INDONESIA perspective - wfsiccm2015.comwfsiccm2015.com/WFSICCM_AB/0920AMOloan TAMPUBOLON.pdf ·...
22
ICU AND HOSPITAL IN INDONESIA 2013 - 2014 INDONESIAN SOCIETY OF INTENSIVE CARE MEDICINE (ISICM) OLOAN E. TAMPUBOLON WFSICCM Congress 2015, Seoul - Korea MANPOWER and ECONOMY in ICU INDONESIA perspective
-
Upload
dinhkhuong -
Category
Documents
-
view
224 -
download
0
Transcript of INDONESIA perspective - wfsiccm2015.comwfsiccm2015.com/WFSICCM_AB/0920AMOloan TAMPUBOLON.pdf ·...
ICU AND HOSPITAL IN INDONESIA 2013 - 2014
INDONESIAN SOCIETY OF INTENSIVE CARE MEDICINE
(ISICM)
OLOAN E. TAMPUBOLON
WFSICCM Congress 2015, Seoul - Korea
MANPOWER and ECONOMY in ICU
INDONESIA perspective
2010 --- 2015

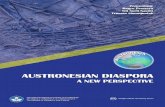
Total Hospital in IndonesiaArea 2013 2014
Sumatera 511 565
Java 1.162 1.252
Borneo 142 151
Celebes 194 209
Bali, Western Lesser Sundas, East Lesser Sundas 121 125
