
A Study on Business Model and Technical Framework for ...
177
A Study on Business Model and Technical Framework for China’s Inclusive Healthcare Services A Thesis Submitted to the University of Manchester for the Degree of Doctor of Business Administration in the Faculty of Humanities Jan. 2019 JIANGNAN LIU MANCHESTER BUSINESS SCHOOL
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of A Study on Business Model and Technical Framework for ...

A Study on Business Model and Technical
Framework for China’s Inclusive Healthcare Services
A Thesis Submitted to the University of Manchester for the Degree of
Doctor of Business Administration
in the Faculty of Humanities
Jan. 2019
JIANGNAN LIU
MANCHESTER BUSINESS SCHOOL
LIST OF CONTENTS
Abstract ............................................................................................................................ I
Keywords ...................................................................................................................... III
Declaration .................................................................................................................... III
Copyright Statement ...................................................................................................... III
Acknowledgements ......................................................................................................... V
Dedication ..................................................................................................................... VI
I. Introduction: Motivation and Research Methodology ............................................. 1
1.1 Background and Motivation .............................................................................. 1
1.2 Significance of the Research ............................................................................. 3
1.3 Research Design ............................................................................................... 7
1.4 Key Contributions ............................................................................................ 8
II. Literature Review ................................................................................................. 11
2.1 Traditional Healthcare Management Frameworks ........................................... 11
2.2 The Concepts and Composition of the Business Model ................................... 12
2.3 Critical success factors for inclusive healthcare services ................................. 17
2.4 The Technical Framework for Inclusive Healthcare Services .......................... 28
III. New Business Model for Inclusive Healthcare Services ........................................ 34
3.1 Inclusive Healthcare System in China: Concepts and Development ................. 34
3.2The Proposed Model: A Coupled Dual-Component Model .............................. 38
3.3Critical Success Factors for the Implementation of the Inclusive Healthcare Services ............................................................................................................... 55
IV. Key Technologies for the Inclusive Healthcare Program ....................................... 83
4.1 Key Technologies of Inclusive Healthcare Based on Evidence Theory ............ 83
4.2 A Cloud-based System and Architecture for Inclusive Healthcare ................... 95
4.3 The Technical Architecture of Medical Image Recognition ........................... 107
V. Case Study: Brain Tumour Image Recognition in the Context of the Inclusive Healthcare program ............................................................................................ 129
5.1 Brain Tumour Image Recognition Based on Morphological Feature Extraction .......................................................................................................................... 130
5.2 Brain Tumour Image Recognition Based on Neural Networks ....................... 134
5.3 Evidential Reasoning for the Diagnosis of Meningioma ................................ 136

VI. Conclusion and Future Research......................................................................... 139
Appendixes .................................................................................................................. 143
Appendix 1. Background Information ................................................................. 143
Appendix 2. Questionnaire on Critical Success Factors for Inclusive Healthcare Services and the Results ..................................................................................... 150
References ................................................................................................................... 160

I
Abstract
China is currently facing a serious conundrum in terms of healthcare availability
and equity (which is characterized by the uneven distribution of medical resources
among urban and rural areas, and a widening gap in medical service standards among
different regions). This has resulted in limited accesses to and high costs of healthcare
services for residences in less developed areas. In view of these issues, China has
planned to launch an initiative called “Inclusive Healthcare” to improve the level of
medical services in less developed areas. To provide such inclusive healthcare
services, we propose a new business model with dual-components and develop a
technical framework for supporting such an initiative.
The proposed business model consists of two parts. The first part is market-
oriented and for-profit, serving as a fund-raising mechanism for the inclusive
healthcare services. The second part is charitable in nature and is responsible for
developing and managing the operations platform for inclusive healthcare services.
From the perspective of governance and funding, we illustrate the key drivers in the
implementation of the inclusive healthcare services, followed by an analysis of the
new business model based on four elements of the business model proposed by
Johnson et al. (2008). These elements include customer value proposition, key
resources, key processes, and profit formula. In the discussion on customer value
proposition, we focus on how the dual-component business model creates value, and
how each participant profits from the new business model. In the discussion on key
resources, we focus on the important roles of technologies such as the Internet and
artificial intelligence (AI) for implementing the inclusive healthcare service systems.
In the discussion on key processes, rather than considering how investors in the
market-oriented part manage the healthcare service system, we emphasize the
business processes of the charitable part and the positive capital inflow from the
market-oriented part to the charitable part. In the discussion on profit formula, we
emphasize how the coupled business model generates profit, right from the interface

II
between the market-oriented part and the charitable part. Finally, building on the
coupled dual business model for inclusive healthcare services, we provide specific
recommendations on the development and implementation of the initiative. To help
put the proposed model into practice, we use the case study approach to study the
critical success factors for implementing inclusive healthcare services in remote and
less developed areas of China. By reviewing the literature on critical success factors
for public-private partnerships (PPP) and healthcare services projects, we summarize
the possible critical success factors for implementing the “inclusive healthcare
services”. Then, through interviews with two government officials, one investment
company executive, four hospital leaders, eight doctors and twenty patients, we
identify six critical success factors which are: medical infrastructure, technology,
funding, government support, external environment, and organization planning and
operations.
In this thesis, we also propose a technical framework for implementing
inclusive healthcare service systems based on cloud computing and artificial
intelligence technologies. At the core of this framework is an integrated architecture
using multi-sources of medical data. The architecture is in line with the diagnostic
logic of evidence-based medicine, and it is implementable using the theory of
evidence-based reasoning. It can make diagnoses by fusing various types of medical
data from multiple sources. Furthermore, we construct a cloud system for inclusive
healthcare services to support the proposed framework, which comprises three layers:
infrastructure, platform service, and platform application. The infrastructure layer
provides basic services for the cloud system to collect and compile basic medical data.
The platform service layer integrates cloud storage, cloud computing and application
development platforms in order to respond to data processing requests and application
development requirements. The application layer is intended for doctors and other
users. It includes a human-computer interface, a comprehensive medical record
processing system, and a comprehensive medical image processing system. Finally,
using multimodality brain tumour imaging as an example, we develop a multimodal
III
brain tumour medical imaging diagnostic methodology, based on evidence fusion
theory. Experiments show the effectiveness of the evidence fusion technology in the
proposed technical framework.
Keywords
Inclusive healthcare service, coupled dual-part business model, critical success factor,
cloud computing, service system architecture, evidence-based reasoning
Declaration
No portion of the work referred to in the thesis has been submitted in support of an
application for another degree or qualification from this or any other university or
other institutes of learning.
Copyright Statement
i. The author of this thesis (including any appendices and/or schedules to this
thesis) owns certain copyright or related rights in it (the “Copyright”) and s/he has
given The University of Manchester certain rights to use such Copyright, including
for administrative purposes.
ii. Copies of this thesis, either in full or in extracts and whether in hard or
electronic copy, may be made only in accordance with the Copyright, Designs and
Patents Act 1988 (as amended) and regulations issued under it or, where appropriate,
in accordance with licensing agreements which the University has, from time to time.
This page must form part of any such copies made.
iii. The ownership of certain Copyright, patents, designs, trademarks and other
intellectual property (the “Intellectual Property”) and any reproductions of copyright
works in the thesis, for example: graphs and tables (“Reproductions”), which may be
described in this thesis, may not be owned by the author and may be owned by third
parties. Such Intellectual Property and Reproductions cannot and must not be made
IV
available for use without the prior written permission of the owner(s) of the relevant
Intellectual Property and/or Reproductions.
iv. Further information on the conditions under which disclosure, publication
and commercialization of this thesis, the Copyright and any Intellectual Property
and/or Reproductions described in it may take place is available in the University
Policy (see http://www.campus.manchester.ac.uk/medialibrary/policies/
intellectualproperty.pdf), in any relevant Thesis restriction declarations deposited in
the University Library, The University Library’s regulations (see
http://www.manchester.ac.uk/library/aboutus/regulations) and in The University’s
policy on presentation of theses.

V
Acknowledgements
I had left my active work responsibilities when I decided to take the DBA
course. I was engaged in a state think tank, while doing some not-so-heavy policy
research work. It was a good friend of mine (Dr. Gao Quanjian) who motivated me to
take the course. In the beginning, I didn’t take it seriously, neither did I think it would
be very useful for me because, by the time of graduation, I would be long retired. By
the same token, I did not believe it would be very difficult, for after all, what I had
been doing was research study.
Nevertheless, the research turned out not as simple as I thought. The experience
I gained in completing the DBA course is not only a honing test, but also a big harvest
for me. DBA training helped me a lot in my systemic study of methodology shaping
my way of thinking and mastering the approach of evidence reasoning (which
provided a reliable tool in my policy research). I put my current work on the inclusive
healthcare in a set of theoretical models for rethinking and argument. As a result, I
somehow obtained fresh inspiration at a higher level. All of these will give me
lifelong benefits. Indeed, I am really grateful for this special piece of my life
experience. It should be a God-sent gift to patronize my knowledge.
Of course, I have more to be thankful for. I want to thank my tutor Prof. Xu
Dongling for the knowledge and competence she gave me. I want to thank Prof. Wan
Guohua and Prof. Jiang Wei for their guidance in my commercial model design and
AI algorithm. I also want to thank other friends (such as Liu Yang, Yan Linping, Lin
Yaqin, Man Yi, Kang Nan) who have offered me assistance; as well as high officials
and my colleagues (Xiao Yi, Xia Linmao, Fang Bin and many hospital directors,
medical workers and patients) who have accepted my interview.
Last but not least, I would like to express my special thank you to my dear wife,
Wang Fei, for her constant encouragement and support, especially when I was
depressed. Without her strong her support, it would have been impossible for me to
make it eventually, after 7 years DBA study.

VI
Dedication
I wish to dedicate my DBA research result to China Insurance Investment Fund
where I work, with the hope that it would be of some use for China’s inclusive
healthcare development.
1
I. Introduction: Motivation and Research Methodology
1.1 Background and Motivation
Healthcare is one of the basic requirements for human beings to live with
dignity and an essential metric for social development. Healthcare reform in China
started in 2003 and has since realized a number of major achievements. However,
quite a few issues remain unsolved. One of such is the availability of healthcare
services in different areas. In other words, an approach to consistent and accessible
healthcare for people all over the country is urgently needed. According toexisting
literature, the status of healthcare availability and equity in China is far from
satisfaction, which is specifically apparent in the following aspects:1
1. A severely unbalanced distribution of healthcare resources among urban and
rural areas. Seventy percent of healthcare resources in China are being allocated in
urban areas. In other words, the urban population have on average more than 2.3
times more healthcare resources than the rural population. The distribution of urban
healthcare institutions and resources is relatively high, dominating the healthcare
market.2 Hospitals of higher levels (Class A hospitals) in Beijing and Shanghai are
particularly well established and well-equipped, resulting in a siphon effect due to the
huge gap between these hospitals and those in less developed areas. There is a relative
shortage of healthcare resources in rural areas, which have only out-of-date facilities
and inefficient healthcare staff who are not able to fulfill the demand for healthcare
services. Thus, patients are forced to seek healthcare services by travelling long
distances (which does not only add to their healthcare expenses, but also worsen the
health conditions). High expenses and lack of access to healthcare services have
become major recurring problems of the society.
2. The availability and equityproblems of healthcare services which result from
uneven economic developments among different areas. Due to differences in
Source:1http://www.docin.com/p-331355683.html PPT: Healthcare Equity and the Role of the Government)
Source:2http://www.sohu.com/a/114880997_488812

2
economic developments, the eastern coasts of China have richer healthcare resources
than the mid-west area. According to the blue paper, China Pharmaceutical Market
Report 2012 (published by the Chinese Academy of Sciences), the overall availability
of material healthcare resources of Eastern China in 2010 was 1.41 times that of
Central China and 1.42 times that of the Western China. The overall healthcare human
resources of Eastern China are 1.19 times those of Central China and 1.27 times those
of Western China.3
3. The “one-size-fits-all” economic development model in China has led to
inequitable healthcare services between urban and rural areas. Since the founding of
the People’s Republic of China in 1949, there has been rapid industrial development
through lowered agricultural products, prices and the implementation of the
“developing industry with agriculture” policy, which effectively transformed China,
but at the same time, widened the gap between urban and rural areas, including
healthcare services.
In short, the gap between Eastern and West China and between urban and rural
China naturally was as portrayed in the above-mentioned availability and equity
problems in healthcare services. The policies of “fixing farm output quotas at the
household level” in rural areas and “working years buyout” in urban areas have
essentially disintegrated the healthcare insurance systems that connected the “barefoot
doctor” in rural areas and “free healthcare services” in urban areas. Also, the policies
have greatly reduced healthcare accessibility. Apart from healthcare expenses, the
public has to incur high travel costs to receive healthcare services in urban areas. This
further aggravates the social problem of limited access to the high cost of healthcare
services. This has become an important driver of poverty resulting from the illnesses
of the rural poor people, and a major barrier in the way of China’s efforts towards a
comprehensively well-off society. The ultimate objective of a successful healthcare
reform in China is healthcare accessibility and equity, rather than just solving the
problem of the high cost of healthcare (which is a major requirement in the new era
Source:3http://news.163.com/12/1228/10/8JQ9QAKP00014JB6.html
3
and an inevitable result of social development). Without solutions to healthcare
availability and equity, full healthcare insurance coverage or the universal sharing of
fair, accessible, high quality and continuous healthcare services will be impossible.
And the attempt to address the problem of limited access to and the high cost of
healthcare will not be able to solve this conundrum.
1.2 Significance of the Research
1.2.1 Theoretical Significance
In view of the current lack of equity in healthcare in remote areas of China, we
propose a dual-component business model for inclusive healthcare initiative to the
government, investors and medical institutions at the core. And to make a viable
solution, we identify the critical success factors for implementing the initiative. This
thesis then analyzes the key technologies needed in the implementation of the
inclusive healthcare services and demonstrates their feasibility using the example of
brain image recognition. These two parts aim to enable implementation of the
inclusive healthcare services in remote areas of China, to improve the status of
medical inequity inthese areas.
Based on the above research objectives, the theoretical significance of this
thesis is as follows:
(1) The coupled dual-component business model proposed in this thesis
provides a sustainable organization and operation modality for charitable
healthcareprojects and provides a scientific theoretical methodology for addressing
the operation of such projects.
The coupled dual-component business model proposed in this thesis is a
powerful combination of a market component and a charitable component: the former
is for-profit and provides funds for the latter; the latter is responsible for the
development and management of the inclusive healthcare system.
Government-led public healthcare services are generally not profit-oriented and
therefore relies on continuous public funding. This has limited the development and
4
improvement of charitable healthcare, rending many such projects unsustainable. The
coupled dual-component business model for inclusive healthcare makes use of
government resources to tightly link a non-profit charitable project with a profitable
commercial project to create a new community of shared interests, allowing the for-
profit component to fund the charitable component, hence forming a short-chain
redistribution mechanism that increases the people’s sense of gratification. Integrating
public and private efforts will enable the government to develop the market and
improve people’s livelihood at the same time. It not only supports the grand vision of
an “all-round well-off society”, but also prevents “falling into/returning to poverty
due to illness.” It equally ensures the consolidation of the achievements in building a
well-off society. The model effectively circumvents the inherent drawbacks of
government and market, maximizes the response to the needs of all stakeholders, and
provides a viable organization and operation mode for similar charitable medical
projects in the future.
(2) Based on the coupled dual-component business model, this thesis identifies
the critical success factors for the inclusive healthcare services and provides
recommendations for implementation.
From a project management perspective, the proposed coupled dual-component
business model for inclusive healthcare is essentially to establish a special long-term
public-private partnership (PPP). In this partnership, public hospitals provide the
medical services for residents, while the medical equipment and various technical
support services are provided by private institutions. In addition, hospitals receive
funding from the government or other non-governmental groups. It is necessary to
understand the critical success factors to ensure a smooth implementation of such a
project. By reviewing the literature on critical success factors for public-private
partnerships (PPP) and healthcare service projects and by considering the relationship
between various participants, this thesis summarizes the possible critical success
factors for implementing the inclusive healthcare services. Then, through interviews
with two government officials, one executive of an investment organization, four

5
hospital leaders, eight doctors and twenty patients, the thesis identifies six critical
success factors, each having one to four sub-categories. Under each sub-category,
some success factors require special attention and are so highlighted in this article.
Finally, this thesis provides management recommendations, based on the business
model for inclusive healthcare, the relationship between all participants and the
outcomes of the interviews.
On the other hand, cloud technology and artificial intelligence technologies are
developing rapidly. Their theoretical bases are constantly enriched and improved. And
their application has become increasingly widespread. At present, research on medical
technology mainly focuses on the improvement of the accuracy of a certain indicator
for various types of diseases. However, to implement inclusive healthcare, it is
necessary to first propose a technical system framework to provide a platform that
accommodates multiple technologies. First of all, the framework needs to be well
targeted. This is a fundamental requirement for the realization of the inclusive
healthcare services. With its wide coverage, inclusive healthcare requires a high level
of technical capability, without which the value of the inclusive healthcare cannot be
brought into full play. Therefore, it is necessary to develop a special technical system
for it. Secondly, the technical framework should be able to accommodate multiple
technologies and be able to scale beyond the current set of technologies by enabling
access to newer technologies.
Based on the above research objectives, the theoretical significance of this
thesis is as follows:
(1) This thesis uses evidence theory to establish a core technical framework
applicable to inclusive healthcare. The technical framework fully reflects the rationale
of evidence-based medicine, so that the diagnosis results derived from various
technologies can be integrated to improve the diagnostic accuracy.
At present, intelligent diagnosis is achieved mostly by feature engineering,
followed by classification of features using classifiers. With the rise of deep learning
in recent years, some scholars have applied such methods as multi-layer neural

6
networks and convolutional neural networks to analyze and classify medical data.
Although diagnostic accuracy is increasing with the development of technologies,
such technologies often apply only to a certain type of data, such as image data. The
doctor’s diagnosis is based on the theory of evidence-based medicine. The judgment
logic of evidence-based medicine is realized by the technical framework (which
advances the technical system theories of inclusive healthcare and even intelligent
medicine).
(2) This thesis establishes a cloud system applicable to inclusive healthcare. The
system is applicable to inclusive healthcare by supporting the core technology
framework through the base layer, the middle layer and the application layer.
Cloud technologies have become mature and are being used in various
applications. Currently, the development of a medical cloud system is mostly focused
on healthcare information systems (HIS) and picture archiving and communication
systems (PACS), without support for intelligent analysis and inclusive healthcare. A
medical cloud system (equipped with the above-mentioned core technologies) can
perform data acquisition, intelligent analysis, data iteration and other functions for
medical data, and it will be able to promote the theoretical basis for medical cloud
systems.
1.2.2 Practical Significance
The coupled dual-component business model proposed in this thesis opens up a
market segment in a field of full competition that solves the dilemma faced by the
government and the market. Investment-led development is an important part of
China’s economic growth. The capital market has already entered a stage of the
heated competition, and low prices have become a key factor in winning projects.
Beside the cost factor, the coupled dual-component business model (proposed in this
thesis) brings in an additional criterion, i.e., contribution to society, such as inclusive
healthcare. Only by having the ability to implement inclusive healthcare and meeting
the current requirements of the government can a player win the competition with the
same price. This model not only meets the current needs of all stakeholders, but also

7
maximizes social benefits and unlocks the hidden value of government projects. In
2017, the gross debt surplus of the Chinese government was 30 trillion yuan. If the
government could encourage all investment companies to allocate 1% of their profits
to feedback to the society, there will be 30 billion yuan available as public welfare
funds for people’s livelihood improvement. In so doing, the hidden value can be
unlocked by market mechanisms, especially for poor areas that require the targeted
support. This approach can also help the government address some difficult problems
in an intensive manner.
Promoting a balanced social development: China is undergoing rapid
urbanization, although the urbanization rate of China is still far behind that of
developed countries, which is 70%. Therefore, the government tend to strengthen
infrastructure development through borrowing. However, this has little to do with
farmers in remote areas after all. Redistributing economic benefits through the
coupled dual-component model (such as by developing public healthcare in counties
and townships and providing subsidies for medical expenditures, etc.) is able to raise
the happiness index and promote social equity in these remote areas where ordinary
people can also enjoy the benefits brought by urbanization.
1.3 Research Design
Firstly, through a literature review and synthesis and based on the definition and
characteristics of the business models mentioned in the literature, this thesis proposes
and elaborates a coupled dual-component business model applicable to the inclusive
healthcare services by summarizing its main features.
With regard to the critical success factors of the business model for inclusive
healthcare, this research conducted in-depth interviews with government officials, one
investment company executive, hospital leaders, doctors and patients using an
interview questionnaire designed by considering various factors mentioned in the
relevant literature (which were individually verified in the interviews). Further, data
were extracted from news articles, reports and other sources and were analyzed for
final identification of the critical success factors for implementing the inclusive
8
healthcare services.
With regard to the technical framework of inclusive healthcare, this thesis
develops a data fusion framework applicable to medical diagnosis based on evidence
fusion theory. At the same time, after a review of existing cloud architectures, a cloud
architecture for inclusive healthcare diagnosis is established. Finally, this thesis
presents an algorithm for comprehensive medical image diagnosis of multimodal
brain tumour, and presents a case study to verify the effectiveness of the technical
framework proposed in this thesis.
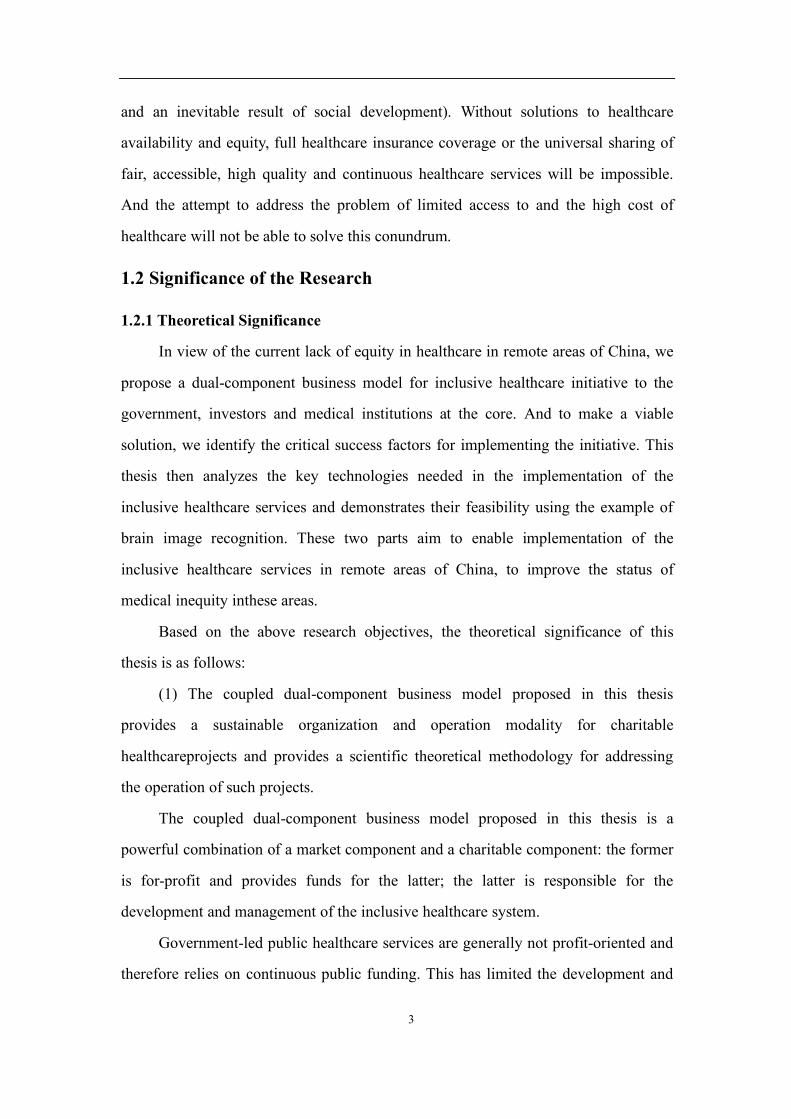
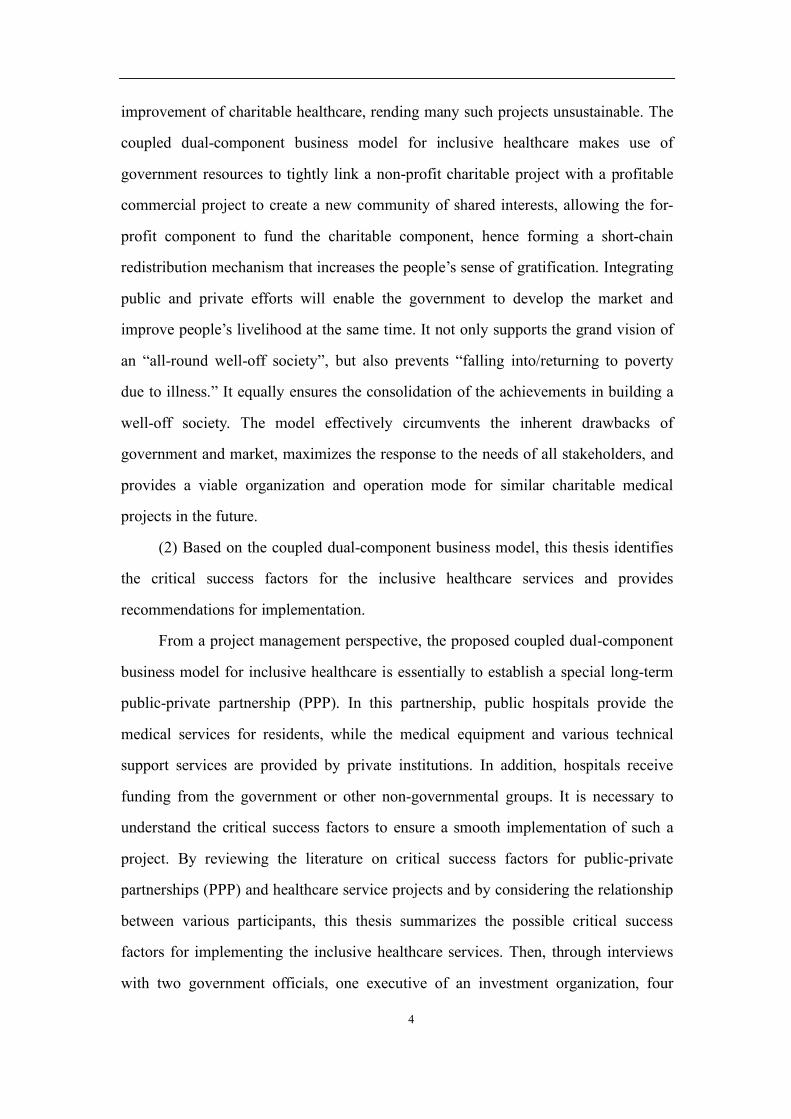
The technical pathway proposed in this thesis can be illustrated by the
conceptual diagram below:
Figure 1-1. The technical pathway presented in this thesis
1.4 Key Contributions
The major innovations of this study, compared with extant literature on
charitable medical service projects, are as follows:
1. Establishing a coupled dual-component business model to enable the
Establishment of a technical framework
Core technical framework based on evidential reasoning
Cloud framework for inclusive healthcare
An intelligent diagnosis method for brain tumour based on multi-modal images
Establishment of a business model
The proposed model: a coupled dual-component model
Stakeholders in business model and their relationships
Key success factors for the implementation of the model

9
inclusive healthcare services to operate sustainably and providing critical success
factors for implementing the business model. This complements the literature in
business model research (in the area of strategic management) and provides new ideas
for extending the traditional business models by linking different business models
together to fit business models in different settings.
Currently, there is a lack of research in the academic community on the mode of
operation of charitable healthcare projects. Particularly, there is no way to ensure the
sustainability of these projects. This research creatively links a non-profit charitable
project with a profitable commercial project to create a new community of shared
interests, allowing the for-profit component to fund the charitable component, hence
forming a short-chain redistribution mechanism that integrates public and private
efforts to enable the government to develop the market and improve people’s
livelihood at the same time. It effectively addresses the issue of funding availability in
charitable healthcare services while considering the interests of government, investors,
medical institutions and patients.
After presenting the business model for inclusive healthcare, this thesis
proposes the critical success factors that should be given attention to in implementing
this business model. Research on critical success factors for various healthcare
projects is not uncommon in the existing literature. However, these critical success
factors do not have viable portability. For example, when implementing telemedicine
services, the success factors for developed and developing countries vary greatly
(Zhang, 2005). Moreover, the inclusive healthcare services also make use of some
emerging technologies such as big data and artificial intelligence. At present, there is
a lack of research on how to apply such advanced technologies in charitable
healthcare projects. Therefore, the critical success factors for the coupled dual-
component business of inclusive healthcare summarized in this thesis are crucial for
the smooth implementation of the project.
In essence, the proposed coupled dual-component business model establishes a
special, long-term public-private partnership (PPP). Therefore, this thesis undertakes

10
case study analyses to summarize the lessons learned and critical success factors in
implementing general PPP projects and similar medical projects in the available
literature. The critical success factors of the coupled dual-component business model
for inclusive healthcare are then summarized, taking into consideration the medical
status in China’s remote and poor areas, and based on synthesizing results of in-depth
interviews with government leaders, an investment company executive, hospital
leaders, doctors and patients.
2. A diagnostic framework for inclusive healthcare is established. The
framework is suitable for a variety of data sources and for the diagnosis of a variety of
diseases and conditions.
It includes three major components: (1) the core technical framework based on
evidence theory; (2) a cloud system framework applicable to inclusive healthcare; and
(3) a diagnostic methodology suitable for multimodal brain tumour imaging. The core
technical framework based on evidence theory is established based on the theories of
evidence fusion and evidence-based medicine. So far, there have been few studies in
this field. The judgment logic of the evidence fusion theory is similar to that of
evidence-based medicine, which is mainly used to prepare diagnostic guides used in
regular human diagnosis. Intelligent diagnosis is possible by combining evidence-
based medicine with evidence theory and algorithms. Further, this thesis establishes a
cloud system framework for inclusive healthcare. The integration of a cloud system
and the above-mentioned core framework allows for a higher level of intelligence
beyond the basic functions of PACS or HIS systems. In addition, this thesis proposes
an algorithm for multi-modal brain tumour image analysis that combines artificial
neural network and data fusion theory. Finally, through an empirical analysis, this
thesis confirms the effectiveness of the proposed core technology framework based on
data fusion theory.
This thesis establishes a business model for healthcare and its accompanying
core technical framework (whose effectiveness has been confirmed by research and
empirical study, and therefore promotes the development of inclusive healthcare).
11
II. Literature Review
2.1 Traditional Healthcare Management Frameworks
The inclusive healthcare service initiative is a kind of telemedicine services.
Specifically, remote monitoring (e.g., monitoring patients’ heartbeat data),
consultation, prevention, diagnosis, and disease treatment are realized for patients
with the help of information technology (IT) so that they can consult doctors at the
targeted hospitals without long distance relocation. Such a new service is especially
appropriate for regions and developing countries that are in high demand for quality
healthcare resources. Furthermore, the service covers all age groups and has
experienced enormous growth in the past decades, showing attractive prospects
(McColl-Kennedy et al., 2012).
Generally, telemedicine service is a kind of complex service network that
involves a number of stakeholders. It is also a combination of IT service (which
involves the transfer of data from a telemedicine service device to a monitoring
facility, which can be highly standardized) and non-IT service (which refers to
knowledge-intensive and individualized service) (e.g., the conversation records
between the patient and the doctor in charge of the case, etc.) (Berry et al., 2007).
Although telemedicine service is technologically realizable, few telemedicine service
innovations have been put into practice due to its complex organizational structure
and longer service period (Bardhan et al., 2010). Finally, it is extremely difficult to
design a successful and sustainable business model for telemedicine with a clear
structure (Cho et al., 2008).
In some literature, telemedicine service involves four different entities: patients,
health care providers (doctors or hospitals), insurance companies (Peters et al., 2015),
and IT service providers. The objective of telemedicine service is to improve the
quality of healthcare service and reduce the expenses of patients (end customers).
However, the value proposition defining such telemedicine service has not been
broadly accepted because the value creation of health care service depends on the
successful integration of customers and service providers. This reveals the

12
inseparability between the production and consumption of telemedicine service, for
which its created value is highly heterogeneous. It also depends on the efforts of the
consumers. Thus, essential differences exist between the business models of
telemedicine services and those commonly used by manufacturers.
Peters et al. (2015) applied design research approaches to develop a special
business model framework that is able to analyze, describe, and classify telemedicine
service with a complex structure. The framework can be expressed as a morphological
box, which is capable of decomposing a complex service system into basic
components and forming parameters by accurately offering a single definition of each
component. From the 16 existing business models of telemedicine service, the value
of each parameter of each component is extracted, and then different types of business
models are identified. The framework can offer inspiration for the design of business
models of subsequent relevant healthcare services.
However, different from a healthcare service that obtains profits from the
investments of several private companies (or individuals) and price adjustment
mechanisms of the market, the services provided by the inclusive healthcare initiative
are intended for public welfare through public hospitals run by the government. In
establishing the business model, the public welfare nature of the services provided by
this project should be given priority.
2.2 The Concepts and Composition of the Business Model
In the past decade, the term “business model” has attracted wide attention
among researchers and practitioners, but a clear and widely accepted definition has
yet to be established. Previous researches have revealed the characteristics of business
models from different perspectives such as strategic management, business processes,
etc. (Coombes et al., 2013). These characteristics have triggered different views on
what essential factors a business model should have. The imprecision of a definition
hinders the development of the business model theories and their application, to some
extent.
Definitions of business model from some reviewed literature (Coombes et al.,

13
2013; Chen et al., 2013) indicate that scholars’ awareness of business models is
essentially related to strategy. For instance, Casadesus-Masanell et al. (2010) stated
that “a firm’s business model is a reflection of its realized strategy,” and “essentially,
[the] strategy coincides with [the] business model, so that an outside observer can [see]
the firm's strategy by looking at its business model.” However, even though business
models can be used to analyze, check, and verify the existing strategies of a company.
Some researchers (Magretta, 2002; Morris et al., 2005) asserted that it is impossible to
equalize these two concepts. Compared with the strategy at the higher level and
tactics at the lower level, the business model is more like a bridge in between, while
the customer value proposition is the critical factor for the connection (Johnson et al.,
2008). Additionally, Amit et al. (2012) stressed the importance of product or process
innovation in business models. By analyzing journal articles with “business model” or
“business models” in the titles that were published on the Web of Science during
1977-2011,Coombes et al. (2013) discovered that the definitions of several business
models contain the following factors: (1) customer value proposition; (2) value
creation, value capture, and value delivery inside the enterprise; (3) value co-creation
process of stakeholders, including customers and enterprises; (4) communication
among stakeholders; and (5) in the marketing field, business models also contain
value exchange under the profiting environment and the non-profiting environment.
In conclusion, at the core of a business model is the value (co-)creation and value-
delivery processes.
In recent years, research has focused on business model innovation. Because of
the changing environment and the impact of new technologies and concepts,
companies need to continuously recognize and overcome various problems (resource
shortage, knowledge barrier, etc.) and update their business models in order to gain
competitive advantages and achieve long-term success(Chesbrough, 2010). Zottet al.
(2011) reported that the business model itself is not independent. Specifically, they
found that the innovation of the business model requires a systematic and historical
perspective to demonstrate how enterprises should operate and create more value,
14
rather than merely capture value. Girotra and Netessine (2013) determined that the
innovation of business models assists companies to realize the sustainable utilization
of products and services. In other words, a new business model promotes the
application of advanced technologies and services. When measuring an innovated
business model for sustainable development, it is essential to consider information
inefficiencies and alignment inefficiencies in the value chain. According to these
principles, they proposed a pedagogical approach which applied design properties
(what, when, who, and why) to develop new business models.
Apart from the innovation of the business model, value co-creation is another
topic that has attracted attention of researchers. Actually, some scholars claimed that
the stakeholder is an inevitable link in the business model, especially in some service
industries (Gao, 2016; Sorescu et al., 2011). Dahan et al. (2010) pointed out that, due
to the operational challenges in developing countries and the continuous application
of advanced technologies, many transnational corporations have considered
deepening cooperation with non-profit nongovernmental organizations (NGOs) for
value co-creation. Such cooperation produces the multi-organizational business model.
Value co-creation originates from companies’ efforts to market new technologies and
new concepts (Ballantyne et al., 2011). In this process, the corporations are not able to
reform their own business models. Therefore, they need to cooperate with other
stakeholders, including customers, governments, research institutions, business
partners and suppliers, to create new products and values. Communication among the
stakeholders plays a vital role in the process of value co-creation. The form of
communication varies according to profits, cash, important resources, abilities, and
even different value propositions (Ballantyne et al., 2011). Recently, researchers have
attached more importance to the research of business models under open
environments (Saebi et al., 2015), where communication between enterprises and the
external world becomes more frequent, and more stakeholders should be considered.
In this process, value co-creation was initially accepted as a means through which
value is created in conjunction with customers, rather than being created entirely
15
inside of the boundaries of a single firm. This concept acknowledges the increasing
role of consumers as innovators in the development of value propositions (von Hippel
et al., 2011). In addition, stakeholders, (other than corporations, e.g., governments,
etc.) will also play a positive role in the business model under open circumstances.
Generally, the stakeholders inside or outside of the enterprises (or organizations)
constitute a network that describes multilateral relations among various stakeholders
based on value co-creation.
As can be noted, quite a lot of definitions and descriptions of business models
are proposed in the literature. Some of them include too many elements in a business
model and seem too complicated. As the most concise ones, Johnson et al. (2008) and
Coombes and Nicholoson (2012) summarize the elements of the business model as
the following four dimensions, which we think are clear, compact and all-inclusive.
Customer value proposition (CVP): This mainly refers to the process in which
companies (or organizations) analyze customers’ demands and create values for them,
which are the core of the business model (Teece, 2010). A successful company must
be able to create values for customers, namely, to obtain what customers need (a job).
The job may be a specific product (real economy) or a solution to a problem (service
industry). Once a company knows the job and understands how to provide it, they can
design the offering. The customer value proposition depends on the following three
aspects (Johnson et al., 2008): (1) whether your offering is important to costumers –
the more important it is, the greater the CVP; (2) whether customers can obtain the
job from existing sales channels –the harder it is for customers to obtain it, or the
lower the level of the customer satisfaction with current options for getting the job
done, the greater the CVP; and (3) the better your solution is than existing alternatives
at getting the job done (lower price, better quality, etc.), the greater the CVP. The
optimal situation is one in which there is no substitute for the product or service that
you can provide well.
Key resources (Casadesus-Masanell et al., 2010): The successful operation of
the business model cannot be separated from the investment of some key resources,

16
including (but not limited to) human resources, technology, products, equipment,
channels, trademarks, etc., which constitute the foundation of delivering the value
proposition to specific customers. The premise for the success of a business model is
identifying and utilizing these key resources to create values for customers and
enterprises themselves (during which the connections and interactions among these
key resources must be made clear).
Profit formula: This mainly refers to the profits that enterprises can obtain for
themselves while creating values for customers. Some scholars also term this as value
capture (Zott et al., 2011). Profit formula depends on two aspects: revenue and cost
structure, where revenue = price * volumes and costs are directly determined by direct
costs, indirect costs, and scale economy (Johnson et al., 2008). Cost structure
generally depends on the characteristics of key resources. During a company’s
operation process, marginal revenue and resource velocity (how fast inventory must
be turned over, fixed assets, and other assets) need to be taken into consideration.
Since price is of great importance to customers, enterprises can start by setting the
price required to deliver the CVP, and then work backwards from there to determine
what the variable costs and gross margins must be. This then establishes the scale and
resource velocity needed to achieve the desired profits.
Key processes: the value that enterprises create and capture for customers’
needs to be transformed and delivered to customers through the designed processes,
including recurrent tasks such as training, development, manufacturing, budgeting,
planning, sales, service, etc. From a broader perspective, key business processes also
comprise a company’s rules, metrics, and norms (Girotra et al., 2013). A great
business process design can assist enterprises to lower costs, increase profits, and
expand the operation scale. It is worth noting that business process reengineering
(BPR) is also an important topic when considering and designing key processes
(Cosenz et al., 2017).
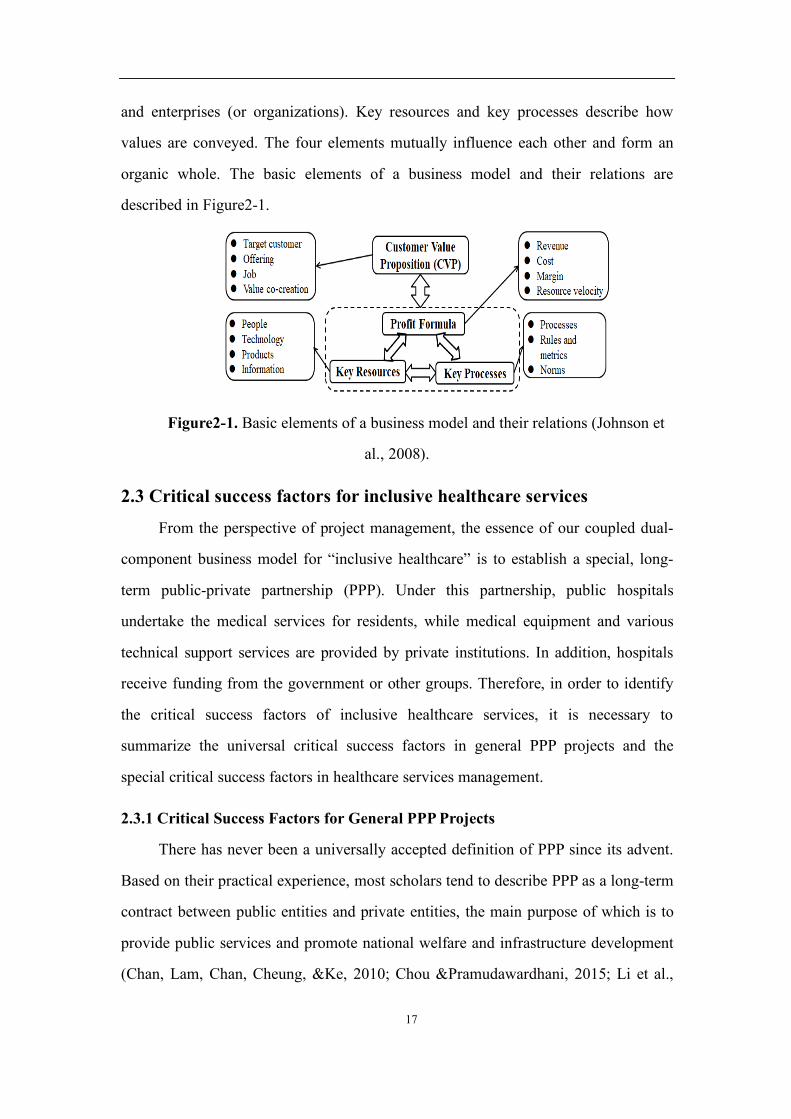
The four elements above must be considered when designing the business
model. Customer value proposition and profit formula define the values of customers
17
and enterprises (or organizations). Key resources and key processes describe how
values are conveyed. The four elements mutually influence each other and form an
organic whole. The basic elements of a business model and their relations are
described in Figure2-1.
Figure2-1. Basic elements of a business model and their relations (Johnson et
al., 2008).
2.3 Critical success factors for inclusive healthcare services
From the perspective of project management, the essence of our coupled dual-
component business model for “inclusive healthcare” is to establish a special, long-
term public-private partnership (PPP). Under this partnership, public hospitals
undertake the medical services for residents, while medical equipment and various
technical support services are provided by private institutions. In addition, hospitals
receive funding from the government or other groups. Therefore, in order to identify
the critical success factors of inclusive healthcare services, it is necessary to
summarize the universal critical success factors in general PPP projects and the
special critical success factors in healthcare services management.
2.3.1 Critical Success Factors for General PPP Projects
There has never been a universally accepted definition of PPP since its advent.
Based on their practical experience, most scholars tend to describe PPP as a long-term
contract between public entities and private entities, the main purpose of which is to
provide public services and promote national welfare and infrastructure development
(Chan, Lam, Chan, Cheung, &Ke, 2010; Chou &Pramudawardhani, 2015; Li et al.,

