
2020_mokhtari_phd_mat.pdf - AURA - Alfred University
166
DEVELOPMENT OF NOVEL COPPER GLASS CONTAINING BONE ADHESIVES FOR ORTHOPAEDIC APPLICATIONS: STRUCTURAL, MECHANICAL, AND BIOLOGICAL EVALUATION BY SAHAR MOKHTARI A THESIS SUBMITTED TO THE FACULTY OF ALFRED UNIVERSITY IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF DOCTOR OF PHILOSOPHY IN MATERIALS SCIENCE AND ENGINEERING ALFRED, NEW YORK DECEMBER, 2020
-
Upload
khangminh22 -
Category
Documents
-
view
8 -
download
0
Transcript of 2020_mokhtari_phd_mat.pdf - AURA - Alfred University
DEVELOPMENT OF NOVEL COPPER GLASS CONTAINING BONE
ADHESIVES FOR ORTHOPAEDIC APPLICATIONS:
STRUCTURAL, MECHANICAL, AND BIOLOGICAL EVALUATION
BY
SAHAR MOKHTARI
A THESIS
SUBMITTED TO THE FACULTY OF
ALFRED UNIVERSITY
IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF
DOCTOR OF PHILOSOPHY
IN
MATERIALS SCIENCE AND ENGINEERING
ALFRED, NEW YORK
DECEMBER, 2020

DEVELOPMENT OF NOVEL COPPER GLASS CONTAINING BONE
ADHESIVES FOR ORTHOPAEDIC APPLICATIONS:
STRUCTURAL, MECHANICAL, AND BIOLOGICAL EVALUATION
BY
SAHAR MOKHTARI
B.S. UNIVERSITY OF TABRIZ (2010)
M.S. IRAN UNIVERSITY OF SCIENCE AND TECHNOLOGY (2013)
SIGNATURE OF AUTHOR _____________________________________
APPROVED BY _______________________________________________
ANTHONY W. WREN, ADVISOR ________________________________________________
ALEXIS G. CLARE, ADVISORY COMMITTEE ________________________________________________
WILLIAM C. LACOURSE, ADVISORY COMMITTEE ________________________________________________
S.K. SUNDARAM, ADVISORY COMMITTEE ________________________________________________
WILLIAM M. CARTY, ADVISORY COMMITTEE ________________________________________________
TIMOTHY KEENAN, CHAIR, ORAL THESIS DEFENSE
ACCEPTED BY _______________________________________________ GABRIELLE G. GAUSTAD, DEAN
KAZUO INAMORI SCHOOL OF ENGINEERING
signature on file
signature on file
signature on file
signature on file
signature on file
signature on file
signature on file
signature on file

Alfred University theses are copyright protected and may be used for education or personal research only. Reproduction or distribution in part or whole is prohibited without written permission from the author. Signature page may be viewed at Scholes Library, New York State College of Ceramics, Alfred University, Alfred, New York.
iii
ACKNOWLEDGMENTS
The time has come where I reflect on my past few years’ experience in this strange
yet wonderful little town called Alfred and think about all the wonderful people I met and
created some of my best and most amazing memories. I am forever grateful for their
contribution, either big or small, that helped me to shape a truly unforgettable experience
to grow, both personally and professionally.
First and foremost, I would like to express my deepest appreciation to my advisor
Dr. Anthony Wren for providing me the opportunity to continue my academic career by
pursuing my PhD. Dear Dr. Wren, I am deeply indebted and forever grateful for your
guidance, patience, dedication, and continuous encouragement during my studies. I am
thankful for providing me the freedom to work my way, and to always be available and
attentive to offer all possible assistance. Without your knowledge, guidance, and persistent
help this dissertation would have not been possible. I would also like to thank and express
my sincere gratitude to my committee members; Dr. Clare, Dr. LaCourse, Dr. Sundaram,
and Dr. Carty, for their continued support, and encouragement. Thank you for your
insightful comments and suggestions that have been an invaluable part to this work. I would
like to acknowledge the assistance of Jim Thiebaud, Gerald Wynick, Darren Stohr, Swavek
Zdzieszynski, and Dr. Keenan for training me to use the instruments and giving their
valuable inputs for my work. I am also thankful to the School of Engineering and all its
member’s staff for all the considerate support.
These past five years would not have been the same without the excellent company
of all my dear friends; Special thanks to my good friend Kaveh for his unconditional
support. Thank you for always finding a way to come and visit me. Ramin for your positive
and encouraging conversations, Iva for many memorable days in our “Good Place”, David
and Vignesh my now “European” friends, Priyatham, Nurila, Keyur, Saturday night’s game
group, and the ladies of ABC.
Last but certainly not least, I would like to express my gratitude to my loving and
caring family members; Ebi, Ehsan, Sahar, Mahsa, and Artin. You have always been there
for me through the good times and the bad, motivating me to be better. Finally, I am

iv
thankful to my mom and dad for their unwavering support. Words cannot express how
much gratitude I have for your endless love and patience throughout these many years far
away from home. None of these would have been possible if it were not for your support.
I am forever grateful.
v
TABLE OF CONTENTS
Page
Acknowledgments ....................................................................................................... iii
Table of Contents ......................................................................................................... v
List of Tables .............................................................................................................. ix
List of Figures .............................................................................................................. x
Abstract ..................................................................................................................... xiv
1 OBJECTIVES ........................................................................................................... 1
2 INTRODUCTION..................................................................................................... 2
2.1 BONE TISSUE ........................................................................................................... 2
2.1.1 Bone Microstructure ....................................................................................... 3
2.1.2 Bone Tissue Diseases ...................................................................................... 5
2.1.3 Vertebral Augmentation .................................................................................. 6
2.1.4 Hip and Knee Arthroplasty ............................................................................. 8
2.2 PMMA BONE CEMENT .......................................................................................... 10
2.2.1 Issues with Current Bone Cements ............................................................... 11
2.3 GLASS POLYALKENOATE CEMENTS ....................................................................... 13
2.3.1 Historical Development ................................................................................ 13
2.3.2 Clinical Applications .................................................................................... 14
2.3.3 Chemistry of Glass Polyalkenoate Cements ................................................. 15
2.3.4 Setting Reaction ............................................................................................ 16
2.3.5 The Glass Component ................................................................................... 17
2.3.6 Polyacrylic Acid ............................................................................................ 18
2.3.7 Adhesion of GPCs to Tooth Structure ........................................................... 19
2.3.8 Transition from Dental to Skeletal Adhesive GPCs ...................................... 20
2.4 COPPER INCORPORATED GLASS POLYALKENOATE CEMENTS ................................ 22
2.5 REFERENCES .......................................................................................................... 25
vi
3 COPPER CONTAINING GLASS POLYALKENOATE CEMENTS BASED
ON SIO2-ZNO-CAO-SRO-P2O5 GLASSES: GLASS CHARACTERIZATION,
PHYSICAL AND ANTIBACTERIAL PROPERTIES ............................................... 33
3.1 ABSTRACT ............................................................................................................. 34
3.2 INTRODUCTION ...................................................................................................... 34
3.3 MATERIALS & METHODS ....................................................................................... 37
3.3.1 Glass Synthesis.............................................................................................. 37
3.3.2 X-Ray Diffraction (XRD) .............................................................................. 38
3.3.3 Differential Thermal Analysis (DTA)............................................................ 38
3.3.4 Scanning Electron Microscopy & Energy Dispersive X-ray Analysis
(SEM/EDS) ................................................................................................................ 38
3.3.5 Advanced Surface Area and Porosity (ASAP) .............................................. 38
3.3.6 Particle Size Analysis (PSA) ......................................................................... 39
3.3.7 X-Ray Photoelectron Spectroscopy (XPS) .................................................... 39
3.3.8 Magic Angle Spinning-Nuclear Magnetic Resonance (MAS-NMR) ............. 39
3.3.9 Ion Release Profiles ...................................................................................... 40
3.3.10 pH Measurements ..................................................................................... 40
3.3.11 Glass Polyalkeonate Cements Formulation.............................................. 40
3.3.12 Rheological Evaluation ............................................................................. 40
3.3.13 Compressive Strength ............................................................................... 41
3.3.14 Shear Bond Strength Test.......................................................................... 41
3.3.15 Antibacterial Testing ................................................................................. 42
3.4 RESULTS ................................................................................................................ 43
3.5 DISCUSSION ........................................................................................................... 56
3.6 CONCLUSION .......................................................................................................... 60
3.7 REFERENCES .......................................................................................................... 61
4 INVESTIGATING THE EFFECT OF COPPER ADDITION ON GLASS
POLYALKENOATE CEMENTS: PHYSICAL, MECHANICAL AND
BIOLOGICAL BEHAVIOR.......................................................................................... 66

vii
4.1 INTRODUCTION ...................................................................................................... 67
4.2 MATERIALS & METHODS ....................................................................................... 71
4.2.1 Glass Synthesis.............................................................................................. 71
4.2.2 Cement Formulation ..................................................................................... 72
4.2.3 Rheological Evaluation ................................................................................. 72
4.2.4 Compressive Strength ................................................................................... 73
4.2.5 Biaxial Flexural Strength .............................................................................. 73
4.2.6 Shear Bond Strength ..................................................................................... 73
4.2.7 Laser Profilometry ........................................................................................ 74
4.2.8 Ion Release Profile ........................................................................................ 74
4.2.9 Simulated Body Fluid Trial ........................................................................... 74
4.2.10 Scanning Electron Microcopy (SEM) ....................................................... 75
4.2.11 Antibacterial Analysis - Agar Diffusion .................................................... 75
4.2.12 Antibacterial Analysis - Bacterial Broth................................................... 75
4.2.13 Cytotoxicity - MTT assay .......................................................................... 76
4.2.14 Statistical Analysis .................................................................................... 77
4.3 RESULTS ................................................................................................................ 77
4.4 DISCUSSION ........................................................................................................... 90
4.5 CONCLUSION .......................................................................................................... 98
4.6 REFERENCES .......................................................................................................... 99
5 COPPER CONTAINING GLASS-BASED BONE ADHESIVES FOR
ORTHOPAEDIC APPLICATIONS: GLASS CHARACTERIZATION AND
ADVANCED MECHANICAL EVALUATION. ....................................................... 105
5.1 INTRODUCTION .................................................................................................... 106
5.2 MATERIALS & METHODS ..................................................................................... 111
5.2.1 Synthesis of Glass Powders ........................................................................ 111
5.2.2 Fabrication of Glass/PAA Hybrid Adhesives ............................................. 111
5.2.3 Scanning Electron Microscopy & Energy Dispersive X-ray Analysis
(SEM/EDS) .............................................................................................................. 111
5.2.4 X-Ray Diffraction (XRD) ............................................................................ 111
viii
5.2.5 X-Ray Photoelectron Spectroscopy (XPS) .................................................. 112
5.2.6 Raman Spectroscopy ................................................................................... 112
5.2.7 ATR-FTIR Spectroscopy ............................................................................. 112
5.2.8 Rheological Evaluation ............................................................................... 112
5.2.9 Mechanical Properties ................................................................................ 113
5.3 RESULTS .............................................................................................................. 113
5.4 DISCUSSION ......................................................................................................... 125
5.5 CONCLUSION ........................................................................................................ 131
5.6 REFERENCES ........................................................................................................ 131
6 CONCLUSION ..................................................................................................... 136
7 APPENDIX ............................................................................................................ 138
7.1 APPENDIX A - PUBLICATIONS .............................................................................. 138
7.2 APPENDIX B – GE CONTAINING GLASS POLYALKENOATE CEMENTS ................... 139

ix
LIST OF TABLES
Page
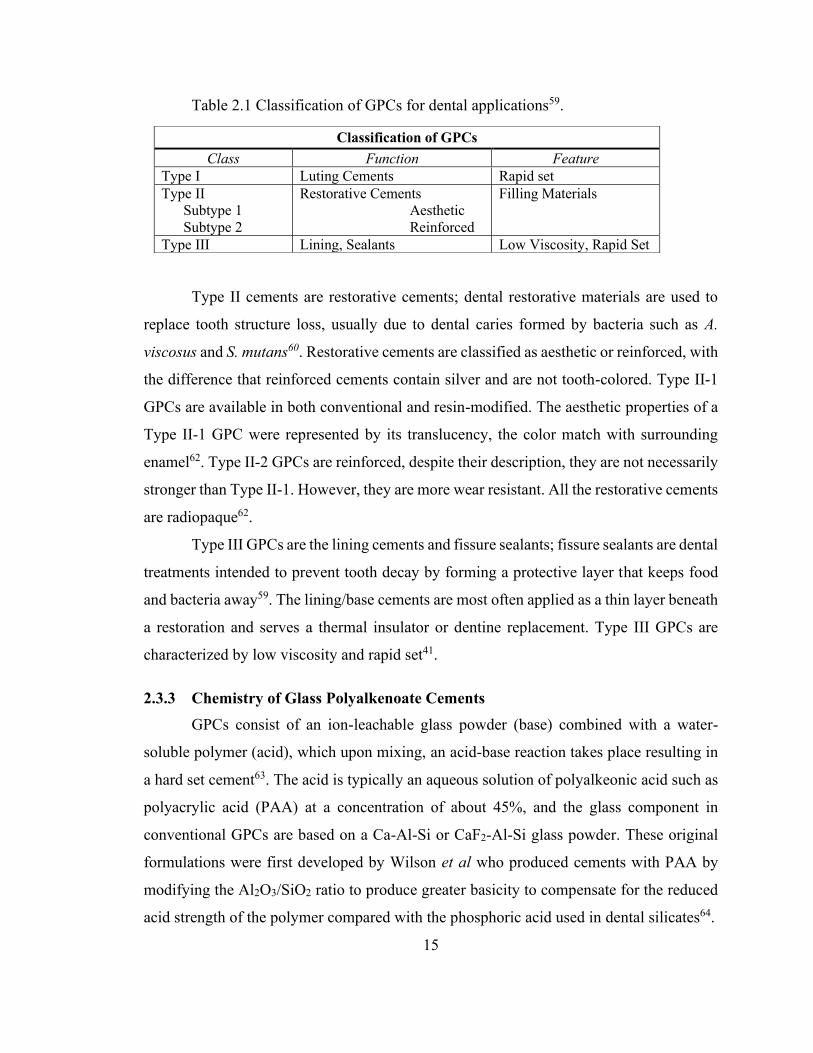
Table 2.1 Classification of GPCs for dental applications59. ............................................. 15
Table 3.1 Glass compositions (Mol. %) where SiO2 is substituted with CuO.................. 38
Table 3.2 Particle size analysis of each glass composition. .............................................. 44
Table 3.3 BET surface area (m2/g) for each glass composition. ....................................... 44
Table 3.4 Working (Tw) and Setting (Ts) times of ConC, Cu6C and Cu12C formulated with 40, 50 and 60wt% PAA. ............................................ 51
Table 4.1 Glass compositions (Mol. Fr). .......................................................................... 72
Table 4.2 Cement formulation for variable P:L ratios and with 40 wt.% concentration of PAA ........................................................................... 72
Table 4.3 Working (Wt) and Setting (St) times of ConC, Cu6C, and Cu12C formulated with 40wt% PAA, and variable P/L ratios. ........................ 77
Table 4.4 Summary of mechanical properties of ConC, Cu6C, and Cu12C after incubation in DI water for 1, 7, 14, and 21 days .......................... 80

x
LIST OF FIGURES
Page
Figure 2.1 Bone tissue structure.......................................................................................... 2
Figure 2.2 The hierarchical structure of typical bone at various length scales. .................. 4
Figure 2.3. (a) Healthy Bone and (b) Osteoporotic Bone ................................................... 6
Figure 2.4. vertebroplasty and kyphoplasty. (a) radiograph showing the trocar inserted into the three vertebrae that are to be treated. (b) The top and bottom vertebrae have undergone vertebroplasty, with the injected PMMA radio-opaque cement visible. The middle vertebral body is undergoing a kyphoplasty, with the balloon tamp being inflated. ............................................................... 7
Figure 2.5 Example of radiographic results before and after cement injection. ................. 9
Figure 2.6. Schematic of cemented total hip replacement. ............................................... 11
Figure 2.7 Setting reaction of a conventional glass polyalkenoate cement. ..................... 17
Figure 2.8 Types of carboxylic acid units used in GPCs liquids. ..................................... 19
Figure 2.9. Schematic of glass polyalkenoate cement adhesion to tooth mineral. ........... 20
Figure 2.10. Mechanisms of Cu antibacterial properties (a) Cu causes cell damage, (b) cell membrane rupture, (c) generation of ROS, and (d) DNA degradation. ..................................................................................... 23
Figure 3.1 Bonded Cu6C cylinders to hydroxyapatite substrates for shear bond strength testing ....................................................................................... 42
Figure 3.2 X-ray Diffraction (XRD) patterns for each powdered glass sample ............... 43
Figure 3.3 DTA thermograms Control, CuG6, and CuG12 powdered glass samples. ..... 45
Figure 3.4 Energy-dispersive X-ray (EDX) and Scanning Electron Microscopy (SEM) of Control, CuG6, and CuG12 powdered glass samples. ................... 46
xi
Figure 3.5 (a) X-ray photoelectron spectroscopy (XPS) survey scans of Control and CuG12 and (b) high-resolution O1s scans of Control, CuG6, and CuG12. ..................................................................................................... 47
Figure 3.6 (a) 29Si MAS-NMR spectrum of Control glass, and (b) corresponding Q-species. ........................................................................................................ 48
Figure 3.7 (a) 29Si MAS-NMR spectrum of CuG12 glass, and (b) corresponding Q-species. ........................................................................................................ 48
Figure 3.8 Ion release profiles of Control, CuG6, and CuG12, investigating (a) silica, (b) zinc, (c) calcium, and (d) strontium release after 1, 10, 100 and 1000 hours incubation in deionized water. ............................. 50
Figure 3.9 pH of extracts from samples release after 1, 10, 100 and 1000 hours incubation in deionized water ......................................................................... 51
Figure 3.10 (a) Working times and (b) setting times of ConC, Cu6C and Cu12C mixed with 40, 50 and 60 wt% PAA. ............................................................. 52
Figure 3.11 Compressive strength of GPC series using 40wt%, 50wt% and 60wt% PAA after 7 days soaking in de-ionized water. .................................. 53
Figure 3.12 Shear bond strength of ConC, Cu6C and Cu12C in addition to SEM imaging of fracture surfaces. ................................................................. 53
Figure 3.13 Antibacterial testing of ConC, Cu6C and Cu12C in a.) E. coli, b.) S. epidermidis, c.) Vancomycin Resistant S. aureus and d.) S. aureus (UMAS-1). ...................................................................................................... 54
Figure 3.14 Antibacterial testing plates presented in rows a.) E. coli, b.) S. epidermidis, Vancomycin Resistant S. aureus and d.) S. aureus (UAMS-1) and columns with samples i.) ConC, ii.) Cu6C and iii.) Cu12C. .................... 55
Figure 4.1 Schematic overview of setting reaction in GPCs, and structure after maturation adhesion to bone tissue. ................................................................ 69
Figure 4.2 (a) Compressive strength of ConC and Cu-GPCs using variable P/L ratios after 14 days incubation in DI water, and (b) Compressive strength with P/L ratio of 2:2.5 after 1, 7, 14, and 21 days incubation in DI water. ..................................................................................................... 78

xii
Figure 4.3 Biaxial flexural strength (BFS) of ConC and Cu-GPCs after 1, 7, 14, and 21 days incubation in DI water. ................................................. 79
Figure 4.4 Shear bond strength of ConC and Cu-GPCs after 1, 7, 14, and 21 days incubation in DI water. ............................................................... 80
Figure 4.5 Laser profilometry images of the fracture surface of ConC and Cu6C after adhesive shear bond analysis, 1 and 21 days incubation in DI water. ................................................................................... 81
Figure 4.6 Projected scan areas of laser profilometry images (Figure 3.5) of ConC and Cu6C fracture surface after 1 and 21 days incubation in DI water, analyzing vertical height (Z) range and corresponding % of total area. ......... 82
Figure 4.7 (a) Shear bond strength testing setup and (b) optical microscopy images of fracture surface of Cu6C after 1, and 21 days. ............................... 83
Figure 4.8 Ion release profiles of ConC and Cu-GPCs, investigating Si, Zn, P, Sr, Ca and Cu release after 1, 7, 14 and 21 days incubation in DI water. ................................................................................... 85
Figure 4.9 SEM micrographs of surface of ConC and Cu-GPCs and corresponding EDX after 21 days incubation in SBF............................................................. 86
Figure 4.10 (a) Agar diffusion antibacterial testing of ConC, Cu6C, and Cu12C in E. coli, S. epidermidis, and S. aureus, (b, c, d) Inhibition Zone (IZ) of ConC, Cu6C, and Cu12C employing the antibacterial agar diffusion method. .................... 88
Figure 4.11 Bacterial viability of ConC and Cu6C, Cu12C extracts after, 1, 7, 14 and 21 days incubation in DI water employing the bacterial broth method. Each test analyzed the GPCs efficacy in (a) E. coli, (b) S.epidermidis, and (c) S. aureus. ............................................................................................. 89
Figure 4.12 MC3T3-E1 cell viability of ConC and Cu6C, Cu12C extracts after 1, 7, 14, and 21 days incubation in DI water .................................................. 90
Figure 5.1 (a) Schematic illustration of the bone cement used in the augmentation of damaged vertebra, (b) Preparation process, where the glass powder, PAA and water were homogeneously mixed and set within 15 minutes. The SEM image shows the microstructure of the of the porous set cement. The unreacted glass particles are labeled. (c) Schematic of the setting reaction of the glass particle and polyacrylic acid in atomic level. Water deprotonates the COOH groups on

xiii
the acid chain, which further crosslinks withs ions released from the surface of the glass. The covalently crosslinked hybrid adhesive is shown where Cu2+ ion crosslinks two groups of COO- on the PAA......... 110
Figure 5.2 SEM images of the glass powders; Control, and Cu-BG glasses before (Cu-BG), and after annealing (Cu-BG A) with the corresponding EDX spectra. ......................................................................... 114
Figure 5.3 SEM images of the Cu-BG glass powder after annealing, and the mapping of the surface showing the distribution of Cu, and Si. ............. 116
Figure 5.4 (a) XRD patterns of the glass powders, and (b) High resolution Cu2p in annealed powder of Cu-BG. ............................................................ 117
Figure 5.5 (a) Raman spectra of the glass powders and (b) Raman spectrum of crystallized Cu-BG, and attributed fitting curves within spectra ranges of 800-1200 cm-1; (c) Control, (d) Cu-BG before annealing, and (e) Cu-BG after annealing. ..................................................................... 119
Figure 5.6 ATR-FTIR spectra within the first 15 minutes of setting reactions (a) Con/PAA and (b) CuG/PAA adhesives. ................................................... 121
Figure 5.7 (a) Typical compressive load-extension for the Con/PAA and (b) CuG/PAA (c) Recovery of the CuG/PAA specimen after compression loading, (c) Projected recovery of CuG/PAA within the first 250 minutes. .................................................................................................. 123
Figure 5.8 Compressive properties of CuG/PAA (a,b) Stress–strain curves during loading–unloading cycles in sequence of increasing strain amplitude of 25, 50, and 75% after 1 and 10 hours incubation in deionized water, (c) corresponding compressive strength of CuG/PAA adhesives. ................ 124
Figure 5.9 Cross section SEM micrographs of the (a-d) Con/PAA, and (e-h) CuG/PAA adhesives. ............................................................................ 125

xiv
ABSTRACT
The main objective of this thesis was to design and develop new formulations of
hybrid organic-inorganic bone cements based on Cu incorporated glasses, that could be
utilized for orthopedic applications and, by doing so, expand their clinical indications. Cu-
containing glass polyalkenoate cements (GPCs) were developed through modification of
the glass composition, and were characterized by their physical, mechanical, and biological
behavior. Three separate glass compositions were synthesized, and the effect of Cu
addition was investigated in relation to the glass structure, morphology, and composition.
In vitro biological behavior was initially evaluated by studying the solubility profiles of
the glass compositions and the resultant cements. Each composition encouraged bone
bonding and provided positive therapeutic effects, such as skeletal tissue mineralization
which was confirmed using Simulated Body Fluid (SBF) trials, and osteoblast cell viability
studied using cytotoxicity assays. Bacterial testing of the GPCs assessed against three
prevalent strains of bacteria and indicated superior antibacterial efficacy of the Cu
incorporated GPCs which could substantially minimize medical device complications
triggered by bacterial infections. The mechanical properties were evaluated by studying
the compressive, flexural, and shear bond strength of the GPCs, and as a function of their
maturation time. Interfacial studies performed between hydroxyapatite (mineralized bone
tissue) and the cements, suggested extensive chemical bonding has occurred leading to
strong interfacial bonding at the material/bone tissue interface. Further studies on the
mechanical properties of GPCs synthesized from crystallized Cu containing glasses,
revealed a viscoelastic behavior of the GPCs with exceptional compressibility, which is
believed that could benefit a wide range of requirements in the development of bone tissue
cements.

1
1 Objectives
The primary goals of this research were to develop glass-based bone cements with
improved physical, mechanical properties, and biocompatibility for orthopedic
applications. The cements must have a similar strength to human bone and have an
adequate host response when introduced into the body; in this case the cement must
promote healthy bone growth. Traditional bone cements based on acrylics such as
polymethylmethacrylate (PMMA) lack chemical bonding to mineralized bone tissue and
rely exclusively on mechanical interaction to achieve implant fixation which routinely
leads to aseptic loosening (failure in absence of infection) of implant. Highly exothermic
setting reaction, thermal necrosis of surrounding bone tissue, release of unreacted toxic
monomer of methylmethacrylate, and volumetric shrinkage are some of the major issues
with available acrylate bone cements. Consequently, these drawbacks have prompted the
need to develop alternative synthetic bone substitute materials such as bioactive glass-
based compositions, which have proven to be an effective material at regenerating bone.
Conventional glass polyalkenoate cements (GPCs) were originally developed for
use as restorative dental materials and have been applied to numerous areas in dentistry.
GPCs are able to chemically bond to bone tissue and provide strong interfacial bonding.
The use of GPCs for orthopaedic applications is of great interest due to their excellent
biocompatibility, lack of significant volumetric shrinkage, lack of heat evolution while
setting, and their ability to chemically adhere to bone mineral. The truly adhesive nature of
GPCs and their superior biological performance make them a promising candidate for
orthopedic applications and as possible alternatives to currently used acrylic cements.
This thesis aims to address issues with currently used bone cements by producing
novel compositions of glass polyalkenoate cements with improved bone bonding and
biological behavior to serve as skeletal adhesive GPCs. To this end, understanding the
chemistry, structure, mechanical, and biological performance of these materials for bone
tissue regeneration, is critical. The next chapter will review general information on bone
tissue microstructure and diseases, commercially available acrylate bone cements,
chemistry and clinical application of glass polyalkenoate cements, and lastly, the rational
of incorporation of Cu in the chemistry of the GPCs.

2
2 Introduction
2.1 Bone Tissue
The initial steps in development of biomedical materials for orthopedic applications
is to understand the composition, microstructure, and function of bone tissue at different
hierarchical levels. The human skeletal system is highly specialized form of connective
tissue, and is composed of bones, tendons, ligaments, and cartilage1. Our skeletal
framework is made up from 206 individual bones that provides body the support and the
protection1. Natural bone is a composite material composed of organic matrix (~30%) that
is reinforced with inorganic components (~70%) of bone minerals (Figure 2.1)2. The
unique composition, design, and assorted arrangement of structures at various levels of
hierarchy assembles into the heterogenous and anisotropic bone to perform diverse
mechanical, chemical, and biological functions3. The main organic component is type І
collagen with the inorganic mineral content deposited as plate-like crystals of calcium
phosphate or hydroxyapatite (HA); Ca10 (PO4)6 (OH)23. Together the organic and inorganic
constituents enable bone to sustain the physical stresses imposed on it by everyday
activities2. Based on reports of wet and dry specimens of human lumbar spine trabecular
bone, the percentage weights of the inorganic and organic phases and water content have
been calculated at approximately 54wt%, 26wt% and 20wt% respectively3.
Figure 2.1 Bone tissue structure. Bone is a self-regenerative material and delivers strength and rigidity yet allows
flexibility for movement and impact resistance2. Morphologically there are two types of

3
bone: cortical (dense), and cancellous (spongy) bone4. In cross section of long bones, such
as femur, the end has a dense cortical shell with porous structure of cancellous bone inside4.
Cortical bone, also called compact or lamellar bone, carries the majority of load in major
bones, and is characterized by dense outer surface that builds a protective layer around the
internal spongy bones, cavity, and canals5. Around 80% of human skeletal mass is
composed of cortical bone and is characterized by 5-10% porosity with pores measuring
up to 10-50 µm in diameter5. Cancellous bone, on the other hand, has a loosely organized
open-cell, foam like structure, is more flexible and optimized to transfer the loads through
bone5. Cancellous bone, also called trabecular bone, is the internal tissue of skeletal bone,
where is typically located at the end of long bone, and the interiors of joints and vertebrae3.
Unlike cortical bone, cancellous bone has much greater porosity and surface area, with 75-
85% porosity with 300-600 µm pores in diameter. In general, cancellous bone is more
dynamic, and is remodeled more often than cortical bone5.
2.1.1 Bone Microstructure Osteon is the basic functional unit of mature cortical bone3. In an osteon, the
osteocytes (matured osteoblasts) are arranged in concentric layers around a central canal
or haversian canal6. These canals run parallel to the surface of the bone, and contain blood
vessels that carry blood to and from the osteon6. Blood vessels in these canals supply blood
to osteons deeper in the bone and tissues of the marrow cavity. Bone is a form of supporting
connective tissue and includes specialized cells such as osteoblasts and osteoclasts, protein
fibres, and ground substance of extracellular matrix7. Collectively, the extracellular protein
fibres and ground substance compose the matrix, which encloses the skeletal system’s
cells. The matrix typically forms most of the volume of connective tissues. The matrix of
bone tissue is solid and sturdy due to the deposition of HA, around the protein fibres6.

4
Figure 2.2 The hierarchical structure of typical bone at various length scales8.
Microstructurally, bone tissue is composed of a mineral and a collagenous phase7.
Figure 2.2 demonstrates the different levels of bone micro and nanostructure. At the
microstructural level, mineralized collagen fibres arrange into planar configuration called
lamellae (7 m wide). An osteon or a haversian system (200 m in diameter), consists of
lamellaes bundled in concentric layers around a central osteonic canal9. Osteons are
cylinders running roughly parallel to the long axis of the bone9.
The nanostructure of bone consists of three main components, hydroxyapatite
crystals, collagen fibres, and non-collagenous organic proteins8. The mature mineralized
crystals are not needle-shaped, but plate-shaped. Plate-like apatite crystals of bone appear
within the distinct spaces within the collagen fibrils3. These crystals are made of carbonated
hydroxyapatite8. The hydroxyapatite crystals grow over time eventually expanding out of
the holes and creating continuous sheets throughout the fibres10. Water initially fills the
space between the fibres and is gradually replaced as the hydroxyapatite crystal
concentration increases10.
The hydroxyapatite is composed of calcium phosphate Ca3 (PO4)2 and accounts for
about 66% of bone weight8. The hydroxyapatite crystals are deposited by the osteoblast
cells onto the preformed collagen fibres. The calcium phosphate crystals are initially
deposited by matrix vesicles at particular areas on the collagen fibres containing bone
nucleus for the formation of first apatite crystals. These vesicles, often referred to matrix
5
vesicles, are rich in calcium and phosphate ions, and included within the osteoblast9. Once
the calcification has begun, the matrix vesicles are no longer needed to support
mineralization and are consumed by the advancing mineralization front in which pre-
formed crystals serve as nuclei for the formation of new crystals10.
2.1.2 Bone Tissue Diseases Osteoporosis is most common bone disease that emerges when bone mineral
density and bone mass decreases, or when the quality of bone structure changes.
Osteoporosis can result in the bone tissue strength reduction, that can in turn, increase the
risk of fractures or broken bones11. Osteoporosis is an immense public health problem,
estimated to afflict 200 million worldwide, and responsible for at least 1.2 million fractures
in the United States each year12. The most common sites of these fractures are the vertebrae
in 538,000 cases, the hip in 227,000 cases. By extreme old age, one of every three women
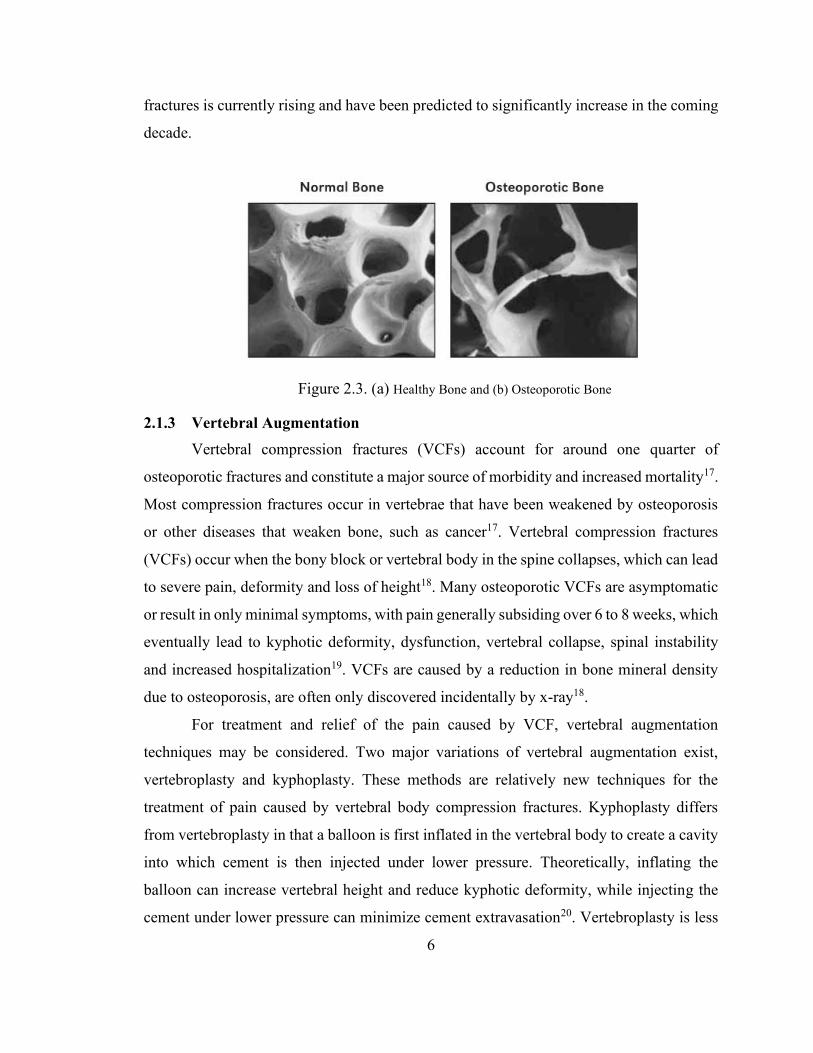
and one of every six men will have had a hip fracture12. Figure 2.3 shows the
morphological difference between healthy and osteoporotic bone13. Not all parts of the
skeleton are equally affected by osteoporosis. Epiphyses of the long bones, vertebrae and
the jaws are more heavily affected which results in fragile limbs, a reduction in height and
a loss of teeth13. More serious fractures that can occur are collapse of the vertebral body
and fracture of the femoral head which require reconstructive surgery (vertebroplasty or
kyphoplasty in the case of vertebral fractures) or fixation of an implant (total hip
replacement in the case of femoral fracture), which, require bone cementation14. In a report
published by Mayo clinic in 2015, the volume of primary and revision orthopedic surgeries
which require bone adhesives, is significantly high in United States and studies show an
exponential growth in the coming decades15. According to the American Academy of
Orthopedic Surgeons (AAOS), in 2017 there were 370,770 total hip replacements (THR)
and 680,150 total knee replacements (TKR) performed only in the United States16. By
2060, primary THR is expected to reach 1.23 million (330 percent increase), primary TKR
is expected to reach 2.60 million (382 percent increase), revision THR is expected to reach
110,000 (219 percent increase), and revision TKR is expected to reach 253,000 (400
percent increase)16. An estimated number of 700,000 patients undergo vertebroplasty and
kyphoplasty in the United States, each year16. The annual incidence of osteoporotic
6
fractures is currently rising and have been predicted to significantly increase in the coming
decade.
Figure 2.3. (a) Healthy Bone and (b) Osteoporotic Bone
2.1.3 Vertebral Augmentation Vertebral compression fractures (VCFs) account for around one quarter of
osteoporotic fractures and constitute a major source of morbidity and increased mortality17.
Most compression fractures occur in vertebrae that have been weakened by osteoporosis
or other diseases that weaken bone, such as cancer17. Vertebral compression fractures
(VCFs) occur when the bony block or vertebral body in the spine collapses, which can lead
to severe pain, deformity and loss of height18. Many osteoporotic VCFs are asymptomatic
or result in only minimal symptoms, with pain generally subsiding over 6 to 8 weeks, which
eventually lead to kyphotic deformity, dysfunction, vertebral collapse, spinal instability
and increased hospitalization19. VCFs are caused by a reduction in bone mineral density
due to osteoporosis, are often only discovered incidentally by x-ray18.
For treatment and relief of the pain caused by VCF, vertebral augmentation
techniques may be considered. Two major variations of vertebral augmentation exist,
vertebroplasty and kyphoplasty. These methods are relatively new techniques for the
treatment of pain caused by vertebral body compression fractures. Kyphoplasty differs
from vertebroplasty in that a balloon is first inflated in the vertebral body to create a cavity
into which cement is then injected under lower pressure. Theoretically, inflating the
balloon can increase vertebral height and reduce kyphotic deformity, while injecting the
cement under lower pressure can minimize cement extravasation20. Vertebroplasty is less
7
invasive and very effective for pain relief14. Kyphoplasty offers greater control of cement
placement and the potential for greater height restoration or kyphosis correction21. Both
procedures are performed via fluoroscopic or CT guided needle placement accompanied
by high quality imaging equipment21. Once the insertion site is identified a trocar is inserted
through the pedicle into the vertebral body22. This is achieved by applying moderate
pressure to the trocar at which point the insert is removed and replaced with a drill to create
a path for the balloon (kyphoplasty) and subsequently, the cement. Trocar is a surgical
instrument with a three-sided cutting point enclosed in a tube, used for withdrawing fluid
from a body cavity. In kyphoplasty a balloon is inserted into the vertebrae and inflated
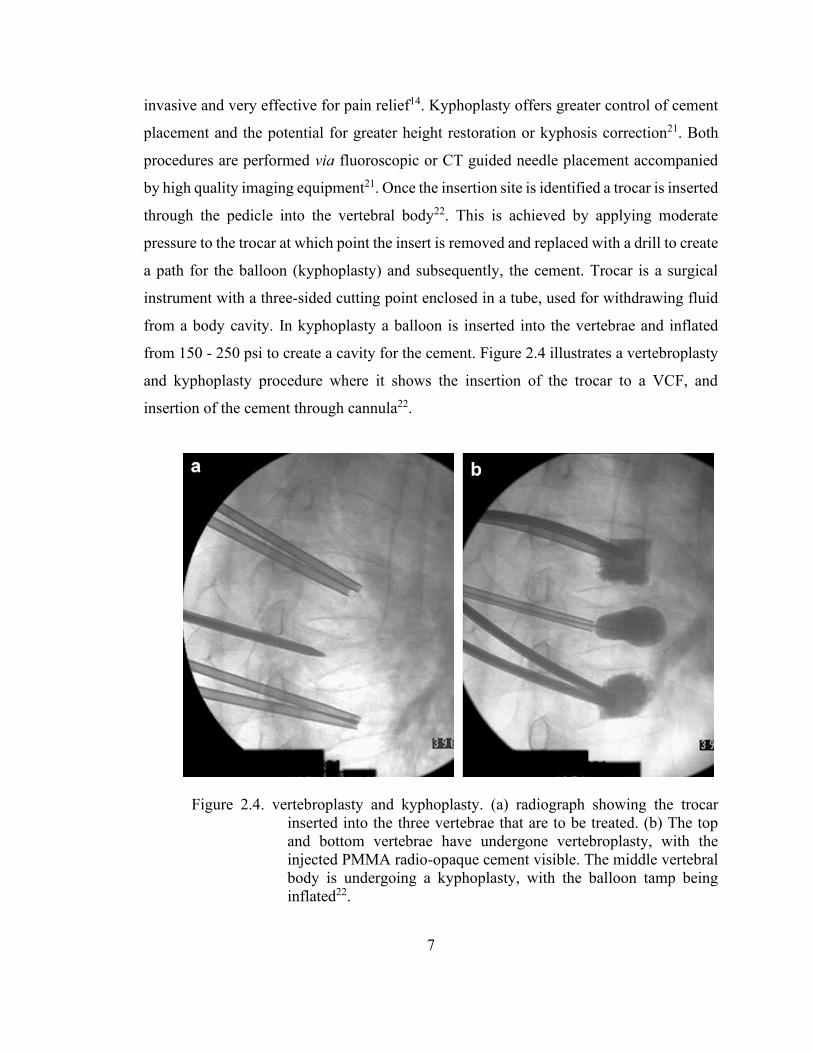
from 150 - 250 psi to create a cavity for the cement. Figure 2.4 illustrates a vertebroplasty
and kyphoplasty procedure where it shows the insertion of the trocar to a VCF, and
insertion of the cement through cannula22.
Figure 2.4. vertebroplasty and kyphoplasty. (a) radiograph showing the trocar inserted into the three vertebrae that are to be treated. (b) The top and bottom vertebrae have undergone vertebroplasty, with the injected PMMA radio-opaque cement visible. The middle vertebral body is undergoing a kyphoplasty, with the balloon tamp being inflated22.
8
2.1.4 Hip and Knee Arthroplasty The incidence of joint replacement procedures is high, with over 1 million total hip
and total knee replacement procedures performed each year in the United States23. Joint
replacement orthopaedic surgeries are generally performed to relieve arthritis pain or some
hip fractures. Bone fractures are among the most common diagnoses that require inpatient
hospitalization23. Therapeutic bone cements are widely used in various orthopaedic and
trauma surgeries to restore the functional capacity of the bone tissue. Some of their
common clinical uses include applications in total hip replacement (THR) or total knee
replacements (TKR). Hip replacement is a surgical procedure in which the hip joint is
replaced by a prosthetic implant. THR consists of replacing both the acetabulum and the
femoral head, and TKR consists of replacing the diseased or damaged joint surfaces of the
knee to allow continued motion of the knee.23 THR surgery is performed by implanting a
metallic stem which is inserted into the medullary cavity of the proximal epiphysis of the
femur with either a metal or ceramic femoral head24. There is also an acetabular component
which is composed of a metal shell with a polymer (polyethylene)/ceramic
(zirconia/alumina) liner25. There are many variations on the materials used for the
articulating surfaces in an effort to reduce wear debris which contributes to aseptic
loosening of the implant which is the primary mode of failure for THR25-26. Osteoporotic
bone provides a unique challenge to reconstructive orthopaedic procedures in surgery and
particularly fracture repair3. Today surgeons use both cemented and cementless stems for
hip arthroplasty, however a cemented stem is preferred in treating the elderly population
with osteoporotic bone27.
A cemented prosthesis is designed to have a layer of bone cement, typically an
acrylic cement, in between the patient's natural bone and the prosthetic joint component28.
Cemented THR, for example, uses acrylate cement to function as a grout, producing an
interlocking fit between cancellous bone and prosthesis. The cement is used to create
instant stability of the femoral stem to permit early load bearing (Figure 2.5). Bone
cementation forms a bond between the prosthesis and the endosteal surface of the bone,
where fixation of the prosthesis is typically achieved by mechanical interlock in case of
acrylate cements25, 28. Research has shown that increased pressurisation enhances

