A Pilot Study of Integral Yoga for Menopausal Hot Flashes
9
Menopause: The Journal of The North American Menopause Society Vol. 21, No. 8, pp. 846/854 DOI: 10.1097/gme.0000000000000191 * 2014 by The North American Menopause Society Pilot study of integral yoga for menopausal hot flashes Nancy E. Avis, PhD, 1 Claudine Legault, PhD, 2 Gregory Russell, MS, 2 Kathryn Weaver, PhD, 1 and Suzanne C. Danhauer, PhD 1 Abstract Objective: This study aims to obtain preliminary data on the efficacy of yoga for reducing self-reported meno- pausal hot flashes in a randomized study including an attention control group. Methods: We randomized 54 late perimenopausal women (2-12 mo of amenorrhea) and postmenopausal women (912 mo of amenorrhea)Vaged 45 to 58 years and who experienced at least four hot flashes per day, on average, for at least 4 weeksVto one of three groups: yoga, health and wellness education (HW), and wait list (WL). Yoga and HW classes consisted of weekly 90-minute classes for 10 weeks. All women completed daily hot flash diaries throughout the trial (10 wk) to track the frequency and severity of hot flashes. The mean hot flash index score is based on the number of mild, moderate, severe, and very severe hot flashes. Results: Hot flash frequency declined significantly across time for all three groups, with the strongest decline occurring during the first week. There was no overall significant difference in hot flash frequency decrease over time by treatment groups, but the yoga and HW groups followed similar patterns and showed greater decreases than the WL group. On week 10, women in the yoga group reported an approximately 66% decrease in hot flash frequency, women in the HW group reported a 63% decrease, and women in the WL group reported a 36% decrease. The hot flash index showed a similar pattern. Conclusions: Results suggest that yoga can serve as a behavioral option for reducing hot flashes but may not offer any advantage over other types of interventions. Key Words: Vasomotor symptoms Y Yoga Y Hot flashes Y Menopause. H ot flashes and/or night sweats (vasomotor symptoms) are the most common and troubling symptoms associ- ated with menopause and are experienced by 64% to 80% of women undergoing natural menopause and by almost all women who undergo surgical menopause. 1<3 For many women, these symptoms are frequent and severe enough to become de- bilitating and impact their quality of life (QOL). 4<10 Hot flashes are one of the chief menopausal complaints for which women in Western societies seek medical treatment 11 and are the primary reason that women begin hormone therapy (HT). 12<16 HT is currently the gold standard for treating vasomotor symptoms. A Cochrane Database systematic review showed a 75% reduction in hot flash frequency with HT compared with placebo. 17 However, findings from the Women’s Health Initiative trial suggest that benefits of HT can be outweighed by risks such as coronary heart disease, stroke, pulmonary embolism, breast cancer, and probable dementia. 18 The widespread publicity of the Women’s Health Initiative results has heightened women’s concerns about taking HT and led to a decrease in HT use. 19,20 Many women have sought alternative treatments for hot flashes, including other pharmaceutical agents, herbal or die- tary remedies, and behavioral therapies, 21,22 but these treat- ments have shown mixed results. Pharmaceutical agents are often ineffective or yield a high incidence of adverse effects, though some antidepressants show promising results. 23 Two reviews of randomized controlled clinical trials of complemen- tary health approaches for hot flashes did not find evidence that herbs and nutritional supplements were beneficial. 24,25 Behavioral interventions involving relaxation and slow, deep abdominal breathing, however, have been found to be use- ful for reducing mild- to moderate-intensity hot flashes. 26<28 Such breathing forms the most integral core of any yoga practice. 29,30 Yoga practice involves the combination of physical postures (asanas), breathing (pranayama), and deep relaxation (savasana). Two uncontrolled studies of yoga interventions found reductions in hot flashes. 31,32 Studies using various control groups have also shown promising results but have used very intensive yoga in- terventions (at least 5 d/wk), 33,34 did not measure daily hot flashes, 33<35 combined the yoga intervention with education, 33 or lacked an attention control group. 36 Received October 3, 2013; revised and accepted November 19, 2013. From the Departments of 1 Social Sciences and Health Policy and 2 Bio- statistical Sciences, Wake Forest School of Medicine, Winston-Salem, NC. Funding/support: This research was supported by grant R21AT004234 from the National Center for Complementary and Alternative Medicine, National Institutes of Health. Clinical trial registration: ClincalTrials.gov identifier: NCT01073397. Financial disclosure/conflicts of interest: None reported. Address correspondence to: Nancy E. Avis, PhD, Department of Social Sci- ences and Health Policy, Wake Forest School of Medicine, Medical Center Boulevard, Winston-Salem, NC 27157. E-mail: [email protected] 846 Menopause, Vol. 21, No. 8, 2014 Copyright © 2014 The North American Menopause Society. Unauthorized reproduction of this article is prohibited.
Transcript of A Pilot Study of Integral Yoga for Menopausal Hot Flashes

Menopause: The Journal of The North American Menopause SocietyVol. 21, No. 8, pp. 846/854DOI: 10.1097/gme.0000000000000191* 2014 by The North American Menopause Society
Pilot study of integral yoga for menopausal hot flashes
Nancy E. Avis, PhD,1 Claudine Legault, PhD,2 Gregory Russell, MS,2 Kathryn Weaver, PhD,1
and Suzanne C. Danhauer, PhD1
AbstractObjective: This study aims to obtain preliminary data on the efficacy of yoga for reducing self-reported meno-
pausal hot flashes in a randomized study including an attention control group.Methods:We randomized 54 late perimenopausal women (2-12 mo of amenorrhea) and postmenopausal women
(912 mo of amenorrhea)Vaged 45 to 58 years and who experienced at least four hot flashes per day, on average, forat least 4 weeksVto one of three groups: yoga, health and wellness education (HW), and wait list (WL). Yoga andHW classes consisted of weekly 90-minute classes for 10 weeks. All women completed daily hot flash diariesthroughout the trial (10 wk) to track the frequency and severity of hot flashes. The mean hot flash index score isbased on the number of mild, moderate, severe, and very severe hot flashes.
