Age Ageing 2011 Banerjee 7 13
7
Click here to load reader
-
Upload
dewi-djasmi -
Category
Documents
-
view
218 -
download
0
Transcript of Age Ageing 2011 Banerjee 7 13

8122019 Age Ageing 2011 Banerjee 7 13
httpslidepdfcomreaderfullage-ageing-2011-banerjee-7-13 17
REVIEW
Human stem cell therapy in ischaemic stroke
a review
SOMA BANERJEE 1dagger DEBORAH W ILLIAMSON 2dagger NAGY HABIB 3 MYRTLE GORDON 4 JEREMY CHATAWAY 1
1Department of Neurology St Mary rsquos Hospital Imperial College Healthcare NHS Trust Praed Street London W21NY UK 2Department of Virology and Immunology Auckland City Hospital Auckland New Zealand3Department of Surgery and 4Department of Haematology Faculty of Medicine Imperial College London UK
Address correspondence to S Banerjee Tel (+44) 20 7886 6889 Fax (+44) 20 7886 1541 Email sbanerjee73hotmailcom
somabanerjee08imperialacuk
Abstract
Stroke is a leading cause of death and disability Globally 15 million people suffer a stroke each year of whom more than 5million die and a further 5 million are left permanently disabled Current treatment options offer modest bene 1047297ts andthere is a pressing need for new and effective treatmentsStem cell therapy is a well-established treatment modality for various haematological diseases with its use now being explored in different disease processes including various neurological diseases as well as vascular conditions such as ischae-mic heart disease and peripheral vascular disease Promising results have been seen in animal models of stroke with evi-dence of signi1047297cant functional bene1047297ts Translation to the bedside however is in its early stages This review will discussthe scienti1047297c background to stem cell therapy in ischaemic stroke including evidence from current clinical trials
Keywords stroke stem cells clinical trials elderly
Introduction
Stroke is the second most common single cause of death worldwide (after ischaemic heart disease) and is the com-monest cause of adult disability In the UK there is astroke every 5 min and on a global basis it causes over1047297 ve million deaths in the world each year Moreover inEurope a quarter of a million people will become disabledafter their 1047297rst stroke each year Even if age-speci1047297c strokeincidence remains stable or falls slightly as more peoplelive into old age the number of new cases of acute strokeper year will rise
Although recent advances have substantially improvedstroke management current acute treatment options offeronly modest effects Aspirin provides only a 1 absolutereduction in death and recurrent ischaemic stroke
Thrombolysis with tissue plasminogen activator is only applicable within a narrow time window and until recently fewer than 1 of stroke patients in England received thistreatment annually [ 1 ]
Most patients show some spontaneous recovery after astroke which can be further improved by interventionssuch as neurorehabilitation However this recovery is oftenincomplete Stroke therefore remains a major source of adult disability and there continues to be a compelling needfor effective treatments for severe disabling stroke
Regenerative potential of the brain
Cells of the brain and central nervous system were until recently thought to be incapable of regeneration However
in the last decade evidence of neurogenesis in the humanadult brain has been demonstrated in the dentate nucleusof the hippocampus and the sub-ventricular zone [ 2 3 ]
This has formed the basis for experimental work investi-gating the potential role of cell transplantation therapy inthe treatment of various neurological diseases in particularischaemic stroke
Ischaemic strokes make up the majority of all strokesaccounting for 80 of the total A recent study of patients
with ischaemic stroke was able to demonstrate evidence of neurogenesis in the ischaemic penumbra where cells were
daggerSoma Banerjee and Deborah Williamson are lead authors both authors haveequally contributed to this work
Age and Ageing 2011 40 7 ndash 13doi 101093ageingafq133
copy The Author 2010 Published by Oxford University Press on behalf of the British Geriatrics SocietyAll rights reserved For Permissions please email journalspermissionsoxfordjournalsorg
Published electronically 10 November 2010
7
8122019 Age Ageing 2011 Banerjee 7 13
httpslidepdfcomreaderfullage-ageing-2011-banerjee-7-13 27
found to preferentially localise to the vicinity of blood vessels [ 4 ] The 1047297ndings are suggestive of stroke-inducedcompensatory neurogenesis where it may contribute topost-ischaemic recovery and therefore represent a potential target for stroke therapy
Approaches to stem cell therapy in ischaemic
stroke
Human stem cell transplantation therapy is a now a well-established treatment for various malignant and non-malignant haematological diseases and some autoimmunedisorders Pre-clinical studies over the last decade havedemonstrated signi1047297cant bene1047297ts of stem cell therapy inrodent models of ischaemic stroke Translation to thebedside however is in its early stages
Clinical approaches to stem cell therapy in stroke can bebroadly divided into endogenous and exogenousapproaches The endogenous approach aims to stimulatemobilisation of stem cells already present within the indi-
vidual Examples of this approach include the use of
granulocyte-colony stimulating factor (G-CSF) which is rou-tinely used to mobilise stem cells for transplantation in hae-matological malignancies G-CSF has been shown to bebene1047297cial in rodent models of stroke (exhibiting neuropro-tective and neuroregenerative activities) [ 5 6 ] and further-more has been shown to be safe in phase I clinical trials of human stroke when used within 7 days [ 7 8 ] or 7 ndash 30 dayspost-stroke [ 9 ] Of note G-CSF appears to have direct bene1047297ts beyond simply mobilisation of stem cells A
number of phase II trials are currently underway to investi-gate its ef 1047297cacy in patients with ischaemic stroke
The exogenous approach involves the transplantation of the patient with stem cells delivered locally (eg direct intra-cerebral implantation) or systemically (eg intravenous) andmay involve in vitro culture of cells for the expansion of cell numbers prior to administration
This review will discuss the exogenous approaches to
stem cell therapy in ischaemic stroke in particular the various types of human stem cells being considered fortherapy and results of the early clinical studies
Stem cells overview
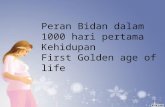
Stem cells can be de1047297ned as clonogenic cells that have thecapacity to self-renew and differentiate into multiple cell lineages [ 10 ] Stem cells are present throughout life thoughdifferences in differentiation potential (potency) allow forfurther sub-classi1047297cation (Figure 1 )
Totipotent stem cells are capable of giving rise to an
entire organism and can be derived from fertilised oocytesand cells of the developing zygote up to the eight-cell stagePluripotent stem cells can give rise to all tissue types fromany of the three embryonic germ layers but unlike totipo-tent cells cannot give rise to an entire organismMultipotent stem cells are more differentiated less plasticcells They are able to differentiate into multiple types of cells but within one organ system (eg blood) Oligopotent and unipotent stem cells have more restricted differentiation
Figure 1 Potency of different stages of stem cells [ 11 ]
S Banerjee et al
8
8122019 Age Ageing 2011 Banerjee 7 13
httpslidepdfcomreaderfullage-ageing-2011-banerjee-7-13 37
potential with the former capable of producing more thanone type of cell (eg clonal common myeloid progenitor)and the latter capable of producing only one mature cell type
Progenitor cells are those cells generated by stem cells which go on to differentiate into mature cells (eg endo-thelial progenitor cells) Unlike stem cells which can repli-cate inde1047297nitely they can only divide a limited number of
times and therefore lie at an intermediate position betweenstem cells and mature fully differentiated cells
Source of stem cells
Stem cells can be classi1047297ed according to their source withthe two major types being embryonic stem (ES) cells andadult stem cells The relative merits of each are presentedin Table 1
Human ES cells are pluripotent and are isolated from5-day-old human blastocysts The major limiting factor to
their widespread use includes ethical concerns regarding theuse of unwanted embryos Furthermore ES cells can becharacterised by their ability to form teratomas [ 12 ] andtherefore there is concern regarding their tumorigenicity
Adult stem cells are multipotent stem cells found indeveloped organisms which are used to replace cells that have died or lost function They can be obtained fromadults as well as children including from umbilical cordblood They have been identi1047297ed within many different organ systems including bone marrow brain heart skinand bone Adult stem cells make up 1 ndash 2 of the total cell population within a particular tissue type They are usually quiescent and held in an undifferentiated state until they receive a stimulus to differentiate
Recent advances in stem cell research have seen theability to transform adult stem cells from human skin 1047297bro-blasts into pluripotent stem cells (ES cell-like) in aphenomenon known as induced pluripotency [ 13 ndash 15 ] Thisis in its very early stages of research but has the potential advantage of obtaining pluripotent stem cells from individ-uals without the ethical dilemmas associated with the useof ES cells
Stem cell transplantation for ischaemic
stroke
Following a stroke all brain tissue elements are lost unlikeParkinsonrsquos disease for example where a speci1047297c neuronal type is damaged After an episode of ischaemia a character-istic pathophysiological change ensues in affected braintissue At the core of the infarct cavity the affected cells die
rapidly by necrosis and an area of surrounding tissue thelsquopenumbrarsquo contains tissue in which neurones and glia vari-ably survive or die by a mixture of ischaemic degenerationand apoptosis over an extended time course of several hours to days and even weeks [ 16 ]
Stem cell therapy for ischaemic stroke thereforefocuses on a regenerative strategy required to restore not only neural elements but also supporting structures such asblood vessels A variety of stem cell types from humanshave been tested in stroke both in experimental and inclinical studies These are discussed below
Neural stemprogenitor cells
It is now generally accepted that active neurogenesis orig-inating from neural stem cells (NSCs) occurs in discreteareas of the mammalian adult brain throughout life giving rise to new populations of neurones and glia [ 17 ]Neurogenesis can be physiological or can be subject toexternal modulation by certain conditions eg CNSdamage such as ischaemia
Preclinical experiments
NSCs can be isolated from foetal as well as adult mammals Several studies have documented the isolation of NSCs from the adult rodent brain [ 18 19 ] and more recent
work has extended to the adult human brain [ 20 21 ]Human NSCs delivered intravenously or stereotactically sur-rounding the lesion have been shown to survive migratetowards the lesion and differentiate (mainly neurones andastrocytes) while improving functional recovery in rodent models of stroke [ 22 ndash 24 ]
Clinical studies
The practicability of routine brain biopsies for isolation of adult human NSCs and autologous transplantation post-stroke remains to be seen and no clinical trials utilising adult NSCs have been undertaken
Immortalised NSC lines can be developed howeverfrom ES or foetal stem cells by the addition of speci1047297cgrowth factors There is currently a phase I trial plannedusing a commercially developed (foetally derived) NSC linedesignated CTX to be delivered by stereotactic injection inpatients with ischaemic stroke (ReNeuron UK) [ 25 ]
Table 1 Relative merits of different sources of stem cells
Cell type Advantages Disadvantages
ES cells Pluripotent Ethical issues
Immortal in vitro Insufficient availability
Highly expandable Unknown risk of tumour
formation
Adult stem
cells
Multipotent Immunosuppression required for
allografting
Potential for induced
pluripotency
Certain types difficult to obtain
eg NSCs
Suitable for autologous and
allogeneic use
Expansion issues
Human stem cell therapy in ischaemic stroke
9
8122019 Age Ageing 2011 Banerjee 7 13
httpslidepdfcomreaderfullage-ageing-2011-banerjee-7-13 47
NT2 cell line
Immortalised cell lines are attractive for use in cellulartherapy as they form an abundant source of cells for trans-plantation in addition to the relative ease of preparationand long-term maintenance The immortalised cell lineNTera-2 (NT2) was derived from a human teratocarcinomaover 20 years ago [ 21 ] After several weeks of exposure toretinoic acid and mitotic inhibitors these cells differentiate
into post-mitotic neurone-like cells named NT2N cells which display a variety of neuronal features [ 26 ] Thesecells maintain their neuronal phenotype both in vitro andin vivo for over a year without reverting to a neoplasticstate [ 27 28 ]
Preclinical experiments
The transplantation of NT2N cells into the ipsilateral stria-tum of ischaemic rat brains improved functional recovery
with some parameters of behavioural improvement persist-ing for up to 6 months post-transplantation [ 29 30 31]Moreover no evidence of tumorigenicity was found follow-ing post-mortem examination of the rats an important consideration given the derivation of this cell line [32]
Clinical studies
NT2N cells were the 1047297rst human cells to be tested instroke clinical trials A phase I trial examined the safety of stereotactic transplantation of cells into patients with basal ganglia stroke which had occurred 6 months to 6 years pre-
viously [33] Twelve patients with stable motor de1047297citsreceived the treatment along with an immunosuppressiveregimen of cyclosporine-A for 8 weeks post-transplantation
The small study population size limited any meaningful interpretation of ef 1047297cacy though there was a trend towardsimproved functional outcome in four patients Autopsy onone patient who died of myocardial infarction 27 monthspost-transplantation showed apparent survival of NT2Ncells in the brain [34] Furthermore positron emission tom-ography scanning at 6 months post-transplantation showedincreased metabolic activity at the site of infarct in sixpatients [35] although this may have indicated an in1047298am-matory response rather than graft survival however nosigns of in1047298ammation were seen on MRI
This initial safety trial led to a Phase II study assessing the effect of NT2N cell transplantation in 18 patients with
substantial 1047297
xed motor de1047297
cits (between 1 and 6 yearspost-stroke) associated with a basal ganglia infarct [36] Theauthors compared stereotactic cellular transplantation plustwo months of rehabilitation ( n = 14) against control patients who received rehabilitation alone ( n = 4) Againthe study was not powered to demonstrate ef 1047297cacyalthough 6 of the 14 patients who received a transplant appeared to show improvement on a standardised strokescale but this was not statistically signi1047297cant against control patients Of note this trial included ischaemic ( n = 9) andhaemorrhagic strokes ( n = 9)
