
An Official Publication of Indian Dental Association, Ludhiana ...
411
Vol. 1 Issue 11 L.E.D. E-Journal Page 1 L.E.D. E-Journal IDA Ludhiana Branch
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of An Official Publication of Indian Dental Association, Ludhiana ...

Vol. 1 Issue 11 L.E.D. E-Journal Page 1
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

L.E.D. E-Journal November 2016 Vol. 1 Issue 11
Contents Index
S. No.
Title Details Page No. From–To
1. Introduction Welcome 5 – 8 Basic Info & Contact Us
5 – 7
Mission & Vision 8 2. Insight into the Journal Information 9 3. Advisory & Editorial Board The Stalwarts 10 – 11 4. Feedback Suggestions 12 5. From the Editor’s Desk Dr. Bhavdeep
Singh Ahuja 13 – 22
6. CBCT in Endodontics – Aboon for effective treatment
and cure
Dr. Edwin Roberto Hernandez Molina
24 – 40
7. Sialolithiasis of Submandibular Gland duct
– A Rare Case Report
Dr. S.P.S. Sodhi, Dr. Gursimrat Kaur Brar & Dr. Dikshit
Behal
42 – 52
8. Power Scaling – Boon orBane – Part III
Dr. Ajay Kakar 54 – 60
9. Early Infancy Teeth – ACase Report
Dr. Parajeeta Dikshit & Dr.
Senchhema Limbu
62 – 69
10. Ridge Split Technique andBone Expansion Osteotomy
– For SuccessfulRehabilitation
Dr. Abhijeet Bhasin
71 – 82
11. Photodontics – Part XIIntroduction to the World
of Lenses – An Enigma or a Reality
Dr. Mayur Davda 84 – 94
12. Infections resulting fromBone Graft Materials – A
Review
Dr. Rita Singh, Dr. Lanka Mahesh &
Dr. Sagrika Shukla
96 – 106
13. Efficacy of 980nm DiodeLaser as an adjunct to
Stannous Fluoride in the management of Dentinal
Hypersensitivity – A controlled prospective
clinical study
Dr. Rajeev Ranjan 108 – 120
14. Radix Entomolaris inPermanent Mandibular
First Molar – An Endodontic Challenge – A
Dr. Meenu Bhola, Dr. Geetika Jindal & Dr. Aashana Goel
122 – 129
Vol. 1 Issue 11 L.E.D. E-Journal Page 2
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bran
ch
Case Report 15. Nanodentistry – A Novel
Approach Dr. Parminder
Singh Grover & Dr. Supreet Kapoor
131 – 135
16. Managing Better – An Art and a Science – Part XI
Dr. Bhavdeep Singh Ahuja
137 – 142
17. Feedback Prize Winning 144 18. Manuscripts Invited For Publishing 147 19. Appendices E-Journal 148 – 411
Author Guidelines For Publishing 150 – 154 DCI - Revised Code of
Ethics Dental Council of
India 155 – 165
DCI – Right to Information - Handbook
Dental Council of India
166 – 191
DCI – Establishment Scheme for Opening of New
Dental Colleges
Dental Council of India
192 – 196
WHO Guidelines on Dengue & Chikungunya
World Health Organization
197 – 227
Dental Trauma Guidelines – Revised
International Association of
Dental Traumatology
228 – 254
Revised Bio Medical Waste Management Rules 2016
Govt. of India Gazette Notification
255 – 292
Introduction and Guidelines for Starting a Diagnostic Installation
AERB - Atomic Energy Regulatory
Board
293 – 296
Revised Guidelines for obtaining Regulatory
Consents for Diagnostic Equipment
AERB - Atomic Energy Regulatory
Board
297 – 299
Guidelines for shielding of X-ray Installations
AERB - Atomic Energy Regulatory
Board
300 – 303
Guidelines for applying for License Diagnostic
Radiology Equipment
AERB - Atomic Energy Regulatory
Board
304 – 329
Checklist for submission of application form for
registration
AERB - Atomic Energy Regulatory
Board
330 – 335
National Treatment Guidelines for
Antimicrobial Use
Antibiotics in Infectious Diseases
336 – 399
Registration and Import of Medical Devices in India –
Frequently Asked Questions
Central Drugs Standard Control
Organization
400 – 411
Vol. 1 Issue 11 L.E.D. E-Journal Page 3
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
Happy GURPURAB
Vol. 1 Issue 11 L.E.D. E-Journal Page 4
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
Vol. 1 Issue 11 L.E.D. E-Journal Page 5
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

L.E.D. E–Journal
Let’s Enjoy Dentistry, Ludhiana
The August Voice of Dentiana L.E.D. E–Journal is the Official Monthly Publication of IDA (Indian Dental Association) Ludhiana Branch, launched w.e.f. 1st January, 2016. L.E.D. stands for Let’s Enjoy Dentistry. The name has no direct reference to any individual, corporate, society etc. and is just a means to inform and enlighten about the visual dentistry amongst dental professionals & in particular, the IDA Members through this medium. The contents in the ‘L.E.D. E–Journal’ is for information purposes only. It is the users’ discretion to follow the path & procedures enlisted within, blindly or under proper guidance or using their own wit & judgment and IDA Ludhiana holds no responsibility for the same. ‘L.E.D. E–Journal’ is the August Voice of Dentiana, where the word ‘Dentiana’ is a short combined word for Dental (Dentists of) + Ludhiana. The Name ‘L.E.D. E–Journal’, ‘Dentiana’ and the Logo are copyrighted properties of IDA (Indian Dental Association) Ludhiana Branch. The contents remain the property of the copyright owner & all rights are reserved. Any misuse of the name & logo for any purpose and without valid permissions from the Editor, Publisher or IDA Ludhiana Branch shall make the user at risk of violation under copyright laws. Published & Printed by: Dr. Bhavdeep Singh Ahuja on
behalf of IDA Ludhiana Branch
Owned by: IDA Ludhiana Branch
IDA Ludhiana Email: [email protected]
IDA Ludhiana Websites & Mirror Links: www.idaludhiana.org, www.idaludhiana.com, www.ludhianaida.com
Editor-in-Chief: Dr. Bhavdeep Singh Ahuja
Editorial Office: Dr. Bhavdeep Singh Ahuja, c/o Dr. Ahuja’s Dentech Smiles Dental Clinic & Implant Centre, # 363-B, B.R.S. Nagar, Main Road, Ludhiana – 141 012 Punjab INDIA Tel: +91 161 5099 039 Mobile: + 91 98761 93039 Website: www.drbhavdeep.com (E-Journal available here also) Email: [email protected]
Vol. 1 Issue 11 L.E.D. E-Journal Page 6
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Templates Design: Nishtha Computers, Satya Printing, Creative Publishing, Raju Cyber Print & Gagan Printing. Templates Final Binding & Design: Creative Publishing House & Raju Cyber Print. Cover Page Design: Big Ideas Inc. Cover Page Conceptualized, Designed & Compiled by: Dr. Bhavdeep Singh Ahuja Creative Framework & Lay out: Dr. Bhavdeep Singh Ahuja, Dr. Navjot Singh Khurana & Dr. Manjot Singh
Copyright©2016 by IDA Ludhiana All rights reserved. No part of this publication may be reposted, reproduced, reprinted, transmitted or otherwise used in any form or by any means, electronic or mechanical, without the express written permission from the Editor/Publisher. The opinions expressed in the articles and advertisements are those of the authors/companies/ dealers and don’t necessarily reflect those of the Editor or Publisher or the Members of the Editorial or Advisory Board of L.E.D. E–Journal. IDA Ludhiana makes every effort to report clinical information and manufacturer’s product news accurately but cannot assume responsibility for the validity of product claims or for typographical errors. The publisher also does not assume responsibility for product names, claims or statements made by advertisers. The views & opinions expressed by authors/companies/dealers published in L.E.D. E–Journal are their own and do not necessarily reflect the policy or position of the Editor or Publisher or the Members of the Editorial or Advisory Board of L.E.D. E–Journal. This E-Journal is sent free of charge to IDA Ludhiana Branch Members via their email and for others; it is available for free download from www.idaludhiana.org, www.idaludhiana.com & from the Editor’s personal website www.drbhavdeep.com (as a tribute to IDA Ludhiana Branch). Acknowledgments The Gyaan snippets & Images have been copied from www.ida.org.in in the L.E.D. E–Journal by IDA Ludhiana, being a small tributary of the big river, the IDA Head Office with the sole aim of creating awareness of IDA Head office activities through an entertaining mode. P.S. It is essential to read this E–Journal under a screen resolution of 1600 x 1200 dpi or more, and preferably on a 17" or bigger monitor (as it contains several tables and high resolution graphics). If the resolution is less than this, you may see broken or overlapping tables/graphics, graphics overlying text or other anomalies. It is strongly advised to switch over to this resolution to read this E–Journal. These pages are viewed best in Internet Explorer 8 and above, Google Chrome etc. The IDA Ludhiana website has been constructed and maintained by IDA Ludhiana Branch. You may want to give me the feedback to make this E–Journal better. Please be kind enough to write your comments/feedback/ suggestions & email it to the Editor, Dr. Bhavdeep S. Ahuja through [email protected]. These feedbacks would help us grow further & become better.
Vol. 1 Issue 11 L.E.D. E-Journal Page 7
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

About L.E.D.: L.E.D. Journal, a multi-specialty & peer reviewed journal coming out every month Online, free & Print on demand and is a compilation of articles, case reports, research reviews etc. published to provide a platform for the presentation and criticism of interesting, innovative and thought provoking ideas in dentistry. L.E.D. Journal is open to publish new, challenging and radical ideas, along with re-publishing of any old but contemporary ideas as long as they are logical, rational, coherent and reasonably expressed. The re-publishing of the old cases would be however, done with the prior permission & consent of the Author & the Publisher and with proper acknowledgment to both in the contribution itself. The main idea behind publishing not only new but old & interesting cases is that India is a diverse country with varied cultural & geographical distributions. Just to quote an example here, that many a times, an interesting case report or a dynamic study presented in Kerala (South) in a Print Journal might not have its far spread reach in Punjab (North). We would like to keep the number of articles around to 10-12 per issue. We would also like L.E.D. Journal to be a medium for discussing varied issues like ethics in dentistry, Informed consent, Medico-Legal issues in Dentistry etc. as well. It is also indented to present this as a form suitable to the general practitioner. The journal’s full text will be available online free at http://www.idaludhiana.org, http://www.idaludhiana.com & on the Editor’s personal website http://www.drbhavdeep.com. The E-Journal allows free access (Open Access) to its contents. The Print Version of L.E.D. Journal, however, would be available on demand for the Authors at a nominal payment. Submitted papers must be in technical English, suitable for scientific publication. All articles submitted will be passed on to the Members of the Editorial Board and will be peer reviewed by them. Receipt of the manuscript will be acknowledged by email. Every effort will be made to complete the review process within 2-4 weeks and communicated to the corresponding author. The Editorial board will strive for the quality and also will try for indexing the journal in various indexing bodies and if successful, the information will be updated on the IDA Ludhiana website from time to time. We welcome all of you and we hope you will consider L.E.D. Journal for your next submission. Papers should be submitted to the Editor, Dr. Bhavdeep Singh Ahuja @ [email protected].
Mission & Vision: The Mission of L.E.D. Journal is to serve as a platform for stimulating, guiding, motivating & support young upcoming dentists to rub shoulder to shoulder with senior professional colleagues & thereby find a footing for themselves in hard working, yet a lot competitive dental world. We wish to promote research & developmental activities in the world of Dentistry manifold. We also intend to increase the scientific contribution & promote development of Dentistry in Punjab especially Ludhiana. through increased exchange of knowledge & ideas. L.E.D. Journal will strive to be a high quality medium which aims to increase the understanding of new upcoming dental technologies & revolutions every month, thus with the overall goal of improving dentistry standards in Punjab especially Ludhiana.
Vol. 1 Issue 11 L.E.D. E-Journal Page 8
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Insight into L.E.D. E–Journal Dear Fellow IDA Members,
Here is an insight into the basic format for the L.E.D. E–Journal: 1. The E–Journal is in a safe, secure & encrypted PDF format & all
the E–Journal download website links (from IDA Ludhiana and the
Editor-in-Chief) are compatible with all the digital devices viz.
Desktop, Laptop, Tablets, All Cell Phones (with internet) & i-Phones
as well. The encrypted format is to ensure against plagiarism.
2. The E–Journal content has been watermarked and guarded against
printing so as the authors can feel safe whilst publishing with us.
However, Authors can request the Editor-in-Chief for a printable
copy for their record, inspection or any other purposes.
3. The print version of the E–Journal would be available on request
and payment (even for authors).
4. The size lay out of the E–Journal is around 11" by 20" (A normal
A4 paper is 8" by 11") with body text size 20 and font Bookman Old
Style with 1.5 line spacing in the text. The body text is justified.
For headings, the body text size is 22 (in Red/Orange Colour).
5. The colour of the body text in the E–Journal is Plum & for
headings, images, bullets and numbering, it is Red/Orange/Pink.
For headings & images, body text with ‘Bold’ has been used.
6. The E–Journal will be available on the IDA Ludhiana Websites &
Mirror Links and also on the Editor-in-Chief’s personal website
(www.drbhavdeep.com) and across all the member emails (if
provided and on request). So, if you still haven't updated your
email id with Hon. Secretary/Hon. Treasurer, please do so at the
earliest.
7. It will be a monthly outing and would release around the first week
of every month.
8. Each issue will have around 11 articles - 8 by the crème de la
crème (best of the best) of the dentistry (National Authors from
India) which includes some of the top notch speakers and 3 from
the members of IDA Ludhiana Branch.
9. There will be some special issues in the calendar year (approx. 2-
3), in which the volume of scientific content would be huge & rich.
10. A few of the best known names are writing a series of articles as
well for the E-Journal.
11. The E-Journal will be available standalone as well as
coupled/combined with the E–Newsletter, Page 3 OLA D.
Vol. 1 Issue 11 L.E.D. E-Journal Page 9
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Editorial Board Editor-in-Chief: Dr. Bhavdeep Singh Ahuja Associate Editors:
1. Dr. Navjot Singh Khurana (Conservative Dentistry & Endodontics) 2. Dr. Harsimran Singh Sethi (Pedodontics & Preventive Dentistry)
Editorial Board:
1. Dr. A. Kumarswamy (Periodontics & Implants) 2. Dr. Adwait Aphale (Dental Photography) 3. Dr. Ajay Chhabra (Conservative Dentistry & Endodontics) 4. Dr. Ajay Kakar (Periodontics & Implants) 5. Dr. Gautam Madan (Oral Surgery & Implants) 6. Dr. Kanwal Bir Singh Kuckreja (Prosthodontics & Implants) 7. Dr. Komal Khatri Majumdar (Implant Dentistry) 8. Dr. Lanka Mahesh (Implant Dentistry) 9. Dr. Navdeep Saini (Conservative Dentistry & Endodontics)
10. Dr. Neeru Singh (Pedodontics & Preventive Dentistry) 11. Dr. Rajan Jairath (Orthodontics) 12. Dr. Sameer Kaura (Oral Surgery & Implants) 13. Dr. Sanghmittra Dasgupta (Oral Surgery & Implants) 14. Dr. Sumeet Rajpal (Pedodontics & Preventive Dentistry) 15. Dr. Surinder Pal Singh Sodhi (Oral Surgery & Implants) 16. Dr. Vijay Deshmukh (Oral & Maxillofacial Surgery) 17. Dr. Vivek Saggar (Pedodontics & Preventive Dentistry)
Advisory Board:
1. Principal, Christian Dental College, Dr. Abi M. Thomas 2. Principal, Baba Jaswant Singh Dental College, Dr.
D.S.Kalsi 3. Principal, Sardar Kartar Singh Sarabha Dental College, Dr.
Rajesh Bhanot 4. President, IDA Ludhiana Branch, Dr. Tarun Kumar 5. Hon. Secretary, IDA Ludhiana Branch, Dr. Rajan Bir Singh
Thind 6. Hon. Treasurer, IDA Ludhiana Branch, Dr. Abhijit Kathpal 7. Immediate Past President, IDA Ludhiana Branch, Dr.
Jaidev Singh Dhillon 8. President-Elect, IDA Ludhiana Branch, Dr. Vandana
Chhabra 9. Dental Council Member from Punjab, Dr. Vikas Jindal
10. President, IDA Punjab State Branch, Dr. Pankaj Shiv 11. Hon. Secretary, IDA Punjab State Branch, Dr. Sachin Dev
Mehta 12. Dr. Puneet Girdhar - Past President, IDA Punjab State, &
Past Vice President IDA Head Office
Vol. 1 Issue 11 L.E.D. E-Journal Page 10
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Editorial & Advisory Board, L.E.D. E-Journal – The Selected 32 Gems & Pearls
Editor-in-Chief, L.E.D. Associate Editor 1, L.E.D. Associate Editor 2, L.E.D. Dr. A. Kumarswamy
Dr. Bhavdeep Singh Ahuja Dr. Navjot Singh Khurana Dr. Harsimran Singh Sethi Periodontics & Implants [email protected]
98761 93039 Conservative Dentistry &
Endodontics Pedodontics & Preventive
Dentistry Editorial Board
Dr. Adwait Aphale Dr. Ajay Chhabra Dr. Ajay Kakar Dr. Gautam Madan
Dental Photography Conservative Dentistry & Endodontics
Periodontics & Implants Oral Surgery & Implants
Editorial Board Editorial Board Editorial Board Editorial Board
Dr. Kanwal Bir Singh Kuckreja Dr. Komal Majumdar Dr. Lanka Mahesh Dr. Navdeep Saini Prosthodontics & Implants Implant Dentistry Implant Dentistry Conservative Dentistry &
Endodontics Editorial Board Editorial Board Editorial Board Editorial Board
Dr. Neeru Singh Dr. Rajan Jairath Dr. Sameer Kaura Dr. Sanghmitra Dasgupta
Pedodontics & Preventive Dentistry
Orthodontics Oral Surgery & Implants Oral Surgery & Implants
Editorial Board Editorial Board Editorial Board Editorial Board
Dr. Sumeet Rajpal Dr. Surinder Pal Singh Sodhi Dr. Vijay Deshmukh Dr. Vivek Saggar
Pedodontics & Preventive Dentistry
Oral Surgery & Implants Oral & Maxillofacial Surgery
Pedodontics & Preventive Dentistry
Editorial Board Editorial Board Editorial Board Editorial Board
Dr. Abi Mathai Thomas Dr. Devinder Singh Kalsi Dr. Rajesh Bhanot Dr. Tarun Kumar
Principal, CDC Principal, BJSDCH Principal, SKSSDC President, IDA Ludhiana Advisory Board Advisory Board Advisory Board Advisory Board
Dr. Rajan Bir Singh Thind Dr. Abhijit Kathpal Dr. Jaidev Singh Dhillon Dr. Vandana Chhabra
Honorary Secretary, IDA Ludhiana Branch
Honorary Treasurer, IDA Ludhiana Branch
Immediate. Past President, IDA Ludhiana Branch
President-Elect. IDA Ludhiana Branch
Advisory Board Advisory Board Advisory Board Advisory Board
Dr. Vikas Jindal Dr. Pankaj Shiv Dr Sachin Dev Mehta Dr. Puneet Girdhar
Member, Dental Council of India (Punjab)
President, IDA Punjab State
Honorary Secretary, IDA Punjab State
Ex-Vice President, IDA HO
Advisory Board Advisory Board Advisory Board Advisory Board
Vol. 1 Issue 11 L.E.D. E-Journal Page 11
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Your (the reader’s) opinion matters to us the most. For striving to
improve continuously, we solicit your earnest support in the form of
suggestions. The suggestions can be bouquets or brickbats as both
will be lapped up in equal measure by us. There might be areas
where, in trying to not put a wrong foot forward, we have treaded the
safe path/zone, however, in certain other sections; we might have
ruffled quite a few feathers. We do request you to just put in a few
lines to the Editor-in-Chief, Dr. Bhavdeep Singh Ahuja’s email at
[email protected] regarding what is your opinion about:
1. The design
2. The layout
3. The content and
4. other sections of the E–Journal L.E.D. (Let’s Enjoy Dentistry)
The suggestions/feedback by the members would be published with
due credits in the next issue of the E–Journal L.E.D. (Let’s Enjoy
Dentistry). However, if the Branch Member wishes to keep his/her
identity secret/hidden, the same would be given respect and the
feedback published under the heading Anonymous. Please get going,
pick up your finger and type out your feedback/suggestions and
send to the Editor-in-Chief, Dr. Bhavdeep Singh Ahuja’s email at
Vol. 1 Issue 11 L.E.D. E-Journal Page 12
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
From the EDITOR’s Desk
Dr. Bhavdeep Singh Ahuja is a Dentist in Ludhiana, Punjab, having graduated in 1998 from Punjabi University, Patiala. He has specialized in Implants from BioHorizons Inc. USA in 2004-05 & in an Advanced Course from LACE-ICOI, USA in 2006. Apart from Dentistry, he holds a Triple M.B.A. in Hospital Management, Human Resource Management & Marketing from three premier Institutes /Universities of India viz. the IIMM Pune, IGNOU New Delhi & Annamalai University. He holds Post Graduate Diploma’s in various specialties viz. Medical Law & Ethics (NLSIU), Clinical Research, Cyber Law, Disaster Management, Financial Management, Bioinformatics amongst many more from different Universities. He is a Certified Health Care Waste Manager from IGNOU & is qualified in Consumer Law as well. He is an academically oriented dentist & has many Original Scientific Publications to his credit in many International & National journals. Presently, he is into 17th year of Clinical Practice in Ludhiana, Punjab & is reachable on www.drbhavdeep.com
Dear Peers in Profession, Colleagues & My Dear Friends,
Warm Greetings from the Editor
You must have read the Part I of this Editorial in L.E.D.
October 2016, Vol. 1 Issue 10
The below is the concluding Part II of the same Editorial
Part II of II
Are Corporate Hospitals becoming the real Villain of the
society?
Asking about the rising corporate hospital sector is a question
that needs no answer. It is not just rising, but is now firmly
established. Government health services have been weakened due
to government indifference and that is why there is scope for
corporate hospitals to prosper. Due to the entry of corporate
hospitals, the order of priorities has changed. As most of the
patients believe, the doctors’ priority is no longer the best
interests of the patients, but the profit earned by the
shareholders of the company.
People’s sensitivities have also become numbed due to certain
corporate hospitals. Once bills in these hospitals start mounting
up to Rs. 10-20 lakh, people began to consider the bills of Rs.
40,000-50,000 as trivial. These hospitals have become more like
malls.
Does our society really need them?
Isn’t the provision of all tertiary health care should be provided by
the Government like the Western World?
Vol. 1 Issue 11 L.E.D. E-Journal Page 13
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
When we try to imitate everything else from the West from clothes
to eatables to ‘live-in’ relationships, why not the healthcare
concept as well?
Public relations officers of many corporate hospitals keep roaming
around to visit doctors; they entice doctors to send patients (to
their hospitals) by tempting them with cuts. Sad to say sooner or
later, most fall prey to such cuts (practices).
Is it Legal?
What about Hippocratic Oath?
Loud call, but won’t it be right to suggest that there is no
humanism to be found in corporate hospitals. Some believe that
small hospitals are being destroyed due to these corporate
hospitals. Going by the patients’ belief; in small hospitals, there is
at least the possibility that the doctor has not lost his basic sense
of humanism as they wait for the patient to make the payment
and give concessions and none of that happens in corporate
hospitals.
Partly true, I believe!!!!
As one of my patients told me, corporate hospitals do maintain
everything five-star style, but forget about the patient. When the
patient comes, they give him lemonade or tea advertising that
they have the latest hi-tech gadgets viz. the optics or for e.g. the
pair of specs. The patient melts because of the free lemonade and
he buys a pair of spectacles that have an actual value of Rs. 200
or so, for Rs. 3000–5000 in the name of high-tech gadgets. He
further told me that the in-house sales shop (medicine or optics)
is the main income avenue of corporate hospitals, by sometimes
offering a free check-up with a 20% off offer, just like in a mall
and the whole corporate atmosphere is just designed to tempt.
Corporate hospitals easily implement government schemes and
insurance schemes as small private clinics and hospitals
sometimes can’t afford those as the government reimbursements
are delayed, and they usually don’t have the time to keep making
trips back and forth to get their payment from the insurance
company.
Corporate hospitals vie for tie-ups with large public sector
companies and the officials are more than eager to oblige as these
Vol. 1 Issue 11 L.E.D. E-Journal Page 14
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

public enterprises give exorbitant reimbursement to their
employees; Rs. 5000 for a normal PFM Crown, Rs. 2000 for a
restoration (filling), Rs. 5000 for just a pair of spectacles, of
course made available from corporate hospitals. The big corporate
hospitals in Mumbai draw in cases from all over Maharashtra.
But junior trainee doctors operate on those cases! Further, often
the quality of these corporate hospitals is not as good as they
claim in their advertisements.
Just recently, the Congress MP of Rajya Sabha, Mr. M.A. Khan
made a complaint to CM of Telangana State and Medical Council
of India that the private hospitals have nothing like humanity. He
charged that corporate hospitals have changed the noble
profession of health into business. He said that his wife had fever
and dysentery and he took her to Yashoda Hospital, Malakpet. He
had already contacted the doctor of the Parliament. The
management of Yashoda Hospital asked him to deposit Rs. 25000
in advance. When he showed his CGHS Health Card, they did not
accept it. Despite this, she was admitted after paying Rs. 15000
as advance. He had already told the doctor that she had only
fever and dysentery and all the pathological tests have already
been done 8 days back and everything is normal. However,
doctors unnecessarily got her HIV, Brain, Kidney and other tests.
When his wife refused to get these tests done, she was threatened
danger to her life. The second day, when he went to hospital, he
was surprised to get a bill of Rs. 25000.
You all can see if this is the attitude of the management of a
corporate hospital with an MP, we can understand how the poor
people are treated in these hospitals. He has made a complaint
with the technical committee of Medical Council of India and
raised objections in Rajya Sabha against the looting of corporate
hospitals.
Nowadays people want glamour and marketing. They have
become used to the mall culture. The concept of ‘master check-
up’ (packages of large number of tests, of which many may be
unnecessary) has gotten into their heads and Doctors who
practice ethically and scientifically are now looked upon with
contempt, because they obviously can’t afford this glitter. But
Vol. 1 Issue 11 L.E.D. E-Journal Page 15
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
people often don’t know what they are getting into by going to
corporate hospitals.
The book “Dissenting Diagnosis” also quotes a general
practitioner: “Corporate hospitals often engage in marketing in a
variety of ways like ‘Buy one, get one free’, ‘Discount week’, full-
page advertisements, mostly full of falsehood promises. They
throw parties for general practitioners, and they give them cuts.
On top of this, they throw parties and supply liquor to keep
politicians in their thrall. Some corporate and large hospitals
admit bogus patients under the Rajiv Gandhi Health Scheme (a
publicly funded health insurance scheme). They give the admitted
person money and plenty to eat and drink. They prepare records
showing that an angioplasty or angiography has been done on
that person, when actually nothing has been done”.
The fault here in lies with the governments first who should first
regulate private hospitals as without it, the basic objectives of
such schemes are lost and they become mechanisms for
corporate hospitals to loot public funds.
Failure of regulation is a common notion and is no longer a
guarded secret.
The regulator of medical profession, the Medical Council of India,
itself stood discredited after the CBI arrested its former president,
Ketan Desai, on April 22, 2010, in a Rs. 2 crore bribery case. The
bribe was paid for securing permission to enroll students in a
Patiala college.
How could the regulator of Dental profession, the Dental Council
of India, be left far behind? The Ex-DCI President, Dr. Anil Kohli
was accused by the CBI of allegedly amassing huge wealth
disproportionate to his known sources of income in September
2011. The CBI was probing Dr. Kohli's role as DCI chairman
between 2006 and 2010 following allegations that he received
favours from dental colleges for verification and cancellation of
certain institutes. He had resigned from the DCI post in 2010.
After registering the case against Dr. Kohli, the CBI had carried
out searches at six places and found that Dr. Kohli had allegedly
made huge investments in properties, including a palatial house
at Gulmohar Park, four shops at Lajpat Nagar and a farmhouse
Vol. 1 Issue 11 L.E.D. E-Journal Page 16
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
at Chhawla (near Najafgarh). CBI also claimed to have recovered
Rs. One crore in cash during the searches at his places, besides
documents showing that he had purchased a house worth Rs. 82
lakh in Lajpat Nagar.
Now there is a move to scrap both the MCI and DCI and replace it
with a commission to regulate medical and dental education and
practices.
Hospital wrongdoings rarely surface since doctors who are aware
of these choose to keep quiet. Even those who are above board
become a party to a wrong if they maintain silence. Like other
corporate czars, hospital bosses cultivate politicians and
whosoever matters. Political patronage has helped hospital
business flourish in North India. For a clean-up job and putting
the fear of law in corporate heads, it requires a herculean effort.
Recently, the Delhi CM, Mr. Arvind Kejriwal slapped a fine of Rs.
600 crore on five Delhi hospitals, which had got land on
concessional rates but did not treat the poor as required under
the deal.
Chennai has recently seen a rise as a medical capital of India;
more than two lakh cataract surgeries in a year, a two-fold jump
in caesarean section, a sharp spiral in hysterectomies. They also
belie an uncomfortable truth: Doctors are increasingly becoming
scalpel-happy. Wide-ranging interviews with surgeons who
testified before an NGO on corrupt practices in corporate
hospitals revealed that often patients are forced to undergo
unnecessary surgeries.
A senior orthopedic surgeon in a corporate hospital explained the
reason behind this unsettling trend: "We have a quota to meet
every month. Many of us see patients as a potential candidate on
our operating table. Only two out of five, however, agree. Many go
for a second opinion and don't return. Many of these surgeries
don't involve too many risks, while at the same time fetches more
revenue for the hospitals".
A doctor on condition of anonymity said in an interview that he
was pulled up by the hospital administration for having only a
10% 'conversion rate' referring to the number of patients who
were advised to undergo surgery. To be fair, the doctors are not
Vol. 1 Issue 11 L.E.D. E-Journal Page 17
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

entirely at fault. For a Rs. 2 lakh surgery, the doctor, probably
gets Rs. 25,000, while the rest goes to the hospital.
Our country has very few guidelines to check the
ethical practices. Any system that rewards a doctor for the
number procedures he does is liable to abuse. Patients as they
say are becoming smarter like the smartphones and not every one
of them is falling prey to the corporate hospital ‘modus operandi’
as many go for a second opinion. Many patients have had
harrowing experiences and sleepless nights when for their
shoulder pain, a cardiac surgery was prescribed and how they got
better just with exercise and also for some, physiotherapy cured
their back pain for which a surgery was recommended.
Doctors can’t be blamed every time though as not all elective
procedures are unnecessary and sometimes early surgery is
recommended as a precautionary measure for the elderly as they
have a lot of other conditions like diabetes and hypertension that
could aggravate their problem later. In some cases, the patients'
themselves ask for a surgery like in the case of many cesarean
sections.
Corruption has many names and one of the civil society isn't
innocent either. Professionals and businessmen of various sorts
indulge in unscrupulous practices, and so do the doctors. The
allegedly unfair ‘trade’ practices by doctors/dentists enlisted
below are all flashed in the print media or the internet by various
sources, however, some of them I found pretty unrealistic:
1. 40-60% kickbacks for lab tests.
2. 30-40% for referring to consultants, specialists & surgeons.
3. 30-40% of total hospital charges.
4. Sink tests – Some tests prescribed by doctors are not needed.
They are there to inflate bills and commissions as the
pathology lab understands what is unnecessary, that’s why
these are called "sink tests" and blood, urine, stool samples
collected will be thrown ‘in the sink’.
Vol. 1 Issue 11 L.E.D. E-Journal Page 18
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

5. Admitting the patient to "keep him under observation" as
some people go to cardiologists feeling unwell and anxious
and most of them aren't really having a heart attack and
cardiologists and family doctors are well aware of this. They
admit such safe patients, put them on a saline drip with mild
sedation, send them home after 3-4 days after charging them
a fat amount for ICU, bed charges, visiting doctors’ fees etc.
6. ICU minus intensive care - Nursing homes all over the
suburbs are run by doctor couples or as one-man-shows. In
such places, nurses and ward boys are 10th class drop-outs in
ill-fitting uniforms and bare feet. These "nurses" sit at the
reception counter, give injections and saline drips, perform
ECG’s, apply dressings and change bandages, and assist in
the operation theatre. At night, they even sit outside the
Intensive Care Units as there is no resident doctor. In case of
a crisis, the doctor who usually lives in the same building will
turn up after 20 minutes after a call from the nurse. Such
ICUs admit safe patients to fill up beds. Genuine patients who
require emergency care are sent elsewhere to hospitals having
a Resident Medical Officer (RMO) round-the-clock.
7. Unnecessary caesarean surgeries and hysterectomies - Many
surgical procedures are done to keep the cash register ringing.
Caesarean deliveries and hysterectomy (removal of uterus) are
high on the list. While the woman with labour pains is
screaming and panicking, the obstetrician who gently
suggests that caesarean is best seems like an angel sent by
God! Menopausal women experience bodily changes that
make them nervous and gullible. They can be frightened by
words like "hemorrhoids and fibroids" that are in almost every
normal woman's radiology reports. When a gynaecologist
gently suggests womb removal "as a precaution", most women
and their husbands agree without a second thought.
8. Cosmetic surgery advertised through newspapers like
Liposuction and plastic surgery are not minor procedures.
Vol. 1 Issue 11 L.E.D. E-Journal Page 19
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Some are life-threateningly major, but advertisements make
them appear as easy as a facial and waxing.
9. Indirect kickbacks from doctors to prestigious hospitals – To
be on the panel of a prestigious hospital, there is give-and-
take involved. The hospital expects the doctor to refer many
patients for hospital admission. If he fails to send a certain
number of patients, he is quietly dumped and so he likes to
admit patients even when there is no need.
10. "Emergency surgery" on a dead body – If a surgeon hurriedly
wheels your patient from the Intensive Care Unit to the
operation theater, refuses to let you go inside and see him,
and wants your signature on the consent form for "an
emergency operation to save his life", it is likely that your
patient is already dead. The "emergency operation" is for
inflating the bill; if you agree for it, the surgeon will come out
15 minutes later and report that your patient died on the
operation table and then, when you take delivery of the dead
body, you will pay OT charges, anesthesiologist's charges,
blah-blah-
I was myself shocked when I heard a few of these on National
Television News (‘Aaj ka Sabse Bada Khulaasa’) or read on the
Internet about these above.
I just wondered how widespread this is or, is it a matter of a
few black sheep giving a bad name to the entire fraternity? The
media have also segregated the same into 2 categories:
1. Young surgeons and old ones: The young ones who are setting
up nursing home etc. have heavy loans to settle. To pay back
the loan, they have to perform as many operations as possible.
Also, to build a reputation, they have to perform a large
number of operations and develop their skills. So, at first,
every case seems fit for cutting. But with age, experience and
prosperity, many surgeons lose their taste for cutting, and stop
recommending operations.
Vol. 1 Issue 11 L.E.D. E-Journal Page 20
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

2. Physicians and surgeons: To a man with a hammer, every
problem looks like a nail. Surgeons like to solve medical
problems by cutting, just as physicians first seek solutions
with drugs. So, if you take your medical problem to a surgeon
first, the chances are that you will unnecessarily end up on the
operation table.
It’s up to our inner conscience that we don’t resort to any of the
above. Doctors too are humans and mistakes happen. But when
payment before treatment is the rule and relations become
commercial, as in corporate hospitals, then forgiving a blunder
becomes difficult.
So, have you guys ever wondered, why is this greed culture
setting in?
Thoughts generate desires and then thinking about the
methods to fulfill them, we tread the wrong path. The energy
called ‘desire’ has been condemned for centuries. Almost all the
so-called saints have been against it, because desire is the very
source of all that you see and they were against all that which is
visible. They wanted to sacrifice the visible at the feet of the
invisible; they wanted to cut the roots of desire so there would no
longer be any possibility of life. Firstly, desire itself is God. Desire
without any object, desire without being goal-oriented,
unmotivated desire, pure desire, is God.
Your very being is desire; to be against it is to be against
yourself and against all. Desire is creativity. God created the
world because a great desire arose in him — a desire to create, a
desire to manifest, a desire to make many from one, a desire to
expand. Desire means a longing, a great longing, to expand, to
become huge, and to be enormous as huge as the sky. In fact,
what the man who wants to have more and more money really
wants is not money but expansion, because money can help you
expand. The man who is after money may not know why he is
after the money. He may himself think and believe that he loves
money, but that is only on the surface of his consciousness. Men
want more power, more fame, longer life, better health, but what
do they desire in these different things? They don’t want to
Vol. 1 Issue 11 L.E.D. E-Journal Page 21
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
remain confined; they don’t want to be limited. It hurts that you
have limitations, because to have limitations means to be
imprisoned. But all these objects of desire, sooner or later,
disappoint. Money has brought a few blessings, but in the same
measure it has brought many curses too. You can have a bigger
house, but now you will have less peace. You can have a bigger
bank balance, but you will also have a bigger madness, anxiety,
neurosis, psychosis. Money has brought a few things which are
good; in the wake of it many other things have arrived which are
not good at all. And if you look at the whole thing, the whole effort
has been a sheer wastage and now you cannot have even the
‘hope’ that the poor man can have. The rich man becomes
hopeless as he has tasted all kinds of things; now he only feels
tastelessness. A kind of death has already happened, because he
cannot conceive of how to fulfill that desire for expansion. But
desire in itself is not wrong. The desire for money, the desire for
power and the desire for prestige are all wrong objects for desire.
You can have a sword and you can kill somebody; that does not
make the sword wrong as you can also save somebody with the
same sword. Poison can kill and poison can become medicine too.
In the right hands, poison is nectar; in the wrong hands, nectar is
poison. This is the essential
wisdom of all the ‘Buddhas’ of all the ages. Intelligence means the
insight that no object can fulfill your desire. The intelligent person
stops desiring objects. He makes his desire pure of all objects
worldly, other worldly. He starts living his desire in its purity,
moment to moment. Desire is beautiful, as there is nothing wrong
in it; just free it from objects. With freedom from objects, desire is
divine and pure; close to GOD.
What do you think about the desires of mankind?
Thank You, See you ALL in the FINALE issue!!!!!
Yours truly,
Bhavdeep
The above is the Second part of two (II) parts of the Editorial.
For reading Part I of this Editorial, check out L.E.D. October
2016, Vol. 1 Issue 10
Vol. 1 Issue 11 L.E.D. E-Journal Page 22
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
Vol. 1 Issue 11 L.E.D. E-Journal Page 23
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
Dr. Edwin Roberto Hernandez Molina graduated in 1995 from University of El Salvador, Central America. He started his private practice from 1997 and after that; he attended to Real World Endo course at Baylor College, Dallas TX in 2004. He has taken Implant courses from Brasseler and Zimmer in 2008 and 2009. He started studies and National University of Colombia, Bogotá branch in 2011 and graduated from a 2 years full time specialty program in Endodontics in 2013. He practiced for 3 years in Bogotá, Colombia. He has been a lecturer in El Salvador and also has been a teacher at national universities for pre-graduate students & for 3 years as a Co-Coordinator of diplomat studies in endodontics for Universidad Evangelica from El Salvador. He has a private practice limited to Endodontics and is presently working as an Endodontist in the Central Military Hospital of El Salvador, Central America.
CBCT in ENDODONTICS A Boon for Effective Treatment & Cure
Author: Dr. Edwin Roberto Hernandez Molina
ABSTRACT
The Radiography is an essential tool to correct diagnosis and
endodontic management related to odontogenic and non-
odontogenic pathologies, treatment planning, intra operative
assessment, recording and appraisement of the endodontic
procedure end result and outcome. Until recently most of the
imaging information in endodontics was obtained through film
based or digital radiographs, these provided useful information:
as the presence and location of peri-radicular lesions, root and
root canal anatomy, proximity with adjacent anatomical
structures. But these types of images have inherent limitations.
The main limitation is, that conventional or digital radiographs
comprise a two dimensional image of a tri-dimensional object,
with an effect on diagnostic capacity. The important features of a
tooth and surrounding hard tissues are viewed only in a proximal
plane (mesio - distal), and can not be valued in a buccal-lingual
plane.
The spatial relation of the dental root with its surrounding
anatomical structures and associated peri-radicular lesions can
not always be assessed with conventional radiographs. As an
alternative to some disadvantages from conventional radiography,
exposures with 10º-15º horizontal angles shifts can be made. This
Vol. 1 Issue 11 L.E.D. E-Journal Page 24
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

might be necessary in diagnosis of traumatic dental lesions as
radicular fractures, avulsions, luxations or judgement of internal
or external resorptions.
It is important to consider that’s not always possible to obtain
an ideal position of the dental X-ray film or digital sensor, as a
consequence could happen variations angles and increase or
reduce the root’s length of the tooth under investigation or even
hide and hinder the appearance of peri-radicular lesions.
Imaging, thus forms the most essential part of all steps in
Endodontics.
INTRODUCTION
Cone Beam Computed Tomography (CBCT) is a diagnostic
imaging modality that provides high-quality, accurate three-
dimensional (3D) representations of the hard tissues and osseous
elements of the maxillofacial skeleton. This extraoral imaging
system was created at the end of the 90’s, to produce
tridimensional scans of the maxillofacial skeleton with a
considerable less radiation dose compared to the computed
tomography.
A single scan is made, where source and sensor rotates the
patient’s head in 180º or 360º (Fig. 1).
Fig-1: CBCT Details
(Image Source: Google)
Vol. 1 Issue 11 L.E.D. E-Journal Page 25
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
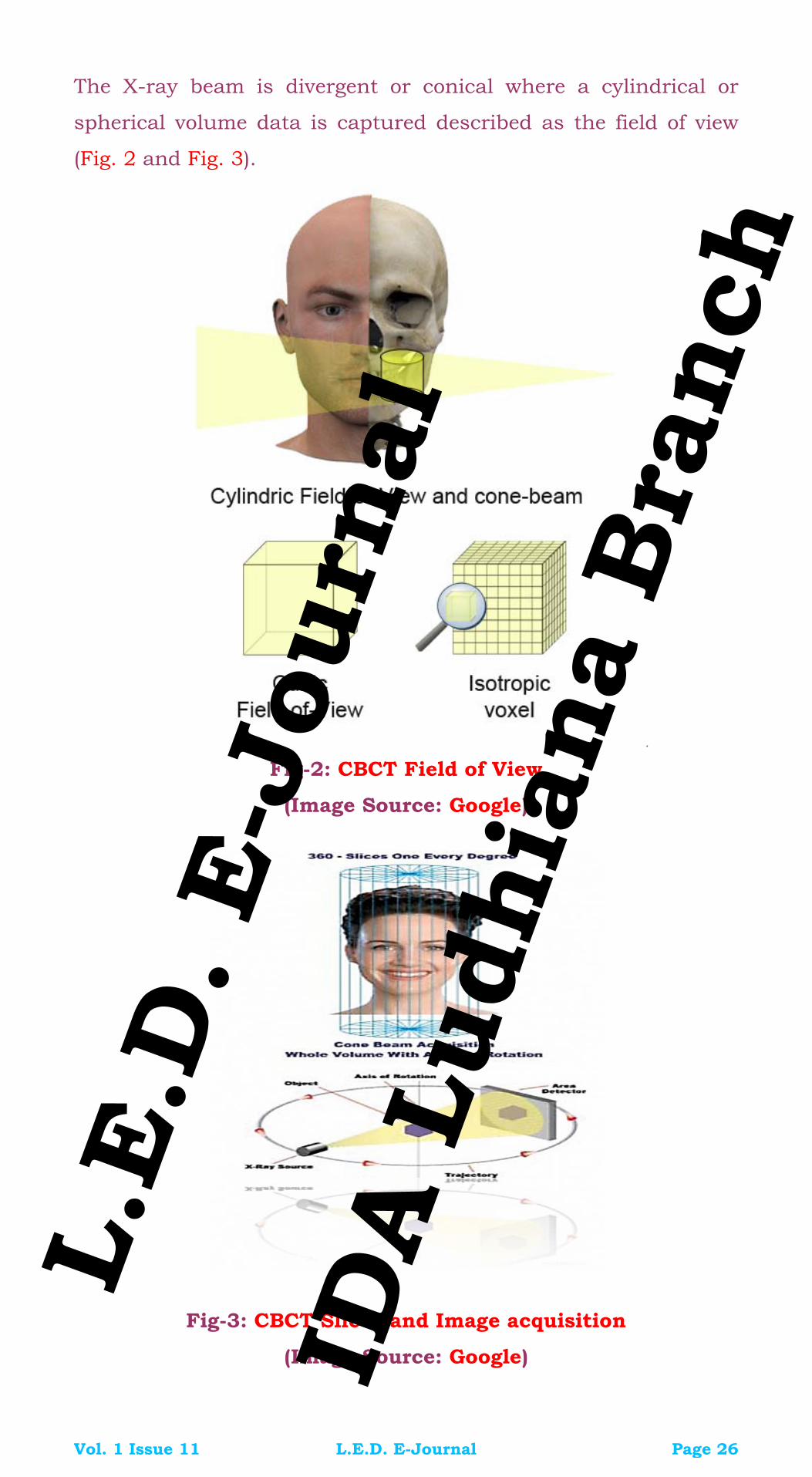
The X-ray beam is divergent or conical where a cylindrical or
spherical volume data is captured described as the field of view
(Fig. 2 and Fig. 3).
.
Fig-2: CBCT Field of View
(Image Source: Google)
Fig-3: CBCT Slices and Image acquisition
(Image Source: Google)
Vol. 1 Issue 11 L.E.D. E-Journal Page 26
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Fig-4: Image Display in 3 Orthogonal Planes
(Image Source: Google)
Images are displayed simultaneously in three orthogonal planes:
Transverse, Sagittal and Coronal (Fig. 4).
Cone Beam Computed Tomography with a limited Field of View
(FOV) may be considered in the following situations:
1. Diagnosis of radiographic signs of periapical pathosis when
there are contradictory (nonspecific) signs and/or symptoms;
2. Confirmation of nonodontogenic causes of pathosis;
3. Assessment and/or management of complex dento-alveolar
trauma, such as severe luxation injuries, suspected fracture of
the overlying alveolar complex and horizontal root fractures,
which may not be readily evaluated with conventional
radiographic views;
4. Appreciation of extremely complex root canal systems prior to
endodontic management (for example, class III & IV dens
invaginatus);
5. Assessment of extremely complex root canal anatomy in teeth
treatment planned for non-surgical endodontic re-treatment;
6. Assessment of endodontic treatment complications (for
examples, [post] perforations) for treatment planning purposes
when existing conventional radiographic views have yielded
insufficient information;
7. Assessment and/or management of root resorption, which
clinically appears to be potentially amenable to treatment;
Vol. 1 Issue 11 L.E.D. E-Journal Page 27
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

8. Pre-surgical assessment prior to complex peri-radicular surgery
(for example posterior teeth).
Clinicians must have core knowledge of CBCT radiography before
requesting CBCT scans and must regularly update their
knowledge. The principles of radiation protection must also be
adhered to. A CBCT scan should have a net benefit to the
management of a patient’s (suspected) endodontic problem. A
comprehensive discussion must take place between the clinician
and patient; only then is the patient’s consent to undergo a CBCT
procedure valid.
As with any ionizing radiation imaging device, the radiation dose
must be kept ‘as low as reasonably achievable’. Indeed, when
considering whether to use CBCT, there is a much greater
responsibility on clinicians to justify its use due to the increased
ionizing radiation.
The entire volume of data must be assessed and reported on. This
would normally be completed by the clinician who has prescribed
the scan, or the practitioner who has taken the scan; however, it
is essential to refer the CBCT image data to a competent person if
the interpretation of the scan is beyond the competence of the
clinician who has prescribed it.
Successful management of endodontic problems is
reliant on diagnostic imaging techniques to provide critical
information about the teeth under investigation, and their
surrounding anatomy. Since its inception, conventional
radiography has remained the mainstay of imaging in
Endodontics.
Cone beam computed tomography reconstructed scans are
invaluable for assessing teeth with unusual anatomy, such as
teeth with an unusual number of roots, dilacerated teeth and
dens in dente. The exact location and anatomy of the root canal
system can be assessed, allowing successful management of the
case.
Previously, even with the aid of magnification, the anatomy of
such a tooth may not be truly appreciated, making treatment
more unpredictable. CBCT systems are available that now provide
Vol. 1 Issue 11 L.E.D. E-Journal Page 28
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

small field of view images at low dose with sufficient spatial
resolution for applications in endodontic diagnosis, treatment
guidance and post treatment evaluation.
This case report provides a perfect example of CBCT as
an imaging adjunct for Endodontics and proves that CBCT has
become a gold standard in diagnosis and treatment planning in
Endodontics now.
CASE REPORT
HISTORY
A female patient 70 years of age referred to our Military Dental
hospital for root canal treatment of the upper right first molar
right.
DIAGNOSIS
Symptomatic Irreversible Pulpitis
RADIOGRAPHIC EXAMINATION
The preoperative radiographic image showed us only two roots
(upper right first molar) instead of the usual three.
Fig-5: Pre-Operative Radiographic View of 16
Vol. 1 Issue 11 L.E.D. E-Journal Page 29
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
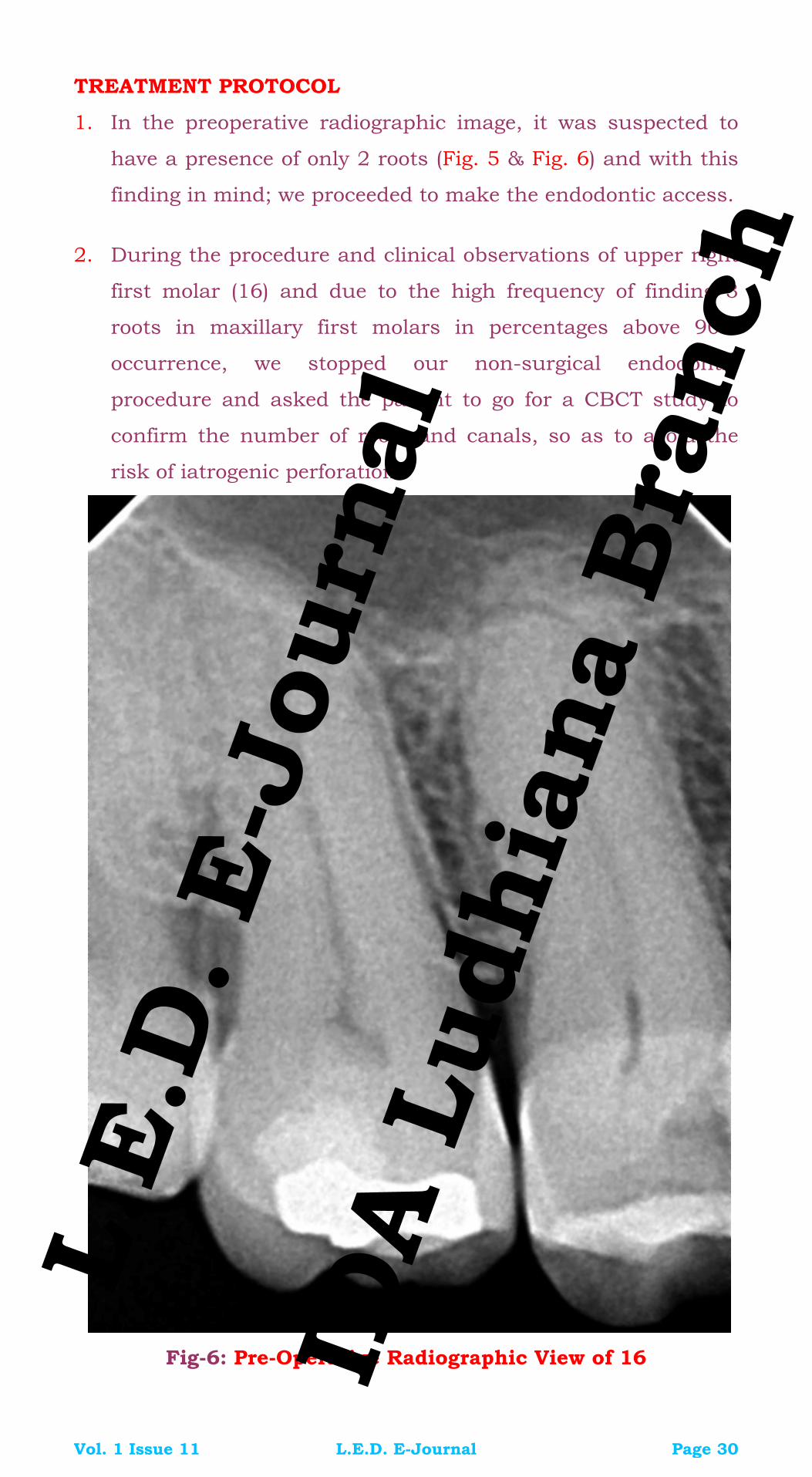
TREATMENT PROTOCOL
1. In the preoperative radiographic image, it was suspected to
have a presence of only 2 roots (Fig. 5 & Fig. 6) and with this
finding in mind; we proceeded to make the endodontic access.
2. During the procedure and clinical observations of upper right
first molar (16) and due to the high frequency of finding 3
roots in maxillary first molars in percentages above 90%
occurrence, we stopped our non-surgical endodontic
procedure and asked the patient to go for a CBCT study to
confirm the number of roots and canals, so as to avoid the
risk of iatrogenic perforation.
Fig-6: Pre-Operative Radiographic View of 16
Vol. 1 Issue 11 L.E.D. E-Journal Page 30
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

3. In 2015, the American Association of Endodontists (AAE) and
the American Academy of Oral and Maxillofacial Radiology
(AAOMR) made an update to the position statement on the
use of computed tomography cone beam (CBCT) to provide
clinicians a science-based guide the use of CBCT in
endodontic treatment.
Fig-7: Working length X-ray of 16
4. As has been demonstrated radiographic images (intraoral and
panoramic) only provide two-dimensional representations of
three-dimensional anatomical structures, but the complex
Vol. 1 Issue 11 L.E.D. E-Journal Page 31
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

anatomies and surrounding structures can hinder the
interpretation of planar images.
Fig-8: Access Opened with 16
Fig-9: Clinical View of Prepared canals with 16
5. Knowing that there may be anatomical variations between
different types of teeth and in this case that concerns us, the
two-dimensional X-ray did not meet the requirements;
therefore an intra-operative CBCT study for the identification
and location of the root canal system in the first upper right
molar was recommended.
Vol. 1 Issue 11 L.E.D. E-Journal Page 32
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

6. Finally, in CBCT images from the study in TRIDENTAL, the
presence of 2 root and 2 lines in the first upper right molar
was confirmed (Fig. 10, Fig. 11, Fig. 12, Fig. 13, Fig. 14, Fig.
15, Fig. 16 and Fig. 17).
Fig-10: 3D Representation with 16
Fig-11: 3D Model reconstructed
Fig-12: Multiplanar of Buccal Canal is marked with Purple arrow and remnants of obturation with Yellow arrow
Vol. 1 Issue 11 L.E.D. E-Journal Page 33
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Fig-13: Another View of above
Fig-14: Occlusal View of Buccal Canal
Fig-15: Multiplanar of Palatal Canal is marked with Purple
arrow and remnants of obturation with Yellow arrow
Vol. 1 Issue 11 L.E.D. E-Journal Page 34
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
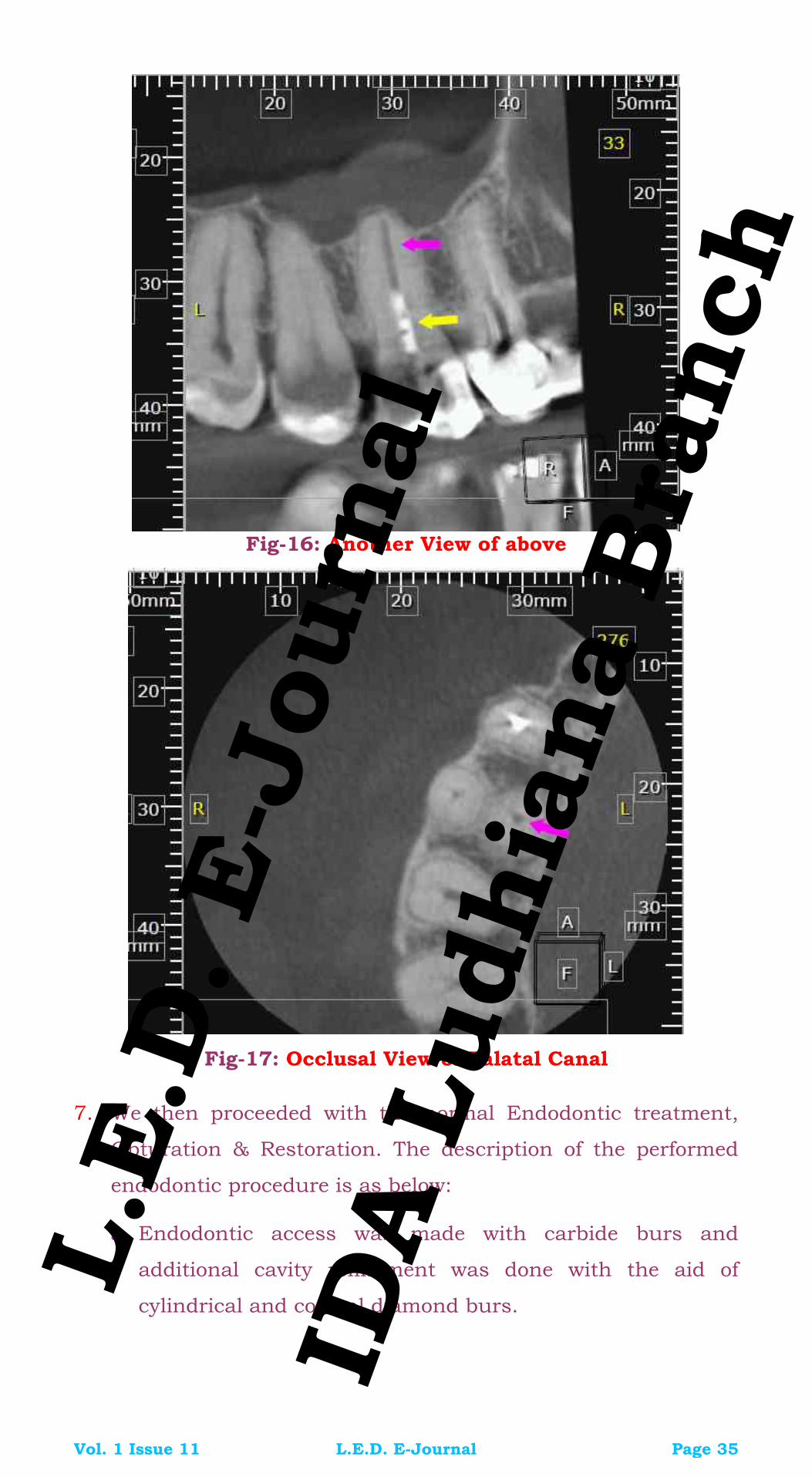
Fig-16: Another View of above
Fig-17: Occlusal View of Palatal Canal
7. We then proceeded with the normal Endodontic treatment,
Obturation & Restoration. The description of the performed
endodontic procedure is as below:
a. Endodontic access was made with carbide burs and
additional cavity refinement was done with the aid of
cylindrical and conical diamond burs.
Vol. 1 Issue 11 L.E.D. E-Journal Page 35
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

b. Search of root canals over the pulp floor with endodontic
explorer and further refinement with CAP2 and CAP
ultrasonic tips from Acteon Satelec.
c. Palatal canal prepared up to Revo S, AS40 file.
d. The buccal canal found and prepared up to Revo S, AS35
file (thought was the DB canal).
e. Search for Canal MB1 canal was made.
f. Irrigation with 5% sodium hypochlorite and active
ultrasonic irrigations with Irrisafe tip (Acteon Satelec).
g. Intracanal medication with calcium hydroxide based paste
(Metapaste, Meta Biomed), CBCT scan indicated.
Fig-18: Completed Obturation with 16
Vol. 1 Issue 11 L.E.D. E-Journal Page 36
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
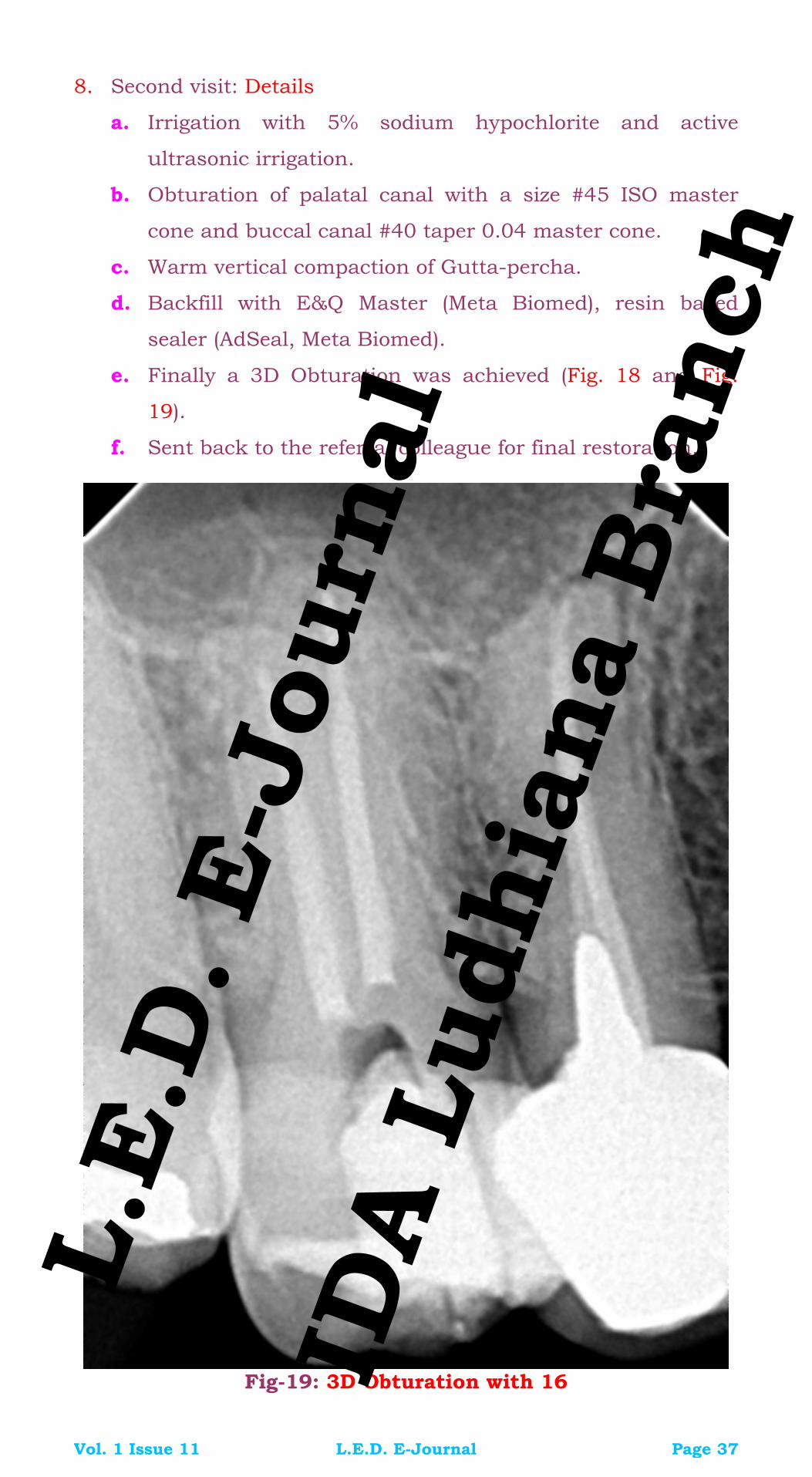
8. Second visit: Details
a. Irrigation with 5% sodium hypochlorite and active
ultrasonic irrigation.
b. Obturation of palatal canal with a size #45 ISO master
cone and buccal canal #40 taper 0.04 master cone.
c. Warm vertical compaction of Gutta-percha.
d. Backfill with E&Q Master (Meta Biomed), resin based
sealer (AdSeal, Meta Biomed).
e. Finally a 3D Obturation was achieved (Fig. 18 and Fig.
19).
f. Sent back to the referral colleague for final restoration.
Fig-19: 3D Obturation with 16
Vol. 1 Issue 11 L.E.D. E-Journal Page 37
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

REVIEW of LITERATURE
B. Cleghorn, W. Christie and C. Dong in 2006 (Root and Root
morphology of the human maxillary molar first permanent
channel: A literature review, JOE, Volume 32, Number 9
September 2006) did a literature review of the anatomy root and
ductwork permanent maxillary first molar; for which four
anatomical studies were taken into account, where indicated that
the maxillary molar NORMALLY has 3 roots in 96.2% of cases
(416 teeth). The presence two roots was found in 16 (3.8%) of the
teeth studied (Fig. 20). Variations may be a result of ethnicity, age
and gender of the population studied.
Fig-20: Review of Literature
CONCLUSION
In conclusion, the success of non-surgical endodontic
treatment depends on the accurate identification of root
canals, cleaning, shaping and obturation of root canal
systems and the quality of the final restoration. 2-D images
result reveals not the actual number of roots and root
canals. In studies, the data acquired by CBCT have shown
a strong correlation between reconstructions and sectioning
through the CBCT and histological examination (J Michetti,
Maret D, JP Mallet, F. Diemer Validation of cone beam
computed tomography as a tool to explore root canal
anatomy Endod J 2010; 36 (7):. 1187-1190).
Vol. 1 Issue 11 L.E.D. E-Journal Page 38
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

SUMMARY
Radiography is an integral part of dental diagnosis and most
commonly used radiograph is IOPA X-ray. IOPA though has
varied implications in dentistry but the biggest drawback is
that it gives only a 2-dimensional aspect of the area in
question. Cone Beam Computed Tomography or the C-arm CT
or Cone Beam Volume CT or CBCT is a medical imaging
technique which gives an accurate idea of canal anatomy and
anatomical landmarks can be marked out as well so that
clinician is able to make his own judgment. CBCT’s scope in
Endodontics is beginning to gain much popularity now such
as to study the accessory canals in a teeth or to see vertical
root fractures in teeth. CBCT is also used effectively for pre-
surgical assessment of position of root apices with respect to
structures like Inferior Alveolar Nerve/Canal (IAN) and
maxillary sinus being most accurate. CBCT plays an
important role in planning for periapical microsurgery on the
palatal roots of maxillary first molars. The distance between
the cortical plate and the palatal root apex can be measured,
and the presence or absence of the maxillary sinus between
the roots could be assessed. CBCT is an excellent tool to see
variations in root canal anatomy and to check the exact
positioning of the apical foramen. CBCT is also helpful in
providing valuable information for determination of type and
severity of dental trauma, horizontal root fractures, alveolar
fractures and other radiolucencies which are otherwise
difficult to find in a normal X-ray. CBCT is of extreme help in
torturous root canal anatomy cases or repeated failure of root
canal treatment. The reason why CBCT is getting popular in
dentistry over the regular CT is very low radiation exposure in
CBCT when compared to a regular CT Scan. Successful
management of endodontic problems is reliant on diagnostic
imaging techniques to provide critical information about the
teeth under investigation, and their surrounding anatomy and
Vol. 1 Issue 11 L.E.D. E-Journal Page 39
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
CBCT is fast becoming the mainstay of imaging in
Endodontics.
REFERENCES
1. B. Cleghorn, W. Christie and C. Dong in 2006 (Root and Root
morphology of the human maxillary molar first permanent
channel: A literature review, JOE, Volume 32, Number 9
September 2006)
2. J Michetti, Maret D, JP Mallet, F. Diemer Validation of cone
beam computed tomography as a tool to explore root canal
anatomy Endod J 2010; 36 (7):. 1187-1190).
3. S. Patel, C. Durack, F. Abella, M. Roig, H. Shemesh, P.
Lambrechts, K. Lemberg. European Society of endodontology
position statement: The use of CBCT in endodontics.
International endodontic journal 47, 502-504, 2014.
P.S. Any feedback/compliments/queries for the Author/s should
be emailed to the Editor-in-Chief, Dr. Bhavdeep Singh Ahuja at
his email id: [email protected]
Vol. 1 Issue 11 L.E.D. E-Journal Page 40
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
Pehla Gyaan
Vol. 1 Issue 11 L.E.D. E-Journal Page 41
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
Dr.S.P.S.Sodhi is the Principal, DIRDS, Faridkot. He passed both his BDS (1983) & MDS in Oral Surgery (1988) from GDC Amritsar. He is practicing Oral Surgery actively since 25 years & Dental Implants since 17 years. He has been a Keynote speaker at various International & National Conferences in India & abroad. He is a recognized Inspector of the Dental Council of India & is also the Editor of Baba Farid University Dental Journal. He has been very active in IDA as well & has held key positions in the past at Local & State Level as well. Dr. Gursimrat Kaur Brar did both her Graduation (BDS – 2001) & Post Graduation (MDS in Oral Surgery – 2015) from DIRDS, Faridkot. Presently, she is working as a Senior Lecturer in Department of Oral & Maxillofacial Surgery in DIRDS, Faridkot.
Dr. Dikshit Behal passed his BDS from Gian Sagar Dental College & Hospital, Ram Nagar, Banur. Presently, he is a Post Graduate Student in the Department of Oral & Maxillofacial Surgery in DIRDS, Faridkot.
Sialolithiasis of Submandibular Gland Duct
A Rare Case Report
Author: Dr. S.P.S.Sodhi
Co-Author 1: Dr. Gursimrat Kaur Brar
Co-Author 2: Dr. Dikshit Behal
ABSTRACT
Sialolithiasis is one of the most common diseases of the salivary
glands and is characterized by the obstruction of salivary gland or
its duct due to the formation of calcareous plaque. It most
frequently occurs in the submandibular salivary gland due to its
anatomic features. The term giant sialolith is used for the stones
over 15 millimeters in any one dimension. It is rarely reported in
the literature. Although, large sialoliths have been described in
the body of salivary glands, they are rarely found in the salivary
ducts. We report a rare case of a giant sialolith of submandibular
gland duct in a 36 year old female. The sialolith was removed
surgically via intra-oral approach. No recurrence was seen on
follow-up.
KEYWORDS
Sialolith, Sialolithiasis, Submandibular gland, Submandibular
duct
Vol. 1 Issue 11 L.E.D. E-Journal Page 42
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
INTRODUCTION
The word ‘sialolith’ literally means calculus in a salivary gland or
duct. Sialolithiasis is defined as the formation of calcific
concretions within the parenchyma or the ductal system of a
major or minor salivary gland. Sialolithiasis is the second most
common disease of the salivary glands after mumps and is
characterized by the obstruction of a salivary gland or its
excretory duct by a calculus or sialolith associated with swelling,
pain, and infection of the affected gland, resulting in salivary
ectasia. The submandibular gland is the most common site for
sialolithiasis (80% - 90%), followed by the parotid gland (5% -
20%). The sublingual gland and minor glands are very rare sites
for sialolithiasis (1% - 2%).
The sialolith are calcium – rich crystallized minerals
typically composed of calcium phosphate or calcium carbonate in
association with other salts and organic material such as
glycoproteins, mucopolysaccharides and desquamated cellular
residue. Bacterial elements have not been identified at the core of
a sialolith.
Demographically, sialolithiasis affects 12 in 100 of the
adult population with male preponderance being twice as much
as females. All age may be affected, although patients in their
third to sixth decade represent the majority of cases, children are
very rarely affected (3%). Simultaneous sialolithiasis in more than
one salivary gland is rare, occurs in fewer than 3% of cases. Also,
70 to 80% of cases feature solitary stones; only about 5% of
patients have three or more stones. There is no left or right
predominance.
Sialoliths can lead to retrograde infection of the duct systems,
strictures, neoplasms, and local trauma are to be considered as
etiological factors. Submandibular sialolithiasis occurs as a
consequence of a hampered flow due to inflammatory stenosis of
Wharton’s duct; moreover, there are some anatomical factors
associated with formation of sialoliths in the submandibular
gland, such as: Wharton’s duct is the longest among the salivary
glands’ ducts; The path of Wharton’s duct goes in an upgoing
direction and the main portion of the duct is wider than the
Vol. 1 Issue 11 L.E.D. E-Journal Page 43
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
orifice; Along with these anatomical factors, the peculiar
composition of the submandibular gland saliva, that is alkaline
and rich of mucin, is relevant for the beginning of sialolith
formation. There is stasis of saliva, precipitation of salts and
organic matrix formation. Dehydration, allergic states, infection of
the oral cavity make saliva denser and start the accumulation of
ductal debris which in turn allow the precipitation of mucoid
elements and salts in order to form the organic matrix. When the
stone reaches a size to obstruct the duct the secretion in the
gland is hampered. This condition facilitates destruction of the
gland.
In this present case report, we present a case of giant sialolith in
the submandibular gland duct, which was successfully treated
via intra-oral approach. No recurrence was seen on follow-up.
CASE REPORT HISTORY & CHIEF COMPLAINT
A 36 year old female patient reported to the Department of
Oral and Maxillofacial Surgery at Dasmesh Institute of Research
and Dental Sciences, Faridkot with the chief complaint of
irritation on the under surface of tongue on right side since 15
days.
History dates back to 3 months when patient started feeling
irritation and swelling in the floor of the mouth on right side.
Patient went to a private dental practitioner, where according to
her, a small piece of stone was removed from the floor of the
mouth and medication was prescribed. Now, about 15 days prior
to this visit, she again started feeling the same irritation and
swelling in the same region and reported to our department for
the treatment of the same. There was no history of any
spontaneous discharge.
INTRA-ORAL EXAMINATION
Clinical examination revealed a yellowish irregular mass with
inflamed sublingual mucosa with respect to the right side of the
floor of the mouth, measuring 2.5cm x 1.5cm in size (Fig.1).
Vol. 1 Issue 11 L.E.D. E-Journal Page 44
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Palpation of the area indicated a nodular, slightly tender mass,
which was stony hard in consistency.
Fig-1: Pre-Operative Intra-Oral View
RADIOGRAPHIC EXAMINATION
We went in for the mandibular occlusal radiograph of the
patient which revealed a radio opaque mass w.r.t. floor of mouth
on the right side (Fig. 2). Provisional diagnosis of sialolith with
respect to right submandibular gland duct was made.
Fig-2: Pre-Operative Mandibular Occlusal Radiographic View
INVESTIGATIONS
All the routine blood investigations of the patient were within
normal range and viral markers were negative.
Vol. 1 Issue 11 L.E.D. E-Journal Page 45
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
TREATMENT PLAN
Surgical excision of the mass was planned under local anesthesia
under strict aseptic conditions.
TREATMENT PROTOCOL
1. Part preparation was done and patient was draped in the usual
manner.
2. Local anesthesia was achieved using 2% lignocaine with
1:80,000 adrenaline using right lingual nerve block and local
infiltration.
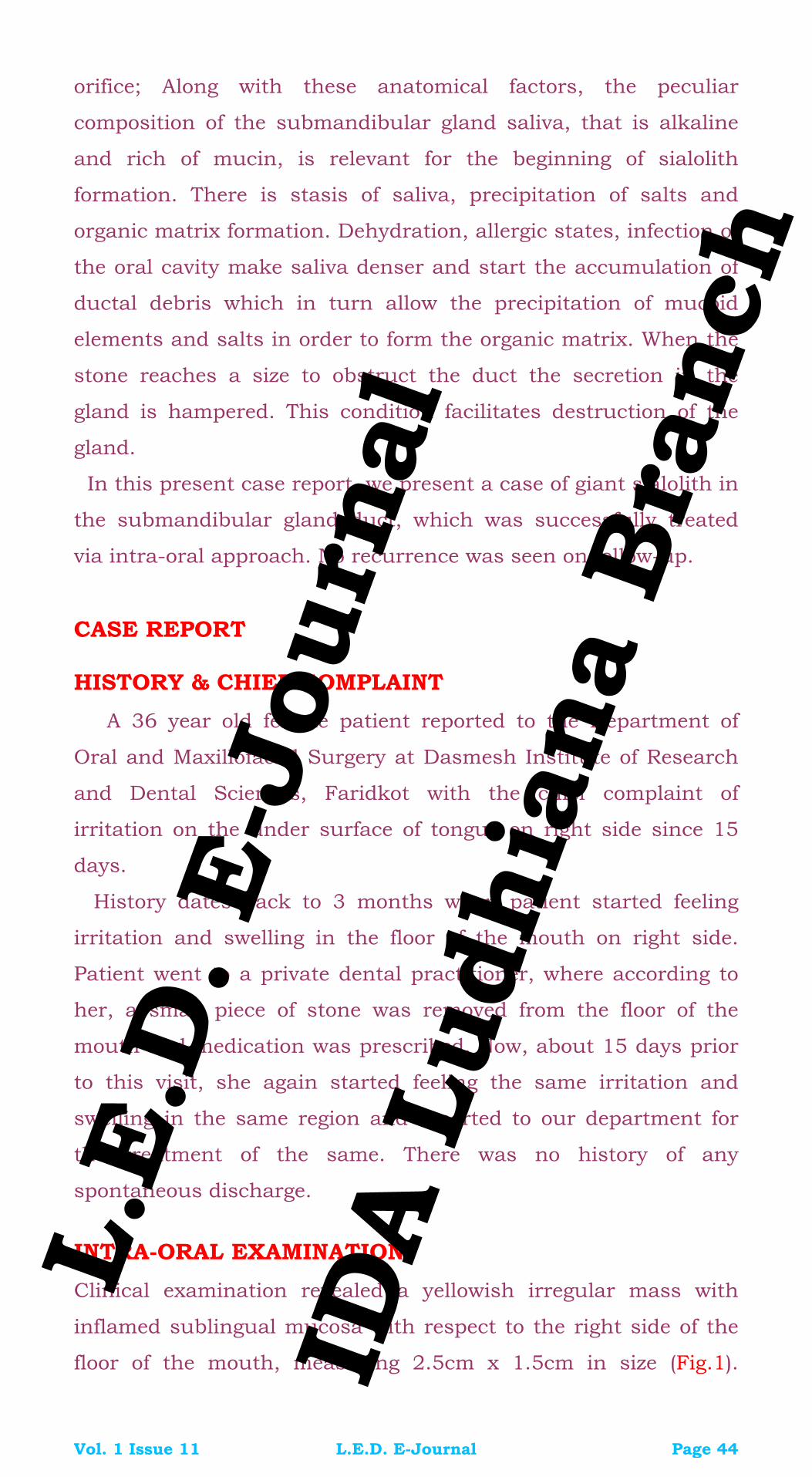
3. A stay suture was tied distal to the opening of submandibular
gland duct (Fig. 3).
Fig-3: A Stay Suture tied to the Opening of Submandibular Duct
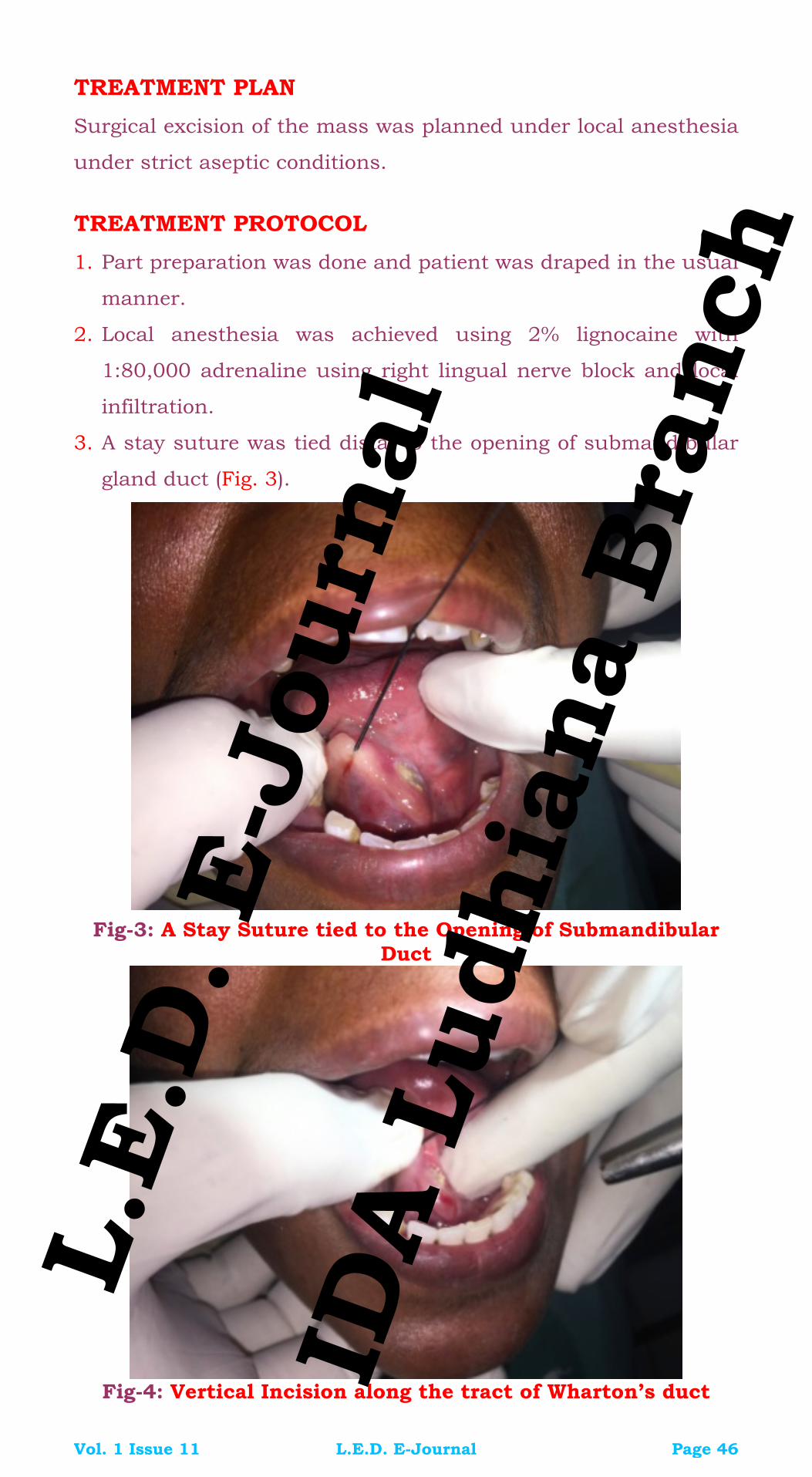
Fig-4: Vertical Incision along the tract of Wharton’s duct
Vol. 1 Issue 11 L.E.D. E-Journal Page 46
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

4. h
grasped with Allis forceps and with the
With bi-digital manipulation and with stay suture, the sialolit
was reflected and vertical incision was given along the tract of
Wharton’s duct (Fig. 4).
5. Then the sialolith was
help of a periosteal elevator (Fig. 5), the sialolith was popped
out (Fig. 6) and primary closure was achieved using 3-0
Mersilk suture (Fig. 7).
Fig-5: Elevation of Sialolith with Periosteal Elevator
Fig-6: Popped out Sialolith
Vol. 1 Issue 11 L.E.D. E-Journal Page 47
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Fig-7: Primary Closure with 3-0 Mersilk Suture
6. The extracted sialolith was then sent for histopathological
examination to confirm the diagnosis (Fig. 8) and biopsy
confirmed the clinical diagnosis.
Fig-8: Retrieved Sialolith sent for Histopathological
Examination
Vol. 1 Issue 11 L.E.D. E-Journal Page 48
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

7. Healing was uneventful.
8. The patient was followed up for 2 months post operatively and
there had been no recurrence.
9. Salivary flow was found to be normal and patient was relieved
of the symptoms.
DISCUSSION
Sialolithiasis is the most common non-neoplastic disease of the
salivary gland and autopsy reports show a 1.2% incidence across
the population. Sialoliths occur most frequently in adults during
the 4th, 5th and 6th decades, but can occurs at any age. Diagnosis
of sialoliths is both clinical and radiographic.
Patients generally develop symptoms when the sialolith
begins to obstruct salivary flow, leading to swelling and eventually
pain that occurs before or during meals. Sialoliths present with
painfu only
(12%), stasis of saliva can ding to retrograde flow of
a of the gland, in which the patient
ductal system of the submandibular and
sublingual ducts are located beneath the mucosa of the floor of
the mouth, a stone in the sublingual gland/duct may be
misdiagnosed as of submandibular gland/duct sialolithiasis in
clinical practice especially, when it is in large and near the gland.
The location of the stone and involved gland must be known
preoperatively, because sublingual gland sialolithiasis is usually
treated with resection of the sublingual gland with the stone via
trans-oral approach, in contrast to the submandibular gland,
which is treated with transoral sailolithotomy or excision of the
submandibular gland through an extra-oral approach.
When the stone is located within the gland, it is not difficult to
identify which gland is involved using CT, however; most stones
(75% - 85%) are located in the duct. In our case the stone was
located in the submandibular gland duct (Wharton’s duct). When
l swelling (59%), painless swelling (29%), and pain
also occur lea
bacteria into the parenchym
may present with purulence from the duct, leucocytosis and
fever.
The most prominent complaint of our patient was irritation
under the tongue, which prompted her to seek the treatment.
Since both the s
Vol. 1 Issue 11 L.E.D. E-Journal Page 49
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

an accompanying abscess develops, it is easier to identify which
gland is involved and where the stone is located by physical
ay require
ial diagnosis is important because of the
pation.
If the stone is too large, or located in the proximal duct,
examination because a sublingual gland abscess mainly presents
with painful swelling over the unilateral mouth flow, whereas a
submandibular gland abscess always presents with painful
swelling over the submandibular area of the neck. Our patient
complained of mild irritation with respect to ventral surface of
tongue. Sialolithiasis treatment depends on the localization of the
salivary calculus, for those closer to the ostium, duct
catheterization and dilatation facilitate and allow retrieval of the
sialolith. For those located in the anterior half of the duct,
surgical intervention is the best choice. Finally the ones located in
the posterior region of the duct or within the gland m
total gland removal.
In our patient, the stone was located in a position jutting out
of the orifice so the patient was relieved of her complaining
symptom by a simple outpatient procedure in which a small
incision was given around the orifice of the duct and the stone
popped out by simple bi-digital manipulation of the duct.
Solitary sialoliths usually do not recur; although chronic multiple
recurrence of sialolith has been reported. Lustmann et al
estimated that the recurrence rate of sialolithiasis is 8.9%. In our
patient, the follow-up was for two months post operatively and
there had been no recurrence.
CONCLUSION
Standard mandibular occlusal radiograph is one of the best
diagnostic options to determine the calculus in the
submandibular gland duct. Sialography, Ultrasonography,
Computerized Tomography and MRI may help in diagnosis.
Preoperative different
different surgical approaches. The primary objective of the
treatment of the sialolith is the restoration of the normal salivary
secretions. Different treatment options may be selected according
to the size and location of the sialolith. Small stones often may be
“milked out” through the ductal orifice using bimanual pal
Vol. 1 Issue 11 L.E.D. E-Journal Page 50
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

piezoelectric extracorporal shock wave lithotripsy or surgical
removal of the stone or the gland may be required.
BIBLIOGRAPHY
1. Batori M., G. Mariotta et al: Diagnostic and surgical
management of submandibular gland sialolithiasis: report of a
ual size: ERMPS: 2005; 9:67-68.
5. Eyigor H., Osma U., Yılmaz M.D., Selcuk O. T. Multiple
sialolithiasis in sublingual gland causing dysphagia, Am J
Case Rep, 2012; 13: 44-46
6. Hong KH, Yang YS: Sialolithiasis in the sublingual gland. J
LaryngolOtol, 2003; 117(11): 905–7
zoni D, de Carvalho PS et al: Sialolithiasis of the
literature. J Oral
and a
d]
]
stone of unus
2. Bodner L. Salivary gland calculi: Diagnostic imaging and
surgical management. Compendium 1993; 14:572-86.
3. Cawson RA, Odell EW. Essentials of oral pathology and oral
medicine.6th ed. pp 239-40. Ediburgh: Churchill Livingstone,
1998.
4. Choi J, Kim K, and S. Oh: Multiple sialoliths in sublingual
gland: report of a case. Int J. Oral MaxillofacSurg, 2002; 31(5):
562–63
7. Jardim EC, Pon
submandibular gand. J CraniofacSurg, 2011; 22(3): 1128–31
8. Ledesma-Montes C, Garcés-Ortìz M, Salcido-Garcìa JF, et al.
Giant sialolith: case report and review of the
MaxillofacSurg 2007; 65: 128-30.
9. Leung AK, Choi MC, Wagner GA. Multiple sialoliths
sialolith of unusual size in the submandibular duct. Oral Surg
Oral Med Oral Pathol Oral RadiolEndod 1999; 87: 331-33
[PubMe
10. Levy DM, ReMine WH, Devine KD. Salivary gland calculi. Pain,
swelling associated with eating. JAMA 1962; 181: 1115-1119
[PubMed
11. Liao L.J., Hsiao J. K., Hsu W.C., Sublingual gland sialolithiasis:
a case report Kaohsiung J Med Sci2007;23:590–3)
Vol. 1 Issue 11 L.E.D. E-Journal Page 51
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
12. Lustmann J, Regev E, Melamed Y. Sialolithiasis: A survey on
245 patients and a review of the literature. Int J Oral
of
PubMed]
MaxillofacSurg 1990; 19:135-8.
13. Marchal F, Dulguerov P. Sialolithiasis management: the state
the art. Arch Otolaryngol Head Neck Surg2003; 129:951–6.
14. McKenna JP, Bostock DJ, McMenamin PG. Sialolithiasis. Am
Fam Physician 1987; 36: 119-25. [
15. Nahalieli o, Eliav E, Hasson O, Zagury A, Baruchin AM.
Pediatric sialolithiasis. Oral Surg Oral Med Oral Pathos
OralRadiolEndod 2000; 90: 709-12.
16. Rauch S, Gorlin RJ:Diseases of the salivary glands. In: Gorlin
RJ, Goldman HM, editors. :Thoma’s Oral Pathology (6thedn), vol
2. St Louis: Mosby; 1970. p. 997-1003.
17. Stafne, E. C., and Gibilisco, .I. A.: Oral Roentgenographic
Diagnosis, ed. 4, Philadelphia, 1975, W. B. Saunders
Company,pp. 135-141.
18. Tyler T. Boynton, DMDStuart E. Lieblich, Unusual case of a
sialolith: a case report. 2014;117:1:e9–e10.
19. Williams MF.Sialolithiasis.OtolaryngolClin North Am 1999
Oct;32(5):819-34 [PubMed]
20. Yildirim A. A case of giant sialolith of the submandibular
Six years of practical
eep Singh Ahuja at
his email id: [email protected]
salivary gland. Ear Nose Throat J. 2004 May;83(5):360-1
[PubMed]
21. Ziegler CM, Steveling H, Seubert M et al: Endoscopy: a
minimally invasive procedure for diagnosis and treatment of
diseases of the salivary glands.
experience. Br J Oral MaxillofacSurg, 2004; 42(1): 1–7.
P.S. Any feedback/compliments/queries for the Author/s should
be emailed to the Editor-in-Chief, Dr. Bhavd
Vol. 1 Issue 11 L.E.D. E-Journal Page 52
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
Doosra Gyaan
Vol. 1 Issue 11 L.E.D. E-Journal Page 53
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Dr. Ajay Kakar is a Periodontist from N.H.D.C. Mumbai, 1985. He is the currently, the President of International Academy of Periodontology. He is a Clinical Associate Professor in Stony Brook, SUNY-USA & a faculty in Manchester University for the Distance Education Program. He is the author of a handbook on Splinting (Management of Mobile & Migrating Teeth) published in an International Journal. He is a genius with a thorough & detailed knowledge on Computers and has written a book as well for the beginners. He is the founder director of Bite-In and is a clinician par excellence with current practice in Le-Visage Dental Clinic, Chembur, Mumbai, with practice limited to Periodontology & Implants.
Power Scaling
Boon or Bane
Part III
Author: Dr. Ajay Kakar
POWER DRIVEN SCALERS
The origins of power driven scaling has very unique origins. The
first ultrasonic scaler was intended to be an instrument for cavity
preparation, but the company had not accounted for the
resiliency of the dentinal tubules. Instead of using the instrument
for cavity preparation it worked adroitly as an instrument for the
removal of plaque and calculus.
Effective ultrasonics can be applied when electrical energy
is converted into mechanical energy with surface vibrations in
excess of 20,000 Hz, a level beyond human hearing. Calculus,
dental cementum, stains and other soft and hard deposits that
collect on teeth can be removed with this instrumentation.
Power driven scalers can be classified into three groups based on
the basic design ideology of the equipment. These are
1. Sonic Scalers
2. Magnetostrictive Scalers
3. Piezo Electric Scalers
All the above types of scalers work with slightly different
methodologies and hence have varying degrees of efficiency. A
clinician should be aware of the different characteristics of these
scalers to be able to decide and choose the most suitable
equipment.
Vol. 1 Issue 11 L.E.D. E-Journal Page 54
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

1. Sonic Scalers: Sonic scalers are driven by compressed air and
create vibratory energies from pressure. Sonic scaler
handpieces will generally fit onto the regular air rotor
handpieces. They generally work at frequencies ranging from
1500 to 7000 Khz depending upon the handpiece and the
pressure of the compressed air.
These scalers have a wide range of amplitude which is
upto 1.5 mm from the center and the tip generally moves in an
orbital fashion. Sonic scalers are susceptible to hand-pressure
damping, which limits the amount of energy which can be
applied to the tooth surface and this thereby lessens the
efficiency of the scaler.
Sonic scalers do not even exhibit a phenomenon
known as cavitation. On a comparison level with the other two
kinds of scalers, sonics are not as efficient in removal of
calculus. In spite of the not so great efficiency at removal of
calculus, these units are capable of removing more than 100
um of cementum during routine debridement. The average
width of the cementum is about 150 um and most of this layer
can be lost if extreme care is not taken while scaling with these
units.
The sonic instruments should be used only on supragingival
areas and never in areas of recession or exposed root surfaces.
A few of the commonly available Sonic scalers are available
from JR Rand Corp, Kavo, Kinetic Instruments, Medidenta and
Star Dental. All these scaler handpieces or at least the tips are
autoclavable. Almost all of them operate at a vibratory
frequency of 6000 Mhz. These scalers generally have upto 3
tips in different shapes for accessing various sites in the oral
cavity. These scalers have been in use now for close to 20
years.
2. Magnetostrictive Scalers: These class of scalers can easily
lay claim as the first kind of ultrasonic devices to be made for
power driven scaling. These instruments work on the principle
of conversion of electrical energy to magnetic energy to
vibratory energy. The vibration of the tips of these scalers is
Vol. 1 Issue 11 L.E.D. E-Journal Page 55
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
elliptical in nature which enhances the application of energy to
the tooth for debridement.
Magnetostrictive scalers have a base unit and metal
inserts of different tip shape and sizes. The base unit processes
the electrical energy and applies it to the inserts. The insert
has a stack of metal plates at the base which is inserted into
the socket of the base unit. The other end of the insert is the
actual working tip. The stack is made up of flat metal strips
sandwiched together. When the electrical signal is turned on, a
low voltage mechanical signal is generated in the handpiece,
creating a magnetic field of fluctuating intensity. The metal
stack acts like an attenuated antenna that picks up the
magnetic field and causes a rapid vibration which is in turn
transferred to the tip which shatters the calculus as soon as it
comes in contact with the tip.
These units generally operate at a frequency of
25,000 to 30,000 Hz. The tips of these instruments have four
working surfaces and these four surfaces are active at different
speeds with energy dissipation decreasing in descending order
from the tip end, front surface and the sides. The tips of
magnetostrictive scalers have a large amplitude of stroke which
also results in a higher power. As the power/amplitude
increases the patient comfort decreases.
The tips are available in a variety of ranges
and the thick tips can be used on higher power settings, but
the thin tips should be preferably used only with a very low
power setting. The larger tips make it pretty difficult to access
furcation areas and hence Dentsply has introduced a slim line
series of tips to be able to access such areas.
Of all the classes of power scalers, these
generate the maximum amount of heat. Close to 60% of the
electrical energy is lost in the form of heat energy. A resultant
of this great amount of heat production is the necessity of a
copious amount of water for the purpose of cooling the tip. A
positive fall out of the copious water is the cavitation and
irrigation of the pocket during the debridement.
Cavitation is the phenomenon by which
Vol. 1 Issue 11 L.E.D. E-Journal Page 56
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
numerous bubbles which eventually collapse, producing shock
waves in the liquid causing the cavitation with a flushing
action. This cavitation has been known to demonstrate cell-
wall rupture, which results in removing deposited bacterial
endotoxim from the root surface. Units are available in which
the water can be replaced by a medicated solution to be
delivered into the pocket while debridement from an attached
reservoir. A negative effect is the aerosol which is produced
requiring high speed suction units and controlled asepsis.
These units are standardly available as fixed
frequency units. A few of them are also available with a
variable manual tune frequency mode. This variable frequency
allows for alteration of energy, frequency and the amount of
water. These setting have to be optimized for various uses and
different locations. The technology of these system vibrations
can be detected in the handpiece where the metal stacks are
vibrate at a rapid frequency. Even though the human ear
cannot decipher sound at a range of 25000 Hz the sound
generated by the contact of the tip to the tooth can be quite
bothersome.
A very new system available is the sustained
performance system from Dentsply, which involves the
stabilization of the insert stroke levels at all power settings. A
specially designed dual-loop feedback circuitry allows the
insert to talk to the scaler during prophylaxis. The system
responds immediately to the inserts needs and clinical power is
not lost when the insert tip touches the tooth surface. This
allows the insert tip to maintain its stroke and frequency at all
power settings, even in the presence of tenacious calculus.
With a lower stroke and controlled power settings there is a
greater comfort to the patient. A temporary power boost can be
provided for very tenacious calculus by pressing the foot
control in the fully depressed position.
Dentsply is one of the original companies which
brought out the magnetostrictive scaler. The other major
brands available are the Parkell scaler and the HSP Sonic II. A
unique design of magnetostrictive scaler is the Odontoson from
Vol. 1 Issue 11 L.E.D. E-Journal Page 57
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Goof. It has a ferrite core rod instead of the stacked metal
insert. This scaler operates at a constant 42,000 Hz frequency.
They have a rotational work pattern and all the sides are
equally active. Stacked metal inserts have only about 6 mm of
an active surface; the ferrite rods have upto 13 mm of active
surface length. Another excellent benefit is that less than 3% of
the energy is converted into heat. It does have a water
irrigation line which is basically used for its benefit of
cavitation and irrigation rather than cooling. This scaler does
not require a foot pedal since an electronic swith is located on
the handpiece itself which comes on as soon as the tip touches
the tooth surface. All the components of this scaler are
autoclavable. The reservoir and pump is located outside of the
scaler and only an electrical supply is required to get it up and
running. The insert tips are made of titanium which increases
the life span of the tip. Another unique aspect of this scaler is
the least amount of amplitude, about 0.1 to 0.2 mm from the
centre. One negative of this scaler is that the Ferrite insert is
very brittle and tends to break very easily with the slightest
impact.
3. Piezo Electrical Scalers: This class of scalers uses a crystal
system to transfer electrical energy directly to magnetic energy
without and magnetic interface. The scalers have a piezo
ceramic drive mechanism that produces a horizontal tip
movement in a back and forth stroke. The handpiece of these
class of scalers is the most ergonomic in utility. The units have
crystals within the handpiece that become distorted by the
incoming electrical current to create vibratory energy which is
translated to the insert tip. There is almost no loss of energy in
this process and hence negligible heat production.
These scalers are the first scalers to have the
potential to work at frequencies of upto 45,000 Hz but
generally are available at fixed frequencies of 32,000 Hz. Since
these tips vibrate in a back and forth linear motion, only
lateral surfaces are active. This requires a little bit of
experience and experience in adapting the tip surface properly
Vol. 1 Issue 11 L.E.D. E-Journal Page 58
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

so that the inactive areas are not pressed on the tooth surface.
The scaler creates a vortex action in the periodontal pocket,
allowing the cavitation to progress beyond the tip. The
vibratory motion move plane generates a clean tip motion
without creating interfering vibrations at the lower powers.
This avoids a hammering effect against the root surface while
increasing patient comfort. The crystals expand and contract
about 30000 times per second.
The technique is so important that the more
the lateral force used, the less effective is the instrument due
to the decreased vibratory action. A practical idea is to use the
tip more like a probe rather than a traditional hand scaler or
curette. Newer tips are finer and shaped more like a probe for
easier utility. A new introduction from Satelec has been the
Twiny tip and the Curette tips which are available in two
forms, diamond coated and plain. The twiny tip is a diamond
shaped tip with a larger amplitude of stroke and bilateral water
irrigation. The working surfaces are the lateral surfaces of the
tip. The Twiny is a very efficient tip for excellent and very fast
and efficient removal of gross calculus. A number of clinicians
are of the opinion that the Twiny is the easiest and best tip for
the most rapid removal of supragingival calculus. A word of
caution is that the outer angle of the tip tends to get hot
during actual usage and care should be taken not to allow it to
touch any mucosal surface.
The curette tips are to be used at a low power
setting thereby at a lower amplitude. These tips are to be used
for the final finishing and removal of the very tenacious
calculus which might be supra gingival or subgingival. The
action has to be gentle and very slow. It is imperative not to
allow the fine tip, which is quite sharp to gouge the root
surface and destroy healthy cementum or enamel. These
scalers are generally multifunctional and in addition to
periodontal procedures, they can be used in conventional and
apical endodontic procedures and a few prosthetic procedures.
The leaders of this technology are Satelac and the EMS Piezo
scaler. Other models are the Spartan and the Osada scaler.
Vol. 1 Issue 11 L.E.D. E-Journal Page 59
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Dear Readers: Important Announcement
The above article by Dr. Ajay Kakar has been published in 3 parts - Part I,
II & III. The above is Part III.
Check Issue L.E.D. Issue September 2016 Vol. 1 Issue 9 for the Ist part
of the above article.
Check Issue L.E.D. Issue October 2016 Vol. 1 Issue 10 for the IInd part
of the above article.
P.S. Any feedback/compliments/queries for the Author/s should
be emailed to the Editor-in-Chief, Dr. Bhavdeep Singh Ahuja at
his email id: [email protected]
Vol. 1 Issue 11 L.E.D. E-Journal Page 60
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Teesra Gyaan
Vol. 1 Issue 11 L.E.D. E-Journal Page 61
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
Dr. Parajeeta Dikshit is an Assistant Professor, Department of Pedodontics and Preventive Dentistry (Pediatric Dentistry) at Kantipur Dental College Teaching Hospital and Research Center, Basundhara, Kathmandu and Consultant Pediatric Dentist at Smile Square Dental Care Center, Maharajgunj, Kathmandu, Nepal. She completed her graduation from KGMC Lucknow and MDS from Kathmandu University (KU-MEMG program). She is the joint secretary of Nepalese Association of Pediatric Dentistry. She has a passion for writing and writes articles for online medical journals Medchrome and Pedchrome.
Dr. Senchhema Limbu is an Assistant Professor, Department of Pedodontics and Preventive Dentistry (Pediatric Dentistry) at Kantipur Dental College Teaching Hospital and Research Center, Basundhara, Kathmandu, Nepal. She is also the Consultant Pediatric Dentist at Dharahara dental hospital and Orchid dental clinic in Kathmandu, Nepal. She is the Ex-General Secretary of Nepal Dental Association and presently, General Secretary of Nepalese Association of Pediatric Dentistry.
Early Infancy teeth A Case Report
Author: Dr. Parajeeta Dikshit
Co-Author: Dr. Senchhema Limbu
ABSTRACT
Eruption of teeth in the first three months of birth is a relatively
rare phenomenon. The teeth present in the oral cavity at birth are
known as natal teeth, those which erupt during the first 30 days
after birth as neonatal teeth and the premature teeth that erupt
after 30 days and within 3 months are termed as Early infancy
teeth. The lower incisor region is the most common site of
eruption of these teeth. Early detection and treatment of these
teeth are recommended as they may cause feeding difficulties,
ulceration on the tongue and oral mucosa as well as aspiration or
swallowing. A case of Early Infancy Teeth with healing ulcer on
the tongue in a 40 day old infant is reported in this article.
KEYWORDS
Early Infancy teeth, natal teeth, neonatal teeth, tooth mobility,
extraction.
INTRODUCTION
Eruption of tooth is a major developmental milestone anticipated
by the parents. The timing of eruption though may vary
Vol. 1 Issue 11 L.E.D. E-Journal Page 62
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
depending on hereditary, endocrinal and environmental factors.
At times, first teeth may be present at birth or erupt during the
first or first few months of life. The etiology of this anomaly
remains unknown and is considered to be multifactorial.
Clinically the premature teeth may be normal in size and shape
or may present alterations like conical or shell like crowns, with
enamel hypoplasia or yellow-brownish discoloration. The teeth
may further cause certain complications like pain on suckling to
the mother difficulty in feeding as well as ulcerations on the
tongue for the infants. The early eruption of teeth does not come
easy and is attached to many social taboos considering it to be a
bad omen. In some countries due to various superstitions it
creates anxiety in the parents who want it to be removed at the
earliest.
CASE REPORT
History & Chief Complaint
A 40 days old infant was referred to the department of Pediatric
Dentistry, Kantipur Dental college teaching hospital and research
center, with the chief complaint of erupted lower teeth. The
parents had noticed the teeth 3 days back and reported of ulcer
on the undersurface of the tongue. A Pediatrician had been
consulted for ulceration of the tongue and the infant was under
topical medication for the same. The child was born through
normal delivery with no complications during pregnancy as well
as after birth. He appeared healthy physically and weighed 3
kilograms.
Intra-Oral Examination
The dental examination revealed the presence of two teeth
resembling the central incisors in the mandibular incisor region
(Fig. 1). The crowns of both teeth were rectangular in shape and
white in color without any signs of discolorations (Fig. 2). The
teeth exhibited grade III mobility. The associated gingiva appeared
to be normal. A healing ulcer was present on the ventral surface
of the tongue.
Vol. 1 Issue 11 L.E.D. E-Journal Page 63
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Fig-1: Intra-Oral Examination View
Fig-2: Teeth resembling Central Incisors
Treatment Plan
The treatment planned was extraction of teeth due to chances of
aspiration.
Treatment Protocol followed
1. The teeth were extracted under topical local anesthesia using
forceps.
2. It was followed by curettage of the socket to remove any
odontogenic cellular remnants.
3. The extracted teeth had slightly developed roots (Fig. 3).
Vol. 1 Issue 11 L.E.D. E-Journal Page 64
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Fig-3: Extracted tooth with slightly developed roots
4. The procedure was well tolerated by the child.
5. The teeth were sent for histological investigation and it was
reported to have thin dentin with normal appearing pulp and
a faint amount of cementum.
6. Post operative complications were not reported and the ulcer
had healed completely on the follow up visit after 7 days (Fig.
4).
Fig-4: Healed Ulcer after 7 days
DISCUSSION
Vol. 1 Issue 11 L.E.D. E-Journal Page 65
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
Presence of teeth in the oral cavity in the first three months after
birth is rare. Teeth present at the time of birth are Natal teeth
and the teeth that erupt within 30 days after birth are known as
Neonatal teeth. In the above case the teeth erupted after 35 days
of birth so it was categorized as Early Infancy teeth. Early Infancy
teeth are teeth that do not confirm the criteria described for natal
or neonatal teeth and erupt within one to three and a half months
after birth. Early Infancy teeth have been reported rarely and are
less common than natal or neonatal teeth. Some other synonyms
used by authors are Congenital teeth, Fetal teeth, Pre-deciduous
teeth, Premature teeth, Precociously erupted teeth and Dentitia
praecox.
The exact etiology for the premature eruption or for appearance
of natal and neonatal teeth is not known. Earlier the neonatal
teeth were considered cysts of the dental lamina of the newborn
and would occur due to inheritance as dominant autosomal trait.
Infection, febrile states, trauma, malnutrition, superior placement
of tooth germ is considered to be other factors in its etiology.
Multiple syndromes like Ellis-van Creveld syndrome, Pierre Robin
syndrome, Hallermann-Streiff syndrome have been reported to be
associated with this condition though none were noticed in the
present case.
The prematurely erupted teeth occur most commonly in the
mandibular incisors region (85%), followed by maxillary incisors
(11%), mandibular cuspids (3%) and maxillary cuspids or molars
(1%). Kates et al reported sixty-one percent of the subjects had a
pair of natal or neonatal teeth (or both) like in this case.
Morphologically, the premature teeth maybe well developed
or poorly developed with small cone shaped crowns. They may
have a yellowish-brown or whitish opaque color with hypoplastic
enamel or dentin. In our cases the teeth had well developed crown
resembling deciduous incisors with slight root formation.
Hebling classified natal teeth into 4 clinical categories:
1. Shell-shaped crown poorly fixed to the alveolus by gingival
tissue and absence of a root.
Vol. 1 Issue 11 L.E.D. E-Journal Page 66
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

