
A Descriptive Study To “Assess The Knowledge And Attitude
132
A Descriptive Study To “Assess The Knowledge And Attitude Regarding Self-Administration Of Insulin Injection Among Diabetes Mellitus Patients In Kempa Cheluvamba General Hospital At Malleswaram, Bangalore” By Namita Singha Dissertation submitted to the Rajiv Gandhi University Of Health Sciences, Karnataka, Bangalore In partial fulfillment Of the requirement for the degree of Master of Science In Medical-Surgical Nursing Under the guidance of Asso. Prof. Victorial Selva Kumari C. Medical-Surgical Nursing Sarvodaya College of Nursing Vijayanagar, Bangalore-40 November 2005
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of A Descriptive Study To “Assess The Knowledge And Attitude

A Descriptive Study To “Assess The Knowledge And Attitude
Regarding Self-Administration Of Insulin Injection Among Diabetes
Mellitus Patients In Kempa Cheluvamba General Hospital At
Malleswaram, Bangalore”
By
Namita Singha
Dissertation submitted to the
Rajiv Gandhi University Of Health Sciences, Karnataka, Bangalore
In partial fulfillment
Of the requirement for the degree of
Master of Science
In
Medical-Surgical Nursing
Under the guidance of
Asso. Prof. Victorial Selva Kumari C.
Medical-Surgical Nursing
Sarvodaya College of Nursing
Vijayanagar, Bangalore-40
November 2005

II
Rajiv Gandhi University of Health Sciences
DECLARATION BY THE CANDIDATE
I hereby declare that this dissertation / thesis entitled “A Descriptive Study To
Assess The Knowledge And Attitude Regarding Self-administration of Insulin
Injection Among Diabetes Mellitus Patients In Kempa Cheluvamba General
Hospital At Malleswaram, Bangalore” is a bonafide and genuine research work
carried out by me under the guidance of Mrs. Victorial Selva Kumari C,
Asso. Professor and HOD, Department of Medical-Surgical Nursing.
Date: Signature of the Candidate
Place: Bangalore Ms. Namita Singha

III
CERTIFICATE BY THE GUIDE
This is to certify that the dissertation entitled “A Descriptive Study To Assess The
Knowledge And Attitude Regarding Self-administration of Insulin Injection
Among Diabetes Mellitus Patients In Kempa Cheluvamba General Hospital At
Malleswaram, Bangalore” is a bonafide research work done by Namita Singha in
partial fulfillment of the requirement for the degree of Master of Science in Nursing.
Date: Signature of the Guide
Place: Bangalore Mrs.Victorial Selva Kumari C.
Asso. Professor and HOD
Medical-Surgical Nursing

IV
ENDORSEMENT BY THE HOD, PRINCIPAL/HEAD OF THE
INSTITUTION
This is to certify that the dissertation entitled “A Descriptive Study To Assess
The Knowledge And Attitude Regarding Self-Administration Of Insulin
Injection Among Diabetes Mellitus Patients In Kempa Cheluvamba General
Hospital At Malleswaram, Bangalore” is a bonafide research work done by
Namita Singha under the guidance of Mrs.Victorial Selva Kumari C,
Asso. Professor, Medical-Surgical Nursing.
Seal and Signature of the Seal and Signature of the
HOD Principal
Asso. Prof. Victorial Selva Kumari C. Prof. T. Bheemappa
Date: Date:
Place: Bangalore Place: Bangalore

V
COPYRIGHT
Declaration by the Candidate
I hereby declare that the Rajiv Gandhi University Of Health Sciences, Karnataka shall
have the rights to preserve, use and disseminate this dissertation/thesis in print or
electronic format for academic/research purpose.
Date: Signature of the Candidate
Place: Bangalore Namita Singha
© Rajiv Gandhi University Of Health Sciences, Karnataka

VI
ACKNOWLEDGEMENT
No one can lead a life apart
Untouched by others lives
My life is not just my own design but
Part of all the rest that pass my way
And each of them is part of mine
It is my pleasure and pride to record my gratitude and thanks to those who have
contributed to the successful completion of this endeavor.
A sincere gratitude to Sri. V. Narayanaswamy, Chairman, Sarvodaya College of
Nursing for providing me an opportunity to advance my education in this institution.
I express my heartfelt thanks to Prof. T Bheemappa, Principal, Sarvodaya College of
Nursing for all the timely guidance and help given in completing this study.
The present study was undertaken and completed under the inspiring and valuable
guidance of Mrs. Victorial Selva Kumari, Asso. Professor and HOD, Medical
surgical Nursing and (my) Co-Guide Mr. Amal Einstein Xavier, Principal, Oriental
College of Nursing. I express my deep sense of gratitude to both of them for their
expert guidance, valuable suggestions, constant encouragement and keen interest in
planning and execution of my study.
I am highly obliged to Prof. Hemalatha, Head of the Department, Pediatric Nursing
and Research Methodologist for her expert guidance and help throughout the study.
I am indebted to Prof. Shridhar, Associate Professor, Medical Surgical Nursing
Kempegowda Institute of Nursing for his guidance and expert suggestions.
I express my gratitude to Mrs. Fermina, Lecturer Medical Surgical Nursing and
Ms. Ramya, Lecturer OBG Department for their guidance and support.

VII
I convey my thanks to the Medical Superintendent, Kempa Cheluvamba General
Hospital, Malleswaram for granting me permission to conduct the research study at
K.C.General Hospital.
Heartfelt thanks to Dr.Gangaboraiah, Biostatistician for guiding me in statistical
analysis and interpretation of data.
I express my gratitude to the entire teaching and non-teaching faculty of Sarvodaya
College of Nursing for their support extended during the course of my study.
My sincere thanks and appreciation to all the experts who validated the tool and
provided constructive and valuable opinion.
A note of thanks to Librarians, Sarvodaya College of Nursing and Chief Librarian,
National Institute of Mental Health and Neuro Sciences, Bangalore for their assistance
in library reviews.
A special thanks to the Diabetic Patients, who participated in my study.
Sincere thanks to Ms. Surekha for Kannada translation and to my beloved
classmates and friends.
I extend my thanks to Mr. B. Suraj Shetty for his excellent computer assistance.
I owe depth of gratitude to my loving parents Mr. Harendra Singha and
Mrs. Dipali Singha and my brother Pranjal for their inspiration and encouragement
throughout the study.
My sincere thanks and gratitude to all whose names are not mentioned but who have
directly or indirectly helped in the completion of this thesis.
Above all, I bow my head with profound gratitude in front of 'God Almighty' for the
blessings showered on me throughout.
Date: Signature of the Candidate
Place: Namita Singha

VIII
LISTS OF ABBREVIATIONS USED
(In alphabetical order)
1. χ² - Chi-square
2. = - Equal to
3. > - Greater Than
4. < - Lesser Than
5. % - Percent
6. BC - Before Christ
7. DCCT - Diabetes control and complications Trial
8. DM - Diabetes Mellitus
9. E.g. - For example
10. HBA,C - Glycosylated Haemoglobin
11. IDDM - Insulin Dependant Diabetes Mellitus
12. IDF - International Diabetes Federation
13. i.e - That is
14. NIDDM - Non- Insulin Dependant Diabetes Mellitus
15. OHA - Oral Hypoglycemic Agent
16. SD -Standard Deviation
17. WHO - World Health Organization

IX
ABSTRACT
Statement of The Problem
A Descriptive Study To “Assess The Knowledge And Attitude Regarding Self-
administration of Insulin Injection Among Diabetes Mellitus Patients In Kempa
Cheluvamba General Hospital At Malleswaram, Bangalore”.
Objectives of The Study
1. To assess the knowledge of patients regarding the Self-administration of
Insulin Injection.
2. To assess the attitude of patients regarding Self-administration of Insulin
Injection
3. To correlate the knowledge and attitude of diabetic patients regarding self-
administration of insulin injection.
4. To associate the knowledge with selected demographic variables.
5. To associate the attitude with selected demographic variables.
6. To develop an information booklet on self-administration of insulin injection
for diabetes mellitus patients.
Research Approach
A descriptive survey approach was used for assessing the knowledge and attitude of
Diabetes Mellitus patients regarding Self-Administration of insulin injection.
Population
The target population consisted of 60 Diabetic patients who were on Insulin Therapy
within the age group of 40-70 years. Half of the patients were admitted and a few
were attending the OPD services in Kempa Cheluvamba General Hospital at
Malleswaram, Bangalore.

X
Sample And Sampling Technique
A sample of 60 Diabetic patients, were selected according to the availability and
convenience of the researcher. Non-probability Convenient sampling technique was
used.
Tool
A Structured Self-Administered Questionnaire and a Likert type of Attitude Scale was
used for the data collection.
The tool consisted of three parts.
Part I : Demographic Data (11questions)
Part II : Knowledge Questionnaire (30 questions)
Part III : Attitude Scale (20 statements)
An information booklet on self-administration of insulin injection was prepared and
distributed among the insulin dependent patients
Data Collection
After obtaining an informed consent from the respondents, the investigator collected
the data from 60 Diabetic patients by means of self administered questionnaire.
Major Findings Of The Study
1. Out of 60 diabetic patients 81.7% had average knowledge, 13.3% had poor
knowledge and only 5% had good knowledge regarding self administration of
insulin injection. The overall mean value of the diabetic patients knowledge
regarding self administration of insulin injection was 14.45 with a standard
deviation of 3.326.
2. Out of 60 diabetic patients, only 18.3% had most favourable and 81.7% had a
favourable attitude towards self administration of insulin injection. It revealed

XI
the mean percentage of the positive attitude, which was 69.05 with a standard
deviation of 5.585.
3. There is no significant association between the level of knowledge and
selected demographic variables.
4. Age, gender, education, religion, occupation, marital status, duration of
diagnosis of diabetes mellitus, number of years on insulin therapy and family
history of diabetes mellitus are not significantly associated with the level of
attitude of diabetic patients.
5. There is a highly significant association between the level of attitude and the
family income of diabetic patients.
In view of the nature of the present study and to accomplish the objectives of the
study, an informational booklet was prepared on self administration of insulin
injection.
Interpretation and Conclusion
The study showed that the theoretical knowledge of diabetic patients regarding self
administration of insulin injection were average and the attitude towards self
administration of insulin injections were favourable.
Key Words
Diabetes Mellitus; Insulin Therapy; Self Administration; Diabetic Patients; Insulin
Injection
XII
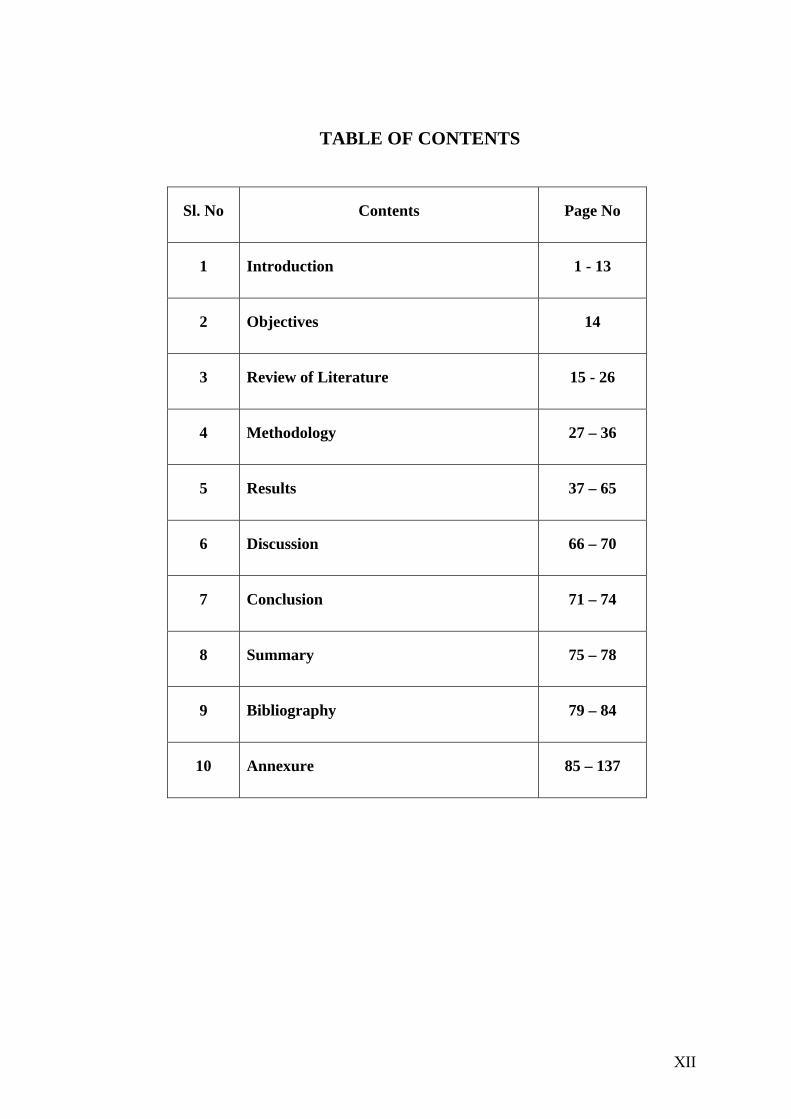
TABLE OF CONTENTS
Sl. No Contents Page No
1 Introduction 1 - 13
2 Objectives 14
3 Review of Literature 15 - 26
4 Methodology 27 – 36
5 Results 37 – 65
6 Discussion 66 – 70
7 Conclusion 71 – 74
8 Summary 75 – 78
9 Bibliography 79 – 84
10 Annexure 85 – 137
XIII
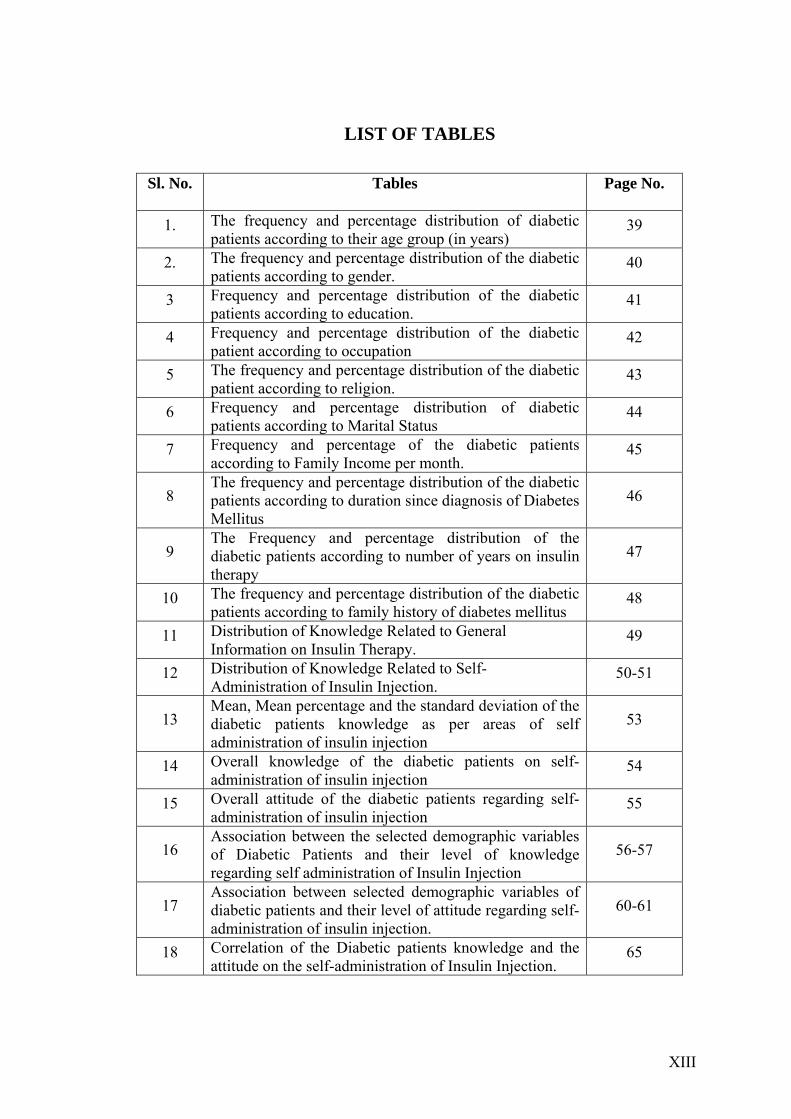
LIST OF TABLES Sl. No. Tables Page No.
1. The frequency and percentage distribution of diabetic patients according to their age group (in years)
39
2. The frequency and percentage distribution of the diabetic patients according to gender.
40
3 Frequency and percentage distribution of the diabetic patients according to education.
41
4 Frequency and percentage distribution of the diabetic patient according to occupation
42
5 The frequency and percentage distribution of the diabetic patient according to religion.
43
6 Frequency and percentage distribution of diabetic patients according to Marital Status
44
7 Frequency and percentage of the diabetic patients according to Family Income per month.
45
8 The frequency and percentage distribution of the diabetic patients according to duration since diagnosis of Diabetes Mellitus
46
9 The Frequency and percentage distribution of the diabetic patients according to number of years on insulin therapy
47
10 The frequency and percentage distribution of the diabetic patients according to family history of diabetes mellitus
48
11 Distribution of Knowledge Related to General Information on Insulin Therapy.
49
12 Distribution of Knowledge Related to Self-Administration of Insulin Injection.
50-51
13 Mean, Mean percentage and the standard deviation of the diabetic patients knowledge as per areas of self administration of insulin injection
53
14 Overall knowledge of the diabetic patients on self-administration of insulin injection
54
15 Overall attitude of the diabetic patients regarding self-administration of insulin injection
55
16 Association between the selected demographic variables of Diabetic Patients and their level of knowledge regarding self administration of Insulin Injection
56-57
17 Association between selected demographic variables of diabetic patients and their level of attitude regarding self-administration of insulin injection.
60-61
18 Correlation of the Diabetic patients knowledge and the attitude on the self-administration of Insulin Injection.
65

XIV
LIST OF FIGURES Sl. No. Figures Page No.
1. Conceptual Framework 13
2. Schematic Representation of Research Design 28
3. Distribution of diabetic patients according to their Age 39
4. Pie chart representing percentage distribution of the diabetic patient according to gender
40
5. Bar Diagram representing Percentage Distribution of the Diabetic Patients according to Education.
41
6. Bar Diagram Representing Percentage Distribution of the Diabetic Patients according to Occupation
42
7. Bar diagram representing Percentage Distribution of the Diabetic patient according to Religion.
43
8. Bar Diagram representing Percentage Distribution of Diabetic Patient according to Marital Status
44
9. Pie diagram Representing Percentage Distribution of the Diabetic Patients according to Family Income per month.
45
10 Bar Diagram representing Percentage Distribution of the Diabetic Patients according to duration since diagnosis of diabetes Mellitus
46
11 Bar diagram representing Percentage Distribution of the Diabetic Patients according to Numbers of years on Insulin Therapy
47
12 Bar Diagram representing Percentage Distribution of the Diabetic Patients according to Family History of Diabetes Mellitus
48
13 Cone Diagram representing Mean Percentage of Diabetic Patients in both the areas of Self - administration of Insulin Injection
53
1 4 Pie diagram representing overall knowledge of the Diabetic patients regarding Self-administration of Insulin Injection
54
15 Pie Diagram Representing overall attitude level of the diabetic patients regarding self-administration of insulin injection
55
16 Scattered diagram representing relationship between knowledge and attitude 65

