let petrol become costly and unaffordable. Let cars be not sold and stop
fuming the environment with carcinogens. Light weight aluminium bikes are
good enough for Indians. We should learn from western mistakes.
Prof. Ramaswamy , the Cartman of India was promoting bullock carts. Since I
hate to hurt animals, I prefer the bikes …even solar driven bikes would do.
Let us run our public transport with biodiesel and our essential factories with
solar and wind energy. There are farmers in Maharashtra manufacturing bio-
diesel with a local oilseed.
All that is essential to life does not take much energy to manufacture nor does
it take imports.
And many of the things that are imported are superfluous to life and health.
To see this reality, I guess people will have to open their third eye.
They have to know that they will be coming back again on this planet.
The web of causation and the web of prevention:
Interactions between chronic disease and health care system
The interactions are very complex. If everyone reflects on the causative
factors even for a week, they are bond to make lasting changes.
risk factors
counselling
disease
screening
outcomes
rehabilitation
1.Synergy:
Several concurrent interventions generate larger gains than individual
interventions.
For example, diet, exercise and mind management in obesity
Cost effective measures to combat obesity in children:
Awareness through health information and communication about healthy food
and exercise… starting young
Reduce the cost of healthy food
Whole grain should cost significantly less than polished cereals
Fiscal measures that increase the price of unhealthy food content
Restrict the marketing of unhealthy foods to children
Regulation of food advertising to children is a more effective and efficient
measure than can school-based health promotion
2. Outcome expectation should be health and well being and not medical
care.
e.g.The hospital should be asked to not only measure how many diabetic
patients were treated but how many normalized their sugars
3. Measure years of healthy life and quality of life and not just life
expectancy
4. Health care spending
Three alternatives are possible
Spend less achieve more
Spend less and achieve as before
Spend more and achieve much more
The more we spend now the less we will spend for years to come.
‘A stitch in time prevents nine’
It is imperative to protect naïve populations.

CHAPTER 8
INTERVENTIONS
Broad Guidelines
Health Education
Evidence indicates that with education, social support, healthy policies and
environments, people can and will take charge of their health. Strategies are
needed to facilitate and support individual responsibility and behaviour change
at schools and workplaces and in other places where people are collectively
present as community and medical-based settings.
Health Policing:
To have a desirable outcome in health parameters, we need a stable political
context. At least the major policy decisions should not be changed for political
gains. It takes time for any policy change to take roots …even to think about
outcomes.
Although I have highlighted the economic benefits and the evidence for it, I
would like to clarify that economics should not be the reason for health
policies.
Economics should not define health but health and well being should define
economics.
Fairness of distribution of available resources and health outcomes among
different sectors should be considered.
For example, if the Land Acquisition Bill is going to undermine future food
security, health and well being, we need shift our focus from large scale
industries to small scale and home- based village industries.
Pre-independence era, everyone was clear about this concept but the same
has disappeared from society today.
Nothing coming out of top IIMs and Financial analysts theory has been able to
sustain the economy. Only traditional wisdom has stood ground.
This quick money business will starve people and cause social in terms of riots
and increased crime. Take a look at Europe and you will realize that even
peaceful populations become restless when insecure.
Legislation as a tool for behaviour change is not a very desirable measure
because it leaves or drives the underprivileged sector away from the delivery
of care when they need it the most.
I would consider empowering the masses, they desire a change and then
demand a legislation that facilitates that change.
For example,
People decide that they want to eat more ragi and get the PDS to supply it,
Government to incentivize the ragi farmers.
Everything should start with the people and end in Parliament and not vice
versa.
Shifting Policy: getting public health and prevention in general practice
The world over, prevention and health promotion is not what doctors like to
address. The pains are much more than the gains. Consequently, it is relegated
to a few activist doctors who choose to swim against the current.
At the DHS, prevention is handled mainly by ancillary workers while doctors
are busy with treatment.
Doctors do give attention to secondary prevention in the form of tablets plus
screening and immunization.
