
Activation of aerobic metabolism by Amaranth oil improves heart rate variability both in athletes...
11
47 Background Pathogenesis of many chronic illnesses is strongly related to oxidative stress (OS), which is defined as excessive production of free radicals (FR) overwhelming the capacity of antioxidant reserve to withstand increas- ing oxidative damage (Cohen et al., 2007; Eizirik, 2008; Henriksen, 2011; Negre-Salvayre et al., 2010; Sarsour et al., 2009; Weseler and Bast, 2010). However, what is fre- quently not recognized is the intensity of redox reactions, which underlies and determines OS manifestations. Namely, mild and reversible disturbances of oxidative homeostasis are necessary for the maintenance of the optimal pro-/antioxidant balance and the overall oxygen metabolism. ese mechanisms underlie widely recog- nized effect of preconditioning or hormesis, stating that moderate activation of FR reactions facilitates assimila- tion of oxidative waste products and improves functional metabolic potential (Jones, 2006; Mandl, 2009; Manoli et al., 2007; Packer, 2007; Tymochko et al., 1998; Voeikov et al., 2009). ere is accumulating evidence that the hor- metic response is achieved not only because a wide range of antioxidant signalling pathways is being initiated, but also because production of endogenous oxygen in FR reactions takes place. Higher intensity of redox reactions is associated with more frequent oscillations in endog- enous oxygen production, improvement in oxygenase/ oxydase reactions balance and subsequently better self- regulation of the living system (Tymochko et al., 1998). In the present study we aimed to achieve desirably mild pro-oxidant activity (hormetic effect) in diabetic patients and in healthy athletes, giving them the oil derived from the seeds of Amaranthus cruentus L., which has been demonstrated to have numerous metabolic effects (Martirosyan et al., 2007; Sirota et al., 2008; Yelisyeyeva ORIGINAL ARTICLE Activation of aerobic metabolism by Amaranth oil improves heart rate variability both in athletes and patients with type 2 diabetes mellitus Olha Yelisyeyeva 1 , Khrystyna Semen 1 , Neven Zarkovic 2 , Danylo Kaminskyy 1 , Olexander Lutsyk 1 , and Volodymyr Rybalchenko 3 1 Danylo Halytsky Lviv National Medical University, Lviv, Ukraine, 2 Rudjer Boskovic Institute, Zagreb, Croatia, and 3 Taras Shevchenko National University of Kyiv, Ukraine Abstract The aim of present research was to study the effects of Amaranth oil (AmO) supplementation on aerobic metabolism and heart rate variability (HRV) in type 2 diabetes mellitus patients and in athletes. Several parameters of aerobic metabolism and HRV were assessed. Supplementation with AmO caused mild pro-oxidant activity resulting in improved uptake of oxidative destruction products and modulation of catalase and SOD activity with subsequent development of an antioxidant effect. These findings were very distinct in athletes but less pronounced in diabetics. Redistribution of haemoglobin ligands in athletes indicates involvement of haemoproteins in free radical reactions during AmO supplementation. Improvement in HRV by daily consumption of AmO as observed in both study groups suggested increased production of endogenous oxygen and enhancement of the cardio-respiratory function. The advantage of activation of aerobic metabolism in OS-related disorders resulting in improved self-organization of the living system and hormetic reaction mechanisms are discussed. Keywords: Amaranth oil, aerobic metabolism, heart rate variability, correlations, metabolic syndrome, type 2 diabetes mellitus, athletes, hormesis, oxidative stress correction Address for Correspondence: Yelisyeyeva Olha, Department of Histology, Cytology and Embryology Danylo Halystky Lviv National Medical University, Lviv, Ukraine; 69, Pekarska str., Lviv, 79010, Ukraine. E-mail: [email protected] (Received 02 December 2011; revised 13 January 2012; accepted 16 January 2012) Archives of Physiology and Biochemistry, 2012; 118(2): 47–57 © 2012 Informa UK, Ltd. ISSN 1381-3455 print/ISSN 1744-4160 online DOI: 10.3109/13813455.2012.659259 Archives of Physiology and Biochemistry Downloaded from informahealthcare.com by University of Calgary on 05/22/12 For personal use only.
Transcript of Activation of aerobic metabolism by Amaranth oil improves heart rate variability both in athletes...
47
Background
Pathogenesis of many chronic illnesses is strongly related to oxidative stress (OS), which is defined as excessive production of free radicals (FR) overwhelming the capacity of antioxidant reserve to withstand increas-ing oxidative damage (Cohen et al., 2007; Eizirik, 2008; Henriksen, 2011; Negre-Salvayre et al., 2010; Sarsour et al., 2009; Weseler and Bast, 2010). However, what is fre-quently not recognized is the intensity of redox reactions, which underlies and determines OS manifestations. Namely, mild and reversible disturbances of oxidative homeostasis are necessary for the maintenance of the optimal pro-/antioxidant balance and the overall oxygen metabolism. These mechanisms underlie widely recog-nized effect of preconditioning or hormesis, stating that moderate activation of FR reactions facilitates assimila-tion of oxidative waste products and improves functional
metabolic potential (Jones, 2006; Mandl, 2009; Manoli et al., 2007; Packer, 2007; Tymochko et al., 1998; Voeikov et al., 2009). There is accumulating evidence that the hor-metic response is achieved not only because a wide range of antioxidant signalling pathways is being initiated, but also because production of endogenous oxygen in FR reactions takes place. Higher intensity of redox reactions is associated with more frequent oscillations in endog-enous oxygen production, improvement in oxygenase/oxydase reactions balance and subsequently better self-regulation of the living system (Tymochko et al., 1998).
In the present study we aimed to achieve desirably mild pro-oxidant activity (hormetic effect) in diabetic patients and in healthy athletes, giving them the oil derived from the seeds of Amaranthus cruentus L., which has been demonstrated to have numerous metabolic effects (Martirosyan et al., 2007; Sirota et al., 2008; Yelisyeyeva
original arTiClE
Activation of aerobic metabolism by Amaranth oil improves heart rate variability both in athletes and patients with type 2 diabetes mellitus
Olha Yelisyeyeva1, Khrystyna Semen1, Neven Zarkovic2, Danylo Kaminskyy1, Olexander Lutsyk1, and Volodymyr Rybalchenko3
1Danylo Halytsky Lviv National Medical University, Lviv, Ukraine, 2Rudjer Boskovic Institute, Zagreb, Croatia, and 3Taras Shevchenko National University of Kyiv, Ukraine
abstractThe aim of present research was to study the effects of Amaranth oil (AmO) supplementation on aerobic metabolism and heart rate variability (HRV) in type 2 diabetes mellitus patients and in athletes. Several parameters of aerobic metabolism and HRV were assessed. Supplementation with AmO caused mild pro-oxidant activity resulting in improved uptake of oxidative destruction products and modulation of catalase and SOD activity with subsequent development of an antioxidant effect. These findings were very distinct in athletes but less pronounced in diabetics. Redistribution of haemoglobin ligands in athletes indicates involvement of haemoproteins in free radical reactions during AmO supplementation. Improvement in HRV by daily consumption of AmO as observed in both study groups suggested increased production of endogenous oxygen and enhancement of the cardio-respiratory function. The advantage of activation of aerobic metabolism in OS-related disorders resulting in improved self-organization of the living system and hormetic reaction mechanisms are discussed.
Keywords: Amaranth oil, aerobic metabolism, heart rate variability, correlations, metabolic syndrome, type 2 diabetes mellitus, athletes, hormesis, oxidative stress correction
Address for Correspondence: Yelisyeyeva Olha, Department of Histology, Cytology and Embryology Danylo Halystky Lviv National Medical University, Lviv, Ukraine; 69, Pekarska str., Lviv, 79010, Ukraine. E-mail: [email protected]
(Received 02 December 2011; revised 13 January 2012; accepted 16 January 2012)
Archives of Physiology and Biochemistry, 2012; 118(2): 47–57© 2012 Informa UK, Ltd.ISSN 1381-3455 print/ISSN 1744-4160 onlineDOI: 10.3109/13813455.2012.659259
Archives of Physiology and Biochemistry
118
2
47
57
02December2011
13January2012
16January2012
1381-3455
1744-4160
© 2012 Informa UK, Ltd.
10.3109/13813455.2012.659259
2012
Activation of aerobic metabolism by Amaranth oil improves heart rate variability
O. Yelisyeyeva et al.
Arc
hive
s of
Phy
siol
ogy
and
Bio
chem
istr
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Cal
gary
on
05/2
2/12
For
pers
onal
use
onl
y.

48 O. Yelisyeyeva et al.
Archives of Physiology and Biochemistry
et al., 2008a). These are considered to be mostly due to the high content of linoleic acid and several other minor components, such as, squalene, tocotrienols, tocoph-erols and phytosterins (Gamel, 2007; Kaminskyy et al., 2002). The presence of conjugated double bounds allows these substances to act simultaneously as active modu-lators of FR reactions and as inducers of the antioxidant defence (AOD).
