adult circumcision practices of traditional surgeons and
85
ADULT CIRCUMCISION PRACTICES OF TRADITIONAL SURGEONS AND NURSES IN RELATION TO THE INITIATES’ HEALTH OUTCOMES/MORBIDITY IN THE EASTERN CAPE. by SIYAMTHEMBA DALASA A dissertation submitted in fulfilment of the requirements for the degree of MAGISTER CURATIONIS DEPARTMENT OF NURSING SCIENCE FACULTY OF HEALTH SCIENCES UNIVERSITY OF FORT HARE Supervisor: Prof DT Goon April 2019
-
Upload
khangminh22 -
Category
Documents
-
view
5 -
download
0
Transcript of adult circumcision practices of traditional surgeons and

ADULT CIRCUMCISION PRACTICES OF TRADITIONAL SURGEONS ANDNURSES IN RELATION TO THE INITIATES’ HEALTH OUTCOMES/MORBIDITY
IN THE EASTERN CAPE.
by
SIYAMTHEMBA DALASA
A dissertation submitted in fulfilment of the requirements for the degree of
MAGISTER CURATIONIS
DEPARTMENT OF NURSING SCIENCE
FACULTY OF HEALTH SCIENCES
UNIVERSITY OF FORT HARE
Supervisor: Prof DT Goon
April 2019

i
DECLARATION
I, Siyamthemba Dalasa, hereby declare that the study on, “Adult circumcision
practices of traditional surgeons and nurses in relation to the initiates’ health
outcomes/morbidity in the eastern cape” is my original work. This study has not been
submitted to any other University for the completion of any degree purposes. The
researcher has revealed and acknowledged all the citations used or quoted from
other people’s work by means of complete referencing.
Name: Siyamthemba Dalasa
Signature: …………………………………..
Date: …………………………………………

ii
DECLARATION ON PLAGIARISM
I, Siyamthemba Dalasa, student number 200902505, confirm that the content
contained in this document is my own work, is not copied from any other author’s
work. I know that plagiarism is wrong and is against the University of Fort Hare’s
policy on plagiarism. In any case where other people’s work has been used in this
document, appropriate citations and references have been provided. I have not
permitted, and I will not consent to anyone copying my work with the aim of making it
their own work.
Signature:……………………….

iii
CERTIFICATION
This study was completed under the guidance and supervision of Professor DT
Goon at the University of Fort Hare, East London.
Supervisor: Professor DT Goon (University of Fort Hare, Department of Nursing
Science, Faculty Sciences)
Signature:…………………………………..
Date:………………………………………...

iv
ACKNOWLEGEMENTS
My sincerest gratitude goes to my supervisor Professor DT Goon, (University of Fort
Hare).
I would to thank the people of the OR Tambo District (KSD, Nyandeni and Qawukeni
municipalities), for allowing me, the opportunity to collect data in order to complete
my research study at the University of Fort Hare. I further thank Mr. Merile, acting on
behalf of the Eastern Cape Department of Health and to Chief Tyhali, representing
the Eastern Cape house of traditional leaders in O.R. Tambo for providing me with
the opportunity to proceed with the collection of data in the district.
I highly appreciate Dr I. Ajayi (University of Fort Hare) for his dedicated help,
guidance, support and mentoring during the process of completing my paper.
To my cousin brother, Sinekhaya Xibiya, and my younger brothers, I thank you for
the help you offered in accompanying me to all those hard-to-reach areas of the
Nyandeni and Qawukeni municipalities.
A very special word of thanks goes to Dr. Yako who, while she was still working for
the University of Fort Hare, helped me to initiate this research process. I deeply
appreciate the assistance I received from all other parties involved, including Ms. N.
Rala (University of Fort Hare,) who helped me when I desperately needed help.

v
LIST OF ACRONYMS
COGTA - Co-operative Governance and Traditional Affairs
DoH - Department of Health
EC DoH - Eastern Cape Department Of Health
HIV - Human Immunodeficiency Virus
KSD - King Sabatha Dalindyebo (municipality)
LRC - Lusikisiki Rescue Centre
MEC - Member of the Executive Council
MMC - Male Medical Circumcision
PIDAC - Provincial Infectious Diseases Advisory Committee.
TMC - Traditional Male Circumcision
UNAIDS - Joint United Nations Programme on HIV and AIDS
WHO - World Health Organisation

vi
ABSTRACT
BACKGROUND
Despite the adverse outcomes associated with traditional male circumcision, the
practice remains prevalent, especially in the Eastern Cape, South, Africa. This study
seeks to assess the practices of traditional surgeons and nurses in relation to the
prevention and control of infections and their understanding of human physiological
mechanisms during circumcision processes.
METHOD
This study has adopted a qualitative design, which involved conducting 115 semi-
structured interviews among traditional surgeons, traditional nurses and traditionally
circumcised men, and one focus group discussion among traditional nurses. The
data generated were transcribed and subjected to thematic content analysis.
RESULTS
The analysis revealed that both traditional surgeons and nurses demonstrated both
poor aseptic techniques and a lack of knowledge of how the human body functions.
Their lack of knowledge of basic human physiology meant that they trivialised sepsis
in the penile wound. In addition, the seclusion lodges for circumcision and initiates
living were unclean and uninhabitable.
CONCLUSION
The poor aseptic techniques of traditional surgeons and nurses, as well as the
uncleanliness of their environment during traditional male circumcision procedures,
could expose initiates to infections and morbidity. Environmental health officers
should regularly supervise traditional surgeons and nurses in order to prevent the
adverse health outcomes associated with the traditional male circumcision practice.
KEY WORDS: Aseptic Technique, Traditional Male Circumcision, Initiates,
Traditional Surgeons and Nurses.

vii
TABLE OF CONTENTS
DECLARATION.........................................................................................................................i
DECLARATION ON PLAGIARISM....................................................................................... ii
CERTIFICATION.....................................................................................................................iii
ACKNOWLEGEMENTS........................................................................................................ iv
LIST OF ACRONYMS.............................................................................................................v
ABSTRACT..............................................................................................................................vi
TABLE OF CONTENTS................................................................................................vii
LIST OF TABLES........................................................................................................... xi
LIST OF FIGURES........................................................................................................ xii
CHAPTER ONE.......................................................................................................................1
1. 1 INTRODUCTION AND BACKGROUND OF THE STUDY............................... 1
1.2 PROBLEM STATEMENT........................................................................................7
1.3PURPOSE OF THE STUDY....................................................................................8
1.4 OBJECTIVES.....................................................................................................8
1.5 RESEARCH QUESTIONS......................................................................................9
1.6SIGNIFICANCE OF THE STUDY........................................................................... 9
1.7DELIMITATIONS OF THE STUDY.......................................................................10
1.8 THEORETICAL FRAMEWORK........................................................................... 10
1.9DEFINITION OF TERMS....................................................................................... 14
1.10OUTLINE OF THE DISSERTATION..................................................................16

viii
CHAPTER TWO....................................................................................................................18
LITERATURE REVIEW................................................................................................18
2.1 INTRODUCTION...................................................................................................18
2.2 CULTURAL AND SOCIAL SIGNIFICANCE OF “ULWALUKO”
(CIRCUMCISION). 18
2.3 TRADITIONAL LEGAL CONSIDERATIONS OF ‘’ULWALUKO”
(CIRCUMCISION).........................................................................................................19
2.4SECRECY OF MALE CIRCUMCISION...............................................................21
2.5 FOOD TABOOS...................................................................................................22
2.6HEALING MEDICINE..............................................................................................23
2.7CONTROL AND PREVENTION OF INFECTION.............................................. 23
2.8COMPLICATIONS OF “ULWALUKO” (CIRCUMCISION)................................ 24
2.9RISKS OF CONTRACTING HUMAN IMMUNODEFICIENCY VIRUS............25
2.10 SUMMARY...................................................................................................28
CHAPTER THREE............................................................................................................... 29
RESEARCH METHODS.............................................................................................. 29
3.1 INTRODUCTION...................................................................................................29
3.2 RESEARCH DESIGN............................................................................................ 29
3.3 POPULATION...................................................................................................29
3.4SAMPLE AND SAMPLING PROCEDURE..........................................................29
3.4.1Inclusion and exclusion criteria..................................................................30
3.5MEASUREMENT INSTRUMENT........................................................................ 30

ix
3.6DATA COLLECTION...............................................................................................31
3.7TRUSTWORTHINESS........................................................................................... 32
3.7.1 Credibility..................................................................................... 32
3.7.2 Confirmability..................................................................................... 32
3.7.3 Transferability..................................................................................... 33
3.7.4 Dependability..................................................................................... 33
3.8ETHICAL CONSIDERATIONS..............................................................................33
3.8.1The principle of respect for persons..........................................................34
3.8.2Principle of no harm to subjects.................................................................34
3.8.3 Principle of justice..................................................................................... 34
3.8.4The principle of anonymity and confidentiality.........................................35
3.8.5 Informed consent..................................................................................... 35
3.9 DATA ANALYSIS...................................................................................................35
CHAPTER FOUR..................................................................................................................37
PRESENTATION OF FINDINGS............................................................................... 37
4.1 INTRODUCTION...................................................................................................37
4.2DEMOGRAPHIC CHARACTERISTICS OF STUDY PARTICIPANTS........... 37
4.3ASSESSMENT OF ASEPTIC TECHNIQUES USED BY TRADITIONAL
SURGEONS AND NURSES DURING TRADITIONAL CIRCUMCISION
PROCESSES 39
4.3.1Use of surgical gloves................................................................................. 39
4.3.2Cleanliness and sterilisation of circumcision instrument........................39

x
4.3.3Cleanliness of the seclusion lodge............................................................40
4.3.4 Wound dressings..................................................................................... 41
4.3.5Treatment of penile wound......................................................................... 42
4.3.6Experience of purulent penile wound........................................................43
4.4 Summary..................................................................................................................43
CHAPTER 5...........................................................................................................................44
DISCUSSION OF FINDINGS, CONCLUSION AND RECOMMENDATIONS.....44
5.1 INTRODUCTION...................................................................................................44
5.2DISCUSSION OF FINDINGS................................................................................ 44
5.3STUDY LIMITATIONS............................................................................................ 47
5.4 CONCLUSION...................................................................................................48
5.5RECOMMENDATIONS.......................................................................................... 48
REFERENCES.............................................................................................................. 50
APPENDIX A: Letter of approval from the University of Fort Hare ethics
committee.......................................................................................................................58
APPENDIX B: Letter of approval from the Eastern Cape Department of Health60
APPENDIX C: Letter of approval from the sub-district house of traditional
leaders in Mthatha.........................................................................................................61
APPENDIX D: Informed Consent by participant/parent/guardian......................... 62
APPENDIX E: Letter for ethical clearance to the University of Fort Hare...........65
APPENDIX F: Researcher’s declaration and conflict of interest declaration.......66
APPENDIX G: Questionnaire guide...........................................................................70

xi
LIST OF TABLES
Table 1.1: Death toll of initiates in the Eastern Cape associated with circumcision
from 2006-2013.
Table 4.1. Demographic characteristics of the participants.

xii
LIST OF FIGURES
Figure 1.1: The Health Belief Model

1
CHAPTER ONE
1. 1 INTRODUCTION AND BACKGROUND OF THE STUDY
According to the World Health Organisation and Joint United Nations Programme
(2007), globally, roughly 30% of males are circumcised, of whom about two thirds
are Muslim. Some common factors of male circumcision are ethnicity, observed
health and sexual fulfilment and the preference to fit into social norms (WHO &
UNAIDS, 2007). Neonatal circumcision is commonly practised in the following
countries: Israel, the United States of America, Canada, Australia and New Zealand
and in the greater part of the Middle East, Central Asia and West Africa (WHO &
UNAIDS, 2007). However, it is less common in East and Southern Africa, where the
average age of circumcision differs from boyhood to the late teens or twenties (WHO
& UNAIDS, 2007).
In several countries, the prevalence of non-religious circumcision has undergone
both rapid increases and decreases, revealing cultural mixing and varying
perceptions of health and sexual benefits (WHO & UNAIDS, 2007). It is also claimed
that male circumcision protects against several diseases that include urinary tract
infections, syphilis, chancroid, invasive penile cancer, and HIV (WHO & UNAIDS,
2007). However, as with any surgical procedure, there are potential risks entailed,
such as cross infection, complete removal of the foreskin or even glans penis.
The benefits of male circumcision are well documented (Connolly et al., 2008; Auvert
et al., 2013; Tobian et al., 2014; Kripke et al., 2016). Available evidence suggests
that male circumcision is protective against the acquisition of HIV and other sexually
transmitted diseases (Connolly et al., 2008; Auvert et al., 2013; Tobian et al., 2014;
Kripke et al., 2016). According to the WHO and UNAIDS (2011), 22% of HIV
infections between 2011 and 2025 among the 14 priority countries of eastern and
southern Africa could be averted if 80% of males between the ages of 15 and 49
years were to be circumcised by 2015. South Africa has a heavy burden of HIV, and
the HIV prevalence rate is disproportionately high among young people. However,
the rate of male circumcision is low in the country (Govender et al., 2013/14; Shisana

