
Locus of control as a measure of ineffectiveness in anorexia nervosa
Upload
independentCategory
view
5download
0
An Examination of the Concept of Central Coherence inWomen with Anorexia Nervosa
Carolina Lopez, MSc1*Kate Tchanturia, PhD1
Daniel Stahl, PhD2
Rhonda Booth, PhD3
Joanna Holliday, PhD4
Janet Treasure, MD, PhD, FRCP,FRCPsych5
ABSTRACT
Objective: To examine central coher-
ence (local and global processing) in
women with anorexia nervosa (AN).
Method: 42 women with AN and 42
healthy women (HC) completed neuro-
psychological testing measuring visuo-
spatial and verbal aspects of central co-
herence: Rey-Osterrieth Complex Figure
(RCFT), Embedded Figures Test (EFT),
Homograph Reading Test (HRT), and Sen-
tence Completion Task (SCT).
Results: People with AN displayed
superior performance on the EFT and
poorer performance in RCFT with the
exception of accuracy in the copy trial.
Long hesitations in the SCT were
observed. Verbal coherence tasks were
not sensitive enough to detect coherence
anomalies in AN.
Conclusion: Women with AN have
strengths in tasks requiring local process-
ing (EFT) and weaknesses on tasks bene-
fited by global processing (RCFT and SCT).
These results are consistent with the
weak central coherence account. This
trait might play a role in the mainte-
nance of AN and can be addressed in
specific clinical interventions. VVC 2007 by
Wiley Periodicals, Inc.
Keywords: central coherence; anorexia;
cognition; information processing; local
processing; global processing; neuro-
psychology
(Int J Eat Disord 2008; 41:143–152)
Introduction
Developmental problems as well as obsessive-com-pulsive disorders (OCD) and obsessive-compulsivepersonality traits (OCPD) might be considered tobe enduring risk factors of relevance to the onsetand prognosis of eating disorders (EDs).1 It is possi-ble that neurocognitive anomalies may underpinOCD and OCPD traits. For example, in a systematicreview of the literature, the overall conclusiondrawn from a meta-analysis of data pertaining toset-shifting (switching between strategies and stim-uli) was that there was moderate sized evidencethat difficulties in set-shifting was associated with
anorexia nervosa (AN). Difficulties in set-shiftingwere found to be linked to childhood perfectionismin people with AN.2
This and other neurocognitive abnormalities areof interest as they support the argument that EDsare neurodevelopmental in origin.3–5
Gillberg et al.6 raised the possibility that AN mightbe considered to be part of the autistic spectrum ofdisorders (ASD). He and his colleagues have col-lected data on neurocognitive and social functioningin a cohort of cases prospectively studied over 20years that support this hypothesis. They found that20% of their AN group met criteria for ASD comor-bidity including social impairments and deficits inempathy.7 They also observed normal to superiorperformance in local processing dependent tasks(e.g. the Block Design subtest of the WAIS-R) andpoor function on tasks requiring global processingstrategies (e.g. the Object Assembly subscale of theWAIS-R).6 Furthermore, the group with ASD comor-bidity performed poorly in the picture arrangementtest.6 This pattern of performance fits with what hasbeen termedweak central coherence.8–10
Weak central coherence refers to a cognitive stylein which there is a bias towards local or detailed-focus processing of information over the naturaltendency to integrate information into a context.8,9
Weak central coherence is thought to explain some
Supported by Nina Jackson Foundation.
*Correspondence to: Carolina Lopez, Department of Academic
Psychiatry, 5th Floor, Thomas Guy House, Guy’s Hospital, London,
SE1 9RT, UK. E-mail: [email protected]
Accepted 31 July 2007
1 Division of Psychological Medicine, King’s College London,
Institute of Psychiatry, IoP, United Kingdom2 Department of Biostatistics and Computing, King’s College
London, IoP, United Kingdom3 SGDP Centre, King’s College London, IoP, United Kingdom4 Oxford Doctoral Course in Clinical Psychology, The Isis
Education Centre, Warneford Hospital, Oxford, United Kingdom5 Department of Academic Psychiatry, Guy’s, King’s and
St. Thomas’s Medical School, London, United Kingdom
Published online 15 October 2007 in Wiley InterScience
(www.interscience.wiley.com). DOI: 10.1002/eat.20478
VVC 2007 Wiley Periodicals, Inc.
International Journal of Eating Disorders 41:2 143–152 2008—DOI 10.1002/eat 143
REGULAR ARTICLE

of the cognitive abnormalities in ASD.9,11 A recentreview of more than 50 studies measuring aspectsof central coherence in ASD concluded that therewas strong evidence for a bias to local processingbut mixed findings with regard to weak global co-herence in this group.9
The concept of weak central coherence is new inthe field of EDs.10 However, it would fit with thefindings from the neurocognitive literature where apreoccupation with detail and a narrow style of in-formation processing have been described.10,12,13
Also it may explain some aspects of the symptoma-tology such as the preoccupation with rules anddetails captured by the Yale-Brown-Cornell EatingDisorder Scale (YBC-EDS).14
Happe and colleagues have described, developed,and adapted various tests that measure the conceptof central coherence in the visuospatial, verbal, andauditory domains.15 These tests have been used in apopulation of ASD and some also in first degree rela-tives.9,16 It is still unclear whether the concept ofcentral coherence is the result of an integratedmechanism that affects information processing fromacross different systems/domains or if it should beconsidered a variable feature within each system/do-main. Hence, there is a need to research into centralcoherence using tasks addressing different domains(e.g. verbal, visuospatial, auditory, etc.).9
An important finding in ASD literature is that theclassical symptom groups of autism (social impair-ments, communication impairments, and re-stricted repetitive behaviors and interests) are etio-logically independent. Thus, the verbal communi-cation deficits in autism and the compulsivesymptoms have distinct causal pathways.17 EDsmight therefore only have some of the symptomclusters in common with ASD. For example, theymay be more akin to high functioning Aspergersand have fewer verbal difficulties.
The aim of this study was to measure central co-herence in people with AN using some of the testsfor central coherence that have been used previ-ously in the ASD population. Our hypothesis wasthat people with AN would display a local process-ing bias and/or weak global processing. A secondaryhypothesis was that this would be most pronouncedin visuospatial tasks rather than verbal tasks.