The key points in the community based prevention are
Behaviour change
Community engagement
Identifying and supporting those at risk of dying prematurely.
Emergent themes and concepts in promotive health:
• Clear leadership and chains of accountability
• Investment in training and development
• Use of information and intelligence for service development – learning
systems
• Partnerships and the concept of ‘connectedness’.

CHAPTER 9
HARD DECISIONS FOR THE COMMUNITY
A. General Population Interventions
1.Fiscal interventions/ Legislation and Regulation
There are some areas where fiscal interventions work.
E.g. Regulating Salt and trans fat (Dalda)
Advantages of Regulation
1. More equitable-poor and rich alike
2. Cost saving to health services plus work place attendance
3. Results are seen rapidly
2. Mass Media Campaigns:
e.g. breast feeding
Generate awareness- more effective
These are not found to be cost saving. Expenditure is more than costs saved
B. Targeting Groups or individuals
1. Community based or primary care led interventions for those at high risk
e.g.Intensive dietary counselling at primary care - Largest impact but very high
costs
For example- Group therapy in Obesity
Group motivation is strong in obesity but lacks continuity
Group intervention in elderly, pregnant women, preschool children have not
found to be effective.
A holistic program is needed to tackle obesity because the disease is very
complex.
Family therapy, cooking skills besides other measures are known to improve
outcomes.
(I have given more details in my book on obesity)
2. Effects of Social and Cultural factors
Example –physical activity
Three factors have repeatedly documented positive associations with physical
activity:
• Physician influence: I have already elaborated on this.
• Social support from friends/peers
• Social support from spouse/family
Negative associations:
• Cost of equipment or access to a gym does influence physical activity
(Many rich people don’t go the gym …..next door.)
• Weather does affect physical activity.. a chill does not allow us to get up
in the morning… forget about exercising……
• Mood- Depression and stress makes you exercise less when you need it
the most.
3. Motivation:
Motivating people requires
• Communication skills- right time, right message, right place
• Knowledge of expectations and cultural aspects
• Consider ethical strain – community versus individual
Goa Can Be A Role Model for Health Promotion:
There are different models of health. I prefer the holonomic model.
The holonomic model is similar to the eudaimonistic model of ancient Greeks
but minus the intangible elements like spirits and the addition of quantum
concepts in physics.
In the holonomic model, you consider the human being as having a body ,
mind , intellect and consciousness (which extends into the environment) as a
spectrum from gross to subtle with inter-convertibility which though not
apparent, invariably exists.
The radionuclide Carbon 12
from the environment does get settled in our cells,
like it or not.
Plus, every single chemical in which the human body comes in contact with is
capable of introducing an epigenetic change and may cause diabetes, cancer
etc.
Since Goa is a small state and many of the aanganwadi workers are computer
literate, we could start a program which could be immediately effective
without being burdensome.

If Rs 50,00,000 is transferred to the aanganwadi under the NP S scheme ,
in twenty years, we would see the trend reversing as in the ECD program.
Additionally, start with a one year total ban on Dalda etc. both at the
aaganwadi and open market.
A chronic disease tax on pure ghee or butter and on products containing
saturated fat. All pedas, burfis and pastries should be billed and tax. Give
subsidized whole wheat flour to the Bakers’ association .
Any products which has salt applied from outside should be taxed.
Locally manufactured parboiled rice as an option at the PDS; whole wheat
bread etc.
Just a few such measures as these will help shape the future.
Even if the Government announces the policy and is going to implement it next
year, the debate will start immediately. Remaining work can be done by the
aaganwadis.
Is the promotive program very difficult?
Not at all.
It is very easy for the Government machinery
Let us take the examples of progressive Goa, business-minded Gujarat, poor
rural Andhra threatened by the naxal movement , poor marginalized farmers
of Maharashtra and Karnataka as a group .
Each group has different needs and it is for the social scientists to collate
various requirements. We need people’s involvement. Right now, everyone is
feeling helpless.
“What can we do?”