Moluccas, Papua 45 46
Total 2.175 2.348
2013 : 452014 : 46
2013 : 1.162
2014 : 1.2522013 : 121
2014 : 125
2013 : 511
2014 : 565
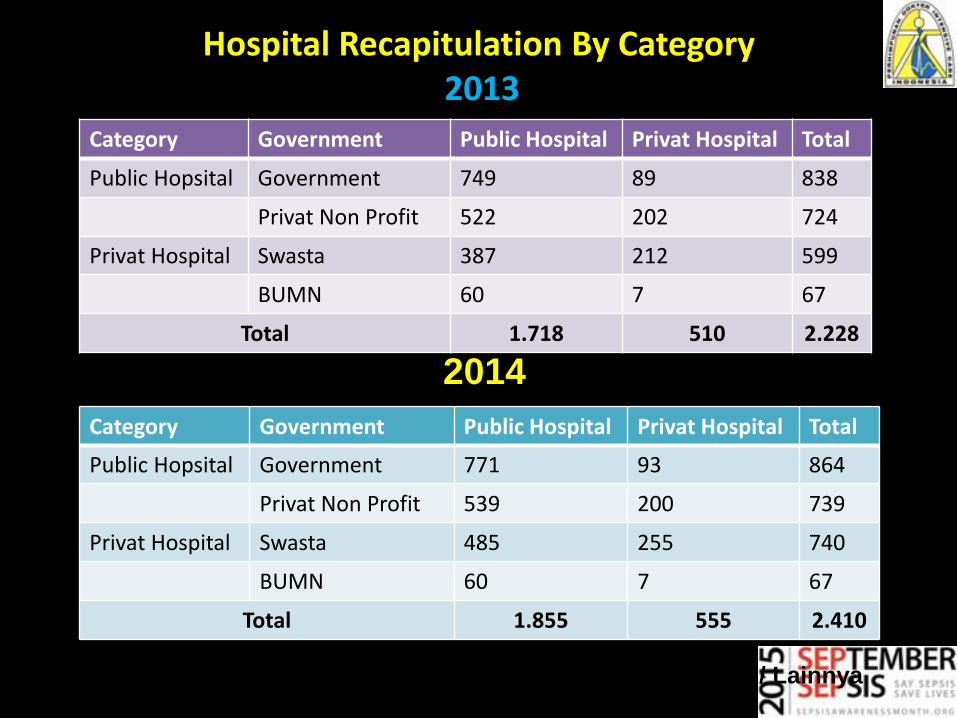
Hospital Recapitulation By Category2013
Category Government Public Hospital Privat Hospital Total
Public Hopsital Government 749 89 838
Privat Non Profit 522 202 724
Privat Hospital Swasta 387 212 599
BUMN 60 7 67
Total 1.718 510 2.228
Keterangan :
RS. Swasta Terdiri Dari : Perusahaan, Perorangan dan Swasta / Lainnya
Category Government Public Hospital Privat Hospital Total
Public Hopsital Government 771 93 864
Privat Non Profit 539 200 739
Privat Hospital Swasta 485 255 740
BUMN 60 7 67
Total 1.855 555 2.410
Per 1 January 20142014
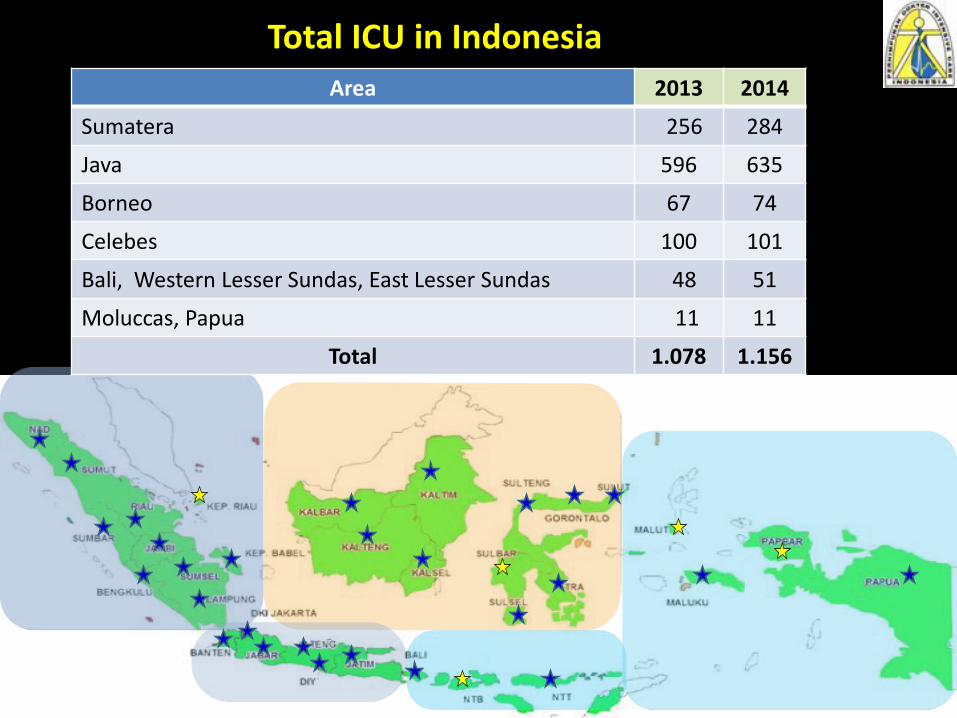
= has provided ICU
= none
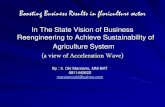
Total ICU in Indonesia
Area 2013 2014
Sumatera 256 284
Java 596 635
Borneo 67 74