9
penetration into bone interstices, which increases tensile and shear strengths at the bone-
cement interface29. A breakdown of the cement can cause the artificial joint to come loose,
which may prompt the need for another joint replacement surgery (revision surgery). The
cement debris can also irritate the surrounding soft tissue and cause inflammation30. One
recognized problem with cementation is that leakage can cause complications ranging from
cardiopulmonary events, to hypotension which in some instances can be fatal30. However
strict adherence to cementing techniques combined with careful monitoring can reduce the
risk of cement associated complications.
Figure 2.5 Example of radiographic results before and after cement injection31.
The mechanical properties of implanted materials that reside alongside living tissue
must be similar in order to distribute the body’s natural forces3. Some of the forces that are
experienced by bone, and must be considered in materials design, are compressive strength,
tensile strength and Young’s modulus32. However, the biocompatibility of an implanted
material is one of the primary concerns when designing bone cements33. Modern bone
cements can be bioactive, which means that they evoke a positive biological response, or

10
bioinert, where they remain inert when implanted into the body. Poymehylmethacrylate
(PMMA) is the most widely used bone cement and it is used to correct both vertebral
compression fractures, knee and hip arthroplasty34. The following section is a review of
this cement for various clinical applications.
2.2 PMMA Bone Cement
The PMMA bone cement had been the gold standard in various orthopaedic
surgeries. The knowledge about the bone cement is of paramount importance to all
orthopaedic surgeons. Bone cements are primarily used for the fixation of artificial joints
but are also used in spinal procedures such as vertebroplasty and kyphoplasty. In joint
arthroplasty the basic function of the bone cement is to fill the free space between the
prosthesis and the bone. The first clinical bone cement used in orthopaedics, was an
acrylate cement based on Polymethylmethacrylate (PMMA), which was used for hip
arthroplasty in 195835. The majority of the bone cements available in the market today, are
based on Polymethylmethacrylate (PMMA) cements. These cements are produced by
mixing PMMA powder with a liquid monomer in the presence of initiators and activators
which set to form a hard cement mass in less than 15 minutes. Bone cement acts as a space-
filler that creates a tight space which holds the implant against the bone and thus acts as a
‘grout’35. One other type of bone cement materials, under development, is based on calcium
phosphate cements (CPCs). However, after more than 60 years from the introduction of
PMMA cements, they have still remained as the gold standards in the field of orthopaedic
cements.
PMMA cements are self-polymerizing, two component (powder and liquid)
systems which are prepared upon mixing in the operating room36. The solid phase is the
polymer of PMMA provided in small balls (1-125 µm) plus the initiator of benzyl peroxide
(BPO) for radical polymerization. The powder of commercial PMMA cements usually
consist of copolymers, radiopacifiers such as zirconium dioxide and barium sulphate, and
various antibiotics37-39. The main ingredient of liquid suspension is the monomer of MMA,
accompanied by different additives such as dimethyl-para-toluidine (DMpT) as activator,
hydroquinone as stabilizer, and possibly a colorant. The composition of powder, liquid

11
component, and the powder to liquid ratio vary based on the specific application and
insertion technique38.
Figure 2.6. Schematic of cemented total hip replacement.
2.2.1 Issues with Current Bone Cements According to the American Academy of Orthopedic Surgeons (AAOS), over
250,000 total hip replacements and 550,000 total knee replacements are performed in the
United States each year40, and orthopedic cements are used for anchoring of artificial joints.
Since 1960, Polymethymethacrylates (PMMA) have been prominently used for fixation of
implants as self-curing bone cements41. The clinical use and availability of various types
of PMMA bone cements have been greatly expanded over the past 60 years, it is not
without its major drawbacks. The primary concern associated with PMMA bone cements
is the weak interface between cement and the bone28. PMMA’s functionality as an in vivo
material has come under speculation due to a number of factors.
One of the primary concerns is the high exotherm reached during the setting
reaction. Highly exothermic reaction of their setting process has been reported for thermal
necrosis of surrounding bone cells42. The exotherm generated during the setting reaction

12
also has serious effects on the body’s natural defense against foreign materials43. This
exotherm can reach up to 120°C, which exceeds ISO requirements for acrylic bone
cements, and results in damaging bone tissue which ultimately causes aseptic loosening of
the implant43. Aseptic loosening is the failure of the bond between an implant and bone in
the absence of infection. The aseptic loosening is the most common mode of failure for an
implant and reported to be the most prevalent cause of failure44. It is estimated that over 25%
of all prosthetic implants will demonstrate evidence of aseptic loosening, often leading to the
need for surgical revision41. Aseptic loosening can be caused by a number of factors
primarily involving cement failure, interfacial failure, bond failure and bone remodeling45. The
PMMA cements lack any chemical bonding to host bone tissue and rely primarily on
mechanical interlocking through penetration of cement in the irregularities in the surface
of bone41. The cement is bonded to the bone by a mechanical interlock which is formed by
the application of pressure to the cement during the operation46. This bond is compromised
by bone tissue necrosis, which occurs during the setting reaction and also by the natural
volumetric shrinkage that occurs in situ47. Research by Orr et al. has calculated that up to
7% shrinkage can occur due to the exothermic polymerisation reaction and subsequent
cooling47. This action can also induce thermal stresses that are sufficient to cause cracking
around the hip replacement femoral stems at the stem/cement interface. Modulus mismatch
or stress shielding can also occur due to the mechanical properties of the cement and bone
being different48. Consequently, bone cement fracture contributes to loss of mechanical
integrity by aseptic loosening of cemented total hip implants. Another concern associated with PMMA cements is the biological and inflammatory
response that is triggered by these materials. The leaching of unreacted monomer, methyl
methacrylate (MMA), which is toxic to the human body results in chemical necrosis of
bone49. Some toxic effects that occur during surgery involve both the heart and lungs. Any
leftover monomer can also present long-term dangers to postoperative healing and may induce
the formation of fibrous connective tissue between cement and bone, which in turn leads to
aseptic loosening49. Unreacted monomer produced during the setting reaction has been found
to disrupt chemotactic signals required for an appropriate immune response hence preventing
bacterial infection50. Unreacted MMA can impair the immune system by disrupting the
chemotactic signals required for an appropriate immune response51. One primary concern when
13
implanting a foreign material into the body is bacterial infection, which can lead to failure of
total hip and knee arthroplasty.
The poor biocompatibility associated with the use of PMMA has generated an
interested in developing alternative cements for use in orthopaedics. As a result of the
foregoing problems, the use of Glass Polyalkenoate Cements (GPCs) in place of the
PMMAs for orthopaedic applications is of great interest due to their excellent
biocompatibility, lack of significant volumetric shrinkage and lack of heat evolution while
setting, their ability to chemically adhere to bone mineral. The truly adhesive nature of
GPCs and non-exothermic setting reaction make them a promising candidate for orthopedic
applications and as possible alternatives to currently used acrylic cements. The next section
describes the functions, properties and chemistry of glass polyalkenoate cements.
2.3 Glass Polyalkenoate Cements
2.3.1 Historical Development Dental carie formation is one the most frequent chronic disease affecting millions
of people each year. Increasing demand has led to the development of different types of
restorative materials for daily dental practice. The most common are amalgams, composite
resins and glass polyalkenoate cements52-53. Dental amalgams have a long clinical history
as a practical and inexpensive dental filling. However, the use of dental amalgams is
limited due to the potential allergic and toxic effects attributed to the release of mercury54.
Moreover, amalgams and other metallic fillers are not tooth colored and their usage has
decreased dramatically over past few years. Resin composites are more esthetically
satisfactory in comparison to amalgams, but their durability is their main shortcoming.
Typical lifespans for composites range from three to ten years, depending on their
applications54. Adhesive cements are more reliable candidates as they are tooth colored and
esthetically acceptable and they are able to chemically bond to tooth and to promote its
remineralization53. Glass polyalkenoate cements, were originally developed as dental
restorative materials but since then they have found other versatile clinical applications55.
Introduction of dental adhesive cements was initially formulated from zinc
phosphate cements, where, zinc oxide powder reacts with an aqueous solution of

14
phosphoric acid and the resultant cements set by an acid-base reaction55. Later, the powder
was substituted by combination of zinc oxide and silicate glass to produce zinc-silico-
phosphate cements and the liquid component were substituted with eugenol to produce zinc
eugenol cements (ZOE)56. Smith developed the first family of zinc polyalkenoate cements
in 1968. He substituted eugenol with polyalkenoic acid and discovered that resultant
cement can bond to tooth structure. Zinc polycarboxylate (ZPCs) cements marketed in the
late 1960s as chemically adhesive materials56.
Shortly after this discovery, the glass polyalkenoate cements (GPCs) were
introduced by Wilson and Kent at the Laboratory of the Government Chemist in London,
in 197257. These cements consisted of an alumino-silcate glass powder and aqueous
solution of polyalkenoic acid such as polyacrylic acid at concentration of 45%57. The glass
composition of conventical GPCs was originally derived from the composition that was
used in dental silicate cements. Wilson modified the aluminum to silicate ratio of the glass
powder to produce glasses that were more susceptible to acid degradation58. These early
materials showed stable chemical adhesion to tooth structure, good biocompatibility and
well balanced physical properties53.
2.3.2 Clinical Applications Glass polyalkenoate cements are currently used for various dental clinical
applications (Table 2.1). They were first developed as restorative dental materials and
adapted as luting agents, filling materials for anterior and posterior teeth, linings, bases and
cores, fissure protection materials for prevention of caries59. Additionally, they are also
used as sealants for patients with allergic reactions to resin based materials, bonding agents
for composite resins, root canal fillings and adhesive cements for orthodontic brackets60.
The chemistry is essentially the same for all three categories, but there are
variations in powder/liquid ratio and powder particle size to accommodate the desired
function60. Type I GPCs are the luting cements; in dentistry, luting agent is viscous material
that placed between tooth structure and prosthesis and acts as an adhesive to bond together
the casting to the tooth. Luting agents are characterized to ensure low film thickness (~10-
20 μm)59 and also to set rapidly61.
15
Table 2.1 Classification of GPCs for dental applications59.
Type II cements are restorative cements; dental restorative materials are used to
replace tooth structure loss, usually due to dental caries formed by bacteria such as A.
viscosus and S. mutans60. Restorative cements are classified as aesthetic or reinforced, with
the difference that reinforced cements contain silver and are not tooth-colored. Type II-1
GPCs are available in both conventional and resin-modified. The aesthetic properties of a
Type II-1 GPC were represented by its translucency, the color match with surrounding
enamel62. Type II-2 GPCs are reinforced, despite their description, they are not necessarily
stronger than Type II-1. However, they are more wear resistant. All the restorative cements
are radiopaque62.
Type III GPCs are the lining cements and fissure sealants; fissure sealants are dental
treatments intended to prevent tooth decay by forming a protective layer that keeps food
and bacteria away59. The lining/base cements are most often applied as a thin layer beneath
a restoration and serves a thermal insulator or dentine replacement. Type III GPCs are
characterized by low viscosity and rapid set41.
2.3.3 Chemistry of Glass Polyalkenoate Cements GPCs consist of an ion-leachable glass powder (base) combined with a water-
soluble polymer (acid), which upon mixing, an acid-base reaction takes place resulting in
a hard set cement63. The acid is typically an aqueous solution of polyalkeonic acid such as
polyacrylic acid (PAA) at a concentration of about 45%, and the glass component in
conventional GPCs are based on a Ca-Al-Si or CaF2-Al-Si glass powder. These original
formulations were first developed by Wilson et al who produced cements with PAA by
modifying the Al2O3/SiO2 ratio to produce greater basicity to compensate for the reduced
acid strength of the polymer compared with the phosphoric acid used in dental silicates64.
Classification of GPCs Class Function Feature
Type I Luting Cements Rapid set Type II Subtype 1 Subtype 2
Restorative Cements Aesthetic Reinforced
Filling Materials
Type III Lining, Sealants Low Viscosity, Rapid Set

16
Since the early introduction of GPCs, a number of modifications were made to these
cements to improve their properties65:
- The choice of alternative polymers such as acrylic/maleic acids were used to serve
as copolymer component.
- Use of dried polymer powders for a better shelf life. The blend of acid and glass
powder was then activated by the addition of water66.
- The incorporation of metallic components such as silver, tin alloys or stainless steel
in the glass powder for improved mechanical strength of cements for use in high stress
sites67-68.
- The development of resin-modified glass ionomer cements (RMGICs)69, in which
the conventional glass polyalkenoate cements also contain hydrophilic photopolymerizable
monomers like hydroxyethyl methacrylate (HEMA) and their associated photo-initiators,
allowing the set cement to be cured by exposure to light70. They have been characterized
as having rapid setting behavior, good strength and improved wear resistance compared to
conventional GPCs70.
2.3.4 Setting Reaction The setting mechanism of all GPCs is based on an acid-base reaction55. Fine
powdered alumino-silicate glass, which is designed to be degradable by relatively weak
acids is mixed with an acidic solution such as PAA to form a set cement. The reaction is
schematically shown in Figure 2.7. The reaction involves three different stages:
dissolution, gelation and maturation66. During the first stage of the setting process, with the
presence of water, the surface of glass particles is attacked by hydrogen ions from the acid
chains. The acid acts as proton donor and the glass powder acts as proton acceptor71.
Degradation starts from glass particles surface, while the core remains intact and exists as
a filler in the set cement. Metal cations, principally Al3+ and Ca2+ are released into solution
and the pH of aqueous phase increases rapidly with release of cations72. This results in
greater ionization of carboxylic acid and their spatial arrangement changes. Due to
electrostatic repulsion, the polymer chains become more polar and uncoil, and finally take
a more linear configuration63. The gel structure starts to form through weak ionic
crosslinking of polyacrylate chains to form a three-dimensional network63. The cation
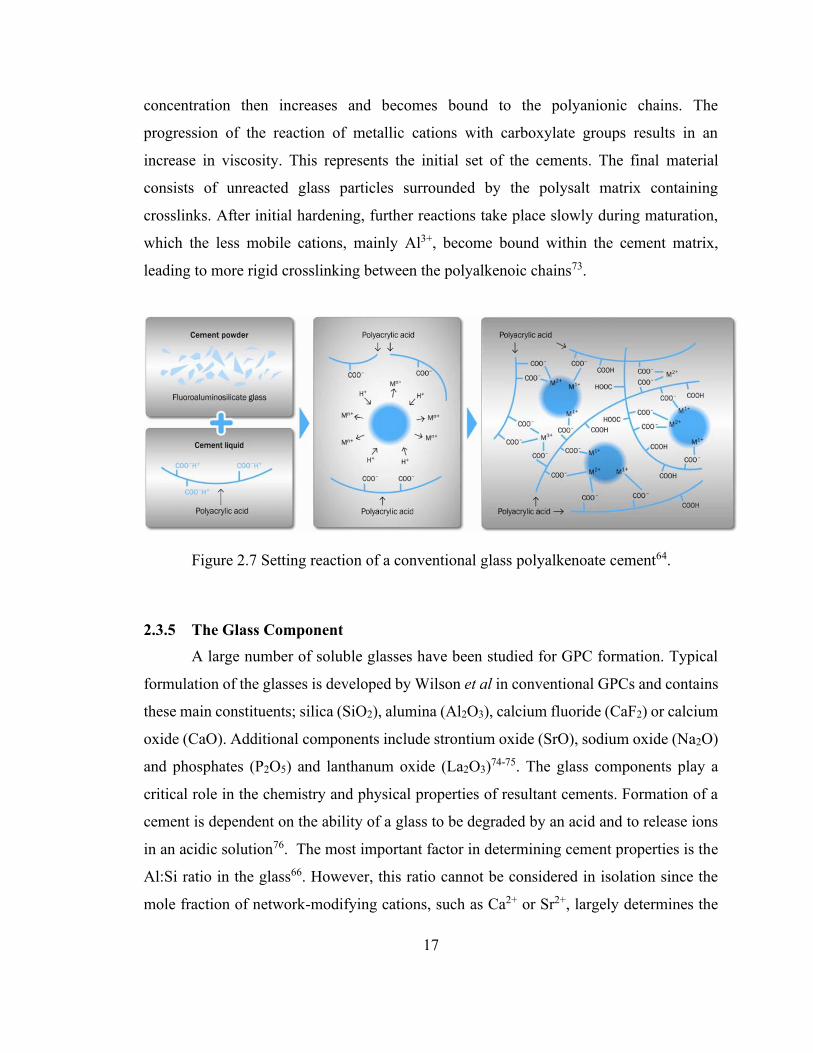
17
concentration then increases and becomes bound to the polyanionic chains. The
progression of the reaction of metallic cations with carboxylate groups results in an
increase in viscosity. This represents the initial set of the cements. The final material
consists of unreacted glass particles surrounded by the polysalt matrix containing
crosslinks. After initial hardening, further reactions take place slowly during maturation,
which the less mobile cations, mainly Al3+, become bound within the cement matrix,
leading to more rigid crosslinking between the polyalkenoic chains73.
Figure 2.7 Setting reaction of a conventional glass polyalkenoate cement64.
2.3.5 The Glass Component A large number of soluble glasses have been studied for GPC formation. Typical
formulation of the glasses is developed by Wilson et al in conventional GPCs and contains
these main constituents; silica (SiO2), alumina (Al2O3), calcium fluoride (CaF2) or calcium
oxide (CaO). Additional components include strontium oxide (SrO), sodium oxide (Na2O)
and phosphates (P2O5) and lanthanum oxide (La2O3)74-75. The glass components play a
critical role in the chemistry and physical properties of resultant cements. Formation of a
cement is dependent on the ability of a glass to be degraded by an acid and to release ions
in an acidic solution76. The most important factor in determining cement properties is the
Al:Si ratio in the glass66. However, this ratio cannot be considered in isolation since the
mole fraction of network-modifying cations, such as Ca2+ or Sr2+, largely determines the

18
structural role of aluminum within the glass network. In the alumino-silicate glasses,
aluminum can be either a network modifier or network former with six or four-fold co-
ordination, respectively64. If the the Al:Si ratio does not exceed 1:1, Al3+ is able to replace
Si4+ in the glass network because they have a similar ionic radius. The glass network will
consist of linked [AlO4] and [SiO4] tetrahedrons. In such case, the glass network forming
units have a negative charge that should be balanced by network-modifying cations. But if
there are insufficient network-modifying cations to balance the charge such as Ca2+, not all
of Al ions can go into four-fold coordination. Some of Al ions adopt six-fold coordination,
and the resulting non-bridging oxygens (NBO) between adjacent aluminum and silicon
tetrahedrons is vulnerable to acid attack40. Calcium fluoride (CaF2) is commonly
incorporated in conventional glass compositions due to its anti-cariogenic properties60.
CaF2 can be substituted in place of CaO as it further disrupts the glass network77. CaF2 is
a powerful network modifier and its incorporation into glasses may result in the formation
of NBOs. Replacement of CaO by CaF2 increases the susceptibility of a glass towards acid
attack77.
2.3.6 Polyacrylic Acid The PAA that reacts with the glass powder in a GPC is usually in an aqueous form,
however it can also be added to the glass as a dried powder and activated by the addition
of water. The polyacrylic acids are homo-polymers of acrylic acid and its copolymer can
contain itaconic acid, maleic acid78 and other additional monomers as shown in Figure 2.8.
By using homopolymers of maleic or itaconic acid, the number of carboxylic groups
(COO) will increase in relative to the total molecular weight, so even more reactive liquids
can be made. Either used alone or as a mixture with polyacrylic acid, GPCs will set rapidly
with degradable glasses which results in materials with higher mechanical properties57.
However, these polyacids show poor adhesion to calcified tissues. The molecular weight
and the concentrations of PAA influences the viscosity of the liquid and so greatly affects
the resulting set cement properties, such as the mechanical strength60. Higher molecular
weights PAA solutions increases the strength of set cements, but it also increases the liquid
viscosity and makes them more difficult to mix63. Therefore, the alterations in molecular
weights are chosen to balance these competing effects to obtain optimum properties.

19
Figure 2.8 Types of carboxylic acid units used in GPCs liquids78.
2.3.7 Adhesion of GPCs to Tooth Structure The chemical adhesion of GPCs to enamel and dentin is complex and it achieved
through an ionic exchange at the GPC/HAp interface79. Initially, when freshly mixed GPC
is placed on dentine or enamel, an ionic bond occurs between the carboxylate functional
groups on the polyalkenoic acid molecules and calcium ions in the HAp-like mineral of
enamel and dentine79. The ionic bonding mechanism between the acid and the HAp is
supported by observations that the bond strength to enamel is greater than to dentin, in
correspondence with relatively higher amounts of HAp in enamel74. Furthermore, an
intermediate layer of calcium and aluminum phosphates and polyacrylates will be formed
at the GPC/HAp interface (Figure 2.9). The thickness of this layer appears to be in the
order of few micrometers and merges to the GPC on one side and to dentin/enamel on the
other side79. In longer term, there are substantial changes at the interface between the GPC
and tooth as ions from the cement and tooth surface diffuse into the interfacial zone. The
interaction zone is a physically evident interface, and its chemical analysis confirmed that
both calcium and strontium were present within it74.

20
Figure 2.9. Schematic of glass polyalkenoate cement adhesion to tooth mineral.
2.3.8 Transition from Dental to Skeletal Adhesive GPCs GPCs have been employed in the repair of tooth tissue for many years. Their history
of good biocompatibility and their chemical bonding to HAp, led researchers to consider
them for medical applications such as bone cements. During past few years, extensive
studies have been conducted on GPCs to improve their properties and to enable their
transition to orthopedics. The main concerns are related to bond strength, mechanical
properties, handling and the bioactivity of the cements. Studies in the field of GPCs fall
into three main categories; modification of glass component, modification of acid phase
and introduction of second phase particles to synthesize GPC composites. In the latter case,
various bioactive particles80 such as Hydroxyapatite81-82, Bioglass83, and Silver nano
particles84 have been successfully incorporated in GPCs. Studies by Porter et al suggested
AgNPs cross-linked within glass ionomer cement (GIC) matrices generated antibiofilm
effects at the nanocomposite surface. He also reported AgNP-containing GPCs had higher
compressive strengths and equivalent flexural strengths to unmodified GPCs85. GPCs are
highly versatile material in the sense that their properties can be modified by several
methods. However, our focus for this study will be to initially investigate the modification
of the glass composition and to understand how these modifications will affect cements
properties.

21
Since the development of GPCs by Wilson et al, many formulations of glasses have
been investigated from a glass structure perspective to determine their resultant cement
properties. One of the primary concerns with the use of conventional GPCs in skeletal
applications, is the presence of Al3+ in the glass composition86. As mentioned earlier, Al3+
plays an important role as network former in the glass structure, however, it has several
well-known toxic effects and negatively affects bone mineralization87. Long term exposure
to Al3+ ions in body fluid can cause neurological disorders such as Alzheimer’s and
Parkinson disease88. Al3+ is unable to cross cell membranes, it is a small ion of high charge
density and consequently binds strongly to anionic ligands inside cells and interfere with
their metabolism89. Due to its toxic behavior, many efforts have been made to remove Al3+
from the glass composition and to replace it by non-toxic components86. To solve this
problem, attempts have been made by Hill et al, where they introduced zinc-silicate glasses
for the base composition90. Further development of calcium-zinc-silicate glasses was
achieved by Towler et al with the production of novel Al3+ free-GPCs91-93. Zinc oxide can
act both as a network modifying oxide and as an intermediate oxide, in a similar fashion to
Al3+. Ternary systems of zinc silicates glasses often have extensive regions of glass
formation. Also, Zinc (Zn) is an essential element needed in the body and can impart
antibacterial properties94. Studies conducted on the role of Zn in bone formation has
revealed positive results95. Studies by Yamaguchi et al, demonstrated that Zn, like bone
growth factors, has a stimulatory effect on bone DNA synthesis96. Therefore, Zn based
GPCs have potential for skeletal applications.
Furthermore, research on Zn-GPCs was expanded by the addition of strontium
oxide (SrO) within the glass composition. Extensive studies have been done on the addition
of strontium to glasses by Hill and Brauer97. Strontium (Sr2+) acts in a very similar fashion
to Ca2+ in the glass structure because they both have similar polarity and atomic size. Where
the strontium substitution doesn’t have adverse effects on structure. Wren et al reported
improved mechanical properties and bioactivity of the resultant GPCs using Sr2+ containing
glasses98-100. In an study by Wren et al, SEM images and corresponding quantitative EDX
analysis of SiO2–CaO–ZnO–SrO GPCs clearly showed calcium phosphate deposition on
the surface of cements after 7 days immersion in SBF, however, no deposition were
22
observed on two commercially available dental cements, Fuji IX and Ketak Molar after 90
days immersion in SBF99. Sr is incorporated in glass for three main reasons: to impart
radiopacity, to improve bioactivity, and it is also known to stimulate bone mineralization
in vivo97, 101-103.
Studies by Hill et al showed Introduction of phosphorus in the form of phosphate
into the glass network is therefore likely to modify the acid degradability of glasses by
changing the susceptibility of bonds in the glass structure to acid hydrolysis75. Phosphate
groups in the polysalt matrix of glass polyalkenoate cements are also likely to compete
with the carboxylate groups for the crosslinking cations such as Zn2+, Ca2+ and are therefore
strongly influence the rheology of the setting cement paste, as well as the mechanical
properties of the hardened cement104.
2.4 Copper Incorporated Glass Polyalkenoate Cements
The primary objective of this work is to reformulate glass composition used in the
Al-free GPCs by incorporating Cu in the glass composition, and to investigate the effect of
Cu on the rheology, mechanical properties and in vitro suitability of zinc based GICs. Glass
composition modification based on Cu incorporation is performed for two main reasons:
1.) to improve physical properties and mechanical strength between cement and bone
mineral, and 2.) to improve biological behavior and the antibacterial efficacy of the
resultant GPCs. Divalent cations in the glass have the potential to link two polyanion
chains. Where the ionic strength of the bond proceeds as M=Al3+>Cu2+>Zn2+>Ca2+>Mg2+
63, Cu2+ can act as a strong ionic crosslink to carboxylic acid (COO-) side groups, resulting
in hardened set materials, which suggests the Cu is a mechanically relevant ion when
formulating GPCs.
Cu has been widely cited as an antibacterial material in health care settings105. The
study of the antibacterial properties of metallic Cu surfaces is a relatively recent
development and has gained momentum. Prior to that, a number of studies have already
dealt with the kinetics of contact killing upon exposure of bacteria to Cu surfaces. The
disruption of microbes due to the presence of Cu ions appears to occur in three parallel

23
ways (Figure 2.10) and as such, prevents the risk of bacterial resistance106. As it is depicted
in Figure 2.10, there are four possible mechanisms for antibacterial effects of Cu; (a) Cu
dissolves from the copper surface and causes cell damage, (b) The cell membrane ruptures
because of Cu and other stress phenomena, leading to loss of membrane potential and
cytoplasmic content, (c) Cu ions induce the generation of reactive oxygen species (ROS),
which cause further cell damage, and (d) Genomic and plasmid DNA becomes degraded.
Contact with Cu surfaces has been shown to damage the integrity of bacterial membranes,
Cu ions can directly damage bacterial proteins and they can also induce the formation of
highly damaging hydroxyl radicals via a Fenton-like chemistry, which can then damage
the cells via their interactions with DNA, enzymes and other proteins, as well as the
peroxidation of lipids and subsequent membrane damage106-107.
Figure 2.10. Mechanisms of Cu antibacterial properties (a) Cu causes cell damage, (b) cell membrane rupture, (c) generation of ROS, and (d)
DNA degradation107.
Cu ions have been reported to be an essential component of the angiogenic
response106, 108. Cu ions have been reported to stimulate the proliferation of endothelial
cells in a dose dependent manner during in vitro culture, and the ability of Cu ions to
promote wound healing in rats has been linked to the upregulation of VEGF expressed by
stimulated cells which plays a very important role in cell differentiation and in blood vessel
formation105, 109. Another important benefit of Cu ions is the low cost and the high stability

24
when are compared with growth factors. Furthermore, these metallic ions are vital in
human metabolism due to the significant amount found in human endothelial cells in the
course of physiological angiogenesis110.
For the reasons mentioned above, Cu has been combined with biomaterials in order
to improve the biological effect. Previous studies suggested that incorporation of Cu ions
in bioactive materials is a feasible way to improve antibacterial properties and
angiogenesis. In some recent studies, various concentrations, up to 10 mol% of copper
oxide were used, in order to demonstrate the properties of this metal oxide in various glass
systems111-113. Popescu et al. reported highly antibacterial, bioactive, and biocompatible
glass ceramics by incorporation of 4 mol% CuO114. In another study, Lin et al showed that
Cu-BGC scaffolds significantly facilitated the regeneration of cartilage and osteochondral
interface, as well as inhibited inflammatory response, which may prevent the development
of osteoarthritis associated with osteochondral defects113. Bernhardt et al directly mixed
Cu2+ solutions with calcium phosphate cements and found that Cu2+ ions could enhance
cell activity and proliferation of osteoblastic cells115. It was found that Cu has a positive
influence on the angiogenic mechanisms of blood vessel formation, enhances bone
metabolic activity, has a valuable antibacterial action, and could play the role of an
enzymatic cofactor in metabolic signals during tissue formation116-117.
The research contained herein, covers four main tasks:
1. Development of novel Cu incorporated glasses for synthesizing GPCs, by
incorporating of Cu in the base glass composition and furthermore characterizing
glasses with respect to structural changes and glass solubility.
2. Synthesizing GPCs and investigating their rheological behavior, evaluating their
mechanical properties and bond strength as outlined by relevant ISO standards.
3. Analyzing solubility and biocompatibility of GPCs with respect to their ion release
profiles, antibacterial activity, mineralization potential through SBF trials and
cytocompatibility with respect to maturation times in DI water.

25
4. Investigating the surface crystallization of the of heat-treated glass particles, to
modify the cross-linking mechanism in the setting reaction, and to improve the
mechanical properties of the resultant GPCs.
Next chapter is focused on the structural characterization of the novel Cu-
containing glass series and extrapolating their potential to form glass-based adhesives,
traditionally known as glass polyalkenoate cement (GPC). The first part of the next chapter
describes the chemistry and morphology of the glasses, and the structural effects of Cu
incorporation in glass, using DTA, MAS-NMR, XPS. Later on, GPCs will be formulated,
and some of the preliminary results regarding the rheological, compressive strength, and
antibacterial properties of will be examined.
2.5 References
1. Zreiqat, H.; Dunstan, C. R.; Rosen, V., A tissue regeneration approach to bone and cartilage repair. Springer: 2015.
2. Bronner, F.; Farach-Carson, M. C.; Mikos, A. G., Engineering of functional skeletal tissues. Springer: 2007.
3. Stevens, M. M., Biomaterials for bone tissue engineering. Materials today 2008, 11 (5), 18-25.
4. Luyten, F. P.; Dell'Accio, F.; De Bari, C., Skeletal tissue engineering: opportunities and challenges. Best Practice & Research Clinical Rheumatology 2001, 15 (5), 759-769.
5. Ortner, D. J.; Turner-Walker, G., The biology of skeletal tissues. In Identification of pathological conditions in human skeletal remains, Elsevier: 2003; pp 11-35.
6. Webster, T. J., Nanotechnology for the regeneration of hard and soft tissues. World Scientific: 2007.
7. Roodman, G. D., Advances in bone biology: the osteoclast. Endocrine reviews 1996, 17 (4), 308-332.
8. Sadat-Shojai, M.; Khorasani, M.-T.; Dinpanah-Khoshdargi, E.; Jamshidi, A., Synthesis methods for nanosized hydroxyapatite with diverse structures. Acta biomaterialia 2013, 9 (8), 7591-7621.
9. Walmsley, G. G.; McArdle, A.; Tevlin, R.; Momeni, A.; Atashroo, D.; Hu, M. S.; Feroze, A. H.; Wong, V. W.; Lorenz, P. H.; Longaker, M. T., Nanotechnology in bone tissue engineering. Nanomedicine: Nanotechnology, Biology and Medicine 2015, 11 (5), 1253-1263.
10. Kobayashi, T.; Nakamura, S.; Yamashita, K., Enhanced osteobonding by negative surface charges of electrically polarized hydroxyapatite. Journal of Biomedical

26
Materials Research: An Official Journal of The Society for Biomaterials, The Japanese Society for Biomaterials, and The Australian Society for Biomaterials and the Korean Society for Biomaterials 2001, 57 (4), 477-484.
11. Barinov, S. M.; Komlev, V. S., Calcium phosphate based bioceramics for bone tissue engineering. Trans Tech Publ: 2008.
12. Downey, P. A.; Siegel, M. I., Bone biology and the clinical implications for osteoporosis. Physical therapy 2006, 86 (1), 77-91.
13. General, O. o. t. S., The basics of bone in health and disease. In Bone Health and Osteoporosis: A Report of the Surgeon General, Office of the Surgeon General (US): 2004.
14. Apt, W. L.; Fierro, J. L.; Calderón, C.; Pérez, C.; Mujica, P., Vertebral hydatid disease: clinical experience with 27 cases. Journal of neurosurgery 1976, 44 (1), 72-76.
15. Maradit Kremers, H.; Larson, D. R.; Crowson, C. S.; Kremers, W. K.; Washington, R. E.; Steiner, C. A.; Jiranek, W. A.; Berry, D. J., Prevalence of Total Hip and Knee Replacement in the United States. J Bone Joint Surg Am 2015, 97 (17), 1386-1397.
16. Surgeons, A. A. o. O., Projected volume of primary and revision total joint replacement in the US 2030 to 2060. Research News 2018.
17. Mathis, J. M.; Barr, J. D.; Belkoff, S. M.; Barr, M. S.; Jensen, M. E.; Deramond, H., Percutaneous vertebroplasty: a developing standard of care for vertebral compression fractures. American journal of neuroradiology 2001, 22 (2), 373-381.
18. Mokhtari S, Wren A (2018) Bioactive glasses 2: Composite bone void fillers, Bioactive Glasses, Elsevier2018, pp. 365-380. doi: https://doi.org/10.1016/B978-0-08-100936-9.00018-6
19. Lieberman, I.; Dudeney, S.; Reinhardt, M.-K.; Bell, G., Initial outcome and efficacy of “kyphoplasty” in the treatment of painful osteoporotic vertebral compression fractures. spine 2001, 26 (14), 1631-1637.
20. Truumees, E.; Hilibrand, A.; Vaccaro, A. R., Percutaneous vertebral augmentation. The Spine Journal 2004, 4 (2), 218-229.
21. Hulme, P. A.; Krebs, J.; Ferguson, S. J.; Berlemann, U., Vertebroplasty and kyphoplasty: a systematic review of 69 clinical studies. Spine 2006, 31 (17), 1983-2001.
22. Wiles, M. D.; Nowicki, R. W.; Hancock, S. M.; Boszczyk, B., Anaesthesia for vertebroplasty and kyphoplasty. Current Anaesthesia & Critical Care 2009, 20 (1), 38-41.
23. Tsukayama, D. T.; Estrada, R.; Gustilo, R., Infection after total hip arthroplasty. J Bone Joint Surg Am 1996, 78 (4), 512-523.
24. Bozic, K. J.; Kurtz, S. M.; Lau, E.; Ong, K.; Vail, T. P.; Berry, D. J., The epidemiology of revision total hip arthroplasty in the United States. JBJS 2009, 91 (1), 128-133.
25. Howard, D.; Wall, P.; Fernandez, M.; Parsons, H.; Howard, P., Ceramic-on-ceramic bearing fractures in total hip arthroplasty: an analysis of data from the National Joint Registry. The Bone & Joint Journal 2017, 99 (8), 1012-1019.

27
26. Kavanagh, B. F.; Ilstrup, D. M.; Fitzgerald Jr, R. H., Revision total hip arthroplasty. JBJS 1985, 67 (4), 517-526.
27. Callaghan, J. J.; Albright, J. C.; Goetz, D. D.; Olejniczak, J. P.; Johnston, R. C., Charnley total hip arthroplasty with cement: minimum twenty-five-year follow-up. Jbjs 2000, 82 (4), 487.
28. Sandiford, N.; Jameson, S.; Wilson, M. J.; Hubble, M.; Timperley, A. J.; Howell, J. R., Cement-in-cement femoral component revision in the multiply revised total hip arthroplasty: results with a minimum follow-up of five years. The bone & joint journal 2017, 99 (2), 199-203.
29. Abdel, M. P.; Ollivier, M.; Parratte, S.; Trousdale, R. T.; Berry, D. J.; Pagnano, M. W., Effect of postoperative mechanical axis alignment on survival and functional outcomes of modern total knee arthroplasties with cement: a concise follow-up at 20 years. JBJS 2018, 100 (6), 472-478.
30. Bergh, M. S.; Gilley, R.; Shofer, F.; Kapatkin, A., Complications and radiographic findings following cemented total hip replacement. Veterinary and Comparative Orthopaedics and Traumatology 2006, 19 (03), 172-179.
31. Andreykiv, A.; Janssen, D.; Nelissen, R.; Valstar, E., On stabilization of loosened hip stems via cement injection into osteolytic cavities. Clinical Biomechanics 2012, 27 (8), 807-812.
32. Gao, C.; Peng, S.; Feng, P.; Shuai, C., Bone biomaterials and interactions with stem cells. Bone research 2017, 5 (1), 1-33.
33. Kenny, S.; Buggy, M., Bone cements and fillers: a review. Journal of Materials Science: Materials in Medicine 2003, 14 (11), 923-938.
34. Kuehn, K.-D.; Ege, W.; Gopp, U., Acrylic bone cements: composition and properties. Orthopedic Clinics 2005, 36 (1), 17-28.
35. Magnan, B.; Bondi, M.; Maluta, T.; Samaila, E.; Schirru, L.; Dall'Oca, C., Acrylic bone cement: current concept review. Musculoskelet Surg 2013, 97 (2), 93-100.
36. Kuehn, K. D.; Ege, W.; Gopp, U., Acrylic bone cements: composition and properties. The Orthopedic clinics of North America 2005, 36 (1), 17-28, v.
37. Stanczyk, M., Study on modelling of PMMA bone cement polymerisation. J Biomech 2005, 38 (7), 1397-403.
38. Kuehn, K.-D., Bone cements: up-to-date comparison of physical and chemical properties of commercial materials. Springer Science & Business Media: 2012.
39. Provenzano, M. J.; Murphy, K. P.; Riley, L. H., 3rd, Bone cements: review of their physiochemical and biochemical properties in percutaneous vertebroplasty. AJNR. American journal of neuroradiology 2004, 25 (7), 1286-90.
40. Brauer, D. S.; Gentleman, E.; Farrar, D. F.; Stevens, M. M.; Hill, R. G., Benefits and drawbacks of zinc in glass ionomer bone cements. Biomedical Materials 2011, 6 (4), 045007.
41. Vaishya, R.; Chauhan, M.; Vaish, A., Bone cement. Journal of clinical orthopaedics and trauma 2013, 4 (4), 157-163.
42. Stańczyk, M., Study on modelling of PMMA bone cement polymerisation. Journal of Biomechanics 2005, 38 (7), 1397-1403.
43. Farrar, D.; Rose, J., Rheological properties of PMMA bone cements during curing. Biomaterials 2001, 22 (22), 3005-3013.

