







Bahasa
Halaman
Hukum


2/26/2014
1
Preventing Unnecessary Hospital Readmissions
Wednesday, February 26th, 2014
2
SpeakerSue Dill Calloway RN, Esq.
CPHRM, CCMSCP
AD, BA, BSN, MSN, JD
President of Patient Safety and Education
Board Member Emergency Medicine Patient Safety Foundation www.empsf.org
614 791-1468
22

2/26/2014
2
3
1. Explain measures a hospital can take to reduce unnecessary readmissions
2. Describe the financial penalties associated with readmissions
Learning Objectives
Hospitals Penalized for Excess Readmissions
First year started October 2012 and Medicare penalized 2,217 hospitals for excess readmission rates
Hospitals forfeited $280 million dollars in the first year which was 2 out of every 3 hospitals
2 million Medicare patients are readmitted within 30 days per year
Second year, starting with October, 2013, hospitals forfeited $217 million dollars
Still about 2 out of every 3 with 2,225 hospitals penalized
4

2/26/2014
3
Bonuses and Penalties for HospitalsMedicare has two payment incentive programs for
hospitals
Medicare cut payments by 1% and this money was set aside for a bonus pool ($850 million) for those that did better than average on a number of measures
One given bonuses and penalties for how well they perform on 24 quality measures called VBP or value based purchasing
The second penalties hospitals with excess readmission rates
Hospitals could gain up to 1.25% in payment or lose as much as 3.25% for the programs combined
5
Hospitals Penalized for Excess Readmissions
6

2/26/2014
4
Chart Shows Readmission Penalty in 2014
7
www.kaiserhealthnews.org/Stories/2013/November/14/value-based-purchasing-medicare-hospitals-chart.aspx
2014 List of Hospitals
8
http://capsules.kaiserhealthnews.org/index.php/2014/01/n
ew-medicare-data-show-hospitals-with-high-rates-of-
readmissions/
2/26/2014
5
Hospital Wide All Cause Unplanned Readmits
9
ww.qualitynet.org/dcs/ContentServer?c=Page&pagename=QnetPublic%2FPage%2FQnetTier4&cid=122877250
4318
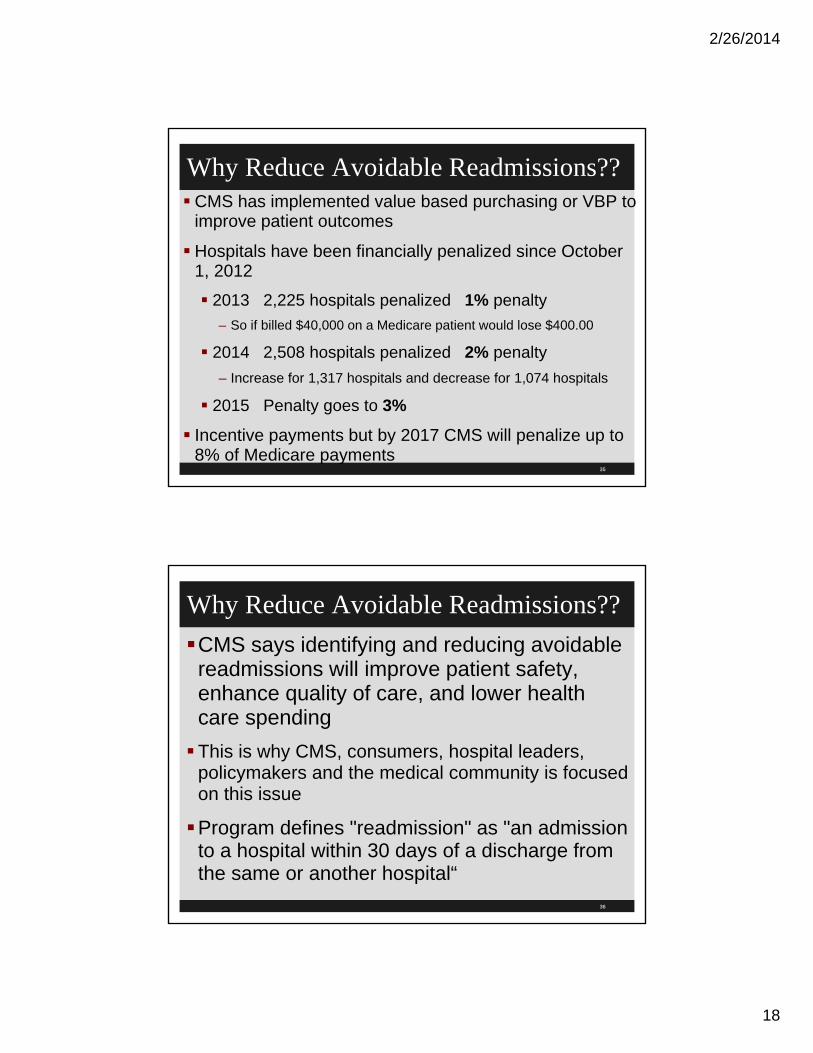
Readmission Rates All Conditions
10

2/26/2014
6
Readmission Reduction Program CMS established a policy of using the risk adjustment
methodology endorsed by the National Quality Forum (NQF) for the readmissions measures for AMI, HF and PN to calculate the excess readmission ratios
See CMS website on readmission reduction program
Also higher rates of readmission for all causes increases chance of being selected for third pilot of CMS worksheets
All cause readmission rates are important because Medicare Payment Advisory Board (MedPAC) is advising Congress to use this measure when determining financial penalties
11
12
www.qualityforum.org/Projects/NQF_All-
Cause_Readmissions_Project.aspx

2/26/2014
7
CMS Readmission Program Website
13
www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/Readmissions-
Reduction-Program.html
CMS Website Hospital Readmissions
14
www.medicare.gov/hospitalcompare/readmission-reduction-
program.html

2/26/2014
8
CMS Website Hospital Readmissions Lists the following:
Name of hospital
Provider number and state
Measure (readmission PN, AMI, HF etc.)
Number of discharges
Excess readmission rate
Predicted readmission rate
Expected readmission rate
Number of readmissions with start and end date of data
15
CMS Readmissions Reduction Program
16
www.cms.gov/Medicare/Medicare-Fee-for-Service-
Payment/AcuteInpatientPPS/Readmissions-Reduction-Program.html

2/26/2014
9
CMS Readmissions Reduction ProgramFY 2012 (starting Oct 2012) IPPS rules defined
readmission as admission within 30 days
Adopted for measures for MI, pneumonia and heart failure
Established methodology to calculate excess readmission rate compared to national average
Risk adjusted as endorsed by National Quality Forum which included patient demographic characteristics, comorbidities, and patient frailty
Used 3 years of discharge data and at least 25 cases
17
CMS Readmissions Reduction Program
FY 2013 rate based on discharges for 3 year period from July 1, 2008 to June 30, 2011
FY 2014 based on 3 years discharges from July 1, 2009 and June 2012
In expanding conditions for FY 2015 to include:
(1) patients admitted for an acute exacerbation of chronic obstructive pulmonary disease (COPD) and
(2) patients admitted for elective total hip arthroplasty (THA) and total knee arthroplasty (TKA)
18

2/26/2014
10
CMS Readmissions Reduction Program
CMS said about 1.4 million TKA and THA procedures are performed on Medicare patients per year
CMS found significant variation in readmission rates of these patients
CMS said readmission rate for COPD was 22% and ranged from 18 to 25% across 4,546 hospitals
19
Formula to Calculate Readmission Adj Factor
20

