







Bahasa
Halaman
Hukum

www.elsevier.com/locate/schres
Schizophrenia Research
Specific cognitive deficits and differential domains of social
functioning impairment in schizophrenia
Alex S. Cohen *, Courtney B. Forbes, Monica C. Mann, Jack J. Blanchard
University of Maryland, College Park, College Park, MD 20742, United States
Received 11 April 2005; received in revised form 30 August 2005; accepted 6 September 2005
Available online 2 November 2005
Abstract
There is considerable inconsistency in findings regarding the relationship between specific cognitive deficits and social
impairment in patients with schizophrenia. This inconsistency may relate to variability across studies in how social functioning
is measured and preliminary evidence suggests that different indices of social functioning (e.g., laboratory test, community
assessment) may have different cognitive correlates. The present study examined this issue by evaluating the relationships
between cognitive deficits (including social cognitive deficits), role-play test performance, and community social functioning in
28 inpatients with schizophrenia. We expected the two measures of social functioning to have only modest convergence with
each other. Moreover, informed by the literature on cognitive functioning in schizophrenia, we identified specific cognitive
processes that were hypothesized to be associated with role-play performance (delayed verbal memory and attentional
vigilance) and social functioning in the community (delayed verbal memory and executive functioning). As expected, the
two measures of social functioning were modestly correlated with each other. Community social functioning was associated
with a relatively constrained pattern of cognitive deficits and received a significant contribution (Dr2=0.24) from specific
cognitive processes beyond that of general cognitive functioning and symptom severity. In contrast to our hypotheses, role-play
test performance was associated with a wide range of cognitive impairments and received little contribution from the specific
cognitive processes beyond the effects of general cognitive functioning. Community social functioning, but not role-play test
performance, was significantly associated with social cognition. These findings highlight the importance of conceptualizing
social functioning as a multidimensional construct for schizophrenia research.
D 2005 Elsevier B.V. All rights reserved.
Keywords: Schizophrenia; Social; Cognition; Functioning; Community; Symptom
0920-9964/$ - see front matter D 2005 Elsevier B.V. All rights reserved.
doi:10.1016/j.schres.2005.09.007
* Corresponding author. Tel.: +1 301 405 7184; fax: +1 301 405
0367.
E-mail address: [email protected] (A.S. Cohen).
1. Introduction
There is considerable evidence to suggest that
cognitive deficits are related to poor social functioning
in patients with schizophrenia. Efforts to identify
specific cognitive deficits that underlie these social
81 (2006) 227–238
A.S. Cohen et al. / Schizophrenia Research 81 (2006) 227–238228
impairments are vital for the development of standar-
dized cognitive assessment batteries (e g., see Green et
al., 2004) and for the advancement of effective cogni-
tive remediation interventions. As yet however, the
identification of specific cognitive correlates that reli-
ably predict social functioning has been hampered due
to inconsistent findings across studies. For example,
the Wisconsin Card Sorting Task, a measure of execu-
tive functioning, has been associated with impaired
social functioning in some (e.g., Penades et al., 2003;
Penn et al., 1996), but not most (e.g., Addington and
Addington, 1999; Addington et al., 1998; Dickerson et
al., 1996; Fujii and Wylie, 2003; Simon et al., 2003;
van Beilen et al., 2003; Woonings et al., 2003) studies.
When attempting to resolve this inconsistency, it is
important to note that there is considerable variability
across studies in how social functioning is measured.
Thus, the aforementioned inconsistency of findings
could reflect, at least in part, the use of different
measures of functioning across studies. The present
study examined whether different social functioning
domains would show divergent cognitive correlates in
patients with schizophrenia.
Recent findings have raised questions about the
utility of conceptualizing social functioning within
the context of a single, isomorphic construct. First,
studies that have examined the convergence between
laboratory and community based measures of social
functioning have generally found only modest levels of
inter-correlation (e.g., Mueser et al., 1990; Penn et al.,
1995; Addington and Addington, 1999 but see also
Bellack et al., 1990). Conceptually speaking, there
are differences between these two measures in that
laboratory-based measures typically assess social com-
petence or social skill ability (Bellack et al., 1990),
whereas community functioning-based instruments
measure the degree to which an individual actually
engages in social activities. Second, preliminary find-
ings from a recent review of 39 published studies
provide tentative evidence that different types of cog-
nitive deficits are associated with different domains of
functioning (Green et al., 2000). Across studies, defi-
cits in delayed verbal memory and attentional vigilance
have tended to be associated with role-play test impair-
ment, whereas deficits in executive functioning,
delayed verbal memory, and verbal fluency have
tended to be associated with impairment on instruments
that measured community social functioning. It is
important to note that the results of Green et al.
(2000) were based on a frequency count of the numbers
of replicated findings, and thus, should be interpreted
cautiously because the numbers of null and
bparadoxicalQ findings were not reported. Nonetheless,these findings support the notion that a meaningful
understanding of the cognitive underpinnings of social
dysfunction requires separate consideration for differ-
ent domains of social functioning.
As yet, the hypothesis that specific cognitive
factors are differentially related to different domains
of social functioning has received limited examina-
tion because few studies have included simultaneous
and multidimensional assessments of functioning
when examining cognitive dysfunction in schizo-
phrenia. Milev et al. (2005) found evidence for
cognitive specificity in relation to different domains
of functional outcome, however, the measures used
in these studies each assessed different aspects of
community functioning, and a laboratory-based mea-
sure was not included. Only two studies that have
simultaneously used both laboratory and community-
based social functioning assessments (Addington and
Addington, 1999; Addington et al., 1998) in exam-
ining correlates of cognitive deficits in schizophrenia
could be identified. Generally speaking, results from
these studies provide support for the notion that
laboratory and community-based social functioning
have different cognitive correlates, although there
was mixed support for the specific cognitive sub-
strates reported in Green et al. (2000). In both
Addington and Addington (1999) and Addington et
al. (1998), the magnitudes of correlations between
role-play test and cognitive impairments tended to be
in the small-to-moderate effect size range, whereas
the magnitudes of correlations between community
social functioning and cognitive impairment tended
to be small and nonsignificant.
When looking at cognitive functioning in patients,
one encounters the additional problem of contrasting
traditional bnonsocialQ measures of cognition with
social-based measures of cognition (Penn et al.,
1997). Social cognition, defined as the mental opera-
tions underlying the ability and capacity to perceive
the intentions and dispositions of others (Brothers,
1990), is relevant to the present discussion because it
has been associated with poorer nonsocial cognitive
functioning (e.g., Bryson et al., 1997; Kee et al., 1998,

A.S. Cohen et al. / Schizophrenia Research 81 (2006) 227–238 229
but see Lancaster et al., 2003) and poorer social func-
tioning across multiple domains in schizophrenia
patients, including role-play performance (Bellack et
al., 1992; Ihnen et al., 1998, but see Mueser et al.,
1996), social functioning in an inpatient setting (Penn
et al., 1996), and community social functioning (Hoo-
ker and Park, 2002; Poole et al., 2000). Recent theor-
ists (e.g., Green and Nuechterlein, 1999; Penn et al.,
1997) have proposed that social cognition reflects a
higher order cognitive function that is dependent on
more basic nonsocial cognitive processes, thus ser-
ving as a mediator between basic cognitive processes
and social functioning. However, the relationships
between these variables are presently unclear because
only a few studies have statistically examined the
independent contributions of social vs. nonsocial cog-
nition to functional outcome (e.g., Kee et al., 2003;
Vauth et al., 2004). Thus far, findings suggest that
social cognition deficits uniquely account for a lim-
ited, but significant amount of variance in community
functioning. It has yet to be determined whether social
cognition is related to role-play test performance
beyond that of nonsocial cognition.