If you are employed and earning well, you can choose and eat.
If you are on the margin of poor and middle-class you cannot afford healthy
food. But you have the power of thought to change things. It may not help now
but your children or grand children will get healthy food.


CHAPTER 10
FUNDING AND VOLUNTEERS:
There are few aspects of a Comprehensive Promotive Health Initiative:
Mainly, it requires funding and it requires volunteers.
Secondly, it has to be holistic, integrated and at grass-roots.
Who will deliver?
Whatever funds we may divert for aaganwadi training , 90% will get siphoned
into administration.
For example,
For a single days training, 50 workers will be included and it will cost the
administration minimum of Rs 50,000 in terms of direct and indirect costs.
We waste time and money right from fixing the program to conducting the
program and a lot of paperwork.
In Goa, training every aaganwadi for one day will cost 12,00,00 (1200x 1000).
And this expense is borne by the tax-payer.
The outcome of the training is measured as trainee satisfaction of the program
right from content delivered to quality of meal served. At some programs,
even a test is given. But this need not translate into desirable outcomes.
But in terms of community benefit what we need to find out is what impact
the training had after one year or five years.
What happens when the general community gets involved in the distribution
of public funds.

We will have volunteers ready to work on a one to one basis. I keep meeting
retired nurses, teachers, members of NGOs who are ready to share their
expertise.
I have not founded any NGO because I don’t want paper work but I keep
networking and a help people to give and take. Most of the work is either done
free or a very small remuneration to meet basic needs.
When people understand that everything comes from public funds and all
positive effort goes to general public welfare, we will get more volunteers.
The dictum is ‘Whatever goes around, comes back’
I add, ‘with interest’
Government Funds:
The only place where Government funding is required for the program is in
drawing up a pension fund for the aaganwadi workers.
In other areas , social , spiritual and religious organizations which are already
doing yeoman service to the nation can be included in the responsibility of
empowerment.
One advantage is that it will be delivered at the doorstep.
The effect of an Isha Yoga volunteer telling you that milk is not the best food is
different than when a Government official tells you.
When someone spends from his or pocket to come to your door-step to tell
you something which is good for you, you react with scepticism.
But the seed of doubt is sown in your sub-conscious mind.
Invariably, you try reading and finding out more on the topic.
Dropping a clue, creating interest, generating curiosity is the best way to make
change happen.
Celebrities can also help by endorsing health.

When we start seeing Aaganwadi workers on Lok Sabha TV and Rajya Sabha
TV discussing problems and solutions, more people will listen.
Third hand information by board room panelists gets muffled in the noise of
cultivated consumerism.
The following organizations in my opinion are doing very good work in the field
of holistic health and there are many more. Others are catering to spiritual
health and may be requested to help in holistic health. They have the finances
and they have volunteers. People are ready to donate to these organizations
because of their credibility.
Each State has at least one prominent organization. If we do a collective effort,
it will take less than two years to get the message across.
Isha yoga
SSY
AOL
Oneness University
Shirdi Saibaba
Satya Saibaba
Tirupati Devasthan
Tej Guru foundation
Lal Baag Ganapati
Siddhivinayak temple
Roman Catholic Church
Syrian Christian Church
Ajmer Darga
Akshardham Temple
Divya Yoga Trust
Retired nurses, school teachers, Government servants etc.
But we will have to inform the doctors first.
For example,
Recently, I heard an obstetrician, a panelist on the RCH program on TV say that
milk is one of the best sources of calcium.
It is obvious that she has not really looked at the charts. I can’t blame her
because nutrition is considered a ‘side’ topic in medical college. If I had not
studied nutrition, I would have also repeated such outdated information that I
was taught 20 years back.
CHAPTER 11
SUMMARY:
What are the health messages they will be giving and reinforcing?
• Breast Feeding
• Immunization for all
• Maternal Nutrition
• Nutrition of the adolescent girl child
• Increasing consumption of fruits and vegetables- seasonal and local.
