
Amphetamine Excretion Profile Following Multidose ...
12
Journal of Analytical Toxicology,Vol. 28, October 2004 Amphetamine Excretion Profile Following Multidose Administration of Mixed Salt Amphetamine Preparation* John T. Cody1,t, Sandra Valtier 2, and Stephen t. Nelson 3 1Academy of Health Sciences,MCCS-HMP PA Branch, FortSam Houston, Texas 78234-6138; 2Clinical Research Squadron, Wilford Hall Medical Center, Lackland AFB, Texas; and 3Department of Pediatrics, Wilford Hall Medical Center, Lackland AFB, Texas [ Abstract ] Interpretation of drug testing results requires detailed scientific information, particularly in those cases where the question of legitimate use versus illicit use arises. Amphetamine remains a widely abused drug throughout the world, although it is also used therapeutically for weight loss, narcolepsy, and attention-deficit disorder with hyperactivity (ADHD). Treatment of ADHD using stimulant drugs is much more common now than it was in even the recent past. Increasingly, older individuals are diagnosed and treated for ADHD, and treatment often continues into adulthood. Amphetamine is commonly used for the treatment of ADHD and is available by prescription as either the d-enantiomer or a mixture of enantiomers. Although used for many years, there are no data available to describe the excretion profile of amphetamine and its enantiomers following repeated use of the drug. As a result, medical review officers (MROs) and forensic toxicologists have no direct evidence to base their decisions on when it comes to evaluation of use of these drugs. The current study was designed to determine the concentration and enantiomer excretion profile following repeated daily administration of mixed enantiomers of amphetamine. Twenty milligrams of Adderall was administered daily to five healthy subjects with all subsequent ad lib urine samples collected for at least five days following administration of the five-dose regimen. Adderall is a 3:1 mixture of d- and I. enantiomers of amphetamine salts and represents the mixed enantiomer proportion of amphetamine available in the United States through pharmaceutical channels. Peak amphetamine concentrations ranged from 5739 to 19,172 ng/mL. Samples containing _> 500 ng/mL amphetamine (the administrative cutoff for a positive result by gas chromatography-mass spectrometry) were seen up to 60:15 (h:min) following administration of the last dose. Enantiomer analysis showed the d-enantiomer to be in excess of the I-enantiomer for as long as the drug was administered. After administration of the last dose of drug, the proportion of I-enantiomer increased over time. Not all samples that contained * This work was supported by the USAF SurgeonGeneral's Office (FWH20020056H). The voluntary fully informed consentof the subjects used in lhis researchwas obtained as required by AFI 40-403. The views expressed in this article are those of the authors and do not reflect the official policy of the Department of Defenseor other Departmentsof the U.S. Government * Author to whom correspondenceshould be addressed: JohnT. Cody, Ph.D,, AMEDD C&S, MCCS-HMP PA Branch, 315] Scott Road, Ft. Sam Houston, TX 78234-6138. >- 500 ng/mL total amphetamine were positive when tested by immunoassay because of the differing cross-reactivity of the enantiomers. This study provides the first description of the excretion of amphetamine following repeated administration of Adderall. The presence of the I-enantiomer separates this drug from other formulations composed of only the d-enantiomer (i.e., Dexedrine and much illicit amphetamine), thus readily differentiating them from Adderall use. Some illicit and medicinal amphetamine is, however, a mixture of amphetamine enantiomers. Because the enantiomers are metabolized at different rates, their proportion offers the opportunity to describe excretion versus time. Coupling this data with drug concentration makes it possible for forensic toxicologists and MROs to come to an informed decision regarding the involvement of this drug in a positive drug test result. Introduction Medical use of amphetamine has a long history. Currently approved clinical indications for the use of amphetamine in- clude narcolepsy, attention-deficit disorder with hyperactivity (ADHD), and as a short-term adjunct to a weight-reduction program. Because of tolerance and the significant potential for abuse, use of amphetamines as part of a weight-reduction pro- gram is limited in scope, and, when prescribed, the duration of treatment is generally limited to weeks rather than being a long-term treatment. The use of amphetamine for the treat- ment of narcolepsy and ADHD are long-standing uses and, unlike the weight-reduction regimen, are often prescribed on a chronic basis. The use of amphetamines for ADHD is common medical practice and can involve dextroamphetamine, dextromethamphetamine, or mixed isomer salts of am- phetamine (1). Amphetamines have a clearly recognized high abuse po- tential. Sources of the abused amphetamine include diver- sion of pharmaceutical amphetamine and illicit synthesis. The presence of a single asymmetric center gives rise to two possible enantiomers, most commonly referred to as d- and Reproduction (photocopying) of editorialcontent of thisjournalis prohibited withoutpublisher's permission. 563 Downloaded from https://academic.oup.com/jat/article/28/7/563/744513 by guest on 03 June 2022
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Amphetamine Excretion Profile Following Multidose ...

Journal of Analytical Toxicology, Vol. 28, October 2004
Amphetamine Excretion Profile Following Multidose Administration of Mixed Salt Amphetamine Preparation*
John T. Cody 1,t, Sandra Valtier 2, and Stephen t. Nelson 3 1Academy of Health Sciences, MCCS-HMP PA Branch, Fort Sam Houston, Texas 78234-6138; 2Clinical Research Squadron, Wilford Hall Medical Center, Lackland AFB, Texas; and 3Department of Pediatrics, Wilford Hall Medical Center, Lackland AFB, Texas
[ Abstract ] Interpretation of drug testing results requires detailed scientific information, particularly in those cases where the question of legitimate use versus illicit use arises. Amphetamine remains a widely abused drug throughout the world, although it is also used therapeutically for weight loss, narcolepsy, and attention-deficit disorder with hyperactivity (ADHD). Treatment of ADHD using stimulant drugs is much more common now than it was in even the recent past. Increasingly, older individuals are diagnosed and treated for ADHD, and treatment often continues into adulthood. Amphetamine is commonly used for the treatment of ADHD and is available by prescription as either the d-enantiomer or a mixture of enantiomers. Although used for many years, there are no data available to describe the excretion profile of amphetamine and its enantiomers following repeated use of the drug. As a result, medical review officers (MROs) and forensic toxicologists have no direct evidence to base their decisions on when it comes to evaluation of use of these drugs. The current study was designed to determine the concentration and enantiomer excretion profile following repeated daily administration of mixed enantiomers of amphetamine. Twenty milligrams of Adderall was administered daily to five healthy subjects with all subsequent ad lib urine samples collected for at least five days following administration of the five-dose regimen. Adderall is a 3:1 mixture of d- and I. enantiomers of amphetamine salts and represents the mixed enantiomer proportion of amphetamine available in the United States through pharmaceutical channels. Peak amphetamine concentrations ranged from 5739 to 19,172 ng/mL. Samples containing _> 500 ng/mL amphetamine (the administrative cutoff for a positive result by gas chromatography-mass spectrometry) were seen up to 60:15 (h:min) following administration of the last dose. Enantiomer analysis showed the d-enantiomer to be in excess of the I-enantiomer for as long as the drug was administered. After administration of the last dose of drug, the proportion of I-enantiomer increased over time. Not all samples that contained
* This work was supported by the USAF Surgeon General's Office (FWH20020056H). The voluntary fully informed consent of the subjects used in lhis research was obtained as required by AFI 40-403. The views expressed in this article are those of the authors and do not reflect the official policy of the Department of Defense or other Departments of the U.S. Government
* Author to whom correspondence should be addressed: John T. Cody, Ph.D,, AMEDD C&S, MCCS-HMP PA Branch, 315 ] Scott Road, Ft. Sam Houston, TX 78234-6138.
>- 500 ng/mL total amphetamine were positive when tested by immunoassay because of the differing cross-reactivity of the enantiomers. This study provides the first description of the excretion of amphetamine following repeated administration of Adderall. The presence of the I-enantiomer separates this drug from other formulations composed of only the d-enantiomer (i.e., Dexedrine and much illicit amphetamine), thus readily differentiating them from Adderall use. Some illicit and medicinal amphetamine is, however, a mixture of amphetamine enantiomers. Because the enantiomers are metabolized at different rates, their proportion offers the opportunity to describe excretion versus time. Coupling this data with drug concentration makes it possible for forensic toxicologists and MROs to come to an informed decision regarding the involvement of this drug in a positive drug test result.
