Serious Violent Offenders: An Exploration of Offender - the ...
Upload
independentCategory
view
2download
0
Available online at www.sciencedirect.com
ScienceDirect
Comprehensive Psychiatry 55 (2014) 40–50www.elsevier.com/locate/comppsych
Aggression–impulsivity, mental pain, and communication difficulties inmedically serious and medically non-serious suicide attemptersYari Gviona,b,⁎, Netta Horresha, Yossi Levi-Belzc, Tsvi Fischeld,e, Ilan Trevese, f,
Mark Weiserg, Haim Shem Davidg, Orit Stein-Reizerh, Alan Aptere, iaDepartment of Clinical Psychology, Bar Ilan University, Ramat Gan, Israel
bDepartment of Clinical Psychology, Tel Aviv-Jaffa Academic Center, Tel Aviv, IsraelcDepartment of Behavioral Sciences, Ruppin Academic Center, Netanya, Israel
dGeha Psychiatric Hospital, Petah Tiqva, IsraeleSackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel
fShalvata Mental health Center, Hod Hasharon, IsraelgPsychiatric Ambulatory Services, Sheba Medical Center, Ramat Gan, Israel
hLev Hasharon Psychiatric Hospital, Pardesia, IsraeliFeinberg Child Study Center, Schneider's Children's Medical Center of Israel, Petach Tikvah, Israel
Abstract
Background: Unbearable mental pain, depression, and hopelessness have been associated with suicidal behavior in general, whiledifficulties with social communication and loneliness have been associated with highly lethal suicide attempts in particular. The literaturealso links aggression and impulsivity with suicidal behavior but raises questions about their influence on the lethality and outcome of thesuicide attempt.Objectives: To evaluate the relative effects of aggression and impulsivity on the lethality of suicide attempts we hypothesized thatimpulsivity and aggression differentiate between suicide attempters and non-attempters and between medically serious and medically non-serious suicide attempters.Method: The study group included 196 participants divided into four groups: 43 medically serious suicide attempters; 49 medically non-serious suicide attempters, 47 psychiatric patients who had never attempted suicide; and 57 healthy control subjects. Data onsociodemographic parameters, clinical history, and details of the suicide attempts were collected. Participants completed a battery ofinstruments for assessment of aggression–impulsivity, mental pain, and communication difficulties.Results: The medically serious and medically non-serious suicide attempters scored significantly higher than both control groups on mentalpain, depression, and hopelessness (p b .001 for all) and on anger-in, anger-out, violence, and impulsivity (p b .05 for all), with nosignificant difference between the two suicide attempter groups. Medically serious suicide attempters had significantly lower self-disclosure(p b .05) and more schizoid tendencies (p b .001) than the other three groups and significantly more feelings of loneliness than the medicallynon-serious suicide attempters and nonsuicidal psychiatric patients (p b .05). Analysis of aggression–impulsivity, mental pain, andcommunication variables with suicide lethality yielded significant correlations for self-disclosure, schizoid tendency, and loneliness. Theinteraction between mental pain and schizoid traits explained some of the variance in suicide lethality, over and above the contribution ofeach component alone.Conclusions: Aggression–impulsivity and mental pain are risk factors for suicide attempts. However, only difficulties in communicationdifferentiate medically serious from medically non-serious suicide attempters. The combination of unbearable mental pain and difficulties incommunication has a magnifying effect on the risk of lethal suicidal behavior.© 2014 Elsevier Inc. All rights reserved.
⁎ Corresponding author. Department of Clinical Psychology, Bar IlanUniversity, Ramat Gan, Israel. Tel.: +972 52 2340520.
E-mail address: [email protected] (Y. Gvion).
0010-440X/$ – see front matter © 2014 Elsevier Inc. All rights reserved.http://dx.doi.org/10.1016/j.comppsych.2013.09.003
1. Introduction
Suicide is often the end result of a complex interaction ofa very many diverse variables, including demographics,personality traits, clinical symptoms and disorders,

41Y. Gvion et al. / Comprehensive Psychiatry 55 (2014) 40–50
environmental pressures, social support, and history ofsuicide attempt as well as biological factors such as genetics,medications, and concordant illness [1–13]. Suicide may bepreceded by suicidal thoughts, threats, gestures, nonsuicidalself-injuries, and suicide attempts of various degrees oflethality, all of which are generally lumped together underthe rubric of “suicidality.” Recently, researchers haveattempted to define these behaviors more clearly [14].Interest has focused on individuals who make nearly lethalsuicide attempts, as the study of this subgroup can best shedlight on actual suicide attempters [15–18].
As such, it is important to identify risk factors thatdistinguish nearly lethal from less serious forms of suicide.Our earlier study showed that mental pain and depression aremore associated with suicidal behavior in general whereasproblems with social communication and loneliness are moreassociated with more lethal suicide attempts [19]. However,more research is necessary to determine the role ofaggression and impulsivity in the lethality of suicide (forreview, see Gvion and Apter [20]).
Aggression has been linked to the act of suicide inmultiple epidemiologic, clinical, retrospective, prospective,and family studies [21], Furthermore low serotoninturnover appears to be common to both aggressive andsuicidal behaviors [22,23] suggesting a common neurobi-ology [24]. Regarding its effect on the lethality of suicide,one study yielded significantly higher levels of aggressionin medically serious suicide attempters than in healthycontrols [25], and others reported that individuals withpersonality disorders, particularly those related to impul-sive and aggressive tendencies and a co-morbid depressivedisorder were at higher risk for more frequent and moremedically severe suicidal behavior than subjects with majordepressive disorder or bipolar depression alone [26,27].From the aspect of choice of method, one study found thatviolent methods of suicide may serve as a behavioralmarker of a higher level of lifetime impulsive–aggressivebehaviors [28]. More violent methods were used more oftenby males and by suicide completers with psychosis. Conneret al. [29] showed that violence during the last year of lifewas more frequent among suicide victims than accidentvictims, suggesting that aggression may be indirectly linkedto high lethality attempts. By contrast, Soloff et al. [30]found no difference in level of aggression between high-and low-lethality suicide attempters.
Impulsivity encompasses a broad range of behaviors thatreflect impaired self-regulation, such as poor planning,responding prematurely before considering the conse-quences, sensation seeking, risk taking, poor inhibition ofresponses, and preference for immediate over delayedrewards [31,32]. Although many studies have identifiedimpulsivity as a common correlate and risk factor for suicidalbehavior [33,34], it is not known if it increases the risk ofsuicide independently of aggressive traits [35] or if it isrelated to the medical severity of suicide attempts. Someauthors reported evidence of higher levels of impulsivity in
individuals who died by suicide than those who did not[28,36] whereas others found that although people whoattempt suicide tend to be more impulsive than people whodo not, the actual act of completed suicide is often not madeimpulsively (e.g., Anestis et al. 37]). Simon et al. [38]reported that only 24% of survivors of near-lethal suicideattempts had thought about their attempt for less than5 minutes. Those who made their attempt within 5 minutesof deciding to do so were less likely to have consideredanother method of suicide. They also had a greater likelihoodof discovery and a lower expectation of death. Baca-Garciaet al. [39,40] claimed that impulsivity is a characteristic ofnonlethal suicide attempts or suicide gestures whereasplanned suicide involves a more subjective element drawnfrom the desired outcome and the perceived lethality of theact of self-harm. Other authors emphasized the mediatoryrole of the intent to die at the time of the suicide attempt.Hawton [41] observed that less than 50% of subjects with ahistory of suicide attempts really wanted to die; he definedtheir attempts as little-planned impulsive acts. Motivesreported in impulsive suicides ranged from escaping from anintolerable situation to manipulation [42].