Celebes 100 101
Bali, Western Lesser Sundas, East Lesser Sundas 48 51
Moluccas, Papua 11 11
Total 1.078 1.156
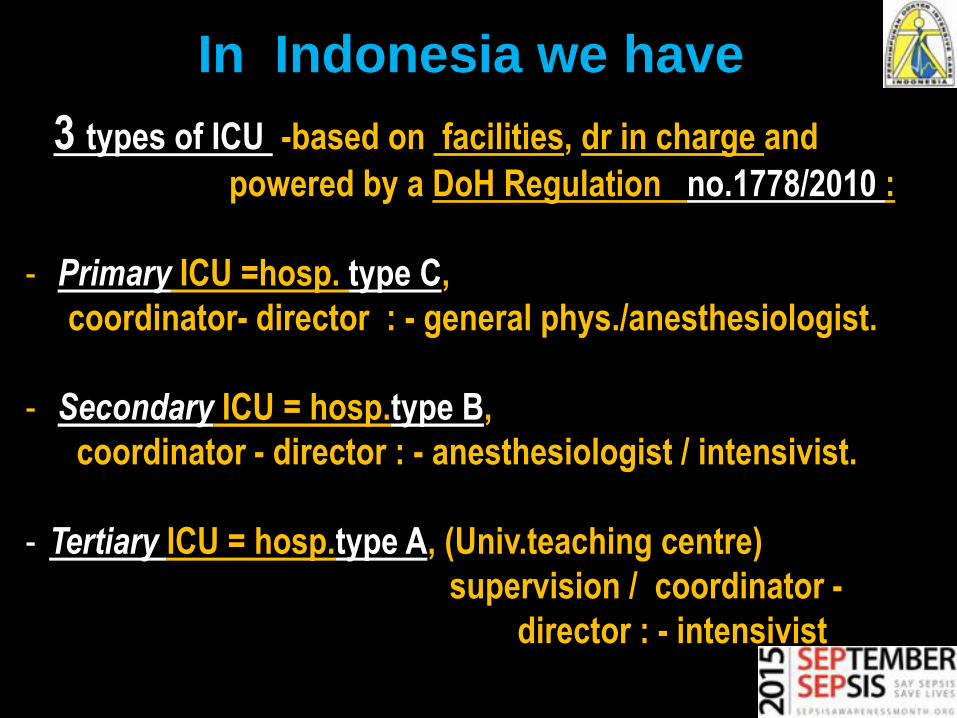
3 types of ICU -based on facilities, dr in charge and
powered by a DoH Regulation no.1778/2010 :
- Primary ICU =hosp. type C,
coordinator- director : - general phys./anesthesiologist.
- Secondary ICU = hosp.type B,
coordinator - director : - anesthesiologist / intensivist.
- Tertiary ICU = hosp.type A, (Univ.teaching centre)
supervision / coordinator -
director : - intensivist.
In Indonesia we have
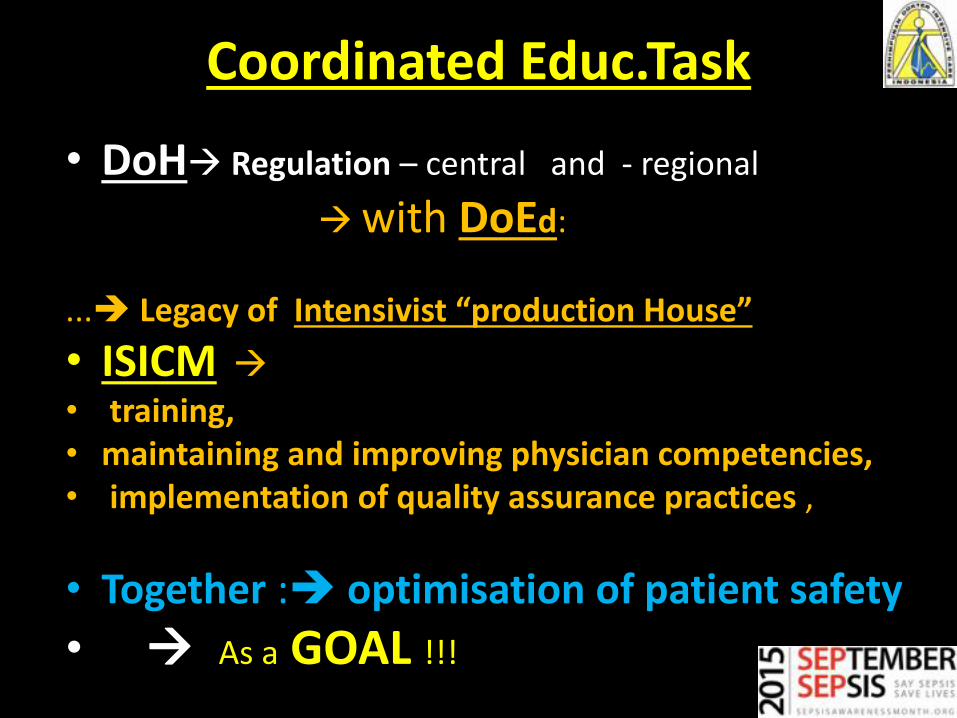
Coordinated Educ.Task
• DoH Regulation – central and - regional
with DoEd:
... Legacy of Intensivist “production House”
• ISICM
• training, • maintaining and improving physician competencies,• implementation of quality assurance practices ,
• Together : optimisation of patient safety
• As a GOAL !!!