Introduction
Medical use of amphetamine has a long history. Currently approved clinical indications for the use of amphetamine in- clude narcolepsy, attention-deficit disorder with hyperactivity (ADHD), and as a short-term adjunct to a weight-reduction program. Because of tolerance and the significant potential for abuse, use of amphetamines as part of a weight-reduction pro- gram is limited in scope, and, when prescribed, the duration of treatment is generally limited to weeks rather than being a long-term treatment. The use of amphetamine for the treat- ment of narcolepsy and ADHD are long-standing uses and, unlike the weight-reduction regimen, are often prescribed on a chronic basis. The use of amphetamines for ADHD is common medical practice and can involve dextroamphetamine, dextromethamphetamine, or mixed isomer salts of am- phetamine (1).
Amphetamines have a clearly recognized high abuse po- tential. Sources of the abused amphetamine include diver- sion of pharmaceutical amphetamine and illicit synthesis. The presence of a single asymmetric center gives rise to two possible enantiomers, most commonly referred to as d- and
Reproduction (photocopying) of editorial content of this journal is prohibited without publisher's permission. 563
Dow
nloaded from https://academ
ic.oup.com/jat/article/28/7/563/744513 by guest on 03 June 2022

l- IS(+) and R(-) are also used to describe these enantiomers, respectively].
Many studies investigating the metabolism and factors that influence metabolism and excretion of amphetamines were completed in the 1960s and 1970s (2-16). Several studies ex- amined the effect of pH by administering agents to maintain acid or alkaline urine, which can be contrasted to uncontrolled conditions (6,8,12,14,15). Results of these studies demonstrated that little of the drug is reabsorbed from the filtrate under acid conditions and was, therefore, excreted more rapidly. The op- posite result was observed under alkaline conditions, in which more of the drug was reabsorbed. This results in lower con- centrations of the drug in the urine and increased metabolism of the drug. One report showed averages of 54.5% of a 10-15- mg dose of amphetamine was excreted intact in 16 h under acid conditions, but only an average of 2.9% was excreted intact when the urine was maintained at an alkaline pH (15).
Differences in the metabolism of amphetamine enantiomers have been investigated by a number of investigators (8,12,14,16). These studies were constrained by a number of factors that limit their use in interpretation of individual sam- ples, as described in the present study. Despite these limita- tions, these studies demonstrated the d-enantiomer is metab- olized more rapidly than the l-, causing the proportion of /-amphetamine to increase in the urine over time following the administration of racemic amphetamine.
The purpose of the present study is to examine the excretion profile of amphetamine following daily administration of the drug Adderall. Adderall is a single-entity (amphetamine) product composed of d-amphetamine saccharate, d,l-am- phetamine aspartate, d-amphetamine sulfate, and d,l-am- phetamine sulfate. The drug is available in 5-, 7.5-, 10-, 12.5-, 15-, 20-, and 30-rag tablets, as well as extended-release cap- sules. Adderall is designed to provide slow onset and offset, thus minimizing potential undesirable effects and the potential for abuse. It also often provides effective control of ADHD with a single daily dose, eliminating the necessity of dosing during the school or work day, making it a popular option of the drugs available to treat this condition. The target dosage of Adderall, as with most stimulant drugs, is the lowest effective dose. Ini- tial recommended dosing for adults is typically 10 rag, fol- lowed by monitoring for effect and escalating the dose if nec- essary to get the desired effect. Typical adult ADHD patients are treated twice a day with 20 mg of the drug.
Materials and Methods
Materials Amphetamine, methamphetamine, amphetamine-d6 (1-
phenyl-2-aminopropane- l,l,2,3,3,3-d6), methamphetamine- dn (1-phenyl-@2-methyl-d3-aminopropane-3,3,3-d3), d-am- phetamine, d-methamphetamine, /-amphetamine, d-methamphetamine, d,l-amphetamine-d5 (1-phenyl-2-amino- propane- l,2,3,3-ds), and d,l-methamphetamine-d5 (1-phenyl- 2-methyl-d3-aminopropane-l,2-d2) were obtained from Ceril- liant (Austin, TX). Heptafluorobutyric anhydride (HFBA) was
564
Journal of Analytical Toxicology, Vol. 28, October 2004
obtained from Sigma Chemical Company (St. Louis, MO). The N-trifluoroacetyl4-prolyl-chloride (I-TPC) used for enan- tiomer analysis was obtained from Aldrich Chemical Com- pany (Milwaukee, WI) and Regis Technologies, Inc. (Morton Grove, IL). Immunoassay reagents were obtained from Roche Diagnostics Corporation (Indianapolis, IN). Adderall (Shire Richwood, Florence, KY), administered to experimental sub- jects, was obtained through the Wilford Hall Medical Center (Lackland AFB, TX) pharmacy.
Drug administration and sample collection Twenty-milligram doses of Adderall (equivalent to approxi-
mately 9.6 and 3.1 mg of d- and l-amphetamine base, respec- tively, per dose) in the form of a single tablet was administered to five healthy male volunteers on each of five consecutive days. Subjects ranged in age from the early 30's to 50's and had no history of drug abuse. The initial dose was administered in the morning. Subjects were instructed to administer subse- quent doses at the same time on successive days. A pre-dose urine sample was collected from each subject to ensure no in- terfering substances were present. Urine samples were col- lected for each day of drug administration and the next five days. Samples were collected ad lib in order to best simulate what would be seen in random drug testing. Likewise, no at- tempt was made to physiologically control urine pH to best em- ulate the situation normally encountered in sample collection for random drug testing. Once collected, the samples were re- frigerated until analysis.
Sample preparation and analysis Sample pH was measured using a Fisher Accumet 50 pH
meter (Houston, TX) and specific gravity determined using an AO Scientific Instruments (Keene, NY) refractometer. Creati- nine levels were determined at the Wilford Hall Medical Center clinical laboratory using standard clinical laboratory proce- dures. Immunoassay analysis was accomplished using Roche Diagnostics Corporation On-Line reagents on an Olympus AU800 (Melville, NY) automated analyzer using standard pro- cedures. Gas chromatographic-mass spectrometric (GC-MS) analyses were performed using a Hewlett-Packard (Agilent, Palo Alto, CA) 6890 GC coupled with an IIP 5973 MS using a 7683 autoinjector.
Quantitative analysis. Two-milliliter aliquots were extracted, derivatized with heptafluorobutyric anhydride (HFBA), and analyzed by GC-MS, as previously described (17), with the ad- ditional option of using a ZB-50 (DB-17 equivalent) capillary column (15 m x 0.25-mm i.d., 0.25-1Jm film thickness) (Phe- nomenex, Torrance, CA), as well as the HP-1 column (12 m x 0.2-ram i.d., 0.33-1Jm film thickness). Instrumental conditions were as follows: splitless injection with injection port and in- terface temperatures at 270~ Conditions for the HP-1 con- sisted of a temperature program with an initial time of 1 rain at 80~ programmed to 180~ at 20~ a with a 2-rain final time. Conditions for the ZB-50 column consisted of a temperature program with an initial time of 2 rain at 80~ programmed to 125~ at 20~ then programmed to 150~ at 25~ with a final time of 0. Quantitation was based on single-point calibration using a calibration standard
Dow
nloaded from https://academ
ic.oup.com/jat/article/28/7/563/744513 by guest on 03 June 2022

Journal of Analytical Toxicology, Vol. 28, October 2004
containing 500 ng/mL amphetamine and methamphetamine with 500 ng/mL deuterium-labeled isotopomer internal stan- dards. Low concentration samples were quantitated based on single-point calibration using a standard at 25 ng/mL am- phetamine and methamphetamine and with 50 ng/mL of each internal standard. Detection limits for this assay were 5 ng/mL for amphetamine and methamphetamine. The assay is linear to 10,000 ng/mL for amphetamine and methamphetamine, with a limit of quantitation (LOQ) of 5 ng/mL for both amphetamine and methamphetamine. Ions monitored were m/z 240, 118, 91 for amphetamine; m/z 254, 210, 118 for methamphetamine; m/z 244, 123 for amphetamine-d6; and m/z 260, 213 for methamphetamine-dll. Acceptance criteria were quantitative values within + 20% of the target concentration with proper qualitative identification as determined by ion ratios within + 20% and retention time within • 2% of the calibration stan- dard while exhibiting acceptable chromatography.
