Dengue
13
Dengue James Whitehorn † and Jeremy Farrar ‡* † London School of Hygiene and Tropical Medicine, London, UK, and ‡ Hospital for Tropical Diseases, Oxford University Clinical Research Unit, Wellcome Trust Major Overseas Programme, Ho Chi Minh City, Vietnam Introduction: Dengue is a vector-borne viral infection that endangers an estimated 2.5 billion people. Disease caused by dengue ranges from a relatively minor febrile illness to a life-threatening condition characterized by extensive capillary leak. A greater understanding of dengue has the potential to improve both the clinical management of individual cases and the control of the disease. Sources of data: We searched the available literature using PubMed, Embase and Web of Science for relevant articles and abstracts. Areas of agreement: Addressing our gaps in the understanding of disease pathogenesis and improving our knowledge of dengue virus biology are necessary in order to develop tools to effectively control, diagnose and treat the disease. Areas of controversy: The pathogenesis of dengue is multifactorial and depends on both host and virus factors. A more integrated understanding of disease pathogenesis is necessary. Areas timely for developing research: There are many questions related to disease pathogenesis, development of diagnostics, drug and vaccine development and individual case management that need addressing if the disease is to be successfully tackled. Keywords: dengue/dengue haemorrhagic fever/dengue shock syndrome/ pathogenesis/vaccine/drug development Introduction Dengue is a viral infection transmitted by Aedes mosquitoes. 1 Dengue is a flavivirus with four different antigenically distinct serotypes (DENV1-4). 2,3 It is a rapidly growing health problem with an estimated 2.5 billion people at risk, mainly in countries of south and south-east Asia, the Caribbean, Central and South America, and more recently in Africa. 4,5 The spread of dengue is thought to be due to a combination of factors: increased urbanization, population growth, migration and inter- national travel and the difficulties of effective vector control. 6 Climate change may be a contributing factor in the global spread of dengue. 7 British Medical Bulletin 2010; 95: 161–173 DOI:10.1093/bmb/ldq019 & The Author 2010. Published by Oxford University Press. All rights reserved. For Permissions, please e-mail: [email protected] Accepted: June 14, 2010 *Correspondence address. Hospital for Tropical Diseases, Oxford University Clinical Research Unit, Wellcome Trust Major Overseas Programme, Ho Chi Minh City, Vietnam. E-mail: [email protected] Published Online July 8, 2010 at Iowa State University on October 19, 2014 http://bmb.oxfordjournals.org/ Downloaded from
Transcript of Dengue

Dengue
James Whitehorn† and Jeremy Farrar‡*
†London School of Hygiene and Tropical Medicine, London, UK, and ‡Hospital for TropicalDiseases, Oxford University Clinical Research Unit, Wellcome Trust Major Overseas Programme,Ho Chi Minh City, Vietnam
Introduction: Dengue is a vector-borne viral infection that endangers an
estimated 2.5 billion people. Disease caused by dengue ranges from a relatively
minor febrile illness to a life-threatening condition characterized by extensive
capillary leak. A greater understanding of dengue has the potential to improve
both the clinical management of individual cases and the control of the disease.
Sources of data: We searched the available literature using PubMed, Embase
and Web of Science for relevant articles and abstracts.
Areas of agreement: Addressing our gaps in the understanding of disease
pathogenesis and improving our knowledge of dengue virus biology are necessary
in order to develop tools to effectively control, diagnose and treat the disease.
Areas of controversy: The pathogenesis of dengue is multifactorial and depends
on both host and virus factors. A more integrated understanding of disease
pathogenesis is necessary.
Areas timely for developing research: There are many questions related to disease
pathogenesis, development of diagnostics, drug and vaccine development and
individual case management that need addressing if the disease is to be
successfully tackled.
Keywords: dengue/dengue haemorrhagic fever/dengue shock syndrome/pathogenesis/vaccine/drug development
Introduction
Dengue is a viral infection transmitted by Aedes mosquitoes.1 Dengue isa flavivirus with four different antigenically distinct serotypes(DENV1-4).2,3 It is a rapidly growing health problem with an estimated2.5 billion people at risk, mainly in countries of south and south-eastAsia, the Caribbean, Central and South America, and more recently inAfrica.4,5 The spread of dengue is thought to be due to a combination offactors: increased urbanization, population growth, migration and inter-national travel and the difficulties of effective vector control.6 Climatechange may be a contributing factor in the global spread of dengue.7
British Medical Bulletin 2010; 95: 161–173
DOI:10.1093/bmb/ldq019
& The Author 2010. Published by Oxford University Press. All rights reserved.
For Permissions, please e-mail: [email protected]
Accepted: June 14, 2010
*Correspondence address.
