A preliminary report of an outbreak of kala-azar in a battalion of king's African rifles*1
10
TRANSACTIONSOF THE ROYAL SOCIETYOF TROPICAL MEDICINE AND HYGIENE. Vol. XXXVI. No. I. June, 1942. 25 A PRELIMINARY REPORT OF AN OUTBREAK OF KALA-AZAR IN A BATTALION OF KING'S AFRICAN RIFLES. BY A. C. E. COLE, M.D., M.R.C.P., MAIOR E.A.A.M.C. * P. C. COSGROVE, M.B., M.R.C.P., CAPT. R.W.A.F.F., AND G. ROBINSON, M.B., DIP.BACT. (LoNo,), ~fAIOR R.W.A.F.F. INTRODUCTION. The occurrence of an outbreak of kala-azar in a K.A.R. battalion which has been operating in Northern Kenya is described. This preliminary report is presented, in its present incomplete form, because although kala-azar has been adequately described in the Sudan, little.is known of the disease in Kenya or in Abyssinia. Now that bodies of troops are moving about these areas, it is hoped that a description of this outbreak may make clear the possibility and the danger of infection and may help in diagnosis at a more early stage of the disease. Thirty cases of the disease have occurred in the battalion in question and one in an auxiliary unit ; and since all were under medical care from the outset a more accurate picture of the disease can be obtained than would be possible from the study of sporadic cases entering civil hospitals. The entire * We are indebted to the DIRECTOR OF MEDICAL SERVICE.S, East Africa Command, for permission to publish this paper, and to Col. A. D. J. B. WILLXAMS, the C.O. of the hospital. The clinical observations were made by the first two authors (A.C.E.C. and P.C.C.) and the laboratory observations by the third (G.R.).
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of A preliminary report of an outbreak of kala-azar in a battalion of king's African rifles*1
TRANSACTIONS OF THE ROYAL SOCIETY OF TROPICAL MEDICINE AND HYGIENE. Vol. XXXVI. No. I. June, 1942.
25
A PRELIMINARY REPORT OF AN OUTBREAK OF KALA-AZAR IN A BATTALION OF KING'S AFRICAN RIFLES.
BY
A. C. E. COLE, M.D., M.R.C.P., MAIOR E.A.A.M.C. * P. C. COSGROVE, M.B., M.R.C.P., CAPT. R.W.A.F.F.,
AND
G. ROBINSON, M.B., DIP.BACT. (LoNo,), ~fAIOR R.W.A.F.F.
INTRODUCTION.
The occurrence of an outbreak of kala-azar in a K.A.R. battalion which has been operating in Northern Kenya is described. This preliminary report is presented, in its present incomplete form, because although kala-azar has been adequately described in the Sudan, little.is known of the disease in Kenya or in Abyssinia. Now that bodies of troops are moving about these areas, it is hoped that a description of this outbreak may make clear the possibility and the danger of infection and may help in diagnosis at a more early stage of the disease.
Thir ty cases of the disease have occurred in the battalion in question and one in an auxiliary unit ; and since all were under medical care from the outset a more accurate picture of the disease can be obtained than would be possible from the study of sporadic cases entering civil hospitals. The entire
* We are indebted to the DIRECTOR OF MEDICAL SERVICE.S, East Africa Command, for permission to publish this paper, and to Col. A. D. J. B. WILLXAMS, the C.O. of the hospital.
The clinical observations were made by the first two authors (A.C.E.C. and P.C.C.) and the laboratory observations by the third (G.R.).
26 KALA-AZAR.
history of the unit can be traced and the time of entry into the probable area of infection is known as well as the" approximate date of the onset of symptoms. In these circumstances the length of the incubation period can be assessed with a fair degree of accuracy.
The study of these cases has revealed certain inconsistencies in the usual description of kala-azar and definite difficulties in laboratory diagnosis in the early stages of the disease. So far in only some of the cases of the series has the diagnosis been confirmed by the discovery of .the parasite, while only a few have been cured.
