KULIAH-Blok18-2012
63
Pemeriksaan Laboratorium Pada Kelainan Sistem Respirasi Dr. Sanarko Lukman Halim, SpPK Bagian Patologi Klinik F.K. UKRIDA
-
Upload
anonymous-qwse0yvwf -
Category
Documents
-
view
225 -
download
1
Transcript of KULIAH-Blok18-2012

Pemeriksaan Laboratorium Pada
Kelainan Sistem Respirasi
Dr. Sanarko Lukman Halim, SpPKBagian Patologi Klinik
F.K. UKRIDA

Tujuan PembelajaranSetelah mempelajari topik ini, mahasiswa memahamitentang berbagai pemeriksaan laboratorium yangdiperlukan pada berbagai kelainan/penyakit saluranpernafasan serta interpretasi hasil pemeriksaan1. Respiratory Acidosis dan Respiratory Alkalosis
akibat penyumbatan saluran pernafasan atau pada kelainan paru,rongga torak.
2. Kelainan paru yang disebabkan infeksi, alergi, trauma, kelainan koagulasi, cystic Fibrosis atau penyakit sistemik

Fungsi Sistem Respiratorik• Oxygen transport• Respiration• Ventilation
– Air Pressure Variances– Airway Resistance– Compliance
• Lung Volumes and Capacities• Diffusion• Perfusion• Ventilation and Perfusion Balance and
ImbalanceThe act of moving air into and out of the lungs is called breathing.

Respiratory Structures and Organs

Transpor Gas• Oxygen is carried in
the blood in two forms: dissolved and attached to hemoglobin
• PaO2 represents the level of dissolved oxygen in plasma (about 3%)
• Rest is carried on hemoglobin - oxyhemoglobin

Human Respiration• Works together with the circulatory system• Exchange of gases between atmosphere, blood,
and cells• If respiratory system and/or circulatory system
fails, death will occur• Cells need O2 for work; release CO2 as a waste
product• Accumulation of excess CO2 is toxic to cells and
MUST be removed

Respiratory System• Intakes oxygen• Releases carbon
dioxide waste
Circulatory system• Transports gases
in blood between lungs and cells

Kelainan Paru dan Saluran Pernafasan pCO2 ↑, pO2 ↓ → Respiratory Acidosis
• Airway obstruction • Asthma• Bronchitis, bronchiectasi, pneumonia,
Aspiration pneumonia, Hospital acquired pneumonia, Pneumonia in Immuno-supressed pneumonia.
• TBC• Chronic Obstructive Pulmonary Disease
(COPD)• Pulmonary Embolism

Kelainan Paru dan Saluran Pernafasan pCO2 ↑, pO2 ↓ → Respiratory Acidosis
• Environment Lung DiseasesAsbestosis, Building-related Diseases
• Atelectasis• Abcess in the Lungs• Lung Cancer• Hyalin Membrane Disease

FAKTOR-FAKTOR yang MENGURANGI FUNGSI RESPIRASI
• Positioning• Environment• Air pollution• Pollens and allergens• Smoking• Drugs and alcohol• Nutrition• Restricted lung movement• Airway obstruction

Gagal PernafasanRespiratory FailurePaO2<60mmHg respiratory failure
Notice: sea level, quiet, inspire air rule off other causes ( heart disease)
PaCO2: The carbon dioxide partial pressure of
arterial bloodNormal: 35-45mmHg (4.7-6.0kPa) mean: 40mmHgSaO2: Saturation of arterial blood oxygenNormal: 0.95-0.98Significance: a parameter to evaluate hypoxia,but not sensitive

Penyebab2 Asidosis RespiratorikRespiratory pathophysiology
respiratory arrestairway obstructionsevere pneumoniachest traumapneumothorax
Acute drug intoxicationespecially narcotics, sedatives
Residual neuromuscular blockadeHead trauma

Penyebab2 Asidosis Respiratorik menahun
Chronic lung disease Neuromuscular diseaseExtreme obesity Chest wall deformity

