







Bahasa
Halaman
Hukum


DR NIGARISH FATIMADEPARTMENT OF DERMATOLOGY
CIVIL HOSPITAL KARACHI

Presenting complaintRecurrent Joint pain in both hands and feet since childhood.
Multiple reddish scaly lesions on trunk and limbs for 8yrs.
Weepy ulcerated lesions on both legs for 2.5 yrs.


History of presenting complaints
Patient has recurrent episodes of joint pain in both hands and feet since childhood , associated with mild fever and swelling.

For the last 8 years patient has developed reddish lesions on shins, which started as small elevations and then coalesced to form larger lesion. He also developed similar lesions on trunk and limbs with in the period of 2-3 years. Lesions were initially asymptomatic but later on became slightly itchy with no noticeable aggravating factor. .
History of presenting complaints
History of presenting complaintHe also noticed burning sensation on face after sun exposure. Lesions on shins showed ulceration at the site of trauma . They were painless and very slow to heal. There was no associated neurosensory deficit noted in lower legs.
F0r these complaints he had received treatments from different hospitals but there was no improvement, so he was referred to civil hospital karachi .
Systemic reviewSystemic reviewCNS: loss of vision since the age of 12 years. No h/o syncope, seizures, motor or sensory loss. Memory intact.
Endocrine system:Enlargement of both breasts and absence of hair in beard, axillary and pubic areas .No known thyroid problem no diabetes.
GIT: Loss of appetite, no vomiting, abdominal pain, or diarrhea. No polydipsia.
Respiratory system: Breathlessness and cough, No sputum or hemoptysis.

Systemic reviewSystemic reviewLocomotor system: Restricted movement of finger joints of both hands.
Urinary system: No h/o ,polyuria ,dysuria, frequency or flank pain.
CVS: No palpitation, orthopnoea or chest pain.

Past HistoryPast HistoryMedical: Loss of vision due to Medical: Loss of vision due to uveitis and glaucoma.uveitis and glaucoma.
No history of mumpsNo history of blood transfusion.
Surgical : eye operations for Surgical : eye operations for glaucoma (trabeculectomy).glaucoma (trabeculectomy).

Personal historyPersonal historyAppetite Appetite : Decreased. : Decreased. Sleep Sleep : Decreased. : Decreased.
Micturition : Normal.Micturition : Normal.
Bowel HabitsBowel Habits : Normal. : Normal.
Addiction Addiction : 12yrs h/o : 12yrs h/o tobacco chewing andtobacco chewing and 2 years h/o Naswar2 years h/o Naswar
No history of sexual contact or travelling.No history of sexual contact or travelling.

Drug historyDrug historyPt is on treatment of depression since 2011 and takingBromazepam 3mgDoxipram hydrochloride 25mg.
Tab Diamox for glaucoma at the age of 10 yrs
(for 2 yrs)

Family historyFamily history
1 brother and 2 sisters all alive and healthy.
Mother died of diabetes and renal failure.
Father died of heart attack .
Socioeconomic HistorySocioeconomic History
He belongs to a lower middle class family.

General physical examination
My patient is a blind middle aged man of average height and weight, well oriented with time, space and person.
VITALS:Pulse :76 beats/ minBP : 120/85 mm of HgR/R : 16 breaths/minTemp : afebrile

General physical examinationGeneral physical examinationAnemia Anemia : : -veJaundice Jaundice : : -veJVP JVP : N/R Clubbing Clubbing : : ++veCyanosis Cyanosis : : -vePedal EdemaPedal Edema : : -veDehydration Dehydration : : -veKoilonychia Koilonychia : : -veThyroid Thyroid : : -ve Lymph Nodes Lymph Nodes : : PalpablePalpable

Apical axillary nodes of right side palpable.
The nodes were about 1 to 2 cm in size, firm in consistency, non tender, not fixed to underlying structures or overlying skin.
Lymph node examination

Systemic examination Abdominal ExaminationNormal in shape.
No tenderness on superficial palpation.
Liver not palpable, span is 8 cm.
Spleen not palpable.
No shifting dullness present.
Gut sounds audible.

Systemic examination Cardiovascular System
Apex beat palpable in 5 th IC space, 6cm from midsternal line.
No parasternal heave.
S1 & S2 audible in all four areas. No added sound heard.