18
2005). Such a partnership requires both parties to have common goals and an
appropriate risk sharing mechanism (Xu, Chan & Yeung, 2010). This is because PPP
involves a variety of actors such as governments, private entities, consumers,
operators, subcontractors, financial organizations, etc. The different goals of these
actors have led to a complex relationship among them, which results in a challenging
implementation process. In China’s rapid marketization process (despite this
constraint), PPP is a very effective way to develop infrastructure projects to meet huge
demands (Chan et al., 2010), although certain conditions or critical success factors
(CSF) have to be met.
Rockart (1979) defines CSF as those few key areas of activity in which
favourable results are absolutely necessary for a particular company to reach its goals.
That is, they are areas where “things must go right” — if there is a deviation in an
activity under these key areas, the entire organization will get half the result with
twice the effort over a period of time. In addition, business failures are often
associated with companies not paying attention to or addressing critical success
factors. Therefore, in management activities, these critical success factors must
receive sufficient attention. According to Rockard’s research (Freund, 1988), critical
success factors have the following characteristics:
• They are crucial to the achievement of a company’s mission;
• They are measurable and controllable in an organization;
• Their number is limited — not every factor is important;
• They are something that must be done;
• They are applicable to all companies in a particular industry with similar goals
and strategies;
• They are stratified — some critical success factors are related to a company’s
overall strategy, while others are related to its day-to-day operations.
Since 1990, the PPP model has been widely used in infrastructure development
projects in developing and developed countries alike. Many scholars have also
summarized the critical success factors in PPP projects (Al-Saadi& Abdou, 2016;
19
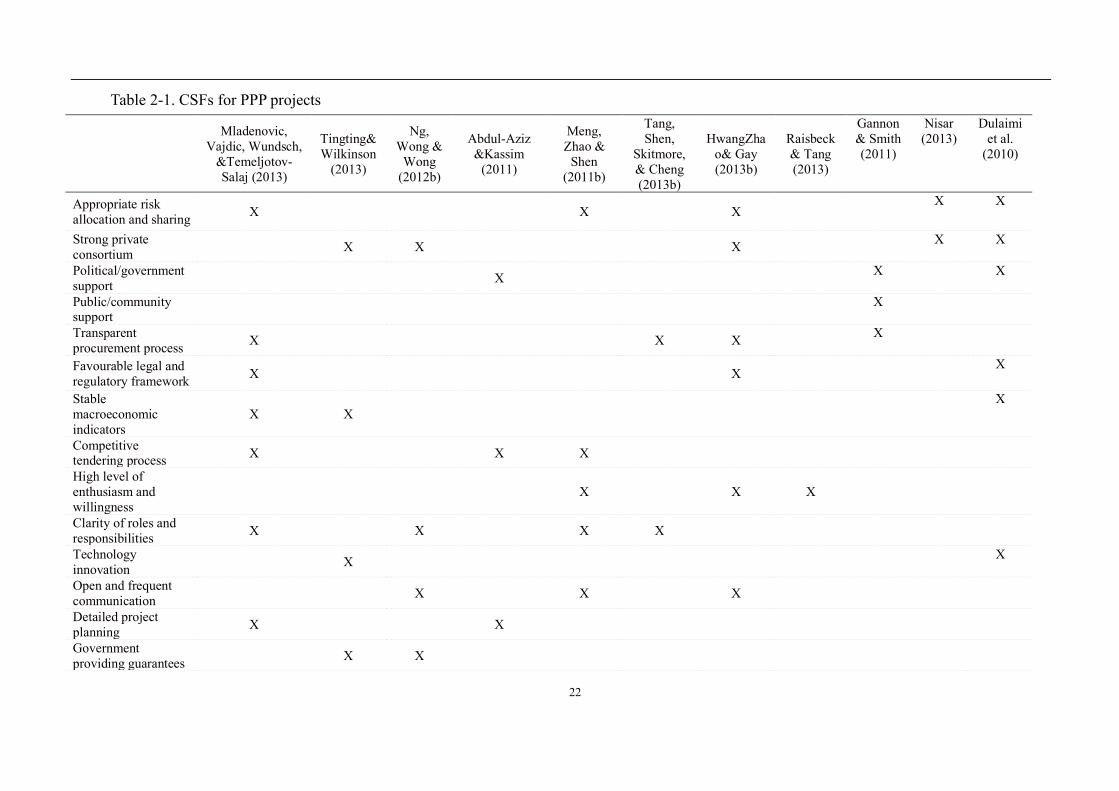
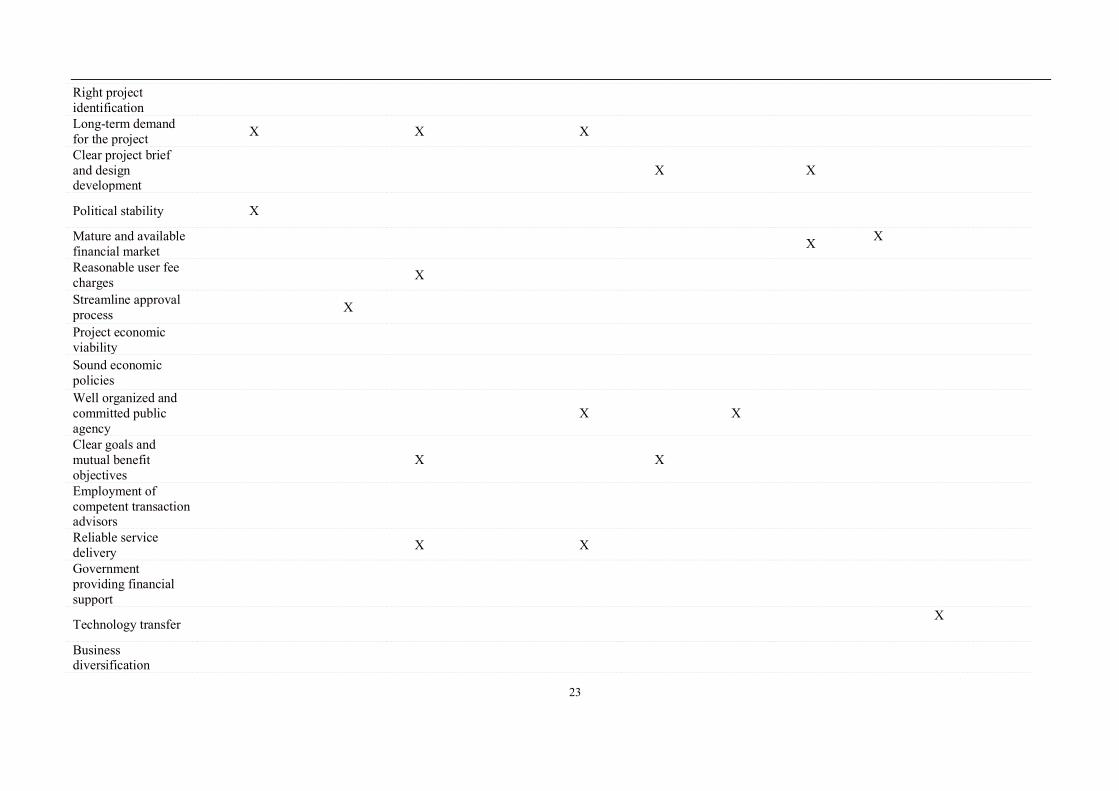
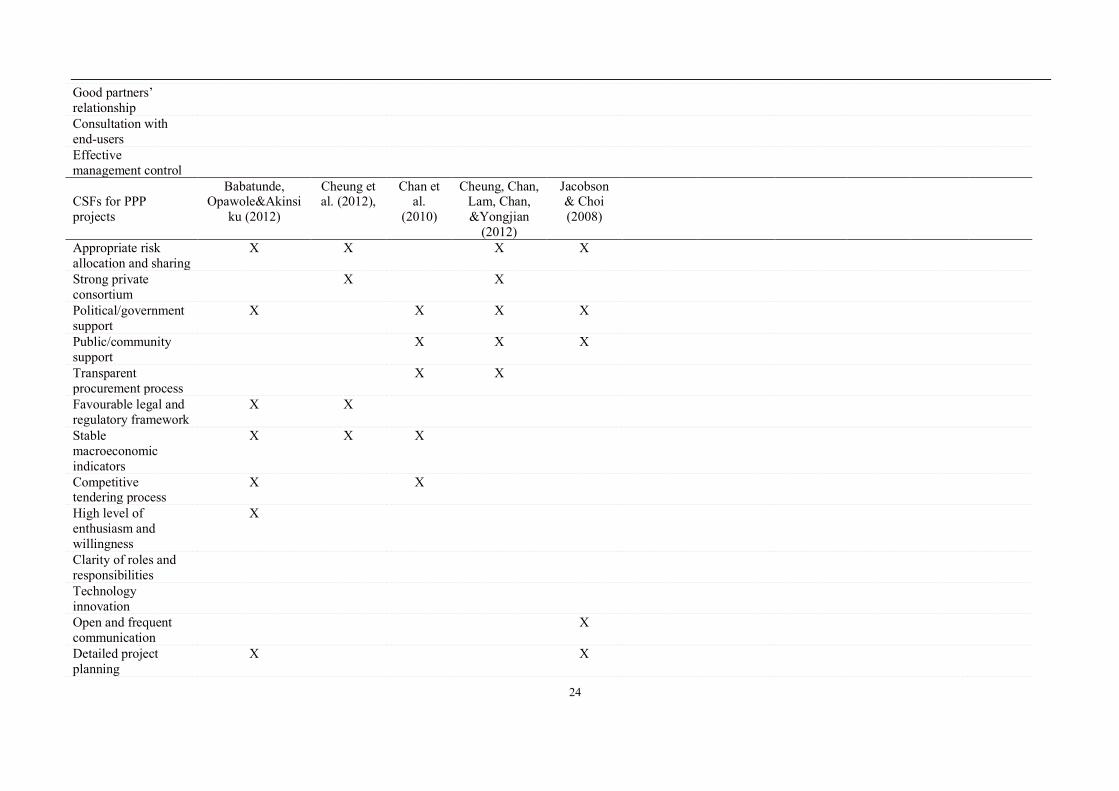
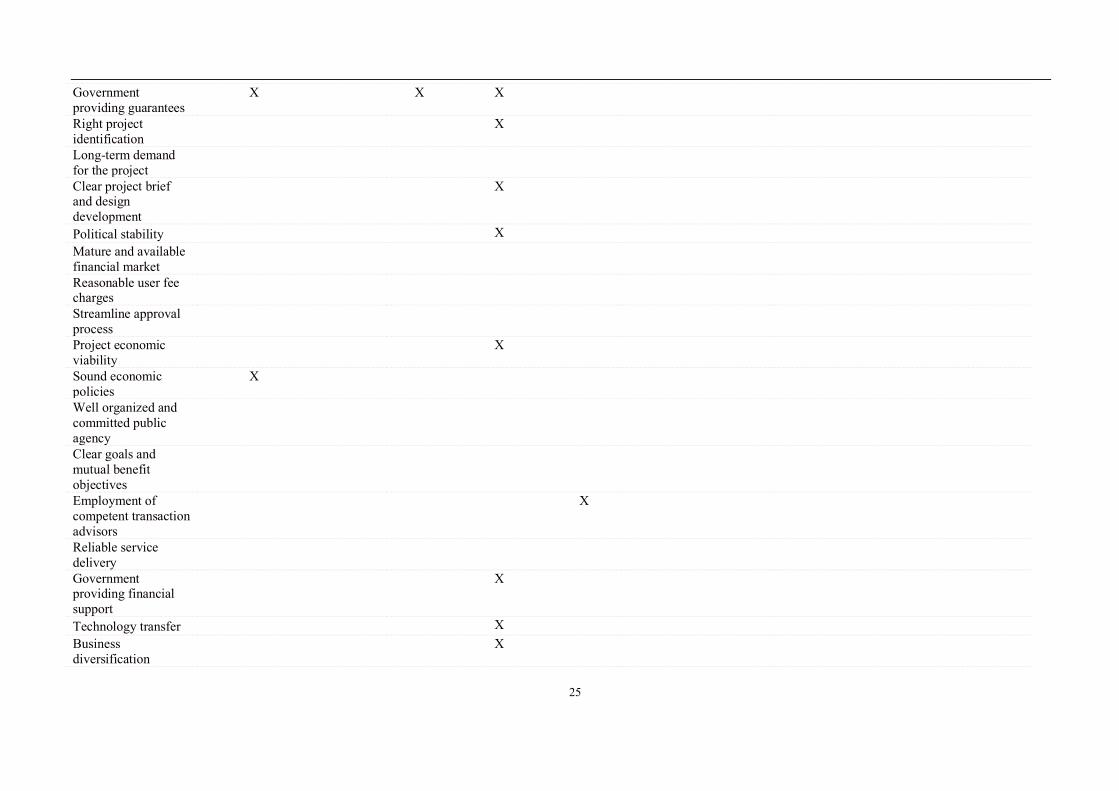
Chan et al., 2010; Hwang, Zhao & Gay, 2013a; Li et al., 2005). Table 1 summarizes
the critical success factors of PPP mentioned in the literature in the last decade (2007-
2017). In this table, there are 35 specific critical success factors, which include
external environment for project implementation, planning, design and management
of the project itself, government (or public sector) support, reliable concession
consortia, technological innovation and transfer, macroeconomic and social support,
economic feasibility of the project, risk factors of the project, among others.
It is essential to note that critical success factors of the PPP model vary in
different countries. For example, in developing countries (especially China), political
stability and government support are crucial (Chan et al., 2010; Osei-Kyei& Chan,
2017). However, in developed countries, this factor is clearly not fairly important
(Cheung, Chan &Kajewski, 2012; Li et al., 2005). The reason may be the lack of
stability in the political and economic environment in many developing countries,
resulting in frequent cancellations and changes in PPP projects implemented in these
countries (Osei-Kyei et al., 2017). Therefore, some researches have called for political
leaders to commit themselves to providing a stable environment to ensure the smooth
implementation of PPP projects. The government should provide appropriate
compensation if private investors suffer a loss of interest in a volatile political
situation (Cheung et al., 2012). In addition, a successful PPP project in most
developing countries requires a stable and sound macroeconomic environment (Qiao
et al., 2001; Osei-Kyei and Chan, 2015b; Ismail, 2013). In terms of the
macroeconomic environment, interest and inflation rates should remain stable for a
period of time to enable project operators to better manage and implement their
projects. The critical success factors for the smooth operation of PPP projects in
developing countries also include: appropriate project election, sound legal and
regulatory framework, community support, mature financial markets, technology
transfer, competitive procurement processes, etc. (Askar & Gab-Allah, 2002; Chan et
al., 2010; Dulaimi, Alhashemi, Ling & Kumaraswamy, 2010; Meng, Zhao & Shen,
2011a; Osei-Kyei& Chan, 2016). While in developed countries, critical success

20
factors for PPP projects include project scale, operational factors (such as clear project
brief and design development), reasonable risk allocation and sharing mechanisms,
effective procurement processes, long-term needs, strong private consortia, clear
objectives, environmental impact of the project, ongoing project monitoring and the
minimization of contract modifications, etc. (Aziz, 2007; Hwang et al., 2013a; Li et
al., 2005; Ng, Wong & Wong, 2012a; Tang, Shen, Skitmore, & Cheng, 2013a; Tiong,
Yeo & McCarthy, 1992). Obviously, due to different cultural, socio-political and
economic backgrounds, the factors that need to be considered when implementing
PPP projects in developed countries differ significantly from those in developing
countries.
2.3.2 Critical Success Factors for Hospital Management
Information technology (IT) in the medical industry can effectively improve a
hospital’s service quality and effectiveness and efficiency. The effective use of IT has
resulted in telemedicine projects being implemented in many countries (Al-Qirim,
2005; Jennett, Yeo, Pauls& Graham, 2003; Kodukula&Nazvia, 2011). With the
increasing application of big data and artificial intelligence technologies in the
medical field, governments and enterprises in many countries are actively exploring
the role of technological innovation in promoting public healthcare services. As a
result, more public medical service initiatives utilizing the latest technologies are
being implemented (Al-Qirim, 2005; De Marco, Mangano, Cagliano, & Grimaldi,
2012b). Without exception, all the researches referred to financial constraints as an
issue that must be considered in these new medical initiatives.
As early as the 1990s, developed countries in Europe and North America have
already implemented various PPP project models such as franchising, DBFO (design,
build, finance and operate), BOO (build, own and operate), BOOT (build, own,
operate and transfer), and BOLB (buy, own, and lease back) in the medical field
(McKee, Edwards &Atun, 2006). For instance, Australia and New Zealand have
applied almost all of the above PPP models (Al-Qirim, 2005). The Private Finance
Initiative (PFI) model in the UK is also a kind of DBFO, which, over the past two

21
decades, has addressed major capital investment issues in healthcare. The key ideas of
this model are: a company—usually in the construction industry—becomes a general
contractor to provide non-clinical services to hospitals by establishing a “special
purpose vehicle”, which serves as a basis for contracting with a health authority. This
model has also been used in Canada, Portugal, Spain and Greece (Atun&Mckee,
2005). Unlike the above countries, Sweden and Italy mainly rely on the franchising
model (De Marco, Mangano, Cagliano, & Grimaldi, 2012b), which was first applied
in the Alzira Hospital in Spain. Under this model, a private company manages a
public hospital, which only serves a specific group of people to maintain the
expenditures of the private group, in return for an annual per capita payment.
However, due to the public nature of the medical expense reimbursement system,
privately funded BOT hospitals are rare in Europe. This is why most projects require a
significant portion of public funds in its capital structure, which on average is
equivalent to more than 30% of the initial investment (Zhang, 2005).
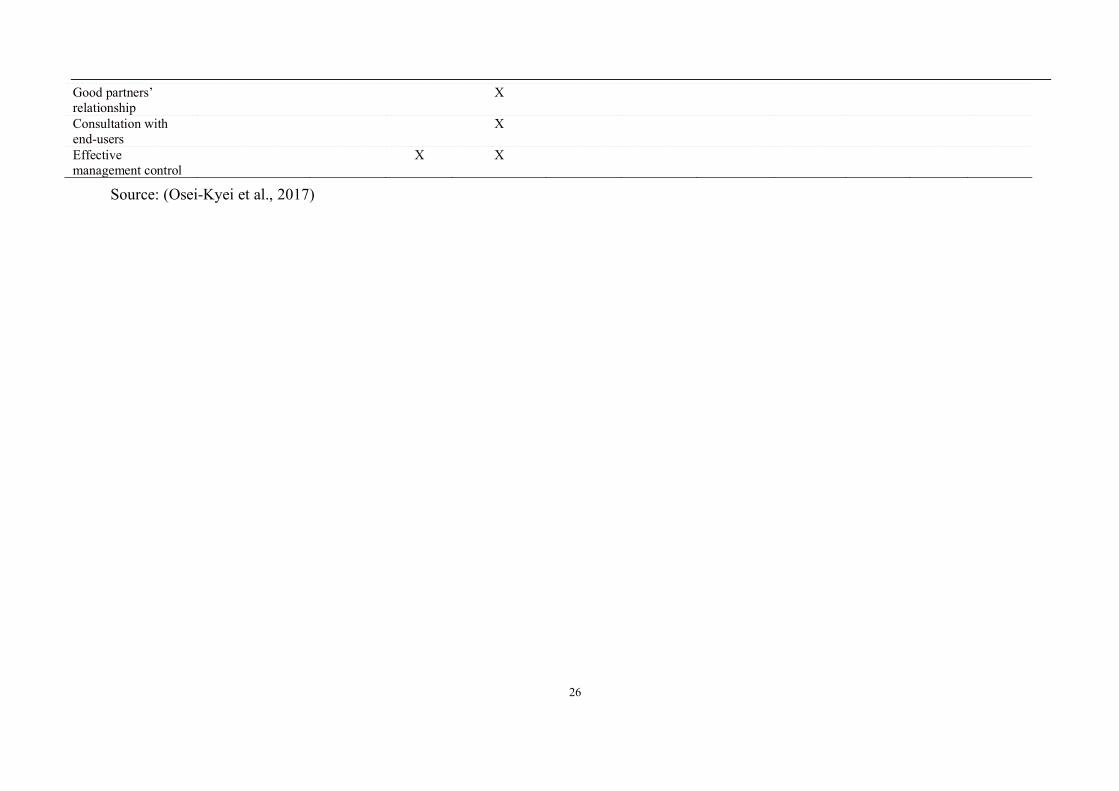
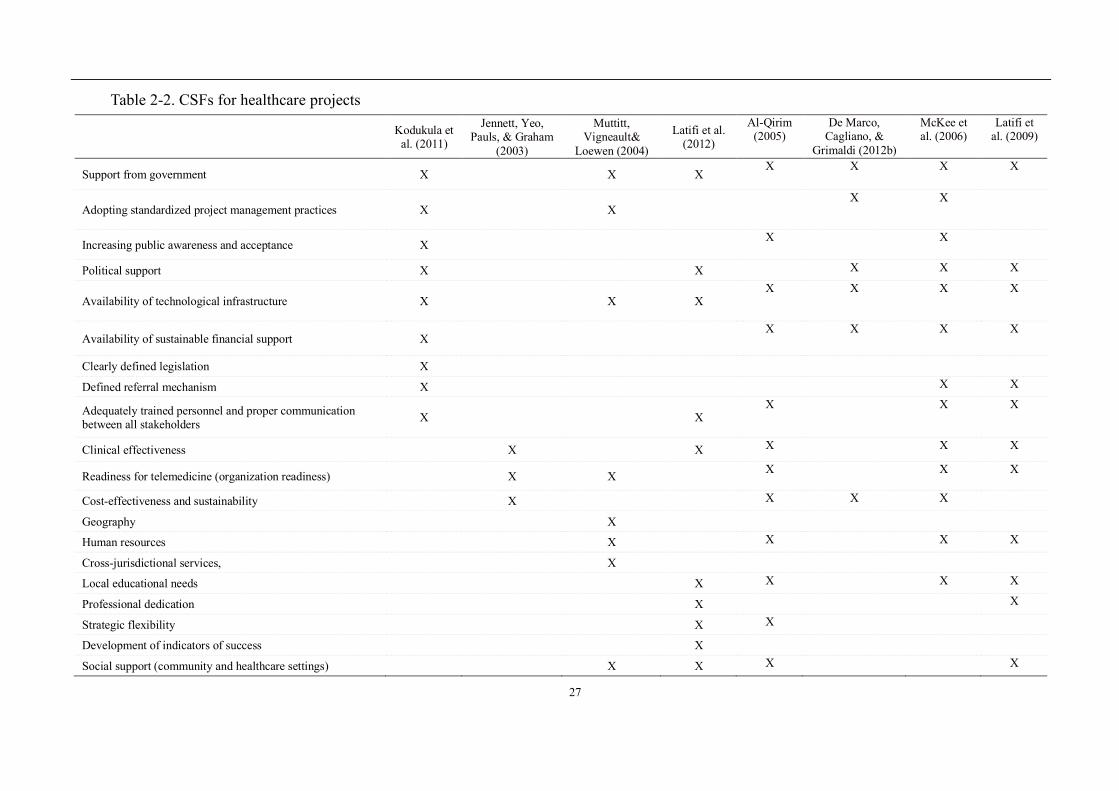
Based on the above literature, Table 2-2 summarizes the critical success factors
in implementing public health projects.
In recent years, smart data-driven healthcare has received increasing attention
and will be playing an important role in comparative studies of clinical practices,
clinical decision support systems, medical data transparency, remote patient
monitoring, effectively reducing mistakes in decisions (based on advanced analysis of
patient files) and reducing avoidable harm to patients (Ahmad, Paul & Rathore, 2016;
Fan, Han & Liu, 2014; Xu, Shen, & Yu, 2017). Leading in this new wave of artificial
intelligence are China’s Alibaba, Baidu and Tencent and America’s Google, Microsoft
and IBM (Miller & Brown, 2018; Chen, Argentinis& Weber, 2016).These have
increasingly been using AI in medical imaging, auxiliary diagnosis, disease risk
prediction, drug extraction, health management, hospital management, assisted
medicine and other areas.
22
Table 2-1. CSFs for PPP projects
Mladenovic,
Vajdic, Wundsch, &Temeljotov-Salaj (2013)
Tingting& Wilkinson
(2013)
Ng, Wong &
Wong (2012b)
Abdul-Aziz &Kassim
(2011)
Meng, Zhao &
Shen (2011b)
Tang, Shen,
Skitmore, & Cheng (2013b)
HwangZhao& Gay (2013b)
Raisbeck& Tang (2013)
Gannon & Smith (2011)
Nisar (2013)
Dulaimi et al.
(2010)
Appropriate risk allocation and sharing X X X X X
Strong private consortium
X X X X X
Political/government support
X X X
Public/community support
X
Transparent procurement process X X X X
Favourable legal and regulatory framework X X X
Stable macroeconomic indicators
X X X
Competitive tendering process X X X
High level of enthusiasm and willingness
X X X
Clarity of roles and responsibilities X X X X
Technology innovation
X X
Open and frequent communication
X X X
Detailed project planning X X
Government providing guarantees
X X
23
Right project identification
Long-term demand for the project X X X
Clear project brief and design development
X X
Political stability X
Mature and available financial market X X
Reasonable user fee charges
X
Streamline approval process
X
Project economic viability
Sound economic policies
Well organized and committed public agency
X X
Clear goals and mutual benefit objectives
X X
Employment of competent transaction advisors
Reliable service delivery
X X
Government providing financial support
Technology transfer X
Business diversification
24
Good partners’ relationship
Consultation with end-users
Effective management control
CSFs for PPP projects
Babatunde, Opawole&Akinsi
ku (2012)
Cheung et al. (2012),
Chan et al.
(2010)
Cheung, Chan, Lam, Chan, &Yongjian
(2012)
Jacobson & Choi (2008)
Appropriate risk allocation and sharing
X X X X
Strong private consortium
X X
Political/government support
X X X X
Public/community support
X X X
Transparent procurement process
X X
Favourable legal and regulatory framework
X X
Stable macroeconomic indicators
X X X
Competitive tendering process
X X
High level of enthusiasm and willingness
X
Clarity of roles and responsibilities
Technology innovation
Open and frequent communication
X
Detailed project planning
X X
25
Government providing guarantees
X X X
Right project identification
X
Long-term demand for the project
Clear project brief and design development
X
Political stability X Mature and available financial market
Reasonable user fee charges
Streamline approval process
Project economic viability
X
Sound economic policies
X
Well organized and committed public agency
Clear goals and mutual benefit objectives
Employment of competent transaction advisors
X
Reliable service delivery
Government providing financial support
X
Technology transfer X Business diversification
X
26
Good partners’ relationship
X
Consultation with end-users
X
Effective management control
X X
Source: (Osei-Kyei et al., 2017)
27
Table 2-2. CSFs for healthcare projects
Kodukula et al. (2011)
Jennett, Yeo, Pauls, & Graham
(2003)
Muttitt, Vigneault&
Loewen (2004)
Latifi et al. (2012)
Al-Qirim (2005)
De Marco, Cagliano, &
Grimaldi (2012b)
McKee et al. (2006)
Latifi et al. (2009)
Support from government X X X X X X X
Adopting standardized project management practices X X X X
Increasing public awareness and acceptance X X X
Political support X X X X X
Availability of technological infrastructure X X X X X X X
Availability of sustainable financial support X X X X X
Clearly defined legislation X
Defined referral mechanism X X X
Adequately trained personnel and proper communication between all stakeholders X X
X X X
Clinical effectiveness X X X X X
Readiness for telemedicine (organization readiness) X X X X X
Cost-effectiveness and sustainability X X X X
Geography X
Human resources X X X X
Cross-jurisdictional services, X
Local educational needs X X X X
Professional dedication X X
Strategic flexibility X X
Development of indicators of success X
Social support (community and healthcare settings) X X X X

28
Among these, medical imaging and disease risk management are currently the
most popular use cases(Miller et al., 2018). Similarly, many countries around the
world have launched medical projects based on AI technologies. In 2015, the Dutch
government began using AI technologies to find the most effective treatment for
specific patient groups and to reduce mistreatment by analyzing digital medical
records. In 2016, the health authorities in Las Vegas, USA used AI technologies for
public health monitoring, and identified sources of disease outbreaks by tracking
social media. In 2017, the Ruijin Hospital affiliated to the School of Medicine,
Shanghai Jiao Tong University (in collaboration with the University of York in the
UK) launched the world’s largest single-centre clinical study to verify the use of
wearable devices in helping the diagnosis and monitoring of Parkinson’s disease. Also,
in 2017, at the Yunqi Conference held in Hangzhou, Alibaba announced entering the
AI medical field, with a focus on doctors, patients, and hospital management (Cao &
Gu, 2018). However, there has so far been no research on the critical success factors
for these projects. Therefore, the inclusive healthcare services are unable to draw
experience and lessons from such projects at this moment.
In essence, inclusive healthcare is also a medical project that combines the PPP
model with new technologies such as big data and artificial intelligence. In view of
the above characteristics, we can see that the critical success factors for the PPP
projects and similar medical projects mentioned in the literature are potential critical
success factors for inclusive healthcare services.
2.4 The Technical Framework for Inclusive Healthcare Services
2.4.1 A Multi-Source Data Fusion Method based on Evidence Theory
Evidential reasoning is an important means of intelligent reasoning and
information fusion in the field of artificial intelligence. Yang and Xu (2013) pointed
out that this method was widely used in the fields of decision science, control science,
information system and operational research. The term “evidential reasoning” first
appeared in an article published on AI by Gordon and Shortliffe (1985), which

29
proposed a method of applying the traditional Dempster-Shafer (D-S) evidence
merging rule of Sentz and Ferson (2002) to the hypothesis space for evidence merging.
Inglis (1977) argues that D-S rule of evidence fusion was based on a framework
composed of exhaustive and mutually exclusive hypotheses, and that the allocation
mechanism was designed to allocate the confidence interval in the entire hypothetical
space and the combination of basic assumptions. It was not just limited to a single
hypothesis. Murphy (2000) indicated that although the traditional D-S evidence fusion
rule was based on probability theory and constructed the complete probability
inference process, the merging precision would be greatly affected when dealing with
highly contradictory evidence. In addition, the D-S evidence fusion rule assumed that
all evidence sources were totally reliable and of equal importance. This means that if a
single piece of evidence is against a hypothesis, the hypothesis will be rejected
(whether or not it is supported by other evidence). Yang and Xu (2002) pointed out
that, although this processing mechanism was effective in some special cases, it was
better to simulate the reality in most cases by characterizing an evidential reasoning
model where all sources complemented each other and each acted as a finite role in
the hypothetical space. In this context, Yang and Xu (2013) constructed a generalized
ER evidential reasoning model, adding weights and reliability to each piece of
evidence, and optimized the performance of the evidence fusion theory in dealing
with some highly conflicting evidence. Further, based on the ER theory, Xu et al.
(2017) proposed a machine learning classification method based on evidential
reasoning rules in small sample reasoning. This method constructed the classification
model using ER rules and uses the quasi-linear optimization algorithm to fit the
parameters, and obtains competitive results in the open standard source dataset test.
The D-S evidential reasoning theory does not work as well as the ER rule when the
evidence is paradoxical.
2.4.2 Large Cloud Architecture for Medical Services
Armbrust et al. (2010) stated that, in order to implement cloud computing, it is
necessary to build a set of reliable softwares and hardwares to store the massive data

30
and host the service applications. Compared with traditional solutions, cloud
computing has better economic benefits when processing massive data. Galante and
Bona (2013) argued that computational elasticity is a very important factor in
evaluating a cloud architecture. The research synthesized relevant work on
computational elasticity mechanisms in cloud systems. Hashem et al. (2015) argued
that a lot of time is needed to build a cloud computing infrastructure that can be used
for massive data processing. The framework includes multiple features such as data
storage and computing, and involves data fusion, data quality assessment, privacy and
security and many other issues. Assunção et al. (2015) introduced a framework for
managing massive data on the cloud by building a data warehouse at the bottom layer
for data storage and pre-processing; a cloud computing component to process data
using models at the middle layer; and applications for behaviour analysis, prediction,
visualization and other purposes based on the data processed. Chang et al. (2016)
established a cloud computing framework suitable for commercial applications, which
is able to prevent virus intrusions and cyber-attacks through a new security
architecture. Page et al. (2016) proposed a structure for providing remote health
monitoring and decision support for digital healthcare (D-health), which includes a
data collection module using Internet of Things (IoT) devices; a system-level
encrypted data storage module, and a data analysis module that uses statistical
inference algorithms. Sivarajah et al. (2017) believe that processing massive data has
the following challenges: (1) data itself, including the value, volume, diversity, etc. of
data; (2) the processing of data, such as the acquisition and storage of data, data
cleansing and value extraction; and (3) data management, including data security,
privacy and other issues.
At the infrastructure layer of the cloud system, an appropriate strategy for
obtaining medical data is needed. Ahmed and Abdullah (2012) established a data
acquisition and management framework for electronic medical records, in which a
wireless sensor network was deployed for medical data acquisition. Shahzad et al.
(2014) developed the SCADA (supervisory control and data acquisition) system,

31
which, if deployed in a cloud environment, could effectively improve the cost of data
acquisition and data security in the cloud system. The data will be monitored and
managed by the master site during the acquisition and transmission process. Reichert
et al. (2014) designed a cloud-based automated data acquisition model that provides
data acquisition services and data snapshots through infrastructure monitoring.
The middle layer of the cloud system should support the application layer using
secure cloud storage and efficient cloud computing solutions and cloud application
development platforms. To improve the security of cloud storage, Wang et al. (2010)
introduced a third-party auditor (TPA), which does not add burden on the network,
nor bring any new vulnerabilities that compromise the data. Kumar et al. (2011) used
a Sobol sequence to verify the integrity of erasure coded data, which provides better
security for cloud storage than traditional protocols. Selvakumar et al. (2013)
proposed a partition-based cloud storage solution, which prevents clients to copy data
locally, thereby improving the efficiency and security of cloud storage. Ren et al.
(2016) used a hashing operation to improve the storage efficiency of cloud storage
while ensuring security. Compared with traditional third-party auditing solutions, this
solution increases the speed of generating and checking security labels to nearly a
thousand times that of traditional methods. In terms of cloud computing, Gong and
Gu (2010) proposed a new pattern-driven application consolidation system that
dynamically discovers important patterns through signal processing techniques and
performs dynamic application consolidation based on the patterns identified, thereby
achieving effective sharing of resource in the cloud computing infrastructure and
improving its efficiency. Iosup et al. (2011) analyzed the performance of cloud
computing services for scientific computing workloads and optimized the device load
in many-task computing to meet the computing requirements. Mastelic et al. (2014)
defined a systematic approach to analyzing the energy efficiency of cloud computing
centres and applied it to the energy efficiency analysis of data centres and their
equipment. Xu et al. (2016) proposed a heuristic technique called PASS (pre-
processing based on a small sample) to pre-process small sample data that frequently

32
occur in big data to improve the efficiency of cloud computing. Reddy et al. (2016)
discussed load balancing and the performance of various algorithms on addressing
this issue. And he proposed an algorithm for balancing the load and computing power
for each node in cloud computing system.
In terms of cloud application platforms, Iosup et al. (2011) discussed the
challenges of the software development process for cloud platforms. Nasui et al.
(2013) proposed a secure, intelligent, connected and interactive cloud-based
application development platform that collects and transmits information from a
variety of data sources in multiple wireless communication systems. The system is
built on a three-layer scalable architecture that promotes interoperability.
2.4.3 Medical Image Recognition Technology for Brain Tumour Diagnosis
This research focused on medical image recognition of the brain. Related
literature can be divided into two groups: the first group aims to identify medical
images through morphological and characteristic engineering; and the other group
aims to use neural networks (including Convolutional Nerual Network: CNN) to
recognize medical images. First, when using morphological, feature engineering for
brain image recognition, Zacharaki et al. (2009) used several steps including defining
the region of interest, feature extraction, feature selection and classification to identify
different types of brain tumours (such as metastatic primary glioma and glioma
grading). Thapaliya and Kwon (2012) introduced an effective framework for
extracting brain tumours from magnetic resonance (MR) images. A median filter was
used to filter the image, and then morphological gradients were used to calculate the
enhanced intensity of the image. Last, a flood-filled algorithm and pixel replacement
algorithms were used to extract brain tumours. Bergner et al. (2013) collected 39
kinds of Raman images from six cases of glioma brain tumour specimens. And
through analyzing the different types of tumour cells’ morphological characteristics
and chemical expression, he developed a classification method based on the Raman
spectrum of brain glioma. Ulku and Camurcu (2014) used histogram equalization and
morphological image processing to perform computer-aided detection of brain images.

33
The accuracy of this method was validated by processing and identifying 125 MR
images of 11 patients. Shanthakumar and Ganesh Kumar (2016) (while adopting the
histogram equalization, the gray level co-occurrence matrix and wavelets as features),
used the SVM classifier to train and classify the extracted features. Brain tumour
detection methods based on neural network has become a hotspot in recent years.
Abdullah et al. (2012) used a cellular neural network to detect and identify tumours in
brain MRI images, with an algorithm developed in MATLAB. Pan et al. (2015) used
artificial neural networks (ANN) and CNN to identify and classify brain MRI tumours.
The classification performance of CNN was 18% higher than that of ANN. Pereira et
al. (2016) used CNN to segment the brain MRI images. A 3*3 kernel was adopted in
that study, and intensity normalization was used to pre-process the data. Kamnitsas et
al. (2016) used a two-channel 3D CNN for brain MR tumour segmentation. In order
to remove false positives, a Conditional Random Field (CRF) was subsequently used
for further analysis. Zhao et al. (2017) combined Fully Convolutional Neural Network
(FCNN) and CRF to form a unified framework to segment brain tumour images. The
precision of traditional brain image methods is limited by the medical knowledge as
the features, which need to be defined by humans. As the era of big data for healthcare
arrives, neural networks start to demonstrate their benefits for the sector.