Enantiomer analysis. Two-milliliter urine samples con- taining 500 ng/mL each of amphetamine-d5 and metham- phetamine-ds were extracted and derivatized with I-TPC, as previously described (18). Instrumental conditions were as fol- lows: splitless injection, with injection port and interface tem- peratures set at 270~ Conditions for the HP-1 column (12 m x 0.2-mm i.d., 0.33-1Jm film thickness) consisted of a temper- ature program with initial temperature at 130~ programmed to 170~ at 4~ then to 240~ at 35~ with a final time of 0. Given that Adderall is amphetamine only, the run time for sample analysis was modified after elution of am- phetamine to decrease overall run time. Ions monitored were m/z 237, 241, 251,255 for d- and/-amphetamine, d,l -am- phetamine-ds; d- and l-methamphetamine and d,l-metham- phetamine-ds, respectively. This assay was developed to provide qualitative determination of the enantiomeric composition of amphetamine, methamphetamine, and related analogues. Each batch of samples was calibrated using a sample containing 50% of both enantiomers of amphetamine and metham- phetamine and analyzed with control samples containing 0% l-enantiomer plus 100% d-enantiomer of amphetamine and methamphetamine and 100% l-enantiomer plus 0% d-enan- tiomer of amphetamine and methamphetamine, along with a control containing no amphetamine or methamphetamine. Acceptance criteria were enantiomer ratios of the deuterated internal standards for all control and unknown samples within • 20% of calibrator, drug enantiomer ratios of controls within + 20% of target percentages, and negative control (0 ng/mL) showed no detectable amphetamine or methamphetamine, with acceptable chromatography and retention times within + 2% of calibrator.
Results and Discussion
Samples collected from subjects in this study (Table I) showed peak levels ranging from 5739 to 19,172 ng/mL. The first sample provided by each subject contained am- phetamine at concentrations over 500 ng/mL (the adminis- trative cutoff for a positive result by GC-MS). This is con-
sistent with the results of a previous study using a single dose of this drug (19). Samples containing ___ 500 ng/mL am- phetamine were seen up to 60:15 (h:min) following admin- istration of the last dose of the drug. Peak concentrations were reached anywhere from 6:45 to 108:00 h after the ad- ministration of the first dose. During the time, subjects were administered drug on a daily basis, nearly all individual sam- ples were positive for amphetamine. These results suggest that individuals on a routine regimen of this drug will very likely test positive for amphetamine. However, not all sam- ples that contained _ 500 ng/mL of amphetamine were positive by immunoassay. This is consistent, given the cross- reactivity of the immunoassay reagents to racemic am- phetamine (62%) and the l-enantiomer (5%) compared to 100% for d-amphetamine (20). Amphetamine could be de- tected [limit of detection (LOD) = 5 ng/mL] in at least one subject, up to approximately 167 h following the last dose, which is comparable to the detection time following a single dose of the drug (19).
Results of a study involving a single 20-mg dose showed peak levels ranging from 2645 to 5948 ng/mL. Peak concen- trations were reached from 5:25 to 22:00 h following adminis- tration of the drug (19). As seen in the current study, the first sample provided by each subject contained amphetamine at concentrations over 500 ng/mL.
As expected, the urine concentration of amphetamine was greatly effected by urine pH. Amphetamine concentrations also varied because of dilution of the urine as reflected by creatinine and specific gravity concentrations. The effects of pH change and creatinine concentration on the concentration of amphetamine are revealed by review of Table I, confirming the difficulty of assessing dose or time since dose based on concentration. Contrasting the extensive variability seen in drug concentrations, the enantiomer proportions were much more consistent and predictable despite changes in specific gravity, creatinine, and pH. The 3:1 ratio of d- to/-am- phetamine in the tablet is reflected in the proportion of enan- tiomers found in the first urine samples collected following administration of the drug that showed 23.47 + 1.42%/-am- phetamine. Following the first sample, the proportion of/-am- phetamine increased with time until administration, and sub- sequent absorption, of the second dose, which resulted in a decrease in proportion of l-enantiomer. This change in pro- portion was repeated with each subsequent administration of the drug until after the last dose, when the proportion of l- enantiomer continued to increase over time. This pattern of enantiomer proportions reflects the metabolism of the drug rather than its rate of excretion (influenced by pH) or volume of urine excretion (reflected by creatinine and specific gravity). These results are consistent with previous studies that show enantiomer ratios are not influenced by pH changes (6) and further supported by another study that evaluated pH, creati- nine, and specific gravity effects (19).
Amphetamine from pharmaceutical sources in the U.S. is either only d-amphetamine or a mixture of d- and/-am- phetamine (1,21) and is not available as/-amphetamine alone. Currently available mixed enantiomer amphetamines in the U.S. are manufactured in the ratio of 3:1 d- to l-enantiomer.
565
Dow
nloaded from https://academ
ic.oup.com/jat/article/28/7/563/744513 by guest on 03 June 2022
Journal of Analytical Toxicology, Vol. 28, October 2004
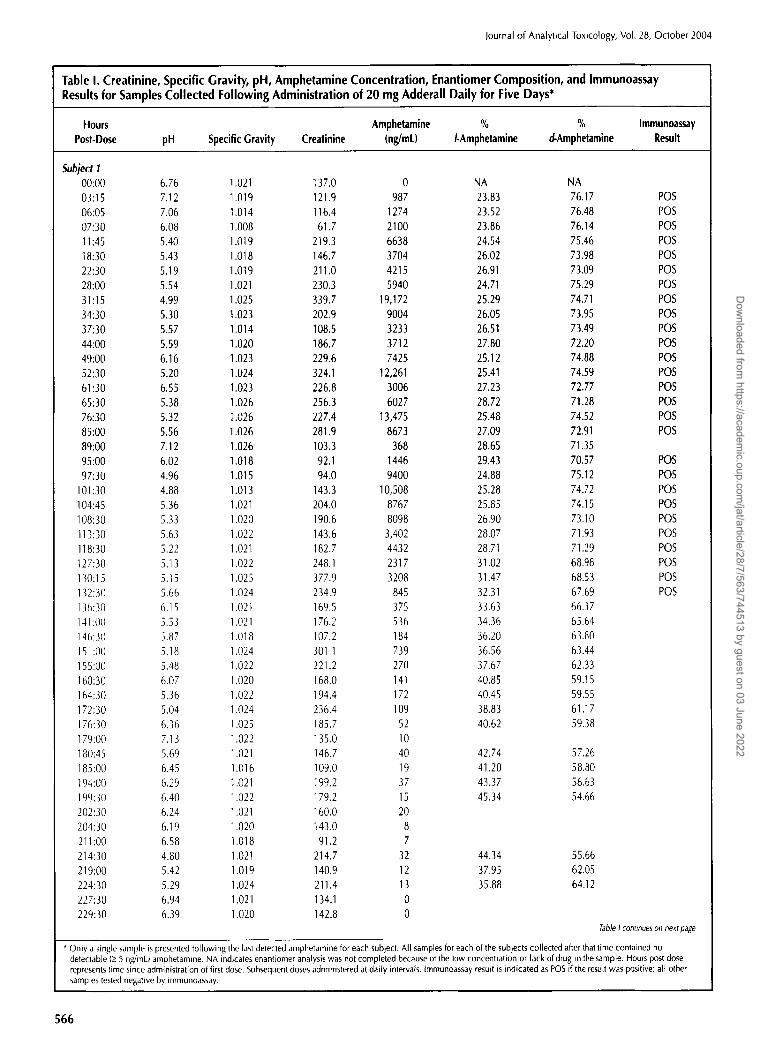
Table I. Creatinine, Specific Gravity, pH, Amphetamine Concentration, Enantiomer Composition, and Immunoassay Results for Samples Collected Following Administration of 20 mg Adderall Daily for Five Days*