Finally, when attempting to understand the relation-
ship between cognitive and social functioning in
patients, it is important to consider the impact of
symptom severity. Negative symptoms in particular,
have been associated with impairments in both cogni-
tive and social functioning (Earnst and Kring, 1997),
although cognitive deficits have contributed to social
functioning impairment beyond the effects of negative
symptoms (Addington and Addington, 1999; Velligan
et al., 1997). The relationships between other symp-
toms and social and cognitive functioning have been
less substantive (Green, 1996), although a few studies
have reported significant associations between disor-
ganization symptom severity and impairment in non-
social (Kerns and Berenbaum, 2002) and social
cognition (Kee et al., 2003) and community social
functioning (Smith et al., 2002) abilities. However,
the differential contribution that symptoms and cogni-
tive impairments make to social functioning across
multiple domains has not been assessed.
The primary purpose of the present study was to
examine the extent to which laboratory and commu-
nity-based social functioning measures differ in their
cognitive and symptom correlates. Given prior
research on the topic, we expected the two measures
of social functioning to have only modest levels of
correlation with each other, and to show different
cognitive correlates. Using the findings of Green et
al. (2000) to inform our hypotheses, we predicted that
deficits on tests of delayed verbal memory and atten-
tional vigilance would be associated with poorer role-
play test performance beyond the effects of other
cognitive tests, and that impairment on tests of delayed
verbal memory and executive functioning would be
associated with poorer community social functioning
beyond the effects of other cognitive tests. We
hypothesized that social cognition scores would
uniquely contribute to the variance of both types of
social functioning above and beyond that of nonsocial
cognition scores. Finally, we examined the relationship
between symptoms and social functioning with the
expectation that cognitive deficits would uniquely
contribute to social functioning score variance beyond
the contribution made by symptoms.
2. Method
2.1. Participants
This study was part of a larger investigation into
affective disturbances in schizophrenia (see Blanchard
et al., 2001). Patients were recruited from an inpatient
hospital, and were in a state of clinical stability when
they enrolled in the current study. Patients met criteria
for Diagnostic and Statistical Manual of Mental Dis-
orders-fourth edition (DSM-IV; American Psychiatric
Association, 1994) schizophrenia based on informa-
tion obtained from a structured clinical interview
(Structured Clinical Interview for DSM-IV; Spitzer
et al., 1990) that was administered by trained mas-
ters-level doctoral students. Patients with evidence of
a history of neurological disorder or serious head
trauma were excluded from the original study. Inter-
rater agreement for diagnosis, based on a review of 14
videotaped interviews, was acceptable (Kappa values
range from 0.85 to 1.00). The methodology and par-
ticipant characteristics are more fully described in
Blanchard et al. (2001).
Not all data were available for each case due to
several factors, such as the inclusion of the role-play
tests late in the study and missing cognitive test data
for some patients. For the present study, cases were

A.S. Cohen et al. / Schizophrenia Research 81 (2006) 227–238230
excluded if there was missing data for any of the
cognitive or social functioning measures. Twenty-
eight of the 55 schizophrenia patient cases were
selected for analysis. There were no significant differ-
ences between those patients that were included and
those that were excluded (n =27) from the present
study in age, education, ethnicity, sex, symptom
severity or intellectual functioning variable scores
(all p values N0.05).
The final sample was composed of 24 males and
four females with an average (meanF standard devia-
tion=mFSD) age of mFSD=33.36F1.26 years
and education of mFSD=12.21F2.42 years. Twelve
of the patients were Caucasian, four were African-
American, 11 were Hispanic and one was Asian-
American/Pacific Islander. Each of these patients
was being prescribed antipsychotic medication.
2.2. Measures
2.2.1. Social functioning
Social functioning was assessed using two different
measures. The first, a Role-Play Test (Bellack et al.,
1994), was used as a measure of laboratory-based
social skill. The version of the role-play test that was
used in this study included two practice, two conver-
sational (e.g., initiating conversation with a new
neighbor) and two assertiveness (e.g., speaking to a
landlord about a ceiling leak that has not been fixed)
role-play situations. The role-plays were enacted with
one of five confederates whose responses were stan-
dardized. Role-play test were videotaped and rated by
one of two raters who independently coded patients’
performance on each of the conversation and asser-
tiveness scenes for a variety of skills, including con-
versational fluency, conversational clarity, number of
social norm violations, positive and negative valance,
and level of arousal (for a review of each of the
measures, see Bellack et al., 1994). For the present
study, the overall skill rating, which is a likert-type
scale from 1 (very poor overall skill) to 5 (very good
overall skill) was used. The overall skill ratings from
the conversational and assertiveness conditions were
highly correlated (r[28]=0.71, p N0.00), suggesting
there was considerable convergence in what they
were measuring. For data reduction purposes, the
four individual overall skill ratings (two from the
conversation scenes and two from the assertiveness
scenes) were averaged together yielding one overall
skill rating. Intra-class Correlation Coefficient (ICC)
for the average overall skill ratings from the role-play
test, computed from independent ratings by both raters
for 24% of the original cases (13 of 55), was adequate
(ICC=0.87).
The second measure of social functioning, a mea-
sure of community functioning, was the Social Adjust-
ment Scale-second edition (SAS-II; Schooler and
Weissman, 1979). The SAS-II is an instrument meant
to assess a wide range of social functioning in the
preceding month. For the present study, we were
most interested in those items that directly tapped
into social behavior as opposed to satisfaction or com-
fort with social relationships. Following the methods
of Blanchard et al. (1998), scores from the five ques-
tions that were related to social behavior were
summed, including frequency of leisure, social, peer
and romantic contacts and degree of activity in social
contacts. The SAS-II has shown adequate reliability
and convergent validity in prior studies with patients
(Blanchard et al., 1998; Glazer et al., 1980; Mueser
et al., 1990). SAS-II scores ranged from 5 to 25, and
were reverse-coded so that higher scores on this mea-
sure would reflect better functioning. This allowed
consistency across measures so that higher scores for
each of the social functioning and cognitive tests
reflected better performance.