34
III. New Business Model for Inclusive Healthcare Services
The successful implementation of inclusive healthcare necessitates financial
support and the allocation of various resources to create and deliver the values needed
by patients. Then, the enterprises or individuals that provide values obtain
corresponding returns or profits. This process is similar to the operation of companies.
Therefore, the successful implementation of inclusive healthcare services requires a
reference to the successful experience of businesses. In the business domain, the
business model is the tool for resource configuration, profit acquisition, and
distribution of profit to stakeholders (Chesbrough, 2007). Business models vary
because each enterprise has its own characteristics and market positioning. Moreover,
the business model plays a crucial role in the future development of an enterprise. As
Bob Higgins of Highland Capital Partners puts it, “... looking back, we believe
technology is to blame in every failure, while the business model is attributable to
every success.”4 Thus, an appropriate business model is bound to ensure the success
of the inclusive healthcare services.
3.1 Inclusive Healthcare System in China: Concepts and Development
In view of medical inequity in remote areas of China, the Chinese government
partnered with companies to implement an inclusive healthcare initiative to address
the issue of “falling into/returning to poverty due to illness” and to reduce inequality
of access to health services. This initiative aims at eliminating the differences in
medical resources between urban and rural areas, promoting the popularization of
quality medical resources, and improving healthcare in poor areas. The goal is to
eliminate the need for patients to travel beyond counties for severe illnesses and
achieve basic medical services for all. The initiative will provide financial support for
the development of medical facilities in poor areas. Relying on telemedicine and
artificial intelligence, the initiative provides advanced disease screening and diagnosis
to poor areas, and ensures the poor’s equal access to fair medical treatment as China

35
implements the new rural cooperative medical insurance scheme and the serious
illness insurance scheme in rural areas. As of July 2017, the inclusive healthcare
services have been piloted in the Guangxi Zhuang Autonomous Region, with plans for
further rollouts in other underdeveloped regions in China such as Xinjiang, Tibet,
Qinghai, Gansu and Ningxia.
The first step in developing inclusive healthcare is to establish necessary
information collection points in primary medical institutions. Modern evidence-based
medicine is premised on the sharing and analyzing of medical data. And the
digitization of patient information collection forms the basis of modern medical
standardization. Only with standardized, informative and reliable patient information
can subsequent medical diagnosis and treatment be reliably carried out. In China,
there is a clear lack of inspection equipment deployed at county-level hospitals,
especially in poor areas (preventing these hospitals from providing patients with
quality medical services). Therefore, the establishment of primary medical
information collection points is a prerequisite for accurate diagnosis and effective
treatment. The collection points will be located in rural and township hospitals in
remote areas, and the key information collection equipment (such as imaging
equipment) will be procured collectively by the inclusive healthcare services team.
Once the information is collected, the existing high-speed broadband network at the
rural and township areas will then be used to transmit it to the remote diagnostic
centre of the inclusive healthcare services, which will ultimately reduce medical
examination expenses. Unified training will also be provided to equipment personnel
so that standardized and complete digital medical file information can be ensured to
assist in subsequent medical diagnosis.
After establishing a complete network of primary medical information
collection points, the inclusive healthcare services will use the remote diagnosis
centre for diagnosis at the remote end. This approach relies on the Internet and big
data on the cloud to remove the barrier of distance and optimize treatment solutions.
The remote diagnostic centre will make full use of quality medical resources in large
36
cities to provide an accurate medical diagnosis for patients in remote areas. The cloud
data centre will integrate advanced technologies such as the Internet and AI to assist
in medical diagnosis and treatment. The medical information processed will
eventually be returned to the information collection point at the grassroots level,
ultimately ensuring that patients in remote areas receive the same quality medical
services available in large cities.
Regarding medical expenses, the remote diagnosis system of universal
healthcare and cloud data platform will ensure reasonable pricing through massive
case data and real-time remote data processing. By combining patient satisfaction
evaluation and using big data to accurately set prices, the initiative is expected to
establish a fully transparent and assessable medical services management approach.
At this stage, the realization of inclusive healthcare can be divided into three steps,
namely (1) the immediate term: promoting the popularization of high-value medical
equipment; closing the gap between urban and rural areas; and significantly reducing
the cost of high-end medical examinations; (2) the short term: remote diagnosis,
intelligent triage, precision fee setting, and resource allocation; (3) the long-term:
replacing today’s traditional medicine with big data driven medicine that transcends
individual experience, and ultimately achieving equity in universal healthcare.
In terms of technology, the overall development plan for the inclusive
healthcare services can be summarized as “one cloud and three ends,” namely a cloud
platform and a cloud-end, a remote-end and a front-end. Work at the front-end
involves the all-round deployment of equipment according to the needs of hospitals at
all levels (provincial/municipal, county/district, and township/community levels). In
this process, the principle of “gap filling” will be followed in order to establish a
telemedicine diagnostic system, which is generally divided into four layers: provincial
support centres, prefectural support (sub) centres, county (district) centres, and
township health centres. This system when in place can handle remote diagnosis,
remote consultation, two-way referral, distance education training, unified medical
data quality control, and remote technical support service. The cloud, on the other

37
hand, is mainly used for developing medical data centres, including a cloud-based
radiographic film repository, a patient portal, a cloud-based 3D advanced impact
analysis, a big data platform for scientific research, etc., as the brain of the entire
inclusive healthcare services. The entire inclusive healthcare services are based on the
cloud platform and uses the “three ends” as service portals. In so doing, “grassroots
treatment and cloud-based diagnosis” can be achieved through innovative
technological means. The details of front-end and remote-end development of the
inclusive healthcare services are shown in Figures 3.1–3.3.
Figure 3-1. The front end of the inclusive healthcare services: the information
network.
Figure 3-2. The remote end of the inclusive healthcare service project: the remote
medical centre.
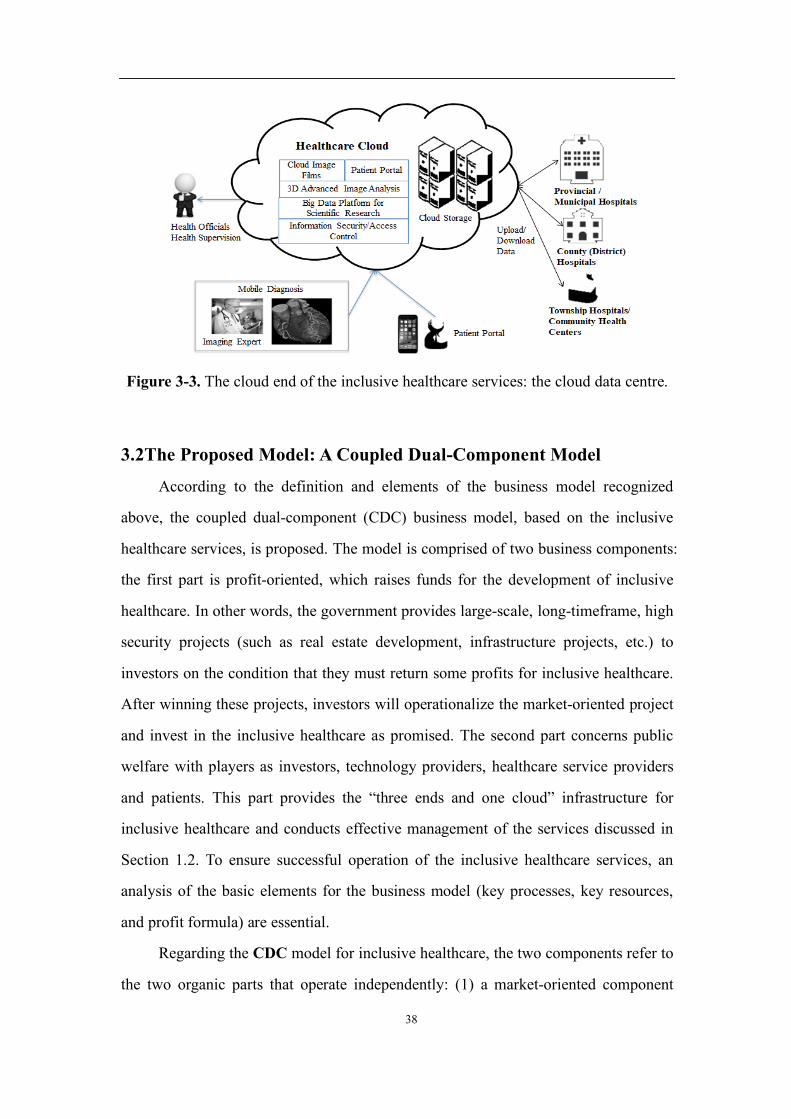
38
Figure 3-3. The cloud end of the inclusive healthcare services: the cloud data centre.
3.2The Proposed Model: A Coupled Dual-Component Model
According to the definition and elements of the business model recognized
above, the coupled dual-component (CDC) business model, based on the inclusive
healthcare services, is proposed. The model is comprised of two business components:
the first part is profit-oriented, which raises funds for the development of inclusive
healthcare. In other words, the government provides large-scale, long-timeframe, high
security projects (such as real estate development, infrastructure projects, etc.) to
investors on the condition that they must return some profits for inclusive healthcare.
After winning these projects, investors will operationalize the market-oriented project
and invest in the inclusive healthcare as promised. The second part concerns public
welfare with players as investors, technology providers, healthcare service providers
and patients. This part provides the “three ends and one cloud” infrastructure for
inclusive healthcare and conducts effective management of the services discussed in
Section 1.2. To ensure successful operation of the inclusive healthcare services, an
analysis of the basic elements for the business model (key processes, key resources,
and profit formula) are essential.
Regarding the CDC model for inclusive healthcare, the two components refer to
the two organic parts that operate independently: (1) a market-oriented component
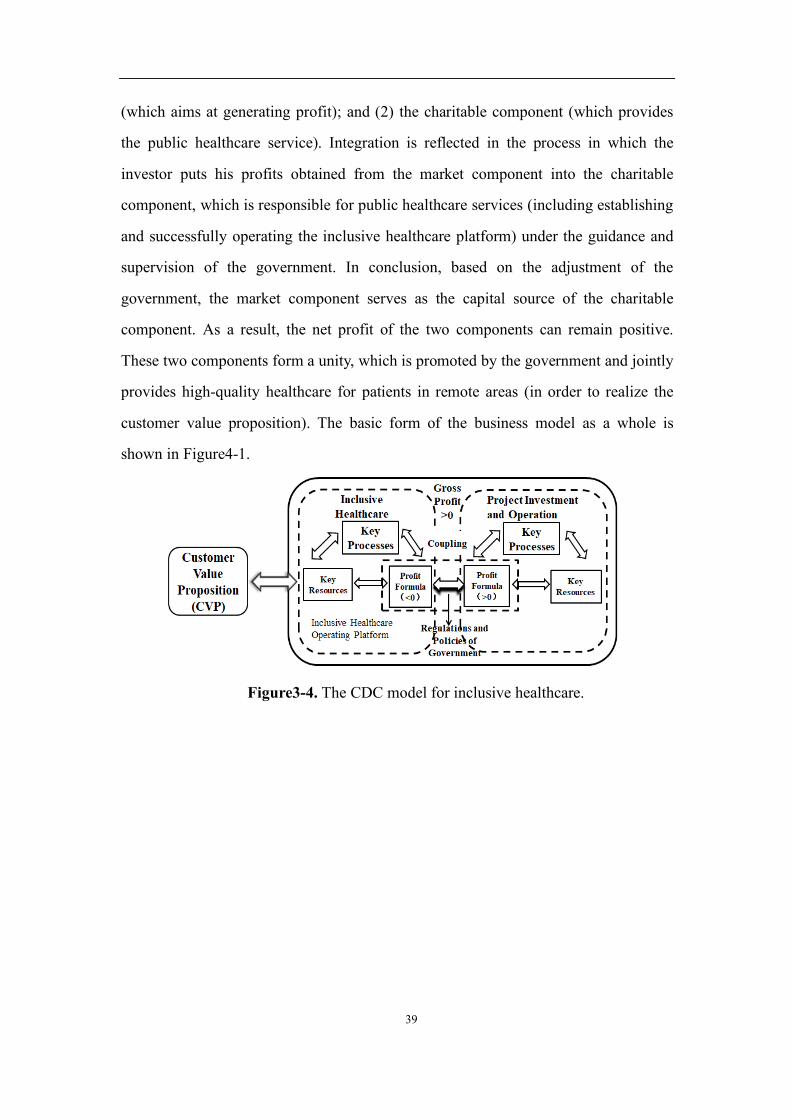
39
(which aims at generating profit); and (2) the charitable component (which provides
the public healthcare service). Integration is reflected in the process in which the
investor puts his profits obtained from the market component into the charitable
component, which is responsible for public healthcare services (including establishing
and successfully operating the inclusive healthcare platform) under the guidance and
supervision of the government. In conclusion, based on the adjustment of the
government, the market component serves as the capital source of the charitable
component. As a result, the net profit of the two components can remain positive.
These two components form a unity, which is promoted by the government and jointly
provides high-quality healthcare for patients in remote areas (in order to realize the
customer value proposition). The basic form of the business model as a whole is
shown in Figure4-1.
Figure3-4. The CDC model for inclusive healthcare.

40
Note that the proposed CDC model is different from traditional pure charity model
with respect to the sustainability of the business models. In fact, if there are no
continuous capitals flowing into the operations of inclusive healthcare services, the
pure charity model cannot run forever. As discussed before, in less developed areas in
China, the government is normally not able to provide enough funds for the purpose
of inclusive healthcare services. However, in the CDC model, there is another part
which generates profits and provides continuous capital flows for charity of
healthcare services, thus the business model may be sustained, and this makes the
inclusive healthcare services feasible for a long timeframe.
3.2.1 Critical Drivers
3.2.1.1 The critical roles of the government
Healthcare service, especially public healthcare service, is a kind of social
guarantee as well as a criterion to evaluate social systems. In China, the government
exerts a unique effect on providing public healthcare services.
Under the specific government system in China, the ideas and determination of
the governing party represent the direction and approaches of social development, and
it can achieve the efficiency and impact unattainable by market-based systems within
a short term, which is a result of the high level of administrative mobilization. For
instance, at the founding of the People’s Republic of China, infectious diseases and
parasitic diseases were rampant. Most people were malnourished with an average life
expectancy of fewer than 35 years. In view of this, the Chinese government
established the rural cooperative medical care system and urban and rural preventive
healthcare network and invested great efforts to develop the publicly funded
healthcare and prevention system. This greatly improved the health of the Chinese
population and made outstanding achievements, in which the healthcare problem of
20% of the world’s population was solved by 2% of the healthcare resources available
in the world with 100% healthcare accessibility. The “barefoot doctor” system in rural
areas is especially praised by the World Health Organization and the World Bank as a
pioneering undertaking of “obtaining the maximum healthcare profits with the least

41
investment”. During this period, with the powerful and effective administrative ability
of the public healthcare system in China, schistosomiasis (bilharziasis), a disease that
had existed for one hundred years at a large scale in Yuhang, Zhejiang was eliminated.
In the first 30 years after the founding of the People’s Republic of China, the Chinese
government successfully implemented comprehensive coverage of healthcare
accessibility. During the 40-year reform and opening-up effort since 1978, the
government has set higher objectives for public healthcare services which include
equity, accessibility, systemization and continuity. Especially, equity in public
healthcare was assigned the top priority.
However, the public welfare healthcare service system led by the government
cannot aim to make profits. Therefore, such a service system requires continuous
financial support, which limits further development and improvement. Indeed, the
low-level operation of free medical services under the planned economic system and
the imbalance between rural and urban areas are a pointer to this disadvantage. The
market economy reform since 1978 has provided institutional conditions for the
development of public healthcare by means of a market mechanism.
In this thesis, we focus on how to ensure the sustainability of public healthcare.
Based on the advantages and disadvantages of public healthcare and private
investment, the CDC model organically connects a non-profit public welfare project
and a for-profit commercial project through the utilization of government resources in
order to form a new interest community. Specifically, the for-profit component
provides financial support for the charitable component to form a short-chain
reallocation system. Finally, the CDC model integrates the power of the government
and the market into civil projects for realizing a “comprehensive well-off society” and
preventing “falling into/returning to poverty due to illness”. The model effectively
avoids the innate disadvantages of the government and the market to satisfy the
demands of all stakeholders.
Different from other privately-operated telemedicine systems that exclude the
role of the government, China’s central or local governments play a pivotal role in the
42
inclusive healthcare services. First, the government has an administrative organization
that extends to all corners of society and can determine the medical status and patient
needs of remote areas to a large extent. China’s one-party state system ensures the
effective execution of the will of the ruling party, and the disciplinary oversight
mechanism of the ruling party ensures that the actions of the government will not
deviate from its governing philosophy, which indirectly ensures the public welfare
nature of inclusive healthcare. In addition, the government can adjust the
implementation of inclusive healthcare through policymaking. Finally, the central
government and local governments connect the implementation process of the
inclusive healthcare. Only through government adjustment are investors willing to
invest profits obtained from the project operation process in the inclusive healthcare
services. Essentially, without the government, it is impossible to connect the two
different components or organically connect the charity project to the market.
In a broad sense, the CDC model constitutes a public-private partnership (PPP)
for healthcare service, which could be compared to a PPP designed for a long-term
infrastructure development. To date, numerous types of PPP have been applied for
public infrastructure construction. These include BOT (Build-Operate-Transfer), BOO
(Build-Own-Operate), BOOT (Build-Own-Operate-Transfer), etc. Without a loss
of generality, PPP often involves a contract between a public sector authority and a
private party, in which the private party provides a public service or project, and
assumes substantial financial, technical, and operational risk in the project. The
government may provide a capital subsidy in the form of a one-time grant or may
support the project by providing revenue subsidies, which include tax breaks or
guaranteed annual revenues for a fixed time period. In the PPP, the government
exchanges the progress of infrastructure construction and realizes effective operation
and management by offering private companies long-term franchise and income rights.
Similar to PPPs in the infrastructure sector, the government authorizes private
companies to build a profitable project with some preferential policies, while the
private companies can achieve satisfactory commercial profits for a long time under
43
the CDC model. In contrast, the private consortium in the above PPPs is responsible
for building, operating, and managing the infrastructure project, while the investor in
the inclusive healthcare only takes care of funding for the healthcare service and is
independent of other participants. In addition, in the inclusive healthcare services,
when the government provides an investor with high-quality projects, it includes the
condition that the investor has to return some profits to the healthcare services for
public welfare. Therefore, the regulation effect of the government is of more
significance in the CDC model.
It should be emphasized that in the fierce market competition, whether the
investment fund can obtain the "prince charming" project is the key embodiment of
the viability." A coupled dual-component model" fully considers the government's
demands and value proposition. Not only can it meet the demands of project funds of
the government (under the same condition), but also provides extra premium to
improve local public health. The result is to make the investment funds in the same
business under the condition of priority for government support and improve the
competitive ability.
3.2.1.2 The characteristics of the insurance fund
The inclusive healthcare initiative plans to cooperate with state-owned
enterprises or investment platforms in provinces and autonomous regions in mid and
west China to establish a fund, whose size in each phase is no less than 10 billion
yuan. Especially, the fund is jointly managed by the investor of the inclusive
healthcare services and local state-owned enterprises. The fund is divided into two
sub-funds: the “Industrial Fund A” and the “Inclusive Healthcare Fund B” at a 5 to 1
combination. Sub-fund A is a profitable fund supported by the government with a
longer investment period, larger scale and more stable profits, whose annualized rate
of return is no higher than the level of the market rate for financing. Meanwhile, Sub-
fund B is generated from the reduced profits of the limited partners of each insurance
enterprise under the guidance of the China Insurance Regulatory Commission (CIRC),
aiming at providing public health services to patients (buying equipment from
44
suppliers and donating them to primary hospitals, developing and managing the “three
ends and one cloud” platform, etc.). These two sub-funds are mutually interdependent
and mutually conditional. Specifically, sub-fund B is the purpose of sub-fund A, while
sub-fund A is the condition of sub-fund B. In other words, the interest margin
obtained by sub-fund A is the source of funding for sub-fund B, while sub-fund B is
the capital investment of the inclusive healthcare.
Overall, in the CDC model, the fund of the public welfare part (sub-fund B) =
project scale × interest margin × investment term × (1-discount rate). The interest
margin originates from the reduced profits of each limited partner (insurance
enterprise). Such an operation system not only guarantees the efficiency of market
competition and operation (the investor must compete for the government’s high-
quality projects with other enterprises), but can also obtain the support of the
government with sustainable capital sources. It is worth noting that the profit formula
of the market-oriented component and the non-profit component constitute a causal
relationship: without sustainable and stable investment from the market model, it is
impossible to continue the development of high-quality charitable healthcare services
in remote areas advocated by inclusive healthcare (its profit can be zero or even
negative). Similarly, if the investor does not invest in the charitable component of the
inclusive healthcare services, he or she will not be able to obtain high-quality
investment projects from the government (and by extension, long-term and stable
profits).
Insurance companies own huge amount of capitals and are always seeking
investment opportunities with characteristics of long-term and stable returns with very
low risks. The government projects such as building infrastructures and utilities just
fit the requirements of investment of the insurance companies. Thus, it is possible to
attract insurance companies to adopt the CDC model. On the other hand, the
governments only act as initiators in CDC model: they provide profitable projects and
ask for running inclusive healthcare services as the premise for obtaining the projects.
After that, the governments only surveil the execution of the contracts and cannot

45
intervene the operations of both the projects and inclusive healthcare services. Thus
this model is consistent with the ideology of market economy.
3.2.2 Key Components of the Business Model
3.2.2.1 Value proposition
The inclusive healthcare is a complex service network involving several
stakeholders who possess different appeals. However, the value creation of the CDC
model aims at answering one question: why would people like to use the proposed
model of healthcare services?
Regarding the inclusive healthcare project, it is possible to deliver advanced
healthcare services to patients in remote areas through IT, AI, and other technical
means. For patients in remote areas, the problem of limited access to and the high cost
of medical service can be mitigated. In China, healthcare resources that are unevenly
distributed (especially healthcare devices) can be reasonably redistributed via the
diagnosis and treatment system of the inclusive healthcare services to improve the
status quo. Additionally, the information management system and cloud centre of the
diagnosis and treatment system will assure the optimal sharing of healthcare
information, improve the accuracy of diagnosis and treatment, and it will reduce
unnecessary costs for patients.
All of the values above need to be created by all actors of the inclusive
healthcare services. In this process, they will benefit from different interests:
For patients (especially patients in remote areas), the CDC model provides them
with advanced healthcare services at a reasonable cost. On the one hand, due to the
unbalanced distribution of healthcare resources (devices, level of the healthcare staff,
etc.) in urban and rural areas in China, these patients could not receive proper
treatment locally and had to travel long distances to first class hospitals in big cities,
incurring higher medical expenses compared to patients with the same disease in big
cities. On the other hand, the CDC model can assist these patients to enjoy relatively
accurate disease diagnosis and convenient treatment service, except for operations
locally, saving transfer fees, repeated examination fees, and travel expenses. If these

46
patients can be treated in local hospitals, the queuing problem in large hospitals could
also be alleviated. Of course, for patients who really need to receive treatment in large
hospitals, the inclusive healthcare system can provide a convenient transfer service.
For healthcare providers (doctors or hospitals) in remote areas, the CDC model
provides advanced healthcare devices and training at a lower price, improving the
amount of healthcare resources of these areas and reducing inequalities of healthcare
resource distribution in China. Meanwhile, if the patients receive healthcare service
locally, the operation situations of the primary level hospitals will improve.
Concerning healthcare service providers (doctors or hospitals) in big cities, the
hierarchical diagnosis and treatment system established by the inclusive healthcare
can help them to disperse the overcrowded patient flow and reduce the workload so
that each patient can obtain a relatively satisfactory healthcare experience.
In conclusion, the inclusive healthcare services can redistribute and balance
healthcare resources to meet the demand of patients in different areas through “three
ends, one cloud”. Patients in each area can enjoy high-quality healthcare service
locally, ameliorating the overburden of first-class hospitals in big cities and improving
patients’ satisfaction.
From the perspective of the government, the CDC model can guarantee the
sustainable operation (positive overall profits) of healthcare services, realize
healthcare equity, and obtain higher public satisfaction without spending government
revenue by searching for appropriate project investment and operators. Actually, the
CDC model integrates the equity and accessibility of public health service and the
high efficiency of the market mechanism, which is quite attractive to the government.
In regard to project investors, the high-quality projects with a large scale, long
duration, and stable profits provided by the government with satisfactory conditions
can be easily obtained through the CDC model, in order to establish a conducive
cooperative relationship with the government (further guaranteeing priority in
obtaining other high-quality government projects). At the same time, it is possible to
enter the promising healthcare industry through investments and establish connections
47
with healthcare service providers, IT providers, and AI providers.
3.2.2.2 Key resources
In this thesis, some key resources that have to be provided to complete the
public health service in the CDC model are critically examined. The market
component acts as the capital source of the public-oriented business model without
considering its operation details, because resources in the market component vary
with different investment projects. Therefore, it is only necessary to know that the
market component has provided sufficient capital for public welfare healthcare
services, rather than a specific analysis of its key resources. In addition, although the
government plays a connecting role between the charitable component and the market
component in the CDC model, it does not directly participate in the development and
operation of inclusive healthcare. Therefore, resources that are closely related to the
government are not regarded as key resources. Government’s policymaking will be
discussed in future research on the mechanism design of the inclusive healthcare
services.
As discussed in the introduction to inclusive healthcare above, successful
implementation of the project cannot be separated from some key techniques such as
information technology (IT), big data analysis, and artificial intelligence (AI).
With high-speed broadband connection over all urban and rural areas as the
physical foundation, IT transmits the basic information of patients and disease
information faithfully in real time to the remote diagnosis and treatment centre via
networks. After the professional analysis of doctors with the assistance of big data
analysis, new diagnosis and treatment information is transmitted to patients through
the Internet in real time as feedback. After this, the patients can discuss subsequent
treatment with the doctors based on their own situation. Without healthcare
information transmission through the Internet, remote diagnosis and cloud data
integration will not be impossible. In addition, IT is also linked to the realization of
healthcare equity in inclusive healthcare. First, online services eliminate identity
differences. On the Internet, the status difference of people in secular society can be
48
minimized or even eliminated. Second, the Internet removes geographical barriers.
Specifically, some patients do not have to travel long distances to communicate with
doctors, which means the distance between each patient and the doctor is equal on the
Internet. Therefore, as long as online services are reliable, human beings have equal
access to healthcare.
Compared to IT, big data analysis and AI can directly improve the quality of
healthcare services. Compared to the doctors’ knowledge and experience, AI that is
driven by deep learning will be able to integrate the common wisdom of human
beings in all professional fields and form a general doctor whose knowledge surpasses
that of all of the experts. Although this general doctor has not yet emerged, the
deduction method based on deep learning of big data and evidence fusion not only
satisfies the requirements of modern evidence-based medicine, but also greatly
extends the thinking ability of human beings. It can be predicted that a general doctor
who replaces individual experts will soon enter the field of healthcare services. And
an online healthcare popularization without differences will fundamentally alter health
inequity. The modern Chinese society has a high degree of informatization, and
theories on deep learning and evidence fusion have gradually matured. This, coupled
with the government’s initiatives to accelerate the technical transformation of the
medical field, inclusive healthcare is feasible from a technology perspective.
According to the theory of the business model, the operation of the inclusive
healthcare cannot succeed without other resources provided by different stakeholders.
The stakeholders of the inclusive healthcare services in this thesis mainly comprise
patients, investors, operators of healthcare instruments, communication network
operators, and data centreoperators. The resources they provide include:
Patients: the end targets of the CDC model who provide specific medical data
(e.g., videos, examination bills, etc.), which are of critical importance to the
development of the cloud data centre of healthcare services.
Hospitals at all levels: the provider of healthcare staff, healthcare diagnosis,
and rendering service of different qualities. Generally, the higher the level of the
49
hospital and the more qualified the medical staff, the more accurate the diagnosis
results. Additionally, senior hospitals can provide remote diagnosis, remote
consultation, remote education training, and other advanced services. A two-
way referral system is also available between the two hospitals.
Project investors: entities that possess mature project management experience
to obtain long-term and stable profits from the market-oriented business model,
ultimately providing capital for the public-oriented business model.
Operators of healthcare instruments: the provider of high-end healthcare
instruments for primary hospitals and for achieving better diagnosis and treatment and
breaking the high-price monopoly of foreign operators.
Operators of communication network and data centre: the developer and
maintainer of the “three ends and one cloud” platform for inclusive healthcare.
3.2.2.3 Key processes
In the market component, the investor searches for high-quality projects
provided by the government with preferential conditions when promising to invest a
part of the revenue in public healthcare services. After that, the investor applies a
mature fund operation mode to obtain long-term and stable profits with a low
investment return rate. The capital of this part is equivalent to the “Industrial Fund A”
mentioned above (whose annual rate of return is not higher than the level of market
financing). Then, under the guidance of the CIRC, sub-fund B emerges from the
reduced profits of the limited partners of each insurance enterprise. The specific
business process of sub-fund A is not a focus of this thesis. Therefore, we assume it
provides a stable and continuous capital flow to sub-fund B.
From the perspective of constructors, the key process of the charitable model
includes: fund-investment (sub-fund B) by the investor; delivery of high-end
healthcare instruments (including radiology, ultrasound, inspection, electrocardiogram,
and other instruments) to primary hospitals in remote areas; and the development,
operation, and management of remote hierarchical medical diagnosis systems
(including intelligent matching, two-way referral system, and intelligent charging

50
system), cloud data centre, and daily healthcare diagnosis and treatment services.
For patients in remote areas, the daily diagnosis and treatment business
processes of the inclusive healthcare include:
1. Patient registration, standardized examinations, and first treatment in primary
hospitals (which transmit patient information to the cloud data centre of the inclusive
healthcare services). After the comprehensive decision of doctors and cloud platforms,
patients are categorized according to disease severity. Patients who can be effectively
treated in primary hospitals will continue their treatment locally. If the patient’s
disease is beyond the service level of primary hospitals, the remote hierarchical
diagnosis system will be applied, and the patient will be transferred to an appropriate
higher-level hospital through the two-way referral system.
2. The business processes of the remote hierarchical diagnosis of the inclusive
healthcare include: the primary hospital transmits all of the healthcare information of
the patient to the provincial remote diagnosis and treatment centre through the
Internet and makes a remote appointment (including contact information of
the applicant), and confirmation of the hospital, department, and doctors for the
patient. After contacting the target experts, the online consultation appointment will
be arranged, after which the primary hospitals and patients are informed to prepare for
the consultation. During the consultation, doctors at primary hospitals need to
describe the patient’s basic information and communicate with remote experts. In
addition, communication between the expert and the patient is critical. In the remote
hierarchical diagnosis and treatment system, the adaption problem of healthcare
resources requires special concern. From this perspective, the inclusive healthcare
initiative comprehensively applies the Internet, big data analysis, AI, and other
technologies to develop the intelligent adaption system which includes: (1) accurately
matching healthcare resources through a “demand-supply” model; (2) reasonably
distributing healthcare resources and avoid resource waste through market-adjusted
prices; (3) establishing appropriate incentives and punishment mechanisms for
medical service institutions and employees; (4) establishing an evaluating system for

51
patients to evaluate the technical ability, professional quality, and service attitude of
healthcare staff in real time; and (5) a two-way referral system that guarantees the
rights and interests of the patients who need to transfer.
3. Based on the remote hierarchical diagnosis system, the cloud end forms high-
level treatment plans by learning and accumulating a great deal of medical structural
data and non-structural data, as well as by a profound understanding of patient,
disease, and medicines. The treatment plan, based on the adaption ability of the big
data model, cloud computing (in addition to customizable and Internet service
standards with individualization, intelligence and continuity) is able to provide
convenient, fast, and controllable healthcare service in order to make the patients and
their family members satisfied and form cooperative and harmonious doctor-patient
relationships. Generally, the cloud end is equipped with cognition healthcare services,
auxiliary healthcare decision-making, and intelligent supervision and alerting, acting
as the brain of the whole inclusive healthcare system.
4. After developing the high-level individualized treatment plan, the inclusive
healthcare initiative calculates the healthcare expenses of each patient through the
intelligent charging system, and patients pay with their own medical insurance.
Finally, the patients can provide a satisfaction score of the medical process. The
general diagnosis and treatment procedures of the inclusive healthcare initiative are
shown in Figure3-5.
Figure3-5. The diagnosis and treatment procedures of the inclusive healthcare.

52
3.2.2.4 Profit formulae
The foundation for inclusive healthcare to provide charitable healthcare services
is that the government provides projects with a large scale, long term, and high
security to the investor on the condition that the investor must invest some part of the
profits in the charitable healthcare services. Then, the government completely lets the
investor run the project in accordance with market rules.
There is also a business model in the market part to ensure that the investor can
obtain satisfactory profits based on special key resources and processes. However, in
this thesis, we do not examine the details of this business model while knowing the
sources and amounts of profits obtained by the investor. After operating the project,
the investor puts some of the long-term and stable profits into public healthcare
services and searches for appropriate business partners to establish the “three ends and
one cloud” platform. The financing model is termed CDC business model, in which
dual components refer to the fact that the market and charitable processes are
separated, while coupling refers to the consistent objective and mutual
complementation. The flow of capital is shown in section 3.2.2. In the CDC model,
the profit formula in different components acts as the coupled junction and bridge.
Specifically, the profits from the market component to the charitable component make
public medical services, which were originally operating at a loss, sustainable.
3.2.3 Implications of the Business Model
3.2.3.1 Expected results of the proposed model
As discussed above, the CDC model for inclusive healthcare comprises a
market-oriented component and a charitable component. The market component
provides sustainable and stable capital to the operation of the charitable component so
that charitable healthcare services can continue. Generally, the investor does not
actively invest profits into a non-profiting public welfare project. Thus, in the CDC
model, the government must serve as the glue for the two components by
promulgating regulations and policies to encourage the investor to invest his or her
profits to the charitable component from which patients can benefit and the

53
government can achieve political goals. The investors themselves can run the high-
quality projects (with a higher investment amount, longer term and lower investment
return rate, but with security and stability) to obtain satisfactory profits and a better
social reputation by supporting the public healthcare service. Meanwhile, it is also a
good opportunity for the investor to enter a promising field of investment (healthcare
service) and expand its future business.
In the CDC model, the values need to be realized with the joint efforts of each
stakeholder. For patients (especially those in remote areas), they can obtain high-
quality healthcare service with a reasonable price nearby, which is the ultimate
objective of the inclusive healthcare services. For healthcare providers (doctors or
hospitals), primary hospitals can be equipped with high-end healthcare devices (e.g.,
X-ray scanners, ultrasonic detectors, etc.), and the professional skills of doctors in
remote areas will also be improved through remote consultation, resource sharing, and
healthcare instruction. With the improvement of resource availability in primary
hospitals, patients in remote areas will be willing to seek healthcare services locally.
Thus, the operation situations of hospitals in remote areas are improved, and the
queuing issue in Class A hospitals in large cities is ameliorated. For the government,
the inclusive healthcare services provide a path for public welfare healthcare services
to be sustainable while reducing financial pressure (followed by higher public
satisfaction towards healthcare and better performance). As for the investor, the CDC
model makes it easier to obtain high-quality projects and establish beneficial
cooperative relationships with the government. For AI and IT providers, the inclusive
healthcare services constitute a good opportunity to establish relationships with
powerful investors and the government, and also to provide a broad stage for the
application of advanced technology.
3.2.3.2 Important steps for implementing the proposed model
The implementation of inclusive healthcare is tightly correlated with the
resources provided by stakeholders.
Among all key resources, the application of AI, big data, and Internet

54
technology is critically important. Specifically, Internet technology connects the
healthcare institutions of each level from the village, town, and county to the city, so
as to ensure the sharing of healthcare information in these institutions (which
constitutes the foundation of remote hierarchical diagnosis). In addition, the Internet
can eliminate patients’ identity differences and regional barriers, and thus promote
healthcare equity. Big data analysis and AI technology that is based on deep learning
and evidence fusion theory (as the foundation of cloud platform development) can
integrate the joint wisdom of human beings in the professional medicine field and
form a general doctor who surpasses any individual expert. This is necessary in order
to provide patients with high-quality and equitable healthcare services that are highly
individualized and intelligent with continuity.
Apart from key technologies, the incentive mechanism provided by the
government also plays a critical role in the implementation process of inclusive
healthcare. Considering the specific political system in China, the ruling party can
implement reform with the assistance of effective administrative mobilization.
Nevertheless, public welfare healthcare services led by the government do not target
profits and thus require continuous financial support. In order to relieve the
government of financial pressure, the government seeks to provide inclusive
healthcare with sustainable development, depending on market regulations. Different
from BOT, BOO and BOOT, which are mainly designed for infrastructure projects,
the government attracts investors with some high-quality investment projects through
open bidding while adding the condition of investing in charitable healthcare service.
In this way, the investor can obtain long-term, stable, and low-risk profits to realize
business success; on the other hand, the charitable healthcare service will be
supported by a continuous cash flow to not only provide high-quality healthcare
services for patients in remote areas, but also avoid huge financial expenditures.
Therefore, the market component can be organically connected with charitable
healthcare services so as to form a new co-existence relationship. Additionally, the
government can supervise the investor and adjust the implementation of the inclusive
55
healthcare through policymaking. On the whole, without the government, it is
impossible to build and manage the inclusive healthcare services.
The successful implementation of inclusive healthcare also requires the support
of some external conditions. First, the government needs to provide attractive high-
quality projects. Generally, the investor pursues long-term, stable and low-risk
investment returns, based on which projects provided by the government must be
guaranteed by the government’s credit with low risk and certain commercial potential,
considerable profit space, and provision of appropriate laws and regulations to ensure
the profits of the investor. Government supervision can guarantee that the investor’s
investment and operation of profitable projects comply with relevant laws and
regulations, and ensure the investor’s ability to fulfill the promise to invest parts of
the profits (sub-fund B) in the public welfare service. Finally, the implementation of
the inclusive healthcare also requires a favourable trend of economic development
and continuous progress of science and technology. Only with a favourable economic
development trend can the projects undertaken by investors have profit space. The
level of science and technology is also directly related to the overall development of
the inclusive healthcare system. Specifically, the front-end healthcare instruments, the
remote-end hierarchical diagnosis system, and the cloud-end healthcare cloud data
centre require the most up-to-date research achievements of several disciplines,
including information, management, and medicine.
The operation of inclusive healthcare cannot be separated from other resources
provided by different stakeholders (patients, hospitals, project investors, medical
device suppliers, communication network providers, and operators of data centres).
Regardless of the differences in the resources they provide (see section 3.2), all of the
resources serve as the premise for the successful implementation of the inclusive
healthcare services.
3.3Critical Success Factors for the Implementation of the Inclusive Healthcare Services
As inferable from the CDC model, actors in the core component of the program
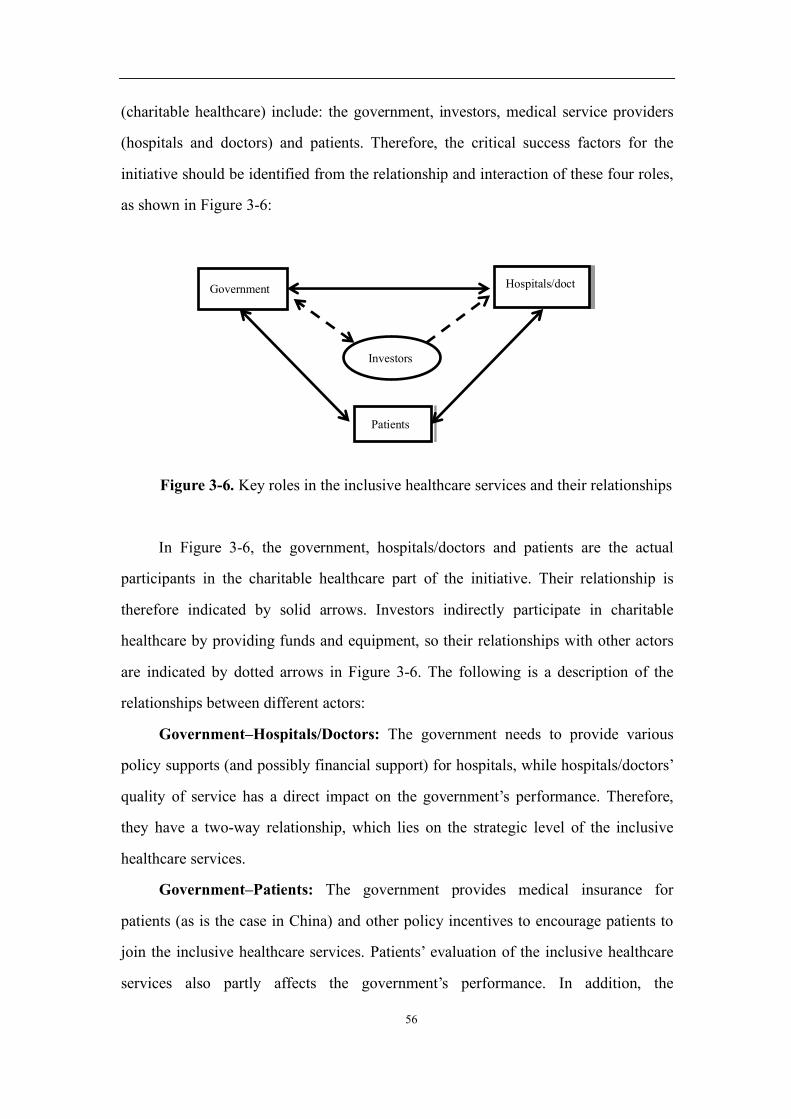
56
(charitable healthcare) include: the government, investors, medical service providers
(hospitals and doctors) and patients. Therefore, the critical success factors for the
initiative should be identified from the relationship and interaction of these four roles,
as shown in Figure 3-6:
Figure 3-6. Key roles in the inclusive healthcare services and their relationships
In Figure 3-6, the government, hospitals/doctors and patients are the actual
participants in the charitable healthcare part of the initiative. Their relationship is
therefore indicated by solid arrows. Investors indirectly participate in charitable
healthcare by providing funds and equipment, so their relationships with other actors
are indicated by dotted arrows in Figure 3-6. The following is a description of the
relationships between different actors:
Government–Hospitals/Doctors: The government needs to provide various
policy supports (and possibly financial support) for hospitals, while hospitals/doctors’
quality of service has a direct impact on the government’s performance. Therefore,
they have a two-way relationship, which lies on the strategic level of the inclusive
healthcare services.
Government–Patients: The government provides medical insurance for
patients (as is the case in China) and other policy incentives to encourage patients to
join the inclusive healthcare services. Patients’ evaluation of the inclusive healthcare
services also partly affects the government’s performance. In addition, the
Investors
Government Hospitals/doct
ors
Patients
57
government (and hospitals/doctors) can learn from the patient’s evaluation of the
initiative in order to timely revise policies or inform similar medical programs in the
future. Therefore, the connection and interaction between patients and the government
is also a two-way relationship, which sits at both strategic and operational levels.
Doctors–Patients: The connection between doctors/hospitals and patients is at
the heart of the entire initiative. Patients need hospitals/doctors for their medical
services, and hospitals/doctors provide high-quality medical services to patients using
a variety of technical means (telemedicine, AI-driven diagnosis and treatment systems)
in the initiative, which represents a direct supply and demand relationship. In the
course of diagnosis and treatment, patients and doctors/hospitals need timely
consultation and communication in order to optimize results. Therefore, such
connections are very strong and work at the operational level.
Government–Investors: Unlike the first three types of relationships, the
relationship between investors and the government indirectly affects the inclusive
healthcare services. Their connection mainly occurs in the market operation part of
the CDC model for inclusive healthcare: the government entrusts profitable public
projects to investors while providing various supports (mainly policy supports); and
investors not only need to ensure profitability as required in regular PPP projects, but
also need to meet government requirement for such projects. Further, they also
commit to allocating part of their profit and invest it in the charitable component of
the inclusive healthcare services. As a result, the government’s supervision of
investors is two-fold: the operation of the profitable project (the market component of
the business model) and the capital investment of the charitable component (the
charitable healthcare component of the business model), with the latter being more
important in implementing the inclusive healthcare services. Therefore, the links
between these two actors are two-way and multi-faceted. They relate not only to the
strategic aspects of universal healthcare, but also the operational aspects of the
initiative.
Investors–Hospital: According to the “three-ends and one cloud” development
58
plan for inclusive healthcare, investors need to provide hosipitals with funds and
equipment (i.e. donating all types of equipment to hospitals after purchase it from
various providers). Further training/technical support may be needed in the future.
The beneficiary hospitals can then use these funds and equipment to provide services
for patients. Therefore, the link between investors and hospitals is one-way, which
also involves both strategic and operational aspects.
As shown in Figure 3-6, the relationship between investors and charitable
healthcare is critical, albeit indirect: the inclusive healthcare services are not able to
sustain without the funds provided by investors. Therefore, both direct and indirect
links in Figure 3-6should be given equal attention in implementing inclusive
healthcare.
By summarizing the critical success factors mentioned in the literature (taking
into consideration the actors of inclusive healthcare and their interconnections), this
thesis designs a list of potential critical success factors for implementing inclusive
healthcare services (see Appendix 2), which has been verified in subsequent case
studies.
3.3.1 Research Methodology for the Critical Success Factors
As of the end of April 2018, inclusive healthcare has not yet been fully
implemented in China’s remote and poor areas. It was therefore not possible to
conduct detailed statistical investigations, and hence the critical success factors for
implementing the inclusive healthcare services can only be summarized through case
studies and literature review.
As mentioned above, the government, investors, hospitals and patients are the
main actors in implementing the inclusive healthcare services. Their attitudes and
behavours directly influence the outcomes of the project. As a result, starting from an
analysis of the above-mentioned actors, this thesis explores, summarizes and compiles
several critical success factors for inclusive healthcare. We conducted in-depth
interviews with government officials, one investment company executive, hospital
leaders, doctors and patients using an interview questionnaire designed by considering

59
various factors mentioned in the relevant literature, which were individually verified
in the interviews. Further, data were extracted from news articles, reports and other
sources and were analyzed for finally identifying the critical success factors for
implementing the inclusive healthcare services.
In order to have a deeper understanding of the current situation and problems
facing primary public healthcare in remote and poor areas, to understand the views of
local government departments, medical organizations and citizens on the inclusive
healthcare model, and to analyze the critical success factors for inclusive healthcare,
the following people have been interviewed within a seven-day timeframe:
� Two government officials: Party Secretary of Fuzhou City, Jiangxi Province;
and Party Secretary of the District Committee, Miyun District, Beijing.
� Head of an investment company: Chief Investment Officer, China Insurance
Investment Fund.
� Four hospital administrators: Deputy Director of Pingnan County Hospital,
Fujian Province; Chief of Medical Section, Zherong County Hospital, Fujian
Province; Vice President of Yonghe County People’s Hospital, Shanxi
Province; and Vice President of Yonghe County TCM Hospital, Shanxi
Province.
� Eight doctors: Director of internal medicine and a surgeon at Pingnan County
Hospital, Fujian Province; Chief of the Emergency Section and an internal
medical doctor at Zherong County Hospital, Fujian Province; an internal
medical doctor and an inpatient doctor at Yonghe County People’s Hospital,
Shanxi Province; and an internal medical doctor and a surgeon at Yonghe
County TCM Hospital, Shanxi Province.
� Twenty patients (from each of the above hospitals).
The author and his assistant interviewed government officials, an investment
company leader, hospital leaders, doctors, and patients for this research. The author
interviewed government officials and the investment company leader, each for 1.5-2
hours.

