A Qualitative Evaluation of the Barriers and Facilitators Toward Implementation of the WHO Surgical...
11
ORIGINAL ARTICLE A Qualitative Evaluation of the Barriers and Facilitators Toward Implementation of the WHO Surgical Safety Checklist Across Hospitals in England Lessons From the “Surgical Checklist Implementation Project” Stephanie J. Russ, PhD, Nick Sevdalis, PhD, Krishna Moorthy, MD, FRCS, Erik K. Mayer, PhD, FRCS, Shantanu Rout, MRCS, Jochem Caris, MD, Jenny Mansell, MSc, Rachel Davies, BA, Charles Vincent, PhD, and Ara Darzi, MD, FACS Objectives: To evaluate how the World Health Organization (WHO) surgical safety checklist was implemented across hospitals in England; to identify barriers and facilitators toward implementation; and to draw out lessons for implementing improvement initiatives in surgery/health care more generally. Background: The WHO checklist has been linked to improved surgical out- comes and teamwork, yet we know little about the factors affecting its suc- cessful uptake. Methods: A longitudinal interview study with operating room personnel was conducted across a representative sample of 10 hospitals in England between March 2010 and March 2011. Interviews were audio recorded over the phone. Interviewees were asked about their experience of how the checklist was introduced and the factors that hindered or aided this process. Transcripts were submitted to thematic analysis. Results: A total of 119 interviews were completed. Checklist implementation varied greatly between and within hospitals, ranging from preplanned/phased approaches to the checklist simply “appearing” in operating rooms, or staff feeling it had been imposed. Most barriers to implementation were specific to the checklist itself (eg, perceived design issues) but also included prob- lematic integration into preexisting processes. The most common barrier was resistance from senior clinicians. The facilitators revealed some positive steps that can been taken to prevent/address these barriers, for example, modifying the checklist, providing education/training, feeding-back local data, fostering strong leadership (particularly at attending level), and instilling accountability. Conclusions: We identified common themes that have aided or hindered the introduction of the WHO checklist in England and have translated these into recommendations to guide the implementation of improvement initiatives in surgery and wider health care systems. Keywords: WHO surgical safety checklist, implementation, barriers and facilitators, patient safety, interview study, surgery, operating room, operating theatre (Ann Surg 2014;00:1–11) T he World Health Organization’s (WHO) surgical safety check- list was a key output of their 2007 “Safe Surgery Saves Lives” campaign. 1,2 The checklist comprises 3 components: “sign-in,” From the Department of Surgery and Cancer, Imperial College London, UK. Disclosure: Supported by the National Institute for Health Research (NIHR), UK, funds. The authors declare no conflicts of interest. The funders had no role in the design and conduct of the study; the collection, management, analysis, and interpretation of the data; or the preparation, review, and approval of the manuscript. Reprints: Stephanie Jane Russ, PhD, Department of Surgery and Cancer, Imperial College London, Room 504, 5th floor, Wright Fleming Building, Norfolk Place, London W2 1PG, United Kingdom. E-mail: [email protected]. Copyright C 2014 by Lippincott Williams & Wilkins ISSN: 0003-4932/14/00000-0001 DOI: 10.1097/SLA.0000000000000793 “time-out,” and “sign-out,” which are carried out when the patient arrives into the operating room (OR) complex, just before the surgi- cal procedure starting and upon completion of the procedure, respec- tively. The purpose of this tool was to create a standardized framework to improve patient safety and reduce the morbidity and mortality as- sociated with potential deviations from best practice, for example, with regard to antibiotic and deep vein thrombosis prophylaxis, as well as avoidable error in the surgical setting. 3,4 The checklist was pilot-tested in a global study across 8 hos- pitals in the developed and developing world. The results were pub- lished in January 2009 and showed a significant reduction in mortality and morbidity after checklist implementation. 5 As a result of these findings, a modified version of the checklist was mandated by the UK’s Department of Health (through the then called “National Pa- tient Safety Agency,” NPSA) for use in all surgical procedures carried out within the National Health Service (NHS) in England and Wales (including day surgery). 6 Hospitals were given 12 months to fully implement the checklist (until January 2010). Some guidance regard- ing implementation, modification, and the correct use of the checklist was made available online 7 and the checklist was also highlighted as part of the “Patient Safety First” campaign, which was active be- tween June 2008 and March 2010 and aimed to promote patient safety across the NHS. 8 To date, the WHO checklist, or a version of it, has been introduced as best practice in several other countries, including the United States. 9 To prospectively evaluate how the checklist was introduced and implemented within England, after the introduction of the WHO checklist as national policy our research team set up the “Surgical Checklist Implementation Project” in 2009. Here, we report longi- tudinal interview data collected between 2010 and 2011 on how the checklist was received across a nationally representative sample of hospitals in England. The following specific research questions were addressed: 1. How was the WHO checklist initially implemented within English hospitals? 2. What were the key barriers and facilitators to its implementation? 3. What lessons can we extract for informing how to optimize the diffusion and uptake of improvement initiatives in surgery and wider health care systems? METHODS Setting and Participants The Surgical Checklist Implementation Project was a multi- phase large research program. For this study, OR personnel were sampled from 10 English hospitals to take part in the interviews. The 10 hospitals were selected to be nationally representative using the following stratification criteria: Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. Annals of Surgery Volume 00, Number 00, 2014 www.annalsofsurgery.com | 1
-
Upload
independent -
Category
Documents
-
view
5 -
download
0
Transcript of A Qualitative Evaluation of the Barriers and Facilitators Toward Implementation of the WHO Surgical...

ORIGINAL ARTICLE
A Qualitative Evaluation of the Barriers and Facilitators TowardImplementation of the WHO Surgical Safety Checklist Across
Hospitals in EnglandLessons From the “Surgical Checklist Implementation Project”
Stephanie J. Russ, PhD, Nick Sevdalis, PhD, Krishna Moorthy, MD, FRCS, Erik K. Mayer, PhD, FRCS,Shantanu Rout, MRCS, Jochem Caris, MD, Jenny Mansell, MSc, Rachel Davies, BA, Charles Vincent, PhD,
and Ara Darzi, MD, FACS
Objectives: To evaluate how the World Health Organization (WHO) surgicalsafety checklist was implemented across hospitals in England; to identifybarriers and facilitators toward implementation; and to draw out lessons forimplementing improvement initiatives in surgery/health care more generally.Background: The WHO checklist has been linked to improved surgical out-comes and teamwork, yet we know little about the factors affecting its suc-cessful uptake.Methods: A longitudinal interview study with operating room personnel wasconducted across a representative sample of 10 hospitals in England betweenMarch 2010 and March 2011. Interviews were audio recorded over the phone.Interviewees were asked about their experience of how the checklist wasintroduced and the factors that hindered or aided this process. Transcriptswere submitted to thematic analysis.Results: A total of 119 interviews were completed. Checklist implementationvaried greatly between and within hospitals, ranging from preplanned/phasedapproaches to the checklist simply “appearing” in operating rooms, or stafffeeling it had been imposed. Most barriers to implementation were specificto the checklist itself (eg, perceived design issues) but also included prob-lematic integration into preexisting processes. The most common barrier wasresistance from senior clinicians. The facilitators revealed some positive stepsthat can been taken to prevent/address these barriers, for example, modifyingthe checklist, providing education/training, feeding-back local data, fosteringstrong leadership (particularly at attending level), and instilling accountability.Conclusions: We identified common themes that have aided or hindered theintroduction of the WHO checklist in England and have translated these intorecommendations to guide the implementation of improvement initiatives insurgery and wider health care systems.
Keywords: WHO surgical safety checklist, implementation, barriers andfacilitators, patient safety, interview study, surgery, operating room, operatingtheatre
(Ann Surg 2014;00:1–11)
T he World Health Organization’s (WHO) surgical safety check-list was a key output of their 2007 “Safe Surgery Saves Lives”
campaign.1,2 The checklist comprises 3 components: “sign-in,”
From the Department of Surgery and Cancer, Imperial College London, UK.Disclosure: Supported by the National Institute for Health Research (NIHR), UK,
funds. The authors declare no conflicts of interest.The funders had no role in the design and conduct of the study; the collection,
management, analysis, and interpretation of the data; or the preparation, review,and approval of the manuscript.
Reprints: Stephanie Jane Russ, PhD, Department of Surgery and Cancer, ImperialCollege London, Room 504, 5th floor, Wright Fleming Building, Norfolk Place,London W2 1PG, United Kingdom. E-mail: [email protected].
Copyright C© 2014 by Lippincott Williams & WilkinsISSN: 0003-4932/14/00000-0001DOI: 10.1097/SLA.0000000000000793
“time-out,” and “sign-out,” which are carried out when the patientarrives into the operating room (OR) complex, just before the surgi-cal procedure starting and upon completion of the procedure, respec-tively. The purpose of this tool was to create a standardized frameworkto improve patient safety and reduce the morbidity and mortality as-sociated with potential deviations from best practice, for example,with regard to antibiotic and deep vein thrombosis prophylaxis, aswell as avoidable error in the surgical setting.3,4
The checklist was pilot-tested in a global study across 8 hos-pitals in the developed and developing world. The results were pub-lished in January 2009 and showed a significant reduction in mortalityand morbidity after checklist implementation.5 As a result of thesefindings, a modified version of the checklist was mandated by theUK’s Department of Health (through the then called “National Pa-tient Safety Agency,” NPSA) for use in all surgical procedures carriedout within the National Health Service (NHS) in England and Wales(including day surgery).6 Hospitals were given 12 months to fullyimplement the checklist (until January 2010). Some guidance regard-ing implementation, modification, and the correct use of the checklistwas made available online7 and the checklist was also highlightedas part of the “Patient Safety First” campaign, which was active be-tween June 2008 and March 2010 and aimed to promote patient safetyacross the NHS.8 To date, the WHO checklist, or a version of it, hasbeen introduced as best practice in several other countries, includingthe United States.9
To prospectively evaluate how the checklist was introducedand implemented within England, after the introduction of the WHOchecklist as national policy our research team set up the “SurgicalChecklist Implementation Project” in 2009. Here, we report longi-tudinal interview data collected between 2010 and 2011 on how thechecklist was received across a nationally representative sample ofhospitals in England. The following specific research questions wereaddressed:
1. How was the WHO checklist initially implemented within Englishhospitals?
2. What were the key barriers and facilitators to its implementation?3. What lessons can we extract for informing how to optimize the
diffusion and uptake of improvement initiatives in surgery andwider health care systems?