2. Solid crown poorly fixed to the alveolus by gingival tissue and
little or no root.
3. Eruption of the incisal margin of the crown through gingival
tissue.
4. Edema of gingival tissue with an unerupted but palpable
tooth.
Histologically, these teeth have dysplastic or hypomineralized
enamel, irregular dentin and osteodentin in the cervical portions
and interglobular dentin in the coronal regions with rich
vascularization of pulp. The incisal edge might lack enamel.
Hertwig’s sheath and cementum might be absent. In the present
case, histologically dentin and pulp appeared normal while only a
faint amount of cementum could be noted.
Traumatic ulceration occurring on the tongue due to
repetitive trauma by the premature teeth has been termed Riga-
Fede disease. It frequently involves the ventral surface of the
tongue or the lingual frenum as tongue constantly rakes over the
teeth.
For the determination of treatment options, it is essential to
perform radiographic examination to check the amount of root
development and to confirm if the teeth belong to primary
dentition. It was suggested in this case but was declined by the
parents. Excessive mobility, risk of aspiration or swallowing and
discomfort to the infant and to the mother are other factors that
determine the treatment protocol. If the degree of tooth mobility is
more than 2 mm, the natal teeth of category (1) or (2) usually
need extraction. The risk of swallowing and aspiration
necessitated extraction as the treatment of choice for the present
case.
Extraction does not usually pose any difficulties as these teeth
can be removed with forceps or even with the fingers. However,
precautions have been recommended when extracting these teeth
in a child up to the 10th day of life. Vitamin K needs to be
administered before extraction to prevent hemorrhage and
unnecessary injury to the gingiva should be avoided and one has
to be alert during extraction to avoid aspiration.
Vol. 1 Issue 11 L.E.D. E-Journal Page 67
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Prematurely erupted true deciduous teeth if diagnosed as
a tooth of the normal dentition without any complications should
not be extracted. Incisal edges causing the trauma to mother or
child can be rounded off and the tooth retained. The mobility of
some premature teeth has been noted to decrease with time.
Kates et al found good prognosis for natal and neonatal teeth that
survived beyond 4 months.
CONCLUSION
Premature teeth are relatively rare with multiple causes
attributed to its development. They may or may not be associated
with syndromes. The treatment should be based on the symptoms
or complications presenting with it. A multidisciplinary approach
between pediatricians and pediatric dentist is required to manage
such cases appropriately.
REFERENCES
1. Jingarwar MM, Bajwa NK., Pathak A. Riga Fede Disease:
Fibrous Hyperplasia Associated with Natal Teeth in an Infant –
A Case Report and Clinical Update. Indian Journal of Neonatal
Medicine and Research Jul 2014; 2(1): 11-13.
2. Mamta Malik, Ravinder Singh Saini, Rahul Jain, Sanjeev
Laller. A Comprehensive Update: Predecidous Teeth (Natal and
Neonatal). Journal of Advanced Medical and Dental Sciences
Research April-June 2014;2( 2) :90-94.
3. Anegundi RT, Sudha P, Kaveri H, Sadanand K. Natal and
neonatal teeth: A report of four cases. J Indian Soc Pedod Prev
Dent 2002; 20(3):86-92.
4. Ertas ET , Sekerci AE, Sisman Y, Sahman H, Etoz M. Natal
Teeth: A Report of Three Cases. J Oral Health Comm Dent
2013;7(2):127-131.
5. Nitin Sharma, Subhash Chander, Shweta Soni, Shamsher
Singh, Madan Gopal Chodhary.Riga-Fede Disease Due to
Neonatal Tooth: A Case Report. International Journal of Oral &
Maxillofacial Pathology 2012; 3(2):43-44.
Vol. 1 Issue 11 L.E.D. E-Journal Page 68
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

6. Shubhangi Mhaske, Monal B. ,Yuwanati, Ashok Mhaske, Raju
Ragavendra, Kavitha Kamath and Swati Saawarn. Natal and
Neonatal Teeth: An Overview of the Literature. ISRN Pediatrics
2013; vol 2013(Article ID 956269): 11 pages.
7. Cunha RF, Boer FAC, Torriani DD. Natal and neonatal teeth:
review of the literature. American Academy of Pediatric
Dentistry 2001; 23: 158-162.
8. Sumedh S. Khare, Rahul Hegde, Namrata Mathrawala.
Neonatal Teeth: A Report of Three Cases. Indian Journal of
Dental Sciences June 2014;6 (2):89-90.
9. Nalam Sai Gautam, N. Radhika Gautham. Natal Teeth – Report
of Two Cases. Adv Hum Biol 2014; 4(2):81-84.
10. Chow MH: Natal and neonatal teeth. J Am Dent Assoc 1980;
100: 215-6.
11. Vaishali Shende,Sandhya Srivastava, Aruna Holani, Ranjit
Patil. Natal Teeth: Clinical study of seven cases. Journal of
Indian Academy of Oral Medicine and radiology Oct-Dec
2011;23(4) : 654-5.
12. Kates GA, Needleman HL, Holmes LB. Natal and neonatal
teeth: a clinical study. J Am Dent Assoc 1984; 109:441-3.
13. Swati Chowdhary,Sandeep Tandon. Congenital teeth:
Superstition and Reality – A Case Report and Review of
Literature. International Journal of Scientific Study Feb 2014;
1(5):53-56.
14. Shalini Gupta, Kavita Nitish Garg, Divya Mehrotra and O P
Gupta. Natal Teeth: A Clinical Report. Asian Journal of Oral
Health & Allied Sciences Jul-Sep 2011;1(3): 205-8.
15. Hebling J, Zuanon ACC, Vianna DR. Dente Natal-A case of
natal teeth.Odontol Clín 1997; 7(1): 37-40.
P.S. Any feedback/compliments/queries for the Author should be
emailed to the Editor-in-Chief, Dr. Bhavdeep Singh Ahuja at his
email id: [email protected]
Vol. 1 Issue 11 L.E.D. E-Journal Page 69
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Chautha Gyaan
Vol. 1 Issue 11 L.E.D. E-Journal Page 70
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
Dr. Abhijeet Bhasin completed his graduation from Modern Dental College and Research Center, Indore in 2007. He had his basic and advance implantology training from Goethe University, Germany and has been practicing Oral Implantology since the past 8 years. He is Member, Indian Society of Oral Implantology (ISOI). He is Vice President (WAUPS) South East Asia. He maintains a dedicated Dental Implant Center and an Implant Training Academy in Indore.
Ridge Split Technique and Bone Expansion Osteotomy
For Successful Rehabilitation
Author: Dr. Abhijeet Bhasin
ABSTRACT
Lack of sufficient bone to place an implant in a functionally and
esthetically appropriate position is a common problem in a
narrow edentulous alveolar ridge. Less than 5 mm bucco-
palatally/bucco-lingually posses a problem for the implant
supported restorations. Ridge split technique seems to be a
reliable and simple option with less morbidity and satisfactory
rehabilitation. Survival and the success of the implants placed
with this technique were consistent with those placed in non
reconstructed bone.
KEYWORDS
Ridge Split, Bone Expansion, Tooth Loss.
INTRODUCTION
Dr. Hilt Tatum 1970’s introduced a method of the ridge splitting
or bone spreading which over a period has been used in implant
dentistry for esthetic rehabilitation and implant bed preparation
in cases of deficient alveolar ridges to satisfy the basic ideal need
for the hard tissue augmentation for functional and esthetic
outcome of implants. Ridge split procedures are commonly
performed for horizontal augmentation of narrow ridges which
would otherwise preclude implant placement.
The labial alveolar bone often undergoes rapid reconstruction
after natural tooth loss with approximately 25% decrease in
volume during 1st year, followed by 40-60% decrease in width in
following next 3 years leading to the labial cortex of bone more
medial than its original position. Loss of bucco-palatal dimension
of ridge further necessitates calls for additional procedure to
receive optimum implant borne prosthesis. Management of such
Vol. 1 Issue 11 L.E.D. E-Journal Page 71
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

defect becomes still critical in esthetic zone. Thus due to this
sequel of resorption after tooth loss jeopardizes the functional and
esthetic outcome of treatment.
SEIBERT’S CLASSIFICATION OF RIDGE DEFORMITIES
1. Class I – Bucco-lingual loss of tissue contour with a normal
apico-coronal height.
2. Class II – Apico-coronal loss of tissue with normal bucco-
lingual contour.
3. Class III – A combination of bucco-lingual and apico-coronal
loss.
4. Ridge described according to the depth of loss: Mild
Less than 3 mm.
5. Ridge described according to the depth of loss: Moderate
Around 3-6 mm
6. Ridge described according to the depth of loss: Severe
Greater than 6 mm
7. Class N: Normal: Minimal height and deformity 9% of all
edentulous ridges
The segmental ridge split procedure (SRSP) creates a crypt
surrounded by bone and periosteum into which implants and
bone graft material can be introduced with reasonable
predictability so that new bone can be constructed which
provides a solid base for dental implant to seat in.
PRE SURGICAL ASSESSMENT
Patient should be healthy and mentally adjusted for the
placement of implants. Patient with poor oral hygiene is NOT the
candidate for the procedure. Patients radiographic records e.g.
OPG, CBCT help in proper assessment of the bone width and
bone quality. The pre-operative intra-oral picture showed thin
and narrow ridge with significant reduction in the bucco-lingual
dimensions (Fig. 1 & Fig. 2).
Vol. 1 Issue 11 L.E.D. E-Journal Page 72
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
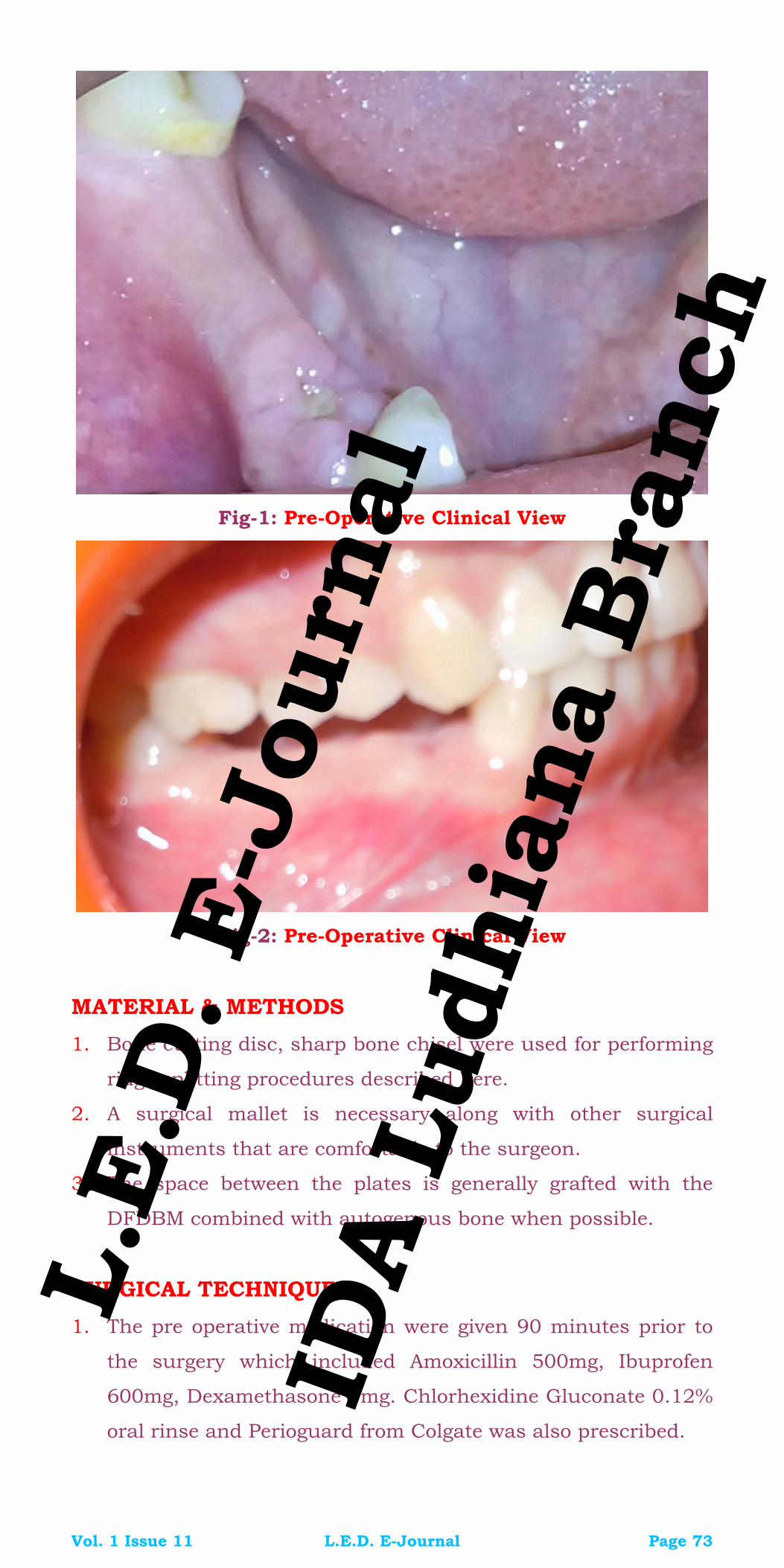
Fig-1: Pre-Operative Clinical View
Fig-2: Pre-Operative Clinical View
MATERIAL & METHODS
1. Bone cutting disc, sharp bone chisel were used for performing
ridge splitting procedures described here.
2. A surgical mallet is necessary along with other surgical
instruments that are comfortable to the surgeon.
3. The space between the plates is generally grafted with the
DFDBM combined with autogenous bone when possible.
SURGICAL TECHNIQUE
1. The pre operative medication were given 90 minutes prior to
the surgery which included Amoxicillin 500mg, Ibuprofen
600mg, Dexamethasone 4mg. Chlorhexidine Gluconate 0.12%
oral rinse and Perioguard from Colgate was also prescribed.
Vol. 1 Issue 11 L.E.D. E-Journal Page 73
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

2. A mid-crestal incision was given with BP Blade No. 15
through out the edentulous area (Fig. 3).
Fig-3: Mid-Crestal Incision
3. A gentle full thickness flap reflection was done and the bone
was measured with bone measuring caliper at different sites
which helped in determining the amount of available bone bed
and the requisite bone expansion to be done (Fig. 4).
Fig-4: Bone Measuring with the Caliper
Vol. 1 Issue 11 L.E.D. E-Journal Page 74
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

4. Crestal corticotomy was done with bone trimming burs (by
ADL Bio) to create a platform for the split with rotary disc (Fig.
5).
Fig-5: Crestal Corticotomy
Fig-6: Horizontal Cut over the prepared bone bed
Vol. 1 Issue 11 L.E.D. E-Journal Page 75
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

5. The horizontal cut was given over the prepared bone bed, with
the use of the sharp chisel and the initial separation of the
two cortical plates was done (Fig. 6).
Fig-7: Ridge Expansion in Progress
Fig-8: Ridge Expanded with Chisel and Mallet
Vol. 1 Issue 11 L.E.D. E-Journal Page 76
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

6. The use of a narrow chisel is recommended which upon
penetrating (by impacting) into the marrow spaces induces
vestibular expansion of the oral cortical process (Fig. 7 and
Fig. 8).
7. The pilot drill was used to prepare the osteotomy site.
Fig-9: Noris Implant being inserted into Osteotomy Site
Fig-10: Noris Implant being inserted into Osteotomy Site
8. On confirmation with the X-ray, the sequential drilling till the
required length and width of the implant is been done
Vol. 1 Issue 11 L.E.D. E-Journal Page 77
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

simultaneously Three Noris Medical Implants of sizes 3.75 by
11.5mm ONYX (44), 3.75 by 11.5mm TUFF (45) and 4.2 by
11.5mm TUFF (46) were placed followed by cover screw
placement (Fig. 9, Fig. 10, Fig. 11 & Fig. 12). Bone graft from
Allograft from Tata Memorial Hospital was used.
Fig-11: Noris Implants with cover screws
Fig-12: Implants as seen on the Post-Operative X-ray
Vol. 1 Issue 11 L.E.D. E-Journal Page 78
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
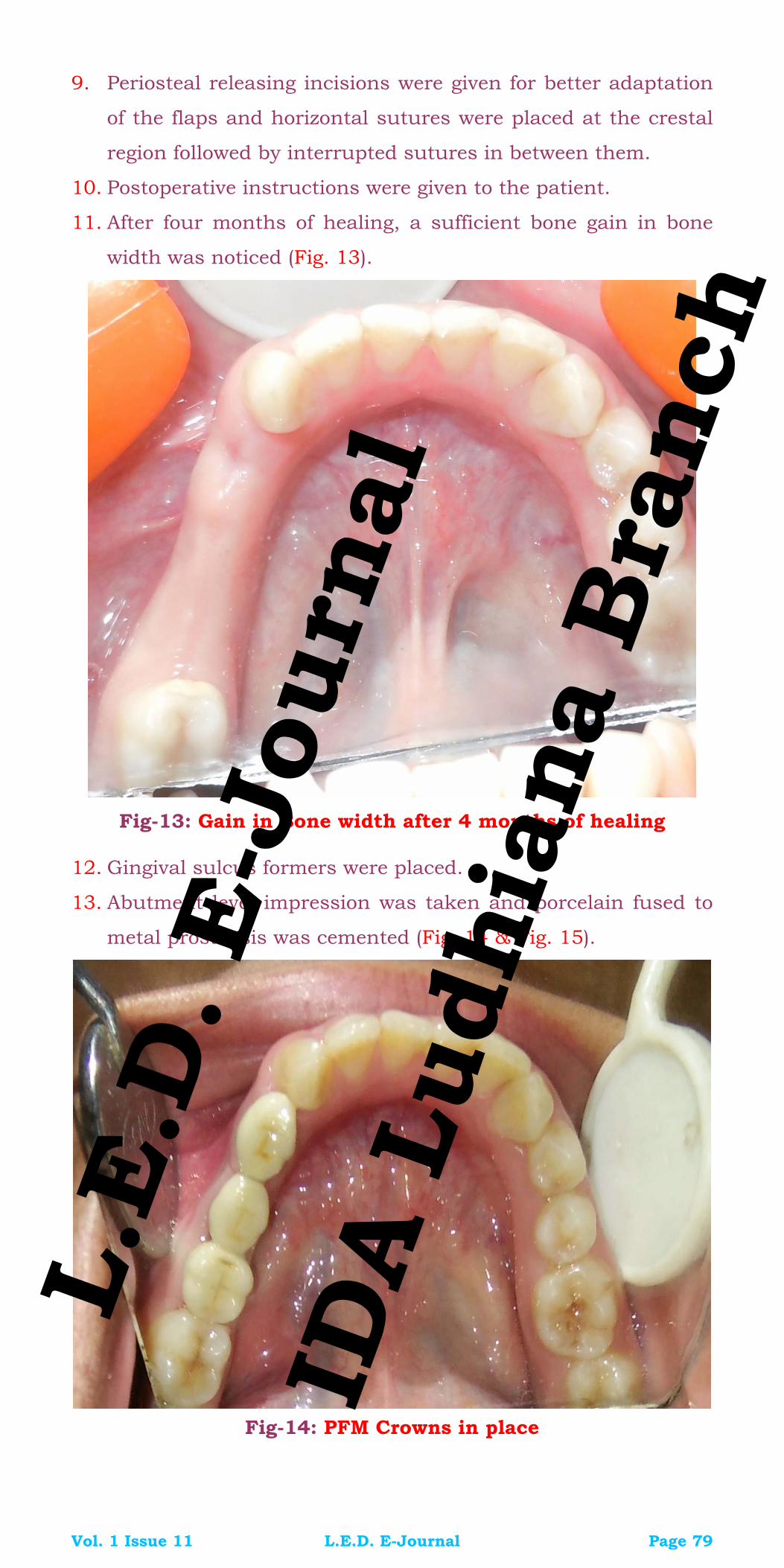
9. Periosteal releasing incisions were given for better adaptation
of the flaps and horizontal sutures were placed at the crestal
region followed by interrupted sutures in between them.
10. Postoperative instructions were given to the patient.
11. After four months of healing, a sufficient bone gain in bone
width was noticed (Fig. 13).
Fig-13: Gain in Bone width after 4 months of healing
12. Gingival sulcus formers were placed.
13. Abutment level impression was taken and porcelain fused to
metal prosthesis was cemented (Fig. 14 & Fig. 15).
Fig-14: PFM Crowns in place
Vol. 1 Issue 11 L.E.D. E-Journal Page 79
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
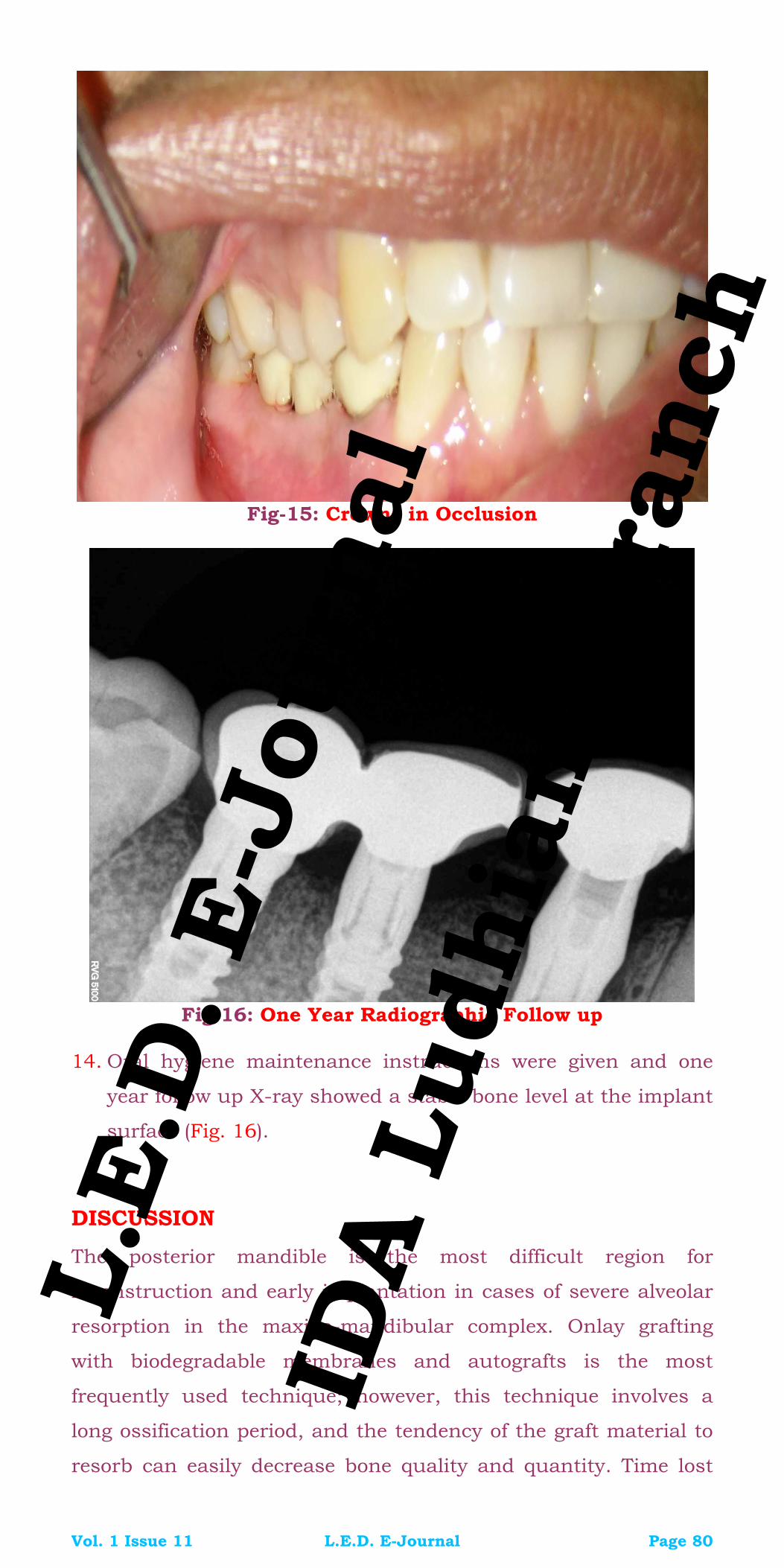
Fig-15: Crowns in Occlusion
Fig-16: One Year Radiographic Follow up
14. Oral hygiene maintenance instructions were given and one
year follow up X-ray showed a stable bone level at the implant
surface (Fig. 16).
DISCUSSION
The posterior mandible is the most difficult region for
reconstruction and early implantation in cases of severe alveolar
resorption in the maxillo-mandibular complex. Onlay grafting
with biodegradable membranes and autografts is the most
frequently used technique; however, this technique involves a
long ossification period, and the tendency of the graft material to
resorb can easily decrease bone quality and quantity. Time lost
Vol. 1 Issue 11 L.E.D. E-Journal Page 80
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

and donor-side morbidity are the main disadvantages of this
reconstructive approach. The split-crest technique should be
delineated as a bone expansion procedure, which potentially
eliminates the overall disadvantages of Onlay grafting for esthetic
and functional demand, with the advantage of a shorter treatment
time. Careful preparation of the bone and maintenance of an
attached periosteum are critical to the formation of new bone
around the interproximal surfaces of the implants. Wound
healing in these cases is similar to the fracture repair of bone.
The gap is filled with a blood clot, which is organized and
replaced with woven bone and further matures into load-bearing
lamellar bone at the implant interface. The ridge splitting
technique is used to expand the edentulous ridge for implantation
or insertion of inter-positional bone graft.
Significant advantages of ridge expansion rather than Onlay
grafting include simultaneous implant placement and grafting,
lower cost, lower possibility of cross-infection from graft materials
and lower morbidity. This technique has greater predictability,
since the grafted area is essentially a five-wall bony defect, with
excellent blood supply. This technique is only suitable for
enhancing ridge width. There must be adequate available bone
height for implant placement, and no vertical bone defect should
be present. A minimum of 3 mm of bone width, including at least
1 mm of cancellous bone is desired to insert a bone chisel
between cortical plates and consequently expanding the cortical
bones. The thinner cortical plates and softer medullary bone
make the maxillary ridge easier to expand. The risk of malfracture
of the osteotomized segment is high in the mandible due to
thicker cortical plates.
The disadvantage of this procedure is that if the
complication arises and bone loss occurs, the patient is left with a
larger bone defect than before. If favorable conditions are not
present, clinician might prefer Onlay augmentation. Therefore,
appropriate case selection and surgical technique is of great
importance when considering the application of this technique.
CONCLUSION
The present case demonstrated that none of the implants placed
in the bone gap created by ridge expansion was lost and all were
successfully osseointegrated. Hard as well as soft tissue
Vol. 1 Issue 11 L.E.D. E-Journal Page 81
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

structures revealed favourable and stable results with a follow-up
of one year. Overall, the advantage of this treatment procedure
was the ability to insert dental implants into a much
compromised bony site in a simultaneous procedure, meaning
only one operation in total with less total healing time compared
to the established treatment methods. But like with other delicate
surgical techniques, the ridge splitting stabilization technique
appears to be more user sensitive.
REFERENCES
1. Basa S, Varol A, Turker N. Alternative bone expansion
technique for immediate placement of implants in the
edentulous posterior mandibular ridge: a clinical report. Int J
Oral Maxillofac Implants. 2004;19(4):554–8.
2. Misch CM. Implant site development using ridge splitting
techniques. Oral Maxillofac Surg Clin North Am. 2004;16(1):65–
74.
3. Ignatius AA, Ohnmacht M, Claes LE, Kreidler J, Palm F. A
composite polymer/tricalcium phosphate membrane for guided
bone regeneration in maxillofacial surgery. J Biomed Mater Res.
2001;58(5):564–9.
4. Hollinger J, Wong ME. The integrated processes of hard tissue
regeneration with special emphasis on fracture healing. Oral
Surg Oral Med Oral Pathol Oral Radiol Endod. 1996;82(6):594–
606.
P.S. Any feedback/compliments/queries for the Author/s should
be emailed to the Editor-in-Chief, Dr. Bhavdeep Singh Ahuja at
his email id: [email protected].
Vol. 1 Issue 11 L.E.D. E-Journal Page 82
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Paanchwaa Gyaan
Vol. 1 Issue 11 L.E.D. E-Journal Page 83
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
Dr. Mayur Davda is the pioneer of training and research at dental photography school and has extensively lectured on documentation at various dental associations and universities across India. He has a long list of firsts to his credit like, the first dentist to exhibit at India’s most prestigious art gallery – The Jehangir, first dentist to exhibit at Kalaghoda art festival, first dentist to be interviewed by Better Photography and Smart Photography magazines & first dentist to be interviewed on national television just to name a few. Considered as one of the finest dental photography experts in the world he has also participated in Portugal dental congress dental photography art exhibition and the only one to represent India. He has won several awards for fine art and wildlife photography and was invited by the Consulate General of Turkey on the National day (2015) for commendable contribution in the field of photography. Famdent Awards has honored him as the highly commended Indian dental talent of the year 2015. He is currently the photomentor for GPS smile design (Las Vegas, USA) and CANON India. To know more about Dr. Mayur Davda you can visit www.mayurdavda.com, www.dentalphotogrraphyschool.in, www.thedentaleducation.com, www.liquidcanvas.in.
PHOTODONTICS – XI
Introduction to the World of Lenses!!!!!!
An Enigma or a Reality?
Author: Dr. Mayur Davda
Continued from Vol. 1 Issue 10
In our previous articles we have discussed about DSLR cameras,
intra oral accessories etc. It is equally (or probably more)
important to have a good lens for dental photography.
We discussed in short about the basics of lenses in L.E.D.
March 2016 Vol. 1 Issue 3; let’s explore the world of Lenses
in a bit more elaborate manner.
INTRODUCTION
A 100 mm macro lens is considered ideal for dental photography.
DSLR cameras have an edge over other cameras like point and
shoot/bridge cameras because of the capability to interchange
lenses. This makes the entire DSLR system extremely versatile.
Once you buy a DSLR Camera, you can specialize in ANY genre of
photography and you just need to have the right lens for it.
(which you can buy separately as per your requirement)
A lens is made up of concave/convex/concavo-convex
glasses and motor inside it. There are a large number of lenses
available in the market hence you need to understand lenses
before you buy one.
This article shall try to focus on what are the different options
available for good dental documentation and in order to
Vol. 1 Issue 11 L.E.D. E-Journal Page 84
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
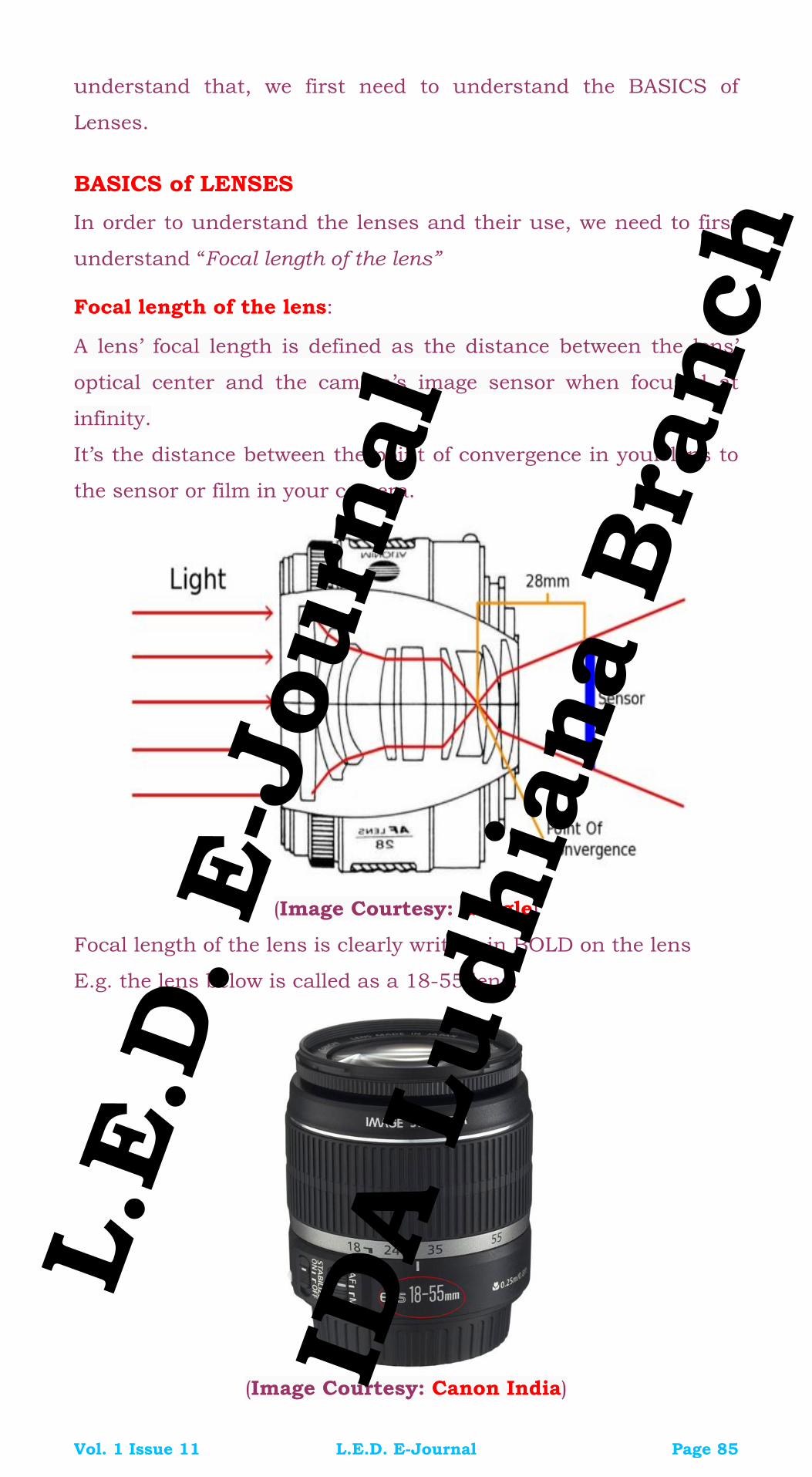
understand that, we first need to understand the BASICS of
Lenses.
BASICS of LENSES
In order to understand the lenses and their use, we need to first
understand “Focal length of the lens”
Focal length of the lens:
A lens’ focal length is defined as the distance between the lens’
optical center and the camera’s image sensor when focused at
infinity.
It’s the distance between the point of convergence in your lens to
the sensor or film in your camera.
(Image Courtesy: Google)
Focal length of the lens is clearly written in BOLD on the lens
E.g. the lens below is called as a 18-55 lens.
(Image Courtesy: Canon India)
Vol. 1 Issue 11 L.E.D. E-Journal Page 85
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Based on the focal length lenses are classified as follows:
1. Wide Angle Lenses
2. Standard Lenses
3. Telephoto Lenses
Wide Angle lenses: Lenses having a focal length of less than 45
mm.
(Image Courtesy: Canon India)
Standard/Normal Lenses: Lenses having a focal length of 45 –
55 mm
(Image Courtesy: Canon India)
Vol. 1 Issue 11 L.E.D. E-Journal Page 86
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Telephoto Lenses: Lenses having focal length of more than 55
mm
(Image Courtesy: Canon India)
USES
1. Wide Angle lenses have a wider angle of view and hence they
cover a larger area in front of the camera.
2. These lenses are used for Landscape photography/
architecture photography/taking images of a large group of
people etc.
3. A standard lens is useful for Portraits/ food photography etc.
4. A telephoto lens has a very narrow angle of view and is useful
to shoot objects which are far away from us for e.g. in wild life
photography, photography of birds, craters of the moon etc.
Prime Lenses:
1. Lenses having a SINGLE focal length.
E.g: Canon 50 mm
2. Note that these lenses could be wideangle, standard or
telephoto.
Vol. 1 Issue 11 L.E.D. E-Journal Page 87
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
(Image Courtesy: Canon India)
Zoom Lenses:
1. Lenses with zoom in-zoom out options and which can be
focused at various focal lengths.
E.g. Canon 18- 55 lens
2. Although it might be tempting to buy a ZOOM lens
(considering it is more versatile) but it’s important to know
that these lenses are “Jack of all trades and master of none”.
(Image Courtesy: Canon India)
It’s always advisable to buy a prime lens for a particular use
(genre of photography) than buy a zoom lens which can cover a
lot of versatile uses.
This may increase the number of lenses that you need to carry
but the images captured by a prime lens are way more superior to
a zoom lens.
Vol. 1 Issue 11 L.E.D. E-Journal Page 88
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Parts of a Lens
(Image Courtesy: Canon India)
1. Focusing ring helps you focus manually in manual focusing
mode.
2. Focal length ring helps you set your lens at the desired focal
length.
3. Auto focus button / auto focus focuses automatically when
you half click the shutter release button on your camera.
4. In a PRIME lens there is NO focal length ring as we cannot
change focal lengths.
5. The only ring in a PRIME lens is the focusing ring with which
you can focus on the object.
(Image Courtesy: Canon India)
Vol. 1 Issue 11 L.E.D. E-Journal Page 89
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Now coming back to Dental Photography
6. We use a SPECIAL lens called a MACRO lens in dental
photography. But WHY is this lens called a SPECIAL LENS?
7. Macro lens is the only lens which is capable of shooting
objects at a very close distance. In other words the lens is
engineered in such a way that the minimum focusing
distance of the lens is very short. Sounds confusing?
The following example will help you understand it better…
(Image Courtesy: Dr. Mayur Davda)
Suppose we had to make an image of 2 central incisors like in the
image above.
8. A macro lens allows us to come as close to 6 inches to the
tooth and shoot the image. (The above image was made using
a Canon 100 mm MACRO lens at a magnification of 1:1.)
9. On the contrary if we would have shot the same image using a
routine (NON MACRO) 100 mm lens then the closest we could
have come to the patient would be approximately 2 feet.
10. The huge distance of 2 feet (approx.) would make it extremely
difficult for us to make dental images.
(Imagine making an image of a third molar from a distance of
2 feet!!)
11. Also note that the flash power falling on the teeth would be
very feeble as the distance (2 feet) would be too large and this
would result in underexposed images (at desired camera
settings).
Vol. 1 Issue 11 L.E.D. E-Journal Page 90
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

12. Another advantage of MACRO lenses is that it gives razor
sharp images of the object in focus; way more than a non-
macro lens could.
13. The major advantage of a MACRO Lens is that it can give us
consistently similar looking images which is a pre requisite for
our before after documentation protocol.
14. This magic happens by the help of MAGNIFICATION ratios.
15. MACRO LENSES are the only lenses in the world which can
help you work in what is called as magnification ratios.
What is MAGNIFICATION RATIO and how to use it for
dental photography?
(Image Courtesy: Canon India)
Every macro lens is equipped with a dial which looks like this
(Image Courtesy: Canon India)
Vol. 1 Issue 11 L.E.D. E-Journal Page 91
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

The “1: in yellow” is the magnification ratio indicator. When you
rotate the focusing ring you will see that the magnification rations
can be changed from 1:1 (extreme close up) to infinity. Thus you
can make images at various magnification ratios of your choice
like 1:1, 1:1.5, 1:2, 1:3, 1:5 etc.
Typically, 1:1 is used for extreme close up images
(the area of coverage at 1:1 is only 4 teeth)
(Image Courtesy: Dr. Mayur Davda)
As we reduce the magnification ratio, the number of teeth keeps
on increasing in our image. The following (below) image was made
at 1:1.5 magnification:
(Image Courtesy: Dr. Mayur Davda)
Vol. 1 Issue 11 L.E.D. E-Journal Page 92
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

At 1:2 you get to see more number of teeth as compared to 1:1.5
(Image Courtesy: Dr. Mayur Davda)
At 1:3 you get to see the entire arches
(Image Courtesy: Dr. Mayur Davda)
This is how we apply magnification ratios in dental photography.
(Image Courtesy: Aum Dental Clinic)
Vol. 1 Issue 11 L.E.D. E-Journal Page 93
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
Thus if you want consistently similar looking images, JUST SET
THE MAGNIFICATION FIRST using the focusing ring and then
shoot.
Consistently similar looking series of images do better justice
to the work a dentist has done. In order to compare the pre-
operative and post-operative image it is imperative that both
images look the same in composition.
This is possible by the use of magnification ratios and macro
lenses only.
Hence if you have made a pre-operative image using a
magnification ratio of 1:1, it is suggested that you make the entire
operative and post-operative images at the same magnification.
Dear Readers: Important Announcement
As all good things come to an end one day, Dr. Mayur Davda,
the Dentist Photography Guru of India will be winding up his
dedicated column on Photography next month with his last article
in December 2016 in our E-Journal.
We will Miss You!!!! Mayur
P.S. Any feedback/compliments/queries for the Author/s should
be emailed to the Editor-in-Chief, Dr. Bhavdeep Singh Ahuja at
his email id: [email protected]
Vol. 1 Issue 11 L.E.D. E-Journal Page 94
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
Chhathaa Gyaan
Vol. 1 Issue 11 L.E.D. E-Journal Page 95
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Dr. Rita Singh is a graduate of Bangalore in 1997 and a Post graduate in Periodontics in 2001 from Rajiv Gandhi University of Health & Sciences, India. She has also completed her Masters in Implantology with Dental XP and Stony Brook School of Dental Medicine. Currently, She is an Associate Professor in the Department of Periodontics in Kathmandu Medical College, Sinamangal. Dr. Lanka Mahesh is an implantologist practicing in New Delhi. He is a Fellow and Diplomate of International College of Oral Implantologists (USA) and the Indian Society of Oral Implantologists. He has undergone advanced surgical training at USA and Spain. He has also authored “Practical Guide to Implant Dentistry” published by Quintessence. He has lectured extensively in India and abroad and has numerous publications on implant related topics.
Dr. Sagrika Shukla is an MDS in Periodontology and is presently attached as a Senior Lecturer in Seema Dental College and Hospital, Rishikesh. She has many national and international publications to her credit. She is also a Fellow and Diplomate of the International Congress of Oral Implantologists (ICOI-USA)
Infections Resulting from Bone Grafting
Biomaterials A Review
Author: Dr. Rita Singh
Co-Author 1: Dr. Lanka Mahesh
Co-Author 2: Dr. Sagrika Shukla
ABSTRACT
Use of bone grafting is a boon in saving ailing and failing bony
structure. Today in dentistry all types of grafts are used,
autogenous, xenografts, allografts alloplasts, all giving favorable
results. Yet, all have demerits. Xenografts and allografts have
high chances of transmission of infection. This article highlights
grafts and transmission of such infections.
KEYWORDS
Infections, Xenografts, Allografts
INTRODUCTION with DISCUSSION
Bone grafts are extensively used in dentistry for reconstruction of
atrophied alveolar ridges, around endosseous implants for
regeneration of missing bony wall to provide support and stability
to implants, for sinus floor elevation procedures, for healing of
intrabony peri-implantitis defects, in periradicular surgery and
Vol. 1 Issue 11 L.E.D. E-Journal Page 96
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

large periapical lesions, in periodontal bony defects and for
reconstruction of maxillofacial defects. There are various bone
grafts used in dentistry. The best being autografts, however, the
chance of second surgical site, limited amount and their rapid
resorption has encouraged clinicians to use xenografts or
allografts.
XENOGRAFTS
Xenografts are grafts shared between different species. There are
many available sources of xenografts used as bone replacement
grafts: Bovine bone, porcine bone, horse bone and natural coral.
The advantage of theses grafts is that they are osteoconductive
and undergo through extensive processing techniques, providing
products which are biocompatible and structurally similar to
human bone. Other advantages include readily availability and
risk free of disease transmission; however ‘risk free of disease
transmission quotient’ has been questioned with the discovery of
bovine spongiform encephalopathy (BSE) and porcine endogenous
retroviruses (PERVs). Xenotransplantation may allow such
organisms to infect xenograft recipients, who may, consequently,
contract previously unknown diseases.
There is also a risk that the infectious organisms might cause
disease and destroy the transplanted organ, even if they do not
harm the human recipient. Even if not infected with disease-
causing organisms when transplanted, the xenografted organ may
remain susceptible to infectious organisms of animals. Also, if a
xenograft recipient is infected, there is a possibility that the
resultant disease might then be passed on to the public. In this
way, xenografting may pose a risk to public health as well as to
individual health.
ANORGANIC BOVINE-DERIVED BONE XENOGRAFT (BDX)
The BDX is a xenograft consisting of deproteinized, sterilized
bovine bone with 75 to 80% porosity and a crystal size of
approximately 10 mm in the form of cortical granules. The
advantage of BDX is that it has osteoconductive properties and
according to Cohen et al and Callan et al use of this graft material
Vol. 1 Issue 11 L.E.D. E-Journal Page 97
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

is considered safe since all the proteins are removed and is 100%
crystalline hydroxyapatite grafting material. Yet, there are
reported cases of BSE (Bovine Spongiform Encephalopathy).
Infectious particles cause BSE in cattle, when these are
accidentally transplanted in humans through bone grafts they
cause Creutzfeldt-Jakob disease (CJD) and a variant of
Creutzfeldt-Jakob disease (vCJD). CJD is a rare, fatal
neurodegenerative disorder of old age, but its variant vCJD can
occur at any age. The occurrence of CJD is rare approximately
one case per million populations. The disease is caused by prions,
which are considered to be composed mainly of an altered normal
protein (prion protein). It is also known as the prion disease. It
was first discovered by Stanley B Prusiner, and he defined prions
as infectious, transmissible proteinaceous particles that lack
nucleic acid and are composed exclusively of a modified isoform
of the noninfectious cellular prion protein (PrPC). The pathogenic
(also called scrapie or PrPSc) form of the prion protein (PrP) has
the same amino acid content but a higher -sheet content than
PrPC. These prions get deposited in cerebrum and cerebellum
causing sponge-like degenerative changes in the brain. Clinical
features include psychiatric symptoms such as depression,
anxiety, apathy, withdrawal, delusions; there is persistent painful
sensory symptoms pain and/or dysesthesia, ataxia, chorea/
dystonia or myoclonus, dementia. Oral manifestations include
pseudobulbar palsy which may cause dysphagia and dysarthria
in patients with transmissible spongiform encephalopathies
(TSEs), orofacial dysesthesia or paresthesia, as well as loss of
taste and smell. There are various types of CJD:
Table 1 below describes those types.
Table:1 – Various forms of Creutzfeldt-Jakob Disease
Vol. 1 Issue 11 L.E.D. E-Journal Page 98
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

There are many reported case of transmission of BSE, although
the risk of transmission of CJD through dentistry is unclear, the
theoretical risk of transmission through any contaminated
instruments or contaminated bovine bone graft can take place.
Incidence of transmission of BSE with bovine xenograft is
estimated to be far less than the incidence of being hit by
lightning. Therefore, the risk of getting disease transmission from
allograft and xenograft is relatively low as long as the
disinfection/sterilization protocols are followed by the suppliers.
World Health Organization stated that bone is labeled as type IV
(no transmission) for proteinaceous infectious particles (prions)
diseases. All current available bone graft materials are safe and
reliable instead of disease transmission potential. According to
Sogal and Tofe, the risk of TSE transmission from a commercially
available bovine-derived xenogenic bone substitute was
insignificant. In animal studies, Adams and Edgar assessed the
possibility of transmission of scrapie through dental burs. They
found no clinical or histological findings of scrapie when the
healthy mice were killed and examined 15 months later. Ingrosso
et al conducted a study on the possibility of prion infection
through dental procedures. They found a significant level of
infectivity in the trigeminal ganglia and in the gingival and pulpal
tissues of scrapie-affected hamsters after intraperitoneal
inoculation, suggesting possible transmission from the central
nervous system through trigeminal nerves toward the oral cavity.
PORCINE BONE GRAFTS
The pig has a number of advantages as a renewable source of
donor tissue including a vast experience in its husbandry and
health care, as well as the advancing technologies to engineer
transgenic animals thus, porcine bone grafts are widely used in
dentistry, selective breeding and screening of the pig can reduce
the risk of animal-human infections, from xenotransplantation.
However, pigs harbor many viruses or ghosts of viruses, some
active, some latent and others represented only by a partial
genetic sequence embedded in the pig genome such as
endogenous retroviruses PERV, which are encoded in their
Vol. 1 Issue 11 L.E.D. E-Journal Page 99
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
genomic DNA and are thus in every cell of every pig, and are
therefore less susceptible to exclusion by careful breeding. There
are at least three variants of PERVs (A, B, B1 and C) in native pig
cells. PERV-A and PERV-B can infect several species including
humans, while PERV-C tropism is limited to pig cells. However,
recombination between PERV-A and PERV-C occurs frequently
producing a high titer, human tropic PERVA/C, these are
considered to be most problematic as they use the same cell
receptor as PERV-A and are the forms derived from co-cultivation
of porcine primary cells and human cells. PERVs infect human
cells in vitro and have been cloned. Recent data suggest that
despite the presence of many fragmentary copies of virus
sequences, there are relatively few; full length copies of the viral
DNA in each cell that are capable of producing infective virus. In
addition, some genomic sites produce incomplete viral
transcripts, which are not thought to be infective. This small
number of intact genes might allow inactivation of proviruses of
PERVs through genetic manipulation. Gammaretrovirus particles
are released by pig cell lines, yet only recently have investigators
looked into the potential risk of human infection by PERV. Two of
the three identified receptor classes of PERV, distinguished by
their envelope sequence and tropism, have been shown to be
capable of replicating in human cells in vitro. In vivo, they may
cause infection and may give rise to two possible effects:
mutagenesis and immuno-suppression. The first may induce
cancer. The second will damage the human immune system and
in analogy to HIV and SIV, high titer virus replication may cause
an AIDS-like disease in the immuno-suppressed human
transplant recipient. Pig cells can survive for many years in the
human body and micro-chimerism has been detected. In
microchimerism, the pig cells in the human body contain PERV
but—if no infection has occurred—no virus particles have been
incorporated rated in the human genome. This however does not
decrease the risk that PERV may cause. Whether one can really
distinguish between microchimerism and an infection is not clear.
Another infection that humans can acquire from pigs is Ebola
virus (EBOV). EBOV causes extremely severe disease in humans
Vol. 1 Issue 11 L.E.D. E-Journal Page 100
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

and in nonhuman primates in the form of viral hemorrhagic fever.
EBOV is a select agent, World Health Organization Risk Group 4
Pathogen (requiring Biosafety Level 4-equivalent containment).
EBOV was first described in 1976 by David Finkes. Today, the
virus is the single member of the species Zaire ebolavirus, which
is included into the genus Ebolavirus, family Filoviridae, order
Mononegavirales. The name EBOV is derived from the Ebola River
(a river that was at first thought to be in close proximity to the
area in Zaire where the first recorded EBOV disease outbreak
occurred) and the taxonomic suffix viruses. It causes a
fulminating hemorrhagic fever syndrome resulting in the death of
most patients within a few days. Human immune responses have
as yet been poorly investigated, mainly due to the fact that most
outbreaks occur in remote areas of central Africa. In infected
humans, there is fatal outcome in humans and is associated with
aberrant innate immunity characterized by a ‘cytokine storm,’
with hypersecretion of numerous pro-inflammatory mediators and
by the noteworthy absence of antiviral interferon. The adaptive
response is globally suppressed, showing a massive loss of CD4
and CD8 lymphocytes and the immune mediators they produce.
EQUINE DERIVED BONE GRAFT
There is always search for better bone grafts resembling human
bone matrix and capable of osteoconductive properties. With
discovery of PERV through porcine bone grafts and CJD through
bovine bone grafts, use of equine bone grafts has become popular.
However, research on risk on disease transmission through
equine is still being investigated. El-Sabban et al stated that there
are no studies on bone substitutes of equine origin, apart from
few papers on an equine bone protein extract, which was capable
of inducing osteoblastic differentiation of human bone marrow-
derived mesenchymal stem cells and ectopic bone formation in a
rat model. According to Stefano et al equine graft material is
biocompatible, and its usage is associated with new blood vessels
ingrowth during healing, which has been found to be extremely
important in bone formation. The status still remains the same.
There is rapid increase in use of equine bone grafts; however,
Vol. 1 Issue 11 L.E.D. E-Journal Page 101
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

research disease transmission through this material needs more
attention.
HUMAN DURA MATTER
Allografts have been successfully used for intraosseous defects,
most common being decalcified freeze dried bone allograft
(DFDBA), however, controversy exists with respect to the
osteoinductive potential of these materials. It has been shown
that inductive capacity varies from bone bank to bone bank and
also from different batches of the same bone bank. The bioactivity
is also dependent on the age of the donor, the younger the donor,
the more osteoinductive graft material will be. Also there are
chances of disease transmission, the most common being
Creutzfeldt-Jakob disease, which can be transferred from an
infected donor. The main disadvantage is that this disease
transcripts as a preclinical state in which it can lie dormant in
the individual for decades (1-40 years), also it cannot be detected
in human blood. These factors increase the chances of
transmission as it goes undetectable on screening. According to
Gajdusek et al, another subacute spongiform encephalopathy,
survived room temperature in 10% formalin for 7 months in the
form of a brain suspension.
CONCLUSION
With various bone grafts in has now become possible to reach the
goal of bone regeneration and achieving ultimate results providing
both function and esthetics. However with the use of xenografts
the risk of disease transmission increases. Although till now no
case of infection from xenotransplantation in dentistry has been
reported, but there is a risk. And to avoid certain precautions can
be taken by the dentist. Patients with confirmed prion disease
should be scheduled at the end of the day to permit more
extensive cleaning and decontamination. It is preferable to avoid
activating waterlines because of the risk of retraction of prions in
oral fluids. Also, a stand-alone suction unit with disposable
reservoir, rather than the suction component of the dental unit,
and a disposable bowl instead of the dental unit spittoon should
Vol. 1 Issue 11 L.E.D. E-Journal Page 102
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

be used. To avoid environmental contamination, dental
equipment should be adequately shielded using disposable,
impermeable cover sheets.
REFERENCES
1. Cohen RE, Mullarky RH, Noble B, Comeau RL, Neiders ME.
Phenotypic characterization of mononuclear cells following
anorganic bovine bone implantation in rats. J Periodontol 1994
Nov;65(11):1008-1015.
2. Dumitrescu AL. Bone grafts and bone graft substitutes in
periodontal therapy. In: Dumitrescu AL, editor. Chemicals in
surgical periodontal therapy. Berlin Heidelberg: Springer-Verlag
2011. p. 73-144.
3. Nasr HF, Aichelmann-Reidy ME, Yukna RA. Bone and bone
substitutes. Periodontol 2000 1999 Feb;19:74-86.
4. Nairne SP. Nuffield council on bioethics. Animal-to-human
transplants: the ethics of xenotransplantation. London: Nuffield
Council on Bioethics; 1996
5. Hurzeler MB, Quinones CR, Kirsch A, Gloker C, Schupbach P,
Strub JR, Caffesse RG. Maxillary sinus augmentation using
different grafting materials and dental implants in monkeys.
Part I. Evaluation of anorganic bovine-derived bone matrix. Clin
Oral Implants Res 1997 Dec;8(6):476-486.
6. Piattelli M, Favero GA, Scarano A, Orsini G, Piattelli A. Bone
reactions to anorganic bovine bone (Bio-Oss) used in sinus
augmentation procedures: a histologic long-term report of 20
cases in humans. Int J Oral Maxillofac Implants 1999 Nov-
Dec;14(6):835-840.
7. Callan DP, Rohrer MD. Use of bovine-derived hydroxyapatite in
the treatment of edentulous ridge defects: a human clinical and
histologic case report. J Periodontol 1993 Jun;64(6): 575-582.
8. Wenz B, Oesch B, Horst M. Analysis of the risk of transmitting
bovine spongiform encephalopathy through bone grafts derived
from bovine bone. Biomaterials 2001 Jun;22(12):1599-1606.
9. Barash JA, Johnson BT, Gregorio DI. Is Surgery a risk factor for
Creutzfeldt-Jakob disease? Outcome variation by control choice
Vol. 1 Issue 11 L.E.D. E-Journal Page 103
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
and exposure assessments. Infect Control Hosp Epidemiol 2008
Mar;29(3):212-218
10. Prusiner SB. Prions. Proc Natl Acad Sci USA 1998
Nov;95(23):13363-13383.
11. Porter SR. Prions and dentistry. JR Soc Med 2002
Apr;95(4):178-181.
12. Porter S, Scully C, Ridgway GL, Bell J. The human
transmissible spongiform encephalopathies (TSEs): implications
for dental practitioners. Br Dent J 2000 Apr;188(8):432-436
13. Azarpazhooh, Leake JL. Prions in dentistry—what are they,
should we be concerned, and what can we do? J Can Dent
Assoc 2006 Feb;72(1):53-60.
14. Li J, Wang HL. Common implant-related advanced bone
grafting complications: classification, etiology, and
management. Implant Dent 2008 Dec;17(4):389-401.
15. Sogal A, Tofe AJ. Risk assessment of bovine spongiform
encephalopathy transmission through bone graft material
derived from bovine bone used for dental applications. J
Periodontol 1999 Sep;70(9):1053-1063.
16. Adams D, Edgar WM. Transmission of agent of Creutzfeldt-
Jakob disease. Br Med J 1978 Apr;1(6118):987.
17. Ingrosso L, Pisani F, Pocchiari M. Transmission of the 263K
scrapie strain by the dental route. J Gen Virol 1999 Nov;80(Pt
11):3043-3047.
18. Ritzhaupt A, Van Der Laan LJ, Salomon DR, Wilson CA. Porcine
endogenous retrovirus infects but does not replicate in
nonhuman primate primary cells and cell lines. J Virol 2002
Nov;76(22):11312-11320.
19. Bach FH, Ivinson AJ. A shrewd and ethical approach to
xenotransplantation. Trends Biotechnol 2002 Mar;20(3):129-31.
20. Todaro GJ, Benveniste RE, Lieber MM, Sherr CJ.
Characterization of a type C virus released from the porcine cell
line PK(15).Virology 1974 Mar;58(1):65-74.
21. Tristem M, Kabat P, Lieberman L, Linde S, Karpas A, Hill F.
Characterization of a novel murine leukemia virus-related
subgroup within mammals. J Virol 1996 Nov;70(11):8241-8246.
Vol. 1 Issue 11 L.E.D. E-Journal Page 104
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
22. Takeuchi Y, Patience C, Magre S, Weiss RA, Banerjee PT, Le
Tissier P, Stoye JP. Host range and interference studies of three
classes of pig endogenous retrovirus. J Virol 1998
Dec;72(12):9986-9991.
23. Wilson CA, Wong S, VanBrocklin M, Federspiel MJ. Extended
analysis of the in vitro tropism of porcine endogenous
retrovirus. J Virol 2000 Jan;74(1):49-56.
24. Oldmixon BA, Wood JC, Ericsson TA, Wilson CA, White- Scharf
ME, Andersson G, Greenstein JL, Schuurman HJ, Patience C.
Porcine endogenous retrovirus transmission characteristics of
an inbred herd of miniature swine. J Virol 2002
Mar;76(6):3045-3048.
25. Denner J. Recombinant porcine endogenous retroviruses (PERV-
A/C): a new risk for xenotransplantation? Arch Virol
2008;153(8):1421-1426.
26. Wilson CA, Wong S, Muller J, Davidson CE, Rose TM, Burd P.
Type C retrovirus released from porcine primary peripheral
blood mononuclear cells infects human cells. J Virol 1998
Apr;72(4):3082-3087.
27. Patience C, Takeuchi Y, Weiss RA. Infection of human cells by
an endogenous retrovirus of pigs. Nat Med 1997 Mar;3(3):276-
282.
28. Akiyoshi DE, Denaro M, Zhu H, Greenstein JL, Banerjee P,
Fishman J. Identification of a full-length cDNA for an
endogenous retrovirus of miniature swine. J Virol 1998
May;72(5):4503-4507.
29. Dobson R. Scientists show that vCJD can be transmitted
through blood. BMJ 2000 Sep;321(7263):721.
30. Armstrong JA, Porterfield JS, De Madrid AT. C-type virus
particles in pig kidney cell lines. J Gen Virol 1971
Feb;10(2):195-198.
31. Denner J. Immunosuppression by retroviruses: implications for
xenotransplantation. Ann N Y Acad Sci 1988 Dec;862:75-86.
32. Weiss RA. Xenografts and retroviruses. Science 1999;285:
1221-1222; US FDA. Transcript from biological response
modifiers committee, xenotransplantation subcommittee. June
3-4 1999. Washington: Millers Reporting Company Inc, 1999.
Vol. 1 Issue 11 L.E.D. E-Journal Page 105
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

33. Pattyn S, Jacob W, van der Groen G, Piot P, Courteille G.
Isolation of Marburg-like virus from a case of haemorrhagic
fever in Zaire. Lancet 1977 Mar;1(8011):573-574.
34. Bowen ETW, Lloyd G, Harris WJ, Platt GS, Baskerville A, Vella
EE. Viral haemorrhagic fever in southern Sudan and northern
Zaire. Preliminary studies on the aetiological agent. Lancet
1977 Mar;1(8011):571-573.
35. Johnson KM, Webb PA, Lange JV, Murphy FA. Isolation and
partial characterisation of a new virus causing haemorrhagic
fever in Zambia. Lancet 1977 Mar;1(8011):569-571.
36. El-Sabban ME, El-Khoury H, Hamdan-Khalil R, Sindet-Pedersen
S, Bazarbachi A. Xenogenic bone matrix extracts induce
osteoblastic differentiation of human bone marrow-derived
mesenchymal stem cells. Regen Med 2007 Jul;2(4):383-390.
37. Li H, Springer M, Zou X, Briest A, Bunger C. Ectopic bone
induction by equine bone protein extract. Adv Exp Med Biol
2006;585:393-402.
38. Sanchez AR, Sheridan PJ, Kupp LI. Is platelet-rich plasma
perfect enhancement factor? A current review. Int J Oral
Maxillofac Implants 2003 Jan-Feb;18(1):93-103.
{Dear Readers: The above article was first published in ‘International Journal
of Implantology and Clinical Research’ Vol. 4 Issue 2 May–August 2013 issue
and has been republished with prior permission from the author Dr. Lanka
Mahesh et al & the Publishing House, Jaypee Journals with due
acknowledgment.}
P.S. Any feedback/compliments/queries for the Author/s should
be emailed to the Editor-in-Chief, Dr. Bhavdeep Singh Ahuja at
his email id: [email protected].
Vol. 1 Issue 11 L.E.D. E-Journal Page 106
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Saatwaa Gyaan
Vol. 1 Issue 11 L.E.D. E-Journal Page 107
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Dr. Rajeev Ranjan graduated from Bharti Vidyapeeth Dental College, Pune in 2008 & did his post graduation in Periodontics from K.L.E. Institute of Dental Sciences, Bangalore in 2013. He is working as a Senior Lecturer in Kalinga Institute of Dental Sciences, Bhubaneshwar since 2013. He has many Original research publications to his credit in National & International Journals. He is apart of many ongoing research activities in his institute; KIDS, Bhubaneshwar. He likes to listen to music, watch movies, read interesting topics both online and in print; in his free time.
Efficacy of 980 nm DIODE LASER as an adjunct to
Stannous Fluoride (SnF2) in the management of
DENTINAL HYPERSENSITIVITY
A controlled prospective clinical study Author: Dr. Rajeev Ranjan
ABSTRACT
Aims and Objectives: The purpose of this prospective clinical
study was to evaluate and compare the clinical effectiveness of
GaAlAs Diode laser alone and with topical 2% Stannous fluoride
gel in the management of Dentinal hypersensitivity.
Materials and Methods Used: 30 patients (14 Males and 16
Females, age 19–70years), contributing 534 teeth with DH were
assessed by air stimuli and measured by Verbal Rating Scale
(VRS). For each patient, the sensitive sites were randomly divided
into G1 (267 teeth), treated by application of 2% Stannous
fluoride gel followed by application of GaAlAs diode laser (Sunny
Germany, 980 nm, 2W, 25 Hz) in continuous mode and G2 (267
teeth), Subjected to only diode laser at the same parameters
employed in G1. VRS recordings were assessed before treatment,
15 min after the laser application and at the end of 2, 7, 14 and
30 days after treatment.
Results: Both Groups have shown significant reduction in DH
after the laser irradiation but reduction in DH was more evident
in GI than G2.
Conclusion: Diode laser is a useful device for DH management
and addition of Stannous fluoride has synergistic effect on laser
desensitization effect.
Vol. 1 Issue 11 L.E.D. E-Journal Page 108
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

KEYWORDS
Diode laser, Dentinal Hypersensitivity, Stannous fluoride gel,
Verbal rating scale
INTRODUCTION
Dentin hypersensitivity (DH) can be described as an adverse
reaction or pain in one or more teeth resulting from either a
thermal, mechanical, or chemical stimulus. Hypersensitive dentin
is an uncommonly sensitive or painful response of exposed dentin
to an irritation. It is one of the most painful, ubiquitous and least
satisfactory treated chronic problems of teeth. Depending on the
population samples studied, 4% to 57% prevalence of DH has
been reported in literature, with higher prevalence of DH ranging
between 60 to 98% in patients suffering from periodontal disease.
Advancement of laser technology and its growing utilization
in dentistry has given an additional therapeutic option for the
treatment of DH. Different types of low (He–Ne, diode) and
middle output power (CO2, Nd:YAG) lasers have been tested for
the reduction of DH but available literature are not sufficient to
give any definitive conclusive remarks. Low output power (low-
level) lasers have shown significant anti-inflammatory effects,
while excessive effects on pulp have been shown by middle output
power lasers.
Diode lasers are the most studied laser in management of DH.
In various studies, different wavelengths of diode lasers have been
used and have shown the best results in several clinical protocols
even in high- grade DH cases.
An additional therapeutic option could be the combination of
laser irradiation with the application of specific products for the
treatment of DH, with the intention of achieving an accumulation
of effects from both treatments. In various clinical studies,
combinations of different types of laser with chemical agents such
as sodium fluoride and stannous fluoride have been evaluated;
with promising results and effectiveness have been found more
than 20% over the laser treatment only.
The aim of the present prospective clinical study was to
evaluate and compare the clinical effectiveness of 980nm Diode
Vol. 1 Issue 11 L.E.D. E-Journal Page 109
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

laser (Fig. 1) alone and in combination with topical Stannous
fluoride (SnF2) gel in the management of DH.
Fig-1: Diode Laser
MATERIALS and METHODS
The patients recruited for this study were selected from the out-
patient division of Department of Periodontics, KLE Society’s
institute of Dental Sciences, Bangalore, Karnataka. Thirty
patients (14 males and 16 females), aged between 19-70 years
(mean age: 41.67 years) with the complaint of DH, contributing
534 teeth were enrolled for the study by convenience sampling
method. Written informed consent was obtained from patients
and it was made clear to the potential subjects that participation
was voluntary. This randomized controlled trial with split mouth
design was carried out from October 2011 to February 2012, with
the follow up of 30 days.
The exclusion criteria for patient enrolment were based on:
carious lesions on the selected or neighbouring teeth, any
desensitizing therapy on the selected teeth during the last 6
months, cervical fillings on the selected teeth, teeth undergone
extensive restoration or endodontic treatment and history of need
to continuously take analgesic medication.
Vol. 1 Issue 11 L.E.D. E-Journal Page 110
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Phase 1 periodontal therapy in form of Scaling and root
planing followed by Oral hygiene instructions were given to each
and every selected patient and the tooth vitality of all sites was
assessed. The degree of sensitivity to an evaporative stimulus
before and after treatment was determined qualitatively with an
air stimulus (Fig. 2). To check the cold air stimulus, the selected
tooth was isolated, dried and a jet of cold air was applied from a
distance of 1 cm for 1 second (Fig. 3). To avoid any discrepancy
during testing, the dentist’s gloved fingers shielded the
neighboring teeth.
Fig-2: Air Stimulus Application
Fig-3: Isolation & Drying of Teeth
Vol. 1 Issue 11 L.E.D. E-Journal Page 111
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Patient responses to air stimuli was recorded according to the
Verbal Rating Scale (VRS) scale in four degrees as given by Tarbet
et al and Collins et al.
0: No discomfort, but patient felt stimulus.
1: Slight discomfort, but not painful.
2: Painful during application of stimulus.
3: Painful during application of stimulus and immediately
afterwards.
Air stimulus recordings were assessed before treatment, 15
min after the laser application and at the end of 2, 7, 14 and 30
days after treatment.
For each patient, the sensitive sites were randomly divided into
two groups:
1. Group 1 (G1) (267 teeth) - treated by application of 2%
Stannous fluoride gel followed by application of GaAlAs diode
laser (Sunny Germany, 980 nm, 2W, 25 Hz) in continuous
mode (Fig. 4 and Fig. 5).
2. Group 2 (G2) (267 teeth) – Subjected to diode laser at the
same parameters employed in Group 1.
Fig-4: Fluoride Gel Application
Vol. 1 Issue 11 L.E.D. E-Journal Page 112
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Fig-5: Diode Laser Application + Stannous Fluoride Gel
Application
In Group 1, 2% Stannous fluoride gel was applied with
cotton pellet and left on tooth surface for 60 seconds before the
irradiation. Application of 980 nm diode laser (2W, 25 Hz,
continuous mode) at three points on the facial surface and at one
point on the lingual surface of incisors and canine and at two
points on the facial and lingual surface of premolars and molars
were performed respectively. Each site received one application
for 30 seconds each at baseline. Laser application was kept
perpendicular to the long axis of the tooth.
In Group 2, teeth were subjected to diode laser irradiation with
the same parameters employed for Group 1 at baseline.
STATISTICAL ANALYSIS
Site prevalence was assessed by Chi square test. Intervisit-
intergroup comparison was done by Mann-Whitney Test and
intervisit-intragroup comparison was done by Kruskal Wallis
Test.
Vol. 1 Issue 11 L.E.D. E-Journal Page 113
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

RESULT
Both Group 1 and Group 2 have shown significant reduction
in DH (Dentine Hypersensitivity) after the diode laser application.
Statistically there was no difference in both groups w. r. t. age
and gender. Site specific reduction in sensitivity estimated by chi
square test showed increased reduction in premolars followed by
incisors, canines and molars (Graph-1).
Graph-1: Site specific reduction in Dentine Hypersensitivity
The mean values of DH in group 1 was 0.96 0.84, 0.80
0.84, 0.72 0.82, 0.73 0.82 and 0.63 0.73, as assessed 15
minutes post-treatment and on days 2, 7, 14 and 30 after the
treatment respectively. In the same way, observed mean values of
DH in group 2 was 1.54 0.81, 1.28 0.81, 1.28 0.81, 1.26
0.81 and 1.29 0.77 at various time intervals post-treatment
respectively. Thus although a decrease in mean values in DH was
observed in both the groups, decrease observed was higher in
Group 1.
Reduction in DH from baseline to at the end of 30 days was
highly significant (P < 0.001) in both group 1 and group 2. When
intergroup comparison of DH between group 1 and group 2 was
done, the value obtained was highly significant (P < 0.001) at
each time interval after intervention.
Vol. 1 Issue 11 L.E.D. E-Journal Page 114
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
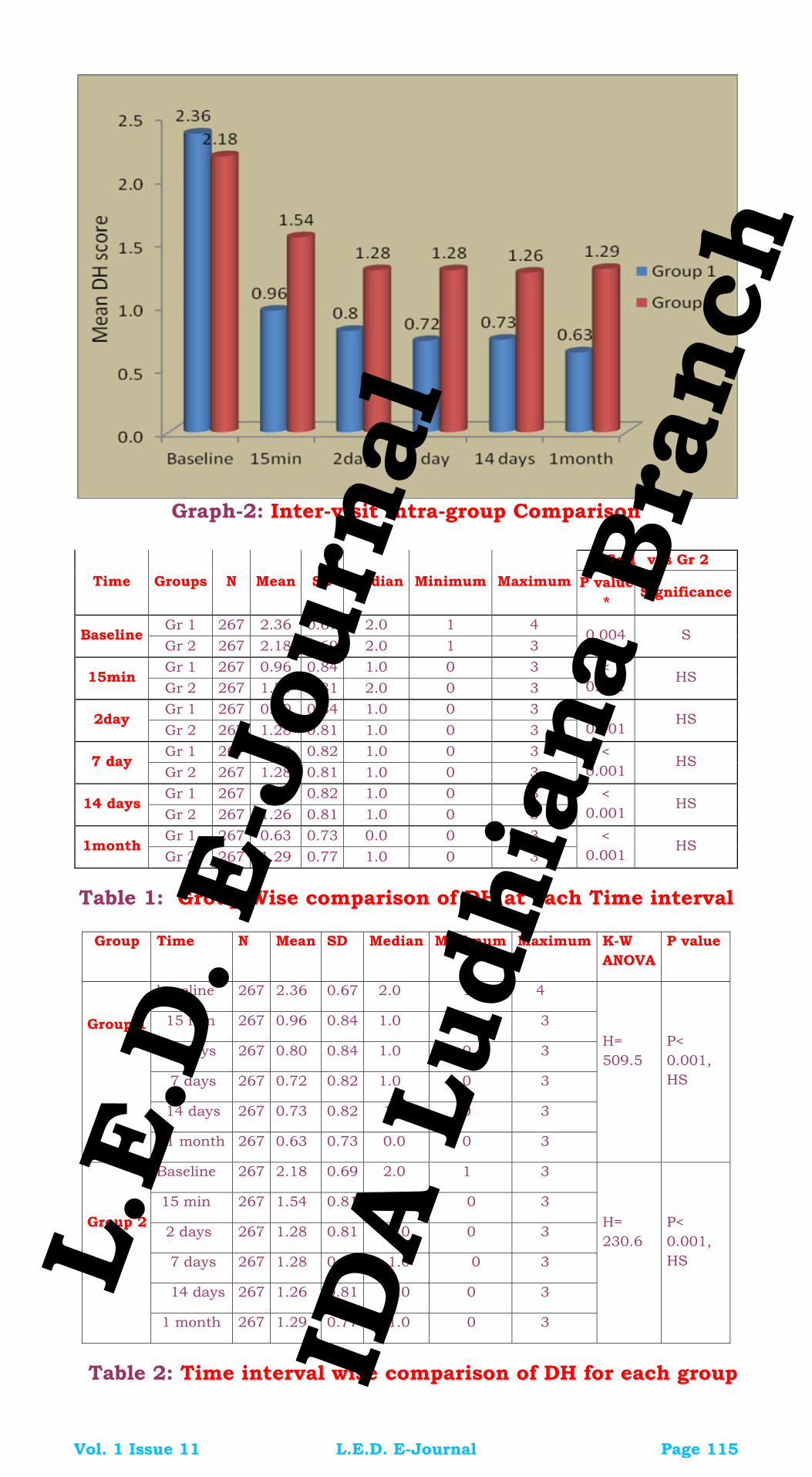
Graph-2: Inter-visit Intra-group Comparison
Gr 1 v/s Gr 2
Time Groups N Mean SD Median Minimum Maximum P value *
Significance
Gr 1 267 2.36 0.67 2.0 1 4 Baseline
Gr 2 267 2.18 0.69 2.0 1 3 0.004 S
Gr 1 267 0.96 0.84 1.0 0 3 15min
Gr 2 267 1.54 0.81 2.0 0 3 <
0.001 HS
Gr 1 267 0.80 0.84 1.0 0 3 2day
Gr 2 267 1.28 0.81 1.0 0 3 <
0.001 HS
Gr 1 267 0.72 0.82 1.0 0 3 7 day
Gr 2 267 1.28 0.81 1.0 0 3 <
0.001 HS
Gr 1 267 0.73 0.82 1.0 0 3 14 days
Gr 2 267 1.26 0.81 1.0 0 3 <
0.001 HS
Gr 1 267 0.63 0.73 0.0 0 3 1month
Gr 2 267 1.29 0.77 1.0 0 3 <
0.001 HS
Table 1: Group Wise comparison of DH at each Time interval
Group Time N Mean SD Median Minimum Maximum K-W
ANOVA P value
baseline 267 2.36 0.67 2.0 1 4
15 min 267 0.96 0.84 1.0 0 3
2 days 267 0.80 0.84 1.0 0 3
7 days 267 0.72 0.82 1.0 0 3
14 days 267 0.73 0.82 1.0 0 3
Group 1
1 month 267 0.63 0.73 0.0 0 3
H= 509.5
P< 0.001, HS
Baseline 267 2.18 0.69 2.0 1 3
15 min 267 1.54 0.81 2.0 0 3
2 days 267 1.28 0.81 1.0 0 3
7 days 267 1.28 0.81 1.0 0 3
14 days 267 1.26 0.81 1.0 0 3
Group 2
1 month 267 1.29 0.77 1.0 0 3
H= 230.6
P< 0.001, HS
Table 2: Time interval wise comparison of DH for each group
Vol. 1 Issue 11 L.E.D. E-Journal Page 115
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

DISCUSSION
Studies have shown slightly higher incidence of DH in females
than males, which could be due to be overall oral hygiene &
healthcare awareness in women and is common between the age
group of 20 to 40 years with the peak incidence at the end of
third decades. However in the present study, there was no
statistically significant difference in both groups w. r. t. age and
gender. Interestingly, site specific prevalence showed increased
predilection in premolars followed by incisors, canines and
molars. This was in accordance with the study of Flynn J et al
who also reported the same DH predilection order.
Even though numerous modes of treatments for DH have
been discussed in literature, it is clear that, the ideal treatment
for DH does not exist. This can be true even in case of
combination of different protocols. Traditional methods for the
management of DH comprehend the topical use of desensitizing
agents, either professionally or at home such as protein
precipitants, tubule-occluding agents, tubule sealants, and,
recently, lasers. Various studies describe a synergistic action of
lasers in association with desensitizing agents. It has been noted
that the laser system can favor the permanence of the
desensitizer for longer time than when they are used alone.
Matsumoto et al and Yamaguchi et al have reported
decrease in hypersensitivity by 85% and 60% respectively in teeth
treated with laser. In a double-blind clinical study Gerschman et
al have found significant reduction in treated group in
comparison to the placebo group: sensitivity to thermal stimuli
was reduced by 67%, whereas the placebo group had a reduction
of 17%, sensitivity to tactile stimuli was reduced by 65%, while
the placebo group showed a reduction of 21%. In a systematic
review by Kimaru et al on management of DH by laser has
concluded GaAlAs laser of wavelength 800 nm has 30%-100%
and GaAlAs laser of wavelength 900nm has 73.3%-100%
effectiveness in management of DH.
Better results were obtained by combined intervention of
laser and stannous fluoride (SnF2) gel therapy (G1) in
management of DH in the current study. It is possible that the
Vol. 1 Issue 11 L.E.D. E-Journal Page 116
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

better performance of combined treatment was due to the higher
stannous fluoride gel adhesion to the dentinal tubules when
combined with laser energy. Even in consideration of the short
sample analyzed, it is possible to speculate that the laser-induced
superficial melting permits longer tubules occlusion by stannous
fluoride gel emphasizing the reduction of DH-related pain.
There was also a significant reduction in sensitivity at 15
minutes followed by further reduction at 2,7,14 and 30 days post-
treatment. These findings were in accordance with Lin and Lan
who reported that the combined use of the GaAlAs laser (830 nm
wavelength) with fluoridation enhances treatment effectiveness by
more than 20% over that of laser treatment only. The added
advantages of combination of dental laser with stannous fluoride
has been reported in another in vivo study by Moritz et al and
suggested that the combined laser treatment and fluoridation
result in permanent integration of fluoride on the dentinal
tubules. The present clinical study has shown that, addition of
fluoride with laser had more significant reduction and reduction
was seen immediately after 15 min. Inter visit comparison shows
greater change on day 30 with mean value 0.63 in group 1 and
1.29 in group 2. This result might be due to the synergistic effect
of fluoride when used along with the diode laser.
CONCLUSION
1. Dentin Hypersensitivity is an age old problem. Plethoras
of treatment modalities are available amongst which
laser seems to be more effective, and has rapid and
lasting effect.
2. When satisfactory oral hygiene is maintained laser plays
vital role in reduction of sensitivity which is common
problem to patient and dentist and causes crippling
discomfort.
3. Addition of fluoride has synergistic effect on laser
desensitization.
Vol. 1 Issue 11 L.E.D. E-Journal Page 117
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
REFERENCES
1. Collins JF, Gingold J, Stanley H, Simring M. Reducing dentinal
hypersensitivity with strontium chloride and potassium
nitrate. General Dentistry 1984; 32: 40–43.
2. Grossman LI. A systematic method for the treatment of
hypersensitive dentin. Journal of American Dental Association
1934; 22: 592–602.
3. Rees J.S, Addy M. A cross-sectional study of dentine
hypersensitivity. Journal of Clinical Periodontology 2002; 29:
997–1003.
4. M. B. Chabanski, D. G. Gillam, J. S. Bulman, and H. N.
Newman. The prevalence, distribution and severity of cervical
dentine sensitivity (CDS) in a population of patients referred to
a specialist periodontology department. Journal of Clinical
Periodontology 1996; 23: 989–992.
5. Renton-Harper P. & Midda M. NdYAG laser treatment of
dentinal hypersensitivity. British Dental Journal 1992; 172:
13–16.
6. Zhang C., Matsumoto K., Kimura, Y., Harashima T., Takeda F.
H., Zhou H. Effects of CO2 laser in treatment of cervical
dentinal hypersensitivity. Journal of Endodontics 1998; 24:
595–597.
7. Kimura Y., Wilder-Smith P., Yonaga K.,Matsumoto K.
Treatment of dentine hypersensitivity by lasers: a review.
Journal of Clinical Periodontology 2000; 27: 715–721.
8. Zanirato R., Curti F., Prezzotto G., De Carvalho E., Pelizon J.
E., Bagnato V. S. Clinical effects of low-intensity laser vs light-
emitting diode therapy on dentin hypersensitivity. Journal of
Oral Laser Applications 2007; 7: 129–136.
9. Launay Y., Mordon S., Cornil A., Brunetaud J. M., Moschetto,
Y. Thermal effects of lasers on dental tissues. Lasers in
Surgery and Medicine 1987; 7: 473–477.
10. Matsumoto K, Tomonari H, Wakabayashi H. Study on the
treatment of hypersensitive dentine by laser. J Conservat Dent
1985; 28: 1366-1371.
Vol. 1 Issue 11 L.E.D. E-Journal Page 118
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

11. Yamaguchi M, Ito M, Miwata T, Horiba N, Matsumoto T,
Nakamura H, Fukaya M. Clinical study on the treatment of
hypersensitive dentin by GaAlAs laser diode using the double
blind test. Aichi-Gakuin J Dent Sci 1990; 28: 703-707.
12. Gerschman JA, Ruben J, Gebart-Eaglemont J. Low level laser
therapy for dentinal tooth hypersensitivity. Aust Dent J 1994;
39: 353-357.
13. Kumar N. G. & Mehta D. S. Short-term assessment of the
Nd:YAG laser with and without sodium fluoride varnish in the
treatment of dentin hypersensitivity – a clinical and scanning
electron microscopy study. Journal of Periodontology 2005;
76:1140–1147.
14. Goharkhay K., Wernisch J., Schoop U., Moritz A. Laser
treatment of hypersensitive dentin: comparative ESEM
investigations. Journal of Oral Laser Applications 2007; 7:
211–223.
15. Tarbet W. J., Silverman, G., Stolman J. M., Fratarcangelo P. A.
Clinical evaluation of a new treatment for dentinal
hypersensitivity . Journal of Periodontology 1980; 51: 535–
540.
16. Collins J. F., Gingold J., Stanley H., Simring, M. Reducing
dentinal hypersensitivity with strontium chloride and
potassium nitrate. General Dentistry 1984; 32:40–43.
17. Flynn J, Galloway R, Orchardson R. The incidence of
hypersensitive teeth in the west of Scotland. J Dent 1985; 13:
230-236.
18. Graf H, Galasse R. Morbidity, prevalence and intraoral
distribution of hypersensitive teeth. J Dent Res 1977; 56 (Spec
Issue A) 162, abstr 479.
19. Kerns D.G, Scheidt M.J, Pashley D.H, Horner J.A, Strong
S.L, Van Dyke T.E. Dentinal tubule occlusion and root
hypersensitivity. Journal of Periodontology 1991; 62: 421–428.
20. Wichgers T.G, Emert R.L. Dentin hypersensitivity. General
Dentistry 1996; 44: 225–232.
21. Lan W.H, Liu H.C, Lin C.P. The combined occluding effect of
sodium fluoride varnish and Nd:YAG laser irradiation on
Vol. 1 Issue 11 L.E.D. E-Journal Page 119
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
human dentinal tubules. Journal of Endodontics 1999; 25:
424–426.
22. Moritz A, Gutknecht N, Schoop U, Goharkhay K, Ebrahim D,
Wernisch J et al. The advantage of CO2-treated dental necks,
in comparison with a standard method: results of an in vivo
study. J Clin Laser Med Surg. 1996; 14 :27-32.
{Dear Readers: The above article was first published in ‘Journal of Dental
Lasers’ Vol. 7 Issue 2 (2013) issue and has been republished with prior
permission from the author Dr. Rajeev Ranjan & the Publishing House,
Wolters Kluwer – Medknow Publication with due acknowledgment.}
P.S. Any feedback/compliments/queries for the Author/s should
be emailed to the Editor-in-Chief, Dr. Bhavdeep Singh Ahuja at
his email id: [email protected]
Vol. 1 Issue 11 L.E.D. E-Journal Page 120
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Aathwaa Gyaan
Vol. 1 Issue 11 L.E.D. E-Journal Page 121
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Dr. Meenu Bhola has passed her BDS from Govt. Dental College, Amritsar and finished her Post Graduation in Pediatric and Preventive Dentistry from Christian Dental College, Ludhiana. She has many national and international publications to her credit. She has presented many scientific papers in various conferences. Currently, she is working as Professor at DIRDS, Faridkot and practicing as Pediatric dentist at Ludhiana. Dr. Geetika Jindal has passed her BDS from Guru Nanak Dev Dental College and Research Institute, Sunam and finished her Post Graduation in Pediatric and Preventive Dentistry from DIRDS, Faridkot. She has many national publications to her credit. She has presented many scientific papers in various conferences. Currently, she is working as a Senior Lecturer at DIRDS, Faridkot. Dr. Aashana Goel has passed her BDS from DIRDS, Faridkot and is pursuing her Post Graduation in Pediatric and Preventive Dentistry from DIRDS, Faridkot. She has presented scientific papers and posters in various conferences. Currently, she is a Post Graduate student at DIRDS, Faridkot.
RADIX ENTOMOLARIS in PERMANENT
MANDIBULAR FIRST MOLAR
An Endodontic Challenge?
A Case Report
Author: Dr. Meenu Bhola
Co-Author 1: Dr. Geetika Jindal
Co-Author 2: Dr. Aashana Goel
ABSTRACT
Comprehensive knowledge of the root canal anatomy is a basic
pre-requisite for endodontic treatment. The success of endodontic
treatment depends upon the proper identification of all canals,
thorough chemo-mechanical preparation followed by a three-
dimensional obturation with a hermetic seal. The endodontic
treatment of a mandibular molar with an aberrant canal
configuration (anatomy) can be diagnostically and technically
challenging.
Radix Entomolaris is one such aberration where an extra
root is usually present on the disto-lingual aspect of mandibular
first molar. This article presents a case report of mandibular first
molar with extra root which was successfully treated.
Vol. 1 Issue 11 L.E.D. E-Journal Page 122
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
KEYWORDS
Endodontic Treatment, Mandibular First Molar, Radix
Entomolaris.
INTRODUCTION
The American Association of Endodontics (AAE) has defined root
canal obturation as “the three dimensional filling of the entire root
canal system as close to the cemento-dentinal junction as
possible”. A tight apical seal is considered desirable to prevent
remaining bacteria and their endotoxins from invading the apex.
The main objective of the root canal treatment is thorough
mechanical and chemical cleaning of all the canals before the
obturation with an inert filling material. Thus, the treatment of
the entire root canal system is essential to maximize the
possibility of obtaining success in endodontic therapy. For this
purpose, knowledge about the anatomy of the pulp chamber and
root canal system along with its potential variations are an
indispensable part of endodontics. It is very well known that
mandibular first molar may display several anatomical variations
in its configuration. Most mandibular first and second molars in
Caucasians have roots with two mesial canals and one distal
canal. Presence of a third root in the permanent first molar is the
major variant of this group.
An additional root, firstly mentioned in literature by
Carabelli in year 1844 is called Radix Entomolaris. The presence
of extra root on lingual side of mandibular first molar is Radix
Entomolaris. Apart from mandibular first molars, it may be rarely
found in mandibular third molars but has not been reported in
mandibular second molar yet. The other variant is Radix
Paramolaris which indicate presence of extra root on the buccal
side.
This case report highlights Radix Entomolaris, a developmental
variation occurring in mandibular molar which is associated with
an extra lingual root, its diagnosis and the endodontic
management.
Vol. 1 Issue 11 L.E.D. E-Journal Page 123
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
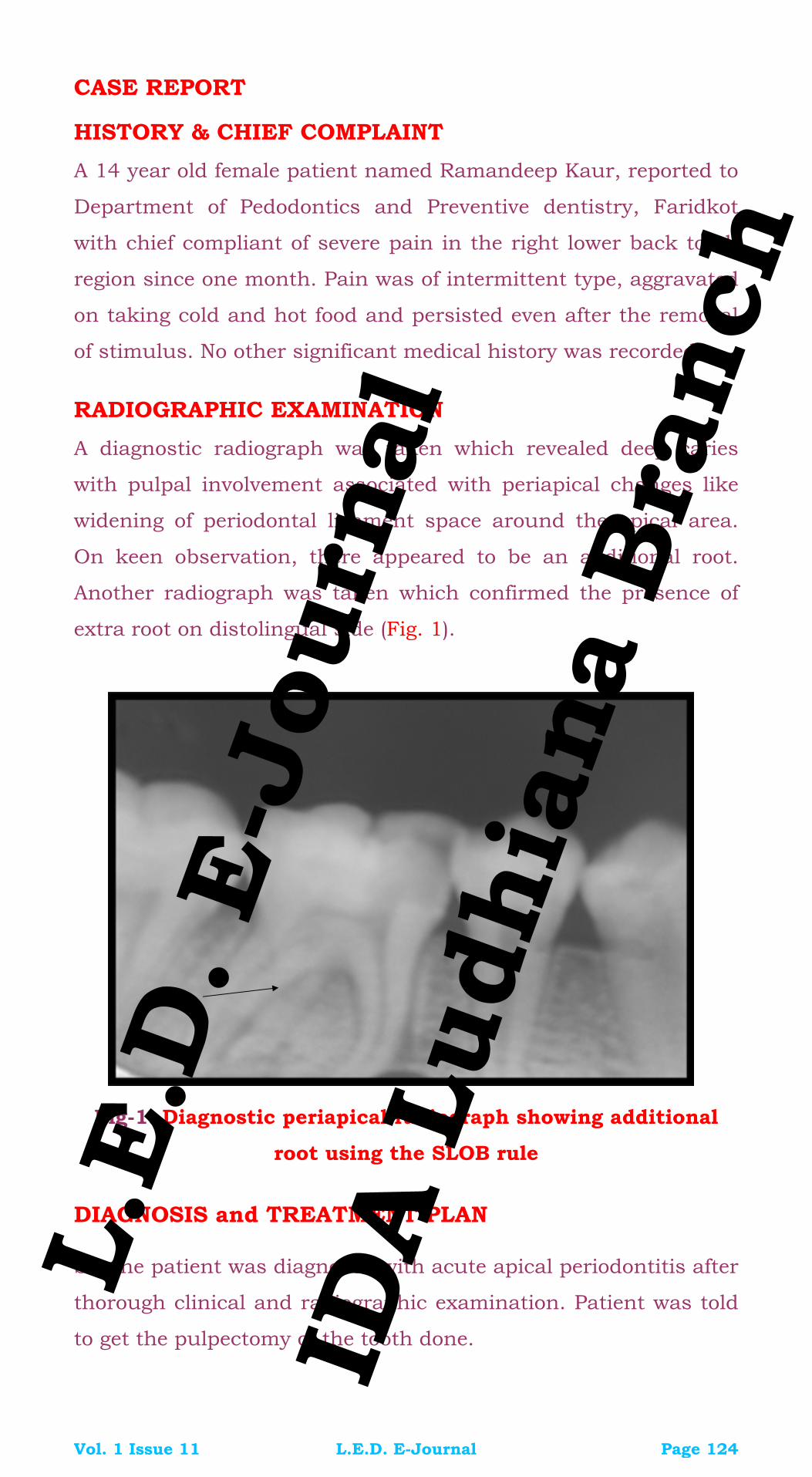
CASE REPORT
HISTORY & CHIEF COMPLAINT
A 14 year old female patient named Ramandeep Kaur, reported to
Department of Pedodontics and Preventive dentistry, Faridkot
with chief compliant of severe pain in the right lower back tooth
region since one month. Pain was of intermittent type, aggravated
on taking cold and hot food and persisted even after the removal
of stimulus. No other significant medical history was recorded.
RADIOGRAPHIC EXAMINATION
A diagnostic radiograph was taken which revealed deep caries
with pulpal involvement associated with periapical changes like
widening of periodontal ligament space around the apical area.
On keen observation, there appeared to be an additional root.
Another radiograph was taken which confirmed the presence of
extra root on distolingual side (Fig. 1).
Fig-1: Diagnostic periapical radiograph showing additional
root using the SLOB rule
DIAGNOSIS and TREATMENT PLAN
So, the patient was diagnosed with acute apical periodontitis after
thorough clinical and radiographic examination. Patient was told
to get the pulpectomy of the tooth done.
Vol. 1 Issue 11 L.E.D. E-Journal Page 124
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

