PPT PAK MUNDAKIR-EBN
54
Evidence-Based Practice
-
Upload
iratonisiyah -
Category
Documents
-
view
57 -
download
9
description
EBN punya peran penting dalam memajukan dunia keperawatan
Transcript of PPT PAK MUNDAKIR-EBN

Evidence-Based Practice

What is - Evidence?Segala sesuatu yang memberikan materi/bahan atau informasi yang pada akhirnya dapat dijadikan bukti atau mungkin menjadi dasar, sebagai kebenaran, yang dapat digunakan mendukung atau membantah tentang suatu issu/kasus
(Webster)• EBN can be defined as the application of valid, relevant, research-based information in
nurse decision-making. • Research-based information is not used in isolation, however, and research findings
alone do not dictate our clinical behaviour• Rather, reseach evidence is used alongside our knowledge of our patients (their
symptoms, diagnoses, and expressed preferences),

Evidence-Based Practice
• Evidence-Based Practice Ketelitian, keterbukaan, kejelasan, dan kebijaksanaan yang sekarang digunakan sebagai bukti terbaik dari tenaga-tenaga kesehatan yang ahli, dan nilai-nilai pasien untuk membuat keputusan tentang pelayanan kepada pasien.
(Sackett, 2000)
• Evidence-based nursing practice adalah suatu penyampain proses keputusan yang dibuat diantara praktisi, pasien dan pihak penting lain yang yang di dasarkan pada bukti penelitian, pengalaman dan yang disukai pasien, clinical expertise, dan sumber informasi penting lainnya. (STTI , 2007)
Evidence-Based Practice
• EBP diartikan sebagai penggunaan evidence yang terbaik dalam membuat keputusan terhadap perawatan pasien (Sackett et al. 2000 dalam Moule dan Goodman 2009).

Evidence-Based Practice
Dalam membuat keputusan tentang evidence-based tentang perawatan pasien perawat seharusnya:
1.menggunakaan evidence terkini yang tersedia2.mempertimbangkan dengan mengutamakan
pasien3.menggunakan pengalaman dan keahliannya
untuk membuat sebuah keputusan.

The components of EBN decision
1. Judgement and expertise of the Nurse2. Valid, Relevant Research Evidence3. Patient Preferences and Circumstances4. Available Resources
Langkah2 penerapan EBP
• Langkah pertama yang seharusnya dalam menerapkan EBP adalah dengan membuat sebuah fokus pertanyaan. Sacket et al. (1997) dalam Craig dan Smyth (2007) menjelaskan bahwa untuk membuat pertanyaan lebih fokus dapat menggunakan sebuah kerangka metoda yang diberi nama P-I-C-O (population, intervention, comparison, dan outcome).