2
et al., 2014) and in parts of South Africa where the rate is high, most of the male
circumcisions are done after sexual debuts (Peltzer et al., 2008b; Peltzer & Kanta,
2009; Maughan-Brown et al., 2011). Consequently, the South African Government
introduced voluntary medical male circumcision as one of the methods of preventing
HIV (SANAC, 2012).
The issue of male circumcision continues to generate attention among policy makers
and scholars. In the South African context, the debate about male circumcision is
two-fold, arising from the cultural divergence in the country. In the Kwa-Zulu Natal
province, and in other provinces, where culturally males are not circumcised, the
priority remains on how to scale up voluntary medical male circumcision (Scott,
Weiss & Viljoen, 2005: 305; Naidoo, Dawood, Driver, Narainsamy, Ndlovu & Ndlovu,
2012). However, in provinces where traditional male circumcision is prevalent, the
need to make the process medically safe overrides the promotion of voluntary
medical male circumcision, which is often resisted by custodians of traditions
(Vincent, 2008b; Kepe, 2010). Among the AmaXhosa people of South Africa (the
majority of whom live in the country's Eastern Cape province), traditional male
circumcision symbolises the “rite of passage of boys to manhood” (Mavundla et al.,
2009). It is viewed as an important process of socialisation, necessary for
maintaining social order and the organisation of groups into hierarchies, renewing
group unity and a means for the transmission of values across generations (Vincent,
2008b; Vincent, 2008a).
Over the past two decades, following the traditional male circumcision ritual,
thousands of young men have been admitted to hospitals, hundreds have undergone
penile amputations and, consequently, died (Kepe, 2010). For instance, a study
conducted in the Mthatha area of South Africa shows that 25 deaths related to
traditional circumcisions were recorded at the Mthatha General Hospital during 2005
and 2006. Another study which assesses the extent of circumcision-related
complications and fatalities in the Eastern Cape shows that the incidence rate
remain unchanged (Meissner & Buso, 2007).
Despite the adverse outcomes associated with traditional male circumcision, the
practice still remains prevalent (Mark et al., 2012). This could be attributable to a
number of factors such as fear of stigmatisation (Mavundla et al., 2010, Peltzer &

3
Kanta, 2009; Mshana et al., 2011), religion/culture, notions of manhood, and social
disapproval (Mark et al., 2012; Kepe, 2010). Meissner & Buso (2007) assert that
unqualified traditional surgeons, negligent traditional nurses, irresponsible parents
and youth medically unfit for the hardships of initiation school contribute to the tragic
outcomes. Anecdotally, the ritual circumcision-related deaths are attributable to poor
hygiene at the initiation schools and failure to adopt proper aseptic techniques. The
South African Regulation 328 of 2007 gives the environmental health practitioners
(EHPs) an ethical opportunity and supremacy to enter every premise,
accommodation or structure for the purpose of health inspections. However,
available evidence suggests that initiation schools are not regularly inspected for
safety due to fear of interference with the traditional value systems (Rathebe, 2018).
Training of traditional nurses and surgeons has been suggested as a means of
reducing the adverse health outcomes associated with traditional male circumcision.
However, the results of studies assessing its effectiveness are mixed (Peltzer et al.,
2008b; Peltzer et al., 2008a). The political will to address the traditional circumcision
related-deaths and complications is lacking; however, the importance of providing
compelling scientific evidence demonstrating the need to make changes cannot be
overemphasised. This study thus seeks to assess the adult circumcision practices of
traditional surgeons and nurses in relation to the initiates’ health outcomes/morbidity
in the Eastern Cape.
In South Africa, more especially in the Eastern Cape, as is often shown on television
news and newspapers, in particular during the winter and summer seasons, when e
the practice of initiation schools normally takes place, it seems that traditional male
circumcision has become a crisis of morbidity and death. The number of deaths of
the initiates associated with circumcision each year has been on the increase (Table
1.1).

4
Table 1.1: Death toll of initiates in the Eastern Cape associated withcircumcision from 2006-2013.
YEAR NUMBER OF DEATHS PER YEAR
2006 58
2007 32
2008 34
2009 91
2010 62
2011 62
2012 74
2013 86
Total 499
Source: Daily Dispatch (Feni, 2014b: 01).
A 16-year-old initiate was interviewed in the Nelson Mandela Academic Hospital
after he was visited by The Daily Dispatch. He explained that he had been
pressurised by from peers and had been tortured by his seniors in the practice and
was attacked by so-called friends. The young man told The Daily Dispatch that as
initiates, they were made to sing all day long, denied water to drink for eight days
and did not eat for two days. They were given food after two days of starvation and
were only given a half-cooked stiff pap. In addition, they were beaten and mocked
when they cried. They were told that they were not real men, but as weak as women.
This explains why some initiates die from dehydration, heart failure and septicaemia.
They are not permitted normal daily diets and emotional, psychological and social
support is denied them. There is no sense of love, kindness or care. Rather, they

5
are judged and tortured, as well as being deprived of the general living conditions
normal for human beings. Even plants cannot survive without water, necessary
nutrients and need suitable environmental conditions to survive. Then how much
more so for human beings? Thus, the focus of this study is to examine the
circumcision practices of traditional surgeons and nurses in relation to the initiates’
health outcomes/morbidity in the Eastern Cape.
In the AmaXhosa tradition, the “abakhwetha” (initiates) are placed away from view
of the public in a temporary lodge called “ibhuma”, which is made from tree branches
and layered with grass to shelter the house of the “abakhweta”. In the middle of the
lodge, there is usually a tall straight pole either from the tree, named in isiXhosa,
“umthathi” or “umnquma”. This is believed to be symbolically linked to the ancestors,
and so provide protection to the “abakhwetha” (initiates). The lodge is generally
located in a wooded area near to water to provide favourable conditions for the
initiates (Dold & Cocks, 2012: 94).
However, urbanisation and environmental factors have precipitated certain changes
in the practice of the traditional circumcision in association with the health conditions
that the ‘’abakhwetha’’ are prone to contract in the process of ‘’ulwaluko’’, for
example, HIV and pneumonia. This is often because resources are scarce in the
urban settlements with the result that the lodge is covered with plastic sheets instead
of grass. However, the central pole from “umnquma” or “umthathi” is still used for the
protection of the ancestors (Dold et al., 2012: 93).
The day before AmaXhosa boys undergo traditional circumcision a goat is
slaughtered and traditional beer is made for clansmen attending the ritual called
“ukubingelelwa” (a greeting ceremony). Only men are allowed to attend this
ceremony in a barn where seating arrangements are in order of seniority. This is
crucial in the AmaXhosa tradition, for example, those who initiated first are senior to
those who initiated later, hence, and the sequence starts from the left, next to the
exit extending towards the junior men. This ritual is performed to request blessings
from the ancestors before the initiates go to the temporary seclusion lodge (Dold et
al., 2012: 93).
The boys eat only the meat from the forelegs which is temporally placed on fire
made from trees called ‘’umthathi (sneezewood)’’ or ‘’umnquma’’. These trees give

6
off a bitter taste, which is symbolic - to strengthen the boys in preparation of the ritual
to follow the next day. The initiates’ hair is remove and burnt to avoid reuse by the
sorcerers. The regrowth of the hair of the initiates symbolises the “rebirth” of
someone in the AmaXhosa tradition (Dold et al., 2012: 96).
Before the sacrifice begins, the initiates perform a dance called “umguyo”. In the past,
the dance costume was made from palm tree leaves and the boys painted their
bodies with clay and ochre. However, nowadays, traditional initiates in the
AmaXhosa culture wear an old shirt and hat that have been cut into many long
ribbons to draw attention to the dance (Dold et al., 2012: 96).
In the hours of the morning on the day of “ulwaluko” (circumcision), following the day
of the sacrifice, the initiates go to the nearest water stream in which they wash
themselves to purify themselves from the ritual uncleanliness called “ubunqalathi” in
AmaXhosa. Physiologically, the cold water helps constrict the blood vessels,
reducing the lowering blood flow to the site of the operation during circumcision, thus
minimising bleeding.
The vital phase of the ritual is that boys run to the nearest stream to wash. On return,
each boy is given an “intambo yabakhwetha” (charm necklace), which is believed to
protect initiates from the evil spirits of the sorcerers, and an “ityeba” (strap) (Dold et
al., 2012: 96). Both of these are made from “uluzi” (a string made from the roots of
fig veld tree) by either the parents or the guardians of each boy, using forest material
(Dold et al., 2012: 96). After the initiates have been given the “intambo yabakhwetha”,
they immediately leave the home and go to the forest where the “ibhuma” has
already been built to shelter the initiates (Dold et al., 2012: 96).
As the initiates invade the forest, they are led by the young boys, called
‘’amanqalath”, of around ten years of age who stay with the initiates during the
period of seclusion and do run odd jobs for the initiates. Following these boys is the
“Ingcibi” (Surgeon), the “Ikhankatha” (traditional nurse), fathers and the elders of the
clan (Dold et al., 2012: 97).
All females are strictly forbidden to attend this phase of the ritual. However, all family
members (including both genders of any age, except the very young who might not
understand what is about to happen) of the clan of each initiate do know that one or

7
more of their family sons is a few hours away from changing from boyhood to
manhood (Dold et al., 2012: 97).
Even though the women and daughters left at home do not attend the ritual in the
forest, they do have mixed emotions of ‘’happiness’’ and ‘’sadness’’ because their
boy children are now going to be groomed into manhood. It makes them happy on
one hand, but on the other, the fact that their child is going to be away from home
for a certain period of time with no idea of what really happens in the ‘’forest’’
(‘’ebhomeni’’) brings them sadness. During this time, the women enjoy themselves
with their traditional songs and playing drums to rejoice in the proceedings of the
ritual in the forest (Dold et al., 2012: 97). Immediately after the surgeon has finished
the operation, the young boys on top of the mountains make the noises of whistling
and shouting, to inform the women at home that their sons are no longer boys (Dold
et al., 2012: 97).
1.2 PROBLEM STATEMENT
Over the past years, a rise in the death of initiates has been noted, especially in the
Eastern Cape. Between 2006 and 2013 about 499 initiates died (table 1.1). There is
no clarity as to whether the initiates’ ill-health and deaths could be attributed to
traditional surgeons’ and nurses’ failure to do their job properly. Initiate deaths are an
ongoing crisis. It was reported by the Social Development MEC that the main focus
in the department is to prioritise the initiative to offer emotional support to young men,
some of whom have had their penises amputated. The report indicated that 19
initiates had died and 134 had been rescued from illegal initiation schools for
hospitalisation. Among those initiates, 11 were from Mount Ayliff, two from Lusikisiki
and the rest from Bizana in the Pondoland region. They were taken to the Lusikisiki
Rescue Centre (LRC). Government statistics from Bisho reveal that 437 initiates
have died, some having lost their penises and thousands more have been
hospitalised. Most of initiate deaths occurred in the O R Tambo region/ district (Nini,
2014: 04).

8
There have also been cases of initiates’ deaths in Mthatha. A 17 -year old initiate
from Qweqwe village died of septicaemia and hypothermia on 23 June 2014. Yet,
another 18-year old initiate from Ncise village died of septicaemia and heart failure
on 30 June 2014 (Feni, 2014a: 05).
The problem of deaths of initiates is exacerbated by the way in which the traditional
surgeons and nurses perform their duties, as well as by the conditions of the
environment in which initiates cared for. It is therefore imperative to investigate the
circumcision practices of traditional surgeons and nurses in relation to the initiates’
health outcomes/morbidity in the Eastern Cape. There is little information in this
regard.
1.3 PURPOSE OF THE STUDY
The aim of this study is to investigate the circumcision practices of traditional
surgeons and nurses in relation to the initiates’ health outcomes/morbidity in the
Eastern Cape, in order to unravel the factors associated with the negative health
outcomes of many initiates.
1.4 OBJECTIVES
The objectives of the study are to:
Determine the sterile procedures, to prevent infection, by traditional surgeons
and nurses before, during and after circumcision..
Assess the human physiological and anatomical knowledge of the traditional
surgeons and nurses in relation to male circumcision and its complications.
Determine the environmental conditions under which the circumcision takes
place.

9
1.5 RESEARCH QUESTIONS
The following research questions have been posed:
What sterile procedures, to prevent infection, do traditional surgeons and
nurses use before, during and after circumcision?
Are the traditional surgeons and nurses knowledgeable about human
physiology and anatomy in relation to male circumcision and its
complications?
Is the environment in which the circumcisions take place hygienically safe
for the circumcisions?
1.6 SIGNIFICANCE OF THE STUDY
Young boys are at risk of losing their gender identity, or even of death, during
traditional circumcision. Thus, this study will benefit the youth, especially those
young males who are still considered boys since they have not yet been circumcised.
With proper research findings, analysis, recommendations and implementation the
young males are more likely to survive the circumcision ceremony without
permanent physical damage or ill health. Further, pre-education of young males
prior to circumcision or initiation school will empower them by teaching them about
what to expect in the process that they are about to undertake.
In addition, this study will benefit the family members through providing
recommendations that could successfully prevent or reduce the morbidity of initiates
from the initiation schools. Hence, the families will be relieved of the unnecessary
loss of their loved ones and the financial stresses of the burial services.
Community members will benefit through the centralisation of circumcision or
initiation schools and they will know to choose right person to circumcise their
children, who will take good care of them. This study will promote community
solidarity to ensure safe circumcision and to eradicate the illegal practices of unsafe
circumcision.

10
The findings and recommendations of the study will help the Eastern Cape
Department of Health (DoH) in the implementation of new strategies to help save the
lives of initiates.
1.7 DELIMITATIONS OF THE STUDY
This study examines the role of traditional surgeons and nurses and their practice
based on what they do to control infections, it assesses the knowledge based of the
physiology l and anatomy of the human body, linked to the practice and its
complications. Further, it assesses the suitability of the environment for the survival
of initiates in which the practice takes place.
1.8 THEORETICAL FRAMEWORK
This study is guided by Hochbaum’s (1958) framework participation in medical
screening programmes. This framework comprises major elements of perception
such as perceived threat, perceived benefits of an action, perceived barriers to an
action and cues to an action (stimulus). Perceived threat is formed by two more
elements, perceived susceptibility and perceived seriousness of the condition.
Perceived susceptibility is defined as one’s judgement or belief whether one is
vulnerable to contracting a condition (Hochbaum, 1958: 09; Glanz, Rimer & Lewis,
2002: 48). According to Hochbaum (1958: 10), a person may believe that he or she
is prone to contracting a disease or may have it without noticing symptoms However,,
the person may not believe in the benefits of early diagnosis. For example, there is
the likelihood that traditional surgeons and nurses might believe that initiates are
prone to certain conditions but, due to socio-cultural stereotypical values, attitudes
and norms or other social influences, they do not consider ways to prevent such
conditions.
Moreover, with education-based knowledge and prioritising the health of the initiates
as a human being, rather than focusing on the social and cultural influences behind
the practice, the boys or their parents would probably opt for other safer means of
circumcision.