Penyebab2 Alkalosis RespiratorikPainAnxietyHyperventilationHypoxemiaRestrictive lung
diseaseSevere
congestive heart failure
Pulmonary emboli
DrugsSepsisFeverThyrotoxicosisPregnancyOveraggressive
mechanical ventilation
Hepatic failure

Four primary conditions are possible 1. Respiratory acidosis
+ acute blood response+ chronic renal response
2. Respiratory alkalosis + acute blood response + chronic renal response
3. Metabolic acidosis+ respiratory response
4. Metabolic alkalosis+ respiratory response

Blood Gas Alterations 1/2• Respiratory Acidosis
– Lower pH due to CO2 accumulation or retention in the blood greater than the high normal value
– Controlled by the lungs– Compensation attempts
• Kidneys attempt to excrete nonvolatile acids and retain HCO3
-Caused by inefficient respiration and/or hypoventilation-Can be acute or chronic–Tachycardia and cardiac arrythmias seen in acute respiratory acidosis

Blood Gas Alterations 2/2• Respiratory Alkalosis
–pH is high due to low CO2–Increased respiratory rate blows
off CO2–Blood contains too little carbonic
acid (carbonic acid deficits)–Compensation
• Kidneys will excrete bicarbonate

Management of Alterations Respiratory Acidosis
–Determine underlying cause of hypoventilation and treat the cause
• Respiratory Alkalosis –Determine underlying cause of
hyperventilation and treat the cause

Sampel utk Analisa Gas Darah
clean procedure (gloves, alco wipe)Have gauze for application of pressure post
arterial puncture4 mins of pressure is idealEspecially in patients who are
anticoagulated23G needle easier, but use what you preferROTATION and INVERSION of the tube for 20
seconds to dissolve and mix the heparin Ice only necessary if there will be a delay from
sampling to testing.

Hasil tes AGDpH - measures acidity/alkalinitypCO2 (partial pressure of CO2)
measures respiratory component[HCO3-] – (bicarbonate concentration)
measures metabolic componentderived value (H-H equation)
pO2 (partial pressure of O2)BE (base excess)O2 saturationSometimes AG (anion gap)Sometimes electrolytes and glucose

Nilai Rujukan Gas Darah
Blood Gas Parameter Parameter Reported and Symbol Used
Normal Value
Carbon dioxide tension*
PCO2 35 – 45 mm Hg (average, 40)
Oxygen tension* PO2 80 – 100 mm Hg
Oxygen percent saturation
SO2 97
Hydrogen ion concentration (–Log CH+)*
pH 7.35 – 7.45
Bicarbonate HCO3- 22 – 26 mmol/L
Analisa Gas Darah/Arterial Blood Gases (ABG)
* Indicates measured parameter Normal values may differ slightly in exams

High pH Low pH
Alkalosis Acidosis
HighPaCO2
LowPaCO2
HighPaCO2
LowPaCO2
Metabolic Respiratory Respiratory Metabolic

Perlu di Tanya? Is the patient acidotic or alkalotic?
If pH < 7.35, the patient is acidoticIf pH > 7.45, the patient is alkalotic? Is the primary cause respiratory or
metabolic?? Is there compensation?? Is the patient hypoxic?
? (oxygen status, A-a)? What is going on?

Oxygen status• Hypoxaemia
• decreased oxygen content of blood • pO2 less than 60 mmHg and
saturation is less than 90%
• Hypoxia• Levels of pO2 sufficiently low to
have an adverse effect on tissue function

Jenis-jenis Hipokia Hypoxic hypoxia
due to low blood pO2e.g. due to lung disease processes
Anaemic hypoxiainadequate O2 delivery to tissues
e.g. in anaemia or CO poisoning Circulatory hypoxia
inadequate blood flow to tissuese.g. shock
Histotoxic hypoxiainability of tissue to use the oxygen
classically, in cyanide poisoning

