






Bahasa
Halaman
Hukum


http://nnr.sagepub.com/Repair
Neurorehabilitation and Neural
http://nnr.sagepub.com/content/early/2014/01/06/1545968313517757The online version of this article can be found at:
DOI: 10.1177/1545968313517757
published online 9 January 2014Neurorehabil Neural RepairReinhart
Georg Kerkhoff, Leandra Bucher, Michael Brasse, Eva Leonhart, Manfed Holzgraefe, Volker Völzke, Ingo Keller and StefanLiving in Neglect: A Randomized Controlled Trial
Smooth Pursuit ''Bedside'' Training Reduces Disability and Unawareness During the Activities of Daily
Published by:
http://www.sagepublications.com
On behalf of:
American Society of Neurorehabilitation
can be found at:Neurorehabilitation and Neural RepairAdditional services and information for
http://nnr.sagepub.com/cgi/alertsEmail Alerts:
http://nnr.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Jan 9, 2014OnlineFirst Version of Record >>
at Schon Klinik Verwaltung GmbH on January 13, 2014nnr.sagepub.comDownloaded from at Schon Klinik Verwaltung GmbH on January 13, 2014nnr.sagepub.comDownloaded from

Neurorehabilitation andNeural Repair201X, Vol XX(X) 1 –10© The Author(s) 2013Reprints and permissions: sagepub.com/journalsPermissions.navDOI: 10.1177/1545968313517757nnr.sagepub.com
Original Article
Introduction
Spatial neglect is a challenging disorder,1 defined as the inability to respond to sensory stimuli in the contralesional hemispace and hemibody of a neurological patient.1 Despite spontaneous recovery, one-third of all neglect patients develop chronic neglect.2 Moreover, the associated unaware-ness impairs recovery,3 predicts poor functional outcome,4 and interferes with the treatment of hemiparesis.5 Unawareness is defined as the impaired insight into left-sided sensory (visual, auditory, haptic, body-related) and motor impairments (hemiparesis) after stroke. As a major source of long-term disability after stroke, neglect and unawareness are associated with an adverse rehabilitation outcome,4,6 espe-cially for functional tasks in peripersonal space, such as find-ing/grasping objects on a table, finding pictures, perceiving the midline in space, or gaze orientation.7,8 Although neglect rehabilitation is effective,9 a reduction in the number of ses-sions by more effective therapies might reduce rehabilitation
costs. Moreover, few RCTs have been conducted,10,11 espe-cially in the acute stage.12 At this stage, patients are immobi-lized in bed, show an ipsilesional gaze deviation,13 and unawareness,14 making treatment difficult. Though much is known about the effects of neglect therapy on test measures,9 little is known about its effects on disability,15 functional neglect measures, and (in)dependence in activities of daily living (ADLs). A recent treatment study, however, clearly
517757 NNRXXX10.1177/1545968313517757Neurorehabil Neural RepairKerkhoff et alresearch-article2013
1Saar Universität, Saarbruecken, Germany2Ambulantes Neurologisches Rehazentrum, Hildesheim, Germany3Asklepios Klinik Schildautal, Seesen, Germany4Helios Klinik, Hattingen, Germany5Schön Klinik, Bad Aibling, Germany
Corresponding Author:Georg Kerkhoff, PhD, Clinical Neuropsychology Unit and Outpatient Service, Saarland University, Building A 1 3, D-66123 Saarbruecken, Germany. Email: [email protected]
Smooth Pursuit “Bedside” Training Reduces Disability and Unawareness During the Activities of Daily Living in Neglect: A Randomized Controlled Trial
Georg Kerkhoff, PhD1, Leandra Bucher, MA1, Michael Brasse, MA2,3, Eva Leonhart, MA1, Manfed Holzgraefe, MD3, Volker Völzke, MA4, Ingo Keller, PhD5, and Stefan Reinhart, MA1
AbstractBackground. Neglect is associated with disability, unawareness, poor long-term outcome, and dependence from caregivers. No randomized trial has evaluated the effects of smooth pursuit eye movement training (SPT) and visual scanning training (VST) at the bedside on these variables. Objective. To compare the effects of SPT and VST in postacute stroke at 1 month with left neglect. Methods: We carried out an assessor-blinded, randomized controlled trial. The 24 participants were randomly allocated to either SPT or VST (n = 12 each). They received 20 treatment sessions lasting 30 minutes each at the bedside over 4 weeks. Outcome measures included the Functional Neglect Index (FNI) based on 4 tasks: find objects on a tray, stick bisection, picture search, and gaze orientation. In addition, the Unawareness and Behavioral Neglect Index (UBNI) with 6 items about unawareness and 4 about neglect in activities of daily living, the Help index (required assistance in 10 functional activities), the Barthel Index, and the rehabilitation phase were rated by treatment-blinded assessors. Outcome measures were obtained before and immediately after the end of the interventions and at a 2-week follow-up. Results. Significantly greater improvements were obtained after SPT versus VST treatment in the FNI and UBNI, and there were continued improvements selectively in the SPT group 2 weeks later. Conclusions. SPT accelerates recovery from functional neglect and reduces unawareness significantly. Bedside neglect treatment using SPT is effective and feasible early after stroke.