11
The perceived seriousness of a condition refers to the extent of severity of the
condition based on biological or physical changes and its impact on socio-economic
engagements (Hochbaum 1958: 12; Glanz et al., 2002: 48).This is, for instance,
evident in the case of initiates who develop sepsis while in the lodge and there is no
consideration of early medical help to prevent complications. Some of those initiates
might end up having their penises amputated, resulting in social stigma, low self-
esteem, inability to meet sexual needs, changes in urine passage. This may result in
psychological stress that could be suicidal in nature.
Glanz et al. (2002:47) define perceived benefits as the belief in the effectiveness of
the proposed action to reduce the risk or seriousness of impact. When public
communities are made aware of crises, they make sound decisions. Social
influences from friends, neighbours and co-workers might play a role in the choice of
circumcision practices, be it in a positive or negative manner (Hochbaum, 1958: 18-
19).
Evidence-based knowledge can be obtained through reading newspapers, watching
television news, attending official awareness programmes in the community, and
reading research articles about the practices of “ulwaluko” (circumcision).
Perceived barriers to an action are generally one’s perception or judgement about
the extent of the difficulty of the set of various factors that may interfere with the
achievement of certain proposed behaviours. For example, when knowledge is
minimal or absent about professionally trained traditional surgeons and nurses, and
social stigma dominates in those who undergo a certain method of circumcision, it
may block bringing changes to healthy behavioural practices. Glanz et al. (2002:47)
define this element as the belief about the physical and psychological costs of the
advised action.
However, Glanz et al. (2002) does not consider the socio-economical aspect in his
definition. Some barriers might be socially or financially related, or sometimes the
culture might be personal to the individual himself. For example, someone might opt
to undergo traditional male circumcision, not because he likes the aspect of it, but
because of his fear that he will be regarded as a boy if he were to undergo medical

12
male circumcision, or else he might be from a remote area where health care centres
are not easily accessed.
Hochbaum’s cues to action or the stimulus refers to an individual’s motivation when
he or she realises that there is a benefit to the action he or she is about to take.
Actual change mostly occurs when an external or internal cue generate an action.
Two types of cues to action have been identified: (a) physical changes noticed by the
individual and (b) cues from the external situation, such as posters, articles,
television and radio programmes (Hochbaum, 1958: 10). Cues to action trigger
‘readiness’ (Glanz et al., 2002:49).
The degree of the required stimulus to activate an action would be determined by the
levels of motivation to change, together with the perceived benefits weighed against
the costs. Change is more likely to happen with improved education in communities
as a way to motivate youth and to advantage traditional surgeons and traditional
nurses who have undergone a proper training about the practice. They are more
likely to practise in a safer way, understanding the social, psychological and
biological changes in the human body and the impact of poor practices of
circumcision and caring for initiates’ wounds in the lodge. In addition, they would
have a better understanding of the physiological and pathological mechanisms
behind the development of certain conditions that at times lead to disability or even
death.
Self-efficacy is defined shortly as confidence in one’s potential to take action (Glanz
et al., 2002: 48).
As based on the framework of this study, the perceived threat of disease with the
help of cues to an action, such as raised awareness, can motivate communities to
consider other ways of preventing complications and deaths of initiates. However,
the likelihood of individuals in the communities considering recommended health
actions may depend on the benefits weighed against the barriers to action and
modifying factors such as age, level of education, personality, social class,
knowledge about the disease and related experiences of that disease. Therefore,
this theoretical framework is focuses more on prevention and bringing about a

13
change in health behavioural practices in communities and in health-care related
settings.
Perceived
susceptibility to
disease
Perceived
seriousness of the
disease
CUES TO ACTION
1. Raised awareness - for example,
mass media campaigns,
newspapers etc.
2. Personal advice - for instance a
reminder from a health
professional.
3. Personal symptoms
4. Illness of a friend or family
member
Perceived benefits of
taking action against
barriers to action

14
Figure 1.1: The health belief model (Hochbaum 1958: 09-19; Glanz 2002: 49).
1.9 DEFINITION OF TERMS
Adverse outcomes
In this study, adverse outcomes refer to ill-health, loss of genital organs or death,
resulting from surgical removal of the foreskin and poor post-surgery management of
circumcision in a traditional setting.
“Unintended injuries caused by medical management rather than the disease
process” (Vincent, Neale, Woloshynowych, 2001).
Circumcision
The surgical removal of the prepuce by a surgeon usually for medical or cultural
reasons. In AmaXhosa tradition, circumcision refers to a ritual that is routinely
performed to mark the boy’s maturity, and it indicates a rite of passage for the
adolescent male from boyhood to manhood (Mogotlane, Ntlangulela & Ogunbanjo,
2004: 60).
Control and prevention of infection
Control and prevention of infection depends on a knowledge-based approach and
applicable methods planned to prevent damage caused by an infection to initiates
and those who take care of them (WHO, 2019).
“Evidence based practices and procedures that, when applied consistently in health
care settings, can prevent or reduce the risk of infection in clients/patients/residents,
health care providers and visitors” (PIDAC, 2009).

15
Infection
The invasion of an organism’s body tissues by disease caused by either bacterial or
viral agents.
“The entry and multiplication of an infectious agent in the tissues of the host”(PIDAC,
2009).
Prevalent
Refers to something that is widespread or existing commonly in a certain area at a
specific time (Smith, 2000).
Traditional male circumcision
The surgical removal of the male’s foreskin out of a hospital environment, by a non-
medically trained surgeon for traditional reasons.
Meissner and Buso (2007) define traditional male circumcision as “a rite of passage
that prepares the initiate for transition to manhood”.
Traditional Nurse
A male person who is usually selected by the community members to look after
initiates. A traditional nurse performs wound dressings and regularly monitors the
progress of wound healing. Mogotlane, Ntlangulela and Ogunbanjo (2004) refer to
traditional nurses as “traditional attendants”.
Traditional Surgeon
A traditional surgeon is someone who performs the surgical removal of the foreskin
in fulfilment of the ritual without having a formal education qualification.
16
According to WHO (2010), a traditional surgeon is a traditional provider who
performs traditional male circumcision in a non-clinical setting for cultural reasons
without any formal medical training.
Traditionally Circumcised Men
These men have undergone traditional circumcision as a rite of passage from
boyhood to manhood. They are meant to take above average social responsibilities,
make sound decisions, respect the elderly, bring order in family disagreements and
do away with childish behaviour (Vincent, 2008a: 438).
“Ulwaluko”
Ulwaluko is the isiXhosa term used to describe traditional male circumcision. It is
defined as an initiation into manhood and is an ancient initiation rite of passage from
boyhood to manhood. This ritual is traditionally intended to teach and prepare young
males for the responsibilities of manhood (Rijken & Dakwa, 2013: 01).
“Umdlanga”
“Umdlanga” refers to the spear that is used by traditional surgeons to cut the foreskin
from an uncircumcised male for traditional reasons. Mogotlane, Ntlangulela &
Ogunbanjo (2004) describe “umdlanga” as the “traditional spear”.
1.10 OUTLINE OF THE DISSERTATION
Chapter One provides an introduction and gives the background of the study, the
problem statement, purpose of the study, objectives, research questions,
significance of the study, delimitations, theoretical framework, definition of key
functional terms and an outline of the study.

17
Chapter Two presents the literature review of the study. Under the review of
literature the cultural significance of traditional male circumcision, traditional legal
considerations of circumcision, the secrecy of traditional male circumcision, food
restrictions, traditional medicine used for wound healing, prevention and control of
infections, complications of circumcision and the risks of contracting HIV in the
process of circumcision are discussed.
Chapter Three - the research methodology of the study is described in this chapter.
The research design, target population, sample, and sampling procedure,
measurement or instrument, data collection, trustworthiness, ethical considerations
and data analysis are provided.
Chapter Four discusses the divergent responses concerning aseptic techniques and
the extent of knowledge of traditional surgeons and nurses about human anatomy
and the physiological process during circumcision.
Chapter Five presents and discusses the findings emerging from the study. It then
draws the conclusion, based on the study findings.

18
CHAPTER TWO
LITERATURE REVIEW
2.1 INTRODUCTIONThe review of literature for this study focuses on investigations of traditional
surgeons’ and amakhankathas’ (traditional nurses’) practices and their impact on the
outcomes or morbidity during circumcision in the initiation schools in the Eastern
Cape. The literature review critically discusses previous studies under the following
subheadings: (1) cultural and social aspects of “ulwaluko” (circumcision); (2) legal
considerations of ulwaluko; (3) secrecy of “ulwaluko”;. (4) food “taboos”; (5) healing
medicine; (6) control of infection by traditional surgeons and nurses (7)
Complications of “ulwaluko”; and (8) the risk of contracting HIV.
2.2 CULTURAL AND SOCIAL SIGNIFICANCE OF “ULWALUKO”(CIRCUMCISION).
Culturally and socially, male circumcision is assumed to signify the rite of passage
from boyhood into manhood, the gaining of social status, the right to take certain
responsibilities at home and in the community. It is believed to be a mark of identity.
For example, a man who has not undergone traditional male circumcision in the
AmaXhosa culture, is less likely to inherit his father’s possessions.
Traditional male circumcision is mainly performed by experienced traditional
surgeons who, the community believes, is good at his job. It is traditionally believed
that AmaXhosa men do not have to be attended to by female nurses in hospitals.
The initiates are not allowed to be seen by women of the community, understandably,
because in AmaXhosa tradition, male circumcision is a secret ritual (Dold & Cocks,
2012: 97).
However, the tradition seems to be ignorant of the prevalent complications and
morbidity associated with “ulwaluko”. Ironically, the complications that occur from
the traditional circumcision practice are eventually more likely to result in the initiates
being attended to by clinical nurses and clinical surgeons. This suggests that

19
working together with trained clinical surgeons and nurses at an early stage could
reduce the common complications and deaths.
According to the study conducted at St Lucy’s Hospital by Anike, Govender,
Ndimand & Tumbo (2013/14: 05), genital sepsis is the most common complication
among the initiates who are hospitalised; and there is a need for traditional surgeons
to be trained on safe techniques and the use of hygienic practices to reduce
complications commonly identified in the study.
2.3 TRADITIONAL LEGAL CONSIDERATIONS OF ‘’ULWALUKO”(CIRCUMCISION).
Originally, traditional surgeons were individuals who were recognised by the
communities as experienced surgeons in the practice of traditional circumcision.
However, the prevalence of complications and deaths of young boys undergoing
traditional male circumcisions among the AmaXhosa has resulted in government
intervening in the process. This has led to some conflict between the government
and the traditional leaders who complain that they were not part of the conclusions
reached by the government, based on traditional circumcision changes (Kepe, 2010:
732). One example of changes government has made, is that traditional surgeons
must be registered with the Department of Health in order to perform traditional male
circumcision. The same author further states that those who illegally perform the
surgical practice of male circumcision should be arrested and illegal initiation schools
should be shut down. Hospitalisation of initiates has increased in numbers, most
probably because initiates found with illnesses resulting from illegal initiation schools
are taken to hospital by the health monitors of the Department of Health (Kepe, 2010:
732; WHO, 2008: 28).
However, there still seem to be illegal practices of traditional male circumcision. For
example, 20 initiates died in Mpumalanga Province in 2013 and the causes of death
were haemorrhage, and hypothermia, which are preventable conditions (Sapa, 2013:
01). Moreover, health workers are still not fully involved in the traditional male
circumcision. The increase in number of initiation schools is linked to financial
benefits to those who claim to be traditional surgeons. It is well known that

20
traditional circumcision is taken care of by traditional leaders, but some misuse the
word “culture” and led the health minister to pronounce these surgeons
“culturepreneurs” because they profit from the practice (Sapa, 2013: 01).
Further, it was stated by the COGTA deputy minister, Obed Bapela, that there is
currently no legislative provision enabling the state to prosecute illegal circumcision.
However, the government is working to develop legislation that will deal with illegal
circumcision and initiation schools (Feketha, 2014: 05).
The age at which young boys are legally permitted to undergo male circumcision is
16 or older with the signed consent of a legal guardian or parent or with the relevant
religious or medical reasons. However, a boy of 18 or more was given the legal right
to sign consent for himself (WHO, 2010: 11). The same author states that it is
recommended in the policy, that those who are about to undergo the process of
circumcision should first undergo a physical examination by an authorised physician
to ensure that his health is good enough for him to be circumcised.
However, there seems to be no clarity on specific medical conditions that might
exclude an individual from the ritual. It is also not clear whether the choice remains
with the client or his parents, in the case of minors, to undergo the circumcision
regardless of his health status as per the medical examination.
According to Deacon and Thomson (2012: 13), some boys are forced to undergo
traditional circumcision at puberty, even though they might prefer a medical
circumcision. This violates the South African Children’s Right Charter that stipulates
children have the right to freedom to practise their own culture, religion and beliefs
without fear.
According to Deacon et al. (2012); The Sunday Times, 27 Jan (2008); and Huisman
(2009) an 18 year-old boy was forced by his father to go for traditional male
circumcision. The boy maintained that his Christian religion did not allow any
procedure involving blood in association with the ancestors (The Sunday Times, 27
Jan 2008). This is basically the violation of the young man’s rights to freely perform
his religious and cultural practices without being interfered with. In this instance, the
case was open by the boy against his father (The Sunday Times, 27 Jan 2008). It is
also stated that traditional leaders themselves did not acknowledge that a child has

21
the right to decide on the type of circumcision he wants to follow. Those who refuse
to undergo traditional circumcision are often totally exorcised by their community
(Huisman, 2009). This is clearly in contradiction of the South African Children’s Right
Charter.
2.4 SECRECY OF MALE CIRCUMCISION
The ritual teachings are not shared with the uncircumcised or with men who have
undergone male medical circumcision (MMC). They are excluded from the important
gatherings of men about the initiation schools and other important cultural practices.
AmaXhosa traditional male circumcision is sacred and there is much secrecy that it
is respected by those who practise it. There are limitations imposed within the
context of traditional male circumcision practice among the isiXhosa speaking tribe.
These include the involvement of women, uncircumcised males and medically
circumcised males. Male medical circumcision practice is stigmatised because it
involves anaesthesia and is assumed to be performed in the presence of female
nurses and female doctors.
It is for instance, believed that women are associated with uncleanliness (“umlaza”)
and in association with this statement, men who have recently been involved in
sexual practice are not allowed to attend the initiates because they carry those
impurities from their female partners (Kepe, 2010: 732).
However, Kepe (2010) continues with the argument that, “the very concepts of
tradition and ritual imply that there is a history to the practice, yet it would be foolish
to assume that traditions and rituals do not change as societies change”.
This indicates that traditional circumcision should go along with the present research
to improve the practice of health- based care to avoid putting initiates at risk of
infections, complications and morbidity.