• CO2 and PCO2
– Pulmonary function & CO2 homeostasis– CO2 elimination
• Hyperventilation– Lowering PCO2
– Alveolar hyperventilation– Causes of alveolar hyperventilation
• Hypoventilation– Raising PCO2
– Alveolar hypoventilation– Causes of alveolar hypoventilation

EquivalencesDisorder Cause Mechanism
Respiratory acidosis
Hypercapnia Alveolar hypoventilation
pH PCO2 CO2 retention
Respiratory alkalosis
Hypocapnia Alveolar hyperventilation
pH PCO2 blow off CO2

Respiratory Compensation for Preventing Change in pH
AcidosisCO2 H+
AcidaemiapH , PCO2
CO2 removalVia respiration
Normal pH
Normal or CO2 removal
Slow or CO2 removal
Cells/Tissue Blood
Lungs
Blood
Hypoventilate
Hyperventilate
Acidosis may be accompanied by acidaemia.The change in pH may be prevented by respiratory removal of CO2.

Respiratory Compensation for Preventing Change in pH
AlkalosisCO2
HCO3-
AlkalaemiapH , PCO2 , HCO3
-
CO2 retentionVia respiration
Normal pH
Normal or CO2 retention
Slow or CO2 retention
Cells/Tissue Blood
Lungs
BloodHypoventilate
Hyperventilate
Alkalosis will not be accompanied by alkalaemia if enough CO2 has been retained to prevent the change in pH.

Terms used for describing compensation• Compensated
– The compensatory mechanisms have come into play in a normal manner; does not necessarily imply that the plasma pH is within the normal range
• Uncompensated– Compensation cannot occur due to some
abnormality; patient may show no sign of compensation
• Partially compensated– Intermediate state where compensation is
occurring but is not yet as complete as it should be

Metabolic and Respiratory Acid-Base Changes in Blood
pH pCO2 HCO3-
Acidosis1. Acute metabolic N 2. Compensated metabolic N 3. Acute respiratory N4. Compensated respiratory N
Alkalosis1. Acute metabolic N 2. Chronic metabolic 3. Acute respiratory N4. Compensated respiratory N
=decreased; =increased; N=normal

Sputum (bukan Ludah) Collection• Proper patient instruction
– Food should not have been ingested for 1-2 h prior to expectoration
– The mouth should be rinsed with saline or water
– Patient should breathe and cough deeply– Patient should expectorate into a
sterile container• Transport container immediately to lab• Perform Gram stain and plant specimen as
soon as possible

Sputum collection
• Sputum of less than 2ml should not be processed unless obviously purulent
• Only 1 sputum per 24hr .submitted • Some scoring system should be used to
reject specimen that re oral contamination.

Sputum collection
• Transportation in <2 hr is recommended with refrigeration if delays anticipated.
• Handle all samples using universal precautions.
• Perform Gram stain and plant specimen as soon as possible

Induced sputumPatients who are unable to produce sputum maybe assisted by respiratory therapy technician.Aerosol induced specimen are collected byallowing the patient to breath aerosolized dropletsof a solution of 15% sodium chloride and 10%glycerin for approximately 10 minute . Obtainingsuch specimen may avoid the need for a moreinvasive procedures ,such as bronchoscopy orneedle aspiration, in many cases.

Sputum Gram Stain and CultureProponents• Demonstration of
predominant morphotype on Gram stain guides therapy
• Accuracy is good when strict criteria are used
• Cheap, so why not?
Antagonists• Poor specimen
collection• Intralaboratory
variability (Gram stain interpretation)
• Low sensitivity and specificity
• Empiric treatment guidelines
• Not cost effective

Gastric aspirationThe gastric aspiration is used exclusively forisolation of acid-fast bacilli and may be collectedfrom patients who are unable to produce sputum,particularly young children. The relative resistanceof mycobacteria allows them to remain viable for ashort period. Gastric lavage must be delivered tothe lab immediately so that the acidity can beneutralized. Specimen can be first neutralized andthen transported if immediate delivery is notpossible.