Some of the data collected to date on the role ofaggression and impulsivity in suicide and suicide lethalityneed to be reconsidered in light of differences among thestudies in definitions used, methods employed, and theselected population. Most did not include a nonsuicidalpsychiatric group or psychiatric patients with aggressive–impulsive features [43], and even studies that investigatedmore specific aspects of aggression [44,45] failed to controlfor level of the medical seriousness of the attempt.Furthermore, the concept of aggression is complicated bythe interchangeable use of the terms aggression, violence,irritability, and anger in the literature. Indeed, Spielberger[46] has emphasized that the expression of anger differswhen it is directed toward others or self; this difference hasbeen explored extensively in the classic psychoanalyticliterature [47]. The concept of impulsivity is complicatedby the confusion in the literature between the state and traitdimensions (see Gvion and Apter [20] for review); that is,between the impulsivity of the suicidal act and impulsivityas an individual personality trait [40]. Finally, bothaggression and impulsivity may be related to mental painand other risk factors of suicide.
Clinical and research experience suggests that people whoare in agony and depression may often be irritable and angry[48]. This, in turn, raises the likelihood of distancing andrejection from family and peers [49], augmenting lonelinessand the risk of suicidal behaviors.
The aim of the present study was to further evaluate therelative effects of aggression and impulsivity on the lethalityof suicide attempts. Five hypotheses were tested: (1)aggression, defined by anger-in, anger-out, and violence,differentiates suicide attempters from non-attempters andmedically serious suicide attempters from medically non-serious suicide attempters; (2) impulsivity differentiates

42 Y. Gvion et al. / Comprehensive Psychiatry 55 (2014) 40–50
suicide attempters from non-attempters and medicallyserious suicide attempters from medically nonsuicideattempters; (3) based on our previous study [19], mentalpain, depression, and hopelessness differentiate suicideattempters from non-attempters but not medically seriousfrom medically non-serious suicide attempters; (4) based onour previous study [19], communication problems, definedby low self-disclosure, loneliness, and schizoid features,differentiates medically serious from medically non-serioussuicide attempters; and (5) aggression and impulsivity have acatalyzing effect on the lethality of suicide attempts, over andabove the mental pain and communication difficulties.
2. Methods
2.1. Study sample
The study included 196 participants (72 women and 124men) aged 16 –71 years, divided into four groups: (1)medically serious suicide attempters (MSSA)—43 consecu-tive patients admitted to a general or psychiatric hospital in2005–2009 for a suicide attempt that required hospitaladmission for longer than 24 hours and treatment either in aspecialized medical unit (including the intensive care or burnunit) or surgery under general anesthesia (e.g. for tendonrepair, stabbing injuries [15]; (2) medically non-serious suicideattempters (MNSSA)—49 patients who had made a suicideattempt that warranted emergency room attention or hospital-ization (e.g., for an overdose, or surface injuries) but did notmeet the criteria for amedically serious attempt; (3) psychiatriccontrol group—47 consecutive patients admitted to apsychiatric facility with a psychiatric diagnosis but no historyof suicidal behavior; and (4) healthy control group—57volunteer subjects without any psychiatric diagnosis and nohistory of suicidal behavior. All groups were matched for ageand sex.
2.2. Interviews and self-rating questionnaires
Data on age, sex, religion, marital status, number ofchildren, education, and employment were collected byquestionnaire. Psychiatric diagnoses were based on theStructured Clinical Interview for DSM-IV (SCID-IV) [50].
The lethality of the suicide attempt was evaluated withone instrument.
• The Lethality Rating Scale (LRS) [22] is aninterviewer-administered instrument that includesthe Medical Damage Rating Scale (MDRS) designedby Beck and colleagues [51]. The LRS rates themedical severity of a suicide attempt on a scale from0 (fully conscious and alert) to 8 (death). Each of itseight subscales may be rated according to the methodof the attempt (shooting, jumping, drug overdose,etc.). The MDRS incorporates data on the attempter'sphysical condition at hospital admission and medicalrecord. Previous research has established an adequate
level of inter-rater reliability (r = .80) [52] andadequate concurrent validity with the Risk RescueRating Measure [53].
Aggressive–impulsive tendencies were evaluated withfour instruments:
• The State-Trait Anger Expression Inventory (STAXI)[46,54] is a 44-item, multidimensional psychometricinstrument comprising five scales: The STAXI StateAnger scale (S-Anger) measures the intensity of angryfeelings experienced “right now, at this moment” or ata designated time; the STAXI Trait Anger scale (T-Anger) measures individual differences in dispositionto experience anger; the STAXI AX/Out, AX/In, andAX/Con scales measure, respectively, the frequencywith which anger is expressed toward other persons orenvironmental objects, the frequency with which angeris experienced but suppressed and the frequency withwhich anger is controlled. For the present study, weused only the 24-item T-Anger scale. In our sample,Cronbach's alpha coefficient for the T-Anger scalewas .88.
• Past Feelings and Acts of Violence (PFAV) [55] is aself-report standardized questionnaire designed tomeasure the risk of engaging in violence on the basisof past violent behavior, use of weapons, and feelingsof anger. It consists of 11 items scored on a 4-pointLikert-type scale ranging from never to very often. ThePFAV has shown good internal consistency (0.78), anditem specificity has been previously reported [55,56].In our sample, item specificity was 0.75.
• The Impulse Control Scale (ICS) [57] consists of 15items scored on a 4-point Likert-type scale rangingfrom never to very often. The ICS was designed tomeasure the tendency to engage in impulsive, spur-of-the-moment behaviors and lack of patience, all ofwhich reflect loss of control. It has an internalreliability of 0.77 [58]. In our sample, item specificitywas 0.85.
• The Suicide Intent Scale (SIS) [59] is a 15-iteminterviewer-administered instrument designed to ret-rospectively capture the circumstances surrounding asuicide attempt. Items are scored from 0 to 2, withhigher scores reflecting more intense expectations orplanning. The SIS has been found to have adequateinternal consistency, excellent inter-rater reliability,and adequate construct validity [59,60]. A factoranalysis conducted by Mieczkowski et al. [61]revealed that two factors explain the variance inscores. For the present study, we used only the eight-item Objective Planning Subscale of the SIS, on whichhigher scores represent higher levels of premeditation,organization, and preparation for death. The subscalehas been found to have good internal consistency andgood predictive validity [61]. In the present sample,

43Y. Gvion et al. / Comprehensive Psychiatry 55 (2014) 40–50
Cronbach's alpha coefficient for the Objective Plan-ning Subscale was .73.
Mental pain was evaluated with three instruments.
• The Orbach and Mikulincer Mental Pain Scale(OMMP) [62] consists of 45 items divided into eightscales: Irreversibility, Loss of Control, NarcissistWounds, Emotional Flooding, Freezing, Self-Es-trangement, Confusion, Emptiness, and Social Dis-tancing. Each item is scored on a 5-point Likert scale.Higher values reflect higher mental pain. In oursample, Cronbach's alpha coefficient for the OMMPscale was .89. The Social Distancing scale wasexcluded from the analysis because of a lowCronbach's value (.42).
• The Beck Depression Inventory (BDI) [63] is a 21-item self-report instrument for analysis of the cogni-tive, affective, physiological, and motivational symp-toms of depression that the individual experiencedover the past month. Each item is scored on a 4-pointscale, with higher scores reflecting more severesymptoms. In the present sample, Cronbach's alphacoefficient was .94.