Results: Hot flash frequency declined significantly across time for all three groups, with the strongest declineoccurring during the first week. There was no overall significant difference in hot flash frequency decrease over timeby treatment groups, but the yoga and HW groups followed similar patterns and showed greater decreases than theWL group. On week 10, women in the yoga group reported an approximately 66% decrease in hot flash frequency,women in the HW group reported a 63% decrease, and women in the WL group reported a 36% decrease. The hotflash index showed a similar pattern.
Conclusions: Results suggest that yoga can serve as a behavioral option for reducing hot flashes but may notoffer any advantage over other types of interventions.
Key Words: Vasomotor symptoms Y Yoga Y Hot flashes Y Menopause.
Hot flashes and/or night sweats (vasomotor symptoms)are the most common and troubling symptoms associ-ated with menopause and are experienced by 64% to
80% of women undergoing natural menopause and by almost allwomen who undergo surgical menopause.1<3 For many women,these symptoms are frequent and severe enough to become de-bilitating and impact their quality of life (QOL).4<10 Hot flashesare one of the chief menopausal complaints for which women inWestern societies seek medical treatment11 and are the primaryreason that women begin hormone therapy (HT).12<16
HT is currently the gold standard for treating vasomotorsymptoms. A Cochrane Database systematic review showed a75% reduction in hot flash frequency with HT compared withplacebo.17 However, findings from the Women’s HealthInitiative trial suggest that benefits of HT can be outweighed
by risks such as coronary heart disease, stroke, pulmonaryembolism, breast cancer, and probable dementia.18 Thewidespread publicity of the Women’s Health Initiative resultshas heightened women’s concerns about taking HT and led toa decrease in HT use.19,20
Many women have sought alternative treatments for hotflashes, including other pharmaceutical agents, herbal or die-tary remedies, and behavioral therapies,21,22 but these treat-ments have shown mixed results. Pharmaceutical agents areoften ineffective or yield a high incidence of adverse effects,though some antidepressants show promising results.23 Tworeviews of randomized controlled clinical trials of complemen-tary health approaches for hot flashes did not find evidence thatherbs and nutritional supplements were beneficial.24,25
Behavioral interventions involving relaxation and slow,deep abdominal breathing, however, have been found to be use-ful for reducing mild- to moderate-intensity hot flashes.26<28 Suchbreathing forms the most integral core of any yoga practice.29,30
Yoga practice involves the combination of physical postures(asanas), breathing (pranayama), and deep relaxation (savasana).Two uncontrolled studies of yoga interventions found reductionsin hot flashes.31,32 Studies using various control groups have alsoshown promising results but have used very intensive yoga in-terventions (at least 5 d/wk),33,34 did not measure daily hotflashes,33<35 combined the yoga intervention with education,33 orlacked an attention control group.36
Received October 3, 2013; revised and accepted November 19, 2013.
From the Departments of 1Social Sciences and Health Policy and 2Bio-statistical Sciences, Wake Forest School of Medicine, Winston-Salem, NC.
Funding/support: This research was supported by grant R21AT004234from the National Center for Complementary and Alternative Medicine,National Institutes of Health.
Clinical trial registration: ClincalTrials.gov identifier: NCT01073397.
Financial disclosure/conflicts of interest: None reported.
Address correspondence to: Nancy E. Avis, PhD, Department of Social Sci-ences and Health Policy, Wake Forest School of Medicine, Medical CenterBoulevard, Winston-Salem, NC 27157. E-mail: [email protected]
846 Menopause, Vol. 21, No. 8, 2014
Copyright © 2014 The North American Menopause Society. Unauthorized reproduction of this article is prohibited.

The objective of the current study was to obtain prelimi-nary data on the efficacy of yoga for reducing self-reportedmenopausal hot flashes in a randomized study that included anattention control group and measured daily hot flashes. At-tention control groups are important to help understand thetrue impact of an active intervention. We hypothesized thatwomen participating in a yoga intervention would achieve agreater reduction in subjective hot flash frequency and se-verity than women in an educational control group or a waitlist (WL) control group. In this pilot study, we also sought toexamine the effects of yoga on self-reported hot flash inter-ference, sleep, anxiety, depressive symptoms, perceivedstress, and QOL, and to track recruitment, retention, and ad-herence to the protocol.
METHODS
Study designWe conducted a randomized study consisting of three
groups: yoga, health and wellness education (HW), and WL.The HW group controlled for attention, time, and social aspectsof the yoga intervention. The WL group controlled for placeboeffects because randomized controlled trials of estrogen therapytypically show, on average, that hot flash frequencies and hotflash scores diminish by about 20% to 30% with 4 weeks ofplacebo.37 This reduction may be attributable to the naturaldecline in symptoms across time or to the placebo effects ofbeing in a trial. It is therefore critical to have an inactive controlgroup to assess the effects of the natural decline in symptoms.
ProcedureEligible participants included late perimenopausal and early
postmenopausal women, aged 45 to 58 years, who experiencedat least four hot flashes per day, on average, for at least 4 weeksand at least 2 months since the last menses. Women werestratified on menopause status based on the criteria developedby the Stages of Reproductive Aging Workshop.38 Late peri-menopause was defined as 2 to 12 months of amenorrhea, andpostmenopause was defined as more than 12 months of amen-orrhea. Women who had surgical menopause were classified aspostmenopausal. Women who had taken HT within the past12 weeks were not eligible. Because hormone-modulatingtherapies can impact ovarian function and increase hot flashes,women taking such therapies (eg, tamoxifen) within the past6 months were not eligible. Women with a history of cancerneeded to be at least 5 years postdiagnosis and off chemother-apy for at least 1 year. We also excluded women who had everused yoga specifically for hot flashes, had used yoga or acu-puncture in the past 3 months, or had untreated thyroid disease,which can increase hot flashes. Women who had initiated her-bal or nutritional remedies within the past 4 weeks were ex-cluded as these remedies may take several weeks to have aneffect. We initially excluded women taking psychoactive med-ications, including antidepressants and anxiolytics, as thesemedications may reduce hot flashes. However, because manywomen were taking antidepressants, we subsequently elimi-nated antidepressants as a criterion but required that women had
been on a stable dose for 3 months at enrollment. The ability toread and understand English was an additional requirement.
