KATA PENGANTAR - Universitas Indonesia
117
Transcript of KATA PENGANTAR - Universitas Indonesia



Ii
KATA PENGANTAR
Puji syukur kita panjatkan kehadirat Tuhan Yang Maha Esa, atas berkat rahmat-Nya “Petunjuk Teknis Kesiapsiagaan Kondisi Darurat dan/atau Bencana di Rumah Sakit” dapat diselesaikan. Indonesia merupakan negara yang sangat rawan bencana, baik bencana alam,bencana non alam dan bencana sosial (akibat ulah manusia). Upaya mengurangi dampak yang ditimbulkan akibat kejadian bencana tersebut, Rumah Sakit perlu meningkatkankesiapsiagaan dalam menghadapi keadaan darurat dan/atau bencana.
Buku petunjuk teknis ini menjelaskan lebih rinci tentang standar kesiapsiagaan menghadapi kondisi darurat dan/atau bencana yang merupakan salah satu standar yang ada di Permenkes No. 66 Tahun 2016 tentang Keselamatan dan Kesehatan Kerja Rumah Sakit.Peningkatan kualitas program khususnya kesiapsiagaan menghadapi kondisi darurat dan/atau bencana di Rumah Sakit selalu menjadi prioritas kami, untuk itu kritik dan saran membangun dari semua pihak sangat kami harapkan demi penyempurnaan buku ini.
Terima kasih kami sampaikan kepada tim penyusun dan semua pihak yang telah berkontribusi dalam penyelesaian panduan ini. Diharapkan buku ini dapat memberikan informasi bagi semua Rumah Sakit dalam menghadapi keadaan darurat dan/atau bencana.
Jakarta, Juni 2020Direktur Kesehatan Kerja dan Olahraga
drg. Kartini Rustandi, M.Kes

II

III
DAFTAR ISI
DAFTAR TABEL DAN BAGAN .......................................................................... vBAB I PENDAHULUAN ................................................................................... 1 A. Latar Belakang .................................................................................... 1 B. Tujuan ................................................................................................... 2 C. Sasaran ................................................................................................ 2 D. Ruang Lingkup ...................................................................................... 2BAB II KONDISI DARURAT DAN/ATAU BENCANA ............................................ 3 A. Pengertian ............................................................................................ 3 B. Kriteria Kondisi darurat di Rumah Sakit ................................................... 3 C. Jenis bencana yang dapat berdampak pada kesiapan Rumah Sakit ........... 4BAB III IDENTIFIKASI DAN PENILAIAN RISIKO KONDISI DARURAT DAN/ATAU BENCANA DI RUMAH SAKIT ......................................................... 5 A. Proses Manajemen Risiko ...................................................................... 5 B. Metode Penilaian Risiko ......................................................................... 7 1) Hazard Identification, Risk Assessment, and Determining Control (HIRADC) .......................................................................................................... 7 2) Hazard and Vulnerability Analysis (HVA) ................................................ 9 3) Hospital Safety Index (HSI) ................................................................ 13 4) Fire Safety Risk Assesment (FSRA) ...................................................... 15BAB IV KESIAPSIAGAAN KONDISI DARURAT DAN/ATAU BENCANADI RUMAH SAKIT ......................................................................................... 17 A. Tim tanggap darurat dan/atau bencana .................................................. 17 B. Standar Prosedur Operasional (SPO) ...................................................... 22 C. Sistem Kode Darurat di Rumah Sakit ..................................................... 24 D. Tingkat Kesiapsiagaan Kondisi darurat dan/atau bencana ....................... 26
E. Rambu-rambu mengenai keselamatan dan tanda darurat sesuai dengan standar dan pedoman teknis ................................................................ 26
F. Kedaruratan Kesehatan Masyarakat ....................................................... 29 BAB VI PELATIHAN DAN SIMULASI KONDISI DARURATDAN/ATAU BENCANA DI RUMAH SAKIT ......................................................... 39 A. Pelatihan .............................................................................................. 39 B. Simulasi ............................................................................................... 39 C. Evaluasi Simulasi Kondisi darurat dan/atau bencana ............................... 40 BAB VII PENUTUP ....................................................................................... 41 DAFTAR PUSTAKA ....................................................................................... 42 LAMPIRAN .................................................................................................. 43

IV

V
iv
DAFTAR TABEL DAN BAGAN
Tabel 1. Formulir Identifikasi Bahaya, Penilaian dan Pengendalian Risiko di Rumah Sakit
Tabel 2. Contoh Matriks Risiko berdasarkan hasil identifikasi dan penilaian risiko
Tabel 3. Contoh Kategori Dampak terhadap keselamatan dan kesehatan
Tabel 4. Contoh Kategori Kemungkinan/ Probabilitas
Tabel 5. Hazard and Vulnerability Analysis (HVA) Kondisi darurat dan/atau bencana
Tabel 6. Kategori Hasil Perhitungan HSI
Tabel 7. Tingkat Status Kondisi Darurat dan/atau Bencana
Tabel 8. Contoh Desain dan Penempatan Rambu-rambu Keselamatan dan Tanda Darurat
Bagan 1. Struktur tim tanggap darurat dan/atau bencana

VI

1
1
BAB I PENDAHULUAN
A. Latar Belakang Bencana adalah peristiwa atau rangkaian peristiwa yang mengancam dan mengganggu kehidupan dan penghidupan masyarakat, yang disebabkan baik oleh faktor alam dan/atau faktor nonalam maupun faktor manusia. Bencana yang disebabkan faktor alam sering kali terjadi di Indonesia. Hal ini disebabkan secara geografis Indonesia terletak di cincin api pasifik (wilayah dengan banyak aktivitas tektonik), sehingga terus menghadapi risiko bencana berupa letusan gunung berapi, gempa bumi, banjir, dan tsunami. Data BNPB tahun 2019, mengungkapkan bahwa kejadian bencana alam mengalami peningkatan jumlah tiap tahunnya. Bencana ini berpotensi merusak bahkan menghancurkan pemukiman, tempat kerja, tempat ibadah, termasuk fasilitas pelayanan kesehatan. Sebagai contoh, gempa bumi di Kota Padang pada tahun 2009 menghancurkan 85 Rumah Sakit dan fasilitas pelayanan kesehatan. Gempa bumi dan tsunami yang terjadi di Sulawesi Tengah tahun 2018 mengakibatkan 18 Rumah Sakit dan 167 fasyankes (117 Pustu dan 50 Puskesmas) mengalami kerusakan (Data Dinkes Provinsi Sulawesi Tengah, Februari 2019).
Selain bencana yang disebabkan oleh alam, bencana juga bisa disebabkan oleh faktor non alam diantaranya adalah outbreak, epidemic dan wabah penyakit. Bencana epidemi yangmenular hingga lintas negara berubah menjadi pandemi sehingga perlu diwaspadai.Bencana pandemic sering disebabkan oleh Penyakit Infeksi Emerging dan Re-emerging(PINERE) atau new - emerging infectious diseases. Setiap bencana akan menimbulkan kerugian baik harta benda, kerusakan lingkungan bahkan korban jiwa. Rumah Sakitsebagai salah satu fasilitas yang memberikan layanan kesehatan bagi korban bencana diharuskan memiliki kesiapan dan rencana mitigasi untuk menghadapi bencana yang akan terjadi, mengingat kejadian bencana dapat menimbulkan korban jiwa massal dan kemungkinan Rumah Sakit tersebut juga terkena dampak bencana.
Manajemen darurat dan/atau bencana harus dapat dilakukan oleh Rumah Sakit sehinggapada saat terjadi bencana, Rumah Sakit dapat diakses, dapat memberikan layanan kesehatan terhadap korban bencana dan berfungsi maksimum dengan infrastruktur yang sama sebelum terjadi bencana, selama bencana, dan segera setelah bencana (WHO, 2015). Program manajemen bencana Rumah Sakit mengarahkan perkembangan dan eksekusi kegiatan yang mampu memitigasi, mempersiapkan, merespon, dan pemulihan situasi dari suatu bencana.
Kementerian Kesehatan telah mengeluarkan Permenkes nomor 66 tahun 2016 tentang Keselamatan dan Kesehatan Kerja Rumah Sakit (K3RS) yang mengatur tentang penyelenggaraan SMK3RS (Sistem Manajemen Keselamatan dan Kesehatan Kerja Rumah Sakit) dan melakukan penerapan standar K3RS, termasuk didalamnya kesiapsiagaan Rumah Sakit menghadapi kondisi darurat dan/atau bencana. Dalam proses akreditasi, Rumah Sakit diharuskan dapat mengembangkan dan memelihara program manajemen

2 2
bencana untuk menanggapi becana baik bencana non alam, bencana alam atau lainnya yang memiliki potensi terjadi dimasyarakat (SNARS edisi 1.1).
Sehubungan dengan pertimbangan tersebut, perlu disusun petunjuk teknis kesiapsiagaan menghadapi kondisi darurat dan/atau bencana di Rumah Sakit.
B. Tujuan Sebagai acuan Rumah Sakit dalam melakukan upaya kesiapsiagaan menghadapi kondisi darurat dan/atau bencana.
C. Sasaran 1) Pimpinan Rumah Sakit2) Manajemen Rumah Sakit3) Pengelola K3 4) Pegawai Rumah Sakit5) Pasien6) Pihak ketiga di Rumah Sakit / tenant7) Pengunjung/ keluarga pasien
D. Ruang lingkupPetunjuk teknis ini mengatur ketentuan-ketentuan yang dianjurkan untuk dilakukan oleh Rumah Sakit dalam menghadapi kondisi darurat dan/atau bencana dari aspek pengelolaan sumber daya yang ada untuk menghadapi bencana baik internal maupun bencana eksternal Rumah Sakit. Lingkup kesiapsiagaan Rumah Sakit dalam menghadapi bencana ekternal sebatas fungsi Rumah Sakit yaitu menerima rujukan korban bencana dari luar.

33
BAB II KONDISI DARURAT DAN/ATAU BENCANA
A. Pengertian• Darurat adalah suatu keadaan tidak normal/tidak diinginkan yang terjadi pada
suatu tempat/kegiatan yang cenderung membahayakan manusia, merusak peralatan/harta benda atau merusak lingkungan sekitarnya yang masih dapat ditangani oleh sumber daya internal Rumah Sakit.
• Bencana adalah peristiwa atau rangkaian peristiwa yang mengancam dan mengganggu kehidupan dan penghidupan masyarakat yang disebabkan, baik oleh faktor alam dan/atau faktor nonalam maupun faktor manusia sehingga mengakibatkan timbulnya korban jiwa manusia, kerusakan lingkungan, kerugian harta benda, dan dampak psikologi yang tidak dapat ditangani sendiri oleh sumber daya internal Rumah Sakit.
• Kesiapsiagaan adalah serangkaian kegiatan yang dilakukan untuk mengantisipasi kondisi darurat dan/atau bencana melalui pengorganisasian serta melalui langkah yang tepat guna dan berdaya guna.
• Tanggap darurat dan bencana adalah serangkaian upaya yang dilakukan dengan segera pada saat kejadian darurat dan bencana untuk menangani dampak buruk yang ditimbulkan, meliputi kegiatan penyelamatan dan evakuasi korban, harta benda, pemenuhan kebutuhan dasar, perlindungan, pengurusan korban, penyelamatan, dan pemulihan sarana prasarana.
• Rumah Sakit adalah institusi pelayanan kesehatan yang menyelenggarakan pelayanan kesehatan perorangan secara paripurna yang menyediakan pelayanan rawat inap, rawat jalan dan gawat darurat.
• Penyakit Infeksi Emerging (PIE) adalah penyakit yang muncul dan menyerang suatu populasi manusia untuk pertama kalinya atau telah ada sebelumnya namun meningkat dengan sangat cepat, baik dalam jumlah kasus baru di dalam satu populasi, ataupun penyebarannya ke daerah geografis yang baru (re-emerging infectious disease) yang dapat berasal dari virus, bakteri dan parasit. Termasuk kelompok PIE adalah penyakit yang pernah terjadi di suatu daerah di masa lalu, kemudian menurun atau telah dikendalikan, namun kemudian dilaporkan lagi dalam jumlah yang meningkat. Bentuk lainnya lagi adalah penyakit lama yangmuncul dalam bentuk klinis yang baru, yang bisa jadi lebih parah atau fatal.
• Kedaruratan Kesehatan Masyarakat adalah kejadian kesehatan masyarakat yang bersifat luar biasa dengan ditandai penyebaran penyakit menular dan/atau kejadian yang disebabkan oleh radiasi nuklir, pencemaran biologi, kontaminasi kimia, bioterorisme dan pangan yang menimbulkan bahaya kesehatan dan berpotensi menyebar ke lintas wilayah atau lintas negara.
B. Kriteria Kondisi darurat di Rumah SakitBeberapa kondisi darurat yang terjadi di Rumah Sakit antara lain

44
1. Kedaruratan keselamatan dan keamanan (demonstrasi/ huru-hara, penculikan bayi, kekerasan dalam Rumah Sakit dan risiko kecelakaan yang diakibatkan oleh kondisi gedung)
2. Tumpahan bahan dan limbah Bahan Berbahaya dan Beracun (B3)3. Kegagalan peralatan medik dan non medik4. Kedaruratan utilitas Rumah Sakit meliputi kegagalan kelistrikan, kegagalan
ketersediaan air, kegagalan informasi teknologi/ IT, dan kegagalan sistem tata udara
5. Outbreak/wabah/pandemi penyakit
Kondisi darurat di Rumah Sakit dapat berkembang menjadi bencana apabila tidak dapat ditangani oleh sumber daya internal Rumah Sakit.
C. Jenis bencana yang dapat berdampak pada kesiapan Rumah SakitPotensi bahaya yang terjadi di Indonesia berdasarkan UU Nomor 24 tahun 2007 dikelompokkan menjadi 3 (tiga) jenis bencana yaitu bencana alam, bencana non alam, dan bencana sosial. 1) Bencana Alam
− Gempa bumi − Letusan gunung berapi − Tsunami − Tanah longsor− Kekeringan− Angin topan− Gelombang pasang/badai− Likuifaksi− Banjir
2) Bencana Non Alam − Kecelakaan transportasi− Kegagalan konstruksi/teknologi− Kebakaran hutan yang disebabkan oleh manusia− Ledakan nuklir− Dampak industri (kimia/biologi, dll)− Pencemaran lingkungan− Outbreak/Wabah/pandemi penyakit
3) Bencana Sosial− Konflik sosial dipicu oleh kecemburuan sosial, budaya, ekonomi dan SARA− Demonstrasi/ huru-hara− Aksi teror− Sabotase

5 5
BAB III IDENTIFIKASI DAN PENILAIAN RISIKO KONDISI DARURAT DAN/ATAU BENCANA DI RUMAH SAKIT
A. Proses Manajemen RisikoRisiko adalah peluang peristiwa atau kondisi tidak pasti, apabila terjadi dapat memberikan dampak positif atau negatif yang dapat mempengaruhi perubahan terhadap biaya, ruang lingkup, dan kualitas pelayanan Rumah Sakit. Manajemen risiko adalah proses perumusan dan pelaksanaan tindakan untuk memitigasi bahaya berdasarkan hasil penilaian risiko (NRC 1983). Manajemen risiko bertujuan untuk meningkatkan peluang dan dampak positif, serta mengurangi peluang dan dampak yang merugikan, misalnya menurunkan kualitas pelayanan Rumah Sakit atau mengganggu fungsi operasional Rumah Sakit saat kondisi darurat dan/atau bencana.
Program manajemen risiko keadaan darurat dan/ atau bencana Rumah Sakit dilakukan melalui beberapa tahapan, sebagai berikut:1. Penetapan Konteks
Manajemen bencana Rumah Sakit dimulai dari penetapan konteks yaitu menetapkan ruang lingkup jenis kondisi darurat dan/atau bencana yang akan dikendalikan.
2. Identifikasi risikoIdentifikasi risiko meliputi segala jenis bahaya dan kelemahan sistem yang dapat menyebabkan kondisi darurat dan/atau bencana dan berdampak pada penghentian proses kerja atau layanan Rumah Sakit serta identifikasi sumber daya internal dan ekternal yang dimiliki atau telah dipersiapkan oleh Rumah Sakit untuk menghadapai kondisi darurat dan/ataubencana. Beberapa dokumen dan sumber data yang perlu dipersiapkan saat melakukan identifikasi diantaranya sebagai berikut:a. Analisis catatan rekaman data kejadian darurat dan/atau bencana
Analisis data insiden/kejadian darurat dan/atau bencana yang pernah terjadi sebelumnya baik pada Rumah Sakit itu sendiri maupun di tempat lain termasuk wabah/endemi.
b. Survey potensi risikoSurvey terhadap semua kondisi yang dapat menimbulkan kejadian darurat dan/atau bencana. Survey dapat dilakukan dengan menggunakan daftar periksa yang tidak terbatas pada :1) Bahan
Melakukan analisis potensi risiko yang berasal dari bahan-bahan yang ada di Rumah Sakit seperti Bahan Berbahaya dan Beracun (B3) dan limbahnya.
2) Peralatan Melakukan analisis semua peralatan yang berpotensi untuk terjadinya kondisi darurat dan/atau bencana seperti peralatan radiologi/radioterapi, instalasi gas medis sentral, peralatan laboratorium, genset, boiler, panel listrik dan sebagainya.
3) Proses/ MetodeMelakukan analisis semua proses dan metode kerja yang berpotensi untuk terjadinya kondisi darurat dan/atau bencana seperti tidak menutup dengan

6 6
rapat tabung gas medis, proses penyimpanan tabung gas yang tidak tepat, ketidakpatuhan terhadap SPO, pengujian alat yang tidak sesuai standar dan sebagainya.
4) Kondisi Lingkungan Melakukan analisis semua kondisi lingkungan kerja yang berpotensi menimbulkan kondisi darurat dan/atau bencana seperti suhu ekstrim, penataan ruangan kerja yang tidak sesuai standar dan sebagainya.
5) Faktor manusiaMelakukan analisis faktor manusia yang mempunyai kemungkinan menimbulkan kondisi darurat dan/atau bencana seperti perilaku yang tidak aman dan sebagainya.
Penilaian risiko adalah kegiatan untuk menilai tingkat kemungkinan dan tingkat keparahan/kerusakan/penghentian proses pelayanan Rumah Sakit akibat kondisidarurat dan/atau bencana. Ada beberapa metode penilaian risiko, diantaranya sebagai berikut:
a. What if analysis (Analisis ‘Bagaimana Jika’);b. Process Hazard Analysis (PHA);c. Hazard Identification Risk Assessment and Determine Control (HIRADC);d. Failure Mode and Effects Analysis (FMEA);e. Hazard Vulnerability Analysis (HVA);f. Hospital Safety Index (HSI); g. Fire Safety Risk Assesment (FSRA); dan lainnya
3. Analisis RisikoHasil penilaian risiko dilakukan analisis sehingga didapatkan informasi yang menjadi dasar Rumah Sakit dalam menentukan prioritas bahaya yang perlu segera dikendalikan, serta menentukan cara pengendalian terbaik untuk meminimalkan risiko. Informasi hasil analisis penilaian risiko juga dapat menghasilkan data yang digunakan untuk pengukuran kinerja, akreditasi fasilitas, peningkatan layanan, dan penilaian kepatuhan terhadap peraturan.
4. Evaluasi RisikoLangkah pertama dalam evaluasi risiko adalah menyusun rencana penanganan risiko. Beberapa hal yang masuk dalam rencana penanganan risiko yaitu hasil identifikasi danpenilaian risiko, penanggung jawab penanganan risiko, dan rencana aksi untuk menguatkan peluang positif dan meminimalkan risiko yang tidak diinginkan. Berdasarkan rencana penanganan risiko kemudian disepakati upaya penanganan risiko, diantaranya sebagai berikut:
a. Mitigasi, tindakan pencegahan awal untuk mencegah atau mengurangi peluang terjadinya risiko yang tidak diharapkan.
b. Kontigensi, tindakan yang diambil dalam merespon pencetus terjadinya risiko sehingga dapat mengurangi dampak risiko yang tidak diinginkan.
c. Transfer, tindakan menggeser/memindahkan risiko ke dalam tanggung jawab bagian lain.
d. Menolak risiko, yaitu tindakan merubah proses kerja atau sistem kerja atau alat kerja sehingga hal tersebut tidak ada lagi dalam draft identifikasi risiko.

7 7
e. Menerima risiko, yaitu kesadaran bahwa risiko tersebut merupakan bagian dari pekerjaan dan menerima konsekuansi yang ditimbulkan.
5. Penanganan RisikoMengidentifikasi pilihan penanganan risiko dan memilih penanganan terbaik.
6. Monitoring dan reviewManajer yang ditunjuk untuk mengelola risiko harus memastikan setiap risiko yang berhasil diidentifikasi dalam pemantauannya. Monitoring risiko meliputi proses identifikasi, analisis, rencana pengendalian risiko, analisis ulang risiko yang masih tersisa, pemantauan pemicu terjadinya risiko, mereview hasil intervensi terhadap risiko.
7. Komunikasi RisikoMelaporkan hasil pemantauan risiko secara berkala untuk menyesuaikan setiap perubahan terkini.
B. Metode Penilaian RisikoUntuk memudahkan identifikasi dan penilaian risiko kondisi darurat dan/atau bencana di Rumah Sakit, terdapat beberapa instrumen yang dapat digunakan antara lain• Hazard Identification, Risk Assessment, and Determine Control (HIRADC)• Hazard Vulnerability Analysis (HVA)• Hospital Safety Index (HSI)• Fire Safety Risk Assesment (FSRA)
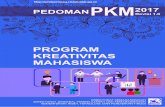
1) Hazard Identification, Risk Assessment, and Determining Control (HIRADC)Salah satu instrumen yang dapat digunakan untuk identifikasi dan penilaian risiko adalah HIRADC (Hazard Identification, Risk Assessment, and Determine Control) atau Identifikasi Bahaya, Penilaian, dan Pengendalian Risiko. Penggunaan instrumen ini secara praktis dapat disesuaikan dengan kondisi Rumah Sakit masing-masing.
Penetapan konteks
Proses Manajemen Risiko
Identifikasi risiko
Pe
nil
aia
n r
isik
o
Ko
min
uka
si d
an k
on
sult
asi
Mo
nit
ori
ng
dan
rev
iu
Analisa risiko
Evaluasi risiko
Penanganan risiko
1. Penetapan Konteks latar belakang, ruang lingkup, tujuan, dan lingkungan pengendalian2. Identifikasi Risiko mengidentifikasi risiko, waktu, sebab, dan proses terjadinya peristiwa risiko3. Analisa risiko mencermati risiko dan tingkat pengendalian serta menilai risiko4. Evaluasi risiko dilakukan untuk pengambilan keputusan mengenai penanganan risiko
5. Penanganan risiko mengidentifikasi opsi penanganan risiko dan memilih opsi terbaik6. Monitoring dan reviu memastikan penanganan dan langkah-langkah lanjutan yang diperlukan7. Komunikasi dan konsultasi dilakukan terus menerus dengan cara mengembangkan metode komunikasi dan pelaporan kepada stakeholder internal maupun eksternal

8 8
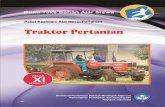
Tabel 1. Formulir Identifikasi Bahaya, Penilaian dan Pengendalian Risiko di Rumah Sakit
Tabel 2. Contoh Matriks Risiko berdasarkan hasil identifikasi dan penilaian risiko
KONSEKUENSI / SEVERITY PELUANG /
PROBABILITY
FORMULIR IDENTIFIKASI BAHAYA, PENILAIAN, DAN PENGENDALIAN RISIKORS. ABC
LOKASI: PoliSkrining
TANGGAL PENILAIAN: DIBUAT OLEH:
DISAHKAN OLEH:
No
1
2
Skrining Awal Pasienmenggubakan thermoscanner dan oxymetri
Registrasi Pasien
Biologi Kontak dengan pasienDroplet
Diskusi dengan pasien,penyerahan form isian
Bekerja dengan komputer
Terkontaminasibakteri atauvirus.
Terkontaminasibakteri atauvirus.
NyeriPinggangMSDS
Pembuatan SPOPenggunaan APDberupa maskerbedah, apsron.
Pembuatan SPOPenggunaan APDberupa maskerbedah.
Pembuatan SPObekerja dengankomputer
PekatihanPenambahan APD berupaface shieldpembuatan sign jaga jarak
PelatihanPemasangan barrierMengubah form isianmenggunakan aplikasi digital
Pelatihan ergonomiPeregangan
Rendah
Rendah
Rendah
Kepala Unit
Kepala UnitSarpras
KoordinatorRegistrasi
5 2 10
4 3 12
3 2 6
3 1 3
2 1 2
2 1 2
Biologi
Ergonimi
Aktivitas PekerjaanBahaya
Jenis DetailRisiko
Risiko Awal Risiko Akhir PIC
Risiko Saat IniRekomendasi Pengendalian
P S RPengendalian Saat
Ini

99
Tabel 3. Contoh Kategori Dampak terhadap keselamatan dan kesehatan
KATEGORI DAMPAK TERHADAP KESELAMATAN & KESEHATAN
1 Tidak ada dampak
2 Membutuhkan P3K
3 Membutuhkan perawatan medis
4 Menyebabkan cacat permanent
5 Menyebabkan kematian
Catatan : Untuk kategori dampak dapat disesuaikan definisi operasionalnya dengan kondisi dan kejadian yang dapat ditimbulkan baik untuk keselamatan maupun kesehatan
Tabel 4. Contoh Kategori Kemungkinan/ Probabilitas
KATEGORI KETERANGAN
1 = sangat jarang Terjadi sekali dalam lima tahun
2= jarang Terjadi sekali dalam 1-2 tahun
3= mungkin Terjadi sekali dalam 1-2 tahun
4= sering Terjadi beberapa kali dalam setahun
5= sangat sering Terjadi dalam hitungan minggu atau bulan
Catatan : Untuk kategori kemungkinan/probabilitas dapat disesuaikan definisi operasionalnya dengan kondisi dan kejadian yang dapat ditimbulkan baik untuk keselamatan/kesehatan
Pada kondisi bencana berupa outbreak/wabah/pandemi penyakit, Rumah Sakit akanmelakukan berbagai penyesuaian untuk memastikan operasional dapat berjalan, namun tetap aman bagi karyawan, pasien, maupun pengunjung. Terjadinya wabah yang mengakibatkan perubahan alur, penambahan kapasitas, atau penambahan SDM, akan menyebabkan timbulnya risiko baru.
2) Hazard and Vulnerability Analysis (HVA)Hazard and Vulnerability Analysis (HVA) merupakan instrumen untuk menilai kerentanan Rumah Sakit terhadap kondisi darurat dan/atau bencana baik yang berasal dari internal maupun eksternal Rumah Sakit. Pengisian instrumen HVA harus melibatkan berbagai berbagai satuan kerja/unit/instalasi yang terkait.
Penilaian risiko kondisi darurat dan/atau bencana dilakukan dengan instrumen HVA dengan langkah-langkah sebagai berikut :a. Menyiapkan instrumen HVA seperti pada tabel 1b. Mengumpulkan data potensi bahaya yang ada di Rumah Sakitc. Memasukkan data potensi bahaya ke dalam tabel HVA

10 10
d. Menginput data yang menggambarkan situasi dan kondisi yang sebenarnya di Rumah Sakit
e. Menghitung tingkat risiko semua kondisi darurat dan/atau bencana yang telah diidentifikasi
f. Menentukan prioritas kondisi darurat dan/atau bencana sesuai dengan hasil HVAg. Menyelenggarakan pertemuan untuk penyebaran informasi prioritas hasil HVA
dengan melibatkan pimpinan dan satuan kerja/unit/instalasi terkaith. Melaporkan hasil penilaian HVA kepada pimpinan tertinggi Rumah Sakiti. Melakukan review hasil penilaian HVA minimal 1 (satu) tahun sekali atau jika
terjadi perubahan/ kejadian yang berdampak pada HVA
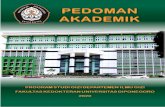
Proses penilaian risiko dengan instrumen HVA di Rumah Sakit sesuai tabel dibawah ini : Tabel 5. Hazard and Vulnerability Analysis (HVA) Kondisi darurat dan/atau bencana
DAMPAK = (LUAS KEJADIAN - MITIGASI)
KEJADIAN
PROBABILITAS DAMPAK MANUSIA
DAMPAK PROPERTI
DAMPAK BISNIS KESIAPAN RESPON
INTERNALRESPON
EXTERNAL
RISIKO
Probabilitas akan terjadi
Kemungkian meninggal atau cedera
Kehilangan dan kerusakan
fisik
Gangguan pelayanan
PraPerencanaan
Waktu, efektifitas,
sumberdaya
Masyarakat/Bantuan
umum dan suplai
Ancaman relatif*
NILAI
0 = N/A 1 = Rendah 2 = Moderat 3 = Tinggi
0 = N/A 1 = Rendah 2 = Moderat 3 = Tinggi
0 = N/A 1 = Rendah 2 = Moderat 3 = Tinggi
0 = N/A 1 = Rendah 2 = Moderat 3 = Tinggi
0 = N/A 1 = Tinggi
2 = Moderat 3 = Rendah
atau tidak ada
0 = N/A 1 = Tinggi
2 = Moderat 3 = Rendah atau tidak
ada
0 = N/A 1 = Tinggi
2 = Moderat 3 = Rendah atau tidak
ada
0 - 100%
Untuk HVA diisi dengan masing-masing menilai kerentanan Rumah Sakit terhadap kondisi darurat dan/atau bencana baik yang berasal dari internal maupun eksternal Rumah Sakit yang diantara terkait dengan human disaster, natural disaster, technological disaster, hazard material disaster termasuk disease disaster.
HVA diisi oleh tim kewaspadaan bencana yang Sebagian besar terdiri dari unsur direksi, manajemen, K3, Mutu, PPI (terkait wabah) bagian umum/logistik, IGD/Medis, pemeliharaan sarana, sanitasi, penunjang medik dan penunjang non medik serta yang dimungkinkan terlibat dalam kondisi bencana.
Pengisian angka dalam kolom dapat mengacu beberapa hal antara lain:• Probabilitas (kemungkinan) terjadinya suatu kondisi darurat dan/atau
bencana. Untuk menentukan probabilitas dapat dipertimbangkan risiko yang diketahui, dan data historis (apakah pernah terjadi sebelumnya).- Poin 0 tidak pernah (NA) : kondisi darurat atau bencana tidak mungkin terjadi- Poin 1 jarang (rare) : kondisi darurat atau bencana terjadi < 30 tahun sekali
10
d. Menginput data yang menggambarkan situasi dan kondisi yang sebenarnya di Rumah Sakit
e. Menghitung tingkat risiko semua kondisi darurat dan/atau bencana yang telah diidentifikasi
f. Menentukan prioritas kondisi darurat dan/atau bencana sesuai dengan hasil HVAg. Menyelenggarakan pertemuan untuk penyebaran informasi prioritas hasil HVA
dengan melibatkan pimpinan dan satuan kerja/unit/instalasi terkaith. Melaporkan hasil penilaian HVA kepada pimpinan tertinggi Rumah Sakiti. Melakukan review hasil penilaian HVA minimal 1 (satu) tahun sekali atau jika
terjadi perubahan/ kejadian yang berdampak pada HVA
Proses penilaian risiko dengan instrumen HVA di Rumah Sakit sesuai tabel dibawah ini : Tabel 5. Hazard and Vulnerability Analysis (HVA) Kondisi darurat dan/atau bencana
DAMPAK = (LUAS KEJADIAN - MITIGASI)
KEJADIAN
PROBABILITAS DAMPAK MANUSIA
DAMPAK PROPERTI
DAMPAK BISNIS KESIAPAN RESPON
INTERNALRESPON
EXTERNAL
RISIKO
Probabilitas akan terjadi
Kemungkian meninggal atau cedera
Kehilangan dan kerusakan
fisik
Gangguan pelayanan
PraPerencanaan
Waktu, efektifitas,
sumberdaya
Masyarakat/Bantuan
umum dan suplai
Ancaman relatif*
NILAI
0 = N/A 1 = Rendah 2 = Moderat 3 = Tinggi
0 = N/A 1 = Rendah 2 = Moderat 3 = Tinggi
0 = N/A 1 = Rendah 2 = Moderat 3 = Tinggi
0 = N/A 1 = Rendah 2 = Moderat 3 = Tinggi
0 = N/A 1 = Tinggi
2 = Moderat 3 = Rendah
atau tidak ada
0 = N/A 1 = Tinggi
2 = Moderat 3 = Rendah atau tidak
ada
0 = N/A 1 = Tinggi
2 = Moderat 3 = Rendah atau tidak
ada
0 - 100%
Untuk HVA diisi dengan masing-masing menilai kerentanan Rumah Sakit terhadap kondisi darurat dan/atau bencana baik yang berasal dari internal maupun eksternal Rumah Sakit yang diantara terkait dengan human disaster, natural disaster, technological disaster, hazard material disaster termasuk disease disaster.
HVA diisi oleh tim kewaspadaan bencana yang Sebagian besar terdiri dari unsur direksi, manajemen, K3, Mutu, PPI (terkait wabah) bagian umum/logistik, IGD/Medis, pemeliharaan sarana, sanitasi, penunjang medik dan penunjang non medik serta yang dimungkinkan terlibat dalam kondisi bencana.
Pengisian angka dalam kolom dapat mengacu beberapa hal antara lain:• Probabilitas (kemungkinan) terjadinya suatu kondisi darurat dan/atau
bencana. Untuk menentukan probabilitas dapat dipertimbangkan risiko yang diketahui, dan data historis (apakah pernah terjadi sebelumnya).- Poin 0 tidak pernah (NA) : kondisi darurat atau bencana tidak mungkin terjadi- Poin 1 jarang (rare) : kondisi darurat atau bencana terjadi < 30 tahun sekali

1111
- Poin 2 kadang-kadang (occasional) : bencana terjadi setiap 5 tahun sekali tapi lebih dari sekali dalam setiap 30 tahun
- Poin 3 sering (frequent) : bencana terjadi lebih sering dari sekali setiap 5 tahun
• Dampak manusia yaitu potensi cedera atau kematian pada staf atau pada pasien- Poin 0 tidak ada dampak : Tidak ada dampak yang berarti/bahaya yang
mempengaruhi masyarakat, kalaupun terjadi pengaruhnya minimal- Poin 1 rendah : Dampak rendah berarti kejadian bencana umumnya
melibatkan ancaman terhadap sejumlah masyarakat. Mungkin ada beberapa penduduk yang luka ringan dan membutuhkan pertolongan pertama.
- Poin 2 moderat : Dampak sedang berarti kejadian bencana menyebabkan sejumlah besar penduduk cidera yang membutuhkan perawatan medis lebih lanjut.
- Poin 3 tinggi : Dampak yang lebih besar berarti kejadian bencana terjadi pada masyarakat luas atau daerah yang terkonsentrasi dengan dampak yang parah. Ini dapat mengakibatkan sejumlah besar kematian dan cidera yang melibatkan evakuasi besar-besaran dan atau membutuhkan tempat penampungan.
• Dampak properti yaitu adanya biaya untuk menggantikan atau membangun kembali, biaya untuk penggantian sementara (sewa, pembelian), biaya untuk memperbaiki, waktu untuk pulih/bertahan dalam bisnis melanjutkan pelayanan secara normal - Poin 0 tidak ada dampak : Tidak ada dampak berarti, ada kemungkinan sedikit
atau tidak ada bahaya yang mempengaruhi masyarakat atau, jika itu terjadi, kerusakan terhadap kalaupun terjadi pengaruhnya minimal
- Poin 1 rendah : Dampak terbatas berarti kejadian bencana umumnya melibatkan hanya kerusakan properti publik atau swasta. Sumber daya lokal dapat memperbaiki atau mengganti properti yang rusak
- Poin 2 moderat : Dampak sedang berarti kejadian bencana menyebabkan kerusakan moderat di area yang luas atau terkonsentrasi. Kerusakan terhadap properti publik dan swasta dapat melebihi sumber daya lokal untuk memperbaiki atau mengganti
- Poin 3 tinggi : Dampak yang lebih luas berarti dampak kejadian menyebabkan kerusakan berat pada properti publik dan swasta di area yang luas atau daerah terkonsentrasi dengan dampak yang parah. Besarnya bencana dapat menghasilkan deklarasi pemerintah bencana besar/ nasional atau darurat
• Dampak bisnis yaitu gangguan bisnis, staf tidak dapat melaporkan pekerjaan, pelanggan tidak dapat mencapai fasilitas, perusahaan yang melanggar perjanjian kontrak, pengenaan denda dan hukuman atau biaya hukum, gangguan pasokan yang kritis, gangguan distribusi pada produk, reputasi dan citra publik, dan dampak keuangan/beban- Poin 0 tidak ada dampak : Tidak ada dampak berarti, ada kemungkinan sedikit
atau tidak ada bahaya yang mempengaruhi masyarakat atau, jika itu terjadi, tidak akan mengganggu jalannya pelayanan

12 12
- Poin 1 rendah : Dampak rendah berarti kejadian bencana umumnya mempengaruhi pelayanan namun hanya dalam waktu kurang dari 2 jam
- Poin 2 moderat : Dampak sedang berarti kejadian bencana umumnya mempengaruhi pelayanan namun hanya dalam waktu kurang lebih dari 8 jam
- Poin 3 tinggi : Dampak yang lebih luas berarti dampak kejadian umumnya mempengaruhi pelayanan namun hanya dalam waktu kurang lebih dari 24 jam
• Kesiapan meliputi status rencana saat ini, frekuensi latihan, status pelatihan, asuransi, ketersediaan sumber alternatif untuk pelayanan- Poin 0 tidak ada : Tidak ada kesiapan sama sekali untuk menghadapi bencana
yang akan terjadi- Poin 1 tinggi : Kesiapan yang dilakukan sudah terbentuk, bisa dilihat dari
adanya dokumen, SDM, dan simulasi risiko bencana yang terjadi- Poin 2 sedang : Kesiapan yang dilakukan sudah terbentuk, namun hanya
berupa dokumen dan SDM- Poin 3 rendah : Kesiapan yang dilakukan sudah terbentuk namun hanya
berupa dokumen• Respon internal meliputi jenis persediaan yang ada apakah memenuhi
kebutuhan, volume persediaan yang ada, distribusi pasokan, ketersediaan staf, ketersediaan sistem cadangan, kemampuan sumber daya internal untuk bertahan terhadap bencana.- Poin 0 tidak ada : Tidak ada sama sekali- Poin 1 tinggi : Respon tinggi yaitu sudah ada tim darurat dan sudah mengikuti
pelatihan kegawatdaruratan- Poin 2 sedang : Respon sedang yaitu sudah ada tim darurat namun belum
diikutsertakan pelatihan- Poin 3 rendah : Respon rendah yaitu belum ada tim darurat yang jelas
• Respon eksternal meliputi jenis perjanjian dengan lembaga masyarakat/latihan, koordinasi dengan lembaga lokal/nasional, koordinasi dengan fasilitas perawatan kesehatan yang lebih tinggi, koordinasi dengan fasilitas pengobatan khusus, sumber daya masyarakat- Poin 0 tidak ada : Tidak ada sama sekali- Poin 1 tinggi : Respon tinggi yaitu Rumah Sakit sudah melakukan kerjasama
dengan semua instansi terkait adanya bencana yang terjadi- Poin 2 sedang : Respon sedang yaitu Rumah Sakit sudah melakukan
kerjasama dengan beberapa instansi- Poin 3 rendah : Respon rendah yaitu Rumah Sakit belum melakukan kerjasama
namun sudah ada rencana untuk melakukan kerjasama.
Nilai Risiko adalah pengkalian probabilitas dengan dampak.
Dalam menentukan prioritas penanganan kondisi darurat dan/atau bencana, dapatmempertimbangkan:
a. Kondisi darurat dan/atau bencana dengan nilai total risiko > 55%

1313
b. Kondisi darurat dan/atau bencana dengan nilai total risiko dibawah 55% tetapi harus dibuat penanganan sesuai rekomendasi dan ketentuan dari hasil akreditasi
c. Kondisi darurat dan/atau bencana dengan nilai total risiko dibawah 55% tetapi merupakan kondisi darurat dan/atau bencana dengan nilai total terbesar pertama dan kedua
Setelah perhitungan menggunakan tabel, selanjutnya dilakukan analisis dengan membandingkan hasil identifikasi HVA yang dilakukan di satuan kerja/unit/instalasidengan standar yang wajib dipenuhi didalam proses penanggulangan terjadinya bencana.
3) Hospital Safety Index (HSI)Hospital Safety Index (HSI) merupakan salah satu instrumen yang digunakan untuk menilai suatu Rumah Sakit atau fasilitas pelayanan kesehatan tetap beroperasi,berfungsi dan memberikan pelayanan dalam kondisi darurat dan/atau bencana. HSImembantu pengambil kebijakan untuk menentukan secara cepat tindakan yang diambil untuk meningkatkan keamanan dan kemampuan Rumah Sakit dalam merespon kondisi darurat dan/atau bencana dengan fokus kepada pencegahan, mitigasi, respon darurat dan pemulihan.
Penilaian menggunakan Hospital Safety Index (HSI) dibagi menjadi 4 (empat) bagian penilaian yaitu :
a. Bahaya yang berdampak pada keamanan Rumah Sakit dan peran Rumah Sakit dalam pengelolaan kondisi darurat dan/atau bencanaPada aspek ini menilai secara cepat bahaya internal dan eksternal Rumah Sakitdan keadaan geoteknik tanah yang dapat mempengaruhi keamanan dan fungsi Rumah Sakit. Pada aspek ini juga mengidentifikasi risiko bencana alam yang mungkin terjadi pada geografis layanan kesehatan, contohnya apakah memiliki risiko terjadi gempa bumi, gunung meletus atau bencana alam lainnya.
b. Keamanan Struktur BangunanPada aspek ini Rumah Sakit akan dievaluasi bagaimana keamanan struktur fasilitas yang melibatkan penilaian dari jenis struktur, bahan, dan paparan sebelumnya terhadap bencana alam dan lainnya. Tujuannya adalah untuk mengetahui apakah struktur memenuhi standar untuk memberikan pelayanan kepada penduduk bahkan dalam kasus bencana besar, atau apakah bisa berdampak dengan membahayakan integritas struktural, dan kapasitas fungsional pada saat terjadinya bencana.Keamanan struktur bangunan dibagi menjadi 2 (dua) bagian yaitu apakah Rumah Sakit atau fasilitas pelayanan kesehatan terdampak bahaya dan kerentanan terhadap bencana. Penilaian kedua apakah struktur fasilitas berdampak atau rusak dan bagaimana kerusakan dapat diperbaiki.

14 14
c. Keamanan Non-StrukturalKegagalan non-struktural biasanya tidak membahayakan stabilitas bangunan, tetapi bisa membahayakan orang dan isi bangunan. Pada aspek ini akan dilakukan evaluasi dan verifikasi stabilitas elemen non-struktural dan apakah peralatan dapat berfungsi selama dan setelah bencana. Analisis ini meliputi akses dan rute keluar dari Rumah Sakit, keamanan jaringan kritis seperti sistem air, listrik, komunikasi,sistem HVAC (Heating, Ventilation and Air-Conditioning), serta peralatan diagnostik, dan perawatan medis.
d. Pengelolaan kondisi darurat dan/atau bencanaAspek pengelolaan kondisi darurat dan/atau bencana, Rumah Sakit akan melakukan evaluasi kesiapan sumber daya manusia Rumah Sakit dalam merespon kondisi darurat dan/atau bencana. Hal ini dapat diketahui dari koordinasi tim Rencana Hospital Disaster Management, pusat komando bencana, respon dan rencana pemulihan Rumah Sakit, manajemen komunikasi dan informasi, ketersediaan SDM, logistik dan keuangan, layanan dan dukungan pasien, dekontaminasi, manajemen korban, keselamatan dan keamanan staf.
Perhitungan nilai Hospital Safety Index (HSI)
Perhitungan nilai HSI menggunakan formulir (kalkulator HSI) yang dikeluarkan oleh WHO dan dapat diunduh di media elektronik (https://www.who.int/hac/techguidance/preparedness/hospital_safety_index_forms.pdf). Langkah pertama yaitu tim evaluasi mengisi dengan lengkap semua aspek penilaian berdasarkan situasi dan kondisi sebenarnya di Rumah Sakit. Selanjutnya, hasil penilaian semua aspek dimasukkan dalam instrumen dalam link yang berisi formula rumus perhitungan. Perhitungan berdasarkan bagaimana penilaian setiap item pertanyaan, pentingnya item dalam masing-masing aspek penilaian dan kepada keseluruhan keamanan Rumah Sakit dalam menghadapi kondisi darurat dan/atau bencana. Dalam melakukan perhitungan, tim evaluasi harus mendapatkan pelatihan terlebih dahulu.
HSI diisi oleh tim kewaspadaan bencana yang didalamnnya ada yang sudah mendapatkan pelatihan HSI dan Sebagian besar terdiri dari unsur direksi/ manajemen, K3, Mutu, PPI (terkait wabah) bagian umum/logistik, IGD/Medis, pemeliharaan sarana, sanitasi, penunjang medik dan penunjang non medik serta yang dimungkinkan terlibat dalam kondisi bencana.
Hasil perhitungan akhir HSI akan mendapatkan 3 (tiga) kategori kesiapsiagaan Rumah Sakit dalam menghadapi bencana yaitu kategori A, B, dan C.

1515
Tabel 6. Kategori Hasil Perhitungan HSISafety Index Klasifikasi Implementasi
0 – 0,35 C Keselamatan suatu fasilitas kesehatan dan isinya berada dalam risiko saat menghadapi situasi bencana
0,36 – 0,65 B Fasilitas kesehatan dinilai dapat bertahan pada situasi bencana tapi peralatan dan pelayanan penting lainnya berada dalam risiko
0,66 – 1 A Fasilitas kesehatan dapat melindungi hidup manusia yang ada di dalamnya dan dinilai dapat tetap berfungsi dalam situasi bencana
4) Fire Safety Risk Assesment (FSRA)Rumah Sakit harus merencanakan dan menerapkan suatu program untuk pencegahan, penanggulangan bahaya kebakaran, serta penyediaan sarana jalan keluar yang aman sebagai respons terhadap kebakaran dan keadaan darurat lainnya. Rumah Sakit perlu melakukan penilaian risiko terjadinya kebakaran secara berkala.
Penilaian risiko kebakaran harus mencakup identifikasi sumber potensi bahaya kebakaran berdasarkan setiap proses kerja yang mungkin dilakukan di Rumah Sakit,identifikasi orang yang berisiko untuk terkena bahaya, melakukan evaluasi, eliminasi, reduksi dan proteksi terhadap potensi risiko. Instrumen penilaian risiko kebakaran dapat disesuaikan dengan kebutuhan masing-masing Rumah Sakit.