Hours Amphetamine % % Immunoassay Post-Dose pH Specific Gravity Creatinine (ng/mL) /-Amphetamine d-Amphetamine Result
Subject I 00:00 6.76 1.021 ] 37.0 0 NA NA 03:15 7.12 1.019 121.9 987 23.83 76.17 06:05 7.06 1.014 116.4 1274 23.52 76.48 07:30 6.08 1.008 61.7 2100 23.86 76.t4 11:45 5.40 1.019 219.3 6638 24.54 75.46 18:30 5.43 1.018 146.7 3704 26.02 73.98 22:30 5.19 1.019 211.0 4215 26.91 73.09 28:00 5.54 1.021 230.3 5940 24.71 75.29 31:15 4.99 1.025 339.7 19,172 25.29 74.71 34:30 5.30 1.023 202.9 9004 26.05 73.95 37:30 5.57 1.014 108.5 3233 26.51 73.49 44:00 5.59 1.020 186.7 3712 27.80 72.20 49:00 6.16 1.023 229.6 7425 25.12 74.88 52:30 5.20 1.024 324.1 12,261 25.41 74.59 61:30 6.55 1.023 226.8 3006 27.23 72.77 65:30 5.38 1.026 256.3 6027 28.72 71.28 76:30 5.32 1.026 227.4 13,475 25.48 74.52 85:00 5.56 1.026 281.9 8673 27.09 72.91 89:00 7.12 1.026 103.3 368 28.65 71.35 95:00 6.02 1.018 92.1 1446 29.43 70.57 97:30 4.96 1.015 94.0 9400 24.88 75.12
101:30 4.88 1.013 143.3 10,508 25.28 74.72 104:45 5.36 1.021 204.0 8767 25.85 74.15 108:30 5.33 1.020 190.6 8098 26.90 73.10 113:30 5.63 1.022 143.6 3,402 28.07 71.93 118:30 5.22 1.021 182.7 4432 28.71 71.29 ] 27:30 5.13 1.022 248.1 2317 31.02 68.98 130:15 5.15 1.025 377.9 3208 31.47 68.53 132:30 5.66 1.024 234.9 845 32.31 67.69 136:30 6.15 1 .(12 t 169.5 375 33.63 66.37 141:00 5.53 1.021 176.2 536 34.36 65.64 146:30 5.87 1.018 107.2 184 36.20 63.80 151:00 5.18 1.024 301.1 739 36.56 63.44 155:00 5.48 1.022 221.2 270 37.67 62.33 160:30 6.07 1.020 168.0 141 40.85 59.15 164:30 5.36 1.022 194.4 172 40.45 59.55 172:30 5.04 1.024 236.4 109 38.83 61.17 176:30 6.36 1.025 185.7 52 40.62 59.38 179:00 7.13 1.022 135.0 10 180:45 5.69 1.021 146.7 40 42.74 57.26 185:00 6.45 1.016 109.0 19 41.20 58.80 194:00 6.29 1.021 199.2 37 43.37 56.63 199:3(/ 6.40 1.022 179.2 15 45.34 54.66 202:30 6.24 1.021 160.0 20 204:30 6.19 1.020 143.0 8 211:00 6.58 1.018 91.2 7 214:30 4.80 1.021 214.7 32 44.34 55.66 219:00 5.42 1.019 140.9 12 37.95 62.05 224:30 5.29 1.024 211.4 13 35.88 64.12 227:30 6.94 1.021 134.1 0 229:30 6.39 1.020 142.8 0
POS POS POS POS POS POS POS POS POS POS POS POS POS POS POS POS POS
POS POS POS POS POS POS POS POS POS POS
Table I continues on next page
* Only a single sample is presented following the last detected amphetamine for each subject. All samples for each of the subjects collected after that time contained no detectable (_> 5 ng/mL) amphetamine. NA indicates enantiomer analysis was not completed because of the low concentration or lack of drug in the sample. Hours post dose represents time since administration of first dose. Subsequent doses administered at daily intervals. Immunoassay resu[t is indicated as POS if the result was positive; all other samples tested negative by immunoassay.
566
Dow
nloaded from https://academ
ic.oup.com/jat/article/28/7/563/744513 by guest on 03 June 2022

Journal of Ahalytical Toxicology, Vol. 28, October 2004
Table I. Creatinine, Specific Gravity, pH, Amphetamine Concentration, Enantiomer Composition, and Immunoassay Results for Samples Collected Following Administration of 20 mg Adderall Daily for Five Days*
Hours Amphetamine % % Immunoassay Post-Dose pH Specific Gravity Creatinine (ng/mL) /-Amphetamine d-Amphetamine Result
233:30 5.58 1.021 139.2 6 238:30 5.21 1.021 136.4 6 243:00 5.71 1.022 198.7 7 249:00 5.66 1.025 237.1 8 252:30 5.30 1.028 241.3 9 258:00 5.54 1.021 151.1 0
Subject 2
00:00 5.49 1.028 250.2 0 NA NA 03:30 5.58 1.021 158.4 6003 25.50 74.50 POS 07:40 5.58 1,014 94.5 4219 23.35 76.65 POS 10:20 6.00 1.009 85.3 1669 25.63 74.37 POS 13:30 6.15 1.015 139.0 2152 25.70 74.30 POS 21:15 5.40 1.026 276.3 6318 26.35 73.65 POS 27:50 5.52 1.030 261.1 10,412 25.52 74.48 POS 32:50 5.46 1.026 203.6 7779 26.36 73.64 POS 34:40 5.35 1.019 220.0 7243 27.08 72.92 POS 37:30 5.76 1.023 180.4 3442 27.91 72.09 POS 45:00 5.42 1.024 200.8 4416 29.08 70.92 POS 51:00 5.38 1,025 176.5 8364 26.41 73.59 POS 54:30 5.75 1,012 82.1 3554 25.46 74.54 POS 56:00 5.87 1.006 45.4 1820 26.00 74.00 POS 59:30 5.28 1,015 142.5 5705 26.26 73.74 POS 61:25 5.44 1,020 175.1 4812 27.05 72.95 POS 69:00 5.33 1.021 200.7 5317 28.43 71.57 POS 73:00 5.70 1,018 145.8 5901 24.88 75.12 POS 76:15 5.72 1.015 106.0 4620 24.92 75.08 POS 79:45 7.07 1.014 99.2 1004 26.92 73.08 POS 81:50 6.76 1.015 109.1 1427 26.54 73.46 POS 85:30 6.68 1.018 129.9 1358 28.68 71.32 POS 87:30 5.82 1.007 54.7 1866 27.03 72.97 POS 95:00 5.60 1.018 178.0 3950 29.83 70.17 POS
101:15 5.20 1.017 186.0 8552 26.06 73.94 POS 107:00 5.40 1.023 224.5 7856 27.44 72.56 POS 108:10 5.54 1.027 293.3 11,226 28.05 71.95 POS 113:30 5.50 1.009 74.0 3192 27.87 72.13 POS 121:40 5.52 1.021 223.1 4142 29.72 70.28 POS 124:30 5.30 1.020 199.7 2505 32.31 67.69 POS 130:30 5.16 1.019 151.5 1895 33.68 66.32 POS 134:00 4.97 1.016 140.4 1589 33.36 66.64 POS 144:00 5.19 1.024 243.1 1373 37.76 62.24 POS 146:20 5.t 3 1.015 117.6 507 39.17 60.83 147:20 5.20 1.014 34.5 135 38.93 61.07 151:00 5.05 1.015 148.5 485 40.12 59.88 152:50 5.38 1.018 136.3 348 41.03 58.97 154:50 5.t9 1.016 126.6 304 4t.74 58.26 156:45 5.78 1,019 162.1 166 43.10 56.90 165:00 5.45 1.022 209.1 264 43.63 56.37 167:30 5.19 1,021 167.0 206 44.47 55.53 170:00 5,63 1.016 89.8 66 44,50 55.50 172:20 5.69 1.016 92.2 65 44.29 55.71 175:45 6.09 1.019 134.3 51 45,74 54.26
Table I continues on next page
�9 Only a single sample is presented following the last detected amphetamine for each subject. All samples for each of the subjects collected after that time contained no detectable (_> 5 ng!mL) amphetamine. NA indicates enantiomer analysis was not completed because of the low concentration or lack of drug in the sample. Hours post dose represents time since administration of first dose. Subsequent doses administered at daily intervals. Immunoassay result is indicated as POS if the result was positive; all other samples tested negative by immunoassay.