Diabetes mellitus (DM) is an increasingly recognized illness caused by insulin deficiency associated with hyperglycaemia, metabolic misbalance and dysfunction of vital organs. Currently, it is believed, that destabiliza-tion of lipid bilayers, distortion of transmembrane phos-pholipid asymmetry and the resulting change in activity of membrane-bound enzymes underlie multiple cellular disorders and insulin resistance associated with progres-sive oxidative destruction (Bochkov et al., 2010; Chang, 2010). Signs of OS in DM are prominent and require complex and long-term correction. Interestingly, OS can develop also in athletes experiencing continuous physi-cal overload (Bosquet et al., 2008; Fisher-Wellman, 2009; Kaikkonen et al., 2010; Radak et al., 2008; Yelisyeyeva et al., 2008a). Hence, comparing these two pathophysi-ologically opposite groups of subjects with OS it should be kept in mind that similar OS signs are attributed to different functional reserves and intensity of redox reac-tions. Namely, drastic decrease in the redox reactions intensity in diabetes and persisting hyperglycaemia promote mechanisms of glucose auto-oxidation and oxi-dative non-enzymatic glycosylation of proteins with sub-sequent accumulation of poorly degradable advanced glycation end-products (Angulo, 2002; Chang, 2010; Ellis, 2007; Negre-Salvayre et al., 2009; Sarsour et al., 2009) worsening further redox imbalance, which does not hap-pen in elite healthy athletes under exhaustive physical load.
Taking into account jeopardy of the avalanche-like branching nature of FR reactions it is extremely impor-tant to use fast and simple analytical diagnostic methods that could rapidly assess changes of the O
2-dependent
metabolism and give information about functional metabolic state of an organism. In this regard, heart rate variability (HRV), which is a modern non-invasive diagnostic tool, reflecting physiological and biochemical regulatory mechanisms can be used (Aubert et al., 2003; Heart, 1996; Lahiri, 2008). It is well known, that heart rate is regulated by the autonomic nervous system, which, in turn, depends upon central nervous and endocrine systems. Thus, functional activity of the pacemaker cells of the sinoatrial node is regulated by the ability of the metabolic system to maintain such integrative homeo-static constants as рО
2, рН, рСО
2 in blood, as well as,
Δμ of the membranes (Del Rio et al., 2010; Mangoni, 2008). On the other hand, their resulting influence on the sinoatrial node could reflect activity of the aerobic metabolism (Yelisyeyeva et al., 2005). There is increasing data proving close relationships between HRV and some metabolic parameters (Connes et al., 2008; Haensel et al.,
2008; Semen et al., 2010). Moreover, it seems likely that improvement of aerobic metabolism and OS resistance and development of higher HRV are closely connected with similar biochemical mechanisms being involved.
Therefore, the aim of present research was to study the effects of Amaranth oil (AmO) supplementation on aerobic metabolism and heart rate variability in type 2 diabetes mellitus patients and in athletes.
Materials and methods
Thirty six patients with verified type 2 DM (aged 57 ± 7 years, male 20 (55.6%), female 16 (44.4%)) were enrolled into the study. Body mass index ranged from 26 to 30 kg/m2 in 22 (61.1%) subjects and from 30 to 35 kg/m2 in 14 (38.9%). The disease duration ranged from 1 to 10 years: 18 (50%) subjects had 1 to 5 years history of diabetes and 18 (50%) were ill from 6 to 10 years. All patients were diagnosed with moderately severe diabetes (by European Diabetes Policy Group, 1998) with fasting glucose 6.7 ± 1.4 mmol/L and Hb
A1c 7.76 ± 0.83%. Signs of retinopathy
were observed in 16 (44.4%) subjects, nephropathy in six (16.7%), subclinical neuropathy in 15 (41.6%) patients. Exclusion criteria included macro-angiopathic com-plication of diabetes, arrhythmia excluding occasional extrasystole, congestive heart failure, liver disorders classified as class B or C by Child-Pugh score. Before inclusion and during the study patients had a compen-sated course of DM and were taking standard therapy including stable doses of oral hypoglycaemic agents (biguanides or sulfonylureas), anti-hypertensive (ACE-inhibitors) and lipid lowering drugs (statins). As a com-parison group served 24 national level athletes (aged 22 ± 3 years, male 16 (66.7%), female 8 (33.3%)) with body mass index ranging from 18 to 22 kg/m2. Enrolment of the athletes into the study as the controls was reasoned by the fact that they also had signs of OS, which, however, were associated with higher functional metabolic reserve (Bosquet et al., 2008; Kaikkonen et al., 2010; Yelisyeyeva et al., 2008a), opposite to the DM patients.
Athletes were not participating in any competitions, had no injuries or diseases and were continuing their usual training regimen for one week before and during the study. All investigations and blood samplings were performed on the first day and at the end of the study (28 ± 2 days for DM subjects, 22 ± 2 days for athletes) in the morning hours between 9 a.m. and 11 a.m. before a meal. Informed consent was obtained before enrolment. Design of the study was approved by the Local Ethics Committee of the Danylo Halytsky Lviv National Medical University.
Preparation of Amaranth oil and regimen of administrationLipid fraction from the seeds of Amaranthus cruentus L. was obtained with the method of vacuum CO
2 cold
extraction by “NVO Danika” (Kharkiv, Ukraine). One mil-lilitre of concentrated AmO was administered orally once
Arc
hive
s of
Phy
siol
ogy
and
Bio
chem
istr
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Cal
gary
on
05/2
2/12
For
pers
onal
use
onl
y.

Activation of aerobic metabolism by Amaranth oil improves heart rate variability 49
© 2012 Informa UK, Ltd.
a day in the evening at least two hours after meal for 28 ± 2 days for DM subjects and for 22 ± 2 days for athletes. Slightly unequal duration of the AmO treatment between the two groups (6 days) was caused by sudden profes-sional engagements of these athletes, which limited their availability for the study. However, due to the fact that already after 3 weeks of treatment the results were obvious this obstacle did not prevent successful end-ing of the study. The fatty acid composition of AmO was as follows: palmitic acid (С
16:0) 18%, linoleic acid (С
18:2)
41%, oleic acid (С18:1
) 37%. It also contained squalene – 3% and minor components of AmO included carot-enoids – 40 mg%; tocopherols and tocotrienols – 94.5 mg% (Kaminskyy et al., 2002).
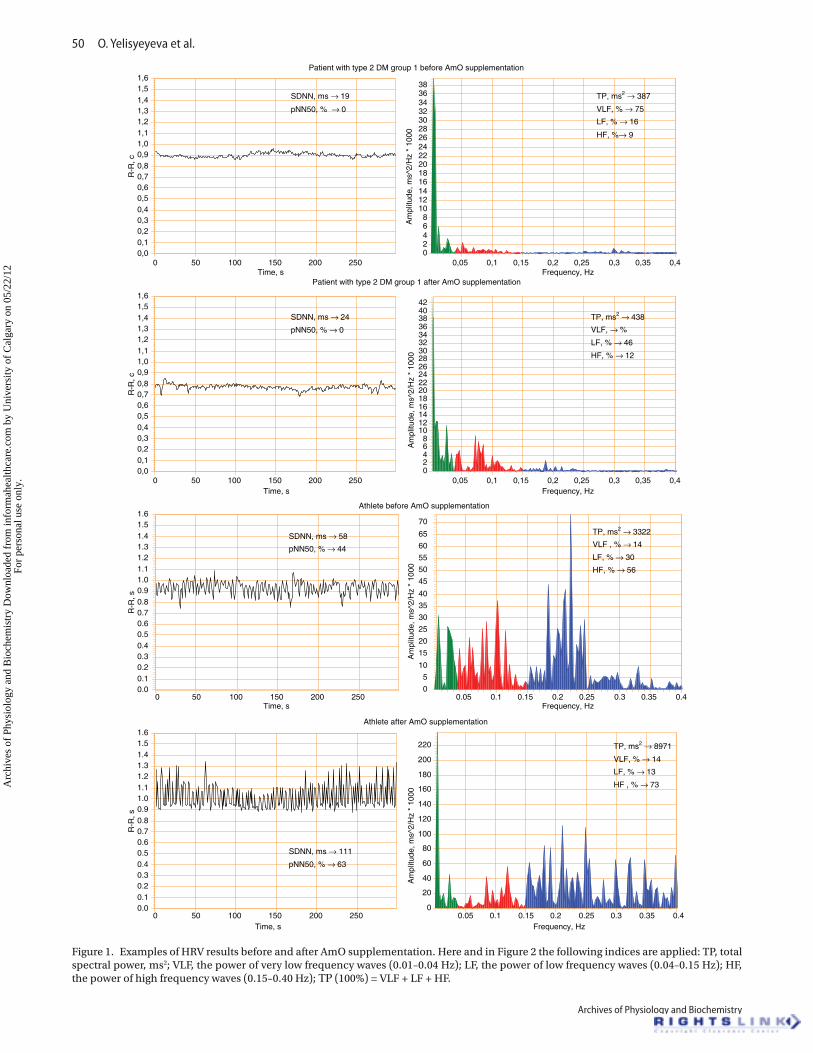
Study of heart rate variabilityDuring quiet wakefulness, not less than 24 hours after the last training, the short-time records of ECG were per-formed using computer electrocardiograph “VNS-Micro” (Neurosoft®, Russia). After 20 minutes of rest, subjects were asked to stay supine quietly for 5 minutes for station-ary condition HRV recording; afterwards they were asked to stand up rapidly and they remained in the standing position for 6 minutes (orthostatic test). RR intervals were determined with a sampling frequency of 2 kHz and were analysed with “Poly-Spectrum” (Neurosoft®, Russia) soft-ware designed according to HRV standards (Heart, 1996). The time-domain indices such as standard deviation of normal RR intervals (SDNN) and percentage of differ-ences between adjacent normal RR intervals exceeding 50 milliseconds (pNN50) were determined. In the presence of normal sinus rhythm and normal atrio-ventricular-nodal function, each of these measurements quantifies parasympathetic regulation of normal RR intervals. The power spectral analysis was performed sequentially with a fast Fourier transformation. The following frequency-domain variables were studied: total power (TP, 0.01 to 0.40 Hz, quantifies regulation of the heart rate in general), high frequency power (HF, 0.15 to 0.40 Hz, reflects pre-dominantly vagal regulation), low frequency power (LF, 0.04 to 0.15 Hz, reflects sympathetic and parasympathetic regulation), and very low frequency power (VLF, 0.01 to 0.04 Hz, reflects central regulatory mechanisms). For typi-cal examples obtained see Figure 1.