Method
Participants
Women meeting the DSM-IV criteria for AN (N 5 42)
and healthy controls (HC, N 5 42) matched for sex and
equivalent in age and intellectual ability participated in
this study.
Participants with AN were ascertained from the South
London and Maudsley NHS Trust and local community:
29 (69%) had AN restrictive subtype and 13 (31%) purging
subtype of AN. Also, 17 (40.5%) were taking psychoactive
medication (58.8% SSRI antidepressants) and 15 (35.7%)
were undergoing inpatient treatment at the time of the
study.
HC were recruited from the staff and student popula-
tion of the Institute of Psychiatry and King’s College of
London, from advertisements on the Eating Disorders
Unit website, and local community. Inclusion criteria
included a body mass index (BMI) between 19 and 26
(kg/m2), no psychoactive medicines, and no personal or
family history of psychiatric illness or EDs.
The exclusion criteria for all participants were as fol-
lows: a history of head injury, neurological diseases, psy-
chosis, and learning disabilities. All participants were
English speakers.
Following a complete description of the study, written
informed consent was obtained from all participants.
Ethical approval was obtained from the South London
and Maudsley Trust (SLAM) Research Ethics Committee.
Measures
ED Diagnosis. Participants in the AN group were
assessed with the semi-structured diagnostic interview
EATATE for ED (part I).18 HC completed the Eating Disor-
der Examination-Questionnaire (EDE-Q19) modified to
provide a lifetime screening for ED symptoms. Addition-
ally, parts II and III of EATATE were administered to all
participants to examine for a history of other psychiatric
problems.
Information Processing. The neuropsychological bat-
tery consisted of four instruments, selected to demon-
strate either predominant global or local information
processing at both verbal and visuospatial levels.9
The Rey-Osterrieth Complex Figure Test - recallform. Recall form (RCFT) is an open-ended measure
of visual perceptual organization and nonverbal mem-
ory.20 In this study, participants were provided with a
blank sheet of paper, colored pencils, and a sheet with
the figure. They were asked to copy and then recall the
figure after a 20-min interval without previous warning.
Pencils were proffered when the participant completed
any element of the figure. The drawing process was video-
recorded and scored using procedures described by Taylor
(adapted from Osterrieth, 1944) for accuracy.20–22 The
Accuracy score (range 0–36) comprises a total of 18 ele-
ments awarded a 0 to 2 quality score (see Fig. 1). The
intraclass correlation coefficient for inter-rater agree-
ment in accuracy score was .89 with an average Kappa
LOPEZ ET AL.
144 International Journal of Eating Disorders 41:2 143–152 2008—DOI 10.1002/eat

coefficient (j) of .85, ranging from .72 to .95 for the indi-
vidual elements, in this study. The percentage of recall
(recall/copy*100) was calculated as a measure of recall
accuracy.
Drawing style was also assessed using both Savage’s23
and Booth’s scoring systems (2006).
Savage’s scoring system addressing organizational
strategy (OS) scores the five main elements of the figure
(0–6 points). Higher scores are awarded to better OS.
Details of this system have been described elsewhere.23
In contrast, Booth’s scoring was specifically designed to
measure central coherence and it addresses not only the
continuity of drawing but also whether the drawing pro-
cess beings with the detail or the global elements.
Following Booth (2006) the degree of coherence in the
drawing process was measured in two independent ele-
ments: (i) Order of Construction Index (mean range 0–
3.3): the first six elements drawn are awarded 0–4 points
according to the following hierarchical categories: (a)
global external structure (elements 2 and 13) 5 4 points;
(b) global internal structure (elements 3, 4, 5, and 16) 5 3
points; (c) local perimeter elements (elements 1, 9, 14,
17, and 18) 5 1 point; and (d) local internal elements
(elements 6, 7, 8, 10, 11, 12, and 15) 5 0 points. The sum
of these scores is averaged leading to the order index. A
higher score is given if the first stage of the drawing
involves the global features rather than the detail. The
intraclass correlation coefficient for the order index was
.93. (ii) Style Index (mean range 0–2): six specific ele-
ments are scored according the ‘‘degree of continuity’’ of
the drawing process: 2 points given where lines are
drawn in a continuous stroke or drawn consecutively, 1
point where the element was partially fragmented or
drawn separately, and 0 points where the line was clearly
disjointed or drawn in a fragmented manner. The sum of
these scores is averaged, leading to the style index. A
higher score indicates more continuity in the drawing
style. The intraclass correlation coefficient for the style
index was .94 in this study with an average Kappa coeffi-
cient of .89 (ranging from .84 to .96).
(3) Coherence Index (CI 5 0–2) was obtained by add-
ing the proportion of the total possible scores in order
(score/3.3) and style indices (score/2). A higher score in
the coherence index means a more coherent drawing
style, e.g. drawing of global elements initially and a con-
tinuous (versus fragmented) drawing style for the main
elements of the figure. The intraclass correlation coeffi-
cient for central coherence index was .97.
The Embedded Figures Test—form B (EFT).24 This
perceptual test measures the time taken to find 12 simple
shapes embedded in complex, colored designs. In this
study, the memory element of the task was omitted by
displaying the simple shape and the complex design
simultaneously. Participants are given a period of 60 s to
find each simple shape. Timing is stopped while the par-
ticipant demonstrates the position of the figure. If the
participant is wrong a ‘‘false claim’’ is noted, the partici-
pant is asked to keep looking and timing is resumed up
to 60 s. After 60 s the item is reported as an ‘‘error’’ and
given the maximum score. The score for each item ranges
from 0 to 60. The total score is the median of the 12 item
scores. A shorter time and fewer errors suggest stronger
local processing as participants need to ignore the back-
ground (context) and focus just on the detail of the
shape. Reliability in populations over 16 years old ranges
from .61 and .90.24
The Sentence Completion Task (SCT) (modified fromHappe et al., 200116). This verbal test consists of 25
sentences, 18 constructed to provoke conflict between
local and global processing and 7 without that tension.
This version was modified in consultation with Happe
and co-workers. Four of the 15 original items that were
found to be insensitive in trials with ASD were removed
and 14 new items were added. New items were selected
after a pilot study that demonstrated they were valid for
the purpose of the task.
