Alienation in the patient role: source of ambivalence and humor in comic get well cards
22
Roslyn Wallach Bologh Alienation in the patient role: source of ambivalence and humor in comic get well cards Abstract The humorous themes of over 300 comic get well cards are analyzed to reveal sources of tension or strain in the patient role. The author uses a model of alienation as a way of categorizing these themes. Corre- sponding to the four aspects of alienated labor as specified by Marx, alienation in the patient role is divided into the following four aspects: alienation from medical providers (domination and indifference), alien- ation of self from body (poweriessness or impotence), alienation from treatment (meaninglessness), alienation from responsibilities (self- estrangement). Each of these categories gets further broken down into sub-categories reflecting the specific sources of ambivalence and humor expressed in the comic get well cards. Using Merton's scheme of social structure and anomie, the author develops the logical possibilities in the patient role: compliant patient, 'problem' patient, malingerer, fatalist and rebel. These categories refer to the consequences of either accepting or rejecting the goal of getting well and the (alienating) means as indicated above required by the American system of medical care. Most of the humor of the get well cards falls primarily under the category that characterizes the 'problem' patient: accepting the goal of getting well but rejecting or ridiculing the alienating means. Jokes are one way that a culture reveals areas of tension or conflict, attitudes and perceptions that might call forth negative sanctions if expressed directly. With the aim of examining areas of tension in the sick role, this study focuses on jokes related to illness. We may assume that such jokes are culturally specific. Therefore, it is hoped that others might contribute to cross-cultural comparisons. This study examines a large sample of American humorous get well cards in order to reveal sources of tension and conflict in the sick role in America. In addition to indicating sources of tensions, humor related to illness may be therapeutic in helping patients to cope with and over- come on some level the stresses and tensions associated with being sick.^ Freud^ analyzed humor as a way of denying a threatening reality Sociology of Health and Illness Vol. 1 No. 2 1979 ©R.K.P. 1979 0141-9889/79/0102-0137 ?1.50/l
Transcript of Alienation in the patient role: source of ambivalence and humor in comic get well cards

Roslyn Wallach Bologh
Alienation in the patient role:source of ambivalence and humorin comic get well cards
Abstract The humorous themes of over 300 comic get well cards are analyzed toreveal sources of tension or strain in the patient role. The author uses amodel of alienation as a way of categorizing these themes. Corre-sponding to the four aspects of alienated labor as specified by Marx,alienation in the patient role is divided into the following four aspects:alienation from medical providers (domination and indifference), alien-ation of self from body (poweriessness or impotence), alienation fromtreatment (meaninglessness), alienation from responsibilities (self-estrangement). Each of these categories gets further broken down intosub-categories reflecting the specific sources of ambivalence and humorexpressed in the comic get well cards.
Using Merton's scheme of social structure and anomie, the authordevelops the logical possibilities in the patient role: compliant patient,'problem' patient, malingerer, fatalist and rebel. These categories referto the consequences of either accepting or rejecting the goal of gettingwell and the (alienating) means as indicated above required by theAmerican system of medical care. Most of the humor of the get wellcards falls primarily under the category that characterizes the 'problem'patient: accepting the goal of getting well but rejecting or ridiculing thealienating means.
Jokes are one way that a culture reveals areas of tension or conflict,attitudes and perceptions that might call forth negative sanctions ifexpressed directly. With the aim of examining areas of tension in thesick role, this study focuses on jokes related to illness. We may assumethat such jokes are culturally specific. Therefore, it is hoped that othersmight contribute to cross-cultural comparisons.
This study examines a large sample of American humorous get wellcards in order to reveal sources of tension and conflict in the sick rolein America. In addition to indicating sources of tensions, humor relatedto illness may be therapeutic in helping patients to cope with and over-come on some level the stresses and tensions associated with beingsick.^ Freud^ analyzed humor as a way of denying a threatening reality
Sociology of Health and Illness Vol. 1 No. 2 1979©R.K.P. 1979 0141-9889/79/0102-0137 ?1.50/l
138 Bologh
and asserting the invulnerability of the ego. Furthermore, medicalattention has recently been directed to the therapeutic effects of humorand laughter in reducing stress and the sensation of pain.''
If there are sources of tension in the sick role, and if tension hindersthe healing process, as may be surmised from the studies of stress as itaffects health^ then the sick role itself may be exacerbating the illness.Therefore changes in the sick role may reduce stress thereby enablingpatients to recover more easily. For example eliminating or reducingsome of the causes of strain involved in being hospitalized (which mayimplicate the whole health care delivery system) may aid in therecovery of patients. Research has found that the survival rate of heartpatients treated in an intensive care unit of a hospital was no higherthan the survival rate of similar patients treated at home. In fact thepatients who were suffering from hypertension did better at home.*
The present study examines humorous get well cards in order toidentify areas of tension or conflict in the patient role. The theoreticalmodel that I have adopted for this analysis goes beyond Merton'sadmittedly sociographic approach'^ (using concepts from everyday life)for the study of ambivalence in the client-professional relationship toan analytic approach using formulations derived from the theory ofahenation. Using a model of alienation, the situation of the patient isconceptualized as analogous to that of the alienated v^^orker. Just asalienated workers have little or no control over the process of work,alienated patients have little or no control over their medical treatmentand hence over their bodies. A recent nevk^spaper account (New YorkTimes, January, 1977) illustrates the extent to which a patient may bealienated from medical practitioners, from medical treatment and con-sequently from his own body:
'My two legs got to stay on - I won't have the operation. I got tocure my ovi n self.' So said a 58 year old Alabama bom ^derelict' at ahearing called to determine whether the man was 'mentally competent'to veto a medical decision requiring the amputation of his right legbelow the knee and part of his left foot.
'He is incompetent to understand the consequences of the illness orof his refusal to take it seriously,' said the attending psychiatrist at thehospital.