TREATMENT PROTOCOL FOLLOWED
1. Tooth was isolated using rubber dam.
2. Root canal treatment was initiated after administering local
anaesthesia.
3. Access preparation was done using an Endo access bur.
4. Careful exploration of the pulp chamber floor of access cavity
using endodontic explorer revealed two distal canal orifices
and two mesial canal orifices.
5. There was a modification done in the access cavity
preparation from triangular shape to trapezoidal form.
Fig-2: Working Length Radiograph w.r.t. 46
6. Patency of canals was made with 15 K-file (Mani Japan).
7. Working length was determined radiographically (Fig. 2).
8. Cleaning and shaping was done with rotary ProTaper
instruments in a step-back manner.
9. EDTA was used as a lubricant and alternate irrigation with
sodium hypochlorite and normal saline was done.
10. Master Cone Working Length X-Ray was recorded (Fig. 3) and
Obturation was performed with gutta percha using lateral
condensation technique (Fig. 4 & Fig. 5).
11. Access cavity was restored with light cure GIC and a post-
obturation radiograph was taken.
Vol. 1 Issue 11 L.E.D. E-Journal Page 125
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Fig-3: Master Cone Radiograph w.r.t. 46
Fig-4: Post Obturation Radiograph w.r.t. 46
Fig-5: Post Obturation Radiograph w.r.t. 46 (Another Angle)
Vol. 1 Issue 11 L.E.D. E-Journal Page 126
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
DISCUSSION
A thorough knowledge of root canal morphology and configuration
of teeth plays an important role in the success of endodontic
therapy. The prevalence of Radix Entomolaris in mandibular first
molar has been well documented in literature. It is associated
with various ethnical groups with the highest frequency (5%-30%)
being observed in population with Mongoloid trait such as
Chinese, Eskimos and American Indians. In African populations,
it is around 3% with least occurrence among Indians (0.2%). A
bilateral occurrence in the population ranges from 50%-67%.
The etiology behind the formation of Radix Entomolaris is
still uncertain. It can be related to certain external factors during
odontogenesis or the penetration of the atavic/atopic gene or a
polygenic system. Third root anomalies may develop during bud
morpho-differentiation as a result of the developmental aberration
of both ectoderm and mesoderm. Curzon suggested that three-
rooted molar trait has a high degree of genetic penetrance
(penetration).
A classification was given by Carlsen & Andersen based on
the location of the cervical part. They are types A, B, C, AC.
a. Type A & Type B refers to a distally located cervical part.
b. Type C refers to a mesially located cervical part.
c. Type AC refers to the location of the cervical part in the
central location in between the mesial and distal components.
De Moor et al had given other classification based on the
curvature of Radix Entomolaris variants in the bucco-lingual
direction.
a. Type I which refers to straight root / canals
b. Type II refers to a curvature at the entrance of the orifice
c. Type III refers to Radix Entomolaris with two curvatures, one
at the coronal level and the other at the middle third.
Once a diagnosis of additional root is reached and an
access cavity has to be prepared, care should be taken to
Vol. 1 Issue 11 L.E.D. E-Journal Page 127
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

establish a “straight-line” access. With the disto-lingually located
orifice of the Root Canal, a modification of the classical triangular
access cavity to a trapezoidal form is required to locate and
access the root canal. The laws of orifice location may aid in the
location of extra orifices. Diagnostic measures such as multiple,
pre-operative radiographs, examination of the pulp chamber floor
with a sharp explorer, troughing of the grooves with ultrasonic
tips, staining the chamber floor with 1% methylene blue dye,
performing the sodium hypochlorite “champagne bubble test,”
and visualizing canal bleeding points are all important aids in
location of the root canal orifices. An endodontic explorer can be
used as a pathfinder to determine the angle at which the canals
depart from the main chamber. Other advanced diagnostic aids
may also help in the better identification and visualization of all
the canals.
Some of the most common problems encountered during
the treatment of Radix Entomolaris are:
1. Difficulty in Radiographic interpretation.
2. Inability to locate the fourth canal.
3. Modification in access cavity preparation.
4. Confusion in working length determination.
Apart from these difficulties, clinicians are prone to
commit some iatrogenic errors like straightening of a root canal
resulting in loss of working length, ledge formation, zipping,
transportation or even perforation.
CONCLUSION
The prognosis of the root canal treatment depends upon the
careful observation and interpretation of radiographs to avoid
missing any extra canals. A number of variations can occur which
might pose a challenge to the clinician. This particular variation
Radix Entomolaris may be a challenge to those who don’t have
proper diagnostic aids and lack in proper knowledge of root canal
anatomy. Hence, knowledge about the unusual root canal
morphologies in terms of root inclination and root canal
curvatures among various ethnical groups is important.
Vol. 1 Issue 11 L.E.D. E-Journal Page 128
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
REFERENCES
1. Balasubramanian, A, Bhosale, S, Kumar3, MR, Jayasree , S
(2013), Endodontic Management of a Tooth with Radix
Entomolaris and Five Root Canal’, Journal of Dental and
Medical Sciences, vol.10, issue.6, pp. 62-65.
2. Bolla, N, Naik, B, Kavuri, SR, Sriram, SK, Radix Entomolaris: A
Case Report, Endodontology.
3. Das, M, Sethi, P, Kavitha, Singh, A (2015), The radix
Entomolaris in permanent Mandibular first molar- An
Endodontic Challenge’, International Journal of Advanced
Multidisciplinary Research, vol.2, issue.5, pg 44-49.
4. Davini, F, Cunha RS, Fontana, ES, Silveira, CF, Silveira Bueno,
CF (2012), Radix entomolaris – A case report’, RSBO, vol. 9,
issue. 3, pg. 340-4.
5. Hegde, V, Kashid, V (2015), Radix Entomolaris-Series Of Case
Reports’, International Journal Of Advances, vol.2, issue.4, pp.
216-220.
6. George, R, Kavyashree, G (2015), Endodontic Management of
Radix Entomolaris’, Journal of Dental and Medical Sciences,
vol.14, issue. 12, pp. 12-14.
7. Kamath, U, Sheth, H, Mohan, N, Reddy, D (2015), Endodontic
management of radix entomolaris: Case reports, International
Journal of Applied Dental Sciences, vol. 2, issue. 1, pp. 15-19.
8. Mahalakshmi, S, Shenoy MA, Shubha, B, Chandy, CJ (2014),
Radix Entomolaris – a rare case series’, SADJ, vol. 69, no. 8.
9. Pai, AR, Jain, R, Colaco, AS (2016), Detection and endodontic
management of radix entomolaris: Report of case series’, Saudi
Endodontic Journal, vol. 4, Issue. 2, pp. 77-82.
P.S. Any feedback/compliments/queries for the Author/s should
be emailed to the Editor-in-Chief, Dr. Bhavdeep Singh Ahuja at
his email id: [email protected]
Vol. 1 Issue 11 L.E.D. E-Journal Page 129
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
Nauwaa Gyaan
Vol. 1 Issue 11 L.E.D. E-Journal Page 130
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Dr. Parminder Singh Grover is a graduate of 2002 from Himachal Dental College, Sundernagar (H.P.). He started his own clinical practice in 2003. Presently, he is a Consultant at SPS, Apollo Hospital Ludhiana and currently runs his practice in two different operatories in Ludhiana.
Dr. Supreet Kapoor is a dentist from Ludhiana, and is a graduate from Christian Dental College Ludhiana. Currently, she is practicing with Dr. Parminder Singh Grover at his clinic in Ludhiana.
NANODENTISTRY
A Novel Approach
Author: Dr. Parminder Singh Grover
Co-Author: Dr. Supreet Kapoor
INTRODUCTION
Nanotechnology, a term though new in surroundings but yet has
its root long back which lies when the concept was first given by
late Nobel physicist Richard P. Feynman - “plenty of room at the
bottom”.
This idea though not accepted at that time but was later taken
forward by Eric Drexler who introduced this term, henceforth
making better materials with much better properties.
As per Norio Tsaniguchi - Nanotechnology mainly consists of
processing, separation, integration and deformation of materials
at atomic level, furthermore integration of above concept into
dentistry thus making upgradation of oral hygiene leads to
emergence of new term – Nanodentistry.
This branch mainly involves concepts of nanotechnology which in
general is understood by following 4 approaches:
1. Bottom-up Approach
2. Top down Approach
3. Functional Approach
4. Biomimetic Approach
Vol. 1 Issue 11 L.E.D. E-Journal Page 131
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

a. Bottom-up Approach: This approach mainly involves a
smaller to bigger complex making entity, the bonds of
resultant being extremely strong. This approach has its
influence in dentistry as follows:
1. Nano-anesthesia: This technique involves use of active,
analgesic micrometer dental nano-robots which within
100 seconds reaches pulp through dentinal tubules all
under control of nano-robot .This solution is available in a
colloidal suspension for local anesthesia.
2. Hypersensitivity cure: This being a newer concept involves
occlusion of selected dentinal tubules by reconstructive
dental nano-robots thus making cure for hypersensitivity.
3. Denti-frobots: This is a concept involving nano-robotic
dentifrice delivered by mouth washes etc. These denti-
frobots through metabolization debride calculus and
further destroying pathogenic bacteria giving rise to
healthy oral ecosystem.
4. Cancer diagnosis: A less invasive means of identifying
cancer cells through identification and quantification of
cancer markers is provided through nanotechnology .This
involves use of Physiochemical nanoscale modification
through the following:
i. Nano-texturing
ii. Quantum dots
iii. Bio barcode assay
iv. Nanometer scale tubes and wire
v. Nanoelectromecahnical systems
vi. Therapeutic nanotechnology
This approach makes use of localize delivery of multiple
and complimentary therapeutic agents. They possess site
specific targeting ability thus making more effective use of
drugs .
Vol. 1 Issue 11 L.E.D. E-Journal Page 132
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

5. Dental durability and cosmetics: Fracture resistant nano-
structured composite nano-material including nano-tubes
are being used for upper layer enamel replacement in
cosmetic dentistry.
6. Orthodontic nano-robots: Nano-robots because of high
positional accuracy can complete the desired action and
then can be easily removed by human excretory channels.
These orthodontic nano-robots can manipulate structures
surrounding tooth like periodontal ligament, alveolar bone
etc thus allowing rapid painless tooth movement.
b. Top down Approach: It seeks to produce smaller devices, as
the name suggest, from bigger ones with precision in
structure. It mainly involves:
1. Nanotechnology for composite: It involves idea to improve
the properties of composite material in terms of
polymerization shrinkage, wear resistance etc.
2. Glass Ionomer Cement: It mainly involves formulation of
cement based on bonded filler with high fluoride release, it
also has shown ability to create caries inhibition zone after
acid exposure because of integration with nanomaterial.
3. Improving Endodontics: By the concept of N.E.R.P. -
Nanomaterial enhanced retrofiller polymer - with the
advantage of better strength and adaptability. These
materials were significantly found to reduce the
microleakage of bacteria compared to conventional
materials thus demonstrating their sealing ability.
4. Impression material: These materials are integrated with
nano-fillers thus making better flow along with improved
properties such as tear strength.
5. Nano-titanium implants: They are highly compatible with
20 times faster bonding and improved strength.
Vol. 1 Issue 11 L.E.D. E-Journal Page 133
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

6. Other techniques involve nano-needles and nano-tweezers
and biodegradable nano-fillers.
c. Functional Approach: It involves development of components
of desired functionality without regard of how they are
assembled. E.g. Synthetic chemical methods used to create
synthetic molecular motors.
d. Biomimetic Approach: A system of imitation of models and
systems for purpose of solving complex human problem. In
other words, the use of concepts to create newer materials.
There is use of this approach at micro-molecular level –
NANO-BIOMIMETICS
Though four approaches are in use, the maximum output in
dentistry is through first two.
Various Nano-materials and Devices:
1. Nanopores
2. Quantum dots
3. Nanoshells
4. Dendromers
5. Liposomes
6. Nanorods
7. Fullerene
NANO-ROBOTS in GENERAL
It is the creation of robots at microscopic scale of nanometers (0.5
- 3 micrometer in diameter) with main element as carbon with
increased strength and chemical inertness.
ELEMENTS of NANO-ROBOTS
The bulk of it is carbon in form of diamond or fullerene. Though it
is much in acceptance and is an emerging field, this technique
still involves many challenges viz. below:
1. Biocompatibility
2. Precision
Vol. 1 Issue 11 L.E.D. E-Journal Page 134
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

3. Coordination of activities
4. Economical status
5. Social issue of acceptance
6. Though with above issues risk posed by molecular
manufacturing and social risk need further investigation
SCOPE of NANOTECHNOLOGY
This is now the third highest booming field with a new scope in
upcoming generations but India is still in the development stage
for nanotechnology.Though research labs are doing excellent jobs
but it may still take a few years to settle as an established field.
CONCLUSION
Mutidisciplinary approach of nanotechnology offers great
potential in dentistry ranging from our restorative materials to
implants. Though it opens a huge range still a need to critically
examine its risk and potential toxicity lies at par.
REFERENCES
1. Sneha sundar rajan shashmi rashmi and vidya saraswath
2. Gribbin and gribbin 1997
3. Das etal
4. Freitas robot 2000
5. Shetty etal 2013
6. Uysal etal
7. Chogle etal
8. Kumar and vijaylakshmi 006
9. Albrektssonet al 2008
10. Gaurav chaudhary tarun Sharma tarun rana
P.S. Any feedback/compliments/queries for the Author/s should
be emailed to the Editor-in-Chief, Dr. Bhavdeep Singh Ahuja at
his email id: [email protected]
Vol. 1 Issue 11 L.E.D. E-Journal Page 135
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Daswaa Gyaan
Vol. 1 Issue 11 L.E.D. E-Journal Page 136
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Dr. Bhavdeep Singh Ahuja is a Dentist in Ludhiana, Punjab, having graduated in 1998 from Punjabi University, Patiala. He has specialized in Implants from BioHorizons Inc. USA in 2004-05 & in an Advanced Course from LACE-ICOI, USA in 2006. Apart from Dentistry, he holds a Triple M.B.A. in Hospital Management, Human Resource Management & Marketing from three premier Institutes /Universities of India viz. the IIMM Pune, IGNOU New Delhi & Annamalai University. He holds Post Graduate Diploma’s in various specialties viz. Medical Law & Ethics (NLSIU), Clinical Research, Cyber Law, Disaster Management, Financial Management, Bioinformatics amongst many more from different Universities. He is a Certified Health Care Waste Manager from IGNOU & is qualified in Consumer Law as well. He is an academically oriented dentist & has many Original Scientific Publications to his credit in many International & National journals. Presently, he is into 17th year of Clinical Practice in Ludhiana, Punjab & is reachable on www.drbhavdeep.com
Managing Better – An Art & a Science – XI
A few Rules – None too Many
Author: Dr. Bhavdeep Singh Ahuja
Continued from Vol. 1 Issue 10 22. Rule 22: Follow marketing strategies which are time
tested and which never fail
No matter what we do, where we operate from or what
we offer our patients, for any business, ensuring that we have
a relevant and stable marketing strategy is crucial. Not only
will it keep us actively in the limelight of our sector, it will
make sure we attract as many people as possible to our
practices online. Regardless of the any type of professional
business or services we offer, there are a few time tested and
solid marketing strategies which usually never fail and are
critical in creating a fruitful venture and we becoming a
successful entrepreneur. There is nothing wrong with creating
an environment of anticipation, but the experience better pay
off. There are a few golden rules or marketing strategies which
we have to bear in mind when approaching the marketing of
our business and we should make sure we follow them to
optimize our marketing needs because these will help us
create a stronger brand and attract more patients to our
practice. However, a word of caution, as these are only the
basics and offer an introduction to creating a solid marketing
Vol. 1 Issue 11 L.E.D. E-Journal Page 137
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
structure; the rest is down to dedicated and consistent work.
Here are a few of them:
a. What is/are your USP (Unique Selling Proposition);
highlight it (the uniqueness). Having a practice already set
up, we should be well aware of what our USP is/are (can be
more than one also). Without any of the above, many
practices eventually fall at the first hurdle, as they simply
can’t offer new patients something an established
practice/clinic can. Keep this in mind and make sure we
mention what makes us different as much as we can,
where we Professionals especially doctors/dentists in
private practice (particularly the medium ones) often
struggle to find something different to say about our
services. We only talk about what we do; so what makes
our services unique compared to our competitors? Rather
than what we offer, we have to think about the way (how)
we offer it, and how this benefits our patients. We might
have a special way of attending to our patients for
assessing their problems and troubles. Once we start
focusing on this, we would have created our unique selling
proposition (USP).
b. Keep it Fresh: Even though it is unlikely that what our
intentions as a practice are and what we offer to change,
keep the marketing fresh. Update your website with good
intelligent content whenever possible, keep an active
presence on social media sites and let people know you are
a living breathing existent individual. Appearing interested,
and not leaving old messages or posts to go stale will show
the patients that we have a passion to provide, not to
mention, it will encourage them to want to connect with us
on a more personal level.
c. Stay Connected: Hand in hand with keeping your
marketing fresh is staying connected. Posting regularly on
Facebook or Twitter is all but pointless if we aren’t willing
to put the effort into what comes next – the contact.
Vol. 1 Issue 11 L.E.D. E-Journal Page 138
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Patients will feel connected and respected if they comment
on a post, for example, and receive a reply.
d. Standardization: Consistency is crucial, we can’t expect
others to be okay when they expect a connection to happen
but no one was there to reply to them, like they were for
others. We have to be consistent and once we have worked
out our USP, we have to apply it to everything with the new
uniqueness. Shun off the old issues as the ghosts of the
past can rise from closet any day. New prospective patients
can come to you from all kinds of routes viz. business
cards, website, phone call, newsletters, blogs, print or
online ads and so on. If we are not consistent in our
uniqueness, we may run the risk of confusing our patients
with mixed messages. We can engage and then only hope
to reap the awards.
e. KISS: Follow the KISS principle; keep it sweet and simple
while writing Editorials or Blogs. Don’t over-complicate the
working style. We may understand the intricate workings of
our services, but may not be entirely relevant, useful or
interesting to our patients. Potential patients are more
inclined to read the ads or marketing blog if it is simple, to
the point and straightforward. Wordy explanations and
flowery writing loses its attention before we can actually get
our point across. Whatever, we need to pass on, should be
done in a creative, yet concise manner.
f. Branding: When branding our practices, create a look that
is different from the others which forms the basis of the
web design or logo which helps us ensure standing out
from the competition.
g. Stay away from fake information: Build the brand from a
position of truth (not hype) and keeping it real is the first
step. Usually, patients can spot hype from far off, so it is
always better to offer them real content, real benefits with
real value for money. We have to demonstrate our ability to
Vol. 1 Issue 11 L.E.D. E-Journal Page 139
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
do this through case studies and testimonials. Don’t offer
the moon, if you can't operate a space ship.
h. Know your Key words: Search Engine Optimization (SEO) is
a way to learn the secrets of using keywords to get the
clinic and services listed higher on search engine listings. If
we know, how to use keywords to generate more hits on
our blog or website, it will bring in the patients who need
what we have to offer.
i. Blogs: Create a blog and write about your offerings and
services in a new and an engaging way. This can be linked
to your clinic website and learn how to blog effectively to
bring in more hits and to get more business. Advertising on
your blog also opens the doors to more cash flow options.
j. Learn how marketing is constantly evolving: Online
marketing is always changing and developing and it’s a
keep up or get left behind situation. Keep up to date with
changes to social media sites, SEO, blogger platforms and
occasionally check marketing blogs for fresh information. It
can actually surprise us that it is easy to pick up and
execute the knowledge and is priceless keeping us ahead of
the competition with the information base we already have.
k. Promise only what you can deliver, keeping it truthful:
Patients know what they want, when and how they want it
usually before they even come onto our website. This
means we need to be fully prepared for anything they may
have queries on beforehand. Offering FAQ’s on the website,
customer reviews and links to social media profiles always
helps a great deal showing that we care about patients and
the services they receive. Patient service should start the
second they click onto your website, not just on the
appointment date. A big mistake is to try to boost the
online appearance by tweaking or essentially lying about
things. Don’t say what you can’t deliver on a promise. If
some materials or components (like Implants) have to be
Vol. 1 Issue 11 L.E.D. E-Journal Page 140
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

outsourced, don’t tell the patient, it will be there in 2 days.
Do not make up customer reviews and never use services
like pay for likes or queue jumping to bump up the website.
Online users are extremely good at sniffing out rats, and a
rat is not something we want to be when trying to run a
successful, healthy and developing clinical practice.
(To be Continued)
REFERENCES
1. Phillip Kotler, Gary Armstrong, John Saunders, Veronica
Wrong et al. Principles of Marketing, 2nd European Edition
2. Phillip Kotler, Kevin Lane Keller et al. Marketing
Management, Twelfth Edition
3. Laura Lowell; 42 rules of marketing
4. The Expert Guide to Affiliate Marketing;
http://Rags2RichesSystem.biz
5. http://www.beckershospitalreview.com/hospital-
management-administration/
6. http://www.ducttapemarketing.com/
7. http://www.bloomberg.com/visual-data/best-
andworst/most-efficient-health-care-2014-countries
8. http://www.forbes.com/
9. https://www.qualitylogoproducts.com/blog/
10. http://www.macquarie.com/
11. http://marketingland.com/
12. http://www.inc.com/
13. http://www.brandfactory.com.au/
14. http://www.brandfactory.com.au/
15. https://www.entrepreneur.com
16. http://www.cision.com/
17. http://www.managementhelp.org/
18. Wikipedia; https://en.wikipedia.org/wiki/
Vol. 1 Issue 11 L.E.D. E-Journal Page 141
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
Dear Readers: Important Announcement
As all good things come to an end one day, Dr. Bhavdeep Singh
Ahuja, the Editor-in-Chief of L.E.D. E-Journal will wind up this
series of articles on ‘Managing Better – An Art & a Science’ next
month with his last article in December 2016 in L.E.D. E-
Journal.
Dear Readers: Important Announcement
The above article by Dr. Bhavdeep S. Ahuja will be published in XII parts.
The above is Part XI.
Check out L.E.D. Issue Jan. 2016 Vol. 1 Issue 1, Feb. 2016 Vol. 1 Issue 2,
Mar. 2016 Vol. 1 Issue 3, Apr. 2016 Vol. 1 Issue 4, May 2016 Vol. 1 Issue 5,
June 2016 Vol. 1 Issue 6, July 2016 Vol. 1 Issue 7, August 2016 Vol. 1 Issue
8 , September 2016 Vol. 1 Issue 9 & October 2016 Vol. 1 Issue 10 for the Ist,
IInd, IIIrd, IVth, Vth, VIth, VIIth, VIIIth , IXth & Xth parts of the above article.
Check out L.E.D. Issue December 2016 Vol. 1 Issue 12 for the XIIth and the
LAST part of the above article in this series.
P.S. Any feedback/compliments/queries for the Author/s should
be emailed to the Editor-in-Chief, Dr. Bhavdeep Singh Ahuja at
his email id: [email protected].
Vol. 1 Issue 11 L.E.D. E-Journal Page 142
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
HAPPY CHILDREN’s DAY
Vol. 1 Issue 11 L.E.D. E-Journal Page 143
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
for
Your honest opinion is of immense value to us. For encouraging the
same, we are starting an award for ‘Best Feedback Series’ every
month. Send your feedback to the Editor in-Chief, Dr. Bhavdeep
Singh Ahuja’s email at [email protected] regarding what is
your overall opinion on E-Journal L.E.D. (Let’s Enjoy Dentistry) or on
the current issue or any particular section of it. The feedback can be
like a performance appraisal, critique review, criticism, applause,
appreciation etc. In short both, bouquets and brickbats are welcome
in equal measure by us. We would be happy to publish with due
credits (both critique review and admiration), the award winning
feedbacks in the next issue of the Publication. However, if the
Branch Member wishes to keep his/her identity secret/hidden, the
feedback would be published under the heading Anonymous. The
best feedback (every month) stands to win a surprise gift at the next
CDE/GBM of IDA Ludhiana Branch. So, if you want to win a prize,
get going, type out your honest feedback and send it to the Editor-in-
Chief, Dr. Bhavdeep Singh Ahuja’s email at [email protected].
Vol. 1 Issue 11 L.E.D. E-Journal Page 144
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Vol. 1 Issue 11 L.E.D. E-Journal Page 145
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Vol. 1 Issue 11 L.E.D. E-Journal Page 146
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

L.E.D. E-Journal
Manuscripts Invited
Would you like to publish in the most happening IDA Local
Branch (IDA Ludhiana) official publication, ‘L.E.D.’ – ‘Let’s
Enjoy Dentistry’, a monthly E-Journal with 11 scientific
articles every month (the first for any local branch dental
journal; both the frequency and the number of articles) in the
ratio of 8 National/International Authors, 2 Local (Ludhiana)
Authors & 1 by the Editor-in-Chief apart from the Editorial.
The first 6 month slots are already gone and out of the 66
articles by 71 authors in the first 6 months since January
2016 launch, even a single Author has not been repeated yet
(again a first) except for the articles in split parts or articles in
series. LED Ludhiana requests original submissions about any
aspect of dentistry in the broadest sense, including, limited
not only to teeth but all aspects of oral health. LED is an
open-access, peer-reviewed journal focused on enlightenment
with enjoyment, but what makes LED truly unique is that it is
multi-disciplinary in scope, publishing articles from all
including young budding authors and is exclusively outreach
oriented. Do you have an interesting case presentation,
research/ review article or a short communication? If so, then
LED could be your perfect outlet. LED could be the
quintessential journal for disseminating your information to a
broad audience that increasingly relies on the Internet for
information. So, what are you waiting for, pick up your pen or
keyboard, punch in & send it across to the Editor-in-Chief, Dr.
Bhavdeep Singh Ahuja at [email protected]. This is
your ticket to ‘Hall of Fame’; the author guidelines are already
attached along with. If you wish to discuss a potential
manuscript idea, please contact the Editor-in-Chief, Dr.
Bhavdeep Singh Ahuja at [email protected] or at his
phone no. 98761-93039.
We look forward to receiving your next manuscript.
Vol. 1 Issue 11 L.E.D. E-Journal Page 147
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

E-Journal
1. Author Guidelines
2. Dental Council of India – Revised Code of Ethics
3. Dental Council of India – Right to Information - Handbook
4. Dental Council of India – Notification – Establishment
Scheme for Opening of New Dental Colleges
5. WHO – Guidelines for Dengue & Chikungunya
6. Dental Trauma Guidelines (Revised) – International
Association of Dental Traumatology
7. Govt. of India Gazette Notification - Revised Bio Medical
Waste Management Rules 2016
8. Atomic Energy Regulatory Board (AERB) – Introduction &
Guidelines for Starting a Diagnostic Installation
9. Atomic Energy Regulatory Board (AERB) – Revised
Guidelines for obtaining Regulatory Consents for
Diagnostic Equipment
10. Atomic Energy Regulatory Board (AERB) – Guidelines for
shielding of X-ray Installations
11. Atomic Energy Regulatory Board (AERB) – Guidelines for
applying for License Diagnostic Radiology Equipment
12. Atomic Energy Regulatory Board (AERB) – Checklist for
submission of application form for registration
13. National Treatment Guidelines for Antimicrobial Use in
Infectious diseases
14. Central Drugs Standard Control Organization – Frequently
Asked Questions on ‘Registration and Import of Medical
Devices in India’
* New from this Issue
Vol. 1 Issue 11 L.E.D. E-Journal Page 148
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

L.E.D. E-Journal November 2016 Vol. 1 Issue 11
APPENDICES Index
S. No.
Title Details Page No. From – To
1. Author Guidelines For Publishing 150 – 154 2. DCI - Revised Code of
Ethics Dental Council of
India 155 – 165
3. DCI – Right to Information - Handbook
Dental Council of India
166 – 191
4. DCI – Establishment Scheme for Opening of
New Dental Colleges
Dental Council of India
192 – 196
5. WHO Guidelines on Dengue & Chikungunya
World Health Organization
197 – 227
6. Dental Trauma Guidelines – Revised
International Association of
Dental Traumatology
228 – 254
7. Revised Bio Medical Waste Management Rules
2016
Govt. of India Gazette
Notification
255 – 292
8. Introduction & Guidelines for Starting a Diagnostic Installation
AERB - Atomic Energy Regulatory
Board
293 – 296
9. Revised Guidelines for obtaining Regulatory
Consents for Diagnostic Equipment
AERB - Atomic Energy
Regulatory Board
297 – 299
10. Guidelines for shielding of X-ray Installations
AERB - Atomic Energy Regulatory
Board
300 – 303
11. Guidelines for applying for License Diagnostic Radiology Equipment
AERB - Atomic Energy
Regulatory Board
304 – 329
12. Checklist for submission of application form for
registration
AERB - Atomic Energy
Regulatory Board
330 – 335
13. National Treatment Guidelines for
Antimicrobial Use
Antibiotics in Infectious Diseases
336 – 399
14. Registration and Import of Medical Devices in
India – Frequently Asked Questions
Central Drugs Standard Control
Organization
400 – 411
Vol. 1 Issue 11 L.E.D. E-Journal Page 149
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Author Guidelines The Editor invites contributions for the IDA Ludhiana Branch E-Journal:
1. Systemized Review articles 2. Original Research articles 3. Short Communications 4. Clinical Case Reports Review articles: These provide an in-depth review of a specific topic by systematic critical assessments of literature and data sources. Appropriate use of tables and figures is encouraged. Where relevant, key messages and salient features may be provided up to 4000 words excluding references and abstract. Research articles: These scientific reports give results of original research. These should have a structured abstract (consisting of Background, Aims, Methods, Results & Conclusions) and should follow the IMRAD (Introduction, Methods, Results and Discussion) format (upto 2500 words). Short Communications: These are brief reports on research (approx. 1200 to 1500 words). A short report may include up to 3 tables or figures and 15 to 20 references. Clinical case reports: Previously undocumented disease process, a unique unreported manifestation or treatment of a known disease condition. (approx. 700 to 1200 words) will be given priority. Covering Letter The covering letter should outline the importance of the paper and its appropriateness for publication in the Journal. It should specify the section of the Journal for which the submitted article is to be considered. It should also explain, with reasons, if there is any deviation from the IMRAD format. If the work has been previously published in part or whole (e.g. as an abstract or proceedings of a conference), this must be stated. Any conflicts of interest, or their absence, must be stated in writing. Title Page This should contain the title, running title, 3-5 Keywords, names of all the authors (without degrees or diplomas), names and full location of the departments and institutions where the work was performed, name of the corresponding author, acknowledgement of financial support and abbreviations used. Superscripted numbers should be used after each authors name and the department and institution corresponding to each number should be specified on the page. Names of authors should appear in the order of authorship The title should be brief but complete and should represent the major theme of the manuscript. It should include the animal species if appropriate. A subtitle can be added if necessary. Abbreviations should not be used. The short title should not exceed 60 characters (including inter-word spaces). It will be used as a running head. The name, telephone and fax numbers, and complete e-mail and postal addresses of the author to whom communications and requests for off prints are to be sent should be mentioned in the title page. In general, the use of abbreviations is discouraged unless they help in improving the readability of the text. The expanded form of each abbreviation should precede its first use in the text unless it is a standard unit of measurement.
Vol. 1 Issue 11 L.E.D. E-Journal Page 150
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Abstract The abstract (250 words) should be structured and a concise and accurate summary of the article and should not contain abbreviations, tables, figures, footnotes or references. It should not draw conclusions stronger or more expansive than those in the body of the paper. Briefly, the background should explain why the study was done, the methods provide how the study was done, the results provide the salient results along with important data and the conclusions briefly highlight the message of the study. Introduction The introduction should state why the study was carried out and what the specific aims of the study were. It should describe the background for the study (the available knowledge), its importance and its goals. It should be brief but complete enough for the reader to understand the reasons for the study without having to read previous publications on the subject. Methods The validity of a study is judged by the methods used. These should be described in sufficient detail to permit evaluation and duplication of the work by others. The following should be described in this section: Study design Setting Selection of participants (Sampling Technique) Interventions (Randomization & blinding, if applicable) Methods of measurement Data collection and processing Loss of data such as dropouts or patients lost to follow up Statistical methods used Ethical guidelines followed by the investigators Consort guidelines in cases of randomized control trials Results These should be concise and include only the tables and figures necessary to enhance understanding of the text. Suitable labels referring to the specific tables and figures must be mentioned in the text. Results should be presented in a logical, sequential order that parallels the organization of the methods section. The text should be used to highlight the most important aspects of the figures and tables, and to convey unique information. Data presented in tables and figures should not be duplicated in the text. Drug names, wherever used, should be generic. If the use of proprietary names is deemed a must for the study, generic names should be mentioned in parentheses. Units of Measurement SI units should be used. Temperature should be expressed in degrees Celsius and blood pressure in mmHg. Discussion The discussion should summarize how the study findings add to the current knowledge, provide explanations for the findings, compare the study’s findings with available studies, discuss the limitations of the study and the implications for future research. Only those published articles directly relevant to interpreting the results and placing them in context should be referenced. Do not repeat the results in the discussion. This section should conclude with a brief summary statement. The conclusion should be based on and justified by the results of the study. The particular relevance of the results to healthcare in India should be stressed. Conclusions regarding cost-benefit should be drawn only if a specific economic analysis formed a part of the study design.
Vol. 1 Issue 11 L.E.D. E-Journal Page 151
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

References References should be numbered in the order in which they appear in the text and these numbers should be inserted above the lines (superscripted) on each occasion the reference is cited (e.g. Sinha12 confirmed other reports13,14...). References included at the end of a sentence or part of a sentence should be placed after the punctuation mark. (Superscripting of the references is excusable/can be done away in some cases) References cited only in tables or in legends to figures should be numbered in accordance with the sequence established by the first identification in the text of the particular table or figure. Avoid using abstracts as references. For papers accepted but not yet published mention the name of the journal, the year of publication and add in press in parentheses. Information from papers submitted for publication but not accepted should be cited in the text as unpublished observations with written permission from the source. Avoid citing a personal communication unless it is essential; such citations must list in parentheses in the text the name of the person and date of communication. Written permission, obtained from the author of such communications for their use in the manuscript, must be submitted to the Journal. Do not include personal communications in the list of references. At the end of the article, the full list of references should include the names of authors, the full title of the journal article or book chapters; the title of journals abbreviated according to the Index Medicus style (www.nlm.nih.gov/bsd/uniform_requirements.html) the year of publication, the volume number and the first and final page numbers of the article or chapter. If there are six or fewer authors in the study being cited, the names of all the authors should be given. If there are more than six authors, the names of the first six authors should be given followed by et al. The authors should check that the references are accurate; lack of accuracy may result in the rejection of an otherwise adequate manuscript. Tables These should be typed in double space, each table on a separate page with the table number (in Roman numerals) and title above the table, and explanatory notes below the table. Tables should be so arranged that comparisons of interest are horizontal (across columns) and from left-to-right. The numbers of observations for each column or row (n) and marginal totals should be provided where appropriate. All abbreviations and symbols in the table must be explained in the footnote(s) to the table, even if the expanded forms have already been mentioned in the text. The units of measure must be mentioned. Figures Each image should be less than 400 kb in size. Size of the image can be reduced by decreasing the actual height and width of the images (keep up to 1024x760 pixels or 5 inches). All image formats (jpeg, tiff, gif, bmp, png, eps, etc.) are acceptable; jpeg is most suitable. Do not zip the files. Legends to figures These should be typed in double space on a separate sheet and figure numbers (in Arabic numerals), should correspond with the order in which the figures are presented in the text. The legend must include enough information to permit interpretation of the figure without reference to the text. Any labels or abbreviations within the figure must be explained in the legend. Authors All authors should have participated sufficiently in the work to take public responsibility for the content. All authors must sign an undertaking accepting responsibility for the submitted manuscript.
Vol. 1 Issue 11 L.E.D. E-Journal Page 152
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Authors are required to state their exact contribution to the study; the Journal may print this information. The order of authorship should be decided by all the authors. The journal strongly discourages alterations in the sequence or deletion/addition of authors at any time after submission of the manuscript. Acknowledgements All contributors who do not meet the criteria for authorship should be listed in an Acknowledgements section. Examples of those who might be acknowledged include a person who provided purely technical help, or statistical or writing assistance. Financial and material support should also be acknowledged. Conflict of interest A conflict of interest exists when a financial or personal relationship of the author may inappropriately influence his or her actions. Conflicts may be personal, commercial, political, academic, or financial. Some examples of financial conflicts of interest include employment; research funding (received or pending), stock or share ownership, payment for lectures or travel, consultancies and non-monetary support. Conflicts, or their absence, must be stated in writing by all authors at the time of submission of the article. The Journal may use information disclosed in conflict of interest and financial interest statements as a basis for editorial decisions. Sources of full or partial funding or other support for the research must be declared. Copyright Authors must agree in writing to transfer to the Journal the copyright for all material submitted, in case of its publication by the Journal. The published manuscript may not be reproduced elsewhere, wholly or in part, without the prior written permission of the Journal. Plagiarism Plagiarism is the use of others published and unpublished ideas or words (or other intellectual property) without attribution or permission, and presenting them as new and original rather than derived from an existing source. This applies to all forms of documents, published (print or electronic) or unpublished. Authors should make sure that their manuscripts are free from plagiarized material. Providing a reference to the material quoted verbatim from previously published material does not absolve the user of plagiarism. Detection of plagiarism would lead to rejection of the manuscript and debar the publication of any material from the concerned authors for at least three years. The Journal may also send this information to the head of the institution where the authors work with a request for an inquiry in the matter. The Journal may also publish such correspondence in its pages to inform its readers of scientific misconduct. Editorial Process A manuscript will be reviewed for possible publication with the understanding that it is being submitted to L.E.D. E- Journal alone at that point in time and has not been published anywhere, simultaneously submitted, or already accepted for publication elsewhere. The journal expects that authors would authorize one of them to correspond with the Journal for all matters related to the manuscript. All manuscripts received are duly acknowledged. On submission, editors review all submitted manuscripts initially for suitability for formal review. Manuscripts with insufficient originality, serious scientific or technical flaws, or lack of a significant message are rejected before proceeding for formal peer-review. Manuscripts that are unlikely to be of interest to the L.E.D. E- Journal readers are also liable to be rejected at this stage itself.
Vol. 1 Issue 11 L.E.D. E-Journal Page 153
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
Manuscripts that are found suitable for publication in L.E.D. E- Journal are sent to two or more expert reviewers. During submission, the contributor is requested to provide names of two or three qualified reviewers who have had experience in the subject of the submitted manuscript, but this is not mandatory. The reviewers should not be affiliated with the same institutes as the contributor/s. However, the selection of these reviewers is at the sole discretion of the editor. The journal follows a double-blind review process, wherein the reviewers and authors are unaware of each other’s identity. Every manuscript is also assigned to a member of the editorial team, who based on the comments from the reviewers takes a final decision on the manuscript. The comments and suggestions (acceptance/ rejection/ amendments in manuscript) received from reviewers are conveyed to the corresponding author. If required, the author is requested to provide a point by point response to reviewers’ comments and submit a revised version of the manuscript. This process is repeated till reviewers and editors are satisfied with the manuscript. Manuscripts accepted for publication are copy edited for grammar, punctuation, print style, and format. Page proofs are sent to the corresponding author. The corresponding author is expected to return the corrected proofs within three days. It may not be possible to incorporate corrections received after that period. The whole process of submission of the manuscript to final decision and sending and receiving proofs is completed online. Copyright form The undersigned author transfers all copyright ownership of the manuscript (Title) to (IDA Journal Ludhiana print and online version) both–in the event the work is published. The undersigned author warrants that the article is original, is not under consideration for publication by another journal and has not been previously published. I sign for and accept responsibility for releasing this material on behalf of any and all co-authors. I declare that there is neither a direct quote from any other copyrighted material or author nor are there any tables or pictures. The laboratory work is done by (Name of the Laboratory) and the name, credential and address have been duly attributed at the end of the article. {If Applicable} Appropriate references to the various published articles from scientific publications with the name of the author and name of publication are given at the end of the article in a numbered fashion as well as the appropriate reference numbers are mentioned. We give the rights to the corresponding author to make necessary changes as per the request of the journal, do the rest of the correspondence on our behalf and he/she will act as the guarantor for the manuscript on our behalf. All persons who have made substantial contributions to the work reported in the manuscript, but who are not contributors, are named in the Acknowledgment and have given me/us their written permission to be named. If I/we do not include an Acknowledgment that means I/we have not received substantial contributions from non-contributors and no contributor has been omitted. Signatures (Digital)
Vol. 1 Issue 11 L.E.D. E-Journal Page 154
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

L.E.D. E-Journal
In our constant endeavour to keep you updated with the latest in
Dentistry, the IDA Ludhiana Branch official publication, ‘L.E.D.’ –
‘Let’s Enjoy Dentistry’, a monthly E-Journal brings you the Revised
Dentists (Code of Ethics) Regulations, 2014 brought about by
The Dental Council of India to regulate dental education & the
profession throughout India. Its main objectives are:
1. Maintain uniform standards of dental education in India – both at
Undergraduate and Postgraduate levels.
2. Regulate the curriculum and prescribe the standard curricula in
the training of dentists, dental hygienists and dental mechanics
3. Regulate the level of examinations and prescribe the standards of
examinations and other requirements to be satisfied to secure for
qualifications
To achieve these objectives, the needs are:
1. Uniformity of curriculum standards of technical and clinical
requirements, standards of examinations;
2. Affiliation of every dental college to an University;
3. Supervision over all the dental institutions to ensure that they
maintain the prescribed standards;
4. Regulation of the profession of dentistry.
The word "moral" is defined as relating to the principles of right and
wrong in behavior and "ethics" is defined as a system of moral values
or the principles of conduct governing an individual or a group and
deals with the values relating to human conduct, with respect to the
rightness and wrongness of certain actions and to the goodness and
badness of the motives and ends of such actions. Dentists should
build their reputation on their professional ability and integrity and
should abide by the regulations put forth by the Dental Council of
India (DCI). Hence, the need for the Code of Ethics for every dentist
in India.
Vol. 1 Issue 11 L.E.D. E-Journal Page 155
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
KDJ – Vol. 37 • No. 3 • July 2014 217
DENTAL COUNCIL OF INDIANOTIFICATION
New Delhi, the 27th June, 2014No. DE-97-2014.—In exercise of the powers conferred by Section 20 read with Section 17A of the Dentists Act, 1948(16 of 1948), the Dental Council of India with the previous sanction of the Central Government, in supersession of theDentists (Code of Ethics) Regulations 1976, except as respects things done or omitted to be done before suchsupersession, hereby makes the following Dental Council of India (Code of Ethics) Regulations :—1. Short title and Commencement :
1.1 These regulations may be called the Revised Dentists (Code of Ethics) Regulations, 2014.1.2 They shall come into force on the date of their publication in the Official Gazette of India.
2. Definitions :In these regulations, unless the context otherwise requires;2.1 ‘Act’ means the Dentists Act, 1948 (16 of 1948);2.2 ‘Council’ means the Dental Council of India;2.3 Dentist means any person with a register able dental degree (in Part A or Part B of the State Dental Register)
either by virtue of a prior registration with the Council or one who has been conferred a Bachelor of DentalSurgery (BDS) from any university recognized by the Council and shall be referred to as a Dentist or DentalSurgeon;
2.4 Post graduate dental degree refers to any postgraduate qualification such as M.D.S. in any discipline ofdentistry received by convocation from a University recognized by the Dental Council of India or any otherpost graduate qualification equivalent to MDS that is recognized by the Council;
2.5 All expressions used and not defined in these regulations shall have the meanings assigned to them in theAct and the regulations made there under from time to time.
CHAPTER 13. Code of Dental Ethics
A. Declaration :Every dentist who has been registered (either on Part A or Part B of the State Dentists Register) shall, withina period of thirty days from the date of commencement of these regulations, and every dentist who getshimself registered after the commencement of these regulations shall, within a period of thirty days fromsuch registration, make, before the Registrar of the State Dental Council, a declaration in the form set out forthe purpose in the Schedule to these regulations and shall agree to have read, understood and thence toabide by the same.
Revised Dentists (Code of Ethics) Regulations – 2014
Vol. 1 Issue 11 L.E.D. E-Journal Page 156
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
KDJ – Vol. 37 • No. 3 • July 2014218
B. Duties and Obligation of Dentists in General3.1 Character of Dentist / Dental Surgeon
In view of the important role of a Dentist/ Dental Surgeon as a health professional educated and trained insurgical and medical treatment of diseases of the Oral cavity, he shall:(3.1.1) Be mindful of the high character of his mission and the responsibilities he holds in the discharge of
his duties as an independent health-care professional and shall always remember that care of thepatient and treatment of the disease depends upon the skill and prompt attention shown by him andalways remembering that his personal reputation, professional ability and fidelity remain his bestrecommendations;
(3.1.2) Treat the welfare of the patients as paramount to all other considerations and shall conserve it tothe utmost of his ability;
(3.1.3) Be courteous, sympathetic, friendly and helpful to, and always ready to respond to, the call of hispatients, and that under all conditions his behaviour towards his patients and the public shall bepolite and dignified;
3.2 Maintaining good Clinical Practices :The Principal objective of the Dental profession is to render service to humanity with full respect for thedignity of profession and man. Dental Surgeons should merit the confidence of patients entrusted to theircare, rendering to each a full measure of service and devotion. They should try continuously to improvemedical knowledge and skills and should make available to their patients and colleagues the benefits oftheir professional attainments. The Dentist/ Dental Surgeon should practice methods of healing foundedon scientific basis and should not associate professionally with anyone who violates this principle. Thehonoured ideals of the dental profession imply that the responsibilities of the Dental Professionals extendnot only to individuals but also to Society.(3.2.1) The Principal objective of the Dental profession is to render service to humanity with full respect
for the dignity of profession and man. Dental Surgeons should merit the confidence of patientsentrusted to their care, rendering to each a full measure of service and devotion. They should trycontinuously to improve medical knowledge and skills and should make available to their patientsand colleagues the benefits of their professional attainments. The Dentist/ Dental Surgeon shouldpractice methods of healing founded on scientific basis and should not associate professionallywith anyone who violates this principle. The honoured ideals of the dental profession imply thatthe responsibilities of the Dental Professionals extend not only to individuals but also to Society.
(3.2.2) Membership in Dental and Medical Associations and Societies: For the advancement of his/herprofession, a Dental Surgeon should be encouraged to affiliate with associations and societies ofdental, oral and allied medical professionals and play a proactive role in the promotion of oral healthin particular and health of an individual in general.
(3.2.3) A Dentist/Dental Surgeon should enrich his professional knowledge by participating in professionalmeetings as part of Continuing Dental and Medical Education programs/Scientific Seminars/Workshopsas stipulated by the regulations made by the statutory bodies from time to time and should registerany mandatory requirements with the state registration bodies or any other body as stipulated.
3.3 Maintenance of Dental/Medical records :(3.3.1) Every Dental surgeon shall maintain the relevant records pertaining to his out- patients and inpatients
(wherever applicable). These records must be preserved for a minimum period of three years fromthe date of commencement of the treatment in a format determined by the Council or accepted as astandard mode of documentation.
(3.3.2) If any request is made for medical or dental records either by the patients/authorized attendant orlegal authorities involved, the same may be issued to the competent authority within 72 hours afterhaving obtained a valid receipt for all documents. It is prudent to keep certified photocopies /carbon copies of such submissions.
(3.3.3) A Registered Dental practitioner shall maintain a Register of Medical Certificates giving full detailsof certificates issued. When issuing a medical certificate he shall always enter the identificationmarks of the patient and keep a copy of the certificate. He shall not omit to record the signature and/or thumb mark, address and at least one identification mark of the patient on the medical certificatesor report. The medical certificate shall be prepared as in Appendix 2 of this document, RevisedDentists Code of Ethics Regulations, 2012.
(3.3.4) Efforts shall be made to digitalize dental/ medical records for quick retrieval.3.4 Display of Registration Numbers :
(3.4.1) Every Dental practitioner shall display the registration number accorded to him by the State DentalCouncil in his clinic and in all his prescriptions, certificates and money receipts given to his patients.
(3.4.2) Dental Surgeons shall display as suffix to their names only recognized Dental degrees which arerecognized by the Council or other qualifications such as certificates/diplomas and memberships/
Revised Dentists (Code of Ethics) Regulations – 2014
Vol. 1 Issue 11 L.E.D. E-Journal Page 157
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

KDJ – Vol. 37 • No. 3 • July 2014 219
honours/ fellowships which are conferred by recognized Universities/ recognized bodies approvedby the Council and obtained by convocation in person or in absentia. Any other qualificationssuch as medical degrees, doctorates, post-doctoral degrees or any degree that has bearing on theperson’s knowledge or exemplary qualification may be used as suffix in a manner that does notconvey to the observer or patient a false impression regarding the practitioner’s knowledge orability as a dental professional. Abbreviations of memberships in association or organizations ofprofessionals should not be used as abbreviations in a manner that is misleading to the public[refer to Article 8.9.3 of this document, Revised Dentists Code of Ethics Regulations, 2012 forrelevant details].
3.5 Prescription of Drugs :Every dental surgeon should take care to prescribe and administer drugs in a responsible manner andensure safe and rational use of drugs. He should as far as possible, prescribe drugs in a generic form.
3.6 Highest Quality Assurance in patient care :Every Dental practitioner should ensure quality treatment that does not compromise the outcome of treatment.He must be vigilant about malpractice by other practitioners that may jeopardize the lives of others and whichare likely to cause harm to the public. All practitioners should be aware of unethical practices and practices byunqualified persons. Dentists/ Dental Surgeons shall not employ in connection with their professional practiceany attendant who is neither registered nor enlisted under the Dentists Act and shall not permit such personsto attend, treat or perform operations upon patients wherever professional discretion or skill is required.
3.7 Exposure of Unethical Conduct :A Dental Surgeon should expose, without fear or favour, incompetent or corrupt, dishonest or unethicalconduct on the part of members of the profession. It is the responsibility of the dental surgeon to report tothe competent authorities’ instances of quackery and any kind of abuse including doctor-patient sexualmisconduct, misuse of fiduciary relationship, child abuse and other social evils that may come to theirattention.
3.8 Payment of Professional Services :The Dental Surgeon, engaged in the practice of his profession shall give priority to the interests ofpatients. The personal financial interests of a dental surgeon should not conflict with the medical interestsof patients. A dental practitioner should announce his fees before rendering service and not after theoperation or treatment is under way. Remuneration received for such services should be in the form andamount specifically announced to the patient at the time the service is rendered. It is unethical to enter intoa contract of “no cure - no payment”. Dental Surgeons rendering service on behalf of the State shall refrainfrom anticipating or accepting any consideration. While it is not mandatory to offer free consultations tofellow dental or medical professionals and their immediate family, it will be deemed a courtesy to offer freeor subsidized consultations and treatment to them in situations where no significant expenses are incurred.
3.9 Observation of Statutes :The Dental Surgeon shall observe the laws of the country in regulating the practice of his professionincluding the Dentists’ Act 1948 and it’s amendments and shall also not assist others to evade such laws.He should be cooperative in observance and enforcement of sanitary laws and regulations in the interestof public health. He should observe the provisions of the State Acts like Drugs and Cosmetics Act, 1940;Pharmacy Act, 1948; Narcotic Drugs and Psychotropic substances Act, 1985; Environmental ProtectionAct, 1986; Drugs and Magic Remedies (Objectionable Advertisement) Act, 1954; Persons with Disabilities(Equal Opportunities and Full Participation) Act, 1995 and Bio-Medical Waste (Management and Handling)Rules, 1998 and such other Acts, Rules, Regulations made by the Central/State Governments or localAdministrative Bodies or any other relevant Act relating to the protection and promotion of public health.
3.10 Signing Professional Certificates, Reports and other Documents :A Registered Dental Surgeon involved independently in the treatment of dental and oral surgical problemsmay be called upon to sign certificates, notifications, reports etc. He is bound to issue such certificates andto sign them. Documents relating to disability, injury in the oral and maxillofacial region and deaths occurringwhile under the care of such dental surgeons should be signed by them in their professional capacity forsubsequent use in the courts or for administrative purposes etc. Such documents, among others, includethe ones given at Appendix 4. Any registered dental surgeon who is shown to have signed or given underhis name and authority any such certificate, notification, report or document of a similar character which isuntrue, misleading or improper, is liable to have his name deleted from the Register.
CHAPTER 24 DUTIES OF DENTAL PRACTITIONERS TO THEIR PATIENTS
4.1 Obligations to Patients(4.1.1) Though a Dental Surgeon is not bound to treat each and every person asking his services, he
should attend emergencies reporting to the clinic and should be mindful of the high character of
Revised Dentists (Code of Ethics) Regulations – 2014
Vol. 1 Issue 11 L.E.D. E-Journal Page 158
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
KDJ – Vol. 37 • No. 3 • July 2014220
his/her mission and the responsibility he discharges in the course of his professional duties. TheDental Surgeon should see patients at their hour of appointment as far as possible unless he isunable to do so due to unforeseen delays. He should never forget that the health and the lives ofthose entrusted to his care depend on his skill and attention. A Dental Surgeon should endeavourto add to the comfort of the sick by making his visits at the hour indicated to the patients. A Dentalsurgeon advising a patient to seek service of another Dental Surgeon or physician is acceptable.However in the case of medical emergency a Dental Surgeon must institute standard care includingresuscitation in case of cardiac episodes, for which all dental surgeons must be adequately trainedin basic life support.
(4.1.2) A Dental Surgeon can refuse treatment using his discretion but it should not be on the basis of anydiscrimination of colour, caste, religion, nationality or the presence of ailments such as HIV or othercontagious diseases. However in keeping with the dictum of medical care, the dental surgeon must‘continue to treat’ if he/she has accepted the patient for treatment. Treatment can be terminated on thewishes of the patient or with the resolution of the complaint for which the patient sought treatment.Treatment can also be terminated if the patient is in need of additional or expert care for which the Dentalsurgeon is not equipped to treat or if it falls outside the range of his expertise. In such instances, thepatient should be referred to such specialists or higher centres where treatment is possible.
(4.1.3) A Dental Practitioner having any incapacity detrimental to the patient or which can affect hisperformance vis-a-vis the patient is not permitted to practice his profession.
4.2 Confidentiality :Confidences concerning individual or domestic life entrusted by patients to a Dental Surgeon and defectsin the disposition or character of patients observed during professionally attending to a patient shouldnever be revealed unless such a revelation is required by the laws of the State. Sometimes, however, aclinician must determine whether his duty to society requires him to employ knowledge, obtained throughconfidence as a health care provider to protect a healthy person against a communicable disease to whichhe is about to be exposed. In such instance, the Dental Surgeon should act as he would wish another to acttoward one of his own family in like circumstances.
4.3 Prognosis :The Dental Surgeon should neither exaggerate nor minimize the gravity of a patient’s disease. He shouldensure himself that the patient, his relatives or his responsible friends have such knowledge of the patient’scondition as will serve the best interests of the patient and the family.
4.4 The Patient must not be neglected :A Dental surgeon is free to choose whom he will serve. He should, however, respond to any request for hisassistance in an emergency. Once having undertaken a case, the Dental Surgeon should not neglect the patient,nor should he withdraw from the case without giving adequate notice to the patient and his family. He shall notwilfully commit an act of negligence that may deprive his patient or patients from necessary Dental/Medical care.
CHAPTER 35 DUTIES OF DENTAL SURGEONS AND SPECIALISTS IN CONSULTATIONS
5.1 Consultation Etiquettes:(5.1.1) A Dental Surgeon should ordinarily be able to deal with all common diseases of the Oral cavity by
virtue of his qualification and training. However, if the patient requires expert care of a specialist,appropriate references to Dental or Medical specialists may be made according to the nature of theproblem. It is the duty of a specialist to refer the patient back to the patient’s original dentist afterthe treatment for which the referral was made. While the specialist can collect his or her fees itwould be unethical to pay commissions or any kind of gratuity to the referring dental surgeon.
(5.1.2) A Dental Surgeon shall not receive from the radiologist, laboratory or dispensing chemist any kindof commission in the form of money, gifts or gratuity for referrals. All referrals for investigationshould be judicious, justifiable and done in the best interests of the patient to arrive at a diagnosis.
5.2 Consultation for Patient’s Benefit:In every consultation, the benefit to the patient is of foremost importance. All Dental Surgeons engaged inthe case should be frank with the patient and his attendants.
5.3 Punctuality in Consultation:Punctuality for consultations should be observed by a Dental Surgeon except in the case of unavoidableprofessional delays which are justifiable.
5.4 Opinions and Disclosure:(5.4.1) All statements to the patient or his representatives made by any Consulting Healthcare Professional
and/or the paramedical staff(nurses, etc.,) should take place in the presence of the Dental Surgeon,except as otherwise agreed. The disclosure of the opinion to the patient or his relatives or friendsshall rest with the Dental Surgeon.
Revised Dentists (Code of Ethics) Regulations – 2014
Vol. 1 Issue 11 L.E.D. E-Journal Page 159
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

KDJ – Vol. 37 • No. 3 • July 2014 221
(5.4.2) Differences of opinion should not be divulged to the patient unnecessarily but when there isirreconcilable difference of opinion the circumstances should be frankly and impartially explained to thepatient or his relatives or friends. It would be up to them to seek further advice, if they so desire.
5.5 Treatment after Consultation:No decision should restrain the attending Dental Surgeon from making such subsequent variations in thetreatment if any unexpected change occurs, but at the next consultation, reasons for the variations shouldbe discussed/ explained. The same privilege, with its obligations, belongs to the consultant when sent forin an emergency during the absence of attending Dental surgeon. The attending Dental Surgeon mayprescribe medicine at any time for the patient, whereas the consultant may prescribe only in case ofemergency or as an expert when called for.
5.6 Patients Referred to Specialists:When a patient is referred to a specialist by the attending Dental surgeon, a case summary of the patientshould be given to the specialist, who should communicate his opinion in writing to the attending Dentalsurgeon.
5.7 Fees and other charges:(5.7.1) A Dental Surgeon or the Clinic run by him shall clearly indicate the cost of treatment for the procedure
and make an estimate of all costs likely to be incurred. Any increase in subsequent cost should bejustified by the Dental surgeon. There is no bar on the display of fees and other charges in the DentalClinic. Prescription should also make it clear if the Dental Surgeon himself dispensed any medicine.
(5.7.2) A Dental Surgeon shall write his name and designation in full along with the recognized dentaldegrees and the registration particulars in his prescription letter head.
Note: In Government hospitals where the patient-load is heavy, the name of the prescribing doctor must bewritten below his signature.
CHAPTER 46 RESPONSIBILITIES OF DENTAL SURGEONS TO ONE ANOTHER
6.1 Dependence of Dental Surgeons to each other:A Dental Surgeon should consider it as a pleasure and privilege to render gratuitous service to otherdentists, physicians and their immediate family dependants. However there is no mandatory bar on oneaccepting fees particularly when it involves expensive materials and time.
6.2 Conduct in Consultation:In consultations, no insincerity, rivalry or envy should be indulged in. All due respect should be observedtowards the Dental Surgeon/physician in-charge of the case and no statement or remark be made, whichwould impair the confidence reposed in him. For this purpose no discussion should be carried on in thepresence of the patient or his representatives.
6.3 Consultant not to take charge of the case:When a specialist Dental Surgeon has been called for consultation, the Consultant should normally nottake charge of the case, especially on the solicitation of the patient or friends. The Consultant shall notcriticize the referring Dental Surgeon. He shall discuss the diagnosis treatment plan with the referringDental Surgeon.
6.4 Appointment of Substitute:Whenever a Dental Surgeon requests another Dental Surgeon to attend his patients during his temporaryabsence from his practice, professional courtesy requires the acceptance of such appointment only whenhe has the capacity to discharge the additional responsibility along with his other duties. The DentalSurgeon acting under such an appointment should give the utmost consideration to the interests andreputation of the absent Dental Surgeon and all such patients should be restored to the care of the latterupon his return.
6.5 Visiting another Case:When it becomes the duty of a Dental Surgeon occupying an official position to see and report upon acondition and appropriate treatment, he should communicate to the Dental Surgeon in attendance so as togive him an option of being present. The Medical Officer/Dental Surgeon occupying an official positionshould avoid remarks upon the diagnosis or the treatment that has been adopted.
CHAPTER 57 DUTIES OF DENTAL SURGEONS TO THE PUBLIC AND TO THE PARAMEDICAL PROFESSION
7.1 Dental Surgeons as Citizens:Dental Surgeons, as good citizens, possessed of special training should disseminate advice on publichealth issues. They should play their part in enforcing the laws of the community and in sustaining theinstitutions that advance the interests of humanity. They should particularly co-operate with the authoritiesin the administration of sanitary/public health laws and regulations.
Revised Dentists (Code of Ethics) Regulations – 2014
Vol. 1 Issue 11 L.E.D. E-Journal Page 160
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

KDJ – Vol. 37 • No. 3 • July 2014222
7.2 Public and Community Health:Dental Surgeons, especially those engaged in public health dentistry, should enlighten the public concerningoral health and prevention of oral diseases such as dental caries, periodontal health, precancerous lesionsand oral cancer. At all times the dental surgeons should notify the constituted public health authorities orhospitals of every case of communicable disease under his care, in accordance with the laws, rules andregulations of the health authorities.
7.3 Pharmacists /Nurses:Dental Surgeons should recognize and promote the practice of different paramedical services such asDental Hygienist, Dental Mechanic, Pharmacy and Nursing as professions and should seek their cooperationwherever required.
CHAPTER 68 UNETHICAL ACTS:
A Dental Surgeon shall not aid or abet or commit any of the following acts which shall be construed as unethical.For the purpose of this regulations a dental surgeon refers to all registered practitioners whether they are inindividual private practice, attached to hospitals, teaching hospitals or employed by others whether they arecorporate or otherwise:8.1 Advertisement:
The global position on the issue of Ethics of Advertisement by Dental/Medical professionals has drasticallychanged over the last few decades. A Dentist or a group of Dentists may advertise provided that theymaintain decorum, keeping in mind the high moral obligations and the value that society places on theimportant nature of their work and the moral character and integrity expected of them. Dental Surgeons areexpected to exhibit integrity, honesty, fidelity and selfless service. Monetary commitments can only besecondary to the welfare of his patients. Under these circumstances it is unethical:(8.1.1) To indulge in demeaning solicitation and false promises through advertisements or direct marketing
of individuals, clinics or hospitals in contravention of the National Advertising Council or anyother body regulating advertising in the country;
(8.1.2) To advertise, whether directly or indirectly or being associated or employed with any organizationor company including corporate bodies that indulges in such activities in a manner which givesunfair professional advantage by cold targeting vulnerable groups and conducting camps andother promotional activity in schools, colleges, old age homes and distributing handbills, claimvouchers and other business promotional activities. Registered charitable organizations includingregistered body of Dental or Medical persons which provide fully free dental care and treatment outof altruism are however exempted;
(8.1.3) To be associated with or employed by those who procure or sanction such false and misleadingadvertisements or publication through press reports that promise inducements, rebates and falsebenefits;
(8.1.4) To employ any agent or canvasser for the purpose of obtaining patients in a manner that iscommercial; or being associated with or employed by those who procure or sanction of suchemployment;
(8.1.5) To use or exhibit any disproportionately large sign, other than a sign which in its character, position,size and wording is merely such as may reasonably be required to indicate to persons seeking theexact location of, and entrance to, the premises at which the dental practice is carried on, andnowhere else;
(8.1.6) To allow the Dental Surgeon’s name to be used to designate commercial articles such as toothpaste, tooth brush, tooth powder, mouth washes liquid cleaners, or the like except if such articlesare fabricated in the dental clinic e.g. dentures, crowns, bridges, etc.;
(8.1.7) To permit publication of the Dental Surgeon’s opinion on any procedure, equipment, in the generalor lay papers or lay journals except when validated or supported by evidence based studies;
(8.1.8) To indulge in surrogate advertisements in the garb of educating the public through TV programs,magazines or periodicals. Any public information disseminated to the public in good faith andintention should not carry addresses telephone numbers, e-mail addresses etc., of the DentalSurgeon or the clinic employing him to attract patients to their establishment;
(8.1.9) To advertise in the electronic media, such as in television programs, that display names, addressesand telephone number of dentists as on-screen ‘scrollers’, or, of the clinics employing such dentists,etc.
8.2 Soliciting:Soliciting of patients, directly or indirectly, by a Dental Surgeon, by a group of Dental Surgeons or byinstitutions or organizations is unethical except when permitted under the provisions mentioned later (vide8.2.1 to 8.2.10 of this document, Revised Dentists Code of Ethics Regulations, 2012). A Dental Surgeon shall
Revised Dentists (Code of Ethics) Regulations – 2014
Vol. 1 Issue 11 L.E.D. E-Journal Page 161
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

KDJ – Vol. 37 • No. 3 • July 2014 223
not make use of himself (or his name) as subject of any form or manner of advertising or publicity through anymode either alone or in conjunction with others which is of such a character as to invite attention to him or tohis professional position, skill, qualification, achievements, attainments, specialties, appointments,associations, affiliations or honors and/or of such character as would ordinarily result in his self-aggrandizement.A Dental Surgeon shall not give to any person, whether for compensation or otherwise, any approval,recommendation, endorsement, certificate, report or statement with respect of any drug, medicine, nostrumremedy, surgical, or therapeutic article, apparatus or appliance or any commercial product or article withrespect of any property, quality or use thereof or any test, demonstration or trial thereof, for use in connectionwith his name, signature, or photograph in any form or manner of advertising through any mode nor shall heboast of cases, operations, cures or remedies or permit the publication of report thereof through any mode.A Dental Surgeon is however permitted as an ethically acceptable practice to make a formal announcementin press regarding the following:(8.2.1) On starting practice.(8.2.2) On change of type of practice.(8.2.3) On changing address.(8.2.4) On temporary absence from duty for a prolonged period of time.(8.2.5) On resumption of practice after a break a prolonged period.(8.2.6) On succeeding to another practice.(8.2.7) About the availability of new equipment or services without boastful claims of being the ‘best’ or
‘first’ especially if such services are already available in other facilities.(8.2.8) Through insertion in Telephone directories, Yellow pages or on the internet is permissible and will
only serve as public information. However any claim to superiority or special skills over others willbe construed as unethical practice.
(8.2.9) Through maintenance of websites about dentists or dental clinics where all information is factualwill not be construed as unethical practice. Websites can also carry details of treatment facilitiesavailable and the fees for the same. This will in fact help patients to make informed choices througha transparent system. However websites should not make claims or statements that are not factualand therefore misleading to the public.
8.3 Publicity and Signage:(8.3.1) Printing of self-photograph, or any such material of publicity in the letter head or on sign board of
the consulting room or any such clinical establishment shall be regarded as acts of self-advertisementand unethical conduct on the part of the physician. However, printing of sketches, diagrams,picture of human system shall not be treated as unethical;
(8.3.2) Using or exhibition of any sign, other than a sign which in its character, position, size and wordingis merely such as may reasonably be required to indicate to persons seeking the exact location of,and entrance to, the premises at which the dental practice is carried on is considered unethical.These include:(8.3.2.1) Use of sign-board with the use of such words which trivialize the dignity of the profession
or notices in regard to practice on premises other than those in which a practice is actuallycarried on, or show cases, or flickering light signs and the use of any sign showing anymatter other than his name and qualifications as defined under Clause (j) of Section 2 ofthe Act;
(8.3.2.2) Affixing a sign-board on a Chemist’s shop or in places where the dentist does not resideor work.
(8.3.3) A Dental Surgeon shall not claim to be a specialist either through displayed signs on the nameboard and / or the office stationary (visiting cards, letterheads, etc.,) unless he has a specialqualification (which is recognized by the Council) in that Specialty. A Dental Surgeon can howeverpractice all branches of Dentistry provided he shows adequate qualification, competence and bonafide training in the concerned branch or branches.
8.4 Patent and Copyrights:A Dental Surgeon may patent surgical instruments, appliances and medicine or Copyright applications,methods and procedures. However, it shall be unethical if the benefits of such patents or copyrights are notmade available in situations where the interest of large population is involved.
8.5 Running an Open Shop (Dispensing of Drugs and Appliances by Physicians):A Dental Surgeon should not run an open shop for sale of medicine for dispensing prescriptions prescribedby doctors other than him or for sale of dental medical or surgical appliances. It is not unethical for a DentalSurgeon to prescribe, supply or sell drugs, remedies or dental appliances in his clinic as long as there is noexploitation of the patients. Drugs prescribed by a Dental Surgeon or brought from the market for a patientshould explicitly state the proprietary formulae as well as generic name of the drug.
Revised Dentists (Code of Ethics) Regulations – 2014
Vol. 1 Issue 11 L.E.D. E-Journal Page 162
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

KDJ – Vol. 37 • No. 3 • July 2014224
8.6 Rebates and Commission:(8.6.1) A Dental Surgeon shall not give, solicit, or receive nor shall he offer to give solicit or receive, any
gift, gratuity, commission or bonus in consideration of or return for the referring, recommending orprocuring of any patient for dental, medical, surgical or other treatment. A Dental Surgeon shall notdirectly or indirectly, participate in or be a party to act of division, transference, assignment,subordination, rebating, splitting or refunding of any fee for medical, surgical or other treatment.
(8.6.2) Provisions of Section 8.6.1 (of this document, Revised Dentists Code of Ethics Regulations, 2012)shall apply with equal force to the referring, recommending or procuring by a physician or anyperson, specimen or material for diagnostic purposes or other study / work. Nothing in this section,however, shall prohibit payment of salaries by a qualified physician to other duly qualified personrendering medical care under his supervision.
8.7 Secret Remedies:The prescribing or dispensing by a physician of secret remedial agents of which he does not know thecomposition, or the manufacture or promotion of their use is unethical and as such prohibited. All the drugsprescribed by a dental surgeon should always carry a proprietary formula and clear name.
8.8 Human Rights:The physician shall not aid or abet torture nor shall he be a party to either infliction of mental or physicaltrauma or concealment of torture inflicted by some other person or agency in clear violation of humanrights.
8.9 Unethical Practices:The following shall also be the unethical practices for a Dentist:(8.9.1) A Dental Surgeon shall not employ a Dentist / Dental Surgeon in the professional practice or any
other professional assistant (not being a registered dental hygienist or a registered dental mechanic)whose name is not registered in the State Dentists Register, to practice Dentistry as defined inClause (d) of Section 2 of the Act. He may however retain the services of a medical practitioner oranaesthetist as necessary;
(8.9.2) Signing under his name and authority any certificate which is untrue, misleading or improper, orgiving false certificates or testimonials directly or indirectly to any person or persons;
(8.9.3) Use of abbreviations after the Dental Surgeon’s name except those indicating dental qualificationsas earned by him during his academic career in dentistry and which conform to the definition of‘recognized dental qualification’ as defined in Clause (j) of Section 2 of the Act, or any otheracademic qualifications from a recognized university obtained through a convocation indicatingexemplary achievement. Any degree conferred on an honorary basis should be suffixed with thewords “Honoris Causa”. Such unacceptable abbreviations include, but not necessarily restrictedto the following which are not academic qualifications:(8.9.3.1) R.D.P. for Registered Dental Practitioner;(8.9.3.2) M.I.D.A. for Member, Indian Dental Association;(8.9.3.3) F.I.C.D. for Fellow of International College of Dentists;(8.9.3.4) M.I.C.D. for Master of International College of Dentists;(8.9.3.5) F.A.C.D. for Fellow or American College of Dentists;(8.9.3.6) M.R.S.H. for Member of Royal Society of Hygiene;(8.9.3.7) F.A.G.E. for Fellow of Academy of General Education, etc.;
(8.9.4) Submission of false information in declaration form at the time of assessment of Dental College.(8.9.5) Serving as (Duplicate faculty) i.e. working simultaneously in two/more Dental Colleges.(8.9.6) Conviction for any crime by any court will constitute unethical act.
8.10 Naming and Styling of Dental Establishments:A Dental Surgeon or a group of Dentists/ Dental Surgeons shall refer to their establishment as a dentalclinic. It may however be referred to as a dental hospital if the practice involves surgical treatment of oraland dental diseases under local or general anaesthesia and if the patients need to be maintained as an in-patient for part of a day or for several days for post-operative care provided the hospital fulfils the statutoryrequirements for such hospitals or establishments in the respective States.
8.11 Contravention of Statutory Provisions:A Dental Surgeon shall not contravene any of the acts referred to in Article 3.9 of this document, RevisedDentists Code of Ethics Regulations, 2014, and named in Annexure 3 of the same document and the rulesmade there under as amended from time to time, involving an abuse of privileges conferred there underupon a dentist, whether such contravention has been the subject of criminal proceedings or not.
8.12 Signing of Certificates:A Registered Dental Surgeon is bound by law to give, or may from time to time be called upon or requestedto give certain certificates, notification, reports and other documents of similar character signed by them in
Revised Dentists (Code of Ethics) Regulations – 2014
Vol. 1 Issue 11 L.E.D. E-Journal Page 163
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

KDJ – Vol. 37 • No. 3 • July 2014 225
their professional capacity for subsequent use in the courts, or elsewhere for administrative purposes, etc.Such documents, among others, include the ones given at Appendix 4 of this document, Revised DentistsCode of Ethics Regulations, 2014. A Dental Surgeon shall not sign under his name and authority anycertificate which is untrue, misleading or improper, or give false certificates or testimonials directly orindirectly to any person or persons. He shall however deem it his duty to sign all necessary certificatesrelating to health of the patients.
8.13 Doctor-Patient Sexual Misconduct:A Dental Surgeon shall not be involved in immorality involving abuse of professional relationship andinvolve in sexual misconduct with a patient by misusing fiduciary relationship.
8.14 Abiding by all Laws of the Land:A Dental Surgeon shall not aid or abet in any violation of the laws of the land or be involved in any matterthat is against public policy. He shall not be convicted by a court of law for offences involving moralturpitude/ criminal acts.
8.15 Relationship with Pharmaceutical Companies and Medical and Dental Industry:8.15.1Gifts, Travel, Hospitality, Monetary Grants:
A Dental Surgeon shall not receive any gift from any pharmaceutical or allied health care industryand their sales people or representatives. A Dental Surgeon shall not accept any travel facilityinside the country or outside, including rail, air, ship, cruise tickets, paid vacations etc. from anypharmaceutical or allied healthcare industry or their representatives for self and family members forvacation or for attending conferences, seminars, workshops, CDE/CME program etc., as a delegate.A Dental Surgeon shall not receive any cash or monetary grants from any pharmaceutical and alliedhealthcare industry for individual purpose in individual capacity under any pretext. Funding formedical research, study etc. can only be received through approved institutions and ProfessionalOrganizations by modalities laid down by law / rules / guidelines adopted by such approvedinstitutions, in a transparent manner. It shall always be fully disclosed.
8.15.2Dental / Medical Research:A Dental Surgeon may carry out, participate in, and work in research projects funded bypharmaceutical and allied healthcare industries. A Dental Surgeon is obliged to know that thefulfillment of the following items [8.15.2.1 to 8.15.2.7 of this document, Revised Dentists Code ofEthics Regulations, 2012] will be an imperative for undertaking any research assignment / projectfunded by industry - for being proper and ethical. Thus, in accepting such a position a Dentalsurgeon shall:(8.15.2.1)Ensure that the particular research proposal(s) has the due permission from the competent
concerned authorities.(8.15.2.2)Ensure that such a research project(s) has the clearance of national/state/ institutional
ethics committees/bodies.(8.15.2.3) Ensure that it fulfils all the legal requirements prescribed for medical research.(8.15.2.4) Ensure that the source and amount of funding is publicly disclosed at the beginning
itself.(8.15.2.5) Ensure that proper care and facilities are provided to human volunteers, if they are
necessary for the research project.(8.15.2.6) Ensure that undue animal experimentations are not done and when these are necessary
they are done in a scientific and a humane way.(8.15.2.7) Ensure that while accepting such an assignment a Dental Surgeon shall have the freedom
to publish the results of the research in the greater interest of the society by insertingsuch a clause in the MOU (Memorandum of Understanding) or any other document /agreement for any such assignment.
8.15.3 Maintaining Professional Autonomy:In dealing with pharmaceutical and allied healthcare industry, a Dental Surgeon shall always ensurethat there shall never be any compromise either with his/her own professional autonomy and / orwith the autonomy and freedom of the medical institution.
8.15.4 Affiliation:A Dental Surgeon may work for pharmaceutical and allied healthcare industries in advisorycapacities, as consultants, as researchers, as treating doctors or in any other professional capacity.In doing so, a medical practitioner shall always:(8.15.4.1) Ensure that his professional integrity and freedom are maintained.(8.15.4.2) Ensure that patients’ interest is not compromised in any way.(8.15.4.3) Ensure that such affiliations are within the law.(8.15.4.4) Ensure that such affiliations/employments are fully transparent and disclosed.
Revised Dentists (Code of Ethics) Regulations – 2014
Vol. 1 Issue 11 L.E.D. E-Journal Page 164
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

8.15.5 Endorsement:A Dental surgeon shall not endorse any drug or product of the industry publically. Any studyconducted on the efficacy or otherwise of such products shall be presented to and / or throughappropriate scientific bodies or published in appropriate scientific journals in a proper way.
CHAPTER 79 PUNISHMENTS AND DISCIPLINARY ACTIONS:
A Dental Surgeon shall not aid or abet or commit any acts which shall be construed as unethical.9.1 It must be clearly understood that the instances of offences and unethical conducts which are given above
do not constitute and are not intended to constitute a complete list of the infamous acts which calls fordisciplinary action, and that by issuing this notice the Dental Council of India and or State Dental Councilsare in no way precluded from considering and dealing with any other form of professional misconduct onthe part of a registered practitioner. Circumstances may and do arise from time to time in relation to whichthere may occur questions of professional misconduct which do not come within any of these categories.Every care should be taken that the code is not violated in letter or spirit. In such instances as in all others,the Dental Council of India and/or State Dental Councils have to consider and decide upon the factsbrought before the Dental Council of India and/or State Dental Councils.
9.2 It is made clear that any complaint with regard to professional misconduct can be brought before theappropriate Dental Council for Disciplinary action. Upon receipt of any complaint of professional misconduct,the appropriate Dental Council would hold an enquiry and give opportunity to the registered Dentalpractitioner to be heard in person or by pleader. If the Dentist/ Dental Surgeon is found to be guilty ofcommitting professional misconduct, the appropriate Dental Council may award such punishment as deemednecessary or may direct the removal altogether or for a specified period, from the register the name of thedelinquent registered practitioner. Deletion from the Register shall be widely publicized in local press aswell as in the publications of different Medical and Dental Associations/ Societies/Bodies.
9.3 In case the punishment of removal from the register is for a limited period, the appropriate Council may alsodirect that the name so removed shall be restored in the register after the expiry of the period for which thename was ordered to be removed.
9.4 Decision on complaint against delinquent Dental Surgeons shall be taken within a time limit of 6 months.9.5 During the pendency of the complaint the appropriate Council may restrain the Dental Surgeon from
performing the procedure or practice which is under scrutiny.9.6 Professional incompetence shall be judged by peer group as per guidelines prescribed by State Dental
Council. For this purpose the State Dental Council shall institute an Ethics Committee consisting of qualifiedpersons of integrity and good name from amongst prominent registered Dental Surgeons in the State.
9.7 Where either on a request or otherwise the State Government or any competent authority is informed thatany complaint against a delinquent practitioner has not been decided by a State Dental Council within aperiod of six months from the date of receipt of complaint by it and further the State Government or anycompetent authority has reason to believe that there is no justified reason for not deciding the complaintwithin the said prescribed period, the State Government or any competent authority may.(9.7.1) Impress upon the concerned State Dental Council to conclude and decide the complaint within a
time bound schedule.(9.7.2) May decide to refer the said complaint pending with the concerned State Dental Council straightaway
or after the expiry of the period which had been stipulated by the Regulation in accordance withpara (9.7.1 of this document, Revised Dentists Code of Ethics Regulations, 2012) above, to itselfand refer the same to the Ethical Committee of the State Dental Council for its expeditious disposalin a period of not more than six months from the receipt of the complaint with the State Government.
9.8 Any person aggrieved by the decision of the State Dental Council on any complaint against a delinquentDental Surgeon, shall have the right to file an appeal to the State Government within a period of 60 daysfrom the date of receipt of the order passed by the said State Dental Council. Provided that the StateGovernment may, if it is satisfied that the appellant was prevented by sufficient cause from presenting theappeal within the aforesaid period of 60 days, allow it to be presented within a further period of 60 days.
Col. (Retd.) Dr. S.K. OJHA, Officiating Secy.[ADVT. III/4/Exty./98/14]
Foot Note : The Principal Regulations, namely, the “Dentists (Code of Ethics) Regulations, 2014”, were published inPart II, Section 3, Sub-sec (1) of the Gazette of India, Extraordinary, on 21.08.1976.
KDJ – Vol. 37 • No. 3 • July 2014226
Revised Dentists (Code of Ethics) Regulations – 2014
Vol. 1 Issue 11 L.E.D. E-Journal Page 165
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
INFORMATION HAND BOOK
a AnR- RIGHT TO
INFORMATION
ti-Tr-t-thzr gRaq DENTAL COUNCIL OF INDIA
4-efff 45, ROI - 110 002 Aiwan-E-Galib Marg, Kotla Road,
New Delhi — 110 002
s 23238542, 23236740 Telephone 2 23238542, 23236740
E-mail tAR s [email protected] Website s www.dciindia.org.in
Vol. 1 Issue 11 L.E.D. E-Journal Page 166
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
INDEX
Sr. No. Topic Page No.
1 CHAPTER -1 The Particulars of its organisation, function and duties
2 CHAPTER -2 The powers and duties of officers and employees
3 CHAPTER -3 Procedure followed in decision making process, including channels of supervision and accountability
4 CHAPTER -4 The norms set by it for discharge of its functions
5 CHAPTER -5 The rules, regulations, instruction, manuals and records, held by its or under its control or used by its employees for discharging its functions
6 CHAPTER -6 A statement of the categories of documents that are held by it or under its control
7 CHAPTER -7 The particulars of any arrangement that exists for consultation with, or representation by, the members of the public in relation to the formulation of its policy or implementation thereof
8 CHAPTER -8 Boards, Councils, Committees and other Bodies consisted as part of Public Authority.
9 CHAPTER -9 A directory of its officers and employees and their monthly remuneration received by each of its officers and employees, including the system of compensation as provided in its regulations
Vol. 1 Issue 11 L.E.D. E-Journal Page 167
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

INDEX
Sr. No. Topic Page No.
10 CHAPTER -10 The budget allocated to each of its agency, indicating the particulars of all plans, proposed expenditure and reports on disbursements made and etc.
11 CHAPTER -11 Particulars of recipients of concessions, permits or authorization granted by the Public Authority
12 CHAPTER -12 Details in respect of the information, available to or held by it, reduced in an electronic form
13 CHAPTER -13 The names, designations and other particulars of the Public Information Officers;
14 CHAPTER -14 The particulars of facilities available to citizens for obtaining information, including the working hours of a library or reading room, if maintained for public use
Vol. 1 Issue 11 L.E.D. E-Journal Page 168
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

CHAPTER -1
The particulars of its organisation, function and duties
1. Brief History
The Dental Council of India - a statutory body - was constituted on 12th April
1949 under an Act of Parliament - the Dentists Act, 1948 (XVI of 1948). The
amendments were made through an ordinance promulgated by the President
of India on 27th August 1992. Through this ordinance, new sections i.e.
section 10A, section 10B, section 10C were introduced in the Dentists Act,
1948 mainly to restrict mushroom growth of dental colleges, increase of the
seats in any of the course and starting of new higher courses without the
prior permission of the Central Govt., Ministry of Health & Family Welfare. The
amendment was duly notified by the Govt. of India in Extraordinary Gazette
of India, Part II, Section I on 3rd April 1993 with effective date 1st June 1992
The Dental Council of India is constituted by an Act of Parliament 'The
Dentist Act 1948 (XVI of 1948) with a view to regulate the Dental Education,
Dental Profession and Dental Ethics, thereto-which came into existence in
March, 1949. The Dentists Act 1948 has been amended in the year 1993,
2010.
2. Objectives
The Council has been constituted to achieve the following objectives:
a) Maintenance of uniform standards of dental educational, both under
graduate and post graduate.
b) Recommendation for recognition/de-recognition of dental qualification
of dental institutions of India or foreign countries.
c) Maintenance of Indian Dental Register by the concerned State Dental
Councils.
d) Reciprocity with foreign countries in the matter of mutual recognition
of dental qualifications.
Vol. 1 Issue 11 L.E.D. E-Journal Page 169
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

3. Functions and Duties
a) Recommendation to the Central Government for grant of permission to
establish a new Dental College or opening of a new of higher course of
study or training or increase in admission capacity in any course of
study or training.
b) Inspection/visitation with a view to maintain minimum standard of
dental education in India.
c) Recommendation to the Central Government for Recognition/
withdrawal of recognition of dental qualifications awarded by dental
institutions in India and abroad.
d) Maintenance of Indian Dental Register by the concerned State Dental
Councils.
e) Grant of Eligibility Certificate to Indian Citizens and Overseas Citizen of
India going overseas for obtaining primary dental qualifications.
4. Constitution and Composition of Council
The Council is constituted by the Central Government under Section 3 of the
Dentists Act, 1948. The composition of the Council is laid down in Section 3 of
the Act. [http://dciindia.org.in/Dentistact1948.aspx].
5. Address
The Dental Council of India has its office at New Delhi and does not have any
subordinate office anywhere in India. The particulars are as under:-
Dental Council of India Aiwan-E-Galib Marg Kotla Road, New Delhi-110002
Tel.: 011-23236740, 23238542 Website: www.dciindia.org.in Email: secretary(&dciindia.orq
Vol. 1 Issue 11 L.E.D. E-Journal Page 170
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Opening hours of the Office: 9:30 AM to 6:00 PM
Timings for Public Dealing: 11:00 to 5:00 PM
Working Days: Monday to Friday.
Vol. 1 Issue 11 L.E.D. E-Journal Page 171
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
CHAPTER -2
Powers and Duties of Officers and Employee
1. Dental Council of India
Dental Council of India is a Statutory Body incorporated under an Act of
Parliament viz. The Dentists Act, 1948 (XVI of 1948) to regulate the Dental
Education and the profession of Dentistry throughout India and it is financed
by the Govt. of India in the Ministry of Health & Family Welfare (Department
of Health) through Grant-in-aid. The General Body of the Dental Council of
India representing various State Governments, Universities, Dental Colleges,
Central Government, etc.
The Dental Council of India is the recommendatory body to the Central
Government for grant of permission for establishment of a dental college,
opening of a new or higher course of study, increase in in-take capacity at the
Under Graduate and Post Graduate level.
2. Powers and Duties of the Council
The Council in order to discharge of its functions is empowered to:
(i) Constitute Committees for general or special purposes at it
deems necessary to carry out the purposes of the Dentists Act;
(ii) appoint a Secretary who may also, if so decided by the Council,
act as Treasurer;
(iii) appoint such other officers and servants as the Council deems
necessary to enable it to carry out its functions under this Act;
(iv) Determine the conditions of the services of the employees.
The Council discharges its statutory functions and duties conferred upon it by
the Dentists Act.
Vol. 1 Issue 11 L.E.D. E-Journal Page 172
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
3. Powers and Duties of Employees
Section 8(1) of the Dentists Act, 1948 inter alia provides that the Council shall
(a) appoint a Secretary who may also, if so decided by the Council, act as
Treasurer; (b) appoint such other officers and servants as the Council deems
necessary to enable it to carry out its functions under this Act; (c) require and
take from the Secretary or from any other officer or servant such security for
the due performance of his duties as the Council considers necessary; and (d)
With the previous sanction of the Central Government, fix the fees and
allowances of the President Vice-President and other members of the Council,
and the pay and allowances and other conditions of service of officers and
servants of the Council.
Section 52 to 56 of the Regulations of the Dental Council of India, 1956
(as modified upto February, 1982) lays down the "powers and duties of
Secretary and other officers and servants of the Council". The provision reads
as under:-
"Secretary
52. The term of office of the Secretary shall be fixed by the Council
at the time of appointment. He shall normally retire on attaining the
age of superannuation as applicable to the Central Government
employees of the corresponding rank. Extension of service beyond the
date of superannuation may be granted by the Council in exceptional
cases on the recommendations of the Executive Committee but no
such extension shall be given without the prior approval of the
Government of India."
53. He shall perform such duties as have been given in the Act and
the Regulations. He shall also be responsible for the safety of the
property of the Council and the control and management of the office,
accounts and correspondence, and shall see that the office staff attend
Vol. 1 Issue 11 L.E.D. E-Journal Page 173
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

punctually, and generally fulfill all such duties as may be required of
him by the Council for the purposes of the Act. He shall attend and
the notes of the proceedings of meetings of the Council and Executive
Committee and any Sub-Committee.
The Secretary, shall not less than 90 days before the expiration of the
term of any existing appointment, draw the attention of the President
to the approaching vacancy, in order that a new appointment may be
made to take effect from the day on which the existing appointment
will expire.
Staff
54. Members of the Ministerial and non-ministerial staff and Class IV
servants shall retire on attaining the age of superanuation as applicable
to the Central Government employees of the corresponding rank.
Extention of service beyond the date of superanuation may be granted
by the Executive Committee in accordance with the Central
Government's general orders on the subject issued from time to time.
55. The powers and duties of the staff will be such as may be laid
down from time to time in the standing orders as framed for the
purpose by the Council.
56. (i) Subject to the approval of the President, the Secretary
shall appoint the ministerial staff and class IV servants and may
engage such temporary personnel as may be required from time
to time, and pay a reasonable rate of remuneration to such
personnel, provided it does not exceed the rate sanctioned by
the Central Government for corresponding permanent staff.
These appointments shall be subject to conformation by the
Executive Committee.
Vol. 1 Issue 11 L.E.D. E-Journal Page 174
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
(ii) The Council may, on the advice of the Executive
Committee, recommend to the Central Government to convert
any existing sanctioned temporary post of an officer, a member
of the ministerial staff or a class IV employees into a permanent
one after taking into account the volume of work of permanent
nature attached to the post and orders on the subject issued by
the Central Government from time to time and that the orders
of the Central Government in this respect shall be final."
The Secretary is assisted in the discharge of his duties, by officers in
the rank of Joint Secretary, Deputy Secretary, Law Officer, Accounts Officer,
Assistant Secretary, Section Incharge, Assistants and other staff in various
categories. The staff serves as the Secretariat of the Dental Council of India
and performs such duties as envisaged under the Dentist Act and the Rules
and Regulations made thereunder. The powers and duties of the staff will be
such as may be laid down from time to time in the standing orders as framed
for the purpose by the Council.
Vol. 1 Issue 11 L.E.D. E-Journal Page 175
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

CHAPTER -3
Procedure followed in decision making process, including channels of supervision and accountability
The Council constituted under Section 3 (Chapter II) of the Dentists Act is the
supreme decision making of the Organisation. The President, Vice-President,
Executive Committee of the Council is elected by the members of the Council from
amongst themselves.
Section 9 of the Dentists Act 1948 provides for the Executive Committee. The
Executive Committee consist of the President and Vice-President ex officio [and the
Director-General of Health Services ex officio] and five other members elected by the
Council. The Executive Committee in addition to the powers and duties conferred
upon it by the Dentists Act 1948, exercises and discharges such powers and duties
as the Council may confer or impose upon it by any regulations which may be made
in this behalf.
The decisions of the Council, Executive Committee and the Sub-Committee
are implemented by the Secretary through the respective sections of the Council
office. The work of the DCI is carried out through the following sections:-
(i) Administration (ii) Accounts (iii) Legal (iv) Under Graduate (v) Post Graduate (vi) Miscellaneous-I,II,III (vii) Inspection (viii) Computer/Admission (ix) Complaint Cell (x) Record (xi) Dairy & Dispatch (xii) Rn Section (xiii) Anti Ragging Cell
Vol. 1 Issue 11 L.E.D. E-Journal Page 176
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

The Secretary of the Council and other staffs are employed by the Council to
carry out the purposes of the Act. The Secretary is assisted in the discharge of its
functions & duties by officers & staffs as provided under Chapter 9 of this handbook.
On receipt of a proposal, the entry level staffs open up a file or process the
proposal in the existing file. The Section Officer/ Assistant scrutinize the proposal
with reference to the relevant Rules and place it before the Section Head/ Assistant
Secretary/ Deputy Secretary. The Assistant Secretary/ the Deputy Secretary review
the proposal and with his comments/observations places before the Secretary in
accordance with Office Orders. The Secretary decides the course of action to be
taken thereon, including placing the matter before the concerned Sub-Committee or
Executive Committee, with the approval of the President as and when required. The
respective superior officers have supervisory control over their subordinates.
Vol. 1 Issue 11 L.E.D. E-Journal Page 177
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

CHAPTER -4
The norms set by it for discharge of its functions
The Council in the performance of its functions is bound by the various Rules
and Regulations (refer Chapter 5 of this handbook) enacted under the Dentists Act,
1948.
L
Vol. 1 Issue 11 L.E.D. E-Journal Page 178
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
CHAPTER -5
The rules, regulations, instructions, manuals and records, held by it or under its control or used by its employees in
discharge of its functions
The following Dental Council of India Rules & Regulations is uploaded on DCI
website as per the specified links given under. It may be looked into on the official
website of Dental Council of India ww.dciindia.org.in.
1. The Dentists Act, 1948
2. The Dentists (Amendment) Act, 1993
3. Revised Dentists (Code of Ethics) Regulations, 2014
4. Dental Council (Election) Regulations, 1952
5. Dental Council of India Regulations, 1956
6. The Dentists (Amendment) Ordinance, 1992
7. Dental Council of India (Establishment of New Dental Colleges,
Opening of New or Higher Course of Study or Training and
Increase of Admission Capacity in Dental Colleges) Regulations,
2006 (alongwith Amendments)
8. Dental Council of India Revised BDS Course Regulations, 2007
(alongwith Amendments)
9. Dental Council of India Revised MDS Course Regulations, 2007
(alongwith Amendments)
10. Dental Council of India Post Graduate Diploma Course
Regulations, 2008
11. Dental Council of India Post Graduate Diploma Course
Regulations (Dental Material), 2008
12. Dental Council of India Dental Hygienists Course Regulations,
2008
13. Dental Operating Room Asstt. Course Regulation,
2007(alongwith Amendments)
Vol. 1 Issue 11 L.E.D. E-Journal Page 179
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
14. Dental Council of India (Miscellaneous) Regulations, 2007
15. Dental Council of India Screening Test Regulations, 2009
(alongwith Amendments)
16. Continuing Dental Education Regulations, 2007
17. DCI Regulations on Curbing the Menace of Ragging in Dental
Colleges, 2009
Vol. 1 Issue 11 L.E.D. E-Journal Page 180
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

CHAPTER -6
A statement of the categories of documents that are held by it or under its control
Scheme received by the Council for Establishment of Dental College for Opening a
New or Higher Course of Study or Training and Increase of Admission Capacity in
dental colleges.
Recommendations
Recommendations by the Council to the Government of India for Establishment of
Dental College for Opening a New or Higher Course of Study or Training and
Increase of Admission Capacity in any dental college.
Recommendation made by the Council to the Central Government for inclusion of a
dental qualification in the Schedules of the Dentists Act 1948.
Eligibility Certificates
Application made by the students/candidates and record of communication with the
concerned authorities.
Staff Related
Employment Record of the Employees
Admission
List of students admitted in Dental Institutions approved/recognised by Dental Council of India.
Issuance of NOC
Vol. 1 Issue 11 L.E.D. E-Journal Page 181
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
CHAPTER -7
The particulars of any arrangement that exists for consultation with, or representation by, the members of the public in relation to the formulation of its policy or implementation thereof
The Council offers services primarily for the dental colleges and Dental professionals.
There is no direct interaction with the public at any point of time. Therefore, at times
meetings with Stakeholders are organized. The Secretary meets visitors only with
prior appointment during the visiting hours.
Vol. 1 Issue 11 L.E.D. E-Journal Page 182
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
CHAPTER -8
Council constituted under Section 3 of the Dentists Act, 1948
1. Council Members
[http://dciindia.org.in/CouncilMember.aspx]
2. Executive Committee Members
[http://dciindia.org.in/ExecutiveCommitteeMembers.aspx]
3. Ex-Officio Member U/S 3(g) of the Dentists Act
[http://dciindia.org.in/CouncilMember.aspx?id=g]
4. Other Committees.
Note: - Information as regards above is available on DCI website as per the specified links.
Vol. 1 Issue 11 L.E.D. E-Journal Page 183
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
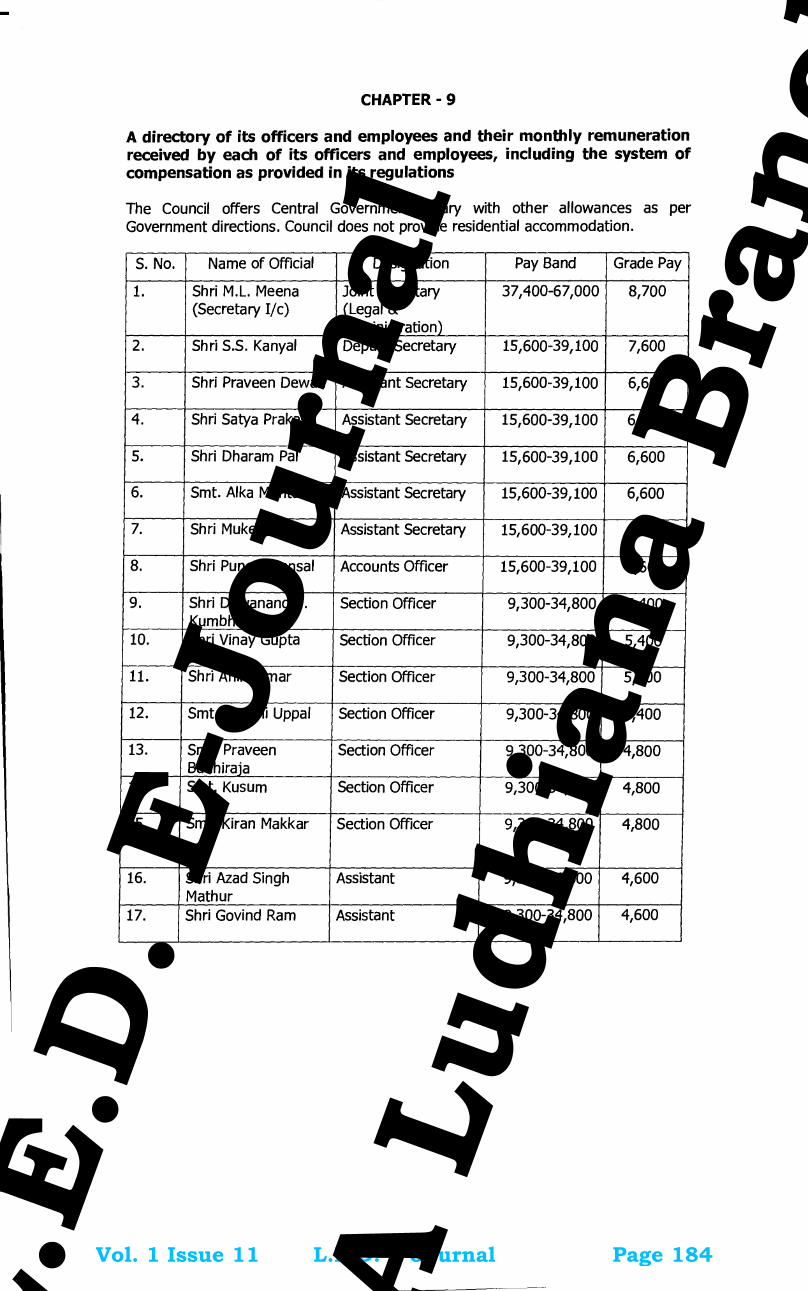
CHAPTER - 9
A directory of its officers and employees and their monthly remuneration received by each of its officers and employees, including the system of compensation as provided in its regulations
The Council offers Central Government salary with other allowances as per Government directions. Council does not provide residential accommodation.
S. No. Name of Official Designation Pay Band Grade Pay
1. Shri M.L. Meena (Secretary I/c)
Joint Secretary (Legal & Administration)
37,400-67,000 8,700
2. Shri S.S. Kanyal Deputy Secretary 15,600-39,100 7,600
3. Shri Praveen Dewan Assistant Secretary 15,600-39,100 6,600
4. Shri Satya Prakash Assistant Secretary 15,600-39,100 6,600
5. Shri Dharam Pal Assistant Secretary 15,600-39,100 6,600
6. Smt. Alka Mehta Assistant Secretary 15,600-39,100 6,600
7. Shri Mukesh Kumar Assistant Secretary 15,600-39,100 6,600
8. Shri Puneet Bansal Accounts Officer 15,600-39,100 6,600
9. Shri Dewanand T. Kumbhare
Section Officer 9,300-34,800 5,400
10. Shri Vinay Gupta Section Officer 9,300-34,800 5,400
11. Shri Anil Kumar Section Officer 9,300-34,800 5,400
12. Smt. Kamini Uppal Section Officer 9,300-34,800 5,400
13. Smt. Praveen Budhiraja
Section Officer 9,300-34,800 4,800
14. Smt. Kusum Section Officer 9,300-34,800 4,800
15. Smt. Kiran Makkar Section Officer 9,300-34,800 4,800
16. Shri Azad Singh Mathur
Assistant 9,300-34,800 4,600
17. Shri Govind Ram Assistant 9,300-34,800 4,600
Vol. 1 Issue 11 L.E.D. E-Journal Page 184
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

18. Shri Naveen Sharma Assistant 9,300-34,800 4,600
19. Smt. Savita Assistant 9,300-34,800 4,600
20. Shri Ram Gahan Prajapati
Assistant 9,300-34,800 4,600
21. Shri Mohinder Singh Assistant 9,300-34,800 4,600
22. Smt. Deepa Chauhan
Assistant 9,300-34,800 4,600
23. Shri Madan Lal U.D. Clerk 5,200-20,200 2,400
24. Shri Mangal Sain U.D. Clerk 5,200-20,200 2,400
25. Shri Indra Raj U.D. Clerk 5,200-20,200 2,400
26. Shri Rakesh Kumar U.D. Clerk 5,200-20,200 2,400
27. Shri Gaurav Dixit U.D. Clerk 5,200-20,200 2,400
28. Shri Sanjay Kumar U.D. Clerk 5,200-20,200 2,400
29. Shri Yogesh Kumar Bhorwal
U.D. Clerk 5,200-20,200 2,400
30. Smt. Jyoti U.D. Clerk 5,200-20,200 2,400
31. Shri Pramod Kumar U.D. Clerk 5,200-20,200 2,400
32. Shri Prem Chand Kargati
L.D. Clerk 5,200-20,200 1,900
33. Shri Avinash Chhabbarwal
L.D. Clerk 5,200-20,200 1,900
34. Shri Piyush Tanwar L.D. Clerk 5,200-20,200 1,900
35. Shri Umesh Singh Bisht
L.D. Clerk 5,200-20,200 1,900
36. Shri Sachin Gupta L.D. Clerk 5,200-20,200 1,900
37. Shri Sant Lal Gupta L.D. Clerk 5,200-20,200 1,900
38. Shri Ram Chander Pandey
L.D. Clerk 5,200-20,200 1,900
39. Shri Dhiraj Singh L.D. Clerk 5,200-20,200 1,900
40. Shri Punit Kumar Staff Car Driver 5,200-20,200 1,900
Vol. 1 Issue 11 L.E.D. E-Journal Page 185
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
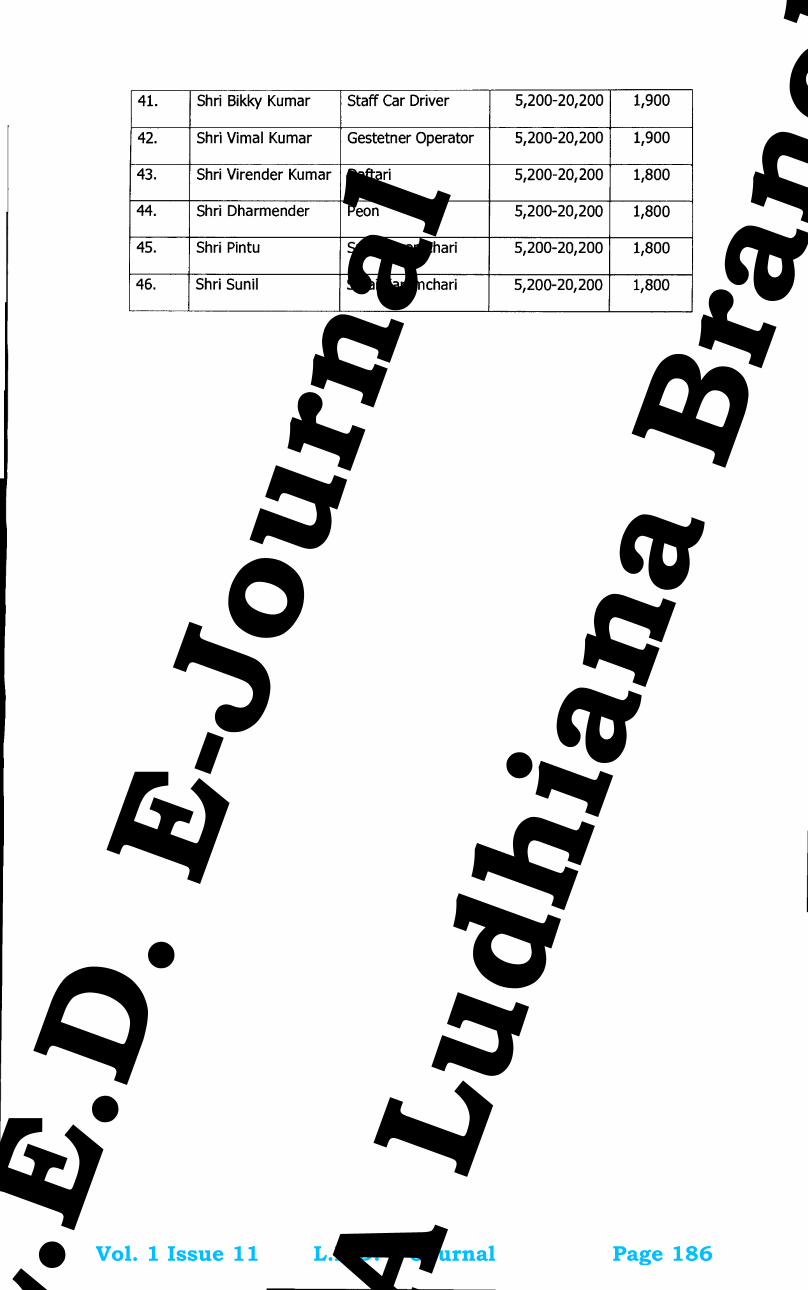
41. Shri Bikky Kumar Staff Car Driver 5,200-20,200 1,900
42. Shri Vimal Kumar Gestetner Operator 5,200-20,200 1,900
43. Shri Virender Kumar Daftari 5,200-20,200 1,800
44. Shri Dharmender Peon 5,200-20,200 1,800
45. Shri Pintu Safai Karamchari 5,200-20,200 1,800
46. Shri Sunil Safai Karamchari 5,200-20,200 1,800
Vol. 1 Issue 11 L.E.D. E-Journal Page 186
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