PICOPopulationBisa merujuk ke usia tertentu, jenis kelamin, jenis penyakit, tingkat keparawatan panyakit. Populasi ini tegantung dengan apakah hasil yang diharapkan sangat luas ataukah tingkat populasi tertentu. Intervention :dapat berupa sebuah tes atau sebuah paparan dan comparison intervention jika memang ada. Memutuskan sebuah outcome tidak harus diptuskan secara langsung tapi dapat difasilitasi dengan mempertimbangkan perspektif pasien.
• Outcome secara umum kemungkinan adalah susah untuk diukur sehingga untuk mendapatkan objektifitas outcome harus lebih spesifik (Craig dan Smyth 2007). Pertanyaan ini dapat dibangun dengan menggunakan tiga atau empat bagian (untuk lebih jelas bisa dilihat di tabel 1).
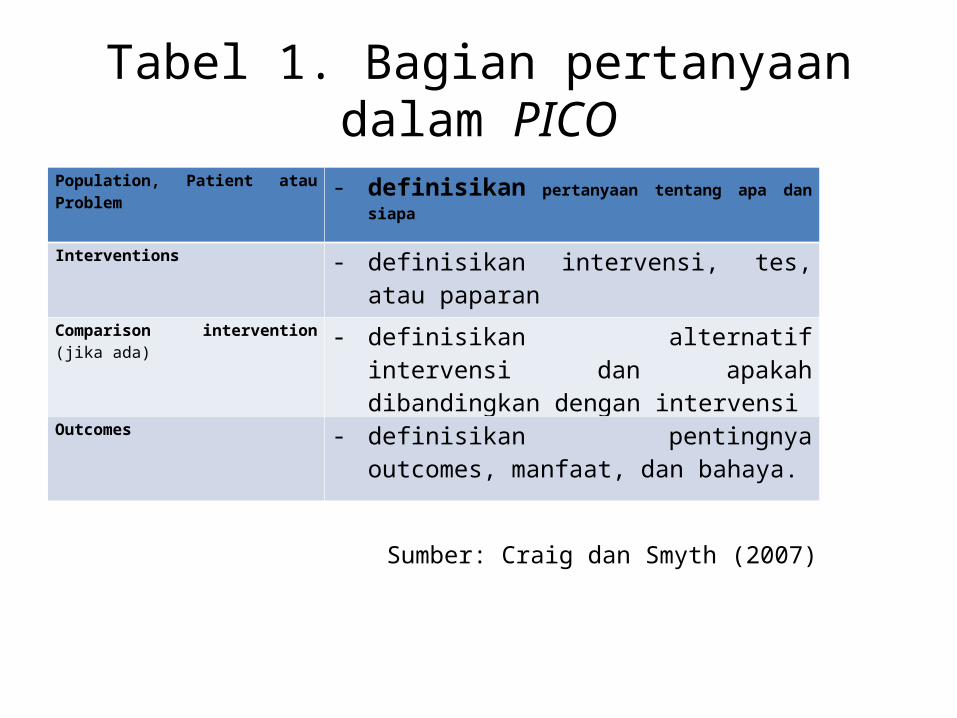
Tabel 1. Bagian pertanyaan dalam PICO
Population, Patient atau Problem - definisikan pertanyaan tentang apa dan siapa
Interventions - definisikan intervensi, tes, atau paparan
Comparison intervention (jika ada) - definisikan alternatif intervensi dan apakah dibandingkan dengan intervensi
Outcomes - definisikan pentingnya outcomes, manfaat, dan bahaya.
Sumber: Craig dan Smyth (2007)
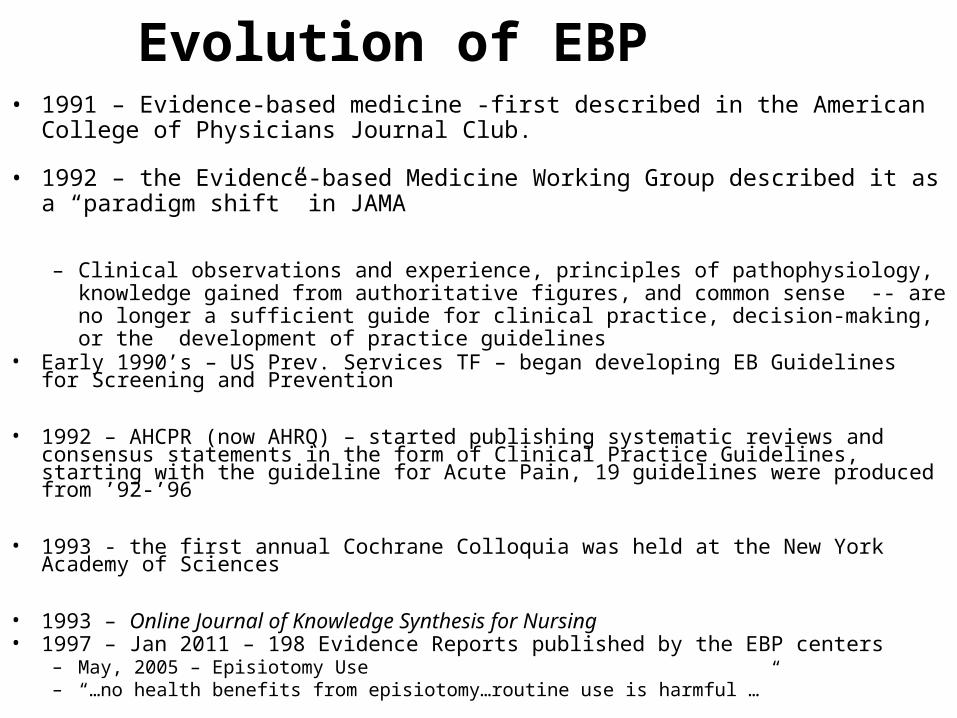
Evolution of EBP• 1991 – Evidence-based medicine -first described in the American College of
Physicians Journal Club.
• 1992 – the Evidence-based Medicine Working Group described it as a “paradigm shift” in JAMA
– Clinical observations and experience, principles of pathophysiology, knowledge gained from authoritative figures, and common sense -- are no longer a sufficient guide for clinical practice, decision-making, or the development of practice guidelines
• Early 1990’s – US Prev. Services TF – began developing EB Guidelines for Screening and Prevention
• 1992 – AHCPR (now AHRQ) – started publishing systematic reviews and consensus statements in the form of Clinical Practice Guidelines, starting with the guideline for Acute Pain, 19 guidelines were produced from ’92-’96
• 1993 - the first annual Cochrane Colloquia was held at the New York Academy of Sciences
• 1993 – Online Journal of Knowledge Synthesis for Nursing • 1997 – Jan 2011 – 198 Evidence Reports published by the EBP centers
– May, 2005 – Episiotomy Use – “…no health benefits from episiotomy…routine use is harmful …”