Neurological Examination
GCS : 15/15
Cranial nerves : Intact (except optic oculomotor, abducent)Motor system : Intact
Sensory system : Intact
Cerebellar system : Intact
Sign of meningeal irritation : Absent
Systemic examination
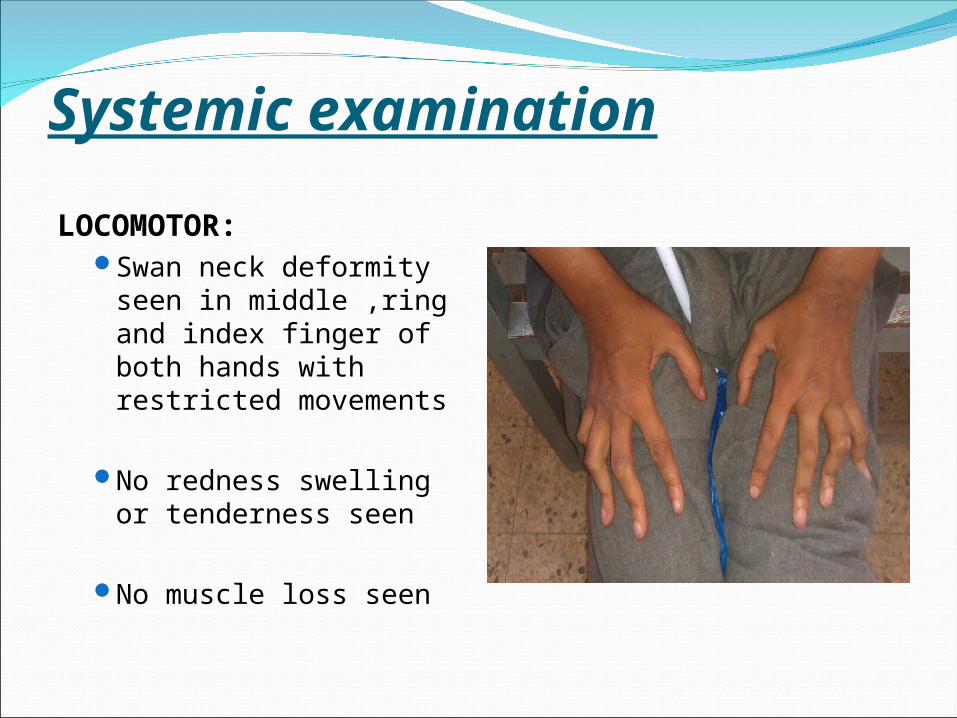
Systemic examinationLOCOMOTOR:
Swan neck deformity seen in middle ,ring and index finger of both hands with restricted movements
No redness swelling or tenderness seen
No muscle loss seen
Systemic examinationRESPIRATORY SYSTEMINSPECTION: Reduced chest movement bilaterally. No obvious deformity seen
PALPATION; Trachea central and apex beat palpable in 5th inter costal space. Decreased chest expansion
PERCUSSION: Liver dullness starting from right 5th InterCostal space. Resonant note all over chest.
AUSCULTATION: Harsh vesicular breathing with prolonged expiration. Vocal resonance normal bilaterally. Occasional rhonchi & end inspiratory crepitations present in the middle & lower zones.

Secondary sexual characteristics
Genitals normal.
Testes normally placed.
Absence of hair in pubic, axillary and beard areas.
Gynaecomastia.


Cutaneous examinationMultiple non tender , scaly, erythematous infiltrated plaques of variable size and shapes present on trunk and limbs.
Margins well defined and central clearing seen in few plaques.
Nerves around the plaques were not palpable.
Redness and mild scaling over nose and cheeks.

Cutaneous examinationMultiple ulcerated lesions of about 2-5 cm present on anterior and medial side of both legs.
Edges undermined with some granulation tissue seen at the base.
Some healed ulcer with atrophy and scarring.

Cutaneous examinationSwelling of both breast with no nipple discharge.
Breast non tender and few erythematous plaques present on both breasts.