• Plenty of water
• Increasing consumption of high fiber ,unpolished ,traditionally cultivated
cereals
• Limited intake of salted foods ,saturated fat & limited unsaturated fat
and sugar sweetened drinks
• Eradication of TFAs in the form of hydrogenated vegetable fats or
partially hydrogenated vegetable fats generally called Dalda which
essentially would translate as ‘ As far as possible do not eat food fried
outside the home’
• Consider milk as an ‘emergency food’ and not as an essential part of
nutrition.
• Eat calcium rich foods like ragi instead.
• Shift from floriculture to horticulture
• Kitchen or balcony gardens
• Take enough of healthy exercise
• Gender Equality
• Social inclusiveness
• Healthy inner child
• Developing self esteem and a resilient mind in the child.
• Improving the power of concentration and discrimination(viveka)
• Instilling assertive capabilities in the child
• Subliminal learning through positive associations.NLP training.
• Balancing right and left brain functions
• Helping children find their soul agenda.
Exercise:
Children will participate in physical activity only if they enjoy it or they get
some tangible benefits in the present.
You can’t tell them that it will save them from heart disease in the future.
Coco Drinks:
Eliminate sugar sweetened coco drinks even if they contain vitamin D calcium
or proteins. They are specifically not NEEDED and can prove to be harmful
They should be made prescription food additives and the doctor prescribing
them should come under consumer act if in future the patient is harmed.
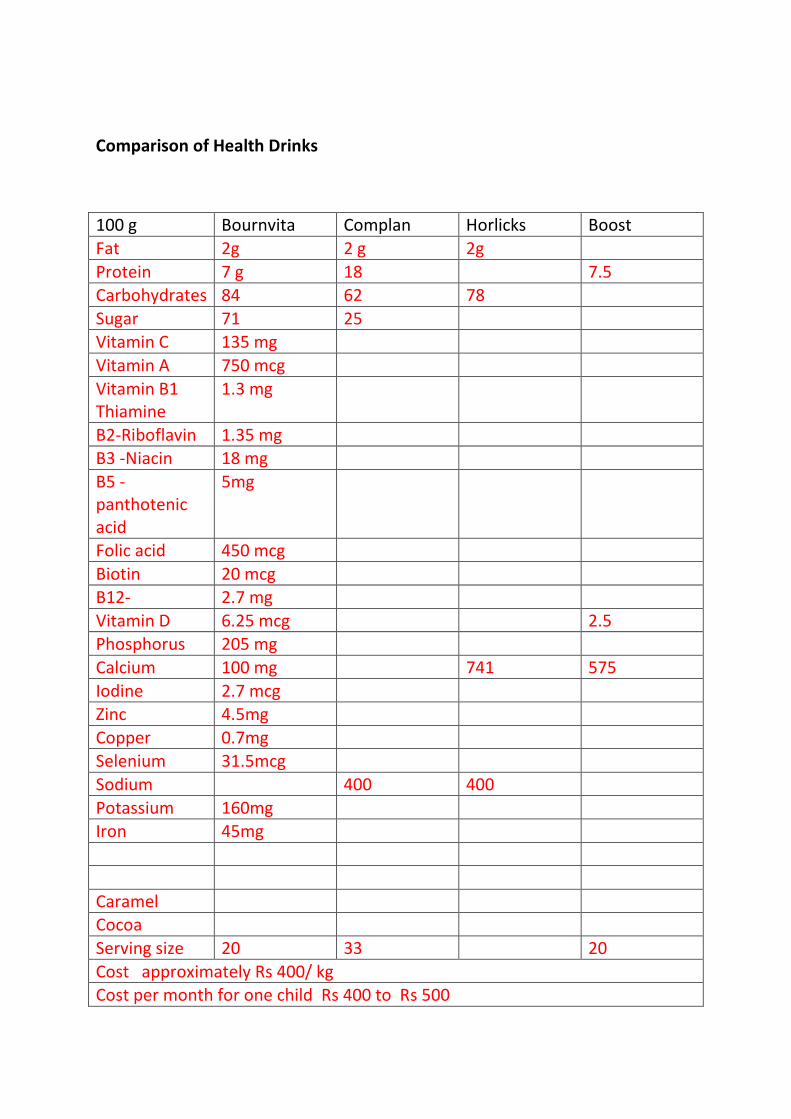
Comparison of Health Drinks
100 g Bournvita Complan Horlicks Boost
Fat 2g 2 g 2g
Protein 7 g 18 7.5
Carbohydrates 84 62 78
Sugar 71 25
Vitamin C 135 mg
Vitamin A 750 mcg
Vitamin B1
Thiamine
1.3 mg
B2-Riboflavin 1.35 mg
B3 -Niacin 18 mg
B5 -
panthotenic
acid
5mg
Folic acid 450 mcg
Biotin 20 mcg
B12- 2.7 mg
Vitamin D 6.25 mcg 2.5
Phosphorus 205 mg
Calcium 100 mg 741 575
Iodine 2.7 mcg
Zinc 4.5mg
Copper 0.7mg
Selenium 31.5mcg
Sodium 400 400
Potassium 160mg
Iron 45mg
Caramel
Cocoa
Serving size 20 33 20
Cost approximately Rs 400/ kg
Cost per month for one child Rs 400 to Rs 500
This is a partial list. Every pack has a different combination. Some have RDA
numbers too.
What we need to consider is whether
1. All the needed micronutrients are supplied?
2. Is the quantity optimum?
3. Is anything there which can cause harm?
4. Who is monitoring the contents?
5. Is a Federal Health Agency like USDA who will take responsibility?
Not just to recommend but to say sorry if they have given a wrong
recommendation.