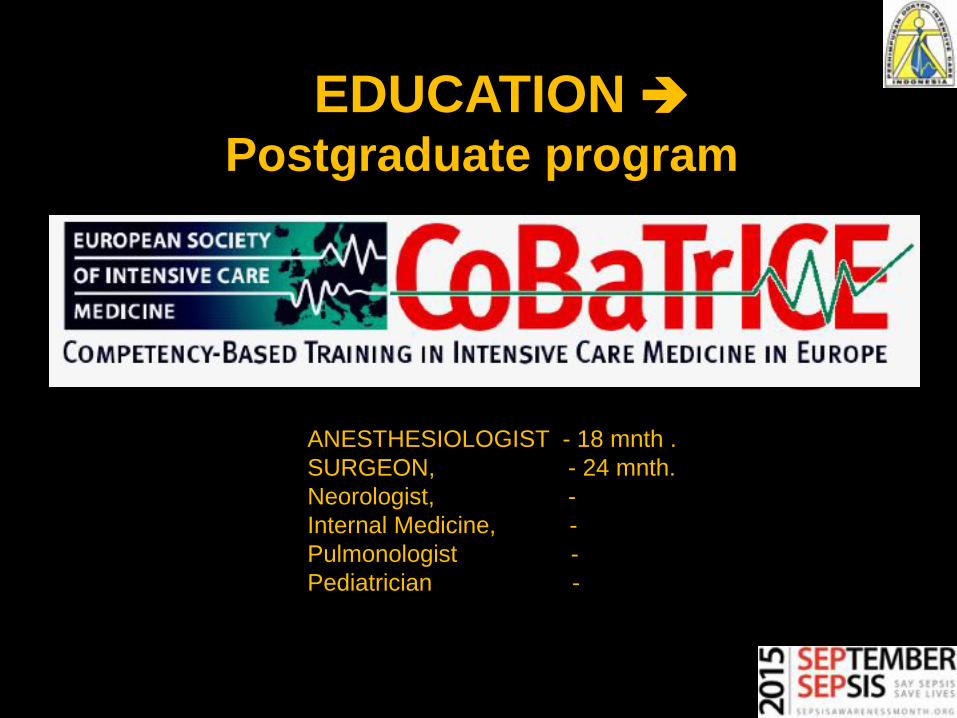
ANESTHESIOLOGIST - 18 mnth .
SURGEON, - 24 mnth.
Neorologist, -
Internal Medicine, -
Pulmonologist -
Pediatrician -
EDUCATIONPostgraduate program
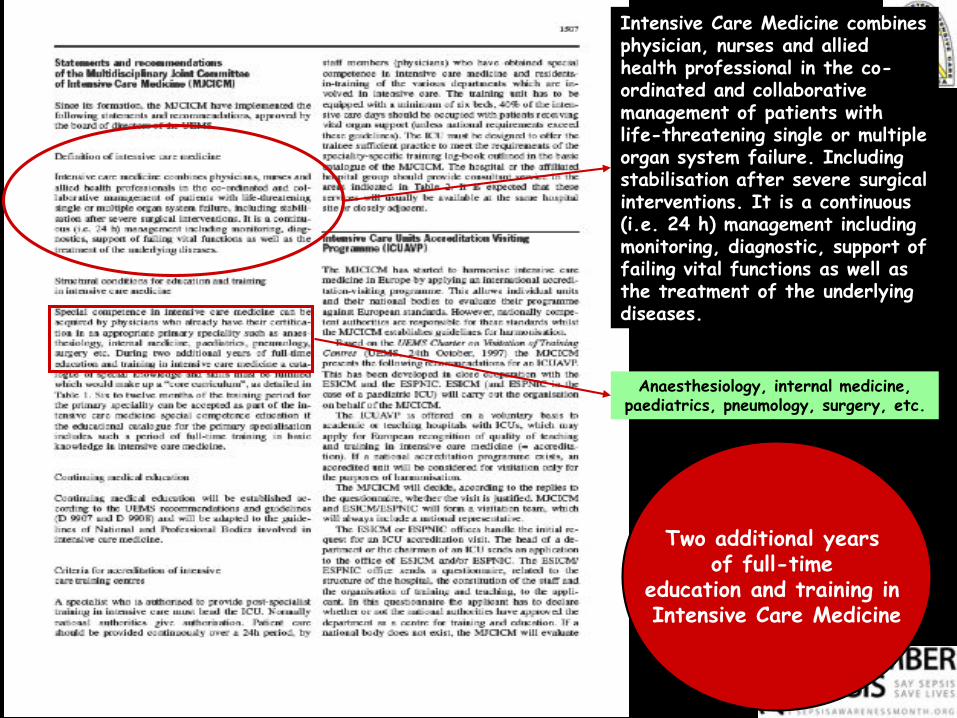
Intensive Care Medicine combines physician, nurses and allied health professional in the co-ordinated and collaborative management of patients with life-threatening single or multiple organ system failure. Including stabilisation after severe surgical interventions. It is a continuous (i.e. 24 h) management including monitoring, diagnostic, support of failing vital functions as well as the treatment of the underlying diseases.