28
44. Lewis, G., Properties of Acrylic Bone Cements:State of the art review. Journal of Biomedical Materials Research 1997, 38, 155-182.
45. Ota, J.; Cook, J. L.; Lewis, D. D.; Tomlinson, J. L.; Fox, D. B.; Cook, C. R.; Schultz, L. G.; Brumitt, J., Short‐term aseptic loosening of the femoral component in canine total hip replacement: effects of cementing technique on cement mantle grade. Veterinary Surgery 2005, 34 (4), 345-352.
46. Shi, Z.; Neoh, K.; Kang, E.; Wang, W., Antibacterial and mechanical properties of bone cement impregnated with chitosan nanoparticles. Biomaterials 2006, 27 (11), 2440-2449.
47. Orr, J.; Dunne, N. In Measurement of shrinkage stresses in PMMA bone cement, Applied Mechanics and Materials, Trans Tech Publ: 2004; pp 127-132.
48. Karimzadeh, A.; Ayatollahi, M., Investigation of mechanical and tribological properties of bone cement by nano-indentation and nano-scratch experiments. Polymer Testing 2012, 31 (6), 828-833.
49. Mousa, W. F.; Kobayashi, M.; Shinzato, S.; Kamimura, M.; Neo, M.; Yoshihara, S.; Nakamura, T., Biological and mechanical properties of PMMA-based bioactive bone cements. Biomaterials 2000, 21 (21), 2137-2146.
50. Hendriks, J.; Van Horn, J.; Van Der Mei, H.; Busscher, H., Backgrounds of antibiotic-loaded bone cement and prosthesis-related infection. Biomaterials 2004, 25 (3), 545-556.
51. Swearingen, M. C.; Granger, J. F.; Sullivan, A.; Stoodley, P., Elution of antibiotics from poly (methyl methacrylate) bone cement after extended implantation does not necessarily clear the infection despite susceptibility of the clinical isolates. Pathogens and disease 2016, 74 (1).
52. Tyas, M.; Burrow, M., Adhesive restorative materials: a review. Australian dental journal 2004, 49 (3), 112-121.
53. Chen, L.; Shen, H.; Suh, B. I., Bioactive dental restorative materials: a review. American journal of dentistry 2013, 26 (4), 219-227.
54. Shenoy, A., Is it the end of the road for dental amalgam? A critical review. Journal of Conservative Dentistry 2008, 11 (3), 99.
55. Davidson, C. L.; Mjör, I. A., Advances in glass-ionomer cements. Quintessence Publishing Co, Inc: 1999.
56. Ladha, K.; Verma, M., Conventional and contemporary luting cements: an overview. The Journal of Indian Prosthodontic Society 2010, 10 (2), 79-88.
57. Khoroushi, M.; Keshani, F., A review of glass-ionomers: From conventional glass-ionomer to bioactive glass-ionomer. Dental research journal 2013, 10 (4), 411.
58. Nicholson, J. W., Chemistry of glass-ionomer cements: a review. Biomaterials 1998, 19 (6), 485-494.
59. Mount, G. J., An atlas of glass-ionomer cements: a clinician's guide. CRC Press: 2003.
60. Sidhu, S. K.; Nicholson, J. W., A review of glass-ionomer cements for clinical dentistry. Journal of functional biomaterials 2016, 7 (3), 16.
61. Sidhu, S. K., Glass-ionomers in Dentistry. Springer: 2016.

29
62. Verdonschot, E.; Oortwijn, J.; Roeters, F., Aesthetic properties of three type II glass polyalkenoate (ionomer) cements. Journal of dentistry 1991, 19 (6), 357-361.
63. Nicholson, J. W.; Wilson, A. D., Acid-Base cements - Their biomedical and industrial applications. Cambridge: 1993; Vol. 3.
64. Lohbauer, U., Dental glass ionomer cements as permanent filling materials?–properties, limitations and future trends. Materials 2009, 3 (1), 76-96.
65. Nagaraja Upadhya, P.; Kishore, G., Glass ionomer cement: the different generations. Trends Biomater Artif Organs 2005, 18 (2), 158-165.
66. Nicholson, J. W., Chemistry of Glass Ionomer Cements. Biomaterials 1998, 19, 485-494.
67. Xie, D.; Brantley, W.; Culbertson, B.; Wang, G., Mechanical properties and microstructures of glass-ionomer cements. Dental Materials 2000, 16 (2), 129-138.
68. Williams, J.; Billington, R.; Pearson, G., The comparative strengths of commercial glass-ionomer cements with and without metal additions. British dental journal 1992, 172 (7), 279-282.
69. Smith, D. C., Development of glass-ionomer cement systems. Biomaterials 1998, 19 (6), 467-478.
70. Wan, A. C.; Yap, A. U.; Hastings, G. W., Acid–base complex reactions in resin‐modified and conventional glass ionomer cements. Journal of biomedical materials research 1999, 48 (5), 700-704.
71. Wilson, A. D., Resin-modified glass-ionomer cements. International Journal of Prosthodontics 1990, 3 (5).
72. Collado-González, M.; Pecci-Lloret, M. R.; Tomás-Catalá, C. J.; García-Bernal, D.; Oñate-Sánchez, R. E.; Llena, C.; Forner, L.; Rosa, V.; Rodríguez-Lozano, F. J., Thermo-setting glass ionomer cements promote variable biological responses of human dental pulp stem cells. Dental Materials 2018, 34 (6), 932-943.
73. Croll, T. P.; Nicholson, J., Glass ionomer cements in pediatric dentistry: review of the literature. Pediatric dentistry 2002, 24 (5), 423-429.
74. Tyas, M. J.; Burrow, M. F., Adhesive restorative materials: a review. Australian dental journal 2004, 49 (3), 112-21; quiz 154.
75. Griffin, S.; Hill, R., Influence of glass composition on the properties of glass polyalkenoate cements. Part II: influence of phosphate content. Biomaterials 2000, 21 (4), 399-403.
76. Najeeb, S.; Khurshid, Z.; Zafar, M. S.; Khan, A. S.; Zohaib, S.; Martí, J. M. N.; Sauro, S.; Matinlinna, J. P.; Rehman, I. U., Modifications in glass ionomer cements: nano-sized fillers and bioactive nanoceramics. International journal of molecular sciences 2016, 17 (7), 1134.
77. De Barra, E.; Hill, R., Influence of glass composition on the properties of glass polyalkenoate cements. Part III: influence of fluorite content. Biomaterials 2000, 21 (6), 563-569.
78. Hu, Y.; Jiang, X.; Ding, Y.; Ge, H.; Yuan, Y.; Yang, C., Synthesis and characterization of chitosan–poly (acrylic acid) nanoparticles. Biomaterials 2002, 23 (15), 3193-3201.

30
79. Nicholson, J. W., Adhesion of glass-ionomer cements to teeth: A review. International Journal of Adhesion and Adhesives 2016, 69, 33-38.
80. Gjorgievska, E.; Nicholson, J. W.; Gabrić, D.; Guclu, Z. A.; Miletić, I.; Coleman, N. J., Assessment of the Impact of the Addition of Nanoparticles on the Properties of Glass–Ionomer Cements. Materials 2020, 13 (2), 276.
81. Gu, Y.; Yap, A.; Cheang, P.; Khor, K., Effects of incorporation of HA/ZrO 2 into glass ionomer cement (GIC). Biomaterials 2005, 26 (7), 713-720.
82. Moshaverinia, A.; Ansari, S.; Moshaverinia, M.; Roohpour, N.; Darr, J. A.; Rehman, I., Effects of incorporation of hydroxyapatite and fluoroapatite nanobioceramics into conventional glass ionomer cements (GIC). Acta Biomaterialia 2008, 4 (2), 432-440.
83. Chen, S.; Cai, Y.; Engqvist, H.; Xia, W., Enhanced bioactivity of glass ionomer cement by incorporating calcium silicates. Biomatter 2016, 6 (1), e1123842.
84. Siqueira, P.-C.; Ana-Paula-Rodrigues Magalhães, W.-C.; Pires, F.-C. P.; Silveira-Lacerda, E.-P.; Carrião, M.-S.; Bakuzis, A.-F.; Souza-Costa, C.-A.; Lopes, L.-G.; Estrela, C., Cytotoxicity of glass ionomer cements containing silver nanoparticles. Journal of clinical and experimental dentistry 2015, 7 (5), e622.
85. Porter, G.; Tompkins, G.; Schwass, D.; Li, K.; Waddell, J.; Meledandri, C., Anti-biofilm activity of silver nanoparticle-containing glass ionomer cements. Dental Materials 2020.
86. Nicholson, J. W.; Czarnecka, B., Role of Aluminium in Glass-ionomer Dental Cements and its Biological Effects. Journal of biomaterials applications 2009.
87. Blades, M.; Moore, D.; Revell, P.; Hill, R., In vivo skeletal response and biomechanical assessment of two novel polyalkenoate cements following femoral implantation in the female New Zealand White rabbit. Journal of materials science: materials in medicine 1998, 9 (12), 701-706.
88. Polizzi, S.; Pira, E.; Ferrara, M.; Bugiani, M.; Papaleo, A.; Albera, R.; Palmi, S., Neurotoxic effects of aluminium among foundry workers and Alzheimer’s disease. Neurotoxicology 2002, 23 (6), 761-774.
89. Visser, W.; Van de Vyver, F., Aluminium-induced osteomalacia in severe chronic renal failure (SCRF). Clinical nephrology 1985, 24, S30.
90. Darling, M.; Hill, R., Novel polyalkenoate (glass-ionomer) dental cements based on zinc silicate glasses. Biomaterials 1994, 15 (4), 299-306.
91. Towler, M.; Crowley, C.; Murphy, D.; O'Callaghan, A., A preliminary study of an aluminum-free glass polyalkenoate cement. Journal of materials science letters 2002, 21 (14), 1123-1126.
92. Towler, M.; Kenny, S.; Boyd, D.; Pembroke, T.; Buggy, M.; Hill, R., Zinc ion release from novel hard tissue biomaterials. Bio-medical materials and engineering 2004, 14 (4), 565-572.
93. Boyd, D.; Li, H.; Tanner, D.; Towler, M.; Wall, J., The antibacterial effects of zinc ion migration from zinc-based glass polyalkenoate cements. Journal of Materials Science: Materials in Medicine 2006, 17 (6), 489-494.
94. Boyd, D.; Towler, M., The processing, mechanical properties and bioactivity of zinc based glass ionomer cements. Journal of Materials Science: Materials in Medicine 2005, 16 (9), 843-850.

31
95. Ma, Z. J.; Yamaguchi, M., Role of endogenous zinc in the enhancement of bone protein synthesis associated with bone growth of newborn rats. Journal of bone and mineral metabolism 2001, 19 (1), 38-44.
96. Yamaguchi, M.; Ma, Z. J., Role of endogenous zinc in the enhancement of bone protein synthesis associated with bone growth of newborn rats. Journal of Mineral Metaboilsm 2001, 19, 38-44.
97. Brauer, D. S.; Karpukhina, N.; Kedia, G.; Bhat, A.; Law, R. V.; Radecka, I.; Hill, R. G., Bactericidal strontium-releasing injectable bone cements based on bioactive glasses. Journal of The Royal Society Interface 2012, rsif20120647.
98. Wren, A.; Hansen, J.; Hayakawa, S.; Towler, M., Aluminium-free glass polyalkenoate cements: ion release and in vitro antibacterial efficacy. Journal of Materials Science: Materials in Medicine 2013, 24 (5), 1167-1178.
99. Wren, A.; Coughlan, A.; Hall, M.; German, M.; Towler, M., Comparison of a SiO2–CaO–ZnO–SrO glass polyalkenoate cement to commercial dental materials: ion release, biocompatibility and antibacterial properties. Journal of Materials Science: Materials in Medicine 2013, 24 (9), 2255-2264.
100. Boyd, D.; Towler, M. R.; Watts, S.; Hill, R. G.; Wren, A. W.; Clarkin, O. M., The role of Sr2+ on the structure and reactivity of SrO–CaO–ZnO–SiO2 ionomer glasses. Journal of Materials Science: Materials in Medicine 2008, 19 (2), 953-957.
101. Wren, A. W.; Boyd, D.; Towler, M. R., The processing, mechanical properties and bioactivity of strontium based glass polyalkenoate cements. J Mater Sci: Mater Med 2008, 19, 1737-1743.
102. Marie, P. J., Strontium ranelate; a novel mode of action optimizing bone formation and resorption. Osteoporosis International 2005, 16, S7-S10.
103. Guida, A.; Towler, M.; Wall, J.; Hill, R.; Eramo, S., Preliminary work on the antibacterial effect of strontium in glass ionomer cements. Journal of materials science letters 2003, 22 (20), 1401-1403.
104. Garcia, L. d. F. R.; Pires-de-Souza, F. d. C.; Teófilo, J. M.; Cestari, A.; Calefi, P. S.; Ciuffi, K. J.; Nassar, E. J., Synthesis and biocompatibility of an experimental glass ionomer cement prepared by a non-hydrolytic sol-gel method. Brazilian dental journal 2010, 21 (6), 499-507.
105. Wu, C.; Zhou, Y.; Xu, M.; Han, P.; Chen, L.; Chang, J.; Xiao, Y., Copper-containing mesoporous bioactive glass scaffolds with multifunctional properties of angiogenesis capacity, osteostimulation and antibacterial activity. Biomaterials 2013, 34 (2), 422-433.
106. Mary, G.; Bajpai, S.; Chand, N., Copper (II) ions and copper nanoparticles‐loaded chemically modified cotton cellulose fibers with fair antibacterial properties. Journal of Applied Polymer Science 2009, 113 (2), 757-766.
107. Grass, G.; Rensing, C.; Solioz, M., Metallic copper as an antimicrobial surface. Applied and environmental microbiology 2011, 77 (5), 1541-1547.
108. Romero-Sánchez, L. B.; Marí-Beffa, M.; Carrillo, P.; Medina, M. Á.; Díaz-Cuenca, A., Copper-containing mesoporous bioactive glass promotes angiogenesis in an in vivo zebrafish model. Acta biomaterialia 2018, 68, 272-285.

32
109. Malhotra, A.; Habibovic, P., Calcium phosphates and angiogenesis: implications and advances for bone regeneration. Trends in Biotechnology 2016, 34 (12), 983-992.
110. Vimalraj, S.; Rajalakshmi, S.; Preeth, D. R.; Kumar, S. V.; Deepak, T.; Gopinath, V.; Murugan, K.; Chatterjee, S., Mixed-ligand copper (II) complex of quercetin regulate osteogenesis and angiogenesis. Materials Science and Engineering: C 2018, 83, 187-194.
111. Bari, A.; Bloise, N.; Fiorilli, S.; Novajra, G.; Vallet-Regí, M.; Bruni, G.; Torres-Pardo, A.; González-Calbet, J. M.; Visai, L.; Vitale-Brovarone, C., Copper-containing mesoporous bioactive glass nanoparticles as multifunctional agent for bone regeneration. Acta biomaterialia 2017, 55, 493-504.
112. Wang, X.; Cheng, F.; Liu, J.; Smått, J.-H.; Gepperth, D.; Lastusaari, M.; Xu, C.; Hupa, L., Biocomposites of copper-containing mesoporous bioactive glass and nanofibrillated cellulose: Biocompatibility and angiogenic promotion in chronic wound healing application. Acta biomaterialia 2016, 46, 286-298.
113. Lin, R.; Deng, C.; Li, X.; Liu, Y.; Zhang, M.; Qin, C.; Yao, Q.; Wang, L.; Wu, C., Copper-incorporated bioactive glass-ceramics inducing anti-inflammatory phenotype and regeneration of cartilage/bone interface. Theranostics 2019, 9 (21), 6300.
114. Popescu, R.; Magyari, K.; Vulpoi, A.; Trandafir, D.; Licarete, E.; Todea, M.; Ştefan, R.; Voica, C.; Vodnar, D.; Simon, S., Bioactive and biocompatible copper containing glass-ceramics with remarkable antibacterial properties and high cell viability designed for future in vivo trials. Biomaterials science 2016, 4 (8), 1252-1265.
115. Bernhardt, A.; Schamel, M.; Gbureck, U.; Gelinsky, M., Osteoclastic differentiation and resorption is modulated by bioactive metal ions Co2+, Cu2+ and Cr3+ incorporated into calcium phosphate bone cements. PloS one 2017, 12 (8), e0182109.
116. Jacobs, A.; Pr, G. R.; Forestier, C.; Nedelec, J.-M.; Descamps, S., Biological properties of copper-doped biomaterials for orthopedic applications: A review of antibacterial, angiogenic and osteogenic aspects. Acta Biomaterialia 2020.
117. Mokhtari, S.; Wren, A.W. Copper Containing Glass-Based Bone Adhesives for Orthopaedic Applications: Glass Characterization and Advanced Mechanical Evaluation. bioRxiv 2020.11.19.390138. doi: 10.1101/2020.11.19.390138

33
3 Copper containing Glass Polyalkenoate Cements based on SiO2-ZnO-CaO-SrO-P2O5 Glasses:
Glass Characterization, Physical and Antibacterial Properties
Journal of Materials Science 52 (15), 8886–8903
DOI 10.1007/s10853-017-0945-5
S. Mokhtari1, K.D. Skelly1, E.A. Krull2, A. Coughlan2, N.P. Mellott3, Y. Gong1, R. Borges4, *A.W. Wren1.
1 Kazuo Inamori School of Engineering, Alfred University, Alfred NY, USA. 2 Department of Bioengineering, University of Toledo, Toledo, OH, USA. 3 Department of Chemical Engineering and Materials Science, Michigan State University, East
Lansing, MI, USA. 4Department of Materials Science and Engineering, Universidade Federal do ABC, Sao Paulo,
Brazil.
Keywords: Glass Polyalkenoate Cement, Copper, Bioglass, Antibacterial, MAS-NMR.
*Address for Correspondence: Dr. Anthony William Wren Kazuo Inamori School of Engineering, Alfred University, Alfred, New York 14802, USA. Tel: 607-871-2183 Email: [email protected]

34
3.1 Abstract
A series of copper (Cu) containing glasses were synthesized and incorporated into
a SiO2-ZnO-CaO-SrO-P2O5 based glass system. Additions of 6 and 12mol% CuO retained
the amorphous character and glasses were processed to possess similar particle sizes and
surface areas. Glass characterization using X-ray Photoelectron spectroscopy (XPS) and
Magic Angle Spinning Nuclear Magnetic Resonance (MAS-NMR) determined the
addition of 12mol% CuO increased the fraction of Q4-speciation and the concentration of
Bridging Oxygens (BO). Each glass presented solubility profiles for the release of Si4+ (18-
31mg/L), Ca2+ (13-16mg/L), Zn2+ (<3mg/L) and Sr2+(2-10mg/L), however no Cu2+ or P5+
were released. Cu-GICs were formulated and the working time (Tw) and setting times (Ts)
were found to be dependent on both Polyacrylic Acid (PAA) concentration and CuO
addition. The mechanical properties, i.e. the compressive strength (18–30 MPa) and the
adhesive bond strength (0.79–1.32 MPa), were relatively low which is likely due to the
glass structure. Antibacterial properties were evaluated in E. coli (4mm), S. epidermidis
(10mm), S. aureus (UMAS-1) and Vancomycin Resistant S. aureus (2mm), presented
antibacterial effects in each microbe tested.
3.2 Introduction
The applicability of bioactive glasses and derivatives thereof have stimulated much
interest in the field of orthopedics as they present significant potential for restoration of
host bone mineral. Skeletal restorative bioactive materials were initially developed with
the pioneering efforts of Prof. Larry Hench in the late 1960’s1-3. The invention of 45S5
Bioglass® (45SiO2-24.5CaO-24.5Na2O-6P2O5) stimulated interest in vitreous materials for
both dental and orthopedic repair as the glass chemistry can be controlled to cause
precipitation of minerals such as calcium and phosphate from the surrounding fluids on the
surface of the bioactive glass implant1, 2, 4. The deposition of this CaP mineral occurs
initially as an amorphous surface layer, but will subsequently crystallize to form the
crystalline mineral phase hydroxyapatite (HaP), a synthetically induce analogue to the
mineral phase of healthy bone tissue3, 5, 6. This process has been cited to eventually lead to

35
bone bonding in vivo and is widely regarded as a positive indicator of bioactivity. Early
studies on the 45S5 Bioglass® formulation determined that a permanent bone to bone tissue
occurred in animal models2. This led to Bioglass® being commercially applied as an
osteoconductive bone graft/void filler or both skeletal and dental applications. They are
used currently for craniofacial defects including periodontal defects, alveolar ridge
augmentation and dental extraction sites in bone tissue2, 3, 7-9.
The applicability of bioactive glasses and ceramics have increased since the success
of 45S5 Bioglass®. Many glass-based medical materials such as glass-ceramic scaffolds
for bone void repair3, 10-15, composites materials16, 17, glass microspheres18-20 and bone
cements21-23 have been investigated. Glass has previously been applied for bone
cementation to improve the bioactivity. Conventional bone cements are primarily based on
acrylic polymers that are used for applications that include total hip and total knee
arthroplasty (THA/TKA), in addition to spinal surgical procedures such as Vertebroplasty
and Kyphoplasty23. Polymers such as polymetylmethacrylate (PMMA)23 and Bisphenyl-a
glycidyal di-methacrylate (Bis-GMA)24 have appropriate mechanical properties for load
bearing applications however, they lack any chemical interaction in vivo, and anchor
implant materials through mechanical interaction with the surrounding bone tissue22, 23, 25.
However, this lack of chemical integration will eventually lead to micro-motion within the
joint space which can lead to the formation of fibrous tissue at the bone-bone cement
interface. In addition, the curing of acrylic materials leads to high exothermic reactions
which is known to damage the surrounding cell and soft tissues25. This has led to the
inclusion of bioactive glass particles being incorporated into the materials to improve
osseointegration with the host tissue. One commercially available composite material
based on Bis-GMA chemistry included combeite (SiO2-Na2O-CaO) glass particles which
resulted in the precipitation of a CaP surface layer when tested using Simulated Body Fluid
(SBF) which greatly improved the bioactive response5, 26. Bioactive glasses are
characterized by this ability which promotes osseous healing within the body. This process
involves partial dissolution of the glass particulate surface which promotes ion exchange
upon exposure to an aqueous physiological medium. The specific mechanism includes the
release of soluble Si4+ into the surrounding medium in the form of silicic acid due to

36
exchange with H+ and H3O. This mechanism results in the precipitation of an initial
amorphous calcium phosphate layer which subsequently crystallizes to HaP3, 5, 27.
Additionally, it is known that the ionic dissolution products from bioactive glasses can
stimulate many critical physiological processes such as angiogenesis, and expression and
upregulation several genes in osteoblasts28, which suggested that their applicability may
influence many important processes in addition to mineral deposition in osseous tissue29.
Therefore, the solubility of the glass particles is critical to promoting the desired bioactive
response. An important characteristic that is critical to controlling glass solubility is related
to the concentration of network formers/network modifiers within the glass30, 31. This will
greatly influence the distribution of bridging oxygens (BO) and non-bridging oxygens
(NBO) in the glass30, 32. It has previously been determined that the concentration of NBO
(Si-NBO) has a significant effect on the glass solubility, and these NBO species are created
by the inclusion of alkali/ alkali earth cations in the glass. This facilitates the ion exchange
process and promotes the rate of Si4+ dissolution, and the bioactive response overall30, 31,
33.
The first part of this chapter aims to study the structure of glass compositions of
SiO2-ZnO-CaO-SrO-P2O5-CuO used in novel glass-based adhesives, traditionally known
as glass polyalkenoate cement (GPC). This composition was selected as it contains
components that can serve a therapeutic value in vivo. Briefly, zinc has been cited to
increase the rate of DNA synthesis in rat models34-36. Strontium is known to have a dual
effect on the metabolism of bone cells where it increases the activity of osteoblast cells
while at the same time decreasing the activity of osteoclast cells, which results in a net
increase in bone mineral density37, 38. Silica, calcium and phosphate are primary
components of the 45S5 Bioglass system and are critical determinants of the mineralization
process. However, for this study the primary goal is to develop Cu containing glasses that
can be used to form a skeletal adhesive. Cu has previously been cited as having promising
bone metabolic properties in addition to being an antibacterial agent. The materials formed
will be a novel class of glass polyalkenoate cements. GPCs are materials that were
originally developed for use in restorative dentistry for lining, luting and filling
applications. Traditional GPCs employ an aluminosilicate or fluoro-aluminosilicate based

37
glass system as the aluminum (Al3+) plays a critical role in the setting of the materials39,
however, neurotoxic concerns and claims of imparting defective mineralization has limited
its use for GPC based bone adhesives40-42. When the glass component is mixed with
Polyacrylic acid (PAA) and water, the surface of the glass partially degrades and releases
cations that serve to crosslink the ionized PAA chains43. This results in a hard cement like
material that can bond to both HaP in bone and tooth, in addition to bonding to surgical
metals44. This acid-base setting reaction is non-exothermic and with the degradation of the
glass, ionic species are liberated into the polysalt matrix43, 45-47. This study investigates the
replacement of Si4+ with Cu2+ as Cu is cited as forming strong bonds with carboxylic acid
groups on the PAA chains during setting48. This study investigates the effect that Cu has
on the glass structure and solubility, characterizing important physical properties such as
rheological and mechanical trends, in addition to determining the antibacterial effects49, 50
of Cu-GPCs in a range of relevant bacteria species. Bioactive Cu-GPCs could potentially
be a safer and more practical alternative to antibiotic doped bone cements23, as the
evolution of antibiotic resistant microbes such as methicillin resistant Staphylococcus
aureus (MRSA) and vancomycin resistant Staphylococcus aureus (VRSA) are a persistent
cause for concern when developing implantable bone cements.
3.3 Materials & Methods
3.3.1 Glass Synthesis Three glasses were formulated for this study, two Cu containing glasses (CuG6,
CuG12) in addition to a CuO free SiO2-CaO-SrO-ZnO-P2O5 glass (Control). The Cu
containing glasses contain incremental concentrations of CuO at the expense of Silica
(SiO2) (Table 3.1). The powdered mixes of analytical grade reagents (Fisher Scientific, PA,
USA) were oven dried (100ºC, 1 h) and fired (1350ºC, 2 h) in platinum crucibles and shock
quenched into water. The resulting frits were dried, ground and sieved to retrieve glass
powders with a maximum particle size of 45μm.

38
Table 3.1 Glass compositions (Mol. %) where SiO2 is substituted by CuO.
SiO2 CuO ZnO CaO SrO P2O5 Control 48 0 36 6 8 2 CuG6 42 6 36 6 8 2 CuG12 36 12 36 6 8 2
3.3.2 X-Ray Diffraction (XRD) Diffraction patterns were collected using a Phaser D2 X-ray Diffraction Unit
(Bruker AXS Inc., WI, USA). Glass powder samples were packed into zero background
sample holders. A generator voltage of 40 kV and a tube current of 30 mA was employed.
Scattering patterns were collected in the range 10˚<2θ<80˚, at a scan step size 0.02˚ and a
step time of 10 s.
3.3.3 Differential Thermal Analysis (DTA) A SDT Q600 Simultaneous Thermal Gravimetric Analyser-Differential Scanning
Calorimetry (TGA-DSC) (TA Instruments, DW, USA) was used to obtain a thermal profile
of each glass, specifically the glass transition temperature (Tg) and crystallization
temperatures. A heating rate of 10°C/min was employed in an air atmosphere using
alumina as a reference in a matched platinum crucible. Sample measurements were carried
out every 0.5 s between 30˚C and 1200˚C. TA Universal Analysis software (TA
Instruments, DW, USA) was used to plot and obtain the temperatures of interest.
3.3.4 Scanning Electron Microscopy & Energy Dispersive X-ray Analysis (SEM/EDS) Imaging was carried out with an FEI Co. Quanta 200F Environmental Scanning
Electron Microscope. Additional compositional analysis was performed with an EDAX
Genesis Energy-Dispersive Spectrometer (EDS). All EDS spectra were collected at 20 kV
using a beam current of 26 nA. Quantitative EDS spectra were subsequently converted into
relative concentration data.
3.3.5 Advanced Surface Area and Porosity (ASAP) In order to determine the surface area of each glass, Advanced Surface Area and
Porosimetry, Micromeritics ASAP 2020 (Micrometrics Instrument Corporation, Norcross,

39
USA) was employed. Approximately 60 mg of each glass was analyzed and the specific
surface area was calculated using the Brunauer-Emmett-Teller (BET) method.
3.3.6 Particle Size Analysis (PSA) Particle size was analyzed using a Multisizer 4 Particle Size Analyzer (Beckman
Coulter, CA, USA). Glass powder samples (n = 3) were loaded into 20°C Isoton II Diluent
at a concentration <10%. Samples were evaluated using a 280 μm standard to a final count
of 30000.
3.3.7 X-Ray Photoelectron Spectroscopy (XPS) Prior to surface analysis, samples were kept in a vacuum desiccator. The chemical
bonding environment of each glass was characterized by X-ray photoelectron spectroscopy
carried out with a Quantera (Physical Electronics, Minnesota, US), using a monochromatic
Al kα radiation (hv=1486.6 eV) at an output of 25.5 watts. All survey spectra were recorded
at constant pass energy of 140 eV and step size of 0.5 eV. Na1s, O1s, Ca2p, C1s and Si2p
high resolution scans were collected with a pass energy of 26 eV, step size of 0.05 eV, and
beam dwell time of ~ 300 ms to yield a signal to noise ratio > 100:1. Analysis area for each
sample is ~ 2 to 3 mm in diameter using a 100 μm beam. Spectra analysis was performed
on CasaXPS (Casa Software Ltd.). Peak positions were calibrated through normalization
of the C1s peak to 284.6 eV.
3.3.8 Magic Angle Spinning-Nuclear Magnetic Resonance (MAS-NMR) Glass powdered samples were tested using a MAS-NMR Bruker Avance III 600
coupled with an Ultrasheild Plus solid state NMR magnet with a 4mm diameter probe. The 29Si and proton channels had a frequency of 600.20 MHz and 119.29 MHz
respectively. Tetrakis (trimethylsiyl)-silane was used for reference with the chemical shift
at -9.843 ppm. Each sample underwent low power decoupling and was spun at 5.0 kHz for
300 scans. The relaxation time was 15 s and the pulse length 75°. Additionally, the
spectrum reference frequency was 498.23 Hz.
40
3.3.9 Ion Release Profiles Each glass (Control, CuG6 and CuG12, where n=3) was immersed in sterile de-
ionised H2O for 1, 10, 100 and 1000 hours. Approximately 1.0 m2 surface area of glass
powder was submerged in 10 ml of de-ionised H2O and rotated on an oscillating platform
at 37ºC. The ion release profile of each glass was measured using Inductively Coupled
Plasma – Atomic Emission Spectroscopy (ICP – AES) on a Perkin-Elmer Optima 5300UV
(Perkin Elmer, MA, USA). ICP – AES calibration standards for Ca, Si, Sr, Zn, P and Cu
ions were prepared from a stock solution on a gravimetric basis. Three target calibration
standards were prepared for each ion and de-ionized water was used as a control.
3.3.10 pH Measurements
Changes in pH of solutions were monitored using a Corning 430 pH meter. Prior to
testing, the pH meter was calibrated using pH buffer solution 4.00 ±0.02 and 7.00±0.02
(Fisher Scientific, Pittsburgh, PA). Sample solutions were prepared by exposing 1m2
surface area of each glass (where n=3) in 10ml de-ionized water. Measurements were
recorded over t = 1, 10 and 100 and 1000 hours. De-ionized water was used as a control
and was measured at each time period.
3.3.11 Glass Polyalkeonate Cements Formulation GPCs were prepared by thoroughly mixing the glass powders (<45 µm) with
polyacrylic acid (E11 PAA—Mw, 210,000, <90 m, Advanced Healthcare Limited, Kent,
UK) and deionized water on a glass plate. The cements were formulated with a powder to
liquid (P:L) ratio of 2:1.5 with 40%, 50%, and 60 wt% additions of PAA. Complete mixing
was undertaken within 20 s.
3.3.12 Rheological Evaluation The setting times (Ts) of the cement series were tested in accordance with
ISO991751 which specifies the standard for dental water-based cements. Ts was measured
by lowering a 400 g mass attached to a Gilmore needle into a cement filed mold measuring
8x9x10mm internal diameter. Cements were stored at 37oC during setting and the Ts was
taken as the time the needle failed to make a complete indent in the cement surface, (where
n = 3). The working time (Tw) of the cements was measured under standard laboratory
41
conditions (Ambient Temp, 25oC), and was defined as the period of time from the start of
mixing during which it was possible to manipulate the material without having an adverse
effect on its properties. Each sample (where n = 3), was measured using a stopwatch on a
clean glass plate with a sterile spatula. Each measurement was conducted under the same
mixing conditions to ensure reproducibility.
3.3.13 Compressive Strength The compressive strengths (σc) of the cements (6x4mm, where n = 5) were
evaluated in accordance with ISO991751. Cylindrical samples were tested after 7 days’
incubation in de-ionized water. Samples were stored in sterile de-ionized water in an
incubator at 37oC. After the incubation time has expired the cements were removed and
tested while wet on an Instron 4082 Universal Testing Machine (Instron Ltd., High
Wycombe, Bucks, UK) using a 5 kN load cell at a crosshead speed of 1 mm/min. The σc
was calculated using Equation 1. where q is the maximum applied load (N) and is the
diameter of sample (mm).
𝐶 =4𝜌
𝜋𝑑2 (1)
3.3.14 Shear Bond Strength Test Shear bond strength testing was conducted according to ISO 2902252. Briefly,
cylindrical samples (6x4ømm, where n = 3) were mounted on hydroxyapatite (HaP) plates
which were pre-mounted in resin and ground using 125 m grit size. Cylindrical Cu-GPC
samples were bonded to the HaP surface and left for 1 hour to set (Figure 3.1). The split
ring molds were then removed, and the bonded samples were incubated in de-ionized water
for 24 hours at 37oC before testing. The test was conducted at a crosshead speed of
1.0mm/min until failure. The bond strength was calculated using Equation. 2. Where σ is
stress expressed in MPa, F is the force, expressed in N and Ab is the bonding area expressed
in mm2.
𝜎 =𝐹
𝐴𝑏 (2)

42
Figure 3.1 Bonded Cu6C cylinders to hydroxyapatite substrates for shear bond strength testing
3.3.15 Antibacterial Testing The antibacterial activity of the GPCs (8x2ømm, where n = 5) were evaluated using
E. coli strain ATCC 8739 (LB agar and broth), S. epidermidis strain ATCC 14990 (BHI
agar and broth), S. aureus (TSB agar and broth) and Vancomycin Resistant S. aureus (TSB
agar and broth) using the agar diffusion method. Each cement sample was placed in
inoculated plates and the plates were cultured for 24 hours at 37oC. Each microbe was
initially grown aerobically in liquid broth at 37oC for 24 hours. Preparation of the agar disc
diffusion plates involved seeding agar plates with a sterile swab dipped in a 1/50 dilution
of the appropriate 24-hour culture of bacteria. The agar diffusion test was performed under
standard laboratory sterile conditions in a fumigation hood using sterile swabs for
inoculation of bacteria. Symbiosis protocol 3 colony counter was used for imaging of the
bacterial plates. Calipers were used to measure zones of inhibition where each sample was
analyzed in triplicate and mean zone sizes ± standard deviations were calculated.
Inhibition Zone (mm) =Halo∅ − Disc∅
2

43
3.4 Results
Glass compositions were formulated by replacing the SiO2 concentration with 6
and 12 mol% CuO into a glass with a starting composition of 48SiO2-36ZnO-6CaO-8SrO-
2P2O5, which is presented in Table 3.1. Initial characterization of the glass includes X-ray
Diffraction (XRD) to determine the amorphicity/crystallinity of the materials. Figure 3.2
presents X-Ray diffraction patterns of Control, CuG6 and CuG12. The characteristic
amorphous hump is presented in Figure 3.2 for each glass composition.
Figure 3.2 X-ray Diffraction (XRD) patterns for each powdered glass sample
Glass frit was pulverized to fine particulates and sieved through a <45µm sieve.
Particle size analysis (PSA) was conducted to determine the mean particle size distribution
and to ensure consistency of material processing. The particle size distribution of each glass
is presented in Table 3.2. The particle size distribution was determined to be similar for
each glass where the D10 ranged from 6.3-6.4µm, D50 8.2-8.5µm and D90 15.9-16.9µm
for Control, CuG6, and CuG12. The mean particle size distribution for the glass series was
similar where the Control was found to have a mean particle size of 10.4µm, CuG6 was
10.7µm and CuG12 was 10.1µm.

44
Table 3.2 Particle size analysis of each glass composition.
D10 D50 D90 Mean Control 6.3 8.4 16.8 10.4 CuG6 6.4 8.5 16.9 10.7 CuG12 6.3 8.2 15.9 10.1
The mean surface area of each glass composition was also determined using
Advanced Surface Area and Porosity (ASAP). Table 3.3 presents the BET surface area
measurements which were found to be similar for each glass at 0.32 m2/g for the Control,
0.88 m2/g for CuG6 and 0.64 m2/g for CuG12.
Table 3.3 BET surface area (m2/g) for each glass composition.
Surface Area (m2/g) S.D. Control 0.32 0.0096 CuG6 0.88 0.0093 CuG12 0.64 0.0097
The thermal profiles of each glass composition were analyzed using Differential
Thermal Analysis (DTA) to determine any differences in the thermal transition point as a
function of CuO concentration. The resulting thermograms are presented in Figure 3.3. The
thermal profile of Control presented in Figure 3.3 shows the glass transition temperature
(Tg) at 661°C and the first primary crystallization temperature (Tc1) evident at a
temperature of 856°C. Addition of 6mol% CuO (CuG6) increased the Tg to 773°C and
also increased crystallization temperature to 1047°C. By further increasing the CuO
concentration to 12 mol% (CuG12), the Tg of the glass increased to 786°C and also
increased Tc1 to 994°C.
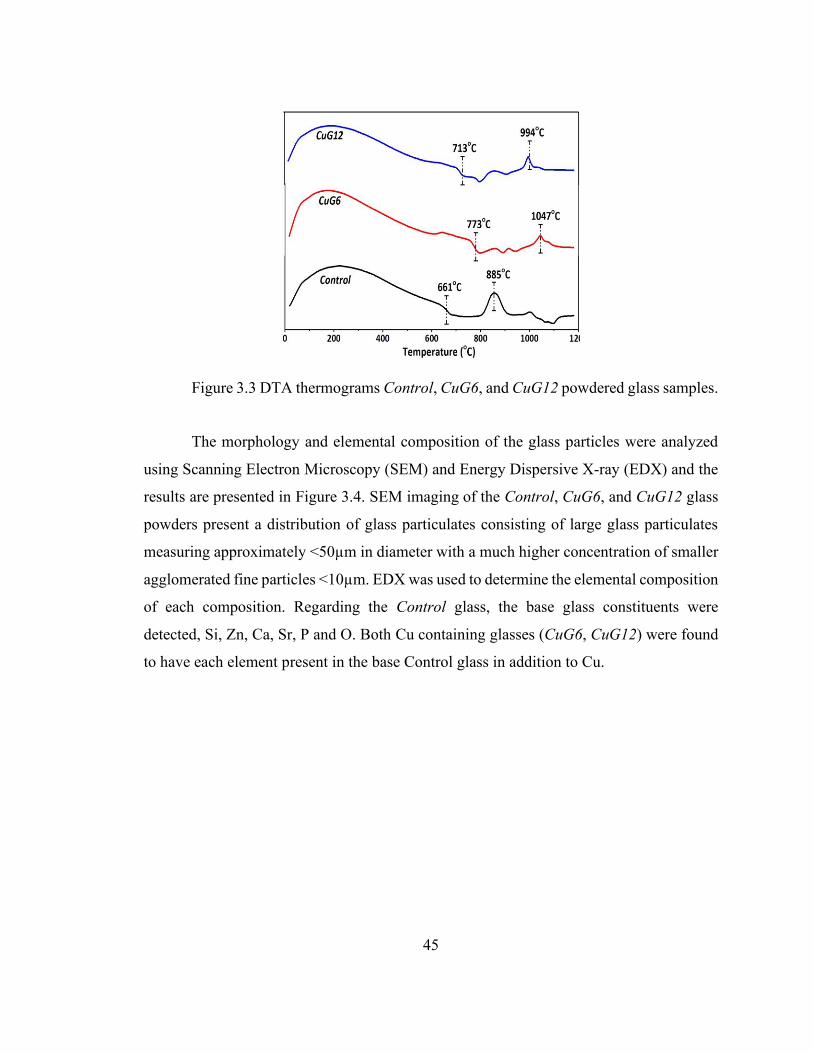
45
Figure 3.3 DTA thermograms Control, CuG6, and CuG12 powdered glass samples.
The morphology and elemental composition of the glass particles were analyzed
using Scanning Electron Microscopy (SEM) and Energy Dispersive X-ray (EDX) and the
results are presented in Figure 3.4. SEM imaging of the Control, CuG6, and CuG12 glass
powders present a distribution of glass particulates consisting of large glass particulates
measuring approximately <50µm in diameter with a much higher concentration of smaller
agglomerated fine particles <10µm. EDX was used to determine the elemental composition
of each composition. Regarding the Control glass, the base glass constituents were
detected, Si, Zn, Ca, Sr, P and O. Both Cu containing glasses (CuG6, CuG12) were found
to have each element present in the base Control glass in addition to Cu.