567
Dow
nloaded from https://academ
ic.oup.com/jat/article/28/7/563/744513 by guest on 03 June 2022

Journal of Analytical Toxicology, Vol. 28, October 2004
Table I. Creatinine, Specific Gravity, pH, Amphetamine Concentration, Enantiomer Composition, and Immunoassay Results for Samples Collected Following Administration of 20 mg Adderall Daily for Five Days*
Hours Amphetamine % % Jmmunoassay Post-Dose pH Specific Gravity Creatinine (ng/mL) /-Amphetamine d-Amphetamine Result
181:00 6.13 1.023 192.0 47 46.68 53.32 189:10 5.38 1.026 259.7 131 45.95 54.05 191:50 5.33 1.025 220,5 81 46.69 53.31 194:15 5.59 1.018 127.6 33 46.84 53.16 197:25 5.57 1.018 106.8 31 46.60 53.40 198:40 5.96 1.007 48.8 13 45.51 54.49 202:20 5.48 1.009 158.6 42 46.68 53.32 206:00 6.38 1.015 127.4 15 46.51 53.49 213:45 5.46 1.019 209.7 39 45.59 54.41 217:10 5.57 1.010 95.0 13 44.74 55.26 218:15 5.72 1.005 28.1 0 219:10 5.75 1.004 25.2 0 221:00 5.69 1.006 42.8 0 223:00 6.10 1.006 39.0 0 224:30 6.18 1.004 26,0 0 226:10 5.59 1.009 79.3 7 228:15 5.56 1.015 123.7 10 237:00 5.69 1.021 186.6 13 41.61 58.39 241:00 5.45 1.026 194.7 0 243:00 5.38 1.020 122.1 11 37.38 62.62 246:30 5.67 1.017 108,5 7 249:00 5.68 1.007 40.2 0 252:15 5.87 1.017 144.9 0 254:45 5.75 1.019 162.3 6 263:00 5.56 1.016 120.1 6 265:40 5.61 1,012 69.3 0
Subject 3 00:00 6.14 1.005 61,5 0 NA NA 01:00 6.65 1.003 31.2 930 21.55 78.45 POS 02:00 6.49 1.007 75.5 2290 23.33 76.67 POS 04:15 6.22 1.006 74.8 2636 23.94 76.06 POS 06:45 6.04 1.020 184.1 6692 26.13 73.87 POS 12:15 5.81 1.006 100.0 3536 26.40 73.60 POS 13:45 6.46 1.002 20.7 691 26.50 73.50 18:45 5.81 1.005 84.2 1702 28.02 71.98 POS 21:30 6.07 1.010 143.3 1488 29.40 70.60 POS 22:45 6.84 1.001 43.5 363 30.09 69.91 25:00 6.29 1.005 46.6 404 30.78 69.22 26:00 6.80 1.001 23.9 349 29.29 70.71 27:45 6.70 1.010 79.1 1197 25.30 74.70 POS 30:30 6.06 1.007 89.5 2347 25.25 74.75 POS 33:30 5.53 1.011 134.4 5312 26.66 73.34 POS 34:30 6.84 1.002 24.2 737 25.81 74.19 36:30 6.30 1.003 28.8 1234 26.62 73.38 POS 44:30 6.30 1.005 148.4 3128 28.94 71,06 POS 46:30 6.43 1.002 37.2 826 20.29 79.71 POS 50:45 6.65 1.002 85.4 2719 26.03 73.97 POS 52:30 6.33 1.001 32.1 2190 24.08 75.92 POS 54:30 6.08 1.002 59.2 2913 25.96 74.04 POS 55:45 6.80 1.003 54.1 1525 26.82 73.18 POS 67:15 6,16 1.004 153.7 4416 30.05 69.95 POS
Table I continues on next page
* Only a single sample is presented following the last detected amphetamine for each subject. All samples for each of the subjects collected after that time contained no detectable (> S ng/mL) amphetamine. NA indicates enantiomer analysis was not completed because of the low concentration or lack of drug in the sample. Hours post dose represents time since administration of first dose. Subsequent doses administered at daily intervals. Immunoassay result is indicated as POS if the result was positive; all other samples tested negative by immunoassay.
568
Dow
nloaded from https://academ
ic.oup.com/jat/article/28/7/563/744513 by guest on 03 June 2022

Journal of Analytical Toxicology, Vol. 28, October 2004
Table I. Creatinine, Specific Gravity, pH, Amphetamine Concentration, Enantiomer Composition, and Immunoassay Results for Samples Collected Following Administration of 20 mg Adderall Daily for Five Days*
Hours Amphetamine % % Immunoassay Post-Dose pH Specific Gravity Creatinine (ng/mL) /-Amphetamine d-Amphetamine Result
69:45 6.23 1.007 197.9 2442 31.12 68.88 POS 71:30 6.62 1.006 41.3 757 31.42 68.58 PO5 72:30 6.55 1.008 74.2 1182 34.40 65.60 POS 73:30 6.54 1.002 20,9 413 31.59 68.41 76:00 6.64 1.005 44.9 1070 28.32 71.68 POS 79:45 6,97 1,012 126.7 1075 26,96 73.04 POS 81:15 5.99 1.017 170,9 3338 27.70 72.30 POS 83:30 6.43 1.005 46.7 1560 27.55 72.45 POS 90:45 5.99 1.016 150.8 5873 30.13 69.87 POS 92:45 6.65 1.008 88.3 1929 29.95 70,05 POS 94:15 7,11 1.007 53.3 837 31.36 68.64 POS 96:30 6.52 1.005 35.2 898 30.86 69.14 POS 99:15 6.25 1.005 32.5 885 31.41 68.59 POS
100:15 6.70 1.003 20.7 1125 26.69 73.31 POS 102:00 6.46 1,004 34.9 1944 26.02 73,98 POS 105:45 7.01 1,007 56.9 1019 26,78 73.22 POS 109:00 6.29 1.005 45.1 2164 27.53 72.47 POS 118:30 6.89 1.015 146.6 1603 29.05 70.95 POS 121:00 6.61 1.022 250.8 3434 32.35 67,65 POS 123:00 6.58 ].006 47.5 1140 31,51 68.49 POS 124:15 6.34 1.004 27.0 909 31.35 68.65 POS 126:15 6.19 1.008 55.2 1162 33.42 66.58 POS 127:45 6.31 1.007 54.5 1150 33.59 66.41 POS 129:30 6.59 1.004 27.4 451 33,82 66.18 133:15 6.26 1.004 30,6 572 35.98 64,02 138:00 6.71 1.009 85.1 562 37.90 62.10 POS 140:00 7.08 1,005 41.4 258 38.48 61,52 141:15 7,18 1,003 17.5 128 38.01 61.99 142:00 7.27 1.002 13.9 66 37.10 62.90 145:15 7.04 1.005 35.0 185 39.02 60.98 149:15 6.42 1.014 126.5 439 42.03 57.97 POS 151:30 6,54 1.011 78.7 308 41,29 58.71 PO5 153:00 6.31 1.005 32.6 300 41.51 58.49 154:15 6.38 1.003 22.5 174 41.30 58.70 156:15 5.71 1.013 96.1 573 42.94 57.06 POS 158:30 5.86 1.008 63,2 381 40.31 59.69 164:15 6.64 1.008 78.6 224 43.75 56.25 167:30 6.90 1,013 ] 43.4 174 45.12 54,88 POS 170:00 6.40 1,006 56.8 116 46,13 53.87 171:45 6.04 1.005 42.3 116 46.54 53.46 174:00 6.67 1.004 34.5 48 47.39 52.61 176:30 6.55 1,008 62.2 58 47,81 52.19 178:30 6.95 1.005 38.8 25 48.20 51.80 187:30 5.92 1.0] 2 132.6 153 48.85 51.15 POS 189:30 6.40 1.003 41.8 46 48.86 51.14 190:15 6.88 1.003 26.6 21 48.00 52.00 191:30 6.66 1.002 22.4 20 49.00 51.00 192:30 6.85 1.002 20.7 18 48.38 51.62 194:30 6.44 1.004 35.5 25 48,99 51.01 197:00 6.77 1.005 40.7 18 49.10 50.90 200:00 6.65 1.005 47.2 16 49.02 50.98 201:00 6.56 1.002 20.0 16 48.61 51.39
Table I continues on next page
* Only a single sample is presented following the last detected amphetamine for each subject. All samples for each of the subjects collected after that time contained no detectable (_> 5 ng/mL) amphetamine. NA indicates enantiomer analysis was not completed because of the low concentration or lack of drug in the sample. Hours post dose represents time since administration of first dose. Subsequent doses administered at daily intervals. Immunoassay result is indicated as POS if the result was positive; all other samples tested negative by immunoassay.