Keywordshemineglect, visual smooth pursuit, stroke rehabilitation, anosognosia, visual scanning, hemianopsia
at Schon Klinik Verwaltung GmbH on January 13, 2014nnr.sagepub.comDownloaded from
2 Neurorehabilitation and Neural Repair XX(X)
indicates that theta-burst neglect therapy significantly reduces neglect in ADLs.16 It is important to note that no RCT has evaluated treatments capable of reducing the unawareness in neglect.17 Interestingly, caloric-vestibular stimulation18 tran-siently reduces unawareness, and galvanic-vestibular stimu-lation permanently reduces left-hand tactile extinction.19 This suggests that repetitive application of neglect-effective treat-ments might cure unawareness.20
Smooth pursuit eye movement training (SPT) using opto-kinetic stimulation significantly reduces visual, auditory, and haptic neglect more than other treatments.21-24 Although VST is a well-established treatment, it shows poor transfer to nontrained tasks,25,26, requires numerous treatment ses-sions (20-40),27,28 does not improve nonvisual neglect,9 and requires partial awareness by the patient, which is impaired in early neglect.14 In contrast, SPT requires less voluntary, top-down guided orientation toward contralesional stimuli. Patients follow moving stimuli with their eyes toward the neglected hemispace, which is easier than performing left-ward saccades in acute stroke.29 Although few treatments are feasible in early stroke at the bedside, patients might benefit from treatments adapted to this situation. Moreover, to date, it is unknown whether SPT and VST reduce disabil-ity, unawareness, and dependence on caregivers. Disability measures are more sensitive to behavioral neglect than paper-pencil tests,30 and, therefore, show the patient’s func-tional (in)capacities in everyday life. In addition, improved awareness would be extremely beneficial because this could increase the unfavorable rehabilitation outcome.3,17
Here, we compared SPT and VST in early stroke reha-bilitation as bedside treatments, with a particular emphasis on functional neglect measures, unawareness, and ADLs. Three kinds of measurements were specifically designed for this purpose: First, a functional neglect index (FNI) was derived based on 4 functional tasks assessing the patient’s performance in peripersonal space. These included find-ing/reaching for objects on a large tray (see Figure 1), pic-ture search, stick bisection, and the patient’s gaze orientation (appendix). Conjugate gaze deviation is a fre-quent epiphenomenon of acute spatial neglect, which recovers in parallel to the disturbed visual exploration behavior, thus making it a sensitive measure of neglect severity.31 Second, ratings of unawareness and behavioral neglect in 10 daily activities as well as the help needed with the execution of 10 daily functional tasks were obtained by treatment-blinded caregivers. Third, the patients’ overall rehabilitation status was documented by the Barthel Index (BI)32 and the current rehabilitation phase (acute, early, or continuing rehabilitation, see the appen-dix), both rated as well by treatment-blinded medical staff. Based on our recent RCT, which showed significant and large improvements in visual and auditory neglect after SPT but not VST,22 we expected significantly greater improvements after SPT than following VST also in the functional outcome measures used in the present study.
SPT relies, as a bottom-up, sensory stimulation treatment, less on the awareness and compliance of the neglect patient. Because of its greater and multimodal efficacy on neglect (visual, auditory, and haptic), we hypothesized further that SPT might reduce unawareness to a greater extent than VST. Finally, from a practical-clinical viewpoint, we sought to explore whether neglect therapy can be con-ducted successfully at the patient’s bedside in this early phase of rehabilitation. As a matter of fact, some neglect treatments like visuomotor feedback training are feasible and effective as bedside trainings in acute patients,33,34 whereas others appear more variable in their efficacy in this early stage (prism adaptation, see Turton et al35 for negative results and Gossmann et al12 for positive results).
Methods
Patients
Inclusion criteria were a single right-hemisphere stroke, visual neglect in 2 screening tests (horizontal line bisection of a 200 mm long × 10 mm broad black line, number cancel-lation),22 and the ability to execute daily neglect training for 30 minutes. Neglect was diagnosed when bisection deviated >5 mm to the right side and when >1 omissions were found on the left side than on the right side of the cancellation test (see Table 1 for individual data). Exclusion criteria were
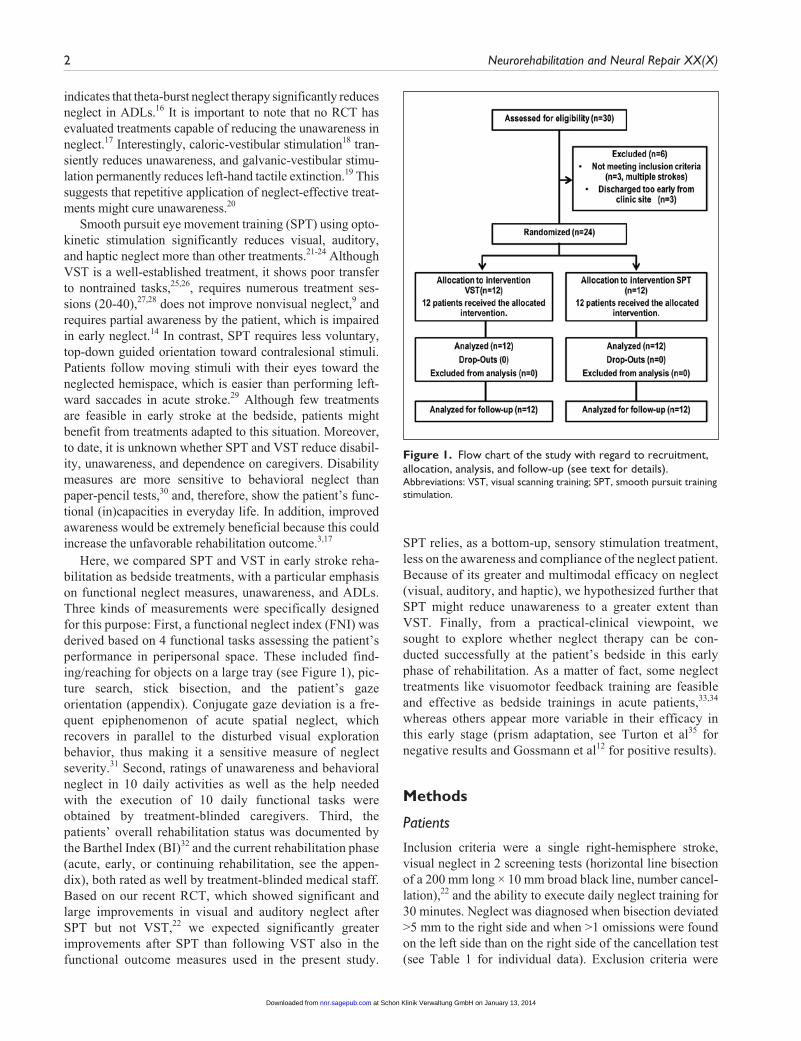
Figure 1. Flow chart of the study with regard to recruitment, allocation, analysis, and follow-up (see text for details).Abbreviations: VST, visual scanning training; SPT, smooth pursuit training stimulation.
at Schon Klinik Verwaltung GmbH on January 13, 2014nnr.sagepub.comDownloaded from

3
Tab
le 1
. D
emog
raph
ical
and
Clin
ical
Dat
a of
24
Patie
nts
With
Lef
t-Si
ded
Spat
ial N
egle
ct in
the
2 T
reat
men
t G
roup
s D
urin
g Ba
selin
e A
sses
smen
ts B
efor
e T
reat
men
t.
