Heparinas de Bajo Peso Molecualr
7
FEATURE ARTICLE Extended Thromboprophylaxis after Hip or Knee Replacement Richard j . Friedman, MD, Guest Editor Abstract Early discharge from the hospital after total joint arthro- plasty has increased the need for extended outpatient thromboprophylaxis. Multiple controlled clinical trial s and several meta-analyses of these data have examined vari- ous agents in different regimens. These data indicate th at extended prophylaxis with a low-molecular-weight heparin after knee or hip arthroplasty sign ificantly reduces the number of venous thromboembolic episodes with no increases in major bleeding. The data also show that >98% of patients given long-term low-molecular-weight heparin prophylaxis remain free from symptomatic deep venous thrombosis and pulmonary embolism. Therefore, to minim ize patient risk saf ely and cost-effectively, extend- ed prophylaxis with low-molecular-weight heparin once- daily for 4 weeks after surgery should be considered for patients undergoing total joint arthroplasty. Without thromboprophylaxis, 45%- 57 % of patients who have undergone total hip replacement (THR) and 40%- 84 % of patients who have had total knee replacement (TKR) experience deep venous thrombosis.' Up to 30% of patients who have had hip replace- ments and up to 7% of patients who have had knee replacements may expe- rience pulmonary embolism.' Both deep venous thrombosis and pul- monary embolism are associated with significant morbidity; the postoperative mortality rate due to pulmonary embolism following THR can be as high as 3%-6%.^ For these reasons, prophylaxis has become an accepted strategy for pre- venting thromboembolic complications after joint replacement surgery. An antithrombotic agent, such as warfarin From Charleston Orthopaedic Associates. Charleston. SC. or a low-tnolecular-weight heparin, was typically administered through the 5- to 14-day period of hospitalization. However, lengths of stay are decreasing dramatically at most institutions. Patients who have undergone TKR are now released from the hospital after 3-4 days, and patients who have had THR are discharged 4-5 days after surgery. As hospital stays decrease, so too does the opportunity for appropriate prophylaxis. This reduction in hospitalization invokes a significant risk for throm- boembolism in the outpatient environ- ment. Results of prospective clinical trials using objective venography indi- cate a 19%-39% incidence of deep venous thrombosis 3 weeks after THR in patients who have received conven- tional inpatient prophylaxis after surgery.-^"* Venous thromboembolism is the most common cause of emergency rehospitalization after THR."" The risk of pulmonary embolism continues throughout the postoperative period. In a survey of approximately 8000 patients who had received thromboprophylaxis during THR, the mortality rate from pulmonary emboHsm was 1.04%. More than 50% of these patients died during the second postoperative week, almost 75% during the third week, 8% during the fourth week, and 5% five weeks after surgery.^ A strategy of extended prophylaxis (ie, prophylactic therapy administered daily for several weeks after dis- charge) has evolved in response to the changing institutional environment. Increasing awareness of other throm- botic risks has also stimulated interest in extended outpatient prophylaxis. These risks include the possibility of persistent activation of coagulation in certain patients,^ the presence of deep venous thrombosis of uncertain clinical significance at discharge, and the risk of postthrombotic syndrome, which is a long-term complication that www.orthobluejournal.com s225
Transcript of Heparinas de Bajo Peso Molecualr

8/8/2019 Heparinas de Bajo Peso Molecualr
http://slidepdf.com/reader/full/heparinas-de-bajo-peso-molecualr 1/7
rd j . Friedman, M D , Guest Editor
Early discharge from the hospital after total joint arthro-
plasty has increased the need for extended outpatient
thrombop rophylaxis. Mu ltiple controlled clinical trials and
several meta-analyses of these data have examined vari-
ous agents in different regimens. These data indicate that
extended prophylaxis with a low-molecular-weight
heparin after knee or h ip arthroplasty sign ificantly reduces
the number of venous thromboembolic episodes with no
increases in major bleeding. The data also show that
> 9 8 % of patients given long-term low-molecular-weight
heparin prophylaxis remain free from symptomatic deep
venous thrombosis and pulmonary embolism. Therefore,
to minim ize patient risk safely and cost-effectively, extend-
ed prophylaxis with low-molecular-weight heparin once-
daily for 4 weeks after surgery should be considered for
patients undergoing total joint arthroplasty.
of patients who have undergone
of patients who have had total
sis.' U p to 30% of
ficant morbidity; the postoperative
or a low-tnolecular-weight heparin,
was typically administered through the
5- to 14-day period of hospitalization.