Despite the initial promise of using NT2N cells for cel-lular transplantation much remains to be seen about theirutility particularly in a clinical setting Following an ischae-mic stroke damage is rarely restricted to the striatum withmany patients having cortical damage Furthermore thefeasibility of NT2N cellular transplantation in the acutestroke setting has yet to be examined
Bone-marrow-derived stem cells
Broadly speaking bone-marrow-derived stem cells consist of both haematopoietic stem cells (HSCs) and mesenchy-mal stem cells (MSCs) HSCs are the precursors of all blood and lymphoid lineages MSCs give rise to the stromal cells of the bone marrow including the formation of osteo-blasts chondrocytes and adipocytes Bone marrow is anattractive source of stem cells being easily accessible andsuitable for autologous (obviating the need for immunosup-pression) as well as allogeneic use
Bone marrow cells have been shown to be able tomigrate to the brain and differentiate into cells that express
neuron-speci1047297c markers [37] Both populations of bonemarrow cells have been studied extensively with regard totheir potential for neuronal differentiation and possible usein neuroregenerative therapy
Mesenchymal stem cells
These cells are probably the most widely studied in exper-imental models of neurotransplantation post-stroke
Preclinical experiments Several studies have demonstratedthat MSCs can improve functional recovery after middle cer-ebral artery occlusion in rats This recovery occurs when theMSCs are delivered by a variety of routes intravenous intra-carotid and intrastriatal starting 1 day post-ischaemia [38 ndash 40] In addition delayed delivery of MSCs even up until onemonth post-infarct can also improve long-term functional outcome [41] Following transplantation however very few cells are actually found in the brain and even fewer of thesecells express neural markers [42] Despite this animals whichreceived MSCs did have some amelioration of functional recovery strongly suggesting a mechanism of action otherthan integration into the host rsquos neural circuitry
Clinical studies The extensive pre-clinical work on MSCsled to a phase III clinical trial using autologous culture-expanded MSCs in patients with ischaemic stroke Five
patients with established stroke (gt1 month post-infarct)received MSCs by the intravenous route following ex vivo culture expansion of the cells [43] Cells were extracted by bone marrow aspiration and culture-expanded There wasno cell-related toxicity related to the MSCs administrationand the authors suggested that functional improvement may have been better in the transplanted group compared
with the control group although this was not statistically signi1047297cant There were no signi1047297cant differences betweenthe two groups in relation to changes in infarct volume at 1-year follow-up
S Banerjee et al
10
8122019 Age Ageing 2011 Banerjee 7 13
httpslidepdfcomreaderfullage-ageing-2011-banerjee-7-13 57
Further to the above trial a phase II trial of intravenousautologous MSC therapy in patients within 6 weeks of carotid territory ischaemic stroke is due to commencerecruiting shortly
Haematopoietic stem cells
The use of HSCs for bone marrow transplantation is well established and the therapeutic potential of stem cells in
bone marrow in the regeneration of other non-haematopoietic tissue such as heart and skeletal muscle hasalso been explored [44 ndash 46]
Preclinical experiments Much of the preclinical work exam-ining the use of HSCs for stroke therapy has focused onthe potential mechanisms of functional recovery Twostudies in particular have demonstrated increased angiogen-esis in penumbral tissue following CD34+ cell transplan-tation whether given systemically or by the intracerebral route [47 48] CD34+ bone marrow-derived cells includepopulations of haematopoietic and endothelial stem andprogenitor cells Both the aforementioned studies showed
evidence of functional recovery as well as reduced infarct size The authors of one of these studies also used an anti-angiogenic compound endostatin administered 7 days afterCD34+ cell transplantation and demonstrated that endogen-ous neurogenesis was suppressed by diminishing angiogen-esis thus suggesting a possible role for CD34+ cells inangiogenesis-mediated neural plasticity post-stroke
Clinical studies A number of clinical trials are currently underway investigating the role of bone-marrow-derivedstem cell therapy at different stages of ischaemic stroke uti-lising different methods of delivery (Table 2 ) Three trials
utilising autologous bone marrow mononuclear cells areongoing Further three trials are underway utilising autolo-gous CD34+ cells in acute as well as chronic ischaemicstroke patients Results from these trials are awaited
Potential mechanisms of recovery
The functional recovery seen in many experimental modelsfollowing stem cell transplantation is likely to be mediatedby several overlapping mechanisms and understanding them is crucial in order to determine the best approach fortranslation into the clinical setting
The integration of transplanted cells into the ischaemicbrain with the replacement of lost cells is an unlikely mech-anism of repair Most studies have shown the survival of
very few transplanted cells following neurotransplantationdespite evidence of signi1047297cant functional recovery Morelikely is the stimulation of a trophic effect on the ischaemicbrain (eg by secretion of various growth factors) including the recruitment of endogenous repair processes
Anti-in1047298ammatory effects may also play a role [49]
Unresolved issues
As is evident from the diversity among the various com-pleted and ongoing trials (Table 2 ) there are a number of unresolved issues in the translation of stem cell therapy
These include
(1) choice of cell type(2) cell numbers to be given(3) optimum timing of treatment(4) optimum route of delivery
Table 2 Overview of published and ongoing clinical trials of human stem cell therapy in ischaemic stroke (exogenous
approaches)
Cell type Study design Number of
patients
Timing of
delivery
post-stroke
Route of
delivery
Trial outcome Trial
status
Neural cells
NT2N [ 28 ] PI NR-SB 12 6 months ndash 6
years
Intracerebral Safe and feasible trend towards functional
improvement with higher dose (6 times 106 versus
2 times 106 cells)
Complete
NT2N [31] PII R-SB 18 1 ndash 6 years Intracerebral Safe and feasible no significant functional
improvement in treated group (14 treated
versus 4 controls) ischaemic and
haemorrhagic strokes included
Complete
Bone marrow-derived cells
MSC [38] PIII R-OL 30 gt1 month Intravenous Safe and feasible non-significant trend towardsfunctional improvement in treated group (5
treated versus 25 controls)
Complete
BMMNC (NCT00859014) PI NR-OL 10 24 ndash 72 h Intravenous Awaited Ongoing
BMMNC (NCT00473057) PI NR-OL 10 3 ndash 90 days Intra-arterial Awaited Ongoing
BMMNC (CTRI2008091
000046)
PIII R-SB 120 7 ndash 30 days Intravenous Awaited Ongoing
CD34+ (NCT00535197) PIII NR-OL 10 7 days Intra-arterial Awaited Ongoing
CD34+ (NCT00761982) PIII NR-SB 20 5 ndash 9 days Intra-arterial Awaited Ongoing
CD34+ (NCT00950521) PII R-OL 30 6 ndash 60 months Intracerebral Awaited Ongoing
Abbreviations BMMNC bone-marrow mononuclear cells NR non-randomised NT2N NTera-2 immortalised neurone-like cell line OL open label PI and II
phase I and II trials R randomised SB single blind
Human stem cell therapy in ischaemic stroke
11
8122019 Age Ageing 2011 Banerjee 7 13
httpslidepdfcomreaderfullage-ageing-2011-banerjee-7-13 67
These issues are discussed in more detail inSupplementary data available in Age and Ageing online
Tracking of stem cells is another area of interest whichis essential to our further understanding of distribution andmechanism of action of cells Potential approaches to thisinclude labelling of cells with a magnetic label (eg super-paramagnetic iron oxide particles) allowing MRI tracking of the cells This has yet to enter the clinical arena in stroke
studies though it has shown promise in rodent models of stroke [51] The ideal method of tracking delivered stemcells is yet to be established though it will probably involvea combination of different imaging modalities and is likely to evolve with emerging imaging technologies
Another important consideration regarding cellulartherapy for stroke is safety in terms of both the cell typeused and the mechanism for extracting preparing andadministering the cells Long-term biosafety studies areessential in this respect particularly with regard to thepotential for tumorigenicity mdash this will become increasingly important if prolonged secretion of trophic factors by genetically modi1047297ed cells enters the clinical arena In
addition the potential for tumour formation in otherorgans must be considered particularly with systemic deliv-ery of cells Furthermore appropriate quality assurance andcontrol standards must be in place to allow the standardis-ation of cell preparations
Conclusions
Stem cell therapy for the treatment ischaemic stroke is anexciting emerging area of research in the clinical arena of stroke therapy Animal studies have shown promising results in induced models of stroke though translation to
the bedside is still in its infancy A number of issues remainunanswered and further investigation of these will beimperative in the ongoing quest for an effective feasibleand safe cell-based therapy
Key points
bull Stem cell therapy has been explored in pre-clinical modelsof acute and chronic ischaemic stroke with evidence of signi1047297cant functional bene1047297ts in animal studies
bull A number of clinical trials of stem cell treatment inischaemic stroke are now underway though translation to
clinical practice remains a long way offbull A number of unanswered questions remain including
questions regarding type and quantity of stem cells to begiven ideal mode of delivery and tracking of cells
Supplementary data
Supplementary data mentioned in the text is available tosubscribers in Age and Ageing online
Conflicts of interest
All authors are involved in an ongoing clinical trial of auto-logous CD34+ stem cell therapy in ischaemic stroke NHand MG have shares in OmniCyte Ltd
References
The long list of references supporting this review hasmeant that only the most important are listed here and arerepresented by bold text throughout the paper The full list of references is available at Age and Ageing online
1 Bourn J Hudson J Scharaschkin A et al National Audit Of 1047297ce Reducing Brain Damage Faster Access to BetterStroke Care 2005 1 ndash 60
2 Eriksson PS Per1047297lieva E Bjork-Eriksson T et al
Neurogenesis in the adult human hippocampus Nat Med1998 4 1313 ndash 7
3 Curtis MA Kam M Nannmark U et al Human neuroblastsmigrate to the olfactory bulb via a lateral ventricular exten-sion Science 2007 315 1243 ndash 9
4 Jin K Wang X Xie L et al Evidence for stroke-inducedneurogenesis in the human brain Proc Natl Acad Sci 2006103 13198 ndash 202
5 Shyu WC Lin SZ Yang HI et al Functional recovery of stroke rats induced by granulocyte colony-stimulating factor-stimulated stem cells Circulation 2004 110 1847 ndash 54
6 Schabitz WR Kollmar R Schwaninger M et al
Neuroprotective effect of granulocyte colony stimulating factor after focal cerebral ischemia Stroke 2003 34 745
7 Shyu WC Lin SZ Lee CC Liu DD Li H Granulocytecolony-stimulating factor for acute ischaemic stroke a ran-domised controlled trial CMAJ 2006 174 927 ndash 33
8 Zhang JJ Deng M Zhang Y et al A short-term assessment of recombinant granulocyte-stimulating factor (RHG-CSF) intreatment of acute cerebral infarction Cerebrovasc Dis 200622 323
9 Sprigg N Bath PM Zhao L e t al Granulocyte-colony-stimulating factor mobilises bone marrow stem cells inpatients with subacute ischemic stroke The STEMS pilot randomised controlled trial Stroke 2006 37 2979 ndash 83
10 Weissman IL Anderson DJ Gage F Stem and progenitorcells origins phenotypes lineage commitments and transdif-ferentiations Annu Rev Cell Dev Biol 2001 17 387 ndash 403
11 Jones M The source of pluripotent stems cells from develop-ing embryos Original work Wikipedia 2006 enwikipediaorg
wikiStem cell ( creativecommonsorglicensesby-sa25 )12 Thomson JA Itskovitz-Eldor J Shapiro SS et al Embryonic
stem cell lines derived from human blastocysts Science 1998
282 1145 ndash 713 Tahashi K Tanabe K Ohruki M et al Induction of pluripo-tent stem cells from adult human 1047297broblasts by de1047297nedfactors Cell 2007 131 861 ndash 72
14 Meissner A Wernig M Jaenisch R Direct reprogramming of genetically undmodi1047297ed 1047297broblasts into pluripotent stemcells Nat Biotechnol 2007 25 1177 ndash 81
15 Yu J Vodyanik MA Smuge-Otto K et al Induced pluripotent stem cell lines derived from human somatic cells Science2007 318 1917 ndash 20
16 Mattson MP Culmsee C Yu ZF Apoptotic and antiapoptoticmechanisms in stroke Cell Tissue Res 2000 301 173 ndash 87
S Banerjee et al
12
8122019 Age Ageing 2011 Banerjee 7 13
httpslidepdfcomreaderfullage-ageing-2011-banerjee-7-13 77
17 Temple S The development of neural stem cells Nature2001 414 112 ndash 7
18 Reynolds BA Weiss S Generation of neurons and astrocytesfrom isolated cells of the adult mammalian central nervoussystem Science 1992 255 1707 ndash 10
19 Wachs FP Couillard-Despres S Engelhardt M et al High ef 1047297-cacy of clonal growth and expansion of adult neural stemcells Lab Invest 2003 83 949 ndash 62
20 Nunes MC Roy NS Keyoung HM et al Identi1047297cation and
isolation of multipotential neural progenitor cells from thesubcortical white matter of the adult human brain Nat Med2003 9 439 ndash 47
21 Arsenijevic Y Villemure JG Brunet JF et al Isolation of mul-tipotent neural precursors residing in the cortex of the adult human brain Exp Neurol 2001 170 48 ndash 62
22 Chu K Kim M Jeong SW Kim SU Yoon BW Humanneural stem cells can migrate differentiate and integrateafter intravenous transplantation in adult rats with transient forebrain ischemia Neurosci Lett 2003 343 129 ndash 33
23 Chu K Kim M Park KI et al Human neural stem cellsimprove sensorimotor de1047297cits in the adult rat brain withexperimental focal ischemia Brain Res 2004 1016145 ndash 53
24 Kelly S Bliss TM Shah AK et al Transplanted human fetal neural stem cells survive migrate and differentiate inischemic rat cerebral cortex Proc Natl Acad Sci USA 2004101 11839 ndash 44
25 ReNeuron receives UK ethics committee Favourable Opinionfor stroke clinical trialReNeuron2009 wwwreneuroncomnews__eventsnewsdocument_196_237php
26 Andrews PW Damjanov I Simon D et al Pluripotent embry-onal carcinoma clones derived from the human teratocarci-noma cell line Tera-2 Differentiation in vivo and in vitroLab Invest 1984 50 147 ndash 62
27 Pleasure SJ Lee VM NTera 2 cells a human cell line which displays characteristics expected of a human com-
mitted neuronal progenitor cell J Neurosci Res 1993 35585 ndash 602
28 Trojanowski JQ Mantione JR Lee JH et al Neurons derivedfrom a human teratocarcinoma cell line establish molecularand structural polarity following transplantation into therodent brain Exp Neurol 1993 122 283 ndash 94
29 Kleppner SR Robinson KA Trojanowski JQ Lee VM Transplanted human neurons derived from a teratocarcinomacell line (NTera-2) mature integrate and survive for over 1 yearin the nude mouse brain J Comp Neurol 1995 357 618 ndash 32
30 Borlongan CV Tajima Y Trojanowski JQ Lee VM Sanberg PR Transplantation of cryopreserved human embryonal carcinoma-derived neurons (NT2N cells) promotes functional recovery in ischemic rats Exp Neurol 1998 149 310 ndash 21