CHAPTER -10
The budget allocated to each of its agency, indicating the particulars of all plans, proposed expenditure and reports on disbursements made and etc.
To obtain this information from accounts
Vol. 1 Issue 11 L.E.D. E-Journal Page 187
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
CHAPTER -11
Particulars of recipients of concessions, permits or authorization granted by the Public Authority
The Dental Council of India is the recommendatory body to the Central
Government u/s 10A of the Dentists Act, 1948 for grant of letter of permission for
the establishment of dental college, increase of intake capacity, opening of a new or
higher course of study, renewal of permission. Such records are maintained in the
concerned file of the college by the respective Section.
The details of number of registered dentists are maintained by the Misc.
Section-II, as per data or information received from the respective State Dental
Councils.
The grant of Eligibility Certificate to Indian Citizen/OCI interested to pursue
foreign dental qualification is maintained by the Misc. Section-I.
Vol. 1 Issue 11 L.E.D. E-Journal Page 188
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
CHAPTER -12
Details in respect of the information, available to or held by it, reduced in an electronic form
Information relating to the Dental Colleges imparting UG & PG dental courses along with admission capacity. [http://dciindia.org .in/CollegeSearch.aspx?ColName=&CourseId =&SplId=O&StateId =&Hospital=&Type=0&Status=--Select--]
Details of Council Members [http://dciindia.org.in/CouncilMemberaspx]
Details of Executive Committee Members [http://dciindia.org.in/ExecutiveCommitteeMembers.aspx]
Details of Ex-Officio Member U/S 3(g) of the Dentists Act [http://dciindia.org.in/CouncilMemberaspx?id=g]
List of students submitted by the colleges [http://dciindia.org.in/StudentDetailsList.aspx]
List of Act & Regulations [http://dciindia.org.in/Dentistact1948.aspx]
Vol. 1 Issue 11 L.E.D. E-Journal Page 189
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

CHAPTER -13
The names, desicinations and other particulars of the Public Information Officers
The following officers are as on date the First Appellate Authority and Public Information Officer of the Dental Council of India under Section 5(1) and under Section 19(1) of Right to Information Act, 2005:
Name with Designation Ph. (Office) & Email
Detail of First Appellate Authority of DCI in respect of RTI Act 2005
Dr. Dibyendu Mazumder President Dental Council of India Aiwan-E-Galib Marg Kotla Road, New Delhi-110002
011-23236740 011-23238542 email:[email protected]
Detail of Public Information Officer of DCI in respect of RTI Act 2005
Mrs. Alka Mehta Assistant Secretary Dental Council of India Aiwan-E-Galib Marg Kotla Road, New Delhi-110002
011-23236740 011-23238542 email:[email protected]
Note: The fee under RTI Act, if paid through Indian Postal Order/Demand Draft should be in favour of the Secretary, Dental Council of India, payable at New Delhi.
Vol. 1 Issue 11 L.E.D. E-Journal Page 190
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

CHAPTER -14
The particulars of facilities available to citizens for obtaining information, including the working hours of a library or reading room, if maintained for public use
1. During, the public dealing hours [11:00 AM to 5:00 PM] on official working
days applicants/ citizens can visit to obtain information.
2. Information on other matters can be obtained from the Public Information
Officer, designated under Rn Act.
3. The Council's Library is meant for the Council's Employees only.
Vol. 1 Issue 11 L.E.D. E-Journal Page 191
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
1214 GI/2016 (1)
jftLVªh laö Mhö ,yö&33004@99 REGD. NO. D. L.-33004/99
vlk/kj.k EXTRAORDINARY
Hkkx III—[k.M 4 PART III—Section 4
izkf/dkj ls izdkf'kr PUBLISHED BY AUTHORITY
la- 89] ubZ fnYyh] 'kqØokj] ekpZ 11] 2016@iQkYxqu 21] 1937 No. 89] NEW DELHI, FRIDAY, MARCH 11, 2016/ PHALGUNA 21, 1937
Hkkjrh; naR; ifj"knHkkjrh; naR; ifj"knHkkjrh; naR; ifj"knHkkjrh; naR; ifj"kn
vf/klwpukvf/klwpukvf/klwpukvf/klwpuk
ubZ fnYyh] 7 ekpZ] 2016
lalalala---- MhbZ&218&2016MhbZ&218&2016MhbZ&218&2016MhbZ&218&2016.—narfpfdRld vf/kfu;e] 1948 ¼1948 dk 16oka½ dh /kkjk 20 ds lkFk ifBr /kkjk 10, }kjk iznRr 'kfDr;ksa dk iz;ksx djrs gq,] Hkkjrh; naR; ifj"kn le; vuqlwph rS;kj djus ds fy, fjV ;kfpdk la[;k 76@2015 ds laca/k esa ekuuh; loksZPp U;k;ky; ds fnukad 24-03-2015 ds funs'k ds vuqlj.k esa Mhth,p,l dh flQkfj'k ij] dsUnzh; ljdkj ds iwokZuqeksnu ls eq[; fofu;eksa ;Fkk ^^Hkkjrh; naR; ifj"kn ¼u, nar dkyst [kksyus] v/;;u vFkok izf'k{k.k ds u, rFkk mPprj ikB~;Øe 'kq: djus rFkk nar dkystksa dh izos'k {kerk c<+kus½ ls lacaf/kr fofu;e] 2006** esa fuEukuqlkj la'kks/ku djrh gS%&
1. laf{kIr uke vkSj izorZu%&laf{kIr uke vkSj izorZu%&laf{kIr uke vkSj izorZu%&laf{kIr uke vkSj izorZu%&
(i) bu fofu;eksa dks ^^Hkkjrh; naR; ifj"kn ¼u, nar dkyst [kksyus] v/;;u vFkok izf'k{k.k ds u, rFkk mPprj ikB~;Øe 'kq: djus vkSj nar dkystksa dh izos'k {kerk½ c<+kus ls lacaf/kr ¼8oka la'kks/ku½ fofu;e] 2016** dgk tk,xkA
(ii) ;s fofu;e ljdkjh jkti= esa buds izdk'ku dh rkjh[k ls ykxw gksaxsA
2. eq[; MhlhvkbZ fofu;e] 2016 ds fofu;e 4¼2½ esa ^^Hkkjrh; naR; ifj"kn ¼u, nar dkyst [kksyus] v/;;u vFkok izf'k{k.k ds mPprj ikB~;Øe 'kq: djus vkSj nar dkystksa dh izos'k {kerk½ c<+kus ls lacaf/kr ¼izFke la'kks/ku½ }kjk tks 16-01-2006** dks ljdkjh jkti= esa vf/klwfpr fd;k x;k] }kjk lfUufo"V ekStwnk ^vuqlwph* ,rn~}kjk fudky nh tkrh gS vkSj fuEu ubZ vuqlwph }kjk izfrLFkkfir dh tkrh gSA
Vol. 1 Issue 11 L.E.D. E-Journal Page 192
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
2 THE GAZETTE OF INDIA : EXTRAORDINARY [PART III —SEC. 4]
^^vuqlwph**^^vuqlwph**^^vuqlwph**^^vuqlwph**
[ns[ksa fofu;e ns[ksa fofu;e ns[ksa fofu;e ns[ksa fofu;e 4(2)]
u, nar dkyst [kksyus@Lukrd&iwoZ lhVksa dh la[;k esa o`f)@vuqefr ds uohdj.k rFkk dsUnzh; ljdkj }kjk Hkkjrh; naR; u, nar dkyst [kksyus@Lukrd&iwoZ lhVksa dh la[;k esa o`f)@vuqefr ds uohdj.k rFkk dsUnzh; ljdkj }kjk Hkkjrh; naR; u, nar dkyst [kksyus@Lukrd&iwoZ lhVksa dh la[;k esa o`f)@vuqefr ds uohdj.k rFkk dsUnzh; ljdkj }kjk Hkkjrh; naR; u, nar dkyst [kksyus@Lukrd&iwoZ lhVksa dh la[;k esa o`f)@vuqefr ds uohdj.k rFkk dsUnzh; ljdkj }kjk Hkkjrh; naR; ifj"kn }kjifj"kn }kjifj"kn }kjifj"kn }kjk vkosnu&i=ksa ij dkjZokbZ ds fy, le;&lwphk vkosnu&i=ksa ij dkjZokbZ ds fy, le;&lwphk vkosnu&i=ksa ij dkjZokbZ ds fy, le;&lwphk vkosnu&i=ksa ij dkjZokbZ ds fy, le;&lwph
Øe Øe Øe Øe la[;kla[;kla[;kla[;k
dkjZokbZ dk pj.k vafre rkjh[kvafre rkjh[kvafre rkjh[kvafre rkjh[k
1. dsUnzh; ljdkj }kjk vkosnu&i=ksa dh izkfIr fdlh Hkh o"kZ 15 twu vkSj 7 tqykbZ ds chp ¼nksuksa fnol 'kkfey½
2. dsUnzh; ljdkj }kjk Hkkjrh; naR; ifj"kn dks vkosnu&i=ksa dk vxzs"k.k
31 tqykbZ rd
3. Hkkjrh; naR; ifj"kn }kjk rduhdh laoh{kk] vkdyu vkSj flQkfj'ksa 31 fnlacj rd
4. dsUnzh; ljdkj }kjk vkosnd ls mRrj@vuqikyu dh izkfIr rFkk rRlaca/kh oS;fDrd lquokbZ ds fy,] ;fn dksbZ gks rks rFkk dsUnzh; ljdkj }kjk Hkkjrh; naR; ifj"kn dks vuqikyu dk vxzs"k.k
MhlhvkbZ ls flQkfj'k dh izkfIr ls nks eghus rd ysfdu 31 tuojh ds ckn ugha
5. Hkkjrh; naR; ifj"kn dh vafre flQkfj'ksa 30 vizSy rd
6. dsUnzh; ljdkj }kjk vuqefr dk i= tkjh djuk 31 ebZ rd
7. ’kS{kf.kd l=@vof/k dh 'kq:vkr 1 vxLr
8. vafre rkjh[k ftl rd fdlh dkj.k mRiUu gksus okyh vkdfLed fjfDr;ksa ij Nk=ksa dks nkf[ky fd;k tk ldrk gS@muds }kjk ’kS{kf.kd l= vkjaHk fd;k tk ldrk gSA
15 flracj rd
fVIi.kh%fVIi.kh%fVIi.kh%fVIi.kh%
(1) vuqefr ds uohdj.k ds laca/k esa vkosnd viuk vkosnu&i= 31 tqykbZ rd Hkkjrh; naR; ifj"kn dks HkstsaxsA
(2) dsUnzh; ljdkj }kjk mi;qZDr le;&lwph] vkosndksa ds fdlh oxZ vFkok Js.kh ds fy, la'kksf/kr dh tk ldrh gS] ftlds dkj.k fyf[kr :i esa fjdkMZ fd, tk,axsA
v/;;u ds mPprj ikB~;Øe ’kq: djus@LukrdksRrj lhVksa dh la[;k c<+kus@vuqefr dk uohdj.k v/;;u ds mPprj ikB~;Øe ’kq: djus@LukrdksRrj lhVksa dh la[;k c<+kus@vuqefr dk uohdj.k v/;;u ds mPprj ikB~;Øe ’kq: djus@LukrdksRrj lhVksa dh la[;k c<+kus@vuqefr dk uohdj.k v/;;u ds mPprj ikB~;Øe ’kq: djus@LukrdksRrj lhVksa dh la[;k c<+kus@vuqefr dk uohdj.k djus vkSj dsUnzh; ljdkj djus vkSj dsUnzh; ljdkj djus vkSj dsUnzh; ljdkj djus vkSj dsUnzh; ljdkj rFkk Hkkjrh; naR; ifj"kn }kjk vkosnu&i=rFkk Hkkjrh; naR; ifj"kn }kjk vkosnu&i=rFkk Hkkjrh; naR; ifj"kn }kjk vkosnu&i=rFkk Hkkjrh; naR; ifj"kn }kjk vkosnu&i=ksa ij dkjZokbZ ds fy, le;&lwphksa ij dkjZokbZ ds fy, le;&lwphksa ij dkjZokbZ ds fy, le;&lwphksa ij dkjZokbZ ds fy, le;&lwph
Øe Øe Øe Øe la[;kla[;kla[;kla[;k
dkjZokbZ dk pj.k vafre rkjh[kvafre rkjh[kvafre rkjh[kvafre rkjh[k
1. dsUnzh; ljdkj }kjk vkosnu&i=ksa dh izkfIr fdlh Hkh o"kZ 15 ekpZ vkSj 7 vizSy ds chp ¼nksuksa fnol 'kkfey½
2. dsUnzh; ljdkj }kjk Hkkjrh; naR; ifj"kn dks vkosnu&i=ksa dk vxzs"k.k 30 vizSy rd
3. Hkkjrh; naR; ifj"kn }kjk rduhdh laoh{kk] vkdyu vkSj flQkfj'ksa 15 vDrwcj rd
4. dsUnzh; ljdkj }kjk vkosnd ls mRrj@vuqikyu dh izkfIr rFkk rRlaca/kh oS;fDrd lquokbZ ds fy,] ;fn dksbZ gks rks rFkk dsUnzh; ljdkj }kjk Hkkjrh; naR; ifj"kn dks vuqikyu dk vxzs’k.k
MhlhvkbZ ls flQkfj'k dh izkfIr ls nks eghus rd ysfdu 15 uoacj ds ckn ugha
5. Hkkjrh; naR; ifj"kn dh vafre flQkfj'ksa 31 tuojh rd
6. dsUnzh; ljdkj }kjk vuqefr dk i= tkjh djuk 28 Qjojh rd
7. ’kS{kf.kd l=@vof/k dh 'kq:vkr 1 ebZ
8. vafre rkjh[k ftl rd fdlh dkj.k mRiUu gksus okyh vkdfLed fjfDr;ksa ij Nk=ksa dks nkf[ky fd;k tk ldrk gS@muds }kjk 'kS{kf.kd l= vkjaHk fd;k tk ldrk gSA
31 ebZ rd
fVIi.kh%fVIi.kh%fVIi.kh%fVIi.kh%
(1) vuqefr ds uohdj.k ds laca/k esa vkosnd viuk vkosnu&i= 30 vizSy rd Hkkjrh; naR; ifj"kn dks HkstsaxsA
(2) dsUnzh; ljdkj }kjk mi;qZDr le;&lwph] vkosndksa ds fdlh oxZ vFkok Js.kh ds fy, la’kksf/kr dh tk ldrh gS] ftlds dkj.k fyf[kr :i esa fjdkMZ fd, tk,axsA
,e- ,y- ehuk] izHkkjh lfpo [foKkiu&III@4@vlk-@395(98)]
Vol. 1 Issue 11 L.E.D. E-Journal Page 193
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
¹Hkkx IIIµ[k.M 4º Hkkjr dk jkti=k % vlk/kj.k 3
ikn fVIi.kh%ikn fVIi.kh%ikn fVIi.kh%ikn fVIi.kh%
1- eq[; fofu;e ;Fkk Hkkjrh; naR; ifj"kn ¼u, nar dkyst [kksyus] v/;;u vFkok izf’k{k.k ds mPprj ikB~;Øe 'kq: djus
vkSj nar dkystksa dh nkf[kyk {kerk c<+kus½ ls lacaf/kr fofu;e] 2006 tks Hkkjr ds vlk/kkj.k jkti= ds Hkkx III, [kaM 4 esa 12-01-2006 dks izdkf'kr fd, x, FksA
2- eq[; fofu;e dk igyk la'kks/ku tks Hkkjr ds vlk/kkj.k jkti= ds Hkkx III, [kaM 4 esa 16-01-2006 dks izdkf'kr fd, x, FksA
3- eq[; fofu;e dk nwljk la'kks/ku tks Hkkjr ds vlk/kkj.k jkti= ds Hkkx III, [kaM 4 esa 22-02-2006 dks izdkf'kr fd, x, FksA
4- eq[; fofu;e dk rhljk la'kks/ku tks Hkkjr ds vlk/kkj.k jkti= ds Hkkx III, [kaM 4 esa 02-11-2006 dks izdkf'kr fd, x, FksA
5- eq[; fofu;e dk pkSFkk la'kks/ku tks Hkkjr ds vlk/kkj.k jkti= ds Hkkx III, [kaM 4 esa 21-05-2012 dks izdkf'kr fd, x, FksA
DENTAL COUNCIL OF INDIA
NOTIFICATION
New Delhi, the 7th March, 2016
No. DE-218-2016.—In exercise of the powers conferred by Section 10A read with Section 20 of the
Dentists Act, 1948 (16 of 1948), the Dental Council of India, on the recommendation of DGHS pursuant to
the direction of the Hon’ble Supreme Court in its order dated 24.03.2015 in W.P. No. 76/2015 for framing
Time Schedule, with the previous approval of the Central Government, hereby amend the Principal
Regulations, namely, “Dental Council of India (Establishment of New Dental Colleges, Opening of New or
Higher Course of Study or Training and Increase of Admission Capacity in Dental Colleges) Regulations,
2006” as under:-
1. Short title and commencement:-
(iii) These Regulations may be called the “Dental Council of India (Establishment of New Dental
Colleges, Opening of New of Higher Course of Study or Training and Increase of Admission
Capacity in Dental Colleges) (8th Amendment) Regulations, 2016”.
(iv) They shall come into force from the date of their publication in the Official Gazette.
2. In regulation 4(2) of the principal DCI regulations 2006, the existing ‘Schedule’ inserted by “Dental
Council of India (Establishment of New Dental Colleges, Opening of New of Higher Course of Study
or Training and Increase of Admission Capacity in Dental Colleges) (1st Amendment) Regulations,
2006”, notified in the Official Gazette on 16.01.2006 is hereby deleted and substituted with the
following new schedule:-
“SCHEDULE”
[See Regulation 4(2)]
TIME SCHEDULE FOR RECEIPT OF APPLICATION FOR ESTABLISHMENT OF NEW
DENTAL COLLEGES / INCREASE OF UNDER GRADUATE SEATS / RENEWAL OF
PERMISSION AND PROCESSING OF THE APPLICATIONS BY THE CENTRAL GOVERNMENT
AND THE DENTAL COUNCIL OF INDIA.
Sl. No. Stage of processing Last Date
1. Receipt of applications by the Central Government. Between 15th June to 7th July (both
days inclusive) of any year
2. Forwarding of applications by the Central Government to
Dental Council of India.
By 31st July
Vol. 1 Issue 11 L.E.D. E-Journal Page 194
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

4 THE GAZETTE OF INDIA : EXTRAORDINARY [PART III —SEC. 4]
3. Technical Scrutiny, Assessment and Recommendations by
the Dental Council of India.
By 31st December
4. Receipt of reply/compliance from the applicant by the
Central Government and for personal hearing thereto, if any
and forwarding of compliance by the Central Government to
the Dental Council of India.
Two months from receipt of
recommendation from DCI but
not after 31st January.
5. Final recommendations by the Dental Council of India. By 30th April
6. Issue of Letter of Permission by the Central Government. By 31st May
7. Commencement of academic session/term 1st of August
8. Last date upto which students can be admitted/Joined
against stray vacancies arising due to any reason
By 15th September
Note:
(1) In case of renewal permission, the applicants shall submit the application to the Dental Council of
India by 31st July.
(2) The time schedule indicated above may be modified by the Central Government, for reasons to be
recorded in writing, in respect of any class or category of applications.
TIME SCHEDULE FOR RECEIPT OF APPLICATION FOR OPENING OF HIGHER COURSES OF
STUDY / INCREASE OF POST GRADUATE SEATS / RENEWAL OF PERMISSION AND
PROCESSING OF THE APPLICATIONS BY THE CENTRAL GOVERNMENT AND THE DENTAL
COUNCIL OF INDIA.
Sl.
No.
Stage of processing Last Date
1. Receipt of applications by the Central Government. Between 15th March to 7
th April
(both days inclusive of any year)
2. Forwarding of applications by the Central Government to
Dental Council of India.
By 30th April
3. Technical Scrutiny, Assessment and Recommendations by the
Dental Council of India.
By 15th October
4. Receipt of reply/ compliance from the applicant by the Central
Government and for personal hearing thereto, if any and
forwarding of compliance by the Central Government to the
Dental Council of India
Two months from receipt of
recommendation from DCI but
not after 15th November
5. Final recommendations by the Dental Council of India. By 31st January
6. Issue of Letter of Permission by the Central Government. By 28th February
7. Commencement of academic session/term 1st May
8. Last date upto which students can be admitted/Joined against
stray vacancies arising due to any reason
By 31st May
Note:
(1) In case of renewal permission, the applicants shall submit the application to the Dental Council of
India by 30th April.
(2) The time schedule indicated above may be modified by the Central Government, for reasons to be
recorded in writing, in respect of any class or category of applications.
M. L. MEENA, Secy. I/c
[ADVT.III/4/Exty./395(98)]
Vol. 1 Issue 11 L.E.D. E-Journal Page 195
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

¹Hkkx IIIµ[k.M 4º Hkkjr dk jkti=k % vlk/kj.k 5
Foot note:
1. The Principal Regulations, namely, the Dental Council of India (Establishment of New Dental Colleges,
Opening of New of Higher Course of Study or Training and Increase of Admission Capacity in Dental
Colleges) Regulations, 2006, published in Part III, Section 4 of the Gazette of India, Extraordinary, on
12.01.2006.
2. The 1st Amendment of the Principal Regulations, published in Part III, Section 4 of the Gazette of India,
Extraordinary, on 16.01.2006.
3. The 2nd
Amendment of the Principal Regulations, published in Part III, Section 4 of the Gazette of
India, Extraordinary, on 22.02.2006.
4. The 3rd
Amendment of the Principal Regulations, published in Part III, Section 4 of the Gazette of India,
Extraordinary, on 02.11.2006.
5. The 4th Amendment of the Principal Regulations, published in Part III, Section 4 of the Gazette of India,
Extraordinary, on 21.05.2012.
Uploaded by Dte. of Printing at Government of India Press, Ring Road, Mayapuri, New Delhi-110064
and Published by the Controller of Publications, Delhi-110054.
Vol. 1 Issue 11 L.E.D. E-Journal Page 196
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Dengue and Chikungunya
Vol. 1 Issue 11 L.E.D. E-Journal Page 197
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

What is Dengue?
• Dengue (pronounced den' gee)
is a viral disease.
• Dengue can be caused by infection with any
one of four closely related dengue viruses.
• DENV 1, DENV 2, DENV 3 or DENV 4.
Vol. 1 Issue 11 L.E.D. E-Journal Page 198
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

How does it spread?
The dengue viruses are transmitted to humans
by the bite of an infected Aedes mosquito.
Vol. 1 Issue 11 L.E.D. E-Journal Page 199
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

• One distinct physical
feature (black and
white stripes on its
body and legs)
hence also called as
‘Tiger mosquito’.
• Bites during the day.
• Lays its eggs in
clean, stagnant
water.
Characteristics of the
Aedes Mosquito
Vol. 1 Issue 11 L.E.D. E-Journal Page 200
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Did you know?
• Only the female Aedes mosquito bites as it needs the
protein in blood to develop its eggs.
• The mosquito becomes infective approximately
seven days after it has bitten a person carrying the
virus.
• Once infected, a mosquito remains infective for life
and passes on the virus to the eggs it lays.
• Peak biting time is at dawn and dusk – 2 hours after
sunrise and 2 hours before sunset.
Vol. 1 Issue 11 L.E.D. E-Journal Page 201
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
Aedes mosquito: Fast facts
• The average lifespan of an Aedes mosquito is
2 weeks.
• The mosquito can lay eggs about 3 times in
its lifetime, and about 100 eggs are produced
each time.
• The eggs can withstand very dry conditions
(desiccation) and remain viable for many
months in the absence of water.
– Repopulation will occur as soon as the eggs in the
containers are flooded with water.
Vol. 1 Issue 11 L.E.D. E-Journal Page 202
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
Aedes mosquito: Fast facts (contd.)
• Adult mosquitoes “usually” rests indoors in dark
areas (closets, under beds, behind curtains).
• They have limited flight range – can fly an average of
400metres looking for water-filled containers to lay
their eggs. This means that people, rather than
mosquitoes, rapidly move the virus within and
between communities and places.
• A few mosquitoes per household can produce large
dengue outbreaks. The dengue mosquito does not
lay eggs in ditches, drainages, canals, wetlands,
rivers or lakes.
Vol. 1 Issue 11 L.E.D. E-Journal Page 203
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
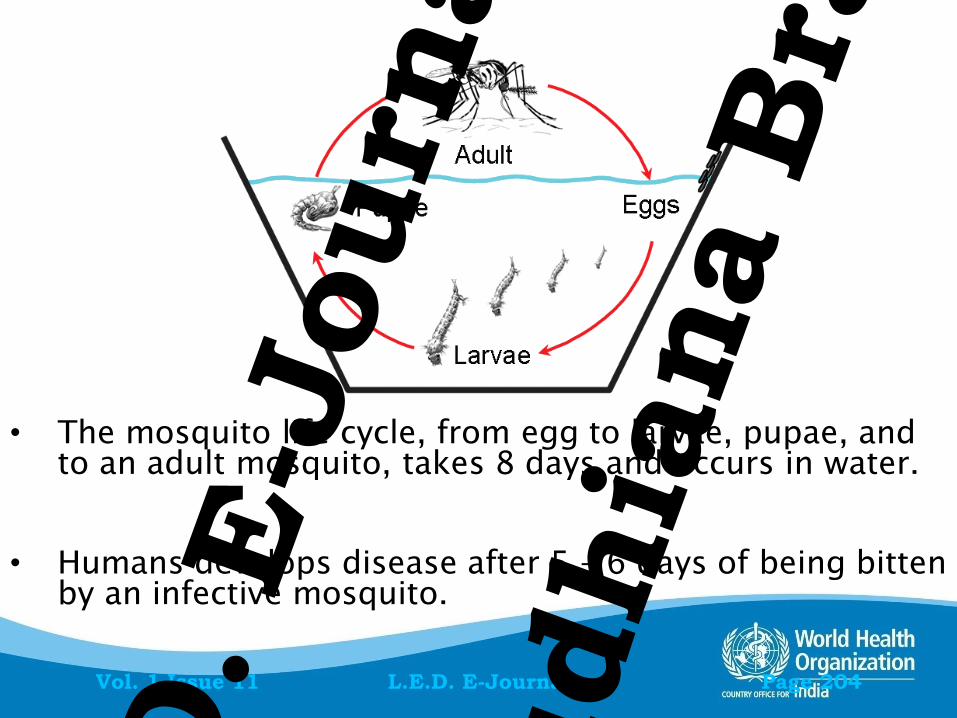
• The mosquito life cycle, from egg to larvae, pupae, and
to an adult mosquito, takes 8 days and occurs in water.
• Humans develops disease after 5 – 6 days of being bitten
by an infective mosquito.
Vol. 1 Issue 11 L.E.D. E-Journal Page 204
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
What can you do to reduce risk of
acquiring dengue?
PROTECT YOURSELF FROM MOSQUITO BITES
• Dengue mosquitoes bite during the day time. Highest
biting intensity is about 2 hours after sunrise and
before sunset.
• Wear full sleeves clothes and long dresses to cover as
much of your body as possible.
• Use repellents, mosquito coils, electric vapor mats
during the daytime also to prevent dengue.
• Use mosquito nets to protect children, elderly and
others who may rest during the day.
Vol. 1 Issue 11 L.E.D. E-Journal Page 205
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Clinical description :
Dengue fever (classical)
An acute onset high fever of 2-7 days duration with
2 or more of the following manifestations:
Headache (often severe)
Retro-orbital pain (severe eye pain behind eyes)
Myalgia (muscle pain)
Arthralgia (joint pain)
Rash
Hemorrhagic manifestations: nose or gum bleed,
easy bruising
All the above symptoms and signs may not be present in the patient.
Vol. 1 Issue 11 L.E.D. E-Journal Page 206
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

What to do if you think you have
dengue
Bed rest- acute phase
Cold sponging for reducing fever
X Avoid aspirin, brufen etc – these can cause gastritis,
vomiting, platelet dysfunction
Paracetamol is preferable for fever management.
Oral electrolyte therapy: for excessive sweating,
vomiting
• Avoid mosquito bites
– wear full sleeves; Place patient under bed net or
use insect repellent on the patient while they have
a fever, Put screens on windows and doors to
prevent mosquitoes from coming into house.
• Consult a physician.
TAKE PLENTY OF FLUIDS
Vol. 1 Issue 11 L.E.D. E-Journal Page 207
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Laboratory findings in
dengue: Blood picture
• If a patient is suspected to be having dengue,
the doctor may ask the patient to get a blood
test done.
• Findings such as reduced platelets or an
increase in blood haematocrit makes
dengue more likely.
(Platelets are cells in blood that help to stop bleeding.
Haematocrit indicates the thickness of blood).
Vol. 1 Issue 11 L.E.D. E-Journal Page 208
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Dengue specific Tests
• Dengue specific tests done in a blood sample
can confirm a diagnosis of dengue.
• There are two basic types of tests:
1. Detecting Dengue antigen in
blood( within first 5 days of
onset of symptoms): NS1
antigen based assays
2. Detecting Dengue antibodies
in blood( after first 5 days of
onset of symptoms)
Vol. 1 Issue 11 L.E.D. E-Journal Page 209
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
Most people who suffer from
dengue fever recover in
1–2 weeks time.
Vol. 1 Issue 11 L.E.D. E-Journal Page 210
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
PREVENT DEHYDRATION
• Dehydration can occur when a person loses too much
fluid (from high fevers, vomiting, or poor oral intake).
• Give plenty of fluids- ORS and juices are preferable to
water
• Watch for any signs of dehydration
Decrease in urination
Few or no tears when child cries
Dry mouth, tongue or lips
Sunken eyes
Listlessness or overly agitated or confused
Fast heart beat (more than 100/min)
Cold or clammy fingers and toes
Vol. 1 Issue 11 L.E.D. E-Journal Page 211
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

The critical period may be
after 3-5 days of fever
• In a few patients, the smallest blood
vessels (capillaries) may become excessively
permeable (“leaky”), allowing the fluid
component to escape from the blood
vessels into body cavities.
• This may lead to failure of the circulatory
system and shock if properly not managed
with fluid resuscitation.
Vol. 1 Issue 11 L.E.D. E-Journal Page 212
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
Can people die from dengue fever?
• People who suffer from dengue fever have no risk of death
but rarely some of them may develop Dengue Hemorrhagic
Fever (DHF) or Dengue Shock Syndrome(DSS).
• Patients suspected to be suffering from DHF/DSS should be
admitted to a hospital without delay.
• Infants and young children are more likely than adults to
develop DHF/DSS or manifestations of severe clinical illness.
Parents need to be vigilant.
• With proper treatment, the patients with Dengue
hemorrhagic fever and dengue shock syndrome can
recover fully.
– Good treatment provided in time can save lives.
Vol. 1 Issue 11 L.E.D. E-Journal Page 213
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Warning signs
Immediate medical attention !
Severe abdominal pain or persistent vomiting
Red spots or patches on the skin
Bleeding from nose or gums
Vomiting blood
Black, tarry stools (feces, excrement)
Drowsiness or irritability
Pale, cold, or clammy skin
Difficulty in breathing
Vol. 1 Issue 11 L.E.D. E-Journal Page 214
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
What does the treating doctor
need to do in such cases?
Monitor progress of patients regularly at 1-2
hours interval.
Platelet counts and haematocrit need to be
monitored repeatedly to review the progress
of patients.
The doctor may advise IV fluids or platelet
transfusion.
All patients do not require platelet
transfusion.
Vol. 1 Issue 11 L.E.D. E-Journal Page 215
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Can you get dengue again
after suffering from it once?
YES
• If a person has suffered from one virus, there can be a
repeat occurrence of dengue if a different strain is
involved subsequently.
• Being affected by one strain offers no protection
against the others.
• A person could suffer from dengue more than once in
her/his lifetime.
Vol. 1 Issue 11 L.E.D. E-Journal Page 216
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Can people suffer from
dengue and not appear ill?
YES
• There are many people who are infected
with the virus and do not suffer from any
signs or symptoms of the disease.
• For every patient with symptoms and
signs there may be 4-5 persons with no
symptoms or with very mild symptoms.
Vol. 1 Issue 11 L.E.D. E-Journal Page 217
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
Can dengue fever patient be treated
at home?
• Most patients with dengue fever can be
treated at home.
• They should take rest, drink plenty of fluids that
are available at home and eat nutritious diet.
• Whenever available, Oral Rehydration Salt/ORS
(commonly used in treating diarrhea) is
preferable. Fruit juices are also good.
• It is important to look for danger signs and
contact the doctor as soon as any one or more
of these are found.
Vol. 1 Issue 11 L.E.D. E-Journal Page 218
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

What is Chikungunya ?
• Chikungunya is a viral illness spread by bite
of infected mosquitoes and clinically
resembles dengue fever.
• The name comes from the African language
meaning “that which bends up”and aptly
describes the stooped appearance of
sufferers with joint pain due to the disease.
Vol. 1 Issue 11 L.E.D. E-Journal Page 219
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
How does Chikungunya spread?
• Through bite of female infected mosquitoes Aedes
aegypti and Aedes albopictus.
• Mosquito usually transmits the disease by biting an
infected person and then biting someone else.
– An infected person cannot spread the infection
directly to other persons (i.e. it is not a
contagious disease).
• Aedes aegypti mosquitoes bite during the day time.
They breed in anything that holds clean water
including tyres, coconut shells, flower pots, storage
pans and cooling systems.
Vol. 1 Issue 11 L.E.D. E-Journal Page 220
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Chikungunya
Clinical signs and Symptoms
• Typical symptoms are similar to that of dengue:
sudden onset fever, severe headache, chills, nausea
and vomiting, and severe joint pains.
• Most patients recover fully, but in some cases the
joint pains may persist for weeks or months.
• Children less than 1 year and elderly are at greater
risk of severe disease
– Underlying medical conditions have also been
identified as a risk factor for poor disease
outcome.
Vol. 1 Issue 11 L.E.D. E-Journal Page 221
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
Chikungunya
Management of patient
• Chikungunya is diagnosed by blood tests (ELISA).
• Symptomatic management
– adequate rest; medicines to reduce joint pains
and fever. Some patients may require long term
pain management medication.
• Patients should avoid further mosquito exposure,
either by staying in places with screens or by using
mosquito nets.
Vol. 1 Issue 11 L.E.D. E-Journal Page 222
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Prevention and control are entirely dependent on taking
steps to avoid mosquito bites and eliminating mosquito
breeding sites.
Vol. 1 Issue 11 L.E.D. E-Journal Page 223
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Prevent mosquito breeding
•Discard/ Destroy unused items.
•Drain out water from various containers.
•Regularly change water and clean flower vases and
other items.
•Empty coolers.
•Cover water storage containers.
Vol. 1 Issue 11 L.E.D. E-Journal Page 224
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

To stop or to slow down the dengue transmission "thermal
fogging", using fogging machines is a supplemental
measure.
In fogging, we should use an insecticide that has an
immediate knock-down effect on adult mosquitoes.
Vol. 1 Issue 11 L.E.D. E-Journal Page 225
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
Individual and household
protection
• Wear full sleeves and full-length clothes to cover limbs.
• Repellents may be applied to exposed skin or to clothing,
in strict accordance with label instructions.
• Insecticide-treated mosquito nets afford good protection
for those who sleep during the day (e.g. infants, elderly).
• Household insecticide aerosol products, mosquito coils or
insecticide vaporizers may also reduce biting activity.
• Household fixtures such as window and door screens and
air-conditioning can also reduce biting.
Vol. 1 Issue 11 L.E.D. E-Journal Page 226
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Controlling Dengue and
Chikungunya is everyone’s
responsibility.
Vol. 1 Issue 11 L.E.D. E-Journal Page 227
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

International Association of Dental Traumatology
DENTAL TRAUMA GUIDELINES
Revised 2012
CONTENT: Section 1. Fractures and luxations of permanent teeth Section 2. Avulsion of permanent teeth Section 3. Traumatic injuries to primary teeth Disclaimer: These guidelines are intended to provide information for health care providers caring for patients with dental injuries. They represent the current best evidence based on literature research and professional opinion. As is true for all guidelines, the health care provider must apply clinical judgment dictated by the conditions present in the given traumatic situation. The IADT does not guarantee favorable outcomes from following the Guidelines, but using the recommended procedures can maximize the chances of success.
THESE GUIDELINES ARE ENDORSED BY THE AMERICAN ASSOCIATION OF ENDODONTISTS
Vol. 1 Issue 11 L.E.D. E-Journal Page 228
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

INTRODUCTION Traumatic dental injuries (TDIs) occur frequently in children and young adults, comprising 5% of all injuries. Twenty‐five percent of all school children experience dental trauma and 33% of adults have experienced trauma to the permanent dentition, with the majority of the injuries occurring before age 19. Luxation injuries are the most common TDIs in the primary dentition, whereas crown fractures are more commonly reported for the permanent teeth. Proper diagnosis, treatment planning and follow‐up are important to assure a favorable outcome. This update includes a review of the current dental literature using EMBASE, MEDLINE, PUBMED and Scopes searches from 1996‐2011, as well as a search of Dental Traumatology from 2000‐2011. The goal of these guidelines is to provide information for the immediate and urgent care of TDIs. It is understood that some of the subsequent treatment may require secondary and tertiary interventions involving specialists with experience in dental trauma. The IADT published its first set of guidelines in 2001, and updated them in 2007. As with previous guidelines, the working group included experienced investigators and clinicians from various dental specialties and general practice. The current revision represents the best evidence based on the available literature and expert professional judgment. In cases where the data did not appear conclusive, recommendations are based on the consensus opinion of the working group, followed by review by the members of the IADT Board of Directors.
It is understood that guidelines are to be applied with evaluation of the specific clinical circumstances, clinicians’ judgment and patients’ characteristics, including but not limited to compliance, finances and understanding of the immediate and long‐term outcomes of treatment alternatives versus non‐treatment. The IADT cannot and does not guarantee favorable outcomes from adherence to the Guidelines, but believe that their application can maximize the chances of a favorable outcome. These Guidelines offer recommendations for diagnosis and treatment of specific TDIs; however, they provide neither the comprehensive nor the detailed information found in textbooks, in the scientific literature, and most recently in the Dental Trauma Guide (DTG), which can be accessed @ http://www.dentaltraumaguide.org and the IADT website, http://www.iadt‐dentaltrauma.org provides connection to the journal Dental Traumatology and other dental trauma information.
GENERAL RECOMMENDATIONS Special considerations for trauma to primary teeth A young child is often difficult to examine and treat due to lack of cooperation and because of fear. The situation is distressing for both the child and the parents. It is important to keep in mind that there is a close relationship between the apex of the root of the injured primary tooth, and the underlying permanent tooth germ. Tooth malformation, impacted teeth, and eruption disturbances in the developing permanent dentition are some of the consequences that can occur following severe injuries to primary teeth and/or alveolar bone. A child’s maturity and ability to cope with the emergency situation, the time for shedding of the injured tooth and the occlusion, are all important factors that influence treatment. Repeated trauma episodes are frequent in children. Immature versus Mature Permanent Teeth
Vol. 1 Issue 11 L.E.D. E-Journal Page 229
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Every effort should be made to preserve pulpal vitality in the immature permanent tooth to ensure continuous root development. The vast majority of TDIs occur in children and teenagers where loss of a tooth has lifetime consequences. The immature permanent tooth has considerable capacity for healing after traumatic pulp exposure, luxation injury and root fractures. Avulsion of Permanent Teeth The prognosis for avulsed permanent teeth is very much dependent on the actions taken at the place of accident. Promotion of public awareness of first‐aid treatment for the avulsed tooth is strongly encouraged. Treatment choices and prognosis for the avulsed tooth are largely dependent on the vitality of the periodontal ligament (PDL), and the maturity of the root. Patient/Parent Instructions
Patient compliance with follow‐up visits and home care contributes to better healing following a TDI. Both the patients and the parents of young patients should be advised regarding care of the injured tooth/teeth for optimal healing, prevention of further injury by avoidance of participation in contact sports, meticulous oral hygiene, and rinsing with an antibacterial such as Chlorhexidine Gluconate 0.1% alcohol free for 1‐2 weeks. Alternatively, with a young child, it is desirable to apply Chlorhexidine Gluconate to the affected area with a cotton swab. The use of pacifiers should be restricted.
Vol. 1 Issue 11 L.E.D. E-Journal Page 230
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
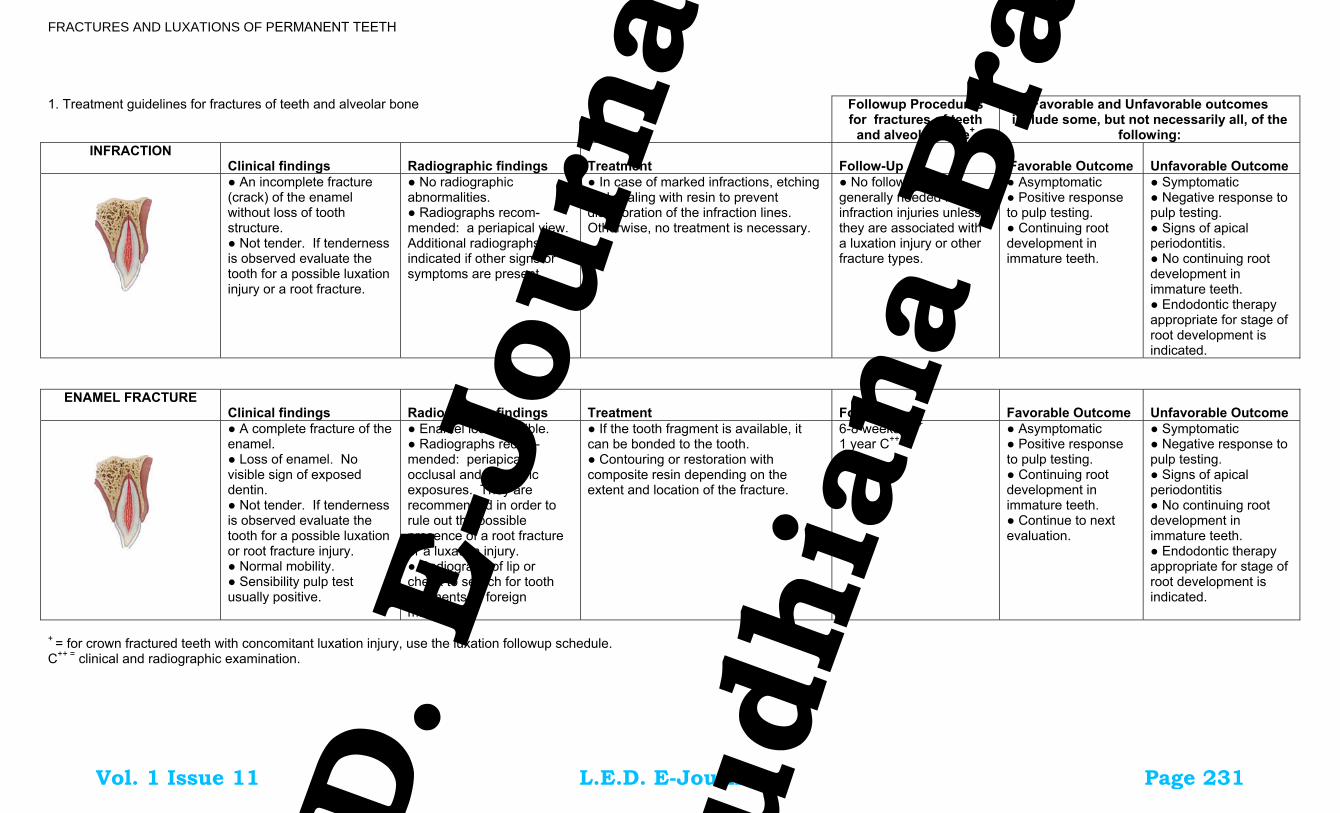
FRACTURES AND LUXATIONS OF PERMANENT TEETH 1. Treatment guidelines for fractures of teeth and alveolar bone Followup Procedures
for fractures of teeth and alveolar bone+
Favorable and Unfavorable outcomes include some, but not necessarily all, of the
following: INFRACTION
Clinical findings Radiographic findings
Treatment
Follow-Up
Favorable Outcome
Unfavorable Outcome
● An incomplete fracture (crack) of the enamel without loss of tooth structure. ● Not tender. If tenderness is observed evaluate the tooth for a possible luxation injury or a root fracture.
● No radiographic abnormalities. ● Radiographs recom- mended: a periapical view. Additional radiographs are indicated if other signs or symptoms are present.
● In case of marked infractions, etching and sealing with resin to prevent discoloration of the infraction lines. Otherwise, no treatment is necessary.
● No follow-up is generally needed for infraction injuries unless they are associated with a luxation injury or other fracture types.
● Asymptomatic ● Positive response to pulp testing. ● Continuing root development in immature teeth.
● Symptomatic ● Negative response to pulp testing. ● Signs of apical periodontitis. ● No continuing root development in immature teeth. ● Endodontic therapy appropriate for stage of root development is indicated.
ENAMEL FRACTURE Clinical findings
Radiographic findings
Treatment
Followup
Favorable Outcome
Unfavorable Outcome
● A complete fracture of the enamel. ● Loss of enamel. No visible sign of exposed dentin. ● Not tender. If tenderness is observed evaluate the tooth for a possible luxation or root fracture injury. ● Normal mobility. ● Sensibility pulp test usually positive.
● Enamel loss is visible. ● Radiographs recom-mended: periapical, occlusal and eccentric exposures. They are recommended in order to rule out the possible presence of a root fracture or a luxation injury. ● Radiograph of lip or cheek to search for tooth fragments or foreign materials.
● If the tooth fragment is available, it can be bonded to the tooth. ● Contouring or restoration with composite resin depending on the extent and location of the fracture.
6-8 weeks C++ 1 year C++
● Asymptomatic ● Positive response to pulp testing. ● Continuing root development in immature teeth. ● Continue to next evaluation.
● Symptomatic ● Negative response to pulp testing. ● Signs of apical periodontitis ● No continuing root development in immature teeth. ● Endodontic therapy appropriate for stage of root development is indicated.
+ = for crown fractured teeth with concomitant luxation injury, use the luxation followup schedule. C++ = clinical and radiographic examination. Vol. 1 Issue 11 L.E.D. E-Journal Page 231
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Follow-Up Procedures for fractures of teeth and alveolar bone+
Favorable and Unfavorable outcomes include some, but not necessarily all, of the
following: ENAMEL-DENTIN-
FRACTURE Clinical findings
Radiographic findings
Treatment
Follow-Up
Favorable Outcome
Unfavorable Outcome
● A fracture confined to enamel and dentin with loss of tooth structure, but not exposing the pulp. ● Percussion test: not tender. If tenderness is observed, evaluate the tooth for possible luxation or root fracture injury. ● Normal mobility. ● Sensibility pulp test usually positive.
● Enamel-dentin loss is visible. ● Radiographs recom-mended: periapical, occlusal and eccentric exposure to rule out tooth displacement or possible presence of root fracture. ● Radiograph of lip or cheek lacerations to search for tooth fragments or foreign materials.
● If a tooth fragment is available, it can be bonded to the tooth. Otherwise perform a provisional treatment by covering the exposed dentin with glass- Ionomer or a more permanent restoration using a bonding agent and composite resin, or other accepted dental restorative materials ● If the exposed dentin is within 0.5mm of the pulp (pink, no bleeding) place calcium hydroxide base and cover with a material such as a glass ionomer.
6-8 weeks C++ 1 year C++
● Asymptomatic ● Positive response to pulp testing. ● Continuing root development in immature teeth ● Continue to next evaluation
● Symptomatic ● Negative response to pulp testing. ● Signs of apical periodontitis. ● No continuing root development in immature teeth. ● Endodontic therapy appropriate for stage of root development is indicated.
ENAMEL-DENTIN-PULP FRACTURE
Clinical findings
Radiographic findings
Treatment
Favorable Outcome
Unfavorable Outcome
● A fracture involving enamel and dentin with loss of tooth structure and exposure of the pulp. ● Normal mobility ● Percussion test: not tender. If tenderness is observed, evaluate for possible luxation or root fracture injury. ● Exposed pulp sensitive to stimuli.
● Enamel – dentin loss visible. ● Radiographs recommended: periapical, occlusal and eccentric exposures, to rule out tooth displacement or possible presence of root fracture. ● Radiograph of lip or cheek lacerations to search for tooth fragments or foreign materials.
● In young patients with immature, still developing teeth, it is advantageous to preserve pulp vitality by pulp capping or partial pulpotomy. Also, this treatment is the choice in young patients with completely formed teeth. ● Calcium hydroxide is a suitable material to be placed on the pulp wound in such procedures. ● In patients with mature apical development, root canal treatment is usually the treatment of choice, although pulp capping or partial pulpotomy also may be selected. ● If tooth fragment is available, it can be bonded to the tooth. ● Future treatment for the fractured crown may be restoration with other accepted dental restorative materials.
6-8 weeks C++ 1 year C++
● Asymptomatic. ● Positive response to pulp testing. ● Continuing root development in immature teeth. ● Continue to next evaluation.
● Symptomatic. ● Negative response to pulp testing. ● Signs of apical periodontitis. ● No continuing root development in immature teeth. ● Endodontic therapy appropriate for stage of root development is indicated.
+ = for crown fractured teeth with concomitant luxation injury, use the luxation followup schedule C++ = clinical and radiographic examination. Vol. 1 Issue 11 L.E.D. E-Journal Page 232
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
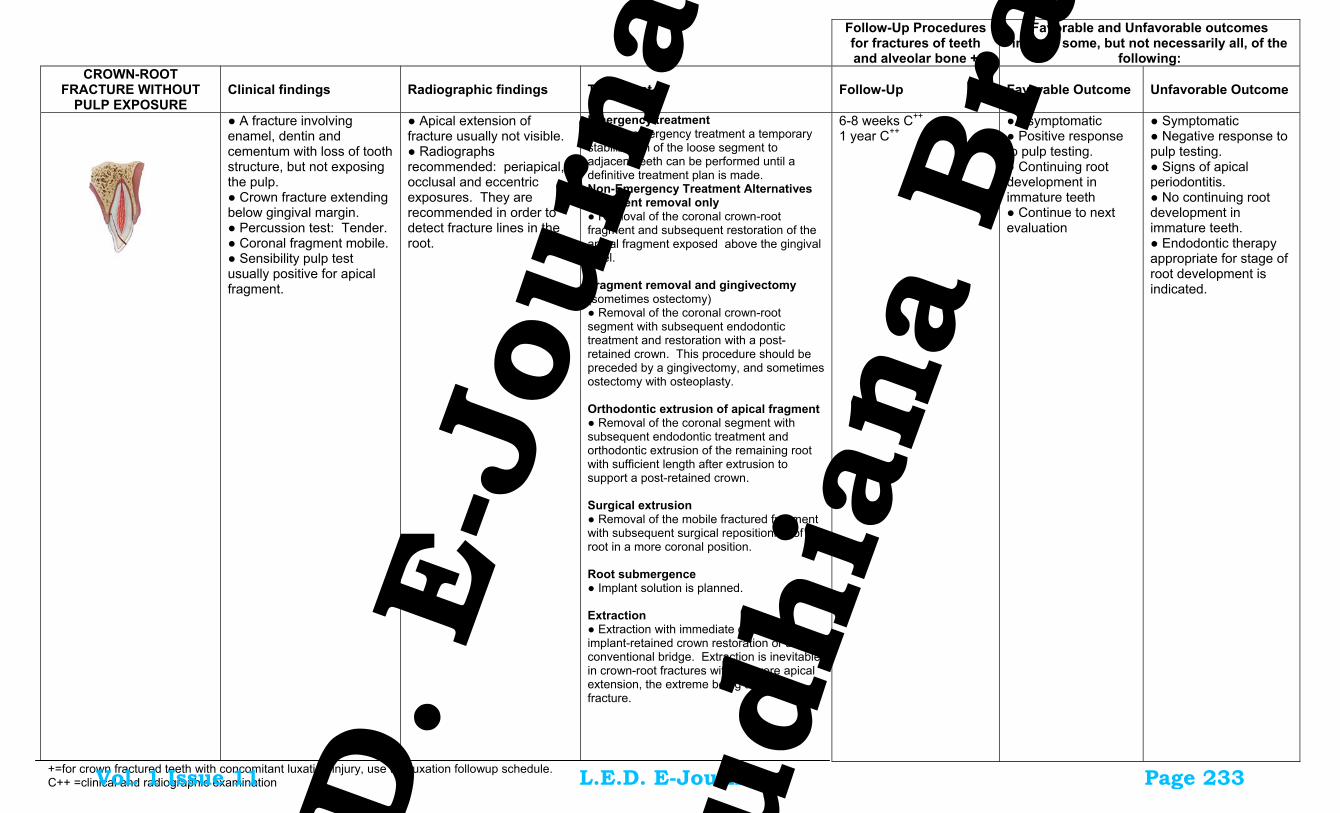
Follow-Up Procedures for fractures of teeth and alveolar bone +
Favorable and Unfavorable outcomes include some, but not necessarily all, of the
following: CROWN-ROOT
FRACTURE WITHOUT PULP EXPOSURE
Clinical findings
Radiographic findings
Treatment
Follow-Up
Favorable Outcome
Unfavorable Outcome
● A fracture involving enamel, dentin and cementum with loss of tooth structure, but not exposing the pulp. ● Crown fracture extending below gingival margin. ● Percussion test: Tender. ● Coronal fragment mobile. ● Sensibility pulp test usually positive for apical fragment.
● Apical extension of fracture usually not visible. ● Radiographs recommended: periapical, occlusal and eccentric exposures. They are recommended in order to detect fracture lines in the root.
Emergency treatment ● As an emergency treatment a temporary stabilization of the loose segment to adjacent teeth can be performed until a definitive treatment plan is made. Non-Emergency Treatment Alternatives Fragment removal only ● Removal of the coronal crown-root fragment and subsequent restoration of the apical fragment exposed above the gingival level. Fragment removal and gingivectomy (sometimes ostectomy) ● Removal of the coronal crown-root segment with subsequent endodontic treatment and restoration with a post-retained crown. This procedure should be preceded by a gingivectomy, and sometimes ostectomy with osteoplasty. Orthodontic extrusion of apical fragment ● Removal of the coronal segment with subsequent endodontic treatment and orthodontic extrusion of the remaining root with sufficient length after extrusion to support a post-retained crown. Surgical extrusion ● Removal of the mobile fractured fragment with subsequent surgical repositioning of the root in a more coronal position. Root submergence ● Implant solution is planned. Extraction ● Extraction with immediate or delayed implant-retained crown restoration or a conventional bridge. Extraction is inevitable in crown-root fractures with a severe apical extension, the extreme being a vertical fracture.
6-8 weeks C++
1 year C++
● Asymptomatic ● Positive response to pulp testing. ● Continuing root development in immature teeth ● Continue to next evaluation
● Symptomatic ● Negative response to pulp testing. ● Signs of apical periodontitis. ● No continuing root development in immature teeth. ● Endodontic therapy appropriate for stage of root development is indicated.
+=for crown fractured teeth with concomitant luxation injury, use the luxation followup schedule. C++ =clinical and radiographic examination
Vol. 1 Issue 11 L.E.D. E-Journal Page 233
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
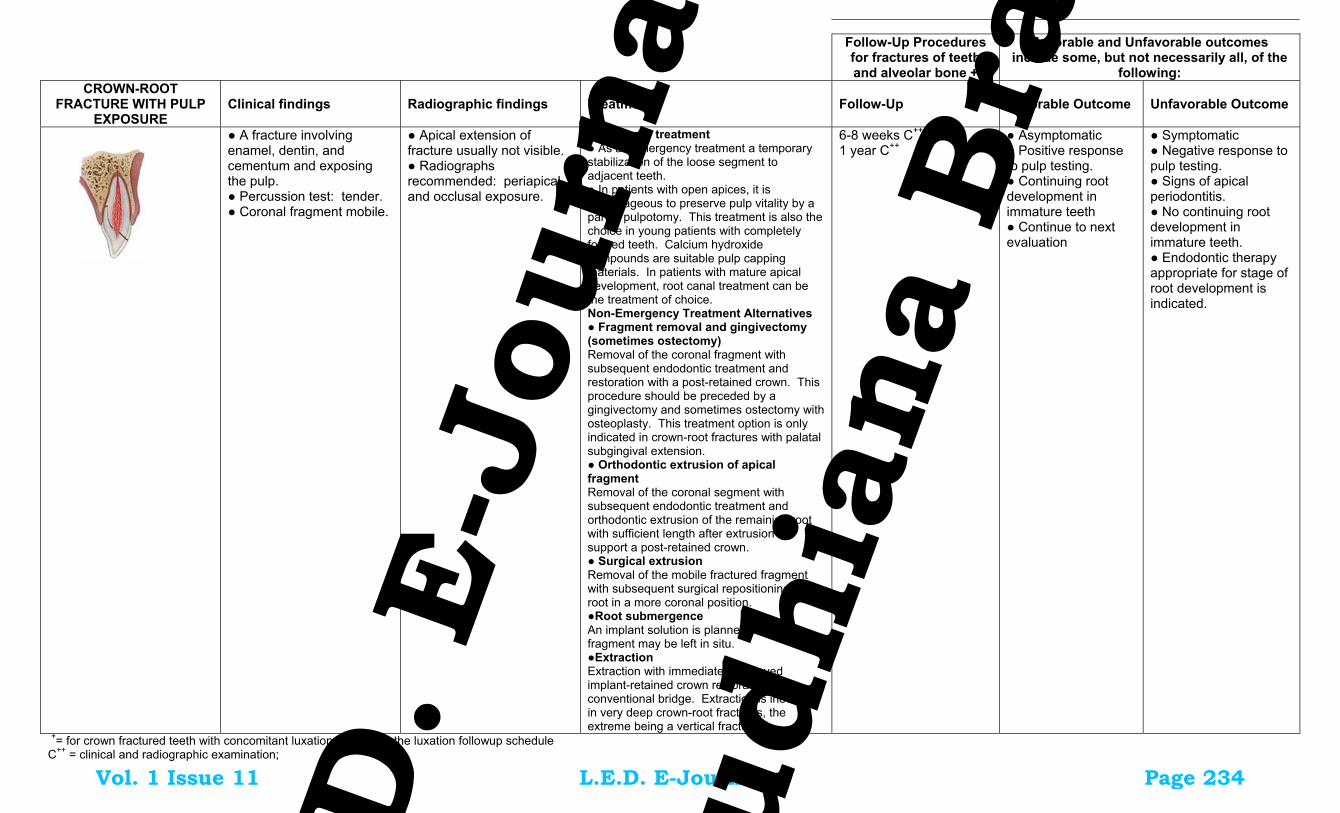
Follow-Up Procedures for fractures of teeth and alveolar bone +
Favorable and Unfavorable outcomes include some, but not necessarily all, of the
following: CROWN-ROOT
FRACTURE WITH PULP EXPOSURE
Clinical findings
Radiographic findings
Treatment
Follow-Up
Favorable Outcome
Unfavorable Outcome
● A fracture involving enamel, dentin, and cementum and exposing the pulp. ● Percussion test: tender. ● Coronal fragment mobile.
● Apical extension of fracture usually not visible. ● Radiographs recommended: periapical and occlusal exposure.
Emergency treatment ● As an emergency treatment a temporary stabilization of the loose segment to adjacent teeth. ● In patients with open apices, it is advantageous to preserve pulp vitality by a partial pulpotomy. This treatment is also the choice in young patients with completely formed teeth. Calcium hydroxide compounds are suitable pulp capping materials. In patients with mature apical development, root canal treatment can be the treatment of choice. Non-Emergency Treatment Alternatives ● Fragment removal and gingivectomy (sometimes ostectomy) Removal of the coronal fragment with subsequent endodontic treatment and restoration with a post-retained crown. This procedure should be preceded by a gingivectomy and sometimes ostectomy with osteoplasty. This treatment option is only indicated in crown-root fractures with palatal subgingival extension. ● Orthodontic extrusion of apical fragment Removal of the coronal segment with subsequent endodontic treatment and orthodontic extrusion of the remaining root with sufficient length after extrusion to support a post-retained crown. ● Surgical extrusion Removal of the mobile fractured fragment with subsequent surgical repositioning of the root in a more coronal position. ●Root submergence An implant solution is planned, the root fragment may be left in situ. ●Extraction Extraction with immediate or delayed implant-retained crown restoration or a conventional bridge. Extraction is inevitable in very deep crown-root fractures, the extreme being a vertical fracture
6-8 weeks C++
1 year C++
● Asymptomatic ● Positive response to pulp testing. ● Continuing root development in immature teeth ● Continue to next evaluation
● Symptomatic ● Negative response to pulp testing. ● Signs of apical periodontitis. ● No continuing root development in immature teeth. ● Endodontic therapy appropriate for stage of root development is indicated.
+= for crown fractured teeth with concomitant luxation injury, use the luxation followup schedule C++ = clinical and radiographic examination; Vol. 1 Issue 11 L.E.D. E-Journal Page 234
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Follow-Up Procedures
for fractures of teeth and alveolar bone
Favorable and Unfavorable outcomes include some, but not necessarily all, of the
following:++ ROOT FRACTURE Clinical findings Radiographic findings Treatment Favorable Outcome Unfavorable Outcome ●The coronal segment may be
mobile and may be displaced. ● The tooth may be tender to percussion. ● Bleeding from the gingival sulcus may be noted. ● Sensibility testing may give negative results initially, indicating transient or permanent neural damage. ● Monitoring the status of the pulp is recommended. ● Transient crown discoloration (red or grey) may occur.
● The fracture involves the root of the tooth and is in a horizontal or oblique plane. ● Fractures that are in the horizontal plane can usually be detected in the regular periapical 90o angle film with the central beam through the tooth. This is usually the case with fractures in the cervical third of the root. ● If the plane of fracture is more oblique which is common with apical third fractures, an occlusal view or radiographs with varying horizontal angles are more likely to demonstrate the fracture including those located in the middle third.
● Reposition, if displaced, the coronal segment of the tooth as soon as possible. ● Check position radiographically. ● Stabilize the tooth with a flexible splint for 4 weeks. If the root fracture is near the cervical area of the tooth, stabilization is beneficial for a longer period of time (up to 4 months). ● It is advisable to monitor healing for at least one year to determine pulpal status. ● If pulp necrosis develops, root canal treatment of the coronal tooth segment to the fracture line is indicated to preserve the tooth.
4 Weeks S+, C++
6-8 Weeks C++
4 Months S++*, C++ 6 Months C++
1 Year C++ 5 Years C++
● Positive response to pulp testing (false negative possible up to 3 months). ● Signs of repair between fractured segments. ● Continue to next evaluation.
● Symptomatic ● Negative response to pulp testing (false negative possible up to 3 months). ● Extrusion of the coronal segment. ● Radiolucency at the fracture line. ● Clinical signs of periodontitis or abscess associated with the fracture line. ● Endodontic therapy appropriate for stage of root development is indicated.
ALVEOLAR FRACTURE Clinical findings Radiographic findings Treatment Follow-Up Favorable Outcome Unfavorable Outcome ● The fracture involves the
alveolar bone and may extend to adjacent bone. ● Segment mobility and dislocation with several teeth moving together are common findings. ● An occlusal change due to misalignment of the fractured alveolar segment is often noted. ● Sensibility testing may or may not be positive.
● Fracture lines may be located at any level, from the marginal bone to the root apex. ● In addition to the 3 angulations and occlusal film, additional views such as a panoramic radiograph can be helpful in determining the course and position of the fracture lines.
● Reposition any displaced segment and then splint. ● Suture gingival laceration if present. ● Stabilize the segment for 4 weeks.
4 Weeks S+, C++ 6-8 Weeks C++ 4 Months C++ 6 Months C++
1 Year C++
5 Years C++
● Positive response to pulp testing (false negative possible up to 3 months). ● No signs of apical periodontitis. ●Continue to next evaluation.
● Symptomatic ● Negative response to pulp testing (false negative possible up to 3 months). ● Signs of apical periodontitis or external inflammatory root resorption. ● Endodontic therapy appropriate for stage of root development is indicated.
S+=splint removal; S++=splint removal in cervical third fractures. C++ = clinical and radiographic examination. ++=Whenever there is evidence of external inflammatory root resorption, root canal therapy should be initiated immediately, with the use of calcium hydroxide as an intra-canal medication. Vol. 1 Issue 11 L.E.D. E-Journal Page 235
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

2. Treatment Guidelines for Luxation Injuries
Follow-Up Procedures for luxated permanent teeth
Favorable and Unfavorable outcomes include some, but not necessarily all, of the following:++
CONCUSSION Clinical findings Radiographic findings Treatment Favorable Outcome Unfavorable Outcome ● The tooth is tender to touch
or tapping; it has not been displaced and does not have increased mobility. ● Sensibility tests are likely to give positive results.
●No radiographic abnormalities
● No treatment is needed. ● Monitor pulpal condition for at least one year.
4 Weeks C++
6-8 Weeks C++ 1 Year C++
● Asymptomatic ● Positive response to pulp testing ● False negative possible up to 3 months. ● Continuing root development in immature teeth ● Intact lamina dura
● Symptomatic ● Negative response to pulp testing ● False negative possible up to 3 months ●No continuing root development in immature teeth, signs of apical periodontitis. ● Endodontic therapy appropriate for stage of root development is indicated.
SUBLUXATION Clinical findings Radiographic findings Treatment Follow-Up Favorable Outcome Unfavorable Outcome ● The tooth is tender to touch
or tapping and has increased mobility; it has not been displaced. ● Bleeding from gingival crevice may be noted. ● Sensibility testing may be negative initially indicating transient pulpal damage. ● Monitor pulpal response until a definitive pulpal diagnosis can be made.
●Radiographic abnormalities are usually not found.
● Normally no treatment is needed, however a flexible splint to stabilize the tooth for patient comfort can be used for up to 2 weeks.
2 Weeks S+, C++
4 Weeks C++
6-8 Weeks C++
6 Months C++
1 Year C++
● Asymptomatic ● Positive response to pulp testing ● False negative possible up to 3 months. ● Continuing root development in immature teeth ● Intact lamina dura
● Symptomatic ● Negative response to pulp testing ● False negative possible up to 3 months ● External inflammatory resorption. ● No continuing root development in immature teeth, signs of apical periodontitis. ● Endodontic therapy appropriate for stage of root development is indicated.
EXTRUSIVE LUXATION Clinical Findings Radiographic findings Treatment Follow-Up Favorable Outcome Unfavorable Outcome ● The tooth appears elongated
and is excessively mobile. ● Sensibility tests will likely give negative results.
●Increased periodontal ligament space apically.
● Reposition the tooth by gently re-inserting It into the tooth socket. ● Stabilize the tooth for 2 weeks using a flexible splint. ● In mature teeth where pulp necrosis is anticipated or if several signs and symptoms indicate that the pulp of mature or immature teeth became necrotic, root canal treatment is indicated.
2 Weeks S+, C++ 4 Weeks C++
6-8 Weeks C++ 6 Months C++
1 Year C++
Yearly 5 years C++
● Asymptomatic ● Clinical and radiographic signs of normal or healed periodontium. ● Positive response to pulp testing (false negative possible up to 3 months). ● Marginal bone height corresponds to that seen radiographically after repositioning. ● Continuing root development in immature teeth.
● Symptoms and radiographic sign consistent with apical periodontitis. ● Negative response to pulp testing (false negative possible up to 3 months). ● If breakdown of marginal bone, splint for an additional 3-4 weeks. ● External inflammatory root resorption. ● Endodontic therapy appropriate for stage of root development is indicated.
S+=splint removal; C++ = clinical and radiographic examination. ++=Whenever there is evidence of external inflammatory root resorption, root canal therapy should be initiated immediately, with the use of calcium hydroxide as an intra-canal medication. Vol. 1 Issue 11 L.E.D. E-Journal Page 236
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Follow-Up Procedures for luxated permanent
teeth
Favorable and Unfavorable outcomes include some, but not necessarily all, of the following:++
LATERAL LUXATION Clinical findings Radiographic findings Treatment Favorable Outcome Unfavorable Outcome ● The tooth is displaced,
usually in a palatal/lingual or labial direction. ● It will be immobile and percussion usually gives a high, metallic (ankylotic) sound. ● Fracture of the alveolar process present. ● Sensibility tests will likely give negative results
● The widened periodontal ligament space is best seen on eccentric or occlusal exposures.
● Reposition the tooth digitally or with forceps to disengage it from its bony lock and gently reposition it into its original location. ● Stabilize the tooth for 4 weeks using a flexible splint. ● Monitor the pulpal condition. ● If the pulp becomes necrotic, root canal treatment is indicated to prevent root resorption.
2 Weeks, C++ 4 Weeks S+, C++ 6-8 Weeks C++
6 Months C++ 1 Year C++
Yearly for 5 years C++
● Asymptomatic ● Clinical and radiographic signs of normal or healed periodontium. ● Positive response to pulp testing (false negative possible up to 3 months). ● Marginal bone height corresponds to that seen radiographically after repositioning. ●Continuing root development in immature teeth
● Symptoms and radiographic signs consistent with apical periodontitis. ● Negative response to pulp testing (false negative possible up to 3 months). ● If breakdown of marginal bone, splint for an additional 3-4 weeks. ● External inflammatory root resorption or replacement resorption ● Endodontic therapy appropriate for stage of root development is indicated.
INTRUSIVE LUXATION Clinical findings Radiographic findings Treatment Follow-Up Favorable Outcome Unfavorable ● The tooth is displaced axially
into the alveolar bone. ● It is immobile and percussion may give a high, metallic (ankylotic) sound. ● Sensibility tests will likely give negative results.
●The periodontal ligament space may be absent from all or part of the root. ● The cemento-enamel junction is located more apically in the intruded tooth than in adjacent non-injured teeth, at times even apical to the marginal bone level.
Teeth with incomplete root formation ● Allow eruption without intervention ● If no movement within few weeks, initiate orthodontic repositioning. ● If tooth is intruded more than 7mm, reposition surgically or orthodontically. Teeth with complete root formation: ● Allow eruption without intervention if tooth intruded less than 3mm. If no movement after 2-4 weeks, reposition surgically or orthodontically before ankylosis can develop. ● If tooth is intruded 3-7 mm, reposition surgically or orthodontically. ● If tooth is intruded beyond 7mm, reposition surgically. ● The pulp will likely become necrotic in teeth with complete root formation. Root canal therapy using a temporary filling with calcium hydroxide is recommended and treatment should begin 2-3 weeks after repositioning. ● Once an intruded tooth has been repositioned surgically or orthodontically, stabilize with a flexible splint for 4 weeks.
2 Weeks, C++ 4 Weeks S+, C++
6-8 Weeks C++
6 Months C++
1 Year C++
Yearly for 5 years C++
● Tooth in place or erupting. ● Intact lamina dura ● No signs of resorption. ● Continuing root development in immature teeth.
● Tooth locked in place/ankylotic tone to percussion. ● Radiographic signs of apical periodontitis ● External inflammatory root resorption or replacement resorption. ● Endodontic therapy appropriate for stage of root development is indicated.
S+=splint removal; C++ = clinical and radiographic examination. ++= whenever there is evidence of external inflammatory root resorption, root canal therapy should be initiated immediately, with the use of calcium hydroxide as an intra-canal medication. Vol. 1 Issue 11 L.E.D. E-Journal Page 237
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
Page 1 of 11
Avulsion of permanent teeth
Avulsion of permanent teeth is seen in 0.5‐3% of all dental injuries (1,2). Numerous studies show that this injury is one of the most serious dental injuries and the prognosis is very much dependent on the actions taken at the place of accident and promptly after the avulsion (2‐27). Replantation is in most situations the treatment of choice, but cannot always be carried out immediately. An appropriate emergency management and treatment plan are important for a good prognosis. There are also individual situations when replantation is not indicated (e.g. severe caries or periodontal disease, non‐cooperating patient, severe medical conditions (e.g. immunosuppression and severe cardiac conditions) which must be dealt with individually. Replantation may successfully save the tooth, but it is important to realize that some of the replanted teeth have lower chances of long term survival and may even be lost or extracted at a later stage.
Guidelines for the emergency management are useful for delivering the best care possible in an efficient manner. The International Association of Dental Traumatology (IADT) has developed a consensus statement after an update of the dental literature and discussions in expert groups. Experienced international researchers and clinicians from various specialties and general dentistry were included in the groups. In cases in which the data did not appear conclusive, recommendations were based on the consensus opinion and in some situations on majority decision among the IADT board members. All recommendations are not evidence based on a high level. The guidelines should therefore be seen as the current best evidence and practice based on literature research and professionals’ opinion.
Guidelines should assist dentists, other health care professionals and patients in decision making. Also, they should be credible, readily understandable and practical with the aim of delivering appropriate care as effectively and efficiently as possible.It is understood that guidelines are to be applied with judgment of the specific clinical circumstances, clinicians’ judgments and patients’ characteristics, including but not limited to compliance, finances and understanding of the immediate and long‐term outcomes of treatment alternatives versus non‐treatment. The IADT cannot and does not guarantee favorable outcomes from strict adherence to the Guidelines, but believe that their application can maximize the chances of a favorable outcome. Guidelines undergo periodic updates. The following guidelines by the International Association of Dental Traumatology (IADT) represent an updated set of guidelines based on the original guidelines published in 2007 (28‐30).
Vol. 1 Issue 11 L.E.D. E-Journal Page 238
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Page 2 of 11
In these IADT Guidelines for management of avulsed permanent teeth the literature has been searched using Medline and Scopus databases using the search words: avulsion, exarticulation and replantation. The task group has then discussed the emergency treatment in detail and reached consensus of what to recommend today as best practice for the emergency management. This text is aiming at giving the concise, short necessary advice for treatment in the emergency situation. More detailed description of protocols, methods and documentation for clinical assessment and diagnosis of different dental injuries can be found in articles, textbooks and manuals (2,24) and in the interactive web site Dental Trauma Guide http://dentaltraumaguide.org
The final decision regarding patient care remains primarily in the hand of the treating dentist. For ethical reasons it is important that the dentist provides the patient and guardian with pertinent information relating to treatment so also the patient and guardian has as much influence in the decision making process as possible.
First aid for avulsed teeth at the place of accident (2,10,24,25,31‐55)
Dentists should always be prepared to give appropriate advice to the public about first aid for avulsed teeth. An avulsed permanent tooth is one of the few real emergency situations in dentistry. In addition to increasing the public awareness by, e.g. mass media campaigns, healthcare professionals. Guardians and teachers should receive information on how to proceed following these severe unexpected injuries. Also, instructions may be given by telephone to people at the emergency site. Immediate replantation is the best treatment at the place of accident. If for some reasons this cannot be carried out, there are alternatives such as using various storage media
If a tooth is avulsed, make sure it is a permanent tooth (primary teeth should not be replanted)
• Keep the patient calm. • Find the tooth and pick it up by the crown (the white part). Avoid touching the root. • If the tooth is dirty, wash it briefly (max 10 seconds) under cold running water and
reposition it. Try to encourage the patient/guardian to replant the tooth. Once the tooth is back in place, bite on a handkerchief to hold it in position.
• If this is not possible, or for other reasons when replantation of the avulsed tooth is not possible (e.g. an unconscious patient), place the tooth in a glass of milk or another suitable storage medium and bring with the patient to the emergency clinic. The tooth can also be transported in the mouth, keeping it inside the lip or cheek if the patient is conscious. If the patient is very young, he/she could swallow the tooth – therefor it is advisable to get the patient to spit in a container and place the tooth in it. Avoid storage in water!
• If there is access at the place of accident to special storage or transport media (e.g. tissue culture/transport medium, Hanks balanced storage medium (HBSS or saline) such media can preferably be used.
• Seek emergency dental treatment immediately.
Vol. 1 Issue 11 L.E.D. E-Journal Page 239
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
Page 3 of 11
The poster ‘Save a Tooth’ is written for the public and is available in several languages: English, Spanish, Portuguese, French, Icelandic, Italian, Arabic and Turkish and can be obtained at the IADT website: http://www.iadt‐dentaltrauma.org.
Treatment guidelines for avulsed permanent teeth (56‐96)
Choice of treatment is related to the maturity of the root (open or closed apex) and the condition of the periodontal ligament cells. The condition of the cells is depending on the storage medium and the time out of the mouth, especially the dry time is critical for survival of the cells. After a dry time of 60 minutes or more all PDL cells are non‐viable. For this reason, the dry time of the tooth, before it was placed replanted or placed in a storage medium, is very important to assess from the patient’s history.
From a clinical point of view it is important for the clinician to roughly assess the condition of the cells by classifying the avulsed tooth into one of the following three groups before starting treatment:
o The PDL cells are most likely viable (i.e. the tooth has been replanted immediately or after a very short time at the place of accident)
o The PDL cells may be viable but compromised. The tooth has been kept in storage medium (e.g. tissue culture medium, HBSS, saline, milk or saliva and the total dry time has been less than 60 min).
o The PDL cells are non‐viable. Examples of this is when the trauma history tells us that the total extra‐oral dry time has been more than 60 min regardless of if the tooth was stored in an additional medium or not, or if the storage medium was non‐physiologic.
1. Treatment guidelines for avulsed permanent teeth with closed apex
1a. The tooth has been replanted before the patient’s arrival at the clinic
• Leave the tooth in place. • Clean the area with water spray, saline or chlorhexidine. • Suture gingival lacerations, if present. • Verify normal position of the replanted tooth both clinically and radiographically. • Apply a flexible splint for up to 2 weeks (see Splinting). • Administer systemic antibiotics. (see Antibiotics).
Vol. 1 Issue 11 L.E.D. E-Journal Page 240
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
Page 4 of 11
• Check tetanus protection (see Tetanus). • Give patient instructions (See Patient instructions). • Initiate root canal treatment 7–10 days after replantation and before splint removal. ( See
Endodontic considerations). Follow‐up See: Follow‐up procedures
1b. The tooth has been kept in a physiologic storage medium or osmolality balanced medium and/or stored dry, the extraoral dry time has been less than 60 minutes
Physiologic storage media include e.g. tissue culture medium and cell transport media. Examples of osmolality balanced media are HBSS, saline and milk. Saliva can also be used.
• Clean the root surface and apical foramen with a stream of saline and soak the tooth in saline thereby removing contamination and dead cells from the root surface.
• Administer local anesthesia. • Irrigate the socket with saline. • Examine the alveolar socket. If there is a fracture of the socket wall, reposition it with a suitable
instrument. • Replant the tooth slowly with slight digital pressure. Do not use force. • Suture gingival lacerations, if present. • Verify normal position of the replanted tooth both clinically and radiographically. • Apply a flexible splint for up to 2 weeks, keep away from the gingiva. • Administer systemic antibiotics (see: Antibiotics). • Check tetanus protection (see Tetanus). • Give patient instructions (See Patient instructions). • Initiate root canal treatment 7–10 days after replantation and before splint removal (See
Endodontic considerations). Follow‐up See: Follow‐up procedures
1c. Dry time longer than 60 minutes or other reasons suggesting non‐viable cells
Delayed replantation has a poor long‐term prognosis. The periodontal ligament will be necrotic and not expected to heal. The goal in delayed replantation is, in addition to restoring the tooth for aesthetic, functional and psychological reasons, to maintain alveolar bone contour However, the expected eventual outcome is ankylosis and resorption of the root and the tooth will be lost eventually.
The technique for delayed replantation is:
Vol. 1 Issue 11 L.E.D. E-Journal Page 241
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Page 5 of 11
• Remove attached non‐viable soft tissue carefully e.g. with gauze. The best way to this has not yet been decided (See Future areas of research).
• Root canal treatment to the tooth can be carried out prior to replantation or later (See Endodontic considerations).
• In cases of delayed replantation, root canal treatment should be done either on the tooth prior to replantation, or it can be done 7–10 days later like in other replantation situations (See Endodontic considerations).
• Administer local anesthesia. • Irrigate the socket with saline. • Examine the alveolar socket. If there is a fracture of the socket wall, reposition it with a suitable
instrument. • Replant the tooth. • Suture gingival lacerations, if present. • Verify normal position of the replanted tooth clinically and radiographically. • Stabilize the tooth for 4 weeks using a flexible splint (See Splinting). • Administration of systemic antibiotics (See Antibiotics). • Check tetanus protection (See Tetanus). • Give patient instructions (See Patient instructions).
In order to slow down osseous replacement of the tooth, treatment of the root surface with fluoride
prior to replantation has been suggested (2% sodium fluoride solution for 20 min) but it should not be seen as an absolute recommendation Follow‐up See: Follow‐up procedures
In children and adolescents ankylosis is frequently associated with infraposition. Careful follow up is required and good communication is necessary to ensure the patient and guardian of this likely outcome. Decoronation may be necessary later when infraposition (>1mm) is seen. For more detailed information of this procedure the reader if referred to textbooks.
2. Treatment guidelines for avulsed permanent teeth with an open apex
Vol. 1 Issue 11 L.E.D. E-Journal Page 242
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
Page 6 of 11
2a. The tooth has been replanted before the patient’s arrival at the clinic
• Leave the tooth in place. • Clean the area with water spray, saline or chlorhexidine. • Suture gingival lacerations, if present. • Verify normal position of the replanted tooth both clinically and radiographically. • Apply a flexible splint for up to 2 weeks (see Splinting). • Administer systemic antibiotics (see Antibiotics). • Check tetanus protection (see Tetanus). • Give patient instructions (see Patient instructions). • The goal for replanting still‐developing (immature) teeth in children is to allow for possible
revascularization of the pulp space. If that does not occur, root canal treatment may be recommended (see Endodontic considerations).
Follow‐up See: Follow‐up procedures
2b. The tooth has been kept in a physiologic storage medium or osmolality balanced medium and/or stored dry, the extraoral dry time has been less than 60 minutes
Physiologic storage media include e.g. tissue culture medium and cell transport media. Examples of osmolality balanced media are HBSS, saline and milk. Saliva can also be used.
• If contaminated, clean the root surface and apical foramen with a stream of saline. • Topical application of antibiotics has been shown to enhance chances for revascularization of
the pulp and can be considered if available (See Antibiotics). • Administer local anesthesia. • Examine the alveolar socket. • If there is a fracture of the socket wall, reposition it with a suitable instrument. • Remove the coagulum in the socket and replant the tooth slowly with slight digital pressure. • Suture gingival lacerations, especially in the cervical area. • Verify normal position of the replanted tooth clinically and radiographically. Apply a flexible
splint for up to 2 weeks (see splinting). • Administer systemic antibiotics (see Antibiotics). • Check tetanus protection (see Tetanus). • Give patient instructions (see Patient instructions). • The goal for replanting still‐developing (immature) teeth in children is to allow for possible
revascularization of the pulp space. The risk of infection related root resorption should be weighed up against the chances of revascularization. Such resorption is very rapid in teeth of children. If revascularization does not occur, root canal treatment may be recommended (see Endodontic considerations).
Vol. 1 Issue 11 L.E.D. E-Journal Page 243
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
Page 7 of 11
Follow‐up See Follow‐up procedures.
2c. Dry time longer than 60 minutes or other reasons suggesting non‐viable cells
Delayed replantation has a poor long‐term prognosis. The periodontal ligament will be necrotic and not expected to heal. The goal in delayed replantation is to restore the tooth to the dentition for aesthetic, functional and psychological reasons and to maintain alveolar contour. The eventual outcome will be ankylosis and resorption of the root. The technique for delayed replantation is:
• Remove attached non‐viable soft tissue carefully e.g. with gauze. The best way to this has not yet been decided (See Future areas of research).
• Root canal treatment to the tooth can be carried out prior to replantation or later (See Endodontic considerations).
• Administer local anesthesia. • Remove the coagulum from the socket with a stream of saline. Examine the alveolar socket. If
there is a fracture of the socket wall, reposition it with a suitable instrument. • Replant the tooth slowly with slight digital pressure. Suture gingival laceration. Verify normal
position of the replanted tooth clinically and radiographically. • Stabilize the tooth for 4 weeks using a flexible splint (See Splinting). • Administer systemic antibiotics (See Antibiotics). • Check tetanus protection (See Tetanus). • Give patient instructions (See Patient instructions).
In order to slow down osseous replacement of the tooth, treatment of the root surface with fluoride prior to replantation (2% sodium fluoride solution for 20 min) has been suggested but it should not be seen as an absolute recommendation
Follow‐up See Follow‐up procedures.
Ankylosis is unavoidable after delayed replantation and must be taken into consideration. In children and adolescents ankylosis is frequently associated with infraposition. Careful follow up is required and good communication is necessary to ensure the patient and guardian of this likely outcome. Decoronation may be necessary when infraposition (>1mm) is seen. For more detailed information of this procedure the reader if referred to textbooks.
Anesthetics (64‐66)
Patients and guardians are recommended by us to do replantation at the place of accident without anesthesia. In the clinic however, where local anesthetics is available, there is no need not to
Vol. 1 Issue 11 L.E.D. E-Journal Page 244
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Page 8 of 11
omit local anesthesia, especially since there are often concomitant injuries. Concern is sometimes raised whether there are risks of compromising healing by using vasoconstrictor in the anesthesia. Evidence is weak for omitting vasoconstrictor in the oral & maxillofacial region and must be further documented before any recommendations against the use of it can be given (see suggested future areas of research at the end of this article). Block anesthesia (e.g. infraorbital nerve block) may be considered as an alternative to infiltration anesthesia in more severely injured areas and must be related to the clinicians’ experience of such blocking techniques.
Antibiotics (67‐76)
The value of systemic administration of antibiotics in human after replantation is still questionable as clinical studies have not demonstrated its value. Experimental studies have however, usually shown positive effects upon both periodontal and pulpal healing especially when administered topically. For this reason antibiotics are in most situations recommended after replantation of teeth. In addition, the patient’s medical status or concomitant injuries may warrant antibiotic coverage.
For systemic administration tetracycline is the first choice in appropriate dose for patient age and weight the first week after replantation. The risk of discoloration of permanent teeth must be considered before systemic administration of tetracycline in young patients. In many countries tetracycline is not recommended for patients under 12 years of age. A penicillin phenoxymethylpenicillin (Pen V,) or amoxycillin, in an appropriate dose for age and weight the first week, can be given as alternative to tetracycline.
Topical antibiotics (minocycline or doxycycline,1mg per 20ml of saline for 5 minutes soak) appear experimentally to have a beneficial effect in increasing the chance of pulpal space revascularization and periodontal healing and may be considered in immature teeth (2b).
Tetanus ( 2,24,25 ) Refer the patient to a physician for evaluation of need for a tetanus booster if the avulsed tooth
has contacted soil or tetanus coverage is uncertain.
Splinting of replanted teeth (77‐83)
It is considered best practice to maintain the repositioned tooth in correct position, provide patient comfort and improve function Current evidence supports short‐term, flexible splints for splinting of replanted teeth. Studies have shown that periodontal and pulpal healing is promoted if the replanted tooth is given a chance for slight motion and the splinting time is not too long. Given this there is so far no specific type of splint related to healing outcomes. The splint should be placed on the buccal surfaces of the maxillary teeth to enable lingual access for endodontic procedures and to avoid occlusal interference.
Vol. 1 Issue 11 L.E.D. E-Journal Page 245
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Page 9 of 11
Replanted permanent teeth should be splinted up to 2 weeks. Various types of acid etch bonded splints have been widely used to stabilize avulsed teeth because they allow good oral hygiene and are well tolerated by the patients. For a detailed description of how to make a splint the reader is referred to articles, textbooks and manuals and the web site Dental Trauma Guide www.dentaltraumaguide.org
Patient instructions (2,24,25)
Patient compliance with follow‐up visits and home care contributes to satisfactory healing following an injury. Both patients and guardians of young patients should be advised regarding care of the replanted tooth for optimal healing and prevention of further injury.
• Avoid participation in contact sports. • Soft diet for up to 2 weeks. Thereafter normal function as soon as possible • Brush teeth with a soft toothbrush after each meal • Use a chlorhexidine (0.1%) mouth rinse twice a day for 1 week.
Endodontic considerations (84‐94)
If root canal treatment is indicated (teeth with closed apex), the ideal time to begin treatment is 7–10 days post replantation. Calcium hydroxide is recommended as an intra‐canal medication for up to 1 month followed by root canal filling with an acceptable material. Alternatively if an antibiotic‐corticosteroid paste is chosen to be used as an anti‐inflammatory, anti‐clastic intra‐canal medicament, it may be placed immediately or shortly following replantation and left for at least 2 weeks. If the antibiotic in the paste is dechlortetracycline, there is a risk of tooth discoloration and care should be taken to confine the paste to the root canal and avoid contact of the paste with the pulp chamber walls
If the tooth has been dry for more than 60 min before replantation. The root canal treatment may be done extra‐orally prior to replantation
In teeth with open apexes, which have been replanted immediately or kept in appropriate storage media prior to replantation, pulp revascularization is possible. The risk of infection related root resorption should be weighed up against the chances of obtaining pulp space revascularization. Such resorption is very rapid in teeth of children. For very immature teeth root canal treatment should be avoided unless there is clinical or radiographic evidence of pulp necrosis.
Follow‐up procedures (2, 6‐9,24,25)
Clinical control
Vol. 1 Issue 11 L.E.D. E-Journal Page 246
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
Page 10 of 11
Replanted teeth should be monitored by clinical and radiographic control after 4 weeks, 3 months, 6 months, one year and yearly thereafter. Clinical and radiographic examination will provide information to determine outcome. Evaluation may include the findings described as follows.
Favorable outcome
Closed apex. Asymptomatic, normal mobility, normal percussion sound. No radiographic evidence of resorption or periradicular osteitis: the lamina dura should appear normal.
Open apex. Asymptomatic, normal mobility, normal percussion sound. Radiographic evidence of arrested or continued root formation and eruption. Pulp canal obliteration is to be expected.
Unfavorable outcome
Closed apex. Symptomatic, excessive mobility or no mobility (ankylosis) with high‐pitched percussion sound. Radiographic evidence of resorption (inflammatory, infection‐related resorption, or ankylosis‐related replacement resorption). When ankylosis occurs in a growing patient, infraposition of the tooth is highly likely leading to disturbance in alveolar and facial growth over the short, medium and long term.
Open apex. Symptomatic, excessive mobility or no mobility (ankylosis) with high‐pitched percussion sound. In the case of ankylosis, the crown of the tooth will appear to be in an infraposition. Radiographic evidence of resorption (inflammatory, infection‐related resorption, or ankylosis‐related replacement resorption) or absence of continued root formation. When ankylosis occurs in a growing patient, infraposition of the tooth is highly likely to occur leading to disturbance of alveolar and facial growth over the short, medium and long term.
Loss of tooth In cases where teeth are lost in the emergency phase or will be lost later after trauma, discussions with colleagues, where available, who have expertise with managing such cases is prudent especially in growing patients. Ideally these discussions should take place before the tooth shows signs of infraposition. Appropriate treatment options may include decoronation, autotransplantation, resin retained bridge, denture, orthodontic space closure with composite modification and sectional osteotomy. Such treatment decisions are based on a full discussion with the child and parents, clinician’s expertise and aim to keep all options open until maturity is reached. After growth is completed implant treatment can also be considered. The clinician is referred to textbooks and articles for further readings regarding these procedures.
Future areas of research ‐ methods discussed but not included as recommendations in the guidelines this time
Vol. 1 Issue 11 L.E.D. E-Journal Page 247
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Page 11 of 11
A number of promising treatment procedures for avulsed teeth have been discussed in the consensus group. Some of these treatment suggestions do have certain experimental evidence and some of them are even used today in clinical practice: According to the group members, there is currently insufficient weight or quality of clinical and/or experimental evidence for some of these methods to be recognized as recommendations in the guidelines this time. These and some other important fields are examples where the group advocates further research and documentation:
⋅ Methods for removal of non‐viable PDL ⋅ Conditioning the PDL with extra oral storage in tissue culture media prior to replantation ⋅ Conditioning the PDL with enamel matrix protein prior to replantation for teeth with short
extra oral periods ⋅ Topical treatment of root surface with fluoride for teeth with long extra oral period ⋅ Revascularization of pulp space and methods promoting this ⋅ Optimal splint types with regards to periodontal and pulpal healing ⋅ Effect on adrenaline content of local anesthesia on healing ⋅ Reducing the inflammation with corticosteroids ⋅ Extra oral root filling of teeth with less than a 60 min drying period ⋅ Use of titanium posts for root elongation and as alternatives to conventional root canal
treatment ⋅ Long term development of alveolar crest following replantation and decoronation
Acknowledgment: The authors wish to express their gratefulness to the Dental Trauma Guide team in Copenhagen, Denmark www.dentaltraumaguide.org for permission to use their illustrations for these Guidelines.
Vol. 1 Issue 11 L.E.D. E-Journal Page 248
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Primary dentition Guidelines
INJURIES IN THE PRIMARY DENTITION 1. Treatment guidelines for fractures of teeth and alveolar bone Follow-up Procedures
for fractures of teeth and alveolar bone
Favorable and Unfavorable outcomes include some, but not necessarily all, of the
following: ENAMEL FRACTURE
Clinical findings Radiographic findings
Treatment
Favorable Outcome Unfavorable Outcome
● Fracture involves enamel. ● No radiographic abnormalities
● Smooth sharp edges.
ENAMEL DENTIN FRACTURE
Clinical findings
Radiographic findings
Treatment
Favorable Outcome Unfavorable Outcome
● Fracture involves enamel and dentin; the pulp is not exposed.
● No radiographic abnormalities The relation between the fracture and the pulp chamber will be disclosed
If possible, seal completely the involved dentin with glass ionomer to prevent microleakage. In case of large lost tooth structure, the tooth can be restored with composite.
3-4 weeks C
CROWN FRACTURE
WITH EXPOSED PULP Clinical findings
Radiographic findings
Treatment
Followup
Favorable Outcome
Unfavorable Outcome
● Fracture involves enamel and dentin and the pulp is exposed.
● The stage of root development can be determined from one exposure.
● If possible preserve pulp vitality by partial pulpotomy. Calcium hydroxide is a suitable material for such procedures. A well-condensed layer of pure calcium hydroxide paste can be applied over the pulp, covered with a lining such as reinforced glass ionomer. Restore the tooth with composite.
● The treatment is depending on the child´s maturity and ability to cope. Extraction is usually the alternative option.
1 week C 6-8 weeks C+R 1 year C+R
● Continuing root development in immature teeth and a hard tissue barrier.
● Signs of apical periodontitis; no continuing root development in immature teeth. Extraction or root canal treatment
C=Clinical examination; R=Radiographic examination Vol. 1 Issue 11 L.E.D. E-Journal Page 249
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Primary dentition Guidelines
Follow-Up Procedures for fractures of teeth
and alveolar bone
Favorable and Unfavorable outcomes include some, but not necessarily all, of the
following: CROWN-ROOT FRACTURE Clinical findings Radiographic findings Treatment Favorable Outcome Unfavorable Outcome
● Fracture involves enamel, dentin and root structure; the pulp may or may not be exposed. ● Additional findings may include loose, but still attached, fragments of the tooth. ● There is minimal to moderate tooth displacement
● In laterally positioned fractures, the extent in relation to the gingival margin can be seen. One exposure is necessary to disclose multiple fragments
Depending on the clinical findings, two treatment scenarios may be considered:
● Fragment removal only. If the fracture involves only a small part of the root and the stable fragment is large enough to allow coronal restoration.
● Extraction in all other instances
In cases of fragment removal only: 1 week C 6-8 weeks C+R 1 year C(*)
● Asymptomatic; continuing root development in immature teeth
● Symptomatic; signs of apical periodontitis; no continuing root development in immature teeth. .
ROOT FRACTURE Clinical findings Radiographic findings Treatment Follow-Up Favorable Outcome Unfavorable Outcome
●The coronal fragment may be mobile and may be displaced.
● The fracture is usually located mid-root or in the apical third.
• If the coronal fragment is not displaced no treatment is required.
• If the coronal fragment is displaced, extract only that fragment. The apical fragment should be left to be resorbed
• No displacement: 1 week C, • 6-8 weeks C, • 1 year C+R and C(*) each subsequent year until exfoliation. • Extraction 1 year C+R and C(*)each subsequent year until exfoliation.
● Signs of repair between fractured segments. ● Continuous resorption of the left apical fragment
.
None
ALVEOLAR FRACTURE Clinical findings Radiographic findings Treatment Follow-Up Favorable Outcome Unfavorable Outcome
● The fracture involves the alveolar bone and may extend to adjacent bone. ● Segment mobility and dislocation are common findings. ● Occlusal interference is often noted. .
● The horizontal fracture line to the apices of the primary teeth and their permanent successors will be disclosed. ● A lateral radiograph may also give information about the relation between the two dentitions and if the segment is displaced in labial direction
● Reposition any displaced segment and then splint. ● General anesthesia is often indicated. ● Stabilize the segment for 4 weeks. ● Monitor teeth in fracture line
1 week C 3-4 weeks S+C+R 6-8 weeks C+R 1 year C+R and C(*) each subsequent year until exfoliation.
● Normal occlusion ● No signs of apical periodontitis. • No signs of disturbances in the permanent successors
● Signs of apical periodontitis or external inflammatory root resorption of primary teeth. ● Signs of disturbances in the permanent successors require follow-up until full eruption.
S=Splint removal C=Clinical examination; R=Radiographic examination; (C*)=Clinical and radiographic monitoring until eruption of the permanent successor Vol. 1 Issue 11 L.E.D. E-Journal Page 250
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Primary dentition Guidelines
2. Treatment guidelines for luxation injuries
Follow-Up Favorable and Unfavorable outcomes include some, but not necessarily all, of the
following: CONCUSSION Clinical findings Radiographic findings Treatment Favorable Outcome Unfavorable Outcome
● The tooth is tender to touch. It has normal mobility and no sulcular bleeding. .
No radiographic abnormalities. Normal periodontal space.
● No treatment is needed. Observation. .
1 week C 6-8 weeks C
● Continuing root development in immature teeth
● No continuing root development in immature teeth, periradicular radiolucencies. ● Crown dark discoloration. No treatment is needed unless a fistula develops.
SUBLUXATION Clinical findings Radiographic findings Treatment Follow-Up Favorable Outcome Unfavorable Outcome
● The tooth has increased mobility but has not been displaced. ● Bleeding from gingival crevice may be noted.
Radiographic abnormalities are usually not found. Normal periodontal space. An occlusal exposure is recommended in order to screen for possible signs of displacement or the presence of a root fracture. The radiograph can furthermore be used as a reference point in case of future complications.
● No treatment is needed. Observation. Brushing with a soft brush and use of chlorhexidine 0.12% alcohol-free topically to the affected area with cotton swabs twice a day for one week.
1 week C 6-8 weeks C Crown discoloration might occur. No treatment is needed unless a fistula develops. Dark discolored teeth should be followed carefully to detect sign of infection as soon as possible
● Continuing root development in immature teeth ● Transient red/gray discoloration. A yellow discoloration indicates pulp obliteration and has a good prognosis
● No continuing root development in immature teeth, periradicular radiolucencies. ● A dark persisting discoloration indicating pulp necrosis.
EXTRUSIVE LUXATION Clinical Findings Radiographic findings Treatment Follow-Up Favorable Outcome Unfavorable Outcome
● Partial displacement of the tooth out of its socket. ● The tooth appears elongated and can be excessively mobile. .
Increased periodontal ligament space apically.
• Treatment decisions are based on the degree of displacement, mobility, root formation and the ability of the child to cope with the emergency situation. ● For minor extrusion (< 3mm) in an immature developing tooth, careful repositioning or leaving the tooth for spontaneous alignment can be treatment options.
• Extraction is the treatment of choice for severe extrusion in a fully formed primary tooth.
1 week C 6-8 weeks C+R 6 months C+R 1 year C+R Discoloration might occur. Dark discolored teeth should be followed carefully to detect sign of infection as soon as possible.
● Continuing root development in immature teeth. ● Transient red/gray discoloration. A yellow discoloration indicates pulp obliteration and has a good prognosis.
● No continuing root development in immature teeth, periradicular radiolucencies. ● A dark persisting discoloration indicating pulp necrosis.
C=Clinical examination; R=Radiographic examination
Vol. 1 Issue 11 L.E.D. E-Journal Page 251
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Primary dentition Guidelines
Follow-Up Favorable and Unfavorable outcomes include some, but not necessarily all, of the
following:
LATERAL LUXATION Clinical findings Radiographic findings Treatment Favorable Outcome Unfavorable Outcome ● The tooth is displaced,
usually in a palatal/lingual or labial direction. ● It will be immobile.
Increased periodontal ligament space apically is best seen on the occlusal exposure. And an occlusal exposure can sometimes also show the position of the displaced tooth and its relation to the permanent successor
● If there is no occlusal interference, as is often the case in anterior open bite, the tooth is allowed to reposition spontaneously.
● If minor occlusal interference, slight grinding is indicated.
● When there is more severe occlusal interference, the tooth can be gently repositioned by combined labial and palatal pressure after the use of local anesthesia.
● In severe displacement, when the crown is dislocated in a labial direction, extraction is the treatment of choice.
.
1 week C 2-3 weeks C 6-8 weeks C+R 1 year C+R
● Asymptomatic ● Clinical and radiographic signs of normal or healed periodontium. ● Transient discoloration might occur
● Symptoms and radiographic sign consistent with periodontitis. ● Grey persistent discoloration
INTRUSIVE LUXATION Clinical findings Radiographic findings Treatment Follow-Up Favorable Outcome Unfavorable Outcome ● The tooth is usually
displaced through the labial bone plate, or can be impinging upon the succedaneous tooth bud
When the apex is displaced toward or through the labial bone plate, the apical tip can be visualized and appears shorter than its contra lateral.
When the apex is displaced towards the permanent tooth germ, the apical tip cannot be visualized and the tooth appears elongated
If the apex is displaced toward or through the labial bone plate, the tooth is left for spontaneous repositioning
If the apex is displaced into the developing tooth germ, extract
1 week C 3-4 weeks C + R 6-8 weeks C 6 months C+R ● 1 year C+R and (C*)
● Tooth in place or erupting. ● No or transient discoloration.
● Tooth locked in place ● Radiographic signs of apical periodontitis ● Persistent discoloration ● Damage to the permanent successor.
C=Clinical examination; R=Radiographic examination; (C*)=Clinical and radiographic monitoring until eruption of the permanent successor
Vol. 1 Issue 11 L.E.D. E-Journal Page 252
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Primary dentition Guidelines
AVULSION Clinical findings Radiographic findings Treatment Follow-Up Favorable Outcome Unfavorable Outcome
The tooth is completely out of the socket
A radiographic examination is essential to ensure that the missing tooth is not intruded.
It is not recommended to replant avulsed primary teeth.
1 week C 6 months C + R • 1 year C + R and (C*)
Damage to the permanent successor.
C=Clinical examination; R=Radiographic examination; (C*)=Clinical and radiographic monitoring until eruption of the permanent successor
Vol. 1 Issue 11 L.E.D. E-Journal Page 253
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