Women were recruited through newspaper advertisements,radio announcements, and hospital postings and screened forinitial eligibility over the telephone. Women who met initialeligibility criteria were scheduled for a baseline clinic visit. Atthe baseline clinic visit, an informed consent form wasobtained, and baseline questionnaires were administered. Toconfirm that women had a sufficient number of hot flashes forstudy eligibility, we asked the participants to complete theDaily Diary of Hot Flashes (DDHF) on a daily basis for thenext 2 weeks and to mail it to the study coordinator. Womenwho met the criterion of an average of at least four hot flashesper day, based on the DDHF, were randomized to one of thethree study groups. Participants assigned to the two interven-tion groups could begin class participation at any time withinthe next 4 weeks (women were encouraged to begin within2 wk). Women assigned to the WL group were told that theywould be contacted in 10 weeks to begin either yoga or HWclasses. Women in the WL group were subsequently ran-domized to yoga or education to avoid the expectation thatone intervention was preferable and to provide an incentivefor staying in the study.
All study participants completed questionnaires 5 weeksafter baseline, at the end of the trial (10 wks after baseline),and 2 months after completion of the trial. All women com-pleted weekly hot flash diaries throughout the trial (10 wk).All study participants agreed not to take hormonal medica-tions or not to initiate other treatments for their hot flashesduring the study. The study protocol was approved by theWake Forest School of Medicine institutional review board.
Study groupsYoga
The study intervention consisted of 10 weekly 90-minuteintegral yoga classes. Classes were offered on a continuousbasis with rolling admission. The basic elements of any yogapractice involve the combination of breathing (pranayama),physical postures (asanas), and deep relaxation (savasana).We chose integral yoga as it is particularly well-suited towomen experiencing hot flashes largely because of its majoremphasis on stress reduction and decreased likelihood ofincreasing heat (an undesirable effect in women with hotflashes).39 Each class was adjusted to the mixture of abilitiesof those present but included the same basic elements (adaptedfrom Satchidananda39) in the following three categories: (1)breathing (pranayama; 15 min)Vcentering meditation (1-2 min;aligning the body in a comfortable seated position, paying at-tention to any physical sensations, and noticing the breath)and deep three-part breathing; (2) physical postures (asanas;45 min)Vwarm-up (eg, cat pose), modified sun salutations,standing poses (eg, warrior I or II, king dancer), brief deeprelaxation, backward bending (eg, cobra, boat pose, optionalbow pose), forward bending (eg, head-to-knee pose, forwardbend, half spinal twist), inverted poses (eg, half shoulder stand,legs up the wall, downward-facing dog), fish pose or supine
Menopause, Vol. 21, No. 8, 2014 847
INTEGRAL YOGA FOR MENOPAUSAL HOT FLASHES
Copyright © 2014 The North American Menopause Society. Unauthorized reproduction of this article is prohibited.

spinal twist, upright spinal twist, and yoga mudra; and (3)deep relaxation (savasana; 30 min)Vyoga nidra and additionalpranayama (alternate nostril breathing).
In addition to the group classes, participants were asked topractice yoga at home for 15 minutes three or more times perweek using a DVD videorecording produced for this study.Home practice consisted of the following: warm-up (circlinghands and feet to warm up the wrist and ankle joints, rotatingshoulder joints, and cat/cow stretch on hands and knees intochild pose to stretch the lower back), backward bend (cobrapose), forward bend (head-to-knee pose), inversion (modifiedshoulder stand), gentle twist (reclining spinal twist), deeprelaxation, deep three-part breathing, and a final period ofstillness and silence.
The yoga instructor was a registered Yoga Alliance teacherand certified integral yoga instructor. In addition, a consultantfrom the New York Integral Yoga Institute reviewed theprotocol and DVD that we made for home practice.
HW control groupThis group was designed to control for time, attention, and
social aspects of the yoga intervention. It was designed to beBbelievable[ without being efficacious for reducing hot flashes.Classes consisted of 10 weekly 90-minute didactic educationalclasses on different topics: menopause, stress management (twosessions), bone health, cardiovascular health, nutrition, financialplanning, skin care, aging and long-term health planning, andcancer prevention and screening. Similar to the yoga classes,women could enter the group at any time. Women were givenmaterials to read at home in an attempt to match the time spentin home yoga practice.
WL control groupParticipants in this group did not participate in any classes
for 10 weeks and were instructed not to initiate any newtreatments for their hot flashes during this time. They com-pleted weekly hot flash diaries and study questionnaires onweeks 5 and 10. We selected a WL control design rather thanusual care because we had learned40 that women do not likebeing assigned to a group that does not receive any treatment.With a WL control design, these women were assured of re-ceiving some intervention, thereby enhancing recruitment andretention. The data of interest for this group were obtainedduring weeks 1 to 10 while the women were waiting to par-ticipate in the yoga or HW classes.
MeasuresThe primary study outcome was frequency and severity of
hot flashes, as measured by the DDHF developed by Sloanet al.37 The DDHF records the frequency and severity of hotflashes using a four-point scaleVmild (sensation of heat with-out perspiration), moderate (sensation of heat with perspirationbut able to continue activity), severe (sensation of heat withsweating, causing cessation of activity or disrupting sleep), verysevere (sensation of heat with severe sweating, disrupting ac-tivity and requiring a change of sheets or clothes)Vto provide ahot flash index (the sum of the number of hot flashes multiplied
by severity). This diary has been used in multiple trials on hotflashes and has exhibited consistency and reliability.37
Secondary study outcomes included hot flash interference,sleep quality, anxiety, depressive symptoms, perceived stress,and QOL. The Hot Flash Related Daily Interference Scale(HFRDIS) is a 10-item psychometrically sound measure forassessing the impact of vasomotor symptoms on daily activi-ties in nine specific domains within the past week (work, so-cial activities, leisure activities, sleep, mood, concentration,relation with others, sexuality, and enjoyment of life) andoverall QOL.41 Item responses range from 1 (not at all) to 10(extremely). The Global Sleep Quality Index of the 19-itemPittsburgh Sleep Quality Index was used to measure sleeppatterns and quality.42,43 Scores range from 0 to 16, with scoresof 5 or higher indicating poor sleep quality and high sleepdisturbances. Depressive symptoms were assessed using theCenter for Epidemiological Studies Depression Scale, shortform (CESD-10),44 a validated self-report questionnaire thatmeasures the frequency of 10 depressive symptoms Bduring thepast week.[ Total scores range from 0 to 30, with higher scoresindicating greater depressive symptoms. Scores higher than 10are indicative of clinically significant depressive symptoms.