Spectrophotometrical methodsAerobic metabolism was assessed according to the parameters of lipid peroxidation/antioxidant activity sys-tem and blood haemoproteins as described previously (Semen et al., 2010; Yelisyeyeva et al., 2008).
Catalase (CAT) (EC 1.11.1.6) activity was determined spectrophotometrically (Korolyuk et al., 1998) with absorbance recorded at 410 nm. The method was based on the ability of hydrogen peroxide to produce stable coloured complexes with ammonium molybdate.
Superoxide dismutase (SOD) (EC 1.15.1.1) activity was assessed by its ability to dismutate superoxide pro-duced during quercetin auto-oxidation in an alkaline
medium (pH = 10.0) (Kostyuk et al., 1990), with absor-bance measured at 406 nm.
Lipid peroxidation products were assayed as ‘thio-barbituric acid reactive species’ (TBARS) (Timirbulatov and Seleznev, 1986). The method is based on induction of lipid peroxidation by iron with the subsequent produc-tion of the coloured complex (predominantly of malonic dialdehyde) with thiobarbituric acid. Absorbance was determined at 532 nm.
Oxidatively modified proteins (OMP) were measured by the reaction between the oxidized carbonyl amino-acid residues and 2,4-dinitrophenylhydrazine (2,4-DNFH) with formation of 2,4-dinitrohydrazones, which were determined spectrophotometrically (Dubinina et al., 1995) at 370 nm.
Determination of conjugated dienes was based on the measurement of absorbance of the lipid phase after its extraction in heptane/isopropanol system at 233 nm (Kamyshnikov, 2000).
The level of β-LP was determined by the turbidimetric assay with spectrophotometric completion (at 700 nm) (Kamyshnikov, 2000). In the presence of CaCl
2 and hepa-
rin the colloid protein stability is affected, which causes the precipitation of β- and pre-β-lipoproteins with the development of insoluble heparin complex (turbid dis-persed solution is formed). The amount of β-LP was cal-culated from the difference of absorbance values (before and after heparin), multiplied by 100. С = (D
2 − D
1)*100,
where С, amount of β-LP, in CU; D2, absorbance of the
turbid solution after reaction with heparin; D1, absor-
bance of the solution before reaction. Normal values of β-LP range from 35 to 55 CU.
The level of haemoglobin (Hb) and its ligands (oxyHb-, carboxyHb, sulfHb, and metHb) were determined by the simultaneous analysis method using absorptive spectros-copy as proposed by (Bilyi et al., 1998). Spectrophotometrical measurement of multi-component solutions was based on the Beer–Lambert–Bouguer law and requires the precise determination of absolute values of molar indices for each solution component. The absorbance of a sample was stud-ied at the following wavelengths: 577.4 nm (for HbO
2); 569.5
nm (for HbCO); 620.3 nm (for SHb); 500.0 nm (for metHb). Percentage of HbNO was not determined due to the limita-tions of the method. The concentration of haemoglobin is expressed in g/L, ligand Hb forms of each sample are given in %. For calculations the inverse matrix of absorbance at the chosen wavelengths, transmission density, and com-plex of formulations were used (Bilyi et al., 1998).
Statistical analysisAll data were processed using the statistical package STATISTICA 6.0. Normal distribution of the obtained val-ues was confirmed with Shapiro–Wilk’s W-test. Normally distributed data were presented as means ± standard error mean (M ± SEM) and compared by t-test for dependent and independent variables. Abnormally dis-tributed parameters were processes by nonparametric Mann–Whitney U-test. The linear correlation coefficient
Arc
hive
s of
Phy
siol
ogy
and
Bio
chem
istr
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Cal
gary
on
05/2
2/12
For
pers
onal
use
onl
y.
50 O. Yelisyeyeva et al.
Archives of Physiology and Biochemistry
Patient with type 2 DM group 1 before AmO supplementation
250200150100500
R-R
, c
1,61,51,41,31,21,11,00,90,80,70,60,50,40,30,20,10,0
0,40,350,30,250,20,150,10,05
Am
plitu
de, m
s^2/
Hz
* 10
00
38363432302826242220181614121086420
Patient with type 2 DM group 1 after AmO supplementation
Time, s250200150100500
R-R
, c
1,61,51,41,31,21,11,00,90,80,70,60,50,40,30,20,10,0
0,40,350,30,250,2Frequency, Hz
Time, s Frequency, Hz
0,150,10,05
Am
plitu
de, m
s^2/
Hz
* 10
00
424038363432302826242220181614121086420
Athlete before AmO supplementation
Time, s250200150100500
R-R
, s
1.61.51.41.31.21.11.00.90.80.70.60.50.40.30.20.10.0
Frequency, Hz0.40.350.30.250.20.150.10.05
Am
plitu
de, m
s^2/
Hz
* 10
00
70
65
60
55
50
45
40
35
30
25
20
15
10
5
0
Athlete after AmO supplementation
Time, s250200150100500
R-R
, s
1.61.51.41.31.21.11.00.90.80.70.60.50.40.30.20.10.0
Frequency, Hz0.40.350.30.250.20.150.10.05
Am
plitu
de, m
s^2/
Hz
* 10
00
220
200
180
160
140
120
100
80
60
40
20
0
SDNN, ms → 19
pNN50, % → 0
TP, ms2 → 387
VLF, % → 75
LF, % → 16
HF, %→ 9
SDNN, ms → 24
pNN50, % → 0TP, ms2 → 438
VLF, → %
LF, % → 46
HF, % → 12
SDNN, ms → 58
pNN50, % → 44
TP, ms2 → 3322
VLF , % → 14
LF, % → 30
HF, % → 56
SDNN, ms → 111
pNN50, % → 63
TP, ms2 → 8971
VLF, % → 14
LF, % → 13
HF , % → 73
Figure 1. Examples of HRV results before and after AmO supplementation. Here and in Figure 2 the following indices are applied: TP, total spectral power, ms2; VLF, the power of very low frequency waves (0.01–0.04 Hz); LF, the power of low frequency waves (0.04–0.15 Hz); HF, the power of high frequency waves (0.15–0.40 Hz); ТР (100%) = VLF + LF + HF.
Arc
hive
s of
Phy
siol
ogy
and
Bio
chem
istr
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Cal
gary
on
05/2
2/12
For
pers
onal
use
onl
y.

Activation of aerobic metabolism by Amaranth oil improves heart rate variability 51
© 2012 Informa UK, Ltd.
(r) and its p level were calculated to estimate relation-ships between HRV and oxygen metabolism parameters (p < 0.05 was considered as significant) (MATLAB version R2006a).
results
The study of HRV in type 2 diabetes patients demon-strated a wide range of individual values with TP rang-ing from 200 ms2 to 1200 ms2. Among them those with dramatically low HRV (TP ≤ 400 ms2) were assigned into very low resistance group 1, while low resistance group 2 comprised the individuals with slightly higher HRV (TP > 400 ms2). Regional and national level athletes with TP ranging from 3500 ms2 to 7000 ms2 formed group 3.