Hospital for Tropical
Diseases, Oxford
University Clinical
Research Unit, Wellcome
Trust Major Overseas
Programme, Ho Chi Minh
City, Vietnam. E-mail:
Published Online July 8, 2010
at Iowa State U
niversity on October 19, 2014
http://bmb.oxfordjournals.org/
Dow
nloaded from

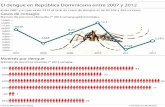
It is estimated that there are between 50 and 100 million cases of dengueeach year, of which �500 000 are severe life-threatening infections.8
There have been numerous urban outbreaks of dengue with significanthealth and economic impacts.9–11 Studies in Thailand and Brazil haveshown that the social and economic impact is equivalent to that ofmalaria in these countries.12,13 However, globally dengue research hasnot received the same level of funding as other tropical infectious dis-eases.8 There are currently no available drugs and no licensed vaccine,and diagnosis in endemic areas is largely clinical.14 Dengue also poses arisk to those who travel to endemic areas and is increasingly beingreported in travellers returning from trips to endemic countries.15
Dengue viruses cause a variety of clinical syndromes ranging fromasymptomatic infection to a self-limiting febrile illness to severe dengue,a life-threatening condition characterized by increased capillary per-meability and shock.16–18 There are concerns that the old WHOdefinitions of dengue that are still in widespread use may lead to under-diagnosis of severe dengue.19 In clinically apparent dengue infectionsymptoms develop after an incubation period of 4–7 days with an abruptonset of fevers often accompanied by headache with severe retro-orbitalpain.20,21 Some patients develop severe arthralgia, explaining the histori-cal name of break-bone fever.22 Early in the illness the skin may appearflushed, with petechiae appearing during the ‘critical phase’ and amacular rash appearing in early convalescence. Even after uncomplicateddengue recovery may be complicated by fatigue and depression.Thrombocytopenia is almost universal in dengue infection and minorbleeding from skin and mucosal surfaces may be seen in uncomplicatedinfections—this can be severe in patients with peptic ulcer disease.23
Biochemical hepatitis is frequently seen in dengue infection, but severeliver pathology, encephalitis and renal dysfunction are relatively rare.21,24
Data from Taiwan show differences in disease manifestations betweenadults and children observed during an outbreak in 2002.25 Arthralgia,headache, gastrointestinal bleeding and significantly severe dengue weremore common in adult patients. The reasons for these differences are notclear but could reflect differences in the host response to infection.Significant and disabling fatigue has been described after recovery fromdengue.26 It is thought that host factors may contribute to the develop-ment of this condition. Vertical transmission of dengue can occur if infec-tion of the mother occurs within 8 days of delivery.27 The WHO haverecently published new guidelines on dengue management.28 The newguidelines indicate that disease caused by dengue encompasses a wideclinical spectrum and that the previously used classifications for severedengue were not always helpful. Dengue is classified in the new systemas either uncomplicated or severe.28 Severe disease is characterizedby plasma leak, haemorrhage and organ impairment. Recognizing the
J. Whitehorn and J. Farrar
162 British Medical Bulletin 2010;95
at Iowa State U
niversity on October 19, 2014
http://bmb.oxfordjournals.org/
Dow
nloaded from
warning signs for severe disease is important for successful clinicalmanagement. Warning signs include abdominal pain, evidence of fluidaccumulation, hepatomegaly and increases in haematocrit accompaniedby a fall in the platelet count.28 The mechanisms that lead to severedengue are not completely understood although various hypotheses exist.Perhaps the most widely accepted hypothesis explaining the developmentof severe dengue is that of antibody-mediated immune enhancement,where antibodies developed to a previous infection lead to enhanced viraluptake with a new infection of a different serotype.29,30 This and otherhypotheses will be discussed in a later section of this review.
Sources of data
We searched the available literature up to April 2010 using PubMed, Webof Science and Embase and making use of the following terms: ‘dengue’;‘dengue fever’; ‘dengue haemorrhagic fever (DHF)’; and ‘dengue viruses’.
Areas of agreement
As dengue has emerged as a global health threat, it has receivedincreased attention from the international public health community.14
Essentially areas of agreement are based around addressing the lack ofeffective diagnostic and therapeutic options, improving clinical care ofaffected patients and developing tools to prevent dengue infection.
Areas of controversy
Is the virus itself or the host response to infection the main cause of severe disease?
The four serotypes of dengue can be further classified into differentgenotypes based on nucleotide variation.31 Different genotypes havebeen associated with different levels of virulence.32,33 It appears thatthe virus may evolve during epidemics to cause more severe disease asseen in disease outbreaks in Cuba and Australia.34,35 It has beensuggested that structural differences in strains of the virus lead to dif-fering abilities to infect different cell types or cause severe disease.36,37
However, given that only a small percentage of patients infected withdengue develop severe disease, it is clear that host factors have a majorrole to play in dengue pathogenesis.31
Many of the clinical features of dengue infection may be due to thepatients’ immune response. The increased vascular permeability seen in
Dengue
British Medical Bulletin 2010;95 163
at Iowa State U
niversity on October 19, 2014
http://bmb.oxfordjournals.org/
Dow
nloaded from
dengue is associated with high levels of cytokines including tumournecrosis factor alpha (TNF-a), interferon gamma (IFN-g), interleukin 6(IL-6) and interleukin 2 (IL-2).38,39 However, it is important to notethat these cytokines are elevated in many diseases, yet dengue is a veryspecific clinical entity. Therefore the clinical features of dengue couldbe due to a specific constellation of these cytokines or a more complexinteraction between host and virus that is yet to be characterized.Polymorphisms in TNF-a are associated with more severe disease.40
Various other genetic factors have been associated with more severedisease: for example, polymorphisms in the vitamin D receptor gene,the mannose-binding lectin gene, and various HLA class I and IIalleles.41–44 However, none of these studies have been large enough toindicate a clear association and the question of host susceptibilityremains unanswered. Cytokine dysregulation and endothelial injurycontribute to the pathogenesis of yellow fever, another flavivirus.45
The pathophysiology of severe yellow fever infection remains unclear,but given similarities with severe dengue, there may be an overlap inthe host and virus determinants of susceptibility.