2.2.2. Cognitive measures
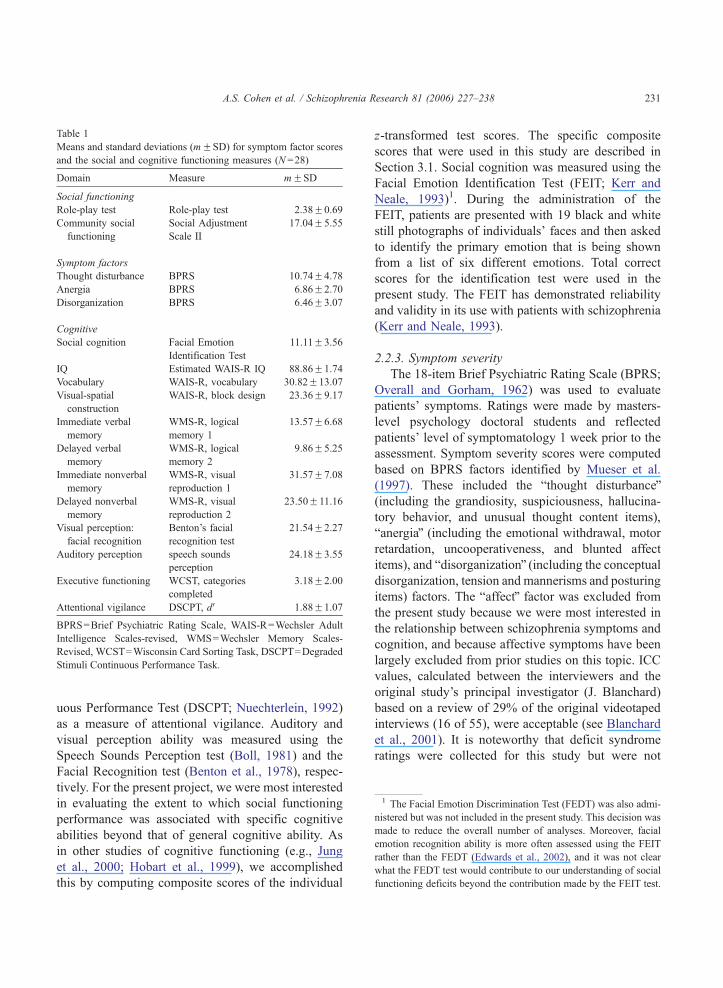
A battery of cognitive tests was used to assess
patients’ cognitive functioning. The cognitive domains
and their corresponding tests are listed in Table 1.
These tests included: the Vocabulary test from
the Wechsler Adult Intelligence Scales-Revised
(WAIS-R; Wechsler, 1981) as a measure of verbal
ability, the Block Design test from the WAIS-R
(Wechsler, 1981) as a measure of visual-spatial con-
struction ability, Logical Memory I and II from the
Wechsler Memory Scales-Revised (WMS-R; Wechs-
ler, 1987) as measures of immediate and delayed ver-
bal memory respectively, Visual Reproduction I and II
from the WMS-R (Wechsler, 1987) as measures of
immediate and delayed non-verbal memory respec-
tively, the categories completed score from the Wis-
consin Card Sorting Task (Heaton et al., 1993) as a
measure of executive functioning and cognitive flex-
ibility, and the d’ from the Degraded Stimuli-Contin-
1 The Facial Emotion Discrimination Test (FEDT) was also admi-
nistered but was not included in the present study. This decision was
made to reduce the overall number of analyses. Moreover, facial
emotion recognition ability is more often assessed using the FEIT
rather than the FEDT (Edwards et al., 2002), and it was not clear
what the FEDT test would contribute to our understanding of social
functioning deficits beyond the contribution made by the FEIT test.
Table 1
Means and standard deviations (mFSD) for symptom factor scores
and the social and cognitive functioning measures (N =28)
Domain Measure mFSD
Social functioning
Role-play test Role-play test 2.38F0.69
Community social
functioning
Social Adjustment
Scale II
17.04F5.55
Symptom factors
Thought disturbance BPRS 10.74F4.78
Anergia BPRS 6.86F2.70
Disorganization BPRS 6.46F3.07
Cognitive
Social cognition Facial Emotion
Identification Test
11.11F3.56
IQ Estimated WAIS-R IQ 88.86F1.74
Vocabulary WAIS-R, vocabulary 30.82F13.07
Visual-spatial
construction
WAIS-R, block design 23.36F9.17
Immediate verbal
memory
WMS-R, logical
memory 1
13.57F6.68
Delayed verbal
memory
WMS-R, logical
memory 2
9.86F5.25
Immediate nonverbal
memory
WMS-R, visual
reproduction 1
31.57F7.08
Delayed nonverbal
memory
WMS-R, visual
reproduction 2
23.50F11.16
Visual perception:
facial recognition
Benton’s facial
recognition test
21.54F2.27
Auditory perception speech sounds
perception
24.18F3.55
Executive functioning WCST, categories
completed
3.18F2.00
Attentional vigilance DSCPT, dV 1.88F1.07
BPRS=Brief Psychiatric Rating Scale, WAIS-R=Wechsler Adult
Intelligence Scales-revised, WMS=Wechsler Memory Scales-
Revised, WCST=Wisconsin Card Sorting Task, DSCPT=Degraded
Stimuli Continuous Performance Task.
A.S. Cohen et al. / Schizophrenia Research 81 (2006) 227–238 231
uous Performance Test (DSCPT; Nuechterlein, 1992)
as a measure of attentional vigilance. Auditory and
visual perception ability was measured using the
Speech Sounds Perception test (Boll, 1981) and the
Facial Recognition test (Benton et al., 1978), respec-
tively. For the present project, we were most interested
in evaluating the extent to which social functioning
performance was associated with specific cognitive
abilities beyond that of general cognitive ability. As
in other studies of cognitive functioning (e.g., Jung
et al., 2000; Hobart et al., 1999), we accomplished
this by computing composite scores of the individual
z-transformed test scores. The specific composite
scores that were used in this study are described in
Section 3.1. Social cognition was measured using the
Facial Emotion Identification Test (FEIT; Kerr and
Neale, 1993)1. During the administration of the
FEIT, patients are presented with 19 black and white
still photographs of individuals’ faces and then asked
to identify the primary emotion that is being shown
from a list of six different emotions. Total correct
scores for the identification test were used in the
present study. The FEIT has demonstrated reliability
and validity in its use with patients with schizophrenia
(Kerr and Neale, 1993).
2.2.3. Symptom severity
The 18-item Brief Psychiatric Rating Scale (BPRS;
Overall and Gorham, 1962) was used to evaluate
patients’ symptoms. Ratings were made by masters-
level psychology doctoral students and reflected
patients’ level of symptomatology 1 week prior to the
assessment. Symptom severity scores were computed
based on BPRS factors identified by Mueser et al.