Case summaryCase summary39 year old blind male , came with the recurrent joint pain of both hands and feet since childhood, multiple reddish, non tender, slightly itchy plaques with fine scaling on trunk and limbs for last 8 yrs. Ulcerated lesion on both legs for last 2 yrs.
On examination patient was dyspneic and there was clubbing, right axillary lymphadenopathy, gynaecomastia. Absent hair growth in beard, axillary and pubic areas. Decreased chest expansion and harsh vesicular breathing and occasional fine bilateral crepts especially on right side. Swan neck deformity with restricted movement in lateral three fingers of both hands. Rest of the examinations were in normal limits.
Differential Diagnosis•

Differential diagnosisConnective tissue disorder
Tuberculosis
Sarcoidosis
Leprosy
Mycosis Fungoides
Tertiary Syphilis
Atypical mycobacterial infection
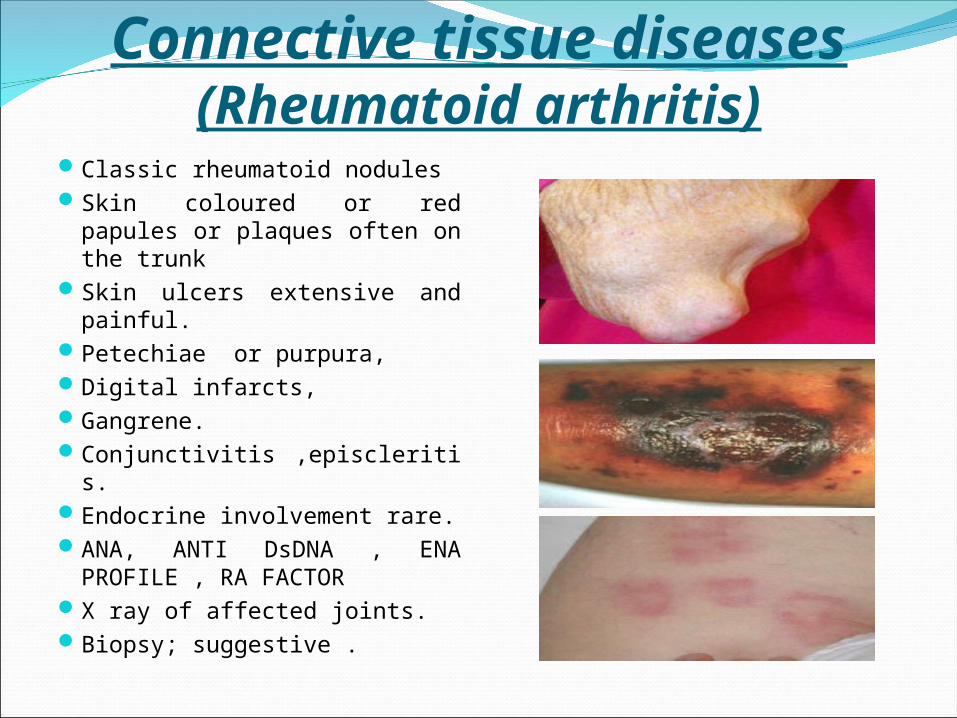
Connective tissue diseases(Rheumatoid arthritis)
Classic rheumatoid nodules Skin coloured or red papules or plaques often on the trunk
Skin ulcers extensive and painful.
Petechiae or purpura,Digital infarcts,Gangrene.Conjunctivitis ,episcleritis.
Endocrine involvement rare.ANA, ANTI DsDNA , ENA PROFILE , RA FACTOR
X ray of affected joints.Biopsy; suggestive .

Cutaneous tuberculosisNon itchy reddish-brown, flat infiltrated nodule or plaque of soft gelatinous consistency .
Lesion shows slow peripheral extension with areas of atrophy.
Multi system involvement is rare.
Diagnosed by smear and culture.
Biopsy is diagnostic (caseating granulomas are seen).

LeprosyMulti system diorder involves skin, peripheral nerves and mucous membranes.
Dry anesthetic and hair less patch.
Thickened sensory nerve can be felt in the vicinity.
Thickening of peripheral nerves with sensory and motor loss.
Deformities are typically associated.
Slit-skin smear shows acid-fast bacilli (AFB).

SarcoidosisMulti system disorder.
Most commonly lungs ,eye and skin are involved
Can usually present with papule ,nodule or plaque.
Investigations; Chest X ray, ACE level, S. calcium ,gallium scan.
Biopsy is diagnostic.