Is the hypothesis of antibody-mediated enhancement sufficient to explain thedevelopment of severe disease?
Epidemiological studies have shown that severe disease is more com-monly seen after secondary infections.46 Infection with one serotype isthought to result in brief protection against all serotypes. As the levelsof neutralizing antibodies fall over time the non-neutralizing or sub-neutralizing antibodies form complexes with the new infecting virusand these complexes are taken up by Fc-receptor bearing cells. Thisresults in increased uptake of virus, increased replication and viralload, and hence a postulated increased likelihood of complications.30
This phenomenon explains the severe disease observed in infants agedbetween 6 and 9 months, where the low non-neutralizing levels ofmaternally derived antibodies are thought to play a crucial role in thedevelopment of severe disease.47,48 These observations have led to con-cerns that a vaccine may potentially result in more severe disease bypriming the immune system and putting individuals at risk when theyare subsequently infected. These fears are ungrounded if such a vaccineproduces long-term neutralizing protection to all four serotypes andthose serotypes do not change over time.3 However, severe disease canoccur in primary infections and most secondary infections do not resultin severe disease indicating that other factors contribute.49–51 Directevidence for antibody-dependent enhancement (ADE) contributing tothe development of severe disease in humans has been difficult to
J. Whitehorn and J. Farrar
164 British Medical Bulletin 2010;95
at Iowa State U
niversity on October 19, 2014
http://bmb.oxfordjournals.org/
Dow
nloaded from

demonstrate, although recent work in infants and elegant in vitro andclinical studies have started to yield crucial insights into how ADE maycontribute to pathogenesis.51,52,53
The pathogenesis of dengue is complex and multifactorial. No hypoth-esis in isolation is sufficient to explain the development of severe disease.It is the interplay between virus factors and genetically determined hostfactors that determine the disease outcome in the individual patient.
Growing points—areas timely for developing research
Increased understanding of dengue pathogenesis
As discussed above the mechanisms that lead to severe dengue are incom-pletely understood. A greater and clearer understanding of disease patho-genesis including host genetics, virus biology and immunopathology,would help the development of targeted clinical interventions.14 Clarifyinghow dengue virus virulence varies between serotypes and evolves withinepidemics would be helpful. Do different serotypes vary in their tissuetropism thus explaining differences in disease severity? Elucidating howthe different factors within the immune system interact and contribute todisease development is essential. Too often research focuses on a singleaspect of the immune response, be it antibody-mediated enhancement,T and B cell responses or the role of complement when a more integratedview, including consideration of the virus, is required.31
Non structural protein-1 (NS1) is a glycoprotein secreted bydengue-infected cells. Early detection of NS1 has demonstrated efficacyas a diagnostic tool.54 Its role in dengue pathogenesis is unclear—defin-ing this role may lend weight to its use in diagnostics. It is possible thatit activates complement at endothelial surfaces thus contributing to thevascular leak that occurs in severe disease.55 Clarifying the events thatoccur at the endothelial surface in dengue infection would be a majoradvance—the development of a suitable animal model of dengue infec-tion would aid this progress.56
An increased understanding of genetic factors that contribute todisease development would help define more clearly populations atrisk. Within populations an increased understanding of differing sus-ceptibilities to disease development is necessary.31
Optimization of clinical management
The commonly used WHO guidelines for the management of denguewere developed after observations in children hospitalized in Bangkok
Dengue
British Medical Bulletin 2010;95 165
at Iowa State U
niversity on October 19, 2014
http://bmb.oxfordjournals.org/
Dow
nloaded from
in the 1960s with dengue.19 These guidelines have evolved over theyears and have been adopted into clinical practice in endemic areas. Anattempt to validate the WHO classifications for severe disease has beenrecently published.57 This study showed that while the WHO classifi-cations had good specificity for severe disease the sensitivity was lower.There is no doubt that the use of the guidelines have led to substantialmortality reductions, yet are guidelines originally developed for Thaichildren 40 years ago still applicable today or, for example, in theincreasing number of adult patients seen globally?19,58
One of the difficulties diagnosing DHF using the old WHO defi-nitions was that the criteria were too rigid.16 Studies have shown thatmany cases of dengue that resulted in shock or death did not meet theWHO case definitions.59,60 These problems have led to the develop-ment of the new WHO guidelines that categorize dengue cases intouncomplicated or severe.28 These guidelines emphasize the importanceof recognizing the warning signs of severe dengue—abdominal pain,vomiting, fluid accumulation, mucosal bleeding, lethargy or restlessness,hepatomegaly, rising haematocrit in conjunction with falling platelets.28
These 2009 WHO guidelines include a detailed description of the clinicalmanagement of dengue including an algorithm for the management(http://whqlibdoc.who.int/publications/2009/9789241547871_eng.pdf).A challenge is educating health-care workers about the new guidelinesand ensuring that they result in better clinical care.
The mortality in severe dengue remains significant particularly ininfants.50,61 In addition higher mortality rates are seen when denguenewly emerges in regions where there is less experience in clinical man-agement of cases, for example, as seen in the epidemics in India andBrazil.10,62 Fluid management in dengue is difficult—the balancebetween too much and too little is critical and getting it wrong can belife-threatening.63 Fluid resuscitation is not without risk and fluid over-load in the recovery phase can cause acute respiratory distress syn-drome.28 Fluid management in patients with co-morbidities orpregnancy is difficult and would benefit from further research.