The fonner dishwasher and World War II veteran expressed determi-nation to 'take medicine to cure my legs' (antibiotics to halt theinfection) or to 'go ahead and die' rather than undergo amputation. Theman had been hospitalized when his badly frostbitten feet developedgangrene. Doctors ordered the infected portions amputated.
On January 10, over objections from hospital physicians, a StateSupreme Court justice ruled that the man had the right to refuse the
Alienation in the patient role: 139
amputation. In April, the man was back on the streets of mid townManhattan. With antiobiotic treatment, the infection was halted. Hehad lost two toes on his left foot and part of his right foot {New YorkTimes, April 1977).
Admittedly an extreme case, in some respects, this report doesreveal a not-so-unusual attitude on the part of the medical profession.Physicians and surgeons are trained to make decisions on the basis of'sound medical practices' which often means treating the illness and notthe patient. This means that treatment is not determined in collabor-ation with the patient taking into consideration his or her way of life.The only thing considered is the illness and its most effective cure ortreatment regardless of the patient's particular needs, life concerns orpriorities. I contend that this is the case more often than not in spite ofthe recognition and emphasis given by the profession to the need totreat the 'whole patient'. A recent study of the socialization of medicalstudents supports this view in its finding that despite the importancegiven to the physician-patient relationship, a great deal of ambivalenceexists regarding this aspect of the doctor's role due to the crosspressures experienced or conflicting messages received.^ The lack ofconsideration or respect for the patient's way of life, in prescribingtreatment may account for the relatively great amount of non-compliance cited in the literature.
In the case described above the physicians felt competent and con-fident to make decisions about the patient's body as a thing separatedfrom the totality of the patient's life. The patient, who alone knewmost about his life, was supposed to trust the competence of thephysician to make such decisions. This is precisely the premise ofmodern medicine and the doctor-patient relationship. The doctor is theauthority in whom patients must have trust and confidence. If that islacking, they should go to a different physician whom they can trustand on whose judgment they must rely. In this type of medical system,the body becomes a thing, an object for medical science and medicalpractice, and not the self of a patient. The body becomes divorced fromthe self.
This treatment by physicians of the body as a thing or object that istheir responsibility exclusively becomes particularly objectionable whenviewed from the existentialist perspective of Jose Ferrater Mora'according to whom, 'Man does not have a body, but is his body - hisowtT body . . . Man is a way of being a body'. Treating a living being, abody, as having no self transforms it into a thing.^° As a thing, itinspires no respect, it has no dignity. Perhaps the greatest indictmentand paradox of modern society is its treatment of people as things atthe same time that it provides the possibility for the greatest develop-
140 Bologh
ment of the self, of individuality. In non-modern societies, the self maybe treated with greater regard, yet its development is infinitelyrestricted and constrained within narrow parameters.
This paradox of modemity is captured by medicine in the concept of'patient', according to one dictionary, 'one who is acted upon'. Whereasmodern medicine can bring to bear on curing the illness all kinds ofsophisticated technology, it tends to ignore the patient's way of being abody, his or her particular life situation. Rather, medical decisions,including the over-sedating of patients in nursing homes and mentalinstitutions as well as the unnecessary surgery found in the US, may bemade in terms of convenience or self-interest of the physician orhospital. Even more intolerable is that while these decisions are justifiedin terms of contributing to the patient's health, these decisions oftenresult in iatrogenic disease. Whereas Illich'' suggests that people foregoprofessional treatment for this reason, the present analysis suggests thatwe should be working toward transforming the patient role in a non-alienated direction by eliminating or reducing the sources of alienation.
Alienation as used here means lack of control over aspects of one'slife. Although the concept, alienation, has not generally been used todescribe the sick role, Tagliacozzo and Mauksch'^ report on the help-lessness in relations with medical personnel that was repeatedly andconsistently expressed by patients who were interviewed on their viewsof the patient role. Brown and Rawlinson" have defined and measuredthe sick role in terms of dependency, lack of power and inactivity.Although some of these elements must be attributed to the effects ofthe illness itself, some of them derive from institutionalized aspects ofthe patient role.
In order to specify the alienating aspects that are built into thepatient role. Figure 1 compares the patient role with that of alienated
Figure 1 Comparison of patient alienation with worker alienation
Patient alienation Theme Worker alienation
From health care providers Domination and From employer and
and from other patients Indifference co-workers
From body Poweriessness From product
From medical treatment Meaninglessness From process ofproduction
From ordinary responsi- Self-Estrangement From what it is to bebilities and roles human: free, willed,
conscious activity.
Alienation in the patient role 141
Alienation in the patient role as presented in Figure 1 has somewhatdifferent components from the classical case of alienated labor. How-ever, we can see the similarity if we substitute alienation from healthcare provider and other patients for alienation from employer and co-workers. The theme here would be domination and indifference.
Continuing the analogy and suggesting that the worker's alienationfrom the product parallels the patient's alienation from his or her bodymay seem odd. In Marx's analysis, the property relation that makes theproduct an alien one belonging to the capitalist (i.e. ownership of themeans of production) results in the product confronting the worker notas the worker's product, that which embodies or realizes the worker'spurposes, but as something that appears to be independent of andforeign to the worker. Marx calls this relationship, the fetishism ofcommodities.
Just as workers are not one with their work, when people become illpatients, it is as if they were not one with their bodies. The ill bodybecomes an 'interesting case', and medical science becomes a fetish.One source of this alienation from the body is the illness which seems to'take possession' of the body making the body appear to be an alien orforeign thing. The theme here is poweriessness.
In addition, the medical profession seems to 'take possession' of thecase'. This can happen because the practices, knowledge and technicalresources that constitute the means of medical practice belongexclusively and legally to the medical profession whose relative wealthand status derive in good part from maintaining this state of affairs. Wecan see the similarity between the patient's alienation from medicaltreatment and the worker's alienation from the process or production.The theme here would be meaninglessness.