In this task, the participant is asked to ‘‘finish off’’ the
ending of a pre-recorded sentence, presented on a tape-
recorder. 18 of the sentences end with a word which is of-
ten paired with another, such as ‘‘up and. . .(down)’’. This
common pairing is a ‘‘local’’ association and in the con-
text of the whole sentence it is incorrect. For example,
‘‘In the morning the sun went up and. . .’’ the local associ-
ation ‘‘down’’ is nonsensical whereas ‘‘shone all day’’ is
an ending that is correct in the overall global context.
The verbal response and the time taken to produce it are
recorded. The scoring is as follows: local completions 5 2
points; answers given after a delay of 10 s, ‘‘odd’’ answers
but not clear local completions, or no answer 5 1 point;
meaningful completions given within 10 s 5 0 points.
Higher scores reflect a preference for local processing or
difficulties in global processing.15 The maximum time
FIGURE 1. Rey-Osterrrieth Complex Figure.
CENTRAL COHERENCE IN ANOREXIA
International Journal of Eating Disorders 41:2 143–152 2008—DOI 10.1002/eat 145

allowed for each completion is 20 s and scoring is based
on participants’ first response.
The Homograph Reading Task (HRT).25,26 This
verbal task tests the ability to process a sentence as a
whole rather than on a local level. The participant is
asked to read out a set of 16 sentences where the context
of the sentence determines how a homograph within it
should be pronounced. The position of the homograph
in the sentences varies (after or before the context) and
the level of usage of the word (rare or frequent) varies.
Thus there are four different conditions i.e. after or
before frequent usage and after or before rare usage. All
responses were recorded. One point was awarded for
each sentence read correctly based on participants’ ini-
tial pronunciation. The total score ranges from 0 to 16,
where higher scores indicate strong coherence.
IQ Levels and Comorbidity. The National Adult Reading
Test (NART)27 was used as an estimate of intellectual ability.
The level of comorbidity was assessed in terms of trait
measures of the common comorbid symptoms (anxiety,
depression, obsessive-compulsive symptoms) by the
Hospital Anxiety and Depression Inventory (HADS28) and
the Obsessive Compulsive Inventory-Revised (OCI-R29).
Procedure
Weight and height were measured on the day of test-
ing. All the neuropsychological measures were adminis-
tered in the same session in this order: RFCT (copy), SCT,
EFT, HRT, and RCFT (recall). Questionnaires were com-
pleted a week before or after the testing session. The
NART test was not obtained from the first 20 participants.
However, as they were recruited from the same sources
as the rest of the sample we do not expect IQ differences.
Three women from the AN group and one HC did not
return all or part of the questionnaires. Their data were
included in the analyses of the main outcomes measures.
Data analysis
Sample size power calculation was conducted using
NQuery 4.0 Advisor program30 based on a pilot study for
this project. It was found that a sample size of 42 partici-
pants in each group would have an 80% power to detect
significant differences between groups with a .05 two-
tailed significance level.
Independent sample t-tests were used for group com-
parisons and means (M) and standard deviations (SD) are
reported. For those measures without a normal distribu-
tion of the data (SCT, HRT, EFT, depression (HADS), and
OCI-R), nonparametric Mann-Whitney U tests were used
and medians (Mdn) and 25 and 75% quartiles (Q) reported.
Additionally, Kruskal-Wallis tests were performed on the
mean score for the four conditions of the HRT.
To explore the relationship between neuropsychologi-
cal, demographic, and clinical variables, Pearson’s corre-
lation coefficient (r) was used for normally distributed
data and Spearman’s rank (rs) correlation was used other-
wise. All correlation analyses were conducted separately
in each group and Cohen’s d was calculated to obtain the
effect size for each variable. For those variables with non-
normally distributed data, d was calculated by transform-
ing the effect-size correlation r 5 Zffiffiffi
Np (from Ref. 31) in d
using an effect size calculator.
We were also interested to measure the process in-
volved to RCFT. Sherman and colleagues (2006) argued
that the poor visual memory performance in AN could
be partly explained by an anomaly in OS. We first repli-
cated Sherman et al.’s study and second, tested an
adapted hypothesis which was to examine whether cen-
tral coherence indices (CI) could also explain poor vis-
ual memory. A series of regression analyses were used to
examine mediating/moderating effects of organiza-
tional strategy, order, style and coherence indices on
recall in the RCFT.32,33 Group was entered as an inde-
pendent dummy-coded variable, percentage of recall as
the dependent variable and CI as well as OS score as the
potential mediators.32 We present standardized beta
(st.b) for a comparison of the effects of independent var-
iables in regressions with a different measurement
range of observations. The assumptions of the linear
regression models were assessed by a visual inspection
of the residuals.34
As this was a novel study, two-tailed tests were used
throughout. The nominal significance level was chosen
to be 5%. Hochberg’s improved Bonferroni correction for
multiple testing was applied on the main outcome meas-
ures.35 All analyses were carried out using SPSS 13.0.
Results
Demographic and Clinical Characteristics
The results of demographic and clinical charac-teristics are shown in Table 1. People with AN havefewer years of education than HC group (U 5558.5, p 5 .01) despite having equivalent levels intheir estimated IQ (t 5 .4, p 5 .65). The AN grouphad had a prolonged illness (M 5 13.08 years, SD 511.2) with profound emaciation and high levels ofdepressive, anxiety and obsessive-compulsivesymptoms. The mean age of onset for the AN groupwas 15.7 years (SD 5 4.0).
Neuropsychological Function
The results of the neuropsychological tests areshown in Table 2.
Rey-Osterrieth Complex Figure Test. The AN grouphad lower scores on the RCFT drawing process var-
LOPEZ ET AL.
