
Agenda - GOV.UK
178
Page 1 of 2 Health and Social Care Information Centre Board Agenda: Part 1 (Public Session) 27 January 2016 – 12:30 to 14:30 Venue: (Nightingale Suite) 110 Rochester Row, Victoria, London, SW1P 1JP Ref No Agenda Item Time Presented By HSCIC 16 06 01 Chair’s Introduction and Apologies (oral) 12:30 – 12:35 Chair HSCIC 16 06 02 Declaration of Interests and minutes 12:34 – 12:45 (a) Register of Interests (paper) – for information (b) Minutes of Board Meeting on 25 November 2015 (paper) – to ratify (c) Matters Arising (oral) – for comment (d) Progress on Action Points (paper) – for information Chair HSCIC 16 06 03 Business and Performance Reporting 12:45 – 13:30 (a) Board Performance Pack (paper) – for information (b) Business Plan and Budget 2015-16 Report (paper) – for information (c) Comprehensive Spending Review (CSR) and Corporate Business Plan 2016-17 Progress Update (paper) – for information (d) Data Release Review: Audit Status Update (paper) – for information (e) Staff Survey Results (paper) – for information (f) Staff Personal Development Review (PDR) Report (paper) – for information CEO Director of Finance and Corporate Services 2 items b, c Lead Clinician and Interim Director of Information and Analytics (Caldicott Guardian) Director of Human Resources and Transformation 2 items e, f HSCIC 16 06 04 Supporting the Health and Social Care System 13:30 – 14:00 (a) Breast Implant Registry Direction (paper) – for acceptance (b) Pulmonary Hypertension Direction (paper) – for acceptance (c) Patient Objection Management System Direction (oral) – for information (d) Cancer Waiting Times Direction (paper) – for acceptance Lead Clinician and Interim Director of Information and Analytics (Caldicott Guardian) 3 items a, b, c Director Of Operations and Assurance Services Agenda Page 1 of 159
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Agenda - GOV.UK
Page 1 of 2
Health and Social Care Information Centre Board
Agenda: Part 1 (Public Session)
27 January 2016 – 12:30 to 14:30
Venue: (Nightingale Suite) 110 Rochester Row, Victoria, London, SW1P 1JP
Ref No Agenda Item Time Presented By HSCIC 16 06 01
Chair’s Introduction and Apologies (oral)
12:30 – 12:35
Chair
HSCIC 16 06 02 Declaration of Interests and minutes
12:34 – 12:45
(a) Register of Interests (paper) – for information (b) Minutes of Board Meeting on 25 November 2015
(paper) – to ratify (c) Matters Arising (oral) – for comment (d) Progress on Action Points (paper) – for information
Chair
HSCIC 16 06 03 Business and Performance Reporting
12:45 – 13:30
(a) Board Performance Pack (paper) – for information
(b) Business Plan and Budget 2015-16 Report (paper) – for information
(c) Comprehensive Spending Review (CSR) and Corporate Business Plan 2016-17 Progress Update (paper) – for information
(d) Data Release Review: Audit Status Update (paper) – for information
(e) Staff Survey Results (paper) – for information
(f) Staff Personal Development Review (PDR) Report (paper) – for information
CEO
Director of Finance and Corporate
Services 2 items b, c
Lead Clinician and Interim Director of Information and
Analytics (Caldicott Guardian)
Director of Human Resources and Transformation
2 items e, f
HSCIC 16 06 04 Supporting the Health and Social Care System
13:30 – 14:00
(a) Breast Implant Registry Direction (paper) – for acceptance
(b) Pulmonary Hypertension Direction (paper) – for acceptance
(c) Patient Objection Management System Direction (oral)
– for information
(d) Cancer Waiting Times Direction (paper) – for acceptance
Lead Clinician and Interim Director of Information and
Analytics (Caldicott Guardian)
3 items a, b, c
Director Of Operations and Assurance
Services
Age
nda
Page 1 of 159

Page 2 of 2
HSCIC 16 06 05 Transparency and Governance
14:00 – 14:25
(a) Committee Reports: i. Assurance and Risk Committee: 13 January 2016
(oral) ii. Information Assurance and Cyber Security
Committee: 13 January 2016 (oral) (b) Arrangements for the Annual Review of Board
Effectiveness (oral) – for information (c) Board Forward Business Schedule 2015-16 (paper) –
for information (d) Board Forward Business Schedule 2016-17 (paper) –
for information
Committee Chair
Committee Chair
Sir Ian Andrews, Non-Executive Director
(Senior Independent Director)
Chair
HSCIC 16 06 06 Any other Business (subject to prior agreement with Chair)
14:25 – 14:30 Chair
HSCIC 16 06 07 Background Paper(s) (for information)
(a) Forthcoming Statistical Publications (paper) – for information
(b) Programme Definitions (paper) – for reference
Date of next meeting 30 March 2016 – Southport (to include morning seminar/presentations)
Page 2 of 159

Page 1 of 4
Board meeting – Public session
Title of paper: HSCIC Board Members Register of Interests
Board meeting date: 27 January 2016
Agenda item no: HSCIC 16 06 02 a
Paper presented by:
Chair
Paper prepared by:
Annabelle McGuire, Secretary to the Board
Paper approved by: (Sponsor Director) N/A
Purpose of the paper: The HSCIC is required by its Standing Orders to maintain a publically available Register of Members’ Interests.
The Register contains, as they become available, the Declarations of Interest made by Board members.
Key risks and issues:
N/A
Patient/public interest:
Corporate Governance
Transparency and Openness
Actions required by the board: For information
02 (
a) R
egis
ter
of In
tere
sts
Page 3 of 159

Page 2 of 4
HSCIC Board Register of Interests 2015-16
Name
Declared Interest
Non-Executive Directors
Kingsley Manning: Chair
Director – Newchurch Limited (non-trading since 01 June 2013)
Director – Hennig UK Limited
Trustee and Board member - Royal Philharmonic Society
Director of Spectrum (General Partner) Limited, the investment advisory board for the Rainbow Seed Fund, which is an investment fund, funded by a number of the research councils.
Sir Ian Andrews: Non-Executive Director Senior Independent Director
Director of IMA Partners Ltd (formerly known as Abis Partnership Ltd) provision of legal and management consultancy services to government, academia (KCL1) and Transparency International UK
Consultancy advice to DH on aspects of governance of NHS Transformation, renegotiation of Connecting for Health contracts with CSC2, and oversight of Fujitsu Arbitration process
Other Offices:
Conservator of Wimbledon and Putney Commons
Trustee Chatham Historic Dockyard
Member of UK Defence Academy Academic Advisory Board
Dr Sarah Blackburn: Non-Executive Director
Director - The Wayside Network Limited
Director - IIA3 Inc
Independent member of the Management Board, RICS4
Non-Executive Partner, The Green Practice, Bristol
Employment (other than with the HSCIC): The Wayside Network Limited
Other Offices:
Audit Committee member, RAC Pension Fund Trustee
Contracts held in last 2 years: The Wayside Network Limited has:
a contract to supply GP and primary care nursing services to Avon and Wiltshire NHS Partnership
a zero hours contract with the Chartered Institute of Internal Auditors
1 King's College London
2 Computer Sciences Corporation
3 The Institute of Internal Auditors
4 Royal Institution of Chartered Surveyors
Page 4 of 159

Page 3 of 4
Name
Declared Interest
Shareholdings:
50% of The Wayside Network Limited
Sir John Chisholm: Non-Executive Director
Executive Chair – Genomics England Ltd.
Chair – Nesta (the charity)
Director – Historic Grand Prix Cars Association Ltd.
Professor Maria Goddard: Non-Executive Director
Member of Board of Directors for the York Health Economics Consortium at the University of York.
Professor of Health Economics at the University of York and head of department/director of the Centre for Health Economics at the University of York
Sir Nick Partridge: Non-Executive Director Vice-Chair
Other Offices:
Chair - Clinical Priorities Advisory Group, NHS England
Deputy Chair - UK Clinical Research Collaboration
Deputy Chair, Sexual Health Forum, DH
Executive Directors
Andy Williams: Chief Executive Officer (CEO)
None
Rachael Allsop: Executive Director of Human Resources and Transformation
None
Rob Shaw: Executive Director of Operations and Assurance Services
None
Carl Vincent: Executive Director of Finance and Corporate Services
None
Directors
Peter Counter: Chief Technology Officer (CTO)
Director at Canary Wharf College Limited
02 (
a) R
egis
ter
of In
tere
sts
Page 5 of 159
Page 4 of 4
Name
Declared Interest
Tom Denwood: National Provider Support and Integration Director
British Computer Society (BCS) Health, Vice Chair Policy and Strategy (a voluntary role at this registered charity)
Senior Responsible Owner (SRO) for Local Service Provider (LSP) Programmes on behalf of Department of Health
James Hawkins: Director of Programme Delivery
Parent Governor at St Peters Church of England Primary School, Harrogate
Isabel Hunt: Director of Customer Relations
Trustee, Thackray Medical Museum (Leeds)
Council Member, Leeds Minster
Director - Barry Wades Estates Ltd
Professor Martin Severs: Lead Clinician and Interim Director of Information and Analytics (Caldicott Guardian)
Trustee of Dunhill Medical Trust, a research charity
Consultant Geriatrician with Portsmouth Hospitals NHS Trust
Professor of Health Care for Older People with University of Portsmouth
Other Offices:
Member of SoS5 Independent Information Governance Oversight Panel
Other relevant interests:
Medical consultant and member of the Royal College of Physicians, British Geriatrics Society and the Faculty of Public Health Medicine
Linda Whalley: Director of Policy and Strategy
None
Director of Information and Analytics
Vacancy
5 Secretary of State
Page 6 of 159

Health and Social Care Information Centre
Minutes of Board Meeting – Wednesday 25 November 2015
Part 1 - Public Session
Present:
Vice-Chair Sir Nick Partridge
Non-Executive Director Sir Ian Andrews
Non-Executive Director Sir John Chisholm
Non-Executive Director Prof. Maria Goddard
Non-Executive Director Dr Sarah Blackburn Chief Executive Officer Andy Williams Director of Operations and Assurance Services Rob Shaw Director of Human Resources and Transformation Rachael Allsop Director of Finance and Corporate Services Carl Vincent In attendance: Chief Technology Officer Peter Counter National Provider Support and Integration Director Tom Denwood Director of Programmes James Hawkins Interim Director of Information and Analytics and Lead Clinician (Caldicott Guardian)
Prof. Martin Severs
Director of Customer Relations Isabel Hunt Secretary to the Board Annabelle McGuire
02 (
b) M
inut
es o
f the
Boa
rd M
eetin
g on
25th
Nov
embe
r 20
15
Page 7 of 159

Page 2 of 6
1. Chair’s Introduction and Apologies (HSCIC 15 05 01)
1.1 The Vice Chair convened a meeting of the HSCIC Board.
1.2 HSCIC Chair, Kingsley Manning, HSCIC Chair and Linda Whalley, Assistant Director for
Strategy and Policy had registered their apologies. Sir Nick Partridge, Non-Executive Director
and Vice Chair of the HSCIC chaired the Board meeting.
2. Declaration of Interests and Minutes (HSCIC 15 05 02)
2.1 (a) Register of Interests (paper): HSCIC 15 05 02 (a) The Board agreed the Register of Interests was correct.
2.2 (b) Minutes of Board meeting on 23 September 2015 (paper): HSCIC 15 05 02 (b)
The Board ratified the minutes of the meeting on 23 September 2015 as correct.
2.3
(c) Progress on action points (paper): HSCIC 15 05 02 (c) The Board noted the progress on action points resulting from the previous meeting.
2.4 (d) Matters Arising: HSCIC 15 05 02 (d): There were no matters arising discussed.
3.
Business and Performance Reporting (HSCIC 15 05 03)
3.1 (a) Board Performance Pack (paper): HSCIC 15 05 03 (a) The CEO presented this item, he highlighted by exception items to be brought to the Boards attention. The purpose was to provide the Board with a summary of performance in October. The status of the electronic referral service (e-RS) was improving overall. The Director of Operations and Assurance Services stated that the Calculating Quality Reporting Service (CQRS) has had a number of High Severity Incidents over a number of months. Mitigating action was underway including service improvement plans and commercial discussions to ensure close monitoring of the situation. Sir Ian Andrews suggested engagement with the Crown commercial representative might be helpful. The CEO highlighted the successful exit of the BT Local Service provider (LSP) contracts. The schedule for the completion of the final Trust was the end of November. The Director of Human Resources and Transformation provided an update on organisational health update, status now green. She highlighted a number of initiatives that were underway. The Board requested sight of the results of the recent staff survey when finalised.
Action: Director of Human Resources and Transformation The CEO said that the status of the data quality indicator is green though he did not consider that reflected the position accurately. This indicator is subject to progressive development. The CEO stated that the addressing of the time delay in reporting to the Board was developing and this meant going forward that the Board would see a more timely set of indicators. The Board noted and received the update.
3.2 (b) Mid-Year review of Corporate Business Plan 2015-16 (paper): HSCIC 15 05 03 (b) The Director of Finance and Corporate Services presented this item. The purpose was to provide the Board with an update of the latest financial position against budget for 2015-16, an update on progress against the Business Plan for 2015-16, an overview of resourcing and the impact on delivery and a forward look at the landscape for future funding expectations, and the HSCIC’s response to expected financial pressures in coming years. He highlighted the budget setting and business planning timetable, and noted the currently uncertain environment in which this process would take place.
Page 8 of 159

Page 3 of 6
He conveyed that the process would take into account the organisations transformation programme, which would lead to a different organisational structure. He said that dialogue was underway with the Department of Health and NHS England to ensure that work prioritisation is correct and aligned. The Board discussed the form of the organisation and if it was prepared for the future, and observed that the delivery of efficiencies was critically important. The Director of Finance and Corporate Services said that the work would be demanding to deliver, however the executive team were aware of this and were focussing on the challenges. The Board noted and received the update.
4. Supporting the Health and Social Care System (HSCIC 15 05 04)
4.1 (a) Streamlining the Independent Information governance Advice to HSCIC (paper): HSCIC 15 05 04 (a)
The interim Director of Information and Analytics and Lead Clinician presented this item. The purpose was to update the Board on progress to establish the Independent Group Advising on the Release of Data (IGARD). The Board observed that the appointment of the IGARD chair was crucial. The Board agreed they would take a proactive role and propose names for the National Data Guardian to consider for the position.
Action: Board Members The Board agreed the implementation of a ‘class action’ approach meaning that following the establishment of a precedent by IGARD future decisions should then go through officials. The Board observed that it was important that the staff are supported, as this was a cultural change for the team. The Board approved the HSCIC response to the IGARD consultation, the IGARD terms of reference and the first stages of the IGARD implementation.
4.2 (b) Directions for Patient Objection Management System – Update and proposed mechanism for formal consultation with the (paper): HSCIC 15 05 04 (b) The interim Director of Information and Analytics and Lead Clinician presented this item. The purpose was to provide the Board with an update on the patient objections programme and the development of the draft Directions. The proposal was that the management of the acceptance of the Directions would be progressed by Chair’s action. This was because the draft was not ready for the November Board and the January Board was scheduled too late to enable the programme delivery timescales (which have been agreed with the Secretary of State for Health) to be met. The Vice Chair informed the Board the Chair supported this approach. The interim Director of Information and Analytics and Lead Clinician confirmed that work is ongoing to draft the Directions within the Department of Health, and that it would be ready for implementation in January. The Board discussed the method by which other organisations would apply the objections. The Board approved the management of the Directions via a Chairs action.
4.3 (c) Update on HSCIC (Immigration Health Charge) Directions (paper): HSCIC 15 05 04 (c) The Director of Operations and Assurance Services presented this item. The purpose was to
provide the Board with an update on the Department of Health Visitor and Migrant cost recovery programme, a request from the Board at its April meeting. He confirmed that the migrant programme would fund the associated costs. He said this had been positive work in conjunction with the Department of Health. He stated that no NHS patient data goes to the Home Office, and the work did not directly support the collection of payments. The Board noted and received the update.
4.4 (d) 100,000 Genomes Project: Proposal for a Secretary of State direction to cover HSCIC
Provision of informatics support (paper): HSCIC 15 05 04 (d) Non-Executive Director Sir John Chisholm registered his interest and took no part in the
discussion or decision on this item.
02 (
b) M
inut
es o
f the
Boa
rd M
eetin
g on
25th
Nov
embe
r 20
15
Page 9 of 159
Page 4 of 6
The Chief Technology Officer presented this item. The HSCIC requires legal cover in the form of a Direction to commence operational management of a selection of services to provide informatics support to Genomics England’s 100,000 Genomes (research) project. The purpose was to obtain the Board’s acceptance of the Direction. The Board were supportive and accepted the Direction.
5. Transparency and Governance (HSCIC 15 05 05)
5.1 (a) Committee Reports: HSCIC 15 05 05 (a)
(a) i Assurance and Risk Committee (ARC) (oral): HSCIC 15 05 05 (a) i The Chair of the Assurance and Risk Committee Dr Sarah Blackburn, reported that the
Committee had met on 10 November 2015. Gerry Murphy (Chair of the Department of Heath Audit and Risk Committee) and Karen Wheeler (NHS England’s National Director for Transformation and Corporate Operations) had joined the Committee. The Committee had considered a risk deep dive on cyber security and the cyber security internal audit report, rated as moderate. There had been a progress report on risk management, assurance mapping and the internal audit plan’s progress, alongside three other internal audit reports. The Committee had reviewed follow-ups on recommendations and actions in respect to internal audits reports and Gateway reviews, where there was still work to be undertaken. There was a first look at the yearend planning, and an update on financial controls. The National Audit Office (NAO) presented their initial thoughts in respect to their external audit plan. The consensus of the Committee was that the HSCIC was doing the right things but could be doing them faster. The next meeting of the Committee would be on 13 January 2016.
(a) ii Information Assurance and Cyber Security Committee (oral): HSCIC 15 05 05 (a) ii The Committee Chair, Sir Ian Andrews, reported that the Committee had met on 12 November
2015. There had been good support from other government departments and agencies but, disappointingly, no representation from the Department of Health. The Committee had received an update on the National Data Guardian’s work with the Care Quality Commission (CQC) on the review of security standards across the health and social care system. Significant support was being provided by the HSCIC and other government departments. The Committee had also received an update from the Department of Health chaired Information Security and Risk Board (ISRB) held on 14 October which had included a briefing on the threat landscape. The Committee had discussed progress on the HSCIC’s cyber security programme, and the implementation of CareCERT. The Security Incident and Compliance Manager provided a useful report, which led to a wide-ranging discussion and an invitation to the executive directors to consider the recommendations, particularly on the formation of a protective working group which should include clinical and technical expertise. This had been the most successful meeting so far with open discussion and constructive challenge. The next meeting of the Committee would be on 13 January 2016.
5.2 (b) Board Forward Business Schedule 2015-16: HSCIC 15 05 05 (b)
The Board noted the forward business schedule.
6. 6.1
Any Other Business The Vice Chair informed the Board of the following items of any other business:
a. A set of draft minutes from the public session of the Board will be agreed by Kingsley Manning (Chair), Andy Williams (CEO), and Annabelle McGuire (Secretary to the Board) and will be published as provisional/unconfirmed minutes on the HSCIC’s web site within ten working days of the meeting taking place. Approval of the minutes will take place the subsequent public Board meeting and republished as ratified minutes. The Board approved
Page 10 of 159
Page 5 of 6
the proposal. b. Approval of the minutes from the Board Business meetings would take place at the following
part 2 session of the public Board. Publication would be of an abridged set of minutes, agreed by Kingsley Manning (Chair) and Andy Williams (CEO), on the HSCIC’s web site. The Board noted the update.
7. Background Papers (HSCIC 15 05 07)
7.1 (a) Forthcoming Statistical Publications (paper): HSCIC 15 05 07 (a)
The Board noted this paper for information.
7.2 (b) Programme Definitions (paper): HSCIC 15 05 07 (b) The Board noted this paper for information.
7.3 (c) Correspondence from the Information Commissioner’s Office to the Chair of the HSCIC
(paper): HSCIC 15 05 07 (c) The Board noted this paper for information.
The arranged date of the next public Board meeting was for 27 January 2016.
8 Date of Next Meeting
8.1 The next statutory Board meeting was scheduled for 27 January 2016.
The Board resolved that pursuant to the Public Bodies (Admission to Meetings) Act 1960 that representatives of the press and other members of the public be excluded from the remainder of this meeting having regard to the confidential nature of the business to be transacted, publicity on which would be prejudicial to the public interest’ (Section 1 (2) Public Bodies (Admission to Meetings) Act 1960).
Table of Actions:
Action Action Owner
The Director of Human Resources and Transformation provided an update on organisational health update, status now green. She highlighted a number of initiatives that were underway. The Board requested sight of the results of the recent staff survey when finalised.
Director of Human Resources and Transformation
The Board observed that the appointment of the IGARD chair was crucial. The Board agreed they would take a proactive role and propose names for the National Data Guardian to consider for the position.
Board Members
02 (
b) M
inut
es o
f the
Boa
rd M
eetin
g on
25th
Nov
embe
r 20
15
Page 11 of 159

Page 6 of 6
Agreed as an accurate record of the meeting
Date:
Signature:
Name: Kingsley manning
Title: HSCIC Chair
Page 12 of 159

Page 1 of 2
Board meeting – Public session
Title of paper: Update on action points from the previous meeting
Board meeting date: 27 January 2016
Agenda item no: HSCIC 16 06 02 d
Paper presented by: Chair
Paper prepared by: Annabelle McGuire, Secretary to the Board
Paper approved by: (Sponsor Director) Action Updates as submitted by the relevant Executive Management Team director.
Purpose of the paper: To share an update on action points from the previous meeting for information.
Key risks and issues: As stated in the action and commentary
Patient/public interest: Corporate Governance
Actions required by the board: To note for information
02 (
d) P
rogr
ess
on A
ctio
n P
oint
s
Page 13 of 159

Pag
e 2
of
2
Su
mm
ary
of
pro
gre
ss
ag
ain
st
Bo
ard
mee
tin
g a
cti
on
s
=
com
ple
ted
c/f
= o
n-g
oin
g
S
tatu
s
Su
mm
ary
of
Acti
on
C
om
men
tary
R
esp
on
sib
le D
irecto
r F
or
Info
rmati
on
On
ly
Org
an
isati
on
al H
ealt
h: T
he D
irecto
r of
Hum
an R
esourc
es a
nd T
ransfo
rmation
pro
vid
ed a
n u
pdate
on o
rganis
ational health
update
, sta
tus n
ow
gre
en.
She h
ighlig
hte
d a
num
ber
of
initia
tives t
hat w
ere
underw
ay.
The B
oard
req
ueste
d s
ight
of th
e r
esults o
f th
e r
ecent sta
ff s
urv
ey w
hen f
inalis
ed.
On the a
genda
Dir
ecto
r o
f H
um
an
R
eso
urc
es a
nd
T
ran
sfo
rmati
on
Y
es
c/f
Ind
ep
en
den
t G
rou
p A
dvis
ing
on
th
e
Rele
ase o
f D
ata
(IG
AR
D):
The B
oard
observ
ed t
hat th
e a
ppoin
tment
of th
e
IGA
RD
chair w
as c
rucia
l. T
he B
oard
ag
reed
they w
ould
take a
pro
active r
ole
and
pro
pose n
am
es f
or
the N
ational D
ata
G
uard
ian to c
onsid
er
for
the p
ositio
n.
Corr
espondence h
as b
een s
ent to
th
e B
oard
advis
ing
the follo
win
g:
A p
roposal fo
r th
e a
ppoin
tment
of
an inte
rim
IG
AR
D C
hair h
as b
een
made, subje
ct to
the B
oard
sendin
g
its lis
t of
nom
inees to D
am
e F
iona
Cald
icott
for
her
revie
w.
M
art
in S
evers
has info
rmed t
he
Board
that th
is a
ppoin
tment
would
als
o b
e h
is n
om
inee to b
ecom
e the
firs
t in
dependent C
hair o
f IG
AR
D,
subje
ct to
ong
oin
g d
iscussio
ns a
nd
oth
er
pote
ntial nom
inations.
A p
roposed p
rocess for
the
appoin
tment of
new
independent
mem
bers
Bo
ard
mem
bers
Y
es
Page 14 of 159
Page 1 of 1
Board meeting – Public session
Title of paper:
HSCIC Board Performance Pack (public)
Board meeting date:
27 January 2016
Agenda item no: HSCIC 16 06 03 a
Paper presented by:
Carl Vincent, Director of Finance and Corporate Services
Paper prepared by:
John Willshere, Portfolio Director
Paper approved by:
Carl Vincent, Director of Finance and Corporate Services
Purpose of the paper:
To provide the Board with a summary of performance in December 2015.
Key risks and issues:
The corporate performance framework monitors HSCIC performance including information governance and security.
Patient/public interest:
The public interest is in ensuring the HSCIC manages its business in an effective way.
Actions required by the board:
To note
03
(a)
Boa
rd P
erfo
rman
ce P
ack
Page 15 of 159


Copyright ©
201
5, H
ealth a
nd S
ocia
l C
are
Info
rma
tion
Cen
tre. A
ll R
ights
Re
serv
ed
Bo
ard
Pe
rfo
rma
nc
e P
ac
k
De
cem
ber
2015
Data
ww
w.h
sc
ic.g
ov.u
k
e
nq
uir
ies
@h
sc
ic.g
ov.u
k
@
hs
cic
03 (
a) B
oard
Per
form
ance
Pac
k
Page 16 of 159

Conte
nts
HS
CIC
Perf
orm
an
ce
Su
mm
ary
3
Pro
gra
mm
e A
ch
ievem
en
t K
PI R
ep
ort
4
IT S
erv
ice P
erf
orm
an
ce
KP
I R
ep
ort
5
Org
an
isa
tio
nal H
ealt
h K
PI R
ep
ort
6
Da
ta Q
uality
KP
I R
ep
ort
7
Fin
an
cia
l M
an
ag
em
en
t (H
SC
IC)
KP
I R
ep
ort
8
Ap
pen
dix
1 -
Man
ag
em
en
t A
cc
ou
nts
9-1
2
Ap
pen
dix
2 -
Pro
gra
mm
e D
elivery
Das
hb
oard
13
-16
Page 17 of 159
Pe
rfo
rma
nc
e I
nd
ica
tor
Ow
ne
rC
urr
en
t
Peri
od
Cu
rren
t
Fo
recast
Pre
vio
us
Fo
recast
Jan
-15
Feb
-15
Mar-
15
Ap
r-15
May-1
5Ju
n-1
5Ju
l-15
Au
g-1
5S
ep
-15
Oct-
15
No
v-1
5D
ec-1
5
Pro
gra
mm
e A
ch
ieve
me
nt
Ja
me
s H
aw
kin
sA
/GA
/GA
/GA
AA
/GA
/GA
/GA
/GA
/GA
/GA
/GA
/GA
/GA
/G
IT S
erv
ice
Pe
rfo
rma
nc
eR
ob
Sh
aw
GA
GG
AG
GG
GG
AG
GG
G
Org
an
isa
tio
na
l H
ea
lth
Ra
ch
ae
l A
lls
op
AA
GG
AA
AA
AA
AA
GG
A
Da
ta Q
ua
lity
Ma
rtin
Se
ve
rsG
GG
GA
AG
GG
GG
GG
GG
Fin
an
cia
l M
an
ag
em
en
t: H
SC
ICC
arl
Vin
ce
nt
AR
AG
GR
GG
GG
GA
AA
HS
CIC
Perf
orm
an
ce S
um
mary Pe
rfo
rma
nc
e T
rac
ke
r: R
oll
ing
12
mo
nth
sP
erf
orm
an
ce
Th
is P
eri
od
2A0T
Pro
gra
mm
e A
ch
ieve
men
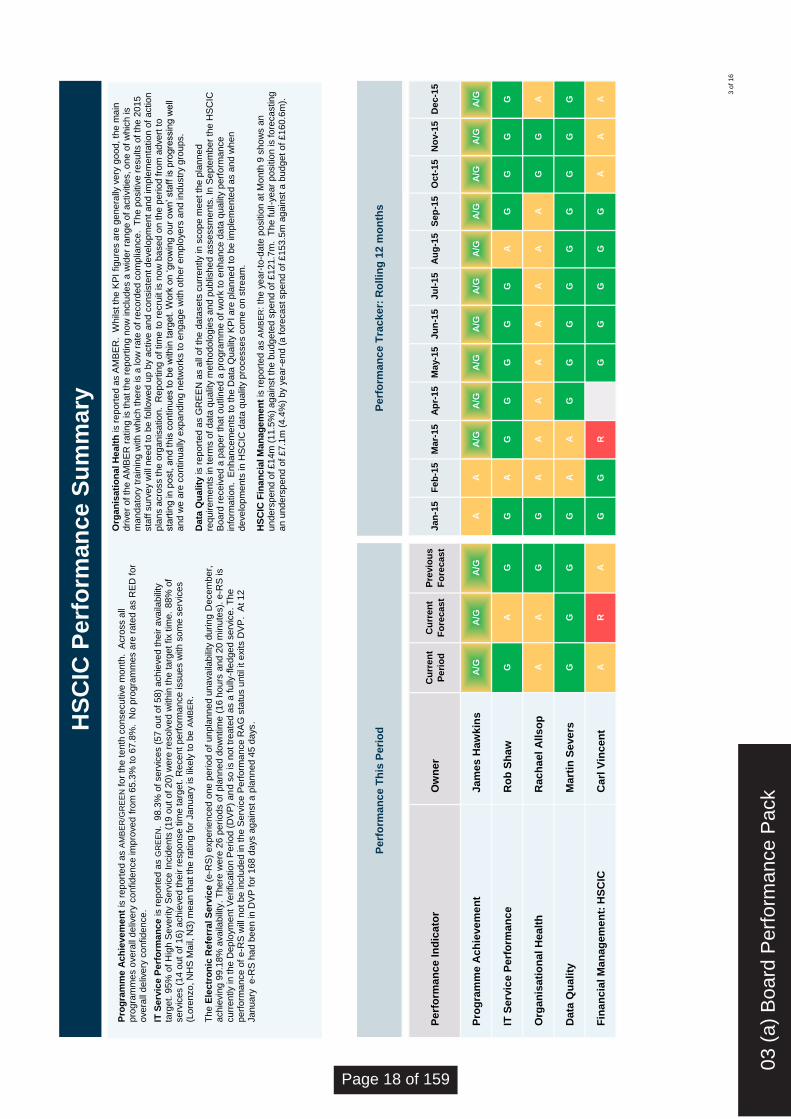
t is
re
port
ed
as A
MB
ER
/GR
EE
N fo
r th
e te
nth
co
nse
cu
tive
mo
nth
. A
cro
ss a
ll p
rog
ram
me
s o
ve
rall
de
live
ry c
on
fid
en
ce
im
pro
ve
d f
rom
65
.3%
to
67
.8%
. N
o p
rog
ram
me
s a
re r
ate
d a
s R
ED
fo
r o
ve
rall
de
live
ry c
on
fide
nce
.
IT S
erv
ice
Perf
orm
an
ce
is r
ep
ort
ed
as G
RE
EN
. 9
8.3
% o
f se
rvic
es (
57
ou
t o
f 5
8)
ach
ieve
d th
eir a
va
ilab
ility
ta
rge
t. 9
5%
of H
igh
Se
ve
rity
Se
rvic
e I
ncid
en
ts (
19
ou
t o
f 2
0)
we
re r
eso
lve
d w
ith
in th
e ta
rge
t fix t
ime
. 8
8%
of
se
rvic
es (
14
ou
t o
f 1
6)
ach
ieve
d th
eir r
esp
on
se
tim
e ta
rge
t. R
ece
nt p
erf
orm
an
ce
issu
es w
ith
so
me
se
rvic
es
(Lo
ren
zo
, N
HS
Ma
il, N
3)
me
an th
at th
e r
atin
g fo
r Ja
nua
ry is lik
ely
to
be
AM
BE
R.
Th
e E
lec
tro
nic
Re
ferr
al S
erv
ice
(e-R
S)
exp
erie
nce
d o
ne p
erio
d o
f u
npla
nn
ed
un
ava
ilab
ility
du
rin
g D
ece
mb
er,
a
ch
ievin
g 9
9.1
8%
ava
ilab
ility
. T
he
re w
ere
26
pe
rio
ds o
f p
lan
ne
d d
ow
ntim
e (
16
ho
urs
an
d 2
0 m
inu
tes).
e-R
S is
cu
rren
tly in th
e D
ep
loym
en
t V
erifica
tio
n P
erio
d (
DV
P)
an
d s
o is n
ot tr
ea
ted
as a
fu
lly-f
led
ge
d s
erv
ice
. T
he
p
erf
orm
an
ce
of e
-RS
will
no
t b
e inclu
de
d in t
he
Serv
ice
Pe
rfo
rma
nce
RA
G s
tatu
s u
ntil it e
xits D
VP
. A
t 1
2
Ja
nua
ry e-R
S h
ad b
een
in D
VP
fo
r 1
68 d
ays a
ga
inst a
pla
nne
d 4
5 d
ays.
Org
an
isa
tio
na
l H
ea
lth
is r
ep
ort
ed
as A
MB
ER
. W
hils
t th
e K
PI fig
ure
s a
re g
ene
rally
ve
ry g
ood
, th
e m
ain
d
rive
r o
f th
e A
MB
ER
ra
ting
is th
at th
e r
ep
ort
ing
no
w in
clu
des a
wid
er
ran
ge
of a
ctivitie
s, o
ne o
f w
hic
h is
ma
nd
ato
ry t
rain
ing
with
wh
ich
th
ere
is a
lo
w r
ate
of re
co
rde
d c
om
plia
nce
. T
he
po
sitiv
e r
esu
lts o
f th
e 2
01
5
sta
ff s
urv
ey w
ill n
ee
d to
be
fo
llow
ed
up
by a
ctive
an
d c
on
sis
ten
t d
eve
lop
me
nt
an
d im
ple
me
nta
tio
n o
f a
ctio
n
pla
ns a
cro
ss th
e o
rgan
isa
tio
n. R
ep
ort
ing
of tim
e to
re
cru
it is n
ow
ba
se
d o
n th
e p
erio
d fro
m a
dve
rt t
o
sta
rtin
g in p
ost,
an
d t
his
co
ntinu
es to
be
with
in t
arg
et.
Wo
rk o
n ‘gro
win
g o
ur
ow
n’ sta
ff is p
rogre
ssin
g w
ell
an
d w
e a
re c
on
tinu
ally
exp
and
ing
ne
two
rks to
en
ga
ge w
ith
oth
er
em
plo
ye
rs a
nd ind
ustr
y g
roup
s.
Da
ta Q
ua
lity
is r
ep
ort
ed
as G
RE
EN
as a
ll o
f th
e d
ata
se
ts c
urr
en
tly in
sco
pe
me
et th
e p
lan
ne
d
req
uire
me
nts
in te
rms o
f d
ata
qu
alit
y m
eth
od
olo
gie
s a
nd p
ublis
he
d a
sse
ssm
en
ts. In
Sep
tem
be
r th
e H
SC
IC
Boa
rd r
ece
ive
d a
pa
pe
r th
at o
utlin
ed a
pro
gra
mm
e o
f w
ork
to
en
ha
nce
da
ta q
ualit
y p
erf
orm
an
ce
in
form
atio
n. E
nh
an
ce
me
nts
to
th
e D
ata
Qu
alit
y K
PI a
re p
lan
ne
d to
be
im
ple
me
nte
d a
s a
nd w
he
n
de
ve
lop
me
nts
in
HS
CIC
da
ta q
ua
lity p
roce
sse
s c
om
e o
n s
tre
am
.
HS
CIC
Fin
an
cia
l M
an
ag
em
en
t is
re
port
ed
as A
MB
ER
: th
e y
ea
r-to
-da
te p
ositio
n a
t M
on
th 9
sh
ow
s a
n
un
de
rsp
en
d o
f £
14m
(1
1.5
%)
ag
ain
st th
e b
udg
ete
d s
pe
nd
of £
121
.7m
. T
he fu
ll-y
ea
r p
ositio
n is fo
reca
stin
g
an
un
de
rsp
en
d o
f £
7.1
m (
4.4
%)
by y
ea
r-e
nd
(a
fo
reca
st sp
en
d o
f £
15
3.5
m a
ga
inst a
bu
dg
et o
f £
16
0.6
m).
3 o
f 16
03 (
a) B
oard
Per
form
ance
Pac
k
Page 18 of 159

A/G
A/G
A/G
A/G
A/G
KP
IP
rog
ram
me
Ac
hie
ve
me
nt
Pre
vio
us
RA
G6
5.8
%
KP
I O
wn
er
Ja
me
s H
aw
kin
sC
urr
en
t R
AG
67
.8%
1 M
on
th F
utu
re F
ore
ca
st
RA
G6
6.9
%
2 M
on
th F
utu
re F
ore
ca
st
RA
G6
9.0
%
3 M
on
th F
utu
re F
ore
ca
st
RA
G7
3.7
%
Ba
se
d o
n N
ove
mb
er
20
15 H
igh
lig
ht
Re
po
rts
O
ve
rall
de
live
ry c
on
fid
en
ce
:
- w
as 6
7.8
%, w
hic
h g
ives a
rating o
f A
MB
ER
-GR
EE
N.
- has b
een A
MB
ER
-GR
EE
N s
ince M
arc
h 2
015, te
n c
onsecutive m
onth
s.
F
or
the fourt
h c
onsecutive m
onth
no p
roje
cts
or
pro
gra
mm
es r
eport
ed a
deliv
ery
con
fidence
of
RE
D.
Ga
tew
ay R
evie
ws
20 G
ate
way R
evie
ws t
oo
k p
lace
be
twe
en
De
ce
mb
er
201
4 a
nd
No
ve
mb
er
20
15
. 1
1 o
f th
ese
(55%
) re
ce
ive
d a
n o
utc
om
e o
f A
MB
ER
o
r b
ett
er.
2 G
ate
way R
evie
ws w
ere
ca
rrie
d o
ut in
Nove
mb
er
20
15
: N
atio
na
l D
ata
Se
rvic
e
De
velo
pm
ent a
nd
CS
C L
SP
.
61.8
63.1
66.0
69.0
68.4
66.3
68.4
66.7
67.7
68.5
65.3
67.8
66.1
64.8
67.4
73.9
75.0
72.4
74.8
74.8
74.2
71.2
73.3
76.9
Dec-1
4Jan-1
5F
eb
-15
Mar-
15
Apr-
15
May-1
5Jun-1
5Jul-
15
Aug
-15
Sep
-15
Oct-
15
Nov-1
5
Pro
gra
mm
e A
ch
ievem
en
t: O
vera
ll D
eli
ve
ry C
on
fid
en
ce (
%)
Actu
al (t
his
mo
nth
)F
ore
ca
st
(th
ree
mo
nth
s a
go
)
0%
0
%
40
%
29
%
50
%
50
%
53
%
56
%
56
%
50
%
50
%
55
%
De
c-1
4Jan-1
5F
eb
-15
Ma
r-1
5A
pr-
15
Ma
y-1
5Jun-1
5Jul-1
5A
ug-1
5S
ep-1
5O
ct-
15
No
v-1
5
Ga
tew
ay R
evie
ws
: %
Am
be
r o
r b
ett
er
% A
mb
er>
to
da
te
2
16
9
2
02468
10
12
14
16
18
Novem
be
r 2
01
5
RA
/RA
A/G
G
4
7
12
7
5
02468
10
12
14
16
18
Novem
be
r 2
01
4
RA
/RA
A/G
G
Dis
trib
uti
on
of
Deli
very
Co
nfi
den
ce R
AG
s d
uri
ng
th
e
las
t 1
2 m
on
ths (
se
e c
ha
rts o
pp
osite
) T
he
nu
mb
er
of
pro
jects
an
d p
rog
ram
me
s r
ep
ort
ing
a
deliv
ery
confidence o
f R
ED
an
d A
MB
ER
-RE
D h
as falle
n.
Ho
we
ve
r, t
he
nu
mb
er
of p
roje
cts
an
d p
rog
ram
me
s r
ep
ort
ing
a d
eliv
ery
confidence o
f G
RE
EN
has a
lso falle
n.
The n
um
ber
of pro
jects
and p
rogra
mm
es r
eport
ing
a
deliv
ery
confidence o
f A
MB
ER
has incre
ased . C
urr
ently,
55%
of th
e p
roje
cts
and p
rogra
mm
es a
re A
MB
ER
(t
he d
iffe
rence in the n
um
ber
of pro
gra
mm
es s
how
n in t
he
two
ch
art
s r
efle
cts
th
e t
ran
sitio
n o
f so
me
pro
gra
mm
es to
se
rvic
e s
ince
No
ve
mb
er
20
14
an
d a
re
fin
em
en
t w
ha
t is
in
clu
ded in the p
rogra
mm
es d
eliv
ery
dashboard
).
4 o
f 16
Page 19 of 159

KP
I IT
Serv
ice P
erf
orm
an
ce
G
KP
I O
wn
er
Ro
b S
haw
G A
Jan-1
5F
eb-1
5M
ar-
15
Apr-
15
May-1
5Jun-1
5Jul-15
Aug-1
5S
ep-1
5O
ct-
15
Nov-1
5D
ec-1
5
66
68
66
65
67
74
62
63
64
62
58
57
20
00
01
31
00
01
00
00
00
00
00
00
68
68
66
65
67
75
65
64
64
62
58
58
26
25
24
23
23
24
22
22
22
19
16
14
01
11
11
10
00
11
11
11
12
22
24
11
27
27
26
25
25
27
25
24
24
23
18
16
33
34
12
15
14
25
17
31
21
18
24
20
30
34
11
14
14
22
17
31
20
17
24
19
91%
100%
92%
93%
100%
88%
100%
100%
95%
94%
100%
95%
% H
SS
Is a
chie
vin
g F
ix T
imes targ
et
Pre
vio
us R
AG
Cu
rren
t R
AG
Fo
recast
RA
G
No. of S
erv
ices a
chie
vin
g A
vaila
bili
ty targ
et
Perf
orm
an
ce In
dic
ato
rs
No. of S
erv
ices b
reachin
g A
vaila
bili
ty targ
et at a c
ritical le
vel
No. of S
erv
ices b
reachin
g A
vaila
bili
ty targ
et, b
ut not to
a c
ritical le
vel
No. of S
erv
ices a
chie
vin
g R
esponse T
imes targ
et
Tota
l N
o. of S
erv
ices m
easure
d for
Availa
bili
ty P
erf
orm
ance >
>>
>
No. of S
erv
ices b
reachin
g R
esponse T
imes targ
et at a c
ritical le
vel
No. of S
erv
ices b
reachin
g R
esponse T
imes targ
et, b
ut not to
a c
ritical le
vel
Tota
l N
o. of S
erv
ices m
easure
d for
Response T
imes P
erf
orm
ance >
>>
>
Tota
l num
ber
of H
igher
Severity
Serv
ice Incid
ents
(H
SS
Is)
Tota
l num
ber
of H
SS
Is a
chie
vin
g F
ix T
imes targ
et
Availab
ilit
y:
57 o
ut of 58 s
erv
ices a
chie
ved t
heir a
vaila
bili
ty t
arg
et
in D
ecem
ber
2015.
CS
C N
ME
's L
ore
nzo s
erv
ice b
reached its
availa
bili
ty t
arg
et at
a n
on
-critical le
vel due t
o a
sin
gle
outa
ge o
n 0
1/1
2/1
5 w
hic
h
impacte
d o
ne N
HS
Hospital T
rust.
T
he c
ause o
f th
is a
vaila
bili
ty b
reach i
s s
till
under
investigation.
How
ever,
we a
re
agre
ein
g a
positio
n w
ith C
SC
on o
ther
Lore
nzo p
erf
orm
ance issues o
n 1
7 a
nd 1
8 D
ecem
ber.
T
he N
HS
e-R
efe
rral S
erv
ice a
chie
ved 9
9.1
8%
availa
bili
ty in D
ecem
ber
2015.
There
was o
nly
one u
npla
nned o
uta
ge:
on
03/1
2/1
5 f
or
a d
ura
tion o
f 6 h
rs a
nd 1
1 m
inute
s w
hen
e-R
S w
as u
navaila
ble
to a
ll users
nationally
. T
he r
oot cause o
f th
is
outa
ge w
as a
data
base issue, re
solv
ed v
ia a
resta
rt o
f th
e e
-RS
applic
ation.
There
were
als
o 2
6 p
lanned e
-RS
changes
imple
mente
d d
uring D
ecem
ber
2015,
whic
h r
esulted in 1
6 h
ours
and 2
0 m
inute
s o
f pla
nned d
ow
ntim
e.
These 2
6 p
lanned
changes inclu
ded t
he s
uccessfu
l deplo
ym
ent
of a m
ajo
r re
lease (
R4.6
) on 1
1/1
2/1
5.
It s
hould
be n
ote
d t
hat e
-RS
is c
urr
ently in t
he D
eplo
ym
ent
Verification P
eriod
(DV
P)
whic
h m
eans t
hat perf
orm
ance w
ill
not
be inclu
ded in t
he S
erv
ice P
erf
orm
ance R
AG
sta
tus u
ntil D
VP
exit.
e-R
S h
as c
urr
ently b
een in D
VP
for
168 w
ork
ing
days a
gain
st
a p
lanned 4
5 d
ays a
t th
e t
ime o
f re
port
pro
duction (
12 J
anuary
2016).
S
ince t
he in
-housin
g o
f S
pin
e S
erv
ices, availa
bili
ty h
as b
een c
onsis
tently h
igh,
inclu
din
g t
hese a
chie
vem
ents
: -
All
4 S
pin
e C
ore
Serv
ices h
ave a
chie
ved 1
00%
availa
bili
ty e
very
month
, sin
ce D
VP
exit in N
ovem
ber
2014.
- S
US
has a
chie
ved 1
00%
availa
bili
ty e
very
month
except
Novem
ber
2015,
sin
ce D
VP
exit in J
une 2
015.
- A
ll 7 C
IS S
erv
ices h
ave a
chie
ved 1
00%
availa
bili
ty e
very
month
except
July
2015,
sin
ce D
VP
exit in J
une 2
015.
Fix
Tim
es:
Hig
h S
everi
ty S
erv
ice I
ncid
en
ts (
HS
SIs
):
20 H
SS
Is w
ere
report
ed in D
ecem
ber
2015,
few
er
than t
he
pre
vio
us m
onth
and low
er
than t
he 1
2 m
onth
avera
ge o
f 22.
Only
one H
SS
I fa
iled its
fix
tim
e targ
et
in the m
onth
: G
DIT
Severity
2, re
lating t
o a
n issue w
ith d
uplic
ate
paym
ents
bein
g
inadvert
ently p
rocessed f
ollo
win
g t
he d
eplo
ym
ent
of B
uild
58 o
n 0
8/1
2/1
5.
Scripts
were
run o
n a
daily
basis
fro
m 1
0/1
2/1
5
in o
rder
to c
aptu
re a
nd r
em
ove a
ll duplic
ate
valu
es, until a p
erm
anent
fix w
as d
eplo
yed o
n 2
2/1
2/1
5.
This
HS
SI to
ok 9
8
hours
and 2
8 m
inute
s t
o r
esolv
e,
again
st
a F
ix T
ime targ
et of
6 h
ours
. 3 S
ecurity
Incid
ents
and 5
Clin
ical S
afe
ty incid
ents
were
rais
ed a
s H
SS
Is in t
he m
onth
.
e-R
S e
xperienced o
ne S
everity
1 H
SS
I in
Decem
ber
2015,
rela
ting t
o the u
npla
nned o
uta
ge r
efe
renced in the A
vaila
bili
ty
com
menta
ry a
bove a
nd o
ne f
urt
her
Severity
2 H
SS
I, w
hic
h d
id n
ot
result in a
ny u
npla
nned d
ow
ntim
e.
Resp
on
se T
imes
14 o
ut of 16 s
erv
ices r
eport
ed a
gain
st
achie
ved o
r exceeded t
heir t
arg
et.
The C
alc
ula
ting Q
ualit
y R
eport
ing S
erv
ice (
CQ
RS
) experienced r
epeat
failu
res a
t a c
ritical le
vel on
Message T
ypes 2
and 7
.
Whils
t th
e M
essage T
ype (
MT
) 2 m
etr
ic c
ontinues t
o fail
serv
ice levels
, it s
hould
be n
ote
d t
hat
follo
win
g t
he r
em
edia
tion a
ctivitie
s s
om
e p
erf
orm
ance im
pro
vem
ents
have b
een o
bserv
ed,
but
not
to a
degre
e w
here
the O
SL (
Opera
ting S
erv
ice L
evel) h
as b
een a
chie
ved.
G
DIT
continue t
o u
ndert
ake low
-level analy
sis
of th
ese b
reaches,
with a
meeting s
chedule
d f
or
mid
-January
2016 t
o d
iscuss t
he late
st
positio
n.
Additio
nally
, B
uild
58 w
as d
eplo
yed o
n 0
8/1
2,
whic
h r
esulted in f
urt
her
impro
vem
ents
in a
num
ber
of M
T2 R
esponse T
ime m
etr
ics.
For
the r
epeat
MT
7 failu
re:
The r
etr
y q
ueue s
ize is b
ein
g m
anaged a
ctively
, id
entify
ing f
urt
her
bott
lenecks in t
he C
usto
mer
Record
Outp
ut
(CR
O)
pro
cessin
g,
whic
h G
DIT
are
investigating.
How
ever,
as y
et
no r
esolu
tion h
as b
een identified.
In p
ara
llel, t
he M
T7 S
erv
ice L
evel
measure
ments
are
bein
g d
iscussed w
ith G
DIT
, an a
ltern
ative p
roposal to
the m
easure
ment
of th
is
serv
ice level is
curr
ently w
ith G
DIT
for
revie
w a
nd a
ccepta
nce.
Sig
nific
ant
pla
nnin
g f
or
year-
end a
ctivitie
s is u
nderw
ay w
ithin
both
GD
IT a
nd H
SC
IC, to
ensure
th
at th
e y
ear-
end Q
OF
(Q
ualit
y a
nd O
utc
om
es F
ram
ew
ork
) calc
ula
tion is d
eliv
ere
d s
uccessfu
lly.
Response T
imes for
CS
C N
ME
’s iP
M N
on
-Acute
serv
ice f
aile
d a
t a n
on
-critical le
vel in
Decem
ber
2015,
again
st
Tra
nsaction T
ype 8
on the iP
M510 I
nsta
nce (
Derb
yshire P
CT
) and a
gain
st
Tra
nsaction T
ype 7
on the iP
M527 I
nsta
nce (
Worc
este
r). T
he R
oot C
ause o
f both
these b
reaches
is s
till
under
investigation,
at th
e t
ime o
f th
is r
eport
's p
roduction.
There
were
no insta
nces o
f e
-RS
Response T
ime / p
erf
orm
ance d
egra
dation in D
ecem
ber
2015.
e-R
S is n
ot
inclu
ded in the R
AG
sta
tus for
this
Perf
orm
ance I
ndic
ato
r, d
ue t
o t
he s
erv
ice c
urr
ently
bein
g in the D
eplo
ym
ent
Verification P
eriod.
Incid
en
ts o
f n
ote
ou
tsid
e t
he r
ep
ort
ing
peri
od
S
ince t
he r
eport
ing p
eriod o
f D
ecem
ber
2015,
the follo
win
g H
SS
Is h
ave b
een r
eport
ed w
hic
h a
re
wort
hy o
f note
: 06/0
1/1
6 -
Vodafo
ne -
In
term
itte
nt
connection issues f
or
som
e N
HS
users
, re
solv
ed b
y
rem
ovin
g a
nd r
epla
cin
g t
he im
pacte
d C
AS
(C
lient
Access S
erv
er)
.
08/0
1/1
6 -
TP
P (
GP
ES
) -
Sin
gle
TP
P s
ite issue p
revente
d t
he
re
turn
of
all
QR
s (
Qu
ery
Re
su
lts)
for
the
PO
M (
Pa
tie
nt
Ob
jectio
ns M
an
ag
em
en
t) e
xtr
act
fro
m t
ha
t su
pp
lier.
Site
wa
s r
em
ove
d f
rom
th
e
extr
act
wh
ich
allo
we
d t
he
extr
act
to c
on
tin
ue
, ro
ot
ca
use
still
un
de
r in
ve
stig
atio
n a
t th
e t
ime
of
rep
ort
pro
du
ctio
n (
12
Ja
nu
ary
20
16
).
Fo
recast:
It is
fore
cast th
at an A
MB
ER
RA
G s
tatu
s w
ill b
e a
chie
ved in J
anuary
2016.
Ca
ve
ats
: 1
.C
urr
en
t m
on
th's
Re
spo
nse
Tim
e a
chie
ve
me
nt
for
the N
HS
an
d E
SG
(E
Secu
rity
Gate
way)
serv
ices is y
et
to b
e r
eceiv
ed
at th
e t
ime o
f re
port
pro
duction.
Data
to b
e inclu
ded
in n
ext
mon
th's
KP
I.
2.
All
da
ta in
this
re
port
is u
nverified
an
d s
ub
ject to
ch
ang
e,
as n
one
of it h
as y
et
been
thro
ugh
Se
rvic
e R
evie
ws w
ith S
upplie
rs.
3.
If a
ny c
ha
ng
es a
re n
ee
de
d f
ollo
win
g t
he
co
mp
letio
n o
f a
ll S
up
plie
r S
erv
ice
Re
vie
ws,
the
se
will
be
re
fle
cte
d in
ne
xt
mo
nth
's K
PI.
03 (
a) B
oard
Per
form
ance
Pac
k
Page 20 of 159