We found that the very low resistance group 1 even-tually comprised mostly patients with long duration of the disease (more than 5 years) and with more promi-nent clinical manifestations of diabetes. The VLF band was dominating in the HRV spectrum (59.5%) in this group suggesting malfunction of central regulatory mechanisms. Their autonomic balance (LF/HF) showed sympathetic predominance (Table 1). During the ortho-static test nearly twofold increase in TP and autonomic bands associated with fourfold elevation of LF/HF index were demonstrated in this group (Figure 2). Patients with higher HRV, comprising the low resistance group 2 had predominantly shorter course of the disease (less than 5 years) and were found with similar structure of HRV spectrum both in supine and orthostatic position (Table 1, Figure 2).
The HRV of the athletes differed from that of diabetic patients by higher indices of TP accompanied by low activity of VLF band (26.8%) and increased vagal activ-ity (HF = 42.8%). Moreover, index of autonomic balance (LF/HF) in this group showed slight parasympathetic predominance in clinostasis. During the orthostatic test lowering of TP with high sympathetic and slightly dimin-ished vagal activity was found (Table 1, Figure 2).
The study of aerobic metabolism found prominent signs of OS in diabetic patients from both groups and much less significant manifestation in athletes (Figure 3).
In particular, markedly increased levels of the oxidative destruction products (TBARS, ОМP, conjugated dienes, β-lipoproteins) in the groups 1 and 2 in comparison to respective values in healthy volunteers (Yelisyeyeva et al., 2008a; Semen et al., 2010) were associated with increased activity of catalase. It is worth noting, that both groups of patients showed significantly elevated OMP levels (more than twofold higher than that of healthy subjects), while TBARS level in athletes was even slightly lower than control values. Such findings suggest possible convenience of OMP as an OS marker, which might be even better than TBARS.
The use of AmO was accompanied by an increase in HRV time and frequency domain indices, most prominent in athletes group (Table 1). Interestingly, the increase in TP in group 1 was 180 ms2, in group 2 – 394
Table 1. Influence of AmO on HRV in supine position in type 2 DM patients and in athletes.
Parameters
Very low resistance DM patients (group 1, ТР ≤ 400), n = 18
Low resistance DM patients (group 2, TP > 400), n = 18 Athletes (group 3), n = 24
1 2 1 2 1 2SDNN, ms 16 ± 1 29 ± 4* 26 ± 1 30 ± 2* 69 ± 6 78 ± 7*pNN50, % 0.09 ± 0.05 0.97 ± 0.33* 1.5 ± 0.7 3.1 ± 1.5 35 ± 4 42 ± 4*TP, ms2 311 ± 17 491 ± 66 779 ± 34 1174 ± 167* 5430 ± 1049 6905 ± 1113*VLF, ms2 185 ± 12 289 ± 37* 396 ± 41 577 ± 50* 1456 ± 302 1363 ± 146LF, ms2 82 ± 12 142 ± 34 242 ± 28 366 ± 76* 1649 ± 453 2390 ± 639*HF, ms2 44 ± 5 60 ± 13 141 ± 32 231 ± 72* 2324 ± 487 3153 ± 537LF/HF 2.3 ± 0.4 2.6 ± 0.3 2.2 ± 0.2 2.4 ± 0.3 0.8 ± 0.1 0.8 ± 0.1The values are given as mean ± SEM. Note: 1, before; 2, after AmO use. *Difference before and after AmO supplementation is significant (p < 0.05); ms, milliseconds; SDNN, standard deviation of normal RR intervals; pNN50, the percent of RR intervals with the difference of more than 50 ms between consecutive cardiac intervals; TP, total spectral power, ms2; VLF, the power of very low frequency waves (0.0–0.04 Hz); LF, the power of low frequency waves (0.04–0.15 Hz); HF, the power of high frequency waves (0.15–0.40 Hz); TP (100%) = VLF + LF + HF.
Figure 2. Influence of AmO on HRV in standing position in type 2 DM patients and in athletes. Note: difference before and after AmO supplementation was significant only for HF in group 1 DM patients and in athletes (p < 0.05).
Arc
hive
s of
Phy
siol
ogy
and
Bio
chem
istr
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Cal
gary
on
05/2
2/12
For
pers
onal
use
onl
y.
52 O. Yelisyeyeva et al.
Archives of Physiology and Biochemistry
ms2, whilst in athletes from group 3 it reached 1476 ms2. Moreover, AmO supplementation in DM patients caused significant increase in VLF associated with the activity of central regulatory mechanisms with insufficient activa-tion of the sympathetic nervous system and worsening of the autonomic balance. Such results of AmO supplemen-tation support our previous findings demonstrating pro-gressive HRV worsening in diabetic patients, who did not use antioxidants in complex therapy (Yelisyeyeva et al., 2005). Increase in HRV in athletes was achieved through activation of the autonomic components with limited involvement of central regulatory mechanisms (decrease in VLF band).
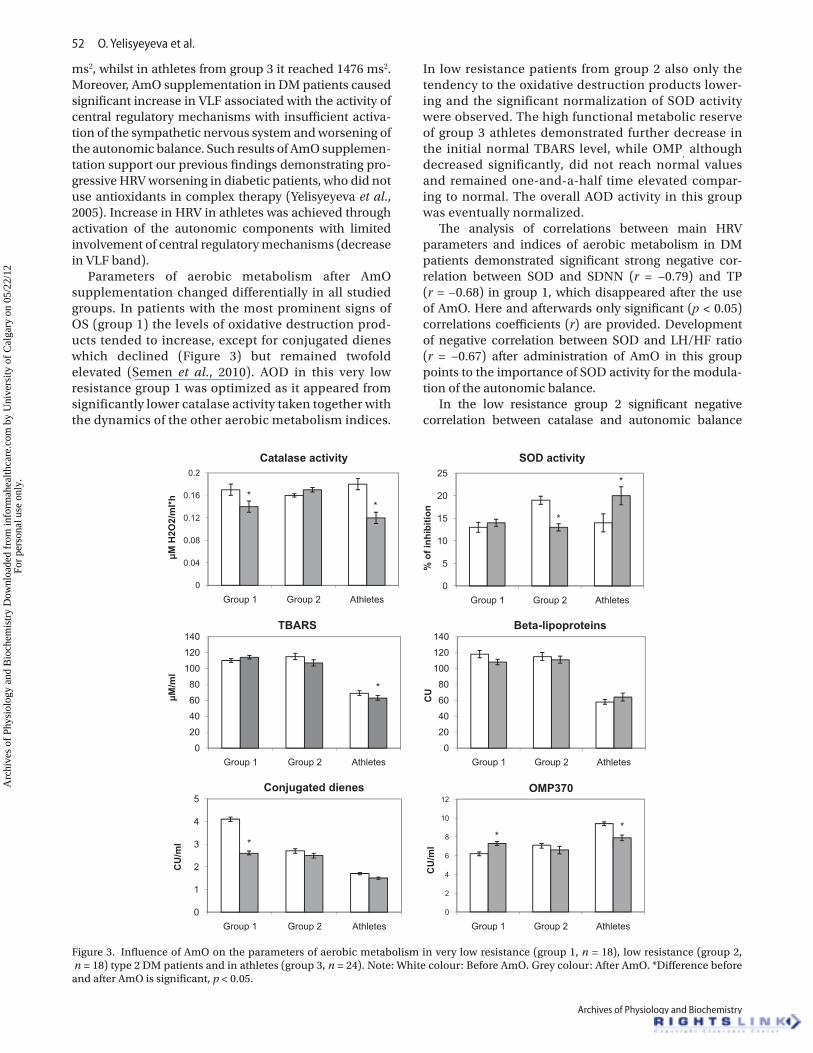
Parameters of aerobic metabolism after AmO supplementation changed differentially in all studied groups. In patients with the most prominent signs of OS (group 1) the levels of oxidative destruction prod-ucts tended to increase, except for conjugated dienes which declined (Figure 3) but remained twofold elevated (Semen et al., 2010). AOD in this very low resistance group 1 was optimized as it appeared from significantly lower catalase activity taken together with the dynamics of the other aerobic metabolism indices.
In low resistance patients from group 2 also only the tendency to the oxidative destruction products lower-ing and the significant normalization of SOD activity were observed. The high functional metabolic reserve of group 3 athletes demonstrated further decrease in the initial normal TBARS level, while OMP
, although
decreased significantly, did not reach normal values and remained one-and-a-half time elevated compar-ing to normal. The overall AOD activity in this group was eventually normalized.
The analysis of correlations between main HRV parameters and indices of aerobic metabolism in DM patients demonstrated significant strong negative cor-relation between SOD and SDNN (r = −0.79) and TP (r = −0.68) in group 1, which disappeared after the use of AmO. Here and afterwards only significant (р < 0.05) correlations coefficients (r) are provided. Development of negative correlation between SOD and LH/HF ratio (r = −0.67) after administration of AmO in this group points to the importance of SOD activity for the modula-tion of the autonomic balance.