2/26/2014
11
Formula to Compute Payment Adjustment
21
Meaningful Use Stage 2 and Readmissions
Hospitals that want to get incentive money for developing electronic health records have to follow the standards for meaningful use
Stage 2 has one element that could help reduce unnecessary readmissions
This is referenced in the CMS discharge planning worksheet
Also in the revised CMS 39 pages of discharge planning standards
22

2/26/2014
12
Meaningful Use Stage 2 and Readmissions
The Eligible Professional (EP) who transitions their patient to another setting of care or provider of care or refers their patient to another provider of care should provide a summary care record for each transition of care or referral
Most hospitals send a continuity of care form or transfer form if transfer to another hospital or LTC
This one has three measures
Details available off the CMS website at http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/downloads/Stage2_EPCore_15_SummaryCare.pdf
23
24

2/26/2014
13
Discharge Planning Revisions
25
www.cms.gov/SurveyCertificationGenInfo/PMSR/list.asp#Top
OfPage
Third Revised Worksheets
26
www.cms.gov/SurveyCertificationGenInfo/PMSR/list.asp#TopOfPage

2/26/2014
14
Discharge Planning Worksheet If transferred to another inpatient facility was the
discharge summary ready and sent with patient?
The following controversial section was changed in the 3rd revision
Was discharge summary sent before first post-discharge appointment or within 7 days of discharge?
Was follow up appointment scheduled?
Now says send necessary medical record information to providers the patient was referred prior to the first post-discharge appointment or 7 days, whichever comes first
27
Discharge Planning WorksheetWas the necessary medical record information
ready at the time of transfer if patient sent to another facility
Was there any part of the discharge plan that the hospital failed to implement that resulted in a delay in discharge
Was there documentation in the medical record of results of tests pending at the time of discharge both to the patient and the post hospital provider?
Was patient readmitted within 30 days?
28

2/26/2014
15
ACGME 6 Core Areas Include Care Transitions
Accreditation Council for Graduate Medical Education has released a guidance for assessing the clinical learning environment in US teaching hospitals
Includes 6 core areas which include care transitions
Other areas include patient safety; health care quality; supervision; duty hours, fatigue management and mitigation; and professionalism
29
30
www.acgme.org/acgmeweb/Portals/0/PDFs/CLER/ACGMECLERNewsRelease.pdf

2/26/2014
16
ACA Driving Drop in Readmission Rates
After holding steady at 19% from 2007 to 2011,
The all-cause 30-day hospital readmission rate among Medicare fee-for-service beneficiaries fell to 18.5% in 2012,
It continued to fall in 2013
According to an entry posted on The CMS Blog website.
Preliminary claims data shows the Medicare readmission rate averaged less than 18% through August.
Dec 201331
32
http://blog.cms.gov/2013/12/06/new-data-shows-affordable-care-act-reforms-are-leading-to-lower-hospital-readmission-rates-for-
medicare-beneficiaries/

2/26/2014
17
49 States Reduced All Cause Readmissions
33
The only state that did not see a decrease – Utah –already had one of the
lowest readmission rates in the country
FY 2014 Hospital Readmission Program
34
2/26/2014
18
Why Reduce Avoidable Readmissions?? CMS has implemented value based purchasing or VBP to
improve patient outcomes
Hospitals have been financially penalized since October 1, 2012
2013 2,225 hospitals penalized 1% penalty
– So if billed $40,000 on a Medicare patient would lose $400.00
2014 2,508 hospitals penalized 2% penalty
– Increase for 1,317 hospitals and decrease for 1,074 hospitals
2015 Penalty goes to 3%
Incentive payments but by 2017 CMS will penalize up to 8% of Medicare payments
35
Why Reduce Avoidable Readmissions??
CMS says identifying and reducing avoidable readmissions will improve patient safety, enhance quality of care, and lower health care spending
This is why CMS, consumers, hospital leaders, policymakers and the medical community is focused on this issue
Program defines "readmission" as "an admission to a hospital within 30 days of a discharge from the same or another hospital“
36

2/26/2014
19
CMS Hospital Value Based Purchasing VBP
37
www.cms.gov/apps/media/press/factsheet.asp?Counter=3947
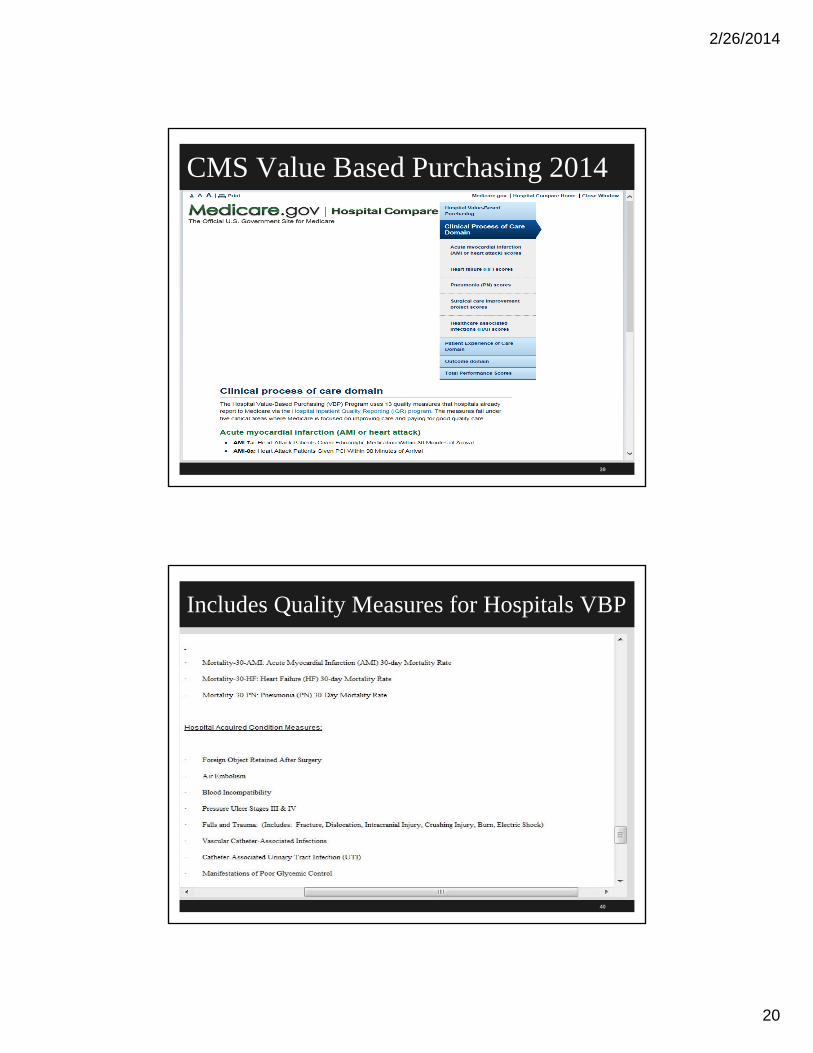
CMS Value Based Purchasing 2014
38
www.medicare.gov/hospitalcompare/data/hospital-vbp.html
2/26/2014
20
CMS Value Based Purchasing 2014
39
Includes Quality Measures for Hospitals VBP
40

2/26/2014
21
CMS Quality Measures for Hospitals VBP
41
To see final rule go to www.cms.gov/HospitalQualityInits/
NQF Readmissions Measures
42
All-cause hospital-wide readmissions measure