146 International Journal of Eating Disorders 41:2 143–152 2008—DOI 10.1002/eat
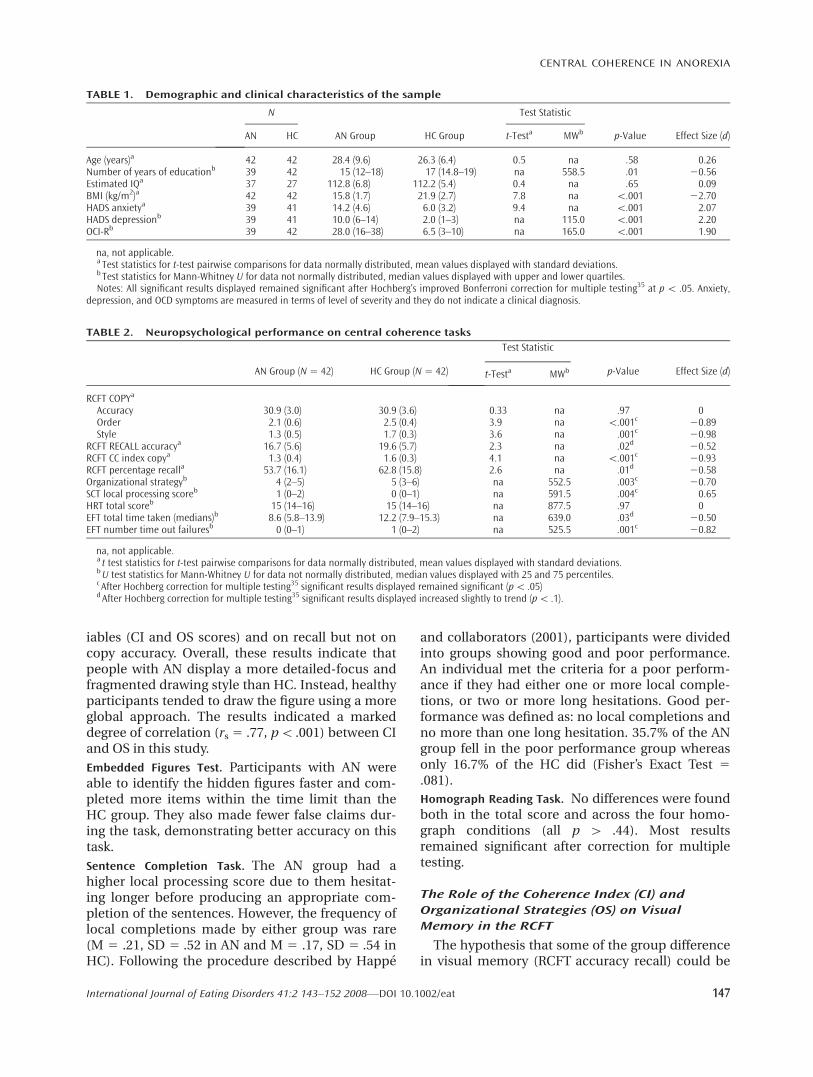
iables (CI and OS scores) and on recall but not oncopy accuracy. Overall, these results indicate thatpeople with AN display a more detailed-focus andfragmented drawing style than HC. Instead, healthyparticipants tended to draw the figure using a moreglobal approach. The results indicated a markeddegree of correlation (rs 5 .77, p\ .001) between CIand OS in this study.
Embedded Figures Test. Participants with AN wereable to identify the hidden figures faster and com-pleted more items within the time limit than theHC group. They also made fewer false claims dur-ing the task, demonstrating better accuracy on thistask.
Sentence Completion Task. The AN group had ahigher local processing score due to them hesitat-ing longer before producing an appropriate com-pletion of the sentences. However, the frequency oflocal completions made by either group was rare(M 5 .21, SD 5 .52 in AN and M 5 .17, SD 5 .54 inHC). Following the procedure described by Happe
and collaborators (2001), participants were dividedinto groups showing good and poor performance.An individual met the criteria for a poor perform-ance if they had either one or more local comple-tions, or two or more long hesitations. Good per-formance was defined as: no local completions andno more than one long hesitation. 35.7% of the ANgroup fell in the poor performance group whereasonly 16.7% of the HC did (Fisher’s Exact Test 5.081).
Homograph Reading Task. No differences were foundboth in the total score and across the four homo-graph conditions (all p [ .44). Most resultsremained significant after correction for multipletesting.
The Role of the Coherence Index (CI) and
Organizational Strategies (OS) on Visual
Memory in the RCFT
The hypothesis that some of the group differencein visual memory (RCFT accuracy recall) could be
TABLE 1. Demographic and clinical characteristics of the sample
N
AN Group HC Group
Test Statistic
p-Value Effect Size (d)AN HC t-Testa MWb
Age (years)a 42 42 28.4 (9.6) 26.3 (6.4) 0.5 na .58 0.26Number of years of educationb 39 42 15 (12–18) 17 (14.8–19) na 558.5 .01 20.56Estimated IQa 37 27 112.8 (6.8) 112.2 (5.4) 0.4 na .65 0.09BMI (kg/m2)a 42 42 15.8 (1.7) 21.9 (2.7) 7.8 na \.001 22.70HADS anxietya 39 41 14.2 (4.6) 6.0 (3.2) 9.4 na \.001 2.07HADS depressionb 39 41 10.0 (6–14) 2.0 (1–3) na 115.0 \.001 2.20OCI-Rb 39 42 28.0 (16–38) 6.5 (3–10) na 165.0 \.001 1.90
na, not applicable.a Test statistics for t-test pairwise comparisons for data normally distributed, mean values displayed with standard deviations.b Test statistics for Mann-Whitney U for data not normally distributed, median values displayed with upper and lower quartiles.Notes: All significant results displayed remained significant after Hochberg’s improved Bonferroni correction for multiple testing35 at p\ .05. Anxiety,
depression, and OCD symptoms are measured in terms of level of severity and they do not indicate a clinical diagnosis.
TABLE 2. Neuropsychological performance on central coherence tasks
AN Group (N5 42) HC Group (N5 42)
Test Statistic
p-Value Effect Size (d)t-Testa MWb
RCFT COPYa
Accuracy 30.9 (3.0) 30.9 (3.6) 0.33 na .97 0Order 2.1 (0.6) 2.5 (0.4) 3.9 na \.001c 20.89Style 1.3 (0.5) 1.7 (0.3) 3.6 na .001c 20.98
RCFT RECALL accuracya 16.7 (5.6) 19.6 (5.7) 2.3 na .02d 20.52RCFT CC index copya 1.3 (0.4) 1.6 (0.3) 4.1 na \.001c 20.93RCFT percentage recalla 53.7 (16.1) 62.8 (15.8) 2.6 na .01d 20.58Organizational strategyb 4 (2–5) 5 (3–6) na 552.5 .003c 20.70SCT local processing scoreb 1 (0–2) 0 (0–1) na 591.5 .004c 0.65HRT total scoreb 15 (14–16) 15 (14–16) na 877.5 .97 0EFT total time taken (medians)b 8.6 (5.8–13.9) 12.2 (7.9–15.3) na 639.0 .03d 20.50EFT number time out failuresb 0 (0–1) 1 (0–2) na 525.5 .001c 20.82
na, not applicable.a t test statistics for t-test pairwise comparisons for data normally distributed, mean values displayed with standard deviations.bU test statistics for Mann-Whitney U for data not normally distributed, median values displayed with 25 and 75 percentiles.c After Hochberg correction for multiple testing35 significant results displayed remained significant (p\ .05)dAfter Hochberg correction for multiple testing35 significant results displayed increased slightly to trend (p\ .1).