1
1. INTRODUCTION
"A wonderful affection not very frequent among men, being a melting down of
the flesh and limbs into urine… life is short, disgusting and painful, thirst
unquenchable, death is inevitable." Areatus, the Greek physician thus described the
clinical features of Diabetes Mellitus, almost 4000 years ago.
Diabetes Mellitus is an endocrine disorder, characterized by hyperglycemia that is,
high blood sugar levels. This is caused due to a relative or absolute insulin deficiency,
a hormone produced by the pancreas. Lack of insulin, either relative or absolute
affects metabolism or breaking down of carbohydrates, proteins, fat, water and
electrolytes leading to an accumulation of glucose in the blood.1 Till the earlier part of
this century, it was believed that there was no effective treatment for this condition,
until the discovery of insulin, in 1922, by Fredrick Banting and his student, John
McCleod 2
PREVALENCE OF DIABETES MELLITUS:
Global Scenario:- The International Diabetes Federation estimated that the
worldwide prevalence of diabetes mellitus in the year 2003 is 194 million.3 The
World Health Organization (WHO) has projected that this number would increase
to 300 million by the year 2025.4
Indian Scenario:- Prevalence of Diabetes Mellitus in India has been growing by
leaps and bounds. In the last 20 years there has been a three fold increase in the
prevalence of Diabetes and today it is estimated that there are over 20 million diabetic
patients in India. India’s diabetic population now ranks first in the world5.
2
A recent national population based study conducted by Ramachandran A,
Snehalatha C, Kapur A, Vijay V, Mohan V, Das AK et al in six urban cities
revealed astonishing results. This study suggested that the prevalence of diabetes
among Chennai residents to be 13.5%, Bangalore – 12.4%, Hyderabad – 16.6%,
Calcutta –11.7%, New Delhi – 11.6% and Mumbai - 9.3%. Thus it is clear that in the
last two decades, there has been a marked increase in the prevalence of diabetes
among urban Indians.6 Ramaiya KL, Kodali VRR, Alberti KGMM had mentioned
that there is a wide urban – rural difference, the prevalence being 2.4% in rural and
11.6% in the urban population.7
Diabetes Mellitus is commonly divided into two main categories namely Type I
diabetes earlier referred as Insulin – Dependent diabetes, and Type II diabetes also
known as Non-Insulin Dependent diabetes. Although both are characterised by
abnormalities in glucose metabolism, there are significant differences in etiology,
pathology and treatment of the two conditions.8
Type II diabetes or Non-Insulin dependent diabetes occurs at a later age, usually after
age of 40, and has a large hereditary component. It is caused by a combination of beta
cell (of the islets of Langerhans) dysfunction and insulin resistance. Management of
Type II diabetes in the majority of patients is with diet, exercise with or without Oral
Hypoglycemic Agents. Even though the disease is prolonged and in the process
certain diabetes complications are associated with the illness requiring insulin, Non-
Insulin Dependent diabetes is often asymptomatic and ketoacidosis is rare.9
Type I diabetes is typically diagnosed at childhood, with peak incidence at puberty. It
is characterized by complete Beta cell failure, requiring exogenous insulin
3
replacement by injection for survival.10 There is evidence to suggest that Type I
diabetes is a slow auto-immune disease, in which insulin producing beta cells of the
pancreas are destroyed by the body’s fight against infection. As in type II the resulting
insulin deficiency leads to the accumulation of glucose in the blood stream,
accompanied by the classical symptoms of polyuria (excessive urination), polydypsia
(excessive thirst), weight loss, fatigue and tiredness. In addition, compensatory fat
metabolism produces ketone bodies, leading to ketoacidosis and coma. The treatment
of Type I diabetes is often complex. In addition to daily injection, it involves many
other life style adjustments such as timing and nature of food consumption, regular
exercise and blood glucose monitoring.11 These life style changes place unique
demands on the individuals as well as the family, as failure to follow any of these
could lead to serious short term and long term consequences (hypoglycemia,
ketoacidosis, heart disease, neuropathy, retinopathy, nephropathy). Both Type I and
Type II diabetes could lead to macro and micro vascular complications, if not
controlled adequately. The long term prognosis of Type I diabetes is said to improve
with a complex demanding and often intensive regimen and maintenance of lower
blood glucose levels is said to reduce the risk of long term complications by as much
as 60%12.
The maintenance of lower blood glucose level is dependent on many factors,
including compliance or adherence to treatment. Insulin has become cornerstone of
diabetes treatment since its initial discovery.13
Insulin therapy in any form is effective in restoring normoglycemia, suppressing
ketogenesis, and delaying or arresting diabetes complications in all patients with
diabetes.13

4
Regular Insulin Therapy is life saving in Type I diabetes. Non-obese, early onset
patients with Type II diabetes respond poorly to Oral Hypoglycemic Agents (OHA)
due to hypoinsulinaemia and low insulin reserve (latent autoimmune diabetes in
adults) hence require Insulin Therapy. The commonest indication of regular Insulin
Therapy in Type II diabetes is OHA failure, which can be primary in 30% or
secondary in 5% - 10% Patients on OHA per year. Regular Insulin Therapy is also
indicated in patients of diabetes associated with renal or hepatic disease, where OHA
is contraindicated.14
Different type and species of insulin have different pharmacological properties.
Human insulin is preferred, for use in pregnant women considering pregnancy,
individuals with allergies or immune resistance to animal derived insulin, those
initiating insulin therapy, and those expected to use insulin only intermittently.14
Conventional insulin administration involves subcutaneous injections with syringes
marked in insulin units. These syringes must be matched with concentration of insulin
in vials.15
Several alternative methods of insulin administration are available like jet injectors
that inject insulin as a fine stream into the skin. Several pen-like devices and insulin
containing cartridge are available, which are easy to operate, improve accuracy and
more convenient. Several new insulin delivery systems are under development that
may eliminate the need for needle-based introduction. This includes insulin pumps,
insulin inhalers. Preliminary studies have shown very promising results but they are
not yet available in India.16
5
Even after discovery of so many alternative devices and newer technologies,
conventional Insulin Therapy with a needle and syringe is still one of the most
popular, convenient, and cost effective method for insulin administration.
Subcutaneous insulin administration is the only insulin administration technique,
which can be done at home environment and can be done by patients themselves.
NEED FOR THE STUDY
Diabetes is widely recognized as one of the leading causes of death and disability
worldwide. Diabetes is not new to the medical world as it is known since antiquity
(1500BC), but now Diabetes has become a major health threat to the whole world.17
The explosion of diabetes in India and other developing countries has been viewed
with serious concern by the World Health Organization (WHO) and the International
Diabetes Federation (IDF) 5.
Increasing prevalence of Diabetes will put a heavy burden not only on health system
but a health worker also have to spend a lot of his professional time on Diabetes care.
Majority of Diabetes population in India belong to Type II (NIDDM) group. Strict
long-term glycemic control reduces the complications associated with Diabetes
Mellitus. This has been established in the recent Diabetes Control and Complications
Trial (DCCT).
Maia FFR, Araujo LR in their study “ Insulin pen injector for the treatment of
Type I Diabetes Mellitus” has mentioned that the treatment of Type I Diabetes
mellitus (DM) has had some breakthroughs over the last few decades. The exogenous
administration of insulin has been the only available treatment for millions of
Diabetics all over the world. After Banting and Best discovered insulin in 1921, the
6
possibility of obtaining an ideal sugar control was more likely, offering Diabetics a
better survival rate and quality of life.18
Mollema ED, Snock FJ, Pouwer F in their study “Diabetes; fear of injecting and self
testing questionnaire” has found that extreme fear of self injecting insulin (Injection
Phobia) is likely to compromise glycemic control as well as emotional well being.19
Cramer JA, Pugh MJ in their study “The influence of Insulin use on glycemic
control” has described numerous barriers to use of insulin e.g., fear of self-injections,
and hypoglycemic events, burden of injections and timings in relation to meals etc.20
According to Diabetes Control and Complication Trial (DCCT) the strict control of
blood sugar level reduces the risks of microangiopathy, retinopathy, and nephropathy
in Diabetic patients. The treatment should be conducted on an individual basis and
requires participation of a multiprofessional team, commitment of the patient and help
from family members.21
It is obvious that in a country like India, the rising prevalence of diabetes with its
attendant complications is likely to produce severe constraints on health care budgets
in the future.5
Considering all the above factors and had having witnessed while posting in clinical
areas the investigator felt that there is a need for assessing the knowledge and attitude
regarding self-administration of insulin injection among Diabetes Mellitus patients.
The Diabetic patients who are on Insulin need to be knowledgeable regarding the
disease and Insulin Therapy and also they must have a positive attitude towards self-
administration of insulin injection to overcome the barriers of insulin injection.

7
Therefore, the researcher is keenly interested to undertake this study. This will help
in avoiding complications besides improving quality of life of the patients.
STATEMENT OF THE PROBLEM
A Descriptive Study To Assess The Knowledge And Attitude Regarding
Self-Administration Of Insulin Injection Among Diabetes Mellitus Patients In Kempa
Cheluvamba General Hospital At Malleswaram, Bangalore.
OBJECTIVES OF THE STUDY
1. To assess the knowledge of patients regarding self-administration of insulin
injection.
2. To assess the attitude of patients regarding self-administration of insulin
injection.
3. To correlate the knowledge and attitude of Diabetic patients regarding self-
administration of insulin injection.
4. To associate the knowledge with selected demographic variables.
5. To associate the attitude with selected demographic variables.
6. To develop an information booklet on self-administration of insulin for
Diabetes Mellitus patients.
OPERATIONAL DEFINITIONS
1. Knowledge: It refers to the level of understanding of Diabetic Patients
regarding self-administration of insulin injection as measured by the correct
responses to the items.
8
2. Attitude: These are feelings and beliefs expressed by patients towards
self-administration and are evident from scores obtained by their response in a
validated rating scale.
3. Self-Administration: The injection expected to be administered by the
patients at home without assistance. This includes preparation of article,
withdrawal of injection, administration and after care.
ASSUMPTIONS
Patients who are on Insulin Therapy of Kempa Cheluvamba General Hospital
will posses some knowledge regarding self-administration of insulin injection.
The increased knowledge of the Diabetes Mellitus patients will show a
positive attitude towards self-administration of Insulin injection.
HYPOTHESIS
H1 : There is a significant relationship between knowledge and attitude of
Diabetes Mellitus patients regarding self-administration of insulin injection.
H2 : There is a significant association between levels of knowledge with
selected demographic variables.
H3 : There is a significant association between the attitudes of diabetes
mellitus patients with selected demographic variables.
SAMPLING CRITERIA
Inclusion Criteria
1. Patients who are diagnosed with diabetes mellitus in K. C. General Hospital
2. Those who are in the age of 40 to 70 years
3. Patients who are on Insulin Therapy.
4. Both male and female are included.
9
Exclusion criteria
1. Diabetic patients who are on Oral Hypoglycemic Agents.
2. Diabetic patients who are on Intravenous Insulin Therapy.
Conceptual Frame Work
A concept is a thought, idea or mental image formed in the mind in response to
learning something new. A framework is a basic structure supporting anything. 22
Conceptual framework deals with the interrelated concepts that assembled together in
some rational scheme by virtue of their relevance to a common theme. 23
One of the important purposes of conceptual framework is to communicate clearly the
interrelationship of various concepts. It guides an investigator to know what data
needs to be collected and gives direction to entire research process.24
The conceptual framework for this study was based on Orem’s self-care model as
cited in Potter and Perry.25 This conceptual framework identifies and defines the
factor or phenomena of work in a nursing situation and describes their relationships.
Each individual has an innate ability to care for oneself. It is a theoretical model
which values individual responsibility and belives in health education as key aspect of
nursing intervention.(Dorothea E.Orem)
This study is aimed at assessing the knowledge and attitude on self-administration of
insulin injection among diabetes Mellitus patients. This study will focus on to find the
association if any, between knowledge and attitude with selected demographic
10
variables and so also will find association if any between the knowledge and attitudes
of Diabetic patients regarding self-administration of insulin injection.
The main concepts that are enumerated in this study are Self-care requisites and self-
care agency. Self-care is the practice of the activities that individuals perform in their
own behalf in maintaining life, health and well-being. In this study self-care
comprises all the activities related to self-administration of insulin injection which in
turn contribute to healthy practices and general health maintenance.
Self-care requisites are the demands of Diabetic patient’s specific of their needs. The
self-care requisites arise from a variety of conditions, which pose as a threat to the life
of an individual .In this study this refers to those conditions where Diabetic patients
need assistance due to wrong self-administration practices, which are detrimental to
their life.
The nurse posses the ability to identify the self-care requisites so as to render
comprehensive nursing care. Self-care agency refers to the human ability for engaging
in self-care. Normally adults voluntarily care for themselves. In this study self-care
agency refers to nursing activities (Nursing Agency) when assessing and determining
client’s needs, one should identify which are the areas where self-care deficits exists.
At the same time, one must gather sufficient information why there is self-care deficit.
The ability of Diabetic patients to meet the self-care demands depends partly on their
knowledge, beliefs, tradition, education, religion, socio-economic background,
making use of skills and available resources. Once the nurses are able to identify the
reasons for the client’s self-care deficits it is possible to plan for intervention.
11
Orem identifies three basic types of nursing systems to meet the client’s needs for
nursing assistance.
1. Wholly compensatory system
2. Partly compensatory system
3. Supportive educative system
The above first two systems plays a vital role in maintaining health of Diabetic
patients. In supportive educative system the client has the resources to meet their
demands, but needs nursing assistance in decision making, behavior control and
acquisition of knowledge and skill.
The investigator assumes that some demographic variables could affect knowledge
and attitude of diabetic patients and further knowledge about self-administration of
insulin injection will have clear association with their behaviors. Based on their
knowledge and background the diabetic patients will possess a positive attitude
towards self-administration of insulin injection. After assessment the findings will
focus on the extent of the problem in these areas.
In this study supportive–educative system is selected for developing framework of the
study. So, in order to educate the diabetic patients, their existing knowledge and
attitude is assessed and guidelines for health teaching is developed according to the
unified unhealthy attitudes (not contributing to healthful living) which are the main
objectives of the study.
In this conceptual model, the self-care agents are the diabetic patients who are on
insulin therapy in K. C. General Hospital at Malleswaram, Bangalore. The identified
Diabetic patient’s attitudes are taken into account and a guide for health teaching will
12
enable them for healthful living. Based on the Orem’s Self-care model the supportive-
educative system is within a client-centered system, where health teaching material is
considered to be an appropriate teaching strategy. The following model represents the
conceptual framework, which the investigator constructed before attempting the
study.

13

14
2. OBJECTIVES
STATEMENT OF THE PROBLEM
A descriptive study to assess the knowledge and attitude regarding self-administration
of insulin injection among Diabetes Mellitus patients in Kempa Cheluvamba General
Hospital at Malleswaram, Bangalore.
OBJECTIVES OF THE STUDY
1. To assess the knowledge of patients regarding self-administration of insulin
injection.
2. To assess the attitude of patients regarding self-administration of insulin
injection.
3. To correlate the knowledge and attitude of Diabetic patients regarding self-
administration of insulin injection.
4. To associate the knowledge with selected demographic variables.
5. To associate the attitude with selected demographic variables.
6. To develop an information booklet on self-administration of insulin for
Diabetes Mellitus patients.
15
3. REVIEW OF LITERATURE
Review of literature is an integral component of any study or research project. It
equips the investigator to be familiar with the existing studies, provides basis for
future investigation and also helps in development of methodology, tool and research
design.
Review of literature involves the systematic identification, location, scrutiny and
summary of written materials that contain information on a research problem.23
Abdellah, Levine states that the review of literature provides basis for future
investigation, justifies the need for replication, throws light upon the feasibility of the
study, indicates constraints of data collection and help to relate findings of one to
another.26
The literature review was based on an extensive survey of books, journals,
international nursing studies and Medline search. A review of research and non-
research literature relevant to the study was taken, which helped the investigator to
develop deeper insight into the problem and gain information on what has been done
in the past. The review of literature related to the purpose of the present study has
been organized and presented under the following headings
Part A: Literature related to Insulin Therapy
Part B: Literature related to insulin administration devices and patient’s preferences
Part C: Literature related to complications of insulin therapy
Part D: Literature related to the knowledge and attitude regarding Insulin Therapy and
patient’s compliance

16
Part A: Literature related to Insulin Therapy
Insulin injections are given to replace endogenous insulin in patients with absolute or
relative deficiencies in insulin secretion.
The aims of insulin therapy are-
Abolish hyperglycemic symptoms
Maintain ideal body weight
Optimize glucose control
Avoid hypoglycemia
Maintain as near normal a blood glucose as practical and safe for the
individual.27
Cramer JA, Pugh MJ conducted a study on ‘‘The influence of Insulin Use on
Glycemic Control’’ to determine the relationship between the self-management and
glycemic control and to identify patient characteristics associated with better control.
In their study they found that adults prescribed a specific insulin regimen averaged
using 77% of prescribed doses, demonstrating good intention to follow the
prescription. However, glycosylated hemoglobin (HbA1C) higher than the
recommended level suggested that the rate of insulin use, the prescribed regimen, or
both were inadequate to achieve good glycemic control in patients with long-term
insulin use.20
Franeine RK in the article ‘‘Intensive Management of Type 1 diabetes in young
children” had mentioned that many pediatric diabetes specialists do not place their
very young patients on continuous subcutaneous insulin injection or flexible bolus
therapy with multiple daily injections. It was shown that very young children with
supportive knowledgeable families can lower glycosylated hemoglobin (HbA1C) to

17
under 80% with multiple injections without increasing episodes of hypoglycemia.
This will enable these very young children to survive into adulthood with minimum
risk for the devastating long-term complications of this disease.28
Another article published by Dewitt DE, Dugedale DC ‘‘Using New Insulin
Strategies in the out patient treatment of Diabetes’’ had commented that when to use
insulin and how to apply the principles of physiologic insulin replacement, using
existing and new insulin is a key step for improving diabetes care. Insulin analogues
and premixed insulin increase physician’s and patient’s ability to lower glycosylated
hemoglobin (HbA1C) levels with fewer episodes of hypoglycemia. Earlier use of
insulin and more aggressive dose escalation are important steps in achieving treatment
goals.29
Garg MK in the article ‘‘Current perspective in Insulin Therapy in the management
of Diabetes Mellitus’’ had mentioned about the effectiveness of Insulin Therapy
among Diabetes Mellitus patients. In the article it was concluded that the efficacy of
human insulin has been proved beyond doubt by two large long term trials in both
Type I and Type II diabetes in controlling hyperglycemia, maintaining
normoglycemia and delaying onset and progression of diabetes complications.24
The Diabetes Control and Complications Trial/ Epidemiology of Diabetes
Interventions and Complications Research Group conducted a study on
‘‘Retinopathy and Neuropathy in patients with type I diabetes four years after a trial
of Insulin Therapy’’ and concluded that among patients with type I diabetes mellitus,
intensive therapy markedly reduces the risk of micro vascular complications as
compared with Conventional Therapy and reduction in the risk of progressive

18
retinopathy and nephropathy persists for at least four years despite increasing
hyperglycemia.30
Hayward RA, Manning WG, Kaplan SH, Wagner EH, Greenfield S did a study
on ‘‘Starting Insulin Therapy in Patients with Type II Diabetes’’ to determine the
effectiveness, complication rates and resource utilization of Insulin Therapy in
clinical practice. They conducted an extensive survey and found that for patients with
Type II Diabetes who were cared for by generalist physicians, starting Insulin
Therapy was generally safe and effective in achieving moderate glycemic control.
However Insulin Therapy was associated with increases in resource use and was
rarely effective in achieving tight glycemic control, even for those with moderate
control.31
Saudek CD, Duckworth WC, Giobbie-Hurder A, Henderson WG, Henry RR,
Kelly DE et al conducted a study on ‘‘Implantable Insulin Pump vs. Multiple-Dose
Insulin for Non Insulin Dependent Diabetes Mellitus’’ to determine whether
Implantable Insulin Pump (IIP) Therapy and Multiple Daily Insulin (MDI) injections
could equally attain improved blood glucose control, and to compare the 2 treatments
with respect to reducing daily blood glucose fluctuations, reducing severe
hypoglycemic insulin reactions and improving patient’s quality of life. After
analyzing the results they concluded that Intensive Insulin Therapy with Implant able
Insulin Pump and Multiple Daily Injection is effective in controlling Non-Insulin
Dependent Diabetes Mellitus.32