2/26/2014
22
NQF Readmissions Measures 1789
NQF Board endorses all-cause hospital wide readmission measure developed by Yale University and CMS
CMS agreed to defer this readmission reason in readmission reduction program until MAP recommended
MAP (Measure Application Partnership) has role to advise on best use of measures in payment and public reporting
Steering committee voted to endorse this measure within one year
43
The Cost of ReadmissionsMedicare wants to pay less to hospitals with higher
than average costs for patient care stating that readmissions cost $26 billion dollars in a decade
Part of the push to make hospitals the hub for coordinating care
Traditionally when hospitals discharged the patient they saw their job as done
But hospitals could be on the hook with what happens after discharge
CMS thinks hospitals are best able to take the lead in overseeing patient care
44

2/26/2014
23
Is This Fair?Hospitals argue that it could punish them for things
they can not control like patients who can not afford their medications
Many feel this is not a quality measure for a hospital
Evidence is mounting that the link between readmission and quality of care is more complex than assumed
Role of other factors such as patient’s demographics, socioeconomic characteristics, social support structure, and co-morbid conditions and risk adjustment is not fully understood
45
Patient Protection and Affordable Care Act
The Patient Protection and Affordable Care Act or PPACA (also abbreviated ACA) was the law that set up the financial penalties for hospitals with excessive readmissions
The new law establishes a VBP program, or value-bases purchasing, to pay hospitals for their actual performance
Included initiatives to prevent hospital readmission through a comprehensive program for hospital discharge planning
46
2/26/2014
24
Hospital Readmissions Sec 3015
Expected to save $7.1 billion over ten years
Beginning in fiscal year 2013 hospitals (started Oct 1, 2012) with higher than expected readmission rates will experience decreased Medicare payments for all Medicare discharges
Secretary of HHS must make available a program to improve their readmission rates through PSO
CAH and post-acute care providers are exempt
Performance data are based on 30 day readmission
47
Hospital Readmissions and CMS
Beginning in 2015, hospitals with certain hospital acquired conditions (HACs) will receive additional payment reductions from Medicare.
CMS will evaluate performance based on achievement and improvement on selected measures
In FY 2013 CMS will measure hospital performance using two domains;
Clinical process of care domain (12 process of care)
Patient experience (patient satisfaction or HCAHPS)
48

2/26/2014
25
AMI, HF, and Pneumonia FY 2013
49
HAI and Surgical Care Improvement
50

2/26/2014
26
Patient Experience of Care Measures
51
HCAHPS
52
www.hcahpsonline.org/home.aspx

2/26/2014
27
Sign Up for Free Newsletter
53
To view and subscribe to other e-Newsletters go to www.HealthCareeNewsletters.com
Readmission Update Newsletter TopicsSome hospitals have a RED team or a committee to
reduce unnecessary readmissions
Following the evidenced based literature for tips to help reduce the unnecessary readmission rate can help
Medicare identifies the best and worst hospitals for THA and TKA
Hospitals with more elderly and poor patients likely to face readmission penalties
Hospitals prohibit early elective C-sections54

2/26/2014
28
Readmission Update Newsletter TopicsHospital compare offers data on % of patients with
THA and TKA who were readmitted and excess readmission data
24 evidenced based practice competencies to ensure staff have knowledge and skills which can reduce complications and costs by 30%
Role of chronic conditions in readmissions
20 item tool that predicts patients with increased risk of readmissions
Called the 8P scale of the target screen of BOOST
55
56

2/26/2014
29
Readmission Update Newsletter Topics 13 most frequent primary diagnoses for
readmissions
COPD, CHF, cardiac ischemic disease, arrhythmia, CV disease, ADE, renal failure, nutritional and metabolic disorders, venous thromboembolism, liver disorders, GI disorders, infectious diseases and neoplasm
Some hospital readmissions are avoidable
Most common reason for readmission related to chronic medical conditions
Hospital reduces readmissions by 37% by using analytics to help which course of treatment is most effective
57
Readmission Update Newsletter TopicsReadmissions for Medicare patients fall for a
second year
Average avoidable readmission rate for first 8 months of 2013 was 18%
Rate had been at 19% for five years
This means 130,000 fewer readmissions
New model predicts risk for readmission from LTC
Indiana Health Information Exchange (IHIE) details its use of predictive analysis to reduce readmission rates
58

2/26/2014
30
Recent Articles in Readmission Update
Racial and economic disparities are prevalent in hospital readmission rates
Hospital readmissions for COPD highest among black patients
A shorter delay to primary PCI for STEMI patients was associated with a reduced rate of readmission
Ten proven ways to reduce readmission
www.beckershospitalreview.com/quality/10-proven-ways-to-reduce-hospital-readmissions.html
59
Ten proven Ways to Reduce Readmission
Understand which patient populations are at greatest risk of readmission
Healthcare Cost and Utilization Project suggest that Medicaid and uninsured patients are at higher risk
Target patients with limited English proficiency
Join a readmission prevention focus collaborative such as a state hospital initiative
Ensure patients schedule a seven day follow up appointment
Implement a robust home healthcare program60

2/26/2014
31
Ten proven Ways to Reduce Readmission
Clearly communicate post-discharge instructions
Install telemonitoring technology in the homes of chronically ill patients
Effectively staff nurses during patient care
Researchers found higher RN overtime staffing increased readmissions as well as ED visits
Meanwhile, higher non-overtime RN staffing was found to decrease ED visits indirectly due to improved discharge teaching quality and discharge readiness
61
Why Patients Are ReadmittedThey do not know their diagnosis and do not
understand what is wrong with them
Confused on what medications to take and when
Primary care physicians are not provided with important information about hospitalization or test results
A follow up appointment is not scheduled
Patient or family members lack proper knowledge to provide needed care
Dartmouth Institute Study 4 page document 201362

2/26/2014
32
Readmission Rates to Hospital and EDReadmission rates to hospitals within 30 days
Medical conditions national average is 16.1%
Surgical procedures national average is 12.7%
ED visit rate within 30 days
Medical conditions national average is 18.8%
Surgical procedures national average is 15.2%
14 days outpatient visit rate national average 62.5%
Dartmouth Institute study 2013 and based on 2009 data
63
64
www.dartmouthatlas.org/downloads/reports/Atlas_CAYC_092811.pdf

2/26/2014
33
Recent Articles in Readmission Update It takes a team approach to reduce readmissions
VA Hospital Readmission Rates Deal a Blow to Medicare
Home Monitoring Reduces Readmissions
Heart Failure Program Cuts Readmission Rates by 30%
Is Reducing Hospital Admissions an Answer?
Care by Hospitalist Offset by Higher Readmissions
A Look at the 7 Hospitals with Highest Rates of Readmissions
65
Recent Articles in Readmission UpdateStudy published Dec 2013 in BMJ found the
following;
Studies 11,000 adult discharges from Boston Medical Center
22.3% were readmitted within 30 days
Only 8% were potentially avoidable readmissions
Comorbidities were the most common cause of readmission and most common readmits were infection, neoplasm, heart failure, GI disorders and liver disorders
Study concluded need to have a strategy that focuses on managing chronic comorbidities and not just the primary reason for admission
66

2/26/2014
34
Post Hospital SyndromeReadmissions can be due to post hospital
syndrome
Readmissions due to stress, sleep loss, pain, discomfort, malnutrition and inactivity that occurs with hospitalization
Discharge assessments need to go beyond the cause of the initial hospitalization
Need implement interventions to eliminate sleep disturbances, minimize pain, address nutritional deficiencies and increase physical activity
NEJM January 10, 201367
68
www.nejm.org/doi/full/10.1056/NEJMp1212324