Though literature on the subject is not available it is felt that there is sufficient justification for presenting this preliminary report.
HISTORY AND EPIDEMIOLOGY.
The battalion was recruited in July, 1940, mainly from the Wakamba and Kipsigis tribes. It was in training in the Nairobi area until 5th December, 1940. No cases of kala-azar have been reported from these areas during the past five years. From 5th to 12th December the battalion was travelling to the northern Lake Rudolph area (Turkana) and reached Kal in on the 12th. It remained in the area Kalin-Lokitaung until 10th February, 1941. This district is dry and there were no mosquitoes, but flies were numerous.
On 10th February it moved to the area Todenyang-Namaraputh on the shore of the northern end of the lake, near to a point where the frontiers of Kenya, the Sudan and Abyssinia meet. Here there are grassy mudflats and reeds, the heat is humid and flies and mosquitoes occur.
From 6th to 19th March the battalion moved in convoy to Nanyuki and then returned to Kalin, where it remained one week.
On 30th March it moved to Kibesh Wells on the Kibesh river, a humid district with numerous mosquitoes, both anopheline and culicine.
" A " Coy. of the battalion remained at Kibesh Wells not more than three nights and then moved on to Washwaha at the foot of the Maji escarpment.
The battalion moved to Todenyang on 18th May, except " D " Coy., which went to Kalam, a district 20 miles north of Todenyang in low lying ground near the Omo river, and " B " Coy., which was at Shunguru.
On 1st June the whole battalion concentrated at Todenyang and then returned by Lokitaung and Kitale to Nyeri.
ADMISSION AND DIAGNOSIS.
When the battalion became exposed to the cold and damp of its camp near Nyeri there was an outbreak of respiratory disease of influenzal type, and a number of cases of malaria also declared themselves. In addition to these, from the second half of June onwards, there were admitted to hospital a number of cases which, did not conform to any known type of disease.
A. C. E. COLE, P. C. COSGROVE AND G. ROBINSON. 27
These were characterized by certain clinical and pathological features as follows : - -
1. High pyrexia (104-105 ° F.) continuous or remittent. 2. Lack of toxaemia or malaise such as might b e expected with
hyperpyrexia. 3. Negative blood cultures, absence of blood parasites and negative serum
reactions for enteric, brueella or typhus fevers. 4. Enlargement of the spleen of varying degree from the barely palpable
to the gross. To the time of writing, thirty-one cases have been admitted. The date
of onset of symptoms has ranged from 11.6.41 to 30.8.41. Further eases may yet occur.
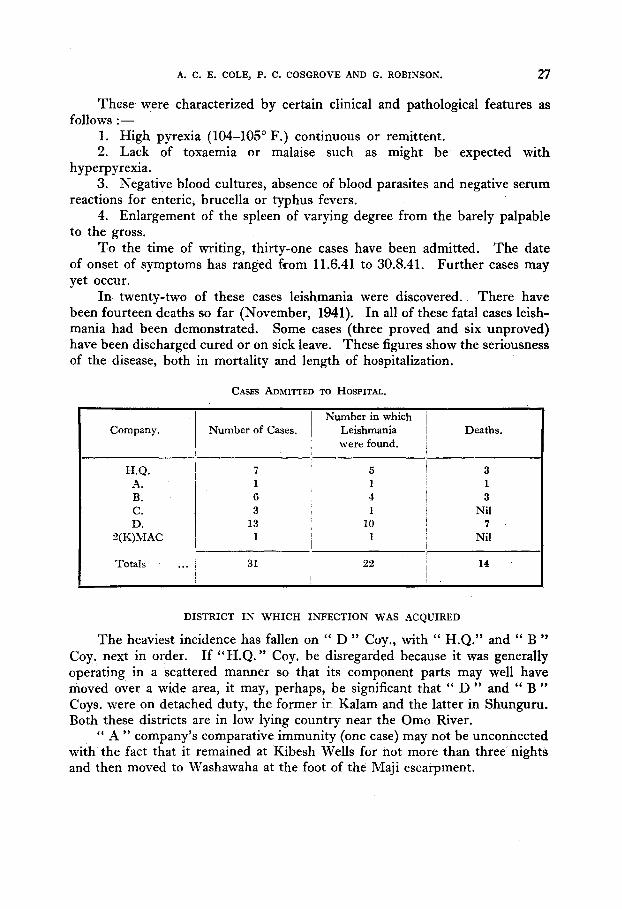
In twenty-two of these eases leishmania were discovered. There have been fourteen deaths so far (November, 1941). In all of these fatal cases leish- mania had been demonstrated. Some eases (three proved and six unproved) have been discharged cured or on sick leave. These figures show the seriousness of the disease, both in mortality and length of hospitalization.