• The Beck Hopelessness Scale (BHS) [64] consists of20 items, each rated on a 5-point Likert scale. The sumof the scores on individual items yields a totalhopelessness score with a possible range of 20 to100. The lower the score, the more hopeless theindividual feels. In this sample, Cronbach's alphacoefficient was .94.
Communication difficulties were evaluated with threeinstruments.
• The Jourard Self-Disclosure Questionnaire (JSDQ)[65] assesses the degree to which subjects share sixareas of self-knowledge (attitudes and positions,personality, interests, study and work, finance andbody) with others (father, mother, girlfriend, boyfriendand stranger). Each item is rated on a 4-point scale. Forthe present study, we used a short version of this scaleconsisting of 40 items and one target individual: closeperson. The internal reliability of the short versionwas .95.
• The Structured Clinical Interview for DSM-IV (SCID-II) Personality Disorders [50] was used to evaluateschizoid traits. The whole interview covers the 11Axis II personality disorders. We used the only theseven-item section on symptoms and behaviors ofschizoid personality disorder. Each item is rated on a3-point scale, with higher scores indicating a greaterschizoid tendency.
• The UCLA Loneliness Scale [66] was designed todetect variations in loneliness in everyday life. Itconsists of 20 statements, such as “I lack companion-ship,” which are rated on a scale of 1 to 4 by the
frequency with which they are true. For the presentstudy, we calculated the mean grade for all items,yielding a final score ranging from 1 to 4. Cronbach'salpha in our sample was .94.
2.3. Procedure
The study was conducted in accordance with the 1989revision of the Helsinki Declaration and was approved byour institutional review board. After candidates for thesuicide and psychiatric groups were deemed medically fit bythe medical staff and were enrolled in the study, they metwith a postgraduate psychologist student who explained theaims and purposes of the project and asked for their writtenconsent to participate. The interviews and questionnaireswere administered in two sessions of approximately 1 houreach. If candidates expressed acute distress, the interviewerconsulted the medical staff for further assistance.
2.4. Data analysis
First, multivariate analyses of variance (MANOVAs)were performed to determine group differences in measuresof impulsive–aggressive tendencies, mental pain, andcommunication difficulties. This was followed by analysesof the relationships among the clinical (aggressive–impul-sive, mental pain variables) and interpersonal variables(communication difficulties) and the medical lethality of theattempt using a series of Pearson correlation tests andhierarchical multiple regression analysis.
2.4.1. Power analysisIn order to examine if our study design had the sufficient
power to detect the assumed group effects, we conducted apower analysis [67]. The power analysis indicated 97%power to detect medium effect size f2(0. 15) with 10predictors and 196 participants (fc(10,192) = 1.597, L =29.40) at α = .05.
The Statistical Package for the Social Sciences (SPSS,version 18.0 forWindows)was used for all analyses, except forpower analysis whichwas conducted byGpower (version 3.1).
3. Results
3.1. Demographic characteristics
Table 1 presents the demographic characteristics of thestudy participants. There were no differences in age, sex, ormarital status among the four study groups or the threesuicide/psychiatric groups. Compared to the other groups,the healthy control subjects had a significantly higherincome (p b .001) and more years of education (p b .001),and most of them (89.5%) lived with families or partners.
3.2. Psychiatric and clinical characteristics
Table 2 presents the psychiatric and clinical characteris-tics of the suicide and psychiatric groups. The two suicide

Table 1Demographic characteristics of the study groups (n = 196).
Characteristic MSSA(n = 43)
MNSSA(n = 49)
Psychiatric controls(n = 47)
Healthy controls(n = 57)
Analysis
Sex, n (%) χ2 = 3.07Male 26 (60.5) 34 (69.4) 33 (70.2) 31 (54.4)Female 17 (39.5) 15 (30.6) 14 (29.8) 26 (45.6)
Age (yr) M = 37.37 M = 40.31 M = 40.96 M = 37.28 F = .98SD = 13.31 SD = 13.76 SD = 14.07 SD = 12.34
Marital status, n (%)Single 27 (62.8) 21 (42.9) 21 (44.7) 30 (52.6) χ2 = 5.33Married 9 (20.9) 17 (34.7) 12 (25.5) 20 (35.1)Div/Wid/Sep 7 (16.3) 11 (22.4) 14 (29.8) 7 (12.3)
Living status, n (%) χ2 = 15.62a
Alone 10 (23.3) 7 (14.3) 14 (29.8) 6 (10.5)Not alone 26 (60.5) 37 (75.5) 29 (61.7) 51 (89.5)Hostel/street 7 (16.3) 5 (10.2) 4 (8.5) 0 (0.0)
Income (1–5 scale) M = 2.5 M = 2.43 M = 2.26 M = 3.39 F = 22.6b
SD = 1.0 SD = 1.1 SD = 0.9 SD = 0.92Education (yr) M = 12.9 M = 12.0 M = 12.4 M = 14.9 F = 26.1b
SD = 2.9 SD = 2.8 SD = 2.1 SD = 1.9
MSSA = medically serious suicide attempters; MNSSA = medically non-serious suicide attempters; Div/Wid/Sep = Divorced/Widowed/Separated.a p b .05.b p b .001.
44 Y. Gvion et al. / Comprehensive Psychiatry 55 (2014) 40–50
groups were similar in the distribution of the diagnoses.However, when comparing the distribution of diagnosesamong three groups (two suicide groups and the nonsuicidalpsychiatric group) there were significant differences(p b .01).
3.3. Suicide attempt characteristics
Table 3 compares the characteristics of the suicideattempts between the two suicide groups. As expected, the
Table 2Psychiatric and clinical characteristics of suicide and psychiatric groups(n = 139).
Characteristic MSSA(n = 43)
MNSSA(n = 49)
Psychiatric Controls(n = 47)
Analysis
Diagnosis—current, n (%)Affective dis.⁎ 23 (53.4) 24 (48.9) 20 (42.6) χ2 = 16.68a
Schizoid dis.⁎ 13 (30.2) 11 (22.4) 25 (53.2)Anxiety dis. 4 (9.3) 10 (20.4) 1 (2.1)Addiction 3 (7.0) 4 (8.2) 1 (2.1)
Comorbid diagnosis, n (%)Axis I 2 (22.4) 1 (10.0) 1 (50.0) χ2 = 1.83Axis I + II 7 (77.8) 9 (90.0) 1 (50.0)
Psychiatric hospitalizationYes 42 (97.7) 46 (93.9) 46 (97.9) χ2 = 1.39No 1 (2.3) 3 (6.1) 1 (2.1)
Psychiatric medicationYes 38 (88.4) 42 (87.5) 44 (93.6) χ2 = 0.16No 5 (11.6) 6 (12.5) 3 (6.4)
MSSA = medically serious suicide attempters; MNSSA = medically non-serious suicide attempters.
⁎ Affective disorder = unipolar depression or bipolar affective dis-order; schizoid disorder = schizophrenia, schizoaffective disorder.
a p b .05.
medically serious suicide attempters had a significantlyhigher mean score on the LRS (p b .01). The most commonsuicide method used by both groups was sedative overdose(51.3%). The medically serious suicide attempters weremore likely to use violent methods (immolation, jumping),but the difference did not reach statistical significance. Therewere no between-group differences in days from the attemptto the interview, number of suicide attempts, and familyhistory of suicide attempts.
Table 3Suicide attempt characteristics and association with lethality (n = 92).