16

17
17
BAB IV KESIAPSIAGAAN KONDISI DARURAT DAN/ATAUBENCANA DI RUMAH SAKIT
Kesiapsiagaan kondisi darurat dan/atau bencana berdasarkan hasil penilaian menggunakan instrumen HIRADC, HVA, HSI, dan FSRA dapat dilakukan dengan menyusun rencana tanggap darurat dan/atau bencana. Rencana tanggap darurat dan/atau bencana merupakansuatu rencana formal tertulis yang dibuat dan disusun oleh tim tanggap darurat dan/ataubencana Rumah Sakit yang disahkan oleh Pimpinan Tertinggi Rumah Sakit, dilanjutkan dengan sosialisasi dan pelatihan.
A. Tim tanggap darurat dan/atau bencanaTim tanggap darurat dan/atau bencana atau Incident Command System harus terdiri dari sumber daya manusia yang yang memiliki pengetahuan atau sudah terlatih, dengan jumlah anggota yang memadai dan menunjuk seorang pemimpin/ ketua tim. Setiap satuan kerja/ unit/ instalasi menugaskan 1 (satu) orang sebagai anggota tim tanggap darurat dan/ atau bencana.
Tim tanggap darurat dan/atau bencana dapat terdiri atas: 1. Pimpinan kondisi darurat dan/atau bencana/ Incident Commander2. Penanggung jawab informasi publik/Public Information Officer3. Penanggungjawab pusat dan penghubung/ koordinasi/ Liaision Officer4. Tim Ahli/ Expert team5. Penanggung jawab keselamatan kerja/Safety Officer6. Penanggung jawab operasional medis dan/atau non medis/ Operations Section
Chief7. Penanggung jawab perencanaan/ Planning Section Chief8. Penanggung jawab logistik/ Logistics Section Chief9. Penanggung jawab keuangan/administrasi/ Finance/Administration Section Chief
Tim dapat dikembangkan sesuai dengan sumber daya yang ada di Rumah Sakit.Bagan 1. Struktur tim tanggap darurat dan/atau bencana
Pimpinan kondisi darurat/Incident Commander Commander
Humas/ Public Information Officer
Pusat dan Informasi/ Liason Officer PJ K3/ Safety Officer
PJ Operasional/ Operations Section Chief
PJ Perencanaan/ Planning Section Chief
PJ Logistic/ Logistic Section Chief
PJ Keuangan/administrasi/ Finance/Administration Section Chief
Expert Team/Tim Ahli

18
18
Uraian tugas masing-masing penanggung jawab sebagai berikut:
No Nama Jabatan Tugas Jabatan
1 Pimpinan kondisi darurat dan/atau bencana/ Incident Commander
• Pimpinan kondisi darurat dan/atau bencana berasal dari jajaran direksi yang dapat dihubungi pada saat bencana
• Memberikan arahan seluruh kegiatan yang dilakukan di pusat komando, mengatur waktu operasional tim, merencanakan strategi dan prioritas dalam melaksanakan rencana tanggap darurat dan/atau bencana
• Memiliki wewenang untuk menunjuk penanggung jawab pusat informasi publik, penanggung jawab penghubung, penanggung jawab K3, penanggung jawaboperasional medis dan/atau non medis, penanggung jawab logistik, penanggung jawab keuangan/administrasi, penanggung jawab perencanaan
• Membuat keputusan untuk pembatasan akses
2 Penanggung jawab pusat informasi publik/ Public Information Officer
• Penanggung Jawab Pusat Informasi Publik adalah Kepala Bagian Pemasaran/Humas/Promkes atau yang dedelegasikan oleh direksi
• Penanggung jawab informasi publik bertanggung jawab dalam penyebaran informasi kedalam dan keluar Rumah Sakit
• Merupakan juru bicara Rumah Sakitterhadap pihak eksternal (media, LSM dan organisasi lainnya)
• Pengendali dan penghubung pesan baik dari internal maupun eksternal Rumah Sakit dan atau tim lapangan
3 Petugas penghubung/koordinasiLiaison Officer
• Petugas penghubung melakukan hubunganantara pihak luar untuk memberikan bantuan/dukungan dengan Rumah Sakitpada saat terjadi bencana
• Pada beberapa kasus, dapat menjadi Pusat Komando Rumah Sakit
• Menyediakan informasi dan kebutuhan sumber daya dari Rumah Sakit lainnya
• Menginformasikan kepada yang berwenang terkait data kesakitan dan kematian korban

1919
3 Tim Ahli / Expert Team • Penanggung jawab terkait dengan kejadian adanya wabah/endemic.
• Penanggung jawab pencegahan dan pengendalian wabah/epidemi denganmemonitor respon Rumah Sakit dalam mengidentifikasi dan memperbaiki kondisi darurat.
• Berkewajiban menentukan potensi bahaya terkait wabah/epidemi yang membahayakan pasien, karyawan, pengunjung dan lingkungan Rumah Sakit
• Bertanggungjawab untuk memastikan keselamatan semua sumber daya manusia yang sedang bertugas
• Bertanggungjawab untuk mengidentifikasi, melakukan evaluasi dan memecahkan masalah pengendalian dan pencegahanyang berhubungan fasilitas dan sarana prasarana
• Mengidentifikasi Alat Pelindung Diri (APD) yang dibutuhkan oleh karyawan berdasarkan potensi bahaya saat terjadi kondisi darurat dan/atau bencana yang terkait dengan wabah/endemi
• Memiliki tugas untuk melakukan koordinasi dengan Tim Medis Reaksi Cepat (TMRC) dan mengaktifkan satuan kerja yang ada diKelompok Staf Medis ( KSM ), rawat jalan, rawat inap, rawat intensif, kamar operasi,penunjang medis dan non medis, dan Forensik untuk kesiapan pelayanan pasien bila terjadi darurat wabah/epidemi.
• Mendata kapasitas medis yang berupa jumlah dokter, perawat dan bidan, kapasitas rawat jalan, kapasitas rawat inap, kapasitas ICU, kapasitas alat kedokteran, kapasitas alat kesehatan dan APD untuk tim medis
4 Penanggung jawab keselamatan kerja/ Safety Officer
• Penanggung jawab keselamatan kerja adalah Kepala Instalasi/Unit/Tim Keselamatan dan Kesehatan Kerja (K3)
• Penangung jawab keselamatan kerja memonitor respon Rumah Sakit dalam

2020
mengidentifikasi dan memperbaiki kondisi darurat.
• Berkewajiban menentukan potensi bahaya keselamatan yang membahayakan pasien, karyawan, pengunjung dan lingkungan Rumah Sakit
• Bertanggungjawab untuk memastikan keselamatan semua sumber daya manusia yang sedang bertugas
• Bertanggungjawab untuk mengidentifikasi, melakukan evaluasi dan memecahkan masalah keselamatan dan kesehatan yang berhubungan dengan struktur bangunan
• Mengidentifikasi Alat Pelindung Diri (APD) yang dibutuhkan oleh karyawan berdasarkan potensi bahaya saat terjadi kondisi darurat dan/atau bencana
• Memiliki tugas untuk melakukan koordinasi dengan Tim Medis Reaksi Cepat (TMRC) dan mengaktifkan Tim rawat jalan, Tim Rawat inap, Tim rawat intensif, Tim kamar operasi, Tim Rawat khusus, Tim penunjang medis, tim evakuasi radiasi, Tim Evakuasi KLB/wabah dan Tim Forensik serta Departemen Medik untuk kesiapan pelayanan pasien bila terjadi darurat bencana
• Mendata kapasitas medis yang berupa jumlah dokter, perawat dan bidan, kapasitas rawat jalan, kapasitas rawat inap, kapasitas ICU, kapasitas alat kedokteran, kapasitas alat kesehatan dan APD untuk tim medis
• Berkoordinasi dengan Koordinator Manajemen Operasional dalam menentukan alternatif lokasi untuk tambahan Rumah Sakit darurat
5 Penanggung jawab operasional medis dan/atau non medis/Operations Section Chief
• Penanggung jawab operasional medis dan/atau non medis mengatur semua kegiatan yang sesuai dengan rencana tanggap darurat dan/atau bencana.
• Memiliki tugas mengkoordinasikan kegiatan operasional tanggap darurat yang terdiri dari infrastruktur, pengamanan,

2121
penyelamatan, pendampingan pasien dan SDM untuk mendukung manajemen medis
6 Penanggung jawab perencanaan/ Planning Section
• Penanggung jawab perencanaan mengumpulkan, mengevaluasi dan menyebarluaskan informasi
• Menyiapkan rencana tanggap darurat dan/atau bencana secara berkala
• Menyiapkan laporan status kondisi darurat dan/atau bencana
• Mendata sumber daya yang ada dan mengidentifikasi kekurangan sumber daya yang dibutuhkan
7 Penanggung jawab logistic /Logistics Section Chief
• Penanggung jawab logistik menyediakan semua kebutuhan pada saat kondisi darurat dan/atau bencana
• Bertanggung jawab dalam penyediaan sumber daya termasuk memperoleh bantuan sumber daya dari dalam dan luar Rumah Sakit, organisasi lain dan pusat krisis kesehatan setempat
• Penanggung jawab logistik adalah Kepala Bagian Unit Layanan Pengadaan
• Mendata ketersediaan sumber daya di Rumah Sakit
• Mendata kapasitas obat-obatan dan alat kesehatan yang ada di Instalasi Farmasi
• Menyiapkan fasilitas dan sarana darurat meliputi kemungkinan pengadaan alat kedokteran, obat-obatan dan makanan
• Penanggung jawab logistik dibagi menjadi Bagian Pelayanan dan Bagian Pendukung
• Bagian Pelayanan bertanggung jawab untuk mendukung komunikasi dan informasi, dan pemberian bantuan makanan untuk pasien dan karyawan
• Bagian Pendukung bertanggung jawab untuk memperoleh semua dukungan, mengkoordinasikan transportasi, memperoleh tambahan sumber daya tenaga kesehatan
8 Penanggung jawab keuangan/administrasi/ Finance /Administration Section Chief
• Penanggung jawab keuangan/administrasi mengkoordinasikan bagian pengadaan, kompensasi, dan pembayaran
• Menghitung anggaran yang dibutuhkan dalam rencana tanggap darurat dan/atau bencana
• Membuat kontrak, kebutuhan pengadaan dan pembayaran seluruh sumber daya

2222
• Penanda Tim Tanggap Darurat dan/atau Bencana
Tim tanggap darurat dan/atau bencana atau wabah/endemi menggunakan penanda yang menjelaskan tugas dan fungsinya. Penanda dapat berupa tanda pengenal yang ditempel dan dapat dilihat oleh karyawan, helm, jaket atau pin. Jenis penanda disesuaikan dengan kondisi dan kebutuhan Rumah Sakitmasing-masing.
B. Standar Prosedur Operasional (SPO)Standar Prosedur Operasional (SPO) berisikan informasi mengenai pengertian, tujuan, kebijakan, prosedur dan unit terkait. Beberapa SPO umum yang minimal harus ada berdasarkan jenis kondisi darurat dan/atau bencana antara lain:1) Pada Semua kondisi darurat dan/atau bencana:
a. Pedoman Kewasapadaan Bencana Rumah Sakitb. SPO Aktivasi Tim Hospital Disaster Plan (HDP)c. SPO Briefing dan SPO Debriefingd. SPO Pelimpahan Wewenang (Transfer of Command) dari Direktur kepada Ketua
HDPe. SPO Layanan Kritisf. SPO Sistem Rujukang. SPO Keamanan dan Keselamatanh. SPO Komunikasi Internali. SPO Pencatatan dan Pelaporanj. SPO Aktivasi Tim Lapangank. SPO Triase Mass Casualty Incidentl. SPO Penyediaan Logistikm. SPO Pengadaan dan Penyediaan Barangn. SPO Manajemen Bantuano. SPO Manajemen Relawanp. SPO Mobilisasi Internal (SDM, Sarana dan Prasarana)q. SPO Manajemen Media (Humas)r. SPO Administrasi dan Keuangans. SPO Pemulangan Pasient. SPO Pemulasaraan Jenazah (terutama bencana terkait infeksi)u. SPO Pelaporan Insiden dan Investigasi
2) Natural Disaster :a. SPO Gempa Bumib. SPO Tsunamic. SPO Banjird. SPO Gunung Meletuse. SPO Kebakaran Hutanf. SPO Tanah Longsorg. SPO Angin Kencang

2323
h. SPO Suhu Ekstrimi. SPO Kekeringan
3) Human Disaster :a. SPO Kejadian Penculikan Bayib. SPO Ancaman Bomc. SPO Huru-hara dan demonstrasid. SPO Sabotase dan Terorismee. SPO Kecelakaan Masalf. SPO Kerusuhan Sipil g. SPO Penyanderaanh. SPO Konflik Bersenjatai. SPO Kerumunan Massa
4) Technological Disater:a. SPO Kejadian Kebakaran/ Code Redb. SPO Penggunaan APARc. SPO Penggunaan Hidrand. SPO Penggunaan sensor asap dan pemadam otomatise. SPO Penggunaan APD Fire Fighterf. SPO Mitigasi Kebakarang. SPO Kegagalan Kelistrikanh. SPO Kegagalan Generatori. SPO Kecelakaan Industrij. SPO Kegagalan Transportasik. SPO Kegagalan Sistem Persediaan Airl. SPO Kekurangan Gas Medism. SPO Kekurangan Supplyn. SPO Kerusakan Struktur Bangunano. SPO Kecelakaan Transportasi
5) Hazmat Disaster:a. SPO Tumpahan B3b. SPO Tanggap Darurat Tumpahan B3c. SPO Penggunaan Spillkitd. SPO Penggunaan APD terkait Disaster Hazmate. SPO Kebocoran Radiasif. SPO Tanggap Darurat Bencana Radiasig. SPO Penggunaan APD terkait Bencana Radiasi
6) Disease Disaster:a. SPO Keracunan makanan Masalb. SPO KLBc. SPO Penggunaan APD terkait Wabah

2424
d. SPO Epidemi, Pandemi dan Emerging Diseasese. SPO Serangan Hama
Apabila kondisi darurat meningkat menjadi bencana, pihak Rumah Sakit memiliki SPO untuk mengelola komunikasi dengan pihak eksternal yang terkait.
C. Sistem Kode Darurat di Rumah Sakit• Kode darurat
Kode darurat di Rumah Sakit digunakan untuk menginformasikan petugas dan pengunjung akan terjadinya suatu kondisi darurat dan bencana yang terjadi. Kode darurat dibuat singkat dan dipahami oleh seluruhnya, sehingga dianggap lebih gampang apabila dipresentasikan dalam warna. Di Rumah Sakit ada beberapa kode kedaruratan yang secara umum digunakan antara lain:1. Kode Biru (Code Blue) : Kedaruratan Medik / resusitasi
Kode Biru (Code Blue) adalah kode yang mengumumkan adanya pasien,keluarga pasien, pengunjung, dan karyawan yang mengalami kegawatan medis atau henti jantung atau henti nafas dan membutuhkan tindakan bantuan hidup dasar / resusitasi segera. Pengumuman ini utamanya adalah untuk memanggil tim medis reaksi cepat atau tim code blue yang bertugas pada saat tersebut, untuk segera berlari secepat mungkin (Respon time < 10 menit) menuju ke tempat lokasi/ ruangan yang diumumkan dan melakukan resusitasi jantung dan paru pada pasien.
2. Kode Merah (Code Red) : KebakaranKode Merah (Code Red) adalah kode yang mengumumkan adanya ancaman kebakaran di lingkungan Rumah Sakit (api maupun asap), sekaligus mengaktifkan tim siaga bencana Rumah Sakit untuk khusus kebakaran. Dimana tim ini terdiri dari seluruh personel Rumah Sakit, yang masing-masing memiliki peran spesifik yang harus dikerjakan sesuai dengan panduan kebakaran/tanggap darurat bencana/Disaster plan Rumah Sakit.
3. Kode Merah Muda (Code Pink) : Penculikan bayiKode Merah Muda (Code Pink) adalah kode yang mengumumkan adanya penculikan bayi/ anak atau kehilangan bayi/ anak di lingkungan Rumah Sakit.Secara universal, pengumuman ini seharusnya diikuti dengan lock down (menutup akses keluar-masuk) Rumah Sakit secara serentak oleh petugas keamanan.
4. Kode Hijau (Code Green) : Kejadian Gempa BumiKode Hijau (Code Green) adalah kode yang mengumumkan adanya kejadian gempa bumi yang terjadi di Rumah Sakit yang diumumkan setelah kejadian gempa dengan maksud agar segera dilakukan penilaian awal dan mencegah kepanikan yang tidak terkendali.

25
25
5. Kode Hitam (Code Black) : Ancaman bomKode Hitam (Code black) adalah kode yang mengumumkan adanya ancaman bom atau ditemukan benda yang dicurigai bom di lingkungan Rumah Sakit.
6. Kode Abu-abu (Code Grey) : Kedaruratan keamananKode Abu-abu (Code Grey) adalah kode yang mengumumkan adanya kedaruratan keamanan seperti huru-hara, ancaman orang yang membahayakan (ancaman orang bersenjata atau tidak bersenjata yang mengancam akan melukai seseorang atau melukai diri sendiri), kekerasan terhadap karyawan, pengunjung dan ancaman lain.
7. Kode Kuning (Code Yellow) : Kedaruratan massal / emergensi internal Kode Kuning (Code Yellow) adalah kode yang mengumumkan adanya kejadian kedaruratan masal / emergensi baik itu yang terjadinya berasal dari luar maupun dari dalam Rumah Sakit, diantaranya adanya kejadian kecelakaan massal, keracunan masal, wabah/epidemic, KLB dari suatu penyakit baik menular/tidak menular.
8. Kode Coklat (Code Brown) : Kehilangan/PencurianKode Coklat (Code Brown) adalah kode yang mengumumkan adanya kejadian kehilangan barang atau adanya kejadian pencurian di dalam / diluar gedung pada area Rumah Sakit.
9. Kode Oranye (Code Orange) : Ancaman akibat bahan kimia, zat biologis, radioaktif / nuklirKode Oranye (Code Orange) adalah kode yang mengumumkan adanya kejadian tumpahan bahan kimia yang kritikal (berpotensi massif) / Zat biologis / kemoterapi/ Radioaktif / Nuklir yang terjadi pada ruangan atau gedung di area lingkungan Rumah Sakit.
10. Kode Ungu ( Code Purple ) : EvakuasiKode Ungu (Code Purple) adalah kode yang mengumumkan pengaktifan evakuasi pasien, pengunjung dan karyawan Rumah Sakit pada titik-titik kumpul / aman yang telah ditentukan setelah ada komando akibat adanya kegawat daruratan kebakaran ataupun bencana. Pada intinya, menginisiasi tim evakuasi untuk melaksanakan tugasnya.
Untuk kode bencana lainnya yang berupa tambahan selain yang ada pada kode bencana tersebut diatas dapat ditambahkan sesuai dengan kesepakatan, pemahaman dan kebijakaan dari Rumah Sakit tersebut. Kejadian-kejadian bencana tersebut seperti :- Tsunami- Banjir bandang

26
26
- Tanah longsor- Angin Puting Beliung/Badai- Kebakaran hutan dan lahan- Kejadian bencana lainnya
• Nomor pentingNomor penting yang dapat dihubungi dibagi menjadi nomor internal Rumah Sakitdan nomor eksternal Rumah Sakit.
Nomor internal Rumah Sakit yang dapat dihubungi antara lain nomor operator, pos satpam, pimpinan kondisi darurat dan/atau bencana, penanggung jawab pengamanan dan penyelamatan, penanggung jawab pusat dan dinformasi, penanggungjawab operasional medis dan non medis penanggung jawab logistik, penanggung jawab keuangan/administrasi, dan penanggungjawab perencanaan/ SDM. Nomor penting internal disesuaikan dengan kebijakan Rumah Sakit.
Nomor penting eksternal Rumah Sakit ketika terjadi bencana antara lain Pusat krisis Kementerian Kesehatan (Public Safety Center), Ambulan gawat darurat, Polisi/ Kodim, SAR, PLN, Pemadam kebakaran, Posko bencana, PMI atau nomor lain sesuai dengan kondisi darurat dan/atau bencana di Rumah Sakit.
D. Tingkat Kesiapsiagaan Kondisi darurat dan/atau bencana Penanganan kondisi darurat dan/atau bencana dilakukan berdasarkan tingkatan kesiapsiagaan. Untuk kejadian adanya bencana wabah/endemic atau pandemik maka tingkatannya mengikuti kebijakan Rumah Sakit dan juga mengacu dari kebijakan pemerintah pusat.
Tabel 7. Tingkat Status Kondisi Darurat dan/atau Bencana
Status Kondisi darurat dan/atau bencana
Istilah Dalam Bahasa Penjelasan
I Awas/ Merah Kondisi darurat dan/atau bencana yang dapat diselesaikan dengan bantuan pihak luar
II Siaga/ Orange Kondisi darurat dan/atau bencana yang dapat diselesaikan oleh internal Rumah Sakit
III Waspada/ Kuning Kondisi darurat dan/atau bencana yang dapat diselesaikan oleh satuan kerja/unit/instalasi terkait

27
27
E. Rambu-rambu mengenai keselamatan dan tanda darurat sesuai dengan standar dan pedoman teknisRambu-rambu keselamatan dan tanda darurat harus diletakkan pada tempat yang mudah dilihat baik oleh petugas Rumah Sakit maupun pengunjung. Beberapa contoh rambu-rambu standar, penempatan dan dasar regulasi antara lain:
Tabel 8. Contoh Desain dan Penempatan Rambu-rambu Keselamatan dan Tanda Darurat
No. Rambu-rambu
Contoh Desain( Antara lain )
Penempatan Dasar Regulasi
1 Arah Jalur Evakuasi
Minimal 20cm - 40cm dari lantai, ditempatkan pada persimpangan koridor, jalan ke luar menuju ruang tangga darurat, balkon atau teras dan pintu menuju tangga darurat.
Rambu evakuasi yang terpasang harus mudah diidentifikasi, mudah terlihat dan tidak terhalang dengan warna dasar hijau dan tulisan warna putih serta dapat berpendar dalam gelap ( glow in the dark / fosforisensi ) dengan ukuran tulisan, jarak antara rambu evakuasi yang proporsional dan beberapa rekomendasi untuk penempatannya adalah :
Dalam ruangan, dapat dikombinasikan sesuai dengan keadaan penempatan barang dan kondisi dari lay out ruangan tersebut. Kombinasi bisa
SNI 03-1746-2000
EVAKUASI
JALUREVAKUASI

28
28
Pada koridor yang panjang dan lurus ( lebih dari 40 meter )
dilakukan pada dinding.
1. Terpasang di dinding dengan ketinggian dari lantai antara 20cm - 40cm
2. Dan/Atau terpasang di dinding dengan ketinggian dari lantai antara 140cm -170 cm
3. Dan/Atau di gantung pada area tertentu yang menunjukkan arahevakuasi menuju titik kumpul aman
Di luar ruangan atau area koridor dapat dikombinasikan dengan keadaan dan kondisi dari layout ruangan dan gedung, yaitu :
1. Terpasang di dinding dengan ketinggian dari lantai kurang lebih 20cm -40cm
2. Dan/Atau terpasang di dinding dengan ketinggian dari lantai antar 140cm -170 cm
3. Atau di gantung pada area tertentu dimana rambu tersebut dapat mudah diidentifikasi, dilihat dan tidak terhalang
4. Jika menggunakan tiang
EVAKUASI

29
29
pada area menuju lapangan atau titik kumpul aman dengan ketinggian antara 175cm – 200cm. Tiang tidak mudah bergeser dan kuat
2 Tanda Exit Maksimal 20 cm di atas pintu darurat/ akses menuju keluar gedung
Permen PUPR Nomor 14 Tahun 2017 Lampiran
3 Rambu Titik kumpul
Dipasang pada lokasi titik kumpul yang sudah ditentukan pada lokasi yang aman
Permen PUPR Nomor 14 Tahun 2017 Lampiran
4 Rambu Penanda APAR
Tinggi pemberian rambu/tanda APARadalah 125 cm dari dasar lantai tepat diatas satu atau kelompok alat pemadam api ringan bersangkutan
Permenakertrans No PER.04/MEN/1980
5 Sign Kotak P3K
Ditempat yang mudah dilihat dan ditempat yang cukup cahaya
Permenakertrans No PER.15/MEN/VIII/2008
Untuk rambu yang terkait dengan adanya bencana wabah/endemic/pandemic dapat disesuaikan dengan kondisi, lokasi dan ruangan yang digunakan dengan petunjuk/rambu yang jelas dan informatif.
F. Kedaruratan Kesehatan Masyarakat Dalam menyelenggarakan pelayanan pasien dalam keadaan darurat tersebut, setiap pasien yang dicurigai menderita penyakit menular terkait kedaruratan kesehatan

30
30
masyarakat harus diterima di Rumah Sakit melalui satu pintu yang telah ditetapkan misalnya IGD atau poliklinik yang khusus ditetapkan sebagai pusat penanganan penyakit tersebut, baik bagi pasien rujukan maupun bukan rujukan. Rumah Sakit menyusun alur penanganan pasien yang efektif dan efisien untuk mempercepat proses penanganan dan mencegah penularan penyakit.
Untuk mengantisipasi dan menanggulangi lonjakan pasien terkait kedaruratan kesehatan masyarakat ini, maka diperlukan prosedur tanggap darurat dan mempersiapkan adanya kemungkinan eskalasi dengan menjalankan rencana Penanggulangan Bencana Rumah Sakit (Hospital Disaster Plan). Alur pengaktifan tim bencana Rumah Sakit adalah sebagai berikut :
1. Kepala IGD melapor sampai dengan Pimpinan Rumah Sakit berdasarkan informasi dari lapangan
2. Pimpinan Rumah Sakit memberikan instruksi kepada tim investigasi KLB untuk melakukan asesmen lapangan secara cepat
3. Diluar jam kerja, Duty Manager mengaktifkan tim investigasi dan memimpin koordinasi pada saat itu untuk laporan segera pada Pimpinan Rumah Sakit.
4. Tim investigasi melaporkan hasil asesmen cepat kepada Pimpinan Rumah Sakit.5. Pimpinan Rumah Sakit mengaktifkan tim penanggulangan bencana Rumah Sakit
dengan Direktur Medik dan Keperawatan sebagai Incident Commander6. Tim bencana segera melakukan koordinasi di posko yang sudah ditetapkan
Pimpinan Rumah Sakit memberikan instruksi kepada jajaran tim penanggulangan bencana untuk mempersiapkan1. Pemetaan Area/Pos Kegiatan (Staging)
Melakukan pengkajian kebutuhan area atau pos kegiatan utama meliputi area pelayanan utama, pembagian zona pelayanan pasien, maupun kebutuhan area lainnya diatur berdasarkan kajian di lapangan.
2. Alur Penanganan Pasien1) Prosedur penanganan pasien
a. Pasien rujukan penyakit menular terkait kedaruratan kesehatan masyarakat− Petugas menerima informasi rujukan pasien yang dicurigai menderita
penyakit menular kedaruratan kesehatan masyarakat kemudian berkoordinasi dengan ruang perawatan isolasi dan melaporkan
− PJ Ruang mengumumkan situasi code yellow bagi para petugas diikuti briefing koordinasi cepat dipimpin oleh Kepala/PJ untuk persiapan mengantisipasi kedatangan ambulans perujuk terkait
− Saat ambulans perujuk tiba di halaman (dropzone), petugas triase melakukan konfirmasi rujukan secara cepat dengan petugas yangmengantar pasien. Pasien tetap berada di dalam ambulans. Petugas triase menentukan level triase pasien dengan mengacu pada

31
31
Emergency Severity Index (ESI) sesuai kondisi pasien menurut laporan petugas perujuk
− Tim keamanan mengawal dan ambulans perujuk menuju ruang isolasisesuai jalur yang ditetapkan
− PJ memberitahu tim jaga di ruang perawatan isolasi untuk bersiap menerima pasien
− Kepala Ruangan melaporkan situasi ke Pimpinan Rumah Sakitb. Pasien datang sendiri (bukan rujukan)
− Petugas triase melakukan asesmen triase cepat termasuk skrining kemungkinan penyakit menular udara akibat infeksi virus terkaitkedaruratan kesehatan masyarakat saat pasien datang. Sedapatmungkin skrining dilakukan sebelum pasien masuk ke dalam areautama. Kriteria skrining disesuaikan dengan gejala penyakit menular terkait kedaruratan kesehatan masyarakat tersebut
− Berdasarkan hasil skrining awal, apabila pasien dicurigai menderita penyakit menular kedaruratan kesehatan masyarakat maka petugastriase mengarahkan pasien masuk ke ruang isolasi transit untuk dilakukan asesmen triase lebih lanjut
− Proses asesmen triase dilanjutkan dengan asesmen medis dan resusitasi-stabilisasi (bila diperlukan) oleh tim dokter spesialis jaga onsite berkolaborasi dengan perawat jaga
− Tim dokter spesialis jaga onsite yang bertanggung jawab melakukan asesmen medis dalam hali ini terdiri atas dokter jaga anestesi, penyakit dalam, dan anak. Keterlibatan bidang medis lain sesuai prioritas kebutuhan klinis pasien.
− Proses asesmen dan asuhan pasien di ruang isolasi transit dilakukansecara efektif dan efisien mengacu pada panduan praktik klinis. Hanya petugas berkepentingan yang melakukan kontak dengan pasien dalam rangka meminimalkan risiko penularan.
− Berdasarkan hasil asesmen awal, dokter spesialis jaga onsite berkoordinasi dan memutuskan tindak lanjut dalam waktu paling lama2 jam sejak pasien datangApabila pasien mengarah ke suspek penyakit menular kedaruratan kesehatan masyarakat maka pasien segera diputuskan masuk rawatinap di ruang isolasi. Bila bukan suspek, maka pasien dikelola sesuai alur rutin.
− Perawat jaga melapor ke Kepala untuk diteruskan ke Pimpinan Rumah Sakit
− PJ mengumumkan situasi code yellow bagi para petugas diikuti briefing koordinasi cepat untuk merespon situasi terkait
− Petugas memberitahu tim jaga di ruang isolasi untuk bersiap menerima pasien
− Pemindahan pasien ke ruang isolasi dilakukan dengan menggunakan ambulans

32
32
c. Prosedur penanganan pasien di ruang perawatan isolasi− Ruang perawatan isolasi yang digunakan untuk perawatan pasien
penyakit menular kedaruratan kesehatan masyarakat adalah bangsal yang telah ditetapkan menggunakan prinsip Kohorting
− Tim jaga di ruang perawatan isolasi menerima informasi mengenai kedatangan pasien terkait penyakit menular kedaruratan kesehatan masyarakat
− SDM dan fasilitas ruang perawatan isolasi dipersiapkan sesuai antisipasi kebutuhan perawatan pasien, terutama kebutuhan perawatan intensif (dengan ventilator)
− Tim medis utama yang bertanggung jawab mengelola penanganan pasien di ruang perawatan isolasi terdiri atas dokter anestesi, paru, dan anak. Keterlibatan bidang medis lain sesuai prioritas kebutuhan klinis pasien
− Untuk pasien rujukan eksternal, tim medis yang bertugas di ruang perawatan isolasi melanjutkan asesmen awal gawat darurat kemudiandiikuti dengan asesmen rawat inap. Sedangkan untuk pasien bukanrujukan yang sebelumnya sudah dikelola maka tim medis ruang isolasi langsung melanjutkan dengan asesmen rawat inap
− Tatalaksana kasus penyakit sesuai dengan panduan praktik klinis yangberlaku
3. Pelayanan Penunjang MedisPelayanan penunjang medis perlu disiapkan dan menyesuaikan alurnya. Pertimbangan untuk mengintegrasikan pelayanan di satu pintu sangat penting agar penanganan pasien tidak bercampur dengan pelayanan pasien umum. Pelayanan penunjang medis meliputi:a. Laboratorium
− Sebagai penunjang medis, laboratorium juga perlu disiapkan dalam membantu klinisi untuk menentukan diagnosa penyakit sesuai panduan praktik klinik. Pemeriksaan laboratorium meliputi pemeriksaan darah rutin, dan pemeriksaan lainnya yang diperlukan sesuai standar yang telah ditetapkan Kementerian Kesehatan
− Melakukan pengambilan spesimen sesuai standar fasilitas laboratorium dan pedoman pengambilan, pengepakan, pengiriman dan pemeriksaan spesimen serta bila diperlukan adanya koordinasi dengan laboratorium rujukan yang ditunjuk oleh Kementerian Kesehatan untuk pemeriksaanspesimen
b. RadiologiProses pemeriksaan sampai hasil radiologi sebaiknya dilaksanakan di ruangisolasi. Pelaksanaan rontgen dilakukan di ruang isolasi dengan menggunakan alat rontgen portable, kemudian imaging plate dibungkus dengan plastik dan didesinfeksi, selanjutnya di proses seperti biasa dengan menerapkan kaidah proteksi radiasi

33
33
c. Kamar operasiPelayanan operasi emergensi pada pasien penyakit menular kedaruratan kesehatan masyarakat dilakukan sesuai indikasi medis dengan memperhatikan standar PPI. Untuk tata udara, dapat digunakan hepafilter yang sudah ada pada ruang tersebut atau digunakan hepafilter portable di kamar operasi
d. HemodialisisPelayanan hemodialisis bagi pasien penyakit menular kedaruratan kesehatan masyarakat dengan memperhatikan standar PPI
4. Pencegahan Dan Pengendalian InfeksiPenanganan pasien penyakit menular kedaruratan kesehatan masyarakat di Rumah Sakit harus memperhatikan prinsip kewaspadaan isolasi menurut panduan PPI, yang secara umum meliputi :a. Kewaspadaan standar/ Standard Precaution
- Merupakan gabungan dari Universal Precaution dan Body Substain Isolation- Waspada terhadap darah, cairan tubuh, sekresi dan ekskresi kecuali
keringat- Ditujukan kepada semua pasien tanpa memandang infeksi atau tidak
infeksi Kewaspadaan standar meliputi :1) Kebersihan tangan2) Penggunaan APD3) Pengelolaan limbah dan benda tajam4) Pengendalian lingkungan5) Penyuntikan yang aman6) Kebersihan pernapasan/etika batuk7) Praktek pungsi lumbal8) Perawatan peralatan kesehatan9) Pengelolaan linen10) Kesehatan pegawai11) Penempatan pasien
b. Kewaspadaan transmisi- Merupakan kewaspadaan tambahan- Ditujukan kepada pasien yang terinfeksi atau diduga infeksi- Meliputi kewaspadaan airborne, kontak, blood borne dan droplet.
c. Pemakaian APDPenyediaan dan penggunaan APD (alat pelindung diri) atau PPE (personal protection equipment) menyesuaian dengan Panduan yang ditetapkan oleh WHO maupun Kementerian Kesehatan sesuai tingkat risiko penularan penyakit. Penyediaan APD sesuai area, untuk area yang masuk zona merah, kuning maupun area hijau. Penyediaan APD diprioritaskan kepada petugas kesehatan di Rumah Sakit yang termasuk kelompok risiko tinggi, seperti :1. APD untuk petugas Rumah Sakit di ruang isolasi adalah APD lengkap
(penutup kepala, kaca mata goggle, masker N95, sarung tangan, apron/

34
34
pakaian pelindung, sepatu pelindung)2. APD untuk petugas Rumah Sakit di ruang Instalasi Gawat Darurat (IGD)
yang melakukan kontak langsung dengan pasien menggunakan APDlengkap
3. APD untuk petugas kesehatan yang tidak kontak langsung dengan pasien minimal terdiri dari masker N95 dan sarung tangan
4. APD untuk petugas laboratorium adalah APD lengkap (penutup kepala, kaca mata goggle, masker N95, sarung tangan, apron/pakaian pelindung, sepatu pelindung)
5. Pada situasi dimana telah terjadi penularan wabah penyakit menular udara antar manusia di dalam Rumah Sakit maka semua petugas kesehatan, baik yang kontak dengan pasien secara langung maupun tidak, diharuskan menggunakan APD lengkap
Untuk ketentuan APD terkait dengan risiko penularan penyakit dapat mengikuti apa yang direkomendasikan dari PPI pada instansi masing-masing yang mengacu pada standar yang ada.
d. Dekontaminasi AmbulansSebelum keluar dari Rumah Sakit, mobil ambulans yang mengantar pasien penyakit menular kedaruratan kesehatan masyarakat harus didekontaminasi di lokasi yang disiapkan.1. Persiapan
a. Petugas menggunakan APD sarung tangan rumah tangga lateks, celemek kedap air, kacamata pelindung, sepatu boot
b. Menyiapkan perlengkapan desinfeksi udara dan Spill Kit darah serta cairan tubuh
2. Prosedura. Petugas cuci tangan dan menggunakan APDb. Langkah pertama dilakukan desinfeksi udarac. Selanjutnya jika ada tumpahan darah atau muntah maka dilakukan
pembersihan sesuai prosedur penanganan tumpahan darah dan cairan tubuh (Spill Kit)
d. Terakhir dilakukan desinfeksi permukaan
5. Kebutuhan LogistikLogistik yang perlu dipersiapkan meliputi :a. Kebutuhan peralatan medis (ventilator, bed side monitor, tabung oksigen,
tiang infus, dsb) sesuai kebutuhanb. Kebutuhan obat untuk pasienc. Kebutuhan obat profilaksis untuk petugas sesuai kebutuhand. Rekam medise. Kebutuhan APD lengkapf. Kebutuhan spill kitg. Kebutuhan forensik

3535
h. Kebutuhan pakaian harian jaga petugasi. Makanan untuk pasien dan keluarga yang berada di Rumah Sakitj. Makanan untuk petugask. Kebutuhan logistik lainnya
6. Penyiapan Infrastruktura. Menyiapkan ruang isolasi perawatan pasienb. Menyiapkan eskalasi ruang isolasi bila diperkirakan akan kapasitas terlampauic. Menyiapkan ruang triage darurat bila diperlukand. Menyiapkan ruang dekontaminasi ambulans e. Menyiapkan ruang istirahat bagi petugas kesehatan dan non kesehatan bila
diberlakukan penutupan terbatas dalam Rumah Sakitf. Menyiapkan Rumah Sakit lapangan, bila diperlukang. Menyiapkan infrastruktur terkait gas medis, air, pembuangan limbah, listrik,
telepon, dan sistem informasi, termasuk jaringan internet untuk memenuhi kebutuhan di lapangan
7. Manajemen Dan Mobilisasi SDMa. Pendataan tenaga, baik tenaga kesehatan maupun nonkesehatan di Rumah
Sakitb. Menyiapkan tenaga cadangan baik tenaga kesehatan maupun non kesehatanc. Pengerahan bantuan SDM untuk eskalasi di IGD maupun ruang isolasi
mengutamakan SDM yang on site di Rumah Sakitd. Apabila dibutuhkan SDM yang lebih banyak maka Rumah Sakit memberikan
instruksi bagi petugas yang sedang libur untuk membantu penanganan pasiene. Rekruitmen dan kredensialing tenaga bantuan atau relawan dari eksternal
dilakukan sesuai prosedur dengan akses koordinasi satu pintu
f. Sebelum terjun ke lapangan dilakukan program pembekalan/pelatihan cepat terkait penanganan kasus bagi para tenaga bantuan
8. Prosedur Keamanana. Memaksimalkan tim petugas keamanan Rumah Sakit untuk meningkatkan
keamanan Rumah Sakitb. Meningkatkan keamanan wilayah IGD dan ruang isolasic. Mengamankan jalur masuk dan keluar ambulans rujukand. Melakukan pengawalan bagi ambulans perujuk menuju ruang isolasi.e. Mengamankan jalur petugas yang mentranspor pasien penyakit menular
terkait kedaruratan kesehatan masyarakatf. Berkoordinasi dengan pihak kepolisiang. Apabila dilakukan penutupan Rumah Sakit untuk karantina maka akses
masuk/keluar pengunjung Rumah Sakit melalui satu pintu dan semua orang yang masuk/keluar Rumah Sakit harus dicatat, termasuk alamat rumah yang

36
36
jelas sesuai dengan tanda pengenal yang sah
9. Komunikasi dan Informasia. Menyiapkan satu orang juru bicara Rumah Sakitb. Melakukan koordinasi dengan pemerintah pusat dan daerah, dalam hal ini
melalui pusat komunikasi publik, mengenai informasi yang akan diberikan kepada media yang diatur sesuai dengan aturan yang berlaku
c. Menyiapkan bahan yang akan disampaikan kepada pusat media pemerintahd. Menyiapkan pesan yang akan disampaikan kepada pasien dan seluruh staf
Rumah Sakite. Menyiapkan hotline atau nomor telepon penting Rumah Sakit dan petugas
medis
10. Transportasia. Menyiapkan kendaraan untuk operasional Rumah Sakitb. Menyiapkan ambulans untuk rujukan
11. Pemulasaran JenazahPenatalaksanaan terhadap jenazah pasien penyakit menular terkait kedaruratan kesehatan masyarakat dilakukan secara khusus:a. Memperhatikan norma agama atau kepercayaan dan perundangan yang
berlakub. Pemeriksaan terhadap jenazah dilakukan oleh petugas kesehatanc. Perlakuan terhadap jenazah dan penghapushamaan bahan dan alat yang
digunakan dalam penatalaksanaan jenazah dilakukan oleh petugas kesehatand. Transportasi jenazah dari ruang isolasi menuju kamar jenazah menggunakan
brankar jenazah tertutupPengelolaan Kamar Jenazah:a. Seluruh petugas pemulasaraan jenazah telah mempersiapkan kewaspadaan
standard (standard precaution)b. Sebelumnya mencuci tangan dengan sabun, serta sebelum dan sesudah
sarung tangan dilepasc. perlakuan terhadap jenazah: luruskan tubuh, tutup mata, telinga, dan mulut
dengan kapas/plester kedap air, lepaskan alat kesehatan yang terpasang, setiap luka harus diplester dengan rapat
d. Jika diperlukan untuk memandikan jenazah (air pencuci dibubuhi bahan desinfektan) atau perlakuan khusus terhadap jenazah maka hanya dapat dilakukan oleh petugas khusus dengan tetap memperhatikan universalprecaution
e. Jenazah pasien pandemi ditutup dengan kain kafan dan bahan dari plastic (yang tidak dapat tembus air). Dapat juga jenazah ditutup dengan bahan kayu atau bahan lain yang tidak mudah tercemar
f. Jenazah tidak boleh dibalsem atau disuntik pengawetg. Jika akan diautopsi hanya dapat dilakukan oleh petugas khusus, autopsi dapat

37
37
dilakukan jika sudah ada izin dari pihak keluarga dan manajemen Rumah Sakit
h. Jenazah yang sudah dibungkus tidak boleh dibuka lagii. Jenazah sebaiknya hanya diantar/diangkut dengan mobil jenazahj. Jenazah sebaiknya disemayamkan tidak lebih dari 4 jam dari ruang
pemulasaraan jenazahk. Jenazah langsung dibawa ke tempat pemakaman umum
12. Surveilans kesehatan terhadap tenaga kesehatan dan pekerja di Rumah SakitDalam pelaksanaan surveilans kesehatan terhadap tenaga kesehatan dan pekerja di Rumah Sakit dilakukan beberapa hal sebagai berikut:a. Surveilans harian terhadap tenaga kesehatan dan pekerja di Rumah Sakit karena
penyakit menular terkait kedaruratan kesehatan masyarakat selama masa penanggulangan episenter.
b. Surveilans harian terhadap tenaga kesehatan dan pekerja yang kontak dengankasus kedaruratan kesehatan masyarakat di Rumah Sakit.− Lakukan pemeriksaan terhadap gejala penyakit yang terkait kedaruratan
kesehatan masyarakat dan pekerja yang kontak dengan pasien, setelah dilakukan investigasi dan dicurigai menderita penyakit menular kedauratan kesehatan masyarakat maka dilakukan perawatan di ruang isolasi
− Pemantauan keluhan kesehatan selanjutnyac. Berkoordinasi dengan dokter yang merawat dalam melakukan pemantauan
kasus harian (dokumentasi klinis, radiologi, dan lab kasus)d. Hasil surveilans dilaporkan setiap hari ke Pimpinan Rumah Sakit selaku
Incident Commander. Jika pasien meninggal, segera laporkan ke IncidentCommander
13. Penutupan Rumah SakitDilaksanakan mengacu pada peraturan perundangan.
14. Alur Pelaporana. Ke luar
Pimpinan Rumah Sakit melaporkan setiap saat kepada DinasKesehatan Provinsi/Kabupaten/Kota dengan tembusan ke Posko Pusat yangakan diteruskan ke Menteri.
b. Ke dalamSistem pelaporan di dalam Rumah Sakit disesuaikan dengan sistem yang berlaku di masing-masing Rumah Sakit, dengan pimpinan Rumah Sakitsebagai penanggung jawab.
15. Sumber Daya AlternatifApabila Rumah Sakit tidak dapat melakukan upaya apabila eskalasi penyakit terjadi lebih luas sehingga kapasitas dan sumber daya yang dimiliki terlampaui

38
38
maka Pimpinan Rumah Sakit selaku incident commander menempuh upaya :a. Koordinasi dengan Rumah Sakit rujukan lainnya untuk merujuk pasien penyakit
menular terkait kedaruratan kesehatan masyarakat yang tidak dapat ditanganib. Koordinasi dengan Rumah Sakit sekitarnya terkait pengaturan rujukan bagi
pasien selain yang terkait wabah penyakit menular udara selama masa tanggap darurat bencana
c. Koordinasi dengan Dinas Kesehatan kabupaten/kota/ provinsi lokal maupun sekitar, pemerintah daerah, serta Kementerian Kesehatan untuk pemenuhan semua kebutuhan yang diperlukan dalam penanganan pasien
16. Demobilisasia. Pengakhiran masa tanggap darurat bencana Rumah Sakit terkait kedaruratan
kesehatan masyarakat dan pengembalian ke fungsi normal Rumah Sakitditetapkan oleh Pimpinan Rumah Sakit dengan memperhatikan masa tanggap darurat bencana yang ditetapkan secara regional atau nasional.
b. Rumah Sakit melakukan debriefing untuk mengevaluasi keseluruhan prosesyang berlangsung selama masa tanggap darurat dan menyusun rencana perbaikan untuk masa mendatang
c. Segala keperluan administratif terkait keuangan/pembiayaan diproses sesuai regulasi yang berlaku

3937
BAB VI PELATIHAN DAN SIMULASI KONDISI DARURAT DAN/ATAUBENCANA DI RUMAH SAKIT
Pelatihan dan simulasi kondisi darurat mencakup dua hal penting, yaitu mengenai penanggulangan pada saat kondisi darurat dan setelah kondisi darurat terjadi. Simulasi dapat dilakukan secara internal dan eksternal. Simulasi internal dilakukan oleh staf dan manajemen Rumah Sakit, di dalam satu area gedung atau untuk keseluruhan area gedung yang ada di Rumah Sakit tanpa melibatkan pihak luar / eksternal terkait. Simulasi eksternal dilakukan oleh staf dan manajemen Rumah Sakit dengan melibatkan pihak-pihak eksternal seperti diantaranya dinas penanggulangan pemadam kebakaran dan penanggulangan bencana, kepolisian, BPBD/BNPB, dan lainnya.
A. PelatihanPelatihan kesiapsiagaan yang dilakukan Rumah Sakit antara lain:• Pelatihan HVA Dan HSI• Pelatihan Darurat Dan Bencana Wabah Internal Dan Eksternal Di Rumah Sakit• Pelatihan Penanganan Kebakaran Di Ruang Perawatan Rumah Sakit• Pelatihan Darurat Dan Bencana Di Tumpahan B3 Di Rumah Sakit• Pelatihan Darurat Keamanan Di Rumah Sakit• Pelatihan Darurat Peralatan Medis Di Rumah Sakit• Pelatihan Darurat Sistem Utilitas Di Rumah Sakit• Pelatihan Darurat Sistem IT Di Rumah Sakit• Pelatihan Basic Life Support (BLS)• Pelatihan Triase• Pelatihan Evakuasi Pasien
Pelatihan yang dibutuhkan dapat disesuaikan berdasarkan hasil penilaian HVA masing-masing Rumah Sakit.
B. SimulasiSimulasi dapat dilakukan dengan table top excercise dan simulasi lapangan. Setiap pegawai Rumah Sakit setidaknya mengikuti simulasi 1 (satu kali) dalam setahun. Pelaksanaan simulasi menggunakan skenario umum dan detail. Skenario disesuaikan dengan kondisi masing-masing Rumah Sakit.
Dalam simulasi perlu dilakukan - identifikasi pihak-pihak (sumber daya manusia) yang harus terlibat mulai dari menit-menit
pertama kejadian- Identifikasi kebutuhan sarana dan prasarana / fasilitas yang dibutuhkan mulai dari awal
sampai dengan akhir (sebelum, saat dan setelah) simulasi- Membuat langkah pemecahan masalah untuk menanggulangi bencana tersebut (siapa
berbuat apa)• Sistem komando• Alur komando / struktur organisasi• Koordinasi

4038
• Tim respon cepat• Triase• Tim Medik / Treatment • Tim Logistik• Evakuasi ( Dokumen, barang dan sistem transportasi )
C. Evaluasi Simulasi Kondisi darurat dan/atau bencana Pada akhir simulasi, Rumah Sakit melakukan diskusi (debriefing) mengenai simulasi yangtelah dilakukan untuk dibuat laporan dan tindak lanjut.

4139
BAB VII PENUTUP
Rumah Sakit merupakan salah satu fasilitas pelayanan kesehatan yang dapat memberikan pelayanan kesehatan secara paripurna kepada masyarakat. Rumah Sakit dengankarakteristik padat karya, pada modal, padat teknologi dan padat pakar mempunyai risiko terhadap keselamatan dan kesehatan kerja terhadap karyawan yang berdampak terhadap kualitas layanan bagi pengguna. Kondisi darurat dan/atau bencana yang dapat terjadi di Rumah Sakit merupakan suatu kejadian yang dapat mengancam jiwa dan keselamatan bagi pekerja dan pengguna Rumah Sakit, sehingga perlu adanya berbagai upaya dalam melakukan identifikasi risiko dan kesiapsiagaandi Rumah Sakit.
Petunjuk teknis kesiapsiagaan kondisi darurat dan/atau bencana di Rumah Sakit merupakan suatu upaya bagaimana pekerja dapat memahami dan melakukan tindakan yang semestinya jika terjadi kondisi darurat dan/atau bencana. Semoga dengan adanya petunjuk teknis ini dapat menciptakan Rumah Sakit yang aman, tetap beroperasi dan memberikan pelayanan dalam kondisi darurat dan/atau bencana.

4240
DAFTAR PUSTAKA
WHO. Hospital Safety Index Guide for Evaluators Second Edition. 2015
KARS. Standar Nasional Akreditasi Rumah Sakit (SNARS) edisi 1.1
EMSA. Hospital Incident Command System Guidebook. 2014
WHO. Hospital Preparedness checklist for pandemic influenza. Focus on Pandemic (H1N1). 2009. Regional Office for Europe.

43
42
LAM
PIR
AN
Lam
pira
n 1
. Tab
el H
SI
42
LAM
PIR
AN
Lam
pira
n 1
. Tab
el H
SI
Hos
pita
l Saf
ety
Inde
x G
UID
E FO
R EV
ALU
ATO
RS
148
Mod
ule
1: H
azar
ds a
ffect
ing
the
safe
ty o
f the
hos
pita
l an
d th
e ro
le o
f the
hos
pita
l in
emer
genc
y an
d di
sast
er m
anag
emen
t
1.1
Haz
ards
Haz
ard
Leve
lSh
ould
the
hosp
ital
be p
repa
red
to
resp
ond
to th
is
haza
rd?
If ye
s, m
ark
the
box.
Obs
erva
tions
(e
valu
ator
’s co
mm
ents
)N
o
haza
rd
Haz
ard
leve
l
LOW
AVERAGE
HIGH
1.1.
1 G
eolo
gica
l haz
ards
Eart
hqua
kes
Refe
r to
regi
onal
and
loca
l haz
ard
map
s or o
ther
haz
ard
info
rmat
ion,
and
rate
the
leve
l of e
arth
quak
e ha
zard
for t
he
hosp
ital’s
loca
tion
(incl
udin
g ca
tchm
ent a
rea)
in te
rms o
f ge
otec
hnic
al so
il an
alys
es. D
eter
min
e w
heth
er th
e ho
spita
l sh
ould
be
prep
ared
to re
spon
d to
an
emer
genc
y or
disa
ster
du
e to
ear
thqu
akes
(bas
ed o
n ex
posu
re o
f the
cat
chm
ent
popu
latio
n or
the
spec
ializ
ed ro
le o
f the
hos
pita
l for
the
trea
t-m
ent o
f inj
ured
pat
ient
s).
Volca
nic a
ctiv
ity an
d er
uptio
nRe
fer t
o re
gion
al a
nd lo
cal h
azar
d m
aps o
r oth
er h
azar
d in
for-
mat
ion,
and
rate
the
leve
l of v
olca
nic
haza
rd fo
r the
hos
pita
l’s
loca
tion.
Thi
s sho
uld
take
into
acc
ount
pro
xim
ity to
vol
cano
es,
volc
anic
act
ivity
, rou
tes o
f lav
a flo
w, p
yroc
last
ic fl
ow a
nd a
sh
fall.
Det
erm
ine
whe
ther
the
hosp
ital s
houl
d be
pre
pare
d to
re
spon
d to
an
emer
genc
y or
disa
ster
due
to v
olca
nic
activ
ity
and
erup
tion
(bas
ed o
n ex
posu
re o
f the
cat
chm
ent p
opul
a-tio
n or
the
spec
ializ
ed ro
le).
Dry m
ass m
ovem
ent −
land
slide
sRe
fer t
o re
gion
al a
nd lo
cal h
azar
d m
aps o
r oth
er h
azar
d in
for-
mat
ion
for t
he re
gion
, and
rate
the
leve
l of l
ands
lide
haza
rd
for t
he h
ospi
tal’s
loca
tion.
Not
e th
at la
ndsli
des m
ay b
e ca
used
by
uns
tabl
e so
ils. D
eter
min
e w
heth
er th
e ho
spita
l sho
uld
be p
repa
red
to re
spon
d to
an
emer
genc
y or
disa
ster
due
to
land
slide
s (ba
sed
on e
xpos
ure
of th
e ca
tchm
ent p
opul
atio
n).
Tsun
amis
Refe
r to
regi
onal
haz
ard
map
s or o
ther
haz
ard
info
rmat
ion,
an
d ra
te th
e le
vel o
f tsu
nam
i haz
ard
caus
ed b
y su
bmar
ine
seism
ic o
r vol
cani
c ac
tivity
for t
he h
ospi
tal’s
loca
tion.
Det
er-
min
e w
heth
er th
e ho
spita
l sho
uld
be p
repa
red
to re
spon
d to
an
emer
genc
y or
disa
ster
due
to ts
unam
is (b
ased
on
expo
sure
of t
he c
atch
men
t pop
ulat
ion)
.
Oth
er g
eolo
gica
l haz
ards
(e.g
. roc
kfal
ls, su
bsid
ence
, deb
ris
and
mud
flow
s (s
peci
fy) .
........
........
........
........
........
........
........
........
........
........
........
........
........
........
....Re
fer t
o re
gion
al a
nd lo
cal h
azar
d m
aps o
r oth
er h
azar
d in
-fo
rmat
ion
to id
entif
y ot
her g
eolo
gica
l phe
nom
ena
not l
isted
ab
ove.
Spe
cify
the
haza
rd a
nd ra
te th
e co
rresp
ondi
ng h
azar
d le
vel f
or th
e ho
spita
l. D
eter
min
e w
heth
er th
e ho
spita
l sho
uld
be p
repa
red
to re
spon
d to
an
emer
genc
y or
disa
ster
due
to
the
iden
tified
geo
logi
cal h
azar
ds (b
ased
on
expo
sure
of t
he
catc
hmen
t pop
ulat
ion)
.
Con
tinue
>>

44
Hos
pita
l Saf
ety
Inde
x G
UID
E FO
R EV
ALU
ATO
RS
148
Mod
ule
1: H
azar
ds a
ffect
ing
the
safe
ty o
f the
hos
pita
l an
d th
e ro
le o
f the
hos
pita
l in
emer
genc
y an
d di
sast
er m
anag
emen
t
1.1
Haz
ards
Haz
ard
Leve
lSh
ould
the
hosp
ital
be p
repa
red
to
resp
ond
to th
is
haza
rd?
If ye
s, m
ark
the
box.
Obs
erva
tions
(e
valu
ator
’s co
mm
ents
)N
o
haza
rd
Haz
ard
leve
l
LOW
AVERAGE
HIGH
1.1.
1 G
eolo
gica
l haz
ards
Eart
hqua
kes
Refe
r to
regi
onal
and
loca
l haz
ard
map
s or o
ther
haz
ard
info
rmat
ion,
and
rate
the
leve
l of e
arth
quak
e ha
zard
for t
he
hosp
ital’s
loca
tion
(incl
udin
g ca
tchm
ent a
rea)
in te
rms o
f ge
otec
hnic
al so
il an
alys
es. D
eter
min
e w
heth
er th
e ho
spita
l sh
ould
be
prep
ared
to re
spon
d to
an
emer
genc
y or
disa
ster
du
e to
ear
thqu
akes
(bas
ed o
n ex
posu
re o
f the
cat
chm
ent
popu
latio
n or
the
spec
ializ
ed ro
le o
f the
hos
pita
l for
the
trea
t-m
ent o
f inj
ured
pat
ient
s).
Volca
nic a
ctiv
ity an
d er
uptio
nRe
fer t
o re
gion
al a
nd lo
cal h
azar
d m
aps o
r oth
er h
azar
d in
for-
mat
ion,
and
rate
the
leve
l of v
olca
nic
haza
rd fo
r the
hos
pita
l’s
loca
tion.
Thi
s sho
uld
take
into
acc
ount
pro
xim
ity to
vol
cano
es,
volc
anic
act
ivity
, rou
tes o
f lav
a flo
w, p
yroc
last
ic fl
ow a
nd a
sh
fall.
Det
erm
ine
whe
ther
the
hosp
ital s
houl
d be
pre
pare
d to
re
spon
d to
an
emer
genc
y or
disa
ster
due
to v
olca
nic
activ
ity
and
erup
tion
(bas
ed o
n ex
posu
re o
f the
cat
chm
ent p
opul
a-tio
n or
the
spec
ializ
ed ro
le).
Dry m
ass m
ovem
ent −
land
slide
sRe
fer t
o re
gion
al a
nd lo
cal h
azar
d m
aps o
r oth
er h
azar
d in
for-
mat
ion
for t
he re
gion
, and
rate
the
leve
l of l
ands
lide
haza
rd
for t
he h
ospi
tal’s
loca
tion.
Not
e th
at la
ndsli
des m
ay b
e ca
used
by
uns
tabl
e so
ils. D
eter
min
e w
heth
er th
e ho
spita
l sho
uld
be p
repa
red
to re
spon
d to
an
emer
genc
y or
disa
ster
due
to
land
slide
s (ba
sed
on e
xpos
ure
of th
e ca
tchm
ent p
opul
atio
n).
Tsun
amis
Refe
r to
regi
onal
haz
ard
map
s or o
ther
haz
ard
info
rmat
ion,
an
d ra
te th
e le
vel o
f tsu
nam
i haz
ard
caus
ed b
y su
bmar
ine
seism
ic o
r vol
cani
c ac
tivity
for t
he h
ospi
tal’s
loca
tion.
Det
er-
min
e w
heth
er th
e ho
spita
l sho
uld
be p
repa
red
to re
spon
d to
an
emer
genc
y or
disa
ster
due
to ts
unam
is (b
ased
on
expo
sure
of t
he c
atch
men
t pop
ulat
ion)
.
Oth
er g
eolo
gica
l haz
ards
(e.g
. roc
kfal
ls, su
bsid
ence
, deb
ris
and
mud
flow
s (s
peci
fy) .
........
........
........
........
........
........
........
........
........
........
........
........
........
........
....Re
fer t
o re
gion
al a
nd lo
cal h
azar
d m
aps o
r oth
er h
azar
d in
-fo
rmat
ion
to id
entif
y ot
her g
eolo
gica
l phe
nom
ena
not l
isted
ab
ove.
Spe
cify
the
haza
rd a
nd ra
te th
e co
rresp
ondi
ng h
azar
d le
vel f
or th
e ho
spita
l. D
eter
min
e w
heth
er th
e ho
spita
l sho
uld
be p
repa
red
to re
spon
d to
an
emer
genc
y or
disa
ster
due
to
the
iden
tified
geo
logi
cal h
azar
ds (b
ased
on
expo
sure
of t
he
catc
hmen
t pop
ulat
ion)
.
Con
tinue
>>