Received 8 January 2010 accepted in revised form 28 July
2010
Human stem cell therapy in ischaemic stroke
13

8122019 Age Ageing 2011 Banerjee 7 13
httpslidepdfcomreaderfullage-ageing-2011-banerjee-7-13 27
found to preferentially localise to the vicinity of blood vessels [ 4 ] The 1047297ndings are suggestive of stroke-inducedcompensatory neurogenesis where it may contribute topost-ischaemic recovery and therefore represent a potential target for stroke therapy
Approaches to stem cell therapy in ischaemic
stroke
Human stem cell transplantation therapy is a now a well-established treatment for various malignant and non-malignant haematological diseases and some autoimmunedisorders Pre-clinical studies over the last decade havedemonstrated signi1047297cant bene1047297ts of stem cell therapy inrodent models of ischaemic stroke Translation to thebedside however is in its early stages
Clinical approaches to stem cell therapy in stroke can bebroadly divided into endogenous and exogenousapproaches The endogenous approach aims to stimulatemobilisation of stem cells already present within the indi-
vidual Examples of this approach include the use of
granulocyte-colony stimulating factor (G-CSF) which is rou-tinely used to mobilise stem cells for transplantation in hae-matological malignancies G-CSF has been shown to bebene1047297cial in rodent models of stroke (exhibiting neuropro-tective and neuroregenerative activities) [ 5 6 ] and further-more has been shown to be safe in phase I clinical trials of human stroke when used within 7 days [ 7 8 ] or 7 ndash 30 dayspost-stroke [ 9 ] Of note G-CSF appears to have direct bene1047297ts beyond simply mobilisation of stem cells A
number of phase II trials are currently underway to investi-gate its ef 1047297cacy in patients with ischaemic stroke
The exogenous approach involves the transplantation of the patient with stem cells delivered locally (eg direct intra-cerebral implantation) or systemically (eg intravenous) andmay involve in vitro culture of cells for the expansion of cell numbers prior to administration
This review will discuss the exogenous approaches to
stem cell therapy in ischaemic stroke in particular the various types of human stem cells being considered fortherapy and results of the early clinical studies
Stem cells overview
Stem cells can be de1047297ned as clonogenic cells that have thecapacity to self-renew and differentiate into multiple cell lineages [ 10 ] Stem cells are present throughout life thoughdifferences in differentiation potential (potency) allow forfurther sub-classi1047297cation (Figure 1 )
Totipotent stem cells are capable of giving rise to an
entire organism and can be derived from fertilised oocytesand cells of the developing zygote up to the eight-cell stagePluripotent stem cells can give rise to all tissue types fromany of the three embryonic germ layers but unlike totipo-tent cells cannot give rise to an entire organismMultipotent stem cells are more differentiated less plasticcells They are able to differentiate into multiple types of cells but within one organ system (eg blood) Oligopotent and unipotent stem cells have more restricted differentiation
Figure 1 Potency of different stages of stem cells [ 11 ]
S Banerjee et al
8
8122019 Age Ageing 2011 Banerjee 7 13
httpslidepdfcomreaderfullage-ageing-2011-banerjee-7-13 37
potential with the former capable of producing more thanone type of cell (eg clonal common myeloid progenitor)and the latter capable of producing only one mature cell type
Progenitor cells are those cells generated by stem cells which go on to differentiate into mature cells (eg endo-thelial progenitor cells) Unlike stem cells which can repli-cate inde1047297nitely they can only divide a limited number of
times and therefore lie at an intermediate position betweenstem cells and mature fully differentiated cells
Source of stem cells
Stem cells can be classi1047297ed according to their source withthe two major types being embryonic stem (ES) cells andadult stem cells The relative merits of each are presentedin Table 1
Human ES cells are pluripotent and are isolated from5-day-old human blastocysts The major limiting factor to
their widespread use includes ethical concerns regarding theuse of unwanted embryos Furthermore ES cells can becharacterised by their ability to form teratomas [ 12 ] andtherefore there is concern regarding their tumorigenicity
Adult stem cells are multipotent stem cells found indeveloped organisms which are used to replace cells that have died or lost function They can be obtained fromadults as well as children including from umbilical cordblood They have been identi1047297ed within many different organ systems including bone marrow brain heart skinand bone Adult stem cells make up 1 ndash 2 of the total cell population within a particular tissue type They are usually quiescent and held in an undifferentiated state until they receive a stimulus to differentiate
Recent advances in stem cell research have seen theability to transform adult stem cells from human skin 1047297bro-blasts into pluripotent stem cells (ES cell-like) in aphenomenon known as induced pluripotency [ 13 ndash 15 ] Thisis in its very early stages of research but has the potential advantage of obtaining pluripotent stem cells from individ-uals without the ethical dilemmas associated with the useof ES cells
Stem cell transplantation for ischaemic
stroke
Following a stroke all brain tissue elements are lost unlikeParkinsonrsquos disease for example where a speci1047297c neuronal type is damaged After an episode of ischaemia a character-istic pathophysiological change ensues in affected braintissue At the core of the infarct cavity the affected cells die
rapidly by necrosis and an area of surrounding tissue thelsquopenumbrarsquo contains tissue in which neurones and glia vari-ably survive or die by a mixture of ischaemic degenerationand apoptosis over an extended time course of several hours to days and even weeks [ 16 ]
Stem cell therapy for ischaemic stroke thereforefocuses on a regenerative strategy required to restore not only neural elements but also supporting structures such asblood vessels A variety of stem cell types from humanshave been tested in stroke both in experimental and inclinical studies These are discussed below
Neural stemprogenitor cells
It is now generally accepted that active neurogenesis orig-inating from neural stem cells (NSCs) occurs in discreteareas of the mammalian adult brain throughout life giving rise to new populations of neurones and glia [ 17 ]Neurogenesis can be physiological or can be subject toexternal modulation by certain conditions eg CNSdamage such as ischaemia
Preclinical experiments
NSCs can be isolated from foetal as well as adult mammals Several studies have documented the isolation of NSCs from the adult rodent brain [ 18 19 ] and more recent
work has extended to the adult human brain [ 20 21 ]Human NSCs delivered intravenously or stereotactically sur-rounding the lesion have been shown to survive migratetowards the lesion and differentiate (mainly neurones andastrocytes) while improving functional recovery in rodent models of stroke [ 22 ndash 24 ]
Clinical studies
The practicability of routine brain biopsies for isolation of adult human NSCs and autologous transplantation post-stroke remains to be seen and no clinical trials utilising adult NSCs have been undertaken
Immortalised NSC lines can be developed howeverfrom ES or foetal stem cells by the addition of speci1047297cgrowth factors There is currently a phase I trial plannedusing a commercially developed (foetally derived) NSC linedesignated CTX to be delivered by stereotactic injection inpatients with ischaemic stroke (ReNeuron UK) [ 25 ]
Table 1 Relative merits of different sources of stem cells
Cell type Advantages Disadvantages
ES cells Pluripotent Ethical issues
Immortal in vitro Insufficient availability
Highly expandable Unknown risk of tumour
formation
Adult stem
cells
Multipotent Immunosuppression required for
allografting
Potential for induced
pluripotency
Certain types difficult to obtain
eg NSCs
Suitable for autologous and
allogeneic use
Expansion issues
Human stem cell therapy in ischaemic stroke
9
8122019 Age Ageing 2011 Banerjee 7 13
httpslidepdfcomreaderfullage-ageing-2011-banerjee-7-13 47
NT2 cell line
Immortalised cell lines are attractive for use in cellulartherapy as they form an abundant source of cells for trans-plantation in addition to the relative ease of preparationand long-term maintenance The immortalised cell lineNTera-2 (NT2) was derived from a human teratocarcinomaover 20 years ago [ 21 ] After several weeks of exposure toretinoic acid and mitotic inhibitors these cells differentiate
into post-mitotic neurone-like cells named NT2N cells which display a variety of neuronal features [ 26 ] Thesecells maintain their neuronal phenotype both in vitro andin vivo for over a year without reverting to a neoplasticstate [ 27 28 ]
Preclinical experiments
The transplantation of NT2N cells into the ipsilateral stria-tum of ischaemic rat brains improved functional recovery
with some parameters of behavioural improvement persist-ing for up to 6 months post-transplantation [ 29 30 31]Moreover no evidence of tumorigenicity was found follow-ing post-mortem examination of the rats an important consideration given the derivation of this cell line [32]
Clinical studies
NT2N cells were the 1047297rst human cells to be tested instroke clinical trials A phase I trial examined the safety of stereotactic transplantation of cells into patients with basal ganglia stroke which had occurred 6 months to 6 years pre-
viously [33] Twelve patients with stable motor de1047297citsreceived the treatment along with an immunosuppressiveregimen of cyclosporine-A for 8 weeks post-transplantation
The small study population size limited any meaningful interpretation of ef 1047297cacy though there was a trend towardsimproved functional outcome in four patients Autopsy onone patient who died of myocardial infarction 27 monthspost-transplantation showed apparent survival of NT2Ncells in the brain [34] Furthermore positron emission tom-ography scanning at 6 months post-transplantation showedincreased metabolic activity at the site of infarct in sixpatients [35] although this may have indicated an in1047298am-matory response rather than graft survival however nosigns of in1047298ammation were seen on MRI
This initial safety trial led to a Phase II study assessing the effect of NT2N cell transplantation in 18 patients with
substantial 1047297
xed motor de1047297
cits (between 1 and 6 yearspost-stroke) associated with a basal ganglia infarct [36] Theauthors compared stereotactic cellular transplantation plustwo months of rehabilitation ( n = 14) against control patients who received rehabilitation alone ( n = 4) Againthe study was not powered to demonstrate ef 1047297cacyalthough 6 of the 14 patients who received a transplant appeared to show improvement on a standardised strokescale but this was not statistically signi1047297cant against control patients Of note this trial included ischaemic ( n = 9) andhaemorrhagic strokes ( n = 9)
Despite the initial promise of using NT2N cells for cel-lular transplantation much remains to be seen about theirutility particularly in a clinical setting Following an ischae-mic stroke damage is rarely restricted to the striatum withmany patients having cortical damage Furthermore thefeasibility of NT2N cellular transplantation in the acutestroke setting has yet to be examined
Bone-marrow-derived stem cells
Broadly speaking bone-marrow-derived stem cells consist of both haematopoietic stem cells (HSCs) and mesenchy-mal stem cells (MSCs) HSCs are the precursors of all blood and lymphoid lineages MSCs give rise to the stromal cells of the bone marrow including the formation of osteo-blasts chondrocytes and adipocytes Bone marrow is anattractive source of stem cells being easily accessible andsuitable for autologous (obviating the need for immunosup-pression) as well as allogeneic use
Bone marrow cells have been shown to be able tomigrate to the brain and differentiate into cells that express
neuron-speci1047297c markers [37] Both populations of bonemarrow cells have been studied extensively with regard totheir potential for neuronal differentiation and possible usein neuroregenerative therapy
Mesenchymal stem cells
These cells are probably the most widely studied in exper-imental models of neurotransplantation post-stroke
Preclinical experiments Several studies have demonstratedthat MSCs can improve functional recovery after middle cer-ebral artery occlusion in rats This recovery occurs when theMSCs are delivered by a variety of routes intravenous intra-carotid and intrastriatal starting 1 day post-ischaemia [38 ndash 40] In addition delayed delivery of MSCs even up until onemonth post-infarct can also improve long-term functional outcome [41] Following transplantation however very few cells are actually found in the brain and even fewer of thesecells express neural markers [42] Despite this animals whichreceived MSCs did have some amelioration of functional recovery strongly suggesting a mechanism of action otherthan integration into the host rsquos neural circuitry
Clinical studies The extensive pre-clinical work on MSCsled to a phase III clinical trial using autologous culture-expanded MSCs in patients with ischaemic stroke Five
patients with established stroke (gt1 month post-infarct)received MSCs by the intravenous route following ex vivo culture expansion of the cells [43] Cells were extracted by bone marrow aspiration and culture-expanded There wasno cell-related toxicity related to the MSCs administrationand the authors suggested that functional improvement may have been better in the transplanted group compared
with the control group although this was not statistically signi1047297cant There were no signi1047297cant differences betweenthe two groups in relation to changes in infarct volume at 1-year follow-up
S Banerjee et al
10
8122019 Age Ageing 2011 Banerjee 7 13
httpslidepdfcomreaderfullage-ageing-2011-banerjee-7-13 57
Further to the above trial a phase II trial of intravenousautologous MSC therapy in patients within 6 weeks of carotid territory ischaemic stroke is due to commencerecruiting shortly
Haematopoietic stem cells
The use of HSCs for bone marrow transplantation is well established and the therapeutic potential of stem cells in
bone marrow in the regeneration of other non-haematopoietic tissue such as heart and skeletal muscle hasalso been explored [44 ndash 46]
Preclinical experiments Much of the preclinical work exam-ining the use of HSCs for stroke therapy has focused onthe potential mechanisms of functional recovery Twostudies in particular have demonstrated increased angiogen-esis in penumbral tissue following CD34+ cell transplan-tation whether given systemically or by the intracerebral route [47 48] CD34+ bone marrow-derived cells includepopulations of haematopoietic and endothelial stem andprogenitor cells Both the aforementioned studies showed
evidence of functional recovery as well as reduced infarct size The authors of one of these studies also used an anti-angiogenic compound endostatin administered 7 days afterCD34+ cell transplantation and demonstrated that endogen-ous neurogenesis was suppressed by diminishing angiogen-esis thus suggesting a possible role for CD34+ cells inangiogenesis-mediated neural plasticity post-stroke