Ow
ner:
KP
I:
Fo
recast
A
Pre
vio
us
G
Cu
rren
tA
Org
an
isati
on
Healt
h
Rach
ael
All
so
p
Ove
rall
Po
sit
ion
: A
mber
rate
d. W
hils
t th
e K
PI fig
ure
s a
re g
enera
lly v
ery
good, th
e low
rate
of com
plia
nce w
ith m
andato
ry tra
inin
g is a
sig
nific
ant concern
. T
he lo
west
com
plia
nce r
ate
is f
or
Info
rmation
Govern
ance tra
inin
g a
nd m
ay b
e lin
ked to a
n intr
anet announcem
ent advis
ing
that th
e tra
inin
g h
as to b
e c
om
ple
ted b
y t
he e
nd o
f January
, ra
ther
than o
n a
'ro
lling
' basis
. W
e s
hould
there
fore
expect
bett
er
results n
ext
month
. T
he p
ositiv
e r
esults of th
e s
taff
surv
ey f
or
2015 w
ill n
eed to b
e f
ollo
wed u
p b
y a
ctive a
nd c
onsis
tent develo
pm
ent
and im
ple
menta
tion o
f action p
lans a
cro
ss the o
rganis
ation to
main
tain
the c
urr
ent ra
ting
. W
e h
ave n
ow
tra
nsitio
ned to r
eport
ing
tim
e to r
ecru
it b
ased o
n a
dvert
to s
tart
ing
in p
ost,
whic
h c
ontinues to b
e w
ithin
targ
et.
Work
on ‘g
row
ing
our
ow
n’ sta
ff is
pro
gre
ssin
g w
ell
and w
e a
re c
ontinually
expandin
g n
etw
ork
s to e
ng
ag
e w
ith o
ther
em
plo
yers
and industr
y g
roups. I
mpro
vem
ents
in d
ata
qualit
y w
ill s
upport
the e
ffective m
anag
em
ent of,
in p
art
icula
r, long
-term
absence.
Net
Mo
vem
en
t
•C
urr
ent head
count is
2755
.
•W
ithin
this
fin
ancia
l year,
our
avera
ge m
onth
ly n
et m
ovem
ent is
21. If th
is c
ontinues w
e w
ould
in
cre
ase b
y a
furt
her
63ft
e b
y the
end o
f M
arc
h w
hic
h w
ould
brin
g
our
tota
l in
cre
ase to 2
55 a
cro
ss
2015
/16.
Att
racti
ng
an
d G
row
ing
Tale
nt
•A
s p
art
of
our
involv
em
ent in
the L
eed
s D
igital S
kill
s G
roup w
e a
re a
main
part
ner
in the L
eed
s D
igital S
tory
- a
cam
paig
n p
roduced b
y H
ebe W
ork
s in
part
ners
hip
with L
eed
s C
ity C
ouncil
. F
ilmin
g a
nd p
roduction o
f a s
hort
film
to
show
case the L
eed
s d
igital scene is b
ein
g c
arr
ied o
ut in
Janua
ry -
a m
em
ber
of H
SC
IC s
taff
will
be inte
rvie
wed. A
dig
ital and n
ational prin
t cam
paig
n w
ill then r
un f
rom
Fe
bru
ary
and the H
SC
IC w
ill featu
re in a
ll of th
e c
am
paig
n's
paid
for
advert
isin
g a
nd w
ill a
lso h
ave the o
ppo
rtunity to lis
t a n
um
ber
of our
key v
acancie
s.
•W
e a
re w
ork
ing w
ith the c
orp
ora
te a
nd d
igital com
munic
ations team
s to d
evelo
p m
ate
ria
ls for
gra
duate
advert
isin
g
sta
rtin
g in J
anua
ry. W
e w
ill a
dvert
ise a
cro
ss a
range
of m
edia
and to u
niv
ers
itie
s d
irectly to m
axim
ise o
ur
audie
nce.
•F
eedba
ck o
n o
ur
entr
y level pro
gra
mm
es c
ontinues to b
e p
ositiv
e fro
m the tra
inees a
nd their
manag
ers
. G
radua
tes,
train
ees a
nd inte
rns w
ere
the h
ighest scorin
g g
roup for
enga
gem
ent w
ithin
the s
taff
surv
ey.
•G
overn
ment ta
rgets
indic
ate
that
we w
ill n
eed
to r
ecru
it to 6
0 a
ppre
nticeship
s n
ext year,
whic
h w
ill b
e c
halle
ngin
g.
Tra
nsacti
on
al R
ecru
itm
en
t
•T
he a
vera
ge tim
e to h
ire a
cro
ss the o
rganis
ation in D
ecem
ber
rose s
lightly b
ut re
main
s w
ithin
the K
PI ta
rget . W
e
are
work
ing w
ith d
irecto
rate
s to b
uild
on p
revio
us im
pro
vem
ents
.
•A
thoro
ugh r
evie
w o
f active r
ecru
itm
ent has found
that a s
ignific
ant num
ber
at sele
ction s
tage h
ad b
een
u
nsu
cce
ssfu
l bu
t h
ad
no
t p
revio
usly
be
en
re
po
rte
d a
s s
uch
. T
his
will
be
fo
llow
ed
up
to
im
pro
ve
re
po
rtin
g .
•A
s a
result o
f th
e r
evie
w, and a
season
al d
eclin
e in r
ecru
itm
ent activity g
ene
rally
, th
ere
are
now
52%
few
er
vacancie
s in s
ele
ction s
tage than w
hen w
e r
eport
ed last m
onth
and a
reduce
d n
um
ber
out to
advert
.
•39 e
xte
rnal new
sta
rters
are
curr
ently e
xpecte
d in J
anua
ry b
ut th
e v
olu
me o
f active r
ecru
itm
ent is
not suff
icie
nt to
m
eet th
e f
inance
fore
caste
d h
ead
count in
cre
ase for
the r
em
ain
der
of th
e y
ear.
T
he n
um
ber
of exte
rnal new
sta
rters
in F
ebru
ary
and M
arc
h is e
xpecte
d to b
e low
er
than in N
ovem
ber
and D
ecem
ber
becau
se o
f th
e r
educe
d
recru
itm
ent activity.
En
gag
em
en
t
•A
report
on the 2
015
sta
ff s
urv
ey r
esults w
as c
onsid
ere
d b
y E
MT
on 0
7
Janua
ry. T
his
inclu
ded
a d
ete
rmin
ation o
f th
e futu
re a
ppro
ach to a
ction
pla
nnin
g, i.e. w
ithin
Directo
rate
s, P
rofe
ssio
nal G
roups o
r P
rofe
ssio
nal P
ools
.
•T
he r
eport
inclu
des a
dra
ft E
MT
respon
se to the k
ey m
essage
s fro
m the s
urv
ey,
whic
h is g
ene
rally
positiv
e a
nd w
hic
h r
efe
rences a
num
ber
of actions a
lready in
pro
gre
ss o
r pla
nne
d.
•R
eport
ing
of pro
gre
ss o
n e
ng
ag
em
ent actions is e
xpecte
d to c
om
mence
from
April 2016.
Sic
kn
ess A
bsen
ce
•
Th
e 1
2-m
onth
rolli
ng a
vera
ge a
bsen
ce r
ate
rem
ain
s s
table
.
•T
he intr
oductio
n o
f A
BR
will
pro
vid
e a
n o
ppo
rtunity to t
est w
heth
er
rate
s a
re g
enu
inely
lo
w o
r re
flect unde
r-re
port
ing o
f sic
kness a
bsen
ce.
•A
furt
her
11 a
bsen
ces r
olle
d into
longe
r te
rm (
28 d
ays+
), w
hic
h is a
net in
cre
ase o
f 5
over
the p
revio
us m
onth
. W
e a
re im
pro
vin
g the q
ualit
y o
f th
e d
ata
and c
ontinue to
revie
w c
ase m
anag
em
ent at
regula
r case c
onfe
rence s
essio
ns.
•A
lmost 20%
of lo
ng
-term
absen
ce c
ase a
re lin
ked to a
nxie
ty, str
ess, depre
ssio
n o
r psychia
tric
illn
ess. W
e a
re d
evelo
pin
g a
range
of health a
nd w
ell
bein
g initia
tives,
inclu
din
g m
indfu
lness s
essio
ns for
sta
ff.
Tra
inin
g a
nd
Develo
pm
en
t
Tra
inin
g D
ays (
Civ
il S
erv
ice L
earn
ing)
•A
n a
vera
ge o
f 1.0
4 t
rain
ing d
ays p
er
pers
on h
ave b
een b
ooked this
year
on C
SL.
Ind
ucti
on
•O
f people
who s
tart
ed in t
he last
6 m
onth
s 5
7%
have a
ttended C
orp
ora
te I
nduction a
nd 6
6%
have
accessed the o
nlin
e induction.
•39%
of
the o
nlin
e induction h
as b
een c
om
ple
ted
by
people
who h
ave s
tart
ed in t
he last
6 m
onth
s.
Man
dato
ry T
rain
ing
•F
ire S
afe
ty c
om
plia
nce s
core
: 69%
•In
form
ation S
ecurity
com
plia
nce s
core
: 37%
•In
form
ation G
overn
ance c
om
plia
nce s
core
: 35%
Learn
ing
an
d D
evelo
pm
en
t L
ead
s S
ati
sfa
cti
on
Sco
re
•L&
D L
eads a
re 9
3%
satisfied w
ith t
he s
erv
ice t
hey r
eceiv
e f
rom
OD
.
Cum
ula
tive fro
m A
pril 2015
Live
Cam
paig
ns%
Tot
al T
ime
Wor
king
Day
s
Ad
vert
isin
g
122.
9%1.
75
Sel
ectio
n
6862
.6%
37.6
8
Ap
po
intm
ent
18.7
%11
.24
15.9
%9.
56
Rec
ruitm
ent S
um
mar
y
app
rova
l to
adve
rt
ad
vert
to
ou
tco
me
ou
tco
me
to c
hec
ks
54ch
ecks
to a
gre
ed s
tart
dat
e
Gro
win
g T
ale
nt
Su
mm
ary
Pla
ced
14/1
5
Curr
ent
positi
on,
cum
ula
tive
15/1
6
Pro
jecte
d
pla
cem
ents
for
15/1
6
Wo
rk E
xp
eri
en
ce
Unpaid
work
shadow
ing u
p t
o 2
weeks
25
58
Ap
pre
nti
ce
sh
ip
Paid
sta
tic t
rain
ing r
ole
up t
o 2
years
with
qualif
ication
47
15
Inte
rnsh
ip
Paid
8 w
eek p
lacem
ent
01
81
8
Un
de
rgra
du
ate
pla
ce
me
nt
year
Paid
9-1
2 m
onth
sandw
ich p
lacem
ent
11
1
Gra
du
ate
fix
ed
tra
inin
g p
osts
Paid
post
up t
o 3
years
within
a p
rofe
ssio
n0
55
Gra
du
ate
ro
tati
on
al tr
ain
ing
sch
em
e
Paid
2 y
ear
schem
e w
ithin
pro
fessio
nal gro
up
10
99
Su
mm
ary
Ta
ble
Ta
rge
tJ
an
-15
Fe
b-1
5M
ar-
15
Ap
r-1
5M
ay
-15
Ju
n-1
5J
ul-
15
Au
g-1
5S
ep
-15
Oc
t-1
5N
ov
-15
De
c-1
5
Eng
ag
em
ent S
co
re>
=7
0
Eng
ag
em
ent A
ctio
ns C
om
ple
ted
>=
90
%#
10
0%
##
90
%9
5%
96
%9
9%
96
%9
6%
N/A
N/A
Pro
fessio
nal G
roup
Me
mb
ers
hip
>=
90
%8
1%
81
%8
0%
80
%8
2%
81
%8
1%
83
%8
4%
87
%9
1%
95
%
PD
R C
om
ple
tio
n>
=9
0%
76
%7
7%
78
%5
%3
8%
87
%8
9%
89
%9
1%
12
%8
7%
90
%
Annual T
rain
ing
Sp
end
/ H
ead
£2
75
/Ye
ar
£2
50
£2
95
£3
53
--
£3
7£
96
£1
61
£1
92
£2
06
£2
28
£3
25
12
Mo
nth
Ave
rag
e S
ickne
ss A
bse
nce
%
<=
3%
2.5
%2
.2%
2.1
%2
.0%
1.9
%1
.8%
1.8
%2
.0%
2.3
%2
.3%
2.3
%2
.3%
Mand
ato
ry T
rain
ing
(c
om
po
site
)T
BC
45
%
Tim
e to
Hire
- I
n p
ost
>=
70
71
70
69
60
54
64
62
62
69
Turn
ove
r9
% -
11
%1
0%
10
%1
1%
11
%1
1%
9%
8%
8%
8%
8%
8%
8%
Ne
t M
onth
ly M
ove
me
nt
TB
C4
52
06
02
58
33
45
12
31
14
31
2
73
75
6 o
f 1
6
Page 21 of 159
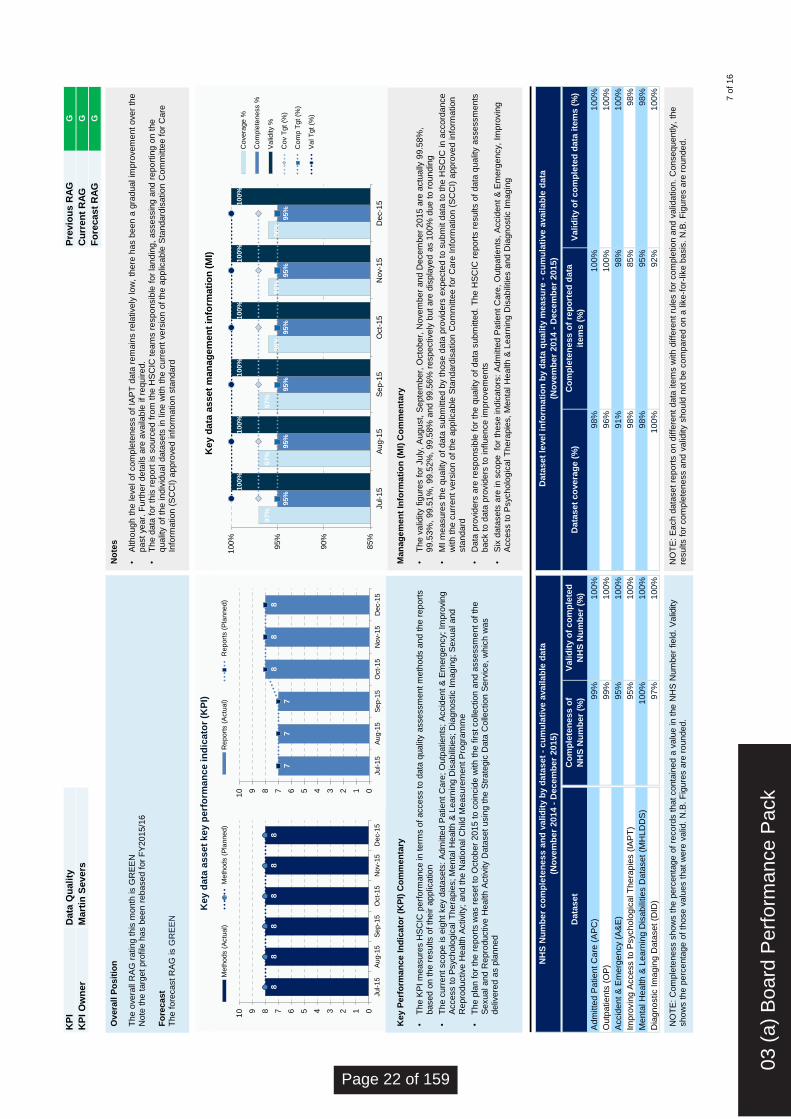
KP
I
D
ata
Qu
ali
tyP
revio
us R
AG
G
KP
I O
wn
er
M
art
in S
evers
Cu
rren
t R
AG
G
Fo
recast
RA
GG
NH
S N
um
ber
co
mp
lete
ness
an
d v
alid
ity b
y d
ata
se
t -
cu
mu
lati
ve a
vaila
ble
data
(No
vem
ber
20
14 -
Dece
mb
er
20
15)
Data
se
t le
vel in
form
ati
on
by d
ata
qu
ality
meas
ure
- c
um
ula
tive a
vaila
ble
data
(No
vem
ber
20
14 -
Dece
mb
er
20
15)
Data
se
tC
om
ple
ten
ess
of
NH
S N
um
ber
(%)
Valid
ity o
f co
mp
lete
d
NH
S N
um
ber
(%)
Data
se
t co
vera
ge (
%)
Co
mp
lete
ness
of
rep
ort
ed
data
item
s (
%)
Valid
ity o
f co
mp
lete
d d
ata
ite
ms (
%)
10
0%
Adm
itte
d P
atient
Care
(A
PC
)9
9%
10
0%
98
%1
00
%1
00
%
Outp
atients
(O
P)
99
%1
00
%9
6%
10
0%
98
%
Accid
en
t &
Em
erg
en
cy (
A&
E)
95
%1
00
%9
1%
98
%1
00
%
Impro
vin
g A
ccess to P
sycholo
gic
al T
hera
pie
s (
IAP
T)
95
%1
00
%9
8%
85
%
10
0%
Menta
l H
ealth &
Le
arn
ing D
isabili
ties D
ata
set (M
HLD
DS
)1
00
%1
00
%9
8%
95
%9
8%
Dia
gn
ostic Im
agin
g D
ata
set (D
ID)
97
%1
00
%1
00
%9
2%
Key P
erf
orm
an
ce I
nd
icato
r (K
PI)
Co
mm
en
tary
•
The K
PI
measure
s H
SC
IC p
erf
orm
ance in t
erm
s o
f access to d
ata
qualit
y assessm
ent m
eth
ods a
nd t
he r
eport
s
based o
n t
he r
esults o
f th
eir a
pplic
ation
•T
he c
urr
ent scope is e
ight
key
data
sets
: A
dm
itte
d P
atient
Care
; O
utp
atients
; A
ccid
ent
& E
merg
ency;
Impro
vin
g
Access to P
syc
holo
gic
al T
hera
pie
s;
Menta
l H
ealth &
Learn
ing D
isabili
ties;
Dia
gnostic I
magin
g;
Sexual and
Repro
ductive H
ealth A
ctivity;
and t
he N
ational C
hild
Measure
ment
Pro
gra
mm
e
•T
he p
lan f
or
the r
eport
s w
as r
eset to
Octo
ber
2015 t
o c
oin
cid
e w
ith t
he f
irst colle
ction a
nd a
ssessm
ent of th
e
Sexual and R
epro
ductive H
ealth A
ctivity
Data
set
usin
g t
he S
trate
gic
Data
Colle
ction S
erv
ice,
whic
h w
as
deliv
ere
d a
s p
lanned
Ov
era
ll P
os
itio
n
The o
vera
ll R
AG
rating t
his
month
is G
RE
EN
N
ote
the t
arg
et
pro
file
has b
een r
ebased f
or
FY
2015/1
6
Fo
recast
The f
ore
cast R
AG
is G
RE
EN
No
tes
•A
lth
ou
gh
th
e le
ve
l o
f co
mp
lete
ness o
f IA
PT
data
rem
ain
s r
ela
tively
lo
w,
there
has b
een a
gra
du
al im
pro
ve
me
nt
over
the
past
ye
ar.
Fu
rth
er
deta
ils a
re a
va
ilable
if
req
uired.
•T
he d
ata
fo
r th
is r
epo
rt is s
ourc
ed f
rom
th
e H
SC
IC t
eam
s r
esp
on
sib
le f
or
land
ing,
assessin
g a
nd
repo
rtin
g o
n t
he
qua
lity o
f th
e in
div
idua
l d
ata
se
ts in lin
e w
ith
the c
urr
ent
ve
rsio
n o
f th
e a
pp
lica
ble
Sta
nd
ard
isa
tio
n C
om
mitte
e for
Care
In
form
atio
n (
SC
CI)
app
rove
d in
form
ation s
tandard
Ma
na
ge
me
nt
Info
rma
tio
n (
MI)
Co
mm
en
tary
•
Th
e v
alid
ity f
igure
s f
or
Ju
ly,
August,
Se
pte
mb
er,
Octo
ber,
No
ve
mb
er
and
De
cem
ber
2015 a
re a
ctu
ally
99.5
8%
, 9
9.5
3%
, 9
9.5
1%
, 9
9.5
2%
, 9
9.5
8%
and 9
9.5
6%
re
sp
ective
ly b
ut
are
dis
pla
ye
d a
s 1
00
% d
ue
to
ro
un
din
g
•M
I m
easu
res th
e q
ua
lity o
f d
ata
su
bm
itte
d b
y t
hose
data
pro
vid
ers
expecte
d t
o s
ubm
it d
ata
to
th
e H
SC
IC in
accord
an
ce
with
th
e c
urr
ent
ve
rsio
n o
f th
e a
pp
licable
Sta
ndard
isa
tion C
om
mitte
e fo
r C
are
In
form
ation (
SC
CI)
app
roved in
form
atio
n
sta
nd
ard
•D
ata
pro
vid
ers
are
re
sp
on
sib
le f
or
the q
ua
lity o
f data
su
bm
itte
d.
Th
e H
SC
IC r
epo
rts r
esu
lts o
f d
ata
qua
lity a
ssessm
ents
b
ack to
data
pro
vid
ers
to
in
fluen
ce im
pro
ve
ments
•S
ix d
ata
se
ts a
re in
sco
pe
fo
r th
ese
in
dic
ato
rs:
Ad
mitte
d P
atie
nt
Care
, O
utp
atie
nts
, A
ccid
en
t &
Em
erg
en
cy,
Imp
rovin
g
Acce
ss to P
sych
olo
gic
al T
hera
pie
s,
Me
nta
l H
ealth &
Learn
ing D
isa
bili
tie
s a
nd D
iagn
ostic I
magin
g
8
8
8
8
8
8
0123456789
10
Jul-1
5A
ug-1
5S
ep-1
5O
ct-
15
Nov-1
5D
ec-1
5
Meth
ods (
Actu
al)
Meth
ods (
Pla
nned)
97%
97%
97%
96%
96%
96%
95%
95%
95%
95%
95%
95%
10
0%
100%
1
00
%
100%
100%
100%
85%
90%
95%
100%
Jul-
15
Au
g-1
5S
ep-1
5O
ct-
15
Nov-1
5D
ec-1
5
Key d
ata
asset
man
ag
em
en
t in
form
ati
on
(M
I)
Covera
ge %
Com
ple
tene
ss %
Va
lidity %
Cov T
gt (%
)
Com
p T
gt (%
)
Va
l T
gt (%
)
NO
TE
: C
om
ple
teness s
how
s t
he p
erc
enta
ge o
f re
co
rds t
hat
conta
ined a
valu
e in t
he N
HS
Num
ber
field
. V
alid
ity
show
s t
he p
erc
enta
ge o
f th
ose v
alu
es t
hat
were
valid
. N
.B.
Fig
ure
s a
re r
ounded.
NO
TE
: E
ach
data
se
t re
po
rts o
n d
iffe
ren
t data
ite
ms w
ith
diffe
ren
t ru
les f
or
co
mp
letion a
nd
va
lidatio
n.
Co
nse
qu
en
tly,
the
resu
lts f
or
co
mp
lete
ness a
nd
va
lidity s
hou
ld n
ot
be c
om
pare
d o
n a
lik
e-f
or-
like
basis
. N
.B.
Fig
ure
s a
re r
ounded.
7
7
7
8
8
8
0123456789
10
Jul-1
5A
ug-1
5S
ep-1
5O
ct-
15
Nov-1
5D
ec-1
5
Report
s (
Actu
al)
Report
s (
Pla
nned)
Key d
ata
asset
key p
erf
orm
an
ce in
dic
ato
r (K
PI)
7 o
f 1
6
03 (
a) B
oard
Per
form
ance
Pac
k
Page 22 of 159

Pre
vio
us R
AG
Cu
rren
t R
AG
Fo
recast
RA
G
Co
re G
iA
Year
to D
ate
: A
ctu
al v B
udget
Year
to D
ate
: A
ctu
al v B
udget
Full
Year
Fore
cast
v B
udget
Full
Year
Fore
cast
v B
udget
Lastr
ow
tag
Rin
g-f
en
ced
GiA
Year
to D
ate
: A
ctu
al v B
udget
Fo
recast
Accu
racy
Act
(£m
)F
'cast
(£m
)
2.3
%F
ull
Year
Fore
cast
v B
udget
12.6
12.3
0.3
9.5
9.3
0.2
2.6
%
Bud (
£m
)A
ct
(£m
)V
ar
(£m
)
In-m
onth
: F
ore
cast
v A
ctu
al
9.5
13.4
3.9
28.9
%
160.6
153.5
7.1
4.4
%148.0
Var
(£m
)V
ar
(%)
98.4
13.8
12.3
%
6.8
4.6
%141.2
Var
(%)
121.7
107.7
14.0
11.5
%112.2
R
Reven
ue S
pen
d -
Co
re &
Rin
g-F
en
ced
Bud (
£m
)A
ct
(£m
)V
ar
(£m
)V
ar
(%)
Bud (
£m
)A
ct
(£m
)V
ar
(£m
)V
ar
(%)
KP
IA
KP
I O
wn
er
AC
arl
Vin
cen
t
Fin
an
cia
l M
an
ag
em
en
t (H
SC
IC)
- fo
r p
ub
lic s
essio
n o
f th
e B
oard
-
20
40
60
80
100
120
140
160
180
£m
Rev
en
ue S
pen
d:
Year
to D
ate
- A
ctu
al
v B
ud
get
Bu
dg
et
Actu
al
Annual B
udg
et (£
161m
)
-12.0
-10.0
-8.0
-6.0
-4.0
-2.0
0.0
2.0
4.0%
Re
ve
nu
e S
pe
nd
: Y
ear
to D
ate
v B
ud
ge
t -
Va
riati
on
Overspending Underspending -
20
40
60
80
100
120
140
160
180
£m
Re
ve
nu
e S
pe
nd
: F
ull
Ye
ar
Fo
rec
as
t v
Bu
dg
et
Fo
recast
Ann
ual S
pen
dA
nnu
al B
ud
get
(£16
1m
)
-8.0
-6.0
-4.0
-2.0
0.0
2.0
4.0%
Re
ve
nu
e S
pe
nd
: F
ull
Ye
ar
Fo
rec
as
t v
Bu
dg
et
- V
ari
ati
on
Overspending Underspending
HS
CIC
Op
era
tin
g c
os
ts
T
he
ye
ar-
to-d
ate
ou
ttu
rn fo
r th
e f
irst n
ine
mo
nth
s o
f th
e y
ea
r is
£1
4.0
m/ 1
1.5
% b
elo
w b
ud
ge
t.
Th
e v
arian
ce
of £
14
.0m
co
mp
rise
s £
13
.8m
un
de
r b
ud
ge
t o
n c
ore
GIA
an
d £
0.2
m u
nd
er
on
rin
g-
fen
ce
d G
iA. T
he
£1
3.8
m u
nd
ers
pe
nd
on
co
re G
iA is la
rge
ly d
ue
to
de
lays t
o r
ecru
itm
en
t to
va
ca
nt ro
les,
pa
rtia
lly o
ffse
t b
y r
esu
lta
nt d
ecre
ase
s to
in
co
me
T
he
£0
.2m
un
de
rsp
en
d o
n r
ing-
fen
ce
d G
iA is a
lso
du
e to
va
ca
ncie
s n
ot b
ein
g f
illed
as e
arly a
s p
red
icte
d.
Th
e fo
reca
st o
utt
urn
fo
r th
e f
ull
ye
ar
is £
7.1
m/ 4
.4%
un
de
r b
ud
ge
t; th
is c
om
prise
s £
6.8
m u
nd
er
bu
dge
t fo
r co
re G
iA (
red
uce
d f
ore
ca
st fo
r sta
ff c
osts
an
d a
n in
cre
ase
in
in
co
me
, p
art
ially
off
se
t b
y r
ele
ase
of ce
ntr
al co
ntin
ge
ncy a
nd
in
cre
ase
in
no
n-s
taff
a
nd
£0
.3m
un
de
r b
ud
ge
t fo
r ring-
fen
ce
d G
iA (
red
ucin
g s
taff
co
sts
as r
ecru
itm
en
t d
ate
s fo
r va
ca
ncie
s m
ove
to
la
ter
in t
he
ye
ar
than
bu
dgete
d).
A
to
p-d
ow
n e
stim
ate
for
the e
nd o
f yea
r, a
dju
stin
g f
or
expe
cte
d r
ecru
itm
en
t ,
pro
cu
rem
en
t a
nd
in
co
me
assu
mp
tio
ns, in
dic
ate
s a
po
ten
tia
l fo
reca
st o
ut-
turn
fo
r co
re G
iA o
f £
10
.9m
. N
on
-GiA
in
co
me
is c
lose
to
bu
dge
t fo
r th
e y
ea
r-to
-da
te a
nd
th
e f
ull
ye
ar
fore
ca
st.
How
eve
r, t
his
co
mp
rise
s a
nu
mb
er
of a
rea
s th
at a
re b
oth
un
de
r a
nd
ove
r b
ud
ge
t -
the
re is a
dd
itio
na
l in
co
me
fr
om
D
SfC
, G
PE
S, S
SD
, S
pin
e 2
an
d C
ross-G
ove
rnm
en
t P
rogra
mm
es, b
ut lo
we
r in
co
me
on
C
ho
ice
s (
inclu
din
g D
AS
), c
are
.da
ta, S
tan
da
rds, S
olu
tio
n A
ssu
ran
ce
, In
form
ation
An
aly
sis
, P
ath
wa
ys a
nd
Te
ch
nic
al A
rch
ite
ctu
re.
Sta
ff C
osts
are
£1
0.0
m u
nd
er
bu
dge
t fo
r th
e y
ea
r-to
-da
te a
nd
fo
reca
st to
be
£1
1.4
m u
nd
er
bu
dge
t fo
r th
e f
ull
ye
ar.
Th
is m
ain
ly r
efle
cts
re
cru
itm
en
t ru
nn
ing b
eh
ind
bu
dge
ted
va
ca
ncie
s -
m
ost o
f th
e v
aca
ncie
s h
ave
no
w b
ee
n r
ep
rofile
d in
th
e fo
reca
st to
la
ter
in th
e y
ea
r. T
he
bu
dge
t in
clu
de
d a
n in
cre
ase
of 4
65
FT
E o
ve
r M
1-9
; h
ow
eve
r, p
erm
an
en
t h
ea
dco
un
t o
nly
in
cre
ase
d b
y
a n
et 2
03
FT
E o
ve
r th
e p
eriod
V
aca
ncie
s h
ave
be
en
mo
vin
g t
o th
e r
igh
t o
ve
r th
e c
ou
rse
of th
e
ye
ar
so
fa
r, w
ith
th
e p
ea
k o
f re
cru
itm
en
t n
ow
be
ing s
ee
n in
Fe
bru
ary
. T
he
fo
reca
st n
ow
in
clu
de
s 1
34
pe
rma
ne
nt e
mp
loye
es to
jo
in d
uring th
e r
em
ain
de
r o
f th
e y
ea
r.
Non
-Sta
ff C
osts
are
fo
reca
st to
be
£1
.0m
ab
ove
bu
dge
t fo
r th
e f
ull
ye
ar.
Th
is in
clu
de
s £
3.6
m o
n
Sp
ine
2 f
or
ad
ditio
na
l w
ork
pa
cka
ge
s (
RF
), £
1.3
m in
ce
ntr
al IC
T a
nd
£0
.5m
fo
r G
S1
lic
en
ce
s in
A
SI,
pa
rtia
lly o
ffse
t b
y u
nd
ers
pe
nd
s in
oth
er
are
as. A
n a
dd
itio
na
l fo
reca
st o
f £
2.5
m h
as b
ee
n
ad
de
d in
Marc
h f
or
co
sts
of th
e M
AR
sch
em
e.
Th
e £
(1.1
)m fu
ll ye
ar
va
rian
ce
on
Una
lloca
ted
Costs
is d
ue
to
sp
ecific
sa
vin
gs h
avin
g b
ee
n
reco
gn
ise
d/ id
en
tifie
d in
all
directo
rate
s th
at in
clu
de
d th
is in
th
eir b
ud
ge
t, o
ffset b
y t
he
re
du
ctio
n
in t
he
ce
ntr
al co
ntin
ge
ncy t
o n
il a
t M
5.
Man
ag
em
en
t a
cti
on
A
lth
ou
gh
tig
hte
r b
ud
ge
ts w
ere
se
t fo
r D
ire
cto
rate
s f
or
15
/16
, th
e d
eta
iled
bu
dge
ts c
on
tain
ed
a
sig
nific
an
t am
ou
nt of re
cru
itm
en
t in
the
first ha
lf o
f th
e y
ea
r, m
uch
of w
hic
h d
id n
ot m
ate
rialis
e
an
d h
as b
ee
n r
efo
reca
st in
to Q
4. S
om
e o
f th
is u
nd
ers
pe
nd
on
sta
ff is b
ein
g u
se
d to
fu
nd
wo
rk
thro
ugh
wo
rkp
acka
ge
s in
pla
ce
of re
cru
itm
en
t, o
r is r
esu
ltin
g in
re
du
ce
d in
co
me
wh
ere
th
e s
taff
w
ere
to
su
pp
ort
exte
rna
lly-f
un
de
d w
ork
. W
ith
th
e r
em
ova
l o
f th
e c
orp
ora
te c
on
tin
ge
ncy f
ore
ca
st,
p
ressu
res w
ill n
ee
d to
be
fu
nd
ed
by D
irecto
rate
s r
ele
asin
g u
nd
ers
pe
nd
s fro
m th
eir r
esp
ective
fo
reca
sts
.
8 o
f 16
Page 23 of 159

20
15
/16
HS
CIC
Ma
na
ge
me
nt
Ac
co
un
ts a
s a
t 3
1s
t D
ec
em
be
r 2
01
5S
um
ma
ry P
os
itio
n
£'m
Bu
dg
et
Actu
al
Var
Bu
dg
et
F'c
ast
Var
Core
GiA
(112.2
)(1
12.2
)(0
.0)
(148.0
)(1
48.0
)(0
.0)
Rin
g-F
enced G
iA(9
.5)
(9.3
)(0
.2)
(12.6
)(1
2.3
)(0
.3)
Exte
rnal In
com
e(4
6.6
)(4
6.4
)(0
.2)
(63.3
)(6
3.7
)0.3
Sta
ff C
osts
121.2
111.2
10.0
162.2
150.8
11.4
Non-s
taff C
osts
48.0
42.8
5.2
62.5
66.0
(3.5
)
Unallo
cate
d C
osts
(0.9
)0.0
(0.9
)(0
.8)
0.4
(1.1
)
Su
rplu
s/ (D
efi
cit
)0.0
(13.8
)13.8
0.0
(6.8
)6.8
Depre
cia
tion G
iA(1
1.9
)(1
1.9
)0.0
(16.3
)(1
6.3
)0.0
Depre
cia
tion C
ost
11.9
11.2
0.7
16.3
15.6
0.7
Su
rplu
s/ (D
efi
cit
)0.0
(0.7
)0.7
0.0
(0.7
)0.7
NO
TE
: figure
s t
hro
ughout
may n
ot
sum
due t
o r
oundin
gs t
o £
0.1
m.
Exact
figure
s a
re a
vailable
if
requir
ed
Ap
pe
nd
ix 1
- M
an
ag
em
en
t A
cc
ou
nts
Year-
to-D
ate
Fu
ll Y
ear
The y
ear-
to-d
ate
outturn
for
the first nin
e m
onth
s o
f th
e y
ear
is £
14.0
m/ 11.5
% b
elo
w b
udget. T
he v
ariance o
f £14.0
m c
om
prises £
13.8
m u
nder
budget
on c
ore
GIA
and £
0.2
m u
nder
on r
ing-f
enced G
iA. T
he £
13.8
m u
nders
pend o
n c
ore
GiA
is larg
ely
due to d
ela
ys to r
ecru
itm
ent to
vacant ro
les, part
ially
offset by
resultant decre
ases to incom
e T
he £
0.2
m u
nders
pend o
n r
ing-f
enced G
iA is a
lso d
ue to v
acancie
s n
ot bein
g fill
ed a
s e
arly
as p
redic
ted.
The fore
cast outturn
for
the full
year
is £
7.1
m/ 4.4
% u
nder
budget; this
com
prises £
6.8
m u
nder
budget fo
r core
GiA
(re
duced fore
cast fo
r sta
ff c
osts
and
an incre
ase in incom
e, part
ially
offset by
rele
ase o
f centr
al contingency
and incre
ase in n
on-s
taff and £
0.3
m u
nder
budget fo
r ring-f
enced G
iA
(reducin
g s
taff c
osts
as r
ecru
itm
ent date
s for
vacancie
s m
ove to late
r in
the y
ear
than b
udgete
d).
A top-d
ow
n e
stim
ate
for
the e
nd o
f ye
ar,
adju
sting for
expecte
d r
ecru
itm
ent , pro
cure
ment a
nd incom
e a
ssum
ptions, in
dic
ate
s a
pote
ntial fo
recast out-
turn
for
core
GiA
of £10.9
m.
Non-G
iA incom
e is c
lose to b
udget fo
r th
e y
ear-
to-d
ate
and the full
year
fore
cast. H
ow
ever,
this
com
prises a
num
ber
of are
as that are
both
under
and
over
budget -
there
is a
dditio
nal in
com
e fro
m D
SfC
, G
PE
S, S
SD
, S
pin
e 2
and C
ross-G
overn
ment P
rogra
mm
es, b
ut lo
wer
incom
e o
n C
hoic
es
(inclu
din
g D
AS
), c
are
.data
, S
tandard
s, S
olu
tion A
ssura
nce, In
form
ation A
naly
sis
, P
ath
ways
and T
echnic
al A
rchitectu
re.
Sta
ff C
osts
are
£10.0
m u
nder
budget fo
r th
e y
ear-
to-d
ate
and fore
cast to
be £
11.4
m u
nder
budget fo
r th
e full
year.
This
main
ly r
eflects
recru
itm
ent
runnin
g b
ehin
d b
udgete
d v
acancie
s -
most of th
e v
acancie
s h
ave n
ow
been r
epro
file
d in the fore
cast to
late
r in
the y
ear.
The b
udget in
clu
ded a
n
incre
ase o
f 465 F
TE
over
M1-9
; how
ever,
perm
anent headcount only
incre
ased b
y a n
et 203 F
TE
over
the p
eriod V
acancie
s h
ave b
een m
ovin
g to the
right over
the c
ours
e o
f th
e y
ear
so far,
with the p
eak o
f re
cru
itm
ent now
bein
g s
een in F
ebru
ary
. T
he fore
cast now
inclu
des 1
34 p
erm
anent em
plo
yees
to join
during the r
em
ain
der
of th
e y
ear.
Non-S
taff C
osts
are
fore
cast to
be £
1.0
m a
bove b
udget fo
r th
e full
year.
This
inclu
des £
3.6
m o
n S
pin
e 2
for
additio
nal w
ork
packages (
RF
), £
1.3
m in
centr
al IC
T a
nd £
0.5
m for
GS
1 lic
ences in A
SI, p
art
ially
offset by
unders
pends in o
ther
are
as. A
n a
dditio
nal fo
recast of £2.5
m h
as b
een a
dded in
Marc
h for
costs
of th
e M
AR
schem
e.
The £
(1.1
)m full
year
variance o
n U
nallo
cate
d C
osts
is d
ue to s
pecific
savin
gs h
avin
g b
een r
ecognis
ed/ id
entified in a
ll directo
rate
s that in
clu
ded this
in
their b
udget, o
ffset by
the r
eduction in the c
entr
al contingency
to n
il at M
5.
Month
ly tre
nd o
f gro
ss e
xpenditure
for
the o
rganis
ation for
the o
rigin
al budget, the late
st
fore
cast (9
month
s o
f actu
al costs
and 3
month
s o
f expecte
d c
osts
) and a
n e
xtr
apola
tion
(runra
te)
of th
e p
ositio
n if th
e c
urr
ent sta
ff p
ositio
n r
em
ain
ed a
t D
ecem
ber
levels
for
the
rem
ain
der
of th
e y
ear.
Actu
al (t
o D
ecem
ber)
and fore
cast sta
ff c
osts
, show
ing p
erm
anent sta
ff b
y curr
ent esta
blis
hm
ent and futu
re r
ecru
itm
ent, p
lus fore
cast non-p
erm
anent
sta
ff. T
he r
ed lin
e s
how
s the o
rigin
al budget.
14
16
18
20
22
Apr
Ma
yJun
Jul
Aug
Sep
Oct
No
vD
ec
Jan
Feb
Ma
r
Mo
nth
ly s
taff
& n
on
-sta
ff e
xp
en
dit
ure
(in
cl
co
nti
ng
en
cy)
£'m
Bud
get
Actu
al/ F
ore
ca
st
Fo
recast
@ r
un
rate
11.3
1
1.3
11.3
11.5
11.5
11.7
11.9
12.1
11.8
1
1.8
11.8
11.8
0.7
1
.0
1.2
0.9
0.9
0.6
0.7
1.1
0.7
0.6
0.8
0.4
0.4
0.4
0.4
- 2 4 6 8
10
12
14
16
Ap
r-14
Ma
y-1
4Jun
-14
Jul-
14
Au
g-1
4S
ep-1
4O
ct-
14
No
v-1
4D
ec-1
4Jan
-15
Fe
b-1
5M
ar-
15
Mo
nth
s
Mo
nth
ly S
taff
Ex
pe
nd
itu
re £
'm
In P
ost (p
erm
)F
ore
cast
In P
ost (n
on-p
erm
)2
01
5/1
6 B
udg
et
9 o
f 16
03 (
a) B
oard
Per
form
ance
Pac
k
Page 24 of 159

2015/1
6 H
SC
IC M
an
ag
em
en
t A
cco
un
ts a
s a
t 31st
Decem
ber
2015
£'m
Bu
dg
et
Ac
tua
lV
ar
Bu
dg
et
F'c
as
tV
ar
In
co
me
Gra
nt in
Aid
(11
2.2
)(1
12
.2)
(0.0
)(1
48
.0)
(14
8.0
)(0
.0)
Gra
nt in
Aid
(rin
g-f
en
ce
d)
(9.5
)(9
.3)
(0.2
)(1
2.6
)(1
2.3
)(0
.3)
Inco
me
(46
.6)
(46
.4)
(0.2
)(6
3.3
)(6
3.7
)0
.3
To
tal In
co
me
(16
8.3
)(1
67
.9)
(0.5
)(2
23
.9)
(22
4.0
)0
.0
Sta
ff C
osts
£1
1.4
m f
ull y
ea
r va
ria
nc
e in
clu
de
s:
Pe
rma
ne
nt S
taff
11
2.7
10
4.4
8.2
15
2.0
14
1.4
10
.64
.0O
&A
S d
ire
cto
rate
(re
cru
itm
en
t d
ela
ys p
lus fu
nd
ing
tra
nsfe
rre
d to
wo
rkp
acka
ge
s)
No
n P
erm
an
en
t S
taff
8.5
6.8
1.8
10
.19
.30
.81
.3H
DS
(d
ela
ye
d r
ecru
itm
en
t a
ga
inst b
ud
ge
t)
To
tal S
taff
Co
sts
12
1.2
11
1.2
10
.01
62
.21
50
.81
1.4
1.5
Info
rma
tio
n &
An
aly
tics d
ire
cto
rate
(d
ela
ye
d r
ecru
itm
en
t a
ga
inst b
ud
ge
t)
1.4
Fin
an
ce
& C
orp
ora
te S
erv
ice
s (
red
uctio
n in
Co
ntr
acto
rs)
1.4
PS
I (
sta
ff r
ed
ep
loym
en
t a
nd
de
lays to
HS
CN
re
cru
itm
en
t)
0.7
Cu
sto
me
r R
ela
tio
ns d
ire
cto
rate
1.0
11
.4
Oth
er C
osts
Pro
fessio
na
l F
ee
s1
8.8
13
.35
.52
4.2
22
.51
.7
Info
rma
tio
n T
ech
no
log
y1
3.2
13
.3(0
.1)
17
.21
9.2
(2.0
)
Tra
ve
l &
Su
bsis
ten
ce
3.5
3.9
(0.4
)4
.75
.2(0
.5)
Acco
mm
od
atio
n8
.59
.0(0
.5)
11
.21
1.3
(0.0
)
Ma
rke
tin
g, T
rain
ing
& E
ve
nts
1.4
1.3
0.1
1.8
2.1
(0.3
)
Offic
e S
erv
ice
s2
.22
.00
.22
.92
.9(0
.1)
Oth
er
0.4
0.1
0.3
0.6
2.8
(2.2
)
To
tal O
the
r C
os
ts4
8.0
42
.85
.26
2.5
66
.0(3
.5)
Un
allo
ca
te
d C
osts
Dire
cto
rate
Co
ntin
ge
ncy/ S
avin
gs
(2.1
)0
.0(2
.1)
(3.2
)0
.4(3
.6)
Ce
ntr
al C
on
tin
ge
ncy
1.2
0.0
1.2
2.4
0.0
2.4
De
pre
cia
tio
n
De
pre
cia
tio
n G
ran
t-in
-Aid
(11
.9)
(11
.9)
0.0
(16
.3)
(16
.3)
0.0
De
pre
cia
tio
n C
osts
11
.91
1.2
0.7
16
.31
5.6
0.7
0.0
(0.7
)0
.70
.0(0
.7)
0.7
Mo
st D
ire
cto
rate
s a
re r
ep
ort
ing
/ fo
reca
stin
g T
&S
co
sts
ab
ove
bu
dg
et.
£0
.3m
ove
r b
ud
ge
t fo
r tr
ain
ing
/ e
xte
rna
l co
urs
e fe
es
Fo
reca
st in
clu
de
s £
2.5
m in
Ma
rch
fo
r M
AR
S
£(5
.5)m
of b
ud
ge
ted
"S
avin
gs to
be
fo
un
d"
ha
ve
all
be
en
re
lea
se
d in
th
e fo
reca
st a
cro
ss P
SI, F
&C
S, H
DS
, O
AS
, C
R a
nd
AS
I.
£4
.0m
of co
ntin
ge
ncy (
bo
th c
en
tra
l a
nd
in
dire
cto
rate
s)
ha
s b
ee
n r
ele
ase
d in
th
e fo
reca
st.
Fu
ll ye
ar
va
ria
nce
in
clu
de
s £
1.5
m IC
T , £
0.7
m C
yb
ers
ecu
rity
an
d £
0.5
m in
Te
ch
Arc
hs (
un
bu
dg
ete
d G
S1
lic
en
ce
s)
Ap
pen
dix
1 -
Man
ag
em
en
t A
cco
un
ts
Deta
il b
y In
co
me/ E
xp
en
dit
ure
Typ
e
Ye
ar-
to-D
ate
Fu
ll Y
ea
r
Rin
g-f
en
ce
d G
iA -
£(0
.2)m
YT
D a
nd
£(0
.1)m
fo
reca
st va
ria
nce
s r
efle
ct th
at e
xp
ecte
d s
pe
nd
is n
ow
ap
pro
ach
ing
bu
dg
et a
fte
r a
slo
we
r sta
rt to
th
e y
ea
r; a
ny o
ve
rsp
en
d w
ou
ld h
ave
to
be
fo
un
d fro
m c
ore
GiA
No
n-G
iA in
co
me
is £
0.2
m u
nd
er
bu
dg
et fo
r th
e y
ea
r-to
-da
te. T
he
fo
reca
st is
£0
.3m
ab
ove
bu
dg
et fo
r th
e fu
ll ye
ar.
Th
is is
prim
arily
drive
n fro
m a
dd
itio
na
l in
co
me
fro
m D
SfC
, G
PE
S, S
pin
e 2
an
d C
ross-G
ove
rnm
en
t P
rog
ram
me
s, b
ut lo
we
r in
co
me
on
Ch
oic
es (
inclu
din
g D
AS
), c
are
.da
ta, S
tan
da
rds, S
olu
tio
n A
ssu
ran
ce
an
d In
form
atio
n A
na
lysis
.
Oth
er
Fu
ll ye
ar
fore
ca
st o
ve
rsp
en
d a
ga
inst b
ud
ge
t in
clu
de
s £
3.7
m fo
r S
pin
e 2
wo
rkp
acka
ge
s a
nd
HS
CN
£0
.4m
, p
art
ially
offse
t b
y
va
rio
us r
ed
uctio
ns, in
clu
din
g £
1.0
m P
op
ula
tio
n H
ea
lth
, £
0.7
m C
yb
ers
ecu
rity
, £
0.5
m C
PIS
an
d £
0.5
m S
CIP
10
of
16
Page 25 of 159

20
15
/16
HS
CIC
Ma
na
ge
me
nt
Ac
co
un
ts a
s a
t 3
1s
t D
ec
em
be
r 2
01
5D
eta
il b
y D
ire
cto
rate
£'m
Bu
dg
et
Actu
al
Var
Bu
dg
et
F'c
ast
Var
Pro
vid
er S
up
po
rt &
In
te
gra
tio
n
Inco
me
(3.6
)(4
.1)
0.4
(4.8
)(5
.4)
0.6
Sta
ff C
osts
14
.11
2.2
2.0
18
.31
6.8
1.4
Oth
er
Co
sts
2.6
2.1
0.4
3.6
3.6
0.0
Con
tin
ge
ncy /
Vir
em
en
ts(0
.8)
0.0
(0.8
)(1
.3)
0.0
(1.3
)
Net
GiA
fu
nd
ed
12
.31
0.2
2.1
15
.71
5.0
0.7
He
alth
D
ig
ita
l S
ervic
es
Inco
me
(12
.0)
(12
.2)
0.2
(16
.0)
(16
.5)
0.4
Sta
ff C
osts
18
.61
7.4
1.2
24
.92
3.6
1.3
Oth
er
Co
sts
6.4
5.8
0.6
8.4
8.1
0.4
Con
tin
ge
ncy /
Vir
em
en
ts(1
.6)
0.0
(1.6
)(2
.1)
0.0
(2.1
)
Net
GiA
fu
nd
ed
11
.41
1.0
0.5
15
.21
5.2
0.0
Op
era
tio
ns &
A
ssu
ra
nc
e S
ervic
es
Inco
me
(24
.8)
(24
.8)
0.1
(33
.0)
(33
.6)
0.6
Sta
ff C
osts
39
.33
6.1
3.2
53
.04
8.9
4.0
Oth
er
Co
sts
14
.61
5.4
(0.8
)1
8.3
22
.9(4
.6)
Con
tin
ge
ncy /
Vir
em
en
ts0
.80
.00
.81
.20
.01
.2
Net
GiA
fu
nd
ed
29
.92
6.7
3.3
39
.43
8.2
1.2
In
fo
rm
atio
n &
A
na
lytic
s
Inco
me
(10
.2)
(8.4
)(1
.7)
(14
.7)
(11
.7)
(3.0
)
Sta
ff C
osts
18
.71
7.4
1.3
25
.02
3.5
1.5
Oth
er
Co
sts
7.5
6.6
1.0
10
.59
.70
.8
Con
tin
ge
ncy /
Vir
em
en
ts0
.40
.00
.40
.60
.00
.6
Net
GiA
fu
nd
ed
16
.51
5.5
1.0
21
.52
1.5
(0.0
)
Arc
hite
ctu
re
, S
ta
nd
ard
s &
In
no
va
tio
n
Inco
me
(3.7
)(4
.6)
0.9
(4.9
)(6
.8)
1.8
Sta
ff C
osts
13
.41
3.0
0.4
18
.31
7.5
0.8
Oth
er
Co
sts
3.3
1.6
1.7
4.3
3.7
0.6
Con
tin
ge
ncy /
Vir
em
en
ts0
.20
.00
.2(0
.0)
0.4
(0.4
)
Net
GiA
fu
nd
ed
13
.11
0.0
3.1
17
.71
4.9
2.8
Fin
an
ce
&
C
orp
ora
te
S
ervic
es
(e
xc
l E
sta
te
s)
Inco
me
(0.8
)(0
.6)
(0.2
)(1
.1)
(0.8
)(0
.3)
Sta
ff C
osts
11
.11
0.1
1.0
14
.71
3.3
1.4
Oth
er
Co
sts
3.7
2.3
1.4
4.6
3.4
1.2
Con
tin
ge
ncy /
Vir
em
en
ts(0
.8)
0.0
(0.8
)(1
.2)
0.0
(1.2
)
Net
GiA
fu
nd
ed
13
.21
1.8
1.4
17
.01
6.0
1.1
Es
tate
s7
.47
.7(0
.3)
9.8
9.9
(0.1
)
HR
&
T
ra
nsfo
rm
atio
n2
.62
.10
.53
.43
.20
.2
Cu
sto
me
r R
ela
tio
ns
3.8
3.1
0.6
5.0
4.5
0.5
Clin
ic
al P
ro
fe
ssio
na
l L
ea
de
rsh
ip
0.7
0.6
0.1
0.9
0.9
0.1
HS
CIC
C
orp
ora
te
(11
1.0
)(1
12
.6)
1.6
(14
5.6
)(1
45
.9)
0.4
Prim
arily
du
e t
o lo
we
r th
an
bu
dg
ete
d s
taff
co
sts
Bu
dg
et
for
co
ntin
ge
ncy f
un
din
g h
as b
ee
n r
ed
uce
d t
o n
il, g
ive
n t
he
cu
rre
nt
leve
l o
f fo
reca
st
sp
en
d a
nd
pre
ssu
res f
or
the
org
an
isa
tio
n.
£(0
.4)m
of
ce
ntr
al a
ccru
als
rele
ase
d f
rom
prio
r ye
ars
. F
ore
ca
st
inclu
de
s £
2.5
m in
Ma
rch
fo
r M
AR
S
£0
.6m
ad
ditio
na
l in
co
me
in
clu
de
s in
cre
ase
s t
o S
pin
e 2
£2
.6m
(a
dd
itio
na
l re
ch
arg
e o
f co
sts
to
DH
to
be
ca
pita
lise
d a
nd
rin
g-f
en
ce
d G
iA)
, p
art
ially
off
se
t b
y
red
uctio
ns in
in
co
me
fo
r N
HS
Pa
thw
ays £
(0.3
)m,
Se
rvic
e M
an
ag
em
en
t £
(0.5
)m,
Cyb
ers
ecu
rity
£(0
.7)m
an
d S
olu
tio
n A
ssu
ran
ce
£(1
.1)m
.
£4
.0m
fo
reca
st
red
uctio
n in
Sta
ff C
osts
is d
ue
to
exp
ecte
d r
ecru
itm
en
t b
ein
g d
ela
ye
d u
ntil la
ter
in t
he
ye
ar,
so
me
of
wh
ich
re
late
s t
o in
co
me
re
du
ctio
ns a
s a
bo
ve
,
with
so
me
sa
vin
gs b
ein
g u
se
d t
o f
un
d w
ork
pa
cka
ge
s (
se
e b
elo
w)
£(4
.6)m
in
cre
ase
in
no
n-s
taff
co
sts
is p
rim
arily
du
e t
o £
3.7
m in
cre
ase
on
Pro
fessio
na
l F
ee
s f
or
Sp
ine
2 w
ork
pa
cka
ge
s (
rela
ted
to
th
e in
cre
ase
d in
co
me
fro
m D
H
an
d r
ed
uce
d s
taff
co
sts
ab
ove
) a
nd
£1
.5m
ad
ditio
na
l fo
reca
st
for
ce
ntr
al IC
T.
Th
e f
ull
ye
ar
inco
me
va
ria
nce
of
£(3
.0)m
is p
rim
arily
du
e t
o r
ed
uctio
n in
exp
ecte
d in
co
me
on
In
form
atio
n A
na
lysis
£(1
.5)m
, ca
re.d
ata
£(0
.9)m
, M
CD
S £
(0.4
)m
an
d
Da
ta D
isse
min
atio
n £
(0.3
)m.
£(0
.9)m
of
the
IA
va
ria
nce
is f
rom
Po
pu
latio
n H
ea
lth
( C
hild
ren
an
d Y
ou
ng
er
Pe
op
le M
en
tal H
ea
lth
Su
rve
y)
- co
sts
ha
ve
als
o
red
uce
d a
cco
rdin
gly
.
£1
.5m
fo
reca
st
un
de
rsp
en
d o
n s
taff
co
sts
in
clu
de
s £
0.5
m r
ed
uctio
n o
n c
are
.da
ta/
MC
DS
(re
late
d t
o in
co
me
va
ria
nce
s a
bo
ve
), £
0.4
m D
ata
Dis
se
min
atio
n s
erv
ice
s
an
d £
0.5
m In
form
atio
n A
na
lysis
£0
.8m
un
de
rsp
en
d o
n n
on
-sta
ff c
osts
is d
ue
to
ad
ditio
na
l IT
co
sts
on
ca
re.d
ata
/ M
CD
S a
nd
Pa
tie
nt
Pre
fere
nce
s o
ffse
t b
y r
ed
uctio
n in
pro
fessio
na
l fe
es/
su
rve
ys
on
Po
pu
latio
n H
ea
lth
( C
hild
ren
an
d Y
ou
ng
er
Pe
op
le M
en
tal H
ea
lth
Su
rve
y)
£1
.9m
fo
reca
st
va
ria
nce
on
In
co
me
is d
ue
to
in
cre
ase
d in
co
me
£2
.3m
on
DS
fC ,
off
se
t b
y £
(0.5
)m r
ed
uctio
n in
exp
ecte
d e
xte
rna
l fu
nd
ing
to
co
ve
r IH
TS
DO
me
mb
ers
hip
.
£0
.8m
fu
ll ye
ar
va
ria
nce
on
sta
ff c
osts
in
clu
de
s f
ore
ca
st
un
de
rsp
en
d o
f £
1.3
m o
n S
tan
da
rds,
pa
rtia
lly o
ffse
t b
y in
cre
ase
d c
osts
of
£(0
.4)m
on
DS
fC &
NT
S.
£0
.6m
fu
ll ye
ar
va
ria
nce
on
no
n-s
taff
co
sts
in
clu
de
s £
1.1
m r
ed
uctio
n in
co
sts
in
Sta
nd
ard
s,
pa
rtia
lly o
ffse
t b
y in
cre
ase
d c
osts
in
DS
fC a
nd
Te
ch
Arc
hite
ctu
re.
£1
.4m
un
de
rsp
en
d o
n s
taff
co
sts
is p
rim
arily
du
e t
o r
ed
uctio
n in
co
ntr
acto
r co
sts
in
Co
mm
erc
ial.
£1
.2m
un
de
rsp
en
d o
n n
on
-sta
ff c
osts
is d
ue
th
e r
ed
uctio
n in
fo
reca
st
leg
al fe
es
Th
e "
Co
ntin
ge
ncy/
Vire
me
nts
" lin
e s
ho
ws D
ire
cto
rate
Sa
vin
gs t
o b
e F
ou
nd
to
be
re
alis
ed
th
rou
gh
ou
t th
e y
ea
r. F
ore
ca
st
ha
s b
ee
n r
ele
ase
d d
ue
to
sa
vin
gs f
ou
nd
on
re
du
ce
d c
on
tra
cto
r co
sts
an
d le
ga
l fe
es.
Inco
me
- £
0.4
m f
ull
ye
ar
fore
ca
st
va
ria
nce
in
clu
de
s £
2.0
m r
ed
uctio
n o
n C
ho
ice
s/
DA
S,
pa
rtia
lly o
ffse
t b
y
£1
.8m
in
cre
ase
d in
co
me
on
GP
ES
.
Sta
ff c
osts
- f
ull
ye
ar
fore
ca
st
va
ria
nce
of
£1
.3m
in
clu
de
s£
1.5
m C
ho
ice
s,
pa
rtia
lly o
ffse
t b
y in
cre
ase
d c
osts
of
£0
.5m
on
GP
So
C R
an
d £
0.4
m o
n R
eso
urc
e P
oo
l
Th
e "
Co
ntin
ge
ncy/
Vire
me
nts
" lin
e s
ho
ws D
ire
cto
rate
Sa
vin
gs t
o b
e F
ou
nd
to
be
re
alis
ed
th
rou
gh
ou
t th
e y
ea
r. F
ore
ca
st
ha
s b
ee
n r
ele
ase
d d
ue
to
sa
vin
gs r
ea
lise
d
to d
ate
£(2
.1)m
Ap
pe
nd
ix 1
- M
an
ag
em
en
t A
cc
ou
nts
Year-
to-D
ate
Fu
ll Y
ear
NO
TE
: B
elo
w i
nc
lud
es
tra
ns
fer
of
bu
dg
ets
@ M
6 f
rom
HD
S t
o P
SI fo
r C
ros
s-G
ove
rnm
en
t p
rog
ram
me
s a
nd
fro
m O
&A
S t
o I&
A f
or
Dem
og
rap
hic
s a
nd
@ M
7,
fro
m H
DS
to
PS
I fo
r H
SC
N
£0
.6m
in
cre
ase
d f
ore
ca
st
for
inco
me
is d
ue
to
£0
.2m
ad
ditio
na
l in
co
me
on
Cro
ss G
ovt
pro
jects
an
d £
0.4
m a
dd
itio
na
l in
co
me
fo
r se
co
nd
me
nts
, P
roto
n B
ea
m
Th
era
py a
nd
bu
sin
ess c
ase
assu
ran
ce
re
vie
w s
erv
ice
.
£1
.4m
fo
reca
st
un
de
rsp
en
d o
n s
taff
co
sts
du
e t
o d
ela
ye
d r
ecru
itm
en
t a
nd
le
ave
rs n
ot
rep
lace
d.
Th
e "
Co
ntin
ge
ncy/
Vire
me
nts
" lin
e s
ho
ws D
ire
cto
rate
Sa
vin
gs t
o b
e F
ou
nd
to
be
re
alis
ed
th
rou
gh
ou
t th
e y
ea
r. F
ore
ca
st
ha
s b
ee
n r
ele
ase
d d
ue
to
sa
vin
gs r
ea
lise
d
to d
ate
£(1
.3)m
11 o
f 16
03 (
a) B
oard
Per
form
ance
Pac
k
Page 26 of 159

2015/1
6 H
SC
IC M
an
ag
em
en
t A
cco
un
ts a
s a
t 31st
Decem
ber
2015
Head
co
un
t
Ap
pen
dix
1 -
Man
ag
em
en
t A
cco
un
ts
Th
e b
ud
ge
t in
clu
de
d a
n in
cre
ase
of
46
5 F
TE
ove
r M
1-9
; h
ow
eve
r, p
erm
an
en
t h
ea
dco
un
t o
nly
in
cre
ase
d b
y a
ne
t 2
03
FT
E o
ve
r th
e p
erio
d
Va
ca
ncie
s h
ave
be
en
mo
vin
g t
o t
he
rig
ht
ove
r th
e c
ou
rse
of
the
ye
ar
so
fa
r, w
ith
th
e
pe
ak o
f re
cru
itm
en
t n
ow
be
ing
se
en
in
Fe
bru
ary
. T
he
fo
reca
st
no
w in
clu
de
s 1
34
pe
rma
ne
nt
em
plo
ye
es t
o jo
in d
urin
g t
he
re
ma
ind
er
of
the
ye
ar.
No
te:
FT
E in
cre
ase
fig
ure
is a
s a
t p
ayro
ll d
ate
th
ere
fore
ma
y d
iffe
r fr
om
HR
fig
ure
s f
or
the
wh
ole
of
the
mo
nth
.
2,4
40
2
,45
8
2,4
82
2,5
27
2,5
62
2,5
69
2,5
89
2,6
09
2,6
41
2,6
85
2,7
46
2
,77
6
13
16
15
11
12
8
10
8
9
10
10
10
57
57
45
4
7
43
41
49
44
3
8
39
37
37
67
68
5
8
65
74
69
66
65
57
61
68
67
2,0
00
2,2
00
2,4
00
2,6
00
2,8
00
3,0
00
3,2
00
Apr-
15
Act
Ma
y-1
5A
ct
June
-15
Act
Jul-1
5A
ct
Aug-1
5A
ct
Sept-
15
Act
Oct-
15
Act
No
v-1
5A
ct
De
c-1
5A
ct
Jan-1
6F
ct
Feb
-16
Fct
Ma
r-1
6F
ct
Wo
rkfo
rce:
Bu
dg
et
vs F
ore
cast
[FT
E]
(note
: axis
sta
rts fro
m 2
,000)
Perm
an
ent
Sta
ffS
econd
ee
Tem
pora
ry S
taff
Co
ntr
acto
rH
eadcou
nt B
udg
et
Apr-
15
Act
Ma
y-1
5A
ct
June
-15
Act
Jul-
15
Act
Aug
-15
Act
Sept-
15
Act
Oct-
15
Act
No
v-1
5A
ct
De
c-1
5A
ct
Jan-1
6F
ct
Feb
-16
Fct
Ma
r-1
6F
ct
Fore
cast In
cre
ase (
FT
E)
2.0
17
.924
.344
.535
.37.6
19
.919
.432
.543
.961
.229
.4
Budg
ete
d Incre
ase
(F
TE
)52
.288
.612
5.2
68
.833
.05
2.5
23
.412
.19.0
(3.5
)2
.84.4
-
20
.0
40
.0
60
.0
80
.0
10
0.0
12
0.0
14
0.0
Perm
an
en
t S
taff
- F
ore
cast
Incre
ase v
s B
ud
gete
d I
ncre
ase [
FT
E]
Fore
cast In
cre
ase (
FT
E)
Budg
ete
d Incre
ase
(F
TE
)
844
855
854
85
9
87
6
87
8
895
905
913
920
940
95
3
397
396
397
40
6
41
0
41
5
431
431
435
436
44
3
44
2
514
509
518
52
0
52
5
52
2
530
533
535
54
7
567
57
5
225
233
239
24
8
258
25
5
250
252
256
25
8
272
27
7
223
230
226
236
23
1
226
227
220
216
22
1
22
3
22
4
229
231
225
23
3
233
23
3
235
238
241
25
3
25
6
25
8
84
85
80
87
85
8
6
82
84
85
96
9
5
96
54
53
54
54
68
6
7
60
58
60
59
60
6
0
6
7
6
6
6
5
5
5
5
5
5
5
0
50
0
1,0
00
1,5
00
2,0
00
2,5
00
3,0
00
Ap
r-1
5A
ct
Ma
y-1
5A
ct
June
-15
Act
Jul-1
5A
ct
Aug-1
5A
ct
Sep
t-1
5A
ct
Oct-
15
Act
No
v-1
5A
ct
De
c-1
5A
ct
Jan-1
6F
ct
Feb
-16
Fct
Ma
r-1
6F
ct
Wo
rkfo
rce:
Bu
dg
et
vs F
ore
cast
by D
irecto
rate
[F
TE
]
Ope
ratio
ns &
Assu
ran
ce
Se
rvic
es
He
alth
D
igital S
erv
ice
sIn
form
atio
n &
An
aly
tics
Arc
hite
ctu
re,
Sta
nd
ard
s &
Inn
ova
tion
Fin
ance &
Corp
ora
te S
erv
ices
Pro
vid
er
Sup
port
& In
teg
ratio
n
Cu
sto
mer
Rela
tio
ns
HR
& T
ran
sfo
rmatio
nC
linic
al
He
adcou
nt
Budg
et
12
of
16
Page 27 of 159
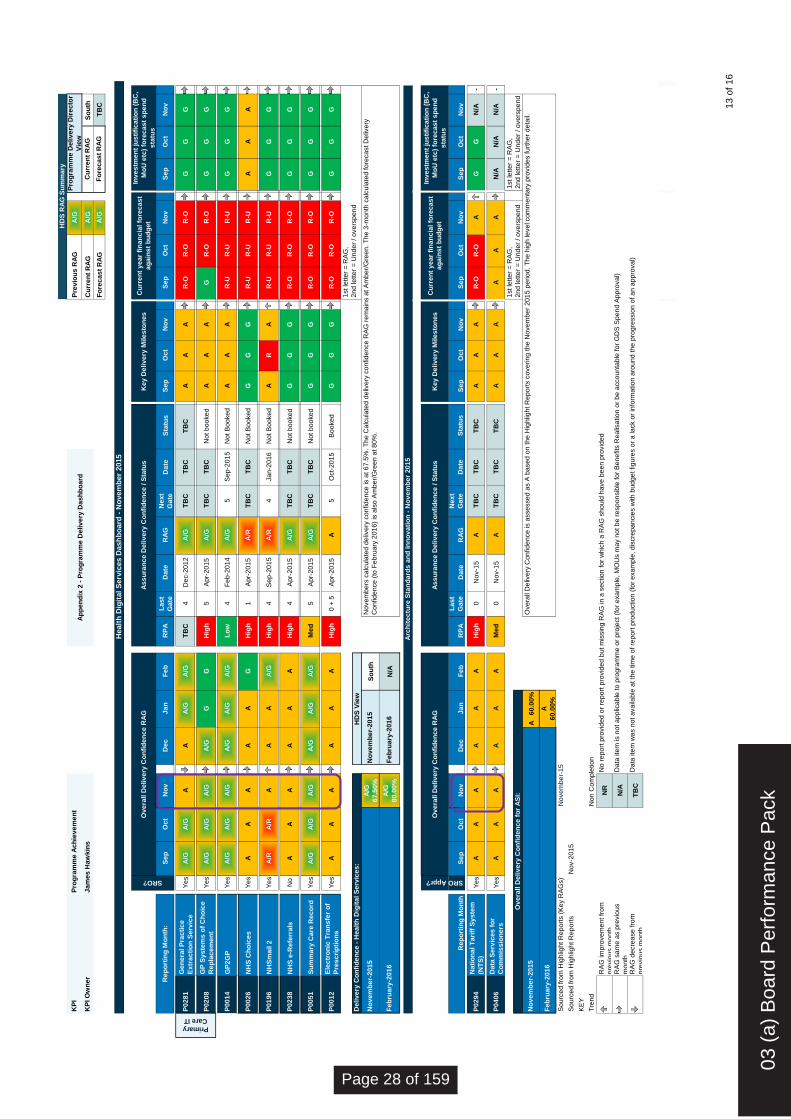
Pre
vio
us
RA
GA
/G
Cu
rre
nt
RA
GA
/GS
ou
th
Ju
lyF
ore
ca
st
RA
GA
/GT
BC
Se
pO
ct
No
vD
ec
Ja
nF
eb
RP
AL
as
t
Ga
teD
ate
RA
GN
ex
t
Ga
teD
ate
Sta
tus
Se
pO
ct
No
vS
ep
Oc
tN
ov
Se
pO
ct
No
v
P0
28
1G
en
era
l P
rac
tic
e
Ex
tra
cti
on
Se
rvic
eY
es
A/G
A/G
AA
A/G
A/G
TB
C4
De
c-2
01
2A
/GT
BC
TB
CT
BC
AA
AR
-OR
-OR
-OG
GG
P0
20
8G
P S
ys
tem
s o
f C
ho
ice
Re
pla
ce
me
nt
Ye
sA
/GA
/GA
/GA
/GG
GH
igh
5A
pr-
20
15
A/G
TB
CT
BC
No
t b
oo
ke
dA
AA
GR
-OR
-OG
GG
P0
01
4G
P2
GP
Ye
sA
/GA
/GA
/GA
/GA
/GA
/GL
ow
4F
eb
-20
14
A/G
5S
ep
-20
15
No
t B
oo
ke
dA
AA
R-U
R-U
R-U
GG
G
P0
02
6N
HS
Ch
oic
es
Y
es
AA
AA
AG
Hig
h1
Ap
r-2
01
5A
/RT
BC
TB
CN
ot B
oo
ke
dG
GG
R-U
R-U
R-U
AA
A
P0
19
6N
HS
ma
il 2
Ye
sA
/RA
/RA
AA
A/G
Hig
h4
Se
p-2
01
5A
/R4
Ja
n-2
01
6N
ot B
oo
ke
dA
RA
R-U
R-U
R-U
GG
G
P0
23
8N
HS
e-R
efe
rra
lsN
oA
AA
AA
AH
igh
4A
pr-
20
15
A/G
TB
CT
BC
No
t b
oo
ke
dG
GG
R-O
R-O
R-O
GG
G
P0
05
1S
um
ma
ry C
are
Re
co
rdY
es
A/G
A/G
A/G
A/G
A/G
A/G
Me
d5
Ap
r-2
01
5A
/GT
BC
TB
CN
ot b
oo
ke
dG
GG
R-O
R-O
R-O
GG
G
P0
01
2E
lec
tro
nic
Tra
ns
fer
of
Pre
sc
rip
tio
ns
Ye
sA
AA
AA
AH
igh
0 +
5A
pr-
20
15
A5
Oct-
20
15
Bo
oke
dG
GG
R-O
R-O
R-O
GG
G
A/G
67
.50
%S
ou
th
A/G
80
.00
%N
/A
Se
pO
ct
No
vD
ec
Ja
nF
eb
RP
A
La
st
Ga
teD
ate
RA
G
Ne
xt
Ga
teD
ate
Sta
tus
Se
pO
ct
No
vS
ep
Oc
tN
ov
Se
pO
ct
No
v
P0
29
4N
ati
on
al T
ari
ff S
ys
tem
(NT
S)
Ye
sA
AA
AA
AH
igh
0N
ov-1
5A
TB
CT
BC
TB
CA
AA
R-O
R-O
AG
GN
/A-
P0
40
6D
ata
Se
rvic
es
fo
r
Co
mm
iss
ion
ers
Ye
sA
AA
AA
AM
ed
0N
ov-1
5A
TB
CT
BC
TB
CA
AA
AA
AN
/AN
/AN
/A-
A 6
0.0
0%
A
60
.00
%
So
urc
ed
fro
m H
igh
ligh
t R
ep
ort
s (
Ke
y R
AG
s)
So
urc
ed
fro
m H
igh
ligh
t R
ep
ort
s
KE
Y
Tre
nd
N
on
Co
mp
letio
n
3R
AG
im
pro
ve
me
nt fr
om
pre
vio
us m
on
thN
R
2R
AG
sa
me
as p
revio
us
mo
nth
N/A
1R
AG
de
cre
ase
fro
m
pre
vio
us m
on
thT
BC
HD
S R
AG
Su
mm
ary
KP
IP
rog
ram
me
Ac
hie
ve
me
nt
Pro
gra
mm
e D
eliv
ery
Dir
ec
tor
Vie
w
KP
I O
wn
er
Ja
me
s H
aw
kin
sC
urr
en
t R
AG
Ap
pe
nd
ix 2
- P
rog
ram
me
De
liv
ery
Da
sh
bo
ard
Healt
h D
igit
al
Serv
ices D
ash
bo
ard
- N
ovem
ber
2015
Fo
rec
as
t R
AG
1st le
tte
r =
RA
G,
2n
d le
tte
r =
Un
de
r / o
ve
rsp
en
dD
eliv
ery
Co
nfi
de
nc
e -
He
alt
h D
igit
al S
erv
ice
s:
HD
S V
iew
Re
po
rtin
g M
on
th:
Primary
Care IT
SRO?
Ov
era
ll D
eliv
ery
Co
nfi
de
nc
e R
AG
As
su
ran
ce
De
liv
ery
Co
nfi
de
nc
e / S
tatu
sK
ey
De
liv
ery
Mile
sto
ne
sC
urr
en
t y
ea
r fi
na
nc
ial fo
rec
as
t
ag
ain
st
bu
dg
et
Inv
es
tme
nt
jus
tifi
ca
tio
n (
BC
,
Mo
U e
tc)
fore
ca
st
sp
en
d
sta
tus
Fe
bru
ary
-20
16
Fe
bru
ary
-20
16
No
ve
mb
er-
20
15
No
ve
mb
er-
20
15
No
ve
mb
ers
ca
lcu
late
d d
eliv
ery
co
nfid
en
ce
is a
t 6
7.5
%. T
he
Ca
lcu
late
d d
eliv
ery
co
nfid
en
ce
RA
G r
em
ain
s a
t A
mb
er/
Gre
en
. T
he
3-m
on
th c
alc
ula
ted
fo
reca
st D
eliv
ery
Co
nfid
en
ce
(to
Fe
bru
ary
20
16
) is
als
o A
mb
er/
Gre
en
at 8
0%
.
Re
po
rtin
g M
on
th
Arc
hit
ec
ture
Sta
nd
ard
s a
nd
In
no
va
tio
n -
No
ve
mb
er
20
15
SRO Appr?
Ov
era
ll D
eliv
ery
Co
nfi
de
nc
e R
AG
As
su
ran
ce
De
liv
ery
Co
nfi
de
nc
e / S
tatu
sK
ey
De
liv
ery
Mile
sto
ne
sC
urr
en
t y
ea
r fi
na
nc
ial fo
rec
as
t
ag
ain
st
bu
dg
et
Inv
es
tme
nt
jus
tifi
ca
tio
n (
BC
,
Mo
U e
tc)
fore
ca
st
sp
en
d
sta
tus
1st le
tte
r =
RA
G,
2n
d le
tte
r =
Un
de
r / o
ve
rsp
en
d
1st le
tte
r =
RA
G,
2n
d le
tte
r =
Un
de
r / o
ve
rsp
en
dO
ve
rall D
eliv
ery
Co
nfi
de
nc
e f
or
AS
I:
No
ve
mb
er-
20
15
Ove
rall
De
live
ry C
on
fid
en
ce
is a
sse
sse
d a
s A
ba
se
d o
n th
e H
igh
ligh
t R
ep
ort
s c
ove
rin
g th
e N
ove
mb
er
20
15
pe
rio
d. T
he
hig
h le
ve
l co
mm
en
tary
pro
vid
es fu
rth
er
de
tail.
Da
ta ite
m w
as n
ot a
va
ilab
le a
t th
e tim
e o
f re
po
rt p
rod
uctio
n (
for
exa
mp
le, d
iscre
pa
ncie
s w
ith
bu
dg
et fig
ure
s o
r a
la
ck o
r in
form
atio
n a
rou
nd
th
e p
rog
ressio
n o
f a
n a
pp
rova
l)
No
re
po
rt p
rovid
ed
or
rep
ort
pro
vid
ed
bu
t m
issin
g R
AG
in
a s
ectio
n fo
r w
hic
h a
RA
G s
ho
uld
ha
ve
be
en
pro
vid
ed
Da
ta ite
m is n
ot a
pp
lica
ble
to
pro
gra
mm
e o
r p
roje
ct (f
or
exa
mp
le, M
OU
s m
ay n
ot b
e r
esp
on
sib
le fo
r B
en
efits
Re
alis
atio
n o
r b
e a
cco
un
tab
le fo
r G
DS
Sp
en
d A
pp
rova
l)
No
v-2
01
5
Fe
bru
ary
-20
16
No
ve
mb
er-
15
13 o
f 16
03 (
a) B
oard
Per
form
ance
Pac
k
Page 28 of 159