METHODSSetting and Participants
The Surgical Checklist Implementation Project was a multi-phase large research program. For this study, OR personnel weresampled from 10 English hospitals to take part in the interviews. The10 hospitals were selected to be nationally representative using thefollowing stratification criteria:
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Annals of Surgery � Volume 00, Number 00, 2014 www.annalsofsurgery.com | 1

Russ et al Annals of Surgery � Volume 00, Number 00, 2014
– Geographic spread: hospitals were selected to cover multiple re-gions. These were determined using the 10 (at the time of the study)health care administrative entities within England as provided bythe Department of Health.
– Type and size: the Department of Health has a hospital classifica-tion “clustering” system based on hospital type (eg, teaching vscommunity) and size (small vs medium vs large)—the latter basedon number of beds/admissions.
– Safety incident reporting levels: all English hospitals are linkedinto a national incident reporting system, termed the “NationalReporting and Learning System,” NRLS (www.nrls.npsa.nhs.uk).A database is maintained of the volume of incidents reported byeach hospital, which classifies them into low, medium, and highreporting hospitals. This criterion was used in light of the evidencethat shows that increased reporting to the NRLS is positively linkedto safety culture within hospitals,10 which can affect how a safetyintervention like the WHO checklist is implemented.
– Checklist implementation early response: after introduction of theWHO checklist as national policy in 2009, the Department ofHealth maintained a database of hospitals regarding where theywere on their implementation pathway (not acknowledged, ac-knowledged, ongoing, completed). Hospitals were required to havereached the stage of “completed” by February 2010.
To achieve representativeness of responses, the sampling tookplace in 2 stages. In the first stage a random set of hospitals acrossthe above criteria was generated by the NPSA. In the second stage,the research team cross-tabulated the criteria, identified hospitals thatfulfilled the cross-stratification as much as this was feasible (eg, therewere only 2 institutions that were listed as not having acknowledgedthe checklist policy, as should be expected), and then randomly se-lected within those. Hospitals were identified with a 3-letter acronymprovided by the Department of Health, to which the research teamwas kept blinded until after the final selection had been made.
Within the 10 selected hospitals, all OR personnel were identi-fied via the human resources department. All personnel subsequentlyreceived an electronic survey of their views on the WHO checklist(data not reported here). Participants who completed the survey hadthe option to provide their details so they could be interviewed regard-ing the checklist—that is, an “opt in” sampling strategy for this study.All of those who “opted in” were contacted for interview. Participat-ing personnel fell under the following professional groups: surgeons,anesthesiologists, OR nurses (including OR managers), operating de-partment practitioners (ODPs; they perform the role of an anestheticnurse or technician in English ORs), and radiographers.
Design and ProcedureInterviews were carried out longitudinally over the course of
1 year (March 2010–March 2011) to capture staff perceptions of thechecklist over time following its formal mandatory introduction intoEnglish ORs. All interviews were carried out over the phone by atrained interviewer from the market research company Ipsos MORI(www.ipsos.com). Interviews lasted approximately 30 minutes each,were audio-recorded, and later were transcribed verbatim for dataanalysis. Before data collection, the study was reviewed by the UK’sIntegrated Research Application System for health research and wasformally approved as a quality improvement study (September 28,2009).
Data Collection InstrumentA semistructured interview schedule was designed by our re-
search team, reviewed by Ipsos MORI experts, and subsequentlypiloted for feasibility at one of the study sites. The interviews com-prised a series of open-ended questions and prompts, which were
designed to capture detailed accounts of the following aspects ofchecklist implementation:
– how the checklist had been implemented within each hospital (eg,“How was the checklist introduced in your hospital?” “Did youreceive any training?”)
– barriers and/or facilitators toward its implementation (eg, “Whatwere your initial reactions upon hearing about the WHO check-list?” “Do you feel that staff are using the checklist as intended?Why/Why not?,” “Is it always possible to use the WHO checklist?,”“What sorts of things make it easier/more difficult to use?”).
The semistructured approach to the interviews was selectedas a method to allow exploration of interviewees’ full range of im-plementation experiences across the sample. An abridged version ofinterview schedule is available in the Appendix (a full version isavailable from the authors on request).
AnalysesAudio-recorded interviews were anonymized and responses
were transcribed verbatim. All transcripts were analyzed by a trainedpsychologist researcher (S.J.R.) using an inductive approach, evolv-ing an interpretive framework to fit the data. Thematic analysis wasundertaken, extracting specific themes from the transcripts regarding(1) how the checklist had been implemented and (2) the perceived bar-riers (factors that hinder uptake) and facilitators (factors that improveuptake) surrounding its implementation. Themes were extracted un-til the standard criterion for qualitative studies of “saturation” wasreached—that is, no further codes were needed to describe the partic-ipants’ views. A senior psychologist with expertise in surgical safety(N.S.) reviewed the analyses to control for bias in theme extraction.
To provide a framework for the coding of the interviews,themes representing barriers and facilitators were grouped accordingto whether they related to organizational, systems, team, or checklist-specific factors. These were based on the large evidence base onfactors affecting safety in surgery and were defined as follows:
– Organizational: Themes relating to financial resources and con-straints; organizational structure; policy, standards, and goals; strat-egy and planning; safety culture and priorities.11,12
– Systems: Themes relating to the integration of the checklistinto existing systems, protocols, and procedures (eg, efficiency,repetition).11–13
– Team: Themes relating to teamwork (eg, communication, cohe-sion), team structure/membership (eg, leadership), and team buy-inand ownership of the checklist.11–15
– Checklist-specific: Themes relating specifically to either checklistdesign, content, applicability or process, and/or the evidence basebehind the checklist.13,15
RESULTS
Participant Demographic InformationA total of 141 participants “opted in” to be interviewed, of
whom a final sample of 119 OR personnel across 10 NHS hospitalswere interviewed (response rate: 84.4%). Participants who were notinterviewed were unable to be contacted due to logistical problems—that is, holidays, lack of availability of time for the interview, orcancelation of interview due to clinical commitments. The 119 par-ticipants who were interviewed varied widely in their experience ofworking in ORs, ranging from 6 months to more than 30 years. Table1 displays respondent numbers according to professional group andhospital size. All hospitals had implemented the checklist 6 to 12months before data collection.
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
2 | www.annalsofsurgery.com C© 2014 Lippincott Williams & Wilkins

Annals of Surgery � Volume 00, Number 00, 2014 Implementing Change in Health Care: The WHO Checklist
TABLE 1. Respondent Profiles
N = 119 N (% of Sample)
Professional groupSurgeon 37 (31)
Attending 19 (16)Other 18 (15)
Anesthesiologist 31 (26)Attending 18 (15)Other 13 (11)
Nurse 23 (19)Operating department practitioner (anesthetic
nurse/technician)18 (15)
Radiographer 10 (8)Trust size
Small 34 (29)Medium 27 (23)Large 25 (21)Acute teaching 33 (28)
How Was the WHO Checklist Initially Implemented?The manner in which the checklist was initially implemented
varied greatly, both between and within hospitals, and fell under 3broad themes:
1. Planned implementation approach2. Limited/no implementation approach3. Imposed implementation approach
Each of these themes is described in Table 2 with illustrativequotes.
Planned implementation refers to interviewees’ reports thatoutlined a clear, articulated strategy for introducing the checklistwith senior leadership and local facilitation—including producingearly modifications of the form, trialling implementation in 1 or 2ORs initially to allow troubleshooting, electing “checklist champions”who acted as local leaders and also a “go-to” person for frontlinepersonnel regarding queries, and providing education and trainingsessions around the importance and use of the checklist. In contrast,limited/no implementation emerged from interviewees’ reports thatemphasized a lack of awareness of any preplanned implementationstrategy and a perception that the checklist had simply “appeared” oneday in ORs. Some staff mentioned that they had received an e-mailor saw posters relating to the checklist’s introduction but that this wasnot formally consolidated by any further implementation exercises.Finally, imposed implementation refers to interviewees’ reports offeeling forced to use the checklist or of an overtly top-down approach(ie, from hospital senior management or the Department of Health)with no opportunity for frontline personnel feedback or involvement.Individuals within the same hospital often reported quite differentimplementation experiences, depending on what professional groupthey belonged to, or what shifts they worked. For example, certainspecialties may have provided some training and education aroundthe initiative during audit days whereas other specialties did not,and individuals working night shifts often reported missing relevantmeetings and education sessions.
Barriers and Facilitators to WHO ChecklistImplementation
A total of 11 themes were extracted that represented barriers tochecklist implementation and 9 themes that represented facilitators.These themes are presented in Tables 3 and 4 along with illustrativequotes. We found no apparent differences between the responsesof individuals who were interviewed at the start of the 1-year data
collection period compared with those interviewed at the end, nordid we find a difference between those who had implemented thechecklist earlier rather than later after the initial mandate.