Characteristic MSSA(n = 43)
MNSSA(n = 49)
Analysis
Method, n (%)Sedative overdose 20 (46.4) 27 (55.2) χ2 = 7.24Not sedative overdose 6 (14.0) 8 (16.3)Immolation 4 (9.4) 1 (2.0)Cutting/Stabbing 4 (9.3) 8 (16.3)Jumping 8 (18.6) 3 (6.1)Hanging 1 (2.3) 2 (4.1)
Lethality Rating Scale Score M = 6.37 M = 2.49 t = 17.60a
SD = 0.93 SD = 1.16Objective PlanningSubscale Score⁎
M = 1.78 M = 1.66 t = 1.12SD = 0.52 SD = 0.55
Interval from attempt tointerview (days)
M = 28.3 M = 22.92 t = 1.08SD = 26.85 SD = 22.70
Number of suicide attempts M = 3.95 M = 5.27 t = .92SD = 5.94 SD = 7.03
Family history of suicide attemptsYes 11 (25.6) 13 (26.5) χ2 = .01No 32 (74.4) 36 (73.5)
MSSA = medically serious suicide attempters; MNSSA = medically non-serious suicide attempters.
⁎ Subscale of the Suicide Intent Scale.a p b .01.

Table 4Means and standard deviations of scale scores and MANOVAs of dependent measures (n = 196).
Measures Groups Analysis
MSSA (1) MNSSA (2) Psychiatric controls (3) Healthy controls (4) F(3,192) Eta2 Scheffe
Aggression–impulsivitySTAXI-In M = 2.63 M = 2.55 M = 2.39 M = 2.04 9.22a .13 1,2 N 3,4
SD = .64 SD = .71 SD = .72 SD = .51STAXI-Out M = 2.29 M = 2.35 M = 2.18 M = 1.96 3.42b .05 1 N 4
SD = .82 SD = .76 SD = .70 SD = .41PFAV M = 1.59 M = 1.57 M = 1.42 M = 1.32 7.50c .12 1,2 N 3,4
SD = .46 SD = .38 SD = .31 SD = .17ICS M = 2.47 M = 2.42 M = 2.14 M = 1.84 16.45c .20 1,2 N 3,4
SD = .66 SD = .49 SD = .57 SD = .34Mental painOMMP M = 3.83 M = 3.65 M = 3.32 M = 2.52 31.40c .33 1,2 N 3 N 4
SD = .74 SD = .70 SD = .87 SD = .68BDI M = 1.62 M = 1.50 M = 1.04 M = .27 64.27c .50 1,2 N 3 N 4
SD = .59 SD = .63 SD = .67 SD = .29BHS M = 3.52 M = 3.29 M = 2.72 M = 2.03 38.82c .38 1,2 N 3 N 4
SD = .81 SD = .84 SD = .90 SD = .48Communication difficultiesJSDQ M = 1.97 M = 2.15 M = 2.14 M = 2.27 2.85a .04 1 b 2,3,4
SD = .44 SD = .58 SD = .59 SD = .39SCID-II⁎ M = 1.88 M = 1.50 M = 1.47 M = 1.27 11.95c .16 1 N 2,3,4
SD = .68 SD = .50 SD = .48 SD = .35UCLA M = 2.74 M = 2.45 M = 2.34 M = 1.53 38.20c .37 1 b 2,3 b 4
SD = .69 SD = .63 SD = .67 SD = .40
STAXI = State-Trait Anger Expression Inventory; PFAV = Past Feelings and Acts of Violence; ICS = Impulse Control Scale; OMMP = Orbach &MikulincerMental Pain Scale; BDI = Beck Depression Inventory; BHS = Beck Hopelessness Scale; JSDQ = Jourard Self-Disclosure Questionnaire; SCID-II = StructuredClinical Interview for DSM-II; UCLA = UCLA Loneliness Scale.
⁎ SCID-II personality assessment items in schizoid trait.a p b .01 Scheffe post hoc test.b p b .05 Scheffe post hoc test.c p b .001 Scheffe post hoc test.
45Y. Gvion et al. / Comprehensive Psychiatry 55 (2014) 40–50
3.4. Group differences in aggression–impulsivity, mentalpain, and communication difficulties
3.4.1. Aggression–impulsivityThe first MANOVA showed a significant group effect of
aggression and trait impulsivity [Wilks F approximation(12,380) = 5.25, p b .001, eta2 = .14]. Table 4 shows themean scores and standard deviations for the variousquestionnaires. Univariate analysis revealed a significantgroup effect for all measures of aggression and traitimpulsivity. On post hoc tests, the two suicide-attemptergroups (MSSA and MNSSA) scored higher than thenonsuicidal psychiatric and healthy groups on level ofanger-in (STAXI-In) (p b .01), violence (PFAV) (p b .001),and trait impulsivity (ICS) (p b .001). The medically serioussuicide attempt group scored higher than the healthy controlson level of anger-out (STAXI-Out) (p b .05). Separatecomparison of the two suicide groups yielded no significantdifferences in any of these measures or in state impulsivity(SIS Objective Planning Subscale, Table 3).
3.4.2. Mental painThe second MANOVA yielded a significant group effect
of mental pain [Wilks F approximation (3,576) = 18.17,
p b .001, eta2 = .23]. Table 4 shows the mean scores andstandard deviations for the various questionnaires. Univar-iate analysis revealed a significant group effect for allsubjective measures of mental pain: mental pain (OMMP),depression (BDI), and hopelessness (BHS). On post hoctests, the two suicide groups (MSSA and MNSSA) scoredsignificantly higher than both control groups on all threemeasures (p b .001, for all). There was no differencebetween the two suicide groups on any of these measures.
3.4.3. Communication difficultiesThe third MANOVA yielded a significant group effect
for communication difficulties [Wilks F approximation(9,576) = 12.40, p b .0001, eta2 = .16]. Table 4 shows themean scores and standard deviations for the variousquestionnaires. Univariate analysis revealed a significantgroup effect for all three measures of communicationdifficulties: self-disclosure (JSDQ), schizoid tendencies(SCID-II), and loneliness (UCLA). On post hoc tests, themedically serious suicide attempters scored significantlylower than the other groups on level of self-disclosure(p b .05) and had more schizoid tendencies (p b .001). Inaddition, they reported more feelings of loneliness than the

46 Y. Gvion et al. / Comprehensive Psychiatry 55 (2014) 40–50
medically non-serious attempters and the nonsuicidalpsychiatric subjects. The healthy controls had a signifi-cantly lower loneliness score than the other three groups(p b .001).
3.5. Relationships among study variables
We tested the association of the aggression–impulsivityvariables (anger-in, anger-out, violence, impulsivity trait,and planning), mental pain variants (mental pain, depression,hopelessness), and communication difficulties (self-disclo-sure, schizoid tendencies, loneliness) with the lethality of thesuicide (Table 5). A significant correlation with lethality wasnoted for communication difficulties. Specifically, signifi-cant positive correlations were found for schizoid tendenciesand loneliness, and a significant negative correlation for self-disclosure. Findings for mental pain and aggressive–impulsive variables were not significant.
3.6. Mental pain, aggressive–impulsive tendencies, andcommunication difficulties as predictors of suicide lethality
To assess the contribution of aggression–impulsivityvariables to the medical lethality of suicide, above andbeyond mental pain variables and communication diffi-culties, we conducted a hierarchical regression analysis,as recommended by Cohen et al. [68]. A regressionequation was constructed with the LRS score as thedependent variable. In the first step, mental pain variables(mental pain, depression, and hopelessness) were enteredinto the equation. In the second step, the aggression–impulsivity variables (anger-in, anger-out, impulsivitytrait, and objective planning) were added, and in the thirdstep, the main effects of the communication variables(self-disclosure, schizoid tendencies, loneliness) wereadded. For this purpose, the self-disclosure scores were
Table 5Inter-correlations among study variables.