60
The author’s assistant interviewed hospital administrators, doctors and patients.
Each hospital leaders were interviewed for about one hour, while 30-45 minutes was
allocated for doctors and about 15 minutes for patients. The interview process was as
follows:
1. Understanding the current status and issues of local public healthcare: reading
(before the interview);
2. Introducing the purpose of the interview and a brief description of the
inclusive healthcare services (goals, activities, methodology, etc.);
3. Assessing interviewees’ understanding and opinions on the inclusive
healthcare services;
4. Inquiring and verifying each of the critical success factors listed in the
questionnaire on critical success factors for inclusive healthcare (see Appendix);
5. Including additional critical success factors that were not listed in the
questionnaire.
All interviews were conducted face-to-face, except the one with the Vice
President of Yonghe County TCM Hospital, which was conducted over the telephone
due to a schedule conflict. In addition, except for the interviews with the leadership,
doctors and patients at the Nanping County Hospital, all interviews were audio-
recorded and transcribed with the consent of the interviewees. These include a
government official (the Party Secretary of Miyun District, Beijing), the head of the
investment company, and all interviewees at Zherong County Hospital, Yonghe
County People’s Hospital and Yonghe County TCM Hospital.
Before conducting the interviews, we designed a questionnaire on critical
success factors for inclusive healthcare. The content of the questionnaire was derived
from the critical success factors summarized in the existing literature and based on the
characteristics of the CDC model of inclusive healthcare. During the interviews, we
asked the interviewees to go through each of the critical success factors on the
questionnaire. (If a factor was considered to be a key success factor for the inclusive
healthcare services, the interviewee would place a tick-mark “√” in the corresponding
61
cell. Otherwise, the cell would be marked with a “×”. If the interviewee would like to
highlight a factor, he/she would draw a double tick-mark “√√” in the corresponding
cell. In view of their different statuses and roles played in inclusive healthcare,
different questionnaires were developed for government officials, investors, hospital
leaders, doctors, patients.) See Appendix 2 for details.
The background materials required in this interview include basic information
about each hospital (its level, equipment, organization structure, number of doctors
and their education, number of beds, etc.) and the basic conditions of the area where
the hospital is located and the area within the jurisdiction of government officials
concerned. Further, we also collected information from China’s “13th Five-Year Plan”
as it relates to the reform of the Chinese healthcare system, information on the central
government’s expenditures on medical insurance in recent years, and information on
similar initiatives in other countries, in order to identify more critical success factors
for the inclusive healthcare services.
It should be added that in May 2016, the author submitted the "couple dual-
component" to the then “National Insurance Supervision and Administration
Commission," which obtained recognition and support. On November 25, at the time
of the chairman of "National Insurance Supervision and Administration Commission,
together with the three main directors of departments of NISAC and five large
insurance companies, and the author's work unit: China Insurance Investment Fund
formed “Insurance Capital Support FOR the Development of the Xinjiang.” In
Urumqi, the capital of Xinjiang autonomous region, the delegation with the party
secretary of Xinjiang and thirty heads of department held a seminar titled "Insurance
Capital Support for the Development of Xinjiang". At the meeting, the author made a
special presentation on "How to Use Insurance Funds to Support the Development of
Xinjiang and the Business Model of Inclusive Medicine." This was recognized and
praised by the participants. After the meeting, the China Insurance Fund and the
government of Xinjiang autonomous region set up the leading group of "inclusive
healthcare" and began to carry out in-depth research on the specific implementation of

62
projects. But it is a pity that after, the main leadership of the NISAC was caught in a
corruption scandal and was forced to run aground.
3.3.2 Results and Analysis of the Interviews
Based on the background information (Appendix 1) and interviewees’ responses,
and using data from the questionnaire on critical success factors (Appendix 2), we
group the critical success factors for inclusive healthcare into six clusters, namely: (1)
medical infrastructure; (2) technology; (3) financial support; (4) government support;
(5) external support; (6) organization, operation and planning.
3.3.2.1 Medical infrastructure
The critical success factors under this cluster are primarily related to hospital
infrastructure. For any hospital, infrastructure is always a measure of its service level:
hospitals cannot provide quality medical services without a capable medical
infrastructure. The medical infrastructure development referred to in this thesis is
mainly divided into two subcategories: doctors and equipment. Hospital leaders are
the subjects of this type of questions.
Doctors
At the interviews, the leaders of all four primary hospitals identified “high
proportion of middle and senior doctors in various departments” as a key success
factor for inclusive healthcare. Patients preferred doctors with a high level of
professionalism, and they believed that a doctor’s reputation and professional title
reflect the doctor’s technical skills. Unfortunately, many departments in these primary
hospitals often lack doctors with middle and senior titles. As a result, some well-to-do
patients would spend large amounts of money to see a doctor in big cities.
Leaders of two hospitals believed that the fact that “the number of doctors in
various departments meets local medical needs” is also an important key success
factor. Judging from the population and the number of hospital personnel in these two
places, there is a lack of doctors in some departments (such as cardiology and
emergency department) in these hospitals, which cannot meet the needs of local

63
residents, hence this factor was considered important.
Based on the background information of the above four hospitals and the
interviews with their leaders, their doctors generally do not have high education
qualification. Each of these hospitals has at most two doctors with a postgraduate
degree, while some do not have any. Most doctors hold a bachelor’s degree, and many
others only completed college education. Some doctors are even non-medical
graduates. Moreover, all the doctors in these hospitals who have received formal
medical education graduated from second-tier medical schools. None of them
graduated from a first-tier medical school. To make things worse, all these hospitals
have encountered difficulties in recruitment: fresh graduates of medical schools are
reluctant to work in these primary hospitals, which also cannot recruit doctors from
other hospitals. In addition, limited financial resources have prevented these hospitals
from providing doctors with reasonable remuneration and comfortable living
conditions, or any further vocational training opportunities. Therefore, many doctors
resign from these hospitals every year, most of whom are young and middle-aged
doctors between 30 and 45 years of age, and are the backbone of primary hospitals. In
short, difficulties in recruiting and retaining talents have become a nightmare for
primary hospitals in these underdeveloped areas, even in the rural areas of Miyun
District, Beijing.
Medical equipment
In this interview, we investigated the attitude of hospital leaders on examination
equipment, beds, surgical equipment, first-aid equipment, and other equipment (such
as disinfection chambers). The results are as follows:
1. All hospital leaders identified that “the hospital is equipped with the
necessary inspection equipment (especially high-end CT and MRI devices)” as a key
success factor for the inclusive healthcare services;
2. The leaders of three hospitals believed that “the hospital’s first-aid facilities
can meet the basic local medical needs” and “the hospital’s other facilities (such as
disinfection chambers) can meet the basic local medical needs” are critical success
64
factors for the inclusive healthcare services;
3. The leaders of two hospitals believed that “the hospital beds can meet the
basic local medical needs” is a key success factor for the initiative.
The above results show that primary hospital leaders generally believed that
some necessary examination equipment, especially high-end examination equipment,
is critical to the implementation of the inclusive healthcare services. However, since
these hospitals generally do not have this equipment, they cannot perform certain
examinations for patients, which has greatly affected the range of medical services
available and has exacerbated the difficulty of local people to access healthcare. As a
hospital leader pointed out:
"The foundation of contemporary hospitals is evidence-based medicine. Doctors
must use these examination devices to diagnose and track patients’ conditions."
Therefore, the deployment of medical examination equipment in primary
hospitals is a key issue to be addressed in the inclusive healthcare services.
Without a doubt, primary hospitals’ need for first-aid equipment and other
supporting equipment cannot be ignored. It is recommended that the inclusive
healthcare services team should carefully examine the needs of such equipment in
hospitals and, where appropriate, fill in the gap in these hospitals by installing the
much-neededequipment. Further, hospital beds are not a key consideration for some
hospitals. It may be attributed to the small local population and the limited capacity of
doctors in these hospitals. As a result, the number of patients that need treatment in
primary hospitals is small. It is therefore recommended that hospitals in need of beds
can seek support directly from the local medical authorities.
3.3.2.2 Critical success factors concerning various technologies
The success of inclusive healthcare is inseparable from the support of key
technologies such as information technology, big data analytics and artificial
intelligence (AI). At the operational level, these technologies require specific software
and hardware to run. In the interviews, we included the concept of information system
availability (Johnston et al., 1988; Lu et al., 2006) and the Technology Acceptance
65
Model (TAM), with a focus on the attitude of hospital leadership and doctors towards
these technologies.
In 1989, Davis F. proposed TAM (Davis, 1989) based on rational behavour
theory, which was first used to provide an explanation of the determinants of the wide
acceptance of computers. The TAM proposes two main determinants: 1) perceived
usefulness, which reflects the extent to which a person believes that using a specific
system improves his job performance; and 2) perceived ease of use, which reflects a
person’s perception of the degree of easiness to use a specific system. We have taken
these two factors into account when designing the questionnaire. Hospital leaders and
doctors are the subjects of this type of questions.
Hardware availability
The main hardware systems of the inclusive healthcare services include:
Internet devices (monitors, mainframe computers, switches, gateways, routers, etc.)
and big data and artificial intelligence hardware (solid state drives, cloud computing
servers, and various types of terminal AI chips, etc.). The former are used to build an
information network for primary medical institutions, and the latter are mainly used to
develop remote diagnostic systems and medical cloud data centres. In the interview:
1. All hospital leaders and doctors believed that “high-quality Internet devices
(for developing primary healthcare information networks)” is very important for
implementing inclusive healthcare. This is also the foundation of telemedicine. The
authors believe that the attitude of interviewed leaders and doctors is, to a large extent,
influenced by the positive effects of an earlier telemedicine project undertaken in
remote and poor areas. The project exposed medical staff and patients in remote and
poor areas to advanced medical technology and hence attracted more patients to these
hospitals, giving doctors an opportunity to learn more advanced technologies.
Therefore, remote and poor areas welcome similar projects.
2. Compared with investment in high-quality Internet devices, fewer hospital
leaders and doctors believed that “high-quality big data and artificial intelligence
hardware systems are important for implementing inclusive healthcare”: two doctors
66
believed that new technologies such as big data and artificial intelligence is
unnecessary in inclusive healthcare because these technologies are “unfamiliar” and
“impractical.”
Software availability
The software required in the inclusive healthcare system includes various types
of medical applications (such as equipment management software, digital medical
imaging, health management software, etc.) and information management systems
(regional health information platform, hospital management information system,
electronic case management system, etc.). In the interviews, we focused on
respondents’ attitude towards software effectiveness and efficiency:
1. All hospital leaders and doctors believed that “the ability of medical software
(including operating systems) to quickly and smoothly complete defined tasks” is a
key success factor for the inclusive healthcare services. Among them, two doctors
highlighted this point.
2. All hospital leaders and doctors believed that “medical software applications
are easy to learn and use” is a key success factor for the inclusive healthcare services.
Among them, two doctors highlighted this point.
3. All hospital leaders and doctors believed that “medical software applications
have a low failure rate and well-established error correction features” is a key success
factor for the inclusive healthcare services.
Technological development, innovation and dissemination
This subcategory mainly examines the attitude of hospital leaders and doctors
towards technology and advanced medical treatment methods that may be applied in
healthcare. The results are as follows:
1. All hospital leaders and seven doctors believed that “the rapid development of
technology (big data, artificial intelligence) in other fields and their application in the
medical field have a positive effect on the implementation of inclusive healthcare.” Of
these interviewees, one doctor highlighted this point and noted that these technologies
should focus on customizing treatment options. There is, however, one doctor who did
67
not believe this is an important point.
2. All hospital leaders and doctors believed that “the development and
dissemination of advanced treatment methods have a positive impact on the
implementation of inclusive healthcare” is a key success factor for the inclusive
healthcare services. Among them, one doctor highlighted this point.
Technical acceptance
In the inclusive healthcare services, the application of various technologies
(Internet, big data, artificial intelligence and diagnostic technology) requires the
engagement and cooperation of all actors. Therefore, the attitude of these actors
towards various technologies is particularly important.
1. All hospital leaders and doctors believed that “public acceptance of various
technologies and their participation” is a key success factor for the inclusive
healthcare services.
2. All hospital leaders and doctors believed that “medical workers’ acceptance
of various technologies and their participation” is a key success factor for the
inclusive healthcare services. Among them, three doctors highlighted this point.
3. All hospital leaders and doctors believed that “government authorities’
acceptance of various technologies and their participation” is a key success factor for
the inclusive healthcare services. Among them, two doctors highlighted this point.
However, there was also one doctor who believed that the government’s attitude
towards technologies does not affect the implementation of the inclusive healthcare
services because the government is not a direct participant in the initiative.
In summary, all hospital leaders and doctors believed that hardware is crucial in
developing the primary healthcare system for inclusive healthcare, and confirmed the
importance of the software system. They also believed that the development and
popularization of advanced medical treatment are indispensable in implementing
inclusive healthcare. At the same time, most of them had a positive attitude towards
the application of big data, artificial intelligence and other technologies in medical
applications. However, some doctors had doubts about the prospect of these new

68
technologies in the medical field, and they do not care about the advancement of these
technologies.
All hospital leaders and doctors believed that the acceptance of various
technologies by patients and medical workers and their participation is a key success
factor for the inclusive healthcare services. Only when both doctors and patients
accept and actively apply these emerging technologies can they achieve optimal
results. China’s specific conditions determine that most public resources are managed
by the government who is also responsible for their allocation. In other words, any
public health services must be supported by the government in order to be able to run
smoothly. Therefore, most hospital leaders and doctors believed that the government’s
attitude towards the application of big data, artificial intelligence and other
technologies in the medical field is a key success factor for the implementation of the
inclusive healthcare services. However, some doctors did not believe the
government’s attitude would have a major impact on the implementation of the
initiative.
3.3.2.3 Critical success factors concerning financial support
The importance of funding is self-evident for any project. A project will not
function smoothly without sufficient and continuous financial support (De Marco et
al., 2012b). Our proposed CDC model focuses on solving the sustainability and
profitability of public healthcare funding. When it comes to funding, investors must
have direct contact with the government. Hospitals, doctors and patients therefore are
not aware of the funding aspects of the initiative. Therefore, only government officials
and investors were asked about funding related issues.
Investor strength
Both government officials believed that “the investor’s financial strength" is a
key success factor for the inclusive healthcare services. The Secretary of the CPC
Committee of Fuzhou, Jiangxi Province specifically highlighted this point, while the
Secretary of the CPC Committee of Miyun District, Beijing, did not give particular
importance to it. This is probably attributable to the different levels of economic

69
development in different regions of China, resulting in different financial strengths in
governments: In poorer areas, the government is unable to provide any further
financial support for such charitable healthcare services. Therefore, it is important for
investors to be financially capable in order to implement inclusive healthcare services
in these areas.
In addition to their own funds, investors can also partner with local financial
institutions. When they encounter financial difficulties, they can continue to provide
funds for the inclusive healthcare services through such financial institutions. This
kind of partnership is very common in PPP projects, and the two government officials
also believed that “investors’ cooperation with local financial institutions” is a key
success factor for the inclusive healthcare services.
From the perspective of investors, their financial strength and the linkage with
financial institutions must naturally be highly valued.
Investment in the for-profit component
According to business model for inclusive healthcare, the for-profit component
provides stable financial support for the charitable healthcare component. Therefore,
the investment and operation of the for-profit component will inevitably have a major
impact on the entire inclusive healthcare services.
Among factors under this category, the most valued one by government officials
and investors is “the scale of investment of the for-profit component”: Both
government officials and the head of investment company highlighted this as one of
the critical success factors for the inclusive healthcare services that deserve the most
attention. The director of the investment company noted that “The scale of investment
in the for-profit component directly determines the income of the project, which funds
the charitable component of the inclusive healthcare services. Therefore, the scale of
investment of the for-profit component is almost no doubt the most critical indicator
of all.”
In addition to the scale of the investment, the “investment cycles of the for-
profit component” is also identified as one of the critical success factors for the

70
inclusive healthcare services. However, its level of importance is considered lower
than the scale of investment, especially from the government’s perspective (neither of
the government’s officials highlighted it, although the head of the investment
company did so). In addition, all government officials believed that the investment
cycle of such for-profit projects is preferably over ten years, so that the charitable
healthcare component can be sustainable.
As for the “profitability of the for-profit component”, although government
officials and the head of investment company confirmed it as a key success factor for
the inclusive healthcare services, none of them believed it should be focused. It
should be noted that the assets of the investors of the inclusive healthcare services
belong to insurance assets, which are characterized by their preference for low-
profitability, stable-return investment and almost risk-free investment projects.
Charitable medical fund
The charitable medical fund for inclusive healthcare requires sustainable
funding sources. In short, there are three main sources: 1. investors allocation of parts
of their income from the for-profit component to investing in charitable healthcare; 2.
funding support from other non-government organizations for the initiative; and 3.
financial support from the government. In this section, we mainly consider the first
two sources of funding. The government’s financial support is addressed in the next
section.
According to results of the interviews, government officials and the head of the
investment company all believed that 0.5% of the revenues from the for-profit
component should be set aside for investing in the in the charitable component of the
inclusive healthcare services. In addition, “funding support from other non-
government organizations” is also identified as a key success factor for the inclusive
healthcare services, although none of the interviewees highlighted this factor.
In summary, in implementing the inclusive healthcare services, due
consideration must be given to the strength of investors (including their own financial
strength and their relationship with the financial sector), the investment of the for-

71
profit component, and the funding sources for the charitable component.
3.3.2.4 Government support
For any PPP project, companies need to work with the government. Therefore,
support from the government is particularly important, as evidenced by numerous
research outputs (see Table 1). This thesis focuses on the specific types of
government’s supports that are required for the successful implementation of the
inclusive healthcare services.
To answer this question, hospital leaders, government officials and investors
were interviewed (see Appendix 2): these actors are able to answer such strategic
issues because they are responsible for the governance of the inclusive healthcare
services.
Policy support
The interviews reveal that:
1. All hospital leaders, government’s officials and the head of the investment
company believed that “medical policy support”, particularly health insurance policy,
is a key success factor for the inclusive healthcare services. Among them, two
government officials and one hospital leader specifically highlighted this point and
considered it to be the most important support of the government. A government
official responded, “In China, the government takes care of much more work than
their foreign counterparts, especially in the public health sector. Very few projects, if
any, can succeed without supporting medical policies.”
2. All government officials and the head of the investment company (the only
two types of target respondents of this question) believed that “policy support for
investors’ investment in profitable projects” is also a key success factor because such
policies support the smooth implementation of the for-profit component, which in turn
guarantees funding for the charitable component.
3. All hospital leaders, government officials, and the leader of the investment
company believed that “policy stability” is a key success factor for the inclusive
healthcare services. In this article, policy stability refers to the continued support and

72
facilitation accorded to the inclusive healthcare services within its authority,
regardless of whether the (central or local) government reshuffles its leadership or
have other changes. Since the inclusive healthcare services is a long-term endeavour,
it is highly in need of policy stability, and volatile policy changes are especially
unacceptable. This is an experience from India4 highlighted by a government official.
Legal and regulatory support
The laws and regulations involved in the inclusive healthcare services include
those in the field of medical and health management, as well as those pertaining to the
investment of the for-profit project. In terms of legal and regulatory support by the
government, this research interviewed government officials, investors and hospital
leaders. Results of the interviews are as follows:
1. All hospital leaders, government officials and the leader of the investment
company believed that “legal and regulatory support for charitable healthcare projects”
is a key success factor for the inclusive healthcare services, especially when it comes
to medical disputes. In contrast, hospital leaders valued this more than government
officials.
2. Similarly, two government officials and the head of investment company also
believed that “legal and regulatory support for the for-profit investment projects” is
also a key success factor for the inclusive healthcare services, which is consistent with
the results in the literature.
Financial support for the charitable healthcare component
Government officials, the head of the investment company and hospital leaders
all believed that “appropriate financial support by the government for charitable
healthcare” is a key success factor for the inclusive healthcare services, and one
hospital leader highlighted this point. In addition, the head of the investment company
also expressed the hope that government financial support during the implementation
of the inclusive healthcare services can be provided to spread the financial burden
facing investors when they invest in the charitable healthcare component. In this
4 http://www.who.int/global_health_histories/seminars/Raman_presentation.pdf?ua=1

73
regard, both government officials said that local finance authorities are able to provide
support for some charitable healthcare projects, but some governments in remote and
poor areas may face certain financial difficulties and therefore may not be able to
provide such funding.
In summary, stable and sustainable policy support is considered the most
important form of government support (whether it is for the charitable healthcare
component or for investors), which is followed by laws and regulations. In addition,
the government also needs to provide corresponding financial support to the
charitable healthcare component.
4.2.2.5 Critical success factors concerning the external environment
The external environment related to inclusive healthcare mainly includes local
non-government support (natural environment, judicial environment, demand for
medical service and community support); public awareness and acceptance of the
initiative; local macroeconomic performance; and market conditions for investors
investing in the for-profit component. For any PPP project, a favourable external
environment guarantees successful operations (Azarmina, Prestwich, Rosenquist, &
Singh, 2008; Kodukula et al., 2011; McKee et al., 2006; Moehr et al., 2006).
For this type of questions, hospital leaders, government officials and the
investor were interviewed based on the reasons mentioned in section 4.4 above.
Local non-government support
Several articles on medical project management identified that the support from
non-government factors in implementing medical projects includes, but is not limited
to: Sound geographical environment (it is apparently difficult to carry out quality
medical projects in mountainous areas); a guaranteed judicial environment; local
medical education needs (medical education, medical knowledge popularization); and
community support. Through the interviews, we found that:
1. Government officials, the investor and hospital leaders all believed that “the
geographical conditions of the region (i.e. the impact of the geographical environment
on the distribution of medical resources)” is a factor worth considering in the
74
inclusive healthcare services. In China’s remote and mountainous provinces (such as
Shanxi, Guizhou, Yunnan, Sichuan, Chongqing, among others), modern medical
technology represented by telemedicine has enabled local residents to have better
access to diagnostic services. Therefore, people in these areas need and welcome the
inclusive healthcare services, and look forward to its launch as early as possible.
Therefore, in remote mountainous areas, there is a stronger incentive to implement
inclusive healthcare.
2. All interviewees believed that “local judicial environment” is a key success
factor for the inclusive healthcare services. This judicial environment here refers to
whether the local society has a fair and just law enforcement environment, whether
the courts and other organs can impartially enforce the law, and whether the citizens
adhere to the rule of law. In today’s China, doctor-patient disputes are an acute
problem for the society. A fair and just judicial environment is very important to the
healthcare sector, which is also a needed guarantee for the development of the
inclusive healthcare services.
3. All interviewees highlighted that “local medical education needs” is a key
success factor for the inclusive healthcare services. Medical education needs to
include formal medical education and the dissemination of medical knowledge for the
general public. Formal medical education is linked to the supply of human resources
in the inclusive healthcare services (especially in remote and poor areas with a lack of
medical personnel); the dissemination of medical knowledge for the public is also an
outreach opportunity for the inclusive healthcare services. If successful, it will help
clear the doubts of the public on the initiative.
4. Government officials and the head of the investment company believed that
“local community support” is a key success factor for the inclusive healthcare services.
At the same time, two of the four hospital leaders did not believe that community
support is helpful to the implementation of the inclusive healthcare services. Rather,
they believed that, although community healthcare services do play a certain role in
some developed countries and developed regions of China, community medical

75
functions are almost ineffective in some remote and poor areas of China due to the
low generally inadequate medical service. Therefore, they did not believe this kind of
support would support the implementation of the inclusive healthcare services.
Other external environmental factors
In some literature on PPP implementation, the public’s perception and
acceptance of the project, stable macroeconomic indicators, and market environment
(for the for-profit project) are critical success factors. Through the interviews, we
found that:
1. Government officials, the head of the investment company and four hospital
leaders believed that “public awareness and acceptance of the inclusive healthcare
services” is a key success factor, and one government official highlighted this.
Although the other four hospital leaders did not highlight this point. They noted the
rejection of similar initiatives by people in poor mountain areas due to the lack of
understanding of telemedicine technology and artificial intelligence technology:
“Many patients still trust more experienced doctors and prefer face-to-face
consultation and treatment. They are doubtful about telemedicine and artificial
intelligence—especially the elderly.” “The people in this area are relatively
conservative, so projects similar to the inclusive healthcare services cannot be
implemented because people simply don't accept it."
Therefore, this thesis believes that “public awareness and acceptance of the
inclusive healthcare services” is a factor that should be given due attention by all
actors.
2. “Stable macroeconomic indicators” is also a key success factor identified by
all interviewees, although none of them highlighted this. However, it can be inferred
from the literature that stable macroeconomic indicators are at least conducive to the
operation of the for-profit component, which indirectly guarantees the source of
funding for the charitable component of the inclusive healthcare services.
3. Government officials and the head of the investment company all believed
that “market environment (for the for-profit project)” is a key success factor for

76
inclusive healthcare.
In summary, favourable external environments are also needed for the inclusive
healthcare services to be successfully implemented. Specifically, local medical
education needs and public awareness and acceptance of the inclusive healthcare
services are factors that should be given particular attention.
3.3.2.6 Critical success factors related to organization, planning and operations
This category of factors is mostly summarized from the literature. According to
the CDC model, the critical success factors related to organization, planning, and
operation include at least four aspects: organization, planning and operations related
to the charitable model; organization, planning and operations related to the market
model; top-level design and management of the inclusive healthcare services; and the
exchange and cooperation among stakeholders. In the interviews, we made the
following arrangements based on the role of each interviewee: we asked hospital
leaders, doctors and patients about the organization, planning and management of the
charitable model. We asked government officials and the investor about the other
three aspects.
Organization, planning and operations management of the business model
for charitable component
For patients in remote and poor areas, they were mostly concerned about
whether the inclusive healthcare services have a “reasonable charging system (for
patients)”: Seventeen of the 20 interviewees highlighted it as a key success factor for
inclusive healthcare. In addition, patients believed that “high-standard hospital
management (including human resources management, business process management,
etc.)” and “communication and consultation among doctors, nurses and patients” are a
key success factor worthy of attention. Of course, “a reasonable transfer/referral
system” is also considered an essential key success factor.
The above four factors are considered as critical success factors by all patients
interviewed. The other five factors were not identified by all patients, but some
patients believed that it is (or even highlighted it as) a key success factor for inclusive
77
healthcare. These five factors listed as follows, sorted by the number of approvals
received: “uniform and reliable medical service standards and evaluation system;”
“clinical effectiveness;” “cost-effectiveness and sustainability of the medical system;”
“appropriateness of business processes for graded diagnosis and treatment systems;”
and “the development of ‘three-ends and one cloud’ infrastructure.”
Most hospital leaders and doctors believed that the nine factors mentioned under
“organization, planning and operation management of the business model for
charitable healthcare” in the questionnaire are all critical success factors for the
inclusive healthcare services. Among them, “a reasonable charging system”, “high-
standard hospital management”, “communication and consultation among doctors,
nurses and patients” are most highlighted.
Organization, planning and operation management of the business model
for the market component
Both government officials and the head of the investment company believed
that the following factors must be considered (i.e. are critical success factors) in
implementing inclusive healthcare.
1. Reasonable project organization structure;
2. Proper project positioning;
3. Reasonable project development plan;
4. Detailed project implementation plan;
5. Transparent tendering and procurement process;
6. Standardized project management measures (including project certification
and quality management);
7. Business diversity.
The market component of the inclusive healthcare services is a typical PPP
project, and the above-mentioned factors are also critical success factors for typical
PPP projects and have been confirmed by various research (see Table 1). In this article,
government officials and the head of the investment company reconfirmed it. Among
the above factors, “standardized project management measures” is considered the

78
most important by government officials (it was highlighted by a government official).
The head of the investment company did not highlight any of the above factors.
Top-level design and management of the inclusive healthcare services
The top-level design and management of the inclusive healthcare services
includes five aspects:
1. The strategic positioning of the inclusive healthcare services—to address the
problem of limited access to and high cost of medical service for people in remote and
poor areas, taking into consideration the requirements of the medical and health
system reform under the “13th Five-Year Plan” (treatment of major disease without
crossing county boundaries);
2. The strategic flexibility of the inclusive healthcare services—actors in the
initiative are required to remain agile and resilient at all times, embrace new
information, evaluate past decisions and change directions and make timely
adjustments based on the latest development. Today, artificial intelligence is
increasingly used in the medical sector, significantly changing the industry landscape
(Miller & Brown, 2018), which is still undergoing rapid changes. In this environment,
the managers of the inclusive healthcare services need certain strategic flexibility to
ensure they keep up with the changes over time;
3. The development of indicators of success—achievable management
objectives and criteria are essential links between the strategic and operational aspects
of the initiative;
4. The effective control and management of the entire initiative by the
leadership—this includes project control and management in the market component
and the development and management of the “three ends and one cloud” platform;
5. The demonstration role of other successful charitable healthcare projects.
The interview results show that government officials in different regions value
different factors. The Secretary of the CPC Committee of Fuzhou City believed that
the first two factors should be highlighted, and that the “development of indicators of
success” and the “effective control and management of the entire initiative by the

79
leadership” are also indispensable critical success factors, although the
“demonstration role of other successful charitable healthcare projects” is not deemed
important. The Secretary of the CPC Committee of Miyun District believed that all
five factors are critical success factors for the inclusive healthcare services, and the
“demonstration role of other successful charitable healthcare projects” should be
highlighted.
The head of the investment company believed that the first four factors are the
critical success factors, among which the “development of indicators of success” is
considered the most important one. Similar to the Secretary of the CPC Committee of
Fuzhou City, he did not consider the “demonstration role of other successful
charitable healthcare projects” a key success factor for the inclusive healthcare
services.
Cooperation and communication among stakeholders
In this section, the stakeholders we examined do not include patients (in the
questionnaire on critical success factors for inclusive healthcare designed by the
author, the communication and consultation between doctors and patients was
classified into the organization of the “organization, planning and operation
management of the business model for charitable component” section). Previous
researches found in the literature revealed that, in PPP projects, the exchange and
cooperation among stakeholders are very important. Such exchange and cooperation
include:
1. The development of a good partnership and a reasonable risk sharing
mechanism;
2. The commitment and willingness of all stakeholders in the initiative;
3. Clearly defined roles, tasks and responsibilities of all stakeholders in the
inclusive healthcare services;
4. The form of cooperation between investors and the government (BOT, BOO,
etc.);
5. Communication among stakeholders.
80
In addition, based on the characteristics of the inclusive healthcare services, we
believe that government supervision of investors (ensuring input and usage of sub-
fund B) should also be considered.
The interviews found that all three interviewees (two government officials and
the leader of the investment company) believed the first three factors listed in the
questionnaire are critical success factors for the inclusive healthcare services, which is
in line with findings of previous research in the literature. For the remaining three
items in the list, the interviewees’ opinions vary: the Party Secretary of Fuzhou and
the head of the investment company believed that these three factors are critical
success factors, among which “government’s supervision of investors” was
considered the most important (both interviewees highlighted this factor). The Party
Secretary of Miyun District did not believe that “the form of cooperation between
investors and the government” and “interactions among stakeholders” are critical
success factors for inclusive healthcare. “Government supervision of investors” was
considered just an ordinary key success factor that does not require special
highlighting.
3.3.3 Critical success factors to be highlighted
Based on the results summarized in sections 4.1–4.6, Table 3 summarizes those
critical success factors that are considered particularly important by interviewees
(government officials, the investment company leader, hospital leaders, doctors, and
patients). The selection criteria are as follows: the factor in question has been
identified by all interviewees of the same type as a key success factor for the inclusive
healthcare services and was highlighted by more than two or half of them.
Specifically: the factor should be highlighted by at least one of the two government
officials, at least two of the four hospital leaders, at least two of the eight doctors, and
at least two of the 20 patients. All factors highlighted by the leader of the investment
company appear in Table 3-1.