In the low resistance group 2 significant negative correlation between catalase and autonomic balance
Figure 3. Influence of AmO on the parameters of aerobic metabolism in very low resistance (group 1, n = 18), low resistance (group 2, n = 18) type 2 DM patients and in athletes (group 3, n = 24). Note: White colour: Before AmO. Grey colour: After AmO. *Difference before and after AmO is significant, p < 0.05.
Arc
hive
s of
Phy
siol
ogy
and
Bio
chem
istr
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Cal
gary
on
05/2
2/12
For
pers
onal
use
onl
y.
Activation of aerobic metabolism by Amaranth oil improves heart rate variability 53
© 2012 Informa UK, Ltd.
index LF/HF (r = −0.82) was seen before administration of AmO. Also negative correlations between the level of β-lipoproteins and SDNN (r = −0.91) and ТР (r = −0.83) were observed vanishing after AmO treatment. Other correlation coefficients were not significant.
In the athletes correlation coefficients predominantly of moderate strength were found between HRV and aerobic metabolism. Before administration of AmO such relationships appeared for SOD (positive with SDNN (r = 0.44), pNN50 (r = 0.72), TP (r = 0.41), HF (r = 0.70)), being negative with LH/HF index (r = −0.48). The TBARS gave negative correlation with SDNN (r = −0.51), pNN50 (r = −0.52), TP (r = −0.47), VLF (r = −0.48). After use of AmO these correlations changed, the SOD correlations disappeared, while new, negative correlations between OMP and HRV were noticed for SDNN (r = −0.48), pNN50 (r = −0.48), TP (r = −0.45), LF (r = −0.45). Similarly, new correlations were observed between activity of catalase and VLF (r = −0.42), β-lipoproteins and pNN50 (r = −0.46). Correlations between TBARS and HRV remained negative, further increasing after administra-tion of AmO (SDNN (r = −0.55), pNN50 (r = −0.59), TP (r = −0.54), VLF (r = −0.41), HF (r = −0.55)).
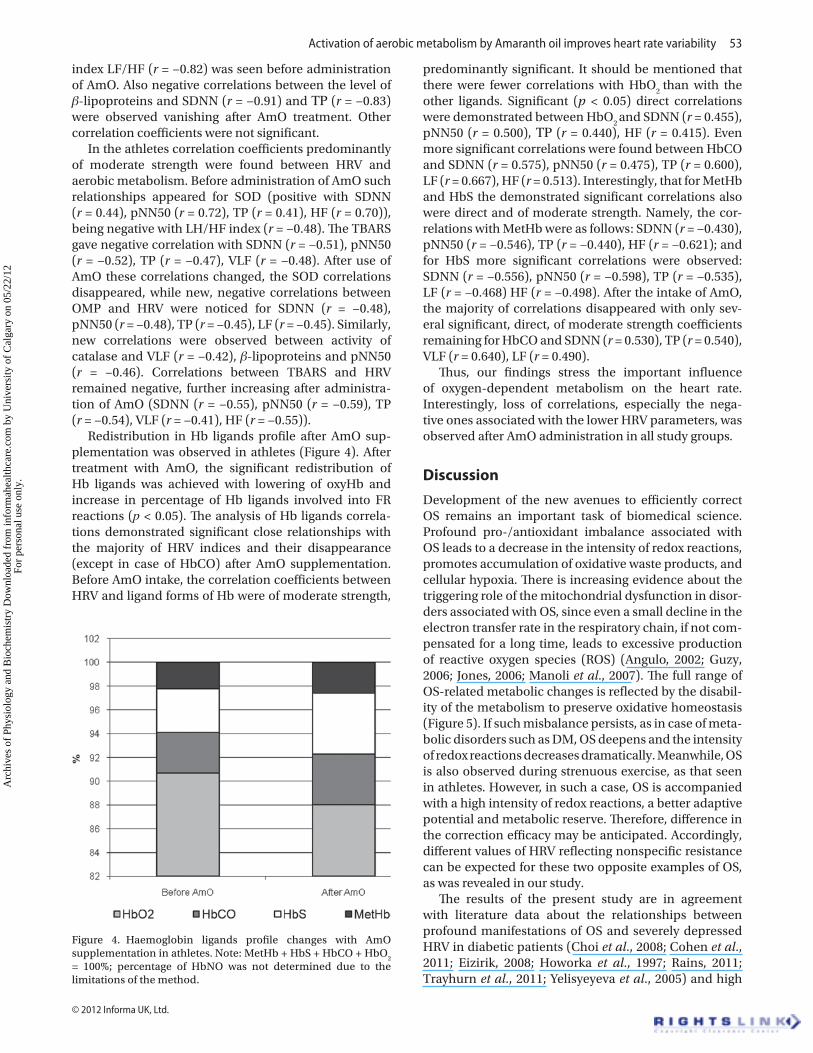
Redistribution in Hb ligands profile after AmO sup-plementation was observed in athletes (Figure 4). After treatment with AmO, the significant redistribution of Hb ligands was achieved with lowering of oxyHb and increase in percentage of Hb ligands involved into FR reactions (р < 0.05). The analysis of Hb ligands correla-tions demonstrated significant close relationships with the majority of HRV indices and their disappearance (except in case of HbCO) after AmO supplementation. Before AmO intake, the correlation coefficients between HRV and ligand forms of Hb were of moderate strength,
predominantly significant. It should be mentioned that there were fewer correlations with HbO
2 than with the
other ligands. Significant (p < 0.05) direct correlations were demonstrated between HbO
2 and SDNN (r = 0.455),
pNN50 (r = 0.500), ТР (r = 0.440), HF (r = 0.415). Even more significant correlations were found between HbCO and SDNN (r = 0.575), pNN50 (r = 0.475), TP (r = 0.600), LF (r = 0.667), HF (r = 0.513). Interestingly, that for MetHb and HbS the demonstrated significant correlations also were direct and of moderate strength. Namely, the cor-relations with MetHb were as follows: SDNN (r = −0.430), pNN50 (r = −0.546), TP (r = −0.440), HF (r = −0.621); and for HbS more significant correlations were observed: SDNN (r = −0.556), pNN50 (r = −0.598), TP (r = −0.535), LF (r = −0.468) HF (r = −0.498). After the intake of AmO, the majority of correlations disappeared with only sev-eral significant, direct, of moderate strength coefficients remaining for HbCO and SDNN (r = 0.530), TP (r = 0.540), VLF (r = 0.640), LF (r = 0.490).
Thus, our findings stress the important influence of oxygen-dependent metabolism on the heart rate. Interestingly, loss of correlations, especially the nega-tive ones associated with the lower HRV parameters, was observed after AmO administration in all study groups.
Discussion
Development of the new avenues to efficiently correct OS remains an important task of biomedical science. Profound pro-/antioxidant imbalance associated with OS leads to a decrease in the intensity of redox reactions, promotes accumulation of oxidative waste products, and cellular hypoxia. There is increasing evidence about the triggering role of the mitochondrial dysfunction in disor-ders associated with OS, since even a small decline in the electron transfer rate in the respiratory chain, if not com-pensated for a long time, leads to excessive production of reactive oxygen species (ROS) (Angulo, 2002; Guzy, 2006; Jones, 2006; Manoli et al., 2007). The full range of OS-related metabolic changes is reflected by the disabil-ity of the metabolism to preserve oxidative homeostasis (Figure 5). If such misbalance persists, as in case of meta-bolic disorders such as DM, OS deepens and the intensity of redox reactions decreases dramatically. Meanwhile, OS is also observed during strenuous exercise, as that seen in athletes. However, in such a case, OS is accompanied with a high intensity of redox reactions, a better adaptive potential and metabolic reserve. Therefore, difference in the correction efficacy may be anticipated. Accordingly, different values of HRV reflecting nonspecific resistance can be expected for these two opposite examples of OS, as was revealed in our study.
The results of the present study are in agreement with literature data about the relationships between profound manifestations of OS and severely depressed HRV in diabetic patients (Choi et al., 2008; Cohen et al., 2011; Eizirik, 2008; Howorka et al., 1997; Rains, 2011; Trayhurn et al., 2011; Yelisyeyeva et al., 2005) and high
Figure 4. Haemoglobin ligands profile changes with AmO supplementation in athletes. Note: MetHb + HbS + HbCO + HbO
2
= 100%; percentage of HbNO was not determined due to the limitations of the method.
Arc
hive
s of
Phy
siol
ogy
and
Bio
chem
istr
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Cal
gary
on
05/2
2/12
For
pers
onal
use
onl
y.