However, lengths of stay are decreasing
dramatically at most institutions.
Patients who have undergone TKR are
now released from the hospital after
3-4 days, and patients who have had
THR are discharged 4-5 days after
surgery. As hospital stays decrease, so
too does the opportunity for appropriate
prophylaxis.
This reduction in hospitalization
invokes a significant risk for throm-
boembolism in the outpatient environ-
ment. Results of prospective clinical
trials using objective venography indi-
cate a 19%-39% incidence of deep
venous thrombosis 3 weeks after THR
in patients who have received conven-
tional inpatient prophylaxis after
surgery.-^"* Venous thromboembolism isthe most common cause of emergency
continues throughout the postoperative
period. In a survey of approximately
8000 patients who had received
thromboprophylaxis during THR,
the mortality rate from pulmonary
emboHsm was 1.04%. More than 50%
of these patients died during the second
postoperative week, almost 75% during
the third week, 8% during the fourth
week, and 5% five weeks after surgery.^
A strategy of extended prophylaxis
(ie, prophylactic therapy administered
daily for several weeks after dis-
charge) has evolved in response to the
changing institutional environment.
Increasing awareness of other throm-
botic risks has also stimulated interest
in extended outpatient prophylaxis.
These risks include the possibility
of persistent activation of coagulation
in certain patients,^ the presence of
deep venous thrombosis of uncertainclinical significance at discharge, and
the risk of postthrombotic syndrome,

8/8/2019 Heparinas de Bajo Peso Molecualr
http://slidepdf.com/reader/full/heparinas-de-bajo-peso-molecualr 2/7
ORTHOPEDICS FEBRUARY 2003 V O L 26 NO 2 / S U P P L
Incidence (
4 0 - 1 • Placeoo
• Enoiapann
Atl DVT Pro i ima l DV T
Incidence (%)
2 0 - , P=01B
1 5 -
1 0 -
5 -
0 -
All
••LJDVT
2n Paceoo
• Enoxapatin
PromnalDvr
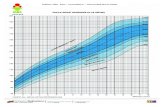
Figure 1: Incidence of thromboembolic events detected on venography in 233 evaluable patients receiving extended prophyla
enoxaparin versus placebo. (Data from Bergqvist et al.") Figure 2: Incidence of thromboembol ic events detected on venography
evaluable patients receiving extended prophylaxis w ith enoxaparin versus placebo followin g hiparthroplasty. (Data from Planes et al.^
3: Incidence of thromboembolic events detected onvenography: enoxaparin versus placebo following hip or knee arthroplasty. (Da
Comp et al ." ) A bbreviations: DVT^deep venous thrombosis and PE=pulmonary embolism.
First Autho r, Year
Bergqvist, 1996
Planes, 1996Dahl, 1997Lassen, 1998Manganell i , 1998
Haentjens, 2000Heit, 2000
Hull, 2000Comp, 2001
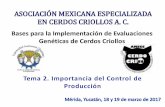
TABLE 1
Overview of Nine Trials Included in a
Procedure
THRTHRTHRTHRTHRTHRTHR or TKR
THRTHR or TKR
Agent
Enoxaparin
EnoxaparinDalteparinDalteparinUFHNadroparinArdeparin
DalteparinEnoxaparin
Abbreviations: THR=totaI hip replacement TKR = total knee reptacmenentAdapted from Eilcelboom JW, et alJ- Copyright 2001. with permission fron
Meta-Analysis of Thromboprophylaxis
In-hospital
N
288
21030 830 080346
1320
99196 8
Duration (d'
10-11
13-157U )71516-174-10
6(2)7-10
and VFH-unfractionated heparin.Elsevier Science.