81
Table 3-1. Critical success factors to be highlighted Type of interviewee
Category Subcategory Factor
Government officials
3. Critical success factors concerning financial support
3.1 Investor strength 3.1.1 Investor’s own financial strength
3.2 Investment in the for-profit component
3.2.1 Scale of investment
4. Government support 4.1 Policy support 4.1.1 Medical policy support 4.1.3 Policy stability
5. Critical success factors concerning the external environment
5.1 Local non-government support
5.1.2 Local judicial environment 5.1.3 Local medical education needs
5.2 Other External Environmental Factors
5.2.1 Public awareness and acceptance of the initiative
6. Organization, planning and operation
6.2 Organization, planning and operation management of the business model for the market component
6.2.6 Standardized project management measures (including project certification and quality management);
6.3 Top-level design and management of the inclusive healthcare services
6.3.1 Strategic positioning of the inclusive healthcare services 6.3.2 Strategic flexibility of the inclusive healthcare services
6.4 Cooperation and communication among stakeholders
6.4.2 The commitment and willingness of all stakeholders in the initiative; 6.4.6 Government supervision of investors
Leader of the investment company
3. Critical success factors concerning financial support
3.2 Investment in the for-profit component
3.2.1 Scale of investment 3.2.2 Project investment cycle
5. Critical success factors concerning the external environment
5.1 Local non-government support
5.1.3 Local medical education needs
6. Organization, planning and operation
6.3 Top-level design and management of the inclusive healthcare services
6.3.3 Development of indicators of success
6.4 Cooperation and communication among stakeholders
6.4.6 Government supervision of investors
Hospital leaders 1.Medical infrastructure 1.1Doctors 1.1.2High proportion of middle and senior-level professionals in various departments
1.2Equipment 1.2.1The hospital is equipped with the necessary inspection equipment (especially high-end CT and MRI devices)
6. Organization, planning and operation
6.1 Organization, planning and operation management of the business model for charitable component
6.1.4 A reasonable charging system 6.1.5 High-standard hospital management
Doctors 2. Critical success factors concerning various technologies
2.2 Software availability 2.2.1 the ability of medical software (including operating systems) to quickly and smoothly complete defined tasks 2.2.2 medical software applications are easy to learn and use
2.4 Technical acceptance 2.4.2 medical workers’ acceptance of various technologies and their participation
6. Organization, planning and operation
6.1 Organization, planning and operation management of the business model for
6.1.4 A reasonable charging system 6.1.9 Communication and consultation among doctors, nurses and patients
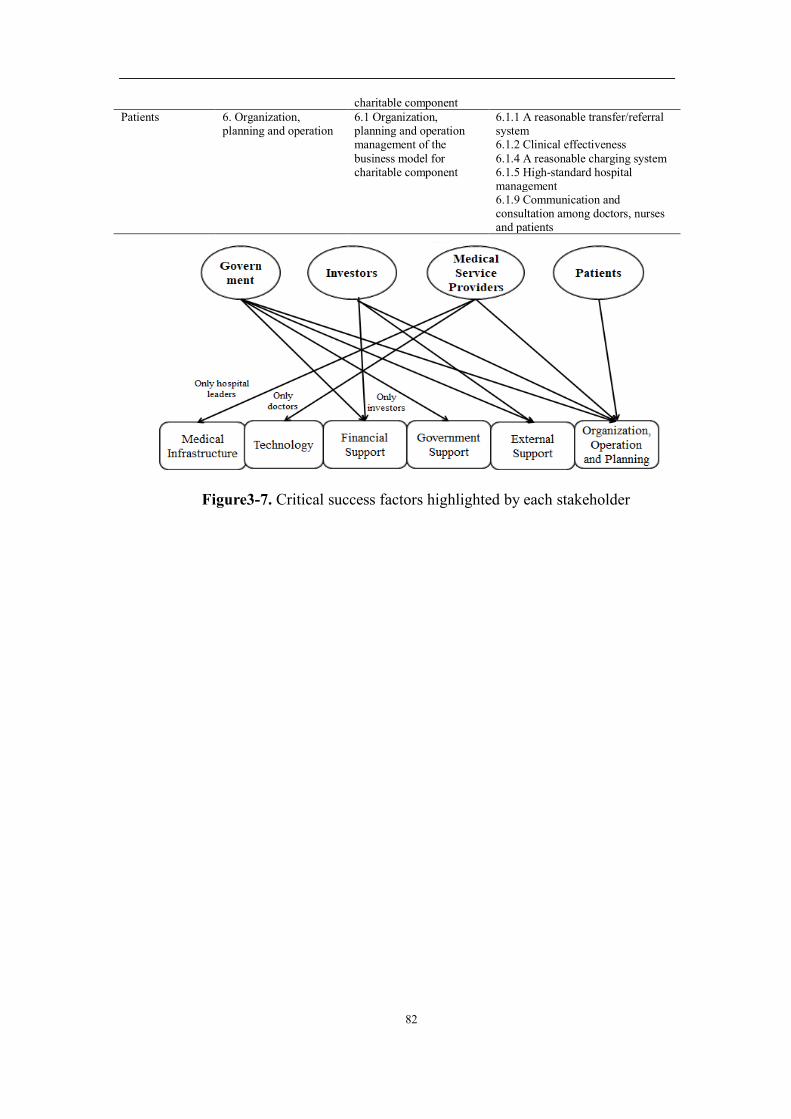
82
charitable component Patients 6. Organization,
planning and operation 6.1 Organization, planning and operation management of the business model for charitable component
6.1.1 A reasonable transfer/referral system 6.1.2 Clinical effectiveness 6.1.4 A reasonable charging system 6.1.5 High-standard hospital management 6.1.9 Communication and consultation among doctors, nurses and patients
Figure3-7. Critical success factors highlighted by each stakeholder
83
IV. Key Technologies for the Inclusive Healthcare Program
4.1 Key Technologies of Inclusive Healthcare Based on Evidence Theory
From Evidence-based Medicine to Evidence Theory
The diagnostic system of Inclusive healthcare is based on remote diagnosis
through a cloud-based infrastructure. Therefore, it differs greatly compared with
traditional clinical diagnosis. Cases need to be diagnosed using a different approach
from traditional clinical medicine to increase diagnostic efficiency with limited
evidence. An efficient inclusive healthcare service can be established using an
inclusive healthcare diagnosis and treatment framework based on the theoretical
framework of evidence-based medicine.
Evidence-based medicine (EBM) is a set of medical concepts and
methodologies based on evidence. The main difference between EBM and clinical
medicine is that the ideas and concepts of EBM are based on the framework of logical
reasoning and evidence, while the latter tends to rely on a combination of experience
and experimental results. The core idea of EBM is to judge the condition or effect of
treatment by carefully, accurately and wisely applying the most reliable evidence
available.
It is generally believed that EBM was first introduced by epidemiologists in the
1970s represented by Archie (Cochrane, 1989), who believed that more than half of
the clinical measures were ineffective or even harmful. These scholars believed that it
is far from sufficient to rely on medical experience for clinical treatment, and that
reliable evidence should be used to prove the effectiveness of these measures. Back
then, people started to realize that many diseases are not caused by a single factor, and
it is difficult and ineffective to diagnose from experience alone. At the same time,
clinical medicine has accumulated substantial cases information after years of
development, although with mixed quality, which makes it difficult for clinicians to
determine their authenticity. Through a large number of random medical experiments,
doctors can now have more knowledge of their reliability and actual effects, enabling
easy screening. After that, large-scale randomized and controlled trials have received

84
increased attention and have been widely conducted. These experiments have greatly
promoted the development of both clinical medicine and EBM. From the perspective
of EBM, a large number of randomized clinical medical experiments provide rich
material for its development, and solidify the foundation of its later development. In
the 1990s, the concept of EBM was proposed and elaborated (Group, 1992), forming
a new systematic framework, which in turn accelerated its development.
EBM is closely related to clinical decision-making. The starting point is that
clinicians need scientific and reliable evidence to support their judgment. The basis of
this judgment is mainly from past research conclusions in the medical field, not just
the clinical experience of the clinicians themselves. The core goal of EBM is to
provide objective and comprehensive decision support for clinical diagnosis through
existing medical research results. Therefore, the EBM system actually contains three
elements. First, researchers in clinical medicine have obtained scientific research
results in clinical medicine using experiments and other methods. These findings
provide a large amount of medical evidence for the EBM system. Second, building on
relevant EBM research and results of current clinical medical research, these pieces of
medical evidence are transformed into clinic practitioners’ practical operational
framework and standards. Third, clinicians refer to the relevant EBM framework to
make decisions on clinical issues and apply EBM to patients. These three elements
constitute the complete process and system of EBM, as shown below.
Figure 4-1. The three elements of EBM

85
New Trends of EBM in the Context of Inclusive Healthcare
The current medical guidelines for therapeutic diagnosis are based primarily on
existing EBM theory systems. The guidelines were written based on existing medical-
related cases and experimental results, using the “If-Then” judgment method to guide
doctors’ diagnosis and treatment. However, the traditional EBM system has several
challenges in the context of inclusive healthcare that need to be addressed:
First of all, currently, the medical evidence used in EBM mainly comes from
medical cases and experimental results, which often take a long time to come to a
usable conclusion. For many chronic diseases, this process often takes years or even
more than a decade. Therefore, traditionally, the preparation and update of the medical
guide is slow, and it is often difficult to update and prepare new iterations of medical
guidelines in a short time. The guidelines-based empirical methods will even remain
an experience from a few decades ago. However, in actual clinical operations, doctors
often need to diagnose according to existing technical tools, medical conditions,
patient conditions and other factors. The knowledge and experience of clinicians are
largely derived from practice in addition to the methodological guidance. However,
these experiences are often difficult to reflect in guidelines written using traditional
EBM methods. The problem is more acute in the case of inclusive healthcare. The
cloud-based medical technology framework for inclusive healthcare identifies and
diagnoses a large number of remote cases through a medical clinic that handles a
much larger number of cases than individual doctors. How to use these cases to
update operational guidelines has therefore become even more important. The
diagnosis and judgment of cases only through traditional EBM guidelines cannot
improve the accuracy and quality of treatment. Only through iterative training using a
large number of time-sensitive cases can the level of diagnosis and treatment be
improved.
Secondly, at present, the EBM guide for treatment follows an “if-then” logic,
which mainly uses the simple reasoning to evaluate each evidence and then provides
judgment for the next judging criteria or judgment result. The diagnostic process is

86
one-dimensional, returning either “yes” or “no”. In the case of traditional EBM, the
duality of 0 and 1 helps human doctors to determine the next treatment or judgment
without complicated reasoning. However, at the same time, a large amount of
information is lost in such judgment, which could lead to biases in judgment or
diagnosis. For example, when presented with the likelihood of 51% and 49%,
traditional EBM guide would point to the 51% path. However, under the cloud
computing system of the inclusive healthcare program, the distributed computing
system can perform much more complicated computations in a very short time. With
this background, the logic judgment framework that pursues judgment speed at the
cost of a large amount of information increasingly appears to be inaccurate and
therefore needs to be improved.
In addition, medical evidence and experimental results used in EBM are
currently often considered effective and reliable. Therefore, in the logical judgment of
EBM, the reliability of each form of evidence is considered to be equal. However, in
EBM guidelines, some medical experiments or cases deviate greatly from clinical
practice due to their small sample sizes or simple methods. However, they have been
treated as reliable evidence and included in the system of EBM guidelines due to slow
iterations or the lack of other similar evidence. This leads to a difference between the
actual clinical judgment and treatment. As a result, clinicians must give their own
judgment and adjust the treatment based on their own experience. However, as cloud-
based automatic intelligent diagnosis will be used in the inclusive healthcare program,
more accurate diagnosis models or guidelines will be required, and the reliability of
evidence must be considered. The traditional EBM system, however, does not reflect
the reliability or credibility of evidence, nor is it able to provide more information for
the computing system, therefore the accuracy of judgment will be affected.
In summary, traditional EBM theory iterates and evolves slowly. And, in order
to enable human doctors to make faster judgments, many multi-dimensional
information such as probability distribution and evidence credibility has been
discarded, thus affecting its accuracy. As a result, clinicians often need to make
87
judgments based on their own experience. In contrast, the inclusive healthcare
program will rely on the cloud medical system for judgment, which behaves
differently from human beings: on the one hand, its logical reasoning has great
advantages over humans; but on the other hand, it does not have the intuition or
experience possessed by human clinicians. Therefore, new evidence-based reasoning
methods must be used to diagnose and make judgments in the context of inclusive
healthcare.
EBM and Evidence Theory
EBM requires a large amount of medical evidence for the final medical
diagnosis. Therefore, it is necessary to develop appropriate methods for evidence
fusion. The evidence fusion theory proposed by Yang, J.B. and Xu, D.L. (Yang & Xu,
2013) provides a very good path for multi-evidence fusion for EBM for the following
three reasons:
First, the EBM system in the context of inclusive healthcare handles a large
amount of data and, building on the existing evidence of traditional medicine, is able
to continuously train the model using new data that is being fed into the system. This
requires a machine learning method to train the model through continuous input of
data. In the Evidential Reasoning (ER) theory proposed by Yang, J.B. and Xu, D.L.,
an algorithm that can train and adjust the model using data through a machine
learning method is presented. At the same time, according to the characteristics of
medicine, the data fusion method generally requires to be transparent and traceable.
Although some machine learning algorithms can enable data fusion, the process itself
often remains a black box. The ER rule proposed by Yang and Xu can ensure
transparency and traceability for each evidence, and therefore is a method that can be
used to achieve the fusion of multi-source medical evidence.
Secondly, the output the ER model is a distribution of values rather than the 0-1
result in the “if-then” logic network of traditional EBM. Therefore, its result is more
accurate when it comes to machine identification. The EBM system based on the ER
evidence fusion method proposes a new method of assisted decision making that uses

88
quantitative information and incomplete or inaccurate subjective information provided
by experts. The traditional inferential method of the EBM system is similar to the
Bayesian method based on probability theory. Its inference mode relies more on
quantitative information and requires a large amount of historical data to determine
the prior distribution, and cannot effectively use qualitative knowledge. This simple
inference method works well when dealing with probability uncertainty. But its
performance needs to be improved when it comes to ambiguity. With ER rules, both
the probability and the ambiguity are considered. This allows the various forms of
evidence to be simulated and improved in the extended confidence space and included
in the ER model. The ER model inherits the confidence distribution mechanism in the
D-S evidence theory, which also allows evidence to more closely resemble reality, so
that all the information of the original evidence can be retained as much as possible
under the ambiguous scenario. Compared with the “yes or no” Bayesian inference, the
D-S evidence theory framework introduces ambiguity while retaining empirical
knowledge, which also results in a more robust inference outcome relative to the
Bayesian approach in scenarios where the evidence is highly conflicted or incomplete.
In addition, the ER evidence theory takes the reliability and weight of evidence
into consideration. In actual application scenarios, such as clinical diagnosis of EBM,
the relative importance of each clinical indicator is not necessarily equal. In other
words, the contribution of different evidence is usually different in the final inference
result. In the traditional D-S evidence theory, although the ambiguity of evidence has
been considered, their relative importance is not fully defined. In the improved ER
model, the weight and reliability of each evidence are parameterized and included. In
the reasoning process of the ER model, all evidence and inference results constitute a
weighted directed acyclic graph. If this directed graph is fully connected, then the
time complexity of the inference will increase exponentially with the addition of
evidence. Meanwhile, because not every piece of evidence has a significant impact on
the final inference result, the evidence matrix in the fully connected state tends to be
89
sparse. In order to reduce the time cost for inference, experts can intervene by
providing guidance on the connection of the initial evidence nodes, upon which
training on evidence weights and reliability can be conducted. The traditional guide-
based EBM diagnosis process can be abstracted into a fixed ER model, while the ER
model provides a training model based on inference examples. In so doing, the
inference process combines the advantages of data-driven methods and knowledge-
driven methods.
Compared with traditional machine learning algorithms such as neural networks,
although the core idea is to train the topological relationship and connection weights
of nodes to optimize training error, the ER learning algorithm gives each node
(evidence) and connection (weight) actual meaning that can be referred to. Although
neural network algorithms can achieve a satisfactory recall rate with large sample
learning, their “black box” reasoning model makes it difficult to provide the basis for
inference in clinical medicine and other practical fields. At the same time, since the
empirical knowledge is not needed, the training of the neural network requires a large
amount of sample input. In the case of rare diseases, the number of samples is not
enough to support the scale of training needed for the neural network, and therefore
inference results are easily limited. The ER model uses the initial evidence framework
provided by experts as the empirical knowledge input, and parameterized learning is
performed on the weight and reliability of each case of evidence based on data input.
In so doing, the data-driven method requires less sample input, and therefore provides
a more adaptive diagnostic solution for various diseases.
Core Technology Framework for Inclusive Healthcare Based on Evidential
Reasoning Theory
The Theoretical Basis of the ER Theory
Evidential Reasoning (ER) rule is a classical information fusion rule in the field
of artificial intelligence. It is inclusive and perfected based on the traditional D-S
evidence theory. In the ER rule, it is assumed that there is a set Θ = {ℎ&, ℎ(, … , ℎ*}
containing a set of mutually exclusive and exhaustive hypotheses, which is called a

90
domain. The power set of the domain Θ is expressed as P(Θ) or20. One piece of
evidence can be expressed by the following:
12 = 345, 67,28|∀5 ⊆ Θ, ∑ 67,2 = 17⊆0 >(4-1)
where 45, 67,28 is the manifestation of evidence 12, which means that the confidence
of 67,2is assigned to the assumption 5. 5 can be any non-empty set in the domain, if
67,2 > 0,45, 67,28 is called the focus element of 12.
ER rules create a new definition of the reliability A2 and weight B2 of evidence12.
The weights reflect the relative importance of the evidence and the reliability reflects
the evaluation of the reliability of the information source. The ER rules improve the
expression of evidence and confidence as shown in the following formula:
CD7,2 = E05 = F
GHI,2C7,25 ⊆ Θ, 5 ≠ F
GHI,241 − A285 = P(Θ)(4-2)
ofwhichmS,T = wTpS,T ,cVW,T = 1/(1 + wT − rT) . cVW,T is a normalized factor,
which makes the sum of all confidence 1. In the case of fusing two pieces of the
evidence following the ER rule, the rules may be expressed as:
67,[(() = \0, 5 = ϕ
_̂`,a(b)
∑ _̂c,a(b)c⊆d, 5 ⊆ e, 5 ≠ ∅(4-3)
C_7,[(() = g(1 − A()C7,& + (1 − A&)C7,(h + ∑ Ci,&Cj,(i∩jl7 ∀5 ⊆ Θ(4-4)
So, for the fusing tasks of two or more than two forms of evidence, the
application of repeated use of ER rules can be adopted. Compared with the traditional
D-S fusion rule, the combination effect of the ER rule was greatly improved when
dealing with evidence with high conflicts or incomplete information, which was an
efficient and practical reasoning rule.
A Multi-Source Data Classifier Based on ER Theory
For an N-class classification problem, if there are K samples in the training data
set, and each data sample has M characteristics, then the ER rule can abstract the
domain Θ as a set containing N categories, and the realization of ER classifier can be

91
divided into four steps: extracting evidence from training data, evaluating the
reliability and weight of evidence, and combining evidence and training classifier
model.
Firstly, the training data can be constructed as a set S = {[opq, rq]op
q ∈ up, rq ∈
Θ} of the feature and category label, and the feature up was constructed according to
the range of values of the training set data. Then, select the points of each feature
interval according to the expert experience, and transform the characteristic of the
numerical model into the category character.
Secondly, the statistical data can be classified directly by compiling a certain
feature, and the reliability of the evidence can be evaluated. The initial value of the
evidence weight can be approximated by the initial reliability. After preprocessing all
M evidence, the ER rules can be used to combine the evidence and eventually obtain
the confidence-merging results as shown in the following formula:
O(oq) = 3rw, 6w,[(x), y = 1,2,… ,z>(4-5)
After setting the initial parameters of the ER classifier, it needs to be trained and
optimized. The training parameters selected here are the sum of the Euclidean
distances between the merged result and the reference of confidence vector. The cost
functions to be optimized are as follows:
ξ(P) = ∑ |}(~(oq), �q)ÄÅql& (4-6)
P represents the weight and reliability parameters to be optimized. In order to
minimize the cost function, the algorithm of sequential linear programming can be
adopted to distinguish from traditional classification algorithms, and ER classification
algorithm focuses on the contribution of the characteristics of training data make to
the final classification result. As a pure data-driven algorithm, the ER classification
algorithm avoids the distortion of the original training data caused by the modal itself.
And it has a concise algorithm structure and a mature training method, which reduces
the time and space complexity. On some classical machine learning test data sets, ER
92
classifier has been proven to be very competitive in classification precision. It is
believed that the classification method that is based on evidential reasoning will be
applied to more pattern recognition situations in the future.
A Multi-source ER Data Classifier for Multimodal Medical Images
At present, neural network classifier is the most widely used classifier in
medical image recognition. The classification results (based on various kinds of
evidence) can be obtained by pre-classification of multimodal images conducted by
neural network. Then the evidence fusion classifier can be used to classify the
multimodal data again to realize the merging of multi-source data.
First, the data are pre-classified using neural networks. Because of the better
effect of the BP neural network on the simulation of small sample training data, the
classification accuracy in this case was often met with the bottleneck. Considering
that the probability of the sample belonging to each class Ç2(É = 1,2,… ,C) was
finally computed in the classification of the op(Ñ = 1,2,… , y) in the BP neural
network, the final classification was used to classify the samples in the category Çq
with the highest probability.
Çq = max2l&,(,…,^
á(op ∈ Ç2)(4-7)
In the re-classification results of neural networks, we can get the probability set
Ç2(É = 1,2,… ,C) of different categories for a particular sample op(Ñ = 1,2,… , y):
up = {áp&, … , áp^}. For two different data sources à& and à( , the probability set
obtained by the neural network classification can be considered as the initial data
classification of confidence degree of two data sources.
After the initial classification, confidence distribution of different data sources
finished by neural network, for L different data sources, the initial confidence
allocation set for the sample classification for each data source is uq =
{áq&, … , áq^}(â = 1,2,… , ä), where m is the number of target categories. Assuming
the number of training samples is N, according to the ER rule in chapter 2, we can
express the confidence degree of the article j of sample i=1,2,..., N) as follows:

93
CD7,p2 = E05 = F
GHI,p2C7,p25 ⊆ Θ, 5 ≠ F
GHI,p241 − Ap285 = P(Θ)(4-8)
The initial value of evidence weight Bp2 and evidence reliability Ap2can be set as
&
ã. According to the multiple evidence fusion rule, the fusion confidence distribution of
L evidence sources can be expressed as:
C_7,[(ã) = g(1 − Apã)C7,p(ãå&) + 41 − Ap(ãå&)8C7,pãh
+∑ Ci,p(ãå&)Cj,pãi∩jl7 ∀5 ⊆ Θ(4-9)
By using recursion algorithm, we can get the fusion result of all L pieces of
evidence of sample i.
Obviously, the fusion confidence of a sample containing L pieces of evidence in
the evidence fusion model depends on the selection of the reliability and weight of the
evidence. The reliability and weight parameters of the initial setting may not be able
to accurately model the relative importance and reliability of different evidences.
Therefore, it is necessary to train the weight parameter Bp2 and the reliability
parameter Gp2 using the existing sample data in order to simplify the complexity of the
model and to describe the coincidence degree of the evidence fusion network
prediction result and the real classification situation. We can use the optimized model
based on MSE: miné
è(á). The objective function here is:ξ(P) = ∑ |}(~4op8, �p)*pl& ,
where ~4op8 represents the fusion result of the first sample, �p represents the true
classification of the i sample, |} represents the Euclidean distance, and P represents
the set of parameters to be optimized 3Ap2, Bp2|Ñ = 1,2,… ,z; É = 1,2,… , ä>. For the
description of the restricted conditions, because the sum of the weights of each
evidence equals to 1, and the weight is non-negative, there are: ∑ Bp2 = 1x2l& , 4Bp2 ≥
08, and the reliability of the evidence can be limited to Ap2 = Bp2 considering the
higher the weight is, the more reliable the evidence is.
In order to solve this parameter cum optimization problem, we choose the

94
sequential linear programming algorithm (SLP). The sequential linear programming
algorithm uses the first-order of Taylor’s expansion to do linear approximation,
targeting nonlinear programming problems (which is the first choice to solve the
optimization problem because of its fast convergence and mature application). After
the linear approximation of the initial optimization problem, we can solve multiple
linear programming problems with simplex method or interior point algorithm.
Sequential linear programming and algorithm implementation can be summarized as
follows:
First, a ladder degree of initial objective function was computed, and the initial
objective function can be approximated as follows: ξ(P) ≈ ξ(áì) + ξ′(áì)(P − áì),
where áì is a given initial point. The original planning problem can thus be
transformed into a linear programming problem: miné
ξ′(áì)P.
Secondly, determine the iteration step size. To determine the appropriate step
size plays a vital role in the realization of the algorithm. An overly large step size may
result in an approximate reduction in accuracy, resulting in an algorithm convergence
failure. On the other hand, an overly small step can lead to excessive accumulation of
iterations and thus greatly increase the time cost of the computation. Usually, we get
the upper bound UB(wóT)=1 of the parameters to be optimized by using constraint
condition, and the initial step can be set to 10% of the upper bound of the parameter.
Then, the optimal solution was obtained by using the linear programming
method and after the first and second steps, the nonlinear function ξ (P) can be
linearly approximated at áì, and the initial search space can be formed around this
initial point. The interior point algorithm can be used to extend the search space until
an optimal solution point is obtained to approximate the original objective function.
The algorithm repeats the process until a stop condition is reached.
Finally, the stop condition of the algorithm can be set to two kinds of case: (1)
The iteration step size of all variables was reduced to below a certain threshold value;
(2) The value of the objective function and the value of the variable were smaller than

95
a threshold after two consecutive iterations. At the stop condition, it can be concluded
that there is no significant difference between the linear approximation of the original
programming problem and the target function value.
The model parameters of the optimal fitting state of the training data can be
obtained by using the training data of the neural network to optimize the evidence
fusion model, and the model parameters of the two-level classifier are taken as
evidence fusion.
4.2 A Cloud-based System and Architecture for Inclusive Healthcare
Second is the development of the cloud system for inclusive healthcare. Primary
medical resources are known to be unevenly distributed and medical data are difficult
to collect. On the one hand, the uneven distribution of medical resources means that
people at the grassroots usually have less access to high-quality medical resources,
mainly due to the scarcity of doctor availability, and also due to the difficulty to
timely identification of some complicated diseases. After multiple referrals and
examinations in hospitals at different levels, the best time for treatment is often
missed when final diagnosis is made. In addition, this multi-level referral process
usually incurs high costs of transportation, accommodation, etc., which are often close
to or more than the medical expenses themselves.
Therefore, it is necessary to establish a cloud system that is applicable to the
specific context of inclusive healthcare. On the one hand, the cloud system collects,
stores and pre-processes data from primary hospitals, upon which the fusion analysis
of various types of data can be conducted. By applying machine learning to the
massive medical data collected by the cloud system combined with existing data, the
accuracy of the machine learning and therefore that of remote diagnosis can be
improved through iterations. Ultimately, the level of diagnostic accuracy will match
top experts in the field, so that healthcare can be made more equitable. On the other
hand, with remote diagnosis, the cloud system eliminates the need for multiple visits
and referrals, and therefore reduces the need for relocations, cutting down expenses
not associated with the medical treatment itself, and ultimately reducing the overall

96
medical expenses for people at the grassroots.
Overall Framework for the Cloud-based System for Inclusive Healthcare
First of all, a framework for the cloud-based system must be developed. The
goal of the cloud system is to build a technology framework for inclusive healthcare
through cloud technology, based on the actual need for inclusive healthcare.
Combined with the existing cloud computing system frameworks, the overall
framework of the cloud-based system for inclusive healthcare can be divided into
three parts: (1) a framework for the medical cloud infrastructure layer, (2) a
framework for the medical service layer, and (3) a framework for the application layer.
The first component, namely the framework for the cloud infrastructure layer
for inclusive healthcare, has three sub-components. The first sub-component is a
framework for retrieving structured data, since some data generated at primary
hospitals during the diagnosis and treatment process (such as electronic medical
records and test results) are stored in the form of structured data (which can be
retrieved with the development of this framework for structured data). The second
sub-component is the acquisition framework for unstructured text data. Before using
the cloud system, most of the text data are handwritten or non-standardized
unstructured (which require appropriate methods for recognition and application in
the machine learning process). The third sub-component is designed for a large
amount of unstructured data stored in medical images. Such data contain massive
information, but it needs to be collected and pre-processed using appropriate methods.
The second component, namely the framework for the medical service layer for
inclusive healthcare, also has three sub-components. The first sub-component is the
big data storage platform for inclusive healthcare. Medical data collected through the
infrastructure layer must be securely stored for safe reading and storage and further
analysis. This can be implemented by using existing cloud storage solutions such as
Hadoop. The second sub-component is the cloud computing platform for inclusive
healthcare. The massive medical resources in the cloud storage platform need to be
processed in computing platform with ultra high-speed computing power. Due to the
97
high computational flexibility requirements for each data node, the platform must be
managed efficiently and flexibly from a remote location. This should be addressed by
building a cloud computing platform for inclusive healthcare. The third sub-
component is an application development platform for inclusive healthcare. Medical
data is highly technical, and its reading and analysis rely on the dedicated medical
software system. All software applications within this system are required to be able
to communicate seamlessly. With the continuous improvement of the platform system,
extended features will be added to the platform in the future. For this reason, an
application development platform needs to be built for the efficient development and
management of relevant applications.
The third component of the cloud platform is the framework for the medical
application layer for inclusive healthcare. Firstly, it is necessary to develop a remote
interactive system for the base layer and the platform layer. The system provides a set
of interfaces for the human-machine interface. On one end is a patient-oriented
system, which provides diagnosis suggestions for patients, who can provide
supplementary information input. On the other end is a doctor-oriented system. For
certain tasks that require doctors’ involvement, the system provides the doctor with
relevant information of the patient, together with the diagnosis suggestion given by
the intelligent diagnosis system. The doctor can provide diagnosis suggestion through
this system so that patients receive supplementary diagnostic information. In addition,
the interactive system can provide continuous input to the background diagnostic
system. Such input is derived from the doctor’s diagnosis and based on the
development of the patient’s condition. Secondly, a comprehensive medical record
diagnosis system (based on textual medical history, medical records and test results)
will be established. This part of the data is mostly text-based data, including both
structured and unstructured text. Firstly, it is necessary to perform natural language
recognition on unstructured text data using a cyclic neural network and other methods
to extract key information and convert these unstructured text data into structured data.
Then, using the structuralized data combined with other structured data, deep learning

98
can be performed to make a diagnosis from patients’ medical records and test results.
Thirdly, a medical imaging diagnostic system will be established. Because medical
imaging plays a very important role in the diagnosis of major diseases, understanding
medical images requires very specialized medical knowledge. In addition, some
medical features are difficult to be recognized by the human eyes. Hospitals at the
grassroots level often fail to efficiently and accurately read medical images. Through
machine learning methods such as convolutional neural networks, multimodal
medical images can be interpreted to give diagnostic recommendations to improve the
accuracy and efficiency of remote diagnosis.
The overall framework of the above medical cloud system is shown below:
Figure 4-2. The overall framework of the cloud-based medical platform for
inclusive healthcare
Framework for the Infrastructure Layer for Inclusive Healthcare.
The core functions of the infrastructure layer for inclusive healthcare are the
collection and analysis of massive amount of data. However, in clinical diagnosis, the
diagnosis decision-making is often supported by multimodal data from multiple data
sources. Therefore, it is necessary to establish a multimodal data acquisition and
processing mechanism.
Framework for structured data acquisition
For clinical diagnosis and decision making, patients’ basic information and
medical record information are usually the first information available to the doctor.
However, the current mainstream electronic medical record management systems can
usually record the clinical symptoms in text-based files, which is not convenient for

99
extraction without the participation of doctors (Informatics and Inc, 1990). Therefore,
this thesis proposes an electronic case system that systematically and hierarchically
records patients’ clinical indicators guided by doctors to support the diagnosis and
decision-making system.
The main challenge in structuring medical record data is that the clinical
indicators for different diseases often differ greatly. Adding too many features to the
system will result in higher feature dimensions and sparse data, which inevitably leads
to the problem of waste of resources. Therefore, this thesis proposes a tree-like
multilayer medical record information storage mechanism, which will be maintained
and improved dynamically under the guidance of doctors, so that medical record data
can be structuralized for subsequent information processing.
For example, for a patient with intracranial tumours, their medical record
information can be classified under “surgery – neurosurgery – intracranial derivative,”
and basic data on breathing, blood pressure, spinal strength and vision can be
provided. In this way, a patient’s unstructured data can be processed in a structured
manner, which makes it easier to standardize its storage and presentation.
Another challenge in the structuralizing medical record data is the
representation of some non-quantitative indicators. For example, a patient’s vertigo
condition is often difficult to quantify. To address this problem, this thesis intends to
use the idea of ordering and grading of non-quantitative indicators under the guidance
of doctors, which stores and quantitatively represents those indicators that are difficult
to quantify. For example, for the conditions of vertigo, they can be classified into the
following five grades based on the patient’s vision and movement impairment: severe,
heavy, moderate, light, and negligible. Through this approach, the massive text data
from the medical record of many patients can be transformed into structured data for
storage, in order to meet the performance requirements of high-speed automatic
information processing of the inclusive healthcare diagnostic system.
Processing unstructured data such as text
Using the hierarchical processing and storage methods described above, a large

100
amount of unstructured data in patients’ medical records can be structuralized.
However, due to limits in the speed of computer operations, storing all the
information in this way will inevitably lead to an increase in the dimension of data,
thereby reducing the operation speed. To address this problem, this thesis proposes a
machine learning method based on natural language processing to train the residual
text in the patients’ medical record, which is coupled with feature extraction to create
abstractions of these data for generating new indicators for comparison with the old
ones (Savova et al., 2008). In this way, patients’ historical diagnostic data can be
retained and structured to the greatest extent, thereby reducing the distortion and loss
of information during processing.
Processing unstructured data such as medical images
Currently, medical images have become an important source of information in
clinical diagnosis. At present, the rapid development of signal processing and nuclear
magnetic technology also enables medical images to accurately record human tissue
conditions to a greater extent. MRI technology is used for medical imaging based on
the difference in the absorption rate of radio frequency signals among tissues with
different water contents in the human body (Jiang, 2013). However, the original data
may be lost due to smoothing and filtering operations in the reconstruction process by
the signal processing and image processing modules of the nuclear magnetic receiver,
which affects the fidelity of the final images. In order to improve the accuracy of
processing and judgment, this thesis intends to take the original signal received by the
nuclear magnetic receiver as a new data source and combine it with the image-based
data source for joint analysis, thereby improving the accuracy of assisted clinical
diagnosis based on medical images.
Framework for the Medical Application Layer for Inclusive Healthcare
A framework for the service layer for inclusive healthcare will be developed
based on the medical cloud infrastructure framework. The medical cloud service layer
is a middle layer that connects the infrastructure layer and the application layer of the
inclusive healthcare cloud system. Three functions will be implemented on the service

101
layer of the cloud platform for inclusive healthcare. The first function is cloud storage,
which stores the three types of data collected by the infrastructure layer using
distributed storage and other storage technologies. The second function is cloud
computing, which processes data by establishing a cloud computing platform. The
third function is the cloud application development platform, which provides a
platform for developing applications for inclusive healthcare.
Cloud storage
Cloud storage function should be first developed. The cloud infrastructure for
inclusive healthcare will provide a large amount of structured and unstructured
medical data, which are large in volume, complex in structure, and require high
collection cost. In addition, citizens’ medical data are confidential information.
Therefore, the cloud storage system needs to have the following features.
First, sufficient storage speed and bandwidth must be ensured to store, read, and
transmit massive amounts of medical data under cost-constrained conditions. We can
optimize the cost by setting and fulfilling storage requirements (Wang et al., 2014).
By establishing a set of multiple data blocks for cloud storage, a heat function can be
defined to determine the level of activity of each data block. Using this heat function,
a cost function can be constructed to achieve cost optimization. In practical
applications, an algorithm is needed to perform real-time optimization of storage and
reading activities. In addition, security is a required feature for medical cloud storage
systems. (Mansfield-Devine 2008; Cachin et al. 2009; Shacham and Waters, 2013).
Here, the meaning of security is two-folded. On the one hand, data security refers to
the prevention of data loss, which can be effectively achieved using multi-site backup
using distributed storage. On the other hand, it also refers to the prevention of data
breach. For this purpose, it is necessary to encrypt and decrypt using the appropriate
technologies. In addition, the fault tolerance and scalability of the cloud storage
system are also important features to be considered.
Based on the above characteristics, the following cloud storage structure can be
developed. Firstly, the access layer through which the cloud storage system can
102
interact with other applications and users. For example, PACS image data can use
standard interface protocols such as NFS and CIFS. The application layer establishes
a connection with the storage system through the access layer, thereby enabling read,
write and other operations on the content of the storage system. Secondly, the basic
administration layer, which integrates related algorithms and models for storing,
reading and writing. By developing appropriate algorithms, this layer enables fast and
low-cost retrieval of background data so as to achieve a balance between efficiency
and cost. In addition, the stored data is encrypted and decrypted using various
algorithms in the basic administration layer to ensure system security. Thirdly, the
storage layer, as a hardware layer, comprises an array of massive storage devices that
hold the data. Storage efficiency is improved by appropriate storage network layout
configuration.
Cloud computing platform
Secondly, the system requires the ability to process and analyze massive data.
The cloud computing facility consists of a large number of basic hardwares, which
require considerations of energy consumption and computational flexibility while
ensuring computing speed. Therefore, the cloud computing platform should have the
following features.
First is fast computing speed. The cloud computing platform must be able to
analyze and process data quickly. This can be done by extending hardware and/or
using efficient data processing technology and programming methods. For example,
Google’s MapReduce programming model divides a large number of jobs into Map
and Reduce tasks, where the former reads input files through and analyzes them using
parallel computing techniques, and the latter is used to combine the results of multiple
Map tasks to quickly process large-scale data. (Cachin et al., 2009). On the other hand,
the platform should have flexible and universal calculation methods applicable to
various types of data. For example, the Dryad Framework based on the directed
acyclic graph (DAG) can handle complex processes more easily and efficiently, by
encapsulating the underlying complexity and enhancing flexibility and adaptability.
103
Therefore, based on the above-mentioned characteristics, a distributed
computing framework should be built by referring to innovative technologies such as
MapReduce and Hadoop. Considering the characteristics of medical data structure, it
is necessary to further develop the scheduling algorithm for hardware and establish an
effective computing node scheduling strategy to reduce data transmission loss and
ensure efficient data computation. On the other hand, it is necessary to establish a
fault tolerance mechanism for medical data tasks and establish a reasonable abnormal
task discovery mechanism for the heterogeneous environment with mixed medical
text and image data, in order to enhance the flexibility and adaptability of the
computing system.
Cloud application development platform
Finally, a development platform for cloud applications needs to be built on the
healthcare cloud system. Through the overall management and detailed design of the
cloud application development platform, application developers can easily and
efficiently develop and implement related applications. As a result, the application
development platform for the medical cloud system must have the following
characteristics.
First, the application development platform must be convenient enough to
enable developers to quickly develop and implement systems and applications.
Second, the long development cycle of some features of the medical cloud means high
development cost. Therefore, open source resources can be directly incorporated into
the platform where appropriate. This requires the application development platform to
provide an interface to a variety of programming languages and modules. Third, due
to the distributed nature of the storage and computing layers of the cloud platform, the
application development platform must be portable so as to enable rapid migration
and replication.
Based on the above considerations, an integrated functional component package
(consisting of integrated development tools, basic service framework and application
development kit) can be developed relying on the best practices of existing

104
development platforms such as Eclipse and Soft Console, etc.
Framework for the Medical Application Layer for Inclusive Healthcare
The data acquisition and hardware architecture design of the cloud platform for
inclusive healthcare has been introduced in previous sections. In this section, we
present the conceptual design of the application layer of the cloud platform, with the
hope that a practical inclusive healthcare tool can be developed to facilitate doctor-
patient interaction and assist clinical diagnosis.
The doctor-patient remote interaction system
The main target group of inclusive healthcare is patients in the underdeveloped
regions of central and western China who have limited access to medical resources
compared to developed regions due to economic status, geographic location and other
reasons. To address this issue, a doctor-patient remote interaction system can be
developed building on the cloud platform for inclusive healthcare. After their
information has been collected at the local medical institutions using the information
collection terminals for inclusive healthcare, patients can participate in multi-party
remote consultations and receive treatment suggestions and treatment plans by experts.
Relative to conventional remote interactive systems, the doctor-patient
interaction system (which is based on the cloud platform for inclusive healthcare)
integrates data analysis and doctor diagnosis, where doctors can retrieve patient data
in real time through the cloud platform and make a diagnosis by combining their own
professional knowledge with system-assisted diagnosis information. Under this model,
doctors can quickly judge the basic condition of the patient according to the assisted
diagnosis by the cloud platform and relieve the burden of high-level hospitals by
saving time. Meanwhile, the doctor’s diagnosis can be adopted by the assisted
diagnosis system for self-training to improve the accuracy of assisted diagnosis in the
future.
The case-based comprehensive diagnosis system
As the number of patients increases, the cloud platform’s data storage
component will accumulate a large number of medical records. As a data-driven

105
intelligent medical platform, it is necessary to establish a comprehensive diagnosis
system based on medical records as an important way for diagnosis and assisted
decision-making.
In order to extract important diagnostic features from text data, the
comprehensive diagnosis system should have strong natural language processing and
analysis capabilities. By accumulating cloud data and updating historical diagnosis
results, the natural language processing algorithm will continuously optimize
performance during the iterative process, so that it is able to faithfully extract features
from medical records during the production phase.
After extracting useful information from the text, the comprehensive diagnosis
system can combine text-based record with imaging diagnosis, pathological data and
patient medical history data to form evidence reasoning system through hypothesis
generation (Moisl, 2011). This will finally provide doctors with supporting diagnostic
opinions through using evidence fusion theory.
The image-based intelligent diagnosis system
As an important source of information in clinical diagnosis, the multimodal
medical images of a large number of patients available in the cloud storage platform
can be used to build an image-based intelligent diagnosis system and provide
important supporting diagnostic information for doctors as important evidence for
reasoning.
The image-based intelligent diagnosis system includes several subsystems,
namely, modal management, image preprocessing, feature extraction and
classification. Since patients’ MRI or tomographic images have scan sequences with
different modes (which represent different indications of the disease), the image
modal management system selects different image processing methods based on
different sequences, so as to maximize the retention of indicators and improve
diagnostic accuracy. In addition, the image diagnosis system needs to perform
denoising and averaging operations on the image according to the morphological
features of different image sequences. For brain MRI images, it is also necessary to
106
perform such operations as skull stripping, registration, and segmentation of regions
of interest. Thanks to a pre-processing module, the processing range of the image is
reduced, thereby cutting the time complexity of feature extraction and improving
system efficiency. Because medical images are unstructured data, it is necessary to
design a feature extraction network according to the morphological features of the
images and extract the pathological indication of the regions of interest, thereby
reducing data dimension and achieving data structuralizing. In terms of the features
extracted, multi-source data classification can be realized by using evidence-based
reasoning machine learning. The results can be summarized as evidence and fed into
the evidence fusion processor.
On the basis of the cloud system for inclusive healthcare, modern artificial
intelligence is needed to perform remote diagnosis using primary medical data. For
example, IBM’s Watson is already able to learn and make judgments on a massive
number of medical records. Currently, the most difficult task in remote diagnosis is
the processing and diagnosis of medical images. This is because medical images are
unstructured data, and are different from structured diagnostic results. Structured
diagnosis results can be directly fed into pathological models for analysis. For
unstructured data such as medical images, however, it is difficult to use traditional
methods to analyze and make judgments directly. Therefore, they are usually
interpreted and analyzed by radiologists. However, since the medical resources of
primary medical care are relatively limited, remote human intervention requires a
large amount of manpower and capital input, not to mention the difficulty in
recruiting a large number of medical personnel in a short period of time.
Therefore, in the context of the inclusive healthcare program, it is necessary to
develop an AI-based telemedicine imaging diagnostic method suitable for this
scenario. On the one hand, using AI to process images can reduce the unit cost of
medical image recognition. Because inclusive healthcare has a very broad coverage, a
large amount of medical image data needs to be processed and recognized on the
cloud. When compared with outstanding AI algorithms, the speed and cost of
107
conventional human identification will be at a disadvantage. Therefore, outstanding
medical image recognition methods will be able to achieve the same performance at a
faster speed and lower cost, thereby promoting the development of inclusive
healthcare. On the other hand, the accuracy of medical image recognition can be
improved by the AI-driven method. Currently, manual identification of lung nodules
and gliomas in medical images remains a challenge. Moreover, working on a large
amount of medical image data for an extended period is prone to fatigue and a
decrease in accuracy. For many tumours, late discovery for a few months would mean
a doubling of treatment difficulty and a significant drop in prognosis quality. Medical
image reading by deep neural networks, convolutional neural networks, etc. have in
some respects exceeded human precision. In summary, we need to develop a rapid,
continuous and high-precision interpretation of primary medical images by
developing AI-driven methods for medical image recognition, thereby improving the
standard of primary healthcare.
4.3 The Technical Architecture of Medical Image Recognition
The technical architecture for medical image recognition is a very important
part of the inclusive healthcare program. The goal of the framework is to identify and
make judgments on medical images using AI theory and methods (such as computer
vision and deep learning, combined with the existing expertise of the medical field).
Building on existing medical image recognition methods, the technology
architecture for medical image recognition is mainly comprised of three parts: (1) pre-
processing of medical image data, (2) feature extraction from medical image data, and
(3) pattern recognition of features in medical image data.
The first part has two sub-processes, namely the pre-processing of medical
image data (using computer technology) and the preprocessing of medical image data
based on existing medical knowledge. Combined, these two processes form a set of
basic data that can be used for AI-driven feature extraction and pattern recognition.
The second part also includes two aspects. First, the feature extraction of medical
image data is based on medical knowledge. Using the expertise in the medical field,

108
we can extract the features known to humans from medical image data and create
structuralized data. Secondly, the feature extraction is based on AI-driven deep
learning. Deep neural network and other AI-driven methods can be used to extract
features that can be used as diagnostic criteria but are still unknown to human. The
third part is pattern recognition based on data features. In this part, the features in the
extracted medical image data are evaluated by classification methods to determine
whether a tumour is present. And if so, is it benign or malignant. Since the medical
image data can be structured in the feature extraction process, the pattern recognition
method supported by AI theory can directly classify and evaluate these structured data
and give conclusions. The technical architecture for medical image recognition is
shown in the figure below.
Figure 4-3. Technology architecture for medical image recognition
As a first step, computer images are pre-processed using computer technology
such as computer vision and morphology. Generally, it is necessary to standardize the
format of the medical image data for screening, after which registration can be
performed using imaging algorithms before subsequent morphological processing can
be completed. In order to facilitate computer-based medical image recognition, the
images should be further processed after the above-mentioned pre-processing.
In the second step, namely, feature extraction, medical image data is processed
based on existing medical knowledge to extract features such as brain tissue symmetry,
the shape of brain chamber, brain tissue texture, etc. The medical image feature
extraction method mainly simulates the key indicators that professional radiologists
use to diagnose brain tumours and thereby automating the process. Based on this
109
method, machine learning is carried out by developing a deep neural network or a
convolutional neural network. The computer then extracts features from the medical
images using data convolution and pooling. In this step, the machine autonomously
learns and analyzes the data with the aim to achieve intelligent extraction of features
on the basis of automated feature extraction.
In the third step, the features extracted are analyzed for pattern recognition to
determine the presence of any disease, and if so, its status. In the second step, data is
extracted by combining medical expertise. Afterwards, the original unstructured data
is structuralized through feature extraction. Then, pattern recognition and diagnosis
classification were applied to the structured data using machine learning algorithms.
Data Pre-processing Method for Medical Image Recognition
The image data of inclusive healthcare often comes from multiple sources. This
results in varying quality of medical image data and very often diverse types of
medical treatment. Taking brain NMR spectroscopy as an example, in some areas
with better medical conditions, the magnetic field strength of NMR instruments can
reach the level of 3T ensuring a good resolution; however, for poorer areas, these
instruments generally have a magnetic field strength of 1.5T, resulting in average
resolutions. In addition, some hospitals produce enhanced sequence scans during
NMR to normal scans while other hospitals do not. This results in the absence of
enhanced sequences in some images. Since each patient uses a different posture when
taking NMR scans, the resulting images also do not conform to a unified angle.
Therefore, it is necessary to pre-process the data for better recognition. In this thesis,
we use data from neuroimaging as an example to illustrate the pre-processing process.
Standardization of medical image data formats
It is necessary to standardize the operation of medical image data. Generally,
grayscale formats such as DICOM 3.0 is used when analyzing medical image data.
Using DICOM 3.0 and other grayscale formats have two advantages. Firstly, with the
grayscale format (since each pixel is composed of one-dimensional darkness level,
rather than a three-dimensional vector as in RGB format) the dimensions are

110
effectively reduced in image processing and hence the amount of data to be processed
is reduced. The images are usually converted to grayscale format before feature
extraction, RGB images can be converted to just 256 levels, while the grayscale
format can be up to 65,536 levels, which provides richer and more helpful effective
information and therefore facilitates image processing and feature extraction in the
ensuing stages. Secondly, medical image data are three-dimensional sequences, unlike
non-professional formats which do not support three-dimensional analyses. However,
the identification of many lesions requires a combination of feature extraction and
analyses of spatial characteristics such as shapes, textures, and squeeze displacement
effects. Therefore, it is necessary to standardize the format of medical image data.
There are many software tools available for this process, notably including micron.
Medical image data preprocessing with morphology analysis
Pre-processing of medical images using morphology-based computer vision
algorithms typically involves the following key steps.
Histogram equalization: by calculating the number of occurrences of each
grayscale value (0-65536), the cumulative distribution rates of each grayscale value
are calculated, which are then used to determine the new value after equalization of
the original values. For most natural images, their level of detail is limited because the
grayscale values of these natural images are distributed in a narrow region. After
correction by histogram equalization, the grayscale levels of the image can be
expanded so that they are evenly distributed with increased contrast, making the
image sharper. For example, let the original image be ò(o), then:
ô(o, r) = ö
G,0 ≤ ò(o, r) < ùûåü
†å°ò(o, r) + G,ù ≤ ò(o, r) < ¢
|,¢ ≤ ò(o, r) < £ò
(4-10)
With the above formula, the range of the original image range is stretched from
[a, b] to [c, d].
Filtering: suppression of noise in the image while maintaining the integrity of
the details as much as possible. Common filtering methods include Gaussian filtering,

111
mean filtering, median filtering, bilateral filtering, and linear neighborhood filtering.
Filtering operations must ensure that the details of the image are preserved as much as
possible, important information such as image contour is not damaged, and the image
must be clear. The following figure illustrates the principle of linear neighborhood
filtering, which is similar to the convolution operation in a convolutional neural
network. The part to the left forms a smaller part to the right after the filtering
operation. Let the input pixel value to the left be ò(o, r), the middle filter (core) be
ℎ(o, r), and the output pixel value to the right be ô(o, r), theng(Ñ, j) = ∑ ò(Ñ +q,2
â, É + ®)ℎ(â, ®).
Figure 4-4. Linear neighborhood filtering
Morphological erosion/dilation operations: two basic operations in morphology.
The combination of erosion and dilation allows for operations that separate discrete
regions or join adjacent regions of the image. From a mathematical point of view,
erosion can be expressed as and dilation can be expressed as
. The former can also be understood as a search for local
minimum, and the latter a search for local maximum. Opening and closing operations
in morphology are constructed based on these two types of operations. Generally,
opening operation is often used in brain image processing, that is, erosion is first
applied before dilation. Through these kinds of operation, small voids in the image
can be eliminated and various types of brain tissue can be separated to facilitate
further processing.
{ | ( ) }A B z B z A= Í!
| }0{ ( )BA B z z AÅ = ¹!