Clinical studies A number of clinical trials are currently underway investigating the role of bone-marrow-derivedstem cell therapy at different stages of ischaemic stroke uti-lising different methods of delivery (Table 2 ) Three trials
utilising autologous bone marrow mononuclear cells areongoing Further three trials are underway utilising autolo-gous CD34+ cells in acute as well as chronic ischaemicstroke patients Results from these trials are awaited
Potential mechanisms of recovery
The functional recovery seen in many experimental modelsfollowing stem cell transplantation is likely to be mediatedby several overlapping mechanisms and understanding them is crucial in order to determine the best approach fortranslation into the clinical setting
The integration of transplanted cells into the ischaemicbrain with the replacement of lost cells is an unlikely mech-anism of repair Most studies have shown the survival of
very few transplanted cells following neurotransplantationdespite evidence of signi1047297cant functional recovery Morelikely is the stimulation of a trophic effect on the ischaemicbrain (eg by secretion of various growth factors) including the recruitment of endogenous repair processes
Anti-in1047298ammatory effects may also play a role [49]
Unresolved issues
As is evident from the diversity among the various com-pleted and ongoing trials (Table 2 ) there are a number of unresolved issues in the translation of stem cell therapy
These include
(1) choice of cell type(2) cell numbers to be given(3) optimum timing of treatment(4) optimum route of delivery
Table 2 Overview of published and ongoing clinical trials of human stem cell therapy in ischaemic stroke (exogenous
approaches)
Cell type Study design Number of
patients
Timing of
delivery
post-stroke
Route of
delivery
Trial outcome Trial
status
Neural cells
NT2N [ 28 ] PI NR-SB 12 6 months ndash 6
years
Intracerebral Safe and feasible trend towards functional
improvement with higher dose (6 times 106 versus
2 times 106 cells)
Complete
NT2N [31] PII R-SB 18 1 ndash 6 years Intracerebral Safe and feasible no significant functional
improvement in treated group (14 treated
versus 4 controls) ischaemic and
haemorrhagic strokes included
Complete
Bone marrow-derived cells
MSC [38] PIII R-OL 30 gt1 month Intravenous Safe and feasible non-significant trend towardsfunctional improvement in treated group (5
treated versus 25 controls)
Complete
BMMNC (NCT00859014) PI NR-OL 10 24 ndash 72 h Intravenous Awaited Ongoing
BMMNC (NCT00473057) PI NR-OL 10 3 ndash 90 days Intra-arterial Awaited Ongoing
BMMNC (CTRI2008091
000046)
PIII R-SB 120 7 ndash 30 days Intravenous Awaited Ongoing
CD34+ (NCT00535197) PIII NR-OL 10 7 days Intra-arterial Awaited Ongoing
CD34+ (NCT00761982) PIII NR-SB 20 5 ndash 9 days Intra-arterial Awaited Ongoing
CD34+ (NCT00950521) PII R-OL 30 6 ndash 60 months Intracerebral Awaited Ongoing
Abbreviations BMMNC bone-marrow mononuclear cells NR non-randomised NT2N NTera-2 immortalised neurone-like cell line OL open label PI and II
phase I and II trials R randomised SB single blind
Human stem cell therapy in ischaemic stroke
11
8122019 Age Ageing 2011 Banerjee 7 13
httpslidepdfcomreaderfullage-ageing-2011-banerjee-7-13 67
These issues are discussed in more detail inSupplementary data available in Age and Ageing online
Tracking of stem cells is another area of interest whichis essential to our further understanding of distribution andmechanism of action of cells Potential approaches to thisinclude labelling of cells with a magnetic label (eg super-paramagnetic iron oxide particles) allowing MRI tracking of the cells This has yet to enter the clinical arena in stroke
studies though it has shown promise in rodent models of stroke [51] The ideal method of tracking delivered stemcells is yet to be established though it will probably involvea combination of different imaging modalities and is likely to evolve with emerging imaging technologies
Another important consideration regarding cellulartherapy for stroke is safety in terms of both the cell typeused and the mechanism for extracting preparing andadministering the cells Long-term biosafety studies areessential in this respect particularly with regard to thepotential for tumorigenicity mdash this will become increasingly important if prolonged secretion of trophic factors by genetically modi1047297ed cells enters the clinical arena In
addition the potential for tumour formation in otherorgans must be considered particularly with systemic deliv-ery of cells Furthermore appropriate quality assurance andcontrol standards must be in place to allow the standardis-ation of cell preparations
Conclusions
Stem cell therapy for the treatment ischaemic stroke is anexciting emerging area of research in the clinical arena of stroke therapy Animal studies have shown promising results in induced models of stroke though translation to
the bedside is still in its infancy A number of issues remainunanswered and further investigation of these will beimperative in the ongoing quest for an effective feasibleand safe cell-based therapy
Key points
bull Stem cell therapy has been explored in pre-clinical modelsof acute and chronic ischaemic stroke with evidence of signi1047297cant functional bene1047297ts in animal studies
bull A number of clinical trials of stem cell treatment inischaemic stroke are now underway though translation to
clinical practice remains a long way offbull A number of unanswered questions remain including
questions regarding type and quantity of stem cells to begiven ideal mode of delivery and tracking of cells
Supplementary data
Supplementary data mentioned in the text is available tosubscribers in Age and Ageing online
Conflicts of interest
All authors are involved in an ongoing clinical trial of auto-logous CD34+ stem cell therapy in ischaemic stroke NHand MG have shares in OmniCyte Ltd
References
The long list of references supporting this review hasmeant that only the most important are listed here and arerepresented by bold text throughout the paper The full list of references is available at Age and Ageing online
1 Bourn J Hudson J Scharaschkin A et al National Audit Of 1047297ce Reducing Brain Damage Faster Access to BetterStroke Care 2005 1 ndash 60
2 Eriksson PS Per1047297lieva E Bjork-Eriksson T et al
Neurogenesis in the adult human hippocampus Nat Med1998 4 1313 ndash 7
3 Curtis MA Kam M Nannmark U et al Human neuroblastsmigrate to the olfactory bulb via a lateral ventricular exten-sion Science 2007 315 1243 ndash 9
4 Jin K Wang X Xie L et al Evidence for stroke-inducedneurogenesis in the human brain Proc Natl Acad Sci 2006103 13198 ndash 202
5 Shyu WC Lin SZ Yang HI et al Functional recovery of stroke rats induced by granulocyte colony-stimulating factor-stimulated stem cells Circulation 2004 110 1847 ndash 54
6 Schabitz WR Kollmar R Schwaninger M et al
Neuroprotective effect of granulocyte colony stimulating factor after focal cerebral ischemia Stroke 2003 34 745
7 Shyu WC Lin SZ Lee CC Liu DD Li H Granulocytecolony-stimulating factor for acute ischaemic stroke a ran-domised controlled trial CMAJ 2006 174 927 ndash 33
8 Zhang JJ Deng M Zhang Y et al A short-term assessment of recombinant granulocyte-stimulating factor (RHG-CSF) intreatment of acute cerebral infarction Cerebrovasc Dis 200622 323
9 Sprigg N Bath PM Zhao L e t al Granulocyte-colony-stimulating factor mobilises bone marrow stem cells inpatients with subacute ischemic stroke The STEMS pilot randomised controlled trial Stroke 2006 37 2979 ndash 83
10 Weissman IL Anderson DJ Gage F Stem and progenitorcells origins phenotypes lineage commitments and transdif-ferentiations Annu Rev Cell Dev Biol 2001 17 387 ndash 403
11 Jones M The source of pluripotent stems cells from develop-ing embryos Original work Wikipedia 2006 enwikipediaorg
wikiStem cell ( creativecommonsorglicensesby-sa25 )12 Thomson JA Itskovitz-Eldor J Shapiro SS et al Embryonic
stem cell lines derived from human blastocysts Science 1998
282 1145 ndash 713 Tahashi K Tanabe K Ohruki M et al Induction of pluripo-tent stem cells from adult human 1047297broblasts by de1047297nedfactors Cell 2007 131 861 ndash 72
14 Meissner A Wernig M Jaenisch R Direct reprogramming of genetically undmodi1047297ed 1047297broblasts into pluripotent stemcells Nat Biotechnol 2007 25 1177 ndash 81
15 Yu J Vodyanik MA Smuge-Otto K et al Induced pluripotent stem cell lines derived from human somatic cells Science2007 318 1917 ndash 20
16 Mattson MP Culmsee C Yu ZF Apoptotic and antiapoptoticmechanisms in stroke Cell Tissue Res 2000 301 173 ndash 87
S Banerjee et al
12
8122019 Age Ageing 2011 Banerjee 7 13
httpslidepdfcomreaderfullage-ageing-2011-banerjee-7-13 77
17 Temple S The development of neural stem cells Nature2001 414 112 ndash 7
18 Reynolds BA Weiss S Generation of neurons and astrocytesfrom isolated cells of the adult mammalian central nervoussystem Science 1992 255 1707 ndash 10
19 Wachs FP Couillard-Despres S Engelhardt M et al High ef 1047297-cacy of clonal growth and expansion of adult neural stemcells Lab Invest 2003 83 949 ndash 62
20 Nunes MC Roy NS Keyoung HM et al Identi1047297cation and
isolation of multipotential neural progenitor cells from thesubcortical white matter of the adult human brain Nat Med2003 9 439 ndash 47
21 Arsenijevic Y Villemure JG Brunet JF et al Isolation of mul-tipotent neural precursors residing in the cortex of the adult human brain Exp Neurol 2001 170 48 ndash 62
22 Chu K Kim M Jeong SW Kim SU Yoon BW Humanneural stem cells can migrate differentiate and integrateafter intravenous transplantation in adult rats with transient forebrain ischemia Neurosci Lett 2003 343 129 ndash 33
23 Chu K Kim M Park KI et al Human neural stem cellsimprove sensorimotor de1047297cits in the adult rat brain withexperimental focal ischemia Brain Res 2004 1016145 ndash 53
24 Kelly S Bliss TM Shah AK et al Transplanted human fetal neural stem cells survive migrate and differentiate inischemic rat cerebral cortex Proc Natl Acad Sci USA 2004101 11839 ndash 44
25 ReNeuron receives UK ethics committee Favourable Opinionfor stroke clinical trialReNeuron2009 wwwreneuroncomnews__eventsnewsdocument_196_237php
26 Andrews PW Damjanov I Simon D et al Pluripotent embry-onal carcinoma clones derived from the human teratocarci-noma cell line Tera-2 Differentiation in vivo and in vitroLab Invest 1984 50 147 ndash 62
27 Pleasure SJ Lee VM NTera 2 cells a human cell line which displays characteristics expected of a human com-
mitted neuronal progenitor cell J Neurosci Res 1993 35585 ndash 602
28 Trojanowski JQ Mantione JR Lee JH et al Neurons derivedfrom a human teratocarcinoma cell line establish molecularand structural polarity following transplantation into therodent brain Exp Neurol 1993 122 283 ndash 94
29 Kleppner SR Robinson KA Trojanowski JQ Lee VM Transplanted human neurons derived from a teratocarcinomacell line (NTera-2) mature integrate and survive for over 1 yearin the nude mouse brain J Comp Neurol 1995 357 618 ndash 32
30 Borlongan CV Tajima Y Trojanowski JQ Lee VM Sanberg PR Transplantation of cryopreserved human embryonal carcinoma-derived neurons (NT2N cells) promotes functional recovery in ischemic rats Exp Neurol 1998 149 310 ndash 21
Received 8 January 2010 accepted in revised form 28 July
2010
Human stem cell therapy in ischaemic stroke
13

8122019 Age Ageing 2011 Banerjee 7 13
httpslidepdfcomreaderfullage-ageing-2011-banerjee-7-13 37
potential with the former capable of producing more thanone type of cell (eg clonal common myeloid progenitor)and the latter capable of producing only one mature cell type
Progenitor cells are those cells generated by stem cells which go on to differentiate into mature cells (eg endo-thelial progenitor cells) Unlike stem cells which can repli-cate inde1047297nitely they can only divide a limited number of
times and therefore lie at an intermediate position betweenstem cells and mature fully differentiated cells
Source of stem cells
Stem cells can be classi1047297ed according to their source withthe two major types being embryonic stem (ES) cells andadult stem cells The relative merits of each are presentedin Table 1
Human ES cells are pluripotent and are isolated from5-day-old human blastocysts The major limiting factor to
their widespread use includes ethical concerns regarding theuse of unwanted embryos Furthermore ES cells can becharacterised by their ability to form teratomas [ 12 ] andtherefore there is concern regarding their tumorigenicity
Adult stem cells are multipotent stem cells found indeveloped organisms which are used to replace cells that have died or lost function They can be obtained fromadults as well as children including from umbilical cordblood They have been identi1047297ed within many different organ systems including bone marrow brain heart skinand bone Adult stem cells make up 1 ndash 2 of the total cell population within a particular tissue type They are usually quiescent and held in an undifferentiated state until they receive a stimulus to differentiate
Recent advances in stem cell research have seen theability to transform adult stem cells from human skin 1047297bro-blasts into pluripotent stem cells (ES cell-like) in aphenomenon known as induced pluripotency [ 13 ndash 15 ] Thisis in its very early stages of research but has the potential advantage of obtaining pluripotent stem cells from individ-uals without the ethical dilemmas associated with the useof ES cells
Stem cell transplantation for ischaemic
stroke
Following a stroke all brain tissue elements are lost unlikeParkinsonrsquos disease for example where a speci1047297c neuronal type is damaged After an episode of ischaemia a character-istic pathophysiological change ensues in affected braintissue At the core of the infarct cavity the affected cells die
rapidly by necrosis and an area of surrounding tissue thelsquopenumbrarsquo contains tissue in which neurones and glia vari-ably survive or die by a mixture of ischaemic degenerationand apoptosis over an extended time course of several hours to days and even weeks [ 16 ]
Stem cell therapy for ischaemic stroke thereforefocuses on a regenerative strategy required to restore not only neural elements but also supporting structures such asblood vessels A variety of stem cell types from humanshave been tested in stroke both in experimental and inclinical studies These are discussed below
Neural stemprogenitor cells
It is now generally accepted that active neurogenesis orig-inating from neural stem cells (NSCs) occurs in discreteareas of the mammalian adult brain throughout life giving rise to new populations of neurones and glia [ 17 ]Neurogenesis can be physiological or can be subject toexternal modulation by certain conditions eg CNSdamage such as ischaemia
Preclinical experiments
NSCs can be isolated from foetal as well as adult mammals Several studies have documented the isolation of NSCs from the adult rodent brain [ 18 19 ] and more recent
work has extended to the adult human brain [ 20 21 ]Human NSCs delivered intravenously or stereotactically sur-rounding the lesion have been shown to survive migratetowards the lesion and differentiate (mainly neurones andastrocytes) while improving functional recovery in rodent models of stroke [ 22 ndash 24 ]
Clinical studies
The practicability of routine brain biopsies for isolation of adult human NSCs and autologous transplantation post-stroke remains to be seen and no clinical trials utilising adult NSCs have been undertaken