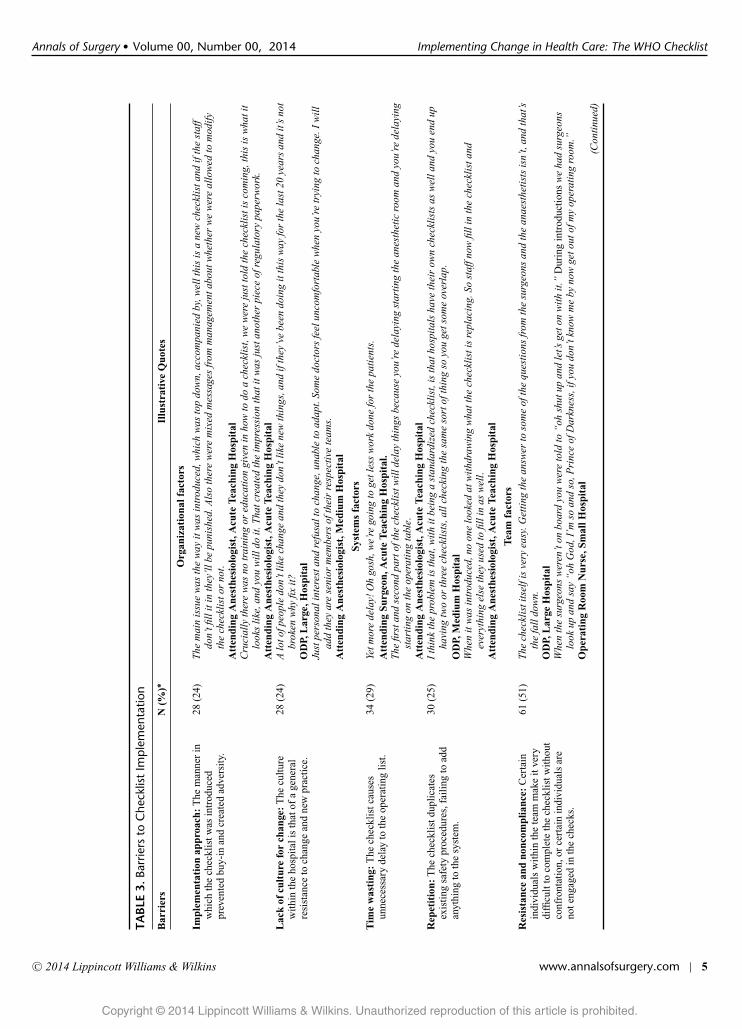
BarriersOrganizational Barriers
Two themes reflected organizational barriers. The first, re-ported by 24% of the sample, related to the style in which the check-list was initially implemented within the hospital. When there was noplanned approach to implementation (eg, a lack of education or train-ing, a perceived lack of support from management, no customizationto the local context), or indeed an imposed approach, staff buy-into the tool was jeopardized because of a lack of ownership over theinitiative and because the local relevance of the tool had not beencommunicated. The second, reported by the same proportion of thesample (but not the same individual staff members), centered aroundthe culture within the hospital. Staff described a general resistance tothe introduction of change, whatever form it takes, particularly frommore senior members of staff. Some stated that this had resulted fromtoo many changes being made to recommended practice in England,and the feeling that “if it’s not broke, why fix it.”
Systems BarriersTwo further barriers related to problems integrating the check-
list into existing systems. Almost a third of the sample (29%) reportedthat the checklist took too long to complete, creating inefficiency inthe running of the operating list. And a quarter of the sample per-ceived the checklist to be directly repetitive of existing safety practicesalready in place, therefore failing to contribute anything “extra” interms of safety to the system (eg, where local checklists had alreadybeen developed and were not removed before the WHO checklist wasintroduced).
Team BarriersThe most common barrier to checklist implementation, re-
ported by 51% of the sample, was active resistance or passive non-compliance from individuals in the OR team, most frequently (84%of the time) from senior surgeons and/or anesthesiologists. This oftenmade it very challenging for the person leading the checks (often anurse) to complete them in the intended manner, or without feelingpersonally attacked.
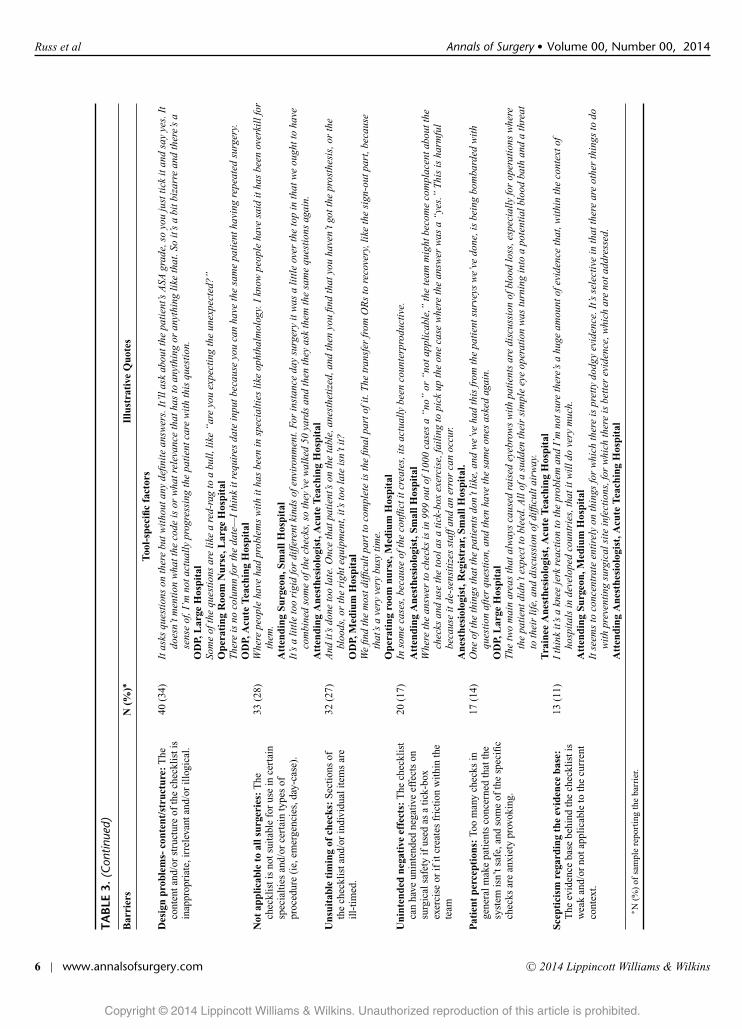
Checklist-Specific BarriersThe majority of barriers that emerged were specific to the
checklist itself. A third of the sample (34%) reported design issueswith regard to the checklist’s content (eg, the awkward wording of cer-tain checks such as “are there any unexpected steps?”—intervieweescommented that if something is unexpected it follows it cannot beanticipated in advance), or physical structure/layout (eg, there beingno space to write answers to questions or to provide the date). Others(27%) perceived there to be issues with the timing at which certainchecks are carried out, for example, with the time-out often beingperceived as being too late to correct errors or disrupting staff at acritical time, and the sign-out suffering from staff leaving the ORbefore the end of the procedure. The checklist was also perceivedby 28% of the sample to be inappropriate for certain surgical pro-cedures; either specific surgical specialties (eg, ophthalmic surgery,obstetrics) or certain contexts (eg, time-pressured emergencies, rapidturnover day-cases). Similarly, some respondents (14%) were con-cerned about the reaction patients might have toward the checks. Forexample, some stated that patients often did not understand why theyhad to confirm their ID/procedure, etc, so many times during theirsurgical pathway, and others felt that specific questions around blood
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
C© 2014 Lippincott Williams & Wilkins www.annalsofsurgery.com | 3

Russ et al Annals of Surgery � Volume 00, Number 00, 2014
TAB
LE2.
Rep
orte
dC
heck
list
Imp
lem
enta
tion
Ap
pro
ache
s
Impl
emen
tati
onA
ppro
ach
Illu
stra
tive
Quo
tes
Pla
nned
impl
emen
tati
onap
proa
ch:
Aw
ell-
plan
ned
and
arti
cula
ted
stra
tegy
was
inpl
ace
for
intr
oduc
ing
the
chec
klis
tin
am
anne
rth
atw
ould
opti
miz
eit
ssm
ooth
inte
grat
ion
and/
orst
aff-
buy-
into
the
tool
.
Itw
asin
trod
uced
into
one
ofth
eor
thop
aedi
cO
Rs
and
sow
hatt
hey
did
isth
ey,j
usto
non
eof
the
Att
endi
ngsu
rgeo
n’s
list
they
used
that
asan
earl
yim
plem
ente
rth
eatr
e.A
ndso
that
team
did
itan
dw
orke
dth
roug
hw
hatw
eha
dto
mak
esu
reth
atw
hatw
eha
dw
orke
dan
dth
atpe
ople
wer
eha
ppy
and
then
they
roll
edit
out.
Ope
rati
ngR
oom
Man
ager
(Nur
se),
Smal
lHos
pita
lW
est
arte
dst
raig
htaw
ay.W
ese
tup
aco
mm
itte
egr
oup.
We
look
edat
the
form
and
how
we
mig
htpo
ssib
lyal
ter
itfo
rou
row
nho
spit
al.W
epu
tasu
gges
tion
box
whe
repe
ople
coul
dw
rite
note
sab
outw
hatt
hey
thou
ghta
ndw
eto
okth
ose
onbo
ard
and
prod
uced
ase
cond
draf
tto
opti
miz
eal
lthe
seco
mm
ents
.The
upta
kew
as10
0%I
wou
ldsa
yw
ithi
n8
or9
mon
ths.
Att
endi
ngSu
rgeo
n,M
ediu
mH
ospi
tal
Itw
asth
eag
enda
for
mos
tmee
ting
s.A
ndth
efo
rmw
aspu
tout
ther
e,w
eta
lked
abou
tita
tsta
ffm
eeti
ngs
befo
reit
wen
tout
for
peop
leto
com
men
ton.
We
took
the
DV
Dth
atw
asof
fere
dfr
omPa
tien
tSaf
ety
Fir
stan
dpl
ayed
iton
educ
atio
naf
tern
oons
,the
good
,the
bad
and
the
ugly
sort
ofth
ing,
soth
atev
eryo
neun
ders
tood
whe
reit
had
com
efr
om’.
We
also
elec
ted
loca
lche
ckli
stch
ampi
ons
who
acte
das
a‘g
oto
’po
intf
orqu
esti
ons
and
quer
ies
and
real
lydr
ove
use
ofth
eto
olon
the
grou
nd.
Ope
rati
ngR
oom
Man
ager
(Nur
se),
Med
ium
Hos
pita
lL
imit
ed/n
oim
plem
enta
tion
appr
oach
:S
taff
wer
eun
awar
eof
any
stru
ctur
edap
proa
chto
impl
emen
tati
onot
her
than
wha
tthe
yhe
ard
via
e-m
ail/
post
ers
orw
ord
ofm
outh
.In
man
yca
ses
the
chec
klis
tjus
tsee
med
to“a
ppea
r”in
OR
s.
Itju
stap
pear
edra
ther
than
ther
ere
ally
bein
gan
yki
ndof
form
alin
trod
ucti
onof
the
chec
klis
t.N
owI
may
have
mis
sed
that
and
that
ispa
rtof
the
prob
lem
isn’
tit,
whe
nyo
u’re
atr
aine
ean
dyo
u’re
noti
nev
ery
day,
that
ther
em
ayha
vebe
ena
sche
dule
dm
eeti
ngth
atw
edi
dn’t
gett
ogo
to,I
don’
tkno
w.