54 O. Yelisyeyeva et al.
Archives of Physiology and Biochemistry
HRV in athletes (Aubert et al., 2003; Iellamo et al., 2002; Yelisyeyeva et al., 2008a). Because, some of diabetic patients in this study showed critically low HRV (TP ≤ 400 ms2), they were identified as very low resistance group 1 for further discussion. These subjects had longer disease duration (5–10 years), the most prominent clini-cal manifestations, and the lowest adaptive potential and resistance to OS. Analysis of their aerobic metabo-lism parameters revealed significant disorders in the pro-/antioxidant balance (twofold increase of TBARS, fourfold increase in conjugated dienes, and the three-fold increase in the amount of β-lipoproteins, together with shifts in the activity of catalase and SOD, which are indicative for chronic severe OS in this group. The other diabetic patients i.e. with a shorter disease duration (up to 5 years) and less prominent clinical manifesta-tions demonstrated slightly higher HRV (ТР > 400 ms2) and were classified as low resistance group 2. Similar to group 1 these patients had significant disorders in the pro-/antioxidant balance. However, they showed only twofold increase in conjugated dienes and had an increased SOD activity which suggests a less prominent OS and consequently a slightly higher intensity of redox reactions.
In the athletes the signs of OS (according to the level of OMP and conjugated dienes) were also shown, but they were accompanied with substantially higher HRV. Disorders of pro-/antioxidant balance in athletes are attributed to insufficient ability of redox processes to control excessive ROS flow caused by physical overload (Aubert et al., 2003; Iellamo et al., 2002; Kaikkonen et al., 2010; Martinmäki and Rusko, 2008; Radak et al., 2008; Yelisyeyeva et al., 2008a). Such OS is not health endan-gering as was also observed in our study since the level of TBARS remained low while activity of catalase and SOD were elevated. High OMP level, which is generally recog-nized as an OS marker, in this group was associated with high HRV and allowed the assumption that it reflects the activity of signalling pathways and production of the wide range of AOD proteins necessary for the efficient maintenance of the mobilization phase of adaptation or the hormetic response.
The dependence of the heart pace-making activity and HRV upon the functional metabolic potential of the organism is being more and more widely discussed (Del Rio et al., 2010; Heart, 1996; Lahiri, 2008; Mangoni, 2008; Semen et al., 2010; Yelisyeyeva et al., 2005). Therefore, activation of aerobic metabolism aimed at correction of OS could be adequately reflected by HRV indices, as was done in our study using the AmO that was shown to induce mild pro-oxidant activity and beneficiary influence aerobic metabolism (Sirota et al., 2008; Yelisyeyeva et al., 2008a, Martirosyan et al., 2007). It serves as a source of PUFAs (up to 50% of linoleic acid) and contains minor components such as carotenoids, tocopherols, tocotrienols, and 3–8% of squalene, which is involved into the synthesis of cholesterol, biologically active steroids, ubiquinone (Gamel, 2007; Kaminskyy et al., 2002; Mattson, 2008; Stuchlik and Zak, 2002). Double bonds in oil components might take a part in FR reactions and provide ω3-mimetic activity of AmO (Das, 2000). Moreover, squalene is able to replace lipid structures in the membranes and to act as superoxide anion scavenger during the FR destruction (Kaminskyy et al., 2002; Martirosyan et al., 2007; Shin et al., 2004). Tocotrienols provide antiradical defence which is even better than that of tocopherols (Sen, 2007). Moreover, they have the unique ability to decrease production of thromboxane B
2 and platelet aggregation factor,
activate proteasomes, and to exhibit cardioprotective effects during ischemia-reperfusion injury (Valko et al., 2007).
AmO increases the amount of С20:5
and С22:6
(ω3 PUFAs) and thus ω3/ω6 ratio in the membranes (Martirosyan et al., 2007) promotes modulation of the eicosanoids syn-thesis with more intensive production of another potent anti-platelet substance – prostacyclin I
3 derived from
eicosapentaienic acid (С20:5
) and, as a result, increases the PGI
3/TXA
2 ratio. On the other hand, in the presence
of С18:2
Hb acquires quasilipoxygenase properties and induces its oxidation by the lipoxygenase pathway (Kuhn et al., 1981). This, in turn, facilitates accumulation of
Figure 5. Changes of main homeostatic constants and biochemical processes involved into development of oxidative stress in DM and exhaustive physical exercise. Mitochondrial dysfunction is a primary event involved in the onset of OS. A decrease in the velocity of the electron transfer in the respiratory chain causes leakage of electrons with subsequent production of superoxide, which is further promoted by activation of mitochondrial uncoupling proteins. Consequently, a switch of the mitochondrial function from ATP-synthesis to excessive ROS generation, resulting in significant oxidative damage to lipids, proteins, and nucleic acids occurs. Deficit of ATP, lowering of the membrane potential (Δµ), and spread of oxidative destruction to all membrane structures and biologically active environments change their physical chemical properties (colloid state) by increasing their viscosity and coagulation. This, in turn, results in decrease in the activity of the microsomal and peroxisomal oxidation, shift in the pro-/antioxidant balance to the left, accumulation of oxidative waste products, cellular hypoxia, and exhaustion of AOD. Importantly, under such circumstances pro-inflammatory signalling path-ways (р38MAPK/PI3, NFkB/Nrf2, SREBR-1/PPARs, etc) are also activated. Finally, an inability to maintain main biochemical constants (pO, pH, pCO
2, ATP/ADP, NADH/NAD+, ω3/ω6 PUFAs)
with time will lead to progressive decrease in the intensity of redox reactions and worsening of OS signs.
Arc
hive
s of
Phy
siol
ogy
and
Bio
chem
istr
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Cal
gary
on
05/2
2/12
For
pers
onal
use
onl
y.

Activation of aerobic metabolism by Amaranth oil improves heart rate variability 55
© 2012 Informa UK, Ltd.
signalling lipid peroxidation end-products, as, for exam-ple, 4-hydroxy-2,3-trans-nonenal (4-HNE) (Cherkas et al., 2009; Cohen et al., 2011; Eckardt et al., 2008; Sasson et al., 2006; Zarkovic, 2003). Because 4-HNE is a potent chemo-attractant, even a slight increase in its amount activates chemotaxis of granulocytes and promotes mild pro-oxidation in particular in the tissues affected by OS. It was shown, that С
18:2, as well as 4-HNE (a product of С
18:2
peroxidation) is a PPAR ligands (Riahi et al., 2010) and induce ARE-mediated (antioxidant response element) signalling. The latter results in induction of hemoxygen-ase and many other antioxidant enzymes (Wang, 2009), which could be an additional mechanism for the benefi-cial effects of the AmO. Our preliminary data indicate that AmO contains also vacenic acid (1.8%), which is readily transformed into conjugated linoleic acid (predomi-nantly 9-cis,11-trans-С
18:2) acting as an efficient PPAR
ligand and antioxidant (Churruca, 2009). Simultaneous activation of peroxisomal and mitochondrial oxidation by AmO provides efficient background for pro-oxidant activity required for hormetic effect.
Supplementation with AmO activated aerobic metabo-lism, improved utilization of the oxidation waste products, and caused modulation of the catalase and SOD activity. However, these effects were limited in patients with dia-betes and low intensity of redox reaction and much more pronounced in athletes with higher intensity of redox reactions; i.e. in group 1 and 2 only a tendency to reduce OS signs was noted with the most prominent finding being lowering of conjugated dienes, which contribute to OS persistence. Moreover, only slight improvement of HRV especially in orthostasis was found in both diabetic groups. A serious pro-/antioxidant imbalance and a low intensity of redox reactions were evident in both diabetic groups. In the very low resistance group 1 of the DM patients AmO supplementation abolished the significant correlations between low HRV indices and high beta-LP values. In the low resistance group 2 of the DM subjects significant cor-relations between slightly higher HRV parameters and low activity of SOD were demonstrated before but not after treatment with AmO. Thus, it can be assumed that some level of superoxide production during FR reactions is a necessary mechanism involved in prevention of their dec-rement. Of note is that in case of sluggish redox reactions production of ROS is markedly reduced. At the same time oxidative destruction products cannot be consumed so they accumulate resulting in further inhibition of FR reac-tions, progression of OS and cellular hypoxia.
In athletes the use of AmO triggered more evidently the hormetic response. Decrease in the TBARS level was accompanied by a mild raise in SOD activity after AmO in accordance with the existing functional needs of the metabolic system. Moreover, increase in HRV in athletes after AmO intake was attributed to further activation of the already initially high autonomic components (HF and LF bands), which are closely related with the high intensity redox reactions and ability to maintain main homeostatic constants (pO
2, pH, pCO
2). Correlations
analysis in athletes demonstrated that high HRV indices positively correlated with low TBARS level but significant correlations with SOD activity indicate some metabolic pattern typical for athletes. Administration of AmO influ-enced this, as was shown by disappearance of correlation between SOD and HRV and development of negative correlations between OMP and majority of HRV indices.