CENTRAL COHERENCE IN ANOREXIA
International Journal of Eating Disorders 41:2 143–152 2008—DOI 10.1002/eat 147

partly explained by the use of strategies poor in co-herence, was supported by regression analyses.
Simple regressions showed that the ‘‘group’’ vari-able accounted for the 7.8% of the overall variance(B 5 9.14, SE 5 3.5, st.b 5 .28, t 5 2.63, p 5 .01) inpercentage of RCFT recall.
We tested the hypothesis of mediation usingboth OS scores (mediation hypothesis 1) and CIindices (mediation hypothesis 2) as potential medi-ators.
Mediation Hypothesis 1: OS scores had a directeffect on recall (B 5 3.8, SE 5 1.02, st.b 5 .38, t 53.8, p \ .001, R2 5 .15). In the multiple regressionanalysis, OS maintained its effect on the percentageof recall (B 5 3.28, SE 5 1.06, st.b 5 .33, t 5 3.08, p5 .003) whereas the effect of group fell to non-sig-nificant levels (B 5 25.7, SE 5 3.5, st.b 5 2.17, t 521.6, p 5 .10). This model explained twice theamount of the variance in percentage of recall thanthe direct model (F(2,81) 5 8.57, p\ .001, R2 5 .18).The Sobel test showed that this mediating effectwas significant (t 5 22.16, p 5 .03). There were nointeractions between group effect and OS, that is,no moderator effects were found (F(5,84) 5 .79, p 5.56).
Mediation Hypothesis 2: The central coherenceindex (CI) also had a direct effect on recall (B 5 18,SE 5 4.74, st.b 5 .39, t 5 3.8, p\ .001, R2 5 .15). Inthe multiple regression analysis, CI maintained itseffect on the percentage of recall (B 5 15.24, SE 55.24, st.b 5 .33, t 5 2.9, p 5 .005) whereas the effect
of group fell to nonsignificant levels (B 5 4.5, SE 53.7, st.b 5 .14, t 5 1.2, p 5 .2). This model alsoexplained a bigger amount of the variance of per-centage of recall than the direct model (F(2,81) 58.0, p\ .001, R2 5 .17). The Sobel test showed thatthis mediating effect was significant (t 5 2.86, p 5.004) and no moderator effects were found (F(1,80)5 .975, p5 .3).
However, the order index was a better predictorthan CI and OS in mediating percentage of recall,explaining 23% of the variance (see Fig. 2). TheSobel test showed that the mediating effect of orderin the copy trial was significant (t 5 3.05, p 5 .002).Again, no moderator effects were found (F(1,80) 5.26, p 5 .6). The role of style index in a mediatingmodel did not reach significance (p 5 .15) neitherwas it a moderator (F(1,80) 5 1.8, p5 .2).
The Impact of Demographic and Clinical
Variables on Neuropsychological Performance
Correlation analyses between demographic, clin-ical and neuropsychological variables were per-formed separately for each group. Only significantresults in each group are described below.
In the AN group, age and illness duration corre-lated with EFT performance: older participantsmade more false claims (rs 5 .40, p\ .05) and tooklonger to complete the test (rs 5 .39, p\ .01) as didthose with a long duration of illness (rs 5 .38, p\.05). The number of false claims increased with agein the EFT (B 5 .027, SE 5 .10, st.b 5 .41, t 5 2.8, p\ .01) and there was a trend for an age effect ontime for EFT (B 5 .18, SE 5 .9, st.b 5 .29, t 5 1.90, p5 .065) in a regression analysis. No differences inperformance were found between subtypes of ANand between medicated and nonmedicatedpatients (all p values[ .09).
In the HC group, the number of years of educa-tion and IQ were negatively correlated to the timetaken in completing the EFT (rs 52.40, p\ .01 andrs 5 2.42, p \ .05, respectively). The number ofyears in education was also negatively correlatedwith false claims (rs 5 2.34, p\ .05). No age effectson neuropsychological results were found in theHC group (all p[ .9).
Interestingly, the level of starvation measured byBMI only correlated with the number of errors inthe initial pronunciation in HRT (rs 5 2.33, p \.05) in the AN group. No other significant correla-tions were found between BMI and all the otherneuropsychological variables in either AN or HCgroups.
FIGURE 2. Direct and mediational model to explaingroup effect on percentage of recall in RCFT. (a) Groupeffect on percentage of recall; (b) Order of constructionindex mediates the effect of the group on percentage ofrecall.
LOPEZ ET AL.
148 International Journal of Eating Disorders 41:2 143–152 2008—DOI 10.1002/eat

Influence of Comorbid Symptoms on
Neuropsychological Performance
Obsessive-compulsive traits as measured byscores on the OCI-R correlated negatively withboth of the recall parameters: percentage of recall(rs 5 2.42, p 5 .009) and accuracy of RCFT (rs 52.41, p\ .05).
Neuropsychological performance did not corre-late with levels of anxiety and depression (all p [.28).
Conclusion
The objective of this study was to examine centralcoherence in people with AN. In general, our find-ings support the hypothesis that people with ANhave weak central coherence with strengths in localprocessing and a relative weakness in global proc-essing, particularly in the visuospatial domain. Spe-cifically, we found that people with AN show higherspeed and accuracy in the EFT, suggestive of supe-rior detail-focused processing. The poor recall inthe RCFT is accounted for by their use of detail-focused rather than global strategies to constructthe figure. This profile is similar to the cognitiveprocessing style shown by people with high func-tioning autism9 and Aspergers.36 In tasks tappingverbal coherence, people with AN hesitate more inthe SCT, suggestive of difficulties in global process-ing, but there were no differences either in thenumber of local completions or in the scores onthe homograph reading task. In terms of comorbidsymptomatology, obsessive-compulsive traits wereassociated with some indices of weak central co-herence, especially in RCFT recall. Thus, peoplewith higher levels of obsessive symptoms displayedweaker central coherence. However, there was noassociation between neuropsychological perform-ance and depression or anxiety. BMI was weaklynegatively correlated with the error score in theHRT but there were no correlations between thedegree of starvation and performance in the othertasks, suggesting that weak central coherencemight be a trait independent of the BMI.
