Acute supra-therapeutic oral terbutaline administration has no ergogenic effect in non-asthmatic...
10
1 23 European Journal of Applied Physiology ISSN 1439-6319 Volume 113 Number 2 Eur J Appl Physiol (2013) 113:411-418 DOI 10.1007/s00421-012-2447-0 Acute supra-therapeutic oral terbutaline administration has no ergogenic effect in non-asthmatic athletes Anthony M. J. Sanchez, Fabio Borrani, Marie Amélie Le Fur, Anais Le Mieux, Virgile Lecoultre, Guillaume Py, Christophe Gernigon, et al.
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Acute supra-therapeutic oral terbutaline administration has no ergogenic effect in non-asthmatic...
1 23
European Journal of AppliedPhysiology ISSN 1439-6319Volume 113Number 2 Eur J Appl Physiol (2013) 113:411-418DOI 10.1007/s00421-012-2447-0
Acute supra-therapeutic oral terbutalineadministration has no ergogenic effect innon-asthmatic athletes
Anthony M. J. Sanchez, Fabio Borrani,Marie Amélie Le Fur, Anais Le Mieux,Virgile Lecoultre, Guillaume Py,Christophe Gernigon, et al.

1 23
Your article is protected by copyright and
all rights are held exclusively by Springer-
Verlag. This e-offprint is for personal use only
and shall not be self-archived in electronic
repositories. If you wish to self-archive your
work, please use the accepted author’s
version for posting to your own website or
your institution’s repository. You may further
deposit the accepted author’s version on a
funder’s repository at a funder’s request,
provided it is not made publicly available until
12 months after publication.

ORIGINAL ARTICLE
Acute supra-therapeutic oral terbutaline administrationhas no ergogenic effect in non-asthmatic athletes
Anthony M. J. Sanchez • Fabio Borrani • Marie Amelie Le Fur •
Anais Le Mieux • Virgile Lecoultre • Guillaume Py •
Christophe Gernigon • Katia Collomp • Robin Candau
Received: 29 February 2012 / Accepted: 16 June 2012 / Published online: 6 July 2012
� Springer-Verlag 2012
Abstract This study aimed to investigate the effects on a
possible improvement in aerobic and anaerobic performance
of oral terbutaline (TER) at a supra-therapeutic dose in 7
healthy competitive male athletes. On day 1, ventilatory
threshold, maximum oxygen uptake ð _VO2 maxÞ and corre-
sponding power output were measured and used to determine
the exercise load on days 2 and 3. On days 2 and 3, 8 mg of
TER or placebo were orally administered in a double-blind
process to athletes who rested for 3 h, and then performed a
battery of tests including a force–velocity exercise test, run-
ning sprint and a maximal endurance cycling test at D50 %
(50 % between VT and _VO2 max). Lactatemia, anaerobic
parameters and endurance performance ( _VO2; _VE and time
until exhaustion) were raised during the corresponding tests.
We found that TER administration did not improve any of the
parameters of aerobic performance (p [ 0.05). In addition,
no change in _VO2 kinetic parameters was found with TER
compared to placebo (p [ 0.05). Moreover, no enhancement
of the force–velocity relationship was observed during sprint
exercises after TER intake (p [ 0.05) and, on the contrary,
maximal strength decreased significantly after TER intake
(p \ 0.05) but maximal power remained unchanged
(p [ 0.05). In conclusion, oral acute administration of TER at
a supra-therapeutic dose seems to be without any relevant
ergogenic effect on anaerobic and aerobic performances in
healthy athletes. However, all participants experienced
adverse side effects such as tremors.
Keywords b2-Agonist � Doping � Force–velocity
relationship � Endurance performance � Anaerobic
performance � Healthy athletes
Introduction
The prevalence of asthma is higher in athletes than in the
general population. b2-adrenergic agonists (b2-agonists)
are the most commonly prescribed medication for
bronchospasm and exercise-induced asthma, affectingCommunicated by Fabio Fischetti.
A. M. J. Sanchez (&) � M. A. Le Fur � A. Le Mieux �G. Py � R. Candau
Faculte des Sciences du Sport, Universite Montpellier
Sud-de-France, 700 avenue du Pic Saint Loup,
34060 Montpellier, France
e-mail: [email protected];
A. M. J. Sanchez � M. A. Le Fur � A. Le Mieux � G. Py �R. Candau
INRA, UMR866-Dynamique Musculaire Et Metabolisme,
2 Place Viala, 34060 Montpellier, France
F. Borrani
Department of Sport and Exercise Science,
University of Auckland, Auckland, New Zealand
V. Lecoultre
Department of Physiology, University of Lausanne,
Lausanne, Switzerland
C. Gernigon
Faculty of Sport and Physical Education Sciences, Southern
France University of Montpellier, Laboratory Epsylon,
Montpellier, France
K. Collomp
Laboratoire CIAMS, Universite Paris Sud-Universite Orleans,
Orleans cedex, France
K. Collomp
Departement des Analyses, AFLD, Paris, France
123
Eur J Appl Physiol (2013) 113:411–418
DOI 10.1007/s00421-012-2447-0
Author's personal copy
&10–20 % of all athletes (Weiler et al. 1998). b2-agonists
such as salbutamol, fenoterol and terbutaline (TER) have
pharmacological effects on smooth and skeletal muscles
(Tashkin 1995). Consequently, b2-agonists have been
prohibited by the World Anti-Doping Agency’s (WADA)
prohibited list. In 2010, all b2-agonists were prohibited
except salbutamol and salmeterol which were authorized
only by inhalation, and for which a declaration of use was
no longer required from January 2011. In January 2012, the
list prohibited the administration of all b2 agonists with the
exception of salbutamol (maximum 1,600 lg over 24 h),
salmeterol and also formoterol (maximum 36 lg over
24 h) when taken by inhalation. The issue of b2-agonists
will continue to be a focus of WADA’s research activity in
order to ensure that the administration of large doses, or by
systemic routes, of these substances is prevented and pro-
hibited, but that the appropriate care and treatment of
asthmatic athletes is facilitated.