(1997). These included the bthought disturbanceQ(including the grandiosity, suspiciousness, hallucina-
tory behavior, and unusual thought content items),
banergiaQ (including the emotional withdrawal, motor
retardation, uncooperativeness, and blunted affect
items), and bdisorganizationQ (including the conceptualdisorganization, tension and mannerisms and posturing
items) factors. The baffectQ factor was excluded from
the present study because we were most interested in
the relationship between schizophrenia symptoms and
cognition, and because affective symptoms have been
largely excluded from prior studies on this topic. ICC
values, calculated between the interviewers and the
original study’s principal investigator (J. Blanchard)
based on a review of 29% of the original videotaped
interviews (16 of 55), were acceptable (see Blanchard
et al., 2001). It is noteworthy that deficit syndrome
ratings were collected for this study but were not
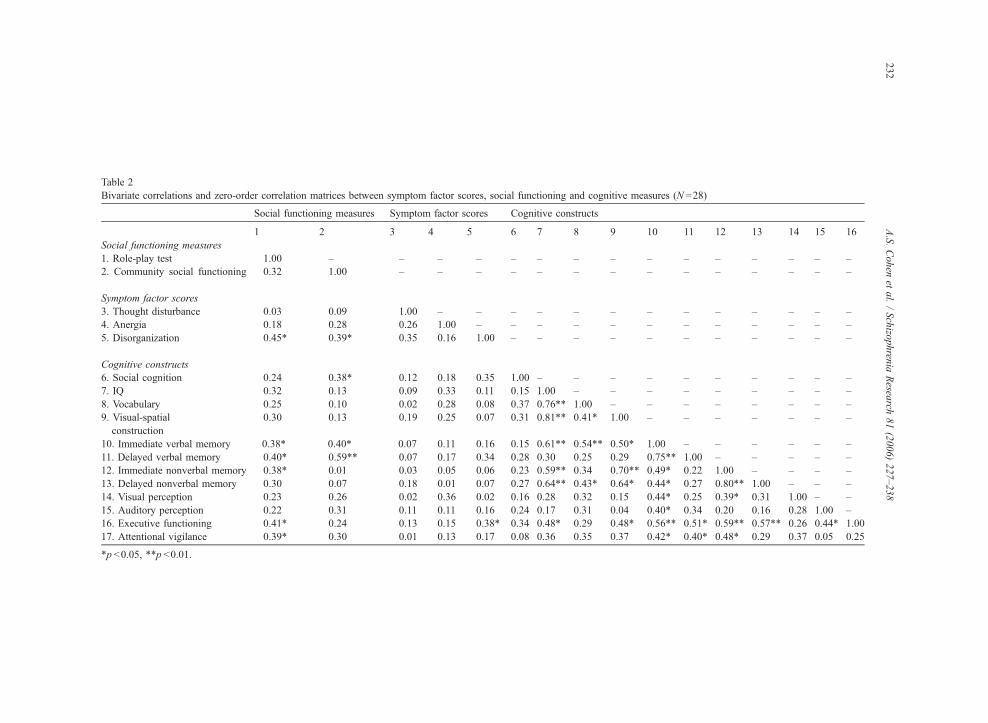
Table 2
Bivariate correlations and zero-order correlation matrices between symptom factor scores, social functioning and cognitive measures (N =28)
Social functioning measures Symptom factor scores Cognitive constructs
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
Social functioning measures
1. Role-play test 1.00 – – – – – – – – – – – – – – –
2. Community social functioning 0.32 1.00 – – – – – – – – – – – – – –
Symptom factor scores
3. Thought disturbance �0.03 0.09 1.00 – – – – – – – – – – – – –
4. Anergia �0.18 �0.28 �0.26 1.00 – – – – – – – – – – – –
5. Disorganization �0.45* �0.39* 0.35 0.16 1.00 – – – – – – – – – – –
Cognitive constructs
6. Social cognition 0.24 0.38* �0.12 �0.18 �0.35 1.00 – – – – – – – – – –
7. IQ 0.32 0.13 �0.09 �0.33 �0.11 0.15 1.00 – – – – – – – – –
8. Vocabulary 0.25 0.10 0.02 �0.28 �0.08 0.37 0.76** 1.00 – – – – – – – –
9. Visual-spatial
construction
0.30 0.13 0.19 �0.25 �0.07 0.31 0.81** 0.41* 1.00 – – – – – – –
10. Immediate verbal memory 0.38* 0.40* 0.07 �0.11 �0.16 0.15 0.61** 0.54** 0.50* 1.00 – – – – – –
11. Delayed verbal memory 0.40* 0.59** �0.07 �0.17 �0.34 0.28 0.30 0.25 0.29 0.75** 1.00 – – – – –
12. Immediate nonverbal memory 0.38* 0.01 0.03 �0.05 0.06 0.23 0.59** 0.34 0.70** 0.49* 0.22 1.00 – – – –
13. Delayed nonverbal memory 0.30 0.07 �0.18 �0.01 �0.07 0.27 0.64** 0.43* 0.64* 0.44* 0.27 0.80** 1.00 – – –
14. Visual perception 0.23 0.26 �0.02 �0.36 �0.02 0.16 0.28 0.32 0.15 0.44* 0.25 0.39* 0.31 1.00 – –
15. Auditory perception 0.22 0.31 0.11 0.11 �0.16 0.24 0.17 0.31 0.04 0.40* 0.34 0.20 0.16 0.28 1.00 –
16. Executive functioning 0.41* 0.24 �0.13 �0.15 �0.38* 0.34 0.48* 0.29 0.48* 0.56** 0.51* 0.59** 0.57** 0.26 0.44* 1.00
17. Attentional vigilance 0.39* 0.30 �0.01 �0.13 �0.17 0.08 0.36 0.35 0.37 0.42* 0.40* 0.48* 0.29 0.37 0.05 0.25
*p b0.05, **p b0.01.
A.S.Cohen
etal./Schizo
phren
iaResea
rch81(2006)227–238
232

A.S. Cohen et al. / Schizophrenia Research 81 (2006) 227–238 233
used in the present study. This is because the results of
many of the cognitive and social functioning
comparisons between deficit and non-deficit patients
are presented elsewhere (Horan and Blanchard, 2003),
and because we were primarily interested in examining
symptoms dimensionally so that we could employ
correlational and regression analyses.
2.2.4. Analyses
The analyses were conducted in four steps. First, we
wanted to understand the relationships between each of
the demographic variables, and symptom factor, cog-
nitive and social functioning scores. Bivariate correla-
tions were computed between each of these variables.
Informed by our literature search, we predicted that the
magnitude of association between the two measures of
social functioning would be modest. We also hypothe-
sized that, of the cognitive variables, only the atten-
tional vigilance, verbal memory and social cognition
test scores would be significantly correlated with role-
play test performance, and that only the executive
functions, verbal memory and social cognition mea-
sures would be significantly associated with commu-
nity social functioning scores. Second, in order to
determine the extent to which social functioning
impairment reflected deficits in the specific cognitive
processes outlined in Green et al. (2000), hierarchical
regressions were computed. Our expectation for these
analyses was that the scores of the specific cognitive
processes would contribute to the variance of social
functioning scores above and beyond that of the more
general cognitive composite scores. Third, we hypothe-
sized that social cognition ability would contribute to
the variance in social functioning scores above and
beyond that of nonsocial cognitive functioning scores
using hierarchical regressions. Finally, using hierarch-
ical regressions, we examined whether cognitive func-
tioning contributed to either social functioning domain
above and beyond the effects of symptoms.
3. Results
Means and standard deviations were computed for the
symptom factor scores and the cognitive and social function-
ing measures. These results are presented in Table 1. The
sample, on average, showed mild levels of thought distur-
bance, anergia and disorganization symptoms. Impairment on
the community social functioning measure was comparable
to that evidenced in a prior study of outpatients with schizo-
phrenia (Blanchard et al., 1998). The skew value for each of
these variables was less than 1.5 suggesting that parametric
statistics were appropriate for statistical computation.