Out-of-hospital
N
26 2
17926528 179296
1195
56 9873
Duration
30(2)
35(2)35(2)353037-382
35(2)27-29
can compromise functional improve-
This review will examine efficacy
and safety data from multiple controlled
clinical trials, explore pharmaco-
economic analyses of extended throm-
boprophylaxis, and apply these findings
to clinical recommendations. Because
enoxaparin is the only low-molecular-
weight heparin that is approved for
extended prophylaxis after THR. we
emphasize data emerging from an array
of controlled clinical trials that focus on
this indication.
CLINICAL TRIALS WITHENOXAPARIN
Three prospective, randomized,double-blind, placebo-controlled stud-
have evaluated the efficacy and safety
of extended prophylaxis with enoxa-
parin in preventing deep venous throm-
bosis."*••*" The three trials featured sim-
ilar study designs, although specific
dosage andduration varied slightly.
Bergqvist et al"^ treated 262 patients
undergoing THR with enoxaparin
(40 mg per day subcutaneously) for
10-11 days (range, 6-12 days) of hospi-
talization. Upon discharge, 131 patients
received 40 mgof enoxaparin subcuta-
neously once a day and 131 patients
received daily subcutaneous injections
of placebo. The protocol dictated that
on day 21 (range, day 19-23) postdis-
charge, prophylaxis would be stopped
and patients would undergo bilateralvenography to screen for deep venous
thrombosis. Patients treated with
is remained >98% free of symp
deep venous thrombosis."^ Th
(P<.CK)1) of deep venous thro
and proximal deep venous thro
in patients whoreceived proph
enoxaparin were significantly
than the rates in patients who re
placebo (Figure 1)."^
Other investigators reported
fmdings.^ One hundred seven
patients undergoing THR r
40 mg of enoxaparin subcutan
once-daily for 13-15 days of h
ization. After bilateral venograp
performed todetect patients wit
venous thrombosis, patients w
charged and randomly assigned t
extended prophylaxis with enoor placebo. Injections continue
until the next venographic evalu

8/8/2019 Heparinas de Bajo Peso Molecualr
http://slidepdf.com/reader/full/heparinas-de-bajo-peso-molecualr 3/7
DMAN EXTENDED THROMBOPROPHYLAXIS
in patients given placebo
The rate of proximal deep
was comparable intwo groups.•*
who underwent THR or
All patients received 30 mg of
urs for the 7-10 days of hospital-
873 patients
to receive daily sub-
of either enoxa-
(40 mg) or placebo until the
ay 21 ±2 days. The results of thisa significantly lower
in the THR patients treated
(8%) than in patients
to a relative risk reduction of
(Figure 3 )." Also, rates of prox-
in the enoxaparin group
e 3 )."
of patients in
c events, whereas > 96 % of patients
did not require rebospitalization
of enoxaparin in
in
in comparison with
Tbe
of hemorrhagic orother drug-
was similar
in the
the prevalence of deep venous
in patients undergoing
META-ANALYSESet al'- analyzed data
com-
TABLE 2
Incidence of Out-of-Hospital Asymptomatic VenousThromboembolism in a Meta-Analysis of Thromboprophylaxis
OutcomeLMWH or
UFHPlacebo or
Untreated Control OR (95 % Cl)
No.Neededto Treat
Distal DVTProximal DVTAny DVT
6.8% (71/1047)2.9% (30/1047)9.6% (101/1047)
10.4% (89/854)
9.1% (78/854)
19.6% (167/854)
0.69 (0.49-0.96) 28
0.33 (0.21-0.51) 16
0.48(0.36-0.63) 10
Abbreviations: Cl=confidence interval. DVT=dL'ep venous thrombosis, LMWH=low-molecutar-weight heparin. OR=odds ratio, andUFH=unfracfionated heparin.Adapted from Eikeiboom JW. et al.'- Copyright 2001. with permission from Elsevier Science.