46
Figure 3.4 Energy-dispersive X-ray (EDX) and Scanning Electron Microscopy (SEM) of Control, CuG6, and CuG12 powdered glass samples.
To further confirm the composition of the glass samples and to investigate the
structure of the glass, X-ray Photoelecton Spectroscopy (XPS) was employed. Figure 3.5
present the XPS survey scans of Control and CuG12 glass (CuG6 not presented). The
Control glass was found to contain zinc, calcium, strontium, silicon and phosphorus in
addition to oxygen. No contamination was found for any of the glass compositions.
Addition of CuO resulted in the presence of Cu2p peaks (Cu 2p1, Cu 2p3) for CuG6, and
CuG12 glasses. Additionally, the high-resolution oxygen signal was further analyzed to
determine the effect that the addition of CuO has on the structure of the oxygen bonds. It
is evident in Figure 3.5 that the binding energy of Control was centred at 531.5eV however

47
the addition of CuO shifts the binding energy of CuG6 to 533.9eV and the binding energy
of CuG12 to 534.3eV.
Figure 3.5 (a) X-ray photoelectron spectroscopy (XPS) survey scans of Control and CuG12 and (b) high-resolution O1s scans of Control, CuG6, and CuG12.
29Si Magic Angle Spinning Nuclear Magnetic Resonance (MAS-NMR) was
performed on the Control and CuG12 glasses. MAS-NMR was employed to determine the
effect that the addition of CuO has on the connectivity of the glass structure, in particular
the bonding of Si to O. Figure 3.6 presents the 29Si MAS-NMR spectra for Control glass
in addition to the relative fraction of Q species. The 29Si MAS-NMR spectrum of Control
presents asymmetrical peak centred at -81 ppm. The corresponding distribution of different
Q species are presented in Figure 3.6 a. The relative fraction of Q-species was determined
within the spectral region of -40 to-120 ppm where the Q-species are centred at -47 ppm
for Q0, -65 ppm for Q1, -79 ppm for Q2, -91 ppm for Q3 and -112 ppm for Q4. The
percentage of Q-species present in the Control glass includes approximately 5% Q0, 8%
Q1, 57% Q2, 28% Q3 and 2% Q4. The 29Si MAS-NMR spectrum for CuG12 is presented
in Figure 3.7. It is evident from Figure 3.7 that for CuG12 a higher degree of asymmetry
exists around the region of -110 ppm compared to the Control glass. The 29Si MAS-NMR
spectrum of CuG12 composed of Q-species are centred at -55 ppm for Q0, -76 ppm for Q1,

48
-85 ppm for Q2, -95 ppm for Q3 and -112 ppm for Q4. The relative fraction of Q-speciation
for CuG12 presented in Figure 3.7 presents 2% Q0, 24% Q1, 25% Q2, 36% Q3 and 13% Q4.
Figure 3.6 (a) 29Si MAS-NMR spectrum of Control glass, and (b) corresponding Q-species.
Figure 3.7 (a) 29Si MAS-NMR spectrum of CuG12 glass, and (b) corresponding Q-species.

49
Ion release profiles were determined for each component of the glass including Si,
Zn, Ca, and Sr, however, no ion release was detected for Cu or P. Each glass powder was
incubated in de-ionized water for 1, 10, 100 and 1000 hours, and the ion release profiles of
liquid glass extracts presented in Figure 3.8. Regarding Si release, presented in Figure 3.8a,
the level of Si release from the Control was found to increase from 18-31mg/L after
incubating over 1-1000 hours. CuG6 was also found to increase with respect to time and
experienced similar release levels from 20-30mg/L. CuG12 presented slightly lower final
Si levels after 1000 hours, which ranged from 20-25mg/L. Zn release was relatively low
for each of the glasses and was below 3mg/L for each glass tested at each time period. Ion
release profiles for Ca and Sr are presented in Figure 3.8c-d. with respect to Ca release,
similar profiles were evident for Control, CuG6 and CuG12, where Control ranged from
13-16mg/L, CuG6 ranged from 13-15mg/L and CuG12 also ranged from 13-15mg/L with
each glass exhibiting an increase with respect to incubation time. Sr release is presented in
Figure 3.8c. Sr release was also found to increase with respect to incubation time for each
glass composition. Control Sr release ranged from 2-8 mg/L, CuG6 ranged from 1-7 mg/L
and CuG12 ranged from 2-10mg/L, with the maximum Sr release being evident after 1000
hours incubation.
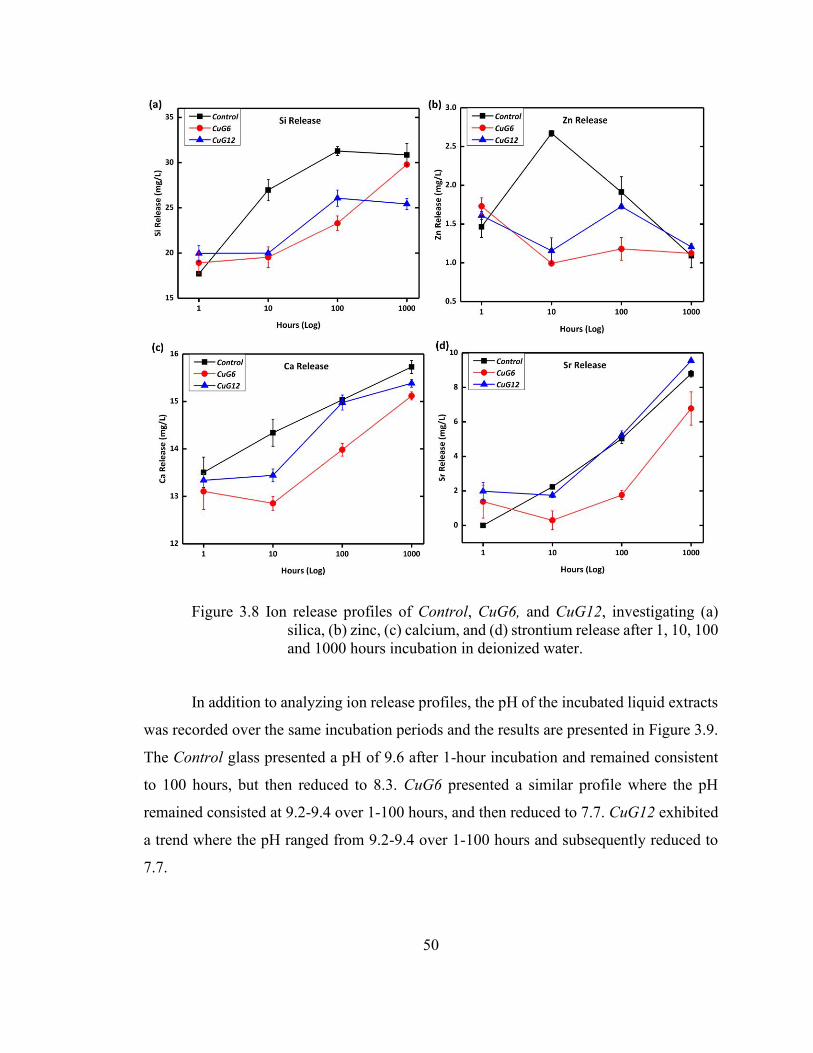
50
Figure 3.8 Ion release profiles of Control, CuG6, and CuG12, investigating (a) silica, (b) zinc, (c) calcium, and (d) strontium release after 1, 10, 100 and 1000 hours incubation in deionized water.
In addition to analyzing ion release profiles, the pH of the incubated liquid extracts
was recorded over the same incubation periods and the results are presented in Figure 3.9.
The Control glass presented a pH of 9.6 after 1-hour incubation and remained consistent
to 100 hours, but then reduced to 8.3. CuG6 presented a similar profile where the pH
remained consisted at 9.2-9.4 over 1-100 hours, and then reduced to 7.7. CuG12 exhibited
a trend where the pH ranged from 9.2-9.4 over 1-100 hours and subsequently reduced to
7.7.

51
Figure 3.9 pH of extracts from samples release after 1, 10, 100 and 1000 hours incubation in deionized water
GPCs were formulated with 40, 50 and 60wt% PAA concentrations for the
rheological and mechanical property evaluation. GPCs were labelled with their
corresponding glass compositions as ConC, Cu6C, and Cu12C, attributed to glass
compositions of Control, CuG6, and CuG12, respectively. The working (Tw) and setting
(Ts) times of the GPCs were conducted according to ISO9917 and the results are presented
in Figure 3.10 and also in Table 3.4.
Table 3.4 Working (Tw) and Setting (Ts) times of ConC, Cu6C and Cu12C formulated with 40, 50 and 60wt% PAA.
Working Times (min,sec) Setting Times (min,sec) ConC Cu6C Cu12C ConC Cu6C Cu12C
40wt% PAA 1m, 58s 1m, 38s 1m, 10s 10m, 16s 7m, 45s 6m, 04s 50wt% PAA 1m, 40s 1m, 11s 1m, 00s 16m, 15s 14m, 10s 8m, 35s 60wt% PAA 1m, 07s 1m, 01s 0m 54s 18m, 05s 24m, 45s 11m, 07s
From Figure 3.10 it is evident that the Tw of the GPCs were found to decrease as
the PAA concentration increased. The Tw of ConC reduced from 1m, 58s to 1m, 07s as the
PAA concentration increased from 40-60wt% PAA. The Cu6C experienced a similar trend

52
where Tw reduced from 1m, 38s to 1m, 01s and Cu12C also reduced from 1m, 10s – 0m,
54s as the PAA concentration increased from 40-60wt%. The Ts of the GPCs are presented
in Figure 3.10 and Table 3.4. Conversely, the Ts were found to increase as the PAA
concentration increase from 40-60wt%. Regarding the ConC, the Ts increased from
10m,16s to 18m, 05s. The Cu-GPCs experienced shorter Ts, however a similar trend is
evident. The Ts of Cu6C increased from 7m, 45s to 24m, 45s and Cu12C increased from
6m, 04s to 11m, 07s.
Figure 3.10 (a) Working times and (b) setting times of ConC, Cu6C and Cu12C mixed with 40, 50 and 60 wt% PAA.
Mechanical testing was conducted on each cement formulation, specifically
compressive and shear bond strength testing. Compressive testing was conducted after 7
days immersion in deionized water considering 40wt%, 50wt% and 60wt% PAA and the
results are presented in Figure 3.11. It is evident from Figure 3.11 that the concentration of
PAA did not have a significant effect on the compressive strength of the GPCs. The highest
compressive strength was attributed to the ConC with 50% PAA with a strength of 35 MPa,
and the lowest strength was found to be Cu12C with 40wt% PAA at 18 MPa. Additionally,
a shear bond strength test was conducted to determine the GPCs ability to adhere to
hydroxyapatite (Hap). The shear bond strength was measured after 24-hours incubation in
water and the results are presented in Figure 3.12. Cements were formulated with 40wt%

53
PAA and attained bond strengths of 0.85 MPa, 1.32 MPa and 0.79 MPa for ConC, Cu6C
and Cu12C respectively.
Figure 3.11 Compressive strength of GPC series using 40wt%, 50wt% and 60wt% PAA after 7 days soaking in de-ionized water.
Figure 3.12 Shear bond strength of ConC, Cu6C and Cu12C in addition to SEM imaging of fracture surfaces.

54
Antibacterial testing was conducted employing a range of bacteria including E. coli,
S. epidermidis, S. aureus (UMAS-1) and Vancomycin Resistant S. aureus (VRSA). Agar
diffusion testing was conducted using GPCs formulated with 40wt% PAA and the results
are presented in Figure 3.13 and Figure 3.14. From Figure 3.13a, it can be observed that
the Cu-GPC presented higher inhibition zones in E. coli than the ConC. The ConC
presented an inhibition zone of 1.7mm which Cu6C and Cu12C presented inhibition zones
of 3.2mm and 3.8mm, respectively. Testing in S. epidermidis is presented in Figure 3.13b
which presented the highest inhibition zones of any bacteria tested. The ConC did not
present any inhibition, however, Cu6C and Cu12C GPCs presented inhibition zones of
9.6mm and 7.5mm respectively. The GPCs were also tested in VRSA and the results are
presented in Figure 3.13c. No inhibition was observed with the ConC while Cu6C and
Cu12C presented inhibition zones of <1mm and 2.1mm respectively. Testing in S. aureus
(UMAS-1) is presented in Figure 3.13d. No inhibition was observed for the ConC and
inhibition zones were inconsistent for Cu6C and Cu12C (3.9mm).
Figure 3.13 Antibacterial testing of ConC, Cu6C and Cu12C in a.) E. coli, b.) S. epidermidis, c.) Vancomycin Resistant S. aureus and d.) S. aureus (UMAS-1).

55
Figure 3.14 Antibacterial testing plates presented in rows a.) E. coli, b.) S. epidermidis, Vancomycin Resistant S. aureus and d.) S. aureus (UAMS-1) and columns with samples i.) ConC, ii.) Cu6C and iii.) Cu12C.

56
3.5 Discussion
For this study three glass compositions were synthesized, and the addition of
6mol% and 12mol% CuO was investigated with respect to glass structure and solubility.
The glass composition was selected based on components that can have positive
therapeutic effect in vivo, and also with respect to formation of glass-based bone adhesives.
A low SiO2 concentration is a known characteristic of soluble bioactive glasses2, in
addition to Si being one of the key components that initiates CaP/apatite mineralization
when tested in synthetic physiological fluids through the formation of Si-OH- groups on
the glass surface26, 29. ZnO, CaO and SrO are known to form bonds with carboxylic acid
(COO-) side groups on the PAA chains which results in these divalent cations (Zn2+, Ca2+,
Sr2+) forming metal-ligand complexes which crosslink the polyacid chains resulting in a
hardened set material. In addition, each of these components are known to have positive
effects on osseous tissue metabolism and repair. The addition of CuO can be justified
through two possible advantages. Firstly, it has been cited in numerous publications to
possess broad spectrum antibacterial properties10, 50, 53-56, which suggests it may prove a
safer alternative to antibiotic doping of medical materials and secondly, Cu has been cited
to have a structural role within a traditional GPC where the ionic strength of the bond
proceeds from M=Al3+>Cu2+>Zn2+>Ca2+>Mg2+, which suggests the Cu is a mechanically
relevant ion when formulating Al-free glasses used in GPCs48. However, the solubility and
structure of the underlying glass structure plays a critical role in the setting of GPCs. Initial
glass characterization determined that each of the starting glasses were amorphous in
structure (Figure 3.2). This is beneficial as crystalline materials tend to be less soluble than
their amorphous counterparts57. Additionally, the BET surface area of glass particles in
Table 3.2 (0.32-0.88m2/g) and the particle size distribution (10.1-10.7µm) of each glass
(Control, CuG6, CuG12) are similar. The particle size distribution is an important
characteristic in the setting and strengthening of GPCs as a higher distribution of smaller
particles results in increased dissolution of the glass particles. Larger particles are also
beneficial as they can act as reinforcing particles that, over extended periods, can result in

57
increased hardening with respect to maturation. Studies conducted by Tyas et al58 and
Mitsuhashi et al59 on the setting, compressive strength and fracture toughness on GPCs and
resin modified GPCs both conclude that GPCs benefit from having a distribution of
particles sizes, where the finer particles initial the setting and the larger unreacted glass
particles result in increasing the fracture energy of the materials.
The structure of the glasses was analyzed using a number of techniques including
Differential Thermal Analysis (DTA), X-ray Photoelectron Spectroscopy (XPS) and Magic
Angle Spinning Nuclear Magnetic Resonance (MAS-NMR). DTA profiles show that the
glass transition temperature (Tg) of the Control (661°C) is significantly lower than that of
the Cu containing glasses (Cu6C 773°C, Cu12C 786°C, Figure 3.3). The increase in Tg is
indicative of increasing the network connectivity within the glass resulting in a less soluble
material. This could be due to the role Cu plays in the glass. Cu has previously been
reported to exist in glass systems as network modifier60. The increase in Tg is indicative of
increasing the Bridging Oxygen (BO) concentration within the glasses. The addition of
6mol% and 12mol% Cu increased the Tg by approximately 110-120°C, which suggests
that the role Cu assumes in the glass is independent with respect to concentration. Both
XPS and MAS-NMR are techniques routinely employed to investigate the structure of
glasses. High resolution O1s XPS results show that the binding energy increases from
531eV to 534eV with as the concentration of Cu in the glass increases (Figure 3.5). This is
indicative of increasing the concentration of BO within the glass structure and the region
of 534eV can be attributed to bridging oxygen in P2O5 and P2O5/ZnO. The binding energy
of Cu2p at 952.53eV can be attributed to valence state of Cu like Cu1+ and Cu2+. MAS-
NMR data presented in Figure 3.6 and Figure 3.7 also suggest that with the addition of
12mol% CuO, the bridging oxygen concentration in the glass is increasing as this technique
probes the local environment of the Si atom. tThese trends are indicative of increasing the
BO connectivity within the glass network. Glasses that have Q-structures with lower BO
concentrations, or higher non bridging oxygen concentrations (NBOs), facilitate a higher
degree of acid degradability when mixed with polyacrylic acids, thus providing ion
dissolution required for crosslinking the acid chains48.

58
Ion release profiles of Si4+, Zn2+, Ca2+ and Sr2+, each as a function of incubation
time in fluids are presented in Figure 3.8. With respect to Cu and P, no ion release was
recorded, or they were below the instruments detection limit. Si4+ levels were found to
increase with respect to incubation time, and the effect of Cu replacement for Si4+ result in
similar levels of Si release which ranged from 20-30mg/L. Si4+ release in this range are
cited to increase osteoblast cell proliferation rate and stimulates genes in osteoblasts that
play a critical role in bone metabolism29. Zn2+ levels were found to be low (<3mg/L) for
each time period, however, toxicity limits for Zn2+ are cited to be 16mg/L for cytotoxic
effects, or even lower at 8 mg/L have been reported to cause oxidative stress in human
osteoblasts29, however Zn2+ at lower levels can have important roles in bone formation and
protein synthesis61. Ca2+ release was found to increase over time for each glass, and
similarly to Si4+, the addition of 6mol% and 12mol% CuO slightly reduced the release
rates, however, each ranged between 13-16mg/L. Ca2+ release is essential for processes
such bioactive glass surface mineralization, GPC formation and from physiological
perspective Ca2+ has been attributed to increasing osteoblast proliferation, differentiation
and extracellular matrix mineralization29. The Ca2+ levels reported here are low compared
to cited cytotoxicity limits which can be up to 120mg/L29. Sr2+ release is known to have
excellent bone metabolic potential and has been implicated for treating osteoporosis29.
Studies by Gentleman et al from silicate glasses (SiO2-P2O5-Na2O-CaO), where the Ca2+
content was substituted with Sr2+, showed enhanced osteoblast activity and osteoblast
activity and inhibited osteoclast activity in the range of 5-23mg/L29. The Sr2+ release from
this glass system is within the region of 2-10mg/L and is highest with the highest Cu
containing glass, CuG12. In addition, the solution pH of the glass series was found to be
slight higher for the Control glass compared to CuG6 and CuG12. However, all glasses
were in the region of 9.4-9.6 until 1000 hours had expired. At this stage, the pH of the
Control reduced to 8.3 while CuG12 reduced to 7.7, close to neutral. This is a positive
attribute as it may suggest that mineral solubility limits are reached and that precipitation
reactions are occurring within the solution which would be a positive attribute as
precipitation of minerals on bioceramics in vitro, via Simulated body fluid (SBF) testing,
is widely regarded as a precursor to bone bonding in vivo5, 26.
59
GPCs were formulated with a range of PAA concentrations (40, 50, 60wt%) and
the Tw and Ts were evaluated. The addition of higher concentration of PAA typically
reduced the rheological properties as the increase in COO- groups facilitates chelation of
the metal cations from the polysalt matrix at a much more rapid rate. The Tw for each GPC
were found to follow this trend, the addition of Cu was found to reduce the Tw. The Ts,
however, did not follow this expected trend, conversely the setting times were found to
increase as the PAA concentration increased. This effect is independent of Cu addition as
the ConC also experienced this trend. The addition of Cu did however, reduce the Ts to
levels that are more representative of the Ts outlined by the ISO9917 standard for water
based cements51. This effect may be related to changes in local pH of the cement matrix
through dissolution of the glass particles in response to PAA. The acid-base setting reaction
attributed to these cements setting and mechanical properties can be heavily influenced by
the setting pH48.
Mechanical properties were evaluated using compressive strength testing and shear
adhesion bond strength testing which were also testing according to ISO standards.
Compressive strength testing (Figure 3.11) was conducted after 7 days’ incubation in
deionized water. The mechanical properties of conventional GPCs are known to increase
with an increasing the polyacrylic acid concentration, however, this effect is highly
dependent on the solubility of the glass and the time it takes for the GPCs to set48. With
regard to the GPC series tested here, little trends were evident and the strengths were in the
region of 18-35MPa, far less than the required 50MPa for luting and lining applications
and even more compared to the 100MPa for restorative applications. The strengths
recorded for this work were found to be both independent of PAA concentration and of Cu
addition. Further bond strength testing was conducted to provide insight into the failure
mechanism. The adhesive bond strengths were 0.85, 1.32 and 0.79 MPa for ConC, Cu6C
and Cu12C respectively (Figure 3.12). These values are lower than reported bonding agents
Clearfil New Bond and Histocaryl, which reported values of 5.2MPa and 1.9MPa
respectively44. The failure of the mechanical properties in these GPCs is likely due to the
reduced dissolution rate of the glass particles. SEM imaging of the shear bond strength
fracture samples suggest that the Cu12C in particular does not fail adhesively, but fails

60
cohesively. Upon examining the fracture surface, a high concentration of unreacted glass
particles is present in addition to a high degree of porosity. Both of these factors may
account for the reduced strengths of this GPCs series.
Antibacterial evaluation was conducted using the 40wt% addition of PAA with
ConC, Cu6C and Cu12C (Figure 3.13 and Figure 3.14). The presence of Cu in Cu6C and
Cu12C presented antibacterial properties in E. coli, which were concentration dependant.
The Cu-GPCs showed the greatest inhibition in S. epidermidis and presented notable effect
in Vancomycin Resistant S. aureus and UMAS-1. This suggests that the addition of Cu to
GPC based skeletal adhesives or other bone cements may be an adequate alternative to
loading cements with antibiotics such as vancomycin, streptomycin and gentamycin. The
overuse of these antibiotics has led to the evolution of resistant strains of microbes which
pose serious issues in immunocompromised patients62-64. The mechanism of action of Cu
ion is cited to be related to the ions ability to adhere to the negatively charges bacterial cell
wall causing it to rupture, thereby leading to protein denaturation and eventual cell death65.
3.6 Conclusion
The study focused on synthesizing Cu containing GPC series that could potentially
employed for skeletal applications. Amorphous materials were synthesized with suitable
particle size characteristics for GPC formation. Glasses presented ICP solubility profiles
that could potentially exhibit bioactive properties, however, the addition of CuO to the
glass increased the concentration of BO such that the particles surface dissolution, when
mixed with PAA, was compromised. This factor is likely the reason that the mechanical
properties suffered. The Cu-GPCs did however, present good antibacterial properties when
tested in a range of microbes. Future work will include synthesizing Cu containing GPC to
improve the mechanical properties and the adhesive bond strength, in addition to
performing Simulated body fluid (SBF) and cytocompatibility testing on the resulting Cu-
GPCs.
Chapter 3 investigated the Cu containing glasses for their use in GPCs. Structural
characterization of the novel Cu-containing glass series, and preliminary results on

61
rheological, mechanical, and antibacterial properties, extrapolated their potential to form
glass-based cements. Next chapter (chapter 4) is extensively focused on rheological,
mechanical, and biological behavior of GPCs. The rheological behavior of GPCs will be
investigated as a function of different formulations. Mechanical properties of GPCs will be
analyzed using compressive, flexural, and shear bond strength testing. Moreover, to
analyze the bond strength, the fracture surface area will be analyzed using laser
profilometry. Later on, in vitro biocompatibility of GPCs will be studied using different
approaches, such as ion release prolife, simulated body fluid trails, antibacterial efficacy in
agar and broth, and finally osteoblast cell cytotoxicity will be evaluated.
3.7 References
1. Gerhardt, L.-C.; Boccaccini, A. R., Bioactive glass and glass-ceramic scaffolds for bone tissue engineering. MATERIALS 2010, 3 (7), 3867-3910.
2. Hench, L. L., The story of Bioglass. J MATER SCI-MATER M 2006, 17, 967-978. 3. Jones, J. R., Review of bioactive glass: from Hench to hybrids. ACTA BIOMATER
2013, 9, 4457-4486. 4. Chen, X.; Meng, Y.; Li, Y.; Zhao, N., Investigation on bio-mineralization of melt
and sol-gel derived bioactive glasses. APPL SURF SCI 2008, 255 (2), 562-564. 5. Kokubo, T.; Takadama, H., How useful is SBF in predicting in vivo bone
bioactivity. BIOMATERIALS 2006, 27, 2907-2915. 6. Bellucci, D.; Bolelli, G.; Cannillo, V.; Cattini, A.; Sola, A., In situ Raman
spectroscopy investigation of bioactive glass reactivity: Simulated body fluid solution vs TRIS-buffered solution. MATER CHARACT 2011, 62 (10), 1021-1028.
7. Kaur, G.; Pandey, O. P.; Singh, K.; Homa, D.; Scott, B.; Pickrell, G., A review of bioactive glasses: their structure, properties, fabrication and apatite formation. J BIOMED MATER RES A 2014, 102 (1), 254-274.
8. Rahaman, M. N.; Day, D. E.; Sonny Bal, B.; Fu, Q.; Jung, S. B.; Bonewald, L. F.; Tomsia, A. P., Bioactive glass in tissue engineering. ACTA BIOMATER 2011, 7 (6), 2355-2373.
9. Vargas, G. E.; Mesones, R. V.; Bretcanu, O.; López, J. M. P.; Boccaccini, A. R.; Gorustovich, A., Biocompatibility and bone mineralization potential of 45S5 Bioglass®-derived glass-ceramic scaffolds in chick embryos. ACTA BIOMATER 2009, 5 (1), 374-380.
10. Wu, C.; Zhou, Y.; Xu, M.; Han, P.; Chen, L.; Chang, J.; Xiao, Y., Copper-containing mesoporous bioactive glass scaffolds with multifunctional properties of angiogenesis capacity, osteostimulation and antibacterial activity. Biomaterials 2013, 34 (2), 422-433.

62
11. Baino, F.; Vitale-Brovarone C., Three-dimensional glass-derived scaffolds for bone tissue engineering: current trends and forecasts for the future. J BIOMED MATER RES A 2011, 97 (4), 514-35.
12. Cannillo, V.; Chiellini, F.; Fabbri, P.; Sola, A., Production of Bioglass® 45S5–Polycaprolactone composite scaffolds via salt-leaching. COMPOS STRUCT 2010, 92 (8), 1823-1832.
13. Chen, Q. Z.; Thompson, I. D.; Boccaccini, A. R., 45S5 Bioglass®-derived glass-ceramic scaffolds for bone tissue engineering. BIOMATERIALS 2006, 27 (11), 2414-2425.
14. Chen, Q.-Z.; Rezwan, K.; Françon, V.; Armitage, D.; Nazhat, S. N.; Jones, F. H.; Boccaccini, A. R., Surface functionalization of Bioglass®-derived porous scaffolds. ACTA BIOMATER 2007, 3 (4), 551-562.
15. Haimi, S.; Gorianc, G.; Moimas, L.; Lindroos, B.; Huhtala, H.; Raty, S.; Kuokkanen, H.; Sandor, G. K.; Schmid, C.; Miettinen, S.; Suuronen, R., Characterization of zinc-releasing three-dimensional bioactive glass scaffolds and their effect on human adipose stem cell proliferation and osteogenic differentiation. ACTA BIOMATER 2009, 5 (8), 3122-3131.
16. Goller, G.; Demirkiran, H.; Oktar, F. N.; Demirkesen, E., Processing and characterization of bioglass reinforced hydroxyapatite composites. CERAM INT 2003, 29 (6), 721-724.
17. Habibe, A. F.; Maeda, L. D.; Souza, R. C.; Barboza, M. J. R.; Daguano, J. K. M. F.; Rogero, S. O.; Santos, C., Effect of bioglass additions on the sintering of Y-TZP bioceramics. MATER SCI ENG C 2009, 29 (6), 1959-1964.
18. Anderson, J. H.; Goldberg, J. A.; Bessent, R. G.; Kerr, D. J.; McKillop, J. H.; Stewart, I.; Cooke, T. G.; McArdle, C. S., Glass yttrium-90 microspheres for patients with colorectal liver metastases. RADIOTHER ONCOL 1992, 25 (2), 137-139.
19. Bortot, M.; Prastalo, S.; Prado, M., Production and characterization of glass microspheres for hepatic cancer treatment. PROCEDIA MAT SCI 2012, 1, 351-358.
20. da Costa Guimaraes, C.; Moralles, M.; Roberto Martinelli, J., Monte Carlo simulation of liver cancer treatment with 166Ho-loaded glass microspheres. RADIAT PHYS CHEM 2014, 95, 185-187.
21. Wren, A. W.; Cummins, N. M.; Towler, M. R., Comparison of antibacterial properties of commercial bone cements and fillers with a zinc-based glass polyalkenoate cement. J MATER SCI 2010, 45, 5244-5251.
22. Smeets, R.; Marx, R.; Kolk, A.; Said-Yekta, S.; Grosjean, M. B.; Stoll, C.; Tinschert, J.; Wirtz, D. C.; Riediger, D.; Endres, K., In Vitro Study of Adhesive Polymethylmethacrylate Bone Cement Bonding to Cortical Bone in Maxillofacial Surgery. J ORAL MAXIL SURG 2010, 68 (12), 3028-3033.
23. Lewis, G., Properties of Acrylic Bone Cements:State of the art review. J BIOMED MATER RES 1997, 38, 155-182.
24. Palussiere, J.; Berge, J.; Gangi, A.; Cotten, A.; Pasco, A.; Bertagnoli, R.; Jaksche, H.; Carpeggiani, P.; Deramond, H., Clinical results of an open prospective study of a Bis-GMA composite in percutaneous vertebral augmentation. Eur Spine J 2005, 14, 982-991.
63
25. Farrar, D. F.; Rose, J., Rheological properties of PMMA bone cements during curing. Biomaterials 2001, 22 (22), 3005-3013.
26. Kokubo, T.; Kim, H.-M.; Kawashita, M., Novel bioactive materials with different mechanical properties. BIOMATERIALS 2003, 24, 2161-2175.
27. Filho, O. P.; LaTorre, G. P.; Hench, L. L., Effect of crystallization on apatite-layer formation of bioactive glass 45S5. J BIOMED MATER RES 1996, 30, 509-514.
28. Hench, L. L., Genetic design of bioactive glass. J EUR CERAM SOC 2009, 29 (7), 1257-1265.
29. Hoppe, A.; Guldal, N. S.; Boccaccini, A. R., A review of the biological response to ionic dissolution products from bioactive glasses and glass-ceramics. BIOMATERIALS 2011, 32 (11), 2757-2774.
30. Serra, J.; Gonzalez, P.; Liste, S.; S. Chiussi; Leon, B.; Perez-amor, M.; Ylanen, H. O.; Hupa, M., Influence of the non-bridging oxygen groups on the bioactivity of silicate glasses. J MATER SCI: MATER MED 2002, 13, 1221-1225.
31. Yamanaka, H.; Nakahata, K.; Terai, R., Structure of Na2O-TiO2-SiO2 glasses from the viewpoint of non-bridging oxygens measured by XPS. J NON-CRYST SOLIDS 1987, 95 & 96, 405-410.
32. Wren, A. W.; Laffir, F. R.; Kidari, A.; Towler, M. R., The structural role of titanium in Ca–Sr–Zn–Si/Ti glasses for medical applications. J NON-CRYST SOLIDS 2011, 357 (3), 1021-1026.
33. Calas, G.; Cormier, L.; Galoisy, L.; Jollivet, P., Structure–property relationships in multicomponent oxide glasses. CR CHIM 2002, 5 (12), 831-843.
34. King, J. C., Does poor zinc nutriture retard skeletal growth and mineralization in adolescents. EUR J CLIN NUTR 1994, 64, 375-376.
35. Rico, H.; Villa, L. F., Zinc, a new coherent therapy for osteoporosis. CALCIFIED TISSUE INT 2000, 67, 422-423.
36. Yamaguchi, M.; Ma, Z. J., Role of endogenous zinc in the enhancement of bone protein synthesis associated with bone growth of newborn rats. J BONE MINER METAB 2001, 19, 38-44.
37. Marie, P. J., Strontium ranelate: new insights into its dual mode of action. BONE 2007, 40 (5), S5-S8.
38. Marie, P. J., Strontium ranelate; a novel mode of action optimizing bone formation and resorption. OSTEOPOROSIS INT 2005, 16, S7-S10.
39. Carter, D. H.; Sloan, P.; Brook, I. M.; Hatton, P. V., Role of exchanged ions in the integration of ionomeric (glass polyalkenoate) bone substitutes. Biomaterials 1997, 18, 459-466.
40. Bush, A., Aluminium and Alzheimers Disease. ALZHEIMERS AUST 2004, 1-5. 41. Polizzi, S.; Pira, E.; Ferrara, M.; Bugiani, M.; Papaleo, A.; Albera, R.; Palmi, S.,
Neurotoxic effects of Aluminium among foundry workers and Alzheimers disease. NEUROTOXICOLOGY 2002, 23, 761-774.
42. Reusche, E.; Pilz, P.; Oberascher, G.; Linder, B.; Egensperger, R.; Gloeckner, K.; Trinka, E.; Iglseder, B., Subacute fatal Aluminium Encephalopathy after Reconstructive Otoneurosurgery: A Case Report. HUM PATHOL 2001, 32 (10), 1136-1139.

64
43. Nicholson, J. W., Chemistry of glass-ionomer cements: a review. BIOMATERIALS 1998, 19, 485-494.
44. Maurer, P.; Bekes, K.; Gernhardt, C. R.; Schaller, H. G.; Schubert, J., Comparison of the bond strength of selected adhesive dental systems to cortical bone under in vitro conditions. INT J ORAL MAX SURG 2004, 33 (4), 377-381.
45. Griffin, S.; Hill, R., Influence of poly(acrylic acid) molar mass on the fracture properties of glass polyalkenoate cements. J MATER SCI 1998, 33, 5383-5396.
46. Kandalam, U.; Bouvier, A. J.; Casas, S. B.; Smith, R. L.; Gallego, A. M.; Rothrock, J. K.; Thompson, J. Y.; Huang, C. Y. C.; Stelnicki, E. J., Novel bone adhesives: a comparison of bond strengths in vitro. INT J ORAL MAX SURG 2013, 42 (9), 1054-1059.
47. Stamboulis, A.; Law, R. V.; Hill, R. G., Characterisation of commercial ionomer glasses using magic angle nuclear magnetic resonance (MAS-NMR). Biomaterials 2004, 25 (17), 3907-3913.
48. Nicholson, J. W.; Wilson, A. D., Acid-Base cements - Their biomedical and industrial applications. Cambridge: 1993; Vol. 3.
49. Chan, Y.-H.; Huang, C.-F.; Ou, K.-L.; Peng, P.-W., Mechanical properties and antibacterial activity of copper doped diamond-like carbon films. SURF COAT ENG 2011, 206 (6), 1037-1040.
50. Pramanik, A.; Laha, D.; Bhattacharya, D.; Pramanik, P.; Karmakar, P., A novel study of antibacterial activity of copper iodide nanoparticle mediated by DNA and membrane damage. COLLOID SURFACE B 2012, 96 (0), 50-55.
51. International Organization for Standardization 9917, Dental Water Based Cements (E). In Case Postale 56, Geneva, Switzerland, 1991; pp CH-11211.
52. International Organization for Standardization - ISO 29022. Dentistry - Adhesion - Notched edge shear bond strength test 2013, E.
53. Aina, V.; Cerrato, G.; Martra, G.; Malavasi, G.; Lusvardi, G.; Menabue, L., Towards the controlled release of metal nanoparticles from biomaterials: Physico-chemical, morphological and bioactivity features of Cu-containing sol–gel glasses. APPL SURF SCI 2013, 283, 240-248.
54. Bonici, A.; Lusvardi, G.; Malavasi, G.; Menabue, L.; Piva, A., Synthesis and characterization of bioactive glasses functionalized with Cu nanoparticles and organic molecules. J EUR CERAM SOC 2012, 32 (11), 2777-2783.
55. Nan, L.; Yang, K., Cu Ions Dissolution from Cu-bearing Antibacterial Stainless Steel. J MATER SCI TECHNOL 2010, 26 (10), 941-944.
56. Singh, S.; Joshi, H. C.; Srivastava, A.; Sharma, A.; Verma, N., An efficient antibacterial multi-scale web of carbon fibers with asymmetrically dispersed Ag–Cu bimetal nanoparticles. COLLOID SURFACE A 2014, 443, 311-319.
57. Li, Y.; Coughlan, A.; Wren, A. W., Investigating the surface reactivity of SiO2–TiO2–CaO–Na2O/SrO bioceramics as a function of structure and incubation time in simulated body fluid. J MATER SCI: MATER MED 2014, 25 (8), 1853-1864.
58. Tyas, M. J.; Burrow, M. F., Adhesive restorative materials: A review. AUST DENT J 2004, 49 (3), 112-121.

65
59. Mitsuhashi, A.; Hanaoka, K.; Teranaka, T., Fracture toughness of resin modified glass ionomer restorative materials: effects of powder/liquid ratio and powder particle size reduction on fracture toughness. DENT MATER 2003, 19, 747-757.
60. Abou-Zeid, Y. M., The effect of copper oxide on the structural and somephysical properties of Li2B4O7 containing Pb3O4 glasses. MIDDLE EAST J APPL SCI 2012, 2 (1), 1-7.
61. Raibee, S. M.; Nazparvar, N.; Azizian, M.; Vashaee, D.; Tayebi, L., Effect of ion substitution on proterties of bioactive glass: a review. CERAM INT 2015, 41, 7241-7251.
62. Henderson, B.; Nair, S. P., Hard labour: bacterial infection of the skeleton. TRENDS MICROBIOL 2003, 11 (12), 570-577.
63. Sterling, G. J.; Crawford, S.; Potter, J. H.; Koerbin, G.; Crawford, R., The pharmokinetics of Simplex-tobramycin bone cement. J BONE JOINT SURG 2003, 85 (B), 646-649.
64. Witte, W.; Cuny, C.; Klare, I.; Nubel, U.; Strommenger, B.; Werner, G., Emergence and spread of antibiotic resistant gram-positive bacterial pathogens. INT J MED MICROBIOL 2008, (298), 365-377.
65. Valodkar, M.; Modi, S.; Pal, A.; Thakore, S., Synthesis and antibacterial activityof Cu, Ag and Cu-Ag alloy nanoparticles: a green approach. MATER RES BULL 2011, 46 (3), 384-389.