45
149
(Con
tinue
d) 1
.1 H
azar
ds
Haz
ard
Leve
lSh
ould
the
hosp
ital b
e pr
epar
ed to
resp
ond
to th
is
haza
rd?
If ye
s, m
ark
the
box.
Obs
erva
tions
(e
valu
ator
’s co
mm
ents
)N
o
haza
rd
Haz
ard
leve
l
LOW
AVERAGE
HIGH
1.1.
2 H
ydro
-met
eoro
logi
cal h
azar
ds
1.1.
2.1
Met
eoro
logi
cal h
azar
dsCy
clone
s/hu
rrica
nes/
typh
oons
Refe
r to
regi
onal
haz
ard
map
s or o
ther
haz
ard
info
rmat
ion,
an
d ra
te th
e ha
zard
leve
l for
the
hosp
ital l
ocat
ion
in te
rms o
f cy
clon
es, h
urric
anes
and
typh
oons
. Det
erm
ine
whe
ther
the
hosp
ital s
houl
d be
pre
pare
d to
resp
ond
to a
n em
erge
ncy
or
disa
ster
due
to c
yclo
nes,
hurr
ican
es o
r typ
hoon
s (ba
sed
on
expo
sure
of t
he c
atch
men
t pop
ulat
ion)
.
Torn
adoe
s Re
fer t
o re
gion
al h
azar
d m
aps o
r oth
er h
azar
d in
form
atio
n,
and
rate
the
torn
ado
haza
rd le
vel f
or th
e ho
spita
l’s lo
catio
n.
Det
erm
ine
whe
ther
the
hosp
ital s
houl
d be
pre
pare
d to
re
spon
d to
an
emer
genc
y or
disa
ster
due
to to
rnad
oes (
base
d on
exp
osur
e of
the
catc
hmen
t pop
ulat
ion)
.
Loca
l sto
rms
Rate
the
haza
rd le
vel f
or th
e ho
spita
l in
rela
tion
to fl
oodi
ng
and
othe
r dam
age
due
to in
tens
ive
(or t
orre
ntia
l) ra
infa
ll fro
m
loca
l sto
rms b
ased
on
the
hist
ory
of su
ch e
vent
s. D
eter
min
e w
heth
er th
e ho
spita
l sho
uld
be p
repa
red
to re
spon
d to
an
emer
genc
y or
disa
ster
due
to lo
cal s
torm
s (ba
sed
on e
xpos
ure
of th
e ca
tchm
ent p
opul
atio
n).
Oth
er m
eteo
rolo
gica
l haz
ards
(e.g
. san
d-st
orm
s, w
ind
gust
s) (s
peci
fy) .
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
.Ra
te th
e ha
zard
leve
l for
the
hosp
ital i
n re
latio
n to
risk
of o
ther
m
eteo
rolo
gica
l haz
ards
bas
ed o
n th
e hi
stor
y of
such
eve
nts.
Det
erm
ine
whe
ther
the
hosp
ital s
houl
d be
pre
pare
d to
re-
spon
d to
an
emer
genc
y or
disa
ster
due
to o
ther
met
eoro
logi
-ca
l haz
ards
(bas
ed o
n ex
posu
re o
f the
cat
chm
ent p
opul
atio
n).
1.1.
2.2
Hyd
rolo
gica
l haz
ards
Rive
r floo
dsRe
fer t
o re
gion
al a
nd lo
cal h
azar
d m
aps o
r oth
er h
azar
d in
for-
mat
ion,
and
rate
the
river
floo
d ha
zard
leve
l of t
he h
ospi
tal’s
lo
catio
n (in
clud
ing
catc
hmen
t are
a) in
term
s of r
iver
floo
ds
(and
oth
er w
ater
cour
ses,
such
as c
reek
s). D
eter
min
e w
heth
er
the
hosp
ital s
houl
d be
pre
pare
d to
resp
ond
to a
n em
erge
ncy
or d
isast
er d
ue to
rive
r floo
ds (b
ased
on
expo
sure
of t
he
catc
hmen
t pop
ulat
ion)
.
Flas
h flo
ods
Refe
r to
regi
onal
and
loca
l haz
ard
map
, oth
er h
azar
d in
form
a-tio
n an
d pa
st in
cide
nts,
and
rate
the
flash
floo
d ha
zard
leve
l for
th
e ho
spita
l’s lo
catio
n. D
eter
min
e w
heth
er th
e ho
spita
l sho
uld
be p
repa
red
to re
spon
d to
an
emer
genc
y or
disa
ster
bas
ed o
n fla
sh fl
oods
(due
to e
xpos
ure
of th
e ca
tchm
ent p
opul
atio
n).
Stor
m su
rge
Refe
r to
regi
onal
haz
ard
map
s or o
ther
haz
ard
info
rmat
ion,
an
d ra
te th
e st
orm
surg
e ha
zard
leve
l ass
ocia
ted
with
risk
s of
cyc
lone
s, hu
rric
anes
, typ
hoon
s and
oth
er st
orm
s for
the
hosp
ital’s
loca
tion.
Det
erm
ine
whe
ther
the
hosp
ital s
houl
d be
pre
pare
d to
resp
ond
to a
n em
erge
ncy
or d
isast
er d
ue to
st
orm
surg
e an
d re
late
d flo
ods (
base
d on
exp
osur
e of
the
catc
hmen
t pop
ulat
ion)
.
Con
tinue
>>
ANN
EX 2
: FO
RM 2
: SAF
E H
OSP
ITAL
S CH
ECKL
IST
Mod
ule
1: H
azar
ds a
ffect
ing
the
safe
ty o
f the
hos
pita
l and
the
role
of t
he h
ospi
tal i
n em
erge
ncy
and
disa
ster
man
agem
ent

46
149
(Con
tinue
d) 1
.1 H
azar
ds
Haz
ard
Leve
lSh
ould
the
hosp
ital b
e pr
epar
ed to
resp
ond
to th
is
haza
rd?
If ye
s, m
ark
the
box.
Obs
erva
tions
(e
valu
ator
’s co
mm
ents
)N
o
haza
rd
Haz
ard
leve
l
LOW
AVERAGE
HIGH
1.1.
2 H
ydro
-met
eoro
logi
cal h
azar
ds
1.1.
2.1
Met
eoro
logi
cal h
azar
dsCy
clone
s/hu
rrica
nes/
typh
oons
Refe
r to
regi
onal
haz
ard
map
s or o
ther
haz
ard
info
rmat
ion,
an
d ra
te th
e ha
zard
leve
l for
the
hosp
ital l
ocat
ion
in te
rms o
f cy
clon
es, h
urric
anes
and
typh
oons
. Det
erm
ine
whe
ther
the
hosp
ital s
houl
d be
pre
pare
d to
resp
ond
to a
n em
erge
ncy
or
disa
ster
due
to c
yclo
nes,
hurr
ican
es o
r typ
hoon
s (ba
sed
on
expo
sure
of t
he c
atch
men
t pop
ulat
ion)
.
Torn
adoe
s Re
fer t
o re
gion
al h
azar
d m
aps o
r oth
er h
azar
d in
form
atio
n,
and
rate
the
torn
ado
haza
rd le
vel f
or th
e ho
spita
l’s lo
catio
n.
Det
erm
ine
whe
ther
the
hosp
ital s
houl
d be
pre
pare
d to
re
spon
d to
an
emer
genc
y or
disa
ster
due
to to
rnad
oes (
base
d on
exp
osur
e of
the
catc
hmen
t pop
ulat
ion)
.
Loca
l sto
rms
Rate
the
haza
rd le
vel f
or th
e ho
spita
l in
rela
tion
to fl
oodi
ng
and
othe
r dam
age
due
to in
tens
ive
(or t
orre
ntia
l) ra
infa
ll fro
m
loca
l sto
rms b
ased
on
the
hist
ory
of su
ch e
vent
s. D
eter
min
e w
heth
er th
e ho
spita
l sho
uld
be p
repa
red
to re
spon
d to
an
emer
genc
y or
disa
ster
due
to lo
cal s
torm
s (ba
sed
on e
xpos
ure
of th
e ca
tchm
ent p
opul
atio
n).
Oth
er m
eteo
rolo
gica
l haz
ards
(e.g
. san
d-st
orm
s, w
ind
gust
s) (s
peci
fy) .
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
.Ra
te th
e ha
zard
leve
l for
the
hosp
ital i
n re
latio
n to
risk
of o
ther
m
eteo
rolo
gica
l haz
ards
bas
ed o
n th
e hi
stor
y of
such
eve
nts.
Det
erm
ine
whe
ther
the
hosp
ital s
houl
d be
pre
pare
d to
re-
spon
d to
an
emer
genc
y or
disa
ster
due
to o
ther
met
eoro
logi
-ca
l haz
ards
(bas
ed o
n ex
posu
re o
f the
cat
chm
ent p
opul
atio
n).
1.1.
2.2
Hyd
rolo
gica
l haz
ards
Rive
r floo
dsRe
fer t
o re
gion
al a
nd lo
cal h
azar
d m
aps o
r oth
er h
azar
d in
for-
mat
ion,
and
rate
the
river
floo
d ha
zard
leve
l of t
he h
ospi
tal’s
lo
catio
n (in
clud
ing
catc
hmen
t are
a) in
term
s of r
iver
floo
ds
(and
oth
er w
ater
cour
ses,
such
as c
reek
s). D
eter
min
e w
heth
er
the
hosp
ital s
houl
d be
pre
pare
d to
resp
ond
to a
n em
erge
ncy
or d
isast
er d
ue to
rive
r floo
ds (b
ased
on
expo
sure
of t
he
catc
hmen
t pop
ulat
ion)
.
Flas
h flo
ods
Refe
r to
regi
onal
and
loca
l haz
ard
map
, oth
er h
azar
d in
form
a-tio
n an
d pa
st in
cide
nts,
and
rate
the
flash
floo
d ha
zard
leve
l for
th
e ho
spita
l’s lo
catio
n. D
eter
min
e w
heth
er th
e ho
spita
l sho
uld
be p
repa
red
to re
spon
d to
an
emer
genc
y or
disa
ster
bas
ed o
n fla
sh fl
oods
(due
to e
xpos
ure
of th
e ca
tchm
ent p
opul
atio
n).
Stor
m su
rge
Refe
r to
regi
onal
haz
ard
map
s or o
ther
haz
ard
info
rmat
ion,
an
d ra
te th
e st
orm
surg
e ha
zard
leve
l ass
ocia
ted
with
risk
s of
cyc
lone
s, hu
rric
anes
, typ
hoon
s and
oth
er st
orm
s for
the
hosp
ital’s
loca
tion.
Det
erm
ine
whe
ther
the
hosp
ital s
houl
d be
pre
pare
d to
resp
ond
to a
n em
erge
ncy
or d
isast
er d
ue to
st
orm
surg
e an
d re
late
d flo
ods (
base
d on
exp
osur
e of
the
catc
hmen
t pop
ulat
ion)
.
Con
tinue
>>
ANN
EX 2
: FO
RM 2
: SAF
E H
OSP
ITAL
S CH
ECKL
IST
Mod
ule
1: H
azar
ds a
ffect
ing
the
safe
ty o
f the
hos
pita
l and
the
role
of t
he h
ospi
tal i
n em
erge
ncy
and
disa
ster
man
agem
ent

47
Hos
pita
l Saf
ety
Inde
x G
UID
E FO
R EV
ALU
ATO
RS
150
(Con
tinue
d) 1
.1 H
azar
ds
Haz
ard
Leve
lSh
ould
the
hosp
ital b
e pr
epar
ed to
resp
ond
to th
is
haza
rd?
If ye
s, m
ark
the
box.
Obs
erva
tions
(e
valu
ator
’s co
mm
ents
)N
o
haza
rd
Haz
ard
leve
l
LOW
AVERAGE
HIGH
Wet
mas
s mov
emen
ts –
land
slide
sRe
fer t
o re
gion
al a
nd lo
cal h
azar
d m
aps o
r oth
er h
azar
d in
for-
mat
ion,
and
rate
the
leve
l of h
azar
d du
e to
land
slide
s cau
sed
by sa
tura
ted
soils
for t
he h
ospi
tal’s
loca
tion.
Det
erm
ine
whe
ther
the
hosp
ital s
houl
d be
pre
pare
d to
resp
ond
to a
n em
erge
ncy
or d
isast
er d
ue to
land
slide
s cau
sed
by sa
tura
ted
soils
(bas
ed o
n ex
posu
re o
f the
cat
chm
ent p
opul
atio
n).
Oth
er h
ydro
logi
cal h
azar
ds (e
.g. h
igh
tides
, ava
lanc
hes,
coas
tal fl
oods
)(s
peci
fy) .
........
........
........
........
........
........
........
........
........
........
........
........
........
........
......
Refe
r to
regi
onal
and
loca
l haz
ard
map
s or o
ther
haz
ard
in-
form
atio
n to
iden
tify
othe
r hyd
ro-m
eteo
rolo
gica
l haz
ards
not
lis
ted
abov
e. S
peci
fy th
e ha
zard
and
rate
the
corre
spon
ding
ha
zard
leve
l for
the
hosp
ital’s
loca
tion.
Det
erm
ine
whe
ther
the
hosp
ital s
houl
d be
pre
pare
d to
resp
ond
to a
n em
erge
ncy
or
disa
ster
due
to o
ther
hyd
rolo
gica
l haz
ard
(bas
ed o
n ex
posu
re
of th
e ca
tchm
ent p
opul
atio
n).
1.1.
2.3
Clim
atol
ogic
al h
azar
dsEx
trem
e te
mpe
ratu
re (e
.g. h
eat w
ave,
cold
wav
e, ex
trem
e w
inte
r con
ditio
ns –
dzud
)Re
fer t
o re
gion
al a
nd lo
cal h
azar
d m
aps o
r oth
er h
azar
d in
form
atio
n, a
nd ra
te th
e le
vel o
f haz
ard
due
to e
xtre
me
tem
-pe
ratu
re o
r wea
ther
con
ditio
n. S
peci
fy th
e ha
zard
and
rate
th
e co
rresp
ondi
ng h
azar
d le
vel f
or th
e ho
spita
l’s lo
catio
n. D
e-te
rmin
e w
heth
er th
e ho
spita
l sho
uld
be p
repa
red
to re
spon
d to
an
emer
genc
y or
disa
ster
due
to e
xtre
me
tem
pera
ture
s (b
ased
on
expo
sure
of t
he c
atch
men
t pop
ulat
ion)
.
Wild
fires
(e.g
. for
ests
, cro
plan
ds, p
opul
ated
area
s)Re
fer t
o re
gion
al a
nd lo
cal h
azar
d m
aps o
r oth
er h
azar
d in
form
atio
n, a
nd ra
te th
e w
ildfir
e ha
zard
leve
l for
the
hosp
ital’s
loca
tion.
Det
erm
ine
whe
ther
the
hosp
ital s
houl
d be
pre
pare
d to
resp
ond
to a
n em
erge
ncy
or d
isast
er d
ue to
w
ildfir
es (b
ased
on
expo
sure
of t
he c
atch
men
t pop
ulat
ion
or
the
spec
ializ
ed ro
le o
f the
hos
pita
l for
the
trea
tmen
t of b
urns
pa
tient
s).
Drou
ght
Refe
r to
regi
onal
and
loca
l haz
ard
map
s or o
ther
haz
ard
info
r-m
atio
n, a
nd ra
te th
e dr
ough
t haz
ard
leve
l for
the
hosp
ital’s
lo
catio
n. D
eter
min
e w
heth
er th
e ho
spita
l sho
uld
be p
repa
red
to re
spon
d to
an
emer
genc
y or
disa
ster
due
to d
roug
ht
(bas
ed o
n ex
posu
re o
f the
cat
chm
ent p
opul
atio
n or
the
spe-
cial
ized
role
of t
he h
ospi
tal f
or th
e tr
eatm
ent o
f mal
nutr
ition
).
Oth
er cl
imat
olog
ical h
azar
ds in
cludi
ng th
ose
attri
buta
ble
to
clim
ate
chan
ge (e
.g. s
ea-le
vel r
ise)
(spe
cify
) .....
........
........
........
........
........
........
........
........
........
........
........
........
........
........
..Ra
te th
e ha
zard
leve
l for
the
hosp
ital i
n re
latio
n to
the
risk
of o
ther
clim
atol
ogic
al h
azar
ds b
ased
on
haza
rd m
aps,
the
hist
ory
of su
ch e
vent
s and
haz
ard
mod
ellin
g. D
eter
min
e w
heth
er th
e ho
spita
l sho
uld
be p
repa
red
to re
spon
d to
an
emer
genc
y or
disa
ster
due
to o
ther
clim
atol
ogic
al h
azar
ds
(bas
ed o
n ex
posu
re o
f the
cat
chm
ent p
opul
atio
n).
Con
tinue
>>
Mod
ule
1: H
azar
ds a
ffect
ing
the
safe
ty o
f the
hos
pita
l and
the
role
of t
he h
ospi
tal i
n em
erge
ncy
and
disa
ster
man
agem
ent

48
Hos
pita
l Saf
ety
Inde
x G
UID
E FO
R EV
ALU
ATO
RS
150
(Con
tinue
d) 1
.1 H
azar
ds
Haz
ard
Leve
lSh
ould
the
hosp
ital b
e pr
epar
ed to
resp
ond
to th
is
haza
rd?
If ye
s, m
ark
the
box.
Obs
erva
tions
(e
valu
ator
’s co
mm
ents
)N
o
haza
rd
Haz
ard
leve
l
LOW
AVERAGE
HIGH
Wet
mas
s mov
emen
ts –
land
slide
sRe
fer t
o re
gion
al a
nd lo
cal h
azar
d m
aps o
r oth
er h
azar
d in
for-
mat
ion,
and
rate
the
leve
l of h
azar
d du
e to
land
slide
s cau
sed
by sa
tura
ted
soils
for t
he h
ospi
tal’s
loca
tion.
Det
erm
ine
whe
ther
the
hosp
ital s
houl
d be
pre
pare
d to
resp
ond
to a
n em
erge
ncy
or d
isast
er d
ue to
land
slide
s cau
sed
by sa
tura
ted
soils
(bas
ed o
n ex
posu
re o
f the
cat
chm
ent p
opul
atio
n).
Oth
er h
ydro
logi
cal h
azar
ds (e
.g. h
igh
tides
, ava
lanc
hes,
coas
tal fl
oods
)(s
peci
fy) .
........
........
........
........
........
........
........
........
........
........
........
........
........
........
......
Refe
r to
regi
onal
and
loca
l haz
ard
map
s or o
ther
haz
ard
in-
form
atio
n to
iden
tify
othe
r hyd
ro-m
eteo
rolo
gica
l haz
ards
not
lis
ted
abov
e. S
peci
fy th
e ha
zard
and
rate
the
corre
spon
ding
ha
zard
leve
l for
the
hosp
ital’s
loca
tion.
Det
erm
ine
whe
ther
the
hosp
ital s
houl
d be
pre
pare
d to
resp
ond
to a
n em
erge
ncy
or
disa
ster
due
to o
ther
hyd
rolo
gica
l haz
ard
(bas
ed o
n ex
posu
re
of th
e ca
tchm
ent p
opul
atio
n).
1.1.
2.3
Clim
atol
ogic
al h
azar
dsEx
trem
e te
mpe
ratu
re (e
.g. h
eat w
ave,
cold
wav
e, ex
trem
e w
inte
r con
ditio
ns –
dzud
)Re
fer t
o re
gion
al a
nd lo
cal h
azar
d m
aps o
r oth
er h
azar
d in
form
atio
n, a
nd ra
te th
e le
vel o
f haz
ard
due
to e
xtre
me
tem
-pe
ratu
re o
r wea
ther
con
ditio
n. S
peci
fy th
e ha
zard
and
rate
th
e co
rresp
ondi
ng h
azar
d le
vel f
or th
e ho
spita
l’s lo
catio
n. D
e-te
rmin
e w
heth
er th
e ho
spita
l sho
uld
be p
repa
red
to re
spon
d to
an
emer
genc
y or
disa
ster
due
to e
xtre
me
tem
pera
ture
s (b
ased
on
expo
sure
of t
he c
atch
men
t pop
ulat
ion)
.
Wild
fires
(e.g
. for
ests
, cro
plan
ds, p
opul
ated
area
s)Re
fer t
o re
gion
al a
nd lo
cal h
azar
d m
aps o
r oth
er h
azar
d in
form
atio
n, a
nd ra
te th
e w
ildfir
e ha
zard
leve
l for
the
hosp
ital’s
loca
tion.
Det
erm
ine
whe
ther
the
hosp
ital s
houl
d be
pre
pare
d to
resp
ond
to a
n em
erge
ncy
or d
isast
er d
ue to
w
ildfir
es (b
ased
on
expo
sure
of t
he c
atch
men
t pop
ulat
ion
or
the
spec
ializ
ed ro
le o
f the
hos
pita
l for
the
trea
tmen
t of b
urns
pa
tient
s).
Drou
ght
Refe
r to
regi
onal
and
loca
l haz
ard
map
s or o
ther
haz
ard
info
r-m
atio
n, a
nd ra
te th
e dr
ough
t haz
ard
leve
l for
the
hosp
ital’s
lo
catio
n. D
eter
min
e w
heth
er th
e ho
spita
l sho
uld
be p
repa
red
to re
spon
d to
an
emer
genc
y or
disa
ster
due
to d
roug
ht
(bas
ed o
n ex
posu
re o
f the
cat
chm
ent p
opul
atio
n or
the
spe-
cial
ized
role
of t
he h
ospi
tal f
or th
e tr
eatm
ent o
f mal
nutr
ition
).
Oth
er cl
imat
olog
ical h
azar
ds in
cludi
ng th
ose
attri
buta
ble
to
clim
ate
chan
ge (e
.g. s
ea-le
vel r
ise)
(spe
cify
) .....
........
........
........
........
........
........
........
........
........
........
........
........
........
........
..Ra
te th
e ha
zard
leve
l for
the
hosp
ital i
n re
latio
n to
the
risk
of o
ther
clim
atol
ogic
al h
azar
ds b
ased
on
haza
rd m
aps,
the
hist
ory
of su
ch e
vent
s and
haz
ard
mod
ellin
g. D
eter
min
e w
heth
er th
e ho
spita
l sho
uld
be p
repa
red
to re
spon
d to
an
emer
genc
y or
disa
ster
due
to o
ther
clim
atol
ogic
al h
azar
ds
(bas
ed o
n ex
posu
re o
f the
cat
chm
ent p
opul
atio
n).
Con
tinue
>>
Mod
ule
1: H
azar
ds a
ffect
ing
the
safe
ty o
f the
hos
pita
l and
the
role
of t
he h
ospi
tal i
n em
erge
ncy
and
disa
ster
man
agem
ent

49
151
(Con
tinue
d) 1
.1 H
azar
ds
Haz
ard
Leve
lSh
ould
the
hosp
ital b
e pr
epar
ed to
resp
ond
to th
is
haza
rd?
If ye
s, m
ark
the
box.
Obs
erva
tions
(e
valu
ator
’s co
mm
ents
)N
o
haza
rd
Haz
ard
leve
l
LOW
AVERAGE
HIGH
1.1.
3 Bi
olog
ical
haz
ards
Epid
emics
, pan
dem
ics an
d em
ergi
ng d
iseas
esW
ith re
fere
nce
to a
ny ri
sk a
sses
smen
ts, p
ast i
ncid
ents
at t
he
hosp
ital a
nd sp
ecifi
c pa
thog
ens,
rate
the
haza
rd le
vel o
f the
ho
spita
l rel
ated
to e
pide
mic
s, pa
ndem
ics a
nd e
mer
ging
di
seas
es. D
eter
min
e w
heth
er th
e ho
spita
l sho
uld
be p
repa
red
to re
spon
d to
an
emer
genc
y or
disa
ster
due
to e
pide
mic
s, pa
ndem
ics a
nd e
mer
ging
dise
ases
(bas
ed o
n ex
posu
re o
f the
ca
tchm
ent p
opul
atio
n or
the
spec
ializ
ed ro
le o
f the
hos
pita
l fo
r the
trea
tmen
t of p
atie
nts w
ith in
fect
ious
dise
ases
).
Food
born
e ou
tbre
aks
With
refe
renc
e to
any
risk
ass
essm
ents
and
pas
t inc
iden
ts a
t th
e ho
spita
l loc
atio
n (in
clud
ing
catc
hmen
t are
a), r
ate
the
haz-
ard
leve
l of t
he h
ospi
tal r
elat
ed to
food
born
e ou
tbre
aks.
De-
term
ine
whe
ther
the
hosp
ital s
houl
d be
pre
pare
d to
resp
ond
to a
n em
erge
ncy
or d
isast
er d
ue to
food
-bor
ne o
utbr
eaks
(b
ased
on
expo
sure
of t
he c
atch
men
t pop
ulat
ion)
.
Pest
atta
cks (
e.g.
infe
stat
ions
)W
ith re
fere
nce
to a
ny ri
sk a
sses
smen
ts a
nd p
ast i
ncid
ents
at
the
hosp
ital,
rate
the
hosp
ital’s
exp
osur
e to
haz
ards
from
pes
t at
tack
s or i
nfes
tatio
ns (fl
ies,
fleas
, rod
ents
, etc
.). D
eter
min
e w
heth
er th
e ho
spita
l sho
uld
be p
repa
red
to re
spon
d to
an
emer
genc
y or
disa
ster
due
to p
est a
ttac
ks o
r inf
esta
tions
(b
ased
on
expo
sure
of t
he c
atch
men
t pop
ulat
ion)
.
Oth
er b
iolo
gica
l haz
ards
(spe
cify
) .....
........
........
........
........
........
........
........
........
........
........
........
........
........
........
.W
ith re
fere
nce
to a
ny ri
sk a
sses
smen
ts, r
ate
the
haza
rd le
vel
for t
he h
ospi
tal i
n re
latio
n ot
her b
iolo
gica
l haz
ards
. Det
erm
ine
whe
ther
the
hosp
ital s
houl
d be
pre
pare
d to
resp
ond
to a
n em
erge
ncy
or d
isast
er d
ue to
oth
er b
iolo
gica
l haz
ards
(bas
ed
on e
xpos
ure
of th
e ca
tchm
ent p
opul
atio
n or
the
spec
ializ
ed
role
of t
he h
ospi
tal f
or th
e tr
eatm
ent o
f pat
ient
s exp
osed
to
biol
ogic
al h
azar
ds).
Hum
an-m
ade
haza
rds
1.1.
4 Te
chno
logi
cal h
azar
dsIn
dust
rial h
azar
ds (e
.g. c
hem
ical, r
adio
logi
cal)
Refe
r to
regi
onal
and
loca
l haz
ard
map
s of i
ndus
tria
l fac
ilitie
s or
oth
er h
azar
d in
form
atio
n an
d an
y pa
st in
cide
nts i
nvol
v-in
g in
dust
rial h
azar
ds, a
nd ra
te th
e in
dust
rial h
azar
d le
vel f
or
the
hosp
ital’s
loca
tion
and
pote
ntia
l con
tam
inat
ion
of th
e ho
spita
l’s sy
stem
s. D
eter
min
e w
heth
er th
e ho
spita
l sho
uld
be
prep
ared
to re
spon
d to
an
emer
genc
y or
disa
ster
due
to in
-du
stria
l haz
ards
(bas
ed o
n ex
posu
re o
f the
cat
chm
ent p
opul
a-tio
n or
the
spec
ializ
ed ro
le o
f the
hos
pita
l for
the
trea
tmen
t of
patie
nts e
xpos
ed to
indu
stria
l haz
ards
).
Fire
s (e.
g. b
uild
ing)
Refe
r to
loca
l haz
ard
map
s or o
ther
haz
ard
info
rmat
ion
on
build
ing
fires
insid
e an
d ou
tsid
e th
e ho
spita
l and
any
pas
t in
cide
nts i
nvol
ving
bui
ldin
g fir
es, a
nd ra
te th
e fir
e ha
zard
le
vel f
or th
e ho
spita
l. D
eter
min
e w
heth
er th
e ho
spita
l sho
uld
be p
repa
red
to re
spon
d to
an
emer
genc
y or
disa
ster
due
to
build
ing
fires
(bas
ed o
n ex
posu
re o
f the
cat
chm
ent p
opul
a-tio
n or
the
spec
ializ
ed ro
le o
f the
hos
pita
l for
the
trea
tmen
t of
burn
s pat
ient
s).
Con
tinue
>>
ANN
EX 2
: FO
RM 2
: SAF
E H
OSP
ITAL
S CH
ECKL
IST
Mod
ule
1: H
azar
ds a
ffect
ing
the
safe
ty o
f the
hos
pita
l and
the
role
of t
he h
ospi
tal i
n em
erge
ncy
and
disa
ster
man
agem
ent

50
151
(Con
tinue
d) 1
.1 H
azar
ds
Haz
ard
Leve
lSh
ould
the
hosp
ital b
e pr
epar
ed to
resp
ond
to th
is
haza
rd?
If ye
s, m
ark
the
box.
Obs
erva
tions
(e
valu
ator
’s co
mm
ents
)N
o
haza
rd
Haz
ard
leve
l
LOW
AVERAGE
HIGH
1.1.
3 Bi
olog
ical
haz
ards
Epid
emics
, pan
dem
ics an
d em
ergi
ng d
iseas
esW
ith re
fere
nce
to a
ny ri
sk a
sses
smen
ts, p
ast i
ncid
ents
at t
he
hosp
ital a
nd sp
ecifi
c pa
thog
ens,
rate
the
haza
rd le
vel o
f the
ho
spita
l rel
ated
to e
pide
mic
s, pa
ndem
ics a
nd e
mer
ging
di
seas
es. D
eter
min
e w
heth
er th
e ho
spita
l sho
uld
be p
repa
red
to re
spon
d to
an
emer
genc
y or
disa
ster
due
to e
pide
mic
s, pa
ndem
ics a
nd e
mer
ging
dise
ases
(bas
ed o
n ex
posu
re o
f the
ca
tchm
ent p
opul
atio
n or
the
spec
ializ
ed ro
le o
f the
hos
pita
l fo
r the
trea
tmen
t of p
atie
nts w
ith in
fect
ious
dise
ases
).
Food
born
e ou
tbre
aks
With
refe
renc
e to
any
risk
ass
essm
ents
and
pas
t inc
iden
ts a
t th
e ho
spita
l loc
atio
n (in
clud
ing
catc
hmen
t are
a), r
ate
the
haz-
ard
leve
l of t
he h
ospi
tal r
elat
ed to
food
born
e ou
tbre
aks.
De-
term
ine
whe
ther
the
hosp
ital s
houl
d be
pre
pare
d to
resp
ond
to a
n em
erge
ncy
or d
isast
er d
ue to
food
-bor
ne o
utbr
eaks
(b
ased
on
expo
sure
of t
he c
atch
men
t pop
ulat
ion)
.
Pest
atta
cks (
e.g.
infe
stat
ions
)W
ith re
fere
nce
to a
ny ri
sk a
sses
smen
ts a
nd p
ast i
ncid
ents
at
the
hosp
ital,
rate
the
hosp
ital’s
exp
osur
e to
haz
ards
from
pes
t at
tack
s or i
nfes
tatio
ns (fl
ies,
fleas
, rod
ents
, etc
.). D
eter
min
e w
heth
er th
e ho
spita
l sho
uld
be p
repa
red
to re
spon
d to
an
emer
genc
y or
disa
ster
due
to p
est a
ttac
ks o
r inf
esta
tions
(b
ased
on
expo
sure
of t
he c
atch
men
t pop
ulat
ion)
.
Oth
er b
iolo
gica
l haz
ards
(spe
cify
) .....
........
........
........
........
........
........
........
........
........
........
........
........
........
........
.W
ith re
fere
nce
to a
ny ri
sk a
sses
smen
ts, r
ate
the
haza
rd le
vel
for t
he h
ospi
tal i
n re
latio
n ot
her b
iolo
gica
l haz
ards
. Det
erm
ine
whe
ther
the
hosp
ital s
houl
d be
pre
pare
d to
resp
ond
to a
n em
erge
ncy
or d
isast
er d
ue to
oth
er b
iolo
gica
l haz
ards
(bas
ed
on e
xpos
ure
of th
e ca
tchm
ent p
opul
atio
n or
the
spec
ializ
ed
role
of t
he h
ospi
tal f
or th
e tr
eatm
ent o
f pat
ient
s exp
osed
to
biol
ogic
al h
azar
ds).
Hum
an-m
ade
haza
rds
1.1.
4 Te
chno
logi
cal h
azar
dsIn
dust
rial h
azar
ds (e
.g. c
hem
ical, r
adio
logi
cal)
Refe
r to
regi
onal
and
loca
l haz
ard
map
s of i
ndus
tria
l fac
ilitie
s or
oth
er h
azar
d in
form
atio
n an
d an
y pa
st in
cide
nts i
nvol
v-in
g in
dust
rial h
azar
ds, a
nd ra
te th
e in
dust
rial h
azar
d le
vel f
or
the
hosp
ital’s
loca
tion
and
pote
ntia
l con
tam
inat
ion
of th
e ho
spita
l’s sy
stem
s. D
eter
min
e w
heth
er th
e ho
spita
l sho
uld
be
prep
ared
to re
spon
d to
an
emer
genc
y or
disa
ster
due
to in
-du
stria
l haz
ards
(bas
ed o
n ex
posu
re o
f the
cat
chm
ent p
opul
a-tio
n or
the
spec
ializ
ed ro
le o
f the
hos
pita
l for
the
trea
tmen
t of
patie
nts e
xpos
ed to
indu
stria
l haz
ards
).
Fire
s (e.
g. b
uild
ing)
Refe
r to
loca
l haz
ard
map
s or o
ther
haz
ard
info
rmat
ion
on
build
ing
fires
insid
e an
d ou
tsid
e th
e ho
spita
l and
any
pas
t in
cide
nts i
nvol
ving
bui
ldin
g fir
es, a
nd ra
te th
e fir
e ha
zard
le
vel f
or th
e ho
spita
l. D
eter
min
e w
heth
er th
e ho
spita
l sho
uld
be p
repa
red
to re
spon
d to
an
emer
genc
y or
disa
ster
due
to
build
ing
fires
(bas
ed o
n ex
posu
re o
f the
cat
chm
ent p
opul
a-tio
n or
the
spec
ializ
ed ro
le o
f the
hos
pita
l for
the
trea
tmen
t of
burn
s pat
ient
s).
Con
tinue
>>
ANN
EX 2
: FO
RM 2
: SAF
E H
OSP
ITAL
S CH
ECKL
IST
Mod
ule
1: H
azar
ds a
ffect
ing
the
safe
ty o
f the
hos
pita
l and
the
role
of t
he h
ospi
tal i
n em
erge
ncy
and
disa
ster
man
agem
ent

51
Hos
pita
l Saf
ety
Inde
x G
UID
E FO
R EV
ALU
ATO
RS
152
(Con
tinue
d) 1
.1 H
azar
ds
Haz
ard
Leve
lSh
ould
the
hosp
ital b
e pr
epar
ed to
resp
ond
to th
is
haza
rd?
If ye
s, m
ark
the
box.
Obs
erva
tions
(e
valu
ator
’s co
mm
ents
)N
o
haza
rd
Haz
ard
leve
l
LOW
AVERAGE
HIGH
Haza
rdou
s mat
eria
ls (c
hem
i-ca
l, bio
logi
cal, r
adio
logi
cal)
Refe
r to
loca
l haz
ard
map
s or
oth
er h
azar
d in
form
a-tio
n on
haz
ardo
us m
ater
ials
(inci
dent
s and
spill
s) in
side
and
outs
ide
the
hosp
ital a
nd
any
past
inci
dent
s inv
olvi
ng
haza
rdou
s mat
eria
l spi
lls o
r le
aks,
and
rate
the
haza
rd-
ous m
ater
ial h
azar
d fo
r the
ho
spita
l and
the
pote
ntia
l co
ntam
inat
ion
of it
s sys
tem
s. D
eter
min
e w
heth
er th
e ho
spita
l sho
uld
be p
repa
red
to re
spon
d to
an
emer
genc
y or
disa
ster
due
to h
azar
dous
m
ater
ials
(bas
ed o
n ex
posu
re
of th
e ca
tchm
ent p
opul
atio
n or
the
spec
ializ
ed ro
le o
f the
ho
spita
l for
the
trea
tmen
t of
patie
nts e
xpos
ed to
haz
ard-
ous m
ater
ials)
.
Chem
ical
Biol
ogica
l
Radi
olog
ical
Pow
er o
utag
esRe
fer t
o an
y pa
st in
cide
nts i
nvol
ving
pow
er o
utag
es fo
r the
ho
spita
l loc
atio
n, a
nd ra
te th
e po
wer
out
age
haza
rd fo
r the
ho
spita
l. Det
erm
ine
whe
ther
the
hosp
ital s
houl
d be
pre
pare
d to
resp
ond
to a
n em
erge
ncy
or d
isast
er d
ue to
pow
er o
utag
es.
Wat
er su
pply
disr
uptio
nRe
fer t
o an
y pa
st in
cide
nts i
nvol
ving
the
disr
uptio
n of
the
wa-
ter s
uppl
y fo
r the
hos
pita
l loc
atio
n, a
nd ra
te th
e ha
zard
for t
he
hosp
ital.
Det
erm
ine
whe
ther
the
hosp
ital s
houl
d be
pre
pare
d to
resp
ond
to a
n em
erge
ncy
or d
isast
er d
ue to
disr
uptio
n of
th
e w
ater
supp
ly.
Tran
spor
tatio
n in
ciden
ts (e
.g. a
ir, ro
ad, r
ail, w
ater
tran
spor
t)Re
fer t
o re
cord
s of p
ast m
ajor
tran
spor
t inc
iden
ts, a
nd d
eter
-m
ine
whe
ther
the
hosp
ital s
houl
d be
pre
pare
d to
resp
ond
to
an e
mer
genc
y or
disa
ster
due
to tr
ansp
ort i
ncid
ents
(bas
ed
on e
xpos
ure
of th
e ca
tchm
ent p
opul
atio
n).
Oth
er te
chno
logi
cal h
azar
ds (e
.g. a
ir po
llutio
n, st
ruct
ural
co
llaps
es, f
ood/
wat
er co
ntam
inat
ion,
nuc
lear
) (s
peci
fy) .
........
........
........
........
........
........
........
........
........
........
........
........
........
........
...Re
fer t
o re
gion
al a
nd lo
cal h
azar
d m
aps,
or o
ther
haz
ard
info
rmat
ion
and
past
inci
dent
s to
iden
tify
othe
r tec
hnol
ogic
al
haza
rds f
or th
e ho
spita
l. Sp
ecify
the
haza
rd a
nd ra
te th
e co
r-re
spon
ding
haz
ard
leve
l for
the
hosp
ital’s
loca
tion.
Det
erm
ine
whe
ther
the
hosp
ital s
houl
d be
pre
pare
d to
resp
ond
to a
n em
erge
ncy
or d
isast
er d
ue to
oth
er te
chno
logi
cal h
azar
ds
(bas
ed o
n ex
posu
re o
f the
cat
chm
ent p
opul
atio
n or
any
sp
ecia
lized
role
of t
he h
ospi
tal f
or th
e tr
eatm
ent o
f pat
ient
s ex
pose
d to
oth
er te
chno
logi
cal h
azar
ds).
1.1.
5 So
ciet
al h
azar
dsSe
curit
y thr
eat t
o ho
spita
l bui
ldin
g an
d st
affRe
fer t
o ris
k/th
reat
ass
essm
ents
and
pas
t sec
urity
inci
dent
s aff
ectin
g th
e ho
spita
l and
staff
, and
rate
the
secu
rity
haza
rd
leve
l to
the
hosp
ital a
nd st
aff. D
eter
min
e w
heth
er th
e ho
spita
l sh
ould
be
prep
ared
to re
spon
d to
an
emer
genc
y or
disa
ster
du
e to
secu
rity
thre
ats t
o th
e ho
spita
l bui
ldin
g an
d st
aff.
Con
tinue
>>
Mod
ule
1: H
azar
ds a
ffect
ing
the
safe
ty o
f the
hos
pita
l and
the
role
of t
he h
ospi
tal i
n em
erge
ncy
and
disa
ster
man
agem
ent

52
Hos
pita
l Saf
ety
Inde
x G
UID
E FO
R EV
ALU
ATO
RS
152
(Con
tinue
d) 1
.1 H
azar
ds
Haz
ard
Leve
lSh
ould
the
hosp
ital b
e pr
epar
ed to
resp
ond
to th
is
haza
rd?
If ye
s, m
ark
the
box.
Obs
erva
tions
(e
valu
ator
’s co
mm
ents
)N
o
haza
rd
Haz
ard
leve
l
LOW
AVERAGE
HIGH
Haza
rdou
s mat
eria
ls (c
hem
i-ca
l, bio
logi
cal, r
adio
logi
cal)
Refe
r to
loca
l haz
ard
map
s or
oth
er h
azar
d in
form
a-tio
n on
haz
ardo
us m
ater
ials
(inci
dent
s and
spill
s) in
side
and
outs
ide
the
hosp
ital a
nd
any
past
inci
dent
s inv
olvi
ng
haza
rdou
s mat
eria
l spi
lls o
r le
aks,
and
rate
the
haza
rd-
ous m
ater
ial h
azar
d fo
r the
ho
spita
l and
the
pote
ntia
l co
ntam
inat
ion
of it
s sys
tem
s. D
eter
min
e w
heth
er th
e ho
spita
l sho
uld
be p
repa
red
to re
spon
d to
an
emer
genc
y or
disa
ster
due
to h
azar
dous
m
ater
ials
(bas
ed o
n ex
posu
re
of th
e ca
tchm
ent p
opul
atio
n or
the
spec
ializ
ed ro
le o
f the
ho
spita
l for
the
trea
tmen
t of
patie
nts e
xpos
ed to
haz
ard-
ous m
ater
ials)
.
Chem
ical
Biol
ogica
l
Radi
olog
ical
Pow
er o
utag
esRe
fer t
o an
y pa
st in
cide
nts i
nvol
ving
pow
er o
utag
es fo
r the
ho
spita
l loc
atio
n, a
nd ra
te th
e po
wer
out
age
haza
rd fo
r the
ho
spita
l. Det
erm
ine
whe
ther
the
hosp
ital s
houl
d be
pre
pare
d to
resp
ond
to a
n em
erge
ncy
or d
isast
er d
ue to
pow
er o
utag
es.
Wat
er su
pply
disr
uptio
nRe
fer t
o an
y pa
st in
cide
nts i
nvol
ving
the
disr
uptio
n of
the
wa-
ter s
uppl
y fo
r the
hos
pita
l loc
atio
n, a
nd ra
te th
e ha
zard
for t
he
hosp
ital.
Det
erm
ine
whe
ther
the
hosp
ital s
houl
d be
pre
pare
d to
resp
ond
to a
n em
erge
ncy
or d
isast
er d
ue to
disr
uptio
n of
th
e w
ater
supp
ly.
Tran
spor
tatio
n in
ciden
ts (e
.g. a
ir, ro
ad, r
ail, w
ater
tran
spor
t)Re
fer t
o re
cord
s of p
ast m
ajor
tran
spor
t inc
iden
ts, a
nd d
eter
-m
ine
whe
ther
the
hosp
ital s
houl
d be
pre
pare
d to
resp
ond
to
an e
mer
genc
y or
disa
ster
due
to tr
ansp
ort i
ncid
ents
(bas
ed
on e
xpos
ure
of th
e ca
tchm
ent p
opul
atio
n).
Oth
er te
chno
logi
cal h
azar
ds (e
.g. a
ir po
llutio
n, st
ruct
ural
co
llaps
es, f
ood/
wat
er co
ntam
inat
ion,
nuc
lear
) (s
peci
fy) .
........
........
........
........
........
........
........
........
........
........
........
........
........
........
...Re
fer t
o re
gion
al a
nd lo
cal h
azar
d m
aps,
or o
ther
haz
ard
info
rmat
ion
and
past
inci
dent
s to
iden
tify
othe
r tec
hnol
ogic
al
haza
rds f
or th
e ho
spita
l. Sp
ecify
the
haza
rd a
nd ra
te th
e co
r-re
spon
ding
haz
ard
leve
l for
the
hosp
ital’s
loca
tion.
Det
erm
ine
whe
ther
the
hosp
ital s
houl
d be
pre
pare
d to
resp
ond
to a
n em
erge
ncy
or d
isast
er d
ue to
oth
er te
chno
logi
cal h
azar
ds
(bas
ed o
n ex
posu
re o
f the
cat
chm
ent p
opul
atio
n or
any
sp
ecia
lized
role
of t
he h
ospi
tal f
or th
e tr
eatm
ent o
f pat
ient
s ex
pose
d to
oth
er te
chno
logi
cal h
azar
ds).
1.1.
5 So
ciet
al h
azar
dsSe
curit
y thr
eat t
o ho
spita
l bui
ldin
g an
d st
affRe
fer t
o ris
k/th
reat
ass
essm
ents
and
pas
t sec
urity
inci
dent
s aff
ectin
g th
e ho
spita
l and
staff
, and
rate
the
secu
rity
haza
rd
leve
l to
the
hosp
ital a
nd st
aff. D
eter
min
e w
heth
er th
e ho
spita
l sh
ould
be
prep
ared
to re
spon
d to
an
emer
genc
y or
disa
ster
du
e to
secu
rity
thre
ats t
o th
e ho
spita
l bui
ldin
g an
d st
aff.
Con
tinue
>>
Mod
ule
1: H
azar
ds a
ffect
ing
the
safe
ty o
f the
hos
pita
l and
the
role
of t
he h
ospi
tal i
n em
erge
ncy
and
disa
ster
man
agem
ent

53
153
(Con
tinue
d) 1
.1 H
azar
ds
Haz
ard
Leve
lSh
ould
the
hosp
ital b
e pr
epar
ed to
resp
ond
to th
is
haza
rd?
If ye
s, m
ark
the
box.
Obs
erva
tions
(e
valu
ator
’s co
mm
ents
)N
o
haza
rd
Haz
ard
leve
l
LOW
AVERAGE
HIGH
Arm
ed co
nflic
tsRe
fer t
o ris
k ass
essm
ents
of a
rmed
con
flict
s and
pas
t inc
iden
ts th
at
have
affe
cted
the
hosp
ital, a
nd ra
te th
e ho
spita
l’s h
azar
d le
vel in
re
latio
n to
arm
ed c
onfli
cts.
Det
erm
ine
whe
ther
the
hosp
ital s
houl
d be
pre
pare
d to
resp
ond
to a
n em
erge
ncy
or d
isast
er d
ue to
arm
ed
confl
icts
(bas
ed o
n ex
posu
re o
f the
cat
chm
ent p
opul
atio
n).
Civi
l unr
est (
inclu
ding
dem
onst
ratio
ns)
Refe
r to
risk
asse
ssm
ents
and
pas
t inc
iden
ts o
f civ
il un
rest
th
at h
ave
affec
ted
the
hosp
ital,
and
rate
the
hosp
ital’s
haz
ard
leve
l in
rela
tion
to d
emon
stra
tions
and
civ
il un
rest
. Det
erm
ine
whe
ther
the
hosp
ital s
houl
d be
pre
pare
d to
resp
ond
to a
n em
erge
ncy
or d
isast
er d
ue to
dem
onst
ratio
ns a
nd c
ivil
unre
st
(bas
ed o
n ex
posu
re o
f the
cat
chm
ent p
opul
atio
n).
Mas
s gat
herin
g ev
ents
Det
erm
ine
whe
ther
the
hosp
ital s
houl
d be
pre
pare
d to
re
spon
d to
an
emer
genc
y or
disa
ster
due
to m
ass g
athe
rings
(b
ased
on
expo
sure
of t
he c
atch
men
t pop
ulat
ion)
.
Disp
lace
d po
pula
tions
Refe
r to
risk
asse
ssm
ents
and
rate
the
hosp
ital’s
haz
ard
leve
l in
term
s of p
eopl
e w
ho h
ave
been
disp
lace
d as
a re
sult
of c
on-
flict
, com
mun
ity u
nres
t and
oth
er so
ciop
oliti
cal c
ircum
stan
c-es
, or d
ue to
hig
h le
vels
of im
mig
ratio
n. D
eter
min
e w
heth
er
the
hosp
ital s
houl
d be
pre
pare
d to
resp
ond
to a
n em
erge
ncy
or d
isast
er d
ue to
disp
lace
d po
pula
tions
.
Oth
er so
cieta
l haz
ards
(e.g
. exp
losio
ns, t
erro
rism
)(s
peci
fy) .
........
........
........
........
........
........
........
........
........
........
....Re
fer t
o ris
k as
sess
men
ts, r
egio
nal a
nd o
ther
haz
ard
info
rma-
tion
and
past
inci
dent
s to
iden
tify
othe
r soc
ieta
l haz
ards
. Sp
ecify
the
haza
rd a
nd ra
te th
e co
rresp
ondi
ng h
azar
d le
vel
for t
he h
ospi
tal’s
loca
tion.
Det
erm
ine
whe
ther
the
hosp
ital
shou
ld b
e pr
epar
ed to
resp
ond
to a
n em
erge
ncy
or d
isast
er
due
to o
ther
soci
etal
haz
ards
(bas
ed o
n ex
posu
re o
f the
ca
tchm
ent p
opul
atio
n or
any
spec
ializ
ed ro
le o
f the
hos
pita
l in
trea
tmen
t of p
atie
nts e
xpos
ed to
soci
etal
haz
ards
).
1.2
Geo
tech
nica
l pro
pert
ies
of s
oils
Liqu
efac
tion
With
refe
renc
e to
the
geot
echn
ical
soil
anal
ysis
at th
e ho
spita
l sit
e, ra
te th
e le
vel o
f the
faci
lity’s
exp
osur
e to
haz
ards
from
sa
tura
ted
and
loos
e su
bsoi
l.
Clay
soils
With
refe
renc
e to
soil
map
s or o
ther
haz
ard
info
rmat
ion,
rate
th
e ho
spita
l’s e
xpos
ure
to h
azar
ds fr
om c
lay
soil.
Unst
able
slop
esRe
fer t
o ge
olog
ical
map
s or o
ther
haz
ard
info
rmat
ion
and
spec
ify th
e ho
spita
l’s e
xpos
ure
to h
azar
ds fr
om th
e pr
esen
ce
of sl
opes
.
Com
men
ts o
n th
e re
sults
of F
orm
2, M
odul
e 1:
......
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
..
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
....
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
....
Nam
e/sig
natu
re o
f eva
luat
or(s
) ......
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
.......
ANN
EX 2
: FO
RM 2
: SAF
E H
OSP
ITAL
S CH
ECKL
IST
Mod
ule
1: H
azar
ds a
ffect
ing
the
safe
ty o
f the
hos
pita
l and
the
role
of t
he h
ospi
tal i
n em
erge
ncy
and
disa
ster
man
agem
ent

54
153
(Con
tinue
d) 1
.1 H
azar
ds
Haz
ard
Leve
lSh
ould
the
hosp
ital b
e pr
epar
ed to
resp
ond
to th
is
haza
rd?
If ye
s, m
ark
the
box.
Obs
erva
tions
(e
valu
ator
’s co
mm
ents
)N
o
haza
rd
Haz
ard
leve
l
LOW
AVERAGE
HIGH
Arm
ed co
nflic
tsRe
fer t
o ris
k ass
essm
ents
of a
rmed
con
flict
s and
pas
t inc
iden
ts th
at
have
affe
cted
the
hosp
ital, a
nd ra
te th
e ho
spita
l’s h
azar
d le
vel in
re
latio
n to
arm
ed c
onfli
cts.
Det
erm
ine
whe
ther
the
hosp
ital s
houl
d be
pre
pare
d to
resp
ond
to a
n em
erge
ncy
or d
isast
er d
ue to
arm
ed
confl
icts
(bas
ed o
n ex
posu
re o
f the
cat
chm
ent p
opul
atio
n).
Civi
l unr
est (
inclu
ding
dem
onst
ratio
ns)
Refe
r to
risk
asse
ssm
ents
and
pas
t inc
iden
ts o
f civ
il un
rest
th
at h
ave
affec
ted
the
hosp
ital,
and
rate
the
hosp
ital’s
haz
ard
leve
l in
rela
tion
to d
emon
stra
tions
and
civ
il un
rest
. Det
erm
ine
whe
ther
the
hosp
ital s
houl
d be
pre
pare
d to
resp
ond
to a
n em
erge
ncy
or d
isast
er d
ue to
dem
onst
ratio
ns a
nd c
ivil
unre
st
(bas
ed o
n ex
posu
re o
f the
cat
chm
ent p
opul
atio
n).
Mas
s gat
herin
g ev
ents
Det
erm
ine
whe
ther
the
hosp
ital s
houl
d be
pre
pare
d to
re
spon
d to
an
emer
genc
y or
disa
ster
due
to m
ass g
athe
rings
(b
ased
on
expo
sure
of t
he c
atch
men
t pop
ulat
ion)
.
Disp
lace
d po
pula
tions
Refe
r to
risk
asse
ssm
ents
and
rate
the
hosp
ital’s
haz
ard
leve
l in
term
s of p
eopl
e w
ho h
ave
been
disp
lace
d as
a re
sult
of c
on-
flict
, com
mun
ity u
nres
t and
oth
er so
ciop
oliti
cal c
ircum
stan
c-es
, or d
ue to
hig
h le
vels
of im
mig
ratio
n. D
eter
min
e w
heth
er
the
hosp
ital s
houl
d be
pre
pare
d to
resp
ond
to a
n em
erge
ncy
or d
isast
er d
ue to
disp
lace
d po
pula
tions
.
Oth
er so
cieta
l haz
ards
(e.g
. exp
losio
ns, t
erro
rism
)(s
peci
fy) .
........
........
........
........
........
........
........
........
........
........
....Re
fer t
o ris
k as
sess
men
ts, r
egio
nal a
nd o
ther
haz
ard
info
rma-
tion
and
past
inci
dent
s to
iden
tify
othe
r soc
ieta
l haz
ards
. Sp
ecify
the
haza
rd a
nd ra
te th
e co
rresp
ondi
ng h
azar
d le
vel
for t
he h
ospi
tal’s
loca
tion.
Det
erm
ine
whe
ther
the
hosp
ital
shou
ld b
e pr
epar
ed to
resp
ond
to a
n em
erge
ncy
or d
isast
er
due
to o
ther
soci
etal
haz
ards
(bas
ed o
n ex
posu
re o
f the
ca
tchm
ent p
opul
atio
n or
any
spec
ializ
ed ro
le o
f the
hos
pita
l in
trea
tmen
t of p
atie
nts e
xpos
ed to
soci
etal
haz
ards
).
1.2
Geo
tech
nica
l pro
pert
ies
of s
oils
Liqu
efac
tion
With
refe
renc
e to
the
geot
echn
ical
soil
anal
ysis
at th
e ho
spita
l sit
e, ra
te th
e le
vel o
f the
faci
lity’s
exp
osur
e to
haz
ards
from
sa
tura
ted
and
loos
e su
bsoi
l.
Clay
soils
With
refe
renc
e to
soil
map
s or o
ther
haz
ard
info
rmat
ion,
rate
th
e ho
spita
l’s e
xpos
ure
to h
azar
ds fr
om c
lay
soil.
Unst
able
slop
esRe
fer t
o ge
olog
ical
map
s or o
ther
haz
ard
info
rmat
ion
and
spec
ify th
e ho
spita
l’s e
xpos
ure
to h
azar
ds fr
om th
e pr
esen
ce
of sl
opes
.
Com
men
ts o
n th
e re
sults
of F
orm
2, M
odul
e 1:
......
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
..
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
....
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
....
Nam
e/sig
natu
re o
f eva
luat
or(s
) ......
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
.......
ANN
EX 2
: FO
RM 2
: SAF
E H
OSP
ITAL
S CH
ECKL
IST
Mod
ule
1: H
azar
ds a
ffect
ing
the
safe
ty o
f the
hos
pita
l and
the
role
of t
he h
ospi
tal i
n em
erge
ncy
and
disa
ster
man
agem
ent