The final aspect of alienation in terms of which we compare theworker and the patient implicates the theme of self-estrangement.Instead of (self) alienation of the worker from what it is to be human:free, willed, conscious activity, we may substitute alienation of thepatient from the ordinary responsibilities and relationships that makeup the self. This means the patient becomes relieved of other roles andreduced in some ways to the status of an infant leading to ambivalenceabout being 'babied'.
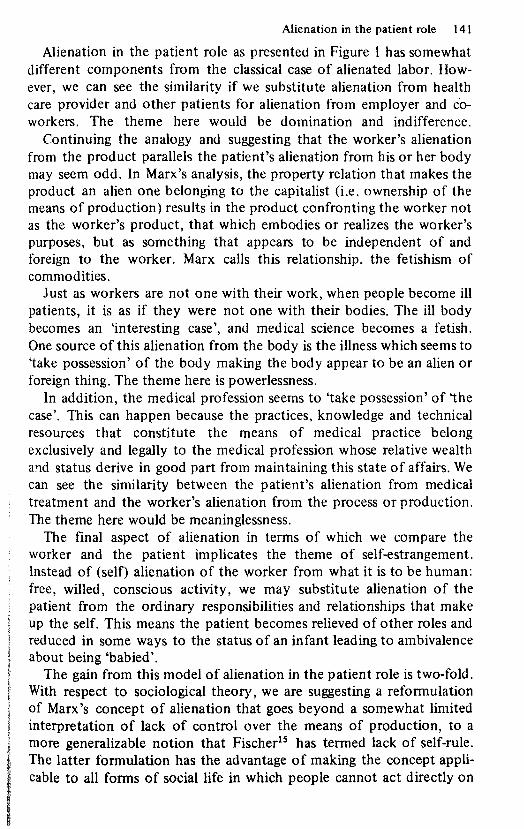
The gain from this model of alienation in the patient role is two-fold.With respect to sociological theory, we are suggesting a reformulationof Marx's concept of alienation that goes beyond a somewhat limitedinterpretation of lack of control over the means of production, to amore generalizable notion that Fischer** has termed lack of self-rule.The latter formulation has the advantage of making the concept appli-cable to all forms of social life in which people cannot act directly on

142 Bologh
the conditions of their lives but must depend on the mediation ofothers who maintain exclusive control over those conditions, a situationMarx calls private property. In other words to the extent that othershave exclusive control (private property rights) over the conditions of aperson's life, that person is alienated.**
The second gain from using this model of alienation applies to thegreater understanding it provides with respect to the patient role.Merton's approach'^ fails to recognize the patient role, and hence theambivalence, as something that can be changed. Therefore, his approachcannot account for social movements that aim to radically change orsubvert the traditional patient role in Westem society. The presentanalysis suggests that such change can be accomplished by treatingmedical knowledge about the illness and the treatment (possible risks,alternatives, etc.) as social property available through the profession tothe patient as opposed to treating it as the private property of theprofession to be used exclusively by the profession on behalf of thepassive patient.
The approach of medical sociology generally has failed to accountfor movements like the numerous self-help groups that have sprung upsuch as the cancer patients self-help organization aimed at combattingthe silence with which their condition is treated by their physicians aswell as by their families and friends, the mental patients organizationand movement challenging the traditional mental health system, themovement toward greater control over the child-birth process, themovement for consumer control over (or participation on) boards ofdirectors of public hospitals and over the expenditures of federal fundsfor medical care, the movement by parents to allow them to stay over-night with their hospitalized children, etc. The Hst keeps expanding.**
Gold and Johnson*^ suggest that the paucity of theoretical develop-ments within medical sociology is due to its identification with themedical profession and the domination ofthe medical perspective. Thisidentification may explain its failure to develop theoretical models thatmight explain the social movements mentioned above or that mightexplain patient ambivalence as something other than a necessary andsomewhat unavoidable consequence of the patient's anxiety.
For Marx, alienated labor is a contradictory condition; hence a tenseor revolutionary form.^" Although posited as free, conscious subjects,in that they are free to sell their labor power as their own privateproperty, the workers are treated as an object in the process of pro-duction. Contradiction similarly characterizes the patient role. Associal beings or subjects patients are expected to seek treatment, tocooperate with treatment, and to compensate the physician for theservice. However, patients are also expected to give themselves up to
Alienation in the patient role 143
the physician, to relinquish their subjectivity and become objects to beworked on and cured by the physician without their comprehension ofor active participation in that process, except for the chronically ill whomust take an active part in their treatment.^'
The patient role may be understood as contradictory in that thepatient is treated as and is expected to be a subject at one point and nota subject at another point. I contend that it is this contradiction thatmakes for strain and ambivalence (conflicting norms) in the patientrole.
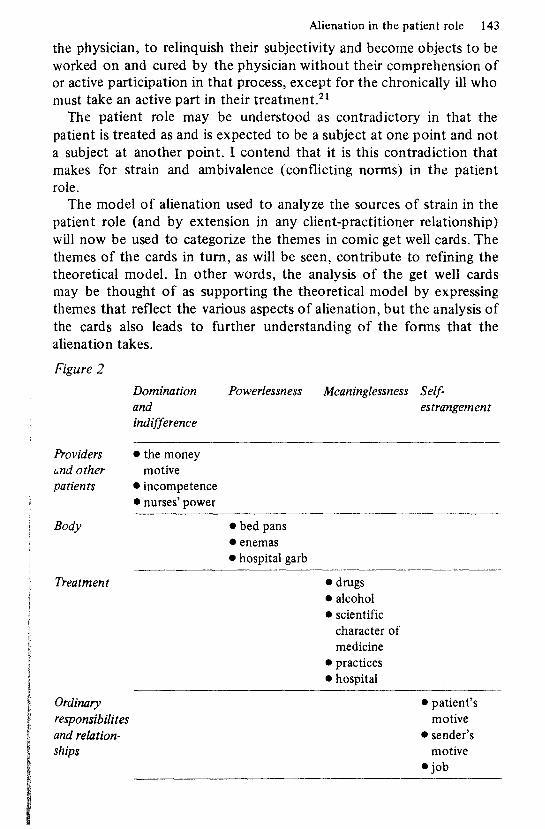
The model of alienation used to analyze the sources of strain in thepatient role (and by extension in any client-practitioner relationship)will now be used to categorize the themes in comic get well cards. Thethemes of the cards in turn, as will be seen, contribute to refining thetheoretical model. In other words, the analysis of the get well cardsmay be thought of as supporting the theoretical model by expressingthemes that reflect the various aspects of alienation, but the analysis ofthe cards also leads to further understanding of the forms that thealienation takes.