Tra
inee
Ane
sthe
siol
ogis
t,C
T1–
3,Sm
allH
ospi
tal
Mos
tly
wor
dof
mou
th,I
thin
k.I
don’
tkno
wab
outa
nyot
her
OR
sbu
twe
just
diss
emin
ated
itam
ongs
tour
selv
es,a
ndI
had
abi
tofa
read
,and
ther
ew
asa
fair
amou
ntfr
omth
em
atro
non
her
emai
ls,a
ndth
ere
was
apo
ster
up.
OD
P,A
cute
Tea
chin
gH
ospi
tal
I’m
nots
ure,
it’s
just
som
ethi
ngth
at,a
sfa
ras
Iw
asco
ncer
ned
inm
yro
le,i
twas
just
som
ethi
ngth
atth
eyw
ere
sudd
enly
doin
gon
eda
y.R
adio
grap
her,
Lar
geH
ospi
tal
Impo
sed
impl
emen
tati
onap
proa
ch:
The
chec
klis
tw
asim
pose
don
staf
ffr
omth
eto
p-do
wn
(eg,
hosp
ital
man
agem
ent/
Dep
artm
ento
fH
ealt
h)an
dth
ere
was
litt
leor
noop
port
unit
yfo
rfr
ontl
ine
staf
fto
bein
volv
edor
tom
odif
yth
eto
olea
rly
on.
Our
man
ager
just
said
,Ith
ink
this
was
onth
eT
hurs
day,
asof
Mon
day
we’
reus
ing
the
WH
Och
eckl
ist,
and
that
’sth
at.
OD
P,M
ediu
mH
ospi
tal
It’s
like
man
yot
her
dire
ctiv
esfr
omth
eD
epar
tmen
tofH
ealt
hth
atw
ege
tthe
seda
ys,t
here
isno
,or
very
litt
ledi
scus
sion
abou
twha
tha
ppen
s,w
e’re
just
told
todo
thin
gsan
dth
at’s
the
end
ofit
.A
tten
ding
Surg
eon,
Med
ium
Hos
pita
lI
don’
tkno
ww
heth
erit
was
pres
ente
das
afa
itac
com
plit
oth
emas
wel
lbut
,cer
tain
ly,o
urch
iefe
xec
had
gota
bee
inth
eir
bonn
etan
dit
was
,no,
you
wil
ldo
this
.A
tten
ding
Ane
sthe
siol
ogis
t,Sm
allH
ospi
tal.
Yeah
exac
tly
from
the
surg
ical
staf
fpoi
ntof
view
cert
ainl
yI
don’
tkno
ww
heth
erth
eth
eatr
est
affg
otan
ybr
iefin
gin
term
sof
filli
ngou
tthe
chec
klis
tbut
from
asu
rgic
alpo
into
fvie
wit
was
very
muc
hju
ston
eda
yth
ere
itis
,rea
dth
ebo
xes
and
filli
tout
.The
rew
asno
disc
ussi
onor
intr
oduc
tion
oran
ythi
ng.T
ypic
al.
Tra
inee
Surg
eon,
Acu
teT
each
ing
Hos
pita
l
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
4 | www.annalsofsurgery.com C© 2014 Lippincott Williams & Wilkins
Annals of Surgery � Volume 00, Number 00, 2014 Implementing Change in Health Care: The WHO Checklist
TAB
LE3.
Barr
iers
toC
heck
list
Imp
lem
enta
tion
Bar
rier
sN
(%)∗
Illu
stra
tive
Quo
tes
Org
aniz
atio
nalf
acto
rs
Impl
emen
tati
onap
proa
ch:
The
man
ner
inw
hich
the
chec
klis
twas
intr
oduc
edpr
even
ted
buy-
inan
dcr
eate
dad
vers
ity.
28(2
4)T
hem
ain
issu
ew
asth
ew
ayit
was
intr
oduc
ed,w
hich
was
top
dow
n,ac
com
pani
edby
,wel
lthi
sis
ane
wch
eckl
ista
ndif
the
staf
fdo
n’tfi
llit
inth
ey’l
lbe
puni
shed
.Als
oth
ere
wer
em
ixed
mes
sage
sfr
omm
anag
emen
tabo
utw
heth
erw
ew
ere
allo
wed
tom
odif
yth
ech
eckl
isto
rno
t.A
tten
ding
Ane
sthe
siol
ogis
t,A
cute
Tea
chin
gH
ospi
tal
Cru
cial
lyth
ere
was
notr
aini
ngor
educ
atio
ngi
ven
inho
wto
doa
chec
klis
t,w
ew
ere
just
told
the
chec
klis
tis
com
ing,
this
isw
hati
tlo
oks
like
,and
you
wil
ldo
it.T
hatc
reat
edth
eim
pres
sion
that
itw
asju
stan
othe
rpi
ece
ofre
gula
tory
pape
rwor
k.A
tten
ding
Ane
sthe
siol
ogis
t,A
cute
Tea
chin
gH
ospi
tal
Lac
kof
cult
ure
for
chan
ge:
The
cult
ure
wit
hin
the
hosp
ital
isth
atof
age
nera
lre
sist
ance
toch
ange
and
new
prac
tice
.
28(2
4)A
loto
fpeo
ple
don’
tlik
ech
ange
and
they
don’
tlik
ene
wth
ings
,and
ifth
ey’v
ebe
endo
ing
itth
isw
ayfo
rth
ela
st20
year
san
dit
’sno
tbr
oken
why
fixit
?O
DP,
Lar
ge,H
ospi
tal
Just
pers
onal
inte
rest
and
refu
salt
och
ange
,una
ble
toad
apt.
Som
edo
ctor
sfe
elun
com
fort
able
whe
nyo
u’re
tryi
ngto
chan
ge.I
wil
lad
dth
eyar
ese
nior
mem
bers
ofth
eir
resp
ecti
vete
ams.
Att
endi
ngA
nest
hesi
olog
ist,
Med
ium
Hos
pita
l
Syst
ems
fact
ors
Tim
ew
asti
ng:
The
chec
klis
tcau
ses
unne
cess
ary
dela
yto
the
oper
atin
gli
st.
34(2
9)Ye
tmor
ede
lay!
Oh
gosh
,we’
rego
ing
toge
tles
sw
ork
done
for
the
pati
ents
.A
tten
ding
Surg
eon,
Acu
teT
each
ing
Hos
pita
l.T
hefir
stan
dse
cond
part
ofth
ech
eckl
istw
illd
elay
thin
gsbe
caus
eyo
u’re
dela
ying
star
ting
the
anes
thet
icro
oman
dyo
u’re
dela
ying
star
ting
onth
eop
erat
ing
tabl
e.A
tten
ding
Ane
sthe
siol
ogis
t,A
cute
Tea
chin
gH
ospi
tal
Rep
etit
ion:
The
chec
klis
tdup
lica
tes
exis
ting
safe
typr
oced
ures
,fai
ling
toad
dan
ythi
ngto
the
syst
em.
30(2
5)I
thin
kth
epr
oble
mis
that
,wit
hit
bein
ga
stan
dard
ized
chec
klis
t,is
that
hosp
ital
sha
veth
eir
own
chec
klis
tsas
wel
land
you
end
upha
ving
two
orth
ree
chec
klis
ts,a
llch
ecki
ngth
esa
me
sort
ofth
ing
soyo
uge
tsom
eov
erla
p.O
DP,
Med
ium
Hos
pita
lW
hen
itw
asin
trod
uced
,no
one
look
edat
wit
hdra
win
gw
hatt
hech
eckl
isti
sre
plac
ing.
Sost
affn
owfil
lin
the
chec
klis
tand
ever
ythi
ngel
seth
eyus
edto
filli
nas
wel
l.A
tten
ding
Ane
sthe
siol
ogis
t,A
cute
Tea
chin
gH
ospi
tal
Tea
mfa
ctor
sR
esis
tanc
ean
dno
ncom
plia
nce:
Cer
tain
indi
vidu
als
wit
hin
the
team
mak
eit
very
diffi
cult
toco
mpl
ete
the
chec
klis
twit
hout
conf
ront
atio
n,or
cert
ain
indi
vidu
als
are
note
ngag
edin
the
chec
ks.
61(5
1)T
hech
eckl
isti
tsel
fis
very
easy
.Get
ting
the
answ
erto
som
eof
the
ques
tion
sfr
omth
esu
rgeo
nsan
dth
ean
aest
heti
sts
isn’
t,an
dth
at’s
the
fall
dow
n.O
DP,
Lar
geH
ospi
tal
Whe
nth
esu
rgeo
nsw
eren
’ton
boar
dyo
uw
ere
told
to“
ohsh
utup
and
let’s
geto
nw
ith
it.”
Dur
ing
intr
oduc
tion
sw
eha
dsu
rgeo
nslo
okup
and
say
“oh
God
,I’m
soan
dso
,Pri
nce
ofD
arkn
ess,
ifyo
udo
n’tk
now
me
byno
wge
tout
ofm
yop
erat
ing
room
.”O
pera
ting
Roo
mN
urse
,Sm
allH
ospi
tal
(Con
tinu
ed)
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
C© 2014 Lippincott Williams & Wilkins www.annalsofsurgery.com | 5
Russ et al Annals of Surgery � Volume 00, Number 00, 2014
TAB
LE3.
(Con
tinue
d)
Bar
rier
sN
(%)∗
Illu
stra
tive
Quo
tes
Too
l-sp
ecifi
cfa
ctor
s
Des
ign
prob
lem
s-co
nten
t/st
ruct
ure:
The
cont
enta
nd/o
rst
ruct
ure
ofth
ech
eckl
isti
sin
appr
opri
ate,
irre
leva
ntan
d/or
illo
gica
l.
40(3
4)It
asks
ques
tion
son
ther
ebu
twit
hout
any
defin
ite
answ
ers.
It’l
lask
abou
tthe
pati
ent’s
ASA
grad
e,so
you
just
tick
itan
dsa
yye
s.It
does
n’tm
enti
onw
hatt
heco
deis
orw
hatr
elev
ance
that
has
toan
ythi
ngor
anyt
hing
like
that
.So
it’s
abi
tbiz
arre
and
ther
e’s
ase
nse
of,I
’mno
tact
uall
ypr
ogre
ssin
gth
epa
tien
tcar
ew
ith
this
ques
tion
.O
DP,
Lar
geH
ospi
tal
Som
eof
the
ques
tion
sar
eli
kea
red-
rag
toa
bull
,lik
e“
are
you
expe
ctin
gth
eun
expe
cted
?”O
pera
ting
Roo
mN
urse
,Lar
geH
ospi
tal
The
reis
noco
lum
nfo
rth
eda
te—
Ith
ink
itre
quir
esda
tein
putb
ecau
seyo
uca
nha
veth
esa
me
pati
enth
avin
gre
peat
edsu
rger
y.O
DP,
Acu
teT
each
ing
Hos
pita
lN
otap
plic
able
toal
lsur
geri
es:
The
chec
klis
tis
nots
uita
ble
for
use
ince
rtai
nsp
ecia
ltie
san
d/or
cert
ain
type
sof
proc
edur
e(i
e,em
erge
ncie
s,da
y-ca
se).