6.Is there a Government body whom the common people can approach?
7. Who is clearing the advertisements? Is there a certified nutritionist on the
panel?
And lastly
8. How many can afford nutritional supplements?
Could we replace these with a sprouted ragi- white maize-malt? Or a porridge?
To illustrate…..
Too much artificial vitamin D intake can cause harm.
It is much more important to have alkaline ash foods that load with calcium
and vitamin D to build and maintain strong bones. I have addressed this in
detail in my book, “A to Z FAQs on Health and Wellbeing”.

Compare this with ragi or semolina used in porridge and roasted gram.
100g Ragi Semolina Gram roasted
Carbohydrates 72 74.8 58.1
Free Sugars - - -
Protein 7.3 10.4 22.5
Fats 1.3 0.8 5.2
Vitamin D
Calcium 344 16 58
Iron 3.9 1.6 9.5
Sodium 11 21
Cost per 100g Rs 2/- Rs 4/- Rs 10/-
Natural foods may lack vitamin D but it can be manufactured with the help of
Sunlight.
It is stored in the body .So don’t worry if you don’t see the Sun every day.
Natural foods have no free sugars, so cause less harm. They have low sodium
so less risk of hypertension.
If we use food intelligently we don’t need supplements. They can be totally
eliminated from the market in future. But if someone wishes to have them in
spite of knowing the truth, it is a personal choice.
Taking 100g of the above everyday is easily possible for a middle class family.
The BPL families will get the required amount of cereal through PDS.
We need to somehow increase the protein content of diet in some parts of
India, where there is more of protein deficiency. Sprouting of ragi increases the
protein quality.
So far, the medical people have been directing the nutrition in our country in
top down approach and we have failed miserably. We are in places worse than
other countries with poor GDP.
It is time to hand over charge to the people.…..Empower, empower, empower.

And learn from people……..
First things first
Implement the proven interventions first. Learn from the success and failures
of other countries.
In India, we have neither the inclination nor the infrastructure to carry out
such studies. Even if we focus on two areas heart disease and low birth weight
we will see results.
We have rules for occupational health and road traffic accidents in place but
they are broken because the perpetrators get away scot-free.
Imagine, a film star running over a pedestrian and goes free in public and the
most disgusting fact is that people watch his films. The person who lost his life
is a non –entity so no one cares. Next time, it could be your son. We are
become so numb to a poor mother’s pain.