1 2 3 4 5
1. Anger-In –2. Anger-Out .04 –3. PFAV .15a .50c –4. ICS .30c .48c .59c –5. OOMP .39c .31c .31c .53c –6. BDI .41c .25c .37c .54c .35c
7. BHS .34c .19b .29c .48c 48c
8. JSDQ −.17a .15⁎ −.04 −.01 −.069. SCID-II⁎ .21b −.05 .06 .12 −.17a
10. UCLA .44c .16a .32c .48c .56c
11. Lethal −.08 .02 .04 .01 .1112. SIS-plan⁎ .14 −.04 −.04 −.21a .02
PFAV = Past Feelings and Acts of Violence; ICS = Impulse Control Scale; OOInventory; BHS = Beck Hopelessness Scale; JSDQ = Jourard Self-DisclosureInterview for DSM-IV personality disorders; UCLA = UCLA Loneliness Scale; L
⁎ SCID-II—items on schizoid trait only. SIS—Objective Planning Scale onla p b .05.b p b .01.c p b .001.
reversed to fit the direction of response of the otherquestionnaires. In the final step, the two-way interactionof schizoid tendencies and mental pain were entered intothe equation (Table 6).
The model was significant overall, and together allvariables accounted for 22% of the variance in suicidelethality. Specifically, in step 1, the mental pain variablesaccounted for 3% of the variance and did not significantlypredict lethality [F)2,88) = 1.12 p N .05]. In step 2, theaggression–impulsivity variables accounted for 2% of thevariance and did not significantly predict lethality [F)4,84) = .51 p N .05]. In step 3, the communicationdifficulties variables accounted for 12% of the variance,over and above the contribution of mental pain andaggressive–impulsive variables [F)3,81) = 3.68 p N .05].In the final step, the interaction of mental pain andschizoid tendencies significantly predicted medical lethal-ity after all other variables had been entered, accountingfor another 5% of the total variance in lethality[F(1,80) = 5.36 p b .02].
4. Discussion
Our previous studies showed that communication prob-lems have a significant effect on the lethality of suicideattempts whereas mental pain, depression, and hopelessnessdo not [19,69]. The purpose of the present study was toevaluate the relative effects of two additional risk factors,aggression and impulsivity. We compared medically serioussuicide attempters with medically non-serious suicideattempters and control groups of nonsuicidal psychiatricpatients and healthy volunteers. Most of our hypotheses wereconfirmed. Indices of mental pain, aggression and impul-sivity, along with communication difficulties, distinguished
6 7 8 9 10 11 12
–.59c –−.12 −.20a –.25c .32b .38c –.62c .61c .32c .50c –.15a .15a −.18a .34c .21b –.17 .18 −.11 .21a −.02 .12 –
MP = Orbach & Mikuliner Mental Pain Scale; BDI = Beck DepressionQuestionnaire; SIS = Suicide Intent Scale; SCID-II = Structural Clinicalethal = Lethality.y.
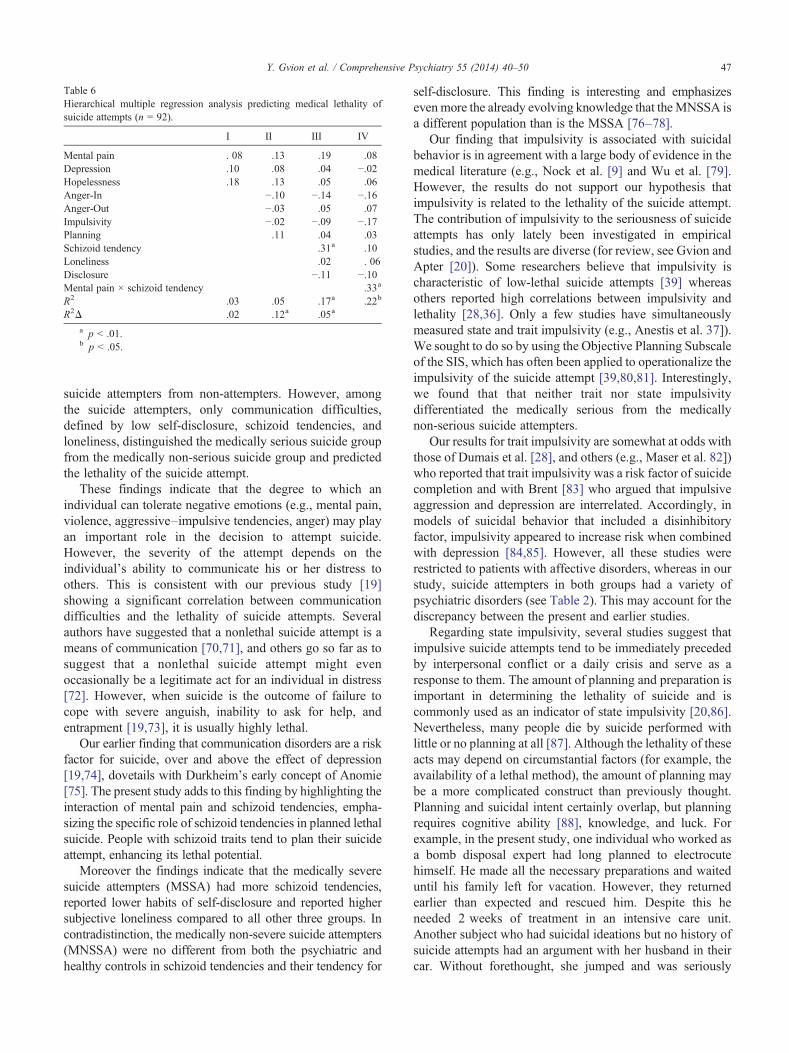
Table 6Hierarchical multiple regression analysis predicting medical lethality ofsuicide attempts (n = 92).
I II III IV
Mental pain . 08 .13 .19 .08Depression .10 .08 .04 −.02Hopelessness .18 .13 .05 .06Anger-In −.10 −.14 −.16Anger-Out −.03 .05 .07Impulsivity −.02 −.09 −.17Planning .11 .04 .03Schizoid tendency .31a .10Loneliness .02 . 06Disclosure −.11 −.10Mental pain × schizoid tendency .33a
R2 .03 .05 .17a .22b
R2Δ .02 .12a .05a
a p b .01.b p b .05.
47Y. Gvion et al. / Comprehensive Psychiatry 55 (2014) 40–50
suicide attempters from non-attempters. However, amongthe suicide attempters, only communication difficulties,defined by low self-disclosure, schizoid tendencies, andloneliness, distinguished the medically serious suicide groupfrom the medically non-serious suicide group and predictedthe lethality of the suicide attempt.
These findings indicate that the degree to which anindividual can tolerate negative emotions (e.g., mental pain,violence, aggressive–impulsive tendencies, anger) may playan important role in the decision to attempt suicide.However, the severity of the attempt depends on theindividual's ability to communicate his or her distress toothers. This is consistent with our previous study [19]showing a significant correlation between communicationdifficulties and the lethality of suicide attempts. Severalauthors have suggested that a nonlethal suicide attempt is ameans of communication [70,71], and others go so far as tosuggest that a nonlethal suicide attempt might evenoccasionally be a legitimate act for an individual in distress[72]. However, when suicide is the outcome of failure tocope with severe anguish, inability to ask for help, andentrapment [19,73], it is usually highly lethal.