Figure 2
Providersend otherpatients
Body
Treatment
Ordinaryresponsibilitesand relation-ships
Dominationandindifference
• the moneymotive
• incompetence• nurses' power
Powerlessness
• bed pans• enemas• hospital garb
Meaninglcssness
• drugs• alcohol• scientific
character ofmedicine
• practices• hospital
Self-estrangement
• patient'smotive
• sender'smotive
• job
144 Bologh
Over three hundred comic get well card messages were collected withthe aim of identifying those aspects of the patient role that appear asthemes for the humor. Those cards whose humor did not derive fromthe patient role such as those in which the humor stemmed from a playon words which did not refer to the role of patient were eliminated.The remaining messages were then analyzed and classified. The classifi-cations in Figure 2 highlight the different aspects of alienation andtension in the patient role.
Domination and indifference: alienation from medical personnel
In a non-alienated relationship, the patient and physician would unitein the single goal of overcoming ill health. Instead we find that theirunity is mediated by factors that estrange them and subordinate thepatient to the physician. One such mediating and alienating factor maybe conceived as the money motive or what Merton calls 'living off theprofession.'
In order for physicians to provide medical care, they must be re-compensed for their services. This leads to the possibility that they maytreat their work as means for receiving income with primary interest inthe income and not in the practice of medicine. Such an orientationleads to relative indifference to the patient. Many physicians in the USrefuse to accept indigent patients whose source of payment is Medicareor Medicaid. Even without this reversal of priorities, we may find amixing of the two motives. Because the money motive of the physicianclass confiicts with the interests of the patient class, the patient may bealienated from the physician. As one might expect, the cost of medicalcare, the money motive and the wealth of physicians appears as one ofthe most frequent sources of humor in comic get well cards. Typicaljokes in this category are:
Know what doctors carry in their little black bags?Tens and twenties.
To feel better, take what nine out of ten doctors take.Take a bag of money to the bank!
Heard your doctor uses the latest techniques available?Tax dielters, fee splitting, computer billing.
Sorry you're not well. You should see my doctor. He got rid of what I had . . .My bank account.
HI? Don't worry! Modern medicine is a wonder!You wonder how you'll pay for it.

Alienation in the patient role 145
Don't begrudge your doctor his fee.He has a wife and family. . . Touring Europe!
The cards indicate another source of ambivalence toward physicians -incompetence. Because of the total dependence on the medicalpractitioner, the competence of the physician becomes of immenseimportance to the patient. Not being able to assess the competence ofthe physician adds an element of distrust to a relationship predicatedon trust: the patient puts himself or herself into the hands of thephysician. The ambivalence about the one-sidedness of the relationship- the patients depend on the physician but have no way to evaluate orcontrol the quality of care received - makes possible the followingexamples of humor.
Do what nine out of ten doctors do when they get sick . . .Ask the clerk in the drug store for his opinion.
I told your doctor this was your first operation. •You know what he said? . . . Mine too!
Your doctor examined you thoroughly and was unable to find the cause of yourillness. He said that it was probably due to excessive drinking . . .So he'll examine you when he's sober.
Cheer up. Your doctor says you're going to get better. . . And he's bound to be right one of these times.
Take a close look at your operation and see if you notice anything unusual . . .The surgeon is missing the lower half of his necktie.
Your doctor would have been one of the greatest surgeons of all times if itweren't for two things. . .His hands.
In the day to day existence of hospital patients, the nurse loomslarge as an important and powerful status. Present more than thedoctor, supposedly available at almost any time, responsible for thecare and comfort of patients, she (where female) evokes mixed f eelings.Her inability or unwillingness to devote herself fully to the welfare ofthe patient (as she has many patients and responsibilities) means thatthe patients become dependent for their care on someone who may notconcern herself fully with each one's needs. This may lead to ambiv-alence on the part of the patient.
However, it turns out that neither the nurse's competence nor motive(inability or unwillingness to give adequate care) appears as a theme inthe cards. Rather, something very interesting shows itself. This has todo with the depiction of the nurse as a female. Presenting the nurse as a

146 Bologh
sexual object seems to be most common. Yet a similar treatment of thetypically male physician as a sex object for a female patient rarelyoccurs. Humor directed at the physician, as we have seen, usually refersto the doctor's competence or motive (money). He is often depicted indiminutive size or as an obvious quack. Rarely does the humor refer tosexuality in the male-physician, female-patient relationship. How do weaccount for the finding that the humor aimed at the nurse most fre-quently alludes to sexuahty?
The depiction of the nurse as a sexual object may have the effect ofboosting the male patient's status as a dominant, hence potent male at atime when his potency is questionable in two ways. First, his illness oraccident reduces his physical potency. Second, and more significant forthe ambivalence, his dependence on and subordination to the femalereduces his sense of potency in a society where the female occupies alow prestige, relatively powerless and subordinate status vis a vis themale. Hence, ambivalence toward the nurse as a powerful figure takestwo typical forms. One form reduces the nurse to a sex object. Theother form depicts her as a powerful person determined to infiictphysical discomfort or pain on the vulnerable patient. The following areinstances of picturing the nurse as powerful and menacing:
Sick? They'll have you up and around in no time.(Picture of nurse happily chasing a patient with a needle)Your nurse likes a moving target.