Tertiary SyphilisMulti system disorder in tertiary stage .
Nodules consist of granulomatous rubbery tissue with a necrotic centre.
Chronic skin ulceration, gummas and nodular infiltration.
Cardiovascular and CNS involvement
(murmur of aortic regurgitation).
Charcot joint(severe osteoarthritis with loss of pain).
Diagnosis-VDRL/TPHA and biopsy

Mycosis fugoides(Cutaneous T-cell lymphoma )
Cutaneous T-cell lymphoma Well demarcated and raised.
characteristic pattern is of horse shoe shaped.
Annular, angulated and serpiginous
Categorized as patch ,plaque and tumor stage
Multisystem involvement unlikely.
Biopsy confirms the diagnosis


InvestigationsInvestigationsCOMPLETE BLOOD COUNT: HAEMOGLOBIN : 12.2gm% HAEMATOCRIT : 37 % R.B.C : 4.0 ml/ul M.C.V : 74 FL M.C.H : 30.0 PG M.C.H.C : 33.10% W.B.C : 11.5 /ul NEUTROPHILS : 78% LYMPHOCYTES : 10% EOSINOPHILS : 03% MONOCYTES : 7.6% BASOPHILIS : 0.4% PLATELETS : 1,42,000 U/L ESR : 32 mm/hr PERIPHERAL FILM Showed no atypical cells

InvestigationsRBS : 74 mg%
BUN : 10.0 mg%
CREATININE : 0.7 mg%
SODIUM : 139 Meq/l
POTASSIUM : 4.4Meq/l
CHLORIDE : 97 Meq/l

Liver function testBILIRUBIN TOTAL : 0.55 mg%
BILIRUBIN DIRECT : 0.4 mg%
SGPT : 11.0 U/L
ALK. PHOSPHATASE : 82 U/L
S.ALBUMIN : 4.3g/dl

Coagulation profilePT : 9.9 seconds (control:10.5 secs)
APTT : 25 seconds(control:26 secs)
INR : 0.94

InvestigationsHBsAg : NON-REACTIVE
ANTI-HCV : NON-REACTIVE

Urine DRSP GRAVITY : 1.025PH : 6.0PROTEINS : -VEGLUCOSE : NEGATIVEHB : NEGATIVERBC : 1-2/HPFWBC : NEGATIVEPUS CELLS : 1-2/HPFEPITHELIAL CELLS : NILGRANULAR CAST : NILAMORPHOUS URATES : -VE
Electrocardiogram Normal ECG with no ischemic changes.

Chest X ray (P/A view)
Bilateral hilar prominence and reticular shadows

X ray hand A/P viewGeneralized bone density reduced.
Reduced joint space and ankylosing at proximal inter phalangeal joints with flexion of middle phalanx and extension of distal phalanx bilaterally, more marked in 4th and 5th digits.

InvestigationsANA : -VE
ANTI Ds DNA : -VE
ENA PROFILE : -VE

RA FACTOR : -VE
ANTI CCP : <7 (<17)
URIC ACID : 4 mg % (upto 7 )
Investigations

InvestigationsVDRL : Non reactive
TPHA : Non reactive
HIV : Non reactive
Investigations Slit skin smear for leprosy : -VE
MT : O mm induration

Hormonal profileT3 :88.0 ng/dl (80-200)
T4 :9.48 ug/dl (4.5-12.5)
TSH :0.93 micro IU/dl (0.5-4.7)
FSH :34.5mIU/ml (0.7-11.1 )
LH :16.9 mIU/ml (0.8-7.6 )
TESTOSTERONE :3.7 ng/dl (249-836) ( for 20- 49yrs)
PROLACTIN :15.9 ng/dl ( 2.o-18 )
Ultra sound Whole Abdomen
Liver normal in size measuring 15.5cm with smooth margins.
Normal size of spleen measuring 10.2cmBoth kidneys were of normal size, Rt kidney is of 9.8cm and Lt kidney of 9.2 cm
IMPRESSION: Normal scan
Ultrasound ScrotumBoth testis normal in size ,shape and position with coarse echotexture.
Right testis measures 1.6x2.2 cm.Left testis measures 1.2x2.5 cm.No cyst ,hydrocele or varicocele seen

Investigations
S. CALCIUM : 9.3 mg/dl(8.5-10.2)
ACE LEVEL : 140U/L(up to 52)

InvestigationsPulmonary function test
InterpretationModerate to severe restrictive pattern
Patient Predicted %Predicted
FVC 1.72 3.17 54%
FEV1 1.69 2.78 61%
FEV1% 98.3 83.2 118%