A/G
A/G
So
uth
A/G
TB
C
Se
pO
ct
No
vS
ep
Oc
tN
ov
Se
pO
ct
No
vS
ep
Oc
tN
ov
Se
pO
ct
No
vS
ep
Oc
tN
ov
Se
pO
ct
No
v
P0
28
1G
en
era
l P
rac
tic
e
Ex
tra
cti
on
Se
rvic
eN
/AN
/AN
/A-
AA
AA
AA
N/A
N/A
N/A
-G
GG
AA
AA
AA
P0
20
8G
P S
ys
tem
s o
f C
ho
ice
Re
pla
ce
me
nt
GG
GG
GG
GG
GG
GG
GG
GA
AA
AA
A
P0
01
4G
P2
GP
AA
AG
GG
AA
AG
GG
N/A
N/A
N/A
-G
GG
GG
G
P0
02
6N
HS
Ch
oic
es
N
/AN
/AN
/A-
AA
AA
AA
AA
AA
GG
GG
GG
GG
P0
19
6N
HS
ma
il 2
GG
GG
GG
AA
AG
GG
GG
GG
GG
AA
A
P0
23
8N
HS
e-R
efe
rra
lsA
AA
GG
GG
GG
GG
GG
GG
AA
AG
GG
P0
05
1S
um
ma
ry C
are
Re
co
rdA
AA
GG
GG
GG
GG
GG
GG
GG
GG
GG
P0
01
2E
lec
tro
nic
Tra
ns
fer
of
Pre
sc
rip
tio
ns
AA
AG
GG
GG
GA
AA
GG
GA
AA
AA
A
A/G
67
.50
%S
ou
th
A/G
80
.00
%N
/A
Se
pO
ct
No
vS
ep
Oc
tN
ov
Se
pO
ct
No
vS
ep
Oc
tN
ov
Se
pO
ct
No
vS
ep
Oc
tN
ov
Se
pO
ct
No
v
P0
29
4N
ati
on
al T
ari
ff S
ys
tem
(NT
S)
N/A
N/A
N/A
-A
AT
BC
--
GG
GG
GA
AA
AA
AG
AA
G
P0
40
6D
ata
Se
rvic
es
fo
r
Co
mm
iss
ion
ers
TB
CT
BC
N/A
-T
BC
TB
CT
BC
--
GG
GN
/AN
/AA
-N
/AN
/AA
-A
AG
GG
G
A
60
.00
%
A
60
.00
%
So
urc
ed
fro
m H
igh
ligh
t R
ep
ort
s (
Ke
y R
AG
s)
So
urc
ed
fro
m H
igh
ligh
t R
ep
ort
s (
Ke
y R
AG
s)
No
v-2
01
5
KE
Y
Tre
nd
N
on
Co
mp
letio
n
3N
R
2N
/A
1T
BC
KP
IP
rev
iou
s R
AG
He
alt
h D
igit
al S
erv
ice
s D
ire
cto
r
Vie
w
KP
I O
wn
er
Ja
me
s H
aw
kin
sC
urr
en
t R
AG
Cu
rre
nt
RA
G
Pro
gra
mm
e A
ch
iev
em
en
tA
pp
en
dix
2 -
Pro
gra
mm
e D
eliv
ery
Da
sh
bo
ard
Healt
h D
igit
al
Serv
ices D
ash
bo
ard
- N
ovem
ber
2015
Pro
gre
ss
ag
ain
st
pla
nn
ed
mit
iga
tio
n f
or
ris
k
Qu
ality
Ma
na
ge
me
nt
ag
ain
st
pla
nP
rog
ram
me
/ P
roje
ct
en
d d
ate
Cu
rre
nt
Inv
es
tme
nt
Ju
sti
fic
ati
on
ap
pro
va
l s
tatu
s
Dig
ita
l &
Te
ch
no
log
y S
pe
nd
Co
ntr
ols
Sta
tus
Re
so
urc
ing
Ag
ain
st
Pla
n
Fo
rec
as
t R
AG
Fo
rec
as
t R
AG
Ov
era
ll D
eliv
ery
Co
nfi
de
nc
e f
or
He
alt
h D
igit
al S
erv
ice
s (
Ca
lcu
late
d):
HD
S V
iew
Re
po
rtin
g M
on
th:
Primary Care IT
Be
ne
fits
re
alis
ati
on
co
nfi
de
nc
e
No
ve
mb
ers
ca
lcu
late
d d
eliv
ery
co
nfid
en
ce
is a
t 6
7.5
%. T
he
Ca
lcu
late
d d
eliv
ery
co
nfid
en
ce
RA
G r
em
ain
s a
t A
mb
er/
Gre
en
. T
he
3-m
on
th c
alc
ula
ted
fore
ca
st D
eliv
ery
Co
nfid
en
ce
(to
Fe
bru
ary
20
16
) is
als
o A
mb
er/
Gre
en
at 8
0%
.
Fe
bru
ary
-20
16
Fe
bru
ary
-20
16
No
ve
mb
er-
20
15
No
ve
mb
er-
20
15
Arc
hit
ec
ture
Sta
nd
ard
s a
nd
In
no
va
tio
n -
No
ve
mb
er
20
15
Be
ne
fits
re
alis
ati
on
co
nfi
de
nc
e
Qu
ality
Ma
na
ge
me
nt
ag
ain
st
pla
nP
rog
ram
me
/ P
roje
ct
en
d d
ate
Cu
rre
nt
Inv
es
tme
nt
Ju
sti
fic
ati
on
ap
pro
va
l s
tatu
s
Dig
ita
l &
Te
ch
no
log
y S
pe
nd
Co
ntr
ols
Sta
tus
Re
so
urc
ing
Ag
ain
st
Pla
nP
rog
res
s a
ga
ins
t p
lan
ne
d
mit
iga
tio
n f
or
ris
k
Ov
era
ll D
eliv
ery
Co
nfi
de
nc
e f
or
AS
I:
No
ve
mb
er-
20
15
RA
G d
ecre
ase
fro
m p
revio
us m
on
thD
ata
ite
m w
as n
ot a
va
ilab
le a
t th
e tim
e o
f re
po
rt p
rod
uctio
n (
for
exa
mp
le, d
iscre
pa
ncie
s w
ith
bu
dg
et fig
ure
s o
r a
la
ck o
r in
form
atio
n a
rou
nd
th
e p
rog
ressio
n o
f a
n a
pp
rova
l)
RA
G im
pro
ve
me
nt fr
om
pre
vio
us m
on
thN
o r
ep
ort
pro
vid
ed
or
rep
ort
pro
vid
ed
bu
t m
issin
g R
AG
in
a s
ectio
n fo
r w
hic
h a
RA
G s
ho
uld
ha
ve
be
en
pro
vid
ed
RA
G s
am
e a
s p
revio
us m
on
thD
ata
ite
m is n
ot a
pp
lica
ble
to
pro
gra
mm
e o
r p
roje
ct (f
or
exa
mp
le, M
OU
s m
ay n
ot b
e r
esp
on
sib
le fo
r B
en
efits
Re
alis
atio
n o
r b
e a
cco
un
tab
le fo
r G
DS
Sp
en
d A
pp
rova
l)
Ove
rall
De
live
ry C
on
fid
en
ce
is a
sse
sse
d a
s A
ba
se
d o
n th
e H
igh
ligh
t R
ep
ort
s c
ove
rin
g th
e N
ove
mb
er
20
15
pe
rio
d. T
he
hig
h le
ve
l co
mm
en
tary
pro
vid
es
furt
he
r d
eta
il.
Fe
bru
ary
-20
16
No
ve
mb
er-
15
14 o
f 16
Page 29 of 159
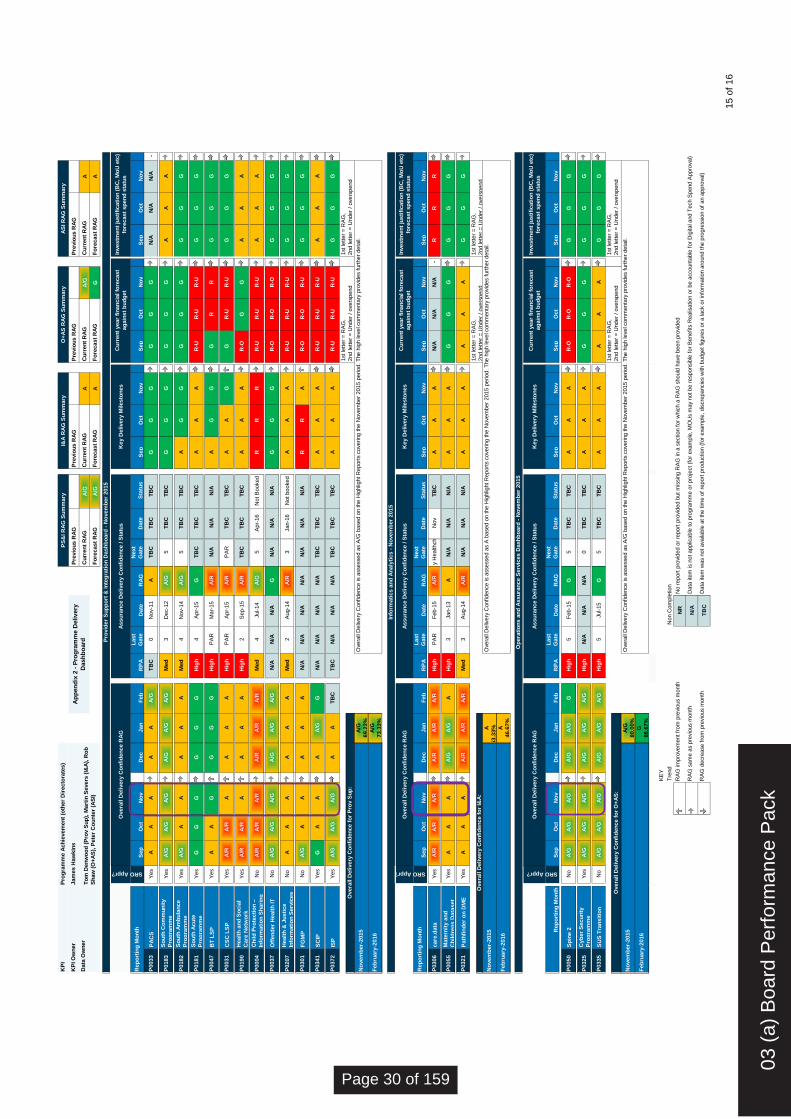
Pre
vio
us R
AG
Pre
vio
us R
AG
Pre
vio
us R
AG
Pre
vio
us R
AG
Cu
rren
t R
AG
A/G
Cu
rren
t R
AG
AC
urr
en
t R
AG
A/G
Cu
rren
t R
AG
A
Fo
recast
RA
GA
/GF
ore
cast
RA
GA
Fo
recast
RA
GG
Fo
recast
RA
GA
Sep
Oct
No
vD
ec
Jan
Feb
RP
A
Last
Gate
Date
RA
G
Next
Gate
Date
Sta
tus
Sep
Oct
No
vS
ep
Oct
No
vS
ep
Oct
No
v
P0033
PA
CS
Yes
AA
AA
AA
/GT
BC
0N
ov-1
1A
TB
CT
BC
TB
CG
GG
GG
GN
/AN
/AN
/A-
P0183
So
uth
Co
mm
un
ity
Pro
gra
mm
eY
es
A/G
A/G
A/G
A/G
A/G
A/G
Med
3D
ec-1
2A
/G5
TB
CT
BC
GG
GG
GG
AA
A
P0182
So
uth
Am
bu
lan
ce
Pro
gra
mm
eY
es
A/G
AA
AA
AM
ed
4N
ov-1
4A
/G5
TB
CT
BC
AG
GG
GG
GG
G
P0181
So
uth
Acu
te
Pro
gra
mm
eY
es
GG
GG
GG
Hig
h4
Apr-
15
GT
BC
TB
CT
BC
AA
AR
-UR
-UR
-UG
GG
P0047
BT
LS
PY
es
AA
GG
GG
Hig
hP
AR
Mar-
15
A/R
N/A
N/A
N/A
AG
GG
RR
GG
G
P0031
CS
C L
SP
Yes
A/R
A/R
AA
AA
Hig
hP
AR
Apr-
15
A/R
PA
RT
BC
TB
CA
AG
GR
-UR
-UG
GG
P0190
Healt
h a
nd
So
cia
l
Care
Netw
ork
Yes
A/R
A/R
AA
AA
Hig
h2
Sep-1
5A
/RT
BC
TB
CT
BC
AA
AR
-OG
GA
AA
P0004
Ch
ild
Pro
tecti
on
–
Info
rmati
on
Sh
ari
ng
No
A/R
A/R
A/R
A/R
A/R
A/R
Med
4Jul-14
A/G
5A
pr-
16
Not B
ooked
RR
RR
-UR
-UR
-UA
AA
P0037
Off
en
der
Healt
h IT
No
A/G
A/G
A/G
A/G
A/G
A/G
N/A
N/A
N/A
GN
/AN
/AN
/AG
GG
R-O
R-O
R-O
GG
G
P0207
Healt
h &
Ju
sti
ce
Info
rmati
on
Serv
ices
No
AA
AA
AA
Med
2A
ug-1
4A
/R3
Jan-1
6N
ot booked
AA
AR
-UR
-UR
-UG
GG
P0301
FG
MP
No
A/G
AA
AA
AN
/AN
/AN
/AN
/AN
/AN
/AN
/AR
RA
R-O
R-O
R-U
GG
G
P0341
SC
IPY
es
GA
AA
A/G
GN
/AN
/AN
/AN
/AT
BC
TB
CT
BC
AA
AR
-UR
-UR
-UA
AA
P0372
ISP
Yes
A/G
A/G
A/G
AA
TB
CT
BC
N/A
N/A
N/A
TB
CT
BC
TB
CA
AA
R-U
R-U
R-U
GG
G
A/G
69.2
3%
A/G
73.3
3%
Sep
Oct
No
vD
ec
Jan
Feb
RP
A
Last
Gate
Date
RA
G
Next
Gate
Date
Sta
tus
Sep
Oct
No
vS
ep
Oct
No
vS
ep
Oct
No
v
P0306
care
.data
Yes
A/R
A/R
A/R
A/R
A/R
A/R
Hig
hP
AR
Feb-1
5A
/R1 d
ay H
ealthcheck N
ov
TB
CA
AA
N/A
N/A
N/A
-R
RR
P0055
Mate
rnit
y a
nd
Ch
ild
ren
s D
ata
set
Yes
AA
AA
/GA
/GA
Hig
h3
Jan-1
3A
N/A
N/A
N/A
AA
AG
GG
GG
G
P0321
Path
fin
der
on
DM
EY
es
AA
AA
/RA
/RA
/RM
ed
3A
ug-1
4A
/RN
/AN
/AN
/AA
AA
AA
AG
GG
A
53.3
3%
A
46.6
7%
Sep
Oct
No
vD
ec
Jan
Feb
RP
A
Last
Gate
Date
RA
G
Next
Gate
Date
Sta
tus
Sep
Oct
No
vS
ep
Oct
No
vS
ep
Oct
No
v
P0050
Sp
ine 2
No
A/G
A/G
A/G
A/G
A/G
GH
igh
5F
eb-1
5G
5T
BC
TB
CA
AA
R-O
R-O
R-O
GG
G
P0325
Cyb
er
Secu
rity
Pro
gra
mm
eY
es
A/G
A/G
A/G
A/G
A/G
A/G
Hig
hN
/AN
/AN
/A0
TB
CT
BC
AA
AG
GG
GG
G
P0335
SU
S T
ran
sit
ion
No
A/G
A/G
A/G
A/G
A/G
A/G
Hig
h5
Jul-15
G5
TB
CT
BC
AA
AA
AA
GG
G
A/G
80.0
0%
G
86.6
7%
KE
Y
Tre
nd
Non C
om
ple
tion
3N
R
2N
/A
1T
BC
Data
Ow
ner
To
m D
en
wo
od
(P
rov S
up
), M
art
in S
evers
(I&
A),
Ro
b
Sh
aw
(O
+A
S),
Pete
r C
ou
nte
r (A
SI)
Pro
vid
er
Su
pp
ort
& In
teg
rati
on
Dash
bo
ard
- N
ovem
ber
2015
KP
I O
wn
er
Jam
es H
aw
kin
s
KP
IP
rog
ram
me A
ch
ievem
en
t (o
ther
Dir
ecto
rate
s)
PS
&I R
AG
Su
mm
ary
I&A
RA
G S
um
mary
O+
AS
RA
G S
um
mary
AS
I R
AG
Su
mm
ary
Ap
pen
dix
2 -
Pro
gra
mm
e D
eliv
ery
Dash
bo
ard
No
vem
ber-
2015
Overa
ll D
eliv
ery
Confidence is a
ssessed a
s A
/G b
ased o
n the H
ighlig
ht R
eport
s c
overing the N
ovem
ber
2015 p
eriod. T
he h
igh level com
menta
ry p
rovid
es f
urt
her
deta
il.
Feb
ruary
-2016
Rep
ort
ing
Mo
nth
1st le
tter
= R
AG
,
2nd letter
= U
nder
/ overs
pend
1st le
tter
= R
AG
,
2nd letter
= U
nder
/ overs
pend
Overa
ll D
elivery
Co
nfi
den
ce f
or
Pro
v S
up
:
SRO Appr?
Overa
ll D
elivery
Co
nfi
den
ce R
AG
Assu
ran
ce D
elivery
Co
nfi
den
ce / S
tatu
sK
ey D
elivery
Milesto
nes
Cu
rren
t year
fin
an
cia
l fo
recast
ag
ain
st
bu
dg
et
Investm
en
t ju
sti
ficati
on
(B
C, M
oU
etc
)
fore
cast
sp
en
d s
tatu
s
Info
rmati
cs a
nd
An
aly
tics -
No
vem
ber
2015
SRO Appr?
Overa
ll D
elivery
Co
nfi
den
ce R
AG
Assu
ran
ce D
elivery
Co
nfi
den
ce / S
tatu
sK
ey D
elivery
Milesto
nes
Cu
rren
t year
fin
an
cia
l fo
recast
ag
ain
st
bu
dg
et
Investm
en
t ju
sti
ficati
on
(B
C, M
oU
etc
)
fore
cast
sp
en
d s
tatu
s
1st le
tter
= R
AG
,
2nd letter
= U
nder
/ overs
pend
1st le
tter
= R
AG
,
2nd letter
= U
nder
/ overs
pend
Overa
ll D
elivery
Co
nfi
den
ce f
or
I&A
:
No
vem
ber-
2015
Overa
ll D
eliv
ery
Confidence is a
ssessed a
s A
based o
n the H
ighlig
ht R
eport
s c
overing the N
ovem
ber
2015 p
eriod. T
he h
igh level com
menta
ry p
rovid
es f
urt
her
deta
il.
Feb
ruary
-2016
Rep
ort
ing
Mo
nth
Feb
ruary
-2016
Rep
ort
ing
Mo
nth
1st le
tter
= R
AG
,
2nd letter
= U
nder
/ overs
pend
1st le
tter
= R
AG
,
2nd letter
= U
nder
/ overs
pend
Overa
ll D
elivery
Co
nfi
den
ce f
or
O+
AS
:
Investm
en
t ju
sti
ficati
on
(B
C, M
oU
etc
)
fore
cast
sp
en
d s
tatu
s
Op
era
tio
ns a
nd
Assu
ran
ce S
erv
ices D
ash
bo
ard
- N
ovem
ber
2015
SRO Appr?
Overa
ll D
elivery
Co
nfi
den
ce R
AG
Assu
ran
ce D
elivery
Co
nfi
den
ce / S
tatu
sK
ey D
elivery
Milesto
nes
Cu
rren
t year
fin
an
cia
l fo
recast
ag
ain
st
bu
dg
et
No
vem
ber-
2015
Data
ite
m w
as n
ot availa
ble
at th
e tim
e o
f re
port
pro
duction (
for
exa
mple
, dis
cre
pancie
s w
ith b
udget figure
s o
r a lack o
r in
form
ation a
round the p
rogre
ssio
n o
f an a
ppro
val)
RA
G im
pro
vem
ent fr
om
pre
vio
us m
onth
No r
eport
pro
vid
ed o
r re
port
pro
vid
ed b
ut m
issin
g R
AG
in a
section f
or
whic
h a
RA
G s
hould
have b
een p
rovid
ed
RA
G s
am
e a
s p
revio
us m
onth
Data
ite
m is n
ot applic
able
to p
rogra
mm
e o
r pro
ject (f
or
exa
mple
, M
OU
s m
ay n
ot be r
esponsib
le f
or
Benefits
Realis
ation o
r be a
ccounta
ble
for
Dig
ital and T
ech S
pend A
ppro
val)
RA
G d
ecre
ase f
rom
pre
vio
us m
onth
Overa
ll D
eliv
ery
Confidence is a
ssessed a
s A
/G b
ased o
n the H
ighlig
ht R
eport
s c
overing the N
ovem
ber
2015 p
eriod. T
he h
igh level com
menta
ry p
rovid
es f
urt
her
deta
il.
15 o
f 16
03 (
a) B
oard
Per
form
ance
Pac
k
Page 30 of 159
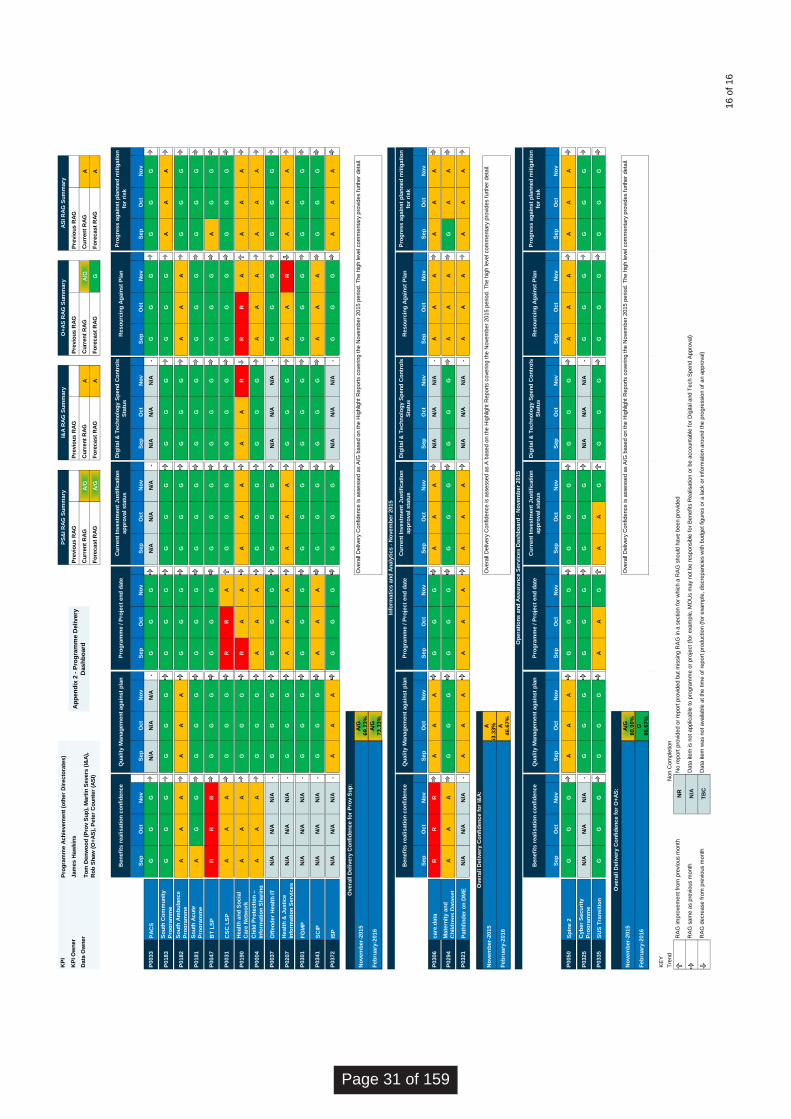
Pro
gra
mm
e A
ch
ievem
en
t (o
ther
Dir
ecto
rate
s)
Jam
es H
aw
kin
sP
revio
us R
AG
Pre
vio
us
RA
GP
revio
us R
AG
0P
revio
us R
AG
0P
revio
us R
AG
0
Cu
rren
t R
AG
A/G
Cu
rren
t R
AG
AC
urr
en
t R
AG
A/G
Cu
rren
t R
AG
A
Fo
recast
RA
GA
/GF
ore
cast
RA
GA
Fo
recast
RA
GG
Fo
recast
RA
GA
Sep
Oct
No
vS
ep
Oct
No
vS
ep
Oct
No
vS
ep
Oct
No
vS
ep
Oct
No
vS
ep
Oct
No
vS
ep
Oct
No
v
P0033
PA
CS
GG
GN
/AN
/AN
/A-
GG
GN
/AN
/AN
/A-
N/A
N/A
N/A
-G
GG
GG
G
P0183
So
uth
Co
mm
un
ity
Pro
gra
mm
eG
GG
GG
GG
GG
GG
GG
GG
GG
GA
AA
P0182
So
uth
Am
bu
lan
ce
Pro
gra
mm
eA
AA
AA
AG
GG
GG
GG
GG
AA
AG
GG
P0181
So
uth
Acu
te
Pro
gra
mm
eA
GG
GG
GG
GG
GG
GG
GG
GG
GG
GG
P0047
BT
LS
PR
RR
GG
GG
GG
GG
GG
GG
GG
GA
GG
P0031
CS
C L
SP
AA
AG
GG
RR
AG
GG
GG
GG
GG
GG
G
P0190
Healt
h a
nd
So
cia
l
Care
Netw
ork
AA
AG
GG
RA
AA
AA
AA
RR
RA
AA
A
P0004
Ch
ild
Pro
tecti
on
–
Info
rmati
on
Sh
ari
ng
AA
AG
GG
AA
AG
GG
GG
GA
AA
AA
A
P0037
Off
en
der
Healt
h IT
N/A
N/A
N/A
-G
GG
GG
GG
GG
N/A
N/A
N/A
-G
GG
GG
G
P0207
Healt
h &
Ju
sti
ce
Info
rmati
on
Serv
ices
N/A
N/A
N/A
-G
GG
AA
AA
AA
GG
GA
AR
AA
A
P0301
FG
MP
N/A
N/A
N/A
-G
GG
GG
GG
GG
GG
GG
GG
GG
G
P0341
SC
IPN
/AN
/AN
/A-
GG
GA
AA
GG
GG
GG
AA
AG
GG
P0372
ISP
N/A
N/A
N/A
-A
AA
GG
GG
GG
N/A
N/A
N/A
-G
GG
AA
A
A/G
69.2
3%
A/G
73.3
3%
Sep
Oct
No
vS
ep
Oct
No
vS
ep
Oct
No
vS
ep
Oct
No
vS
ep
Oct
No
vS
ep
Oct
No
vS
ep
Oct
No
v
P0306
care
.data
RR
RA
AA
GG
GA
AA
N/A
N/A
N/A
-A
AA
AA
A
P0294
Mate
rnit
y a
nd
Ch
ild
ren
s D
ata
set
AA
AG
GG
GG
GG
GG
GG
GA
AA
GA
A
P0321
Path
fin
der
on
DM
EN
/AN
/AN
/A-
AA
AA
AA
AA
AN
/AN
/AN
/A-
AA
AA
AA
A
53.3
3%
A
46.6
7%
Sep
Oct
No
vS
ep
Oct
No
vS
ep
Oct
No
vS
ep
Oct
No
vS
ep
Oct
No
vS
ep
Oct
No
vS
ep
Oct
No
v
P0050
Sp
ine 2
GG
GA
AA
GG
GG
GG
GG
GA
AA
AA
A
P0325
Cyb
er
Secu
rity
Pro
gra
mm
eN
/AN
/AN
/A-
GG
GG
GG
GG
GN
/AN
/AN
/A-
GG
GG
GG
P0335
SU
S T
ran
sit
ion
GG
GG
GG
AA
GA
AG
GG
GG
GG
GG
G
A/G
80.0
0%
G
86.6
7%
KE
Y
Tre
nd
Non C
om
ple
tion
3R
AG
im
pro
vem
ent fr
om
pre
vio
us m
onth
2R
AG
sam
e a
s p
revio
us m
onth
1R
AG
decre
ase f
rom
pre
vio
us m
onth
Data
Ow
ner
To
m D
en
wo
od
(P
rov S
up
), M
art
in S
evers
(I&
A),
Ro
b S
haw
(O
+A
S),
Pete
r C
ou
nte
r (A
SI)
Pro
vid
er
Su
pp
ort
& In
teg
rati
on
Dash
bo
ard
- N
ovem
ber
2015
KP
IP
S&
I R
AG
Su
mm
ary
I&A
RA
G S
um
mary
O+
AS
RA
G S
um
mary
AS
I R
AG
Su
mm
ary
KP
I O
wn
er
Ap
pen
dix
2 -
Pro
gra
mm
e D
eliv
ery
Dash
bo
ard
No
vem
ber-
2015
Overa
ll D
eliv
ery
Confidence is a
ssessed a
s A
/G b
ased o
n the H
ighlig
ht R
eport
s c
overing the N
ovem
ber
2015 p
eriod. T
he h
igh level com
menta
ry p
rovid
es f
urt
her
deta
il.
Feb
ruary
-2016
Pro
gre
ss a
gain
st
pla
nn
ed
mit
igati
on
for
risk
Overa
ll D
elivery
Co
nfi
den
ce f
or
Pro
v S
up
:
Ben
efi
ts r
ealisati
on
co
nfi
den
ce
Qu
ality
Man
ag
em
en
t ag
ain
st
pla
nP
rog
ram
me / P
roje
ct
en
d d
ate
Cu
rren
t In
vestm
en
t Ju
sti
ficati
on
ap
pro
val sta
tus
Dig
ital &
Tech
no
log
y S
pen
d C
on
tro
ls
Sta
tus
Reso
urc
ing
Ag
ain
st
Pla
n
Info
rmati
cs a
nd
An
aly
tics -
No
vem
ber
2015
Ben
efi
ts r
ealisati
on
co
nfi
den
ce
Qu
ality
Man
ag
em
en
t ag
ain
st
pla
n
Overa
ll D
elivery
Co
nfi
den
ce f
or
I&A
:
No
vem
ber-
2015
Pro
gra
mm
e / P
roje
ct
en
d d
ate
Cu
rren
t In
vestm
en
t Ju
sti
ficati
on
ap
pro
val sta
tus
Overa
ll D
eliv
ery
Confidence is a
ssessed a
s A
based o
n the H
ighlig
ht R
eport
s c
overing the N
ovem
ber
2015 p
eriod. T
he h
igh level com
menta
ry p
rovid
es f
urt
her
deta
il.
Feb
ruary
-2016
Dig
ital &
Tech
no
log
y S
pen
d C
on
tro
ls
Sta
tus
Reso
urc
ing
Ag
ain
st
Pla
nP
rog
ress a
gain
st
pla
nn
ed
mit
igati
on
for
risk
Feb
ruary
-2016
Reso
urc
ing
Ag
ain
st
Pla
nP
rog
ress a
gain
st
pla
nn
ed
mit
igati
on
for
risk
Overa
ll D
elivery
Co
nfi
den
ce f
or
O+
AS
:
Ben
efi
ts r
ealisati
on
co
nfi
den
ce
Qu
ality
Man
ag
em
en
t ag
ain
st
pla
nP
rog
ram
me / P
roje
ct
en
d d
ate
Cu
rren
t In
vestm
en
t Ju
sti
ficati
on
ap
pro
val sta
tus
Dig
ital &
Tech
no
log
y S
pen
d C
on
tro
ls
Sta
tus
Op
era
tio
ns a
nd
Assu
ran
ce S
erv
ices D
ash
bo
ard
- N
ovem
ber
2015
TB
CD
ata
ite
m w
as n
ot availa
ble
at th
e tim
e o
f re
port
pro
duction (
for
exa
mple
, dis
cre
pancie
s w
ith b
udget figure
s o
r a lack o
r in
form
ation a
round the p
rogre
ssio
n o
f an a
ppro
val)
NR
No r
eport
pro
vid
ed o
r re
port
pro
vid
ed b
ut m
issin
g R
AG
in a
section f
or
whic
h a
RA
G s
hould
have b
een p
rovid
ed
N/A
Data
ite
m is n
ot applic
able
to p
rogra
mm
e o
r pro
ject (f
or
exa
mple
, M
OU
s m
ay n
ot be r
esponsib
le f
or
Benefits
Realis
ation o
r be a
ccounta
ble
for
Dig
ital and T
ech S
pend A
ppro
val)
No
vem
ber-
2015
Overa
ll D
eliv
ery
Confidence is a
ssessed a
s A
/G b
ased o
n the H
ighlig
ht R
eport
s c
overing the N
ovem
ber
2015 p
eriod. T
he h
igh level com
menta
ry p
rovid
es f
urt
her
deta
il.
16 o
f 16
Page 31 of 159

Page 1 of 1
Board Meeting – Public Session
Title of paper: Update on progress against Budget & Business Plan/ 2015/16
Board meeting date: 27 January 2016
Agenda item no: HSCIC 16 06 03 b
Paper presented by:
Carl Vincent, Director of Finance & Corporate Services
Paper prepared by:
Carl Vincent, Director of Finance & Corporate Services/ Rebecca Giles, Head of Strategic Finance, Reporting & Change/ David O’Brien, Head of Business Intelligence
Paper approved by: (Sponsor Director) Carl Vincent, Director of Finance & Corporate Services
Purpose of the paper: To provide an update to the Board of the latest financial position against budget for the 2015/16 financial year and an update on progress against the 2015/16 Business Plan.
Key risks and issues:
Financial position and delivery of business plan commitments for 2015/16
Patient/public interest:
Indirect
Actions required by the Board: The Board are requested to:
note the reported performance on delivering business plan commitments and mitigating actions
note the current financial forecast outturn for 2015/16
03 (
b) B
usin
ess
Pla
n an
d B
udge
t 201
5-16
Rep
ort
Page 32 of 159


Update on progress against Budget & Business Plan/ 2015/16
Author Carl Vincent
Date 27 January 2016
03 (
b) B
usin
ess
Pla
n an
d B
udge
t 201
5-16
Rep
ort
Page 33 of 159

2015/16 Budget and Business Plan: Q3 Update
Contents
Contents 2
Executive Summary 3
Update on 2015/16 Budget 3
Update on 2015/16 Business Plan 4
Actions Required of the Board 5
Appendix A: 2015/16 Corporate Business Plan monitoring – Q3 summary 6
Appendix B: Business Plan deliverables rated Red or Amber/Red 10
Page 34 of 159

2015/16 Budget and Business Plan: Q3 Update
Executive Summary
This paper provides an update to the Board of the latest financial position against budget for the 2015/16 financial year and an update on progress against the 2015/16 Business Plan.
Update on 2015/16 Budget
As at December month-end, the HSCIC reported an underspend against budget for the first nine months of the year of £14.0m and forecast an underspend against budget for the full year of £7.1m, comprising £6.8m for core GiA and £0.2m for ring-fenced GiA.
The full year forecast, however, still includes optimistic projections of recruitment for the remainder of the year. Net recruitment of permanent staff for the first nine months of the year was 203 FTE (22.5 FTE monthly average) with forecast projections of a net increase of 134 FTE in the remaining three months, peaking in February, as per the following graph:
The net staff increase for the remainder of the year has decreased significantly from previous months but 134 FTE in 3 months is still unlikely to be achievable. If we assume a net increase of 20 FTE per month for the last quester, forecast costs will decrease by a further £0.6m.
Additionally, the more staff that are recruited in the remainder of this year, the higher the cost pressure that is carried forward into 16/17. As Directorates are currently finalising 16/17 to 18/19 budget plans that reflect the expected GiA decrease of 30% over the next 4 years, the future years’ pressures are contributing the reducing forecast recruitment for this year and this may reduce further still next month. Partially offsetting this pressure, the current Mutually Agreed Resignation Scheme (MARS) is expected to reduce headcount, although some of these staff are expected to be replaced.
The forecast for non-staff costs continues to predict expenditure over budget, however, the previously predicted forecast overspends earlier in the year on Professional Fees and ICT have reduced significantly or reversed. An additional forecast has been included this month for the expected cost of the MAR Scheme.
External income is currently forecast to end the year slightly above budget, but within this are fluctuations in both directions across a number of programmes, particularly for programmes that were in the process of being developed/ established or reorganised when the budgets
Apr-15Act
May-15Act
June-15Act
Jul-15Act
Aug-15Act
Sept-15Act
Oct-15Act
Nov-15Act
Dec-15Act
Jan-16Fct
Feb-16Fct
Mar-16Fct
Forecast Increase (FTE) 2.0 17.9 24.3 44.5 35.3 7.6 19.9 19.4 32.5 43.9 61.2 29.4
Budgeted Increase (FTE) 52.2 88.6 125.2 68.8 33.0 52.5 23.4 12.1 9.0 (3.5) 2.8 4.4
-
20.0
40.0
60.0
80.0
100.0
120.0
140.0
Permanent Staff - Forecast Increase vs Budgeted Increase [FTE]
Forecast Increase (FTE) Budgeted Increase (FTE)
03 (
b) B
usin
ess
Pla
n an
d B
udge
t 201
5-16
Rep
ort
Page 35 of 159

2015/16 Budget and Business Plan: Q3 Update
were set, so this remains an area of risk for the organisation. Over-arching Provision of Services Agreements (POSAs) have been signed with DH and NHSE and the underlying work packages for 2015/16 are in most instances either agreed or in an advanced stage of development.
The Capital budget for the year is expected to be £14.0m (final confirmation not yet received from DH); to December, we had spent £7.5m. Capital requirements for the remainder of the year are heavily reliant on the likely requirements of the Data Services Programme. £1.3m has been returned to DH to fund capital development of the Spine asset for CHRIS replacement.
Although the “bottom-up” forecast outturn position is an underspend of £7.1m, a “top down view, adjusting for likely recruitment (as above) and expected spend on professional fees and ICT, gives a more likely out-turn of £11.1m (£10.9m core, £0.2m ring-fenced). This is still subject to any required accounting adjustments at year-end.
Update on 2015/16 Business Plan
The corporate business plan contains 65 commitments to be delivered during 2015/16. Overall the reported delivery progress as at the close of quarter three is good for most deliverables, with few reported as being at significant risk of non-delivery.
Delivery progress of the business plan commitments is monitored by directorates and reported to the corporate business intelligence team on a quarterly basis. The reported information is triangulated with other sources of intelligence such as risk reports, performance data and programme highlights reports.
The table below summarises the reported delivery progress at the close of quarter three. More detail is provided at Appendix A. RAG ratings are applied to each commitment. These ratings are based on the RAG rating definitions for delivery confidence as applied to projects and programmes across the organisation.
RAG Status RAG Definition Number of
Commitments
Green On target for successful in-year delivery 25
Amber/Green Successful in-year delivery is probable 15
Amber Successful in-year delivery is feasible, issues need resolving 9
Amber/Red Successful in-year delivery in doubt, urgent action is required 2
Red Successful in-year delivery appears unachievable 3
2 Blue Delivery has been completed 8
Grey Not reported this quarter 3
Total 65
Note that the RAG ratings in this report refer to the status of work originally planned to be completed within 2015/16. This might be different from the overall status of a multi-year programme. For example, in the case of a large programme with a life cycle of many years, the RAG rating reported here applies to the elements of the programme originally planned
Page 36 of 159
2015/16 Budget and Business Plan: Q3 Update
for delivery during 2015/16 rather than the overall delivery confidence for the entire programme.
Three commitments had a RED delivery status at the close of quarter three, indicating that successful delivery as originally planned will not be achieved in 2015/16:
2.6 Develop and obtain approval for standards necessary to integrate information flows within social care and between health and social care
3.12: Put NHS Mail2 into live service
3.18: Support NHS England to achieve 80% take-up of the Child Protection Information Service (CP-IS)
Two commitments had an AMBER-RED delivery status at the close of quarter three, indicating that successful delivery in 2015/16 is in doubt and that urgent action is required. These are:
3.3: Introduce new assurance processes to enable the HSCIC to open up access and reduce timescales for connectivity to national systems
5.6: Work with DH and the Cabinet Office to design a Centre of Excellence for Big Data and Data Science
More information about these commitments, including the cause of delivery issues and the mitigating actions, is presented in Appendix B.
Actions Required of the Board
The Board are requested to:
note the reported performance on delivering business plan commitments and mitigating actions
note the current financial forecast outturn for 2015/16
03
(b)
Bus
ines
s P
lan
and
Bud
get 2
015-
16 R
epor
t
Page 37 of 159

2015
/16 B
ud
get
an
d B
usin
ess P
lan
: Q
3 U
pd
ate
Ap
pendix
A: 2015/1
6 C
orp
ora
te B
usi
ness
Pla
n m
onito
ring –
Q3 s
um
mary
Ref
Dir
ecto
rate
Sta
tus
Co
mm
en
t (f
or
co
mm
itm
en
ts r
ate
d A
MB
ER
or
wo
rse)
1.1
OA
SA
/G
1.2
OA
SN
RT
his
is a
th
ree
-ye
ar
asp
ira
tio
n in
th
e O
AS
bu
sin
ess p
lan
, n
ot
inte
nd
ed
as a
n in
-
ye
ar
de
live
rab
le fo
r 2
01
5/1
6
1.3
OA
SA
/G
1.4
OA
SA
/G
1.5
OA
SC
1.6
OA
SG
2.1
AS
IA
/G
2.2
AS
IA
/G
2.3
AS
IA
Th
e o
pe
ratio
na
l e
ffe
ctive
ne
ss o
f th
e s
tan
da
rds im
ple
me
nta
tio
n t
ea
m is a
t risk
du
e t
o r
ecru
itm
en
t d
ela
ys.
2.4
AS
IA
De
ve
lop
me
nt
of th
e S
CC
I su
pp
ort
se
rvic
e h
as b
ee
n a
ffe
cte
d b
y s
taff illn
ess
du
rin
g Q
1 a
nd
de
lays in
re
cru
itin
g a
pe
rma
ne
nt
SC
CI
Ch
air.
2.5
OA
SG
2.6
PS
IR
De
lays in
de
ve
lop
ing
th
e s
tan
da
rds a
nd
ob
tain
ing
ap
pro
va
l fr
om
SC
CI
ha
s
pu
sh
ed
th
e d
elive
ry t
ime
sca
le b
eyo
nd
20
15
/16
(to
Au
gu
st
20
16
).
2.7
AS
IA
De
pe
nd
ency o
n t
he
op
era
tio
na
l e
ffe
ctive
ne
ss o
f th
e I
nn
ova
tio
n S
erv
ice
(2
.1
ab
ove
). T
he
co
nce
pt
of a
ph
ysic
al In
no
va
tio
n C
en
tre
is o
n h
old
pe
nd
ing
fu
rth
er
co
nsid
era
tio
n.
2.8
HD
SG
Ensure
that G
P c
linic
al syste
ms c
an d
eliver
the n
ew
GP
2G
P r
equir
em
ents
to s
upport
the e
lectr
onic
tra
nsfe
r of re
cord
s w
hen p
atients
transfe
r th
eir
GP
Co
mm
itm
en
ts
Deliver
a c
yber
securi
ty s
trate
gy a
nd p
rogra
mm
e that m
eet th
e S
ecre
tary
of S
tate
’s r
equir
em
ent to
im
pro
ve d
ata
and s
yste
m s
ecuri
ty
acro
ss the h
ealth a
nd c
are
syste
m, and c
an r
espond to the e
volv
ing n
atu
re o
f cyber
thre
ats
that are
posed
Support
the d
evelo
pm
ent of a s
erv
ice for
managin
g p
eople
’s p
refe
rences for
managin
g the s
hari
ng o
f pers
onal data
, in
lin
e w
ith the
com
mitm
ent giv
en b
y the N
IB
Develo
p the S
CC
I support
serv
ice into
a fully o
pera
tional str
ate
gic
support
function
1. E
NS
UR
E T
HA
T E
VE
RY
CIT
IZE
N’S
DA
TA
IS
PR
OT
EC
TE
D
2. E
ST
AB
LIS
H S
HA
RE
D A
RC
HIT
EC
TU
RE
AN
D S
TA
ND
AR
DS
SO
EV
ER
YO
NE
BE
NE
FIT
S
Revie
w a
nd u
pdate
the s
ecto
r-w
ide Info
rmation G
overn
ance T
oolk
it s
o that it s
upport
s local health a
nd c
are
org
anis
ations d
eliver
inte
gra
ted s
erv
ices
Support
th
e N
ational D
ata
Guard
ian b
y h
osting the independent In
form
ation G
overn
ance O
vers
ight P
anel to
pro
vid
e a
dvic
e, challenge
and s
cru
tiny to the h
ealth a
nd c
are
syste
m r
egard
ing the u
se o
f sensitiv
e d
ata
Deliver
enhanced info
rmation g
overn
ance a
nd s
ecuri
ty o
pera
tions functions for
the s
yste
ms a
nd s
erv
ices d
elivere
d b
y H
SC
IC.
In c
ollabora
tion w
ith o
ur
part
ners
, consolidate
the p
ositio
n o
f th
e Info
rmation G
overn
ance A
llia
nce a
s the s
ingle
auth
ori
tative s
ourc
e o
f
info
rmation g
overn
ance a
dvic
e, guid
ance a
nd b
est pra
ctice for
the h
ealth a
nd c
are
secto
r.
Develo
p the H
SC
IC a
s the s
ecto
r-w
ide c
entr
e o
f com
pete
nce for
technic
al arc
hitectu
re, in
form
ation s
tandard
s a
nd innovation
Work
with the Inte
ropera
bility B
oard
to d
evelo
p n
ew
sta
ndard
s for
the inte
ropera
bility o
f care
docum
ents
and r
ecord
s
Pro
gre
ss the im
ple
menta
tion o
f S
NO
ME
D C
T, pharm
acy s
tandard
s, and inte
ropera
bility s
tandard
s
HS
CIC
Bu
sin
es
s P
lan
Mo
nit
ori
ng
- Q
ua
rte
r 3
Su
mm
ary
Esta
blish n
ew
work
ing p
rocesses for
develo
pm
ent of in
novative ideas in the H
SC
IC a
nd e
xplo
re o
ptions for
the d
evelo
pm
ent of a n
ew
innovation c
entr
e that can s
upport
our
work
Ensure
that clinic
al safe
ty s
tandard
s a
re incorp
ora
ted into
em
erg
ing technolo
gie
s, health a
nd w
ellbein
g r
ecord
s, apps a
nd a
ssis
tive
devic
es u
sed b
y c
itiz
ens a
nd c
are
pro
fessio
nals
, and w
ork
with the R
oyal C
olleges a
nd o
thers
to p
rom
ote
clinic
al safe
ty s
tandard
s
Develo
p a
nd o
bta
in a
ppro
val fo
r sta
ndard
s n
ecessary
to inte
gra
te info
rmation flo
ws w
ithin
socia
l care
and b
etw
een h
ealth a
nd s
ocia
l care
2
Page 38 of 159

2015
/16 B
ud
get
an
d B
usin
ess P
lan
: Q
3 U
pd
ate
Re
fD
irecto
rate
Sta
tus
Co
mm
en
t (f
or
co
mm
itm
en
ts r
ate
d A
MB
ER
or
wo
rse)
3.1
HD
SA
Imple
menta
tion r
e-p
rofile
d t
o t
ake p
lace o
ver
a longer
tim
escale
than o
rigin
ally
pla
nned.
3.2
OA
SG
3.3
OA
SA
/RD
ela
yed b
y r
esourc
e c
onstr
ain
ts:
sta
ff a
ssig
ned t
o t
est
and a
ssura
nce w
ork
on
hig
h p
riority
critical national syste
ms
3.4
HD
SA
HS
CIC
instr
ucte
d b
y N
HS
Engla
nd t
o c
ease w
ork
on C
hoic
es t
ransfo
rmation.
HS
CIC
now
delivering a
liv
e s
erv
ice o
nly
, but
this
inclu
des d
elivery
of a
roadm
ap o
f ongoin
g e
nhancem
ents
.
3.5
OA
SG
3.6
OA
SG
3.7
HD
SC
3.8
OA
SC
3.9
OA
SA
/G
3.1
0O
AS
G
3.1
1O
AS
A/G
3.1
2H
DS
RD
elivery
date
has b
een p
ut
back.
Pilot
pla
nned for
April, e
xit fro
m N
HS
Mail1
pla
nned for
Septe
mber
2016
3.1
3H
DS
C
3.1
4H
DS
C
3.1
5O
AS
G
3.1
6O
AS
G
3.1
7O
AS
G
3.1
8P
SI
RD
eplo
ym
ent
issues c
oncern
suppliers
, pro
cure
ment,
technolo
gy a
nd local
auth
ority
resourc
es.
Delivery
tim
escale
repro
file
d t
o 2
017.
Tra
nsfe
r th
e C
entr
al H
ealth R
egis
try Inquir
y S
yste
m (
CH
RIS
) in
to the S
pin
e s
erv
ice
HS
CIC
Bu
sin
es
s P
lan
Mo
nit
ori
ng
- Q
ua
rte
r 3
Su
mm
ary
Make a
ccess to the S
um
mary
Care
Record
available
to m
ore
clinic
al and s
ocia
l care
settin
gs (
consis
tent w
ith the N
IB fra
mew
ork
) in
ord
er
to im
pro
ve p
atient outc
om
es, avoid
onw
ard
refe
rrals
and e
nhance p
atient experi
ence o
f care
Co
mm
itm
en
ts
3. IM
PL
EM
EN
T N
AT
ION
AL
SE
RV
ICE
S T
HA
T M
EE
T N
AT
ION
AL
AN
D L
OC
AL
NE
ED
S
Allow
“vir
tual sm
art
card
auth
entication”
to m
anage a
ccess to n
ational syste
ms s
uch a
s the S
um
mary
Care
Record
(S
CR
) th
rough m
obile
devic
es
Launch the e
-Re
ferr
als
serv
ice a
nd its
new
vis
ion for
impro
vin
g a
ccess to s
erv
ices
Manage the tra
nsitio
n o
f th
e C
are
Identity
Serv
ice to m
eet th
e r
equir
em
ents
of th
e S
pin
e E
xte
nsio
n b
usin
ess c
ase
Support
nationally r
olled o
ut m
obile a
pplications in lin
e w
ith the N
ational In
form
ation B
oard
’s F
ram
ew
ork
for
Action.
Pro
gre
ss the m
igra
tion o
f th
e S
econdary
Uses S
erv
ice into
the H
SC
IC,
ensuri
ng c
ontinuity o
f serv
ice a
nd d
eliveri
ng the a
nnual P
aym
ent
by R
esults r
equir
em
ents
Mig
rate
, build a
nd o
pera
te a
new
Na
tional P
andem
ic F
lu s
erv
ice
De
velo
p the S
pin
e s
erv
ice a
s a
national hub s
upport
ing the e
xchange o
f in
form
ation a
cro
ss h
ealth, socia
l care
, lo
cal auth
ori
ties a
nd o
ther
org
anis
ations involv
ed in the n
ew
models
of in
tegra
ted c
are
.
Intr
oduce n
ew
assura
nce p
rocesses to e
nable
the H
SC
IC t
o o
pen u
p a
ccess a
nd r
educe tim
escale
s for
connectivity to n
ational syste
ms
Re
desig
n N
HS
Choic
es to d
eliver
a g
row
ing r
ange o
f pers
onal tr
ansactions, to
support
the d
elivery
of th
e N
IB o
bje
ctives
De
velo
p identity
veri
fication s
olu
tions to s
upport
health a
nd s
ocia
l care
work
ers
and p
atient/citiz
en identity
in s
upport
of th
e N
ational
Info
rmation B
oard
’s F
ram
ew
ork
for
Action.
Support
NH
S E
ngla
nd to a
chie
ve 8
0%
take-u
p o
f th
e C
hild P
rote
ction Info
rmation S
erv
ice
Put N
HS
Mail2 into
liv
e s
erv
ice
Impro
ve the e
ffectiveness o
f th
e E
lectr
onic
Pre
scri
ption S
erv
ice for
patients
, pre
scri
bers
, dis
pensers
and the p
rescri
ption r
eim
burs
em
ent
agency b
y e
nsuri
ng a
t le
ast one thir
d o
f all p
rescri
ption ite
ms a
re p
rescri
bed, dis
pensed a
nd c
laim
ed u
sin
g the s
erv
ice
Re
vie
w o
ptions for
the futu
re d
irection o
f th
e G
PE
S s
erv
ice w
ith a
vie
w t
o r
educin
g c
osts
, in
cre
asin
g c
apacity a
nd turn
aro
und o
f extr
act
delivery
Co
ntinue the tra
nsfe
r of serv
ices into
the S
erv
ice Inte
gra
tion a
nd M
anagem
ent envir
onm
ent, to s
trength
en o
ur
serv
ice m
anagem
ent and s
o
build c
onfidence in o
ur
ability to d
eliver
hig
h q
uality
resilie
nt serv
ices w
ith h
igh levels
of availability.
Co
mm
ence the p
rocess o
f decom
mis
sio
nin
g the N
ational H
ealth A
pplication a
nd Infr
astr
uctu
re S
erv
ices(N
HA
IS)
and b
uild n
ew
functionality
into
the S
pin
e s
erv
ice to s
upport
national pri
mary
care
regis
tration
2
03 (
b) B
usin
ess
Pla
n an
d B
udge
t 201
5-16
Rep
ort
Page 39 of 159

2015
/16 B
ud
get
an
d B
usin
ess P
lan
: Q
3 U
pd
ate
Ref
Dir
ecto
rate
Sta
tus
Co
mm
en
t (f
or
co
mm
itm
en
ts r
ate
d A
MB
ER
or
wo
rse)
4.1
PS
IG
4.2
OA
SG
4.3
PS
IC
4.4
HR
A/G
4.5
HD
SC
4.6
HD
SG
4.7
PS
IA
Mile
sto
ne
ta
rge
t d
ate
s h
ave
mo
ve
d b
ack.
Asse
ssm
en
ts o
f te
am
ca
pa
city a
nd
urg
en
cy o
f th
e w
ork
ha
ve
le
d t
o t
his
de
live
rab
le b
ein
g d
e-p
rio
ritise
d.
4.8
PS
IG
4.9
PS
IA
/G
4.1
0P
SI
G
4.1
1P
SI
G
5.1
IAA
/G
5.2
AS
IA
Q3
re
po
rt n
ot
rece
ive
d b
y d
ea
dlin
e.
Am
be
r sta
tus d
erive
d fro
m p
rog
ram
me
hig
hlig
hts
re
po
rt R
AG
ra
tin
gs fo
r d
elive
ry c
on
fid
en
ce
an
d k
ey m
ile
sto
ne
de
live
ry
5.3
IAG
5.4
IAG
5.5
AS
IA
/G
5.6
IAA
/RD
ep
en
de
ncy o
n r
ecru
itm
en
t to
a D
ire
cto
r o
f D
ata
Scie
nce
ro
le
4. S
UP
PO
RT
HE
AL
TH
AN
D C
AR
E O
RG
AN
ISA
TIO
NS
TO
GE
T T
HE
BE
ST
FR
OM
TE
CH
NO
LO
GY
, D
AT
A A
ND
IN
FO
RM
AT
ION
HS
CIC
Bu
sin
es
s P
lan
Mo
nit
ori
ng
- Q
ua
rte
r 3
Su
mm
ary
Co
mm
itm
en
ts
5.
MA
KE
BE
TT
ER
US
E O
F H
EA
LT
H A
ND
CA
RE
IN
FO
RM
AT
ION
Ensure
that all p
art
s o
f th
e H
SC
IC a
re p
rovid
ing e
ffective s
upport
to local health a
nd c
are
inte
gra
tion p
rogra
mm
es
Publish the fir
st sta
ge o
f our
report
to p
rovid
e the S
ecre
tary
of S
tate
with the fin
din
gs fro
m o
ur
thre
e-y
ear
rollin
g r
evie
w o
f national and
local data
collections to m
anage the a
dm
inis
trative b
urd
en o
n fro
nt line s
erv
ices a
ssocia
ted w
ith n
ational data
collections
Pilot th
e “
Oxygen”
app to p
rovid
e c
linic
ians a
nd c
are
pro
fessio
nals
with c
ontr
olled a
nd a
uditable
access to the S
um
mary
Care
Record
Deliver
the N
IB p
riori
ties c
oncern
ing d
evelo
pm
ent of th
e h
ealth info
rmatics p
rofe
ssio
n a
nd s
kills
Pro
vid
e the c
apability for
secure
messagin
g a
nd p
aperl
ess p
rocesses a
cro
ss c
are
settin
gs a
nd into
care
hom
es
Obta
in b
usin
ess c
ase a
ppro
vals
for
the S
outh
Acute
Pro
gra
mm
e, support
ed b
y a
gre
em
ents
betw
een D
H a
nd the p
rovid
ers
Com
ple
te the N
ME
and L
ondon P
AC
S c
ontr
act exits a
nd c
lose the p
rogra
mm
es
Ensure
that th
e e
xit a
nd tra
nsitio
n a
rrangem
ents
for
the B
T a
nd C
SC
LS
P C
ontr
acts
are
managed s
uccessfu
lly
Launch a
tools
et to
help
health a
nd c
are
org
anis
ations d
evelo
p a
nd im
ple
ment a b
enefits
realisation s
trate
gy
Ensure
that th
e im
ple
menta
tions o
f th
e S
outh
Com
munity a
nd C
hild H
ealth P
rogra
mm
e a
re c
om
ple
ted in a
ll tru
sts
Support
the c
om
ple
tion o
f th
e im
ple
menta
tions in b
oth
NH
S T
rusts
for
the S
outh
Am
bula
nce P
rogra
mm
e
Work
with
ou
r part
ners
on
th
e d
evelo
pm
en
t of
the n
ew
paym
en
t an
d t
ari
ff s
trate
gie
s t
hat
will sh
ape t
he f
utu
re r
equ
irem
en
ts o
f
the N
ation
al T
ari
ff S
erv
ice
Desig
n a
nd d
eliver
the f
irst
ph
ase o
f th
e D
ata
Serv
ices P
rogra
mm
e,
sta
rtin
g w
ith
th
e n
ation
al re
pository
for
data
serv
ices
Work
with
th
e D
H a
nd t
he C
abin
et
Off
ice t
o d
esig
n a
Cen
tre o
f E
xcellen
ce f
or
Big
Data
an
d D
ata
Scie
nce
Imple
men
t a “
sin
gle
fro
nt
door”
to m
ake it
easie
r fo
r re
searc
h o
rgan
isation
s t
o a
ccess h
ealth
an
d c
are
data
th
at
is h
eld
in
diffe
ren
t org
an
isation
s (
the H
SC
IC,
Pu
blic H
ealth
En
gla
nd a
nd t
he C
lin
ical P
ractice R
esearc
h d
ata
lin
k,
for
exam
ple
)
Con
solidate
an
d b
ett
er
assu
re t
he r
eport
ing a
nd p
ublication
of,
an
d im
pro
ve p
ublic a
ccess t
o,
indic
ato
rs,
inclu
din
g t
he N
ation
al
Info
rmation
Board
com
mitm
en
t to
deliver
a n
ation
al qu
ality
lib
rary
Work
with
NH
S E
ngla
nd t
o d
evelo
p a
new
nation
al D
ata
Serv
ices f
or
Com
mis
sio
ners
serv
ice
2
Page 40 of 159
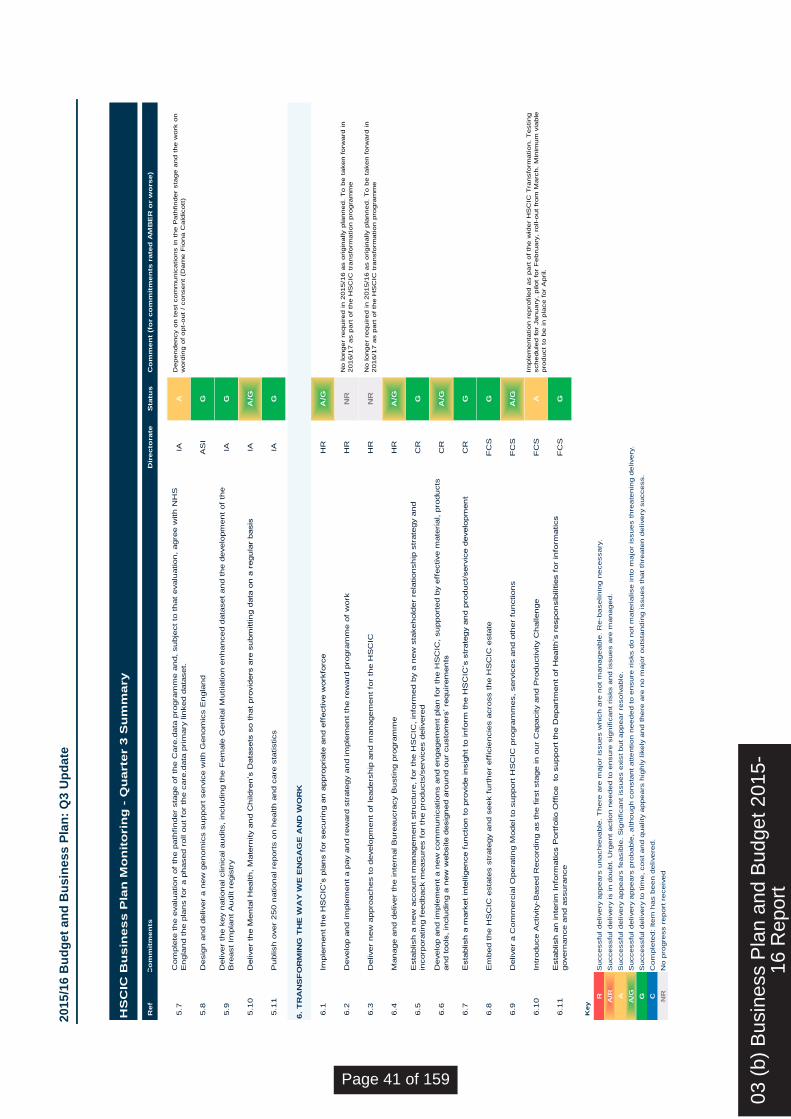
2015
/16 B
ud
get
an
d B
usin
ess P
lan
: Q
3 U
pd
ate
Ref
Dir
ecto
rate
Sta
tus
Co
mm
en
t (f
or c
om
mit
men
ts r
ate
d A
MB
ER
or w
orse)
5.7
IAA
De
pe
nd
ency o
n t
est
co
mm
un
ica
tio
ns in
th
e P
ath
fin
de
r sta
ge
an
d t
he
wo
rk o
n
wo
rdin
g o
f o
pt-
ou
t /
co
nse
nt
(Da
me
Fio
na
Ca
ldic
ott
)
5.8
AS
IG
5.9
IAG
5.1
0IA
A/G
5.1
1IA
G
6.1
HR
A/G
6.2
HR
NR
No
lo
ng
er
req
uire
d in
20
15
/16
as o
rig
ina
lly p
lan
ne
d.
To
be
ta
ke
n fo
rwa
rd in
20
16
/17
as p
art
of th
e H
SC
IC t
ran
sfo
rma
tio
n p
rog
ram
me
6.3
HR
NR
No
lo
ng
er
req
uire
d in
20
15
/16
as o
rig
ina
lly p
lan
ne
d.
To
be
ta
ke
n fo
rwa
rd in
20
16
/17
as p
art
of th
e H
SC
IC t
ran
sfo
rma
tio
n p
rog
ram
me
6.4
HR
A/G
6.5
CR
G
6.6
CR
A/G
6.7
CR
G
6.8
FC
SG
6.9
FC
SA
/G
6.1
0F
CS
AIm
ple
me
nta
tio
n r
ep
rofile
d a
s p
art
of th
e w
ide
r H
SC
IC T
ran
sfo
rma
tio
n.
Te
stin
g
sch
ed
ule
d fo
r Ja
nu
ary
, p
ilo
t fo
r F
eb
rua
ry,
roll-o
ut
fro
m M
arc
h.
Min
imu
m v
iab
le
pro
du
ct
to b
e in
pla
ce
fo
r A
pril.
6.1
1F
CS
G
Ke
y
R
A/R A
A/G G C
NR
Com
ple
ted: Item
has b
een d
elivere
d.
No p
rogre
ss r
eport
receiv
ed
Successfu
l delivery
appears
unachie
vable
. T
here
are
majo
r is
sues w
hic
h a
re n
ot m
anageable
. R
e-b
aselinin
g n
ecessary
.
Successfu
l delivery
is in d
oubt. U
rgent action n
eeded to e
nsure
sig
nific
ant ri
sks a
nd issues a
re m
anaged.
Successfu
l delivery
appears
feasib
le. S
ignific
ant is
sues e
xis
t but appear
resolv
able
.
Successfu
l delivery
appears
pro
bable
, although c
onsta
nt attention n
eeded to e
nsure
ris
ks d
o n
ot m
ate
rialise into
majo
r is
sues thre
ate
nin
g d
elivery
.
Successfu
l delivery
to tim
e, cost and q
uality
appears
hig
hly
lik
ely
and there
are
no m
ajo
r outs
tandin
g issues that th
reate
n d
elivery
success.
6.
TR
AN
SF
OR
MIN
G T
HE
WA
Y W
E E
NG
AG
E A
ND
WO
RK
Pu
blish
over
25
0 n
ation
al re
port
s o
n h
ealth
an
d c
are
sta
tistics
Com
ple
te t
he e
valu
ation
of
the p
ath
fin
der
sta
ge o
f th
e C
are
.data
pro
gra
mm
e a
nd,
su
bje
ct
to t
hat
evalu
ation
, agre
e w
ith
NH
S
En
gla
nd t
he p
lan
s f
or
a p
hased r
oll o
ut
for
the c
are
.data
pri
mary
lin
ked d
ata
set.
Deliver
the k
ey n
ation
al clin
ical au
dits,
inclu
din
g t
he F
em
ale
Gen
ital M
utila
tion
en
han
ced d
ata
set
an
d t
he d
evelo
pm
en
t of
the
Bre
ast
Impla
nt
Au
dit r
egis
try
Desig
n a
nd d
eliver
a n
ew
gen
om
ics s
upport
serv
ice w
ith
Gen
om
ics E
ngla
nd
HS
CIC
Bu
sin
es
s P
lan
Mo
nit
orin
g -
Qu
arte
r 3
Su
mm
ary
Co
mm
itm
en
ts
Esta
blish
an
in
teri
m I
nfo
rmatics P
ort
folio O
ffic
e
to s
upport
th
e D
epart
men
t of
Health
’s r
espon
sib
ilitie
s f
or
info
rmatics
govern
an
ce a
nd a
ssu
ran
ce
Imple
men
t th
e H
SC
IC’s
pla
ns f
or
secu
rin
g a
n a
ppro
pri
ate
an
d e
ffective w
ork
forc
e
Develo
p a
nd im
ple
men
t a p
ay a
nd r
ew
ard
str
ate
gy a
nd im
ple
men
t th
e r
ew
ard
pro
gra
mm
e o
f w
ork
Deliver
new
appro
ach
es t
o d
evelo
pm
en
t of
leaders
hip
an
d m
an
agem
en
t fo
r th
e H
SC
IC
Man
age a
nd d
eliver
the in
tern
al B
ure
au
cra
cy B
ustin
g p
rogra
mm
e
Deliver
a C
om
merc
ial O
pera
tin
g M
odel to
su
pport
HS
CIC
pro
gra
mm
es,
serv
ices a
nd o
ther
fun
ction
s
Intr
odu
ce A
ctivity-B
ased R
ecord
ing a
s t
he f
irst
sta
ge in
ou
r C
apacity a
nd P
rodu
ctivity C
hallen
ge
Develo
p a
nd im
ple
men
t a n
ew
com
mu
nic
ation
s a
nd e
ngagem
en
t pla
n f
or
the H
SC
IC,
su
pport
ed b
y e
ffective m
ate
rial, p
rodu
cts
an
d t
ools
, in
clu
din
g a
new
website d
esig
ned a
rou
nd o
ur
cu
sto
mers
’ re
qu
irem
en
ts
Esta
blish
a m
ark
et
inte
llig
en
ce f
un
ction
to p
rovid
e in
sig
ht
to in
form
th
e H
SC
IC’s
str
ate
gy a
nd p
rodu
ct/
serv
ice d
evelo
pm
en
t
Em
bed t
he H
SC
IC e
sta
tes s
trate
gy a
nd s
eek f
urt
her
eff
icie
ncie
s a
cro
ss t
he H
SC
IC e
sta
te
Esta
blish
a n
ew
accou
nt
man
agem
en
t str
uctu
re,
for
the H
SC
IC,
info
rmed b
y a
new
sta
keh
old
er
rela
tion
sh
ip s
trate
gy a
nd
incorp
ora
tin
g f
eedback m
easu
res f
or
the p
rodu
cts
/serv
ices d
elivere
d
Deliver
the M
en
tal H
ealth
, M
ate
rnity a
nd C
hildre
n’s
Data
sets
so t
hat
pro
vid
ers
are
su
bm
ittin
g d
ata
on
a r
egu
lar
basis
2
03 (
b) B
usin
ess
Pla
n an
d B
udge
t 201
5-16
Rep
ort
Page 41 of 159