The potential ergogenic effects of b2-agonists in athletes
have been the subject of controversy for decades. Systemic
administration of salbutamol is prohibited by the WADA
because of possible positive effects on the user’s perfor-
mance. Experiments performed in animal models using
chronic b2-agonists intakes at doses 10- to 20-fold higher
than therapeutic doses showed a muscle anabolic effect
(Mounier et al. 2007; Douillard et al. 2011, 2012; Ryall and
Lynch 2008; Tonge et al. 2010). But several toxicological
effects such as alterations of trabecular bone or an
increased heart weight associated with inflammation, focal
myocardial necrosis and fibrosis were also described
(Weiler et al. 1998; Bonnet et al. 2005, 2007).
Although many groups have studied the performance
effects of b2-agonists, few studies have revealed an
increase in endurance performance. Several years ago, it
was found that oral and inhaled administration of salbuta-
mol may improve the time until exhaustion during a con-
stant work test or the final sprint during an endurance
exercise (Collomp et al. 2000; van Baak et al. 2004; Bedi
et al. 1988). However, this ergogenic effect has not been
identified for any b2-agonist other than salbutamol with
inhaled administration (Kindermann 2007). Moreover, no
study has evaluated the effects of oral TER administration
on endurance performance.
Concerning anaerobic performance, an increase in the
maximal power output was found with acute and chronic oral
salbutamol treatments (Sanchez et al. 2012) and with
administration by inhalation (Signorile et al. 1992).
Depending on the muscle group considered, this increase
ranges from about 5–13 % (Collomp et al. 2005; Le Panse
et al. 2005, 2006). Interestingly, during leg extension exer-
cise, increase in peak torque was preferentially obtained for
low speeds of shortening (van Baak et al. 2000). This element
suggests that b2-agonists would have more significant effects
on high-load exercise on cyclo-ergocycle, which requires
low speeds of shortening, than on running sprint which
requires high speeds of shortening. Otherwise, the appear-
ance of acute deleterious effects such as tachycardia and
muscular tremors when participants use b2-agonists is fre-
quently observed (van Baak et al. 2000; Ryall and Lynch
2008). van Baak et al. (2000) concluded that oral salbutamol
appears to be an effective ergogenic aid, but only in non-
asthmatic individuals not experiencing adverse side effects.
Interestingly, TER seems to involve fewer side effects than
the other b2-agonists (Whitsett et al. 1981).
TER is a fast-acting b2-agonist available for both inha-
lation and per os therapeutic administration [used at 0.5 and
5 mg, respectively (Vidal 2011)]. TER combines a rapid
onset of action with a long duration of 12 h and represents a
valuable addition to the treatment of asthmatic patients,
especially those with ongoing symptoms. Due to the rapid
onset and long duration of its action and its fewer side effects
compared to other b2-agonists, this drug may be of benefit to
asthmatic athletes performing in endurance sports both for
the prevention of exercise-induced asthma and as a regular
treatment of chronic asthma in athletes. The problem lies in
the potential benefit of the drug in non-asthmatic athletes. A
threshold has been attributed to salbutamol and salmeterol
urinary concentration but not to TER. It is thus important to
consider the potential effects of this drug on performance.
Indeed, the potential ergogenic effects of TER must be
explored in order to encourage studies on the definition of a
urinary threshold. Larsson et al. (1997) have already found
that inhalation of TER at therapeutic doses that yield sig-
nificant bronchodilatation does not influence physical per-
formance at low temperatures in healthy athletes. But, to our
knowledge, no study has investigated the potential ergogenic
effects of oral TER administration at supra-therapeutic doses
in non-asthmatic competitive athletes. Thus, the aim of this
study was to determine whether an acute supra-therapeutic
TER administration (8 mg) improves aerobic and anaerobic
performance in healthy athletes.
Methods
Subjects
Seven well-trained male competitive athletes (mean ± SD;
age 29 ± 6 years; height 180 ± 5 cm; body mass 74 ± 8;
body mass index 22.8 ± 3.2 kg m-2) volunteered to par-
ticipate in this study after being informed of the nature of,
and the possible disadvantages associated with, the
experiment. These subjects engaged in recreational sports
an average of 10 h/week. The study procedures complied
with the Declaration of Helsinki on human experimentation
and were approved by the local human ethics committee.