CASES ADM1TTED TO H O S P I T A L .
Company,
H . Q .
A. B. C. D.
2 ( K) M A C
N u m b e r of Cases.
7 1 6 3
13 1
N u m b e r in which i Leishmania ! were found, i
Deaths .
5 ! 3 1 i 1 4 ! a 1 i Nil
l0 i v 1 Nil
I -! o
Totals ... 31 22 14 I I
DISTRICT IN WHICH INFECTION WAS ACQUIRED
The heaviest incidence has fallen on " D " Coy., with " H.Q." and " B " Coy. next in order. If " H . Q . " Coy. be disregarded because it was generally operating in a Scattered manner so that its component parts may well have moved over a wide area, it may, perhaps, be significant that " D " and " B " Coys. were on detached duty, the former ir_ Kalam and the latter in Shunguru. Both these districts are in low lying country near the Omo River.
" A " company's comparative immunity (one case) may not be unconnected with the fact that it remained at Kibesh Wells for not more than three nights and then moved to Washawaha at the foot of the Maji escarpment.
28 rau~-~.aa.
The following investigations have been carried out by Colonel MACLEAN and others.
1. A survey of the native population revealed microscopically positive cases at Shunguru and Kibesh Wells, and a number of other persons with illness and enlarged spleen and liver.
2. A sandfly (Phlebotomus). survey of the area from Lodwar to Kibesh Wells showed a dry season sandfly infestation of the whole of the Sanderson Gulf area (north of Lake Rudolph) in the vicinity of rivers, particularly at Kalam, Shunguru and Kibesh Wells. The infestation dropped rapidly as the distance from the river increased.
It is noteworthy that no European cases have occurred. A possible explanation is that in drier areas sandfly infestation only occurred or was more intense in the shade of native huts and in the organic pollution around them. African troops would be more likely to frequent these places.
Incubation Period.
Probably the first opportunity for infection was in the Todenyang- Namarabuth area from '10th February onwards.
The date of onset of symptoms in the first recorded case was l lth June, 1941. The symptoms of a number of the subsequent cases started between 26th and 28th June. This would seem to indicate that the incubation period is somewhere in the neighbourhood of 4 months. Confirmation of this figure may be obtained in another way. The first seven cases occurred between l l th and 29th June and were distributed between all five companies, and this probably corresponds with an infection occurring in the period 10th February to 6th March, when the whole battalion was in the Todenyang-Namaraputh area.
Later cases from 7th July to 28th August were distributed as follows: " D " Coy., 12 ; " B" Coy., 3 ; " H.Q." 3. It is not unreasonable to suppose. that this corresponds with infection during the period 18th May to 1st June, when " D " Coy. was on detached duty at Kalam. In this case the incubation period would appear to be about 2 months.
CLINICAL FEATURES ANrD PATHOLOGY.
Onset.--The onset was sudden with headache and high fever rising above 103 ° F. in 24 hours, except in four cases where there was a gradual rise of temperature during the first week, not reaching the maximum until the second week.
Fourteen cases complained mainly of abdominal pain, five of them vomiting. The pain was sometimes over the spleen or liver but more often had a general upper abdominal distribution. Only one case complained of diarrhoea but four others were found to have loose stools containing pus and blood cells.