33(2
8)W
here
peop
leha
veha
dpr
oble
ms
wit
hit
has
been
insp
ecia
ltie
sli
keop
htha
lmol
ogy.
Ikn
owpe
ople
have
said
itha
sbe
enov
erki
llfo
rth
em.
Att
endi
ngSu
rgeo
n,Sm
allH
ospi
tal
It’s
ali
ttle
too
rigi
dfo
rdi
ffere
ntki
nds
ofen
viro
nmen
t.Fo
rin
stan
ceda
ysu
rger
yit
was
ali
ttle
over
the
top
inth
atw
eou
ghtt
oha
veco
mbi
ned
som
eof
the
chec
ks,s
oth
ey’v
ew
alke
d50
yard
san
dth
enth
eyas
kth
emth
esa
me
ques
tion
sag
ain.
Att
endi
ngA
nest
hesi
olog
ist,
Acu
teT
each
ing
Hos
pita
lU
nsui
tabl
eti
min
gof
chec
ks:
Sec
tion
sof
the
chec
klis
tand
/or
indi
vidu
alit
ems
are
ill-
tim
ed.
32(2
7)A
ndit
’sdo
neto
ola
te.O
nce
that
pati
ent’s
onth
eta
ble,
anes
thet
ized
,and
then
you
find
that
you
have
n’tg
otth
epr
osth
esis
,or
the
bloo
ds,o
rth
eri
ghte
quip
men
t,it
’sto
ola
teis
n’ti
t?O
DP,
Med
ium
Hos
pita
lW
efin
dth
em
ostd
iffic
ultp
artt
oco
mpl
ete
isth
efin
alpa
rtof
it.T
hetr
ansf
erfr
omO
Rs
tore
cove
ry,l
ike
the
sign
-out
part
,bec
ause
that
’sa
very
very
busy
tim
e.O
pera
ting
room
nurs
e,M
ediu
mH
ospi
tal
Uni
nten
ded
nega
tive
effe
cts:
The
chec
klis
tca
nha
veun
inte
nded
nega
tive
effe
cts
onsu
rgic
alsa
fety
ifus
edas
ati
ck-b
oxex
erci
seor
ifit
crea
tes
fric
tion
wit
hin
the
team
20(1
7)In
som
eca
ses,
beca
use
ofth
eco
nflic
titc
reat
es,i
tsac
tual
lybe
enco
unte
rpro
duct
ive.
Att
endi
ngA
nest
hesi
olog
ist,
Smal
lHos
pita
lW
here
the
answ
erto
chec
ksis
in99
9ou
tof1
000
case
sa
“no
”or
“no
tapp
lica
ble,
”th
ete
amm
ight
beco
me
com
plac
enta
bout
the
chec
ksan
dus
eth
eto
olas
ati
ck-b
oxex
erci
se,f
aili
ngto
pick
upth
eon
eca
sew
here
the
answ
erw
asa
“ye
s.”
Thi
sis
harm
ful
beca
use
itde
-sen
siti
zes
staf
fand
aner
ror
can
occu
r.A
nest
hesi
olog
ist,
Reg
istr
ar,S
mal
lHos
pita
l.P
atie
ntpe
rcep
tion
s:To
om
any
chec
ksin
gene
ralm
ake
pati
ents
conc
erne
dth
atth
esy
stem
isn’
tsaf
e,an
dso
me
ofth
esp
ecifi
cch
ecks
are
anxi
ety
prov
okin
g.
17(1
4)O
neof
the
thin
gsth
atth
epa
tien
tsdo
n’tl
ike,
and
we’
veha
dth
isfr
omth
epa
tien
tsur
veys
we’
vedo
ne,i
sbe
ing
bom
bard
edw
ith
ques
tion
afte
rqu
esti
on,a
ndth
enha
veth
esa
me
ones
aske
dag
ain.
OD
P,L
arge
Hos
pita
lT
hetw
om
ain
area
sth
atal
way
sca
used
rais
edey
ebro
ws
wit
hpa
tien
tsar
edi
scus
sion
ofbl
ood
loss
,esp
ecia
lly
for
oper
atio
nsw
here
the
pati
entd
idn’
texp
ectt
obl
eed.
All
ofa
sudd
enth
eir
sim
ple
eye
oper
atio
nw
astu
rnin
gin
toa
pote
ntia
lblo
odba
than
da
thre
atto
thei
rli
fe,a
nddi
scus
sion
ofdi
fficu
ltai
rway
.T
rain
eeA
nest
hesi
olog
ist,
Acu
teT
each
ing
Hos
pita
lSc
epti
cism
rega
rdin
gth
eev
iden
ceba
se:
The
evid
ence
base
behi
ndth
ech
eckl
isti
sw
eak
and/
orno
tapp
lica
ble
toth
ecu
rren
tco
ntex
t.
13(1
1)I
thin
kit
’sa
knee
jerk
reac
tion
toth
epr
oble
man
dI’
mno
tsur
eth
ere’
sa
huge
amou
ntof
evid
ence
that
,wit
hin
the
cont
exto
fho
spit
als
inde
velo
ped
coun
trie
s,th
atit
wil
ldo
very
muc
h.A
tten
ding
Surg
eon,
Med
ium
Hos
pita
lIt
seem
sto
conc
entr
ate
enti
rely
onth
ings
for
whi
chth
ere
ispr
etty
dodg
yev
iden
ce.I
t’sse
lect
ive
inth
atth
ere
are
othe
rth
ings
todo
wit
hpr
even
ting
surg
ical
site
infe
ctio
ns,f
orw
hich
ther
eis
bett
erev
iden
ce,w
hich
are
nota
ddre
ssed
.A
tten
ding
Ane
sthe
siol
ogis
t,A
cute
Tea
chin
gH
ospi
tal
∗ N(%
)of
sam
ple
repo
rtin
gth
eba
rrie
r.
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
6 | www.annalsofsurgery.com C© 2014 Lippincott Williams & Wilkins
Annals of Surgery � Volume 00, Number 00, 2014 Implementing Change in Health Care: The WHO ChecklistTA
BLE
4.Fa
cilit
ator
sto
Che
cklis
tIm
ple
men
tatio
n
Faci
litat
ors
N(%
)∗Il
lust
rati
veQ
uote
s
Org
aniz
atio
nalf
acto
rs
1.E
duca
tion
/tra
inin
g:S
taff
buy-
inan
dow
ners
hip
ofth
ech
eckl
isti
sim
prov
edby
educ
atio
nan
dtr
aini
ngar
ound
its
evid
ence
base
,its
loca
lrel
evan
cean
dbe
stpr
acti
ce.
40(3
4)E
duca
tion
’spr
obab
lyth
em
osti
mpo
rtan
tthi
ng.E
duca
tion
prog
ram
sto
ever
ybod
y,no
tjus
tmed
ical
staf
f,bu
tope
rati
ngro
omst
affa
sw
ell.
Itne
eds
tobe
inco
rpor
ated
into
clin
ical
gove
rnan
ceda
ysor
som
ethi
ng,a
bout
why
you’
redo
ing
the
chec
klis
t,an
dw
hat
impr
ovem
ents
itha
sm
ade.
Ane
sthe
siol
ogis
t,C
T1–
3,Sm
allH
ospi
tal.
We
shou
ldha
veal
lhad
trai
ning
init
,exp
lain
ing
wha
tthe
yw
ant,
why
itw
asim
port
ant,
why
they
wan
ted
usto
doit
,and
how
tode
alw
ith
resi
stan
ttea
mm
embe
rs.
Ope
rati
ngR
oom
Nur
se,L
arge
Hos
pita
l2.
Feed
back
onlo
cald
ata:
Reg
ular
feed
back
oflo
cald
ata
and
anec
dota
lev
iden
cesu
ppor
ting
abe
nefi
cial
impa
ctof
the
chec
klis
trei
nfor
ces
that
itis
notj
usta
tick
-box
exer
cise
.
36(3
0)I
thin
kth
atif
you
coul
dpr
oduc
eda
tato
show
that
unto
war
dev
ents
are
bein
gre
duce
dlo
call
y,ev
enin
the
rela
tive
lysh
ortt
ime
it’s
been
roll
edou
t,I
thin
kth
atw
ould
galv
anis
epe
ople
into
usin
git
.A
tten
ding
Surg
eon,
Med
ium
Hos
pita
lW
hatI
’mst
arti
ngto
dono
wis
ask
peop
leto
reco
rdw
hen
itfla
gsso
met
hing
up,s
oI
can
stan
dup
ata
staf
fmee
ting
once
am
onth
and
say
the
surg
ical
safe
tych
eckl
istt
his
mon
thha
spr
even
ted
16ne
arm
isse
s-
this
wou
ldpr
omot
eit
sus
eev
enm
ore.
Ope
rati
ngR
oom
Man
ager
(Nur
se),
Med
ium
Hos
pita
l3.
Acc
ount
abili
tyfo
rno
n-co
mpl
ianc
e:R
amifi
cati
ons
for
activ
eno
ncom
plia
nce
wit
hth
ech
eckl
ista
rede
sire
dan
dth
ough
tto
impr
ove
effe
ctiv
enes
sof
the
tool
.
18(1
5)A
noth
erth
ing
that
coul
dbe
done
isth
ehi
gher
man
agem
entc
ould
star
tto
have
teet
h,if
you
like
,sta
rtto
take
peop
leas
ide
and
say,
you
doth
is,o
rel
se,b
utyo
udo
find
inm
edic
alpr
ofes
sion
sth
atdo
esn’
thap
pen
muc
h.A
tten
ding
Ane
sthe
siol
ogis
t,M
ediu
mH
ospi
tal
The
orga
niza
tion
now
have
puto
utth
atif
the
WH
OC
heck
list
isn’
tdon
ean
dth
ere’
spe
ople
resi
stin
g,th
esu
rgeo
nsan
dth
est
affc
ange
trep
orte
dto
thei
rre
gist
ered
bodi
es.I
t’sa
thre
at,b
utit
wor
ks.