19
Part B: Literature related to Insulin administration devices and patient’s
preferences
Summers KH, Szeinbach SL, Lenox BM conducted a study on “Preference for
Insulin Delivery by systems among current Insulin users and non-users” to examine
the respondent preferences for the vial and syringe and the insulin injection pen
device between current insulin users and non-users. Based on this survey, they
concluded that the overall preference for the insulin injection pen device appeared to
be higher compared with the vial and syringe among both insulin users and non-users
Social acceptability was the strongest predictor of preferences for insulin injection
pen devices for current insulin users. Social acceptability and ease of use were
significant predictors of preference for the vial and syringes. For insulin non –users,
these results suggested that patient discussions about vial and syringe should
emphasize activity interference and ease of use.33
Hill J in the review article “Devices for Insulin Administration” has commented that
the drive to improve blood glucose control to prevent diabetic complications has
resulted in many patient’s with Type II as well as those with type I requiring Insulin
Therapy. Jillian Hill describes the devices now available to deliver insulin, which
enable more people to manage their insulin administration independently.34
Sucic M, Galic E, Cabrijan T, Ivandic A, Petrusic A, Wyatt J et al did a study on
“Patient acceptance and reliability of new Humalin / Humalog 3.0 ml prefilled insulin
pen in ten Croatian diabetes centers’’ to assess preferences patient acceptance
reliability and safety of the new Lilly Humalin / Humalog 3.0 ml prefilled insulin pen
in a clinical setting. Results of the study were majority of patient rated the new
prefilled pen as being more convenient and easier to use and indicated that it

20
represented a significant or modest an improvement over their previous insulin
injection method (i.e., either reusable devices or traditional syringe and vial)35
Another study was conducted by de Sauza CR, Zanetti ML on "The use of
disposable syringes in administration of insulin at home’’ to observe the behavior of
113 people with diabetes mellitus in relation to the utilization and reutilization of
disposable syringes for the administration of insulin at home. The obtained results
showed that 98.2% used a disposable syringe for insulin application and only 5.3%
actually disposed of it. Among these 94.6% re-used the disposable syringe after
application by means of various procedures.36
Robertson KE, Glazer NB, Campabell RK in their article “Latest developments in
Insulin injection devices” had mentioned about the dramatic changes in the treatment
of diabetes. Today patients with diabetes have ready access to more information about
the disease and its treatment options. As a result insulin treated patients have become
more autonomous in the management of their diabetes and may be better prepared to
participate in making informed choices regarding insulin delivery devices.37
Part C: Literature related to complications of Insulin Therapy
Messad D, Outtas O, Demoly P in their article “Hypersensitivity to Insulin” had
commented that the use of purified insulin obtained by genetics has dramatically
lowered the frequency of insulin hypersensitivity, In the case of localized cutaneous
reactions spontaneous regression is generally observed, the association of an oral
antihistamine and / or fractioning of the dose and its injections on several different
sites often leads to disappearance of these reactions.38

21
Saudan B, Gipardot C, Fermon C in their case report ‘‘Extreme subcutaneous
insulin resistance a misunderstood syndrome’’ had mentioned that extreme
subcutaneous insulin resistance (SIR) is a rare syndrome characterized by severe
resistance to subcutaneous insulin with normal intravenous insulin sensitivity.39
Richardson T, Kerr D in their review article ‘‘Skin related complications of Insulin
Therapy-epidemiology and emerging management strategies’’ had reported that
Insulin Therapy is associated with important cutaneous adverse effects which can
affect insulin absorption kinetics causing glycemic excursions above and below target
levels for blood glucose. Common complications of subcutaneous insulin injection
include lipoatrophy and lipohypertrophy. The likelihood of lipoatrophy can be
reduced by regular rotation of injection sites. Local allergic reactions to insulin are
usually erythema, pruritus and indurations. These allergic reactions are usually short-
lived and resolve spontaneously within a few weeks.40
Yokoyama H, Fukumoto S, Koyama H in their case report Insulin Allergy
desensitization with crystalline zinc insulin and steroid tapering had recommended
that the insulin analogues Aspart and Lispro, have been safe alternatives for patients
with insulin allergy, because of their decreased immunogenecity.41
Sola -Grzagnes A, Pecquet C, Radermeker R, Pietri L, Elgrably F, Slama G
et al. did a study on successful treatment of insulin allergy in a type 1 diabetic patient
by means of constant subcutaneous pump infusion of insulin.42
Log win S, Conget I, Jansa M, Vidal M, Nicolan C, Gomis R et al. conducted a
study on “Human Insulin Induced Lipoatrophy; successful treatment using a jet

22
injector device’’ to evaluate the efficacy of the administration of insulin by a jet
injector device in stopping and reversing severe human insulin–induced lipoatrophy.
The results of the study were total loss of subcutaneous tissue in the injection areas
were demonstrated and measured by high frequency ultrasound. Dermatologic exam
demonstrated a severe reduction of fat tissue. So they concluded that jet-injector
devices might constitute a helpful method to treat those patients affected by severe
human insulin induced lipoatrophy. 43
Part D: Literature related to the knowledge and attitude regarding Insulin
Therapy and patient’s compliance.
Reach G, Zerrouki A, Leclereq D, d’Ivernois JF did a study on “Adjusting Insulin
doses from knowledge to decision” to analyze the adjustment of insulin doses in type
1 diabetic patients with poorly controlled diabetes. After analysis they had found that
the fear of hypoglycemia was the most frequently given reason for not adjusting the
insulin doses, when the question asked to the patients with an open answer. This study
illustrates the difference between the thinking and doing. It also shows that the
degree of confidence in one’s own knowledge, the health beliefs, and the fear of
hypoglycemia differently influences the preparation that the patients have of their
behavior and what they really do.44
According to Bergenstal RM one key physician barrier to start insulin is either not
understanding or accepting that over time insulin will be a necessary part of therapy
for most patients with type II diabetes. Diabetes experts feel so strongly that
overcoming barriers to insulin initiation is critical to improve glycemic control and
quality of life outcomes for patients with diabetes. A study conducted by Diabetes
Attitudes, Wishes and Needs (DAWN) shows health care provider should focus as

23
much on patient’s attitudes and environment as on medicine when trying to improve
health.45
Skinner TC in the article “Psychological barriers” had mentioned that type II
diabetes treatment outcomes ultimately depend on patients and their ability to make
long term behavioral changes that support good self care and metabolic control.
Patient’s perception about diabetes and diabetes related complications can have a
strong influence on their emotional well being and quality of metabolic control.
Negative emotions and preconceptions about treatment can also discourage adherence
to treatment plans. “Psychological insulin resistance” caused by fear and concerns
about insulin and daily injections can discourage many patients from starting Insulin
Therapy. Depression, stress and anxiety represent further obstacles to optimum self-
care and the attainment of glucose goals.46
Asakura T did a study on “Research regarding proper use of insulin in diabetic
patients” to determine education and the degree of understanding of insulin self
injection. After analysis it became clear that older patients ability to understand
diminished and that patient’s life style, including psychological factors, exerts a large
influence on continuing the correct treatment. So the researcher recommended giving
guidance about treatment, which fits the patient’s lifestyles.47
Maureen IH conducted a study on “A National sample patients with type 2 diabetes”
in Bethesda, Maryland. Study revealed that 29% Patients were treated with insulin,
65% treated with oral agents, 80% treated with diet alone had never monitored their
blood glucose level. At least once per day blood glucose monitoring was predicted by
39% of those taking insulin.48

24
Mollema ED, Snock FJ, Heine RJ, Vander Ploeg HM conducted a study on
“Phobia of self injecting and self –testing in insulin treated diabetic patient’s
opportunity for screening’’ and found that severe fear of self injection and self-testing
characterized by emotional distress and avoidance behavior seems to occur in a small
group of insulin treated patients with diabetes.49
Pawar BK, Walfard S, Sigh BM conducted a study on ‘‘Type I diabetes mellitus in
a routine diabetes clinic the association of psycho-social factors, diabetes knowledge
and glycemic control to insulin regime’’ and concluded that in routine clinical
practice the use of intensive insulin regimes are associated with worse glycemic
control, despite patients being marginally more knowledgeable and self-directed.50
Almeida HG, Campus JJ, Kfouri C, Tanita MT, Dias AE, Souza MM conducted a
study on ‘‘Profile of patients with diabetes type I: insulin therapy and self-
monitoring’’ to know the insulin treatment and the plan for glycemic self-monitoring
used by these patients, to verify their knowledge as for what they consider the
optimization of these parameters and limitations for use They concluded that although
human insulin is already adopted as the use of choice, the outline of insulin treatment
plan is still traditional and the monitoring is for behind the ideal.51
Lombardo F, Salzano G, Messina MF, Deluka F in their article ‘‘How self
management therapy can improve quality of life for diabetic patients’’ has mentioned
that self control led therapy is vital in the treatment of insulin dependent diabetes
mellitus, allowing as it does, correct insulin therapy, a reduction in hospitalization and
modification of therapy for individual needs in relation to various factors. The
diabetes team (doctors, nurse,5 dietician, psychologist and social assistant) must set
25
objectives making the patient aware of his condition, giving him the knowledge of
what to do and how to do it. In this way quality of life can be improved for the
patients affected by this chronic illness and they can understand how to face the future
with realistic optimism.52
Coates VF, Boore JR conducted a study on ‘‘The influence of psychological factors
on the self management of insulin dependent diabetes mellitus’’ to investigate the
influence of a number of psychological factors upon the practice and outcome of
diabetes self-management among young adults with IDDM health beliefs, perception
of control and knowledge were assessed by scales, questionnaire and glycosylated
hemoglobin values The results demonstrated that the subjects perceived that they
were responsible for the control of their diabetes, that the benefits of following the
treatment is greater than any barriers and that they were knowledgeable about their
diabetes.53
Saunders SA, Wallymahmed M, Macfarlane IA in their study “glycemic control in
a type I diabetes clinic for younger adult’’ had concluded that despite regular
specialist physician, specialist diabetic nurse, and dietician input, encouragement of
multiple daily injection and rapidly following up failed appointments (including home
visits) tight glycemic control is rare in a routine clinic setting.54
Kapoor A conducted a study on ‘‘Diabetes care in India’’ and revealed that among
824 diabetes 69% were on oral agents, 15% were on combination of insulin and oral
hypoglycemic agents, 15% were on insulin alone 1% were on diet exercise and others
on herbal precautions. 58% of insulin users visit doctor monthly compared to 58%
tablet users, 43% self-administer insulin, 33% were given insulin by family members,

26
while 25% depend on health care professional to administer insulin. Only 109 patients
answered to the question “who taught you injection technique?’’ 78% learnt the
technique by themselves, 9%were taught by family members and 13% learnt from
qualified source.55
De Weerdt I, Visser AP, Kok G, Vander Veen KA in their study “Determinants of
active self care behavior of insulin treated patients with diabetes; implications for
diabetes education’’ revealed that most important aim of diabetes education is to alter
the self care behavior of patients with diabetes. In order to change their behavior its
determinants must be known. The attitude was found to be the most important
determinant of active self care, while a sufficient level of knowledge was a
prerequisite for a positive attitude. According to the results of this study diabetes
education should first aim at improving the level the knowledge and the health focus
of control of the patients and second at a positive attitude to active self care. It is
necessary to educate the social environment to create a more supportive atmosphere
for the patients with diabetes.56
An extensive review of related literature both research and non research was carried
out and presented in this chapter. The literature review helped the investigator to
establish the need for the study, state the problem clearly, develop a conceptual
framework, develop the tool, to adopt research methodology, select techniques of data
collection and decide on the plans of statistical analysis in order to achieve the
objectives of the study.
27
4. METHODOLOGY
Research methodology is the systematic way to solve the research problem.
Research methodology aims at helping the researcher to answer the research questions
effectively, accurately and economically, studying how research is done
scientifically.57
This chapter deals with the description of methodology and different steps, which
were undertaken for gathering and organizing date for the investigation. This includes
Research Approach, Research Design, Variables under Study, Settings of the Study,
Population of the Study, Sample, Sample Size, Sampling Technique, Criteria for
selection of Sample, Development and Description of the Tool, Content Validity,
Pilot Study, Method for Data Collection and Data Analysis.
RESEARCH APPROACH
The approach to research is the umbrella that covers the basic procedure for
conducting research.24 The study was intended to assess the knowledge and attitude
of Diabetes Mellitus patients regarding self-administration of insulin injection.
Descriptive survey approach, which is exploratory in nature, was found to be the most
suitable approach for the attainment of the objectives of the study
RESEARCH DESIGN
The research design is concerned with the overall framework for conducting the
study. A research design incorporates the most important methodological decision
that a researcher makes in conducting a research study23. The research design used
for this study is descriptive and exploratory.
The schematic representation of the design used in this study is given in figure (2)

28
K. C. General Hospital
Background Variables
• Age • Sex • Education • Occupation • Religion • Martial
Status • Family
Income • Duration
since diagnosis of Diabetes Mellitus
• Actual number of years on insulin therapy
• Family history of Diabetes M llit
Target
Population
Diabetic Patient who are on Insulin therapy and who are admitted in K.C. G Hospital are also those attending the OPD services in K. C. General Hospital
Samples 60 Diabetic Patients between age of 40 to 70 years and who are on Subcutaneous Insulin Injection Sampling: Convenient Sampling
Tool
Structured Knowledge Questionnaire
Structured
Likert type Attitude Scale
Assessment
Knowledge and Attitude of Diabetic Patients regarding self administration of Insulin Injection
Plan for Intervention
Development of an Information Booklet
K. C. General Hospital
Fig. 2 : Schematic Representation of Research Design

29
VARIABLES UNDER STUDY
Variables are qualities, properties or characteristics of persons things or situation that
change or vary.58
Research Variables
Knowledge and attitude of Diabetic patients regarding self-administration of Insulin
Injection.
Demographic Variables
Age, Gender, Education, Occupation, Religion, Marital Status, Family income per
month, Duration since diagnosis of Diabetes Mellitus, Actual number of years on
Insulin therapy, Family History of Diabetes Mellitus.
SETTING OF THE STUDY
Setting is the physical location and condition in which data collection takes place 23
Setting of this particular study was the ward and OPD of Kempa Cheluvamba General
Hospital, at Malleswaram, Bangalore.
The Kempa Cheluvamba General Hospital is situated in the heart of the city with bed
strength of 450 with daily average of 250 inpatients. The outpatient department
functions daily and average of 80 patients avail the clinical facilities
POPULATION FOR THE STUDY
Population is the entire aggregation of cases that meet a designed set of criteria 23
The target population for the present study includes the diabetic patients who are on
Insulin Therapy and who are aged between 40 to 70 years and those who are admitted
30
in the wards and attending OPD services in Kempa Cheluvamba General Hospital at
Malleswaram, Bangalore.
SAMPLE
Sample is a subset of population selected to participate in a research study.23
SAMPLE SIZE
The sample was arbitrarily decided to be 60 diabetic patients who are on Insulin
Therapy keeping in mind the availability of subjects
SAMPLING TECHNIQUE
Sampling is a process of selecting a portion of the population to represent the entire
population. Non-probability sampling technique was considered appropriate for this
study. According to Kerlinger FN “Non probability samples are selected based on
the judgments of researcher to achieve particular objectives of the research at hand” 59
The convenience sampling technique is a type of non-probability sampling, which
was found to be appropriate for the study
CRITERIA FOR SELECTION OF SAMPLE
Inclusion Criteria
1. Patients who are diagnosed with diabetes mellitus
2. Those who are in the age of 40 to 70 years
3. Patients who are on insulin therapy
4. Both male and female are included

31
Exclusion Criteria
1. Diabetic patients who are on Oral Hypoglycemic Agents
2. Diabetic patients who are on Intravenous Insulin Therapy.
DATA COLLECTION INSTRUMENT
An instrument is a written device that a researcher uses to collect data
Based on the objectives of study a structured questionnaire and an attitude scale were
developed to assess the knowledge and attitude of the diabetes mellitus patients
regarding self-administration of insulin injection.
DEVELOPMENT OF TOOL
The tool was developed based on the following
o Review of related literature
o Preparation of blue print
o Consultation with subject experts
o Researcher’s personal experience in Clinical Setting
The tool was initially prepared in English and was then translated to Kannada
(annexure H and J)
THE BLUE PRINT
The blue print was prepared to construct the tool. There was 30 knowledge
questionnaire featuring to the three domains of learning i.e., knowledge, application
and comprehension were formed. According to the content area, the item were spread
in three domains. There were 11 items on knowledge domain, 10 items on application
and 09 items in comprehension domain.

32
DESCRIPTION OF THE TOOL
The instrument consists of 3 sections
Section I Socio-Demographic Data
The first items of the tool consists of items seeking information about age, sex,
occupation, education, income, religion, duration of years on insulin therapy and
family history of Diabetes Mellitus.
Section II Knowledge Questionnaire
This section comprises of 30 statements regarding self-administration of insulin
injection and is divided into 2 main areas
Part –A : Statement related to general information regarding Insulin Therapy.
Part-B : Statement related to self –administration of insulin injection
The items were of multiple-choice type. Total score is 30. Each correct response will
carry a score of‘ “one’’ and “zero” score for incorrect response.
The knowledge of the respondents was arbitrarily categorized as follows:
Poor : 0-10
Average : 11-20
Good : 21-30
Section III Attitude sale
This section contains 20 statements framed into a Likert type Attitude Scale that gives
the attitude of diabetes mellitus patient regarding self-administration of insulin
injection. Each attitude items are having 5 options i.e., Strongly Agree (SA), Agree
(A), Uncertain (U), Disagree (D) and Strongly Disagree (SD). There were 15
positively stated and 5 negatively stated items
33
The response for each item was measured as a five-point scale as follows
Options Positive statements Negative statements
Strongly agree 5 1
Agree 4 2
Uncertain 3 3
Disagree 2 4
Strongly 1 5
The maximum score is 100 and minimum score is 20
The attitudes of the respondents were arbitrarily categorized as follows:
Unfavorable : Below 50
Favorable : 50-75
Most Favorable : Above 75
TESTING OF THE INSTRUMENT
A. Content Validity:
Validity refers to a complex concept, which broadly concerns the soundness of the
study’s evidence that is, whether the findings are cogent, convincing and well
grounded.23
Content validity represents the universe of contents or the domain of the given
construct. The universe of the content provides the framework and basis of
formulating the items.
The prepared tool was sent to eleven experts for content validity (Annexure D) who
were requested to render their opinion about relevance the items of the study - nine

34
experts in the field of Medical Surgical Nursing, one expert from General Medicine
and one expert from department of Bio-statistics
There were 100% agreements on all items, but suggestions were given to modify
contain questions and the modifications were then made in the tool.
CRITERIA CHECKLIST
A criteria checklist was prepared for content validity. Each criteria has 1-3 response
columns for rating
1) Completely meets the criteria
2) Partially meets the criteria
3) Does not meet the criteria
B. Reliability of the Tool
Reliability is the degree of consistency that the instrument or procedure demonstrates
whatever it is measuring it does so consistently.22
In order to establish the reliability of the tool, split-half method was used. The tool
was administered to 6 diabetic patients and the test was first divided into two
equivalent halves and correlation of the half test was found by using Karl Pearson
Correlation Coefficient formula and the significance of the correlation was tested by
using probable error. The reliability coefficient of the whole test was then estimated
by Spearman’s Brown Prophecy formula. The reliability of the knowledge
questionnaire was 0.94 and reliability of the Likert type Attitude Scale was 0.84. So
the tool was found to be highly feasible and reliable for data collection

35
PILOT STUDY
The pilot study is the trial run study, conducted before actual study in different
population with similar characteristics.
A pilot study was conducted to test the reliability of the tool. The data for the pilot
study was collected from six diabetic patients in K.C.General hospital at
Malleswaram, Bangalore from 02-09-05 to 10-09-05.Administrative approval was
obtained from the hospital administrator.
The pilot study confirmed that the final study was feasible.
METHOD OF DATA COLLECTION
A formal permission for conducting the study was obtained from the Medical
Superintendent and Nursing Superintendent of K.C. General Hospital at
Malleswaram, Bangalore. The method adopted for data collection was Self
Administered Questionnaire method by the investigator. The investigator introduced
herself to the Diabetic patients and explained the purpose of the study. The subjects
were assured confidentiality. They were requested to reply frankly and truly. The
investigator took consent from the Diabetic patients before administering the
questionnaire. Approximately 45-50 minutes were spent with each patient to collect
the complete data. No significant problem was faced by the investigator.
PLAN FOR DATA ANALYSIS
The data will be analyzed on the basis of objectives and hypothesis of the study. The
data obtained will be analyzed by using descriptive and inferential statistics.
36
The planned analysis of raw data is as follows:
Section I Socio Demographic Data
Demographic data would be analyzed in terms of frequency and percentage
distribution.
Section II Knowledge Questionnaire
The knowledge will be analyzed in terms of frequency, percentage, mean, mean
percentage and standard deviation.
Section III Attitude Scale
The attitude of the diabetic patients will be analyzed in terms of frequency,
percentage, mean, mean percentage and standard deviation.
Section IV Relationship between the knowledge and attitude of Diabetes Mellitus
patients with selected demographic variables.
χ² test will be used to find out the association between the knowledge and attitude
with selected demographic variables.
Section V relationship between knowledge and attitude
The relationship between knowledge and attitude of Diabetes Mellitus patients will be
tested by using Product Moment Correlation Co-Efficient.
The level of significance would be set at 0.05 levels to test the significance of
difference. This level is often used as a standard for testing the difference.
SUMMARY
This chapter has dealt with the methodology undertaken for the study. It includes
research approach, research design, description of setting; population, sample and
sampling technique used, development and description of tool, pilot study, procedure
for data collection and plan for data analysis.