2012 GUIDELINES COMMITTEES
FRACTURES AND LUXATIONS OF PERMANENT TEETH: Dr. Jens Andreasen, Denmark Dr. Anthony DiAngelis, USA Dr. Kurt Ebeleseder, Austria Dr. David Kenny, Canada Dr. Asgeir Sigurdsson, Iceland Dr. Martin Trope, USA AVULSION OF PERMANENT TEETH: Dr. Lars Andersson, Kuwait Dr. Jens O Andreasen, Denmark Dr. Peter Day, United Kingdom Dr. Geoffrey Heithersay, Australia Dr. Yango Pohl, Germany Dr. Martin Trope, USA TRAUMATIC INJURIES TO PRIMARY TEETH: Dr. Jens Andreasen, Denmark Dr. Marie Therese Flores, Chile Dr. Barbro Malmgren, Sweden Dr. Agneta Robertson, Sweden IADT, BOARD OF DIRECTORS, 2012 Dr. Lars Andersson, President, Kuwait Dr. Anthony J. DiAngelis, President Elect, USA Dr. Lamar Hicks, Secretary/Treasurer, USA Dr. Mitsuhiro Tsukiboshi, Immediate‐Past President, Japan Dr. Giacomo Cavalleri, Italy Dr. Nestor Cohenca, USA Dr. Peter Day, UK Dr. Olle Malmgren, Sweden Dr. Alex J. Moule, Australia Dr. Juan E. Onetto, Chile Dr. Yango Pohl, Germany
References for all Guidelines can be viewed on the originally published works: Link to > > Section 1. Fractures and luxations of permanent teeth
Link to > > Section 2. Avulsion of permanent teeth
Link to > > Section 3. Traumatic injuries to primary teeth
Vol. 1 Issue 11 L.E.D. E-Journal Page 254
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
L.E.D. E-Journal
Bio-Medical Waste
The IDA Ludhiana Branch official publication, ‘L.E.D.’ – ‘Let’s
Enjoy Dentistry’ strives to keep dentists connected with the
latest rules and regulations. The brand new additions in this
series are the Bio-Medical Waste (Management and Handling)
Rules, 2016.
Bio-Medical Waste is waste that is either putrescible or
potentially infectious. Bio-Medical waste also includes the
waste associated with the generation of biomedical waste that
visually appears to be of medical or laboratory origin (e.g.,
packaging, unused bandages, infusion kits, etc.), as well
research laboratory waste containing biomolecules or
organisms that are restricted from environmental release.
Discarded sharps are considered biomedical waste whether
they are contaminated or not, due to the possibility of being
contaminated with blood and their propensity to cause injury
when not properly contained and disposed of Disposal of this
waste is an environmental concern, as many medical wastes
are classified as infectious or biohazardous & could potentially
lead to the spread of infectious disease.
The Bio-medical Waste (Management and Handling)
Rules, 1998 & further amendments were passed for the
regulation of bio-medical waste management in 1998 & on 28th
Mar 2016 Biomedical Waste Management Rules 2016 were
notified by Central Govt. Each State's Pollution Control Board
or Pollution control Committee will be responsible for
implementing the new legislation.
Biomedical waste must be properly managed and
disposed of to protect the environment, general public and
workers, especially healthcare and sanitation workers who are
at risk of exposure to biomedical waste as an occupational
hazard. Steps in the management of biomedical waste include
generation, accumulation, handling, storage, treatment,
transport and disposal.
Vol. 1 Issue 11 L.E.D. E-Journal Page 255
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

1
[Published in the Gazette of India, Extraordinary, Part II, Section 3, Sub-section (i)]
GOVERNMENT OF INDIA
MINISTRY OF ENVIRONMENT, FOREST AND CLIMATE CHANGE
NOTIFICATION
New Delhi, the 28th
March, 2016
G.S.R. 343(E).-Whereas the Bio-Medical Waste (Management and Handling) Rules, 1998 was published
vide notification number S.O. 630 (E) dated the 20th July, 1998, by the Government of India in the
erstwhile Ministry of Environment and Forests, provided a regulatory frame work for management of
bio-medical waste generated in the country;
And whereas, to implement these rules more effectively and to improve the collection,
segregation, processing, treatment and disposal of these bio-medical wastes in an environmentally sound
management thereby, reducing the bio- medical waste generation and its impact on the environment, the
Central Government reviewed the existing rules;
And whereas, in exercise of the powers conferred by sections 6, 8 and 25 of the Environment
(Protection) Act, 1986 (29 of 1986), the Central Government published the draft rules in the Gazette vide
number G.S.R. 450 (E), dated the 3rd
June, 2015 inviting objections or suggestions from the public within
sixty days from the date on which copies of the Gazette containing the said notification were made
available to the public;
And whereas, the copies of the Gazette containing the said draft rules were made available to the
public on the 3rd
June, 2015;
And whereas, the objections or comments received within the specified period from the public in
respect of the said draft rules have been duly considered by the Central Government;
Now, therefore, in exercise of the powers conferred by section 6, 8 and 25 of the Environment
(Protection) Act, 1986 (29 of 1986), and in supersession of the Bio-Medical Waste (Management and
Handling) Rules, 1998, except as respects things done or omitted to be done before such suppression, the
Central Government hereby makes the following rules, namely:-
1. Short title and commencement.- (1) these rules may be called the Bio-Medical Waste Management
Rules, 2016.
(2) They shall come into force on the date of their publication in the Official Gazette.
2. Application.-
(1) These rules shall apply to all persons who generate, collect, receive, store, transport, treat,
dispose, or handle bio medical waste in any form including hospitals, nursing homes, clinics,
dispensaries, veterinary institutions, animal houses, pathological laboratories, blood banks, ayush
Vol. 1 Issue 11 L.E.D. E-Journal Page 256
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

2
hospitals, clinical establishments, research or educational institutions, health camps, medical or surgical
camps, vaccination camps, blood donation camps, first aid rooms of schools, forensic laboratories and
research labs.
(2). These rules shall not apply to,-
(a) radioactive wastes as covered under the provisions of the Atomic Energy Act, 1962(33 of
1962) and the rules made there under;
(b) hazardous chemicals covered under the Manufacture, Storage and Import of Hazardous
Chemicals Rules, 1989 made under the Act;
(c) solid wastes covered under the Municipal Solid Waste (Management and Handling) Rules,
2000 made under the Act;
(d) the lead acid batteries covered under the Batteries (Management and Handling) Rules, 2001
made under the Act;
(e) hazardous wastes covered under the Hazardous Wastes (Management, Handling and
Transboundary Movement) Rules, 2008 made under the Act;
(f) waste covered under the e-Waste (Management and Handling) Rules, 2011 made under the
Act; and
(g) hazardous micro organisms, genetically engineered micro organisms and cells covered under
the Manufacture, Use, Import, Export and Storage of Hazardous Microorganisms,
Genetically Engineered Micro organisms or Cells Rules, 1989 made under the Act.
3. Definitions.- In these rules, unless the context otherwise requires, -
(a) "Act" means the Environment (Protection) Act, 1986 (29 of 1986);
(b) "animal house" means a place where animals are reared or kept for the purpose of experiments or
testing;
(c) "authorisation" means permission granted by the prescribed authority for the generation, collection,
reception, storage, transportation, treatment, processing, disposal or any other form of handling of
bio-medical waste in accordance with these rules and guidelines issued by the Central Government
or Central Pollution Control Board as the case may be;
(d) "authorised person" means an occupier or operator authorised by the prescribed authority to
generate, collect, receive, store, transport, treat, process, dispose or handle bio-medical waste in
accordance with these rules and the guidelines issued by the Central Government or the Central
Pollution Control Board, as the case may be;
Vol. 1 Issue 11 L.E.D. E-Journal Page 257
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

3
(e) "biological" means any preparation made from organisms or micro-organisms or product of
metabolism and biochemical reactions intended for use in the diagnosis, immunisation or the
treatment of human beings or animals or in research activities pertaining thereto;
(f) "bio-medical waste" means any waste, which is generated during the diagnosis, treatment or
immunisation of human beings or animals or research activities pertaining thereto or in the
production or testing of biological or in health camps, including the categories mentioned in
Schedule I appended to these rules;
(g) "bio-medical waste treatment and disposal facility" means any facility wherein treatment, disposal
of bio-medical waste or processes incidental to such treatment and disposal is carried out, and
includes common bio-medical waste treatment facilities;
(h) “Form” means the Form appended to these rules;
(i) “handling” in relation to bio-medical waste includes the generation, sorting, segregation,
collection, use, storage, packaging, loading, transportation, unloading, processing, treatment,
destruction, conversion, or offering for sale, transfer, disposal of such waste;
(j) “health care facility” means a place where diagnosis, treatment or immunisation of human beings
or animals is provided irrespective of type and size of health treatment system, and research
activity pertaining thereto;
(k) “major accident” means accident occurring while handling of bio-medical waste having potential to
affect large masses of public and includes toppling of the truck carrying bio-medical waste,
accidental release of bio-medical waste in any water body but exclude accidents like needle prick
injuries, mercury spills;
(l) “management” includes all steps required to ensure that bio- medical waste is managed in such a
manner as to protect health and environment against any adverse effects due to handling of such
waste;
(m) "occupier" means a person having administrative control over the institution and the premises
generating bio-medical waste, which includes a hospital, nursing home, clinic, dispensary,
veterinary institution, animal house, pathological laboratory, blood bank, health care facility and
clinical establishment, irrespective of their system of medicine and by whatever name they are
called;
(n) "operator of a common bio-medical waste treatment facility" means a person who owns or controls
a Common Bio-medical Waste Treatment Facility (CBMWTF) for the collection, reception,
storage, transport, treatment, disposal or any other form of handling of bio-medical waste;
(o) “prescribed authority” means the State Pollution Control Board in respect of a State and Pollution
Control Committees in respect of an Union territory;
(p) "Schedule" means the Schedule appended to these rules.
Vol. 1 Issue 11 L.E.D. E-Journal Page 258
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

4
4. Duties of the Occupier.- It shall be the duty of every occupier to-
(a) take all necessary steps to ensure that bio-medical waste is handled without any adverse effect to
human health and the environment and in accordance with these rules;
(b) make a provision within the premises for a safe, ventilated and secured location for storage of
segregated biomedical waste in colored bags or containers in the manner as specified in Schedule I,
to ensure that there shall be no secondary handling, pilferage of recyclables or inadvertent
scattering or spillage by animals and the bio-medical waste from such place or premises shall be
directly transported in the manner as prescribed in these rules to the common bio-medical waste
treatment facility or for the appropriate treatment and disposal, as the case may be, in the manner
as prescribed in Schedule I;
(c) pre-treat the laboratory waste, microbiological waste, blood samples and blood bags through
disinfection or sterilisation on-site in the manner as prescribed by the World Health Organisation
(WHO) or National AIDs Control Organisation (NACO) guidelines and then sent to the common
bio-medical waste treatment facility for final disposal;
(d) phase out use of chlorinated plastic bags, gloves and blood bags within two years from the date of
notification of these rules;
(e) dispose of solid waste other than bio-medical waste in accordance with the provisions of
respective waste management rules made under the relevant laws and amended from time to time;
(f) not to give treated bio-medical waste with municipal solid waste;
(g) provide training to all its health care workers and others, involved in handling of bio medical waste
at the time of induction and thereafter at least once every year and the details of training
programmes conducted, number of personnel trained and number of personnel not undergone any
training shall be provided in the Annual Report;
(h) immunise all its health care workers and others, involved in handling of bio-medical waste for
protection against diseases including Hepatitis B and Tetanus that are likely to be transmitted by
handling of bio-medical waste, in the manner as prescribed in the National Immunisation Policy or
the guidelines of the Ministry of Health and Family Welfare issued from time to time;
(i) establish a Bar- Code System for bags or containers containing bio-medical waste to be sent out of
the premises or place for any purpose within one year from the date of the notification of these
rules;
(j) ensure segregation of liquid chemical waste at source and ensure pre-treatment or neutralisation
prior to mixing with other effluent generated from health care facilities;
(k) ensure treatment and disposal of liquid waste in accordance with the Water (Prevention and
Control of Pollution) Act, 1974 ( 6 of 1974);
Vol. 1 Issue 11 L.E.D. E-Journal Page 259
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

5
(l) ensure occupational safety of all its health care workers and others involved in handling of bio-
medical waste by providing appropriate and adequate personal protective equipments;
(m) conduct health check up at the time of induction and at least once in a year for all its health care
workers and others involved in handling of bio- medical waste and maintain the records for the
same;
(n) maintain and update on day to day basis the bio-medical waste management register and display
the monthly record on its website according to the bio-medical waste generated in terms of
category and colour coding as specified in Schedule I;
(o) report major accidents including accidents caused by fire hazards, blasts during handling of bio-
medical waste and the remedial action taken and the records relevant thereto, (including nil report)
in Form I to the prescribed authority and also along with the annual report;
(p) make available the annual report on its web-site and all the health care facilities shall make own
website within two years from the date of notification of these rules;
(q) inform the prescribed authority immediately in case the operator of a facility does not collect the
bio-medical waste within the intended time or as per the agreed time;
(r) establish a system to review and monitor the activities related to bio-medical waste management,
either through an existing committee or by forming a new committee and the Committee shall
meet once in every six months and the record of the minutes of the meetings of this committee
shall be submitted along with the annual report to the prescribed authority and the healthcare
establishments having less than thirty beds shall designate a qualified person to review and monitor
the activities relating to bio-medical waste management within that establishment and submit the
annual report;
(s) maintain all record for operation of incineration, hydro or autoclaving etc., for a period of five
years;
(t) existing incinerators to achieve the standards for treatment and disposal of bio-medical waste as
specified in Schedule II for retention time in secondary chamber and Dioxin and Furans within two
years from the date of this notification.
5. Duties of the operator of a common bio-medical waste treatment and disposal facility.-It shall be
the duty of every operator to -
(a) take all necessary steps to ensure that the bio-medical waste collected from the occupier is
transported, handled, stored, treated and disposed of, without any adverse effect to the human
health and the environment, in accordance with these rules and guidelines issued by the Central
Government or, as the case may be, the central pollution control board from time to time;
(b) ensure timely collection of bio-medical waste from the occupier as prescribed under these rules;
(c) establish bar coding and global positioning system for handling of bio- medical waste within one
year;
Vol. 1 Issue 11 L.E.D. E-Journal Page 260
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

6
(d) inform the prescribed authority immediately regarding the occupiers which are not handing over
the segregated bio-medical waste in accordance with these rules;
(e) provide training for all its workers involved in handling of bio-medical waste at the time of
induction and at least once a year thereafter;
(f) assist the occupier in training conducted by them for bio-medical waste management;
(g) undertake appropriate medical examination at the time of induction and at least once in a year and
immunise all its workers involved in handling of bio-medical waste for protection against diseases,
including Hepatitis B and Tetanus, that are likely to be transmitted while handling bio-medical
waste and maintain the records for the same;
(h) ensure occupational safety of all its workers involved in handling of bio-medical waste by
providing appropriate and adequate personal protective equipment;
(i) report major accidents including accidents caused by fire hazards, blasts during handling of bio-
medical waste and the remedial action taken and the records relevant thereto, (including nil report)
in Form I to the prescribed authority and also along with the annual report;
(i) maintain a log book for each of its treatment equipment according to weight of batch; categories of
waste treated; time, date and duration of treatment cycle and total hours of operation;
(k) allow occupier , who are giving waste for treatment to the operator, to see whether the treatment is
carried out as per the rules;
(l) shall display details of authorisation, treatment, annual report etc on its web-site;
(m) after ensuring treatment by autoclaving or microwaving followed by mutilation or shredding,
whichever is applicable, the recyclables from the treated bio-medical wastes such as plastics and
glass, shall be given to recyclers having valid consent or authorisation or registration from the
respective State Pollution Control Board or Pollution Control Committee;
(n) supply non-chlorinated plastic coloured bags to the occupier on chargeable basis, if required;
(o) common bio-medical waste treatment facility shall ensure collection of biomedical waste on
holidays also;
(p) maintain all record for operation of incineration, hydroor autoclaving for a period of five years;
and
(q) upgrade existing incinerators to achieve the standards for retention time in secondary chamber and
Dioxin and Furans within two years from the date of this notification.
6. Duties of authorities.-The Authority specified in column (2) of Schedule-III shall perform the
duties as specified in column (3) thereof in accordance with the provisions of these rules.
Vol. 1 Issue 11 L.E.D. E-Journal Page 261
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

7
7. Treatment and disposal.- (1) Bio-medical waste shall be treated and disposed of in accordance
with Schedule I, and in compliance with the standards provided in Schedule-II by the health care
facilities and common bio-medical waste treatment facility.
(2) Occupier shall hand over segregated waste as per the Schedule-I to common bio-medical waste
treatment facility for treatment, processing and final disposal:
Provided that the lab and highly infectious bio-medical waste generated shall be pre-treated by
equipment like autoclave or microwave.
(3) No occupier shall establish on-site treatment and disposal facility, if a service of ` common bio-
medical waste treatment facility is available at a distance of seventy-five kilometer.
(4) In cases where service of the common bio-medical waste treatment facility is not available, the
Occupiers shall set up requisite biomedical waste treatment equipment like incinerator, autoclave
or microwave, shredder prior to commencement of its operation, as per the authorisation given by
the prescribed authority.
(5) Any person including an occupier or operator of a common bio medical waste treatment facility,
intending to use new technologies for treatment of bio medical waste other than those listed in
Schedule I shall request the Central Government for laying down the standards or operating
parameters.
(6) On receipt of a request referred to in sub-rule (5), the Central Government may determine the
standards and operating parameters for new technology which may be published in Gazette by
the Central Government.
(7) Every operator of common bio-medical waste treatment facility shall set up requisite biomedical
waste treatment equipments like incinerator, autoclave or microwave, shredder and effluent
treatment plant as a part of treatment, prior to commencement of its operation.
(8) Every occupier shall phase out use of non-chlorinated plastic bags within two years from the date
of publication of these rules and after two years from such publication of these rules, the
chlorinated plastic bags shall not be used for storing and transporting of bio-medical waste and
the occupier or operator of a common bio-medical waste treatment facility shall not dispose of
such plastics by incineration and the bags used for storing and transporting biomedical waste
shall be in compliance with the Bureau of Indian Standards. Till the Standards are published, the
carry bags shall be as per the Plastic Waste Management Rules, 2011.
(9) After ensuring treatment by autoclaving or microwaving followed by mutilation or shredding,
whichever is applicable, the recyclables from the treated bio-medical wastes such as plastics and
glass shall be given to such recyclers having valid authorisation or registration from the
respective prescribed authority.
(10) The Occupier or Operator of a common bio-medical waste treatment facility shall maintain a
record of recyclable wastes referred to in sub-rule (9) which are auctioned or sold and the same
shall be submitted to the prescribed authority as part of its annual report. The record shall be
open for inspection by the prescribed authorities.
Vol. 1 Issue 11 L.E.D. E-Journal Page 262
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
8
(11) The handling and disposal of all the mercury waste and lead waste shall be in accordance with
the respective rules and regulations.
8. Segregation, packaging, transportation and storage.-(1) No untreated bio-medical waste
shall be mixed with other wastes.
(2) The bio-medical waste shall be segregated into containers or bags at the point of generation in
accordance with Schedule I prior to its storage, transportation, treatment and disposal.
(3) The containers or bags referred to in sub-rule (2) shall be labeled as specified in Schedule IV.
(4) Bar code and global positioning system shall be added by the Occupier and common bio-medical
waste treatment facility in one year time.
(5) The operator of common bio-medical waste treatment facility shall transport the bio-medical waste
from the premises of an occupier to any off-site bio-medical waste treatment facility only in the
vehicles having label as provided in part ‘A’ of the Schedule IV along with necessary information
as specified in part ‘B’ of the Schedule IV.
(6) The vehicles used for transportation of bio-medical waste shall comply with the conditions if any
stipulated by the State Pollution Control Board or Pollution Control Committee in addition to the
requirement contained in the Motor Vehicles Act, 1988 (59 of 1988), if any or the rules made there
under for transportation of such infectious waste.
(7) Untreated human anatomical waste, animal anatomical waste, soiled waste and, biotechnology
waste shall not be stored beyond a period of forty –eight hours:
Provided that in case for any reason it becomes necessary to store such waste beyond
such a period, the occupier shall take appropriate measures to ensure that the waste does not
adversely affect human health and the environment and inform the prescribed authority along with
the reasons for doing so.
(8) Microbiology waste and all other clinical laboratory waste shall be pre-treated by sterilisation to
Log 6 or disinfection to Log 4, as per the World Health Organisation guidelines before packing
and sending to the common bio-medical waste treatment facility.
9. Prescribed authority.-(1) The prescribed authority for implementation of the provisions of these
rules shall be the State Pollution Control Boards in respect of States and Pollution Control Committees in
respect of Union territories.
(2) The prescribed authority for enforcement of the provisions of these rules in respect of all health
care establishments including hospitals, nursing homes, clinics, dispensaries, veterinary
institutions, animal houses, pathological laboratories and blood banks of the Armed Forces under
the Ministry of Defence shall be the Director General, Armed Forces Medical Services, who shall
function under the supervision and control of the Ministry of Defence.
Vol. 1 Issue 11 L.E.D. E-Journal Page 263
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

9
(3) The prescribed authorities shall comply with the responsibilities as stipulated in Schedule III of
these rules.
10. Procedure for authorisation.-Every occupier or operator handling bio-medical waste, irrespective
of the quantity shall make an application in Form II to the prescribed authority i.e. State Pollution
Control Board and Pollution Control Committee, as the case may be, for grant of authorisation and
the prescribed authority shall grant the provisional authorisation in Form III and the validity of
such authorisation for bedded health care facility and operator of a common facility shall be
synchronised with the validity of the consents.
(1) The authorisation shall be one time for non-bedded occupiers and the authorisation in such cases
shall be deemed to have been granted, if not objected by the prescribed authority within a period of
ninety days from the date of receipt of duly completed application along with such necessary
documents.
(2) In case of refusal of renewal, cancellation or suspension of the authorisation by the prescribed
authority, the reasons shall be recorded in writing:
Provided that the prescribed authority shall give an opportunity of being heard to the
applicant before such refusal of the authorisation.
(3) Every application for authorisation shall be disposed of by the prescribed authority within a period
of ninety days from the date of receipt of duly completed application along with such necessary
documents, failing which it shall be deemed that the authorisation is granted under these rules.
(4) In case of any change in the bio-medical waste generation, handling, treatment and disposal for
which authorisation was earlier granted, the occupier or operator shall intimate to the prescribed
authority about the change or variation in the activity and shall submit a fresh application in Form
II for modification of the conditions of authorisation.
11. Advisory Committee.-(1) Every State Government or Union territory Administration shall
constitute an Advisory Committee for the respective State or Union territory under the chairmanship of
the respective health secretary to oversee the implementation of the rules in the respective state and to
advice any improvements and the Advisory Committee shall include representatives from the
Departments of Health, Environment, Urban Development, Animal Husbandry and Veterinary Sciences
of that State Government or Union territory Administration, State Pollution Control Board or Pollution
Control Committee, urban local bodies or local bodies or Municipal Corporation, representatives from
Indian Medical Association, common bio-medical waste treatment facility and non-governmental
organisation.
(2) Notwithstanding anything contained in sub-rule (1), the Ministry of Defence shall constitute the
Advisory Committee (Defence) under the chairmanship of Director General of Health Services of
Armed Forces consisting of representatives from the Ministry of Defence, Ministry of
Environment, Forest and Climate Change, Central Pollution Control Board, Ministry of Health and
Family Welfare, Armed Forces Medical College or Command Hospital.
Vol. 1 Issue 11 L.E.D. E-Journal Page 264
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
10
(3) The Advisory Committee constituted under sub-rule (1) and (2) shall meet at least once in six
months and review all matters related to implementation of the provisions of these rules in the
State and Armed Forces Health Care Facilities, as the case may be.
(4) The Ministry of Health and Defence may co-opt representatives from the other Governmental and
non-governmental organisations having expertise in the field of bio-medical waste management.
12. Monitoring of implementation of the rules in health care facilities.- (1) The Ministry of
Environment, Forest and Climate Change shall review the implementation of the rules in the country
once in a year through the State Health Secretaries and Chairmen or Member Secretary of State Pollution
Control Boards and Central Pollution Control Board and the Ministry may also invite experts in the field
of bio-medical waste management, if required.
(2) The Central Pollution Control Board shall monitor the implementation of these rules in respect of
all the Armed Forces health care establishments under the Ministry of Defence.
(3) The Central Pollution Control Board along with one or more representatives of the Advisory
Committee constituted under sub-rule (2) of rule 11, may inspect any Armed Forces health care
establishments after prior intimation to the Director General Armed Forces Medical
Services.
(4) Every State Government or Union territory Administration shall constitute District Level
Monitoring Committee in the districts under the chairmanship of District Collector or District
Magistrate or Deputy Commissioner or Additional District Magistrate to monitor the compliance
of the provisions of these rules in the health care facilities generating bio-medical waste and in the
common bio-medical waste treatment and disposal facilities, where the bio-medical waste is
treated and disposed of.
(5) The District Level Monitoring Committee constituted under sub-rule (4) shall submit its report
once in six months to the State Advisory Committee and a copy thereof shall also be forwarded to
State Pollution Control Board or Pollution Control Committee concerned for taking further
necessary action.
(6) The District Level Monitoring Committee shall comprise of District Medical Officer or District
Health Officer, representatives from State Pollution Control Board or Pollution Control
Committee, Public Health Engineering Department, local bodies or municipal corporation, Indian
Medical Association, common bio-medical waste treatment facility and registered non-
governmental organisations working in the field of bio-medical waste management and the
Committee may co-opt other members and experts, if necessary and the District Medical Officer
shall be the Member Secretary of this Committee.
13. Annual report.-(1) Every occupier or operator of common bio-medical waste treatment facility
shall submit an annual report to the prescribed authority in Form-IV, on or before the 30th June of every
year.
(2) The prescribed authority shall compile, review and analyse the information received and send this
information to the Central Pollution Control Board on or before the 31st July of every year.
Vol. 1 Issue 11 L.E.D. E-Journal Page 265
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
11
(3) The Central Pollution Control Board shall compile, review and analyse the information received
and send this information, along with its comments or suggestions or observations to the Ministry
of Environment, Forest and Climate Change on or before 31st
August every year.
(4) The Annual Reports shall also be available online on the websites of Occupiers, State Pollution
Control Boards and Central Pollution Control Board.
14. Maintenance of records.- (1) Every authorised person shall maintain records related to the
generation, collection, reception, storage, transportation, treatment, disposal or any other form of
handling of bio-medical waste, for a period of five years, in accordance with these rules and
guidelines issued by the Central Government or the Central Pollution Control Board or the
prescribed authority as the case may be.
(2) All records shall be subject to inspection and verification by the prescribed authority or the
Ministry of Environment, Forest and Climate Change at any time.
15. Accident reporting.- (1) In case of any major accident at any institution or facility or any other
site while handling bio-medical waste, the authorised person shall intimate immediately to the prescribed
authority about such accident and forward a report within twenty-four hours in writing regarding the
remedial steps taken in Form I.
(2) Information regarding all other accidents and remedial steps taken shall be provided in the annual
report in accordance with rule 13 by the occupier.
16. Appeal.-(1) Any person aggrieved by an order made by the prescribed authority under these
rules may, within a period of thirty days from the date on which the order is communicated to him, prefer
an appeal in Form V to the Secretary (Environment) of the State Government or Union territory
administration .
(2) Any person aggrieved by an order of the Director General Armed Forces Medical Services under
these rules may, within thirty days from the date on which the order is communicated to him,
prefer an appeal in Form V to the Secretary, Ministry of Environment, Forest and Climate Change.
(3) The authority referred to in sub-para (1) and (2) as the case may be, may entertain the appeal after
the expiry of the said period of thirty days, if it is satisfied that the appellant was prevented by
sufficient cause from filing the appeal in time.
(4) The appeal shall be disposed of within a period of ninety days from the date of its filing.
17. Site for common bio-medical waste treatment and disposal facility.-(1) Without
prejudice to rule 5 of these rules, the department in the business allocation of land assignment shall be
responsible for providing suitable site for setting up of common biomedical waste treatment and disposal
facility in the State Government or Union territory Administration.
Vol. 1 Issue 11 L.E.D. E-Journal Page 266
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
12
(2) The selection of site for setting up of such facility shall be made in consultation with the prescribed
authority, other stakeholders and in accordance with guidelines published by the Ministry of
Environment, Forest and Climate Change or Central Pollution Control Board.
18. Liability of the occupier, operator of a facility.- (1) The occupier or an operator of a common
bio-medical waste treatment facility shall be liable for all the damages caused to the environment or the
public due to improper handling of bio- medical wastes.
(2) The occupier or operator of common bio-medical waste treatment facility shall be liable for action
under section 5 and section 15 of the Act, in case of any violation.
SCHEDULE I
[See rules 3 (e), 4(b), 7(1), 7(2), 7(5), 7 (6) and 8(2)]
Part-1
Biomedical wastes categories and their segregation, collection, treatment, processing and
disposal options
Category Type of Waste Type of Bag or
Container to be
used
Treatment and Disposal options
(1) (2) (3) (4)
Yellow (a) Human Anatomical
Waste: Human tissues, organs,
body parts and fetus
below the viability
period (as per the
Medical Termination of
Pregnancy Act 1971,
amended from time to
time).
Yellow coloured
non-chlorinated
plastic bags
Incineration or Plasma Pyrolysis or
deep burial*
(b)Animal Anatomical
Waste : Experimental animal
carcasses, body parts,
organs, tissues,
including the waste
generated from
animals used in
experiments or testing
in veterinary hospitals
or colleges or animal
houses.
(c) Soiled Waste: Items contaminated
with blood, body fluids
like dressings, plaster
casts, cotton swabs and
Incineration or Plasma Pyrolysis or
deep burial*
In absence of above facilities,
autoclaving or micro-waving/
Vol. 1 Issue 11 L.E.D. E-Journal Page 267
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
13
bags containing residual
or discarded blood and
blood components.
hydroclaving followed by shredding or
mutilation or combination of
sterilization and shredding. Treated
waste to be sent for energy recovery.
(d) Expired or
Discarded Medicines: Pharmaceutical waste
like antibiotics,
cytotoxic drugs
including all items
contaminated with
cytotoxic drugs along
with glass or plastic
ampoules, vials etc.
Yellow coloured
non-chlorinated
plastic bags or
containers
Expired `cytotoxic drugs and items
contaminated with cytotoxic drugs to be
returned back to the manufacturer or
supplier for incineration at temperature
>1200 0C or to common bio-medical
waste treatment facility or hazardous
waste treatment, storage and disposal
facility for incineration at >12000C Or
Encapsulation or Plasma Pyrolysis at
>12000C.
All other discarded medicines shall be
either sent back to manufacturer or
disposed by incineration.
(e) Chemical Waste:
Chemicals used in
production of biological
and used or discarded
disinfectants.
Yellow coloured
containers or
non-chlorinated
plastic bags
Disposed of by incineration or Plasma
Pyrolysis or Encapsulation in
hazardous waste treatment, storage and
disposal facility.
(f) Chemical Liquid
Waste : Liquid waste generated
due to use of chemicals
in production of
biological and used or
discarded disinfectants,
Silver X-ray film
developing liquid,
discarded Formalin,
infected secretions,
aspirated body
fluids, liquid from
laboratories and floor
washings, cleaning,
house-keeping and
disinfecting activities
etc.
Separate
collection
system leading
to effluent
treatment system
After resource recovery, the chemical
liquid waste shall be pre-treated before
mixing with other wastewater. The
combined discharge shall conform to
the discharge norms given in Schedule-
III.
(g) Discarded linen,
mattresses, beddings
contaminated with
blood or body fluid.
Non-chlorinated
yellow plastic
bags or suitable
packing material
Non- chlorinated chemical disinfection
followed by incineration or Plazma
Pyrolysis or for energy recovery.
In absence of above facilities, shredding
or mutilation or combination of
sterilization and shredding. Treated
waste to be sent for energy recovery or
incineration or Plazma Pyrolysis.
Vol. 1 Issue 11 L.E.D. E-Journal Page 268
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

14
(h) Microbiology,
Biotechnology and
other clinical
laboratory waste: Blood bags, Laboratory
cultures, stocks or
specimens of micro-
organisms, live or
attenuated vaccines,
human and animal cell
cultures used in
research, industrial
laboratories, production
of biological, residual
toxins, dishes and
devices used for
cultures.
Autoclave safe
plastic bags or
containers
Pre-treat to sterilize with non-
chlorinated chemicals on-site as per
National AIDS Control Organisation or
World Health Organisation guidelines
thereafter for Incineration.
Red Contaminated Waste
(Recyclable) (a) Wastes generated
from disposable items
such as tubing, bottles,
intravenous tubes and
sets, catheters, urine
bags, syringes (without
needles and fixed needle
syringes) and
vaccutainers with their
needles cut) and gloves.
Red coloured
non-chlorinated
plastic bags or
containers
Autoclaving or micro-waving/
hydroclaving followed by shredding or
mutilation or combination of
sterilization and shredding. Treated
waste to be sent to registered or
authorized recyclers or for energy
recovery or plastics to diesel or fuel oil
or for road making, whichever is
possible.
Plastic waste should not be sent to
landfill sites.
White
(Translucent) Waste sharps
including Metals: Needles, syringes with
fixed needles, needles
from needle tip cutter or
burner, scalpels, blades,
or any other
contaminated sharp
object that may cause
puncture and cuts. This
includes both used,
discarded and
contaminated metal
sharps
Puncture proof,
Leak proof,
tamper proof
containers
Autoclaving or Dry Heat Sterilization
followed by shredding or mutilation or
encapsulation in metal container or
cement concrete; combination of
shredding cum autoclaving; and sent for
final disposal to iron foundries (having
consent to operate from the State
Pollution Control Boards or Pollution
Control Committees) or sanitary
landfill or designated concrete waste
sharp pit.
Blue (a) Glassware: Broken or discarded and
contaminated glass
including medicine vials
and ampoules except
those contaminated with
cytotoxic wastes.
Cardboard boxes
with blue
colored marking
Disinfection (by soaking the washed
glass waste after cleaning with
detergent and Sodium Hypochlorite
treatment) or through autoclaving or
microwaving or hydroclaving and then
sent for recycling.
Vol. 1 Issue 11 L.E.D. E-Journal Page 269
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
15
(b) Metallic Body
Implants
Cardboard boxes
with blue
colored marking
*Disposal by deep burial is permitted only in rural or remote areas where there is no access to
common bio-medical waste treatment facility. This will be carried out with prior approval from the
prescribed authority and as per the Standards specified in Schedule-III. The deep burial facility
shall be located as per the provisions and guidelines issued by Central Pollution Control Board
from time to time.
Part -2
(1) All plastic bags shall be as per BIS standards as and when published, till then the prevailing Plastic
Waste Management Rules shall be applicable.
(2) Chemical treatment using at least 10% Sodium Hypochlorite having 30% residual chlorine for
twenty minutesor any other equivalent chemical reagent that should demonstrate Log104 reduction
efficiency for microorganisms as given in Schedule- III.
(3) Mutilation or shredding must be to an extent to prevent unauthorized reuse.
(4) There will be no chemical pretreatment before incineration, except for microbiological, lab and
highly infectious waste.
(5) Incineration ash (ash from incineration of any bio-medical waste) shall be disposed through
hazardous waste treatment, storage and disposal facility, if toxic or hazardous constituents are
present beyond the prescribed limits as given in the Hazardous Waste (Management, Handling and
Transboundary Movement) Rules, 2008 or as revised from time to time.
(6) Dead Fetus below the viability period (as per the Medical Termination of Pregnancy Act 1971,
amended from time to time) can be considered as human anatomical waste. Such waste should be
handed over to the operator of common bio-medical waste treatment and disposal facility in yellow
bag with a copy of the official Medical Termination of Pregnancy certificate from the Obstetrician
or the Medical Superintendent of hospital or healthcare establishment.
(7) Cytotoxic drug vials shall not be handed over to unauthorised person under any circumstances.
These shall be sent back to the manufactures for necessary disposal at a single point. As a second
option, these may be sent for incineration at common bio-medical waste treatment and disposal
facility or TSDFs or plasma pyrolys is at temperature >1200 0C.
(8) Residual or discarded chemical wastes, used or discarded disinfectants and chemical sludge can be
disposed at hazardous waste treatment, storage and disposal facility. In such case, the waste should
be sent to hazardous waste treatment, storage and disposal facility through operator of common
bio-medical waste treatment and disposal facility only.
Vol. 1 Issue 11 L.E.D. E-Journal Page 270
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
16
(9) On-site pre-treatment of laboratory waste, microbiological waste, blood samples, blood bags
should be disinfected or sterilized as per the Guidelines of World Health Organisation or National
AIDS Control Organisation and then given to the common bio-medical waste treatment and
disposal facility.
(10) Installation of in-house incinerator is not allowed. However in case there is no common biomedical
facility nearby, the same may be installed by the occupier after taking authorisation from the State
Pollution Control Board.
(11) Syringes should be either mutilated or needles should be cut and or stored in tamper proof, leak
proof and puncture proof containers for sharps storage. Wherever the occupier is not linked to a
disposal facility it shall be the responsibility of the occupier to sterilize and dispose in the manner
prescribed.
(12) Bio-medical waste generated in households during healthcare activities shall be segregated as per
these rules and handed over in separate bags or containers to municipal waste collectors. Urban
Local Bodies shall have tie up with the common bio-medical waste treatment and disposal facility
to pickup this waste from the Material Recovery Facility (MRF) or from the house hold directly,
for final disposal in the manner as prescribed in this Schedule.
SCHEDULE II
[See rule 4(t), 7(1) and 7(6)]
STANDARDS FOR TREATMENT AND DISPOSAL OF
BIO-MEDICALWASTES
1. STANDARDS FOR INCINERATION.-
All incinerators shall meet the following operating and emission standards-
A. Operating Standards
1). Combustion efficiency (CE) shall be at least 99.00%.
2). The Combustion efficiency is computed as follows:
%C02
C.E. = ------------ X 100
%C02 + % CO
3). The temperature of the primary chamber shall be a minimum of 800 0C and the secondary
chamber shall be minimum of 10500C + or - 50
0C.
4). The secondary chamber gas residence time shall be at least two seconds.
B. Emission Standards
Vol. 1 Issue 11 L.E.D. E-Journal Page 271
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
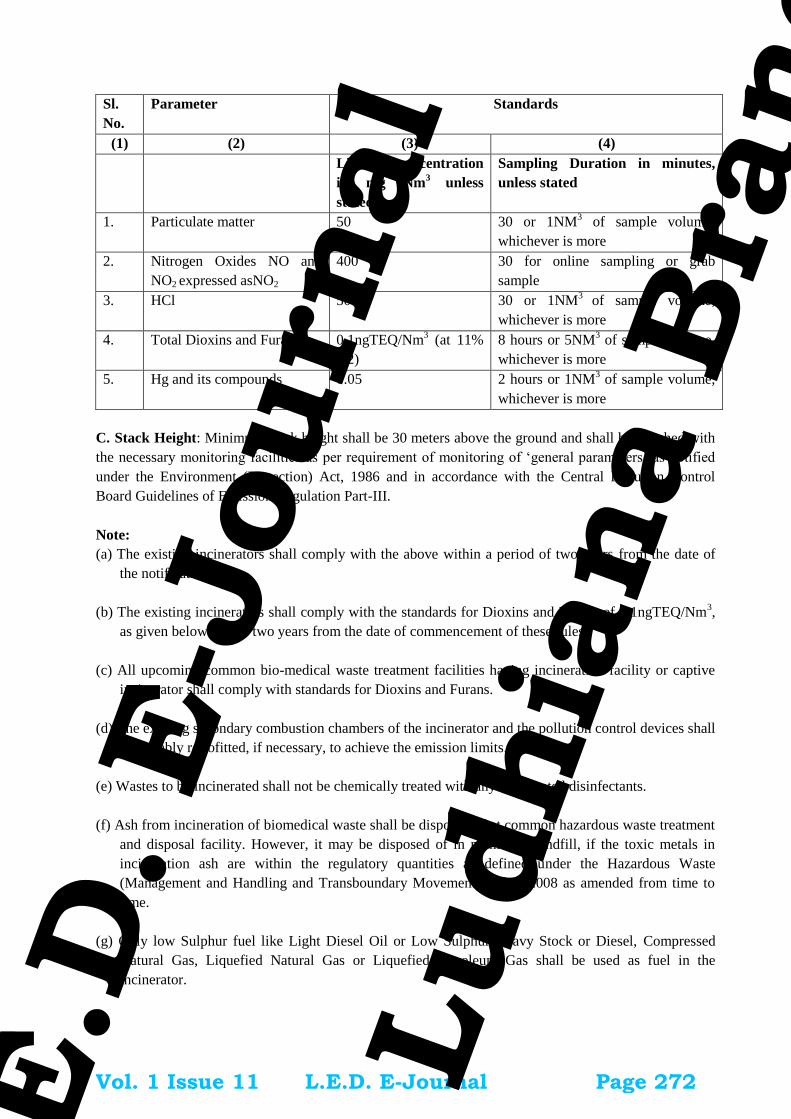
17
Sl.
No.
Parameter Standards
(1) (2) (3) (4)
Limiting concentration
in mg Nm3
unless
stated
Sampling Duration in minutes,
unless stated
1. Particulate matter 50 30 or 1NM3 of sample volume,
whichever is more
2. Nitrogen Oxides NO and
NO2 expressed asNO2
400 30 for online sampling or grab
sample
3. HCl 50 30 or 1NM3
of sample volume,
whichever is more
4. Total Dioxins and Furans 0.1ngTEQ/Nm3 (at 11%
O2)
8 hours or 5NM3 of sample volume,
whichever is more
5. Hg and its compounds 0.05 2 hours or 1NM3 of sample volume,
whichever is more
C. Stack Height: Minimum stack height shall be 30 meters above the ground and shall be attached with
the necessary monitoring facilities as per requirement of monitoring of ‘general parameters’ as notified
under the Environment (Protection) Act, 1986 and in accordance with the Central Pollution Control
Board Guidelines of Emission Regulation Part-III.
Note:
(a) The existing incinerators shall comply with the above within a period of two years from the date of
the notification.
(b) The existing incinerators shall comply with the standards for Dioxins and Furans of 0.1ngTEQ/Nm3,
as given below within two years from the date of commencement of these rules.
(c) All upcoming common bio-medical waste treatment facilities having incineration facility or captive
incinerator shall comply with standards for Dioxins and Furans.
(d) The existing secondary combustion chambers of the incinerator and the pollution control devices shall
be suitably retrofitted, if necessary, to achieve the emission limits.
(e) Wastes to be incinerated shall not be chemically treated with any chlorinated disinfectants.
(f) Ash from incineration of biomedical waste shall be disposed of at common hazardous waste treatment
and disposal facility. However, it may be disposed of in municipal landfill, if the toxic metals in
incineration ash are within the regulatory quantities as defined under the Hazardous Waste
(Management and Handling and Transboundary Movement) Rules, 2008 as amended from time to
time.
(g) Only low Sulphur fuel like Light Diesel Oil or Low Sulphur Heavy Stock or Diesel, Compressed
Natural Gas, Liquefied Natural Gas or Liquefied Petroleum Gas shall be used as fuel in the
incinerator.
Vol. 1 Issue 11 L.E.D. E-Journal Page 272
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

18
(h) The occupier or operator of a common bio-medical waste treatment facility shall monitor the stack
gaseous emissions (under optimum capacity of the incinerator) once in three months through a
laboratory approved under the Environment (Protection) Act, 1986 and record of such analysis
results shall be maintained and submitted to the prescribed authority. In case of dioxins and furans,
monitoring should be done once in a year.
(i) The occupier or operator of the common bio-medical waste treatment facility shall install continuous
emission monitoring system for the parameters as stipulated by State Pollution Control Board or
Pollution Control Committees in authorisation and transmit the data real time to the servers at State
Pollution Control Board or Pollution Control Committees and Central Pollution Control Board.
(j) All monitored values shall be corrected to 11% Oxygen on dry basis.
(k) Incinerators (combustion chambers) shall be operated with such temperature, retention time and
turbulence, as to achieve Total Organic Carbon content in the slag and bottom ashes less than 3% or
their loss on ignition shall be less than 5% of the dry weight.
(l) The occupier or operator of a common bio-medical waste incinerator shall use combustion gas
analyzer to measure CO2, CO and O2.
2. Operating and Emission Standards for Disposal by Plasma Pyrolysis or Gasification:
A. Operating Standards:
All the operators of the Plasma Pyrolysis or Gasification shall meet the following operating and emission
standards:
1) Combustion Efficiency (CE) shall be at least 99.99%.
2) The Combustion Efficiency is computed as follows.
% CO2 C.E =
……………………… X 100
(% CO2 + % CO)
3) The temperature of the combustion chamber after plasma gasification shall be 1050 ± 50 o C with
gas residence time of at least 2(two) second, with minimum 3 % Oxygen in the stack gas.
4) The Stack height should be minimum of 30 m above ground level and shall be attached with the
necessary monitoring facilities as per requirement of monitoring of ‘general parameters’ as
notified under the Environment (Protection) Act, 1986 and in accordance with the CPCB
Guidelines of Emission Regulation Part-III.
B. Air Emission Standards and Air Pollution Control Measures
(i) Emission standards for incinerator, notified at Sl No.1 above in this Schedule, and revised from
time to time, shall be applicable for the Plasma Pyrolysis or Gasification also.
Vol. 1 Issue 11 L.E.D. E-Journal Page 273
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

19
(ii) Suitably designed air pollution control devices shall be installed or retrofitted with the ‘Plasma
Pyrolysis or Gasification to achieve the above emission limits, if necessary.
(iii) Wastes to be treated using Plasma Pyrolysis or Gasification shall not be chemically treated with
any chlorinated disinfectants and chlorinated plastics shall not be treated in the system.
C. Disposal of Ash Vitrified Material: The ash or vitrified material generated from the ‘Plasma
Pyrolysis or Gasification shall be disposed off in accordance with the Hazardous Waste (Management,
Handling and Transboundary Movement) Rules 2008 and revisions made thereafter in case the
constituents exceed the limits prescribed under Schedule II of the said Rules or else in accordance with
the provisions of the Environment (Protection) Act, 1986, whichever is applicable.
3. STANDARDS FOR AUTOCLAVING OF BIO-MEDICAL WASTE.-
The autoclave should be dedicated for the purposes of disinfecting and treating bio-medical
waste.
(1) When operating a gravity flow autoclave, medical waste shall be subjected to:
(i) a temperature of not less than 121° C and pressure of 15 pounds per square inch (psi) for an
autoclave residence time of not less than 60 minutes; or
(ii) a temperature of not less than 135° C and a pressure of 31 psi for an autoclave residence time of
not less than 45 minutes; or
(iii) a temperature of not less than 149° C and a pressure of 52 psi for an autoclave residence time
of not less than 30 minutes.
(2) When operating a vacuum autoclave, medical waste shall be subjected to a minimum of three
pre-vacuum pulse to purge the autoclave of all air. The air removed during the pre-vacuum, cycle should
be decontaminated by means of HEPA and activated carbon filtration, steam treatment, or any other
method to prevent release of pathogen. The waste shall be subjected to the following:
(i) a temperature of not less than 121°C and pressure of 15 psi per an autoclave residence time of
not less than 45 minutes; or
(ii) a temperature of not less than 135°C and a pressure of 31 psi for an autoclave residence time of
not less than 30 minutes;
(3) Medical waste shall not be considered as properly treated unless the time, temperature and
pressure indicators indicate that the required time, temperature and pressure were reached during the
autoclave process. If for any reasons, time temperature or pressure indicator indicates that the required
temperature, pressure or residence time was not reached, the entire load of medical waste must be
autoclaved again until the proper temperature, pressure and residence time were achieved.
Vol. 1 Issue 11 L.E.D. E-Journal Page 274
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

20
(4) Recording of operational parameters: Each autoclave shall have graphic or computer recording
devices which will automatically and continuously monitor and record dates, time of day, load
identification number and operating parameters throughout the entire length of the autoclave cycle.
(5) Validation test for autoclave: The validation test shall use four biological indicator strips, one shall
be used as a control and left at room temperature, and three shall be placed in the approximate center of
three containers with the waste. Personal protective equipment (gloves, face mask and coveralls) shall be
used when opening containers for the purpose of placing the biological indicators. At least one of the
containers with a biological indicator should be placed in the most difficult location for steam to
penetrate, generally the bottom center of the waste pile. The occupier or operator shall conduct this test
three consecutive times to define the minimum operating conditions. The temperature, pressure and
residence time at which all biological indicator vials or strips for three consecutive tests show complete
inactivation of the spores shall define the minimum operating conditions for the autoclave. After
determining the minimum temperature, pressure and residence time, the occupier or operator of a
common biomedical waste treatment facility shall conduct this test once in three months and records in
this regard shall be maintained.
(6) Routine Test: A chemical indicator strip or tape that changes colour when a certain temperature is
reached can be used to verify that a specific temperature has been achieved. It may be necessary to use
more than one strip over the waste package at different locations to ensure that the inner content of the
package has been adequately autoclaved. The occupier or operator of a common bio medical waste
treatment facility shall conduct this test during autoclaving of each batch and records in this regard shall
be maintained.
(7) Spore testing: The autoclave should completely and consistently kill the approved biological
indicator at the maximum design capacity of each autoclave unit. Biological indicator for autoclave shall
be Geobacillusstearothermophilus spores using vials or spore Strips; with at least 1X106 spores. Under no
circumstances will an autoclave have minimum operating parameters less than a residence time of 30
minutes, a temperature less than 121o C or a pressure less than 15 psi. The occupier or operator of a
common bio medical waste treatment and disposal facility shall conduct this test at least once in every
week and records in this regard shall be maintained.
4. STANDARDS OF MICROWAVING.-
(1) Microwave treatment shall not be used for cytotoxic, hazardous or radioactive wastes,
contaminated animal carcasses, body parts and large metal items.
(2) The microwave system shall comply with the efficacy test or routine tests and a performance
guarantee may be provided by the supplier before operation of the limit.
(3) The microwave should completely and consistently kill the bacteria and other pathogenic
organisms that are ensured by approved biological indicator at the maximum design capacity of each
microwave unit. Biological indicators for microwave shall be Bacillus atrophaeusspores using vials or
spore strips with at least 1 x 104sporesper detachable strip. The biological indicator shall be placed with
waste and exposed to same conditions as the waste during a normal treatment cycle.
Vol. 1 Issue 11 L.E.D. E-Journal Page 275
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

21
5. STANDARDS FOR DEEP BURIAL.- (1) A pit or trench should be dug about two meters deep.
It should be half filled with waste, then covered with lime within 50 cm of the surface, before filling the
rest of the pit with soil.
(2) It must be ensured that animals do not have any access to burial sites. Covers of galvanised iron
or wire meshes may be used.
(3) On each occasion, when wastes are added to the pit, a layer of 10 cm of soil shall be added to
cover the wastes.
(4) Burial must be performed under close and dedicated supervision.
(5) The deep burial site should be relatively impermeable and no shallow well should be close to the
site.
(6) The pits should be distant from habitation, and located so as to ensure that no contamination
occurs to surface water or ground water. The area should not be prone to flooding or erosion.
(7) The location of the deep burial site shall be authorised by the prescribed authority.
(8) The institution shall maintain a record of all pits used for deep burial.
(9) The ground water table level should be a minimum of six meters below the lower level of deep
burial pit.
6. STANDARDS FOR EFFICACY OF CHEMICAL DISINFECTION
Microbial inactivation efficacy is equated to “Log10 kill” which is defined as the difference
between the logarithms of number of test microorganisms before and after chemical treatment. Chemical
disinfection methods shall demonstrate a 4 Log10 reduction or greater for Bacillus Subtilis (ATCC
19659) in chemical treatment systems.
7. STANDARDS FOR DRY HEAT STERILIZATION
Waste sharps can be treated by dry heat sterilization at a temperature not less than 1850C, at least
for a residence period of 150 minutes in each cycle, which sterilization period of 90 minutes. There
should be automatic recording system to monitor operating parameters.
(i) Validation test for Shaprs sterilization unit
Waste shaprs sterilization unit should completely and consistently kill the biological indicator
GeobacillusStearothermophillus or Bacillus Atropheausspoers using vials with at least log10 6 spores per
ml. The test shall be carried out once in three months
(ii) Routine test
Vol. 1 Issue 11 L.E.D. E-Journal Page 276
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

22
A chemical indicator strip or tape that changes colour when a certain temperature is reached can
be used to verify that a specific temperature has been achieved. It may be necessary to use more than one
strip over the waste to ensure that the inner content of the sharps has been adequately disinfected. This
test shall be performed once in week and records in this regard shall be maintained.
8. STANDARDS FOR LIQUID WASTE.-
(1) The effluent generated or treated from the premises of occupier or operator of a common bio
medical waste treatment and disposal facility, before discharge into the sewer should conform to the
following limits-
PARAMETERS PERMISSIBLE LIMITS
pH 6.5-9.0
Suspended solids 100 mg/l
Oil and grease 10 mg/l
BOD 30 mg/l
COD 250 mg/l
Bio-assay test 90% survival of fish after 96 hours in 100% effluent.
(2) Sludge from Effluent Treatment Plant shall be given to common bio-medical waste treatment facility
for incineration or to hazardous waste treatment, storage and disposal facility for disposal.
Schedule III
[See rule 6 and 9(3)]
List of Prescribed Authorities and the Corresponding Duties
Sl.
No
.
(1)
Authority
(2)
Corresponding Duties
(3)
1 Ministry of Environment, Forest
and Climate Change, Government
of India
(i) Making Policies concerning bio-medical waste
Management in the Country including notification
of Rules and amendments to the Rules as and
when required.
(ii) Providing financial assistance for training and
awareness programmes on bio-medical waste
management related activities to for the State
Pollution Control Boards or Pollution Control
Committees.
(iii) Facilitating financial assistance for setting up or
up-gradation of common bio-medical waste
treatment facilities.
(iv) Undertake or support operational research and
assessment with reference to risks to environment
and health due to bio-medical waste and
Vol. 1 Issue 11 L.E.D. E-Journal Page 277
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
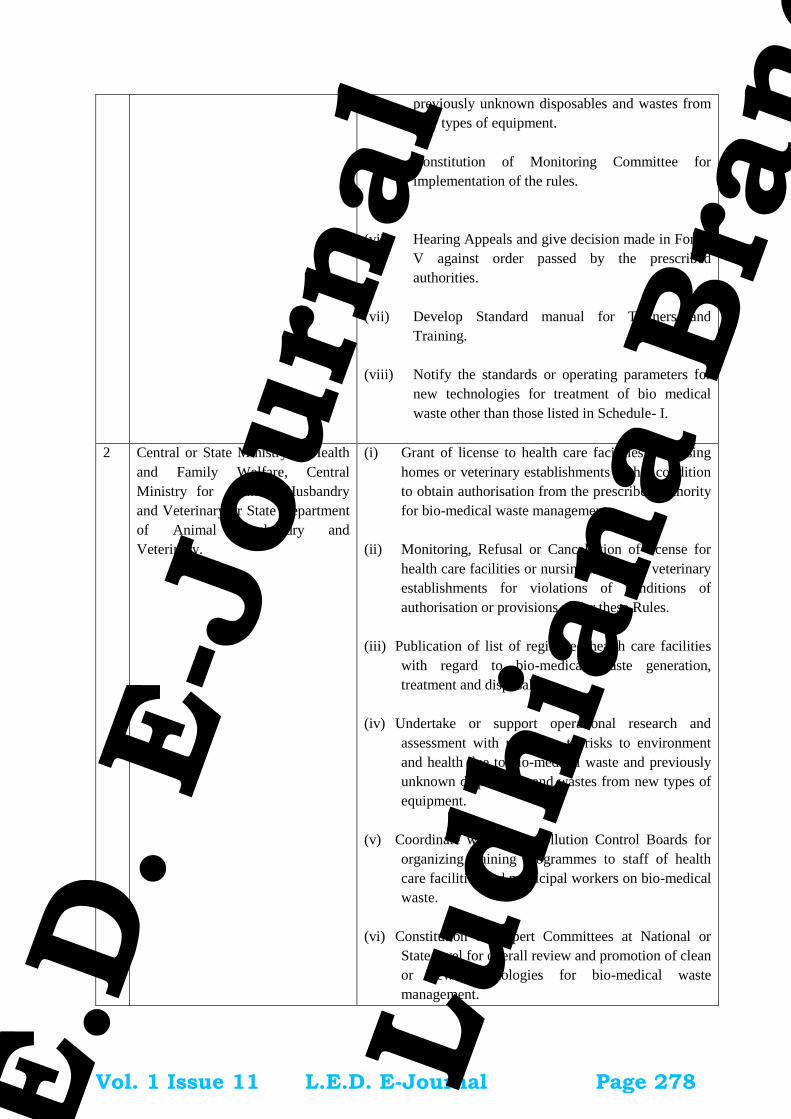
23
previously unknown disposables and wastes from
new types of equipment.
(v) Constitution of Monitoring Committee for
implementation of the rules.
(vi) Hearing Appeals and give decision made in Form-
V against order passed by the prescribed
authorities.
(vii) Develop Standard manual for Trainers and
Training.
(viii) Notify the standards or operating parameters for
new technologies for treatment of bio medical
waste other than those listed in Schedule- I.
2 Central or State Ministry of Health
and Family Welfare, Central
Ministry for Animal Husbandry
and Veterinary or State Department
of Animal Husbandry and
Veterinary.
(i) Grant of license to health care facilities or nursing
homes or veterinary establishments with a condition
to obtain authorisation from the prescribed authority
for bio-medical waste management.
(ii) Monitoring, Refusal or Cancellation of license for
health care facilities or nursing homes or veterinary
establishments for violations of conditions of
authorisation or provisions under these Rules.
(iii) Publication of list of registered health care facilities
with regard to bio-medical waste generation,
treatment and disposal.
(iv) Undertake or support operational research and
assessment with reference to risks to environment
and health due to bio-medical waste and previously
unknown disposables and wastes from new types of
equipment.
(v) Coordinate with State Pollution Control Boards for
organizing training programmes to staff of health
care facilities and municipal workers on bio-medical
waste.
(vi) Constitution of Expert Committees at National or
State level for overall review and promotion of clean
or new technologies for bio-medical waste
management.
Vol. 1 Issue 11 L.E.D. E-Journal Page 278
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
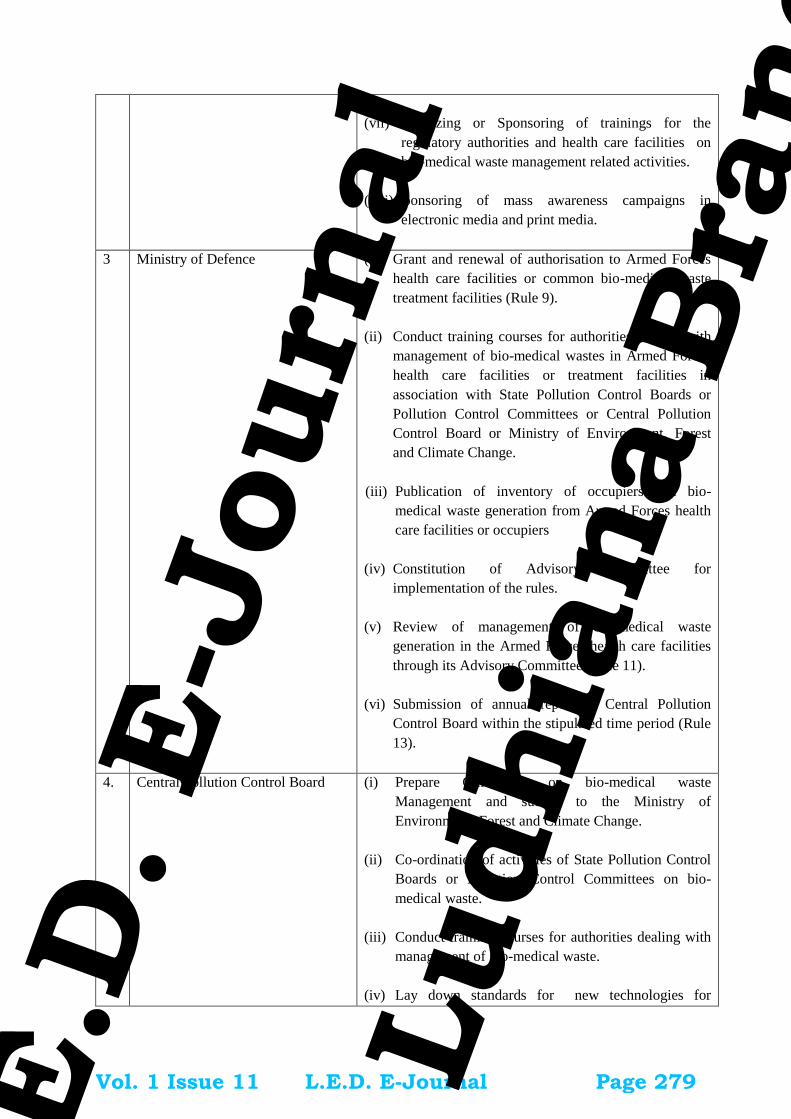
24
(vii) Organizing or Sponsoring of trainings for the
regulatory authorities and health care facilities on
bio-medical waste management related activities.
(viii) Sponsoring of mass awareness campaigns in
electronic media and print media.
3 Ministry of Defence (i) Grant and renewal of authorisation to Armed Forces
health care facilities or common bio-medical waste
treatment facilities (Rule 9).
(ii) Conduct training courses for authorities dealing with
management of bio-medical wastes in Armed Forces
health care facilities or treatment facilities in
association with State Pollution Control Boards or
Pollution Control Committees or Central Pollution
Control Board or Ministry of Environment, Forest
and Climate Change.
(iii) Publication of inventory of occupiers and bio-
medical waste generation from Armed Forces health
care facilities or occupiers
(iv) Constitution of Advisory Committee for
implementation of the rules.
(v) Review of management of bio-medical waste
generation in the Armed Forces health care facilities
through its Advisory Committee (Rule 11).
(vi) Submission of annual report to Central Pollution
Control Board within the stipulated time period (Rule
13).
4. Central Pollution Control Board (i) Prepare Guidelines on bio-medical waste
Management and submit to the Ministry of
Environment, Forest and Climate Change.
(ii) Co-ordination of activities of State Pollution Control
Boards or Pollution Control Committees on bio-
medical waste.
(iii) Conduct training courses for authorities dealing with
management of bio-medical waste.
(iv) Lay down standards for new technologies for
Vol. 1 Issue 11 L.E.D. E-Journal Page 279
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

25
treatment and disposal of bio-medical waste (Rule 7)
and prescribe specifications for treatment and
disposal of bio-medical wastes (Rule 7).
(v) Lay down Criteria for establishing common bio-
medical waste treatment facilities in the Country.
(vi) Random inspection or monitoring of health care
facilities and common bio-medical waste treatment
facilities.
(vii) Review and analysis of data submitted by the State
Pollution Control Boards on bio-medical waste and
submission of compiled information in the form of
annual report along with its observations to Ministry
of Environment, Forest and Climate Change .
(viii) Inspection and monitoring of health care facilities
operated by the Director General, Armed Forces
Medical Services (Rule 9).
(ix) Undertake or support research or operational
research regarding bio-medical waste.
5. State Government of Health or
Union Territory Government or
Administration
(i) To ensure implementation of the rule in all health
care facilities or occupiers.
(ii) Allocation of adequate funds to Government health
care facilities for bio-medical waste management.
(iii) Procurement and allocation of treatment equipments
and make provision for consumables for bio-medical
waste management in Government health care
facilities.
(iv) Constitute State or District Level Advisory
Committees under the District Magistrate or
Additional District Magistrate to oversee the bio-
medical waste management in the Districts.
(v) Advise State Pollution Control Boards or Pollution
Control Committees on implementation of these
Rules.
(vi) Implementation of recommendations of the Advisory
Committee in all the health care facilities.
Vol. 1 Issue 11 L.E.D. E-Journal Page 280
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

26
6. State Pollution Control Boards or
Pollution Control Committees
(i) Inventorisation of Occupiers and data on bio-medical
waste generation, treatment & disposal.
(ii) Compilation of data and submission of the same in
annual report to Central Pollution Control Board
within the stipulated time period.
(iii) Grant and renewal, suspension or refusal cancellation
or of authorisation under these rules (Rule 7, 8 and
10).
(iv) Monitoring of compliance of various provisions and
conditions of authorisation.
(v) Action against health care facilities or common bio-
medical waste treatment facilities for violation of
these rules (Rule 18).
(vi) Organizing training programmes to staff of health
care facilities and common bio-medical waste
treatment facilities and State Pollution Control
Boards or Pollution Control Committees Staff on
segregation, collection, storage, transportation,
treatment and disposal of bio-medical wastes.
(vii) Undertake or support research or operational research
regarding bio-medical waste management.
(viii) Any other function under these rules assigned by
Ministry of Environment, Forest and Climate
Change or Central Pollution Control Board from
time to time.
(ix) Implementation of recommendations of the Advisory
Committee.
(x) Publish the list of Registered or Authorised (or give
consent) Recyclers.
(xi) Undertake and support third party audits of the
common bio-medical waste treatment facilities in
their State.
7 Municipalities or Corporations,
Urban Local Bodies and Gram
Panchayats
(i) Provide or allocate suitable land for development of
common bio-medical waste treatment facilities in
their respective jurisdictions as per the guidelines of
Vol. 1 Issue 11 L.E.D. E-Journal Page 281
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
27
Central Pollution Control Board.
(ii) Collect other solid waste (other than the bio-
medical waste) from the health care facilities as
per the Municipal Solid Waste ( Management and
handling) Rules, 2000 or as amended time to time.
(iii) Any other function stipulated under these Rules.
Vol. 1 Issue 11 L.E.D. E-Journal Page 282
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
28
SCHEDULE IV
[See rule 8(3) and (5)]
Part A
LABEL FOR BIO-MEDICAL WASTE CONTAINERS or BAGS
CYTOTOXIC HAZARDSYMBOL
HANDLE WITH CARE HANDLE WITH CARE
Part B
LABEL FOR TRANSPORTING BIO-MEDICAL WASTE BAGS OR CONTAINERS
Day ............Month ..............
Year ...........
Date of generation ...................
Waste category Number ........
Waste quantity…………
Sender's Name and Address Receiver's Name and Address:
Phone Number ........ Phone Number ...............
Fax Number............... Fax Number .................
Contact Person ........ Contact Person .........
In case of emergency please contact :
Name and Address :
Phone No.
Note :Label shall be non-washable and prominently visible.
FORM – I
[ (See rule 4(o), 5(i) and 15 (2)]
ACCIDENT REPORTING
1. Date and time of accident :
2. Type of Accident :
Vol. 1 Issue 11 L.E.D. E-Journal Page 283
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
29
3. Sequence of events leading to accident :
4. Has the Authority been informed immediately :
5. The type of waste involved in accident :
6. Assessment of the effects of the
accidents on human health and the environment:
7. Emergency measures taken :
8. Steps taken to alleviate the effects of accidents :
9. Steps taken to prevent the recurrence of such an accident :
10. Does you facility has an Emergency Control policy? If yes give details:
Date : …………………… Signature …………………….
Place: …………………… Designation …………………..
FORM - II
(See rule10)
APPLICATION FOR AUTHORISATION OR RENEWAL OF AUTHORISATION
(To be submitted by occupier of health care facility or common bio-medical waste treatment facility)
To
The Prescribed Authority
(Name of the State or UT Administration)
Address.
1. Particulars of Applicant:
(i) Name of the Applicant:
(In block letters & in full)
(ii) Name of the health care facility (HCF) or common bio-medical waste treatment facility
(CBWTF) :
(iii) Address for correspondence:
(iv) Tele No., Fax No.:
Vol. 1 Issue 11 L.E.D. E-Journal Page 284
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

30
(v) Email:
(vi) Website Address:
2. Activity for which authorisation is sought:
Activity Please tick
Generation, segregation
Collection,
Storage
packaging
Reception
Transportation
Treatment or processing or conversion
Recycling
Disposal or destruction
use
offering for sale, transfer
Any other form of handling
3. Application for □ fresh or □ renewal of authorisation (please tick whatever is applicable):
(i) Applied for CTO/CTE Yes/No
(ii) In case of renewal previous authorisation number and date:
------------------------------------------------------
(iii) Status of Consents:
(a) under the Water (Prevention and Control of Pollution) Act, 1974
------------------------------------------------------
(b) under the Air (Prevention and Control of Pollution) Act, 1981:
------------------------------------------------------
4. (i) Address of the health care facility (HCF) or common bio-medical waste treatment facility
(CBWTF):
(ii) GPS coordinates of health care facility (HCF) or common bio-medical waste treatment
facility (CBWTF):
5. Details of health care facility (HCF) or common bio-medical waste treatment facility (CBWTF):
(i) Number of beds of HCF:
(ii) Number of patients treated per month by HCF:
(iii) Number healthcare facilities covered by CBMWTF: ______
(iv) No of beds covered by CBMWTF: ______
(v) Installed treatment and disposal capacity of CBMWTF:_______ Kg per day
(vi) Quantity of biomedical waste treated or disposed by CBMWTF:_____ Kg/ day
(vii) Area or distance covered by CBMWTF:______________
Vol. 1 Issue 11 L.E.D. E-Journal Page 285
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
31
(pl. attach map a map with GPS locations of CBMWTF and area of coverage)
(viii) Quantity of Biomedical waste handled, treated or disposed:
Category Type of Waste Quantity
Generated or
Collected, kg/day
Method of
Treatment and
Disposal
(Refer Schedule-
I)
(1) (2) (3) (4)
Yellow
(a) Human Anatomical Waste:
(b)Animal Anatomical Waste :
(c) Soiled Waste:
(d) Expired or Discarded Medicines:
(e) Chemical Solid Waste:
(f) Chemical Liquid Waste :
(g) Discarded linen, mattresses, beddings
contaminated with blood or body fluid.
(h) Microbiology, Biotechnology and other
clinical laboratory waste:
Red Contaminated Waste (Recyclable)
White
(Translucen
t)
Waste sharps including Metals:
Blue Glassware:
Metallic Body Implants
6. Brief description of arrangements for handling of biomedical waste (attach details):
(i) Mode of transportation (if any) of bio-medical waste:
(ii) Details of treatment equipment (please give details such as the number, type & capacity
of each unit)
No of units Capacity of each unit
Incinerators :
Plasma Pyrolysis:
Autoclaves:
Microwave:
Hydroclave:
Shredder:
Needle tip cutter or
destroyer
Sharps encapsulation or
concrete pit:
Deep burial pits:
Chemical disinfection:
Any other treatment
equipment:
Vol. 1 Issue 11 L.E.D. E-Journal Page 286
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

32
7. Contingency plan of common bio-medical waste treatment facility (CBWTF)(attach documents):
8. Details of directions or notices or legal actions if any during the period of earlier authorisation
9. Declaration
I do hereby declare that the statements made and information given above are true to the best of my
knowledge and belief and that I have not concealed any information.
I do also hereby undertake to provide any further information sought by the prescribed authority in
relation to these rules and to fulfill any conditions stipulated by the prescribed authority.
Date : Signature of the Applicant
Place : Designation of the Applicant
FORM –III
(See rule 10)
AUTHORISATION
(Authorisation for operating a facility for generation, collection, reception, treatment, storage, transport
and disposal of biomedical wastes)
1. File number of authorisation and date of issue……………………………………….
2. M/s __________________ an occupier or operator of the facility located at
______________________ is hereby granted an authorisation for;
Activity Please tick
Generation, segregation
Collection,
Storage
packaging
Reception
Transportation
Treatment or processing or conversion
Recycling
Disposal or destruction
use
offering for sale, transfer
Any other form of handling
3. M/s _____________________________ is hereby authorized for handling of biomedical waste
as per the capacity given below;
(i) Number of beds of HCF:
(ii) Number healthcare facilities covered by CBMWTF: ______
Vol. 1 Issue 11 L.E.D. E-Journal Page 287
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

33
(iii) Installed treatment and disposal capacity:_______ Kg per day
(iv) Area or distance covered by CBMWTF:______________
________________________________________________
(v) Quantity of Biomedical waste handled, treated or disposed:
Type of Waste Category Quantity permitted for
Handling
Yellow
Red
White (Translucent)
Blue
3. This authorisation shall be in force for a period of …………. Years from the date of issue.
4. This authorisation is subject to the conditions stated below and to such other conditions as may
be specified in the rules for the time being in force under the Environment (Protection) Act, 1986.
Date ……………. Signature……………………..
Place: ………………… Designation …………………..
Terms and conditions of authorisation *
1. The authorisation shall comply with the provisions of the Environment (Protection) Act, 1986
and the rules made there under.
2. The authorisation or its renewal shall be produced for inspection at the request of an officer
authorised by the prescribed authority.
3. The person authorized shall not rent, lend, sell, transfer or otherwise transport the biomedical
wastes without obtaining prior permission of the prescribed authority.
4. Any unauthorised change in personnel, equipment or working conditions as mentioned in the
application by the person authorised shall constitute a breach of his authorisation.
5. It is the duty of the authorised person to take prior permission of the prescribed authority to close
down the facility and such other terms and conditions may be stipulated by the prescribed
authority.
Form - IV
(See rule 13)
ANNUAL REPORT
[To be submitted to the prescribed authority on or before 30th June every year for the period from January
to December of the preceding year, by the occupier of health care facility (HCF) or common bio-medical
waste treatment facility (CBWTF)]
Sl.
No.
Particulars
1 . Particulars of the Occupier :
(i) Name of the authorised person (occupier or
operator of facility)
:
Vol. 1 Issue 11 L.E.D. E-Journal Page 288
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
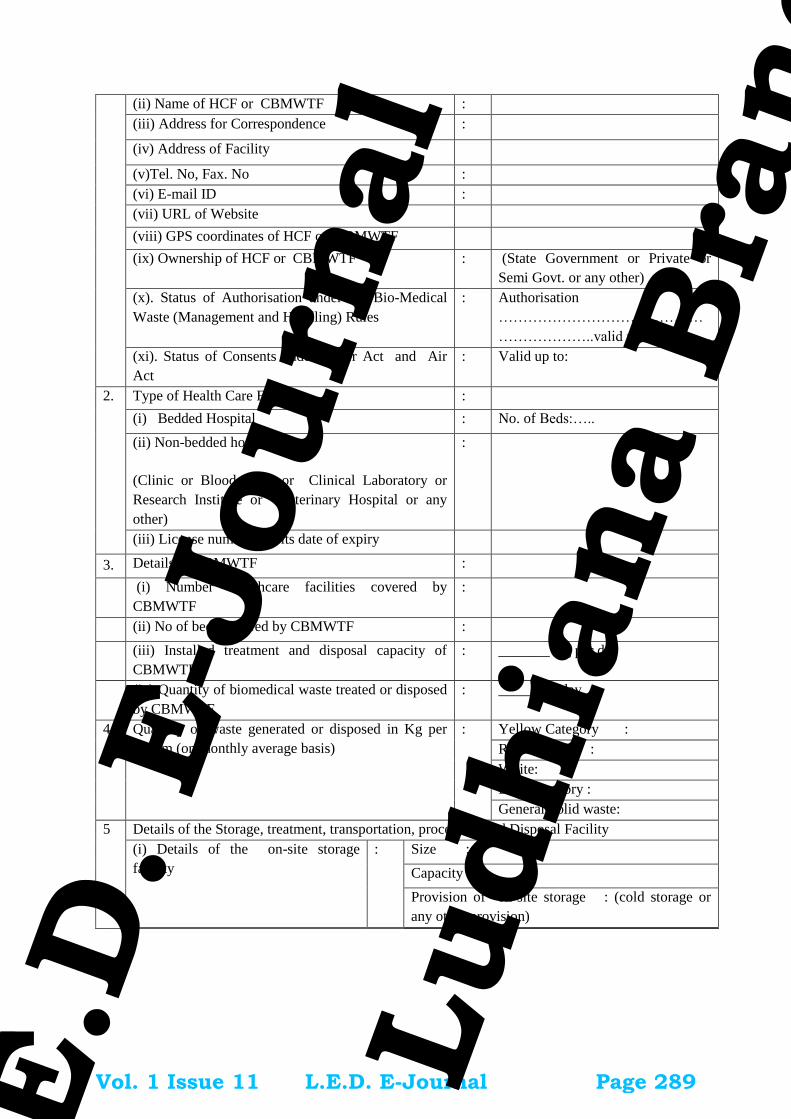
34
(ii) Name of HCF or CBMWTF :
(iii) Address for Correspondence :
(iv) Address of Facility
(v)Tel. No, Fax. No :
(vi) E-mail ID :
(vii) URL of Website
(viii) GPS coordinates of HCF or CBMWTF
(ix) Ownership of HCF or CBMWTF : (State Government or Private or
Semi Govt. or any other)
(x). Status of Authorisation under the Bio-Medical
Waste (Management and Handling) Rules
: Authorisation No.:
……………………………………
………………..valid up to ………..
(xi). Status of Consents under Water Act and Air
Act
: Valid up to:
2. Type of Health Care Facility :
(i) Bedded Hospital : No. of Beds:…..
(ii) Non-bedded hospital
(Clinic or Blood Bank or Clinical Laboratory or
Research Institute or Veterinary Hospital or any
other)
:
(iii) License number and its date of expiry
3. Details of CBMWTF :
(i) Number healthcare facilities covered by
CBMWTF
:
(ii) No of beds covered by CBMWTF :
(iii) Installed treatment and disposal capacity of
CBMWTF:
: _______ Kg per day
(iv) Quantity of biomedical waste treated or disposed
by CBMWTF
: _____ Kg/day
4. Quantity of waste generated or disposed in Kg per
annum (on monthly average basis)
:
Yellow Category :
Red Category :
White:
Blue Category :
General Solid waste:
5 Details of the Storage, treatment, transportation, processing and Disposal Facility
(i) Details of the on-site storage
facility
: Size :
Capacity :
Provision of on-site storage : (cold storage or
any other provision)
(ii) Details of the treatment or :
Vol. 1 Issue 11 L.E.D. E-Journal Page 289
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

35
disposal facilities Type of treatment
equipment
No
of
unit
s
Cap
acit
y
Kg/
day
Quantity
treatedo
r
disposed
in kg
per
annum
Incinerators
Plasma Pyrolysis
Autoclaves
Microwave
Hydroclave
Shredder
Needle tip cutter or
destroyer
-
Sharps
encapsulation or
concrete pit
-
Deep burial pits:
Chemical
disinfection:
-
Any other treatment
equipment:
(iii) Quantity of recyclable wastes
sold to authorized recyclers after
treatment in kg per annum.
: Red Category (like plastic, glass etc.)
(iv) No of vehicles used for collection
and transportation of biomedical
waste
:
(v) Details of incineration ash and
ETP sludge generated and disposed
during the treatment of wastes in Kg
per annum
Quantity
generated
Where
disposed
Incineration
Ash
ETP Sludge
(vi) Name of the Common Bio-
Medical Waste Treatment Facility
Operator through which wastes are
disposed of
:
(vii) List of member HCF not handed
over bio-medical waste.
6 Do you have bio-medical waste
management committee? If yes, attach
minutes of the meetings held during
the reporting period
7 Details trainings conducted on BMW
(i) Number of trainings conducted on
BMW Management.
Vol. 1 Issue 11 L.E.D. E-Journal Page 290
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

36
(ii) number of personnel trained
(iii) number of personnel trained at
the time of induction
(iv) number of personnel not
undergone any training so far
(v) whether standard manual for
training is available?
(vi) any other information)
8 Details of the accident occurred
during the year
(i) Number of Accidents occurred
(ii) Number of the persons affected
(iii) Remedial Action taken (Please
attach details if any)
(iv) Any Fatality occurred, details.
9. Are you meeting the standards of air
Pollution from the incinerator? How
many times in last year could not met
the standards?
Details of Continuous online emission
monitoring systems installed
10
.
Liquid waste generated and treatment
methods in place. How many times
you have not met the standards in a
year?
11 Is the disinfection method or
sterilization meeting the log 4
standards? How many times you have
not met the standards in a year?
12
.
Any other relevant information
: (Air Pollution Control Devices attached with the
Incinerator)
Certified that the above report is for the period from
…………………………………………………………..…………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
……………………………..
Name and Signature of the Head of the Institution
Date:
Place
FORM –V
Vol. 1 Issue 11 L.E.D. E-Journal Page 291
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
37
(See rule 16)
Application for filing appeal against order passed by the prescribed authority
1. Name and address of the person applying for appeal :
2. Number, date of order and address of the authority which passed the order, against which appeal
is being made (certified copy of order to be attached):
3. Ground on which the appeal is being made:
4. List of enclosures other than the order referred in para 2 against which appeal is being filed:
Signature ……………………..
Date : Name and Address……………………..
[F. No. 3-1/2000-HSMD]
(Bishwanath Sinha)
Joint secretary to the Government of India
******
Vol. 1 Issue 11 L.E.D. E-Journal Page 292
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

L.E.D. E-Journal
AERB Guidelines
The IDA Ludhiana Branch publication, ‘L.E.D.’ Ludhiana – ‘Let’s
Enjoy Dentistry’, a monthly E-Journal brings you the latest Atomic
Energy Regulatory Board (AERB) guidelines for radiographic
equipment in dental clinic & institutions in India. AERB has itself
developed and commissioned its computerized e-Governance project
“e-Licensing of Radiation Applications (e-LORA)” for Radiotherapy
facilities. This will facilitate the online submission of applications,
issuance of all regulatory clearances and registration of radiotherapy
institutions/radiation professionals. The system is being rolled out in
a phased manner by AERB and several institutes have already gone
online through e-LORA. All Radiotherapy facilities are expected to be
switched to online mode very shortly. For this purpose, all existing
radiotherapy centers are required to submit the details regarding the
following to AERB for pre-registration in e-LORA.
1. Present Employer
2. Licensee(s)
3. Radiological Safety Officer (s)
The format for details (as an excel file) can be downloaded
from AERB website as shown in the above Picture. Radiotherapy
institutions should ensure that all radiation professionals working in
the institution are registered with AERB through e-LORA. Kindly note
that AERB plans to stop accepting paper based regulatory
applications w.e.f. December 01, 2013 and all regulatory clearances
will be issued based on electronic submissions through e-LORA only.
The guidelines and all the needed details & forms are attached along
with.
Vol. 1 Issue 11 L.E.D. E-Journal Page 293
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Guidelines
GUIDELINES FOR STARTING A DIAGNOSTIC X-RAY INSTALLATION(Applicable for Diagnostic X-Ray/Cathlab/CTScan/C-Arm/Mammography/Dental/OPG/BMD/Mobile Units)
As per Atomic Energy (Radiation Protection) Rules 2004 Section (3) a Licence / Registration isnecessary for establishing a radiation installation. This process involves 3 steps. (i) SiteApproval by DRS (ii) Quality Assurance Test by manufacturer/supplier under intimation to DRS(iii) Licence/Registration by AERB through DRS.
1. Submit completely filled and duly signed “Application for Site Approval of X-Ray InstallationLayout” along with layout plan of the diagnostic x-ray room, drawn to scale 1:50 showing detailsas described in the application form, in original with two copies for approval to the Director,Directorate of Radiation Safety, District Hospital Compound, Thrissur. Pin: 680 001. Separateform should be submitted for each medical diagnostic x-ray unit installation. Mobile units do notrequire plan approval (mobile units should not be used in a room with table) but needRegistration Certificate. Enclose fees in the form of Demand Draft drawn in favour of theDirector of Radiation Safety payable at Thrissur, at the rates prescribed by theGovdownernment.
2. The room housing an x-ray unit shall not be less than 18m2 for general-purposeradiography and conventional fluoroscopy equipment and no single dimension of the x-ray roomshall be less than 4.0m. The room housing the gantry of the computed tomography (CT Scan)unit shall not be less than 25 m 15
and no single dimension of the gantry of CT Scan room shall be less than 4m. The roomhousing an orthopan tomography (OPG) units shall not be less that 15 m2
and no single dimension of the OPG room shall be less than 3.5m. The room housing amammography x-ray unit shall not be less than 10 m2
and no single dimension of x-ray room shall be less than 3m. Also, not more than one unit ofany type shall be installed in the same room. The minimum wall thickness of the x-ray roomshould be 9 inch or 23cm solid brick or equivalent. There shall be no windows and ventilationsshall be above 2m from the floor outside. Table shall be oriented such that the primary (cheststand) is not directed towards the main door or darkroom. The primary wall thickness shall be35 cm of solid brick or 32 cm solid brick + 1.5 mm LEAD
3. The users should install only Atomic Energy Regulatory Board (AERB) “Type Approved”unit or unit with valid NOC for medical diagnostic purpose and obtain a copy of the AERB “Type
1 / 3Vol. 1 Issue 11 L.E.D. E-Journal Page 294
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
Guidelines
Approval” certificate from the supplier/manufacturer of the x-ray unit prior to the procurement ofthe unit. User may verify the Type Approval Certificate Number from AERB in case of anydoubt.
4. The users should procure and use protective accessories such as mobile protective barrier,lead rubber aprons, lead rubber flaps, gloves, thyroid shields, etc.
5. The employer shall provide Personnel Monitoring Badges to all radiation workers of theinstitute. For procuring personnel monitoring badges, please contact Avanttec LaboratoriesPrivate Limited, #31, Kamaraj Street, Srinivasa Nagar, Padi, Chennai-600 050.
6. The users should follow the guidelines given in AERB Safety Code for Medical DiagnosticX-Ray Equipment and Installations [Code No.AERB/SC/MED-2 (Rev.-1)]. The same can bepurchased from AERB or downloaded from AERB website www.aerb.gov.in. The user shallcomply with other regulatory documents related to the use and operation of x-ray units that areavailable in AERB website or DRS website.
i Atomic Energy (Radiation Protection) Rules, 2004 (G.S.R.303)
ii Radiation Surveillance Procedures for Medical Applications of Radiation, 1989(G.S.R.No.388)
iii Performa for “Registration of Diagnostic X-Ray installations and Licence of ComputedTomography (CT)/Cathlab unit Installations”.
iv Documents (i) & (ii) can be purchased from bookstalls selling government publications or canbe downloaded from DRS website. (iii) shall be given by the Directorate of Radiation Safety onSite Approval
7. The users should request the supplier/manufacturer of the diagnostic x-ray units to conductQuality Assurance (QA) tests after the installation of x-ray unit/computed tomographyunit/mammography/ cathlab unit prior to using it for patient diagnosis, under intimation to theDRS. Preserve the QA tests report in the hospital/institution record for further use and submit acopy of QA tests report to the DRS. The unit should be used for patient diagnosis only if itsperformance is found satisfactory.
8. After installation, the users should send the completely filled and duly signed “Applicationfor Registration of Diagnostic X-Ray installations” / “Application for Licence of ComputedTomography (CT) unit / Interventional Radiology (Cathlab) Installations” (as applicable) to theDirector, Directorate of Radiation Safety, District Hospital Compound, Thrissur -680 001 for
2 / 3Vol. 1 Issue 11 L.E.D. E-Journal Page 295
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
Guidelines
onward transmission with recommendation to the Atomic Energy Regulatory Board for obtainingRegistration Certificate for diagnostic x-ray units and/or Licence Certificate for CT Scan/Cathlabunits for operation.
9. The employer shall employ only qualified Radiologist and x-ray Technician. The minimumqualification is given in AERB Safety Code for Medical Diagnostic X-Ray Equipment andInstallations [Code No.AERB/SC/MED-2(Rev-1)]
10. AERB issues notice every year in all leading newspapers in the country (both Hindi andEnglish) regarding “Statutory Requirements for Safe Operation of Medical diagnostic X-ray unitsby Hospitals, Clinics and other Medical Institutions in India”.
3 / 3Vol. 1 Issue 11 L.E.D. E-Journal Page 296
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
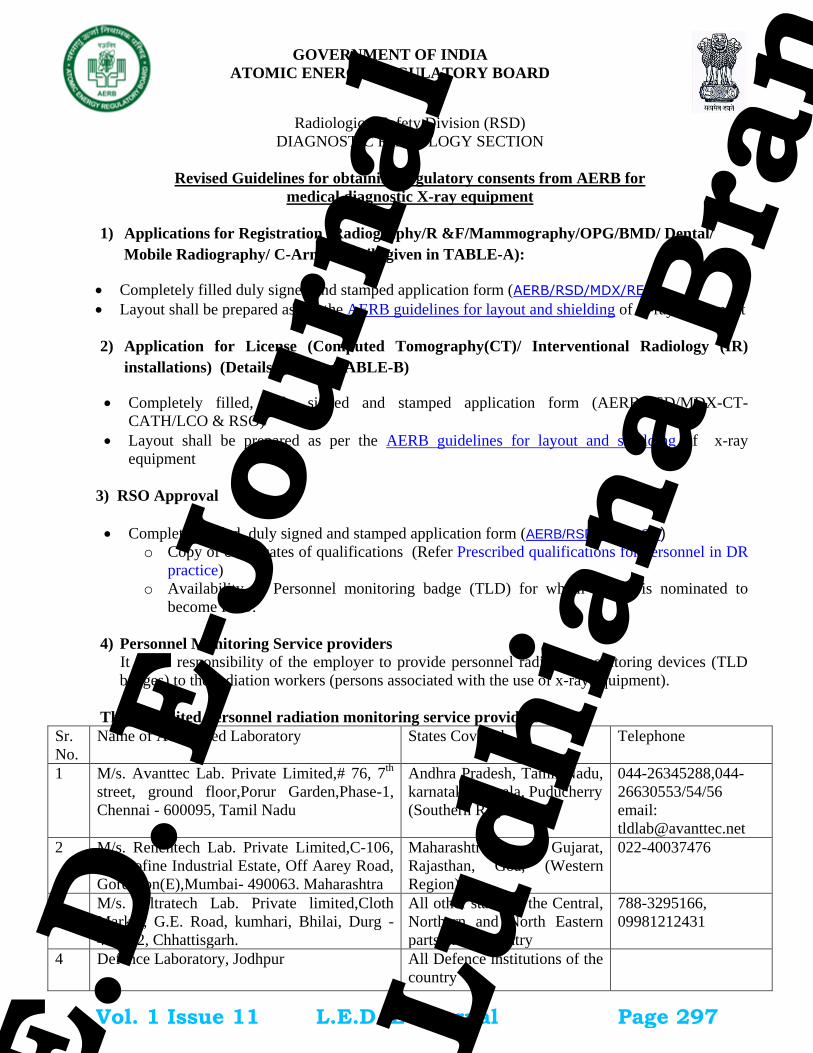
Radiological Safety Division (RSD)
DIAGNOSTIC RADIOLOGY SECTION
Revised Guidelines for obtaining regulatory consents from AERB for
medical diagnostic X-ray equipment
1) Applications for Registration (Radiography/R &F/Mammography/OPG/BMD/ Dental/
Mobile Radiography/ C-Arm) (details given in TABLE-A):
Completely filled duly signed and stamped application form (AERB/RSD/MDX/REG).
Layout shall be prepared as per the AERB guidelines for layout and shielding of x-ray equipment
2) Application for License (Computed Tomography(CT)/ Interventional Radiology (IR)
installations) (Details given in TABLE-B)
Completely filled, duly signed and stamped application form (AERB/RSD/MDX-CT-
CATH/LCO & RSO)
Layout shall be prepared as per the AERB guidelines for layout and shielding of x-ray
equipment
3) RSO Approval
Completely filled, duly signed and stamped application form (AERB/RSD/MDX-RSO) o Copy of certificates of qualifications (Refer Prescribed qualifications for personnel in DR
practice)
o Availability of Personnel monitoring badge (TLD) for which he/she is nominated to
become RSO.
4) Personnel Monitoring Service providers
It is the responsibility of the employer to provide personnel radiation monitoring devices (TLD
badges) to the radiation workers (persons associated with the use of x-ray equipment).
The accredited personnel radiation monitoring service providers:
Sr.
No.
Name of Accredited Laboratory States Covered Telephone
1 M/s. Avanttec Lab. Private Limited,# 76, 7th
street, ground floor,Porur Garden,Phase-1,
Chennai - 600095, Tamil Nadu
Andhra Pradesh, Tamil Nadu,
karnataka, Kerala, Puducherry
(Southern Region)
044-26345288,044-
26630553/54/56
email:
2 M/s. Renentech Lab. Private Limited,C-106,
Synthofine Industrial Estate, Off Aarey Road,
Goregaon(E),Mumbai- 490063. Maharashtra
Maharashtra, Gujarat,
Rajasthan, Goa, (Western
Region)
022-40037476
3 M/s. Ultratech Lab. Private limited,Cloth
Market, G.E. Road, kumhari, Bhilai, Durg -
490042, Chhattisgarh.
All other states in the Central,
Northern and North Eastern
parts of the country
788-3295166,
09981212431
4 Defence Laboratory, Jodhpur All Defence institutions of the
country
GOVERNMENT OF INDIA
ATOMIC ENERGY REGULATORY BOARD
Vol. 1 Issue 11 L.E.D. E-Journal Page 297
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

5) Points to be noted
a) No two X-ray equipment should be installed in the same room
b) X-ray installations should be located as far as feasible from areas of high occupancy such as
maternity, pediatric and ultra sonography rooms and other departments not directly related to
radiation applications in medicine.
c) Periodic safety status reports as per prescribed format on AERB website should be maintained by
registrant/ licensee.
d) Quality Assurance should be conducted once in two years on every x-ray equipment and records
to be maintained by registrant/licensee.
e) Other requirements relevant to medical diagnostic installations are prescribed in AERB safety
Code (AERB/SC/Med-2), 2001 and its amendment.
6) Renewal of Registration/ License: Application for renewal of Registration/ Licence shall be
submitted to Head, RSD, AERB at least 3 months prior to their validity date.
TABLE –A: Requirements for Registration to use/ operate X-ray equipment .
(Ref. Application form AERB/RSD/MDX/REG)
Type of X-ray unit Requirements for layout
of the room to install
X-ray equipment
Requirements for Registration
Radiography/
Fluoroscopy/
Mammography/
OPG/
Dental CBCT
Kindly see layout and
shielding guidelines for
diagnostic x-ray
installations (as applicable)
2 copies of layout of X-ray equipment room (in
1:50 scale)
Copy of valid NOC/ Type Approval certificate of
X-ray equipment
Copy of RSO approval, if already obtained
Availability of protective accessories ( Mobile
protective barrier, protective apron of 0.25mm Pb
equivalent)
List of qualified/ trained personnel with TLD
badges numbers (which should include names of
doctors, operator and RSO )
Copy of authenticated QA report
C-arm/
Mobile
radiography/ Intra
oral dental
equipment/
BMD
Not applicable Copy of valid NOC/ Type Approval certificate of
X-ray equipment
Copy of RSO approval, if already obtained
Availability of protective accessories ( Mobile
protective barrier, protective apron of 0.25mm Pb
equivalent)
List of qualified/ trained personnel with TLD
badges numbers (which should include names of
doctors, operator and RSO)
Copy of authenticated QA report
Vol. 1 Issue 11 L.E.D. E-Journal Page 298
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
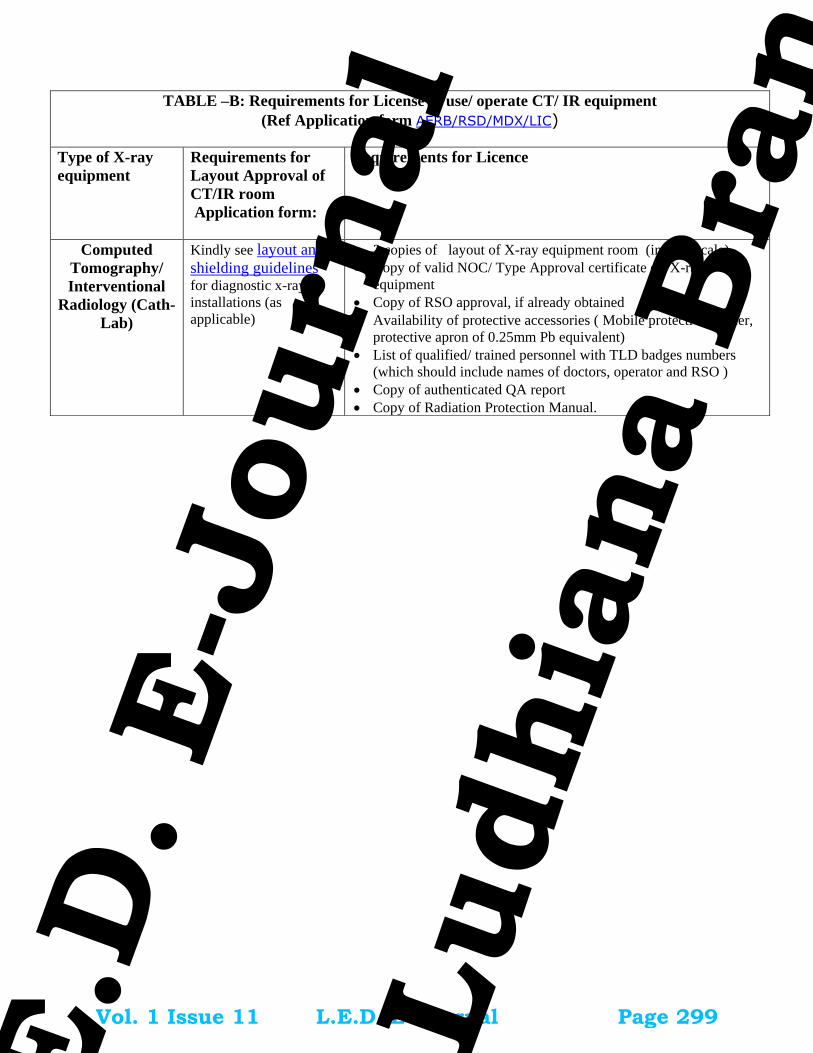
TABLE –B: Requirements for License to use/ operate CT/ IR equipment
(Ref Application form AERB/RSD/MDX/LIC)
Type of X-ray
equipment
Requirements for
Layout Approval of
CT/IR room
Application form:
Requirements for Licence
Computed
Tomography/
Interventional
Radiology (Cath-
Lab)
Kindly see layout and
shielding guidelines
for diagnostic x-ray
installations (as
applicable)
2 copies of layout of X-ray equipment room (in 1:50 scale)
Copy of valid NOC/ Type Approval certificate of X-ray
equipment
Copy of RSO approval, if already obtained
Availability of protective accessories ( Mobile protective barrier,
protective apron of 0.25mm Pb equivalent)
List of qualified/ trained personnel with TLD badges numbers
(which should include names of doctors, operator and RSO )
Copy of authenticated QA report
Copy of Radiation Protection Manual.
Vol. 1 Issue 11 L.E.D. E-Journal Page 299
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Guidelines for shielding of x-ray installations
The utility can hence forth follow the standard layout plans as provided in AERB web-site or customize it as per guidelines given below:
Options in shielding materials
X-ray equipment must be installed in adequately shielded rooms to ensure that public in the vicinity of
the x-ray installations are not unduly exposed to x-ray radiation. The adequacy of shielding depends on
the material and thickness used for this purpose. Different materials can be used for shielding. However,
brick or concrete are considered the best materials, as they are easily available, economical, and have
good structural strength.
While lead is a suitable shielding option for energies encountered in diagnostic x-rays, it is a weak
structural material with tendency to lose uniformity and needs periodic radiation survey to ensure its
continued adequacy. Also, Lead poses a serious environmental hazard and the use of it is being
discouraged the world over. Recently, many new materials are being used/ developed as potential
shielding materials, as an alternate to Lead. AERB would like to promote use of these materials, on
demonstration of shielding adequacy.
Step- by-step guidelines for submission of layout plan in diagnostic radiology facility 1) Decide a suitable room for housing an X-ray unit to facilitate the easy movement of staff and
patient positioning.
2) Room should have preferably one entrance door and window if present, should be above 2m from the finished floor level outside the x-ray room.
3) Door should have a hydraulic mechanism to ensure that door is closed during procedure and
should be provided with overlapping at the joints to avoid streaming.
4) Identify the walls as Wall A, Wall B, Wall C & Wall D (in any sequence)
5) Position the location of the equipment for each modality as follows:
a) Radiography and Fluoroscopy equipment: Couch, Control console and chest stand
- In such a way that chest stand is on the opposite wall of the entrance door and the control console.
- Mobile protective barrier with lead equivalent glass viewing window should be positioned in such a manner that the operator is completely shielded during the exposure.
- Control console should be positioned as far away as possible from the x-ray tube.
b) Computed Tomography and Interventional radiology equipment: Gantry / C-Arm, Couch,
Separate control console room, viewing window,
- Position the gantry and couch such that the patient is completely visible from the control console, during the scanning
- The entrance door to the gantry room from the control console shall have similar requirements as the patient entrance door.
c) Mammography/ OPG/ CBCT: Control console, Equipment and Protective barrier
Positioning of equipment should be as far as possible from the door and the control console.
Vol. 1 Issue 11 L.E.D. E-Journal Page 300
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
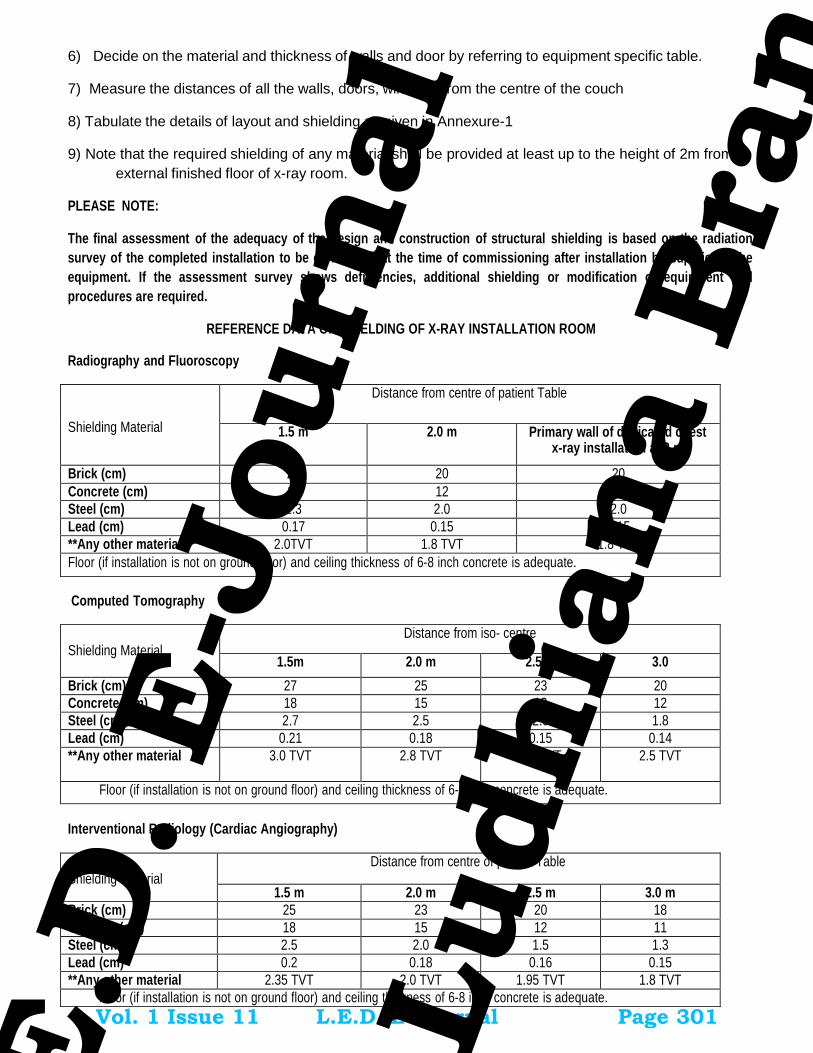
6) Decide on the material and thickness of walls and door by referring to equipment specific table.
7) Measure the distances of all the walls, doors, windows from the centre of the couch
8) Tabulate the details of layout and shielding as given in Annexure-1
9) Note that the required shielding of any material shall be provided at least up to the height of 2m from
external finished floor of x-ray room.
PLEASE NOTE:
The final assessment of the adequacy of the design and construction of structural shielding is based on the radiation
survey of the completed installation to be carried out at the time of commissioning after installation by supplier of the
equipment. If the assessment survey shows deficiencies, additional shielding or modification of equipment and
procedures are required.
REFERENCE DATA ON SHIELDING OF X-RAY INSTALLATION ROOM
Radiography and Fluoroscopy
Shielding Material
Distance from centre of patient Table
1.5 m 2.0 m Primary wall of dedicated chest x-ray installation at 2 m
Brick (cm) 23 20 20
Concrete (cm) 15 12 12
Steel (cm) 2.3 2.0 2.0
Lead (cm) 0.17 0.15 0.15
**Any other material 2.0TVT 1.8 TVT 1.8 TVT
Floor (if installation is not on ground floor) and ceiling thickness of 6-8 inch concrete is adequate.
Computed Tomography
Shielding Material
Distance from iso- centre
1.5m 2.0 m 2.5 m 3.0
Brick (cm) 27 25 23 20
Concrete (cm) 18 15 13 12
Steel (cm) 2.7 2.5 2.0 1.8
Lead (cm) 0.21 0.18 0.15 0.14
**Any other material 3.0 TVT 2.8 TVT 2.6 TVT 2.5 TVT
Floor (if installation is not on ground floor) and ceiling thickness of 6-8 inch concrete is adequate.
Interventional Radiology (Cardiac Angiography)
Shielding Material
Distance from centre of patient Table
1.5 m 2.0 m 2.5 m 3.0 m
Brick (cm) 25 23 20 18
Concrete(cm) 18 15 12 11
Steel (cm) 2.5 2.0 1.5 1.3
Lead (cm) 0.2 0.18 0.16 0.15
**Any other material 2.35 TVT 2.0 TVT 1.95 TVT 1.8 TVT
Floor (if installation is not on ground floor) and ceiling thickness of 6-8 inch concrete is adequate.
Vol. 1 Issue 11 L.E.D. E-Journal Page 301
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Mammography
Shielding Material
Distance from centre of patient Table
Standard gypsum wallboard construction is usually
adequate to shield the walls of mammography facility (as per thickness given below)
Solid core wooden door ( 5 cm thick) leading to corridors outside a mammography room provide adequate shielding. Standard wooden doors may not be sufficient if the shielded area has significant occupancy.
Standard concrete construction provides adequate barriers above and below mammographic facilities
Lead lined walls and doors are usually not required
1.0 m 1.5m
Gypsum Wallboard (cm) 1.5 1.0
Plate Glass (cm) 1.0 1.0
Concrete (cm) 1.0 1.0
Brick (cm) 1.5 1.0
**Any other material 2 TVT 1.68 TVT
Bone Mineral Densitometry
Dose rate at 1m is less than allowable dose limit for public hence no structural shielding is needed even with the smallest
room.
Dental CBCT/OPG (Ref: - Report of HPA working party on dental CBCT (HPA-RPD-065)
Shielding Material
Distance from centre of patient Table
0.5m* 1.0m 1.5 m 2.0m
Brick (cm) 22 17 15 12
Concrete (cm) 15 11 9.5 8
Baryte Plaster (cm) 1.5 1.0 -- --
Lead (cm) 0.22 0.17 0.15 0.12
**Any other material 2.6 TVT 2 TVT 1.72 TVT 1.4TVT
*Considered at this distance as the foot print of this equipment is small 100cm X 150cm Floor (if installation is not on ground floor) and ceiling thickness of 6-8 inch concrete is adequate.
Dental -intra oral radiography (Recommendatory)
Shielding Material
Distance from centre of patient Table
1.0m 2 m 4.0m
Primary wall
Secondary wall
Primary wall
Secondary wall
Primary wall
Secondary wall
Brick (cm) 12 5 10 5 8 --
Concrete (cm) 9 4 7 2 5.0 --
Lead (cm) 0.1 0.04 0.08 0.02 0.06 --
C- Arm and Lithotripsy x-ray equipment:
Mobile C-arm and Lithotripsy equipment should be used in Operation Theater with normal wall thickness of 9” brick/ 6”
concrete and should have 1.0 mm lead lined doors/windows.
**Note: : Lead free shielding materials have been developed by Council of Scientific and Industrial Research (CSIR)- Advanced
Materials & Process Research Institute (AMPRI), Bhopal. These materials may also be used as biological shielding material for
construction of medical diagnostic x-ray installations (X-ray room). For further details of these materials you may visit the website
www.ampri.res.in.
Vol. 1 Issue 11 L.E.D. E-Journal Page 302
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