Recent Evidence Reports
193. Alzheimer's Disease and Cognitive Decline 192. Lactose Intolerance and Health 190. Enhancing Use and Quality of Colorectal Cancer Screening189. Exercise-induced Bronchoconstriction and Asthma188. Impact of Consumer Health Informatics Applications187. Treatment of Overactive Bladder in Women185. Management of Ductal Carcinoma in Situ (DCIS)184. Treatment of Common Hip Fractures151. Nurse Staffing and Quality of Patient Care140. Tobacco Use: Prevention, Cessation, and Control
This is just one example of literature syntheses that are available to support EBP.
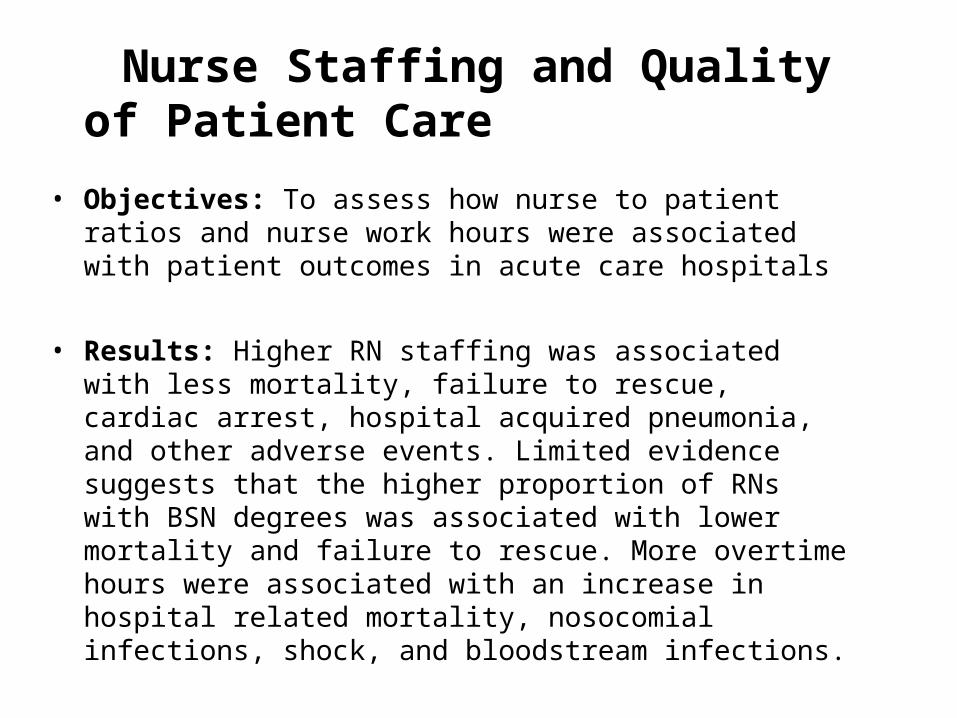
Nurse Staffing and Quality of Patient Care
• Objectives: To assess how nurse to patient ratios and nurse work hours were associated with patient outcomes in acute care hospitals
• Results: Higher RN staffing was associated with less mortality, failure to rescue, cardiac arrest, hospital acquired pneumonia, and other adverse events. Limited evidence suggests that the higher proportion of RNs with BSN degrees was associated with lower mortality and failure to rescue. More overtime hours were associated with an increase in hospital related mortality, nosocomial infections, shock, and bloodstream infections.