37
5. RESULTS
Analysis refers to a number of closely related operations, which are performed with
the purpose of summarizing the collecting data and organizing the data in such a
manner that they answer the research questions.
Descriptive study design with survey approach was used in the present study. The
data was collected from Diabetic patients
Objectives of the study were:
1. To assess the knowledge of patients regarding self-administration of insulin
injection.
2. To assess the attitude of patients regarding self-administration of insulin
injection.
3. To correlate the knowledge and attitude of Diabetic patients regarding self-
administration of insulin injection.
4. To associate the knowledge with selected demographic variables.
5. To associate the attitude with selected demographic variables.
6. To develop an information booklet on self-administration of insulin for
Diabetes Mellitus patients.
The data collected were organized, tabulated, analyzed and interpreted by using
descriptive and inferential statistics and described with the help of tables and graphs.

38
The data presented under the following sections
Section I:
In this section the description of socio-demographic characteristics of the subjects are
drawn.
Section II:
The descriptive statistics such as mean, SD, calculated to average out the knowledge
scores.
Section III:
The descriptive statistics such as mean and SD calculated to average out the attitude
scores
Section IV
Data on association between the selected Demographic variables of the diabetic
patients and knowledge regarding self administration of insulin injection
Section V
Data on association between selected demographic variables of the diabetic patients
and their attitude regarding self administration of insulin injection.
Section VI
This section is to examine the relationship between knowledge and attitude by using
inferential statistical method, the Karl Pearson’s Correlation Co-efficient method.

39
Section - I
Data on Demographic variables of the Diabetic Patients Table - I
The Frequency and Percentage Distribution of Diabetic Patients according to their Age Group (in years)
Age (yrs) No. of subjects Percent
≤ 40 5 8.3
41-50 12 20.0
51-60 20 33.3
61-70 23 38.3
Total 60 100.0
Fig. 3 Distribution of diabetic patients according to their Age
Maximum number of diabetic patients, 38.3% were in the age group of 61 – 70 years,
33.3% were of 51 – 60 years. 20% fell under the age group of 41 – 50 years and 8.3%
were of below 40 years of age. Thus it shows that the maximum number of diabetic
patients participated in the study were between the age group of 61 – 70 years.
38.3
33.3
20
8.3
05
10152025303540
Perc
enta
ge
61-70 51-60 41-50 ? 40
Age
61-7051-6041-50? 40
<
<

40
Table – II
The Frequency and Percentage Distribution of the Diabetic patients according to Gender.
Gender No. of Subjects Percent
Male 44 73.3
Female 16 26.7
Total 60 100.0
26.7
73.3
MaleFemale
Fig. 4 Pie chart representing Percentage Distribution of the Diabetic Patients
according to Gender.
The percentage distribution of the diabetic patient according to gender reveals that
majority of the subjects, 73.3% were male and 26.7% were female.

41
Table - III
The Frequency and Percentage Distribution of the Diabetic Patients according to Education.
Educational status No. of subjects Percent
Primary 44 73.3
Secondary 13 21.7
Higher secondary 2 3.3
Graduate and above 1 1.7
Total 60 100.0
73.3
21.7
3.3 1.7
0
10
20
30
40
50
60
70
80
Perc
enta
ge
Primary Secondary Higher secondary Graduate andabove
Education
Primary
Secondary
Higher secondary
Graduate and above
Fig. 5 Bar Diagram representing Percentage Distribution of the Diabetic Patients according to Education.
The result indicate that only 1.7% of the diabetic patient had completed graduation,
3.3% had completed higher secondary, 21.7% completed secondary education and
73.3 % had completed only primary education. It shows that maximum number of the
diabetic patient who participated in the study had completed their primary education.

42
Table - IV
The Frequency and Percentage Distribution of the Diabetic Patients according to
Occupation
Occupation No. of
Subjects Percent
Unemployed 32 53.3
Private 9 15.0
Government 5 8.3
Self-employed 14 23.3
Total 60 100.0
53.3
158.3
23.3
0
10
20
30
40
50
60
Perc
enta
ge
Unemployed Private Government Self-employed
Occupation
Unemployed
Private
Government
Self-employed
Fig. 6 Bar Diagram Representing Percentage Distribution of the Diabetic
Patients according to Occupation
Table IV (Figure 6) depicts that 53.3% diabetic patients were unemployed, 23% were
self employed, 15% were private employee and only 8.3% were Government
employee.
43
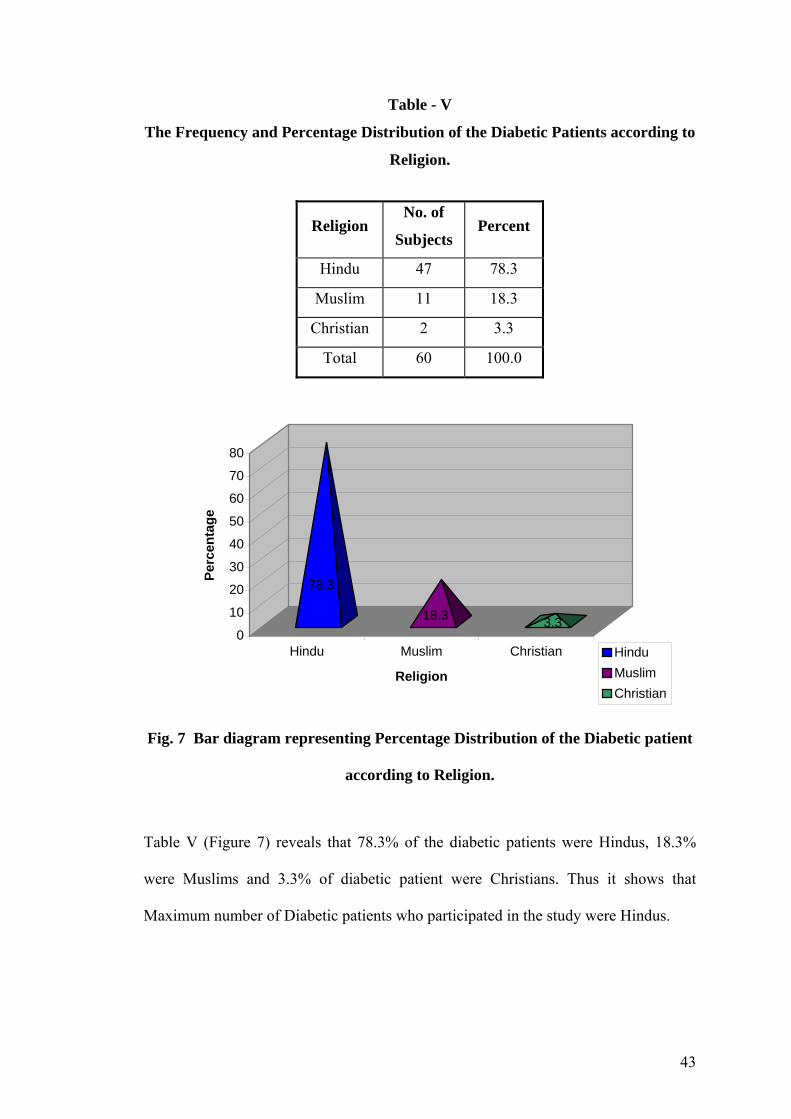
Table - V
The Frequency and Percentage Distribution of the Diabetic Patients according to
Religion.
Religion No. of
Subjects Percent
Hindu 47 78.3
Muslim 11 18.3
Christian 2 3.3
Total 60 100.0
78.3
18.3 3.30
10
20
30
40
50
60
70
80
Perc
enta
ge
Hindu Muslim Christian
Religion
HinduMuslimChristian
Fig. 7 Bar diagram representing Percentage Distribution of the Diabetic patient
according to Religion.
Table V (Figure 7) reveals that 78.3% of the diabetic patients were Hindus, 18.3%
were Muslims and 3.3% of diabetic patient were Christians. Thus it shows that
Maximum number of Diabetic patients who participated in the study were Hindus.

44
Table - VI
The Frequency and Percentage Distribution of Diabetic Patients according to Marital Status
Marital status No. of subjects Percent
Married 52 86.7
Unmarried 1 1.7
Widow(er) 7 11.7
Divorced 0 0
Total 60 100.0
86.7
1.711.7
0
0
10
20
30
40
50
60
70
80
90
Perc
enta
ge
Married Unmarried Widow(er) Divorced
Marital Status
Married
Unmarried
Widow(er)
Divorced
Fig. 8 Bar Diagram representing Percentage Distribution of Diabetic Patient according to Marital Status
Data presented shows that maximum number of the diabetic patients, 86.7% were
married, 11.7% were widow or widower and only 1.7% were unmarried. None of the
subjects were divorced.

45
Table - VII
The Frequency and percentage Distribution of the Diabetic Patient according to
Family Income per month.
Income (Rs) No. of subjects Percent
≤2000 38 63.3
2001-3000 11 18.3
3001-4000 5 8.3
>4001 6 10.0
Total 60 100.0
Fig. 9 Pie diagram Representing Percentage Distribution of the Diabetic Patients according to Family Income per month.
The results indicate that 63.3% of the diabetic patient had a family income less than or
equal to 2,000 per month, 18.3% had between 2001 to 3000, 10.%.were having family
income more than 4001 or above and 8.3% had a family income of 3001 – 4000.
63.318.3
8.310
? 20002001-30003001-4000> 4001
≤

46
Table – VIII
The Frequency and Percentage Distribution of the diabetic patients according to
Duration since diagnosis of Diabetes Mellitus
Distribution of duration
diabetes mellitus
No. of subjects Percent
<3 24 40.0
4-6 13 21.7
7-9 9 15.0
>9 14 23.4
Total 60 100.0
40
21.7
15
23.4
0
5
10
15
20
25
30
35
40
Perc
enta
ge
< 3 4 ~ 6 7 ~ 8 > 9
Duration of Diabetes Mellitus
< 34 ~ 67 ~ 8> 9
Fig 10 Bar Diagram representing Percentage Distribution of the Diabetic Patients according to duration since diagnosis of diabetes Mellitus
The table VIII and Figure 10 reveals that in 40% diabetic patient duration of diagnosis
of Diabetes Mellitus were lesser than or equal to 3 years, 23.4% duration of diagnosis
were greater than or equal to 9 years, 21.7% were within 4 – 6 years and in 15%
duration of diabetes Mellitus were 7 – 9 years.
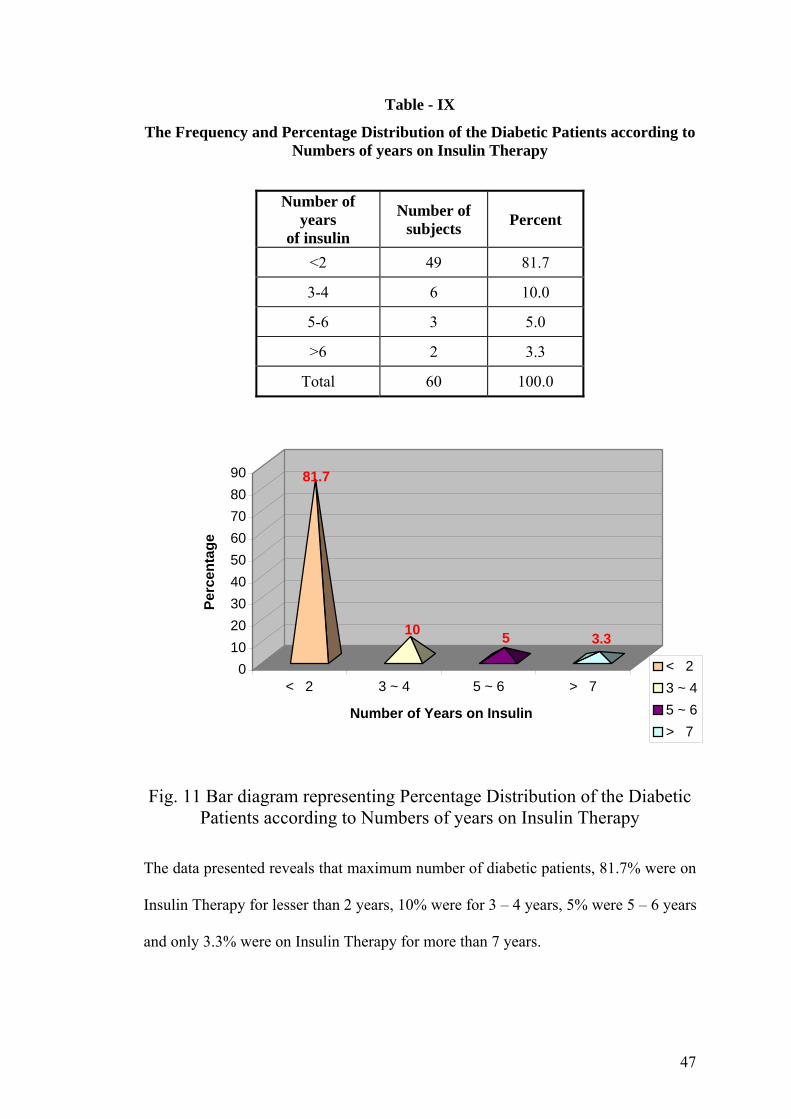
47
Table - IX
The Frequency and Percentage Distribution of the Diabetic Patients according to Numbers of years on Insulin Therapy
Number of years
of insulin
Number of subjects Percent
<2 49 81.7
3-4 6 10.0
5-6 3 5.0
>6 2 3.3
Total 60 100.0
81.7
10 5 3.3
0102030405060708090
Perc
enta
ge
< 2 3 ~ 4 5 ~ 6 > 7
Number of Years on Insulin
< 23 ~ 45 ~ 6> 7
Fig. 11 Bar diagram representing Percentage Distribution of the Diabetic Patients according to Numbers of years on Insulin Therapy
The data presented reveals that maximum number of diabetic patients, 81.7% were on
Insulin Therapy for lesser than 2 years, 10% were for 3 – 4 years, 5% were 5 – 6 years
and only 3.3% were on Insulin Therapy for more than 7 years.
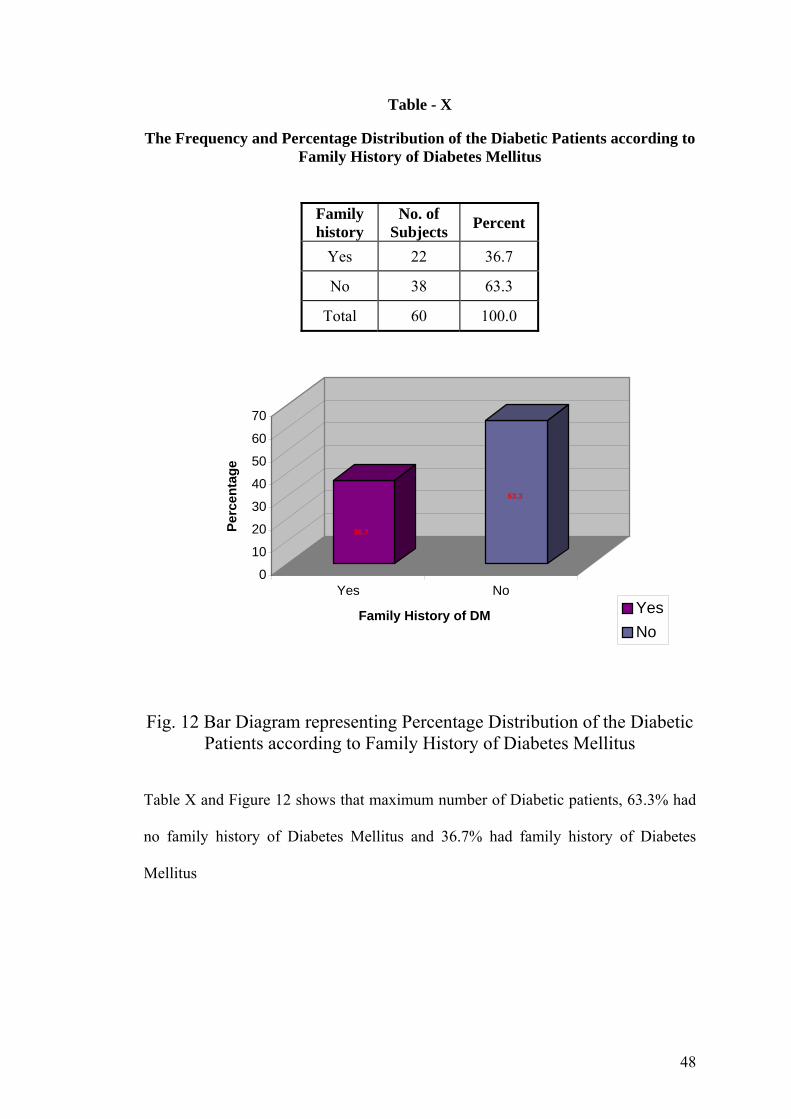
48
Table - X
The Frequency and Percentage Distribution of the Diabetic Patients according to Family History of Diabetes Mellitus
Family history
No. of Subjects Percent
Yes 22 36.7
No 38 63.3
Total 60 100.0
Fig. 12 Bar Diagram representing Percentage Distribution of the Diabetic Patients according to Family History of Diabetes Mellitus
Table X and Figure 12 shows that maximum number of Diabetic patients, 63.3% had
no family history of Diabetes Mellitus and 36.7% had family history of Diabetes
Mellitus
36.7
63.3
0
10
20
30
40
50
60
70
Perc
enta
ge
Yes No
Family History of DM YesNo
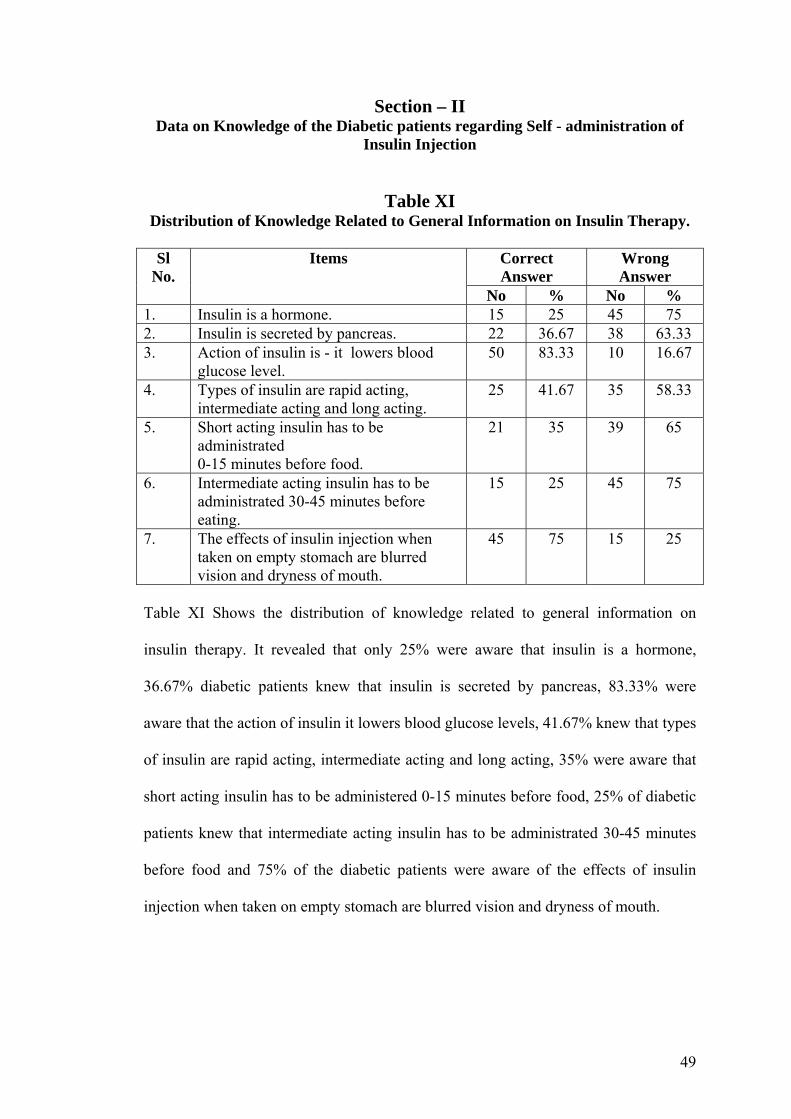
49
Section – II Data on Knowledge of the Diabetic patients regarding Self - administration of
Insulin Injection
Table XI
Distribution of Knowledge Related to General Information on Insulin Therapy.
Correct Answer
Wrong Answer
Sl No.
Items
No % No % 1. Insulin is a hormone. 15 25 45 75 2. Insulin is secreted by pancreas. 22 36.67 38 63.33 3. Action of insulin is - it lowers blood
glucose level. 50 83.33 10 16.67
4. Types of insulin are rapid acting, intermediate acting and long acting.
25 41.67 35 58.33
5. Short acting insulin has to be administrated 0-15 minutes before food.
21 35 39 65
6. Intermediate acting insulin has to be administrated 30-45 minutes before eating.
15 25 45 75
7. The effects of insulin injection when taken on empty stomach are blurred vision and dryness of mouth.
45 75 15 25
Table XI Shows the distribution of knowledge related to general information on
insulin therapy. It revealed that only 25% were aware that insulin is a hormone,
36.67% diabetic patients knew that insulin is secreted by pancreas, 83.33% were
aware that the action of insulin it lowers blood glucose levels, 41.67% knew that types
of insulin are rapid acting, intermediate acting and long acting, 35% were aware that
short acting insulin has to be administered 0-15 minutes before food, 25% of diabetic
patients knew that intermediate acting insulin has to be administrated 30-45 minutes
before food and 75% of the diabetic patients were aware of the effects of insulin
injection when taken on empty stomach are blurred vision and dryness of mouth.