Cod
eT
reat
men
tA
ge,
Gen
der
Etio
logy
, D
ays
Sinc
e Le
sion
Lesi
on
Loca
tion
(Rig
ht)
Mot
or
Stat
us
Vis
ual
Fiel
d (D
efec
t)
Line
Bis
ectio
n,
Dev
iatio
n (m
m)
Can
cella
tion
Om
issi
ons,
Le
ft/R
ight
Tre
atm
ent
Peri
od
(day
s)
Reh
abili
tatio
n St
atus
Bart
hel I
ndex
Reh
abili
tatio
n Ph
asea
Pre
Post
Foll
Pre
Post
Foll
DS
VST
65, f
I, 21
F, T
L pa
resi
sL-
QU
A18
4/1
2650
9595
CD
DM
PV
ST71
, fH
, 33
BG, T
hal
L pl
egia
Nor
mal
187/
259
1010
10B
BB
MS
VST
49, f
H, 1
8BG
Nor
mal
Nor
mal
125/
125
3560
65C
CC
WP
VST
60, m
I, 17
T, P
L pa
resi
sL-
HH
146/
224
2040
40B
CC
PRV
ST53
, mH
, 62
BGL
pare
sis
Nor
mal
195/
230
1010
10B
BB
JFV
ST73
, fI,
47F,
PL
pleg
iaN
orm
al22
6/2
280
00
BB
BEH
VST
65, m
I, 66
F, P,
T, O
L pl
egia
L-H
H13
7/3
295
1010
BB
BG
SV
ST63
, mI,
50F,
TL
pleg
iaN
orm
al17
8/3
275
510
BB
BER
VST
82, m
I, 38
OL
pare
sis
L-H
H9
9/3
1930
3555
BC
CK
DV
ST58
, mI,
33F,
TL
pleg
iaN
orm
al33
6/2
1815
3030
BB
BM
IV
ST69
, fI,
35F,
P, T
L pl
egia
Nor
mal
277/
318
015
35B
BC
DW
VST
59, m
I, 21
O, P
L pl
egia
L-H
H41
10/5
200
020
BB
BM
ean
(SD
)64
(3)
37 (
5)+
20.3
(9)
6.7/
2.4
(1.7
/1.8
)27
(3)
15 (
5)26
(8)
32 (
8)
IKSP
T61
, fI,
51F,
TL-
pleg
iaL-
QU
A13
5/2
3020
3035
BB
CW
FSP
T68
, mI,
30P,
F, T
L-pl
egia
Nor
mal
296/
127
015
30B
BB
JWSP
T73
, mI,
44F,
TL-
pleg
iaN
orm
al37
7/2
315
3030
BB
BW
HSP
T63
, mI,
12F,
TL-
pleg
iaN
orm
al36
5/1
360
510
BB
BR
WSP
T59
, mI,
16P,
F, T
L-pl
egia
Nor
mal
324/
124
015
45B
BC
ME
SPT
74, f
I, 24
F, T
L-pl
egia
Nor
mal
2710
/446
2030
30B
BB
HS
SPT
60, m
I, 11
P, O
L-pa
resi
sN
orm
al14
3/0
210
2525
BB
BG
HSP
T50
, mH
, 44
F, T
L-pl
egia
Nor
mal
174/
135
00
0B
BB
PGSP
T53
, mH
, 56
BGN
orm
alN
orm
al18
5/2
2910
4055
BC
CR
ASP
T61
, mI,
27F,
PL-
pare
sis
L-Q
UA
196/
150
3565
85C
CD
SNSP
T60
, fI,
20F,
P, T
L-pl
egia
Nor
mal
217/
335
1545
70B
CD
NS
SPT
84, f
I, 25
F,P,
TL-
pare
sis
L-H
H27
5/2
3630
4045
BC
CM
ean
(SD
)64
(3)
30 (
4)+
24.2
(8)
5.6/
1.7
(1.8
/1.1
)33
(2)
11 (
4)28
(5)
38 (
7)
Abb
revi
atio
ns: P
re, p
rete
st; P
ost,
post
test
; Fol
l, fo
llow
-up-
test
; VST
, vis
ual s
cann
ing
trai
ning
; f, f
emal
e; m
, mal
e; L
, lef
t; Q
UA
, hom
onym
ous
quad
rano
pia;
I, is
chem
ia; H
, hem
orrh
age;
BG
, bas
al g
angl
ia;
F, fr
onta
l; P,
par
ieta
l; T
, tem
pora
l; O
, occ
ipita
l; T
hal,
Tha
lam
us; H
H, h
omon
ymou
s he
mia
nopi
a; S
D, s
tand
ard
devi
atio
n; S
PT, s
moo
th p
ursu
it tr
aini
ng s
timul
atio
n.a Bo
ld in
dica
tes
patie
nts
with
impr
ovem
ent
in r
ehab
ilita
tion
stat
us d
urin
g or
aft
er n
egle
ct t
reat
men
t. Li
ne b
isec
tion:
pos
itive
val
ues
indi
cate
rig
ht-s
ided
dev
iatio
n (m
axim
um c
utof
f: ±
5 m
m).
Can
cella
tion:
om
itted
dig
its p
er h
emifi
eld
are
give
n (m
axim
um 1
0 pe
r he
mifi
eld;
cut
off:
max
imum
1 o
mis
sion
/hem
ifiel
d). A
lloca
tion
to r
ehab
ilita
tion
phas
e is
bas
ed o
n th
e Ba
rthe
l Ind
ex (
BI).
Phas
e B,
BI
= 0
-35;
pha
se C
, BI =
35-
65; p
hase
D, B
I >65
.
at Schon Klinik Verwaltung GmbH on January 13, 2014nnr.sagepub.comDownloaded from

4 Neurorehabilitation and Neural Repair XX(X)
psychiatric, ophthalmological, or other neurological dis-eases. From 30 eligible patients with left neglect caused by right-hemisphere stroke, 6 were excluded: 3 because of mul-tiple strokes and 3 because of too early a discharge to com-plete the trial (Figure 2). Finally, 24 patients with acute visuospatial neglect, as assessed by the 2 screening tests, were randomly allocated to SPT or VST (by a person not involved in the study who drew lots from a sealed envelope). All patients had corrected-to-normal visual acuity, were right-handed, and gave their informed consent to participate in the study according to the declaration of Helsinki II (see Table 1 for clinical/demographic details).