66
4 Investigating the Effect of Copper Addition on Glass Polyalkenoate Cements: Physical, Mechanical and Biological Behavior
Journal of Biomedical Glasses 5 (1), 13-33
doi.org/10.1515/bglass-2019-0002
*S. Mokhtari1, A.W. Wren1.
1 Kazuo Inamori School of Engineering, Alfred University, Alfred NY, USA.
Keywords: Glass Polyalkenoate Cement, Copper, Mechanical, Antibacterial, MTT, bone.
*Address for Correspondence: Sahar Mokhtari Kazuo Inamori School of Engineering, Alfred University, Alfred, New York 14802, USA. Tel: 607-232-0474 email: [email protected]

67
Abstract:
The physical, mechanical, and biological behavior of Cu containing glass
polyalkenote cements were investigated, where copper (Cu2+) was incorporated into a
SiO2-ZnO-CaO-SrO-P2O5 based glass system. Three GPCs were formulated for this study,
a Control and two Cu-GPCs with 6 (CuG6) and 12 (Cu12G) Mol.% of CuO substituted for
the SiO2 in the glass. Rheological evaluation of GPCs determined that the addition of the
Cu decreases the working (Wt) and setting times (St) in the cements. The mechanical
properties of the cements were evaluated after 1 - 21 days incubation in DI water. The
compressive strength (CS) of the cements were found to range between 21-36 MPa, with
Cu6C having the highest CS. Biaxial flexural strength (BFS) and Shear Bond Strength
(SBS) of the GPCs were found to increase with respect to time and were higher for the Cu-
GPCs at 14 MPa and 2.1 MPa respectively. Bioactivity testing was conducted using
Simulated Body Fluid (SBF) which revealed CaP precipitants on each of the GPCs
surfaces. The effect of Cu addition to the GPCs greatly enhanced the antibacterial
inhibition zone (IZ) when tested in E. coli (3mm), S. aureus (24mm) and S. epidermidis
(22mm). Cytocompatibility testing revealed more favorable MC3T3 osteoblast cell
viability when compared to the Control GPC.
4.1 Introduction
According to American Academy of Orthopaedic Surgeons (AAOS), and as of
2014, more than 7 million Americans live with total knee (4.7 million) or total hip (2.5
million) replacements, with more than one million procedures performed each year1. The
annual volumes of orthopaedic interventions are currently rising and have been predicted
to considerably increase in the coming decade1-2. Despite the early stages of clinical
success with the majority of orthopaedic prostheses, studies show 10 years after
implantation approximately 30% of prostheses require revision surgery with aseptic
loosening being the primary reason for the failure of cemented implants3-5. Aseptic
loosening is the disintegration of the interface between bone tissue and the implant, which
can be induced by inadequate initial fixation, leading to osteolysis5. Until now and among
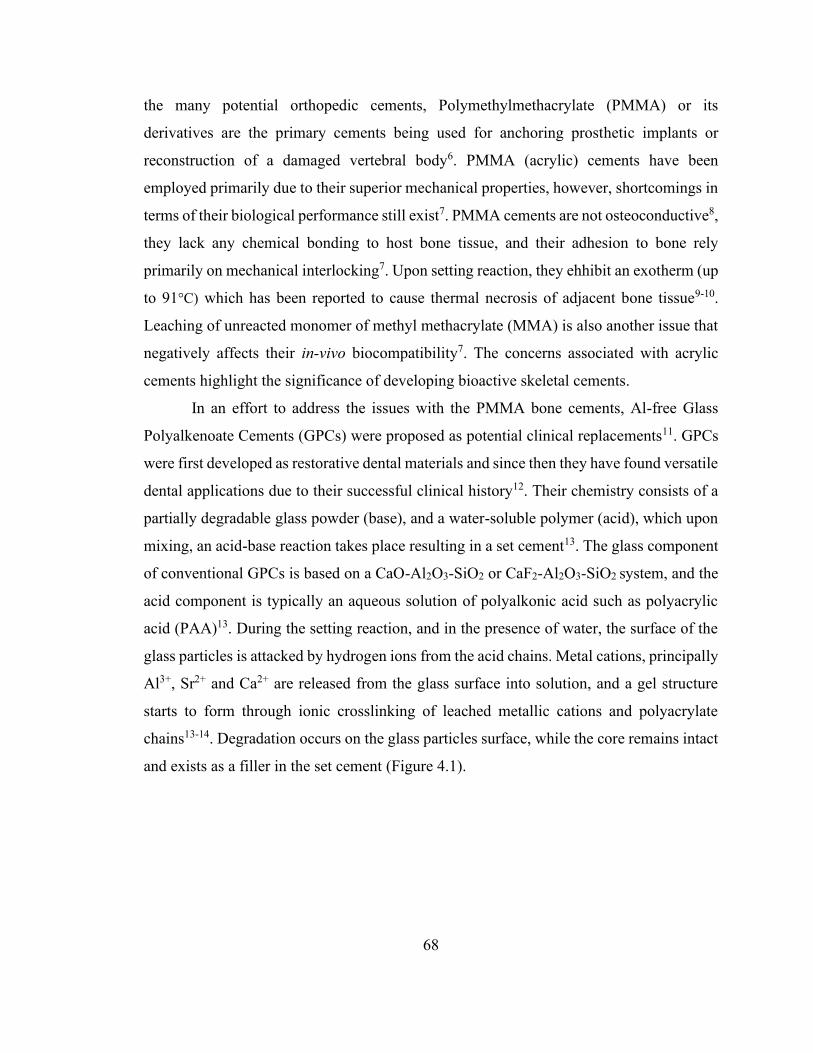
68
the many potential orthopedic cements, Polymethylmethacrylate (PMMA) or its
derivatives are the primary cements being used for anchoring prosthetic implants or
reconstruction of a damaged vertebral body6. PMMA (acrylic) cements have been
employed primarily due to their superior mechanical properties, however, shortcomings in
terms of their biological performance still exist7. PMMA cements are not osteoconductive8,
they lack any chemical bonding to host bone tissue, and their adhesion to bone rely
primarily on mechanical interlocking7. Upon setting reaction, they ehhibit an exotherm (up
to 91°C) which has been reported to cause thermal necrosis of adjacent bone tissue9-10.
Leaching of unreacted monomer of methyl methacrylate (MMA) is also another issue that
negatively affects their in-vivo biocompatibility7. The concerns associated with acrylic
cements highlight the significance of developing bioactive skeletal cements.
In an effort to address the issues with the PMMA bone cements, Al-free Glass
Polyalkenoate Cements (GPCs) were proposed as potential clinical replacements11. GPCs
were first developed as restorative dental materials and since then they have found versatile
dental applications due to their successful clinical history12. Their chemistry consists of a
partially degradable glass powder (base), and a water-soluble polymer (acid), which upon
mixing, an acid-base reaction takes place resulting in a set cement13. The glass component
of conventional GPCs is based on a CaO-Al2O3-SiO2 or CaF2-Al2O3-SiO2 system, and the
acid component is typically an aqueous solution of polyalkonic acid such as polyacrylic
acid (PAA)13. During the setting reaction, and in the presence of water, the surface of the
glass particles is attacked by hydrogen ions from the acid chains. Metal cations, principally
Al3+, Sr2+ and Ca2+ are released from the glass surface into solution, and a gel structure
starts to form through ionic crosslinking of leached metallic cations and polyacrylate
chains13-14. Degradation occurs on the glass particles surface, while the core remains intact
and exists as a filler in the set cement (Figure 4.1).
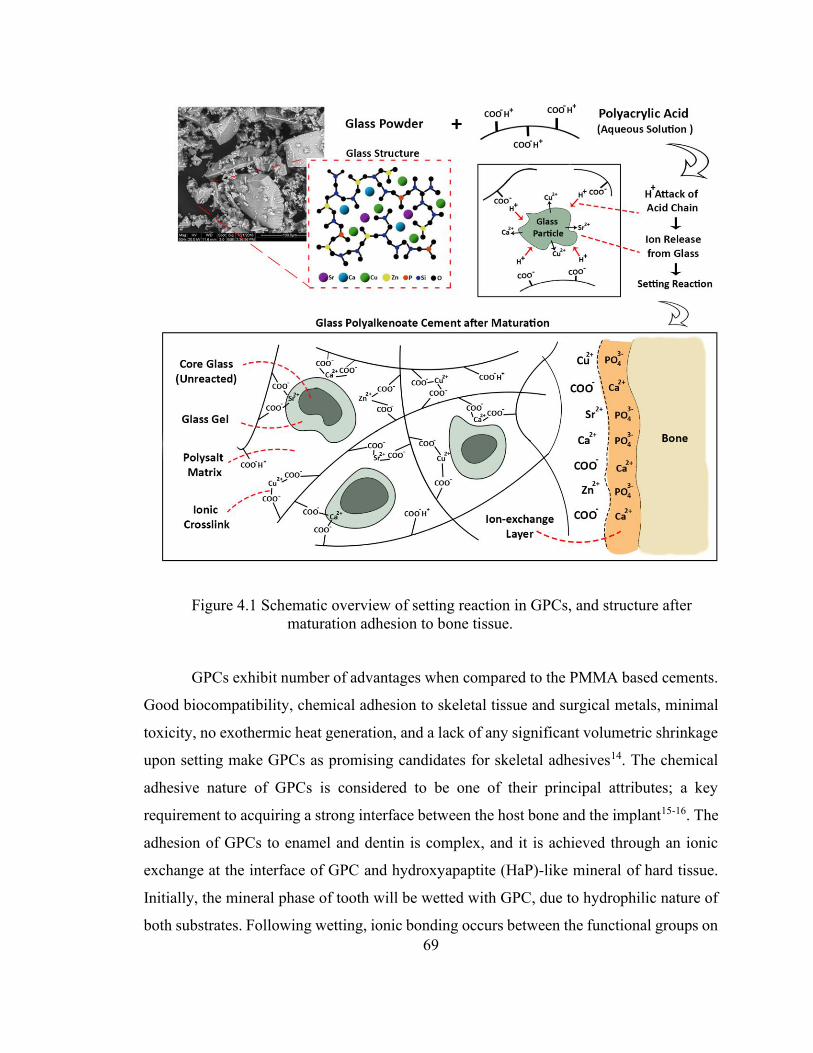
69
Figure 4.1 Schematic overview of setting reaction in GPCs, and structure after maturation adhesion to bone tissue.
GPCs exhibit number of advantages when compared to the PMMA based cements.
Good biocompatibility, chemical adhesion to skeletal tissue and surgical metals, minimal
toxicity, no exothermic heat generation, and a lack of any significant volumetric shrinkage
upon setting make GPCs as promising candidates for skeletal adhesives14. The chemical
adhesive nature of GPCs is considered to be one of their principal attributes; a key
requirement to acquiring a strong interface between the host bone and the implant15-16. The
adhesion of GPCs to enamel and dentin is complex, and it is achieved through an ionic
exchange at the interface of GPC and hydroxyapaptite (HaP)-like mineral of hard tissue.
Initially, the mineral phase of tooth will be wetted with GPC, due to hydrophilic nature of
both substrates. Following wetting, ionic bonding occurs between the functional groups on
70
the acid (typically carboxylate groups) and Ca2+, and PO43- ions on the HaP surface15, 17.
Ultimately, the diffusion of ions such as Ca2+, Sr2+, and PO43- from glass and HaP substrate
within the interfacial zone creates a strongly bonded ion-exchange layer which consists of
ions from both sides (Figure 4.1) 15. Ionic dissolution of glass particles into the surrounding
medium affords GPCs the potential to re-mineralize hard tissue and potentially encourage
physiological processes such as bone regeneration18-19.
One of the primary concerns with the use of conventional GPCs for skeletal
applications, is the presence of Aluminum (Al3+) in the glass. Al3+ plays a critical role in
the glass structure as a network intermediate where it promotes the formation of non-
bridging oxygens (NBO-) and making the glass vulnerable to acid attack20-21. However,
Al3+ is recognized as being neurotoxic and is implicated in diseases such as Alzheimer’s
and Parkinson22-23. Moreover, presence of Al3+ in skeletal tissue negatively affects bone
mineralization24. Therefore, to facilitate the transition from conventional dental GPC to
skeletal adhesive, Al-free GPC were developed by substitution of Al3+ with zinc (Zn2+) 25-
26. Zn2+ provides alternative to Al3+ in the glass with similar structural role as network
intermediate. Additionally, the introduction of Zn2+ improves biocompatibility of cements
as it has been cited to improve osteogenesis27-28. Extensive in vitro and in vivo studies,
suggested encouraging results for the biological performance of Al-free GPCs18, 29. Studies
by Hatton et al showed osteoconduction and new bone formation on the cements (Mp4,
Pilkington, UK) surface after six weeks implantation29-30. Despite GPCs presenting good
biological performance, their poor mechanical strength and poor fracture toughness limit
their application in load-bearing applications31. Different compositions of commercially
available GPCs exhibit compressive strength ranging between 60 to 300 MPa, elastic
moduli of 2 to 10 GPa, and flexural strength up to 50 MPa14.
Modification in chemical composition of the glass, the acid component, and
variations in powder to liquid ratio of GPCs can alter the physical, biological, and
mechanical properties, therefore extending their applications to orthopaedics32. Divalent
cations in the glass have the potential to link two polyanionic chains, where the ionic
strength of the bond proceeds as M=Al3+>Cu2+>Zn2+>Ca2+>Mg2+33. This suggests that
Cu2+ is a mechanically relevant ion when formulating GPCs, because it can act as a strong

71
ionic crosslink to two carboxylic acid (COO-) side groups, resulting in hardened set
materials34. Additionally, Cu2+ has been extensively cited in literature for being an
antibacterial agent35 and has been shown to enhance and stimulate the proliferation of
osteoblast cells and to promote the bone regeneration35-37. Ewald et al. showed enhanced
osteoblastic cell activity and proliferation on the calcium phosphate cements mixed with
Cu2+ solution38. In a study by Wang et al. Cu-doped bioactive borate glass scaffolds showed
a significantly higher capacity to proliferate MC3T3-E1 cells compared to the control
scaffolds39. Several recent studies have demonstrated that Cu2+ stimulates the proliferation
of endothelial cells and promotes angiogenesis, suggesting Cu2+ acts as one of the primary
agents for wound healing applications37, 40-43. Cu2+ can up-regulate the hypoxia-inducible
factor 1 (HIF-1) transcription activity; by stabilizing the expression of hypoxia-inducible
factor 1 (HIF-1α), and the secretion of vascular endothelial growth factor (VEGF)43-44.
Artificially mimicked Hypoxia, has been established as a major pathway to angiogenesis
and vascularization44.
The primary objective of this research will be to investigate the effect that the
Copper (Cu2+) addition has on GPCs formed from a SiO2-CaO-SrO-ZnO-P2O5 glass
system, and the potential as a GPC based bone cement/adhesive. More specifically the
objective of this study is to analyze the effect of Cu2+ on the handling and mechanical
properties, the adhesive bond strength, and in-vitro biological potential of Cu-GPCs.
4.2 Materials & Methods
4.2.1 Glass Synthesis Three glasses were formulated for this study, two Cu containing glasses (CuG6,
CuG12) in addition to a Cu free SiO2-CaO-SrO-ZnO-P2O5 glass (Control). The Cu
containing glasses contain incremental concentrations of CuO at the expense of Silica
(SiO2) (Table 4.1). The powdered mixes of analytical grade reagents (Fisher Scientific, PA,
USA) were oven dried (100°C, 1 h) mixed and fired (1350°C, 2 hr) in platinum crucibles
and shock quenched into water. The resulting frits were dried, ground and sieved to retrieve
glass powders with a maximum particle size of 45μm.

72
Table 4.1 Glass compositions (Mol. Fr).
SiO2 CuO ZnO CaO SrO P2O5 Control 48 0 36 6 8 2 CuG6 42 6 36 6 8 2 CuG12 36 12 36 6 8 2
4.2.2 Cement Formulation Cements were prepared by thoroughly mixing the glass powders (<45μm) with
polyacrylic acid (E11 PAA—Mw, 210,000, <90μm, Advanced Healthcare Limited, Kent,
UK) and de-ionized (DI) water on a clean glass plate. The cements were formulated with
variable powder to liquid (P:L) ratios from 2:1.5 to 2:3.0 with 40wt% additions of PAA
(Table 4.2). Complete mixing was undertaken within 20s.
Table 4.2 Cement formulation for variable P:L ratios and with 40 wt.% concentration of PAA
2:3.0 2:2.5 2:2.0 2:1.5 Glass (g) 1 1 1 1 PAA (g) 0.6 0.5 0.4 0.3
Water (mL) 0.9 0.75 0.6 0.45
4.2.3 Rheological Evaluation The working time (Wt) of the cements was measured under standard laboratory
conditions (Ambient Temp, 25°C), and was defined as the period of time from the start of
mixing during which it was possible to manipulate the material without having an adverse
effect on its properties. Each sample (where n = 5), was measured using a stopwatch on a
clean glass plate with a sterile spatula. The setting time (St) of the cement series was tested
in accordance with ISO991745 which specifies the standard for dental water based cements.
Cements were stored at 37°C during setting period, and St was measured by lowering a 400
g mass attached to a Gilmore needle into a cement filled mould with 8×9×10 mm internal
diameter. St was taken as the time the needle failed to make a complete indent in the cement

73
surface. Each measurement was conducted under the same mixing conditions to ensure
reproducibility.
4.2.4 Compressive Strength The compressive strength (CS) of the cements (6×4mm, where n = 5) were
evaluated in accordance with ISO991745. Cylindrical samples were tested after 1, 7, 14,
and 21 days incubation in DI water. Samples were stored in sterile DI water in an incubator
at 37°C, after the incubation time has expired the cements were removed and tested while
wet on an Instron 4082 Universal Testing Machine using a 5 kN load cell at a crosshead
speed of 1 mm/min. The CS (MPa) was calculated using Equation. 1. Where ρ is the
maximum applied load (N) and d is the diameter of sample (mm).
𝐶𝑆 =4𝜌
𝜋𝑑2 (1)
4.2.5 Biaxial Flexural Strength The biaxial flexural strength (BFS) of the cements (where n = 5) were evaluated
by a method described by Williams et al 46. Cement discs measuring (2×12ømm) were
tested after 1, 7, 14, and 21 days. Samples were stored in sterile DI water in an incubator
at 37°C. At each time period, the cements discs were removed and tested while wet on an
Instron 4082 Universal Testing Machine using a 1 kN load cell at a crosshead speed of 1
mm/min. The BFS (MPa) was calculated using Equation. 2. Where ρ is the fracture load
(N), t is the sample thickness (mm) and r is the radius of the support bearing (mm).
𝐵𝐹𝑆 =𝜌
𝑡2{0.63 ln(𝑟/𝑡) + 1.156} (2)
4.2.6 Shear Bond Strength Shear bond strength (SBS) testing was conducted according to ISO 2902247.
Briefly, cylindrical cement samples (6×4ømm, where n = 15) were mounted on
hydroxyapatite (HaP) plates which were pre-mounted in resin and ground using 125μm
grit size. Samples were bonded to the HaP surface and left for 1 hour to set. The split ring
molds were then removed, and the bonded samples were incubated in DI water for 1, 7, 14,
and 21 days at 37°C before testing. The test was conducted at a crosshead speed of 1.0
74
mm/min until failure. The SBS (MPa) was calculated using Equation. 3. Where ρ is the
fracture load (N) and Ab is the bonding area expressed in mm2.
𝑆𝐵𝑆 =𝜌
𝐴𝑏 (3)
4.2.7 Laser Profilometry Laser Profilometry was performed on a Solarius Laserscan Profilometer (Solarius,
Ca, USA), with a vertical sensor resolution of 10μm, and spot size of 2μm. Analysis of
data was performed using Solar Map Version 5.0.4.5261 software.
4.2.8 Ion Release Profile Each of the cement discs (2×12ømm, where n = 5) were incubated in 10 mL of
sterile DI water and rotated on an oscillating platform at 37°C for 1, 7, 14 and 21 days.
After each time period, the extracts were prepared by removing the cement disc and
filtering the remaining liquid. The ion release profiles of the liquid extracts were measured
using Inductively Coupled Plasma–Optical Emission Spectroscopy (ICP–OES) on a
Perkin- Elmer Optima 3000DV (Perkin-Elmer, MA, USA). ICP–OES calibration standards
for Ca2+, Si4+, Zn2+, PO43-, Sr2+ and Cu2+ were prepared from a stock solution on a
gravimetric basis. Three target calibration standards were prepared for each ion and DI
water was used as a control.
4.2.9 Simulated Body Fluid Trial Simulated body fluid (SBF) was prepared with the ionic concentration similar to
that of human blood plasma, and in accordance with the procedure outlined by Kokubo et
al48. Each cement disc (2×6ømm, where n = 3) was subsequently immersed in a fixed
volume of SBF according to Eq. 4. Where Vs is the volume of SBF used (mL) and Sa is
the exposed surface area of the cement disc (mm2). Specimens were stored in plastic
containers for 1, 7, 14 and 21 days. After the specified incubation time, the specimens were
removed from the SBF, gently rinsed in DI water and oven dried (37˚C, 24 h). Changes in
the surface morphology of the incubated samples after soaking in SBF were characterized
by scanning electron microscopy (SEM).
𝑉𝑠 =𝑆𝑎
10 (4)

75
4.2.10 Scanning Electron Microcopy (SEM) A FEI Co. Quanta 200F Environmental Scanning Electron Microscope (SEM)
equipped with an EDAX Genesis Energy-Dispersive Spectrometer was used to obtain
secondary electron images and carry out chemical analysis of the surface of the discs. All
EDX spectra were collected at 15 kV, using a beam current of 26 nA. Quantitative EDX
converted the collected spectra into concentration data by using standard reference spectra
obtained from pure elements under similar operating parameters.
4.2.11 Antibacterial Analysis - Agar Diffusion The cement discs (2 × 6ømm, where n = 3) were initially sterilized by placing discs
under UV light for 3 hours prior to testing. The antibacterial activity of the cements was
evaluated using E. coli strain ATCC 8739 (LB agar and broth), S. epidermidis strain ATCC
14990 (BHI agar and broth), S. aureus (TSB agar and broth) using the agar diffusion
method. Each microbe was initially grown aerobically in liquid broth at 37˚C for 24 hours.
The agar diffusion test was performed under standard laboratory sterile conditions in a
fumigation hood using sterile swabs for inoculation of bacteria. Each cement disc was
placed within an inoculated plate and cultured for 24 hours at 37˚C. Preparation of the agar
disc diffusion plates involved seeding agar plates with a sterile swab dipped in a 1/50
dilution of the appropriate 24-hour culture of bacteria. Symbiosis protocol 3 colony counter
was used for imaging of the bacterial plates. Calipers were used to measure zones of
inhibition where each sample was analyzed in triplicate and mean zone sizes ± standard
deviations were calculated. Inhibition zone sizes were calculated using Equation. 5.
𝐼𝑛ℎ𝑖𝑏𝑖𝑡𝑖𝑜𝑛 𝑍𝑜𝑛𝑒 (𝑚𝑚) =𝐻𝑎𝑙𝑜∅−𝐷𝑖𝑠𝑐∅
2 (5)
4.2.12 Antibacterial Analysis - Bacterial Broth The antibacterial activity of the cements was evaluated against three strains of
bacteria, using the bacterial broth method. Luria agar and broth were used for the culture
of E. coli, which was grown aerobically at 37 °C. Similarly, S. epidermidis strain ATCC
14990, and S. aureus were also used and were cultured in BHI, and TSB agar and broth,
respectively. Each cement sample (2×12ømm, where n = 5) was exposed to 10 mL of
sterile DI water and rotated on an oscillating platform at 37°C for 1, 7, 14 and 21 days.

76
After each time period expired, liquid extracts were removed. Bacterial solutions were
prepared by growing microbes aerobically in liquid broth at 37˚C for 24 hours. The
antibacterial efficacy was tested in 98 well plates in 9 replicates, where aliquots (20 μL) of
undiluted cement extracts were added into wells containing (80 μL) bacterial solution and
were inoculated over a time period of 24 hours in a sterile incubator at 37 °C. The
experimental extracts were compared against a healthy growing population of E. coli, S.
epidermidis and S. aureus at each time period. A sterile control (sterile DI water and broth)
was also analyzed as the liquid medium background. At each time period, the broth was
examined by UV–Visible light spectroscopy (Pharmacia biotech ultrospec 3000 UV–
Visible light spectrophotometer) at 600 nm for the transmission (%T) through the liquid
medium.
4.2.13 Cytotoxicity - MTT assay The established cell line MCT3T osteoblasts was used in this study as required by
ISO10993 part 549. Cells were maintained on a regular feeding regime in a cell culture
incubator at 37 °C/5 % CO2/95 % air atmosphere. The culture media used was HyClone
MEM Alpha Modification (1X) media (Thermo Scientific, MA, USA), which included L-
glutamine, ribonucleosides, and deoxyribonucleosides, and was supplemented with 10
vol% fetal bovine serum (Thermo Scientific, MA, USA). The cytotoxicity of cement
extracts was evaluated using the methyl tetrazolium (MTT) assay in 96 well plates in 9
replicates. Aliquots (10 μL) of undiluted cement extracts over 1,7,14, and 21 days were
added into wells containing MCT3T cells in (100 μL) culture medium. Cells were seeded
at a density of 10,000 cells per well and incubated for 24 hours. The MTT assay was then
added in an amount equal to 10 % of the culture medium volume/well. The cultures were
then re-incubated for a further 4 h (37 °C/5 % CO2). Next, the cultures were removed from
the incubator and the resultant formazan crystals were dissolved by adding an amount of
MTT Solubilization solution (10 % Triton X-100 in acidic isopropanol (0.1 NHCI)) equal
to the original culture medium volume. Once the crystals were fully dissolved, the
absorbance was measured at a wavelength of 570 nm. Aliquots (100 μl) of tissue culture
water were used as controls, and cells were assumed to have metabolic activities of 100 %.

77
4.2.14 Statistical Analysis Statistical analysis was conducted to compare mechanical properties, antibacterial
efficacy, and cytocompatibility of cements in relation to 1.) maturation time in DI water
over 1, 7, 14 and 21 days, and 2) differences between the cement compositions (ConC,
Cu6C and Cu12C) at each individual time period. SPSS 19.0 Statistics Software was used
to conduct one-way analysis of variance (ANOVA). Comparison of relevant means was
performed using the post hoc Bonferroni test. Differences between groups were deemed
significant when p < 0.05.
4.3 Results
Three different glasses were synthesized as; Control, CuG6 and CuG12, where
CuG6 and CuG12 containing 6 and 12 Mol.% of CuO at the expense of silica (Table 4.1).
Control, CuG6 and CuG12 glasses were used to form GPCs where the cement formulations
(Table 4.2) were prepared by varying the P/L ratio at a PAA concentration of 40wt%. The
GPCs working (Wt) and setting times (St) were analyzed as a function of powder to liquid
(P/L) ratio, ranging from 2:1.5 to 2:3.0. The results are presented in Table 4.3. For Control
and Cu-GPCs (Cu6C, and Cu12C), Wt was decreased by decreasing the P/L ratio from
2:3.0 to 2:1.5, where Wt at P/L of 2:3.0 was found to be 1m, 58s for ConC, 1m, 38s for
Cu6C, and 1m, 10s for Cu12C. At P/L of 2:1.5, the Wt values were found to be 41s, 46s,
29s, for ConC, Cu6C, and Cu12C, respectively. Similar trend was observed for the St of
the cements. The longest St was observed at P/L of 2:3.0 with 10m, 16s for ConC, 7m, 45s
for Cu6C, and 6m, 04s for Cu12C and while the shortest St occurred at P/L of 2:1.5, with
130s, 55s, and 18s, respectively. Within each P/L ratio formulation, the ConC cement
presented the longest Wt and St, and Cu12C showed the shortest Wt and St.
Table 4.3 Working (Wt) and Setting (St) times of ConC, Cu6C, and Cu12C formulated with 40wt% PAA, and variable P/L ratios.
Working Times (min,sec) Setting Times (min,sec) P/ L Ratio ConC Cu6C Cu12C ConC Cu6C Cu12C
2:3.0 1m, 58s 1m, 38s 1m, 10s 10m, 16s 7m, 45s 6m, 04s 2:2.5 1m, 32s 1m, 37s 57s 4m, 32s 5m, 31s 3m, 45s 2:2.0 1m, 06s 1m, 04s 46s 3m, 16s 2m, 56s 1m, 11s 2:1.5 41s 46s 29s 2m, 10s 55s 18s

78
To investigate the mechanical properties of the GPCs, compressive strength, biaxial
flexural strength and shear bond strength testing were performed. Initially, cements with
differing P/L ratios were incubated in DI water for 14 days. Their compressive strengths
(CS) were calculated and the results are presented in Figure 4.2a. The highest CS for
Control and Cu6C were attained at P/L of 2:2.5, with 28 MPa and 30 MPa, respectively.
The highest CS for Cu12C was found to be 25 MPa at P/L ratio of 2:3.0. Based on the
cements handling properties (Wt and St) and preliminary CS results, P/L ratio of 2:2.5 was
chosen for formulating the cement series and to further analyze mechanical properties and
biological behavior. To determine the effects of maturation time on mechanical properties,
each cement was tested for CS after 1, 7, 14, and 21 days incubation in DI water at 37°C
and the results are presented in Figure 4.2b. For each of the cement composition, CS
remained relatively unchanged over the 1 to 21 days incubation period, however, Cu6C
exhibited higher CS compared to ConC and Cu12C. The CS of Control, Cu6C and Cu12C
after 21 days incubation in DI water were at 28, 33, and 25MPa respectively.
Figure 4.2 (a) Compressive strength of ConC and Cu-GPCs using variable P/L ratios after 14 days incubation in DI water, and (b) Compressive strength with P/L ratio of 2:2.5 after 1, 7, 14, and 21 days incubation in DI water.
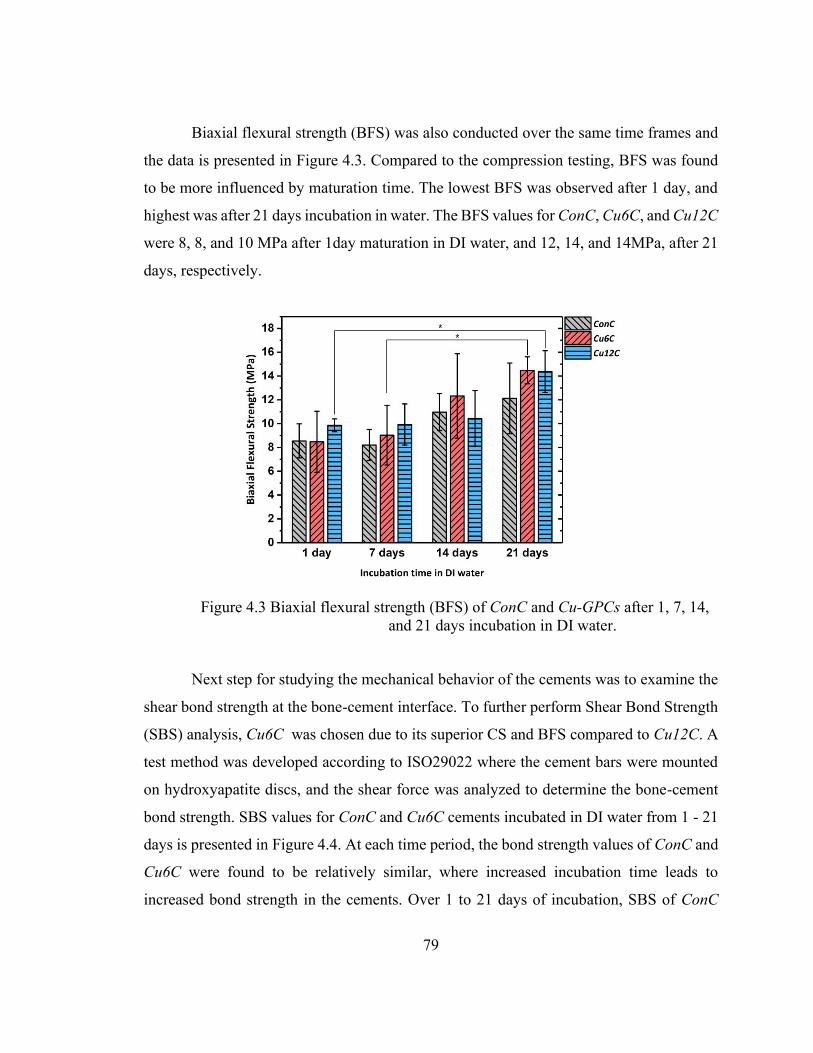
79
Biaxial flexural strength (BFS) was also conducted over the same time frames and
the data is presented in Figure 4.3. Compared to the compression testing, BFS was found
to be more influenced by maturation time. The lowest BFS was observed after 1 day, and
highest was after 21 days incubation in water. The BFS values for ConC, Cu6C, and Cu12C
were 8, 8, and 10 MPa after 1day maturation in DI water, and 12, 14, and 14MPa, after 21
days, respectively.
Figure 4.3 Biaxial flexural strength (BFS) of ConC and Cu-GPCs after 1, 7, 14, and 21 days incubation in DI water.
Next step for studying the mechanical behavior of the cements was to examine the
shear bond strength at the bone-cement interface. To further perform Shear Bond Strength
(SBS) analysis, Cu6C was chosen due to its superior CS and BFS compared to Cu12C. A
test method was developed according to ISO29022 where the cement bars were mounted
on hydroxyapatite discs, and the shear force was analyzed to determine the bone-cement
bond strength. SBS values for ConC and Cu6C cements incubated in DI water from 1 - 21
days is presented in Figure 4.4. At each time period, the bond strength values of ConC and
Cu6C were found to be relatively similar, where increased incubation time leads to
increased bond strength in the cements. Over 1 to 21 days of incubation, SBS of ConC

80
ranged between 1.4 to 1.9 MPa, and for Cu6C it ranged from 1.3 to 2.1 MPa. A summary
of the mechanical properties of the Control and Cu-GPCs after different incubation time
periods is presented in Table 4.4.
Figure 4.4 Shear bond strength of ConC and Cu-GPCs after 1, 7, 14, and 21 days incubation in DI water.
Table 4.4 Summary of mechanical properties of ConC, Cu6C, and Cu12C after incubation in DI water for 1, 7, 14, and 21 days
Compressive Strength (MPa)
Biaxial Flexural Strength (MPa)
Shear Bond Strength (MPa)
ConC Cu6C Cu12C ConC Cu6C Cu12C ConC Cu6C 1 Day 24.14 27.06 20.55 8.55 8.48 9.86 1.42 1.32 7 Days 27.66 36.21 24.24 8.20 9.03 9.93 1.51 1.81
14 Days 28.28 30.26 21.64 10.97 12.33 10.43 1.82 1.95 21 Days 28.85 33.47 25.24 12.12 14.48 14.37 1.91 2.1
To provide further insight into the mechanism of interfacial failure, laser
profilometry was performed on the surface of the tested shear bond strength samples. 3D
micro-topography of the fracture surface of ConC and Cu6C after 1 and 21 days incubation
in DI water is presented in Figure 4.5, where the smooth blue background represents the
HaP surface, and the circular mark illustrates the fractured surface of the cement cylinders.

81
The scale bars in Figure 4.5 represents the vertical height (Z), which is demonstrated at the
same range (0 to 1.5mm) for all the scans (X = 7 mm, Y = 7 mm, Z = 1.5 mm). The surface
topography scans presented in Figure 4.5 highlight the distribution of the residual cements
after failure compared to the smooth HaP surface. Projected scan area in Figure 4.6, shows
the vertical height analysis of the scanned area presented in Figure 4.5, displaying the
change in vertical height (Z) of the surface extending from the residual cement disc to the
edges of the HaP background. For each scan, three ranges of the surface height values (Z)
with the corresponding percentage, are presented. The smoothest surface was observed
after 1day incubation, with approximately 63% and 76% of total area of the sample ≤ 0.25
mm in height, for Conc and Cu6C, respectively.
Figure 4.5 Laser profilometry images of the fracture surface of ConC and Cu6C after adhesive shear bond analysis, 1 and 21 days incubation in DI water.

82
Further analysis of the samples surface after 21 days, shows a significant change in
the topography for Cu6C, displaying distinct circular mark of residual cement. For Cu6C,
approximately 25% of total area of the sample was determined to be higher than 0.85 mm
in height, to maximum of 1.27 mm. After 21 days, ConC showed lower height parameters
compared to Cu6C, with maximum height occurring between 0.55 – 0.83 mm covering
approximately 25% of total area.
Figure 4.6 Projected scan areas of laser profilometry images (Figure 3.5) of ConC and Cu6C fracture surface after 1 and 21 days incubation in DI water, analyzing vertical height (Z) range and corresponding % of total area.

83
Optical microscopy images of the fracture surface of Cu6C cements after 1 and 21
days incubation in DI water are presented in Figure 4.7. In Figure 4.7, the white background
is the HaP surface, and Cu6C cement appeared as darker green.
Figure 4.7 (a) Shear bond strength testing setup and (b) optical microscopy images of fracture surface of Cu6C after 1, and 21 days.
To quantify the ion release from each cement, ICP-OES was performed on the
cements discs incubated in DI water over 1, 7, 14, and 21 days. Ion release profiles were
determined for each cement composition including Si, Zn, Ca, P, Cu, and Sr, and the
corresponding results are illustrated in Figure 4.8. Si release was found to increase with
respect to incubation time for all three GPCs. ConC exhibited higher release of Si compared
to Cu-GPCs, with a high burst of ions over the first 7 days and then a steady release up to
21 days. Si release for ConC ranged from 25 to 104 mg/L. However, Si release for Cu-
CPCs showed a relatively linear trend with consistent release over the 1 - 21 day incubation
period. Si release for Cu6C and Cu12C ranged from 49 to 82 mg/L and 43 to 79 mg/L,
respectively. Zn release was relatively low, with no release in the first 24 hours for all
GPCs. ConC had the lowest Zn release with 0 to 0.1 mg/L. Cu-GPCs exhibited very similar
levels of Zn release, but higher than the ConC cement. Cu6C and Cu12C released 1.9 and
1.6 mg/L Zn after 21 days. Ca release profiles of ConC and Cu-GPCs were similar with

84
none of the cements having significantly higher release than others. All the cements
showed a gradual increase in their Ca release over 1 to 21 days. The same trend was also
observed for Sr release. Over the experimented time period of 1 to 21 days, Ca release was
found to range from 0 to 1.3, 1.7 and 1.4 mg/L, and Sr release ranged from 1.5 to 5.7, 1.9
to 5.9 and 1.7 to 5.3 mg/L for ConC, Cu6C and Cu12C, respectively. On the other hand,
the results of P release from the cements showed higher ion release for the ConC cements
compared to Cu-GPCs, ranging from 3.7 to 8.3 mg/L. However, P release of Cu-GPCs
remained constant over the course of 21 days. P release from Cu6C was found to range
from 4.4 to 5.2 mg/L, and for Cu12C this was found to range from 3.4 to 4.9 mg/L. Cu-
GPCs were also examined for the Cu release. The results from Figure 4.8, indicates steady
release of Cu from GPCs over 1 to 21 days. Cu release reached 2.1 mg/L at day 1 for Cu6C
remained relatively constant for the next 21 days, with 2.1 mg/L at day 21. For Cu12,
highest amount of Cu release was at day one with 2.5 mg/L. After 21 days incubation, Cu
release levels was found to be 2.4 mg/L for Cu12C.

85
Figure 4.8 Ion release profiles of ConC and Cu-GPCs, investigating Si, Zn, P, Sr, Ca and Cu release after 1, 7, 14 and 21 days incubation in DI water.
Simulated Body Fluid (SBF) trials were conducted for each GPC to evaluate their
preliminary in-vitro bioactivity. SBF trials were performed on the cement discs over 1 to
21 days of immersion, and SEM images of the depositions on the surface of ConC, Cu6C,
and Cu12C after 21 days incubation in SBF, along with their corresponding EDX spectra,
are presented in Figure 4.9.