The important hallmark of the metabolic activation in athletes after AmO intake was redistribution of the ligand forms of Hb and changes in their correlations with HRV. Lowering HbO
2 percentage with simultaneous increase
in HbCO, HbS, metHb can be associated with the produc-tion of ROS during haemolysis of old or oxidatively dam-aged erythrocytes and decline of heme with production of superoxide, СО·, Н
2О
2 (Belcher et al., 2010; Cohen et
al., 2007; Kim et al., 2011; Widmer et al., 2010). It can be assumed that oxidative destruction of some amounts of Hb is an essential mechanism of the FR reactions, their maintenance and, simultaneously, control of excessive FR destruction (through bilirubin production). The relation-ship between all HRV parameters (except VLF) and HbСО, which is not able to form ligands and must be utilized, may reflect the adaptation on account of the involvement of Hb into FR reactions. Under such circumstances, the degree of the irreversible oxidative destruction of Hb can presum-ably serve as an early marker of the stress heart rate regu-lation, even if the HRV indices still remain high. Indirect correlations between HbS and metHb and HRV points to intensive reduction of HbS and metHb, which results in increase in the Hb lifespan and improvement of the meta-bolic system feedback control. After AmO supplementa-tion practically all correlations have disappeared with only direct correlation between HbСО and HRV parameters being left. Such changes could be attributed to the involve-ment of Hb into FR reactions and improvement of the endogenous oxygen production (Tymochko et al., 1998). This, in turn, could attenuate dependence of the metabolic system on the transport function of Hb, optimize cardio-respiratory function, and ultimately, reduce the heart rate.
Conclusions
To sum up, AmO was shown to induce a pre-condition-ing effect in subjects experiencing OS, which was less prominent in DM patients with sluggish redox reac-tions and more pronounced in athletes with a higher functional metabolic potential. These effects can be attributed to the ability of AmO to modulate activity of SOD and catalase and therefore to control the produc-tion of superoxide and H
2O
2 on one hand, improving
assimilation of oxidative metabolic products (OMP, conjugated dienes) on the other. Evidently, perva-sive influence of AmO triggered activation of aerobic metabolism with more efficient interaction between all functioning structures (from blood haemoproteins to peroxisomes and mitochondria) leading to improved maintenance of oxygen and FR homeostasis. At the level of an organism this was reflected by modulation
Arc
hive
s of
Phy
siol
ogy
and
Bio
chem
istr
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Cal
gary
on
05/2
2/12
For
pers
onal
use
onl
y.
56 O. Yelisyeyeva et al.
Archives of Physiology and Biochemistry
of the cardio-respiratory function and increase in HRV observed for all studied groups. Finally, AmO caused an antioxidant effect through mild pro-oxidant activity involving all hierarchical functional structures, which could be a principal underlying mechanism of the improved feedback control, self-organization of the liv-ing system and maintenance of oxidative homeostasis through hormetic reaction.
acknowledgement
This article would not appear without the initiative and keen interest of the late Professor Janos Feher, who supported our scientific concept of oxidative stress correction and made us think about its implica-tion in metabolic syndrome. We also have to mention an important role of our teacher Professor Mykhaylo Tymochko, who left us valuable scientific acquirement in the field of free radical and oxygen homeostasis and died too early under tragic circumstances. This research is dedicated to them. The study was sup-ported by COST B35 Action.
Declaration of interest
The authors declare no conflicts of interest.
referencesAngulo P. (2002). Nonalcoholic fatty liver disease. N Engl J Med
346:1221–31.Aubert AE, Seps B, Beckers F. (2003). Heart rate variability in athletes.
Sports Med 33:889–919.Belcher JD, Beckman JD, Balla G, Balla J, Vercellotti G. (2010). Heme
degradation and vascular injury. Antioxid Redox Signal 12:233–48.Bilyi O, Dudok K, Lukyanez V. (1998). Determination of the
hemoglobin content and its ligand forms in blood using the method of absorptive spectroscopy. Lviv: Lviv State University Press (in Ukrainian):24 pp.
Bochkov VN, Oskolkova OV, Birukov KG, Levonen A-L, Binder CJ, Stockl J. (2010). Generation and biological activities of oxidized phospholipids. Antioxid Redox Signal 12:1009–59.
Bosquet L, Mekari S, Arvisais D, Aubert AE. (2008). Is heart rate a convenient tool to monitor overreaching? A systematic review of the literature. Br J Sports Med 42:709–14.
Chang Y-C, Chuang L-M. (2010). The role of oxidative stress in the pathogenesis of type 2 diabetes: from molecular mechanism to clinical implication. Am J Transl Res 2:316–31.
Cherkas A, Yelisyeyeva O, Semen K, Zarkovic K, Kaminskyy D, Gasparovic AC, Jaganjac M, Lutsyk A, Waeg G, Zarkovic N. (2009). Persistent accumulation of 4-hydroxynonenal-protein adducts in gastric mucosa after Helicobacter pylori eradication. Coll Antropol 33:815–21.
Choi SW, Benzie IF, Ma SW, Strain JJ, Hannigan BM. (2008). Acute hyperglycemia and oxidative stress: Direct cause and effect? Free Rad Biol Med 44:1217–31.
Christensen JH, Skou HA, Madsen T, Terring I, Schmidt EB. (2001). Heart rate variability and n-3 polyunsaturated fatty acids in patients with diabetes mellitus. J Int Med 249:545–52.
Churruca I, Fernandez-Quintela A, Portillo MP. (2009). Conjugated linoleic acid isomers: Differences in metabolism and biological effects. Biofactors 35:105–11.
Cohen G, Riahi Y, Alpert E, Gruzman A, Sasson S. (2007). The roles of hyperglycaemia and oxidative stress in the rise and collapse of
the natural protective mechanism against vascular endothelial cell dysfunction in diabetes. Arch Physiol Biochem 113:259–67.
Cohen G, Riahi Y, Sasson S. (2011). Lipid peroxidation of poly-unsaturated fatty acids in normal and obese adipose tissues. Arch Physiol Biochem 117:131–39.
Connes P, Hue O, Hardy-Dessources MD, Boucher JH, Pichot V, Barthelemy JC. (2008). Hemorheology and heart rate variability: is there a relationship? Clin Hemorheol Microcirc 38:257–65.
Das UN. (2000). Beneficial effect(s) of n-3 fatty acids in cardiovascular diseases: but, why and how? Prostagland Leukotrien Essent Fatty Acids 63:351–62.
Del Rio R, Moya EA, Iturriaga R. (2010). Carotid body and cardiorespiratory alterations in intermittent hypoxia: the oxidative link. Eur Respir J 36:143–50.
Dubinina E, Burmistrov S, Khodov D, Porotov I. (1995). Oxidative modification of human blood serum proteins: a method for its estimation. Vopr Med Chimii (in Russian) 41:24–9.
Eckardt K, Sell H, Eckel J. (2008). Novel aspects of adipocyte-induced skeletal muscle insulin resistance. Arch Physiol Biochem 114:287–98.
Eizirik DL, Cardozo AK, Cnop M. (2008). The role for endoplasmic reticulum stress in diabetes mellitus. Endocr Rev 29:42–61.
Ellis EM. (2007). Reactive carbonils and oxidative stress: potential for therapeutic intervention. Pharmacol Therapeutics 115:13–24.
Ezenwaka CE, Nwagbara E, Seales D, Okali F, Sell H, Eckel J. (2009). Insulin resistance, leptin and monocyte chemotactic protein-1 levels in diabetic and non-diabetic Afro-Caribbean subjects. Arch Physiol Biochem 115:22–7.
Fisher-Wellman K, Bell HK, Bloomer RJ. (2009). Oxidative stress and antioxidant defense mechanisms linked to exercise during cardiopulmonary and metabolic disorders. Oxid Med Cell Longevity 2:43–51.
Gamel TH, Mesallam AS, Damir AA, Shekib LA, Linssen JP. (2007). Characterization of Amaranth seed oils. J Food Lipids 14:323–34.
Guzy RD, Schumacker PT. (2006). Oxygen sensing by mitochondria at complex III: The paradox of increased ROS during hypoxia. Exp Physiol 91:807–19.
Haensel A, Mills PJ, Nelesen RA, Ziegler MG, Dimsdale JE. (2008). The relationship between heart rate variability and inflammatory markers in cardiovascular diseases. Psychoneuroendocrinol 33:1305–12.
Henriksen EJ, Diamond-Stanic MK, Marchionne EM. (2011). Oxidative stress and the etiology of insulin resistance and type 2 diabetes. Free Rad Biol Med 51:993–99.
Howorka K, Pumprla J, Haber P, Koller-Strametz J, Mondrzyk J, Schabmann A. (1997). Effects of physical training on heart rate variability in diabetic patients with various degrees of cardiovascular autonomic neuropathy. Cardiovasc Res 34: 206–14.
Iellamo F, Legramante JM, Pigozzi F, Spataro A, Norbiato G, Lucini D, Pagani M. (2002). Conversion from vagal to sympathetic predominance with strenuous training in high-performance world class athlete. Circulation 105:2719–24.
Jones DP. (2006). Disruption of mitochondrial redox circuitry in oxidative stress. Chem Biol Interact 163:38–53.
Kaikkonen P, Hynynen E, Mann T, Rusko H, Nummela A. (2010). Can HRV be used to evaluate training load in constant load exercises? Eur J Appl Physiol 108:435–42.