Think! How she would be feeling when that celebrity’s poster is flashed all over
or when ladies throng to fall all over him.
Do we really have a soul or are worshipping the lowest gods, money and fame?
First aid classes and Cost-effectiveness:
Every school child today learns first aid but in emergency cannot do much
whereas in the village even uneducated people know through experience or
intuitively what to do.
The first aid course is not cost effective and funds could be used for some
better purpose. For years, things will be followed without testing cost
effectiveness.
A lady assisted me in giving CPR to her husband having had watched it on TV.
She gave the CPR while I gave the cardiac massage. The person survived.
So, more TV programs would help.
APPENDIX
RECIPES:
Here are a few recipes to supplement what I have written in the text. You will
find more recipes in my book on Diabetes. Hopefully, I will get the time to
write a full-fledged recipe book in future.
Ketchup:
1 kg tomato pulp
Tie in a muslin bag: 2 medium onions chopped, garlic 4-5 pods,
5g of lavang , velchi, tikhi, jeera
3 g/1tsp red chillie powder
½ tsp black pepper, 3tsp salt, sugar 100g, vinegar-50 ml
Moong Chaat:
Sprouted moong + kulith - steam slightly
Add chopped onions, tomatoes, coriander leaves
Salt, chaat masala, lime, red chillie powder
Baked Cauliflower Leaves
In Goa, cauliflower leaves are usually thrown away. They are rich in calcium.
4- 5 cauliflower leaves
Toss in oil the following
Small onion
Garlic pods 2-3
Salt, pepper
Add leaves- bake 10 minutes
Idli –Sambhar:
In Karnataka, morning starts with idli -chatni and in Tamilnadu they say good
morning with idli-sambhar. I have met people who have had idli- sambhar
almost every morning for 40-50 years and they are never tired of it.
You get readymade idli batter to help the working woman. And king- size plate
idlis save time and LPG.
If the SHGs could supply idli batter and sambhar powder to the working
woman, both will benefit and so will the children’s nutrition.
I have collected many recipes of sambhar and idli. I will give my favourite.
Fluffy Idlis:
1 serving=3 idlis= 1 cereal exchange and 1/2 protein exchange
Rice, parboiled, 100 g -345 Calories
Urad dal/black gram dal, 50 g- 175 Calories
Fenugreek seeds, 1 tsp /5g
Salt to taste, 2 g
In emergency situations replace rice with idli rawa (rawa/dal=3:1 by volume).
Method:
Clean wash and soak , dal and rice separately in two cups water for 4 hours.
Add fenugreek to the rice.
Grind rice coarsely with 1/4 cup water and grind dal very fine with 1/2 cup
water. Mix the two, keep overnight/12 hours to ferment. Add salt and mix
thoroughly till froth appears.
Grease idli moulds with a little oil. Add batter. Steam the idlis in the idli cooker
for 10 minutes.
Makes 10 idlis of medium size.
Total calories:520
Calories per idli is @ 52 Calories.
Sambar:
1 protein exchange, 1 vegetable exchange, 1/2 fat exchange.
Toovar dal, 30 g- 100 Calories
Potato small, 25 g- 25 Cal
Small onion, 50 g- 25 Cal
Coconut 10 g, roasted- 44 Cal
Oil,1 tsp- 45 Cal
Vegetables:
Small tomato- 25 g
Drumstick -1/2
Lady finger -2
Spices:
Cumin seeds -1/4 tsp
Coriander seeds ¼ tsp
Pinch turmeric
1 red chillie
Pinch of hing,
Pinch of fenugreek
Chana dal 1/4 tsp; Black gram/urad dal 1/4 tsp- roast
Tempering: curry leaves 5, shallot 1, mustard seeds, 1/4 tsp.
Seasoning with tamarind paste-20 g.
Method:
Wash and soak dal. Boil to 3 whistles with a green chillie, hing and turmeric.