Treatments
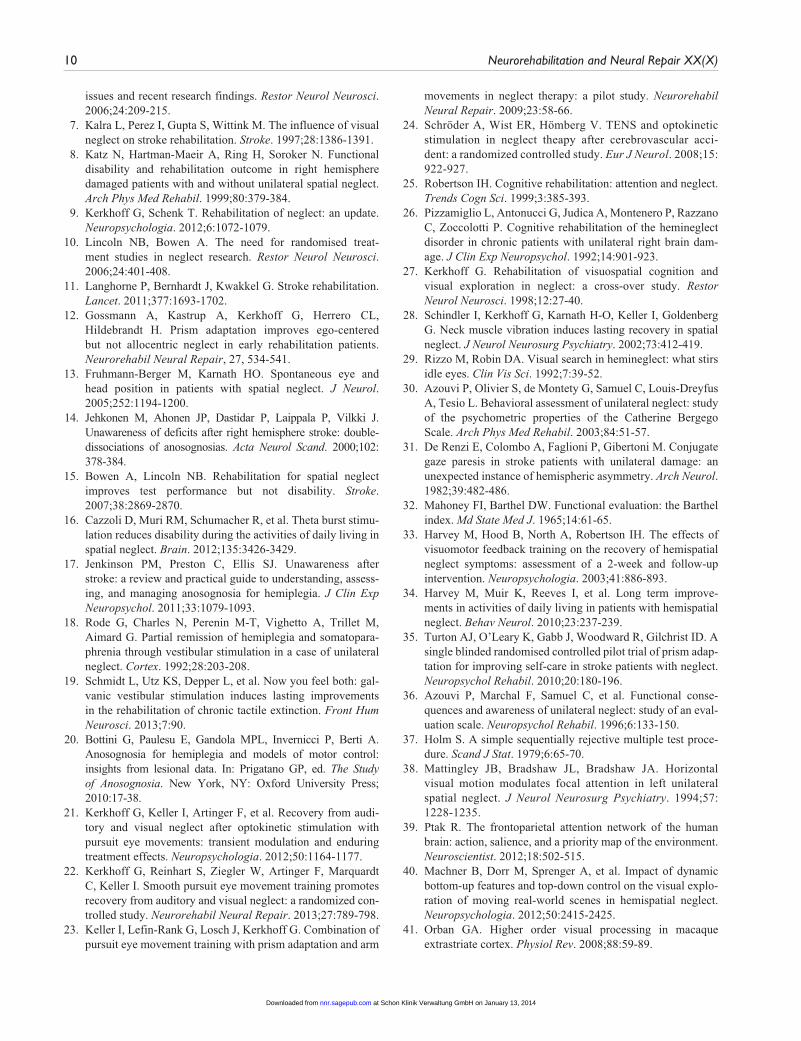
Patients received 20 treatment sessions (30 minutes each) in total (1 session daily, from Monday to Friday) over a period of 1 month (Table 1). Both treatments were realized as bed-side treatments, using a laptop with a 15-inch monitor, cen-trally placed at a viewing distance of 0.40 m (39.2° vs 30.1° horizontal/vertical size) in front of the patient on a board seated solidly across the patient’s bed, with the patient sit-ting upright in the bed (Figure 1).
During SPT, stimuli were random displays of 20 to 60 identically colored and sized squares, moving horizontally from right to left at constant velocity, providing a coherent stimulus pattern (see Figure 1 for exemplary display). The color, size (1°-2.5°), and velocity (3.1-12.6 degrees/s) of the stimuli were varied from time to time. The patient was encouraged to conduct smooth pursuit eye movements, repeatedly following the stimulus pattern from right to left, without head movements. During VST, patients viewed stationary displays of stimuli implemented in the same software. Stimuli were geometrical objects (circles, trian-gles, squares, etc), stars, letters, or digits (see Figure 1 for an example). The number of stimuli (5-60), their size (1°-2.5°), color, and spatial arrangement were varied (sys-tematic versus unordered, with/without line numbering, with/without subsidiary horizontal reference lines, and with/without a red vertical “anchor line” on the leftmost side of the display). Patients were trained to scan systemati-cally from left to right and from top to bottom, naming all objects, or counting certain stimuli. The therapist kept the patient’s head in a straight position in either treatment to promote eye instead of head movements. She watched con-tinuously from the side whether the patient made smooth pursuit eye movements to the contralesional side (SPT) or saccadic eye movements (VST). If patients did not execute the appropriate eye movements, the instructions were repeated. If patients were tired, a short break (2 minutes) was given, adjusted to patients’ individual requirements.
Assessments and Design
The FNI included the following 4 tasks:
Tray test. A total of 18 everyday objects (pen, sponge, tea light, handkerchiefs, etc) were presented on a large ply-wooden tray (size 0.75 m × 0.25 m, 113.3° horizontal eccentricity), at a distance of 0.25 m from the patient (Figure 1). Three target and 3 distractor objects, respectively, were affixed in either of 3 imag-inary segments (left, middle, and right segment) of the tray. Target objects were randomly and succes-sively shown to the patient by the experimenter, using a demonstration object that was identical to the respective target object. Patients were instructed to explore for and subsequently grasp the target object with the right hand. The number of target objects found within a cutoff (maximum) duration of 30 s (hits) and the respective exploration duration was stopped with a stopwatch. Objects not found within 30 s were counted as omissions, with the maximum exploration duration of 30 s. Hits (maximum 3 per segment) and exploration duration for the left, mid-dle, and right segments were recorded separately (see the appendix).
Pointing at drawings. A large test sheet (0.42 m × 0.3 m, 80.06° horizontal × 61.93° vertical size) pre-sented 16 color drawings of animals (each 3.5 cm × 3,5 cm = 8.01° × 8.01°), equally spaced in 4 × 4 rows in both hemispaces, at a distance of 0.25 m from the patient. The patient’s task was to point to 10 (5 in each hemispace) drawings as subsequently and randomly announced by the experimenter. The number of ani-mals correctly pointed to within 20 s (recorded by a stopwatch) was counted as hits. Drawings not found within the maximum exploration duration of 20 s were counted as omissions, with the maximum exploration duration of 20 s. Hits (maximum 5 in each hemifield) and respective exploration duration were documented separately for the left and right hemispaces. For the tray test and animal drawings test, 2 parallel versions were developed (A and B), which were alternated across the 3 time points of measurement to reduce memory effects (see the appendix for details).