2/26/2014
35
CMS Report 2014
CMS says multiple factors contribute to hospital readmission rates
Premature discharge
Poor quality of care
Lack of education to patients before they left
Most common patients returning to the hospital were CHF, COPD, pneumonia and high blood pressure
85% of hospitals had an average readmission rate
8% of hospitals had a higher rate or 364 hospitals69
AHA Publishes Trend Reports
70
www.ahanews.com/ahanews_app/jsp/display.jsp?domain=AHANEWS&dcrpath=AHANEWS/AHANewsNowArticle/data/ann_091411_trendwatch

2/26/2014
36
Hospital Readmission RatesHospitals started reporting hospital readmission
rates voluntarily to CMS in 2009
This is on the hospital compare website at http://hospitalcompare.hhs.gov
Made so the public can review this data
Do you know what the average readmission rate is?
Do you know what your rate of readmission is?
2013 study shows that 7% of acute care hospitals had a higher than expected readmission rates or 307 out of 4,498 and 8% in 2014 data
71
Risk Adjusted 30 day readmission rates for MI, HF, and
pneumonia is risk adjusted
Beginning in FY 2013
Risk adjusted for age, gender, medical diagnosis, and selected medical history
Rate of excess readmission will be penalized
In FY 2009 the follow were the % of inpatients
2.5% of patients had a diagnosis of AMI
4.2% of patients had a diagnosis of pneumonia
5.7% has heart failure72

2/26/2014
37
73
Risk Adjusted Dual Eligible PatientsRisk adjusters proposed for use in the Hospital
Readmission Reduction Program or HRRP does not capture certain important factors
Does not capture dual eligible status where patient qualified for Medicare and Medicaid
There are 9 million patients with dual eligible status
These patients are the most chronically ill
Their healthcare costs are nearly 5 times those of other Medicare beneficiaries
74

2/26/2014
38
Risk Adjusted Dual Eligible PatientsOther challenges in risk adjustment include:
Race and ethnicity
– TJC in the patient centered communication standard requires all hospitals to collect race and ethnicity information on all patients including outpatients
Limited English Proficiency
– There are 50 million patients in the US whose primary language is not English
– Need to ensure there is an interpreter when indicated
– Also standard in the TJC Patient Centered Communication Standards
Source: AHA Trend Watch September 201175
CMS Hospital Compare Website
76
www.medicare.gov/hospitalcompare/search.html

2/26/2014
39
Rate of Readmissions MI, CHF, and Pneumonia
77
Rate of Readmissions MI, CHF, and Pneumonia
78

2/26/2014
40
Rate of Readmission for MI is 18.3% 2014
79
National Rate of Readmission MI 18.3%
80

2/26/2014
41
Rate of Readmission for CHF 23% 2014
81
National Rate of HF Patients is 23%
82

2/26/2014
42
Pneumonia Rate National is 17.6% 2014
83
National Rate Readmission Pneumonia 17.6%
84

2/26/2014
43
Rate of Readmission Pneumonia 20.3% 2013
85
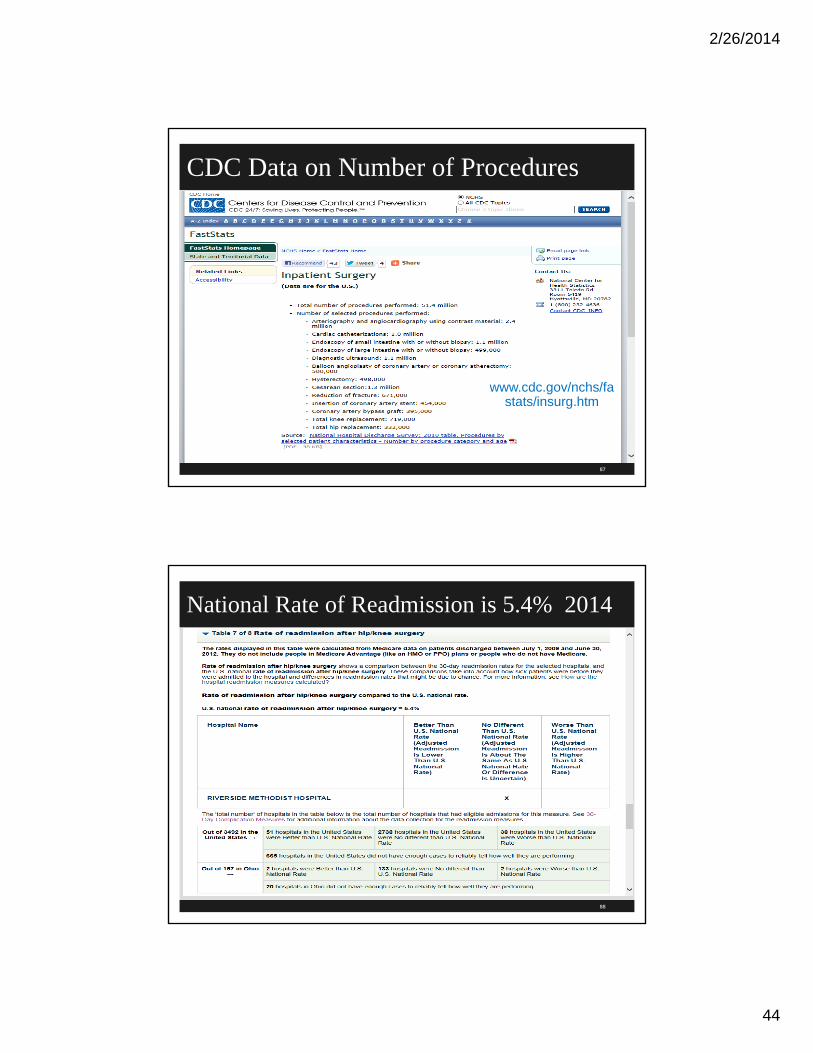
Hip and Knee ReplacementsCMS publishes outcomes of knee and hip
replacement first in Dec 2013
In first report, identified 97 hospitals with best outcomes and 95 with adverse outcomes
Covered surgeries between July 2009 and June 2012
Some hospitals complained assessments outdated
In 2010 there were 719,000 knee replacements costing 12 billion dollars and
332,000 hip replacements costing 8 billion86
2/26/2014
44
CDC Data on Number of Procedures
87
www.cdc.gov/nchs/fastats/insurg.htm
National Rate of Readmission is 5.4% 2014
88
2/26/2014
45
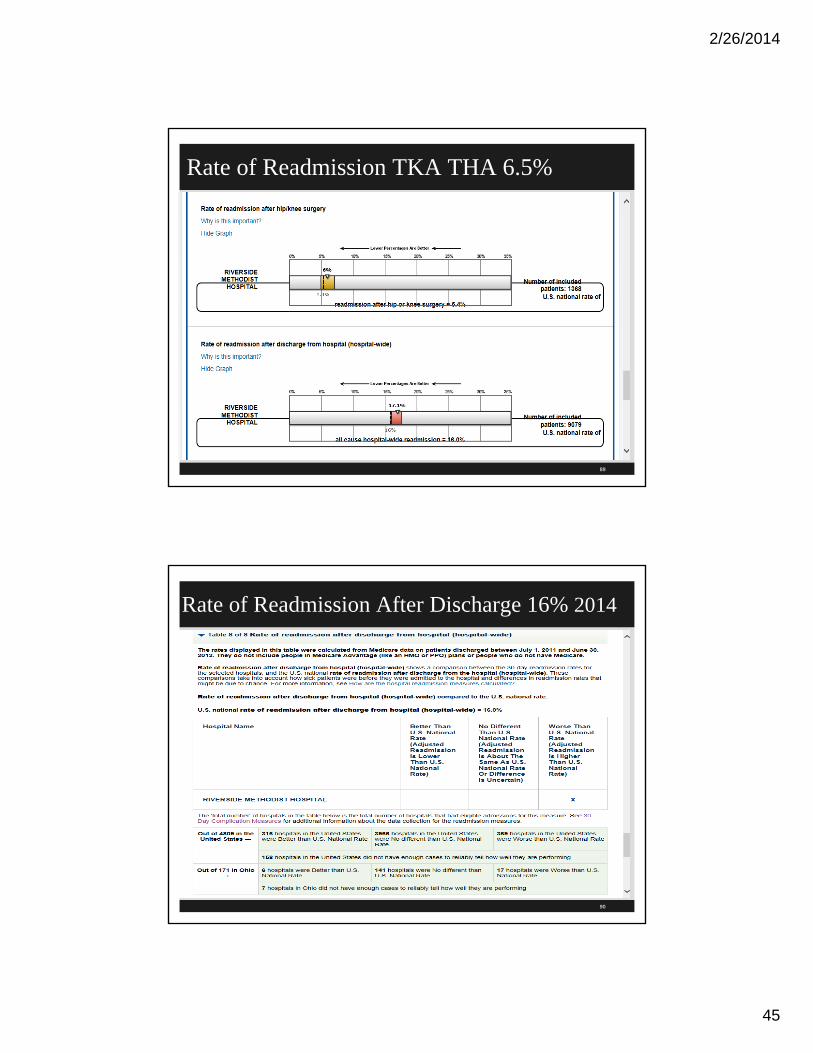
Rate of Readmission TKA THA 6.5%
89
Rate of Readmission After Discharge 16% 2014
90