In order to determine whether differences in gender and
ethnicity were associated with differences in cognitive and
social functioning scores, group comparisons were con-
ducted. T-tests revealed that men had significantly better
vocabulary (t[26]=2.12, p b0.05) and visual spatial con-
struction (t[26]=2.09, p b0.05) performance than females,
but that there were no significant differences between males
and females on any of the other social or cognitive function-
ing variables. It is important to point out that this analysis
was underpowered because there were only four females in
the present sample. None of the social and cognitive func-
tioning variable values were significantly different between
the Caucasian vs. non-Caucasians, suggesting that there
were no demonstrable differences between the ethnic groups
on any of these variables.
Zero-order correlations between the symptom factor,
social functioning and cognitive scores were computed
and presented in Table. 2. Some findings from this table
warrant mention here because they bear relevance to the
present hypotheses. First, the role-play test and community
social functioning were modestly, but not significantly cor-
related (r[28]=0.32, ns). Although the magnitude of corre-
lation was at the moderate size level (Cohen, 1987), the two
measures shared only 9% common variance. Second, neither
the thought disturbance nor the anergia factor scores were
significantly related to any of the cognitive or social func-
tioning scores. The disorganization factor scores were sig-
nificantly and inversely related to both the role-play and
community social functioning measures, and executive
functioning impairment, but not any of the other cognitive
measured scores.
3.1. Bivariate correlations between the social functioning
and cognitive measures
Correlations computed between the role-play and com-
munity social functioning and the cognitive scores are pre-
sented in Table 2. As hypothesized, role-play test scores
were significantly and inversely associated with the delayed
verbal memory and attentional vigilance scores. Role-play
test scores were also significantly associated with immediate
non-verbal and verbal memory and executive function
scores. It is noteworthy that each of the correlations was
of a small to medium effect size. Thus, role-play test impair-
ment was associated with a wider range of cognitive deficits
than anticipated. In contrast, community social functioning
impairments were significantly associated with deficits in
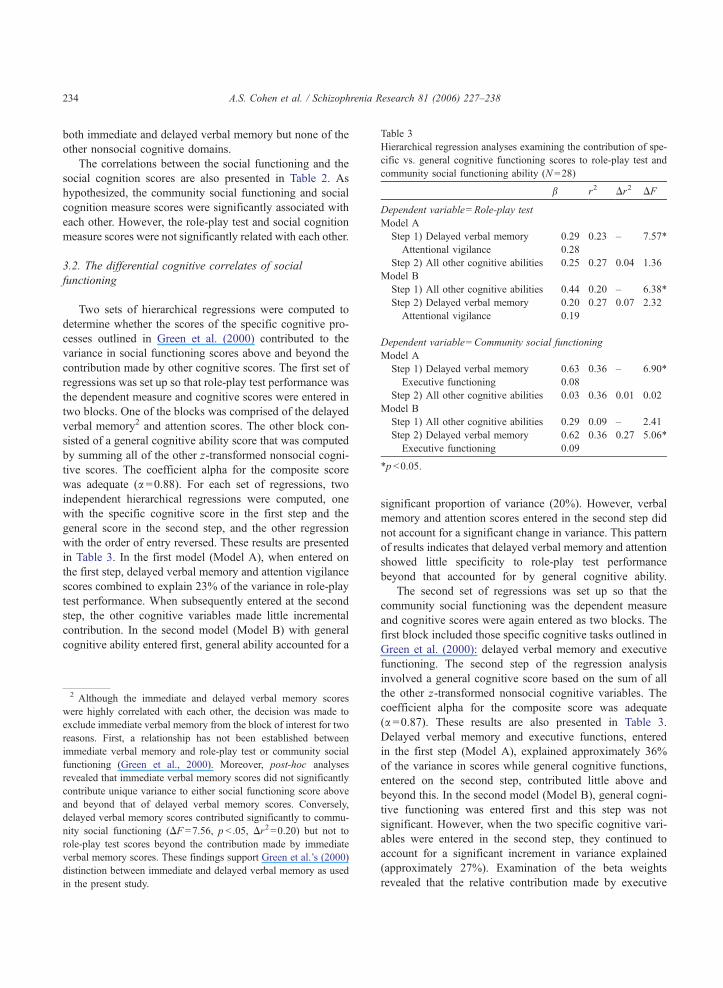
Table 3
Hierarchical regression analyses examining the contribution of spe-
cific vs. general cognitive functioning scores to role-play test and
community social functioning ability (N =28)
b r2 Dr2 DF
Dependent variable=Role-play test
Model A
Step 1) Delayed verbal memory 0.29 0.23 – 7.57*
Attentional vigilance 0.28
Step 2) All other cognitive abilities 0.25 0.27 0.04 1.36
Model B
Step 1) All other cognitive abilities 0.44 0.20 – 6.38*
Step 2) Delayed verbal memory 0.20 0.27 0.07 2.32
Attentional vigilance 0.19
Dependent variable=Community social functioning
Model A
Step 1) Delayed verbal memory 0.63 0.36 – 6.90*
Executive functioning �0.08
Step 2) All other cognitive abilities 0.03 0.36 0.01 0.02
Model B
Step 1) All other cognitive abilities 0.29 0.09 – 2.41
Step 2) Delayed verbal memory 0.62 0.36 0.27 5.06*
Executive functioning �0.09
*p b0.05.
A.S. Cohen et al. / Schizophrenia Research 81 (2006) 227–238234
both immediate and delayed verbal memory but none of the
other nonsocial cognitive domains.
The correlations between the social functioning and the
social cognition scores are also presented in Table 2. As
hypothesized, the community social functioning and social
cognition measure scores were significantly associated with
each other. However, the role-play test and social cognition
measure scores were not significantly related with each other.
3.2. The differential cognitive correlates of social
functioning
Two sets of hierarchical regressions were computed to
determine whether the scores of the specific cognitive pro-
cesses outlined in Green et al. (2000) contributed to the
variance in social functioning scores above and beyond the
contribution made by other cognitive scores. The first set of
regressions was set up so that role-play test performance was
the dependent measure and cognitive scores were entered in
two blocks. One of the blocks was comprised of the delayed
verbal memory2 and attention scores. The other block con-
sisted of a general cognitive ability score that was computed
by summing all of the other z-transformed nonsocial cogni-
tive scores. The coefficient alpha for the composite score
was adequate (a =0.88). For each set of regressions, two
independent hierarchical regressions were computed, one
with the specific cognitive score in the first step and the
general score in the second step, and the other regression
with the order of entry reversed. These results are presented
in Table 3. In the first model (Model A), when entered on
the first step, delayed verbal memory and attention vigilance
scores combined to explain 23% of the variance in role-play
test performance. When subsequently entered at the second
step, the other cognitive variables made little incremental
contribution. In the second model (Model B) with general
cognitive ability entered first, general ability accounted for a
2 Although the immediate and delayed verbal memory scores
were highly correlated with each other, the decision was made to
exclude immediate verbal memory from the block of interest for two
reasons. First, a relationship has not been established between
immediate verbal memory and role-play test or community social
functioning (Green et al., 2000). Moreover, post-hoc analyses
revealed that immediate verbal memory scores did not significantly
contribute unique variance to either social functioning score above
and beyond that of delayed verbal memory scores. Conversely,
delayed verbal memory scores contributed significantly to commu-
nity social functioning (DF =7.56, p b .05, Dr2=0.20) but not to
role-play test scores beyond the contribution made by immediate
verbal memory scores. These findings support Green et al.’s (2000)
distinction between immediate and delayed verbal memory as used
in the present study.
significant proportion of variance (20%). However, verbal
memory and attention scores entered in the second step did
not account for a significant change in variance. This pattern
of results indicates that delayed verbal memory and attention
showed little specificity to role-play test performance
beyond that accounted for by general cognitive ability.