Immortalised NSC lines can be developed howeverfrom ES or foetal stem cells by the addition of speci1047297cgrowth factors There is currently a phase I trial plannedusing a commercially developed (foetally derived) NSC linedesignated CTX to be delivered by stereotactic injection inpatients with ischaemic stroke (ReNeuron UK) [ 25 ]
Table 1 Relative merits of different sources of stem cells
Cell type Advantages Disadvantages
ES cells Pluripotent Ethical issues
Immortal in vitro Insufficient availability
Highly expandable Unknown risk of tumour
formation
Adult stem
cells
Multipotent Immunosuppression required for
allografting
Potential for induced
pluripotency
Certain types difficult to obtain
eg NSCs
Suitable for autologous and
allogeneic use
Expansion issues
Human stem cell therapy in ischaemic stroke
9
8122019 Age Ageing 2011 Banerjee 7 13
httpslidepdfcomreaderfullage-ageing-2011-banerjee-7-13 47
NT2 cell line
Immortalised cell lines are attractive for use in cellulartherapy as they form an abundant source of cells for trans-plantation in addition to the relative ease of preparationand long-term maintenance The immortalised cell lineNTera-2 (NT2) was derived from a human teratocarcinomaover 20 years ago [ 21 ] After several weeks of exposure toretinoic acid and mitotic inhibitors these cells differentiate
into post-mitotic neurone-like cells named NT2N cells which display a variety of neuronal features [ 26 ] Thesecells maintain their neuronal phenotype both in vitro andin vivo for over a year without reverting to a neoplasticstate [ 27 28 ]
Preclinical experiments
The transplantation of NT2N cells into the ipsilateral stria-tum of ischaemic rat brains improved functional recovery
with some parameters of behavioural improvement persist-ing for up to 6 months post-transplantation [ 29 30 31]Moreover no evidence of tumorigenicity was found follow-ing post-mortem examination of the rats an important consideration given the derivation of this cell line [32]
Clinical studies
NT2N cells were the 1047297rst human cells to be tested instroke clinical trials A phase I trial examined the safety of stereotactic transplantation of cells into patients with basal ganglia stroke which had occurred 6 months to 6 years pre-
viously [33] Twelve patients with stable motor de1047297citsreceived the treatment along with an immunosuppressiveregimen of cyclosporine-A for 8 weeks post-transplantation
The small study population size limited any meaningful interpretation of ef 1047297cacy though there was a trend towardsimproved functional outcome in four patients Autopsy onone patient who died of myocardial infarction 27 monthspost-transplantation showed apparent survival of NT2Ncells in the brain [34] Furthermore positron emission tom-ography scanning at 6 months post-transplantation showedincreased metabolic activity at the site of infarct in sixpatients [35] although this may have indicated an in1047298am-matory response rather than graft survival however nosigns of in1047298ammation were seen on MRI
This initial safety trial led to a Phase II study assessing the effect of NT2N cell transplantation in 18 patients with
substantial 1047297
xed motor de1047297
cits (between 1 and 6 yearspost-stroke) associated with a basal ganglia infarct [36] Theauthors compared stereotactic cellular transplantation plustwo months of rehabilitation ( n = 14) against control patients who received rehabilitation alone ( n = 4) Againthe study was not powered to demonstrate ef 1047297cacyalthough 6 of the 14 patients who received a transplant appeared to show improvement on a standardised strokescale but this was not statistically signi1047297cant against control patients Of note this trial included ischaemic ( n = 9) andhaemorrhagic strokes ( n = 9)
Despite the initial promise of using NT2N cells for cel-lular transplantation much remains to be seen about theirutility particularly in a clinical setting Following an ischae-mic stroke damage is rarely restricted to the striatum withmany patients having cortical damage Furthermore thefeasibility of NT2N cellular transplantation in the acutestroke setting has yet to be examined
Bone-marrow-derived stem cells
Broadly speaking bone-marrow-derived stem cells consist of both haematopoietic stem cells (HSCs) and mesenchy-mal stem cells (MSCs) HSCs are the precursors of all blood and lymphoid lineages MSCs give rise to the stromal cells of the bone marrow including the formation of osteo-blasts chondrocytes and adipocytes Bone marrow is anattractive source of stem cells being easily accessible andsuitable for autologous (obviating the need for immunosup-pression) as well as allogeneic use
Bone marrow cells have been shown to be able tomigrate to the brain and differentiate into cells that express
neuron-speci1047297c markers [37] Both populations of bonemarrow cells have been studied extensively with regard totheir potential for neuronal differentiation and possible usein neuroregenerative therapy
Mesenchymal stem cells
These cells are probably the most widely studied in exper-imental models of neurotransplantation post-stroke
Preclinical experiments Several studies have demonstratedthat MSCs can improve functional recovery after middle cer-ebral artery occlusion in rats This recovery occurs when theMSCs are delivered by a variety of routes intravenous intra-carotid and intrastriatal starting 1 day post-ischaemia [38 ndash 40] In addition delayed delivery of MSCs even up until onemonth post-infarct can also improve long-term functional outcome [41] Following transplantation however very few cells are actually found in the brain and even fewer of thesecells express neural markers [42] Despite this animals whichreceived MSCs did have some amelioration of functional recovery strongly suggesting a mechanism of action otherthan integration into the host rsquos neural circuitry
Clinical studies The extensive pre-clinical work on MSCsled to a phase III clinical trial using autologous culture-expanded MSCs in patients with ischaemic stroke Five
patients with established stroke (gt1 month post-infarct)received MSCs by the intravenous route following ex vivo culture expansion of the cells [43] Cells were extracted by bone marrow aspiration and culture-expanded There wasno cell-related toxicity related to the MSCs administrationand the authors suggested that functional improvement may have been better in the transplanted group compared
with the control group although this was not statistically signi1047297cant There were no signi1047297cant differences betweenthe two groups in relation to changes in infarct volume at 1-year follow-up
S Banerjee et al
10
8122019 Age Ageing 2011 Banerjee 7 13
httpslidepdfcomreaderfullage-ageing-2011-banerjee-7-13 57
Further to the above trial a phase II trial of intravenousautologous MSC therapy in patients within 6 weeks of carotid territory ischaemic stroke is due to commencerecruiting shortly
Haematopoietic stem cells
The use of HSCs for bone marrow transplantation is well established and the therapeutic potential of stem cells in
bone marrow in the regeneration of other non-haematopoietic tissue such as heart and skeletal muscle hasalso been explored [44 ndash 46]
Preclinical experiments Much of the preclinical work exam-ining the use of HSCs for stroke therapy has focused onthe potential mechanisms of functional recovery Twostudies in particular have demonstrated increased angiogen-esis in penumbral tissue following CD34+ cell transplan-tation whether given systemically or by the intracerebral route [47 48] CD34+ bone marrow-derived cells includepopulations of haematopoietic and endothelial stem andprogenitor cells Both the aforementioned studies showed
evidence of functional recovery as well as reduced infarct size The authors of one of these studies also used an anti-angiogenic compound endostatin administered 7 days afterCD34+ cell transplantation and demonstrated that endogen-ous neurogenesis was suppressed by diminishing angiogen-esis thus suggesting a possible role for CD34+ cells inangiogenesis-mediated neural plasticity post-stroke
Clinical studies A number of clinical trials are currently underway investigating the role of bone-marrow-derivedstem cell therapy at different stages of ischaemic stroke uti-lising different methods of delivery (Table 2 ) Three trials
utilising autologous bone marrow mononuclear cells areongoing Further three trials are underway utilising autolo-gous CD34+ cells in acute as well as chronic ischaemicstroke patients Results from these trials are awaited
Potential mechanisms of recovery
The functional recovery seen in many experimental modelsfollowing stem cell transplantation is likely to be mediatedby several overlapping mechanisms and understanding them is crucial in order to determine the best approach fortranslation into the clinical setting
The integration of transplanted cells into the ischaemicbrain with the replacement of lost cells is an unlikely mech-anism of repair Most studies have shown the survival of
very few transplanted cells following neurotransplantationdespite evidence of signi1047297cant functional recovery Morelikely is the stimulation of a trophic effect on the ischaemicbrain (eg by secretion of various growth factors) including the recruitment of endogenous repair processes
Anti-in1047298ammatory effects may also play a role [49]
Unresolved issues
As is evident from the diversity among the various com-pleted and ongoing trials (Table 2 ) there are a number of unresolved issues in the translation of stem cell therapy
These include
(1) choice of cell type(2) cell numbers to be given(3) optimum timing of treatment(4) optimum route of delivery
Table 2 Overview of published and ongoing clinical trials of human stem cell therapy in ischaemic stroke (exogenous
approaches)
Cell type Study design Number of
patients
Timing of
delivery
post-stroke
Route of
delivery
Trial outcome Trial
status
Neural cells
NT2N [ 28 ] PI NR-SB 12 6 months ndash 6
years
Intracerebral Safe and feasible trend towards functional
improvement with higher dose (6 times 106 versus
2 times 106 cells)
Complete
NT2N [31] PII R-SB 18 1 ndash 6 years Intracerebral Safe and feasible no significant functional
improvement in treated group (14 treated
versus 4 controls) ischaemic and
haemorrhagic strokes included
Complete
Bone marrow-derived cells
MSC [38] PIII R-OL 30 gt1 month Intravenous Safe and feasible non-significant trend towardsfunctional improvement in treated group (5
treated versus 25 controls)
Complete
BMMNC (NCT00859014) PI NR-OL 10 24 ndash 72 h Intravenous Awaited Ongoing
BMMNC (NCT00473057) PI NR-OL 10 3 ndash 90 days Intra-arterial Awaited Ongoing
BMMNC (CTRI2008091
000046)
PIII R-SB 120 7 ndash 30 days Intravenous Awaited Ongoing
CD34+ (NCT00535197) PIII NR-OL 10 7 days Intra-arterial Awaited Ongoing
CD34+ (NCT00761982) PIII NR-SB 20 5 ndash 9 days Intra-arterial Awaited Ongoing
CD34+ (NCT00950521) PII R-OL 30 6 ndash 60 months Intracerebral Awaited Ongoing
Abbreviations BMMNC bone-marrow mononuclear cells NR non-randomised NT2N NTera-2 immortalised neurone-like cell line OL open label PI and II
phase I and II trials R randomised SB single blind
Human stem cell therapy in ischaemic stroke
11
8122019 Age Ageing 2011 Banerjee 7 13
httpslidepdfcomreaderfullage-ageing-2011-banerjee-7-13 67
These issues are discussed in more detail inSupplementary data available in Age and Ageing online
Tracking of stem cells is another area of interest whichis essential to our further understanding of distribution andmechanism of action of cells Potential approaches to thisinclude labelling of cells with a magnetic label (eg super-paramagnetic iron oxide particles) allowing MRI tracking of the cells This has yet to enter the clinical arena in stroke
studies though it has shown promise in rodent models of stroke [51] The ideal method of tracking delivered stemcells is yet to be established though it will probably involvea combination of different imaging modalities and is likely to evolve with emerging imaging technologies
Another important consideration regarding cellulartherapy for stroke is safety in terms of both the cell typeused and the mechanism for extracting preparing andadministering the cells Long-term biosafety studies areessential in this respect particularly with regard to thepotential for tumorigenicity mdash this will become increasingly important if prolonged secretion of trophic factors by genetically modi1047297ed cells enters the clinical arena In
addition the potential for tumour formation in otherorgans must be considered particularly with systemic deliv-ery of cells Furthermore appropriate quality assurance andcontrol standards must be in place to allow the standardis-ation of cell preparations
Conclusions
Stem cell therapy for the treatment ischaemic stroke is anexciting emerging area of research in the clinical arena of stroke therapy Animal studies have shown promising results in induced models of stroke though translation to
the bedside is still in its infancy A number of issues remainunanswered and further investigation of these will beimperative in the ongoing quest for an effective feasibleand safe cell-based therapy
Key points
bull Stem cell therapy has been explored in pre-clinical modelsof acute and chronic ischaemic stroke with evidence of signi1047297cant functional bene1047297ts in animal studies
bull A number of clinical trials of stem cell treatment inischaemic stroke are now underway though translation to
clinical practice remains a long way offbull A number of unanswered questions remain including
questions regarding type and quantity of stem cells to begiven ideal mode of delivery and tracking of cells
Supplementary data
Supplementary data mentioned in the text is available tosubscribers in Age and Ageing online
Conflicts of interest
All authors are involved in an ongoing clinical trial of auto-logous CD34+ stem cell therapy in ischaemic stroke NHand MG have shares in OmniCyte Ltd
References
The long list of references supporting this review hasmeant that only the most important are listed here and arerepresented by bold text throughout the paper The full list of references is available at Age and Ageing online
1 Bourn J Hudson J Scharaschkin A et al National Audit Of 1047297ce Reducing Brain Damage Faster Access to BetterStroke Care 2005 1 ndash 60
2 Eriksson PS Per1047297lieva E Bjork-Eriksson T et al
Neurogenesis in the adult human hippocampus Nat Med1998 4 1313 ndash 7
3 Curtis MA Kam M Nannmark U et al Human neuroblastsmigrate to the olfactory bulb via a lateral ventricular exten-sion Science 2007 315 1243 ndash 9
4 Jin K Wang X Xie L et al Evidence for stroke-inducedneurogenesis in the human brain Proc Natl Acad Sci 2006103 13198 ndash 202
5 Shyu WC Lin SZ Yang HI et al Functional recovery of stroke rats induced by granulocyte colony-stimulating factor-stimulated stem cells Circulation 2004 110 1847 ndash 54
6 Schabitz WR Kollmar R Schwaninger M et al
Neuroprotective effect of granulocyte colony stimulating factor after focal cerebral ischemia Stroke 2003 34 745
7 Shyu WC Lin SZ Lee CC Liu DD Li H Granulocytecolony-stimulating factor for acute ischaemic stroke a ran-domised controlled trial CMAJ 2006 174 927 ndash 33
8 Zhang JJ Deng M Zhang Y et al A short-term assessment of recombinant granulocyte-stimulating factor (RHG-CSF) intreatment of acute cerebral infarction Cerebrovasc Dis 200622 323