2/26/2014
46
Partnership for PatientsAnother initiative tied to the CMS Hospital Value-
Based Purchasing Program is the Partnership for Patients
This is a public-private partnership to improve the quality, safety, and affordability of healthcare
It has the potential to save up to $35 billion in healthcare cost
It could reduce Medicare costs by up to $50 billion
States that 1 in 20 patients has an infection related to their hospital care
91
Partnership for Patients
92
http://partnershipforpatients.cm
s.gov/

2/26/2014
47
Partnership for PatientsStates 1 in 7 Medicare patients harmed in course of
their care costing 4.4 billion every year
Program may use as much as $1 billion in new funding
To keep patients from getting injured or sicker in the health care system
$500 million for community based care transition program
CMS has a Care Transition website for resources and websites
93
Partnership for PatientsHENS or Hospital Engagement Networks with 26 organizations working with 3,700 hospitals
Also focus on patient and family engagement
The goal is to reduce HACs by 40%
The goal is a 20% reduction in readmission rates
There are 102 organizations participating in the community based transitions program to improve transitions from hospitals to other settings
94

2/26/2014
48
CMS Community Care Transition Program
95
CMS Care Transition Program
96
http://innovation.cms.gov/initiatives/CCTP/?itemID=CMS1239313
2/26/2014
49
Partnership for Patients Focus Areas Resources
97
http://partnershipforpatients.cms.gov/p4p_resources/lpresource
s.html
Readmissions Resources P4P
98
http://partnershipforpatients.cms.gov/p4p_resources/tsp-preventablereadmissions/toolpreventablereadmissions.html

2/26/2014
50
Readmissions Resources Includes link and information on many of the
evidenced based projects to reduce unnecessary readmissions
Updated Project RED (Re-Engineered Discharge)
Care Transitions (Dr Coleman University of Colorado)
Transitional Care Model (TCM, Dr. Mary Naylor, University of Pa)
BOOST or Better Outcomes for Older Americans (Society of Hospital Medicine)
IHI Transforming Care at the Bedside, Medicare Demonstration Project, INTERACT, GRACE, etc.
99
100

2/26/2014
51
/ 40
Partnering to HealOne of the Partnership for Patients is a video every
healthcare practitioner should see
It is related to the hospital initiative to reduce the number of healthcare associated infections (HAIs)
It is a computer-based, video simulation training program
Hospitals should consider making it mandatory for direct care givers it is that good!
Partnering to heal video at http://www.hhs.gov/partneringtoheal
1http://hhs.gov/ophs/initiatives/hai/index.html101
Video on Preventing HAI
102
www.hhs.gov/ash/initiatives/hai/training/

2/26/2014
52
Readmission Rates Vary Readmission rates vary widely in the US
Too often quality of care during transition from hospital to home is not good
Data shows readmission rate for MI and CHF vary
Found only modest association between performance on discharge measures and patient readmission rates
Public reporting unlikely to yield large reductions in unnecessary readmissions
We need to improve in the ambulatory section
See A. K. Jha, E. J. Orav, and A. M. Epstein, Preventing Readmissions with Improved Hospital Discharge Planning, NEJM Dec 31, 2009 361 (27):2637-2645
103
Geographic Variation in Hospital Readmissions
2007 Medicare SAF data

2/26/2014
53
Many Good Resources Commonwealth Website
http://www.commonwealthfund.org/Content/Publications/Literature-Abstracts/2010/Jan/Preventing-Readmissions-with-Improved-Hospital-Discharge-Planning.aspx
105
106