No! No! Nurse!I said snip off his spectacles.
Your nurse is so meanYour bedpan goes from freezer to you!
Be nice to your nurseAfter all she's the one calling the shots.
But more cards derive their humor from depicting the nurse as a sexobject, and in this way, I propose, attempt to reverse and deny thepower of the female nurse over the male patient.
We hear you're giving the nurses a hard time.(Inside the card, the patient is shown chasing the nurse.)So keep at it.
We all want you to get well.(Picture of a patient and nurse in bed.)But with the proper therapy.
The doctor says that he's seen signs of your recovery(Inside is a sign that says:) Memo: Nurse - meet me at shute at 8:30.

Alienation in the patient role 147
Hey Fella - You must be recovering fast from your operation.The nurses have declared your room an erogenous zone.
The next time the nurse brings you rubbing alcoholDrink the alcohol and rub the nurse!
Whereas it is seen as a sign of health and potency for the male patientto treat the female nurse as a sex object, the cards do not indicate aparallel relationship for the female patient and the male physician.(Female doctors and male nurses do not exist in get well cards as yet.)The only card that implied that the female patient might be interestedsexually in the male physician was the following:
Dearie, your doctor say you're responding well. ..But he didn't say to what.
One other card indicated the possibility of the patient's sexual interestin the physician, but it ends with a play on the physician's fee:
I hear that you doctor has a handsome face,handsome build, handsome manner,.. . Handsome fee.
There were several cards that used a sexual theme with respect to themale physician-female patient relationship. It is interesting that theserelatively few cards refer to the physician's sexual interest in thepatient. In contrast, the male patient was depicted as sexually interestedin the nurse. Both cases, therefore, utilize the stereotype of the male astiie sexually interested or aggressive party. Treating the nurse as a sexobject supposedly enhances the patient's status as a potent and domi-nant male. For the female patient, an interest on the part of thephysician supposedly reflects well on her status as a desirable object.
Because of you, the doctor has decided to changeprofessions and be a massager.
When I asked the doctor how you wereHe said you're charming, lovely, cute and recuperating.
I understand your doctor put his finger on your problem.I've heard of medical coverage but this is ridiculous.
Powerlessness: alienation from body
Illness itself is a form of alienation in that the sick body does notI respond to the self the way it usually does when well. The inability of
the body to function normally and the inability of the self to make the
148 Bologh
body respond the way it should leads to the need for external aids,including medical personnel. The body becomes more dependent onthese external forces than on the self. One object of humor thatsymbolizes the alienation of self from (control over) the body is thebedpan as displayed in the following example of 'bedpan humor'.
Feeling better? The nurse tells me you make a big splash.Missed the bedpan, huh?
The other item that the cards assume to have comical elements is theenema:
This is a doctor; he is your friend.This is a nurse; she is your friend.This is your enema ordered and given by your friends.
Humor related to control over the body is not exhausted by bedpansand enemas as the following card indicates:
How does the birdie go - cheep, cheep.How does the doggie go - bow wowHow does the sickie go . . .Too darn often.
An unexpected object of the comic get well cards that was related toahenation from the body was the hospital garb of patients. While aseemingly trivial concern, Goffman^^ has alerted us to the dehumanizingaspect of institutional garb.
Why are hospital gowns like American auto insurance in Mexico?Cause nothing's covered south of the border!
Hope you've got something to cover your incidentals while you're in thehospital. ..You know how short those gowns are.
Meaninglessness: alienation from treatment
We find that cards often rely for their humor on the ambivalence ofpatients to drugs. Because medical knowledge is treated as privateproperty not generally accessible to the patient, except at the discretionof the physician, patients may be ambivalent about the nature ofmedical knowledge. Freidson^^ describes the resentment of patientstoward the control of information by the medical profession. Theyresent not being informed. At the same time that they resent thedoctor's exclusive knowledge, they also respect and depend on it. Thisambivalence gets expressed in the get well cards' ridiculing professional

Alienation in the patient role 149
knowledge and treatment. The following cards highlight the possibledangers of medicine.
Be careful about taking medicine while you're sick.Outdated drugs can be very dangerous.Just last night I cleaned a bunch of them out ofmy medicine cabinet and flushed them.This morning my toilet died.
You're Sick? There's a new miracle drug that hasno side effects.That's the miracle.
Some cards joke that the medicine is really alcohol or that the bestmedicine is alcohol:
Be sure to keep the top on your medicine bottleOtherwise it will get fiat.(Shows a beer cap)
I wanted to send you an appropriate gift while you were sickSo here's something to stir your 'medicine' with.
Your nurse says you're her best patientNot only do you take your medicineYou even lick the spooon.
Sorry you're sick. Have you tried the new wonder drugs?Like scotch, bourbon and vodka?
I was surprised that so many cards made reference to drinking. Formany, alcohol is the best medicine for 'whatever ails you'. Jokes aboutalcohol as medicine may be a way of making light of a problem thatneeds more than alcohol for its cure. It is possible that adages like'There's nothing that a good drink won't cure' make light of the medicalproblem and of the techniques of medical science as well. Some cardsdirectly joke about the scientific character of medical treatment:
Scientists experimenting with mice have come up with anidea that should have you up in no time.They're going to put several of them in your bed!
Every sick room should have one! Whatever kind of bug you've got.This ought to fill the bill. Cause if your doc can't trap those germs. . . This venus fiytrap will.(Picture of a doctor holding a butterfly net, a trap and a locked box)
Other cards that fit into the category of alienation from treatmentwith its theme of meaninglessness focus on specific medical practices.