55
Hos
pita
l Saf
ety
Inde
x G
UID
E FO
R EV
ALU
ATO
RS
154
Mod
ule
2: S
truc
tura
l Saf
ety
2.1
Prio
r eve
nts
affec
ting
hos
pita
l saf
ety
Safe
ty le
vel
Obs
erva
tions
(e
valu
ator
s’ co
mm
ents
)Low
Average
High
1. P
rior m
ajor
stru
ctur
al d
amag
e or
failu
re o
f the
hos
pita
l bui
ldin
g(s)
Safe
ty ra
tings
: Low
= M
ajor
dam
age
and
no re
pairs
; Ave
rage
= M
oder
ate
dam
age
and
build
ing
only
par
tially
repa
ired;
Hig
h =
Min
or o
r no
dam
age,
or
build
ing
fully
repa
ired.
IF S
UCH
AN
EVE
NT
HAS
NO
T O
CCU
RRED
IN T
HE
VICI
NIT
Y O
F TH
E H
OSP
ITAL
, LE
AVE
BOXE
S BL
ANK
AND
PRO
VID
E CO
MM
ENT.
2. H
ospi
tal b
uilt
and/
or re
paire
d us
ing
curre
nt sa
fety
stan
dard
sSa
fety
ratin
gs: L
ow =
Cur
rent
safe
ty st
anda
rds n
ot a
pplie
d; A
vera
ge =
Cur
rent
sa
fety
stan
dard
s par
tially
app
lied;
Hig
h =
Curre
nt sa
fety
stan
dard
s ful
ly a
pplie
d.
3. E
ffect
of r
emod
ellin
g or
mod
ifica
tion
on th
e st
ruct
ural
beh
avio
ur o
f th
e ho
spita
lSa
fety
ratin
gs: L
ow =
Maj
or re
mod
ellin
g or
mod
ifica
tions
hav
e be
en ca
rried
ou
t with
maj
or co
mpr
omisi
ng e
ffect
on
the
perfo
rman
ce o
f the
stru
ctur
e; A
v-er
age
= M
oder
ate
rem
odel
ling
and/
or m
odifi
catio
ns w
ith m
inor
effe
ct o
n th
e pe
rform
ance
of t
he st
ruct
ure;
Hig
h =
Min
or re
mod
ellin
g an
d/or
mod
ifica
tions
; no
mod
ifica
tions
wer
e ca
rried
out
; or m
ajor
rem
odel
ling
and/
or m
odifi
catio
n en
hanc
ing
the
stru
ctur
al b
ehav
iour
or h
avin
g no
neg
ativ
e eff
ect.
2.2
Build
ing
inte
grit
ySa
fety
leve
lO
bser
vatio
ns
(eva
luat
ors’
com
men
ts)
Low
Average
High
4. S
truct
ural
syst
em d
esig
nSa
fety
ratin
gs: L
ow =
Poo
r stru
ctur
al sy
stem
des
ign;
Ave
rage
= M
oder
ate
stru
ctur
al sy
stem
des
ign;
Hig
h =
Goo
d st
ruct
ural
syst
em d
esig
n.
5. C
ondi
tion
of th
e bu
ildin
gSa
fety
ratin
gs: L
ow =
Cra
cks o
n th
e gr
ound
and
firs
t floo
rs; M
ajor
det
erio
ra-
tion
caus
ed b
y wea
ther
ing
or n
orm
al a
gein
g; A
vera
ge =
Som
e de
terio
ratio
n ca
used
onl
y by w
eath
erin
g or
nor
mal
age
ing;
Hig
h =
No
dete
riora
tion
or
crac
ks o
bser
ved.
6. C
ondi
tion
of th
e co
nstru
ctio
n m
ater
ials
Safe
ty ra
tings
: Low
= R
ust w
ith fl
akin
g; c
rack
s lar
ger t
han
3mm
(con
cret
e),
exce
ssiv
e de
form
atio
ns (s
teel
and
woo
d); A
vera
ge =
Cra
cks b
etw
een
1 an
d 3
mm
pre
sent
(con
cret
e), m
oder
ate
and
visib
le d
efor
mat
ions
(ste
el a
nd w
ood)
or
rust
with
no
flaki
ng; H
igh
= C
rack
s les
s tha
n 1
mm
(con
cret
e), n
o vi
sible
de
form
atio
ns; n
o ru
st.
7. In
tera
ctio
n of
non
stru
ctur
al e
lem
ents
with
the
stru
ctur
eSa
fety
ratin
gs: L
ow =
Par
titio
n w
alls
rigid
ly a
ttach
ed to
the
stru
ctur
e, su
s-pe
nded
ceili
ngs o
r fac
ades
inte
ract
ing
with
the
stru
ctur
es, d
amag
e w
ould
ha
ve si
gnifi
cant
effe
ct o
n th
e st
ruct
ure;
Ave
rage
= S
ome
of th
e pr
eced
ing
nons
truct
ural
ele
men
ts in
tera
ctin
g w
ith th
e st
ruct
ures
, dam
age
wou
ld n
ot
affec
t the
stru
ctur
e; H
igh
= T
here
are
no
nons
truct
ural
ele
men
ts a
ffect
ing
the
stru
ctur
e.
8. P
roxi
mity
of b
uild
ings
(for
ear
thqu
ake-
indu
ced
poun
ding
)Sa
fety
ratin
gs: L
ow =
Sep
arat
ion
is le
ss th
an 0
.5%
of t
he h
eigh
t of t
he sh
orte
r of
two
adja
cent
bui
ldin
gs; A
vera
ge =
Sep
arat
ion
is be
twee
n 0.
5% a
nd 1
.5%
of
the
heig
ht o
f the
shor
ter o
f tw
o ad
jace
nt b
uild
ings
; Hig
h =
Sep
arat
ion
is m
ore
than
1.5
% o
f the
hei
ght o
f the
shor
ter o
f tw
o ad
jace
nt b
uild
ings
.
IF T
HE
HO
SPIT
AL IS
NO
T IN
A H
IGH
/MO
DER
ATE
SEIS
MIC
ZO
NE,
TH
EN L
EAVE
BO
XES
BLAN
K AN
D P
ROVI
DE
COM
MEN
T.
Con
tinue
>>

56
Hos
pita
l Saf
ety
Inde
x G
UID
E FO
R EV
ALU
ATO
RS
154
Mod
ule
2: S
truc
tura
l Saf
ety
2.1
Prio
r eve
nts
affec
ting
hos
pita
l saf
ety
Safe
ty le
vel
Obs
erva
tions
(e
valu
ator
s’ co
mm
ents
)Low
Average
High
1. P
rior m
ajor
stru
ctur
al d
amag
e or
failu
re o
f the
hos
pita
l bui
ldin
g(s)
Safe
ty ra
tings
: Low
= M
ajor
dam
age
and
no re
pairs
; Ave
rage
= M
oder
ate
dam
age
and
build
ing
only
par
tially
repa
ired;
Hig
h =
Min
or o
r no
dam
age,
or
build
ing
fully
repa
ired.
IF S
UCH
AN
EVE
NT
HAS
NO
T O
CCU
RRED
IN T
HE
VICI
NIT
Y O
F TH
E H
OSP
ITAL
, LE
AVE
BOXE
S BL
ANK
AND
PRO
VID
E CO
MM
ENT.
2. H
ospi
tal b
uilt
and/
or re
paire
d us
ing
curre
nt sa
fety
stan
dard
sSa
fety
ratin
gs: L
ow =
Cur
rent
safe
ty st
anda
rds n
ot a
pplie
d; A
vera
ge =
Cur
rent
sa
fety
stan
dard
s par
tially
app
lied;
Hig
h =
Curre
nt sa
fety
stan
dard
s ful
ly a
pplie
d.
3. E
ffect
of r
emod
ellin
g or
mod
ifica
tion
on th
e st
ruct
ural
beh
avio
ur o
f th
e ho
spita
lSa
fety
ratin
gs: L
ow =
Maj
or re
mod
ellin
g or
mod
ifica
tions
hav
e be
en ca
rried
ou
t with
maj
or co
mpr
omisi
ng e
ffect
on
the
perfo
rman
ce o
f the
stru
ctur
e; A
v-er
age
= M
oder
ate
rem
odel
ling
and/
or m
odifi
catio
ns w
ith m
inor
effe
ct o
n th
e pe
rform
ance
of t
he st
ruct
ure;
Hig
h =
Min
or re
mod
ellin
g an
d/or
mod
ifica
tions
; no
mod
ifica
tions
wer
e ca
rried
out
; or m
ajor
rem
odel
ling
and/
or m
odifi
catio
n en
hanc
ing
the
stru
ctur
al b
ehav
iour
or h
avin
g no
neg
ativ
e eff
ect.
2.2
Build
ing
inte
grit
ySa
fety
leve
lO
bser
vatio
ns
(eva
luat
ors’
com
men
ts)
Low
Average
High
4. S
truct
ural
syst
em d
esig
nSa
fety
ratin
gs: L
ow =
Poo
r stru
ctur
al sy
stem
des
ign;
Ave
rage
= M
oder
ate
stru
ctur
al sy
stem
des
ign;
Hig
h =
Goo
d st
ruct
ural
syst
em d
esig
n.
5. C
ondi
tion
of th
e bu
ildin
gSa
fety
ratin
gs: L
ow =
Cra
cks o
n th
e gr
ound
and
firs
t floo
rs; M
ajor
det
erio
ra-
tion
caus
ed b
y wea
ther
ing
or n
orm
al a
gein
g; A
vera
ge =
Som
e de
terio
ratio
n ca
used
onl
y by w
eath
erin
g or
nor
mal
age
ing;
Hig
h =
No
dete
riora
tion
or
crac
ks o
bser
ved.
6. C
ondi
tion
of th
e co
nstru
ctio
n m
ater
ials
Safe
ty ra
tings
: Low
= R
ust w
ith fl
akin
g; c
rack
s lar
ger t
han
3mm
(con
cret
e),
exce
ssiv
e de
form
atio
ns (s
teel
and
woo
d); A
vera
ge =
Cra
cks b
etw
een
1 an
d 3
mm
pre
sent
(con
cret
e), m
oder
ate
and
visib
le d
efor
mat
ions
(ste
el a
nd w
ood)
or
rust
with
no
flaki
ng; H
igh
= C
rack
s les
s tha
n 1
mm
(con
cret
e), n
o vi
sible
de
form
atio
ns; n
o ru
st.
7. In
tera
ctio
n of
non
stru
ctur
al e
lem
ents
with
the
stru
ctur
eSa
fety
ratin
gs: L
ow =
Par
titio
n w
alls
rigid
ly a
ttach
ed to
the
stru
ctur
e, su
s-pe
nded
ceili
ngs o
r fac
ades
inte
ract
ing
with
the
stru
ctur
es, d
amag
e w
ould
ha
ve si
gnifi
cant
effe
ct o
n th
e st
ruct
ure;
Ave
rage
= S
ome
of th
e pr
eced
ing
nons
truct
ural
ele
men
ts in
tera
ctin
g w
ith th
e st
ruct
ures
, dam
age
wou
ld n
ot
affec
t the
stru
ctur
e; H
igh
= T
here
are
no
nons
truct
ural
ele
men
ts a
ffect
ing
the
stru
ctur
e.
8. P
roxi
mity
of b
uild
ings
(for
ear
thqu
ake-
indu
ced
poun
ding
)Sa
fety
ratin
gs: L
ow =
Sep
arat
ion
is le
ss th
an 0
.5%
of t
he h
eigh
t of t
he sh
orte
r of
two
adja
cent
bui
ldin
gs; A
vera
ge =
Sep
arat
ion
is be
twee
n 0.
5% a
nd 1
.5%
of
the
heig
ht o
f the
shor
ter o
f tw
o ad
jace
nt b
uild
ings
; Hig
h =
Sep
arat
ion
is m
ore
than
1.5
% o
f the
hei
ght o
f the
shor
ter o
f tw
o ad
jace
nt b
uild
ings
.
IF T
HE
HO
SPIT
AL IS
NO
T IN
A H
IGH
/MO
DER
ATE
SEIS
MIC
ZO
NE,
TH
EN L
EAVE
BO
XES
BLAN
K AN
D P
ROVI
DE
COM
MEN
T.
Con
tinue
>>

57
155
(Con
tinue
d) 2
.2 B
uild
ing
inte
grit
ySa
fety
leve
lO
bser
vatio
ns
(eva
luat
ors’
com
men
ts)
Low
Average
High
9. P
roxi
mity
of b
uild
ings
(win
d tu
nnel
effe
ct an
d fir
e)Sa
fety
ratin
gs: L
ow =
Sep
arat
ion
less
than
5 m
; Ave
rage
= S
epar
atio
n be
twee
n 5
m a
nd 1
5 m
; Hig
h =
Sep
arat
ion
mor
e th
an 1
5 m
.
10. S
truct
ural
redu
ndan
cySa
fety
ratin
gs: L
ow =
Few
er th
an th
ree
lines
of r
esist
ance
in e
ach
dire
ctio
n;
Aver
age
= T
hree
line
s of r
esist
ance
in e
ach
dire
ctio
n or
line
s with
out o
rtho
go-
nal o
rient
atio
n; H
igh
= M
ore
than
thre
e lin
es o
f res
istan
ce in
eac
h or
thog
onal
di
rect
ion
of th
e bu
ildin
g.
11. S
truct
ural
det
ailin
g, in
cludi
ng co
nnec
tions
Safe
ty ra
tings
: Low
= N
o ev
iden
ce o
f eng
inee
red
build
ing
reco
rds,
or b
uilt
acco
rdin
g to
an
old
desig
n st
anda
rd; A
vera
ge =
Bui
lt ac
cord
ing
to p
revi
ous
desig
n st
anda
rds a
nd n
o re
trofit
ting
wor
k to
a cu
rrent
stan
dard
; Hig
h =
Bui
lt ac
cord
ing
to a
cur
rent
stan
dard
.
12. R
atio
of c
olum
n st
reng
th to
bea
m st
reng
thSa
fety
ratin
gs: L
ow =
Stre
ngth
of b
eam
s is o
bvio
usly
gre
ater
than
stre
ngth
of
colu
mns
; Ave
rage
= S
treng
th o
f bea
ms i
s sim
ilar t
o st
reng
th o
f col
umns
; Hig
h =
Stre
ngth
of c
olum
ns is
gre
ater
than
stre
ngth
of b
eam
s.
13. S
afet
y of f
ound
atio
nsSa
fety
ratin
gs: L
ow =
No
evid
ence
that
foun
datio
ns w
ere
desig
ned
acco
rdin
g to
stan
dard
s (fo
unda
tion
size,
soil
surv
ey) a
nd/o
r the
re is
evi
denc
e of
dam
age;
no
pla
ns a
re a
vaila
ble;
Ave
rage
= L
ittle
evi
denc
e (d
raw
ings
, soi
l sur
vey)
that
fo
unda
tions
wer
e de
signe
d ac
cord
ing
to st
anda
rds;
and/
or th
ere
is ev
iden
ce
for m
oder
ate
dam
age;
Hig
h =
Stro
ng e
vide
nce
that
foun
datio
ns w
ere
de-
signe
d ac
cord
ing
to st
anda
rds w
ith st
rong
evi
denc
e of
no
dam
age.
14. Ir
regu
larit
ies i
n bu
ildin
g st
ruct
ure
plan
(rig
idity
, mas
s, re
sista
nce)
Safe
ty ra
tings
: Low
= S
hape
s are
irre
gula
r and
stru
ctur
e is
not u
nifo
rm; A
ver-
age
= S
hape
s on
plan
are
irre
gula
r but
stru
ctur
e is
unifo
rm; H
igh
= S
hape
s on
plan
are
regu
lar a
nd st
ruct
ure
has u
nifo
rm p
lan,
and
ther
e ar
e no
ele
men
ts
that
wou
ld ca
use
signi
fican
t tor
sion.
15. Ir
regu
larit
ies i
n el
evat
ion
of b
uild
ings
Safe
ty ra
tings
: Low
= S
igni
fican
t disc
ontin
uous
or i
rregu
lar e
lem
ents
, sig
nifi-
cant
varia
tion
in e
leva
tion
of b
uild
ings
; Ave
rage
= S
ever
al d
iscon
tinuo
us o
r irr
egul
ar e
lem
ents
, som
e va
riatio
n in
the
elev
atio
n of
bui
ldin
gs; H
igh
= N
o sig
nific
ant d
iscon
tinuo
us o
r irre
gula
r ele
men
ts, li
ttle
or n
o va
riatio
n in
ele
va-
tion
of b
uild
ings
.
16. Ir
regu
larit
ies i
n he
ight
of s
tore
ysSa
fety
ratin
gs: L
ow =
Hei
ght o
f sto
reys
diff
ers b
y mor
e th
an 2
0%; A
vera
ge =
St
orey
s hav
e sim
ilar h
eigh
ts (t
hey d
iffer
by l
ess t
han
20%
but
mor
e th
an 5
%);
Hig
h =
Sto
reys
are
of s
imila
r hei
ght (
they
diff
er b
y les
s tha
n 5%
).
17. S
truct
ural
inte
grity
of r
oofs
Safe
ty ra
tings
: Low
= M
onop
itch
or fl
at li
ght r
oofs,
and
/or l
arge
roof
ove
r-ha
ngs;
Aver
age
= P
re-s
tress
ed co
ncre
te ro
of, g
able
roof
with
gen
tle sl
ope,
sa
tisfa
ctor
ily co
nnec
ted,
no
larg
e ro
of o
verh
angs
; Hig
h =
Rei
nfor
ced
cast
in
plac
e on
conc
rete
roof
dec
k or h
ippe
d lig
ht ro
of, s
atisf
acto
ry co
nnec
tions
, no
larg
e ro
of o
verh
angs
.
18. S
truct
ural
resil
ienc
e to
haz
ards
oth
er th
an e
arth
quak
es an
d st
rong
w
inds
Safe
ty ra
tings
: Low
= Lo
w st
ruct
ural
resil
ienc
e to
haz
ards
pre
sent
at t
he si
te
of th
e ho
spita
l; Ave
rage
= S
atisf
acto
ry st
ruct
ural
resil
ienc
e (ta
king
acc
ount
of
stru
ctur
al ri
sk re
duct
ion
mea
sure
s in
plac
e); H
igh
= G
ood
stru
ctur
al re
silie
nce
(taki
ng a
ccou
nt o
f risk
redu
ctio
n m
easu
res i
n pl
ace)
.
Con
tinue
>>
ANN
EX 2
: FO
RM 2
: SAF
E H
OSP
ITAL
S CH
ECKL
IST
Mod
ule
2: S
truc
tura
l Saf
ety

58
155
(Con
tinue
d) 2
.2 B
uild
ing
inte
grit
ySa
fety
leve
lO
bser
vatio
ns
(eva
luat
ors’
com
men
ts)
Low
Average
High
9. P
roxi
mity
of b
uild
ings
(win
d tu
nnel
effe
ct an
d fir
e)Sa
fety
ratin
gs: L
ow =
Sep
arat
ion
less
than
5 m
; Ave
rage
= S
epar
atio
n be
twee
n 5
m a
nd 1
5 m
; Hig
h =
Sep
arat
ion
mor
e th
an 1
5 m
.
10. S
truct
ural
redu
ndan
cySa
fety
ratin
gs: L
ow =
Few
er th
an th
ree
lines
of r
esist
ance
in e
ach
dire
ctio
n;
Aver
age
= T
hree
line
s of r
esist
ance
in e
ach
dire
ctio
n or
line
s with
out o
rtho
go-
nal o
rient
atio
n; H
igh
= M
ore
than
thre
e lin
es o
f res
istan
ce in
eac
h or
thog
onal
di
rect
ion
of th
e bu
ildin
g.
11. S
truct
ural
det
ailin
g, in
cludi
ng co
nnec
tions
Safe
ty ra
tings
: Low
= N
o ev
iden
ce o
f eng
inee
red
build
ing
reco
rds,
or b
uilt
acco
rdin
g to
an
old
desig
n st
anda
rd; A
vera
ge =
Bui
lt ac
cord
ing
to p
revi
ous
desig
n st
anda
rds a
nd n
o re
trofit
ting
wor
k to
a cu
rrent
stan
dard
; Hig
h =
Bui
lt ac
cord
ing
to a
cur
rent
stan
dard
.
12. R
atio
of c
olum
n st
reng
th to
bea
m st
reng
thSa
fety
ratin
gs: L
ow =
Stre
ngth
of b
eam
s is o
bvio
usly
gre
ater
than
stre
ngth
of
colu
mns
; Ave
rage
= S
treng
th o
f bea
ms i
s sim
ilar t
o st
reng
th o
f col
umns
; Hig
h =
Stre
ngth
of c
olum
ns is
gre
ater
than
stre
ngth
of b
eam
s.
13. S
afet
y of f
ound
atio
nsSa
fety
ratin
gs: L
ow =
No
evid
ence
that
foun
datio
ns w
ere
desig
ned
acco
rdin
g to
stan
dard
s (fo
unda
tion
size,
soil
surv
ey) a
nd/o
r the
re is
evi
denc
e of
dam
age;
no
pla
ns a
re a
vaila
ble;
Ave
rage
= L
ittle
evi
denc
e (d
raw
ings
, soi
l sur
vey)
that
fo
unda
tions
wer
e de
signe
d ac
cord
ing
to st
anda
rds;
and/
or th
ere
is ev
iden
ce
for m
oder
ate
dam
age;
Hig
h =
Stro
ng e
vide
nce
that
foun
datio
ns w
ere
de-
signe
d ac
cord
ing
to st
anda
rds w
ith st
rong
evi
denc
e of
no
dam
age.
14. Ir
regu
larit
ies i
n bu
ildin
g st
ruct
ure
plan
(rig
idity
, mas
s, re
sista
nce)
Safe
ty ra
tings
: Low
= S
hape
s are
irre
gula
r and
stru
ctur
e is
not u
nifo
rm; A
ver-
age
= S
hape
s on
plan
are
irre
gula
r but
stru
ctur
e is
unifo
rm; H
igh
= S
hape
s on
plan
are
regu
lar a
nd st
ruct
ure
has u
nifo
rm p
lan,
and
ther
e ar
e no
ele
men
ts
that
wou
ld ca
use
signi
fican
t tor
sion.
15. Ir
regu
larit
ies i
n el
evat
ion
of b
uild
ings
Safe
ty ra
tings
: Low
= S
igni
fican
t disc
ontin
uous
or i
rregu
lar e
lem
ents
, sig
nifi-
cant
varia
tion
in e
leva
tion
of b
uild
ings
; Ave
rage
= S
ever
al d
iscon
tinuo
us o
r irr
egul
ar e
lem
ents
, som
e va
riatio
n in
the
elev
atio
n of
bui
ldin
gs; H
igh
= N
o sig
nific
ant d
iscon
tinuo
us o
r irre
gula
r ele
men
ts, li
ttle
or n
o va
riatio
n in
ele
va-
tion
of b
uild
ings
.
16. Ir
regu
larit
ies i
n he
ight
of s
tore
ysSa
fety
ratin
gs: L
ow =
Hei
ght o
f sto
reys
diff
ers b
y mor
e th
an 2
0%; A
vera
ge =
St
orey
s hav
e sim
ilar h
eigh
ts (t
hey d
iffer
by l
ess t
han
20%
but
mor
e th
an 5
%);
Hig
h =
Sto
reys
are
of s
imila
r hei
ght (
they
diff
er b
y les
s tha
n 5%
).
17. S
truct
ural
inte
grity
of r
oofs
Safe
ty ra
tings
: Low
= M
onop
itch
or fl
at li
ght r
oofs,
and
/or l
arge
roof
ove
r-ha
ngs;
Aver
age
= P
re-s
tress
ed co
ncre
te ro
of, g
able
roof
with
gen
tle sl
ope,
sa
tisfa
ctor
ily co
nnec
ted,
no
larg
e ro
of o
verh
angs
; Hig
h =
Rei
nfor
ced
cast
in
plac
e on
conc
rete
roof
dec
k or h
ippe
d lig
ht ro
of, s
atisf
acto
ry co
nnec
tions
, no
larg
e ro
of o
verh
angs
.
18. S
truct
ural
resil
ienc
e to
haz
ards
oth
er th
an e
arth
quak
es an
d st
rong
w
inds
Safe
ty ra
tings
: Low
= Lo
w st
ruct
ural
resil
ienc
e to
haz
ards
pre
sent
at t
he si
te
of th
e ho
spita
l; Ave
rage
= S
atisf
acto
ry st
ruct
ural
resil
ienc
e (ta
king
acc
ount
of
stru
ctur
al ri
sk re
duct
ion
mea
sure
s in
plac
e); H
igh
= G
ood
stru
ctur
al re
silie
nce
(taki
ng a
ccou
nt o
f risk
redu
ctio
n m
easu
res i
n pl
ace)
.
Con
tinue
>>
ANN
EX 2
: FO
RM 2
: SAF
E H
OSP
ITAL
S CH
ECKL
IST
Mod
ule
2: S
truc
tura
l Saf
ety

59
Hos
pita
l Saf
ety
Inde
x G
UID
E FO
R EV
ALU
ATO
RS
156
Com
men
ts o
n th
e re
sults
of F
orm
2, M
odul
e 2.
(Inc
lude
refe
renc
e to
the
build
ing
type
(s),
stru
ctur
al sy
stem
(s) a
nd a
ge(s
) of b
uild
ings
.
Atta
ch si
te p
lan,
list
all
build
ings
and
indi
cate
thos
e th
at w
ere
asse
ssed
.)
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
Nam
e/sig
natu
re o
f eva
luat
or(s
) ......
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
...

60
157
Mod
ule
3: N
onst
ruct
ural
safe
ty
3.1.
Arc
hite
ctur
al s
afet
ySa
fety
leve
lO
bser
vatio
ns
(eva
luat
ors’
com
men
ts)
Low
Average
High
19. M
ajor
dam
age
and
repa
ir of
non
stru
ctur
al e
lem
ents
Safe
ty ra
tings
: Low
= M
ajor
dam
age
and
no re
pairs
com
plet
ed; A
vera
ge =
M
oder
ate
dam
age,
bui
ldin
g on
ly p
artia
lly re
paire
d; H
igh
= M
inor
or n
o da
m-
age,
or b
uild
ing
fully
repa
ired.
IF S
UCH
AN
EVE
NT
HAS
NO
T O
CCU
RRED
IN T
HE
VICI
NIT
Y O
F TH
E H
OSP
ITAL
, LE
AVE
BOXE
S BL
ANK
AND
PRO
VID
E CO
MM
ENT.
20. C
ondi
tion
and
safe
ty o
f doo
rs, e
xits
and
entra
nces
Safe
ty ra
tings
: Low
= D
oors
, exi
ts a
nd e
ntra
nces
in p
oor c
ondi
tion,
subj
ect
to d
amag
e w
hich
wou
ld im
pede
the
func
tion
of th
is an
d ot
her e
lem
ents
, sy
stem
s or o
pera
tions
; ent
ranc
e w
idth
is le
ss th
an 1
15cm
; Ave
rage
= In
fair
cond
ition
, sub
ject
to d
amag
e bu
t dam
age
wou
ld n
ot im
pede
the
func
tion
of
this
and
othe
r ele
men
ts, s
yste
ms o
r ope
ratio
ns; o
r ent
ranc
e w
idth
is le
ss th
an
115c
m; H
igh
= In
goo
d co
nditi
on, n
o or
min
or p
oten
tial f
or d
amag
e th
at
wou
ld im
pede
the
func
tion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or o
pera
tions
; an
d en
tranc
e w
idth
is e
qual
to o
r lar
ger t
han
115c
m.
21. C
ondi
tion
and
safe
ty o
f win
dow
s and
shut
ters
Safe
ty ra
tings
: Low
= W
indo
ws a
nd sh
utte
rs in
poo
r con
ditio
n, su
bjec
t to
dam
age
whi
ch w
ould
impe
de th
e fu
nctio
n of
this
and
othe
r ele
men
ts,
syst
ems o
r ope
ratio
ns (e
.g. w
eak p
rote
ctiv
e gl
azin
g); A
vera
ge =
In fa
ir co
ndi-
tion,
subj
ect t
o da
mag
e bu
t dam
age
wou
ld n
ot im
pede
the
func
tion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or o
pera
tions
; Hig
h =
In g
ood
cond
ition
, no
or
min
or p
oten
tial f
or d
amag
e th
at w
ould
impe
de th
e fu
nctio
n of
this
and
othe
r el
emen
ts, s
yste
ms o
r ope
ratio
ns; p
rote
ctiv
e gl
ass (
e.g.
pol
ycar
bona
te g
lazi
ng,
blas
t film
) has
bee
n ad
ded
in c
ritic
al w
ards
.
22. C
ondi
tion
and
safe
ty o
f oth
er e
lem
ents
of t
he b
uild
ing
enve
lope
(e
.g. o
utsid
e w
alls,
facin
gs)
Safe
ty ra
tings
: Low
= B
uild
ing
enve
lope
in p
oor c
ondi
tion,
subj
ect t
o da
mag
e w
hich
wou
ld im
pede
the
func
tion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or
oper
atio
ns; A
vera
ge =
In fa
ir co
nditi
on, s
ubje
ct to
dam
age
but d
amag
e w
ould
no
t im
pede
the
func
tion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or o
pera
tions
; H
igh
= In
goo
d co
nditi
on, n
o or
min
or p
oten
tial f
or d
amag
e th
at w
ould
im
pede
the
func
tion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or o
pera
tions
.
23. C
ondi
tion
and
safe
ty o
f roo
fing
Safe
ty ra
tings
: Low
= R
oofin
g in
poo
r con
ditio
n, su
bjec
t to
dam
age
whi
ch
wou
ld im
pede
the
func
tion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or o
pera
tions
; Av
erag
e =
In fa
ir co
nditi
on, s
ubje
ct to
dam
age
but d
amag
e to
ele
men
t(s)
wou
ld n
ot im
pede
the
func
tion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or o
pera
-tio
ns; H
igh
= In
goo
d co
nditi
on, n
o or
min
or p
oten
tial f
or d
amag
e th
at w
ould
im
pede
the
func
tion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or o
pera
tions
.
24. C
ondi
tion
and
safe
ty o
f rai
lings
and
para
pets
Safe
ty ra
tings
: Low
= R
ailin
gs a
nd p
arap
ets i
n po
or co
nditi
on, s
ubje
ct to
dam
-ag
e w
hich
wou
ld im
pede
the
func
tion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or
oper
atio
ns; A
vera
ge =
Sub
ject
to d
amag
e bu
t dam
age
to e
lem
ent(s
) wou
ld
not i
mpe
de th
e fu
nctio
n of
this
and
othe
r ele
men
ts, s
yste
ms o
r ope
ratio
ns;
Hig
h =
No
or m
inor
pot
entia
l for
dam
age
that
wou
ld im
pede
the
func
tion
of
this
and
othe
r ele
men
ts, s
yste
ms o
r ope
ratio
ns.
25. C
ondi
tion
and
safe
ty o
f per
imet
er w
alls
and
fenc
ing
Safe
ty ra
tings
: Low
= P
erim
eter
wal
ls an
d fe
ncin
g in
poo
r con
ditio
n, su
bjec
t to
dam
age w
hich
wou
ld im
pede
the f
unct
ion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or
ope
ratio
ns; A
vera
ge =
In fa
ir co
nditi
on, s
ubje
ct to
dam
age b
ut d
amag
e to
elem
ent(s
) wou
ld n
ot im
pede
the f
unct
ion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or
ope
ratio
ns; H
igh
= In
goo
d co
nditi
on, n
o or
min
or p
oten
tial f
or d
amag
e tha
t w
ould
impe
de th
e fun
ctio
n of
this
and
othe
r ele
men
ts, s
yste
ms o
r ope
ratio
ns.
Con
tinue
>>
ANN
EX 2
: FO
RM 2
: SAF
E H
OSP
ITAL
S CH
ECKL
IST

61
157
Mod
ule
3: N
onst
ruct
ural
safe
ty
3.1.
Arc
hite
ctur
al s
afet
ySa
fety
leve
lO
bser
vatio
ns
(eva
luat
ors’
com
men
ts)
Low
Average
High
19. M
ajor
dam
age
and
repa
ir of
non
stru
ctur
al e
lem
ents
Safe
ty ra
tings
: Low
= M
ajor
dam
age
and
no re
pairs
com
plet
ed; A
vera
ge =
M
oder
ate
dam
age,
bui
ldin
g on
ly p
artia
lly re
paire
d; H
igh
= M
inor
or n
o da
m-
age,
or b
uild
ing
fully
repa
ired.
IF S
UCH
AN
EVE
NT
HAS
NO
T O
CCU
RRED
IN T
HE
VICI
NIT
Y O
F TH
E H
OSP
ITAL
, LE
AVE
BOXE
S BL
ANK
AND
PRO
VID
E CO
MM
ENT.
20. C
ondi
tion
and
safe
ty o
f doo
rs, e
xits
and
entra
nces
Safe
ty ra
tings
: Low
= D
oors
, exi
ts a
nd e
ntra
nces
in p
oor c
ondi
tion,
subj
ect
to d
amag
e w
hich
wou
ld im
pede
the
func
tion
of th
is an
d ot
her e
lem
ents
, sy
stem
s or o
pera
tions
; ent
ranc
e w
idth
is le
ss th
an 1
15cm
; Ave
rage
= In
fair
cond
ition
, sub
ject
to d
amag
e bu
t dam
age
wou
ld n
ot im
pede
the
func
tion
of
this
and
othe
r ele
men
ts, s
yste
ms o
r ope
ratio
ns; o
r ent
ranc
e w
idth
is le
ss th
an
115c
m; H
igh
= In
goo
d co
nditi
on, n
o or
min
or p
oten
tial f
or d
amag
e th
at
wou
ld im
pede
the
func
tion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or o
pera
tions
; an
d en
tranc
e w
idth
is e
qual
to o
r lar
ger t
han
115c
m.
21. C
ondi
tion
and
safe
ty o
f win
dow
s and
shut
ters
Safe
ty ra
tings
: Low
= W
indo
ws a
nd sh
utte
rs in
poo
r con
ditio
n, su
bjec
t to
dam
age
whi
ch w
ould
impe
de th
e fu
nctio
n of
this
and
othe
r ele
men
ts,
syst
ems o
r ope
ratio
ns (e
.g. w
eak p
rote
ctiv
e gl
azin
g); A
vera
ge =
In fa
ir co
ndi-
tion,
subj
ect t
o da
mag
e bu
t dam
age
wou
ld n
ot im
pede
the
func
tion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or o
pera
tions
; Hig
h =
In g
ood
cond
ition
, no
or
min
or p
oten
tial f
or d
amag
e th
at w
ould
impe
de th
e fu
nctio
n of
this
and
othe
r el
emen
ts, s
yste
ms o
r ope
ratio
ns; p
rote
ctiv
e gl
ass (
e.g.
pol
ycar
bona
te g
lazi
ng,
blas
t film
) has
bee
n ad
ded
in c
ritic
al w
ards
.
22. C
ondi
tion
and
safe
ty o
f oth
er e
lem
ents
of t
he b
uild
ing
enve
lope
(e
.g. o
utsid
e w
alls,
facin
gs)
Safe
ty ra
tings
: Low
= B
uild
ing
enve
lope
in p
oor c
ondi
tion,
subj
ect t
o da
mag
e w
hich
wou
ld im
pede
the
func
tion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or
oper
atio
ns; A
vera
ge =
In fa
ir co
nditi
on, s
ubje
ct to
dam
age
but d
amag
e w
ould
no
t im
pede
the
func
tion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or o
pera
tions
; H
igh
= In
goo
d co
nditi
on, n
o or
min
or p
oten
tial f
or d
amag
e th
at w
ould
im
pede
the
func
tion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or o
pera
tions
.
23. C
ondi
tion
and
safe
ty o
f roo
fing
Safe
ty ra
tings
: Low
= R
oofin
g in
poo
r con
ditio
n, su
bjec
t to
dam
age
whi
ch
wou
ld im
pede
the
func
tion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or o
pera
tions
; Av
erag
e =
In fa
ir co
nditi
on, s
ubje
ct to
dam
age
but d
amag
e to
ele
men
t(s)
wou
ld n
ot im
pede
the
func
tion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or o
pera
-tio
ns; H
igh
= In
goo
d co
nditi
on, n
o or
min
or p
oten
tial f
or d
amag
e th
at w
ould
im
pede
the
func
tion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or o
pera
tions
.
24. C
ondi
tion
and
safe
ty o
f rai
lings
and
para
pets
Safe
ty ra
tings
: Low
= R
ailin
gs a
nd p
arap
ets i
n po
or co
nditi
on, s
ubje
ct to
dam
-ag
e w
hich
wou
ld im
pede
the
func
tion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or
oper
atio
ns; A
vera
ge =
Sub
ject
to d
amag
e bu
t dam
age
to e
lem
ent(s
) wou
ld
not i
mpe
de th
e fu
nctio
n of
this
and
othe
r ele
men
ts, s
yste
ms o
r ope
ratio
ns;
Hig
h =
No
or m
inor
pot
entia
l for
dam
age
that
wou
ld im
pede
the
func
tion
of
this
and
othe
r ele
men
ts, s
yste
ms o
r ope
ratio
ns.
25. C
ondi
tion
and
safe
ty o
f per
imet
er w
alls
and
fenc
ing
Safe
ty ra
tings
: Low
= P
erim
eter
wal
ls an
d fe
ncin
g in
poo
r con
ditio
n, su
bjec
t to
dam
age w
hich
wou
ld im
pede
the f
unct
ion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or
ope
ratio
ns; A
vera
ge =
In fa
ir co
nditi
on, s
ubje
ct to
dam
age b
ut d
amag
e to
elem
ent(s
) wou
ld n
ot im
pede
the f
unct
ion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or
ope
ratio
ns; H
igh
= In
goo
d co
nditi
on, n
o or
min
or p
oten
tial f
or d
amag
e tha
t w
ould
impe
de th
e fun
ctio
n of
this
and
othe
r ele
men
ts, s
yste
ms o
r ope
ratio
ns.
Con
tinue
>>
ANN
EX 2
: FO
RM 2
: SAF
E H
OSP
ITAL
S CH
ECKL
IST

62
Hos
pita
l Saf
ety
Inde
x G
UID
E FO
R EV
ALU
ATO
RS
158
(Con
tinue
d) 3
.1. A
rchi
tect
ural
saf
ety
Safe
ty le
vel
Obs
erva
tions
(e
valu
ator
s’ co
mm
ents
)Low
Average
High
26. C
ondi
tion
and
safe
ty o
f oth
er ar
chite
ctur
al e
lem
ents
(e.g
. cor
nice
s, or
nam
ents
, chi
mne
ys, s
igns
)Sa
fety
ratin
gs: L
ow =
Oth
er a
rchi
tect
ural
elem
ent(s
) in
poor
cond
ition
, sub
ject
to
dam
age w
hich
wou
ld im
pede
the f
unct
ion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or
ope
ratio
ns; A
vera
ge =
In fa
ir co
nditi
on, e
lem
ent(s
) are
subj
ect t
o da
mag
e but
da
mag
e wou
ld n
ot im
pede
the f
unct
ion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or
oper
atio
ns; H
igh
= In
goo
d co
nditi
on, n
o or
min
or p
oten
tial f
or d
amag
e tha
t w
ould
impe
de th
e fun
ctio
n of
this
and
othe
r ele
men
ts, s
yste
ms o
r ope
ratio
ns.
27. S
afe
cond
ition
s for
mov
emen
t out
side
the
hosp
ital b
uild
ings
Safe
ty ra
tings
: Low
= O
bsta
cles
or d
amag
e to
stru
ctur
e or
road
and
wal
kway
s w
ill im
pede
veh
icle
and
ped
estri
an a
cces
s to
build
ings
or e
ndan
ger p
edes
-tri
ans;
Aver
age
= O
bsta
cles
or d
amag
e to
stru
ctur
e or
road
and
wal
kway
s w
ill n
ot im
pede
ped
estri
an a
cces
s, bu
t will
impe
de v
ehic
le a
cces
s; H
igh
= N
o ob
stac
les,
or p
oten
tial f
or o
nly m
inor
or n
o da
mag
e th
at w
ill n
ot im
pede
pe
dest
rian
or v
ehic
le a
cces
s.
28. S
afe c
ondi
tions
for m
ovem
ent i
nsid
e the
bui
ldin
g (e
.g. c
orrid
ors,
stai
rs)
Safe
ty ra
tings
: Low
= O
bsta
cles
and
dam
age
to e
lem
ent(s
) will
impe
de m
ove-
men
t ins
ide
the
build
ing
and
enda
nger
occ
upan
ts; A
vera
ge =
Obs
tacl
es o
r da
mag
e to
ele
men
ts w
ill n
ot im
pede
mov
emen
t of p
eopl
e bu
t will
impe
de
mov
emen
t of s
tretc
hers
, whe
eled
equ
ipm
ent;
Hig
h =
No
obst
acle
s, po
tent
ial
for n
o or
min
or d
amag
e w
hich
will
not
impe
de m
ovem
ent o
f peo
ple
or
whe
eled
equ
ipm
ent.
29. C
ondi
tion
and
safe
ty o
f int
erna
l wal
ls an
d pa
rtiti
ons
Safe
ty ra
tings
: Low
= In
tern
al w
alls
and
part
ition
s in
poor
cond
ition
, sub
ject
to
dam
age
whi
ch w
ould
impe
de th
e fu
nctio
n of
this
and
othe
r ele
men
ts,
syst
ems o
r ope
ratio
ns; A
vera
ge =
In fa
ir co
nditi
on, e
lem
ent(s
) are
subj
ect t
o da
mag
e bu
t dam
age
wou
ld n
ot im
pede
the
func
tion
of th
is an
d ot
her e
le-
men
ts, s
yste
ms o
r ope
ratio
ns; H
igh
= In
goo
d co
nditi
on, n
o or
min
or p
oten
tial
for d
amag
e th
at w
ould
impe
de th
e fu
nctio
n of
this
and
othe
r ele
men
ts,
syst
ems o
r ope
ratio
ns.
30. C
ondi
tion
and
safe
ty o
f fal
se o
r sus
pend
ed ce
iling
sSa
fety
ratin
gs: L
ow =
False
or s
uspe
nded
ceilin
gs in
poo
r con
ditio
n, su
bjec
t to
dam
age w
hich
wou
ld im
pede
the f
unct
ion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or
ope
ratio
ns; A
vera
ge =
In fa
ir co
nditi
on, e
lem
ent(s
) sub
ject
to d
amag
e but
da
mag
e wou
ld n
ot im
pede
the f
unct
ion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or
oper
atio
ns; H
igh
= In
goo
d co
nditi
on, n
o or
min
or p
oten
tial f
or d
amag
e tha
t w
ould
impe
de th
e fun
ctio
n of
this
and
othe
r ele
men
ts, s
yste
ms o
r ope
ratio
ns.
IF T
HE
HO
SPIT
AL D
OES
NO
T H
AVE
FALS
E O
R SU
SPEN
DED
CEI
LIN
GS,
LEA
VE
BOXE
S BL
ANK.
31. C
ondi
tion
and
safe
ty o
f the
ele
vato
r sys
tem
Safe
ty ra
tings
: Low
= E
leva
tor s
yste
m in
poo
r con
ditio
n, su
bjec
t to
dam
age
whi
ch w
ould
impe
de th
e fu
nctio
n of
this
and
othe
r ele
men
ts, s
yste
ms o
r op
erat
ions
; Ave
rage
= In
fair
cond
ition
, ele
men
t(s) s
ubje
ct to
dam
age
but
dam
age
wou
ld n
ot im
pede
the
func
tion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or
oper
atio
ns; H
igh
= In
goo
d co
nditi
on, n
o or
min
or p
oten
tial f
or d
amag
e th
at
wou
ld im
pede
the
func
tion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or o
pera
tions
.
IF T
HER
E AR
E N
O E
LEVA
TORS
, LEA
VE B
OXE
S BL
ANK
AND
PRO
VID
E CO
MM
ENT.
32. C
ondi
tion
and
safe
ty o
f sta
irway
s and
ram
psSa
fety
ratin
gs: L
ow =
In p
oor c
ondi
tion,
subj
ect t
o da
mag
e or
ther
e ar
e ob
-st
acle
s, w
hich
wou
ld im
pede
the
func
tion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or
ope
ratio
ns; A
vera
ge =
In fa
ir co
nditi
on, s
ubje
ct to
dam
age
but d
amag
e an
d ob
stac
les w
ould
not
impe
de th
e fu
nctio
n of
this
and
othe
r ele
men
ts, s
yste
ms
or o
pera
tions
; Hig
h =
In g
ood
cond
ition
, no
obst
acle
s, po
tent
ial f
or n
o or
m
inor
dam
age
that
wou
ld im
pede
the
func
tion
of th
is an
d ot
her e
lem
ents
, sy
stem
s or o
pera
tions
.
IF TH
ERE A
RE N
O ST
AIRS
AND
RAM
PS, L
EAVE
BOX
ES B
LANK
AND
PRO
VIDE
CO
MM
ENT.
Con
tinue
>>
Mod
ule
3: N
onst
ruct
ural
safe
ty

63
Hos
pita
l Saf
ety
Inde
x G
UID
E FO
R EV
ALU
ATO
RS
158
(Con
tinue
d) 3
.1. A
rchi
tect
ural
saf
ety
Safe
ty le
vel
Obs
erva
tions
(e
valu
ator
s’ co
mm
ents
)Low
Average
High
26. C
ondi
tion
and
safe
ty o
f oth
er ar
chite
ctur
al e
lem
ents
(e.g
. cor
nice
s, or
nam
ents
, chi
mne
ys, s
igns
)Sa
fety
ratin
gs: L
ow =
Oth
er a
rchi
tect
ural
elem
ent(s
) in
poor
cond
ition
, sub
ject
to
dam
age w
hich
wou
ld im
pede
the f
unct
ion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or
ope
ratio
ns; A
vera
ge =
In fa
ir co
nditi
on, e
lem
ent(s
) are
subj
ect t
o da
mag
e but
da
mag
e wou
ld n
ot im
pede
the f
unct
ion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or
oper
atio
ns; H
igh
= In
goo
d co
nditi
on, n
o or
min
or p
oten
tial f
or d
amag
e tha
t w
ould
impe
de th
e fun
ctio
n of
this
and
othe
r ele
men
ts, s
yste
ms o
r ope
ratio
ns.
27. S
afe
cond
ition
s for
mov
emen
t out
side
the
hosp
ital b
uild
ings
Safe
ty ra
tings
: Low
= O
bsta
cles
or d
amag
e to
stru
ctur
e or
road
and
wal
kway
s w
ill im
pede
veh
icle
and
ped
estri
an a
cces
s to
build
ings
or e
ndan
ger p
edes
-tri
ans;
Aver
age
= O
bsta
cles
or d
amag
e to
stru
ctur
e or
road
and
wal
kway
s w
ill n
ot im
pede
ped
estri
an a
cces
s, bu
t will
impe
de v
ehic
le a
cces
s; H
igh
= N
o ob
stac
les,
or p
oten
tial f
or o
nly m
inor
or n
o da
mag
e th
at w
ill n
ot im
pede
pe
dest
rian
or v
ehic
le a
cces
s.
28. S
afe c
ondi
tions
for m
ovem
ent i
nsid
e the
bui
ldin
g (e
.g. c
orrid
ors,
stai
rs)
Safe
ty ra
tings
: Low
= O
bsta
cles
and
dam
age
to e
lem
ent(s
) will
impe
de m
ove-
men
t ins
ide
the
build
ing
and
enda
nger
occ
upan
ts; A
vera
ge =
Obs
tacl
es o
r da
mag
e to
ele
men
ts w
ill n
ot im
pede
mov
emen
t of p
eopl
e bu
t will
impe
de
mov
emen
t of s
tretc
hers
, whe
eled
equ
ipm
ent;
Hig
h =
No
obst
acle
s, po
tent
ial
for n
o or
min
or d
amag
e w
hich
will
not
impe
de m
ovem
ent o
f peo
ple
or
whe
eled
equ
ipm
ent.
29. C
ondi
tion
and
safe
ty o
f int
erna
l wal
ls an
d pa
rtiti
ons
Safe
ty ra
tings
: Low
= In
tern
al w
alls
and
part
ition
s in
poor
cond
ition
, sub
ject
to
dam
age
whi
ch w
ould
impe
de th
e fu
nctio
n of
this
and
othe
r ele
men
ts,
syst
ems o
r ope
ratio
ns; A
vera
ge =
In fa
ir co
nditi
on, e
lem
ent(s
) are
subj
ect t
o da
mag
e bu
t dam
age
wou
ld n
ot im
pede
the
func
tion
of th
is an
d ot
her e
le-
men
ts, s
yste
ms o
r ope
ratio
ns; H
igh
= In
goo
d co
nditi
on, n
o or
min
or p
oten
tial
for d
amag
e th
at w
ould
impe
de th
e fu
nctio
n of
this
and
othe
r ele
men
ts,
syst
ems o
r ope
ratio
ns.
30. C
ondi
tion
and
safe
ty o
f fal
se o
r sus
pend
ed ce
iling
sSa
fety
ratin
gs: L
ow =
False
or s
uspe
nded
ceilin
gs in
poo
r con
ditio
n, su
bjec
t to
dam
age w
hich
wou
ld im
pede
the f
unct
ion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or
ope
ratio
ns; A
vera
ge =
In fa
ir co
nditi
on, e
lem
ent(s
) sub
ject
to d
amag
e but
da
mag
e wou
ld n
ot im
pede
the f
unct
ion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or
oper
atio
ns; H
igh
= In
goo
d co
nditi
on, n
o or
min
or p
oten
tial f
or d
amag
e tha
t w
ould
impe
de th
e fun
ctio
n of
this
and
othe
r ele
men
ts, s
yste
ms o
r ope
ratio
ns.
IF T
HE
HO
SPIT
AL D
OES
NO
T H
AVE
FALS
E O
R SU
SPEN
DED
CEI
LIN
GS,
LEA
VE
BOXE
S BL
ANK.
31. C
ondi
tion
and
safe
ty o
f the
ele
vato
r sys
tem
Safe
ty ra
tings
: Low
= E
leva
tor s
yste
m in
poo
r con
ditio
n, su
bjec
t to
dam
age
whi
ch w
ould
impe
de th
e fu
nctio
n of
this
and
othe
r ele
men
ts, s
yste
ms o
r op
erat
ions
; Ave
rage
= In
fair
cond
ition
, ele
men
t(s) s
ubje
ct to
dam
age
but
dam
age
wou
ld n
ot im
pede
the
func
tion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or
oper
atio
ns; H
igh
= In
goo
d co
nditi
on, n
o or
min
or p
oten
tial f
or d
amag
e th
at
wou
ld im
pede
the
func
tion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or o
pera
tions
.
IF T
HER
E AR
E N
O E
LEVA
TORS
, LEA
VE B
OXE
S BL
ANK
AND
PRO
VID
E CO
MM
ENT.
32. C
ondi
tion
and
safe
ty o
f sta
irway
s and
ram
psSa
fety
ratin
gs: L
ow =
In p
oor c
ondi
tion,
subj
ect t
o da
mag
e or
ther
e ar
e ob
-st
acle
s, w
hich
wou
ld im
pede
the
func
tion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or
ope
ratio
ns; A
vera
ge =
In fa
ir co
nditi
on, s
ubje
ct to
dam
age
but d
amag
e an
d ob
stac
les w
ould
not
impe
de th
e fu
nctio
n of
this
and
othe
r ele
men
ts, s
yste
ms
or o
pera
tions
; Hig
h =
In g
ood
cond
ition
, no
obst
acle
s, po
tent
ial f
or n
o or
m
inor
dam
age
that
wou
ld im
pede
the
func
tion
of th
is an
d ot
her e
lem
ents
, sy
stem
s or o
pera
tions
.
IF TH
ERE A
RE N
O ST
AIRS
AND
RAM
PS, L
EAVE
BOX
ES B
LANK
AND
PRO
VIDE
CO
MM
ENT.
Con
tinue
>>
Mod
ule
3: N
onst
ruct
ural
safe
ty