Other versions of the tasks employed in thisstudy have been previously used in AN. Our find-ings in the EFT corroborate those of Kemps andTokley12 who found superior local processing in theAN group. However, the previous literature is moreheterogeneous.37–39 Methodological differencessuch as whether or not memory is a component ofthe task may explain the variation. This is an areathat would merit more attention.
The RCFT has commonly been used in AN andmost research indicates that the accuracy of recallis poor.40–44 Sherman et al.45 examined the processas well as the outcome of this task. We have repli-cated their study and corroborated their results.Their measure of the process is conceptualized asan organizational strategy (OS) attributed to the ex-ecutive functioning (for details review Ref. 23)rather than central coherence. Poor organizationalstrategy might relate to impaired executive func-tions (planning and organization), whereas weakcentral coherence refers to a detailed-focus cogni-tive style (or local bias) not totally explained by ex-ecutive dysfunctions (see Happe and Frith, 2006).Our results are consistent both with the organiza-tional strategy account of Sherman et al. (2006) aswell as the central coherence account. Neuroimag-ing studies using both executive function and cen-tral coherence tasks may help to clarify this rela-tionship.
The mediational role of weak coherence in theRCFT has both research and clinical implications.For example, it could help to explain inconsistentresults from memory tasks in AN46 and perhapssome of their compulsive checking behaviors. Sav-age and collaborators noted that their findings inAN, without comorbid OCD, replicated those theyhad obtained in people with obsessive compulsivespectrum disorders.23,47,48 Interestingly a recentworking party set up to consider diagnostic issuesfor the DSM V relating to OCD have proposed thatboth EDs and autistic spectrum disorders could beencompassed within a broad obsessive compulsivespectrum umbrella.49 In relation to this, it is note-worthy that we found OCI-R scores were related torecall accuracy in the RCFT.
This is the first time that the verbal coherencetasks used in this study (HRT and SCT) have beenadministered to people with AN to our knowledge.People with ASD make more errors on context-appropriate pronunciation when reading thehomographs25,26 and people with high functioningASD have been found to produce more local com-pletions than matched healthy controls in theSCT.15 In our study, there were no major group dif-ferences on this task; however, the longer hesita-tions are similar to what was found in parents,especially fathers, of children with ASD.16
Several theories have been advanced to explainweak central coherence. One theory is that weakcentral coherence is associated with atypical func-tion in specific regions in the brain.9 For example,anomalies in the right hemisphere might impairglobal processing.50,51 Weak visual coherence hasbeen associated with impairments in the magno-
CENTRAL COHERENCE IN ANOREXIA
International Journal of Eating Disorders 41:2 143–152 2008—DOI 10.1002/eat 149

cellular visual pathway52,53 and with anomalies inthe neural mechanisms needed to integrate localmotion information in the dorsal visual pathway. Asecond theory is that weak central coherence iscaused by under-connectivity or a lack of neuralsynchronization.54–56
A pilot neuroimaging study using the EFT foundthat people with autism and healthy controlsshared some but not all patterns of activation.57
People with autism showed more activation in theright ventral occipitotemporal area, whereashealthy controls displayed increased activation inthe right dorsolateral prefrontal and parietalregions. This suggests the employment of differentstrategies to solve the task; people with autismmight use mental imagery and healthy controls usehigher order visual perception and working mem-ory. Moreover, abnormal patterns of activation dur-ing the EFT were also found in parents of peoplewith autism. It will be of interest to examine brainactivation in people with AN while completing thisand other tasks involved in central coherence.
This study has some limitations. First, it is diffi-cult to find neuropsychological tasks that measureonly one conceptual dimension such as central co-herence. For example, even though longer hesita-tions in the SCT might represent a difficulty inglobal processing time they might also be causedby a fear of mistakes or difficulties in set-shifting.
Unfortunately, the verbal coherence tasks used inthis study were insensitive to variation in this highIQ, well educated population (the majority of bothAN and HC populations scored at the extreme endof the scale with little deviation) and ceiling/flooreffects were observed. Thus, the possibility of weakcentral coherence in the verbal domain remainsunproved. There is a need to look for more sensitiveverbal tasks. A suitable alternative task might bethe California Verbal Learning Test which Savageand collaborators have used to investigate verbalorganizational strategies in obsessive-compulsivepopulations with interesting results.47,58 In futurestudies it would be interesting to have a test bat-tery, which taps into these different dimensionsand which has been field tested in a group with anequivalent mean IQ to the AN group.
Finally, this clinical sample had a severe, chronicAN and the results may not generalize to other EDpopulations (e.g. less severe AN or bulimia nerv-osa).
In conclusion, these results suggest that peoplewith AN have weak central coherence with a biastowards local rather than global processing, partic-ularly in the visuospatial domain. This profile
appears to be particularly associated with obses-sive-compulsive symptoms. Obsessive-compulsivetraits have an impact on the prognosis of AN andmay be both moderating and mediating factors intreatment.59
Treasure60 argues that new treatments for ANshould be tailored to specifically address predis-posing or maintaining factors of the illness such asanomalies in information processing. It is possiblethat specific treatment modules to correct informa-tional processing bias, such as weak central coher-ence, may improve the outcome of AN by affectingthe compulsive traits of the illness. We are currentlypiloting a module of cognitive remediation therapy(CRT61) in inpatient settings, addressing set-shift-ing difficulties and weak central coherence.62 Asimilar but less intensive module has also beendeveloped for outpatient settings. These modulesof treatment can be included as part of the stand-ard treatment for patients with AN. More researchis needed to explore the clinical implications ofthese findings.
Carolina Lopez is a PhD student funded by a Chileangovernment scholarship. We would like to thank AndreaHoness for her help in the pilot study and Laura Verneyin the review of the manuscript.