50
Table XII
Distribution of Knowledge Related to Self Administration of Insulin Injection.
Correct Answer
Wrong Answer
Sl No.
Items
No % No % 8. Self administration of insulin is a cost
effective method 20 33.33 40 66.67
9. Insulin injection should be taken according to doctors advice
16 26.67 44 73.33
10. The areas suitable for self administration of insulin injection are arms, thighs, abdomen
32 53.33 28 46.67
11. Insulin injection can be administered just beneath the skin
47 78.33 13 21.67
,12. The sites for insulin injections are selected by rotating pattern.
26 43.33 34 56.67
13. The advantage of site rotation is to prevent tissue damage.
34 56.67 26 43.33
14. An open insulin vial can be preserved by keeping in a cold place
47 78.33 13 21.67
15. One of the complications of insulin injection is decreased blood sugar
52 86.67 8 13.33
16. Insulin syringes are preferred for insulin injection it is easy to calculate the dose
30 50 30 50
17. Before administering insulin injection inspect the vial for changes, like clumping, frosting
15 25 45 75
18. Insulin should be drawn from the vial by injecting a small amount of air
20 33.33 40 66.67
19. Which of the following step is correct when preparing to administer two types of insulin – the regular insulin is with- drawn first
13 21.67 47 78.33
20. An insulin vial should not be shaken vigorously to prevent clumping
15 25 45 75
21. Insulin preloaded syringes should be kept in vertical position
17 28.33 43 71.67
22. Insulin absorption rate increases with exercise
20 33.33 40 66.67
23. Insulin absorption rate decreases with smoking
16 26.67 44 73.33
24. Insulin doses are calculated in units 22 36.67 38 63.33 25. Spirit is used to wipe the insulin
injection site. 50 83.33 10 16.67
26. One should not message the site following insulin injection in order to prevent rapid absorption of insulin.
14 23.33 46 76.67

51
27. Once opened an insulin vial can be used for 30 days
16 26.67 44 73.33
28. The effectiveness of insulin can be measured by checking blood and urine glucose levels
51 85 9 15
29. Taking insulin ensures best control of diabetes
48 80 12 20
30. When experiencing hypoglycemia one should take some sugar dissolved in water.
53 88.33 7 11.67
Table XII depicts the distribution of knowledge related to self-administration of
insulin injection. It revealed that only 33.33% accepts that self-administration of
insulin injection is a cost effective method, 26.67% knew that insulin injection should
be taken according to doctor’s advice, 53.33% diabetic patients were aware that the
areas suitable for insulin injection are arms, thighs, abdomen, 78.33% of them knew
that Insulin injection can be administered just beneath the skin, 43.33% were aware
that the sites for insulin injection are selected by rotating pattern 56.67% were aware
that the advantage of site rotation is to prevent tissue damage 78.33% knew that an
open insulin vial can be preserved by keeping in a cold place, 86.67% knew that one
of the complications of insulin injection is decreased blood sugar, 50% were aware
that insulin syringes are preferred for insulin injection because it is easy to calculate
the dose, 25% knew that before administering insulin injection inspection of the vial
for changes, clumping, frosting should be done. 33.33% were aware that insulin
should be drawn from the vial by injecting a small amount of air 21.67% knew that
while preparing to administer two types of insulin the regular insulin is withdrawn
first, 25% were aware that an insulin vial should not be shaken vigorously to prevent
clumping, 28.33% knew that insulin preloaded syringes should be kept in vertical
position, 33.33% were aware that insulin absorption rate increases with exercise,
26.67% of them knew that insulin absoption rate decreases with smoking, 36.67%

52
were aware that insulin doses are calculated in units, 83.33% were having the idea
that spirit is used to wipe the insulin injection site, 23.33% knew that one should not
massage the site following insulin injection in order to prevent rapid absorption of
insulin. 26.67% were aware that once opened an insulin vial can be used for 30 days,
85% were aware that the effectiveness of insulin can be measured by checking blood
and urine sugar levels, 80% diabetic patient knew that taking insulin ensures best
control of diabetes and 88.33% of the subjects were aware that when experiencing
hypoglycemia one should take some sugar dissolved in water.

53
Table – XIII
Mean, Mean percentage and the Standard Deviation of the diabetic patients knowledge as per areas of self administration of Insulin Injection
Percentage of
Areas Range Max. score Mean SD Mean SD
General information 1-7 7 3.21 1.67 45.85 23.87
Self administration 6-16 23 11.23 2.61 48.82 11.34
Overall 7-23 30 14.45 3.26 48.17 10.87
Fig .13 Cone Diagram representing Mean Percentage of Diabetic Patients
in both the areas of Self - administration of Insulin Injection
The data analysed shows the mean, mean percentage, and the standard deviation of
the knowledge obtained by the diabetic patients in both the areas of self
administration of insulin injection The data reveals that the lowest mean percentage
score is 45.85% with a standard deviation of 1.67 in the area of knowledge related to
insulin therapy, where as the area of knowledge related self administration of insulin
injection the mean percentage of score is 48.82% with a standard deviation of 2.61.
The over all mean percentage was found to be 48.17% with a standard deviation of
3.26
45.85 48.82
05
101520253035404550
Perc
enta
ge
General information Self administration
Areas General informationSelf administration

54
Table - XIV Overall knowledge of the Diabetic Patients on Self-administration of Insulin
Injection
Knowledge No. of subjects Percent
Poor 8 13.3
Average 49 81.7
Good 3 5.0
Total 60 100.0
13.3
81.7
5
Poor Average Good
Fig 14 Pie diagram representing overall knowledge of the Diabetic patients
regarding Self-administration of Insulin Injection
Table XIV and Figure 14 shows the overall knowledge of the diabetic patients
regarding self-administration of insulin injection. Among them 81.7% diabetic
patients possess average knowledge, 13.3% had poor knowledge and only 5% diabetic
patients had good knowledge regarding self-administration of insulin injection

55
Section – III Data on the Attitude of the Diabetic Patients regarding Self-administration of
Insulin Injection
Table - XV Overall Attitude of the Diabetic Patients regarding Self-administration of Insulin
Injection
Attitude No. of subjects Percent
Favourable 49 81.7
Most favourable 11 18.3
Unfavourable 0 0
Total 60 100.0
Fig. 15 Pie Diagram Representing Overall Attitude level of the Diabetic patients
regarding Self-administration of Insulin Injection
The data presented shows the overall attitude level of the diabetic patients regarding
self-administration of insulin injection. This reveals that the maximum number of
diabetic patients 81.7%, has a favorable attitude, and only 18.3% Diabetic patients
had the most favorable attitude towards self-administration of insulin injection.
81.7
18.3 0
FavourableMost favourableUnfavourable

56
Section - IV Data on Association between the selected Demographic variables of the Diabetic
Patients and Knowledge regarding Self administration of Insulin Injection
Table – XVI Association between the selected demographic variables of Diabetic Patients and
their level of Knowledge regarding Self - administration of Insulin Injection
Demographic Variables Below mean
Above mean Total
Chi- Square value
Df p-value Inference
≤40 5 0 5 41-50 9 3 12 51-60 12 8 20 61-70 13 10 23
Age (yrs)
Total 39 21 60
4.166 3 >0.244 Not significant
Male 26 18 44 Female 13 3 16 Gender Total 39 21 60
2.532 1 >0.244 Not significant
Primary 30 14 44 Secondary 7 6 13
Higher secondary 2 0 2
Graduate and above 0 1 1
Education
Total 39 21 60
3.841 3 >0.279 Not significant
Unemployed 20 12 32 Private 6 3 9
Government 3 2 5 Self-
employed 10 4 14 Occupation
Total 39 21 60
0.408 3 >0.939 Not significant
Hindu 30 17 47
Muslim 9 2 11
Christian 0 2 2 Religion
Total 39 21 60
5.11 2 >0.078 Not significant

57
Demographic Variables Below mean
Above mean Total
Chi- Square value
Df p-value Inference
Married 32 20 52
Unmarried 1 0 1
Widow(er) 6 1 7 Marital Status
Total 39 21 60
2.133 2 >0.344 Not significant
<2000 24 14 38
2001-3000 9 2 11
3001-4000 3 2 5
>4001 3 3 6
Income
Total 39 21 60
2.073 3 >0.557 Not Significant
<3 17 7 24
4-6 8 5 13
7-9 8 1 9
>9 6 8 13
Duration of Diabetes Mellitus
Total 39 21 60
5.702 3 >0.127 Not significant
<2 35 14 49
3-4 1 5 6
5-6 2 1 3
>6 1 1 2
Number of years on Insulin
Therapy
Total 39 21 60
7.253 3 >0.064 Not significant
yes 14 8 22
No 25 13 38
Family History of Diabetes Mellitus Total 39 21 60
5.702 3 >0.127 Not significant

58
Table. XVI describes the association between selected demographic variables of the
diabetic patient and their level of knowledge regarding self administration of insulin
injection.
The table reveals that there is no association between the knowledge level of diabetic
patients regarding self administration of insulin injection and their age. At 0.05 level
of significance with 3 degree of freedom the calculated Chi-square value is 4.166 is
(P> 2.44). Hence there is no association between the knowledge level and age of the
diabetic patients.
A chi-square test was done to find out the association between the level of knowledge
and gender. The calculated chi-square value is 2.532 (P> 0.244). So there is no
association between the knowledge level and gender.
To find the association between the level of knowledge and educational status a Chi-
square test was done. The calculated Chi-square value is 3.841 (P>0.279). Hence
there is no significant association between the knowledge level and education.
A Chi-square test was done to find out the association between the knowledge level
and occupation of diabetic patients. The calculated chi-square value is 0.408
(P>0.939) at 3 degree of freedom. Hence there is no association between the
knowledge level and occupation of the diabetic patients.
The association between the knowledge regarding self administration of insulin
injection and their religion were tested by using a Chi-square test. The calculated
value is 5.11 (P>0.078) at 2 degree of freedom. Hence there is no significant
association between the knowledge level and religion.

59
A Chi-square test was done to find out the association between the knowledge level
and marital status. At 2 degree of freedom and 0.05 level of significance calculated
Chi-square value is 2.133 (P>0.344). So there is no significant association between
the level of knowledge and martial status.
To find out the association between the knowledge level and income a chi-square test
was done. The calculated Chi-square value is 2.073 (P>0.557) at 3 degree of freedom
and 0.05 level of significance and there is no association between the knowledge level
and income.
A Chi-square test was done to associate the knowledge and duration of diagnosis of
Diabetes Mellitus. The calculated chi-square value is 5.702 (P> 0.127) at 3 degree of
freedom. Hence the investigator could not elicit any association between the level of
knowledge and duration of diagnosis of diabetes mellitus.
To find out the association between the knowledge level with number of years on
insulin therapy, a Chi-square test was done. The calculated Chi-square value is 7.253
(P>0.064) at 3 degree of freedom. So there is no significant association between the
knowledge and numbers of years on insulin therapy
The table reveals that there is no significant association between the level of
knowledge and family history of Diabetes Mellitus. At 1 degree of freedom the
calculated Chi-square value is 0.028 (P>0.866).
Hence H2 can be rejected, there is no significant association between the level of
knowledge of Diabetic patients and selected demographic variables.

60
Section - V Data on Association between Selected Demographic Variables of the Diabetic
Patients and their Attitude regarding Self - administration of Insulin Injection.
Table - XVII
Association between Selected Demographic Variables of Diabetic Patients and
their level of Attitude regarding Self -administration of Insulin Injection.
Demographic Variables Below mean
Above mean Total
Chi- square value
df p-value Inference
≤40 4 1 5 41-50 9 3 12 51-60 13 7 20 61-70 10 13 23
Age
Total 36 24 60
4.783 3 >0.188 Not significant
Male 26 18 44 Female 10 6 16 Gender Total 36 24 60
0.057 1 >0.812 Not significant
Primary 26 18 44 Secondary 7 6 13
Higher secondary 2 - 2
Graduate and above 1 - 1
Education
Total 36 24 60
2.220 3 >0.528 Not significant
Unemployed 17 15 32 Private 5 4 9
Government 3 2 5
Self-employed 11 3 14 Occupation
Total 36 24 60
2.716 3 >0.437 Not significant
Hindu 28 19 47
Muslim 8 3 11
Christian 2 2 Religion
Total 36 24 60
3.746 2 >0.154 Not significant

61
Demographic Variables Below mean
Above mean Total
Chi- square value
df p-value Inference
Married 31 21 52
Unmarried 1 1
Widow(er) 4 3 7 Marital Status
Total 36 24 60
0.694 2 >0.707 Not significant
<2000 18 20 38
2001-3000 11 11
3001-4000 5 5 Income
>4001 2 4 6
14.917 3 <0.002 Highly significant
<3 17 7 24
4-6 9 4 13
7-9 5 4 9
>9 5 9 14
Duration of diabetes mellitus
Total 36 24 60
5.15 3 >0.161 Not significant
<2 33 16 49
3-4 2 4 6
5-6 1 2 3
>6 2 2
Number of years on insulin therapy
Total 36 24 60
6.769 3 >0.08 Not significant
yes 15 7 22
No 21 17 38
Family History of Diabetes mellitus Total 36 24 60
0.969 1 >0.325 Not significant

62
Table - XVII describe the association between the selected demographic variables of
the diabetic patients and their level of attitude regarding self administration of insulin
injection.
A Chi - square test was done to find out the association between the level of attitude
and their age. At 0.05 level of significance and 3 degree of freedom, the calculated chi
square value is 4.783 (p>0.188). Hence, there is no significant association between the
level of attitude of diabetic patient with their age.
To find out the association between the level of attitude and gender, a chi square test
was done. The findings reveal that at 0.05 level of significance, the calculated chi
square value is 0.057 (p>0.812) at 1 degree of freedom. So there is no significant
association between the level of attitude and gender.
A Chi square test was done to find out the association between the level of attitude
and educational status. The calculated chi square value is 2.220 (p>0.528) at 3 degree
of freedom. Hence, there is no association between the level of attitude and
educational status.
To find out the association between the level of attitude and occupation, a chi square
test was done. The calculated Chi - square value is 2.716 (p>0.437) at 3 degree of
freedom. So there is no association between the level of attitude and occupation of
diabetic patients.

63
A Chi - square test was done to find out the association between the level of attitude
and religion. Here, the calculated chi square value depicts 3.746 which is greater than
the table value (p>0.154). No association between the level of altitude and religion
was elicited.
To find out the association between the level of attitude and marital status of diabetic
patients the calculated Chi-square value is 0.694 which is greater than the table value
(P>0.707) Hence, there is no association between the level of attitude and marital
status.
The table reveals that there is a significant association between the level of attitude
and income of diabetic patients. At 0.05 level of significance and 3 degree of
freedom, the calculated value is 14.917 (p<0.002). Hence there is an association
between the level of attitude and income of diabetic patients.
To find out the association between the level of attitude and duration of diagnosis of
diabetic mellitus a chi square test was done. The calculated chi square value is 5.15
(p>0.161) at 3 degree of freedom. So, there is no significant association between the
level of attitude and duration of diagnosis of diabetic mellitus.
A Chi - square test was done to find out the association between the level of attitude
and number of years in insulin therapy. At 0.05 level of significance and 3 degree of
freedom the calculated chi square value is 6.769 (p>0.08). Hence, there is no
association between the level of attitude and number of years on insulin therapy.

64
To elicit the association between the level of attitude and family history of diabetic
mellitus Chi - square test was done. At 1 degree of freedom and 0.05 level of
significance, the calculated chi square value is 0.969 (p>0.325). Hereby, the
investigator could not elicit any association between the levels of attitude with family
history of diabetic mellitus.
Hence H3 is rejected, there is no significant association between attitude towards self-
administration of insulin injection and selected demographic variables, except for
income of the Diabetic patients. The analysis shows there is a significant association
between attitude of Diabetic patients and Family Income.

65
Section – VI Data on correlation between the Knowledge and Attitude scores of the Diabetic
Patients regarding self-administration of Insulin Injection.
Table - XVIII Correlation of the Diabetic patients Knowledge and the Attitude on the
self administration of Insulin Injection.
Items Mean Standard Deviation
Product moment correlation
coefficient. "r"
Knowledge 14.45 3.326
Attitude 69.05 5.586 0.315
Knowledge score
3020100
Attit
ude
scor
e
90
80
70
60
50
Fig. 16 Scattered diagram representing relationship between Knowledge and
Attitude
The mean value of overall knowledge was 14.45 with a standard deviation of 3.326,
where as mean value of attitude was 69.05 with a standard deviation of 5.586. The
knowledge and attitude correlation value was "r" = 0.315 (p<0.014)by using Karl
Pearson's Product Moment Correlation Coefficient formula . It shows a statistically
positive correlation between the diabetic patients knowledge and attitude regarding
self administration of insulin injection. Hence H1 is accepted.

66
6. DISCUSSION
A hallmark of professional behavior is the personal commitment to the ongoing
acquisition of new knowledge.
The study is focused on assessing the knowledge and attitude regarding self-
administration of insulin injection among diabetes mellitus patients. It was aimed at
the improvement of the knowledge of Diabetic patients, so that they can develop a
positive attitude towards it.
The study attempted to test the following hypothesis:
H1 : There is a significant relationship between knowledge and attitude of
Diabetes Mellitus patients regarding self-administration of insulin injection.
H2 : There is a significant association between levels of knowledge with
selected demographic variables.
H3 : There is a significant association between the attitudes of diabetes
mellitus patients with selected demographic variables.
The findings of the study have been discussed with reference to the objectives and
hypothesis of the study.
Maximum number of diabetic patients, 38.3% was in the age group of 61 – 70
years, 33.3% were of 51 – 60 years. 20% fell under the age group of 41 – 50
years and 8.3% were of below 40 years of age. Thus it shows that the
maximum number of diabetic patients participated in the study were in the age
group of 61 – 70 years.