Study Heparin Control OR [95% Cl]
PlanesBergqvistDahlManganelliLassenHullComp
Total
3/8521/11711/934/333/113
10/29149/315
10/8843/11623/892/28
9/10211/13369/298
101/1047 167/854
0 28 [0 08 . 1.08)
0 37 [0,20, 0 6810 38 [0 18. 0,85)
179 [0,30, 10,61)0.28 [0,07,0.39 [0.16,0.61 [0.41,
1.07)0.95)0.95)
0.48 [0,36, 0.63)
H0,1 1 10
Favors heparin Favors control
Eigure 4: Risk of asymptomatic venous thromboembolism in a meta-analysis of heparinstudies. (Adapted from Eikeiboom jW, et al.'^ Copyright 2001, with permission from Elsevier
Science.)
heparins or unfractionated heparin ver-
sus placebo or untreated control in
approximately 4000 patients undergo-
ing THR or TKR (Table l).3.4.n,i3-!8
The clinical endpoints were sympto-
matic venous thromboembolism
including deep venous thrombosis and
pulmonary embolism, asymptomatic
deep venous thrombosis by venogra-
phy, major or minor bleeding, or any
cause of mortality.
Table 2 demonstrates the signifi-
cant impact of pharmacologic prophy-
laxis with low-molecular-weight
heparins or unfractionated heparin on
the overall rate of venographically
demonstrated deep venous thrombo-
sis. Prophylaxis decreased the rate of
proximal deep venous thromboses by
two-thirds and the rate of distal deepvenous thrombosis by approximately
reduction favored long-term prophy-
laxis with low-molecular-weight
heparin across each study (Figure
4). ' - The rate of risk reduction was
higher in THR than inT KR .' =
The decrease in asymptomatic
venous thromboembolism correlated
with a reduced number of sympto-
matic events. As shown in Table 3,
extended prophylaxis significantly
decreased symptomatic events occur-
ring postdischarge, with >98% of all
patients in the extended prophylaxis
group free from symptomatic deep
venous thrombosis and pulmonary
embolism.' ' Thus, venographic deep
venous thrombosis is a good surrogate
marker for clinical episodes.
All of these benefits were achieved
with no compromise in safety, as mea-
sured by episodes of major bleeding or

8/8/2019 Heparinas de Bajo Peso Molecualr
http://slidepdf.com/reader/full/heparinas-de-bajo-peso-molecualr 4/7
ORTHOPEDICS FEBRUARY 2003 V O L 26 N O 2/ S U P P L
TABLE 3
Incidence of Out-of-Hospital Symptomatic VenousThromboembolism in a Meta-Analysis of Thromboprophylaxis
OutcomeLMWH or
UFHPlacebo or
Untreated Control OR (95% Cl)
No.Neededto Treat
DVT 1.1% (22/1964)P E 0.2% (3/1961)Any VTE 1.3% (25/1 964 )
2.7% (47/1 742)0.6% (11/I 744)3.3% (58/1 744)
0.41 (0.24-0 .68) 620.43 (0.17-1 .06) 2500.38 (0.24-0.61 ) 50
Abbreviations: Cl=confidence inten-at. DVT=deep venous thrombosis, LMWH= low-molecular-weight heparin. OR=odds ratio. PE= pulmonary em bolism. UFH=unfractionated heparin. andVTE=venous thromboembolism.Adapted from Eikelboom JW, et al. '^ Copyright 2001, with permission from Elsevier Science.
following knee or hip arthroplasty sig-
nificantly reduces the number of venousthromboembolic episodes with no
excesses in major bleeding. The data
demonstrate that a decrease in the rate
of asymptomatic venographic deep
venous thrombosis translates into a
decrease in the symptomatic deep
venous thrombosis rate. The reduction
in risk is approximately 20 sympto-
matic events per 1000 treated pa tients.'-
A second meta-analysis of six of
these studies supports these findings
and, therefore, it can be concluded
that extended prophylaxis with low-
molecular-weight heparin results in a
50% odds reduction in the risk of
developing venous thromboembolism
after lower limb arthroplasty.'^ In this
analysis, the overall frequency of
cl inical venous thromboembol ism
was 1.6% after extended prophylaxis
versus 3.3% in patients receiving
placebo. '^ These findings indicate
that >98% of patients receiving long-term prophylaxis with low-molecular-
weight heparin do not experience
clinical symptoms of deep venous
thrombosis and pulmonary embolism.