The second set of regressions was set up so that the
community social functioning was the dependent measure
and cognitive scores were again entered as two blocks. The
first block included those specific cognitive tasks outlined in
Green et al. (2000): delayed verbal memory and executive
functioning. The second step of the regression analysis
involved a general cognitive score based on the sum of all
the other z-transformed nonsocial cognitive variables. The
coefficient alpha for the composite score was adequate
(a =0.87). These results are also presented in Table 3.
Delayed verbal memory and executive functions, entered
in the first step (Model A), explained approximately 36%
of the variance in scores while general cognitive functions,
entered on the second step, contributed little above and
beyond this. In the second model (Model B), general cogni-
tive functioning was entered first and this step was not
significant. However, when the two specific cognitive vari-
ables were entered in the second step, they continued to
account for a significant increment in variance explained
(approximately 27%). Examination of the beta weights
revealed that the relative contribution made by executive

Table 4
Hierarchical regression analyses examining the contribution of spe-
cific vs. general cognitive functioning scores to role-play test and
community social functioning ability, controlling for symptom
severity scores (N =28)
b r2 Dr2 DF
Dependent variable=Role-play test
Step 1) Disorganization symptom factor �0.40 0.19 – 1.77
Anergia symptom factor �0.14
Thought disturbance symptom factor 0.07
Step 2) All other cognitive abilities 0.48 0.41 0.22 8.10**
Step 3) Delayed verbal memory �0.06 0.47 0.07 1.23
Attentional Vigilance 0.30
Dependent variable=Community social functioning
Step 1) Disorganization symptom factor �0.50 0.27 – 2.89
Anergia symptom factor �0.12
Thought disturbance symptom factor 0.23
Step 2) All other cognitive abilities 0.16 0.30 0.02 0.72
Step 3) Delayed verbal memory 0.62 0.54 0.24 5.25*
Executive functioning �0.15
A.S. Cohen et al. / Schizophrenia Research 81 (2006) 227–238 235
functions was not significant, suggesting that the bulk of the
contribution were made by delayed verbal memory scores. In
sum, these results suggest that relatively specific cognitive
impairments predicted community social functioning, but not
role-play test performance.
3.3. The contribution of social cognition to social
functioning
Hierarchical regressions were then used to examine the
relative contributions of social and nonsocial cognition
scores to social functioning. Two separate regressions
were set up with role-play performance and community
functioning as the dependent variables. In each regression
analysis, two cognitive variables were entered: a z-score-
transformed composite of all of the nonsocial cognition
scores and the social cognition measure. The coefficient
alpha for the nonsocial composite score was adequate
(a =0.86). In each regression model (predicting role-play
and community functioning), the general cognitive compo-
site score was entered first, followed by the social cognition
score. Due to space limitations and the lack of significant
findings in these analyses, these results are presented in text.
For the role-play test, nonsocial cognition, entered in the
first step, accounted for a significant proportion of the var-
iance (Dr2[1, 26]=0.24, p b0.01). However, social cognition
did not account for a significant increment in explained
variance on the second step (Dr2[1, 25]=0.01, ns).
For the community social functioning measure, general
cognitive functioning accounted for a modest but nonsigni-
ficant amount of variance (Dr2[1, 26]=0.13, ns). Entered on
the next step, social cognition failed to account for a sig-
nificant increment in explained variance of community func-
tioning (Dr2[1,25]=0.08, ns). In sum, these results suggest
that social cognition explained a modest but nonsignificant
amount of unique variance in community social functioning
scores, and explained little variance beyond nonsocial cogni-
tion ability to role-play test performance.
3.4. Controlling for symptom severity
We sought to examine whether the unique contributions
that the specific nonsocial cognitive factors made to social
functioning would be maintained beyond the effects of symp-
tom severity. In order to examine this issue, the regressions
from Section 3.2 were recomputed with the thought distur-
bance, anergia and disorganization factor scores entered in
the first block. These results are presented in Table 4. When
the role-play test measure was entered as the dependent
measure, the symptom factor scores, entered in the first
step, accounted for 19% of the variance in role-play test
scores. This contribution was not statistically significant.
The general cognitive factor, entered in the second step,
explained approximately 22% of the variance ( p b0.05)
beyond symptom factor scores. The unique contribution of
the delayed verbal memory and attentional vigilance scores,
entered in the third step, was nonsignificant. Thus, general
cognitive functioning remained a significant predictor of
role-play performance even after controlling for symptoms.
When the community social functioning measure was
entered as the dependent measure, approximately 27% of the
variance was accounted for by symptom factor scores ( p of
F change=0.06), entered in the first step. The general
cognitive factor, entered in the second step, explained
approximately 2% of the variance beyond the symptom
severity, and the contribution of the delayed verbal memory
and executive functioning scores, entered in the third step,
remained significant (Dr2=0.24). As before, this contribu-
tion was primarily accounted for by delayed verbal memory
scores. In sum, specific cognitive deficits were associated
with community social functioning deficits beyond the
effects of symptoms and general cognitive functioning.
4. Discussion
Although cognitive dysfunction has been linked to
functional outcome in schizophrenia, the identification
of specific cognitive deficits that contribute to func-
tional impairments has been complicated by inconsis-
tent findings across studies. Preliminary evidence
A.S. Cohen et al. / Schizophrenia Research 81 (2006) 227–238236
(e.g., Green et al., 2000; Addington et al., 1998;
Addington and Addington, 1999) has suggested that
this inconsistency might be due, in part, to different
domains of social functioning being associated with
different types of cognitive processes. Findings
from the present study support this notion. First, the
role-play test and community social functioning mea-
sures were nonsignificantly, but modestly correlated
with each other suggesting that there was unique
variance in each measure. Second, there were appreci-
able differences in the cognitive correlates between
these two social functioning measures. Role-play
test performance tended to have a diverse set of
cognitive correlates, whereas the community social
functioning measure was significantly correlated
with immediate and delayed verbal memory solely.
Third, specific cognitive deficits showed little unique
contribution to role-play test performance, whereas
delayed verbal memory and executive functioning
uniquely contributed over a quarter of the variance
in community social functioning scores beyond
general cognitive ability. These findings were main-
tained even when thought disturbance, anergia and
disorganization symptom severity was controlled for.