67
The percentage distribution of the diabetic patient according to gender reveals
that majority of the subjects, 73.3% were male and 26.7% were female.
The result indicate that only 1.7% of the diabetic patient had completed
graduation, 3.3% had completed higher secondary, 21.7% completed
secondary education and 73.3 % had completed only primary education. It
shows that maximum number of the diabetic patient who participated in the
study had completed their primary education.
It reveled that 53.3% diabetic patients were unemployed, 23% were self
employed, 15% were private employee and only 8.3% were Government
employee.
It depicts that 78.3% of the diabetic patients were Hindus, 18.3% were
Muslims and 3.3% of diabetic patient were Christians. Thus it shows that
maximum number of Diabetic patients who participated in the study were
Hindus.
Data presented shows that maximum number of the diabetic patients, 86.7%
were married, 11.7% were widow or widower and only 1.7% were unmarried.
None of the subjects were divorced.
The results indicate that 63.3% of the diabetic patient had a family income less
than or equal to 2,000 per month, 18.3% had between 2001 to 3000, 10 %.
were having family income more than 4001 or above and 8.3% had a family
income of 3001 – 4000.
This reveals that in 40% diabetic patient duration of diagnosis of Diabetes
Mellitus were lesser than or equal to 3 years, 23.4% duration of diagnosis
were greater than or equal to 9 years, 21.7% were within 4 – 6 years and in
15% duration of diabetes Mellitus were 7 – 9 years.

68
The data presented reveals that maximum number of diabetic patients, 81.7%
were on insulin therapy for lesser than 2 years, 10% were for 3 – 4 years, 5%
were 5 – 6 years and only 3.3% were on insulin therapy for more than 7 years.
It shows that maximum number of diabetic patients, 63.3% had no family
history of diabetes mellitus and 36.7% had family history of diabetes mellitus
The first objective was to assess the knowledge of the diabetic patients regarding
self administration of insulin injection. The level of knowledge regarding self
administration of the insulin injection were assessed and tabulated in tables XI - XIV.
Out of 60 diabetic patients 81.7% had average knowledge, 13.3% had poor
knowledge and only 5% had good knowledge regarding self administration of insulin
injection. The overall mean value of the diabetic patients knowledge regarding self
administration of insulin injection was 14.45 with a standard deviation of 3.326. This
findings showed that the most of the diabetic patients were not much aware of self
administration of insulin injection.
The second objective was to assess the attitude of the diabetic patients regarding
self administration of insulin injection. The level of attitude regarding self
administration of insulin injection was assessed and tabulated in table XV. Out of 60
diabetic patients, only 18.3% had most favourable and 81.7% had a favourable
attitude towards self administration of insulin injection. It revealed the mean
percentage of the positive attitude, which was 69.05 with a standard deviation of
5.585. These results showed that most of the diabetic patients were not having a most
favourable attitude towards self-administration of insulin injection.

69
Third objective was to correlate the knowledge and attitude of diabetic patients
regarding self administration of insulin injection. The relationship between the
knowledge and the attitude was tested and presented in table XVIII. The study
revealed that there was a positive correlation between the knowledge and the attitude
of diabetic patients.
Fourth objective was to find out the association between the knowledge with
selected demographic variables. The association between the diabetic patients
knowledge with the selected demographic variables were listed in table XVI. There
was no significant association between the knowledge level of diabetic patients with
selected demographic variables at 0.05 level of significance.
The fifth objective was to find out the association between the attitude with
selected demographic variables. The association of the attitudes of diabetic patients
and selected demographic variables were tested by using a chi square test and
presented in the table XVII. Statistically no significant association was found between
age, sex, education, occupation, religion, marital status, duration of diagnosis of
diabetes mellitus, number of years on insulin therapy and family history of diabetic
mellitus. There was a highly significant association between the level of attitude
among diabetic patients and their income.
The sixth objective was to prepare an information booklet based on the
knowledge of the diabetic patients. An information booklet was prepared to improve
the knowledge and attitude of diabetic patients regarding self administration of insulin
injection. The present study shows that only 5% diabetic patients had good knowledge
81.7% had average knowledge, and 13.3% had poor knowledge regarding self

70
administration of insulin injection. The study also reveals that 81.7% of the diabetic
patients possess a favourable attitude and only 18.3% diabetic patients possess most
favorable attitude towards self administration of insulin injection. And therefore it is
important to improve their knowledge regarding self administration of insulin
injection to enable them practice self administration of insulin with a more confident
and healthy way.

71
7. CONCLUSION
Education can gradually change people from their wrong unhealthy perceptions and
practices. A major goal of nursing practice is to provide health education that is
culturally sensitive, which fits into health beliefs and practices of the people. Healthy
practices should be encouraged and a positive attitude should be reinforced.
The following conclusions were drawn from the present study.
The Diabetic patients had an average knowledge regarding Self-administration
of insulin injection.
The Diabetic patients had a favourable attitude towards Self-administration of
Insulin injection.
The study findings reveal that there is a significant relationship between the
knowledge and attitude of Diabetic patients.
The study shows that there is no significant association between the
knowledge level and selected demographic variables.
The study findings indicate that there is no significant association between the
attitude level and selected demographic variables, except for the family
income. There is a significant association between the attitude of Diabetic
patients and income.
The implications were given on various aspects like Nursing Practice, Nursing
Administration, Nursing Education and Nursing Research.

72
NURSING IMPLICATIONS
Nursing Practice
The nurses play a key role in patient care. The day of admission to the day of
discharge nurse is with the patient, caring and consoling.
A nurse is expected to give nursing care as well as health teaching regarding
safe practices of insulin administration.
The present study administers an informational booklet to the Diabetic
patients, in order to impart knowledge and to prevent Insulin Therapy
complications.
The nurse needs to prepare self-instructional materials, which can be studied at
home with family members.
The nursing personnel needs to take initiative in directing, teaching and
educating the patients about self-administration practices which can be better
understood by the patients, family members, and the community at large.
Nursing administration
Nursing administrators can play a better role in planning educational
programme for Diabetic patients in order to improve patient’s knowledge and
attitude towards self-administration of insulin injection.
Nurse administrators should be necessarily involve in formulating policies for
health education in the hospital settings as well as community.
Nursing Education
Nursing education and curriculum should be planned in a way that it will
encourage the nursing students to train the diabetic patients especially for
certain tasks.( e.g. self-administration of insulin injection)

73
Along with imparting the knowledge specific attention and motivation can be
given to a specific areas.
Nursing education should emphasize on preparing prospective nurses to
impart health education by using various methods.
Nursing Research
Nursing research is the means by which nursing profession is growing.
More research should be done related to Insulin Therapy and self-
administration, in order to prevent the complications and reduce the rate of
malpractices.
LIMITATIONS
1. The sample size was limited to 60.
2. Only one hospital in Bangalore was included
3. The study was limited to the Diabetic patients who were on subcutaneous
Insulin therapy.
4. There was no experimentation in the study.
5. Generalization could not be made due to small sample size.
RECOMMENDATIONS
On the basis of the study that had been conducted, certain recommendations are
suggested for future students.
1. A similar study can be done on a larger sample
2. An experimental study can be done to assess the effectiveness of planned
teaching programme on insulin therapy.

74
3. An Exploratory study may be conducted to identify the lack of awareness,
knowledge, practices and attitude of Diabetic patients regarding insulin self-
administration.
4. A follow up study could be carried out to find the effectiveness of the study by
evaluating the knowledge in the Diabetic patients.
5. Information Booklet of the present study could be used for educating the
Diabetic patients.

75
8. SUMMARY
Education is evidence based care and handling gives nurses the opportunity to
improve their ability to use theoretical knowledge in clinical practice.
The study was conducted to assess the knowledge and attitude of diabetes mellitus
patients regarding self-administration of insulin injection. The convenience sampling
technique was used for a sample of 60 diabetic patients. The conceptual framework
was based on Orem’s Self Care model.
Objectives of the study were
1. To assess the knowledge of patients regarding self-administration of insulin
injection.
2. To assess the attitude of patients regarding self-administration of insulin
injection.
3. To correlate the knowledge and attitude of Diabetic patients regarding self-
administration of insulin injection.
4. To associate the knowledge with selected demographic variables.
5. To associate the attitude with selected demographic variables.
6. To develop an information booklet on self-administration of insulin for
Diabetes Mellitus patients.
Content validity of the tool was obtained on the basis of expert judgement. Reliabity
of tool was established by using Spearman’s Brown Prophecy Formula.
A structured self-administered questionnaire and a Likert type of attitude Scale was
administered to 60 diabetic patients. The collected data were statistically analyzed by
using both descriptive and inferential statistics.

76
The major findings of the study:
I. Findings regarding demographic variables of the diabetic patients
Maximum number of diabetic patients, 38.3% was in the age group of 61 – 70
years, 33.3% were of 51 – 60 years. 20% fell under the age group of 41 – 50
years and 8.3% were of below 40 years of age. Thus it shows that the
maximum number of diabetic patients participated in the study were in the age
group of 61 – 70 years.
The percentage distribution of the diabetic patient according to gender reveals
that majority of the subjects, 73.3% were male and 26.7% were female.
The result indicate that only 1.7% of the diabetic patient had completed
graduation, 3.3% had completed higher secondary, 21.7% completed
secondary education and 73.3 % had completed only primary education. It
shows that maximum number of the diabetic patient who participated in the
study had completed their primary education.
It reveled that 53.3% diabetic patients were unemployed, 23% were self
employed, 15% were private employee and only 8.3% were Government
employee.
It depicts that 78.3% of the diabetic patients were Hindus, 18.3% were
Muslims and 3.3% of diabetic patient were Christians. Thus it shows that
maximum number of Diabetic patients who participated in the study were
Hindus.
Data presented shows that maximum number of the diabetic patients, 86.7%
were married, 11.7% were widow or widower and only 1.7% were unmarried.
None of the subjects were divorced.

77
The results indicate that 63.3% of the diabetic patient had a family income less
than or equal to 2,000 per month, 18.3% had between 2001 to 3000,
10 %.were having family income more than 4001 or above and 8.3% had a
family income of 3001 – 4000.
This reveals that in 40% diabetic patient duration of diagnosis of diabetes
Mellitus were lesser than or equal to 3 years, 23.4% duration of diagnosis
were greater than or equal to 9 years, 21.7% were within 4 – 6 years and in
15% duration of diabetes Mellitus were 7 – 9 years.
The data presented reveals that maximum number of diabetic patients, 81.7%
were on insulin therapy for lesser than 2 years, 10% were for 3 – 4 years, 5%
were 5 – 6 years and only 3.3% were on insulin therapy for more than 7 years.
It shows that maximum number of diabetic patients, 63.3% had no family
history of diabetes mellitus and 36.7% had family history of diabetes mellitus
II Findings related to the level of knowledge of the diabetic patients regarding self
administration of insulin injection.
Out of 60 diabetic patients 81.7% had average knowledge, 13.3% had poor
knowledge and only 5% had good knowledge regarding self administration of
insulin injection.
The overall mean value of the diabetic patients knowledge regarding self
administration of insulin injection was 14.45 with a standard deviation of
3.326.
This findings showed that the most of the diabetic patients were not aware of the
self administration of insulin injection.

78
III Findings related to the level of attitude of diabetic patients towards self
administration of insulin injection.
Out of 60 diabetic patients, only 18.3% had most favourable and 81.7% had a
favourable attitude towards self administration of insulin injection.
The mean percentage of the positive attitude, which was 69.05 with a standard
deviation of 5.585.
These results showed that most of the diabetic patients were not having a most
favourable attitude towards self-administration of insulin injection.
IV Findings on the association between selected demographic variables and the level
of knowledge of the diabetic patients
The investigator could not elicit any significant association between the
knowledge level of diabetic patients with selected demographic variables at
0.05 level of significance.
V Findings regarding association between selected demographic variables and level
of attitude of the diabetic patients
Statistically no significant association was found between age, gender,
education, occupation, religion, marital status, duration of diagnosis of
diabetes mellitus, numbers of years on insulin therapy and family history of
diabetic mellitus.
There was a highly significant association between the level of attitude among
diabetic patients and their income.
VI Findings on the relationship between the knowledge and attitude of diabetic
patients
There was a positive correlation between the knowledge and the attitude of
diabetic patients.

79
9. BIBLIOGRAPHIC REFERENCES
1. Hanslett C, Chilvers ER, Boon NA, Colledge NR, Hunter JAA. Davidson’s
Principles and Practice of Medicine. 19th ed. Edinburgh: Churchill Livingstone;
2002.
2. Frier B. The hazardous path of diabetes management: Pilgrims’ Progress or
Paradise Lost? Proceedings of The Royal College of Physicians of Edinburgh;
1989 Oct 19; 4:Edinburgh; 1989. p. 449-458.
3. International Diabetes Federation. Diabetes Atlas. [Online]. 2005 [Cited 2005 Oct
17]; Available from: URL:http://www.eatlas.idf.org
4. Pradeepa R, Deepa R, Mohan V. Epidemiology of Diabetes in India-current
perspective and future projections. J Indian Med Assoc 2002 Mar;100(03):144-8.
5. Mohan V. Diabetes Mellitus. [Online]. 2002. [Cited 2005 May 20]: Available
from: URL:http://www.google.com
6. Ramachandran A, Snehalatha C, Kapoor A, Vijay V, Mohan V, Das AK et al.
Diabetes Epidemiology Study Group in India (DESI): high prevalence of diabetes
and impaired glucose tolerance in India -National Urban Diabetes Survey.
Diabetologia 2001; 44:1094-101
7. Ramaiya KL, Kodali VRR, Alberti KGMM. Epidemiology of diabetes in Asians
of the Indian sub-continent. Diabetes Metab Rev 1990;6:125-46.
8. Smeltzer CS, Bare GB. Brunner and Suddarth’s Text book of Medical Surgical
Nursing. 7th ed. Philadelphia: Lippincott; 1999.
9. Cox DJ, Gonder F. Major development in Behavioral Research. Journal of
Consulting and Clinical Psychology 1992;60(4):628-38

80
10. Johnson SB. Insulin Dependent Diabetes Mellitus in childhood. In Michael C,
Roberts (Ed) Handbook of Pediatric Psychology. 2nd ed. The Guildford Press;
1995.
11. La-Greca AM, Auslander WF, Spetter D. “I get by with a little help from my
family and friends”: Adolescent support for diabetes care. J Pediatr Psychology
1992; 20:4. 449- 76
12. DCCT Research Group. Effects of Intensive Diabetes treatment on the
development and progression of long-term complication in adolescent with Insulin
Dependent Diabetes Mellitus. J Pediatr 1994 August;125(2):177-1
13. Garg MK. Current Perspective in Insulin Therapy in the Management of Diabetes
Mellitus. J Indian Med Assoc 2002 Mar ;100(3):194-5,202.
14. Garg MK, Baliga KV.Management of Type-2 Diabetes (NIDDM). Med J Armed
Forces India 2002;58:53-9
15. American Diabetes Association. Insulin Administration. Diabets Care
1999;22:S83-7.
16. Dr. Mohan V. The Hindu. 2005 Nov 14;suppl. Available from:
URL:http://www.thehindu.com
17. Zimmet PZ. Diabetes Epidemiology as a tool to trigger diabetes research and care.
Diabetologia 1999;42:499-518
18. Maia FFR, Araujo LR. Insulin Pen injector for the treatment of type 1 Diabetes
Mellitus. J Paedtr (Rio J) 2002 May-Jun;78(3):189-92.
19. Mollema ED, Snoek FJ, Pouwer F. Diabetes Fear of Injecting and Self-testing
Questionnaire. Diabetes Care 2000 Jun;23(6)
20. Cramer JA, Pugh MJ. The influence of insulin use on Glycemic Control. Diabetes
Care 2005 Jan;28(1)

81
21. The Diabetes Control and Complications Trial. Effect of Intensive Insulin
Therapy on the micro vascular complications of type 1 diabetes mellitus. JAMA
2002;287:2563-9.
22. Best JW, Kahn J. Research in Education. 1st edition. New Delhi: Hall of India Pvt
Limited; 1999.
23. Polit FD, Hungler PB. Nursing Research - Principles and Methods. 6th ed.
Philadelphia: Lippincott Company; 1999.
24. Treece EW, Treece TW. Elements of research in nursing. 2nd ed. St.Louis: Mosby
Company; 1988.
25. Potter PA, Perry AG. Basic Nursing-Theory and Practice. 5th ed. USA: Mosby
Year Book Inc; 1995.
26. Abdellah FG, Levine E. Better patient Care through Nursing Research. London:
The Mac Millan Company; 1965.
27. Brennan G. The Tayside Diabetes Handbook - Treatment with Insulin. [Online]
2004. [Cited 2005 Sep 17]: Available from: URL:http://www.medline.com
28. Francine RK. Intensive Management of Type 1 diabetes in young children. Lancet
2005 Feb 26;365
29. Dewitt DE, Dugdale DC. Using New Insulin Strategies in the Outpatient
Treatment of Diabetes. JAMA 2003 May 7; 289(7)
30. The Diabetes Control and Complications Trial / Epidemiology of Diabetes
Interventions and Complications Research Group. Retinopathy and nephropathy
in patients with type 1 diabetes four years after a trial of Intensive Therapy. N
Engl J Med 2000 Feb 10;342(6)
31. Hayward RA, Manning WG, Kaplan S, Wagner EH, Greenfield S. Starting Insulin
Therapy in Patients with Type 2 Diabetes. JAMA 1997 Nov 26;278(20)
82
32. Saudek CD, Duckworth WC, Giobbie-Hurder A, Henderson WG, Henry RR,
Kelly DE et al. Implantable Insulin v/s Multiple Dose Insulin for Non Insulin
Dependent Diabetes Mellitus, JAMA 1996 Oct 23-30;276(16)
33. Summers KH, Szeinbach SL, Lenox BM. Preference for Insulin Delivery Systems
among current insulin users and non-users. Clin Ther 2004 Sep: 26(9):1498-505.
34. Hill J. Devices for insulin administration. Nurs Times 2003 Apr 15-21;99(15):51-2
35. Sucio M, Galic E, Cabrijan T, Ivandic A, Petrusic A, Wyatt J et al. Patient
acceptance and reliability of new Humalin / Humalog 3.0 ml prefilled insulin pen
in ten Croatian Diabetes Centers. Med. Sci Monit 2002; 8(3): 121-6
36. De Souza CR, Zanetti ML. The use of disposable syringes in the administration of
insulin at home. Rev Lat Am Enfermagem 2001 Jan;9(1):39-45
37. Robertson KE, Glazer NB, Campbell RK. The Latest Developments in Insulin
Injection Devices. Diabetes Edu 2000 Jan –Feb; 26(1)
38. Mersad D, Outtas O, Demoly P. Hypersensitivity to Insulin. Presse Med 2004
May 22;33(9 pt 1):631 – 8
39. Soudan B, Girardot C, Fermon C. Extreme Subcutaneous Insulin Resistance: a
misunderstood syndrome. Diabetes Metab 2003 Nov;29(5):539-46
40. Richardson T, Kerr D. Skin-related complications of Insulin Therapy:
epidemiology and emerging management strategies. Am J Clin Dermatol
2003;4(10):661 - 7
41. Yokoyama H, Fukumoto S, Koyama H. Insulin Allergy; desensitization with
crystalline zinc-insulin and steroid tapering. Diabetes Res Clin Pract 2003
Sep;61(3):161–6
42. Sola-Gazagnes A, Pecquet C, Radermecker R, Pietri L, Elgrably F, Slama G et al.
Successful treatment of Insulin Allergy in a type 1 diabetic patient by means of

83
constant Subcutaneous Pump Infusion of Insulin. Diabetes care 2003
Oct;26(10):2961-2
43. Logwin S, Conget J, Jansa M, Vidal M, Nicolan C, Gomis R. Human insulin
induced Lipoatrophy. Successful treatment using a jet-injector device. Diabetes
care 1997 Jan;20(1);119
44. Reach G, Zeriouki A, Leclercq D, d’Ivernois JF. Adjusting insulin doses: from
knowledge to decision. Patient Educ Cons 2005 Jan;56(1):98-103
45. Bergenstal RM. Effective Insulin Therapy. International textbook of Diabetes
Mellitus. 3rd ed. John Wiley and sons Ltd:ISBN; 2004.
46. Skinner TC. Psychological barriers. Eur J Endocrinol 2004 Oct ;151 Suppl 2 :
T13-7:T29-30
47. Asakura T. Research regarding proper use of insulin in diabetic patients.
Yakugaku Zasshi 2001 Sep;121 (9):653-61
48. Maureen IH. Frequency of blood glucose monitoring in relation to Glycemic
Control in patients in the Type 2 Diabetes. Diabetes Care 2001;24
49. Mollema ED, Snoek FJ, Heine RJ, Van der Ploeg HM. Phobia of self-injecting
and self-testing in insulin treated diabetic patients opportunity for screening.
Diabet Med [11553207] : Available from: URL: http: // www.pubmed.com 2001
Aug ; 18 (8): 671 – 4
50. Power BK, Walford S, Singh BM. Type 1 diabetes mellitus in a routine diabetes
clinic : the association of psycho-social factors, diabetes knowledge and glycemic
control to insulin regime. Diabetes Res Clin Pract 1999 Nov;46(2):151-5
51. Almeida HG, Campos JJ, Kfouri C, Tanita MT, Dias AE, Souza MM. Profile of
patients with diabetes type 1:insulinotherapy and self-monitoring. Rev Assoc Med
Bras 2002 Apr-Jun;48(2):151-5

84
52. Lombardo F, Salzano G, Messina MF, DeLuka F. How self-management therapy
can improve quality of life for diabetic patients? Acta Biomed Ateneo Parmense
2003;74 suppl 1 : 26-8
53. Coates VF, Boore JR. The influence of psychological factors on the self-
management of Insulin-Dependent Diabetes Mellitus. J Adv Nurse 1998
Mar;27(3):528-37
54. Saunders SA, Wallymahmed M, Macfarlane IA. Glycemic control in a type 1
diabetes clinic for younger adults. Q J Med 2004;97:575-80
55. Kapoor A. Diabetes care in India. International Journal of Diabetes in Developing
Countries 1997;17: 5-7.
56. De-weerdt J, Visser AP, Kok G, Vander Veen FA. Determinants of active self-
care behavior of insulin treated patients with diabetes: implications for diabetes
education. Soc Sci Med 1990;30(5):605-15.
57. Kothari CR. Research Methodology. Mumbai: Vishwa Prakashan; 1998.
58. Burns N, Grove SK. The practice of Nursing Research. 2nd ed. Philadelphia: WB
Saunder’s Company; 2002.
59. Kerlinger FN. Foundation of Behavioral Research. New York: Hold International
Edu: 1973.