References
1. Jacobi C, Hayward C, de Zwaan M, Kraemer HC, Agras SW. Com-
ing to terms with risk factors for eating disorders: Application
of risk terminology and suggestions for a general taxonomy.
Psychol Bull 2004;130:19–65.
2. Tchanturia K, Morris R, Anderluh M, Collier D, Nikolaou V,
Treasure J. Set shifting in anorexia nervosa: An examination
before and after weight gain, in full recovery and relationship
to childhood and adult OCPD traits. J Psychiatr Res
2004;38:545–552.
3. Connan F, Campbell I, Katzman M, Lightman S, Treasure J. A
neurodevelopmental model for anorexia nervosa. Physiol
Behav 2003;79:13–24.
4. Treasure J, Southgate L, Tchanturia K, Lopez C, Collier D. Gene
environment and developmental issues in eating disorders.
Assoc Child Adolesc Mental Health 2006;25:51–62.
5. Gillberg C, Rastam M, Gillberg J. Anorexia nervosa: Physical
health and neurodevelopment at 16 and 21 years. Dev Med
Child Neurol 1994;36:567–575.
6. Gillberg I, Gillberg C, Rastam M, Johansson M. The cognitive
profile of anorexia nervosa: A comparative study including a
community-based sample. Compr Psychiatry 1996;37:23–30.
7. Rastam M, Gillberg C, Gillberg IC, Johansson M. Alexithymia in
anorexia nervosa: A controlled study using the 20-item Toronto
Alexithymia Scale. Acta Psychiatr Scand 1997;95:385–388.
8. Frith U. Autism: Explaining the Enigma. Oxford: Basil Blackwell,
1989.
9. Happe F, Frith U. The weak coherence account: Detail-focused
cognitive style in autism spectrum disorders. J Autism Dev Dis-
ord 2006;36:5–25.
LOPEZ ET AL.
150 International Journal of Eating Disorders 41:2 143–152 2008—DOI 10.1002/eat
10. Gillberg I, Rastam M, Wentz E, Gillberg C. Cognitive and execu-
tive functions in anorexia nervosa ten years after onset of eat-
ing disorder. J Clin Exp Neuropsychol 2007;29:170–178.
11. Frith U, Happe F. Autism: beyond ‘‘theory of mind’’. Cognition
1994;50:115–132.
12. Kemps E, Tokley M. Preoccupation with detail contributes to
poor abstraction in anorexia nervosa. J Clin Exp Neuropsychol
(in press).
13. Strupp BJ, Weingartner H, Kaye WH, Gwirstman H. Cognitive
processing in anorexia nervosa. A disturbance in automatic in-
formation processing. Neuropsychobiology 1986;15:89–94.
14. Sunday SR, Halmi KA, Einhorn AM. The Yale-Brown-Cornell Eat-
ing Disorder Scale: a new scale to assess eating disorder symp-
tomatology. Int J Eat Disord 1995;18:237–245.
15. Booth R. Local-Global Processing and Cognitive Style in Autism
Spectrum Disorders and Typical Development. London: King’s
College London, 2006.
16. Happe F, Briskman J, Frith U. Exploring the cognitive pheno-
type of autism: Weak ‘‘central coherence’’ in parents and sib-
lings of children with autism. I. Experimental tests. J Child Psy-
chol Psychiatry 2001;42:299–307.
17. Ronald A, Happe F, Bolton P, Butcher L, Price T, Wheelwright
MA, et al. Genetic heterogeneity between the three compo-
nents of the autism spectrum: A twin study. J Am Acad Child
Adolesc Psychiatry 2006;45:691–699.
18. Anderluh M, Tchanturia K, Rabe-Hesketh S, Treasure J. Child-
hood obsessive-compulsive personality traits in adult women
with eating disorders: Defining a broader eating disorder phe-
notype. Am J Psychiatry 2003;160:242–247.
19. Fairburn C, Beglin S. Assessment of eating disorders: Interview
or self-report questionnaire? Int J Eat Disord 1994;16:363–
370.
20. Osterrieth P. Test of copying a complex figure: Contribution to
the study of perception and memory. Archives de Psychologie
1944;30;206–356.
21. Spreen O, Strauss E. A Compendium of Neuropsychological
Tests: Administration, Norms and Commentary, 2nd ed. New
York: Oxford University Press, 1998.
22. Lezak M, Howieson D, Loring D. Neuropsychological Assess-
ment, 4th ed. New York: Oxford University Press, 2004.
23. Savage CR, Baer L, Keuthen N, Brown HD, Rauch SL, Jenike MA.
Organizational strategies mediate nonverbal memory impair-
ment in obsessive-compulsive disorder. Biol Psychiatry 1999;
45:905–916.
24. Witkin H, Oltman P, Raskin E, Karp S. A Manual for the Embed-
ded Figure Test. California: Consulting Psychologists Press,
1971.
25. Happe F. Central coherence and theory of mind in autism:
Reading homographs in context. Br J Dev Psychol 1997;15:1–
12.
26. Jolliffe T, Baron-Cohen S. A test of central coherence theory:
Linguistic processing in high-functioning adults with autism or
Asperger syndrome: Is local coherence impaired? Cognition
1999;22:149–185.
27. Nelson HE, Willison J. National Adult Reading Test (NART).
Windsor, UK: NFER-NELSON Publishing, 1991.
28. Zigmond A, Snaith R. The hospital anxiety and depression scale.
Acta Psychiatrica Scandinavica 1983;67:361–370.
29. Foa E, Huppert J, Langner R, Leiberg S, Kichic R, Hajcak G, et al.
The Obsessive-compulsive inventory: Development and valida-
tion of a short version. Psychol Assess 2002;14:485–
496.
30. Elashoff J. nQuery Advisor. In: 4.0. V, editor. Statistical Solutions
Ltd. Los Angeles, CA; 2000.
31. Rosenthal R. Meta-Analtytic Procedures for Social Research (Re-
vised). Newbury Park, CA: Sage, 1991.
32. Baron RM, Kenny DA. The moderator-mediator variable distinc-
tion in social psychological research: Conceptual, strategic and
statistical considerations. J Pers Soc Psychol 1986;51:1173–
1182.
33. Kenny DA, Kashy D, Bolger N. Data analysis in social psychol-
ogy. In: Gilbert S, Fiske S, Lindzey G, editors. The Handbook of
Social Psychology, 4th ed. Boston, MA: McGraw-Hill, 1998,
pp. 233–265.