FORMAT FOR SUBMISSION OF LAYOUT DETAILS OF MEDICAL X-RAY INSTALLATION
Type of equipment: Model name:
Wall Identification Distance from exposure
area (from centre of the couch)
Material used for shielding Thickness of the shielding material (cm)
Wall A
Wall B
Wall C
Wall D
Entrance Door
Any other door
Window, if any, if at the height less than 2 m from outside finished floor of x-ray room
Floor
Ceiling
Check list to be filled by applicant Status
1 All the walls are identified and distances of walls from the centre of the couch/equipment are indicated in the layout drawing
2 Layout drawing indicates the location of the mobile protective barrier
3 Layout drawing indicates x-ray machine, couch, control panel/ control room, chest stand, windows, doors, make and model of the x-ray equipment.
4 Layout drawing is signed and stamped by the applicant.
5 Layout drawing is authenticated by supplier.
6 The layout drawing is as per values filled in the above table.
7 Chest Stand is on the opposite wall of control console and entrance door Yes/ No
8 If NO whether, a permanent protective barrier is placed between operator and chest stand
9 Height of the window from outside finished floor of x-ray room is > 2 m Yes/ No
10 If No, whether shielding is provided on the window up to 2m Yes/ No
11 No permanent occupancy behind chest stand is ensured Yes/ No
Attach drawing authenticated by supplier in A4 size sheet (scale 1:50) indicating details given above.
Verified by: Name:
Signature of applicant
Signature of the supplier
Name Designation Company
Vol. 1 Issue 11 L.E.D. E-Journal Page 303
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Page 1 of 26
October 16, 2014 Always visit eLORA for recent guidelines
Guidelines for Applying for Licence of Diagnostic Radiology X-ray Equipments through eLORA System
General Guidelines (Applicable for all types of equipments viz. existing as well as new) ........................... 2
1. Register Your Institute ...................................................................................................................... 2
2. Prerequisites for Licence .................................................................................................................. 4
A. Declare Employees ....................................................................................................................... 4
B. Obtain RSO Approval .................................................................................................................... 6
C. Add Instrument ............................................................................................................................. 9
D. Prepare Layout ...........................................................................................................................10
E. Quality Assurance .......................................................................................................................11
Guidelines for Obtaining Licence for Existing X-ray Equipment .................................................................11
3. Declare Your X-ray Equipments ......................................................................................................11
4. Record Licence Detail .....................................................................................................................12
5. Fill Application Form for Licence ....................................................................................................13
Guidelines for Obtaining Licence for New X-ray Equipment ......................................................................18
6. Procurement of X-ray Equipment ...................................................................................................18
7. Application for Licence ...................................................................................................................18
Guidelines for Other Processes ..................................................................................................................19
8. Change in Layout: ...........................................................................................................................19
9. Safety Status Report .......................................................................................................................20
10. QA Test Summary .......................................................................................................................20
11. Radiation Survey Report .............................................................................................................20
12. Procurement of X-ray Tube ........................................................................................................20
13. Intimation of Receipt ..................................................................................................................20
14. Intimation of Decommissioning .................................................................................................21
Important Message ....................................................................................................................................21
15. NO LICENSE FEE /PROCESSING FEE BY AERB ..............................................................................21
Annexures ...................................................................................................................................................22
Annexure - 1: List of Personnel Monitoring Service (PMS) Providers ....................................................22
Annexure - 2: Standard Layouts .............................................................................................................23
a) Standard Layout of X-ray Installation .....................................................................................23
b) Standard Layout of CT Installation .........................................................................................24
c) Standard Layout of Interventional Radiology Installation ......................................................25
d) Standard Layout of Mammography Installation .....................................................................26
Vol. 1 Issue 11 L.E.D. E-Journal Page 304
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
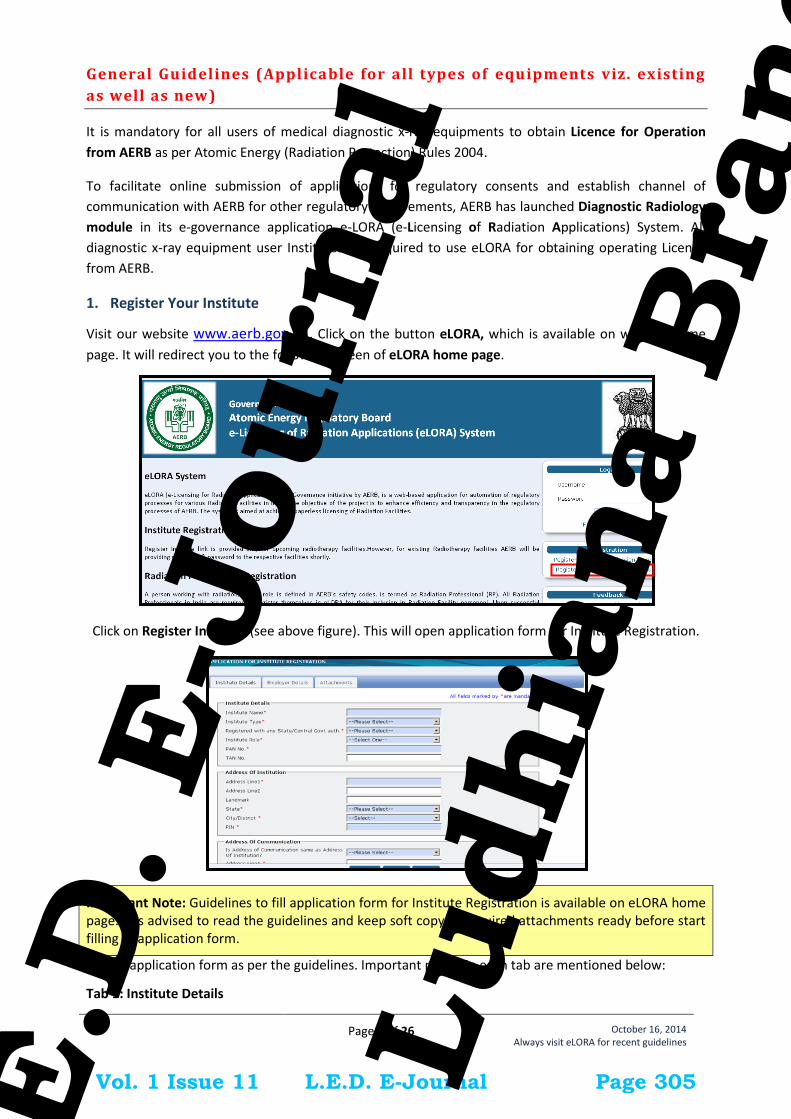
Page 2 of 26
October 16, 2014 Always visit eLORA for recent guidelines
General Guidelines (Applicable for all types of equipments viz. existing
as well as new)
It is mandatory for all users of medical diagnostic x-ray equipments to obtain Licence for Operation
from AERB as per Atomic Energy (Radiation Protection) Rules 2004.
To facilitate online submission of applications for regulatory consents and establish channel of
communication with AERB for other regulatory requirements, AERB has launched Diagnostic Radiology
module in its e-governance application e-LORA (e-Licensing of Radiation Applications) System. All
diagnostic x-ray equipment user Institutes are required to use eLORA for obtaining operating Licence
from AERB.
1. Register Your Institute
Visit our website www.aerb.gov.in . Click on the button eLORA, which is available on website home
page. It will redirect you to the following screen of eLORA home page.
Click on Register Institute (see above figure). This will open application form for Institute Registration.
Important Note: Guidelines to fill application form for Institute Registration is available on eLORA home page. It is advised to read the guidelines and keep soft copy of required attachments ready before start filling of application form.
Fill the application form as per the guidelines. Important points in each tab are mentioned below:
Tab 1: Institute Details
Vol. 1 Issue 11 L.E.D. E-Journal Page 305
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Page 3 of 26
October 16, 2014 Always visit eLORA for recent guidelines
In Type of Facility section, for the field Practice select Diagnostic Radiology and for the field Role of
Institute click on Medical Diagnostic X-ray Facility
Tab 2: Employer Details
Name: Fill the complete name of employer as appearing in his/her document for Proof of Identity/Date
of Birth (DOB) to be attached.
Date of Birth: Fill the DOB as appearing in the proof of identity/DOB to be attached
Document/card for proof of identity and date of birth (of employer): Select one from the drop down.
(Soft copy of this is a mandatory attachment).
Document/Card No. (of Proof of Identity/DOB): Must match with the proof of identity/DOB attached
E-mail (O): Will be used to send USERNAME and PASSWORD of your eLORA account and for all future
communications. (Make sure to provide correct email address).
Tab 3: Attachments
Upload of following attachments are mandatory:
Proof of Identity and Date of Birth (of employer): Acceptable documents are as follows:
o Passport
o PAN card issued by Income Tax Department
o Driving Licence issued by RTO
o Photo identity document/card having serial number and date of birth issued by
Central/State Government or PSU
Proof of Employership: Example: (i) Appointment Letter of Employer, (ii) Board Resolution, (iii)
Any Govt./PUC document substantiating proprietorship (iv) Partnership deed (notorised) or (iv)
Proprietor’s self declaration on institute letter head affixed with institute seal
Upload scan copy of any one of the document (in the relevant position) for the proof of
existence of institute:
o PAN of Institute
o TAN of Institute
o Registration with State/Central/Local Government Authority
Enter the Captch and submit the application form.
Important Note: Fields marked with * in the application form are mandatory. Application form will not be submitted if any mandatory field left blank.
Vol. 1 Issue 11 L.E.D. E-Journal Page 306
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
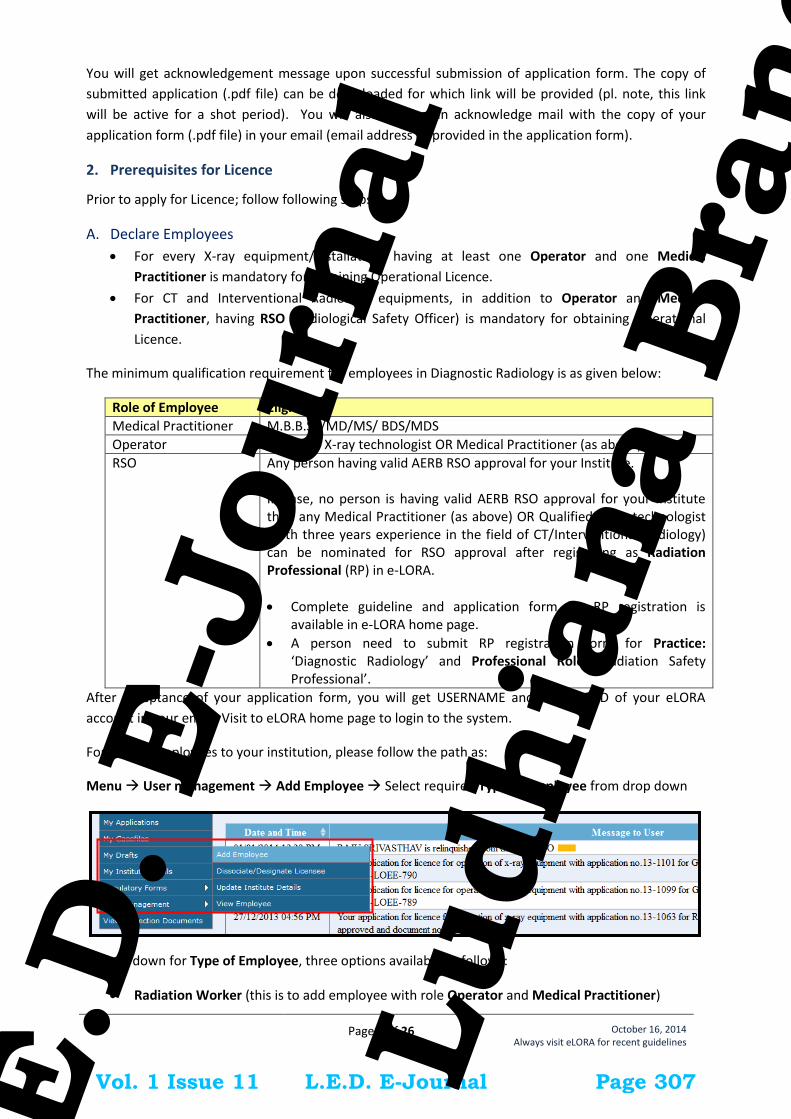
Page 4 of 26
October 16, 2014 Always visit eLORA for recent guidelines
You will get acknowledgement message upon successful submission of application form. The copy of
submitted application (.pdf file) can be downloaded for which link will be provided (pl. note, this link
will be active for a shot period). You will also receive an acknowledge mail with the copy of your
application form (.pdf file) in your email (email address as provided in the application form).
2. Prerequisites for Licence
Prior to apply for Licence; follow following steps:
A. Declare Employees
For every X-ray equipment/installation, having at least one Operator and one Medical
Practitioner is mandatory for obtaining Operational Licence.
For CT and Interventional Radiology equipments, in addition to Operator and Medical
Practitioner, having RSO (Radiological Safety Officer) is mandatory for obtaining Operational
Licence.
The minimum qualification requirement for employees in Diagnostic Radiology is as given below:
Role of Employee Eligibility
Medical Practitioner M.B.B.S. /MD/MS/ BDS/MDS
Operator Qualified X-ray technologist OR Medical Practitioner (as above)
RSO Any person having valid AERB RSO approval for your Institute. In case, no person is having valid AERB RSO approval for your Institute then any Medical Practitioner (as above) OR Qualified X-ray technologist (with three years experience in the field of CT/Interventional Radiology) can be nominated for RSO approval after registering as Radiation Professional (RP) in e-LORA.
Complete guideline and application form for RP registration is available in e-LORA home page.
A person need to submit RP registration form for Practice: ‘Diagnostic Radiology’ and Professional Role: ‘Radiation Safety Professional’.
After acceptance of your application form, you will get USERNAME and PASSWORD of your eLORA
account in your email. Visit to eLORA home page to login to the system.
For adding employees to your institution, please follow the path as:
Menu User management Add Employee Select required Type of Employee from drop down
In drop down for Type of Employee, three options available as follows:
Radiation Worker (this is to add employee with role Operator and Medical Practitioner)
Vol. 1 Issue 11 L.E.D. E-Journal Page 307
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
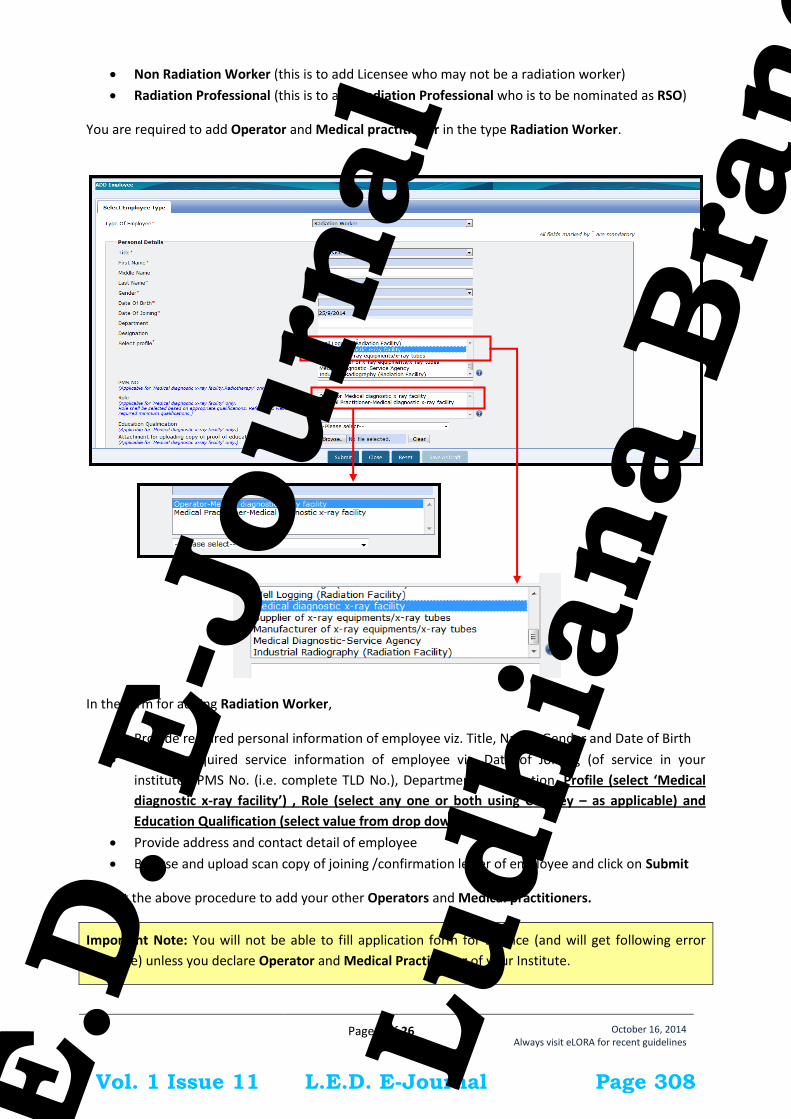
Page 5 of 26
October 16, 2014 Always visit eLORA for recent guidelines
Non Radiation Worker (this is to add Licensee who may not be a radiation worker)
Radiation Professional (this is to add Radiation Professional who is to be nominated as RSO)
You are required to add Operator and Medical practitioner in the type Radiation Worker.
In the form for adding Radiation Worker,
Provide required personal information of employee viz. Title, Name, Gender and Date of Birth
Provide required service information of employee viz. Date of Joining (of service in your
institute), PMS No. (i.e. complete TLD No.), Department, Designation, Profile (select ‘Medical
diagnostic x-ray facility’) , Role (select any one or both using Ctrl key – as applicable) and
Education Qualification (select value from drop down)
Provide address and contact detail of employee
Browse and upload scan copy of joining /confirmation letter of employee and click on Submit
Repeat the above procedure to add your other Operators and Medical practitioners.
Important Note: You will not be able to fill application form for Licence (and will get following error
message) unless you declare Operator and Medical Practitioner of your Institute.
Vol. 1 Issue 11 L.E.D. E-Journal Page 308
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Page 6 of 26
October 16, 2014 Always visit eLORA for recent guidelines
In case your institute is not having valid RSO, you need to obtain RSO approval from AERB. For a person
required to be nominated as RSO, you need to add him/her in the type Radiation Professional (RP).
While adding RP, system will ask RP registration ID and Date of birth of RP. (Obtain these details from
the Radiation Professional)
In the form for adding Radiation Professional,
Enter Registration ID and Date of birth of RP – personal detail of RP will come automatically.
Provide Date of Joining (of service in your institute), PMS No. (i.e. complete TLD No.),
Department and Designation, Profile (i.e. ‘Medical diagnostic x-ray facility’) and Role (i.e.
‘Operator’, Medical Practitioner’ or both)
Provide Email (O)
Browse and upload scan copy of joining /confirmation letter of employee and click on Submit
Important Note: Radiation Professional can subsequently be nominated for the approval of Radiological Safety Officer (RSO). Process of RSO nomination explained in Sr. No.: B
B. Obtain RSO Approval
In case you do not have valid RSO for your CT and Interventional Radiology facility, obtain RSO approval.
For CT and Interventional Radiology facilities, RSO approval is mandatory. For nominating your
employee for RSO approval, follow the path as:
Menu Regulatory Forms Common Forms
Vol. 1 Issue 11 L.E.D. E-Journal Page 309
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
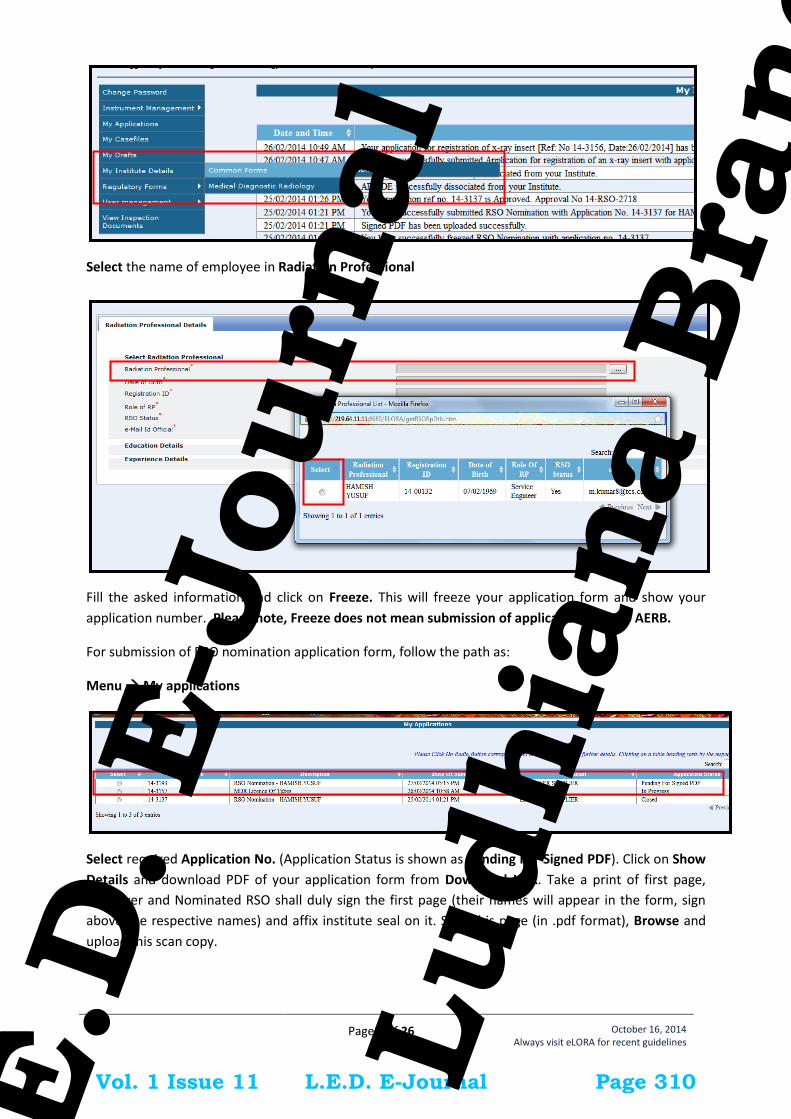
Page 7 of 26
October 16, 2014 Always visit eLORA for recent guidelines
Select the name of employee in Radiation Professional
Fill the asked information and click on Freeze. This will freeze your application form and show your
application number. Please note, Freeze does not mean submission of application form to AERB.
For submission of RSO nomination application form, follow the path as:
Menu My applications
Select required Application No. (Application Status is shown as Pending For Signed PDF). Click on Show
Details and download PDF of your application form from Download Link. Take a print of first page,
Employer and Nominated RSO shall duly sign the first page (their names will appear in the form, sign
above the respective names) and affix institute seal on it. Scan this page (in .pdf format), Browse and
upload this scan copy.
Vol. 1 Issue 11 L.E.D. E-Journal Page 310
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Page 8 of 26
October 16, 2014 Always visit eLORA for recent guidelines
After uploading of scan file, Application Status will change to Signed PDF Uploaded
Select the Application No and click on Submit to complete submission of application form (Application
Status will change to Submitted).
Important Note: The above mentioned procedure of submission of application is applicable for other
Vol. 1 Issue 11 L.E.D. E-Journal Page 311
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
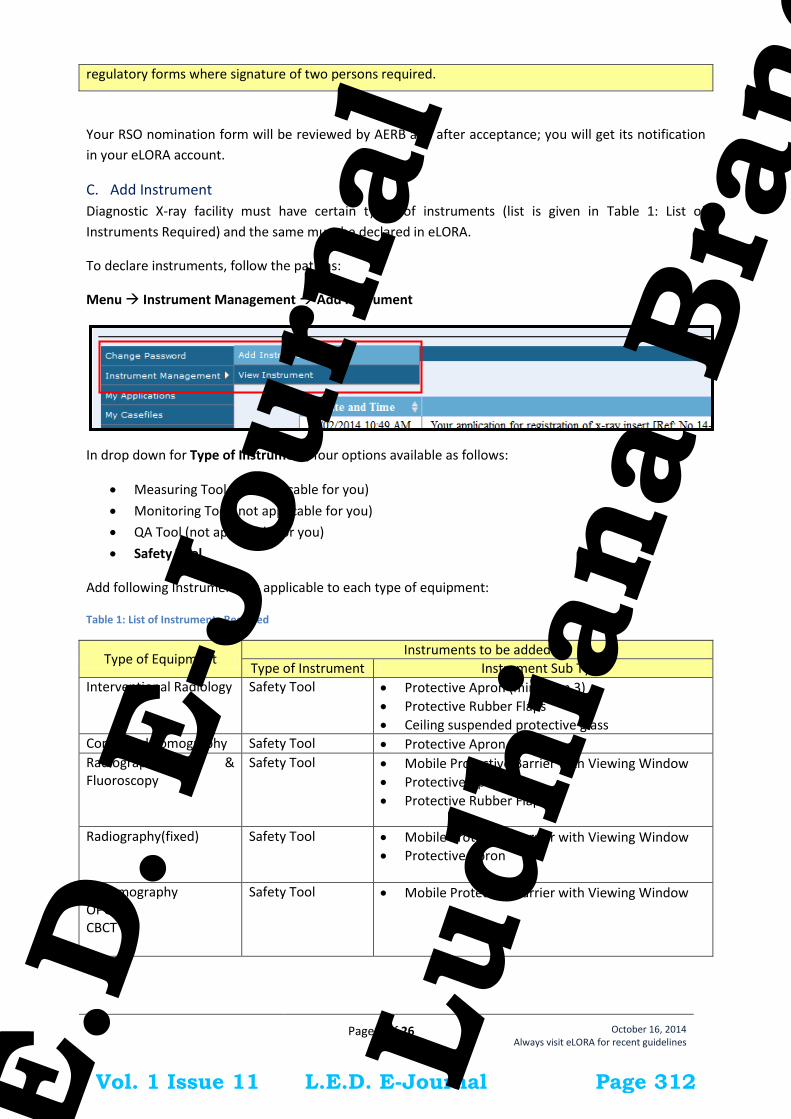
Page 9 of 26
October 16, 2014 Always visit eLORA for recent guidelines
regulatory forms where signature of two persons required.
Your RSO nomination form will be reviewed by AERB and after acceptance; you will get its notification
in your eLORA account.
C. Add Instrument
Diagnostic X-ray facility must have certain types of instruments (list is given in Table 1: List of
Instruments Required) and the same must be declared in eLORA.
To declare instruments, follow the path as:
Menu Instrument Management Add Instrument
In drop down for Type of Instrument, four options available as follows:
Measuring Tool (not applicable for you)
Monitoring Tool (not applicable for you)
QA Tool (not applicable for you)
Safety Tool
Add following Instruments as applicable to each type of equipment:
Table 1: List of Instruments Required
Type of Equipment Instruments to be added
Type of Instrument Instrument Sub Type
Interventional Radiology
Safety Tool Protective Apron (minimum 3)
Protective Rubber Flaps
Ceiling suspended protective glass Computed Tomography Safety Tool Protective Apron
Radiography & Fluoroscopy
Safety Tool Mobile Protective Barrier with Viewing Window
Protective Apron
Protective Rubber Flaps
Radiography(fixed) Safety Tool Mobile Protective Barrier with Viewing Window
Protective Apron
Mammography OPG CBCT
Safety Tool Mobile Protective Barrier with Viewing Window
Vol. 1 Issue 11 L.E.D. E-Journal Page 312
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Page 10 of 26
October 16, 2014 Always visit eLORA for recent guidelines
Radiography (Mobile) Radiography (Portable) C-arm/O-Arm Dental (Intra-oral) Dental (Hand –held)
Safety Tool Protective Apron
Provide the required information while adding equipment.
Important Note: You will not be able to fill application form for Licence (and will get following error
message) unless you declare required Instrument(s).
D. Prepare Layout
Prepare a sketch of layout (1:50 scale) of each x-ray room (not applicable for Radiography (mobile), C-
Arm, O-Arm, Dental (Intra-oral) and Dental (Hand –held) X-ray equipment) providing all the details
about wall dimensions, wall thickness, wall/shielding material, distances of all walls/shielding from x-ray
equipment, relative positions of x-ray equipment, couch, control console/control room, protective
barrier, door(s), window(s) , occupancy around the x-ray room etc. For the preparation layout details,
guidelines and model layout plans are available on AERB website
(http://www.aerb.gov.in/AERBPortal/pages/English/X-Ray/X-Ray_jsp.action) as well as enclosed here as
Annexure - 2: Standard Layouts.
You are required to preserve the duly signed and stamped copy of x-ray room with details of shielding
at your institution and same will be verified during AERB inspection.
There is no requirement to prepare a new layout plan in case you already have AERB approved layout
plan. The same can be used as a record for layout.
If your x-ray room is as per model layout or has AERB approved layout, you need not to submit all
details in the application form for License.
In case your x-ray room does not follow standard requirements,
You will be required to provide the details in the prescribed format in the application form for
operating Licence, as well as
You will have to get radiation survey done from supplier of equipment or authorized agencies as
per prescribed format as given in application form for operating Licence.
Important Note: While submitting Operational Licence application form for CT and Interventional Radiology equipment, you will be asked to upload scan copy of duly signed and stamped layout plan.
Vol. 1 Issue 11 L.E.D. E-Journal Page 313
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Page 11 of 26
October 16, 2014 Always visit eLORA for recent guidelines
E. Quality Assurance
Prior to apply for licence for operation of existing x-ray equipment, conduct its Quality Assurance (QA)
as per AERB prescribed format. The Quality Assurance (QA) formats are available on AERB website
(http://www.aerb.gov.in/AERBPortal/pages/English/X-Ray/XRAYmanfform_jsp.action).
Important Note: While submitting Operational Licence application form for CT and Interventional Radiology equipment, you will be asked to upload scan copy of duly signed and stamped QA.
Guidelines for Obtaining Licence for Existing X -ray Equipment
3. Declare Your X-ray Equipments
After login, you will see following screen with various Menu on left hand side. You will have to declare
your all X-ray equipments one-by-one. Click on Declare Existing X-ray Equipment to declare your
existing x-ray equipment.
Provide the detail as asked in the form and click on Submit.
After successful submission, an acknowledgement message with equipment id will be displayed.
Vol. 1 Issue 11 L.E.D. E-Journal Page 314
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
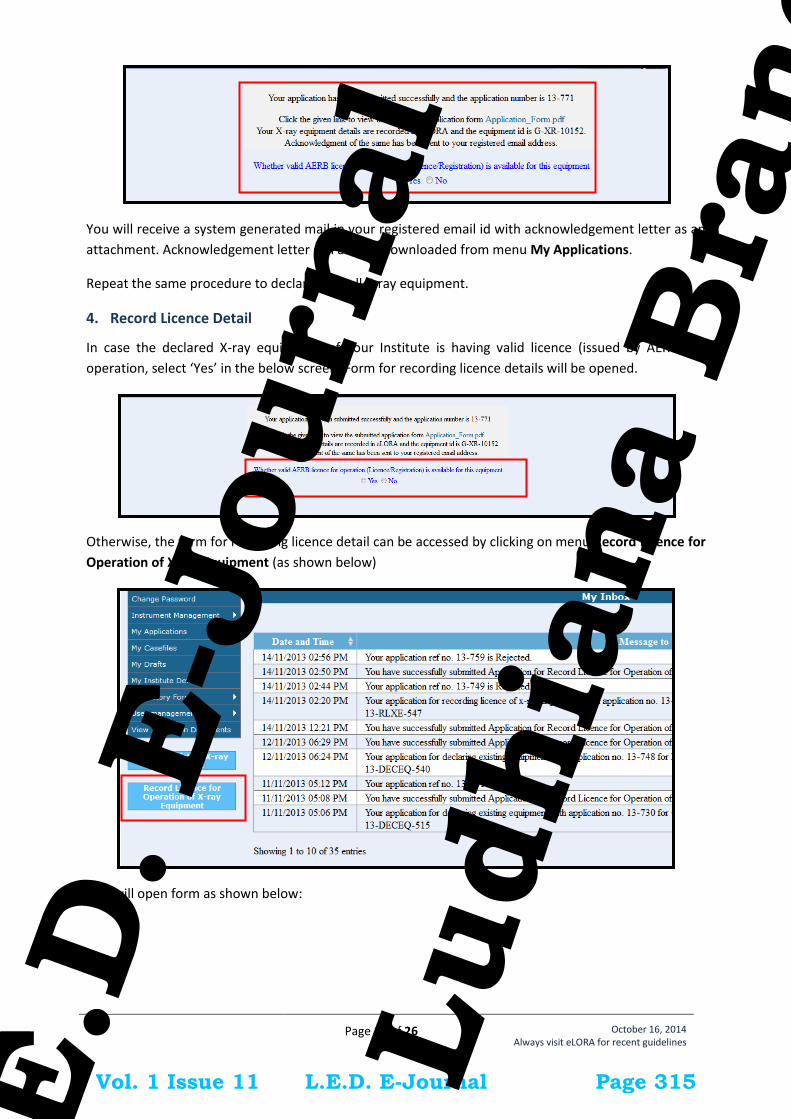
Page 12 of 26
October 16, 2014 Always visit eLORA for recent guidelines
You will receive a system generated mail in your registered email id with acknowledgement letter as an
attachment. Acknowledgement letter can also be downloaded from menu My Applications.
Repeat the same procedure to declare your all X-ray equipment.
4. Record Licence Detail
In case the declared X-ray equipment of your Institute is having valid licence (issued by AERB) for
operation, select ‘Yes’ in the below screen. Form for recording licence details will be opened.
Otherwise, the form for recording licence detail can be accessed by clicking on menu Record Licence for
Operation of X-ray Equipment (as shown below)
This will open form as shown below:
Vol. 1 Issue 11 L.E.D. E-Journal Page 315
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Page 13 of 26
October 16, 2014 Always visit eLORA for recent guidelines
Provide following required details and submit the form:
Equipment Id: To be selected from provided List (all your declared equipments will appear
here)
Reference number of licence for operation: as appearing on AERB licence/registration
Issuance date: as appearing on AERB licence/registration
Expiry date: as appearing on AERB licence/registration
Upload copy of Licence for operation: Browse and upload scanned copy of AERB
licence/registration
After successful submission, following message will be displayed. The submitted application form (.pdf
file) can be downloaded from the link provided therein.
Your Licence record detail will be verified by AERB. After acceptance of your submitted detail, you will
receive a system generated message in your registered email address with an acknowledgement letter
as an attachment. An acknowledgement letter can also be downloaded from menu My Applications.
5. Fill Application Form for Licence
The application form for licence is available in menu.
Menu Licence for Operation of Existing Equipments
Important Note: You won’t be able to fill the application form if required prerequisites are not completed.
Vol. 1 Issue 11 L.E.D. E-Journal Page 316
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Page 14 of 26
October 16, 2014 Always visit eLORA for recent guidelines
A form will be opened as shown below:
Form initially will have three tabs:
1. Employee Detail: This will show the list of employees added as Radiation Professional.
(Employees added as Radiation Worker and Non Radiation Worker will not be show).
2. Safety Tools Detail: This will show the list of Instruments added.
3. General Detail: In the field Application for, select Licence for Operation for first time
application. In future, select Renewal of Licence for Operation for submission of form for
renewal of existing Licence. Then click on Equipment Id, it will show list of equipments
declared by you. Select Equipment for which you wish to submit application form.
Vol. 1 Issue 11 L.E.D. E-Journal Page 317
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Page 15 of 26
October 16, 2014 Always visit eLORA for recent guidelines
Provide Serial Number of Equipment if available.
In case you have approved RSO (RSO approval received on paper), select Yes and provide required
detail and upload scan copy of RSO approval letter.
In case you do not have approved RSO, then select No and select one of your employee in the field
Name of the person designated as RSO for this equipment (this will not be applicable for CT and
Interventional Radiology equipment).
Important Note: Obtain prior approval of RSO for CT and Interventional Radiology equipment if you do not have valid RSO.
After selection of equipment, two more tabs will be displayed (viz. Layout Detail and QA Test Report)
4. Layout Detail: If installation layout of your equipment is as per AERB model layout, then select
Yes
Vol. 1 Issue 11 L.E.D. E-Journal Page 318
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Page 16 of 26
October 16, 2014 Always visit eLORA for recent guidelines
Important Note: While submitting Operational Licence application form for CT and Interventional Radiology equipment, you will be asked to upload scan copy of duly signed and stamped layout plan.
If X-ray equipment installation layout is not as per AERB model layout, then select No.
Provide the detail as per your room layout plan (as explained above in section D: Prepare
Layout)
upload copy of room layout plan (in case of CT and Interventional Radiology)
For Radiation Survey Report: Get radiation survey done from supplier of equipment or authorized
agencies as per prescribed format and provide the details in the application form (as applicable):
The exposure parameters to be selected for while carrying out survey are given in the table:
Type of Equipment Applied Voltage # Applied Current *Exposure time
Vol. 1 Issue 11 L.E.D. E-Journal Page 319
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
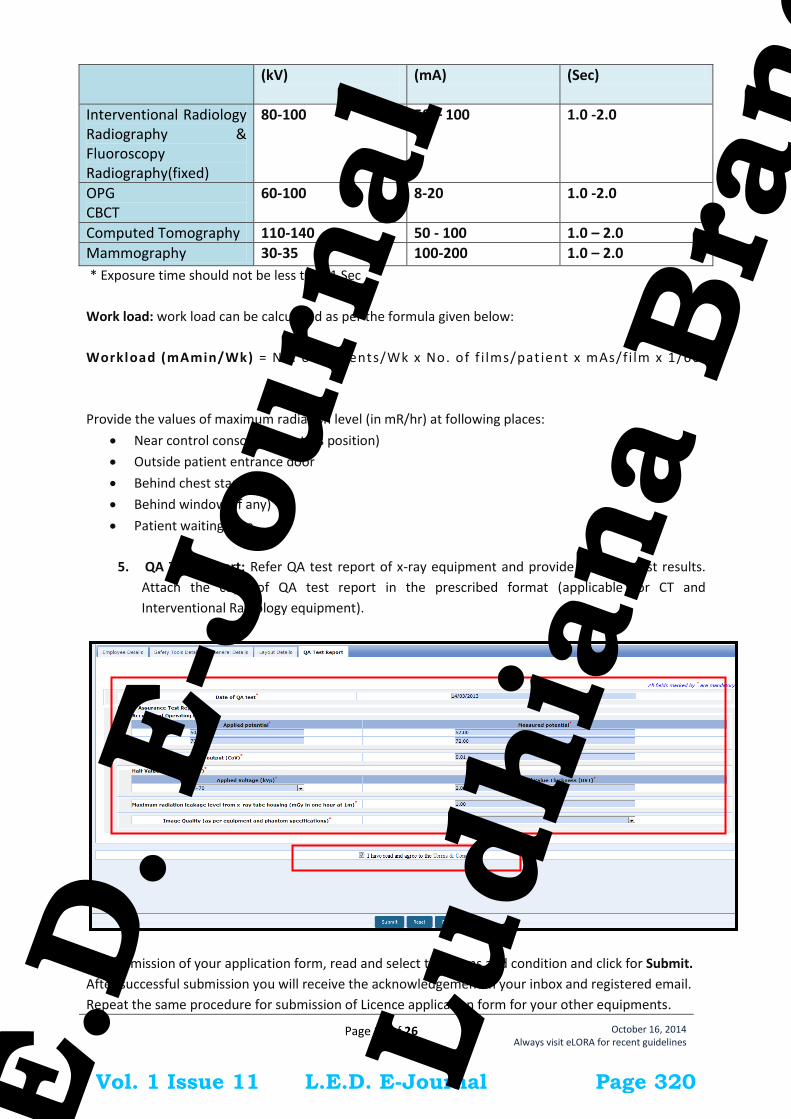
Page 17 of 26
October 16, 2014 Always visit eLORA for recent guidelines
(kV)
(mA) (Sec)
Interventional Radiology Radiography & Fluoroscopy Radiography(fixed)
80-100 50 – 100 1.0 -2.0
OPG CBCT
60-100 8-20 1.0 -2.0
Computed Tomography 110-140 50 - 100 1.0 – 2.0
Mammography 30-35 100-200 1.0 – 2.0
* Exposure time should not be less than 1 Sec
Work load: work load can be calculated as per the formula given below:
Workload (mAmin/Wk) = No. of patients/Wk x No. of f i lms/pat ient x mAs/fi lm x 1/60
Provide the values of maximum radiation level (in mR/hr) at following places:
Near control console (operators position)
Outside patient entrance door
Behind chest stand wall
Behind window (if any)
Patient waiting area
5. QA Test Report: Refer QA test report of x-ray equipment and provide required test results.
Attach the copy of QA test report in the prescribed format (applicable for CT and
Interventional Radiology equipment).
For submission of your application form, read and select the terms and condition and click for Submit.
After successful submission you will receive the acknowledgement in your inbox and registered email.
Repeat the same procedure for submission of Licence application form for your other equipments.
Vol. 1 Issue 11 L.E.D. E-Journal Page 320
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
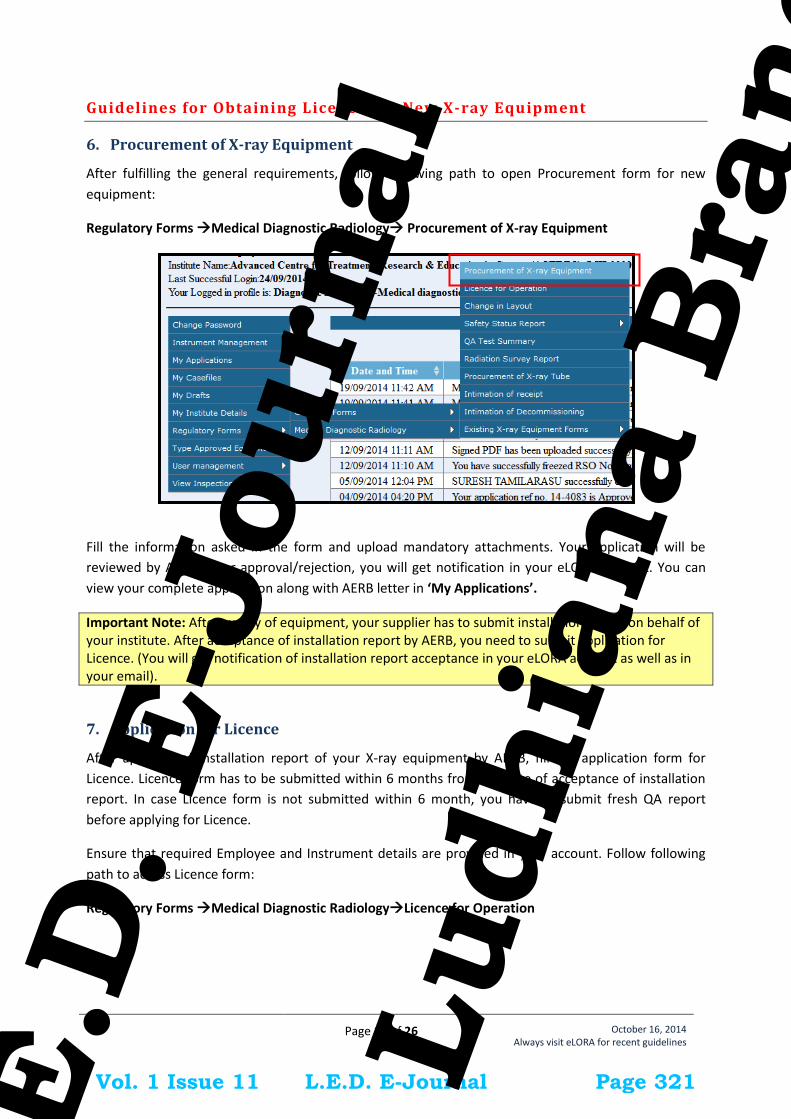
Page 18 of 26
October 16, 2014 Always visit eLORA for recent guidelines
Guidelines for Obtaining Licence for New X-ray Equipment
6. Procurement of X-ray Equipment
After fulfilling the general requirements, follow following path to open Procurement form for new
equipment:
Regulatory Forms Medical Diagnostic Radiology Procurement of X-ray Equipment
Fill the information asked in the form and upload mandatory attachments. Your application will be
reviewed by AERB. After approval/rejection, you will get notification in your eLORA account. You can
view your complete application along with AERB letter in ‘My Applications’.
Important Note: After supply of equipment, your supplier has to submit installation report on behalf of your institute. After acceptance of installation report by AERB, you need to submit application for Licence. (You will get notification of installation report acceptance in your eLORA account as well as in your email).
7. Application for Licence
After approval of installation report of your X-ray equipment by AERB, fill the application form for
Licence. Licence form has to be submitted within 6 months from the date of acceptance of installation
report. In case Licence form is not submitted within 6 month, you have to submit fresh QA report
before applying for Licence.
Ensure that required Employee and Instrument details are provided in your account. Follow following
path to access Licence form:
Regulatory Forms Medical Diagnostic RadiologyLicence for Operation
Vol. 1 Issue 11 L.E.D. E-Journal Page 321
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
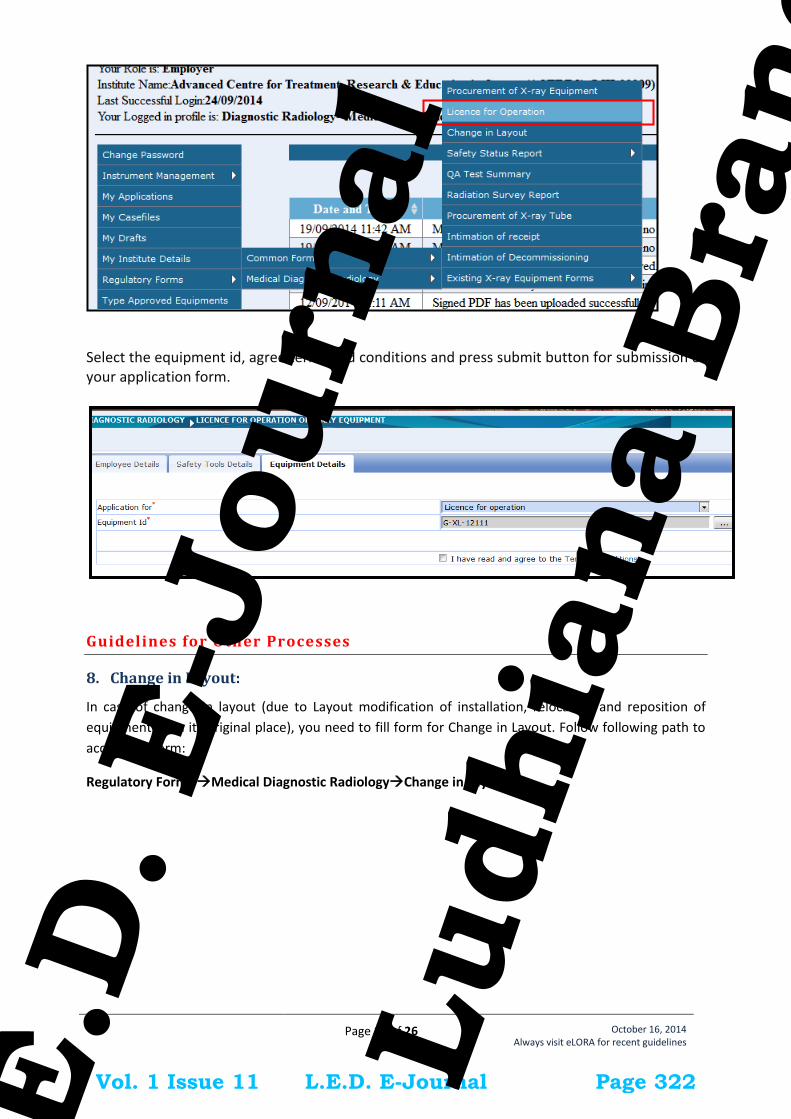
Page 19 of 26
October 16, 2014 Always visit eLORA for recent guidelines
Select the equipment id, agree terms and conditions and press submit button for submission of your application form.
Guidelines for Other Processes
8. Change in Layout:
In case of change in layout (due to Layout modification of installation, relocation and reposition of
equipment from its original place), you need to fill form for Change in Layout. Follow following path to
access this form:
Regulatory Forms Medical Diagnostic RadiologyChange in Layout
Vol. 1 Issue 11 L.E.D. E-Journal Page 322
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Page 20 of 26
October 16, 2014 Always visit eLORA for recent guidelines
Pl. note, in this form you will have to provide detail of shielding around X-ray equipment as asked in
Licence form. Fill the detail as required in the form and submit.
9. Safety Status Report
Use this form to submit safety annual safety status of your Institute. Follow following path to access this
form:
Regulatory Forms Medical Diagnostic RadiologySafety Status Report (Patient Examination Report
/Operation Safety Report)
10. QA Test Summary
Use this form to submit QA test summary of periodic QA or QA done after layout change. Follow
following path to access this form:
Regulatory Forms Medical Diagnostic RadiologyQA Test Summary
11. Radiation Survey Report
In case of change in layout, you need to submit radiation survey around the installation. The same form
is also be used to submit Periodic RSR (RSR – Radiation Survey Report). Follow following path to access
this form:
Regulatory Forms Medical Diagnostic Radiology Radiation Survey Report
12. Procurement of X-ray Tube
This form is used to apply for procurement of X-ray tube (in case of replacement of old/damaged x-ray
tube). Follow following path to access this form:
Regulatory Forms Medical Diagnostic RadiologyProcurement of X-ray Tube
13. Intimation of Receipt
After receipt of new X-ray tube, you need to intimate its receipt through Intimation of Receipt form.
Follow following path to access this form:
Vol. 1 Issue 11 L.E.D. E-Journal Page 323
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Page 21 of 26
October 16, 2014 Always visit eLORA for recent guidelines
Regulatory Forms Medical Diagnostic RadiologyIntimation of Receipt
14. Intimation of Decommissioning
In order to intimate decommissioning of your X-ray equipment, use this form. Follow following path to
access this form:
Regulatory Forms Medical Diagnostic RadiologyIntimation of Decommissioning
Important Message
15. NO LICENSE FEE /PROCESSING FEE BY AERB
It may please be noted that AERB does not charge any fee for issuance of regulatory consents including
license or registration. However, It has been brought to the notice that some of the suppliers/agencies,
while providing services/assistance to the users of Diagnostic X-ray facility for getting their X-ray
equipment licensed or registered by AERB, are demanding money to be paid to AERB. In case anybody
demands for payment to be made to AERB or any of its officials, kindly provide all the details to:
The Vigilance Officer
Atomic Energy Regulatory Board
Niyamak Bhavan, Anushaktinagar
Mumbai – 400094
Telefax: 022-25576255
e-mail: [email protected]
Vol. 1 Issue 11 L.E.D. E-Journal Page 324
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Page 22 of 26
October 16, 2014 Always visit eLORA for recent guidelines
Annexures
Annexure - 1: List of Personnel Monitoring Service (PMS) Providers
The following Accredited Laboratories provide TLD services in the respective states as mentioned
below:
Sr. No. State Name of Accredited Laboratory
1. Andhra Pradesh, Tamil Nadu,
Karnataka, Kerala, Puducherry,
Andaman and Nicobar and
Lakshdeep (Southern Region)
Avanttec Lab. Private Limited
31, Kamraj Street, Srinivasa Nagar, Padi, Chennai,
Tamil Nadu
Pin- 600050
Tel.: 044-26345288, 044-26630553/54/56
2. Maharashtra, Gujarat, Rajasthan,
Goa, Dadra and Nagar Haveli and
Diu (Western Region)
Renentech Lab. Private Limited
C-106, Synthofine Industrial Estate, Off Aarey Road,
Goregaon (E), Mumbai, Maharashtra
Pin- 490063
Tel.: 022-40037476
3. All other states in the Central,
Northern and North Eastern parts of
the country
Ultratech Lab. Private limited
Cloth Market, G.E. Road, kumhari, Bhilai, Durg,
Chhattisgarh
Pin- 490042
Tel.: 0788-3295166, 09981212431
4. All Defence institutions of country Defence Laboratory, Jodhpur
Vol. 1 Issue 11 L.E.D. E-Journal Page 325
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Page 23 of 26
October 16, 2014 Always visit eLORA for recent guidelines
Annexure - 2: Standard Layouts
a) Standard Layout of X-ray Installation
Legend: 1. Examination Table 2. Spot Film Device 3. Column Stand 4. X-ray Tube Head 7. Chest Stand 8. Control Unit 9. Mobile Protective Barrier
with lead glass viewing window of 1.7 mm lead equivalence
Name of Institute:
Complete Address of Institute:
Make of X-ray Equipment:
Model of X-ray Equipment:
Signature of Head of Institute:
[Seal of Institute]
Vol. 1 Issue 11 L.E.D. E-Journal Page 326
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Page 24 of 26
October 16, 2014 Always visit eLORA for recent guidelines
b) Standard Layout of CT Installation
Legend: 1. CT Gantry 2. Examination Table 3, 4. Control Unit 5. Viewing glass window of
100cm x 80cm of 2.0 mm lead equivalence
Name of Institute:
Complete Address of Institute:
Make of X-ray Equipment:
Model of X-ray Equipment:
Signature of Head of Institute:
[Seal of Institute]
Vol. 1 Issue 11 L.E.D. E-Journal Page 327
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Page 25 of 26
October 16, 2014 Always visit eLORA for recent guidelines
c) Standard Layout of Interventional Radiology Installation
Legend: 1. C-arm 2. Examination Table 5. Fixed Radiation Shield 6,7,8. Control Unit 9. Viewing glass window of
120cm x 100cm of 2.0 mm lead equivalence
Name of Institute:
Complete Address of Institute:
Make of X-ray Equipment:
Model of X-ray Equipment:
Signature of Head of Institute:
[Seal of Institute]
Vol. 1 Issue 11 L.E.D. E-Journal Page 328
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Page 26 of 26
October 16, 2014 Always visit eLORA for recent guidelines
d) Standard Layout of Mammography Installation
Legand: 1. Mammography Equipment 2. Control Unit with protective
barrier of 1.5 mm lead equivalence
Name of Institute:
Complete Address of Institute:
Make of X-ray Equipment:
Model of X-ray Equipment:
Signature of Head of Institute:
[Seal of Institute]
Vol. 1 Issue 11 L.E.D. E-Journal Page 329
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Checklist for submission of application form for Registration
*Incomplete submission may cause delay in processing of the application.
Name of the Hospital/Institution: City
State Sr.No.
Checkpoints
Status
1 Application form is completely filled, duly signed and stamped YES/NO
2 Address for correspondence is correctly mentioned with pin code (courier doesn’t reach without pin code)
YES/NO
3 Name of related medical practitioner, operator and RSO is given in the staff list YES/NO
4 TLD badge numbers of radiation workers are provided in the staff list YES/NO
5 Copy of
a) Valid Type Approval/NOC is enclosed b) For nominated RSO, latest qualification certificates are enclosed
c) QA report is enclosed
YES/NO YES/NO
YES/NO
6 Layout report and 2 copies of layout are enclosed YES/NO
7 Undertaking/declaration has been duly signed and stamped YES/NO
Place: Signature:
Date: Name of the Applicant:
Vol. 1 Issue 11 L.E.D. E-Journal Page 330
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Form ID: AERB/RSD/MDX/REG
Government of India Atomic Energy Regulatory Board
Niyamak Bhavan Anushaktinagar,
Mumbai – 400 094
APPLICATION FOR REGISTRATION OF DIAGNOSTIC X-RAY EQUIPMENT [RADIOGRAPHY / RADIOGRAPHY & FLUOROSCOPY (R&F) / DENTAL/
ORTHO-PANTOMOGRAPHY (OPG) / MAMMOGRAPHY/ BONE DENSITOMETER] -----------------------------------------------------------------------------------------------------------------------------------
a) This Application would be considered by the competent authority for issuance of relevant consents, under the Atomic Energy (Radiation Protection) Rules, 2004).
b) The duly filled-in form should be sent to Head, Radiological Safety Division, (RSD) AERB, Niyamak Bhavan, Anushaktinagar, Mumbai-400094 with the necessary documents.
c) Incomplete applications and those without all relevant documents are liable to be rejected. d) All the forms pertaining to this facility can be downloaded from the website www.aerb.gov.in e) Attach extra sheets wherever required ---------------------------------------------------------------------------- -----------------------------------------------------
PART A GENERAL PARTICULARS
A.1 Name of the institution: Address of the institution (for correspondence):
Telephone No Fax No. Institution Personnel Monitoring Number:
A.2 Name of the Head of the institution $: Telephone No Mobile no Fax No. Email
A.3 Name and designation of the applicant#: Telephone No. Mobile No Fax No. Email
(Registrant is also designated as RSO) A.4 In case applicant wish to nominate another Radiological Safety Officer (RSO)*,
Name and Designation
Telephone No. Mobile No. Fax No. Email RSO Approval reference No.: Valid up to
A.5 Address of installation of the X-ray equipment: --------------------------------------------------------------------------------------------------------------------- # Applicant is the person in whose name the licence to handle the source may be issued, under AERPR-2004, and would have the responsibilities of “licencee” prescribed in AERPR-2004 and should be a full time employee of the institution $ The head of the institution is the person who would have the responsibilities of “employer” prescribed in RPR-2004 * RSO is the person who is so designated by employer and approved by competent authority and have the responsibilities of “Radiological Safety Officer”.
Vol. 1 Issue 11 L.E.D. E-Journal Page 331
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

PART B
DETAILS OF THE EQUIPMENT B.1: Whether the equipment is: New/ pre-owned B.2 In case of pre-owned: purchased/received from (name and address): B.3 Type of Equipment
1) Radiography fixed/ R&F combined/ Radiography ( Mobile)/ Mammography/ C-arm/ dental/BMD/ 2) others (please specify) B.4 Purpose Medical Diagnosis/ Research/ Veterinary/ others (please specify) B.5 Details of equipment (Attach extra sheets if required)
Sr. No.
Type of equipment
Model Name Supplier Name Date of installation
NOC / Type Approval No. (attach copy)
Max kVp
Max. mA/mAs
B. 6 Quality Assurance report enclosed: YES/NO
If QA report is not enclosed with this application, Quality Assurance tests on the X-Ray machines to be conducted within six months from the date of application and records to be maintained with the institution.
B. 7 Layout report is enclosed (applicable only for fixed installations): YES/NO B. 8 AVAILABILITY OF RADIATION PROTECTION ACCESSORIES
1. Red light, X-Ray Caution Symbol and Warning Placards 2. Lead aprons 3. Quality Assurance kit (optional)
B.9 WORK LOAD DETAILS
Name of Examination No. of patients/day mAs/exposure kV
Chest
Abdomen
Extremities
Skull
Spinal
Special Procedures
Vol. 1 Issue 11 L.E.D. E-Journal Page 332
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

PART C
STAFF DETAILS (Please attach separate list if required)
Sr.No.
Name Academic/Professional Qualification
Experience PMS (TLD Number)
Full time /Part time
Related medical practitioner
Operators RSO
designate Attach copy
UNDERTAKING BY NOMINATED RSO
I hereby undertake to fulfil Duties and Responsibilities of RSO as follows: a) I have read and understood the AERB guidelines on radiation protection. b) I shall ensure that the radiographer/s operating the x-ray equipment are trained in radiation
protection aspects and provided with adequate protective accessories while operating the equipment c) I shall ensure that suppliers of x-ray equipment will render training to the x-ray technologist/
operator on safe operation of x-ray equipment. d) I shall ensure that the QA of the equipment is carried out once in two years, or as recommended by
AERB and maintain records thereof. e) I shall ensure that the TLD badges are distributed to the radiation workers ( whoever operates the x-
ray equipment /works around the x-ray equipment/ associated with the procedure ) f) I shall ensure that proper instructions on using of TLD badges are given to the radiation workers g) I shall maintain control TLD badge at a location away from the radiation areas h) I shall ensure that the TLD badges are sent periodically for evaluation of doses and maintain the
dose records thereof. i) I shall report any excessive exposures ( above quarterly or annual limit) to AERB j) I shall ensure that proper warning x-ray symbols , are placed on the door to the room housing the
x-ray equipment k) I shall ensure that female radiation workers get alternative employment, away from radiation areas,
on declaration of pregnancy. ( for eg, Darkroom assistant, receptionist, record keeping etc) l) I shall ensure that lead aprons are properly placed on a stand provided for the purpose, when not in
use. m) I shall ensure lead aprons are checked once in a year for integrity. n) I shall prepare and maintain periodic safety status reports which will be made available to
representatives of inspecting agency. o) I shall advise the management about regulatory requirements for installation of any new x-ray
equipment/ decommissioning of old x-ray equipment p) I shall inform the AERB, in case of relinquishing the responsibilities of Radiological Safety
Officer. I have also understood the relevant provisions of the Act, Rules and Safety Code as mentioned above and radiation safety aspects. I am solely responsible for discharging the duties of Radiological Safety Officer of diagnostic radiology department as per rule 22 of AE (RP) R-2004. Place Signature of Registrant/ RSO Date Name of Registrant/ RSO
Vol. 1 Issue 11 L.E.D. E-Journal Page 333
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

PART D
UNDERTAKING BY HEAD OF THE INSTITUTION AND APPLICANT I/ We hereby certify that
a) Quality Assurance tests will be conducted within six months from the date of application and records will be maintained at the premises.
b) All the statement made above are correct to the best of my knowledge and belief c) No activity will be carried out for purposes other than those specified in this form; d) Site and layout shall be as per the approved plan only. e) The equipment shall be put into operation only after obtaining Registration certificate from the
Competent Authority. f) No person below age of 18 years shall be employed as radiation worker (operator and RSO) g) All provisions of the Atomic Energy (Radiation Protection) Rules, 2004 shall be strictly complied with. h) All provisions of AERB Safety Code on Medical Diagnostic X-ray Equipment and Installations,
AERB/SC/MED- 2 (Rev–1) or the revised version thereof currently in force shall be complied with i) The facility shall not be transferred/sold/ rented by me/us to another without the prior permission of the
competent authority; j) The installation / maintenance of the equipment would be done by authorized and trained persons. k) Full facilities will be accorded by me/us to any authorised representatives of the competent authority to
inspect this installations at any time; l) Medical surveillance of all persons engaged in radiation work as required by the competent authority
will be duly carried out at my/our expense m) All recommendations made from time to time by the competent authority in respect of radiation safety
will be duly implemented; n) Duly qualified and trained manpower (including radiological safety officer, shall be appointed before the
commencement of operation of the facility; o) Decommissioning/ dismantling and reuse of the site of the decommissioned facility will be done with
prior intimation to AERB. p) All necessary facilities will be provided to the RSO to discharge his duties and functions effectively. q) Atomic Energy Regulatory Board will be immediately informed in case the RSO is relieved of his duties
and his original certificate would be returned. r) Keep AERB informed about any changes in the information furnished above
In case, it is found, at any stage, that the information provided by me/us is false and/ or not authentic, then I/ we hereby accept that appropriate regulatory actions may be initiated against me/us and our institution, in accordance with the applicable Rules.
Place: Signature: Date: Name of the Applicant: Designation:
Signature: Name of Head of the Institution:
Designation:
DECLARATION BY THE AUTHORISED SUPPLIER
Our company has installed a (type of x-ray unit) x-ray equipment model ________________, which is having a valid NOC/Type Approval certificate from AERB. Its performance/ acceptance test are demonstrated to the user’s representative on……………….
Place: _____________________ Signature of the service engineer Date: _____________________ Name Designation Company
SEAL OF THE COMPANY
Vol. 1 Issue 11 L.E.D. E-Journal Page 334
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

PART E
LAYOUT AND SHIELDING DETAILS OF MEDICAL X-RAY INSTALLATION Name of the hospital: Type of equipment: Model name: Identification of location (Room No.):
(Refer AERB guidelines for layout and shielding of x-ray installations) Wall Identification Distance from exposure area
(from centre of the couch) Material used for shielding
Thickness of the shielding material (cm)
Wall A Wall B Wall C Wall D Entrance Door Any other door Window, if any, if at the height less than 2 m from outside finished floor of x-ray room
Floor Ceiling
Attach drawing authenticated by supplier in A4 size sheet (scale 1:50) indicating details given above.
Verified by: Name:
Signature of applicant Signature of the supplier Name Designation Company
Check list to be filled by applicant Status
1
All the walls are identified and distances of walls from the centre of the couch/equipment are indicated in the layout drawing
2 Layout drawing indicates the location of the mobile protective barrier 3 Layout drawing indicates x-ray machine, couch, control panel/ control room, chest stand, windows,
doors, make and model of the x-ray equipment. 4 Layout drawing is signed and stamped by the applicant. 5 Layout drawing is authenticated by supplier. 6 The layout drawing is as per values filled in the above table. 7 Chest Stand is on the opposite wall of control console and entrance door Yes/ No 8 If NO whether, a permanent protective barrier is placed between operator and chest stand
9 Height of the window from outside finished floor of x-ray room is > 2 m Yes/ No 10 If No, whether shielding is provided on the window up to 2m Yes/ No
11 No permanent occupancy behind chest stand is ensured Yes/ No
Vol. 1 Issue 11 L.E.D. E-Journal Page 335
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
National Treatment Guidelines
for Antimicrobial Use in Infectious Diseases
NATIONAL CENTRE FOR DISEASE CONTROL
Directorate General of Health Services
Ministry of Health & Family Welfare
Government of India
Version 1.0 (2016)
Vol. 1 Issue 11 L.E.D. E-Journal Page 336
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
2
CONTENTS
Chapter 1 .................................................................................................................................................................................................................. 7
Introduction ........................................................................................................................................................................................................ 7
Chapter 2. ................................................................................................................................................................................................................. 9
Syndromic Approach For Empirical Therapy Of Common Infections.......................................................................................................... 9
A. Gastrointestinal & Intra-Abdominal Infections ......................................................................................................................................... 10
B. Central Nervous System Infections ........................................................................................................................................................... 13
C. Cardiovascular Infections .......................................................................................................................................................................... 14
D. Skin & Soft Tissue Infections ................................................................................................................................................................... 15
E. Respiratory Tract Infections ...................................................................................................................................................................... 16
F. Urinary Tract Infections ............................................................................................................................................................................. 17
G. Obstetrics And Gynaecological Infections ................................................................................................................................................ 18
H. Bones And Joint Infections ....................................................................................................................................................................... 22
I. Eye Infections ............................................................................................................................................................................................ 23
J. Ear Infections ............................................................................................................................................................................................ 25
K. Infections in Burn and Plastic Surgery ...................................................................................................................................................... 26
L. Fungal Infections ...................................................................................................................................................................................... 27
M. Febrile Neutropenia .................................................................................................................................................................................. 27
N. Post-Cardiovascular Surgery Infections .................................................................................................................................................... 29
O. Pediatric Infections ................................................................................................................................................................................... 31
P. Neonatal Infections .................................................................................................................................................................................... 39
R. Post Solid Organ Transplant ...................................................................................................................................................................... 40
S. Surgical Antimicrobial Prophylaxis ........................................................................................................................................................... 41
Chapter 3 ................................................................................................................................................................................................................ 42
Treatment Of Muti-Drug Resistant Bacterial Pathogens .............................................................................................................................. 42
1. Methicillin- Resistant S. aureus (MRSA) .................................................................................................................................................. 42
2. Vancomycin Resistant Enterococcus (VRE) ........................................................................................................................................... 42
3. Extended Spectrum Βeta-Lactamases (ESBL) Producing Enterobacteriaceae. .......................................................................................... 42
4. Carbapenem- Resistant Enterobacteriaceae (CRE) .................................................................................................................................... 42
Chapter 4 ................................................................................................................................................................................................................ 44
Guidelines For Optimizing Use Of Key Antimicrobials ................................................................................................................................ 44
A. Antimicrobial Prescribing: Good Practice ................................................................................................................................................ 44
B. Reserve Antimicrobials ............................................................................................................................................................................ 45
C. Hypersensitivity ....................................................................................................................................................................................... 45
D. Alert Antimicrobials.................................................................................................................................................................................. 46
E. Alert Antibiotics And Their Indications .................................................................................................................................................... 46
Chapter 5 ................................................................................................................................................................................................................ 49
Preventive Strategies For Healthcare Associated Infections ......................................................................................................................... 49
A. Healthcare Associated Infections .............................................................................................................................................................. 49
B. Reducing the risk of Health care associated infections.............................................................................................................................. 49
Chapter 6 ................................................................................................................................................................................................................ 50
Monitoring Antimicrobial Use ......................................................................................................................................................................... 50
A. Background ............................................................................................................................................................................................... 50
B. Need For Surveillance To Track Antimicrobial Use And Resistance ....................................................................................................... 50
C. Standardized Methodology And Outcome Measures ................................................................................................................................ 50
D. Situation In Developing Countries ............................................................................................................................................................ 51
High-end Antibiotic Monitoring Sheet .......................................................................................................................................................... 52
Surgical Prophylaxis Monitoring Sheet ......................................................................................................................................................... 52
Chapter 7 ................................................................................................................................................................................................................ 53
Dosage Guide For Commonly Used Antimicrobial Agents ........................................................................................................................... 53
Chapter 8 ................................................................................................................................................................................................................ 57
Link To National Programme Current Guidelines For Treatment Of Specific Infections......................................................................... 57
Chapter 9 ................................................................................................................................................................................................................ 59
Case Definitions And Diagnosis For Common Infections .................................................................................................................................. 59
DIARRHEA ................................................................................................................................................................................................... 59
ENTERIC FEVER ......................................................................................................................................................................................... 59
SPONTANEOUS BACTERIAL PERITONITIS ........................................................................................................................................... 59
ACUTE PANCREATITIS ............................................................................................................................................................................. 59
ACUTE BACTERIAL MENINGITIS ........................................................................................................................................................... 60
BRAIN ABSCESS ......................................................................................................................................................................................... 60
INFECTIVE ENDOCARDITIS ..................................................................................................................................................................... 60
CELLULITIS ................................................................................................................................................................................................. 61
FURUNCULOSIS ......................................................................................................................................................................................... 61
URINARY TRACT INFECTIONS ............................................................................................................................................................... 61
PNEUMONIA ............................................................................................................................................................................................... 61
ABBREVIATIONS ................................................................................................................................................................................................ 63
Vol. 1 Issue 11 L.E.D. E-Journal Page 337
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

3
Vol. 1 Issue 11 L.E.D. E-Journal Page 338
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

4
Vol. 1 Issue 11 L.E.D. E-Journal Page 339
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
5
Vol. 1 Issue 11 L.E.D. E-Journal Page 340
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
6
Vol. 1 Issue 11 L.E.D. E-Journal Page 341
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

7
Chapter 1
INTRODUCTION
Infections caused by microorganisms have threatened human life since time immemorial. During the pre-antibiotic era, these
have been a major concern for the high morbidity and mortality in humans. Some of the virulent organisms with the potential
to spread infection from one infected person to another at a very rapid rate may cause worldwide pandemics, epidemics or
outbreaks. With the discovery of the first antibiotic, "the magic bullet" Penicillin in the year 1943, patients could be effectively
cured of many life-threatening infections. This gave a huge relief to the medical practitioners. Next three decades saw the
development and discovery of a wide variety of antimicrobial agents. Subsequently, the pace of discovery of newer molecules
declined from 1970 to 1987. It has reached a “discovery void” level from 1987 onwards up till now. This is the post-antibiotic
era in which the medical practitioners have to treat and manage all types of infections with equal or greater efficiency.
Spontaneous natural development of antimicrobial resistance in the microorganisms in nature is a slow process. However, the
frequent and inappropriate use of a newly discovered antimicrobial drug leads to the development of altered mechanisms in the
pathophysiology of the concerned microbes as a survival strategy. Such antibiotic selection pressure kills the susceptible
microbes and helps in selective replication of drug resistant bacteria. These resistant bacteria already existed in the population
along with the susceptible ones or susceptible bacteria acquired resistance during antimicrobial treatment. Ultimately, such
resistant bacteria multiply abundantly and entirely replace the susceptible bacterial population. This results in treatment failure
or ineffective management of such infected patients. Antimicrobial resistance has been observed and reported with practically
all the newly discovered antimicrobial molecules till date. Antimicrobial resistance makes the treatment of patients difficult,
costly and sometimes impossible.
Emergence of antimicrobial resistance in pathogens has become a matter of great public health concern. Antimicrobial
resistance is well recognised as a global threat to human health. Infections caused by antimicrobial-resistant micro-organisms
in hospitals are associated with increased morbidity, mortality and healthcare costs. Resistance has emerged even to newer and
more potent antimicrobial agents like carbapenems. Selection and spread of resistant microorganisms in the presence of
antimicrobials is facilitated by:
Irrational use of drugs
Self-medication
Misuse of drugs
Antimicrobial resistance is closely linked to inappropriate antimicrobial use. It is estimated that 50% or more of hospital
antimicrobial use is inappropriate. There is a need for increased education and awareness about antimicrobial resistance among
the public and health-care professionals. One needs to develop and improve the surveillance system for antimicrobial
resistance and infectious diseases in general, particularly through improved linkage of data. Nothing will work unless we
improve diagnostic testing to ensure more tailored interventions and respond to the opportunities afforded by advances in
genomic technologies and point of care testing.
Since ‘post antibiotic era’ is reported to be “discovery void”; antimicrobial resistance is considered to be the most serious
health threats especially for the common infections like sepsis, diarrhea, pneumonia, urinary tract infection, gonorrhea,
malaria, tuberculosis, HIV, influenza. Presently, carbapenem resistance is reported worldwide in more than 50% of strains of
Klebsiella pneumoniae causing health care associated infections like pneumonia, blood stream infections, infections in the
newborn and intensive care units. More than 50% of Escherichia coli strains causing urinary tract infections are reported
worldwide to be resistant to fluoroquinolones. Similarly, patients suffering from gonorrhea are reported to be resistant to the
last resort of antibiotics - third generation cephalosporins. High mortality (64%) was seen among patients infected with
Methicillin resistant Staphylococcus aureus (MRSA). Over all, the antimicrobial resistance is associated with higher mortality
rate, longer hospital stay, delayed recuperation and long term disability.
Similar observations on the emergence of antimicrobial resistance in gram-negative and gram-positive bacteria are reported
also from India. The resistance range varies widely depending on the type of health care setting and the geographical location,
availability of antimicrobials in hospitals and over the counter, prescribing habits of treating clinicians coming from different
streams of medicine like allopathy, homeopathy, ayurvedic or quacks. The drug resistance has been reported to develop in a
microbial population to an antibiotic molecule following its improper and irrational use. To combat the problem of ineffective
management of infections and their complications caused by drug resistant microorganisms, it is imperative to report such
problems and generate national data at all levels of healthcare settings thus leading to a better tracking and monitoring system
in the country.
The published reports in the country reveal an increasing trend of drug resistance in common diseases of public health
importance i.e. Cholera: showing high level of resistance to commonly used antimicrobials e.g. Furazolidone (60-80%),
Cotriamoxazole (60-80%) and Nalidixic Acid (80-90%), Enteric fever: Chloramphenicol, Ampicillin, Cotriamoxazole (30-
50%), Fluoroquinolones (up to 30%), Meningococcal infections: Cotriamoxazole, Ciprofloxacin and Tetracycline (50-100%),
Gonococcal infections: Penicillin (50-80%), Ciprofloxacin (20-80%). Resistance is also seen in Meningococcal infections,
malaria, leprosy, kala-azar, TB, & HIV. Recently, NDM-1 positive bacteria have also been reported. Factors responsible for
emergence of antimicrobial resistance could be widespread use and availability of practically all the antimicrobials over the
counter for human, animal and industrial consumption. There are definite policies/guidelines for appropriate use of
antimicrobials at national level in specific national health programmes (e.g. RNTCP, National AIDS Control Programme,
National Malaria Control Programme etc.). etc
For other pathogens of public health importance like enteric fever, diarrhoeal disease, respiratory infections etc., the individual
hospitals are following their own antimicrobial policies and hospital infection control guidelines.
Reliable Indian data on antimicrobial resistance (AMR)for important pathogens of public health importance is an essential pre-
Vol. 1 Issue 11 L.E.D. E-Journal Page 342
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

8
requisite for developing/modifying appropriate guidelines for use of antimicrobials. Currently, there is no accepted national
database of antimicrobial resistance in different pathogens except for those where there is a specific national health
programme. Despite many microbiology laboratories (in both public as well as private sector) performing routine antibiotic
susceptibility testing (AST) of at least bacterial pathogens, the data is neither analysed regularly nor disseminated for use by
clinicians / public health experts / programme managers. Quality control and data sharing by these laboratories are other
important issues that need attention.
Recently, Ministry of health has launched ‘National programme for AMR Containment’ in 2012-2017, and one of the key
activities initiated under the programme is AMR surveillance with a network of ten laboratories across the country. Currently,
the National programme for Containment of AMR is generating AMR data for common bacterial pathogens from various
surveillance network sites across the country. The data generated from these surveillance sites shall be useful to understand the
magnitude and trend of drug resistance and identify the emergence of resistance, and will enable to accordingly update the
treatment guidelines.
Furthermore, need for antibiotics can be reduced by spreading the knowledge of infection control measures and adopting and
implementing the hospital infection control practices, formation of active hospital infection control teams in each hospital
working round the clock and monitoring and containing the spread of infections. The importance of hand hygiene cannot be
more emphasized in helping to control the spread of infections from one patient to another. Access to clean water also helps in
the containment of waterborne diseases and outbreaks and infections. Lastly, preventing the acquisition of an infection by
vaccination for different microbial infections will also help in reducing the need for prescription of antibiotics.
Implementation of an antibiotic stewardship program - a multidisciplinary program in the country will help to find out the
lacunae and improve upon the rational use of antibiotic with appropriate interventions and strategies.
To contain the further development of antimicrobial resistance with no new drug on the horizon and bring the existing levels of
reported resistance in the country, it is imperative to have standardized national treatment guidelines for the practitioners so
that they rationally use the currently available antimicrobial agents effectively for a long duration and manage their patients
more effectively.
How to use these guidelines?
These guidelines list the recommended treatments for common infectious diseases that are based on scientific evidence,
literature review and are consistent with the already existing international guidelines and formulated with the collective
opinion of a wide group of recognised national experts. The topics covered in this document include empiric treatment choices
for different syndromes, infections of specific body sites, and in certain special settings; antimicrobial choices for multi-drug
resistant bacterial pathogens; optimizing and monitoring use of antimicrobials; preventive strategies for healthcare associated
infections, case definitions and diagnosis of common infections.
It is emphasized that antimicrobials should be prescribed only when they are necessary in treatment following a clear
diagnosis. Not all patients need antibiotics; non−drug treatment may be suitable and this has been emphasized in these
guidelines.
In all cases, the benefit of administering the medicine should be considered in relation to the risk involved. This is particularly
important during pregnancy where the risk to both mother and foetus must be considered.
The content of these treatment guidelines will undergo a process of continuous review. Comments or suggestions for
improvement are welcome.
These suggestions may be sent to: [email protected]
DISCLAIMER: This publication provides only suggestive guidelines and the opinions expressed herein reflect those of the contributors. The
protocols described herein are general and may not apply to a specific patient. They should NOT supplant clinical judgment,
factors like hemodynamics of specific patients, availability of antimicrobials and local antibiogram of healthcare setting.
Vol. 1 Issue 11 L.E.D. E-Journal Page 343
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

9
Chapter 2.
SYNDROMIC APPROACH FOR EMPIRICAL THERAPY OF COMMON INFECTIONS
Empirical or presumptive anti-infective therapy is based on a clinical diagnosis combined with evidence from the literature
and from the educated experience of the probable pathogens causing the infection. To optimize an accurate microbiological
diagnosis, clinicians should ensure that diagnostic specimens are properly obtained and promptly submitted to the
microbiology laboratory, preferably before the institution of antimicrobial therapy. All attempts should be made to establish
diagnosis of the patients based on the facilities available to the treating doctor and affordability of the patients.
Definitive therapy depends on the microbiologic diagnosis by isolation or other direct evidence of pathogen.
According to WHO, presumptive treatment is a one-time treatment given for a presumed infection in a person, or group of
people, at high risk of infection.
Presumptive treatment is prescribed typically while waiting for the culture report or in situations where the facilities for doing
these tests is not available, is difficult or not cost effective or is impractical. However in certain situations the empirical
therapy prescribed as prophylaxis also (e.g surgical prophylaxis, high prevalence, repeated risk of exposure).
The syndromic approach is based on the presence of consistent groups of symptoms and easily recognized signs caused by a
single pathogen or a mixture of pathogens.
Before starting presumptive therapy ensure the following
1. Send and follow up on standard investigations for all suspected infections for correct and accurate diagnosis and
prognosis.
2. Antibiotics SHOULD be started only after after sending appropriate cultures if facilities are available. Similary any
change in antibiotic MUST be guided by sensitivity profile.
3. Assess the factors affecting activity of antimicrobilas such as renal excretion, interactions and allergy before
prescribing antibiotics.
4. Review of antibiotic therapy MUST be done daily and the therapy escalated or deescalated accordinglyespacially
after the culture reports are available.
Empirical Therapy si justified in patients with life threatening infections, in ICU settings and while awaiting results of culture.
The timing of initial therapy should be guided by the patient’s condition and urgency of the situation. In critically ill patients
e.g. patients in septic shock or bacterial meningitis therapy should be initiated immediately after or concurrently with
collection of diagnostic specimens. In other conditions wehere patient is stable, antimicrobial therapy should be deliberately
withheld until appropriate specimens have been collected and submitted to the microbiology laboratory e.g when treating a
patient of osteomyelitis or sub-acute endocarditis. Premature usage of antimicrobial in such cases can preclude opportunity to
establish a microbiological diagnosis, which is critical in the management of these patients.
Merits and limitations of empiric vs definitive antimicrobial therapy should be very clear to the treating doctor prescribing
antimicrobials.As the laboratory results pertaining to microbiological tests do not become available for 24 to 72 hours, initial
therapy for infection is often empiric and guided by the clinical presentation. Therefore, a common approach is to use broad-
spectrum antimicrobial agents as initial empiric therapy with the intent to cover multiple possible pathogens commonly
associated with the specific clinical syndrome. However, once laboratory results of microbiology tests are available with
identification of pathogen alongwith antimicrobial susceptibility data, every attempt should be made to narrow the antibiotic
spectrum. This is a critically helpful and integral component of antimicrobial therapy because it can reduce cost and toxicity
and significantly delay the emergence of antimicrobial resistance in the community. Antimicrobial agents with a narrower
spectrum should be directed at the most likely pathogens for the duration of therapy for infections such as community-acquired
pneumonia, urinary tract infections, soft tissue infections etc. in anOPD setting because specific microbiological tests are not
routinely performed or available or affordable.
Due considerations housld be given to the bactericidal vs bacteriostatic nature of the antimicrobial agents. Bactericidal
drugs, which cause death and disruption of the bacterial cell, include drugs that primarily act on the cell wall (e.g., β-lactams),
cell membrane (e.g., daptomycin), or bacterial DNA (e.g., fluoroquinolones). Bacteriostatic agents (e.g. sulfonamides and
macrolides) inhibit bacterial replication without killing the organismact by inhibiting metabolic pathways or protein synthesis
in bacteria. However, some antimicrobials are bactericidal against certain organisms may act as bacteriostatic against others
and vice versa. Unfortunately such distinction is not significant in vivo. Bactericidal agents are preferred in the case of serious
infections to achieve rapid cure (e.g in cases of meningitis and endocarditis).
There are few conditions where combination antimicrobial therapy is contemplated. These include conditions where
synergism of antimicrobials established or cases of infection withspecific microbes, where monotherapy is not generally
recommended (e.g., treatment of endocarditis caused by Enterococcus species with a combination of penicillin and
gentamicin). It also includes critically ill patients who may require empiric therapy before microbiological etiology and/or
antimicrobial susceptibility can be determined (e.g. suspected healthcare-care associated infections with Acinetobacter
baumannii or Pseudomonas aeruginosa). Other conditions where combination therapy may be required include cases where
Vol. 1 Issue 11 L.E.D. E-Journal Page 344
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
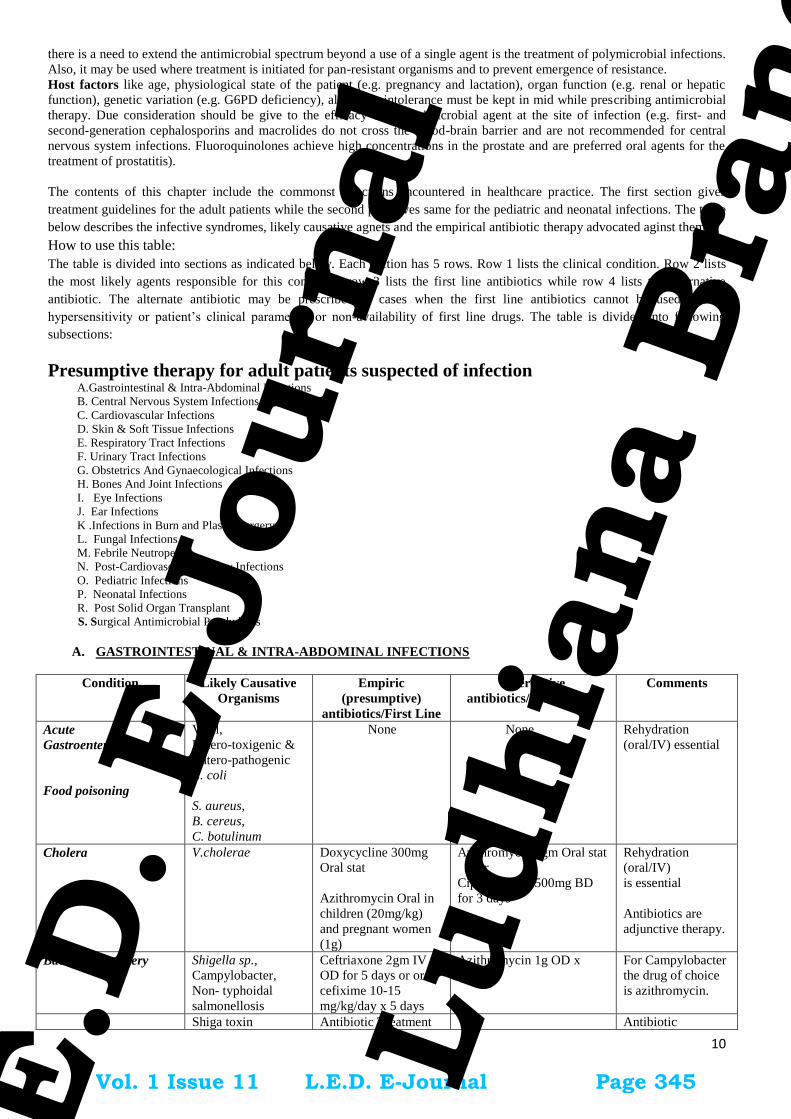
10
there is a need to extend the antimicrobial spectrum beyond a use of a single agent is the treatment of polymicrobial infections.
Also, it may be used where treatment is initiated for pan-resistant organisms and to prevent emergence of resistance.
Host factors like age, physiological state of the patient (e.g. pregnancy and lactation), organ function (e.g. renal or hepatic
function), genetic variation (e.g. G6PD deficiency), allergy or intolerance must be kept in mid while prescribing antimicrobial
therapy. Due consideration should be give to the efficacy of an antimicrobial agent at the site of infection (e.g. first- and
second-generation cephalosporins and macrolides do not cross the blood-brain barrier and are not recommended for central
nervous system infections. Fluoroquinolones achieve high concentrations in the prostate and are preferred oral agents for the
treatment of prostatitis).
The contents of this chapter include the commonst infections encountered in healthcare practice. The first section gives
treatment guidelines for the adult patients while the second part gives same for the pediatric and neonatal infections. The table
below describes the infective syndromes, likely causative agnets and the empirical antibiotic therapy advocated aginst them.
How to use this table:
The table is divided into sections as indicated below. Each section has 5 rows. Row 1 lists the clinical condition. Row 2 lists
the most likely agents responsible for this condition, row 3 lists the first line antibiotics while row 4 lists the alternative
antibiotic. The alternate antibiotic may be prescribed in cases when the first line antibiotics cannot be used due to
hypersensitivity or patient’s clinical parameters or non-availability of first line drugs. The table is divided into following
subsections:
Presumptive therapy for adult patients suspected of infection
A.Gastrointestinal & Intra-Abdominal Infections
B. Central Nervous System Infections
C. Cardiovascular Infections
D. Skin & Soft Tissue Infections
E. Respiratory Tract Infections
F. Urinary Tract Infections
G. Obstetrics And Gynaecological Infections
H. Bones And Joint Infections
I. Eye Infections
J. Ear Infections
K .Infections in Burn and Plastic Surgery
L. Fungal Infections
M. Febrile Neutropenia
N. Post-Cardiovascular Surgery Infections
O. Pediatric Infections
P. Neonatal Infections
R. Post Solid Organ Transplant
S. Surgical Antimicrobial Prophylaxis
A. GASTROINTESTINAL & INTRA-ABDOMINAL INFECTIONS
Condition Likely Causative
Organisms
Empiric
(presumptive)
antibiotics/First Line
Alternative
antibiotics/Second Line
Comments
Acute
Gastroenteritis
Food poisoning
Viral,
Entero-toxigenic &
Entero-pathogenic
E. coli
S. aureus,
B. cereus,
C. botulinum
None None Rehydration
(oral/IV) essential
Cholera V.cholerae Doxycycline 300mg
Oral stat
Azithromycin Oral in
children (20mg/kg)
and pregnant women
(1g)
Azithromycin 1gm Oral stat
or
Ciprofloxacin 500mg BD
for 3 days
Rehydration
(oral/IV)
is essential
Antibiotics are
adjunctive therapy.
Bacterial dysentery
Shigella sp.,
Campylobacter,
Non- typhoidal
salmonellosis
Ceftriaxone 2gm IV
OD for 5 days or oral
cefixime 10-15
mg/kg/day x 5 days
Azithromycin 1g OD x
3days
For Campylobacter
the drug of choice
is azithromycin.
Shiga toxin Antibiotic Treatment Antibiotic
Vol. 1 Issue 11 L.E.D. E-Journal Page 345
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

11
producing E. coli not recommended. use associated with
development of
hemolytic uremic
syndrome.
Amoebic dysentery
E. histolytica
Metronidazole 400mg
Oral TDS for 7-10
days
Tinidazole 2gm Oral OD
for 3 days
Add diloxanide
furoate 500 mg
TDS for 10d
Giardiasis Giardia lamblia Metronidazole 250-
500mg oral
TID x 7-10 d
Tinidazole 2 gm oral x
1 dose
Enteric fever
S.Typhi,
S.Paratyphi A
Outpatients:
Cefixime 20mg/kg/day
for 14 days or
Azithromycin 500 mg
BD for 7 days.
Inpatients: Ceftriaxone
2 g IV BDfor 2 weeks
+/-Azithromycin 500
mg BD for 7 days
Cotrimoxazole 960 mg BD
for 2 weeks
Majority of strains
arenalidixic acid
resistant.
Ceftriaxone to be
changed to oral
cefixime when
patient is afebrile to
finish total duration
of 14days.
Biliary tract infections
(cholangitis,
cholecystitis)
Enterobacteriaceae
(E.coli, Klebsiella
sp.)
Ceftriaxone 2gm IV
OD or
Piperacillin-
Tazobactam 4.5gm IV
8 hourly
or
Cefoperazoe-
Sulbactam 3gm IV
12hourly
For 7-10 days
Imipenem 500mg IV
6hourly
or
Meropenem 1gm IV
8hourly
For 7-10 days
Surgical or
endoscopic
intervention to be
considered if there
is biliary
obstruction.
High prevalence of
ESBL producing
E.coli, Klebsiella
sp.strains. De-
escalate therapy
once antibiotic
susceptibility is
known.
Hospital acquired
diarrhea
C. difficile Metronidazole 400 mg
oral TDSfor 10 days
Severe disease:start
Vancomycin 250 mg oral
6h empirically.
Spontaneous bacterial
Peritonitis
Enterobacteriaceae
(E.coli, Klebsiella
sp.)
Cefotaxime 1-2 gm IV
TDS
or
Piperacillin-
Tazobactam 4.5gm IV
8 hourly
or
Cefoperazone-
Sulbactam 3gm IV
12h
Imipenem 500 mg IV
6hourly or
Meropenem 1gm IV
8hourly
Descalate to
Ertapenem 1 gm IV
OD for 5-7 days
once the patient
improves
Secondary peritonitis,
Intra-abdominal
abscess/ GI perforation
Enterobacteriaceae
(E.coli, Klebsiella
sp.), Bacteroides
(colonic
perforation),
Anaerobes
Piperacillin-
Tazobactam 4.5gm IV
8 hourly
or
Cefoperazone-
Sulbactam 3gm IV
12hourly in severe
infections
In very sickpatients, if
required, addition of
cover for yeast
(fluconazole iv 800
mg loading dose day
1, followed by 400 mg
Imipenem 1g IV 8hourly
or
Meropenem 1gm IV
8hourly
or
Doripenem 500 mg TDS
or
Ertapenem 1 gm IV OD
Source control is
important to reduce
bacterial load.
If excellent source
control – for 5-7
days; other wise 2-
3 weeks suggested.
Vol. 1 Issue 11 L.E.D. E-Journal Page 346
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