64
159
(Con
tinue
d) 3
.1. A
rchi
tect
ural
saf
ety
Safe
ty le
vel
Obs
erva
tions
(e
valu
ator
s’ co
mm
ents
)Low
Average
High
33. C
ondi
tion
and
safe
ty o
f floo
r cov
erin
gsSa
fety
ratin
gs: L
ow =
Floo
r cov
erin
gs in
poo
r con
ditio
n, su
bjec
t to
dam
age
whi
ch w
ould
impe
de th
e fun
ctio
n of
this
and
othe
r ele
men
ts, s
yste
ms o
r ope
ra-
tions
; Ave
rage
= In
fair
cond
ition
, sub
ject
to d
amag
e but
dam
age w
ould
not
im-
pede
func
tion;
Hig
h =
In g
ood
cond
ition
, no
or m
inor
pot
entia
l for
dam
age t
hat
wou
ld im
pede
the f
unct
ion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or o
pera
tions
.
3.2
Infr
astr
uctu
re p
rote
ctio
n, a
cces
s an
d ph
ysic
al
secu
rity
Safe
ty le
vel
Obs
erva
tions
(e
valu
ator
s’ co
mm
ents
)Low
Average
High
34. L
ocat
ion
of h
ospi
tal’s
criti
cal s
ervi
ces a
nd e
quip
men
t in
the
hosp
ital
in re
latio
n to
loca
l haz
ards
Safe
ty ra
tings
: Low
= N
o pr
otec
tion
mea
sure
s tak
en; s
ubje
ct to
dam
age,
fa
ilure
and
disr
uptio
n of
crit
ical
serv
ices
and
hos
pita
l ope
ratio
ns in
em
erge
n-ci
es a
nd d
isast
ers;
Aver
age
= P
artia
l mea
sure
s to
prot
ect c
ritic
al se
rvic
es fr
om
loca
l haz
ards
are
take
n; su
bjec
t to
dam
age
with
som
e di
srup
tion
of c
ritic
al
serv
ices
and
hos
pita
l ope
ratio
ns in
em
erge
ncie
s or d
isast
ers;
Hig
h =
Man
y m
easu
res a
re ta
ken
to p
rote
ct c
ritic
al se
rvic
es; h
igh
prob
abili
ty th
at c
ritic
al
serv
ices
and
hos
pita
l will
ope
rate
with
no
or li
mite
d di
srup
tion
in e
mer
genc
ies
and
disa
ster
s.
35. H
ospi
tal a
cces
s rou
tes
Safe
ty ra
tings
: Low
= A
cces
s rou
tes s
ubje
ct to
obs
tacl
es a
nd d
amag
e th
at
wou
ld im
pede
acc
ess a
nd th
e fu
nctio
n of
oth
er e
lem
ents
, sys
tem
s or o
pera
-tio
ns; A
vera
ge =
Acc
ess r
oute
s sub
ject
to so
me
obst
acle
s and
dam
age
that
w
ould
not
impe
de a
cces
s and
func
tion;
Hig
h =
No
or m
inor
pot
entia
l for
ob
stac
les o
r dam
age
that
wou
ld im
pede
acc
ess a
nd th
e fu
nctio
n of
oth
er
elem
ents
, sys
tem
s or o
pera
tions
.
36. E
mer
genc
y exi
ts an
d ev
acua
tion
rout
esSa
fety
ratin
gs: L
ow =
Exi
t and
eva
cuat
ion
rout
es a
re n
ot c
lear
ly m
arke
d an
d m
any a
re b
lock
ed; A
vera
ge =
Som
e ex
it an
d ev
acua
tion
rout
es a
re m
arke
d an
d m
ost a
re c
lear
of o
bsta
cles
; Hig
h =
All
exit
and
evac
uatio
n ro
utes
are
cl
early
mar
ked
and
free
of o
bsta
cles
.
37. P
hysic
al se
curit
y of b
uild
ing,
equ
ipm
ent,
staff
and
patie
nts
Safe
ty ra
tings
: Low
= N
o m
easu
res a
re in
pla
ce; A
vera
ge =
Som
e ph
ysic
al
secu
rity p
rote
ctio
n is
in p
lace
(e.g
. lock
ed st
orag
e fo
r sup
plie
s and
equ
ipm
ent,
asse
t tra
ckin
g an
d in
vent
ory c
ontro
l); H
igh
= W
ide
rang
e of
secu
rity m
easu
res
in p
lace
(e.g
. des
ign
and
layo
ut, p
hysic
al b
arrie
rs, a
cces
s con
trol a
nd d
oor
secu
rity s
yste
ms,
lock
ed st
orag
e fo
r sup
plie
s and
equ
ipm
ent).
3.3
Crit
ical
sys
tem
sSa
fety
leve
lO
bser
vatio
ns
(eva
luat
ors’
com
men
ts)
Low
Average
High
3.3.
1 El
ectr
ical
sys
tem
s38
. Cap
acity
of a
ltern
ate
sour
ces o
f ele
ctric
ity (e
.g. g
ener
ator
s)Sa
fety
ratin
gs: L
ow =
Alte
rnat
e so
urce
(s) i
s(ar
e) m
issin
g or
cove
rs le
ss th
an
30%
of d
eman
d in
crit
ical
are
as, o
r can
onl
y be
star
ted
man
ually
; Ave
rage
=
Alte
rnat
e so
urce
(s) c
over
s 31–
70%
of d
eman
d in
crit
ical
are
as a
nd st
arts
au-
tom
atic
ally
in le
ss th
an 1
0 se
cond
s in
criti
cal a
reas
; Hig
h =
Alte
rnat
e so
urce
(s)
star
t(s) a
utom
atic
ally
in le
ss th
an 1
0 se
cond
s and
cove
r(s) m
ore
than
70%
of
dem
and
in c
ritic
al a
reas
.
39. R
egul
ar te
sts o
f alte
rnat
e so
urce
s of e
lect
ricity
in cr
itica
l are
asSa
fety
ratin
gs: L
ow =
Test
ed a
t ful
l loa
d ev
ery 3
mon
ths o
r mor
e; A
vera
ge
= Te
sted
at f
ull l
oad
ever
y 1 to
3 m
onth
s; H
igh
= Te
sted
at f
ull l
oad
at le
ast
mon
thly.
40. C
ondi
tion
and
safe
ty o
f alte
rnat
e so
urce
(s) o
f ele
ctric
itySa
fety
ratin
gs: L
ow =
No
alte
rnat
e so
urce
s; ge
nera
tors
are
in p
oor c
ondi
tion,
th
ere
are
no p
rote
ctiv
e m
easu
res;
Aver
age
= G
ener
ator
s are
in fa
ir co
nditi
on,
som
e m
easu
res p
rovi
de p
artia
l pro
tect
ion
and
secu
rity;
Hig
h =
Gen
erat
ors a
re
in g
ood
cond
ition
, wel
l-sec
ured
and
in g
ood
wor
king
ord
er fo
r em
erge
ncie
s.
Con
tinue
>>
ANN
EX 2
: FO
RM 2
: SAF
E H
OSP
ITAL
S CH
ECKL
IST
Mod
ule
3: N
onst
ruct
ural
safe
ty

65
159
(Con
tinue
d) 3
.1. A
rchi
tect
ural
saf
ety
Safe
ty le
vel
Obs
erva
tions
(e
valu
ator
s’ co
mm
ents
)Low
Average
High
33. C
ondi
tion
and
safe
ty o
f floo
r cov
erin
gsSa
fety
ratin
gs: L
ow =
Floo
r cov
erin
gs in
poo
r con
ditio
n, su
bjec
t to
dam
age
whi
ch w
ould
impe
de th
e fun
ctio
n of
this
and
othe
r ele
men
ts, s
yste
ms o
r ope
ra-
tions
; Ave
rage
= In
fair
cond
ition
, sub
ject
to d
amag
e but
dam
age w
ould
not
im-
pede
func
tion;
Hig
h =
In g
ood
cond
ition
, no
or m
inor
pot
entia
l for
dam
age t
hat
wou
ld im
pede
the f
unct
ion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or o
pera
tions
.
3.2
Infr
astr
uctu
re p
rote
ctio
n, a
cces
s an
d ph
ysic
al
secu
rity
Safe
ty le
vel
Obs
erva
tions
(e
valu
ator
s’ co
mm
ents
)Low
Average
High
34. L
ocat
ion
of h
ospi
tal’s
criti
cal s
ervi
ces a
nd e
quip
men
t in
the
hosp
ital
in re
latio
n to
loca
l haz
ards
Safe
ty ra
tings
: Low
= N
o pr
otec
tion
mea
sure
s tak
en; s
ubje
ct to
dam
age,
fa
ilure
and
disr
uptio
n of
crit
ical
serv
ices
and
hos
pita
l ope
ratio
ns in
em
erge
n-ci
es a
nd d
isast
ers;
Aver
age
= P
artia
l mea
sure
s to
prot
ect c
ritic
al se
rvic
es fr
om
loca
l haz
ards
are
take
n; su
bjec
t to
dam
age
with
som
e di
srup
tion
of c
ritic
al
serv
ices
and
hos
pita
l ope
ratio
ns in
em
erge
ncie
s or d
isast
ers;
Hig
h =
Man
y m
easu
res a
re ta
ken
to p
rote
ct c
ritic
al se
rvic
es; h
igh
prob
abili
ty th
at c
ritic
al
serv
ices
and
hos
pita
l will
ope
rate
with
no
or li
mite
d di
srup
tion
in e
mer
genc
ies
and
disa
ster
s.
35. H
ospi
tal a
cces
s rou
tes
Safe
ty ra
tings
: Low
= A
cces
s rou
tes s
ubje
ct to
obs
tacl
es a
nd d
amag
e th
at
wou
ld im
pede
acc
ess a
nd th
e fu
nctio
n of
oth
er e
lem
ents
, sys
tem
s or o
pera
-tio
ns; A
vera
ge =
Acc
ess r
oute
s sub
ject
to so
me
obst
acle
s and
dam
age
that
w
ould
not
impe
de a
cces
s and
func
tion;
Hig
h =
No
or m
inor
pot
entia
l for
ob
stac
les o
r dam
age
that
wou
ld im
pede
acc
ess a
nd th
e fu
nctio
n of
oth
er
elem
ents
, sys
tem
s or o
pera
tions
.
36. E
mer
genc
y exi
ts an
d ev
acua
tion
rout
esSa
fety
ratin
gs: L
ow =
Exi
t and
eva
cuat
ion
rout
es a
re n
ot c
lear
ly m
arke
d an
d m
any a
re b
lock
ed; A
vera
ge =
Som
e ex
it an
d ev
acua
tion
rout
es a
re m
arke
d an
d m
ost a
re c
lear
of o
bsta
cles
; Hig
h =
All
exit
and
evac
uatio
n ro
utes
are
cl
early
mar
ked
and
free
of o
bsta
cles
.
37. P
hysic
al se
curit
y of b
uild
ing,
equ
ipm
ent,
staff
and
patie
nts
Safe
ty ra
tings
: Low
= N
o m
easu
res a
re in
pla
ce; A
vera
ge =
Som
e ph
ysic
al
secu
rity p
rote
ctio
n is
in p
lace
(e.g
. lock
ed st
orag
e fo
r sup
plie
s and
equ
ipm
ent,
asse
t tra
ckin
g an
d in
vent
ory c
ontro
l); H
igh
= W
ide
rang
e of
secu
rity m
easu
res
in p
lace
(e.g
. des
ign
and
layo
ut, p
hysic
al b
arrie
rs, a
cces
s con
trol a
nd d
oor
secu
rity s
yste
ms,
lock
ed st
orag
e fo
r sup
plie
s and
equ
ipm
ent).
3.3
Crit
ical
sys
tem
sSa
fety
leve
lO
bser
vatio
ns
(eva
luat
ors’
com
men
ts)
Low
Average
High
3.3.
1 El
ectr
ical
sys
tem
s38
. Cap
acity
of a
ltern
ate
sour
ces o
f ele
ctric
ity (e
.g. g
ener
ator
s)Sa
fety
ratin
gs: L
ow =
Alte
rnat
e so
urce
(s) i
s(ar
e) m
issin
g or
cove
rs le
ss th
an
30%
of d
eman
d in
crit
ical
are
as, o
r can
onl
y be
star
ted
man
ually
; Ave
rage
=
Alte
rnat
e so
urce
(s) c
over
s 31–
70%
of d
eman
d in
crit
ical
are
as a
nd st
arts
au-
tom
atic
ally
in le
ss th
an 1
0 se
cond
s in
criti
cal a
reas
; Hig
h =
Alte
rnat
e so
urce
(s)
star
t(s) a
utom
atic
ally
in le
ss th
an 1
0 se
cond
s and
cove
r(s) m
ore
than
70%
of
dem
and
in c
ritic
al a
reas
.
39. R
egul
ar te
sts o
f alte
rnat
e so
urce
s of e
lect
ricity
in cr
itica
l are
asSa
fety
ratin
gs: L
ow =
Test
ed a
t ful
l loa
d ev
ery 3
mon
ths o
r mor
e; A
vera
ge
= Te
sted
at f
ull l
oad
ever
y 1 to
3 m
onth
s; H
igh
= Te
sted
at f
ull l
oad
at le
ast
mon
thly.
40. C
ondi
tion
and
safe
ty o
f alte
rnat
e so
urce
(s) o
f ele
ctric
itySa
fety
ratin
gs: L
ow =
No
alte
rnat
e so
urce
s; ge
nera
tors
are
in p
oor c
ondi
tion,
th
ere
are
no p
rote
ctiv
e m
easu
res;
Aver
age
= G
ener
ator
s are
in fa
ir co
nditi
on,
som
e m
easu
res p
rovi
de p
artia
l pro
tect
ion
and
secu
rity;
Hig
h =
Gen
erat
ors a
re
in g
ood
cond
ition
, wel
l-sec
ured
and
in g
ood
wor
king
ord
er fo
r em
erge
ncie
s.
Con
tinue
>>
ANN
EX 2
: FO
RM 2
: SAF
E H
OSP
ITAL
S CH
ECKL
IST
Mod
ule
3: N
onst
ruct
ural
safe
ty

66
Hos
pita
l Saf
ety
Inde
x G
UID
E FO
R EV
ALU
ATO
RS
160
(Con
tinue
d) 3
.3 C
ritic
al s
yste
ms
Safe
ty le
vel
Obs
erva
tions
(e
valu
ator
s’ co
mm
ents
)Low
Average
High
41. C
ondi
tion
and
safe
ty o
f ele
ctric
al eq
uipm
ent,
cabl
es an
d ca
ble d
ucts
Safe
ty ra
tings
: Low
= E
lect
rical
equi
pmen
t, po
wer
lines
, cab
les a
nd d
ucts
are
in
poor
cond
ition
, the
re a
re n
o pr
otec
tive m
easu
res;
Aver
age =
Ele
ctric
al eq
uip-
men
t, po
wer
lines
, cab
les a
nd d
ucts
are
in fa
ir co
nditi
on; s
ome m
easu
res p
rovi
de
parti
al p
rote
ctio
n an
d se
curit
y; H
igh
= El
ectri
cal e
quip
men
t, po
wer
lines
, cab
les
and
duct
s are
in g
ood
cond
ition
, wel
l-sec
ured
and
in g
ood
wor
king
ord
er.
42. R
edun
dant
syst
em fo
r the
loca
l ele
ctric
pow
er su
pply
Safe
ty ra
tings
: Low
= T
here
is o
nly o
ne e
ntra
nce
for t
he lo
cal p
ower
supp
ly;
Aver
age
= T
here
are
two
entra
nces
for t
he lo
cal p
ower
supp
ly; H
igh
= T
here
ar
e m
ore
than
two
entra
nces
for t
he lo
cal p
ower
supp
ly.
43. C
ondi
tion
and
safe
ty o
f con
trol p
anel
s, ov
erlo
ad b
reak
er sw
itche
s an
d ca
bles
Safe
ty ra
tings
: Low
= C
ontr
ol p
anel
s or o
ther
ele
men
ts a
re in
poo
r con
di-
tion,
ther
e ar
e no
pro
tect
ive
mea
sure
s; Av
erag
e =
Con
trol
pan
els o
r oth
er
elem
ents
are
in fa
ir co
nditi
on; s
ome
mea
sure
s pro
vide
par
tial p
rote
ctio
n;
Hig
h =
Con
trol
pan
els o
r oth
er e
lem
ents
are
in g
ood
cond
ition
, wel
l-pr
otec
ted
and
in g
ood
wor
king
ord
er.
44. L
ight
ing
syst
em fo
r crit
ical a
reas
of t
he h
ospi
tal
Safe
ty ra
tings
: Low
= P
oor l
evel
of l
ight
ing,
ther
e ar
e no
pro
tect
ive
mea
sure
s; Av
erag
e =
Lig
htin
g is
satis
fact
ory
in th
e cr
itica
l are
as; s
ome
mea
sure
s pro
vide
par
tial p
rote
ctio
n; H
igh
= G
ood
leve
ls of
ligh
ting
and
prot
ectio
n m
easu
res i
n pl
ace.
45. C
ondi
tion
and
safe
ty o
f int
erna
l and
exte
rnal
ligh
ting
syst
ems
Safe
ty ra
tings
: Low
= In
tern
al a
nd e
xter
nal l
ight
ing
syst
ems a
re in
poo
r co
nditi
on, t
here
are
no
prot
ectiv
e m
easu
res;
Aver
age
= In
fair
cond
ition
; so
me
mea
sure
s pro
vide
par
tial p
rote
ctio
n; H
igh
= In
goo
d co
nditi
on,
wel
l-pro
tect
ed a
nd in
goo
d w
orki
ng o
rder
.
46. E
xter
nal e
lect
rical
syst
ems i
nsta
lled
for h
ospi
tal u
sage
Safe
ty ra
tings
: Low
= N
o el
ectr
ical
subs
tatio
ns in
stal
led
for h
ospi
tal
dem
ands
; Ave
rage
= S
ubst
atio
ns in
stal
led;
som
e m
easu
res p
rovi
de
part
ial p
rote
ctio
n, b
ut w
ould
be
vuln
erab
le to
dam
age
or d
isrup
tion,
do
not p
rovi
de e
noug
h po
wer
to th
e ho
spita
l; H
igh
= E
lect
rical
subs
tatio
ns
inst
alle
d, w
ell-p
rote
cted
, and
pro
vide
eno
ugh
pow
er to
the
hosp
ital i
n an
em
erge
ncy
or d
isast
er.
47. E
mer
genc
y mai
nten
ance
and
rest
orat
ion
of e
lect
ric p
ower
supp
ly
and
alte
rnat
e so
urce
sSa
fety
ratin
gs: L
ow =
Doc
umen
ted
proc
edur
es a
nd m
aint
enan
ce/in
-sp
ectio
n re
cord
s do
not e
xist
; Ave
rage
= D
ocum
ente
d pr
oced
ures
exi
st,
mai
nten
ance
/insp
ectio
n re
cord
s are
up
to d
ate,
per
sonn
el h
ave
been
tr
aine
d, b
ut re
sour
ces a
re n
ot a
vaila
ble;
Hig
h =
Doc
umen
ted
proc
edur
es
exist
, mai
nten
ance
/insp
ectio
n re
cord
s are
up
to d
ate,
per
sonn
el h
ave
been
trai
ned,
and
reso
urce
s are
in p
lace
for i
mpl
emen
ting
emer
genc
y m
aint
enan
ce a
nd re
stor
atio
n.
3.3.
2 Te
leco
mm
unic
atio
ns s
yste
ms
48. C
ondi
tion
and
safe
ty o
f ant
enna
sSa
fety
ratin
gs: L
ow =
Ant
enna
s and
bra
cing
in p
oor c
ondi
tion,
ther
e ar
e no
pr
otec
tive
mea
sure
s; Av
erag
e =
Ante
nnas
and
bra
cing
are
in fa
ir co
nditi
on,
som
e m
easu
res p
rovi
de p
artia
l pro
tect
ion;
Hig
h =
Ante
nnas
and
bra
cing
ar
e in
goo
d co
nditi
on, w
ell-s
ecur
ed a
nd p
rote
ctio
n m
easu
res a
re in
pla
ce.
IF T
HER
E AR
E N
O A
NTE
NN
AS, L
EAVE
BO
XES
BLAN
K AN
D P
ROVI
DE
COM
MEN
T.
49. C
ondi
tion
and
safe
ty o
f low
- and
extra
-low
-vol
tage
syst
ems
(inte
rnet
and
tele
phon
e)Sa
fety
ratin
gs: L
ow =
Low
vol
tage
syst
ems i
n po
or c
ondi
tion,
ther
e ar
e no
pro
tect
ive
mea
sure
s; Av
erag
e =
Low
vol
tage
syst
ems i
n fa
ir co
nditi
on,
som
e m
easu
res p
rovi
de p
artia
l pro
tect
ion;
Hig
h =
Goo
d co
nditi
on, w
ell-
secu
red
and
othe
r pro
tect
ion
mea
sure
s in
plac
e.
Con
tinue
>>
Mod
ule
3: N
onst
ruct
ural
safe
ty

67
Hos
pita
l Saf
ety
Inde
x G
UID
E FO
R EV
ALU
ATO
RS
160
(Con
tinue
d) 3
.3 C
ritic
al s
yste
ms
Safe
ty le
vel
Obs
erva
tions
(e
valu
ator
s’ co
mm
ents
)Low
Average
High
41. C
ondi
tion
and
safe
ty o
f ele
ctric
al eq
uipm
ent,
cabl
es an
d ca
ble d
ucts
Safe
ty ra
tings
: Low
= E
lect
rical
equi
pmen
t, po
wer
lines
, cab
les a
nd d
ucts
are
in
poor
cond
ition
, the
re a
re n
o pr
otec
tive m
easu
res;
Aver
age =
Ele
ctric
al eq
uip-
men
t, po
wer
lines
, cab
les a
nd d
ucts
are
in fa
ir co
nditi
on; s
ome m
easu
res p
rovi
de
parti
al p
rote
ctio
n an
d se
curit
y; H
igh
= El
ectri
cal e
quip
men
t, po
wer
lines
, cab
les
and
duct
s are
in g
ood
cond
ition
, wel
l-sec
ured
and
in g
ood
wor
king
ord
er.
42. R
edun
dant
syst
em fo
r the
loca
l ele
ctric
pow
er su
pply
Safe
ty ra
tings
: Low
= T
here
is o
nly o
ne e
ntra
nce
for t
he lo
cal p
ower
supp
ly;
Aver
age
= T
here
are
two
entra
nces
for t
he lo
cal p
ower
supp
ly; H
igh
= T
here
ar
e m
ore
than
two
entra
nces
for t
he lo
cal p
ower
supp
ly.
43. C
ondi
tion
and
safe
ty o
f con
trol p
anel
s, ov
erlo
ad b
reak
er sw
itche
s an
d ca
bles
Safe
ty ra
tings
: Low
= C
ontr
ol p
anel
s or o
ther
ele
men
ts a
re in
poo
r con
di-
tion,
ther
e ar
e no
pro
tect
ive
mea
sure
s; Av
erag
e =
Con
trol
pan
els o
r oth
er
elem
ents
are
in fa
ir co
nditi
on; s
ome
mea
sure
s pro
vide
par
tial p
rote
ctio
n;
Hig
h =
Con
trol
pan
els o
r oth
er e
lem
ents
are
in g
ood
cond
ition
, wel
l-pr
otec
ted
and
in g
ood
wor
king
ord
er.
44. L
ight
ing
syst
em fo
r crit
ical a
reas
of t
he h
ospi
tal
Safe
ty ra
tings
: Low
= P
oor l
evel
of l
ight
ing,
ther
e ar
e no
pro
tect
ive
mea
sure
s; Av
erag
e =
Lig
htin
g is
satis
fact
ory
in th
e cr
itica
l are
as; s
ome
mea
sure
s pro
vide
par
tial p
rote
ctio
n; H
igh
= G
ood
leve
ls of
ligh
ting
and
prot
ectio
n m
easu
res i
n pl
ace.
45. C
ondi
tion
and
safe
ty o
f int
erna
l and
exte
rnal
ligh
ting
syst
ems
Safe
ty ra
tings
: Low
= In
tern
al a
nd e
xter
nal l
ight
ing
syst
ems a
re in
poo
r co
nditi
on, t
here
are
no
prot
ectiv
e m
easu
res;
Aver
age
= In
fair
cond
ition
; so
me
mea
sure
s pro
vide
par
tial p
rote
ctio
n; H
igh
= In
goo
d co
nditi
on,
wel
l-pro
tect
ed a
nd in
goo
d w
orki
ng o
rder
.
46. E
xter
nal e
lect
rical
syst
ems i
nsta
lled
for h
ospi
tal u
sage
Safe
ty ra
tings
: Low
= N
o el
ectr
ical
subs
tatio
ns in
stal
led
for h
ospi
tal
dem
ands
; Ave
rage
= S
ubst
atio
ns in
stal
led;
som
e m
easu
res p
rovi
de
part
ial p
rote
ctio
n, b
ut w
ould
be
vuln
erab
le to
dam
age
or d
isrup
tion,
do
not p
rovi
de e
noug
h po
wer
to th
e ho
spita
l; H
igh
= E
lect
rical
subs
tatio
ns
inst
alle
d, w
ell-p
rote
cted
, and
pro
vide
eno
ugh
pow
er to
the
hosp
ital i
n an
em
erge
ncy
or d
isast
er.
47. E
mer
genc
y mai
nten
ance
and
rest
orat
ion
of e
lect
ric p
ower
supp
ly
and
alte
rnat
e so
urce
sSa
fety
ratin
gs: L
ow =
Doc
umen
ted
proc
edur
es a
nd m
aint
enan
ce/in
-sp
ectio
n re
cord
s do
not e
xist
; Ave
rage
= D
ocum
ente
d pr
oced
ures
exi
st,
mai
nten
ance
/insp
ectio
n re
cord
s are
up
to d
ate,
per
sonn
el h
ave
been
tr
aine
d, b
ut re
sour
ces a
re n
ot a
vaila
ble;
Hig
h =
Doc
umen
ted
proc
edur
es
exist
, mai
nten
ance
/insp
ectio
n re
cord
s are
up
to d
ate,
per
sonn
el h
ave
been
trai
ned,
and
reso
urce
s are
in p
lace
for i
mpl
emen
ting
emer
genc
y m
aint
enan
ce a
nd re
stor
atio
n.
3.3.
2 Te
leco
mm
unic
atio
ns s
yste
ms
48. C
ondi
tion
and
safe
ty o
f ant
enna
sSa
fety
ratin
gs: L
ow =
Ant
enna
s and
bra
cing
in p
oor c
ondi
tion,
ther
e ar
e no
pr
otec
tive
mea
sure
s; Av
erag
e =
Ante
nnas
and
bra
cing
are
in fa
ir co
nditi
on,
som
e m
easu
res p
rovi
de p
artia
l pro
tect
ion;
Hig
h =
Ante
nnas
and
bra
cing
ar
e in
goo
d co
nditi
on, w
ell-s
ecur
ed a
nd p
rote
ctio
n m
easu
res a
re in
pla
ce.
IF T
HER
E AR
E N
O A
NTE
NN
AS, L
EAVE
BO
XES
BLAN
K AN
D P
ROVI
DE
COM
MEN
T.
49. C
ondi
tion
and
safe
ty o
f low
- and
extra
-low
-vol
tage
syst
ems
(inte
rnet
and
tele
phon
e)Sa
fety
ratin
gs: L
ow =
Low
vol
tage
syst
ems i
n po
or c
ondi
tion,
ther
e ar
e no
pro
tect
ive
mea
sure
s; Av
erag
e =
Low
vol
tage
syst
ems i
n fa
ir co
nditi
on,
som
e m
easu
res p
rovi
de p
artia
l pro
tect
ion;
Hig
h =
Goo
d co
nditi
on, w
ell-
secu
red
and
othe
r pro
tect
ion
mea
sure
s in
plac
e.
Con
tinue
>>
Mod
ule
3: N
onst
ruct
ural
safe
ty

68
161
(Con
tinue
d) 3
.3 C
ritic
al s
yste
ms
Safe
ty le
vel
Obs
erva
tions
(e
valu
ator
s’ co
mm
ents
)Low
Average
High
50. A
ltern
ate
com
mun
icatio
n sy
stem
sSa
fety
ratin
gs: L
ow =
Alte
rnat
e co
mm
unic
atio
ns sy
stem
s do
not e
xist
, are
in
poo
r con
ditio
n, o
r do
not f
unct
ion;
Ave
rage
= H
ospi
tal-w
ide
alte
rnat
e co
mm
unic
atio
ns sy
stem
in fa
ir co
nditi
on, b
ut is
not
test
ed o
n an
ann
ual
basis
; Hig
h =
Alte
rnat
e co
mm
unic
atio
n sy
stem
in g
ood
cond
ition
and
te
sted
at l
east
ann
ually
.
51. C
ondi
tion
and
safe
ty o
f tel
ecom
mun
icatio
ns e
quip
men
t and
cabl
esSa
fety
ratin
gs: L
ow =
Tele
com
mun
icat
ions
equ
ipm
ent a
nd c
able
s are
in
poor
con
ditio
n; th
ere
are
no p
rote
ctiv
e m
easu
res;
Aver
age
= E
quip
men
t an
d ca
bles
are
in fa
ir co
nditi
on; s
ome
mea
sure
s pro
vide
par
tial p
rote
ctio
n;
Hig
h =
In g
ood
cond
ition
, wel
l-sec
ured
and
pro
tect
ed fr
om h
azar
ds.
52. E
ffect
of e
xter
nal t
elec
omm
unica
tions
syst
ems o
n ho
spita
l com
-m
unica
tions
Safe
ty ra
tings
: Low
= E
xter
nal t
elec
omm
unic
atio
ns sy
stem
s cau
se
maj
or in
terfe
renc
e w
ith h
ospi
tal c
omm
unic
atio
ns; A
vera
ge =
Ext
erna
l te
leco
mm
unic
atio
ns sy
stem
cau
se m
oder
ate
inte
rfere
nce
with
hos
pita
l co
mm
unic
atio
ns; H
igh
= E
xter
nal c
omm
unic
atio
ns c
ause
no
inte
rfere
nce
with
hos
pita
l com
mun
icat
ions
.
53. S
afet
y of s
ites f
or te
leco
mm
unica
tion
syst
ems
Safe
ty ra
tings
: Low
= S
ites f
or te
leco
mm
unic
atio
ns sy
stem
s are
in p
oor
cond
ition
, at h
igh
risk
of fa
ilure
due
to h
azar
ds; t
here
are
no
prot
ectiv
e m
easu
res;
Aver
age
= S
ites i
n fa
ir co
nditi
on, s
ome
mea
sure
s pro
vide
par
-tia
l pro
tect
ion;
Hig
h =
Goo
d co
nditi
on, w
ell-s
ecur
ed a
nd o
ther
pro
tect
ive
mea
sure
s in
plac
e.
54. C
ondi
tion
and
safe
ty o
f int
erna
l com
mun
icatio
ns sy
stem
sSa
fety
ratin
gs: L
ow =
Inte
rnal
com
mun
icat
ions
syst
ems d
o no
t exi
st o
r are
in
poo
r con
ditio
n; A
vera
ge =
Inte
rnal
com
mun
icat
ions
syst
ems a
re in
fair
cond
ition
, but
ther
e ar
e no
alte
rnat
e sy
stem
s; H
igh
= In
tern
al c
omm
uni-
catio
ns a
nd b
ack-
up sy
stem
s are
in g
ood
wor
king
ord
er.
55. E
mer
genc
y mai
nten
ance
and
rest
orat
ion
of st
anda
rd an
d al
tern
ate
com
mun
icatio
ns sy
stem
sSa
fety
ratin
gs: L
ow =
Doc
umen
ted
proc
edur
es a
nd m
aint
enan
ce/in
-sp
ectio
n re
cord
s do
not e
xist
; Ave
rage
= D
ocum
ente
d pr
oced
ures
exi
st,
mai
nten
ance
/insp
ectio
n re
cord
s are
up
to d
ate,
per
sonn
el h
ave
been
tr
aine
d, b
ut re
sour
ces a
re n
ot a
vaila
ble;
Hig
h =
Doc
umen
ted
proc
edur
es
exist
, mai
nten
ance
/insp
ectio
n re
cord
s are
up
to d
ate,
per
sonn
el h
ave
been
trai
ned,
and
reso
urce
s are
in p
lace
for i
mpl
emen
ting
emer
genc
y m
aint
enan
ce a
nd re
stor
atio
n.
3.3.
3 W
ater
sup
ply
syst
em56
. Wat
er re
serv
es fo
r hos
pita
l ser
vice
s and
func
tions
Safe
ty ra
tings
: Low
= S
uffici
ent f
or 2
4 ho
urs o
r les
s or w
ater
tank
doe
s not
ex
ist; A
vera
ge =
Suffi
cien
t for
mor
e th
an 2
4 ho
urs b
ut le
ss th
an 7
2 ho
urs;
Hig
h =
Gua
rant
eed
to c
over
at l
east
72
hour
s.
57. L
ocat
ion
of w
ater
stor
age
tank
sSa
fety
ratin
gs: L
ow =
The
site
is v
ulne
rabl
e w
ith h
igh
risk
of fa
ilure
(e.g
. st
ruct
ural
, arc
hite
ctur
al a
nd/o
r sys
tem
vul
nera
bilit
ies)
; Ave
rage
= T
he si
te
is ex
pose
d to
mod
erat
e ris
k of
failu
re (e
.g. s
truc
tura
l, ar
chite
ctur
al a
nd/o
r sy
stem
vul
nera
bilit
ies)
; Hig
h =
The
site
is n
ot e
xpos
ed to
visu
ally
iden
tifi-
able
risk
s (e.
g. st
ruct
ural
, arc
hite
ctur
al a
nd/o
r sys
tem
vul
nera
bilit
ies)
.
IF T
HE
HO
SPIT
AL D
OES
NO
T H
AVE
A W
ATER
STO
RAG
E TA
NK,
LEA
VE B
OXE
S BL
ANK
AND
PRO
VID
E CO
MM
ENT.
58. S
afet
y of t
he w
ater
dist
ribut
ion
syst
emSa
fety
ratin
gs: L
ow =
Les
s tha
n 60
% a
re in
goo
d op
erat
iona
l con
ditio
n;
Aver
age
= B
etw
een
60%
and
80%
are
in g
ood
cond
ition
; Hig
h =
Abo
ve
80%
are
in g
ood
cond
ition
.
Con
tinue
>>
ANN
EX 2
: FO
RM 2
: SAF
E H
OSP
ITAL
S CH
ECKL
IST
Mod
ule
3: N
onst
ruct
ural
safe
ty

69
161
(Con
tinue
d) 3
.3 C
ritic
al s
yste
ms
Safe
ty le
vel
Obs
erva
tions
(e
valu
ator
s’ co
mm
ents
)Low
Average
High
50. A
ltern
ate
com
mun
icatio
n sy
stem
sSa
fety
ratin
gs: L
ow =
Alte
rnat
e co
mm
unic
atio
ns sy
stem
s do
not e
xist
, are
in
poo
r con
ditio
n, o
r do
not f
unct
ion;
Ave
rage
= H
ospi
tal-w
ide
alte
rnat
e co
mm
unic
atio
ns sy
stem
in fa
ir co
nditi
on, b
ut is
not
test
ed o
n an
ann
ual
basis
; Hig
h =
Alte
rnat
e co
mm
unic
atio
n sy
stem
in g
ood
cond
ition
and
te
sted
at l
east
ann
ually
.
51. C
ondi
tion
and
safe
ty o
f tel
ecom
mun
icatio
ns e
quip
men
t and
cabl
esSa
fety
ratin
gs: L
ow =
Tele
com
mun
icat
ions
equ
ipm
ent a
nd c
able
s are
in
poor
con
ditio
n; th
ere
are
no p
rote
ctiv
e m
easu
res;
Aver
age
= E
quip
men
t an
d ca
bles
are
in fa
ir co
nditi
on; s
ome
mea
sure
s pro
vide
par
tial p
rote
ctio
n;
Hig
h =
In g
ood
cond
ition
, wel
l-sec
ured
and
pro
tect
ed fr
om h
azar
ds.
52. E
ffect
of e
xter
nal t
elec
omm
unica
tions
syst
ems o
n ho
spita
l com
-m
unica
tions
Safe
ty ra
tings
: Low
= E
xter
nal t
elec
omm
unic
atio
ns sy
stem
s cau
se
maj
or in
terfe
renc
e w
ith h
ospi
tal c
omm
unic
atio
ns; A
vera
ge =
Ext
erna
l te
leco
mm
unic
atio
ns sy
stem
cau
se m
oder
ate
inte
rfere
nce
with
hos
pita
l co
mm
unic
atio
ns; H
igh
= E
xter
nal c
omm
unic
atio
ns c
ause
no
inte
rfere
nce
with
hos
pita
l com
mun
icat
ions
.
53. S
afet
y of s
ites f
or te
leco
mm
unica
tion
syst
ems
Safe
ty ra
tings
: Low
= S
ites f
or te
leco
mm
unic
atio
ns sy
stem
s are
in p
oor
cond
ition
, at h
igh
risk
of fa
ilure
due
to h
azar
ds; t
here
are
no
prot
ectiv
e m
easu
res;
Aver
age
= S
ites i
n fa
ir co
nditi
on, s
ome
mea
sure
s pro
vide
par
-tia
l pro
tect
ion;
Hig
h =
Goo
d co
nditi
on, w
ell-s
ecur
ed a
nd o
ther
pro
tect
ive
mea
sure
s in
plac
e.
54. C
ondi
tion
and
safe
ty o
f int
erna
l com
mun
icatio
ns sy
stem
sSa
fety
ratin
gs: L
ow =
Inte
rnal
com
mun
icat
ions
syst
ems d
o no
t exi
st o
r are
in
poo
r con
ditio
n; A
vera
ge =
Inte
rnal
com
mun
icat
ions
syst
ems a
re in
fair
cond
ition
, but
ther
e ar
e no
alte
rnat
e sy
stem
s; H
igh
= In
tern
al c
omm
uni-
catio
ns a
nd b
ack-
up sy
stem
s are
in g
ood
wor
king
ord
er.
55. E
mer
genc
y mai
nten
ance
and
rest
orat
ion
of st
anda
rd an
d al
tern
ate
com
mun
icatio
ns sy
stem
sSa
fety
ratin
gs: L
ow =
Doc
umen
ted
proc
edur
es a
nd m
aint
enan
ce/in
-sp
ectio
n re
cord
s do
not e
xist
; Ave
rage
= D
ocum
ente
d pr
oced
ures
exi
st,
mai
nten
ance
/insp
ectio
n re
cord
s are
up
to d
ate,
per
sonn
el h
ave
been
tr
aine
d, b
ut re
sour
ces a
re n
ot a
vaila
ble;
Hig
h =
Doc
umen
ted
proc
edur
es
exist
, mai
nten
ance
/insp
ectio
n re
cord
s are
up
to d
ate,
per
sonn
el h
ave
been
trai
ned,
and
reso
urce
s are
in p
lace
for i
mpl
emen
ting
emer
genc
y m
aint
enan
ce a
nd re
stor
atio
n.
3.3.
3 W
ater
sup
ply
syst
em56
. Wat
er re
serv
es fo
r hos
pita
l ser
vice
s and
func
tions
Safe
ty ra
tings
: Low
= S
uffici
ent f
or 2
4 ho
urs o
r les
s or w
ater
tank
doe
s not
ex
ist; A
vera
ge =
Suffi
cien
t for
mor
e th
an 2
4 ho
urs b
ut le
ss th
an 7
2 ho
urs;
Hig
h =
Gua
rant
eed
to c
over
at l
east
72
hour
s.
57. L
ocat
ion
of w
ater
stor
age
tank
sSa
fety
ratin
gs: L
ow =
The
site
is v
ulne
rabl
e w
ith h
igh
risk
of fa
ilure
(e.g
. st
ruct
ural
, arc
hite
ctur
al a
nd/o
r sys
tem
vul
nera
bilit
ies)
; Ave
rage
= T
he si
te
is ex
pose
d to
mod
erat
e ris
k of
failu
re (e
.g. s
truc
tura
l, ar
chite
ctur
al a
nd/o
r sy
stem
vul
nera
bilit
ies)
; Hig
h =
The
site
is n
ot e
xpos
ed to
visu
ally
iden
tifi-
able
risk
s (e.
g. st
ruct
ural
, arc
hite
ctur
al a
nd/o
r sys
tem
vul
nera
bilit
ies)
.
IF T
HE
HO
SPIT
AL D
OES
NO
T H
AVE
A W
ATER
STO
RAG
E TA
NK,
LEA
VE B
OXE
S BL
ANK
AND
PRO
VID
E CO
MM
ENT.
58. S
afet
y of t
he w
ater
dist
ribut
ion
syst
emSa
fety
ratin
gs: L
ow =
Les
s tha
n 60
% a
re in
goo
d op
erat
iona
l con
ditio
n;
Aver
age
= B
etw
een
60%
and
80%
are
in g
ood
cond
ition
; Hig
h =
Abo
ve
80%
are
in g
ood
cond
ition
.
Con
tinue
>>
ANN
EX 2
: FO
RM 2
: SAF
E H
OSP
ITAL
S CH
ECKL
IST
Mod
ule
3: N
onst
ruct
ural
safe
ty

70
Hos
pita
l Saf
ety
Inde
x G
UID
E FO
R EV
ALU
ATO
RS
162
(Con
tinue
d) 3
.3 C
ritic
al s
yste
ms
Safe
ty le
vel
Obs
erva
tions
(e
valu
ator
s’ co
mm
ents
)Low
Average
High
59. A
ltern
ate
wat
er su
pply
to th
e re
gula
r wat
er su
pply
Safe
ty ra
tings
: Low
= P
rovi
des l
ess t
han
30%
of d
aily
dem
and
in a
n em
er-
genc
y or
disa
ster
scen
ario
; Ave
rage
= P
rovi
des 3
0−80
% o
f dai
ly d
eman
d in
an
emer
genc
y or
disa
ster
scen
ario
; Hig
h =
Pro
vide
s mor
e th
an 8
0% o
f da
ily d
eman
d in
an
emer
genc
y or
disa
ster
scen
ario
.
60. S
uppl
emen
tary
pum
ping
syst
emSa
fety
ratin
gs: L
ow =
The
re is
no
back
-up
pum
p an
d op
erat
iona
l cap
ac-
ity d
oes n
ot m
eet m
inim
um d
aily
dem
and;
Ave
rage
= S
uppl
emen
tary
pu
mps
are
in fa
ir co
nditi
on b
ut w
ould
not
mee
t the
min
imum
dai
ly d
e-m
and
for w
ater
; Hig
h =
All
supp
lem
enta
ry p
umps
and
bac
k-up
syst
ems
are
oper
atio
nal a
nd w
ould
mee
t the
min
imum
dem
and
for w
ater
.
61. E
mer
genc
y mai
nten
ance
and
rest
orat
ion
of w
ater
supp
ly sy
stem
sSa
fety
ratin
gs: L
ow =
Doc
umen
ted
proc
edur
es a
nd m
aint
enan
ce/in
-sp
ectio
n re
cord
s do
not e
xist
; Ave
rage
= D
ocum
ente
d pr
oced
ures
exi
st,
mai
nten
ance
/insp
ectio
n re
cord
s are
up
to d
ate,
per
sonn
el h
ave
been
tr
aine
d, b
ut re
sour
ces a
re n
ot a
vaila
ble;
Hig
h =
Doc
umen
ted
proc
edur
es
exist
, mai
nten
ance
/insp
ectio
n re
cord
s are
up
to d
ate,
per
sonn
el h
ave
been
trai
ned,
and
reso
urce
s are
in p
lace
for i
mpl
emen
ting
emer
genc
y m
aint
enan
ce a
nd re
stor
atio
n.
3.3.
4 Fi
re p
rote
ctio
n sy
stem
62. C
ondi
tion
and
safe
ty o
f the
fire
pro
tect
ion
(pas
sive)
syst
emSa
fety
ratin
gs: L
ow =
Ele
men
t(s) a
re su
bjec
t to
dam
age,
and
dam
age
wou
ld im
pede
the
func
tion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or
oper
atio
ns; A
vera
ge =
Ele
men
t(s) a
re su
bjec
t to
dam
age
but d
amag
e w
ould
not
impe
de fu
nctio
n; H
igh
= N
o or
min
or p
oten
tial f
or d
amag
e th
at w
ould
impe
de th
e fu
nctio
n of
this
and
othe
r ele
men
ts, s
yste
ms o
r op
erat
ions
.
63. F
ire/s
mok
e de
tect
ion
syst
ems
Safe
ty ra
tings
: Low
= N
o sy
stem
has
bee
n in
stal
led;
Ave
rage
= S
yste
m is
pa
rtia
lly in
stal
led,
or i
nfre
quen
tly m
aint
aine
d an
d te
sted
; Hig
h =
Sys
tem
is
inst
alle
d an
d w
ell-m
aint
aine
d an
d te
sted
freq
uent
ly.
64. F
ire su
ppre
ssio
n sy
stem
s (au
tom
atic
and
man
ual)
Safe
ty ra
tings
: Low
= N
o sy
stem
has
bee
n in
stal
led;
insp
ectio
ns d
o no
t oc
cur;
Aver
age
= S
yste
m is
par
tially
inst
alle
d, o
r sys
tem
is in
stal
led,
but
no
mai
nten
ance
or t
estin
g; in
spec
tions
are
inco
mpl
ete
or o
utda
ted;
Hig
h =
Sy
stem
is fu
lly in
stal
led
and
regu
larly
mai
ntai
ned
and
test
ed fr
eque
ntly
; in
spec
tions
are
com
plet
e an
d up
to d
ate.
65. W
ater
supp
ly fo
r fire
supp
ress
ion
Safe
ty ra
tings
: Low
= A
sour
ce o
f per
man
ent s
uppl
y w
hich
cou
ld b
e us
ed
for fi
re su
ppre
ssio
n do
es n
ot e
xist
; Ave
rage
= A
sour
ce o
f per
man
ent
supp
ly o
f wat
er is
ava
ilabl
e fo
r fire
supp
ress
ion;
ther
e is
limite
d ca
paci
ty
avai
labl
e, a
nd n
o m
aint
enan
ce a
nd te
stin
g ha
s bee
n co
nduc
ted;
Hig
h =
A
sour
ce o
f per
man
ent w
ater
supp
ly w
ith si
gnifi
cant
cap
acity
for fi
re su
p-pr
essio
n is
avai
labl
e, re
gula
rly m
aint
aine
d an
d fre
quen
tly te
sted
.
66. E
mer
genc
y mai
nten
ance
and
rest
orat
ion
of th
e fir
e pr
otec
tion
syst
emSa
fety
ratin
gs: L
ow =
Doc
umen
ted
proc
edur
es a
nd m
aint
enan
ce/in
-sp
ectio
n re
cord
s do
not e
xist
; Ave
rage
= D
ocum
ente
d pr
oced
ures
exi
st,
mai
nten
ance
/insp
ectio
n re
cord
s are
up
to d
ate,
per
sonn
el h
ave
been
tr
aine
d, b
ut re
sour
ces a
re n
ot a
vaila
ble;
Hig
h =
Doc
umen
ted
proc
edur
es
exist
, mai
nten
ance
/insp
ectio
n re
cord
s are
up
to d
ate,
per
sonn
el h
ave
been
trai
ned,
and
reso
urce
s are
in p
lace
for i
mpl
emen
ting
emer
genc
y m
aint
enan
ce a
nd re
stor
atio
n.
Con
tinue
>>
Mod
ule
3: N
onst
ruct
ural
safe
ty

71
Hos
pita
l Saf
ety
Inde
x G
UID
E FO
R EV
ALU
ATO
RS
162
(Con
tinue
d) 3
.3 C
ritic
al s
yste
ms
Safe
ty le
vel
Obs
erva
tions
(e
valu
ator
s’ co
mm
ents
)Low
Average
High
59. A
ltern
ate
wat
er su
pply
to th
e re
gula
r wat
er su
pply
Safe
ty ra
tings
: Low
= P
rovi
des l
ess t
han
30%
of d
aily
dem
and
in a
n em
er-
genc
y or
disa
ster
scen
ario
; Ave
rage
= P
rovi
des 3
0−80
% o
f dai
ly d
eman
d in
an
emer
genc
y or
disa
ster
scen
ario
; Hig
h =
Pro
vide
s mor
e th
an 8
0% o
f da
ily d
eman
d in
an
emer
genc
y or
disa
ster
scen
ario
.
60. S
uppl
emen
tary
pum
ping
syst
emSa
fety
ratin
gs: L
ow =
The
re is
no
back
-up
pum
p an
d op
erat
iona
l cap
ac-
ity d
oes n
ot m
eet m
inim
um d
aily
dem
and;
Ave
rage
= S
uppl
emen
tary
pu
mps
are
in fa
ir co
nditi
on b
ut w
ould
not
mee
t the
min
imum
dai
ly d
e-m
and
for w
ater
; Hig
h =
All
supp
lem
enta
ry p
umps
and
bac
k-up
syst
ems
are
oper
atio
nal a
nd w
ould
mee
t the
min
imum
dem
and
for w
ater
.
61. E
mer
genc
y mai
nten
ance
and
rest
orat
ion
of w
ater
supp
ly sy
stem
sSa
fety
ratin
gs: L
ow =
Doc
umen
ted
proc
edur
es a
nd m
aint
enan
ce/in
-sp
ectio
n re
cord
s do
not e
xist
; Ave
rage
= D
ocum
ente
d pr
oced
ures
exi
st,
mai
nten
ance
/insp
ectio
n re
cord
s are
up
to d
ate,
per
sonn
el h
ave
been
tr
aine
d, b
ut re
sour
ces a
re n
ot a
vaila
ble;
Hig
h =
Doc
umen
ted
proc
edur
es
exist
, mai
nten
ance
/insp
ectio
n re
cord
s are
up
to d
ate,
per
sonn
el h
ave
been
trai
ned,
and
reso
urce
s are
in p
lace
for i
mpl
emen
ting
emer
genc
y m
aint
enan
ce a
nd re
stor
atio
n.
3.3.
4 Fi
re p
rote
ctio
n sy
stem
62. C
ondi
tion
and
safe
ty o
f the
fire
pro
tect
ion
(pas
sive)
syst
emSa
fety
ratin
gs: L
ow =
Ele
men
t(s) a
re su
bjec
t to
dam
age,
and
dam
age
wou
ld im
pede
the
func
tion
of th
is an
d ot
her e
lem
ents
, sys
tem
s or
oper
atio
ns; A
vera
ge =
Ele
men
t(s) a
re su
bjec
t to
dam
age
but d
amag
e w
ould
not
impe
de fu
nctio
n; H
igh
= N
o or
min
or p
oten
tial f
or d
amag
e th
at w
ould
impe
de th
e fu
nctio
n of
this
and
othe
r ele
men
ts, s
yste
ms o
r op
erat
ions
.
63. F
ire/s
mok
e de
tect
ion
syst
ems
Safe
ty ra
tings
: Low
= N
o sy
stem
has
bee
n in
stal
led;
Ave
rage
= S
yste
m is
pa
rtia
lly in
stal
led,
or i
nfre
quen
tly m
aint
aine
d an
d te
sted
; Hig
h =
Sys
tem
is
inst
alle
d an
d w
ell-m
aint
aine
d an
d te
sted
freq
uent
ly.
64. F
ire su
ppre
ssio
n sy
stem
s (au
tom
atic
and
man
ual)
Safe
ty ra
tings
: Low
= N
o sy
stem
has
bee
n in
stal
led;
insp
ectio
ns d
o no
t oc
cur;
Aver
age
= S
yste
m is
par
tially
inst
alle
d, o
r sys
tem
is in
stal
led,
but
no
mai
nten
ance
or t
estin
g; in
spec
tions
are
inco
mpl
ete
or o
utda
ted;
Hig
h =
Sy
stem
is fu
lly in
stal
led
and
regu
larly
mai
ntai
ned
and
test
ed fr
eque
ntly
; in
spec
tions
are
com
plet
e an
d up
to d
ate.
65. W
ater
supp
ly fo
r fire
supp
ress
ion
Safe
ty ra
tings
: Low
= A
sour
ce o
f per
man
ent s
uppl
y w
hich
cou
ld b
e us
ed
for fi
re su
ppre
ssio
n do
es n
ot e
xist
; Ave
rage
= A
sour
ce o
f per
man
ent
supp
ly o
f wat
er is
ava
ilabl
e fo
r fire
supp
ress
ion;
ther
e is
limite
d ca
paci
ty
avai
labl
e, a
nd n
o m
aint
enan
ce a
nd te
stin
g ha
s bee
n co
nduc
ted;
Hig
h =
A
sour
ce o
f per
man
ent w
ater
supp
ly w
ith si
gnifi
cant
cap
acity
for fi
re su
p-pr
essio
n is
avai
labl
e, re
gula
rly m
aint
aine
d an
d fre
quen
tly te
sted
.
66. E
mer
genc
y mai
nten
ance
and
rest
orat
ion
of th
e fir
e pr
otec
tion
syst
emSa
fety
ratin
gs: L
ow =
Doc
umen
ted
proc
edur
es a
nd m
aint
enan
ce/in
-sp
ectio
n re
cord
s do
not e
xist
; Ave
rage
= D
ocum
ente
d pr
oced
ures
exi
st,
mai
nten
ance
/insp
ectio
n re
cord
s are
up
to d
ate,
per
sonn
el h
ave
been
tr
aine
d, b
ut re
sour
ces a
re n
ot a
vaila
ble;
Hig
h =
Doc
umen
ted
proc
edur
es
exist
, mai
nten
ance
/insp
ectio
n re
cord
s are
up
to d
ate,
per
sonn
el h
ave
been
trai
ned,
and
reso
urce
s are
in p
lace
for i
mpl
emen
ting
emer
genc
y m
aint
enan
ce a
nd re
stor
atio
n.
Con
tinue
>>
Mod
ule
3: N
onst
ruct
ural
safe
ty