9 Sprigg N Bath PM Zhao L e t al Granulocyte-colony-stimulating factor mobilises bone marrow stem cells inpatients with subacute ischemic stroke The STEMS pilot randomised controlled trial Stroke 2006 37 2979 ndash 83
10 Weissman IL Anderson DJ Gage F Stem and progenitorcells origins phenotypes lineage commitments and transdif-ferentiations Annu Rev Cell Dev Biol 2001 17 387 ndash 403
11 Jones M The source of pluripotent stems cells from develop-ing embryos Original work Wikipedia 2006 enwikipediaorg
wikiStem cell ( creativecommonsorglicensesby-sa25 )12 Thomson JA Itskovitz-Eldor J Shapiro SS et al Embryonic
stem cell lines derived from human blastocysts Science 1998
282 1145 ndash 713 Tahashi K Tanabe K Ohruki M et al Induction of pluripo-tent stem cells from adult human 1047297broblasts by de1047297nedfactors Cell 2007 131 861 ndash 72
14 Meissner A Wernig M Jaenisch R Direct reprogramming of genetically undmodi1047297ed 1047297broblasts into pluripotent stemcells Nat Biotechnol 2007 25 1177 ndash 81
15 Yu J Vodyanik MA Smuge-Otto K et al Induced pluripotent stem cell lines derived from human somatic cells Science2007 318 1917 ndash 20
16 Mattson MP Culmsee C Yu ZF Apoptotic and antiapoptoticmechanisms in stroke Cell Tissue Res 2000 301 173 ndash 87
S Banerjee et al
12
8122019 Age Ageing 2011 Banerjee 7 13
httpslidepdfcomreaderfullage-ageing-2011-banerjee-7-13 77
17 Temple S The development of neural stem cells Nature2001 414 112 ndash 7
18 Reynolds BA Weiss S Generation of neurons and astrocytesfrom isolated cells of the adult mammalian central nervoussystem Science 1992 255 1707 ndash 10
19 Wachs FP Couillard-Despres S Engelhardt M et al High ef 1047297-cacy of clonal growth and expansion of adult neural stemcells Lab Invest 2003 83 949 ndash 62
20 Nunes MC Roy NS Keyoung HM et al Identi1047297cation and
isolation of multipotential neural progenitor cells from thesubcortical white matter of the adult human brain Nat Med2003 9 439 ndash 47
21 Arsenijevic Y Villemure JG Brunet JF et al Isolation of mul-tipotent neural precursors residing in the cortex of the adult human brain Exp Neurol 2001 170 48 ndash 62
22 Chu K Kim M Jeong SW Kim SU Yoon BW Humanneural stem cells can migrate differentiate and integrateafter intravenous transplantation in adult rats with transient forebrain ischemia Neurosci Lett 2003 343 129 ndash 33
23 Chu K Kim M Park KI et al Human neural stem cellsimprove sensorimotor de1047297cits in the adult rat brain withexperimental focal ischemia Brain Res 2004 1016145 ndash 53
24 Kelly S Bliss TM Shah AK et al Transplanted human fetal neural stem cells survive migrate and differentiate inischemic rat cerebral cortex Proc Natl Acad Sci USA 2004101 11839 ndash 44
25 ReNeuron receives UK ethics committee Favourable Opinionfor stroke clinical trialReNeuron2009 wwwreneuroncomnews__eventsnewsdocument_196_237php
26 Andrews PW Damjanov I Simon D et al Pluripotent embry-onal carcinoma clones derived from the human teratocarci-noma cell line Tera-2 Differentiation in vivo and in vitroLab Invest 1984 50 147 ndash 62
27 Pleasure SJ Lee VM NTera 2 cells a human cell line which displays characteristics expected of a human com-
mitted neuronal progenitor cell J Neurosci Res 1993 35585 ndash 602
28 Trojanowski JQ Mantione JR Lee JH et al Neurons derivedfrom a human teratocarcinoma cell line establish molecularand structural polarity following transplantation into therodent brain Exp Neurol 1993 122 283 ndash 94
29 Kleppner SR Robinson KA Trojanowski JQ Lee VM Transplanted human neurons derived from a teratocarcinomacell line (NTera-2) mature integrate and survive for over 1 yearin the nude mouse brain J Comp Neurol 1995 357 618 ndash 32
30 Borlongan CV Tajima Y Trojanowski JQ Lee VM Sanberg PR Transplantation of cryopreserved human embryonal carcinoma-derived neurons (NT2N cells) promotes functional recovery in ischemic rats Exp Neurol 1998 149 310 ndash 21
Received 8 January 2010 accepted in revised form 28 July
2010
Human stem cell therapy in ischaemic stroke
13

8122019 Age Ageing 2011 Banerjee 7 13
httpslidepdfcomreaderfullage-ageing-2011-banerjee-7-13 47
NT2 cell line
Immortalised cell lines are attractive for use in cellulartherapy as they form an abundant source of cells for trans-plantation in addition to the relative ease of preparationand long-term maintenance The immortalised cell lineNTera-2 (NT2) was derived from a human teratocarcinomaover 20 years ago [ 21 ] After several weeks of exposure toretinoic acid and mitotic inhibitors these cells differentiate
into post-mitotic neurone-like cells named NT2N cells which display a variety of neuronal features [ 26 ] Thesecells maintain their neuronal phenotype both in vitro andin vivo for over a year without reverting to a neoplasticstate [ 27 28 ]
Preclinical experiments
The transplantation of NT2N cells into the ipsilateral stria-tum of ischaemic rat brains improved functional recovery
with some parameters of behavioural improvement persist-ing for up to 6 months post-transplantation [ 29 30 31]Moreover no evidence of tumorigenicity was found follow-ing post-mortem examination of the rats an important consideration given the derivation of this cell line [32]
Clinical studies
NT2N cells were the 1047297rst human cells to be tested instroke clinical trials A phase I trial examined the safety of stereotactic transplantation of cells into patients with basal ganglia stroke which had occurred 6 months to 6 years pre-
viously [33] Twelve patients with stable motor de1047297citsreceived the treatment along with an immunosuppressiveregimen of cyclosporine-A for 8 weeks post-transplantation
The small study population size limited any meaningful interpretation of ef 1047297cacy though there was a trend towardsimproved functional outcome in four patients Autopsy onone patient who died of myocardial infarction 27 monthspost-transplantation showed apparent survival of NT2Ncells in the brain [34] Furthermore positron emission tom-ography scanning at 6 months post-transplantation showedincreased metabolic activity at the site of infarct in sixpatients [35] although this may have indicated an in1047298am-matory response rather than graft survival however nosigns of in1047298ammation were seen on MRI
This initial safety trial led to a Phase II study assessing the effect of NT2N cell transplantation in 18 patients with
substantial 1047297
xed motor de1047297
cits (between 1 and 6 yearspost-stroke) associated with a basal ganglia infarct [36] Theauthors compared stereotactic cellular transplantation plustwo months of rehabilitation ( n = 14) against control patients who received rehabilitation alone ( n = 4) Againthe study was not powered to demonstrate ef 1047297cacyalthough 6 of the 14 patients who received a transplant appeared to show improvement on a standardised strokescale but this was not statistically signi1047297cant against control patients Of note this trial included ischaemic ( n = 9) andhaemorrhagic strokes ( n = 9)
Despite the initial promise of using NT2N cells for cel-lular transplantation much remains to be seen about theirutility particularly in a clinical setting Following an ischae-mic stroke damage is rarely restricted to the striatum withmany patients having cortical damage Furthermore thefeasibility of NT2N cellular transplantation in the acutestroke setting has yet to be examined
Bone-marrow-derived stem cells
Broadly speaking bone-marrow-derived stem cells consist of both haematopoietic stem cells (HSCs) and mesenchy-mal stem cells (MSCs) HSCs are the precursors of all blood and lymphoid lineages MSCs give rise to the stromal cells of the bone marrow including the formation of osteo-blasts chondrocytes and adipocytes Bone marrow is anattractive source of stem cells being easily accessible andsuitable for autologous (obviating the need for immunosup-pression) as well as allogeneic use
Bone marrow cells have been shown to be able tomigrate to the brain and differentiate into cells that express
neuron-speci1047297c markers [37] Both populations of bonemarrow cells have been studied extensively with regard totheir potential for neuronal differentiation and possible usein neuroregenerative therapy
Mesenchymal stem cells
These cells are probably the most widely studied in exper-imental models of neurotransplantation post-stroke
Preclinical experiments Several studies have demonstratedthat MSCs can improve functional recovery after middle cer-ebral artery occlusion in rats This recovery occurs when theMSCs are delivered by a variety of routes intravenous intra-carotid and intrastriatal starting 1 day post-ischaemia [38 ndash 40] In addition delayed delivery of MSCs even up until onemonth post-infarct can also improve long-term functional outcome [41] Following transplantation however very few cells are actually found in the brain and even fewer of thesecells express neural markers [42] Despite this animals whichreceived MSCs did have some amelioration of functional recovery strongly suggesting a mechanism of action otherthan integration into the host rsquos neural circuitry
Clinical studies The extensive pre-clinical work on MSCsled to a phase III clinical trial using autologous culture-expanded MSCs in patients with ischaemic stroke Five
patients with established stroke (gt1 month post-infarct)received MSCs by the intravenous route following ex vivo culture expansion of the cells [43] Cells were extracted by bone marrow aspiration and culture-expanded There wasno cell-related toxicity related to the MSCs administrationand the authors suggested that functional improvement may have been better in the transplanted group compared
with the control group although this was not statistically signi1047297cant There were no signi1047297cant differences betweenthe two groups in relation to changes in infarct volume at 1-year follow-up
S Banerjee et al
10
8122019 Age Ageing 2011 Banerjee 7 13
httpslidepdfcomreaderfullage-ageing-2011-banerjee-7-13 57
Further to the above trial a phase II trial of intravenousautologous MSC therapy in patients within 6 weeks of carotid territory ischaemic stroke is due to commencerecruiting shortly
Haematopoietic stem cells
The use of HSCs for bone marrow transplantation is well established and the therapeutic potential of stem cells in
bone marrow in the regeneration of other non-haematopoietic tissue such as heart and skeletal muscle hasalso been explored [44 ndash 46]
Preclinical experiments Much of the preclinical work exam-ining the use of HSCs for stroke therapy has focused onthe potential mechanisms of functional recovery Twostudies in particular have demonstrated increased angiogen-esis in penumbral tissue following CD34+ cell transplan-tation whether given systemically or by the intracerebral route [47 48] CD34+ bone marrow-derived cells includepopulations of haematopoietic and endothelial stem andprogenitor cells Both the aforementioned studies showed
evidence of functional recovery as well as reduced infarct size The authors of one of these studies also used an anti-angiogenic compound endostatin administered 7 days afterCD34+ cell transplantation and demonstrated that endogen-ous neurogenesis was suppressed by diminishing angiogen-esis thus suggesting a possible role for CD34+ cells inangiogenesis-mediated neural plasticity post-stroke
Clinical studies A number of clinical trials are currently underway investigating the role of bone-marrow-derivedstem cell therapy at different stages of ischaemic stroke uti-lising different methods of delivery (Table 2 ) Three trials
utilising autologous bone marrow mononuclear cells areongoing Further three trials are underway utilising autolo-gous CD34+ cells in acute as well as chronic ischaemicstroke patients Results from these trials are awaited
Potential mechanisms of recovery
The functional recovery seen in many experimental modelsfollowing stem cell transplantation is likely to be mediatedby several overlapping mechanisms and understanding them is crucial in order to determine the best approach fortranslation into the clinical setting
The integration of transplanted cells into the ischaemicbrain with the replacement of lost cells is an unlikely mech-anism of repair Most studies have shown the survival of
very few transplanted cells following neurotransplantationdespite evidence of signi1047297cant functional recovery Morelikely is the stimulation of a trophic effect on the ischaemicbrain (eg by secretion of various growth factors) including the recruitment of endogenous repair processes
Anti-in1047298ammatory effects may also play a role [49]
Unresolved issues
As is evident from the diversity among the various com-pleted and ongoing trials (Table 2 ) there are a number of unresolved issues in the translation of stem cell therapy
These include
(1) choice of cell type(2) cell numbers to be given(3) optimum timing of treatment(4) optimum route of delivery
Table 2 Overview of published and ongoing clinical trials of human stem cell therapy in ischaemic stroke (exogenous
approaches)
Cell type Study design Number of
patients
Timing of
delivery
post-stroke
Route of
delivery
Trial outcome Trial
status
Neural cells
NT2N [ 28 ] PI NR-SB 12 6 months ndash 6
years
Intracerebral Safe and feasible trend towards functional
improvement with higher dose (6 times 106 versus
2 times 106 cells)
Complete
NT2N [31] PII R-SB 18 1 ndash 6 years Intracerebral Safe and feasible no significant functional
improvement in treated group (14 treated
versus 4 controls) ischaemic and
haemorrhagic strokes included
Complete
Bone marrow-derived cells
MSC [38] PIII R-OL 30 gt1 month Intravenous Safe and feasible non-significant trend towardsfunctional improvement in treated group (5
treated versus 25 controls)
Complete
BMMNC (NCT00859014) PI NR-OL 10 24 ndash 72 h Intravenous Awaited Ongoing
BMMNC (NCT00473057) PI NR-OL 10 3 ndash 90 days Intra-arterial Awaited Ongoing
BMMNC (CTRI2008091
000046)
PIII R-SB 120 7 ndash 30 days Intravenous Awaited Ongoing
CD34+ (NCT00535197) PIII NR-OL 10 7 days Intra-arterial Awaited Ongoing
CD34+ (NCT00761982) PIII NR-SB 20 5 ndash 9 days Intra-arterial Awaited Ongoing
CD34+ (NCT00950521) PII R-OL 30 6 ndash 60 months Intracerebral Awaited Ongoing
Abbreviations BMMNC bone-marrow mononuclear cells NR non-randomised NT2N NTera-2 immortalised neurone-like cell line OL open label PI and II
phase I and II trials R randomised SB single blind
Human stem cell therapy in ischaemic stroke
11
8122019 Age Ageing 2011 Banerjee 7 13
httpslidepdfcomreaderfullage-ageing-2011-banerjee-7-13 67
These issues are discussed in more detail inSupplementary data available in Age and Ageing online
Tracking of stem cells is another area of interest whichis essential to our further understanding of distribution andmechanism of action of cells Potential approaches to thisinclude labelling of cells with a magnetic label (eg super-paramagnetic iron oxide particles) allowing MRI tracking of the cells This has yet to enter the clinical arena in stroke
studies though it has shown promise in rodent models of stroke [51] The ideal method of tracking delivered stemcells is yet to be established though it will probably involvea combination of different imaging modalities and is likely to evolve with emerging imaging technologies