Ope
rati
ngR
oom
Man
ager
(Nur
se),
Med
ium
Hos
pita
l4.
Supp
ort
from
hosp
ital
man
agem
ent:
Vis
ible
,flex
ible
and
activ
esu
ppor
tfro
mho
spit
alm
anag
emen
tdur
ing
impl
emen
tati
onan
dbe
yond
rein
forc
esth
eim
port
ance
ofus
ing
the
chec
klis
t.
9(8
)M
anag
emen
thav
eto
play
ali
ttle
,man
agem
entm
eans
the
man
ager
s,no
tthe
doct
ors,
they
have
tosh
owcl
inic
ians
allo
ver
the
hosp
ital
that
this
isno
tjus
tthe
irjo
b,bu
tour
job
toge
ther
.A
tten
ding
Ane
sthe
siol
ogis
t,A
cute
Tea
chin
gH
ospi
tal
It’s
afe
wdi
nosa
urs
that
we
have
,but
the
chie
fexe
cuti
veat
this
hosp
ital
istr
ying
toau
ditn
owth
roug
hou
rop
erat
ing
room
man
agem
ents
yste
mso
that
she
can
try
and
addr
ess
it.
Ope
rati
ngR
oom
Man
ager
(Nur
se),
Smal
lHos
pita
l
Syst
ems
fact
ors
5.In
tegr
atio
nw
ith
exis
ting
proc
esse
s:T
hech
eckl
ists
houl
dbe
inco
rpor
ated
into
exis
ting
pape
rwor
k/pr
oces
ses
tost
ream
line
and
rem
ove
repe
titi
on.
19(1
6)It
coul
dbe
impr
oved
byfu
lly
inte
grat
ing
itin
toso
me
sort
ofpe
ri-o
pera
tive
path
way
,whi
chw
ould
redu
ceth
edu
plic
atio
nth
atex
ists
.A
tten
ding
Ane
sthe
siol
ogis
t,Sm
allH
ospi
tal
We
now
prin
tito
nth
eba
ckof
our
pre-
opch
eckl
ist,
soit
’sth
enju
ston
esh
eet.
It’s
now
ona
care
plan
we
also
tick
that
we’
vedo
neit
,so
we’
vego
tevi
denc
eth
atw
e’ve
done
itif
that
shee
tis
also
lost
.O
pera
ting
Roo
mN
urse
,Med
ium
Hos
pita
l
Tea
mfa
ctor
s6.
Seni
orcl
inic
albu
y-in
:W
hen
seni
orsu
rgeo
nsan
dan
esth
esio
logi
sts
driv
eus
eof
the
chec
klis
titi
sus
edm
ore
effe
ctiv
ely.
27(2
3)I
thin
kth
edr
ivin
gfo
rce
has
tobe
from
the
seni
orst
aff,
seni
orsu
rgeo
n,se
nior
anes
thes
iolo
gist
,Att
endi
ngs.
Ifth
eyta
keit
seri
ousl
yev
eryb
ody
does
.Ify
ouse
eth
egu
yon
top
moc
king
it,n
obod
yel
seis
goin
gto
stan
dup
for
it-
nom
atte
rho
wm
uch
we
try
toki
llth
ehi
erar
chy,
Ith
ink
abi
tofi
tmay
stil
lrem
ain.
Tra
inee
Surg
eon,
Smal
lHos
pita
lT
hat’s
beca
use
Ipa
rtic
ular
lydi
dw
ork
wit
hon
eA
tten
ding
surg
eon
who
isin
favo
urof
the
WH
Och
eckl
ista
ndhe
has
been
able
toim
prov
eup
onev
eryb
ody
abou
tthe
impo
rtan
ceof
the
form
.Onc
ew
ege
tthe
surg
ical
team
onbo
ard
it’s
hist
ory
and
itflo
ws
for
ever
yone
.T
rain
eeA
nest
hesi
olog
ist,
Med
ium
Hos
pita
l7.
Lea
ders
hip
skill
s:S
tron
gin
divi
dual
lead
ersh
ipsk
ills
and
pass
iona
tele
ader
sen
gend
erpa
rtic
ipat
ion
from
the
rest
ofth
ete
am.
26(2
2)It
’sab
outa
sser
tive
ness
atth
een
dof
the
day,
you
don’
thav
eto
beag
gres
sive
,but
you
have
tobe
asse
rtiv
ebu
tfirm
,and
give
them
reas
ons
why
you’
resa
ying
wha
tyou
’re
sayi
ng.
OD
P,A
cute
Tea
chin
gH
ospi
tal
Som
epe
ople
are
muc
hbe
tter
atit
than
othe
rs.S
ome
peop
leha
vego
tacl
ear
voic
e,th
ey’r
eco
mm
itte
dto
doin
git
and
they
doit
form
ally
.Oth
erpe
ople
notr
eall
yin
toit
,the
ym
umbl
e,th
eyan
swer
thei
row
nqu
esti
ons,
whi
chco
mpl
etel
yta
kes
away
the
safe
tyas
pect
ofit
.A
tten
ding
Surg
eon
Smal
lHos
pita
l(C
onti
nued
)
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
C© 2014 Lippincott Williams & Wilkins www.annalsofsurgery.com | 7

Russ et al Annals of Surgery � Volume 00, Number 00, 2014
TAB
LE4.
(Con
tinue
d)
Faci
litat
ors
N(%
)∗Il
lust
rati
veQ
uote
s
8.In
volv
ing
the
enti
reO
Rte
am:
Invo
lvem
ento
fal
ltea
mm
embe
rsin
the
impl
emen
tati
onan
dm
odifi
cati
onof
the
chec
klis
tim
prov
esup
take
.
18(1
5)I
thin
kth
eyne
edto
actu
ally
geta
who
lebu
nch
ofpe
ople
from
diffe
rent
back
grou
nds
inan
dsa
y,w
hich
bits
ofth
isdo
and
don’
twor
kfo
ryo
u?T
here
isob
viou
sly
ave
rysu
rgic
ally
desi
gned
form
,the
yne
edm
ore
inpu
tfro
man
esth
esio
logi
sts
and
muc
hm
ore
inpu
tfr
omnu
rsin
gst
aff.
Att
endi
ngA
nest
hesi
olog
ist,
Acu
teT
each
ing
Hos
pita
lSt
affw
ere
brou
ghti
nea
rly
on.I
twas
actu
ally
disc
usse
dat
staf
flev
elas
toho
ww
ew
ere
goin
gto
doit
,and
soth
eyw
ere
alli
nvol
ved
from
the
very
begi
nnin
gan
dso
Ith
ink
from
enga
ging
them
it’s
actu
ally
enco
urag
edth
eir
invo
lvem
enta
ndI
thin
kit
’sbe
enac
cept
edac
ross
allo
pera
ting
room
sin
the
hosp
ital
.O
pera
ting
Roo
mM
anag
er(N
urse
),Sm
allH
ospi
tal
Too
l-sp
ecifi
cfa
ctor
s9.
Mod
ifica
tion
/ada
ptat
ion:
Ow
ners
hip
and
effe
ctiv
eus
eof
the
chec
klis
tim
prov
edby
cust
omiz
atio
nof
the
layo
utan
d/or
cont
ent
toth
esp
ecifi
csu
rgic
alco
ntex
t.
67(5
6)So
we
use
diffe
rent
vers
ions
ofth
ech
eckl
istd
epen
ding
onth
esu
rgic
alsp
ecia
lty
and
role
.And
that
’sm
ade
abi
gdi
ffere
nce
toac
cept
ance
beca
use
wha
tpeo
ple
real
lydi
dn’t
like
abou
tita
tthe
begi
nnin
gw
asth
eon
esi
zefit
sal
lapp
roac
h.A
tten
ding
Ane
sthe
siol
ogis
t,Sm
allH
ospi
tal
Wel
lwe’
reev
olvi
ngit
now
toa
whi
tebo
ard,
soth
atw
ew
illm
ark
iton
aw
hite
boar
dra
ther
than
phys
ical
lyst
and
ther
ew
ith
ash
eet
inou
rha
nd,b
ecau
seI
thin
kth
at’s
wha
tsen
dssu
rgeo
nsan
dan
aest
hesi
olog
ists
cold
real
ly,r
eadi
ngfr
oma
set.
Soit
’sli
kean
aide
mem
oire
inO
Rno
was
oppo
sed
toa
list
.Itm
akes
peop
leth
ink
abi
tmor
e.O
pera
ting
Roo
mM
anag
er(N
urse
),M
ediu
mH
ospi
tal
∗ N(%
)of
sam
ple
repo
rtin
gth
efa
cili
tato
r.
loss and difficult airway (part of the sign-in checks) would be anxietyprovoking for certain patients (this was a particular concern if thepatient was undergoing a local anesthetic procedure and thereforewitnessed all of the checks). Some also felt that the evidence basebehind the checklist was not robust enough, either in general or withregard to the English health care system specifically (eg, several in-terviewees mentioned that English hospitals were noncomparable tothe developing world hospitals that showed the largest improvementin outcomes after introduction of the checklist in the pilot study).5
Finally, 20% of the sample raised the issue that when not used inthe intended manner the checklist could have unintended negativeeffects on care, making it paradoxically less safe for the patient. Forexample, if used as a tick-box exercise with limited buy-in from staff,the checklist could create a false sense of security and, over time,result in complacency—inadvertently causing diminished levels ofteam vigilance in the OR. In addition, staff might be distracted fromtheir routine safety processes if the checklist was initiated at an inap-propriate time, or indeed resistant individuals might cause animosityamong team members having a negative impact on teamworking andteam cohesion.