The 10-item Hopkins Symptom Checklist (HSCL)45,46 as-sesses the presence and intensity of anxiety symptoms duringthe previous week. A total score of 1.55 or higher indicatesmoderate anxiety symptoms, and a score of 1.75 or higherindicates severe anxiety. The HSCL has been used in previousstudies of treatments of menopausal symptoms.47 The four-item Perceived Stress Scale (PSS)48,49 assesses four aspectsof self-reported perceived stress experienced during the past2 weeks (1, never; 5, very often). Items are summed so that thetotal score ranges from 4 to 20.
Global QOL was assessed via a single-item 100-mm visualanalogue scale, where participants rate their overall QOLalong a line (where 0 is the lowest possible QOL and 100 isthe highest possible QOL). Health-related QOL was measuredusing the MOS 36-item Short Form Health Survey (SF-36).50
The SF-36 is one of the most widely used measures of healthstatus consisting of 36 items measuring the following two com-ponents: physical component score (PCS) and mental compo-nent score (MCS). Scores are standardized to a mean of 50.
Statistical analysesStatistical analyses were performed using the SAS statisti-
cal package. This pilot study of 54 participants was conductedto examine trends and to plan a larger clinical trial. Recruit-ment and retention are presented in a Consolidated Standardsof Reporting Trials (CONSORT) diagram. Reasons for drop-outs and the numbers of yoga or HW classes attended weretabulated. Group comparisons of baseline characteristics in-cluded W
2 test and Fisher’s exact test for categorical variables,and analysis of variance for continuous variables. Our primaryaim addressed the effects of yoga on the frequency and severityof reported hot flashes. Log-transformed data were analyzedfollowing an intention-to-treat analysis, and results were back-transformed to original units. A linear mixedmodel with repeated
848 Menopause, Vol. 21, No. 8, 2014 * 2014 The North American Menopause Society
AVIS ET AL
Copyright © 2014 The North American Menopause Society. Unauthorized reproduction of this article is prohibited.

measures (PROC mixed in SAS)51,52 was used, with group,week, and group by week interaction in the model adjusting forbaseline outcome and menopause status (perimenopause orpostmenopause). The adjusted ratio of the frequency and se-verity of hot flashes in a specific week versus baseline values�100, based on log-transformed data, were also plotted.
Secondary outcomes, including hot flash interference (HotFlash Related Daily Interference Scale), sleep quality (GlobalSleep Quality Index), depressive symptoms (CESD-10), an-xiety symptoms (HSCL), perceived stress (Perceived StressScale), general QOL, and mental and physical componentsof QOL (SF-36 MCS and PCS), were analyzed with the samemethods as the primary outcome.
RESULTS
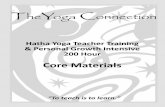
Participant data are shown in Figure 1. A total of 449 womenresponded to advertisements; 288 of these women completed
the telephone screener, and 161 were never reached after atleast three attempts. Of the 288 women who were screened, 133met initial eligibility criteria, and 155 were ineligible. The pri-mary reasons for ineligibility included he following: too fewhot flashes (n = 67), on antidepressants (n = 48; an exclusioncriterion later changed as mentioned in BMethods[), not yetperimenopausal (n = 32), recent yoga practice (n = 29), andrecent cancer (n = 26).
Of the 133 eligible women, 80 completed baseline visits and65 agreed to be randomized, but 11 were ineligible for furtherparticipation after completion of the 2-week hot flash diary,yielding 54 women who were enrolled and randomized. At thefinal follow-up, 79.6% of the women remained in the study(yoga, 15; HW, 14;WL, 14). Reasons for dropping out includedtransportation issues (n = 2), time constraints (n = 2), reportedinability to do yoga (n = 1), and unspecified reasons (n = 6).
At least 8 of 10 classes were attended by 50% of womenin the yoga group and by 47% of women in the HW group.
FIG. 1. Consolidated Standards of Reporting Trials (CONSORT) diagram.
Menopause, Vol. 21, No. 8, 2014 849
INTEGRAL YOGA FOR MENOPAUSAL HOT FLASHES
Copyright © 2014 The North American Menopause Society. Unauthorized reproduction of this article is prohibited.

At least 6 of 10 classes were attended by 61% of womenin the yoga group and by 63% of women in the HW group.
Baseline characteristicsBaseline characteristics by group assignment are shown in
Table 1. There were no differences in demographic variablesamong the three groups. The average number of hot flashesper day was 10.1, 8.7, and 9.1 in the WL, HW, and yogagroups, respectively; 15% of the women were perimeno-pausal, and 40% were African American. All women in theWL group had some comorbidities (most commonly arthritisand hypertension), which were significantly more than thosein the other two groups (61% in both). There was a trendtoward higher depressive symptoms and anxiety scores andlower MCS among women in the yoga group.