Finally, social cognition made a modest (but not
statistically significant) contribution to the variance
of community social functioning scores beyond that
of nonsocial cognition, while the unique contribution
made to the variance in role-play test performance
was negligible. With respect to future research, studies
that focus on the relationship between cognitive
deficits and social functioning could provide a fuller
understanding of social abilities by including multi-
dimensional assessments.
In support of findings from Green et al. (2000),
secondary verbal memory, and to a lesser extent,
executive functions uniquely accounted for over a
quarter of the variance in community social function-
ing scores beyond other cognitive abilities and symp-
toms. Although this finding should be interpreted
cautiously because it is inconsistent with the findings
of some studies (e.g., Addington and Addington,
1999), the notion that secondary verbal memory and
executive functions are highly related to impaired
community social functioning is promising for the
generation of future hypotheses. On the other hand,
role-play test performance was associated with a more
generalized cognitive deficit. This is consistent with
other studies, in that role-play test performance has
shown a diverse and variable set of cognitive associ-
ates (e.g., Addington and Addington, 1999).
Interpretation of the present findings is constrained
by the reality that domains of social functioning mea-
sured in this study (role-play and community func-
tioning) can be further parsed into subdomains that
may also have differential correlates with cognitions.
For example, our measure of community functioning
could be further broken down into community social
functioning in familial, peer-group and professional
settings. Moreover, aspects of bnon-socialQ commu-
nity functioning such as occupational achievement
were not assessed and may well have different rela-
tionships with cognition (e.g., Milev et al., 2005).
Some limitations of the present project warrant
mention. First, although the cognitive battery was
relatively broad in scope, not all domains of cognitive
functioning were represented. For example, the pre-
sent study lacked a measure of verbal fluency. Green
et al. (2000) reported that at least four studies had
found a significant relationship between verbal flu-
ency deficits and impairments in community social
functioning. Second, the measure of social cognition
was limited in that it was based solely on facial
emotion identification ability. Examples of social
cognition measures used in other studies include
theory of mind, vocal affect perception and measures
of bsocial intelligenceQ (Penn et al., 1997). Third,
although each of the patients in the present study
was medicated, we were unable to examine the
effects of differential dosage and type of medication
on social functioning or cognitive performance
because medication status was clinically determined.
Fourth, the sample was predominantly male. Previous
research has suggested that males and females differ
in the cognitive correlates of their social functioning
impairments (Mueser et al., 1995) and we were
unable to effectively address this issue. Fifth, the
small sample size, while comparable to many other
neuropsychological studies of social functioning
(e.g., Addington et al., 1998), may have reduced
power and precluded finding significance in the rela-
tionships between the community social functioning
and cognitive measures. Finally, the current study
involved inpatients and the social functioning mea-
sure covered an epoch prior to hospitalization, so the
degree to which the findings generalize to stabilized
A.S. Cohen et al. / Schizophrenia Research 81 (2006) 227–238 237
outpatients is unclear. Further, the study examined
social functioning cross-sectionally, and it is possible
that measures of longitudinal social functioning may
have yielded different findings (see Milev et al.,
2005).
4.1. Summary
Given recent efforts to develop effective cognitive
and social rehabilitation treatments for patients with
schizophrenia, identifying which, if any, specific cog-
nitive deficits underlie social functional impairments
is important. The present findings suggest that impair-
ment in different domains of social functioning reflect
different cognitive liabilities. Thus, it seems a reason-
able conclusion that more consistent and specific
cognitive correlates of functional outcome could
potentially be identified by focusing on more refined
domains of functioning.
Acknowledgements
This research was supported by National Institute
of Mental Health grant MH51240 to Dr. Blanchard.
References
Addington, J., Addington, D., 1999. Neurocognitive and social
functioning in schizophrenia. Schizophr. Bull. 25, 173–182.
Addington, J., McCleary, L., Munroe-Blum, H., 1998. Relationship
between cognitive and social dysfunction in schizophrenia.
Schizophr. Res. 34, 59–66.
American Psychiatric Association, 1994. Diagnostic and Statistical
Manual of Mental Disorders, Fourth Edn. American Psychiatric
Association, Washington, DC.
Bellack, A.S., Morrison, R.L., Wixted, J.T., et al., 1990. An analysis
of social competence in schizophrenia. Br. J. Psychiatry 156,
809–818.
Bellack, A.S., Mueser, K.T., Wade, J., et al., 1992. The ability of
schizophrenics to perceive and cope with negative affect. Br. J.
Psychiatry 160, 473–480.
Bellack, A.S., Sayers, M., Mueser, K.T., et al., 1994. Evaluation of
social problem solving in schizophrenia. J. Abnorm. Psychology
103, 371–378.
Benton, A.V.M., Hamsher, K., Levin, H., 1978. Test of Facial
Recognition Manual. Benton Laboratory of Neuropsychology,
Iowa City, IA.
Blanchard, J.J., Mueser, K.T., Bellack, A.S., 1998. Anhedonia,
positive and negative affect, and social functioning in schizo-
phrenia. Schizophr. Bull. 24, 413–424.
Blanchard, J.J., Horan, W.P., Brown, S.A., 2001. Diagnostic differ-
ences in social anhedonia: a longitudinal study of schizophrenia
and major depressive disorder. J. Abnorm. Psychology 110,
363–371.
Boll, T.J., 1981. The Halstead-Reitan neuropsychological battery.
Handbook of Clinical Neuropsychology. Wiley-Interscience,
New York, pp. 577–607.
Brothers, L., 1990. The social brain: a project for integrating
primate behavior and neurophysiology in a new domain. Con-
cepts Neurosci. 1, 24–61.
Bryson, G., Bell, M., Lysaker, P., 1997. Affect recognition in
schizophrenia: a function of global impairment or a specific
cognitive deficit. Psychiatry Res. 71, 105–113.
Cohen, J., 1987. Statistical Power Analysis for the Behavioral
Sciences, Rev. Lawrence Erlbaum Associates, Inc.
Dickerson, F., Boronow, J.J., Ringel, N., et al., 1996. Neurocogni-
tive deficits and social functioning in outpatients with schizo-
phrenia. Schizophr. Res. 21, 75–83.
Earnst, K.S., Kring, A.M., 1997. Construct validity of negative
symptoms: an empirical and conceptual review. Clin. Psychol.
Rev. 17, 167–189.
Edwards, J., Jackson, H.J., Pattison, P.E., 2002. Emotion recogni-
tion via facial expression and affective prosody in schizophre-
nia: a methodological review. Clin. Psychol. Rev. 22, 789–832.
Fujii, D.E., Wylie, A.M., 2003. Neurocognition and community
outcome in schizophrenia: long-term predictive validity. Schi-
zophr. Res. 59, 219–223.
Glazer, W.M., Aaronson, H.S., Prusoff, B.A., et al., 1980. Assess-
ment of social adjustment in chronic ambulatory schizophrenics.
J. Nerv. Ment. Dis. 168, 493–497.
Green, M.F., 1996. What are the functional consequences of neu-
rocognitive deficits in schizophrenia? Am. J. Psychiatry. 153,
321–330.
Green, M.F., Nuechterlein, K.H., 1999. Should schizophrenia be
treated as a neurocognitive disorder? Schizophr. Bull. 25,
309–319.