86
Figure 4.9 SEM micrographs of surface of ConC and Cu-GPCs and corresponding EDX after 21 days incubation in SBF.
As shown in Figure 4.9, all three GPCs presented a similar morphology of spherical
precipitants on the surface after 21 days incubation in SBF. The clusters of spherical shaped
particles are attributed to CaP formation on the surface50-51. EDX spectra presents (Figure
4.9) the semi-quantitative elemental composition (wt%) of the CaP depositions which
showed the presence of Si, Sr, P, Ca, Zn, and Cu (only in Cu-GPCs). EDX elemental

87
composition of the spherical surface precipitants after immersion in SBF reveal relatively
low amount concentrations of Si on the surface with 2, 1, and 1 wt% for ConC, Cu6C, and
Cu12C respectively. However, considerably higher concentrations of Ca and P, and Zn are
present when compared to initial glass composition, with 12, 17, and 16 wt% of Ca, and
18, 26 and 26 wt% of P, and 58, 45, and 44 wt% of Zn for ConC, Cu6C, and Cu12C
respectively. Moreover, EDX results confirmed the presence of 2, and 3 wt% of Cu on the
surface depositions of Cu6C and Cu12C, respectively.
To assess the antibacterial efficacy of the cements and to determine the potential of
Cu ions on the cement’s antibacterial properties, two different test methods were employed.
First, agar diffusion testing was conducted on the cement discs with a range of bacteria.
Result of agar diffusion testing is presented in Figure 4.10a. It is evident from Figure 4.10a
that ConC cement showed the smallest inhibition zone (IZ) of any bacteria tested compared
to Cu-GPCs. Measurements of IZ of agar diffusion test are presented in Figure 4.10 (b,
c,d). No inhibition was observed for ConC testing in E. coli, and S. aureus. The only IZ
observed for ConC was 1.7 mm testing in S. epidermidis. In contrast to Control cement,
Cu-GPCs demonstrated significantly higher antibacterial activity, particularly with S.
epidermidis and S. aureus (Figure 4.10). IZ calculated for Cu6C cement was 1.9 mm, 21.3
mm, and 20.5 mm when tested in E. coli, S. epidermidis and S. aureus, respectively Figure
4.10 (b, c,d). Cu12C exhibited 3.0 mm, 21.6 mm, and 23.9 mm IZ when tested in E. coli,
S. epidermidis and S. aureus, respectively.

88
Figure 4.10 (a) Agar diffusion antibacterial testing of ConC, Cu6C, and Cu12C in E. coli, S. epidermidis, and S. aureus, (b, c, d) Inhibition Zone (IZ) of ConC, Cu6C, and Cu12C employing the antibacterial agar diffusion method.
Further, to quantify the antibacterial properties of the cements as a function of time,
bacterial-broth test was performed on the liquid extracts incubated in DI water over 1 - 21
days. The same three bacterium were tested, and the results are presented in Figure 4.11.
Bacterial viabilities for Cu-GPCs were reduced as low as 5% for E. coli, 3% for S.

89
epidermidis, and 2% for S. aureus. For ConC, the viability was found to be lower when
compared to healthy growing E. coli, and S. aureus with 83%, and 95% viability,
respectively. However, the bacterial viability of the ConC in S. epidermidis, was increased
from 96 to 113, 122, and 123% after 1, 7, 14, and 21 days. Apart from the ConC in S.
epidermidis, all the other cements exhibit relatively stable viability with respect to time.
Figure 4.11 Bacterial viability of ConC and Cu6C, Cu12C extracts after, 1, 7, 14 and 21 days incubation in DI water employing the bacterial broth method. Each test analyzed the GPCs efficacy in (a) E. coli, (b) S.epidermidis, and (c) S. aureus.
To analyze the cytotoxicity of the cement series, MTT assay was performed on the
GPC liquid extracts post incubation in DI water after 1, 7, 14, and 21 days. Cell viability
was conducted using MC3T3-E1 osteoblast precursor cell line and the results are presented
in Figure 4.12. All the experimental cements tested, had lower viability compared to
healthy growing osteoblast cells with a metabolic rate of 100%. ConC expressed cell
viability of 90, 77, 78, and 58% at 1, 7, 14, and 21 days incubation time, respectively. Cu-
GPCs induced lower cell viability compared to the ConC at day 1, however their viability
was higher than ConC after 21 days. Cu6C exhibited cell viability of 81, 85, 86 and 71%,
and Cu12C expressed viability of 72, 73, 71, and 69 % after 1, 7, 14, and 21 days
respectively. None of the extracts caused a reduction in cell viability lower than 58%,
which was presented by the Control GPC after 21 days incubation.

90
Figure 4.12 MC3T3-E1 cell viability of ConC and Cu6C, Cu12C extracts after 1, 7, 14, and 21 days incubation in DI water
4.4 Discussion
The glasses used for this study were based on a SiO2-CaO-ZnO-SrO-P2O5 system
with incorporation of CuO. The novel Al-free compositions were designed by
incorporating of Cu2+ in the glass chemistry, such that the resultant GPCs present
satisfactory handling and mechanical properties, and also provide a therapeutic effect upon
release from the GPC. The structure of the glasses were characterized in an earlier study
by the authors34. Control and Cu-GPCs were formulated with a range of different P/L ratios
(2:3.0 to 2:1.5) and their Wt and St is presented in Table 4.3. Two independent trends were
observed for the rheology as a function of 1) glass chemistry and 2) different P/L ratios.
The first observation was that, by incorporating CuO in the glass, the Wt and St decreases.
For all different P/L ratios, ConC had the longest and Cu12C had the shortest Wt and St,
respectively. This may be attributed to number of different physiochemical processes. The
susceptibility of the glass to acid attack is modified by the composition of the glass and
liberation of different metal cations in the aqueous solution. Ions released by the glass
particles interact with charged acid chains, resulting in gelation and further hardening of
the cement. The reduction in setting times as observed in Cu-GPCs is likely due to presence
of divalent cations of Cu2+ which have the potential to crosslink two polyanionic chains.
91
Release of Cu2+ ions from Cu6C, and Cu12C glasses increases the concentration of metal
cations in the solution, which further accelerates the chelation and shortens the setting
times. Accordingly, Cu12C with a higher concentration of CuO, had shorter Wt and St
compared to Cu6C. An additional observation noted was that by increasing the P/L ratio,
the Wt and St increases for all the cements. The liquid component consists of the acid (PAA)
and water. Typically, a higher concentration of PAA results in increasing the number of
COO- groups in the liquid, thus accelerating the setting reaction. However, an opposite
trend was observed here. The Wt and St were delayed by increasing the liquid in
formulation. One possible explanation is that by increasing the liquid content, system
becomes more fluid. This makes the cement mix more dilute, decreases the initial viscosity,
and this decreases the availability of binding sites for chelation thereby delaying the
crosslinking process. An ideal bone cement should have an extended Wt to allow sufficient
manipulating, and a rapid St to reduce the risk of infection33. The experimental GPCs
presented here exhibit typical Wt and St observed for dental GPCs. For commercially
available dental GPCs the Wt is quoted to range from 1.3 - 3.8 minutes and the St is reported
to range between 2.7 - 6.2 minutes33. Yet, the majority of commercially available acrylic
based cements for skeletal applications have longer Wt ranging between 3-8 minutes and
St ranging between 6-14 minutes52. The St of the GPCs formulated in this study is
comparable with commercially available bone cements, however, their Wt falls shorter than
timeframes proposed for Vertebroplasty or Kyphoplasty with a recommended range
between 5-8 minutes52.
The mechanical properties of the cements were evaluated with compression,
flexural, and shear bond strength testing outlined by ISO standards where applicable.
Figure 4.2a illustrates the effect of differing P/L ratio and differing maturation time on the
GPCs compressive strength. The results from Figure 4.2a, indicates that the CS was not
significantly affected by neither P/L ratio nor maturation time (p > 0.05), however, it was
influenced by chemistry of the glasses. Highest strength was obtained by Cu6C with
significantly higher CS values compared to ConC and Cu12C (p=0.000) during 1 to 21
days of incubation period. Cu12C identified as the weakest cement with significantly lower
CS compared to ConC (p=0.003), and Cu6C (p=0.000). Figure 4.2b suggests that cements

92
attain most of their CS in their first 24 hours and then retain their strength with respect to
incubation time. Compressive strengthening in GPCs can be explained by analyzing the
microstructure of cements. As described earlier, after initial stages of setting reaction, the
set cement consists of intact glass particles which are surrounded by a crosslinked polysalt
matrix13. The mechanical strength can be attributed to the magnitude of complexation
within the polysalt matrix. The extent, and the strength of the complexation, depends on
the glass solubility and release of specific cations involved in GPC maturation, the degree
of naturalization, polyacrylic molecular weight and concentration53. With regard to Cu-
GPCs, increased release of Cu2+, facilitates a higher degree of the interaction between the
cations and polyanion chains which increases the extent of crosslinking in the cement
structure which contributes to increased CS as presented for Cu6C (Figure 4.2b). Unreacted
glass particles act as reinforcing agent within the cement matrix. The experimental GPCs
examined here, exhibit lower range of CS (20-35 MPa) compared to commercially
available bone cements which range between 80-100 MPa for Vertebroplasty or
Kyphoplasty52, and conventional dental GPCs which ranging between 60-300 MPa14. CS
of Fuji IX and Ketac Molar, one hour after mixing, has been quoted to be of 84 and 86
MPa, respectively 54.
In studying the mechanical properties of GPCs, CS is not particularly reliable, since
the fracture mode of GPCs at the atomic level is accompanied by tensile or shear failure
rather than compression47, 55. Tensile measurement of brittle materials such as GPCs comes
with its own limitations, therefore, BFS is considered as the more relevant analysis to
assess tensile strength of the GPCs. BFS of ConC and Cu-GPCs as a function of incubation
in DI water is illustrated in Figure 4.3. ConC and Cu-GPCs show similar values (p > 0.05)
at each time period: 12, 14 and 14 MPa for Control, Cu6C, and Cu12C after 21 days
incubation. The BFS for each GPC was observed to slightly increase with respect to
maturation time. This effect may be attributed to the ongoing dissolution of the glass
particles resulting in increased crosslinking. The setting reaction of these cements takes
place in three stages; dissolution, gelation and maturation13. The first two stages are
typically completed within the first 24 hours, however maturation accompanied with
additional crosslinking can take place over extended time periods14. Increased

93
concentration of polysalt crosslinked COO- groups increases the BFS of cements which
range from 8-14 MPa. BFS values attained here can be considered for non-load bearing
skeletal applications, and is comparable with the values for commercially available CPCs
such as Cementek (Teknimed, Toulouse, France) and α-BSM (ETEX Corporation, MA,
USA) that have flexural strengths of 9 MPa and 4 MPa respectively49.
To further evaluate the mechanical and adhesive nature of these Cu-GPCs, shear
bond strength (SBS) testing was performed on the ConC and Cu6C cements which
exhibited higher CS and BFS compared to Cu12C. The SBS results are presented in Figure
4.4. SBS testing can provide an insight into the extent of chemical bonding at the cement-
bone tissue interface. Studies on the adhesion mechanism of GPCs to dentin and enamel
suggest that chemical bonding is developed with the HaP mineral phase, rather than the
collagen component15. Initially when freshly mixed cement paste is placed on surface, it
will be wetted due to the hydrophilic nature of HaP15. Gradually, ionic bonds will develop
between free COO- groups from the PAA and calcium and phosphate ions from HaP. As
time proceeds a diffusion process occurs where ions from the cement and the HaP diffuse
to an interfacial zone. Eventually, the ion exchanged layer consists of calcium and
phosphate ions from HaP in addition to ions liberated from the glass phase of the GPC15,
17. This may explain the increase in SBS of the GPC with respect to time. Glass dissolution
and diffusion of ions over time will contribute to development of a strongly ion exchanged
interface. With respect to this study, surface topography was analyzed with laser
profilometry of cement-HaP interface post fracture, and the effect of incubation time on
the bond strength. The results from Figure 4.5 and accompanying surface characteristics
(Figure 4.6) present visible differences in the topography of the fractured samples after 1
and 21 days incubation. Comparison of each GPC surface after 1 and 21 days presents two
different failure mechanisms. Smooth fracture surface (Figure 4.5) of the GPCs after 1 day
suggests little to no chemical bonding is developed at the interface and thus cements fail
adhesively at the interface. Materials that experience adhesive failure typically exhibit low
bond strength15, 56. However, after 21 days a considerable amount of the GPC was adhered
HaP, post fracture. This suggests an alternative mechanism of failure. Rough fracture
surface of the ConC and Cu6C after 21 days in Figure 4.5 and Figure 4.6, suggests that

94
cohesive failure occurs within the cement rather that at the interface. This observation is
more clear for Cu6C cements after 21 days incubation period. A considerable amount of
residual cement at the interface of Cu6C after 21 days suggests that extensive chemical
bonding has occurred. This can be further confirmed with optical microscopy images taken
from the Cu6C fracture surface after 1 and 21 days incubation (Figure 4.7). It is evident
the incubation time leads to increased crosslinking and maturation within the GPC, and
additionally the addition of Cu to the glass phase of the GPC greatly improves the adhesive
nature of the material.
In order to determine the solubility, and to further analyze potential therapeutic
effects of the cements, ion release profiles were analyzed with respect to incubation time.
Levels of Si, Zn, Ca, Sr, P, and Cu were released from cements after 1, 7, 14 and 21 days
(Figure 4.8). Overall, Cu-GPCs exhibited similar ion release profiles, however, the ConC
and Cu-GPCs presented different behavior for Si, Zn, and P release. Gradual and steady Si
release plays a key role in the process of in vivo mineral formation. Release of Si ions from
the glass into physiological solution results in formation of Si-OH (Silanols) on the surface,
which is known as the first initial step for calcium phosphate deposition 57. ConC and Cu-
GPCs exhibited Si release in the range of 24 to 104 mg/L. Si release, <100 mg/L, is
considered favorable to enhance bone formation through inciting stimulatory effects on
osteoblast cell proliferation58. Zn ions have also proven to positively affect bone
metabolism by promoting its formation and mineralization59. Zn can favorably enhance
alkaline phosphatase activity in bone tissue, however, it has been reported that Zn
concentration higher than 16 mg/L could be cytotoxic for surrounding bone tissue58.
Control cement exhibited low Zn release, ranging from 0 to 0.1 mg/L over 21 days. Cu-
GPCs showed general increase in Zn release which ranged from 0 to 1.9 mg/L over 21
days of incubation. With respect to Ca release, cements showed a similar profile. However,
for P ion release, ConC exhibited a higher rate of P release compared to the Cu-GPCs.
Overall, release of Ca and P from the cements showed a gradual increase with respect to
time. Ca and P are the main inorganic constituents in skeletal tissue and it is widely
established that the release of these ions triggers new bone formation along the bone-
implant interface60. ConC and Cu-GPCs exhibited similar Sr release profiles, with a
95
gradual increase, reaching to 6mg/L after 21 days. In-vivo studies on the therapeutic effects
of Sr revealed enhanced osteoblast cell activity, differentiation, and proliferation61-62. In
general, lower levels of Si and P release from Cu-GPCs may be attributed to structural
effects of Cu addition in the glass structure. In a previous study, MAS-NMR results of
these glasses established that the addition of CuO increased the percentage of Q3 and Q4
species within the glass, indicating an increase in the number of bridging-oxygens (BOs)
in the glass. This effect results in increasing the network connectivity of the glass
structure,34 and makes the glass less soluble, and will likely decrease the release of network
forming ions such as Si and P. However, network modifier cations such as Sr and Ca, which
form crosslinks with PAA groups, are less restricted within the glass structure and more
are available to release upon incubation in an aqueous environment33. This could explain
the similar levels of release attributed to Ca and Sr observed for each GPC. The Cu-GPCs
exhibited a relatively constant Cu release rate over 21 days which may provide a positive
therapeutic benefit as Cu ions possess are known to induce antimicrobial effects, and are
also cited to improve angiogenesis through stimulation of endothelial cells and new bone
formation at implant sites35, 37.
Analyzing the surface depositions of materials incubated in SBF is conducted as a
screening test to study the ability of a materials potential for bone bonding in physiological
fluids48. Precipitation of calcium phosphate on the surface is regarded as a pre-requisite for
the material to bond to living bone and provides the driving force for formation of
biologically active bone-like apatite48. Analysis of SEM images along with their
corresponding EDX spectra (Figure 4.9) of the ConC and Cu-GPCs after 21 days
incubation in SBF identifies the presence of Ca2+ and PO43- containing precipitates on the
materials surface. Similar morphologies of the precipitants suggest that the ConC and Cu-
GPCs exhibit similar behavior when incubated in the SBF. Despite the low amount of Ca
and P in the starting glass composition (Table 4.1), EDX results confirms considerably
higher amounts of Ca and P are deposited on the surface after SBF incubation, acquiring
up to 17 and 26 wt% of Ca and P for Cu-GPCs, respectively. Comparing these values with
the initial glass compositions, suggests high degree of reactions occurred between the
GPCs and the SBF solution resulting in formation of calcium phosphate. Dissolution of the

96
glass particles from the cements and the release of Si ions leads to the formation of silanol
groups (Si-OH) on the surface. Silanol groups are scattered across the surface and
eventually form a silica-rich layer. Si-OH groups from the glass, and COOH groups from
PAA covers the surface as favored sites for continuous absorption of calcium and
phosphate ions from the solution and from the glass63-64. This leads to the formation and
growth of amorphous calcium phosphate on top of the silica-rich layer.65. Low
concentrations of Si, and high concentrations of Ca and P from EDX (Figure 4.9) suggest
the formation of calcium phosphate rich depositions that cover the silica-rich layer on the
surface of the incubated GPCs. Further insight into the surface depositions reveal high
levels of Zn are present. This might be due to high content of Zn in the initial glass
composition. Zn are released into solution and supersaturate the SBF-cement interface,
resulting in formation of zinc rich calcium phosphate depositions on the surface of
cements66. Subsequently, release of Sr and Cu ions (only in Cu-GPCs) into the solution,
results in the precipitation and formation of Sr and Cu containing zinc-calcium-phosphate
depositions, as the EDX elemental composition of the precipitates, confirms presence of
Sr and Cu on the surface of cement discs. The presence of therapeutic ions such as Cu and
Sr on the surface depositions and further releasing to surrounding biological environment
plays a critical role to enhance bioactivity and antibacterial efficacy58.
Next, the cements were analyzed for their antibacterial efficacy. Bacterial infection
remains a major concern in the field of orthopaedics, and negatively impacts the clinical
outcome of the orthopedic devices causing complication such as osteomyelitis (bone
infection)67. The four most common bacterial species causing osteomyelitis are S. aureus,
P. aeruginosa, S. epidermidis and E. coli, while S. aureus remains as the dominant species
accounting for over 45% of all the skeleton infections68. In this study, the antibacterial
efficacy of the cements was tested against three prevalent infectious bacteria was
conducted and the results are presented in Figure 4.10 and Figure 4.11. The images of
bacterial cultures in Figure 4.10, clearly shows enhanced inhibition zone (IZ) for Cu-GPCs,
specifically against S. epidermidis and S. aureus bacteria. The growth of all three species
of bacteria is significantly (p=0.000) reduced for Cu6C and Cu12C, when compared to
ConC cement. Cu12C shows significantly greater IZ than Cu6C when tested in E. coli

97
(p=0.016), and S. aureus (p=0.000). However, no significant change was observed in IZ of
Cu6C and Cu12C when tested in S. epidermidis (p=0.836). The agar-broth test method
results (Figure 4.11) give a clear insight to the cements antibacterial properties over
extended time periods, and when compared to healthy growing bacteria. For all three-
bacterium tested, the bacterial viability of Cu-GPCs was found to be 1) significantly lower
(p=0.000) than healthy growing bacteria, and 2) significantly lower (p=0.000) than the
ConC cement. However, the ConC cement showed different behavior when compared
against the reference bacteria. For the ConC cement, the viability was found to be
significantly lower (p=0.000) than 100% reference bacteria only when tested in E. coli, but
significantly higher (p=0.043) when tested in S. epidermidis. No statistically significant
change in viability was observed for ConC cement when tested in S. aureus (p=0.552). For
all three species of bacteria, Cu-GPCs exhibit a consistent bacterial viability, as their
viabilities do not significantly vary (p < 0.005) at each time period and over 1 to 21 days
of incubation. Wren et al studied the antibacterial properties of the commercially available
bone cements including Simplex P+Tobramycin, Spineplex and Novabone against E. coli,
S. epidermidis and S. aureus69. No inhibition zone was reported for the bone cements
without antibiotics against three different species of bacteria. Maximum IZ of 13mm was
reported for Simplex P + antibiotic when tested in S. epidermidis69. However, experimental
Cu-GPCs exhibited greater IZs even when compared to antibiotic containing bone cements
such as Simplex P. The antibacterial efficacy of the Cu-GPCs is greatly enhanced by
incorporation of the Cu ions within the glass phase. These can be one alternative to
antibiotic-loading of the cements, which has developed serious antibiotic-resistant bacterial
pathogens70. The exact molecular mechanism in which Cu ions act as antibacterial agents
is complex and are not understood completely, however, several pathways are suggested.
High concentration of Cu inside a bacteria cell, induces Cu redox cycling, this leads to
generation of hydrogen peroxide which results in oxidative damage to bacteria. Formation
of reactive oxygen species (ROS) can cause oxidative stress and disrupts the cell
hemostasis71. Cu also obstruct the cell metabolism by disrupting proteins and enzymes in
bacteria, resulting in uncontrolled activation of hydrolytic enzymes and causing membrane
damage to the bacteria72.

98
The MC3T3-E1 cell viability of the untreated GPC extracts are presented in Figure
4.12. The MTT assay determines the number of viable cells based on cell metabolism73.
The results from Figure 4.12 illustrates that the cell viabilities of ConC and Cu-GPCs were
significantly reduced when compared to healthy growing cell population, which was
assumed to have a metabolic rate of 100%, with (p=0.000) for Control, (p=0.000) for
Cu6C, and (p=0.001) for Cu12C. Additionally, analyzing the behavior of the cements over
differing time periods demonstrates that the cell viability of the ConC cement significantly
(p=0.000) decreases over the 1 to 21 days incubation period. However, the Cu-GPCs
exhibited a consistent cell viability profile, with insignificant influence on cell’s
metabolism over 1 to 21 days, with (p=0.063) for Cu6C, and (p=0.870) for Cu12C GPCs.
One possible explanation is higher degree of solubility for ConC compared to Cu-GPCs.
Dissolution products of the glass and acid component of the GPCs can significantly alter
the pH of the surrounding solution and consequently affect the number of viable cells.
Generally, GPCs consist of highly soluble glass particles, and aqueous solutions of
polymeric acids such as PAA, where release of its unreacted monomer is considered as the
main reason for their mild cytotoxicity74.
4.5 Conclusion
To conclude, the incorporation of Cu within GPCs can impart beneficial properties
for materials applied for vertebroplasty and kyphoplasty. Rheological behavior of the
GPCs formulated with P/L of 2:3.0 to 2:2.5 indicated adequate physical properties.
Mechanical properties studies showed time dependent behavior of flexural strength for the
cements; however, the compressive and shear bond strength were not significantly
influenced by maturation time. This series of Cu-GPCs presents solubility profiles that
encourage bioactivity, and antibacterial efficacy. Significantly improved antibacterial
efficacy on Cu-GPCs, shows promising results for developing antibiotic free cements.
Additionally, cell cytotoxicity studies conducted to determine MC3T3 Osteoblast viability,
indicated that the GPCs retain cytocompatibility.
Chapter 4 investigated the Cu containing GPCs, with regard to rheological
mechanical, and biological behavior. In vitro studies on biological behavior of the GPCs,

99
represented adequate biocompatibility of the GPCs. Specifically, the results from
antibacterial testing of the cements were promising indicators of their potential in
orthopedic bone cements. However, the mechanical strength of the cements yet to be
improved. Next chapter (chapter 5) is focused on addressing the issues with the low
compressive strength and brittle fracture nature of these materials. Improving the Cu-GPCs
strength through surface treatment of glass powder and testing their mechanical properties
will be a primary focus. The first part of next chapter will mainly investigate the surface
features of the annealed glasses using SEM, Raman, and XRD. Second part of the study
will analyze the cement formation using FTIR, and provides insights on mechanical
properties, and compressive strength of the GPCs formed with annealed glass powders.
4.6 References
1. Maradit Kremers, H.; Larson, D. R.; Crowson, C. S.; Kremers, W. K.; Washington, R. E.; Steiner, C. A.; Jiranek, W. A.; Berry, D. J., Prevalence of Total Hip and Knee Replacement in the United States. J Bone Joint Surg Am 2015, 97 (17), 1386-97.
2. Culliford, D. J.; Maskell, J.; Kiran, A.; Judge, A.; Javaid, M. K.; Cooper, C.; Arden, N. K., The lifetime risk of total hip and knee arthroplasty: results from the UK general practice research database. Osteoarthritis Cartilage 2012, 20 (6), 519-24.
3. Love, C.; Tomas, M. B.; Marwin, S. E.; Pugliese, P. V.; Palestro, C. J., Role of Nuclear Medicine in Diagnosis of the Infected Joint Replacement. RadioGraphics 2001, 21 (5), 1229-1238.
4. Jiang, Y.; Jia, T.; Wooley, P. H.; Yang, S.-Y., Current research in the pathogenesis of aseptic implant loosening associated with particulate wear debris. Acta Orthop Belg 2013, 79 (1), 1-9.
5. Abu-Amer, Y.; Darwech, I.; Clohisy, J. C., Aseptic loosening of total joint replacements: mechanisms underlying osteolysis and potential therapies. Arthritis research & therapy 2007, 9 (1), S6.
6. Magnan, B.; Bondi, M.; Maluta, T.; Samaila, E.; Schirru, L.; Dall'Oca, C., Acrylic bone cement: current concept review. Musculoskelet Surg 2013, 97 (2), 93-100.
7. Arora, M.; Chan, E. K.; Gupta, S.; Diwan, A. D., Polymethylmethacrylate bone cements and additives: A review of the literature. World J Orthop 2013, 4 (2), 67-74.
8. Wang, W.; Yeung, K. W. K., Bone grafts and biomaterials substitutes for bone defect repair: A review. Bioactive Materials 2017, 2 (4), 224-247.
9. Draenert, K.; Draenert, Y., The Three Interfaces. In The Well-Cemented Total Hip Arthroplasty, Springer: 2005; pp 93-102.

100
10. Kim, S. B.; Kim, Y. J.; Yoon, T. L.; Park, S. A.; Cho, I. H.; Kim, E. J.; Kim, I. A.; Shin, J.-W., The characteristics of a hydroxyapatite–chitosan–PMMA bone cement. Biomaterials 2004, 25 (26), 5715-5723.
11. Towler, M.; Crowley, C.; Murphy, D.; M. C. O'Callaghan, A., A preliminary study of aluminum-free glass polyalkenoate cement. 2002; Vol. 21, p 1123-1126.
12. Croll, T. P.; Nicholson, J., Glass ionomer cements in pediatric dentistry: review of the literature. Pediatric dentistry 2002, 24 (5), 423-429.
13. Nicholson, J. W., Chemistry of glass-ionomer cements: a review. Biomaterials 1998, 19 (6), 485-494.
14. Lohbauer, U., Dental Glass Ionomer Cements as Permanent Filling Materials? – Properties, Limitations and Future Trends. Materials 2009, 3 (1), 76-96.
15. Nicholson, J. W., Adhesion of glass-ionomer cements to teeth: A review. International Journal of Adhesion and Adhesives 2016, 69, 33-38.
16. Hatton, P. V.; Kearns, V. R.; Brook, I. M., 11 - Bone–cement fixation: glass–ionomer cements A2 - Revell, Peter A. In Joint Replacement Technology, Woodhead Publishing: 2008; pp 252-263.
17. Tyas, M. J.; Burrow, M. F., Adhesive restorative materials: a review. Aust Dent J 2004, 49 (3), 112-21; quiz 154.
18. Kovarik, R. E.; Haubenreich, J. E.; Gore, D., Glass Ionomer Cements: A Review of Composition, Chemistry, and Biocompatibility as a Dental and Medical Implant Material. 2005, 15 (6), 655-671.
19. Nicholson, J. W.; Braybrook, J. H.; Wasson, E. A., The biocompatibility of glass-poly(alkenoate) (Glass-Ionomer) cements: A review. Journal of Biomaterials Science, Polymer Edition 1991, 2 (4), 277-285.
20. Nicholson, J. W.; Czarnecka, B., Review paper: Role of aluminum in glass-ionomer dental cements and its biological effects. J Biomater Appl 2009, 24 (4), 293-308.
21. Griffin, S. G.; Hill, R. G., Influence of glass composition on the properties of glass polyalkenoate cements. Part I: influence of aluminium to silicon ratio. Biomaterials 1999, 20 (17), 1579-86.
22. Polizzi, S.; Pira, E.; Ferrara, M.; Bugiani, M.; Papaleo, A.; Albera, R.; Palmi, S., Neurotoxic effects of Aluminium among foundry workers and Alzheimers disease. Neuro Toxicology 2002, 23, 761-774.
23. Shaw, C. A.; Tomljenovic, L., Aluminum in the central nervous system (CNS): toxicity in humans and animals, vaccine adjuvants, and autoimmunity. Immunol Res 2013, 56 (2-3), 304-16.
24. Hurrell-Gillingham, K.; Reaney, I. M.; Brook, I.; Hatton, P. V., In vitro biocompatibility of a novel Fe2O3 based glass ionomer cement. J Dent 2006, 34 (8), 533-8.
25. Lewis, G.; Towler, M. R.; Boyd, D.; German, M. J.; Wren, A. W.; Clarkin, O. M.; Yates, A., Evaluation of two novel aluminum-free, zinc-based glass polyalkenoate cements as alternatives to PMMA bone cement for use in vertebroplasty and balloon kyphoplasty. J Mater Sci Mater Med 2010, 21 (1), 59-66.

101
26. Wren, A. W.; Hansen, J. P.; Hayakawa, S.; Towler, M. R., Aluminium-free glass polyalkenoate cements: ion release and in vitro antibacterial efficacy. J Mater Sci Mater Med 2013, 24 (5), 1167-78.
27. Brauer, D. S.; Gentleman, E.; Farrar, D. F.; Stevens, M. M.; Hill, R. G., Benefits and drawbacks of zinc in glass ionomer bone cements. Biomed Mater 2011, 6 (4), 045007.
28. Yusa, K.; Yamamoto, O.; Takano, H.; Fukuda, M.; Iino, M., Zinc-modified titanium surface enhances osteoblast differentiation of dental pulp stem cells in vitro. Scientific Reports 2016, 6, 29462.
29. Hatton, P. V.; Hurrell-Gillingham, K.; Brook, I. M., Biocompatibility of glass-ionomer bone cements. J Dent 2006, 34 (8), 598-601.
30. Brook, I. M.; Hatton, P. V., Glass-ionomers: bioactive implant materials. Biomaterials 1998, 19 (6), 565-71.
31. Xie, D.; Brantley, W. A.; Culbertson, B. M.; Wang, G., Mechanical properties and microstructures of glass-ionomer cements. Dental Materials 16 (2), 129-138.
32. Najeeb, S.; Khurshid, Z.; Zafar, M. S.; Khan, A. S.; Zohaib, S.; Marti, J. M.; Sauro, S.; Matinlinna, J. P.; Rehman, I. U., Modifications in Glass Ionomer Cements: Nano-Sized Fillers and Bioactive Nanoceramics. Int J Mol Sci 2016, 17 (7).
33. Wilson, A. D.; Nicholson, J. W., Acid-base cements: their biomedical and industrial applications. Cambridge University Press: 2005; Vol. 3.
34. Mokhtari, S.; Skelly, K. D.; Krull, E. A.; Coughlan, A.; Mellott, N. P.; Gong, Y.; Borges, R.; Wren, A. W., Copper-containing glass polyalkenoate cements based on SiO2–ZnO–CaO–SrO–P2O5 glasses: glass characterization, physical and antibacterial properties. Journal of Materials Science 2017, 52 (15), 8886-8903.
35. Bari, A.; Bloise, N.; Fiorilli, S.; Novajra, G.; Vallet-Regi, M.; Bruni, G.; Torres-Pardo, A.; Gonzalez-Calbet, J. M.; Visai, L.; Vitale-Brovarone, C., Copper-containing mesoporous bioactive glass nanoparticles as multifunctional agent for bone regeneration. Acta Biomater 2017, 55, 493-504.
36. D'Mello, S.; Elangovan, S.; Hong, L.; Ross, R. D.; Sumner, D. R.; Salem, A. K., Incorporation of copper into chitosan scaffolds promotes bone regeneration in rat calvarial defects. J Biomed Mater Res B Appl Biomater 2015, 103 (5), 1044-9.
37. Wu, C.; Zhou, Y.; Xu, M.; Han, P.; Chen, L.; Chang, J.; Xiao, Y., Copper-containing mesoporous bioactive glass scaffolds with multifunctional properties of angiogenesis capacity, osteostimulation and antibacterial activity. Biomaterials 34 (2), 422-433.
38. Ewald, A.; Kappel, C.; Vorndran, E.; Moseke, C.; Gelinsky, M.; Gbureck, U., The effect of Cu(II)-loaded brushite scaffolds on growth and activity of osteoblastic cells. Journal of biomedical materials research. Part A 2012, 100 (9), 2392-400.
39. Wang, H.; Zhao, S.; Zhou, J.; Shen, Y.; Huang, W.; Zhang, C.; Rahaman, M. N.; Wang, D., Evaluation of borate bioactive glass scaffolds as a controlled

102
delivery system for copper ions in stimulating osteogenesis and angiogenesis in bone healing. J. Mater. Chem. B 2014, 2 (48), 8547-8557.
40. Li, J.; Zhai, D.; Lv, F.; Yu, Q.; Ma, H.; Yin, J.; Yi, Z.; Liu, M.; Chang, J.; Wu, C., Preparation of copper-containing bioactive glass/eggshell membrane nanocomposites for improving angiogenesis, antibacterial activity and wound healing. Acta Biomaterialia 2016, 36, 254-266.
41. Shi, M.; Chen, Z.; Farnaghi, S.; Friis, T.; Mao, X.; Xiao, Y.; Wu, C., Copper-doped mesoporous silica nanospheres, a promising immunomodulatory agent for inducing osteogenesis. Acta Biomaterialia 2016, 30, 334-344.
42. Stähli, C.; James-Bhasin, M.; Hoppe, A.; Boccaccini, A. R.; Nazhat, S. N., Effect of ion release from Cu-doped 45S5 Bioglass® on 3D endothelial cell morphogenesis. Acta Biomaterialia 2015, 19, 15-22.
43. Gerard, C.; Bordeleau, L. J.; Barralet, J.; Doillon, C. J., The stimulation of angiogenesis and collagen deposition by copper. Biomaterials 2010, 31 (5), 824-31.
44. Feng, W.; Ye, F.; Xue, W.; Zhou, Z.; Kang, Y. J., Copper regulation of hypoxia-inducible factor-1 activity. Mol Pharmacol 2009, 75 (1), 174-82.
45. International Organization for Standardization 9917, Dental Water Based Cements (E). In Case Postale 56, Geneva, Switzerland, 1991; pp CH-11211.
46. Williams, J. A.; Billington, R. W.; Pearson, G. J., The effect of the disc supportsystem on biaxial tensile strength of a glass ionomer cement. Dental Materials 2002, 18 (2002), 376-379.
47. Xie, D.; Brantley, W. A.; Culbertson, B. M.; Wang, G., Mechanical properties and microstructures of glass-ionomer cements. Dental Materials 2000, 16 (2), 129-138.
48. Kokubo, T.; Takadama, H., How useful is SBF in predicting in vivo bone bioactivity. Biomaterials 2006, 27, 2907-2915.
49. Bohner, M., Physical and chemical aspects of calcium phosphates used in spinal surgery. Eur Spine J 2001, 10 Suppl 2, S114-21.
50. Oliveira, J. M.; Silva, S. S.; Malafaya, P. B.; Rodrigues, M. T.; Kotobuki, N.; Hirose, M.; Gomes, M. E.; Mano, J. F.; Ohgushi, H.; Reis, R. L., Macroporous hydroxyapatite scaffolds for bone tissue engineering applications: physicochemical characterization and assessment of rat bone marrow stromal cell viability. J Biomed Mater Res A 2009, 91 (1), 175-86.
51. Simka, W.; Krzakala, A.; Maselbas, M.; Dercz, G.; Szade, J.; Winiarski, A.; Michalska, J., Formation of bioactive coatings on Ti-13Nb-13Zr alloy for hard tissue implants. RSC Advances 2013, 3 (28), 11195-11204.
52. He, Z.; Zhai, Q.; Hu, M.; Cao, C.; Wang, J.; Yang, H.; Li, B., Bone cements for percutaneous vertebroplasty and balloon kyphoplasty: Current status and future developments. Journal of Orthopaedic Translation 2015, 3 (1), 1-11.
53. Gaviria, J.; García, C. G.; Vélez, E.; Quijano, J., The Mechanism of Formation of Glass-Ionomer Cement: A Theoretical Study. Modeling and Numerical Simulation of Material Science 2013, 3 (04), 149.

103
54. Kleverlaan, C. J.; van Duinen, R. N.; Feilzer, A. J., Mechanical properties of glass ionomer cements affected by curing methods. Dental materials : official publication of the Academy of Dental Materials 2004, 20 (1), 45-50.
55. Prosser, H. J.; Powis, D. R.; Wilson, A. D., Glass-ionomer cements of improved flexural strength. J Dent Res 1986, 65 (2), 146-8.
56. Nicholson, A. O. A. W., Glass-ionomer cements as adhesives. Journal of Materials Science: Materials in Medicine 1993, 4 (2), 95-101.
57. Hench, L. L.; Roki, N.; Fenn, M. B., Bioactive glasses: Importance of structure and properties in bone regeneration. Journal of Molecular Structure 2014, 1073, 24-30.
58. Hoppe, A.; Güldal, N. S.; Boccaccini, A. R., A review of the biological response to ionic dissolution products from bioactive glasses and glass-ceramics. Biomaterials 2011, 32 (11), 2757-2774.
59. Du, R. L.; Chang, J.; Ni, S. Y.; Zhai, W. Y.; Wang, J. Y., Characterization and in vitro bioactivity of zinc-containing bioactive glass and glass-ceramics. J Biomater Appl 2006, 20 (4), 341-60.
60. Rahaman, M. N.; Day, D. E.; Bal, B. S.; Fu, Q.; Jung, S. B.; Bonewald, L. F.; Tomsia, A. P., Bioactive glass in tissue engineering. Acta Biomater 2011, 7 (6), 2355-73.
61. Gorustovich, A. A.; Steimetz, T.; Cabrini, R. L.; Porto Lopez, J. M., Osteoconductivity of strontium-doped bioactive glass particles: a histomorphometric study in rats. J Biomed Mater Res A 2010, 92 (1), 232-7.
62. O’donnell, M.; Candarlioglu, P.; Miller, C.; Gentleman, E.; Stevens, M., Materials characterisation and cytotoxic assessment of strontium-substituted bioactive glasses for bone regeneration. Journal of Materials Chemistry 2010, 20 (40), 8934-8941.
63. Li, P.; Ohtsuki, C.; Kokubo, T.; Nakanishi, K.; Soga, N.; Nakamura, T.; Yamamuro, T., Apatite formation induced by silica gel in a simulated body fluid. Journal of the American Ceramic Society 1992, 75 (8), 2094-2097.
64. Chon, S. S.; Piraino, L.; Mokhtari, S.; Krull, E. A.; Coughlan, A.; Gong, Y.; Mellott, N. P.; Keenan, T. J.; Wren, A. W., Synthesis, characterization and solubility analysis of amorphous SiO2-CaO-Na2O-P2O5 scaffolds for hard tissue repair. Journal of Non-Crystalline Solids 2018, 490, 1-12.
65. Kokubo, T., Apatite formation on surfaces of ceramics, metals and polymers in body environment. Acta Materialia 1998, 46 (7), 2519-2527.
66. Boyd, D.; Towler, M., The processing, mechanical properties and bioactivity of zinc based glass ionomer cements. Journal of Materials Science: Materials in Medicine 2005, 16 (9), 843-850.
67. Song, Z.; Borgwardt, L.; Høiby, N.; Wu, H.; Sørensen, T. S.; Borgwardt, A., Prosthesis Infections after Orthopedic Joint Replacement: The Possible Role of Bacterial Biofilms. Orthopedic Reviews 2013, 5 (2), e14.
68. Ribeiro, M.; Monteiro, F. J.; Ferraz, M. P., Infection of orthopedic implants with emphasis on bacterial adhesion process and techniques used in studying bacterial-material interactions. Biomatter 2012, 2 (4), 176-194.