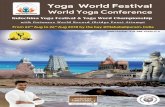
Hot flash changesForty-nine of the 54 participants returned at least one
follow-up diary and were included in the analyses (WL, 15;HW, 17; yoga, 17). On week 10, 13 WL, 14 HW, and 12 yogaparticipants returned their diaries. Means for the hot flash fre-quency and hot flash index, by week and group, are shown inTable 2. Figure 2 shows the percentages of daily hot flashesfrom baseline each week. Hot flash frequency declined signif-icantly across time for all three groups (P G 0.0001), with thestrongest decline occurring during the first week. Differences inhot flash frequency across time tended to be larger between theWL group and the yoga group. By the third week of treatment,women in the yoga group reported an approximately 45% de-crease in hot flash frequency compared with about 22% for theWL group. The HW group showed a decrease similar to that inthe yoga group from weeks 5 to 10. The WL group showed an
TABLE 1. Baseline characteristics of study sample
Yoga (n = 18) Health and wellness education (n = 19) Wait list (n = 17) P
DemographicsAge, mean (SE), y 53.5 (0.7) 52.8 (0.7) 53.5 (0.7) 0.66Race, n (%) 0.83White 11 (65) 12 (63) 9 (52)African American 6 (35) 7 (37) 8 (47)
Education, n (%) 0.49High school or some college 10 (56) 7 (37) 7 (41)College or more 8 (44) 12 (63) 10 (59)
Employed, n (%) 14 (78) 13 (68) 15 (88) 0.43Hard to pay for basics 0.55Somewhat hard or very hard 6 (33) 6 (32) 3 (18)Not very hard at all 12 (67) 13 (68) 14 (82)
Income, n (%) 0.50US$10,000-29,999 3 (17) 6 (32) 2 (12)US$30,000-74,999 9 (50) 6 (32) 6 (35)QUS$75,000 6 (33) 7 (37) 9 (53)
Married/partnered, n (%) 9 (50) 12 (63) 11 (65) 0.65Current smoker, n (%) 0 (0) 1 (5) 1 (6) 0.76Any exercise in the past month, n (%) 15 (83) 17 (89) 12 (71) 0.34
Medical characteristicsAny comorbidity, n (%) 11 (61) 11 (61) 17 (100) 0.01Hysterectomy, n (%) 7 (39) 7 (37) 8 (47) 0.81Oophorectomy, n (%) 0.80No 11 (61) 14 (74) 12 (71)One ovary removed 2 (11) 2 (11) 3 (18)Both ovaries removed 5 (28) 3 (16) 2 (12)
Menopause status, n (%) 0.99Perimenopausal 3 (17) 3 (16) 2 (12)Postmenopausal 15 (83) 16 (84) 15 (88)
Time since last menstrual period, mean (SE), y 2.9 (0.9) 2.5 (0.7) 3.8 (1.1) 0.60a
Time with hot flashes, mean (SE), y 1.6 (0.4) 2.0 (0.4) 2.2 (0.5) 0.68a
Hot flashes per day, mean (SE) 9.1 (1.2) 8.7 (1.2) 10.1 (1.5) 0.59b
Symptoms and quality of lifeHFRDIS, mean (SE) 4.7 (0.5) 4.1 (0.5) 4.6 (0.6) 0.72Sleep quality (GSQI), mean (SE) 10.9 (0.9) 8.5 (0.9) 9.9 (0.9) 0.15Depressive symptoms (CESD-10), mean (SE) 10.8 (1.3) 7.2 (1.2) 7.3 (1.3) 0.08Perceived stress (PSS), mean (SE) 5.4 (0.9) 3.5 (0.8) 4.5 (0.9) 0.27Hopkins Symptom Checklist, mean (SE) 1.6 (0.1) 1.4 (0.1) 1.7 (0.1) 0.06Global quality of life (VAS), mean (SE) 68.4 (5.4) 73.0 (4.1) 72.5 (4.1) 0.68SF-36 MCS, mean (SE) 41.3 (2.4) 50.5 (2.3) 60.4 (2.5) 0.01SF-36 PCS, mean (SE) 54.4 (1.3) 54.1 (1.3) 51.4 (1.4) 0.22
HFRDIS, Hot Flash Related Daily Interference Scale; GSQI, Global Sleep Quality Index; CESD-10, Center for Epidemiological Studies Depression Scale, shortform; PSS, Perceived Stress Scale; VAS, visual analogue scale; SF-36, MOS 36-item Short Form Health Survey; MCS, mental component score; PCS, physicalcomponent score.aFrom log-transformed data.bFrom log-transformed data adjusted for menopause status.
850 Menopause, Vol. 21, No. 8, 2014 * 2014 The North American Menopause Society
AVIS ET AL
Copyright © 2014 The North American Menopause Society. Unauthorized reproduction of this article is prohibited.

initial decline of 22% on week 1 but remained fairly stableuntil week 7 when hot flash frequency decreased slightly more.On week 10, we found a 66% reduction in hot flashes forthe yoga group and a 63% reduction in hot flashes for theHW group, compared with 36% in the WL group. These per-
centages represent a decrease in the mean hot flashes per day:6.5 in the yoga group, 5.9 in the HW group, and 4.2 in theWL group.
Figure 3 shows the results using the hot flash index, whichtakes into account both frequency and severity. This figure
TABLE 2. Frequency and severity index of hot flashes per day adjusted for baseline values and menopause status, by week
Week Yoga (n = 18) Health and wellness education (n = 19) Wait list (n = 17)
P
Group-week interaction Group Week
Frequency 0.91 0.18 G0.00011 5.7 (1.1) 6.5 (1.3) 6.8 (1.4)2 5.1 (1.0) 6.1 (1.2) 7.2 (1.5)3 4.8 (0.9) 6.1 (1.2) 6.8 (1.4)4 4.7 (0.9) 5.5 (1.1) 7.1 (1.5)5 4.9 (0.9) 5.0 (1.0) 6.6 (1.4)6 5.0 (1.0) 4.9 (1.0) 6.8 (1.4)7 4.7 (0.9) 5.0 (1.0) 6.0 (1.3)8 4.3 (0.9) 4.3 (0.9) 5.9 (1.2)9 3.3 (0.7) 3.3 (0.7) 6.1 (1.3)10 3.0 (0.6) 3.2 (0.7) 5.5 (1.2)
Hot flash index 0.70 0.14 G0.00011 10.7 (2.3) 12.6 (2.8) 13.2 (3.1)2 9.7 (2.1) 11.7 (2.6) 13.6 (3.1)3 8.9 (2.0) 11.2 (2.4) 13.1 (3.0)4 8.7 (1.9) 10.2 (2.2) 14.4 (3.4)5 9.5 (2.1) 8.8 (1.9) 13.3 (3.2)6 9.0 (2.0) 8.5 (1.9) 13.5 (3.3)7 8.5 (1.9) 8.7 (2.0) 11.8 (2.8)8 8.3 (2.0) 7.3 (1.6) 11.6 (2.8)9 6.2 (1.5) 5.2 (1.2) 12.3 (2.9)10 5.5 (1.3) 5.1 (1.2) 10.9 (2.6)
Data are presented as mean (SE).Values were transformed back to original units from log-transformed values. Main-effects P values were derived from a model excluding group-week interaction.