Facilitators
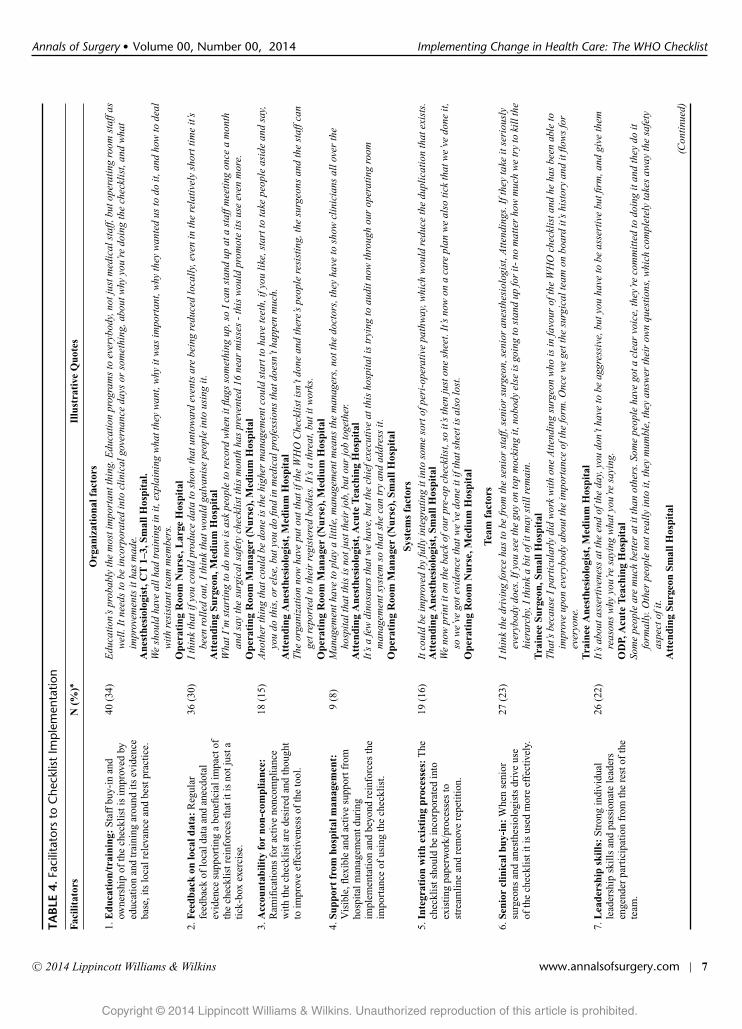
Organizational FacilitatorsFour of the 9 facilitators to checklist implementation repre-
sented organizational factors. A third of the sample reported that theprovision of education and training around the checklist would be apowerful facilitator to its successful implementation. Many expresseda desire to be provided with information about the background to itsdevelopment, the evidence supporting its efficacy and why it wasrelevant to the context of their local OR. Similarly, training sessionsteaching best practice in use of the tool and/or how to deal with re-sistant team members when carrying out the checks were suggested.A comparable proportion of respondents felt that the regular provi-sion of data and feedback (eg, at audit days) regarding benefits thatthe checklist was achieving locally (eg, reductions in complicationsand incidents, improved outcomes, anecdotal clinical stories of nearmisses prevented by the checklist) would significantly increase buy-in to the tool, particularly for those doubting its relevance to EnglishORs. Next, 15% of the sample expressed the desire for there to beconsequences for noncompliance with the checklist such that resis-tant individuals are held accountable at a management level for theiractions. However, it was also mentioned that this kind of enforcedaccountability was rare in the medical profession (although it wasmore applicable to OR nurses). Finally, and related to this, 15% ofstaff mentioned that there being visible support and alignment fromhospital management around the checklist during implementationand beyond was critical to gaining buy-in from frontline staff, be-cause it emphasized that the initiative was a priority throughout theorganization.
Systems FacilitatorsA number of respondents (16%) reported that use of the check-
list could be facilitated by integrating it with existing paperwork andprocesses (eg, integrating it into the patient care plan to avoid lots ofloose pieces of paper and removing existing checks that the checklistwas replicating)—acting to reduce the feeling of too much repetitionand extra workload.
Team FacilitatorsThree facilitators were associated with the OR team and how
they drove use of the checklist. First, participants (22%) reportedthat the checks were completed best when the person leading themhad strong leadership skills and an assertive presence in the OR.
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
8 | www.annalsofsurgery.com C© 2014 Lippincott Williams & Wilkins
Annals of Surgery � Volume 00, Number 00, 2014 Implementing Change in Health Care: The WHO Checklist
This meant that any resistance could be overturned and the entireteam was more likely to engage and listen rather than the checkssimply “happening” in the background. “Checklist champions” (pas-sionate individuals who promoted the tool on the ground and actedas a “go-to” point for queries) were also described as powerful fa-cilitators to uptake. Second, and related to this, an optimal conditionaccording to approximately a quarter of the sample, was if seniorclinicians (ie, surgeons and anesthetists at Attending level) showedvisible leadership of the checklist. In particular, if Attending surgeonsand anesthesiologists led the checks themselves or actively drove useof the checklist, it was said to foster engagement from the team as awhole and impress on everyone the significance of the tool. Finally,although senior clinical leadership was thought to be a key, inclusiveinput around the introduction and customization of the checklist fromthe entire multidisciplinary team was also reported to be important.
Checklist-Specific FacilitatorsThe most commonly reported facilitator to implementation of
the checklist (by 56% of the sample) was modification of the tool tosuit the specific surgical context and/or to make it more user-friendly.A number of respondents reported that the checklist had been suc-cessfully adapted to suit a particular surgical specialty (either throughlocal customization or by adopting one of the modified versions madeavailable by the NPSA), and others outlined more general customiza-tions that had been made to the tool, for example, displaying thechecklist on the OR wall rather than using the paper form (which wasperceived to make it less of a tick-box exercise and more of a safetydiscussion).
What Lessons Can We Extract for Informing How toOptimize the Diffusion and Uptake of ImprovementInitiatives in Surgery/Health Care?
On the basis of the themes extracted from OR personnels’ com-ments, a set of guidelines have been put together that apply broadlyto the implementation of improvement within health care systemsand indicate the strategies that should be considered during the earlyphases of introducing an improvement initiative (Box 1).
Box 1. Lessons for Implementing Change inHealth Care
A plan for implementation should be devised before in-troduction of the initiative, which is tailored toward all relevantstakeholders (aligning all levels of the organization) and takesinto account unusual shift patterns etc. Practical steps that shouldbe considered when formulating this plan are as follows:
� Modification of the initiative to suit the local context is veryimportant (2 or more different versions of the tool or processmay be required). Modifications should focus on how best tointegrate the initiative within existing processes to streamlineand remove repetition. The focus should be making the initia-tive user-friendly. Frontline staff involvement in the processof modification is key for optimizing buy-in.
� Education around the evidence base for the improvement ini-tiative is critical. This education should be tailored to reach allstakeholders and be should hold relevance to the local teamsand organization. Education should include an emphasis ofthe reasons why there is a need for the improvement in thefirst place.
� Training on the practical application of the improvementshould be included. This should focus both on the optimalday to day use of the initiative as well as how to deal with re-sistant members of staff or other potential barriers that mightemerge. Training should be multidisciplinary, rather than be-ing delivered to different professional groups independently.
� Data highlighting the local impact of the initiative should befed-back to staff periodically. This will reinforce the personalrelevance of the initiative for local teams. Anecdotal staffstories highlighting the benefits of the initiative are particu-larly powerful and should be shared within multidisciplinaryforums.
� Champions or early adopters should be identified, elected,and nurtured to promote uptake of the initiative on the groundand to act as a “go to” point for queries around implemen-tation. Social forums or communication channels by whichthese individuals might influence others should be supported.
� Buy-in from senior clinical staff should be sort at the veryearly stages of implementation. Senior staff members are par-ticularly powerful advocates for the introduction of changeand should be harnessed wherever possible to communicateto others their commitment to the new initiative, setting theexample from the top.
� Management should be seen to be involved and support-ive of frontline staff during introduction of the initiative andbeyond, such that it is seen as an organizational priority fromthe outset and all levels of the organization are aligned on acommon goal.
� A system that holds people accountable for improper be-havior or use of the initiative should be considered.
� Auditing of the initiative should be carefully thoughtthrough such that the “how” it is being used can be capturedas well as the “if.” Observations of the use of the initiative inpractice are strongly encouraged. This will inform on specificlocal barriers and facilitators surrounding its use, whether it isbeing used in the intended manner and whether there are anyunintended consequences of its introduction. It will also aidthe provision of comprehensive feedback to team membersfor quality improvement.
DISCUSSIONThis study was part of a national evaluation of the imple-
mentation of the WHO surgical safety checklist across England (theSurgical Checklist Implementation Project). To our knowledge, thisqualitative study is the first of its kind and size to be reported, coveringa representative sample of English hospitals. It aims to understand thebehaviors and strategies that have led to successful implementationof the checklist, and those that have hindered it. Thus, it aims to in-form practical steps that hospitals might take to better embed the toolinto practice and to extract lessons to reduce current variation andbetter inform the implementation and uptake of quality improvementinitiatives more generally.16–18
Key FindingsThere was large variation in how the checklist was initially
implemented, both between and within hospitals. This ranged fromapparently very well-orchestrated strategies in some hospitals, to
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
C© 2014 Lippincott Williams & Wilkins www.annalsofsurgery.com | 9

Russ et al Annals of Surgery � Volume 00, Number 00, 2014
others, where the checklist simply appeared without prior warning,or staff felt like it was being imposed upon them. Although there wasguidance available for implementing the initiative (from the NPSA),not all hospitals utilized this effectively. This is important becausea poor implementation strategy was identified as an important or-ganizational barrier to effective uptake of the checklist. For safetyand quality interventions to realize their potential benefit, a concrete,multiphased implementation plan needs to be developed before theirintroduction.
Numerous additional barriers and facilitators to checklist im-plementation emerged from the interviews, which included organi-zational and system-, team-, and checklist-specific factors. The ma-jority of the barriers concerned the checklist itself (eg, perceiveddesign issues and doubts surrounding the evidence), but duplicationof processes and difficulties in integrating the checklist with existingsystems were also reported. The most common barrier was resistanceor noncompliance from individual members of the OR team (particu-larly at Attending level), which in many cases prevented the checklistfrom being used in the manner it was intended. This supports recentobservational data, which demonstrates poor compliance with thechecklist in practice.19 The checklist is essentially an aid to enhanceteam performance, communication, and vigilance; however, here ithas been demonstrated that when poorly or improperly used withoutadequate buy-in it can adversely affect the OR team.20
The facilitators that emerged demonstrate the positive andproactive strategies that have been developed to mitigate the vari-ous barriers and greatly increase the chances of proper use of thechecklist and of full implementation. These centered around modify-ing the tool to suit the local context to complement existing systems;conveying the relevance and importance of the tool to local teams andindividuals (through education/training and feedback of local data);identifying strong leaders and advocates for the initiative (particularlyat Attending level); considering methods of instilling accountability;and aligning strategic priorities across the hospital (from frontline per-sonnel to hospitals’ executive boards). These steps are evidenced byquotations from the sample and are in line with previous literature.14
They form the basis of our recommendations (Box 1) and should beincorporated into local efforts to aid implementation of the checklistand other surgical safety initiatives.