Evolution of EBP
• 1998 – Evidence-Based Nursing journal debuted
• 1999 – The UK Department of Health stipulated that, to enhance the quality of care, nursing, midwifery, and health visiting practice must be evidence-based
• 2002 - JCAHO begins requiring monitoring of evidence-based core measures
• 2004 – WorldViews on Evidence-Based Nursing
• 2004 – AACN began publishing “Practice Alerts”
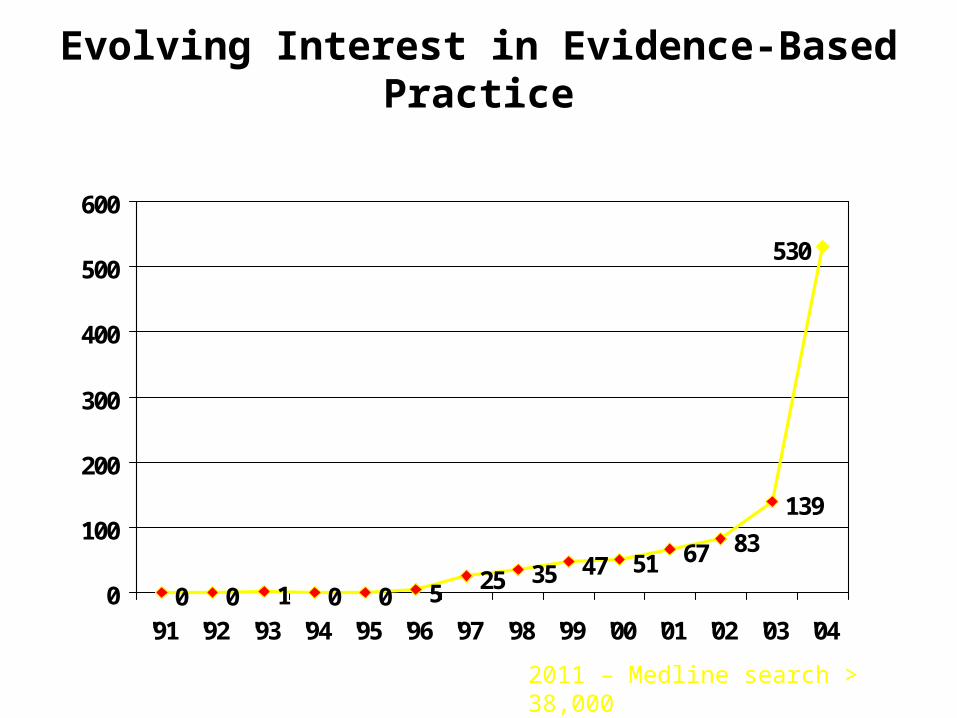
Evolving Interest in Evidence-Based Practice
0 0 1 0 0 5 25 35 47 51 67 83
139
530
0
100
200
300
400
500
600
'91 '92 '93 '94 '95 '96 '97 '98 '99 '00 '01 '02 '03 '04
2011 – Medline search > 38,000

Dalam satu decade, konsep EBP sudah diterima dan digunakan oleh perawat di hampir setiap spesialisasi pelayanan dengan berbagai peran dan posisi perawat di seluruh dunia
EBP – means many things to many people
Factors Contributing to Emphasis on Evidence-Based Nursing Practice
• Scientific knowledge expansion
• Knowledge availability -- The Internet
• Highly educated nurses in clinical settings
Factors Contributing to Emphasis on Evidence-Based Nursing Practice
• Aggressive pursuit of cost-effectiveness• Focus on quality of care, Risk & error reduction• Highly educated consumers • JCAHO/Accreditation expectations• Increased attention to institutional image
– Magnet hospital movement
• Most nurses agree that EBP is important… but how do we make it happen?
What is the 1st step toward EBP for the practicing nurse?
• Asking good clinical questions
• Nurses must be empowered to ask critical questions in the spirit of looking for opportunities to improve nursing care and patient outcomes
• Risk-taking environment