It is likely that there is a significant unreported burden of mortalityin remote health facilities, where clinical management may be poor.Early and careful administration of parenteral fluids is life-saving insevere dengue. Ringer’s lactate has demonstrated efficacy for use indengue shock syndrome and dextran or starch have also been suggestedfor severe disease.64 Successful management of severe dengue requiresfavourable staff-to-patient ratios and the ability to closely monitorpatients.28 Unfortunately the use of parenteral fluids and the intensemonitoring that is required may not always be available and there is aneed for research on the use of oral rehydration therapy aimed at pre-venting the development of shock in severe dengue.14
J. Whitehorn and J. Farrar
166 British Medical Bulletin 2010;95
at Iowa State U
niversity on October 19, 2014
http://bmb.oxfordjournals.org/
Dow
nloaded from

The endothelial leak seen in severe dengue is transient and if appro-priate supportive therapy is given during this period, mortality ratesare low.16 However, in the early stages of disease clinical features arenon-specific and are shared with other infectious aetiologies.61 Makinga diagnosis early in the disease would significantly aid clinical manage-ment. Additionally predicting which patients are at risk of severedisease would be a major advance. Traditionally diagnosis has reliedon serology, which can take time to give useful results, meaning thatdiagnosis is often retrospective.1 IgM against dengue can be detectedafter 5 days of fever—commercially available diagnostic kits based onELISA have been assessed.65 These have potential but have limitations,for example, the persistence of IgM in some patients in endemic areasmaking it difficult to diagnose an acute infection. The detection of thedengue protein NS1 also has proven use in diagnosis.54 Quantifyingthe titre of NS1 early in clinical illness may allow one to predict thoseat risk of developing severe disease.66 Real-time PCR is another poten-tial, highly sensitive diagnostic tool in dengue diagnosis.67 However,the cost of molecular tests such as PCR make it an impractical tool foruse in many settings where dengue is prevalent. A rapid sensitive testthat combines detection of NS1, IgG and IgM allowing diagnosis ofinfection throughout the illness course would be a major advance indengue diagnostics. The development of appropriate clinical algorithmsfor use in resource-limited settings in parallel to the development ofmolecular diagnostic tools is necessary if the burden of dengue is to beadequately dealt with. A study has demonstrated the potential use of adecision tree algorithm using simple clinical and haematological par-ameters.68 Testing the validity of such an algorithm in primary care set-tings have the potential to improve the triage and initial clinicalmanagement of patients with dengue. Detection of plasma leakagethrough serial ultrasound is a useful adjunctive tool in dengue diagno-sis and management, and yet it is unlikely to be of benefit in manyareas due to lack of availability.69 Identifying additional predictors ofdengue would be useful, but making these into diagnostic techniquesthat are practical in resource-limited settings is the challenge.70
Vaccine development
A vaccine against dengue would be a major advance in the control ofthe disease. In view of the potential risks of antibody-mediatedenhancement seen with heterotypic infections, a successful vaccinewould have to offer lasting protection against all four serotypes.2
Based on the success of vaccination against other flaviviruses, forexample, Japanese encephalitis and yellow fever, the development of a
Dengue
British Medical Bulletin 2010;95 167
at Iowa State U
niversity on October 19, 2014
http://bmb.oxfordjournals.org/
Dow
nloaded from

live attenuated vaccine had previously been the most promising pro-spect for vaccinologists.71 However despite encouraging results withmonovalent vaccines in clinical trials the development of a tetravalentformulation has proved problematic and development has been sus-pended.3,72–75 The leading vaccine candidate at present is a chimericvaccine—a recombinant clone based on yellow fever vaccine strainwith dengue virus membrane and envelope protein genes substitutedinto the construct.76,77 This chimeric vaccine has shown promise inPhase II clinical trials and appears safe and immunogenic. It is antici-pated that Phase III trials will start in the near future.
Despite promising progress there remain unanswered questions thatneed to be addressed and are potential areas for research. The lack of asuitable animal model of dengue infection hinders the transfer of lab-oratory findings into clinical practice.31 How do we quantify immuneprotection? Do tetravalent vaccine constructs hinder the developmentof immunity to individual serotypes? Could a dengue vaccine renderpopulations more vulnerable to severe infection, either throughantibody-mediated enhancement or via a mechanism similar to thatseen with vaccines against respiratory syncytial virus?78 How safe aredengue vaccines in different subsets of the population?3
In addition to the science of vaccine development and questionsregarding the safety and efficacy of individual vaccine candidates, thereneeds to be sustained co-ordination between different countries andvaccine developers if a vaccine is to be successfully developed.53,79
Anti-dengue drugs
A greater understanding of dengue virus biology has meant that targetswithin the lifecycle have been identified that could potentially be thesite of a therapeutic agent.80 The staggering success in developingdrugs against HIV is an example of how efficiently effective antiviralscan be developed given appropriate funding.