HRCT
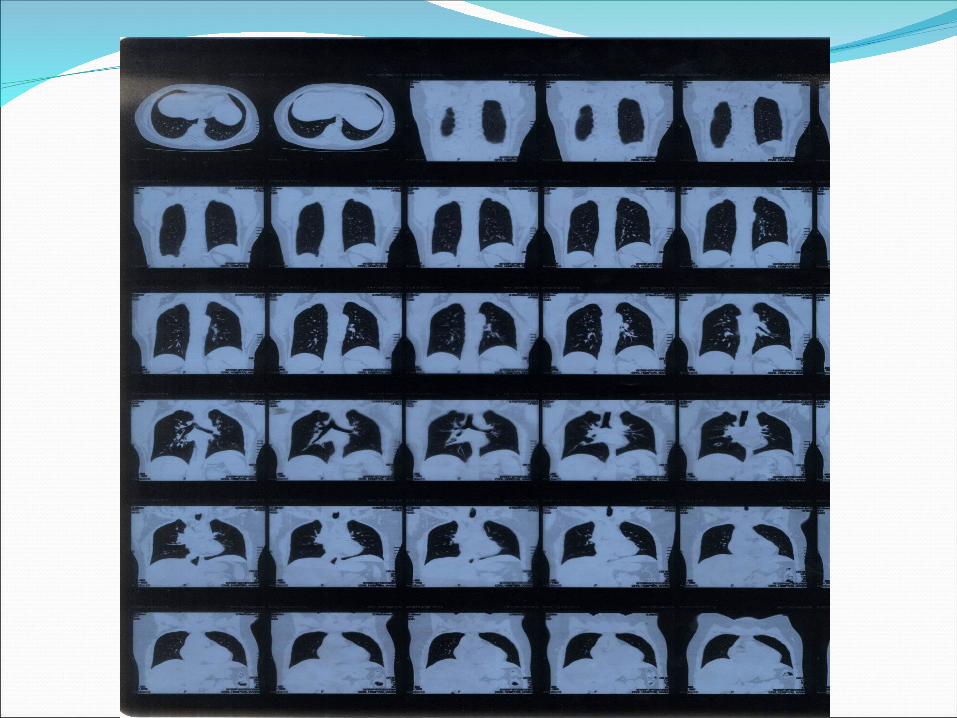

High Resolution Computed Tomography(HRCT)CONCLUSION:
Bilateral focal lower lobe brochiectasis.
Mediastinal and Right Axillary lymphadenopathy.

CT Scan Brain
Normal scan of brain

Investigations
BronchoscopyTesticular biopsy
Patient refused for these procedures.

What Next


Investigations
BIOPSY (skin lesion)
AFB smear -veAFB culture -ve
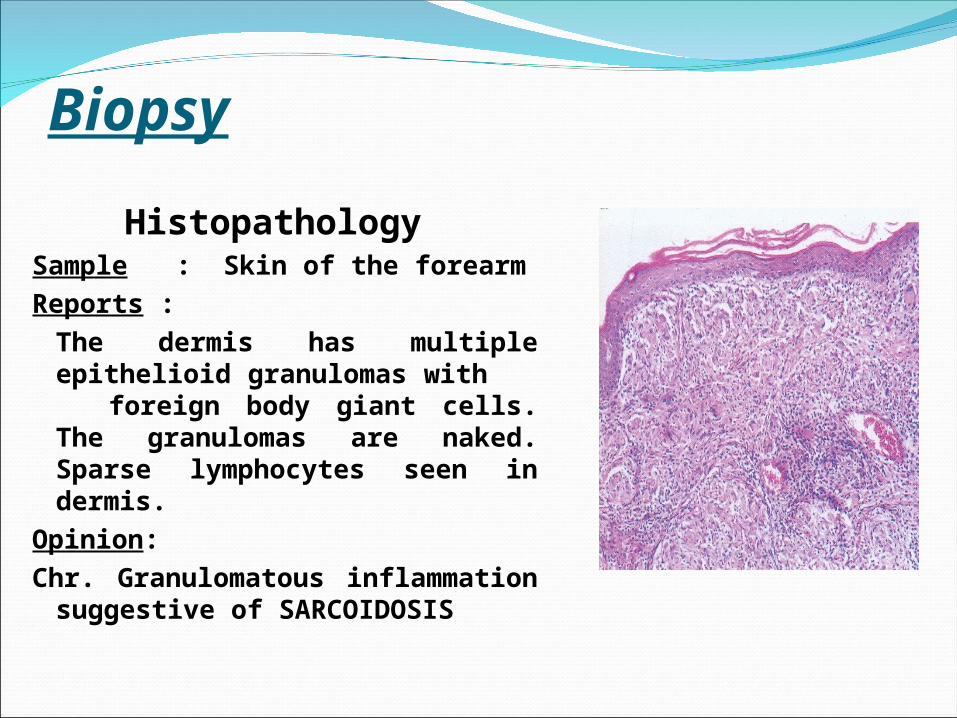
Biopsy HistopathologySample : Skin of the forearmReports : The dermis has multiple epithelioid granulomas with foreign body giant cells. The granulomas are naked. Sparse lymphocytes seen in dermis.
Opinion: Chr. Granulomatous inflammation suggestive of SARCOIDOSIS