12
2nd
day onwards) &
and for Enterococcus
(vancomycin
/teicoplanin) may be
contemplated
Pancreatitis
Mild- moderate
No antibiotics
Post necrotizing
pancreatitis: infected
pseudocyst; pancreatic
abscess
Entrobacteriaceae,
Enterococci, S.
aureus,
S. epidermidis,
anaerobes, Candida
sp.
Piperacillin-
Tazobactam 4.5 gm IV
8 hourly empirically
or
Cefoperazone-
Sulbactam 3gm IV 8
hourly in severe
infections
In very sick patients, if
required, addition of
cover for yeast
(fluconazole iv 800
mg loading dose day
1, followed by 400 mg
2nd
day onwards) &
and for Enterococcus
(vancomycin
/teicoplanin) may be
contemplated
For 7-10 days
Imipenem-Cilastatin 500mg
IV 6hourly
or
Meropenem 1gm IV
8hourly
or
Doripenem 500mg IV 8h
Duration of
treatment is based
on source control
and clinical
improvement
Diverticulitis
Mild-
OPD treatment
Gram-Negative
Bacteria
Anaerobes
Amoxycillin-
Clavulanate 625mg
TDS for 7 days
Ciprofloxacin +
Metronidazole for 7 days
Diverticulitis moderate Gram- Negative
Bacteria
Anaerobes
Ceftriaxone 2gm IV
OD +metronidazole
500 mg IV TDS or
Piperacillin-
Tazobactam 4.5 gm IV
8 hourly empirically
or
Cefoperazoe-
Sulbactam 3gm IV 8
hourly
BL-BLI agents
have very good
anaerobic cover, so
no need to add
metronidazole.
Diverticulitis
Severe
Gram- Negative
Bacteria
Anaerobes
Meropenem 1gm IV
8hrly or Imipenem
Cilastatin 500mg IV 6
hourly
Duration based on
improvement
Liver Abscess Polymicrobial
Amoxycillin-
clavulanate/ 3rd
generation
cephalosporin
+
Metronidazole 500mg
I.V.TID / 800mg oral
TID for 2 weeks
Piperacillin-Tazobactam IV Ultrasound guided
drainage indicated
inlarge abscesses,
signsof imminent
rupture andno
response to
medicaltreatment.
Vol. 1 Issue 11 L.E.D. E-Journal Page 347
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
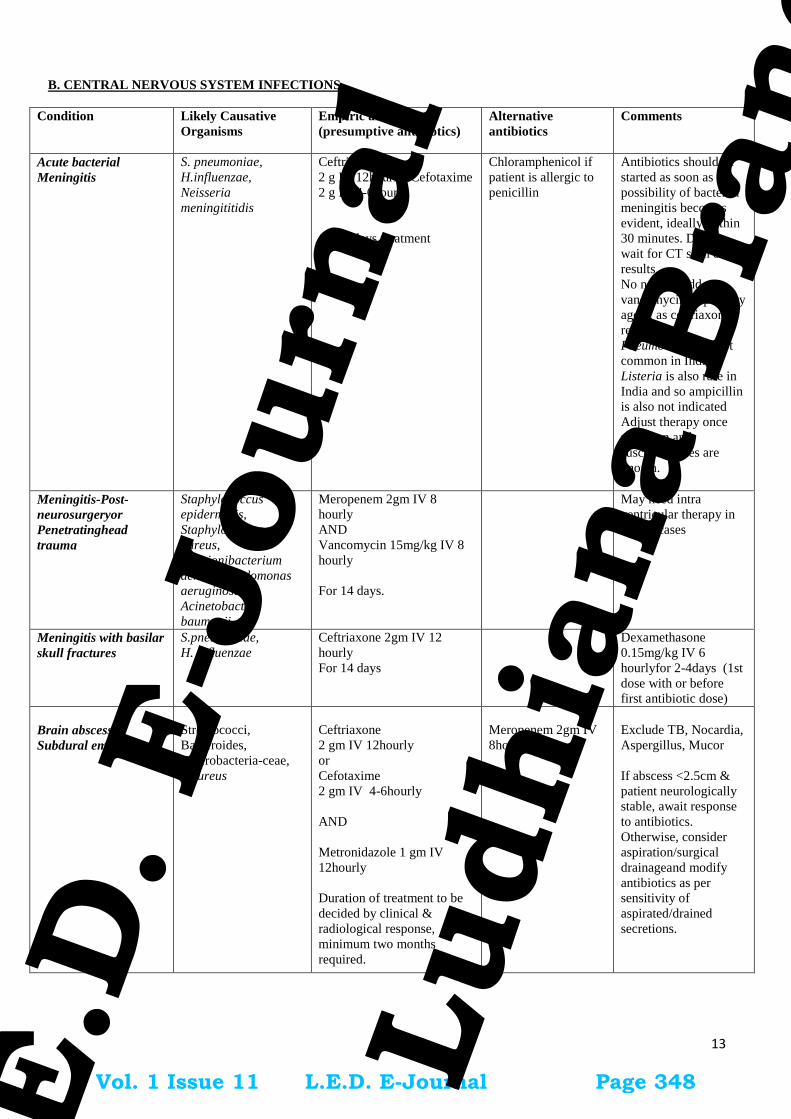
13
B. CENTRAL NERVOUS SYSTEM INFECTIONS
Condition Likely Causative
Organisms
Empiric antibiotics
(presumptive antibiotics)
Alternative
antibiotics
Comments
Acute bacterial
Meningitis
S. pneumoniae,
H.influenzae,
Neisseria
meningititidis
Ceftriaxone
2 g IV 12hourly/ Cefotaxime
2 g IV 4-6hourly
10-14 days treatment
Chloramphenicol if
patient is allergic to
penicillin
Antibiotics should be
started as soon as the
possibility of bacterial
meningitis becomes
evident, ideally within
30 minutes. Do not
wait for CT scan or LP
results.
No need to add
vancomycin as primary
agent, as ceftriaxone
resistant
Pneumococcus is not
common in India.
Listeria is also rare in
India and so ampicillin
is also not indicated
Adjust therapy once
pathogen and
susceptibilities are
known.
Meningitis-Post-
neurosurgeryor
Penetratinghead
trauma
Staphylococcus
epidermidis,
Staphylococcus
aureus,
Propionibacterium
acnes, Pseudomonas
aeruginosa,
Acinetobacter
baumanii
Meropenem 2gm IV 8
hourly
AND
Vancomycin 15mg/kg IV 8
hourly
For 14 days.
May need intra
ventricular therapy in
severe cases
Meningitis with basilar
skull fractures
S.pneumoniae,
H. influenzae
Ceftriaxone 2gm IV 12
hourly
For 14 days
Dexamethasone
0.15mg/kg IV 6
hourlyfor 2-4days (1st
dose with or before
first antibiotic dose)
Brain abscess,
Subdural empyema
Streptococci,
Bacteroides,
Enterobacteria-ceae,
S.aureus
Ceftriaxone
2 gm IV 12hourly
or
Cefotaxime
2 gm IV 4-6hourly
AND
Metronidazole 1 gm IV
12hourly
Duration of treatment to be
decided by clinical &
radiological response,
minimum two months
required.
Meropenem 2gm IV
8hourly
Exclude TB, Nocardia,
Aspergillus, Mucor
If abscess <2.5cm &
patient neurologically
stable, await response
to antibiotics.
Otherwise, consider
aspiration/surgical
drainageand modify
antibiotics as per
sensitivity of
aspirated/drained
secretions.
Vol. 1 Issue 11 L.E.D. E-Journal Page 348
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

14
C. CARDIOVASCULAR INFECTIONS
Condition Likely causative
Organism
Empiric
antibiotics
(presumptive
antibiotics)
Alternative
antibiotics
Comments
Infective Endocarditis:
Native valve (awaiting
cultures) Indolent
Viridans Streptococci,
other Streptococci,
Enterococci
Penicillin G
20MU IV
divided doses, 4
hourly
or
Ampicillin 2gm
iv 4h
AND
Gentamicin
1mg/kg im or iv
8h
Duration: 4-6
weeks
Vancomycin
15mg/kg IV 12
hourly
(maximum 1g 12
hourly)//teicplani
n 12mg/kg IV 12
hourly x 3 doses
followed by 6 -
12 mg once daily
IV depending
upon severity +
Gentamicin
1mg/kg IM or IV
8 hourly
Duration: 4-6
weeks
or
Daptomycin
6mg/kg IV once
a day
Duration: 4-6
weeks
If patient is stable, ideally waitblood
cultures.
Antibiotic choice as per sensitivity
results.
Guidance from Infectious disease
specialist or clinical microbiologist is
recommended
Infective Endocarditis:
Native valve (awaiting
cultures)
In Severe Sepsis
S.aureus
(MSSA or MRSA)
Risk for gram-
negative bacilli
Vancomycin 25-
30 mg/kg
loading followed
by 15-20 mg/kg
IV 12 hourly
(maximum 1gm
12
hourly)/teicoplan
in 12mg/kg IV
12 hourly x 3
doses followed
by 6 -12 mg once
daily IV
depending upon
severity AND
Meropenem 1gm
IV 8h
Duration: 4-6
weeks
Daptomycin
6mg/kg IV once
a day
AND
Meropenem 1gm
IV q8h
Duration: 4-6
weeks
Modify antibiotics based on culture
results and complete 4-6 weeks of
antibiotics
Vol. 1 Issue 11 L.E.D. E-Journal Page 349
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

15
Infective Endocarditis:
Prosthetic Valve
awaiting Cultures
Vancomycin
15mg/kg IV 12
hourly
(maximum 1gm
12
hourly)/teicoplan
in 12mg/kg IV
12 hourly x 3
doses followed
by 6 -12 mg once
daily IV
depending upon
severity +
Gentamicin
1mg/kg q12h IV
Daptomycin can be used in place of Vancomycin/
Teicoplanin for
patients
unresponsive to
or intolerant of
Vancomycin/Tei
coplanin or with
Vancomycin/Gly
copeptide-
resistant isolates
Antibiotic choice as per sensitivity.
Guidance from Infectious disease
specialist or microbiologist is
recommended.
D. SKIN & SOFT TISSUE INFECTIONS
Condition Likely Causative
Organisms
Empiric
antibiotics
(presumptive
antibiotics)
Alternative
antibiotics
Comments
Cellulitis Streptococcus
pyogenes(common),
S.aureus
Amoxicillin-
Clavulanate
1.2gm IV
TDS/625 mg oral
TDS
or
Ceftriaxone 2gm
IV OD
Clindamycin
600-900mg IV
TDS
Treat for 5-7 days.
Furunculosis S.aureus Amoxicillin-
Clavulanate
1.2gm IV/Oral
625 TDS
or
Ceftriaxone 2gm
IV OD
Duration – 5-7
days
Clindamycin
600-900mg IV
TDS
Get pus cultures before starting
antibiotics
Necrotizing
fasciitis
Streptococcus
pyogenes, S. aureus,
anaerobes,
Enterobacteriaceae
(polymicrobial)
Piperacillin-
Tazobactam
4.5gm IV
6hourly
or Cefoperazone-
Sulbactam 3gm
IV 12hourly
AND
Clindamycin
600-900mg IV 8
hourly
Duration
depends on the
progress
Imipenem 1g
IV8hourly
or
Meropenem 1gm
IV 8hourly
AND
Clindamycin
600-900mg IV
TDS/linezolid
600 mg IV
BD/daptomycin
6mg/kg/day
Early surgical intervention crucial
Vol. 1 Issue 11 L.E.D. E-Journal Page 350
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

16
E. RESPIRATORY TRACT INFECTIONS
Condition Likely Causative
Organisms
Empiric
antibiotics
(presumptive
antibiotics)
Alternative
antibiotics
Comments
Community
acquired
Pneumonia
S. pneumoniae,
H.influenzae,
Legionella,
E.coli, Klebsiella sp.,
S.aureus
Mild to moderate
cases
Amoxycillin-
500mg-1 g TDS
oral.
If IV indicated,
amoxycillin-
clavulanate 1.2 g
IV TDS or
Ceftriaxone 2g IV
OD
For
Severe cases
Amoxycillin-
clavulanate 1.2 g
IV TDS
OrCeftriaxone 2g
IV OD
Duration 5-8 days
Piperacillin-
Tazobactam 4.5gm
IV 6 hourly
or
Imipenem 1g IV
6hourly
or
Cefoperazone-
Sulbactam 3gm IV
12 hourly
If MRSA is a concern, add
Linezolid 600mg IV/Oral BD
If atypical pneumonia
suspected, Doxycycline
100mg bd
or
Azithromycin 500 mg oral/IV
OD
Lung abscess,
Empyema
S. pneumoniae,
E.coli,
Klebsiella sp.,
Pseudomonas
aeruginosa,
S.aureus, anaerobes
Piperacillin-
Tazobactam 4.5gm
IV 6hourly
or
Cefoperazone-
Sulbactam 3gm IV
12 hourly
ADD Clindamycin
600-900mg IV
8hourly
3-4 weeks treatment required
Acute pharyngitis
Viral None required As most cases are viral no
antimicrobial therapy required
Group A ß-hemolytic
Streptococci
(GABHS),
Group C, G
Streptococcus,
Oral Penicillin v
500mg BD
or
Amoxicillin 500 mg
Oral TDS for 10
days
In case of penicillin
allergy:
Azithromycin
500mg OD for 5
days
or
Benzathine
penicillin 12 lac
units IM stat
Antibiotics are recommended
to reduce transmission rates
and prevention of long term
sequaelae such as rheumatic
fever
Ludwig’s angina
Vincent’s angina
Polymicrobial
(Cover oral anaerobes)
Clindamycin 600
mg IV 8 hourly
or
Amoxicillin-
Clavulanate 1.2gm
IV
Piperacillin-
Tazobactam 4.5gm
IV 6 hourly
Duration based on
improvement
Acute bacterial
rhinosinusitis
Viral,
S. pneumoniae,
H.influenzae,
M. catarrhalis
Amoxicillin-
clavulanate 1gm
oral BD for 7 days
Moxifloxacin
400mg OD for 5-
7days
Acute bronchitis Viral Antibiotics not
required
- -
Acute bacterial
exacerbation of
COPD
S. pneumoniae
H. influenzae
M. catarrhalis
Amoxicillin-
clavulanate 1gm
oral BD for 7 days
Azithromycin 500
mg oral OD × 3
days
Vol. 1 Issue 11 L.E.D. E-Journal Page 351
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

17
F. URINARY TRACT INFECTIONS
Asymptomatic bacteriuria NOT to be treated except pregnant women and immunocompromised patients. All cases of
dysuria may not be UTI. Refer to Obstetrics and gynaecology infections for treatment of asymptomatic bacteriuira in
pregnant women.
Condition Likely Causative
Organisms
Empiric antibiotics
(presumptive
antibiotics)
Alternative
antibiotics
Comments
Acute
uncomplicated
Cystitis
E.coli, Staphylococcus
saphrophyticus(in
sexually
activeyoungwomen),
Klebsiella pneumoniae
Nitrofurantoin 100
mg BD for 7 days
or Cotrimoxazole
960mg BD for 3-5
days
or
Ciprofloxacin 500
mg BD for 3-5 days
Cefuroxime 250
mg BD for 3-5
days
Get urine cultures before
antibiotics & modify therapy
based on sensitivities.
Acute
uncomplicated
Pyelonephritis
E.coli,
Staphylococcus
saphrophyticus (in
sexually active young
women),
Klebsiella pneumoniae,
Proteus mirabilis
Amikacin 1 g OD
IM/IV
or
Gentamicin 7
mg/kg/day OD
(Monitor renal
function closely and
rationalise according
to culture report)
Complete total
duration of 14 days
Piperacillin-
Tazobactam 4.5g
IV 6 hourly
or
Cefoperazone-
Sulbactam 3g IV
12 hourly
or
Ertapenem 1 g IV
OD
Urine culture and
susceptibilities need to be
collected before starting
antimicrobial treatment to
guide treatment.
Complicated
Pyelonephritis
Escherichia coli,
Klebsiella pneumonia,
Proteus mirabilis,
Pseudomonas
aeruginosa,
Enterococcus sp.
Frequently multi-drug
resistant organisms are
present
Piperacillin-
Tazobactam 4.5gm
IV 6 hourly
or
Amikacin 1 g OD
IV
or
Cefoperazone-
Sulbactam 3gm IV
12 hourly
Imipenem 1g IV 8
hourly
or
Meropenem 1gm
IV 8 hourly
Get urine cultures before
antibiotics & switch to a
narrow spectrum agent based
on sensitivities. Treat for 10-
14 days.
De-escalate to Ertapenem 1
gm IV OD, if
Imipenem/meropenem
initiated.
Monitor renal function if
aminoglycoside is used.
Acute prostatitis
Enterobacteriaceae
(E.coli, Klebsiella sp.)
Doxycline 100 mg
BD
or
Co-trimoxazole 960
mg BD.
In severe cases,
Piperacillin-
Tazobactam
4.5gm IV 6
hourly
or
Cefoperazone-
sulbactam 3gm IV
12 hourly
or
Ertapenem 1 gm
IV OD
or
Imipenem 1g IV 8
hourly
or
Meropenem 1gm
IV 8 hourly
Get urine and prostatic
massagecultures before
antibiotics & switch to narrow
spectrum agent based on
sensitivities and then treat
total for 3-4 weeks.
Use Ciprofloxacin (if
sensitive)
Vol. 1 Issue 11 L.E.D. E-Journal Page 352
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

18
G. OBSTETRICS AND GYNAECOLOGICAL INFECTIONS
Fluoroquinolones are contraindicated in 1st trimester.
Cotrimoxazole is contraindicated in 1st trimester.
Doxycycline is not recommended in nursing mothers. If need to administer doxycycline discontinuation of
nursing may be contemplated.
Infections
Likely organism Primary treatment
(presumptive
antibiotics)
Alternate
treatment
Remarks
Asymptomatic
Bacteriuria
> 1,00,000 cfu/ ml of
bacteria of same
species in 2 urine
cultures obtained 2-7
days apart.
Treat as per
sensitivity result for 7
days.
Nitrofurantoin 100
mg Oral, BD for 7
days
or Amoxicillin 500
mg Oral BD
x 7-10 days .
Oral
cephalosporins,
TMP-SMX or TMP
alone
Screen in 1st trimester.
Can cause pylonephritis
in upto 25% of all
pregnant women.
30 % Chance of
recurrence after
empirical therapy 1. Few
direct effects, uterine
hypo perfusion due to
maternal anemia
dehydration, may cause
fetal cerebral hypo
perfusion.
2. LBW,
prematurity,premature
labour, hypertension,
preeclampsia, maternal
anemia, and amnionitis.
Need to document
pyuria (Pus cells >
10/HPF)
Group B
streptococcal
Disease, Prophylaxis
and Treatment
Group B Streptococci IV Penicillin G 5
million units.
(Loading dose) then
2.5 -3 million units
IV QID until
delivery.
or
Ampicillin 2 gm IV
( Loading dose) then
1 gm QID until
delivery
Cefazolin 2 gm IV
(Loading Dose) and
then 1 gm TID
Clindamycin 900
mg IV TID or
vancomycin IV or
teicoplanin for
penicillin allergy
Prevalance very low so
the prophylaxis may be
required only on culture
documented report
Associated with high
risk of pre-term
labour,still birth,neonatal
sepsis
Chorioamnionitis
Group B streptococcus, Gram negative bacilli,
chlamydiae, ureaplasma and anaerobes, usually
Polymicrobial
Clindamycin/
vancomycin/
teicoplanin and
cefoperazone-
sulbactum
If patient is not in
sepsis then IV
Ampicillin
Preterm Birth, 9-11%
death rate in preterm
infant’s unfavourable
neurologic outcome,
lesser risk to term
infants.
Septic abortion
Bacteroides, Prevotella bivius,
Group B, Group A
Streptococcus,
Enterobactereaceae, C.
trachomatis, Clostridium
perfringens.
Ampicillin 500
mg QID +
Metronidazole
500mg IV TDS if
patient has not
taken any prior
antibiotic (start
antibiotic after
sending cultures)
If patient has been
Ceftriaxone 2g IV
OD
Vol. 1 Issue 11 L.E.D. E-Journal Page 353
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

19
partially treated
with antibiotics,
send blood
cultures and start
Piperacillin-
Tazobactam or
Cefoperazone-
sulbactam till the
sensitivity report
is available.
Endomyometritis
and Septic Pelvic
Vein Phlebitis
Bacteroides, Prevotella bivius,
Group B, Group A
Streptococcus,
Enterobactereaceae, C.
trachomatis, Clostridium
perfringens
Same as above.
Obstetric Sepsis
during pregnancy
Group A beta-haemolytic
Streptococcus,
E.coli, anaerobes.
If patient is in
shock and blood
culture reports are
pending, then start
Piperacillin-
Tazobactam or
Cefoperazone-
sulbactam till the
sensitivity report
is available and
modify as per the
report. If patient
has only fever,
with no features
of severe sepsis
start amoxicillin
clavulanate oral
625TDS/IV 1.2
gm TDS Or
Ceftriaxone 2gm
IV OD+
Metronidazole
500mg IV TDS
+/-gentamicin
7mg/kg/day OD if
admission needed.
MRSA cover
may be required if
suspected or
colonized
(Vancomycin/
Teicoplanin)
Obstetric Sepsis
following pregnancy
S. pyogenes,
E. coli,
S. aureus
S. pneumoniae,
Meticillin-resistant
S. aureus (MRSA),
C. septicum &
Morganella morganii.
Same as above
Sources of sepsis
outside Genital tract
Mastitis
UTI
Pneumonia
Skin and soft tissue
(IV site, surgical
site, drain site etc.)
Syphillis Refer to STD program
guidelines
Tuberculosis in
pregnancy
Similar to NON
PREGNANT
population with
Please refer RNTCP guideline
WHO has advocated that, all the first line drugs are
Very small chance of
transmission of infection
to fetus.
Vol. 1 Issue 11 L.E.D. E-Journal Page 354
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

20
some exceptions
(see comment and
chapter 8)
safe in pregnancy and can be used except
streptomycin. SM causes significant ototoxicity to
the fetus (Pyrazinamide not recommended by US
FDA)
1. Mother and baby should stay together and the
baby should continue to breastfeed.
2. Pyridoxine supplementation is recommended for
all pregnant or breastfeeding women taking
isoniazid as well as to neonate who are being breast
fed by mothers taking INH.
Late diagnosis can
predispose to LBW,
prematurity.
VIRAL INFECTIONS (NO ANTIBIOTICS TO BE GIVEN)
Influenza In
pregnancy
(seasonal And
H1N1)
The best
preventive
strategy is
administration of
single dose of
killed vaccine.
Oseltamivir 75 mg Oral
BD for 5 days
Nebulization with
Zanamvir respules (2)
5 mg each, BD
for 5 days
1. Tendency for severe
including premature labor
&delivery.
2. Treatment should
begin within 48 hrs of
onset of symptoms.
3. Higher doses
commonly used in non
pregnant population (150
mg) are not
recommended in
pregnancy due to safety
concerns.
4. Chemoprophylaxis can
be used in significant
exposures.
5. Live (nasal Vaccine) is
contraindicated in
pregnancy.
Direct fetal infection
rare
Preterm delivery and
pregnancy loss.
PARASITIC INFECTIONS
Acute
Toxoplasmosis
in pregnancy
<18 weeks gestation at diagnosis
Spiramycin 1 gm Oral qid until 16-18
weeks/Pyrimathamine + sulphadizine. Alternate every
two weeks–
Varicella
>20 wks of gestation,
presenting within 24
hours of the onset of the
rash,
Aciclovir 800mg Oral 5
times a day
IV acyclovir
recommended for the
treatment of severe
complications,
> 24 hrs from the onset
of rash, antivirals are not
found to be useful.
VZIG should be offered to susceptible women < 10
days of the exposure. VZIG has no role in treatment
once the rash appears.
The dose of VZIG is 125 units / 10kg not exceeding
625 units, IM.
Chickenpox during
pregnancy does not
justify termination
without prior prenatal
diagnosis as only.
A minority of fetuses
infected develop fetal
varicella syndrome.
Vol. 1 Issue 11 L.E.D. E-Journal Page 355
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

21
If PCR Positive -
>18 weeks gestation and documented fetal infection by
positive amniotic fluid PCR.
Pyremethamine 50 mg Oral BD x 2 days then 50 mg
OD
+
Sulphadiazine 75 mg/kg Oral x 1 dose then 50mg/kg
bd
+
Folinic Acid (10-20 mg Oral daily) for minimum of 4
weeks or for duration of pregnancy.
Malaria In
pregnancy
As per national program
GENITAL TRACT INFECTIONS
Candidiasis Candida species Fluconazole oral 150 mg single dose
For milder cases-
Intravaginal agents as creams or suppositories
clotrimazole, miconazole, nystatin.
Intravaginal azoles, single dose to 7-14 days.
Non-pregnant- If
recurrent candidiasis,
(4 or more
episodes/year) 6
months suppressive
treatment with
fluconazole 150 mg
oral once a week or
clotrimazole vaginal
suppositories 500 mg
once a week.
Bacterial
vaginosis
Polymicrobial Metronidazole500mg Oral BD x 7 days
Or metronidazole vaginal gel 1 HS x 5 days
Or Tinidazole 2 g orally ODx 3 days Or 2%
Clindamycin Vaginal cream 5 gm HS x 5 days
Treat the partner.
Trichimoniasis Trichomonas vaginalis
Metronidazole 2 gm single dose or 500 mg Oral BD X
7 days or
Tinidazole 2 gm Oral single doseFor treatment failure
– retreat with Metronidazole 500 mg Oral BD X 7
Days, if 2nd failure Metronidazole 2 gm Oral OD X 3-
5 days
Treat sexual partner
with metronidazole 2
gm single dose
Cervicitis
/Urethritis
Mucopurulent
gonoccocal
Polymicrobial
Ceftriaxone 250 mg IM Single dose + Azithromycin 1
gm single dose OR Doxycycline 100mg BD x 7 day
Pelvic
Inflammatory
Disease
(Salpingitis &
tubo-ovarian
abscess)
S. aureus,
Enterobacteriacae,
gonococci, gardenella
Outpatient treatment
Ceftriaxone 250 mg IM/IV single dose plus +/-
Metronidazole 500 mg BD x 14 days Plus Doxycycline
100 mg BD x 14 Days
Inpatient Treatment Clindamycin +ceftriaxone till
patient admitted then change to OPD treatment
Drainage of tubo-
ovarian abscess
wherever indicated
Evaluate and treat sex
partner
Mastitis
without abscess
S. aureus
Amoxycillin clavulunate/Cephalexin 500 mg QID/ OR
Ceftriaxone 2 gm OD OR
MRSA- based on sensitivities Add
Clindamycin 300 QID or
Vancomycin I gm IV 12 hourly /teicoplanin 12mg/kg
IV 12 hourly x 3 doses followed by 6 once daily IV
Mastitis with
abscess
Drainage with antibiotic cover for
MRSA
Clindamycin 300 QID or
Vancomycin 15mg/kg IV 12 hourly (maximum 1gm 12
hourly)/teicoplanin 12mg/kg IV 12 hourly x 3 doses
followed by 6 mg once daily IV
Vol. 1 Issue 11 L.E.D. E-Journal Page 356
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

22
H. BONES AND JOINT INFECTIONS
Condition Likely causative
Organisms
Empiric antibiotics Alternative
antibiotics
Comments
Acute
osteomyelitis OR
Septic arthritis
S.aureus,
Streptococcus
pyogenes
Enterobacteriaceae
Ceftriaxone 2g IV OD
Followed by Oral therapy by
Cloxacillin 500mg q 8h
Or
Cephalexin 500mg q 6h
Piperacillin-
tazobactam
4.5gm IV q 6h or
Cefoperazone-
sulbactam 3gm
IV q 12h
AND
Clindamycin 600-
900mg IV TDS
Treat based on culture of
blood/synovial fluid/bone
biopsy
Orthopedic Consultation
is essential for surgical
debridement
Duration: 4-6 weeks
(From initiation or last
major debridement)
Chronic
Osteomyelitis
OR
Chronic synovitis
No empiric therapy
Definitive
treatmentguided by
bone/synovial biopsy
culture.
Treat for 6 weeks
minimum Investigate for TB,
Nocardia, fungi.
Extensive surgical
debridement.
Total duration of
treatment depends on the
joint and the organism.
Choose antibiotic based
on sensitivity.
Prosthetic joint
infection
Coagulase negative
staphylococci,
Staphylococcus
aureus,Streptococci
Gram-negative bacilli,
Enterococcus,
Anaerobes
Ceftriaxone 2g IV OD. Add
Vancomycin1gm IV BD or
Teicoplanin 800mg x 3
doses followed by 400mg
Once daily
4 weeks
Vol. 1 Issue 11 L.E.D. E-Journal Page 357
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

23
I. EYE INFECTIONS
Eyelid infections Likely organisms First line/ Suggested
Regimen
Alternate regimen Remarks
Blephritis
Unclear
S.aureus,
S.epidermidis
Lid margin care with baby
shampoo & warm compresses
24 hourly. Artificial tears if
associated with dry eye.
External Hordeolum S. aureus
Hot pack
Internal Horedeolum
Blephritis
MSSA/
S. epidermidis
Oral Cloxacillin 250-500 mg
qid or
Oral Cephalexin 500mg QID
Lid margin care with
baby shampoo & warm
compresses 24 hourly.
Artificial tears if
associated with dry eye.
MRSA
Oral Trimethoprim
sulphamethoxazole960 mg
BD or
Linezolid 600mg BD
Cunjuctival infections
Viral conjunctivitis
(pink eye)
No antibiotics required treat
for symptoms
Highly contagious.
If pain &
photophobia the
suggestive of
keratitis.
Bacterial
conjunctivitis
S.aureus,
S.pneumoniae,
H.influenzae
Ophthalmologic solution:
Gatifloxacin 0.3%,
levofloxacin 0.5%,
Moxifloxacin 0.5% 1-2 drops
q2h while awake during 1st 2
days, then q4-8h upto 7 days
Uncommon causes-
Chlamydia
trachomatis
N.gonorrhoeae
Corneal infections
Herpes Simplex
keratitis
H.simplex type
1&2
Trifluridine ophthalmic soln
1drop 2 hourly, up to
9times/day until re-epithilised.
then 1 drop 4 hourly upto 5
times/day for total duration of
21days
Ganciclovir 0.15%
ophthalmic gel for
acute herpitic keratitis.
Flurescine staining
shows topical
dendritic
figures.30-50%
recur within 2yr.
Varicella Zoster
ophthalmicus
Varicella–zoster
virus
Famciclovir 500mg BD Or
TID OR Valacyclovir 1gm
oral TID X 10days
Acyclovir 800mg 5
times/d x 10days
.
Acute bacterial
keratitis (No
comorbidities)
S.aureus,
S.pneumoniae,
S.pyogenes,
Haemophilus spp
Moxifloxacin topical(0.5%):1
drop 1 hourly for first
48hr,then reduce as per
response
Gatifloxacin 0.3%
ophthalmic Solution
1drop 1 hourly for 1st
48hrs then reduce as
per response
Moxifloxacin.
Preferable.
Treatment may fail
against MRSA.
Acute Bacterial
(Contact lens users)
P.aeruginosa
Tobramycin or Gentamicin
14mg/ml + Piperacilin or
Ticarcillin eye drops (6-
Ciprofloxacin
ophthalmic 0.3% or
Levofloxacin
Vol. 1 Issue 11 L.E.D. E-Journal Page 358
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
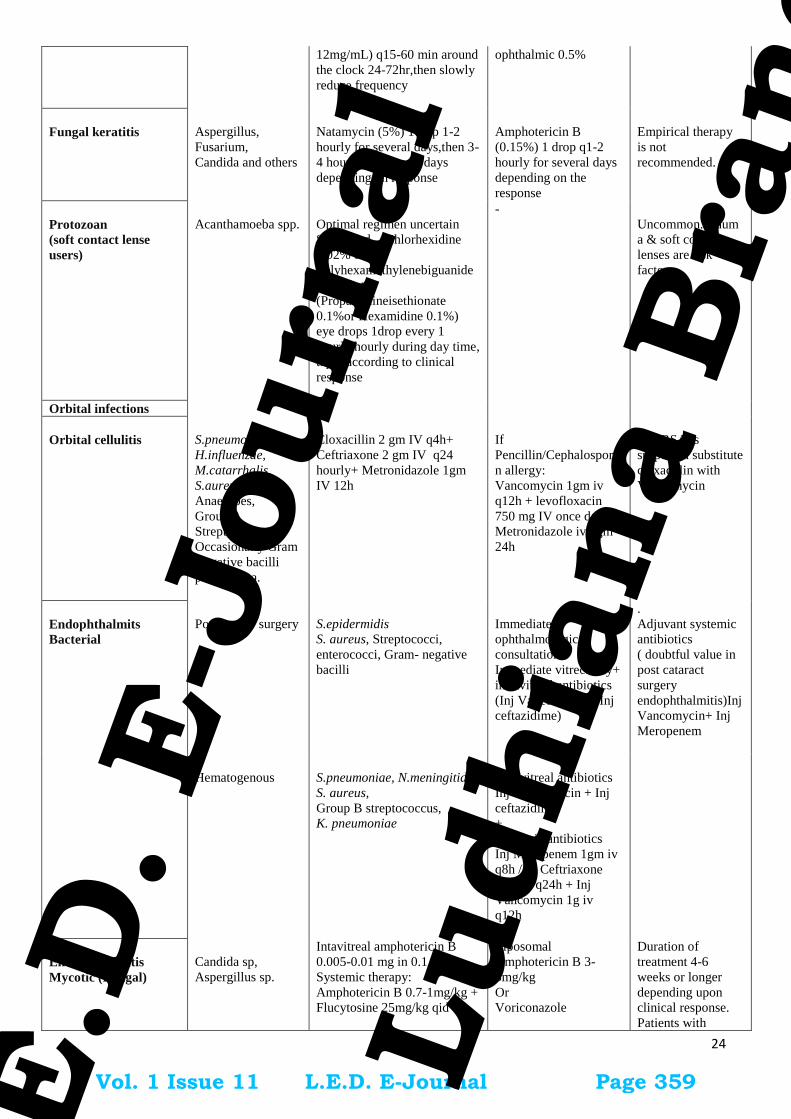
24
12mg/mL) q15-60 min around
the clock 24-72hr,then slowly
reduce frequency
ophthalmic 0.5%
Fungal keratitis
Aspergillus,
Fusarium,
Candida and others
Natamycin (5%) 1drop 1-2
hourly for several days,then 3-
4 hourly for several days
depending on response
Amphotericin B
(0.15%) 1 drop q1-2
hourly for several days
depending on the
response
Empirical therapy
is not
recommended.
Protozoan
(soft contact lense
users)
Acanthamoeba spp.
Optimal regimen uncertain
Suggested –(Chlorhexidine
0.02% or
Polyhexamethylenebiguanide
0.02%) +
(Propamidineisethionate
0.1%or Hexamidine 0.1%)
eye drops 1drop every 1
hourly hourly during day time,
taper according to clinical
response
-
Uncommon.Traum
a & soft contact
lenses are risk
factors
Orbital infections
Orbital cellulitis
S.pneumoniae,
H.influenzae,
M.catarrhalis,
S.aureus,
Anaerobes,
Group A
Streptococcus,
Occasionally Gram
Negative bacilli
post trauma.
Cloxacillin 2 gm IV q4h+
Ceftriaxone 2 gm IV q24
hourly+ Metronidazole 1gm
IV 12h
If
Pencillin/Cephalospori
n allergy:
Vancomycin 1gm iv
q12h + levofloxacin
750 mg IV once daily +
Metronidazole iv 1gm
24h
If MRSA is
suspected substitute
cloxacillin with
Vancomycin
Endophthalmits
Bacterial
Post-ocular surgery
S.epidermidis
S. aureus, Streptococci,
enterococci, Gram- negative
bacilli
Immediate
ophthalmological
consultation.
Immediate vitrectomy+
intravitreal antibiotics
(Inj Vancomycin + Inj
ceftazidime)
.
Adjuvant systemic
antibiotics
( doubtful value in
post cataract
surgery
endophthalmitis)Inj
Vancomycin+ Inj
Meropenem
Hematogenous
S.pneumoniae, N.meningitidis,
S. aureus,
Group B streptococcus,
K. pneumoniae
Intravitreal antibiotics
Inj Vancomycin + Inj
ceftazidime
+
Systemic antibiotics
Inj Meropenem 1gm iv
q8h /Inj Ceftriaxone
2gm iv q24h + Inj
Vancomycin 1g iv
q12h
Endophthalmitis
Mycotic (Fungal)
Candida sp,
Aspergillus sp.
Intavitreal amphotericin B
0.005-0.01 mg in 0.1 ml
Systemic therapy:
Amphotericin B 0.7-1mg/kg +
Flucytosine 25mg/kg qid
Liposomal
Amphotericin B 3-
5mg/kg
Or
Voriconazole
Duration of
treatment 4-6
weeks or longer
depending upon
clinical response.
Patients with
Vol. 1 Issue 11 L.E.D. E-Journal Page 359
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
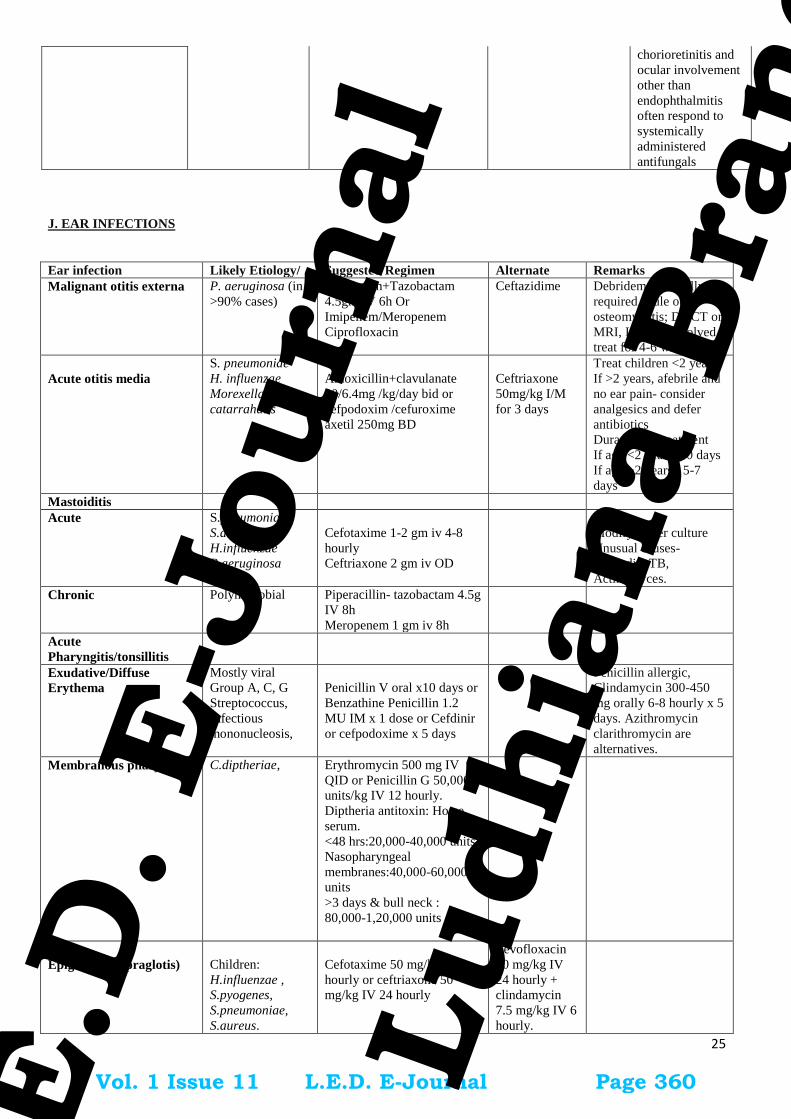
25
chorioretinitis and
ocular involvement
other than
endophthalmitis
often respond to
systemically
administered
antifungals
J. EAR INFECTIONS
Ear infection Likely Etiology/ Suggested Regimen Alternate Remarks
Malignant otitis externa P. aeruginosa (in
>90% cases)
Piperacilin+Tazobactam
4.5gm IV 6h Or
Imipenem/Meropenem
Ciprofloxacin
Ceftazidime Debridement usually
required. Rule out
osteomyelitis; Do CT or
MRI, If bone involved ,
treat for 4-6 wks.
Acute otitis media
S. pneumoniae
H. influenzae
Morexella
catarrahalis
Amoxicillin+clavulanate
90/6.4mg /kg/day bid or
cefpodoxim /cefuroxime
axetil 250mg BD
Ceftriaxone
50mg/kg I/M
for 3 days
Treat children <2 years
If >2 years, afebrile and
no ear pain- consider
analgesics and defer
antibiotics
Duration of treatment
If age <2 years: 10 days
If age >2 years : 5-7
days
Mastoiditis
Acute S.pneumoniae
S.aureus
H.infiuenzae
P.aeruginosa
Cefotaxime 1-2 gm iv 4-8
hourly
Ceftriaxone 2 gm iv OD
Modify as per culture
Unusual causes-
Nocardia, TB,
Actinomyces.
Chronic Polymicrobial Piperacillin- tazobactam 4.5g
IV 8h
Meropenem 1 gm iv 8h
Acute
Pharyngitis/tonsillitis
Exudative/Diffuse
Erythema
Mostly viral
Group A, C, G
Streptococcus,
Infectious
mononucleosis,
Penicillin V oral x10 days or
Benzathine Penicillin 1.2
MU IM x 1 dose or Cefdinir
or cefpodoxime x 5 days
Penicillin allergic,
Clindamycin 300-450
mg orally 6-8 hourly x 5
days. Azithromycin
clarithromycin are
alternatives.
Membranous pharyngitis C.diptheriae, Erythromycin 500 mg IV
QID or Penicillin G 50,000
units/kg IV 12 hourly.
Diptheria antitoxin: Horse
serum.
<48 hrs:20,000-40,000 units,
Nasopharyngeal
membranes:40,000-60,000
units
>3 days & bull neck :
80,000-1,20,000 units
Epiglotitis(Supraglotis)
Children:
H.influenzae ,
S.pyogenes,
S.pneumoniae,
S.aureus.
Cefotaxime 50 mg/kg IV 8
hourly or ceftriaxone 50
mg/kg IV 24 hourly
Levofloxacin
10 mg/kg IV
24 hourly +
clindamycin
7.5 mg/kg IV 6
hourly.
Vol. 1 Issue 11 L.E.D. E-Journal Page 360
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

26
Adult: Group A
Streptococcus ,
H.influenzae
Laryngitis(hoarseness) Viral (90%) No antibiotic indicated
K. INFECTIONS IN BURNS PATIENTS
Condition Likely Causative
Organism
Empiric antibiotics
Alternative
antibiotics
Comments
For burns wound that is
clinically or
microbiologically not
infected
Prophylactic parenteral
antibiotics in burns are
NOT indicated
Topical antibiotics to be
given after debridement
For burns wound that are
clinically or
microbiologically infected
Strep pyogenes,
Enterobacter sp.,
S. aureus,
S. epidermidis,
Pseudomonas,
fungi (rare)
i. Burn wound sepsis
Pipercillin-tazobactam
or
Cefoperazone-sulbactam
or
With or without:
Vancomycin
//Teicoplanin
(if there is suspicion for
MRSA)
Antifunal Therapy –
When extensive burns
and patient not
responding to antibiotics
o If hemodynamically
stable: fluconazole
o If hemodynamically
unstable:
Echinocandin
Burn wound cellulitis
Cefazolin
or
Clindamycin
or
Vancomycin if there is
suspicion for MRSA
With and without (for burns
involving the lower extremity
or feet or burns in patients
with diabetes)
Pipercillin-tazobactam
or
cefoperazone-sulbactam
Carbapenem
+/-
Vancomycin/
Teicoplanin
Antibiotic choices are
dependent on the
antibiogram of the
individual institution.
Surgical debridement as
necessary.
Amphotericin B is toxic
to all burn patient as
renal system
compromised, hence
Caspofungin may be
used.
Prophylaxis in Plastic Surgery
Surgical prophylaxsis: Inj Cefuroxime 1.5 g/ Cefazolin IV just before incision single dose.
Vol. 1 Issue 11 L.E.D. E-Journal Page 361
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

27
L .FUNGAL INFECTIONS
Routine antifungal prophylactic therapy in critically ill patients is NOT recommended. Fungal therapy is usually started
based on positive cultures or systemic evidence of fungal infection. It is advised to take paired cultures if fungal infection is
suspected. Evidence includes persistent sepsis / SIRS despite broad spectrum antibiotic (exclude sepsis, abscess, drug fever,
DVT etc). Treat according to identification and antifungal sensitivity of Candida isolate.
Fluconazole IV/oral 800 mg OD first day (12mg/kg) and then 400 mg OD (6mg/kg from second day) if fluconazole
naïve or sensitive
Or
2nd
line Liposomal Amphotericin B (for Candida krusei and C.glabrata as inherently resistant to Fluconazole.) or
Caspofungin (As Caspofungin is inherently inactive against Zygomycetes, Cryptococcus, Fusarium and
Trichosporon Spp) Liposomal Amphotericin B IV 3mg/kg OD or Caspofungin dose: IV 70mg on Day 1 (loading),
50mg OD (<80kg) or 70mg OD (if >80kg) thereafter.Moderate to severe hepatic dysfunction: reduce the subsequent
daily dose to 35mg OD. Check for drug interactions.
To be decided by Microbiologist/ID physician based on patient’s hepatic / renal functions/Severity of infection /drug
interactions e.g. rifampicin, carbamazepine, phenytoin, efavirenz, nevirapine, cyclosporin, dexamethasone, tacrolimus
etc.
M. FEBRILE NEUTROPENIA
Febrile Neutropenia- definition
Neutropenia-ANC<500/mm3 and expected to fall below 500/mm
3 in 48hrs
Fever -single oral temperature of 38.3oC (101
0 F) on one occasion or 38
oC (100.4
0 F) on at least 2 occasions (1 hour
apart)
Neutropenic patients may not have usual signs of infection. Redness, tenderness and fever may be the only signs.
Protocol:
Critical examination of areas usually harboring infections, including but not limited to, oral cavity, axillary region,
scalp, groin, perineal region.
Send blood Cultures 2 sets (each bottle 10ml x 4 bottles)
Other relevant investigations: urea, creatinine, ALT, urine culture, Chest Xray, separate culture from central line, etc.
Patient-Haemodynamically stable
Blood culture 2 sets
Start IV Ceftazidime
No need to add glycopeptide in the initial regimen (except in specific situations, given below)
Patient-Haemodynamically unstable
Start BL-BLI agent (Cefoperazone-Sulbactam/piperacillin-tazobactam)
OR
Carbapenem (meropenem/imipenem/doripenem)
No need to add glycopeptide in the initial regimen (except in specific situations, given below)
Reassess after 48 hours:
If blood cultures are negative, haemodynamically stable but still febrile
Reculture blood
Add amikacin for 3 days
Add colistin (instead of amikacin) if indicated (see below)
If blood cultures are negative, haemodynamically unstable but still febrile
Inj Colistin (+/-Carbapenem) + glycopeptide + Echinocandin/L-Ampho B
Blood culture growing Gram negative bacilli
Patient afebrile - continue the empirical antibiotic till antibiotic sensitivity is available.
Rationalise as per susceptibility profiles
When to add glycopeptides?
1. Haemodynamic instability, or other evidence of severe sepsis, septic shock or pneumonia
2. Colonisation with MRSA or penicillin-resistant S. pneumonia
Vol. 1 Issue 11 L.E.D. E-Journal Page 362
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
28
3. Suspicion of serious catheter-related infectione.g. chills or rigours with infusion through catheter and cellulitis
around the catheter exit site
4. Skin or soft-tissue infection at any site
5. Positive blood culture for gram-positive bacteria, before final identification and susceptibility testing is available
6. Severe mucositis
When to add empirical colistin in febrile neutropenic patients?
1. Heamodynamic instability.
2. Colonisation with carbapenem resistant gram-negative bacteria.
3. Previous infection with carbapenem resistant gram-negative bacteria.
4. GNB in blood, sensivity pending, persistent fever with haemodynamic instability.
Empirical Antifungal Therapy
No response to broad spectrum antibiotics (3-5 days)-add L-Ampho B / echinocandin
When a patient is located at a remote area and may not have access to emergency healthcare services, febrile
neutropenia can be lifethreatening. Under such circumstances, availability of broad-spectrum oral antibiotics with the
patient can help them gain time to reach emergency healthcare service.
Useful tips
Febrile after 72 hrs-CT chest and consider empirical antifungal.
If fever persists on empirical antibiotics, send two sets blood cultures/day for 2 days
Send further cultures if clinical deteriaration Unexplained persistent fever in otherwise stable patient doesn’t require change in empirical antibiotic regimen.
Continue the regimen till ANC is >500 cells/mm3
If glycopeptide started as a part of empirical regimen, STOP after 48 hrs, if no evidenc of Gram positive infection
Antibiotic treatment should be given for at least seven days with an apparently effective antibiotic, with at least four
days without fever.
Once Neutrophil count has recovered, with no culture positivity and heamodynamically stable; antibiotics can be
stopped and patient observed, even if remains febrile. Evaluate for fungal infection, if at risk.
Antibiotic Prophylaxis
Though quinolone prophylaxis is recommended by International guidleines, it is not useful in Indian scenario due to high
resistance.
Antiviral prophylaxis
For HSV IgG positive patients undergoing allo-HSCT or leukemia induction needs acyclovir prophylaxis
All patients being treated for cancer need to receive annual influenza vaccination with an inactivated vaccine.
Neutropenic patients presenting with influenza like illness should receive empirical treatment with neuraminidase
inhibitor.
Antifungal prophylaxis
a) Induction chemotherapy of Acute Leukemia: Posoconazole
b) Post allo BMT
Pre engraftment: Voriconazole/echinocandin
Post engraftment: Posoconazole
Vol. 1 Issue 11 L.E.D. E-Journal Page 363
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

29
N. POST-CARDIOVASCULAR SURGERY INFECTIONS
Surveillance regarding the Infections following CTVS should be done in each institute
1. Antibiotic Prophylaxis to be guided by the institutional prevalence of MRSA infection and in patients at increased risk for
MRSA colonization
2. Nasal screening before CTV surgery is recommended to rule out MRSA colonization
S.
no.
Surgery
Antibiotic Prophylaxis
Comments
1st line 2
nd line Special
Antibiotic/Combination
1. CABG Cefazolin Cefuroxime - Vancomycin /Teicoplanin to be used
in case of high prevalence of MRSA
infections only
Using only Vancomycin/Teicoplanin
is NOT recommended due to lack of
coverage of GNB
Vancomycin infusion to be given
over 1 hour & to be started 2 hrs
before the surgical incision
Teicoplanin dosing to start with 800
mg x 3 doses and then 6 mg/kg to
complete prophylxis
Duration of Prophylaxis: Continued
till 48 hours after the surgery
Empirical Treatment after appropriate specimen for stain & cultures have been collected
S.
no.
Infection/
Syndrome
Likely
Causative
agents
Antibiotics Comments
1st line 2
nd line Special Antibiotic/
Combination
1 Sternotomy site
infection
Not known BL-BLI
(Piperacillin-
tazobactam,
Cefoperazone-
sulbactam, cefipime-
tazobactam) with or
without amikacin.
With
Vancomycin/
teicoplanin
Daptomycin/
Linezolid with
carbapenem
Consider de-
escalation to
TMP/SMX ,
doxy/minocycline,
cloxacillin, cefazolin,
If these are sensitive
1) Removal of
the foreign
body (steel
wires) should
be considered
2 Infection of
vascular
catheters
Not known BL-BLI
(Piperacillin-
tazobactam,
Cefoperazone-
sulbactam, cefipime-
tazobactam) with or
without amikacin
withVancomycin/
teicoplanin
Carbapenem
(Empirical
anti-MRSA
drug if the
incidence of
MRSA CRBSI
is high)
Consider de-
escalation as per the
isolate,
susceptibility,
MICs, adverse
effects, drug allergy
3 Pneumonia Not known BL-BLI
(Piperacillin-
tazobactam,
Cefoperazone-
sulbactam) with or
without amikacin
Carbapenem
Consider de-
escalation as per the
isolate,
susceptibility,
MICs, adverse
effects, drug allergy
4 Mediastinitis Not known BL-BLI
(Piperacillin-
tazobactam,
Carbapenem
with or
without
Consider de-
escalation as per the
isolate,
Vol. 1 Issue 11 L.E.D. E-Journal Page 364
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
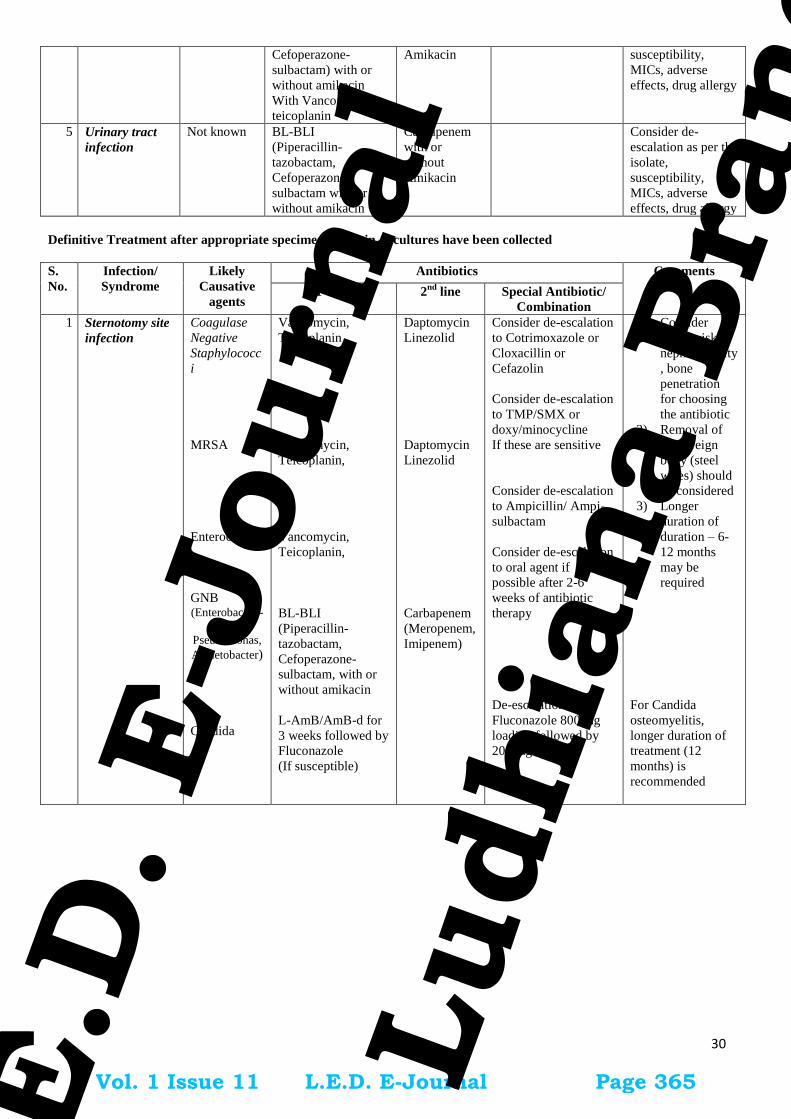
30
Cefoperazone-
sulbactam) with or
without amikacin
With Vancomycin/
teicoplanin
Amikacin
susceptibility,
MICs, adverse
effects, drug allergy
5 Urinary tract
infection
Not known BL-BLI
(Piperacillin-
tazobactam,
Cefoperazone-
sulbactam with or
without amikacin
Carbapenem
with or
without
Amikacin
Consider de-
escalation as per the
isolate,
susceptibility,
MICs, adverse
effects, drug allergy
Definitive Treatment after appropriate specimen for stain & cultures have been collected
S.
No.
Infection/
Syndrome
Likely
Causative
agents
Antibiotics Comments
1st line 2
nd line Special Antibiotic/
Combination
1 Sternotomy site
infection
Coagulase
Negative
Staphylococc
i
MRSA
Enterococcus
GNB (Enterobacteri-
-acae,
Pseudomonas,
Acinetobacter)
Candida
Vancomycin,
Teicoplanin
Vancomycin,
Teicoplanin,
Vancomycin,
Teicoplanin,
BL-BLI
(Piperacillin-
tazobactam,
Cefoperazone-
sulbactam, with or
without amikacin
L-AmB/AmB-d for
3 weeks followed by
Fluconazole
(If susceptible)
Daptomycin
Linezolid
Daptomycin
Linezolid
Carbapenem
(Meropenem,
Imipenem)
Consider de-escalation
to Cotrimoxazole or
Cloxacillin or
Cefazolin
Consider de-escalation
to TMP/SMX or
doxy/minocycline
If these are sensitive
Consider de-escalation
to Ampicillin/ Ampi-
sulbactam
Consider de-escalation
to oral agent if
possible after 2-6
weeks of antibiotic
therapy
De-escalation to
Fluconazole 800 mg
loading followed by
200 mg BD
1) Consider
MICs, risk of
nephrotoxicity
, bone
penetration
for choosing
the antibiotic
2) Removal of
the foreign
body (steel
wires) should
be considered
3) Longer
duration of
duration – 6-
12 months
may be
required
For Candida
osteomyelitis,
longer duration of
treatment (12
months) is
recommended
Vol. 1 Issue 11 L.E.D. E-Journal Page 365
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
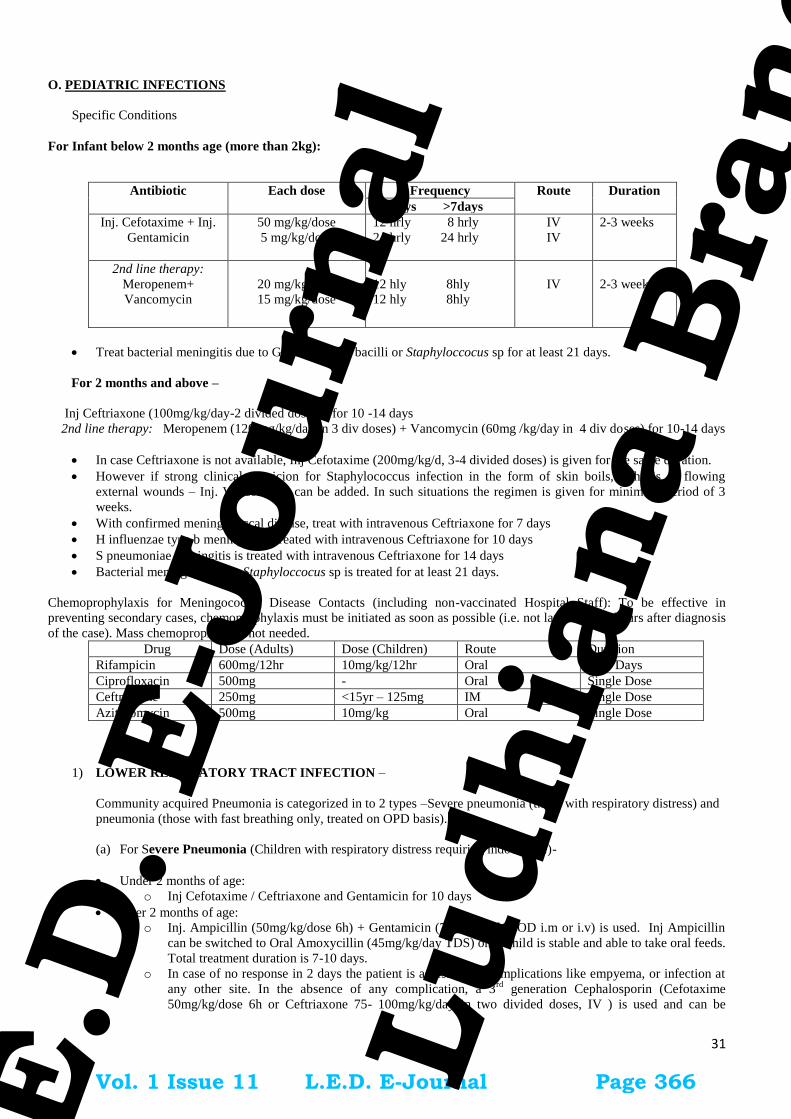
31
O. PEDIATRIC INFECTIONS
Specific Conditions
For Infant below 2 months age (more than 2kg):
Antibiotic Each dose Frequency Route Duration
<7 days >7days
Inj. Cefotaxime + Inj.
Gentamicin
50 mg/kg/dose
5 mg/kg/dose
12 hrly 8 hrly
24 hrly 24 hrly
IV
IV
2-3 weeks
2nd line therapy:
Meropenem+
Vancomycin
20 mg/kg/dose
15 mg/kg/dose
12 hly 8hly
12 hly 8hly
IV
2-3 weeks
Treat bacterial meningitis due to Gram-negative bacilli or Staphyloccocus sp for at least 21 days.
For 2 months and above –
Inj Ceftriaxone (100mg/kg/day-2 divided dosage) for 10 -14 days
2nd line therapy: Meropenem (120 mg/kg/day in 3 div doses) + Vancomycin (60mg /kg/day in 4 div doses) for 10-14 days
In case Ceftriaxone is not available, Inj Cefotaxime (200mg/kg/d, 3-4 divided doses) is given for the same duration.
However if strong clinical suspicion for Staphylococcus infection in the form of skin boils, arthritis or flowing
external wounds – Inj. Vancomycin can be added. In such situations the regimen is given for minimum period of 3
weeks.
With confirmed meningococcal disease, treat with intravenous Ceftriaxone for 7 days
H influenzae type b meningitis is treated with intravenous Ceftriaxone for 10 days
S pneumoniae meningitis is treated with intravenous Ceftriaxone for 14 days
Bacterial meningitis due to Staphyloccocus sp is treated for at least 21 days.
Chemoprophylaxis for Meningococcal Disease Contacts (including non-vaccinated Hospital Staff): To be effective in
preventing secondary cases, chemoprophylaxis must be initiated as soon as possible (i.e. not later than 48 hours after diagnosis
of the case). Mass chemoprophylaxis not needed.
Drug Dose (Adults) Dose (Children) Route Duration
Rifampicin 600mg/12hr 10mg/kg/12hr Oral Two Days
Ciprofloxacin 500mg - Oral Single Dose
Ceftriaxone 250mg <15yr – 125mg IM Single Dose
Azithromycin 500mg 10mg/kg Oral Single Dose
1) LOWER RESPIRATORY TRACT INFECTION –
Community acquired Pneumonia is categorized in to 2 types –Severe pneumonia (those with respiratory distress) and
pneumonia (those with fast breathing only, treated on OPD basis).
(a) For Severe Pneumonia (Children with respiratory distress requiring indoor care)-
Under 2 months of age:
o Inj Cefotaxime / Ceftriaxone and Gentamicin for 10 days
Over 2 months of age:
o Inj. Ampicillin (50mg/kg/dose 6h) + Gentamicin (7.5mg/kg/day OD i.m or i.v) is used. Inj Ampicillin
can be switched to Oral Amoxycillin (45mg/kg/day TDS) once child is stable and able to take oral feeds.
Total treatment duration is 7-10 days.
o In case of no response in 2 days the patient is assessed for complications like empyema, or infection at
any other site. In the absence of any complication, a 3rd
generation Cephalosporin (Cefotaxime
50mg/kg/dose 6h or Ceftriaxone 75- 100mg/kg/day in two divided doses, IV ) is used and can be
Vol. 1 Issue 11 L.E.D. E-Journal Page 366
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

32
switched to oral Cefopodoxime (10mg/kg/day BD) once the child is able to take orally. Total treatment
duration is 7-10 days.
o In case the patient has severe sepsis/ septic shock, Inj. Piperacillin + Tazobactam (90mg/kg/dose 6h) +
MRSA cover with IV Vancomycin (15mg/kg/dose 6h) is recommended.
Whenever Staphyloccus aureus is suspected in children (see Text Box), the various drug options are:
In severe pneumonia, use Inj.Cloxacillin or Inj Clindamycin may be added to the initial regime. OR
Oral or IV Co- Amoxyclavulanic acid can be used.
In very severe necrotizing pneumonia or for a patient in septic shock, MRSA cover should be added with IV
Vancomycin Vancomycin 25-30 mg IV loading followed by 15-20 mg/kg 8-12 Hourly /)/ Teicoplanin 12 mg/kg x3
doses followed by 6 mg/kg once a day or Linezolid (10mg/kg/dose 8h).
The total duration for treatment for uncomplicated Staphylococcal pneumonia is 3-4 weeks.
(b) For pneumonia (OPD)
Oral Amoxicillin (45mg/kg/day TDS) for a period of 5 days is recommended as the first choice. In case of non
availability, one may use oral Co-trimoxazole (8mg/kg/day of TMP component BD).
Routine use of macrolide antibiotics for all cases of pneumonia is not advocated. Recent data suggests that (i) the routine
addition of macrolides to children with CAP does not improve outcome (ii) selective use of macrolides would reduce their
indiscriminate use and reduce antibiotic resistance.
Classically the mycoplasma pneumonia presents in an atypical fashion but literature suggests that it can sometimes be difficult
to distinguish mycoplasma pneumonia from a pyogenic pneumonia.
Macrolide antibiotics should be considered in following clinical scenarios where the likelihood of mycoplasma pneumonia is
high:
a. Children with a subacute presentation with prolonged low grade fever, persistent cough, chest signs out of
proportion to the radiographic abnormality (usually showing perihilar streaky infiltrates).
b. Children with CAP (acute pneumonia like presentation with radiological evidence of patchy or lobar
consolidation) who also have or develop extrapulmonary manifestations like myocarditis, hemolytic
anemias, glomeruonephritis, aseptic arthritis, CNS problems (aseptic meningitis, encephalitis, ataxia), etc.
c. Non response to first line antibiotics in children who are immunized with Hib/PCV and have no suppurative
complications of CAP.
In the first two conditions macrolide antibiotics can be used along with the first line therapy for CAP.
EMPYEMA
• Proper drainage : Forms the main core of treatment.
Antimicrobial Therapy:
Anti- Staphylococcal penicillin (Cloxacillin 100-200 mg/kg/day) along with 3rd generation cephalosporin like
Ceftriaxone may be used as first line drug.
Co-Amoxyclav is alternative first line therapy.
It is important to have high index of suspicion for staphylococcal infection as the initial
choice of antibiotic does not cover this less common but a more severe infection
adequately. Staphylococcal pneumonia is suspected if any child with pneumonia has:
Rapid progression of the disease, or
Pneumatocele, or Pneumothorax, or Effusion on chest X-ray, or
Large skin boils or abscess or infected scabies or
Post-measles pneumonia, which is not responding within 48 hours to the initial
therapy.
To cover for staphylococcal infection, Cloxacillin or other antistaphyloccal drug
should be added to the initial regimen as discussed in the text.
Vol. 1 Issue 11 L.E.D. E-Journal Page 367
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
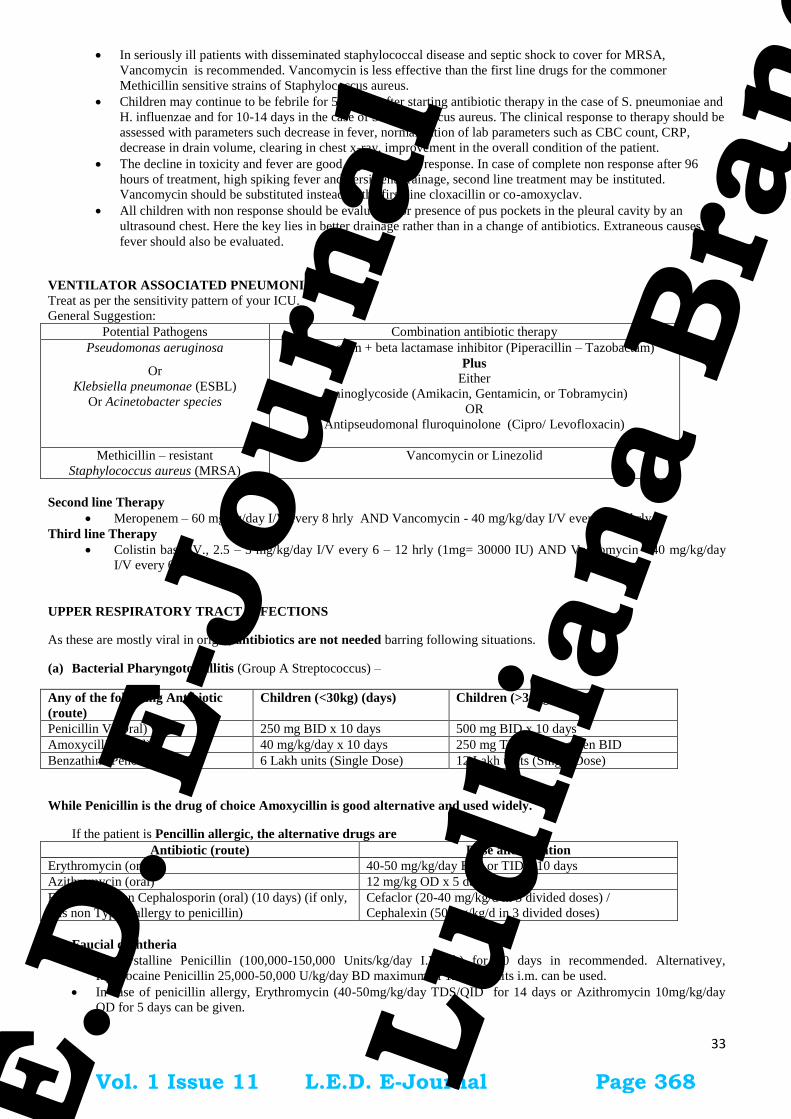
33
In seriously ill patients with disseminated staphylococcal disease and septic shock to cover for MRSA,
Vancomycin is recommended. Vancomycin is less effective than the first line drugs for the commoner
Methicillin sensitive strains of Staphylococcus aureus.
Children may continue to be febrile for 5-7 days after starting antibiotic therapy in the case of S. pneumoniae and
H. influenzae and for 10-14 days in the case of Staphylococcus aureus. The clinical response to therapy should be
assessed with parameters such decrease in fever, normalization of lab parameters such as CBC count, CRP,
decrease in drain volume, clearing in chest x-ray, improvement in the overall condition of the patient.
The decline in toxicity and fever are good signs of likely response. In case of complete non response after 96
hours of treatment, high spiking fever and persistent drainage, second line treatment may be instituted.
Vancomycin should be substituted instead of the first line cloxacillin or co-amoxyclav.
All children with non response should be evaluated for presence of pus pockets in the pleural cavity by an
ultrasound chest. Here the key lies in better drainage rather than in a change of antibiotics. Extraneous causes of
fever should also be evaluated.
VENTILATOR ASSOCIATED PNEUMONIA:
Treat as per the sensitivity pattern of your ICU.
General Suggestion:
Potential Pathogens Combination antibiotic therapy
Pseudomonas aeruginosa
Or
Klebsiella pneumonae (ESBL)
Or Acinetobacter species
Beta Lactam + beta lactamase inhibitor (Piperacillin – Tazobactam)
Plus
Either
Aminoglycoside (Amikacin, Gentamicin, or Tobramycin)
OR
Antipseudomonal fluroquinolone (Cipro/ Levofloxacin)
Methicillin – resistant
Staphylococcus aureus (MRSA)
Vancomycin or Linezolid
Second line Therapy
Meropenem – 60 mg/kg/day I/V every 8 hrly AND Vancomycin - 40 mg/kg/day I/V every 6 - 8 hrly
Third line Therapy
Colistin base IV., 2.5 – 5 mg/kg/day I/V every 6 – 12 hrly (1mg= 30000 IU) AND Vancomycin - 40 mg/kg/day
I/V every 6 - 8 hrly
UPPER RESPIRATORY TRACT INFECTIONS
As these are mostly viral in origin, antibiotics are not needed barring following situations.
(a) Bacterial Pharyngotonsillitis (Group A Streptococcus) –
Any of the following Antibiotic
(route)
Children (<30kg) (days) Children (>30kg) (days)
Penicillin V (Oral) 250 mg BID x 10 days 500 mg BID x 10 days
Amoxycillin (Oral) 40 mg/kg/day x 10 days 250 mg TID, can be given BID
Benzathine Pencillin G (IM) 6 Lakh units (Single Dose) 12 Lakh units (Single Dose)
While Penicillin is the drug of choice Amoxycillin is good alternative and used widely.
If the patient is Pencillin allergic, the alternative drugs are
Antibiotic (route) Dose and duration
Erythromycin (oral) 40-50 mg/kg/day BID or TID x 10 days
Azithromycin (oral) 12 mg/kg OD x 5 days
First Generation Cephalosporin (oral) (10 days) (if only,
it is non Type 1 allergy to penicillin)
Cefaclor (20-40 mg/kg/d in 3 divided doses) /
Cephalexin (50 mg/kg/d in 3 divided doses)
(b) Faucial diphtheria
Inj.Crystalline Penicillin (100,000-150,000 Units/kg/day I.V 6h) for 10 days in recommended. Alternativey,
Inj.Procaine Penicillin 25,000-50,000 U/kg/day BD maximum of 12 lakh units i.m. can be used.
In case of penicillin allergy, Erythromycin (40-50mg/kg/day TDS/QID for 14 days or Azithromycin 10mg/kg/day
OD for 5 days can be given.
Vol. 1 Issue 11 L.E.D. E-Journal Page 368
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

34
(c) Acute otitis media (AOM) –
Oral Amoxicillin (45mg/kg/day TDS/50-60mg/kg/day in two divided doses) for 7 to 10 days is recommended.
For severe cases (Severe Otalgia and/ or Temp >390C), Co-Amoxycillin Clavulanate (45 mg/kg/day po BD) or
Inj.Ceftriaxone 75 mg/kg/day OD can be used.
In case of penicillin allergy, Cefidinir (14 mg/kg/d in 2 divided doses) can be used
Total duration of treatment is recommended for 7 to 10 days.
(d) Mastoiditis And Other Acute Ear Infection
Inj. Amoxicillin-clavulanate OR 3rd Gen Cephalosporin (Ceftriaxone/ cefotaxime).
(e) CSOM
Routinely systemic antibiotic is not recommended until there is exacerbation and these are referred to ENT
(f) Acute Sinusitis with URI-
Oral Amoxycillin (45 mg/kg/day TDS) for 7-10 days is recommended. For severe
cases, Amoxycillin Clavulanate (45 mg/kg/day oral BD) or Inj.Ceftriaxone 75 mg/kg/day OD can be used.
(g) Ludwig’s Angina
1st line : Clindamycin IV 8 hourly or Amoxicillin-Clavulanate IV
2nd
line : Piperacillin-Tazobactam IV 6 hourly
(h) Pertussis
Erythromycin for 14 days, Azithromycin for 5 days, Clarithromycin for 7 days and have similar efficacy but differ in
terms of cost, duration of therapy, side effects, tolerability, likelihood of drug interaction. Considering all factors,
Azithromycin in a dose of 10 mg/kg once a day for 5 days in infants less than 6 months and 10 mg/kg on day 1 and
then 5 mg/kg day on 2 to 5 days is the cheapest, shortest best tolerated and most convenient option and can be safely
given to infants less than 1 month (unlike all other macrolides).
GASTRO-INTESTINAL DISEASES
(1) Dysentery
(a) For inpatients- Inj Ceftriaxone (100mg/kg) for 5-7 days.
(b) For OPD cases
Cefixime (8mg/kg/day BD)
Or
Azithromycin 10-20 mg/ kg (ceiling dose of 1 gm) for 5 days.
In case of non response after 2 antibiotics, investigate for appropriate therapy.
Fluoroquinolones are not preferred due to high level of resistance in many parts of the country.
(2) Cholera
Single dose oral azithromycin 10 mg/ kg (ceiling dose of 1 gm) or Doxycycline (50mg for less than 3 years
and 100 mg for those above).
(3) Enteric Fever
(a) For OPD cases-
Oral Cefixime 20 mg/kg/day (max dose of 1200) for 14 days or azithromycin 10-20 mg/kg (ceiling dose of 1
gm) for 7-10 days. Antibiotic therapy should be continued till one week post-fever defervescence.
(b) For inpatients
Inj Ceftriaxone 100 mg/ kg/day and shift to oral cefixime once fever resolves. Antibiotic therapy should be
continued till one week post-fever defervescence.
Second line:
a) Ofloxacin 15mg/kg/d in two divided doses for 10-14 days. Antibiotic therapy should be continued till one
week post-fever defervescence.
b) Chloramphenicol (50- 75mg/kg/day PO) x 14 days
c) TMP-SMX (8 mg/kg/day of TMP PO) x 14 days
Vol. 1 Issue 11 L.E.D. E-Journal Page 369
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
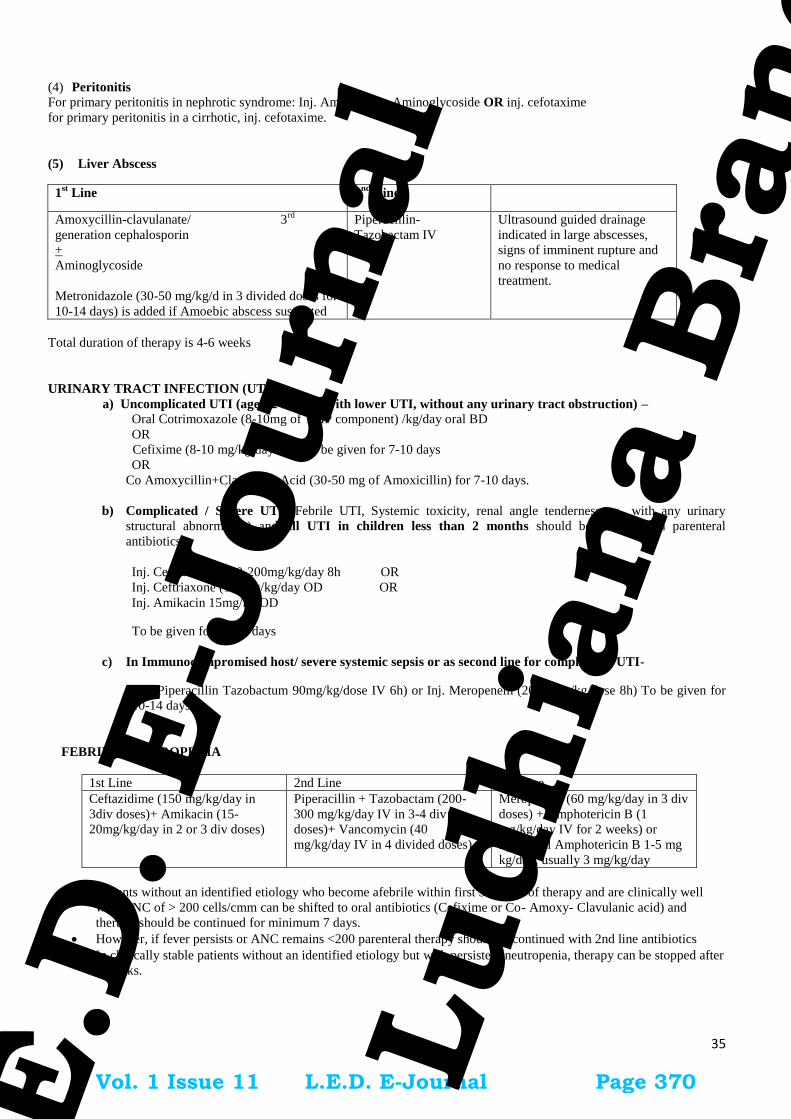
35
(4) Peritonitis For primary peritonitis in nephrotic syndrome: Inj. Ampicillin + Aminoglycoside OR inj. cefotaxime
for primary peritonitis in a cirrhotic, inj. cefotaxime.
(5) Liver Abscess
1st Line 2
nd Line
Amoxycillin-clavulanate/ 3rd
generation cephalosporin
+
Aminoglycoside
Metronidazole (30-50 mg/kg/d in 3 divided doses for
10-14 days) is added if Amoebic abscess suspected
Piperacillin-
Tazobactam IV
Ultrasound guided drainage
indicated in large abscesses,
signs of imminent rupture and
no response to medical
treatment.
Total duration of therapy is 4-6 weeks
URINARY TRACT INFECTION (UTI)
a) Uncomplicated UTI (age> 2 months with lower UTI, without any urinary tract obstruction) – Oral Cotrimoxazole (8-10mg of TMP component) /kg/day oral BD
OR
Cefixime (8-10 mg/kg/day BD) to be given for 7-10 days
OR
Co Amoxycillin+Clavulanic Acid (30-50 mg of Amoxicillin) for 7-10 days.
b) Complicated / Severe UTI (Febrile UTI, Systemic toxicity, renal angle tenderness or with any urinary
structural abnormality) and all UTI in children less than 2 months should be treated with parenteral
antibiotics.
Inj. Cefotaxime (150-200mg/kg/day 8h OR
Inj. Ceftriaxone (100mg/kg/day OD OR
Inj. Amikacin 15mg/kg OD
To be given for 10-14 days
c) In Immunocompromised host/ severe systemic sepsis or as second line for complicated UTI-
Inj. Piperacillin Tazobactum 90mg/kg/dose IV 6h) or Inj. Meropenem (20-40mg/kg/dose 8h) To be given for
10-14 days
FEBRILE NEUTROPENIA
1st Line 2nd Line 3rd Line
Ceftazidime (150 mg/kg/day in
3div doses)+ Amikacin (15-
20mg/kg/day in 2 or 3 div doses)
Piperacillin + Tazobactam (200-
300 mg/kg/day IV in 3-4 div
doses)+ Vancomycin (40
mg/kg/day IV in 4 divided doses)
Meropenem (60 mg/kg/day in 3 div
doses) + Amphotericin B (1
mg/kg/day IV for 2 weeks) or
liposomal Amphotericin B 1-5 mg
kg/day, usually 3 mg/kg/day
Patients without an identified etiology who become afebrile within first 3-5 days of therapy and are clinically well
with ANC of > 200 cells/cmm can be shifted to oral antibiotics (Cefixime or Co- Amoxy- Clavulanic acid) and
therapy should be continued for minimum 7 days.
However, if fever persists or ANC remains <200 parenteral therapy should be continued with 2nd line antibiotics
In clinically stable patients without an identified etiology but with persistent neutropenia, therapy can be stopped after
2 weeks.
Vol. 1 Issue 11 L.E.D. E-Journal Page 370
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
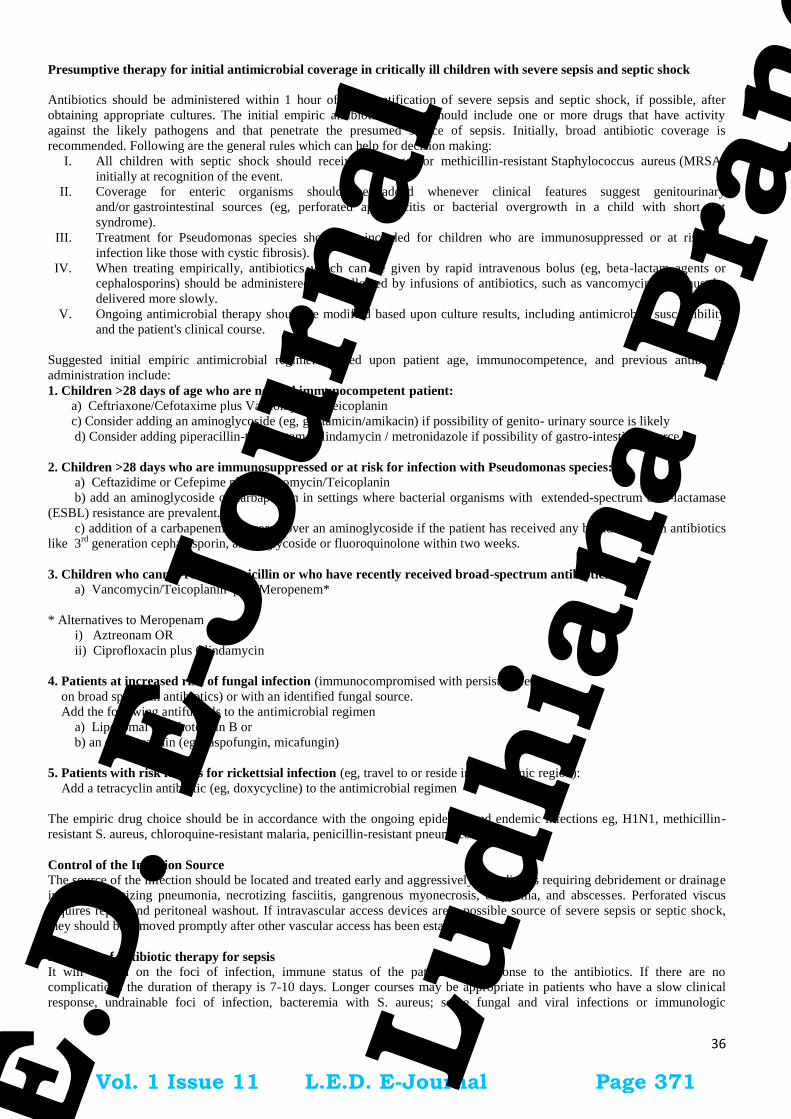
36
Presumptive therapy for initial antimicrobial coverage in critically ill children with severe sepsis and septic shock
Antibiotics should be administered within 1 hour of the identification of severe sepsis and septic shock, if possible, after
obtaining appropriate cultures. The initial empiric antibiotic therapy should include one or more drugs that have activity
against the likely pathogens and that penetrate the presumed source of sepsis. Initially, broad antibiotic coverage is
recommended. Following are the general rules which can help for decision making:
I. All children with septic shock should receive coverage for methicillin-resistant Staphylococcus aureus (MRSA)
initially at recognition of the event.
II. Coverage for enteric organisms should be added whenever clinical features suggest genitourinary
and/or gastrointestinal sources (eg, perforated appendicitis or bacterial overgrowth in a child with short gut
syndrome).
III. Treatment for Pseudomonas species should be included for children who are immunosuppressed or at risk for
infection like those with cystic fibrosis).
IV. When treating empirically, antibiotics which can be given by rapid intravenous bolus (eg, beta-lactam agents or
cephalosporins) should be administered first followed by infusions of antibiotics, such as vancomycin, that must be
delivered more slowly.
V. Ongoing antimicrobial therapy should be modified based upon culture results, including antimicrobial susceptibility
and the patient's clinical course.
Suggested initial empiric antimicrobial regimens based upon patient age, immunocompetence, and previous antibiotic
administration include:
1. Children >28 days of age who are normal immunocompetent patient:
a) Ceftriaxone/Cefotaxime plus Vancomycin //Teicoplanin
c) Consider adding an aminoglycoside (eg, gentamicin/amikacin) if possibility of genito- urinary source is likely
d) Consider adding piperacillin-tazobactam / clindamycin / metronidazole if possibility of gastro-intestinal source
2. Children >28 days who are immunosuppressed or at risk for infection with Pseudomonas species:
a) Ceftazidime or Cefepime plus Vancomycin/Teicoplanin
b) add an aminoglycoside or carbapenem in settings where bacterial organisms with extended-spectrum beta-lactamase
(ESBL) resistance are prevalent.
c) addition of a carbapenem is favored over an aminoglycoside if the patient has received any broad-spectrum antibiotics
like 3rd
generation cephalosporin, aminoglycoside or fluoroquinolone within two weeks.
3. Children who cannot receive penicillin or who have recently received broad-spectrum antibiotics:
a) Vancomycin/Teicoplanin plus Meropenem*
* Alternatives to Meropenam
i) Aztreonam OR
ii) Ciprofloxacin plus Clindamycin
4. Patients at increased risk of fungal infection (immunocompromised with persistent fever
on broad spectrum antibiotics) or with an identified fungal source.
Add the following antifungals to the antimicrobial regimen
a) Liposomal Amphotericin B or
b) an echinocandin (eg, caspofungin, micafungin)
5. Patients with risk factors for rickettsial infection (eg, travel to or reside in an endemic region):
Add a tetracyclin antibiotic (eg, doxycycline) to the antimicrobial regimen
The empiric drug choice should be in accordance with the ongoing epidemic and endemic infections eg, H1N1, methicillin-
resistant S. aureus, chloroquine-resistant malaria, penicillin-resistant pneumococci.
Control of the Infection Source
The source of the infection should be located and treated early and aggressively. Conditions requiring debridement or drainage
include necrotizing pneumonia, necrotizing fasciitis, gangrenous myonecrosis, empyema, and abscesses. Perforated viscus
requires repair and peritoneal washout. If intravascular access devices are a possible source of severe sepsis or septic shock,
they should be removed promptly after other vascular access has been established.
Duration of antibiotic therapy for sepsis
It will depend on the foci of infection, immune status of the patient and response to the antibiotics. If there are no
complications the duration of therapy is 7-10 days. Longer courses may be appropriate in patients who have a slow clinical
response, undrainable foci of infection, bacteremia with S. aureus; some fungal and viral infections or immunologic
Vol. 1 Issue 11 L.E.D. E-Journal Page 371
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

37
deficiencies, including neutropenia Use of procalcitonin levels or similar biomarkers may assist the clinician in the
discontinuation of empiric antibiotics in patients.
Management of Central line/long line catheter-Related Infections -
1. Empirical coverage if suspecting gram-negative bacilli
Choice should be based on local antimicrobial susceptibility and the severity of disease a fourth-generation cephalosporin,
carbapenem, or b-lactam/b-lactamase combination, with or without an aminoglycoside).
2. Empirical antimicrobial therapy if suspecting MRSA
a. for health care settings with an elevated prevalence of MRSA- Vancomycin is recommended
b. for institutions in which the most of MRSA isolates have vancomycin minimum inhibitory concentration (MIC) values
12 mg/mL- Daptomycin, should be used.
c. Linezolid should not be used for empirical therapy.
3. Empirical combination antibiotic coverage for MDR gram-negative bacilli, such as
Pseudomonas aeruginosa, should be used when CRBSI is suspected in
a. Neutropenic patients
b. severely ill patients with sepsis
c. patients known to be colonized with such pathogens, until the culture and susceptibility data are available and de-
escalation of the antibiotic regimen can be done.
4. Empirical therapy for suspected CRBSI involving femoral catheters in critically ill patients should include coverage
for gram-positive pathogens, gram-negative bacilli and Candida species.
5. Empirical therapy if catheter-related candidemia is suspected *-
a. Echinocandin or
b. Fluconazole can be used in patients without azole exposure in the previous 3 months in health care settings where the risk
of Candida krusei or Candida glabratainfection is very low.
*It should be suspected in septic patients with any of the following risk factors: total parenteral nutrition, prolonged use of
broad-spectrum antibiotics, hematologic malignancy, receipt of bone marrow or solid-organ transplant, femoral
catheterization, or colonization due to Candida species at multiple sites.
6. Antibiotic lock therapy should be used for catheter salvage; however, if antibiotic lock therapy cannot be used, systemic
antibiotics should be administered through the colonized catheter.
Duration of antimicrobial therapy:
A. Uncomplicated Short term central venous or arterial catheter related blood stream infection
a. Coagulase negative staph:
i) treat for 5-7 days, if the catheter is removed
ii) treat for 10-14 days, if the catheter is retained
b. Staph aureus :- treat for more than 14 days
c. Enterococcus :- treat for 7-14 days
d. Gram negative bacilli :- treat for 7-14 days
e. Candida sp. :- treat for 14 days after the first negative blood culture,
B. Complicated Short term central venous or arterial catheter related blood stream infection
Four to 6 weeks of antibiotic therapy should be administered to patients with
persistent fungemia or bacteremia after catheter removal (i.e., occurring more than 72
hours after catheter removal), and to patients who are found to have infective endocarditis or suppurative
thrombophlebitis, and to pediatric patients with osteomyelitis.
BRAIN ABSCESS
Inj Ceftriaxone + Vancomycin OR
Inj Teicoplanin + Metronidazole,
Drain pus, rationalize antibiotics according to culture and sensitivity and continue for 3 to 4 week.
1. Remove the catheter
2.Treat with systemic
antibiotics
Vol. 1 Issue 11 L.E.D. E-Journal Page 372
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

38
OSTEOMYELITIS –
Co-Amoxy clavulunic + Gentamicin
SEPTIC ARTHRITIS
1 st line Inj Co-Amoxy clavulunic + Gentamicin
2nd
line Inj Ceftriaxone//cefotaxime +/- Vancomycin
TETANUS – Inj Crystalline Penicillin (2 lac IU /kg/ d /12 hourly) or Inj Metronidazole (mg/kg/d).
ACUTE ENDOCARDITIS – Inj Crystalline Penicillin/ampicillin + Gentamicin for 3-4 weeks is given which is tailored
depending upon culture & sensitivity report.
MALARIA - As per National Malaria Control Program guidelines. See chapter 8.
TUBERCULOSIS IN CHILDREN
Refer to RNTCP guidelines
ACUTE RHEUMATIC FEVER (ARF)
*Contraindicated in penicillin allergy
# maximum dose-500mg; contraindicated in liver disorders; can be given in patients with penicillin allergy; do not use if high
rates of group A streptococal macrolide resistance prevalent.
Duration for secondary prophylaxis:
It depends on the presence of carditis during the acute episode.
Antibiotic Dose Route Frequency Duration
Primary prophylaxis for rheumatic fever (Treatment of group A streptococcal tonsillo-pharyngitis)
The primary goal of treating an ARF attack is to eradicate streptococcal organisms and bacterial antigens from the
pharyngeal region. The antibiotic therapy is very effective if started within 9 days after onset of symptoms to prevent
rheumatic fever specially carditis.
Benzathine Penicillin G*
[After sensitivity testing]
According to weight of the
child
weight ≥ 27 kg :- 1.2 million units
weight < 27 kg :- 0.6 million units
Deep
intramuscular
injection
Only once
Single dose
Single dose
Alternative antibiotics
Azithromycin 12.5 mg/kg/day divided Oral OD 5 days
Amoxicillin 25–50mg/kg/day divided
Adult dose
750-1500 mg/day
Oral TDS 10 days
Cephalexin 15-20 mg/kg/dose Oral BD 10 days
Erythromycin 250 mg #OR
40 mg/kg/day divided
Oral QID 10 days
Penicillin-V 250 mg
Adult dose
500mg
Oral QID 10 days
Secondary prophylaxis for rheumatic fever
It involves continuous administration of antibiotics in patients with a previous attack of RF and/or rheumatic heart
disease. It is mandatory for all patients who have had an attack of RF, whether or not they have residual rheumatic
valvular heart disease.
Benzathine Penicillin G Same as above same same Every 3-4
weeks
Penicillin V Same same BD See below
Sulfadiazine
(patients allergic to penicillin)
weight >27 kg:- 0.5 g
weight ≥27 kg:- 1 g
oral OD See below
Erythromycin
(patients allergic to penicillin &
sufadiazine)
Same same BD See below
Vol. 1 Issue 11 L.E.D. E-Journal Page 373
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

39
1. NO carditis: continue for 5 years after last attack or 18 years of age [whichever is longer]
2. Carditis present (healed carditis or mild mitral regurgitation): continue for 10 yearsafter last attack or 25 years of age
[whichever is longer]
3. Carditis present (established heart disease or following valve surgery or ballon mitral valvotomy): continue lifelong
4. Expert consultation should be sought if want to discontinue after 40 years of age instead of life-long prophylaxis as
recurrence beyond this age is minimal.
PAEDIATRIC SURGICAL CASES
Clean Surgery Clean Surgery likely to be
contaminated
Contaminated/dirty Surgery or
Peritonitis
Surgeries like Uncomplicated
Hernia, cyst excision, hydrocoele
- No Pre-operative prophylaxis
needed
For all other surgeries under
this group:
Inj Ceftriaxone 50 – 75 mg/kg/day
I.V or I/M single dose half an
hour before surgery
For GI surgeries
Inj Ceftriaxone 50 – 75 mg/kg/day,
I.V or I/M 12 hly doses
AND
Metronidazole 20 – 30 mg/kg/day
I/V every 8 hrly
Given for 48hrs only.
Urinary tract surgeries
Inj Ceftriaxone 50 – 75 mg/kg/day
I.V or I/M 12hrly doses
Do not continue beyond 48hrs of
surgery
All surgeries under this group
Inj Ceftriaxone 50 – 75 mg/kg/day, I.V
or I/M 12hrly doses
AND
Metronidazole 20 – 30 mg/kg/day I/V
every 8 hrly
AND
Gentamicin 7.5mg/kg/d 24hrly IV or IM
2nd Line
Piperacillin + Tazobactam (200-300
mg/kg/day IV in 3-4 div doses) +
Vancomycin (40 mg/kg/day IV in 4
divided doses)
Cellulitis/ Abscesses Cloxacillin (50-
100 mg/kg/d) in
3-4 divided
doses
OR
Co- Amoxy-
Clav
OR
Cefazolin (50
mg/Kg/d in 6-8
h doses)
Clindamycin (20-
40mg/Kg/d in 6-8
hly doses)
Treat for 5-7 days.
P. NEONATAL INFECTIONS
a. SEPTICEMIA OR PNEUMONIA
1. In asymptomatic babies at high risk of sepsis eg. presence of foul smelling liquor or two or more risk factors listed
below warrants the initiation of antibiotic therapy.
Risk factors for Early onset sepsis are :
(a) Maternal fever (Temperature > 380C) before delivery or during labor
(b) Membranes ruptured for more than 24 hours before delivery.
(c) More than three vaginal examinations during labor.
(d) Low birth weight (<2500 gms) or preterm babies.
(e) Prolonged and difficult delivery with instrumentation.
Vol. 1 Issue 11 L.E.D. E-Journal Page 374
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

40
(f) Perinatal asphyxia. (Apgar < 4 at 1 min of age)
(g) Meconium stained liquor.
2. A sepsis screen should be done in such infants. If two sepsis screens (NNF protocols) done at 12 hours interval or a
single sepsis screen is negative and infant remains asymptomatic at 48 -72 hours, the antibiotics may be
discontinued.
Antibiotic Each dose Frequency Route Duration(Days)
< 7 days > 7 days
Inj. Ampicillin
And
Inj. Gentamicin
50 mg/kg/dose
5-7.5 mg/kg/dose
12 hrly 8hrly
24 hrly 24hrly
IV
IV
7-10
7-10
o In cases with severe sepsis (Sclerema/ Shock / suspicion of meningitis) Inj Cefotaxime 200 mg/kg/day IV in 4 div doses)
+ Amikacin (15mg/kg/d) is recommended
o If sepsis is suspected to be health care associated or if there is no response in 48-72 hours of initial therapy or if there is
documented resistance then change to injection Piperacillin- Tazobactam (200-300 mg/kg/day IV in 3-4 div doses) and
Amikacin.
o Vancomycin can be added to the regime if staphylococcus is suspected.
b. NEONATAL MENINGITIS
Antibiotic Dose Frequency Route Duration
(Weeks) < 7 days > 7 days
First
Line
Inj. Ampicillin and
Inj. Gentamicin
100 mg/kg/dose
5-7.5 mg/kg/d
12 hrly 8 hrly
5 mg/kg/d 7.5 mg/kg/d
24 hrly 24hrly
IV
IV
3
3
Second
Line
Inj. Cefotaxime
and
Inj. Gentamicin
50 mg/kg/dose
5-7.5 mg/kg/d
12 hrly 8 hrly
5 mg/kg/d 7.5 mg/kg/d
24 hrly 24hrly
IV
IV
3
3
Q. POST SOLID ORGAN TRANSPLANT
Post-operative infections following solid organ transplant (kidney, liver, heart, lung)
Condition Likely causative
Organisms
Empiric antibiotics Alternative
antibiotics
Comments
Post-op fever with
hemodynamic stability
Usually not due to
infection
None
Look for hematoma, DVT,
transfusion related fever
Surgical site infection
S. aureus, Entero-
bacteriaceae,
Pseudomonas spp.
Treat based on culture and
sensitivities
VAP/HAP Entero-bacteriaceae,
Pseudomonas spp.,
Acinetobacter spp.
Piperacillin-
tazobactam 4.5g IV
q6h or Cefoperazone-
sulbactam 3g IVq8h
Imipenem 1g IV
q8h or
meropenem1g IV
q8h
Modify based on culture of
lower respiratory tract
secretions.
Vol. 1 Issue 11 L.E.D. E-Journal Page 375
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