One potential mechanism of action of an anti-dengue drug is throughinhibition of viral entry. The fusion of the viral membrane with the hostmembrane is mediated by dengue virus E protein.81 Research has shownsome promising initial results in laboratory studies with an experimentalentry inhibitor—these findings could pave the way to the development ofsuccessful therapeutic agents.82 Other potential targets receiving researchattention are the viral proteins NS3 and NS5, which play an integral rolein genome replication—their protease domains could be target forprotease inhibitors.83,84 A computer program has been used to identifysuitable molecules that can ‘dock’ into the NS3 protease domain.85 Thechallenge is to bridge the gap between findings in the laboratory and the
J. Whitehorn and J. Farrar
168 British Medical Bulletin 2010;95
at Iowa State U
niversity on October 19, 2014
http://bmb.oxfordjournals.org/
Dow
nloaded from

bedside; however, given the progress in our understanding of denguevirus biology, the future of drug development is encouraging. There arepotential therapeutic developments for the treatment of other flavivirusessuch as hepatitis C.86 In view of structural similarities between differentflaviviruses, these developments could be used in the field of dengue treat-ment. The complications of dengue occur as the virus is cleared from theblood, and so it is possible that an anti-dengue drug will have no ben-eficial role. As the severe manifestations of disease are in part due to theimmune response perhaps the development of an immunomodulatoryagent would be the best therapeutic strategy? Animal studies have shownthe protective effect of monoclonal antibodies against the NS1 protein ofWest Nile virus, and more recent work in mice has shown the therapeuticpotential of a monoclonal antibody directed against a structural epitopein an experimental DENV-1 infection.87,88
Vector control
In addition to vaccination, successful vector control would be a usefuladjunct to controlling dengue. Dengue is closely associated with Aedesaegypti—the global spread of dengue is related to changes in humanbehaviour, in particular the expansion of large urban centres, whichsupport the breeding of A. aegypti.6 Although vector control has pre-viously had success, the persistence of pockets of mosquitoes resultedin disease re-emergence.89 Studies have shown different efficiencies ofdengue transmission between different mosquito strains and differentserotypes of dengue.90,91 A greater understanding of the interactionsbetween mosquitoes and the different serotypes of dengue would giveus a greater understanding of transmission dynamics and would poten-tially lead to better prediction of epidemics, and thus better control ofthe disease. The development of genetically modified mosquitoes thatare less able to transmit dengue is a potential option for diseasecontrol. However, mathematical models have indicated that this strat-egy may select for greater disease virulence, suggesting that measuresthat increase mosquito mortality may be more effective.92 Transgenicmosquitoes are likely to be less reproductively fit—infection of trans-genic mosquitoes with the symbiont Wolbachia potentially confers areproductive advantage, thus allowing the establishment of transgenicsin the environment.93 Cyclopoid copepods are invertebrate predatorsof mosquito larvae. Introduction of copepods into water containers,the typical breeding site of Aedes, can have a major impact on mos-quito populations.94 The roll-out of larvicidal interventions requiresactive community involvement and the success of such measures woulddepend on imaginative public health engagement.94
Dengue
British Medical Bulletin 2010;95 169
at Iowa State U
niversity on October 19, 2014
http://bmb.oxfordjournals.org/
Dow
nloaded from

Conclusions
Successfully tackling the threat of dengue represents a major publichealth challenge for the twenty-first century. A co-ordinated multidisci-plinary approach is necessary. Major advances are possible provideddengue research receives the attention and funding its prevalencedeserves.
References
1 Halstead SB. Dengue. Lancet 2007;370:1644–52.2 Halstead SB. Pathogenesis of dengue: challenges to molecular biology. Science
1988;239:476–81.3 Webster DP, Farrar J, Rowland-Jones S. Progress towards a dengue vaccine. Lancet Infect Dis
2009;9:678–87.4 DengueNet–WHO’s Internet-based system for the global surveillance of dengue fever and
dengue haemorrhagic fever (dengue/DHF). Dengue/DHF—global public health burden. WklyEpidemiol Rec 2002;77:300–4. http://www.who.int/denguenet.
5 Franco L, Caro AD, Carletti F et al. Recent expansion of dengue virus serotype 3 in West
Africa. Euro Surveill 2010;15:19490.6 Gubler DJ. The changing epidemiology of yellow fever and dengue, 1900 to 2003: full circle?
Comp Immunol Microbiol Infect Dis 2004;27:319–30.
7 Hsieh YH, Chen CW. Turning points, reproduction number, and impact of climatologicalevents for multi-wave dengue outbreaks. Trop Med Int Health 2009;14:628–38.
8 Gubler DJ. Epidemic dengue/dengue hemorrhagic fever as a public health, social and econ-
omic problem in the 21st century. Trends Microbiol 2002;10:100–3.9 Gubler DJ. Cities spawn epidemic dengue viruses. Nat Med 2004;10:129–30.
10 Anuradha S, Singh NP, Rizvi SN et al. The 1996 outbreak of dengue hemorrhagic fever inDelhi, India. Southeast Asian J Trop Med Public Health 1998;29:503–6.
11 Vaughn DW. Invited commentary: dengue lessons from Cuba. Am J Epidemiol2000;152:800–3.
12 Clark DV, Mammen MP Jr, Nisalak A et al. Economic impact of dengue fever/dengue
hemorrhagic fever in Thailand at the family and population levels. Am J Trop Med Hyg2005;72:786–91.
13 Luz PM, Grinsztejn B, Galvani AP. Disability adjusted life years lost to dengue in Brazil.
Trop Med Int Health 2009;14:237–46.14 Farrar J, Focks D, Gubler D et al. Towards a global dengue research agenda. Trop Med Int
Health 2007;12:695–9.15 Allwinn R, Hofknecht N, Doerr HW. Dengue in travellers is still underestimated.