At this point, extended prophylaxis
appears to be more effective in THR
than in TKR. However, further studies
in knee surgery are required.
COST-EFFICACYThe extent to which low-molecular-
weight beparins such as enoxaparin can
achieve widespread clinical acceptance
or safety. With managed care resting on
a foundation of cost-efficiency, anyagent used for extended thrombopro-
phylaxis must not place significant bur-
dens on the cost of care.
Enoxaparin has been comprehen-
sively studied from a pharmacoeco-
nomic as well as clinical perspective,
and these studies are reviewed in detail
elsewhere.-^" A French decision analysis
model of data from enoxaparin clinical
trials in extended thrombopropbylaxis
has shown that the outpatient adminis-
tration of enoxaparin for 3 weeks to
patients who have had THR is a cost-
effective alternative to perioperative
thromboprophylaxis when weighed
directly against the costs of sympto-
matic thromboembolic events or death
associated with thromboembolic
events.-" A Swedish decision analysis
model found the same results when
enoxaparin was self-administered in the
majority of p atients.'- A decision tree
model that also included lifelong out-comes and indirect costs of care dem on-
strated that 28 days of extended throm-
boprophylaxis with enoxaparin cost
less and increased life expectancy more
than a similar duration of unfractionat-
ed hepadn prophylaxis.^^
Another study was conducted to
compare the cost of extended prophy-
laxis with enoxaparin versus warfarin
in a decision tree analysis of this strat-
egy in patients undergoing THA.^'*Warfarin therapy was classified as min-
imal, moderate, or maximal, depend-
determinations. The cost of prop
is with enoxaparin was then com
with each of these intensities o
farin therapy and found that the
administering enoxaparin ex
that of administering warfarin
approximately 3 weeks. In p
who required maximal monitor
warfarin, enoxaparin could be gi
31 days before its total costs ex
those of warfarin (Table 4)?'* Th
cal factors that enhanced the cost
tiveness of enoxaparin related d
to the expense of monitoring p
receiving w arfarin and the cost o
plications and treatment failu
those patients. Therefore, althouacquisition cost of enoxaparin w
ically higher than that of warfar
total cost associated with admi
tion of the low-molecular-w
heparin remained below that o
farin because of the need for o
monitoring.24
RISK STRATIFICATIOThe primary goal of risk stra
tion is to aid the surgeon in de
which patients require extende
phylaxis after hosp ital dischar
checklist can be used to rate
patient based on points assigne
variety of risk factors that occur
24 hours of surgery.-^ The s
allows the surgeon an opportun
rate the need for extended proph
based on the patient's risk factor
POSTTHROMBOTIC
S Y N D R O M EExtended prophylaxis should
be considered to reduce the r
postthrombotic syndrome, whic
be a long-term complication o
joint arthroplasty.
Many surgeons do not rec
that this is a significant clinica
cern among their patients, po
because long-term (> 10 years) c
foUow-up focuses on evaluation
joint for symptomatic or radiogfailure, rather than a broader a
ment for vascular conditions. P

8/8/2019 Heparinas de Bajo Peso Molecualr
http://slidepdf.com/reader/full/heparinas-de-bajo-peso-molecualr 5/7
EXTENDED THROMBOPROPHYLAXIS
However, in clinical studies that
RECOMMENDATIONSGiven current knowledge and sur-
ns' desire to safely m inimize patient
Patients undergoing THR may
In TKR, enoxaparin (30 mg subcu-
patients who have preexisting
TABLE 4
Costs of Total Cl inical Pathway of Extended Thromboprophylaxis:Enoxaparin versus Warfarin
Comparison CrossoverDay* Total Costs^
Enoxaparin versus warfarin (minimum follow-up)Enoxaparin versus warfarin (moderate follow-up)Enoxaparin versus warfarin (maximum follow-up)
19 J711 .36 versus $700.9 521 $801.4 9 versus $797 .9031 $1025.49 versus $1010.50
*The day at which one prophylactic regimen cost cur\-e crossed the comparator and. thus, lostits cost-effectiveness a dvantage.fTotal costs in US dollars at crossover day.Adapted with permission from Friedman RJ, et al.-'' Copyright 2000. Lippincott Williams &Wilkins.