Nursing vs. Medical Questions
• Often more exploratory• Less frequently focused on intervention selection• Less evidence to support many nursing interventions• Most nursing interventions have less capacity for
harm• Many nursing challenges often go beyond individual
clinical interventions (e.g. nurse staffing, education, recruitment)

Clinical Nursing Questions
• Pada pasien pasca operasi, apakah analgesik X atau analgesik Y yang lebih baik menurunkan rasa nyeri?
• Diantara pasien sakit kritis, apakah di kontrol atau bebas kunjungan lebih efektif menurunkan kecemasan pasien?
What kind of questions might the Nurse Manager ask?
• Pada unit medical bedah, bekerja dalam 12 jam satu shift atau 8 jam/shif yang lebih sering terjadi kekeliruan pemebrian obat?

Key Questions to Ask When Considering EBP
• Why have we always done “it” this way?
• Do we have evidence-based rationale?
• Or, is this practice merely based on tradition?
• Is there a better (more effective, faster, safer, less expensive, more comfortable) method?
• What approach does the patient (or the target group) prefer?
• What do experts in this specialty recommend?
•What methods are used by leading/benchmark, organizations?•Do the findings of recent research suggest an alternative method?•Are organizational barriers inhibiting the application of best practices in this situation?•Is there a review of the research on this topic?•Are there nationally recognized standards of care, practice guidelines, or protocols that apply?
Steps in the EBP Process
• Mengembangkan pertanyaan yang baik• Menemukan sumber EB untuk menjawab
pertanyaan• Mengevaluasi kekuatan dan penerapan
evidence • Mengimplementasikan evidence to practice• Evaluating the effects
• Apabila kita menilai pertanyaan tersebut dapat menjadi peluang dan meningkatkan layanan/manfaat, berikutnya kita harus menemukan evidance
• Where should we look?
Strength of Evidence
• Level I - meta-analysis of multiple studies• Level II - experimental studies, RCTs• Level III - quasiexperimental studies• Level IV - nonexperiemental studies
• Level V - case reports, clinical examples
• At what level is most nursing evidence?

AACN Levels of Evidence (Armola, et al. , C C Nurse, 2
LEVEL A Meta-analysis or metasynthesis of multiple controlled studies, supporting a specific action
LEVEL B Controlled, randomized, or nonrandomized studies, supporting a specific action
LEVEL C Qualitative, descriptive or correlational studies or systematic reviews with consistent results
LEVEL D Peer-reviewed prof. organ. standards with studies to support them
LEVEL E Theory-based evidence from expert opinion or case studies
LEVEL M Manufacturer’s recommendations only
AACN Levels of Evidence Armola, et al. , C C Nurse (, 2009)
• Level A
• Level B
• Level C
• Level D
• Level E
• Level M
• Meta-analysis or metasynthesis of multiple controlled studies, supporting a specific action
• Controlled, randomized, or nonrandomized studies, supporting a specific action
• Qualitative, descriptive or correlational studies or systematic reviews with consistent results
• Peer-reviewed prof. organ. standards with studies to support them
• Theory-based evidence from expert opinion or case studies
• Manufacturer’s recommendations only

Preprocessed Evidence
(A. DiCenso, 2009)

Resources to Support Evidence-Based Practice
• Government agencies• Cochrane Collaboration• Professional Organizations• Benchmark Institutions
AHRQ – Agency for Healthcare Research and Quality