Another important consideration regarding cellulartherapy for stroke is safety in terms of both the cell typeused and the mechanism for extracting preparing andadministering the cells Long-term biosafety studies areessential in this respect particularly with regard to thepotential for tumorigenicity mdash this will become increasingly important if prolonged secretion of trophic factors by genetically modi1047297ed cells enters the clinical arena In
addition the potential for tumour formation in otherorgans must be considered particularly with systemic deliv-ery of cells Furthermore appropriate quality assurance andcontrol standards must be in place to allow the standardis-ation of cell preparations
Conclusions
Stem cell therapy for the treatment ischaemic stroke is anexciting emerging area of research in the clinical arena of stroke therapy Animal studies have shown promising results in induced models of stroke though translation to
the bedside is still in its infancy A number of issues remainunanswered and further investigation of these will beimperative in the ongoing quest for an effective feasibleand safe cell-based therapy
Key points
bull Stem cell therapy has been explored in pre-clinical modelsof acute and chronic ischaemic stroke with evidence of signi1047297cant functional bene1047297ts in animal studies
bull A number of clinical trials of stem cell treatment inischaemic stroke are now underway though translation to
clinical practice remains a long way offbull A number of unanswered questions remain including
questions regarding type and quantity of stem cells to begiven ideal mode of delivery and tracking of cells
Supplementary data
Supplementary data mentioned in the text is available tosubscribers in Age and Ageing online
Conflicts of interest
All authors are involved in an ongoing clinical trial of auto-logous CD34+ stem cell therapy in ischaemic stroke NHand MG have shares in OmniCyte Ltd
References
The long list of references supporting this review hasmeant that only the most important are listed here and arerepresented by bold text throughout the paper The full list of references is available at Age and Ageing online
1 Bourn J Hudson J Scharaschkin A et al National Audit Of 1047297ce Reducing Brain Damage Faster Access to BetterStroke Care 2005 1 ndash 60
2 Eriksson PS Per1047297lieva E Bjork-Eriksson T et al
Neurogenesis in the adult human hippocampus Nat Med1998 4 1313 ndash 7
3 Curtis MA Kam M Nannmark U et al Human neuroblastsmigrate to the olfactory bulb via a lateral ventricular exten-sion Science 2007 315 1243 ndash 9
4 Jin K Wang X Xie L et al Evidence for stroke-inducedneurogenesis in the human brain Proc Natl Acad Sci 2006103 13198 ndash 202
5 Shyu WC Lin SZ Yang HI et al Functional recovery of stroke rats induced by granulocyte colony-stimulating factor-stimulated stem cells Circulation 2004 110 1847 ndash 54
6 Schabitz WR Kollmar R Schwaninger M et al
Neuroprotective effect of granulocyte colony stimulating factor after focal cerebral ischemia Stroke 2003 34 745
7 Shyu WC Lin SZ Lee CC Liu DD Li H Granulocytecolony-stimulating factor for acute ischaemic stroke a ran-domised controlled trial CMAJ 2006 174 927 ndash 33
8 Zhang JJ Deng M Zhang Y et al A short-term assessment of recombinant granulocyte-stimulating factor (RHG-CSF) intreatment of acute cerebral infarction Cerebrovasc Dis 200622 323
9 Sprigg N Bath PM Zhao L e t al Granulocyte-colony-stimulating factor mobilises bone marrow stem cells inpatients with subacute ischemic stroke The STEMS pilot randomised controlled trial Stroke 2006 37 2979 ndash 83
10 Weissman IL Anderson DJ Gage F Stem and progenitorcells origins phenotypes lineage commitments and transdif-ferentiations Annu Rev Cell Dev Biol 2001 17 387 ndash 403
11 Jones M The source of pluripotent stems cells from develop-ing embryos Original work Wikipedia 2006 enwikipediaorg
wikiStem cell ( creativecommonsorglicensesby-sa25 )12 Thomson JA Itskovitz-Eldor J Shapiro SS et al Embryonic
stem cell lines derived from human blastocysts Science 1998
282 1145 ndash 713 Tahashi K Tanabe K Ohruki M et al Induction of pluripo-tent stem cells from adult human 1047297broblasts by de1047297nedfactors Cell 2007 131 861 ndash 72
14 Meissner A Wernig M Jaenisch R Direct reprogramming of genetically undmodi1047297ed 1047297broblasts into pluripotent stemcells Nat Biotechnol 2007 25 1177 ndash 81
15 Yu J Vodyanik MA Smuge-Otto K et al Induced pluripotent stem cell lines derived from human somatic cells Science2007 318 1917 ndash 20
16 Mattson MP Culmsee C Yu ZF Apoptotic and antiapoptoticmechanisms in stroke Cell Tissue Res 2000 301 173 ndash 87
S Banerjee et al
12
8122019 Age Ageing 2011 Banerjee 7 13
httpslidepdfcomreaderfullage-ageing-2011-banerjee-7-13 77
17 Temple S The development of neural stem cells Nature2001 414 112 ndash 7
18 Reynolds BA Weiss S Generation of neurons and astrocytesfrom isolated cells of the adult mammalian central nervoussystem Science 1992 255 1707 ndash 10
19 Wachs FP Couillard-Despres S Engelhardt M et al High ef 1047297-cacy of clonal growth and expansion of adult neural stemcells Lab Invest 2003 83 949 ndash 62
20 Nunes MC Roy NS Keyoung HM et al Identi1047297cation and
isolation of multipotential neural progenitor cells from thesubcortical white matter of the adult human brain Nat Med2003 9 439 ndash 47
21 Arsenijevic Y Villemure JG Brunet JF et al Isolation of mul-tipotent neural precursors residing in the cortex of the adult human brain Exp Neurol 2001 170 48 ndash 62
22 Chu K Kim M Jeong SW Kim SU Yoon BW Humanneural stem cells can migrate differentiate and integrateafter intravenous transplantation in adult rats with transient forebrain ischemia Neurosci Lett 2003 343 129 ndash 33
23 Chu K Kim M Park KI et al Human neural stem cellsimprove sensorimotor de1047297cits in the adult rat brain withexperimental focal ischemia Brain Res 2004 1016145 ndash 53
24 Kelly S Bliss TM Shah AK et al Transplanted human fetal neural stem cells survive migrate and differentiate inischemic rat cerebral cortex Proc Natl Acad Sci USA 2004101 11839 ndash 44
25 ReNeuron receives UK ethics committee Favourable Opinionfor stroke clinical trialReNeuron2009 wwwreneuroncomnews__eventsnewsdocument_196_237php
26 Andrews PW Damjanov I Simon D et al Pluripotent embry-onal carcinoma clones derived from the human teratocarci-noma cell line Tera-2 Differentiation in vivo and in vitroLab Invest 1984 50 147 ndash 62
27 Pleasure SJ Lee VM NTera 2 cells a human cell line which displays characteristics expected of a human com-
mitted neuronal progenitor cell J Neurosci Res 1993 35585 ndash 602
28 Trojanowski JQ Mantione JR Lee JH et al Neurons derivedfrom a human teratocarcinoma cell line establish molecularand structural polarity following transplantation into therodent brain Exp Neurol 1993 122 283 ndash 94
29 Kleppner SR Robinson KA Trojanowski JQ Lee VM Transplanted human neurons derived from a teratocarcinomacell line (NTera-2) mature integrate and survive for over 1 yearin the nude mouse brain J Comp Neurol 1995 357 618 ndash 32
30 Borlongan CV Tajima Y Trojanowski JQ Lee VM Sanberg PR Transplantation of cryopreserved human embryonal carcinoma-derived neurons (NT2N cells) promotes functional recovery in ischemic rats Exp Neurol 1998 149 310 ndash 21
Received 8 January 2010 accepted in revised form 28 July
2010
Human stem cell therapy in ischaemic stroke
13

8122019 Age Ageing 2011 Banerjee 7 13
httpslidepdfcomreaderfullage-ageing-2011-banerjee-7-13 57
Further to the above trial a phase II trial of intravenousautologous MSC therapy in patients within 6 weeks of carotid territory ischaemic stroke is due to commencerecruiting shortly
Haematopoietic stem cells
The use of HSCs for bone marrow transplantation is well established and the therapeutic potential of stem cells in
bone marrow in the regeneration of other non-haematopoietic tissue such as heart and skeletal muscle hasalso been explored [44 ndash 46]
Preclinical experiments Much of the preclinical work exam-ining the use of HSCs for stroke therapy has focused onthe potential mechanisms of functional recovery Twostudies in particular have demonstrated increased angiogen-esis in penumbral tissue following CD34+ cell transplan-tation whether given systemically or by the intracerebral route [47 48] CD34+ bone marrow-derived cells includepopulations of haematopoietic and endothelial stem andprogenitor cells Both the aforementioned studies showed
evidence of functional recovery as well as reduced infarct size The authors of one of these studies also used an anti-angiogenic compound endostatin administered 7 days afterCD34+ cell transplantation and demonstrated that endogen-ous neurogenesis was suppressed by diminishing angiogen-esis thus suggesting a possible role for CD34+ cells inangiogenesis-mediated neural plasticity post-stroke
Clinical studies A number of clinical trials are currently underway investigating the role of bone-marrow-derivedstem cell therapy at different stages of ischaemic stroke uti-lising different methods of delivery (Table 2 ) Three trials
utilising autologous bone marrow mononuclear cells areongoing Further three trials are underway utilising autolo-gous CD34+ cells in acute as well as chronic ischaemicstroke patients Results from these trials are awaited
Potential mechanisms of recovery
The functional recovery seen in many experimental modelsfollowing stem cell transplantation is likely to be mediatedby several overlapping mechanisms and understanding them is crucial in order to determine the best approach fortranslation into the clinical setting
The integration of transplanted cells into the ischaemicbrain with the replacement of lost cells is an unlikely mech-anism of repair Most studies have shown the survival of
very few transplanted cells following neurotransplantationdespite evidence of signi1047297cant functional recovery Morelikely is the stimulation of a trophic effect on the ischaemicbrain (eg by secretion of various growth factors) including the recruitment of endogenous repair processes
Anti-in1047298ammatory effects may also play a role [49]
Unresolved issues
As is evident from the diversity among the various com-pleted and ongoing trials (Table 2 ) there are a number of unresolved issues in the translation of stem cell therapy
These include
(1) choice of cell type(2) cell numbers to be given(3) optimum timing of treatment(4) optimum route of delivery
Table 2 Overview of published and ongoing clinical trials of human stem cell therapy in ischaemic stroke (exogenous
approaches)
Cell type Study design Number of
patients
Timing of
delivery
post-stroke
Route of
delivery
Trial outcome Trial
status
Neural cells
NT2N [ 28 ] PI NR-SB 12 6 months ndash 6
years
Intracerebral Safe and feasible trend towards functional
improvement with higher dose (6 times 106 versus
2 times 106 cells)
Complete
NT2N [31] PII R-SB 18 1 ndash 6 years Intracerebral Safe and feasible no significant functional
improvement in treated group (14 treated
versus 4 controls) ischaemic and
haemorrhagic strokes included
Complete
Bone marrow-derived cells
MSC [38] PIII R-OL 30 gt1 month Intravenous Safe and feasible non-significant trend towardsfunctional improvement in treated group (5
treated versus 25 controls)
Complete
BMMNC (NCT00859014) PI NR-OL 10 24 ndash 72 h Intravenous Awaited Ongoing
BMMNC (NCT00473057) PI NR-OL 10 3 ndash 90 days Intra-arterial Awaited Ongoing
BMMNC (CTRI2008091
000046)
PIII R-SB 120 7 ndash 30 days Intravenous Awaited Ongoing
CD34+ (NCT00535197) PIII NR-OL 10 7 days Intra-arterial Awaited Ongoing
CD34+ (NCT00761982) PIII NR-SB 20 5 ndash 9 days Intra-arterial Awaited Ongoing
CD34+ (NCT00950521) PII R-OL 30 6 ndash 60 months Intracerebral Awaited Ongoing
Abbreviations BMMNC bone-marrow mononuclear cells NR non-randomised NT2N NTera-2 immortalised neurone-like cell line OL open label PI and II
phase I and II trials R randomised SB single blind
Human stem cell therapy in ischaemic stroke
11
8122019 Age Ageing 2011 Banerjee 7 13
httpslidepdfcomreaderfullage-ageing-2011-banerjee-7-13 67
These issues are discussed in more detail inSupplementary data available in Age and Ageing online
Tracking of stem cells is another area of interest whichis essential to our further understanding of distribution andmechanism of action of cells Potential approaches to thisinclude labelling of cells with a magnetic label (eg super-paramagnetic iron oxide particles) allowing MRI tracking of the cells This has yet to enter the clinical arena in stroke
studies though it has shown promise in rodent models of stroke [51] The ideal method of tracking delivered stemcells is yet to be established though it will probably involvea combination of different imaging modalities and is likely to evolve with emerging imaging technologies
Another important consideration regarding cellulartherapy for stroke is safety in terms of both the cell typeused and the mechanism for extracting preparing andadministering the cells Long-term biosafety studies areessential in this respect particularly with regard to thepotential for tumorigenicity mdash this will become increasingly important if prolonged secretion of trophic factors by genetically modi1047297ed cells enters the clinical arena In
addition the potential for tumour formation in otherorgans must be considered particularly with systemic deliv-ery of cells Furthermore appropriate quality assurance andcontrol standards must be in place to allow the standardis-ation of cell preparations
Conclusions
Stem cell therapy for the treatment ischaemic stroke is anexciting emerging area of research in the clinical arena of stroke therapy Animal studies have shown promising results in induced models of stroke though translation to
the bedside is still in its infancy A number of issues remainunanswered and further investigation of these will beimperative in the ongoing quest for an effective feasibleand safe cell-based therapy
Key points
bull Stem cell therapy has been explored in pre-clinical modelsof acute and chronic ischaemic stroke with evidence of signi1047297cant functional bene1047297ts in animal studies
bull A number of clinical trials of stem cell treatment inischaemic stroke are now underway though translation to
clinical practice remains a long way offbull A number of unanswered questions remain including
questions regarding type and quantity of stem cells to begiven ideal mode of delivery and tracking of cells
Supplementary data
Supplementary data mentioned in the text is available tosubscribers in Age and Ageing online
Conflicts of interest
All authors are involved in an ongoing clinical trial of auto-logous CD34+ stem cell therapy in ischaemic stroke NHand MG have shares in OmniCyte Ltd
References
The long list of references supporting this review hasmeant that only the most important are listed here and arerepresented by bold text throughout the paper The full list of references is available at Age and Ageing online
1 Bourn J Hudson J Scharaschkin A et al National Audit Of 1047297ce Reducing Brain Damage Faster Access to BetterStroke Care 2005 1 ndash 60
2 Eriksson PS Per1047297lieva E Bjork-Eriksson T et al
Neurogenesis in the adult human hippocampus Nat Med1998 4 1313 ndash 7
3 Curtis MA Kam M Nannmark U et al Human neuroblastsmigrate to the olfactory bulb via a lateral ventricular exten-sion Science 2007 315 1243 ndash 9
4 Jin K Wang X Xie L et al Evidence for stroke-inducedneurogenesis in the human brain Proc Natl Acad Sci 2006103 13198 ndash 202
5 Shyu WC Lin SZ Yang HI et al Functional recovery of stroke rats induced by granulocyte colony-stimulating factor-stimulated stem cells Circulation 2004 110 1847 ndash 54