Mash.
Boil onion, potato, tomatoes and drumstick.
Roast all spices with little oil and coconut. Grind to a paste.
Heat the oil. Add mustard seeds, one shallot and curry leaves for tempering.
Add dal and ground masala. Add salt. Served with idlis.
Makes 2 katories, serving per katorie 70 Calories.
All vegetables taken together will make less than 20 calories, hence we can
ignore their calorie count.
Quick Method:
Wash and soak toovar dal for an hour. If you can get use unpolished,
uncoloured dal. Add little hing and haldi powder. Cook the dal and the
vegetables in different vessels but at the same go for 3 whistles.
Add tamarind juice, chiliie powder and salt. Temper w curry leaves and
mustard in a little oil. Add to sambhar. Add homemade sambhar powder.
Garnish with coriander. Varying the vegetables and seasoning will alter the
taste.
It takes around forty five minutes in the morning to prepare idli – sambhar and
tea. And while you eat your breakfast put your rice to boil. So, in 90 minutes
meals are ready for four people.
It is faster than other breakfast options. My friends had timed preparation
time. So, the alarm would be set as per breakfast options.
Ragi Mudde:
Is usually had with sambhar.
Tomato Thokku:
Can be had with chapatti, bread, rice or dosa. Onions and tomatoes are rich in
anti oxidants.
Dice equal number of onions and tomatoes.
Fry onion and tomatoes in minimum oil.
For 2onions and 2 medium tomatoes,
I pinch haldi powder, half teaspoon red chillie powder, salt to taste
Pinch of sugar. Add water, close and cook.
Temper with mustard seeds (sarson,rayee, sansvaa) and curry leaves.
FIRST AID
Herbs:
There are a few herbs which I ask all people to grow in their garden or balcony.
These were herbs that were traditionally grown in Goa.
Aloe Vera:
Aloe Vera is useful in any inflammation or skin lesions.
It works wonders when applied externally in arthritis
It is an immune modulator in cancer and an anti-ageing herb.
Aloe Vera can be eaten as vegetable.
Tulsi
Is a great immune booster in viral colds and fevers.
Ginger:
Used in cold and fever
Brahmi
Is a memory enhancer
Turmeric:
It is useful in common cold, sore throat, and is anti cancer
Punarnava:
Is a liver tonic . The leaves can be eaten as a vegetable and cause an increase in
urine.
Other first aid measures:
Diarrhoea:
Rice water in copious diarrhoea used in Bangladesh.
Burnt toast in black tea
Pomegranate and apple
Pomegranate rind in abdominal colic
Worms:
The small fresh shoots of guava decrease worms.
There are many good books on herbs.
The DHS or AYUSH could compile a list of healthy herbs and give it to the
aaganwadi workers on line at almost no cost.
Indigenous Knowledge:
Preserving indigenous knowledge is important. For example, in the Rural
Health Centre of St John’s medical college there is a stone called the Sadhu
stone or anti venom stone. At least it was there till 1996. My colleagues
informed me that that two stones were gifted by a visiting sadhu and one was
stolen.
My interns used the stone to neutralize snake venom in snake bites.
At that time, I was a die-hard rationalist with an over-inflated ego. Anything
not in my books was false. I had each and every study on snakebite
photocopied from the journals to prove that no one had used stones costing
me almost a few thousands. My senior colleagues were balanced in their
opinions and my interns were almost emotional about the stone.
Every time they mentioned the stone, I would react, “Superstition” and the
poor little ones would almost plead with me, “No Ma’am it really works”
Now, having studied atomic physics, I have a clue of how it could work.
I wish I wasn’t so adamant. I might even got an international research grant for
testing the stone.

Peruchi Fod (पे�चीपे�चीपे�चीपे�ची फोडफोडफोडफोड):
This a Marathi story about sharing. A mother of three children has three
guavas .She cuts each guava into four and gives them to the children. The
eldest realizes that the mother has not kept anything for herself gives two
pieces out of her four (50-50) to the mother.