Cochrane Collaboration
• “an international, independent, not-for-profit organization of over 27,000 contributors from more than 100 countries, dedicated to making up-to-date, accurate information about the effects of health care readily available worldwide.
• Contributors produce systematic assessments of healthcare interventions, known as Cochrane Reviews, which are published online in The Cochrane Library.
• Rely heavily on RCTs• Primarily focused on effectiveness of interventions, more
medical and pharmaceutical than nursing
Cochrane Collaboration http://www.cochrane.org
Substitution of Drs by Nurses in Primary Care
Objectives: to evaluate the impact on patient outcomes, processes of care, and costs. Outcomes included: morbidity; mortality; satisfaction; compliance; and preference.
Studies were included if nurses were compared to doctors providing a similar primary health care service. Doctors included: general practitioners, family physicians, pediatricians, internists or geriatricians. Nurses included: nurse practitioners, clinical nurse specialists, or advanced practice nurses.
Results: 4253 articles were screened, 25 articles met our inclusion criteria. No appreciable differences were found between doctors and nurses in health outcomes, processes of care, or cost; but patient satisfaction was higher with nurse-led care.
Professional Nursing Organizations Supporting Evidence-Based Practice
• AACN• AWHONN• AORN• ONS• Sigma Theta Tau
Am. Assoc. of Critical Care Nurses
Succinct dynamic directives…supported by evidence to ensure excellence in practice and a safe and humane work environment.
• Venous Thromboembolism Prevention• Oral Care in the Critically Ill• Noninvasive BP Monitoring• Verification of Feeding Tube Placement• Ventilator Associated Pneumonia• Dysrthymia Monitoring
• Published since 2005 • Available free on AACN website• Include ppt presentations and audit tools

Oncology Nursing Society
• EBP Resource Center • http://onsopcontent.ons.org/toolkits/evidence/
• Also provides topical toolkits, on specific topics, plus: • How To Find The Evidence • How To Critique Evidence• How To Develop An Evidence Based Presentation• Evidence Based Practice Education Guidelines• Evidence on Clinical Topics• How to Change Practice• Levels of Evidence Table

Sigma Theta Tau EBP Initiatives
• Strategic Plan• Online Resources
– NKI http://www.nursingknowledge.org > 200 resources for EBP – some free, some for purchase
• New Award for EBP (formerly Clin Scholarship)
• Conferences – International EBP and Research Congress– July, 2010 – Orlando– July, 2011 – Cancun– July, 2012 – Australia
Journals Supporting EBP
– Evidence-Based Nursing– Online Journal of Clinical Innovations– WorldViews on Evidence-Based Nursing– The Online Journal of Knowledge Synthesis for Nursing –
(archived, no longer being published)– Reflections on Nursing Leadership (Vol 28, 2)
Local vs. Global Evidence
• Institutional/Local > National/International– CPI Data/Research Results– Standards & Protocols/Practice Guidelines– Expert Advice– Patient/Family Preferences
Values and Preferences
EBN - integration of the best evidence available, nursing expertise, and the values and preferences of the individuals, families and communities …
Yasmin Amarsi, RNL, 2002:
“The crux is to ensure that EBN attends to what is important to nursing and that caring is not sacrificed on the altar of scientific evidence.”
Amy’s Blog • I consulted a well-regarded oncologist in New York. After the tests she
regretfully informed me that my disease was not curable. She recommended an evidence-based course of medications aimed at slowing the progression. Before I committed, I wanted a second opinion. I secured an appointment with the pre-eminent researcher/ clinician in inflammatory breast cancer. …
• The building was beautiful, the staff attentive. …I had no doubt that the care would be top-notch.
• Everything changed when I sat down with the physician. He never asked about my goals for care. He recommended an aggressive approach of chemotherapy, radiation, mastectomy, and more aggressive chemotherapy. My doctor in New York had said this was the standard, evidence-based protocol for patients in Stage III B…But since I am in Stage IV (with mets) she said I wouldn’t get the benefit of this aggressive, curative approach.

• “All of my patients use this protocol,” he said. • I was shocked. “Does this mean I could get better?” I asked.• “No, this is not a cure.” he answered. “But if you respond to the treatment,
you might live longer, although there are no guarantees.”• My goals are to maximize my quality of life so I can live, work, and enjoy my
family … Would I undergo a year or more of grueling, debilitating treatment only to live with spinal fractures if the cancer progressed? … Would I get the possibility of quantity and no quality?
• I pressed him. “Why do the mastectomy? If the cancer has already spread to my spine. You can’t remove it.”
• His brow furrowed. “Well, you don’t want to look at the cancer, do you?” He made it sound like cosmetic surgery.
• Right now, I feel fine. I can work. I am pain free. Did I want to trade that for a slim chance of a little extra time (no guarantees, of course)?