569
Dow
nloaded from https://academ
ic.oup.com/jat/article/28/7/563/744513 by guest on 03 June 2022

Journal of Analytical Toxicology, Vol. 28, October 2004
Table I. Creatinine, Specific Gravity, pH, Amphetamine Concentration, Enantiomer Composition, and Immunoassay Results for Samples Collected Following Administration of 20 mg Adderall Daily for Five Days*
Hours Amphetamine % % Immunoassay Post-Dose pH Specific Gravity Creatinine (ng/mL) /-Amphetamine d-Amphetamine Result
202:15 6.33 1.003 27.2 17 48.54 51.46 212:00 5.61 1.010 142.1 49 49.28 50,72 216:00 6.95 1.016 192.2 21 49.48 50.52 217:00 6.52 1.006 49.4 13 47.49 52.51 219:15 6.57 1.005 43.3 11 46.71 53.29 221:30 7.19 1.005 26.9 0 223:30 6.56 1.007 52.9 13 47.37 52.63 225:30 6.58 1,008 65.0 12 49.25 50.75 229:15 6.46 1,004 30.7 8 45.91 54.09 234:30 5.80 1.010 95.0 22 45.96 54.04 237:00 6.82 1.010 83.2 13 45.04 54.96 238:45 7.48 1.009 55.2 0 240:00 6.71 1.005 28.8 0 242:00 6.17 1.007 57.6 10 44.42 55.58 243:00 7.05 1.003 18.4 0 244:00 7.38 1.007 54.3 0 246:00 7.11 1.011 79.1 0 247:45 6.49 1.009 131.9 12 44.78 55.22 250:15 6.62 1.012 98.8 10 43.37 56.63 255:45 5.59 1.007 65.4 15 39.34 60.66 259:30 5.49 1.010 88.3 17 39.45 60,55 262:00 6.08 1.009 88.8 9
Subject 4 00:00 5.25 1.012 80.1 0 NA NA 09:20 5.21 1,013 93.4 4949 23.23 76.77 POS 11:37 5,78 1.005 35.5 1783 25.25 74.75 POS 13:45 7.19 1.005 36.0 831 25.66 74.34 POS 15:30 7.81 1.003 24.0 269 26.43 73.57 22:50 6.11 1.009 93.7 1883 28.99 71.0l POS 25:00 6.24 1.005 58.2 1054 29.13 70.87 POS 29:50 6.51 1.006 58,9 2446 25.20 74.80 POS 34:00 5.63 1.008 84.7 3871 26.33 73.67 POS 36:30 5.71 1.006 63.4 3089 27.02 72.98 POS 38:00 7.65 1.004 31.1 729 27.66 72.34 POS 40:30 7.68 1.004 28.6 458 29.41 70.59 48:30 5.61 1.007 75.7 2257 30.84 69.16 POS 52:30 6.14 1.008 88.2 2885 25.44 74.56 POS 54:00 6.89 1.005 50.9 1939 26.26 73.74 POS 55:50 7,03 1.004 32.0 1405 2735 72.65 POS 63:20 5.64 ].011 144.6 4445 28.08 71.92 POS 65:45 5.71 1.007 77.3 2368 33.51 66.49 POS 69:00 5.68 1.003 36.5 1385 30.08 69.92 POS 72:40 5.45 1,006 69.4 2146 30.58 69.42 POS 76:10 6.20 1.005 62.3 2705 26.90 73.10 POS 84:00 5.62 1.012 173.1 5739 27.35 72.65 POS 87:00 7.25 1,009 78.5 1443 27.64 72.36 POS 90:40 7.44 1.009 67.0 976 29.68 70.32 POS 94:50 6.11 1.008 68.5 2446 30.67 69.33 POS 97:15 6.09 1.007 56.0 1681 31.28 68.72 POS 99:30 6.32 1,006 48.3 1590 27.56 72.44 POS
102:05 6,13 1,005 39.3 2733 26.08 73.92 POS
Table I continues on next page
* Only a single sample is presented following the last detected amphetamine for each subject. All samples for each of the subjects collected after that time contained no detectable (> 5 ng/mL) amphetamine, NA indicates enantiomer analysis was not completed because of the low concentration or lack of drug in the sample, Hours post dose represents time since administration of first dose. Subsequent doses administered at daily intervals. Immunoassay result is indicated as POS if the result was positive; all other samples tested negative by immunoassay,
570
Dow
nloaded from https://academ
ic.oup.com/jat/article/28/7/563/744513 by guest on 03 June 2022

Journal of Analytical Toxicology, Vol. 28, October 2004
Table I. Creatinine, Specific Gravity, pH, Amphetamine Concentration, Enantiomer Composition, and Immunoassay Results for Samples Collected Following Administration of 20 mg Adderall Daily for Five Days*
Hours Amphetamine % % Immunoassay Post-Dose pH Specific Gravity Creatinine (ngJmL) /-Amphetamine d-Amphetamine Result
104:30 5.73 1.006 52.0 3757 26.62 73.38 111:00 6.71 1.013 138.0 3972 27.94 72.06 113:10 7,23 1.010 83.4 1106 28.76 71.24 118:15 6.60 1.007 44.3 1099 30.26 69.74 121:00 5.93 1.006 44.5 1439 31.52 68.48 123:10 5.80 1.005 31.6 884 31.79 68.21 124:40 5.58 1.005 33.2 958 32.22 67.78 126:30 5.64 1.005 30.0 688 32.87 67.13 144:45 5,50 1,009 84.3 545 39.15 60.85 147:25 5.93 1.005 38.6 185 40.06 59.94 149:40 5.62 1.005 46.4 209 40.72 59.28 150:50 7.28 1.006 58.8 209 37.79 62.21 155:50 5.29 1.015 162.3 523 43.57 56.43 159:15 7.10 1.005 32.2 29 44.64 55.36 161:42 6.73 1.004 30.3 32 46.29 53.71 166:50 5.72 1.008 76.7 134 47.61 52.39 169:40 5.48 1.007 64.0 98 48.16 51.84 172:40 5.36 1.010 86,7 83 50.70 49.30 178:47 5.56 1.009 96.7 66 50.68 49.32 181:20 5.85 1.017 209.6 87 54.86 45.14 184:20 7.26 1.003 20.4 0 190:55 5.59 1.008 90.2 41 52.90 47.10 193:00 6.06 1.002 29.2 11 193:40 6.70 1,002 14.4 0 194:30 6.87 1.002 15.2 0 197:00 6.58 1.004 27.7 0 206:00 6.36 1.017 182.0 18 54.74 45.26 208:30 7.37 1.010 84.6 0 210:50 6.99 1.003 34.4 0 215:40 5.83 1.007 83.0 10 54.79 45.21 219:18 5.59 1.007 78.4 6 220:50 7.50 1.004 35.8 0 224:00 6.90 1.007 75.9 0 226:30 6,02 1.004 62.3 0 240:30 5.82 1.025 313.3 12 29.01 70.99 245:00 6.84 1.007 39.8 0
POS POS POS POS POS POS POS
SubjeU S 00:00 6.78 1.005 33.6 0 NA NA 03:15 6.03 1.009 61.4 2794 23.26 76.74 POS 06:15 5.72 1.008 58.4 4017 23.71 76.29 POS 11:10 5.90 1.015 151.3 3980 24.96 75.04 POS 13:20 5.75 1.010 84,5 2692 26.20 73.80 POS 18:30 5.80 1.016 174.9 3426 29.58 70.42 POS 18:45 5.32 1.010 65.6 2036 26.15 73.85 POS 20:15 5.66 1.007 69.6 2236 25.44 74.56 POS 22:15 6.02 1.007 52.5 4359 23.59 76.41 POS 24:05 5.88 1.006 35.5 3199 24.91 75.09 POS 26:45 5.94 1.009 57.7 3476 24.68 75.32 POS 29:00 6.02 1.002 44.4 2410 25.10 74.90 POS 30:15 6.09 1.005 37.0 1726 25.10 74.90 POS 36:01 6.08 1.014 147.1 2774 26.75 73.25 POS
Table I continues on next page
* Only a single sample is presented following the last detected amphetamine for each subject. All samples for each of the subjects collected after that time contained no detectable (--2 S nglmL) amphetamine. NA indicates enantiomer analysis was not completed because of the low concentration or lack of drug in the sample, Hours post dose represents time since administration of first dose. Subsequent doses administered at daily intervals. Immunoassay result is indicated as POS if the result was positive; all other samples tested negative by immunoassay.