Intervirology 2008;51:96–100.
16 WHO. Dengue haemorrhagic fever: diagnosis, treatment, prevention and control. 2ndEdition Geneva: World Health Organisation, 1997, ed.
17 WHO. In Asia ROfS-E (eds) Guidelines for treatment of dengue fever/dengue haemorrhagicfever in small hospitals. New Delhi: World Health Organisation, 1999, editor.
18 Kalayanarooj S, Vaughn DW, Nimmannitya S et al. Early clinical and laboratory indicators
of acute dengue illness. J Infect Dis 1997;176:313–21.19 Deen JL, Harris E, Wills B et al. The WHO dengue classification and case definitions: time
for a reassessment. Lancet 2006;368:170–3.
20 Endy TP, Chunsuttiwat S, Nisalak A et al. Epidemiology of inapparent and symptomaticacute dengue virus infection: a prospective study of primary school children in Kamphaeng
Phet, Thailand. Am J Epidemiol 2002;156:40–51.
J. Whitehorn and J. Farrar
170 British Medical Bulletin 2010;95
at Iowa State U
niversity on October 19, 2014
http://bmb.oxfordjournals.org/
Dow
nloaded from
21 Kabra SK, Jain Y, Singhal T et al. Dengue hemorrhagic fever: clinical manifestations and
management. Indian J Pediatr 1999;66:93–101.22 McBride JH. Dengue fever. An Australian perspective. Aust Fam Physician 1999;28:319–23.
23 tsai CJ, Kuo CH, Chen PC et al. Upper gastrointestinal bleeding in dengue fever. Am JGastroenterol 1991;86:33–5.
24 thisyakorn U, Thisyakorn C. Dengue infection with unusual manifestations. J Med AssocThai 1994;77:410–3.
25 Wang C, Lee I, Su M et al. Differences in clinical and laboratory characteristics and disease
severity between children and adults with dengue virus infection in Taiwan, 2002. Trans RSoc Trop Med Hyg 2009;103:871–7.
26 Seet RC, Quek AM, Lim EC. Post-infectious fatigue syndrome in dengue infection. J ClinVirol 2007;38:1–6.
27 Chye JK, Lim CT, Ng KB et al. Vertical transmission of dengue. Clin Infect Dis1997;25:1374–7.
28 WHO. Dengue: Guidelines for Diagnosis, Treatment, Prevention and Control, new edn.Geneva: World Health Organisation, 2009.
29 Kliks SC, Nisalak A, Brandt WE et al. Antibody-dependent enhancement of dengue virusgrowth in human monocytes as a risk factor for dengue hemorrhagic fever. Am J Trop MedHyg 1989;40:444–51.
30 Halstead SB. Neutralization and antibody-dependent enhancement of dengue viruses. AdvVirus Res 2003;60:421–67.
31 Martina BE, Koraka P, Osterhaus AD. Dengue virus pathogenesis: an integrated view. ClinMicrobiol Rev 2009;22:564–81.
32 Leitmeyer K, Vaughn D, Watts D et al. Dengue virus structural differences that correlate with
pathogenesis. J Virol 1999;73:4738–47.33 Sanchez I, Ruiz B. A single nucleotide change in the E protein gene of dengue virus 2
Mexican strain affects neurovirulence in mice. J Gen Virol 1996;77:2541–5.34 Streatfield R, Bielby G, Sinclair D. A primary dengue 2 epidemic with spontaneous haemor-
rhagic manifestations. Lancet 1993;342:560–1.
35 Guzman MG, Kouri G, Halstead SB. Do escape mutants explain rapid increases in denguecase-fatality rates within epidemics? Lancet 2000;355:1902–3.
36 Vaughn DW, Green S, Kalayanarooj S et al. Dengue viremia titer, antibody response pattern,and virus serotype correlate with disease severity. J Infect Dis 2000;181:2–9.
37 Diamond M, Edgil D, Roberts T et al. Infection of human cells by dengue virus is modulated
by different cell types and viral strains. J Virol 2000;74:7814–23.38 Kurane I, Innis BL, Nimmannitya S et al. Activation of T lymphocytes in dengue virus infec-
tions. High levels of soluble interleukin 2 receptor, soluble CD4, soluble CD8, interleukin 2,
and interferon-gamma in sera of children with dengue. J Clin Invest 1991;88:1473–80.39 Hober D, Poli L, Roblin B et al. Serum levels of tumor necrosis factor-alpha (TNF-alpha),
interleukin-6 (IL-6), and interleukin-1 beta (IL-1 beta) in dengue-infected patients. Am JTrop Med Hyg 1993;48:324–31.
40 Fernandez-Mestre MT, Gendzekhadze K, Rivas-Vetencourt P et al. TNF-alpha-308A allele, a
possible severity risk factor of hemorrhagic manifestation in dengue fever patients. TissueAntigens 2004;64:469–72.
41 Acioli-Santos B, Segat L, Dhalia R et al. MBL2 gene polymorphisms protect against develop-ment of thrombocytopenia associated with severe dengue phenotype. Hum Immunol2008;69:122–8.