Horizontal stick bisection. Patients were instructed to assess the midpoint of a wooden bar (length 1 m; height/breadth 1 cm), horizontally and centrally placed at a distance of 0.25 m from the patient. A total of 6 trials (3 visual, 3 tactile) were performed. In the visual condition, patients scanned the bar visually. In the tactile condition, patients were blindfolded, and the right index finger was used to explore the bar hap-tically. The order of testing was fixed: first visual, then tactile bisection. In both conditions, the right index finger was used to point to the subjective mid-point. The mean deviation from the objective midpoint across all trials was transformed to a score ranging from 0 to 3, reflecting the magnitude of the deviation (see the appendix).
at Schon Klinik Verwaltung GmbH on January 13, 2014nnr.sagepub.comDownloaded from

Kerkhoff et al 5
Gaze deviation. The researcher stood at the end of the patient’s bed and scored gaze orientation in a “con-frontation” procedure31 in the following way while watching the patient in bed: Does the patient make normal, spontaneous eye/head movements to either side? (score 0). Does he or she show delayed leftward (contralesional) movement of eyes/head? (score 1). Does he or she show leftward movement of eyes/head only after a verbal command? (score 2). Does he or she show no leftward movement of eyes/head despite a verbal command? (score 3).
The patient’s performance in the tests of the FNI was scored (0-3) by 2 independent raters to calculate a composite
score of neglect severity ranging between 0 and 15. Both raters were not involved in the assessments nor in any treat-ment. The scoring procedure (see the appendix) was defined before the rating was implemented. The aim of this proce-dure was to rate the left-to-right-gradient of the patient’s spatial attention as a global measure of neglect severity. The scorings of the 2 examiners were identical (Spearman’s ρ; all r = 1.00) for each neglect test, thus showing perfect objectivity and reliability of the scoring procedure.
Unawareness and behavioral neglect index (UBNI): We used a rating similar to the Catherine Bergego Scale (CBS) to assess behavioral neglect in daily life.30,36 In addition and differing from the CBS, the UBNI includes
Figure 2. Top: Examples of smooth pursuit eye movement training (SPT) and visual scanning training (VST) designs; Arrows indicate the direction of motion on the screen during VST but were not visible during therapy. Bottom: Layout of the bedside treatment setup and spatial layout of the tray test (see text for details).
at Schon Klinik Verwaltung GmbH on January 13, 2014nnr.sagepub.comDownloaded from

6 Neurorehabilitation and Neural Repair XX(X)
6 items assessing the degree of unawareness in daily life. The UBNI was rated by the nurses on the ward (who were blinded to the treatment type) on a 4-point rating scale (behavior occurrence: 0, never; 1, rarely; 2, frequent; 3, daily). From the 10 items, 6 items assessed unawareness and 4 behavioral neglect in ADLs (details in the appendix). The mean rating over all 10 items was calculated and used for statistical analyses.
Help Index, Barthel Index, and Rehabilitation Status
The help which the patient needed to accomplish 8 func-tional ADLs was rated by the nurses on a 5-point scale: 1, no help needed; 2, verbal instruction sufficient for patient to solve the task; 3, little practical help necessary by staff to solve the task; 4, medium help necessary by nurse; 5, patient is completely relying on external help by the nurse to solve the task; see the appendix). The rating nurses were blinded to the treatment type the patients received. The BI includes 10 variables concerning ADL and mobility.32 Following guidelines of the Federal Rehabilitation Council, patients are allocated to rehabilitation phases (B: early; C: continu-ing rehabilitation; D, posthospital curative treatment) based on the BI (appendix, Table 1). The BI and rehabilitation phases were scored by treatment-blinded physicians.
Statistical Analyses
The data were analyzed separately for all dependent variables with ANOVAs with the factors time (baseline, posttreatment, and follow-up) and group (SPT, VST). The α level was set at .05 (2-tailed) and corrected for pairwise comparisons accord-ing to Holm’s procedure,37 where the fist comparison is com-puted with α, the second with α/2, and the third with α/3. The rehabilitation phase data were transferred to a score (B = 1, C = 2, D = 3) and analyzed nonparametrically.
Results
Group Comparison at Baseline
As t tests for independent measurements revealed no signifi-cant differences between the groups at the baseline assessment (smallest P = .28; Help Scale), the 2 groups were assumed as comparable in all clinical/demographic variables assessed (Table 1). Moreover, both groups did not differ significantly in horizontal line bisection (t = −1.088; P = .288) and digit can-cellation at baseline (left-sided omissions: t = 1.492, P = .15; right-sided omissions: t = 1.704, P = .103; all 2 tailed).
Functional Neglect Index
The analysis revealed a significant effect of time point [F(2, 44) = 36.67, P < .001] and a significant Time Point ×
Group interaction [F(2, 44) = 5.84, P = .006]. There was no significant effect of group [F(1, 22) = 0.86, P = .37]. Further pairwise comparisons (Figure 3) revealed significant differ-ences between all time points in the SPT group (Baseline − Posttreatment: mean difference = 5.16, P < .001; Baseline − Follow-up: mean difference = 7.00, P < .001; Posttreatment − Follow-up: mean difference = 1.83, P = .021). For the VST group, there were significant differences between base-line and posttreatment (mean difference = 2.83, P = .041) and baseline and follow-up (mean difference = 2.83, P = .010). There was no significant difference between post-treatment and follow-up (mean difference = 0.00, P = 1.00).
Unawareness and Behavioral Neglect Index
For the UBNI, the effect of time [F(2, 44) = 6.87, P = .003] and the Time × Group interaction [F(2, 44) = 6.39, P = .004] were highly significant. There was no significant effect of group [F(1, 22) = 0.25, P = .63]. Pairwise compari-sons in the SPT group revealed significant differences between the baseline and posttreatment measurement (mean
Figure 3. Results of the 2 treatments (SPT, VST) for the Functional Neglect Index and the Unawareness Behavioral Neglect Index. Asterisks indicate significant differences with P < .05, 2-tailed.Abbreviations: SPT, smooth pursuit training stimulation; VST, visual scanning training.
at Schon Klinik Verwaltung GmbH on January 13, 2014nnr.sagepub.comDownloaded from

Kerkhoff et al 7
difference = 0.37, P = .001) and between baseline and follow-up (mean difference = 0.57, P < .002) but no differ-ence between posttreatment and follow-up (mean differ-ence = 0.20, P = .174). For the VST group, all comparisons failed to reach significance: largest mean difference (Baseline − Posttreatment) = 0.06; smallest P = 1.00.