41
CLABSI
S. aureus, Entero-
bacteriaceae,
Pseudomonas spp.,
Acinetobacter spp.
Candida spp.
Vancomycin loading
of 25-30 mg /kg in
patients of septic
shock followed by
15mg/kg IV 12 hourly
(maximum 1gm 12
hourly)/teicoplanin
12mg/kg IV 12 hourly
x 3 doses followed by
6 -12 mg once daily
IV depending upon
severity + Piperacillin-
tazobactam 4.5g IV
q6h or Cefoperazone-
sulbactam 3g IVq8h
For 2 weeks duration
Daptomycin 6
mg/kg IV od
+Meropenem 1g
IVq8h
Draw 2-3 blood culture sets
with at least one from
peripheral sites before starting
antibiotics and modify based
on culture.
Removal of catheter must be
contemplated.
CAUTI Entero-bacteriaceae,
Enterococci
Candida spp.
Piperacillin-
tazobactam 4.5g IV
q6h or Cefoperazone-
sulbactam 3g IVq8h
Imipenem 1g IV
q8h or
Meropenem 1g IV
q8h
Do blood and urine cultures
before starting antibiotics and
modify based on culture.
Removal of catheter must be
contemplated.
R. SURGICAL ANTIMICROBIAL PROPHYLAXIS
To be administered within 1 hr before the surgical incision.
Single dose is recommended. Consider for second intra-operative dosein prolong surgery based on the choice of
antibiotic used for prophylaxis.
Prophylaxis should not be given beyond surgery duration (except for cardiothoracic surgery, up to 48 hours
permissible)
Choice of the prophylaxis should be based on the local antibiogram.
SURGERY MEDICATION
Breast Inj.Cefazolin 2gm or Inj.Cefuroxime 1.5gm IV stat
Gastroduodenal & biliary Inj.Cefaperazone- Sulbactam 2gm IV stat & BD for 24hrs(maximum)
ERCP Inj.Piperacillin-Tazobactum 4.5gm or Inj.Cefaperazone- Sulbactam 2gm IV stat
Cardiothoracic Inj.Cefuroxime 1.5gm IV stat & BD for 48hrs
Colonic surgery Inj.Cefaperazone- Sulbactam 2gm IV stat & BD for 24hrs(maximum)
Abdominal surgery (hernia) Inj.Cefazolin 2gm or Inj.Cefuroxime 1.5gm IV stat
Head & Neck/ ENT Inj.Cefazolin 2gm IV stat
Neurosurgery Inj.Cefazolin 2gm or Inj.Cefuroxime 1.5gm IV stat
Obstetrics& Gynecology Inj.Cefuroxime 1.5gm IV stat
Orthopaedic
Inj.Cefuroxime 1.5gm IV stat & BD for 24 hrs(maximum)
or
Inj.Cefazolin 2gm IV stat
Open reduction of closed fracture with internal fixation- Inj.Cefuroxime 1.5gm IV stat
and q 12h or Inj.Cefazolin 2gm IV stat and q 12h for 24 hrs
Trauma Inj.Cefuroxime 1.5gm IV stat and q 12h (for 24 hrs)
or Inj.Ceftriaxone 2gm IV OD
Urologic procedures Antibiotics only to patients with documented bacteriuria
Trans- rectal prostatic surgery Inj.Cefaperazone- Sulbactam 2gm IV stat
Vol. 1 Issue 11 L.E.D. E-Journal Page 376
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
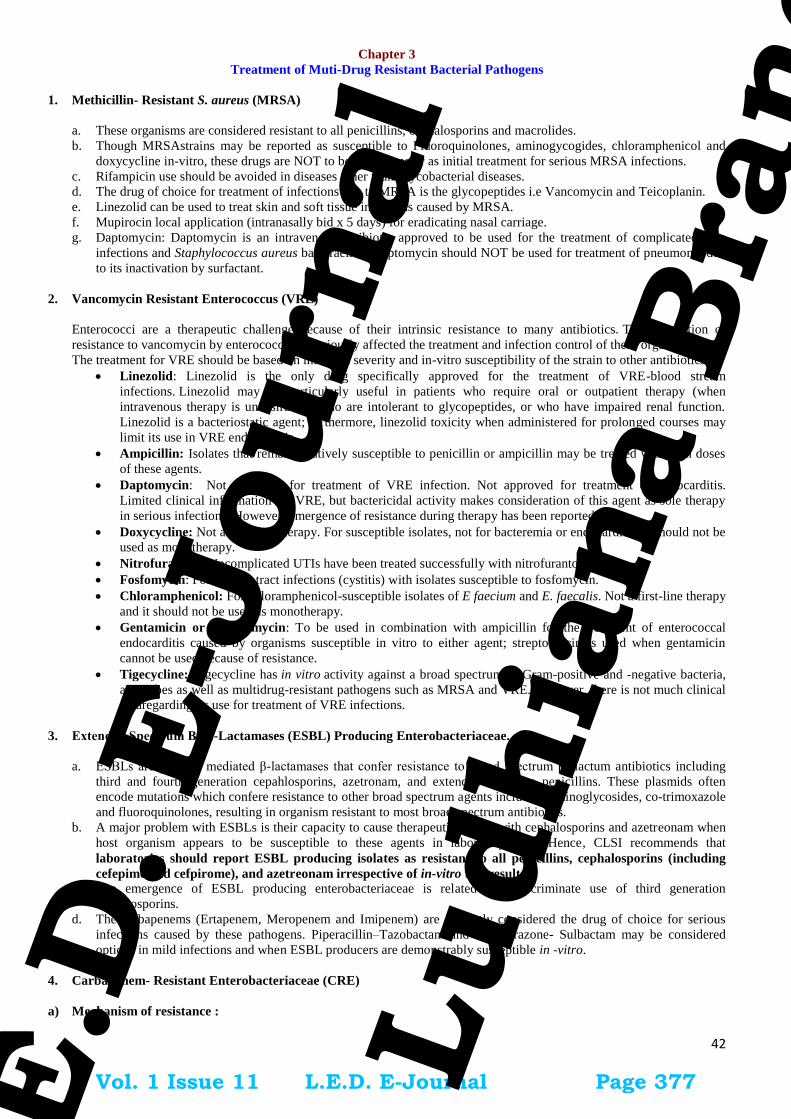
42
Chapter 3
Treatment of Muti-Drug Resistant Bacterial Pathogens
1. Methicillin- Resistant S. aureus (MRSA)
a. These organisms are considered resistant to all penicillins, cephalosporins and macrolides.
b. Though MRSAstrains may be reported as susceptible to Fluoroquinolones, aminogycogides, chloramphenicol and
doxycycline in-vitro, these drugs are NOT to be used alone or as initial treatment for serious MRSA infections.
c. Rifampicin use should be avoided in diseases other than Mycobacterial diseases.
d. The drug of choice for treatment of infections due to MRSA is the glycopeptides i.e Vancomycin and Teicoplanin.
e. Linezolid can be used to treat skin and soft tissue infections caused by MRSA.
f. Mupirocin local application (intranasally bid x 5 days) for eradicating nasal carriage.
g. Daptomycin: Daptomycin is an intravenous antibiotic approved to be used for the treatment of complicated skin
infections and Staphylococcus aureus bacteraemia. Daptomycin should NOT be used for treatment of pneumonia due
to its inactivation by surfactant.
2. Vancomycin Resistant Enterococcus (VRE)
Enterococci are a therapeutic challenge because of their intrinsic resistance to many antibiotics. The acquisition of
resistance to vancomycin by enterococci has seriously affected the treatment and infection control of these organisms.
The treatment for VRE should be based on infection severity and in-vitro susceptibility of the strain to other antibiotics.
Linezolid: Linezolid is the only drug specifically approved for the treatment of VRE-blood stream
infections. Linezolid may be particularly useful in patients who require oral or outpatient therapy (when
intravenous therapy is undesirable), who are intolerant to glycopeptides, or who have impaired renal function.
Linezolid is a bacteriostatic agent; furthermore, linezolid toxicity when administered for prolonged courses may
limit its use in VRE endocarditis.
Ampicillin: Isolates that remain relatively susceptible to penicillin or ampicillin may be treated with high doses
of these agents.
Daptomycin: Not approved for treatment of VRE infection. Not approved for treatment of endocarditis.
Limited clinical information for VRE, but bactericidal activity makes consideration of this agent as sole therapy
in serious infections. However, emergence of resistance during therapy has been reported.
Doxycycline: Not a first line therapy. For susceptible isolates, not for bacteremia or endocarditis. It should not be
used as monotherapy.
Nitrofurantoin:Uncomplicated UTIs have been treated successfully with nitrofurantoin.
Fosfomycin: For urinary tract infections (cystitis) with isolates susceptible to fosfomycin.
Chloramphenicol: For chloramphenicol-susceptible isolates of E faecium and E. faecalis. Not a first-line therapy
and it should not be used as monotherapy.
Gentamicin or streptomycin: To be used in combination with ampicillin for the treatment of enterococcal
endocarditis caused by organisms susceptible in vitro to either agent; streptomycin is used when gentamicin
cannot be used because of resistance.
Tigecycline: Tigecycline has in vitro activity against a broad spectrum of Gram-positive and -negative bacteria,
anaerobes as well as multidrug-resistant pathogens such as MRSA and VRE. However, there is not much clinical
dataregarding its use for treatment of VRE infections.
3. Extended Spectrum Βeta-Lactamases (ESBL) Producing Enterobacteriaceae.
a. ESBLs are plasmid mediated β-lactamases that confer resistance to broad spectrum β- lactum antibiotics including
third and fourth generation cepahlosporins, azetronam, and extended spectrum penicillins. These plasmids often
encode mutations which confere resistance to other broad spectrum agents including aminoglycosides, co-trimoxazole
and fluoroquinolones, resulting in organism resistant to most broad spectrum antibiotics.
b. A major problem with ESBLs is their capacity to cause therapeutic failure with cephalosporins and azetreonam when
host organism appears to be susceptible to these agents in laboratory tests. Hence, CLSI recommends that
laboratories should report ESBL producing isolates as resistant to all penicillins, cephalosporins (including
cefepime and cefpirome), and azetreonam irrespective of in-vitro test results. c. The emergence of ESBL producing enterobacteriaceae is related to indiscriminate use of third generation
cephalosporins.
d. The carbapenems (Ertapenem, Meropenem and Imipenem) are currently considered the drug of choice for serious
infections caused by these pathogens. Piperacillin–Tazobactam and Cefoperazone- Sulbactam may be considered
options in mild infections and when ESBL producers are demonstrably susceptible in -vitro.
4. Carbapenem- Resistant Enterobacteriaceae (CRE)
a) Mechanism of resistance :
Vol. 1 Issue 11 L.E.D. E-Journal Page 377
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

43
i. Combinations of ESBL or AmpC and porin loss: Porin loss is often unstable and may impose afitness cost,
meaning that these strains rarely spread. Ertapenem is particularly affected.
ii. Acquired carbapenemases
b) Treatment :
i. Most carbapenemase producers are extremely drug resistant: being resistant to β-lactam antibiotics, aminogycosides,
and β-lactam–βlactam inhibitor combinations.
ii. Polymyxins, tigecycline & fosfomycin are the agents with most frequent in vitro activity, but all have limitations.
Dosage will vary with the patient and infection site, but should be on the principle of ‘highest safe’ rather than
‘minimum potentially effective; durations should be as standard for the infection type.
iii. Colistin - Case reports of successful use in a range of infections due to carbapenemase producers.
iv. Tigecycline:Active in-vitro vs. most carbapenem-resistant E. coli. Licensed for complicated skin and soft-tissue
Infections and complicated intraabdominal infections. Case reports of success in various infections with
carbapenemase producers. Low blood concentrations; off-label use should be cautious for blood stream infections,
unsuitable in urinary infections as only 22% excreted in urine. Excess deaths in some trials, especially ventilator
associated pneumonia (not a licensed indication).
v. Others: a few isolates are susceptible to other antibiotics including e.g. chloramphenicol, ciprofloxacin and
cotrimoxazole. Most producers, however, are resistant to these drugs.
Recommended measures to control spread of Multi-drug resistant organisms (MDRO) :
i. Improved laboratory detection and reporting of MDRO
ii. Enhanced infection surveillance and control in ICUs
iii. Prevent spread by barrier precautions : Gowns and gloves
iv. Hand Washing
v. Restricted use of 3rd
generation cephalosporins
Vol. 1 Issue 11 L.E.D. E-Journal Page 378
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

44
Chapter 4
Guidelines For Optimizing Use Of Key Antimicrobials
A. Antimicrobial Prescribing: Good Practice
1. Send for the appropriate investigations in all suspected infections as recommended. These are the minimum required for
diagnosis, prognosis and follow up of these infections.
2. All attempts shall be made to send microbiological samples prior to initiating antimicrobial therapy. Rapid tests, such as
Gram stain, can help determine therapeutic choices when decision on empiric therapy is required.
3. Differentiation between contamination, colonization and infection is important to prevent overuse of antimicrobials. Use
hospital guidelines based on local antibiograms when choosing antimicrobial therapy whenever possible. If alternatives to
those recommended as used, reasons in the case records should be documented.
4. Prescribing antibiotics just in case an infection is present is rarely justified. Where patients are in hospital close
observation is usually a better option till the diagnosis is made.
5. Choice of antibiotics: This depends on antibiotic susceptibility of the causative organism. There are some infections,
which can be treated by one of several drugs. The choice can be based on Toxicity, Efficacy, Rapidity of action,
Pharmacokinetics and Cost. Use the most effective, least toxic and least expensive antibiotic for the precise duration of
time needed to cure or prevent infection. Pathogens specific guidance in hospital policy is encouraged.Before
prescribing consider the following:
a. Which organism is likely to cause the disease?
b. What is the clinical diagnosis and what other steps should be taken to reach diagnostic precision?
c. Which antimicrobial agents are available and active against the presumed cause of the illness? Is their range of
antimicrobial activity appropriate and what information is available about the likelihood of drug resistance?
d. Check for factors, which will affect choice of drug and dose, e.g., renal function, interactions, allergy, pregnancy
and lactation.
e. Check that the appropriate dose is prescribed. If uncertain, contact Infectious Diseases Physician or clinical
microbiologist. Alternatively, check in the formulary.
f. What is the duration of treatment?
g. Is treatment working?
6. Clinical Diagnosis: The antibiotic treatment chosen must be based on presumptive diagnosis made on some assumption
regarding the nature of disease. The treating doctor may not have difficulty in choosing the appropriate antibiotic to treat a
disease caused by a single microorganisms e.g scarlet fever, typhoid, anthrax, as microbiological diagnosis is implicit in
clinical diagnosis. However, diseases such as pneumonia, meningitis and urinary tract infection can be caused by spectrum
of bacterial species and doctor may be wrong if he has to guess which antimicrobial agent to use. In such instances one
should seek a bacteriological diagnosis.
7. Empiric Therapy – If the causative agent is not known and where delay in initiating therapy would be life threatening or
risk serious morbidity, antimicrobial therapy based on a clinically defined infection is justified and the following points
should be taken into consideration :
a. Do not rush to treat.
b. Collect the necessary specimens before commencing therapy.
c. Cover all possible microbial causes.
d. Try to attain synergy.
e. Consider possible interaction with other drugs.
f. Accuracy of diagnosis should be reviewed regularly and treatment altered/stopped when microbiological results
become available.
g. Use less costly drugs where possible.
8. The need for antimicrobial therapy should be reviewed on a daily basis. For most infections 5 – 7 days of antimicrobial
therapy is sufficient (simple UTI can be adequately treated with 3 days of antibiotic).
9. All IV antibiotics may only be given for 48 – 72 hours without review and consideration of oral alternatives. New
microbiological or other information (e.g. fever defervescence for at least 24h, marked clinical improvement; low CRP)
should at this stage often permit a switch to oral antibiotic(s), or switch to an IV narrow spectrum alternative, or cessation
of antibiotics (no infection present).
10. Once culture reports are available, the physician should step down to the narrowest spectrum, most efficacious and most
cost effective option. If there is no step down availed, the reason shall be documented and is subjected to clinical audit.
11. Some guiding principles for de-escalation /Escalation:
a. If ESBL +ve: drug choice is monotherapy with carbepenems. Preferably choose group I carbepenem. Piperacillin
–Tazobactum and Cefoperazone –Sulbactam can be used if in-vitro sensitive and for mild infections.
b. Vancomycin should be used only for confirmed MRSA infections and not in MSSA infections.
c. In case of Pan drug resistant Pseudomonas /Acinetobacter spp. combination therapy using colistin along with
beta-lactams (using PK/PD principles) should be discussed with microbiologist / physician.
12. . Treatment with antibiotic combinations: In order to avoid antagonism between drugs and undesirable side effects of
several antibiotics it is advisable to use a single drug where ever possible. There are situations however, when the use of
antibiotic combination is desirable. The situations are:
Vol. 1 Issue 11 L.E.D. E-Journal Page 379
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

45
a. A temporary expedient during the investigation of an obscure illness.
b. To prevent the development of bacterial resistance in long term therapy e.g treatment of tuberculosis.
c. To achieve synergistic effect, e.g. in treating infective endocarditis.
d. Mixed infection, when one drug is not effective against the pathogen.
e. To permit a reduction of the dose of potentially toxic drug.
The choice of the drug should be that they act synergistically. The following combinations are synergistic
1. Aminoglycoside and beta–lactam antibiotic.
2. Beta –lactam antibiotic and beta–lactamase inhibitor.
3. Beta –lactam antibiotic and Glycopeptide (vancomycin/teicoplanin)
4. Sulphamethoxazole and Trimethoprim.
14. Is Treatment working?: Where treatment is apparently failing, advice from an ID physician/clinical microbiologist
should normally be sought rather than blindly changing to an alternative choice of antimicrobial agent.
Antimicrobial drug therapy cannot be considered in isolation and other aspects of therapy must be taken into account in
judging the effect of treatment. Even an appropriate antibiotic may be ineffective unless pus is drained, septic shock
treated and hypoxia and anemia corrected. There are several conditions in which chemotherapy alone cannot eliminate an
infection. Obstructive lesions can cause infection to recur, unless they can be dealt with surgically. Also, chemotherapy
cannot obviate the necessity for draining an abscess or removing sequestra or calculi. Failure of treatment can also be due
to a super-added infection, e.g. phlebitis, development of resistance during therapy or poor tissue penetration.
13. Laboratory control of the effects of treatment: Whether treatment has been successful or not is best judged by clinical
criteria, but it is useful to know whether the infecting organism has been eliminated. Reapeated cultures are, therefore
sometimes indicated.
B. Reserve Antimicrobials
These reserve antimicrobials will be made available following a recommendation from the Microbiology Department as per
culture report or if included in an antimicrobial policy for a clinical specialty that has been agreed with antibiotic management
team. They are held in reserve to maintain their effectiveness in treating certain difficult infections by reducing the spread of
microbial resistance and to encourage cost effective prescribing. Before a reserve antibiotic is issued to the ward, the
pharmacist is instructed to ascertain the indication and if this falls outside the approved policy, to request that the prescriber
consult the ID Physician/clinical microbiologist.
The following criteria has been proposed to protect the Carbapenems and Linezolid from overuse –
1. Severe sepsis as defined by more than one organ failure of new onset and/or elevated serum lactate.
2. Clinical failure of other classes of antibiotics over 48 hours in terms of worsening inflammatory markers, unresolving
fever and new/worsening hemodynamic instability.
3. Underlying severe immuno-suppression – Neutropeniea, immuno-suppressive therapy, Diabetic Ketoacidosis (DKA)
etc.
4. The organism is susceptible to only carbapenems / linezolid, as per culture report.
The following criteria has been proposed for initiating Colistin –
1. Pan-resistant organism as per culture report with evidence of invasive disease – fever/ leucocytosis/elevated
procalcitonin (PCT) or culture from a sterile site.
2. Clinical failure of all other classes of antibiotics over 72 hours.
The following criteria has been proposed for initiating Rifampicin –
1. Empiric or proven TB as a part of ATT (4 drug regimen)
Rifampicin should not be prescribed in our country for any treatment other than for Mycobacteria and for
chemoprophylaxis of meningoccal meningitis in clinically indicated population
Rifampicin should not be prescribed alone as an anti-bacterial.
The following criteria has been proposed for initiating Aminoglycosides –
I. The focus of infection is not lung or an anaerobic abscess.
II. Only as a part of initial empiric regimen of a combination therapy – shall step down to single drug after culture report.
III. Other safer drug options have been ruled out in a culture report.
C. Hypersensitivity
All patients should be asked about drug allergies. This is the responsibility of the doctor caring the patient. If a patient reports a
drug allergy clarify whether this is an allergy or drug intolerance. In some cases there will be an overlap between drug allergy
and drug intolerance.
Clinical features suggestive of drug allergy:
One or more symptoms developed during or following drug administration including difficulty breathing, swelling,
itching, rash, and anaphylaxis, swelling of the lips, loss of consciousness, seizures or congestion involving mucous
membranes of eyes, nose and mouth.
Vol. 1 Issue 11 L.E.D. E-Journal Page 380
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

46
Clinical features suggestive of drug intolerance:
One or more symptoms developed during or following drug administration including gastrointestinal symptoms e.g.
nausea, vomiting, diarrhoea, abdominal pain and feeling faint.
If patients are unable to give an allergy history, the doctor caring in the patient should take reasonable steps to contact
someone who can provide a reliable allergy history. It is the prime responsibility of the prescribing doctor to ensure that:
i. The allergy box on the patient’s drug chart is completed, when a new prescription chart is written or transcribed. If
no allergy - specify "No known allergy". The box should be signed and dated. If allergy history cannot be obtained,
then specify "history not available." Under no circumstances should the allergy box be left blank. A pharmacist or
nurse may complete the allergy box if the allergy status is documented in the clerking in notes.
ii. The allergy box is completed before prescribing a new drug, except in exceptional circumstances. If patients have a
suspected drug allergy then the drug and suspected reaction. Should be documented in the clerking-in notes and the
drug chart.
D. Alert Antimicrobials
To Prevent and Control the Emergence and Spread of Antimicrobial-Resistant Micro-organisms in Hospitals” one major
strategic goal is to “define guidelines for use of key antibiotics”, (“Alert” antibiotics) targeted in these guidelines are
ciprofloxacin, ceftazidime, cefotaxime, ceftriaxone, vancomycin (or teicoplanin), imipenem, levofloxacin, meropenem,
moxifloxacin,piperacillin-tazobactam, linezolid (oral/IV), voriconazole, caspofungin, valganciclovir, ertapenem and
newer preparations of amphotericin.
Collectively, these are among the drugs most frequently prescribed irrationally which is largely responsible for the current
escalation of antibiotic costs. They also account for a significant proportion of serious antibiotic toxicity including Clostridium
difficilediarrhoea and CNS toxicity/seizures as well as the emergence of major antimicrobial resistance. Safer, cheaper and
equally effective alternatives are often available which allow such agents to be kept in reserve for occasions when there are
clear cut microbiological indications. It is critical, therefore, that these Alert antibiotics be prescribed only on the
recommendation of senior medical staff or after discussion with the on-call Clinical Microbiologist or ID physician.
E. Alert Antibiotics And Their Indications
1. CIPROFLOXACIN, INTRAVENOUS
Oral ciprofloxacin is well absorbed and this is therefore the preferred route of administration. Intravenous therapy is only
indicated in the following situations:
When the patient is unable to swallow or the oral route is otherwise compromised.
In serious sepsis (e.g. nosocomial pneumonia in ITU) when the recommended dose is 400mg 8 hourly.
Common indications for ciprofloxacin in the Antibiotic Policy, either alone or in combination, are as follows:
second line therapy in exacerbation of chronic bronchitis
pyelonephritis
acute inflammatory infective diarrhoeas
serious infected diabetic ulcers infected burn wounds with coliforms or Pseudomonas infection present
treatment of documented or presumed gram-ve bacilli resistant to penicillins or cephalosporins or when the patient is
allergic (history of anaphylactic reaction or rash) to these agents
selected haematology patients requiring prophylaxis
severe acute pelvic inflammatory disease
2. CEFTAZIDIME
Limited use only. Main indication is documented or suspected Pseudomonas aeruginosainfection. Other indications currently
listed in the Antibiotic Policy are as follows:
Second line agent in neutropenic patients with septicaemia or pneumonia
Empiric therapy of CAPD associated peritonitis (not children), 1g IV stat then 125mg/litre in each bag
Empiric therapy of post operative, post traumatic or shunt associated meningitis
Empiric therapy of infective exacerbation of cystic fibrosis
3. PIPERACILLIN - TAZOBACTAM
Currently listed in the antibiotic policy for the following:
Pneumonia or septicaemia in neutropenic patients (+ Gentamicin)
As a single agent (or in combination with Gentamicin) for treatment of sepsis which has not responded to first line
treatment or if it is not appropriate for gentamicin to be added to first-line therapy.
4. CEFTRIAXONE
IV Ceftriaxone is currently listed in the antibiotic policy for the following:
Epiglottitis,
Brain abscess,
Vol. 1 Issue 11 L.E.D. E-Journal Page 381
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

47
Bacterial meningitis,
Pyelonephritis in children,
Empiric therapy of septicaemia in children,
In ascites for treatment of sub-acute bacterial peritonitis,
Skin and soft tissue infections managed via out-patients or the home IV antibiotic programme,
Acute septic monoarthritis if penicillin allergic,
Spontaneous bacterial peritonitis.
5. APPROPRIATE USE OF CARBEPENEMS
Very high rates (60-75%) of resistance to 3rd
and 4th
generation cephalosporins {due to extended spectrum beta-
lactamases (ESBL) production} observed in E. coli and Klebsiella species..
This pattern of resistance although seen primarily among nosocomially acquired infections, is also seen isolates of E
coli and Klebsiella species isolated from community acquired infections.
These strains of bacteria are frequently resistant to other major classes of antibiotics (fluoroquinolones, β-lactam + β-
lactamase inhibitor(BL + BLI) combinations and aminoglycosides)
Carbapenems (imipenem, meropenem and ertapenem), beta-lactam antibiotics with exceptionally broad spectrum of
activity, are the only class of antimicrobials which remain effective against ESBL-producing isolates of E coli and
Klebsiella species
Imipenem is susceptible to degradation by the enzyme dehydropeptidase-1 (DHP-1) located in renal tubules and
requires coadministrationwith a DHP-1 inhibitor cilastatin. Meropenem and ertapenem are administered without a
DHP-1 inhibitor.
Indications for carbapenem use:
1. Infections [e.g., bacteremia, pyelonephritis, intra-abdominal infections (peritonitis, cholangitis, abscesses), nosocomial
pneumonia etc.] confirmed (by appropriate culture and susceptibility studies) to be caused by Gram-negative bacteria (E
coli, Klebsiella spp., Enterobacter spp., Pseudomonas aeruginosa, other non-fermenting Gram-negative bacilli) resistant
to other classes of antimicrobials and susceptible only to carbapenemsin-vitro
2. Initial empiric treatment for severe, life-threatening infections (associated with multi-organ dysfunction, septic shock)
caused by Gram-negative bacteria.
Febrile neutropenia
Ventilator associated / nosocomial pneumonia
Pyelonephritis / complicated urinary tract infections
Complicated intra-abdominal infections
Once the culture and susceptibility reports are available, choose the most appropriate antibiotic based on spectrum of
activity, toxicity and cost (‘de-escalation’).
Indications for Ertapenem use:
Ertapenem has excellent in-vitro and in-vivo activity against ESBL producing Enterobacteriaceae, but lacks activity against
Pseudomonas aeruginosa, and is therefore not considered appropriate for the treatment of conditions like febrile neutropenia
and serious nosocomial infections. Ertapenem does not select Carbapenem-resistant Pseudomonas aeruginosa (at least in the
short-term). Its use should be restricted to severe Gram-negative or polymicrobial community acquired infections confirmed to
be caused by susceptible bacterial pathogens. Hence, this drug may be recommended as the initial choice for ESBL producing
strains of E coli and Klebsiella spp..
Indication of Meropenem and Imipenem
Meropenem and Imipenem regarded as third line agents and are reserved for:
serious infections due to multiple resistant strains (e.g. ESBL)
empiric use in the seriously ill patient in either ITU or Haematology
the treatment of infective exacerbations in Cystic fibrosis (CF)
severe acute narcotising pancreatitis
Outside these clinical settings it should only be used after consultation with a Clinical Microbiologist or ID physician.
Unlike imipenem , meropenem has not been associated with CNS toxicity. Also, it is administered by convenient IV bolus
injection. Clinicians must be aware that mechanism of resistance to meropenem and imipenem are different and hence in-vitro
test for one carbapenem cannot be used to interpret the other.
Dose
Imipenem*: 500 mg i.v. Q6H
Meropenem: 1 gmi.v.Q8H
Ertapenem: 1gm i.v. /i.m.Q 24H
*Note Anti-infective sub-committeerecommends use at a more frequent dosing interval. They believe that optimum
plasma concentrations are more reliably maintained with 6-hourly dosing.
Vol. 1 Issue 11 L.E.D. E-Journal Page 382
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

48
6. LINEZOLID (IV AND ORAL FORMS)
Linezolid should only be prescribed after consulting an ID specialist or clinical microbiologist and a mandatory order
form completed.
Restricted indications including infections due to proven glycopeptide-insensitive Staphylococcus aureus or
vancomycin-resistant enterococcus (currently uncommon).
To enable IV/oral switch from IV vancomycin (used for MRSA or MRSE) to oral linezolid (when patient’s discharge
is possible and continuation treatment using combination rifampicin /trimethoprim is inappropriate.
May be an option in surgical site infections (e.g. large bowel surgery, vascular surgery, etc).
Poor IV access and a glycopeptide is indicated.
Use in out-patient home parenteral antibiotic therapy for skin and soft tissue infections as an alternative to IV
teicoplanin.
Rare cases of proven hypersensitivity/allergy to the glycopeptides.
7. VANCOMYCIN
Vancomycin is the drug of choice for in-patient treatment of the following infections.
Serious (e.g. bacteraemia, osteomyelitis) coagulase negative staphylococcal and MRSA infections and penicillin
resistant enterococcal infections
Empiric therapy in febrile neutropenic patients not responding to first line therapy
Continuous ambulatory peritoneal dialysis (CAPD) associated peritonitis
Prosthetic valve endocarditis
8. TEICOPLANIN
Teicoplanin is a suitable alternative to vancomycin for all indications for Vancomycin except meningitis:
patients receiving out-patient/home parenteral therapy with glycopeptidesafter loading dosages
inability to tolerate vancomycin
oncology/haematology patients
Rare cases of vancomycin resistant and teicoplanin sensitive strains.
Vol. 1 Issue 11 L.E.D. E-Journal Page 383
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

49
Chapter 5
Preventive Strategies for Healthcare Associated Infections
A. Healthcare Associated Infections
Health Care Associated Infections or HCAI are a worldwide phenomenon. HCAI have been defined variously at different
times and by different organizations. Current definitions incorporate infections which were neither incubating nor did they
manifest or present, during the period of admission in patients admitted in the hospital but were present on or after the 3rd
calendar day of admission, (the day of hospital admission being calendar day 1).
B. Reducing the risk of Health care associated infections
B1. Development of an effective Infection Prevention and Control Program
Infection Prevention and Control Programs are directed towards patient safety and health care professionals’ safety. Reducing
the preventable part of health care associated infections (HCAI) is central to any Infection Control program.
An effective Infection Prevention and Control Program would have the following components:
1. Infection Control Committee with its defined role and constituents
2. Infection Control Core Team for day to day working with defined roles
3. Infection Control Manual with policies, guidelines, recommendations and working protocols including activities and
practices under the program with Hand hygiene and Standard Precautions being the mainstay
4. Annual Plan for each healthcare setup with prioritization based on risk matrix for that unit and review
5. Should incorporate Antimicrobial Stewardship programs
B2. Hand-hygieneand Standard Precautions’
Health care workers and professionals anywhere and at all levels should be well oriented to concepts of hand hygiene.
Practicing ‘Standard Precautions’, prevents direct contact with all body fluids (including blood), secretions, excretions, non-
intact skin (including rashes), and mucous membranes.
Hand hygiene in the form of tap, sink and appropriate antiseptic/ rubs for washing or hand-rub or surgical scrub should be
facilitated. Atleast hand rubs should be available in all patient care areas including patient’s bed side or easily available within
vicinity.
Indications for hand washing and hand antisepsis should be made known amongst all engaged in providing patient care.
Protocols and procedures of any area should always include hand hygiene as applicable and these should be mandatory step.
B3. Antimicrobial Stewardship Program
Antimicrobial Stewardship Program shall form another main focus of the Infection Prevention and Control Program. This shall
include all components of antimicrobial stewardship so as to stress upon advocacy of safe use of antimicrobials, which shall be
strengthened, with periodic review of antimicrobial guidelines and implementation locally in each of the health care setups.
B4. Educational Programs and Strategies
Appropriate educational material should be made available to all. These shall be based upon recent evidences and part of
relevant national and international guidelines and appropriately indigenized for effective implementation. This would be
augmented by periodic CME or educational interactive programs and awareness drives. Local Health care setup should provide
antimicrobial susceptibility patterns, appropriate usage of antimicrobials and have updates on antimicrobials communicated to
all relevant personnel in patient care, locally and periodically. Specific infectious diseases and their prevention and control
awareness should be made available as and when required to relevant staff locally and may be extended to community if so
desired by the health departments of that district/city/area.
B5. NotificationAll relevant information as required by law on communicable diseases would be notified as appropriate to
relevant authority. Incase of specific reports from public health agencies requiring action on their recommendations,
appropriate action should be taken.
B6. Prophylaxis including Immunization
Staff should be immunized against diseases, which have risk of transmission through exposure from patients and to limit
transmission of diseases from healthcare workers to patients. Immunisation in high-risk group may be required for influenza,
meningococcal infections among exposure prone healthcare workers in outbreak situations, hepatitis B vaccination for all staff,
varicella vaccine to high-risk group etc. Among the diseases that have potential of being transmitted from healthcare workers
to patients typhoid vaccine should be included among the food handling staff. Immunise all health care workers and others
involved in handling of bio-medical waste for protection against diseases including Hepatitis B and Tetanus that are likely to
be transmitted by handling of bio-medical waste. All the under trainee staff including medical and nursing students should be
immunized for potential occupational risk exposures (e.g. hepatitis B vaccination to the students).
Vol. 1 Issue 11 L.E.D. E-Journal Page 384
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

50
Chapter 6
Monitoring Antimicrobial Use
A. Background
World Health Organization’s 2014 report on global surveillance of antimicrobial resistance reveals that antibiotic
resistance is no longer a prediction for the future; it is happening right now, across the world, and is putting at risk the
ability to treat common infections in the community and hospitals. It is an increasingly serious threat to global public
health that requires action across all government sectors and society.
There are high proportions of antimicrobial resistance (AMR) amongst bacteria that cause common infections (e.g. urinary
tract infections, pneumonia, bloodstream infections) throughout the world. Resistant microorganisms (including bacteria,
fungi, viruses and parasites) are able to survive attack by antimicrobial drugs, such as antibacterial drugs (e.g., antibiotics),
antifungals, antivirals, and antimalarials, so that standard treatments become ineffective and infections persist, increasing
the risk of spread to others.
The evolution of resistant strains is a natural phenomenon the use and misuse of antimicrobial drugs accelerates the
emergence of drug-resistant strains. The evolving public health threat of AMR is driven by both appropriate and
inappropriate use of antimicrobial agents. Overuse plays an important role in the emergence of AMR. Paradoxically,
underuse through inappropriate choice, inadequate dosing, poor adherence to treatment, and substandard antimicrobials,
also plays an important role in the emergence and spread of AMR. Hence, there is need to monitor the use of
antimicrobials at all levels of health care, study the antimicrobial use practices in various infections and behavior of
stakeholders for antibiotic use and resistance.
B. Need For Surveillance To Track Antimicrobial Use And Resistance
Increasing levels of antimicrobial resistance correlate with inappropriate antibiotic use as shown at the population and
individual level. Therefore, our goal should be to use antimicrobials rationally and for that we need to know how
antimicrobials are being used. Monitoring of antimicrobial use is a crucial component to identify targets for improving
antimicrobial use and to further correlate with antimicrobial resistance surveillance programmes. World Health Organization
(WHO) highlights the establishment of effective, epidemiologically sound surveillance of antimicrobial use and AMR among
common pathogens in the community, hospitals and other health-care facilities as one of the key public health priorities.
Surveillance systems are required to understand trends in antibiotic use and AMR, as well as the long-term temporal
associations between these two in different areas. Tracking antimicrobial use, and the emergence and spread of resistant strains
of bacteria provides information, insights, and tools needed to guide policy and to evaluate measures taken to promote
appropriate antimicrobial use at all levels, from local to global. Data could also stimulate a sense of urgency to act. Improving
antibiotic use is the key feature in efforts to contain AMR. Strategies for interventions to reduce antibiotic use have to be
prioritized and customized based on local realties. Data from surveillance could help in identifying priorities and processes and
in documenting a baseline for monitoring effects of interventions.
C. Standardized Methodology And Outcome Measures
The use of a standardised methodology allows meaningful comparisons over time and between different facilities or countries.
Expression of antibiotic consumption should be in international accepted formats. Therefore, we need to have a methodology
and a common unit of measurement in each country in order to assure the comparability of the data.
The Anatomical Therapeutic Chemical (ATC) classification and the Defined daily Dose (DDD) as a measuring unit have
become the gold standard for international drug utilization research. ATC/DDD methodology of classification is a tool for
drug utilization research in order to improve quality of drug use. It is an international language for grouping of drugs and
measuring consumption of drug use. The WHO recommends this methodology of classification as their international standard
for drug utilization studies. This methodology is widely used in drug catalogues, drug safety assessment and drug utilization
and pharmacoepidemiology. The ATC/DDD system is a tool for exchanging and comparing data on drug use at international,
national or local levels. When monitoring antimicrobial consumption in pediatric setting, tota antibiotic events
C1. The ATC Classification
The ATC system was initiated in the 1970s by the Norwegian Medicinal Depot, and is now coordinated by the World health
Organization (WHO) Collaborating Centre for Drug Statistics methodology, established in Oslo in 1982. The centre revises the
ATC codes as necessary and maintains an online database and published index. Drugs are divided into different groups
according to the organ or system on which they act and/or their therapeutic and chemical characteristics. Each drug is assigned
at least one ATC code, which are classified into groups at five different levels. Table 1 below shows an illustration using
amoxicillin as an example.
Table1: Classification of amoxicillin of the Anatomical Therapeutic Chemical (ATC) classification system
ATC
Classification
ATC Category Description
J General anti-infectives for systemic use 1st level, anatomical main group
Vol. 1 Issue 11 L.E.D. E-Journal Page 385
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

51
J01 Antibacterials for systemic use 2nd
level, therapeutic main group
J01C Beta-lactam antibacterials, penicillins 3rd
level, therapeutic/pharmacological subgroup
J01C A Penicillins with extended spectrum 4th
level,chemical/therapeutic/pharmacological subgroup
J01C A04 Amoxicillin 5th
level, subgroup for chemical substance
C2. Defined Daily Dose
To facilitate the ability to compare consumption information across time and geography, a technical unit of measurement was
created for use in conjunction with the ATC classification. It is referred as the Defined Daily Dose (DDD) and assigned to
each drug at the 5th
level (chemical substance) classification. It is defined by the ATC as the assumed average maintenance
dose per day for a drug used for its main indication in adults. For antibiotics, the main indication is moderate to severe
infections. The WHO Collaborating Centre using established principles assigns ATC and DDDs. Different DDDs may be
assigned for different drug formulation (ie, parenteral versus oral). Table 2 provides some examples of DDDs for antibiotics.
Table 2: Examples of Defined Daily Doses
ATC Classification ATC Drugs Defined Daily Dose
J01C A04 Amoxicillin 1 g (oral or parenteral)
J01M A06 Norfloxacin 0.8 g (oral)
J01M A02 Ciprofloxacin 1 g (oral)
0.5 g (parenteral)
J01F F01 Clindamycin 1.2 g(oral)
1.8 g (parenteral)
J01C A12 Piperacillin 1.4 g (parenteral)
ATC – Anatomical Therapeutic Chemical
DDDs are useful for measuring and comparing volumes of drug use. DDDs should not be considered as the “correct” dose but
as an international compromise on review of available documentation.
C3. How to use the ATC/DDD classification to quantify the antibiotic consumption?
1. For OPD from administrative prescription claims data, If data are available at the individual claim level and the
antibiotic is identified or mentioned, it is a fairly straightforward process to apply the ATC classification and convert
into a number of DDDs. For example, if the prescription indicates that the particular patient was dispensed 14
ciprofloxacin 500 tablets from a particular pharmacy. The number of DDDs is calculated by multiplying the quantity
by the DDD conversion factor. In this example, the strength of one tablet is 500 mg and the ATC/DDD is 1 g for
ciprofloxacin. Each 500 mg tablet is equivalent to 0.5 DDD. Multiplication of the quantity dispensed (14 tablets) by a
conversion factor of 0.5 equals to total of 7 DDDs dispensed from this prescription. Data can then be collated,
expressed and evaluated based on any other prescriptions record and then merged.
2. Hospital pharmacy data: Most hospital pharmacies have the ability to express their drug dispensing information in
monthly collation of numbers of drugs dispenses by type of drug. ATC/DDD system can be applied in a similar
fashion to the above out-patient prescription example. The usual divisions within a hospital are wards or various
departments. Consumption data can be collated for each department separately from the pharmacy records.
C4. Expressing consumption information
Most commonly, units for antibiotic consumption include DDD per 1000 inhabitant-days for out-patient data and DDD per
100 bed-days in hospitals.
Because the ATC/DDD system is continuously being modified, it is essential that the version (year) of ATC classification in
use is clearly identified. The most recent classification is usually used. However, one must be aware of changes in the
classification or DDD assignment when comparing with earlier information.
D. Situation In Developing Countries
There are wide variations between regions and countries, in their capacity to carry out surveillance system. In resource-poor
countries with comparatively weak health systems, there are constraints related to infrastructure, trained personnel, networking
and coordination. Currently it is not possible in resource-poor countries to quantify the effects of AMR on the individual or the
community, because of lack of availability of good quality data in sufficient quantities. Therefore, developing validated,
reproducible and sustainable surveillance methodologies to quantify AMR and antibiotic use in the community, and to inform
the development of interventions and evaluate their impact is a priority.
The methods for obtaining data are often problematic, especially with regards to data on antimicrobial use. About 80% of
antibiotics are used in the community and the rest are used in hospitals. There is a lack of community-based databases on
AMR and antibiotic use in developing countries. Moreover, antibiotics can be obtained easily from private retail pharmacies
without prescription and pharmacists also advise and dispense antibiotics to patients. Therefore, developing a methodology,
which is reproducible and sustainable, is needed to measure antimicrobial use in the community for developing country.
Vol. 1 Issue 11 L.E.D. E-Journal Page 386
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

52
High-end Antibiotic Monitoring Sheet
Surgical Prophylaxis Monitoring Sheet
Vol. 1 Issue 11 L.E.D. E-Journal Page 387
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

53
Chapter 7
Dosage Guide For Commonly Used Antimicrobial Agents
ANTIBIOTICS ADVERSE REACTION ROUTE PAEDIATRIC
DOSE
ADULT DOSE
Amikacin Nephrotoxicity, Ototoxicity Intravenous 15-22.5 mg/Kg/day
in 2-3 doses
15mg/Kg/day q 8-12
hours, max doses
1.5mg/Kg
Amoxycillin Fever, rash, diarrhea, abdominal cramps,
AST ALT elevation.
Oral 20-50mg/Kg/day, 3-4
doses
250-500mg q 8 hourly
Amoxycillin-
clavunate
(co-amoxyclav)
Rash, diarrhea, abdominal, AST ALT
elevation
Oral,
Intravenous
40mg/kg/day
(amoxicillin) in 2
doses
90mg/kg/day if
penicillin resistant S.
pneumoniaesuspected
in otitis media
100mg/kg/day
375mg 8hourly
625-1000mg 12 hourly
Ampicillin Hypersensitivity reaction, nausea,
diarrhea, exfoliative dermatitis, seizures,
precipitates infectious mononucleosis
rash, interstitial nephritis.
Intravenous
or
Oral
100-400 mg/kg/day
in 4 doses (IV)
500 mg-1gm q 6 hourly
Azithromycin Leukopenia, transient elevation of liver
enzymes, renal toxicity.
Oral 10 mg/kg/day once
daily
Enteric fever 20
mg/kg/day once daily
500mg daily
Azetronam Rash, Diarrhoea , vomiting, AST, ALT
elevation
Intravenous 30 - 120mg/kg/day
Q 6-8 hourly
In cystic fibrosis max
dose 200 mg/kg/day
1-2g q 8 hourly, Max
dose 8gm in 24 hours
Benzathine
penicillin
Hypersensitivity and Jarisch Herxheimer
reaction, haemolytic anemia, seizures
with high doses in renal failure
Intramuscular 1,200,000 units( >30
Kg)
600,000 units ( <30
Kg)
1.2-2.4 million
units/dose
Cefadroxil Rash eosinophilla Oral 30 mg/kg/day in 2
doses
500mg bid or 1 g bid
Cefazolin Leukopenia, eosinophilia, rash, transient
elevation of liver enzymes renal toxicity
Intravenous 100 mg/kg/day 3-4
divided doses
0.52gm q 6-8 hourly
Cefepime Same as third generation cephalosporins.
Adjust dose in renal failure.
Intravenous 1-4gm/day 2-3 doses
Cefixime Diarrhoea, Leukopenia, renal toxicity,
transient elevation of liver enzymes.
Oral 15mg/kg/day in 2
divided doses,
20mg/kg/day in 2
divided doses for
enteric fever.
400mg/day in 1-2
divided doses.
Cefotaxime Arrythmia, transient elevation of liver
enzymes, renal toxicity.
Intravenous 100mg/kg/day in 3-4
divided doses,
200mg/kg/day in 4
divided doses for
meningitis
1-2gm 6-8 hourly
Ceftazidime Hypersensitivity reaction, dizziness, rash,
diarrhea, colitis, exfoliative dermatitis,
thrombocytopenia
Intravenous
Intramuscular
75-100mg/kg/day in
3 divided doses
100mg/kg/day in
meningitis (IV)
1-2g q 8-12 hourly (IV)
Ceftriaxone Gall bladder sludging , transient elevation
of liver enzymes, renal toxicity
Intravenous 50-100 mg/kg/day in
2 divided doses
Meningitis
100mg/kg/day in 2
divided doses
1-2gm q 12-24 hourly
Cefuroxime Leukopenia, eosinophilia, allergic
reaction, transient elevation of liver
enzymes , renal toxicity
Intravenous 75-100mg/kg/day in
3 divided doses
750mg- 1.5g q 8 hourly
Vol. 1 Issue 11 L.E.D. E-Journal Page 388
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
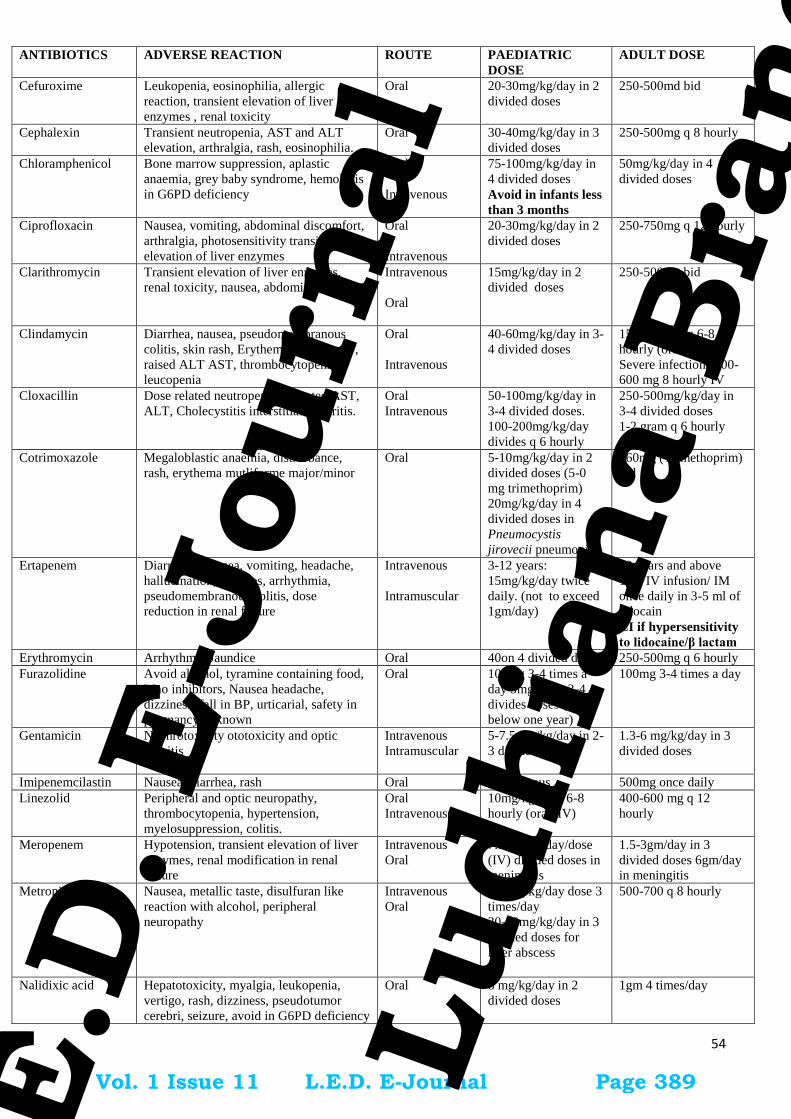
54
ANTIBIOTICS ADVERSE REACTION ROUTE PAEDIATRIC
DOSE
ADULT DOSE
Cefuroxime Leukopenia, eosinophilia, allergic
reaction, transient elevation of liver
enzymes , renal toxicity
Oral 20-30mg/kg/day in 2
divided doses
250-500md bid
Cephalexin Transient neutropenia, AST and ALT
elevation, arthralgia, rash, eosinophilia.
Oral 30-40mg/kg/day in 3
divided doses
250-500mg q 8 hourly
Chloramphenicol Bone marrow suppression, aplastic
anaemia, grey baby syndrome, hemolysis
in G6PD deficiency
Oral
Intravenous
75-100mg/kg/day in
4 divided doses
Avoid in infants less
than 3 months
50mg/kg/day in 4
divided doses
Ciprofloxacin Nausea, vomiting, abdominal discomfort,
arthralgia, photosensitivity transient
elevation of liver enzymes
Oral
Intravenous
20-30mg/kg/day in 2
divided doses
250-750mg q 12 hourly
Clarithromycin Transient elevation of liver enzymes,
renal toxicity, nausea, abdominal cramps
Intravenous
Oral
15mg/kg/day in 2
divided doses
250-500mg bid
Clindamycin Diarrhea, nausea, pseudomembranous
colitis, skin rash, Erythema multiforme ,
raised ALT AST, thrombocytopenia,
leucopenia
Oral
Intravenous
40-60mg/kg/day in 3-
4 divided doses
150-300 mg q 6-8
hourly (oral, iv)
Severe infections 300-
600 mg 8 hourly IV
Cloxacillin Dose related neutropenia, elevated AST,
ALT, Cholecystitis interstitial nephritis.
Oral
Intravenous
50-100mg/kg/day in
3-4 divided doses.
100-200mg/kg/day
divides q 6 hourly
250-500mg/kg/day in
3-4 divided doses
1-2 gram q 6 hourly
Cotrimoxazole Megaloblastic anaemia, distrurbance,
rash, erythema mutliforme major/minor
Oral 5-10mg/kg/day in 2
divided doses (5-0
mg trimethoprim)
20mg/kg/day in 4
divided doses in
Pneumocystis
jirovecii pneumonia
160mg (Trimethoprim)
bid
Ertapenem Diarrhoea, nausea, vomiting, headache,
hallucination, seizures, arrhythmia,
pseudomembranous colitis, dose
reduction in renal failure
Intravenous
Intramuscular
3-12 years:
15mg/kg/day twice
daily. (not to exceed
1gm/day)
13 years and above
1gm IV infusion/ IM
once daily in 3-5 ml of
lidocain
CI if hypersensitivity
to lidocaine/β lactam
Erythromycin Arrhythmia Jaundice Oral 40on 4 divided doses 250-500mg q 6 hourly
Furazolidine Avoid alcohol, tyramine containing food,
Mao inhibitors, Nausea headache,
dizziness, fall in BP, urticarial, safety in
pregnancy unknown
Oral 100mg 3-4 times a
day 5mg/kg in 3-4
divides doses (not
below one year)
100mg 3-4 times a day
Gentamicin Nephrotoxicity ototoxicity and optic
neuritis
Intravenous
Intramuscular
5-7.5 mg/kg/day in 2-
3 divided doses
1.3-6 mg/kg/day in 3
divided doses
Imipenemcilastin Nausea, diarrhea, rash Oral Intravenous 500mg once daily
Linezolid Peripheral and optic neuropathy,
thrombocytopenia, hypertension,
myelosuppression, colitis.
Oral
Intravenous
10mg/kg/dose 6-8
hourly (oral, IV)
400-600 mg q 12
hourly
Meropenem Hypotension, transient elevation of liver
enzymes, renal modification in renal
failure
Intravenous
Oral
7.5 mg/kg/day/dose
(IV) divided doses in
meningitis
1.5-3gm/day in 3
divided doses 6gm/day
in meningitis
Metronidazole Nausea, metallic taste, disulfuran like
reaction with alcohol, peripheral
neuropathy
Intravenous
Oral
7.5 mg/kg/day dose 3
times/day
30-50mg/kg/day in 3
divided doses for
liver abscess
500-700 q 8 hourly
Nalidixic acid Hepatotoxicity, myalgia, leukopenia,
vertigo, rash, dizziness, pseudotumor
cerebri, seizure, avoid in G6PD deficiency
Oral 8 mg/kg/day in 2
divided doses
1gm 4 times/day
Vol. 1 Issue 11 L.E.D. E-Journal Page 389
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

55
ANTIBIOTICS ADVERSE REACTION ROUTE PAEDIATRIC
DOSE
ADULT DOSE
Nitofurantoin Discoloration of urine, vertigo, rash,
methemoglobinemia, cholestatic jaundice,
hepatocellular damage and neuropathy.
Avoid at term and labour.
Oral 8 mg/kg/day in 2
divided doses
50-100 mg q 6 hourly
(5-7mg/kg/day in 4
divided doses max dose
400mg)
Norfloxacin Sam as quinolones Oral 20-30 mg/kg/day in 2
divided doses
200-400 mg twice daily
Ofloxacin Leukopenia, transient of liver enzymes,
renal toxicity. May precipitate
psychosis/seizures,photosensitivity.
Oral
Intravenous
20 mg/kg/day in 2
divided doses
200-400 q 12 hourly
Penicillin G Hypersensitivity reaction like anaphylaxis
rare. nonfatal reactions are like serum
sickness, rash contact dermatitis seen in 1
in 1000 adults. Jarisch Herxheimer
reaction, haemolytic anaemia with high
doses
Oral
Intravenous
50,000units/kg/
dose 6 hourly (Oral)
200,000-400,000
units/kg/day in 4
divided doses (IV)
2-24 million units day
in divided doses q 4-6
hours (IV)
Penicillin V Rash, haemolytic anaemia interstitial
nephritis, seizure with high doses.
Oral 20-50 mg/kg/day in 4
divided doses
250-500 mg every 6-8
hourly.
Piperacillin –
Tazobactum
Leukopenia, transient elevation of liver
enzymes, renal toxicity.
Intravenous 200-400mg/kg/day in
3-4 divided doses
4.5 gm q 8hourly
Teicoplanin Hypersensitivity reactions, rash, less
nephrotoxic as compares to Vancomycin
Intravenous
Intramuscular
10mg/kg/day /dose
every 12 hours for 3
doses the
10mg/kg/day once
daily
400mg once daily (6-
30mg/kg/day)
Tigecycline Nausea, vomiting, allergic reactions,
photosensitivity, pseudo tumor cerebri,
pancreatitis.
No dose adjustment to renal failure
Intravenous Above 10 years 100mg followed by
50mg every 12 hurly
infusion over 30-60
minutes.
Vancomycin Red man syndrome, oto-toxicity,
nephrotoxicity
Intravenous 40-60 mg/kg/day in
3-4 divided doses
0.5gm q 6 hourly or
1gm q 12 hourly
.
Drug doses in Pediatric Age group
Drug name Dose Frequency Maximum
dose
Comments
Cefepime
Infants >14 days of age and Children >40
kg in weight
50 mg/kg q 12 h
Ceftazidime
Infants and children <12 years
100–15
mg/kg/d
Divided q 8 h 6 g
Cefotaxime
Infants and children
a) < 50 kg
b) >12 years and >50 kg
100–200
mg/kg/d
1–2 g
Divided q6-8 h
q 8 h
2 g
Ceftriaxone
Infants and children
50-75 mg/kg/d Divided q 12 h 2 g
Vancomycin
Infants and children
40 mg/kg/d Divided q 6-8
h
2 g
Linezolid
Infants and children <12 years
Children >12 years of age and adolescents
10 mg/kg
10 mg/kg
q 8 h
q 12 h
Piperacillin 100-300
mg/kg/d
q 8 h 4 g
Ciprofloxacin 20–30 mg/kg/d divided every
12 h
800 mg
Levofloxacin
Children 6 months to 5 years of age
Children >5 years of age
10 mg/kg
10 mg/kg
q12 h
q 24 h
500 mg
Vol. 1 Issue 11 L.E.D. E-Journal Page 390
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

56
Amikacin
Infants and children
15–22.5
mg/kg/d
q 24 h
Gentamicin 5-7.5 mg/kg/d q 24 h If normal renal function
Meropenem
Infants ≥3 months of age and children
20 mg/kg q 8 h 1 g
Imepenem-cilastin
Infants < 3 months of age
Infants > 3 months of age and children
100 mg/kg/d
60-100
mg/kg/d
Divided q 6 h
Divided q 6 h
4 g
Fluconazole 12 mg/kg/d q 24 h
Anidulafungin
Children 2– 17 years of age
1.5 mg/kg/day Limited experience
Micafungin
Children >2 years of age
1–4 mg/kg/day 150 mg Limited experience
Caspofungin
Children 3months-17 years
loading dose of
70 mg/m2/day
on day 1
followed by
50 mg/m2/day
thereafter
70 mg; may
increase to 70
mg/m2/day if
clinical
response
is inadequate.
Clindamycin 10 mg/kg/dose q 6-8 h 900 mg Q 8
Vol. 1 Issue 11 L.E.D. E-Journal Page 391
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

57
Chapter 8
Link To National Programme Current Guidelines For Treatment Of Specific Infections
(HIV, RTI& STI, Tuberculosis, Malaria, Dengue, Kala azar, Leptospirosis, Leprosy, Japanese Encphalitis,
Filariasis)
National AIDS control programme (NACP):
In 1986, following the detection of the first AIDS case in the country, the National AIDS Committee was constituted
in the Ministry of Health and Family Welfare. In 1992 India’s first National AIDS Control Programme (1992-1999)
was launched, and National AIDS Control Organisation (NACO) was constituted to implement the programme.
During NACP-II (1999-2006), the free ART (Antiretroviral therapy) programme was rolled out on April 1, 2004 in
eight government hospitals in six high prevalence states has since been scaled up to 400 ART centres where in a total
of around 16,00,000 patients have been registered in HIV care and nearly 6,00,000 patients are currently on ART. The
national programme provides free First line, alternate First line and Second line antiretroviral drugs to adults and
children as per their eligibility. NACO makes available with updated related infections antimicrobial therapy
guidelines on regular basis.
Following links can be refered for further details:
NACO Guidelines for Antiretroviral therapy for HIV-infected Adults and Adolescents 2013
http://www.naco.gov.in/upload/Policies%20&%20Guidelines/Antiretroviral%20Therapy%20Guidelines%20for
%20HIV-Infected%20Adults%20and%20Adolescents.pdf
National Guidelines on Second-line and Alternative First-line ART For Adults and Adolescents 2013
http://www.naco.gov.in/upload/Policies%20&%20Guidelines/National%20Guidelines%20on%20Second-
line%20and%20Alternative%20First-
line%20ART%20For%20Adults%20and%20Adolescents%20May%202013.pdf
Guidelines for Prevention and Management of Common Opportunistic Infections/Malignancies among HIV-
Infected Adult and Adolescent 2007
http://naco.gov.in/upload/Policies%20&%20Guidelines/7-
Guidelines%20for%20Prevention%20and%20Management%20of%20common%20opportunistic%20infections.
National Guidelines on Prevention, Management and Control of Reproductive Tract Infections and Sexually
Transmitted Infections 2014
http://www.naco.gov.in/upload/2014%20mslns/National%20RTI%20STI%20technical%20guidelines%20Sep20
14.pdf
Revised National Tuberculosis Control Programme (RNTCP) DOTS-PLUS:
The Revised National TB Control Programme (RNTCP), an application of the WHO recommended Directly
Observed Treatment, Short Course (DOTS) strategy was launched in 1992 with the objective of detecting at least
70% of new sputum positive TB patients and curing at least 85% of such patients.
However the emergence of resistance to drugs used to treat tuberculosis, and particularly multidrug-resistant TB
(MDR-TB), has become a significant public health problem in a many countries. In India, the available information
from the several studies conducted in the past suggests that the rate of MDR-TB is relatively low in India. Yet this
translates into a large absolute number of cases. Specific measures are being taken within the Revised National
Tuberculosis Control Programme (RNTCP) to address the MDR-TB problem through appropriate management of
patients and strategies to prevent the propagation and dissemination of MDR-TB.
Revised National Tuberculosis Control Programme (RNTCP) DOTS-PLUS Guidelines 2010–
http://health.bih.nic.in/Docs/Guidelines/Guidelines-DOTS-Plus.pdf
National Vector Borne Disease Control Programme (NVBDCP):
NVBDCP Is an umbrella programme for prevention and control of vector borne diseases viz. Malaria, Japanese
Encephalitis (JE), Dengue, Chikungunya, Kala-azar and Lymphatic Filariasis. Out of these six diseases, two diseases
Vol. 1 Issue 11 L.E.D. E-Journal Page 392
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

58
namely Kala-azar and Lymphatic Filariasis have been targeted for elimination by 2015. Malaria, Filaria, Japanese
Encephalitis, Dengue and Chikungunya are transmitted by mosquitoes whereas Kala-azar is transmitted by sand-flies.
The transmission of vector borne diseases depends on prevalence of infective vectors and human vector contact,
which is further influenced by various factors such as climate, sleeping habits of human, density and biting of vectors
etc.
Following links can be referred for further details:
Dengue Clinical Management Guidelines 2014
http://nvbdcp.gov.in/Doc/Dengue-National- Guidelines-2014.pdf
Diagnosis and Treatment of Malaria Guidelines 2013
http://nvbdcp.gov.in/Doc/Diagnosis-Treatment-Malaria-2013.pdf
Operational Guidelineson Kala-Azar (Visceral Leishmaniasis) Elimination in India 2015
http://nvbdcp.gov.in/Doc/opertional-guideline-KA-2015.pdf
National Guidelines Diagnosis, Case Management Prevention and Control of Leptospirosis 2015
http://www.ncdc.gov.in/writereaddata/mainlinkfile/File558.pdf
Operational Guidelines on Disability Prevention & Medical Rehabilitation under National Leprosy
Eradication
Program 2012
http://nlep.nic.in/pdf/Guidelines%20for%20Primary,%20Secondary%20and%20TLC%20(Atul%20Shah%2
0247.2012.pdf
Guidelines on clinical management of acute encephalitis syndrome including Japanese encephalitis 2009
http://nvbdcp.gov.in/Doc/Revised%20guidelines%20on%20AES_JE.pdf
Guidelines on Filariasis Control in India & Its Elimination
http://nvbdcp.gov.in/doc/guidelines-filariasis-elimination-india.pdf
Vol. 1 Issue 11 L.E.D. E-Journal Page 393
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

59
Chapter 9
Case Definitions and Diagnosis for Common Infections
DIARRHEA
“Diarrhea” is an alteration in a normal bowel movement characterized by an increase in the water content, volume, or
frequency of stools. A decrease in consistency (i.e., soft or liquid) and an increase in frequency of bowel movements to ⩾3
stools per day have often been used as a definition for epidemiological investigations.
“Infectious diarrhea” is diarrhea due to an infectious etiology, often accompanied by symptoms of nausea, vomiting, or
abdominal cramps.
“Acute diarrhea” is an episode of diarrhea of <14 days in duration. “Persistent diarrhea” is diarrhea of >14 days in
duration.
ENTERIC FEVER
Acute non-complicated disease: Acute typhoid fever is characterized by prolonged fever, altered bowel function (constipation
in adults, diarrhea in children), headache, malaise and anorexia. Bronchitic cough and exanthem (rose spots on chest ,
abdomen, and trunk) may be seen in the early disease.
Complicated disease: Severe disease can have abdominal pain, occult blood in stools, malena, perforation peritonitis,
myocarditis, pneumonitis and enteric encephalopathy.
Case definition
Confirmed case of typhoid fever
A patient with fever (38°C and above) that has lasted for at least three days, with a laboratory-confirmed positive culture
(blood, bone marrow, bowel fluid) of S. typhi.
Probable case of typhoid fever
A patient with fever (38°C and above) that has lasted for at least three days, with a positive serodiagnosis or antigen detection
test but without S. typhi isolation.
SPONTANEOUS BACTERIAL PERITONITIS
The diagnosis of spontaneous bacterial peritonitis (SBP) is made in transudative ascitis with increased absolute
polymorphonuclear leukocyte (PMN) count (i.e., ≥250 cells/mm3
[0.25 x 109/L]) and without an evident intra-abdominal,
surgically treatable source of infection. An abdominal paracentesis must be performed and ascitic fluid must be analyzed
before a confident diagnosis of ascitic fluid infection can be made.
ACUTE PANCREATITIS
Acute inflammation of pancreas, usually caused by alcohol or gallstone migrating through the common bile duct. Less
commonly caused by trauma, infections like mumps, ascariasis and drugs like diuretic, azathioprine, etc.
Routine use of prophylactic antibiotics in patients with severe AP is not recommended. The use of antibiotics in patients
with sterile necrosis to prevent the development of infected necrosis is not recommended.
Infected necrosis should be considered in patients with pancreatic or extrapancreatic necrosis who deteriorate or fail to
improve after 7 – 10 days of hospitalization. In these patients, either (i) initial CT-guided fi ne-needle aspiration (FNA) for
Gram stain and culture to guide use of appropriate antibiotics or (ii) empiric use of antibiotics after obtaining necessary
cultures for infectious agents, without CT FNA, should be given.
If diarrhoea present WITH vomiting, low grade fever with no mucus in stools think of viral infection.
If diarrhoea present WITH vomiting, abdominal cramps, blood and mucus in stools WITH fever, think
of bacterial infection.
If diarrhoea present WITH blood and mucus in stool WITH no fever, think of amoebiasis.
If profuse diarrhoea present (rice water stools) WITH vomiting, think of cholera.
If diarrhoea present WITH excessive vomiting (especially if in more than one member of the
household or group) think of food poisoning.
Vol. 1 Issue 11 L.E.D. E-Journal Page 394
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

60
In patients with infected necrosis, antibiotics known to penetrate pancreatic necrosis, such as carbapenems, quinolones, and
metronidazole, may be useful in delaying or sometimes totally avoiding intervention, thus decreasing morbidity and mortality.
ACUTE BACTERIAL MENINGITIS
Acute bacterial meningitis (ABM) is a potentially life-threatening neurological emergency.
Patients generally presents with short history of high-grade fever with prominent headache, neck stiffness, photophobia,
nausea, vomiting and altered mental status (lethargy to coma). Infants, elderly, and immunocompromised patients may show
only mild behavioural changes with low-grade fever and little clinical evidence of meningeal inflammation.
Patients with ABM should be rapidly hospitalized and assessed for consideration of lumbar puncture (LP) if clinically safe.
Ideally, patients should have fast-track brain imaging before LP, but initiation of antibiotic therapy should not be delayed
beyond 3 h after first contact of patient with health service.
CSF examination reveals elevated pressure (200-500 mm H2O) and protein (100- 500 mg/dl, normal 15-45 mg/dl), decreased
glucose (<40% of serum glucose) and marked pleocytosis (100-10,000 white blood cells/μl, (normal <5) with 60% or greater
polymorphonuclear leucocytes.
Pyogenic meningitis should be differentiated from tubercular meningitis, which has relatively longer history of low to high
grade of fever, constitutional symptoms, and CSF shows lymphocytic predominance, normal to mildly reduced sugar and
raised proteins.
BRAIN ABSCESS
Brain abscess is defined as a focal suppurative infection within the brain parenchyma, typically surrounded by a well-
vascularized capsule. The most important investigation to diagnose brain abscesses is cranial imaging, either cranial
tomography (CT) or magnetic resonance imaging (MRI).
Headache is the most common presenting symptom of brain abscess. Fever is generally present but its absence does not rule
out the diagnosis. Mostly patients have a focal neurologic deficit such as hemiparesis, apahasia, visual field defects depending
on the location of abscess.
INFECTIVE ENDOCARDITIS
Bacterial endocarditis is a life-threatening infectious disease. Clinical manifestations of bacterial endocarditis include fever,
toxaemia, clubbing, splenomegaly, anaemia, microscopic haematuria, a new onset or changing murmur, evidence of immune
phenomena such as roth spots, osler nodes.
The diagnosis of bacterial endocarditis is based on Modified Duke s criteria which involves clinical, laboratory and
echocardiographic findings.
Definite IE
Pathological criteria
Microorganisms demonstrated by culture or on histological examination of a vegetation, vegetation that has
embolized, or an intracardiac abscess specimen; or
Pathological lesions; vegetation or intracardiac abscess confirmed by histological examination showing active
endocarditis
Clinical criteria
2 major criteria; or
1 major criterion and 3 minor criteria; or
5 minor criteria
Possible IE
1 major criterion and 1 minor criterion; or
3 minor criteria
Rejected IE
Firm alternate diagnosis; or
Resolution of symptoms suggesting IE with antibiotic therapy for ≤4 days; or
No pathological evidence of IE at surgery or autopsy, with antibiotic therapy for ≤4 days; or
Does not meet criteria for possible IE, as above
Modified Duke s criteria for diagnosis of endocarditis
Major Criteria
1. Blood cultures positive
a. Typical microorganisms consistent with IE from 2 separate blood cultures
Vol. 1 Issue 11 L.E.D. E-Journal Page 395
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

61
Viridans streptococci, Streptococcus gallolyticus (Streptococcus bovis), HACEK group, Staphylococcus aureus; or
Community-acquired enterococci, in the absence of a primary focus; or
b. Microorganisms consistent with IE from persistently positive blood culture
≥2 positive blood cultures of blood samples drawn >12 h apart; or
All of 3 or a majority of ≥4 separate cultures of blood (with first and last samples drawn ≥1 h apart); or
c. Single positive blood culture for Coxiella burnetii or phase I IgG antibody titre >1:800
2. Imaging positive for IE
a. Echocardiogram positive for IE
Vegetation;
Abscess pseudoaneurysm, intracardiac fistula
Valvular perforation or aneurysm;
New partial dehiscence of prosthetic valve
b. Abnormal activity around the site of prosthetic valve implantation detected by “F-FDG PET/CT (only if the
prosthesis was implanted for >3 months) or radiolabelled leucocytes SPECT/CT
c. Definite paravalvular lesions by cardiac CT
Minor Criteria
1. Predisposition such as predisposing heart condition, or injection drug use
2. Fever defined as temperature >38°C
3. Vascular phenomena (including those detected by imaging only): major arterial emboli, septic pulmonary infarcts,
infectious (mycotic) aneurysm, intracranial haemorrhage, conjunctival haemorrhages, and Janeway’s lesions
4. Immunological phenomena: glomerulonephritis. Osler’s nodes, Roth’s spots, and rheumatoid factor
5. Microbiological evidence: positive blood culture but does not meet a major criterion as noted above or serological
evidence of active infection with organism consistent with IE
CELLULITIS
Cellulitis is an acute spreading infection that involves subcutaneous tissue, most commonly caused by group a streptococcus
and staph aureus. Trauma and underlying skin lesion can lead to the development of cellulitis. Cellulitis may also develop due
to the spread of adjacent infections like osteomyelitis.
Clinical findings: Clinically rapidly intensifying pain and redness is a common presentation. Fever and lymphadenopathy may
be present. The borders in cellulitis are not well demarcated. Though group A streptococci and staphylococcus are the most
common organisms rarely organisms like H influenza, pneumococcus may also cause cellulitis.
FURUNCULOSIS
Furunculosis is a deep infection of the hair follicle leading to abscess formation with accumulation of pus and necrotic tissue.
Furuncles appear as red, swollen, and tender nodules on hair-bearing parts of the body, and the most common infectious agent
is Staphylococcus aureus, but other bacteria may also be causative. Furunculosis often tends to be recurrent and may spread
among family members.
A carbuncle is a coalescence of several inflamed follicles into a single inflammatory mass with purulent drainage from
multiple follicles.
URINARY TRACT INFECTIONS
The term UTI encompasses a variety of clinical entities viz asymptomatic bacteriuria (ASB), cystitis, prostatitis and
pyelonephritis.
Uncomplicated UTI refers to acute cystitis or pyelonephritis in non pregnant outpatient women without anatomic abnormalities
or instrumentation of urinary tract. Complicated UTI includes all other types of UTI.
Cystitis: The typical symptoms of cystitis are dysuria, urinary frequency, and urgency. Other symptoms are nocturia,
hematuria, suprapubic discomfort, and hesitancy.
Pyelonephritis : severe pyelonephritis present as high fever, rigors, nausea, vomiting, flank or loin pain.symptoms are acute in
onset and symptoms of cystitis may not be present. Fever is the main distinguishing feature between cystitis and
pyelonephritis.
Prostatitis: Acute bacterial prostatitis presents as dysuria, frequency and pain in pelvis or perineal area. Fever and chills are
usually present and symptoms of bladder outlet obstruction are common.
PNEUMONIA
Pneumonia is an inflammation in alveolar tissue, most often caused by a microbial agent. The community acquired pneumonia
is most commonly caused by Streptococcus pneumoniae (typical) and less frequently by Mycoplasma pneumoniae, H.
influenzae, Chlamydia pneumoniae, Staphylococcus aureus or Legionella pneumoniae (atypical). Haemophilus influenzae
infection is seen mostly in patients with chronic bronchitis. Nosocomial pneumonia is likely to be caused by Gram-negative
bacilli or Staphylococcus aureus.
Vol. 1 Issue 11 L.E.D. E-Journal Page 396
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

62
Sudden onset of fever, productive cough, chest pain, shortness of breath and (in some cases) pleuritic chest pain; systemic
symptoms like headache, bodyache and delirium are more severe with atypical pneumonia.
For assessment of the severity of pneumonia “CURB- 65” severity score can be used-
Confusion,
Urea >7 mmol/l,
Respiratory rate ≥30/min,
low Blood pressure (diastolic blood pressure (DBP) ≤ 60 mm Hg or systolic BP ≤ 90 mm Hg) and
Age ≥65 years
Patients with scores 0 and 1 are at low risk of mortality (1.5%) might be suitable for management as hospital outpatients.
Patients with a score of 2 are at intermediate risk of mortality (9%) and should be considered for hospital supervised treatment.
Patients with a score of >2 are at high risk of mortality (>19%) and requires ICU care.
Vol. 1 Issue 11 L.E.D. E-Journal Page 397
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

63
ABBREVIATIONS
AIDS Acute Immuno Deficiency Syndrome
ALT- Alanine Amino Transferase
AM-CL- Amoxicillin/clavulanate
AMR – Antimicrobial Resistance
ANC- Antenetal Care
AOM- Acute otitis media
ART- Anti retroviral treatment
AST- Anti microbial susceptibility test
ATT- Anti Tubercular Treatment
BAL- Broncho Alveolar lavage
BCG- Bacillus Calmette Guerin
BD- Bis in Die (12 hourly)
BL-BLI- Beta lactam-beta-lactam inhibitor
BMT- Bone Marrow Transplantation
BP- Blood Pressure
CABG- Coronary Artery Bypass graft
CAPD- Continuous Ambulatory Peritoneal Dialysis
CI- Confidence Interval
CLSI- Clinical and Laboratory Standards Institute
CME- Continuing medical education
CMV- Cyto Megalo Virus
CNS-Central Nervous System
CRBSI-Catheter Related Bloodstream Infection
CRP- C reactive protein
CRS-Congenital Rubella Syndrome
CSF- Cerebro Spinal Fluid
CSSD- Central Stores and Supply Department
CTVS- Cardio Thoracic and Vascular Surgery
CVS- Cardiovascular System
DS- Double Strength
DT-Dispersible Tablet
DVT- Deep Venous Thrombosis
E.T.O-Ethylene Oxide Sterizilation
ECG- Echo Cardio Gram
ECHO- Echo Cardio Graphy
EGA-Estimated Gestational Age
ENT-Ear Nose Throat
ESBL-Extended-Spectrum Beta- Lactamase
ESRD- End Stage Renal Disease
FDA- Food and Drug Authority
FQ- Fluoroquinolone
G6PD- Glucose 6- phosphate dehydrogenase
GBS- Guillain Barre syndrome
GI-Gastro-Intestinal
HIV-Human Immunodeficiency Virus
HSV- Herpes Simplex virus
ICU-Intensive Care Unit
ID- Infectious disease
IU- International unit
IUD- Intra Uterine Device
IV-Intra Venous
LBW-Low Birth Weight
MDR-Multi Drug Resistant
MIC- Minimum Inhibitory Concentration
MRSA- Methicillin Resistant Staphylococus aureus
MSSA- Methicillin Sensitive Staphylococcus aureus
NICU- Neonatal Intensive Care Unit
OD- Once a day
OPD-Outdoor Patient Department
OT-Operation Theatre
PANDAS- Pediatric Autoimmune Neuropsychiatric
Disorders Associated with Streptococcal Infections
PCR- Polymerase chain reaction
PICU-Pediatric Intensive Care Unit
PJI-Periprosthetic Joint Infection
RNTCP-Revised National Tuberculosis Control Programme
RTI- Reproductive tract infection
SOP- Standard operating procedure
STI-Sexually Transmitted Infection
TB-Tuberculosis
TDS - Ter die sumendum (8 hourly)
TMP-SMX- Trimethoprim sulphamethoxazole
TMP-SMX-DS- Trimethoprim sulphamethoxazole double
strength
URI-Upper Respiratory Infection
UTI-Urinary Tract Infection
VAP-Ventilator Associated Pneumonia
HAP-Hospital Acquired Pneumonia
VDRL-Venereal Disease Research Laboratory
VRE-Vancomycin Associated Enterococci
VZIG- Varicella Zoster immunoglobulin
WBC-White Blood Cell
WHO-World Health Organization
Vol. 1 Issue 11 L.E.D. E-Journal Page 398
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

64
LIST OF EXPERTS
Authors-
Dr..S. Venkatesh, Director, National Centre for Disease Control, New Delhi.
Dr..L.S. Chauhan, Ex-Director, National Centre for Disease Control, New Delhi.
Dr. A. K. Gadpayle, Director PGIMER and Medical Superintendent Dr. RML Hospital, New Delhi
Dr. T. S. Jain, President, Hospital Infection Control Society, India
Dr. Chand Wattal, Senior Consultant, Clinical Microbiology, Sir Ganga Ram Hospital, New Delhi
Dr. S. Aneja, Director Professor, Paediatrics, Kalawati Saran Children Hospital & Lady Hardinge Medical College, New Delhi
Dr. Abdul Ghafur, Consultant Infectious Diseases & Clinical Microbiology, Apollo Hospital, Chennai
Dr. Manju Puri, Professor &Head Gynecology and Obstetrics, Lady Hardinge Medical College and Smt Sucheta Kriplani Hospital, Delhi
Dr. Ajit Sinha, Head Surgery, Safadarjang Hospital, New Delhi
Dr. Varinder Singh, Professor Paediatrics, Kalawati Saran Children Hospital & Lady Hardinge Medical College, New Delhi
Dr. Usha Baveja, Senior Consultant, Microbiology, Medanta-The Medicity, Gurgaon, Haryana
Dr. Renu Dutta, Director Professor, Microbiology, Lady Hardinge Medical College, New Delhi
Dr. Rajni Gaind, Consultant and Professor, Head Microbiology,VMMC & Safdarjang Hospital, New Delhi
Dr. Raman Sardana, Head & Chairman, Hospital Infection Control & Microbiology, Indraprastha Apollo Hospitals, Sarita Vihar, NewDelhi.
Dr. Vikas Manchanda, Assistant Professor, Microbiology, Maulana Azad Medical College, New Delhi
Dr. Anita Kotwani, Ex-Associate Professor, Pharmacology, Vallabhbhai Patel Chest Institute, Delhi
Dr. Charoo Hans, Head Microbiology, PGIMER and associated Dr. RML Hospital, New Delhi
Dr. Sudha Chandelia, Assistant Professor, Pediatrics & Division of Critical care, PGIMER and associated Dr. RML Hospital, New Delhi
Dr. Piyush Jain, Assistant Professor, Medicine, PGIMER and associated Dr. RML Hospital, New Delhi
Dr. Shashi Khare, Ex-Additional Director, Microbiology, National Centre for Disease Control, New Delhi.
Dr. Sarika Jain, Assistant Director, Microbiology, National Centre for Disease Control, New Delhi.
Contributors/Reviewers-
Dr K. K. Aggarwal, Hon’ble Secretary General, Indian Medical Association, Delhi
Dr Jagdish Chandra, Director Professor & Head Paediatrics, Kalawati Saran Children Hospital & Lady Hardinge Medical College, Delhi
Dr.Anupam Prakash, Associate Professor, Medicine, Lady Hardinge Medical College & associated Smt Sucheta Kriplani Hospital, Delhi
Dr. Ravinder Kaur, Director Professor & Head Microbiology, Lady Hardinge Medical College, New Delhi
Dr. Sonal Saxena, Professor Microbiology, Lady Hardinge Medical College, New Delhi
Dr. Anil Garg, C.M.O. (SAG) Medicine, Deen Dayal Upadhayaya Hospital, New Delhi
Dr. Harish Gandhi, C.M.O. (SAG) Ophthalmology, Deen Dayal Upadhayaya Hospital, New Delhi
Dr. K. K. Kumra, C.M.O. (SAG) Orthopedics, Deen Dayal Upadhayaya Hospital, New Delhi
Dr. Manisha Jhawar, President Elect, Surat Ob & Gyn Society, Surat, Gujarat
Dr. Anurag Aggarwal, Assistant Professor, Pediatrics, Maulana Azad Medical College and associated Lok Nayak Hospital, New Delhi
Dr. Narender Saini, Former Hon’ble Secretary General, Indian Medical Association, Delhi
Dr. Rakesk Kumar. Mahajan, Professor & Consultant, Microbiology, PGIMER and associated Dr. RML Hospital, New Delhi
Dr. Kamini Walia, Sr. Scientist, Indian Council of Medical Research, Ansari Nagar, New Delhi
Dr. Padmini Srikantiah, Senior Medical Epidemiologist, Centers for Disease Control and Prevention, Delhi
Dr. S. Roy Choudhury, Professor & Head, Kalawati Saran Children Hospital & Lady Hardinge Medical College, New Delhi
Dr. Sunil Gupta, Additional Director and Head, Microbiology, National Centre for Disease Control, New Delhi.
Vol. 1 Issue 11 L.E.D. E-Journal Page 399
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Central Drugs Standard Control Organization Directorate General of Health Services, Ministry of Health and Family Welfare, Government of India
Page 1 of 12
Frequently asked Questions on Medical Devices
Central Drugs Standard Control Organization
(Medical Devices and Diagnostic Division)
Frequently Asked Questions on
Registration and Import of Medical Devices
in India
Doc No.: CDSCO/MD/FAQ/RC/01/00
Date :21-02-2013
CENTRAL DRUGS STANDARD CONTROL ORGANIZATION
DIRECTORATE GENERAL OF HEALTH SERVICES
MINISTRY OF HEALTH & FAMILY WELFARE
GOVT. OF INDIA
Notice: The replies to the FAQs are aimed only for creating public awareness about In-Vitro Diagnostic Devices Regulation by CDSCO and are not meant to be used for legal or professional purposes. The readers are advised to refer to the statutory provisions of Drugs and Cosmetics Act & Rules and respective Guidelines / Clarifications issued by CDSCO time to time for all their professional needs.
Vol. 1 Issue 11 L.E.D. E-Journal Page 400
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Central Drugs Standard Control Organization Directorate General of Health Services, Ministry of Health and Family Welfare, Government of India
Page 2 of 12
Frequently asked Questions on Medical Devices
MEDICAL DEVICE REGULATIONS
1. What is a medical device in India? Ans:such devices intended for internal or external use in the diagnosis, treatment, mitigation or prevention of disease or disorder in human beings or animals, as may be specified from time to time by the Central Government by notification in the Official Gazette, after consultation with the Board.
2. Whether medical devices are regulated in India? Ans:Yes, import, manufacture, sale and distribution of medical devices are regulated in India under the provisions of the Drugs & Cosmetic Act 1940 & Rules 1945.
3. Where can we get a copy of the Drugs & Cosmetic Act 1940 & Rules 1945?
Ans: The copy of the Drugs & Cosmetic Act 1940 & Rules 1945 is available in Link: http://cdsco.nic.in/Drugs&CosmeticAct.pdf
4. Whether all medical devices are regulated in India?
Ans: No, however only notified medical devices are regulatedin India. The following medical devices are notified under the Drugs and Cosmetics Act.
Name of the Device Notification Number
Date of Notification
Disposable Hypodermic Syringes GSR 365 (E) 17-03-1989
Disposable Hypodermic Needles GSR 365 (E) 17-03-1989
Disposable Perfusion Sets GSR 365 (E) 17-03-1989
In-vitro Diagnostic Devices for HIV, HbsAg and HCV GSR 601(E) 27-08-2002
Cardiac Stents S.O. 1468 (E) 06-10-2005
Drug Eluting Stents S.O. 1468 (E) 06-10-2005
Catheters S.O. 1468 (E) 06-10-2005
Intra Ocular Lenses S.O. 1468 (E) 06-10-2005
I.V. Cannulae S.O. 1468 (E) 06-10-2005
Bone Cements S.O. 1468 (E) 06-10-2005
Heart Valves S.O. 1468 (E) 06-10-2005
Scalp Vein Set S.O. 1468 (E) 06-10-2005
Orthopaedic Implants S.O. 1468 (E) 06-10-2005
Internal Prosthetic Replacements S.O. 1468 (E) 06-10-2005
Vol. 1 Issue 11 L.E.D. E-Journal Page 401
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Central Drugs Standard Control Organization Directorate General of Health Services, Ministry of Health and Family Welfare, Government of India
Page 3 of 12
Frequently asked Questions on Medical Devices
5. Which is the Regulatory Authority that governs the regulations of Import of medical devices in India? Ans:Drugs Controller General (India), Central Drugs Standard Control Organization (CDSCO), Directorate General of Health Services , Ministry of Health and Family Welfare, Government of India , FDA Bhavan, ITO, Kotla Road, New Delhi -110002 Phone: 91-11-23236965 / 23236975, Fax: 91-11-23236973, E-mail:- [email protected]
6. Which division of CDSCO (HQ) is responsible for registration/import of Medical
Devices in India? Ans: Medical Device & Diagnostics Division, Central Drugs Standard Control Organization (CDSCO), Directorate General of Health Services, Ministry of Health and Family Welfare, Government of India FDA Bhavan, ITO, Kotla Road, New Delhi -110002 is responsible for registration/import of Medical Devices in India.
7. What are the requirements for import of medical devices in India?
Ans: For the import of medical devices in India, Registration Certificate in Form 41 and Import License in Form 10 are required as per provisions of the Drugs & Cosmetic Act & Rules. For import of medical device, the manufacturing site and products (medical devices) are required to be registered with Indian drug regulatory agency (i.e. Central Drugs Standards Control Organization).
8. Whether Registration and import license is required for import of non-notified
medical device in India? Ans:No, registration is not required for import of non-notified medical devices in India. However, the followingdevices are regulated as “Drugs” under Drugs and Cosmetics Act and Rules, hence registration and import license is required for import in to India. Blood Grouping Sera Ligatures, Sutures, Staples Intra Uterine Devices (Cu-T) Condoms Tubal Rings Surgical Dressing Umbilical Tapes Blood / Blood Component Bags
9. Who canimport medical devices into India?
Ans: Any person/firm/enterprise etc. having wholesale license and/or manufacturing license issued under Drugs and Cosmetics Act, 1940 and Rules 1945 can be an applicant for Registration and import of medical devices into India.
10. To whom shall the application be submitted for Registration/Import License for
Medical Device in India? Ans. Applications for Registration/ Import Licenseof Medical Device shall be submitted to the Drugs Controller General (India), Central Drugs Standard Control Organization (CDSCO), FDA Bhawan, ITO, Kotla Road, Delhi-110002. Phone: 91-11-23236965 / 23236975. Fax: 91-11-23236973.
Vol. 1 Issue 11 L.E.D. E-Journal Page 402
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Central Drugs Standard Control Organization Directorate General of Health Services, Ministry of Health and Family Welfare, Government of India
Page 4 of 12
Frequently asked Questions on Medical Devices
11. What is the procedure to apply for the "Registration certificate" in Form-41 for Medical Devices in India? Ans:Following steps may be adopted for Registration application STEP 1.Pay the required Registration fee through TR-6 Challan (in triplicate) in Bank of Baroda, Kasturba Gandhi Marg, New Delhi.
A fee of one thousand and five hundred US dollars [or its equivalent in Indian rupees] shall be paid along with the application in Form 40 as registration fee for the manufacturing premises meant for manufacturing of medical device intended for import into and use in India.
A fee of one thousand US dollars [or its equivalent in Indian rupees] shall be paid along with the application in Form 40 for the registration of a single medical device meant for import into and use in India and an additional fee at the rate of one thousand US dollars for each additional medical device:
STEP 2.Compilation of Registration dossier as per the guidance documents available atthe link:http://cdsco.nic.in/Medical_div/guidance.htm
STEP 3.Submit Product Registration application at CDSCO (HQ), New Delhi
12. Whether Device manufacturing site required to be inspected before grant of
Registration Certificate in Form 41? If yes, how much fees for the inspection or visit of the manufacturing premises of Medical Devices? Ans:No, however if required the applicant shall be liable for the payment of a fee of five thousand US dollars [or its equivalent in Indian rupees] for expenditure as may be required for inspection or visit of the manufacturing premises.
13. How the fees shall be paid in India?
Ans: The fees shall be paid through a Challan in the Bank of Baroda, Kasturba Gandhi Marg, New Delhi-110001 or any other branch or branches of Bank of Baroda, or any other bank, as notified, from time to time, by the Central Government, to be credited under the Head of Account “0210-Medical and Public Health, 04-Public Health, 104-Fees and Fines”: Provided that in the case of any direct payment of fees by a manufacturer in the country of origin, the fees shall be paid through Electronic Clearance System (ECS) from any bank in the country of origin to the Bank of Baroda, Kasturba Gandhi Marg, New Delhi, through the Electronic Code of the bank in the Head of Account “0210-Medical and Public Health, 04- Public Health, 104-Fee and Fines”, and the original receipt of the said transfer shall be treated as an equivalent to the bank challan, subject to the approval by the Bank of Baroda that they have received the payment.
14. Is there any system of prescreening of applications for issue of grant of
Registration Certificate/ Import Licence at the time of submission at CDSCO (HQ) New Delhi? Ans: Yes, application will be prescreened as per checklist available under link: http://cdsco.nic.in/Medical_div/medical_device_division.htm
Vol. 1 Issue 11 L.E.D. E-Journal Page 403
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Central Drugs Standard Control Organization Directorate General of Health Services, Ministry of Health and Family Welfare, Government of India
Page 5 of 12
Frequently asked Questions on Medical Devices
15. What is the time period for Grant of Registration Certificate? Ans: If the application is complete in all respects and informations specified in Schedules D-I and D-II are in order, the licensing authority shall, within nine months from the date of receipt of an application, issue such Registration Certificate in From 41.
16. What is the Duration/Validity of "Registration certificate" in Form-41 for Medical
Devices in India? Ans:A Registration Certificate, unless, it is sooner suspended or cancelled, shall be valid for a period of three years from the date of its issue
17. How to register additional device(s) in the already approved/valid Registration
Certificate? Ans.Importer has to apply for endorsement to the existing Registration Certificate along with the requisite documents provided that the additional device(s) is being manufactured at the same manufacturing site as stated in the Registration Certificate for each additional device 1000 USD is to be paid as a Registration fee. The requirements for endorsement of additional Device(s) to the valid Registration Certificate are remains same to the fresh Registration Certificate except Site Registration Fees (1500 USD) and Plant Master File.
18. When should an application for Re-Registration of devices be submitted?
Ans. Applications for Re-Registration should be submitted minimum Nine months ahead of the expiry of the registration certificate.
19. What are the requirements for Re-Registration of devices?
Ans. The requirements for Re-registration of Devices are remains same as fresh Registration requirements except requirement of hard copy of Plant Master File (PMF) and Device Master File (DMF) provided there are no changes in the PMF and DMF, However soft copy of PMF and DMF in the form of compact disc shall be provided along with the application.
20. Is it possible for an applicant to submit their applications for Registration
Certificate (Form 41) and Import License (Form 10) together? Ans.Yes, an applicant can apply for both Registration Certificate (Form 41) and Import License (Form 10) together,provided Indian agent and importer remain same
21. How much fees for issuance of duplicate copy of "Registration certificate" in Form-
41 for Medical Devices in India? Ans: A fee of three hundred US dollars [or its equivalent in Indian rupees] shall be paid for a duplicate copy of the Registration Certificate, if the original is defaced, damaged or lost.
22. What are the requirements for grant of Import license in Form 10 of Medical
Devices? Ans.The requirements for grant of import license in Form 10 are available in the CDSCO web page under link i.ehttp://cdsco.nic.in/Medical_div/medical_device_division.htm
Vol. 1 Issue 11 L.E.D. E-Journal Page 404
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
Central Drugs Standard Control Organization Directorate General of Health Services, Ministry of Health and Family Welfare, Government of India
Page 6 of 12
Frequently asked Questions on Medical Devices
23. What is the Duration/Validity of "Import Licence” in Form-10 for Medical Devices in
India? Ans: Import Licence, unless, it is sooner suspended or cancelled, shall be valid for a period of three years (Till Registration Certificate is valid).
24. When should an application for renewal of Import Licencebe submitted?
Ans.Applications for Import Licence should be submitted along with the application for Re-Registration provided importer and Indian Agent are remain same or minimum three months ahead of the expiry of the Import Licence.
25. Whether Devices, having valid Import Licence, can be imported from any notified
ports of India? Ans.Yes,
26. Whether multiple Import Licences are required for devices that are registered under
one Registration Certificate by the same Indian Agent/ Importer in case he wants to import from different notified ports? Ans. No.Single license may be issued, in respect of the import of more than one drug or class of drugs manufactured by the same manufacturer to the Importer through which importer can import the products thorough any notified port under Drugs and Cosmetics Act and Rules.
27. Whether devices imported under valid import Licence can stocked in any other
wholesale licence premises other than stated in the Import Licence? Ans. Yes
28. What is the time period for Grant of Import licence?
Ans: If the application is complete in all respects and informations are in order, the licensing authority may within three months from the date of receipt of an application, issue an import licence in Form 10.
29. Whether Notified Medical Devices can be imported only for demo purpose into
India? Ans. No,there is no provision to import demo samples in India.
30. What is the Test license in Form 11?
Ans:The Test Licence in Form 11 is to import small quantities of drugs / Medical Devices/ Diagnostic kits, for the purpose of examination, test or analysis provided that Imported Medical Devices under Form 11 shall not be used for any commercial purposes.
31. What are essential documents required for import of medical device for
examination, test and analysis in Form11? Ans:The essential documents required for Import of devices under test Licence are available in CDSCO website under Link: http://cdsco.nic.in/Medical_div/medical_device_division.htm
Vol. 1 Issue 11 L.E.D. E-Journal Page 405
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Central Drugs Standard Control Organization Directorate General of Health Services, Ministry of Health and Family Welfare, Government of India
Page 7 of 12
Frequently asked Questions on Medical Devices
32. What is the Duration/validity of "Test License" in Form-11? Ans:A Test License unless, it is sooner suspended or cancelled, shall be valid for a period of one year from the date of its issue
33. Whether Registration Certificate and Import Licence are required to import
componentsof Medical Devices? Ans.Yes, Devices in assembled form ready for packaging and sterilization are regulated under the provision of Drugs and Cosmetic Act 1940 and Rules thereunder. Hence Registration Certificate and Import Licence are required to import into India.
34. Whether both legal (If any) and actual manufactures name and address should be
stated in the Free Sale Certificate issued by the national Regulatory agency for the purpose of registration of devices in India? Ans.Yes.
35. Any changes in name and/oraddress of Indian agent/ Importer or change in
constitution after issue of Registration Certificate/ Import Licence are required to be communicated to the Licensing Authority? Ans.Yes, Indian agent/ Importer shall inform the licensing authority immediately in writing and shall submit fresh application as per Rules.
36. Any changes in name and/or address of legal and/or actual manufacturer or change
in constitution after issue of Registration Certificate/ Import Licence are required to be communicated to the Licensing Authority? Ans. Yes, the manufacturer or his authorizd agent in india shall inform the licensing authority immediately in writing in the event of any change in the constitution of the firm and / or address of the registered office / factory premises operating under this Registration Certificate. Where any such change in the constitution of the firm and/or address takes place, the current Registration Certificate shall be deemed to be valid for a maximum period of three months from the date on which the change has taken place unless, in the meantime, a fresh Registration Certificate has been taken from the licensing authority in the name of the firm with the changed constitution of the firm and/or changed address of the registered office or factory premises
37. Whether acquisition/merger of one company by another company is considered as
change in constitution of the company? Ans.Yes.
38. What are the changes that require an applicant to make afresh Registration?
Ans.The following changes require a fresh registration – Any change with respect to manufacturer (legal/ actual) like change in constitution, change in name, change in address, etc. Any change with respect to importer/ Indian Agent like change in constitution, change in name, etc.
39. What are the changes which do not require fresh registration and only notification
or amendment may be obtained?
Vol. 1 Issue 11 L.E.D. E-Journal Page 406
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
Central Drugs Standard Control Organization Directorate General of Health Services, Ministry of Health and Family Welfare, Government of India
Page 8 of 12
Frequently asked Questions on Medical Devices
Ans.Change in shelf life, change in the method of testing, minor change in manufacturing process not affecting the final product specifications, updation in IFU like warnings, precautions, additional instructions and safety etc., labels and packaging (provided proper justification should be provided for the above changes).
40. If there is a change in the Indications and/ or Intended use of a registered notified
medical device, does the applicant need to submit a fresh application including Power of Attorney incorporating the changed Indications and/ or Intended use of the registered notified medical device? Ans.Yes, revised Power of Attorney is required to be submitted, reflecting the changes/ modification to indications.
41. What is the procedure for expanding/ modifying the currently registered
indications? Ans.The process for change notification to CDSCO and approval will be followed in such case. Revised Power of Attorney including the expanded/ modified indication will need to be submitted to the CDSCO.
42. Whether any minor change which is notified to the Regulatory Authority but
CDSCO’s response is awaited can be imported in India? Ans.NO.
43. What is the time line for response to a change notification?
Ans. 90 working days. 44. At the time of submitting applications for registration/ re-registration of medical
devices, are original labels as per Rule 96 to be submitted to the CDSCO? Ans. While original labels as per Rule 96 are required however applicants may submit coloured copy of original label incorporating all details as per Rule 96. Labels submitted should include all models for which registration is sought.
45. What are mandatory addresses on the labels of registered notified medical devices
being imported/ marketed in India? Ans. The label of registered notified medical devices being imported must include the names and addresses of the legal manufacturer, actual manufacturer and the name and address of importer on which the Import License in Form 10 has been issued.
46. Can the importers of registered notified medical devices incorporate India-specific
requirements on labels after/post landing in India at customs warehouse or place approved by the Licensing Authority? Ans. Yes, importers of registered notified medical devices are currently allowed to incorporate India-specific requirements like name and address of importer, import Licence Number on imported medical devices post landing in India at customs warehouse or place approved by the CDSCO prior to release into market.
47. Can the Quality Manual as per ISO 13485 be submitted in lieu of the Plant Master
File? Ans.Yes. Provided Quality Manual has same content as prescribed in Plant Master File.
Vol. 1 Issue 11 L.E.D. E-Journal Page 407
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch
Central Drugs Standard Control Organization Directorate General of Health Services, Ministry of Health and Family Welfare, Government of India
Page 9 of 12
Frequently asked Questions on Medical Devices
48. The numbers of employees in the manufacturing premise are required to be
included in the Plant Master File? However, there may be a change in this number by the time the Plant Master File is collated and submitted? Ans.Yes, the number of employees as on the date of preparation of Plant Master File will be considered for the purpose of registration.
49. Whether Certificate of Exportability (which reflects that the proposed products may
not be freely sold in the country of origin but can be exported), is acceptable as Free Sale Certificate? Ans.No
50. Which manufacturing site is considered the manufacturing premise for the purpose
of inclusion in the Form - 40? Ans.The actual site of final batch release of the medical device is considered the manufacturing premise for the purpose of inclusion in the Form – 40.
51. If applicant has applied for Registration Certificate and still not issued but in
between there is the change has happened in the constitution of either Manufacturer or Indian Agent, address of manufacturer whether fresh fees is required for plant registration and product registration? Ans. Yes. The applicant has to submit the Fresh application including fee.
52. If applicant wants to apply for Registration Certificate but the product is not being
sold in any of the following countries i.e. USA, Europe, Japan, Health Canada or Australia. Can he apply for Registration Certificate? Ans. No. However if safety and effectiveness of device is proven by conducting clinical trials in India can apply for registration certificate.
53. If applicant wants to apply for Registration Certificate but the product is not sold in
the country of origin but is registered and marketed in any one of the following countries i.e. USA, Europe, Japan, Health Canada or Australia. Can he apply for Registration Certificate? Ans. Yes.
54. What is the generic name of the medical device?
Ans. The generic name is the name as per the internationally accepted nomenclature for the medical device.
55. What is a “new” medical device?
Ans. A “new” medical device is one which does not have a predicate medical device registered / approved in India.
56. What is a “predicate” medical device?
Ans. A “predicate” medical device is one which is registered / approved in India and has the same indications/ intended use, material of construction and design characteristics as the device which is proposed for registration in India.
Vol. 1 Issue 11 L.E.D. E-Journal Page 408
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Central Drugs Standard Control Organization Directorate General of Health Services, Ministry of Health and Family Welfare, Government of India
Page 10 of 12
Frequently asked Questions on Medical Devices
57. How is the process for registration of a “new” medical device different from that of a medical device for which predicates exist? Ans. Notified medical devices for which predicate devices are not registered in India are classified as “new” medical devices. These medical devices are referred to the Medical Device Advisory Committees (MDAC) to comment on safety, effectiveness, essentiality and desirability of proposed New Devices.
58. Which are the Specialties for which Medical Device Advisory Committees exist?
Ans. Currently, Medical Device Advisory Committees cover the following specialties –Cardiovascular, Dental, Ophthalmic, Orthopaedic, Reproductive and Urology and a miscellaneous devices committee. Further, the CDSCO has also formulated a “General Expert Pool” for Medical Device Advisory Committee to advise the Drugs Controller General of India in matters related to review and regulatory approval of new medical devices and clinical trials.
59. Who will issue Form-9 the manufacturer or the Principle Indian Agent?
Ans.Form-9 can be issued by either the manufacturer OR the Principle Indian Agent. 60. How should the documents be notarized?
Ans.The notary should ensure that documents are properly authenticated by signing each document/page or by providing notarization page (Declaration from notary) having name/number of certificate/documents along with pages eg. “This part includes certificate X (pages), Certificate Y (pages)” etc. and should be intact (Authorized by notary tamper proof) and stapling or pasting not accepted.
61. What is the time limit for submission of Query Response?
Ans. There is no time limit for submission of Query Response as per the provision of Drugs and Cosmetics Act and Rules, however, it should be reasonable and justifiable.
62. Can Third party/Authorized Consultant ask the status of the application?
Ans. No. Only either applicant or his authorized Regular employee may ask the status of their application if it is beyond the time limit prescribed under Drugs and Cosmetics Act and Rules.
63. Who is authorized to make a Technical Presentation, on behalf of applicant, when
asked by the CDSCO? Ans. Only Subject Expert or Technical Person of the company who is equally competent to make technical presentation.
64. Whether the Importer who is having valid Form-10 license but there is some small
change in the name of importer or address of Importer still can he import till another license is granted? Ans. No, at the time of import, the label of the product should comply with details as specified in the Form-10 for the product.
65. Can ISO Symbols such as , , , , etc. be incorporated on the labels of registered notified medical devices being imported into India?
Vol. 1 Issue 11 L.E.D. E-Journal Page 409
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Central Drugs Standard Control Organization Directorate General of Health Services, Ministry of Health and Family Welfare, Government of India
Page 11 of 12
Frequently asked Questions on Medical Devices
Ans.Yes, the ISO Symbols are acceptable on labels of registered notified medical devices being imported into India.
66. Whether shelf life of the device can be stated on the label instead of date of
manufacture? Ans.Yes
67. What are mandatory addresses on the labels of registered notified medical devices
being imported/ marketed in India as per the Drugs and Cosmetics Act, 1940? Ans.Name and address of Legal Manufacturer, Actual manufacturer and importer as stated in Form-10.
68. All certificates with minimum 6 months validity are being asked as per guidance
document. Can the applicant provide the renewed certificates in case the certificate gets expired during the review process? Ans.As per the Guidance document for Registration/ Re-registration, all certificates with minimum 6 months validity are to be submitted. However, if the applicant has a valid reason for not being able to submit the same within stipulated validity, they can provide an undertaking to the CDSCO stating that fresh certificates will be submitted immediately after expiry of such certificates and such instances will be dealt on a case to case basis as per rationale of reason.
69. If my medical device has an adverse event, do I need to report it to CDSCO? Ans. Yes, To find out more about the adverse event reporting criteria, procedure and timeline, please refer to our website on http://cdsco.nic.in/pharmacovigilance.htm
70. If a recall or corrective action is required for my medical device, do I need to report
it to the CDSCO? Ans.Yes
71. Can import of the medical device with brand namebe done in case the Import
License (Form-10) reflecting the product (medical device) with generic name or vice versa? Ans. No
72. Can an importer import a registered notified medical device having residualshelf
life less than 60 % for Commercial or testing purpose? Ans. No.
73. Can one time permission for import of regulated medical device be granted without
having valid Import Licence in Form-10? Ans. No.
74. What are the regulatory requirements for Import, Manufacture and labeling of
Veterinary medical devices? Ans. Same as devices meant for human beings.
Vol. 1 Issue 11 L.E.D. E-Journal Page 410
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch

Central Drugs Standard Control Organization Directorate General of Health Services, Ministry of Health and Family Welfare, Government of India
Page 12 of 12
Frequently asked Questions on Medical Devices
75. Is there a need to register notified products that are imported and locally processed for 100% export only and which will not be marketed in India? Ans. No, However the importer shall comply with requirements specified by DGFT from time to time.
76. Whether local manufacturer needs to obtain an import license for suture raw
material that is used 100% for own manufacturing of final finished Sutures for which state FDA has already issued a manufacturing license. Ans. Yes.
77. Where can I submit my enquiries related to registration, import and manufacture of medical devices? Ans.All enquiries regarding the submission and approvals can be sent to the Drugs Controller General India ([email protected]) - CDSCO, FDA Bhawan, ITO, Kotla Road, New Delhi - 110002. Phone: 91-11-23236965 / 23236975. Fax: 91-11-23236973.
Vol. 1 Issue 11 L.E.D. E-Journal Page 411
L.E.
D. E
-Jou
rnal
IDA
Ludh
iana
Bra
nch




