Our earlier finding that communication disorders are a riskfactor for suicide, over and above the effect of depression[19,74], dovetails with Durkheim's early concept of Anomie[75]. The present study adds to this finding by highlighting theinteraction of mental pain and schizoid tendencies, empha-sizing the specific role of schizoid tendencies in planned lethalsuicide. People with schizoid traits tend to plan their suicideattempt, enhancing its lethal potential.
Moreover the findings indicate that the medically severesuicide attempters (MSSA) had more schizoid tendencies,reported lower habits of self-disclosure and reported highersubjective loneliness compared to all other three groups. Incontradistinction, the medically non-severe suicide attempters(MNSSA) were no different from both the psychiatric andhealthy controls in schizoid tendencies and their tendency for
self-disclosure. This finding is interesting and emphasizesevenmore the already evolving knowledge that theMNSSA isa different population than is the MSSA [76–78].
Our finding that impulsivity is associated with suicidalbehavior is in agreement with a large body of evidence in themedical literature (e.g., Nock et al. [9] and Wu et al. [79].However, the results do not support our hypothesis thatimpulsivity is related to the lethality of the suicide attempt.The contribution of impulsivity to the seriousness of suicideattempts has only lately been investigated in empiricalstudies, and the results are diverse (for review, see Gvion andApter [20]). Some researchers believe that impulsivity ischaracteristic of low-lethal suicide attempts [39] whereasothers reported high correlations between impulsivity andlethality [28,36]. Only a few studies have simultaneouslymeasured state and trait impulsivity (e.g., Anestis et al. 37]).We sought to do so by using the Objective Planning Subscaleof the SIS, which has often been applied to operationalize theimpulsivity of the suicide attempt [39,80,81]. Interestingly,we found that that neither trait nor state impulsivitydifferentiated the medically serious from the medicallynon-serious suicide attempters.
Our results for trait impulsivity are somewhat at odds withthose of Dumais et al. [28], and others (e.g., Maser et al. 82])who reported that trait impulsivity was a risk factor of suicidecompletion and with Brent [83] who argued that impulsiveaggression and depression are interrelated. Accordingly, inmodels of suicidal behavior that included a disinhibitoryfactor, impulsivity appeared to increase risk when combinedwith depression [84,85]. However, all these studies wererestricted to patients with affective disorders, whereas in ourstudy, suicide attempters in both groups had a variety ofpsychiatric disorders (see Table 2). This may account for thediscrepancy between the present and earlier studies.
Regarding state impulsivity, several studies suggest thatimpulsive suicide attempts tend to be immediately precededby interpersonal conflict or a daily crisis and serve as aresponse to them. The amount of planning and preparation isimportant in determining the lethality of suicide and iscommonly used as an indicator of state impulsivity [20,86].Nevertheless, many people die by suicide performed withlittle or no planning at all [87]. Although the lethality of theseacts may depend on circumstantial factors (for example, theavailability of a lethal method), the amount of planning maybe a more complicated construct than previously thought.Planning and suicidal intent certainly overlap, but planningrequires cognitive ability [88], knowledge, and luck. Forexample, in the present study, one individual who worked asa bomb disposal expert had long planned to electrocutehimself. He made all the necessary preparations and waiteduntil his family left for vacation. However, they returnedearlier than expected and rescued him. Despite this heneeded 2 weeks of treatment in an intensive care unit.Another subject who had suicidal ideations but no history ofsuicide attempts had an argument with her husband in theircar. Without forethought, she jumped and was seriously

48 Y. Gvion et al. / Comprehensive Psychiatry 55 (2014) 40–50
injured. Both subjects were included in the medically serioussuicide attempt group.
Another construct classically associated with suicide isaggression. In the present study, both anger-in and anger-out,in addition to violence, differentiated suicide attempters fromnon-attempters. This finding is compatible with the litera-ture, starting from the classic work of Menninger [47], whotermed suicide “murder in the 180th degree” and laterSpielberger [46], who conceptualized suicide as an inher-ently aggressive act. Others have emphasized the role ofaggression, anger-in, and violent behavior in completedsuicide [29]. Most studies focused on personality traits andpsychiatric diagnosis related to self-reported aggression orthe method chosen for the suicide [28]. Our study revealedno significant difference in aggression variables betweenhigh- and low-lethal suicide attempters. The discrepancybetween our results and those of others may be attributable tothe widespread confusion between trait and state aggression,and to the overlap between aggression and impulsivity (seeWilliams [73] for review). Thus, the present study focusedonly on trait aggression and attempted to separate aggressionfrom impulsivity. However it should be stated that in ourstudy too, measures of aggression and measures ofimpulsivity were significantly correlated (see Table 5).
In conclusion, mental pain, communication difficulties, andaggressive–impulsive tendencies all appear to differentiatebetween psychiatric patients who attempt suicide and thosewho do not. Only communication problems, however,differentiate between suicidal individual who make medicallyserious or medically non-serious suicide attempts. Theseconsiderations should enable clinicians to tailor treatmentprograms for psychiatric patients at risk for suicide.
4.1. Limitations of the study
One limitation to the study is its relatively small group ofMSSA. However medical serious suicide attempters(MSSA) are very hard to recruit as this is a relatively rarepopulation, hence the relative small sample. Nevertheless,the study of this subgroup is important as it can shed light onactual suicide completers [15–19].
Recall bias is also a major limitation of retrospective studiesand may compromise the validity of studies based on self-reported data. In the present study, information on suicide intentand other independent variables (aggressive–impulsive;mentalpain variants and loneliness) may have been biased, although itseems reasonable to assume that the bias was equallydistributed among the groups. Another limitation of thisstudy is its cross-sectional design which precluded conclusionsregarding cause and effect. Longitudinal, prospective studiesare recommended for further research in the field.
References
[1] Apter A, Wasserman D. Adolescent attempted suicide. In: King RA, &Apter A, editors. Suicide in children and adolescents. Cambridge:University Press; 2003. p. 63-86.
[2] Brausch AM. Evaluation of factors for depression and suicide in acommunity sample of adolescents: The role of body image, disorderedeating, parent and peer support, and self esteem. Dissertation AbstractsInternational, 69(08), (UMI No.3324866):DAI volume?, 2008.
[3] Cheah D, Schmitt G, Pridmore S. Suicide, misappropriation andimpulsivity. Aust N Z J Psychiatry 2008;42:544-6.
[4] Frattaroli J. Experimental disclosure and its moderators: a meta-analysis. Psychol Bull 2006;132:823-65.
[5] Gvion Y, Apter A. Review on suicide behavior. Publ Health Rev2012;34(2).
[6] Holmstrand C, Niméus A, Träskman-Bendz L. Risk factors of futuresuicide in suicide attempters—a comparison between suicides andmatched survivors. Nord J Psychiatry 2006;60:162-7.
[7] Haukka J, Suominen K, Partonen T, Lönnqvist J. Determinants andoutcomes of serious attempted suicide: a nationwide study in Finland,1996 to 2003. Am J Epidemiol 2008;167:1155-63.
[8] Kõlves K, Värnik A, Tooding LM, Wasserman D. The role of alcoholin suicide: a case-control psychological autopsy study. Psychol Med2006;36:923-30.
[9] Nock MK, Borges G, Bromet EJ, Alonso J, Angermeyer M, BeautraisA, et al. Cross-national prevalence and risk factors for suicidalideation, plans and attempts. Br J Psychiatry 2008;192:98-105.
[10] Routasalo PE, Savikko N, Tilvis RS, Strandberg TE, Pitkala KH.Social contacts and their relationship to loneliness among aged people—a population-based study. Gerontology 2006;52:181-7.