85
10. ANNEXURES ANNEXURE-A
REQUESTING FOR CONDUCTING THE RESEARCH STUDY From,
Namita Singha 2nd year M.Sc. (Nursing) Sarvodaya College of Nursing Vijayanagar, Bangalore
To, The Medical Superintendent K.C. General Hospital Malleswaram Bangalore
Through
The Principal Sarvodaya College of Nursing Vijayanagar Bangalore-560040
Sub: -Seeking permission for conducting the Research Study Respected sir, I am a student of M.Sc. (Nursing) in Sarvodaya College of Nursing affiliated to Rajiv Gandhi University of Health Sciences, Bangalore with Specialization in Medical-Surgical Nursing. I have to conduct a research for the purpose of partial fulfillment of my course. The subject selected for the study is “A Descriptive Study To Assess The Knowledge And Attitude Regarding Self-Administration Of Insulin Injection Among Diabetes Mellitus Patients In K.C. General Hospital, Malleswaram At Bangalore”. Hence, I request you to kindly permit to conduct the research study in your esteemed institution. Hope you will consider my request and will do the needful. Thanking you, Date: Place: Bangalore Your’s Faithfully, Namita Singha

86
ANNEXURE-B
LETTER GRANTING PERMISSION TO CONDUCT THE STUDY
Ref. Letter No: Date:
To,
Namita Singha
IInd year M.Sc. Nursing
Sarvodaya College of Nursing
Bangalore-40
The above candidate who is undergoing M.Sc. Nursing programme in Sarvodaya
College of Nursing, Bangalore is permitted to collect data from Kempa Cheluvamba
General Hospital at Malleswaram, Bangalore in the month of September to October.
Place: Bangalore Yours sincerely
Date:
Medical Superintendent

87
ANNEXURE-C
CONSENT FORM OF THE RESPONDENTS
Dear participants,
I Miss. Namita Singha is a 2nd year M.Sc. (Nursing) student of Sarvodaya
College of Nursing. As part of the partial fulfillment of the course, I have to conduct a
research and the problem selected is A descriptive study to “assess the knowledge and
attitude regarding self administration of Insulin injection among Diabetes Mellitus
patients” in Kempa Cheluvamba General Hospital at Malleshwaram, Bangalore. I
would like get some information and your opinion regarding self administration of
Insulin injection.
This information will be kept confidential and will be only used for study
purpose. This is for your information and kind participation.
Signature of the investigator
I am willing to participate in the study and aware that the information
provided will be kept confidential and used only for the study purpose.
Signature of the participant

89
ANNEXURE - E
LETTER SEEKING EXPERT OPINION ON VALIDITY OF THE TOOL
From
Ms. Namita Singha
2nd Year M.Sc (Nursing)
Sarvodaya College Of Nursing
Bangalore
To
[Through the Principal, Sarvodaya College of Nursing, Bangalore]
Respected Madam/sir,
Sub-Requesting Expert opinion on content validation
I am a final year M.Sc (N) student (Medical-Surgical Nursing) in the above-
mentioned institution. As a part of academic requirement I am undertaking A
Descriptive Study To “Assess The Knowledge And Attitude Regarding Self-
administration of Insulin Injection Among Diabetes Mellitus Patients In Kempa
Cheluvamba General Hospital at Malleswaram, Bangalore”.
Objectives of the study
1. To assess the knowledge of patients regarding the Self-administration of Insulin
Injection.
2. To assess the attitude of patients regarding Self-administration of Insulin Injection
3. To correlate the knowledge and attitude of diabetic patients regarding self-
administration of insulin injection.
4. To associate the knowledge with selected demographic variables.

90
5. To associate the attitude with selected demographic variables.
6. To develop an information booklet on self-administration of insulin injection for
diabetes mellitus patients.
Along with that I am enclosing
a) Structured questionnaire for knowledge assessment
b) Attitude scale for the assessment of attitude
c) Scoring keys
d) Criteria checklist for validation
e) Certificate of content validity
I request you to give your expert opinion and suggestion on the appropriateness
of the items, need for modification or deletion, by using the evaluation criterion
checklist enclosed. This will help me in the systematic conduction of the study.
Kindly sign the certificate of validation stating that you have validated the tool.
Thanking you,
Your’s faithfully
Place:Bangalore
Date:
Namita Singha
91
ANNEXURE - F
CRITERIA FOR VALIDATING THE TOOL
Areas Opinion Item no Suggestions
Relevant
Relevant To Some Extent
SECTION-I
DEMOGRAPHIC DATA
Not Relevant
Relevant
Relevant To Some Extent
SECTION-II
QUESTIONNAIRE
Not Relevant
Relevant
Relevant To Some Extent
SECTION-III
ATTITUDE
SCALE
Not Relevant

92
ANNEXURE - G
CERTIFICATE OF CONTENT VALIDITY
This is to certify that the tool for A Descriptive Study To “Assess The
Knowledge And Attitude Regarding Self-administration of Insulin Injection Among
Diabetes Mellitus Patients In Kempa Cheluvamba General Hospital at Malleswaram,
Bangalore”, prepared by Ms.Namita Singha, II nd Year M.Sc. Nursing student of
Sarvodaya College of Nursing, Bangalore is appropriate and found to be valid.
She has lot /none/few/some/of modifications required to be made in her tool.
Signature
Place:
Date: Seal

93
ANNEXURE - H
TOOL FOR DATA COLLECTION
Section-I Socio-Demographic Data.
Instructions:
The interviewer introduces herself and asks the participants to put a tick (√) mark to
the correct answer in the box given in the right side of each option. The participant is
ensured that the information would be kept confidential and will be used only for the
research purposes
1. Code no: 2. Age in years 2.1) ≤ 40 years [ ] 2.2) 41-50 years [ ] 2.3) 51-60 years [ ] 2.4) 61–70 years [ ]
3. Gender 3.1) Male [ ] 3.2) Female [ ]
4. Education of the participant 4.1) Primary level of education [ ] 4.2) Secondary level of education [ ] 4.3) Higher Secondary level of education [ ] 4.4) Graduate and above [ ]
5. Occupation of the participant 5.1) Unemployed [ ] 5.2) Private [ ]
5.3) Government [ ] 5.4) Self-employed [ ]

94
6. Religion 6.1) Hindu [ ] 6.2) Muslim [ ] 6.3) Christian [ ] 6.4) Others [ ] 7. Marital status 7.1) Married [ ] 7.2) Unmarried [ ] 7.3) Widow (er) [ ] 7.4) Divorced [ ] 8. Family income per month 8.1) Less than 2000 [ ] 8.2) 2001-3000 [ ] 8.3) 3001-4000 [ ] 8.4) 4001 and above [ ] 9. Duration since diagnosis of Diabetes Mellitus 9.1) ≤ 3 Years [ ] 9.2) 4-6 years [ ] 9.3) 7-9 years [ ] 9.4) ≥ 10 years [ ] 10. Actual number of years on Insulin therapy 10.1 ) < 2 yrs. [ ] 10.2) 3 – 4 yrs. [ ] 10.3) 5-6 yrs. [ ] 10.4) 7 yrs. and above [ ] 11. Family history of diabetes 11.1) Yes [ ] 11.2) No [ ]

95
Section-II Self-Administered Questionnaire
Instruction to the participant:
In this section there are questions relating to the knowledge of self-administration of
insulin injection. Please read the questions carefully and give your response that you
feel most relevant to you.
A. General Information regarding Insulin Therapy 1. Insulin is a/an 1.1) Hormone [ ] 1.2) Vitamin [ ] 1.3) Mineral [ ] 1.4) Enzyme [ ]
2. Insulin is secreted by 2.1) Liver [ ] 2.2) Pancreas [ ] 2.3) Kidney [ ] 2.4) Spleen [ ]
3. Action of Insulin is 3.1) It has no action on glucose [ ]
3.2) It increases the blood glucose level [ ] 3.3) It lowers blood glucose level [ ] 3.4) It completely removes glucose from the blood [ ] 4. Types of insulin are
4.1) Rapid acting [ ] 4.2) Intermediate acting [ ] 4.3) Long acting [ ] 4.4) All of the above [ ]
5. Short acting insulin has to be administered 5.1) 0-15 minutes before food [ ] 5.2) 0-30 minutes before food [ ] 5.3) 0-45 minutes before food [ ] 5.4) 15-30 minutes after food [ ]
96
6. Intermediate acting insulin has to be administered 6.1) Along with food [ ] 6.2) 0-15 minutes before eating [ ] 6.3) 30-45 minutes before eating [ ] 6.4) 45-60 minutes before eating [ ]
7. The effects of insulin injection when taken on empty stomach are 7.1) Increased pulse and respiration [ ] 7.2) High fever and rigor [ ] 7.3) High blood pressure [ ]
7.4) Blurred vision and dryness of mouth [ ] B. Regarding Self-Administration of Insulin Injection 8. Self-administration of insulin is
8.1) Dangerous [ ] 8.2) Less painful [ ] 8.3) Time consuming [ ] 8.4) A cost-effective method [ ]
9. Insulin injections should be taken 9.1) Once daily [ ]
Twice a day [ ] 9.2) Three times a day [ ] 9.3) According to doctors advice [ ] 10. The areas suitable for self-administration of insulin injection are 10.1) Arms [ ] 10.2) Thighs [ ] 10.3) Abdomen [ ] 10.4) All of the above [ ]
11. Insulin injection can be administered 11.1) Just beneath the skin [ ] 11.2) Into the vein [ ] 11.3) Into the muscle [ ] 11.4) Into the nerves [ ]

97
12. The site for the insulin injections are selected by 12.1) Rotating pattern [ ] 12.2) Using the different sites haphazardly [ ] 12.3) Using same injection sites daily [ ] 12.4) Using two injection sites [ ]
13. The advantage of site rotation is 13.1) To promote circulation [ ] 13.2) To prevent tissue damage [ ] 13.3) To prevent absorption of insulin [ ] 13.4) To promote lymph flow [ ]
14. An open insulin vial can be preserved by 14.1) Keeping in a cold place [ ] 14.2) Keeping in direct sunlight [ ] 14.3) Keeping in a hot place [ ] 14.4) Keeping in deep freezer [ ]
15. One of the complications of insulin injection is 15.1) Increased blood sugar [ ] 15.2) Decreased blood sugar [ ] 15.3) Increased blood pressure [ ] 15.4) Decreased blood pressure [ ]
16. Insulin syringes are preferred for insulin injection because it is 16.1) Less painful [ ] 16.2) Handy [ ] 16.3) Less expensive [ ] 16.4) Easy to calculate the dose [ ] 17. Before administering insulin injection inspect the vial for changes, like 17.1) Scratches on the vial [ ] 17.2) Size of the vial [ ] 17.3) Clumping, frosting [ ] 17.4) Design of the vial [ ]
18. Insulin should be drawn from the vial
18.1) By injecting a small amounts of air [ ] 18.2) Without injecting a small amount of air [ ] 18.3) By injecting a small amount of water [ ] 18.4) Insulin is poured into the syringe [ ]

98
19. Which of the following step is correct when preparing to administer two types of insulin?
19.1) Two separate syringes must be used [ ] 19.2) The regular insulin is withdrawn first [ ] 19.3) Air is placed in the intermediate acting insulin vial first [ ] 19.4) The intermediate acting insulin is drawn up first [ ]
20. An Insulin vial should not be shaken vigorously to 20.1) Prevent discoloration [ ] 20.2) Prevent clumping [ ] 20.3) Prevent leakage [ ] 20.4) Promote precipitation [ ]
21. Insulin preloaded syringes should be kept in
21.1) Inverted position [ ] 21.2) Horizontal position [ ] 21.3) Vertical position [ ] 21.4) Oblique position [ ]
22. Insulin absorption rate increases with
22.1) Smoking [ ] 22.2) Drinking of water [ ] 22.3) Sleeping [ ] 22.4) Exercise [ ] 23. Insulin absorption rate decreases with
23.1) Drinking of water [ ] 23.2) Smoking [ ] 23.3) Exercise [ ] 23.4) Sleeping [ ]
24. Insulin doses are calculated in
24.1) Milliliters [ ] 24.2) Deciliters [ ] 24.3) Units [ ] 24.4) Milligrams [ ]
25. The following solution is used to wipe the insulin injection site 25.1) Betadine [ ] 25.2) Water [ ] 25.3) Spirit [ ] 25.4) Acriflavine [ ]

99
26. One should not massage the site following insulin injection in order to
26.1) Maintain insulin in the subcutaneous tissue [ ] 26.2) Prevent rapid absorption of insulin [ ] 26.3) Prevent tissue damage [ ] 26.4) Prevent discomfort [ ]
27. Once opened an insulin vial can be used for 27.1) 60 days [ ] 27.2) 45 days [ ] 27.3) 30 days [ ] 27.4) 15 days [ ]
28. The effectiveness of insulin can be measured by
28.1) Checking blood and urine glucose levels [ ] 28.2) Checking blood pressure levels [ ] 28.3) Checking body temperature [ ] 28.4) Checking peripheral pulses [ ]
29. Taking insulin ensures
29.1) Best control of diabetes [ ] 29.2) Damage kidneys [ ] 29.3) Not adequate for diabetes control [ ] 29.4) Damage pancreas [ ]
30. When experiencing hypoglycemia one should
30.1) Take some water [ ] 30.2) Take some sugar dissolved in water [ ] 30.3) Take the next meal [ ] 30.4) Take some milk [ ]

100
Section-III Attitude Scale to Assess the Attitude of Diabetes Mellitus patients
towards Self-Administration of Insulin Injection Instructions: The attitude scale consists of 15 statements. Each statement is provided with a five-
point scale namely Strongly Agree (SA), Agree (A), Uncertain (U), Disagree (D), and
Strongly Disagree (DA). Please read each statement given below and indicate the
response by placing a tick mark against the one of the five points in the appropriate
column.
Sl. no
Statements Strongly Agree
Agree Uncertain Disagree Strongly Disagree
Do you feel /think/believe that
1 Self-administration of insulin is the most convenient method
2 Patients can improve the quality of their life with Diabetes mellitus by self administration of insulin
3 * Self-administration of insulin is time consuming
4 Self-administration of insulin injection does not need supervision
5 Even illiterate can learn self-administration of insulin injection technique more effectively
6 Self administration of insulin therapy will not require much time to learn
7 Patients are the most appropriate persons than others to get involved in the self-administration of insulin injection
8 The stress of frequent visit to hospital is minimized
9 Right technique and site rotation are two important aspects the patient should know regarding self-administration of insulin injection
10 Self-administration of insulin is possible at home environment
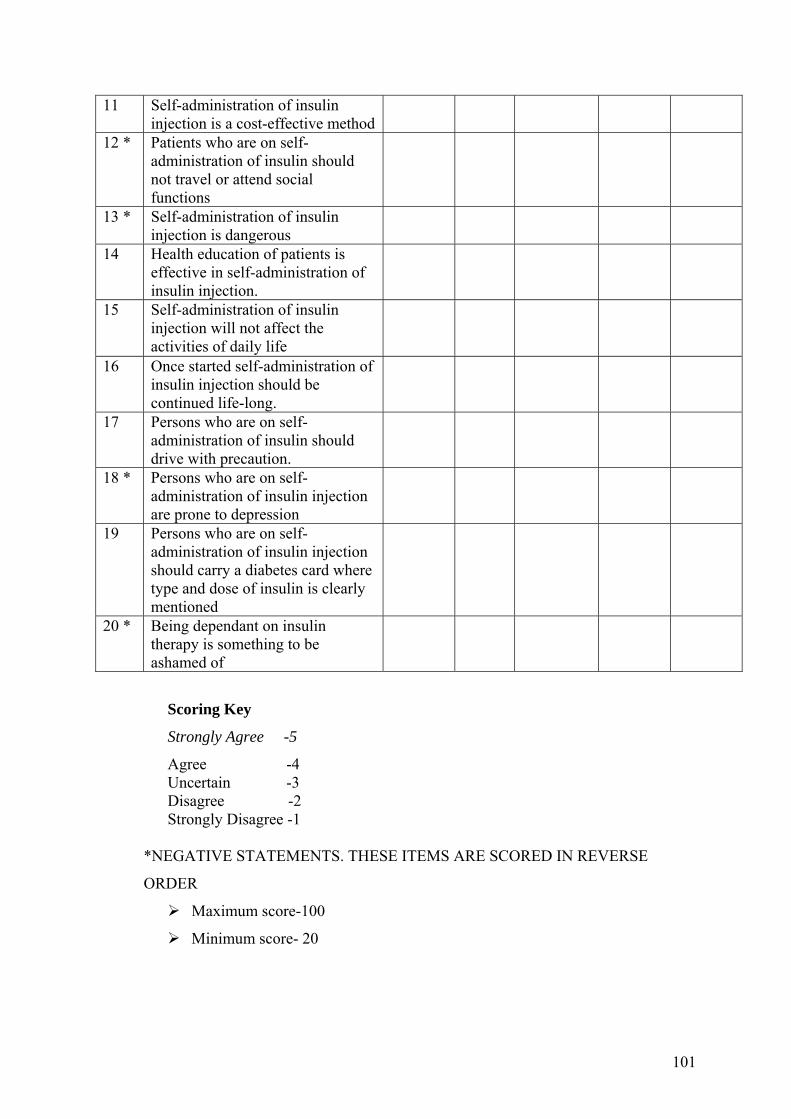
101
11 Self-administration of insulin injection is a cost-effective method
12 * Patients who are on self-administration of insulin should not travel or attend social functions
13 * Self-administration of insulin injection is dangerous
14 Health education of patients is effective in self-administration of insulin injection.
15 Self-administration of insulin injection will not affect the activities of daily life
16 Once started self-administration of insulin injection should be continued life-long.
17 Persons who are on self-administration of insulin should drive with precaution.
18 * Persons who are on self-administration of insulin injection are prone to depression
19 Persons who are on self-administration of insulin injection should carry a diabetes card where type and dose of insulin is clearly mentioned
20 * Being dependant on insulin therapy is something to be ashamed of
Scoring Key
Strongly Agree -5
Agree -4 Uncertain -3 Disagree -2 Strongly Disagree -1
*NEGATIVE STATEMENTS. THESE ITEMS ARE SCORED IN REVERSE
ORDER
Maximum score-100
Minimum score- 20
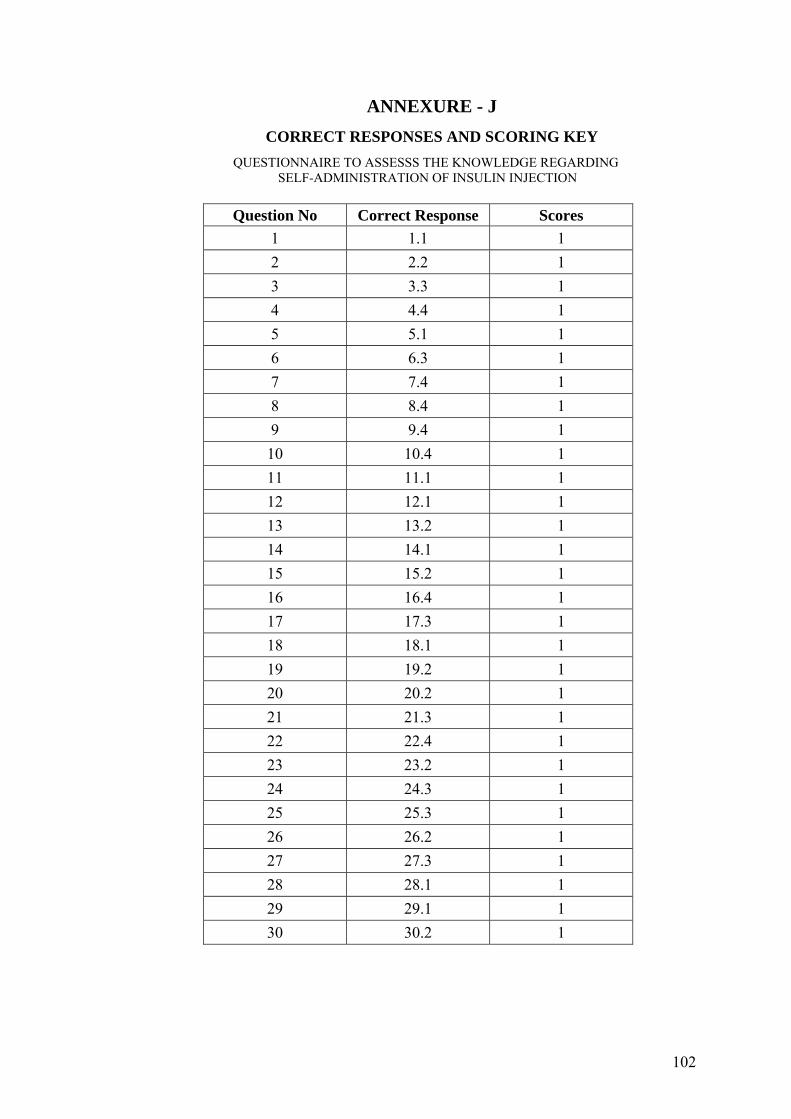
102
ANNEXURE - J CORRECT RESPONSES AND SCORING KEY
QUESTIONNAIRE TO ASSESSS THE KNOWLEDGE REGARDING SELF-ADMINISTRATION OF INSULIN INJECTION
Question No Correct Response Scores
1 1.1 1 2 2.2 1 3 3.3 1 4 4.4 1 5 5.1 1 6 6.3 1 7 7.4 1 8 8.4 1 9 9.4 1 10 10.4 1 11 11.1 1 12 12.1 1 13 13.2 1 14 14.1 1 15 15.2 1 16 16.4 1 17 17.3 1 18 18.1 1 19 19.2 1 20 20.2 1 21 21.3 1 22 22.4 1 23 23.2 1 24 24.3 1 25 25.3 1 26 26.2 1 27 27.3 1 28 28.1 1 29 29.1 1 30 30.2 1