72
163
(Con
tinue
d) 3
.3 C
ritic
al s
yste
ms
Safe
ty le
vel
Obs
erva
tions
(e
valu
ator
s’ co
mm
ents
)Low
Average
High
3.3.
5 W
aste
man
agem
ent s
yste
ms
67. S
afet
y of n
onha
zard
ous w
aste
wat
er sy
stem
sSa
fety
ratin
gs: L
ow =
Sys
tem
for n
onha
zard
ous w
aste
wat
er d
ispos
al d
oes
not e
xist
or i
s in
poor
con
ditio
n; A
vera
ge =
Sys
tem
is in
fair
cond
ition
, but
lit
tle o
r no
evid
ence
of c
ompl
ianc
e an
d m
aint
enan
ce; H
igh
= W
aste
wat
er
disp
osal
syst
em is
in g
ood
cond
ition
with
goo
d ca
paci
ty a
nd e
vide
nce
of
com
plia
nce
and
mai
nten
ance
.
68. S
afet
y of h
azar
dous
was
tew
ater
and
liqui
d w
aste
Safe
ty ra
tings
: Low
= S
yste
m fo
r haz
ardo
us w
aste
wat
er d
ispos
al d
oes n
ot
exist
or i
s in
poor
con
ditio
n; A
vera
ge =
Sys
tem
is in
fair
cond
ition
but
litt
le
or n
o ev
iden
ce o
f com
plia
nce
and
mai
nten
ance
; Hig
h =
Disp
osal
syst
em
has g
ood
capa
city
and
evi
denc
e of
com
plia
nce
and
mai
nten
ance
.
69. S
afet
y of n
onha
zard
ous s
olid
was
te sy
stem
Safe
ty ra
tings
: Low
= S
yste
m fo
r sol
id w
aste
disp
osal
doe
s not
exi
st o
r is
in p
oor c
ondi
tion;
Ave
rage
= S
yste
m is
in fa
ir co
nditi
on, b
ut li
ttle
or n
o ev
iden
ce o
f com
plia
nce
and
mai
nten
ance
; Hig
h =
Disp
osal
syst
em is
in
good
con
ditio
n w
ith g
ood
capa
city
and
evi
denc
e of
com
plia
nce
and
mai
nten
ance
.
70. S
afet
y of h
azar
dous
solid
was
te sy
stem
Safe
ty ra
tings
: Low
= S
yste
m fo
r haz
ardo
us w
aste
disp
osal
doe
s not
exi
st
or is
in p
oor c
ondi
tion;
Ave
rage
= S
yste
m is
in fa
ir co
nditi
on b
ut li
ttle
or
no e
vide
nce
of c
ompl
ianc
e an
d m
aint
enan
ce; H
igh
= D
ispos
al sy
stem
is
in g
ood
cond
ition
with
goo
d ca
paci
ty a
nd e
vide
nce
of c
ompl
ianc
e an
d m
aint
enan
ce.
71. E
mer
genc
y mai
nten
ance
and
rest
orat
ion
of al
l typ
es o
f hos
pita
l w
aste
man
agem
ent s
yste
ms
Safe
ty ra
tings
: Low
= D
ocum
ente
d pr
oced
ures
and
mai
nten
ance
/in-
spec
tion
reco
rds d
o no
t exi
st; A
vera
ge =
Doc
umen
ted
proc
edur
es e
xist
, m
aint
enan
ce/in
spec
tion
reco
rds a
re u
p to
dat
e, p
erso
nnel
hav
e be
en
trai
ned,
but
reso
urce
s are
not
ava
ilabl
e; H
igh
= D
ocum
ente
d pr
oced
ures
ex
ist, m
aint
enan
ce/in
spec
tion
reco
rds a
re u
p to
dat
e, p
erso
nnel
hav
e be
en tr
aine
d, a
nd re
sour
ces a
re in
pla
ce fo
r im
plem
entin
g em
erge
ncy
mai
nten
ance
and
rest
orat
ion.
3.3.
6 Fu
el s
tora
ge s
yste
ms
(e.g
. gas
, gas
olin
e an
d di
esel
)72
. Fue
l res
erve
sSa
fety
ratin
gs: L
ow =
Suffi
cien
t for
24
hour
s or l
ess,
or fu
el ta
nk d
oes n
ot
exist
; Ave
rage
= S
uffici
ent f
or m
ore
than
24
hour
s but
less
than
72
hour
s; H
igh
= G
uara
ntee
d to
cov
er a
t lea
st 7
2 ho
urs.
73. C
ondi
tion
and
safe
ty o
f abo
ve-g
roun
d fu
el ta
nks a
nd/o
r cyl
inde
rsSa
fety
ratin
gs: L
ow =
Tank
s are
in p
oor c
ondi
tion;
ther
e ar
e no
anc
hors
or
tank
enc
losu
re; t
anks
are
not
safe
ly lo
cate
d w
ith re
spec
t to
haza
rds;
Aver
age
= Ta
nks a
re in
fair
cond
ition
, anc
hors
and
bra
cing
are
inad
equa
te fo
r maj
or
haza
rds;
tank
enc
losu
re h
as so
me
safe
ty a
nd se
curit
y m
easu
res;
Hig
h =
Ta
nks a
re in
goo
d co
nditi
on; a
ncho
rs a
nd b
raci
ng a
re in
goo
d co
nditi
on fo
r m
ajor
haz
ards
; the
tank
enc
losu
re h
as a
dequ
ate
safe
ty a
nd se
curit
y.
IF T
HE
HO
SPIT
AL D
OES
NO
T H
AVE
THES
E SE
RVIC
ES, L
EAVE
BO
XES
BLAN
K AN
D P
ROVI
DE
COM
MEN
T.
74. S
afe
loca
tion
of fu
el st
orag
e aw
ay fr
om h
ospi
tal b
uild
ings
Safe
ty ra
tings
: Low
= F
uel s
tora
ge is
not
acc
essib
le a
nd is
not
loca
ted
in a
secu
re si
te; A
vera
ge =
Site
in fa
ir co
nditi
on a
nd in
fair
loca
tion
in
rela
tion
to h
azar
ds; s
ome
mea
sure
s pro
vide
par
tial p
rote
ctio
n; H
igh
= In
go
od c
ondi
tion
and
good
loca
tion,
wel
l-sec
ured
and
oth
er p
rote
ctio
n m
easu
res i
n pl
ace;
fuel
tank
s are
acc
essib
le.
IF T
HER
E IS
NO
FU
EL TA
NK,
LEA
VE B
OXE
S BL
ANK
AND
PRO
VID
E CO
MM
ENT.
Con
tinue
>>
ANN
EX 2
: FO
RM 2
: SAF
E H
OSP
ITAL
S CH
ECKL
IST
Mod
ule
3: N
onst
ruct
ural
safe
ty

73
163
(Con
tinue
d) 3
.3 C
ritic
al s
yste
ms
Safe
ty le
vel
Obs
erva
tions
(e
valu
ator
s’ co
mm
ents
)Low
Average
High
3.3.
5 W
aste
man
agem
ent s
yste
ms
67. S
afet
y of n
onha
zard
ous w
aste
wat
er sy
stem
sSa
fety
ratin
gs: L
ow =
Sys
tem
for n
onha
zard
ous w
aste
wat
er d
ispos
al d
oes
not e
xist
or i
s in
poor
con
ditio
n; A
vera
ge =
Sys
tem
is in
fair
cond
ition
, but
lit
tle o
r no
evid
ence
of c
ompl
ianc
e an
d m
aint
enan
ce; H
igh
= W
aste
wat
er
disp
osal
syst
em is
in g
ood
cond
ition
with
goo
d ca
paci
ty a
nd e
vide
nce
of
com
plia
nce
and
mai
nten
ance
.
68. S
afet
y of h
azar
dous
was
tew
ater
and
liqui
d w
aste
Safe
ty ra
tings
: Low
= S
yste
m fo
r haz
ardo
us w
aste
wat
er d
ispos
al d
oes n
ot
exist
or i
s in
poor
con
ditio
n; A
vera
ge =
Sys
tem
is in
fair
cond
ition
but
litt
le
or n
o ev
iden
ce o
f com
plia
nce
and
mai
nten
ance
; Hig
h =
Disp
osal
syst
em
has g
ood
capa
city
and
evi
denc
e of
com
plia
nce
and
mai
nten
ance
.
69. S
afet
y of n
onha
zard
ous s
olid
was
te sy
stem
Safe
ty ra
tings
: Low
= S
yste
m fo
r sol
id w
aste
disp
osal
doe
s not
exi
st o
r is
in p
oor c
ondi
tion;
Ave
rage
= S
yste
m is
in fa
ir co
nditi
on, b
ut li
ttle
or n
o ev
iden
ce o
f com
plia
nce
and
mai
nten
ance
; Hig
h =
Disp
osal
syst
em is
in
good
con
ditio
n w
ith g
ood
capa
city
and
evi
denc
e of
com
plia
nce
and
mai
nten
ance
.
70. S
afet
y of h
azar
dous
solid
was
te sy
stem
Safe
ty ra
tings
: Low
= S
yste
m fo
r haz
ardo
us w
aste
disp
osal
doe
s not
exi
st
or is
in p
oor c
ondi
tion;
Ave
rage
= S
yste
m is
in fa
ir co
nditi
on b
ut li
ttle
or
no e
vide
nce
of c
ompl
ianc
e an
d m
aint
enan
ce; H
igh
= D
ispos
al sy
stem
is
in g
ood
cond
ition
with
goo
d ca
paci
ty a
nd e
vide
nce
of c
ompl
ianc
e an
d m
aint
enan
ce.
71. E
mer
genc
y mai
nten
ance
and
rest
orat
ion
of al
l typ
es o
f hos
pita
l w
aste
man
agem
ent s
yste
ms
Safe
ty ra
tings
: Low
= D
ocum
ente
d pr
oced
ures
and
mai
nten
ance
/in-
spec
tion
reco
rds d
o no
t exi
st; A
vera
ge =
Doc
umen
ted
proc
edur
es e
xist
, m
aint
enan
ce/in
spec
tion
reco
rds a
re u
p to
dat
e, p
erso
nnel
hav
e be
en
trai
ned,
but
reso
urce
s are
not
ava
ilabl
e; H
igh
= D
ocum
ente
d pr
oced
ures
ex
ist, m
aint
enan
ce/in
spec
tion
reco
rds a
re u
p to
dat
e, p
erso
nnel
hav
e be
en tr
aine
d, a
nd re
sour
ces a
re in
pla
ce fo
r im
plem
entin
g em
erge
ncy
mai
nten
ance
and
rest
orat
ion.
3.3.
6 Fu
el s
tora
ge s
yste
ms
(e.g
. gas
, gas
olin
e an
d di
esel
)72
. Fue
l res
erve
sSa
fety
ratin
gs: L
ow =
Suffi
cien
t for
24
hour
s or l
ess,
or fu
el ta
nk d
oes n
ot
exist
; Ave
rage
= S
uffici
ent f
or m
ore
than
24
hour
s but
less
than
72
hour
s; H
igh
= G
uara
ntee
d to
cov
er a
t lea
st 7
2 ho
urs.
73. C
ondi
tion
and
safe
ty o
f abo
ve-g
roun
d fu
el ta
nks a
nd/o
r cyl
inde
rsSa
fety
ratin
gs: L
ow =
Tank
s are
in p
oor c
ondi
tion;
ther
e ar
e no
anc
hors
or
tank
enc
losu
re; t
anks
are
not
safe
ly lo
cate
d w
ith re
spec
t to
haza
rds;
Aver
age
= Ta
nks a
re in
fair
cond
ition
, anc
hors
and
bra
cing
are
inad
equa
te fo
r maj
or
haza
rds;
tank
enc
losu
re h
as so
me
safe
ty a
nd se
curit
y m
easu
res;
Hig
h =
Ta
nks a
re in
goo
d co
nditi
on; a
ncho
rs a
nd b
raci
ng a
re in
goo
d co
nditi
on fo
r m
ajor
haz
ards
; the
tank
enc
losu
re h
as a
dequ
ate
safe
ty a
nd se
curit
y.
IF T
HE
HO
SPIT
AL D
OES
NO
T H
AVE
THES
E SE
RVIC
ES, L
EAVE
BO
XES
BLAN
K AN
D P
ROVI
DE
COM
MEN
T.
74. S
afe
loca
tion
of fu
el st
orag
e aw
ay fr
om h
ospi
tal b
uild
ings
Safe
ty ra
tings
: Low
= F
uel s
tora
ge is
not
acc
essib
le a
nd is
not
loca
ted
in a
secu
re si
te; A
vera
ge =
Site
in fa
ir co
nditi
on a
nd in
fair
loca
tion
in
rela
tion
to h
azar
ds; s
ome
mea
sure
s pro
vide
par
tial p
rote
ctio
n; H
igh
= In
go
od c
ondi
tion
and
good
loca
tion,
wel
l-sec
ured
and
oth
er p
rote
ctio
n m
easu
res i
n pl
ace;
fuel
tank
s are
acc
essib
le.
IF T
HER
E IS
NO
FU
EL TA
NK,
LEA
VE B
OXE
S BL
ANK
AND
PRO
VID
E CO
MM
ENT.
Con
tinue
>>
ANN
EX 2
: FO
RM 2
: SAF
E H
OSP
ITAL
S CH
ECKL
IST
Mod
ule
3: N
onst
ruct
ural
safe
ty

74
Hos
pita
l Saf
ety
Inde
x G
UID
E FO
R EV
ALU
ATO
RS
164
(Con
tinue
d) 3
.3 C
ritic
al s
yste
ms
Safe
ty le
vel
Obs
erva
tions
(e
valu
ator
s’ co
mm
ents
)Low
Average
High
75. C
ondi
tion
and
safe
ty o
f the
fuel
dist
ribut
ion
syst
em (v
alve
s, ho
ses,
conn
ectio
ns)
Safe
ty ra
tings
: Low
= L
ess t
han
60%
of t
he sy
stem
is in
safe
ope
ratio
nal c
ondi
-tio
n; A
vera
ge =
bet
wee
n 60
% a
nd 9
0% o
f the
syst
em is
in g
ood
oper
atio
nal
cond
ition
and
has
aut
omat
ic sh
ut-o
ff va
lves
; Hig
h =
Mor
e th
an 9
0% o
f the
sy
stem
is in
goo
d op
erat
iona
l con
ditio
n an
d ha
s aut
omat
ic sh
ut-o
ff va
lves
.
IF T
HER
E IS
NO
FU
EL D
ISTR
IBU
TIO
N TA
NK,
LEA
VE B
OXE
S BL
ANK
AND
PR
OVI
DE
COM
MEN
T.
76. E
mer
genc
y mai
nten
ance
and
rest
orat
ion
of fu
el re
serv
esSa
fety
ratin
gs: L
ow =
Doc
umen
ted
proc
edur
es a
nd m
aint
enan
ce/in
-sp
ectio
n re
cord
s do
not e
xist
; Ave
rage
= D
ocum
ente
d pr
oced
ures
exi
st,
mai
nten
ance
/insp
ectio
n re
cord
s are
up
to d
ate,
per
sonn
el h
ave
been
tr
aine
d, b
ut re
sour
ces a
re n
ot a
vaila
ble;
Hig
h =
Doc
umen
ted
proc
edur
es
exist
, mai
nten
ance
/insp
ectio
n re
cord
s are
up
to d
ate,
per
sonn
el h
ave
been
trai
ned,
and
reso
urce
s are
in p
lace
for i
mpl
emen
ting
emer
genc
y m
aint
enan
ce a
nd re
stor
atio
n.
3.3.
7 M
edic
al g
ases
sys
tem
s77
. Loc
atio
n of
stor
age
area
s for
med
ical g
ases
Safe
ty ra
tings
: Low
= N
o sit
es re
serv
ed fo
r med
ical
gas
es, o
r site
s for
med
i-ca
l gas
es a
re a
t hig
h ris
k of
failu
re d
ue to
haz
ards
; the
re a
re n
o pr
otec
tive
mea
sure
s, an
d st
orag
e is
not a
cces
sible
; Ave
rage
= R
eser
ved
area
s in
fair
cond
ition
and
fair
loca
tion;
som
e m
easu
res p
rovi
de p
artia
l pro
tect
ion;
H
igh
= In
goo
d co
nditi
on, w
ell-s
ecur
ed a
nd o
ther
pro
tect
ive
mea
sure
s in
plac
e; st
orag
e is
acce
ssib
le.
78. S
afet
y of s
tora
ge ar
eas f
or m
edica
l gas
tank
s and
/or c
ylin
ders
Safe
ty ra
tings
: Low
= M
edic
al g
as ta
nks a
nd c
ylin
ders
in st
orag
e ar
eas
are
poor
con
ditio
n; n
o pr
otec
tion
mea
sure
s, no
t sec
ured
; per
sonn
el a
re
not t
rain
ed to
ope
rate
med
ical
gas
and
fire
ext
ingu
ishin
g eq
uipm
ent;
Aver
age
= M
edic
al g
as ta
nks a
nd c
ylin
ders
in st
orag
e ar
eas a
re in
fair
con-
ditio
n, so
me
mea
sure
s pro
vide
par
tial p
rote
ctio
n; th
e qu
ality
of a
ncho
rs
and
brac
es is
inad
equa
te; p
erso
nnel
are
trai
ned
to o
pera
te e
quip
men
t; H
igh
= G
ood
cond
ition
, wel
l-sec
ured
and
pro
tect
ed, a
ncho
rs a
re o
f goo
d qu
ality
for m
ajor
haz
ards
; med
ical
gas
and
fire
ext
ingu
ishin
g eq
uipm
ent
oper
ated
by
qual
ified
per
sonn
el.
79. C
ondi
tion
and
safe
ty o
f med
ical g
as d
istrib
utio
n sy
stem
(e.g
. val
ves,
pipe
s, co
nnec
tions
)Sa
fety
ratin
gs: L
ow =
Les
s tha
n 60
% o
f the
syst
em is
in g
ood
wor
king
co
nditi
on; A
vera
ge =
Bet
wee
n 60
% a
nd 8
0% o
f the
syst
em is
in g
ood
wor
king
con
ditio
n; H
igh
= M
ore
than
80%
of t
he sy
stem
is in
goo
d w
ork-
ing
cond
ition
.
80. C
ondi
tion
and
safe
ty o
f med
ical g
as cy
linde
rs an
d re
late
d eq
uip-
men
t in
the
hosp
ital
Safe
ty ra
tings
: Low
= M
edic
al g
as ta
nks a
nd c
ylind
ers i
n ho
spita
l are
as a
re in
po
or c
ondi
tion,
no
prot
ectiv
e m
easu
res;
not s
ecur
ed; A
vera
ge =
Med
ical
gas
ta
nks a
nd c
ylind
ers a
re in
fair
cond
ition
; the
qua
lity
of a
ncho
rs a
nd b
race
s is
inad
equa
te; s
ome
mea
sure
s pro
vide
par
tial p
rote
ctio
n; H
igh
= G
ood
cond
ition
, w
ell-s
ecur
ed a
nd p
rote
cted
; anc
hors
are
of g
ood
qual
ity fo
r maj
or h
azar
ds.
81. A
vaila
bilit
y of a
ltern
ativ
e so
urce
s of m
edica
l gas
esSa
fety
ratin
gs: L
ow =
Alte
rnat
ive
sour
ces a
re n
ot a
vaila
ble;
Ave
rage
=
Alte
rnat
ive
sour
ces i
n pl
ace
but d
eliv
ery
of su
pplie
s tak
es lo
nger
than
15
days
; Hig
h =
Suffi
cien
t alte
rnat
ive
sour
ces a
re a
vaila
ble
at sh
ort n
otic
e (le
ss th
an 1
5 da
ys).
Con
tinue
>>
Mod
ule
3: N
onst
ruct
ural
safe
ty

75
Hos
pita
l Saf
ety
Inde
x G
UID
E FO
R EV
ALU
ATO
RS
164
(Con
tinue
d) 3
.3 C
ritic
al s
yste
ms
Safe
ty le
vel
Obs
erva
tions
(e
valu
ator
s’ co
mm
ents
)Low
Average
High
75. C
ondi
tion
and
safe
ty o
f the
fuel
dist
ribut
ion
syst
em (v
alve
s, ho
ses,
conn
ectio
ns)
Safe
ty ra
tings
: Low
= L
ess t
han
60%
of t
he sy
stem
is in
safe
ope
ratio
nal c
ondi
-tio
n; A
vera
ge =
bet
wee
n 60
% a
nd 9
0% o
f the
syst
em is
in g
ood
oper
atio
nal
cond
ition
and
has
aut
omat
ic sh
ut-o
ff va
lves
; Hig
h =
Mor
e th
an 9
0% o
f the
sy
stem
is in
goo
d op
erat
iona
l con
ditio
n an
d ha
s aut
omat
ic sh
ut-o
ff va
lves
.
IF T
HER
E IS
NO
FU
EL D
ISTR
IBU
TIO
N TA
NK,
LEA
VE B
OXE
S BL
ANK
AND
PR
OVI
DE
COM
MEN
T.
76. E
mer
genc
y mai
nten
ance
and
rest
orat
ion
of fu
el re
serv
esSa
fety
ratin
gs: L
ow =
Doc
umen
ted
proc
edur
es a
nd m
aint
enan
ce/in
-sp
ectio
n re
cord
s do
not e
xist
; Ave
rage
= D
ocum
ente
d pr
oced
ures
exi
st,
mai
nten
ance
/insp
ectio
n re
cord
s are
up
to d
ate,
per
sonn
el h
ave
been
tr
aine
d, b
ut re
sour
ces a
re n
ot a
vaila
ble;
Hig
h =
Doc
umen
ted
proc
edur
es
exist
, mai
nten
ance
/insp
ectio
n re
cord
s are
up
to d
ate,
per
sonn
el h
ave
been
trai
ned,
and
reso
urce
s are
in p
lace
for i
mpl
emen
ting
emer
genc
y m
aint
enan
ce a
nd re
stor
atio
n.
3.3.
7 M
edic
al g
ases
sys
tem
s77
. Loc
atio
n of
stor
age
area
s for
med
ical g
ases
Safe
ty ra
tings
: Low
= N
o sit
es re
serv
ed fo
r med
ical
gas
es, o
r site
s for
med
i-ca
l gas
es a
re a
t hig
h ris
k of
failu
re d
ue to
haz
ards
; the
re a
re n
o pr
otec
tive
mea
sure
s, an
d st
orag
e is
not a
cces
sible
; Ave
rage
= R
eser
ved
area
s in
fair
cond
ition
and
fair
loca
tion;
som
e m
easu
res p
rovi
de p
artia
l pro
tect
ion;
H
igh
= In
goo
d co
nditi
on, w
ell-s
ecur
ed a
nd o
ther
pro
tect
ive
mea
sure
s in
plac
e; st
orag
e is
acce
ssib
le.
78. S
afet
y of s
tora
ge ar
eas f
or m
edica
l gas
tank
s and
/or c
ylin
ders
Safe
ty ra
tings
: Low
= M
edic
al g
as ta
nks a
nd c
ylin
ders
in st
orag
e ar
eas
are
poor
con
ditio
n; n
o pr
otec
tion
mea
sure
s, no
t sec
ured
; per
sonn
el a
re
not t
rain
ed to
ope
rate
med
ical
gas
and
fire
ext
ingu
ishin
g eq
uipm
ent;
Aver
age
= M
edic
al g
as ta
nks a
nd c
ylin
ders
in st
orag
e ar
eas a
re in
fair
con-
ditio
n, so
me
mea
sure
s pro
vide
par
tial p
rote
ctio
n; th
e qu
ality
of a
ncho
rs
and
brac
es is
inad
equa
te; p
erso
nnel
are
trai
ned
to o
pera
te e
quip
men
t; H
igh
= G
ood
cond
ition
, wel
l-sec
ured
and
pro
tect
ed, a
ncho
rs a
re o
f goo
d qu
ality
for m
ajor
haz
ards
; med
ical
gas
and
fire
ext
ingu
ishin
g eq
uipm
ent
oper
ated
by
qual
ified
per
sonn
el.
79. C
ondi
tion
and
safe
ty o
f med
ical g
as d
istrib
utio
n sy
stem
(e.g
. val
ves,
pipe
s, co
nnec
tions
)Sa
fety
ratin
gs: L
ow =
Les
s tha
n 60
% o
f the
syst
em is
in g
ood
wor
king
co
nditi
on; A
vera
ge =
Bet
wee
n 60
% a
nd 8
0% o
f the
syst
em is
in g
ood
wor
king
con
ditio
n; H
igh
= M
ore
than
80%
of t
he sy
stem
is in
goo
d w
ork-
ing
cond
ition
.
80. C
ondi
tion
and
safe
ty o
f med
ical g
as cy
linde
rs an
d re
late
d eq
uip-
men
t in
the
hosp
ital
Safe
ty ra
tings
: Low
= M
edic
al g
as ta
nks a
nd c
ylind
ers i
n ho
spita
l are
as a
re in
po
or c
ondi
tion,
no
prot
ectiv
e m
easu
res;
not s
ecur
ed; A
vera
ge =
Med
ical
gas
ta
nks a
nd c
ylind
ers a
re in
fair
cond
ition
; the
qua
lity
of a
ncho
rs a
nd b
race
s is
inad
equa
te; s
ome
mea
sure
s pro
vide
par
tial p
rote
ctio
n; H
igh
= G
ood
cond
ition
, w
ell-s
ecur
ed a
nd p
rote
cted
; anc
hors
are
of g
ood
qual
ity fo
r maj
or h
azar
ds.
81. A
vaila
bilit
y of a
ltern
ativ
e so
urce
s of m
edica
l gas
esSa
fety
ratin
gs: L
ow =
Alte
rnat
ive
sour
ces a
re n
ot a
vaila
ble;
Ave
rage
=
Alte
rnat
ive
sour
ces i
n pl
ace
but d
eliv
ery
of su
pplie
s tak
es lo
nger
than
15
days
; Hig
h =
Suffi
cien
t alte
rnat
ive
sour
ces a
re a
vaila
ble
at sh
ort n
otic
e (le
ss th
an 1
5 da
ys).
Con
tinue
>>
Mod
ule
3: N
onst
ruct
ural
safe
ty

76
165
(Con
tinue
d) 3
.3 C
ritic
al s
yste
ms
Safe
ty le
vel
Obs
erva
tions
(e
valu
ator
s’ co
mm
ents
)Low
Average
High
82. E
mer
genc
y mai
nten
ance
and
rest
orat
ion
of m
edica
l gas
syst
ems
Safe
ty ra
tings
: Low
= D
ocum
ente
d pr
oced
ures
and
mai
nten
ance
/in-
spec
tion
reco
rds d
o no
t exi
st; A
vera
ge =
Doc
umen
ted
proc
edur
es e
xist
, m
aint
enan
ce/in
spec
tion
reco
rds a
re u
p to
dat
e, a
nd p
erso
nnel
hav
e be
en
trai
ned,
but
reso
urce
s are
not
ava
ilabl
e; H
igh
= P
roce
dure
s exi
st, m
aint
e-na
nce/
insp
ectio
n re
cord
s are
up
to d
ate,
per
sonn
el h
ave
been
trai
ned,
an
d re
sour
ces a
re in
pla
ce fo
r im
plem
entin
g em
erge
ncy
mai
nten
ance
an
d re
stor
atio
n.
3.3.
8 H
eatin
g, v
entil
atio
n, a
nd a
ir-co
nditi
onin
g (H
VAC)
sys
tem
s83
. Ade
quat
e lo
catio
n of
enc
losu
res f
or H
VAC
equi
pmen
tSa
fety
ratin
gs: L
ow =
HVA
C en
clos
ures
are
not
acc
essib
le a
nd th
ey a
re n
ot
loca
ted
in a
safe
site
; the
re a
re n
o pr
otec
tive
mea
sure
s; Av
erag
e =
HVA
C en
clos
ures
are
acc
essib
le, l
ocat
ed a
t a sa
fe si
te; s
ome
mea
sure
s pro
vide
pa
rtia
l pro
tect
ion
from
haz
ards
; Hig
h =
HVA
C en
clos
ures
are
acc
essib
le, i
n a
safe
loca
tion
and
prot
ecte
d fro
m h
azar
ds.
84. S
afet
y of e
nclo
sure
s for
HVA
C eq
uipm
ent
Safe
ty ra
tings
: Low
= H
VAC
equi
pmen
t is n
ot a
cces
sible
; no
prot
ectio
n m
easu
res f
or sa
fe o
pera
tion
and
mai
nten
ance
; Ave
rage
= H
VAC
is ac
ces-
sible
; som
e m
easu
res p
rovi
de p
artia
l pro
tect
ion;
Hig
h =
HVA
C eq
uipm
ent
is ac
cess
ible
, wid
e ra
nge
of p
rote
ctio
n m
easu
res i
n pl
ace.
85. S
afet
y and
ope
ratin
g co
nditi
on o
f HVA
C eq
uipm
ent (
e.g.
boi
ler,
exha
ust)
Safe
ty ra
tings
: Low
= H
VAC
equi
pmen
t in
poor
con
ditio
n, n
ot m
aint
aine
d;
Aver
age
= H
VAC
equi
pmen
t in
fair
cond
ition
; som
e m
easu
res p
rovi
de
part
ial p
rote
ctio
n, b
ut n
o re
gula
r mai
nten
ance
; Hig
h =
Goo
d co
nditi
on,
wel
l-sec
ured
and
pro
tect
ed fr
om h
azar
ds (e
.g. a
ncho
rs a
re o
f goo
d qu
al-
ity);
regu
lar m
aint
enan
ce a
nd te
stin
g of
con
trol
s and
ala
rms c
ondu
cted
.
86. A
dequ
ate
supp
orts
for d
ucts
and
revi
ew o
f flex
ibili
ty o
f duc
ts an
d pi
ping
that
cros
s exp
ansio
n jo
ints
Safe
ty ra
tings
: Low
= S
uppo
rts a
re la
ckin
g an
d co
nnec
tions
are
rigi
d;
Aver
age
= S
uppo
rts a
re in
fair
cond
ition
or c
onne
ctio
ns a
re fl
exib
le; H
igh
= S
uppo
rts a
re in
goo
d co
nditi
on a
nd c
onne
ctio
ns a
re fl
exib
le.
87. C
ondi
tion
and
safe
ty o
f pip
es, c
onne
ctio
ns an
d va
lves
Safe
ty ra
tings
: Low
= Le
ss th
an 6
0% o
f pip
es a
re in
goo
d co
nditi
on; li
mite
d pr
otec
tive
mea
sure
s aga
inst
haz
ards
; Ave
rage
= B
etw
een
60%
and
80%
are
in
good
cond
ition
; som
e m
easu
res p
rovi
de p
artia
l pro
tect
ion
agai
nst h
azar
ds;
Hig
h =
Abo
ve 8
0% a
re in
goo
d co
nditi
on a
nd a
re w
ell-s
ecur
ed a
nd p
rote
cted
ag
ains
t haz
ards
.
88. C
ondi
tion
and
safe
ty o
f air-
cond
ition
ing
equi
pmen
tSa
fety
ratin
gs: L
ow =
Air-
cond
ition
ing
units
in p
oor c
ondi
tion,
not
se
cure
d; A
vera
ge =
Air-
cond
ition
ing
units
are
in fa
ir co
nditi
on; s
ome
mea
sure
s pro
vide
par
tial p
rote
ctio
n (e
.g. q
ualit
y of
anc
hors
and
bra
ces i
s in
adeq
uate
); H
igh
= G
ood
cond
ition
, wel
l-sec
ured
and
pro
tect
ed fr
om
haza
rds (
e.g.
anc
hors
are
of g
ood
qual
ity).
89. O
pera
tion
of ai
r-con
ditio
ning
syste
m (in
cludi
ng n
egat
ive p
ress
ure a
reas
)Sa
fety
ratin
gs: L
ow =
Air-
cond
ition
ing
syst
em h
as n
o ca
pabi
lity
for e
stab
-lis
hing
zon
es o
f the
hos
pita
l; Ave
rage
= A
ir-co
nditi
onin
g sy
stem
can
est
ab-
lish
zone
s, bu
t has
no
capa
city
to se
para
te a
ir ci
rcul
atin
g be
twee
n hi
gh-ri
sk
area
s and
oth
er a
reas
of t
he h
ospi
tal; H
igh
= Ai
r-con
ditio
ning
syst
em c
an
isola
te a
ir fro
m h
igh-
risk
area
s; ne
gativ
e pr
essu
re ro
oms a
re a
vaila
ble.
Con
tinue
>>
ANN
EX 2
: FO
RM 2
: SAF
E H
OSP
ITAL
S CH
ECKL
IST
Mod
ule
3: N
onst
ruct
ural
safe
ty

77
165
(Con
tinue
d) 3
.3 C
ritic
al s
yste
ms
Safe
ty le
vel
Obs
erva
tions
(e
valu
ator
s’ co
mm
ents
)Low
Average
High
82. E
mer
genc
y mai
nten
ance
and
rest
orat
ion
of m
edica
l gas
syst
ems
Safe
ty ra
tings
: Low
= D
ocum
ente
d pr
oced
ures
and
mai
nten
ance
/in-
spec
tion
reco
rds d
o no
t exi
st; A
vera
ge =
Doc
umen
ted
proc
edur
es e
xist
, m
aint
enan
ce/in
spec
tion
reco
rds a
re u
p to
dat
e, a
nd p
erso
nnel
hav
e be
en
trai
ned,
but
reso
urce
s are
not
ava
ilabl
e; H
igh
= P
roce
dure
s exi
st, m
aint
e-na
nce/
insp
ectio
n re
cord
s are
up
to d
ate,
per
sonn
el h
ave
been
trai
ned,
an
d re
sour
ces a
re in
pla
ce fo
r im
plem
entin
g em
erge
ncy
mai
nten
ance
an
d re
stor
atio
n.
3.3.
8 H
eatin
g, v
entil
atio
n, a
nd a
ir-co
nditi
onin
g (H
VAC)
sys
tem
s83
. Ade
quat
e lo
catio
n of
enc
losu
res f
or H
VAC
equi
pmen
tSa
fety
ratin
gs: L
ow =
HVA
C en
clos
ures
are
not
acc
essib
le a
nd th
ey a
re n
ot
loca
ted
in a
safe
site
; the
re a
re n
o pr
otec
tive
mea
sure
s; Av
erag
e =
HVA
C en
clos
ures
are
acc
essib
le, l
ocat
ed a
t a sa
fe si
te; s
ome
mea
sure
s pro
vide
pa
rtia
l pro
tect
ion
from
haz
ards
; Hig
h =
HVA
C en
clos
ures
are
acc
essib
le, i
n a
safe
loca
tion
and
prot
ecte
d fro
m h
azar
ds.
84. S
afet
y of e
nclo
sure
s for
HVA
C eq
uipm
ent
Safe
ty ra
tings
: Low
= H
VAC
equi
pmen
t is n
ot a
cces
sible
; no
prot
ectio
n m
easu
res f
or sa
fe o
pera
tion
and
mai
nten
ance
; Ave
rage
= H
VAC
is ac
ces-
sible
; som
e m
easu
res p
rovi
de p
artia
l pro
tect
ion;
Hig
h =
HVA
C eq
uipm
ent
is ac
cess
ible
, wid
e ra
nge
of p
rote
ctio
n m
easu
res i
n pl
ace.
85. S
afet
y and
ope
ratin
g co
nditi
on o
f HVA
C eq
uipm
ent (
e.g.
boi
ler,
exha
ust)
Safe
ty ra
tings
: Low
= H
VAC
equi
pmen
t in
poor
con
ditio
n, n
ot m
aint
aine
d;
Aver
age
= H
VAC
equi
pmen
t in
fair
cond
ition
; som
e m
easu
res p
rovi
de
part
ial p
rote
ctio
n, b
ut n
o re
gula
r mai
nten
ance
; Hig
h =
Goo
d co
nditi
on,
wel
l-sec
ured
and
pro
tect
ed fr
om h
azar
ds (e
.g. a
ncho
rs a
re o
f goo
d qu
al-
ity);
regu
lar m
aint
enan
ce a
nd te
stin
g of
con
trol
s and
ala
rms c
ondu
cted
.
86. A
dequ
ate
supp
orts
for d
ucts
and
revi
ew o
f flex
ibili
ty o
f duc
ts an
d pi
ping
that
cros
s exp
ansio
n jo
ints
Safe
ty ra
tings
: Low
= S
uppo
rts a
re la
ckin
g an
d co
nnec
tions
are
rigi
d;
Aver
age
= S
uppo
rts a
re in
fair
cond
ition
or c
onne
ctio
ns a
re fl
exib
le; H
igh
= S
uppo
rts a
re in
goo
d co
nditi
on a
nd c
onne
ctio
ns a
re fl
exib
le.
87. C
ondi
tion
and
safe
ty o
f pip
es, c
onne
ctio
ns an
d va
lves
Safe
ty ra
tings
: Low
= Le
ss th
an 6
0% o
f pip
es a
re in
goo
d co
nditi
on; li
mite
d pr
otec
tive
mea
sure
s aga
inst
haz
ards
; Ave
rage
= B
etw
een
60%
and
80%
are
in
good
cond
ition
; som
e m
easu
res p
rovi
de p
artia
l pro
tect
ion
agai
nst h
azar
ds;
Hig
h =
Abo
ve 8
0% a
re in
goo
d co
nditi
on a
nd a
re w
ell-s
ecur
ed a
nd p
rote
cted
ag
ains
t haz
ards
.
88. C
ondi
tion
and
safe
ty o
f air-
cond
ition
ing
equi
pmen
tSa
fety
ratin
gs: L
ow =
Air-
cond
ition
ing
units
in p
oor c
ondi
tion,
not
se
cure
d; A
vera
ge =
Air-
cond
ition
ing
units
are
in fa
ir co
nditi
on; s
ome
mea
sure
s pro
vide
par
tial p
rote
ctio
n (e
.g. q
ualit
y of
anc
hors
and
bra
ces i
s in
adeq
uate
); H
igh
= G
ood
cond
ition
, wel
l-sec
ured
and
pro
tect
ed fr
om
haza
rds (
e.g.
anc
hors
are
of g
ood
qual
ity).
89. O
pera
tion
of ai
r-con
ditio
ning
syste
m (in
cludi
ng n
egat
ive p
ress
ure a
reas
)Sa
fety
ratin
gs: L
ow =
Air-
cond
ition
ing
syst
em h
as n
o ca
pabi
lity
for e
stab
-lis
hing
zon
es o
f the
hos
pita
l; Ave
rage
= A
ir-co
nditi
onin
g sy
stem
can
est
ab-
lish
zone
s, bu
t has
no
capa
city
to se
para
te a
ir ci
rcul
atin
g be
twee
n hi
gh-ri
sk
area
s and
oth
er a
reas
of t
he h
ospi
tal; H
igh
= Ai
r-con
ditio
ning
syst
em c
an
isola
te a
ir fro
m h
igh-
risk
area
s; ne
gativ
e pr
essu
re ro
oms a
re a
vaila
ble.
Con
tinue
>>
ANN
EX 2
: FO
RM 2
: SAF
E H
OSP
ITAL
S CH
ECKL
IST
Mod
ule
3: N
onst
ruct
ural
safe
ty

78
Hos
pita
l Saf
ety
Inde
x G
UID
E FO
R EV
ALU
ATO
RS
166
(Con
tinue
d) 3
.3 C
ritic
al s
yste
ms
Safe
ty le
vel
Obs
erva
tions
(e
valu
ator
s’ co
mm
ents
)Low
Average
High
90. E
mer
genc
y mai
nten
ance
and
rest
orat
ion
of H
VAC
syst
ems
Safe
ty ra
tings
: Low
= D
ocum
ente
d pr
oced
ures
and
mai
nten
ance
/in-
spec
tion
reco
rds d
o no
t exi
st; A
vera
ge =
Doc
umen
ted
proc
edur
es e
xist
, m
aint
enan
ce/in
spec
tion
reco
rds a
re u
p to
dat
e, p
erso
nnel
hav
e be
en
trai
ned,
but
reso
urce
s are
not
ava
ilabl
e; H
igh
= D
ocum
ente
d pr
oced
ures
ex
ist, m
aint
enan
ce/in
spec
tion
reco
rds a
re u
p to
dat
e, p
erso
nnel
hav
e be
en tr
aine
d, a
nd re
sour
ces a
re in
pla
ce fo
r im
plem
entin
g em
erge
ncy
mai
nten
ance
and
rest
orat
ion.
3.4
Equi
pmen
t and
sup
plie
sSa
fety
leve
lO
bser
vatio
ns
(eva
luat
ors’
com
men
ts)
Low
Average
High
3.4.
1 O
ffice
and
sto
rero
om fu
rnis
hing
s an
d eq
uipm
ent (
fixed
and
mov
able
)91
. Saf
ety o
f she
lvin
g an
d sh
elf c
onte
nts
Safe
ty ra
tings
: Low
= S
helv
ing
is no
t saf
ely
loca
ted
(or i
n se
ismic
and
w
ind-
pron
e ar
eas n
ot a
ttac
hed
to w
alls
in m
ore
than
20%
of c
ases
); Av
erag
e =
She
lvin
g is
safe
ly lo
cate
d (a
nd a
ttac
hed
to w
alls
in se
ismic
and
w
ind-
pron
e ar
eas)
and
con
tent
s are
secu
red
in 2
0−80
% o
f cas
es; H
igh
=
Mor
e th
an 8
0% o
f she
lvin
g an
d th
e co
nten
ts o
f she
lves
are
safe
ly lo
cate
d,
atta
ched
to w
alls,
and
con
tent
s are
secu
red.
92. S
afet
y of c
ompu
ters
and
prin
ters
Safe
ty ra
tings
: Low
= N
o m
easu
res t
o pr
otec
t com
pute
rs fr
om h
azar
ds a
re
in p
lace
; Ave
rage
=Co
mpu
ters
are
in sa
fe lo
catio
ns, s
ome
mea
sure
s offe
r pa
rtia
l pro
tect
ion
from
haz
ards
; Hig
h =
Com
pute
rs a
re in
safe
loca
tions
, w
ell-s
ecur
ed a
nd g
ood
prot
ectiv
e m
easu
res i
n pl
ace.
3.4.
2 M
edic
al a
nd la
bora
tory
equ
ipm
ent a
nd s
uppl
ies
used
for d
iagn
osis
and
trea
tmen
t93
. Saf
ety o
f med
ical e
quip
men
t in
oper
atin
g th
eatre
s and
reco
very
ro
oms
Safe
ty ra
tings
: Low
= T
he o
pera
ting
thea
tres
are
in a
n un
safe
loca
tion,
eq
uipm
ent i
s lac
king
or i
n po
or c
ondi
tion
or th
ere
are
no p
rote
ctiv
e m
ea-
sure
s; Av
erag
e =
The
ope
ratin
g th
eatr
es a
re in
a sa
fe lo
catio
n, e
quip
men
t is
in fa
ir co
nditi
on, a
nd so
me
mea
sure
s pro
vide
par
tial p
rote
ctio
n; H
igh
=
Ope
ratin
g th
eatr
es a
re in
a sa
fe lo
catio
n, e
quip
men
t is i
n go
od c
ondi
tion,
is
wel
l-sec
ured
and
mea
sure
s pro
vide
pro
tect
ion.
94. C
ondi
tion
and
safe
ty o
f rad
iolo
gy an
d im
agin
g eq
uipm
ent
Safe
ty ra
tings
: Low
= T
he ra
diol
ogy a
nd im
agin
g eq
uipm
ent i
s not
in a
safe
lo
catio
n, e
quip
men
t is l
acki
ng o
r in
poor
cond
ition
, or t
here
are
no
prot
ectiv
e m
easu
res;
Aver
age
= T
he e
quip
men
t is i
n a
safe
loca
tion,
is in
fair
cond
ition
, an
d so
me
mea
sure
s offe
r par
tial p
rote
ctio
n; H
igh
= E
quip
men
t is i
n a
safe
lo
catio
n, is
in g
ood
cond
ition
, wel
l-sec
ured
and
mea
sure
s pro
vide
goo
d pr
otec
tion.
95. C
ondi
tion
and
safe
ty o
f lab
orat
ory e
quip
men
t and
supp
lies
Safe
ty ra
tings
: Low
= B
iosa
fety
mea
sure
s are
poo
r, la
bora
tory
equ
ipm
ent
is la
ckin
g or
in p
oor c
ondi
tion,
or t
here
are
no
prot
ectiv
e m
easu
res;
Aver
-ag
e =
Bio
safe
ty m
easu
res a
re in
pla
ce, t
he e
quip
men
t is i
n fa
ir co
nditi
on,
and
som
e m
easu
res p
rovi
de p
artia
l pro
tect
ion;
Hig
h =
Bio
safe
ty m
easu
res
are
in p
lace
, equ
ipm
ent i
s in
good
con
ditio
n, w
ell-s
ecur
ed a
nd m
easu
res
prov
ide
good
pro
tect
ion.
96. C
ondi
tion
and
safe
ty o
f med
ical e
quip
men
t in
emer
genc
y car
e se
rvice
s uni
tSa
fety
ratin
gs: L
ow =
The
med
ical
equ
ipm
ent i
s lac
king
or i
n po
or c
ondi
-tio
n or
ther
e ar
e no
pro
tect
ive
mea
sure
s; Av
erag
e =
The
equ
ipm
ent i
s in
fair
cond
ition
and
som
e m
easu
res p
rovi
de p
artia
l pro
tect
ion;
Hig
h =
Equ
ipm
ent i
s in
good
con
ditio
n, w
ell-s
ecur
ed a
nd m
easu
res p
rovi
de
good
pro
tect
ion.
Con
tinue
>>
Mod
ule
3: N
onst
ruct
ural
safe
ty

79
Hos
pita
l Saf
ety
Inde
x G
UID
E FO
R EV
ALU
ATO
RS
166
(Con
tinue
d) 3
.3 C
ritic
al s
yste
ms
Safe
ty le
vel
Obs
erva
tions
(e
valu
ator
s’ co
mm
ents
)Low
Average
High
90. E
mer
genc
y mai
nten
ance
and
rest
orat
ion
of H
VAC
syst
ems
Safe
ty ra
tings
: Low
= D
ocum
ente
d pr
oced
ures
and
mai
nten
ance
/in-
spec
tion
reco
rds d
o no
t exi
st; A
vera
ge =
Doc
umen
ted
proc
edur
es e
xist
, m
aint
enan
ce/in
spec
tion
reco
rds a
re u
p to
dat
e, p
erso
nnel
hav
e be
en
trai
ned,
but
reso
urce
s are
not
ava
ilabl
e; H
igh
= D
ocum
ente
d pr
oced
ures
ex
ist, m
aint
enan
ce/in
spec
tion
reco
rds a
re u
p to
dat
e, p
erso
nnel
hav
e be
en tr
aine
d, a
nd re
sour
ces a
re in
pla
ce fo
r im
plem
entin
g em
erge
ncy
mai
nten
ance
and
rest
orat
ion.
3.4
Equi
pmen
t and
sup
plie
sSa
fety
leve
lO
bser
vatio
ns
(eva
luat
ors’
com
men
ts)
Low
Average
High
3.4.
1 O
ffice
and
sto
rero
om fu
rnis
hing
s an
d eq
uipm
ent (
fixed
and
mov
able
)91
. Saf
ety o
f she
lvin
g an
d sh
elf c
onte
nts
Safe
ty ra
tings
: Low
= S
helv
ing
is no
t saf
ely
loca
ted
(or i
n se
ismic
and
w
ind-
pron
e ar
eas n
ot a
ttac
hed
to w
alls
in m
ore
than
20%
of c
ases
); Av
erag
e =
She
lvin
g is
safe
ly lo
cate
d (a
nd a
ttac
hed
to w
alls
in se
ismic
and
w
ind-
pron
e ar
eas)
and
con
tent
s are
secu
red
in 2
0−80
% o
f cas
es; H
igh
=
Mor
e th
an 8
0% o
f she
lvin
g an
d th
e co
nten
ts o
f she
lves
are
safe
ly lo
cate
d,
atta
ched
to w
alls,
and
con
tent
s are
secu
red.
92. S
afet
y of c
ompu
ters
and
prin
ters
Safe
ty ra
tings
: Low
= N
o m
easu
res t
o pr
otec
t com
pute
rs fr
om h
azar
ds a
re
in p
lace
; Ave
rage
=Co
mpu
ters
are
in sa
fe lo
catio
ns, s
ome
mea
sure
s offe
r pa
rtia
l pro
tect
ion
from
haz
ards
; Hig
h =
Com
pute
rs a
re in
safe
loca
tions
, w
ell-s
ecur
ed a
nd g
ood
prot
ectiv
e m
easu
res i
n pl
ace.
3.4.
2 M
edic
al a
nd la
bora
tory
equ
ipm
ent a
nd s
uppl
ies
used
for d
iagn
osis
and
trea
tmen
t93
. Saf
ety o
f med
ical e
quip
men
t in
oper
atin
g th
eatre
s and
reco
very
ro
oms
Safe
ty ra
tings
: Low
= T
he o
pera
ting
thea
tres
are
in a
n un
safe
loca
tion,
eq
uipm
ent i
s lac
king
or i
n po
or c
ondi
tion
or th
ere
are
no p
rote
ctiv
e m
ea-
sure
s; Av
erag
e =
The
ope
ratin
g th
eatr
es a
re in
a sa
fe lo
catio
n, e
quip
men
t is
in fa
ir co
nditi
on, a
nd so
me
mea
sure
s pro
vide
par
tial p
rote
ctio
n; H
igh
=
Ope
ratin
g th
eatr
es a
re in
a sa
fe lo
catio
n, e
quip
men
t is i
n go
od c
ondi
tion,
is
wel
l-sec
ured
and
mea
sure
s pro
vide
pro
tect
ion.
94. C
ondi
tion
and
safe
ty o
f rad
iolo
gy an
d im
agin
g eq
uipm
ent
Safe
ty ra
tings
: Low
= T
he ra
diol
ogy a
nd im
agin
g eq
uipm
ent i
s not
in a
safe
lo
catio
n, e
quip
men
t is l
acki
ng o
r in
poor
cond
ition
, or t
here
are
no
prot
ectiv
e m
easu
res;
Aver
age
= T
he e
quip
men
t is i
n a
safe
loca
tion,
is in
fair
cond
ition
, an
d so
me
mea
sure
s offe
r par
tial p
rote
ctio
n; H
igh
= E
quip
men
t is i
n a
safe
lo
catio
n, is
in g
ood
cond
ition
, wel
l-sec
ured
and
mea
sure
s pro
vide
goo
d pr
otec
tion.
95. C
ondi
tion
and
safe
ty o
f lab
orat
ory e
quip
men
t and
supp
lies
Safe
ty ra
tings
: Low
= B
iosa
fety
mea
sure
s are
poo
r, la
bora
tory
equ
ipm
ent
is la
ckin
g or
in p
oor c
ondi
tion,
or t
here
are
no
prot
ectiv
e m
easu
res;
Aver
-ag
e =
Bio
safe
ty m
easu
res a
re in
pla
ce, t
he e
quip
men
t is i
n fa
ir co
nditi
on,
and
som
e m
easu
res p
rovi
de p
artia
l pro
tect
ion;
Hig
h =
Bio
safe
ty m
easu
res
are
in p
lace
, equ
ipm
ent i
s in
good
con
ditio
n, w
ell-s
ecur
ed a
nd m
easu
res
prov
ide
good
pro
tect
ion.
96. C
ondi
tion
and
safe
ty o
f med
ical e
quip
men
t in
emer
genc
y car
e se
rvice
s uni
tSa
fety
ratin
gs: L
ow =
The
med
ical
equ
ipm
ent i
s lac
king
or i
n po
or c
ondi
-tio
n or
ther
e ar
e no
pro
tect
ive
mea
sure
s; Av
erag
e =
The
equ
ipm
ent i
s in
fair
cond
ition
and
som
e m
easu
res p
rovi
de p
artia
l pro
tect
ion;
Hig
h =
Equ
ipm
ent i
s in
good
con
ditio
n, w
ell-s
ecur
ed a
nd m
easu
res p
rovi
de
good
pro
tect
ion.
Con
tinue
>>
Mod
ule
3: N
onst
ruct
ural
safe
ty

80
167
(Con
tinue
d) 3
.4 E
quip
men
t and
sup
plie
sSa
fety
leve
lO
bser
vatio
ns
(eva
luat
ors’
com
men
ts)
Low
Average
High
97. C
ondi
tion
and
safe
ty o
f med
ical e
quip
men
t in
inte
nsiv
e or
inte
rme-
diat
e ca
re u
nit
Safe
ty ra
tings
: Low
= T
he m
edic
al e
quip
men
t is l
acki
ng o
r in
poor
con
di-
tion,
or t
here
are
no
prot
ectiv
e m
easu
res;
Aver
age
= T
he e
quip
men
t is
in fa
ir co
nditi
on a
nd so
me
mea
sure
s pro
vide
par
tial p
rote
ctio
n; H
igh
=
Equi
pmen
t is i
n go
od c
ondi
tion,
is w
ell-s
ecur
ed a
nd m
easu
res p
rovi
de
good
pro
tect
ion.
98. C
ondi
tion
and
safe
ty o
f equ
ipm
ent a
nd fu
rnish
ings
in th
e ph
arm
acy
Safe
ty ra
tings
: Low
= T
he e
quip
men
t in
the
phar
mac
y is
lack
ing
or in
poo
r co
nditi
on, o
r the
re a
re n
o pr
otec
tive
mea
sure
s; Av
erag
e =
The
equ
ipm
ent
is in
fair
cond
ition
and
som
e m
easu
res p
rovi
de p
artia
l pro
tect
ion;
Hig
h =
Equ
ipm
ent i
s in
good
con
ditio
n, is
wel
l-sec
ured
and
mea
sure
s pro
vide
go
od p
rote
ctio
n.
99. C
ondi
tion
and
safe
ty o
f equ
ipm
ent a
nd su
pplie
s in
the
ster
iliza
tion
serv
ices
Safe
ty ra
tings
: Low
= E
quip
men
t is l
acki
ng o
r in
poor
con
ditio
n, o
r the
re
are
no p
rote
ctiv
e m
easu
res;
Aver
age
= E
quip
men
t is i
n fa
ir co
nditi
on a
nd
som
e m
easu
res p
rovi
de p
artia
l pro
tect
ion;
Hig
h =
Equ
ipm
ent i
s in
good
co
nditi
on, i
s wel
l-sec
ured
and
mea
sure
s pro
vide
goo
d pr
otec
tion.
100.
Con
ditio
n an
d sa
fety
of m
edica
l equ
ipm
ent f
or o
bste
tric e
mer
gen-
cies a
nd n
eona
tal c
are
Safe
ty ra
tings
: Low
= E
quip
men
t is l
acki
ng o
r in
poor
con
ditio
n, o
r the
re
are
no p
rote
ctiv
e m
easu
res;
Aver
age
= E
quip
men
t is i
n fa
ir co
nditi
on a
nd
som
e m
easu
res p
rovi
de p
artia
l pro
tect
ion;
Hig
h =
Equ
ipm
ent i
s in
good
co
nditi
on, i
s wel
l-sec
ured
and
mea
sure
s pro
vide
goo
d pr
otec
tion.
101.
Con
ditio
n an
d sa
fety
of m
edica
l equ
ipm
ent a
nd su
pplie
s for
em
er-
genc
y car
e fo
r bur
nsSa
fety
ratin
gs: L
ow =
Equ
ipm
ent i
s lac
king
, is i
n po
or c
ondi
tion,
or t
here
ar
e no
pro
tect
ive
mea
sure
s; Av
erag
e =
Equ
ipm
ent i
s in
fair
cond
ition
and
so
me
mea
sure
s pro
vide
par
tial p
rote
ctio
n; H
igh
= E
quip
men
t is i
n go
od
cond
ition
, is w
ell-s
ecur
ed a
nd m
easu
res p
rovi
de g
ood
prot
ectio
n.
102.
Con
ditio
n an
d sa
fety
of m
edica
l equ
ipm
ent f
or n
ucle
ar m
edici
ne
and
radi
atio
n th
erap
ySa
fety
ratin
gs: L
ow =
Equ
ipm
ent i
s lac
king
, is i
n po
or c
ondi
tion,
or t
here
ar
e no
pro
tect
ive
mea
sure
s; Av
erag
e =
Equ
ipm
ent i
s in
fair
cond
ition
and
so
me
mea
sure
s pro
vide
par
tial p
rote
ctio
n; H
igh
= E
quip
men
t is i
n go
od
cond
ition
, is w
ell-s
ecur
ed a
nd m
easu
res p
rovi
de g
ood
prot
ectio
n.
IF T
HE
HO
SPIT
AL D
OES
NO
T H
AVE
THES
E SE
RVIC
ES, L
EAVE
BO
XES
BLAN
K AN
D P
ROVI
DE
COM
MEN
T.
103.
Con
ditio
n an
d sa
fety
of m
edica
l equ
ipm
ent i
n ot
her s
ervi
ces
Safe
ty ra
tings
: Low
= M
ore
than
30%
of e
quip
men
t is a
t risk
of m
ater
ial o
r fu
nctio
nal f
ailu
re a
nd/o
r equ
ipm
ent p
uts t
he e
ntire
serv
ice’s
ope
ratio
n at
di
rect
or i
ndire
ct ri
sk; A
vera
ge =
Bet
wee
n 10
% a
nd 3
0% o
f equ
ipm
ent i
s at
risk
of l
oss;
Hig
h =
Les
s tha
n 10
% o
f equ
ipm
ent i
s at r
isk o
f los
s.
104.
Med
icine
s and
supp
lies
Safe
ty ra
tings
: Low
= N
onex
isten
t; Av
erag
e =
Sup
ply
cove
rs le
ss th
an 7
2 ho
urs a
t max
imum
cap
acity
; Hig
h =
Sup
ply
guar
ante
ed fo
r at l
east
72
hour
s at m
axim
um h
ospi
tal c
apac
ity.
105.
Ste
rilize
d in
stru
men
ts an
d ot
her m
ater
ials
Safe
ty ra
tings
: Low
= N
onex
isten
t; Av
erag
e =
Sup
ply
cove
r les
s tha
n 72
ho
urs a
t max
imum
cap
acity
; Hig
h =
Sup
ply
is gu
aran
teed
for a
t lea
st 7
2 ho
urs a
t max
imum
hos
pita
l cap
acity
.
Con
tinue
>>
ANN
EX 2
: FO
RM 2
: SAF
E H
OSP
ITAL
S CH
ECKL
IST
Mod
ule
3: N
onst
ruct
ural
safe
ty