[11] Orbach I, Iohan-Barak M. Psychopathology and risk factors for suicidein the young, theoretical and empirical. In: Wasserman D, &Wasserman C, editors. Oxford textbook of suicide prevention. Aglobal perspective. Oxford: Oxford University Press; 2009. p. 634-41.
[12] Wasserman D, Sokolowski M, Wasserman J, Rujescu D. Neurobiol-ogy and the genetics of suicide. In: Wasserman D, & Wasserman C,editors. Oxford textbook of suicide prevention. A global perspective.Oxford: Oxford University Press; 2009. p. 165-82.
[13] Brodsky BS, Groves SA, Oquendo MA, Mann JJ, Stanley B.Interpersonal precipitants and suicide attempts in borderline person-ality disorder. Suicide Life Threat Behav 2006;36:313-22.
[14] Apter A. Clinical aspects of suicide behavior relevant to genetics.Europ Psych 2010;25(5):257-9.
[15] Beautrais AL. Suicide and serious suicide attempts in youth: amultiple-group comparison study. Am J Psychiatry 2003;160:1093-9.
[16] Marzano L, Rivlin A, Fazel S, Hawton K. Interviewing survivors ofnear-lethal self-harm: a novel approach for investigating suicideamongst prisoners. J Forensic Leg Med 2009;16:152-5.
[17] Marzano L, Fazel S, Rivlin A, Hawton K. Psychiatric disorders inwomen prisoners who have engaged in near-lethal self-harm: a case-control study. Br J Psychiatry 2010;197:219-26.
[18] Rivlin A, Hawton K, Marzano L, Fazel S. Psychiatric disorders in maleprisoners who made near-lethal suicide attempts: case-control study. BrJ Psychiatry 2010;197:313-9.
[19] Levi Y, Horesh N, Fischel T, Treves I, Or E, Apter A. Mental pain andits communication in medically serious suicide attempts: an “impos-sible situation”. J Affect Disord 2008;111:244-50.
[20] Gvion Y, Apter A. Aggression, impulsivity and suicide behavior: areview of the literature. Suicide Life Threat Behav 2011;15:93-112.
[21] Conner KR, Swogger MT, Houston RJ. A test of reactive aggression-suicidal behavior hypotheses: Is there a case for proactiveaggression? J Abnorm Psychol 2009;118:235-40.
[22] Mann JJ, Malone KM. Cerebrospinal fluid amines and higher lethalitysuicide attempts in depressed inpatients. Biol Psychiatry 1997;41:162-71.
[23] Ninan PT, van Kammen DP, Scheinin M, Linnoila M, Bunney Jr WE,Goodwin FK. CSF 5-hydroxyindoleacetic acid levels in suicidalschizophrenic patients. Am J Psychiatry 1984;141:566-9.
[24] Mann JJ, Currier D. Biological predictors of suicidal behavior in mooddisorders. In: Wasserman D, & Wasserman C, editors. OxfordTextbook of Suicidology and Suicide Prevention: A Global Perspec-tive. Oxford: Oxford University Press; 2009. p. 335-41.

49Y. Gvion et al. / Comprehensive Psychiatry 55 (2014) 40–50
[25] Doihara C, Kawanishi C, Yamada T, Sato R, Hasegawa H, Furuno T,et al. Trait aggression in suicide attempters: a pilot study. PsychiatryClin Neurosci 2008;62:352-4.
[26] McGlashan TH. Borderline personality disorder and unipolar affectivedisorder. Long-term effects of comorbidity. J Nerv Ment Dis1987;175:467-73.
[27] Black DW, Bell S, Hulbert J, Nasrallah A. The importance of Axis II inpatients with major depression. A controlled study. J Affect Disord1988;14:115-22.
[28] Dumais A, Lesage AD, Lalovi A, Séguin M, Tousignant M, ChawkyN, et al. Is violent method of suicide a behavioral marker of lifetimeaggression? Am J Psychiatry 2005;162:1375-8.
[29] Conner KR, Duberstein PR, Conwell Y, Seidlitz L, Caine ED.Psychological vulnerability to completed suicide: a review of empiricalstudies. Suicide Life Threat Behav 2001;31:367-85.
[30] Soloff PH, Fabio A, Kelly TM, Malone KM, Mann JJ. High-lethalitystatus in patients with borderline personality disorder. J Pers Disord2005;19:386-99.
[31] Whiteside SP, Lynam DR. Understanding the role of impulsivity andexternalizing psychopathology in alcohol abuse: application of theUPPS impulsive behavior scale. Exp Clin Psychopharmacol2003;11:210-7.
[32] Evenden J. Impulsivity: a discussion of clinical and experimentalfindings. J Psychopharmacol 1999;13:180-92.
[33] Horesh N, Rolnick T, Iancu I, Dannon P, Lepkifker E, Apter A, et al.Anger, impulsivity, and suicide risk. Psychother Psychosom1997;66:92-6.
[34] Horesh N, Gothelf D, Ofek H, Weizman T, Apter A. Impulsivity as acorrelate of suicidal behavior in adolescent psychiatric patients. Crisis1999;20:8-14.
[35] Baud P. Personality traits as intermediary phenotypes in suicidalbehavior: genetic issues. Am J Med Genet C: Semin Med Genet2005;133:34-42.
[36] Swann AC, Dougherty DM, Pazzaglia PJ, Pham M, Steinberg JL,Moeller FG. Increased impulsivity associated with severity of suicideattempt history in patients with bipolar disorder. Am J Psychiatry2005;162:1680-8.
[37] Anestis MD, Selby EA, Joiner TE. The role of urgency in maladaptivebehaviors. Behav Res Ther 2007;45:3018-29.
[38] Simon OR, Swann AC, Powell KE, Potter LB, KresnowMJ, O'CarrollPW. Characteristics of impulsive suicide attempts and attempters.Suicide Life Threat Behav 2001;32(Suppl):S49-59.
[39] Baca-Garcia E, Diaz-Sastre C, Basurte E, Prieto R, Ceverino A, Saiz-Ruiz J, et al. A prospective study of the paradoxical relationshipbetween impulsivity and lethality of suicide attempts. J Clin Psychiatry2001;62:560-5.
[40] Baca-Garcia E, Diaz-Satre C, Garcia-Resa E, Blasco H, BraquehaisConesa D, Oquendo MA, et al. Suicide attempts and impulsivity. EurArch Psychiatry Clin Neurosci 2005;255:152-6.
[41] Hawton K. Suicidal behavior in children and adolescents. NewburyPark, CA: Sage; 1986.
[42] Carballo JJ, Oquendo MA, Giner L, Zalsman G, Roche AM, She L.Impulsive–aggressive traits and suicidal adolescents and youngadults with alcoholism. International J Adolesc Med Health2006;18:15-9.
[43] Stanford MS, Helfritz LE, Conklin SM, Greve KW, Adams D,Villemarette-Pittman NR, et al. A comparison of anticonvulsants in thetreatment of impulsive aggression. Exp Clin Psychopharm2005;13:72-7.
[44] Giegling I, Olgiati P, Hartmann AM, Calati R, Möller HJ, Rujescu D,et al. Personality and attempted suicide. Analysis of anger, aggressionand impulsivity. J Psychiatr Res 2009;43:1262-71.
[45] Goldston DB, Reboussin BA, Daniel SS. Predictors of suicideattempts: state and trait components. J Abnorm Psychol2006;115:842-9.
[46] Spielberger CD. State-Trait Anger-Expression Inventory. Professionalmanual. Odessa, FL: Psychological Assessment Resources; 1988.