2015
/16 B
ud
get
an
d B
usin
ess P
lan
: Q
3 U
pd
ate
Ap
pendix
B: B
usi
ness
Pla
n d
eliv
era
ble
s ra
ted R
ed o
r Am
ber/R
ed
1.
BU
SIN
ES
S P
LA
N D
EL
IVE
RA
BL
ES
RA
TE
D A
S ‘
RE
D’:
Co
mm
itm
en
t R
oo
t C
au
se a
nd
Im
pact
Ac
tio
ns T
aken
A
cti
on
Du
e D
ate
(w
here
ap
pli
cab
le)
2.6
D
evelo
p a
nd o
bta
in a
ppro
val fo
r sta
ndard
s n
ecessary
to inte
gra
te
info
rmation f
low
s w
ithin
socia
l care
and b
etw
ee
n h
ealth a
nd
socia
l care
(Pro
vid
er
Su
pp
ort
an
d
Inte
gra
tio
n)
The d
eliv
ery
has a
dep
end
ency o
n t
he
com
ple
tion o
f an S
CC
I sta
ndard
s r
evie
w,
whic
h is e
xperi
encin
g d
ela
ys.
As a
resu
lt o
f th
e S
CC
I sta
ndard
s r
evie
w
dela
ys, th
e d
eliv
ery
tim
escale
for
this
w
ork
has b
een e
xte
nd
ed t
o A
ug
ust
20
16.
T
his
means it is
not fe
asib
le to c
om
ple
te
the w
ork
during th
e lifetim
e o
f th
e
2015
/16 C
orp
ora
te B
usin
ess P
lan a
s
origin
ally
pla
nne
d
A T
ole
rance E
xception
Re
port
for
the
pro
ject w
as a
ppro
ved b
y t
he
HS
CIC
C
orp
ora
te A
ppro
va
ls B
oard
on 1
1
January
. T
his
sets
out
a r
evis
ed
meth
od f
or
the d
eve
lopm
en
t of
info
rmation s
tand
ard
s w
hic
h r
eflects
on
lessons learn
t th
rou
gh t
he
develo
pm
ent of
the info
rmation
sta
ndard
for
Assessm
ent, D
ischarg
e
and W
ithdra
wal fr
om
Hospital to
Socia
l C
are
.
The n
ew
meth
odo
log
y w
ill d
eliv
er
the
rem
ain
ing s
tandard
s in a
more
ag
ile
and t
imely
manner,
with less s
taff
ing
resourc
e tha
n o
rigin
ally
an
ticip
ate
d
The d
eliv
ery
tim
efr
am
e h
as b
ee
n
exte
nd
ed t
o A
ugust
201
6.
3.1
2
Put N
HS
Ma
il2 into
liv
e s
erv
ice
(Healt
h D
igit
al
Se
rvic
es)
Deliv
ery
tim
escale
s h
ave e
xte
nde
d
be
yo
nd
those
ori
gin
ally
pla
nned
du
e to
dela
ys in t
he s
ignin
g o
f contr
acts
and
issues p
reventin
g n
etw
ork
connection
betw
een d
ata
centr
es.
A T
ole
rance E
xception
Re
port
(tim
e
and c
ost)
was a
ppro
ve
d b
y t
he H
SC
IC
Corp
ora
te A
ppro
va
ls B
oa
rd in
Novem
ber.
The p
roje
ct has a
gre
ed its
fin
ancia
l and p
roje
ct pla
ns w
ith t
he D
H a
nd
contin
ues to
op
era
te w
ithin
busin
ess
case tole
rances.
The c
om
merc
ial am
endm
ent
with t
he
incum
bent supp
lier
has b
ee
n a
gre
ed
and s
igne
d b
y a
ll part
ies. T
he u
pdate
d
financia
l b
aselin
e h
as a
lso b
een
agre
ed a
nd a
ppro
ved
. A
ch
ievem
ent of
these m
ilesto
nes h
as s
ee
n t
he p
roje
ct
Pilo
t sche
du
led t
o s
tart
in A
pril
Data
mig
ration d
ue t
o c
om
ple
te b
e
end o
f June
NH
S M
ail1
exit p
lan
ned f
or
Septe
mber.
Page 42 of 159
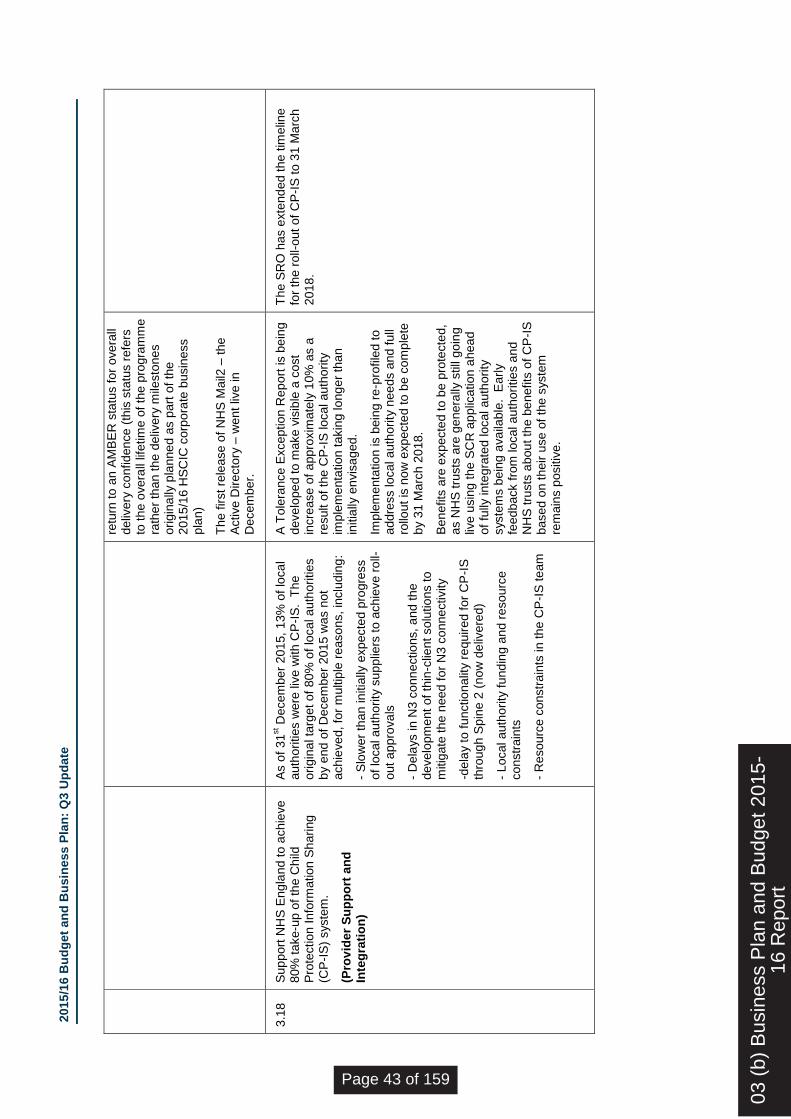
2015
/16 B
ud
get
an
d B
usin
ess P
lan
: Q
3 U
pd
ate
retu
rn to
an A
MB
ER
sta
tus f
or
overa
ll deliv
ery
co
nfidence
(th
is s
tatu
s r
efe
rs
to th
e o
vera
ll lif
etim
e o
f th
e p
rogra
mm
e
rath
er
than t
he d
eliv
ery
mile
sto
nes
origin
ally
pla
nne
d a
s p
art
of
the
2015
/16 H
SC
IC c
orp
ora
te b
usin
ess
pla
n)
The f
irst re
lease o
f N
HS
Mail2
– t
he
Active D
irecto
ry –
went
live
in
Decem
ber.
3.1
8
Sup
port
NH
S E
ng
land t
o a
chie
ve
80%
take
-up o
f th
e C
hild
P
rote
ction I
nfo
rmation S
haring
(CP
-IS
) syste
m.
(Pro
vid
er
Su
pp
ort
an
d
Inte
gra
tio
n)
As o
f 31
st D
ecem
ber
2015,
13%
of
loca
l auth
orities w
ere
liv
e w
ith C
P-I
S.
The
origin
al ta
rget of
80
% o
f lo
cal a
uth
orities
by e
nd o
f D
ecem
ber
2015 w
as n
ot
achie
ve
d, fo
r m
ultip
le r
easo
ns, in
clu
din
g:
- S
low
er
than in
itia
lly e
xpecte
d p
rogre
ss
of
local auth
ority
sup
plie
rs t
o a
chie
ve r
oll-
out a
ppro
va
ls
- D
ela
ys in N
3 c
onn
ectio
ns, a
nd t
he
develo
pm
ent of
thin
-clie
nt solu
tio
ns to
mitig
ate
th
e n
eed
for
N3 c
onnectivity
-dela
y t
o f
unctio
na
lity r
equir
ed f
or
CP
-IS
thro
ug
h S
pin
e 2
(no
w d
eliv
ere
d)
- Local auth
ority
fund
ing a
nd r
esourc
e
constr
ain
ts
- R
esourc
e c
onstr
ain
ts in th
e C
P-I
S te
am
A T
ole
rance E
xception
Re
port
is b
ein
g
develo
pe
d to m
ake v
isib
le a
cost
incre
ase o
f appro
xim
ate
ly 1
0%
as a
re
sult o
f th
e C
P-I
S local auth
ority
im
ple
menta
tion t
akin
g long
er
than
in
itia
lly e
nvis
aged.
Imple
menta
tio
n is b
ein
g r
e-p
rofile
d t
o
addre
ss local auth
ority
nee
ds a
nd f
ull
rollo
ut
is n
ow
expecte
d to
be c
om
ple
te
by 3
1 M
arc
h 2
018.
Ben
efits
are
exp
ecte
d t
o b
e p
rote
cte
d,
as N
HS
tru
sts
are
ge
nera
lly s
till
go
ing
live u
sin
g the
SC
R a
pplic
ation a
hea
d
of
fully
inte
gra
ted local auth
ority
syste
ms b
ein
g a
va
ilable
. E
arl
y
feedback fro
m local au
thori
ties a
nd
NH
S tru
sts
abou
t th
e b
enefits
of
CP
-IS
based o
n t
heir u
se o
f th
e s
yste
m
rem
ain
s p
ositiv
e.
The S
RO
has e
xte
nd
ed t
he
tim
elin
e
for
the r
oll-
out
of
CP
-IS
to 3
1 M
arc
h
2018
.
03 (
b) B
usin
ess
Pla
n an
d B
udge
t 201
5-16
Rep
ort
Page 43 of 159

2015
/16 B
ud
get
an
d B
usin
ess P
lan
: Q
3 U
pd
ate
2
. B
US
INE
SS
PL
AN
DE
LIV
ER
AB
LE
S R
AT
ED
AS
‘A
MB
ER
/ R
ED
’:
Co
mm
itm
en
t R
oo
t C
au
se a
nd
Im
pact
Ac
tio
ns T
aken
A
cti
on
Du
e D
ate
(w
here
ap
pli
cab
le)
3.3
In
troduce
ne
w a
ssura
nce
pro
cesses to e
nab
le t
he H
SC
IC t
o
open
up a
ccess a
nd r
educe
tim
escale
s f
or
connectivity t
o
nationa
l syste
ms
(Op
era
tio
ns a
nd
As
su
ran
ce)
Skill
ed r
esourc
es r
eq
uired
to c
om
ple
te th
is
work
are
als
o a
ssig
ned
to t
he test
and
assura
nce o
f critical natio
nal syste
ms.
These r
esourc
e c
on
str
ain
ts r
em
ain
a r
isk a
s
the s
erv
ices tri
es to b
ala
nce p
lann
ed d
em
and
with u
nsched
ule
d ‘h
igh p
rio
rity
’ an
d ‘m
ust do’
support
in lin
e w
ith a
llocate
d b
udg
ets
and
resourc
e a
vaila
bili
ty.
The d
eliv
ery
tim
escale
has a
lso b
een
im
pacte
d
by t
he ina
bili
ty t
o r
ecru
it to p
erm
anent
positio
ns.
5.6
W
ork
with D
H a
nd th
e C
abin
et
Off
ice to d
esig
n a
Ce
ntr
e o
f E
xcelle
nce f
or
Big
Data
an
d D
ata
S
cie
nce
(In
form
ati
on
an
d A
naly
tic
s)
Work
on the C
entr
e o
f E
xcelle
nce
is
depe
nde
nt o
n th
e a
ppo
intm
ent of
a D
irecto
r of
Data
Scie
nce to le
ad t
his
work
A D
irecto
r of
Data
Scie
nce r
ole
was
appro
ve
d a
nd th
e r
ecru
itm
ent pro
cess
sta
rted,
inte
rvie
ws w
ere
he
ld
Decem
ber
2015.
As a
t 8 J
anuary
2015
a s
uccessfu
l cand
idate
ha
d y
et to
be a
ppo
inte
d.
Work
on the
Centr
e o
f E
xcelle
nce
is d
epen
dent
on
the
appo
intm
ent of
a D
irecto
r o
f D
ata
S
cie
nce
to le
ad t
his
work
Page 44 of 159

Page 1 of 1
Board Meeting – Public Session
Title of paper: Update on Budget and Business Planning/ Future years
Board meeting date: 27 January 2016
Agenda item no: HSCIC 16 06 03 c
Paper presented by:
Carl Vincent, Director of Finance & Corporate Services
Paper prepared by:
Carl Vincent, Director of Finance & Corporate Services. Rebecca Giles, Head of Strategic Finance, Reporting & Change David O’Brien, Head of Business Intelligence
Paper approved by: (Sponsor Director) Carl Vincent, Director of Finance & Corporate Services
Purpose of the paper: To provide an update to the Board on progress on the Business Planning and Budget process for 2016/17 to 2018/19 and future financial position of the HSCIC.
Key risks and issues:
Financial position and delivery of business plan commitments for 2016/17 to 2018/19
Patient/public interest:
Indirect
Actions required by the Board: The Board are requested to:
note the current process for Budget and Business Planning for 2016/17 to 2018/19, including the impact of Transformation.
note the level of uncertainty about future years’ funding and the way we are currently managing that risk
03 (
c) C
ompr
ehen
sive
Spe
ndin
g R
evie
w(C
SR
) an
d C
orpo
rate
Bus
ines
s P
lan
Page 45 of 159

1 Copyright © 2014, Health and Social Care Information Centre.
Update on Budget and Business Planning/ Future years
Author Carl Vincent
Date 27 January 2016
03 (
c) C
ompr
ehen
sive
Spe
ndin
g R
evie
w(C
SR
) an
d C
orpo
rate
Bus
ines
s P
lan
Page 46 of 159

Update on Business Plan & Budget 15/16
2 Copyright © 2014, Health and Social Care Information Centre.
Contents
Contents 2
Executive Summary 3
Business Planning process for 2016/17 – 2018/19 3
Budget process for 2016/17 – 2018/19 3
Future years’ financial risks 4
Actions Required of the Board 4
Appendix A: DH Guidance - Headlines 5
Page 47 of 159

Update on Business Plan & Budget 15/16
3 Copyright © 2014, Health and Social Care Information Centre.
Executive Summary
This paper provides an update to the Board on progress on the Business Planning and Budget process for 2016/17 to 2018/19 and future financial position of the HSCIC. The Board are specifically requested to note the level of uncertainty about future years’ funding, and the way we are currently managing that risk.
Business Planning process for 2016/17 – 2018/19
The Department of Health issued 2016/17 business planning guidance to its Arms-Length Bodies in mid-December. This guidance sets out the planning process and timeline, and provides advice about the required content of business plan documents.
Appendix A presents the main points of the guidance and key milestones. HSCIC is required to submit a draft corporate business plan to DH by the end of January. DH intends to conduct a peer review of business plans across its family of Arms-Length Bodies during February. HSCIC is expected to submit a finalised and approved business plan to DH towards the end of March.
Note that the DH deadline for receipt of a finalised business plan precedes the meeting date on which the HSCIC Board will sign-off its business plan. This scenario has occurred in previous years and it is expected that an arrangement will be found to suit all parties.
It is proposed that the HSCIC Board participates in the corporate business planning process as follows:
24 February: HSCIC Board business meeting (private) - consideration of advanced draft of corporate business plan, Board member input and comments.
30 March: HSCIC Board public meeting: approval and sign-off of finalised plan.
The HSCIC corporate business plan is directly informed by business plans produced at directorate level across the organisation. Initial drafts of these directorate level business plans have been developed as part of an integrated business planning and budget-setting process. This has included consideration of existing work that could be stopped or de-scoped in order to meet financial constraints during the period 2016/17 to 2018/19, and new work for which funding has yet to be identified. These business plans will be refined during the next few weeks, following an internal review and challenge process and in line with the finalisation of budgets.
Budget process for 2016/17 – 2018/19
Directorates are currently working to set detailed budgets for 2016/17 to 2018/19 using targets agreed by EMT, based on an assumption of an SR settlement of 30% reduction over 4 years, taking into account certain known adjustments such as programmes coming to an end and changes in income expectations.
03 (
c) C
ompr
ehen
sive
Spe
ndin
g R
evie
w(C
SR
) an
d C
orpo
rate
Bus
ines
s P
lan
Page 48 of 159

Update on Business Plan & Budget 15/16
4 Copyright © 2014, Health and Social Care Information Centre.
The high level timetable for budgeting is:
Mid November - set provisional directorate targets for 16/17 to 18/19 (complete)
Mid January - EMT review and challenge of draft budgets (complete)
End January - detailed directorate budgets set
Feb/ Mar - identify work that cannot be delivered once efficiency taken into account and agree priorities for stopping work with DH, NHS E and other ALBs
Feb/ Mar - adjust budgets if required if there are changes to funding assumptions from commissioners
Feb/ Mar - recut budget to new post-Transformation structure There are on-going discussions between the HSCIC and DH/ ALBs and we are in the process of establishing senior sign-off arrangements.
Future years’ financial risks
The working assumption of a 30% reduction in core GiA over four years has not yet been formally confirmed by DH but is in line with their current expectations. There remains uncertainty as to our external funding from our commissioners for future years; as an allocation between organisations, these funding streams were not specifically addressed by the outcome of the Spending Review. There will continue to be considerable uncertainty in this area until all of our commissioner organisations have completed their budget and business planning processes for the coming year (predominantly DH, NHS E, PHE). There is further uncertainty as to how much of the funding for the programmes proposed in the Spending Review in response to the publication of Personalised Health and Care 2020 will come to the HSCIC. Dialogue is continuing between the HSCIC and our commissioners to gain more certainty on expected funding for future years and to ensure that all external funding, both for new and on-going work, covers the full costs incurred by the HSCIC.
Actions Required of the Board
The Board are requested to:
note the current process for Budget and Business Planning for 2016/17 to 2018/19, including the impact of Transformation.
note the level of uncertainty about future years’ funding and the way we are currently managing that risk
Page 49 of 159

Update on Business Plan & Budget 15/16
5 Copyright © 2014, Health and Social Care Information Centre.
Appendix A: DH Guidance - Headlines
Overview
ALB business plans should:
Set out clear and achievable plans for delivery in 2016-17.
Indicate the direction of travel needed to live within funding trajectories over the Spending Review period, and any help the ALB might need from DH to achieve this.
General Requirements
ALB business plans should:
Include SMART objectives for 2016-17, including key deliverables and milestones. This should include how the ALB will fulfil any statutory duties.
Show how the ALB contributes to the DH Shared Delivery Plan workstreams.
Demonstrate alignment with and / or dependencies on other ALBs’ plans.
Show that the ALB has the right skills and capabilities in place to deliver its objectives.
Show that the ALB can deliver its objectives within the 2016-17 financial allocation.
Set out (at a high level) how the ALB will respond to the Spending Review challenge over the longer term, including expected impact on finances, workforce, and delivery.
Specific Finance Requirements
ALB plans should satisfy the following financial requirements:
Show credible plans for delivering agreed cost reductions to operate within allocations.
Indicate the likely cost of transition during the year and a statement on how this will be funded.
Identify new work the ALB is being commissioned to undertake and how this is funded.
Include capital plans with a breakdown of component costs.
Headline Timetable
Date Milestone Comment
w/e 29 Jan Draft plan to DH sponsor team HSCIC will submit an ‘early’ draft
Feb (tbc) Peer review of ALB business plans More info to come from DH on this
w/c 22 Feb Final draft to DH sponsor team Unlikely to be ‘final’ draft for HSCIC
Early March Sign-off by ALB Board HSCIC Board sign-off is 30 March
25 March Finalised plan to DH for approval Submit plan as issued to HSCIC Board
31 March DH approval of plan (Subject to changes post-HSCIC Board)
End March Publish plan on ALB website Need to engage with Comms team
03 (
c) C
ompr
ehen
sive
Spe
ndin
g R
evie
w(C
SR
) an
d C
orpo
rate
Bus
ines
s P
lan
Page 50 of 159


Page 1 of 1
Board Meeting – Public Session
Title of paper: Audits of recipients of confidential information Six monthly report on audits of recipients of confidential information under data sharing framework contracts and agreements
Board meeting date: 27 January 2016
Agenda item no: HSCIC 16 06 03 d
Paper presented by:
Martin Severs Caldicott Guardian and Lead Clinician
Paper prepared by:
Nicholas Oughtibridge Head of Information Standards
Paper approved by: (Sponsor Director) Martin Severs Caldicott Guardian and Lead Clinician
Purpose of the paper: For information
Key risks and issues: Mitigation for “we fail to protect data and/or succumb to IT/cyber security threats”
Patient/public interest:
Failure to demonstrate trustworthiness will reduce public trust; this report demonstrates HSCIC is taking its responsibilities seriously
Actions required by the Board: To note for information
03
(d)
Dat
a R
elea
se R
evie
w
Page 51 of 159

1 Copyright © 2016, Health and Social Care Information Centre.
Audits of recipients of confidential information
Six monthly report on audits of recipients of confidential information under data sharing framework contracts and agreements
Nicholas Oughtibridge
27 January 2016
03 (
d) D
ata
Rel
ease
Rev
iew
Page 52 of 159
Audits of recipients of confidential information
2 Copyright © 2016, Health and Social Care Information Centre.
Contents
Contents 2
Background 3
Selection of organisations to audit 3
Planned audits 3
Building capacity 4
Summary 4
Actions Required of the Board 4
Page 53 of 159

Audits of recipients of confidential information
3 Copyright © 2016, Health and Social Care Information Centre.
Background
The HSCIC provides confidential information to a wide variety of organisations to support specific purposes. Each dissemination of these data is subject to a Data Sharing Framework Contract1 and Data Sharing Agreement2. Recipients of data are required to have regard to the HSCIC Code of Practice on Confidential Information3.
The HSCIC has provision through the Data Sharing Framework Contract to audit the recipients of these data to ensure that confidential information is handled appropriately. The audits contribute to our mitigation of the risk that we fail to protect our data. This report is a status update on those audits. It provides the numbers of completed audit visits and the number of reports published on the HSCIC web site.
Selection of organisations to audit
The HSCIC uses a balanced risk approach combined with random sampling to identifying recipients of confidential information to audit. The criteria adopted are:
Complaints
Known issues: concerns which have raised either internally (Information Asset Owners,
customer relationship manager, Data Access Advisory Group, Caldicott Guardian, Senior
Information Risk Owner) or externally (whistle blower, another organisation, patients or an
independent body such as Monitor, Information Commissioners Office, Confidentiality
Advisory Group, Office of National Statistics)
Organisations which have received high media interest for their previous handling of data
Repeated extensions for the same data
Low IG Toolkit scores (or 100% for first year of completion)
Organisations presenting high risk of linking confidential data from two or more different
datasets
Random selection of data recipients
Self-selection by a data recipient who may wish to be seen to have received a positive
audit statement from HSCIC
Planned audits
Nineteen organisations have been audited to date. The reports of audits are published on the HSCIC website4. Once we have achieved a critical mass of audits, we will undertake a lessons learned exercise to ensure we can feed the results in to HSCIC processes and procedures to support continuous improvement. Findings from this will be fed back to the board in the next biannual report in July.
1 Standard Data Sharing Contract - http://www.hscic.gov.uk/media/15728/DARS-Data-Sharing-
Contract/pdf/HSCIC_Data_Sharing_Framework_Contract_Jan2015v_2_(restricted_editing).pdf 2 Template Data Sharing Agreement - http://www.hscic.gov.uk/media/15729/DARS-Data-Sharing-
Agreement/pdf/Data_Sharing_Agreement_2015v2(restricted_editing).pdf 3 Code of Practice on Confidential Information - http://systems.hscic.gov.uk/cop
4 http://www.hscic.gov.uk/dsa
03 (
d) D
ata
Rel
ease
Rev
iew
Page 54 of 159

Audits of recipients of confidential information
4 Copyright © 2016, Health and Social Care Information Centre.
Building capacity
The team is now fully staffed with two qualified auditors. Plans are in place for our policy and process for undertaking internal and external audits to be shared with the recipients of thess data and wider stakeholders. The high level process adopted is illustrated in figure 1. The SIRO may commission additional audits as follow-up.
Figure 1 Steps to deliver an audit
Auditees have found the experience constructive and have taken steps to improve their handling of HSCIC data. One organisation has chosen to no longer use HSCIC data.
Summary
By the end of December we have completed 19 audits. We are on track to complete a total of 25 audits during the current financial year. For the year ending March 2017, we are planning to deliver 30 audits.
Figure 2 Cumulative on-site reviews completed and reports published by month
Actions Required of the Board
The Board is asked to note progress for information.
Recipient and audit team identified based on perceived risk or random sampling
Onsite audit scheduled and available evidence reviewed
Onsite audit. Headline findings shared with SIRO
Report prepared. Opportunity for auditee to correct inaccuracies
Report published on HSCIC website
0
10
20
30
40
50
60
70
Onsite review completed Report published
Page 55 of 159
Page 1 of 1
Board Meeting – Public Session
Title of paper: 2015 HSCIC Staff Survey Results
Board meeting date: 27 January 2016
Agenda item no: HSCIC 16 06 03 e
Paper presented by:
Rachael Allsop, Executive Director of HR and Transformation
Paper prepared by:
Ken Baker, Head of Employment Policy and Practice
Paper approved by: (Sponsor Director) Rachael Allsop, Executive Director of HR and Transformation
Purpose of the paper: To inform the Board of the results of the 2015 staff survey
Key risks and issues:
The main risk relating to the survey is a failure to produce and implement action plans to address issues identified in the survey. This would undermine the credibility of the survey and risk wasting opportunities to improve our reputation as an employer. The production of plans and ongoing progress will be reported as part of the organisational health KPIs.
Patient/public interest:
Indirect: Addressing issues identified in the staff survey will help to improve staff engagement and make the HSCIC a better place to work. Evidence demonstrates that an engaged workforce is a more productive workforce.
Actions required by the Board: To note the results of the staff survey
03 (
e) S
taff
Sur
vey
Res
ults
Page 56 of 159


1 Copyright © 2016, Health and Social Care Information Centre.
2015 HSCIC Staff Survey Results
Author: Ken Baker
Head of Employment Policy and Practice
Date: 27 January 2016
03 (
e) S
taff
Sur
vey
Res
ults
Page 57 of 159

2015 HSCIC Staff Survey Results
2 Copyright © 2016, Health and Social Care Information Centre.
Contents 1 Executive Summary 3
2 Background 3
3 Recommendation 3
4 Implications 3
4.1 Strategy Implications 3
4.2 Financial Implications 3
4.3 Stakeholder Implications 4
4.4 Handling 4
5 Risks and Issues 4
6 Corporate Governance and Compliance 4
7 Management Responsibility 4
8 Actions Required of the Board 4
Page 58 of 159

2015 HSCIC Staff Survey Results
3 Copyright © 2016, Health and Social Care Information Centre.
1 Executive Summary
This paper accompanies the draft report from the employee survey that was conducted during November 2015, for consideration by the HSCIC Board. The report offers a summary of the key issues and an initial corporate response to what is generally an improved outcome overall. This will be followed by detailed action plans within each Professional Pool, to ensure that plans are aligned with our future structure. The report and a summary of staff comments will be published on the intranet. Progress against action plans will be reported as part of our organisational health KPIs.
2 Background
The HSCIC is committed to seeking regular, structured feedback from staff through employee surveys to gauge the degree of staff engagement and our organisational health. This is the fourth survey since the establishment of the HSCIC and has the best response rate to date (70%), with improved results in almost all areas.
3 Recommendation
It is recommended that the Board note the content of the report.
4 Implications
4.1 Strategy Implications
The survey informs our approach to securing an appropriate workforce and transforming the HSCIC to become a high-performing organisation. The overall staff engagement scores have all improved and are now all ‘green-rated’ at 70% or over. Ten of the overall organisational health scores have improved but there is generally more work to do in this area, particularly in terms of performance management. Business areas will undertake further analysis of the free text comments but, once again, they reflect key themes around the commitment, hard work and enthusiasm of staff within teams. There is still a tendency, however, to level criticism at others outside of the immediate team or department, which we will need to address.
4.2 Financial Implications
The financial implications are expected to be minimal as a number of actions are already in progress (e.g. the Transformation Programme, movement to Resource Pools, Talent Management, etc.) or can be implemented without incurring additional costs (e.g. continuing improvements to communication and more effective performance management). Action plans will identify any significant financial implications that may arise from their implementation.
03 (
e) S
taff
Sur
vey
Res
ults
Page 59 of 159

2015 HSCIC Staff Survey Results
4 Copyright © 2016, Health and Social Care Information Centre.
4.3 Stakeholder Implications
The key stakeholders in relation to the survey are our staff. Demonstrating that we are listening to, and taking action on, the issues that they raise will contribute to developing the HSCIC as an employer of choice for existing staff and future job applicants. There is also ample evidence that an engaged workforce is a more productive workforce and this will have benefits for our customers and end-users.
4.4 Handling
The full report will be published on the Intranet and Weekly Review. There will be ongoing communication reporting on the development, implementation and progress of action plans.
5 Risks and Issues
The main risk relating to the survey is a failure to produce action plans, designed to address issues identified in the survey, and to manage progress against those plans. This would undermine the credibility of the survey and risk wasting opportunities to improve our reputation as an employer. The production of plans and ongoing progress will be reported as part of the organisational health KPIs.
6 Corporate Governance and Compliance
The production and delivery of action plans will be reported as part of the organisational health KPIs.
7 Management Responsibility
Rachael Allsop has Executive Director responsibility for the staff survey. Ken Baker, Head of Employment Policy and Practice, is responsible for the day to day management of the survey.
8 Actions Required of the Board
The Board is asked to note the results of the 2016 HSCIC staff survey.
Page 60 of 159
EM
PLO
YE
E
SU
RV
EY
Nove
mber 2
015
RE
SU
LTS
1
03 (
e) S
taff
Sur
vey
Res
ults
Page 61 of 159

Chie
f E
xecutive’s
Fore
word
ma
kin
g c
usto
me
r ca
re o
ur
top p
riority
.
Th
is h
as to
im
pro
ve
durin
g 2
01
6 if w
e
are
to
be tru
ste
d a
cro
ss th
e s
yste
m to
deliv
er
data
, in
form
ation
and
te
chn
olo
gy
se
rvic
es th
at o
ur
cu
sto
me
rs n
ee
d to
me
et
natio
na
l a
nd
lo
cal p
rioritie
s.
I w
as e
nco
ura
ge
d to
se
e th
e la
rge
st
imp
rove
me
nt in
re
spo
nse
s c
once
rne
d
our
str
ate
gic
dire
ction
. H
avin
g a
‘cle
arly
art
icu
late
d s
tra
teg
y’ i
ncre
ase
d b
y 9
poin
ts to
67. I re
cog
nis
e th
is s
till
only
retu
rns a
n ‘a
mb
er’ s
tatu
s o
ve
rall,
but I
hop
e fo
r fu
rth
er
imp
rove
me
nts
as s
taff
are
incre
asin
gly
eng
ag
ed in
Tra
nsfo
rma
tio
n. W
e m
ust p
ush
fo
rwa
rd
and
ensu
re th
at o
ur
vis
ion a
nd
our
go
als
are
cle
ar,
wh
ich
will
be a
ssis
ted b
y a
gre
ate
r u
nd
ers
tand
ing
of o
ur
cu
sto
me
rs.
Ou
r p
rioritie
s d
urin
g 2
01
6/1
7 w
ill r
efle
ct
this
, p
art
icu
larly w
ith
th
e m
ove
to
a n
ew
ope
ratin
g m
ode
l in
Ap
ril th
at w
ill e
nsu
re
we
co
nce
ntr
ate
our
skill
s a
nd
re
sou
rce
s
on d
eliv
ery
prioritie
s.
Th
e a
rea
of m
ost co
nce
rn to
sta
ff
app
ea
rs to
be a
rou
nd th
e m
ana
ge
me
nt
of p
erf
orm
ance
. W
hile
th
e s
co
res a
re
hig
her
than
in
pre
vio
us y
ears
, it is s
till
one
of th
e lo
we
st
sco
ring
in
dic
ato
rs in
eve
ry d
ire
cto
rate
. D
uring
th
e p
ast ye
ar,
we
ha
ve
intr
odu
ced
ta
lent m
ana
ge
me
nt
for
gra
de
s 8
b a
nd
abo
ve
an
d w
e w
ill r
oll
this
out to
oth
er
ban
ds in
th
e c
om
ing
mo
nth
s. T
he im
pact a
nd
vis
ibili
ty o
f th
is
ma
y ta
ke
mo
re tim
e to
em
erg
e a
nd
I
accep
t th
at w
e n
ee
d to
dem
onstr
ate
how
the o
rga
nis
ation
al ch
an
ge
s w
e a
re
ma
kin
g w
ill e
nsu
re th
at p
erf
orm
ance
is
bein
g m
ana
ge
d a
pp
rop
riate
ly.
Ove
rall,
th
e s
urv
ey h
as m
any p
ositiv
es.
Th
ere
are
co
ntin
uin
g im
pro
ve
me
nts
we
ca
n m
ake
and
th
ere
are
so
me
cle
ar
are
as r
eq
uirin
g a
tte
ntio
n. T
he E
xe
cutive
Ma
na
ge
me
nt T
eam
and
I w
ill b
e
deve
lopin
g a
ction
pla
ns in
re
spo
nse
. S
o,
if y
ou h
ave
ide
as a
nd
th
ou
gh
ts o
n h
ow
we
ca
n a
dd
ress s
om
e o
f th
e c
ore
issu
es,
ple
ase
dis
cu
ss th
ese
in
yo
ur
team
s a
nd
with
yo
ur
ma
na
ge
rs a
nd
dire
cto
rs s
o th
at
we
ca
n e
nsu
re th
e r
igh
t ste
ps a
re ta
ke
n.
Th
an
k y
ou
An
dy W
illia
ms
2
Firstly, th
an
k y
ou
to a
ll co
lleag
ues
wh
o r
espo
nd
ed
to
the e
mp
loye
e
su
rve
y. W
e h
ad
a
70 p
er
ce
nt
respo
nse
ra
te
with
50
0 m
ore
sta
ff ta
kin
g p
art
than
last ye
ar.
Th
is in
its
elf is
a s
tro
ng
indic
ation
th
at
em
plo
ye
es w
ant to
part
icip
ate
and
are
active
ly e
ng
ag
ed in
th
e o
rga
nis
ation
.
I a
m d
elig
hte
d c
olle
ag
ues h
ave
re
turn
ed
the h
ighest score
s a
cro
ss the b
oard
sin
ce th
e H
SC
IC w
as c
reate
d. T
his
su
gg
ests
we
are
mo
vin
g in
th
e r
igh
t
dire
ction
. T
he a
ction
s w
e t
ake
in
respo
nse
to
th
e s
urv
ey w
ill n
ee
d to
focus o
n s
usta
inin
g a
nd
, w
here
ve
r
possib
le, b
uild
ing
on th
is m
om
en
tum
.
Over
the p
ast year,
I h
ave c
onsis
tently
em
ph
asis
ed th
e n
ee
d f
or
a s
tro
ng
er
cu
sto
me
r fo
cus a
nd
th
e s
urv
ey s
how
s
that th
ere
is in
cre
ase
d a
wa
ren
ess o
f
wh
o t
he c
usto
me
r is
. H
ow
eve
r, t
here
wa
s n
o c
han
ge
fro
m th
e p
revio
us y
ear
on u
nd
ers
tand
ing
cu
sto
me
r n
ee
ds a
nd
a n
um
ber
of yo
u d
o n
ot fe
el th
at w
e a
re
Page 62 of 159

Intr
oduction
The s
taff
surv
ey s
eeks to m
easure
sta
ff
eng
ag
em
en
t a
nd
org
anis
ation
al h
ea
lth
in th
e H
SC
IC.
Th
e e
ng
ag
em
en
t q
uestio
ns fo
llow
th
e
sa
me
fo
rma
t a
s la
st ye
ar,
exce
pt th
at
two
qu
estio
ns h
ave
be
en a
me
nd
ed
in
respo
nse
to
fe
ed
ba
ck. “
Th
ere
are
frequent opport
unitie
s for
me to s
how
initia
tive
in m
y r
ole
” h
as b
eco
me
“I
have
an a
pp
rop
riate
le
ve
l o
f co
ntr
ol
ove
r m
y w
ork
” a
nd
“T
ime
passe
s
qu
ickly
wh
en
I a
m w
ork
ing
” h
as b
ee
n
repla
ced
by “
I fe
el su
pp
ort
ed b
y m
y lin
e
ma
na
ge
r”.
Th
e H
SC
IC h
as c
han
ge
d s
ince th
e
su
rve
y w
as f
irst d
esig
ned
and
ove
r th
e
next fe
w m
onth
s w
e w
ill r
evie
w o
ptio
ns
to e
nsu
re th
at it is r
ele
va
nt to
th
e
tra
nsfo
rme
d o
rga
nis
ation
.
Th
e s
urv
ey r
esults a
re c
alc
ula
ted
by
giv
ing
a s
co
re to
each
re
spo
nse
– f
rom
five
poin
ts f
or
‘str
ong
ly a
gre
e’ to
one
poin
t fo
r ‘s
tro
ng
ly d
isa
gre
e’. T
he s
um
of th
ose
sco
res fo
r e
ach
qu
estio
n is
div
ided
by t
he n
um
ber
of re
spo
nse
s
and
mu
ltip
lied b
y 2
0 to
giv
e a
n o
ve
rall
sco
re o
ut o
f a
ma
xim
um
possib
le 1
00
.
Benchm
ark
s in
dic
ate
that hig
her
perf
orm
ing o
rga
nis
ation
s te
nd
to
have
an e
ng
ag
em
en
t sco
re o
f 7
0 o
r o
ve
r a
nd
we
ha
ve
ap
plie
d t
he s
am
e ta
rge
t to
th
e
org
anis
ation
al h
ea
lth
sco
res.
All
of th
e q
uestio
ns h
ave
, th
ere
fore
,
bee
n g
ive
n a
RA
G s
tatu
s b
ase
d o
n:
s
co
res b
elo
w 6
5 a
nd
app
lies t
o
issu
es r
eq
uirin
g s
ign
ific
ant
imp
rove
me
nt
s
co
res b
etw
een
65-6
9 a
nd
app
lies
to is
su
es r
eq
uirin
g m
onito
ring
and
slig
ht im
pro
ve
me
nt
s
co
res o
f 7
0 a
nd
abo
ve
an
d
indic
ate
s o
ve
rall
sa
tisfa
ction
Sco
res h
ave
be
en r
oun
de
d to
wh
ole
num
bers
fo
r th
e R
AG
ra
ting
.
Su
pp
lem
en
tary
qu
esti
on
s
To
ca
ptu
re id
ea
s, th
ou
gh
ts a
nd
th
em
es
we
aske
d c
olle
ag
ues t
o c
om
me
nt on
two
su
pp
lem
en
tary
qu
estio
ns:
•W
hat w
ork
s r
eally
we
ll w
ith
in y
our
dire
cto
rate
?
•W
ith
in y
our
dire
cto
rate
: w
hat a
re
the to
p 3
th
ing
s th
at co
uld
be
don
e
to m
ake
th
is a
gre
at p
lace t
o w
ork
?
The s
econd q
uestion is d
esig
ned to
iden
tify
wh
at is
mo
st im
port
ant to
mo
st
peo
ple
, to
help
prio
ritise a
ction
.
All
co
mm
ents
, g
roup
ed
by d
ire
cto
rate
,
are
pub
lish
ed
in
a s
epa
rate
app
en
dix
ava
ilable
here
[a
dd
lin
k]
and
th
ese
will
be a
dd
resse
d a
s p
art
of th
e s
urv
ey
action p
lans.
Co
nfi
den
tia
lity
Th
e s
taff
su
rve
y r
esults a
re r
eceiv
ed
fro
m th
e in
de
pe
nd
en
t P
icke
r In
stitu
te
and
are
ag
gre
ga
ted
by d
ire
cto
rate
,
locatio
n, b
an
d, p
rofe
ssio
na
l g
roup
and
various e
qualit
y s
trands; th
ey d
o n
ot
iden
tify
in
div
idua
ls.
To
pro
tect a
ga
inst p
eo
ple
be
ing
iden
tifie
d b
y c
ross-r
efe
rencin
g d
iffe
ren
t
bre
akd
ow
ns, re
sults fo
r g
roup
s w
ith
sm
all
em
plo
ye
e n
um
bers
or
low
num
bers
of re
spo
nd
en
ts a
re n
ot
pro
vid
ed b
y P
icker.
Wh
ere
possib
le, P
icke
r h
ave
am
alg
am
ate
d r
esults fo
r sm
all
num
bers
with
in o
ther
team
re
po
rts.
3
03 (
e) S
taff
Sur
vey
Res
ults
Page 63 of 159

Response r
ate
s b
y D
irecto
rate
Th
ere
we
re 1
,85
2 r
espo
nse
s to
th
e s
urv
ey –
alm
ost 5
00
mo
re th
an
la
st ye
ar
and
re
pre
sen
ting
70%
of a
ll sta
ff.
Th
is in
clu
de
d:
•1
58
(7
9%
) re
spo
nse
s fro
m F
inan
ce a
nd
Co
rpo
rate
Se
rvic
es
•4
5 (
82%
) re
spo
nse
s fro
m H
R a
nd
Tra
nsfo
rma
tio
n c
om
bin
ed
with
Clin
ica
l a
nd
Pu
blic
Assu
ran
ce
•1
04
(7
2%
) re
spo
nse
s fro
m P
rovid
er
Su
pp
ort
•3
88
(7
3%
) re
spo
nse
s fro
m In
form
atio
n a
nd
An
aly
tics
•536 (
61%
) re
sponses fro
m O
pera
tions a
nd A
ssura
nce S
erv
ices
•3
68
(7
2%
) re
spo
nse
s fro
m H
ealth
Dig
ita
l S
erv
ice
s
•55 (
74%
) re
spo
nse
s fro
m C
usto
me
r R
ela
tion
s
•1
85
(7
4%
) re
spo
nse
s fro
m A
rch
ite
ctu
re, S
tand
ard
s a
nd
In
no
va
tion
•1
3 (
100
%)
respo
nse
s fro
m A
ca
de
my (
gra
du
ate
s, in
tern
s a
nd
tra
inee
s)
No
te: A
s a
re
sult o
f th
e s
ma
ll siz
e o
f th
e C
linic
al a
nd
Pu
blic
Assu
ran
ce
Dire
cto
rate
th
eir d
ire
cto
rate
-le
ve
l re
spo
nse
s h
ave
be
en
co
mb
ined
with
th
e H
R a
nd
Tra
nsfo
rma
tio
n D
ire
cto
rate
fo
r th
e p
urp
ose
s o
f th
is s
urv
ey.
Wo
rk a
rea
s w
ith
sm
all
em
plo
ye
e n
um
bers
have
be
en g
roup
ed
to
ge
the
r w
here
ve
r p
ossib
le t
o e
nsu
re th
at w
e r
eceiv
e a
s m
uch
deta
il in
th
e r
esults a
s p
ossib
le t
o e
na
ble
me
an
ing
ful a
ction
wh
ilst
pro
tecting
th
e a
no
nym
ity o
f re
spo
nd
en
ts. T
he fo
llow
ing
wo
rk
are
as h
ave
be
en g
roup
ed
to
ge
the
r:
•H
R a
nd
Tra
nsfo
rma
tio
n –
oth
er
co
mp
rise
s O
rga
nis
ation
al D
eve
lopm
ent,
Em
plo
ym
ent
Po
licy &
Pra
ctice, D
ISC
and
Clin
ica
l
•P
rovid
er
Su
pp
ort
– o
the
r co
mp
rise
s In
tero
pe
rab
ility
/Dig
ita
l T
echn
olo
gy F
un
d, P
AC
S, a
nd
PS
Dire
cto
rate
Ce
ntr
al S
erv
ice
s
•In
form
atio
n a
nd
An
aly
tics –
oth
er
co
mp
rise
s C
are
.data
and
MC
DS
, B
ene
fits
Ma
na
ge
me
nt a
nd
Utilis
ation
and
Sta
tistical
Govern
ance
•O
pera
tion
s a
nd
Assu
ran
ce
Se
rvic
es –
oth
er
co
mp
rise
s C
entr
al S
erv
ice
s, O
pera
tion
s a
nd
Te
chn
ica
l S
erv
ice
s C
en
tra
l S
erv
ice
s
and
NT
S a
nd
SU
S P
rog
ram
me
s
•A
rch
ite
ctu
re, S
tand
ard
s a
nd
In
no
va
tion
– o
the
r co
mp
rise
s B
usin
ess A
rch
ite
ctu
re, D
ata
Se
rvic
es P
rog
ram
me
and
Co
mm
issio
nin
g a
nd
Fin
an
ce D
ata
Se
rvic
es
4
Page 64 of 159
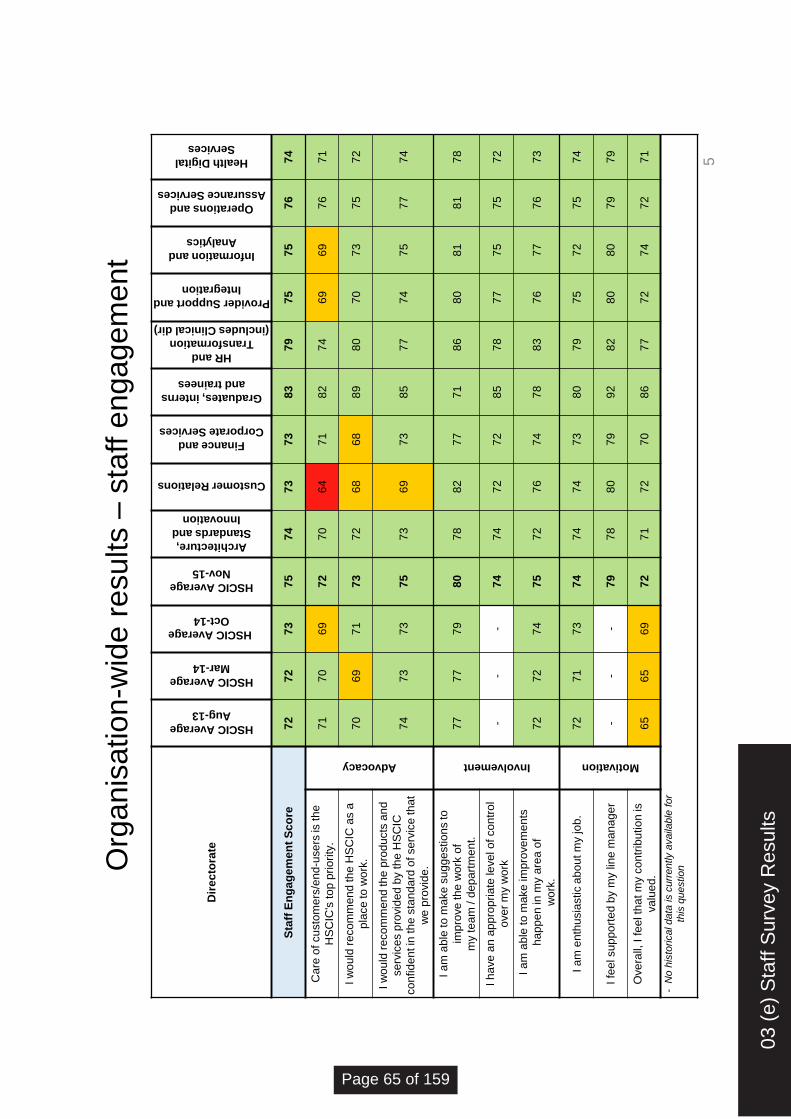
Dir
ec
tora
te
HSCIC Average
Aug-13
HSCIC Average
Mar-14
HSCIC Average
Oct-14
HSCIC Average
Nov-15
Architecture,
Standards and
Innovation
Customer Relations
Finance and
Corporate Services
Graduates, interns
and trainees
HR and
Transformation
(includes Clinical dir)
Provider Support and
Integration
Information and
Analytics
Operations and
Assurance Services
Health Digital
Services
Sta
ff E
ng
ag
em
en
t S
co
re
72
7
2
73
7
5
74
7
3
73
8
3
79
7
5
75
7
6
74
Ca
re o
f cu
sto
me
rs/e
nd
-use
rs is
th
e
HS
CIC
's to
p p
rio
rity
.
Advocacy
71
7
0
69
7
2
70
6
4
71
8
2
74
6
9
69
7
6
71
I w
ou
ld r
eco
mm
en
d th
e H
SC
IC a
s a
pla
ce
to
wo
rk.
70
6
9
71
7
3
72
6
8
68
8
9
80
7
0
73
7
5
72
I w
ou
ld r
eco
mm
en
d th
e p
rod
ucts
an
d
se
rvic
es p
rovid
ed
by t
he
HS
CIC
co
nfid
en
t in
th
e s
tan
da
rd o
f se
rvic
e th
at
we
pro
vid
e.
74
7
3
73
7
5
73
6
9
73
8
5
77
7
4
75
7
7
74
I a
m a
ble
to
ma
ke
su
gg
estio
ns to
imp
rove
th
e w
ork
of
my te
am
/ d
ep
art
me
nt.
Involvement
77
7
7
79
8
0
78
8
2
77
7
1
86
8
0
81
8
1
78
I h
ave
an
ap
pro
pri
ate
leve
l o
f co
ntr
ol
ove
r m
y w
ork
-
- -
74
7
4
72
7
2
85
7
8
77
7
5
75
7
2
I a
m a
ble
to
ma
ke
im
pro
ve
me
nts
ha
pp
en
in m
y a
rea
of
wo
rk.
72
7
2
74
7
5
72
7
6
74
7
8
83
7
6
77
7
6
73
I a
m e
nth
usia
stic a
bo
ut m
y jo
b.
Motivation
72
7
1
73
7
4
74
7
4
73
8
0
79
7
5
72
7
5
74
I fe
el su
pp
ort
ed
by m
y lin
e m
an
ag
er
- -
- 7
9
78
8
0
79
9
2
82
8
0
80
7
9
79
Ove
rall,
I f
ee
l th
at m
y c
on
trib
utio
n is
va
lue
d.
65
6
5
69
7
2
71
7
2
70
8
6
77
7
2
74
7
2
71
- N
o h
isto
rical data
is c
urr
ently a
vaila
ble
for
this
questio
n
Org
anis
atio
n-w
ide
re
su
lts –
sta
ff e
nga
gem
en
t
5
03 (
e) S
taff
Sur
vey
Res
ults
Page 65 of 159

Dir
ec
tora
te
HSCIC Average
Aug-13
HSCIC Average
Mar-14
HSCIC Average
Oct-14
HSCIC Average
Nov-15
Architecture,
Standards and
Innovation
Customer
Relations
Finance and
Corporate
Services
Graduates,
interns and
trainees
HR and
Transformation
(including
Clinical)
Provider Support
and Integration
Information and
Analytics
Operations and
Assurance
Services
Health Digital
Services
Org
an
isa
tio
n H
ea
lth
Sc
ore
6
6
67
6
9
71
7
1
74
7
0
75
7
8
74
6
9
71
7
1
Ge
ne
rally
, I
kn
ow
wh
o t
he
cu
sto
me
rs
of th
e H
SC
IC a
re.
73
7
3
74
7
6
75
8
3
73
7
2
75
7
7
75
7
7
76
I h
ave
a c
lea
r u
nd
ers
tan
din
g o
f th
e
ne
ed
s o
f m
y c
usto
me
rs.
77
7
6
78
7
8
75
8
2
76
6
5
84
7
9
77
7
8
78
Th
e H
SC
IC h
as c
lea
r a
nd
re
leva
nt
org
an
isa
tio
na
l va
lue
s.
- -
67
7
1
70
7
1
70
8
0
80
7
6
69
7
1
70
Th
e H
SC
IC h
as a
cle
arl
y a
rtic
ula
ted
str
ate
gy fo
r its fu
ture
. 5
5
59
5
8
67
6
8
72
6
9
75
7
3
69
6
3
68
6
6
I ca
n s
ee
ho
w m
y w
ork
ob
jective
s
co
ntr
ibu
te to
th
e H
SC
IC a
ch
ievin
g its
sta
ted
pu
rpo
se
.
64
6
5
65
6
9
70
7
7
70
8
2
77
7
2
67
6
9
67
I h
ave
th
e r
igh
t kn
ow
led
ge
an
d s
kill
s
to p
erf
orm
we
ll in
my r
ole
. 7
9
78
7
8
79
8
0
81
7
7
82
8
3
80
7
8
78
7
9
I a
m c
lea
r a
bo
ut th
e k
no
wle
dg
e a
nd
skill
s th
at I
ne
ed
to
pro
gre
ss w
ith
in
the
org
an
isa
tio
n.
65
6
4
66
6
7
67
7
0
66
7
7
73
6
9
67
6
6
66
**I h
ave
th
e o
pp
ort
un
ity to
be
en
ga
ge
d a
nd
in
vo
lve
d in
org
an
isa
tio
na
l ch
an
ge
in
itia
tive
s.
60
6
3
67
6
8
67
6
8
69
8
0
82
7
6
67
6
7
67
I h
ave
ch
alle
ng
ing
wo
rk o
bje
ctive
s.
72
7
3
74
7
6
74
8
1
74
7
8
77
7
6
74
7
7
76
My w
ork
are
a d
iffe
ren
tia
tes b
etw
ee
n
go
od
an
d a
ve
rag
e p
erf
orm
an
ce
. 6
1
60
6
1
63
6
1
59
6
2
77
7
2
66
6
0
63
6
3
My w
ork
are
a m
on
ito
rs it
s
pe
rfo
rma
nce
usin
g K
PIs
or
me
tric
s.
60
6
4
65
6
5
66
6
5
66
6
6
86
6
9
63
6
5
64
My w
ork
are
a p
erf
orm
s w
ell
ag
ain
st
its K
PIs
/ta
rge
ts.
60
6
4
72
7
3
73
7
4
71
6
3
78
7
5
73
7
4
74
- N
o h
isto
rical data
is c
urr
ently a
vaila
ble
for
this
questio
n
Org
anis
atio
n-w
ide
re
su
lts –
org
an
isa
tio
na
l h
ealth
6
Page 66 of 159

Org
an
isation
-wid
e r
esu
lts –
EM
T r
esp
on
se
Th
e E
xe
cutive
Ma
na
ge
me
nt T
eam
is d
elig
hte
d th
at a
lmo
st
500
mo
re s
taff
to
ok th
e tim
e to
re
spo
nd
to
th
e 2
01
5 s
urv
ey,
bring
ing
th
e to
tal to
1,8
52
(7
0%
of a
ll sta
ff).
Y
our
feed
ba
ck is
imp
ort
ant a
nd
will
in
form
wo
rk to
build
on
action
s ta
ke
n in
respo
nse
to
th
e la
st su
rve
y. E
MT
is a
wa
re t
hat a
ction
s a
cro
ss
all
dire
cto
rate
s h
ave
no
t a
lwa
ys b
ee
n c
onsis
tent o
r h
ad
hig
h
vis
ibili
ty b
ut th
ere
has b
ee
n g
ood
pro
gre
ss a
nd
th
is w
ill b
e
me
asu
red
fo
rma
lly a
s p
art
of o
ur
KP
Is.
It is
enco
ura
gin
g to
se
e a
n in
cre
ase
in
th
e o
ve
rall
eng
ag
em
en
t sco
re, p
art
icu
larly d
urin
g a
perio
d o
f ch
an
ge
.
Th
ere
has b
ee
n s
tead
y p
rog
ress in
all
are
as a
nd
th
e fa
ct th
at
Gra
duate
s, T
rain
ees a
nd I
nte
rns h
ave r
eport
ed s
uch p
ositiv
e
results, o
n a
100
% r
espo
nse
ra
te, is
te
sta
me
nt to
th
e s
uccess
of th
e in
itia
tive
to
‘g
row
our
ow
n sta
ff’.
Th
e tw
o h
igh
est sco
ring
eng
ag
em
en
t q
uestio
ns r
ela
te to
th
e
abili
ty t
o m
ake
su
gg
estion
s to
im
pro
ve
th
e w
ork
of th
e a
rea
and
fe
elin
g s
upp
ort
ed b
y t
he lin
e m
ana
ge
r, w
hic
h is a
lso
enco
ura
gin
g.
Our
Org
anis
ational H
ealth S
core
s h
ave a
lso im
pro
ved, w
ith
incre
ase
d s
co
res fo
r a
ll b
ut tw
o q
uestio
ns, w
hic
h r
em
ain
unch
an
ge
d fro
m la
st ye
ar.
T
he r
esults s
ug
ge
st a
bett
er
und
ers
tand
ing
of o
ur
str
ate
gy a
nd
va
lues b
ut th
ere
is s
till
wo
rk
to b
e d
on
e. D
istin
gu
ish
ing
betw
een
go
od
and
poo
r
perf
orm
ance
re
ma
ins a
sig
nific
ant co
nce
rn fo
r m
any o
f yo
u,
desp
ite
a s
ligh
t im
pro
ve
me
nt in
th
e s
co
re.
There
are
severa
l g
ood n
ew
s s
tories in t
hese r
esults, w
hic
h
we
will
build
upo
n, a
nd
we
will
use th
e o
pp
ort
unity p
rese
nte
d
by T
ransfo
rma
tio
n to
add
ress th
ose
are
as th
at yo
u h
ave
to
ld
us m
ost re
qu
ire
deve
lopm
ent:
My w
ork
are
a d
iffe
ren
tia
tes b
etw
een
go
od
an
d a
ve
rag
e
perf
orm
an
ce
The s
core
has im
pro
ved f
rom
61 to 6
3 b
ut th
is r
em
ain
s the
low
est sco
ring
qu
estio
n in
th
e e
ntire
su
rve
y, d
esp
ite
th
e
imp
lem
en
tation
of re
gu
lar
PD
Rs,
Ta
lent M
ana
ge
me
nt a
nd
a
rang
e o
f K
PIs
. I
t is
cle
ar
that m
any p
eo
ple
fe
el th
at th
ey a
re
perf
orm
ing w
ell
but p
oo
r p
erf
orm
ance
in o
thers
is n
ot
ch
alle
ng
ed o
r m
ana
ge
d e
ffe
ctive
ly. W
e n
ee
d to
do m
ore
to
ensu
re th
at p
eo
ple
kn
ow
th
eir c
ontr
ibutio
n is v
alu
ed
.
Recog
nitio
n S
chem
es a
re c
urr
ently b
ein
g p
ilote
d a
t a local
leve
l, w
ith
a v
iew
to
deve
lopin
g a
n o
rga
nis
ation
-wid
e s
ch
em
e
in th
e y
ear
ahe
ad
.
Pe
rfo
rma
nce
ma
na
ge
me
nt, le
d b
y c
are
er
ma
na
ge
rs a
nd
su
pp
ort
ed b
y p
rofe
ssio
na
l g
roup
s, is
a f
und
am
enta
l part
of o
ur
Tra
nsfo
rma
tio
n P
rog
ram
me
. T
here
will
be a
mo
re v
isib
le
focus o
n m
ana
gin
g p
erf
orm
ance
at a
n in
div
idua
l, p
rofe
ssio
na
l
gro
up a
nd o
rganis
ational le
vel, m
easure
d b
y K
PIs
and
und
erp
inne
d b
y I
SO
900
1.
Th
e H
SC
IC h
as
a c
lea
rly a
rtic
ula
ted
str
ate
gy f
or
its
fu
ture
Sin
ce th
e la
st su
rve
y w
e h
ave
ha
d a
se
ries o
f w
ork
sh
op
s to
eng
ag
e s
taff
in d
eve
lopin
g o
ur
str
ate
gy fo
r th
e fu
ture
. I
t h
as
bee
n c
ove
red
in
th
e ‘a
ll h
an
ds c
onfe
ren
ce
’ and
in
a n
um
ber
of
blo
gs a
nd a
rtic
les o
n the Intr
anet. T
he s
trate
gy h
as info
rmed
and
in
spire
d t
he T
ransfo
rma
tio
n P
rog
ram
me
, w
hic
h is n
ow
ente
ring
th
e d
eta
iled d
esig
n a
nd
eng
ag
em
en
t sta
ge
.
03 (
e) S
taff
Sur
vey
Res
ults
Page 67 of 159