81
167
(Con
tinue
d) 3
.4 E
quip
men
t and
sup
plie
sSa
fety
leve
lO
bser
vatio
ns
(eva
luat
ors’
com
men
ts)
Low
Average
High
97. C
ondi
tion
and
safe
ty o
f med
ical e
quip
men
t in
inte
nsiv
e or
inte
rme-
diat
e ca
re u
nit
Safe
ty ra
tings
: Low
= T
he m
edic
al e
quip
men
t is l
acki
ng o
r in
poor
con
di-
tion,
or t
here
are
no
prot
ectiv
e m
easu
res;
Aver
age
= T
he e
quip
men
t is
in fa
ir co
nditi
on a
nd so
me
mea
sure
s pro
vide
par
tial p
rote
ctio
n; H
igh
=
Equi
pmen
t is i
n go
od c
ondi
tion,
is w
ell-s
ecur
ed a
nd m
easu
res p
rovi
de
good
pro
tect
ion.
98. C
ondi
tion
and
safe
ty o
f equ
ipm
ent a
nd fu
rnish
ings
in th
e ph
arm
acy
Safe
ty ra
tings
: Low
= T
he e
quip
men
t in
the
phar
mac
y is
lack
ing
or in
poo
r co
nditi
on, o
r the
re a
re n
o pr
otec
tive
mea
sure
s; Av
erag
e =
The
equ
ipm
ent
is in
fair
cond
ition
and
som
e m
easu
res p
rovi
de p
artia
l pro
tect
ion;
Hig
h =
Equ
ipm
ent i
s in
good
con
ditio
n, is
wel
l-sec
ured
and
mea
sure
s pro
vide
go
od p
rote
ctio
n.
99. C
ondi
tion
and
safe
ty o
f equ
ipm
ent a
nd su
pplie
s in
the
ster
iliza
tion
serv
ices
Safe
ty ra
tings
: Low
= E
quip
men
t is l
acki
ng o
r in
poor
con
ditio
n, o
r the
re
are
no p
rote
ctiv
e m
easu
res;
Aver
age
= E
quip
men
t is i
n fa
ir co
nditi
on a
nd
som
e m
easu
res p
rovi
de p
artia
l pro
tect
ion;
Hig
h =
Equ
ipm
ent i
s in
good
co
nditi
on, i
s wel
l-sec
ured
and
mea
sure
s pro
vide
goo
d pr
otec
tion.
100.
Con
ditio
n an
d sa
fety
of m
edica
l equ
ipm
ent f
or o
bste
tric e
mer
gen-
cies a
nd n
eona
tal c
are
Safe
ty ra
tings
: Low
= E
quip
men
t is l
acki
ng o
r in
poor
con
ditio
n, o
r the
re
are
no p
rote
ctiv
e m
easu
res;
Aver
age
= E
quip
men
t is i
n fa
ir co
nditi
on a
nd
som
e m
easu
res p
rovi
de p
artia
l pro
tect
ion;
Hig
h =
Equ
ipm
ent i
s in
good
co
nditi
on, i
s wel
l-sec
ured
and
mea
sure
s pro
vide
goo
d pr
otec
tion.
101.
Con
ditio
n an
d sa
fety
of m
edica
l equ
ipm
ent a
nd su
pplie
s for
em
er-
genc
y car
e fo
r bur
nsSa
fety
ratin
gs: L
ow =
Equ
ipm
ent i
s lac
king
, is i
n po
or c
ondi
tion,
or t
here
ar
e no
pro
tect
ive
mea
sure
s; Av
erag
e =
Equ
ipm
ent i
s in
fair
cond
ition
and
so
me
mea
sure
s pro
vide
par
tial p
rote
ctio
n; H
igh
= E
quip
men
t is i
n go
od
cond
ition
, is w
ell-s
ecur
ed a
nd m
easu
res p
rovi
de g
ood
prot
ectio
n.
102.
Con
ditio
n an
d sa
fety
of m
edica
l equ
ipm
ent f
or n
ucle
ar m
edici
ne
and
radi
atio
n th
erap
ySa
fety
ratin
gs: L
ow =
Equ
ipm
ent i
s lac
king
, is i
n po
or c
ondi
tion,
or t
here
ar
e no
pro
tect
ive
mea
sure
s; Av
erag
e =
Equ
ipm
ent i
s in
fair
cond
ition
and
so
me
mea
sure
s pro
vide
par
tial p
rote
ctio
n; H
igh
= E
quip
men
t is i
n go
od
cond
ition
, is w
ell-s
ecur
ed a
nd m
easu
res p
rovi
de g
ood
prot
ectio
n.
IF T
HE
HO
SPIT
AL D
OES
NO
T H
AVE
THES
E SE
RVIC
ES, L
EAVE
BO
XES
BLAN
K AN
D P
ROVI
DE
COM
MEN
T.
103.
Con
ditio
n an
d sa
fety
of m
edica
l equ
ipm
ent i
n ot
her s
ervi
ces
Safe
ty ra
tings
: Low
= M
ore
than
30%
of e
quip
men
t is a
t risk
of m
ater
ial o
r fu
nctio
nal f
ailu
re a
nd/o
r equ
ipm
ent p
uts t
he e
ntire
serv
ice’s
ope
ratio
n at
di
rect
or i
ndire
ct ri
sk; A
vera
ge =
Bet
wee
n 10
% a
nd 3
0% o
f equ
ipm
ent i
s at
risk
of l
oss;
Hig
h =
Les
s tha
n 10
% o
f equ
ipm
ent i
s at r
isk o
f los
s.
104.
Med
icine
s and
supp
lies
Safe
ty ra
tings
: Low
= N
onex
isten
t; Av
erag
e =
Sup
ply
cove
rs le
ss th
an 7
2 ho
urs a
t max
imum
cap
acity
; Hig
h =
Sup
ply
guar
ante
ed fo
r at l
east
72
hour
s at m
axim
um h
ospi
tal c
apac
ity.
105.
Ste
rilize
d in
stru
men
ts an
d ot
her m
ater
ials
Safe
ty ra
tings
: Low
= N
onex
isten
t; Av
erag
e =
Sup
ply
cove
r les
s tha
n 72
ho
urs a
t max
imum
cap
acity
; Hig
h =
Sup
ply
is gu
aran
teed
for a
t lea
st 7
2 ho
urs a
t max
imum
hos
pita
l cap
acity
.
Con
tinue
>>
ANN
EX 2
: FO
RM 2
: SAF
E H
OSP
ITAL
S CH
ECKL
IST
Mod
ule
3: N
onst
ruct
ural
safe
ty

82
Hos
pita
l Saf
ety
Inde
x G
UID
E FO
R EV
ALU
ATO
RS
168
(Con
tinue
d) 3
.4 E
quip
men
t and
sup
plie
sSa
fety
leve
lO
bser
vatio
ns
(eva
luat
ors’
com
men
ts)
Low
Average
High
106.
Med
ical e
quip
men
t spe
cifica
lly u
sed
in e
mer
genc
ies a
nd d
isast
ers
Safe
ty ra
tings
: Low
= N
onex
isten
t; Av
erag
e =
Sup
ply
cove
rs le
ss th
an 7
2 ho
urs a
t max
imum
hos
pita
l cap
acity
; Hig
h =
Sup
ply
guar
ante
ed fo
r at
leas
t 72
hour
s at m
axim
um h
ospi
tal c
apac
ity.
107.
Sup
ply o
f med
ical g
ases
Safe
ty ra
tings
: Low
= L
ess t
han
10 d
ays’
supp
ly; A
vera
ge =
Sup
ply
for
betw
een
10 a
nd 1
5 da
ys; H
igh
= S
uppl
y fo
r at l
east
15
days
.
108.
Mec
hani
cal v
olum
e ve
ntila
tors
Safe
ty ra
tings
: Low
= N
onex
isten
t; Av
erag
e =
Sup
ply
cove
rs le
ss th
an 7
2 ho
urs a
t max
imum
hos
pita
l cap
acity
; Hig
h =
Sup
ply
guar
ante
ed fo
r at
leas
t 72
hour
s at m
axim
um h
ospi
tal c
apac
ity.
109.
Ele
ctro
med
ical e
quip
men
tSa
fety
ratin
gs: L
ow =
Non
exist
ent;
Aver
age
= S
uppl
y co
vers
less
than
72
hour
s at m
axim
um h
ospi
tal c
apac
ity; H
igh
= S
uppl
y gu
aran
teed
for a
t le
ast 7
2 ho
urs a
t max
imum
hos
pita
l cap
acity
.
110.
Life
-sup
port
equ
ipm
ent
Safe
ty ra
tings
: Low
= N
onex
isten
t; Av
erag
e =
Sup
ply
cove
rs le
ss th
an 7
2 ho
urs a
t max
imum
hos
pita
l cap
acity
; Hig
h =
Sup
ply
guar
ante
ed fo
r at
leas
t 72
hour
s at m
axim
um h
ospi
tal c
apac
ity.
111.
Sup
plie
s, eq
uipm
ent o
r cra
sh ca
rts f
or ca
rdio
pulm
onar
y arre
stSa
fety
ratin
gs: L
ow =
Non
exist
ent;
Aver
age
= S
uppl
ies a
nd e
quip
men
t fo
r car
diop
ulm
onar
y em
erge
ncie
s (or
cra
sh c
arts
) in
good
con
ditio
n bu
t co
ver l
ess t
han
72 h
ours
at m
axim
um h
ospi
tal c
apac
ity; H
igh
= S
uppl
ies
and
equi
pmen
t for
car
diop
ulm
onar
y em
erge
ncie
s (or
cra
sh c
arts
) gua
r-an
teed
in g
ood
cond
ition
and
ade
quat
e su
pplie
s for
at l
east
72
hour
s at
max
imum
hos
pita
l cap
acity
.
Com
men
ts o
n th
e re
sults
of F
orm
2, M
odul
e 3.
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
Nam
e/sig
natu
re o
f eva
luat
or(s
) ......
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
...
Mod
ule
3: N
onst
ruct
ural
safe
ty

83
Hos
pita
l Saf
ety
Inde
x G
UID
E FO
R EV
ALU
ATO
RS
168
(Con
tinue
d) 3
.4 E
quip
men
t and
sup
plie
sSa
fety
leve
lO
bser
vatio
ns
(eva
luat
ors’
com
men
ts)
Low
Average
High
106.
Med
ical e
quip
men
t spe
cifica
lly u
sed
in e
mer
genc
ies a
nd d
isast
ers
Safe
ty ra
tings
: Low
= N
onex
isten
t; Av
erag
e =
Sup
ply
cove
rs le
ss th
an 7
2 ho
urs a
t max
imum
hos
pita
l cap
acity
; Hig
h =
Sup
ply
guar
ante
ed fo
r at
leas
t 72
hour
s at m
axim
um h
ospi
tal c
apac
ity.
107.
Sup
ply o
f med
ical g
ases
Safe
ty ra
tings
: Low
= L
ess t
han
10 d
ays’
supp
ly; A
vera
ge =
Sup
ply
for
betw
een
10 a
nd 1
5 da
ys; H
igh
= S
uppl
y fo
r at l
east
15
days
.
108.
Mec
hani
cal v
olum
e ve
ntila
tors
Safe
ty ra
tings
: Low
= N
onex
isten
t; Av
erag
e =
Sup
ply
cove
rs le
ss th
an 7
2 ho
urs a
t max
imum
hos
pita
l cap
acity
; Hig
h =
Sup
ply
guar
ante
ed fo
r at
leas
t 72
hour
s at m
axim
um h
ospi
tal c
apac
ity.
109.
Ele
ctro
med
ical e
quip
men
tSa
fety
ratin
gs: L
ow =
Non
exist
ent;
Aver
age
= S
uppl
y co
vers
less
than
72
hour
s at m
axim
um h
ospi
tal c
apac
ity; H
igh
= S
uppl
y gu
aran
teed
for a
t le
ast 7
2 ho
urs a
t max
imum
hos
pita
l cap
acity
.
110.
Life
-sup
port
equ
ipm
ent
Safe
ty ra
tings
: Low
= N
onex
isten
t; Av
erag
e =
Sup
ply
cove
rs le
ss th
an 7
2 ho
urs a
t max
imum
hos
pita
l cap
acity
; Hig
h =
Sup
ply
guar
ante
ed fo
r at
leas
t 72
hour
s at m
axim
um h
ospi
tal c
apac
ity.
111.
Sup
plie
s, eq
uipm
ent o
r cra
sh ca
rts f
or ca
rdio
pulm
onar
y arre
stSa
fety
ratin
gs: L
ow =
Non
exist
ent;
Aver
age
= S
uppl
ies a
nd e
quip
men
t fo
r car
diop
ulm
onar
y em
erge
ncie
s (or
cra
sh c
arts
) in
good
con
ditio
n bu
t co
ver l
ess t
han
72 h
ours
at m
axim
um h
ospi
tal c
apac
ity; H
igh
= S
uppl
ies
and
equi
pmen
t for
car
diop
ulm
onar
y em
erge
ncie
s (or
cra
sh c
arts
) gua
r-an
teed
in g
ood
cond
ition
and
ade
quat
e su
pplie
s for
at l
east
72
hour
s at
max
imum
hos
pita
l cap
acity
.
Com
men
ts o
n th
e re
sults
of F
orm
2, M
odul
e 3.
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
Nam
e/sig
natu
re o
f eva
luat
or(s
) ......
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
...
Mod
ule
3: N
onst
ruct
ural
safe
ty

84
169
Mod
ule
4: E
mer
genc
y an
d di
sast
er m
anag
emen
t
4.1
Coor
dina
tion
of e
mer
genc
y an
d di
sast
er m
an-
agem
ent a
ctiv
itie
sSa
fety
leve
lO
bser
vatio
ns
(eva
luat
ors’
com
men
ts)
Low
Average
High
112.
Hos
pita
l Em
erge
ncy/
Disa
ster
Com
mitt
eeSa
fety
ratin
gs: L
ow =
Com
mitt
ee d
oes n
ot e
xist
, or 1
–3 d
epar
tmen
ts o
r di
scip
lines
repr
esen
ted;
Ave
rage
= C
omm
ittee
exi
sts w
ith 4
–5 d
epar
t-m
ents
or d
iscip
lines
repr
esen
ted,
but
is n
ot fu
lfilli
ng fu
nctio
ns e
ffect
ivel
y;
Hig
h =
Com
mitt
ee e
xist
s with
6 o
r mor
e de
part
men
ts o
r disc
iplin
es
repr
esen
ted
and
is fu
lfilli
ng fu
nctio
ns e
ffect
ivel
y.
113.
Com
mitt
ee m
embe
r res
pons
ibili
ties a
nd tr
aini
ngSa
fety
ratin
gs: L
ow =
Com
mitt
ee d
oes n
ot e
xist
or m
embe
rs a
re u
ntra
ined
an
d re
spon
sibili
ties n
ot a
ssig
ned;
Ave
rage
= M
embe
rs h
ave
rece
ived
tr
aini
ng a
nd h
ave
been
offi
cial
ly a
ssig
ned;
Hig
h =
All
mem
bers
are
trai
ned
and
are
activ
ely
fulfi
lling
thei
r rol
es a
nd re
spon
sibili
ties.
114.
Des
igna
ted
emer
genc
y and
disa
ster
man
agem
ent c
oord
inat
orSa
fety
ratin
gs: L
ow =
The
re is
no
staff
mem
ber w
ho h
as b
een
assig
ned
resp
onsib
ilitie
s as t
he e
mer
genc
y/di
sast
er m
anag
emen
t coo
rdin
ator
; Av
erag
e =
Em
erge
ncy/
disa
ster
man
agem
ent c
oord
inat
ion
task
s hav
e be
en a
ssig
ned
to a
staff
mem
ber,
but i
t is n
ot h
is/he
r mai
n ta
sk; H
igh
=
A st
aff m
embe
r is a
ssig
ned
the
emer
genc
y an
d di
sast
er m
anag
emen
t co
ordi
natio
n re
spon
sibili
ties a
s his/
her m
ain
task
, is f
ulfil
ling
the
role
of
impl
emen
ting
the
hosp
ital’s
pre
pare
dnes
s pro
gram
me.
115.
Pre
pare
dnes
s pro
gram
me
for s
treng
then
ing
emer
genc
y and
disa
s-te
r res
pons
e an
d re
cove
rySa
fety
ratin
gs: L
ow =
A p
rogr
amm
e fo
r str
engt
heni
ng p
repa
redn
ess,
re-
spon
se a
nd re
cove
ry d
oes n
ot e
xist
or,
if it
exist
s, no
pre
pare
dnes
s act
ivi-
ties a
re b
eing
impl
emen
ted;
Ave
rage
= A
pro
gram
me
for s
tren
gthe
ning
pr
epar
edne
ss, r
espo
nse
and
reco
very
exi
sts a
nd so
me
activ
ities
are
bei
ng
impl
emen
ted;
Hig
h =
A p
rogr
amm
e fo
r str
engt
heni
ng p
repa
redn
ess,
resp
onse
and
reco
very
is b
eing
fully
impl
emen
ted
unde
r the
lead
ersh
ip
of th
e H
ospi
tal E
mer
genc
y/D
isast
er C
omm
ittee
.
116.
Hos
pita
l inc
iden
t man
agem
ent s
yste
mSa
fety
ratin
gs: L
ow =
No
arra
ngem
ents
for h
ospi
tal i
ncid
ent m
anag
emen
t ex
ist; A
vera
ge =
Sta
ff as
signe
d to
key
hos
pita
l inc
iden
t man
agem
ent
posit
ions
but
with
no
writ
ten
proc
edur
es to
ope
ratio
naliz
e its
func
tions
; H
igh
= H
ospi
tal i
ncid
ent m
anag
emen
t pro
cedu
res e
xist
and
are
fully
op
erat
iona
l with
pro
perly
trai
ned
pers
onne
l to
assu
me
diffe
rent
coo
rdin
a-tio
n ro
les a
nd re
spon
sibili
ties.
117.
Em
erge
ncy O
pera
tions
Cen
tre (E
OC)
Safe
ty ra
tings
: Low
= T
he E
OC
is no
t des
igna
ted
or is
in a
n un
safe
or
inse
cure
loca
tion;
Ave
rage
= T
he d
esig
nate
d EO
C is
in a
safe
, sec
ure
and
acce
ssib
le lo
catio
n, b
ut w
ould
hav
e lim
ited
oper
atio
nal c
apac
ity im
med
i-at
ely
in a
n em
erge
ncy;
Hig
h =
The
EO
C is
in a
safe
, sec
ure,
and
acc
essib
le
loca
tion
with
imm
edia
te o
pera
tiona
l cap
acity
.
118.
Coo
rdin
atio
n m
echa
nism
s and
coop
erat
ive
arra
ngem
ents
with
lo
cal e
mer
genc
y/di
sast
er m
anag
emen
t age
ncie
sSa
fety
ratin
gs: L
ow =
No
arra
ngem
ents
exi
st; A
vera
ge =
Arr
ange
men
ts
exist
but
are
not
fully
ope
ratio
nal;
Hig
h =
Arr
ange
men
ts e
xist
and
are
fully
op
erat
iona
l.
119.
Coo
rdin
atio
n m
echa
nism
s and
coop
erat
ive
arra
ngem
ents
with
the
heal
th-c
are
netw
ork
Safe
ty ra
tings
: Low
= N
o ar
rang
emen
ts e
xist
; Ave
rage
= A
rran
gem
ents
ex
ist b
ut a
re n
ot fu
lly o
pera
tiona
l; H
igh
= A
rran
gem
ents
exi
st a
nd a
re fu
lly
oper
atio
nal.
ANN
EX 2
: FO
RM 2
: SAF
E H
OSP
ITAL
S CH
ECKL
IST

85
169
Mod
ule
4: E
mer
genc
y an
d di
sast
er m
anag
emen
t
4.1
Coor
dina
tion
of e
mer
genc
y an
d di
sast
er m
an-
agem
ent a
ctiv
itie
sSa
fety
leve
lO
bser
vatio
ns
(eva
luat
ors’
com
men
ts)
Low
Average
High
112.
Hos
pita
l Em
erge
ncy/
Disa
ster
Com
mitt
eeSa
fety
ratin
gs: L
ow =
Com
mitt
ee d
oes n
ot e
xist
, or 1
–3 d
epar
tmen
ts o
r di
scip
lines
repr
esen
ted;
Ave
rage
= C
omm
ittee
exi
sts w
ith 4
–5 d
epar
t-m
ents
or d
iscip
lines
repr
esen
ted,
but
is n
ot fu
lfilli
ng fu
nctio
ns e
ffect
ivel
y;
Hig
h =
Com
mitt
ee e
xist
s with
6 o
r mor
e de
part
men
ts o
r disc
iplin
es
repr
esen
ted
and
is fu
lfilli
ng fu
nctio
ns e
ffect
ivel
y.
113.
Com
mitt
ee m
embe
r res
pons
ibili
ties a
nd tr
aini
ngSa
fety
ratin
gs: L
ow =
Com
mitt
ee d
oes n
ot e
xist
or m
embe
rs a
re u
ntra
ined
an
d re
spon
sibili
ties n
ot a
ssig
ned;
Ave
rage
= M
embe
rs h
ave
rece
ived
tr
aini
ng a
nd h
ave
been
offi
cial
ly a
ssig
ned;
Hig
h =
All
mem
bers
are
trai
ned
and
are
activ
ely
fulfi
lling
thei
r rol
es a
nd re
spon
sibili
ties.
114.
Des
igna
ted
emer
genc
y and
disa
ster
man
agem
ent c
oord
inat
orSa
fety
ratin
gs: L
ow =
The
re is
no
staff
mem
ber w
ho h
as b
een
assig
ned
resp
onsib
ilitie
s as t
he e
mer
genc
y/di
sast
er m
anag
emen
t coo
rdin
ator
; Av
erag
e =
Em
erge
ncy/
disa
ster
man
agem
ent c
oord
inat
ion
task
s hav
e be
en a
ssig
ned
to a
staff
mem
ber,
but i
t is n
ot h
is/he
r mai
n ta
sk; H
igh
=
A st
aff m
embe
r is a
ssig
ned
the
emer
genc
y an
d di
sast
er m
anag
emen
t co
ordi
natio
n re
spon
sibili
ties a
s his/
her m
ain
task
, is f
ulfil
ling
the
role
of
impl
emen
ting
the
hosp
ital’s
pre
pare
dnes
s pro
gram
me.
115.
Pre
pare
dnes
s pro
gram
me
for s
treng
then
ing
emer
genc
y and
disa
s-te
r res
pons
e an
d re
cove
rySa
fety
ratin
gs: L
ow =
A p
rogr
amm
e fo
r str
engt
heni
ng p
repa
redn
ess,
re-
spon
se a
nd re
cove
ry d
oes n
ot e
xist
or,
if it
exist
s, no
pre
pare
dnes
s act
ivi-
ties a
re b
eing
impl
emen
ted;
Ave
rage
= A
pro
gram
me
for s
tren
gthe
ning
pr
epar
edne
ss, r
espo
nse
and
reco
very
exi
sts a
nd so
me
activ
ities
are
bei
ng
impl
emen
ted;
Hig
h =
A p
rogr
amm
e fo
r str
engt
heni
ng p
repa
redn
ess,
resp
onse
and
reco
very
is b
eing
fully
impl
emen
ted
unde
r the
lead
ersh
ip
of th
e H
ospi
tal E
mer
genc
y/D
isast
er C
omm
ittee
.
116.
Hos
pita
l inc
iden
t man
agem
ent s
yste
mSa
fety
ratin
gs: L
ow =
No
arra
ngem
ents
for h
ospi
tal i
ncid
ent m
anag
emen
t ex
ist; A
vera
ge =
Sta
ff as
signe
d to
key
hos
pita
l inc
iden
t man
agem
ent
posit
ions
but
with
no
writ
ten
proc
edur
es to
ope
ratio
naliz
e its
func
tions
; H
igh
= H
ospi
tal i
ncid
ent m
anag
emen
t pro
cedu
res e
xist
and
are
fully
op
erat
iona
l with
pro
perly
trai
ned
pers
onne
l to
assu
me
diffe
rent
coo
rdin
a-tio
n ro
les a
nd re
spon
sibili
ties.
117.
Em
erge
ncy O
pera
tions
Cen
tre (E
OC)
Safe
ty ra
tings
: Low
= T
he E
OC
is no
t des
igna
ted
or is
in a
n un
safe
or
inse
cure
loca
tion;
Ave
rage
= T
he d
esig
nate
d EO
C is
in a
safe
, sec
ure
and
acce
ssib
le lo
catio
n, b
ut w
ould
hav
e lim
ited
oper
atio
nal c
apac
ity im
med
i-at
ely
in a
n em
erge
ncy;
Hig
h =
The
EO
C is
in a
safe
, sec
ure,
and
acc
essib
le
loca
tion
with
imm
edia
te o
pera
tiona
l cap
acity
.
118.
Coo
rdin
atio
n m
echa
nism
s and
coop
erat
ive
arra
ngem
ents
with
lo
cal e
mer
genc
y/di
sast
er m
anag
emen
t age
ncie
sSa
fety
ratin
gs: L
ow =
No
arra
ngem
ents
exi
st; A
vera
ge =
Arr
ange
men
ts
exist
but
are
not
fully
ope
ratio
nal;
Hig
h =
Arr
ange
men
ts e
xist
and
are
fully
op
erat
iona
l.
119.
Coo
rdin
atio
n m
echa
nism
s and
coop
erat
ive
arra
ngem
ents
with
the
heal
th-c
are
netw
ork
Safe
ty ra
tings
: Low
= N
o ar
rang
emen
ts e
xist
; Ave
rage
= A
rran
gem
ents
ex
ist b
ut a
re n
ot fu
lly o
pera
tiona
l; H
igh
= A
rran
gem
ents
exi
st a
nd a
re fu
lly
oper
atio
nal.
ANN
EX 2
: FO
RM 2
: SAF
E H
OSP
ITAL
S CH
ECKL
IST

86
Hos
pita
l Saf
ety
Inde
x G
UID
E FO
R EV
ALU
ATO
RS
170
4.2
Hos
pita
l em
erge
ncy
and
disa
ster
resp
onse
and
re
cove
ry p
lann
ing
Safe
ty le
vel
Obs
erva
tions
(e
valu
ator
s’ co
mm
ents
)Low
Average
High
120.
Hos
pita
l em
erge
ncy o
r disa
ster
resp
onse
pla
nSa
fety
ratin
gs: L
ow =
Pla
n is
not d
ocum
ente
d; A
vera
ge =
Doc
umen
ted
plan
is c
ompl
ete,
but
is n
ot e
asily
acc
essib
le, n
ot u
p to
dat
e (m
ore
than
12
mon
ths s
ince
the
last
upd
ate)
; Hig
h =
Pla
n is
com
plet
e, e
asily
acc
essib
le,
revi
ewed
/upd
ated
at l
east
ann
ually
, and
reso
urce
s are
ava
ilabl
e to
impl
e-m
ent t
he p
lan.
121.
Hos
pita
l haz
ard-
spec
ific s
ubpl
ans
Safe
ty ra
tings
: Low
= H
azar
d-sp
ecifi
c re
spon
se su
bpla
ns a
re n
ot d
ocu-
men
ted;
Ave
rage
= D
ocum
ente
d pl
ans a
re c
ompl
ete
but n
ot e
asily
ac-
cess
ible
, not
up
to d
ate
(mor
e th
an 1
2 m
onth
s sin
ce la
st re
view
/upd
ate)
; H
igh
= D
ocum
ente
d pl
ans a
re c
ompl
ete,
revi
ewed
/upd
ated
at l
east
an
nual
ly, a
nd re
sour
ces a
re a
vaila
ble
to im
plem
ent t
he p
lans
.
122.
Pro
cedu
res t
o ac
tivat
e an
d de
activ
ate
plan
sSa
fety
ratin
gs: L
ow =
Pro
cedu
res d
o no
t exi
st o
r exi
st o
nly
as a
doc
umen
t; Av
erag
e =
Pro
cedu
res e
xist
, per
sonn
el h
ave
been
trai
ned,
but
pro
cedu
res
are
not u
pdat
ed o
r tes
ted
annu
ally
; Hig
h =
Up-
to-d
ate
proc
edur
es e
xist
, pe
rson
nel h
ave
been
trai
ned,
and
pro
cedu
res h
ave
been
test
ed a
t lea
st
annu
ally
.
123.
Hos
pita
l em
erge
ncy a
nd d
isast
er re
spon
se p
lan
exer
cises
, eva
lua-
tion
and
corre
ctiv
e ac
tions
Safe
ty ra
tings
: Low
= R
espo
nse
plan
and
subp
lans
hav
e no
t bee
n te
sted
; Av
erag
e =
Res
pons
e pl
an o
r sub
plan
s are
test
ed, b
ut a
re n
ot te
sted
at
leas
t ann
ually
; Hig
h =
Res
pons
e pl
an o
r sub
plan
s are
test
ed a
t lea
st a
nnu-
ally
and
upd
ated
acc
ordi
ng to
the
exer
cise
resu
lts.
124.
Hos
pita
l rec
over
y pla
nSa
fety
ratin
gs: L
ow =
Rec
over
y pl
an is
not
doc
umen
ted;
Ave
rage
= D
ocu-
men
ted
plan
is c
ompl
ete,
but
not
eas
ily a
cces
sible
, not
up-
to-d
ate
(mor
e th
an 1
2 m
onth
s sin
ce la
st re
view
/upd
ate)
; Hig
h =
Doc
umen
ted
plan
is
com
plet
e, e
asily
acc
essib
le, a
nd re
view
ed/u
pdat
ed a
t lea
st a
nnua
lly.
4.3
Com
mun
icat
ion
and
info
rmat
ion
man
agem
ent
Safe
ty le
vel
Obs
erva
tions
(e
valu
ator
s’ co
mm
ents
)Low
Average
High
125.
Em
erge
ncy i
nter
nal a
nd ex
tern
al co
mm
unica
tion
Safe
ty ra
tings
: Low
= C
entr
al in
tern
al a
nd e
xter
nal c
omm
unic
atio
n sy
stem
fu
nctio
ns in
cons
isten
tly o
r inc
ompl
etel
y; o
pera
tors
are
not
trai
ned
in
emer
genc
y co
mm
unic
atio
n; A
vera
ge =
Sys
tem
func
tions
app
ropr
iate
ly,
oper
ator
s hav
e re
ceiv
ed so
me
trai
ning
in e
mer
genc
y co
mm
unic
atio
n,
test
s are
not
con
duct
ed a
t lea
st a
nnua
lly; H
igh
= S
yste
m fu
nctio
ns c
om-
plet
ely
and
oper
ator
s are
fully
trai
ned
in e
mer
genc
y us
e, a
nd te
sts o
f the
sy
stem
are
con
duct
ed a
t lea
st a
nnua
lly.
126.
Ext
erna
l sta
keho
lder
dire
ctor
ySa
fety
ratin
gs: L
ow =
Dire
ctor
y of
ext
erna
l sta
keho
lder
s doe
s not
exi
st;
Aver
age
= D
irect
ory
exist
s but
is n
ot c
urre
nt (m
ore
than
3 m
onth
s sin
ce
it w
as u
pdat
ed);
Hig
h =
Dire
ctor
y is
avai
labl
e, is
up
to d
ate
and
is he
ld b
y ke
y em
erge
ncy
resp
onse
staff
.
127.
Pro
cedu
res f
or co
mm
unica
ting
with
the
publ
ic an
d m
edia
Safe
ty ra
tings
: Low
= P
roce
dure
s do
not e
xist
, no
spok
espe
rson
nom
i-na
ted;
Ave
rage
= P
roce
dure
s exi
st a
nd n
omin
ated
spok
espe
rson
s hav
e be
en tr
aine
d; H
igh
= P
roce
dure
s exi
st, n
omin
ated
spok
espe
rson
s hav
e be
en tr
aine
d, a
nd p
roce
dure
s hav
e be
en te
sted
at l
east
ann
ually
.
128.
Man
agem
ent o
f pat
ient
info
rmat
ion
Safe
ty ra
tings
: Low
= P
roce
dure
s for
em
erge
ncy
situa
tions
do
not e
xist
; Av
erag
e =
Pro
cedu
res f
or e
mer
genc
y sit
uatio
ns e
xist
and
per
sonn
el h
ave
been
trai
ned
but n
o re
sour
ces a
re a
vaila
ble;
Hig
h =
Pro
cedu
res f
or e
mer
-ge
ncy
situa
tions
exi
st, p
erso
nnel
hav
e be
en tr
aine
d, a
nd re
sour
ces a
re in
pl
ace
for i
mpl
emen
tatio
n.
Mod
ule
4: E
mer
genc
y an
d di
sast
er m
anag
emen
t

87
Hos
pita
l Saf
ety
Inde
x G
UID
E FO
R EV
ALU
ATO
RS
170
4.2
Hos
pita
l em
erge
ncy
and
disa
ster
resp
onse
and
re
cove
ry p
lann
ing
Safe
ty le
vel
Obs
erva
tions
(e
valu
ator
s’ co
mm
ents
)Low
Average
High
120.
Hos
pita
l em
erge
ncy o
r disa
ster
resp
onse
pla
nSa
fety
ratin
gs: L
ow =
Pla
n is
not d
ocum
ente
d; A
vera
ge =
Doc
umen
ted
plan
is c
ompl
ete,
but
is n
ot e
asily
acc
essib
le, n
ot u
p to
dat
e (m
ore
than
12
mon
ths s
ince
the
last
upd
ate)
; Hig
h =
Pla
n is
com
plet
e, e
asily
acc
essib
le,
revi
ewed
/upd
ated
at l
east
ann
ually
, and
reso
urce
s are
ava
ilabl
e to
impl
e-m
ent t
he p
lan.
121.
Hos
pita
l haz
ard-
spec
ific s
ubpl
ans
Safe
ty ra
tings
: Low
= H
azar
d-sp
ecifi
c re
spon
se su
bpla
ns a
re n
ot d
ocu-
men
ted;
Ave
rage
= D
ocum
ente
d pl
ans a
re c
ompl
ete
but n
ot e
asily
ac-
cess
ible
, not
up
to d
ate
(mor
e th
an 1
2 m
onth
s sin
ce la
st re
view
/upd
ate)
; H
igh
= D
ocum
ente
d pl
ans a
re c
ompl
ete,
revi
ewed
/upd
ated
at l
east
an
nual
ly, a
nd re
sour
ces a
re a
vaila
ble
to im
plem
ent t
he p
lans
.
122.
Pro
cedu
res t
o ac
tivat
e an
d de
activ
ate
plan
sSa
fety
ratin
gs: L
ow =
Pro
cedu
res d
o no
t exi
st o
r exi
st o
nly
as a
doc
umen
t; Av
erag
e =
Pro
cedu
res e
xist
, per
sonn
el h
ave
been
trai
ned,
but
pro
cedu
res
are
not u
pdat
ed o
r tes
ted
annu
ally
; Hig
h =
Up-
to-d
ate
proc
edur
es e
xist
, pe
rson
nel h
ave
been
trai
ned,
and
pro
cedu
res h
ave
been
test
ed a
t lea
st
annu
ally
.
123.
Hos
pita
l em
erge
ncy a
nd d
isast
er re
spon
se p
lan
exer
cises
, eva
lua-
tion
and
corre
ctiv
e ac
tions
Safe
ty ra
tings
: Low
= R
espo
nse
plan
and
subp
lans
hav
e no
t bee
n te
sted
; Av
erag
e =
Res
pons
e pl
an o
r sub
plan
s are
test
ed, b
ut a
re n
ot te
sted
at
leas
t ann
ually
; Hig
h =
Res
pons
e pl
an o
r sub
plan
s are
test
ed a
t lea
st a
nnu-
ally
and
upd
ated
acc
ordi
ng to
the
exer
cise
resu
lts.
124.
Hos
pita
l rec
over
y pla
nSa
fety
ratin
gs: L
ow =
Rec
over
y pl
an is
not
doc
umen
ted;
Ave
rage
= D
ocu-
men
ted
plan
is c
ompl
ete,
but
not
eas
ily a
cces
sible
, not
up-
to-d
ate
(mor
e th
an 1
2 m
onth
s sin
ce la
st re
view
/upd
ate)
; Hig
h =
Doc
umen
ted
plan
is
com
plet
e, e
asily
acc
essib
le, a
nd re
view
ed/u
pdat
ed a
t lea
st a
nnua
lly.
4.3
Com
mun
icat
ion
and
info
rmat
ion
man
agem
ent
Safe
ty le
vel
Obs
erva
tions
(e
valu
ator
s’ co
mm
ents
)Low
Average
High
125.
Em
erge
ncy i
nter
nal a
nd ex
tern
al co
mm
unica
tion
Safe
ty ra
tings
: Low
= C
entr
al in
tern
al a
nd e
xter
nal c
omm
unic
atio
n sy
stem
fu
nctio
ns in
cons
isten
tly o
r inc
ompl
etel
y; o
pera
tors
are
not
trai
ned
in
emer
genc
y co
mm
unic
atio
n; A
vera
ge =
Sys
tem
func
tions
app
ropr
iate
ly,
oper
ator
s hav
e re
ceiv
ed so
me
trai
ning
in e
mer
genc
y co
mm
unic
atio
n,
test
s are
not
con
duct
ed a
t lea
st a
nnua
lly; H
igh
= S
yste
m fu
nctio
ns c
om-
plet
ely
and
oper
ator
s are
fully
trai
ned
in e
mer
genc
y us
e, a
nd te
sts o
f the
sy
stem
are
con
duct
ed a
t lea
st a
nnua
lly.
126.
Ext
erna
l sta
keho
lder
dire
ctor
ySa
fety
ratin
gs: L
ow =
Dire
ctor
y of
ext
erna
l sta
keho
lder
s doe
s not
exi
st;
Aver
age
= D
irect
ory
exist
s but
is n
ot c
urre
nt (m
ore
than
3 m
onth
s sin
ce
it w
as u
pdat
ed);
Hig
h =
Dire
ctor
y is
avai
labl
e, is
up
to d
ate
and
is he
ld b
y ke
y em
erge
ncy
resp
onse
staff
.
127.
Pro
cedu
res f
or co
mm
unica
ting
with
the
publ
ic an
d m
edia
Safe
ty ra
tings
: Low
= P
roce
dure
s do
not e
xist
, no
spok
espe
rson
nom
i-na
ted;
Ave
rage
= P
roce
dure
s exi
st a
nd n
omin
ated
spok
espe
rson
s hav
e be
en tr
aine
d; H
igh
= P
roce
dure
s exi
st, n
omin
ated
spok
espe
rson
s hav
e be
en tr
aine
d, a
nd p
roce
dure
s hav
e be
en te
sted
at l
east
ann
ually
.
128.
Man
agem
ent o
f pat
ient
info
rmat
ion
Safe
ty ra
tings
: Low
= P
roce
dure
s for
em
erge
ncy
situa
tions
do
not e
xist
; Av
erag
e =
Pro
cedu
res f
or e
mer
genc
y sit
uatio
ns e
xist
and
per
sonn
el h
ave
been
trai
ned
but n
o re
sour
ces a
re a
vaila
ble;
Hig
h =
Pro
cedu
res f
or e
mer
-ge
ncy
situa
tions
exi
st, p
erso
nnel
hav
e be
en tr
aine
d, a
nd re
sour
ces a
re in
pl
ace
for i
mpl
emen
tatio
n.
Mod
ule
4: E
mer
genc
y an
d di
sast
er m
anag
emen
t

88
171
4.4
Hum
an re
sour
ces
Safe
ty le
vel
Obs
erva
tions
(e
valu
ator
s’ co
mm
ents
)Low
Average
High
129.
Sta
ff co
ntac
t list
Safe
ty ra
tings
: Low
= C
onta
ct li
st d
oes n
ot e
xist
; Ave
rage
= L
ist e
xist
s, bu
t is
not c
urre
nt (m
ore
than
3 m
onth
s sin
ce it
was
upd
ated
); H
igh
= L
ist is
av
aila
ble
and
up to
dat
e.
130.
Sta
ff av
aila
bilit
ySa
fety
ratin
gs: L
ow =
Les
s tha
n 50
% o
f sta
ff ar
e av
aila
ble
to ru
n ea
ch
depa
rtm
ent a
dequ
atel
y; A
vera
ge =
50−
80%
of s
taff
are
avai
labl
e; H
igh
=
80−
100%
of s
taff
are
avai
labl
e.
131.
Mob
iliza
tion
and
recr
uitm
ent o
f per
sonn
el d
urin
g an
em
erge
ncy
or d
isast
erSa
fety
ratin
gs: L
ow =
Pro
cedu
res d
o no
t exi
st o
r exi
st o
nly
in a
doc
umen
t; Av
erag
e =
Pro
cedu
res e
xist
and
per
sonn
el h
ave
been
trai
ned,
but
the
hum
an re
sour
ces f
or a
n em
erge
ncy
situa
tion
are
not a
vaila
ble;
Hig
h =
Pr
oced
ures
exi
st, p
erso
nnel
hav
e be
en tr
aine
d, a
nd th
e hu
man
reso
urce
s ar
e av
aila
ble
to m
eet a
ntic
ipat
ed n
eeds
in a
n em
erge
ncy.
132.
Dut
ies a
ssig
ned
to p
erso
nnel
for e
mer
genc
y or d
isast
er re
spon
se
and
reco
very
Safe
ty ra
tings
: Low
= E
mer
genc
y as
signm
ents
do
not e
xist
or a
re n
ot
docu
men
ted;
Ave
rage
= D
utie
s are
iden
tified
, som
e (b
ut n
ot a
ll) p
erso
n-ne
l rec
eive
writ
ten
assig
nmen
ts o
r tra
inin
g; H
igh
= W
ritte
n du
ties a
re
assig
ned,
and
trai
ning
or a
n ex
erci
se is
con
duct
ed fo
r all
pers
onne
l at
leas
t ann
ually
.
133.
Wel
l-bei
ng o
f hos
pita
l per
sonn
el d
urin
g an
em
erge
ncy o
r disa
ster
Safe
ty ra
tings
: Low
= A
des
igna
ted
spac
e an
d m
easu
res d
o no
t exi
st;
Aver
age
= S
pace
has
bee
n de
signa
ted,
but
mea
sure
s cov
er le
ss th
an 7
2 ho
urs;
Hig
h =
Mea
sure
s are
ens
ured
for a
t lea
st 7
2 ho
urs.
4.5
Logi
stic
s an
d fin
ance
Safe
ty le
vel
Obs
erva
tions
(e
valu
ator
s’ co
mm
ents
)Low
Average
High
134.
Agr
eem
ents
with
loca
l sup
plie
rs an
d ve
ndor
s for
emer
genc
ies a
nd
disa
ster
sSa
fety
ratin
gs: L
ow =
No
arra
ngem
ents
exi
st; A
vera
ge =
Arr
ange
men
ts
exist
, but
are
not
fully
ope
ratio
nal;
Hig
h =
Arr
ange
men
ts e
xist
and
are
fu
lly o
pera
tiona
l.
135.
Tran
spor
tatio
n du
ring
an e
mer
genc
ySa
fety
ratin
gs: L
ow =
Am
bula
nces
and
oth
er v
ehic
les a
nd m
odes
of
tran
spor
tatio
n ar
e no
t ava
ilabl
e; A
vera
ge =
Som
e ve
hicl
es a
re a
vaila
ble,
bu
t not
in su
ffici
ent n
umbe
rs fo
r a m
ajor
em
erge
ncy
or d
isast
er; H
igh
=
Appr
opria
te v
ehic
les i
n su
ffici
ent n
umbe
rs a
re a
vaila
ble
durin
g em
erge
n-ci
es/d
isast
ers.
136.
Food
and
drin
king
-wat
er d
urin
g an
em
erge
ncy
Safe
ty ra
tings
: Low
= P
roce
dure
s for
food
and
drin
king
-wat
er fo
r em
er-
genc
ies a
re n
on-e
xist
ent;
Aver
age
= P
roce
dure
s exi
st, f
ood
and
drin
king
-w
ater
is g
uara
ntee
d fo
r les
s tha
n 72
hou
rs; H
igh
= F
ood
and
drin
king
-w
ater
for e
mer
genc
ies i
s gua
rant
eed
for a
t lea
st 7
2 ho
urs.
137.
Fina
ncia
l res
ourc
es fo
r em
erge
ncie
s and
disa
ster
sSa
fety
ratin
gs: L
ow =
Em
erge
ncy
budg
et o
r mec
hani
sm to
acc
ess
emer
genc
y fu
nds i
s not
in p
lace
; Ave
rage
= F
unds
are
bud
gete
d an
d m
echa
nism
s are
ava
ilabl
e bu
t cov
er le
ss th
an 7
2 ho
urs;
Hig
h =
Suffi
cien
t fu
nds a
re g
uara
ntee
d fo
r 72
hour
s or m
ore.
ANN
EX 2
: FO
RM 2
: SAF
E H
OSP
ITAL
S CH
ECKL
IST
Mod
ule
4: E
mer
genc
y an
d di
sast
er m
anag
emen
t

89
171
4.4
Hum
an re
sour
ces
Safe
ty le
vel
Obs
erva
tions
(e
valu
ator
s’ co
mm
ents
)Low
Average
High
129.
Sta
ff co
ntac
t list
Safe
ty ra
tings
: Low
= C
onta
ct li
st d
oes n
ot e
xist
; Ave
rage
= L
ist e
xist
s, bu
t is
not c
urre
nt (m
ore
than
3 m
onth
s sin
ce it
was
upd
ated
); H
igh
= L
ist is
av
aila
ble
and
up to
dat
e.
130.
Sta
ff av
aila
bilit
ySa
fety
ratin
gs: L
ow =
Les
s tha
n 50
% o
f sta
ff ar
e av
aila
ble
to ru
n ea
ch
depa
rtm
ent a
dequ
atel
y; A
vera
ge =
50−
80%
of s
taff
are
avai
labl
e; H
igh
=
80−
100%
of s
taff
are
avai
labl
e.
131.
Mob
iliza
tion
and
recr
uitm
ent o
f per
sonn
el d
urin
g an
em
erge
ncy
or d
isast
erSa
fety
ratin
gs: L
ow =
Pro
cedu
res d
o no
t exi
st o
r exi
st o
nly
in a
doc
umen
t; Av
erag
e =
Pro
cedu
res e
xist
and
per
sonn
el h
ave
been
trai
ned,
but
the
hum
an re
sour
ces f
or a
n em
erge
ncy
situa
tion
are
not a
vaila
ble;
Hig
h =
Pr
oced
ures
exi
st, p
erso
nnel
hav
e be
en tr
aine
d, a
nd th
e hu
man
reso
urce
s ar
e av
aila
ble
to m
eet a
ntic
ipat
ed n
eeds
in a
n em
erge
ncy.
132.
Dut
ies a
ssig
ned
to p
erso
nnel
for e
mer
genc
y or d
isast
er re
spon
se
and
reco
very
Safe
ty ra
tings
: Low
= E
mer
genc
y as
signm
ents
do
not e
xist
or a
re n
ot
docu
men
ted;
Ave
rage
= D
utie
s are
iden
tified
, som
e (b
ut n
ot a
ll) p
erso
n-ne
l rec
eive
writ
ten
assig
nmen
ts o
r tra
inin
g; H
igh
= W
ritte
n du
ties a
re
assig
ned,
and
trai
ning
or a
n ex
erci
se is
con
duct
ed fo
r all
pers
onne
l at
leas
t ann
ually
.
133.
Wel
l-bei
ng o
f hos
pita
l per
sonn
el d
urin
g an
em
erge
ncy o
r disa
ster
Safe
ty ra
tings
: Low
= A
des
igna
ted
spac
e an
d m
easu
res d
o no
t exi
st;
Aver
age
= S
pace
has
bee
n de
signa
ted,
but
mea
sure
s cov
er le
ss th
an 7
2 ho
urs;
Hig
h =
Mea
sure
s are
ens
ured
for a
t lea
st 7
2 ho
urs.
4.5
Logi
stic
s an
d fin
ance
Safe
ty le
vel
Obs
erva
tions
(e
valu
ator
s’ co
mm
ents
)Low
Average
High
134.
Agr
eem
ents
with
loca
l sup
plie
rs an
d ve
ndor
s for
emer
genc
ies a
nd
disa
ster
sSa
fety
ratin
gs: L
ow =
No
arra
ngem
ents
exi
st; A
vera
ge =
Arr
ange
men
ts
exist
, but
are
not
fully
ope
ratio
nal;
Hig
h =
Arr
ange
men
ts e
xist
and
are
fu
lly o
pera
tiona
l.
135.
Tran
spor
tatio
n du
ring
an e
mer
genc
ySa
fety
ratin
gs: L
ow =
Am
bula
nces
and
oth
er v
ehic
les a
nd m
odes
of
tran
spor
tatio
n ar
e no
t ava
ilabl
e; A
vera
ge =
Som
e ve
hicl
es a
re a
vaila
ble,
bu
t not
in su
ffici
ent n
umbe
rs fo
r a m
ajor
em
erge
ncy
or d
isast
er; H
igh
=
Appr
opria
te v
ehic
les i
n su
ffici
ent n
umbe
rs a
re a
vaila
ble
durin
g em
erge
n-ci
es/d
isast
ers.
136.
Food
and
drin
king
-wat
er d
urin
g an
em
erge
ncy
Safe
ty ra
tings
: Low
= P
roce
dure
s for
food
and
drin
king
-wat
er fo
r em
er-
genc
ies a
re n
on-e
xist
ent;
Aver
age
= P
roce
dure
s exi
st, f
ood
and
drin
king
-w
ater
is g
uara
ntee
d fo
r les
s tha
n 72
hou
rs; H
igh
= F
ood
and
drin
king
-w
ater
for e
mer
genc
ies i
s gua
rant
eed
for a
t lea
st 7
2 ho
urs.
137.
Fina
ncia
l res
ourc
es fo
r em
erge
ncie
s and
disa
ster
sSa
fety
ratin
gs: L
ow =
Em
erge
ncy
budg
et o
r mec
hani
sm to
acc
ess
emer
genc
y fu
nds i
s not
in p
lace
; Ave
rage
= F
unds
are
bud
gete
d an
d m
echa
nism
s are
ava
ilabl
e bu
t cov
er le
ss th
an 7
2 ho
urs;
Hig
h =
Suffi
cien
t fu
nds a
re g
uara
ntee
d fo
r 72
hour
s or m
ore.
ANN
EX 2
: FO
RM 2
: SAF
E H
OSP
ITAL
S CH
ECKL
IST
Mod
ule
4: E
mer
genc
y an
d di
sast
er m
anag
emen
t