412 Eur J Appl Physiol (2013) 113:411–418
123
Author's personal copy

Each participant gave written informed consent before
beginning the tests. The subjects were asked to maintain
their dietary habits throughout the study period, but to
abstain from alcohol and caffeine for a minimum of 24 h
before each laboratory visit to avoid interactions. Partici-
pants were screened with a medical history and physical
examination to exclude those with a history of broncho-
spasm or atopy. Other exclusion criteria were respiratory
tract infection during the previous month, regular tobacco
use, regular use of any medical drug, and recognized
asthma or allergy during the 5 years preceding the study.
Moreover, pulmonary function was tested before the
experiment to ensure that the subjects did not have asthma
or exercise-induced bronchospasm. The highest forced
expiratory volume during 1 s (FEV1) was recorded at rest
in a standing position and after the incremental maximal
test of the preliminary session. None of the subjects
showed a post-exercise fall in FEV1 [10 %.
Drug
In accordance with a double-blind, equilibrated random-
ized crossover study, either 8 mg TER (Bricanyl, UK) or
placebo (sweetener) was administered to each subject 3 h
before the tests. The therapeutic dose in pregnancy is 5 mg
(Vidal 2011; Le Fur et al. 2012). Placebo and TER were
packaged in identical capsules. An independent researcher
was involved and he was the only one to know the order of
the processing. The experimenters questioned the subjects
immediately after the two trials, as to their knowledge of
which of the two treatments they had received first, and
whether they were able to report any difference. The sub-
jects and the experimenters were informed about admin-
istration of the processing only after analysis of the results.
Tests
There were three study days in total. On day 1, all partic-
ipants performed a primary incremental test on a cycl-
oergometer (Monarck 818E, Stockholm, Suede), with no
drug intake, to establish a performance baseline for each
participant and to verify that they satisfied the inclusion
criteria. The power output associated with maximal oxygen
consumption ð _VO2 maxÞ was defined as the minimal work-
load at which ð _VO2 maxÞ occurred. All participants gave
maximum effort and were encouraged to do so.
Participants were then randomized to one of the two
treatment sequences: TER or placebo. Three hours after
treatment, they performed a battery of tests (Fig. 1) starting
with postural sway measures. Immediately after this test,
the participants performed 5 9 4 s cycling sprints inter-
spersed with 3 min of passive recovery, which constituted
the force–velocity exercise test. The parameters measured
were the force–velocity relationship, maximal velocity
ðvmaxÞ, maximal force ðFmaxÞ; maximal power output
ðPmaxÞ; optimal velocity ðvoptÞ and optimal force ðFoptÞ.After 5 min of passive recovery, participants performed a
70-m running sprint during which performance was
measured using a radar (Stalker professional sports
radar, Applied concept, Texas) enabling evaluation of the
instantaneous speeds. The parameters measured were
the maximal velocity ðvmaxÞ mean velocity ðvmeanÞ and the
initial acceleration. The acceleration phase was obtained by
fitting the speed–time curve from the standing start to the
maximal velocity to the following exponential equation
(Chelly and Denis 2001):
vðtÞ ¼ vmaxð1� e�t=sÞ;
where vmax is the maximal velocity, s is the time constant
of the acceleration phase.
The initial acceleration of each sprint was calculated as
the ratio vmax=s.
After 5 min of passive recovery, participants performed
a constant work cycling exercise at D50 % [50 % between
the ventilatory threshold (VT) and _VO2 max] until exhaus-
tion. Aerobic performance was evaluated with _VO2peak;
peak ventilation ð _VEpeakÞ and time until exhaustion.
Finally, the participants completed the Affect Grid.
Force–velocity exercise test
As recommended by Arsac et al. (1996), the subjects were
familiarized with the friction-loaded cycle ergometer by
5 min of submaximal cycling (100–150 W) and sprints of
2–4 s against friction loads of 0.20–1 N kg-1 body mass.
Wash out period
5min 5min
TreatmentPlacebo or8 mg TER
F-v relationship test5 x 4 s repetitions
Running sprint70m
Endurance cycling testTime to exhaustion at Δ50%
3h
Postural sway Affect Grid
Day 1
Incrementaltest
Day 2 or 3
1 week
Fig. 1 Sequence of the
experimental protocol
Eur J Appl Physiol (2013) 113:411–418 413
123
Author's personal copy

After stretching and 5 min of rest, the subjects were asked
to perform five sprints separated by at least 3 min of rest.
Frictional loads of 0.2, 0.6 and 1.0 N kg-1 body mass were
applied to the friction belt in randomized order. The saddle
height and toe clips were adjusted for each subject. The
saddle height was measured and used for the whole tests.
At a signal given by the experimenter, the subjects were
asked to pedal as fast as possible until told to stop at the
signal given 4 s after the start. During the effort, each
subject was vigorously encouraged. The goal of this task
was to create the greatest acceleration of the flywheel, so
the subjects were required to produce the highest explosive
force possible on the pedal.
A standard friction-loaded cycle ergometer (model
918E, Monark-Crescent AB, Stockholm, Sweden) was
used, equipped with a strain gauge (interface MFG type,
Scottsdale, AZ, USA) and an incremental encoder (Engs-
tler type RIS IP50, 100 digits/turn of wheel, Aldingen,
Germany) fixed on a wheel (for details see Arsac et al.
1996). The strain gauge measured the friction force applied
by the belt that surrounds the flywheel. It was calibrated
with a known mass (9.78 kg) hung on the friction belt and
in an unloaded condition to give a 0 value. The strain gauge
was checked after 10 min of switching on the system to
avoid possible effects of temperature shift. The strain
gauge’s non-linearity was no more than 0.3 %. The
incremental encoder measured the displacement with a
precision of 12,060.6 points per pedal revolution or 2,010.1
points m-1.