150 Bologh
Don't worry about that operation.Here's the way it works.The Doctor puts you to sleep.A few hours later you wake up and you're all cured.. . . The rest of it you wouldn't believe!
Cheer up! While you're in the hospital you 11 be thoroughly examined by yourdoctor, the chief resident, an intern, your fioor nurse, a student nurse, the nightnurse, a nurse's aide, orderlies, your friends, your relatives, the newspaper man,the window washer, the janitor, the florist and the Ladies Auxiliary.
Take that thermometer out of your mouth.You don't know where it's been.
Here's something to wear in case they want totake a sample of your blood.(Inside is a sign:) 'I gave at the office'.
Alienation from the process of treatment includes alienation fromthe hospital and its practices, procedures, and policies. One cardexpresses the ambivalence about hospitals this way:
There is a lot to be said about hospitals.And you've probably said them all. 1 hope youget out of that i^''.\$% place soon.
Like the physician, the hospital evokes complaints for its highcharges:
Aren't hospitals classy? Where else can youpay ?3.00 for a Kleenex?
Just let a smile be your umbrellaWhen you're in that hospital!You're going to get soaked anyway!
Cheer up! Hospitals aren't all bad!They give you all the gelatin you caneat for $90 a day.
The following card includes an apology for the hospital after deridingits procedures:
Where else can you get such original clothesOr sleeping pills just when you started to dozeWhere else find a bed that folds with you in itOr an army of interns to brighten each minuteWhere else can you order a great 'Taste-Free Diet'.Or have visitors chase away dull peace and quiet.Where else but in hospitals
Alienation in the patient role 151
Yet when you feel sick
What better place is there to get well quick?
Other cards include no such apology:
You should be happy you're in the hospitalLook at all the service you get.Wake-up service (with a hypo)Breakfast in bed (Yuk)Your own bathroom (bedpan)A lot of company (25 interns staring at your naked body).
Finally the bureaucratization of hospitals becomes an object ofridicule and irony: .
Aren't hospitals wonderful? Where else would theywake you up at 2 A.M. to give you a sleeping pill?
With the hassle of hospital insurance forms,waiting lines, and red tape,. . . you've really got to be in good shapeto be in the hospital these days.
One card graphically illustrates how shut out the patient may befrom hospital procedures. It pictures a patient going around andlooking at what it says on all the doors: 'Private; Doctors only; Nursesonly; No peeking'. The message reads:
While you're in the hospitalThe doors they won't let you into are notworth fussing about. . .So the thing to do is concentrate on findingthe door marked . . . Out.
Self-estrangement: alienation from responsibflities and relationships
The last form of alienation that I use to interpret the humor of comicget well cards refers to the separation of the patient from responsi-bilities and relationships. One common source of humor refers to theexemption from responsibilities (which is an essential element inParsons' original formulation of the sick role^^) as a motive forbecoming, feigning or remaining ill or incapacitated:
Tonsils out?Looks Uke you got rid of your tonsils, sure enough!Boy! You'll do anything to eat ice cream and all that stuff!

152 Bologh
Sorry about your accident.But if I were youMy face would be redAfter all you've gone throughFor breakfast in .bed!
Sorry you're sick.Is it the 24 hour flu.Is it the 36 hour virusOr just the 40 hour week?
To you in the hospital.What fortitude! What stamina!What patience and endurance.Some people will do anythingTo collect their health insurance.
In addition to joking about the patients' motive regarding their ill-ness (malingering) some cards play on the sender's motive for wantingthe patient to get well - to take care of the unpleasant work that thepatient usually does. This may also be a way of telling the patient notto be too eager to come back but to enjoy the time off. It also becomesa way of playing with the expectation that others will help out and takecare of the patient's responsibilities.
Get well soon!The dishes are piling up!
Relax - don't worry, forget all about the tonsof work on your desk,ltll wait till you get back.
Get well soon.It's your turn to drive Tuesday.
In a somewhat different vein are those cards which make light of thepatient's ordinary responsibilities and activities:
Don't worry about your jobSome kid is doing it on his lunch hour.
The boss wants to know how come you're in the hospital.You sure get plenty of rest when you're in the office.
Just relax and take it easy.Pretend you're at work.
The ambivalence in the patient role about the exemption fromresponsibilities stems in part at least from uncertainty about thesecurity of one's job as indicated below:
Alienation in the patient role 153
Get well soon, and please hurry back.No one can take your place.
I At least none of the people they'veI interviewed so far.
I Thus we see that the above cards play on the possible sources ofI ambivalence about missing work and one's ordinary responsibilities and« relationships.
Alienation and anomie
Because we are dealing with norms of the patient role (trust, confidenceand dependency with regard to medical personnel and medical treat-ment as well as exemption from ordinary responsibilities) and theambivalence with regard to these norms, it becomes possible to relatethe concept of alienation to that of anomie. Merton's scheme of therelation between social structure and anomie^^ may be applied to thestructure of the patient role. The patient role consists of two types ofnorms - the goal and the means for realizing the goal. The patient's goalis to get well. The means for getting well include subservience to theauthority of the medical practitioner and suspension of ordinary rolesand responsibilities. Where the patient encounters or learns of incom-petent or indifferent treatment, as expressed in 'atrocity stories',^ thesenorms become strained. Or the patient may find the suspension of ordi-nary roles more appealing than the goal of getting well providing anothersource of confiict between the means and the goal. The logical possi-bilities that follow from the means-end scheme are shown in Figure 3.
Some may accept the goal and the means. This represents the 'good'or compliant patient, Merton's conformist. Some may accept the goalbut reject the means of traditional 'obedience' to medical authority.This represents the 'bad' or 'problem' patient,^' Merton's innovator,who may tend toward non-compliance or membership in a social move-ment asserting patient rights and challenging the domination of phys-ician or hospital over the patient. This category accounts for the jokesabout medical personnel, procedures and treatment.