Unless otherwise contraindicated, all
patients undergoing hip or knee arthro-
plasty should be advised to take onebaby aspirin daily for prevention of
stroke, myocardial infarction, and other
arterial complications.
CONCLUSIONLower extremity total joint arthro-
plasty is associated with a high risk of
postoperative venous thromboem-
bolism. Traditionally, antithrombotic
prophylaxis has been administered dur-
ing hospitalization, typically for 5-14days. Currently, patients are spending
less time in the hospital after surgery.
Therefore, they must continue throm-
boprophylaxis after hospital discharge.
Data from clinical studies suggest
that there is a protracted risk of throm-
boembolic disease that extends many
weeks following the procedure.
Extended thromboprophylaxis has
been show n in m ultiple c linical trials to
be a safe and effective strategy for
reducing the risk of venous throm-boembolism after joint replacement. Of
the therapeutic options (eg, low-molec-
ular-weight heparins, unfractionated
heparin, or warfarin), only enoxaparin
is approved for use in extended pro-
phylaxis following THR. Data from
controlled trials provide evidence sup-
porting the notion that prolonging
thromboprophylaxis with enoxaparin
significantly reduces the prevalence of
deep venous thrombosis. This conclu-sion is supported by several pharma-
coeconomic analyses that confirm the
prophylaxis when compared with the
total cost of a thromboembolic event or
compared with extended prophylaxiswith agents that require extensive labo-
ratory monitoring, such as warfarin or
unfractionated heparin.
REFERENCES1. Geerts WH. Heil JA. Pineo GF. et al.
Prevention of venous thromboembolism. Chest.
2001; 119(sijppU:l32S-175S.2. Clage tt GP. Ande rson FA, Heit J. Levine
MN, Wheeler HB. Prevention of venous throm-boembolism. Chest. 1995; 10S(suppl):312S-334S.
3. Planes A. Vochelle N . Darmon J-Y. FagolaM. Bellaud M. Huet Y. Risk of deep-venousthrombosis after hospital discharge in patientshaving undergone total hip replacement: double-blind randomised comparison of enoxaparin ver-sus placebo. Lancet. 1996; 348:224-228,
4. Bergqvist D. Benoni G. Bjorgeil O. et al.Low-molecular-weigbt heparin (enoxaparin) asprophylaxis against venous thromboembolismafter total hip replacement. N Engl J Med. 1996;335:696-700.
5. Seagroatt V. Tan H S. Golda cre M,Bulstrode C. Nugent I. Gill L. Elective total hipreplacement: incidence, emergency readmissionrate, and postoperative mortality. Br Med J.
1991; 303:1431-1435-6. Johnson R. Green JR. Ch arnley J.Pulmonary embolism and its prophylaxis follow-ing the Charnley total hip replacement. CU nOrthop. 1977; 127:123-132.
7. Kher A. Samama MM. Low-molecular-weight heparins: weeks or months instead ofdays of treatment. Clin Appl Thromb Hemost.
2001:7:314-320.
8. Prandoni P. Lensing AWA. Cogo A, et al.The long-term clinical course of acute deepvenous thrombosis. Ann Intern Med. 1996;125:1-7.
9. Serafini S. Beltram etti C, Siragu sa S,Barone M , Piovclla F. Post-thrombotic syndromeafter asymptomatic post-operative deep vein throm-bosis: an inception cohort study [abstractj. Tlimmb
Haemost. 1997; 77(s uppl):7 l8. AbsU act PS-2930.
10. McNally MA. McAlinden MG, O'Connell

8/8/2019 Heparinas de Bajo Peso Molecualr
http://slidepdf.com/reader/full/heparinas-de-bajo-peso-molecualr 6/7
ORTHOPEDICS FEBRUARY 2003 VOL le NO 2/SUPPLEM
years. Acta Orthop Scand. 1994; 65:595-598.11 . Comp PC, Spiro TE. Friedman RJ, el al.