Org
an
isation
-wid
e r
esu
lts –
EM
T r
esp
on
se
Pe
op
le f
rom
a n
um
ber
of d
iscip
lines,
and
gra
de
s, h
ave
be
en
invo
lve
d in
de
ve
lopin
g o
ur
futu
re s
tru
ctu
re a
nd
new
wa
ys o
f
wo
rkin
g; th
ere
is a
n a
ctive
pro
gra
mm
e o
f co
mm
unic
ation
and
eng
ag
em
en
t, w
hic
h w
as d
iscu
ssed
at JN
CC
on 2
2 D
ecem
ber
and
will
co
ntin
ue
as w
e m
ove
to
th
e first p
ha
se o
f
imp
lem
en
tation
in A
pril th
is y
ear.
Ca
re o
f c
us
tom
ers
/en
d-u
se
rs is
th
e H
SC
IC’s
to
p p
rio
rity
Th
e s
urv
ey s
ug
ge
sts
th
at w
e k
now
th
e n
ee
ds o
f o
ur
cu
sto
me
rs b
ut th
at m
eetin
g th
em
is n
ot o
ur
top p
riority
. T
he
revie
w o
f o
ur
app
roa
ch
to
Cu
sto
me
r R
ela
tion
s a
nd
th
e
appoin
tment of S
trate
gic
Account M
anag
ers
has a
lready h
ad
so
me
positiv
e r
esults. T
here
will
be a
co
ntin
uin
g f
ocus o
n
go
od
cu
sto
me
r se
rvic
e –
in
tern
ally
and
exte
rna
lly –
to
ensu
re
that it is e
mb
ed
de
d a
cro
ss th
e o
rga
nis
ation
.
I w
ou
ld r
ec
om
me
nd
th
e H
SC
IC a
s a
pla
ce
to
wo
rk
Th
e o
ve
rall
sco
re h
as im
pro
ve
d to
73 b
ut ra
ng
es fro
m 6
8 in
two a
reas to a
very
solid
89 f
or
Gra
duate
s, In
tern
s a
nd
Tra
inee
s. A
lo
t o
f w
ork
has g
one
in
to m
akin
g s
ure
th
at th
e
exp
erie
nce
of tr
ain
ee
s is p
ositiv
e a
nd
it se
em
s to
be p
ayin
g
off
. A
num
ber
of sta
ff b
en
efits
and
hea
lth
and
we
ll-b
ein
g
initia
tive
s h
ave
be
en d
eve
lope
d o
ve
r th
e la
st ye
ar
and
th
is w
ill
co
ntin
ue
in
to th
e fu
ture
. E
ffe
ctive
ca
ree
r m
ana
ge
me
nt w
ill b
e
a k
ey f
eatu
re o
f th
e tra
nsfo
rme
d o
rga
nis
ation
, su
pp
ort
ed b
y
pro
fessio
na
l deve
lopm
ent.
I h
ave
th
e r
igh
t k
no
wle
dg
e a
nd
sk
ills
to
perf
orm
we
ll in
my r
ole
Th
is is o
ne
of th
e h
igh
est sco
ring
qu
estio
ns o
ve
rall
(79)
but
would
appear
to b
e s
om
ew
hat at odds w
ith a
score
of 67 in
respo
nse
to
th
e s
tate
me
nt “I
am
cle
ar
abo
ut th
e k
now
ledg
e
and
skill
s t
hat I n
ee
d to
pro
gre
ss w
ith
in t
he o
rga
nis
ation
”.
Th
is m
igh
t su
gg
est th
at w
e n
ee
d to
be c
leare
r a
bo
ut th
e
req
uire
me
nts
and
exp
ecta
tion
s o
f m
ore
se
nio
r ro
les.
Th
ere
is a
sig
nific
ant p
iece o
f w
ork
alre
ad
y u
nd
erw
ay t
o
deve
lop c
are
er
ladd
ers
with
in p
rofe
ssio
na
l g
roup
s, b
ase
d
aro
und n
ew
generic job r
ole
s that are
subje
ct to
a r
igoro
us
co
nsis
tency c
heckin
g p
roce
ss. T
his
will
deliv
er
gre
ate
r cla
rity
aro
un
d h
ow
re
spo
nsib
ilitie
s a
nd
th
e r
eq
uis
ite
kn
ow
ledg
e,
skill
s a
nd
exp
erie
nce
ch
an
ge
fo
r d
iffe
ren
t ro
les w
ith
in –
and
acro
ss –
th
e c
are
er
ladd
ers
.
Wh
ilst E
MT
will
se
t th
e p
rioritie
s f
or
action
in
re
spo
nse
to
th
e
su
rve
y, it is c
ritica
l th
at th
e v
ariou
s b
usin
ess u
nits id
en
tify
th
e
exte
nt to
whic
h e
ach o
f th
e issues a
ffects
their p
art
icula
r are
a.
Actio
n p
lans w
ill n
ee
d to
be ta
ilore
d t
o fit lo
cal circu
msta
nce
s
and
, m
ost im
port
antly, n
ee
d to
be m
ana
ge
d e
ffe
ctive
ly to
ensu
re th
at th
ey a
re d
eliv
ere
d.
Re
sp
on
se
by E
xec
uti
ve
Ma
na
ge
me
nt
Te
am
, J
an
ua
ry 2
01
6
Page 68 of 159
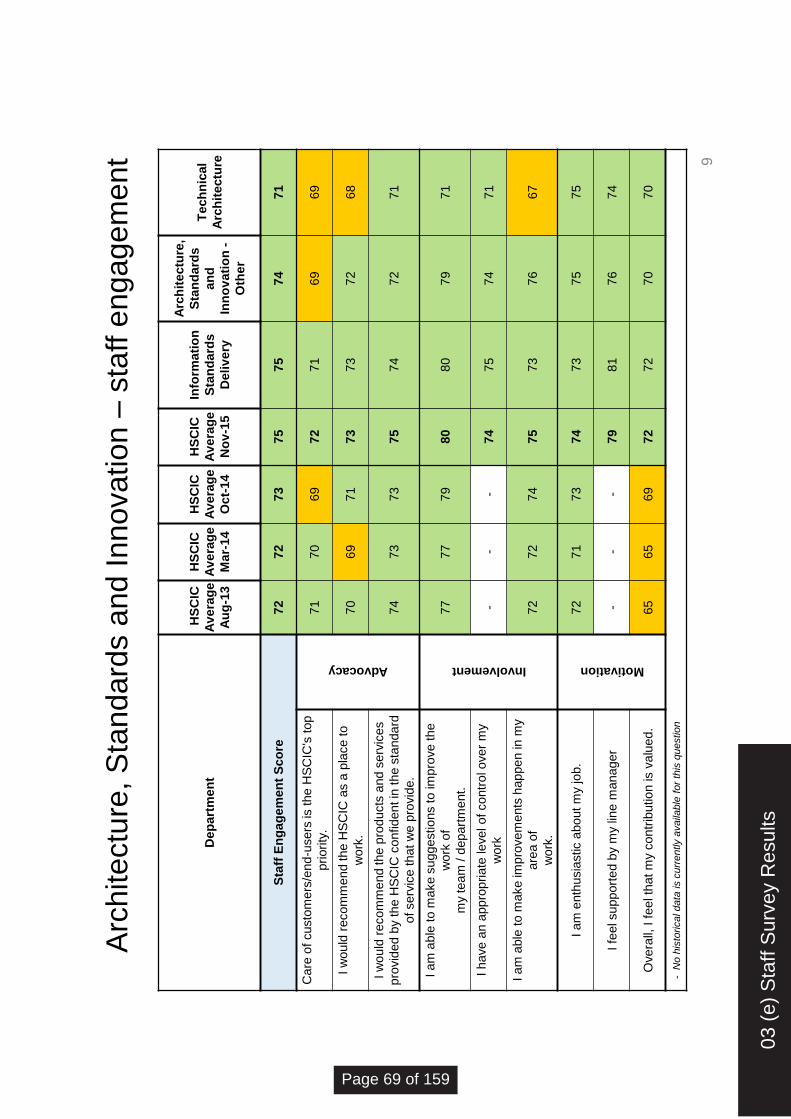
Arc
hite
ctu
re, S
tan
dard
s a
nd I
nn
ova
tio
n –
sta
ff e
ng
ag
em
en
t
De
pa
rtm
en
t
HS
CIC
Av
era
ge
Au
g-1
3
HS
CIC
Av
era
ge
Ma
r-14
HS
CIC
Av
era
ge
Oc
t-14
HS
CIC
Av
era
ge
No
v-1
5
Info
rma
tio
n
Sta
nd
ard
s
De
liv
ery
Arc
hit
ectu
re,
Sta
nd
ard
s
an
d
Inn
ov
ati
on
-
Oth
er
Te
ch
nic
al
Arc
hit
ectu
re
Sta
ff E
ng
ag
em
en
t S
co
re
72
72
73
75
75
74
71
Ca
re o
f cu
sto
me
rs/e
nd
-use
rs is
the
HS
CIC
's t
op
priority
.
Advocacy
71
70
69
72
71
69
69
I w
ould
recom
mend the H
SC
IC a
s a
pla
ce to
wo
rk.
70
69
71
73
73
72
68
I w
ould
re
co
mm
end
th
e p
rod
ucts
and
se
rvic
es
pro
vid
ed
by t
he H
SC
IC c
onfid
en
t in
th
e s
tand
ard
of se
rvic
e th
at
we
pro
vid
e.
74
73
73
75
74
72
71
I a
m a
ble
to
ma
ke
su
gg
estio
ns to
im
pro
ve
th
e
wo
rk o
f
my t
ea
m / d
ep
art
me
nt.
Involvement
77
77
79
80
80
79
71
I h
ave
an
app
rop
ria
te le
ve
l o
f co
ntr
ol o
ve
r m
y
wo
rk
- -
- 74
75
74
71
I a
m a
ble
to
ma
ke
imp
rove
me
nts
hap
pe
n in
my
are
a o
f
wo
rk.
72
72
74
75
73
76
67
I a
m e
nth
usia
stic a
bo
ut m
y jo
b.
Motivation
72
71
73
74
73
75
75
I fe
el su
pp
ort
ed b
y m
y lin
e m
ana
ge
r -
- -
79
81
76
74
Ove
rall,
I f
eel th
at
my c
ontr
ibutio
n is v
alu
ed
. 65
65
69
72
72
70
70
- N
o h
isto
rical data
is c
urr
ently a
vaila
ble
for
this
questio
n
9
03 (
e) S
taff
Sur
vey
Res
ults
Page 69 of 159

Dep
art
me
nt
HS
CIC
Av
era
ge
Au
g-1
3
HS
CIC
Av
era
ge
Ma
r-14
HS
CIC
Av
era
ge
Oc
t-14
HS
CIC
Av
era
ge
No
v-1
5
Info
rma
tio
n
Sta
nd
ard
s
De
liv
ery
Arc
hit
ectu
re,
Sta
nd
ard
s a
nd
Inn
ov
ati
on
- O
the
r
Te
ch
nic
al
Arc
hit
ectu
re
Org
an
isa
tio
n H
ea
lth
Sc
ore
66
67
69
71
72
70
68
Ge
ne
rally
, I
kn
ow
wh
o t
he c
usto
me
rs o
f
the H
SC
IC a
re.
73
73
74
76
76
78
70
I h
ave
a c
lear
und
ers
tand
ing o
f th
e
nee
ds o
f m
y c
usto
me
rs.
77
76
78
78
77
78
69
Th
e H
SC
IC h
as c
lear
and
re
leva
nt
org
an
isa
tio
na
l va
lues.
- -
67
71
70
71
70
Th
e H
SC
IC h
as a
cle
arly a
rtic
ula
ted
str
ate
gy
for
its f
utu
re.
55
59
58
67
69
71
65
I ca
n s
ee h
ow
my w
ork
obje
ctive
s
co
ntr
ibute
to
th
e H
SC
IC a
ch
ievin
g its
sta
ted p
urp
ose
.
64
65
65
69
70
72
69
I h
ave
th
e r
ight
kn
ow
ledg
e a
nd
skill
s t
o
perf
orm
we
ll in
my r
ole
. 79
78
78
79
81
79
79
I a
m c
lear
abo
ut
the
kn
ow
ledg
e a
nd
skill
s th
at
I n
ee
d t
o p
rog
ress w
ith
in t
he
org
an
isa
tio
n.
65
64
66
67
67
68
67
**I h
ave
th
e o
pp
ort
unity
to b
e e
ng
ag
ed
and
invo
lve
d in
org
an
isa
tio
na
l ch
an
ge
initia
tive
s.
60
63
67
68
66
64
71
I h
ave
ch
alle
ng
ing w
ork
obje
ctive
s.
72
73
74
76
74
73
76
My
wo
rk a
rea
diffe
ren
tia
tes b
etw
een
goo
d a
nd
ave
rag
e p
erf
orm
ance
. 61
60
61
63
64
59
56
My
wo
rk a
rea
mo
nito
rs its
perf
orm
ance
usin
g K
PIs
or
me
tric
s.
60
64
65
65
72
57
59
My
wo
rk a
rea
pe
rfo
rms w
ell
aga
inst its
KP
Is/t
arg
ets
. 60
64
72
73
75
71
68
**P
revio
us y
ears
this
was I
have t
he o
pport
unity t
o e
ngage in
org
anis
atio
nal change in
itia
tives.
Arc
hite
ctu
re, S
tan
dard
s a
nd I
nn
ova
tio
n –
org
an
isa
tio
na
l h
ealth
10
Page 70 of 159

Custo
me
r R
ela
tio
ns –
sta
ff e
ng
ag
em
en
t
De
pa
rtm
en
t
HS
CIC
Av
era
ge
Au
g-1
3
HS
CIC
Av
era
ge
Ma
r-14
HS
CIC
Av
era
ge
Oc
t-14
HS
CIC
Av
era
ge
No
v-1
5
Co
mm
un
icati
on
s
Co
nta
ct
cen
tre
Sta
ff E
ng
ag
em
en
t S
co
re
72
72
73
75
71
77
Ca
re o
f cu
sto
me
rs/e
nd
-use
rs is
the
HS
CIC
's top p
riority
.
Advocacy
71
70
69
72
61
69
I w
ould
re
co
mm
end
th
e H
SC
IC a
s a
pla
ce
to w
ork
. 70
69
71
73
63
78
I w
ould
re
co
mm
end
th
e p
rod
ucts
and
se
rvic
es p
rovid
ed
by
the H
SC
IC c
onfid
en
t
in th
e s
tand
ard
of se
rvic
e t
hat w
e p
rovid
e.
74
73
73
75
70
67
I a
m a
ble
to
ma
ke
su
gg
estio
ns to
im
pro
ve
the w
ork
of
my t
ea
m / d
ep
art
me
nt.
Involvement
77
77
79
80
82
82
I h
ave
an
app
rop
ria
te le
ve
l o
f co
ntr
ol o
ve
r
my w
ork
-
- -
74
68
80
I a
m a
ble
to
ma
ke
imp
rove
me
nts
hap
pe
n
in m
y a
rea
of
wo
rk.
72
72
74
75
73
80
I a
m e
nth
usia
stic a
bo
ut m
y jo
b.
Motivation
72
71
73
74
71
81
I fe
el su
pp
ort
ed b
y m
y lin
e m
ana
ge
r -
- -
79
80
79
Ove
rall,
I f
eel th
at
my c
ontr
ibutio
n is
va
lued
. 65
65
69
72
68
81
- N
o h
isto
rical data
is c
urr
ently a
vaila
ble
for
this
questio
n
11
03 (
e) S
taff
Sur
vey
Res
ults
Page 71 of 159

Custo
me
r R
ela
tio
ns –
org
an
isa
tio
na
l h
ealth
De
pa
rtm
en
t
HS
CIC
Av
era
ge
Au
g-1
3
HS
CIC
Av
era
ge
Ma
r-14
HS
CIC
Av
era
ge
Oc
t-14
HS
CIC
Av
era
ge
No
v-1
5
Co
mm
un
icati
on
s
Co
nta
ct
cen
tre
Org
an
isa
tio
n H
ea
lth
Sc
ore
66
67
69
71
72
77
Ge
ne
rally
, I
kn
ow
wh
o t
he c
usto
me
rs o
f th
e
HS
CIC
are
. 73
73
74
76
82
86
I h
ave
a c
lear
und
ers
tand
ing o
f th
e n
ee
ds o
f
my c
usto
me
rs.
77
76
78
78
80
85
Th
e H
SC
IC h
as c
lear
and
re
leva
nt
org
an
isa
tio
na
l va
lues.
- -
67
71
67
80
Th
e H
SC
IC h
as a
cle
arly a
rtic
ula
ted
str
ate
gy
for
its f
utu
re.
55
59
58
67
72
72
I ca
n s
ee h
ow
my w
ork
obje
ctive
s c
ontr
ibute
to th
e H
SC
IC a
ch
ievin
g its
sta
ted p
urp
ose
. 64
65
65
69
76
79
I h
ave
th
e r
ight
kn
ow
ledg
e a
nd
skill
s t
o
perf
orm
we
ll in
my r
ole
. 79
78
78
79
82
80
I am
cle
ar
about th
e k
now
ledge a
nd s
kill
s
that I
ne
ed
to
pro
gre
ss w
ith
in t
he
org
an
isa
tio
n.
65
64
66
67
69
73
**I h
ave
th
e o
pp
ort
unity
to b
e e
ng
ag
ed
and
invo
lve
d in
org
an
isa
tio
na
l ch
an
ge
in
itia
tive
s.
60
63
67
68
68
67
I h
ave
ch
alle
ng
ing w
ork
obje
ctive
s.
72
73
74
76
82
78
My
wo
rk a
rea
diffe
ren
tia
tes b
etw
een
go
od
and
ave
rag
e p
erf
orm
ance
. 61
60
61
63
56
65
My
wo
rk a
rea
mo
nito
rs its
perf
orm
ance
usin
g K
PIs
or
metr
ics.
60
64
65
65
59
76
My
wo
rk a
rea
pe
rfo
rms w
ell
aga
inst its
KP
Is/t
arg
ets
. 60
64
72
73
68
81
- N
o h
isto
rical data
is c
urr
ently a
vaila
ble
for
this
questio
n
**P
revio
us y
ears
this
was I
have t
he o
pport
unity t
o e
ngage in
org
anis
atio
nal change in
itia
tives.
12
Page 72 of 159

Fin
an
ce a
nd C
orp
ora
te S
erv
ice
s –
sta
ff e
ng
ag
em
en
t
De
pa
rtm
en
t
HS
CIC
Av
era
ge
Au
g-1
3
HS
CIC
Av
era
ge
Ma
r-14
HS
CIC
Av
era
ge
Oc
t-14
HS
CIC
Av
era
ge
No
v-1
5
Po
rtfo
lio
B
us
ine
ss
Se
rvic
es
Fin
an
ce
Pro
cu
rem
en
t
& C
on
tra
cts
Sta
ff E
ng
ag
em
en
t S
co
re
72
72
73
75
75
74
75
69
Ca
re o
f cu
sto
me
rs/e
nd
-use
rs is
the
HS
CIC
's t
op
priority
.
Advocacy
71
70
69
72
66
75
73
70
I w
ould
re
co
mm
end
th
e H
SC
IC a
s a
pla
ce to w
ork
. 70
69
71
73
71
72
71
60
I w
ould
re
co
mm
end
th
e p
rod
ucts
and
se
rvic
es p
rovid
ed
by
the H
SC
IC
co
nfid
en
t in
th
e s
tand
ard
of se
rvic
e
that w
e p
rovid
e.
74
73
73
75
72
71
74
71
I a
m a
ble
to
ma
ke
su
gg
estio
ns to
imp
rove
th
e w
ork
of
my t
ea
m / d
ep
art
me
nt.
Involvement
77
77
79
80
82
72
78
75
I h
ave
an
app
rop
ria
te le
ve
l o
f co
ntr
ol
ove
r m
y w
ork
-
- -
74
74
69
74
70
I a
m a
ble
to
ma
ke
imp
rove
me
nts
hap
pe
n in
my a
rea
of
wo
rk.
72
72
74
75
80
71
75
70
I a
m e
nth
usia
stic a
bo
ut m
y jo
b.
Motivation
72
71
73
74
72
76
76
69
I fe
el su
pp
ort
ed b
y m
y lin
e m
ana
ge
r -
- -
79
85
81
78
72
Overa
ll, I f
eel th
at m
y contr
ibution is
va
lued
. 65
65
69
72
70
75
74
64
- N
o h
isto
rical data
is c
urr
ently a
vaila
ble
for
this
questio
n
* N
ot
enough d
ata
to d
ispla
y
**P
revio
us y
ears
this
was I
have t
he o
pport
unity t
o e
ngage in
org
anis
atio
nal change in
itia
tives.
13
03 (
e) S
taff
Sur
vey
Res
ults
Page 73 of 159

Fin
an
ce a
nd C
orp
ora
te S
erv
ice
s –
org
an
isa
tio
na
l h
ealth
De
pa
rtm
en
t
HS
CIC
Av
era
ge
Au
g-1
3
HS
CIC
Av
era
ge
Ma
r-14
HS
CIC
Av
era
ge
Oc
t-14
HS
CIC
Av
era
ge
No
v-1
5
Po
rtfo
lio
B
us
ine
ss
Se
rvic
es
Fin
an
ce
P
rocu
rem
en
t
& C
on
tracts
Org
an
isati
on
Healt
h S
co
re
66
67
69
71
70
72
73
67
Ge
ne
rally
, I
kn
ow
wh
o t
he c
usto
me
rs o
f th
e
HS
CIC
are
. 73
73
74
76
71
73
79
68
I h
ave
a c
lear
und
ers
tand
ing o
f th
e n
ee
ds o
f
my c
usto
me
rs.
77
76
78
78
76
79
80
71
Th
e H
SC
IC h
as c
lear
and
re
leva
nt
org
an
isa
tio
na
l va
lues.
- -
67
71
71
79
70
64
Th
e H
SC
IC h
as a
cle
arly a
rtic
ula
ted
str
ate
gy
for
its f
utu
re.
55
59
58
67
64
78
71
67
I ca
n s
ee h
ow
my w
ork
obje
ctive
s c
ontr
ibute
to th
e H
SC
IC a
ch
ievin
g its
sta
ted p
urp
ose
. 64
65
65
69
65
75
75
68
I h
ave
th
e r
ight
kn
ow
ledg
e a
nd
skill
s t
o
perf
orm
we
ll in
my r
ole
. 79
78
78
79
76
78
81
74
I a
m c
lear
abo
ut
the
kn
ow
ledg
e a
nd
skill
s
that I
ne
ed
to
pro
gre
ss w
ith
in t
he
org
an
isa
tio
n.
65
64
66
67
65
62
70
66
**I h
ave
th
e o
pp
ort
unity
to b
e e
ng
ag
ed
and
invo
lve
d in
org
an
isa
tio
na
l ch
an
ge
in
itia
tive
s.
60
63
67
68
75
55
72
65
I h
ave
ch
alle
ng
ing w
ork
obje
ctive
s.
72
73
74
76
70
73
79
75
My
wo
rk a
rea
diffe
ren
tia
tes b
etw
een
go
od
and
ave
rag
e p
erf
orm
ance
. 61
60
61
63
64
70
60
59
My
wo
rk a
rea
mo
nito
rs its
perf
orm
ance
usin
g K
PIs
or
me
tric
s.
60
64
65
65
68
70
65
63
My
wo
rk a
rea
pe
rfo
rms w
ell
aga
inst its
KP
Is/t
arg
ets
. 60
64
72
73
72
72
70
71
- N
o h
isto
rical data
is c
urr
ently a
vaila
ble
for
this
questio
n
**P
revio
us y
ears
this
was I
have t
he o
pport
unity t
o e
ngage in
org
anis
atio
nal change in
itia
tives.
14
Page 74 of 159
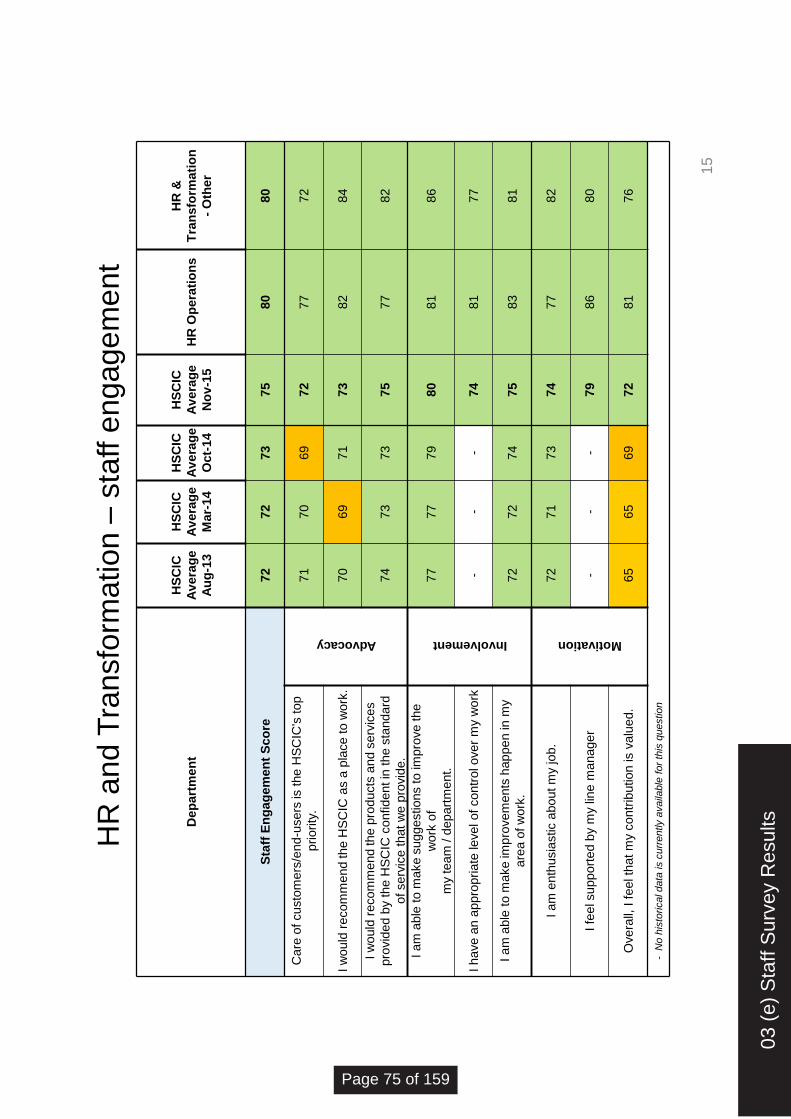
HR
an
d T
ran
sfo
rma
tion
– s
taff e
ng
ag
em
en
t
De
pa
rtm
en
t
HS
CIC
Av
era
ge
Au
g-1
3
HS
CIC
Av
era
ge
Mar-
14
HS
CIC
Av
era
ge
Oct-
14
HS
CIC
Av
era
ge
No
v-1
5
HR
Op
era
tio
ns
HR
&
Tra
ns
form
ati
on
- O
the
r
Sta
ff E
ng
ag
em
en
t S
co
re
72
72
73
75
80
80
Ca
re o
f cu
sto
me
rs/e
nd
-use
rs is
the
HS
CIC
's t
op
priority
.
Advocacy
71
70
69
72
77
72
I w
ould
re
co
mm
end
th
e H
SC
IC a
s a
pla
ce
to
wo
rk.
70
69
71
73
82
84
I w
ould
re
co
mm
end
th
e p
rod
ucts
and
se
rvic
es
pro
vid
ed
by t
he H
SC
IC c
onfid
en
t in
th
e s
tand
ard
of se
rvic
e th
at
we
pro
vid
e.
74
73
73
75
77
82
I am
able
to m
ake s
uggestions to im
pro
ve the
wo
rk o
f
my t
ea
m / d
ep
art
me
nt.
Involvement
77
77
79
80
81
86
I h
ave
an
app
rop
ria
te le
ve
l o
f co
ntr
ol o
ve
r m
y w
ork
-
- -
74
81
77
I a
m a
ble
to
ma
ke
imp
rove
me
nts
hap
pe
n in
my
are
a o
f w
ork
. 72
72
74
75
83
81
I a
m e
nth
usia
stic a
bo
ut m
y jo
b.
Motivation
72
71
73
74
77
82
I fe
el su
pp
ort
ed b
y m
y lin
e m
ana
ge
r -
- -
79
86
80
Ove
rall,
I f
eel th
at
my c
ontr
ibutio
n is v
alu
ed
. 65
65
69
72
81
76
- N
o h
isto
rical data
is c
urr
ently a
vaila
ble
for
this
questio
n
15
03 (
e) S
taff
Sur
vey
Res
ults
Page 75 of 159

Dep
art
men
t
HS
CIC
Avera
ge
Au
g-1
3
HS
CIC
Avera
ge
Mar-
14
HS
CIC
Avera
ge
Oct-
14
HS
CIC
Avera
ge
No
v-1
5
HR
Op
era
tio
ns
HR
&
Tra
nsfo
rmati
on
-
Oth
er
Org
an
isati
on
Healt
h S
co
re
66
6
7
69
7
1
77
7
9
Genera
lly, I know
who the c
usto
mers
of th
e
HS
CIC
are
. 7
3
73
7
4
76
7
2
81
I have a
cle
ar
unde
rsta
ndin
g o
f th
e n
eed
s o
f
my c
usto
mers
. 7
7
76
7
8
78
7
5
89
Th
e H
SC
IC h
as c
lear
and r
ele
vant
org
anis
ational valu
es.
- -
67
7
1
79
8
3
Th
e H
SC
IC h
as a
cle
arl
y a
rtic
ula
ted s
trate
gy
for
its fu
ture
. 5
5
59
5
8
67
7
5
71
I can s
ee h
ow
my w
ork
obje
ctives c
ontr
ibute
to the H
SC
IC a
chie
vin
g its
sta
ted p
urp
ose.
64
6
5
65
6
9
76
8
2
I have the r
ight know
ledge
and s
kill
s to
perf
orm
well
in m
y r
ole
. 7
9
78
7
8
79
8
1
86
I am
cle
ar
abou
t th
e k
now
ledge
and s
kill
s
that I need
to p
rogre
ss w
ithin
the
org
anis
ation.
65
6
4
66
6
7
76
6
9
**I have the o
ppo
rtunity to b
e e
nga
ged a
nd
involv
ed in o
rganis
ational chang
e initia
tives.
60
6
3
67
6
8
80
8
6
I have c
halle
ngin
g w
ork
obje
ctives.
72
7
3
74
7
6
78
7
6
My w
ork
are
a d
iffe
rentiate
s b
etw
een g
ood
and a
vera
ge p
erf
orm
ance.
61
6
0
61
6
3
76
6
7
My w
ork
are
a m
onitors
its
perf
orm
ance
usin
g K
PIs
or
metr
ics.
60
6
4
65
6
5
81
8
3
My w
ork
are
a p
erf
orm
s w
ell
again
st its
KP
Is/targ
ets
. 6
0
64
7
2
73
7
2
79
- N
o h
isto
rical data
is c
urr
ently a
vaila
ble
for
this
questio
n
**P
revio
us y
ears
this
was I
have t
he o
pport
unity t
o e
ngage in
org
anis
atio
nal change in
itia
tives.
HR
an
d T
ran
sfo
rma
tion
– o
rga
nis
atio
na
l h
ealth
16
Page 76 of 159

Pro
vid
er
Su
pp
ort
an
d I
nte
gra
tio
n –
sta
ff e
ng
ag
em
en
t
De
pa
rtm
en
t
HS
CIC
Av
era
ge
Au
g-1
3
HS
CIC
Av
era
ge
Ma
r-14
HS
CIC
Av
era
ge
Oc
t-14
HS
CIC
Av
era
ge
No
v-1
5
CS
C P
S
BT
PS
/So
uth
Lo
cal C
lin
ica
l
Sys
tem
s
Pro
vid
er
Su
pp
ort
Oth
er
Sta
ff E
ng
ag
em
en
t S
co
re
72
72
73
75
75
75
73
Ca
re o
f cu
sto
me
rs/e
nd
-use
rs is
the
HS
CIC
's t
op
priority
.
Advocacy
71
70
69
72
71
70
64
I w
ould
re
co
mm
end
th
e H
SC
IC a
s a
pla
ce
to
wo
rk.
70
69
71
73
70
71
67
I w
ould
re
co
mm
end
th
e p
rod
ucts
and
se
rvic
es p
rovid
ed
by
the H
SC
IC c
onfid
en
t
in th
e s
tand
ard
of se
rvic
e t
hat w
e p
rovid
e.
74
73
73
75
76
72
74
I a
m a
ble
to
ma
ke
su
gg
estio
ns to
im
pro
ve
the w
ork
of
my t
ea
m / d
ep
art
me
nt.
Involvement
77
77
79
80
79
81
84
I h
ave
an
app
rop
ria
te le
ve
l o
f co
ntr
ol o
ve
r
my w
ork
-
- -
74
76
77
76
I a
m a
ble
to
ma
ke
imp
rove
me
nts
hap
pe
n
in m
y a
rea
of
wo
rk.
72
72
74
75
75
77
77
I a
m e
nth
usia
stic a
bo
ut m
y jo
b.
Motivation
72
71
73
74
77
75
72
I fe
el su
pp
ort
ed b
y m
y lin
e m
ana
ge
r -
- -
79
82
81
74
Ove
rall,
I f
eel th
at
my c
ontr
ibutio
n is
va
lued
. 65
65
69
72
73
72
70
- N
o h
isto
rical data
is c
urr
ently a
vaila
ble
for
this
questio
n
17
03 (
e) S
taff
Sur
vey
Res
ults
Page 77 of 159
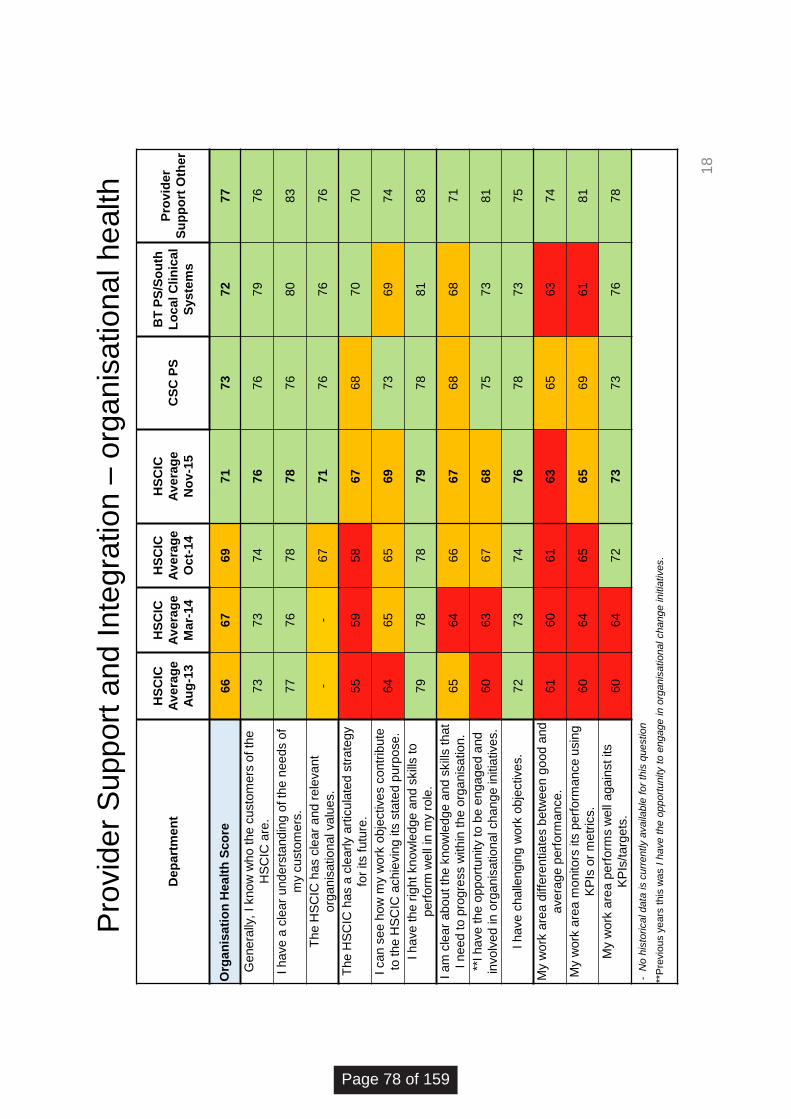
Pro
vid
er
Su
pp
ort
an
d I
nte
gra
tio
n –
org
an
isa
tio
na
l h
ealth
De
pa
rtm
en
t
HS
CIC
Av
era
ge
Au
g-1
3
HS
CIC
Av
era
ge
Ma
r-14
HS
CIC
Av
era
ge
Oc
t-14
HS
CIC
Av
era
ge
No
v-1
5
CS
C P
S
BT
PS
/So
uth
Lo
cal C
lin
ica
l
Sys
tem
s
Pro
vid
er
Su
pp
ort
Oth
er
Org
an
isa
tio
n H
ea
lth
Sc
ore
66
67
69
71
73
72
77
Genera
lly,
I know
who t
he c
usto
mers
of th
e
HS
CIC
are
. 73
73
74
76
76
79
76
I h
ave
a c
lear
und
ers
tand
ing o
f th
e n
ee
ds o
f
my c
usto
me
rs.
77
76
78
78
76
80
83
Th
e H
SC
IC h
as c
lear
and
re
leva
nt
org
an
isa
tio
na
l va
lues.
- -
67
71
76
76
76
Th
e H
SC
IC h
as a
cle
arly a
rtic
ula
ted
str
ate
gy
for
its f
utu
re.
55
59
58
67
68
70
70
I ca
n s
ee h
ow
my w
ork
obje
ctive
s c
ontr
ibute
to th
e H
SC
IC a
ch
ievin
g its
sta
ted p
urp
ose
. 64
65
65
69
73
69
74
I h
ave
th
e r
ight
kn
ow
ledg
e a
nd
skill
s t
o
perf
orm
we
ll in
my r
ole
. 79
78
78
79
78
81
83
I a
m c
lear
abo
ut
the
kn
ow
ledg
e a
nd
skill
s t
hat
I n
ee
d to
pro
gre
ss w
ith
in t
he o
rga
nis
atio
n.
65
64
66
67
68
68
71
**I h
ave
th
e o
pp
ort
unity
to b
e e
ng
ag
ed
and
involv
ed in o
rganis
ational change initia
tives.
60
63
67
68
75
73
81
I h
ave
ch
alle
ng
ing w
ork
obje
ctive
s.
72
73
74
76
78
73
75
My
wo
rk a
rea
diffe
ren
tia
tes b
etw
een
go
od
and
ave
rag
e p
erf
orm
ance
. 61
60
61
63
65
63
74
My
wo
rk a
rea
mo
nito
rs its
perf
orm
ance
usin
g
KP
Is o
r m
etr
ics.
60
64
65
65
69
61
81
My
wo
rk a
rea
pe
rfo
rms w
ell
aga
inst its
KP
Is/t
arg
ets
. 60
64
72
73
73
76
78
- N
o h
isto
rical data
is c
urr
ently a
vaila
ble
for
this
questio
n
**P
revio
us y
ears
this
was I
have t
he o
pport
unity t
o e
ngage in
org
anis
atio
nal change in
itia
tives.
18
Page 78 of 159
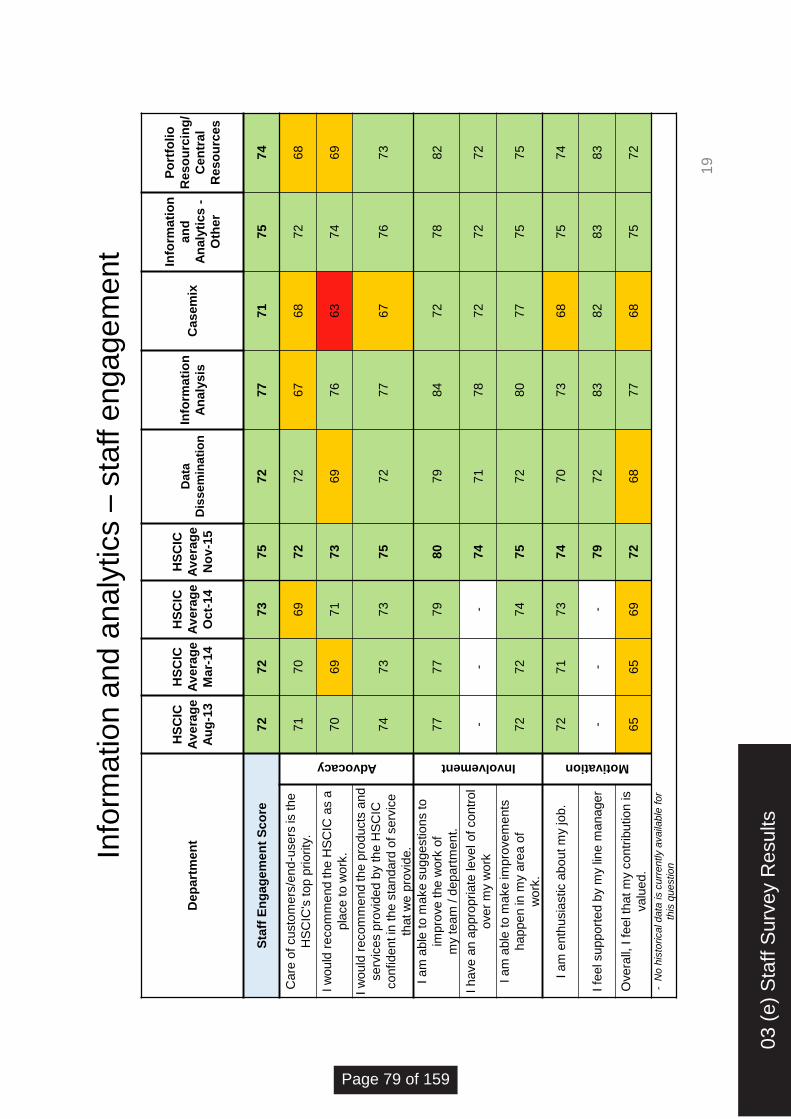
Info
rma
tio
n a
nd a
naly
tics –
sta
ff e
ng
ag
em
en
t
De
pa
rtm
en
t
HS
CIC
Av
era
ge
Au
g-1
3
HS
CIC
Av
era
ge
Ma
r-14
HS
CIC
Av
era
ge
Oc
t-14
HS
CIC
Av
era
ge
No
v-1
5
Data
Dis
sem
inati
on
Info
rma
tio
n
An
aly
sis
C
as
em
ix
Info
rmati
on
an
d
An
aly
tic
s -
Oth
er
Po
rtfo
lio
Re
so
urc
ing
/
Ce
ntr
al
Re
so
urc
es
Sta
ff E
ng
ag
em
en
t S
co
re
72
72
73
75
72
77
71
75
74
Ca
re o
f cu
sto
me
rs/e
nd
-use
rs is
the
HS
CIC
's t
op
priority
.
Advocacy
71
70
69
72
72
67
68
72
68
I w
ould
re
co
mm
end
th
e H
SC
IC a
s a
pla
ce
to
wo
rk.
70
69
71
73
69
76
63
74
69
I w
ould
re
co
mm
end
th
e p
rod
ucts
and
se
rvic
es p
rovid
ed
by
the H
SC
IC
co
nfid
en
t in
th
e s
tand
ard
of se
rvic
e
that w
e p
rovid
e.
74
73
73
75
72
77
67
76
73
I a
m a
ble
to
ma
ke
su
gg
estio
ns to
impro
ve the w
ork
of
my t
ea
m / d
ep
art
me
nt.
Involvement
77
77
79
80
79
84
72
78
82
I h
ave
an
app
rop
ria
te le
ve
l o
f co
ntr
ol
ove
r m
y w
ork
-
- -
74
71
78
72
72
72
I a
m a
ble
to
ma
ke
imp
rove
me
nts
hap
pe
n in
my a
rea
of
wo
rk.
72
72
74
75
72
80
77
75
75
I a
m e
nth
usia
stic a
bo
ut m
y jo
b.
Motivation
72
71
73
74
70
73
68
75
74
I fe
el su
pp
ort
ed b
y m
y lin
e m
ana
ge
r -
- -
79
72
83
82
83
83
Overa
ll, I f
eel th
at m
y contr
ibution is
va
lued
. 65
65
69
72
68
77
68
75
72
- N
o h
isto
rical data
is c
urr
ently a
vaila
ble
for
this
questio
n
19
03 (
e) S
taff
Sur
vey
Res
ults
Page 79 of 159

Info
rma
tio
n a
nd a
naly
tics –
org
an
isa
tio
na
l h
ealth
De
pa
rtm
en
t
HS
CIC
Av
era
ge
Au
g-1
3
HS
CIC
Av
era
ge
Ma
r-14
HS
CIC
Av
era
ge
Oc
t-14
HS
CIC
Av
era
ge
No
v-1
5
Data
Dis
se
min
ati
on
Info
rmati
on
An
aly
sis
C
as
em
ix
Info
rma
tio
n
an
d
An
aly
tic
s-
Oth
er
Po
rtfo
lio
Reso
urc
ing
/
Ce
ntr
al
Re
so
urc
es
Org
an
isa
tio
n H
ea
lth
Sc
ore
66
67
69
71
69
69
67
71
71
Ge
ne
rally
, I
kn
ow
wh
o t
he c
usto
me
rs
of th
e H
SC
IC a
re.
73
73
74
76
74
75
69
73
78
I h
ave
a c
lear
und
ers
tand
ing o
f th
e
nee
ds o
f m
y c
usto
me
rs.
77
76
78
78
79
76
79
75
75
Th
e H
SC
IC h
as c
lear
and
re
leva
nt
org
an
isa
tio
na
l va
lues.
- -
67
71
69
66
65
73
75
Th
e H
SC
IC h
as a
cle
arly a
rtic
ula
ted
str
ate
gy
for
its f
utu
re.
55
59
58
67
67
61
58
65
67
I ca
n s
ee h
ow
my w
ork
obje
ctive
s
co
ntr
ibute
to
th
e H
SC
IC a
ch
ievin
g its
sta
ted p
urp
ose
.
64
65
65
69
67
66
57
75
69
I h
ave
th
e r
ight
kn
ow
ledg
e a
nd
skill
s
to p
erf
orm
we
ll in
my r
ole
. 79
78
78
79
77
79
79
70
79
I a
m c
lear
abo
ut
the
kn
ow
ledg
e a
nd
skill
s th
at
I n
ee
d t
o p
rog
ress w
ith
in
the o
rga
nis
atio
n.
65
64
66
67
66
66
62
68
76
**I h
ave
th
e o
pp
ort
unity
to b
e
engaged a
nd involv
ed in
org
an
isa
tio
na
l ch
an
ge
initia
tive
s.
60
63
67
68
62
68
59
71
75
I h
ave
ch
alle
ng
ing w
ork
obje
ctive
s.
72
73
74
76
68
76
73
78
75
My
wo
rk a
rea
diffe
ren
tia
tes b
etw
een
goo
d a
nd
ave
rag
e p
erf
orm
ance
. 61
60
61
63
60
60
68
64
60
My
wo
rk a
rea
mo
nito
rs its
perf
orm
ance
usin
g K
PIs
or
me
tric
s.
60
64
65
65
69
60
63
62
60
My
wo
rk a
rea
pe
rfo
rms w
ell
aga
inst
its K
PIs
/targ
ets
. 60
64
72
73
71
74
78
73
69
- N
o h
isto
rical data
is c
urr
ently a
vaila
ble
for
this
questio
n
**P
revio
us y
ears
this
was I
have t
he o
pport
unity t
o e
ngage in
org
anis
atio
nal change in
itia
tives.
20
Page 80 of 159

Op
era
tio
ns a
nd
Assu
ran
ce
Se
rvic
es –
sta
ff e
ng
ag
em
en
t
De
pa
rtm
en
t
HSCIC Average
Aug-13
HSCIC Average
Mar-14
HSCIC Average
Oct-14
HSCIC Average
Nov-15
IG and
information
Standards
IT infrastructure
Services
Service
Management
(National)
Solution
Assurance
Spine Services
Systems and
Service Delivery
Operations and
Assurance
Services- Other
Sta
ff E
ng
ag
em
en
t S
co
re
72
72
73
75
71
78
77
77
75
76
81
Ca
re o
f cu
sto
me
rs/e
nd
-use
rs is
the H
SC
IC's
to
p p
rio
rity
.
Advocacy
71
70
69
72
68
77
73
79
80
77
69
I w
ould
re
co
mm
end
th
e H
SC
IC
as a
pla
ce
to
wo
rk.
70
69
71
73
71
75
77
75
73
76
82
I w
ould
re
co
mm
end
th
e p
rod
ucts
and
se
rvic
es p
rovid
ed
by t
he
HS
CIC
co
nfid
en
t in
th
e s
tand
ard
of se
rvic
e th
at
we
pro
vid
e.
74
73
73
75
71
76
75
81
80
79
80
I a
m a
ble
to
ma
ke
su
gg
estio
ns to
imp
rove
th
e w
ork
of
my
team
/ d
epart
ment.
Involvement
77
77
79
80
76
80
83
82
77
82
85
I h
ave
an
app
rop
ria
te le
ve
l o
f
co
ntr
ol o
ve
r m
y w
ork
-
- -
74
68
79
77
75
74
75
80
I am
able
to m
ake im
pro
vem
ents
hap
pe
n in
my a
rea
of
wo
rk.
72
72
74
75
70
77
78
77
76
75
87
I a
m e
nth
usia
stic a
bo
ut m
y jo
b.
Motivation
72
71
73
74
71
77
77
76
74
74
76
I fe
el su
pp
ort
ed b
y m
y lin
e
ma
na
ge
r -
- -
79
77
83
82
78
75
78
89
Ove
rall,
I f
eel th
at
my
co
ntr
ibutio
n is v
alu
ed
. 65
65
69
72
70
76
74
74
68
72
76
- N
o h
isto
rical data
is c
urr
ently a
vaila
ble
for
this
questio
n
21
03 (
e) S
taff
Sur
vey
Res
ults
Page 81 of 159

Op
era
tio
ns a
nd
Assu
ran
ce
Se
rvic
es –
org
an
isa
tio
na
l h
ea
lth
Dep
art
men
t
HSCIC Average
Aug-13
HSCIC Average
Mar-14
HSCIC Average
Oct-14
HSCIC Average
Nov-15
IG and
Information
Standards
IT infrastructure
Services
Service
Management
(National)
Solution
Assurance
Spine Services
Systems and
Service Delivery
Operations and
Assurance
Services- Other
Org
an
isa
tio
n H
ea
lth
Sc
ore
6
6
67
6
9
71
7
0
71
7
3
72
7
1
70
*
Ge
ne
rally
, I
kn
ow
wh
o t
he
cu
sto
me
rs o
f
the
HS
CIC
are
. 7
3
73
7
4
76
7
6
71
8
2
82
8
0
74
7
8
I h
ave
a c
lea
r u
nd
ers
tan
din
g o
f th
e n
ee
ds
of m
y c
usto
me
rs.
77
7
6
78
7
8
75
7
4
76
8
1
75
8
0
82
Th
e H
SC
IC h
as c
lea
r a
nd
re
leva
nt
org
an
isa
tio
na
l va
lue
s.
- -
67
7
1
73
7
1
72
7
1
73
7
0
73
Th
e H
SC
IC h
as a
cle
arl
y a
rtic
ula
ted
str
ate
gy fo
r its fu
ture
. 5
5
59
5
8
67
6
6
65
6
9
69
6
9
67
6
0
I ca
n s
ee
ho
w m
y w
ork
ob
jective
s
co
ntr
ibu
te to
th
e H
SC
IC a
ch
ievin
g its
sta
ted
pu
rpo
se
.
64
6
5
65
6
9
69
6
4
72
6
9
69
6
7
80
I h
ave
th
e r
igh
t kn
ow
led
ge
an
d s
kill
s to
pe
rfo
rm w
ell
in m
y r
ole
. 7
9
78
7
8
79
7
5
76
7
7
77
7
7
81
8
0
I a
m c
lea
r a
bo
ut th
e k
no
wle
dg
e a
nd
skill
s
tha
t I n
ee
d to
pro
gre
ss w
ith
in th
e
org
an
isa
tio
n.
65
6
4
66
6
7
66
6
9
69
6
6
66
6
3
71
**I h
ave
th
e o
pp
ort
un
ity to
be
en
ga
ge
d
an
d in
vo
lve
d in
org
an
isa
tio
na
l ch
an
ge
initia
tive
s.
60
6
3
67
6
8
64
6
7
72
6
7
68
6
6
78
I h
ave
ch
alle
ng
ing
wo
rk o
bje
ctive
s.
72
7
3
74
7
6
76
8
0
77
7
6
76
7
7
80
My w
ork
are
a d
iffe
ren
tia
tes b
etw
ee
n g
oo
d
an
d a
ve
rag
e p
erf
orm
an
ce
. 6
1
60
6
1
63
6
3
65
6
6
63
6
4
60
7
1
My w
ork
are
a m
on
ito
rs it
s p
erf
orm
an
ce
usin
g K
PIs
or
me
tric
s.
60
6
4
65
6
5
63
7
0
68
6
5
62
6
2
80
My w
ork
are
a p
erf
orm
s w
ell
ag
ain
st its
KP
Is/t
arg
ets
. 6
0
64
7
2
73
7
0
74
7
7
74
7
0
75
*
- N
o h
isto
rical data
is c
urr
ently a
vaila
ble
for
this
questio
n
* N
ot
enough d
ata
to d
ispla
y
**P
revio
us y
ears
this
was I
have t
he o
pport
unity t
o e
ngage in
org
anis
atio
nal
change initia
tives.
22
Page 82 of 159
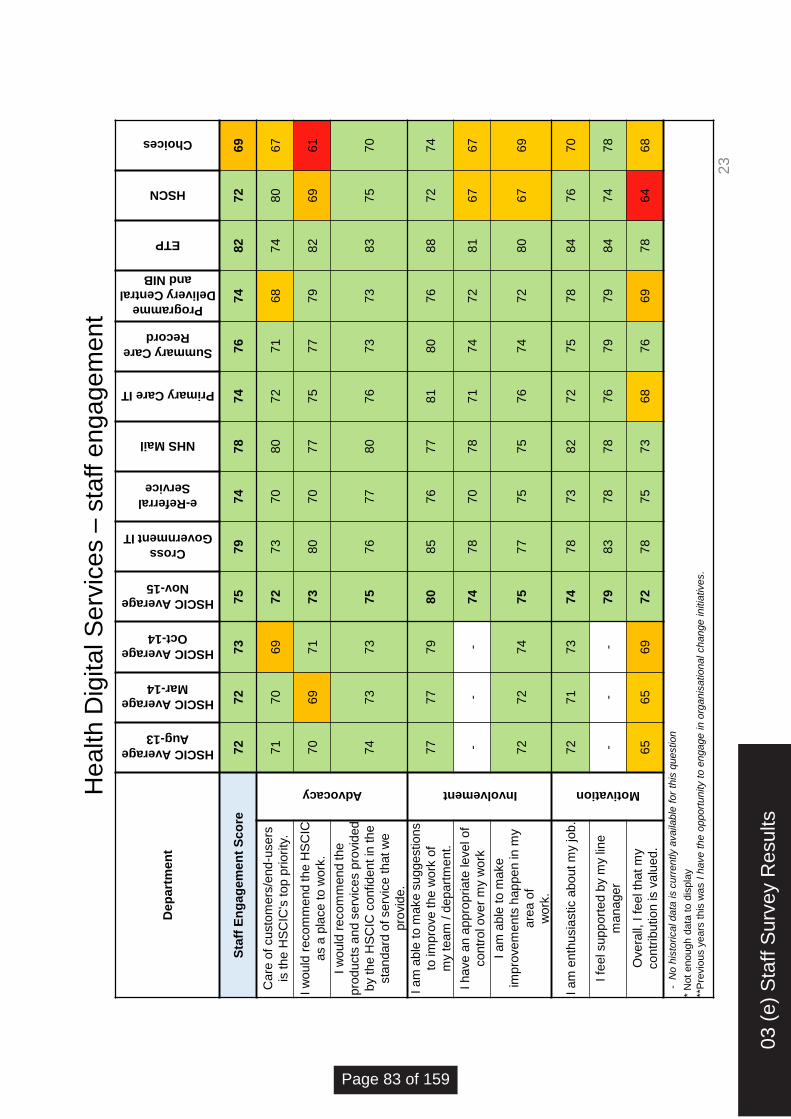
He
alth
Dig
ita
l S
erv
ice
s –
sta
ff e
ng
ag
em
en
t
De
pa
rtm
en
t
HSCIC Average
Aug-13
HSCIC Average
Mar-14
HSCIC Average
Oct-14
HSCIC Average
Nov-15
Cross
Government IT
e-Referral
Service
NHS Mail
Primary Care IT
Summary Care
Record
Programme
Delivery Central
and NIB
ETP
HSCN
Choices
Sta
ff E
ng
ag
em
en
t S
co
re
72
72
73
75
79
74
78
74
76
74
82
72
69
Ca
re o
f cu
sto
me
rs/e
nd
-use
rs
is th
e H
SC
IC's
top
prio
rity
.
Advocacy
71
70
69
72
73
70
80
72
71
68
74
80
67
I w
ould
re
co
mm
end
th
e H
SC
IC
as a
pla
ce
to
wo
rk.
70
69
71
73
80
70
77
75
77
79
82
69
61
I w
ould
recom
mend the
pro
du
cts
and
se
rvic
es p
rovid
ed
by
the H
SC
IC c
onfid
en
t in
th
e
sta
nd
ard
of se
rvic
e t
hat w
e
pro
vid
e.
74
73
73
75
76
77
80
76
73
73
83
75
70
I a
m a
ble
to
ma
ke
su
gg
estio
ns
to im
pro
ve
th
e w
ork
of
my t
ea
m / d
ep
art
me
nt.
Involvement
77
77
79
80
85
76
77
81
80
76
88
72
74
I h
ave
an
app
rop
ria
te le
ve
l o
f
co
ntr
ol o
ve
r m
y w
ork
-
- -
74
78
70
78
71
74
72
81
67
67
I a
m a
ble
to
ma
ke
imp
rove
me
nts
hap
pe
n in
my
are
a o
f
wo
rk.
72
72
74
75
77
75
75
76
74
72
80
67
69
I a
m e
nth
usia
stic a
bo
ut m
y jo
b.
Motivation
72
71
73
74
78
73
82
72
75
78
84
76
70
I fe
el su
pp
ort
ed b
y m
y lin
e
ma
na
ge
r -
- -
79
83
78
78
76
79
79
84
74
78
Ove
rall,
I f
eel th
at
my
co
ntr
ibutio
n is v
alu
ed
. 65
65
69
72
78
75
73
68
76
69
78
64
68
- N
o h
isto
rical data
is c
urr
ently a
vaila
ble
for
this
questio
n
* N
ot
enough d
ata
to d
ispla
y
**P
revio
us y
ears
this
was I
have t
he o
pport
unity t
o e
ngage in
org
anis
atio
nal change in
itia
tives.
23
03 (
e) S
taff
Sur
vey
Res
ults
Page 83 of 159