42 LaFleur C, Granados J, Vargas-Alarcon G et al. HLA-DR antigen frequencies in Mexicanpatients with dengue virus infection: HLA-DR4 as a possible genetic resistance factor for
dengue hemorrhagic fever. Hum Immunol 2002;63:1039–44.43 Loke H, Bethell D, Phuong CX et al. Susceptibility to dengue hemorrhagic fever in Vietnam:
evidence of an association with variation in the vitamin d receptor and Fc gamma receptor
IIa genes. Am J Trop Med Hyg 2002;67:102–6.44 Loke H, Bethell DB, Phuong CX et al. Strong HLA class I–restricted T cell responses in
dengue hemorrhagic fever: a double-edged sword? J Infect Dis 2001;184:1369–73.45 Monath T, Barrett A. Pathogenesis and pathophysiology of yellow fever. Adv Virus Res
2003;60:343–95.
Dengue
British Medical Bulletin 2010;95 171
at Iowa State U
niversity on October 19, 2014
http://bmb.oxfordjournals.org/
Dow
nloaded from
46 Graham RR, Juffrie M, Tan R et al. A prospective seroepidemiologic study on dengue in chil-
dren four to nine years of age in Yogyakarta, Indonesia I. Studies in 1995–1996. Am J TropMed Hyg 1999;61:412–9.
47 Kalayanarooj S, Nimmannitya S. Clinical presentations of dengue hemorrhagic fever ininfants compared to children. J Med Assoc Thai 2003;86:S673–80.
48 Chau TN, Quyen NT, Thuy TT et al. Dengue in Vietnamese infants—results of
infection-enhancement assays correlate with age-related disease epidemiology, and cellularimmune responses correlate with disease severity. J Infect Dis 2008;198:516–24.
49 Guzman MG, Kouri G. Dengue: an update. Lancet Infect Dis 2002;2:33–42.50 Wichmann O, Hongsiriwon S, Bowonwatanuwong C et al. Risk factors and clinical features
associated with severe dengue infection in adults and children during the 2001 epidemic in
Chonburi, Thailand. Trop Med Int Health 2004;9:1022–9.51 Dejnirattisai W, Jumnainsong A, Onsirisakul N et al. Cross-reacting antibodies enhance
dengue virus infection in humans. Science 2010;328:745–8.52 Chau T, Anders K, Lien lB et al. Clinical and virological features of dengue in Vietnamese
infants. PLoS Negl Trop Dis 2010;4:e657.
53 Stephenson JR. Understanding dengue pathogenesis: implications for vaccine design. BullWorld Health Organ 2005;83:308–14.
54 Hang VT, Nguyet NM, Trung DT et al. Diagnostic accuracy of NS1 ELISA and lateral flow
rapid tests for dengue sensitivity, specificity and relationship to viraemia and antibodyresponses. PLoS Negl Trop Dis 2009;3:e360.
55 Avirutnan P, Punyadee N, Noisakran S et al. Vascular leakage in severe dengue virus infec-tions: a potential role for the nonstructural viral protein NS1 and complement. J Infect Dis2006;193:1078–88.
56 Rico-Hesse R. Dengue virus markers of virulence and pathogenicity. Future Virol 2009;4:581.57 Srikiathachorn A, Gibbons R, Green S et al. Dengue haemorrhagic fever: the sensitivity and
specificity of the World Health Organisation definitions for identification of severe cases ofdengue in Thailand, 1994–2005. Clin Infect Dis 2010;50:1135–43.
58 Kalayanarooj S. Standardised clinical management: evidence of reduction of dengue haemor-
rhagic fever case-fatality rate in Thailand. Dengue Bull 1999;23:10–7.59 Sumarmo, Wulur H, Jahja E et al. Clinical observations on virologically confirmed fatal
dengue infections in Jakarta, Indonesia. Bull World Health Organ 1983;61:693–701.60 Phuong CX, Nhan NT, Kneen R et al. Clinical diagnosis and assessment of severity of con-
firmed dengue infections in Vietnamese children: is the world health organization classifi-
cation system helpful? Am J Trop Med Hyg 2004;70:172–9.61 Harris E, Videa E, Perez L et al. Clinical, epidemiologic, and virologic features of dengue in
the 1998 epidemic in Nicaragua. Am J Trop Med Hyg 2000;63:5–11.
62 Teixeira MG, Costa Mda C, Barreto F et al. Dengue: twenty-five years since reemergence inBrazil. Cad Saude Publica 2009;25:S7–18.
63 Moxon C, Wills B. Management of severe dengue in children. Adv Exp Med Biol2008;609:131–44.
64 Wills BA, Nguyen MD, Ha TL et al. Comparison of three fluid solutions for resuscitation in
dengue shock syndrome. N Engl J Med 2005;353:877–89.65 Hunsperger EA, Yoksan S, Buchy P et al. Evaluation of commercially available anti-dengue
virus immunoglobulin M tests. Emerg Infect Dis 2009;15:436–40.66 Libraty DH, Young PR, Pickering D et al. High circulating levels of the dengue virus non-
structural protein NS1 early in dengue illness correlate with the development of dengue
hemorrhagic fever. J Infect Dis 2002;186:1165–8.67 Kong YY, Thay CH, Tin TC et al. Rapid detection, serotyping and quantitation of dengue
viruses by TaqMan real-time one-step RT-PCR. J Virol Methods 2006;138:123–30.68 Tanner L, Schreiber M, Low JG et al. Decision tree algorithms predict the diagnosis and
outcome of dengue fever in the early phase of illness. PLoS Negl Trop Dis 2008;2:e196.