Prolonged enoxaparin therapy to prevent venousthromboembolism after primary hip or kneereplacement. J Bone Joint Siir^^ Am. 2001;83:336-345.
12 . Eikelboom JW. Quinlan DJ, Douketis JD.Extended-duration prophylaxis against venousthromboembolism after total hip or knee replace-ment: a meta-analysis of the randomised trials.Lancer. 2001; 358:9-15.
13. Hull RD. PineoGF. Franci.sC. etal. Low-molecular-wcight heparin prophylaxis using dal-teparin extended out-of-hospital versus in-hospi-tal warfarinVout-of-hospital placebo in hip arthro-plasty patients. A double-blind, randomized com-parison. Arch Intern Med. 2000; 160:2208-2215.
14. Dahl OE. Andreassen G. Aspelin T. et al.Prolonged thromboprophylaxis following hipreplacement surgery - results of a double-btind,prospective, randomised, placebo-controlledstudy with dalteparin (Fragmin). Thromb
Haemosf. 1997; 77:26-31.15 . Lassen MR, Borris LC, Anderson BS, et
al. Efficacy and safety of prolonged thrombopro-phylaxis with a low-molecular-weight heparin(dalteparin) after total hip arthroplasty—the
Danish Prolonged Prophylaxis (DaPP) Study.Thromb Res. 1998; 89:281-287.
16. Heit JA. Elliott CG. Trowbridge AA,MorTey BF, Gent M, Hirsh J, for the ArdeparinArthroplasty Study Group. Ardeparin sodium forextended out-of-hospital prophylaxis againstvenous thromboembolism after total hip or kneereplacement. A randomized, double-blind, place-bo-controlled trial. Ann Intern Med. 2000;132:853-861.
17. Manganelli D, Pazzagli M. Mazzantini D,et al. Prolonged prophylaxis with unfractionatedheparin is effective to reduce delayed deep veinthrombosis in total hip replacement. Respiration.1998; 65:369-374.
18. Haentjens P. Venous thromboembolismafter total hip arthroplasty: a review of incidenceand prevention during hospitalization and afterhospital discharge. Acta Orthop Belg. 20f)0;66:1 -8.
19. Cohen AT. Bailey CS. Alikhan R, CooperDJ. Extended thromboprophylaxis with low-mol-ecular-weight heparin reduces symptomatic
venous thromboembolism following limb arthro-plasty - a meta-analysis [letter] . ThrombHaemost. 2001; 85:940-941.
20 . Bergqvist D. Enoxaparin. A pharmacoeco-nomic review of its use in the prevention and treat-
ment of venous thromboembolism and incoronary syndromes. Pharmacoeconomics20:225-243,
21 . Detournay B, Planes A, VochelFagnani F. Cost effectiveness of a low-moleweight heparin in prolonged prophylaxis adeep vein thrombosis after total hip replacePharmacoeconomics. 1998; 13(1 pt l):81-
22 . Bergqvist D, Jonsson B. Cost-effeness of prolonged out-of-hospital prophwith low-molecular-weight heparin folltotal hip replacement. Haemostasis.3O(.supp!2):13O-l35.
23 . Marchetti M. Liberato NL, RuperBarosi G. Long-term cost-effectiveness omolecular-weight heparin versus unfractioheparin for the prophylaxis of venous tboembolism in elective hip replaceHaematotogica. 1999; 84:730-737.
24 . Friedman RJ, Dunsworth GA. Cost ses of extended prophylaxis with enoxaafter hip arthroplasty. Ctin Orthop.
370:171-182.25 . Caprini JA, Arceius Jl, Hasty JH, Tam
AC, Fabrega F Clinical assessment of vthromboembolic risk in surgical patients.Thromb Hemost. 1991; 17(suppl 3):3O4-312

8/8/2019 Heparinas de Bajo Peso Molecualr
http://slidepdf.com/reader/full/heparinas-de-bajo-peso-molecualr 7/7