571
Dow
nloaded from https://academ
ic.oup.com/jat/article/28/7/563/744513 by guest on 03 June 2022
Journal of Analytical Toxicology, Vol. 28, October 2004
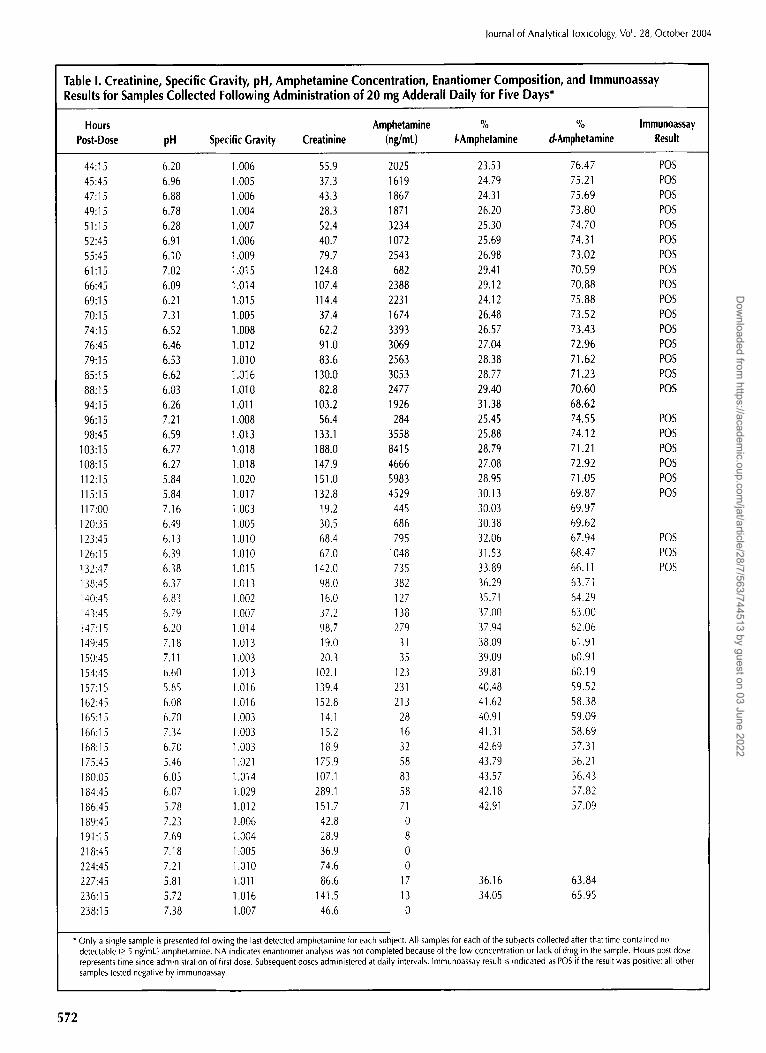
Table I. Creatinine, Specific Gravity, pH, Amphetamine Concentration, Enantiomer Composition, and Immunoassay Results for Samples Collected Following Administration of 20 mg Adderall Daily for Five Days*
Hours Amphetamine % % Immunoassay Post-Dose pH Specific Gravity Creatinine (ng/mL) /-Amphetamine d.Amphetamine Result
44:15 6.20 1.006 55.9 2025 23.53 76.47 45:45 6.96 1,005 37.3 1619 24.79 75.21 47:15 6.88 1,006 43.3 1867 24.31 75.69 49:15 6.78 1,004 28.3 1871 26.20 73.80 51:15 6.28 1,007 52.4 3234 25.30 74.70 52:45 6.91 1,006 40.7 1072 25.69 74.31 55:45 6.10 1.009 79.7 2543 26.98 73.02 61:15 7,02 1.015 124.8 682 29.41 70.59 66:45 6.09 1.014 107.4 2388 29.12 70.88 69:15 6.21 1.015 114.4 2231 24.12 75.88 70:15 7.31 1.005 37.4 1674 26.48 73.52 74:15 6.52 1.008 62.2 3393 26.57 73.43 76:45 6.46 1.012 91.0 3069 27.04 72.96 79:15 6,53 1,010 83.6 2563 28.38 71.62 85:15 6.62 1.016 130.0 3053 28,77 7l .23 88:t5 6.03 1.010 82.8 2477 29.40 70.60 94:15 6.26 1.011 103.2 1926 31.38 68.62 96:15 7,21 1,008 56.4 284 25.45 74.55 98:45 6.59 1,013 133.1 3558 25.88 74.12
103:15 6.77 1.018 188.0 8415 28.79 71.21 108:15 6.27 1.018 t47.9 4666 27.08 72.92 112:15 5.84 1.020 151.0 5983 28.95 71.05 115:15 5.84 1.017 132.8 4529 30.13 69.87 117:00 7.16 1,003 19.2 445 30.03 69.97 120:35 6.49 1.005 30.5 686 30.38 69.62 123:45 6.13 1.010 68.4 795 32.06 67.94 126:15 6.39 1,010 67.0 1048 31.53 68.47 132:47 6.38 1.015 142.0 735 33.89 66.11 138:45 6.37 1.013 98.0 382 36.29 63.71 140:45 6.83 1.002 16.0 127 35.71 64.29 143:45 6.79 1.007 37.2 138 37.00 63.00 147:15 6.20 1.014 98.7 279 37.94 62.06 149:45 7.18 1.013 19.0 31 38.09 61.91 150:45 7.11 1,003 20.3 35 39.09 60.91 154:45 6.60 1.013 102.1 123 39.81 60.19 157:15 5.85 1.016 139.4 231 40.48 59.52 162:45 6.08 1.016 152.8 213 41.62 58.38 165:15 6.70 1.003 14.1 28 40.91 59.09 166:15 7.34 1,003 15.2 16 41.31 58.69 168:15 6.70 1.003 18.9 32 42.69 57.31 175:45 5.46 1.021 175.9 58 43.79 56.21 180:05 6.05 1.014 107.1 83 43.57 56.43 184:45 6.07 1.029 289.1 58 42.18 57.82 186:45 5.78 1.012 151.7 71 42.91 57.09 189:45 7.23 1.006 42.8 0 191 :l 5 7.69 1.004 28.9 8 218:45 7.18 1.005 36.9 0 224:45 7.21 1.010 74.6 0 227:45 5.81 1.011 86.6 17 36.16 63,84 236:15 5.72 1.016 141.5 13 34.05 65.95 238:15 7.38 1,007 46.6 0
POS POS POS POS POS POS POS POS POS POS POS POS POS POS POS POS
POS POS POS POS POS POS
POS POS POS
* Only a single sample is presented following the last detected amphetamine for each subject. All samples for each of the subjects collected after that time contained no detectable (_> 5 ng/mL) amphetamine. NA indicates enantiomer analysis was not completed because of the low concentration or lack of drug in the sample. Hours post (lose represents time since administration of first dose. Subsequent doses administered at daily intervals. Immunoassay result is indicated as POS if the result was positive; all other samples tested negative by immunoassay.