He
alth
Dig
ita
l S
erv
ice
s –
org
an
isa
tio
na
l h
ea
lth
De
pa
rtm
en
t
HSCIC
Average
Aug-13
HSCIC
Average
Mar-14
HSCIC
Average
Oct-14
HSCIC
Average
Nov-15
Cross
Government
IT
e-Referral
Service
NHS Mail
Primary
Care IT
Summary
Care Record
Programme
Delivery
Central and
NIB
ETP
HSCN
Choices
Org
an
isa
tio
n H
ea
lth
Sc
ore
6
6
67
6
9
71
7
4
69
*
71
7
6
72
7
9
* 6
6
Ge
ne
rally
, I
kn
ow
wh
o t
he
cu
sto
me
rs o
f th
e H
SC
IC a
re.
73
7
3
74
7
6
82
8
2
85
7
9
79
7
6
86
8
1
65
I h
ave
a c
lea
r u
nd
ers
tan
din
g o
f
the
ne
ed
s o
f m
y c
usto
me
rs.
77
7
6
78
7
8
79
8
0
88
7
7
85
7
0
89
8
1
74
Th
e H
SC
IC h
as c
lea
r a
nd
rele
va
nt o
rga
nis
atio
na
l va
lue
s.
- -
67
7
1
72
6
8
82
7
4
73
8
0
77
7
7
61
Th
e H
SC
IC h
as a
cle
arl
y
art
icu
late
d s
tra
teg
y fo
r its fu
ture
. 5
5
59
5
8
67
6
8
64
7
3
72
6
9
72
7
5
73
5
7
I ca
n s
ee
ho
w m
y w
ork
ob
jective
s c
on
trib
ute
to
th
e
HS
CIC
ach
ievin
g its
sta
ted
pu
rpo
se
.
64
6
5
65
6
9
74
6
6
75
7
0
73
7
2
81
6
5
59
I h
ave
th
e r
igh
t kn
ow
led
ge
an
d
skill
s to
pe
rfo
rm w
ell
in m
y r
ole
. 7
9
78
7
8
79
8
2
78
8
0
77
7
7
80
8
0
78
7
9
I a
m c
lea
r a
bo
ut th
e k
no
wle
dg
e
an
d s
kill
s th
at I
ne
ed
to
pro
gre
ss
with
in th
e o
rga
nis
atio
n.
65
6
4
66
6
7
71
5
8
67
6
8
66
6
8
76
6
5
62
**I h
ave
th
e o
pp
ort
un
ity to
be
en
ga
ge
d a
nd
in
vo
lve
d in
org
an
isa
tio
na
l ch
an
ge
in
itia
tive
s.
60
6
3
67
6
8
74
6
1
68
7
3
76
7
2
75
6
6
60
I h
ave
ch
alle
ng
ing
wo
rk
ob
jective
s.
72
7
3
74
7
6
82
8
0
73
7
6
87
7
2
85
6
4
72
My w
ork
are
a d
iffe
ren
tia
tes
be
twe
en
go
od
an
d a
ve
rag
e
pe
rfo
rma
nce
.
61
6
0
61
6
3
66
6
1
58
6
2
68
5
8
69
6
0
62
My w
ork
are
a m
on
ito
rs it
s
pe
rfo
rma
nce
usin
g K
PIs
or
me
tric
s.
60
6
4
65
6
5
60
6
4
58
6
1
77
6
7
74
4
8
65
My w
ork
are
a p
erf
orm
s w
ell
ag
ain
st its K
PIs
/ta
rge
ts.
60
6
4
72
7
3
77
6
7
* 6
7
79
7
4
86
*
73
- N
o h
isto
rical d
ata
is c
urr
ently a
vaila
ble
for
this
question
*
Not enough d
ata
to d
ispla
y
**P
revio
us y
ears
this
was I
have the o
pport
unity to e
ngage in
org
anis
ational c
hange in
itia
tives.
24
Page 84 of 159
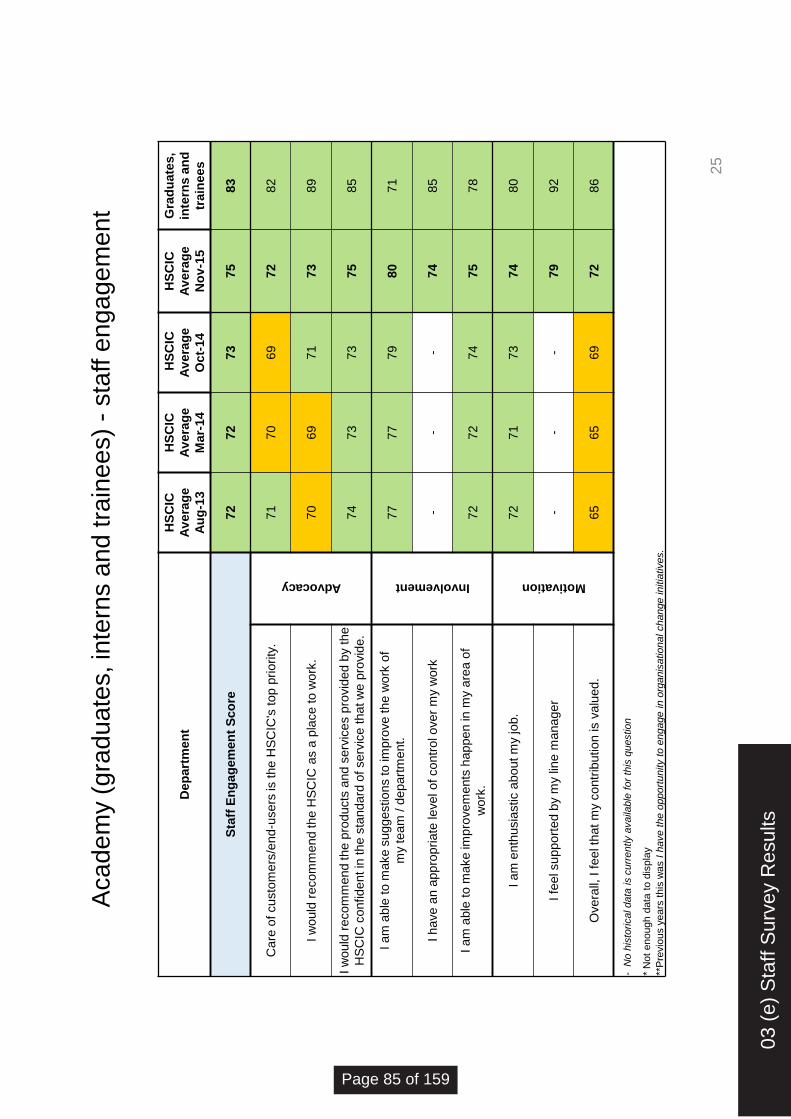
Aca
de
my (
gra
du
ate
s, in
tern
s a
nd
tra
ine
es)
- sta
ff e
ng
ag
em
en
t
25
De
pa
rtm
en
t
HS
CIC
Av
era
ge
Au
g-1
3
HS
CIC
Av
era
ge
Ma
r-14
HS
CIC
Av
era
ge
Oc
t-14
HS
CIC
Av
era
ge
No
v-1
5
Gra
du
ate
s,
inte
rns
an
d
tra
ine
es
Sta
ff E
ng
ag
em
en
t S
co
re
72
72
73
75
83
Ca
re o
f cu
sto
me
rs/e
nd
-use
rs is
the
HS
CIC
's t
op
prio
rity
.
Advocacy
71
70
69
72
82
I w
ould
re
co
mm
end
th
e H
SC
IC a
s a
pla
ce
to
wo
rk.
70
69
71
73
89
I w
ould
re
co
mm
end
th
e p
rod
ucts
and
se
rvic
es p
rovid
ed
by t
he
HS
CIC
co
nfid
en
t in
th
e s
tand
ard
of se
rvic
e t
hat w
e p
rovid
e.
74
73
73
75
85
I a
m a
ble
to
ma
ke
su
gg
estio
ns to
im
pro
ve
th
e w
ork
of
my t
ea
m / d
ep
art
me
nt.
Involvement
77
77
79
80
71
I h
ave
an
app
rop
ria
te le
ve
l o
f co
ntr
ol o
ve
r m
y w
ork
-
- -
74
85
I a
m a
ble
to
ma
ke
imp
rove
me
nts
hap
pe
n in
my a
rea
of
wo
rk.
72
72
74
75
78
I a
m e
nth
usia
stic a
bo
ut m
y jo
b.
Motivation
72
71
73
74
80
I fe
el su
pp
ort
ed b
y m
y lin
e m
ana
ge
r -
- -
79
92
Ove
rall,
I f
eel th
at
my c
ontr
ibutio
n is v
alu
ed
. 65
65
69
72
86
- N
o h
isto
rical data
is c
urr
ently a
vaila
ble
for
this
questio
n
* N
ot
enough d
ata
to d
ispla
y
**P
revio
us y
ears
this
was I
have t
he o
pport
unity t
o e
ngage in
org
anis
atio
nal change in
itia
tives.
03 (
e) S
taff
Sur
vey
Res
ults
Page 85 of 159
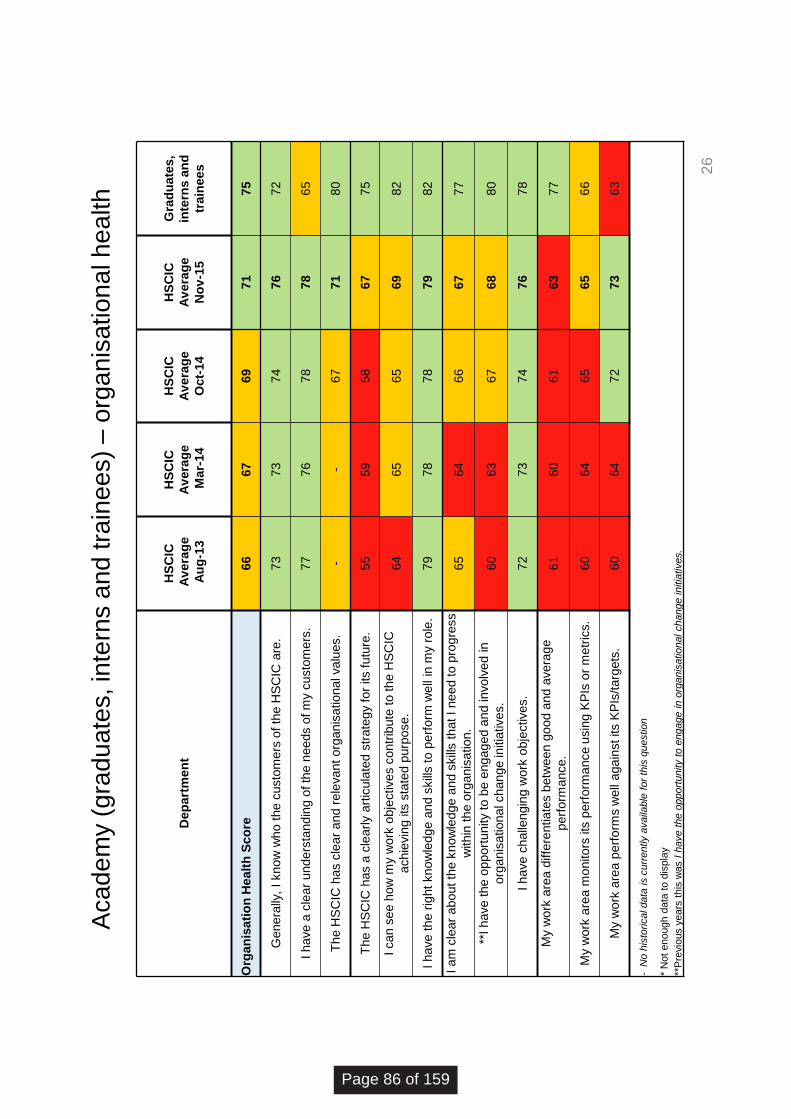
Aca
de
my (
gra
du
ate
s, in
tern
s a
nd
tra
ine
es)
– o
rga
nis
atio
na
l h
ea
lth
26
De
pa
rtm
en
t
HS
CIC
Av
era
ge
Au
g-1
3
HS
CIC
Av
era
ge
Ma
r-14
HS
CIC
Av
era
ge
Oc
t-14
HS
CIC
Av
era
ge
No
v-1
5
Gra
du
ate
s,
inte
rns
an
d
tra
ine
es
Org
an
isa
tio
n H
ea
lth
Sc
ore
66
67
69
71
75
Genera
lly,
I know
who t
he c
usto
mers
of th
e H
SC
IC a
re.
73
73
74
76
72
I h
ave
a c
lear
und
ers
tand
ing o
f th
e n
ee
ds o
f m
y c
usto
me
rs.
77
76
78
78
65
Th
e H
SC
IC h
as c
lear
and
re
leva
nt
org
an
isa
tio
na
l va
lues.
- -
67
71
80
Th
e H
SC
IC h
as a
cle
arly a
rtic
ula
ted
str
ate
gy
for
its f
utu
re.
55
59
58
67
75
I ca
n s
ee h
ow
my w
ork
obje
ctive
s c
ontr
ibute
to
th
e H
SC
IC
ach
ievin
g its
sta
ted p
urp
ose
. 64
65
65
69
82
I h
ave
th
e r
ight
kn
ow
ledg
e a
nd
skill
s t
o p
erf
orm
we
ll in
my r
ole
. 79
78
78
79
82
I a
m c
lear
abo
ut
the
kn
ow
ledg
e a
nd
skill
s t
hat I
ne
ed
to
pro
gre
ss
with
in t
he o
rga
nis
atio
n.
65
64
66
67
77
**I h
ave
th
e o
pp
ort
unity
to b
e e
ng
ag
ed
and
in
vo
lve
d in
org
an
isa
tio
na
l ch
an
ge
initia
tive
s.
60
63
67
68
80
I h
ave
ch
alle
ng
ing w
ork
obje
ctive
s.
72
73
74
76
78
My
wo
rk a
rea
diffe
ren
tia
tes b
etw
een
go
od
and
ave
rag
e
perf
orm
ance
. 61
60
61
63
77
My
wo
rk a
rea
mo
nito
rs its
perf
orm
ance
usin
g K
PIs
or
me
tric
s.
60
64
65
65
66
My
wo
rk a
rea
pe
rfo
rms w
ell
aga
inst its K
PIs
/targ
ets
. 60
64
72
73
63
- N
o h
isto
rical data
is c
urr
ently a
vaila
ble
for
this
questio
n
* N
ot
enough d
ata
to d
ispla
y
**P
revio
us y
ears
this
was I
have t
he o
pport
unity t
o e
ngage in
org
anis
atio
nal change in
itia
tives.
Page 86 of 159

Re
su
lts b
y e
thn
icity –
sta
ff e
ng
ag
em
en
t
Eth
nic
ity
HSCIC Average
Aug-13
HSCIC Average
Mar-14
HSCIC Average
Oct-14
HSCIC Average
Nov-15
A White -
British
C White - Any
other White
background
H Asian or
Asian British -
Indian
J Asian or
Asian British -
Pakistani
N Black or
Black British -
African
Undefined
Z Not Stated
Sta
ff E
ng
ag
em
en
t S
co
re
72
72
73
75
75
73
76
76
78
73
73
Ca
re o
f cu
sto
me
rs/e
nd
-use
rs is
the
HS
CIC
's t
op
priority
.
Advocacy
71
70
69
72
71
68
75
72
79
72
71
I w
ould
re
co
mm
end
th
e H
SC
IC a
s a
pla
ce
to
wo
rk.
70
69
71
73
73
70
78
79
76
70
69
I w
ould
re
co
mm
end
th
e p
rod
ucts
and
se
rvic
es p
rovid
ed
by
the H
SC
IC
co
nfid
en
t in
th
e s
tand
ard
of se
rvic
e
that w
e p
rovid
e.
74
73
73
75
75
74
76
77
81
73
73
I a
m a
ble
to
ma
ke
su
gg
estio
ns to
imp
rove
th
e w
ork
of
my t
ea
m / d
ep
art
me
nt.
Involvement
77
77
79
80
81
78
75
72
78
78
77
I h
ave
an
app
rop
ria
te le
ve
l o
f co
ntr
ol
ove
r m
y w
ork
-
- -
74
75
73
71
72
74
71
74
I a
m a
ble
to
ma
ke
imp
rove
me
nts
hap
pe
n in
my a
rea
of
wo
rk.
72
72
74
75
76
76
72
71
74
72
74
I a
m e
nth
usia
stic a
bo
ut m
y jo
b.
Motivation
72
71
73
74
74
71
78
85
78
74
73
I fe
el su
pp
ort
ed b
y m
y lin
e m
ana
ge
r -
- -
79
79
80
81
87
83
80
75
Ove
rall,
I f
eel th
at
my c
ontr
ibutio
n is
va
lued
. 65
65
69
72
73
69
74
71
80
72
69
27
03 (
e) S
taff
Sur
vey
Res
ults
Page 87 of 159

Eth
nic
ity
HSCIC
Average
Aug-13
HSCIC
Average
Mar-14
HSCIC
Average
Oct-14
HSCIC
Average
Nov-15
A White -
British
C White - Any
other White
background
H Asian or
Asian British -
Indian
J Asian or
Asian British -
Pakistani
N Black or
Black British -
African
Undefined
Z Not Stated
Org
an
isati
on
Healt
h S
co
re
66
6
7
69
7
1
71
7
0
71
7
4
74
6
9
69
Genera
lly, I know
who th
e c
usto
mers
of th
e H
SC
IC a
re.
73
7
3
74
7
6
76
7
6
76
7
9
76
7
0
78
I have a
cle
ar
unde
rsta
nd
ing o
f th
e
need
s o
f m
y c
usto
mers
. 7
7
76
7
8
78
7
8
77
7
5
73
7
8
76
7
6
The H
SC
IC h
as c
lear
and r
ele
vant
org
anis
ational v
alu
es.
- -
67
7
1
71
6
9
76
7
9
75
6
9
67
The H
SC
IC h
as a
cle
arl
y a
rtic
ula
ted
str
ate
gy for
its futu
re.
55
5
9
58
6
7
67
6
5
68
7
1
66
6
5
67
I can s
ee h
ow
my w
ork
obje
ctives
contr
ibute
to the H
SC
IC a
chie
vin
g its
sta
ted p
urp
ose.
64
6
5
65
6
9
69
6
6
72
7
5
74
6
6
70
I have the r
ight know
ledge
and s
kill
s to
perf
orm
well
in m
y r
ole
. 7
9
78
7
8
79
7
9
77
7
7
80
8
5
79
7
9
I am
cle
ar
abou
t th
e k
now
ledge
and
skill
s that I nee
d to p
rogre
ss w
ithin
the
org
anis
ation.
65
6
4
66
6
7
67
6
7
68
7
5
76
6
8
62
**I have the
oppo
rtunity to b
e e
ngag
ed
and involv
ed in o
rganis
ational c
hang
e
initia
tives.
60
6
3
67
6
8
69
6
7
68
6
7
64
6
4
65
I have c
halle
ngin
g w
ork
obje
ctives.
72
7
3
74
7
6
77
7
1
72
7
6
77
7
3
75
My w
ork
are
a d
iffe
rentiate
s b
etw
ee
n
good
and a
vera
ge p
erf
orm
ance.
61
6
0
61
6
3
62
6
6
67
6
9
69
6
3
62
My w
ork
are
a m
onitors
its
perf
orm
ance
usin
g K
PIs
or
metr
ics.
60
6
4
65
6
5
66
6
6
65
6
8
73
6
5
61
My w
ork
are
a p
erf
orm
s w
ell
again
st its
KP
Is/targ
ets
. 6
0
64
7
2
73
7
4
73
7
4
74
7
4
72
6
9
- N
o h
isto
rical data
is c
urr
ently a
vaila
ble
for
this
questio
n
*Not enough d
ata
to d
ispla
y
**P
revio
us y
ears
this
was I
have t
he o
pport
unity t
o e
ngage
in o
rganis
atio
nal change in
itia
tives.
Re
su
lts b
y e
thn
icity –
org
an
isa
tio
na
l h
ea
lth
28
Page 88 of 159

Re
su
lts b
y G
en
de
r –
sta
ff e
ng
ag
em
en
t
Ge
nd
er
HSCIC
Average
Aug-13
HSCIC
Average
Mar-14
HSCIC
Average
Oct 14
HSCIC
Average
Nov 2015
Female
Male
Sta
ff E
ng
ag
em
en
t S
co
re
72
72
73
75
75
75
Ca
re o
f cu
sto
me
rs/e
nd
-use
rs is
the
HS
CIC
's t
op
priority
.
Advocacy
71
70
69
72
71
72
I w
ould
re
co
mm
end
th
e H
SC
IC a
s a
pla
ce
to
wo
rk.
70
69
71
73
73
72
I w
ould
re
co
mm
end
th
e p
rod
ucts
and
se
rvic
es p
rovid
ed
by
the H
SC
IC c
onfid
en
t in
th
e s
tand
ard
of se
rvic
e th
at
we
pro
vid
e.
74
73
73
75
75
75
I a
m a
ble
to
ma
ke
su
gg
estio
ns to
im
pro
ve
th
e w
ork
of
my
team
/ d
epart
ment.
Involvement
77
77
79
80
80
80
I h
ave
an
app
rop
ria
te le
ve
l o
f co
ntr
ol o
ve
r m
y w
ork
-
- -
74
74
74
I a
m a
ble
to
ma
ke
imp
rove
me
nts
hap
pe
n in
my a
rea
of
wo
rk.
72
72
74
75
76
75
I a
m e
nth
usia
stic a
bo
ut m
y jo
b.
Motivation
72
71
73
74
74
75
I fe
el su
pp
ort
ed b
y m
y lin
e m
ana
ge
r -
- -
79
79
80
Ove
rall,
I f
eel th
at
my c
ontr
ibutio
n is v
alu
ed
. 65
65
69
72
72
73
- N
o h
isto
rical data
is c
urr
ently a
vaila
ble
for
this
questio
n
* N
ot
enough d
ata
to d
ispla
y
**P
revio
us y
ears
this
was I
have t
he o
pport
unity t
o e
ngage in
org
anis
atio
nal change in
itia
tives.
29
03 (
e) S
taff
Sur
vey
Res
ults
Page 89 of 159
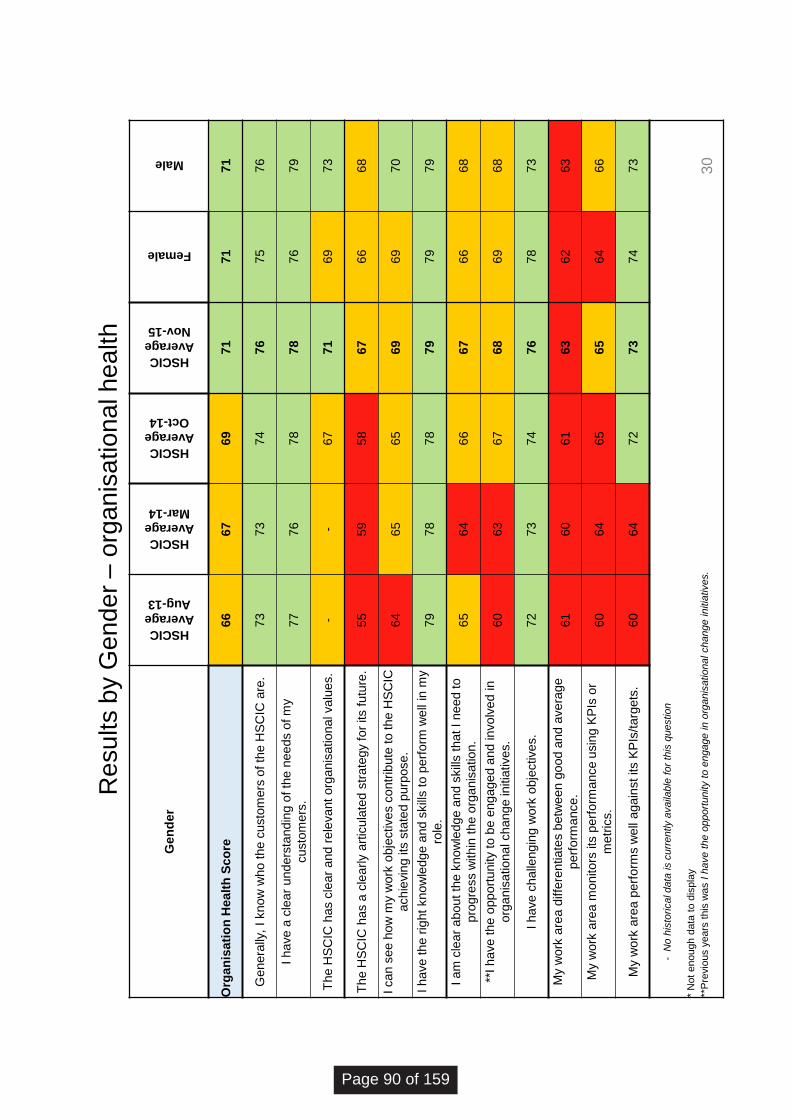
Re
su
lts b
y G
en
de
r –
org
an
isa
tio
na
l h
ea
lth
Ge
nd
er
HSCIC
Average
Aug-13
HSCIC
Average
Mar-14
HSCIC
Average
Oct-14
HSCIC
Average
Nov-15
Female
Male
Org
an
isa
tio
n H
ea
lth
Sc
ore
66
67
69
71
71
71
Genera
lly,
I know
who t
he c
usto
mers
of th
e H
SC
IC a
re.
73
73
74
76
75
76
I h
ave
a c
lear
und
ers
tand
ing o
f th
e n
ee
ds o
f m
y
custo
mers
. 77
76
78
78
76
79
Th
e H
SC
IC h
as c
lear
and
re
leva
nt
org
an
isa
tio
na
l va
lues.
- -
67
71
69
73
Th
e H
SC
IC h
as a
cle
arly a
rtic
ula
ted
str
ate
gy
for
its f
utu
re.
55
59
58
67
66
68
I ca
n s
ee h
ow
my w
ork
obje
ctive
s c
ontr
ibute
to
th
e H
SC
IC
ach
ievin
g its
sta
ted p
urp
ose
. 64
65
65
69
69
70
I h
ave
th
e r
ight
kn
ow
ledg
e a
nd
skill
s t
o p
erf
orm
we
ll in
my
role
. 79
78
78
79
79
79
I a
m c
lear
abo
ut
the
kn
ow
ledg
e a
nd
skill
s t
hat I
ne
ed
to
pro
gre
ss w
ith
in t
he o
rga
nis
atio
n.
65
64
66
67
66
68
**I h
ave
th
e o
pp
ort
unity
to b
e e
ng
ag
ed
and
in
vo
lve
d in
org
an
isa
tio
na
l ch
an
ge
initia
tive
s.
60
63
67
68
69
68
I h
ave
ch
alle
ng
ing w
ork
obje
ctive
s.
72
73
74
76
78
73
My
wo
rk a
rea
diffe
ren
tia
tes b
etw
een
go
od
and
ave
rag
e
perf
orm
ance
. 61
60
61
63
62
63
My
wo
rk a
rea
mo
nito
rs its
perf
orm
ance
usin
g K
PIs
or
me
tric
s.
60
64
65
65
64
66
My
wo
rk a
rea
pe
rfo
rms w
ell
aga
inst its K
PIs
/targ
ets
. 60
64
72
73
74
73
- N
o h
isto
rical data
is c
urr
ently a
vaila
ble
for
this
questio
n
* N
ot
enough d
ata
to d
ispla
y
**P
revio
us y
ears
this
was I
have t
he o
pport
unity t
o e
ngage in
org
anis
atio
nal change in
itia
tives.
30
Page 90 of 159

Re
su
lts b
y W
ork
ing
Pa
tte
rn –
sta
ff e
ng
ag
em
en
t
Fu
ll-P
art
Tim
e s
tatu
s
HSCIC
Average
Aug-13
HSCIC
Average
Mar-14
HSCIC
Average
Oct-14
HSCIC
Average
Nov-15
Full Time
Part Time
Sta
ff E
ng
ag
em
en
t S
co
re
72
72
73
75
75
74
Ca
re o
f cu
sto
me
rs/e
nd
-use
rs is
the
HS
CIC
's t
op
prio
rity
.
Advocacy
71
70
69
72
72
70
I w
ould
re
co
mm
end
th
e H
SC
IC a
s a
pla
ce
to
wo
rk.
70
69
71
73
73
71
I w
ould
re
co
mm
end
th
e p
rod
ucts
and
se
rvic
es p
rovid
ed
by
the H
SC
IC c
onfid
en
t in
th
e s
tand
ard
of se
rvic
e th
at w
e
pro
vid
e.
74
73
73
75
75
74
I a
m a
ble
to
ma
ke
su
gg
estio
ns to
im
pro
ve
th
e w
ork
of
my t
ea
m / d
ep
art
me
nt.
Involvement
77
77
79
80
80
79
I h
ave
an
app
rop
ria
te le
ve
l o
f co
ntr
ol o
ve
r m
y w
ork
-
- -
74
74
75
I a
m a
ble
to
ma
ke
imp
rove
me
nts
hap
pe
n in
my a
rea
of
wo
rk.
72
72
74
75
75
75
I a
m e
nth
usia
stic a
bo
ut m
y jo
b.
Motivation
72
71
73
74
74
74
I fe
el support
ed b
y m
y lin
e m
anager
- -
- 79
79
80
Ove
rall,
I f
eel th
at
my c
ontr
ibutio
n is v
alu
ed
. 65
65
69
72
72
73
- N
o h
isto
rical data
is c
urr
ently a
vaila
ble
for
this
questio
n
* N
ot
enough d
ata
to d
ispla
y
**P
revio
us y
ears
this
was I
have t
he o
pport
unity t
o e
ngage in
org
anis
atio
nal change in
itia
tives.
31
03 (
e) S
taff
Sur
vey
Res
ults
Page 91 of 159

Re
su
lts b
y W
ork
ing
Pa
tte
rn –
org
an
isa
tio
na
l h
ea
lth
Fu
ll-P
art
Tim
e s
tatu
s
HSCIC
Average
Aug-13
HSCIC
Average
Mar-14
HSCIC
Average
Oct-14
HSCIC
Average
Nov-15
Full Time
Part Time
Org
an
isa
tio
n H
ea
lth
Sc
ore
66
67
69
71
71
71
Ge
ne
rally
, I
kn
ow
wh
o t
he c
usto
me
rs o
f th
e H
SC
IC a
re.
73
73
74
76
76
77
I h
ave
a c
lear
und
ers
tand
ing o
f th
e n
ee
ds o
f m
y
cu
sto
me
rs.
77
76
78
78
78
78
Th
e H
SC
IC h
as c
lear
and
re
leva
nt
org
an
isa
tio
na
l va
lues.
- -
67
71
71
71
Th
e H
SC
IC h
as a
cle
arly a
rtic
ula
ted
str
ate
gy
for
its f
utu
re.
55
59
58
67
67
68
I ca
n s
ee h
ow
my w
ork
obje
ctive
s c
ontr
ibute
to
th
e H
SC
IC
ach
ievin
g its
sta
ted p
urp
ose
. 64
65
65
69
69
70
I h
ave
th
e r
ight
kn
ow
ledg
e a
nd
skill
s t
o p
erf
orm
we
ll in
my
role
. 79
78
78
79
79
79
I a
m c
lear
abo
ut
the
kn
ow
ledg
e a
nd
skill
s t
hat I
ne
ed
to
pro
gre
ss w
ith
in t
he o
rga
nis
atio
n.
65
64
66
67
67
69
**I h
ave
th
e o
pp
ort
unity
to b
e e
ng
ag
ed
and
in
vo
lve
d in
org
an
isa
tio
na
l ch
an
ge
initia
tive
s.
60
63
67
68
68
68
I h
ave
ch
alle
ng
ing w
ork
obje
ctive
s.
72
73
74
76
76
73
My
work
are
a d
iffe
rentiate
s b
etw
een g
ood a
nd a
vera
ge
perf
orm
ance
. 61
60
61
63
62
63
My
wo
rk a
rea
mo
nito
rs its
perf
orm
ance
usin
g K
PIs
or
me
tric
s.
60
64
65
65
65
66
My
wo
rk a
rea
pe
rfo
rms w
ell
aga
inst its K
PIs
/targ
ets
. 60
64
72
73
74
72
- N
o h
isto
rical data
is c
urr
ently a
vaila
ble
for
this
questio
n
* N
ot
enough d
ata
to d
ispla
y
**P
revio
us y
ears
this
was I
have t
he o
pport
unity t
o e
ngage in
org
anis
atio
nal change in
itia
tives.
3
2
Page 92 of 159

Re
su
lts b
y A
ge
– s
taff e
ng
ag
em
en
t
Ag
e G
rou
p
HSCIC Average
Aug-13
HSCIC Average
Mar-14
HSCIC Average
Oct-14
HSCIC Average
Nov-15
16-30
31-40
41-50
51+
Sta
ff E
ng
ag
em
en
t S
co
re
72
72
73
75
76
76
74
74
Ca
re o
f cu
sto
me
rs/e
nd
-use
rs is
the
HS
CIC
's t
op
priority
.
Advocacy
71
70
69
72
73
70
71
74
I w
ould
re
co
mm
end
th
e H
SC
IC a
s a
pla
ce
to
wo
rk.
70
69
71
73
77
75
71
70
I w
ould
re
co
mm
end
th
e p
rod
ucts
and
se
rvic
es
pro
vid
ed b
y th
e H
SC
IC c
onfident in
the s
tandard
of se
rvic
e th
at
we
pro
vid
e.
74
73
73
75
75
75
75
75
I a
m a
ble
to
ma
ke
su
gg
estio
ns to
im
pro
ve
th
e
wo
rk o
f
my t
ea
m / d
ep
art
me
nt.
Involvement
77
77
79
80
80
81
80
79
I h
ave
an
app
rop
ria
te le
ve
l o
f co
ntr
ol o
ve
r m
y
wo
rk
- -
- 74
75
74
74
73
I a
m a
ble
to
ma
ke
imp
rove
me
nts
hap
pe
n in
my
are
a o
f
wo
rk.
72
72
74
75
75
76
75
73
I a
m e
nth
usia
stic a
bo
ut m
y jo
b.
Motivation
72
71
73
74
74
74
73
75
I fe
el su
pp
ort
ed b
y m
y lin
e m
ana
ge
r -
- -
79
83
81
78
77
Ove
rall,
I f
eel th
at
my c
ontr
ibutio
n is v
alu
ed
. 65
65
69
72
75
74
71
70
- N
o h
isto
rical data
is c
urr
ently a
vaila
ble
for
this
questio
n
* N
ot
enough d
ata
to d
ispla
y
**P
revio
us y
ears
this
was I
have t
he o
pport
unity t
o e
ngage in o
rganis
ational change initia
tives.
33
03 (
e) S
taff
Sur
vey
Res
ults
Page 93 of 159
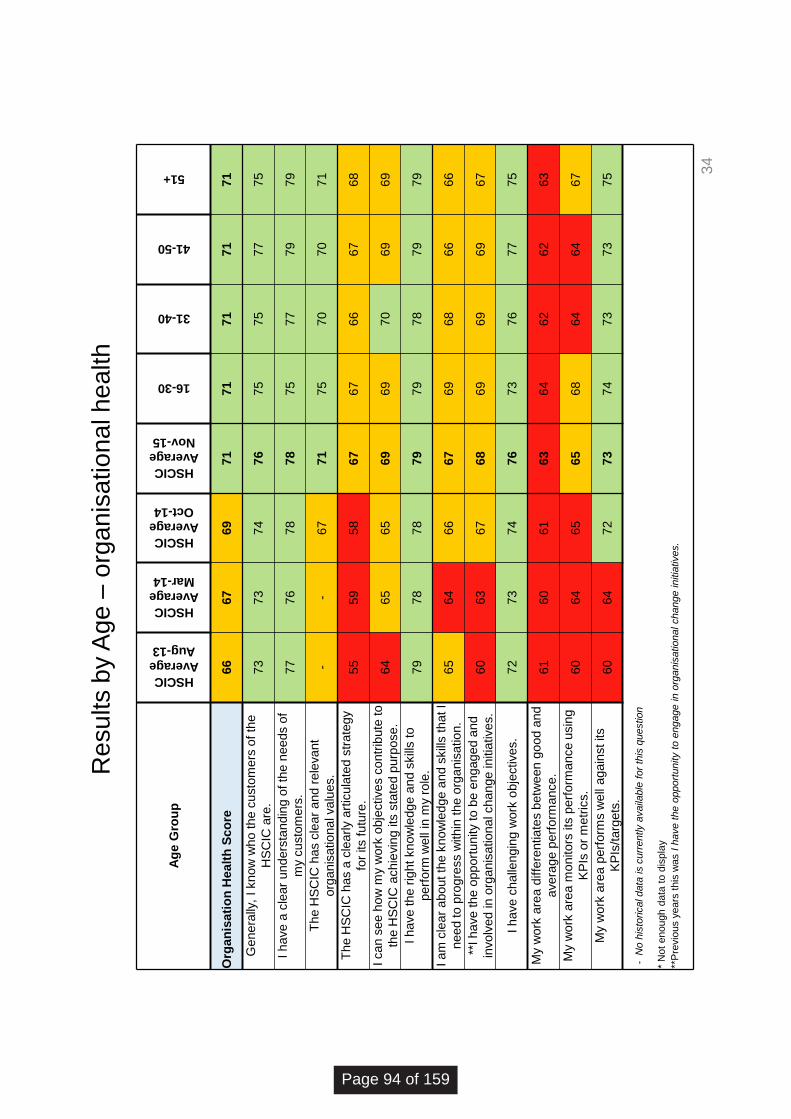
Re
su
lts b
y A
ge
– o
rga
nis
atio
na
l h
ea
lth
Ag
e G
rou
p
HSCIC
Average
Aug-13
HSCIC
Average
Mar-14
HSCIC
Average
Oct-14
HSCIC
Average
Nov-15
16-30
31-40
41-50
51+
Org
an
isa
tio
n H
ea
lth
Sc
ore
66
67
69
71
71
71
71
71
Ge
ne
rally
, I
kn
ow
wh
o t
he c
usto
me
rs o
f th
e
HS
CIC
are
. 73
73
74
76
75
75
77
75
I h
ave
a c
lear
und
ers
tand
ing o
f th
e n
ee
ds o
f
my c
usto
me
rs.
77
76
78
78
75
77
79
79
Th
e H
SC
IC h
as c
lear
and
re
leva
nt
org
an
isa
tio
na
l va
lues.
- -
67
71
75
70
70
71
The H
SC
IC h
as a
cle
arly
art
icula
ted s
tra
tegy
for
its f
utu
re.
55
59
58
67
67
66
67
68
I ca
n s
ee h
ow
my w
ork
obje
ctive
s c
ontr
ibute
to
the H
SC
IC a
ch
ievin
g its
sta
ted p
urp
ose
. 64
65
65
69
69
70
69
69
I h
ave
th
e r
ight
kn
ow
ledg
e a
nd
skill
s t
o
perf
orm
we
ll in
my r
ole
. 79
78
78
79
79
78
79
79
I a
m c
lear
abo
ut
the
kn
ow
ledg
e a
nd
skill
s t
hat I
nee
d to
pro
gre
ss w
ith
in t
he o
rga
nis
atio
n.
65
64
66
67
69
68
66
66
**I h
ave
th
e o
pp
ort
unity
to b
e e
ng
ag
ed
and
invo
lve
d in
org
an
isa
tio
na
l ch
an
ge
in
itia
tive
s.
60
63
67
68
69
69
69
67
I h
ave
ch
alle
ng
ing w
ork
obje
ctive
s.
72
73
74
76
73
76
77
75
My
wo
rk a
rea
diffe
ren
tia
tes b
etw
een
go
od
and
ave
rag
e p
erf
orm
ance
. 61
60
61
63
64
62
62
63
My
wo
rk a
rea
mo
nito
rs its
perf
orm
ance
usin
g
KP
Is o
r m
etr
ics.
60
64
65
65
68
64
64
67
My
wo
rk a
rea
pe
rfo
rms w
ell
aga
inst its
KP
Is/t
arg
ets
. 60
64
72
73
74
73
73
75
- N
o h
isto
rical data
is c
urr
ently a
vaila
ble
for
this
questio
n
* N
ot
enough d
ata
to d
ispla
y
**P
revio
us y
ears
this
was I
have t
he o
pport
unity t
o e
ngage in
org
anis
atio
nal change in
itia
tives.
34
Page 94 of 159

Re
su
lts b
y D
isa
bili
ty –
sta
ff e
ng
ag
em
en
t
Dis
ab
ilit
y
HSCIC
Average
Aug-13
HSCIC
Average
Mar-14
HSCIC
Average
Oct-14
HSCIC
Average
Nov-15
No
Not
Declared
Undefined
Yes
Sta
ff E
ng
ag
em
en
t S
co
re
72
72
73
75
75
74
75
77
Ca
re o
f cu
sto
me
rs/e
nd
-use
rs is
the
HS
CIC
's
top p
riority
.
Advocacy
71
70
69
72
72
73
71
77
I w
ould
re
co
mm
end
th
e H
SC
IC a
s a
pla
ce
to
wo
rk.
70
69
71
73
71
72
74
75
I w
ould
re
co
mm
end
th
e p
rod
ucts
and
se
rvic
es
pro
vid
ed
by t
he H
SC
IC c
onfid
en
t in
th
e
sta
nd
ard
of se
rvic
e t
hat w
e p
rovid
e.
74
73
73
75
75
75
74
79
I a
m a
ble
to
ma
ke
su
gg
estio
ns to
im
pro
ve
th
e
wo
rk o
f
my t
ea
m / d
ep
art
me
nt.
Involvement
77
77
79
80
80
80
80
83
I h
ave
an
app
rop
ria
te le
ve
l o
f co
ntr
ol o
ve
r m
y
wo
rk
- -
- 74
75
73
73
73
I a
m a
ble
to
ma
ke
imp
rove
me
nts
hap
pe
n in
my a
rea
of
wo
rk.
72
72
74
75
75
75
75
79
I a
m e
nth
usia
stic a
bo
ut m
y jo
b.
Motivation
72
71
73
74
73
74
75
77
I fe
el su
pp
ort
ed b
y m
y lin
e m
ana
ge
r -
- -
79
78
78
81
81
Ove
rall,
I f
eel th
at
my c
ontr
ibutio
n is v
alu
ed
. 65
65
69
72
71
70
73
74
- N
o h
isto
rical data
is c
urr
ently a
vaila
ble
for
this
questio
n
* N
ot
enough d
ata
to d
ispla
y
**P
revio
us y
ears
this
was I
have t
he o
pport
unity t
o e
ngage in
org
anis
atio
nal change in
itia
tives.
35
03 (
e) S
taff
Sur
vey
Res
ults
Page 95 of 159

Re
su
lts b
y D
isa
bili
ty –
org
an
isa
tio
na
l h
ea
lth
Dis
ab
ilit
y
HSCIC
Average
Aug-13
HSCIC
Average
Mar-14
HSCIC
Average
Oct 14
HSCIC
Average
Nov-15
No
Not
Declared
Undefined
Yes
Org
an
isa
tio
n H
ea
lth
Sc
ore
66
67
69
71
71
71
71
73
Ge
ne
rally
, I
kn
ow
wh
o t
he c
usto
me
rs o
f th
e
HS
CIC
are
. 73
73
74
76
76
79
75
81
I h
ave
a c
lear
und
ers
tand
ing o
f th
e n
ee
ds o
f
my c
usto
me
rs.
77
76
78
78
78
78
77
83
Th
e H
SC
IC h
as c
lear
and
re
leva
nt
org
an
isa
tio
na
l va
lues.
- -
67
71
70
68
72
72
Th
e H
SC
IC h
as a
cle
arly a
rtic
ula
ted
str
ate
gy
for
its f
utu
re.
55
59
58
67
66
67
67
70
I ca
n s
ee h
ow
my w
ork
obje
ctive
s c
ontr
ibute
to th
e H
SC
IC a
ch
ievin
g its
sta
ted p
urp
ose
. 64
65
65
69
69
70
69
70
I have the r
ight
know
ledge a
nd s
kill
s to
perf
orm
we
ll in
my r
ole
. 79
78
78
79
79
79
79
73
I a
m c
lear
abo
ut
the
kn
ow
ledg
e a
nd
skill
s t
hat
I n
ee
d to
pro
gre
ss w
ith
in t
he o
rga
nis
atio
n.
65
64
66
67
65
63
69
68
**I h
ave
th
e o
pp
ort
unity
to b
e e
ng
ag
ed
and
invo
lve
d in
org
an
isa
tio
na
l ch
an
ge
in
itia
tive
s.
60
63
67
68
69
68
67
70
I h
ave
ch
alle
ng
ing w
ork
obje
ctive
s.
72
73
74
76
77
76
75
78
My
wo
rk a
rea
diffe
ren
tia
tes b
etw
een
go
od
and
ave
rag
e p
erf
orm
ance
. 61
60
61
63
61
61
63
61
My
wo
rk a
rea
mo
nito
rs its
perf
orm
ance
usin
g
KP
Is o
r m
etr
ics.
60
64
65
65
66
65
65
72
My
work
are
a p
erf
orm
s w
ell
again
st its
KP
Is/t
arg
ets
. 60
64
72
73
74
74
73
75
- N
o h
isto
rical data
is c
urr
ently a
vaila
ble
for
this
questio
n
* N
ot
enough d
ata
to d
ispla
y
**P
revio
us y
ears
this
was I
have t
he o
pport
unity t
o e
ngage in
org
anis
atio
nal change in
itia
tives.
36
Page 96 of 159

Re
su
lts b
y B
ase
– s
taff e
ng
ag
em
en
t
Ba
se
HSCIC Average
Aug-13
HSCIC Average
Mar-14
HSCIC Average
Oct-14
HSCIC Average
Nov-15
Bridgewater Place
- Leeds
Durham House
Exeter
Geographic
Hedge End
- Southampton
Leeds
Princes Exchange
– Leeds
Prospect House
- Redditch
Skipton House
- London
Southport
Trevelyan Square
- Leeds
Vantage - Leeds
Whitehall - Leeds
Sta
ff E
ng
ag
em
en
t S
co
re
72
72
73
75
75
74
77
80
68
76
73
72
69
70
74
74
76
Ca
re o
f cu
sto
me
rs/e
nd
-use
rs is
the H
SC
IC's
to
p p
rio
rity
.
Advocacy
71
70
69
72
71
75
78
74
56
72
68
73
66
72
68
72
75
I w
ould
re
co
mm
end
th
e H
SC
IC
as a
pla
ce
to
wo
rk.
70
69
71
73
74
71
77
76
65
75
67
73
62
65
72
71
74
I w
ould
re
co
mm
end
th
e p
rod
ucts
and
se
rvic
es p
rovid
ed
by t
he
HS
CIC
co
nfid
en
t in
th
e s
tand
ard
of se
rvic
e th
at
we
pro
vid
e.
74
73
73
75
75
77
79
77
68
75
71
76
70
73
74
75
77
I a
m a
ble
to
ma
ke
su
gg
estio
ns
to im
pro
ve
th
e w
ork
of
my t
ea
m / d
ep
art
me
nt.
Involvement
77
77
79
80
82
79
82
83
72
81
81
75
76
76
80
78
81
I h
ave
an
app
rop
ria
te le
ve
l o
f
co
ntr
ol o
ve
r m
y w
ork
-
- -
74
71
76
75
81
62
75
76
73
67
70
75
73
76
I am
able
to m
ake im
pro
vem
ents
hap
pe
n in
my a
rea
of w
ork
. 72
72
74
75
74
74
77
81
70
77
78
68
68
68
76
74
77
I a
m e
nth
usia
stic a
bo
ut m
y jo
b.
Motivation
72
71
73
74
77
72
75
79
68
75
71
67
70
70
75
73
77
I fe
el su
pp
ort
ed b
y m
y lin
e
ma
na
ge
r -
- -
79
82
70
79
85
84
81
76
74
78
72
78
79
79
Ove
rall,
I f
eel th
at
my
co
ntr
ibutio
n is v
alu
ed
. 65
65
69
72
71
70
72
79
64
75
68
69
68
66
72
71
72
- N
o h
isto
rica
l dat
a is
cu
rren
tly
avai
lab
le f
or
this
qu
esti
on
*
Th
ere
was
no
t en
ou
gh d
ata
to d
isp
lay
resu
lts
fro
m o
ther
loca
tio
ns
37
03 (
e) S
taff
Sur
vey
Res
ults
Page 97 of 159
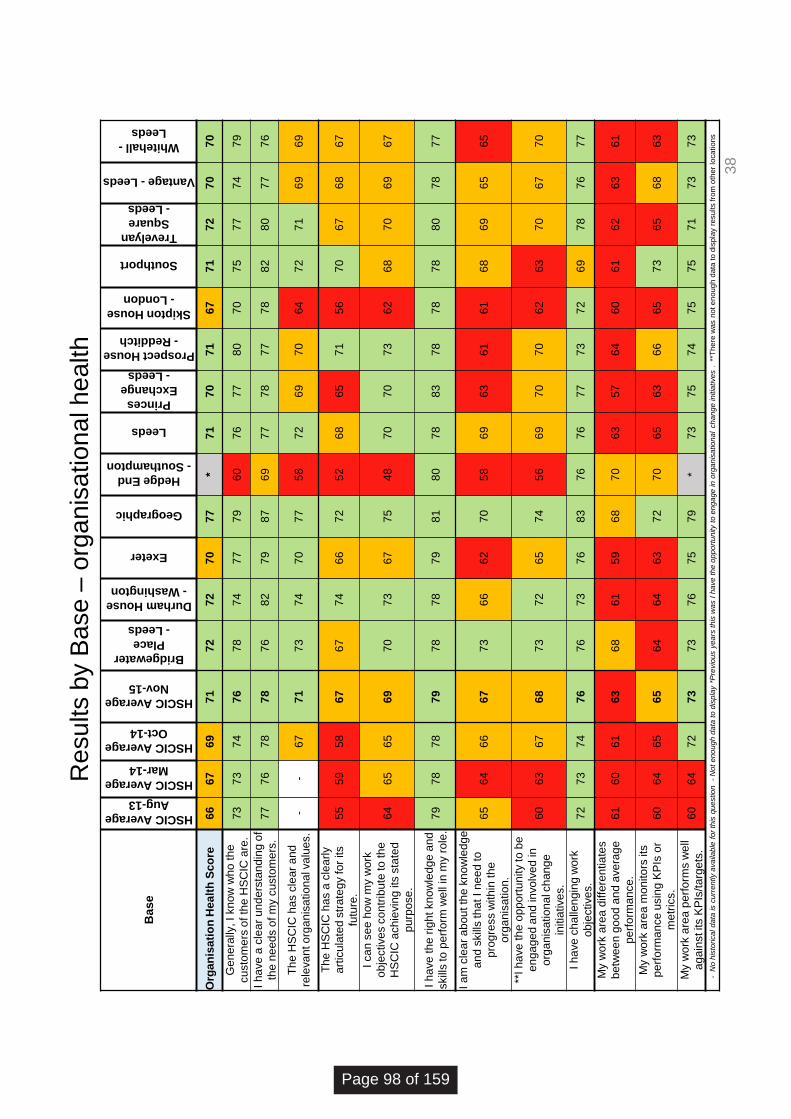
Re
su
lts b
y B
ase
– o
rga
nis
atio
na
l h
ea
lth
38
Base
HSCIC Average
Aug-13
HSCIC Average
Mar-14
HSCIC Average
Oct-14
HSCIC Average
Nov-15
Bridgewater
Place
- Leeds
Durham House
- Washington
Exeter
Geographic
Hedge End
- Southampton
Leeds
Princes
Exchange
- Leeds
Prospect House
- Redditch
Skipton House
- London
Southport
Trevelyan
Square
- Leeds
Vantage - Leeds
Whitehall -
Leeds
Org
an
isa
tio
n H
ea
lth
Sc
ore
6
6
67
6
9
71
7
2
72
7
0
77
*
71
7
0
71
6
7
71
7
2
70
7
0
Ge
ne
rally
, I
kn
ow
wh
o t
he
cu
sto
me
rs o
f th
e H
SC
IC a
re.
73
7
3
74
7
6
78
7
4
77
7
9
60
7
6
77
8
0
70
7
5
77
7
4
79
I h
ave
a c
lea
r u
nd
ers
tan
din
g o
f
the
ne
ed
s o
f m
y c
usto
me
rs.
77
7
6
78
7
8
76
8
2
79
8
7
69
7
7
78
7
7
78
8
2
80
7
7
76
Th
e H
SC
IC h
as c
lea
r a
nd
rele
va
nt o
rga
nis
atio
na
l va
lue
s.
- -
67
7
1
73
7
4
70
7
7
58
7
2
69
7
0
64
7
2
71
6
9
69
Th
e H
SC
IC h
as a
cle
arl
y
art
icu
late
d s
tra
teg
y fo
r its
futu
re.
55
5
9
58
6
7
67
7
4
66
7
2
52
6
8
65
7
1
56
7
0
67
6
8
67
I ca
n s
ee
ho
w m
y w
ork
ob
jective
s c
on
trib
ute
to
th
e
HS
CIC
ach
ievin
g its
sta
ted
pu
rpo
se
.
64
6
5
65
6
9
70
7
3
67
7
5
48
7
0
70
7
3
62
6
8
70
6
9
67
I h
ave
th
e r
igh
t kn
ow
led
ge
an
d
skill
s to
pe
rfo
rm w
ell
in m
y r
ole
. 7
9
78
7
8
79
7
8
78
7
9
81
8
0
78
8
3
78
7
8
78
8
0
78
7
7
I a
m c
lea
r a
bo
ut th
e k
no
wle
dg
e
an
d s
kill
s th
at I
ne
ed
to
pro
gre
ss w
ith
in t
he
org
an
isa
tio
n.
65
6
4
66
6
7
73
6
6
62
7
0
58
6
9
63
6
1
61
6
8
69
6
5
65
**I h
ave
th
e o
pp
ort
un
ity to
be
en
ga
ge
d a
nd
in
vo
lve
d in
org
an
isa
tio
na
l ch
an
ge
initia
tive
s.
60
6
3
67
6
8
73
7
2
65
7
4
56
6
9
70
7
0
62
6
3
70
6
7
70
I h
ave
ch
alle
ng
ing
wo
rk
ob
jective
s.
72
7
3
74
7
6
76
7
3
76
8
3
76
7
6
77
7
3
72
6
9
78
7
6
77
My w
ork
are
a d
iffe
ren
tia
tes
be
twe
en
go
od
an
d a
ve
rag
e
pe
rfo
rma
nce
.
61
6
0
61
6
3
68
6
1
59
6
8
70
6
3
57
6
4
60
6
1
62
6
3
61
My w
ork
are
a m
on
ito
rs it
s
pe
rfo
rma
nce
usin
g K
PIs
or
me
tric
s.
60
6
4
65
6
5
64
6
4
63
7
2
70
6
5
63
6
6
65
7
3
65
6
8
63
My w
ork
are
a p
erf
orm
s w
ell
ag
ain
st its K
PIs
/ta
rge
ts.
60
6
4
72
7
3
73
7
6
75
7
9
* 7
3
75
7
4
75
7
5
71
7
3
73
- N
o h
isto
rica
l d
ata
is c
urr
en
tly a
va
ilab
le f
or
this
qu
estio
n
- N
ot
en
ou
gh
da
ta t
o d
isp
lay *
Pre
vio
us y
ea
rs th
is w
as I
ha
ve
th
e o
pp
ort
un
ity t
o e
ng
ag
e in
org
an
isa
tio
na
l ch
an
ge
in
itia
tive
s .
**
Th
ere
wa
s n
ot e
no
ug
h d
ata
to
dis
pla
y r
esu
lts fro
m o
the
r lo
ca
tio
ns
Page 98 of 159
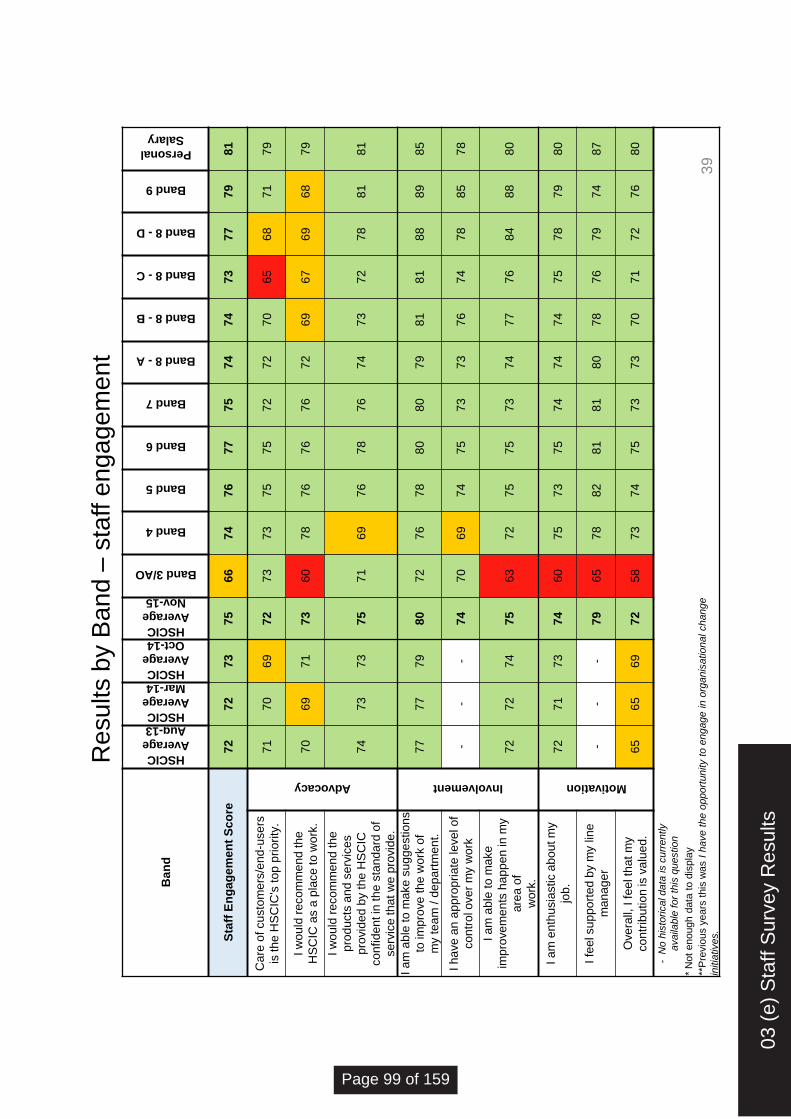
Re
su
lts b
y B
an
d –
sta
ff e
ng
ag
em
en
t
Ban
d
HSCIC
Average
Aug-13 HSCIC
Average
Mar-14 HSCIC
Average
Oct-14 HSCIC
Average
Nov-15
Band 3/AO
Band 4
Band 5
Band 6
Band 7
Band 8 - A
Band 8 - B
Band 8 - C
Band 8 - D
Band 9
Personal
Salary
Sta
ff E
ng
ag
em
en
t S
co
re
72
7
2
73
7
5
66
7
4
76
7
7
75
7
4
74
7
3
77
7
9
81
Care
of custo
mers
/end
-users
is the H
SC
IC's
top p
riority
.
Advocacy
71
7
0
69
7
2
73
7
3
75
7
5
72
7
2
70
6
5
68
7
1
79
I w
ould
recom
mend the
HS
CIC
as a
pla
ce to w
ork
. 7
0
69
7
1
73
6
0
78
7
6
76
7
6
72
6
9
67
6
9
68
7
9
I w
ould
recom
mend the
pro
ducts
and s
erv
ices
pro
vid
ed b
y the H
SC
IC
confident in
the s
tand
ard
of
serv
ice that w
e p
rovid
e.
74
7
3
73
7
5
71
6
9
76
7
8
76
7
4
73
7
2
78
8
1
81
I am
able
to m
ake s
ugge
stions
to im
pro
ve t
he w
ork
of
my team
/ d
epart
ment.
Involvement
77
7
7
79
8
0
72
7
6
78
8
0
80
7
9
81
8
1
88
8
9
85
I have a
n a
ppro
priate
level of
contr
ol o
ver
my w
ork
-
- -
74
7
0
69
7
4
75
7
3
73
7
6
74
7
8
85
7
8
I am
able
to m
ake
impro
vem
ents
happ
en in m
y
are
a o
f
work
.
72
7
2
74
7
5
63
7
2
75
7
5
73
7
4
77
7
6
84
8
8
80
I am
enth
usia
stic a
bout m
y
job.
Motivation
72
7
1
73
7
4
60
7
5
73
7
5
74
7
4
74
7
5
78
7
9
80
I fe
el suppo
rted b
y m
y lin
e
manag
er
- -
- 7
9
65
7
8
82
8
1
81
8
0
78
7
6
79
7
4
87
Overa
ll, I feel th
at
my
contr
ibution is
valu
ed.
65
6
5
69
7
2
58
7
3
74
7
5
73
7
3
70
7
1
72
7
6
80
- N
o h
isto
rical data
is c
urr
ently
availa
ble
for
this
questio
n
* N
ot
enough d
ata
to d
ispla
y
**P
revio
us y
ears
this
was I
have t
he o
pport
unity t
o e
ngage in
org
anis
atio
nal change
initia
tives.
39
03 (
e) S
taff
Sur
vey
Res
ults
Page 99 of 159
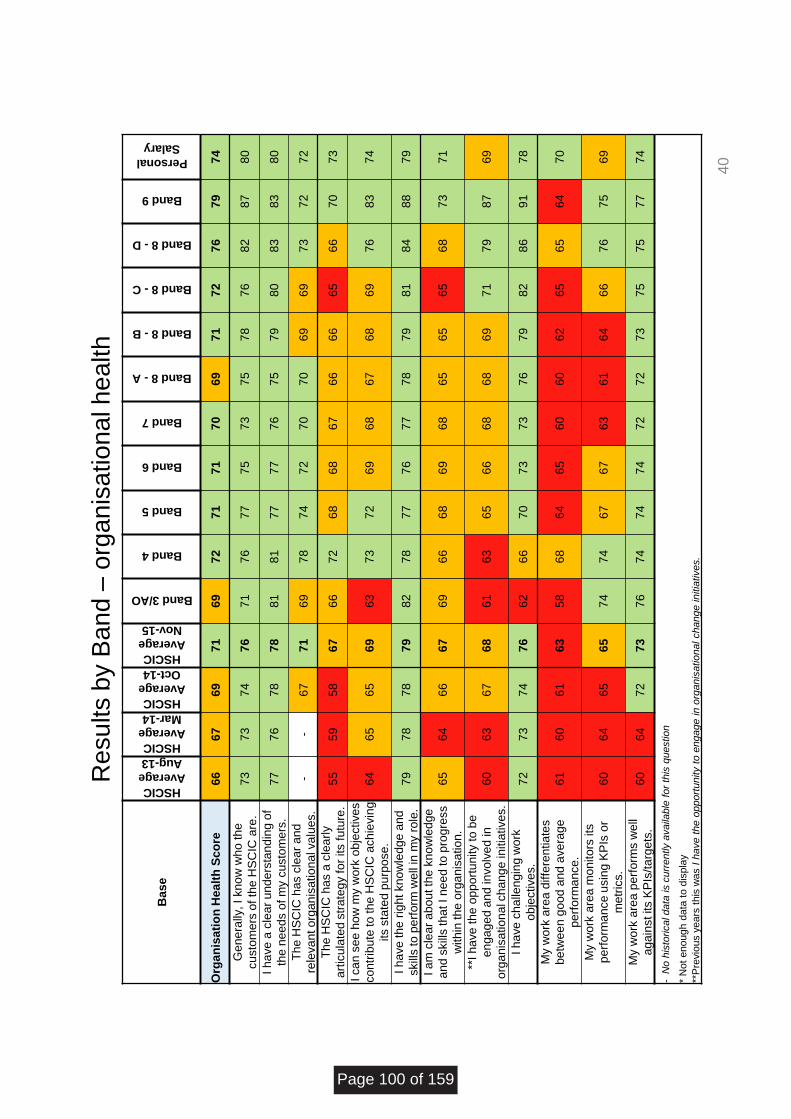
Re
su
lts b
y B
an
d –
org
an
isa
tio
na
l h
ea
lth
Base
HSCIC
Average
Aug-13
HSCIC
Average
Mar-14
HSCIC
Average
Oct-14
HSCIC
Average
Nov-15
Band 3/AO
Band 4
Band 5
Band 6
Band 7
Band 8 - A
Band 8 - B
Band 8 - C
Band 8 - D
Band 9
Personal
Salary
Org
an
isati
on
Healt
h S
co
re
66
6
7
69
7
1
69
7
2
71
7
1
70
6
9
71
7
2
76
7
9
74
Genera
lly, I know
who th
e
custo
mers
of
the H
SC
IC a
re.
73
7
3
74
7
6
71
7
6
77
7
5
73
7
5
78
7
6
82
8
7
80
I have a
cle
ar
unde
rsta
nd
ing o
f
the n
eed
s o
f m
y c
usto
mers
. 7
7
76
7
8
78
8
1
81
7
7
77
7
6
75
7
9
80
8
3
83
8
0
The H
SC
IC h
as c
lear
and
rele
vant org
anis
ational valu
es.
- -
67
7
1
69
7
8
74
7
2
70
7
0
69
6
9
73
7
2
72
The H
SC
IC h
as a
cle
arl
y
art
icula
ted
str
ate
gy for
its futu
re.
55
5
9
58
6
7
66
7
2
68
6
8
67
6
6
66
6
5
66
7
0
73
I can s
ee h
ow
my w
ork
obje
ctives
contr
ibute
to the H
SC
IC a
chie
vin
g
its s
tate
d p
urp
ose.
64
6
5
65
6
9
63
7
3
72
6
9
68
6
7
68
6
9
76
8
3
74
I have the r
ight know
ledge
and
skill
s to p
erf
orm
well
in m
y r
ole
. 7
9
78
7
8
79
8
2
78
7
7
76
7
7
78
7
9
81
8
4
88
7
9
I am
cle
ar
abou
t th
e k
now
ledge
and s
kill
s that I nee
d to p
rogre
ss
within
the o
rganis
ation.
65
6
4
66
6
7
69
6
6
68
6
9
68
6
5
65
6
5
68
7
3
71
**I have the
oppo
rtunity to b
e
en
ga
ge
d a
nd
in
vo
lve
d in
org
anis
ational c
hang
e initia
tives.
60
6
3
67
6
8
61
6
3
65
6
6
68
6
8
69
7
1
79
8
7
69
I have c
halle
ngin
g w
ork
obje
ctives.
72
7
3
74
7
6
62
6
6
70
7
3
73
7
6
79
8
2
86
9
1
78
My w
ork
are
a d
iffe
rentiate
s
betw
ee
n g
ood
and a
vera
ge
perf
orm
ance.
61
6
0
61
6
3
58
6
8
64
6
5
60
6
0
62
6
5
65
6
4
70
My w
ork
are
a m
onitors
its
perf
orm
ance u
sin
g K
PIs
or
metr
ics.
60
6
4
65
6
5
74
7
4
67
6
7
63
6
1
64
6
6
76
7
5
69
My w
ork
are
a p
erf
orm
s w
ell
again
st its K
PIs
/targ
ets
. 6
0
64
7
2
73
7
6
74
7
4
74
7
2
72
7
3
75
7
5
77
7
4
- N
o h
isto
rical data
is c
urr
ently a
vaila
ble
for
this
questio
n
* N
ot
enough d
ata
to d
ispla
y
**P
revio
us y
ears
this
was I
have t
he o
pport
unity t
o e
ngage in
org
anis
atio
nal change in
itia
tives.
40
Page 100 of 159