A. C. E. COLE, P. C. COSGROVE AND G. ROBINSON. 29
Seven cases complained of cough and pain in the chest, or both, and these were found to Lave some physical signs such as an occasional rhonchus or a few r~les at one base. Three cases complained mainly of pain in the neck, two had definite stiffness amounting to rigidity. Four cases complained mainly of sore throat. On examination of the throat there was little to see beyond the general appearance of a moderate degree of pharyngitis.
The Temperature.
The course of the fever in these cases is variable, one constant feature being the high temperatures registered : 104-105 ° F. at one stage or another of the disease.
Some cases commenced with a high almost continuous fever in the first week, changing to a more remittent type in the second, and perhaps dropping in level in the third to a comparatively moderate 100-102 ° F. In others the temperature gradually climbed in the first week as in typhoid and remained high in the second. Even without treatment there seems to be, in some cases, an undulant tendency--the temperature dropping to 99-100 ° F. and perhaps rising again after another week or two. This fall in temperature may be some- times wrongly attributed to therapeutic measures.
Two or more peaks of fever in the 24 hours were not infrequently observed.
Splenomegaly and Hepatomegaly.
In all descriptions of kala-azar extreme enlargement of the spleen is one of the points emphasised. On admission, however, no less than seven cases had no detectable splenic enlargement while in a number of others the spleen was only just palpable. The number of cases which on admission had slight hepatic enlargement was seven, but on subsequent examination 4--6 weeks later this number had increased to twelve. Six weeks after admission there were only two patients in whom the spleen was not palpable and in the remainder the average size of the organ, as measured in fingers' breadth" below the costal margin, had increased. It would appear that while the spleen may enlarge before febrile symptoms occur, it requires some weeks or months of illness for this to become outstanding. It is important to note that the failure to detect enlargement does not exclude kala-azar.
Kidneys.
A point that seems to emerge from a study of these cases is that damage to the kidneys usually occurs. Out of twenty-seven cases where the urine was tested, twenty-four showed albumin presem as a fair cloud, and in fifteen of these granulm" casts were also present. At postmortem examination of the fatal eases the kidneys were found to be swollen under the capsule.
30 KALA-AZAR.
Clinical Appearance.
The majority of the cases have been characterized by a remarkable appear- ance of fitness in spite of the fever. Thus, a man with a temperature of 103 ° F. might be seen walking around the ward and making a pretty fair effort at eating his food ration. On interrogation, he would reply, as often as not , that he had no complaint of any sort beyond a certain diminution of his customary vigour, or he might complain, in addition, of a slight headache.
Examination would show a clean tongue and few physical signs beyond fever, some degree of pallor of the mucous membranes and, in some cases, splenomegaly. In sharp contradistinction to the above, four of the cases were admitted in a definitely typhoidal state, with dirty tongue and apathetic manner. Later, however, the condition of those showing few symptoms might deteriorate seriously.
Blood Counts.
White Cell Count.--The white cell count is included here as it seems to be one of the chief characteristics of the disease and is especially valuable for diagnosis, It is invariably lowered even in the very earliest stages of the disease and a normal or high count excludes a diagnosis of kala-azar, The total white counts of the cases studied in hospital varied between 1,400 and 6,200, with an average of 3,340 w.b.c, per cu. mm.
Even more striking is the change in the polymorphonuclear cells, for not only is there a drop in the total number but the normal ratio of 2/3 poly- morphs to 1/3 lymphocytes is completely reversed. •
The differential polymorphonuclear count averaged 36" per cent., with variation between 18 and 56 per cent. In two cases complete agranulocytosis occurred at one point. This granulocytopenia is undoubtedly the cause of some of the complications of the disease.
Haemoglobin and Red Cell Count.--There is nothing characteristic in the red cell count. Anaemia is frequent and may be extreme but is not invariable. It appears to be hypochromic in type. On admission, haemoglobin varied between 30 and 90 per cent. and unless treated it tended to drop further as the disease progressed, eventually reaching very low levels.