22
2.5 FOOD TABOOS
Initiates are traditionally forbidden to consume salty foods and water for the first eight
days post circumcision. Only hard food is allowed because it is believed that water
causes painful micturition and more bleeding (ukucobela) from the operation site
(Casement, 2018; Bullock, 2015). This evidence shows that lack of education is
having other influences based on the practice of traditional male circumcision. In
their study, Mogotlane, Ntlangulela & Ogunbanjo (2004) report that initiates
verbalised the restrictions on drinking water and eating salty foods, including meat.
Unfortunately, in some regions, initiates are restricted from eating eggs and meat,
which are scientifically proven sources of protein which facilitate the healing process
of wounds. According to the WHO (2008: 29), traditional surgeons and nurses
ignore the anatomical significance of the procedure, wound dressing techniques,
food that is richer in protein to facilitate wound healing, and arising health conditions
are not taken seriously as medical conditions that need urgent medical attention. As
a result, initiates die every year. For example, a 15-year-old initiate from East
London (Duncan Village) died at the Gompo Initiation School after complaining of
severe chest pain and respiratory problems. The traditional surgeon called the father.
However, when the father came to the lodge the initiate told him that he was feeling
much better. Then after a while, the pain and the difficulty in breathing became
worse and the ambulance and police were called in, but when they arrived at the
scene, the initiate has already passed on. This is likely to instil psychological trauma
to the parents as well as fellow initiates, who had to watch their friend dying and
being taken away from them as a corpse (Mukhuthu, 2014: 02).
Despite common practice, the policy of male circumcision in the Eastern Cape,
states that it is illegal to deprive “abakhwetha” (initiates) of water to drink as one of
the common complications among the initiates is dehydration (WHO, 2008: 13).

23
2.6 HEALING MEDICINE
In traditional circumcision, medicinal plants called isichwe (everlasting) are used as
an anti-septic and ishwadi (sore eye flower) is used to heal the wounds of initiates.
The ishwadi plant, which is used to stop bleeding, is normally gathered by a
traditional nurse a month before the circumcision and is left to dry out in the kraal in
readiness for use (Dold & Cocks, 2012: 96).
2.7 CONTROL AND PREVENTION OF INFECTION
In a traditional male circumcision, it is probable that sterility is not maintained. This
might include the use of sterile gloves during the procedure and the use of a sterile
cutting object called ‘’umdlanga”. The changing of wound dressings by one
traditional nurse from the first initiate to the last, without washing his hands can
introduce infection through contamination, the repeated use of ‘’ityeba’’ (bandage)
that has been washed with ordinary soap can also expose initiates to infection of the
circumcision wound. However, there is no scientific evidence to support or criticise
whether traditional surgeons and nurses apply aseptic techniques during the wound
care of initiates.
The assumption that one “umdlanga”(knife or assegai) is used by traditional surgeon
to circumcise many different initiates without its being sterilised is more likely to
expose the boys to infectious diseases, in particular HIV, Hepatitis C Virus (HCV)
and HBV. (Sedar, Derek, Unic, Marijancevic, Markovic, Primorac & Petrovecki, 2013:
150).
Moreover, the unwillingness to use medical equipment and the lack of education,
knowledge and the reluctance of traditional surgeons to work together with the
Department of Health, as well as the scarcity of resources, is likely to interfere with
the control of infection in the AmaXhosa traditional circumcision practice.
Interestingly, the study conducted by Peltzer, Nqeketo, Petros and Kanta (2008a)
reports that most traditional surgeons and nurses who were trained on ten modules
(safe circumcision, infection control, sexual health education, detection and early

24
management of complications, anatomy and post-operative care) over five days
wore gloves during operations and care but did not use the recommended
instruments. High rates of complications were found in this study and as a result, it
showed little support of the benefits of traditional male circumcision.
Currently, no studies showing evidence of the acknowledgement of the importance
of hand hygiene by traditional surgeons and nurses before and after they attend to
initiates. Peltzer et al. (2008a) report that only some of the surgeons and nurses
wore gloves but they did not clarify whether the gloves were changed between
initiates. It was not clear whether the gloves used were sterile or not. The routine
according to which bandages were changed during wound dressings was not
mentioned to their study. The use of dirty bandages can introduce infection to the
initiates’ wounds. The nature of the cutting objects used was different from one
initiate to another. However, it was not clear whether these objects were used
repeatedly on different initiates. Lastly, there is no clarity as to whether the
instruments used were sterile or not.
2.8 COMPLICATIONS OF “ULWALUKO” (CIRCUMCISION)
Traditional surgeons do not usually undergo any formal training to perform their job.
They use their own traditional skills and circumcision techniques. This may result in
initiates’ lives being at risk because of the traditional surgeons’ lack of knowledge
about the anatomical and physiological aspects of the procedure, its complications
and their management.
The extent in which the ‘’ityeba” (bandage) is tightly applied around the penis is likely
to interfere with the blood circulation to the glans penis by severely constricting blood
vessels. As a result, gangrenous penile tissue may form from insufficient
oxygenation.
Wilcken, Keil and Dick (2010: 908) claim that four of the 45 admitted patients lost
the glans of the penis and two patients lost the entire penis. “In this study, 93% of
the 45 subjects presented with some form of penile injury resulting, not necessarily
from the circumcision procedure itself, but from poor post-operative wound care”

25
(Wilcken et al., 2010: 908). Other complications are linked to the poor practice of
traditional surgeons, for instance, excessive bleeding is more likely to be witnessed
when the penile shaft skin is excessively removed or the glans penis is cut off by
surgeon (Wilcken et al., 2010: 908; WHO, 2008: 29).
In AmaXhosa traditional male circumcision fluid intake is normally restricted to
minimal amounts because it is traditionally believed that fluid intake causes more
“icobelo”(bleeding) from the operation site. Based on this belief, initiates may
become dehydrated and eventually die. According to Wilcken et al. (2010: 908)
dehydration was found to be a common cause of death.
2.9 RISKS OF CONTRACTING HUMAN IMMUNODEFICIENCY VIRUS
The Brown, Venkataramani, Nattrass, Phil, Seekings and Whiteside (2011) study
argues that there is more risk of contracting HIV amongst individuals whose
foreskins have not been removed at all and amongst those with partially removed
foreskins. However, complete removal of the foreskin proved to be more important in
the reduction of HIV among males. They further maintain that partial removal of the
foreskin is more common among young men who have experienced traditional male
circumcision. Consequently, medical male circumcision was considered a more
protective and safer practice in reducing the chances of HIV infection among
circumcised men. According to Vincent (2008a), the cutting of the foreskin
contributes to the reduction of HIV infection by removing cells that are particularly
susceptible to contracting HIV. The same authors further state that there is an
impression that the circumcised penis develops a thicker layer of skin, which is
resistant to HIV infection.
The younger the age of the person undergoing male circumcision, the lower the
chances of contracting HIV (Brown et al., 2011: 503). The results of this study, as
indicated above encourages medical male circumcision (MMC) at very young age,
for example, the circumcision of infants is regarded as a more advantageous
practice than those who are circumcised during adolescence.

26
Most men who were traditionally circumcised prefer TMC over male medical
circumcision (Brown et al., 2011: 501). However, with the knowledge of the benefits
of MMC, a few traditionally circumcised men have indicated a preference for
MMC(Brown et al., 2011: 501).
It seems that despite the on-going research knowledge and the existing laws about
circumcision, there are still challenges resulting from traditional male circumcision.
For example, the fact that there are still complications resulting from circumcision
malpractices and unauthorised surgeons circumcise boys as young as eight,
suggests that enforced parental education about the route that they should follow
when their children are about to undergo circumcision is needed to protect their
children against these surgeons. In addition, the children themselves should be
warned (Sapa, 2013: 01).
“Last year, around 400 000 initiates underwent the rites of passage, with just over
20 000 being illegal initiates who were either under age or had no permission from
parents or traditional leaders. Over 80 initiates died, while 31 had their penises
amputated. A further 670 were admitted to hospital and four initiates lost their lives in
East London Hospitals and Qawukeni. The death of initiates was largely caused by
septicaemia, dehydration, gangrene, kidney problems and abuse, according to the
EC DoH” (Ludidi, 2014: 01). Children and communities also need to be empowered
because the lives of the children are at risk of illegal circumcision that might result in
these young boys dying, while measures to prevent these deaths are believed to be
available.
For example, the provincial health spokesperson said that there was a case where
the Department of Health officials were doing random checks and were denied
access by the parents to one of the illegal initiation schools. As a result one initiate
died the following day (Feni, 2014b: 01). These people should be held liable and the
law should take its course to punish them because they are costing the lives of
young men.
In one of the initiation schools at kwa-Dosi village, close to Mthatha, traditional
nurses were found drunk and could hardly manage to move (Feni, 2014b: 01). This
suggests an urgent need for professionally trained traditional nurse to look after
initiates with regulations to guide their practice. No one dealing with life and death

27
situations should be caught drunk at the workplace. These people are not mentally
or physically fit to take care of the initiates.
There also seems to be difficulty in implementing health strategies for the prevention
of infections that occur in the practice of traditional male circumcision. This might be
because of the cultural differences between the Department of Health and the
communities that practise traditional male circumcision as a rite of passage from
boyhood to manhood. Some of the differences may arise a result of the fact that the
ritual is sacred and there is secrecy behind its practice (Nkosi, 2013:126).
Traditional male circumcision should be formalised and centralised to ensure
identifiable initiation school locations. Traditional surgeons and traditional nurses
should undergo proper formal training. The training should be long enough to allow
enough time for both theoretical training and practical exposure to ensure that
initiates will be safe from complications and death related to the traditional practice.
It was stated in The Daily Dispatch newspaper that the government is being urged to
include into policy the availability of first-aid training and kits for traditional surgeons,
traditional healers and clean running water points at circumcision sites and tap water
for nurses who help initiates (Feketha, 2014: 05).
Most of the studies seem to focus on the prevalence of specific conditions that
initiates tend to acquire rather than looking at the major causative factors regarding
the practice of traditional surgeons and nurses. They do not specify the procedures
and curricula, which the training of traditional surgeons and nurses should be
focusing on. Furthermore, it is not clear what practical changes could be made in the
environment where contagious practices are evident. For example, from a medical
perspective, when wound dressing is carried out, a sterile field is normally
considered important to prevent contamination from unsterile objects. Few studies
specify significant physiological mechanisms behind the development of the sepsis
and other complications.
However, bringing change in the traditional circumcision practice among the
AmaXhosa population is not easy. This is because they have been practising this
ritual since the times of their ancestors and the male traditional circumcision is still
considered a valuable practice in AmaXhosa tradition.

28
According to Burns and Grove (1993: 683), within the social system there are forces
that promote social stability as well as forces that resist change.
2.10 SUMMARY
In this chapter, literature was reviewed, and the cultural and social aspects of
circumcision have been discussed, as well as the legal considerations of
circumcision, the secrecy of TMC, food restrictions, healing medicines, control of
infection by traditional surgeons and nurses, medical and surgical complications of
TMC and the risk of contracting HIV was also considered. The design and the
methodology of this study are discussed in the following chapter.

29
CHAPTER THREE
RESEARCH METHODS
3.1 INTRODUCTION
This chapter describes the methodology and design utilised in this study. It further
describes the research design, population, sample and sampling procedure,
instrument of measurement, collection of data, trustworthiness, ethical
considerations and an analysis of the data.
3.2 RESEARCH DESIGN
The study uses a qualitative method and an exploratory research design. Semi-
structured interviews of traditional surgeons, nurses and traditionally circumcised
men, with one focus group interview in the study area, were conducted.
3.3 POPULATION
The target population was both traditional surgeons and nurses aged between 18
and 90, as well as traditionally circumcised males aged between 16 and 35.
3.4 SAMPLE AND SAMPLING PROCEDURE
This study has adopted purposive and snowballing sampling techniques. A
purposive sampling method was used to select 47 traditionally circumcised men.
Purposive sampling was adopted because the researcher wanted to target the most
knowledgeable participants about Male Traditional Circumcision (MTC). Access to
the traditional nurses and surgeons was limited and, given the sensitivity of the topic,
the researcher adopted a snowballing sampling technique to reach this group of
study participants. Thirty traditional surgeons were selected using this technique.
The researcher was able to identify a traditional surgeon in the community after

30
discussion with the community elders. At the end of the interview, this traditional
surgeon was asked to refer the researcher to other traditional surgeons. Every
traditional surgeon was asked to refer the researcher to another traditional surgeon
until the sample size of 30 was reached. The snowballing sampling technique was
also used to select 45 traditional nurses. Data collection ceased when data
saturation was reached.
3.4.1 Inclusion and exclusion criteria
Participants were included in the study if they were registered traditional surgeons
aged between 18 and 90; traditional nurses aged between 18 and 90, and
traditionally circumcised men aged between 16 and 35. Non- circumcised males;
medically circumcised males; non-registered traditional surgeons; women or females
and children; and mentally challenged individuals were excluded from the study.
3.5 MEASUREMENT INSTRUMENT
Focus group interviews and semi-structured interviews with video tapes were used.
The researcher developed interview guides to guide the focus group interview and
the semi-structured interviews. The following questions were asked:
What measures do traditional surgeons use to sterilise their surgical instruments
for circumcision?
What do you do to prevent excessive bleeding?
Do traditional surgeons tighten the bandage around the penis?
Do traditional nurses tighten the bandage during wound dressings?
Are the initiates allowed to drink water?
How would you describe the conditions under which the traditional surgeons
perform circumcision?
31
What measures do traditional nurses used to sterilise their surgical instruments
for circumcision?
What measures are taken to safeguard the health of the initiates after
circumcision?
How would you describe the conditions of the lodge where the initiates are kept
after circumcision?
3.6 DATA COLLECTION
Data was collected through one focus group interview of seven traditional nurses
and 115 semi-structured interviews of 45 traditional nurses, 30 traditional surgeons
and 47 traditionally circumcised men were conducted in a quiet, private setting. The
researcher asked permission from the participants prior to the commencement of
each interview session. The interviews were facilitated by the researcher. During
data collection the researcher asked open-ended questions using a self-structured
questionnaire –interview guide. The questionnaire was written in English, which
meant that the researcher had to translate what was written in the questionnaire for
the participants in order for them to clearly understand the content. The focus group
interview with the traditional nurses lasted for 21 minutes 48 seconds. The semi-
structured interviews with traditional surgeons, nurses and traditionally circumcised
men lasted between 07:37 and 23: 06 minutes per session. Participants were free to
ask questions; share their experiences, views, emotions and wishes about the topic
under investigation without fear of intimidation. Instead of taking notes, the
researcher used video tapes and recording software to record the information from
the participants, but no participants’ images were captured in the process.
The researcher asked the participants about the use of surgical gloves during
surgical removal of the foreskin and wound dressings. He also investigated whether
the circumcision instruments were sterile and whether one circumcision instrument
was used to circumcise more than one initiate without its being sterilised. The
researcher asked about the cleanliness of the environment in which the circumcision