Flywheel inertia varies among ergometers, even for a
specific model. Therefore, to ensure accurate measurement
of the inertia, the method proposed by Lakomy et al.
(Lakomy 1986) was used. Briefly, the inertia of the ergo-
cycle was simply determined from the linear relationship
between the free decelerations of the flywheel and the
corresponding friction loads. The following equation was
obtained to assess the force exerted by the subject when he
accelerated the flywheel (Finertia):
Finertia ¼ 0:1322a� 0:0453;
where the inertia force is expressed in N and a is the
acceleration of the flywheel expressed in rpm s-1.
Force and displacement signals were sampled at 200 Hz
and stored on a PC via an interface (Electronic, Informa-
tique du Pilat, Jonzieux, France). For further calculations,
instantaneous force and displacement data were low-pass
filtered (Butterworth 4th order with no phase lag) with a
cut-off frequency of 10 Hz. The velocity and acceleration
of the flywheel were obtained by 1st and 2nd order digital
derivations of the displacement signal, respectively. The
total external force (F) was the sum of the inertia force and
the friction force (Ffriction):
F ¼ Finertia þ Ffriction:
F and velocity data were averaged for each pedal
downstroke (i.e. 1/2 revolution), which was limited
between two minimal values of instantaneous velocity
corresponding to the top and bottom dead centers of a
crank revolution.
Blood analysis
Blood lactate concentrations were measured 1 min after the
end of the force–velocity exercise test. Capillary blood
samples were collected from the fingertip and analyzed
using the Lactate Pro analyzer (LT-1710, Arkray, Japan).
_VO2 kinetics
Breath-by-breath ventilation and gas exchange were con-
tinuously measured using a calibrated automated gas-
analysis system (VMAX29, Sensormedics).
Data were fitted with a classical serial model including
two components as described previously (e.g. Borrani et al.
2003):
_VO2ðtÞ ¼ _VO2i
þ A1½1� e� ðt�TD1Þ=s1f g�Phase 1 (primary component)
þ A2½1� e� t�TD2ð Þ=s2f g�UPhase 2 (slow component)
where U ¼ 0 for t\TD2 and U ¼ 1 for t� TD2; _VO2i is the
oxygen consumption at rest, A1 and A2 are the asymptotic
amplitudes for the primary and second exponential,
respectively, s1 and s2 are the times constant of each
exponential and TD1 and TD2 represents the time delay to
onset of the primary and the slow component, respectively.
The initial component (cardiodynamic phase) was not
modeled since the focus was on the SC kinetic. The pri-
mary component phase is not distorted by any early car-
diodynamic influence (Paterson and Whipp 1991; Whipp
et al. 1982). As a consequence, the first 20 s were removed
from analysis to ensure that the early initial component did
not influence the result (Whipp et al. 1982).
The magnitude of SC was assigned the value ðA02Þ:
A02 ¼ A2½1� e� ðte�TD2Þ=s2f g�;
where te is the time at the end of exercise.
VT was determined as the power output corresponding
to the point where a systematic increase in the ventilatory
equivalent for O2_VE�
_VO2
� �occurred without an increase
in the ventilatory equivalent for CO2_VE�
_VCO2
� �.
414 Eur J Appl Physiol (2013) 113:411–418
123
Author's personal copy

Postural sway measures and Affect Grid
Before exercises, participants had to stand on a force
platform (Medicapteurs, France). Center of pressure (COP)
displacement data were recorded during 51.2 s at a sample
frequency of 40 Hz. The variability (standard deviation) of
COP time series and their power spectra were computed in
both anteriorposterior (AP) and mediolateral (ML) direc-
tions (Prieto et al. 1996). Immediately after the constant
work cycling exercise, participants completed the Affect
Grid that measures the dimensions of pleasure-displeasure
(from 1 = unpleasant feelings to 9 = pleasant feelings)
and arousal-sleepiness (from 1 = sleepiness to 9 = high
arousal) (Russell 1989).
Statistical analysis
Data are presented as mean values ± standard deviation
(SD). When the normality of distribution was satisfied, a
student-paired test was used to test differences between
placebo and TER treatments. When normality of distribu-
tion was not satisfied, data were evaluated by a paired
Wilcoxon test. The parameters of _VO2 kinetics models
were determined using an iterative procedure by mini-
mizing the sum of the residual mean squares of the dif-
ferences between the _VO2 model and the _VO2 measured.
Statistical significance was accepted at the 0.05 level.
Results
When questioned after the two trials, as to their knowledge
of which of the two treatments they had received, all
subjects were able to identify the TER treatment although
the double-blind protocol was effectively completed. All
participants reported adverse effects such as tremors,
starting 1 h after the 8 mg TER administration, with an
increased magnitude during the following 2 h, just before
performing the exercises.
Incremental test
The mean value for _VO2 max was 57 ± 3 ml min-1 kg-1.
The mechanical power corresponding to _VO2 max was
351 ± 57 W and Delta T50 was 241 ± 36 W.