“मा�या दोन फोडी त ूघे”
Very important to note the altruism. For her, equality is at individual level.
“मा�याह� दोन फोडी तू घे”
The other two children imitate her. Again note the role modelling.
If you change the eldest, the others will follow.
Now, the mother has six pieces…and the children only two.
So, she gives one piece each and they all have three each ending the arithmetic
lesson.
4x 3=12
3x4=12
Apply this fractal to society in general. The effects are just mind blowing.
The next message
Love, sharing…….guava , fruit
‘Guava means love’
‘Guava is tasty’
Next, the NLP message, the story was followed by some rhyme that the
children chanted in class and every time they ate guavas.
Peruchi fod, laagté god
पे�ची फोड,लागत ेगोड
Neem Pesticide:
For kitchen garden and nursery. It requires 80kg leaves per hectare which is
not suited for large scale agriculture. Azadirachtin is the active principle.
5 litres water, 1kg green neem leaves. Spray in late evenings or early morning
once in ten days and alternate days in rainy season. Neem can be used to
protect stored grains.
I used to take a brush and paint the under surface of leaves with the extract.
The waste can be used as green fertilizer.
GLOSSARY:
DALY –DISABILITY ADJUSTED LIFE YEARS
IT- Information Technology
GM-Genetically Modified
SRI- systemic Rice Intensification
CSR- Corporate Social Responsibility
NGO- non Government Organization
ECD -Early Childhood Development
RO -Reverse Osmosis
DHA –Docosa Hexanoic Acid
EPA- Environmental Protection Act
CIKS- Centre For Indigenous Knowledge Systems
SHG- Self Help Groups
Juliennes: small longitudinal strips of a vegetable
Sada: dry land
Dodka:Ridged gourd
Arbi, aalu:Colocasia colocasia antiquorum
References:
Tagore’s poem, ‘Where the head is held high’
Ascherio A, Katan MB, Zock PL, Stampfer MJ, Willett WC. “Trans fatty acids and
coronary heart disease”. N Engl J Med 1999; 340 :1994-1998.
Coronary Artery Disease in Indians – A global perspective, Cardiology society of
India, 1998, edited By Dr Kamal K Sethi.
Dr Satwant Pasricha, “Claims of Reincarnation: An Empirical study of Cases in
India”, Harman Publication House, 1990.
Dr Walter Semkiv, “ Born Again- Reincarnation cases involving Celebrities,
India’s political legends and Film Stars”, Ritana Books,2007.
Dr Brian Weiss, “Many Lives, Many Masters”, Piatkus Publication,1988 and
other books
Dr Bruce Goldberg, “Soul Healing”, Pustak Mahal, 1997 and other books.
Vialatte F.B et al, “EEG paroxysmal gamma waves during Bhramari Pranayama:
A yoga breathing technique” 2008 . Available online at www.sciencedirect.com
About the Author
Dr Kunda Silimkhan, M.D. started her career in Internal Medicine and worked
in various medical colleges both in the urban and rural environment. She also
worked in a public sector undertaking.
During her practice, she was able to meet people in their community setting
and understand the various factors which led to disease and healing.
She now intends taking the message to the larger community through her
many books.
Book by the Author:
My Little book of Understanding and Overcoming Stress
Other e-books by the same author:
FAQs on Health & Well-being with their Honest Answers, Part 1
Reversing Diabetes -The Diabetes Educator’s Training Manual
Obesity Work book - A step by step manual to help you lose weight holistically
Flex your Spiritual Muscle - Concepts in Metaphysical Fitness
How I Healed Myself -My Journey through Asthma
Demystifying the Chakras -An Easy guide to Self- healing
The Mysterious Science of Dowsing
Know my Secret - Study less, Score more
Reflections on the Bhagwad Geeta - Musings of a Scientific Mind
Goodbye Anger
The Doctor’s Theory of Everything - An Insight into Self-healing
Understanding Past Lives
Holonomic Therapy- The Future of Healing