Barthel Index, Rehabilitation Phase, Help Scale
For the BI, there was a significant effect of time [F(2, 44) = 33.66, P < .001] in the ANOVA (Figure 4). Pairwise com-parisons were significant for all differences of time (Baseline − Posttreatment: mean difference = −13.95, P < .001; Baseline − Follow-up: mean difference = −21.87, P < .001; Posttreatment − Follow-up: mean difference = −7.91, P = .002). The effect of group [F(1, 22) = 0.46, P = .83] and the Time Point × Group interaction [F(2, 44) = 1.89, P = .16] were not significant.
Table 1 shows the rehabilitation phases of all patients over the 3 time points of measurements descriptively. Six SPT patients improved in their rehabilitation phase (3 dur-ing, 3 after SPT), whereas 4 VST patient improved (3 dur-ing, 1 after VST). Friedman tests revealed significant effects of time [χ2(2) = 9.58, P = .008] for the SPT group as well as for the VST group [χ2(2) = 6.50, P = .039]. For the SPT
group, pairwise comparisons (Wilcoxon tests) revealed sig-nificant differences between baseline and follow-up (Z = 2.33, P = .020) and posttreatment and follow-up (Z = 2.00, P = .046). The comparison baseline-posttreatment failed to reach statistical significance (Z = 1.73, P = .083). For the VST group, only the comparison between baseline and fol-low-up was significant (Z = 2.00, P = .046). The remaining comparisons were not significant: Baseline − Posttreatment, Z =1.73, P = .083; Posttreatment − Follow-up, Z = 1.00, P = .317. Pairwise comparisons (Mann-Whitney U tests) between both treatment groups were not significant for any time point (all P >.55).
For the Help Scale, the effect of time point [F(2, 44) = 30.05, P < .001] was significant. Pairwise comparisons revealed significant effects between all time points (Baseline − Posttreatment: mean difference = 0.74, P < .001; Baseline − Follow-up: mean difference = 1.01, P < .001; Posttreatment − Follow-up: mean difference = 0.27, P = .004). There was no significant effect of group [F(2, 44) = 0.81, P = .45] and no Time Point × Group interaction [F(2, 44) = 0.81, P = .45].
Discussion
SPT induced significantly greater improvements in the FNI and UBNI than VST. These improvements continued—albeit to a smaller extent—selectively in the SPT group in the posttreatment period, whereas no such effect was observed after VST. Functionally, the progress observed after SPT mainly reflects improvements in finding and grasping objects in the neglected near space, finding more pictures in near space, and improving the perception of the subjective midline (haptically and visually). It is important to note that the ipsilesional gaze deviation, which is so typi-cal and disabling in acute neglect patients, normalized sig-nificantly after both treatments, paralleling recent findings after prism treatment in early neglect.12 These findings in functional neglect tasks were paralleled in significantly greater improvements of the SPT group in the UBNI. Put differently, unawareness and behavioral neglect—as rated by caregivers who were blinded to the treatments and who observed the patients many hours per day on the ward—improved to a significantly greater extent after SPT than VST. After both treatments, the BI and Help Index improved but without a statistical differential treatment effect (as shown by the nonsignificant interaction). However, the per-centage of improvements in the BI over the 3 assessments was hugely different: SPT patients improved by 154% dur-ing treatment and 35.7 % in the follow-up period. In con-trast, VST patients improved by 73% during treatment and by 23 % thereafter. Albeit nonsignificant, this shows that SPT induced more widespread improvements also in the BI, which might reach significance with a larger sample size. Because a patient’s progression in the rehabilitation phase depends on increases in the BI, the greater percentage of patients improving in their rehab phase during or after SPT
Figure 4. Results of the 2 treatments (SPT, VST) in the Barthel Index and the Help Scale.Abbreviations: SPT, smooth pursuit training stimulation; VST, visual scanning training.
at Schon Klinik Verwaltung GmbH on January 13, 2014nnr.sagepub.comDownloaded from

8 Neurorehabilitation and Neural Repair XX(X)
versus VST (50% vs 33.3%) is encouraging because it shows that SPT accelerates functional recovery from neglect more than conventional VST. It is important to note that the improvements achieved in both groups proved to be stable at follow-up.
SPT as neglect therapy probably relies on the reactiva-tion of a cortico-subcortical network related to optokinetic stimulation with smooth pursuit eye movements.22 This modulates and finally reduces neglect in multiple ways: first, it provides sensory information necessary to compute egocentric spatial information required for accurate behav-ior in space.9 Many of the concerned brain regions are involved in gaze and attention shifts (occipitotemporal, parietal, insular, occipital cortex, basal ganglia, cerebel-lum, and brain stem; see details in Kerkhoff et al22), which were explicit features of our SPT therapy. Additionally, SPT may activate the vestibulo-ocular system via optoki-netic nystagmus. By this mechanism, SPT may correct the pathological, ipsilesional bias in functional visual neglect tasks, enabling the detection of more targets in the tray or animal picture task, and induce a more symmetrical gaze orientation. Second, SPT facilitates multimodal attention shifts to the neglected side.38 Interestingly, the frontopari-etal attention network, which is believed to be involved in neglect, contains a modality-independent priority map,39 which may be responsible for this multimodal efficacy of SPT. Third, the dynamic features inherent in moving dis-plays that elicit smooth pursuit eye movements40 may increase perceptual saliency of contralesional targets, and the multiplicity of brain regions involved in visual motion processing41 may further enhance this superior effect as opposed to the static patterns viewed during VST. It is important to note that the superior effect of SPT was not limited to test scores but was also found for behavioral neglect as rated in relevant ADLs. Fourth, and the most
interesting, this is the first study showing that unawareness can be significantly reduced by systematic neglect therapy. This may be also the explanation for the continued improve-ments after the end of SPT as opposed to VST. Our present findings support empirically the hypothesis put forward by Bottini et al20 according to which some neglect therapies might also effectively reduce unawareness. Finally, we found that both neglect therapies are feasible as “bedside” treatments early after stroke, albeit with a hugely differen-tial efficacy. This holds true for some other neglect treat-ments as well (ie, visuomotor feedback training)33,34 but may be more variable for others (ie, prism adaptation: neg-ative35 and positive12 results). Early neglect therapy may speed up functional recovery and benefit from processes of brain reorganization occurring during this early phase after stroke.