Green, M.F., Kern, R.S., Braff, D.L., et al., 2000. Neurocognitive
deficits and functional outcome in schizophrenia: are we mea-
suring the bright stuffQ? Schizophr. Bull. 26, 119–136.
Green, M.F., Nuechterlein, K.H., Gold, J.M., et al., 2004.
Approaching a consensus cognitive battery for clinical trials in
schizophrenia: the NIMH-MATRICS conference to select cog-
nitive domains and test criteria. Biol. Psychiatry 56, 301–307.
Heaton, R.K., Chelune, G.J., Talley, J.L., Kay, G.C., Curtiss, G.,
1993. Wisconsin Card Sorting Test Manual Revised and
Expanded. Psychological Assessment Resources, Odessa, FL.
Hobart, M.P., Goldberg, R., Bartko, J.J., 1999. Repeatable battery
for the assessment of neuropsychological status as a screen-
ing test in schizophrenia: II. Convergent/discriminant validity
and diagnostic group comparisons. Am. J. Psychiatry 156,
1951–1957.
Hooker, C., Park, S., 2002. Emotion processing and its relationship
to social functioning in schizophrenia patients. Psychiatry Res.
112, 41–50.
Horan, W.P., Blanchard, J.J., 2003. Neurocognitive, social, and
emotional dysfunction in deficit syndrome schizophrenia. Schi-
zophr. Res. 65, 125–137.
A.S. Cohen et al. / Schizophrenia Research 81 (2006) 227–238238
Ihnen, G.H., Penn, D.L., Corrigan, P.W., et al., 1998. Social per-
ception and social skill in schizophrenia. Psychiatry Res. 80,
275–286.
Jung, R.E., Yeo, R.A., Chiulli, S.J., 2000. Myths of neuropsychol-
ogy: Intelligence, neurometabolism, and cognitive ability. Clin.
Neuropsychol. 14, 535–545.
Kee, K.S., Kern, R.S., Green, M.F., et al., 1998. Perception of
emotion and neurocognitive functioning in schizophrenia:
what’s the link? Psychiatry Res. 81, 57–65.
Kee, K.S., Green, M.F., Mintz, J., et al., 2003. Is emotion proces-
sing a predictor of functional outcome in schizophrenia? Schi-
zophr. Bull. 29, 487–497.
Kerns, J.G., Berenbaum, H., 2002. Cognitive impairments asso-
ciated with formal thought disorder in people with schizophre-
nia. J. Abnorm. Psychology 111, 211–224.
Kerr, S.L., Neale, J.M., 1993. Emotion perception in schizophrenia:
specific deficit or further evidence of generalized poor perfor-
mance? J. Abnorm. Psychology 102, 312–318.
Lancaster, R.S., Evans, J.D., Bond, G.R., et al., 2003. Social
cognition and neurocognitive deficits in schizophrenia. J.
Nerv. Ment. Dis. 191, 295–299.
Milev, P., Ho, B.C., Arndt, S., 2005. Predictive values of neuro-
cognition and negative symptoms on functional outcome in
schizophrenia: a longitudinal first-episode study with 7-year
follow-up. Am. J. Psychiatry 162, 495–506.
Mueser, K.T., Bellack, A.S., Morrison, R.L., et al., 1990. Gender,
social competence, and symptomatology in schizophrenia: a
longitudinal analysis. J. Abnorm. Psychology 99, 138–147.
Mueser, K.T., Blanchard, J.J., Bellack, A.S., 1995. Memory and
social skill in schizophrenia: the role of gender. Psychiatry Res.
57, 141–153.
Mueser, K.T., Doonan, R., Penn, D.L., et al., 1996. Emotion recog-
nition and social competence in chronic schizophrenia. J.
Abnorm. Psychology 105, 271–275.
Mueser, K.T., Penn, D.L., Blanchard, J.J., et al., 1997. Affect
recognition in schizophrenia: a synthesis of findings across
three studies. Psychiatry 60, 301–308.
Nuechterlein, K.H., Asarnow, R.F., 1992. Manual and computer
program for the UCLA Continuous Performance Test: Version 4.
Overall, J.E., Gorham, D.R., 1962. The brief psychiatric rating
scale. Psychol. Rep. 10, 799.
Penades, R., Boget, T., Catalan, R., et al., 2003. Cognitive mechan-
isms, psychosocial functioning, and neurocognitive rehabilita-
tion in schizophrenia. Schizophr. Res. 63, 219–227.
Penn, D.L., Mueser, K.T., Doonan, R., et al., 1995. Relations
between social skills and ward behavior in chronic schizophre-
nia. Schizophr. Res. 16, 225–232.
Penn, D.L., Spaulding, W., Reed, D., et al., 1996. The relationship
of social cognition to ward behavior in chronic schizophrenia.
Schizophr. Res. 20, 327–335.
Penn, D.L., Corrigan, P.W., Bentall, R.P., et al., 1997. Social
cognition in schizophrenia. Psychol. Bull. 121, 114–132.
Poole, J.H., Tobias, F.C., Vinogradov, S., 2000. The functional
relevance of affect recognition errors in schizophrenia. J. Int.
Neuropsychol. Soc. 6, 649–658.
Schooler, N.H., Weissman, G., 1979. Resource Materials for Com-
munity Mental Health Program Evaluators. National Institute of
Mental Health, Rockville, MD.
Simon, A.E., Giacomini, V., Ferrero, F., et al., 2003. Dysexecutive
syndrome and social adjustment in schizophrenia. Aust. N. Z. J.
Psychiatry 37, 340–346.
Smith, T.E., Hull, J.W., Huppert, J.D., et al., 2002. Recovery from
psychosis in schizophrenia and schizoaffective disorder: symp-
toms and neurocognitive rate-limiters for the development of
social behavior skills. Schizophr. Res. 55, 229–237.
Spitzer, R.L., Williams, J.B.W., Gibbon, M., 1990. User’s guide for
the structured clinical interview for DSM-III-R: SCID: Amer-
ican Psychiatric Association.
van Beilen, M., Kiers, H.A., Bou, A., et al., 2003. Cognitive deficits
and social functioning in schizophrenia: a clinical perspective.
Clin. Neuropsychol. 17, 507–514.
Vauth, R., Rusch, N., Wirtz, M., et al., 2004. Does social cognition
influence the relation between neurocognitive deficits and
vocational functioning in schizophrenia? Psychiatry Res. 128,
155–165.
Velligan, D.I., Mahurin, R.K., Diamond, P.L., et al., 1997. The
functional significance of symptomatology and cognitive func-
tion in schizophrenia. Schizophr. Res. 25, 21–31.
Wechsler, D., 1981. Wechsler Adult Intelligence Scale-Revised.
Psychological Corporation, New York.
Wechsler, D., 1987. Wechsler Memory Scale-Revised. Psychologi-
cal Corporation, New York, NY.
Woonings, F.M., Appelo, M.T., Kluiter, H., et al., 2003. Learning,
potential, and social functioning in schizophrenia. Schizophr.
Res. 59, 287–296.
Top Related
Copyright © 2022 FDOKUMEN