Force–velocity exercise test
No improvement was found in the force–velocity rela-
tionship after TER intake (p [ 0.05). TER was not found
to improve maximal velocity (p [ 0.05) but a significant
decrease of peak force was obtained with TER (p \ 0.05),
without altering the peak power (p [ 0.05). No difference
was found for optimal force and optimal velocity
(p [ 0.05). These results are detailed in Table 1.
Blood lactate
Blood lactate concentrations 1 min after the force–velocity
exercise test were no different between placebo and TER
(p [ 0.05). The values were 7.8 (2.1) and 6.1 (2.1) mM,
respectively.
Running test
During the running test, no difference on mean speed,
maximal speed and initial acceleration was found between
placebo and TER (p [ 0.05) (Table 2).
Endurance test
Table 3 presents kinetic parameters for the curve fitting of_VO2 response during the endurance test. TER was not
found to improve aerobic performance with regard to the
collected variables. Indeed, no significant differences in_VO2peak; _VEpeak and in cycling time until exhaustion at a
power output corresponding to Delta T50 were found
between TER and placebo (p [ 0.05). No significant dif-
ference was found between placebo and TER treatment on
Table 1 Force-velocity test on ergocycle under placebo and 8 mg
TER conditions in the 7 male study participants
Variable Placebo Terbutaline Significance
vmax (rpm) 183 (8) 190 (17) NS
Fmax (N) 245.4 (36.9) 231.1 (38.2) p \ 0.05
Pmax (W kg-1) 25.8 (3.3) 24.7 (2.3) NS
vopt (rpm) 100.1 (7.2) 101.8 (8.9) NS
Fopt (N) 150.2 (34.2) 141.9 (31.1) NS
Results are given as mean values with standard deviation in paren-
theses (SD)
NS not significant, vmax maximal velocity, Fmax maximal force, Pmax
maximal power output, vopt optimal velocity, Fopt optimal force
Table 2 Running sprint performance under placebo and 8 mg TER
conditions in the 7 male study participants
Variable Placebo Terbutaline Significance
vmax (m s-1) 8.6 (0.4) 8.4 (0.5) NS
vmean (m s-1) 6.2 (1.3) 6.3 (1.1) NS
vmax=s (m s-2) 5.1 (1.7) 5.0 (0.6) NS
Results are given as mean values with standard deviation in paren-
theses (SD)
NS not significant, vmax vmean maximal velocity, mean velocity, vmax=sinitial acceleration
Eur J Appl Physiol (2013) 113:411–418 415
123
Author's personal copy
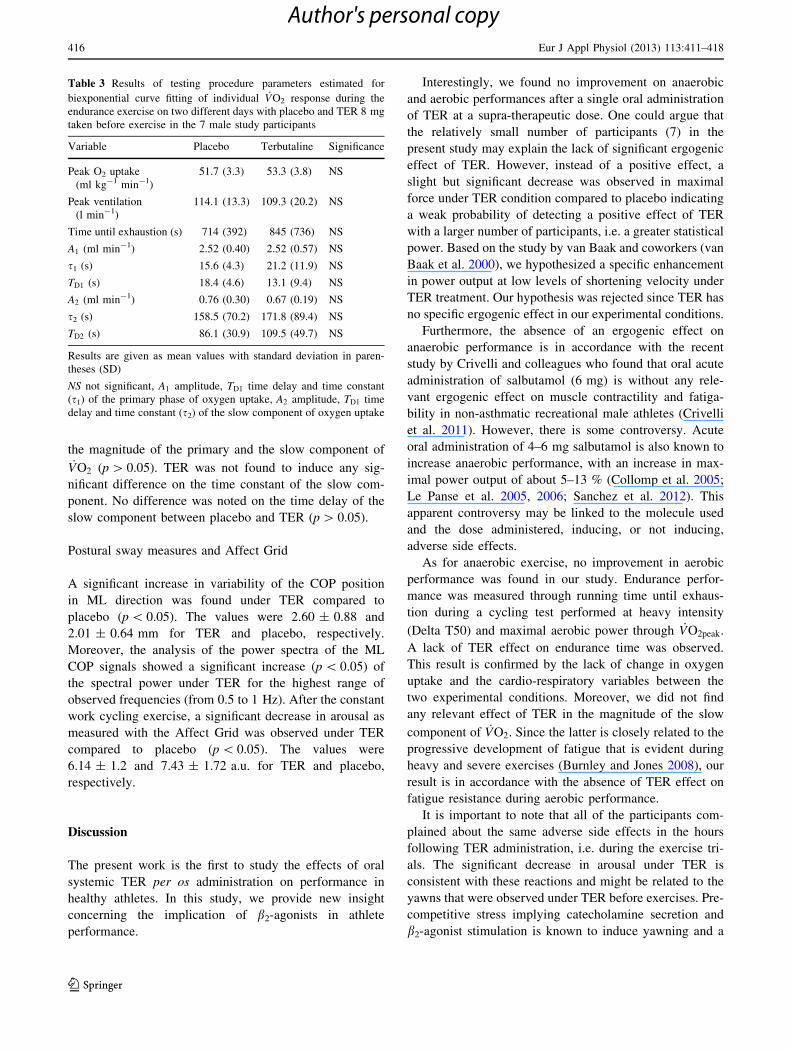
the magnitude of the primary and the slow component of_VO2 (p [ 0.05). TER was not found to induce any sig-
nificant difference on the time constant of the slow com-
ponent. No difference was noted on the time delay of the
slow component between placebo and TER (p [ 0.05).