Our study has limitations: First, it might be argued that improvements over the 3 time points of measurement reflect spontaneous recovery because our study lacks a second baseline. The significantly greater improvements in the FNI and UBNI observed after SPT versus VST argue against this. Moreover, more patients in the SPT than in the VST group showed further improvements in the follow-up period [3 vs 1 patient(s)], although this missed significance. Second, although some patients in the SPT group made quicker progress in their BI and rehabilitation status, both interaction effects were nonsignificant. If this trend can be replicated in larger samples, SPT may accelerate neglect therapy, leading to earlier discharge of patients, thus saving hospital costs.
In conclusion, bedside SPT reduces functional neglect and unawareness significantly more than VST. This cor-roborates the findings of our recent RCT in a different sam-ple22 and shows that SPT effectively reduces multimodal neglect and unawareness after stroke.
Appendix
Scoring of FNI.a
Test Performance Score
Tray test, hits Omissions in the left segment = Omissions middle = Omissions right/No omissions 0 Only omissions on the left segment, no omissions in the middle or right segment 1 Omissions left > Omissions right and no omissions on the right segment 2 Omissions in each segment and a clear left to right gradient (left ≥ middle > right omissions) 3Tray test,
search time (ST)
ST left-sided items = ST middle = ST right (±10% tolerance range) 0ST left > ST middle > ST right 1ST left > ST middle = ST right (±10% tolerance range); 2ST > 90 s 3
Animal picture search, hits
Omissions left = Omissions right/No omissions 0Omissions left − Omissions right = 1 1Omissions left − Omissions right > 1 2Omission of all left-sided targets 3
(continued)
at Schon Klinik Verwaltung GmbH on January 13, 2014nnr.sagepub.comDownloaded from

Kerkhoff et al 9
Test Performance Score
Animal picture search, search time (ST)
ST left = Right (±10%) 0ST left > right (up to 50%) 1ST left > right (more than 50%) 2ST left > 100 s 3
Haptic horizontal rod bisection
Right-sided deviation < 5 cm 0Right-sided deviation 5-10 cm 1Right-sided deviation 10-30 cm 2Right-sided deviation >30 cm 3
Visual horizontal rod bisection
Right-sided deviation <5 cm 0Right-sided deviation 5-10 cm 1Right-sided deviation 10-30 cm 2Right-sided deviation >30 cm 3
Ipsilesional head and gaze deviation (see De Renzi et al31)
Normal head and gaze deviation 0Orientation predominantly normal but preferably deviated toward the right hemispace 1Orientation predominantly to the right hemispace 2Head and gaze completely oriented to the right hemispace 3
aMaximum score = 21.
Appendix (continued)
Tray test. Targets version A: candle light, pen, blue spoon, letter file, red sponge, battery, chewing gum, matches, tesa film. Targets version B: button, tempos, adhesive, sweets, slide, pencil, yellow spoon, lipstick, yellow sponge. In version B, the tray was rotated 180°. Targets from version A served as distractors in version B and vice versa.
Animal picture search. Targets version A, left side: deer, kangaroo, zebra, cat, pig; right side: elephant, lion, cow, rabbit, greyhound. Targets version B: left side: elephant, horse, cow, sheep, bear; right side: pig, monkey, kangaroo, rhinoceros, rabbit.
Unawareness and Behavioral Neglect Index item list 1. The patient’s left arm is displaced, 2. The patient’s left leg is displaced. 3. The patient expresses hate toward his paretic (left) side (misoplegia). 4. The patient per-severes in daily activities. 5. The patient attributes his paresis to an external cause (denial). 6. The patient shows inconsistencies between acting and talking about actions with his left limbs. 7. The patient does not shave/comb his left body side. 8. The patient does not find his room on the ward. 9. The patient does not find his personal belongings in his room. 10. The patient searches for food on the wrong (right) side.
Help Index. Item List: 1. Correct arm placing, 2. Correct leg placing. 3. Dressing. 4. Shaving/combing. 5. Orienting in the rehabilitation ward. 6. Orienting in the patient’s room. 7. Eating. 8. Putting on glasses. 9. Finding persons or objects in the room. 10. Transfers from bed to chair and back. Caregivers rated on a 5-point rating scale to which extent the patient required help in the abovementioned activities (1: no
help needed; 2: verbal instruction sufficient for patient to solve the task; 3: little practical help neces-sary by staff to solve the task; 4: medium help neces-sary by nurse; 5: patient is completely relying on external help by the nurse to solve the task).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, author-ship, and/or publication of this article.
References
1. Husain M. Hemispatial neglect. In: Goldenberg G, Miller BV, eds. Handbook of Clinical Neurology. Amsterdam, Netherlands: Elsevier B V; 2008:359-372.
2. Rengachary J, He BJ, Shulman GL, Corbetta M. A behavioral analysis of spatial neglect and its recovery after stroke. Front Hum Neurosci. 2011;5:29.
3. Gialanella B, Monguzzi V, Santoro R, Rocchi S. Functional recovery after hemiplegia in patients with neglect: the reha-bilitative role of anosognosia. Stroke. 2005;36:2687-2690.
4. Jehkonen M, Laihosalo M, Kettunen J. Anosognosia after stroke: assessment, occurrence, subtypes and impact on functional out-come reviewed. Acta Neurol Scand. 2006;114:293-306.
5. Paolucci S, Antonucci G, Guariglia C, Magnotti L, Pizzamiglio L, Zoccolotti P. Facilitatory effect of neglect rehabilitation on the recovery of left hemiplegic stroke patients: a cross-over study. J Neurol. 1996;243:308-314.
6. Jehkonen M, Laihosalo M, Kettunen JE. Impact of neglect on functional outcome after stroke: a review of methodological
at Schon Klinik Verwaltung GmbH on January 13, 2014nnr.sagepub.comDownloaded from
10 Neurorehabilitation and Neural Repair XX(X)
issues and recent research findings. Restor Neurol Neurosci. 2006;24:209-215.
7. Kalra L, Perez I, Gupta S, Wittink M. The influence of visual neglect on stroke rehabilitation. Stroke. 1997;28:1386-1391.
8. Katz N, Hartman-Maeir A, Ring H, Soroker N. Functional disability and rehabilitation outcome in right hemisphere damaged patients with and without unilateral spatial neglect. Arch Phys Med Rehabil. 1999;80:379-384.
9. Kerkhoff G, Schenk T. Rehabilitation of neglect: an update. Neuropsychologia. 2012;6:1072-1079.
10. Lincoln NB, Bowen A. The need for randomised treat-ment studies in neglect research. Restor Neurol Neurosci. 2006;24:401-408.