2/26/2014
54
Variation of Readmissions Rates
107
http://www.nejm.org/doi/full/10.1056/NEJMsa0803563?siteid=nejm&keytype=ref
&ijkey=3CQjS3yxXjOtY
108
2/26/2014
55
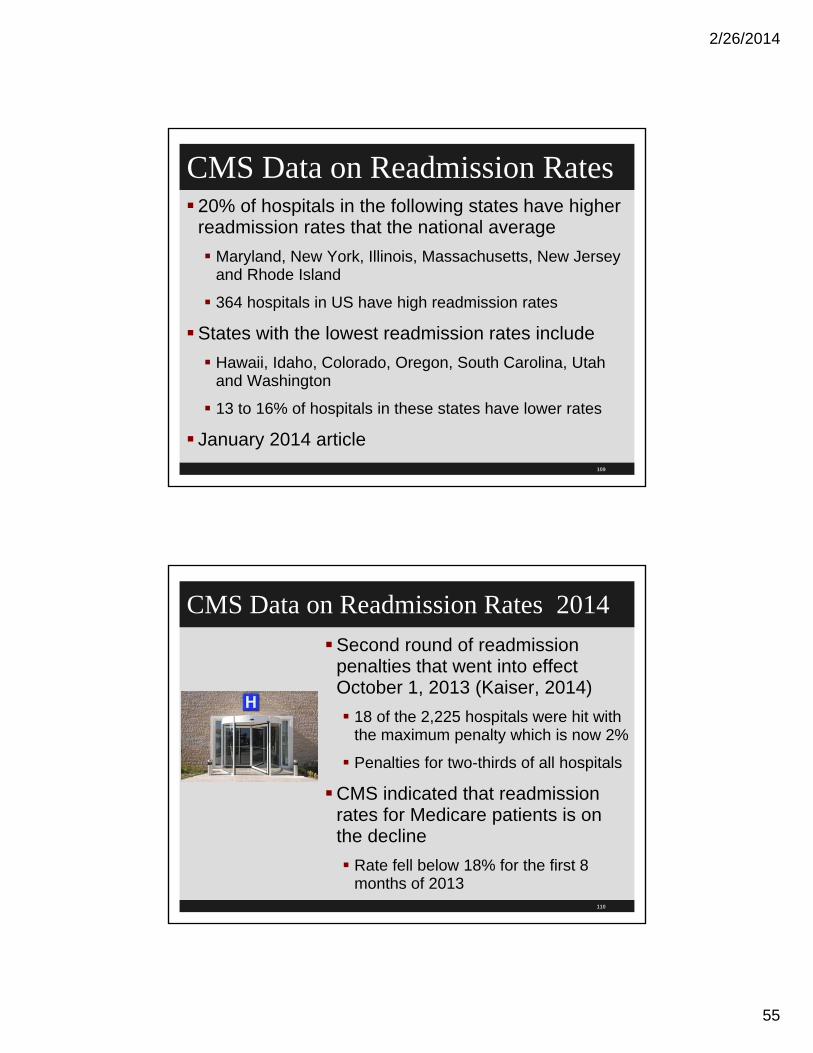
CMS Data on Readmission Rates 20% of hospitals in the following states have higher
readmission rates that the national average
Maryland, New York, Illinois, Massachusetts, New Jersey and Rhode Island
364 hospitals in US have high readmission rates
States with the lowest readmission rates include
Hawaii, Idaho, Colorado, Oregon, South Carolina, Utah and Washington
13 to 16% of hospitals in these states have lower rates
January 2014 article109
CMS Data on Readmission Rates 2014
Second round of readmission penalties that went into effect October 1, 2013 (Kaiser, 2014)
18 of the 2,225 hospitals were hit with the maximum penalty which is now 2%
Penalties for two-thirds of all hospitals
CMS indicated that readmission rates for Medicare patients is on the decline
Rate fell below 18% for the first 8 months of 2013
110

2/26/2014
56
Chart Worst and Best Readmission Rates
111
http://capsules.kaiserhealthnews.org/index.php/2014/01/new-medicare-data-show-hospitals-with-high-rates-
of-readmissions/
Readmissions and DischargesOne in 5 hospital discharges (20%) is complicated
by adverse event within 30 days which is about 2 million Medicare patients per year (March 2011 data)
20% were readmitted within 30 days with 1/3 leading to disability
Often leads to visits to the ED and rehospitalization
6% of these patients had preventable adverse events
66% were adverse drug events so focus on medications when patients discharged The incidence and severity of adverse events affecting patients after discharge from the hospital.
Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. Ann Intern Med. 2003;138:161-167
112

2/26/2014
57
Preventing Readmissions Studies differ on rate of preventable readmissions and
one said 76% of readmissions are thought to be preventable
It is the preventable ones that hospitals need to work on
Medicare data shows that over half of patients readmitted received no follow up care
Recent studies show interventions targeted at post-acute care transition can reduce readmissions by one third (Coleman and Naylor)
Technologies for Improving Post-acute Care Transitions, Center for technology and Aging, Sept 2010
113
Preventing ReadmissionsHHS study finds a high rate of Medicare patient
deaths due to adverse events (AE)
15,000 Medicare patients experience an AE during healthcare delivery that lead to their death every month
Nov 16, 2010 OIG study
Found 1 in every 7 discharges (13.5%) experience an AE and the cost to CMS is $324 million
44% of all AE were preventable and 51% were not
November 2010, OEI-06-09-00090114

2/26/2014
58
115
Preventing ReadmissionsCare Transitions Intervention and Transitional
Care Model are two common interventions that focus on the post-acute care transitions
Guided care and Geriatric Resources for Assessment and Care of Elderly are promising care coordination intervention models
Technologies to improve medication adherence, medication reconciliation, patient monitoring, communication between clinicians, risk assessment are important aspects of care transitions
116

2/26/2014
59
Readmissions and Discharges 40% of patients who were discharged had test results
pending
Many discharged patients had pending workups with interventions to be followed up by outpatient physicians
More than 1/3 of the recommended follow ups were not followed
Frequently because the discharge summary did not contain the details of the necessary work up
But availability of discharge summary increased likelihood of work ups being done
Tying up loose ends: discharging patients with unresolved medical issues. Moore C, McGinn T, Halm E. Arch Intern Med. 2007;167:1305-1311
117
Readmissions and DischargesAnother study finds that 41% of inpatients were
discharged with a study pending
It was also discovered that 2/3 of the physicians were not aware of the results
37% of the tests required some action on behalf of the physician
Inpatient physicians were dissatisfied with system for following up test results returning after discharge
Roy, Christopher etc. Patient Safety Concerns Arising from Test Results that Return after Hospital Discharge, Ann Intern Med 2005; 143(2):121-8
118

2/26/2014
60
Readmissions and DischargesMany were not done because the discharge
summary was not available at the time of the first clinic or office visit
Later study found that 78% of patients who went for the first post hospital visit the primary care physician did not have a discharge summary for the patient
Note NQF 34 Safe Practices to dictate the discharge summary when patient discharged and ensure it gets to the PCP timely and document this communication
Why CMS includes in DP standards and worksheet
Incomplete handoffs lead to unnecessary readmission
Care transition important for high risk and the elderly119
Readmissions and Discharges 37.2% of patients did not know the purpose of their
medication
Only 14% knew the side effects of the medications they were taking
Only 41.9% of patients were unable to state their diagnosis
Hospitals may want to focus on ensuring adequate medication information, discharge diagnosis and plan of care information to the patient Patient Understanding of their Treatment Plans and Discharge Diagnosis at
Discharge, Mayo Clinic Proceedings, Aug 2005;80(8):991-994
120

2/26/2014
61
Readmissions and DischargesThis lead to the development of a formal discharge
checklist to ensure communication at discharge
Transition of care for hospitalized elderly patients—development of a discharge checklist for hospitalists. Halasyamani L, Kripalani S, Coleman E, et al. J Hosp Med. 2006;1:354-360
The Pa Patient Safety Authority has excellent resources including suggested elements for a discharge checklist
See Care at discharge—a critical juncture for transition to posthospital care. Pa Pat Saf Advis 2008 Jun;5(2):39-43
121
PaPSA Checklist
122

2/26/2014
62
123
124
http://patientsafetyauthority.org/EducationalTools/PatientSafetyTools/tk_discharge/Pag
es/home.aspx

2/26/2014
63
PaPSA on Preventing Readmission Had more than 800 reports in 3 ½ year period of
harm from patients from incomplete discharge
30% of patients did not receive verbal or written discharge instructions before they left the facility
Lack of medication reconciliation was evident
Essential parts of the discharge process include Educating the patient and or family including what to do if a problem
occurs
Assessing the patients understanding of the plan
Scheduling follow up appointments
Confirming the medication plan125
PaPSA on Preventing ReadmissionsSome patients received another patients instructions
Many patients did not have their IV access device removed prior to discharge
Many patients returned with an IV site infection and or phlebitis
Discharge of patients before test results were made available to the attending who would have postponed discharge based on the final results
Many medication related issues such as lack of instructions
126

2/26/2014
64
CMS ChecklistCMS, in the QIO 9th scope of work, has 14
states in the care transition project,
Each of the 14 states will summarize their results and these calls are free to listen to
Sign up for upcoming sessions at http://www.cfmc.org/integratingcare/learning_sessions.htm
CMS has published a checklist which is available at www.medicare.gov
127
Care Transitions Resources and Webinars
128
www.cfmc.org/integratingcare/learning_sessions.htm