Some may reject the goal but accept the means. This represents themalingerer, the 'hierarchical'," the 'hospital-oriented',^' and the 'lowerclass' patient* similar to Merton's ritualist. Such patients accept theirperceived subservient role of docile, passive recipient, preferring thissituation to the uncertainties and problems they face when well.Shiloh'* describes a similar type of patient found in mental hospitals.
Those who reject the goal of getting well and the means for ac-
154 Bologh
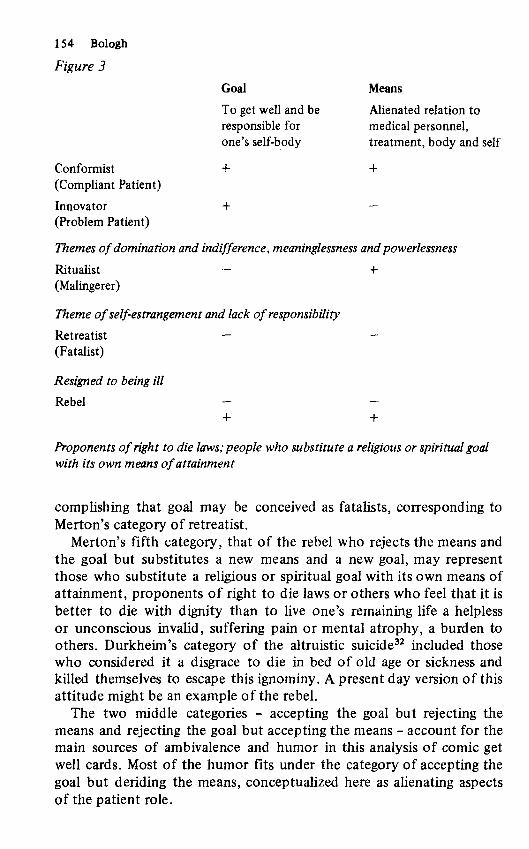
Figure 3
Goal Means
To get well and be Alienated relation toresponsible for medical persormel,one's self-body treatment, body and self
Conformist + +(Compliant Patient)
Innovator + —(Problem Patient)
Themes of domination and indifference, meaninglessness and powerlessness
Ritualist - +(Malingerer)
Theme of self-estrangement and lack of responsibility
Retreatist — —(Fatalist)
Resigned to being ill
Rebel - -4- +
Proponents of right to die laws: people who substitute a religious or spiritual goalwith its own means of attainment
complishing that goal may be conceived as fatalists, corresponding toMerton's category of retreatist.
Merton's fifth category, that of the rebel who rejects the means andthe goal but substitutes a new means and a new goal, may representthose who substitute a religious or spiritual goal with its own means ofattainment, proponents of right to die laws or others who feel that it isbetter to die with dignity than to live one's remaining life a helplessor unconscious invalid, suffering pain or mental atrophy, a burden toothers. Durkheim's category of the altruistic suicide^^ included thosewho considered it a disgrace to die in bed of old age or sickness andkilled themselves to escape this ignominy. A present day version of thisattitude might be an example of the rebel.
The two middle categories - accepting the goal but rejecting themeans and rejecting the goal but accepting the means - account for themain sources of ambivalence and humor in this analysis of comic getwell cards. Most of the humor fits under the category of accepting thegoal but deriding the means, conceptualized here as alienating aspectsof the patient role.
Alienation in the patient role 155
1 Conclusion
This work proposes that where alienation or lack of control over con-ditions affecting one's life (or body) is the expected or required meansfor achieving some important end, such as becoming well or earning aliving, we will find internal confiict and ambivalence as possible conse-quences. Furthermore, that alienation characterizes the patient rolecalls into question the possible exacerbating effect of the patient role,with its attendant strains or tensions, on recovery from illness. Theresearch of Brown and Rawlinson^^ indicates that following cardiacsurgery those people who reject the sick role, defined in terms ofdependency, lack of power and inactivity, had better long term workadjustment than those who did not reject it, suggesting that the patientrole in its present form may be detrimental to post-operative adjust-ment.
Of similar interest is the finding that among Mexican-Americans,higher scores on a measure of alienation, defined as social helplessness,were correlated with higher scores on a scale measuring intensity ofdepression.^ If the patient role is characterized by alienation, asargued in this paper, and if alienation is associated with depression,then the patient role may contribute to the development of depressionand affect the illness status of the patient. Thus alienation in thepatient role expressed as ambivalence and humor in comic get wellcards may have other serious ramifications. These may include, inaddition to effects on health, challenges to the medical profession onsuch matters as its withholding information about possible risks fromprescribed medication and about alternative forms of treatment, aswell as the other targets of the social movements and self-help groupsenumerated earlier.
Department of Sociology and AnthropologySt John's University, New York
Notes
1. For their comments and the opportunity to present a very early draft of thispaper at the Lunch-Bag Seminar, I want to thank my colleagues at St. John'sUniversity. Thanks also to Graves Enck and Edgar W. Mills, Jr. for theirhelpful suggestions.
2. For an account of how fooling around, like humor, provides a way ofI temporarily escaping from the constraints of a given social activity withoutI having to confront or reject those constraints and possibly jeopardize one'sj membership status, see R. W. Bologh, 'On Fooling Around: A Phenomenologi-I cal Analysis of Playfulness',^nna/i of Phenomenotogical Sociology, vol. 1
(1976), pp.113-25.
156 Bologh
3. S. Freud, 'Humor', in J. Strachey (ed.),Sigmund Freud, Coltected Papers,vol. V, New York, Basic Books, 1959, pp.215-21, reprinted from J. Riviere(translatoi),International Journal of Psycho-Analysis, 9,1, 1928.
4. N. Cousins, 'What I Learned from 3,000 Doctors',Prevention, vol. 30, no. 6(June 1978), pp.102-14, excerpted from The Saturday Review, 1978 discussesthe supportive responses by physicians to the article in which he discusses thetherapeutic effects of laughter, 'Anatomy of an Illness (As Perceived by thePatient)', The New England Journal of Medicine, vol. 295, no. 26 (Oct.-Dec.1976), pp.1458-63.