FIG. 2. Percentage of baseline hot flash frequency across time, by intervention group.
Menopause, Vol. 21, No. 8, 2014 851
INTEGRAL YOGA FOR MENOPAUSAL HOT FLASHES
Copyright © 2014 The North American Menopause Society. Unauthorized reproduction of this article is prohibited.

shows a pattern similar to that for frequency alone. There isa general decline across time, and the week 10 mean hotflash index in the yoga and WL groups is half that in theWL group.
QOL outcomesAlthough this small pilot study was not powered to find
small differences, patterns of hot flash interference and de-pressive symptoms (CESD-10) did not change appreciably(Table 3). On week 10, the WL group showed better sleepquality, improved overall QOL, and a tendency for less per-ceived stress, whereas the HW group reported worse sleepquality and global QOL and more perceived stress. Sleep
quality, QOL, and perceived stress did not change meaning-fully in the yoga group.
DISCUSSION
This pilot study sought to obtain data on the feasibility andpreliminary efficacy of yoga as an intervention for reducingmenopausal hot flashes. The physiological rationale for in-vestigating this relationship is based on several complex hy-pothesized pathways, especially pathways mediated by thehypothalamic-pituitary-adrenal axis, through which yoga ishypothesized to decrease arousal in the autonomic nervous sys-tem (ANS).53 In particular, the hormonal changes occurringduring menopause are thought to be associated with a narrowingof the body’s thermoregulatory zone (thermoregulation being
FIG. 3. Percentage of baseline hot flash index across time, by intervention group.
TABLE 3. Quality-of-life outcomes by intervention group and week, after controlling for baseline values
Outcome
Yoga Health and wellness education Wait list
P for group-weekinteraction
Week 5(n = 16)
Week 10(n = 15)
Week 5(n = 15)
Week 10(n = 14)
Week 5(n = 14)
Week 10(n = 14)
HFRDIS 3.15 (0.49) 3.00 (0.51) 2.78 (0.50) 2.65 (0.51) 3.67 (0.53) 3.55 (0.53) 0.99Sleep quality (GSQI) 9.39 (0.73) 8.93 (0.75) 8.07 (0.75) 9.00 (0.77) 9.28 (0.79) 7.64 (0.79) 0.04Depressive symptoms (CESD-10) 8.67 (1.08) 8.11 (1.11) 7.71 (1.09) 8.77 (1.11) 8.79 (1.15) 8.57 (1.15) 0.53Perceived stress (PSS) 3.53 (0.69) 3.68 (0.74) 3.34 (0.68) 4.70 (0.97) 4.02 (0.85) 3.11 (0.66) 0.08Global quality of life 72.37 (4.03) 77.39 (4.22) 80.18 (4.24) 66.11 (4.37) 72.4 (4.35) 79.17 (4.35) 0.01Hopkins Symptom Checklist 1.48 (0.07) 1.38 (0.07) 1.36 (0.07) 1.32 (0.06) 1.51 (0.07) 1.44 (0.07) 0.84SF-36 PCS 50.91 (1.28) 51.17 (1.33) 54.31 (1.31) 52.90 (1.34) 54.25 (1.39) 50.61 (1.43) 0.14SF-36 MCS 51.32 (2.14) 52.61 (2.22) 50.79 (2.16) 50.29 (2.20) 49.42 (2.29) 52.38 (2.33) 0.53
HFRDIS, Hot Flash Related Daily Interference Scale; GSQI, Global Sleep Quality Index; CESD-10, Center for Epidemiological Studies Depression Scale, shortform; PSS, Perceived Stress Scale; SF-36, MOS 36-item Short Form Health Survey; PCS, physical component score; MCS, mental component score.
852 Menopause, Vol. 21, No. 8, 2014 * 2014 The North American Menopause Society
AVIS ET AL
Copyright © 2014 The North American Menopause Society. Unauthorized reproduction of this article is prohibited.

under the control of the ANS) at which the normal physiologicalresponse to heating or cooling occurs. This narrowing means thathot flashes are more likely to result when body temperature in-creases.54 A decrease in arousal of the ANS, hypothesized to bebrought about by yoga, may thus lead to improved thermoreg-ulation.
Our three-group design incorporated both attention (ie,HW) and WL control groups. Sloan et al37 found that a re-duction of 3.5 hot flashes per day corresponded to a 6-pointincrease in QOL on a scale from 0 to 100 points, which isBa conservative estimate of a minimally clinically significantchange.[ All three groups met this threshold.
Our results provide additional support for previous studies’results on the potential benefits of yoga for reducing hotflashes.33<35 Several things are worth noting about our find-ings. First, we found meaningful reductions in hot flashesdespite class attendance being suboptimal and lower than inother studies.33,34 We also found a reduction in hot flashes inthe WL group, consistent with other hot flash interventionstudies that have shown a substantial placebo effect.37 Aparticularly noteworthy finding is the similarity of results be-tween the yoga group and the HW group. Randomized trialsof behavioral interventions are often criticized because greaterexpectations are often created in the intervention group ascompared with the attention control group. We purposelypresented our study as one comparing two types of interven-tions to reduce menopausal symptoms and tried to avoid anysuggestion that the yoga group was of greater interest, thusattempting to equalize expectations in both groupsVa clearmethodological strength of this study.
The findings from the present study are very similar tothose from our previous study on acupuncture for hot flashes.40
The acupuncture study was designed similarly with respect toeligibility and outcomes. In that study, women (n = 56) wererandomized to one of three groups: usual care, placebo (shamacupuncture), or standardized individual acupuncture based ontraditional Chinese medicine principles. Results showed a sig-nificant decrease in the mean frequency of hot flashes similar tothat of the present study. There was a 35% to 40% reduction inhot flashes on week 2 for both the sham group and the tradi-tional Chinese medicine group. There was no difference bytreatment group (P = 0.15). However, when combined, the twoacupuncture groups showed a significantly greater decreasethan the usual care group (P G 0.05).