2/26/2014
65
Toolkit
129
www.cfmc.org/integratingcare/toolkit_PDF.ht
m
130
http://www.cfmc.org/caretransitions/patient_resources.htm

2/26/2014
66
131
132

2/26/2014
67
11 Essential Steps of RED Process
Greenwald etc. identified 11 essential steps to the reengineered discharge process at Boston Medical Center
Educating patients and families about their diagnosis throughout the hospital stay
Assessing the patients’ understanding of the plan by asking them to explain the plan in their own words
Advising the patient and family of any tests completed in the hospital with results pending at time of discharge and identifying the clinician responsible for the results
133
11 Essential Steps of RED Process
Scheduling follow-up appointments and tests to be done following discharge
Organizing services to be initiated following discharge
Confirming the medication plan
Reconciling the discharge plan with national guidelines and critical pathways when relevant
134

2/26/2014
68
11 Essential Steps of RED Process
Reviewing with the patient what to do if a problem occurs
Expediting the transmission of the discharge summary to the healthcare providers who are accepting responsibility for the patient’s care
Giving the patient written discharge instructions
Greenwald JL, Denham CR, Jack BW. The hospital discharge: a review of high risk care transition with highlights of a reengineered discharge process. J Patient Saf 2007 Jun;3(2):97-106.
135
Medication List
136

2/26/2014
69
Outstanding Labs or Tests
137
Appointments for Follow Up
138

2/26/2014
70
Project RED Tools
139
http://www.ahrq.gov/professionals/systems/hospital/red/index.html
Updated RED Program
140
http://www.ahrq.gov/professionals/systems/hospital/red/index.html
http://www.ahrq.gov/professionals/systems/hospital/red/index.html
http://www.ahrq.gov/professionals/systems/hospital/red/index.html

2/26/2014
71
141
http://www.ahrq.gov/professionals/systems/hospital/red/inde
x.html
3 Factors Leading to Errors at Discharge
Greenwald etc identified factors that lead to error at discharge to three types
1. Hospital care system characteristics
Many hospitals don’t get discharge summaries to PCP timely
Many errors around lack of medication reconciliation at discharge
2. Patient characteristics
Factors in literature at risk for hospitalization include lack of social, financial, and familial support and low health literacy, lack of follow up and adherence to treatment
142

2/26/2014
72
3 Factors Leading to Errors at Discharge
3. Clinician characteristics
These focus on quality and effectiveness of communication and
Timeliness and completeness of discharge summaries provided to subsequent caregivers
Clinicians with limited time or lack of effort put into educating patients at discharge lead to lack of patient understanding
This is why studies that used transition coaches to assist and encourage the patient to participate in their care were successful at unnecessary readmissions
143
Transitions ResearchResearch on preventing unnecessary readmissions
looks at the studies on improving transitions
Transitions is the process designed to ensure coordination and continuity of healthcare as patients transfer between different locations or different levels of care
We want to improve the transition to home, long term care, home health, assisted living or other post discharge places
How do we do this right so the patient does not have a unnecessary readmission
144

2/26/2014
73
Patient Characteristics Play a RoleThrough out this presentation are various evidenced
based articles that discuss patient characteristics that increase the patient’s readmission rate
Hospitals should be aware of this research to determine high risk patients
Patients with co-morbidities are high risk for readmissions
The more chronic conditions the patient has the greater the likelihood or readmission
See chart on next page
145
More Chronic Conditions More Readmissions
146

2/26/2014
74
Patient Characteristics Play a Role
MedPAC found Medicare patients with end stage renal disease (ESRD) have a higher rate of readmission
31.6% are readmitted within 30 days
Compared with 16.9% of non-ESRD patients Medicare Payment Advisory Commission. (June 2007). Payment Policy for Inpatient
Readmissions. Report to the Congress: Promoting Greater Efficiency in Medicare. Washington, DC.
Patients with CHF were more likely to be admitted if has PVD, diabetes, CVA, or CAD Aranda, J.M., et al. (2009). Current Trends in Heart Failure
Readmission Rates: Analysis of Medicare Data. Clinical Cardiology, 32(1), 47-52.
147
Patient Characteristics Play a Role
Studies have also shown the following increase the rate of readmission;
Depression especially for patients diagnosed with coronary artery disease
Age
Gender
Race and ethnicity (African Americans had highest rate)
Medicaid coverage (Jiang, 2010, JAMA)
Language barriers (Karline, LS 2010, Journal Hospital Medicine)
Patient in counties with low median income
148
2/26/2014
75
Patient Characteristics Play a Role
In spite of these studies, little agreement on characteristics that might best predict which patients are at greater risk for readmission
Five statistical models intended to predict a patient’s risk of readmission found little consistency among patient characteristics Ross, J.S., et al. (2008). Statistical Models and Patient Predictors of Readmission for
Heart Failure: A Systematic Review. Archives of Internal Medicine, 168(13), 1371-1386.
More work is needed to help hospitals better focus their efforts to determine which patients are likely to benefit
149
Approaches to Reduce Readmissions
One study found that calling CHF patients within 7 days of readmissions reduced readmission
Patients with earlier follow up after discharge were less likely to be readmitted
There are many other studies such as the RED project that resulted in 30% fewer admissions
This will be discussed in detail later
Metro Health in Wyoming cut their CHF rate in half, from 15.5% to 7.4%
Developed educational material, included diet and self care, scheduled appointments, etc.
150

2/26/2014
76
AHA Guide to Reduce Readmissions
151
www.hret.org/readmissions
AHA Health Care Leader Guide
152
www.hret.org/care/projects/guide-to-reduce-readmissions.shtml
2/26/2014
77
AHA Reducing Avoidable Hospital Readmissions
Some readmissions can be avoided by evidenced based practice but the means for achieving this still remains controversial
Preventing readmissions is a complex, system-wide problem that involves hospitals, physicians, other providers, patients and their families
AHA created a framework
AHA included a list of strategies that hospitals might find helpful in both documents
AHA worked with 3 states and got payer data on readmissions
153
AHA 4 StepsFirst, examine your hospital’s current rate of readmissions
Second, assess and prioritize you improvement opportunities
Third, develop an action plan of strategies to implement
Fourth, monitor you hospital’s progress
154

2/26/2014
78
Step 1 Current Rate of Admissions
Compile data on your readmission rate
Hospital compare has 30 day admission rates on CHF, MI, and pneumonia
listed at www.hospitalcompare.hhs.gov
Knowing data will help hospital target strategies for reducing readmissions
First, look at rates for different conditions so examine by diagnosis and significant co-morbidities and correlate with patient’s severity
155
Step 1 Examine Current Rate of Readmissions
For example, MI, CHF, pneumonia, patients with diabetes, obesity, or COPD
Second, look at readmission rate by practitioner to look for patterns or if any type of practitioner is associated with unexpected readmissions
Third, look at readmission rates by readmission source such as nursing homes, home health etc. to determine the places where most often patients are being readmitted
156

2/26/2014
79
Step 1 Examine Current Rate of Readmissions
Lastly, look at readmission rates at different time frames such as 7, 30, 60, and 90 days which can bring into flaws in transitioning patients to the ambulatory setting
Hospitals should also pull the charts of a few patients who were readmitted from various setting
Purpose is to understand why patient was readmitted and what could have been done to prevent the readmission
Look at financial impact on the hospital that reduced payments would have
157
2. Prioritize Improvement Opportunities
AHA recommends to assess and prioritize your improvement opportunities
There are one of more approaches that can be followed
Focus on specific patient populations such as older adults with co-morbidity since need a more rigorous assessment process to determine discharge needs
COPH, diabetes, renal failure, liver failure etc.
158