6 Schabitz WR Kollmar R Schwaninger M et al
Neuroprotective effect of granulocyte colony stimulating factor after focal cerebral ischemia Stroke 2003 34 745
7 Shyu WC Lin SZ Lee CC Liu DD Li H Granulocytecolony-stimulating factor for acute ischaemic stroke a ran-domised controlled trial CMAJ 2006 174 927 ndash 33
8 Zhang JJ Deng M Zhang Y et al A short-term assessment of recombinant granulocyte-stimulating factor (RHG-CSF) intreatment of acute cerebral infarction Cerebrovasc Dis 200622 323
9 Sprigg N Bath PM Zhao L e t al Granulocyte-colony-stimulating factor mobilises bone marrow stem cells inpatients with subacute ischemic stroke The STEMS pilot randomised controlled trial Stroke 2006 37 2979 ndash 83
10 Weissman IL Anderson DJ Gage F Stem and progenitorcells origins phenotypes lineage commitments and transdif-ferentiations Annu Rev Cell Dev Biol 2001 17 387 ndash 403
11 Jones M The source of pluripotent stems cells from develop-ing embryos Original work Wikipedia 2006 enwikipediaorg
wikiStem cell ( creativecommonsorglicensesby-sa25 )12 Thomson JA Itskovitz-Eldor J Shapiro SS et al Embryonic
stem cell lines derived from human blastocysts Science 1998
282 1145 ndash 713 Tahashi K Tanabe K Ohruki M et al Induction of pluripo-tent stem cells from adult human 1047297broblasts by de1047297nedfactors Cell 2007 131 861 ndash 72
14 Meissner A Wernig M Jaenisch R Direct reprogramming of genetically undmodi1047297ed 1047297broblasts into pluripotent stemcells Nat Biotechnol 2007 25 1177 ndash 81
15 Yu J Vodyanik MA Smuge-Otto K et al Induced pluripotent stem cell lines derived from human somatic cells Science2007 318 1917 ndash 20
16 Mattson MP Culmsee C Yu ZF Apoptotic and antiapoptoticmechanisms in stroke Cell Tissue Res 2000 301 173 ndash 87
S Banerjee et al
12
8122019 Age Ageing 2011 Banerjee 7 13
httpslidepdfcomreaderfullage-ageing-2011-banerjee-7-13 77
17 Temple S The development of neural stem cells Nature2001 414 112 ndash 7
18 Reynolds BA Weiss S Generation of neurons and astrocytesfrom isolated cells of the adult mammalian central nervoussystem Science 1992 255 1707 ndash 10
19 Wachs FP Couillard-Despres S Engelhardt M et al High ef 1047297-cacy of clonal growth and expansion of adult neural stemcells Lab Invest 2003 83 949 ndash 62
20 Nunes MC Roy NS Keyoung HM et al Identi1047297cation and
isolation of multipotential neural progenitor cells from thesubcortical white matter of the adult human brain Nat Med2003 9 439 ndash 47
21 Arsenijevic Y Villemure JG Brunet JF et al Isolation of mul-tipotent neural precursors residing in the cortex of the adult human brain Exp Neurol 2001 170 48 ndash 62
22 Chu K Kim M Jeong SW Kim SU Yoon BW Humanneural stem cells can migrate differentiate and integrateafter intravenous transplantation in adult rats with transient forebrain ischemia Neurosci Lett 2003 343 129 ndash 33
23 Chu K Kim M Park KI et al Human neural stem cellsimprove sensorimotor de1047297cits in the adult rat brain withexperimental focal ischemia Brain Res 2004 1016145 ndash 53
24 Kelly S Bliss TM Shah AK et al Transplanted human fetal neural stem cells survive migrate and differentiate inischemic rat cerebral cortex Proc Natl Acad Sci USA 2004101 11839 ndash 44
25 ReNeuron receives UK ethics committee Favourable Opinionfor stroke clinical trialReNeuron2009 wwwreneuroncomnews__eventsnewsdocument_196_237php
26 Andrews PW Damjanov I Simon D et al Pluripotent embry-onal carcinoma clones derived from the human teratocarci-noma cell line Tera-2 Differentiation in vivo and in vitroLab Invest 1984 50 147 ndash 62
27 Pleasure SJ Lee VM NTera 2 cells a human cell line which displays characteristics expected of a human com-
mitted neuronal progenitor cell J Neurosci Res 1993 35585 ndash 602
28 Trojanowski JQ Mantione JR Lee JH et al Neurons derivedfrom a human teratocarcinoma cell line establish molecularand structural polarity following transplantation into therodent brain Exp Neurol 1993 122 283 ndash 94
29 Kleppner SR Robinson KA Trojanowski JQ Lee VM Transplanted human neurons derived from a teratocarcinomacell line (NTera-2) mature integrate and survive for over 1 yearin the nude mouse brain J Comp Neurol 1995 357 618 ndash 32
30 Borlongan CV Tajima Y Trojanowski JQ Lee VM Sanberg PR Transplantation of cryopreserved human embryonal carcinoma-derived neurons (NT2N cells) promotes functional recovery in ischemic rats Exp Neurol 1998 149 310 ndash 21
Received 8 January 2010 accepted in revised form 28 July
2010
Human stem cell therapy in ischaemic stroke
13

8122019 Age Ageing 2011 Banerjee 7 13
httpslidepdfcomreaderfullage-ageing-2011-banerjee-7-13 67
These issues are discussed in more detail inSupplementary data available in Age and Ageing online
Tracking of stem cells is another area of interest whichis essential to our further understanding of distribution andmechanism of action of cells Potential approaches to thisinclude labelling of cells with a magnetic label (eg super-paramagnetic iron oxide particles) allowing MRI tracking of the cells This has yet to enter the clinical arena in stroke
studies though it has shown promise in rodent models of stroke [51] The ideal method of tracking delivered stemcells is yet to be established though it will probably involvea combination of different imaging modalities and is likely to evolve with emerging imaging technologies
Another important consideration regarding cellulartherapy for stroke is safety in terms of both the cell typeused and the mechanism for extracting preparing andadministering the cells Long-term biosafety studies areessential in this respect particularly with regard to thepotential for tumorigenicity mdash this will become increasingly important if prolonged secretion of trophic factors by genetically modi1047297ed cells enters the clinical arena In
addition the potential for tumour formation in otherorgans must be considered particularly with systemic deliv-ery of cells Furthermore appropriate quality assurance andcontrol standards must be in place to allow the standardis-ation of cell preparations
Conclusions
Stem cell therapy for the treatment ischaemic stroke is anexciting emerging area of research in the clinical arena of stroke therapy Animal studies have shown promising results in induced models of stroke though translation to
the bedside is still in its infancy A number of issues remainunanswered and further investigation of these will beimperative in the ongoing quest for an effective feasibleand safe cell-based therapy
Key points
bull Stem cell therapy has been explored in pre-clinical modelsof acute and chronic ischaemic stroke with evidence of signi1047297cant functional bene1047297ts in animal studies
bull A number of clinical trials of stem cell treatment inischaemic stroke are now underway though translation to
clinical practice remains a long way offbull A number of unanswered questions remain including
questions regarding type and quantity of stem cells to begiven ideal mode of delivery and tracking of cells
Supplementary data
Supplementary data mentioned in the text is available tosubscribers in Age and Ageing online
Conflicts of interest
All authors are involved in an ongoing clinical trial of auto-logous CD34+ stem cell therapy in ischaemic stroke NHand MG have shares in OmniCyte Ltd
References
The long list of references supporting this review hasmeant that only the most important are listed here and arerepresented by bold text throughout the paper The full list of references is available at Age and Ageing online
1 Bourn J Hudson J Scharaschkin A et al National Audit Of 1047297ce Reducing Brain Damage Faster Access to BetterStroke Care 2005 1 ndash 60
2 Eriksson PS Per1047297lieva E Bjork-Eriksson T et al
Neurogenesis in the adult human hippocampus Nat Med1998 4 1313 ndash 7
3 Curtis MA Kam M Nannmark U et al Human neuroblastsmigrate to the olfactory bulb via a lateral ventricular exten-sion Science 2007 315 1243 ndash 9
4 Jin K Wang X Xie L et al Evidence for stroke-inducedneurogenesis in the human brain Proc Natl Acad Sci 2006103 13198 ndash 202
5 Shyu WC Lin SZ Yang HI et al Functional recovery of stroke rats induced by granulocyte colony-stimulating factor-stimulated stem cells Circulation 2004 110 1847 ndash 54
6 Schabitz WR Kollmar R Schwaninger M et al
Neuroprotective effect of granulocyte colony stimulating factor after focal cerebral ischemia Stroke 2003 34 745
7 Shyu WC Lin SZ Lee CC Liu DD Li H Granulocytecolony-stimulating factor for acute ischaemic stroke a ran-domised controlled trial CMAJ 2006 174 927 ndash 33
8 Zhang JJ Deng M Zhang Y et al A short-term assessment of recombinant granulocyte-stimulating factor (RHG-CSF) intreatment of acute cerebral infarction Cerebrovasc Dis 200622 323
9 Sprigg N Bath PM Zhao L e t al Granulocyte-colony-stimulating factor mobilises bone marrow stem cells inpatients with subacute ischemic stroke The STEMS pilot randomised controlled trial Stroke 2006 37 2979 ndash 83
10 Weissman IL Anderson DJ Gage F Stem and progenitorcells origins phenotypes lineage commitments and transdif-ferentiations Annu Rev Cell Dev Biol 2001 17 387 ndash 403
11 Jones M The source of pluripotent stems cells from develop-ing embryos Original work Wikipedia 2006 enwikipediaorg
wikiStem cell ( creativecommonsorglicensesby-sa25 )12 Thomson JA Itskovitz-Eldor J Shapiro SS et al Embryonic
stem cell lines derived from human blastocysts Science 1998
282 1145 ndash 713 Tahashi K Tanabe K Ohruki M et al Induction of pluripo-tent stem cells from adult human 1047297broblasts by de1047297nedfactors Cell 2007 131 861 ndash 72
14 Meissner A Wernig M Jaenisch R Direct reprogramming of genetically undmodi1047297ed 1047297broblasts into pluripotent stemcells Nat Biotechnol 2007 25 1177 ndash 81
15 Yu J Vodyanik MA Smuge-Otto K et al Induced pluripotent stem cell lines derived from human somatic cells Science2007 318 1917 ndash 20
16 Mattson MP Culmsee C Yu ZF Apoptotic and antiapoptoticmechanisms in stroke Cell Tissue Res 2000 301 173 ndash 87
S Banerjee et al
12
8122019 Age Ageing 2011 Banerjee 7 13
httpslidepdfcomreaderfullage-ageing-2011-banerjee-7-13 77
17 Temple S The development of neural stem cells Nature2001 414 112 ndash 7
18 Reynolds BA Weiss S Generation of neurons and astrocytesfrom isolated cells of the adult mammalian central nervoussystem Science 1992 255 1707 ndash 10
19 Wachs FP Couillard-Despres S Engelhardt M et al High ef 1047297-cacy of clonal growth and expansion of adult neural stemcells Lab Invest 2003 83 949 ndash 62
20 Nunes MC Roy NS Keyoung HM et al Identi1047297cation and
isolation of multipotential neural progenitor cells from thesubcortical white matter of the adult human brain Nat Med2003 9 439 ndash 47
21 Arsenijevic Y Villemure JG Brunet JF et al Isolation of mul-tipotent neural precursors residing in the cortex of the adult human brain Exp Neurol 2001 170 48 ndash 62
22 Chu K Kim M Jeong SW Kim SU Yoon BW Humanneural stem cells can migrate differentiate and integrateafter intravenous transplantation in adult rats with transient forebrain ischemia Neurosci Lett 2003 343 129 ndash 33
23 Chu K Kim M Park KI et al Human neural stem cellsimprove sensorimotor de1047297cits in the adult rat brain withexperimental focal ischemia Brain Res 2004 1016145 ndash 53
24 Kelly S Bliss TM Shah AK et al Transplanted human fetal neural stem cells survive migrate and differentiate inischemic rat cerebral cortex Proc Natl Acad Sci USA 2004101 11839 ndash 44
25 ReNeuron receives UK ethics committee Favourable Opinionfor stroke clinical trialReNeuron2009 wwwreneuroncomnews__eventsnewsdocument_196_237php
26 Andrews PW Damjanov I Simon D et al Pluripotent embry-onal carcinoma clones derived from the human teratocarci-noma cell line Tera-2 Differentiation in vivo and in vitroLab Invest 1984 50 147 ndash 62
27 Pleasure SJ Lee VM NTera 2 cells a human cell line which displays characteristics expected of a human com-
mitted neuronal progenitor cell J Neurosci Res 1993 35585 ndash 602
28 Trojanowski JQ Mantione JR Lee JH et al Neurons derivedfrom a human teratocarcinoma cell line establish molecularand structural polarity following transplantation into therodent brain Exp Neurol 1993 122 283 ndash 94
29 Kleppner SR Robinson KA Trojanowski JQ Lee VM Transplanted human neurons derived from a teratocarcinomacell line (NTera-2) mature integrate and survive for over 1 yearin the nude mouse brain J Comp Neurol 1995 357 618 ndash 32
30 Borlongan CV Tajima Y Trojanowski JQ Lee VM Sanberg PR Transplantation of cryopreserved human embryonal carcinoma-derived neurons (NT2N cells) promotes functional recovery in ischemic rats Exp Neurol 1998 149 310 ndash 21
Received 8 January 2010 accepted in revised form 28 July
2010
Human stem cell therapy in ischaemic stroke
13

8122019 Age Ageing 2011 Banerjee 7 13
httpslidepdfcomreaderfullage-ageing-2011-banerjee-7-13 77
17 Temple S The development of neural stem cells Nature2001 414 112 ndash 7
18 Reynolds BA Weiss S Generation of neurons and astrocytesfrom isolated cells of the adult mammalian central nervoussystem Science 1992 255 1707 ndash 10
19 Wachs FP Couillard-Despres S Engelhardt M et al High ef 1047297-cacy of clonal growth and expansion of adult neural stemcells Lab Invest 2003 83 949 ndash 62
20 Nunes MC Roy NS Keyoung HM et al Identi1047297cation and
isolation of multipotential neural progenitor cells from thesubcortical white matter of the adult human brain Nat Med2003 9 439 ndash 47
21 Arsenijevic Y Villemure JG Brunet JF et al Isolation of mul-tipotent neural precursors residing in the cortex of the adult human brain Exp Neurol 2001 170 48 ndash 62
22 Chu K Kim M Jeong SW Kim SU Yoon BW Humanneural stem cells can migrate differentiate and integrateafter intravenous transplantation in adult rats with transient forebrain ischemia Neurosci Lett 2003 343 129 ndash 33
23 Chu K Kim M Park KI et al Human neural stem cellsimprove sensorimotor de1047297cits in the adult rat brain withexperimental focal ischemia Brain Res 2004 1016145 ndash 53
24 Kelly S Bliss TM Shah AK et al Transplanted human fetal neural stem cells survive migrate and differentiate inischemic rat cerebral cortex Proc Natl Acad Sci USA 2004101 11839 ndash 44
25 ReNeuron receives UK ethics committee Favourable Opinionfor stroke clinical trialReNeuron2009 wwwreneuroncomnews__eventsnewsdocument_196_237php
26 Andrews PW Damjanov I Simon D et al Pluripotent embry-onal carcinoma clones derived from the human teratocarci-noma cell line Tera-2 Differentiation in vivo and in vitroLab Invest 1984 50 147 ndash 62
27 Pleasure SJ Lee VM NTera 2 cells a human cell line which displays characteristics expected of a human com-
mitted neuronal progenitor cell J Neurosci Res 1993 35585 ndash 602
28 Trojanowski JQ Mantione JR Lee JH et al Neurons derivedfrom a human teratocarcinoma cell line establish molecularand structural polarity following transplantation into therodent brain Exp Neurol 1993 122 283 ndash 94
29 Kleppner SR Robinson KA Trojanowski JQ Lee VM Transplanted human neurons derived from a teratocarcinomacell line (NTera-2) mature integrate and survive for over 1 yearin the nude mouse brain J Comp Neurol 1995 357 618 ndash 32
30 Borlongan CV Tajima Y Trojanowski JQ Lee VM Sanberg PR Transplantation of cryopreserved human embryonal carcinoma-derived neurons (NT2N cells) promotes functional recovery in ischemic rats Exp Neurol 1998 149 310 ndash 21
Received 8 January 2010 accepted in revised form 28 July
2010
Human stem cell therapy in ischaemic stroke
13