32
process took place. In assessing the level of understanding of human physiological
processes, the participants were requested to explain whether the bandage was
tightly applied around the penis, and if the initiates were free to drink clean water.
3.7 TRUSTWORTHINESS
Ensuring data quality in a qualitative study is very important. The researcher
established credibility, confirmability, dependability and transferability of this study
in the following ways:
3.7.1 Credibility
Long lasting engagement: data was collected until there was no more new
information from the participants (data saturation reached). Also, the researcher
established rapport with the participants, which made the interview atmosphere more
relaxed.
Negative case analysis: the researcher ensured that the analysis was done in sucha way that all voices were represented. Both positive and divergent views were
captured in the analysis.
Referral adequacy: the researcher continued to ask for referrals from participants
until the data saturation was reached.
Constant observation was maintained by continually interpreting data in different
ways to determine what added up and what did not.
Peer debriefing: Throughout the period of data collection, the researcher kept in
touch with the supervisor to discuss challenges and to gain insight. Through this, the
researcher modified his techniques and styles of questioning to ensure accurate data
were gathered.
Member checks. The researcher assessed the intentionality of participants torectify noticeable errors and provide additional information.
3.7.2 Confirmability
The idea of confirmability is the qualitative researcher’s comparable concern to
neutrality (Shenton, 2004). The researcher ensured that bias was eliminated from

33
the study by excluding his own ideas about the topic under investigation. Both
positive and negative contributions of ideas from the interviews of participants were
documented without compromising either. The data were collected from participants
with experience and knowledge of the phenomenon under study.
3.7.3 Transferability
According to Lincoln and Guba (1985), transferability is a way of achieving external
validity in qualitative research. The authors explain that by describing a
phenomenon in sufficient detail one can begin to evaluate the extent to which the
conclusions drawn are transferable to other times, settings, situations and people.
To enhance transferability in this study, the researcher provided a full description of
the research context and the assumptions about the phenomenon being studied.
3.7.4 Dependability
According to Shenton (2004), dependability entails the researcher’s applying
techniques that, if the study was to be done once again, in the same setting, using
the same methods, and with similar participants’ comparable results would be
achieved. “External audits involve having a researcher not involved in the research
process examine both the process and product of the research study. The purpose
is to evaluate the accuracy and evaluate whether or not the findings, interpretations
and conclusions are supported by the data” (Lincoln & Guba, 1985).
In this study, dependability was ensured through regular checks for possible errors
that might have occurred during the process of transcription. It was ensured that the
content of transcription did not lose the actual meaning of the original themes. The
researcher also ensured consistency in the presentation of such themes.
3.8 ETHICAL CONSIDERATIONS
The rights of the participants were protected, and the ethical standards were
adhered to. The University of Fort Hare Ethical Review Committee granted ethical
approval (GOO011SDAL01) for the study. All participants signed a written informed
consent form to indicate their willingness to participate in the study. The rights of

34
participants to privacy, anonymity and confidentiality, to be treated fairly, to self-
determination and the right to protection from discomfort and harm were ensured
(Brink, Van Der Walt & Rensburg, 2013: 34).
3.8.1 The principle of respect for persons
The individual participants were aware that their decisions whether to take part in the
study or not carried no risk of punishment or harmful treatment.
The researcher respected the participants’ right to withdraw from the study at any
time in the process or to refuse to provide information or to ask for clarity about the
aim of the study. The participants voluntarily decided whether to participate in the
study or not.
In some rural African communities and religious groups, individuals may not be
regarded as independent, and the researcher had to respect this traditional practice
without ignoring the human rights of vulnerable participants (Brink et al., 2013: 35).
In keeping with the University’s reputation, the researcher treated every participant
with respect and kindness to avoid any negative attitude from the participants
towards the researcher which might eventually impact on the University (Brink et al.,
2013: 35).
3.8.2 Principle of no harm to subjects
The physical, social, emotional or psychological well-being of all the participants was
secured by the researcher to ensure that there was no harm or discomfort to any of
them. This principle was ensured by protecting the image of persons through the use
of voice recordings and temporary names, instead of cameras showing the identity of
persons and using real names. The interviews were conducted in isolation from
peers to allow ease of communication and safety from social criticism and judgement.
3.8.3 Principle of justice
The selection of the participants by the researcher was directly based on individuals
who were able to provide information related to the research problem. There were no
participants taken advantage of just because they could be easily manipulated to be

35
part of the study. The researcher treated each one of the participants in the same
way without any judgements or favours to benefit certain individual participants.
3.8.4 The principle of anonymity and confidentiality
The right to privacy and confidentiality of the participants was adhered to. For
example, in the case where a participant verbally stated the extent to which the
information he gave could be shared, the researcher respected this right. The
researcher explained to the participants that the information received from them
would remain anonymous (nameless or private) and confidential. This was ensured
by using temporary names for each participant with their matching codes to protect
their real names; the list of real names was destroyed. No photographs or video
footage showing faces were used in the process of data collection to protect the
image of the participants. If it happened that a video camera or recordings were used,
then the researcher had to take the responsibility to keep them in a secure place.
During the data discussions temporary names were used to identify the participants
(Brink et al., 2013:36). The researcher kept all the recorded information in a safe
locker to which no one had access without the permission of the participants or the
researcher.
3.8.5 Informed consent
The researcher read and verbally clarified to the participants what was written in the
consent form, with a second official person to witness whether the participant had
understood and agreed to what was explained to him before signing the consent
form. Hence, written consent was obtained from all the participants in this study.
3.9 DATA ANALYSIS
Data were transcribed and translated to English verbatim. To ensure validity, two
independent qualitative researchers assessed the translations to ensure their
accuracy. Thematic content analysis was used for data analysis. All responses were
read for familiarisation with the data. At this stage, codes and themes had not yet
been developed. Two of the authors independently coded the data after reading the
responses. The research team then met to review the codes and themes before

36
agreeing on the themes. Content analysis was used to ensure that all relevant
information was grouped and coded appropriately.
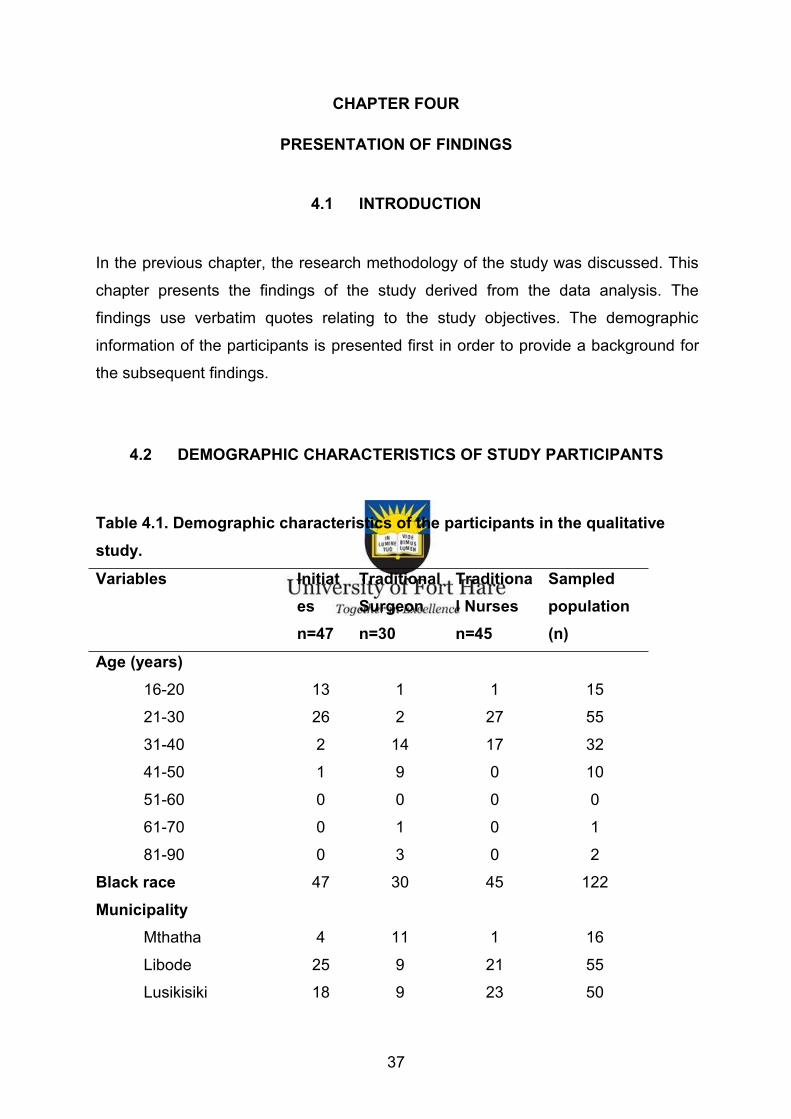
37
CHAPTER FOUR
PRESENTATION OF FINDINGS
4.1 INTRODUCTION
In the previous chapter, the research methodology of the study was discussed. This
chapter presents the findings of the study derived from the data analysis. The
findings use verbatim quotes relating to the study objectives. The demographic
information of the participants is presented first in order to provide a background for
the subsequent findings.
4.2 DEMOGRAPHIC CHARACTERISTICS OF STUDY PARTICIPANTS
Table 4.1. Demographic characteristics of the participants in the qualitativestudy.Variables Initiat
esn=47
TraditionalSurgeonn=30
Traditional Nursesn=45
Sampledpopulation(n)
Age (years)16-20 13 1 1 15
21-30 26 2 27 55
31-40 2 14 17 32
41-50 1 9 0 10
51-60 0 0 0 0
61-70 0 1 0 1
81-90 0 3 0 2
Black race 47 30 45 122
MunicipalityMthatha 4 11 1 16
Libode 25 9 21 55
Lusikisiki 18 9 23 50

38
Level of educationTertiary 8 2 2 12
Grade 12-11 22 6 12 40
Grade 11-10 7 6 9 22
Grade 10-9 8 8 4 19
Grade 9-8 1 2 4 7
Grade 8-7 0 1 3 4
Grade 7-6 0 2 2 3
Grade 6-5 0 0 2 2
Grade 4-3 1 1 0 2
Grade 2-1 0 2 0 2
Did you stay in a shelterwithin the community?
No 31 23 30 84
Yes 13 5 15 33
Did you stay in a hut inthe bush?
No 11 5 9 25
Yes 33 25 29 87
TOTAL n=122
Table 4.1 presents the demographic characteristics of the participants. A total of 122
participants took part in the study; 47 traditionally circumcised men, 30 traditional
surgeons and 45 traditional nurses. Of the 47 traditionally circumcised men, 44 were
between the ages of 16 and 30; 32 had a grade 9 to 12 level of education; and 35
lived in a bush hut during the period of circumcision. Pertaining to the traditional
surgeons, most (22) of them were between the ages of 31 and 50 and 25 lived in a
hut in the bush. Half of the traditional surgeons had a grade 3-4 level of education.
Slightly more than half of the traditional nurses were between the ages of 21 and 30.
A significant majority of the 29 traditional nurses lived in a hut in the bush and all of
them had at least a grade 5 level of education.

39
Amongst the 116 interviews conducted during the study, 115 were semi-structured
interviews with 30 traditional surgeons, 47 traditionally circumcised men, 38
traditional nurses and one interview of seven participants was conducted as a focus
group interview of traditional nurses. All participants were of black South African
origin from the O. R. Tambo region in the Eastern Cape.
4.3 ASSESSMENT OF ASEPTIC TECHNIQUES USED BY TRADITIONALSURGEONS AND NURSES DURING TRADITIONAL CIRCUMCISION
PROCESSES
4.3.1 Use of surgical gloves
Most traditional surgeons stated that they used gloves, and that they changed them
for every initiate they attended. However, the majority of the traditionally circumcised
men disagreed that the traditional surgeons had used gloves. Most of them stated
that those who happened to use gloves did not change them between initiates. One
traditionally circumcised man only realised at the time of the interview that the
traditional surgeon who circumcised him had not used gloves, and he stated that:
“He never used gloves, it is only now that I see that traditional surgeon was stupid,
he was drunk” (In-depth interview, traditional circumcised man, Participant 5).
In contrast, the majority of of both traditionally circumcised men and traditional
nurses maintained that traditional nurses did not use gloves, and the few who
happened to use them, did not change them between initiates attended to during
wound dressings.
4.3.2 Cleanliness and sterilisation of circumcision instrument
When asked whether they sterilised their instruments, most traditional surgeons
claimed that they sterilised their assegai. The traditional surgeons’ responses
confirmed that they cleaned their assegais after use. This is evident from the
response of an old traditional surgeon who had been practising since 1972:
“I clean my assegais using spirit and a soap that I got from health department but I
do not know its name” (In-depth interview, traditional surgeon, participant 1).