Re
su
lts b
y P
rofe
ssio
na
l G
rou
p –
sta
ff e
ng
ag
em
en
t
41
**P
rofe
ss
ion
al G
rou
p
HSCIC Average
Nov 2015
Business
Administration
Clinical
Informatics
Communications
& Stakeholder
Relations
Information
Management
Information
Technology
Project &
Programme
Delivery
N/A
Sta
ff E
ng
ag
em
en
t S
co
re
75
75
75
73
76
76
75
74
Ca
re o
f cu
sto
me
rs/e
nd
-use
rs is
the
HS
CIC
's t
op
priority
.
Advocacy
72
75
73
68
68
75
70
73
I w
ould
re
co
mm
end
th
e H
SC
IC a
s a
pla
ce
to
wo
rk.
73
72
69
70
73
73
72
74
I w
ould
re
co
mm
end
th
e p
rod
ucts
and
se
rvic
es
pro
vid
ed b
y th
e H
SC
IC c
onfident in
the s
tandard
of se
rvic
e th
at
we
pro
vid
e.
75
74
76
73
75
76
75
73
I a
m a
ble
to
ma
ke
su
gg
estio
ns to
im
pro
ve
th
e
wo
rk o
f
my t
ea
m / d
ep
art
me
nt.
Involvement
80
79
76
83
82
80
81
77
I h
ave
an
app
rop
ria
te le
ve
l o
f co
ntr
ol o
ve
r m
y
wo
rk
74
75
75
71
76
75
74
72
I a
m a
ble
to
ma
ke
imp
rove
me
nts
hap
pe
n in
my
are
a o
f
wo
rk.
75
75
75
74
78
75
75
73
I a
m e
nth
usia
stic a
bo
ut m
y jo
b.
Motivation
74
73
76
72
72
76
74
75
I fe
el su
pp
ort
ed b
y m
y lin
e m
ana
ge
r 79
78
82
78
81
79
79
79
Ove
rall,
I f
eel th
at
my c
ontr
ibutio
n is v
alu
ed
. 72
72
74
68
75
72
72
73
- N
o h
isto
rical data
is c
urr
ently a
vaila
ble
for
this
questio
n
* N
ot
enough d
ata
to d
ispla
y
**P
revio
us y
ears
this
was I
have t
he o
pport
unity t
o e
ngage in
org
anis
atio
nal change in
itia
tives.
03 (
e) S
taff
Sur
vey
Res
ults
Page 101 of 159
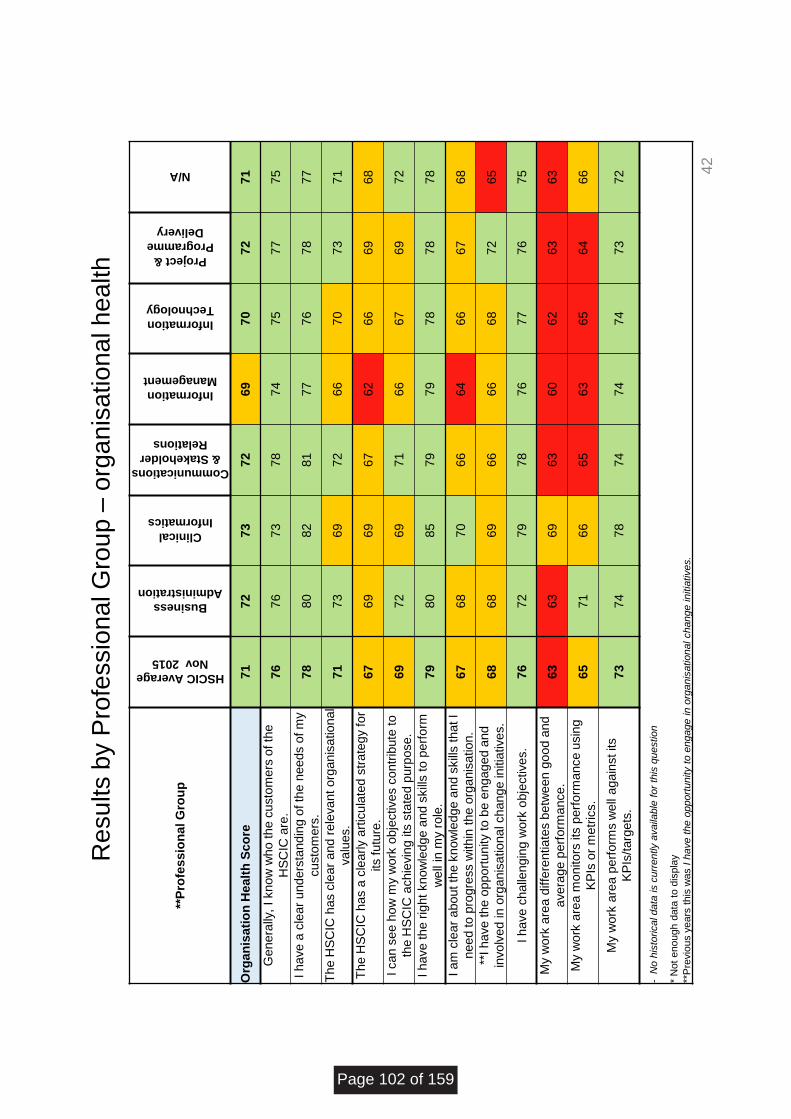
Re
su
lts b
y P
rofe
ssio
na
l G
rou
p –
org
an
isa
tio
na
l h
ea
lth
42
**P
rofe
ss
ion
al G
rou
p
HSCIC Average
Nov 2015
Business
Administration
Clinical
Informatics
Communications
& Stakeholder
Relations
Information
Management
Information
Technology
Project &
Programme
Delivery
N/A
Org
an
isa
tio
n H
ea
lth
Sc
ore
71
72
73
72
69
70
72
71
Ge
ne
rally
, I
kn
ow
wh
o t
he c
usto
me
rs o
f th
e
HS
CIC
are
. 76
76
73
78
74
75
77
75
I h
ave
a c
lear
und
ers
tand
ing o
f th
e n
ee
ds o
f m
y
cu
sto
me
rs.
78
80
82
81
77
76
78
77
Th
e H
SC
IC h
as c
lear
and
re
leva
nt
org
an
isa
tio
na
l
va
lues.
71
73
69
72
66
70
73
71
Th
e H
SC
IC h
as a
cle
arly a
rtic
ula
ted
str
ate
gy
for
its fu
ture
. 67
69
69
67
62
66
69
68
I ca
n s
ee h
ow
my w
ork
obje
ctive
s c
ontr
ibute
to
the H
SC
IC a
ch
ievin
g its
sta
ted p
urp
ose
. 69
72
69
71
66
67
69
72
I h
ave
th
e r
ight
kn
ow
ledg
e a
nd
skill
s t
o p
erf
orm
we
ll in
my r
ole
. 79
80
85
79
79
78
78
78
I a
m c
lear
abo
ut
the
kn
ow
ledg
e a
nd
skill
s t
hat I
nee
d to
pro
gre
ss w
ith
in t
he o
rga
nis
atio
n.
67
68
70
66
64
66
67
68
**I h
ave
th
e o
pp
ort
unity
to b
e e
ng
ag
ed
and
invo
lve
d in
org
an
isa
tio
na
l ch
an
ge
in
itia
tive
s.
68
68
69
66
66
68
72
65
I h
ave
ch
alle
ng
ing w
ork
obje
ctive
s.
76
72
79
78
76
77
76
75
My
wo
rk a
rea
diffe
ren
tia
tes b
etw
een
go
od
and
ave
rag
e p
erf
orm
ance
. 63
63
69
63
60
62
63
63
My
wo
rk a
rea
mo
nito
rs its
perf
orm
ance
usin
g
KP
Is o
r m
etr
ics.
65
71
66
65
63
65
64
66
My
wo
rk a
rea
pe
rfo
rms w
ell
aga
inst its
KP
Is/t
arg
ets
. 73
74
78
74
74
74
73
72
- N
o h
isto
rical data
is c
urr
ently a
vaila
ble
for
this
questio
n
* N
ot
enough d
ata
to d
ispla
y
**P
revio
us y
ears
this
was I
have t
he o
pport
unity t
o e
ngage in o
rganis
ational change initia
tives.
Page 102 of 159

Page 1 of 1
Board Meeting – Public Session
Title of paper: Performance and Development Review Activity: A Summary of Employee Appraisal
Board meeting date: 27 January 2016
Agenda item no: HSCIC 16 06 03 f
Paper presented by:
Rachael Allsop, Executive Director of HR and Transformation
Paper prepared by:
Tim Roebuck, Head of Organisational Development
Paper approved by: (Sponsor Director) Rachael Allsop, Executive Director of HR and Transformation
Purpose of the paper: To inform the Board of Employee Appraisal Activity
Key risks and issues:
The paper is presented for information in recognition of the importance of regular Performance and Development Reviews (PDRs) for employees.
Patient/public interest:
Indirect: There is a wider expectation that publically funded organisations manage performance.
Actions required by the Board: To note the levels of PDR activity
03 (
f) P
erso
nal D
evel
opm
ent R
evie
w(P
DR
)
Page 103 of 159


1 Copyright © 2014, Health and Social Care Information Centre.
Performance and Development Review Activity
A Summary of Employee Appraisals
Author: Tim Roebuck
Date: 8 January 2016
03 (
f) P
erso
nal D
evel
opm
ent R
evie
w(P
DR
)
Page 104 of 159
PDR Activity
2 Copyright © 2014, Health and Social Care Information Centre.
Contents
Contents 2
Background 3
Current PDR Activity by Directorate 3
Table view of mid-year PDRs 4
Page 105 of 159

PDR Activity
3 Copyright © 2014, Health and Social Care Information Centre.
Background
The Board requested information in relation to our commitment that each employee has a PDR. In our last report to the Board we reported that by the end of the last financial year 85% of employees had undergone a PDR.
While we would not anticipate reaching 100% compliance due to the numbers of people who are out of the business at any one time* the levels of activity are greater now compared to the same point of the previous year:
90% of employees have uploaded a PDR since 1st September 2015 as compared to 74% in the previous year.
We are also able to comfirm that this higher rate of compliance has been consistently maintained throughout the year as 87% of employees also received their start of year performance meeting with their manager.
Current PDR Activity by Directorate
2,460 PDRs were uploaded across the organisation out of a possible 2,743.
*Approximately 4% of the workforce are away from the workplace at any one time due to a number of factors such as maternity leave, secondment or health related absence etc.
03 (
f) P
erso
nal D
evel
opm
ent R
evie
w(P
DR
)
Page 106 of 159

PDR Activity
4 Copyright © 2014, Health and Social Care Information Centre.
Table view of mid-year PDRs
Directorate Uploaded Headcount Percentage
928 Architecture, Standards and Innovation (Dir) Total 214 256 83.6%
928 Clinical Professional Leadership (Dir) Total 2 6 33.3%
928 Customer Relations (Dir) Total 72 84 85.7%
928 Finance and Corporate Services (Dir) Total 170 195 87.2%
928 Health Digital Services (Dir) Total 404 446 90.6%
928 HR and Transformation (Dir) Total 55 59 93.2%
928 Information and Analytics (Dir) Total 489 550 88.9%
928 Operations and Assurance Services (Dir) Total 845 914 92.5%
928 Provider Support and Integration (Dir) Total 209 233 89.7%
TOTAL 2,460 2,743 89.7%
*Approximately 4% of the workforce are away from the workplace at any one time due to a number of factors such as maternity leave, secondment or health related absence etc.
Page 107 of 159

Page 1 of 1
Board meeting – Public session
Title of paper: Direction from Department of Health for a Breast Implant Registry – Formal Consultation
Board meeting date: 27 January 2016
Agenda item no: HSCIC 16 06 04 a
Paper presented by:
Martin Severs, Interim Director of Information and Analytics, Caldicott Guardian and Lead Clinician
Paper prepared by:
Alyson Whitmarsh, Clinical Audit & Registries Programme Manager, Information & Analytics Directorate John Varlow, Information Analysis Director, Information & Analytics Directorate
Paper approved by: (Sponsor Director) Professor Martin Severs, Interim Director of Information and Analytics, Caldicott Guardian and Lead Clinician
Purpose of the paper: To enable the views of the Board to be considered as part of the formal consultation on the Direction prior to it being signed by the Department of Health. This consultation is in line with our agreed process.
Key risks and issues:
Obtaining patient consent. Patient consent is
obtained to support some existing audits and opportunities do exist to obtain consent.
Potential delays within the SCII process. The registry is being assessed for burden and considered as a collection.
The Registry will need to be self-funding from March ‘17. Internationally, manufacturers or providers support on a per implant basis.
The Direction provides a legal basis for HSCIC to collect the data and must be in place before data can flow. If the Direction is not approved then there will be reputational risks for the HSCIC in not delivering to the agreed timeframe as the data cannot flow without Directions in place.
Patient/public interest:
Indirect
Actions required by the board: Consider the draft Direction and to identify any issues or concerns as part of the formal consultation process.
04 (
a) B
reas
t Im
plan
t Reg
istr
y
Page 108 of 159

1 Copyright © 2016, Health and Social Care Information Centre.
Direction from the Department of Health to establish and operate a Breast Implant Registry
Formal consultation with the HSCIC Board
Alyson Whitmarsh
7th
January 2016
04 (
a) B
reas
t Im
plan
t Reg
istr
y
Page 109 of 159

Direction from the Department of Health to establish and operate a Breast Implant Registry
2 Copyright © 2016, Health and Social Care Information Centre.
Contents 1 Executive Summary 3
2 Background 3
3 Recommendation 3
4 Implications 3
4.1 Strategy Implications 3
4.2 Financial Implications 4
4.3 Stakeholder Implications 4
4.4 Handling 5
5 Risks and Issues 5
6 Corporate Governance and Compliance 5
7 Management Responsibility 6
8 Actions Required of the Board 6
Page 110 of 159

Direction from the Department of Health to establish and operate a Breast Implant Registry
3 Copyright © 2016, Health and Social Care Information Centre.
1 Executive Summary
The Health and Social Care Information Centre (HSCIC) has been commissioned to develop a Breast Implant Registry on behalf of the Department of Health (DH). The registry is designed to capture all breast implant surgery carried out, both privately and by the NHS, and is being produced in response to the requirements from the Keogh Review of Regulation of Cosmetic Interventions. The registry will allow patients to be traced in the event of a product recall. Information captured by the registry will also be analysed and published by the HSCIC.
A Direction from the DH is needed to provide the legal basis for the data to flow. The draft Direction which has been reviewed by Information Governance is available on request.
2 Background
The registry will support the implementation of Recommendation 21 of the Keogh Review of
the Regulation of Cosmetic Interventions:
“A National Breast and Cosmetic Implant Registry should be established and operational
within 12 months. All cosmetic surgery providers need to keep a minimum data set that
should be defined by the RCS Inter-specialty Group. This should include details of the
implant, the surgeon, the hospital and appropriate outcomes. These data should be easily
accessible in the case of a product recall”.
The priority is to develop and maintain a breast implant registry. The long term vision is to
expand the registry to other types of implant. The registry has the support of the relevant
ministers and a detailed work package between DH and the HSCIC has been agreed.
The registry will be established for England. The HSCIC is asked to work with the devolved
administrations to enable them to request that the HSCIC to collect data on their behalf.
3 Recommendation
The Board is asked to consider this draft Direction and to identify any issues or concerns as part of the formal consultation process. This will provide the legal basis for collection of data to support the registry.
4 Implications
4.1 Strategy Implications
The development and operation of this registry supports the following parts of the HSCIC strategy: Make better use of health and care information
04 (
a) B
reas
t Im
plan
t Reg
istr
y
Page 111 of 159
Direction from the Department of Health to establish and operate a Breast Implant Registry
4 Copyright © 2016, Health and Social Care Information Centre.
• Make available more information, data and insight. • Citizens will make informed choices about their own care. • Care professionals will make better and safer decisions. • Policy makers will better commission health and care, In addition, the 2015-16 HSCIC business plan describes the intention to deliver the registry: ‘Deliver the key national clinical audits, including the Female Genital Mutilation enhanced dataset and the development of the Breast Implant Audit registry ‘.
4.2 Financial Implications
This service is directly funded by the DH (value £395,557 over two years). A POSA work package is in place for the current year. Funding is agreed until the end of March 2017 after which the registry is to be become self-funding. The funding is largely for the staff resources needed to develop, operate and maintain the registry. In the event that a sustainable funding model is not achieved; the HSCIC retain the option to close the service if it becomes financially unviable.
4.3 Stakeholder Implications
The DH is the commissioner however there are several other key stakeholders. The registry is being developed with the guidance of an advisory group which includes representation from the relevant professional bodies (The British Association of Aesthetic Plastic Surgeons (BAAPS) and the British Association of Plastic Reconstructive and Aesthetic Surgeons (BAPRAS)), the Medicines and Healthcare Products Regulatory Authority (MHRA), patient representatives and bodies representing private and NHS providers. Stakeholders are agreed for the need to be able to trace individuals in the event of a product recall. The monitoring of outcomes by brand, hospital and surgeon, highlighting where these fall below an expected performance in order to allow investigation is under discussion. The MHRA regulates medicines, medical devices and blood components for transfusion in the UK. They are responsible for ensuring their safety, quality and effectiveness and will issue safety alerts, if required, for breast implants. Providers will be responsible for patient recall in the event of a patient safety (implant) alert. The HSCIC will conduct track and trace for patients’ latest registered address and for mortality status and disseminate to providers to enable them to conduct recalls. No further disseminations are planned. Any requests for dissemination will be subject appropriate legal gateways and will be charged on a cost recovery basis. Some stakeholders have expressed concern over the need for patient consent however the registry’s commissioners and our own IG advice confirms this is necessary. Other audits have been successful in securing patient consent for data submission. As with other consented collections managed by the audit and registry team, the input and support of HSCIC IG will be required for the development and approval of the consent model and associated fair processing information provided to patients. Stakeholders are keen to see the registry progress due to the Keogh review recommendations, and because other countries are now operating similar registries, on which this one is based.
Page 112 of 159

Direction from the Department of Health to establish and operate a Breast Implant Registry
5 Copyright © 2016, Health and Social Care Information Centre.
Separate working groups have also been established to advise on the detailed content of the registry, analysis and governance.
4.4 Handling
A communications plan has been developed. Communications are being developed in conjunction with the professional bodies and the organisation representing providers to ensure that the responsibilities of providers and clinicians within the scope of the registry are clear, understood and widely communicated to the relevant stakeholders. Patients are being consulted during the registry development. Information and guidance which will support clinicians and patients to have an informed discussion about how the information collected about them will be used will be provided. It is anticipated that publication of a Data Provision Notice will form part of the communications. Communication will take various forms and include direct communication with providers; website development; stakeholder updates and promotion through professional bodies.
5 Risks and Issues
Obtaining patient consent. Patient consent is already obtained to support some audits
and opportunities do exist to obtain consent during pre-operation discussions.
Potential delays within the SCCI process. The registry is currently being assessed for
burden. SCCI have been asked to consider the registry as a collection nonetheless
timescales are challenging.
Most activity takes place within private providers. The organisation representing these
providers is a member of the advisory group.
Funding from DH ends March ‘17. Registry will need to be self-funding.
Internationally, manufacturers or providers support on a per implant basis. Consensus
from the advisory group is that this should be workable in UK.
6 Corporate Governance and Compliance
The Breast Implant Registry has a signed POSA work package approved by the Corporate Approvals Board (CAB) and has a current entry on the Portfolio database. Information Governance has reviewed the draft Direction. Key progress indicators are outlined in the work package between the HSCIC and the DH and are reported to the advisory board and monitored by the commissioner. These can also be reported to the HSCIC Board.
04 (
a) B
reas
t Im
plan
t Reg
istr
y
Page 113 of 159
Direction from the Department of Health to establish and operate a Breast Implant Registry
6 Copyright © 2016, Health and Social Care Information Centre.
7 Management Responsibility
Alyson Whitmarsh, Clinical Audit & Registries Programme Manager, Information & Analytics Directorate. Martin Severs, Interim Director of Information and Analytics, Caldicott Guardian and Lead Clinician.
8 Actions Required of the Board
The Board are asked to consider the draft Direction and to identify any issues or concerns as part of the formal consultation process.
Page 114 of 159
Page 1 of 3
Carolyn Heaney Room 2N16 Quarry House, LS2 7UB Leeds XX January 2016
Andy Williams Chief Executive, Health and Social Care Information Centre 1 Trevelyan Square, Boar Lane Leeds LS1 6AE Dear Andy I am writing to direct the Health and Social Care Information Centre to establish and operate the Breast and Cosmetic Implant Registry. This service will support the implementation of Recommendation 21 of the Keogh Review of the Regulation of Cosmetic Interventions
“A National Breast and Cosmetic Implant Registry should be established and operational within 12 months. All cosmetic surgery providers need to keep a minimum data set that should be defined by the RCS Inter-specialty Group. This should include details of the implant, the surgeon, the hospital and appropriate outcomes, and these data need to be held in electronic format until the registry is operational. These data should be easily accessible in the case of a product recall”.
The priority is to develop and maintain a breast implant registry. However, the long term vision is to expand the registry to other types of implant, for example, buttock and calf implants. The Health and Social Care Act 2012 makes provisions for Secretary of State to direct the Health and Social Care Information Centre to exercise functions on the basis that Secretary of State considers it to be in the interests of the health service in England. Under section 254 of the 2012 Act, HSCIC is directed to:
host a Breast and Cosmetic Implant Registry to support the collection and storage of appropriately consented participant information;
04 (
a) B
reas
t Im
plan
t Reg
istr
y
Page 115 of 159

Page 2 of 3
trace NHS numbers, where not available, and where possible to trace for those patients whose NHS number was not initially supplied to allow unique identification within the registry;
track latest known patient address in the event of a product failure;
monitor the outcomes achieved by ‘brand’ of prosthesis, hospital and surgeon, and highlight where these fall below an expected performance in order to allow prompt investigation and to support follow-up action.
Please accept this letter as a direction given under subsection (1) of section 254 of the 2012 Act to the Health and Social Care Information Centre to establish and manage the Breast and Cosmetic Implant Registry, details of which are set out in the attached schedule. The Health and Social Care Information Centre is directed to publish and disseminate data in line with its responsibilities under relevant legislation and guidance following consultation with DH. The Breast and Cosmetic Implant Registry shall be established for England. The Health and Social Care Information Centre should work with the devolved administrations to enable those administrations to request that the Health and Social Care Information Centre to collect data on their behalf. Implementation Data can be submitted to the Breast and Cosmetic Implant Registry from April 2016 onwards and will follow a schema agreed between the Health and Social Care Information Centre and the Department of Health. The initial dataset schema is attached in the schedule below. Yours sincerely Director name Director title ..Ends
Page 116 of 159

Page 3 of 3
Schedule to Direction Breast and Cosmetic Implant Registry System Scope
1. The Service will enable the Health and Social Care Information Centre (HSCIC) to collect patient identifiable data with the appropriate patient consent on implant devices e.g. breast implants which have been inserted into the body for cosmetic or reconstructive surgery.
2. The data shall be securely stored and managed by the HSCIC acting as an agent for the Department of Health. No one outside HSCIC will have access to the registry. The Breast and Cosmetic Implant Registry will track and trace patients where the Medicines and Healthcare Products Regulatory Agency considers the risk to be high and referral back to a surgeon advisable.
3. The priority is to develop and maintain a breast implant registry. However, the long term vision is to expand the registry to other types of implant, for example, buttock and calf implants.
4. The HSCIC will become the Data Controller for data that is submitted to the registry. The key HSCIC deliverables are as follows;
Develop an appropriate dataset for the Breast Implant Registry. This will include mapping to existing clinical terminologies and classifications as appropriate.
Data will be collected from:
o Private cosmetic surgery clinics, providing breast augmentation services.
o NHS Providers of reconstructive and plastic surgery.
Trace NHS numbers, where not available, and where possible to trace for those patients whose NHS number was not initially supplied to allow unique identification within the registry.
Track latest known patient address in the event of a product failure.
Monitor the outcomes achieved by ‘brand’ of prosthesis, hospital and surgeon, and highlight where these fall below an expected performance in order to allow prompt investigation and to support follow-up action.
Publish data in line with its responsibilities under the Statistics and Registration Services Act 2007 (SRSA) and relevant professional guidance including the UK Statistics Authority Code of Practice for Official Statistics. HSCIC may also publish in other forms, manner and times that it considers appropriate following consultation with DH
Disseminate data in line with its responsibilities under relevant legislation and guidance following consultation with DH.
The initial database schema for a breast implant registry is below. Add in database schema
04 (
a) B
reas
t Im
plan
t Reg
istr
y
Page 117 of 159


Page 1 of 1
Board meeting – Public session
Title of paper: Direction from NHS England for the National Clinical Audit of Pulmonary Hypertension (NAPH) – Formal Consultation
Board meeting date: 27 January 2016
Agenda item no: HSCIC 16 06 04 b
Paper presented by:
Martin Severs, Interim Director of Information and Analytics, Caldicott Guardian and Lead Clinician
Paper prepared by:
Dominic Povey, Clinical Audit & Registries Operations Manager, Information & Analytics Directorate John Varlow, Information Analysis Director, Information & Analytics Directorate
Paper approved by: (Sponsor Director) Professor Martin Severs, Interim Director of Information and Analytics, Caldicott Guardian and Lead Clinician
Purpose of the paper: To enable the views of the Board to be considered as part of the formal consultation on the Direction prior to it being signed by NHS England. This consultation is in line with our agreed process.
Key risks and issues:
The HSCIC relies on Section 251 (NHS Act
2006) to set aside the common law duty of confidence and deliver the National Audit of Pulmonary Hypertension (NAPH).
The office of the Secretary of State, through the Confidentiality Advisory Group (CAG) has questioned the continued use of Section 251 (S251) support and highlighted the statutory powers open to NHS England to ‘Direct’ the HSCIC to complete this work. The continuation of the current route risks the refusal of CAG to renew the S251 support which without Directions would force the HSCIC close the data collection resulting in considerable reputational harm.
Obtaining patient consent. Patient consent is obtained to support some existing audits and opportunities do exist to obtain consent although it has been agreed that this is impractical for this clinical audit.
Patient/public interest: Indirect
Actions required by the board: Consider the draft Direction and to identify any issues or concerns as part of the formal consultation process.
04 (
b) P
ulm
onar
y H
yper
tens
ion
Dire
ctio
n
Page 118 of 159

1 Copyright © 2016, Health and Social Care Information Centre.
Direction from NHS England for the collection of data to support the National Audit of Pulmonary Hypertension (NAPH)
Formal consultation with the HSCIC Board
Dominic Povey / Alyson Whitmarsh
7th
January 2016
04 (
b) P
ulm
onar
y H
yper
tens
ion
Dire
ctio
n
Page 119 of 159

Direction from NHS England for the collection of data to support the National Audit of Pulmonary Hypertension (NAPH)
2 Copyright © 2016, Health and Social Care Information Centre.
Contents 1 Executive Summary 3
2 Background 3
3 Recommendation 3
4 Implications 3
4.1 Strategy Implications 3
4.2 Financial Implications 4
4.3 Stakeholder Implications 4
5 Risks and Issues 4
6 Corporate Governance and Compliance 5
7 Management Responsibility 5
8 Actions Required of the Board 5
Page 120 of 159

Direction from NHS England for the collection of data to support the National Audit of Pulmonary Hypertension (NAPH)
3 Copyright © 2016, Health and Social Care Information Centre.
1 Executive Summary
The HSCIC provides informatics and project management to the National Audit of Pulmonary Hypertension (NAPH) with a report being published on an annual basis covering a range of process and clinical outcome measures. The clinical audit has Section 251 (of the NHS Act 2006) support in place from the Confidentiality Advisory Group (CAG) to allow it to set aside the common law duty of confidence to collect and process the patient information. However, a Direction from NHS England is needed to provide a more appropriate legal basis for the data to flow. The draft ‘Direction’ drafted by NHS England (NHSE) is available on request.
2 Background
The NAPH is a nationwide clinical audit of specialised pulmonary hypertension centres in the UK. The purpose is to, describe clinical practice, measure practice against professionally agreed standards, provide epidemiological information for future service planning, measure clinical outcomes and facilitate quality improvement. The Audit informs PH services which are nationally commissioned by the National Commissioning Group (NCG), which oversees the national commissioning of highly specialised and often high cost healthcare services within NHSE. NHSE has commissioned the clinical audit since 2013 which is supported by a Provision of Services Agreement (POSA). The identifiable flow of data utilises Section 251 of the NHS Act 2006 to set aside the common law of confidence in order to flow the data without patient consent. Advice from CAG to the HSCIC on related clinical audits states this temporary measure needs to cease and be replaced by the more appropriate statutory powers of NHSE to ‘Direct’ the HSCIC to flow. The current CAG approval expires in the middle of April 2016.
3 Recommendation
The Board is asked to consider this draft Direction and to identify any issues or concerns as part of the formal consultation process. This will provide the legal basis for collection of data to support the clinical audit.
4 Implications
4.1 Strategy Implications
The development and operation of this Audit supports the following parts of the HSCIC strategy: Make better use of health and care information • Make available more information, data and insight. • Citizens will make informed choices about their own care. • Care professionals will make better and safer decisions. • Policy makers will better commission health and care,
04 (
b) P
ulm
onar
y H
yper
tens
ion
Dire
ctio
n
Page 121 of 159

Direction from NHS England for the collection of data to support the National Audit of Pulmonary Hypertension (NAPH)
4 Copyright © 2016, Health and Social Care Information Centre.
In addition, the 2015-16 HSCIC business plan describes the intention to deliver the clinical audit: ‘Deliver the key national clinical audits, including the Female Genital Mutilation enhanced dataset and the development of the Breast Implant Audit registry ‘.
4.2 Financial Implications
This service is directly funded by NHSE (current value £83k) and has a Provision of Service Agreement (POSA) work package in place for the current financial year. The commissioner has confirmed that ‘NHSE has currently no intention of discontinuing the contract’. However further details can only be provided after NHSE have finalised the internal funding arrangements for the 2016/17 financial year, expected by the end of January 2016.The funding is largely for the staff resources needed to develop, operate and maintain the clinical audit.
4.3 Stakeholder Implications
The NHSE Commissioner, the NAPH Lead Clinician, the patient representative group and others on the NAPH Project Board have been consulted on the proposal to move the legal basis from S251 support from CAG to ‘Directions’. Without exception all have been extremely supportive in understanding how this will negate the need to seek S251 support from CAG in future years by removing the need for an annual review and placing the audit under the statutory footing of a ‘Direction’. In addition to the implications for this clinical audit the ability to utilise ‘Directions’ for NAPH, it is of considerable interest at a strategic level by colleagues in the NHS England Medical Directorate who manage the National Clinical Audit Programme. This clinical audit has an international standing as the most comprehensive in this area providing vital information to clinicians, patients and commissioners for an extremely complex condition with an expensive treatment pathway.
4.4 Handling
The move from Section 251 support to ‘Directions’ will be communicated to the NAPH Programme Board as well as contacts in all specialised clinical centres. In addition the patient leaflet will be updated and in consultation with the PH Patient Association, patients will be notified of this change via their newsletter and communication routes. Assurances will need to be provided to patients that the move to ‘Directions’ will continue to maintain the stringent safeguards already in place and confirm the move as positive.
5 Risks and Issues
The HSCIC relies on Section 251 (NHS Act 2006) to set aside the common law duty of confidence and deliver the National Audit of Pulmonary Hypertension (NAPH).
The office of the Secretary of State, through the Confidentiality Advisory Group (CAG) has questioned the continued use of Section 251 (S251) support and highlighted the statutory powers open to NHS England to ‘Direct’ the HSCIC to complete this work.
Page 122 of 159

Direction from NHS England for the collection of data to support the National Audit of Pulmonary Hypertension (NAPH)
5 Copyright © 2016, Health and Social Care Information Centre.
The continuation of the current route risks the refusal of CAG to renew the S251 support which without Directions would force the HSCIC close the data collection resulting in considerable reputational harm.
Obtaining patient consent. Patient consent is obtained to support some existing audits and opportunities do exist to obtain consent although it has been agreed that this is impractical for this clinical audit.
6 Corporate Governance and Compliance
The NAPH has a signed POSA work package and has a current entry on the Portfolio database. Information Governance has reviewed the draft Direction and found it to be sound. Key progress indicators are outlined in the work package between the HSCIC and the NHSE and are reported to the advisory board and monitored by the commissioner. These can also be reported to the HSCIC Board.
7 Management Responsibility
Alyson Whitmarsh, Clinical Audit & Registries Programme Manager, Information & Analytics Directorate. Professor Martin Severs, Interim Director of Information and Analytics, Caldicott Guardian and Lead Clinician.
8 Actions Required of the Board
The Board are asked to consider the draft Direction and to identify any issues or concerns as part of the formal consultation process.
04 (
b) P
ulm
onar
y H
yper
tens
ion
Dire
ctio
n
Page 123 of 159


1 Copyright © 2015, Health and Social Care Information Centre
National Audit of Pulmonary Hypertension
(NAPH) Specification
04 (
b) P
ulm
onar
y H
yper
tens
ion
Dire
ctio
n
Page 124 of 159
2 Copyright © 2015, Health and Social Care Information Centre
Document Management Revision History Version Date Summary of Changes
0.1 Sept 2015 Review of initial draft by Dominic Povey – Operations Manager
0.2 Oct 2015 Review by Richard Sewart (NHS England)
Reviewers This document must be reviewed by the following people: author to indicate reviewers
Reviewer name Title / Responsibility Date Version
Dominic Povey Operations Manager – HSCIC Clinical Audit Sept 2015 0.1
Richard Sewart NHS England - Data Sharing and Privacy Specialist Oct 2015 0.2
Document filename: National Audit of Pulmonary Hypertension (NAPH) Specification v1.0 05-01-16
Programme: CASU Project: National Audit of Pulmonary Hypertension
Document Reference: NAPH Spec
Project Manager: Julie Michalowski
Status: Final
Owner: Dominic Povey Version: 1.0
Author: Julie Michalowski Version issue date: 5th Jan 2016
Page 125 of 159

3 Copyright © 2015, Health and Social Care Information Centre
Document Control:
The controlled copy of this document is maintained in the HSCIC corporate network. Any copies of this document held outside of that area, in whatever format (e.g. paper, email attachment), are considered to have passed out of control and should be checked for currency and validity.
04 (
b) P
ulm
onar
y H
yper
tens
ion
Dire
ctio
n
Page 126 of 159
4 Copyright © 2015, Health and Social Care Information Centre
1. Introduction
The National Audit of Pulmonary Hypertension (NAPH) was established in 2010. Initial funding was provided by the patient group Pulmonary Hypertension - UK (PH-UK). HSCIC provides informatics and project management to the audit with a report being published on an annual basis covering a range of process and outcome measures. NHS England and HSCIC act as Data Controllers for the Audit. Clinical leadership is provided by Dr Simon Gibbs, Consultant Cardiologist from Imperial College Healthcare NHS Trust and has been since the audit’s inception. Clinical input into the audit is also provided by the National Pulmonary Hypertension Centres of the UK and Ireland Physicians Committee.
The Audit is now funded by the NHS England Specialised Services Team.
2. The Audit The National Audit of Pulmonary Hypertension (NAPH) is a nationwide audit of specialised pulmonary hypertension centres in the UK. The purpose of the Audit is to describe clinical practice, measure practice against professionally agreed standards, provide epidemiological information for future service planning, measure clinical outcomes and facilitate quality improvement. In addition, in 2015 the Audit provided analysed data for the Pulmonary Hypertension Dashboard, part of NHS E Specialised services quality dashboards.
There are eight centres in the UK, 7 in England trusts and 1 in Scotland (although the de-identified pseudonymised data flow from Scotland is outside of this specification) that are responsible for diagnosis and treatment planning in their own services and any shared care arrangements with other organisations :
Great Ormond Street Hospital for Children NHS Foundation Trust
Imperial College Healthcare NHS Trust
Papworth Hospital NHS Foundation Trust
Royal Brompton and Harefield NHS Foundation Trust
Royal Free London NHS Foundation Trust
Sheffield Teaching Hospitals NHS Foundation Trust
The Newcastle upon Tyne Hospitals NHS Foundation Trust
3. Informatics
The Audit uses the HSCIC’s Clinical Audit Platform (CAP) to collect data from the eight centres. Most centres upload data directly into the system with two manually entering data. Data collection is on a continuous basis with an annual extraction of data forming a cohort of patients who were seen in the pulmonary hypertension service within a specified 12 month period.
Page 127 of 159

5 Copyright © 2015, Health and Social Care Information Centre
4. The Dataset
The dataset was reviewed and revised in 2012/13 by the HSCIC and the clinical lead. Since then minor amends have been made as clinical requirements have developed. A list of data items collected can be found in the NAPH Technical Output Specification (dataset) v1.3.
5. Audit Outputs
5.1 Five annual reports have been published; the sixth is currently in progress. The outputs for the Audit are determined by the clinical lead and approved by the National Pulmonary Hypertension Centres of the UK and Ireland Physicians Committee. PHA UK and the Specialised Commissioning Groups NHS England are consulted on the Audit’s output on an annual basis.
5.2 In 2015, the Audit provided analysed data for the Specialised Services Quality Dashboard to provide assurance on the quality of care by collecting new information about outcomes from healthcare providers. The Pulmonary Hypertension element of the dashboard covers three of the four measures.
04 (
b) P
ulm
onar
y H
yper
tens
ion
Dire
ctio
n
Page 128 of 159


DRAFT V0.1
1
D I R E C T I O N S
NATIONAL HEALTH SERVICE, ENGLAND
The Health and Social Care Information Centre (Establishment of Information Systems for NHS Services:
National Audit of Pulmonary Hypertension) Directions 2016
The National Health Service Commissioning Board gives the following Directions to the Health and Social Care Information Centre in exercise of the powers conferred by sections 254(1), (3) and (6) of the Health and Social Care Act 2012.
In accordance with section 254(5) of the Health and Social Care Act 2012, the National Health Service Commissioning Board has consulted the Health and Social Care Information Centre before giving these Directions.
Citation, commencement and interpretation
1. These Directions may be cited as The Health and Social Care Information Centre (Establishment of Information Systems for NHS Services: National Audit of Pulmonary Hypertension) Directions 2016 and shall come into force on 1 April 2016.
2. In these Directions–
“The 2012 Act” means the Health and Social Care Act 20121;
“The Board” means the National Health Service Commissioning Board2;
“HSCIC” means the Health and Social Care Information Centre3;
“Relevant Organisation”
means the NHS Trusts and NHS Foundation Trusts listed in the Specification;
1 2012 c7 2 The National Health Service Commissioning Board was established by section 1H of the National Health Service Act 2006 (2006 c 41.), and operates as NHS England. 3 The Health and Social Care Information Centre is a body corporate established under section 252(1) of the Health and Social Care Act 2012
04 (
b) P
ulm
onar
y H
yper
tens
ion
Dire
ctio
n
Page 129 of 159

2
“Specification” means the National Audit of Pulmonary Hypertension (NAPH) Specification version 1.0 dated 05/01/2016 and annexed to these Directions at Annex A or any subsequent amended version of the same document;
“Technical Output Specification”
means the NAPH Technical Output Specification version 1.3 dated 07/02/2014 and annexed to these Directions at Annex B or any subsequent amended version of the same document.
Establishing and Operating the National Audit of Pulmonary Hypertension Information System
3. – (1) Pursuant to its powers under sections 254(1) and 254(6) of the 2012 Act, the Board directs the HSCIC to establish and operate a system for the collection of the information described in sub-paragraph (2) from the Relevant Organisations, such system to be known as “the National Audit of Pulmonary Hypertension Information System”.
(2) The information referred to in sub-paragraph (1) is the information described in the Technical Output Specification.
(3) The Board directs HSCIC to carry out the activities described in sub-paragraph (1) in accordance with the Specification and Technical Output Specification.
S254(3) - Requirement for these Directions
4. In accordance with section 254(3) of the 2012 Act, the Board confirms that it is necessary or expedient for it to have the information which will be obtained through the HSCIC complying with these Directions in relation to the Board’s functions in connection with the provision of NHS Services. In particular the information obtained through compliance with these Directions will facilitate or enable the achievement of the purposes that are described in the Specification.
Fees and Accounts
5. Pursuant to sub-section 254(7) of the 2012 Act, HSCIC is entitled to charge the Board a reasonable fee in respect of the cost of HSCIC complying with these Directions and the Board acknowledges such right and agrees to meet such reasonable fee charged by HSCIC.
Page 130 of 159

3
6. The HSCIC must keep proper accounts, and proper records in relation to the accounts, in connection with the National Audit of Pulmonary Hypertension Information System.
Review of these Directions
7. These Directions will be reviewed when the Board approves any amendment to the
Specification or Technical Output Specification. This review will include consultation with the HSCIC as required by sub-section 254(5) of the 2012 Act.
Signed by authority of the NHS Commissioning Board
Sir Bruce Keogh Caldicott Guardian
[INSERT DATE]
Annex A – National Audit of Pulmonary Hypertension – Specification Annex A has been removed and can be provided on request. Annex B – National Pulmonary Hypertension Audit – Technical Output Specification
Annex B has been removed and can be provided on request.
04 (
b) P
ulm
onar
y H
yper
tens
ion
Dire
ctio
n
Page 131 of 159

Page 1 of 1
Board meeting – Public session
Title of paper: Direction from NHS England for National Cancer Waiting Times Monitoring Dataset
Board meeting date: 27 January 2016
Agenda item no: HSCIC 15 06 04 d
Paper presented by: Rob Shaw, Director of Operations and Assurance Services
Paper prepared by: Graham Ambrose, Service Delivery Manager, Operations and Assurance Services
Paper approved by: (Sponsor Director) Rob Shaw, Director of Operations and Assurance Services
Purpose of the paper: To bring the final draft of the Direction to enable the views of the Board to be considered as part of the formal consultation prior to these being signed by NHS England. This consultation is in line with our agreed process.
Key risks and issues:
The Direction provides a legal basis for HSCIC to collect the proposed updated data set through the existing service provided to NHS England. The main risk is that suppliers will not be ready to send the new data items for the 1st April 2016.
Patient/public interest: Indirect
Actions required by the board: Approval of the draft Direction
04 (
d) C
ance
r W
aitin
g T
ime
Dire
ctio
n
Page 132 of 159


1 Copyright © 2015, Health and Social Care Information Centre.
Direction from NHS England for National Cancer Waiting Times Monitoring dataset
Consultation and approval by the HSCIC Board
Rob Shaw
27 January 2016
04 (
d) C
ance
r W
aitin
g T
ime
Dire
ctio
n
Page 133 of 159

Direction from NHS England for National Cancer Waiting Times Monitoring dataset
2 Copyright © 2015, Health and Social Care Information Centre.
Contents
Contents 2
Executive Summary 3
Background 3
Recommendation 3
Implications 3
Strategy Implications 3
Financial Implications 3
Stakeholder Implications 4
Handling 4
Risks and Issues 4
Corporate Governance and Compliance 4
Management Responsibility 4
Actions Required of the Board 5
Page 134 of 159

Direction from NHS England for National Cancer Waiting Times Monitoring dataset
3 Copyright © 2015, Health and Social Care Information Centre.
Executive Summary
The purpose of this paper is to present an updated Direction paper for the National Cancer Waiting Times Monitoring data set to the the HSCIC Board for comment and approval.
Background
The Cancer Waiting Times service is provided by HSCIC as commissioned by NHS England. Following the Department of Health review of Cancer Waiting Times Standards it was confirmed in Improving Outcomes: A Strategy for Cancer that: “overall, cancer waiting time standards should be retained. Shorter waiting times can help to ease patient anxiety and, at best, can lead to earlier diagnosis, quicker treatment, a lower risk of complications, an enhanced patient experience and improved cancer outcomes. The current cancer waiting times standards will therefore be retained.” An updated version of the National Cancer Waiting Times Monitoring Data Set (NCWTMDS) is detailed in the attached specification document. This supports the continued management and monitoring of waiting times standards. This Directions paper supports the enhanced specification which introduces a new file format and two new data items for use from 01 April 2016. HSCIC have completed the changes required to accept the new data items and will release the changes in April 2016 once all suppliers are ready to submit data.
Recommendation
That the Board approve the draft Direction for the National Cancer Waiting Times Monitoring data set.
Implications
Strategy Implications
The National Cancer Waiting Times Monitoring service is an existing service provided by HSCIC under the agreed organisational strategy and business plans.
Financial Implications
There are no additional financial implications as a result of this proposal as the service is fully supported under the existing POSA and the Service Level Agreement. The service is fully funded by NHS England.
04 (
d) C
ance
r W
aitin
g T
ime
Dire
ctio
n
Page 135 of 159

Direction from NHS England for National Cancer Waiting Times Monitoring dataset
4 Copyright © 2015, Health and Social Care Information Centre.
Stakeholder Implications
Trusts that provide data into the National Cancer Waiting Times Monitoring service will need to supply the two additional data items from April 2016 where appropriate. NHS England has communicated details of the changes out to stakeholders and system suppliers. Systems and Service Delivery will work with suppliers to test submissions in readiness for April 2016.
Handling
NHS England has communicated the proposed changes out to stakeholders and suppliers and will continue to update them on progress.
Risks and Issues
The major risk is that suppliers will not be ready to submit the additional data items by April 2016. NHS England are responsible for ensuring that suppliers are ready to send the new data items although HSCIC will assist with testing submissions from suppliers and will work with NHS England and the Standardisation Committee for Care Information (SCCI) to determine the readiness of stakeholders before implementation of the proposed changes.
Corporate Governance and Compliance
The information standard (SCCI0147) in this updated Direction for NCWTMDS has been approved for publication by the Department of Health under section 250 of the Health and Social Care Act 2012. Assurance that this information standard meets the requirements of the Act and is appropriate for the use specified in the specification document has been provided by SCCI, a sub-group of the National Information Board. This information standard comprises the following documents:
Requirements Specification
Change Specification
Implementation guidance. An Information Standards Notice (SCCI0147 Amd 7/2015) has been issued.
Management Responsibility
Rob Shaw, Executive Director, Operations and Assurance Services Sean Walsh, Director, Systems and Service Delivery, Operations and Assurance Services
Page 136 of 159

Direction from NHS England for National Cancer Waiting Times Monitoring dataset
5 Copyright © 2015, Health and Social Care Information Centre.
Graham Ambrose, Service Delivery Manager, Systems and Service Delivery, Operations and Assurance Services
Actions Required of the Board
The Board is asked to consider and approve the draft Direction for the National Cancer Waiting Times Monitoring data set.
04 (
d) C
ance
r W
aitin
g T
ime
Dire
ctio
n
Page 137 of 159


DRAFT V0.2
1
D I R E C T I O N S
NATIONAL HEALTH SERVICE, ENGLAND
The Health and Social Care Information Centre (Establishment of Information Systems for NHS Services: National Cancer Waiting Times Monitoring (SCCI0147))
Directions 2015
The National Health Service Commissioning Board gives the following Directions to the Health and Social Care Information Centre in exercise of the powers conferred by sections 254(1), (3) and (6) of the Health and Social Care Act 2012.
In accordance with section 254(5) of the Health and Social Care Act 2012, the National Health Service Commissioning Board has consulted the Health and Social Care Information Centre before giving these Directions.
Citation, commencement and interpretation
1. These Directions may be cited as The Health and Social Care Information Centre (Establishment of Information Systems for NHS Services: National Cancer Waiting Times Monitoring (SCCI0147)) Directions 2015 and shall come into force on [insert date].
2. In these Directions–
“The 2012 Act” means the Health and Social Care Act 20121;
“The Board” means the National Health Service Commissioning Board2;
“HSCIC” means the Health and Social Care Information Centre3;
"Information means a document containing standards in relation to the
1 2012 c7 2 The National Health Service Commissioning Board was established by section 1H of the National Health Service Act 2006 (2006 c 41.), and operates as NHS England. 3 The Health and Social Care Information Centre is a body corporate established under section 252(1) of the Health and Social Care Act 2012
04 (
d) C
ance
r W
aitin
g T
ime
Dire
ctio
n
Page 138 of 159

2
Standard" processing of information as provided for in section 250(2) of the 2012 Act. References to the number and title of an Information Standard are to the number and title given to a particular Information Standard within the Information Standards Notice;
"Information Standards Notice"
means the document published by or on behalf of the Board or the Secretary of State to confirm the making or amendment of an Information Standard, summarise its purpose and scope, reference the documentation in which the details of the Standard are set out and mandate compliance with it;
“Relevant Organisation”
means an organisation type that is listed under “applies to” in the Specification;
“SCCI0147” is the unique reference number for the National Cancer Waiting Times Monitoring Data Set Information Standard;
“Specification” means the National Cancer Waiting Times Monitoring Dataset V 1.2 Specification that has been published by the Board version 3.3 dated 30/10/2015 and annexed to these Directions at Annex A or any subsequent amended version of the same document published by the Board which supersedes version 3.2;
“Technical Output Specification”
means Part 2 of the Specification.
Establishing and Operating the National Cancer Waiting Times Monitoring Information System
3. – (1) Pursuant to its powers under sections 254(1) and 254(6) of the 2012 Act, the Board directs the HSCIC to establish and operate a system for the collection of the information described in sub-paragraph (2) from the Relevant Organisations, such system to
be known as “the National Cancer Waiting Times Monitoring Information System (SCCI0147)”.
(2) The information referred to in sub-paragraph (1) is the information described in the Technical Output Specification.
(3) The Board directs HSCIC to carry out the activities described in sub-paragraph (1) in accordance with the criteria in part 1 of the Specification and generally in such a way as to enable and facilitate the Concept of Operation specified in part 3 of the Specification and compliance with Information Standards Notice SCCI0147.
Page 139 of 159

3
S254(3) - Requirement for these Directions
4. In accordance with section 254(3) of the 2012 Act, the Board confirms that it is necessary or expedient for it to have the information which will be obtained through the HSCIC complying with these Directions in relation to the Board’s functions in connection with the provision of NHS Services. In particular the information obtained through compliance with these Directions will facilitate or enable the achievement of the purposes of Information Standard SCCI0147 that are described in the Specification.
Fees and Accounts
5. Pursuant to sub-section 254(7) of the 2012 Act, HSCIC is entitled to charge the Board a reasonable fee in respect of the cost of HSCIC complying with these Directions and the Board acknowledges such right and agrees to meet such reasonable fee charged by HSCIC.
6. The HSCIC must keep proper accounts, and proper records in relation to the
accounts, in connection with the National Cancer Waiting Times Monitoring Information System (SCCI0147).
Review of these Directions
7. These Directions will be reviewed when the Board approves any amendment to the
Information Standard SCCI0147. This review will include consultation with the HSCIC as required by sub-section 254(5) of the 2012 Act.
Signed by authority of the NHS Commissioning Board
Sir Bruce Keogh Caldicott Guardian
[INSERT DATE]
04 (
d) C
ance
r W
aitin
g T
ime
Dire
ctio
n
Page 140 of 159

4
Annex A – National Cancer Waiting Times Monitoring Dataset v1.2: Specification
014772015spec.pdf
Page 141 of 159

Pag
e 1
of
1
HS
CIC
– D
raft
Pu
bli
c B
oa
rd B
usin
ess S
ch
ed
ule
20
15-1
6
29
Ap
ril
20
15
*
10
Ju
ne
201
5 *
1
5 J
uly
20
15
*
23
Se
pt
20
15 *
2
5 N
ov 2
01
5 *
2
7 J
an
201
6 *
3
0 M
ar
20
16
*
Ac
co
un
tab
ilit
y
Ac
co
un
tab
ilit
y
Ac
co
un
tab
ilit
y
Ac
co
un
tab
ilit
y
Ac
co
un
tab
ilit
y
Ac
co
un
tab
ilit
y
Ac
co
un
tab
ilit
y
Re
gis
ter
of In
tere
sts
Min
ute
s o
f p
revio
us m
ee
tin
g (
Ma
r) –
to r
ati
fy
Pro
gre
ss o
n A
ctio
n P
oin
ts
Bo
ard
Forw
ard
Bu
sin
ess S
ch
ed
ule
20
15
-16
Re
po
rts f
rom
sub
-co
mm
itte
es
Re
gis
ter
of In
tere
sts
Min
ute
s o
f p
revio
us m
ee
tin
g (
Ap
r) –
to r
ati
fy
Pro
gre
ss o
n A
ctio
n P
oin
ts
Bo
ard
Forw
ard
Bu
sin
ess S
ch
ed
ule
20
15
-16
An
nu
al R
ep
ort
an
d A
cco
unts
fo
r
20
14
-20
15
fo
r H
SC
IC –
fo
r a
pp
rova
l
Re
gis
ter
of In
tere
sts
Min
ute
s o
f p
revio
us m
ee
tin
g (
Ju
ne
) –
to r
ati
fy
Pro
gre
ss o
n A
ctio
n P
oin
ts
Bo
ard
Forw
ard
Bu
sin
ess S
ch
ed
ule
20
15
-16
Re
po
rts f
rom
sub
-co
mm
itte
es
Info
rma
tio
n A
ssu
ran
ce
and
Cyb
er
Se
cu
rity
Co
mm
itte
e T
erm
s o
f
Re
fere
nce
Sch
em
a D
ele
ga
tio
n o
f A
uth
oritie
s –
bri
efin
g n
ote
Re
gis
ter
of In
tere
sts
Min
ute
s o
f p
revio
us m
ee
tin
g (
Ju
ly) –
to r
ati
fy
Pro
gre
ss o
n A
ctio
n P
oin
ts
Bo
ard
Forw
ard
Bu
sin
ess S
ch
ed
ule
20
15
-16
Re
po
rts f
rom
sub
-co
mm
itte
es
Re
gis
ter
of In
tere
sts
Min
ute
s o
f p
revio
us m
ee
tin
g (
Se
p) –
to r
ati
fy
Pro
gre
ss o
n A
ctio
n P
oin
ts
Bo
ard
Forw
ard
Bu
sin
ess S
ch
ed
ule
20
15
-16
Re
po
rts f
rom
sub
-co
mm
itte
es
Re
gis
ter
of In
tere
sts
Min
ute
s o
f p
revio
us m
ee
tin
g (
No
v) –
to r
ati
fy
Pro
gre
ss o
n A
ctio
n P
oin
ts
Bo
ard
Forw
ard
Bu
sin
ess S
ch
ed
ule
20
15
-16
and
201
6-1
7
Arr
an
gem
en
ts fo
r th
e A
nn
ua
l R
evie
w
of
Bo
ard
Eff
ective
ne
ss
Re
po
rts f
rom
sub
-co
mm
itte
es
Re
gis
ter
of In
tere
sts
Min
ute
s o
f p
revio
us m
ee
tin
g (
Ja
n) –
to r
ati
fy
Pro
gre
ss o
n A
ctio
n P
oin
ts
Bo
ard
Forw
ard
Bu
sin
ess S
ch
ed
ule
20
15
-16
and
201
6-1
7
Sch
em
e o
f D
ele
ga
ted
of
Au
thori
ties
20
16
-17
Co
rpo
rate
Go
ve
rna
nce
Ma
nu
al 2
016
-
17
An
nu
al R
evie
w o
f B
oa
rd
Eff
ective
ne
ss (
TB
C)
Re
po
rts f
rom
sub
-co
mm
itte
es
Su
pe
rvis
ing
Ma
na
ge
me
nt
Su
pe
rvis
ing
Ma
na
ge
me
nt
Su
pe
rvis
ing
Ma
na
ge
me
nt
Su
pe
rvis
ing
Ma
na
ge
me
nt
Su
pe
rvis
ing
Ma
na
ge
me
nt
Su
pe
rvis
ing
Ma
na
ge
me
nt
Su
pe
rvis
ing
Ma
na
ge
me
nt
Bo
ard
Pe
rfo
rma
nce
Pack
Fo
rth
co
min
g S
tatistica
l P
ub
lica
tio
ns
Re
vie
w o
f th
e N
atio
nal B
ack O
ffic
e
Tra
cin
g S
erv
ice
– I
nte
rim
Pro
gre
ss
Re
po
rt
Bo
ard
Pe
rfo
rma
nce
Pack –
fo
r in
form
ati
on
on
ly
Fo
rth
co
min
g S
tatistica
l P
ub
lica
tio
ns
– f
or
info
rma
tio
n o
nly
Bo
ard
Pe
rfo
rma
nce
Pack
Fo
rth
co
min
g S
tatistica
l P
ub
lica
tio
ns
Da
ta R
ele
ase
Re
vie
w:
Au
dit S
tatu
s
Re
po
rt
Sta
ff P
ers
ona
l D
eve
lop
me
nt
Re
vie
w
Re
po
rt
Ca
re.d
ata
no
te –
Bo
ard
ap
pro
va
ls
an
d b
ud
get
positio
n
Bo
ard
Pe
rfo
rma
nce
Pack
(i)
Da
ta Q
ua
lity K
ey P
erf
orm
ance
Ind
ica
tor
Pla
n (
pa
pe
r) –
fo
r in
form
ati
on
(ii)
Da
ta Q
ua
lity S
tra
teg
y o
n a
Pag
e
(pa
pe
r) –
fo
r in
form
ati
on
Fo
rth
co
min
g S
tatistica
l P
ub
lica
tio
ns
Tra
nsfo
rma
tion
Pro
gra
mm
e M
id-Y
ea
r R
ep
ort
20
15
-16
Bo
ard
Pe
rfo
rma
nce
Pack
Fo
rth
co
min
g S
tatistica
l P
ub
lica
tio
ns
Ele
ctr
on
ic R
efe
rra
l S
erv
ice
– L
esso
ns
Ide
ntified
(T
BC
)
Re
vie
w o
f th
e N
atio
nal B
ack O
ffic
e
Tra
cin
g S
erv
ice
- F
inal R
epo
rt (
DA
TE
T
O B
E C
ON
FIR
ME
D)
Bo
ard
Pe
rfo
rma
nce
Pack
Fo
rth
co
min
g S
tatistica
l P
ub
lica
tio
ns
Da
ta R
ele
ase
Re
vie
w:
Au
dit S
tatu
s
Up
da
te
Bo
ard
Pe
rfo
rma
nce
Pack
Fo
rth
co
min
g S
tatistica
l P
ub
lica
tio
ns
Info
rma
tio
n A
ssu
ran
ce
and
Cyb
er
Se
cu
rity
An
nu
al R
epo
rt 2
01
5-1
6
Tra
nsfo
rma
tion
Pro
gra
mm
e R
ep
ort
2
01
5-1
6
E-m
ed
3 D
irection
: F
it N
ote
A
gg
reg
ate
d D
ata
: Id
en
tified
Issu
es
Da
ta Q
ua
lity U
pd
ate
Eq
ua
lity a
nd
Div
ers
ity –
fo
r in
form
ati
on
on
ly
Str
ate
gy
Fo
rmu
lati
on
S
tra
teg
y F
orm
ula
tio
n
Str
ate
gy
Fo
rmu
lati
on
S
tra
teg
y F
orm
ula
tio
n
Str
ate
gy
Fo
rmu
lati
on
S
tra
teg
y F
orm
ula
tio
n
Str
ate
gy
Fo
rmu
lati
on
Th
e H
ea
lth
an
d S
ocia
l C
are
In
form
atio
n C
entr
e (
Imm
igra
tion
H
ea
lth
Cha
rge
) D
irection
s 2
015
U
K G
en
etic T
esting
Dir
ectio
ns
Da
ta S
erv
ice
fo
r C
om
mis
sio
ners
D
ire
ctio
ns
Ca
re.d
ata
re
vis
ed
NH
S E
ngla
nd
D
ire
ctio
ns
Dir
ectio
ns:
Da
ta E
xtr
actio
ns f
or
the
D
ep
art
me
nt o
f W
ork
an
d P
en
sio
ns F
it
to W
ork
Pro
gra
mm
e
HS
CIC
So
cia
l C
are
Work
Up
da
te
Typ
e 2
Ob
jectio
ns D
irection
Assu
rin
g T
ransfo
rma
tio
n U
pd
ate
D
ire
ctio
n
Ge
no
mic
s D
ire
ction
Dir
ectio
ns:
Fem
ale
Ge
nita
l M
utila
tio
n
Pre
ve
ntio
n P
roje
ct
E-m
ed
3 D
irection
: F
it N
ote
A
gg
reg
ate
d D
ata
HS
CIC
In
form
ation
Go
ve
rna
nce
S
tra
teg
y
Str
ea
mlin
ing
th
e In
de
pe
nde
nt
Info
rma
tio
n G
ove
rnan
ce
Ad
vic
e t
o
HS
CIC
Up
da
te o
n t
he
HS
CIC
(Im
mig
ratio
n
He
alth
Cha
rge
) D
irection
s
Dir
ectio
ns f
or
Pa
tien
t O
bje
ction
M
an
ag
em
en
t S
yste
m -
Up
da
te
Str
ea
mlin
ing
th
e In
de
pe
nde
nt
Info
rma
tio
n G
ove
rnan
ce
Ad
vic
e t
o
HS
CIC
Ge
no
mic
s D
ire
ction
Da
ta P
rovis
ion
No
tice
s (
TB
C)
Bre
ast Im
pla
nt R
eg
istr
y D
irectio
n
Pu
lmon
ary
Hyp
ert
ensio
n D
irectio
n
Dir
ectio
ns f
or
Pa
tien
t O
bje
ction
M
an
ag
em
en
t S
yste
m -
ra
tifica
tio
n
Str
ea
mlin
ing
th
e In
de
pe
nde
nt
Info
rma
tio
n G
ove
rnan
ce
Ad
vic
e t
o
HS
CIC
Ca
re.d
ata
DH
Direction
on O
bje
ctio
ns
Pla
nn
ing
P
lan
nin
g
Pla
nn
ing
P
lan
nin
g
Pla
nn
ing
P
lan
nin
g
Pla
nn
ing
B
usin
ess P
lan
201
5-1
6 –
fo
r a
pp
rova
l
Bo
ard
Ove
rvie
w a
nd
Pip
elin
e o
f In
ve
stm
en
t D
ecis
ion
s
Mid
-ye
ar
revie
w o
f C
orp
ora
te
Bu
sin
ess P
lan
201
5-1
6
Dra
ft C
orp
ora
te B
usin
ess P
lan 2
01
6-
17
(U
pd
ate
an
d T
imelin
e)
Co
mp
reh
ensiv
e S
pen
din
g R
evie
w
Up
da
te
Co
rpo
rate
Bu
sin
ess P
lan
20
16-1
7
(Fin
al)
Ap
ril
an
d M
ay 2
01
5
Ju
ne
20
15
Ju
ly a
nd
Au
gu
st
20
15
Se
pt
an
d O
ct
20
15
No
v a
nd
De
c 2
01
5
Ja
n a
nd
Fe
b 2
016
Ma
r 2
01
6
Ke
y M
ee
tin
gs
K
ey
Me
eti
ng
s
Ke
y M
ee
tin
gs
Ke
y M
ee
tin
gs
K
ey
Me
eti
ng
s
Ke
y M
ee
tin
gs
Ke
y M
ee
tin
gs
E
xe
cu
tive
Ma
na
ge
me
nt
Te
am
-
we
ekly
B
oa
rd S
trate
gy S
essio
n –
25
F
eb
rua
ry
R
em
un
era
tio
n C
om
mitte
e –
30
Ma
rch
E
xe
cu
tive
Ma
na
ge
me
nt
Te
am
-
we
ekly
B
oa
rd S
trate
gy S
essio
n –
20
M
ay
A
ssu
ran
ce
and
Ris
k C
om
mitte
e –
1
0 J
un
e
E
xe
cu
tive
Ma
na
ge
me
nt
Te
am
-
we
ekly
In
form
atio
n A
ssu
ran
ce
and
C
yb
er
Se
cu
rity
Co
mm
itte
e –
01
Ju
ly
R
em
un
era
tio
n C
om
mitte
e –
07
Au
gu
st
E
xe
cu
tive
Ma
na
ge
me
nt
Te
am
–
we
ekly
B
oa
rd B
usin
ess M
ee
tin
g –
02
S
ep
tem
be
r
In
form
atio
n A
ssu
ran
ce
and
C
yb
er
Se
cu
rity
Co
mm
itte
e –
15
S
ep
tem
be
r
A
ssu
ran
ce
and
Ris
k C
om
mitte
e –
1
6 S
ep
tem
be
r
E
xe
cu
tive
Ma
na
ge
me
nt
Te
am
–
we
ekly
B
oa
rd B
usin
ess M
ee
tin
g –
28
O
cto
be
r
In
form
atio
n A
ssu
ran
ce
and
C
yb
er
Se
cu
rity
Co
mm
itte
e –
12
N
ove
mb
er
A
ssu
ran
ce
and
Ris
k C
om
mitte
e –
1
0 N
ove
mbe
r
E
xe
cu
tive
Ma
na
ge
me
nt
Te
am
–
we
ekly
B
oa
rd B
usin
ess M
ee
tin
g –
16
D
ece
mb
er
A
ssu
ran
ce
and
Ris
k C
om
mitte
e –
1
3 J
an
ua
ry
In
form
atio
n A
ssu
ran
ce
and
C
yb
er
Se
cu
rity
Co
mm
itte
e –
13
Ja
nua
ry
E
xe
cu
tive
Ma
na
ge
me
nt
Te
am
–
we
ekly
B
oa
rd B
usin
ess M
ee
tin
g –
24
F
eb
rua
ry
In
form
atio
n A
ssu
ran
ce
and
C
yb
er
Se
cu
rity
Co
mm
itte
e –
15
M
arc
h
* P
lea
se s
ee
th
e f
inal
age
nd
a fo
r fu
ll d
eta
ils o
f th
e it
em
s d
iscu
sse
d a
t th
e s
tatu
tory
pu
blic
Bo
ard
me
eti
ngs
05 (
c) F
orw
ard
Bus
ines
s S
ched
ule
2015
-16
Page 142 of 159