Anaesthesiology, internal medicine, paediatrics, pneumology, surgery, etc.
Two additional years of full-time
education and training in Intensive Care Medicine
Multidisciplinary team, ONE Management in ICU
• Solid Multidisciplinary team :
• Intensivist/ coord. (SpAnKIC, SpPDKIC, SpBKIC,.)
• Clinical Microbiology
•Pharmasy/clinical pharmacologist
• ICU Nurse
•Fysioterapist
•Dietician
PROFESIONAL org. Gov./DoH
• Hand in hand:
• support the training, updating to improve
physician competencies,
• implementation of quality assurance practices,
regional and centrally through
scheduled sessions over the year.
• There are always third parties coming to
support… :WHO e.o.
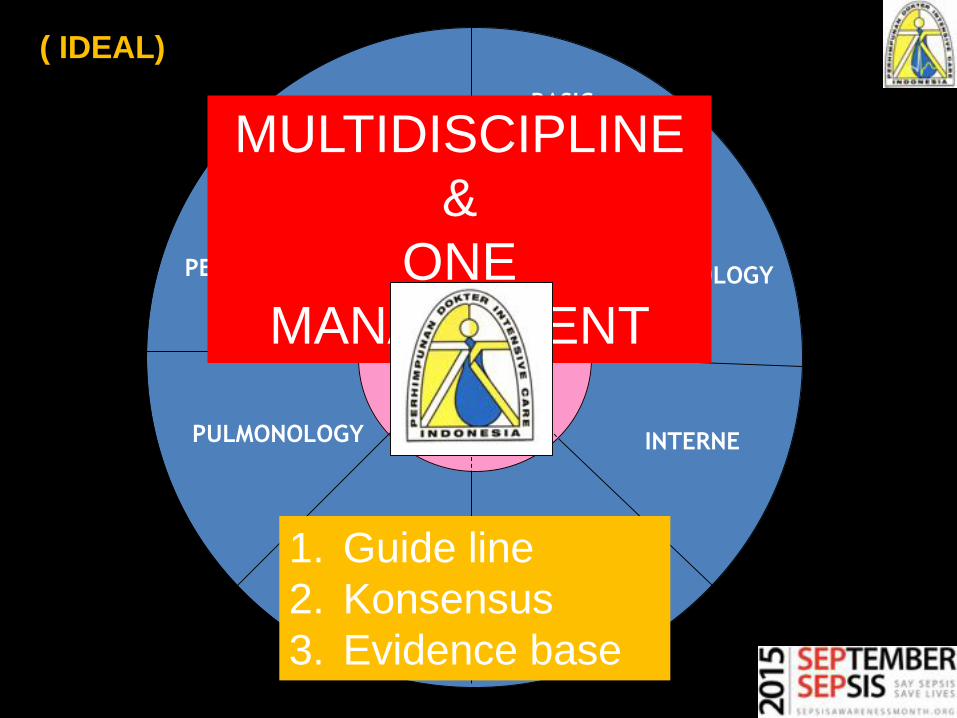
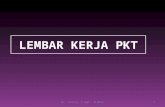
SURGERY
INTERNE
ANESTESIOLO-
GY
CARDIOLOGY
PULMONOLOGY
PEDIATRI
NEUROLO-
GY
BASIC
SCIENCEMULTIDISCIPLINE
&
ONE
MANAGEMENT
1. Guide line
2. Konsensus
3. Evidence base
( IDEAL)
ICU Triage
• Patients should be admitted if they can benefit with decreased risk of death
• patients with reversible medical conditions who have a “reasonable” prospect of substantial recovery
NIH Concensus conference
Prepare referral…
to a larger/higher..better institution…
If the patient is
stabilized and
transportable .