Strengths and LimitationsThe current study has certain limitations. The number of hos-
pitals from which participants were sampled is small compared tothe overall number of English hospitals, thereby potentially limitinggeneralizability. Furthermore, the opt-in sampling strategy may meanthat we have captured the individuals with the strongest views (eitherpositive or negative) around the checklist and who are most passionateabout sharing them, meaning that we may have missed some valuablefeedback from those who are more impartial. In addition, for practi-cal reasons, data collection took place over the period of 1 year afterthe official national deadline for implementing the checklist, whichmeans that some respondents will have been using the checklist forlonger than others at the time of interview; this could have influ-enced some of the responses we collected. We did, however, examinethe themes extracted from earlier versus later interviews and fromearlier versus later implementers and found no apparent patterns ordifferences distinguishing these groups. We therefore conclude thatfactors associated with the timeline of the study are not likely to haveaffected our dataset. Finally, we have captured the views of OR per-sonnel only, and while this is important it might also be instructive tocapture the views of managerial staff and the views of those from thewider regulatory bodies who were involved in implementation of thechecklist, such as the Department of Health. This would provide apotentially fuller picture of the challenges and enablers encountered
throughout the process of implementation. The current research alsohas some notable strengths. First, to the best of our knowledge, thisis the first nationally representative evaluation of the checklist witha multicenter hospital sample and therefore these findings are gener-alizable to a certain level. The themes revealed by this study likelyrepresent the barriers and facilitators at play during the implemen-tation of many change initiatives in health care and hence present avaluable learning opportunity. Second, the qualitative approach un-dertaken allowed for a detailed analysis of the barriers and facilitatorstoward implementation of the checklist, which would not have beenpossible using a broader survey approach. The accounts generatedfrom the interviews were detailed, and reaching saturation in the the-matic extraction of these interviews suggests that the analysis wasexhaustive. Finally, theme extraction was reviewed and checked by2 psychologists with expertise in both the methodology and patientsafety research, to ensure accuracy and control of bias in the analysis.
Future DirectionsSimilar barriers and facilitators to the implementation of the
checklist have been previously identified as factors influencing theimplementation of change in health care and also in other industries,and as such have been translated into recommendations for imple-mentation already.21–23 This presents the difficult question—why aresome institutions failing to take advantage of existing knowledge andguidelines about how to introduce an intervention successfully? Thecentralized structure of the English health care system should allowthe introduction of improvement initiatives, with the potential to pos-itively influence the care of millions of patients, but interventionsoften struggle to achieve full implementation.24 Further systematicresearch can shed light on what differentiates teams and organizationsthat employ an effective implementation strategy from those who failor struggle.
In addition, although getting the implementation strategy rightis key in order for an initiative such as the checklist to fulfil its poten-tial (or conversely to avoid unintended negative impacts on safety),ultimately it must be demonstrated that this variation in implemen-tation has tangible and sustained impacts on patient care at the locallevel. This means that continuous evaluation of an intervention shouldbe part of its implementation (and not an afterthought). Locally col-lected data are more personally relevant and more persuasive to clin-ical teams—and indeed if we are to shift to a culture of intelligentdata usage aimed at continuous quality and safety improvement, wetake the view that data ought to be collected, fed-back, and discussedregularly. This study clearly demonstrates that not doing so ultimatelyjeopardizes buy-in, which we believe applies not just to the checklistbut to any such intervention. It is therefore important to focus ef-forts on developing methods by which the impact of the checklist ondaily, case-by-case team performance can be captured and fed-backto teams. Routinely collected data, observations as well as anecdotalexamples, and clinical stories relating to the benefits brought aboutby the checklist all have a role to play.
CONCLUSIONSThe WHO surgical safety checklist was a high profile and
mandatory safety improvement initiative that was required to be im-plemented throughout English ORs. This nationally representativestudy has identified a large degree of variation in the approach takento introduce the checklist and a number of factors representing bar-riers and facilitators to the success of the implementation across 10hospitals. We have translated these findings into a number of lessonsthat should be considered when implementing change in surgery andhealth care more broadly. Implementation guidance should includeexplicit attention to barriers and facilitators and the developmentof a proactive implementation strategy at a local level. Local data
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
10 | www.annalsofsurgery.com C© 2014 Lippincott Williams & Wilkins

Annals of Surgery � Volume 00, Number 00, 2014 Implementing Change in Health Care: The WHO Checklist
collection and feedback in relation to how initiatives like the check-list work in practice will also be necessary to engage clinical teamsand to highlight areas where further intervention or training is needed.
ACKNOWLEDGMENTSThe authors thank the following individuals who formed the
advisory board for the project: Mr Kevin Cleary, National PatientSafety Agency, UK; Mr Graham Copeland, Warrington and HaltonNHS Trust, UK; Mr Mark Emerton, Leeds Teaching Hospitals NHSTrust, UK; Mr Derek Fawcett, The British Association of UrologicalSurgeons; Professor Atul Gawande, Harvard Medical School, US;Alan Glanz, Department of Health, UK; Professor Michael Horrocks,Association of Surgeons of Great Britain and Ireland; Dr Judith Hulf,Royal College of Anaesthetists, UK; Sir Bruce Keogh, Medical Di-rector, National Health Service, UK; Professor Ravi Mahajan, RoyalCollege of Anaesthetists, UK; Miss Clare Marx, Royal College ofSurgeons of England; Claudia Mcmonagle, Patient Representative,UK; Professor Peter Pronovost, Johns Hopkins Medicine, US; Pro-fessor James Reason, University of Manchester, UK; and ProfessorJane Reid, The International Federation of Perioperative Nurses.
REFERENCES1. World Health Organization. Safe surgery saves lives: second global pa-
tient safety challenge. WHO Web site. Available at: http://www.who.int/patientsafety/safesurgery/knowledge base/SSSL Brochure finalJun08.pdf .Published 2008. Accessed April 13, 2014.
2. World Health Organization. WHO surgical safety checklist. WHO Web site.Available at: http://www.who.int/patientsafety/safesurgery/tools resources/SSSL Checklist finalJun08.pdf . Published 2008. Accessed April 13, 2014.
3. World Health Organization. Implementation manual WHO surgical safetychecklist 2009. WHO Web site. Available at: http://whqlibdoc.who.int/publications/2009/9789241598590 eng.pdf . Published 2009. Accessed April13, 2014.
4. Gawande A. The Checklist Manifesto: How to Get Things Right. New YorkCity, NY: Metropolitan Books of Henry Holt and Co; 2011.
5. Haynes AB, Weiser TG, Berry WR, et al. A surgical safety checklist toreduce morbidity and mortality in a global population. New Engl J Med.2009;360:491–499.
6. Modified version of the WHO checklist for UK. National Reporting and Learn-ing Web site. Available at: http://www.nrls.npsa.nhs.uk/resources/?EntryId45=59860. Published 2009. Accessed on April 13, 2014.
7. Guidance on implementation and correct use of the checklist. Na-tional Reporting and Learning Web site. Available at: http://www.nrls.npsa
.nhs.uk/resources/?EntryId45=59860. Published 2009. Accessed March 13,2014.
8. Patient Safety First Campaign. Patient Safety First Web site. 2008. Availableat: http://www.patientsafetyfirst.nhs.uk/Content.aspx?path=/Campaign-news/current/WHOSafeSurgeryChecklist/. Accessed April 13, 2014.
9. Joint Commission information on implementation of surgical safety checklist.Joint Commission Web site. Available at: http://www.jointcommission.org/standards information/up.aspx. Published 2012. Accessed April 13, 2014.
10. Hutchinson A, Young TA, Cooper KL, et al. Trends in healthcare incidentreporting and relationship to safety and quality data in acute hospitals: resultsfrom the National Reporting and Learning System. Qual Saf Health Care.2009;18:5–10.
11. Taylor-Adams S, Vincent C. Systems Analysis of Clinical Incidents: The Lon-don Protocol. London, UK: Clinical Safety Research Unit, Imperial CollegeLondon.
12. Vincent C, Taylor-Adams S, Chapman EJ, et al. How to investigate and analyseclinical incidents: Clinical Risk Unit and Association of Litigation and RiskManagement Protocol. BMJ. 2000;320:777–781.
13. Fourcade A, Blache JL, Grenier C, et al. Barriers to staff adoption of a surgicalsafety checklist. BMJ Qual Saf. 2012;21:191–197.
14. Russ S, Rout S, Sevdalis N, et al. Do safety checklists improve teamworkand communication in the operating theatre? A systematic review. Ann Surg.2013;258:856–871.
15. Conley DM, Singer S, Edmondson L, et al. Effective surgical safety checklistimplementation. JAMA. 2011;212:873–879.
16. Ovretveit J. Understanding the conditions for improvement: research to dis-cover which context influences affect improvement success. BMJ Qual Saf.2011;20(suppl 1):i18–i23.
17. Alexander J, Herald L. The science of quality improvement implemen-tation: developing capacity to make a difference. Med Care. 2011;49:S6–S20.
18. Kaplan H, Provost L, Froehle CM, et al. The Model for understanding suc-cess in quality (MUSIQ): building a theory of context in healthcare qualityimprovement. BMJ Qual Saf. 2012;21:13–20.
19. Pickering SP, Robertson ER, Griffin D, et al. Compliance and use of theWorld Health Organization checklist in UK operating theatres. Br J Surg.2013;100:1664–1670.
20. Whyte S, Lingard L, Espin S, et al. Paradoxical effects of interprofessionalbriefings on OR team performance. Cogn Technol Work. 2008;10:287–294.
21. Berwick D. Disseminating innovations in health care. JAMA. 2003;289:1969–1975.
22. Rogers EM. Diffusion of Innovations. 5th ed. New York, NY: Free Press; 2003.23. Wilson CB. Adoption of a new surgical technology. BMJ. 2006;332:112–114.24. Ranji SR, Shojania KG. Implementing patient safety interventions in your
hospital: what to try and what to avoid. Med Clin North Am. 2008:92:275–293.
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
C© 2014 Lippincott Williams & Wilkins www.annalsofsurgery.com | 11