Histological differentialsTuberculosisCaseation necrosis Langhan giant cell
Tuberculoid Leprosy Epitheloid cell granuloma around dermal nerves
Granuloma annulareNecrobiosis of ConnectiveTissue,
wall of pallisading histiocytes ,
Multinuleated giant cells.

Final diagnosisFinal diagnosis
SARCOIDOSIS WITH MULTISYSTEM INVOLVEMENT
(Ocular, Respiratory ,Musculoskeletal and Endocrine involvement)

Treatment givenTab. Prednisolone 5mg (initially) 4+2+0
On followup dose increased to 8+4+0
Cap Omeprazole 20 mg 1+0+1
Tab Azathioprine 50 mg 1+0+1
Potent steroid ointment LA Twice daily

Treatment ResponseBeforeBefore AfterAfter

Treatment ResponseBeforeBefore AfterAfter


SarcoidosisSarcoidosis is now most common of the fibrotic lung disorders. Other commonly affected organs include ,
Skin Eye Liver HeartNervous system Musculoskeletal Endocrine system

Types of cutaneous Sarcoidosis
PAPULAR ANNULAR LUPUS PERNIO
PLAQUE ERYTHEMA NODOSUM SCAR SARCOID

Ocular symptomsAny part of the eye can be involved:
granulomatous uveitis: most common, results in blurred vision, watery eyes and photophobia
iris nodulesretinochoroiditisconjunctivitislacrimal gland involvementoptic nervesproptosis Cataracts, glaucoma, and blindness can result.

Anterior uveitis often manifests as the initial presentation of sarcoidosis.
CASE REPORTS: Two patients came in for routine eye examinations, with no symptoms of
anterior uveitis. The first, a 36-year-old man, had a bilateral granulomatous anterior uveitis.
The uveitis was treated with topical corticosteroids, with no complications. The second case involved a 44-year-old woman with chronic, recurrent,
bilateral, non-granulomatous anterior uveitis. Despite treatment with topical and oral corticosteroids. the patient had a prolonged course with recurrent episodes leading to secondary sequelae, including glaucoma and cataract .Later on both patients developed skin lesions and were co-managed with internal medicine, and in each case, systemic workups were consistent with sarcoidosis.
CONCLUSION: Anterior uveitis often manifests as the initial presentation of sarcoidosis.
Without acute symptoms, the detection and diagnosis may be delayed, leading to visual deterioration. The diagnosis of sarcoidosis may be difficult, owing to the lack of definitive diagnostic criteria and a variety of presentations. Histologic confirmation may not always be possible or practical. However, a range of serological and radiological tests, when combined with physical and ophthalmic evaluation, can lead to the presumed diagnosis of sarcoidosis. Aggressive treatment is imperative in order to prevent permanent structural damage to the eye resulting from this idiopathic inflammation.

Rheumatoid like presentations in Sarcoidosis
The most common form of joint involvement is an acute poly arthritis/peri arthritis.
The arthritis may be migratory, intermittent or additive in time. Most common in bones of finger and toes.
Clinical presentations resemble reactive arthritis , rheumatoid arthritis or even spondyloarthropathies . More commonly, however, it is non migratory and accompanied by other signs of sarcoidosis
Sarcoidosis of the reproductive systemMale The frequency of genitourinary sarcoidosis in men is < 0.2% in clinically diagnosed cases, and 5% in autopsy studies.
It can present as An asymptomatic mass in scrotum Acute epididymo-orchitis Primary testicular failure Low testosterone Oligospermia and infertility
Fibrosis and occlusion of the ductus epididymis seen in this disease cause oligospermia and infertility. Leydig cell dysfunction may alter secondary sexual characteristics.
Glucocorticoids are effective in reducing sarcoid-testicular mass and improving gonadal function.

Take home message
Skin and other systemic involvement leads to a diverse range of presentation , clinician must remain vigilant of unusual manifestations of sarcoidosis so that treatment specific to sarcoidosis can be tailored for maximal benefit.

Copyright © 2022 FDOKUMEN