Kaminskyy DV, Yelisyeyeva OP, Chercas AP, Kurkevych AK, Konyk UV, Darmogray RY, Aleksevich YI. (2002). Physical and chemical characteristic of amaranth and peculiarities of its metabolic influence. Medical Chemistry (in Ukrainian) 4:77–85.
Kamyshnikov VS (Ed.). (2000). Reference on clinical biochemical laboratory diagnostics (in 2 volumes). Minsk: Belarus. V.1 495 pp.; V.2 494 pp.
Kim YM, Pae HO, Park JE, Lee YC, Woo JM, Kim NH, Choi YK, Lee BS, Kim SR, Chung HT. (2011). Heme oxygenase in the regulation of vascular biology: from molecular mechanisms to therapeutic opportunities. Antioxid Redox Signal 14:137–167.
Arc
hive
s of
Phy
siol
ogy
and
Bio
chem
istr
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Cal
gary
on
05/2
2/12
For
pers
onal
use
onl
y.
Activation of aerobic metabolism by Amaranth oil improves heart rate variability 57
© 2012 Informa UK, Ltd.
Korolyuk M, Ivanova L, Mayorova I, Tokarev V. (1998). A method for measuring catalase activity. Lab Delo (in Russian) 1:16–9.
Kostyuk V, Potapovich A, Kovaleva Z. (1990). A simple sensitive assay for determination of superoxide dismutase activity based on reaction of quercetin oxidation. Vopr Med Khimii (in Russian) 2:88–91.
Kuhn H, Gotze R, Schewe T, Rapoport S. (1981). Quasi-lipoxygenaze activity of haemoglobin a model for lipoxygenases. Eur J Biochem 120:161–68.
Lahiri MK, Kannankeril PJ, Goldberger JJ. (2008). Assessment of autonomic function in cardiovascular disease: physiological basis and prognostic implications. J Am Coll Cardiol 51:1725–33.
Mandl J, Meszaros T, Banhegyi G, Hunyady L, Csala M. (2009). Endoplasmic reticulum: nutrient sensor in physiology and pathology. Trends Endocrinol Metab 20:194–201.
Mangoni ME, Nargeot J. (2008). Genesis and regulation of the heart automaticity. Physiol Rev 88:919–82.
Manoli I, Alesci S, Blackman MR, Su YA, Rennert OM, Chrousos GP. (2007). Mitochondria as key components of the stress response. Trends Endocrinol Metab 18:190–98.
Martinmäki K, Rusko H. (2008). Time-frequency analysis of heart rate variability during immediate recovery from low and high intensity exercise. Eur J Appl Physiol 102:353–60.
Martirosyan DM, Miroshnichenko LA, Kulakova SN, Pogojeva AV, Zoloedov VI. (2007). Amaranth oil application for coronary heart disease and hypertension. Lipids Health & Disease 6:1–12.
Mattson MP. (2008). Dietary factors, hormesis and health. Ageing Res Rev 7:43–8.
Negre-Salvayre A, Auge N, Ayala V, Basaga H, Boada J, Brenke R, Chapple S, Feher J, et al. (2010). Pathological aspects of lipid peroxidation. Free Radic Res 44:1125–71.
Negre-Salvayre A, Salvayre R, Augé N, Pamplona R, Portero–Otín M. (2009). Hyperglycemia and glycation in diabetic complications. Antioxid Redox Signal 11:3071–109.
Packer L, Cadenas E. (2007). Oxidants and antioxidants revisited. New concepts of oxidative stress. Free Radical Res 41:951–52.
Pollack GH, Figueroa X, Zhao Q. (2009). Molecules, water, and radiant energy: New clues for the origin of life. Int J Mol Sci 10:1419–29.
Radak Z, Chung HY, Goto S. (2008). Systemic adaptation to oxidative challenge induced by regular exercise. Free Rad Biol Med 44:153–59.
Rains JL, Jain SK. (2011). Oxidative stress, insulin signaling, and diabetes. Free Rad Biol Med 50:567–75.
Riahi Y, Sin-Malia Y, Cohen G, Alpert E, Gruzman A, Eckel J, Staels B, Guichardant M, Sasson S. (2010). The natural protective mechanism against hyperglycemia in vascular endothelial cells roles of the lipid peroxidation product 4-hydroxydodecadienal and peroxisome proliferator-activated receptor δ. Diabetes 59:808–18.
Sarsour EH, Kumar MG, Chaudhuri L, Kalen AL, Goswami PC. (2009). Redox control of the cell cycle in health and disease. Antioxid Redox Signal 11:2985–3011.
Sasson S, Eckel J. (2006). Disparate effects of 12-lipoxygenase and 12-hydroxyeicosatetraenoic acid in vascular endothelial and smooth muscle cells and in cardiomyocytes. Arch Physiol Biochem 112:119–29.
Semen KO, Yelisyeyeva OP, Kaminskyy DV, Cherkas AP, Zarkovic K, Lutsyk OO, Cipak A, Jaganjac M, Zarkovic N. (2010). Interval hypoxic training in complex treatment of Helicobacter
pylori–associated peptic ulcer disease. Acta Biochim Pol 57: 199–208.
Sen CK, Khanna S, Roy S. (2007). Tocotrienols in health and disease: the other half of the natural vitamin E family. Mol Aspects Med 28:692–728.
Shin DH, Heo HJ, Lee YJ, Kim HK. (2004). Amaranth squalene reduces serum and liver lipid levels in rats fed a cholesterol diet. Br J Biomed Sci 61:11–4.
Sirota TV, Yelisyeyeva OP, Khunderyakova NV, Makhotina OA. (2008). Amaranth seed oil: effect of oral administration on energetic functions of rat liver mitochondria activated with adrenaline. Biochem (Moscow) Suppl Series A: Memb Cell Biol 2:40–7.
Stuchlik M, Zak S. (2002). Vegetable lipids as components of functional foods. Biomed Papers 146:3–10.
Task Force of the ES of Cardiology and the North AmS of Pacing and Electrophysiology. (1996). Heart rate variability. Standards of measurement, physiological interpretation, and clinical use. Eur Heart J 17:354–81.
Timirbulatov R, Seleznev E. (1986). Methods for increasing intensity of free radical oxidation of blood lipids containing components and its diagnostic value. Lab Delo (in Russian) 4:209–11.
Trayhurn P, Christian A, Drevon CA, Eckel J. (2011). Secreted proteins from adipose tissue and skeletal muscle – adipokines, myokines and adipose/muscle cross-talk. Arch Physiol Biochem 117:47–56.
Tymochko M, Yelisyeyeva O, Kobylinska L, Tymochko I. (1998). Metabolic aspects of the oxygen homeostasis formation in the extremal states. Lviv (Ukraine):Missioner, 142 pp.
Valko M, Leibfrit D, Moncol J, Cronin MT, Mazur M, Telser J. (2007). Free radicals and antioxidants in normal physiological functions and human disease. Int J Biochem Cell Biol 39:44–84.
Voeikov VL, Del Giudice E. (2009). Water respiration – The basis of the living state. Water 1:52–75.
Wang R, Kern JT, Goodfriend TL, Ball DL, Luesch H. (2009). Activation of the antioxidant response element by specific oxidized metabolites of linoleic acid. Prostagland Leukotrien Essent Fatty Acids 81:53–9.
Weseler AR, Bast A. (2010). Oxidative stress and vascular function: implications for phramacologic treatment. Curr Hypertens Rep 12:154–61.
Widmer CC, Pereira CP, Gehrig P, Vallelian F, Schoedon G, Buehler PW, Schaer DJ. (2010). Hemoglobin can attenuate hydrogen peroxide-induced oxidative stress by acting as an antioxidative peroxidase. Antioxid Redox Signal 12:185–198.
Yelisyeyeva O, Cherkas A, Semen K, Kaminskyy D, Lutsyk A. (2008a). Study of aerobic metabolism parameters and heart rate variability and their correlations in elite athletes: a modulatory effect of Amaranth oil. CEMED 3:293–307.
Yelisyeyeva O, Cherkas A, Zarkovic K, Semen K, Kaminskyy D, Waeg G, Zarkovic N. (2008b). The distribution of 4-hydroxynonenal-modified proteins in gastric mucosa of duodenal peptic ulcer patients. Free Rad Res 42:205–11.
Yelisyeyeva O, Serhiyenko O, Cherkas A, Semen K, Kaminskyy D, Kurkevych A. (2005). Heart rate variability in patients with diabetes mellitus: an attempt of metabolic interpretation. Probl Endocr Pathol (in Ukrainian) 1:95–110.
Zarkovic N. (2003). 4-Hydroxynonenal as a bioactive marker of pathophysiological processes. Mol Aspects Med 24:281–91.
Arc
hive
s of
Phy
siol
ogy
and
Bio
chem
istr
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Cal
gary
on
05/2
2/12
For
pers
onal
use
onl
y.




