5. For a review of the literature up to 1974 on health and stress see B. and B.Dohrenwend, Stressful Life Events: Their Nature and Effects, New York,John Wiley and Sons, 1974.
6. H. G. Mather, N. G. Pearson, and K. L. Read, 'Acute Myocardial Infarction:Home and Hospital Treatment', .finVw/i Medical Journat, vol. 3, no. 5770(August 1971), pp.334-38.
7. R. K. Uetton, Sociological Ambivalence,'New York, The Free Press, 1976.8. \. Adler and J. T. Shuval, 'Cross Pressures during Socialization for Medicine',
American Sociological Review, 43, no. 5 (October 1978), pp.693-704.9. J. F. Mora, Being and Death, Berkeley, University of California Press, 1965,
p.147.10. P. Manning and H. Fabrega, Jr., 'The Experience of Self and Body: Health and
Illness in the Chiapas Highlands', in G. Fsathas,Phenomenotogicat Sociotogy,New York, John Wiley and Sons, 1973.
11. I. Illich, Medical Nemesis: The Expropriation of Health, London, Calder andBoyars, 1975.
12. D. L. Tagliacozzo and H. O. Mauksch, 'The Patient's View of the Patient'sRole', in E. G. Jaco, Patients, Physicians and Illness, New York, Free Press,1972,pp.406-12. .
13. J. S. Brown and M. E. Rawlinson, 'Relinquishing the Sick Role FollowingOpen-Heart Surgery',/ourwj/ of Health and Social Behavior, vol. 16, no. 1(March 1975), pp.12-27.
14. K. Marx, 'Alienated Labor' from 'The Economic and Philosophical Manuscriptsin T. B. Bottomore, Karl Marx, Early Writings, New York, McGraw Hill, 1963,pp. 120-34. R. 'Sl&uner, Alienation and Freedom, Chicago, University ofChicago Press, 1964. M. Seeman, 'On the Meaning of Alienation', AmericanSociological Review, vol. 24, no. 6 (December 1959), pp.783-9I.
15. G. Fischer, Ways to Self Rule: Beyond Marxism and Anarchism, New York,Exposition Press, 1978.
16. This elaboration of Marx's concept is presented and the Implications furtherdeveloped in R. W. Bologh, Dialecticat Phenomenology: Marx's Method,London, Routledge & Kegan Paul, 1979. In contrast, Blauner and Seeman(op. cit.) treat alienation as independent of property relations.
17. R.K. Merton, op. cit.18. L. G. Reeder has called attention to such movements. He interprets these move-
ments as indicative of a change from patient-client to consumer, but he doesnot account for this change. L. G. Reeder, 'The Patient-Client as a Consumer:Some Observations on the Changing Professional-Client Relationship', Journalof Health and Social Behavior, vol. 13, no. 4 (December 1972), pp.406-12.
19. M. Gold, 'A Crisis of Identity: The Case of Medical Sociology',/ourna/ ofHealth and Social Behavior, vol. 18, no. 2 (June 1977), pp.160-68;M. Johnson, 'Medical Sociology and Sociological Theory', Social Science and
Alienation in the patient role 157
Medicine, vol. 9, no. 4/5 (April/May 1975), pp.227-32.20. R. W. Bologh (1979), op. cit. develops this notion of a contradictory form of
life as revolutionary.21. T. Szazs and M. HoUender, 'A Contribution to the Philosophy of Medicine:
The Basic Models of the Doctor-Patient Relationship', A.M.A. Archives ofInternal Medicine, vol. 91, (May 1956), p.585; cited in S.W. Bloom, TheDoctor and His Patient, New York, Free Press, 1965, p.41.
22. E. Gotfmsin, Asylums, Garden City, New York, Anchor Books, 1961.23. E. Fieidson, Profession of Medicine, New York, Dodd, Mead, 1970.24. T. Parsons, The Social System, Glencoe, The Free Press, 1951, pp.439-79.25. R. Merton, Social Theory and Social Structure, Glencoe, The Free Press, 1957,
pp.131-60.26. G. Stimson and B. Webb, Going to See the Doctor. The Consultation Process
in General Practice, London, Routledge & Kegan Paul, 1975.27. J. Lorber, 'Good Patients and Problem Patients: Conformity and Deviance in a
General Hospital',/ourna/ of Health and Social Behavior, vol. 16, no. 2(June 1975), pp.213-25.
28. A. Shiloh, 'Equalitarian and Hierarchical Patients: An Investigation amongHadassah Hospital Patients', in E. Freidson and J. Lorber (eds). Medical Menand Their Work, Chicago, Aldine, 1972; reprinted from Medical Care, 3, (1965(1965),pp.87-95.
29. R. L. Coser,Z,i/e in the Ward, East Lansing, Michigan State University Press,1962.
30. L. W. Simmons and H. G. Wolff, Social Science in Medicine, New York,Russell Sage Foundation, 1954.
31. A. Shiloh, 'Sanctuary or Prison - Responses to Life in a Mental Hospital', inA. L. Strauss (ed.). Where Medicine Fails, New Brunswick, Transation, 1973,pp.133-50.
32. E. Durkheim,SMJCjde, New York, Free Press, 1951, pp.217-18.33. J. S. Brown and M. E. Rawlinson, 'Sex Differences in Sick Role Rejection and
Work Performance Following Cardiac Surgery',/ourna/ of Health and SocialBehavior, vol. 18, no. 3 (September 1977), pp.276-92.
34. G. M. Quesada, W. Spears and P. Ramos, 'Interracial Depressive Epidemiologyin the Southwest',/ourna/ of Health and Social Behavior, vol. 19, no. 1(March 1978), pp.77-85.