Definition Pleural Effusions• Increased amount of fluid within the
pleural cavity– Stedman’s Medical Dictionary
• Accumulation of fluid between the layers of the membrane that lines the lungs and the chest cavity– Medline Plus
Urgent pleural disorders• Pleural emergencies: haemorrhage - haemothorax
elevated pleural pressure- tension pneumothorax
- massive pleural effusion

Haemothorax pleural fluid with Ht > 50% blood Ht
CAUSES:• chest trauma: penetrating / non – penetrating
(lung blood vessels, chest wall, diaphragm, pleural adhesions, mediastinum, large vessels, abdomen)
• iatrogenic(pleural biopsy, subclavian or jugular CVC placement, thoracentesis, transthoracic or transbronchial NA, esophageal variceal TH,...)
• nonthraumatic(pleural malignancy, anticoagulant TH, spontaneous rupture of vessel (AO aneurism), bleeding disorder, thoracic endometriosis)

Tipe• Hydrothorax• Hemothorax• Chylothorax• Pyothorax / Empyema
Efusi PleuraKlasifikasi a. Transudate
– Ultrafiltrate of plasma
– Small group of etiologies
b. Exudate– Produced by host
of inflammatory conditions
– Large group of etiologies

DISORDERS• Obstruction of Upper
Airway• Atelectasis• Tracheobronchitis• Pneumonia
– Bacterial– Viral– Fungal– Aspiration– Hypostatic– Chemical
• Tuberculosis• Abscess
• Pleural disorders• Pulmonary edema• Chest Trauma• Pulmonary Emboli
(PE)• Chronic obstructive
pulmonary disease (chronic airflow limitation)– Bronchitis– Emphysema– Asthma– Bronchiectasis

Diagnostic Tests• CBC• Chest x-ray/ CT• MRI/Fluoroscopic studies• Sputum culture and
sensitivity• ABG’s• Pulse oximetry
• Bronchoscopy• Mantoux• Pulmonary
angiography• Pulmonary Function
Test• VQ Scan• Thoracentesis

The Tuberculosis (TB) PandemicTB is spread from an
infectiousperson to a vulnerable personthrough the air
TB usually affects the lungsbut can affect any part of an infected person

HIV/AIDS and TB: A Deadly Combination
• HIV suppresses the human immune system• TB suppresses the human immune system• Each makes the other worse synergistically

Definition of Asthma• Chronic inflammatory disorder of the
airways in which many cells and cellular elements play a role. In susceptible individuals, this inflammation causes recurrent episodes of wheezing, breathlessness, chest tightness, and coughing, particularly at night or in the early morning. These episodes are associated with widespread but variable airflow obstruction that is reversible either spontaneously, or with treatment.

Bronchial Asthma

Risk Factors for COPDHost factors
• Alpha-1-antitrypsin deficiency
• Asthma and airway hyperresponsiveness
• Disordered lung development
Environmental factors• Tobacco smoke• Occupational
dusts/chemicals• Air pollution• Childhood
infections• Lower
socioeconomic status

Chronic Bronchitis• Persistent cough with sputum production
for at least 3 months in ≥ consecutive years
• Simple / Chronic asthmatic / Obstructive• Most frequent in middle-aged men• Higher incidence in urban dwellers• May coexist with emphysema• Presents with exertional dyspnoea and
frequent respiratory tract infections

Komplikasi Bronkhitis Menahun• ↓PaO2 ↑PaCO2 ….Respiratory failure• Respiratory tract infections (H. influenzae,
Strep. Pneumoniae)• Pulmonary hypertension → Cor
pulmonale• Atypical metaplasia / dysplasia of
respiratory epithelium….Bronchogenic carcinoma

Emphysema• Abnormal permanent enlargement of the
airspaces distal to the terminal bronchiole, accompanied by destruction of their walls
• Types: (1) centrilobular(2) panlobular(3) paraseptal(4) irregular
• Associated with heavy cigarette smoking