112
Medical image preprocessing based on medical knowledge algorithm
After the preliminary pretreatment process using morphology, further
pretreatment in conjunction with relevant medical knowledge is required. Taking
brain images as an example, registration of multiple sequences of brain images of the
same case needs to be performed (Nyul et al., 2003) along with skull stripping
operations.
First, multimodal brain image registration is required. The registration of
multimodal three-dimensional brain images can be performed by using mutual
information (Maes et al., 1997; Studholme et al., 1999; Pluim et al. 2001). For
example, in maximum normalized mutual information operations, given a particular
modal image is set as a floating image © and a reference image ™, then the spatial
coordinates of the floating image F and the reference image R are respectively P≠ and
PÆ, and its rigid body transformation can be expressed as:
VÆ(PÆ − CÆ) = R±™≤™≥�¥(ᥠ− à¥) + µ(µ∂, µ≤, µ≥)(4-11)
Rigid body transformation of the image is performed by determining the
rotational centre of gravity CÆ and C≠ of both image and the translation variable t.
Normalized mutual information can be calculated based on this operation. With the
entropy of the image A, B obtained, the calculation can be expressed as follows:
E(A, B) = ((∫(ª)º∫(i)å∫(ª,i))
∫(ª)º∫(i)(4-12)
Subsequently, the Powell multi-parameter optimization algorithm and the Brent
algorithm can be used to perform optimization and approximation of registration
parameters so as to achieve registration.
Skull stripping is a key task in the preprocessing of brain images. The
conventional method for skull stripping is generally based on manual separation or by
a semi-automatic separation algorithm using traditional morphology. Recently, some
highly automated methods have emerged. These include region-based skull stripping
algorithms, threshold-based and morphological techniques, and brain tissue separation
methods using anisotropic diffusion, among others,(Atkins &Mackiewich, 1998;
Lemieux et al., 1999; Lemieux et al., 1999; Meegama&Rajapakse, 2004). There are

113
also some template-based separation methods that use iterative smoothing to achieve
skull stripping,(Dale et al., 1999; Lemieux et al., 1999) These methods are more
robust but still require manual intervention. Some scholars have proposed new
methods that combine these two types of techniques (Kapur et al., 1996). However,
before application, such algorithms require some adaptive correction algorithms for
corrections,(Wells et al., 1996; Shattuck et al., 2001; Shattuck & Leahy, 2002).
By comparison, the BET algorithm is a highly automated algorithm available
(Headington & Oxford; Smith, 2002). Firstly, a grayscale histogram of the whole
brain image is used to determine an upper and lower boundary of the grayscale. The
centre of gravity of the brain is then estimated. Based on this, the brain surface is
moved towards the edge, so as to achieve skull stripping. The algorithm can be
expressed as follows. First, the maximum and minimum grayscale values Iæóø =
MAX ¬t&,MIN4t(, I(0), I(1), , I(d&)8ƒ , Iæ≈± = MAX ¬t(, MAX4t∆, I(0), I(1), . . , I(d()8ƒ ,
where t&,(,∆ is the mediation parameters used by the algorithm to adjust the maximum
and minimum ranges, d&,( represent the search distance from the minimum and
maximum values to construct t» = (…̂ °∂ − µ()¢ + µ(, where bÀis a constant. Then a
mediator fraction is constructed: f = ((ÃÕŒœå –)
ÃÕ—“å b. Using volume features, s , Çw and f&
are defined, and the iterative defection u = 0.5sÀ + ò&Çw + 0.05ò&®Ç̂w can be
determined, which can be used to perform skull stripping operation through iterative
calculation.
Through the above steps, a standardized, pre-processed medical images can be
ready for subsequent feature extraction and feature-based pattern recognition.
Feature extraction from brain tumour images
Feature extraction is a special method of data dimensionality reduction in image
processing. When the data in question is too large and redundant, converting the input
data into a set of indicative feature vectors greatly saves the cost of time and storage
space in data processing. After pre-processing the brain tumour image data, it is often
necessary to perform feature extraction on the target region for tumour recognition,
114
analysis and classification.
Feature extraction of medical images can be divided into two subcategories:
feature extraction that is based on image morphology and deep feature extraction
which is based on the convolutional neural network. Among them, morphology-based
feature extraction is based on theories of computer graphics to quantitatively describe
various visual features such as shape, gradation, symmetry and specific areas, etc.
Morphology-based brain image feature extraction can accurately simulate the doctor’s
observation and evaluation process of medical images. It can be combined with the
doctor’s clinical knowledge to capture deformation, edema and other important
information in brain tissues, (providing important evidence for disease diagnosis).
It is inferable that the quality of feature selection has a significant impact on the
accuracy of diagnosis in practical applications. Therefore, researchers from all over
the world have never stopped their search for features that can be used to increase
classification efficiency. However, since the traditional machine learning algorithms
are sensitive to feature selection, designing a robust feature extraction network is
often a time-consuming task. In recent years, with the development of deep learning
technology, feature extraction based on convolutional neural networks has been
widely used. Different from conventional feature extraction methods, convolutional
neural networks do not require manual intervention in the design of features at
different layers. Instead, they can be learned from training data using a generic
learning process. This section will introduce and analyze feature extraction for brain
tumour image diagnosis based on morphology and deep learning networks, which will
serve as a basis for later diagnosis and classification.
A feature extraction method based on morphology and medical information
The distinct structure of brain tumours, which are different from normal brain
tissues, gives them unique shapes, grayscale and volume in medical imaging. This
section will elaborate on the typical morphological features and representation of
brain tumours.
115
Shape-based feature extraction
Recognizing the shape of an object is the first stage in which human vision
systems work. We can determine the edge and area of the object after edge abstraction
and other operations. Clinically, benign and malignant brain tumours usually exhibit
distinct differences in shape. Most benign tumour tissues have regular shapes, smooth
edges, noticeable outlines and clear boundaries with surrounding brain tissue.
Malignant tumours usually have irregular shapes with a rough edge and blurred
boundaries with the surrounding brain tissue. Therefore, the shape of brain tumours
are important morphological features for the automatic diagnosis of brain tumours,
and the extraction of shape features with strong characterization ability is an effective
way to improve the accuracy of diagnosis.
Compactness is a commonly used method in shape analysis. The parameters can
be normalized to increase along with the complexity of the shape. The value of the
compactness parameter is zero when the shape is circular. This can be expressed as
equation (4-13) below, where p and a are the number of edge pixels and the number of
pixels in the region, respectively:
C = 1 − »◊°b
ÿb (4-13)
Based on the shape characteristics of the moment, all moments can be
calculated using the edge information of the preprocessed target. Generally, the third
moments can be calculated using the following equations:
©& =Ÿ⁄¤∑ [≥(p)å^⁄]b¤Œ‹⁄ ›
⁄b
⁄¤
∑ ≥(p)¤Œ‹⁄
(4-14)
©( =Ÿ⁄¤∑ [≥(p)å^⁄]fi¤Œ‹⁄ ›
⁄fi
⁄¤
∑ ≥(p)¤Œ‹⁄
(4-15)
©∆ =Ÿ⁄¤∑ [≥(p)å^⁄]–¤Œ‹⁄ ›
⁄–
⁄¤
∑ ≥(p)¤Œ‹⁄
(4-16)

116
C& = &
*∑ fl(Ñ)*
pl& (4-17)
These three basic moments, proposed by Gupta et al. (Gupta & Srinath, 1987),
have the following two advantages: first, these three basic moments are dimensionless
moments, which are conducive to comparison and combination. Second, the larger the
F3 value, the rougher is the edge of the target shape. This is useful for characterizing
the roughness of the edge of the tumour.
The Fourier descriptor method (Persoon& Fu, 1986) is a classic method for
describing the shape of a region’s boundary. It is able to convert a 5-D problem into a
1-D problem, which is useful for feature representation. If the points on the edge of
the tumour are represented by a complex number ‡p = ·p + Érp, then the Fourier
descriptor for the edge features of the tumour can be defined as follows:
A(n) = &
*∑ ‡p1o6 Ÿå2(◊p
*›*å&
plì (4-18)
n = 1,2,… ,N − 1
Since only the amplitude of the FD is concerned here, the FD can be normalized
as follows:
NFD(k) = 0k = 0 (4-19)
NFD(k) = ª(q)
ª(&)â = 1,2,… , z/2 (4-20)
MFD(k) = ª(qº*)
ª(&)â = −1, −2,… , −*
(+ 1(4-21)
The following Fourier descriptor is commonly used in image processing tasks:
FD = 1 −∑
‖¤Âc(Ê)‖‖Ê‖
¤b
Ê‹Á¤b
∑ ‖*¥Ë(q)‖¤b
Ê‹Á¤b
(4-22)
Chord length of the closed 5-D curve can effectively distinguish the shape of the
curve (You & Jain, 1984). The chord length Li is defined as the length of the line
segment connecting the two points on a curve, which is normalized with the largest
chord length. All chords of a given closed curve include all chords from any point on
the curve to any other point. Given N points on the boundary, there are N(N+1)/2
different chords. Calculating chord length can effectively distinguish the shape of the

117
contour. Since it is insensitive to operations such as displacement, rotation, and size
transformation, features are usually represented by the mean value features of the
chord length:
£ü = &
Ä∑ äp
Äpl& (4-23)
where K is the number of points on the edge to be processed and Li is the
distance between points on the edge.
R = &
w∑ |jåÈŒ|œŒ‹Í
(4-24)
Radius, where C is the centre of the tumour (xcentre, ycentre), Vi is the point on
the edge of the target (xi, yi):
|à − �p| = Î(op − oü[w [H)( + (rp − rü[w [H)((4-25)
Extraction of grayscale feature
In a normal grayscale image, the grayscale values within a region can describe
the average grayscale level of the region. In medical images, quantified data often
represent a certain physiological characteristic of the target. For example, edema in
the brain tissue around a malignant tumour exhibits low-density, and therefore darker
tones, while calcification exhibits high-density and brighter tones. Therefore, the
feature of mean grayscale value has been given new meanings in medical image
recognition, and has become an important feature for doctors to make an image-
assisted diagnosis.
Mean grayscale value (M)
M = &
*∑ ∑ …(Ñ, É)Ï
2l&∫pl& (4-26)
The mean grayscale value describes the average gray level of the target area.
Grayscale variance (V)
V = &
*∑ ∑ […(Ñ, É) − £](Ï
2l&∫pl& (4-27)
The grayscale variance describes the extent to which the target area deviates
from the mean of the entire image.
Grayscale skewness (S)

118
S = &
*
∑ ∑ [Ã(p,2)åx]fiÌÓ‹⁄
ÔŒ‹⁄
Èfi (4-28)
Grayscale skewness reflects the tendency for the overall grayscale level of the
target area to be higher or lower than the average grayscale value. It can be used to
represent the deviation of the average grayscale level due to a very small number of
extreme values.
Grayscale kurtosis (K)
K = &
*
∑ ∑ [Ã(p,2)åx]–ÌÓ‹⁄
ÔŒ‹⁄
È– (4-29)
The kurtosis represents the steepness of the distribution of the gray value of the
target area. It can be used to characterize the smoothness of the gray level in the target
area.
Grayscale entropy (E)
Given áp =*Œ
*, i = 0,1, … , L − 1, where Ni represents the number of pixels of
gray value i in the image, and L is the gray resolution of the image, the grayscale
entropy can then be expressed as:
E = −∑ áp log( ápãå&plì (4-30)
The grayscale entropy reflects the randomness of the distribution of grayscale
value in the image.
Extraction of volumetric feature
The volumetric feature of brain tumours is an important factor in assisted
diagnosis that influences treatment plans. Volume measurement and 3D visualization
can help doctors develop effective treatment plans. At present, the determination of
tumour volume is mainly based on human judgment and is usually estimated based on
one or more two-dimensional slices. Since the area of different locations of a tumour
varies in MRI image sequences, manual estimation is subjective and can lead to great
ambiguity, and quantitative description is not possible. With the increased
sophistication in 3D image reconstruction, the fuzzy region competition algorithm and
the two-dimensional region superposition technique with high stability and accuracy
can be used to estimate the volume of brain tumours.

119
Figure 4-5 shows the three-dimensional views of three different brain tumours.
As shown in the figure, brain tumours have irregular and highly different shapes. With
such an intuitive view, the incompleteness of the two-dimensional view can be
avoided. Rich three-dimensional information like this can help doctors diagnose brain
tumours more effectively. In Figure 4-5, (a) is a meningioma located in the left frontal
lobe of the brain, (b) is a glioma located in the left posterior part of the brain, and (c)
is an astrocytoma located in the right frontal lobe of the brain.
(a) (b) (c)
Figure 4-5. Three-dimensional views of three different brain tumours
(a) Meningioma (left frontal); (b) glioma (left posterior); (c) astrocytoma (right
frontal)
Extraction of edema feature
Clinically, tumours can cause local brain tissue damage and affect cerebral
blood circulation, often leading to edema around the tumour. The edema in the
medical images, especially the peripheral edema, especially white matter edema,
around the lesion, is a useful indication of malignant tumours. Malignant tumours are
often accompanied by varying degrees of edema. For example, from enhanced scan
sequences of malignant astrocytoma, low-density shadows of peritumoural edema can
be observed. Malignant meningioma can invade the skull and brain tissues, causing
reactive cerebral edema. Peripheral edema of malignant brain metastases is often
more serious and form the shape of fingers.
Therefore, the analysis of edema in brain tumour images also plays a crucial
role in the final diagnosis. However, due to the limitations of medical imaging devices
and the complexity of the causes of tumour edema, edema is not easily represented in

120
medical images by a simple method. In clinical practices, even experienced doctors
may make different analyses and judgments on the presence or absence of edema and
its state. In fact, even the same doctor may not be able to give the same result at
different times. In clinical analysis, doctors usually first judge whether edema exists.
And if so, what is its degree of severity. This is also a problem yet to be solved in
brain tumour feature extraction. A common solution is to first isolate the edema and
then further examine it. Because the shape of brain tumours is complex and
changeable with blurred edges, how to isolate them has always been considered a
major problem. Classical preprocessing algorithms can only isolate the tumour area,
but the isolation of the edema area is close to impossible. At present, the level set
method of Mumford and Shah is often used in brain image processing often used to
isolate the peripheral edema area of brain images. However, further research is still
needed for automatic identification and quantitative analysis.
Feature extraction based on deep learning techniques
Feature extraction methods based on morphology and clinical information can
simulate to the greatest extent the perception of human vision in medical images.
However, due to individual differences, patient information in different modal images
may vary greatly with different features. Therefore, extraction models based on fixed
features tend to be less adaptable when dealing with brain tumour isolation for
different patients.
Convolutional neural network
The convolutional neural network proposed by Yam Lecun (Hinton et al., 2014)
is a supervised deep learning method that has obtained great success in the field of
pattern recognition, such as image recognition, speech recognition and natural
language processing. The convolutional neural network obtains convolution weights
through supervised training by cyclically convolving and downsampling the original
data, to finally extract features that are useful for classification directly from the
original input.
Feature extraction techniques that are based on convolutional neural networks
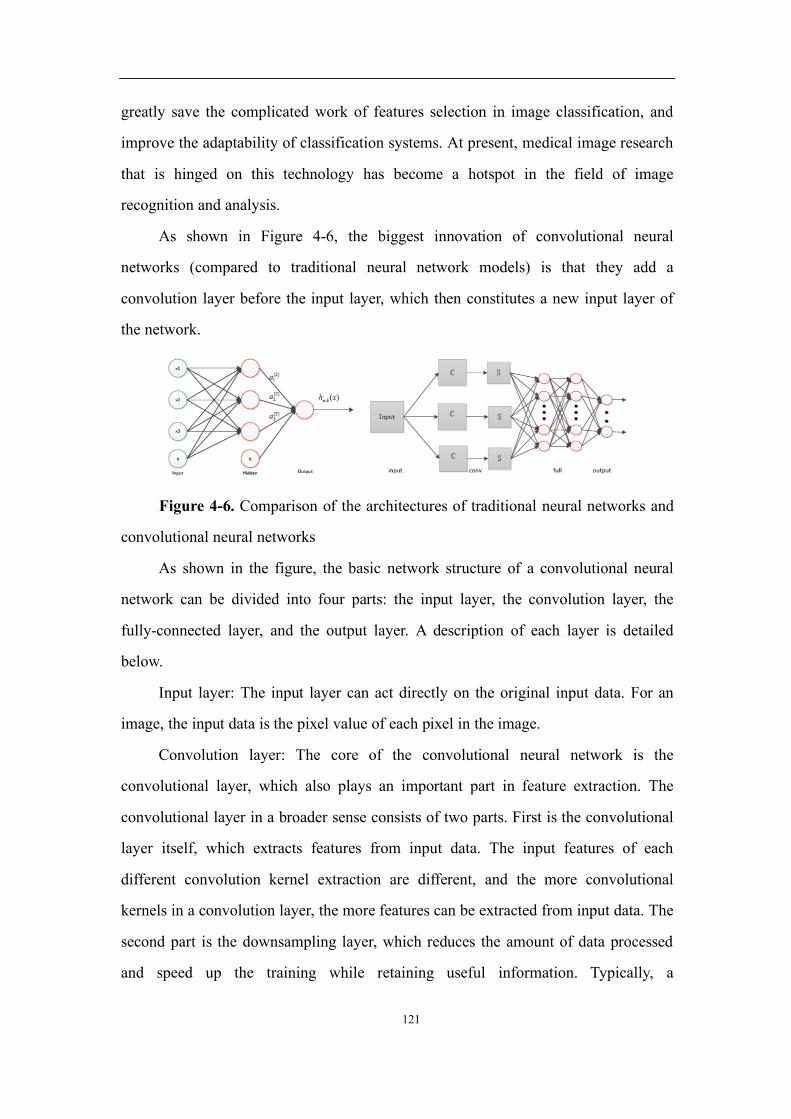
121
greatly save the complicated work of features selection in image classification, and
improve the adaptability of classification systems. At present, medical image research
that is hinged on this technology has become a hotspot in the field of image
recognition and analysis.
As shown in Figure 4-6, the biggest innovation of convolutional neural
networks (compared to traditional neural network models) is that they add a
convolution layer before the input layer, which then constitutes a new input layer of
the network.
Figure 4-6. Comparison of the architectures of traditional neural networks and
convolutional neural networks
As shown in the figure, the basic network structure of a convolutional neural
network can be divided into four parts: the input layer, the convolution layer, the
fully-connected layer, and the output layer. A description of each layer is detailed
below.
Input layer: The input layer can act directly on the original input data. For an
image, the input data is the pixel value of each pixel in the image.
Convolution layer: The core of the convolutional neural network is the
convolutional layer, which also plays an important part in feature extraction. The
convolutional layer in a broader sense consists of two parts. First is the convolutional
layer itself, which extracts features from input data. The input features of each
different convolution kernel extraction are different, and the more convolutional
kernels in a convolution layer, the more features can be extracted from input data. The
second part is the downsampling layer, which reduces the amount of data processed
and speed up the training while retaining useful information. Typically, a

122
convolutional neural network contains at least two convolution layers. The more
convolutional layers, the more abstract features can be extracted from on the previous
layer.
Fully-connected layer: The fully connected layer corresponds to the hidden
layers of the multilayer perceptron. In the fully connected layer, the neural nodes of
the latter layer are connected to each neural node of the previous layer, but there is no
connection between neuron nodes of the same layer. The neuron nodes of each layer
are forwardly propagated based on the weights on each connecting line, and then the
outputs of the neuron nodes for the next layer are obtained by weighted combination.
Output layer: The number of neural nodes in the output layer varies according to
the specific application scenario. If it is a classification task, the output layer of the
convolutional neural network is usually a classifier.
The correlation operations of the convolutional neural network include
convolution, downsampling, and others.
Convolution: Convolution plays an important role in analytical mathematics. It
includes continuous convolution and discrete convolution. The following is the
formula for convolution.
Continuous convolution:
y(t) = ∫ o(6)ℎ(µ − 6)|6 = o(µ)ℎ(µ)ıåı (4-31)
Discrete convolution:
y(n) = ∑ o(Ñ)ℎ(y − Ñ) = o(y)ℎ(y)ıplåı (4-32)
Convolution operations in convolutional neural networks are discrete operations.
But they differ to some extent from the definition of discrete convolution in analytical
mathematics. Convolution is actually a filter, rather than convolution in the true sense.
The convolution kernel of responses can also be considered as a filter. The kernel size
determines the size of the participating sub-regions in the image. The size of the
parameters on the convolution kernel determines the voting ability of pixel points
corresponding to the image region covered by the convolution kernel to the final
result. The greater is the weight, the greater is its voting contribution.
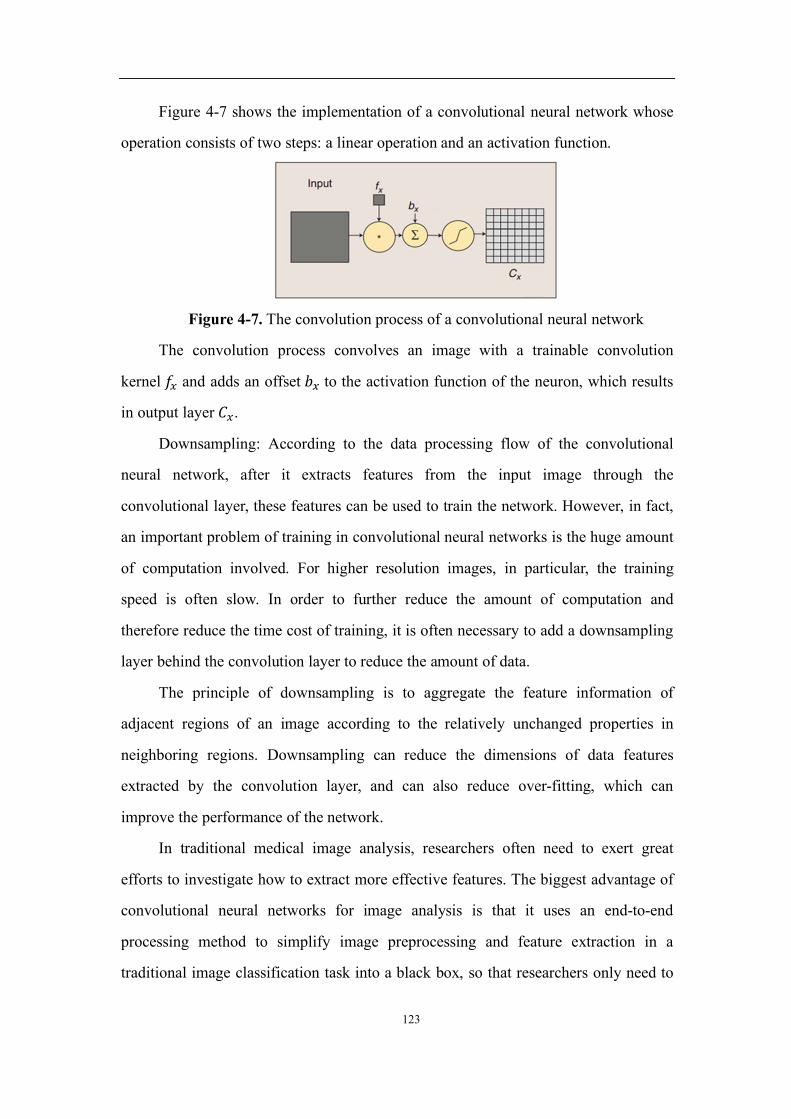
123
Figure 4-7 shows the implementation of a convolutional neural network whose
operation consists of two steps: a linear operation and an activation function.
Figure 4-7. The convolution process of a convolutional neural network
The convolution process convolves an image with a trainable convolution
kernel ò∂ and adds an offset ¢∂ to the activation function of the neuron, which results
in output layer à∂.
Downsampling: According to the data processing flow of the convolutional
neural network, after it extracts features from the input image through the
convolutional layer, these features can be used to train the network. However, in fact,
an important problem of training in convolutional neural networks is the huge amount
of computation involved. For higher resolution images, in particular, the training
speed is often slow. In order to further reduce the amount of computation and
therefore reduce the time cost of training, it is often necessary to add a downsampling
layer behind the convolution layer to reduce the amount of data.
The principle of downsampling is to aggregate the feature information of
adjacent regions of an image according to the relatively unchanged properties in
neighboring regions. Downsampling can reduce the dimensions of data features
extracted by the convolution layer, and can also reduce over-fitting, which can
improve the performance of the network.
In traditional medical image analysis, researchers often need to exert great
efforts to investigate how to extract more effective features. The biggest advantage of
convolutional neural networks for image analysis is that it uses an end-to-end
processing method to simplify image preprocessing and feature extraction in a
traditional image classification task into a black box, so that researchers only need to

124
focus on how to design the network architecture and how to optimize its parameters.
The convolutional neural network forwards the features obtained by convolution, and
then back-propagates the difference between the network output value and the data
tag to adjust network parameters. In so doing, the convolutional neural network can
automatically extract features for classification without human intervention. In
conventional image classification tasks, image preprocessing and feature extraction
require professional processing and clinical knowledge to complete the tasks.
Convolutional neural networks simplify and integrate this process, so that users do not
need to know how to perform image feature extraction to effectively complete image
classification tasks.
However, drawbacks still exist in feature extraction methods based on
convolutional neural networks. At present, feature extraction using convolutional
neural networks mainly depends on the kernel function of the convolutional layer. But,
such feature extraction without human intervention is prone to extracting medical
features with insufficient clinical and medical significance. For the identification and
diagnosis of brain tumours, doctors’ clinical knowledge and experience play a crucial
role in the accuracy of the diagnosis. For deep learning technologies to have a broader
application prospect in the assisted diagnosis of tumours, further optimization of the
convolutional kernel is required. Only then can they really be useful to doctors and
patients and improve the efficiency of diagnosis and treatment.
Methods for the classification of brain tumour images
Pattern recognition is a basic skill of human beings. In daily life, humans can
use vision to easily identify objects based on their feature. For machines, however,
automatic recognition and classification of objects is a complex task. Pattern
recognition technologies emerged in the 1960s with the goal of classifying an object
through a feature shared by the same class. A computer pattern recognition system
consists essentially of three interrelated, yet distinct processes, namely: data
generation, pattern analysis and pattern classification. Among them, pattern analysis is
the core of the tasks. Information obtained by pattern analysis is then used to train the

125
computer to formulate the judging criteria for classifying patterns.
The construction methods of classifiers usually include statistical methods,
machine learning methods (such as support vector machines) and evidence-based
reasoning classification. This article will introduce the principles of several common
classifiers and their characteristics.
Naive Bayes classifier
Bayesian classification is a statistical classification method. It can predict the
likelihood of class membership, i.e., the probability that a given sample belongs to a
particular class.
Bayesian classification is based on Bayes’ theorem. A simple Bayesian
classification algorithm called Naive Bayes classification can achieve high
classification accuracy and speed, particularly when used in large data classification.
The Naive Bayes classifier works as follows.
Each data sample is represented by an N-dimensional feature vector X = {X1,
X2, ..., Xn}, which describes n metrics for n samples of attributes A1, A2, ..., An,
respectively.
Suppose there are m classes: C1, C2, ..., Cm. Given an unknown data sample X,
the classifier will predict that X belongs to the class with the highest posterior
probability (under condition X). In other words, the Naive Bayes classification assigns
an unknown sample to the class Ci, if and only if
p ¬jŒ
ˆƒ 6 ¬
jÓ
ˆƒ 1 ≤ É ≤ C É ≠ Ñ (4-33)
then, maximizeP(àp|·). Class P(àp|·), the largest of àp is called the maximum
posterior hypothesis. According to Bayes’ theorem:
p ¬jŒ
ˆƒ = 6 ¬ˆ
jŒƒ × ÿ(jŒ)
ÿ(ˆ) (4-34)
Only p(ˆ
jŒ) × p(àp) needs to be the largest sincep(·) is a constant for all classes.
Given a data set with multiple attributes, a simple assumption of class
conditional independence can be made.
In order to classify unknown samples, for each class àp , p(ˆ
jŒ) × p(àp) is

126
calculated. Sample X is then assigned to class Ci.
The Naive Bayes classifier is characterized by its simplicity and fast operations.
However, the simple assumption of conditional independence does not hold in many
cases, and as a result, classification accuracy will be affected.
Support vector machines
The support vector machine method is a pattern recognition method derived
from statistical learning methods (Chapelle et al., 2002). The steps that a support
vector machine follows to solve the classification problem can be described as follows:
(a) the input space is transformed into a feature space of a higher dimension by
nonlinear mapping, and (b) a hyperplane that splits the training data is constructed.
For linearly separable data, the support vector machine seeks to find
hyperplanes that minimize training errors while classifying training data, as shown
below:
w ∙ x + b = 0(4-35)
min &
(‖B‖( rp(B ∙ op + ¢) ≥ 1 (4-36)
At this point, the problem is transformed into a classical nonlinear optimization
problem. To solve this problem, the Lagrangian-based Karush-Kuhn-Tucker (KKT)
theorem can be introduced, that is:
maximize ∑ ùp˚pl& − &
(∑ rpr2ùpù2op
¸o2˚p,2l& (4-37)
∑ ùprp = 0˚pl& ùy|ùp ≥ 0 (4-38)
The solution for w can be calculated by:
w = ∑ ùprpop˚pl& (4-39)
among which the non-zero solution is an element that constructs the boundary
distance classification hyperplane, which is also commonly referred to as the support
vector. Here, optimizal hyperplane theory can be applied to nonlinearly overlapping
data by mapping the input support vector to the high-dimensional feature space, as
shown in equation:
op ∈ ™w → fl(o) = [ù&˛&(o), ù(˛((o),… , ùw˛w(o)]¸ ∈ ™ˇ (4-40)

127
maximize ∑ ùp˚pl& − &
(∑ rpr2ùpù2!˚
p,2l& (4-41)
∑ ùprp = 0˚pl& ùy|ùp ≥ 0 (4-42)
where K is the penalty constant.
Under this condition, the optimal hyperplane can be determined by solving the
optimization problem, thus solving the classification problem.
Support vector machine is a new statistical learning method for small sample
with a solid theoretical basis. It basically does not involve the law of large numbers
and probability measure, which also greatly simplifies the classification and
regression based on this method. At the same time, since a small number of support
vectors finally determines the classification result, it will be easy to eliminate
redundant samples by grasping key samples. This also increases the robustness of the
algorithm. However, since the classic support vector machine only provides a solution
to the two-class problem, in the case of a multi-class problem, it is often necessary to
combine multiple types of support vector machines or combine support vector
machines with other algorithms.
Artificial neural networks
Artificial neural networks are inspired by the study of the human brain. These
methods attempt to simulate the nervous system of the human brain with a large
number of processing units (artificial neurons, electronic components, etc.). In
artificial neural networks, information is processed by the interaction of neurons. The
storage of knowledge and information is represented in the distributed connection
between network elements, while the learning and recognition of networks depend on
the evolutionary dynamics of the weights of neuron connections (Hecht & Nielsen,
2002).
As an intelligent bionic model based on physiology, artificial neural networks
are a nonlinear large-scale adaptive dynamic system that is nonlinear, non-local, non-
stationary and non-convex. In recent years, research on artificial neural networks has
made great progress and has become an extremely important research field in artificial
intelligence.
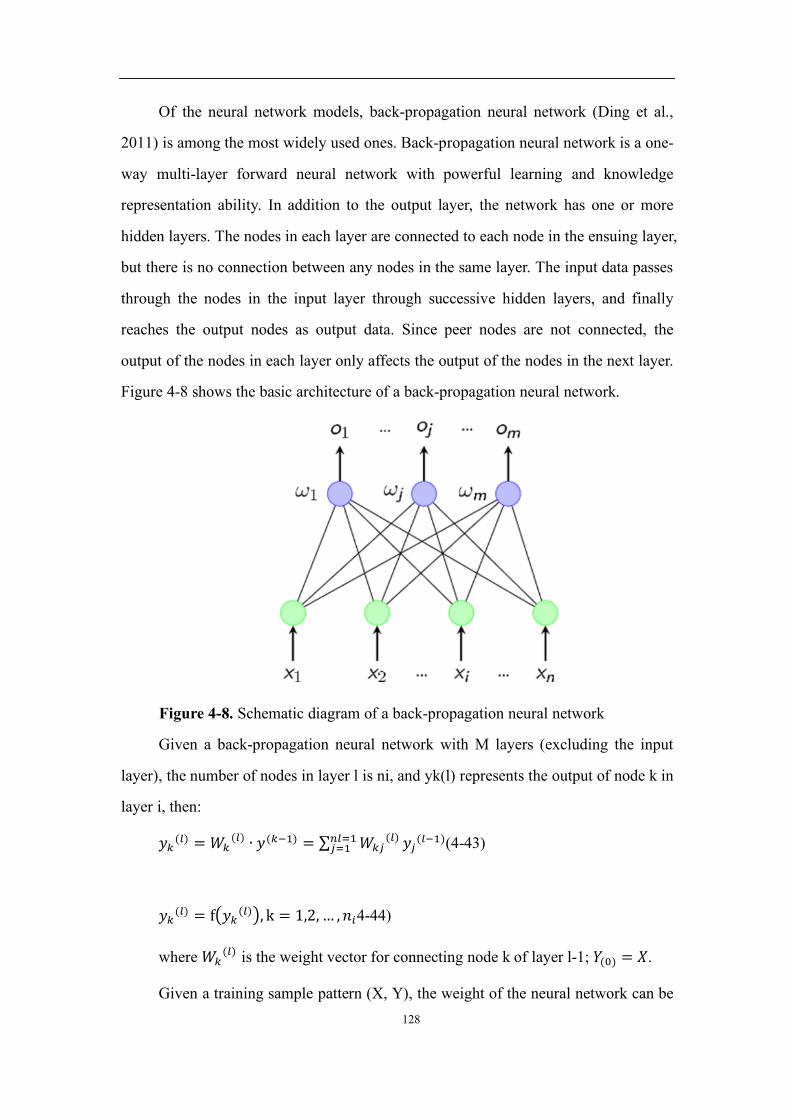
128
Of the neural network models, back-propagation neural network (Ding et al.,
2011) is among the most widely used ones. Back-propagation neural network is a one-
way multi-layer forward neural network with powerful learning and knowledge
representation ability. In addition to the output layer, the network has one or more
hidden layers. The nodes in each layer are connected to each node in the ensuing layer,
but there is no connection between any nodes in the same layer. The input data passes
through the nodes in the input layer through successive hidden layers, and finally
reaches the output nodes as output data. Since peer nodes are not connected, the
output of the nodes in each layer only affects the output of the nodes in the next layer.
Figure 4-8 shows the basic architecture of a back-propagation neural network.
Figure 4-8. Schematic diagram of a back-propagation neural network
Given a back-propagation neural network with M layers (excluding the input
layer), the number of nodes in layer l is ni, and yk(l) represents the output of node k in
layer i, then:
rq(˚) ="q
(˚) ∙ r(qå&) = ∑ "q2(˚)w˚l&
2l& r2(˚å&)(4-43)
rq(˚) = f4rq
(˚)8, k = 1,2, … , yp4-44)
where "q(˚) is the weight vector for connecting node k of layer l-1; #(ì) = ·.
Given a training sample pattern (X, Y), the weight of the neural network can be