104
69. Wren, A.; Cummins, N. M.; Towler, M., Comparison of antibacterial properties of commercial bone cements and fillers with a zinc-based glass polyalkenoate cement. Journal of materials science 2010, 45 (19), 5244-5251.
70. Witte, W.; Cuny, C.; Klare, I.; Nubel, U.; Strommenger, B.; Werner, G., Emergence and spread of antibiotic-resistant Gram-positive bacterial pathogens. Int J Med Microbiol 2008, 298 (5-6), 365-77.
71. Manzl, C.; Enrich, J.; Ebner, H.; Dallinger, R.; Krumschnabel, G., Copper-induced formation of reactive oxygen species causes cell death and disruption of calcium homeostasis in trout hepatocytes. Toxicology 2004, 196 (1), 57-64.
72. Hajipour, M. J.; Fromm, K. M.; Akbar Ashkarran, A.; Jimenez de Aberasturi, D.; Larramendi, I. R. d.; Rojo, T.; Serpooshan, V.; Parak, W. J.; Mahmoudi, M., Antibacterial properties of nanoparticles. Trends in Biotechnology 2012, 30 (10), 499-511.
73. Siqueira, P.-C.; Magalhães, A.-P.-R.; Pires, W.-C.; Pereira, F.-C.; Silveira-Lacerda, E.-P.; Carrião, M.-S.; Bakuzis, A.-F.; Souza-Costa, C.-A.; Lopes, L.-G.; Estrela, C., Cytotoxicity of glass ionomer cements containing silver nanoparticles. Journal of Clinical and Experimental Dentistry 2015, 7 (5), e622-e627.
74. Selimović-Dragaš, M.; Huseinbegović, A.; Kobašlija, S.; Hatibović-Kofman, Š., A comparison of the in vitro cytotoxicity of conventional and resin modified glass ionomer cements. Bosnian journal of basic medical sciences 2012, 12 (4), 273.

105
5 Copper Containing Glass-Based Bone Adhesives for Orthopaedic Applications: Glass Characterization and Advanced Mechanical
Evaluation.
Submitted to Journal of Materials Science
*Sahar. Mokhtari1, Anthony.W. Wren1.
1 Kazuo Inamori School of Engineering, Alfred University, Alfred NY, USA.
Keywords: Bioactive Glass, Raman, Copper, Bone, Adhesive, Viscoelastic
*Address for Correspondence: Sahar Mokhtari Kazuo Inamori School of Engineering, Alfred University, Alfred, New York 14802, USA. Tel: 607-232-0474 email: [email protected]
106
Abstract
This study addresses issues with currently used bone adhesives, by producing novel
glass based skeletal adhesives through modification of the base glass composition to
include copper (Cu) and by characterizing each glass with respect to structural changes.
Bioactive glasses have found applications in fields such as orthopedics and dentistry, where
they have been utilized for the restoration of bone and teeth. The present work outlines the
formation of flexible organic-inorganic polyacrylic acid (PAA) – glass hybrids,
commercial forms are known as glass ionomer cements (GICs). Initial stages of this
research will involve characterization of the Cu-glasses, significant to evaluate the
properties of the resulting adhesives. Scanning electron microscopy (SEM) of annealed Cu
glasses indicates the presence of partial crystallization in the glass. The structural analysis
of the glass using Raman suggests the formation of CuO nanocrystals on the surface. X-
ray diffraction (XRD) pattern and X-ray photoelectron spectroscopy (XPS) further
confirmed the formation of crystalline CuO phases on the surface of the annealed Cu-glass.
The setting reaction between the glass particles and the PAA was studied using Fourier
transform infrared spectroscopy (ATR-FTIR). The mechanical properties of the Cu
containing adhesives exhibited higher strengths and flexibilities when compared with the
control composition. Oscillatory compression data indicated the Cu glass adhesives are
more viscous than the control composition and were efficient at energy dissipation due to
the reversible interactions between CuO nano particles and PAA polymer chains. It is
proposed the strong gel viscoelastic behavior and the enhanced mechanical properties are
attributed to the unique energy dissipation via the rearrangement of Cu/PAA interactions
which facilitate the toughness and extensibility of the polymer matrix.
5.1 Introduction
Bone tissue fractures are one of the most prevalent clinical diagnoses that often
require invasive surgery procedures1. Therapeutic bone adhesives are widely used in
various orthopaedic and trauma surgeries to repair and remodel the operational capacity of
the bone tissue2. Bone adhesives are synthetic, self-curing, non-metallic materials that are
mainly used either to stabilize prostheses, or used as bone fillers to fix damaged bone
107
tissue3. Some of their most common clinical uses include applications in total hip or total
knee replacements for anchoring functions where bone adhesive is implanted together with
the prostheses4. Other common example is their application in treating benign aggressive
bone tumours by regeneration of lost bone tissue created after curettage of tumours5.
Injectable bone adhesives are prevalently used for bone augmentation procedures and
treatment of damaged vertebral body (vertebroplasty and kyphoplasty) where bone
adhesive is injected into cracked or broken vertebral body that is often caused by
osteoporosis 6-8. The principal steps in vertebroplasty and kyphoplasty involves injection
of a paste of the bone adhesive into a cavity of the fractured vertebral body through a
cannula, either directly or by the means of an inflatable balloon9-10. Figure 5.1a presents a
schematic overview of the bone adhesives used in the vertebral body augmentation. The
ultimate goal of using bone adhesive is to obtain optimal functional state of bone tissue by
stabilization, surface adhesion, and ultimately the repair of the damaged bone tissue 11.
Currently, the clinically available bone adhesives are only based on commercially available
materials known as bone cement8. Despite being the current standard of care, the major
clinical shortcomings of traditional bone cement still exist which have necessitated the
need to develop alternate bone adhesives.
The first clinical bone cement used in orthopaedics, was an acrylate cement based
on Polymethylmethacrylate (PMMA), which was first used for hip arthroplasty in 19588.
Although the clinical use and availability of various types of PMMA bone cements, they
are not without major drawbacks6, 12. The primary concern associated with PMMA bone
cement is the lack of any chemical bonding to host bone tissue which relies primarily on
mechanical interlocking through penetration of cement in the irregularities in the surface
of bone, acting more as cement rather than adhesive13-14. Lack of interfacial chemical
bonding or inadequate adhesion leads to aseptic loosening of implant, causing failure, and
eventually requires revision surgeries14. The ideal bone adhesive should possess strong
interfacial adhesion, quick and non-exothermic setting reaction, minimum swelling and
volume shrinkage1. It is also a requirement that the bone adhesive shows biocompatibility
under physiological conditions, with minimal or no cytotoxicity15. The unique
physiochemical properties of conventionally known glass ionomer cements (GICs) could

108
significantly benefit the field of orthopaedics; however, the mechanical properties of such
materials should be addressed first16-18. Among different compositions of biomedical
cements, the GICs showed the most biocompatibility in-vitro, and in-vivo19-20. The GICs
have a complex chemistry of an interpenetrating network consisting of organic and
inorganic components forming a rigid crosslinked structure18. GICs consist of an ion-
leachable glass powder (base) combined with a water-soluble polymer (acid), which upon
mixing, an acid-base reaction takes place resulting in a hard set cement21. Since the early
introduction of GICs, a number of modifications were made to these cements to improve
their properties22. The formulation of its main constituents plays a critical role in the
properties of the resultant cements. Depending on application, formulation can be
modified; variations in the glass, acid, aqueous solution, and powder to liquid ratio can
significantly alter setting reaction, physical, mechanical and biological behavior23-24.
From mechanical perspective, a combination of strong adhesive and cohesive
strength is required. Bone adhesives spread over the entire surface, evenly distribute, and
transmit the physical forces throughout the contact area and effectively minimize stress
localization25. They could also resolve certain drawbacks of metallic implants such as stress
shielding, which is correlated with relatively high stiffness of metallic implants when
compared to the natural bone material14. Natural bone tissue has a unique mechanical
property and exhibits viscoelastic and rate-dependent failure behavior. When strained, it
exhibits both viscous and elastic characteristics depending on its loading condition and
strain rates26-27. The viscoelasticity of bone arises from its complex hierarchal structure,
primarily influenced by porosity and water content28. Compressive experiments on femoral
cortical bone over a range of strain rates, discovered that the bone would be stronger, stiffer,
and more brittle at faster strain rate29-30.
We hereby report the fabrication of a Cu containing glass-based bone adhesive that
shows exceptional viscoelastic properties. In this study, a novel glass formulation was
synthesized that incorporates large quantities of di- and tri-valent cations in order to fully
crosslink the polyacrylic acid polymer matrix, while limiting ion availability so as to allow
control over the setting kinetics of the gel31. This property is mainly provided by inclusion
of divalent ions (Cu) which produce charge balanced, acid-labile tetrahedral structure, as

109
depicted in Figure 5.132-33. Polyacrylic acid was selected because of its excellent
injectability, its chemical and mechanical diversity and its excellent biocompatibility34.
Divalent cations in the glass have the potential to link two polyanion chains, with high
ionic strength of the bond. Cu2+ can act as a strong ionic crosslink to carboxylic acid (COO-
) side groups, resulting in hardened set materials, which suggests the Cu is a mechanically
relevant ion when formulating the adhesives31. In addition, Cu2+ has regularly been cited
for being antibacterial agent34-37.
The setting reaction in these adhesives involves three different stages: dissolution,
gelation and maturation. During the first stage of the setting process, with the presence of
water, the surface of glass particles is attacked by hydrogen ions from the acid chains38.
The acid acts as proton donor and the glass powder acts as proton acceptor. Degradation
starts from glass particles surface, while the core remains intact and exists as a filler in the
set adhesives. Metal cations, principally Cu2+ and Ca2+ are released into solution and the
pH of aqueous phase increases rapidly with release of cations33. This results in greater
ionization of carboxylic acid and their spatial arrangement changes. Due to electrostatic
repulsion, the polymer chains become more polar and uncoil, and finally take a more linear
configuration. The gel structure starts to form through weak ionic crosslinking of
polyacrylate chains to form a three-dimensional network39. The cation concentration then
increases and becomes bound to the polyanionic chains. The advancement of the reaction
of metallic cations with carboxylate groups leads to an increase in viscosity. This represents
the initial set of the adhesives. The final material consists of unreacted glass particles
surrounded by the polysalt matrix containing crosslinks. After initial hardening, further
reactions take place slowly during maturation, which the less mobile cations, mainly Zn,
become bound within the adhesives matrix, leading to more rigid crosslinking between the
polyalkenoic chains40-42. The goal of this research is to address the limitations of currently
used adhesives for skeletal tissue repair, and to produce novel viscoelastic glass-based

110
adhesive that are tailored to encourage bone bonding and to improve the bioactivity of
adhesives.
Figure 5.1 (a) Schematic illustration of the bone cement used in the augmentation of damaged vertebra, (b) Preparation process, where the glass powder, PAA and water were homogeneously mixed and set within 15 minutes. The SEM image shows the microstructure of the of the porous set cement. The unreacted glass particles are labeled. (c) Schematic of the setting reaction of the glass particle and polyacrylic acid in atomic level. Water deprotonates the COOH groups on the acid chain, which further crosslinks withs ions released from the surface of the glass. The covalently crosslinked hybrid adhesive is shown where Cu2+ ion crosslinks two groups of COO- on the PAA.

111
5.2 Materials & Methods
5.2.1 Synthesis of Glass Powders Two glass compositions were formulated for this study, a Cu containing glass (Cu-
BG) in addition to a Cu free control glass (Control). The Cu-BG glass contain 12 mol%
CuO at the expense of Silica (SiO2) (Table 1). The powdered mixes of analytical grade
reagents (Fisher Scientific, PA, USA) were oven dried at 100°C for 1 hour, melted at
1350°C for 3 hours in platinum crucibles, and shock quenched into water. The resulting
frits were dried, ground and sieved to retrieve glass powders with a maximum particle size
of 45μm. Glass powders were then annealed at 10°C/min heating profile below their Tg for
3 hours and cooled down to room temperature at 5°C/min.
5.2.2 Fabrication of Glass/PAA Hybrid Adhesives adhesives were prepared by thoroughly mixing the glass powders with polyacrylic acid
(E11 PAA—Mw, 210,000, <90 µm, Advanced Healthcare Limited, Kent, UK) and distilled
water on a glass plate. The adhesives were formulated with a powder to liquid (P:L) ratio
of 2:3 with 40 wt% additions of PAA.
5.2.3 Scanning Electron Microscopy & Energy Dispersive X-ray Analysis (SEM/EDS) Imaging was carried out with SEM (Quanta 200, FEI Company, Hillsboro, OR).
Additional compositional analysis was performed with an EDAX Genesis Energy-
Dispersive Spectrometer (EDS).
5.2.4 X-Ray Diffraction (XRD) Diffraction patterns were collected using a D2 PHASER (Bruker Corporation,
Billerica, MA), and phase ID was conducted using Diffrac.EVA software (Bruker
Corporation, Billerica, MA). Diffractograms were collected in the range 10˚<2θ<80˚, at a
scan step size 0.02˚ and a step time of 10s.

112
5.2.5 X-Ray Photoelectron Spectroscopy (XPS) The X-ray photoelectron spectroscopy was carried out using a PHI (Physical
Electronics, Minnesota, US) Quantera Scanning X-ray Microprobe, a monochromatic Al
kα radiation (hv=1486.6 eV) at an output of 25.5 watts. Cu2p high resolution scans were
collected with a pass energy of 26 eV, step size of 0.05 eV, and beam dwell time of ~ 300
ms to yield a signal to noise ratio > 100:1. Analysis area for each sample is ~ 2 to 3 mm in
diameter using a 100 μm beam. Spectra analysis was performed on CasaXPS (Casa
Software Ltd.). Peak positions were calibrated through normalization of the C1s peak to
284.6 eV.
5.2.6 Raman Spectroscopy Raman analysis was performed using an Alpha300 R – Confocal Raman
spectrometer (Alpha300 R, WITec, Germany) in the wavenumber range between 200 cm−1
to 1200cm−1 using a continuous wave diode laser with an excitation wavelength of 488 nm
and power of 1 mW. The excitation source was focused on the sample surface using a
Nikon CF Plan ELWD 50x microscope objective. Data were collected using 100
accumulations, integration time of 1 s/accumulation, and an optical grating of 1800
groves/mm.
5.2.7 ATR-FTIR Spectroscopy The infrared spectra were recorded on a Bruker Invenio R – FTIR Spectrometer
with an A225/Q-Pt ATR Multiple Crystals CRY Diamond accessory. The spectral range
recorded was from 4000 cm-1 to 200 cm-1 with a resolution of 2 cm-1 taking the average of
50 scans.
5.2.8 Rheological Evaluation The working time (Tw) of the adhesives were measured under standard laboratory
conditions (Ambient Temp, 25oC). Each sample (where n = 3), was measured using a
stopwatch on a clean glass plate with a sterile spatula. Each measurement was conducted
under the same mixing conditions to ensure reproducibility. The setting times (Ts) of the
adhesive series was measured by lowering a 400 g mass attached to a Gilmore needle into
a adhesive filed mold measuring 8x9x10mm internal diameter. Adhesives were stored at

113
37oC during setting and the Ts was taken as the time the needle failed to make a complete
indent in the adhesive surface, (where n = 3).
5.2.9 Mechanical Properties The compressive strengths (σc) of the adhesives (6x4ømm, where n = 5) were
evaluated in accordance with ISO9917. Cylindrical samples were tested after 1, and 10
hours incubation in de-ionized water. Samples were stored in sterile de-ionized water in an
incubator at 37oC. After the incubation time has expired the adhesives were removed and
tested while wet on an Instron 4082 Universal Testing Machine (Instron Ltd., High
Wycombe, Bucks, UK) using a 1 kN load cell at a crosshead speed of 0.1 mm/min.
5.3 Results
The adhesives materials under investigation as part of this work are hybrid
structures, resultant of in-situ crosslinking between a polyacrylic acid (PAA) matrix and
novel compositions of Cu containing glasses. Thus, the first part of this paper will analyze
the structural properties of the glasses as a result of Cu inclusion which is significant to
evaluate changes observed in the properties of the formed adhesives. The initial step in the
fabrication process was to formulate the glass composition, by tailoring the chemistry
required for the setting reaction. Glasses were prepared via melt quenching technique to
obtain parent glass powders and further post-processed for surface treatment. The physical
and structural properties of these glasses were compared to Cu free annealed Control glass,
and to as prepared Cu-BG before heat treatment. The annealing process of glasses was
performed for 3 hours just below the glass transition temperature (Tg) of each glass
composition.
The morphology and the elemental composition of the Control, and Cu-BG glass
powders before and after annealing were analyzed using scanning electron microscopy
(SEM) and energy-dispersive X-ray (EDX). The SEM micrographs in Figure 5.2 present
unpolished surfaces of glass particles, showing a distribution of glass particulates
measuring approximately 40 µm in diameter with a much higher concentration of smaller
agglomerated fine particles below 10 µm. SEM micrographs of the annealed Control glass
(Figure 5.2) show homogenous surface features with no microscopic evidence of phase
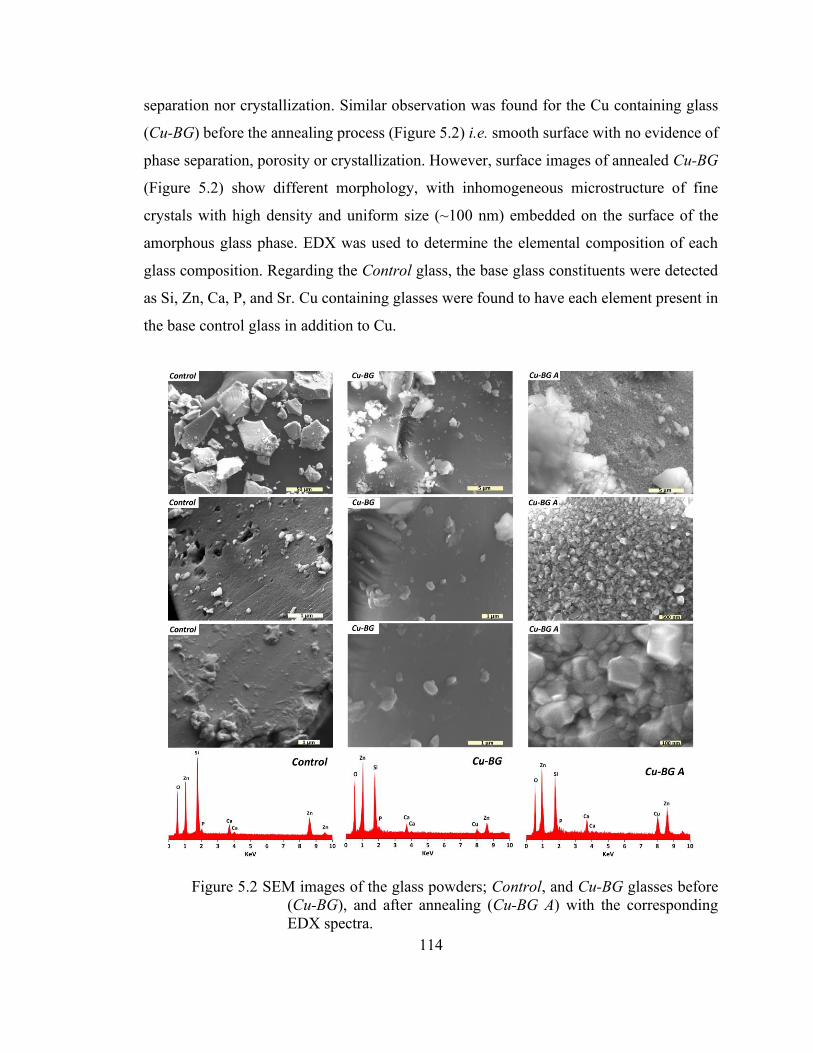
114
separation nor crystallization. Similar observation was found for the Cu containing glass
(Cu-BG) before the annealing process (Figure 5.2) i.e. smooth surface with no evidence of
phase separation, porosity or crystallization. However, surface images of annealed Cu-BG
(Figure 5.2) show different morphology, with inhomogeneous microstructure of fine
crystals with high density and uniform size (~100 nm) embedded on the surface of the
amorphous glass phase. EDX was used to determine the elemental composition of each
glass composition. Regarding the Control glass, the base glass constituents were detected
as Si, Zn, Ca, P, and Sr. Cu containing glasses were found to have each element present in
the base control glass in addition to Cu.
Figure 5.2 SEM images of the glass powders; Control, and Cu-BG glasses before (Cu-BG), and after annealing (Cu-BG A) with the corresponding EDX spectra.

115
To further investigate the crystallization of annealed Cu-BG glass powder, and to
identify the elemental composition correlated with surface nano crystals, combined SEM-
EDX elemental mapping was performed on the surface of annealed Cu-BG sample. Figure
5.3 shows SEM micrographs of annealed Cu-BG glass powder with combined elemental
mapping, containing the signals of Si, and Cu. The SEM micrographs of glass powder
shown in Figure 5.3b, and Figure 5.3c clearly exhibit a crystallized surface feature for the
Cu-BG glass, with the crystals of cubic shape or rounded cubes measuring approximately
100 nm (Figure 5.3c) in size. Figure 5.3b shows two types of morphologies; one shows the
crystalline surface of Cu-BG glass (magnified in Figure 5.3c), and the other displays Cu-
BG glass particulates (marked with arrow) scattered on the surface, which in contrast to
crystallized surface, do not represent any crystallization and seem to be remained
amorphous. Thus, to differentiate the elemental composition of the crystalline and non-
crystalline phases, elemental mapping collected from the frame depicted in Figure 5.3b,
and results are presented in Figure 5.3d-f. Through elemental mapping (Figure 5.3d-f), it
is shown that Cu, and Si are not uniformly distributed on the glassy and crystalline surface;
the crystalline phase on the surface is enriched in Cu but depleted of Si. An opposite
observation was found for the amorphous glass particulates, which were enriched in Si
rather than Cu. This is further confirmed by EDX elemental analysis, revealing that the
crystalline surface of glass contained about 43 at.% of Cu, and 13 at.% of Si.

116
Figure 5.3 SEM images of the Cu-BG glass powder after annealing, and the mapping of the surface showing the distribution of Cu, and Si.
To investigate the crystalline phases observed in the SEM micrographs, glasses
were examined by X-ray diffraction (XRD) analysis (Figure 5.4a). A typical amorphous
feature with a broad XRD halo was observed for the Control, and as prepared Cu-BG glass
before annealing, confirming predominantly amorphous structures for these glasses. XRD
patterns of annealed Cu-BG glass at 672°C, however, revealed the presence of
characteristic peaks corresponding to CuO crystals. An amorphous halo is still present
indicating the remainder of a glassy structure for annealed Cu-BG powder. In order to
analyze the chemical state of Cu atoms in the annealed composition of Cu containing
glasses, and to what extent monovalent and divalent Cu ions exist in the glass, high
resolution XPS measurements were carried out. The core-level spectra in the region of the
Cu2p is shown in Figure 5.4b. The two peaks at binding energies of 933 eV and 954 eV
are due to the spin-orbit doublet of the Cu2p core level transition. Strong satellite peaks
attributed to shake-up transition, are centred around 942 eV, and 960 eV. Each spectrum
of Cu 2p3/2 and Cu 2p1/2 could be deconvoluted into two peaks. The peaks located at
932.8 eV and 953.1 eV correspond to the Cu 2p3/2 and Cu 2p1/2, respectively, indicating
the presence of Cu compounds containing Cu+ ions in the glass. Similarly, the peaks for
Cu 2p3/2 and Cu 2p1/2 located at 934.9 eV and 955.2 eV, respectively, represent the
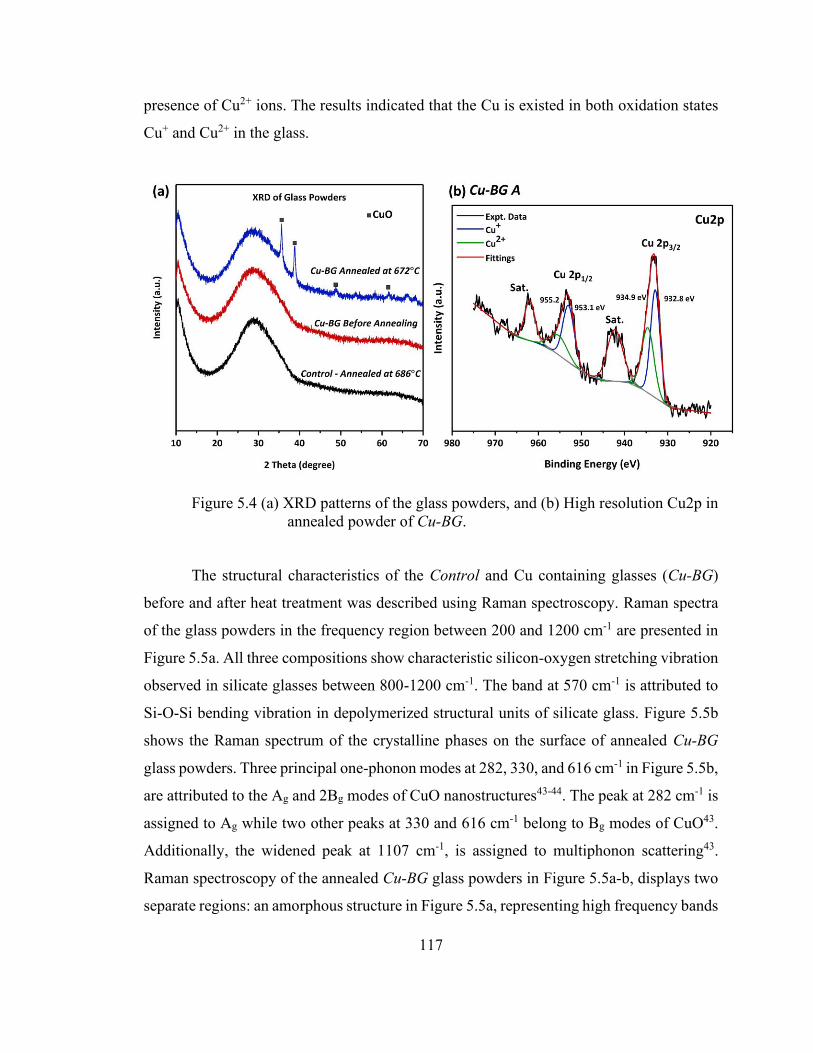
117
presence of Cu2+ ions. The results indicated that the Cu is existed in both oxidation states
Cu+ and Cu2+ in the glass.
Figure 5.4 (a) XRD patterns of the glass powders, and (b) High resolution Cu2p in annealed powder of Cu-BG.
The structural characteristics of the Control and Cu containing glasses (Cu-BG)
before and after heat treatment was described using Raman spectroscopy. Raman spectra
of the glass powders in the frequency region between 200 and 1200 cm-1 are presented in
Figure 5.5a. All three compositions show characteristic silicon-oxygen stretching vibration
observed in silicate glasses between 800-1200 cm-1. The band at 570 cm-1 is attributed to
Si-O-Si bending vibration in depolymerized structural units of silicate glass. Figure 5.5b
shows the Raman spectrum of the crystalline phases on the surface of annealed Cu-BG
glass powders. Three principal one-phonon modes at 282, 330, and 616 cm-1 in Figure 5.5b,
are attributed to the Ag and 2Bg modes of CuO nanostructures43-44. The peak at 282 cm-1 is
assigned to Ag while two other peaks at 330 and 616 cm-1 belong to Bg modes of CuO43.
Additionally, the widened peak at 1107 cm-1, is assigned to multiphonon scattering43.
Raman spectroscopy of the annealed Cu-BG glass powders in Figure 5.5a-b, displays two
separate regions: an amorphous structure in Figure 5.5a, representing high frequency bands

118
(800-1200cm-1) associated with stretching vibrations of mostly depolymerised silicate
species, and Raman signature of the CuO nanocrystals in Figure 5.5b. The high frequency
envelope (800-1200 cm-1) in the Raman spectra of amorphous silicate glasses, contains
information about the tetrahedral silicate units and structure of the glasses45. To assign
different type of silicate species (Qn) and their depolymerization degree, the vibrational
spectra of glasses within the high frequency region of 800-1200 cm-1 were deconvoluted
to four Gaussian bands attributed to vibration of the species Q3, Q2, Q1 and Q0 in the glass46.
Results are presented in Figure 5.5c-d. The band located near 850cm-1 is assigned to
depolymerised orthosilicates (Q0). The region of 900–1000 cm-1, is associated with the Si–
O stretching vibration of Q1 species.1100 cm-1, and 1000 cm-1 are associated with the
symmetric Si–O stretching vibration of the major Q3, and Q2 species, respectively46. The
Raman spectra of the Control, and Cu-BG glasses before and after annealing (Figure 5.5c-
d) indicates the existence of four different types of silicate species: Q2 and Q1 in major
concentrations, and Q3 and Q0 in minor concentrations. Thus, the trend is that the more
depolymerized the silica network, the lower the central frequency of the main band. In
Figure 5.5c-d, it can be seen that the centre of band shifts after the substitution of Cu for
Si from being cantered around 961 cm-1 for the Control to approximately 955 cm-1 for the
Cu containing glasses. By deconvoluting the spectra, it can be examined to see that the
substitution of the Cu leads to destruction of more polymerized units in the structure. First,
the shoulder marked at 1009 cm-1 (Q2 species) loses intensity with Cu substitution
alongside the growth of a new peak from what was originally a small shoulder at 860 cm-1
(Q0 species). Secondly, the shift of the most prominent peak from 1009 cm-1 to 943 cm-1
indicates the general population of silica tetrahedra is overall less connected.

119
Figure 5.5 (a) Raman spectra of the glass powders and (b) Raman spectrum of crystallized Cu-BG, and attributed fitting curves within spectra ranges of 800-1200 cm-1; (c) Control, (d) Cu-BG before annealing, and (e) Cu-BG after annealing.
Glass-based adhesives were formulated at powder to liquid ratio of 2:3, using the
annealed glass powders of Control and CuG with addition of 40 wt% solution of PAA in
deionized water. Hereby, the adhesives are labelled with their corresponding glass
compositions as Con/PAA and CuG/PAA. Due to their similarity in the chemical

120
composition with the glass-based ionomer cements, the working and setting time were
measured according to ISO9917. The working time of the adhesives were found to be at
110s and 355s for Con/PAA and CuG/PAA, respectively. Similar trend was also observed
for the setting time; 8m,46s for Con/PAA, and 15m,5s for CuG/PA. Incorporation of the
Cu into the glass composition of the adhesives increased the working and setting time by
223%, and 72% respectively. To investigate the real-time molecular interactions in setting
reaction of the adhesives, ATR-FTIR spectra were collected at one-minute intervals, and
for over 15 minutes from beginning of the mixing. Results are presented in Figure 5.6. The
characteristic band for free PAA (not coordinated to a metal ion) was identified at c. 1700
cm-1, as was the band for ionized PAA at 1550 cm-1 (Figure 5.6). As the setting reaction
proceeded, the absorbance for the ionized PAA band increased and the absorbance for the
free PAA band decreased from a clear peak into a shoulder.
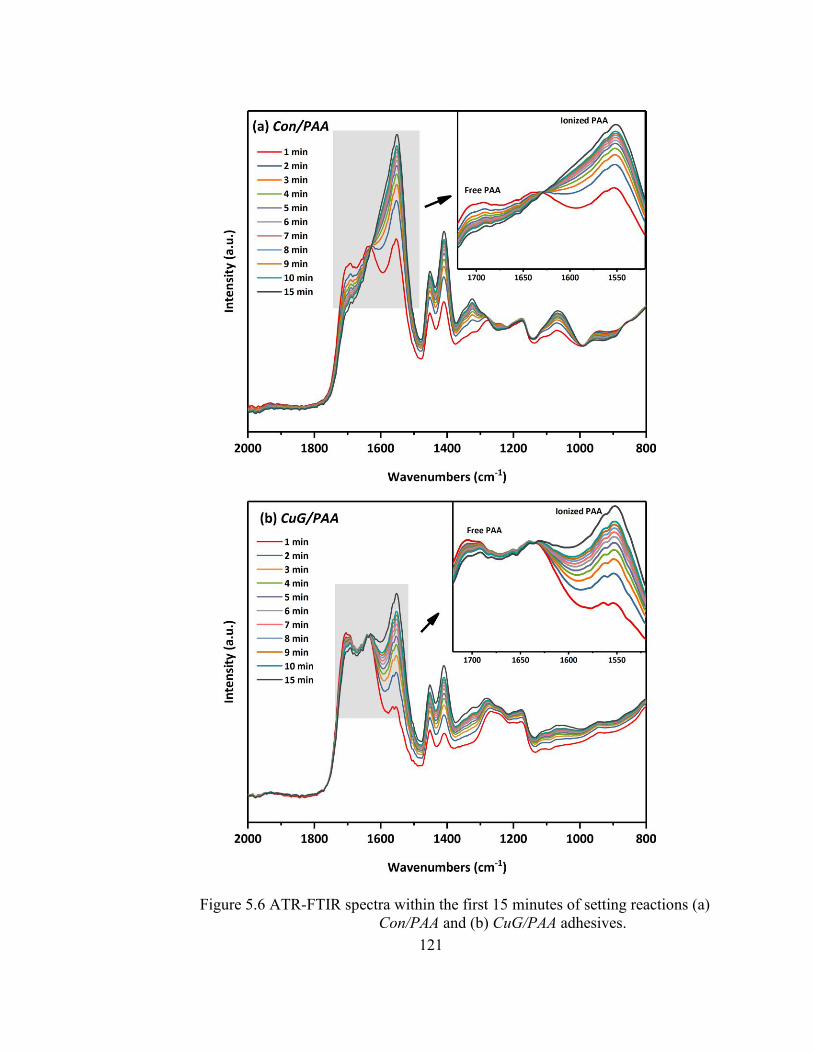
121
Figure 5.6 ATR-FTIR spectra within the first 15 minutes of setting reactions (a) Con/PAA and (b) CuG/PAA adhesives.

122
To analyze the mechanical properties of the adhesives, series of compressive
measurements were performed. Figure 5.7a shows a typical stress-strain curve for
Con/PAA. The average compressive strength calculated to be at 30.7 ± 0.9 MPa. The stress-
strain curve for Con/PAA represents the typical behavior of brittle fracture, similar to
compressive fracture of glass ionomer cements. In contrast, the compressive stress-strain
curve for CuG/PAA in Figure 5.7b, shows a different behavior. A nonlinear viscoelastic
behavior was observed for CuG/PAA adhesives, with exceptional compressibility and full
recovery even after large compressive strains (~75%). The inset shows the sample before
test, and immediately after releasing the compressive stress. Figure 5.7a and Figure 5.7d
show the uniaxial recovery percentage as a function of time for the CuG/PAA adhesives
after samples were 75% compressed. The uniaxial recovery percentage was calculated as
the ratio of the recovered height to the initial height of the sample. As it can be seen from
Figure 5.7d, the adhesives quickly recover after releasing the compressive stress. The
recovery rate is approximately at 52%, 15 minutes after test, and it reaches 61% within the
next 45 minutes. After this point, the recovery process slows down, and it exhibits a
plateau. The recovery rate of the adhesives 48 hours after performing compressive test, was
measured to be at 69% of their initial height.

123
Figure 5.7 (a) Typical compressive load-extension for the Con/PAA and (b) CuG/PAA (c) Recovery of the CuG/PAA specimen after compression loading, (c) Projected recovery of CuG/PAA within the first 250 minutes.
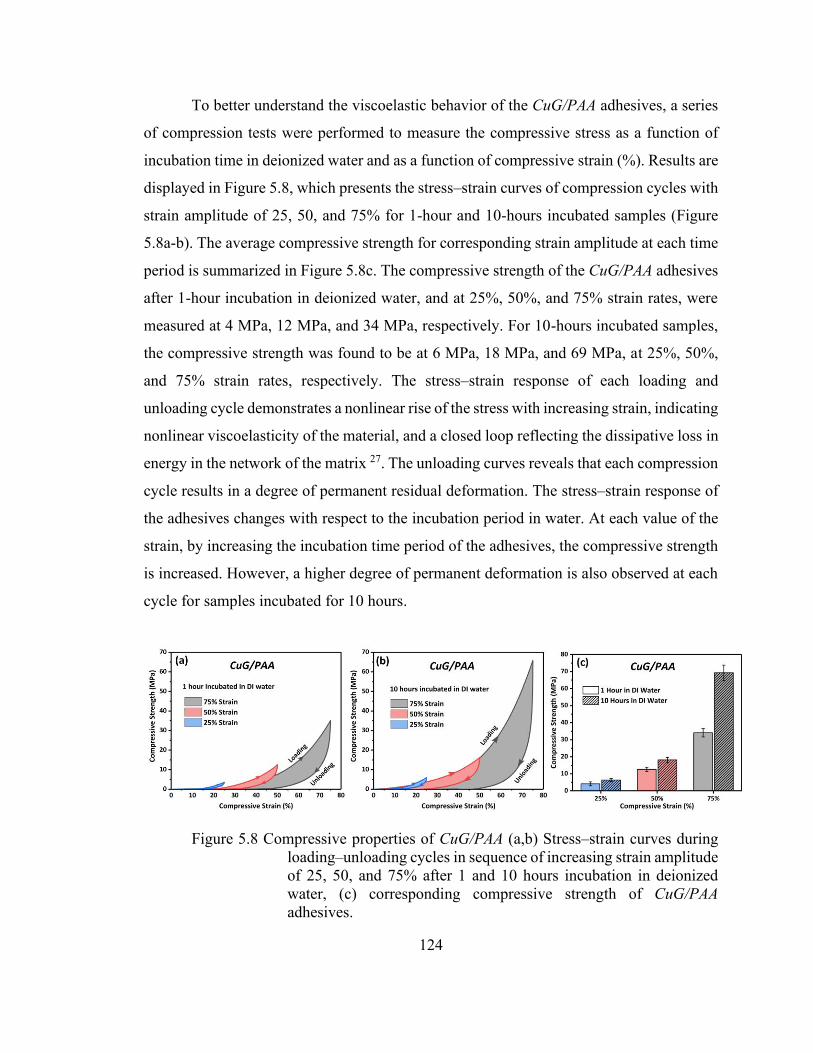
124
To better understand the viscoelastic behavior of the CuG/PAA adhesives, a series
of compression tests were performed to measure the compressive stress as a function of
incubation time in deionized water and as a function of compressive strain (%). Results are
displayed in Figure 5.8, which presents the stress–strain curves of compression cycles with
strain amplitude of 25, 50, and 75% for 1-hour and 10-hours incubated samples (Figure
5.8a-b). The average compressive strength for corresponding strain amplitude at each time
period is summarized in Figure 5.8c. The compressive strength of the CuG/PAA adhesives
after 1-hour incubation in deionized water, and at 25%, 50%, and 75% strain rates, were
measured at 4 MPa, 12 MPa, and 34 MPa, respectively. For 10-hours incubated samples,
the compressive strength was found to be at 6 MPa, 18 MPa, and 69 MPa, at 25%, 50%,
and 75% strain rates, respectively. The stress–strain response of each loading and
unloading cycle demonstrates a nonlinear rise of the stress with increasing strain, indicating
nonlinear viscoelasticity of the material, and a closed loop reflecting the dissipative loss in
energy in the network of the matrix 27. The unloading curves reveals that each compression
cycle results in a degree of permanent residual deformation. The stress–strain response of
the adhesives changes with respect to the incubation period in water. At each value of the
strain, by increasing the incubation time period of the adhesives, the compressive strength
is increased. However, a higher degree of permanent deformation is also observed at each
cycle for samples incubated for 10 hours.
Figure 5.8 Compressive properties of CuG/PAA (a,b) Stress–strain curves during loading–unloading cycles in sequence of increasing strain amplitude of 25, 50, and 75% after 1 and 10 hours incubation in deionized water, (c) corresponding compressive strength of CuG/PAA adhesives.