40
However, most traditionally circumcised men were of the opinion that the
circumcision instruments were unclean and unsterilised.
4.3.3 Cleanliness of the seclusion lodge
The results generally showed that the temporary seclusion lodge was dirty and not fit
for habitation. One traditionally circumcised man explained that they were made to
sit and sleep on the ground and that insects bit them. Others simply stated that the
environment was dirty. Another traditionally circumcised man described the
environment as unclean. He said that he did not think that a professional doctor
would approve of any human beings staying in the temporary seclusion lodges. This
is because initiates excreted urine inside the lodge. Despite urinating in the seclusion
lodge, their food was served and eaten in the dirty environment. Moreover, the
processes such as wound dressings and caring for the initiates goes on concurrently
in the same place. This, according to the participant, would indicate to anyone that
the place itself was not a hygienic place because some individuals used the place to
smoke, rest and to sleep over night. He maintained that when people are all sleeping
in one place, it becomes foul-smelling. In addition, the traditional nurses stayed there
without bathing, which further indicates that it was not fitting place for anyone to stay.
“I don’t think a doctor would agree with the way people live there because you will
remember that initiates excrete urine there inside, eating is done there and all that
process of looking after initiates, the dressing of wounds of initiates, everything is
done there inside and that tells you that it should not be a neat place where
everything is done in one place because others are smoking, others are staying
there and others are sleeping. You will remember that when people are sleeping
there is too much odours and the traditional nurses are staying there and they do not
bath, everything which informs you that if there would be a visit from the people who
are experts, they would tell you that it is not a proper place for anyone to stay” (In-
depth interview, traditionally circumcised man, participant 2).
However, one participant, who was initiated covertly, stated that he made an effort to
clean the environment using cow dung before he was circumcised. According to
him, the once-off use of the cow dung kept the place clean for the entire two weeks
of his stay in the lodge. He went further to describe the further improvements made
to the lodge after his initiation by stating that the floor had been cemented in order to

41
store the maize and it became even neater (In-depth interview; traditional
circumcised man participant 1).
In the focus group discussion interview among traditional nurses, it was emphatically
stated that the seclusion lodge was not clean because there was no sweeping of the
floor. While some supported this statement, one traditional nurse stated on behalf of
the group that:
“Oowh! It is dirty, it is dirty, it is dirty in the seclusion lodge so that is clear that there
is work done! There is no sweeping of the floor in there you too know about that,
they said while laughing. One of them returning the question, “Was yours got
cleaned up?” The researcher laughed without responding. They continued
confirming, ‘It is dirty in the lodge, there is no cleaning done’. Laughing throughout.
They repeatedly asked the researcher the same question and laughing at the same
time, “Wait, was yours getting cleaned up?”( Focus group interview, traditional
nurses, participant 3).”
On the other hand, one among the traditionally circumcised men, participant 5, said
that his place was cleaned up before he entered as a newly circumcised initiate.
However, there was no clarity on continuous cleaning of the lodge during his period
of stay.
4.3.4 Wound dressings
Wound dressing is the main duty of the traditional nurses. In terms of the cleanliness
of the environment where wound dressing is performed, over half of the traditionally
circumcised men and traditional nurses indicated that the environment in which
traditional nurses work is not hygienically prepared prior to wound dressing. However,
the traditional surgeons stated that the main surgery of traditional male circumcision
is done in a clean environment. Most traditionally circumcised men corroborated this
view. A vast majority of the traditional surgeons and traditional nurses claimed that
the bandages are not tightly applied. However, when water appears from the penile
wound, the water is squeezed out from underneath the penis (where the wound is)
by tightening of the bandage known as ‘ityeba’ (Semi structured interview, traditional
surgeon 1).

42
In contrast, most traditionally circumcised men responded that the bandage was
tightly applied. This was confirmed repeatedly during the interviews. In describing
the effect of the tightening of the bandage, one traditionally circumcised man said:
The bandage is tightly tied around the penile wound and often make the wound to
get very sore (Semi-Structured Interview, Traditionally circumcised man, participant
3).
The tightening of the bandage often leads to the initiate experiencing pain, as
described by one of the participants: While you urinating yes it is fine and then after
traditional bandage is applied it is painful but it goes away with time and also when it
is painful on urination it gets fixed and you get better (Semi-Structured Interview,
Traditionally circumcised man, participant 4)
Likewise, participant 5 revealed that during the first two days of the seclusion period,
t felt normal, however, from the third to the eighth day, things got worse as the
bandage was tightly applied, a process he described as “ukutyanywa”.
You can feel that it is painful and some tend to consider loosening their own
bandages and therefore it becomes difficult even to pass urine because you have to
be tightly dressed with the traditional bandage (Semi structured interview,
traditionally circumcised man, participant 5).
4.3.5 Treatment of penile wound
In order to facilitate healing of septic wounds, all participants stated that there were
traditional medicines or leaves that are used; among which are ‘isichwe’ (traditional
leaf), ‘ishwadi’ (traditional medicine) and ‘ityeba’ (traditional bandage). The traditional
bandages are made from used, old clothes, cut into small strips of bandage. The
leaves and the often-used traditional bandages are not sterilised. This poses the risk
of exposure to infection. In trying to heal the wounds, the importance of aseptic
techniques is ignored by the traditional surgeons and nurses. This is possibly due to
a lack of knowledge.
“To eliminate the pus, there is one thing that is usually used within the Xhosa tribe
which is ‘isichwe’ (traditional medicinal leaf) to mention one that is used to drain the
pus completely” (In-depth interview, traditionally circumcised man, participant 2).

43
In addition, one traditionally circumcised man added that cotton wool, surgical
bandages and betadine were not used in the bush.
“There are certain leaves that are used which we cannot mention my honourable
chairperson. Yes things that are meant for treatment in accordance with the tradition.
Surgical bandages, cotton wools and beta-dines are not used there”(In-depth
interview, traditionally circumcised man, participant 5).
4.3.6 Experience of purulent penile wound
Most traditionally circumcised men stated that they had had purulent penile wounds
when they were circumcised. To some, the presence of pus in the wounds of the
initiates was taken lightly as it is perceived as an expectation of traditional
AmaXhosa male circumcision.
“Yes there was pus (ubugqutsu) and we will have to understand that it is expected
when you are there inside, more especially when you circumcised in AmaXhosa
tradition” (In-depth interview, traditionally circumcised man, participant 2).
Another participant stated that it is a must to have an infected penile wound while in
the initiation school. This indicates how lightly the presence of infection is viewed in
the tradition of AmaXhosa male circumcision.
Laughing, “It is a must that there is a pus while you are there” (In-depth interview,
traditionally circumcised man, participant 5).
4.4 SummaryThe demographic characteristics of the participants are presented in this chapter, as
well as the findings of the study, using verbatim quotes. The next chapter discusses
the findings and offers a conclusion and recommendations resulting from the study.

44
CHAPTER 5
DISCUSSION OF FINDINGS, CONCLUSION AND RECOMMENDATIONS
5.1 INTRODUCTION
The study results were interpreted in the previous chapter. The discussion of the
findings, the limitations of the study, conclusion and the study recommendations are
presented in this chapter.
5.2 DISCUSSION OF FINDINGS
This study assesses the aseptic techniques of traditional surgeons and nurses and
the cleanliness of the circumcision environment. The study has produced mixed
results. While traditional surgeons described their environment and instruments as
clean, the traditionally circumcised men disagreed. Further, the traditional surgeons
claimed that they used surgical gloves and changed the gloves for each initiate.
However, the traditionally circumcised men disagreed and often maintained that they
did not use gloves. An intervention study, which trained traditional surgeons and
nurses in the Eastern Cape on safe circumcision, infection control, anatomy, post-
operative care, detection and early management of complications and sexual health,
reveals that most traditional surgeons and nurses wore gloves during operation and
care, but did not use the recommended circumcision instruments (Peltzer, Nqeketo,
Petros & Kanta., 2008b). It is possible that many of the above-mentioned traditional
surgeons and nurses gave the response they felt was socially desirable in view of
the fact that they had been trained on the importance of using surgical gloves. The
traditionally circumcised men had no reason to misrepresent the facts considering
that they had nothing to lose, unlike the traditional surgeons. For this reason, there is
a need for proper inspection of the traditional circumcision process in the study
settings. Many circumcision-related deaths and complications could be prevented
with the proper use of gloves and a clean environment.
45
The majority of both traditionally circumcised men and traditional nurses stated that
traditional nurses did not use surgical gloves, and the few who did use them, did not
change the gloves between initiates. Rijken and Dakwa (2013) also found, in their
study of ulwaluko, that traditional nurses in Pondoland did not use gloves, and did
not wash their hands prior to circumcision. This posed the risk of infection to the
initiates. The application of universal precautions and aseptic techniques play a vital
role in the prevention of cross infections by reducing the microbial load on the wound
surface (Orsted et al., 2018).
It is strongly recommended that, when carrying out any procedures that involve the
presence of bodily fluids, such as blood, purulence, exudate, excretions and invasive
procedures, attendants wear surgical gloves to reduce the risks of acquiring
infections from either the patients or transmitting them to the patients. Surgical
gloves are a way of preventing hands from being in direct contact with the sterile
sites (Brooker & Waugh, 2013). When dressing wounds, surgical gloves must be
worn, changed and hands must be washed before and after each initiate attended to
by either traditional surgeon or nurse in order to prevent cross infections among the
initiates. This is applicable in both traditional settings and government or private
sectors that offer health care services of any kind that involve risks related to
bacterial or viral infections (Burns et al., 2006). Brooker & Waugh (2013) argue that it
is crucial to treat gloves as single use items, and then discard them immediately after
removal.
Most responses of traditional nurses and traditionally circumcised men in the study
clearly show that the temporary seclusion lodges were dirty, and that traditional
nurses and traditionally circumcised men stayed in the lodges for days without
bathing resulting in the lodges becoming foul smelling. None of the published
studies has reported on environmental cleanliness during traditional male
circumcision. According to Jill (1986), the reservoirs of environmental infections are
the air, direct contact and cross infection. This was further clarified in a hospital
setting where the air contains droplets from the nasal passages of patients, staff
personnel and visitors, as well as skin shed as they move around. When the wound
is not covered, it is exposed to microbial substances. When an occlusive dressing is
applied in a sterile environment, it helps by completely isolating the wound from the
environmental contaminants (Jill, 1986). However, there are further chances of

46
further infection through openings, such as drains, interference with the dressing or
moisture penetrating through the dressing (David, 1986).
Most traditional surgeons and traditional nurses claimed that the penile bandage was
not tightly applied and that it was only tightened when the wound was wet. However,
more than half of traditionally circumcised men responded that the bandage was
tightly applied. When muscle tissue is compressed, blood supply to the peripheral
tissues becomes diminished or they are completely deprived of oxygenation and
nutrient supply, requirements for healthy survival of such tissues (Copstead &
Banasik, 1995). Exposing muscle cells to such conditions can lead to either infection
or dry, shrunken and dark reddish to black tissue being affected. These may be
signs and symptoms of gangrene (Copstead & Banasik, 1995). Eventually the line of
separation might bring about complete separation followed by the total fall off the
gangrenous tissue, a process called auto-amputation. This happens when there is
no surgical intervention (Copstead & Banasik, 1995).
At least one study on ‘relative contributions of compression and hypoxia to
development of muscle tissue damage’ suggested that hypoxia does not evidentially
lead to cell death in a 22-hour period. Nevertheless, muscle tissue compression has
been tested further and found conclusively to cause prompt cell death which
worsened with time (Rijken & Dakwa, 2013). Dry gangrene is the result of chronic
ischemia without infection.
The results of the current study indicate that most traditionally circumcised men
developed wound sepsis while in the initiation school, and for some, it was perceived
to be a normal phase a wound had to undergo before healing.There is a delay in
wound healing and increased pain when sepsis develops. The oxygen needed for
the vital functioning of body cells is compromised for both body cells and the bacteria
present in the body; when the wound is infected, a rise in body temperature, redness
and inflammation and/or pain is normally manifested. This may also lead to extreme
anxiety, sorrow, ill health and the possibility of the patient’s death.. Furthermore, the
rendering of nursing care might be costly (Van Rooyen et al., 2009, Gethin, 2009:
05). Individuals with septic wounds experience more pain than those with non-septic
wounds (White, 2009). Hence, it is important to control infection to prevent infection
in active wounds.

47
Based on the findings of this study, close supervision of traditional surgeons and
nurses by environmental health officers and infection control personnel would be a
key factor in ensuring the use of surgical gloves and the adoption of aseptic
techniques during circumcision and post-surgery wound care. This would possibly
reduce the rate of morbidity and deaths in the process of circumcision.
A multiple-disciplinary team involved in the process of traditional male circumcision,
including environmental health officers and infection control personnel, needs to be
closely engaged in these processes. There is a need for legal seclusion lodges to be
built in places that are officially chosen by government officials. Notwithstanding,
these lodges would have to be in line with the general practices of traditional male
circumcision. Initiates should be looked after by well-trained staff, with appropriate
security measures. Strict rules on cleanliness are needed and the number of visitors
to the lodge should be limited to minimise avoidable infections.
Community leaders and government stakeholders need to encourage the public to
participate positively for such implementations to be made. It should be made clear
that the changes implemented are not meant to interfere with the processes of
traditional circumcision but to save the lives of the initiates.
5.3 STUDY LIMITATIONS
Even though this study makes an important contribution to the body of knowledge on
traditional circumcision, the findings should be interpreted within its limitations. First,
this study utilised a qualitative approach thus limiting the generalisability of the
findings. Qualitative studies are context specific, and as such, the findings of this
study may not reflect the practice of traditional surgeons throughout South Africa.
However, this study provides rich data on the aseptic techniques of traditional
surgeons and nurses in the Eastern Cape. Further, the responses are self-reported,
thus, social desirability bias cannot be ruled out in the responses of the traditional
nurses and surgeons. Nonetheless, the combination of responses of traditionally
circumcised men with that of traditional surgeons helps to mitigate this limitation.