90
Hos
pita
l Saf
ety
Inde
x G
UID
E FO
R EV
ALU
ATO
RS
172
4.6
Pati
ent c
are
and
supp
ort s
ervi
ces
Safe
ty le
vel
Obs
erva
tions
(e
valu
ator
s’ co
mm
ents
)Low
Average
High
138.
Con
tinui
ty o
f em
erge
ncy a
nd cr
itica
l car
e se
rvice
sSa
fety
ratin
gs: L
ow =
Pro
cedu
res d
o no
t exi
st o
r exi
st o
nly
as a
doc
umen
t; Av
erag
e =
Pro
cedu
res e
xist
, per
sonn
el h
ave
been
trai
ned
but w
ould
not
be
ava
ilabl
e at
all
times
; Hig
h =
Pro
cedu
res e
xist
, per
sonn
el h
ave
been
tr
aine
d, a
nd re
sour
ces a
re a
vaila
ble
to im
plem
ent p
roce
dure
s at m
axi-
mum
hos
pita
l cap
acity
for e
mer
genc
y an
d di
sast
er si
tuat
ions
at a
ll tim
es.
139.
Con
tinui
ty o
f ess
entia
l clin
ical s
uppo
rt se
rvice
sSa
fety
ratin
gs: L
ow =
Pro
cedu
res d
o no
t exi
st o
r exi
st o
nly
as a
doc
umen
t; Av
erag
e =
Proc
edur
es e
xist
and
per
sonn
el h
ave
been
trai
ned
but w
ould
no
t be
avai
labl
e at
all
times
; Hig
h =
Proc
edur
es e
xist
s, pe
rson
nel h
ave
been
tra
ined
, and
reso
urce
s are
ava
ilabl
e to
impl
emen
t pro
cedu
res a
t max
imum
ho
spita
l cap
acity
for e
mer
genc
y an
d di
sast
er si
tuat
ions
at a
ll tim
es.
140.
Exp
ansio
n of
usa
ble
spac
e fo
r mas
s cas
ualty
incid
ents
Safe
ty ra
tings
: Low
= S
pace
for e
xpan
sion
has n
ot b
een
iden
tified
; Ave
r-ag
e =
Spa
ce h
as b
een
iden
tified
; equ
ipm
ent,
supp
lies a
nd p
roce
dure
s ar
e av
aila
ble
to c
arry
out
the
expa
nsio
n an
d st
aff h
ave
been
trai
ned,
but
te
stin
g ha
s not
bee
n co
nduc
ted;
Hig
h =
Pro
cedu
res e
xist
and
hav
e be
en
test
ed, p
erso
nnel
hav
e be
en tr
aine
d, a
nd e
quip
men
t, su
pplie
s and
oth
er
reso
urce
s are
ava
ilabl
e to
car
ry o
ut th
e ex
pans
ion
of sp
ace.
141.
Tria
ge fo
r maj
or e
mer
genc
ies a
nd d
isast
ers
Safe
ty ra
tings
: Low
= D
esig
nate
d tr
iage
loca
tion
or p
roce
dure
s do
not
exist
; Ave
rage
= T
riage
loca
tion
and
proc
edur
es e
xist
and
per
sonn
el h
ave
been
trai
ned,
but
pro
cedu
res h
ave
not b
een
test
ed fo
r em
erge
ncy
and
disa
ster
situ
atio
ns; H
igh
= L
ocat
ion
and
proc
edur
es e
xist
and
hav
e be
en
test
ed, p
erso
nnel
hav
e be
en tr
aine
d, a
nd re
sour
ces a
re in
pla
ce to
impl
e-m
ent a
t max
imum
hos
pita
l cap
acity
in e
mer
genc
y an
d di
sast
er si
tuat
ions
.
142.
Tria
ge ta
gs an
d ot
her l
ogist
ical s
uppl
ies f
or m
ass c
asua
lty in
ciden
tsSa
fety
ratin
gs: L
ow =
Non
exist
ent;
Aver
age
= S
uppl
y co
vers
less
than
72
hour
s of m
axim
um h
ospi
tal c
apac
ity; H
igh
= S
uppl
y gu
aran
teed
for a
t le
ast 7
2 ho
urs o
f max
imum
hos
pita
l cap
acity
.
143.
Syst
em fo
r ref
erra
l, tra
nsfe
r and
rece
ptio
n of
pat
ient
sSa
fety
ratin
gs: L
ow =
Pro
cedu
res d
o no
t exi
st o
r exi
st o
nly
as a
doc
umen
t; Av
erag
e =
Pro
cedu
res e
xist
and
per
sonn
el h
ave
been
trai
ned,
but
pro
-ce
dure
s hav
e no
t bee
n te
sted
for e
mer
genc
y or
disa
ster
situ
atio
ns; H
igh
= P
roce
dure
s exi
st a
nd h
ave
been
test
ed, p
erso
nnel
hav
e be
en tr
aine
d,
and
reso
urce
s are
ava
ilabl
e to
impl
emen
t mea
sure
s at m
axim
um h
ospi
tal
capa
city
in e
mer
genc
y or
disa
ster
situ
atio
ns.
144.
Infe
ctio
n su
rvei
llanc
e, p
reve
ntio
n an
d co
ntro
l pro
cedu
res
Safe
ty ra
tings
: Low
= P
olic
ies a
nd p
roce
dure
s do
not e
xist
; sta
ndar
d pr
e-ca
utio
ns fo
r inf
ectio
n pr
even
tion
and
cont
rol a
re n
ot fo
llow
ed ro
utin
ely;
Av
erag
e =
Pol
icie
s and
pro
cedu
res e
xist
, sta
ndar
d pr
ecau
tions
are
rou-
tinel
y fo
llow
ed, p
erso
nnel
hav
e be
en tr
aine
d, b
ut th
e le
vel o
f res
ourc
es
requ
ired
for e
mer
genc
y an
d di
sast
er si
tuat
ions
, inc
ludi
ng e
pide
mic
s, is
not a
vaila
ble;
Hig
h =
Pol
icie
s and
pro
cedu
res e
xist
, inf
ectio
n pr
even
tion
and
cont
rol m
easu
res a
re in
pla
ce, p
erso
nnel
hav
e be
en tr
aine
d, a
nd
reso
urce
s are
ava
ilabl
e to
impl
emen
t mea
sure
s at m
axim
um h
ospi
tal
capa
city
in e
mer
genc
y an
d di
sast
er si
tuat
ions
.
145.
Psy
chos
ocia
l ser
vice
sSa
fety
ratin
gs: L
ow =
Pro
cedu
res d
o no
t exi
st o
r exi
st o
nly
as a
doc
u-m
ent;
Aver
age
= P
roce
dure
s exi
st a
nd p
erso
nnel
hav
e be
en tr
aine
d, b
ut
the
leve
l of r
esou
rces
requ
ired
for e
mer
genc
y an
d di
sast
er si
tuat
ions
is
not a
vaila
ble;
Hig
h =
Pro
cedu
res e
xist
, per
sonn
el h
ave
been
trai
ned,
and
re
sour
ces a
re a
vaila
ble
for i
mpl
emen
tatio
n of
pro
cedu
res a
t max
imum
ho
spita
l cap
acity
in e
mer
genc
y an
d di
sast
er si
tuat
ions
.
Mod
ule
4: E
mer
genc
y an
d di
sast
er m
anag
emen
t

91
Hos
pita
l Saf
ety
Inde
x G
UID
E FO
R EV
ALU
ATO
RS
172
4.6
Pati
ent c
are
and
supp
ort s
ervi
ces
Safe
ty le
vel
Obs
erva
tions
(e
valu
ator
s’ co
mm
ents
)Low
Average
High
138.
Con
tinui
ty o
f em
erge
ncy a
nd cr
itica
l car
e se
rvice
sSa
fety
ratin
gs: L
ow =
Pro
cedu
res d
o no
t exi
st o
r exi
st o
nly
as a
doc
umen
t; Av
erag
e =
Pro
cedu
res e
xist
, per
sonn
el h
ave
been
trai
ned
but w
ould
not
be
ava
ilabl
e at
all
times
; Hig
h =
Pro
cedu
res e
xist
, per
sonn
el h
ave
been
tr
aine
d, a
nd re
sour
ces a
re a
vaila
ble
to im
plem
ent p
roce
dure
s at m
axi-
mum
hos
pita
l cap
acity
for e
mer
genc
y an
d di
sast
er si
tuat
ions
at a
ll tim
es.
139.
Con
tinui
ty o
f ess
entia
l clin
ical s
uppo
rt se
rvice
sSa
fety
ratin
gs: L
ow =
Pro
cedu
res d
o no
t exi
st o
r exi
st o
nly
as a
doc
umen
t; Av
erag
e =
Proc
edur
es e
xist
and
per
sonn
el h
ave
been
trai
ned
but w
ould
no
t be
avai
labl
e at
all
times
; Hig
h =
Proc
edur
es e
xist
s, pe
rson
nel h
ave
been
tra
ined
, and
reso
urce
s are
ava
ilabl
e to
impl
emen
t pro
cedu
res a
t max
imum
ho
spita
l cap
acity
for e
mer
genc
y an
d di
sast
er si
tuat
ions
at a
ll tim
es.
140.
Exp
ansio
n of
usa
ble
spac
e fo
r mas
s cas
ualty
incid
ents
Safe
ty ra
tings
: Low
= S
pace
for e
xpan
sion
has n
ot b
een
iden
tified
; Ave
r-ag
e =
Spa
ce h
as b
een
iden
tified
; equ
ipm
ent,
supp
lies a
nd p
roce
dure
s ar
e av
aila
ble
to c
arry
out
the
expa
nsio
n an
d st
aff h
ave
been
trai
ned,
but
te
stin
g ha
s not
bee
n co
nduc
ted;
Hig
h =
Pro
cedu
res e
xist
and
hav
e be
en
test
ed, p
erso
nnel
hav
e be
en tr
aine
d, a
nd e
quip
men
t, su
pplie
s and
oth
er
reso
urce
s are
ava
ilabl
e to
car
ry o
ut th
e ex
pans
ion
of sp
ace.
141.
Tria
ge fo
r maj
or e
mer
genc
ies a
nd d
isast
ers
Safe
ty ra
tings
: Low
= D
esig
nate
d tr
iage
loca
tion
or p
roce
dure
s do
not
exist
; Ave
rage
= T
riage
loca
tion
and
proc
edur
es e
xist
and
per
sonn
el h
ave
been
trai
ned,
but
pro
cedu
res h
ave
not b
een
test
ed fo
r em
erge
ncy
and
disa
ster
situ
atio
ns; H
igh
= L
ocat
ion
and
proc
edur
es e
xist
and
hav
e be
en
test
ed, p
erso
nnel
hav
e be
en tr
aine
d, a
nd re
sour
ces a
re in
pla
ce to
impl
e-m
ent a
t max
imum
hos
pita
l cap
acity
in e
mer
genc
y an
d di
sast
er si
tuat
ions
.
142.
Tria
ge ta
gs an
d ot
her l
ogist
ical s
uppl
ies f
or m
ass c
asua
lty in
ciden
tsSa
fety
ratin
gs: L
ow =
Non
exist
ent;
Aver
age
= S
uppl
y co
vers
less
than
72
hour
s of m
axim
um h
ospi
tal c
apac
ity; H
igh
= S
uppl
y gu
aran
teed
for a
t le
ast 7
2 ho
urs o
f max
imum
hos
pita
l cap
acity
.
143.
Syst
em fo
r ref
erra
l, tra
nsfe
r and
rece
ptio
n of
pat
ient
sSa
fety
ratin
gs: L
ow =
Pro
cedu
res d
o no
t exi
st o
r exi
st o
nly
as a
doc
umen
t; Av
erag
e =
Pro
cedu
res e
xist
and
per
sonn
el h
ave
been
trai
ned,
but
pro
-ce
dure
s hav
e no
t bee
n te
sted
for e
mer
genc
y or
disa
ster
situ
atio
ns; H
igh
= P
roce
dure
s exi
st a
nd h
ave
been
test
ed, p
erso
nnel
hav
e be
en tr
aine
d,
and
reso
urce
s are
ava
ilabl
e to
impl
emen
t mea
sure
s at m
axim
um h
ospi
tal
capa
city
in e
mer
genc
y or
disa
ster
situ
atio
ns.
144.
Infe
ctio
n su
rvei
llanc
e, p
reve
ntio
n an
d co
ntro
l pro
cedu
res
Safe
ty ra
tings
: Low
= P
olic
ies a
nd p
roce
dure
s do
not e
xist
; sta
ndar
d pr
e-ca
utio
ns fo
r inf
ectio
n pr
even
tion
and
cont
rol a
re n
ot fo
llow
ed ro
utin
ely;
Av
erag
e =
Pol
icie
s and
pro
cedu
res e
xist
, sta
ndar
d pr
ecau
tions
are
rou-
tinel
y fo
llow
ed, p
erso
nnel
hav
e be
en tr
aine
d, b
ut th
e le
vel o
f res
ourc
es
requ
ired
for e
mer
genc
y an
d di
sast
er si
tuat
ions
, inc
ludi
ng e
pide
mic
s, is
not a
vaila
ble;
Hig
h =
Pol
icie
s and
pro
cedu
res e
xist
, inf
ectio
n pr
even
tion
and
cont
rol m
easu
res a
re in
pla
ce, p
erso
nnel
hav
e be
en tr
aine
d, a
nd
reso
urce
s are
ava
ilabl
e to
impl
emen
t mea
sure
s at m
axim
um h
ospi
tal
capa
city
in e
mer
genc
y an
d di
sast
er si
tuat
ions
.
145.
Psy
chos
ocia
l ser
vice
sSa
fety
ratin
gs: L
ow =
Pro
cedu
res d
o no
t exi
st o
r exi
st o
nly
as a
doc
u-m
ent;
Aver
age
= P
roce
dure
s exi
st a
nd p
erso
nnel
hav
e be
en tr
aine
d, b
ut
the
leve
l of r
esou
rces
requ
ired
for e
mer
genc
y an
d di
sast
er si
tuat
ions
is
not a
vaila
ble;
Hig
h =
Pro
cedu
res e
xist
, per
sonn
el h
ave
been
trai
ned,
and
re
sour
ces a
re a
vaila
ble
for i
mpl
emen
tatio
n of
pro
cedu
res a
t max
imum
ho
spita
l cap
acity
in e
mer
genc
y an
d di
sast
er si
tuat
ions
.
Mod
ule
4: E
mer
genc
y an
d di
sast
er m
anag
emen
t

92
173
146.
Pos
t-mor
tem
pro
cedu
res i
n a m
ass f
atal
ity in
ciden
tSa
fety
ratin
gs: L
ow =
Pro
cedu
res f
or a
mas
s fat
ality
inci
dent
do
not e
xist
or
exist
onl
y as
a d
ocum
ent;
Aver
age
= Pr
oced
ures
exi
st a
nd p
erso
nnel
hav
e be
en tr
aine
d, b
ut th
e le
vel o
f res
ourc
es re
quire
d fo
r em
erge
ncy
and
disa
ster
sit
uatio
ns is
not
ava
ilabl
e; H
igh
= Pr
oced
ures
exi
st, p
erso
nnel
hav
e be
en
train
ed, a
nd re
sour
ces a
re a
vaila
ble
for i
mpl
emen
tatio
n of
pro
cedu
res a
t m
axim
um h
ospi
tal c
apac
ity in
em
erge
ncy
and
disa
ster
situ
atio
ns.
4.7
Evac
uati
on, d
econ
tam
inat
ion
and
secu
rity
Safe
ty le
vel
Obs
erva
tions
(e
valu
ator
s’ co
mm
ents
)Low
Average
High
147.
Evac
uatio
n pl
anSa
fety
ratin
gs: L
ow =
Pla
n do
es n
ot e
xist
or e
xist
s onl
y as
a d
ocum
ent;
Aver
age
= P
lan
exist
s and
per
sonn
el h
ave
been
trai
ned
in p
roce
dure
s, bu
t tes
ts a
re n
ot c
ondu
cted
regu
larly
; Hig
h =
Pla
n ex
ists,
pers
onne
l hav
e be
en tr
aine
d, a
nd e
vacu
atio
n dr
ills a
re h
eld
at le
ast a
nnua
lly.
148.
Dec
onta
min
atio
n fo
r che
mica
l and
radi
olog
ical h
azar
dsSa
fety
ratin
gs: L
ow =
No
pers
onal
pro
tect
ive
equi
pmen
t is a
vaila
ble
for i
mm
edia
te u
se b
y ho
spita
l sta
ff, o
r no
deco
ntam
inat
ion
area
exi
sts;
Aver
age
= P
erso
nal p
rote
ctiv
e eq
uipm
ent i
s ava
ilabl
e fo
r im
med
iate
use
, de
cont
amin
atio
n ar
eas a
re e
stab
lishe
d, st
aff tr
aini
ng a
nd d
rills
are
not
cond
ucte
d an
nual
ly; H
igh
= P
erso
nal p
rote
ctiv
e eq
uipm
ent i
s ava
ilabl
e fo
r im
med
iate
use
, dec
onta
min
atio
n ar
eas a
re e
stab
lishe
d an
d pe
rson
nel
are
trai
ned
and
test
ed a
t lea
st a
nnua
lly.
149.
Per
sona
l pro
tect
ion
equi
pmen
t and
isol
atio
n fo
r inf
ectio
us d
is-ea
ses a
nd e
pide
mics
Safe
ty ra
tings
: Low
= N
o pe
rson
al p
rote
ctiv
e eq
uipm
ent i
s ava
ilabl
e fo
r im
med
iate
use
by
hosp
ital s
taff,
or n
o iso
latio
n ar
ea e
xist
s; Av
erag
e =
Sup
-pl
y is
avai
labl
e fo
r im
med
iate
use
, but
is su
ffici
ent f
or le
ss th
an 7
2 ho
urs o
f m
axim
um h
ospi
tal c
apac
ity, i
sola
tion
area
s are
est
ablis
hed,
staff
trai
ning
an
d te
stin
g of
pro
cedu
res a
re n
ot c
ondu
cted
ann
ually
; Hig
h =
Sup
ply
is gu
aran
teed
for a
t lea
st 7
2 ho
urs o
f max
imum
hos
pita
l cap
acity
and
alte
r-na
te so
urce
s are
in p
lace
for r
esup
ply,
isola
tion
area
s are
est
ablis
hed,
staff
tr
aini
ng a
nd te
stin
g of
pro
cedu
res a
re c
ondu
cted
at l
east
ann
ually
.
150.
Em
erge
ncy s
ecur
ity p
roce
dure
sSa
fety
ratin
gs: L
ow =
Em
erge
ncy
secu
rity
proc
edur
es d
o no
t exi
st o
r exi
st
only
as a
doc
umen
t; Av
erag
e =
Doc
umen
ted
proc
edur
es e
xist
and
per
-so
nnel
hav
e be
en tr
aine
d in
em
erge
ncy
secu
rity
proc
edur
es b
ut te
stin
g is
not c
ondu
cted
at l
east
ann
ually
; Hig
h =
Per
sonn
el a
re tr
aine
d an
d te
sts o
f th
e do
cum
ente
d pr
oced
ures
are
hel
d at
leas
t ann
ually
.
151.
Com
pute
r sys
tem
net
wor
k sec
urity
Safe
ty ra
tings
: Low
= T
he h
ospi
tal d
oes n
ot h
ave
a co
mpu
ter s
ecur
ity sy
s-te
m p
lan
and
proc
edur
es in
pla
ce; A
vera
ge =
The
hos
pita
l has
a b
asic
cyb
er
secu
rity
plan
in p
lace
but
it is
not
mon
itore
d an
d up
date
d re
gula
rly; H
igh
=
The
hosp
ital h
as a
cyb
er se
curit
y pl
an in
pla
ce a
nd it
is u
pdat
ed re
gula
rly.
Com
men
ts o
n th
e re
sults
of F
orm
2, M
odul
e 3.
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
Nam
e/sig
natu
re o
f eva
luat
or(s
) ......
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
...
ANN
EX 2
: FO
RM 2
: SAF
E H
OSP
ITAL
S CH
ECKL
IST
Mod
ule
4: E
mer
genc
y an
d di
sast
er m
anag
emen
t

93
173
146.
Pos
t-mor
tem
pro
cedu
res i
n a m
ass f
atal
ity in
ciden
tSa
fety
ratin
gs: L
ow =
Pro
cedu
res f
or a
mas
s fat
ality
inci
dent
do
not e
xist
or
exist
onl
y as
a d
ocum
ent;
Aver
age
= Pr
oced
ures
exi
st a
nd p
erso
nnel
hav
e be
en tr
aine
d, b
ut th
e le
vel o
f res
ourc
es re
quire
d fo
r em
erge
ncy
and
disa
ster
sit
uatio
ns is
not
ava
ilabl
e; H
igh
= Pr
oced
ures
exi
st, p
erso
nnel
hav
e be
en
train
ed, a
nd re
sour
ces a
re a
vaila
ble
for i
mpl
emen
tatio
n of
pro
cedu
res a
t m
axim
um h
ospi
tal c
apac
ity in
em
erge
ncy
and
disa
ster
situ
atio
ns.
4.7
Evac
uati
on, d
econ
tam
inat
ion
and
secu
rity
Safe
ty le
vel
Obs
erva
tions
(e
valu
ator
s’ co
mm
ents
)Low
Average
High
147.
Evac
uatio
n pl
anSa
fety
ratin
gs: L
ow =
Pla
n do
es n
ot e
xist
or e
xist
s onl
y as
a d
ocum
ent;
Aver
age
= P
lan
exist
s and
per
sonn
el h
ave
been
trai
ned
in p
roce
dure
s, bu
t tes
ts a
re n
ot c
ondu
cted
regu
larly
; Hig
h =
Pla
n ex
ists,
pers
onne
l hav
e be
en tr
aine
d, a
nd e
vacu
atio
n dr
ills a
re h
eld
at le
ast a
nnua
lly.
148.
Dec
onta
min
atio
n fo
r che
mica
l and
radi
olog
ical h
azar
dsSa
fety
ratin
gs: L
ow =
No
pers
onal
pro
tect
ive
equi
pmen
t is a
vaila
ble
for i
mm
edia
te u
se b
y ho
spita
l sta
ff, o
r no
deco
ntam
inat
ion
area
exi
sts;
Aver
age
= P
erso
nal p
rote
ctiv
e eq
uipm
ent i
s ava
ilabl
e fo
r im
med
iate
use
, de
cont
amin
atio
n ar
eas a
re e
stab
lishe
d, st
aff tr
aini
ng a
nd d
rills
are
not
cond
ucte
d an
nual
ly; H
igh
= P
erso
nal p
rote
ctiv
e eq
uipm
ent i
s ava
ilabl
e fo
r im
med
iate
use
, dec
onta
min
atio
n ar
eas a
re e
stab
lishe
d an
d pe
rson
nel
are
trai
ned
and
test
ed a
t lea
st a
nnua
lly.
149.
Per
sona
l pro
tect
ion
equi
pmen
t and
isol
atio
n fo
r inf
ectio
us d
is-ea
ses a
nd e
pide
mics
Safe
ty ra
tings
: Low
= N
o pe
rson
al p
rote
ctiv
e eq
uipm
ent i
s ava
ilabl
e fo
r im
med
iate
use
by
hosp
ital s
taff,
or n
o iso
latio
n ar
ea e
xist
s; Av
erag
e =
Sup
-pl
y is
avai
labl
e fo
r im
med
iate
use
, but
is su
ffici
ent f
or le
ss th
an 7
2 ho
urs o
f m
axim
um h
ospi
tal c
apac
ity, i
sola
tion
area
s are
est
ablis
hed,
staff
trai
ning
an
d te
stin
g of
pro
cedu
res a
re n
ot c
ondu
cted
ann
ually
; Hig
h =
Sup
ply
is gu
aran
teed
for a
t lea
st 7
2 ho
urs o
f max
imum
hos
pita
l cap
acity
and
alte
r-na
te so
urce
s are
in p
lace
for r
esup
ply,
isola
tion
area
s are
est
ablis
hed,
staff
tr
aini
ng a
nd te
stin
g of
pro
cedu
res a
re c
ondu
cted
at l
east
ann
ually
.
150.
Em
erge
ncy s
ecur
ity p
roce
dure
sSa
fety
ratin
gs: L
ow =
Em
erge
ncy
secu
rity
proc
edur
es d
o no
t exi
st o
r exi
st
only
as a
doc
umen
t; Av
erag
e =
Doc
umen
ted
proc
edur
es e
xist
and
per
-so
nnel
hav
e be
en tr
aine
d in
em
erge
ncy
secu
rity
proc
edur
es b
ut te
stin
g is
not c
ondu
cted
at l
east
ann
ually
; Hig
h =
Per
sonn
el a
re tr
aine
d an
d te
sts o
f th
e do
cum
ente
d pr
oced
ures
are
hel
d at
leas
t ann
ually
.
151.
Com
pute
r sys
tem
net
wor
k sec
urity
Safe
ty ra
tings
: Low
= T
he h
ospi
tal d
oes n
ot h
ave
a co
mpu
ter s
ecur
ity sy
s-te
m p
lan
and
proc
edur
es in
pla
ce; A
vera
ge =
The
hos
pita
l has
a b
asic
cyb
er
secu
rity
plan
in p
lace
but
it is
not
mon
itore
d an
d up
date
d re
gula
rly; H
igh
=
The
hosp
ital h
as a
cyb
er se
curit
y pl
an in
pla
ce a
nd it
is u
pdat
ed re
gula
rly.
Com
men
ts o
n th
e re
sults
of F
orm
2, M
odul
e 3.
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
Nam
e/sig
natu
re o
f eva
luat
or(s
) ......
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
........
...
ANN
EX 2
: FO
RM 2
: SAF
E H
OSP
ITAL
S CH
ECKL
IST
Mod
ule
4: E
mer
genc
y an
d di
sast
er m
anag
emen
t

94
68

9567
Lampiran 2 Contoh Prinsip Prosedur yang harus ada dalam SPO
PRINSIP PROSEDUR YANG HARUS ADA DI SPO TERKAIT DISEASE DISASTER
PEMANTAUAN KESEHATAN MANDIRI UNTUK PEKERJA RUMAH SAKIT
Prinsip prosedur
Sebelum masuk kerja, ada kebijakan yang menerapkan pemantauan kesehatan mandiri (self assessment) bagi seluruh pekerja Rumah Sakit sebagai skrining kesehatan kerja. Pelaksanaan pemantauan kesehatan mandiri ini bersifat wajib.
Tujuan
Tujuan pemantauan kesehatan mandiri adalah untuk memastikan pekerja yang akan memasuki tempat kerja dan melakukan kegiatan kerja dalam kondisi tidak terjangkit atau bergejala
Instruksi Umum untuk semua Pekerja Rumah Sakit
a. Pekerja Rumah Sakit wajib melakukan pemantauan kesehatan mandiri ini dengan mengisi
form yang telah ditetapkan
b. K3 melaksanakan pemantauan hasil pengisian form pemantauan kesehatan mandiri
c. K3 melakukan koordinasi lebih lanjut untuk penanganan bila ditemukan masalah klinis
Pemulihan
a. Apabila hasil pemantauan kesehatan mandiri tidak ditemukan masalah klinis, pekerja bisa
melanjutkan tugas sesuai profesinya
b. Pada temuan hasil pemantauan dengan masalah klinis, setelah melalui tindak lanjut
sesuai masalah kesehatan yang dialami akan masuk dalam dalam program rehabilitasi
kesehatan kerja

96
68
PENENTUAN ZONASI TEMPAT KERJA
Prinsip Prosedur
Identifikasi jenis pekerjaan dan kaitannya dengan potensi bahaya penularan perlu dilakukan dalam rangka membuat upaya pengendalian risiko yang lebih terstruktur. Penilaian risiko dilakukan berdasarkan hasil identifikasi risiko kerja.
Tujuan
Untuk bisa dilaksanakan pengendalian risiko yang lebih efektif dan efisien.
Pengelompokan Pekerja Berisiko
a. Risiko Pajanan Rendah
Adalah pekerjaan yang aktifitas kerjanya tidak berhubungan langsung dengan sumber risiko infeksi
b. Risiko Pajanan Sedang
Adalah pekerjaan yang sering berhubungan/kontak dengan sumber risiko infeksi namun bukan sumber risiko yang sudah terkonfirmasi positif terinfeksi
c. Risiko Pajanan Tinggi
Adalah pekerjaan yang berpotensi tinggi untuk kontak dekat atau kontak langsung dengan sumber risiko yang diduga atau sudah terkonfirmasi positif terinfeksi
Keluaran/Output
- Narasi zonasi risiko kerja
- Peta risiko kerja
69
KEBAKARAN ( CODE MERAH)
Prinsip prosedur bila terjadi kebakaran di Rumah Sakit
1. Tenang. bertindak cepat. Jangan berteriak kebakaran (Teriakan “ Kode Merah” )2. Pindahkan semua pasien dari daerah yang terkena langsung atau yang dekat sumber
asap/api3. Aktifkan alarm kebakaran terdekat (jika tersedia) dan hubungi nomor keadaan
darurat pada masing masing Rumah Sakit untuk mengaktifkan kode merah/red dan melaporkan lokasi serta keparahan api
4. Membatasi api dengan menutup semua pintu dan jendela5. Memadamkan api dengan segera jika mungkin, jika tidak: evakuasi semua orang ke
daerah yang aman sementara bila terus membesar, evakuasi melalui pintu darurat yang sudah diberi tanda EXIT
Instruksi umum untuk semua Pegawai Rumah Sakit
1. Pastikan semua pintu darurat dan keluar, koridor dan ruang tertutup bebas dari halangan apapun
2. Tidak boleh menggunakan lift3. Menjaga dan tidak boleh mempergunakan saluran telepon kecuali untuk pengendalian
kebakaran. Mengaktifkan sistem komunikasi Rumah Sakit4. Semua personil Tanggap Darurat Kebakaran Gedung dan Korporat di Rumah Sakit harus
diaktifkan5. Bila suara alarm dan pengumuman tidak ada atau didengar dalam waktu 60 detik,
hubungi supervisor perawat, jika tidak ada respon dalam 120 detik, mengevakuasi orang di bagian bangunan ke luar gedung
6. Menenangkan pasien dan rekan kerja
Pemulihan Keadaan
1. Tidak boleh masuk ke area yang terkena sampai ada pengarahan dari Personil Tanggap Daruarat Gedung Rumah Sakit
2. Setelah diperbolehkan masuk kembali, memberitahukan petugas yang bertanggung jawab (supervisor perawat) kerusakan di masing-masing tempat atau barang-barang pribadi
3. Menjamin semua sistem darurat berfungsi penuh kembali4. Meyakinkan staf dan pasien tentang kondisi yang sudah aman

97
69
KEBAKARAN ( CODE MERAH)
Prinsip prosedur bila terjadi kebakaran di Rumah Sakit
1. Tenang. bertindak cepat. Jangan berteriak kebakaran (Teriakan “ Kode Merah” )2. Pindahkan semua pasien dari daerah yang terkena langsung atau yang dekat sumber
asap/api3. Aktifkan alarm kebakaran terdekat (jika tersedia) dan hubungi nomor keadaan
darurat pada masing masing Rumah Sakit untuk mengaktifkan kode merah/red dan melaporkan lokasi serta keparahan api
4. Membatasi api dengan menutup semua pintu dan jendela5. Memadamkan api dengan segera jika mungkin, jika tidak: evakuasi semua orang ke
daerah yang aman sementara bila terus membesar, evakuasi melalui pintu darurat yang sudah diberi tanda EXIT
Instruksi umum untuk semua Pegawai Rumah Sakit
1. Pastikan semua pintu darurat dan keluar, koridor dan ruang tertutup bebas dari halangan apapun
2. Tidak boleh menggunakan lift3. Menjaga dan tidak boleh mempergunakan saluran telepon kecuali untuk pengendalian
kebakaran. Mengaktifkan sistem komunikasi Rumah Sakit4. Semua personil Tanggap Darurat Kebakaran Gedung dan Korporat di Rumah Sakit harus
diaktifkan5. Bila suara alarm dan pengumuman tidak ada atau didengar dalam waktu 60 detik,
hubungi supervisor perawat, jika tidak ada respon dalam 120 detik, mengevakuasi orang di bagian bangunan ke luar gedung
6. Menenangkan pasien dan rekan kerja
Pemulihan Keadaan
1. Tidak boleh masuk ke area yang terkena sampai ada pengarahan dari Personil Tanggap Daruarat Gedung Rumah Sakit
2. Setelah diperbolehkan masuk kembali, memberitahukan petugas yang bertanggung jawab (supervisor perawat) kerusakan di masing-masing tempat atau barang-barang pribadi
3. Menjamin semua sistem darurat berfungsi penuh kembali4. Meyakinkan staf dan pasien tentang kondisi yang sudah aman

98

9970
KEAMANAN (CODE GREY )
Prinsip Prosedur Keselamatan Keamanan Di Rumah Sakit
1. Mengamankan fasilitas dan kejadian yang tidak diinginkan dan membatasi akses dan gerakan di dalam Rumah Sakit.
2. Bila ada situasi yang mengganggu keamanan dan diumumkan "kode ...." disampaikan melalui sistem komunikasi Rumah Sakit ke Pos Komando keamanan Rumah Sakit
3. Bila mendengar "kode ...." pusat komando keamanan Rumah Sakit segera menutup semua pintu keluar dan masing-masing gedung mengunci lobi Gedung Rumah Sakit
4. Bila mendengar "Kode ...." semua staf /pegawai yang berada didekat pintu keluar ruangan, lantai, lobi harus segera menutup dan mengunci semua pintu dan memastikan semua pasien, pengunjung, dan staf tetap ditempat.
5. Hidupkan sistem komunikasi untuk instruksi lebih lanjut.6. Staf / pegawai Rumah Sakit harus melaporkan semua orang asing ke supervisor
keperawatan. 7. Staf / pegawai akan menginstruksikan pengunjung untuk tinggal di lokasi sampai
petunjuk lebih lanjut dari staf/pegawai Rumah Sakit.8. Rumah Sakit tetap pada "waspada" sampai dinyatakan kode... selesai.
Penanggung jawab gedung Rumah Sakit yang bertanggung jawab
1. Sesuai dengan situasi, langsung menghubungi dan berkomunikasi dengan Bagian Informasi Gedung untuk mengumumkan "Kode..." (dengan HT / telepon ), menempatkan seluruh staf/pegawai Rumah Sakit pada peringatan keamanan tinggi.
2. Memeriksa bahwa semua pintu luar tertutup dan terkunci.3. Memberitahukan dan berkomunikasi untuk tindak lanjut dengan: polisi, Direktur / CEO,
staf , dan Instalasi Gawat Darurat (IGD).4. Selama waktu "waspada" menetapkan 2 orang tim dengan radio (HT) untuk memeriksa
pintu dan area bangunan dimasing-masing gedung.
Pemulihan
1. Pusat komunikasi masing-masing gedung langsung mengumumkan "pemulhan" pada saat yang tepat, untuk memungkinkan kembali ke kegiatan normal.
2. Meyakinkan, menginformasikan staf dan pasien.
Situasi PenyanderaanA. Bila mengetahui situasi ini:
1. Memberitahukan supervisor perawat yang akan memberitahu polisi2. Mendeklarasikan sebuah "Kode ..."3. Menjaga semua orang menjauh dari daerah tersebut
B. Administrator yang bertanggung jawab (CEO atau supervisor perawat shift)1. Admistrator yang bertanggung jawab dan departement polisi akan memutuskan
bagaimana untuk melanjutkan atau bernegosiasi. Pusat komando akan dibentuk2. Administrator yang bertanggung jawab dan represetative polisi akan tetap di daerah
tersebut selama negosiasi.3. Mengaktifkan insiden kritis dan tim stres pembekalan
C. Pemeliharaan / penjaga keamanan1. Mengamankan daerah

100 71
GEMPA ( CODE GREEN)
Selama gempa bumiTetap tenang, bersikap menenangkan pasien dan berlindung ditempat yang aman
Kalau di luar: berdiri jauh dari pohon gedung, telepon dan saluran listrik.
Jika mengemudi: berkendara dari underpass, jalan layang, berhenti di daerah yang aman; tetap di dalam kendaraan, radio atau telepon Rumah Sakit untuk melaporkan status dan lokasi, jika mungkin.
Pemulihan setelah gempa/kerusakan struktur
1. Gunakan alat pemadam kebakaran untuk memadamkan kebakaran kecil. Aktifkan rencana keselamatan kebakaran (Code red) dan mengumumkan Code Green jika dan pindah ke lokasi yang aman.
2. Memeriksa cedera pada diri sendiri, karyawan lain, pasien, pengunjung, memberikan pertolongan pertama jika diperlukan.
3. Menjamin keselamatan karyawan lain dan pasien di unit Anda / departemen / daerah.
4. Melakukan pemeriksaan kerusakan unit Anda, departemen, atau daerah. Melaporkan semua temuan kepada pengawas / supervisor keperawatan Anda.
5. Mengaktifkan sistem komunikasi Rumah Sakit dan menunggu instruksi lebih lanjut.
6. Tidak menggunakan saluran telepon kecuali dalam keadaan darurat untuk mencegah overloading sistem telepon.

10172
TUMPAHAN BAHAN BERBAHAYA (CODE ORANGE)
Prinsip Prosedur Tumpahan Bahan Berbahaya dan Penyebarannya
Bila mengetahui adanya tumpahan bahan berbahaya, atau melepaskan debu(termasuk asbes) harus segera memberitahu supervisor perawat / tim tanggap darurat Rumah Sakit yang bertanggung jawab dan mengisolasi daerah tersebut
Instruksi Umum
1. Pemberitahuan semua orang di daerah tumpahan langsung tentang bahaya paparan
2. Semua staf/pegawai harus menutup di daerah tumpahan dengan menutup semua pintu masuk / keluar ke daerah tersebut dan diberikan penandaan keselamatan pasca peringatan bahaya
3. Perawat supervisor atau penanggung jawab ruangan harus memberitahu pusat komunikasi tumpahan atau pelepasan debu Rumah Sakit dan tingkat bahaya untuk pengumuman kode darurat
4. Pemeriksaan MSDS untuk penanganan yang tepat, membersihkan dan informasi pembuangan yang benar
• menutupi atau membuang penyerap tumpahan (menggunakan Spill kit)• memanggil pegawai terlatih dan kompeten untuk penanganan lebih lanjut

102
73
Lampiran 3. Contoh Skenario Umum untuk Simulasi
KEBAKARAN AKIBAT GEMPA SKALA INTENSITAS VII MMI
Pada tanggal 8 November 2016 terjadi gempa skala intensitas VII MMI pegawai dan tamugedung RS X panik masing-masing menyelamatkan diri mencari tempat perlindungan yang aman. Para pegawai dan perawat berteriak instruksi kepada para pegawai dan tamumenunjukkan tempat aman. Pegawaipun berteriak kepada pegawai lainnya agar berlindung dari reruntuhan.
Tiba-tiba salah satu pegawai lt 3 melihat listrik yang memercik karena colokan renggang akibat kabel yang tertindih tas yang jatuh. Api menyambar dokumen, pegawai bertambah panik teriak kebakaran kebakaran.
Setelah gempa berhenti, pegawai segera menuju lokasi sambil membawa APAR, namun karena api dekat dengan pasien, maka pegawai mencoba menyelamatkan tamu sambil teriak minta tolong. Mendengar teriakan, pegawai lain segera teriak code red,menghubungi Dinas Kebakaran dan pegawai membunyikan alarm .... Alarm .... lalu pegawai yang membawa APAR mencoba memadamkan api , pegawai lain menghubungi KKD gedung RSUD. KKD gedung instruksi umumkan kondisi emergency dengan code red. Mendengar pengumuman maka seluruh tim tanggap darurat siaga laksanakan tugasnya. Karena asap mulai menyebar, maka pegawai yang memadamkan api dengan APAR menjadi gagal karena jarak semprot yang jauh menghindari asap. Tindakan evakuasi parsial di instruksikan regu evakuasi lt 3,menuju tangga darurat kanan dan kiri
KKD menghubungi koordinator semua lantai perawatan dan staf Medik untuk mengevakuasi penghuni menuju titik berkumpul, selanjutnya memonitor kesiagaan seluruh timnya melalui ……. Api membesar membakar kasur dan mulai merambat ke benda lain di dalam kamar ………., regu pemadam sekuriti yang tiba mulai menggelar hidran, dan kesulitan mengarahkan pancaran air hidran ke dalam ruangan karena pandangannya terhalang asap yang tebal. Pendinginan dengan melokalisir area terbakar dilakukan, dan karena asap mulai naik melalui shaf, maka KKD instruksikan evakuasi (code purple) seluruh pasien lantai 3 s/d 7. Semua Koordinator Lantai memimpin timnya mengevakuasi pasien, dengan memperhatikan klasifikasi : semua pasien mobile, limited mobile, dan not mobile beserta keluarganya ke area pengungsian di dekat pintu taangga darurat, pasien not mobile beserta keluarganya ke titik berkumpul melalui ramp.
Pada saat pompa hidran utama diaktifkan tiba-tiba mesin mati, maka tehnisi segera mengaktifkan pompa diesel. KKD melaporkan kepada Direktur Emergency dan minta bantuan koordinasi area parkir diluar gedung dan tambahan tenaga bantuan (perawat, dokter, tehnik, dll).
Kondisi parkir mobil yang padat menghalangi masuknya Fire Truck Dinas Kebakaran, semua crew Fire Truck Dinas Pemadam menuju Poskotis berkoordinasi dengan KKD dan mengambil alih operasi pemadaman. Dengan menggunakan alat bantu pernafasan mandiri (SCBA) maka crew Dinas Pemadam berhasil memadamkan kebakaran dalam tempo 15 menit.
Tanda-tanda interior dan struktur bangunan dinyatakan aman oleh KKD setelah berkoordinasi dengan Direktur Emergency, maka KKD memberi instruksi : Pasien lantai 2 kamar 206 di pindahkan ke ruang perawatan lain, sementara pasien dari kamar lainnya di lantai 2 dan lantai 3 s/d 8 kembali memasuki ruang perawatan setelah kondisi dinyatakan steril dari asap. Koordinator Titik berkumpul melaporkan kepada KKD dan diketahui 1 pasien trauma, 1 meninggal karena shock.
74
Contoh skenario terjadi kedaruratan bencana (multiple code) di Rumah Sakit
1. Terjadi Gempa berkekuatan 5,8 SR2. Paging dibunyikan telah terjadi CODE GREEN3. Semua orang yang ada di RS melindungi diri gempa sampai gempa selesai , 4. Tiba-tiba terdengaar teriakan dari salah satu pegawai di salah satu ruang perawatan
yang memberikan peringatan jika ada kebakaran akibat Konsleting listrik5. Komando lantai mengaktifkan kode red dan menghubungi operator untuk
memberitahukan telah terjadi kode red6. Tim kode Red melakukan tugas masing-masing sesuai tugasnya 7. Petugas Helm Merah dibantu oleh karyawan lainnya dan security berusaha
memadamkan kebaaran api dengan memakai APAR 8. Petugas Helm Kuning memberi komando dalam evakuasi pasien dengan meminta
bantuan orang yang berada di tempat tersebut 9. Petugas Helm biru memberi komando dalam penyelamatan asset dibantu petugas lainnya 10. Jika api padam api evakuasi tidak dilakukan
Simulasi selesai
11. Jika api tidak bisa dikendalikan komando lantai melakukan evakuasi sesuai arahan komandan bencana
12. pegawai dan pengunjung melakukan evakuasi menuju assembly point, namun ada sebagian pasien dan pengunjung yang masih berada di ruangan sambil menunggu perkembangan dan instruksi dari komando bencana
13. komando bencana mengintruksikan untuk dilakukan evakuasi14. Karyawan dan penunggu pasien yang ada di Ruangan melakukan evakuasi terhadap
pasien, asset dan dokumen.15. Disaat proses evakuasi masih berlangsung kondisi agak tegang16. Tiba2 ada yang pingsan orang yang ada didekatnya melakukan bhd dan segera berteriak
code blue tim code blue segera melakukan tindakan sampai pasien dapat di amankan17. Sementara itu pasien-pasien yang dievakusi di assembly point mendapat tindakan
darurat oleh petugas medis sebelum dipindah dengan ambulance ke IGD/gedung lainOperasi Tanggap Darurat Kebakaran (Code Red), Tanggap Darurat Medis (Code Blue) dan Evakuasi total dinyatakan selesai dilaksanakan.

103
74
Contoh skenario terjadi kedaruratan bencana (multiple code) di Rumah Sakit
1. Terjadi Gempa berkekuatan 5,8 SR2. Paging dibunyikan telah terjadi CODE GREEN3. Semua orang yang ada di RS melindungi diri gempa sampai gempa selesai , 4. Tiba-tiba terdengaar teriakan dari salah satu pegawai di salah satu ruang perawatan
yang memberikan peringatan jika ada kebakaran akibat Konsleting listrik5. Komando lantai mengaktifkan kode red dan menghubungi operator untuk
memberitahukan telah terjadi kode red6. Tim kode Red melakukan tugas masing-masing sesuai tugasnya 7. Petugas Helm Merah dibantu oleh karyawan lainnya dan security berusaha
memadamkan kebaaran api dengan memakai APAR 8. Petugas Helm Kuning memberi komando dalam evakuasi pasien dengan meminta
bantuan orang yang berada di tempat tersebut 9. Petugas Helm biru memberi komando dalam penyelamatan asset dibantu petugas lainnya 10. Jika api padam api evakuasi tidak dilakukan
Simulasi selesai
11. Jika api tidak bisa dikendalikan komando lantai melakukan evakuasi sesuai arahan komandan bencana
12. pegawai dan pengunjung melakukan evakuasi menuju assembly point, namun ada sebagian pasien dan pengunjung yang masih berada di ruangan sambil menunggu perkembangan dan instruksi dari komando bencana
13. komando bencana mengintruksikan untuk dilakukan evakuasi14. Karyawan dan penunggu pasien yang ada di Ruangan melakukan evakuasi terhadap
pasien, asset dan dokumen.15. Disaat proses evakuasi masih berlangsung kondisi agak tegang16. Tiba2 ada yang pingsan orang yang ada didekatnya melakukan bhd dan segera berteriak
code blue tim code blue segera melakukan tindakan sampai pasien dapat di amankan17. Sementara itu pasien-pasien yang dievakusi di assembly point mendapat tindakan
darurat oleh petugas medis sebelum dipindah dengan ambulance ke IGD/gedung lainOperasi Tanggap Darurat Kebakaran (Code Red), Tanggap Darurat Medis (Code Blue) dan Evakuasi total dinyatakan selesai dilaksanakan.

104
75
Lampiran 4. Contoh Skenario Detil untuk Simulasi
SKENARIO DETIL SIMULASI GEMPA & KEBAKARAN
No Waktu KEJADIAN PEMERAN AKTIF K E G I A T A N PEMERAN PASIFA X : 00 Guncangan
gempaKaryawan Masing-masing
menyelamatkan diri menuju tempat aman, melindungi kepala dari reruntuhan
Seluruh pengguna
Semua KL. Y&S Ingatkan prosedur saat terjadi gempa
RE.1-4 Y
Semua RE.1 Y Teriak tunjukkan tempat aman terdekat bagi keluarga pasien
Keluarga pasien
Semua RE.2 Y Teriak tunjukkan cara melindungi kepala & badan dari reruntuhan
s.d.a
Semua RE.3 Y Teriak pada pasien yang limited mobile agar turun dari ranjang dan tiarap di samping ranjang
Pasien Limited mobil
Semua RE.4 Y Teriak tunjukkan cara berlindung pasien yang menggunakan oksigen dan infus, agar tidak lari.
Pasien
B X : 02 Guncangan KKD Instruksi via HT lihat hasil receiver skala MMI, atau telpon BMKG
Tim Teknik
Berhenti Tim Teknik Melaporkan dengan HT informasi skala intensitas & kondisi gempa
KKD
KKD Instruksi periksa struktur bangunan &laporkan segera, umumkan code brown
Tim Teknik
Tim Teknik Instruksi umumkan code brown
TI
Tim Teknik Instruksi periksa seluruh lantai
TTL
TI Umumkan code brown 0Semua KL.Y Instruksi tenangkan pasien
dan stabilkan kondisinyaSemua RE.Y
Semua RE.1-4Y Tenangkan pasien dan stabilkan kondisinya
Pasien
TPP Menghubungi KKD menanyakan perlu evakuasi atau tidak
KKD
RTB.A Menghubungi KKD menanayakan perlu evakuasi atau tidak
KKD
76
Asst.1KKD/RTB.B Melaporkan kondisi pasien, menanyakan perlu evakuasi atau tidak
KKD
Asst.2KKD/RTB.C Melaporkan kondisi operasional, menanyakan perlu evakuasi atau tidak
KKD
Asst.3KKD Melaporkan kondisi support, membantu operasional komunikasi darurat
KKD
KL Gempa sudah selesai, pasien harap kembali ke tempat tidur
RE. Pasien
R.E Memandu pasien kembali ke tempat tidur
Pasien & kel. pasien
C X : 03 Kebakaran di
Pasien …… Teriak kebakaran-kebakaran
RE.1,2,3, KL.3 Y
Lantai 3 RE.1 Y lt.3 Mengambil APAR menuju ruang….
Keluarga pasien
RE.2 Y lt.3 Tekan tombol fire alarm, dan bantu evakuasi pasien ….
Pasien
RE.3 Y lt.3 Evakuasi pasien yang dekat dengan api ke area pengungsian
RE.2 Y lt.3,
KL.3 Y Lapor terjadi kebakaran di ruang….
KKD
KKD Instruksi umumkan code red ruang…..
TI
TI Umumkan code red PenggunaTim Teknik Memanggil dan membagi
tugas kepada timnyaTim Teknik Lantai
Pemadam.1 Lapor kepada TKP, telah mendengar code red di lantai 3
TKP
TKP Lapor regu pemadam telah menuju lokasi, dan TKP Merapat ke lantai 3
KKD
KKD Hubungi tim tanggap darurat, dan minta ke lantai 3
TT,TPP,AsKKD123
Tim Teknik Instruksi buka pintu darurat lantai dasar ramp
TTL
Tim Teknik Instruksi padamkan listrik & AC lantai 3, non aktifkan lift
TTL
TTL Non aktifkan lift, dan siaga di depan emergency lift lobby utama no.8
-
TTL Padamkan MCB zona A listrik & AC lantai 3
-
Catatan : Skenario dapat disesuaikan dengan kondisi dan keadaan yang ada di setiap institusi

105
76
Asst.1KKD/RTB.B Melaporkan kondisi pasien, menanyakan perlu evakuasi atau tidak
KKD
Asst.2KKD/RTB.C Melaporkan kondisi operasional, menanyakan perlu evakuasi atau tidak
KKD
Asst.3KKD Melaporkan kondisi support, membantu operasional komunikasi darurat
KKD
KL Gempa sudah selesai, pasien harap kembali ke tempat tidur
RE. Pasien
R.E Memandu pasien kembali ke tempat tidur
Pasien & kel. pasien
C X : 03 Kebakaran di
Pasien …… Teriak kebakaran-kebakaran
RE.1,2,3, KL.3 Y
Lantai 3 RE.1 Y lt.3 Mengambil APAR menuju ruang….
Keluarga pasien
RE.2 Y lt.3 Tekan tombol fire alarm, dan bantu evakuasi pasien ….
Pasien
RE.3 Y lt.3 Evakuasi pasien yang dekat dengan api ke area pengungsian
RE.2 Y lt.3,
KL.3 Y Lapor terjadi kebakaran di ruang….
KKD
KKD Instruksi umumkan code red ruang…..
TI
TI Umumkan code red PenggunaTim Teknik Memanggil dan membagi
tugas kepada timnyaTim Teknik Lantai
Pemadam.1 Lapor kepada TKP, telah mendengar code red di lantai 3
TKP
TKP Lapor regu pemadam telah menuju lokasi, dan TKP Merapat ke lantai 3
KKD
KKD Hubungi tim tanggap darurat, dan minta ke lantai 3
TT,TPP,AsKKD123
Tim Teknik Instruksi buka pintu darurat lantai dasar ramp
TTL
Tim Teknik Instruksi padamkan listrik & AC lantai 3, non aktifkan lift
TTL
TTL Non aktifkan lift, dan siaga di depan emergency lift lobby utama no.8
-
TTL Padamkan MCB zona A listrik & AC lantai 3
-
Catatan : Skenario dapat disesuaikan dengan kondisi dan keadaan yang ada di setiap institusi

106

107
77
PENGARAH
drg. Kartini Rustandi, M.Kes
PENYUSUN
Ali Syahrul Chairuman, SKM, MKKK (RSUP Fatmawati)Imarsan, ST (RSUPN dr Cipto Mangunkusumo)
Meilissa Rahmadani, SKM (RS Universitas Indonesia)Ai Siti Rokhayah, SKM (RSUD Budhi Asih)
Kurniawan Arif M, SKM, MMRS (RSUP dr Hasan Sadikin)Taufik Herdiansyah, SKM, MMRS (RSUP dr Hasan Sadikin)
Wahyu Damayanti, SKM, MM (RSUP dr Sardjito)Tasripin, SKM, MKM (Dit. Kesehatan Kerja dan Olahraga)
dr Astuti, MKKK (Dit. Kesehatan Kerja dan Olahraga)dr Inne Nutfiliana, MKK (Dit. Kesehatan Kerja dan Olahraga)
Syahrul Efendi Panjaitan, SKM, MKKK (Dit. Kesehatan Kerja dan Olahraga)Iman Surahman, SKM, MKM (Dit. Kesehatan Kerja dan Olahraga)
RR Winda Kusumaningrum, MKKK (Jabfung Pembimbing Kesehatan Kerja)Dara Puspita Dewi, SKM (Dit. Kesehatan Kerja dan Olahraga)
KONTRIBUTOR
Chaterina Welong, SKM, MARS (RSUP dr M Djamil)Lina Sari, SKM, MARS (RSUP dr M Djamil)
dr. Tri Wahyu Kusumawati, MARS (Dit. Mutu dan Akreditasi Yankes)Ika Ratnawati, SKM, MKKK (Dit. Kesehatan Kerja dan Olahraga)
Dr. Selamet Riyadi, MKKK (Jabfung Pembimbing Kesehatan Kerja)dr Puspita Tri Utami (Jabfung Pembimbing Kesehatan Kerja)
dr Yunita Arihandayani, MKM (Dit. Kesehatan Kerja dan Olahraga)Retno Juli Siswantari, SKM, MKM (Jabfung Pembimbing Kesehatan Kerja)dr. Suryo Wibowo, SpOK (Perhimpunan Kedokteran Okupasi Indonesia)
Hendra, SKM, MKKK (Perhimpunan Ahli Kesehatan Kerja Indonesia)Dr. dr. Daru Lestantyo, MS (Komunitas Ahli K3 Rumah Sakit)
Komite Akreditasi Rumah SakitDirektorat Pelayanan Kesehatan RujukanDirektorat Fasilitas Pelayanan Kesehatan
Pusat Krisis Kesehatan

108