572
Dow
nloaded from https://academ
ic.oup.com/jat/article/28/7/563/744513 by guest on 03 June 2022

Journal of Analytical Toxicology, Vol. 28, October 2004
50
40 '
30"
S
20 '
1 0
x = x
�9 W l ' ' O 0
�9 "
0
Q0:Q0 24:00 48:00 7'2:00 98:00 120;GO 144:00 1 B0:Q0 192:00 21 B:O0
Hours Pe~-Rrxt...Bom
Subj=ct o l A2 e 3 =4 ==5
Figure 1. Excretion profile of/-amphetamine following administration of a single 20-mg dose of Adderall on each of five consecutive days to five healthy male subjects.
This results in the same 3:1 proportion of the enantiomers ini- tially following administration of this product. Illicit am- phetamine in the U.S. is either only the d-enantiomer or a racemic mixture. These products result in a different enan- tiomer excretion pattern. The absence of l-enantiomer clearly would demonstrate that Adderall could not be the source of the amphetamine. Initially, racemic amphetamine results in essentially equal amounts of both enantiomers shortly after administration of the drug, followed thereafter by a progres- sively increasing proportion of the l-enantiomer. As shown in Figure 1, following the administration of Adderall, the pro- portion of d- to l-enantiomer did not approach 1:1 while the drug is still being administered on a daily basis. Following se- cession of dosing, the proportion of l-enantiomer increased, approaching a 1:1 ratio, but not for at least three days fol- lowing the last dose of the drug. Four of the five subject sam- ples approached, but never actually exceeded, a 1:1 ratio prior to their concentration dropping below the LOD (Figure 1). This is consistent with the single dose study, which showed the proportion did not reach 1:1 in four of five subjects until after 132 h post dose.
Other than a single entity mixed enantiomer formulation, the only scenario that would give this proportion would be to administer d-amphetamine and racemic amphetamine in the appropriate proportions and timing to attain those seen in this study. Although unlikely, this possibility should be con- sidered when interpreting results.
To assess the use of racemic versus d-amphetamine, Tetlow and Merrill (22) used enantiomer ratios to monitor compliance with treatment of amphetamine abuse with d-amphetamine. These investigators were able to differentiate use of d-am- phetamine from use of racemic amphetamine. In addition, the investigators were able to identify individuals that used both d- and racemic amphetamine. In a similar study, George and Braithwaite (23) were also able to differentiate the use of am- phetamine sources based on the average ratio of 1- to d-am- phetamine.
Conclusions
The current study presents the first published data on the excretion of amphetamine following multi-dose administra- tion of a mixed enantiomer amphetamine product available in the U.S. under a variety of brand names. Evaluation of these data allow for differentiation of the use of this formulation from both common forms of illicit amphetamine. The mere presence of l-enantiomer eliminates the possibility of the in- dividual using medicinal or illicit d-amphetamine. Racemic amphetamine (not legally marketed in the U.S.) yields enan- tiomer proportions different than those found following the use of mixed amphetamine isomer preparations such as Adderall.
Acknowledgments
The authors acknowledge the assistance provided by Donna Hensley for assistance with processing and analysis of samples. Immunoassay analysis of these samples was accomplished at the Air Force Drug Testing Laboratory, and the authors wish to thank those individuals that assisted with that analysis and to Dr. Mobley and Ms. Sobecki for their administrative assistance.
References
1. Physician's Desk Reference, 57th ed. Medical Economics Com- pany, Montvale N J, 2003.
2. E. Anggard, L.E. Jonsson, A.L. Hogmark, and L.M. Gunne. Am- phetamine metabolism in amphetamine psychosis. Clin. Phar- macol. Ther. 14(5): 870-880 (1973).
3. M.A. Evans, G. Wimbish, L. Griffis, R. Martz, D.J. Brown, B.E. Rodda, L. Lemberger, and R.B. Forney. Subjective responses and excretion patterns of dextroamphetamine after the administra-
573
Dow
nloaded from https://academ
ic.oup.com/jat/article/28/7/563/744513 by guest on 03 June 2022

Journal of Analytical Toxicology, Vol. 28, October 2004
tion of therapeutic doses. J. Forensic Sci. 22(1): 197-201 (1977). 4. M. Rowland and A.H. Beckett. The amphetamines: clinical and
pharmacokinetic implications of recent studies of an assay pro- cedure and urinary excretion in man. Arzneimittelforschung 16(11): 1369-1373 (1966).
5. J.M. Davis, I.J. Kopin, L. Lemberger, and J. Axelrod. Effects of uri- nary pH on amphetamine metabolism. Ann. N. Y. Acad. Sci. 179:493-501 (1971).
6. L.M. Gunne. The urinary output of d- and I-amphetamine in man. Biochem. Pharmacol. 16:863-869 (1967).
7. M. Rowland. Amphetamine blood and urine levels in man. J. Pharm. Sci. 58(4): 508-509 (1969).
8. A.H. Beckett and M. Rowland. Urinary excretion kinetics of am- phetamine in man. J. Pharm. Pharmacol. 17:628-639 (1965).
9. E. Anggard, L.M. Gunne, L.E. Jonsson, and F. Niklasson. Phar- macokinetic and clinical studies on amphetamine dependent subjects. Eur. J. Clin. Pharmacol. 3:3-11 (1970).
10. S.H. Wan, S.B. Matin, and D.L. Azarnoff. Kinetics, salivary ex- cretion of amphetamine isomers, and effect of urinary pH. Clin. Pharmacol. Ther. 23(5): 585-590 (1978).
11. J. Gal. Stereochemistry of metabolism of amphetamines: use of (-)-alpha-methoxy-alpha-(trifluoromethyl)phenylacetyl chloride for GLC resolution of chiral amines. J. Pharm. Sci. 66(2): 169-172 (1977).
12. A.H. Beckett and M. Rowland. Rhythmic urinary excretion of amphetamine in man. Nature 204(4964): 1203-1204 (1964).
13. KS. Sever, J. Caldwell, L.G. Dring, and R.T. Williams. The metabolism of amphetamine in dependent subjects. Eur. J. Clin. Pharmacol. 6(3): 177-180 (1973).
14. A.H. Beckett, J.A. Salmon, and M. Mitchard. The relation between blood levels and urinary excretion of amphetamine under con- trolled acidic and under fluctuating urinary pH values using
[14C]amphetamine. J. Pharm. Pharmacol. 21 (4): 251-258 (1969). 15. A.H. Beckett, M. Rowland, and P. Turner. Influence of urinary pH
on excretion of amphetamine. Lancet 1:303 (1965). 16. L.G. Dring, R.L. Smith, and R.T. Williams. The metabolic fate of
amphetamine in man and other species. Biochem. J. 116: 425~135 (1970).
17. S. Valtier and J.T. Cody. Evaluation of internal standards for the analysis of amphetamine and methamphetamine. J. Anal. Toxicol. 19(6): 375-380 (1995).
18. D. Hensley and J.T. Cody. Simultaneous determination of am- phetamine, methamphetamine, methylenedioxyamphetamine (MDA), methylenedioxymethamphetamine (MDMA), and methylenedioxyethylamphetamine (MDEA) enantiomers by GC-MS. J. Anal. Toxicol. 23(6): 518-523 (1999).
19. J.T. Cody, S. Valtier, and S.L. Nelson. Amphetamine enantiomer excretion profile following administration of Adderall. J. Anal. Toxicol., In press.
20. Roche Diagnostics Corporation. Online Automated Assays for Drug Abuse: Amphetamines (package insert). Roche Diagnos- tics Corporation, Indianapolis, IN, 2001.
21. Wolter Kluwer Co. Drug Facts and Comparisons. Wolter Kluwer Co., St. Louis, MO, 2002.
22. V.A. Tetlow and J. Merrill. Rapid determination of amphetamine stereoisomer ratios in urine by gas chromatography-mass spec- trometry. Ann. Clin. Biochem. 33:50-54 (1996).
23. S. George and R.A. Braithwaite. Using amphetamine isomer ra- tios to determine the compliance of amphetamine abusers pre- scribed dexedrine. J. Anal. Toxicol. 24(3): 223-227 (2000).
Manuscript received August 8, 2003; revision received January 13, 2004.
574
Dow
nloaded from https://academ
ic.oup.com/jat/article/28/7/563/744513 by guest on 03 June 2022




