48
Access to the community was not easy because traditional male circumcision is
secret amongst those who practise it and particularly among circumcised men.
5.4 CONCLUSION
This study has established that both traditional surgeons and nurses poorly maintain
aseptic techniques, thus, exposing initiates to infections, morbidity or death.
Concerning the issue of bandage tightening, the findings have shown mixed results.
Hence, this study concludes that instances of bandage tightening during wound
dressing be strongly discouraged.
Based on the findings of this study, it is evident that the environment in which
circumcision processes take place is exceptionally dirty. These results suggest that
the adverse outcomes resulting from traditional male circumcision are costly to both
the initiates and the government health services. Their cleanliness would benefit
both the government’s wastage of resources and the citizens’ vulnerable lives.
5.5 RECOMMENDATIONS
Traditional male circumcision stakeholders should work closely with government
departments to improve the conditions under which the traditional circumcision
practice is performed to meet acceptable standards of general health care settings.
This should, however, be done in a way that respects the tradition of male
circumcision among the AmaXhosa and AmaMpondo tribes in the Eastern Cape.
There is a need for professionally trained and knowledgeable individuals to take over
the performance of circumcision surgery and the continued nursing care of initiates
following the surgical removal of the prepuce. Traditional male circumcision should
be done in clean and well-ventilated, spacious and warm surroundings. A close
supervision of traditional surgeons and nurses by environmental health officers and
infection control personnel is therefore recommended.

49
The public of the Eastern Cape need to be convincingly educated about the current
risks of traditional male circumcisions and the significance of their threat to lives. The
pressures arising from the stereotypes of traditional male circumcision need to be
revealed. This could be achieved through health promotions and safety talk shows
on radios or through other relevant community stakeholders, such as churches,
schools and chief gatherings. The aim is to spread awareness so that young people
can make sound and independent decisions about their choice of circumcision,
without feeling pressured by either peers or family members or the community at
large.
Finally, Traditional Male Circumcision (TMC) should keep abreast of present
research to reduce the practice of health-based activities that put initiates at risk of
infections, complications or morbidity.

50
REFERENCES
Anike, U., Govender, I., Ndimande, J.V. & Tumbo, J. (2013). Complications of
traditional circumcision amongst young Xhosa males seen at St Lucy’s Hospital.
African Health Care and Family Medicine, 5(1), 5.
Auvert, B., Taljaard, D., Rech, D., Lissouba, P., Singh, B., Bouscaillou, J., Peytavin,
G., Mahiane, S.G., Sitta, R. & Puren, A. (2013). Association of the ANRS-12126
male circumcision project with HIV levels among men in a South African township:
evaluation of effectiveness using cross-sectional surveys. Plos Medicine, 10(9),
e1001509.
Brink, H., Van De Walt, C. & Van Rensburg, G. (2013). Fundamentals of research
methodology for healthcare professionals. Third edition. Cape Town, South Africa:
Juta & Company.
Brooker, C. & Waugh, A. (2013). Foundations of Nursing Practice. 2nd Edition.
Fundamentals of Holistic Care, Mosby Ltd. Available from:
https://www.elsevier.com/books/foundations-of-nursing-practice/brooker/978-0-7234-
3661-4
Brown, B.M., Venkataramani, A.S., Nattrass, N., Phil, D., Seekings, J. & Whiteside,
W.A. (2011). A cut above the rest: Traditional male Circumcision and HIV risk
among Xhosa men in Cape Town, South Africa. Journal of Acquired Immune
Deficiency Syndrome, 58(5), 501-503.
Bullock, R. (2015). It’s hard to be a man. A month with three initiates during the
Xhosa circumcision ritual. Africa geographic stories. Available from:
https://magazine.africageographic.com/weekly/issue-48/xhosa-circumcision-ritual-
south-africa-its-hard-to-be-a-man/
Burns, N. & Grove, K. (1993). The Practice of Nursing Research Conduct, Critique &
Utilization. 2ND Edition. Philadelphia: W. B. Saunders Company.

51
Burns, A.A., Niemann, S. & Metcalf, E. (2006). Where women have no doctor: A
health guide for women. United States of America: Hesperian Foundation.
Casement, A. (2018). Who owns the Jung. 2nd edition. New York: Routledge.
Connolly, C., Simbayi, L.C., Shanmugam, R. & Nqeketo, A. (2008). Male
circumcision and its relationship to HIV infection in South Africa: results of a national
survey in 2002. SAMJ: South African Medical Journal, 98(10), 789-794.
Copstead, L.E.C. & Banasik, J.L. (1995). Pathophysiology: Evolve learning
system.4th edition. Saunders: Elsevier.
David, J.A. (1986). Wound management: a comprehensive guide to dressing and
healing. United States: Springhouse Corporation.
Deacon, H. & Thomson, K. (2012). The social penis: Traditional Male Circumcision
and Initiation in Southern Africa, 1800-2000: A literature review. Centre for Social
Sciences Research, working paper no. 304. Available from:
http://cssr.uct.ac.za/pub/wp/304/
Dold, T. & Cocks, M. (2012). Voices from the forest: Celebrating nature and culture
in Xhosa land. Sunnyside, Auckland Park, South Africa: Jacana Media.
Feketha, S. (2014). Democratic Alliance calls for initiation death probe. Eastern
Cape Daily Dispatch News, p.05
Feni, L. (2014a). Emotional return of initiates: not all families can celebrate after
deaths. Eastern Cape Daily Dispatch news, p.05. Retrieved from: Traditional affairs
correspondent.
Feni, L. (2014b). Soaring initiate deaths ‘a crisis’: calls for tougher action as death
toll climbs to eight. Eastern Cape Daily Dispatch News, p.01. Retrieved from:
Traditional affairs correspondents.

52
Gethin, G. (2009). Role of topical antimicrobials in wound management. Journal of
Wound Care, 4-7.
Glanz, K., Rimer, B.K. & Lewis, F.M. (2002). Health behaviour and education:
Theory research and practice. San Francisco: Wiley & Sons.
Govender, K., George, G., Mucheuki, C. & Strauss, M. (2013/14). Voluntary medical
male circumcision in South Africa: challenges and opportunities, SAHR KWIK
SKWIZ SERIES. South African Health Review (SAHR), 3(12), p.05. Available from
URL:http://www.hst.org.za/publications/Kwik%20Skwiz/KWIK%20SKWIZ_Vol3_Iss1
2.pdf
Hochbaum, G.M. (1958). Public participation in medical screening programs: A
socio-psychological study. Public health services, United States: Washington, D. C.
Government Printing Office.
Huisman, B. (2009). Son takes parents to court over circumcision. Sunday Times,
n/p.
Jill, A.D. (1986). Wound Management: A comprehensive guide to dressing and
healing- (practical nursing handbook). Pennsylvania: Springhouse Pub Co.
Kepe, T. (2010). ‘Secrets’ that kill: Crisis, custodianship and responsibility in ritual
male circumcision in the Eastern Cape Province, South Africa. Social Science and
Medicine, 70(5), p.732.
Kripke, K., Chen, P.-A., Vazzano, A., Thambinayagam, A., Pillay, Y., Loykissoonlal,
D., Bonnecwe, C., Barron, P., Kiwango, E. & Castor, D. (2016). Cost and impact of
voluntary medical male circumcision in South Africa: Focusing the program on
specific age groups and provinces. PLoS One, 11: e0157071.
Lincoln, Y. & Guba, E. (1985). Naturalistic Inquiry. Beverly Hills, Calif: Sage
Publications.
Ludidi, V. (2014). Initiation season around the corner: deaths and injuries are still the
major concern for authorities and parents. Eastern Cape Today Newspaper, p.01.

53
Mark, D., Middelkoop, K., Black, S., Roux, S., Fleurs, L., Wood, R. & Bekker, L.
(2012). Low acceptability of medical male circumcision as an HIV/AIDS prevention
intervention within a South African community that practices traditional circumcision.
South African Medical Journal, 102, 571-573.
Maughan-Brown, B., Venkataramani, A., Nattrass, N., Seekings, J. & Whiteside, A.
(2011). A cut above the rest: traditional male circumcision and HIV risk among
Xhosa men in Cape Town, South Africa. AIDS Journal of Acquired Immune
Deficiency Syndromes, 58 (5), 499-505.
Mavundla, T.R., Netswera, F. G., Bottoman, B. & Toth, F. (2009). Rationalization of
indigenous male circumcision as a sacred religious custom: health beliefs of Xhosa
men in South Africa. Journal of Transcultural Nursing, 20 (4), 395-404.
Mavundla, T., Netswera, F., Toth, F., Bottoman, B. & Tenge, S. (2010). How boys
become dogs: Stigmatization and marginalization of uninitiated Xhosa males in East
London, South Africa. Qualitative Health Research, 20 (7), 931-941.
Meissner, O. & Buso, D.L. (2007). Traditional male circumcision in the Eastern Cape:
Scourge or blessing? South African Medical Journal, 97(5), 371-373.
Mogotlane, S. Ntlangulela, J. & Ogunbanjo, B. (2004). Mortality and morbidity among
traditionally circumcised Xhosa boys in the Eastern Cape Province, South Africa.
Department of Health Studies, UNISA, 27(2), 57-62
Mshana, G., Wambura, M., Mwanga, J., Mosha, J., Mosha, F. & Changalucha, J.
(2011). Traditional male circumcision practices among the Kurya of North-eastern
Tanzania and implications for national programmes. Aids Care, 23 (9), 1111-1116.
Available from: https://doi.org/10.1080/09540121.2011.554518
Mukhuthu, Z. (2014). Initiate, 15, dies in his father’s arms: Dad watches helplessly as
teen with chest took his last breath. Daily Dispatch News. p.02.
Naidoo, P.V., Dawood, F., Driver, C., Narainsamy, M., Ndlovu, S. & Ndlovu, V.
(2012). Knowledge, attitudes and perceptions of pharmacy and nursing students

54
towards male circumcision and HIV in a KwaZulu Natal University, South Africa.
African Journal of Primary Health Care and Family Medicine, 4(1), 327.
Nini, A. (2014, July). More Aid for Eastern Cape initiation victims: Help for those who
suffered injuries. Eastern Cape Daily Dispatch News. p.04.
Nkosi, M. (2013). The nature and causes of Male Circumcision in Clermont-
kwaDabeka in KwaZulu-Natal, South Africa: School of education, University of
KwaZulu-Natal, South Africa. Journal of Human Ecology, 41(2), 119-130.
Orsted, H., Keast, D., Forest-Lalande, L., Kuhnke, J., O’Sullivan-Drombolis, D., Jin,
S., Haley, J. & Evans, R. (2018). Foundations of Best Practice for Skin and Wound
Management: Best Practice Recommendations for the Prevention and Management
of Wounds. Canada: Canadian Association of Wound Care.
Peltzer, K., Nqeketo, A., Petros, G. & Kanta, X. (2008a). Evaluation of a safer male
circumcision training programme for traditional surgeons and nurses in the Eastern
Cape, South Africa. African Journal of Traditional, Complementary and Alternative
Medicines, 5 (4), 346-354.
Peltzer, K. & Kanta, X. (2009). Medical circumcision and manhood initiation rituals in
the Eastern Cape, South Africa: a post intervention evaluation. Culture, Health &
Sexuality, 11 (1): 83-97. Available from: doi: 10.1080/13691050802389777.
Peltzer, K., Nqeketo, A., Petros, G. & Kanta, X. (2008b). Traditional circumcision
during manhood initiation rituals in the Eastern Cape, South Africa: A pre-post
intervention evaluation. BMC Public Health, 8 (1): 64.
Provincial Infectious Diseases Advisory Committee (2009). Best practices for
environmental cleaning for prevention and control of infections in all health care
settings. 2nd edition. Queen’s Printer for Ontario.
Rathebe, P.C. (2018). The role of environmental health in the Basotho male initiation
schools: neglected or restricted? BMC Public Health, 18, 994.
Rijken, D.J. & Dakwa, P.J.H. (2013). Ulwaluko: problem analysis of the situation in
Pondoland. 6(12), 2.

55
Scott, B.E., Weiss, H.A. & Viljoen, J.I. (2005). The acceptance of male circumcision
as an HIV intervention among a rural Zulu population, KwaZulu- Natal, South Africa.
Aids Care, 17(3): 304-313.
Sedar, T., Derek, L., Unic, A., Marijancevic, D., Markovic, D., Primorac, A. &
Petrovecki, M. (2013). Occupational exposures in healthcare workers in University
Hospital Dubrava-10 year follow up study. European Journal of Public Health, 21(3),
150-4.
Shenton, A.K. (2004). Strategies for ensuring trustworthiness in qualitative research
projects. Education for information, 22(2004), 63-75.
Shisana, O., Rehle, T., Simbayi, L.C., Zuma, K., Jooste, S., Zungu, N., Labadarios,
D. & Onoya, D. (2014). South African national HIV prevalence, incidence and
behaviour survey, 2012 output type. HIV/AIDS, STIs and TB (HAST), Population
Health Systems and Innovation (PHHSI), Human Science Research Council (HSRC).
Smith, T. (2000). Concise Oxford English Dictionary. Tenth Edition. Oxford University
Press. Great Clarendon Street, Oxford, UK.
South African National AIDS Council (2012). National strategic plan on HIV, STIs
and TB, 2012-2016, South African National AIDS Council. South Africa: Government
Document.
South African Press Association, (2013). Minister denounces ‘culturepreneurs’: IOL
news. Available from: https://mg.co.za/article/2013-07-08-initiation-has-become-
criminal-says-motsolaedi
The Sunday Times (2008). Teen sues father after forced circumcision. 27 January.
Tobian, A.A., Kacker, S. & Quinn, T.C. (2014). Male circumcision: a globally relevant
but under-utilized method for the prevention of HIV and other sexually transmitted
infections. Annual Review of Medicine, 65: 293-306. Available from:
10.1146/annurev-med-092412-090539