Pag
e 1
of
1
H
SC
IC –
Dra
ft P
ub
lic B
oa
rd B
usin
ess S
ch
ed
ule
20
16-1
7 i
04
Ma
y 2
01
6 ii
0
8 J
un
e 2
01
6
07
Se
pt
20
16
30
No
v 2
01
6
01
Fe
b 2
017
29
Ma
r 2
017
Go
ve
rna
nc
e a
nd
Ac
co
un
tab
ilit
y
Go
ve
rna
nc
e a
nd
Ac
co
un
tab
ilit
y
Go
ve
rna
nc
e a
nd
Ac
co
un
tab
ilit
y
Go
ve
rna
nc
e a
nd
Ac
co
un
tab
ilit
y
Go
ve
rna
nc
e a
nd
Ac
co
un
tab
ilit
y
Go
ve
rna
nc
e a
nd
Ac
co
un
tab
ilit
y
Re
gis
ter
of In
tere
sts
Min
ute
s o
f p
revio
us m
ee
tin
g
Pro
gre
ss o
n A
ctio
n P
oin
ts
Bo
ard
Forw
ard
Bu
sin
ess S
ch
ed
ule
20
16-1
7
Re
po
rts f
rom
Su
b-C
om
mitte
es
An
nu
al R
evie
w o
f B
oa
rd E
ffective
ne
ss
Re
po
rt 2
01
5-1
6
Re
gis
ter
of In
tere
sts
Min
ute
s o
f p
revio
us m
ee
tin
g
Pro
gre
ss o
n A
ctio
n P
oin
ts
Bo
ard
Forw
ard
Bu
sin
ess S
ch
ed
ule
20
16-1
7
Re
po
rts f
rom
Su
b-C
om
mitte
es
* H
SC
IC A
nn
ua
l R
ep
ort
an
d A
ccou
nts
fo
r
20
15
-16
Re
gis
ter
of In
tere
sts
Min
ute
s o
f p
revio
us m
ee
tin
g
Pro
gre
ss o
n A
ctio
n P
oin
ts
Bo
ard
Forw
ard
Bu
sin
ess S
ch
ed
ule
20
16-1
7
Re
po
rts f
rom
Su
b-C
om
mitte
es
Sch
em
a D
ele
ga
tio
n o
f A
uth
oritie
s U
pd
ate
s
Re
gis
ter
of In
tere
sts
Min
ute
s o
f p
revio
us m
ee
tin
g
Pro
gre
ss o
n A
ctio
n P
oin
ts
Bo
ard
Forw
ard
Bu
sin
ess S
ch
ed
ule
20
16-1
7
Re
po
rts f
rom
Su
b-C
om
mitte
es
Re
gis
ter
of In
tere
sts
Min
ute
s o
f p
revio
us m
ee
tin
g
Pro
gre
ss o
n A
ctio
n P
oin
ts
Bo
ard
Forw
ard
Bu
sin
ess S
ch
ed
ule
20
16-1
7
Re
po
rts f
rom
Su
b-C
om
mitte
es
Re
gis
ter
of In
tere
sts
Min
ute
s o
f p
revio
us m
ee
tin
g
Pro
gre
ss o
n A
ctio
n P
oin
ts
Bo
ard
Forw
ard
Bu
sin
ess S
ch
ed
ule
20
16-1
7
an
d 2
01
7-1
8
Arr
an
gem
en
ts fo
r th
e A
nn
ua
l R
evie
w o
f
Bo
ard
Effe
ctive
ne
ss 2
01
6-1
7
Co
rpo
rate
Go
ve
rna
nce
Ma
nu
al 2
017
-18
Sch
em
e o
f D
ele
ga
ted
Au
tho
ritie
s 2
01
7-1
8
Re
po
rts f
rom
Su
b-C
om
mitte
es
Su
pe
rvis
ing
Ma
na
ge
me
nt
Su
pe
rvis
ing
Ma
na
ge
me
nt
Su
pe
rvis
ing
Ma
na
ge
me
nt
Su
pe
rvis
ing
Ma
na
ge
me
nt
Su
pe
rvis
ing
Ma
na
ge
me
nt
Su
pe
rvis
ing
Ma
na
ge
me
nt
Bo
ard
Pe
rfo
rma
nce
Pack
Tra
nsfo
rma
tion
Pro
gra
mm
e P
lan
201
6-1
7
Bo
ard
Pe
rfo
rma
nce
Pack
Bo
ard
Pe
rfo
rma
nce
Pack
Sta
ff P
ers
ona
l D
eve
lop
me
nt
Re
vie
w R
ep
ort
Bo
ard
Pe
rfo
rma
nce
Pack
Tra
nsfo
rma
tion
Pro
gra
mm
e M
id-Y
ea
r R
ep
ort
20
16
-17
Bo
ard
Pe
rfo
rma
nce
Pack
Sta
ff S
urv
ey R
esu
lts 2
01
6-1
7
Sta
ff P
ers
ona
l D
eve
lop
me
nt
Re
vie
w R
ep
ort
M
id-Y
ea
r R
ep
ort
Bo
ard
Pe
rfo
rma
nce
Pack
Tra
nsfo
rma
tion
Pro
gra
mm
e F
ina
l R
epo
rt
20
16
-17
Info
rma
tio
n A
ssu
ran
ce
an
d C
yb
er
Secu
rity
A
nn
ua
l R
ep
ort
20
16
-17
Str
ate
gy
Fo
rmu
lati
on
S
tra
teg
y F
orm
ula
tio
n
Str
ate
gy
Fo
rmu
lati
on
S
tra
teg
y F
orm
ula
tio
n
Str
ate
gy
Fo
rmu
lati
on
S
tra
teg
y F
orm
ula
tio
n
Dir
ectio
ns (
to b
e c
on
firm
ed
)
Str
ea
mlin
ing
th
e In
de
pe
nde
nt
Info
rma
tion
G
ove
rna
nce A
dvic
e t
o H
SC
IC U
pd
ate
Dir
ectio
ns (
to b
e c
on
firm
ed
)
Dir
ectio
ns (
to b
e c
on
firm
ed
)
Str
ea
mlin
ing
th
e In
de
pe
nde
nt
Info
rma
tion
G
ove
rna
nce A
dvic
e t
o H
SC
IC U
pd
ate
Dir
ectio
ns (
to b
e c
on
firm
ed
)
Dir
ectio
ns (
to b
e c
on
firm
ed
)
Str
ea
mlin
ing
th
e In
de
pe
nde
nt
Info
rma
tion
G
ove
rna
nce A
dvic
e t
o H
SC
IC U
pd
ate
Dir
ectio
ns (
to b
e c
on
firm
ed
)
Pla
nn
ing
P
lan
nin
g
Pla
nn
ing
P
lan
nin
g
Pla
nn
ing
P
lan
nin
g
iii B
usin
ess P
lan
201
6-1
7 (
* F
inal)
*
Mid
-ye
ar
revie
w o
f C
orp
ora
te B
usin
ess
Pla
n 2
01
6-1
7
* C
orp
ora
te B
usin
ess P
lan
201
7-1
8 (
Dra
ft)
* C
orp
ora
te B
usin
ess P
lan
201
7-1
8 (
Fin
al)
Pa
pe
rs f
or
Info
rma
tio
n O
nly
P
ap
ers
fo
r In
form
ati
on
On
ly
Pa
pe
rs f
or
Info
rma
tio
n O
nly
P
ap
ers
fo
r In
form
ati
on
On
ly
Pa
pe
rs f
or
Info
rma
tio
n O
nly
P
ap
ers
fo
r In
form
ati
on
On
ly
Da
ta R
ele
ase
Au
dit S
tatu
s R
ep
ort
Fo
rth
co
min
g S
tatistica
l P
ub
lica
tio
ns
Fo
rth
co
min
g S
tatistica
l P
ub
lica
tio
ns
Da
ta R
ele
ase
Au
dit S
tatu
s R
ep
ort
Fo
rth
co
min
g S
tatistica
l P
ub
lica
tio
ns
Fo
rth
co
min
g S
tatistica
l P
ub
lica
tio
ns
Da
ta R
ele
ase
Au
dit S
tatu
s R
ep
ort
Fo
rth
co
min
g S
tatistica
l P
ub
lica
tio
ns
Fo
rth
co
min
g S
tatistica
l P
ub
lica
tio
ns
Ap
ril
an
d M
ay 2
01
6
Ju
ne
an
d J
uly
20
16
A
ug
us
t a
nd
Se
pte
mb
er
20
16
Oc
tob
er
an
d N
ove
mb
er
201
6
De
ce
mb
er
20
16
an
d J
an
ua
ry 2
01
7
Fe
bru
ary
an
d M
arc
h 2
01
7
Ke
y M
ee
tin
gs
K
ey
Me
eti
ng
s
Ke
y M
ee
tin
gs
Ke
y M
ee
tin
gs
K
ey
Me
eti
ng
s
Ke
y M
ee
tin
gs
E
xe
cu
tive
Ma
na
ge
me
nt
Te
am
– w
ee
kly
B
oa
rd B
usin
ess M
ee
tin
g –
13
Ap
ril
20
16
A
ssu
ran
ce
and
Ris
k C
om
mitte
e –
24
Ma
y 2
01
6
In
form
atio
n A
ssu
ran
ce
and
Cyb
er
Se
cu
rity
Co
mm
itte
e –
18
Ma
y 2
01
6
P
ub
lic B
oa
rd M
ee
tin
g –
4 M
ay 2
01
6
E
xe
cu
tive
Ma
na
ge
me
nt
Te
am
– w
ee
kly
P
ub
lic B
oa
rd (
Acco
un
ts)
- 0
8 J
un
e
20
16
B
oa
rd B
usin
ess M
ee
tin
g –
27
Ju
ly 2
01
6
A
ssu
ran
ce
and
Ris
k C
om
mitte
e –
08
Ju
ne 2
016
In
form
atio
n A
ssu
ran
ce
and
Cyb
er
Se
cu
rity
Co
mm
itte
e –
20
Ju
ly 2
01
6
R
em
un
era
tio
n C
om
mitte
e –
12 J
uly
2
01
6
E
xe
cu
tive
Ma
na
ge
me
nt
Te
am
- w
ee
kly
P
ub
lic B
oa
rd M
ee
tin
g –
7 S
ep
tem
be
r 2
01
6
A
ssu
ran
ce
and
Ris
k C
om
mitte
e –
31
Au
gu
st 2
01
6
In
form
atio
n A
ssu
ran
ce
and
Cyb
er
Se
cu
rity
Co
mm
itte
e –
28
Se
pte
mb
er
20
16
E
xe
cu
tive
Ma
na
ge
me
nt
Te
am
– w
ee
kly
B
oa
rd B
usin
ess M
ee
tin
g 2
6 O
cto
be
r 2
01
6
P
ub
lic B
oa
rd S
em
ina
r –
30
Nove
mb
er
20
16
A
ssu
ran
ce
and
Ris
k C
om
mitte
e
- 1
6
No
ve
mb
er
20
16
In
form
atio
n A
ssu
ran
ce
and
Cyb
er
Se
cu
rity
Co
mm
itte
e -
16 N
ove
mb
er
20
16
R
em
un
era
tio
n C
om
mitte
e –
22
No
ve
mb
er
20
16
E
xe
cu
tive
Ma
na
ge
me
nt
Te
am
– w
ee
kly
B
oa
rd B
usin
ess M
ee
tin
g –
14
D
ece
mb
er
20
16
A
ssu
ran
ce
and
Ris
k C
om
mitte
e –
18
Ja
nua
ry 2
01
7
In
form
atio
n A
ssu
ran
ce
and
Cyb
er
Se
cu
rity
Co
mm
itte
e -
18 J
an
uary
20
17
E
xe
cu
tive
Ma
na
ge
me
nt
Te
am
– w
ee
kly
P
ub
lic B
oa
rd M
ee
tin
g –
1 F
eb
rua
ry
20
17
B
oa
rd B
usin
ess M
ee
tin
g 0
1 M
arc
h
20
17
A
ssu
ran
ce
and
Ris
k C
om
mitte
e –
15
M
arc
h 2
01
7
In
form
atio
n A
ssu
ran
ce
and
Cyb
er
Se
cu
rity
Co
mm
itte
e -
15 M
arc
h 2
01
7
R
em
un
era
tio
n C
om
mitte
e –
14 M
arc
h
20
17
i This
is a
liv
ing d
ocum
ent a
nd is s
ubje
ct to
re
gula
r up
date
s
ii P
lease s
ee
th
e f
ina
l ag
end
a f
or
the f
ull
deta
ils o
f th
e ite
ms d
iscussed a
t th
e s
tatu
tory
public
HS
CIC
Bo
ard
meetings
iii O
ccasio
nally
docum
ents
will
no
t be
rele
ased into
th
e p
ublic
dom
ain
alo
ngsid
e t
he B
oard
pack u
ntil th
ey h
ave b
een
ap
pro
ved b
y t
he B
oard
. *
The r
ele
vant
docum
ents
will
subseq
uen
tly b
e p
ublis
hed s
ep
ara
tely
on t
he H
SC
IC w
ebsite
05 (
d) F
orw
ard
Bus
ines
s S
ched
ule
2016
-17
Page 143 of 159


Page 1 of 1
Board meeting – Public session
Title of paper: HSCIC Statistical Publications
Board meeting date: 27 January 2016
Agenda item no: HSCIC 16 06 07 a
Paper presented by: For information only
Paper prepared by: Claire Thompson, Statistical Governance Manager
Paper approved by: (Sponsor Director) Chris Roebuck, Interim Director and Head of Profession for Statistics
Purpose of the paper:
This paper describes HSCIC Official (and National) Statistics publications planned for January – March 2016, and media and web coverage for publications released in October and November 2015.
Key risks and issues:
N/A
Patient/public interest: Overview of HSCIC Statistical Publications
Actions required by the board: For information
07
(a)
For
thco
min
g S
tatis
tical
Pub
licat
ions
Page 144 of 159


Copyright © 2015, Health and Social Care Information Centre
HSCIC Statistical Publications
Author Chris Roebuck
Date 14 January 2016
07 (
a) F
orth
com
ing
Sta
tistic
alP
ublic
atio
ns
Page 145 of 159

HSCIC Statistical Publications
1 Copyright © 2015, Health and Social Care Information Centre.
Contents
Contents 1
Purpose 2
Background to HSCIC Official Statistics 2
Forthcoming Publications 2
Official and National Statistics 2
Clinical Audits 6
User and Media Activity 7
Actions Required of the Board 11
Page 146 of 159

HSCIC Statistical Publications
2 Copyright © 2015, Health and Social Care Information Centre.
Purpose
This paper describes:
HSCIC Official (and National) Statistics publications planned for January – March 2016;
Media coverage for press released Official Statistics publications;
Web activity for publications released in October and November 2015.
Background to HSCIC Official Statistics
As at 13 November 2015, the HSCIC is responsible for 88 active (currently published or planned for future release) series of Official Statistics of which 25 are designated as National Statistics, which means that the UK Statistics Authority (UKSA) recognises them as being compliant with the Code of Practice for Official Statistics.
Official Statistics are expected to evolve and improve over time, to meet the changing needs of our users, to improve their quality and utility and to respond to changes in their administrative and management data sources.
“Experimental statistics” are new Official Statistics that are undergoing evaluation. A key part of this evaluation is user engagement whereby the HSCIC invites readers to comment on the publications, which helps to inform future releases.
Most HSCIC Official Statistics are published annually or more frequently. Generally, each edition is similar in content to previous versions but any substantial changes are noted below (note: no such changes are yet planned).
National Statistics are identified below with [NS].
Forthcoming Publications
Official and National Statistics
Dates for forthcoming publications are confirmed approximately six to eight weeks ahead of publication; until this point, the HSCIC announces only the planned month of publication.
January 2016
New releases
None scheduled for January.
Biennial
None scheduled for January.
Annual
13 January 2016 General Ophthalmic Services activity statistics - Selected statistics for England, April 2015 to September 2015 [NS]
28 January 2016 Accident and Emergency Attendances in England - 2014-15
07 (
a) F
orth
com
ing
Sta
tistic
alP
ublic
atio
ns
Page 147 of 159

HSCIC Statistical Publications
3 Copyright © 2015, Health and Social Care Information Centre.
Biannual
None scheduled for January.
Quarterly
13 January 2016 Statistics on NHS Stop Smoking Services in England - April 2015 to September 2015
19 January 2016 Numbers of Patients Registered at a GP Practice - January 2016
27 January 2016 Summary Hospital-level Mortality Indicator (SHMI) - Deaths associated with hospitalisation, England, July 2014 - June 2015
27 January 2016 Data on written complaints in the NHS - 2015/16 Quarter 2, Experimental [NS]
29 January 2016 Seven-day Services - England, Provisional, Experimental statistics
Monthly
07 January 2016 HES-DID Data Linkage Report - Provisional Summary Statistics, April 2014 to August 2015 (Experimental Statistics)
08 January 2016 HES-MHLD Data Linkage Report - Summary Statistics, September 2015
08 January 2016 Maternity Services Monthly Statistics - Maternity Services Statistics – May & June 2015
08 January 2016 NHS Safety Thermometer Report - England December 2014 - December 2015
14 January 2016 Provisional Monthly Patient Reported Outcome Measures (PROMs) in England - April 2014 to March 2015 - January 2016 Release
14 January 2016 Provisional Monthly Patient Reported Outcome Measures (PROMs) in England - April 2015 to August 2015
15 January 2016 Quality Outcomes Framework (QOF) Recorded Dementia Diagnoses - December 2015
20 January 2016 Improving Access to Psychological Therapies Report - October Final, November Primary 2015 and Quarter 2 2015/16
20 January 2016 Mental Health and Learning Disabilities Statistics - Monthly report: Final October 2015 and Provisional November 2015
21 January 2016 Learning Disability Services Monthly Statistics - Commissioner Census (Assuring Transformation), December 2015, Experimental Statistics
22 January 2016 NHS Sickness Absence Rates - September 2015 Provisional Statistics
22 January 2016 NHS Workforce Statistics - October 2015 Provisional Statistics
26 January 2016 Provisional Accident and Emergency Quality Indicators for England - October 2015, by provider
26 January 2016 Provisional Monthly Hospital Episode Statistics for Admitted Patient Care, Outpatient and Accident and Emergency data - April 2015 - October 2015
27 January 2016 Maternity Services Monthly Statistics - Maternity Services Statistics – July & August 2015
Page 148 of 159

HSCIC Statistical Publications
4 Copyright © 2015, Health and Social Care Information Centre.
Other
12 January 2016 NICE Technology Appraisals in the NHS in England (Innovation Scorecard) - to June 2015
15 January 2016 Health Survey for England 2014 report - new chapters
19 January 2016 Focus on Dementia
February 2016
New releases
03 February 2016 Care Information Choices, England December 2015
Biennial
None scheduled for February.
Annual
04 February 2016 Adult Critical Care in England 2014-15
10 February 2016 Personal Social Services: Staff of Social Services Departments, England September 2015
24 February 2016 Breast Screening Programme, England Statistics for 2014-15
Biannual
None scheduled for February.
Quarterly
11 February 2016 Patient Reported Outcome Measures (PROMs) in England - Special Topic PROMs Quarterly Topic of Interest Q2 2015-16
16 February 2016 NHS Dental Statistics for England 2015-16, Second quarterly report
19 February 2016 Learning Disability Services Quarterly Statistics Commissioner Census (Assuring Transformation), Q3 2015/16, Experimental Statistics
25 February 2016 NHS Outcomes Framework indicators February 2016 release
Monthly
04 February 2016 HES-Diagnostic Imaging Dataset Data Linkage Report Provisional Summary Statistics, April to September 2015 (Experimental Statistics)
05 February 2016 HES-MHLD Data Linkage Report Summary Statistics, October 2015
10 February 2016 NHS Safety Thermometer Report England January 2015 - January 2016
11 February 2016 Provisional Monthly Patient Reported Outcome Measures (PROMs) in England April 2014 to March 2015 - February 2016 Release
11 February 2016 Provisional Monthly Patient Reported Outcome Measures (PROMs) in England April 2015 to September 2015
07 (
a) F
orth
com
ing
Sta
tistic
alP
ublic
atio
ns
Page 149 of 159

HSCIC Statistical Publications
5 Copyright © 2015, Health and Social Care Information Centre.
12 February 2016 Quality Outcomes Framework (QOF) Recorded Dementia Diagnoses January 2016
19 February 2016 Learning Disability Services Monthly Statistics Commissioner census (Assuring Transformation), January 2016, Experimental Statistics
23 February 2016 Improving Access to Psychological Therapies Report November Final, December Primary 2015 and most recent quarterly data (Quarter 2 2015/16)
23 February 2016 Mental Health and Learning Disabilities Statistics Monthly report: Final November 2015 and Provisional December 2015
23 February 2016 NHS Sickness Absence Rates October 2015, Provisional statistics
23 February 2016 NHS Workforce Statistics November 2015, Provisional Statistics
24 February 2016 Provisional Accident and Emergency Quality Indicators for England November 2015, by provider
24 February 2016 Provisional Monthly Hospital Episode Statistics for Admitted Patient Care, Outpatient and Accident and Emergency data April 2015 - November 2015
Other
25 February 2016 NHS Vacancies Statistics England 2015, Provisional, Experimental statistics
March 2016
New releases
Mental Health Services Monthly Statistics Provisional January 2016
Biennial
None scheduled for March.
Annual
General Ophthalmic services workforce statistics 31 December 2015
General and Personal Medical Services, England 2005-2015, as at 30 September
Biannual
General Ophthalmic services workforce statistics 31 December 2015
Quarterly
NHS Continuing Healthcare Activity England, Quarter 3, 2015-16
Statistics on Women's Smoking Status at Time of Delivery: England Quarter 3, October 2015 to December 2015
CCG Outcomes Indicator Set March 2016 release
NHS Staff Earnings Estimates December 2015, Provisional statistics
Page 150 of 159

HSCIC Statistical Publications
6 Copyright © 2015, Health and Social Care Information Centre.
Female Genital Mutilation October-December 2015, Experimental Statistics, Enhanced Dataset
Summary Hospital-level Mortality Indicator (SHMI) Deaths associated with hospitalisation, England, October 2014 - September 2015
Monthly
HES-Diagnostic Imaging Dataset Data Linkage Report Provisional Summary Statistics, April to October 2015 (Experimental Statistics)
HES-MHLD Data Linkage Report Summary Statistics, November 2015
Improving Access to Psychological Therapies Report December 2015 Final, January Primary 2016 and most recent quarterly data (Quarter 2 2015/16)
Learning Disability Services Monthly Statistics Commissioner census (Assuring Transformation), February 2016, Experimental Statistics
Maternity Services Monthly Statistics September 2015 and October 2015, Experimental statistics
NHS Safety Thermometer Report England February 2015 - February 2016
NHS Sickness Absence Rates November 2015, Provisional statistics
NHS Workforce Statistics September 2015
NHS Workforce Statistics December 2015, Provisional Statistics
Provisional Accident and Emergency Quality Indicators for England December 2015, by provider
Provisional Monthly Hospital Episode Statistics for Admitted Patient Care, Outpatient and Accident and Emergency data April 2015 - December 2015
Provisional Monthly Patient Reported Outcome Measures (PROMs) in England April 2014 to March 2015 - March 2016 Release
Provisional Monthly Patient Reported Outcome Measures (PROMs) in England April 2015 to October 2015
Quality Outcomes Framework (QOF) Recorded Dementia Diagnoses February 2016
Other
None scheduled for March.
Clinical Audits
Clinical Audits are not currently classified as Official Statistics. The Code of Practice for Official Statistics is followed as best practice during the production cycle but the release processes differ.
January 2016
27 January 2016 National Diabetes Audit - National Diabetes Audit Core Report 1 2014-2015
February 2016 12 February 2016 National Pulmonary Hypertension Audit 2015 March 2016 National Diabetes Input Audit
National Diabetes Footcare Audit
07 (
a) F
orth
com
ing
Sta
tistic
alP
ublic
atio
ns
Page 151 of 159

HSCIC Statistical Publications
7 Copyright © 2015, Health and Social Care Information Centre.
User and Media Activity
The following tables show web and media coverage figures for Official (and National) Statistics released by the HSCIC during October and November 2015. Audits are not included.
Unique page views are the number of times the publication page was viewed during the two-week period following its release. Note that one user could generate more than one unique visit.
Media Units are the total articles or other media coverage for example print, online articles or broadcasts for the publication (each is counted separately i.e. an article appearing in both a newspaper’s print and online instances will count as two citations) . The totals in the table include all media units for the month of publication plus the following month.
Bars in the tables below indicate the scale of interest generated by each publication.
October 2015
Note that media activity shown above for Community Care Statistics may also cite the two other Social Care reports published on the same day (Measures from the Adult Social Care Outcomes Framework and Personal Social Services Adult Social Care Survey).
Publication Date Unique page views Media units
NICE Technology Appraisals in the NHS in England, Innovation Scorecard - to
March 2015, Experimental statistics01/10/2015 672
HES-MHLDDS Data Linkage Report, Summary Statistics - Jun 15 02/10/2015 282
Quality Outcomes Framework (QOF) Recorded Dementia Diagnoses - August
201502/10/2015 308
Community Care Statistics, Social Services Activity, England - 2014-15 [NS]06/10/2015 956 39
Measures from the Adult Social Care Outcomes Framework, England - 2014-15,
Final release 06/10/2015 791
Personal Social Services Adult Social Care Survey, England - 2014-1506/10/2015 666 3
NHS Safety Thermometer Report - September 2014 to September 201507/10/2015 183
Provisional Monthly Patient Reported Outcome Measures (PROMs) in England -
April 2014 to March 2015, October 2015 release08/10/2015 214
Page 152 of 159
HSCIC Statistical Publications
8 Copyright © 2015, Health and Social Care Information Centre.
Publication Date Unique page views Media units
Provisional Monthly Patient Reported Outcome Measures (PROMs) in England –
April 2015 to May 201508/10/2015 458
HES-DID Data Linkage Report - Provisional Summary Statistics, April 2015-May
2015 (Experimental Statistics) 09/10/2015 81
Estates Returns Information Collection (ERIC) - England, 2014-1514/10/2015 767 23
Sexual and Reproductive Health Services, England - 2014-15 [NS]14/10/2015 477
Number of Patients Registered at a GP Practice - October 201515/10/2015 642
Quality Outcomes Framework (QOF) Recorded Dementia Diagnoses - September
2015 16/10/2015 432
Improving Access to Psychological Therapies Report, July 2015 Final, August
2015 Primary and Quarter 1 2015/16 20/10/2015 515
Mental Health and Learning Disabilities Statistics Monthly Report: Final July and
Provisional August 20/10/2015 387
Learning Disability Services Monthly Statistics - England Commissioner Census
(Assuring Transformation) - September 2015, Experimental Statistics21/10/2015 181
NHS Sickness Absence Rates April 2015 to June 201522/10/2015 180
NHS Staff Earnings Estimates to July 2015 - Provisional statistics 22/10/2015 94
NHS Workforce Statistics - July 2015, Provisional statistics 22/10/2015 130
Inpatients Formally Detained in Hospitals Under the Mental Health Act 1983 and
Patients Subject to Supervised Community Treatment, England - 2014-2015,
Annual figures23/10/2015 1,058 19
Mental Health Bulletin, Annual Report - 2014-1523/10/2015 859
Quality Outcomes Framework (QOF) Recorded Dementia Diagnoses - July 201523/10/2015 282
07 (
a) F
orth
com
ing
Sta
tistic
alP
ublic
atio
ns
Page 153 of 159

HSCIC Statistical Publications
9 Copyright © 2015, Health and Social Care Information Centre.
November 2015
Publication Date Unique page views Media units
Data on written complaints in the NHS - 2015/16 Quarter 1, Experimental [NS] 03/11/2015 536 6
Quality Outcomes Framework (QOF) Recorded Dementia Diagnoses - June 2015 06/11/2015 302
Cervical Screening Programme, England - 2014-2015 [NS] 10/11/2015 467 11
HES-DID Data Linkage Report - Provisional Summary Statistics, April 2015 to
June 2015 (Experimental Statistics) 11/11/2015 55
NHS Safety Thermometer Report - England October 2014 - October 201511/11/2015 339
Prescribing Costs in Hospitals and the Community - England, 2014-1512/11/2015 296
Provisional Monthly Patient Reported Outcome Measures (PROMs) in England -
April 2014 to March 2015 - November 2015 Release 12/11/2015 294
Provisional Monthly Patient Reported Outcome Measures (PROMs) in England –
April 2015 to June 201512/11/2015 655
Provisional Monthly Patient Reported Outcome Measures (PROMs) in England -
Special Topic: Time Series Analysis from 2009-10 to 2014-1512/11/2015 197
Quality Outcomes Framework (QOF) Recorded Dementia Diagnoses - October
2015 13/11/2015 295
General Pharmaceutical Services - 2005/6 - 2014/15 [NS]18/11/2015 273
NHS Outcome Framework Indicators – November 2015 release19/11/2015 290
Learning Disability Services Monthly Statistics - England Commissioner Census
(Assuring Transformation) - October 2015, Experimental Statistics 20/11/2015 145
Learning Disability Services Quarterly Statistics - England Commissioner Census
(Assuring Transformation) – Quarter 2 2015/16, Experimental Statistics 20/11/2015 67
Quality Outcomes Framework (QOF) Recorded Dementia Diagnoses - May 201520/11/2015 181
Page 154 of 159

HSCIC Statistical Publications
10 Copyright © 2015, Health and Social Care Information Centre.
Publication Date Unique page views Media units
Improving Access to Psychological Therapies Report, August 2015 Final,
September 2015 Primary and most recent Quarterly data (Quarter 1 2015/16) 24/11/2015 359
Mental Health and Learning Disabilities Statistics Monthly Report: Final August
and Provisional September24/11/2015 346
Psychological Therapies, Annual Report on the use of IAPT services - England,
2014-15 24/11/2015 650 9
Hospital Episode Statistics, Admitted Patient Care - England, 2014-15 [NS] 25/11/2015 211 3
Maternity Services Monthly Statistics, England – April 2015, Experimental
statistics25/11/2015 501
NHS Maternity Statistics - England, 2014-1525/11/2015 240 21
National Child Measurement Programme - England, 2014-15 [NS]26/11/2015 1,475 78
NHS Dental Statistics for England - 2015/16, First Quarterly Report26/11/2015 166
Personal Social Services: Expenditure and Unit Costs, England - 2014-15, Final
release [NS] 26/11/2015 629
NHS Sickness Absence Rates July 201527/11/2015 192
NHS Staff Earnings Estimates to August 2015 - Provisional statistics27/11/2015 154
NHS Workforce Statistics - August 2015, Provisional statistics27/11/2015 148
Quality Outcomes Framework (QOF) Recorded Dementia Diagnoses - April 201527/11/2015 234
07 (
a) F
orth
com
ing
Sta
tistic
alP
ublic
atio
ns
Page 155 of 159

HSCIC Statistical Publications
11 Copyright © 2015, Health and Social Care Information Centre.
Actions Required of the Board
None - For information only.
Page 156 of 159

Page 1 of 1
Board meeting – Public session
Title of paper: Programme Definitions
Board meeting date: 27 January 2016
Agenda item no: HSCIC 16 06 07 b
Paper presented by:
Carl Vincent, Director of Finance and Corporate Services
Paper prepared by:
John Willshere, Portfolio Director
Paper approved by: (Sponsor Director) Carl Vincent, Director of Finance and Corporate Services
Purpose of the paper: To provide the Board with a summary of each programme listed on the programme dashboards.
Key risks and issues:
The programme dashboards monitor the performance of each programme. This document gives a brief overview of what each programme was set up to do.
Patient/public interest:
The public interest is in ensuring the HSCIC manages its programmes in an effective way. This document gives patients and members of the public a useful overview of each programme on the dashboard.
Actions required by the board: For reference only
07 (
b) P
rogr
amm
e D
efin
ition
s
Page 157 of 159
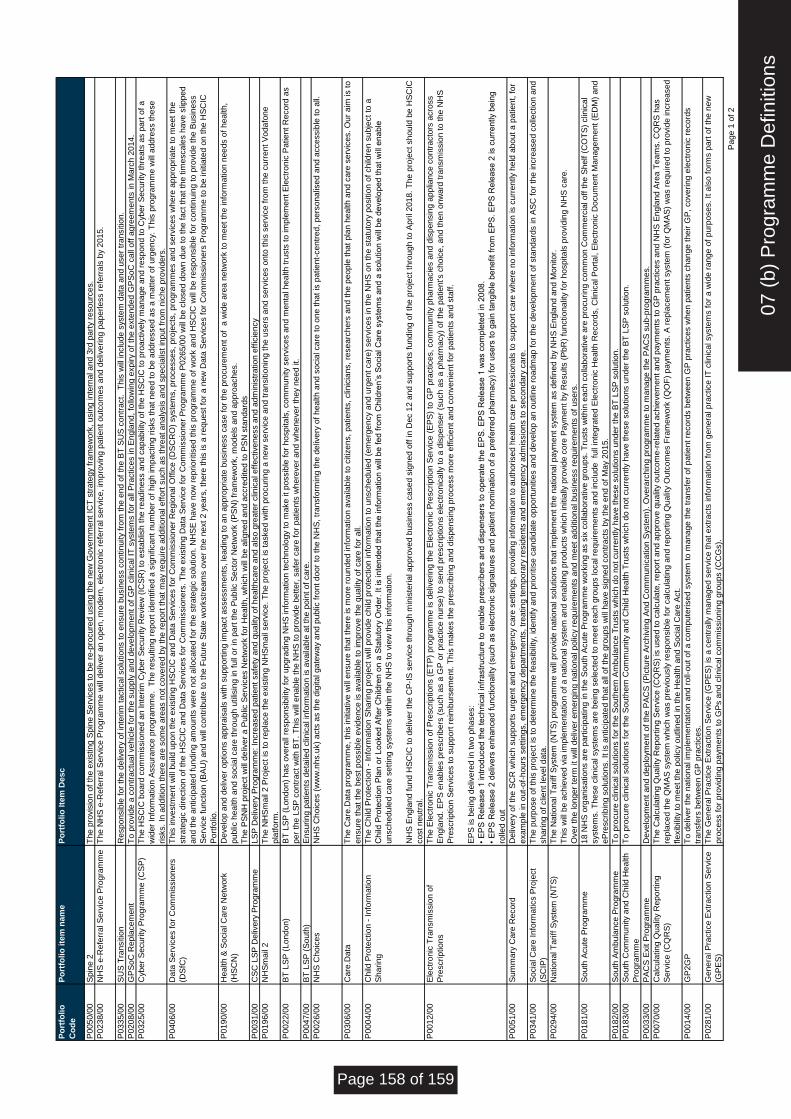
Po
rtfo
lio
Co
de
Po
rtfo
lio
ite
m n
am
eP
ort
foli
o I
tem
De
sc
P0
05
0/0
0S
pin
e 2
Th
e p
rovis
ion o
f th
e e
xis
tin
g S
pin
e S
erv
ice
s t
o b
e r
e-p
rocu
red
usin
g t
he
ne
w G
ove
rnm
ent
ICT
str
ate
gy
fra
me
wo
rk,
usin
g in
tern
al a
nd
3rd
pa
rty r
eso
urc
es.
P0
23
8/0
0N
HS
e-R
efe
rra
l S
erv
ice
Pro
gra
mm
eT
he N
HS
e-R
efe
rra
l S
erv
ice
Pro
gra
mm
e w
ill d
eliv
er
an
op
en
, m
ode
rn,
ele
ctr
onic
re
ferr
al se
rvic
e, im
pro
vin
g p
atie
nt
ou
tco
me
s a
nd
de
live
ring
pa
pe
rless r
efe
rra
ls b
y 2
01
5.
P0
33
5/0
0S
US
Tra
nsitio
n
Re
sp
on
sib
le f
or
the
deliv
ery
of
inte
rim
tactica
l so
lutio
ns t
o e
nsu
re b
usin
ess c
ontin
uity
fro
m t
he
en
d o
f th
e B
T S
US
co
ntr
act.
T
his
will
in
clu
de
syste
m d
ata
and
use
r tr
ansitio
n.
P0
20
8/0
0G
PS
oC
Re
pla
ce
me
nt
To
pro
vid
e a
co
ntr
actu
al ve
hic
le f
or
the
su
pp
ly a
nd
de
ve
lopm
ent
of
GP
clin
ica
l IT
syste
ms f
or
all
Pra
ctice
s in
En
gla
nd
, fo
llow
ing e
xp
iry o
f th
e e
xte
nd
ed
GP
So
C c
all
off
agre
em
ents
in
Ma
rch
20
14
.
P0
32
5/0
0C
yb
er
Se
cu
rity
Pro
gra
mm
e (
CS
P)
Th
e H
SC
IC b
oa
rd c
om
mis
sio
ne
d a
n I
nte
rim
Cyb
er
Se
cu
rity
Re
vie
w (
ICS
R)
to e
sta
blis
h th
e r
ead
iness a
nd
ca
pa
bili
ty o
f th
e H
SC
IC t
o p
roa
ctive
ly m
ana
ge
an
d r
esp
on
d t
o C
yb
er
Se
cu
rity
thre
ats
as p
art
of
a
wid
er
Info
rma
tio
n A
ssu
ran
ce
pro
gra
mm
e. T
he r
esu
ltin
g r
epo
rt id
en
tifie
d a
sig
nific
ant
nu
mb
er
of
hig
h im
pactin
g r
isks t
ha
t n
ee
d t
o b
e a
dd
resse
d a
s a
ma
tte
r o
f u
rge
ncy.
Th
is p
rog
ram
me
will
add
ress t
he
se
risks.
In a
dd
itio
n t
he
re a
re s
om
e a
reas n
ot
co
ve
red
by t
he
re
port
tha
t m
ay
requ
ire
ad
ditio
na
l e
ffo
rt s
uch
as t
hre
at
an
aly
sis
and
sp
ecia
list
inpu
t fr
om
nic
he p
rovid
ers
.
P0
40
6/0
0D
ata
Se
rvic
es f
or
Co
mm
issio
ne
rs
(DS
fC)
Th
is in
ve
stm
ent
will
build
up
on
th
e e
xis
tin
g H
SC
IC a
nd
Data
Se
rvic
es f
or
Co
mm
issio
ne
r R
eg
iona
l O
ffic
e (
DS
CR
O)
syste
ms,
pro
ce
sse
s,
pro
jects
, pro
gra
mm
es a
nd
se
rvic
es w
here
ap
pro
pria
te t
o m
eet
the
str
ate
gic
dire
ctio
n o
f th
e H
SC
IC a
nd
Data
Se
rvic
es f
or
Co
mm
issio
ne
rs.
Th
e e
xis
tin
g D
ata
Se
rvic
e f
or
Co
mm
issio
ne
r P
rog
ram
me
P0
26
5/0
0 w
ill b
e c
lose
d d
ow
n d
ue t
o t
he
fa
ct
tha
t th
e t
ime
sca
les h
ave
slip
pe
d
and the a
nticip
ate
d f
undin
g a
mounts
were
not allo
cate
d f
or
the s
trate
gic
solu
tion. N
HS
E h
ave n
ow
reprioritised this
pro
gra
mm
e o
f w
ork
and H
SC
IC w
ill b
e r
esponsib
le f
or
continuin
g to p
rovid
e the B
usin
ess
Se
rvic
e f
unctio
n (
BA
U)
and
will
co
ntr
ibute
to
th
e F
utu
re S
tate
wo
rkstr
eam
s o
ve
r th
e n
ext
2 y
ears
, th
ere
th
is is a
re
qu
est
for
a n
ew
Da
ta S
erv
ice
s f
or
Co
mm
issio
ne
rs P
rogra
mm
e to
be
in
itia
ted
on
th
e H
SC
IC
Po
rtfo
lio.
P0
19
0/0
0H
ea
lth
& S
ocia
l C
are
Ne
two
rk
(HS
CN
)
De
ve
lop a
nd
de
live
r o
ptio
ns a
pp
rais
als
with
su
pp
ort
ing im
pact
asse
ssm
ents
, le
ad
ing t
o a
n a
pp
rop
ria
te b
usin
ess c
ase
fo
r th
e p
rocu
rem
ent
of
a w
ide a
rea
ne
two
rk t
o m
eet
the
in
form
atio
n n
ee
ds o
f h
ea
lth
,
pub
lic h
ea
lth
and
so
cia
l ca
re t
hro
ugh
utilis
ing in
fu
ll o
r in
pa
rt t
he P
ublic
Se
cto
r N
etw
ork
(P
SN
) fr
am
ew
ork
, m
ode
ls a
nd
ap
pro
ach
es.
Th
e P
SN
H p
roje
ct
will
deliv
er
a P
ublic
Se
rvic
es N
etw
ork
fo
r H
ea
lth
, w
hic
h w
ill b
e a
ligne
d a
nd
accre
dite
d t
o P
SN
sta
nd
ard
s
P0
03
1/0
0C
SC
LS
P D
eliv
ery
Pro
gra
mm
eL
SP
De
live
ry P
rogra
mm
e: In
cre
ase
d p
atie
nt
sa
fety
and
qu
alit
y o
f h
ea
lth
ca
re a
nd
als
o g
reate
r clin
ica
l e
ffe
ctive
ne
ss a
nd
ad
min
istr
atio
n e
ffic
iency
P0
19
6/0
0N
HS
ma
il 2
Th
e N
HS
ma
il 2
Pro
ject
is t
o r
epla
ce
th
e e
xis
tin
g N
HS
ma
il se
rvic
e. T
he p
roje
ct
is t
aske
d w
ith
pro
cu
ring
a n
ew
se
rvic
e a
nd t
ran
sitio
nin
g t
he
use
rs a
nd
se
rvic
es o
nto
th
is s
erv
ice
fro
m t
he
cu
rre
nt
Vo
da
fone
pla
tfo
rm.
P0
02
2/0
0B
T L
SP
(L
on
do
n)
BT
LS
P (
Lon
do
n)
has o
ve
rall
resp
on
sib
ility
fo
r u
pgra
din
g N
HS
in
form
atio
n t
ech
no
logy t
o m
ake
it
po
ssib
le f
or
ho
sp
ita
ls,
co
mm
unity
se
rvic
es a
nd
me
nta
l h
ea
lth
tru
sts
to im
ple
me
nt
Ele
ctr
onic
Pa
tie
nt
Re
co
rd a
s
per
the
LS
P c
ontr
act
with
BT
. T
his
will
ena
ble
th
e N
HS
to p
rovid
e b
ett
er,
sa
fer
ca
re f
or
pa
tie
nts
wh
ere
ve
r a
nd w
hen
eve
r th
ey
nee
d it.
P0
04
7/0
0B
T L
SP
(S
outh
)E
nsu
ring
pa
tie
nts
deta
iled c
linic
al in
form
atio
n is a
va
ilable
at
the
po
int o
f ca
re.
P0
02
6/0
0N
HS
Ch
oic
es
NH
S C
ho
ice
s (
ww
w.n
hs.u
k)
acts
as t
he
dig
ita
l g
ate
wa
y a
nd
pu
blic
fro
nt
do
or
to t
he
NH
S,
tra
nsfo
rmin
g t
he
de
live
ry o
f h
ea
lth
and
so
cia
l ca
re t
o o
ne
th
at
is p
atie
nt-
ce
ntr
ed,
pe
rso
na
lise
d a
nd
acce
ssib
le to
all.
P0
30
6/0
0C
are
.Data
Th
e C
are
.Da
ta p
rog
ram
me
, th
is in
itia
tive
will
ensu
re t
hat
the
re is m
ore
ro
un
de
d in
form
atio
n a
va
ilable
to
citiz
ens,
pa
tie
nts
, clin
icia
ns,
rese
arc
hers
and
th
e p
eo
ple
th
at
pla
n h
ea
lth
and
ca
re s
erv
ice
s.
Ou
r a
im is t
o
ensu
re t
hat
the
be
st
po
ssib
le e
vid
en
ce
is a
va
ilable
to
im
pro
ve
th
e q
ua
lity
of
ca
re f
or
all.
P0
00
4/0
0C
hild
Pro
tectio
n -
Info
rma
tio
n
Sh
arin
g
Th
e C
hild
Pro
tectio
n -
Info
rma
tio
n S
harin
g p
roje
ct
will
pro
vid
e c
hild
pro
tectio
n in
form
atio
n t
o u
nsch
ed
ule
d (
em
erg
en
cy a
nd
urg
en
t ca
re)
se
rvic
es in
th
e N
HS
on t
he
sta
tuto
ry p
ositio
n o
f ch
ildre
n s
ubje
ct
to a
Ch
ild P
rote
ctio
n P
lan o
r L
ooke
d A
fte
r C
hild
ren
on
a S
tatu
tory
Ord
er.
It is
in
ten
de
d t
ha
t th
e in
form
atio
n w
ill b
e f
ed f
rom
Ch
ildre
n’s
So
cia
l C
are
syste
ms a
nd
a s
olu
tio
n w
ill b
e d
eve
lope
d t
ha
t w
ill e
na
ble
unsch
ed
ule
d c
are
se
ttin
g s
yste
ms w
ith
in th
e N
HS
to v
iew
this
in
form
atio
n.
NH
S E
ngla
nd
fu
nd
HS
CIC
to
deliv
er
the
CP
-IS
se
rvic
e th
rou
gh m
inis
teria
l a
pp
rove
d b
usin
ess c
ase
d s
igne
d o
ff in
Dec 1
2 a
nd
su
pp
ort
s f
und
ing o
f th
e p
roje
ct
thro
ug
h t
o A
pril 2
01
8.
Th
e p
roje
ct
sh
ou
ld b
e H
SC
IC
co
st
ne
utr
al.
P0
01
2/0
0E
lectr
onic
Tra
nsm
issio
n o
f
Pre
scrip
tio
ns
Th
e E
lectr
onic
Tra
nsm
issio
n o
f P
rescrip
tio
ns (
ET
P)
pro
gra
mm
e is d
eliv
ering
th
e E
lectr
onic
Pre
scrip
tio
n S
erv
ice
(E
PS
) to
GP
pra
ctice
s,
co
mm
unity
pha
rma
cie
s a
nd
dis
pen
sin
g a
pp
liance
co
ntr
acto
rs a
cro
ss
En
gla
nd
. E
PS
ena
ble
s p
rescrib
ers
(su
ch
as a
GP
or
pra
ctice
nu
rse
) to
se
nd
pre
scrip
tio
ns e
lectr
onic
ally
to a
dis
pen
se
r (s
uch
as a
pha
rma
cy)
of
the
pa
tie
nt's c
hoic
e, a
nd
th
en
on
wa
rd t
ransm
issio
n t
o t
he
NH
S
Pre
scrip
tio
n S
erv
ice
s t
o s
upp
ort
re
imb
urs
em
ent.
Th
is m
ake
s t
he
pre
scrib
ing a
nd
dis
pen
sin
g p
roce
ss m
ore
eff
icie
nt
an
d c
onve
nie
nt
for
pa
tie
nts
and
sta
ff.
EP
S is b
ein
g d
eliv
ere
d in
tw
o p
hase
s:
• E
PS
Re
lease
1 in
tro
duce
d t
he
te
ch
nic
al in
fra
str
uctu
re t
o e
na
ble
pre
scrib
ers
and
dis
pen
se
rs t
o o
pe
rate
th
e E
PS
. E
PS
Re
lease
1 w
as c
om
ple
ted
in
20
08
.
• E
PS
Re
lease
2 d
eliv
ers
enh
an
ce
d f
unctio
na
lity (
su
ch
as e
lectr
onic
sig
na
ture
s a
nd
pa
tie
nt
no
min
atio
n o
f a
pre
ferr
ed p
ha
rma
cy)
for
use
rs t
o g
ain
ta
ng
ible
be
ne
fit
fro
m E
PS
. E
PS
Re
lease
2 is c
urr
ently b
ein
g
rolle
d o
ut
P0
05
1/0
0S
um
ma
ry C
are
Re
co
rdD
eliv
ery
of
the
SC
R w
hic
h s
upp
ort
s u
rge
nt
an
d e
me
rge
ncy c
are
se
ttin
gs,
pro
vid
ing in
form
atio
n t
o a
uth
orise
d h
ea
lth
ca
re p
rofe
ssio
na
ls t
o s
upp
ort
ca
re w
here
no
in
form
atio
n is c
urr
ently h
eld
ab
ou
t a
pa
tie
nt,
fo
r
exa
mp
le in
ou
t-o
f-h
ou
rs s
ettin
gs,
em
erg
en
cy d
ep
art
me
nts
, tr
ea
tin
g t
em
pora
ry r
esid
en
ts a
nd
em
erg
en
cy a
dm
issio
ns t
o s
eco
nd
ary
ca
re.
P0
34
1/0
0S
ocia
l C
are
In
form
atics P
roje
ct
(SC
IP)
Th
e p
urp
ose
of
this
pro
ject
is t
o d
ete
rmin
e t
he
fe
asib
ility
, id
en
tify
and
prio
ritise
ca
nd
idate
opp
ort
unitie
s a
nd
de
ve
lop a
n o
utlin
e r
oad
ma
p f
or
the
deve
lopm
ent
of
sta
nd
ard
s in
AS
C f
or
the
in
cre
ase
d c
olle
ctio
n a
nd
sh
arin
g o
f clie
nt
leve
l d
ata
.
P0
29
4/0
0N
atio
na
l T
ariff
Syste
m (
NT
S)
Th
e N
atio
na
l T
ariff
Syste
m (
NT
S)
pro
gra
mm
e w
ill p
rovid
e n
atio
na
l so
lutio
ns t
ha
t im
ple
me
nt
the
na
tio
na
l p
aym
ent
syste
m a
s d
efin
ed
by N
HS
En
gla
nd
an
d M
on
ito
r.
Th
is w
ill b
e a
ch
ieve
d v
ia im
ple
me
nta
tio
n o
f a
natio
na
l syste
m a
nd
en
ab
ling p
rod
ucts
wh
ich
in
itia
lly p
rovid
e c
ore
Pa
yme
nt
by R
esu
lts (
Pb
R)
functio
na
lity
for
ho
sp
ita
ls p
rovid
ing N
HS
ca
re.
Ove
r th
e lo
ng
er
term
it
will
deliv
er
em
erg
ing n
atio
na
l p
olic
y r
equ
ire
me
nts
and
me
et
ad
ditio
na
l b
usin
ess r
equ
ire
me
nts
of
use
rs.
P0
18
1/0
0S
outh
Acu
te P
rogra
mm
e1
8 N
HS
org
anis
atio
ns a
re p
art
icip
atin
g in
th
e S
outh
Acu
te P
rogra
mm
e w
ork
ing a
s s
ix c
olla
bo
rative
gro
up
s.
Tru
sts
with
in e
ach
co
llabo
rative
are
pro
cu
ring
co
mm
on C
om
me
rcia
l o
ff t
he
Sh
elf (
CO
TS
) clin
ica
l
syste
ms.
Th
ese
clin
ica
l syste
ms a
re b
ein
g s
ele
cte
d t
o m
eet
ea
ch
gro
up
s lo
ca
l re
qu
ire
me
nts
and
in
clu
de
fu
ll in
teg
rate
d E
lectr
onic
He
alth
Re
co
rds,
Clin
ica
l P
ort
al, E
lectr
onic
Do
cu
me
nt
Ma
na
ge
me
nt
(ED
M)
an
d
eP
rescrib
ing s
olu
tio
ns.
It is a
nticip
ate
d t
ha
t a
ll o
f th
e g
roup
s w
ill h
ave
sig
ne
d c
ontr
acts
by
the
en
d o
f M
ay 2
01
5.
P0
18
2/0
0S
outh
Am
bula
nce
Pro
gra
mm
eT
o p
rocu
re c
linic
al so
lutio
ns f
or
the
So
uth
ern
Am
bula
nce
Tru
sts
wh
ich
do
no
t cu
rre
ntly h
ave
th
ese
so
lutio
ns u
nd
er
the
BT
LS
P s
olu
tio
n.
P0
18
3/0
0S
outh
Co
mm
unity
and
Child
Hea
lth
Pro
gra
mm
e
To
pro
cu
re c
linic
al so
lutio
ns f
or
the
So
uth
ern
Com
mu
nity
and
Child
Hea
lth
Tru
sts
wh
ich
do
no
t cu
rre
ntly h
ave
th
ese
so
lutio
ns u
nd
er
the
BT
LS
P s
olu
tio
n.
P0
03
3/0
0P
AC
S E
xit P
rogra
mm
eD
eve
lopm
ent
an
d d
ep
loym
ent
of
the
PA
CS
(P
ictu
re A
rch
ivin
g A
nd C
om
mu
nic
atio
n S
yste
m).
Ove
rarc
hin
g p
rog
ram
me
to
ma
na
ge
th
e P
AC
S s
ub-p
rog
ram
me
s.
P0
07
0/0
0C
alc
ula
tin
g Q
ualit
y R
epo
rtin
g
Se
rvic
e (
CQ
RS
)
Th
e C
alc
ula
tin
g Q
ualit
y R
epo
rtin
g S
erv
ice
(C
QR
S)
is u
se
d t
o c
alc
ula
te,
rep
ort
and
ap
pro
ve
qu
alit
y o
utc
om
e-r
ela
ted
ach
ieve
me
nt
an
d p
aym
ents
to G
P p
ractice
s a
nd
NH
S E
ngla
nd
Are
a T
eam
s.
CQ
RS
has
repla
ce
d t
he
QM
AS
syste
m w
hic
h w
as p
revio
usly
re
sp
on
sib
le f
or
ca
lcu
latin
g a
nd
re
port
ing Q
ualit
y O
utc
om
es F
ram
ew
ork
(Q
OF
) p
aym
ents
. A
re
pla
ce
me
nt
syste
m (
for
QM
AS
) w
as r
equ
ire
d t
o p
rovid
e in
cre
ase
d
fle
xib
ility
to m
eet
the
po
licy o
utlin
ed
in
th
e H
ealth
and
So
cia
l C
are
Act.
P0
01
4/0
0G
P2
GP
To
de
live
r th
e n
atio
na
l im
ple
me
nta
tio
n a
nd
ro
ll-o
ut
of
a c
om
pute
rise
d s
yste
m t
o m
ana
ge
th
e t
ran
sfe
r o
f p
atie
nt
reco
rds b
etw
een
GP
pra
ctice
s w
hen
pa
tie
nts
ch
an
ge
th
eir G
P,
co
ve
ring
ele
ctr
onic
re
co
rds
tra
nsfe
rs b
etw
een
GP
pra
ctice
s.
P0
28
1/0
0G
ene
ral P
ractice
Extr
actio
n S
erv
ice
(GP
ES
)
Th
e G
ene
ral P
ractice
Extr
actio
n S
erv
ice
(G
PE
S)
is a
ce
ntr
ally
ma
na
ge
d s
erv
ice
th
at
extr
acts
in
form
atio
n f
rom
gen
era
l p
ractice
IT
clin
ica
l syste
ms f
or
a w
ide r
ang
e o
f p
urp
ose
s.
It a
lso
fo
rms p
art
of
the
ne
w
pro
ce
ss f
or
pro
vid
ing p
aym
ents
to G
Ps a
nd
clin
ica
l co
mm
issio
nin
g g
rou
ps (
CC
Gs).
Pa
ge
1 o
f 2
07 (
b) P
rogr
amm
e D
efin
ition
s
Page 158 of 159

P0
20
7/0
0H
ea
lth
& J
ustice
In
form
atio
n
Se
rvic
es
He
alth
and
Ju
stice
In
form
atio
n S
erv
ice
s (
HJIS
) fo
cu
se
s o
n t
he
fu
ture
in
form
atio
n s
erv
ice
s r
equ
ire
d t
o s
upp
ort
the
sta
tuto
ry r
esp
on
sib
ilitie
s o
f N
HS
En
gla
nd
(H
ea
lth
& J
ustice
) in
th
e d
ire
ct
pro
vis
ion a
nd
co
mm
issio
nin
g o
f h
ea
lth
ca
re f
or
all
pla
ce
s o
f d
ete
ntio
n,
an
d S
exu
al A
ssa
ult R
efe
rra
l C
entr
es,
in E
ngla
nd
.
P0
03
7/0
0O
ffe
nd
er
He
alth
IT
To
de
plo
y a
clin
ica
l syste
m t
o a
ll p
riso
ns in
th
e S
outh
and
Lo
nd
on
so
th
at
the
y ca
n lin
k u
p w
ith
exis
tin
g d
ep
loym
ent
pla
ns in
NM
E t
o f
orm
a n
atio
na
l n
etw
ork
. T
he s
yste
m c
hose
n T
PP
Systm
On
e,
pro
vid
es a
sin
gle
pa
tie
nt
reco
rd w
hic
h is a
llow
ing p
atie
nts
in
form
atio
n t
o b
e t
ran
sfe
rre
d w
hen
th
ey a
re m
ove
d a
rou
nd
th
e p
riso
n e
sta
te. T
hus p
rovid
ing c
ontin
uity o
f ca
re a
nd
im
pro
vin
g h
ea
lth
ca
re f
or
priso
ne
rs a
s w
ell
as
wo
rkin
g e
nviro
nm
ent
for
sta
ff.
P0
30
1/0
0F
em
ale
Ge
nita
l M
utila
tio
n P
reve
ntio
n
– D
ata
and
Syste
ms B
usin
ess C
ase
De
ve
lopm
ent
Th
e o
bje
ctive
of
this
docu
me
nt
is t
o d
efin
e a
nd
au
tho
rise
th
e w
ork
packa
ge
to
pro
du
ce
a f
easib
ility
stu
dy o
n in
form
atio
n c
olle
ctio
n a
nd
sh
arin
g b
y th
e N
HS
on F
em
ale
Ge
nita
l M
utila
tio
n (
FG
M).
Th
e w
ork
packa
ge
will
deliv
er
an
asse
ssm
ent
of
the
fe
asib
ility
of
ach
ievin
g t
he
fo
llow
ing o
bje
ctive
s:
- H
ow
ca
n t
he
NH
S s
upp
ort
the
mu
lti-a
ge
ncy o
bje
ctive
of
pro
tectin
g a
nd
ca
ring
fo
r th
ose
cu
rre
ntly a
ffe
cte
d b
y, o
r a
t im
min
en
t risk o
f, F
GM
;
- H
ow
ca
n t
he
NH
S s
upp
ort
the
lo
ng
te
rm h
ea
lth
edu
ca
tio
n a
nd
he
alth
pro
mo
tio
n c
om
pon
en
ts o
f a
mu
lti-a
ge
ncy s
tra
teg
y o
n t
he
era
dic
atio
n o
f F
GM
An
asse
ssm
ent
of
feasib
ility
will
be f
orm
ula
ted
in
a f
inal d
ocu
me
nt
wh
ich
will
co
nta
in a
stu
dy in
ve
stig
atin
g m
ultip
le o
ptio
ns f
or
ach
ievin
g t
he
ob
jective
.
Th
e o
ptio
ns w
ill c
onsid
er
tho
se
re
quire
me
nts
, risks a
nd
be
ne
fits
re
leva
nt
to t
he
ob
jective
s,
sta
rtin
g f
rom
a ‘d
o n
oth
ing’ sta
te, to
one
wh
ich
fu
lly a
dd
resse
s t
he
ob
ligatio
ns o
n t
he
NH
S a
nd
he
alth
ca
re
pro
fessio
na
ls a
s o
utlin
ed
in
th
e m
ulti-a
ge
ncy p
ractice
gu
idelin
es o
n F
GM
.
All
the
op
tio
ns t
og
eth
er
will
id
en
tify
a c
om
mo
n s
et o
f re
qu
ire
me
nts
, ag
ain
st
wh
ich
ea
ch
in
div
idua
l o
ptio
n w
ill b
e a
sse
sse
d.
Ea
ch
op
tio
n w
ill a
lso
sp
ecify t
he
estim
ate
d r
eso
urc
es,
in te
rms o
f tim
e, co
st
an
d
ma
teria
ls,
req
uire
d t
o r
ealis
e th
e o
ptio
n.
P0
05
5/0
0M
ate
rnity
and
Child
ren
s D
ata
se
tsT
o c
olle
ct
an
d r
epo
rt o
n d
ata
fo
r m
ate
rnity,
ch
ild h
ealth
and
ad
ole
sce
nt
me
nta
l h
ea
lth
se
rvic
es.
P0
37
2/0
0In
form
atio
n S
erv
ice
fo
r P
are
nts
at
Po
int o
f C
are
Th
e H
SC
IC C
ross-G
ove
rnm
ent
Pro
gra
mm
es t
ea
m h
as b
ee
n a
ske
d t
o in
itia
te a
nd
su
bse
qu
en
tly m
ana
ge
th
e d
eliv
ery
of
a p
roje
ct
to d
eve
lop in
form
atio
n s
harin
g b
etw
een
ma
tern
ity s
yste
ms a
nd
a c
entr
al
repo
sito
ry o
wn
ed
by P
HE
. T
he p
roje
ct
will
fa
cili
tate
PH
E in
pro
vid
ing a
n in
form
atio
n s
erv
ice
(h
igh q
ua
lity
dig
ita
l a
dvic
e)
at
po
int o
f ca
re (
ma
tern
ity)
fo
r n
ew
and
exp
ecta
nt
pa
ren
ts.
Th
is w
ork
is b
ein
g
co
mm
issio
ne
d,
an
d f
und
ed
, b
y P
HE
and
alig
ns w
ith
th
e P
HE
Mark
etin
g S
tra
teg
y (a
dd
ressin
g k
ey
pub
lic h
ea
lth
issu
es,
incre
asin
g q
ua
lity
and
co
st-
eff
ective
ne
ss a
nd
be
ing e
vid
en
ce
ba
se
d)
as w
ell
as b
ein
g a
dire
ct
min
iste
ria
l re
qu
ire
me
nt
(Da
n P
oulte
r) t
o p
rovid
e d
ire
ct
acce
ss t
o a
co
he
ren
t se
rvic
e a
t po
int o
f ca
re f
or
this
patie
nt
gro
up
.
P0
32
1/0
0P
ath
fin
de
rs o
n D
ME
(fo
rme
rly
Str
ate
gic
Ca
pa
bili
ty P
latf
orm
(S
CP
)
P1
)
A p
ub
lic c
om
mitm
ent
ha
s b
ee
n m
ade
to
extr
act
prim
ary
ca
re d
ata
fro
m G
P S
yste
ms in
ea
rly
201
4 a
nd
to
lin
k a
nd
dis
se
min
ate
th
at
da
ta in
an
on
ymis
ed f
orm
fro
m J
uly
201
4.
Th
is,
alo
ng
with
oth
er
sh
ort
term
co
mm
itm
ents
asso
cia
ted
with
pro
gra
mm
es,
inclu
din
g c
are
.data
, re
su
lts in
a r
equ
ire
me
nt
for
a n
ew
Inte
rim
Pla
tfo
rm t
o m
eet
the
re
quire
me
nts
of
NH
S E
ngla
nd
as L
ea
d C
om
mis
sio
ne
r a
hea
d o
f a
ny s
ignific
ant
inve
stm
ent
in th
e S
tra
teg
ic C
apa
bili
ty P
latf
orm
. T
he S
tra
teg
ic C
apa
bili
ty is p
lann
ed
to
be
th
e p
latf
orm
tha
t e
na
ble
s t
he
HS
CIC
to
ca
rry o
ut
its s
tatu
tory
re
qu
ire
me
nts
fo
r th
e p
roce
ssin
g a
nd
dis
se
min
atio
n o
f
data
in
a s
afe
an
d s
ecu
re e
nviro
nm
ent.
P0
01
0/0
0D
efe
nce
Me
dic
al S
erv
ice
s (
DM
S)
Su
pp
ort
De
fence
Me
dic
al S
erv
ice
s t
o d
eliv
er
the
fu
lly o
pe
ratin
g c
apa
bili
ty o
f th
eir P
ers
onn
el C
are
Re
co
rd S
yste
m P
rogra
mm
e (
DM
ICP
). T
his
in
clu
de
s in
teg
ratin
g w
ith
th
e s
erv
ice
s a
nd
syste
ms o
f th
e N
HS
,
pro
vis
ion o
f re
leva
nt
SM
E,
skill
s a
nd
pro
gra
mm
e r
eso
urc
e. In
th
is c
onte
xt
NH
S s
yste
ms in
clu
de
pa
tie
nt
reg
istr
atio
n,
sta
ff a
uth
en
tica
tio
n a
nd
pa
tie
nt
ch
oic
e to
ge
the
r w
ith
activity
rela
ted
ma
na
ge
me
nt
info
rma
tio
n.
Pa
ge
2 o
f 2
Page 159 of 159




