Postural sway measures and Affect Grid
A significant increase in variability of the COP position
in ML direction was found under TER compared to
placebo (p \ 0.05). The values were 2.60 ± 0.88 and
2.01 ± 0.64 mm for TER and placebo, respectively.
Moreover, the analysis of the power spectra of the ML
COP signals showed a significant increase (p \ 0.05) of
the spectral power under TER for the highest range of
observed frequencies (from 0.5 to 1 Hz). After the constant
work cycling exercise, a significant decrease in arousal as
measured with the Affect Grid was observed under TER
compared to placebo (p \ 0.05). The values were
6.14 ± 1.2 and 7.43 ± 1.72 a.u. for TER and placebo,
respectively.
Discussion
The present work is the first to study the effects of oral
systemic TER per os administration on performance in
healthy athletes. In this study, we provide new insight
concerning the implication of b2-agonists in athlete
performance.
Interestingly, we found no improvement on anaerobic
and aerobic performances after a single oral administration
of TER at a supra-therapeutic dose. One could argue that
the relatively small number of participants (7) in the
present study may explain the lack of significant ergogenic
effect of TER. However, instead of a positive effect, a
slight but significant decrease was observed in maximal
force under TER condition compared to placebo indicating
a weak probability of detecting a positive effect of TER
with a larger number of participants, i.e. a greater statistical
power. Based on the study by van Baak and coworkers (van
Baak et al. 2000), we hypothesized a specific enhancement
in power output at low levels of shortening velocity under
TER treatment. Our hypothesis was rejected since TER has
no specific ergogenic effect in our experimental conditions.
Furthermore, the absence of an ergogenic effect on
anaerobic performance is in accordance with the recent
study by Crivelli and colleagues who found that oral acute
administration of salbutamol (6 mg) is without any rele-
vant ergogenic effect on muscle contractility and fatiga-
bility in non-asthmatic recreational male athletes (Crivelli
et al. 2011). However, there is some controversy. Acute
oral administration of 4–6 mg salbutamol is also known to
increase anaerobic performance, with an increase in max-
imal power output of about 5–13 % (Collomp et al. 2005;
Le Panse et al. 2005, 2006; Sanchez et al. 2012). This
apparent controversy may be linked to the molecule used
and the dose administered, inducing, or not inducing,
adverse side effects.
As for anaerobic exercise, no improvement in aerobic
performance was found in our study. Endurance perfor-
mance was measured through running time until exhaus-
tion during a cycling test performed at heavy intensity
(Delta T50) and maximal aerobic power through _VO2peak.
A lack of TER effect on endurance time was observed.
This result is confirmed by the lack of change in oxygen
uptake and the cardio-respiratory variables between the
two experimental conditions. Moreover, we did not find
any relevant effect of TER in the magnitude of the slow
component of _VO2. Since the latter is closely related to the
progressive development of fatigue that is evident during
heavy and severe exercises (Burnley and Jones 2008), our
result is in accordance with the absence of TER effect on
fatigue resistance during aerobic performance.
It is important to note that all of the participants com-
plained about the same adverse side effects in the hours
following TER administration, i.e. during the exercise tri-
als. The significant decrease in arousal under TER is
consistent with these reactions and might be related to the
yawns that were observed under TER before exercises. Pre-
competitive stress implying catecholamine secretion and
b2-agonist stimulation is known to induce yawning and a
Table 3 Results of testing procedure parameters estimated for
biexponential curve fitting of individual _VO2 response during the
endurance exercise on two different days with placebo and TER 8 mg
taken before exercise in the 7 male study participants
Variable Placebo Terbutaline Significance
Peak O2 uptake
(ml kg-1 min-1)
51.7 (3.3) 53.3 (3.8) NS
Peak ventilation
(l min-1)
114.1 (13.3) 109.3 (20.2) NS
Time until exhaustion (s) 714 (392) 845 (736) NS
A1 (ml min-1) 2.52 (0.40) 2.52 (0.57) NS
s1 (s) 15.6 (4.3) 21.2 (11.9) NS
TD1 (s) 18.4 (4.6) 13.1 (9.4) NS
A2 (ml min-1) 0.76 (0.30) 0.67 (0.19) NS
s2 (s) 158.5 (70.2) 171.8 (89.4) NS
TD2 (s) 86.1 (30.9) 109.5 (49.7) NS
Results are given as mean values with standard deviation in paren-
theses (SD)
NS not significant, A1 amplitude, TD1 time delay and time constant
(s1) of the primary phase of oxygen uptake, A2 amplitude, TD1 time
delay and time constant (s2) of the slow component of oxygen uptake
416 Eur J Appl Physiol (2013) 113:411–418
123
Author's personal copy

state of febrility. Moreover, the analysis of postural control
may provide further insight into TER side effects. The
increase in variability of the center of pressure and power
spectrum in ML direction under TER may be related to
tremor, the most characteristic adverse effect following
administration of b2-adrenergic agonists (Cazzola and
Matera 2012). It can therefore be hypothesized that these
marked adverse effects may prevent a possible ergogenic
effect of TER. Indeed, van Baak et al. (2000) reported that
oral salbutamol intake appears to be an effective ergogenic
aid, only in non-asthmatic individuals not experiencing
adverse side effects.