111
ANNEXURE - K
Blue Print – Knowledge regarding Self Administration of insulin injection
Sl.No Content Knowledge Comprehension Application Total no of Questions
Percentage (%)
1. General Information 1,2,3 4,7 5,7 7 23.33%
2. Insulin Self-administration 10,12,13,15,22,23,28,30 8,9,16,19,24,26,29 11,14,17,18,20,21,25,27 23 76.67%
Total 11 9 10 30 100%
Knowledge – 36.67%
Comprehension – 30%
Application – 33.33%

111
“Successful patient discharge depends on Successful Medical Team Work”
Margaret Foster - 1883

111
Information Booklet
On
Self - Administration of Insulin
Injection
Prepared in partial fulfillment for the
DEGREE OF MASTER OF SCIENCE IN NURSING FROM
Rajiv Gandhi University of Health Sciences, Karnataka,
Bangalore.
By Ms. Namita Singha
FINAL YEAR M.SC. NURSING STUDENT

112
1. Basic Concepts 1.1. What is Insulin ?
Insulin is a hormone secreted by groups of cells within the pancreas
called Islet cells.
1.2. What is the action of Insulin?
Insulin lowers the blood glucose level by
- Promoting the transport of glucose into the cells and
- Inhibiting the conversion of glycogen and amino acids to
glucose.
1.3. What do you mean by Insulin Therapy or Insulin Treatment ?
Administration of insulin in the treatment of both type 1 and type2
diabetes
2. Treatment with Insulin
2.1. Aims of Insulin Treatment
- Abolish hyperglycemic symptoms
- Maintain ideal body weight
- Optimize glucose control
- Avoid hypoglycemia
- Maintain as near normal a blood glucose as is practical and safe
for the individual
- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -
Starting insulin is best managed as an outpatient, with input from a
Diabetes Specialist Nurse.
- - - - - - - - - - - - - - - - - - - - - - - - - - -- - -- - - - - - - - - - - - - - - - - -
2.2. Insulin therapy in Type 1 Diabetes
Regular insulin therapy is life saving in type 1 diabetes. Patients are
usually seen urgently after the diagnosis is made and insulin
started, preferably as an out-patient, with input from one of the
Diabetes Specialist Nurses.
2.3. Insulin Therapy in type 2 Diabetes
The most common indication for insulin in these patients is
worsening glycemic control on Oral Hypoglycemic Agents.

113
2.4. Insulin in the Elderly
Chronological age is not a contraindication to insulin therapy.
3. Starting Insulin
All patients starting insulin should have the following :
Review of dietary intake, with emphasis on regular and
consistent carbohydrate intake.
An individualized regime, which must take account of life style
factors such as shift work, holidays, exercise etc.
Appropriate education on self-management of insulin
administration.
Education on avoidance of hypoglycemia
Education on “sick day rules”, including avoidance of diabetic
ketoacidosis for people with type 1 Diabetes.
4. Timing of Injections in relation to meals
Standard insulin preparations should be injected subcutaneously
usually 15-30 minutes before meals
Analogue insulins have a rapid onset of action and an early
peak response. In view of this, they should be injected
immediately (usually within 5-10 minutes) before eating or just
after. Delays between injection and eating with these
preparations will predispose a patient to hypoglycemia.
Examples of short-acting analogues include insulin Lispro
(Humalog) or Insulin Aspart (NOVORAPID)
Insulin analogue mixtures are also available (e.g. Human
Mixtard, Humalog Mix 25 or Novomix)
5. Insulin presentation
- Rapid acting
- Intermediate working
- Long acting

114
6. Identification of insulin preparation
Please check the carton and the vial for the name and type of
insulin prescribed to you. In the event of any doubt, always seek
clarification from your physician.
7. Clearness or Clarity of Insulin
The Human Long acting and Human Mix acting insulin preparation
should look uniformly milky after mixing. The regular insulin is
always clear.
8. Storage
Insulin should be stored in a refrigerator but never in a freezer.
Do not use insulin if it is frozen.
If it is not possible to store it in a refrigerator, it should be kept
cool as possible below 300 C while in use. At this temperature
the preparation are likely to remain stable for about a month.
Do not use a vial of insulin beyond the date of expiry mentioned
on the label..
9. Insulin Administration devices
9.1 Syringes
The dose of insulin is always expressed in International Human
Units (IHU). Please study the markings made on the insulin
syringes carefully and understand calculation of the dose in ML.
Do make sure that you use only a syringe calibrated to 40 IHU
per ML.
The volume of insulin has to be injected, depends upon the dose
required by the patient. Hence, do use a syringe marked for the
use of insulin. If proper syringe is not used, it may lead to an
error in the dosage. This may cause serious problems such as
blood glucose may become too low or high.
Syringes are suitable for
• Patients using two different insulin preparation that need to be
mixed

115
• Patients using large volumes of insulin which cannot be
accommodated in a pen
• Patients whose injections are given by a 3rd party. Eg. Carer or
Community Nurse
• Injections for use with syringes should be prescribed in vials.
9.2 Pen devices
Many patients use a pen injection device for insulin administration.
This is available in two forms, either a reusable form for use with a
cartridge or a prefilled (disposable) type. Both are available on
prescription.
Pen devices are designed for self use only.
The advantages of pen injection devices is the convenience of
carrying and administering the insulin
Disposable (pre filled) pens are particularly useful for patients
who are not so dexterous.
All cartridges for re-usable pens at present come in 3ml size.
However a few patients receiving Porkine insulin. (Hypurin
preparations) use 1.5 ml cartridges.
Pen needles are available on prescription. 8 mm, 6mm or 5 mm needles
are recommended. Needles should be changed for each injection.
Storage of Insulin pen devices.
Insulin pens that are “in use” may be kept at room temperature, but
spare cartridges or disposable pens should be kept in a fridge.
10. Injection sites
Assess each patient individually for suitable areas to inject.
This include :
• Arms - upper, outer parts of arms
• Abdomen - lower abdomen below umbilicus
• Thighs - upper outer thighs
• Buttocks - upper outer buttocks
Recommend sites that are easiest to reach
Rotate sites at each injection.

116
Injection sites.
Injection Site Rotation
• Do not mix site and time, each side has a different absorption
pattern
• Advise patients to keep a consistence side for each time a day,
which helps to reliably predict the effect of a dose of insulin
• It is important however to rotate injections within the same site
each day
11. Injection Technique
11.1. Preparing the Dose and injection
1. Wash your hands with soap and water
2. Insert the plunger into the syringe, fix the needle with a slight
twist. Push the plunger in and out several times to remove all the
water that might have remained inside. Now, the syringe is ready
for use. However, this step is not necessary while using a sterile
disposable syringe and a needle.
3. Thoroughly but gently mix the insulin by upending the bottle and
rolling it between the palms (fig A). Shaking the bottle creates
bubbles. This step is particularly important for long acting and Mix

117
Fig. A
type of insulin. Do not use the insulin if anything unusual is
detected in the appearance of the vial.
• Begin by turning the bottle of
insulin upside down and rolling it
between the plans. The purpose of
this step is to mix the insulin
thoroughly.
(When using a new vial, remove the plastic protective cap on the stopper.
However do not remove the stopper)
4. Wipe the insulin bottle top with 70% alcohol immediately before
drawing insulin into the syringe and allow it to dry.
5. Draw air into the insulin syringe in the same amount as the insulin
to be withdrawn (fig B). If 10 units are to be removed, leave 10
units of air in the syringe.
• Carefully wipe off the top of the bottle with alcohol-soaked
cotton
• The next step is vital
• Draw air into the syringe in the
same amount as the insulin dose to
be taken.
• In other words, if you need 20 units
of insulin, you fill the syringe with
20 units of air, which is left in the
syringe temporarily,
• The reason for this is that a vacuum
exists in the insulin bottle, and in order to remove insulin you
must first inject same amount of air.
6. Insert the needle in the bottle, and push
the plunger down (fig C)
Fig. B
Fig. C

118
• With the air still in the syringe, carefully insert the needle
through the diaphragm top into the bottle
• Push the plunger down
7. Invert the bottle and draw more insulin into the syringe than
needed. Push the plunger up, expelling the insulin and air bubbles.
Do this several times to get rid of all air bubbles in the syringe (fig
D)
• Turn the bottle upside down and pull
back the plunger to a point
considerably past the amount of
insulin needed
• Push the insulin and air back into
bottle several times.
• The purpose of this step is to push all
of the air bubbles back into the bottle of insulin.
8. Pull the plunger down slowly to the right amount of insulin (fig E)
• Now that all the air bubbles are out of
the syringe, carefully pull the plunger
down to the correct amount of insulin
9. Holding the syringe at an angle to the skin (15 to 20 degrees
straight up-and-down), plunge the needle into the site that has
been prepared by cleaning with alcohol (fig F). Push the plunger
down all the way.
• The syringe now has the precise
amount of insulin required.
• Wipe the spot to be injected with
cotton and alcohol, and pinch the
skin
Fig. D
Fig E
Fig F

119
• Holding the syringe like a pencil, push the needle straight into
the skin and push the plunger down.
• Release the pinched skin, press the cotton ball next to the
needle, and pull out
10. Quickly withdraw the needle apply gentle pressure over the
injection site with an alcohol swab. Do not rub the area.
If you doctor advised you to mix different types of insulin, ensure to
follow the same sequence for drawing insulin from the vials. The rapid
acting is always drawn first.
1. Inject an amount of air equal to the dose of intermediate insulin
into the NPH or Lente insulin bottle. Withdraw the empty syringe at
this time without removing any insulin.
2.Ignore the previous bottle for a moment, inject an amount of air
equal to the desired dose of regular insulin in to the bottle and
remove the proper amount of regular insulin getting out the
bubbles as usual
3. Return to the intermediate insulin bottle but do not inject any air
this time. Simply insert the needle and withdraw the correct
amount of NPH or Lente insulin.
4.This final amount in the syringe is the sum of the regular
(crystalline) insulin plus the intermediate insulin for the total
measured dose.
Patients become very adapt it this procedure and have very little
trouble with the technique
The insulin mixture should be prepared just prior to injection
12. Sterilization of insulin syringes:
Do not share your syringe or needles with anyone else. Reusable syringes
and needles must be sterilized before each injection. Separate the
syringe, plunger (piston) and the needle. Place them in water in a covered

120
container. Bring the water to boiling and continue to boil it at least for 5
minutes. Allow it to cool completely. Follow all the instructions mentioned
on the package of the syringe.
Whenever disposable syringes and needles are used, use them only once
and then discard.
13. Dosage:
The insulin requirement of every patient is different and your doctor will
decide the dose considering your blood glucose values, age, daily
activities etc.
Insulin dose may be affected by various factors. Hence, it is necessary to
anticipate change in the dose of insulin required and seek your doctor’s
advice well on time.
Some of such factors are as follows:
13.1 Illness:
During an illness your requirement may actually go up, even if you are not
eating well.
13.2 Pregnancy:
During pregnancy it is important that your diabetes is controlled for you
as well as your baby.
13.3 Exercise:
Exercise may lower body’s need for insulin during and for some time after
activity. Exercise may also speed up the effect of an insulin dose,
especially if it involves the area of injection site.
13.4 Medication:
Insulin requirements may be modified by the effect of a number of
medications you may require to take during illness.

121
13.5 Travel:
When traveling across two or more time zones, consult your doctor well in
advance and seek his advice about dosage adjustments and schedule.
14. Common problems associated with Insulin:
14.1 Hypoglycemia:
Excessive lowering of blood glucose is called as hypoglycemia. This
problem is most frequent and can occur due to the following reasons:
• Taking higher doses of insulin than is required
• Missing or delaying meals
• Exercising or working more than usual
• An infection or illness (especially with diarrhoea or vomiting)
• A change in body’s need for insulin
• Consumption of alcoholic beverages.
The symptoms of mild to moderate hypoglycemia may include - sweating,
dizziness, palpitation, tremors, hunger, restlessness, tingling in the hands,
feet, lip or tongue, light headedness, inability to concentrate, headache,
drowsiness, sleep disturbance, anxiety, blurred vision, slurred speech,
depressive mood, abnormal behavior, unsteady movements and
personality changes
Signs and symptoms of severe hypoglycemia can include disorientation,
seizures, unconsciousness and death.
Mild to moderate hypoglycemia may be treated by -
- Consuming food or drinks that contain sugar. Patients should always
carry a quick source of sugar, such as sugar candies or glucose tablets.
More severe hypoglycemia may require assistance of another person and /
or hospitalization.
If you have frequent episodes of hypoglycemia or experience difficulty in
recognizing the symptoms, you should consult you doctor to discuss the
possible changes in therapy, meal plans and /or exercise program to help
you avoid hypoglycemia.

122
14.2 Hyperglycemia and Diabetic Acidosis: Hyperglycemia or high glucose levels in the blood may develop if your
body has too little insulin
Hyperglycemia can be brought about by:
• Omitting your insulin or taking less than the doctor has prescribed
• Eating significantly more than your meal plan suggests
• Developing a fever or infection
In patients with type I diabetes prolonged hyperglycemia can result in
diabetes acidosis usually come on gradually, over a period of hours or
days and include a drowsy feeling, flushed face, thirst, loss of appetite
and breath smelling of fruity odor. Urine tests would show large amounts
of glucose and acetone. Heavy breathing and rapid pulse are more severe
symptoms. It uncorrected, prolonged, hyperglycemia or diabetic acidosis
can result in loss of consciousness or death. Therefore it is important that
you obtain medical assistance immediately.
14.3 Lipodystophy:
Administration of insulin subcutaneonsly may result in lipotrophy
(depression in the skin) or lipohypertrophy (enlargement of thickening of
tissue). If you notice either of these conditions, consult your doctor. A
change in your injection technique may help alleviate the problem.
14.4 Allergy to insulin:
Local allergy: patients occasionally experience redness, swelling and
itching at the site of injection of insulin. If you have local reactions contact
your doctor.
Systemic Allergy: Less common, but potentially more serious is
generalized allergy to insulin which may cause rash over the whole body,
shortness of breath, wheezing, reduction in blood pressure, fast pulse or
sweating. Severe case of generalized allergy may be life threatening, if
you think you are having a generalized allergic reaction to insulin, seek
medical help immediately.

123
In conclusion each person is unique. The insulin requirement of every
patient is different considering the blood glucose values, age, daily
activities etc. Knowing how to inject and calculate the insulin dose is very
important. If you do your injections will be more comfortable. So, this
booklet is designed and given to diabetes mellitus patients who are on
insulin injection to increase their knowledge regarding self-administration
of insulin injection and to develop a positive attitude towards it and to
practice the insulin administration accurately.

135
ANNEXURE - N
Lists of Experts
1. Dr. B.A.Pataliah
Professor of Medical Surgical Nursing
The Oxford College of Nursing
J.P Nagar
Bangalore-75
2. Dr. K.P. Neeraja
Professor
Navodaya College of Nursing
Raichur
3. Mrs. Mosphea Khanam
Professor of Medical – Surgical Nursing
Regional College of Nursing
Guwahati, Assam
4. Mr. Amal Einstein Xavier
Principal
Oriental College of Nursing
Rajajinagar
5. Prof. S. Chitra
Principal
East-west College of Nursing
Rajajinagar
6. Mrs. Unmona Borgohain
Joint Director Nursing cum
Vice-Principal
Asian Institute of Nursing Education
G.N.R.C. Campus
Dispur, Guwahati – 06

137
7. Prof. N.N. Yalayyaswamy
Professor, Medical surgical Nursing
Kempa gowda Institute of Nursing
Bangalore – 4
8. Dr. Gangaboraih
Associate Professor of Statistics
Department of Community Medicine
Kempe gowda Institute of Medical Sciences
Bangalore – 4
9. Mr. Shridhar K.V
Associate Professor, Medical Surgical Nursing
Kempe gowda Institute of Nursing
Bangalore – 4
10. Dr. Dayanant.
Consultant Physician
Geetha Nursing Home
Bangalore.
11. Mr. S.N. Nanjunde Gowda
Associate Professor, Medical Surgical Nursing
Icon College of Nursing
Bangalore.




