129
adjusted to minimize the following criteria function.
E(W) = &
(%# − #&%( = &
(∑ (#q − #q' )(wx
ql& (4-45)
At the same time, the weight can be corrected using the gradient descent method,
i.e., the correction amount of the weight vector "p(˚):
∆"p(˚) = −ù )}
)ÏŒ(*) = ù+p(˚)r(˚å&)(4-46)
Here, for input layer M:
+p(˚) = ∑ "p2(˚º&)w˚º&
2l& +2(˚º&)ò,(#p(˚))(4-47)
For other layers:
+p(˚) = (#p − #p(x)ò,(-Œ→(x)))(4-48)
This is the famous back-propagation algorithm. For a given input sample, the
neural network will adaptively adjust the weight based on this algorithm to generate
an output close to the ideal value.
Back-propagation neural networks have a strong ability to self-learn and adapt
and generalize, and are characterized by a large fault tolerance space. However,
network training failure may happen because the weights of local search optimization
methods of back-propagation algorithms tend to converge to a local minimum. At the
same time, the gradient descent method used by the back-propagation neural networks
to optimize the target function results in slow convergence speed. At present, the
improvement of back-propagation neural network mainly relies on the combination
with simulated annealing algorithms and other genetic algorithms, which play a
complementary role in optimization.
V. Case Study: Brain Tumour Image Recognition in the Context of the Inclusive Healthcare program
In this chapter, we provide an example of brain tumour image recognition in the
context of inclusive healthcare using artificial intelligence. Data of brain tumour
patients in a hospital in China were analyzed. Machine learning methods were used to

130
detect tumours from the image data.
In this study, 145 brain tumour cases were used for image recognition, where
both morphology-based methods and neural network-based methods were used.
5.1 Brain Tumour Image Recognition Based on Morphological Feature Extraction
Structured operation on medical images
Firstly, the medical images need to be converted into a data matrix that can be
used for analysis. By using the "imread" function of MATLAB, each pixel point can
be converted to a number ranging from 0 to 255, which represents the gray level of
the pixel. Then we can get a data matrix. If the original image is 256 by 256 pixels,
then it can be converted into a 256 by 256 data matrix, each element ranging from 0 to
255. For example, the matrix in the following figure to the right is part of the content
of the left one, but is represented in the form of data.
Figure 5-1 Morphological preprocessing of medical images
Subsequently, the image is preprocessed using morphological methods. After
normalizing the image size, the image undergoes a smoothing and sharpening
procedure. Then, quadrature equalization is applied, as shown below:

131
Figure 5-2. An image after smoothing, sharpening, and quadrature equalization
operations
Through the above operations, the details are preserved and the contrast is
enhanced to the level required for analysis. Further, by calculating the number of
occurrences of each grayscale value (0-255), the cumulative distribution ratio of each
gradation value is calculated, which can be used to determine the new value after
equalization. Since the grayscale values of most natural images are distributed in a
narrow area, the image details are not sharp enough. After histogram equalization, the
grayscale of the image is widened and more evenly distributed while the contrast is
increased, resulting in a sharper image.
Feature extraction from medical images
After image preprocessing, feature extraction is conducted for the image. Here,
seven features are extracted from the image: contrast, correlation value, energy,
homogeneity, entropy, as well as the mean and variance of the above features. Each
feature corresponds to a separate morphological meaning: (1) contrast reflects the
sharpness of the image and the depth of the texture and grooves. The larger the value
is, the higher is the sharpness and the deeper is the texture and grooves; (2) correlation
value reflects the local grayscale correlation of an image, which helps to rapidly
detect local grayscale changes in an image, etc.; (3) homogeneity reflects the
homogeneity of texture and measures the extent to which image textures change
locally. A high value indicates a lack of variation between different regions of the
image, that is, local regions have uniform characteristics; (4) energy value is a concept
of energy in morphology, which reflects the degree of uniformity of the gray level
distribution of the image and the thickness of the texture; (5) entropy is a measure of
the amount of information existing in an image. It represents the level of evenness or
complexity of textures in an image; (6-7) the features above are further classified by
calculating their mean and variance values.
The above features once extracted can be included in a matrix, as shown in the
figure below:
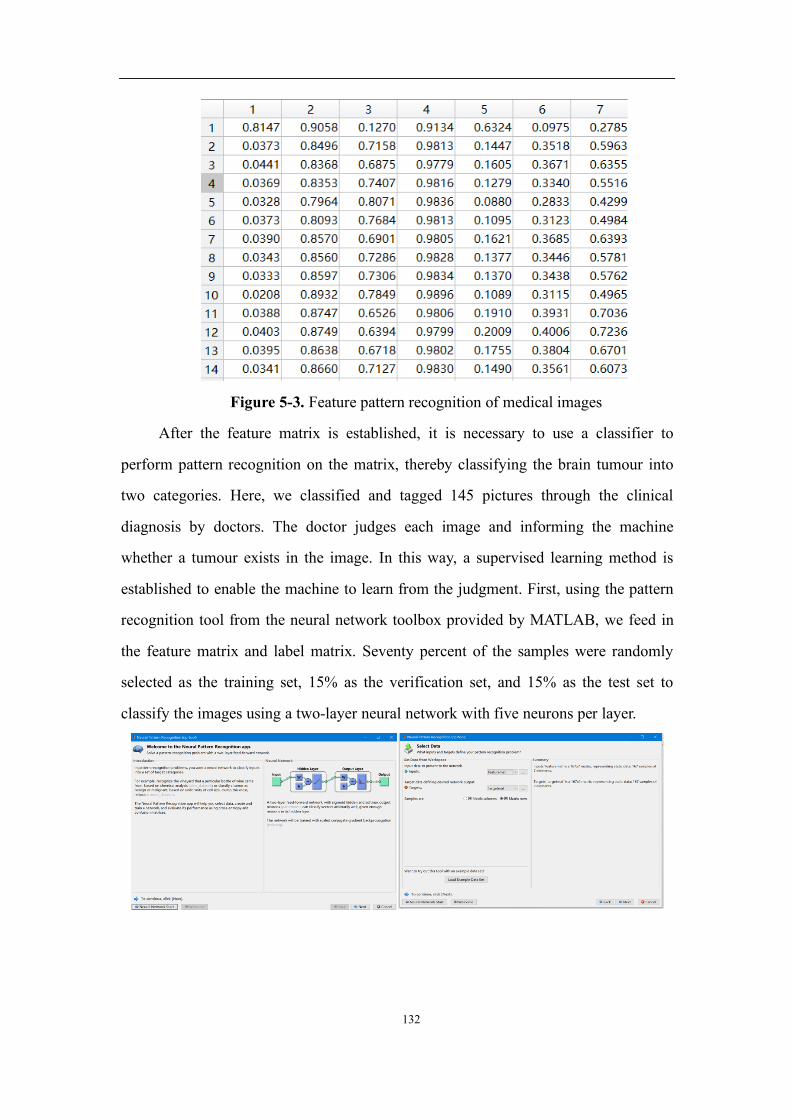
132
Figure 5-3. Feature pattern recognition of medical images
After the feature matrix is established, it is necessary to use a classifier to
perform pattern recognition on the matrix, thereby classifying the brain tumour into
two categories. Here, we classified and tagged 145 pictures through the clinical
diagnosis by doctors. The doctor judges each image and informing the machine
whether a tumour exists in the image. In this way, a supervised learning method is
established to enable the machine to learn from the judgment. First, using the pattern
recognition tool from the neural network toolbox provided by MATLAB, we feed in
the feature matrix and label matrix. Seventy percent of the samples were randomly
selected as the training set, 15% as the verification set, and 15% as the test set to
classify the images using a two-layer neural network with five neurons per layer.

133
Figure 5-4. Establishement of the Neural Network
The trained classifier was used to produce the confusion matrix, which shows
that the classification accuracy of the test set is 81.4%. Among these images, 10 were
classified as cancerous, achieving a 40% accuracy; 135 were classified as cancer-free,
with an accuracy of 84.4%.
Figure 5-5. One of the results of feature extraction and reclassification of
medical images experiment
Feature extraction and reclassification of medical images through
morphological feature engineering can achieve relatively good results. By extracting 7
basic morphological features, an accuracy of about 80% can be achieved. Feature
extraction incorporating medical expertise will be able to achieve better results.
However, the limitation of feature engineering is that the extracted features must be
based on medical knowledge that is known to humans. Therefore, it is limited by the

134
extent of current manual detection. Nevertheless, image recognition work can be
performed rapidly on a large scale using massive computing power.
5.2 Brain Tumour Image Recognition Based on Neural Networks
At present, feature extraction and classification using feature engineering
combined with classifiers is a sophisticated method that can achieve relatively good
results. In the meantime, neural networks have become a powerful tool with the rapid
development of machine learning algorithms in image recognition and classification.
Next, we will describe a supervised learning of medical images using a neural
network model for classification and recognition.
Grouping and labeling of medical images
Firstly, the data should be grouped into training sets, validation sets and test sets.
The training set is used to fit the model and train the classification model by setting
the parameters of the classifier. Later, when combining the validation set, the different
values of the same parameter are chosen, and several classifiers are fitted out. The
validation set uses each model to predict the validation set data and record the model
accuracy rate after the training set finishing making several models in order to find
most effective model. The parameters of the model with the best effect are chosen to
adjust the model parameters, such as parameters and kernel functions in SVM. Finally,
after selecting the optimal model through the training set and the validation set, we
need to use the test set to predict the model and measure the performance and
classification capabilities of the optimal model. That is, the test set can be treated as a
data set that never existed, and when the model parameters have been determined, the
model performance is evaluated using the test set.
Structured operation on medical images
Subsequently, the medical image needs to be converted into a data matrix that
can be used for analysis. By using the “imread” function in MATLAB, each pixel
point can be converted to a number ranging from 0 to 255, whose value size
represents the gray level of the pixel.

135
Figure 5-6. Structured operation on medical images
Because of the need to build a multiple neural network and since the neural
network toolbox can only build a single layer neural network, we need to use the
MATLAB newff command to build a multiple neural network. Here, we use newff [5
10 8] to build a three-layer neural network, in which the first layer uses 5 neurons, the
second layer uses 10 neurons, and the third layer uses 8 neurons to classify images.
Using multiple neural networks enables neurons in different layers to identify and
classify different levels of detail. Considering the number of samples, it is not
advisable to use neural networks with too many layers and too many neurons to
prevent overfitting.
In this neural network, the conjugate gradient method is used as its training
method. The conjugate gradient method is one of the conjugate methods. And the
conjugate method constructs the vector group á(&), á((), ……á(w) with the symmetric
positive definite matrix conjugate, followed by a search in n directions and after n
steps, the minimum point is reached. The conjugate gradient method considers adding
the component of negative gradient direction in each search direction, and ensures
that each search direction is conjugate, thus synthesizing the advantages of gradient
method and conjugate method.
In this neural network, the cross-entropy function is used as the performance
functions, which can be used to measure the error between the predicted value and the
actual value of the artificial neural network, and the cross-entropy function can
promote the training of the artificial neural network effectively. By measuring the
error between the predicted value and the actual value, the speed of the parameter can
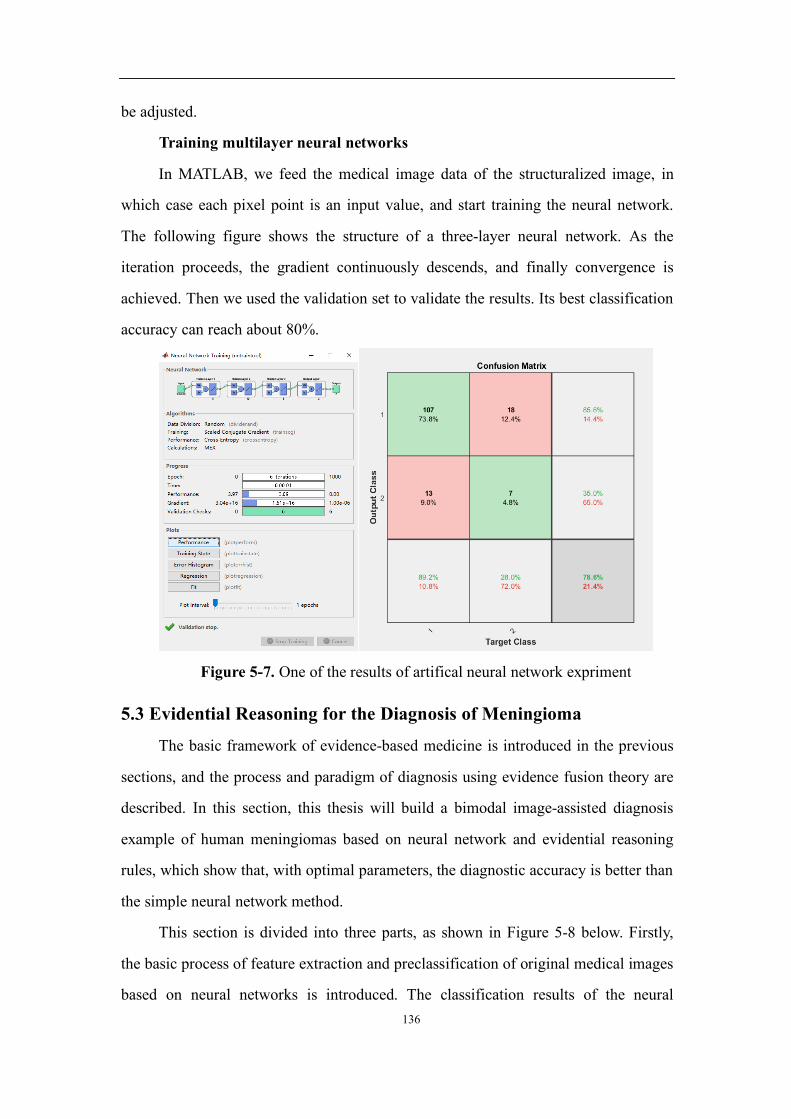
136
be adjusted.
Training multilayer neural networks
In MATLAB, we feed the medical image data of the structuralized image, in
which case each pixel point is an input value, and start training the neural network.
The following figure shows the structure of a three-layer neural network. As the
iteration proceeds, the gradient continuously descends, and finally convergence is
achieved. Then we used the validation set to validate the results. Its best classification
accuracy can reach about 80%.
Figure 5-7. One of the results of artifical neural network expriment
5.3 Evidential Reasoning for the Diagnosis of Meningioma
The basic framework of evidence-based medicine is introduced in the previous
sections, and the process and paradigm of diagnosis using evidence fusion theory are
described. In this section, this thesis will build a bimodal image-assisted diagnosis
example of human meningiomas based on neural network and evidential reasoning
rules, which show that, with optimal parameters, the diagnostic accuracy is better than
the simple neural network method.
This section is divided into three parts, as shown in Figure 5-8 below. Firstly,
the basic process of feature extraction and preclassification of original medical images
based on neural networks is introduced. The classification results of the neural
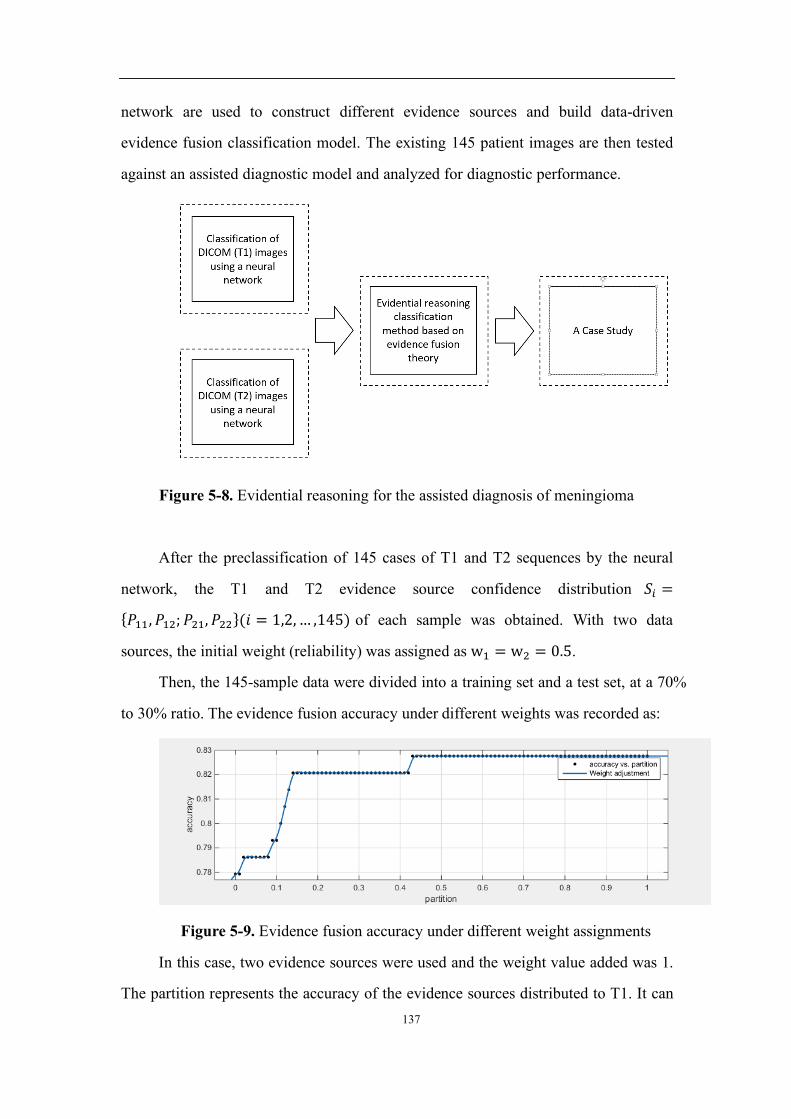
137
network are used to construct different evidence sources and build data-driven
evidence fusion classification model. The existing 145 patient images are then tested
against an assisted diagnostic model and analyzed for diagnostic performance.
Figure 5-8. Evidential reasoning for the assisted diagnosis of meningioma
After the preclassification of 145 cases of T1 and T2 sequences by the neural
network, the T1 and T2 evidence source confidence distribution up =
{á&&, á&(; á(&, á((}(Ñ = 1,2,… ,145) of each sample was obtained. With two data
sources, the initial weight (reliability) was assigned as w& = w( = 0.5.
Then, the 145-sample data were divided into a training set and a test set, at a 70%
to 30% ratio. The evidence fusion accuracy under different weights was recorded as:
Figure 5-9. Evidence fusion accuracy under different weight assignments
In this case, two evidence sources were used and the weight value added was 1.
The partition represents the accuracy of the evidence sources distributed to T1. It can

138
be seen from the test result that when T1 and T2 data sources weight proportion were
0.45/0.55, the accuracy can reach 82.8%, which was significantly higher than using
the back-propagation neural network.
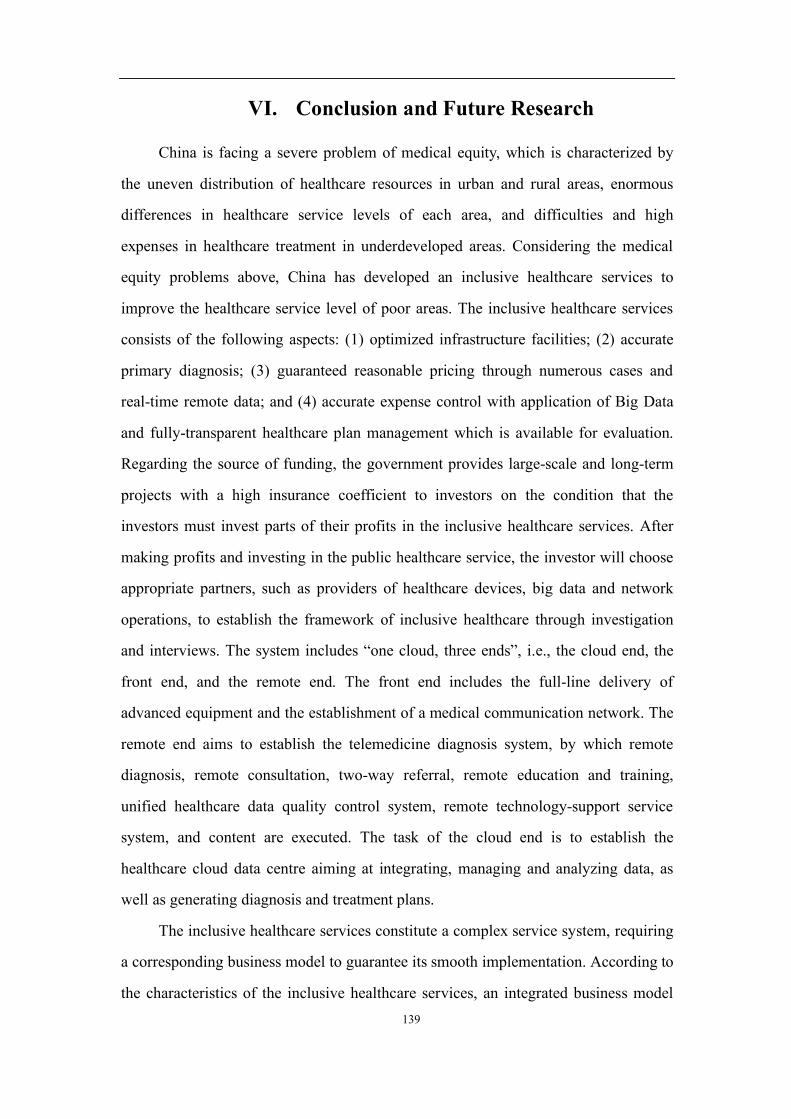
139
VI. Conclusion and Future Research
China is facing a severe problem of medical equity, which is characterized by
the uneven distribution of healthcare resources in urban and rural areas, enormous
differences in healthcare service levels of each area, and difficulties and high
expenses in healthcare treatment in underdeveloped areas. Considering the medical
equity problems above, China has developed an inclusive healthcare services to
improve the healthcare service level of poor areas. The inclusive healthcare services
consists of the following aspects: (1) optimized infrastructure facilities; (2) accurate
primary diagnosis; (3) guaranteed reasonable pricing through numerous cases and
real-time remote data; and (4) accurate expense control with application of Big Data
and fully-transparent healthcare plan management which is available for evaluation.
Regarding the source of funding, the government provides large-scale and long-term
projects with a high insurance coefficient to investors on the condition that the
investors must invest parts of their profits in the inclusive healthcare services. After
making profits and investing in the public healthcare service, the investor will choose
appropriate partners, such as providers of healthcare devices, big data and network
operations, to establish the framework of inclusive healthcare through investigation
and interviews. The system includes “one cloud, three ends”, i.e., the cloud end, the
front end, and the remote end. The front end includes the full-line delivery of
advanced equipment and the establishment of a medical communication network. The
remote end aims to establish the telemedicine diagnosis system, by which remote
diagnosis, remote consultation, two-way referral, remote education and training,
unified healthcare data quality control system, remote technology-support service
system, and content are executed. The task of the cloud end is to establish the
healthcare cloud data centre aiming at integrating, managing and analyzing data, as
well as generating diagnosis and treatment plans.
The inclusive healthcare services constitute a complex service system, requiring
a corresponding business model to guarantee its smooth implementation. According to
the characteristics of the inclusive healthcare services, an integrated business model
140
with two components is proposed. The first component targets the market and profits
in order to raise capital for the implementation of charitable healthcare, while the
second component establishes and manages the operation platform of the inclusive
healthcare services. Then, the key driving forces for the implementation of the
inclusive healthcare services are demonstrated from the perspectives of the
government and insurance funds. The coupled dual-component business model for
inclusive healthcare is then analyzed according to four dimensions of a business
model (customer value proposition, key resources, key processes, and profit formula)
proposed by Johnson et al. For customer value proposition, we critically answer how
the coupled dual-component model for inclusive healthcare creates values and how
each actor obtains benefits from the service model. For key resources, the importance
of the Internet, AI, and other technologies to the implementation of the inclusive
healthcare are demonstrated. For the key processes, this thesis does not consider how
the investor operates the profitable component. Instead, we stressed the business
processes of the charitable healthcare service and cash flow, which is generated by the
market-oriented business model to the public-oriented component and guarantees the
successful implementation of the inclusive healthcare services. As for-profit formula,
we point out that the coupled model refers to the connection of the profit formula of
two different components: the market-oriented one and the charitable one. Specifically,
the investor obtains long-term and stable market profits through operating large-scale
and long-cycle projects with a high insurance coefficient, and then invests some part
of the profits in the inclusive healthcare services under the guidance and supervision
of the government. Then, the investor seeks appropriate business partners to establish
the “three ends, one cloud” system of the inclusive healthcare services. In this process,
the complete business separation between the market and the public welfare part is
realized, making net profit ability of the whole inclusive healthcare services positive
and ensure the sustainability of the charitable healthcare component. We also
proposes specific suggestions for the initiative’s prospects and steps of
implementation.

141
This thesis uses a case study approach to explore the critical success factors of
implementing inclusive healthcare services in remote and poor areas of China. By
reviewing the literature on critical success factors for public-private partnerships (PPP)
and healthcare projects, this thesis summarizes the possible critical success factors for
implementing the “inclusive healthcare services”. Then, through interviews with two
government officials, one investment company executive, four hospital leaders, eight
doctors and twenty patients, the thesis identifies six critical success factors, namely:
medical infrastructure, technology, funding, government support, external
environment, as well as organization, planning and operations. With one to four
subcategories in each major category, a total of eighteen subcategories were identified.
Under each sub-category, some success factors require special attention and are
highlighted in this thesis. One of the main contributions of this research is the
identification, classification and description of the critical success factors of the
implementation of the coupled dual-component business model for inclusive
healthcare.
This thesis establishes a technical framework for the implementation of
inclusive healthcare based on cloud technology and artificial intelligence. At the core
of this framework is an integrated methodology using multi-source medical data
based on evidence fusion theory. The methodology is in line with the diagnostic logic
of evidence-based medicine and is implementable using algorithms. It can make
diagnoses through merging various types of medical data from multiple sources.
Further, this thesis constructs a cloud system for inclusive healthcare to support the
core technology framework, which comprises three layers: infrastructure, platform
service, and platform application. The infrastructure layer provides basic services for
the cloud system to collect and compile basic medical data. The platform service layer
integrates cloud storage, cloud computing and application development platforms to
respond to data processing requests and application development requirements. The
application layer is intended for doctors and other users and includes a human-
computer interaction system, a comprehensive medical record diagnosis system, and a

142
comprehensive medical image diagnostic system. Finally, using multimodality brain
tumour imaging as an example, a multimodal brain tumour medical imaging diagnosis
methodology (based on evidence fusion theory) was developed. Experiments have
shown the effectiveness of the core evidence fusion technology in the technical
framework proposed.
There are a few limitations in the research of this thesis. First, due to resource
and time limitation, the feasibility of AI doctor and related applications of AI
technologies are not implemented, thus they are not shown in details. Second, the
details of using the evidential reasoning theory in evidence-based medicine such as
guidelines and rules for diagnosis and treatments are not provided. Third, how the
CDC model is implemented, in reality, still has a long way to go. All these limitations
can be the future research direction extending the research in this thesis.

143
Appendixes
Appendix 1. Background Information
1. Basic information on the surveyed areas
1. Pingnan County, Fujian Province
Pingnan County belongs to Ningde City, Fujian Province. It is located in the
upper reaches of Huotong Creek and Gutian Creek in the northeast of Ningde City.
The county has an area of 1,487 square kilometers in a humid subtropical monsoon
climate. As of the end of 2017, there are 140,000 residents in its 4 towns, 7 townships,
152 administrative villages and 7 administrative communities. Pingnan is one of the
economically underdeveloped areas in Fujian Province. In 2017, its regional gross
domestic product (GDP) was 743,564 yuan, and the average disposable income of all
residents is 17,921 yuan. Public finance income was 609,830,000 yuan, of which
medical and health expenditure was 196,620,000 yuan. As of year-end 2017, the
county had 10 nursing homes and 400 welfare hospital beds. Seven community
service centres have been established.
2. Zherong County, Fujian Province
Zherong County belongs to Ningde City, Fujian Province. With a population of about
103,000 in a total land area of 571 square kilometers, Zherong County is the county
with the lowest population in Fujian Province. Since ancient times it has been an
important trading point between Fujian and Zhejiang provinces. And it is one of the
55 open counties and cities approved by the State Council. In 2017, the county's GDP
was 5.462 billion yuan. As of the end of 2017, the county’s registered population is
108,769 with a total public finance income of 376 million yuan. Out of this, local
public finance income was 243 million yuan, of which 151 million yuan was tax
revenue, accounting for 61.8% of the total local public finance income. The public
budget expenditure was 1.444 billion yuan, and the average disposable income of all
residents was 19,840 yuan.
There are 110 medical and health institutions in the county, including 7 county-
144
level institutions, 1 community healthcare centre, 8 township healthcare centres (1
Class B hospital, and 7 Class C hospitals), 81 village clinics and 13 private clinics.
There are 412 registered healthcare workers, including 41 senior professionals and 93
intermediate-level professionals. On average, there are 3.8 healthcare workers per
1,000 residents. In total, there are 100 village doctors and 454 hospital registered beds
and 484 actual beds in the county.
3. Yonghe County, Shanxi Province
Yonghe County is located in Linyi City, Shanxi Province, at the southern tip of
Luliang Mountain Range and the east side of the Shanxi-Shaanxi Grand Canyon in
the middle reaches of the Yellow River. The county has a total area of 1,212 square
kilometers with two 2 towns, 5 townships and 79 villages under its administration and
a residence population of 65,700 (as of year-end 2016). Having harsh natural
conditions, underdeveloped economy and a lack of cultural facilities, the county was
designated by the state as a national key target for poverty alleviation.
In 2016, Yonghe County’s total GDP was 794.55 million yuan, with a total
fiscal revenue of 157.77 million yuan and a general budgetary income of 74.29
million yuan. Tax revenue was 58.4 million yuan, and the general budgetary
expenditure is 790.68 million yuan. The annual per capita disposable income of urban
and township residents was 19,366 yuan. The per capita net income of rural residents
was 3,221 yuan. As of the end of 2016, there were 97 healthcare institutions
(including clinics) in the county, including one maternal and child health centre. There
are 202 beds in all health institutions (including clinics) and 235 health workers
across the country.
4. Fuzhou City, Jiangxi Province
Fuzhou is a prefecture-level city in Jiangxi Province located in the eastern part
of the province. It is about 222 kilometers long from north to south and 169
kilometers wide from east to west. The total area is 18,816.92 square kilometers
divided into 2 districts and 9 counties, which all together accounts for 11.27% of the
total area of the province. In 2016, the total population is 4 million and the common

145
language is Gan Chinese. As of the end of 2016, the city’s total population was
4,001,819, an increase from 17,132 from the end of 2015. Among them, urban
population is 1,871,053, accounting for 46.65% of the total population.
Fuzhou is one of the 20 cities in the Western Taiwan Straits Economic Zone
identified by the State Council. It is the first city in Jiangxi to be included in the state-
level Poyang Lake Eco-Economic Zone and one of the important cities in the former
Central Soviet Area. In December 2016, it was listed as one of the third batch of
comprehensive national new urbanization pilot areas. In 2017, the city’s total
production value exceeded 130 billion yuan and reached135.457 billion yuan. In 2017,
the city’s total fiscal revenue was 18.364 billion yuan, of which tax revenue was
15.190 billion yuan. The per capita disposable income of urban residents was 29,463
yuan. And the per capita disposable income of rural residents was 13,563 yuan.
5. Miyun District, Beijing
Miyun District is located in the northeast of Beijing, with a longitude of
116°39′33′′E and a latitude of 40°13′7′′N. The east and the north are respectively
bordered by Xinglong, Chengde and Luanping counties of Chengde City, Hebei
Province, and the west and south of the country borders Huairou, Shunyi and Pinggu
districts, respectively. As the largest district in Beijing, Miyun is an important
drinking water source and ecological conservation development area for the capital.
The total area of the district is 2229.45 square kilometers, with a registered population
of 436,000 (as of year-end 2016). It administers 17 towns, 2 subdistricts and 1 district
office. It is home to the Miyun Reservoir, Simatai Great Wall, Black Dragon Pool,
Yunmengshan Forest Park, and Gubei Water Town, and other attractions.
In 2017, the district’s GDP reached 27.82 billion yuan, with an annual per capita
disposable income of 32,165 yuan: 40,031 yuan among urban residents and 22,604
yuan among rural residents. The general public budget revenue of the whole district
was 3.3 billion yuan, up by 6% over the previous year. The annual general public
budget expenditure was 15.09 billion yuan, up by 33% over the previous year. The
growth of expenditure mainly comes from education, agriculture, healthcare and other
146
areas related to residents’ livelihood, which have been given top priority by the
district.
2. Basic information of surveyed hospitals
1. Pingnan County Hospital, Fujian Province
The Pingnan County Hospital is the only comprehensive hospital in the county
that integrates medical care, nursing, teaching, scientific research, healthcare and
rehabilitation. The hospital is responsible for the healthcare of over 300,000 residents
in the county and surrounding areas. It is also responsible for providing guidance for
the diagnosis and treatment of critical illnesses and difficult diseases, emergency
rescue, and medical technology of the county. As of the end of 2017, the hospital had
320 beds, 14 clinical departments, 12 medical technology departments and 13
administrative functional departments. There are 374 employees, most of whom have
a bachelor’s degree, including 38 people with senior professional titles and 68 with
intermediate professional titles. Responding to request from the new leadership of the
hospital, the county government decided to invest 740 million yuan to build modern,
new facilities for the hospital in a three-year period.
2. Zherong County Hospital, Fujian Province
Established in 1937, Zherong County Hospital is the only Class 2 Category B
comprehensive hospital in Zherong County that integrates medical treatment, teaching,
scientific research, first aid, healthcare and rehabilitation.
It is a national-level “baby-friendly hospital”, a designated hospital supported
by the Fuzhou General Hospital of the Nanjing Military Region, and a member
hospital of the East-Fujian Medical Group. It covers an area of 15,793 square meters,
with a total floor area of 23,000 square meters. The total value of hospital assets is
95.05 million yuan, with 15 clinical departments, 12 medical technology departments
and 15 functional departments. In recent years, the hospital has made the development
of specialties a priority. Based on the existing capabilities, rehabilitation medicine is
being developed as a priority. At present, satisfactory results have been achieved in
the treatment of peripheral nerve injury rehabilitation, neck and shoulder pain, stroke,

147
brain trauma sequelae, bone and joint lesions, among others. At the same time, the
hospital actively introduces advanced methods and modern medical methodologies,
and extensively carries out advanced treatments such as painless treatment (including
painless delivery), TST minimally invasive surgery, hip replacement, laparoscopy,
postpartum rehabilitation, and myocardial infarction. In terms of human resources,
more than 30 professionals with a bachelor’s degree have been recruited from inside
and outside the province. And more than 70 people have been selected to join Class 3
Category A hospitals for training. The main medical equipment in the hospital include
16-row spiral computed tomography, DR machine, laparoscope, mobile C-arm X-ray
machine, full body colour ultrasound scanner, electronic gastroscope, electronic
bronchoscope, electronic colonoscope, cystoscope and prostate resectoscope systems,
electronic colposcope, LEEP knife, Q-switched dual-wavelength YAG laser, bone
density scanner, Hemodiafiltration system, extracorporeal shock wave lithotripsy,
anorectal treatment devices, otoacoustic emission analyzer, and vision screening
instrument, etc.
3. Yonghe County People’s Hospital, Shanxi Province
Yonghe County People’s Hospital is located in Zhengda Street, Yonghe County.
It was established on November 1, 2000. Currently, it has 79 formal employees and
55 temporary employees. Among the formal staff members, there are 9 employees
with full-time undergraduate degrees and more than 20 employees with in-service
education (undergraduate) degrees. In 2016, the hospital was designated as a Class 2
Category B hospital.
In April 2018, the hospital was listed as one of the pilot hospitals for precision
poverty alleviation in medical institutions in Shanxi Province. In April 2018, six
medical teams from Shanxi Hospital and Linfen Fourth People’s Hospital were
assigned to the hospital for training and support. In order to address the problems of
limited scale, disrepair and lack of equipment for clinical treatment, the medical teams
decided to work with the hospital to strive for qualification of Class 2 Category B
hospitals in the annual review this year. They first set up a special working group and

148
signed target performance letters with heads of each department. Subsequently, the
heads of the medical department, the hospital infection department, the clinical
laboratory department, and the pharmacy department were selected to study at the
Linfen Fourth Hospital.
By the time of writing this thesis, the hospital has improved some rules and
regulations and revised the nursing work regulations, the job description for nurses,
emergency nursing plans and treatment process. And it has established a hospital
quality control committee and a three-level quality control system. Under the
supervision of the head nurse Zhang Jianwei of the Nursing Department of Shanxi
Hospital, the hospital carried out night inspection by the head nurse; standardized the
head nurse’s work manual, the nursing style and nurse’s appearance, the management
of the awarding of professional certificate for nurses.
4. Yonghe County TCM Hospital, Shanxi Province
Yonghe County TCM Hospital was founded in 1984. It is located in the centre
of Zhengda Street of the county. It covers an area of 4,510 square meters and has a
floor area of 2,390 square meters, including 1,670 square meters of operational area.
It has 64 employees, among which there are 2 deputy chief doctors and 19 attending
doctors. There are 18 outpatient departments and 40 beds. In rural areas, there is a
general lack of medical services and medicine. Based on an evaluation of its current
conditions, the hospital carried forward the spirit of hard work and diligence, and
adheres to the policy of “targeting the rural area and farmers, and serving agricultural
production”. Considering the high cost of medical services in rural areas, the hospital
has been implementing five “convenience measures”: First, the hospital remains open
on holidays. Second, it waives registration fees and allows free selection of doctors.
Third, deposit is not collected to ensure patients with financial difficulties receive
timely treatment. Four, low fees and high-quality services, with small but effective
prescriptions, simple and convenient procedures characterized by integrity and
accountability, with the goal to allow patients to spend less money for effective
treatment. Five, deferred, reduced or waived payment for patients with financial

149
difficulties. Its efforts to reduce patients’ burden and provide high quality services
have been welcomed by all patients. Over the years, making use of the fact that
people in the mountainous areas favour TCM treatment and the abundance of local
wild herbal medicines, the hospital has been highlighting the characteristics of TCM
and promoting the combination of Chinese and Western medicines. Based on this
concept, it has established specialties such as in bone injury, TCM skin and external
diseases, cerebrovascular disease, acute abdomen, etc. And, it has created
considerable impact in the local communities. In terms of management, we applied
stringent management policies in managing its staff and the operations of the hospital.
It has developed regulations consisting 45 chapters and 503 paragraphs, and 117
performance evaluation criteria so that every position is accountable and every
operation has rules to follow.
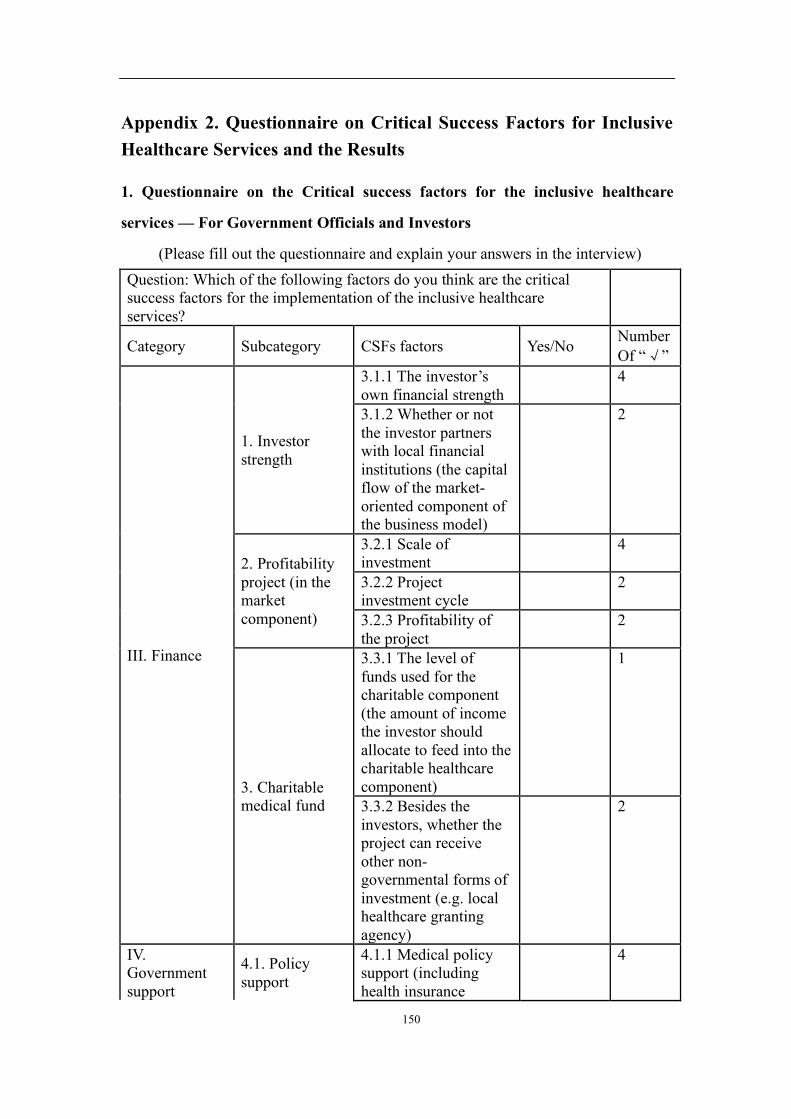
150
Appendix 2. Questionnaire on Critical Success Factors for Inclusive Healthcare Services and the Results
1. Questionnaire on the Critical success factors for the inclusive healthcare
services — For Government Officials and Investors
(Please fill out the questionnaire and explain your answers in the interview) Question: Which of the following factors do you think are the critical success factors for the implementation of the inclusive healthcare services?
Category Subcategory CSFs factors Yes/No Number Of “ ”
III. Finance
1. Investor strength
3.1.1 The investor’s own financial strength 4
3.1.2 Whether or not the investor partners with local financial institutions (the capital flow of the market-oriented component of the business model)
2
2. Profitability project (in the market component)
3.2.1 Scale of investment 4
3.2.2 Project investment cycle 2
3.2.3 Profitability of the project 2
3. Charitable medical fund
3.3.1 The level of funds used for the charitable component (the amount of income the investor should allocate to feed into the charitable healthcare component)
1
3.3.2 Besides the investors, whether the project can receive other non-governmental forms of investment (e.g. local healthcare granting agency)
2
IV. Government support
4.1. Policy support
4.1.1 Medical policy support (including health insurance
4