[47] Menninger KA. Psychoanalytic aspects of suicide. Int J Psychoanal1933;14:376-90.
[48] Rutz W, Rihmer Z. Suicide in men. Suicide prevention for the maleperson. In: Wasserman D, & Wasserman C, editors. Oxford textbookof suicide prevention. A global perspective. Oxford University Press;2009. p. 249-55.
[49] Werner NE, Crick NR. Relational aggression and social-psychologicaladjustment in a college sample. J Abnorm Psychol 1999;108:615-23.
[50] First MB, Spitzer RL, Gibbon M, Williams JBW. Structured ClinicalInterview for DSM-IVAxis I Disorders with Psychotic Screen. NewYork:New York State Psychiatric Institute, Biometrics Research Unit; 1995.
[51] Beck AT, Beck R, Kovacs M. Classification of suicidal behaviors: I.Quantifying intent and medical lethality. Am J Psychiatry 1975;132:285-7.
[52] Lester D, Beck A. Suicidal intent, medical lethality of the suicideattempt, and components of depression. J Clin Psychol 1975;31:11-2.
[53] Weisman AD, Worden JW. Risk-rescue rating in suicide assessment.Arch Gen Psychiatry 1972;26:553-60.
[54] Spielberger CD, Sydeman SJ. State-trait anxiety inventory and state-trait anger expression inventory. In: & Maurish ME, editor. The use ofpsychological testing for treatment planning and outcome assessment.Hillsdale, NJ: Lawrence Erlbaum; 1994. p. 292-321.
[55] Plutchick R, van-Praag HM. A self-report measure of violence risk, II.Compr Psychiatry 1990;31:450-6.
[56] Brent DA, Kolko DJ, Allan MJ, Brown RV. Suicidality in affectivelydisordered adolescent inpatients. J Am Acad Child Adolesc Psychiatry1990;29:586-93.
[57] Plutchik R, Van Praag H. The measurement of suicidality, aggressivityand impulsivity. Prog Neuropsychopharmacol Biol Psychiatry1989;13(Suppl):S23-34.
[58] Kotler M, Finkelstein G, Molcho A, Botsis AJ, Plutchik R, Brown SL,et al. Correlates of suicide and violence risk in an inpatient population:coping styles and social support. Psychiatry Res 1993;47:28-290.
[59] Beck RW, Morris JB, Beck AT. Cross-validation of the Suicide IntentScale. Psychol Rep 1974;34:445-6.
[60] Beck AT, Schuyler D, Herman I. Development of Suicide Intent Scales.In: Beck AT, Resnick HLP, & Lettieri D, editors. The prediction ofsuicide. Bowie, MD: Charles Press Publishers; 1974. p. 45-56.
[61] Mieczkowski TA, Sweeney JA, Haas GL, Junker BW, Brown RP,Mann JJ. Factor composition of the suicide intent scale. Suicide LifeThreat Behav 1993;23:37-45.
[62] Orbach I, Mikulincer M, Sirota P, Gilboa-Schechtman E. Mental pain:a multidimensional operationalization and definition. Suicide LifeThreat Behav 2003;33:219-30.
[63] Beck AT. The Beck Depression Inventory. San Antonio, TX:Psychological Corporation; 1978.
[64] Beck AT, Weissman A, Lester D, Trexler L. The measurement ofpessimism: The Hopelessness Scale. J Consult Clin Psychol 1974;42:861-5.
[65] Jouard SM. The disclosure: an experimental analysis of the transparentself. New York: Wiley-Interscience; 1971.
[66] Russell D, Peplau LA, Cutrona CE. The revised UCLA LonelinessScale: concurrent and discriminant validity evidence. J Pers SocPsychol 1980;39:472-80.
[67] Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed.Lawrence Erlbaum As: Hillsdale, NJ; 1988.
[68] Cohen J, Cohen P, West SG, Aiken LS. Applied multiple regression/correlation analysis for the behavioral sciences. 3rd ed. Routledge; 2003.
[69] Horesh N, Levi J, Apter A. Medically serious versus non-serioussuicide attempts: relationships of lethality and intent to clinical andinterpersonal characteristics. J Affect Disord 2012;136:286-93.
[70] Shneidman ES. Suicide as psychache: a clinical approach to self-destructive behavior. Northvale, NJ: Jason Aronson; 1993.
[71] Kreitman N. Parasuicide. New York, NY: Wiley; 1977.[72] Hjelmeland H, Hawton K, Nordvik H, Bille-Brahe U, De Leo D,
Fekete S, et al. Why people engage in parasuicide: a cross-culturalstudy of intentions. Suicide Life Threat Behav 2002;32:380-93.

50 Y. Gvion et al. / Comprehensive Psychiatry 55 (2014) 40–50
[73] Williams JMG. Cry of pain: understanding suicide and self-harm.London: Penguin Books; 1997.
[74] Apter A, Horesh N, Gothelf D, Graffi H, Lepkifker E. The relationshipbetween self disclosure and serious suicidal behavior. ComprPsychiatry 2001;42:70-5.
[75] Durkheim E. Suicide: a study in sociology. Spoulding JA, Simpson G,translators. New York: Free Press; 1951 (original work published 1897).
[76] Beautrais AL. Suicide and serious suicide attempts: two populations orone? Psychol Med 2001;31:837-45.
[77] Dejong TM, Overholser JC, Stockmeie CA. Apples to oranges? Adirect comparison between suicide attempters and suicide com-pleters. J Affect Disord 2010;124:90-7.
[78] Hawton K. Studying survivors of nearly lethal suicide attempts: animportant strategy in suicide research. Suicide Life Threat Behav2001;32:76-85.
[79] Wu CS, Liao SC, Lin KM, Tseng MM, Wu EC, Liu SK.Multidimensional assessments of impulsivity in subjects with historyof suicidal attempts. Compr Psychiatry 2009;50:315-21.
[80] Beck AT, Schuyler D, Herman I. Development of suicidal intentscales. In: Beck AT, Resnick CL, & Lettieri D, editors. The predictionof suicide. Bowie, MD: Charles Press; 1986. p. 45-56.
[81] Soloff PH, Lynch KG, Kelly TM, Malone KM, Mann JJ. Character-istics of suicide attempts of patients with major depressive episode andborderline personality disorder: a comparative study. Am J Psychiatry2000;157:601-8.
[82] Maser JD, Akiskal HS, Schettler P, Scheftner W,Mueller T, Endicott J,et al. Can temperament identify affectively ill patients who engage inlethal or near-lethal suicidal behavior? A 14-year prospective study.Suicide Life Threat Behav 2002;32:10-32.
[83] Brent DA. In search of endophenotypes for suicidal behavior. Am JPsychiatry 2009;133:13-24.
[84] Apter A, Plutchik R, van Praag HM. Anxiety, impulsivity anddepressed mood in relation to suicidal and violent behavior. ActaPsychiatr Scand 1993;87:1-5.
[85] Baumeistar RF. Suicide as escape from self. Psychol Rev 1990;97:90-113.[86] Witte TK, Merril KA, Stellrecht NE, Bernert RA, Hollar DL,
Schatschneider C, et al. Impulsive youth suicide attempters are notnecessarily all that impulsive. J Affect Dis 2008;107:107-16.
[87] Conner KR. A call for research on planned vs. unplanned suicidalbehavior. Suicide Life Threat Behav 2004;34:89-99.
[88] Freedenthal S. Challenges in assessing intent to die: can suicideattempters be trusted? Omega (Westport) 2007;55:57-70.
Copyright © 2022 FDOKUMEN