Complications.
The more important complications noted were as follows : - - 1. Haemorrhage,--There appears to be an increased tendency to bleed
from mucous surfaces, although skin petechiae were only once seen. It appeared very commonly as a terminal manifestation. Epistaxis occurred in five cases,~once terminally. Haemorrhage into or from the gums occurred in four cases. Haematemesis and urethral haemorrhage occttrred once each. In five cases severe bowel haemorrhages occurred terminally.
A. C. E. COLE, P. C. COSGROVE AND G. ROBINSON. 31
2. Diarrhoea.--Although only one case complained of dysenteric symptoms on entry, four others were found to have blood and pus in ~heir stools. Diarrhoea occurred at some stage or another during eve.ry patient's illness, and recurred frequently in those cases not doing well.
Five fatal cases had severe bloody, dysentery amounting to bowel haemor- rhage as a terminal symptom.
The administration of therapeutic tartar emetic frequently has the effect of producing diarrhoea.
3. Pharyngitis.--Sore throat, dysphagia, and cough with the expectoration of muco-pus occurred in fifteen cases at one time or other during their illness. The throat appearances were indefinlte--the pharynx appearing dryish, granular or gelatinous. This condition is probably associated with granulocytopenia.
4. Pneumonia and Bronchitis.---In addition to-the seven cases complaining of cough and pain in the chest, four others were found during their illness to have rhonchi or r~les in their chests--presumably due to bronchitis.
Two cases developed a definite pneumonia and recovered. In one a white cell count of 2,000 (all lymphocytes) improved to 3,600 with 30 per cent. poly- morphonuclears ; in the other no alteration occurred.
Other Features Noted.
Glandular Enlargement occurred in seven cases, generally only the femoral or inguinal group. A generalized enlargement was found in two cases, in both of which the Kahn test was negative.
Skin Rashes.--A fine papular eruption of the face was noted in four cases. In one, scraping of a papule showed leishmania associated with pus cells, while culture yielded a growth of cocci.
Terminal Condition.
Inanition (five cases).--Four patients died in a state of inanition resembling typhoid, in which there was a gradual loss of vitality till death occurred ; a fifth died with a combination of terminal pneumonia and inanition.
Heart Failure (three cases).--One died unexpectedly of collapse and heart failure while comparatively well; another of heart failure following a serous pericarditis ; a third had a pericarditis of pneumococcal origin asso- ciated with pneumococcal septicaemia. In all fatal cases the heart had a flabby, oedematous or gelatinous appearance.
Dysentery (four eases).mFour had severe dysentery with considerable bowel haemorrhage as a terminal phenomenon ; one had in addition broncho- pneumonia, and one epistaxis.
Epistaxis (two cases).--Two cases presented epistaxis as a terminal pheno- menon, one in addition suffering from haemorrhagic dysentery.
Delirium.--One died in febrile delirium.
32 KALA-AZAR.
Results of Treatment.
These have been very disappointing. The only antimonial drug available was sodium antimonyl tartrate~. Tryparsamide was also tried but with no success.
Tartar emetic was used in a course of about 25 to 27 grains in 12 to 14 intra- venous injections on alternate days. In every case it succeeded in bringing the temperature down to normal or nearly so, but on stopping it the fever usually returned after 2 or 3 weeks except in the few successful cases.
A second course might again reduce the fever, b u t the condition of the patient might then have deteriorated to such an extent that he might not be able to tolerate the relatively toxic ~lrug.
Some got tired of injections and flatly refused further treatment. So far three cases diagnosed microscopically have been discharged to sick
leave, and six unconfirmed cases have been discharged. Clinical cure in these cases merely consisted in absence of fever for 3 or more
weeks, and in general well-being, gain in weight etc. The spleen did not decrease markedly in size, and in the confirmed cases a second examination for leishmania was not done. The blood count remains abnormal with low haemo- globin red cell count, and also a low white cell count with relative lymphocytosis.