Patogenesis Emfisema

Bronchiectasis• A chronic necrotising infection of the
bronchi and bronchioles associated with abnormal permanent dilation of these airways
• Presents with cough, productive of large amounts of foul-smelling, purulent sputum, hamoptysis and digital clubbing
• Pooled secretions in lower lobes → respiratory tract infections

Bronchiectasis Aetiology • Bronchial obstruction
Tumour, foreign bodies, mucous impactionAsthma / Chronic bronchitis
• InfectionTuberculosis, Staphylococcus aureus, Measles, Pertussis
• CongenitalCongenital bronchiectasis, Cystic fibrosis, Intralobar sequestration, Immunodeficiency, Kartagener’s syndrome, Yellow nail syndrome

Cystic Fibrosis Genetic defect


Lung Abscess
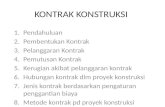
Figure 16-1. Lung abscess. A, Cross-sectional view of lung Figure 16-1. Lung abscess. A, Cross-sectional view of lung abscess. abscess. AFC,AFC, Air-fluid cavity; Air-fluid cavity;
RB,RB, ruptured bronchus (and drainage of the liquified contents ruptured bronchus (and drainage of the liquified contents of the cavity); of the cavity); EDA,EDA, early development of abscess; early development of abscess; PM,PM, pyogenic membrane. Consolidation (B) and excessive pyogenic membrane. Consolidation (B) and excessive
bronchial secretions (C) are common secondary anatomic bronchial secretions (C) are common secondary anatomic alterations of the lungs.alterations of the lungs.
A
AFC
RB
EDAPM
B
C

Atelectasis Assessment and Diagnostic Findings
• SpO2 < 90%• PaO2 < 80• PaCO2 > 45• HCO3- to
compensate

Evaluasi Laboratorium• Deteksi berkurangnya fungsi saluran
pernafasan dan alveoli → Analisa Gas Darah.• Deteksi adanya infeksi dengan memperhatikan
1. Petanda hematologi adanya infeksi/inflamasi:* Jumlah Leukosit, Gambaran Darah Tepi,
LED, CRP, IgE. 2. Deteksi kuman: pembiakan, preparat,secara
imunologis• Periksa adanya cystic fibrosis sebagai
penyebab sputum kental→ infeksi, sesak nafas (DD/ Asma)

Retensi CO2 PCO2
• Meningkatnya CO2 → H+ → AsidosisAnalisa gas darah Respiratory Acidosis
Reaction shifts right
Retention of CO2 by the lungs CO2, PCO2
CO2 + H2O H2CO3 H+ + HCO3-
Reaction shifts right [H+], pH, acidosis

Mikrobiologi• The culture of lower respiratory specimens may
result in more unnecessary microbiologic effort than any other type of specimen.”
• Overtreatment has lead to resistance – Multidrug resistant Streptococcus
pneumoniae– Resistance among hospital acquired
pathogens such as Acinetobacter, Pseudomonas aeruginosa E.coli K.pneumonia (ESBLs) MRSA and others

Categories of Lower Respiratory Tract Infections
• Acute bronchitis• Community acquired pneumonia• Hospital acquired pneumonia• Pneumonia in the
immunocompromised host

Community Acquired Pneumonia Diagnosis Available Test Methodologies
• Sputum Gram stain and culture• Blood cultures• Serologic studies• Antigen detection tests• Nucleic acid amplification tests

McPherson RA., Pincus MR., Editors Henry’s Clinical Diagnosis and Management by Laboratory Methods 21st edition, ISBN-13:978-1-4260-0287-1 Saunders Elsevier 2007
Daftar Kepustakaan
1. Gaw A, Clinical Biochemistry, ISBN 0-443-04481-3 Churchill Living Stone New York, 1995, 92-93 Churchill Living Stone New York ISBN 0-443-04481-3. 1995
2. Abraham P. editor, Physiology, ISBN-13: 978-1-905704-64-4, Amber Books London , 2007 6
3. Johnston SL, Holgate ST, Asthma: Critical Debate, ISBN 0-632-05721-1 Oxford,England, Blackwell Science,2002.