MUST....
Working hours hours
• Team 24/7 available,
• Dedication… for a better time nationwide
• depends on type of ICU/ Hospital/ area,
• Gov. take care of monthly income(remuneration) of
GP’s and Specialist., central or regional.
National Insurance, Private Insurances co.
• Take care of standard & private hospital
ICU finance,
• Monthly/annual based contributions,
• Fixed contribution,
• Clinical ICU pathway set up by
prof.organisation.
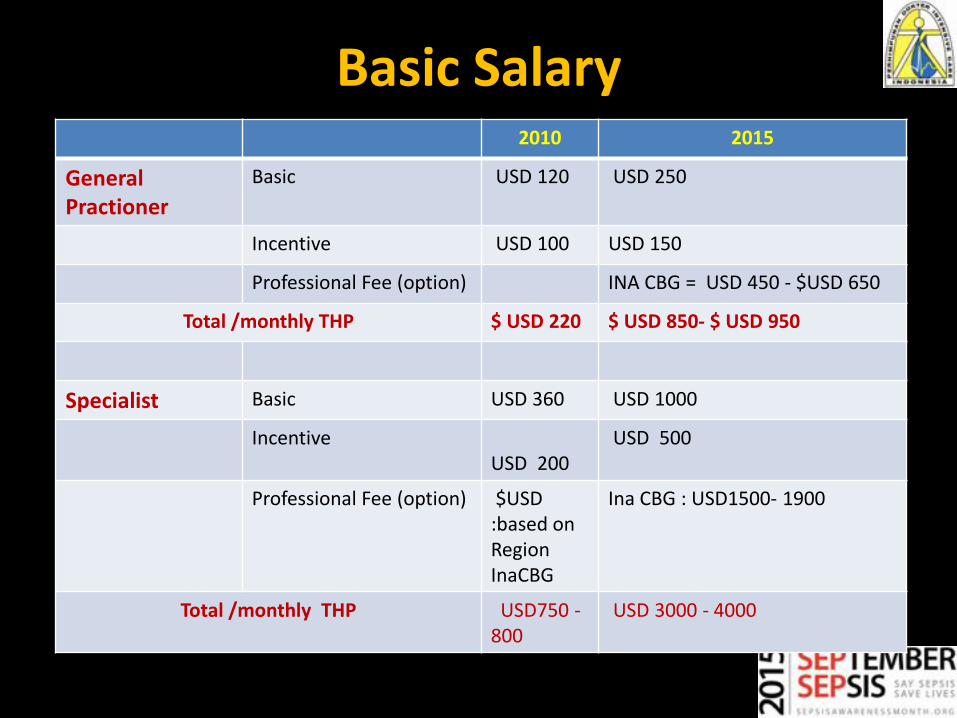
Basic Salary2010 2015
GeneralPractioner
Basic USD 120 USD 250
Incentive USD 100 USD 150
Professional Fee (option) INA CBG = USD 450 - $USD 650
Total /monthly THP $ USD 220 $ USD 850- $ USD 950
Specialist Basic USD 360 USD 1000
IncentiveUSD 200
USD 500
Professional Fee (option) $USD :based on RegionInaCBG
Ina CBG : USD1500- 1900
Total /monthly THP USD750 -800
USD 3000 - 4000
Attention & stay focused
• We call for attention to remain focused on the major hurdles facing all physicians in modern-day intensive care medicine:
• defining, training, maintaining and improving physician competencies,
• implementation of quality assurance practices and, ultimately,
• our collective goal of the optimisation of patient safety.
TEAM WORK !!!
In darkness
Light up a candle
When you can not bring in the sun………