• “But what about the side effects of radiation?” I asked. “I’ve heard they are terrible.”
• He frowned and seemed annoyed by my questions. “My patients don’t complain to me about it,” he replied.
• Inwardly, I shook my head. Of course his patients never complained to him. Most of them were probably unaware that less aggressive treatments were viable options. To me, there were real drawbacks. Undergo aggressive therapy that might buy me a longer life…at what cost? I might never recover my health for the limited period of time I have.
• This doctor, top in his field, was reflecting the bias of our medical system towards focusing (evidence-based) survival. He was focused only on quantity and forgot about quality.
• The patient’s goals and desires, hopes and fears, were not part of the equation. He was practicing one-size-fits-all (cookbook?) medicine that was not going to be right for me, even though scientific studies showed it was statistically more likely to lengthen life.
• Based on a perverse set of metrics, this oncologist was offering technically the “best” care America had to offer.
• Yet this good care was not best for me. It wouldn’t give me health. Instead, it might take away what health I had. It doesn’t matter if care is cutting-edge, technologically advanced, (and evidence-based); if it doesn’t take the patient’s goals into account, it may not be worth doing.
• I returned to my original New York oncologist.
• I was determined not only to choose treatment that would maximize the healthy time I had remaining, but also to use that time to call on our health care institutions and professionals to make a real commitment to listening to their patients.

Moving Toward our Destiny
Evidence-based practice is every nurses’ responsibility
What can you do to make this goal a reality?

Educator’s Role Educator’s Role– EB Education for EB
Practice– Base educational content
on evidence– Seek the most current
forms of evidence, e.g. journals & online sources vs. texts
– Encourage students to question and challenge
– Teach research content in a manner that is interesting and useful
Manager/Administrator’s Role• Encourage inquisitive minds• Promote risk-taking and
flexibility in the clinical environment
• Incorporate EBP activities into performance evals
• Provide time & resources – unit internet access
• Provide support personnel• Empower staff to make EB
practice changes• Acknowledge and reward EB
improvements
Researcher’s RoleResearcher’s Role– Remain clinically in touch– Conduct clinically useful
studies– Support clinicians in
accessing and synthesizing the evidence
– Collaborate with clinicians and patients
– Disseminate findings that are understandable and accessible
– Emphasize clinical implications
Nurse Clinician’s RoleNurse Clinician’s Role– “Worry and Wonder”– Be the Inquiring Mind– Question clinical traditions– Stay abreast of the literature -
guidelines– Find your niche – and become the
expert– Collaborate with APNs &
researchers– Be an advocate for evidence-based
changes– LISTEN to your PATIENTS – to guard
patient & family preferences

Institute of Medicine October 2010 Report: The Future of Nursing Leading Change, Advancing
Health
1. Remove scope-of-practice barriers2. Expand opportunities for nurses to lead and diffuse collaborative
improvement efforts3. Implement nurse residency programs4. Increase the proportion of nurses with a baccalaureate degree to
80% in 20205. Double the number of nurses with a doctorate by 20206. Ensure that nurses engage in lifelong learning7. Prepare and enable nurses to lead change to advance health8. Build an infrastructure for the collection and analysis of
interprofessional health care workforce data
The Problem – Transition to Practice: Promoting Public Safety
• 35 to 60% new nurses leave position in first year of practice, estimated replacement cost $46,000 to $64,000 per nurse
• 10% typical hospital’s nursing staff comprised of new graduates
• New nurses experience increased stress 3-6 months after hire, increased stress levels are risk factors for patient safety and practice errors
• NCSBN – transition programs reduce 1st year turnover from 35-60% to 6-13%, results in positive return on investment from 67 to 885%
What is the Residency Research Showing?
Retention nationally 94.4% for new grad first year vs. about 73% without residency
Surveys completed initially, 6 months, and 12 months; scores improve in new graduate’s ability to› organize and prioritize› communicate and be leaders at bedside› decreased stress over the year (less so at Kentucky)