Otherwise, participants in the present study took this
drug for the first time. Taking these substances repeatedly
can involve a reduction in b2-receptor contents and side
effect manifestations (Sato et al. 2010). Anabolic effects
have been reported in animals with chronic salbutamol
treatment. These observations have not been reported for
humans in scientific literature but it is well known that
bodybuilders frequently use clenbuterol at high doses
because of their anabolic and lipolytic properties (e.g.
http://www.musclesprod.com/steroid-profiles/axiolabs/clen
butaplex/). The apparent discrepancy between studies with
respect to ergogenic effects may be due primarily to the
nature and the mode of intake and more particularly the
distribution of b2-agonists in the organism. All the studies
that found no ergogenic effect of salbutamol on force pro-
duction used inhalation administration; in contrast, studies
that noted an ergogenic effect used oral administration.
Inhalation is associated with a more marked local effect on
pulmonary b2-adrenoceptors than on peripheral skeletal
muscle adrenoceptors. To the best of our knowledge, no
study has evaluated the anabolic effects of oral TER at high
doses. Thus, taking all these factors into account, we cannot
exclude a potential effect on anaerobic performance with a
chronic treatment of TER, especially at therapeutic doses.
Conclusions
In conclusion, acute supra-therapeutic dose of TER seems
to be without any relevant ergogenic effect on anaerobic
and aerobic performances in healthy athletes. The absence
of an ergogenic effect for an amount of 8 mg is concom-
itant with the occurrence of marked adverse side effects
and does not exclude a potential ergogenic effect of a lower
dose, where the deleterious effects could be reduced. Nor
does it exclude potential effects of short-term treatment. In
the anti-doping fight, these elements must be highlighted in
preventive action.
Acknowledgments We give special thanks to the participants for
their great effort, compliance and enthusiasm when participating in
the study. We would like to thank Drs Sofiane Ramdani and Benoit
Seigle for their analysis and helpful discussions related to postural
sway data. This work was supported by the World Anti-Doping
Agency and by a fellowship from the Ministere de la Recherche et de
la Technologie (to AMJS).
Conflict of interest The authors declare no conflict of interest.
References
Arsac LM, Belli A, Lacour JR (1996) Muscle function during brief
maximal exercise: accurate measurements on a friction-loaded
cycle ergometer. Eur J Appl Physiol Occup Physiol 74(1–2):
100–106
Bedi JF, Gong H Jr, Horvath SM (1988) Enhancement of exercise
performance with inhaled albuterol. Can J Sport Sci (Journal
canadien des sciences du sport) 13(2):144–148
Bonnet N, Brunet-Imbault B, Arlettaz A, Horcajada MN, Collomp K,
Benhamou CL, Courteix D (2005) Alteration of trabecular bone
under chronic beta2 agonists treatment. Med Sci Sports Exerc
37(9):1493–1501
Bonnet N, Laroche N, Beaupied H, Vico L, Dolleans E, Benhamou
CL, Courteix D (2007) Doping dose of salbutamol and exercise
training: impact on the skeleton of ovariectomized rats. J Appl
Physiol 103(2):524–533. doi:10.1152/japplphysiol.01319.2006
Borrani F, Candau R, Perrey S, Millet GY, Millet GP, Rouillon JD
(2003) Does the mechanical work in running change during the
VO2 slow component? Med Sci Sports Exerc 35(1):50–57
Burnley M, Jones AM (2008) Viewpoint: fatigue mechanisms
determining exercise performance: integrative physiology is
systems physiology. J Appl Physiol 104(5):1545–1546
Cazzola M, Matera MG (2012) Tremor and beta(2)-adrenergic agents:
is it a real clinical problem? Pulm Pharmacol Ther 25(1):4–10.
doi:10.1016/j.pupt.2011.12.004
Chelly SM, Denis C (2001) Leg power and hopping stiffness:
relationship with sprint running performance. Med Sci Sports
Exerc 33(2):326–333
Collomp K, Candau R, Lasne F, Labsy Z, Prefaut C, De Ceaurriz J
(2000) Effects of short-term oral salbutamol administration on
exercise endurance and metabolism. J Appl Physiol
89(2):430–436
Collomp K, Le Panse B, Portier H, Lecoq AM, Jaffre C, Beaupied H,
Richard O, Benhamou L, Courteix D, De Ceaurriz J (2005)
Effects of acute salbutamol intake during a Wingate test. Int J
Sports Med 26(7):513–517. doi:10.1055/s-2004-821223
Crivelli G, Millet GP, Gremion G, Borrani F (2011) Effects of
salbutamol on the contractile properties of human skeletal
muscle before and after fatigue. Acta Physiol (Oxf)
203(2):311–320. doi:10.1111/j.1748-1716.2011.02302.x
Douillard A, Galbes O, Rossano B, Vernus B, Bonnieu A, Candau R,
Py G (2011) Time course in calpain activity and autolysis in
slow and fast skeletal muscle during clenbuterol treatment. Can J
Physiol Pharmacol 89(2):117–125. doi:10.1139/y10-114
Douillard A, Galbes O, Begue G, Rossano B, Levin J, Vernus B,
Bonnieu A, Candau R, Py G (2012) Calpastatin overexpression
in the skeletal muscle of mice prevents clenbuterol-induced
muscle hypertrophy and phenotypic shift. Clin Exp Pharmacol
Physiol 39(4):364–372. doi:10.1111/j.1440-1681.2012.05677.x
Kindermann W (2007) Do inhaled beta(2)-agonists have an ergogenic
potential in non-asthmatic competitive athletes? Sports Med
37(2):95–102
Lakomy HK (1986) Measurement of work and power output using
friction-loaded cycle ergometers. Ergonomics 29(4):509–517.