The results of our present study, in combination with those ofthe acupuncture study, found a similar reduction in hot flashesfor women in four different treatment groups: yoga, HW, trueacupuncture, and sham acupuncture. Both studies controlledfor treatment expectations with the inclusion of active controlgroups. Taken together, these findings point to the importance ofincluding active control groups in randomized interventionstudies for menopausal hot flashes. They also raise the questionof why these control groups are equally effective as the presumedactive intervention. The question remains as to whether the activeinterventions are indeed efficacious or whether their efficacy is aresult of the expectations that participants have of them.
This pilot study raises some questions about feasibility.Recruitment was challenging because we could only offer theyoga and HW classes one time during the week. Providingmore options for classes would enhance both recruitment andclass attendance. Furthermore, it was initially a challenge topresent the HW intervention as one to reduce hot flashes,which led us to revise our study presentation more generally toreduce menopausal symptoms.
The present study had several limitations. The sample sizewas, by design, underpowered to detect important differencesbetween groups. As previously mentioned, recruitment andclass attendance were challenging largely owing to the in-ability to offer more flexible and varied class days and times.
Despite these limitations, the present study has severalstrengths and important findings. Our three-group design is animportant advance over studies that lack groups that controlfor time or attention. Although larger studies are needed, thisdesign and our results suggest that yoga can serve as a be-havioral option for reducing hot flashes but may not offer anyadvantage over other types of interventions.
CONCLUSIONS
This study suggests that yoga, as well as education, may bebehavioral interventions that help reduce hot flashes.
REFERENCES
1. Avis NE, Crawford SL, McKinlay SM. Psychosocial, behavioral, andhealth factors related to menopause symptomatology. Womens Health1997;3:103-120.
2. Williams RE, Kalilani L, DiBenedetti DB, et al. Frequency and severityof vasomotor symptoms among peri- and postmenopausal women in theUnited States. Climacteric 2008;11:32-43.
3. Woods NF, Mitchell ES. Symptoms during the perimenopause: preva-lence, severity, trajectory, and significance in women’s lives. Am J Med2005;118(suppl 12B):14-24.
4. Avis NE, Ory M, Matthews KA, Schocken M, Bromberger J, Colvin A.Health-related quality of life in a multiethnic sample of middle-agedwomen: Study of Women’s Health Across the Nation (SWAN). MedCare 2003;41:1262-1276.
5. Daly E, Gray A, Barlow D, McPherson K, Roche M, Vessey M. Mea-suring the impact of menopausal symptoms on quality of life. Br Med J1993;307:836-840.
6. Ledesert B, Ringa V, Breart G. Menopause and perceived health statusamong the women of the French GAZEL cohort.Maturitas 1994;20:113-120.
7. Fuh JL, Wang SJ, Lee SJ, Lu SR, Juang KD. Quality of life and meno-pausal transition for middle-aged women on Kinmen island. Qual LifeRes 2003;12:53-61.
8. Kumari M, Stafford M, Marmot M. The menopausal transition was as-sociated in a prospective study with decreased health functioning inwomen who report menopausal symptoms. J Clin Epidemiol 2005;58:719-727.
9. Utian WH. Psychosocial and socioeconomic burden of vasomotorsymptoms in menopause: a comprehensive review. Health Qual LifeOutcomes 2005;3:47.
10. Williams RE, Levine KB, Kalilani L, Lewis J, Clark RV. Menopause-specific questionnaire assessment in US population-based study shows neg-ative impact on health-related quality of life. Maturitas 2009;62:153-159.
11. Williams RE, Kalilani L, DiBenedetti DB, Zhou X, Fehnel SE, Clark RV.Healthcare seeking and treatment for menopausal symptoms in theUnited States. Maturitas 2007;58:348-358.
12. Johannes CB, Crawford SL, Posner JG, McKinlay SM. Longitudinalpatterns and correlates of hormone replacement therapy use in middle-aged women. Am J Epidemiol 1994;140:439-452.
Menopause, Vol. 21, No. 8, 2014 853
INTEGRAL YOGA FOR MENOPAUSAL HOT FLASHES
Copyright © 2014 The North American Menopause Society. Unauthorized reproduction of this article is prohibited.

13. Kuh D, Hardy R, Wadsworth M. Social and behavioural influences on theuptake of hormone replacement therapy among younger women. BJOG2000;107:731-739.
14. Kuh DL, Wadsworth M, Hardy R. Women’s health in midlife: theinfluence of the menopause, social factors and health in earlier life.Br J Obstet Gynaecol 1997;104:923-933.
15. Hunter MS, O’Dea I, Britten N. Decision-making and hormone replace-ment therapy: a qualitative analysis. Soc Sci Med 1997;45:1541-1548.
16. Porter M, Penney GC, Russell D, Russell E, Templeton A. A populationbased survey of women’s experience of the menopause. Br J ObstetGynaecol 1996;103:1025-1028.
17. Maclennan AH, Broadbent JL, Lester S, Moore V. Oral oestrogen andcombined oestrogen/progestogen therapy versus placebo for hot flushes.Cochrane Database Syst Rev 2004;CD002978.
18. Rossouw JE, Anderson GL, Prentice RL, et al. Risks and benefits ofestrogen plus progestin in healthy postmenopausal women: principal re-sults from the Women’s Health Initiative randomized controlled trial.JAMA 2002;288:321-333.
19. Haas JS, Kaplan CP, Gerstenberger EP, Kerlikowske K. Changes in theuse of postmenopausal hormone therapy after the publication of clinicaltrial results. Ann Intern Med 2004;140:184-188.
20. Tsai SA, Stefanick ML, Stafford RS. Trends in menopausal hormonetherapy use of US office-based physicians, 2000-2009. Menopause2011;18:385-392.
21. Nedrow A, Miller J, Walker M, Nygren P, Huffman LH, Nelson HD.Complementary and alternative therapies for the management of meno-pause-related symptoms: a systematic evidence review. Arch Intern Med2006;166:1453-1465.
22. Kessel B, Kronenberg F. The role of complementary and alternativemedicine in management of menopausal symptoms. Endocrinol MetabClin North Am 2004;33:717-739.