151
policies)
4.1.2 Policy support for investors investing in the for-profit project
2
4.1.3 Policy Stability 4
4.2 Legal and regulatory support
4.2.1 Legal and regulatory support for inclusive healthcare (to be filled by government officials)
4
4.2.2 Legal and regulatory support for the for-profit projects
4
4.3 Financial support provided by the government for the charitable healthcare component
2
V. External task environment
1. Local non-government support
5.1.1 Local geographical conditions (the impact of geographical restrictions on the distribution of medical resources)
3
5.1.2 Local judicial environment (effective legal implementation frameworks, criminal law authority)
4
5.1.3 Local medical education needs 4
5.1.4 Social support (support that local communities can provide)
2
3. Other external environmental factors
5.2.1 Public awareness and acceptance of the initiative
3
5.2.2 Stable macroeconomic indicators
2
5.2.3 Market environment (for the
1
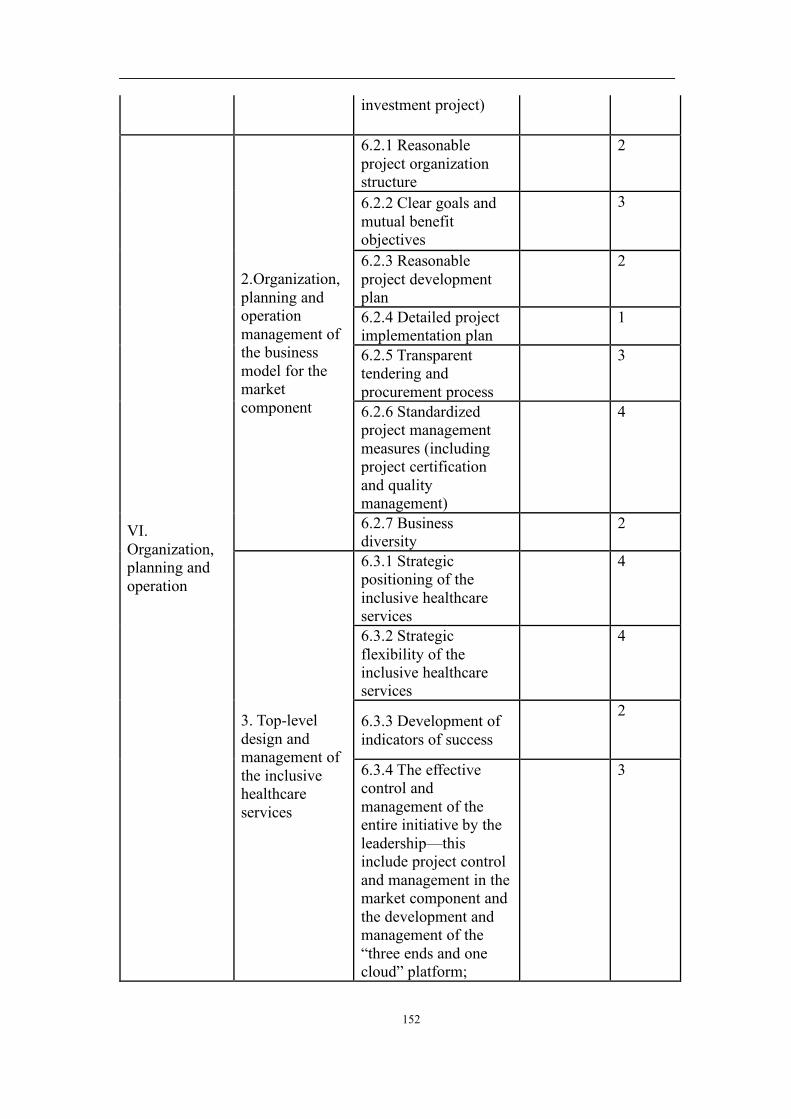
152
investment project)
VI. Organization, planning and operation
2.Organization, planning and operation management of the business model for the market component
6.2.1 Reasonable project organization structure
2
6.2.2 Clear goals and mutual benefit objectives
3
6.2.3 Reasonable project development plan
2
6.2.4 Detailed project implementation plan 1
6.2.5 Transparent tendering and procurement process
3
6.2.6 Standardized project management measures (including project certification and quality management)
4
6.2.7 Business diversity 2
3. Top-level design and management of the inclusive healthcare services
6.3.1 Strategic positioning of the inclusive healthcare services
4
6.3.2 Strategic flexibility of the inclusive healthcare services
4
6.3.3 Development of indicators of success
2
6.3.4 The effective control and management of the entire initiative by the leadership—this include project control and management in the market component and the development and management of the “three ends and one cloud” platform;
3

153
6.3.5 The demonstration role of other successful charitable healthcare projects.
3
4. Cooperation and communication among stakeholders
6.4.1 A good partnership and a reasonable risk sharing mechanism among stakeholders;
1
6.4.2 The commitment and willingness of all stakeholders in the initiative;
4
6.4.3 Clearly defined roles, tasks and responsibilities of all stakeholders in the inclusive healthcare services;
3
6.4.4 The form of cooperation between investors and the government (BOT, BOO, etc.);
2
6.4.5 Communication among stakeholders.
2
6.4.6 Government supervision of investors (ensuring input and usage of sub-fund B)
4
2. Questionnaire on the Critical success factors for the Inclusive healthcare
services — For Hospital Leadership and Doctors
(Please fill out the questionnaire and explain your answers in the interview) Question: Which of the following factors do you think are the critical success factors for the implementation of the inclusive healthcare services?
Category Sub-category CSFs factors Yes/No Number Of “ ”
I. Medical infrastructure (for hospital
1. Doctors 1.1.1 The number of doctors in various
3
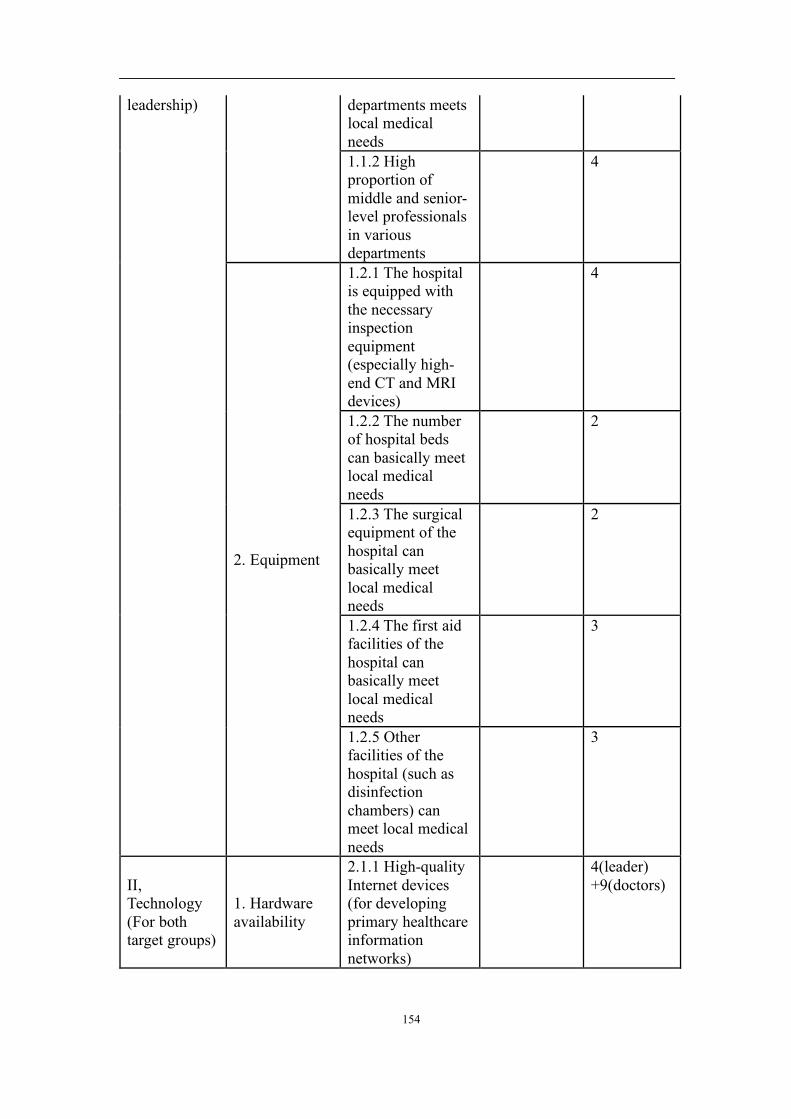
154
leadership) departments meets local medical needs 1.1.2 High proportion of middle and senior-level professionals in various departments
4
2. Equipment
1.2.1 The hospital is equipped with the necessary inspection equipment (especially high-end CT and MRI devices)
4
1.2.2 The number of hospital beds can basically meet local medical needs
2
1.2.3 The surgical equipment of the hospital can basically meet local medical needs
2
1.2.4 The first aid facilities of the hospital can basically meet local medical needs
3
1.2.5 Other facilities of the hospital (such as disinfection chambers) can meet local medical needs
3
II, Technology (For both target groups)
1. Hardware availability
2.1.1 High-quality Internet devices (for developing primary healthcare information networks)
4(leader) +9(doctors)
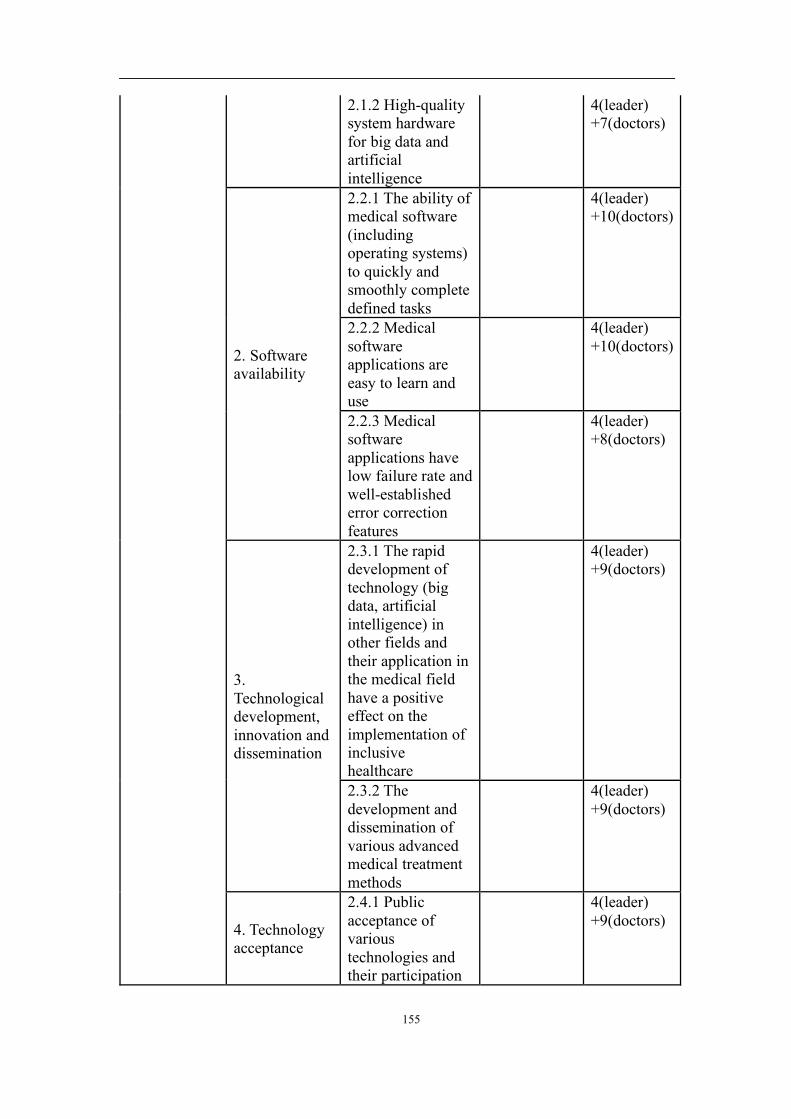
155
2.1.2 High-quality system hardware for big data and artificial intelligence
4(leader) +7(doctors)
2. Software availability
2.2.1 The ability of medical software (including operating systems) to quickly and smoothly complete defined tasks
4(leader) +10(doctors)
2.2.2 Medical software applications are easy to learn and use
4(leader) +10(doctors)
2.2.3 Medical software applications have low failure rate and well-established error correction features
4(leader) +8(doctors)
3. Technological development, innovation and dissemination
2.3.1 The rapid development of technology (big data, artificial intelligence) in other fields and their application in the medical field have a positive effect on the implementation of inclusive healthcare
4(leader) +9(doctors)
2.3.2 The development and dissemination of various advanced medical treatment methods
4(leader) +9(doctors)
4. Technology acceptance
2.4.1 Public acceptance of various technologies and their participation
4(leader) +9(doctors)
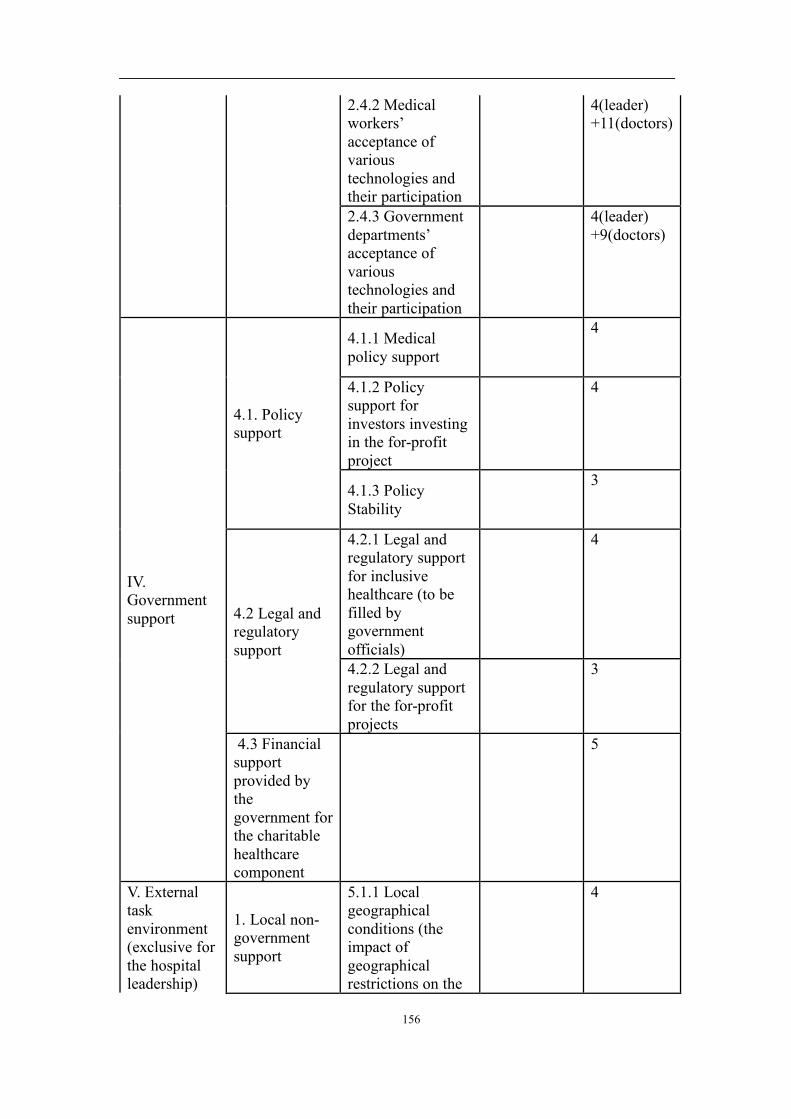
156
2.4.2 Medical workers’ acceptance of various technologies and their participation
4(leader) +11(doctors)
2.4.3 Government departments’ acceptance of various technologies and their participation
4(leader) +9(doctors)
IV. Government support
4.1. Policy support
4.1.1 Medical policy support
4
4.1.2 Policy support for investors investing in the for-profit project
4
4.1.3 Policy Stability
3
4.2 Legal and regulatory support
4.2.1 Legal and regulatory support for inclusive healthcare (to be filled by government officials)
4
4.2.2 Legal and regulatory support for the for-profit projects
3
4.3 Financial support provided by the government for the charitable healthcare component
5
V. External task environment (exclusive for the hospital leadership)
1. Local non-government support
5.1.1 Local geographical conditions (the impact of geographical restrictions on the
4

157
distribution of medical resources) 5.1.2 Local judicial environment (effective legal implementation frameworks, criminal law authority)
4
5.1.3 Local medical education needs
5
5.1.4 Social support (support that local communities can provide)
5
2. Other external environmental factors
5.2.1 Public awareness and acceptance of the initiative
4
5.2.2 Stable macroeconomic indicators
3
5.2.3 Market environment (for the investment project)
4
VI. Organization, planning and operation (For both target groups)
1. Organization, planning and operation management of the business model for charitable component
6.1.1 A reasonable transfer/referral system
4(leader) +8(doctors)
6.1.2 Clinical effectiveness
4(leader) +8(doctors)
6.1.3 Cost-effectiveness and sustainability
5(leader) +8(doctors)
6.1.4 (For patients) A reasonable charging system
6(leader) +10(doctors)
6.1.5 High-standard hospital management (including human resources management, operational process management, etc.)
6(leader) +9(doctors
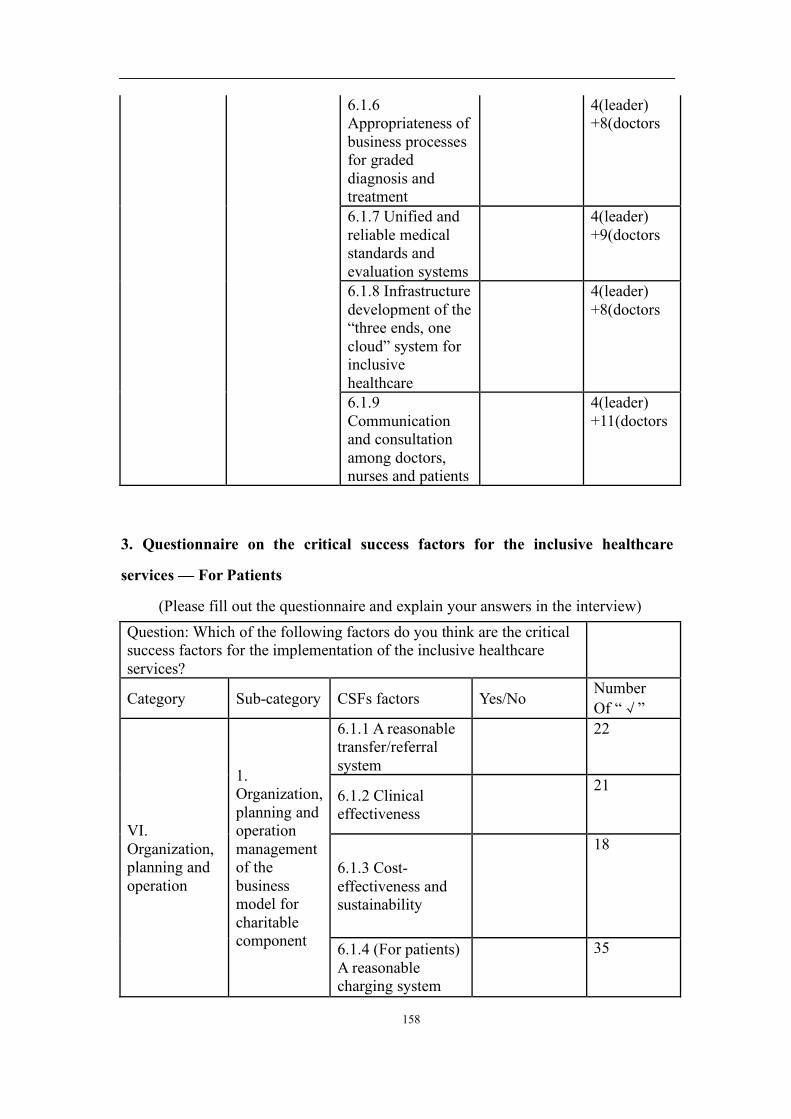
158
6.1.6 Appropriateness of business processes for graded diagnosis and treatment
4(leader) +8(doctors
6.1.7 Unified and reliable medical standards and evaluation systems
4(leader) +9(doctors
6.1.8 Infrastructure development of the “three ends, one cloud” system for inclusive healthcare
4(leader) +8(doctors
6.1.9 Communication and consultation among doctors, nurses and patients
4(leader) +11(doctors
3. Questionnaire on the critical success factors for the inclusive healthcare
services — For Patients
(Please fill out the questionnaire and explain your answers in the interview) Question: Which of the following factors do you think are the critical success factors for the implementation of the inclusive healthcare services?
Category Sub-category CSFs factors Yes/No Number Of “ ”
VI. Organization, planning and operation
1. Organization, planning and operation management of the business model for charitable component
6.1.1 A reasonable transfer/referral system
22
6.1.2 Clinical effectiveness
21
6.1.3 Cost-effectiveness and sustainability
18
6.1.4 (For patients) A reasonable charging system
35
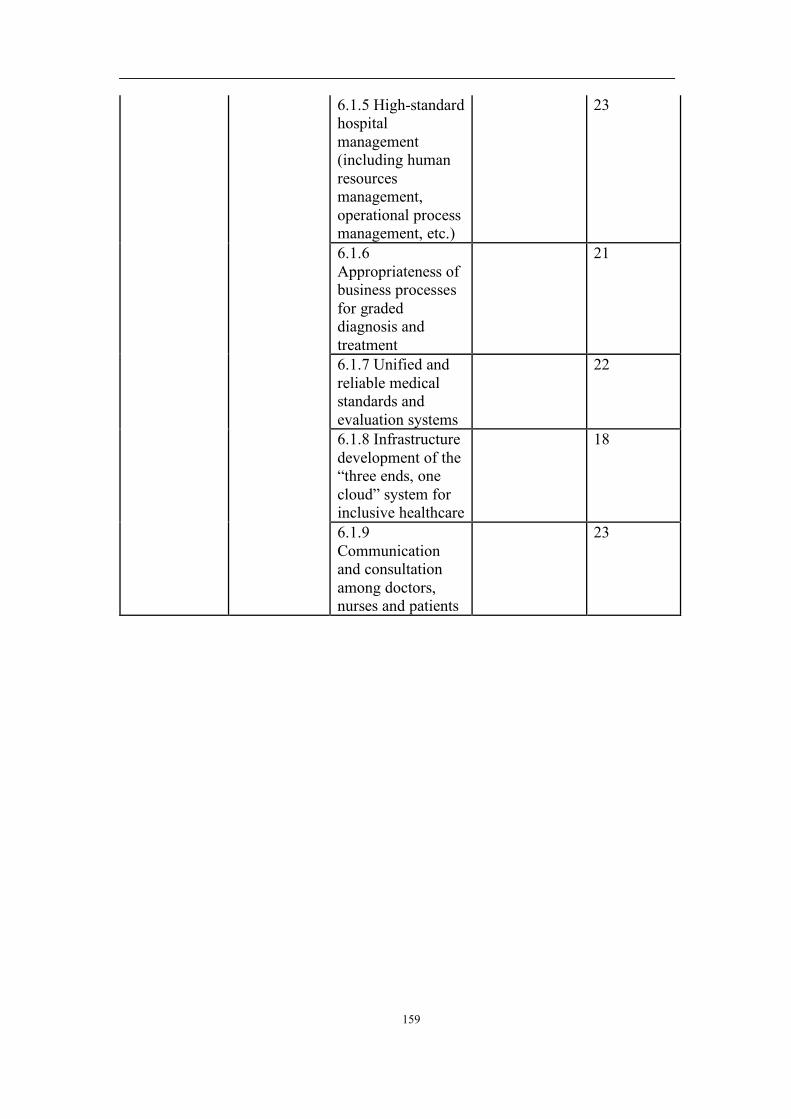
159
6.1.5 High-standard hospital management (including human resources management, operational process management, etc.)
23
6.1.6 Appropriateness of business processes for graded diagnosis and treatment
21
6.1.7 Unified and reliable medical standards and evaluation systems
22
6.1.8 Infrastructure development of the “three ends, one cloud” system for inclusive healthcare
18
6.1.9 Communication and consultation among doctors, nurses and patients
23
160
References
Abdullah, A. A., Chize, B. S., & Zakaria, Z. (2012). Design of Cellular Neural
Network Simulator based on Matlab for Brain Tumour Detection. Journal of
Medical Imaging & Health Informatics, 2(3), 296-306.
Ahmed, S., & Abdullah, A. (2012). E-healthcare and data management services in a
cloud. Paper presented at the High Capacity Optical Networks and Enabling
Technologies.
Amit, R., & Zott, C. (2012). Creating value through business model innovation. MIT
Sloan Management Review, 53(3), 41.
Armbrust, M., Fox, A., Griffith, R., Joseph, A. D., Katz, R., Konwinski, A., Zaharia,
M. (2010). A view of cloud computing. Commun. ACM, 53(4), 50-58.
Assunção, M. D., Calheiros, R. N., Bianchi, S., Netto, M. A. S., & Buyya, R. (2015).
Big data computing and clouds: Trends and future directions. Journal of
Parallel and Distributed Computing, 79-80 (Supplement C), 3-15.
Atkins, M. S., & Mackiewich, B. T. (1998). Fully automatic segmentation of the brain
in MRI. IEEE Transactions on Medical Imaging, 17(1), 98-107
Ballantyne, D., Frow, P., Varey, R. J., & Payne, A. (2011). Value propositions as
communication practice: Taking a wider view. Industrial Marketing
Management, 40(2SI), 202-210.
Bardhan, I. R., Demirkan, H., Kannan, P. K., Kauffman, R. J., & Sougstad, R. (2010).
An interdisciplinary perspective on IT services management and service science.
Journal of Management Information Systems, 26(4SI), 13-64.
Bergner, N., Medyukhina, A., Geiger, K. D., Kirsch, M., Schackert, G., Krafft, C.,
Popp, J. (2013). Hyperspectral unmixing of Raman micro-images for
assessment of morphological and chemical parameters in non-dried brain
tumour specimens. Analytical & Bioanalytical Chemistry, 405(27), 8719-8728.
Berry, L. L., & Bendapudi, N. (2007). Health care: A fertile field for service research.
Journal of Service Research, 10(2), 111-122.
Cachin, C., Keidar, I., & Shraer, A. (2009). Trusting the cloud. ACM SIGACT News,

161
40(2), 81-86.
Casadesus-Masanell, R., & Ricart, J. E. (2010). From strategy to business models and
onto tactics. Long Range Planning, 43(2), 195-215.
Chang, V., Kuo, Y., & Ramachandran, M. (2016). Cloud computing adoption
framework: A security framework for business clouds. Future Generation
Computer Systems, 57 (Supplement C), 24-41.
Chapelle, O., Vapnik, V., & Bengio, Y. (2002). Model selection for small sample
regression. Machine Learning, 48(1-3), 9-23.
Chesbrough, H. (2010). Business model innovation: Opportunities and barriers.
[Article]. Long Range Planning, 43(2-3SI), 354-363.
Cho, S., Mathiassen, L., & Gallivan, M. (2008). Open it-based innovation: Moving
towards cooperative it transfer and knowledge diffusion. Springer.
Cochrane, A. L. (1989). Archie Cochrane in his own words: Selections arranged from
his 1972 introduction to “effectiveness and efficiency: Random reflections on
the health services”. Controlled Clinical Trials, 10(4), 428-433
Coombes, P. H., & Nicholson, J. D. (2013). Business models and their relationship
with marketing: A systematic literature review. Industrial Marketing
Management, 42(5), 656-664.
Cosenz, F., & Noto, G. (2017). A dynamic business modelling approach to design and
experiment new business venture strategies. Long Range Planning.
Dahan, N. M., Doh, J. P., Oetzel, J., & Yaziji, M. (2010). Corporate-NGO
collaboration: Co-creating new business models for developing markets.
[Article]. Long Range Planning, 43(2-3SI), 326-342.
Dale, A. M., Fischl, B., & Sereno, M. I. (1999). Cortical surface-based analysis. I.
Segmentation and surface reconstruction. Neuroimage, 9(2), 179-194.
Ding, S., Su, C., & Yu, J. (2011). An optimizing BP neural network algorithm based
on genetic algorithm. Artificial Intelligence Review, 36(2), 153-162.
Galante, G., & Bona, L. C. E. D. (2013). A Survey on Cloud Computing Elasticity.
Paper presented at the IEEE Fifth International Conference on Utility and Cloud
162
Computing.
Gao, J. C. (2016). The innovation trend research of retail business model in the
internet plus age. In H. Xu & Z. Zhang (Eds.).Advances in Social Science
Education and Humanities Research (54, pp. 1356-1360). PARIS: ATLANTIS
PRESS.
Girotra, K., & Netessine, S. (2013). Business model innovation for sustainability.
Manufacturing & Service Operations Management, 15(4SI), 537-544.
Gong, Z., & Gu, X. (2010). PAC: Pattern-driven Application consolidation for
efficient cloud computing. Paper presented at the IEEE International
Symposium on Modeling, Analysis and Simulation of Computer and
Telecommunication Systems.
Gordon, J., & Shortliffe, E. H. (1985). A method for managing evidential reasoning in
a hierarchical hypothesis space. Elsevier Science Publishers Ltd.
Group, E. B. M. W. (1992). Evidence-based medicine: A new approach to teaching the
practice of medicine. Jama the Journal of the American Medical Association,
268(17), 2420-2425.
Gupta, L., & Srinath, M. D. (1987). Contour sequence moments for the classification
of closed planar shapes. Pattern Recognition, 20(3), 267-272.
Hashem, I. A. T., Yaqoob, I., Anuar, N. B., Mokhtar, S., Gani, A., Ullah Khan, S.
(2015). The rise of “big data” on cloud computing: Review and open research
issues. Information Systems, 47 (Supplement C), 98-115.
Headington, & Oxford, O. X. BET: Brain Extraction Tool Stephen M. Smith
Hecht-Nielsen. (2002). Theory of the backpropagation neural network. Paper
presented at the International Joint Conference on Neural Networks.
Hinton, G. E., Osindero, S., & Teh, Y. W. (2014). A fast learning algorithm for deep
belief nets. Neural Computation, 18(7), 1527-1554.
Informatics, H., & Inc, H. D. A. (1990). Healthcare informatics: the business
magazine for information and communication systems.
Iosup, A., Ostermann, S., Yigitbasi, M. N., Prodan, R., Fahringer, T., Epema, D.
163
(2011). Performance analysis of cloud computing services for many-tasks
scientific computing. IEEE Transactions on Parallel & Distributed Systems,
22(6), 931-945.
JamesInglis. (1977). A mathematical theory of evidence. Technometrics, 20(1), 106
Jiang, B. L. (2013). Principle of MRI and its clinical application. China Medical
Equipment
Johnson, M. W., Christensen, C. M., & Kagermann, H. (2008). Reinventing your
business model. Harvard Business Review, 86(12), 50-59.
Kamnitsas, K., Ledig, C., Newcombe, V. F. J., Simpson, J. P., Kane, A. D., Menon, D.
K., Glocker, B. (2016). Efficient multi-scale 3D CNN with fully connected CRF
for accurate brain lesion segmentation. Medical Image Analysis, 36, 61.
Kapur, T., Grimson, W. E., & Kikinis, R. (1996). Segmentation of brain tissue from
magnetic resonance images. Medical Image Analysis, 1(2), 109.
Kumar, P. S., Subramanian, R., & Selvam, D. T. (2011) Ensuring data storage
security in cloud computing using Sobol Sequence. Paper presented at the
International Conference on Parallel Distributed and Grid Computing.
Lemieux, L., Hagemann, G., Krakow, K., & Woermann, F. G. (1999). Fast automatic
segmentation of the brain in T1-weighted volume MRI data. Paper presented at
the Medical Imaging.
Lemieux, L., Hagemann, G., Krakow, K., & Woermann, F. G. (1999). Fast, accurate,
and reproducible automatic segmentation of the brain in T1-weighted volume
MRI data. Magnetic Resonance in Medicine, 42(1), 127
Maes, F., Collignon, A., Vandermeulen, D., Marchal, G., & Suetens, P. (1997). Multi-
modality image registration by maximizing of mutual information. IEEE Trans
Med Imaging, 16(2), 187-198
Magretta, J. (2002). Why business models matter?Harvard Business Review, 80(5), 86.
Mansfield-Devine, S. (2008). Danger in the clouds. Network Security, 2008(12), 9-11.
Mastelic, T., Oleksiak, A., Claussen, H., Brandic, I., Pierson, J. M., Vasilakos, A. V.
(2014). Cloud Computing:Survey on energy efficiency. Acm Computing Surveys,
164
47(2), 1-36.
McColl-Kennedy, J. R., Vargo, S. L., Dagger, T. S., Sweeney, J. C., &Kasteren, V. Y.
(2012). Health care customer value co-creation practice styles. Journal of
Service Research, 15(4), 370-389.
MEEGAMA, R. G. N., & RAJAPAKSE, J. C. (2004). Fully automated peeling
technique for t1-weighted, high-quality mr head scans. International Journal of
Image & Graphics, 4(02), 141-156.
Mohsin, S., Sajjad, S., Malik, Z., & Abdullah, A. H. (2012). Efficient way of skull
stripping in mri to detect brain tumour by applying morphological operations,
after detection of false background. Raffles Bulletin of Zoology, 28(28), 335-337.
Moisl, H. (2011). Hypothesis Generation. Springer US.
Murphy, C. K. (2000). Combining belief functions when evidence conflicts. Decision
Support Systems, 29(1), 1-9.
Nasui, D., Sgarciu, V., & Cernian, A. (2013). Cloud-based application development
platform for secure, intelligent, interlinked and interactive infrastructure. Paper
presented at the IEEE International Symposium on Applied Computational
Intelligence and Informatics.
Nyul, L. G., Udupa, J. K., & Saha, P. K. (2003). Incorporating a measure of local
scale in voxel-based 3-D image registration. IEEE Trans Med Imaging, 22(2),
228-237.
Page, A., Hijazi, S., Askan, D., Kantarci, B., & Soyata, T. (2016). Research directions
in cloud-based decision support systems for health monitoring using internet-of-
things driven data acquisition. Working Paper.
Pan, Y., Huang, W., Lin, Z., Zhu, W., Zhou, J., Wong, J.,& Ding, Z. (2015). Brain
tumour grading based on Neural Networks and Convolutional Neural Networks.
Conf Proc IEEE Eng Med Biol Soc, 2015, 699-702.
Pereira, S., Pinto, A., Alves, V., & Silva, C. A. (2016). brain tumour segmentation
using convolutional neural networks in mri images. IEEE Transactions on
Medical Imaging, 35(5), 1240-1251.

165
Persoon, E., & Fu, K. S. (1986). Shape discrimination using fourier descriptors. IEEE
Transactions on Systems Man & Cybernetics, 7(3), 170-179.
Peters, C., Blohm, I., & Leimeister, J. M. (2015). anatomy of successful business
models for complex services: Insights from the telemedicine field. Journal of
Management Information Systems, 32(3), 75-104.
Pluim, J. P. W., Maintz, J. B. A., & Viergever, M. A. (2001). Mutual information
matching in multiresolution contexts. Image & Vision Computing, 19(1), 45-52
Reddy, V. K., Surya, K. D., Praveen, M. S., Lokesh, B., Vishal, A., &Akhil, K. (2016).
Performance analysis of load balancing algorithms in cloud computing
environment. Telkomnika Indonesian Journal of Electrical Engineering, 9(18),
1-6.
Reichert, Z., Richards, K., & Yoshigoe, K. (2014). Automated forensic data
acquisition in the cloud. Paper presented at the IEEE International Conference
on Mobile Ad Hoc and Sensor Systems.
Ren, Y., Shen, J., Zheng, Y., Wang, J., & Chao, H. C. (2016). Efficient data integrity
auditing for storage security in mobile health cloud. Peer-to-Peer Networking
and Applications, 9(5), 854-863.
Saebi, T., & Foss, N. J. (2015). Business models for open innovation: Matching
heterogeneous open innovation strategies with business model dimensions.
European Management Journal, 33(3), 201-213.
Savova, G. K., Ogren, P. V., Duffy, P. H., Buntrock, J. D., & Chute, C. G. (2008).
Mayo clinic nlp system for patient smoking status identification. Journal of the
American Medical Informatics Association, 15(1), 25.
Selvakumar, C., Rathanam, G. J., & Sumalatha, M. R. (2013). PDDS - Improving
cloud data storage security using data partitioning technique. Paper presented at
the Advance Computing Conference.
Sentz, K., & Ferson, S. (2002). Combination of evidence in dempster-shafer theory.
Contemporary Pacific, 11(2), 416-426.
Shacham, H., & Waters, B. (2013). Compact proofs of retrievability. Journal of
166
Cryptology, 26(3), 442-483.
Shahzad, A., Musa, S., Aborujilah, A., & Irfan, M. (2014). A new cloud based
supervisory control and data acquisition implementation to enhance the level of
security using testbed. Journal of Computer Science, 10(4), 652-659.
Shanthakumar, P., & Ganesh Kumar, P. (2016). Computer aided brain tumour
detection system using watershed segmentation techniques. International
Journal of Imaging Systems & Technology, 25(4), 297-301.
Shattuck, D. W., Sandor-Leahy, S. R., Schaper, K. A., Rottenberg, D. A., & Leahy, R.
M. (2001). Magnetic resonance image tissue classification using a partial
volume model. Neuroimage, 13(5), 856-876.
Shattuck, D. W., & Leahy, R. M. (2002). Brainsuite: An automated cortical surface
identification tool. Medical Image Analysis, 6(2), 129-142.
Sivarajah, U., Kamal, M. M., Irani, Z., & Weerakkody, V. (2017). Critical analysis of
big data challenges and analytical methods. Journal of Business Research, 70
(Supplement C), 263-286.
Smith, S. M. (2002). Fast robust automated brain extraction. Human Brain Mapping,
17(3), 143.
Sorescu, A., Frambach, R. T., Singh, J., Rangaswamy, A., & Bridges, C. (2011).
Innovations in retail business models. Journal of Retailing, 871(SI), S3-S16.
Studholme, C., Hill, D. L. G., & Hawkes, D. J. (1999). An overlap invariant entropy
measure of 3d medical image alignment. Pattern Recognition, 32(1), 71-86.
Teece, D. J. (2010). Business models, business strategy and innovation. Long Range
Planning, 43(2), 172-194.
Thapaliya, K., & Kwon, G. R. (2012). Extraction of brain tumour based on
morphological operations. Paper presented at the International Conference on
Computing Technology and Information Management.
Ulku, E. E., & Camurcu, A. Y. (2014). Computer aided brain tumour detection with
histogram equalization and morphological image processing techniques. Paper
presented at the International Conference on Electronics, Computer and
167
Computation.
von Hippel, E., Ogawa, S., & de Jong, J. P. J. (2011). The age of the consumer-
innovator. MIT Sloan Management Review, 53(1), 27-35.
Wang, C., Wang, Q., Ren, K., & Lou, W. (2010). Privacy-preserving public auditing
for data storage security in cloud computing, 62(2), 525-533.
Wang, N., Yang, Y., Meng, K., Chen, Y., & Ji, Q. (2014). A customer experience-
based cost minimization strategy of storing data in cloud computing. Acta
Electronica Sinica, 42(1), 20-27.
Wells, W. M., Grimson, E. L., Kikinis, R., & Jolesz, F. A. (1996). Adaptive
segmentation of mri data.
Xu, G., Ding, Y., Wu, C., Zhai, Y., & Zhao, J. (2016). Explore maximal frequent item
sets for big data preprocessing based on small sample in cloud computing. Paper
presented at the International Congress on Ultra Modern Telecommunications
and Control Systems and Workshops.
Xu, X., Zheng, J., Yang, J. B., Xu, D. L., & Chen, Y. W. (2017). Data classification
using evidence reasoning rule. Knowledge-Based Systems, 116(C), 144-151.
Yang, J. B., & Xu, D. L. (2002). On the evidential reasoning algorithm for multiple
attribute decision analysis under uncertainty. IEEE Transactions on Systems
Man & Cybernetics: Part A Systems & Humans, 32(3), 289-304.
Yang, J. B., & Xu, D. L. (2013a). Evidential reasoning rule for evidence combination.
Artificial Intelligence, 205(205), 1-29.
Yang, J. B., & Xu, D. L. (2013b). Evidential reasoning rule for evidence combination.
Artificial Intelligence, 205(205), 1-29.
You, Z., & Jain, A. K. (1984). Performance evaluation of shape matching via chord
length distribution. Computer Vision Graphics & Image Processing, 28(2), 185-
198.
Zacharaki, E. I., Wang, S., Chawla, S., Soo Yoo, D., Wolf, R., Melhem, E. & Davatz.
(2009). Classification of brain tumour type and grade using MRI texture and
shape in a machine learning scheme. Magnetic Resonance in Medicine Official

168
Journal of the Society of Magnetic Resonance in Medicine, 62(6), 1609-1618.
Zhao, X., Wu, Y., Song, G., Li, Z., Zhang, Y.,... Fan, Y. (2017). A deep learning model
integrating FCNNs and CRFs for brain tumour segmentation. Medical Image
Analysis, 43(12).
Zott, C., Amit, R., & Massa, L. (2011). The business model: Recent developments and
future research. Journal of Management, 37(4), 1019-1042.




