doi:10.1080/00140138608968287
Eur J Appl Physiol (2013) 113:411–418 417
123
Author's personal copy

Larsson K, Gavhed D, Larsson L, Holmer I, Jorfelt L, Ohlsen P
(1997) Influence of a beta2-agonist on physical performance at
low temperature in elite athletes. Med Sci Sports Exerc
29(12):1631–1636
Le Fur MA, Sanchez AMJ, Candau R (2012) Effets ergogeniques des
b2 agonistes: mode d’action et enjeux pour la lutte antidopage.
Mov Sport Sci/Sci Mot. http://dx.doi.org/10.1051/sm/2012003
Le Panse B, Collomp K, Portier H, Lecoq AM, Jaffre C, Beaupied H,
Richard O, Benhamou L, De Ceaurriz J, Courteix D (2005)
Effects of short-term salbutamol ingestion during a Wingate test.
Int J Sports Med 26(7):518–523. doi:10.1055/s-2004-821224
Le Panse B, Arlettaz A, Portier H, Lecoq AM, De Ceaurriz J,
Collomp K (2006) Short term salbutamol ingestion and supra-
maximal exercise in healthy women. Br J Sports Med
40(7):627–631. doi:10.1136/bjsm.2006.026237
Mounier R, Cavalie H, Lac G, Clottes E (2007) Molecular impact of
clenbuterol and isometric strength training on rat EDL muscles.
Pflugers Arch 453(4):497–507. doi:10.1007/s00424-006-0122-1
Paterson DH, Whipp BJ (1991) Asymmetries of oxygen uptake
transients at the on- and offset of heavy exercise in humans.
J Physiol 443:575–586
Prieto TE, Myklebust JB, Hoffmann RG, Lovett EG, Myklebust BM
(1996) Measures of postural steadiness: differences between
healthy young and elderly adults. IEEE Trans Biomed Eng
43(9):956–966. doi:10.1109/10.532130
Russell JA (1989) Affect grid: a single-item scale of pleasure and
arousal. J Pers Soc Psychol 57(3):493–502
Ryall JG, Lynch GS (2008) The potential and the pitfalls of beta-
adrenoceptor agonists for the management of skeletal muscle
wasting. Pharmacol Ther 120(3):219–232. doi:10.1016/j.pharm
thera.2008.06.003
Sanchez AM, Collomp K, Carra J, Borrani F, Coste O, Prefaut C,
Candau R (2012) Effect of acute and short-term oral salbutamol
treatments on maximal power output in non-asthmatic athletes.
Eur J Appl Physiol. doi:10.1007/s00421-011-2307-3
Sato S, Nomura S, Kawano F, Tanihata J, Tachiyashiki K, Imaizumi
K (2010) Adaptive effects of the beta2-agonist clenbuterol on
expression of beta2-adrenoceptor mRNA in rat fast-twitch fiber-
rich muscles. J Physiol Sci 60(2):119–127. doi:10.1007/s12576-
009-0075-1
Signorile JF, Kaplan TA, Applegate B, Perry AC (1992) Effects of
acute inhalation of the bronchodilator, albuterol, on power
output. Med Sci Sports Exerc 24(6):638–642
Tashkin DP (1995) Multiple dose regimens. Impact on compliance.
Chest 107(5 Suppl):176S–182S
Tonge DP, Jones SW, Parr T, Bardsley R, Doherty M, Maciewicz RA
(2010) Beta2-adrenergic agonist-induced hypertrophy of the
quadriceps skeletal muscle does not modulate disease severity in
the rodent meniscectomy model of osteoarthritis. Osteoarthritis
Cartilage 18(4):555–562. doi:10.1016/j.joca.2009.11.014
van Baak MA, Mayer LH, Kempinski RE, Hartgens F (2000) Effect
of salbutamol on muscle strength and endurance performance in
nonasthmatic men. Med Sci Sports Exerc 32(7):1300–1306
van Baak MA, de Hon OM, Hartgens F, Kuipers H (2004) Inhaled
salbutamol and endurance cycling performance in non-asthmatic
athletes. Int J Sports Med 25(7):533–538. doi:10.1055/s-2004-
815716
Vidal (2011) Le dictionnaire. Editeur Vidal, 2012
Weiler JM, Layton T, Hunt M (1998) Asthma in United States
Olympic athletes who participated in the 1996 Summer Games.
J Allergy Clin Immunol 102(5):722–726
Whipp BJ, Ward SA, Lamarra N, Davis JA, Wasserman K (1982)
Parameters of ventilatory and gas exchange dynamics during
exercise. J Appl Physiol 52(6):1506–1513
Whitsett TL, Manion CV, Wilson MF (1981) Cardiac, pulmonary and
neuromuscular effects of clenbuterol and terbutaline compared
with placebo. Br J Clin Pharmacol 12(2):195–200
418 Eur J Appl Physiol (2013) 113:411–418
123
Author's personal copy