23. Pachman DR, Jones JM, Loprinzi CL. Management of menopause-associated vasomotor symptoms: current treatment options, challenges andfuture directions. Int J Womens Health 2010;2:123-135.
24. Kronenberg F, Fugh-Berman A. Complementary and alternative medi-cine for menopausal symptoms: a review of randomized, controlled trials.Ann Intern Med 2002;137:805-813.
25. Huntley AL, Ernst E. A systematic review of herbal medicinal products forthe treatment of menopausal symptoms. Menopause 2003;10:465-476.
26. Sood R, Sood A, Wolf SL, et al. Paced breathing compared with usualbreathing for hot flashes. Menopause 2013;20:179-184.
27. Freedman RR, Woodward S. Behavioral treatment of menopausal hotflushes: evaluation by ambulatory monitoring. Am J Obstet Gynecol1992;167:436-439.
28. Keefer L, Blanchard EB. Hot flash, hot topic: conceptualizing menopausalsymptoms from a cognitive-behavioral perspective. Appl PsychophysiolBiofeedback 2005;30:75-82.
29. Farhi D. Yoga Mind, Body and Spirit: A Return to Wholeness, 1st ed. NewYork, NY: Holt Paperbacks and Henry Holt and Company, LLC, 2000.
30. Fried R, Grimaldi J. The psychology and physiology of breathing. In:Behavioral Medicine, Clinical Psychology and Psychiatry. New York,NY: Plenum Press, 1993.
31. Cohen BE, Kanaya AM, Macer JL, Shen H, Chang AA, Grady D. Fea-sibility and acceptability of restorative yoga for treatment of hot flushes: apilot trial. Maturitas 2007;56:198-204.
32. Booth-LaForce C, Thurston RC, Taylor MR. A pilot study of a Hathayoga treatment for menopausal symptoms. Maturitas 2007;57:286-295.
33. Chattha R, Raghuram N, Venkatram P, Hongasandra NR. Treating theclimacteric symptoms in Indian women with an integrated approach toyoga therapy: a randomized control study. Menopause 2008;15:862-870.
34. Joshi S, Khandwe R, Bapat D, Deshmukh U. Effect of yoga on meno-pausal symptoms. Menopause Int 2011;17:78-81.
35. Elavsky S, McAuley E. Physical activity and mental health outcomesduring menopause: a randomized controlled trial. Ann Behav Med2007;33:132-142.
36. Carson JW, Carson KM, Porter LS, Keefe FJ, Seewaldt VL. Yoga ofAwareness program for menopausal symptoms in breast cancer survi-vors: results from a randomized trial. Support Care Cancer 2009;17:1301-1309.
37. Sloan JA, Loprinzi CL, Novotny PJ, Barton DL, Lavasseur BI,Windschitl H. Methodologic lessons learned from hot flash studies.J Clin Oncol 2001;19:4280-4290.
38. Soules MR, Sherman S, Parrott E, et al. Executive summary: Stages ofReproductive Aging Workshop (STRAW). Fertil Steril 2001;76:874-878.
39. Satchidananda YSS. Integral Yoga Hatha. Buckingham, VA: IntegralYoga Publications, 1970.
40. Avis NE, Legault C, Coeytaux RR, et al. A randomized, controlled pilotstudy of acupuncture treatment for menopausal hot flashes. Menopause2008;15:1070-1078.
41. Carpenter JS. The Hot Flash Related Daily Interference Scale: a tool forassessing the impact of hot flashes on quality of life following breastcancer. J Pain Symptom Manage 2001;30:979-989.
42. Owens JF, Matthews KA. Sleep disturbance in healthy middle-agedwomen. Maturitas 1998;30:41-50.
43. Buysse DJ, Reynolds CF III, Monk TH, Berman SR, Kupfer DJ. ThePittsburgh Sleep Quality Index: a new instrument for psychiatric practiceand research. Psychiatry Res 1989;28:193-213.
44. Andresen EM, Malmgren JA, Carter WB, Patrick DL. Screening for de-pression in well older adults: evaluation of a short form of the CES-D(Center for Epidemiologic Studies Depression Scale). Am J Prev Med1994;10:77-84.
45. Derogatis LR, Lipman RS, Rickels K, Uhlenhuth EH, Covi L. TheHopkins Symptom Checklist (HSCL): a self-report symptom inventory.Behav Sci 1974;19:1-15.
46. Winokur A, Winokur DF, Rickels K, Cox DS. Symptoms of emotionaldistress in a family planning service: stability over a four-week period.Br J Psychiatry 1984;144:395-399.
47. Shantha S, Brooks-Gunn J, Locke RJ, Warren MP. Natural vaginal pro-gesterone is associated with minimal psychological side effects: a pre-liminary study. J Womens Health Gender Based Med 2001;10:991-997.
48. Cohen S, Kamarck T, Mermelstein R. A global measure of perceivedstress. J Health Soc Behav 1983;24:385-396.
49. Cohen S, Williamson GM. Perceived stress in a probability sample of theUnited States. In: Spacapan S, Oskamp S, ed. The Social Psychology ofHealth. Newbury Park, CA: Sage, 1988.
50. Ware JE Jr, Sherbourne CD. TheMOS 36-item short form health survey (SF-36), 1: conceptual framework and item selection.Med Care 1992;6:473-483.
51. Jennrich RI, Schluchter MD. Unbalanced repeated-measures models withstructured covariance matrices. Biometrics 1986;42:805-820.
52. Laird NM, Ware JH. Random-effects models for longitudinal data. Bio-metrics 1982;38:963-974.
53. Browne RP, Gerbarg PL. Sudarshan Kriya yogic breathing in the treat-ment of stress, anxiety, and depression, 1: neurophysiologic model.J Altern Complement Med 2005;11:189-201.
54. Freedman RR. Pathophysiology and treatment of menopausal hot flashes.Semin Reprod Med 2005;23:117-125.
854 Menopause, Vol. 21, No. 8, 2014 * 2014 The North American Menopause Society
AVIS ET AL
Copyright © 2014 The North American Menopause Society. Unauthorized reproduction of this article is prohibited.