LABORATORY INVESTIGATION.
Diagnostic Puncture.--The spleen, liver, bone marrow, and tonsils were all, in one or other of the cases, submitted to diagnostic puncture. Superficial scrapings of the skin were also examined but with negative result. The parasite was found in the spleen, liver, bone marrow and lymph gland, the spleen having yielded the most successful results.
Parasites are very scanty in the early stages and it is only later in the disease that they can be demonstrated more easily. In every postmortem examination careful search showed a few parasites in the spleen o r liver or bone marrow, although puncture during life often did not collect enough tissue to reveal them.
Material from thirty-one cases was examined in the Laboratory, corn- prising : -
Cases. Cases. Sp_leen smears ... in 11 Blood culture ... in 10 Liver smears ... ,, 6 Spleen culture . . . . . 2 Bone marrow smears ,, 8 Postmortem material ,, 11 Lymph gland smears ,, 3 Tonsil and nasal swabs ,, 6
Leishmania were found in twenty-two cases. Spleen Smears.--Seven showed parasites and in only one case were they
at all numerous. Usually they were extremely scanty and found only af ter a prolonged search (1 hour in some cases).
A. C. E. COLEj P. C. COSGROVE AND G. ROBINSON. 33
Liver Smears.--Four were positive. The parasites were scanty. Bone Marrow Smears.--One only showed very scanty extracellular parasites. Lymph Gland Sraears.--Two out of three examined showed very scanty
parasites. Blood Cultures.--None was positive. The media used for blood culture
were: (1) N.N.N., us ing human blood. (2) Citrated blood. (3) A mixture of laked blood and 1-2 per cent. saline.
Spleen Culture.--Material from two postmortems was cultured in citrated blood medium. In one case flagellate forms were seen on the 17th day. They gradually increased in number for about 14 days when the culture became con- taminated. The body from which the culture was made had been lying in the mortuary for 18 hours. The second culture was contaminated from the start.
Postmortem Material.--Parasites were found in smears of spleen and bone marrow in all cases which came to postmortem. They were very scanty a n d on this account were not seen in sections stained with haematoxylin and eosin. They were found in liver smears in three of the cases. In one case of kala-azar (not in the present series) parasites were very numerous in sections of spleen liver and lymph glands.
Tonsillar and Nasal Swabs.--Smears from six cases were examined. All were negative.
Skin Scrapings.--Smears from a proved case (spleen puncture) were examined. No leishmania were seen. In another case leishmania were found in scrapings from a facial papule.
APPEARANCE OF THE PARASITE.
In most cases the parasites were scanty and often distorted. They w e r e
rarely intracellular. Four types were seen : - - (a) A round swollen parasite with well-marked body and nuclei. (b) An elongated parasite in which the body and nuclei stained well. (c) A parasite in which the body did not show up at all. All that could
be seen being the trophonucleus and kinetoplast. A group of these in a cell gave a very characteristic picture.
(d) The typical text-book parasite. These were scarcely ever seen, The above appearances were seen in both Leishman and Giemsa stained
preparations. Generally speaking the kinetoplast was very conspicuous and drew one's
attention to the parasite. It must be emphasised that prolonged search is necessary before reporting
a smear as negative. Some of the distortion and bad staining may have been due to a little of
the local anaesthetic getting into the needle. For this reason the later punctures were done without an anaesthetic and the results were noticeably better.
O
34 gaLA-,~.,,m.
FORMOL-GEL REACTION.
This test was done in twenty-one cases in the present series and was completely negative. The test was positive in one case from another unit in whom the disease was of long standing (7 months).
iV[I$CELLANEOUS POSTMORTEM APPEARANCES.
In all cases the heart was pale and flabby and the myocardium oedematous. The kidneys in two cases showed necrosis and partial disintegration of the
epithelium of the convoluted tubules. All cases showed oedema of the peri- nephric tissue, and cloudy swelling of the kidney.
Splenomegaly was a feature of all the cases, though frequently not very marked.