69 Srikiatkhachorn A, Krautrachue A, Ratanaprakarn W et al. Natural history of plasmaleakage in dengue hemorrhagic fever: a serial ultrasonographic study. Pediatr Infect Dis J2007;26:283–90; discussion 91–2.
70 Srikiatkhachorn A, Green S. Markers of dengue disease severity. Curr Top MicrobiolImmunol 2010;338:67–82.
J. Whitehorn and J. Farrar
172 British Medical Bulletin 2010;95
at Iowa State U
niversity on October 19, 2014
http://bmb.oxfordjournals.org/
Dow
nloaded from
71 Edelman R. Dengue vaccines approach the finish line. Clin Infect Dis 2007;45:S56–60.
72 Innis BL, Eckels KH. Progress in development of a live-attenuated, tetravalent dengue virusvaccine by the United States Army Medical Research and Materiel Command. Am J TropMed Hyg 2003;69:1–4.
73 Edelman R, Wasserman SS, Bodison SA et al. Phase I trial of 16 formulations of a tetravalentlive-attenuated dengue vaccine. Am J Trop Med Hyg 2003;69:48–60.
74 Sun W, Edelman R, Kanesa-Thasan N et al. Vaccination of human volunteers with mono-valent and tetravalent live-attenuated dengue vaccine candidates. Am J Trop Med Hyg2003;69:24–31.
75 Halstead SB, Marchette NJ. Biologic properties of dengue viruses following serial passage inprimary dog kidney cells: studies at the University of Hawaii. Am J Trop Med Hyg2003;69:5–11.
76 Guirakhoo F, Kitchener S, Morrison D et al. Live attenuated chimeric yellow fever dengue
type 2 (ChimeriVax-DEN2) vaccine: Phase I clinical trial for safety and immunogenicity:effect of yellow fever pre-immunity in induction of cross neutralizing antibody responses toall 4 dengue serotypes. Hum Vaccin 2006;2:60–7.
77 Guirakhoo F, Pugachev K, Zhang Z et al. Safety and efficacy of chimeric yellowFever-dengue virus tetravalent vaccine formulations in nonhuman primates. J Virol2004;78:4761–75.
78 Castilow E, Olson M, Varga S. Understanding respiratory syncytial virus (RSV)vaccine-enhanced disease. Immunol Res 2007;39:225–39.
79 Edelman R, Hombach J. “Guidelines for the clinical evaluation of dengue vaccines inendemic areas”: summary of a World Health Organisation Technical Consultation. Vaccine2008;26:4113–9.
80 Swaminathan S, Khanna N. Dengue: recent advances in biology and current status of transla-tional research. Curr Mol Med 2009;9:152–73.
81 Heinz F, Allison S. The machinery for flavivirus fusion with host cell membranes. Curr OpinMicrobiol 2001;4:450–5.
82 Wang Q, Patel S, Vangrevelinghe E et al. A small-molecule dengue virus inhibitor.
Antimicrob Agents Chemother 2009;53:1823–31.83 Lescar J, Luo D, Xu T et al. Towards the design of antiviral inhibitors against flaviviruses:
the case for the multifunctional NS3 protein from Dengue virus as a target. Antiviral Res2008;80:94–101.
84 Melino S, Paci M. Progress for dengue virus diseases. Towards the NS2B-NS3pro inhibition
for a therapeutic-based approach. FEBS J 2007;274:2986–3002.85 Tomlinson SM, Malmstrom RD, Watowich SJ. New approaches to structure-based discovery
of dengue protease inhibitors. Infect Disord Drug Targets 2009;9:327–43.
86 Webster D, Klenerman P, Collier J et al. Development of novel treatments for hepatitis C.Lancet Infect Dis 2009;9:108–17.
87 Chung K, Nybakken G, Thompson B et al. Antibodies against West Nile Virus nonstructuralprotein NS1 prevent lethal infection through Fc gamma receptor-dependent and -independentmechanisms. J Virol 2006;80:1340–51.
88 Shrestha B, Brien J, Sukupolvi-Petty S et al. The development of therapeutic antibodies thatneutralize homologous and heterologous genotypes of dengue virus type 1. PLoS Pathog2010;6:e1000823.
89 Ooi EE, Goh KT, Gubler DJ. Dengue prevention and 35 years of vector control in Singapore.Emerg Infect Dis 2006;12:887–93.
90 Gubler DJ, Nalim S, Tan R et al. Variation in susceptibility to oral infection with dengueviruses among geographic strains of Aedes aegypti. Am J Trop Med Hyg 1979;28:1045–52.
91 Hanley K, Nelson J, Schirtzinger E et al. Superior infectivity for mosquito vectors contributesto competitive displacement among strains of dengue virus. BMC Ecol 2008;8:1.
92 Medlock J, Luz PM, Struchiner CJ et al. The impact of transgenic mosquitoes on dengue
virulence to humans and mosquitoes. Am Nat 2009;174:565–77.93 Rasgon J. Using predictive models to optimize Wolbachia-based strategies for vector-borne
disease control. Adv Exp Med Biol 2008;627:114–25.94 Marten G, Reid J. Cyclopoid copepods. J Am Mosq Control Assoc 2007;23:65–92.
Dengue
British Medical Bulletin 2010;95 173
at Iowa State U
niversity on October 19, 2014
http://bmb.oxfordjournals.org/
Dow
nloaded from