34. Tabachnick BG, Fidell LS. Using Multivariate Statistics, 4th ed.
New York: Allyn & Bacon, 2001.
35. Hochberg Y. A sharper Bonferroni procedure for multiple test
of significance. Biometrika 1988;75:800–802.
36. Jolliffe T, Baron-Cohen S. Are people with autism and Asperger
syndrome faster than normal on the Embedded Figures Test?
J Am Acad Child Adolesc Psychiatry 1997;38:527–534.
37. Sours JA. The anorexia nervosa syndrome: Phenomenologic
and psychodinamic components. Clinical heterogeneity in four
cases. Psychiatr Q 1969;43:240–256.
38. Basseches HI, Karp SA. Field dependence in young anorectic
and obese women. Psychother Psychosom 1984;41:33–37.
39. McLaughlin EF, Karp SA, Herzog DB. Sense of ineffectiveness in
women with eating disorders: A clinical study of anorexia nerv-
osa and bulimia. Int J Eat Disord 1985;4:511–523.
40. Thompson S. Implications of neuropsychological test results of
women in a new phase of anorexia nervosa. Eur Eat Disord Rev
1993;1:152–165.
41. Jones B, Duncan C, Brouwers P, Mirsky A. Cognition in eating
disorders. J Clin Exp Neuropsychol 1991;13:711–728.
42. Mathias J, Kent P. Neuropsychological consequences of extreme
weight loss and dietary restriction in patients with anorexia
nervosa. J Clin Exp Neuropsychol 1998;20:548–564.
43. Kingston K, Szmukler G, Andrewes D, Tress B, Desmond P.
Neuropsychological and structural brain changes in anorexia
nervosa before and after refeeding. Psychol Med 1996;26:15–
28.
44. Murphy R, Nutzinger DO, Paul T, Leplow B. Dissociated condi-
tional-associative learning in anorexia nervosa. J Clin Exp Neu-
ropsychol 2002;24:176–186.
45. Sherman BJ, Savage CR, Eddy KT, Blais MA, Deckersbach T, Jack-
son SC, et al. Strategic memory in adults with anorexia nervosa:
Are there similarities to obsessive compulsive spectrum disor-
ders? Int J Eat Disord 2006;39:468–476.
46. Southgate L, Tchanturia K, Treasure J. Neuropsychological stud-
ies in eating disorders: A review. In: Swain PI, editor. Progress in
Eating Disorders. USA: Nova Science Publisher, 2005, pp 1–69.
47. Savage CR, Deckersbach T, Wilhelm S, Rauch SL, Baer L, Reid T,
et al. Strategic processing and episodic memory impairment in
obsessive-compulsive disorder. Neuropsychology 2000;14:141–
151.
48. Deckersbach T, Savage CR, Philips W, Wilhelm S, Buhlmann U,
Rauch SL, et al. Characteristics of memory dysfunction in body
dysmorphic disorder. J Int Neuropsychol Soc 2000;6:673–
681.
49. Hollander E, Kim S, Khanna S, Pallanti S. Obsessive-compulsive
disorder and obsessive-compulsive spectrum disorders: Diagnostic
and dimensional issues. CNS Spectr 2007;12(Suppl 3):5–13.
50. Fink GR, Halligan PW, Marshall JC, Frith CD, Frackowiak RS,
Dolan RJ. Neural mechanisms involved in the processing of
global and local aspects of hierarchically organized visual stim-
uli. Brain 1997;120(Pt 10):1779–1791.
51. Heinze HJ, Hinrichs H, Scholz M, Burchert W, Mangun GR. Neu-
ral mechanisms of global and local processing. A combined
PET and ERP study. J Cogn Neurosci 1998;10:485–498.
52. Spencer J, O’Brien J, Riggs K, Braddick O, Atkinson J, Wattam-
Bell J. Motion processing in autism: Evidence for a dorsal
stream deficiency. NeuroReport 2000;11:2765–2767.
CENTRAL COHERENCE IN ANOREXIA
International Journal of Eating Disorders 41:2 143–152 2008—DOI 10.1002/eat 151

53. Milne E, Swettenham J, Hansen P, Campbell R, Jeffries H,
Plaisted K. High motion coherence thresholds in children with
autism. J Child Psychol Psychiatry 2002;43:255–263.
54. Brock J, Brown CC, Boucher J, Rippon G. The temporal binding
deficit hypothesis of autism. Dev Psychopathol 2002;14:209–
224.
55. Frith CD. Is autism a disconnection disorder? Lancet Neurol
2004;3:577.
56. Just MA, Cherkassy VL, Keller TA, Minshew NJ. Cortical activa-
tion and synchronization during sentences comprehension in
high-functioning autism: Evidence for underconnectivity. Brain
2004;127(Pt 8):1811–1821.
57. Ring HA, Baron-Cohen S, Wheelwright S, Williams SCR,
Brammer M, Andrew C, et al. Cerebral correlates of pre-
served cognitive skills in autism: A functional MRI study of
Embedded Figures Task performance. Brain 1999;1222:1305–
1315.
58. Savage CR, Deckerbach T, Heckers S, Wagner AD, Schacter D,
Alpert NM, et al. Prefrontal regions supporting spontaneous
and directed application of verbal learning strategies. Evidence
from PET. Brain 2001;124:219–231.
59. Crane AM, Roberts ME, Treasure J. Are obsessive-compulsive
personality traits associated with a poor outcome in anorexia
nervosa? A systematic review of randomized controlled trials
and naturalistic outcome studies. Int J Eat Disord (in press).
60. Treasure J. Getting beneath the phenotype of anorexia nervosa:
The search for viable endophenotypes and genotypes. Can J
Psychiatry 2007;52:212–209.
61. Tchanturia K, Whitney J, Treasure J. Can cognitive exercises help
treat anorexia nervosa? J Eat Weight Disord 2006;11:e112–116.
62. Baldock E, Tchanturia K. Translating laboratory research into
clinical practice: foundations, functions and future of cognitive
remediation therapy for anorexia nervosa. Therapy 2007; 4:
285–292.
LOPEZ ET AL.
152 International Journal of Eating Disorders 41:2 143–152 2008—DOI 10.1002/eat
Copyright © 2022 FDOKUMEN




