56
Van Rooyen, D., Jordan, P., Brooker, C. & Waugh, A. (2009). Foundation of nursing
practice: Fundamentals of holistic care. African edition. Edinburgh, Elsevier.
Vincent, C., Neale, G. & Woloshynowych, M. (2001). Adverse events in British
hospitals: preliminary retrospective record review. British Medical Journal, 322(7285),
517-519.
Vincent, L. (2008a). Boys will be boys: traditional Xhosa male circumcision, HIV and
sexual socialisation in contemporary South Africa, Culture, health and sexuality.
International Journal for Research, Intervention and Care,10(5), 431-446. Available
from: https://doi.org/10.1080/13691050701861447
Vincent, L. (2008b). Cutting tradition: The political regulation of traditional
circumcision rites in South Africa's liberal democratic order. Journal of Southern
African Studies, 34 (1), 77-91.
White, R. (2009). Wound infection-associated pain. Journal of Wound Care, 18(6),245-249.
World Health Organisation (2008). Male Circumcision Policy, Practices and Services
in the Eastern Cape Province of South Africa: Case study.
World Health Organisation (2010). Male Circumcision Policy Practices and Services
in the Eastern Cape Province of South Africa. Case Study.
World Health Organisation (2009). Prevention and control of infection: Clean care is
safer care. Available from: https://www.who.int/gpsc/ipc/en/
World Health Organisation & The Joint United Nations Programme on HIV/AIDS
(2007). Male Circumcision: global trends and determinants of prevalence, safety and
acceptability. Geneva, Switzerland, WHO Press. p.35
World Health Organisation & The Joint United Nations Programme on HIV/AIDS.
(2011). Progress in scale-up of male circumcision for HIV prevention in Eastern and
Southern Africa: Focus on service delivery. Geneva, Switzerland, WHO Press.
Wilcken, A., Keil, T. & Dick, B. (2010). Traditional male circumcision in the Eastern
Cape and Southern Africa: A systematic review of prevalence and complications.
Institute for Social Medicine, Epidemiology and Health Economics, Charity University

57
Medical Centre, Berlin, German, 88912), 907-914. Available from: DOI:
10.2471/BLT.09.072975

58
APPENDIX A: Letter of approval from the University of Fort Hare ethicscommittee

59

60
APPENDIX B: Letter of approval from the Eastern Cape Department of Health
61
APPENDIX C: Letter of approval from the sub-district house of traditionalleaders in Mthatha

62
APPENDIX D: Informed Consent by participant/parent/guardian
Ethics Research Confidentiality and Consent Form
Please note:
This form is to be completed by the researcher(s) as well as by the intervieweebefore the commencement of the research. Copies of the signed form must befiled and kept on record
(To be adapted for individual circumstances/needs)
Our University of Fort Hare / Department is asking people from your community /
sample / group to answer some questions, which we hope will benefit your
community and possibly other communities in the future.
I ---------------Master’s degree student at the University of Fort Hare, School of
Health Sciences, Department of Nursing Sciences is conducting research regarding
Research Project: -----We are carrying out this research to help improve the quality
of patient care. .
Please understand that you are not being forced to take part in this study and the
choice whether to participate or not is yours alone. However, we would really
appreciate it if you do share your thoughts with us. If you choose not take part in
answering these questions, you will not be affected in any way. If you agree to
participate, you may stop me at any time and tell me that you don’t want to go on

63
with the interview. If you do this, there will also be no penalties and you will NOT be
prejudiced in ANY way. Confidentiality will be observed professionally.
I will not be recording your name anywhere on the questionnaire and no one will be
able to link you to the answers you give. Only the researchers will have access to the
unlinked information. The information will remain confidential and there will be no
“come-backs” from the answers you give.
The interview will last around (X?) minutes (this is to be tested through a pilot). I will
be asking you questions and ask that you are as open and honest as possible in
answering these questions. Some questions may be of a personal and/or sensitive
nature. I will be asking some questions that you may not have thought about before,
and which also involve thinking about the past or the future. We know that you
cannot be absolutely certain about the answers to these questions but we ask that
you try to think about these questions. When it comes to answering questions there
are no right and wrong answers. When we ask questions about the future we are not
interested in what you think the best thing would be to do, but what you think would
actually happen. (adapt for individual circumstances)
If possible, our organisation would like to come back to this area once we have
completed our study to inform you and your community of what the results are and
discuss our findings and proposals around the research and what this means for
people in this area.
CONSENT
I hereby agree to participate in research
regarding …………………………………………………. I understand that I am
participating freely and without being forced in any way to do so. I also understand
that I can stop this interview at any point should I not want to continue and that this
decision will not in any way affect me negatively.
I understand that this is a research project whose purpose is not necessarily to
benefit me personally.

64
I have received the telephone number of a person to contact should I need to speak
about any issues which may arise in this interview.
I understand that this consent form will not be linked to the questionnaire, and that
my answers will remain confidential.
I understand that if at all possible, feedback will be given to my community on the
results of the completed research.
……………………………..
Signature of participant Date:…………………..
I hereby agree to the tape recording of my participation in the study
……………………………..
Signature of participant Date:…………………..

65
APPENDIX E: Letter for ethical clearance to the University of Fort Hare
SECTION 1: DETAILS OF APPLICANT/PRINCIPAL INVESTIGATOR
Name:SIYAMTHEMBA
Surname:
DALASA
Professional Status:PROFESSIONAL NURSE
University Division / Faculty and Department: FACULTY OF SCIENCE AND
AGRICULTURE: NURSING
SCIENCES
Telephone No: 043 7092448 (w)
Fax No: Cell No: 0812188044
E-mail address: [email protected]
SECTION 2: TITLE OF STUDY
Title of Research Project:
ADULT CIRCUMCISION PRACTICES OF TRADITIONAL SURGEONS AND NURSES IN
RELATION TO THE INITIATES’ HEALTH OUTCOMES/MORBIDITY IN THE EASTERN
CAPE.
Sponsor’s Protocol No (if applicable)
Sponsor’s Details (if applicable)
SECTION 3: STUDY FOR DEGREE PURPOSES Not applicable
Name of Degree: MASTER OF CURATIONIS Supervisor: PROF. T. GOON
Division/Department: NURSING SCIENCES E-mail:

66
APPENDIX F: Researcher’s declaration and conflict of interest declaration
RESEARCH ETHICS COMMITTEE
RESEARCHER'S DECLARATION AND CONFLICT OF INTERESTDECLARATION
(To be completed in typescript)
The principal investigator, as well as all sub- & co-investigators must each sign a
separate declaration.
A. RESEARCHER
Surname Initial TitlCapacity Principal X Sub- Co-Department Nursing SciencesPresent E-Telephone (w Ce Fa
B. PROJECT TITLE (MAXIMUM OF 250 CHARACTERS FOR DATABASE
PURPOSES)

67
I, (Title, Full
name) …………………………………………………………………………………………
declare that:
I have read through the submitted version of the research protocol and allsupporting documents and am satisfied with their contents
I am suitably qualified and experienced to perform and/or supervise the above
research study.
I agree to conduct or supervise the described study personally in accordance withthe relevant, current protocol and will only change the protocol after approval by
the UREC, except when urgently necessary to protect the safety, rights, or welfareof subjects. In such a case, I am aware that I should notify the UREC without delay.
I agree to timeously report to the UREC serious adverse events that may occur
in the course of the investigation.
I agree to maintain adequate and accurate records and to make those records
available for inspection by the appropriate authorised agents when and if
necessary.
I agree to comply with all other requirements regarding the obligations of clinical
investigators and all other pertinent requirements in the Declaration of Helsinki, as
well as South African and ICH GCP Guidelines and the Ethical Guidelines of the
Department of Health as well as applicable regulations pertaining to health and
other research.
I agree to comply with all regulatory and monitoring requirements of the UREC.
I agree that I am conversant with the above guidelines.
I will ensure that every research subject or other involved persons, such as
relatives, shall at all times be treated in a dignified manner and with respect.
I will submit all required reports within the stipulated time frames.
Principal / Sub- / Co-investigator /Supervisor: …………………………………….……….………………
(print name)

68
Signature :…………………………………….……….………………
Date :…………………………………….……….………………
CONFLICT OF INTEREST DECLARATION (OBLIGATORY)
The researcher is expected to declare to the University Research Ethics Committee(UREC) the presence of any potential or existing conflict of interest that maypotentially pose a threat to the scientific integrity and ethical conduct of any researchin the University.
The UREC will decide whether such conflicts are sufficient as to warrantconsideration of their impact on the ethical conduct of the study.
Disclosure of conflict of interest does not imply that a study will be deemed unethical,as the mere existence of a conflict of interest does not mean that a study cannot beconducted ethically. However, failure to declare to the UREC a conflict of interestknown to the researcher at the outset of the study
will be deemed to be unethical conduct.
Researchers are therefore expected to sign either of the two declarations below:
a) As the Principal Researcher in this study (name: )
I hereby declare that I am not aware of any potential conflict of interest which
may influence my ethical conduct of this study.
Signature: _____________________________ Date: ________________________

69
b) As the Principal Researcher in this study (name: SIYAMTHEMBA DALASA)
I hereby declare that I am aware of potential conflicts of interest which
should be considered by the UREC:
Signature: _____________________________ Date:_________________________
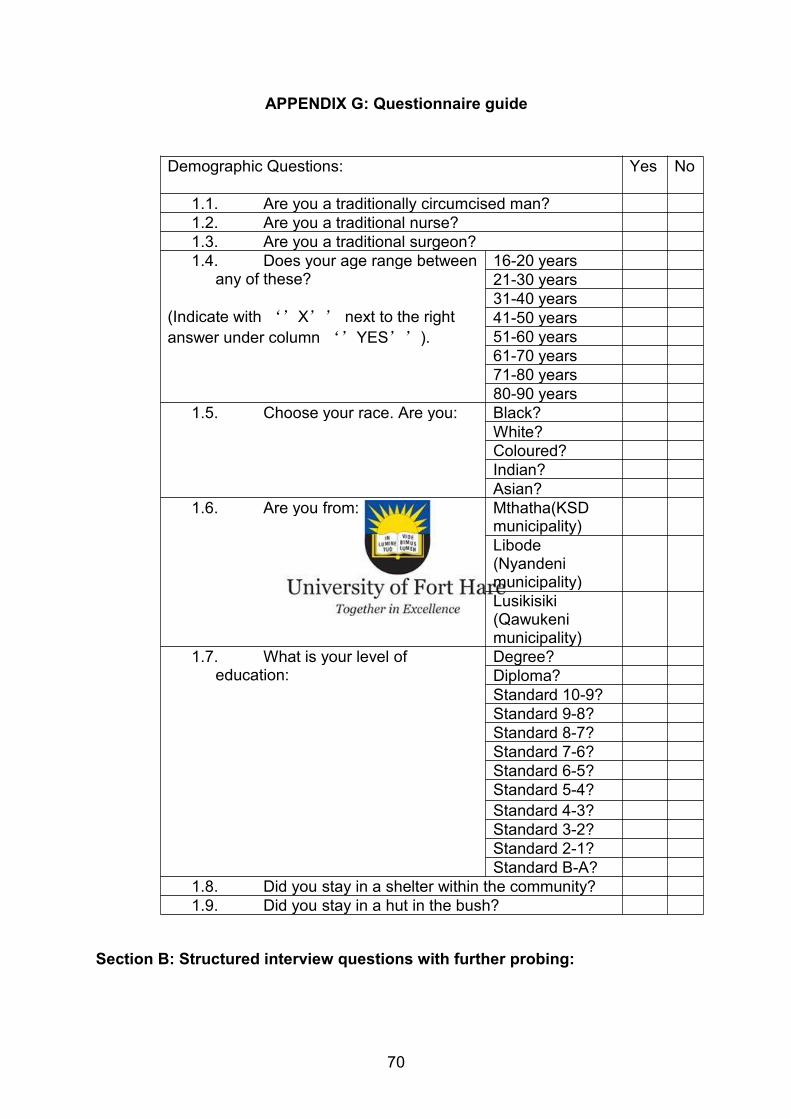
70
APPENDIX G: Questionnaire guide
Demographic Questions: Yes No
1.1. Are you a traditionally circumcised man?1.2. Are you a traditional nurse?1.3. Are you a traditional surgeon?1.4. Does your age range between
any of these?
(Indicate with ‘’X’’ next to the rightanswer under column ‘’YES’’).
16-20 years21-30 years31-40 years41-50 years51-60 years61-70 years71-80 years80-90 years
1.5. Choose your race. Are you: Black?White?Coloured?Indian?Asian?
1.6. Are you from: Mthatha(KSDmunicipality)Libode(Nyandenimunicipality)Lusikisiki(Qawukenimunicipality)
1.7. What is your level ofeducation:
Degree?Diploma?Standard 10-9?Standard 9-8?Standard 8-7?Standard 7-6?Standard 6-5?Standard 5-4?Standard 4-3?Standard 3-2?Standard 2-1?Standard B-A?
1.8. Did you stay in a shelter within the community?1.9. Did you stay in a hut in the bush?
Section B: Structured interview questions with further probing:

71
What measures do traditional surgeons use to sterilise their surgical instruments
for circumcision?
What do you do to prevent excessive bleeding?
Do traditional surgeons tighten the bandage around the penis?
Do traditional nurses tighten the bandage during wound dressings?
Are the initiates allowed to drink water?
How would you describe the conditions under which the traditional surgeons
perform circumcision?
What measures do traditional nurses used to sterilise their surgical instruments
for circumcision?
What measures are taken to safeguard the health of the initiates after
circumcision?
How would you describe the conditions of the lodge where the initiates are kept
after circumcision?
Probed questionsPsychological counsellingDo initiates get psychological counselling about the conditions of the customduring and after seclusion period prior to circumcision?Support from the traditional surgeons (family, traditional surgeons, traditionalnurses); any form of maltreatment?
QuestionsDo traditional surgeons work in a neatly prepared environment prior tocircumcision procedure?The use of traditional surgeons use gloves; changing of the gloves before theyattend to the next initiate; the use of blades or knife to cut the foreskin; whethersealed blades; use of an assegai; the sterilisation of the assegai or the knife afteruse; use of the same blade, knives or assegai on more than one initiate?The traditional surgeons use new sealed bandages to cover the wound;application of ointment after the foreskin cut or when dressing out the wound;wound dressing; the neatness of the environment; use and changing of glovesbefore attending to the next initiate; use of new sealed bandages to cover thewound?

72
Human physiological and anatomical knowledge of the traditional surgeonsabout male circumcision and its complications
Do traditional surgeons tightly apply the bandage around the penis? How are themeals cooked-well cooked or half done? Allow to drink water? Get enough rest?
Environmental conditions in which the circumcision takes placeThe state of the initiates lodge (cold hut, wet when raining, hot, dirty, small,overcrowded); mountainous setting?