11. Langhorne P, Bernhardt J, Kwakkel G. Stroke rehabilitation. Lancet. 2011;377:1693-1702.
12. Gossmann A, Kastrup A, Kerkhoff G, Herrero CL, Hildebrandt H. Prism adaptation improves ego-centered but not allocentric neglect in early rehabilitation patients. Neurorehabil Neural Repair, 27, 534-541.
13. Fruhmann-Berger M, Karnath HO. Spontaneous eye and head position in patients with spatial neglect. J Neurol. 2005;252:1194-1200.
14. Jehkonen M, Ahonen JP, Dastidar P, Laippala P, Vilkki J. Unawareness of deficits after right hemisphere stroke: double-dissociations of anosognosias. Acta Neurol Scand. 2000;102: 378-384.
15. Bowen A, Lincoln NB. Rehabilitation for spatial neglect improves test performance but not disability. Stroke. 2007;38:2869-2870.
16. Cazzoli D, Muri RM, Schumacher R, et al. Theta burst stimu-lation reduces disability during the activities of daily living in spatial neglect. Brain. 2012;135:3426-3429.
17. Jenkinson PM, Preston C, Ellis SJ. Unawareness after stroke: a review and practical guide to understanding, assess-ing, and managing anosognosia for hemiplegia. J Clin Exp Neuropsychol. 2011;33:1079-1093.
18. Rode G, Charles N, Perenin M-T, Vighetto A, Trillet M, Aimard G. Partial remission of hemiplegia and somatopara-phrenia through vestibular stimulation in a case of unilateral neglect. Cortex. 1992;28:203-208.
19. Schmidt L, Utz KS, Depper L, et al. Now you feel both: gal-vanic vestibular stimulation induces lasting improvements in the rehabilitation of chronic tactile extinction. Front Hum Neurosci. 2013;7:90.
20. Bottini G, Paulesu E, Gandola MPL, Invernicci P, Berti A. Anosognosia for hemiplegia and models of motor control: insights from lesional data. In: Prigatano GP, ed. The Study of Anosognosia. New York, NY: Oxford University Press; 2010:17-38.
21. Kerkhoff G, Keller I, Artinger F, et al. Recovery from audi-tory and visual neglect after optokinetic stimulation with pursuit eye movements: transient modulation and enduring treatment effects. Neuropsychologia. 2012;50:1164-1177.
22. Kerkhoff G, Reinhart S, Ziegler W, Artinger F, Marquardt C, Keller I. Smooth pursuit eye movement training promotes recovery from auditory and visual neglect: a randomized con-trolled study. Neurorehabil Neural Repair. 2013;27:789-798.
23. Keller I, Lefin-Rank G, Losch J, Kerkhoff G. Combination of pursuit eye movement training with prism adaptation and arm
movements in neglect therapy: a pilot study. Neurorehabil Neural Repair. 2009;23:58-66.
24. Schröder A, Wist ER, Hömberg V. TENS and optokinetic stimulation in neglect theapy after cerebrovascular acci-dent: a randomized controlled study. Eur J Neurol. 2008;15: 922-927.
25. Robertson IH. Cognitive rehabilitation: attention and neglect. Trends Cogn Sci. 1999;3:385-393.
26. Pizzamiglio L, Antonucci G, Judica A, Montenero P, Razzano C, Zoccolotti P. Cognitive rehabilitation of the hemineglect disorder in chronic patients with unilateral right brain dam-age. J Clin Exp Neuropsychol. 1992;14:901-923.
27. Kerkhoff G. Rehabilitation of visuospatial cognition and visual exploration in neglect: a cross-over study. Restor Neurol Neurosci. 1998;12:27-40.
28. Schindler I, Kerkhoff G, Karnath H-O, Keller I, Goldenberg G. Neck muscle vibration induces lasting recovery in spatial neglect. J Neurol Neurosurg Psychiatry. 2002;73:412-419.
29. Rizzo M, Robin DA. Visual search in hemineglect: what stirs idle eyes. Clin Vis Sci. 1992;7:39-52.
30. Azouvi P, Olivier S, de Montety G, Samuel C, Louis-Dreyfus A, Tesio L. Behavioral assessment of unilateral neglect: study of the psychometric properties of the Catherine Bergego Scale. Arch Phys Med Rehabil. 2003;84:51-57.
31. De Renzi E, Colombo A, Faglioni P, Gibertoni M. Conjugate gaze paresis in stroke patients with unilateral damage: an unexpected instance of hemispheric asymmetry. Arch Neurol. 1982;39:482-486.
32. Mahoney FI, Barthel DW. Functional evaluation: the Barthel index. Md State Med J. 1965;14:61-65.
33. Harvey M, Hood B, North A, Robertson IH. The effects of visuomotor feedback training on the recovery of hemispatial neglect symptoms: assessment of a 2-week and follow-up intervention. Neuropsychologia. 2003;41:886-893.
34. Harvey M, Muir K, Reeves I, et al. Long term improve-ments in activities of daily living in patients with hemispatial neglect. Behav Neurol. 2010;23:237-239.
35. Turton AJ, O’Leary K, Gabb J, Woodward R, Gilchrist ID. A single blinded randomised controlled pilot trial of prism adap-tation for improving self-care in stroke patients with neglect. Neuropsychol Rehabil. 2010;20:180-196.
36. Azouvi P, Marchal F, Samuel C, et al. Functional conse-quences and awareness of unilateral neglect: study of an eval-uation scale. Neuropsychol Rehabil. 1996;6:133-150.
37. Holm S. A simple sequentially rejective multiple test proce-dure. Scand J Stat. 1979;6:65-70.
38. Mattingley JB, Bradshaw JL, Bradshaw JA. Horizontal visual motion modulates focal attention in left unilateral spatial neglect. J Neurol Neurosurg Psychiatry. 1994;57: 1228-1235.
39. Ptak R. The frontoparietal attention network of the human brain: action, salience, and a priority map of the environment. Neuroscientist. 2012;18:502-515.
40. Machner B, Dorr M, Sprenger A, et al. Impact of dynamic bottom-up features and top-down control on the visual explo-ration of moving real-world scenes in hemispatial neglect. Neuropsychologia. 2012;50:2415-2425.
41. Orban GA. Higher order visual processing in macaque extrastriate cortex. Physiol Rev. 2008;88:59-89.
at Schon Klinik Verwaltung GmbH on January 13, 2014nnr.sagepub.comDownloaded from
Top Related
Copyright © 2022 FDOKUMEN