125
Cross section SEM micrographs of the adhesives are shown in Figure 5.9. Both
compositions show porous microstructure of unreacted glass particulates within the PAA
matrix. The Con/PAA exhibits a fracture surface containing visible microcracks (Marked
in Figure 5.9b), and gaps at the interface of the glass particles and PAA matrix; glass
particles are encapsulated within PAA matrix where there is a visible gap debonded matrix
from particle creating voids. (Figure 5.9c-d). The SEM micrographs of CuG/PAA shows a
different microstructure (Figure 5.9e-h), where a homogenous matrix is observed with no
visible microcracks and no interfacial disconnections between the glass particles and PAA
matrix (Figure 5.9h).
Figure 5.9 Cross section SEM micrographs of the (a-d) Con/PAA, and (e-h) CuG/PAA adhesives.
5.4 Discussion
A combination of good mechanical properties, bio-adhesion, and biocompatibility
is required to achieve an ideal bone adhesive 1, 47. The bone adhesives used for orthopaedic
applications, should promote regeneration of bone tissue, encourage chemical bone-
bonding and provide sufficient adhesive and cohesive mechanical strength15. In clinical
dentistry, glass-based adhesives such as glass ionomer cements have shown exceptional
126
properties and have been developed for various dental applications. The excellent
biological performance of these materials such as bone tissue mineralization, minimal
cytotoxicity, and superior biocompatibility suggests that they could provide a better and
safer alternative to commercially available bone adhesives for orthopaedic applications16.
In this study, we synthesized novel glass-based bone adhesives through modification of the
glass composition and surface treatment of the glass powders. Shock quenching of the glass
melt during the glass-making process introduces structural thermal stresses, which in turn
influences the glass particles reactivity which affects the mechanical strength of the formed
glass-based adhesive48. Decreased compressive strength could be attributed to the
unreacted core of glass particles which acts as a reinforcing filler within the adhesive matrix 49. When the thermally stressed glass is heat-treated to its glass transition temperature, at
such viscosity, residual internal stresses in the glass structure are relieved, provided that
the stress-relieved glass is cooled slowly to minimize internal stress48. Glass powder treated
in this manner significantly improves the compressive strength of the adhesives50. In
addition, heat treatment of the glass powders could cause a decrease in the reactivity of the
glass powder through crystallization, which in turn gives the adhesives longer working and
setting times and much improved handling characteristics48. The effects of Cu
incorporation in the chemistry of these glasses, is structurally characterized in previously
published studies by the authors32-33. Earlier structural investigations on this glass system,
suggested that the incorporation of 12 mol.% of CuO at the expense of SiO2 caused the
glasses to undergo amorphous phase separation32. In this study, we reported the
development of surface crystallized Cu containing glass powders, in an approach to design
a glass-based bone adhesive with improved physical and mechanical properties. The
SEM/EDX analysis of the glass powders presented in Figure 5.2 and Figure 5.3, discern
surface morphologies and the elemental composition of the glass powders differentiated
by composition and the heat treatment profile. The Control and Cu-BG glass powder (prior
to annealing) showed no evidence of crystallization, maintaining their amorphous nature.
However, upon annealing of the Cu-BG glass just below its Tg, the glass began to
crystallize, with uniformly dispersed nano-sized cubic crystals on the surface of glass
particles. Glasses show a very distinct behavior with respect to their crystallization
127
mechanisms51. The heterogeneous surface contains two phases: an amorphous glassy phase
embedded with homogeneously distributed crystals52. Since the crystallization behavior
of the glasses is greatly influenced by the crystallization temperature in crystal growth
stage, it is necessary to clarify the formation of various crystalline phases created in the
glass powders at the different thermal treatment temperatures, which could influence the
mechanical and structural properties of resultant adhesives.
XRD was used to identify the crystal system of nanocrystals upon heat treatment.
XRD patterns of control glass (Figure 5.4a) shows the presence of characteristic broad
hump, confirming a predominantly amorphous glass structure. XRD pattern of the annealed
Cu-BG glass shows an amorphous halo, and diffraction peaks corresponding to CuO,
whereas it is not evident in the spectra of the as prepared Cu-BG glass. XRD results of Cu-
BG glasses demonstrating partial crystallization has occurred upon heat treatment. Cu may
exist in different oxidation states within glass. XPS is commonly used to identify the
chemical states of constituents and to analyze transition metal complexes with localized
valence d-orbitals53 De-convoluted XPS core spectra of Cu2p3/2 and Cu2p1/2 peaks are
presented in Figure 5.4b. It has been reported that the shakeup satellites peaks are indicator
of CuO presence at the surface54. As it was also shown with XRD the presence of CuO
phase in the glass, XPS analysis revealed the presence of surface Cu2+ ions and therefore
suggested that the Cu compounds were predominately present at the surface as CuO
nanoparticles. XRD analyzes the bulk of the material, whereas, XPS measurements
primarily reveal the surface information 55. The presence of satellite peaks in Figure 5.4b
is an indication of compounds having Cu2+ ions, as it is attributed to materials having
partially filled 3d9 shell configuration in the ground state. For metallic Cu, or Cu2O, with
a completely filled shell (3d10), the satellite peak is reportedly absent due to the fact that
the ligand-to-metal 3d charge transfer is not allowed55. Thus, in our prepared nanoparticles
too, we are affirmative of obtaining CuO phase, formed on the outer amorphous structure
of the glass particles.
Different Raman signatures involve different silicate networks around the origin46.
The Raman spectra focuses on the band between 800 cm-1 and 1200 cm-1 where the silica
tetrahedra display distinct characteristic vibrations in accordance with their network
128
connectivity56. Deconvolution of the band between 800 cm-1 and 1200 cm-1, indicated that
the incorporation of the modifier cations such as Cu into the structure disrupts the Si–O
connectivity, resulting in the creation of non-bridging oxygens (NBOs) within the silicate
structure. The notation Qn, where n is the number of bridging oxygens, is frequently used
to distinguish between the different tetrahedral species in the network: Q3 corresponds to
silicate species with one NBO (Si2O5), Q2 to silicate species with two NBOs (SiO3) and Q1
to silicate species with three NBO (SiO2), and Q0 is the Orthosilicate with no bridging
oxygen56. The effect of the annealing does not significantly impact the Cu glass structure,
although there is an increase in the relative intensity and broadening to lower frequency of
the band associated with the Si-O-Si bending vibrations57. Control and Cu-BG glasses
exhibited only the bands associated with the silica tetrahedra vibration, however, the
Raman spectra of the annealed Cu-BG (Figure 5.5b) glasses show the evidence of Cu-O
vibration bands, as well. We observed two different domains of Raman vibrations in
annealed Cu-glasses indicating of an amorphous matrix with the formation of CuO crystals
on the surface of the glass44. Raman spectrum of annealed Cu-glass (Figure 5.5b) contains
the strong intensity of vibrations of nano crystalline CuO bands if compared to those of not
annealed Cu-BG43. Raman spectrum of cupric oxide (CuO) includes 12 vibration modes
with only 3 modes, Ag and 2Bg, active in Raman 54-55. In our case and according to the
Raman spectra, we observed the appearance of all three Raman active modes located at
282, 330 and 616 cm-1, corresponding to the standard modes Ag, Bg(1) and Bg(2)
respectively. Increase in the Raman intensities for the CuO with the heat treatment (Figure
5.5b) may be due to the partial crystallization of CuO in the glass. This is in agreement
with the previous results suggesting on formation of the Cu-rich domain in the surface and
nano crystallization of CuO. The results from the structural analysis of the glasses, suggests
that the Cu addition in the structure of control glass leads to formation of amorphous phase
separation of Cu-rich domains, and further development of nanocrystals of CuO on the
surface of the glass particles upon heat treatment.
The setting reaction of the glass-based adhesives is determined by several factors
including the chemistry of the glass composition (base), the type of acid, and the powder
to liquid ratio in the formulation39. However, the setting reaction between glass and PAA
129
is predominantly influenced by the chemistry of the glass regarding the degradation rate,
and release of multivalent cations to crosslink with polymeric acid58. The setting reaction
of the adhesives is an in-situ reaction between the glass powder and the PAA solution
which takes place immediately upon mixing different components59. Hence, it is very
important to characterize the working and setting times of these adhesive as these
properties are significant to their clinical applicability. The setting profile was plotted as
the ratio of the absorbance for the ionized PAA to free PAA over time, as described in
Figure 5.6. The gel formation seemed to occur within several minutes, judging from the
setting time of the adhesive60. For both adhesive compositions the conversion ratio
followed a smooth increase over time, with the rate of conversion increasing in Con/PAA.
This trend was also observed for the final conversion ratio at 15 min. The Cu containing
adhesive CuG/PAA (Figure 5.6b) followed a different setting profile than Con/PAA (Figure
5.6a), with a smooth increase in the conversion ratio (Figure 5.6b). The ionization ratio for
the Con/PAA was 32% higher than that of the adhesive containing Cu. These FTIR results
are consistent with noted increases in working and setting times with increasing Cu content.
The setting mechanism in glass-based adhesives is an acid-base reaction61. The reaction
involves three different stages: dissolution, gelation and maturation18. During the first stage
of the setting process, with the presence of water, the surface of glass particles is attacked
by hydrogen ions from the acid chains, where the acid acts as proton donor and the glass
powder acts as proton acceptor22. Degradation starts from glass particles surface, while the
core remains intact and exists as a filler in the set cement22. In case of annealed Cu-BG
glasses, the degradation is slowed down due to surface crystallization and therefore the
setting reaction between glass particle and the acidic solution is delayed.
The mechanical properties of the glass-based adhesives are well understood by
virtue of the formation of a continuous crosslink in the network. It is considered that the
interactions between polymer−polymer, polymer−filler, and filler−filler contribute to the
mechanical properties of adhesives. The high compressive strength is related to the high
cross-linking density. The rigid network is mainly ascribed to the strong covalent
interactions of COO- chains and metallic cations released from glass particles 62. The
control adhesive of Con/PAA exhibits a typical brittle fracture (Figure 5.7a) at low stress

130
of the stress−strain curve63. This yielding phenomenon reveals the network structural
changes beyond a certain strain, which is related to plastic deformation63. Owing to
chemically covalently cross-linked networks in Con/PAA, a rigid microstructure with a
clear yielding point was observed. Also, in the SEM micrograph of the fractured surfaces
of the Con/PAA (Figure 5.9a-d), there are more glass particles–matrix debonded sites
visible due to the weakness of the glass–matrix interface compared to CuG/PAA. The glass
particle–matrix interface is considered to be the weakest component of glass-based
adhesives which may act as a stress concentration center and decreases mechanical
properties where, the fracture is primarily occurred in the glass particle–matrix interface63-
64. However, the CuG/PAA shows a different mechanical response under compressive
strains exhibiting unique nonlinear viscoelastic behavior. By homogeneous distribution of
CuO nanocrystals on the surface of the glass, multifunctional cross-links occurs at the
interface with PAA matrix due to the combination of Cu2+/COO- covalent cross-links
(related to the plastic properties) and physical CuO/COO interactions (related to the
viscoelastic properties)65. The debonding and rebonding of the physical cross-links such as
hydrogen interactions are an effective means to dissipate deformation energy65-66. The high
flexibility of the CuG/PAA adhesives, arises from its unique crystalline surface with the
reversible rearrangement of Cu/COO, resulting of efficient energy dissipation: when a
crack occurs at deformations, conformations dissipate the energy and increase crack
propagation resistance52. The loading-unloading hysteresis loops of the adhesives shown
in Figure 5.8, also indicates the influence of incubation period of the adhesives. A bigger
hysteresis loop means a larger energy dissipated during the cyclic compression experiments
and the adhesive possesses a lower elasticity with poorer repeatability67. Nonlinear
mechanical response of networks can change dramatically when these networks are
repeatedly strained, provided the bonds are not permanently cross-linked67. From the
loading-unloading curves (Figure 5.8), we can find each compression leads to a degree of
permanent residual deformation, and the recoverability of the adhesive slightly decreases
as a function of incubation time. This might be due to maturation process of the adhesives
where it increases the ratio of chemical crosslinking between the glass particles and PAA
matrix, therefore decreasing the viscoelasticity of the adhesives64. CuG/PAA has a
131
pronounced tendency for self-association on recovery under high strain rates, which is
advantageous for the formation of load-bearing networks within the host polymer matrix68.
5.5 Conclusion
In summary, this work reports the viscoelastic behavior of glass-based adhesives
through surface crystallization of the glass particles. In order to establish the required
properties that could offer a suitable material for glass-based bone adhesives, surface
crystallization was obtained upon heat treatment in Cu-BG. A viscoelastic behavior was
accomplished in CuG/PAA adhesives during compressive measurement compared with
Con/PAA. The CuG/PAA exhibits exceptional viscoelastic behavior, which is believed that
could benefit a wide range of requirements in the development of bone tissue adhesives.
5.6 References
1. Böker, K. O.; Richter, K.; Jäckle, K.; Taheri, S.; Grunwald, I.; Borcherding, K.; von Byern, J.; Hartwig, A.; Wildemann, B.; Schilling, A. F., Current State of Bone Adhesives—Necessities and Hurdles. Materials 2019, 12 (23), 3975.
2. Augat, P.; von Rüden, C., Evolution of fracture treatment with bone plates. Injury 2018, 49, S2-S7.
3. Fedak, P. W. M.; Kasatkin, A., Enhancing Sternal Closure Using Kryptonite Bone Adhesive: Technical Report. Surgical Innovation 2011, 18 (4), NP8-NP11.
4. Bai, S.; Zhang, X.; Lv, X.; Zhang, M.; Huang, X.; Shi, Y.; Lu, C.; Song, J.; Yang, H., Bioinspired Mineral–Organic Bone Adhesives for Stable Fracture Fixation and Accelerated Bone Regeneration. Advanced Functional Materials 2019, 1908381.
5. Marsell, R.; Einhorn, T. A., The biology of fracture healing. Injury 2011, 42 (6), 551-555.
6. Arora, M.; Chan, E. K.; Gupta, S.; Diwan, A. D., Polymethylmethacrylate bone cements and additives: A review of the literature. World J Orthop 2013, 4 (2), 67-74.
7. Culliford, D. J.; Maskell, J.; Kiran, A.; Judge, A.; Javaid, M. K.; Cooper, C.; Arden, N. K., The lifetime risk of total hip and knee arthroplasty: results from the UK general practice research database. Osteoarthritis Cartilage 2012, 20 (6), 519-24.
8. Magnan, B.; Bondi, M.; Maluta, T.; Samaila, E.; Schirru, L.; Dall'Oca, C., Acrylic bone cement: current concept review. Musculoskelet Surg 2013, 97 (2), 93-100.

132
9. Wang, W.; Yeung, K. W. K., Bone grafts and biomaterials substitutes for bone defect repair: A review. Bioactive Materials 2017, 2 (4), 224-247.
10. He, Z.; Zhai, Q.; Hu, M.; Cao, C.; Wang, J.; Yang, H.; Li, B., Bone cements for percutaneous vertebroplasty and balloon kyphoplasty: Current status and future developments. Journal of Orthopaedic Translation 2015, 3 (1), 1-11.
11. Maradit Kremers, H.; Larson, D. R.; Crowson, C. S.; Kremers, W. K.; Washington, R. E.; Steiner, C. A.; Jiranek, W. A.; Berry, D. J., Prevalence of Total Hip and Knee Replacement in the United States. J Bone Joint Surg Am 2015, 97 (17), 1386-97.
12. Kim, S. B.; Kim, Y. J.; Yoon, T. L.; Park, S. A.; Cho, I. H.; Kim, E. J.; Kim, I. A.; Shin, J.-W., The characteristics of a hydroxyapatite–chitosan–PMMA bone cement. Biomaterials 2004, 25 (26), 5715-5723.
13. Zhang, Q.-H.; Cossey, A.; Tong, J., Stress shielding in bone of a bone-cement interface. Medical Engineering & Physics 2016, 38 (4), 423-426.
14. Bousnane, T.; Benbarek, S.; Sahli, A.; Serier, B.; Bouiadjra, B. A. B., Damage of the bone-cement interface in finite element analyses of cemented orthopaedic implants. Periodica Polytechnica Mechanical Engineering 2018, 62 (2), 173-178.
15. Farrar, D. F., Bone adhesives for trauma surgery: A review of challenges and developments. International journal of adhesion and adhesives 2012, 33, 89-97.
16. Sidhu, S. K.; Nicholson, J. W., A Review of Glass-Ionomer Cements for Clinical Dentistry. Journal of Functional Biomaterials 2016, 7 (3).
17. Nicholson, A. O. A. W., Glass-ionomer cements as adhesives. Journal of Materials Science: Materials in Medicine 1993, 4 (2), 95-101.
18. Nicholson, J. W., Chemistry of glass-ionomer cements: a review. Biomaterials 1998, 19 (6), 485-494.
19. Hatton, P. V.; Hurrell-Gillingham, K.; Brook, I. M., Biocompatibility of glass-ionomer bone cements. Journal of Dentistry 2006, 34 (8), 598-601.
20. Hatton, P. V.; Kearns, V. R.; Brook, I. M., 11 - Bone–cement fixation: glass–ionomer cements In Joint Replacement Technology, Woodhead Publishing: 2008; pp 252-263.
21. Tyas, M. J.; Burrow, M. F., Adhesive restorative materials: a review. Australian dental journal 2004, 49 (3), 112-21; quiz 154.
22. Kovarik, R. E.; Haubenreich, J. E.; Gore, D., Glass Ionomer Cements: A Review of Composition, Chemistry, and Biocompatibility as a Dental and Medical Implant Material. J Long Term Eff Med Implants 2005, 15 (6), 655-671.
23. Nicholson, J. W.; Sidhu, S. K.; Czarnecka, B., Enhancing the Mechanical Properties of Glass-Ionomer Dental Cements: A Review. Materials 2020, 13 (11), 2510.
24. Bezerra, I. M.; Brito, A. C. M.; de Sousa, S. A.; Santiago, B. M.; Cavalcanti, Y. W.; de Almeida, L. d. F. D., Glass ionomer cements compared with composite resin in restoration of noncarious cervical lesions: A systematic review and meta-analysis. Heliyon 2020, 6 (5), e03969.
25. Mousa, W. F.; Kobayashi, M.; Shinzato, S.; Kamimura, M.; Neo, M.; Yoshihara, S.; Nakamura, T., Biological and mechanical properties of PMMA-based bioactive bone cements. Biomaterials 2000, 21 (21), 2137-2146.
133
26. Iyo, T.; Maki, Y.; Sasaki, N.; Nakata, M., Anisotropic viscoelastic properties of cortical bone. Journal of Biomechanics 2004, 37 (9), 1433-1437.
27. Garner, E.; Lakes, R.; Lee, T.; Swan, C.; Brand, R., Viscoelastic dissipation in compact bone: implications for stress-induced fluid flow in bone. J. Biomech. Eng. 2000, 122 (2), 166-172.
28. Lakes, R. S.; Katz, J. L.; Sternstein, S. S., Viscoelastic properties of wet cortical bone—I. Torsional and biaxial studies. Journal of Biomechanics 1979, 12 (9), 657-678.
29. Johnson, T.; Socrate, S.; Boyce, M., A viscoelastic, viscoplastic model of cortical bone valid at low and high strain rates. Acta biomaterialia 2010, 6 (10), 4073-4080.
30. Lakes, R. S.; Katz, J. L., Viscoelastic properties of wet cortical bone—II. Relaxation mechanisms. Journal of Biomechanics 1979, 12 (9), 679-687.
31. Wilson, A. D.; Nicholson, J. W., Acid-base cements: their biomedical and industrial applications. Cambridge University Press: 2005; Vol. 3.
32. Mokhtari, S.; Skelly, K. D.; Krull, E. A.; Coughlan, A.; Mellott, N. P.; Gong, Y.; Borges, R.; Wren, A. W., Copper-containing glass polyalkenoate cements based on SiO2–ZnO–CaO–SrO–P2O5 glasses: glass characterization, physical and antibacterial properties. Journal of Materials Science 2017, 52 (15), 8886-8903.
33. Mokhtari, S.; Wren, A. W., Investigating the effect of Copper Addition on SiO2-ZnO-CaO-SrO-P2O5 Glass Polyalkenoate Cements: Physical, Mechanical and Biological Behavior. In Biomedical Glasses, 2019; Vol. 5, p 13.
34. Wang, X.; Cheng, F.; Liu, J.; Smått, J.-H.; Gepperth, D.; Lastusaari, M.; Xu, C.; Hupa, L., Biocomposites of copper-containing mesoporous bioactive glass and nanofibrillated cellulose: Biocompatibility and angiogenic promotion in chronic wound healing application. Acta Biomaterialia 2016, 46, 286-298.
35. Stähli, C.; James-Bhasin, M.; Hoppe, A.; Boccaccini, A. R.; Nazhat, S. N., Effect of ion release from Cu-doped 45S5 Bioglass® on 3D endothelial cell morphogenesis. Acta Biomaterialia 2015, 19, 15-22.
36. Li, J.; Zhai, D.; Lv, F.; Yu, Q.; Ma, H.; Yin, J.; Yi, Z.; Liu, M.; Chang, J.; Wu, C., Preparation of copper-containing bioactive glass/eggshell membrane nanocomposites for improving angiogenesis, antibacterial activity and wound healing. Acta Biomaterialia 2016, 36, 254-266.
37. Manzl, C.; Enrich, J.; Ebner, H.; Dallinger, R.; Krumschnabel, G., Copper-induced formation of reactive oxygen species causes cell death and disruption of calcium homeostasis in trout hepatocytes. Toxicology 2004, 196 (1), 57-64.
38. Prosser, H. J.; Powis, D. R.; Wilson, A. D., Glass-ionomer cements of improved flexural strength. Journal of dental research 1986, 65 (2), 146-8.
39. Mokhtari, S.; Krull, E. A.; Sanders, L. M.; Coughlan, A.; Mellott, N. P.; Gong, Y.; Borges, R.; Wren, A. W., Investigating the effect of germanium on the structure of SiO2-ZnO-CaO-SrO-P2O5 glasses and the subsequent influence on glass polyalkenoate cement formation, solubility and bioactivity. Materials Science and Engineering: C 2019, 103, 109843.

134
40. Wren, A. W.; Hansen, J. P.; Hayakawa, S.; Towler, M. R., Aluminium-free glass polyalkenoate cements: ion release and in vitro antibacterial efficacy. J Mater Sci Mater Med 2013, 24 (5), 1167-78.
41. Du, R. L.; Chang, J.; Ni, S. Y.; Zhai, W. Y.; Wang, J. Y., Characterization and in vitro bioactivity of zinc-containing bioactive glass and glass-ceramics. J Biomater Appl 2006, 20 (4), 341-60.
42. Lewis, G.; Towler, M. R.; Boyd, D.; German, M. J.; Wren, A. W.; Clarkin, O. M.; Yates, A., Evaluation of two novel aluminum-free, zinc-based glass polyalkenoate cements as alternatives to PMMA bone cement for use in vertebroplasty and balloon kyphoplasty. J Mater Sci Mater Med 2010, 21 (1), 59-66.
43. Goldstein, H.; Kim, D.-s.; Peter, Y. Y.; Bourne, L.; Chaminade, J.; Nganga, L., Raman study of CuO single crystals. Physical Review B 1990, 41 (10), 7192.
44. Xu, J.; Ji, W.; Shen, Z.; Li, W.; Tang, S.; Ye, X.; Jia, D.; Xin, X., Raman spectra of CuO nanocrystals. Journal of Raman spectroscopy 1999, 30 (5), 413-415.
45. González, P.; Serra, J.; Liste, S.; Chiussi, S.; León, B.; Pérez-Amor, M., Raman spectroscopic study of bioactive silica based glasses. Journal of non-crystalline solids 2003, 320 (1-3), 92-99.
46. Yadav, A. K.; Singh, P., A review of the structures of oxide glasses by Raman spectroscopy. RSC advances 2015, 5 (83), 67583-67609.
47. Donkerwolcke, M.; Burny, F.; Muster, D., Tissues and bone adhesives—historical aspects. Biomaterials 1998, 19 (16), 1461-1466.
48. Neve, A.; Piddock, V.; Combe, E., The effect of glass heat treatment on the properties of a novel polyalkenoate cement. Clinical materials 1993, 12 (2), 113-115.
49. Yli-Urpo, H.; Lassila, L. V.; Närhi, T.; Vallittu, P. K., Compressive strength and surface characterization of glass ionomer cements modified by particles of bioactive glass. Dental Materials 2005, 21 (3), 201-209.
50. Karimi, A. Z.; Rezabeigi, E.; Drew, R. A., Glass ionomer cements with enhanced mechanical and remineralizing properties containing 45S5 bioglass-ceramic particles. Journal of the mechanical behavior of biomedical materials 2019, 97, 396-405.
51. Müller, R.; Zanotto, E.; Fokin, V., Surface crystallization of silicate glasses: nucleation sites and kinetics. Journal of non-crystalline solids 2000, 274 (1-3), 208-231.
52. Abo-Mosallam, H.; Park, H., Crystallization characteristics of La2O3-containing glasses for glass ionomer cement. Materials Letters 2012, 72, 137-140.
53. Panzner, G.; Egert, B.; Schmidt, H. P., The stability of CuO and Cu2O surfaces during argon sputtering studied by XPS and AES. Surface science 1985, 151 (2-3), 400-408.
54. Sahai, A.; Goswami, N.; Kaushik, S.; Tripathi, S., Cu/Cu2O/CuO nanoparticles: Novel synthesis by exploding wire technique and extensive characterization. Applied Surface Science 2016, 390, 974-983.
55. Wei, B.; Yang, N.; Pang, F.; Ge, J., Cu2O–CuO Hollow Nanospheres as a Heterogeneous Catalyst for Synergetic Oxidation of CO. The Journal of Physical Chemistry C 2018, 122 (34), 19524-19531.

135
56. Notingher, I.; Boccaccini, A.; Jones, J.; Maquet, V.; Hench, L., Application of Raman microspectroscopy to the characterisation of bioactive materials. Materials characterization 2002, 49 (3), 255-260.
57. Aguiar, H.; Solla, E.; Serra, J.; González, P.; León, B.; Malz, F.; Jäger, C., Raman and NMR study of bioactive Na2O–MgO–CaO–P2O5–SiO2 glasses. Journal of non-crystalline solids 2008, 354 (45-46), 5004-5008.
58. Moshaverinia, A.; Roohpour, N.; Chee, W. W.; Schricker, S. R., A review of powder modifications in conventional glass-ionomer dental cements. Journal of materials chemistry 2011, 21 (5), 1319-1328.
59. Wetzel, R.; Eckardt, O.; Biehl, P.; Brauer, D.; Schacher, F., Effect of poly (acrylic acid) architecture on setting and mechanical properties of glass ionomer cements. Dental Materials 2020, 36 (3), 377-386.
60. Valliant, E.; Dickey, B.; Price, R.; Boyd, D.; Filiaggi, M., Fourier transform infrared spectroscopy as a tool to study the setting reaction in glass-ionomer cements. Materials Letters 2016, 185, 256-259.
61. de Oliveira, B. M.; Agostini, I. E.; Baesso, M. L.; Menezes-Silva, R.; Borges, A. F. S.; Navarro, M. F. L.; Nicholson, J. W.; Sidhu, S. K.; Pascotto, R. C., Influence of external energy sources on the dynamic setting process of glass-ionomer cements. Dental Materials 2019, 35 (3), 450-456.
62. Charrier, E. E.; Pogoda, K.; Wells, R. G.; Janmey, P. A., Control of cell morphology and differentiation by substrates with independently tunable elasticity and viscous dissipation. Nature communications 2018, 9 (1), 449.
63. Xie, D.; Brantley, W.; Culbertson, B.; Wang, G., Mechanical properties and microstructures of glass-ionomer cements. Dental Materials 2000, 16 (2), 129-138.
64. Yamazaki, T.; Schricker, S. R.; Brantley, W. A.; Culbertson, B. M.; Johnston, W., Viscoelastic behavior and fracture toughness of six glass-ionomer cements. The Journal of prosthetic dentistry 2006, 96 (4), 266-272.
65. Yang, J.; Han, C.-R.; Duan, J.-F.; Xu, F.; Sun, R.-C., Mechanical and viscoelastic properties of cellulose nanocrystals reinforced poly (ethylene glycol) nanocomposite hydrogels. ACS applied materials & interfaces 2013, 5 (8), 3199-3207.
66. Chaudhuri, O., Viscoelastic hydrogels for 3D cell culture. Biomaterials science 2017, 5 (8), 1480-1490.
67. Zhu, C.; Han, T. Y.-J.; Duoss, E. B.; Golobic, A. M.; Kuntz, J. D.; Spadaccini, C. M.; Worsley, M. A., Highly compressible 3D periodic graphene aerogel microlattices. Nature communications 2015, 6 (1), 1-8.
68. Lei, Z.; Wang, Q.; Sun, S.; Zhu, W.; Wu, P., A bioinspired mineral hydrogel as a self‐healable, mechanically adaptable ionic skin for highly sensitive pressure sensing. Advanced Materials 2017, 29 (22), 1700321.
136
6 Conclusion
Despite the evident advantages of GPCs for orthopedic applications, the ideal GPC
remains to be developed. The primary issue with these materials is their mechanical
properties, all of which has restricted their indications in the operating to non-load bearing
sites. To this end, this thesis focused on designing and developing a new generation of Cu
incorporated GPCs with improved physical, mechanical and biological response, to expand
their clinical relevance.
In this project, we investigated novel glass polyalkenoate cement (GPC)
formulations that could be utilized for orthopedic applications. We synthesized three
separate glass compositions with incorporation of Cu and analyzed the glass structure and
solubility in relation to the chemistry. We further synthesized the glass polyalkenoate
cements (GPC) or skeletal adhesives using the glass compositions, and investigated the
physical, mechanical, and in vitro biological behavior.
The first part of this work in chapter 3, studied the structure of Cu containing glasses
with suitable characteristics for GPC formation. Addition of CuO to the glass increased the
concentration of BO in the glass network. Glasses presented ICP solubility profiles that
could potentially exhibit bioactive properties. Next, GPCs were formulated using the Cu
incorporated glass compositions in chapter 4. Rheological behavior of the GPCs indicated
adequate physical properties outlined by ISO standards for vertebroplasty or kyphoplasty.
Mechanical properties studies showed time dependent behavior of flexural strength for the
cements; however, the compressive and shear bond strength were not significantly
influenced by maturation time. Simulated Body Fluid (SBF) trials of the cements revealed
a layer of hydroxyapatite, an analogue of the natural bone mineral, was deposited on the
surface of the cements, indicating of in vitro biocompatibility. Additionally, Osteoblast cell
viability techniques were performed on the bone cements which suggested minimal
cytotoxicity. Synthesized glass-based cements showed excellent antibacterial properties
when tested against different strains of bacteria over extended time periods. The promising
results of antibacterial efficacy of GPCs indicates their great potential in minimizing
complications attributed to the antibiotic loaded cements. Later, in chapter 5, GPCs were
developed using annealed composition of Control, and Cu12G glasses. Glasses were
137
annealed below their Tg, and surface crystallization was achieved through heat treatment
of the Cu containing glasses. GPCs formulated with annealed CuBG composition, showed
exceptional viscoelastic behavior. It is proposed the strong gel viscoelastic behavior and
the enhanced mechanical properties are attributed to the unique energy dissipation via the
rearrangement of Cu/PAA interactions which facilitate the extensibility of the polymer
matrix.
To conclude, the glass-based hybrid cements investigated here, encouraged
chemical bone bonding and hence provided strong mechanical interface. Moreover, their
good biological behavior such as bone mineralization, minimal cytotoxicity, and their
superior antibacterial properties suggested these materials provide a better and safer
alternative to commercially available bone adhesives for orthopaedic application. GPCs
formed with annealed Cu containing glasses exhibited viscoelastic behavior, of which is
believed could benefit a wide range of requirement in development of the bone tissue
cements.
Future work may include analysing the mechanical properties of these cements
under cyclic conditions and determining the fatigue strength. Most of mechanical tests
reported in the literature for these materials, were conducted under static conditions, and
have been performed in compression rather than tension. To properly assess the mechanical
effectiveness of these cements, and their clinical relevance towards load bearing defects,
the materials should be tested using clinically relevant mechanical tests, including the
cyclic conditions.
Lastly, in order to transition GPCs with improved to commercially feasible bonce
cement products, future research should focus on performing comprehensive in vivo
studies. This includes animal trials to evaluate the performance of these materials,
considering immunological complications that might arise from glass particles dissolution.
In addition, the bone bonding ability between the cement and the bone mineral, should be
evaluated using animal models.

138
7 Appendix
7.1 Appendix A - Publications
List of publications related to this thesis:
Book Chapter
• S. Mokhtari, A.W. Wren. Bioactive Glass Composite Bone Void Fillers. Bioactive Glasses: Materials, Properties and Applications. 2nd ed., Elsevier, 2017.
Journal Publications
• Mokhtari S, Skelly KD, Krull EA, Coughlan A, Mellott NP, Gong Y, Borges R, Wren AW. Copper-containing glass polyalkenoate cements based on SiO2-ZnO-CaO-SrO-P2O5 glasses: glass characterization, physical and antibacterial properties. Journal of Materials Science: Special Larry Hench Edition. 52 (15) 2017.
• S. Mokhtari, A.W. Wren, Investigating the effect of Copper Addition on SiO2-ZnO-CaO-SrO-P2O5 Glass Polyalkenoate Cements: Physical, Mechanical and Biological Behaviour, Biomedical Glasses, 5 (1), 2019, 13-33.
• S. Mokhtari, E.A. Krull, L.M. Sanders, A. Coughlan, N.P. Mellott, Y. Gong, R. Borges, A.W. Wren, Investigating the effect of germanium on the structure of SiO2-ZnO-CaO-SrO-P2O5 glasses and the subsequent influence on glass polyalkenoate cement formation, solubility and bioactivity, Materials Science and Engineering: C, Volume 103, 2019.
• S. Mokhtari, A.W. Wren. Novel Glass Based Bone Cements Showing Viscoelastic Behaviour: Glass Characterization and Mechanical Properties. Journal of Materials Science. 2020. Submitted manuscript
Conference Presentations
• S. Mokhtari, A.W. Wren. ZrO2 addition in SiO2-CaO-Na2O-P2O5 bioactive glass system: Effects on the network structure and solubility 25th International Congress on Glass, June 2019, Boston, MA, USA.
• S. Mokhtari, A. G. Clare, W. C. LaCourse, A.W. Wren Development of novel zirconium containing bioactive glass fibers: physical and mechanical properties. 43rd International Conference and Exposition on Advanced Ceramics and Composites, Jan 2019, Daytona Beach, FL, USA.
139
• S. Mokhtari, A.W. Wren. Germanium Based Glass Polyalkenoate Cements for Skeletal Applications: Glass Characterization and Physical and Bioactive Properties. Materials Science and Technology Conference, Oct 2018, Columbus, OH, USA.
• S. Mokhtari, A.W. Wren. Copper based Glass Polyalkenoate Bone Cements: effect of copper substitution on physical, mechanical, and antibacterial properties. Materials Science and Technology Conference, Oct 2017, Pittsburgh, PA, USA.
• S. Mokhtari, L.M. Placek, A.W. Wren. Addition of Ge, Ti and Cu on the structure of SiO2-CaO-SrO-ZnO-P2O5 Glasses for Orthopedic Application. 42nd Annual Northeast Bioengineering Conference (NEBEC), April 2016, Binghamton, NY, USA.
7.2 Appendix B – Ge Containing Glass Polyalkenoate Cements
Initially, as a part of this thesis proposal, our approach was to investigate potential
incorporation of Cu, Ge, and Ti in the glass composition of GPCs. Candidate glasses were
synthesized and characterized with respect to their cement formation. Ti containing glasses
showed minimal glass solubility, and slow kinetics of degradation, therefore not ideally
suitable for the acid-base setting reaction of GPCs. On the other hand, Ge containing
glasses were highly soluble and could degrade in the process of GPCs formation.
Preliminary studies were conducted on Ge containing glasses and their resultant cements,
and results are published in a paper presented in the following appendix. Ge containing
GPCs, showed substantial amount of hydroxyapatite deposition when incubated in
simulated body fluid, due to their highly soluble glass composition. However, their
rheological, mechanical, and specifically antibacterial properties suffered when compared
to Cu containing GPCs. Therefore, Cu containing glass series were selected for the
remainder of this thesis.

140

141

142

143

144

145
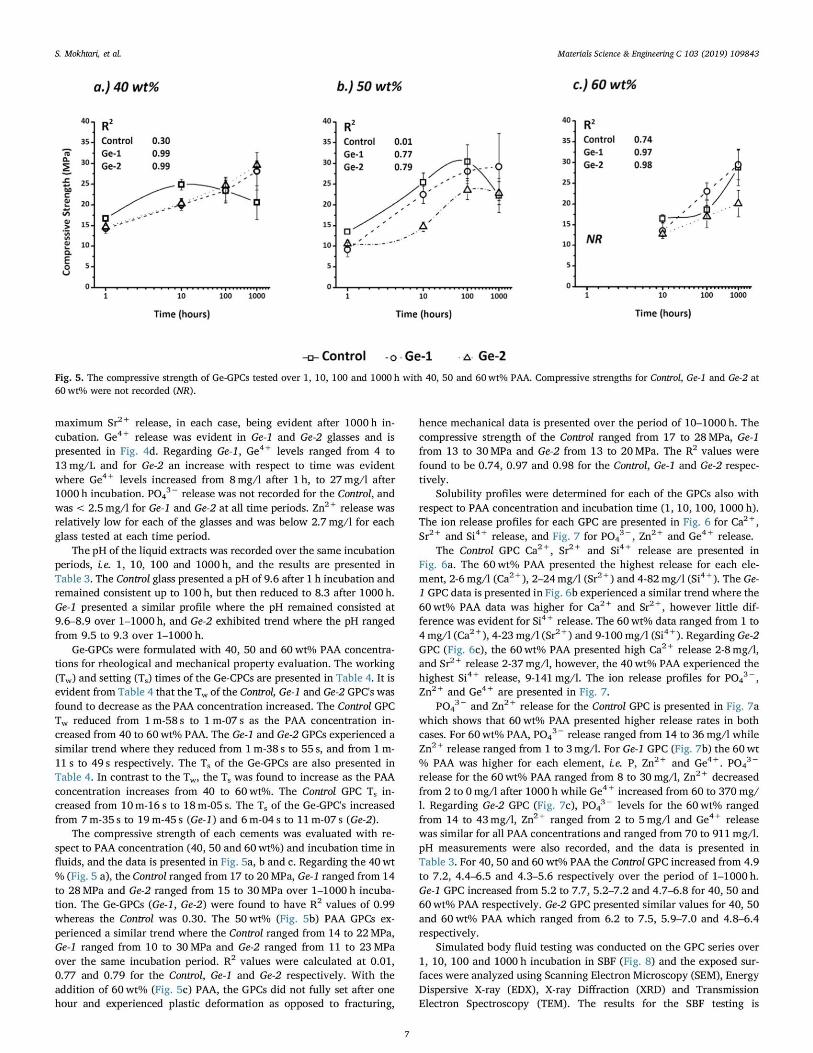
146
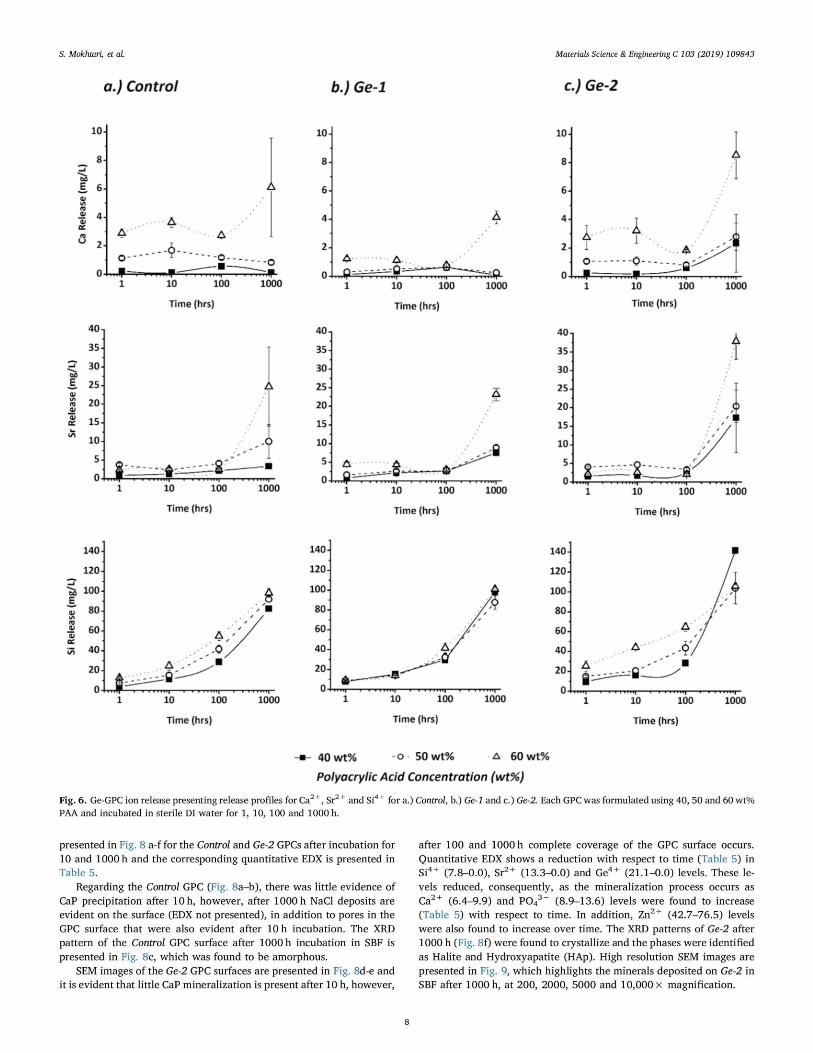
147

148

149

150

151




