2/26/2014
80
2. Prioritize Improvement OpportunitiesFocus on stages of the delivery process so if you
identify patients being admitted for the same reason look at the resources available
Such as CHF patient , MI, asthma, diabetes, renal failure and pneumonia
Patient and family education can help patients take care of their care
Focus on the hospital’s priority areas and current PI initiatives
Look at current PI program and can redesign fundamental care processes
See AHA list of past and current PI programs159
3. Develop Action Plan of Strategies
Develop an action plan of strategies to implement
This is why doing a literature search and have librarian obtain articles from evidence based research
Need many in the community to work together to prevent unnecessary readmissions to the hospital
See list of major strategies to reduce avoidable readmissions
Need to use technology such as remote monitoring, electronic medical records and telehealth
160

2/26/2014
81
Strategies During Hospitals
Risk screen patients and tailor care
Tailor patient care needs based on evidenced based guidelines, clinical practice guidelines, care path
– Develop pathways that include discharge steps consistent with these evidenced based guidelines
– CHF CPG, CABG, Pneumonia pathways, Total hip and total knee pathways
– Pathways are not cook book medicine but assist in ensuring evidenced based practice is followed
– Include actions to take if variances occur with CPG161
162

2/26/2014
82
Strategies During Hospitals
– Get with the guidelines!!!
– www.ahrq.gov and www.guidelines.gov
Have healthcare worker responsible for discharge planning and define scope of their responsibility
Have a social worker or nurse case manager to provide discharge planning services
Some have discharge advocate
Remember to include education to patients and families about their disease
Provide patient with disease specific, low literacy and language and age appropriate educational material
163
Strategies During HospitalsBe aware of research that shows patients at
increased risk of readmission such as patients with low health literacy
20% of population reads at the 5th grade level
½ of adults have trouble understanding simple health information (consent, prescriptions, oral instructions)
– Can not tell health literacy by looking so observe closely in elderly, unemployed, did not finish high school, born in US but English a second language, noncompliant, immigrant, can’t name medications, forgot glasses and will read later, etc.
High risk patients also include history of readmission, failed teach back, longer stay than expected, high risk conditions, poor, disabled or on dialysis
164

2/26/2014
83
Strategies During HospitalsRespond to patient needs for early ambulation,
early nutritional interventions, PT, social work etc
– Nursing assessment and identified criteria to see dietician timely
– Quality and patient safety initiatives to improve surgical outcomes such as prevention of PE and DVT
Develop a multidisciplinary team to evaluate and implement discharge needs– Consider a checklist of things to consider in the discharge process
– See Society of Hospital Medicine at http://www.hospitalmedicine.org/AM/Template.cfm?Section=Quality_Improvement_Tools&Template=/CM/ContentDisplay.cfm&ContentID=8363 165
166

2/26/2014
84
167
168

2/26/2014
85
Strategies During HospitalizationConsider putting together a hospital team to
evaluate the literature and reengineer the discharge process in your hospital– Research shows increased number of readmissions due to phlebitis
so consider annual orientation and credentialing of nurses to start IV
– Strict adherence to the IV standards such as the IV Nurses Infusion Society Standards of Practice
– Consider infusion nurses
– Restarting IVs started by squad under less than ideal circumstances
– Strict adherence to how long IVs can stay in
– Have a process to ensure all IVs and IV access devices are removed prior to discharge
169
Strategies During HospitalizationEvaluate all patients on admission and throughout
hospitalization for discharge planning
Physical therapist can assess ability to do ADL and environmental barriers in postdischarge care area and what services will be needed after discharge
Discuss end of life care wishes
Some hospitals require code status of all patients upon admission
Studies found that often RRT or code called and then after wards patient was made a DNR
Pneumonia readmissions may reflect need for end of life care
170

2/26/2014
86
Strategies During HospitalizationDevelop community connections to eliminate
barriers to successful transition
Need to build relationships with other healthcare providers, and public and private groups
Parish nurse programs, meals on wheels, etc.
Community partners that can help with nonmedical such as behavioral, health literacy, and cultural issues
Engage families, patients and caregivers
Get their active participation, teach back,
Get their feedback in addressing healthcare delivery issues such as understanding discharge instructions
171
Strategies at Discharge Implement comprehensive discharge planning
Should be written out so the patient can understand
Should be comprehensive to include medication use, activity level, symptoms that patient should call the physician or return,
TJC has a discharge tracer
Provide discharge plan to patient
Make sure PCP gets discharge summary
172

2/26/2014
87
Strategies at Discharge Implement comprehensive discharge planning
(continued)
Reconcile discharge plan with national guidelines/CPGs
Standardized checklist of transitional services
Give patient care record including pending tests
The detailed written discharge plan should include how to fill prescription along with a list of all medical problems
Instruct patient to bring plan to all appointments173
Strategies at DischargeUse teach back method to educate the patient and
their care giver
Have the patient repeat back the instructions in their own words to make sure they understand the discharge instructions
Focus handoff information on patient and family
Make sure patient repeats back what to do if a problem arises
Make sure patient has it in writing the signs and symptoms to watch for
174

2/26/2014
88
Strategies at DischargeSchedule the patient’s follow up appointment
Make the appointment for all follow up appointments before the patient is discharged
Provide times and information and directions to the patient in writing
The nurse case manager or discharge planner can also schedule any further diagnostic tests that were ordered
Also want to confirm services to be received before the patient leaves the hospital
175
Strategies at DischargeDevelop standardized checklist to assess that all
discharge components are completed
Finalize the plan with the patient and make sure patient verbalizes understanding
Perform a final physical assessment with attention to the removal of all IV lines or other access ports
Want to get a timely transfer of the discharge summary to the primary care physician and
Follow up by telephone 2 to 3 days after discharge to assess optimal care and recovery
176

2/26/2014
89
Strategies at DischargeStandardize the discharge instruction document and
include:
primary and secondary diagnosis, patient education, services to be provided
dietary and other lifestyle modifications, medications, follow-up appointments
pending tests
adverse events or complications to watch for, and provider contact information for any problems that occur
177
Strategies at DischargeAssist the patient in managing their medications
Give patient complete list of medications at discharge
Include times to take and reason
Pharmacist role in assisting with understanding new medications or high risk medications
Some use MAR to have patient document when meds given
Use transitional coach to help
RARE program has recommendations for mental health patient
178

2/26/2014
90
Strategies at DischargeDon’t just focus attention on the admitting diagnosis
but also on the comorbidities patients have
Patients with neoplasm, heart failure, and chronic kidney disease had a higher risk of potentially avoidable readmissions
When patient is admitted determine if admitted within last 90 days
If so some hospitals are doing a RCA or assessment of the reason for readmission
50% to 60% more likely to be admitted again
179
Strategies at DischargeTiming of the physician follow up appointment may
be important
One hospital found if patient saw doctor day 1-4 the chance of readmission is less than 6%
If appointment 6-10 days after discharge readmission rate was 6 to 13%
If visits on day 25 then chance went up to 29%
Readmission rate increased 1% for every day between discharge and the first physician visit
Article published Jan 8, 2014, Detroit Medical Center, Media Health Leaders
180

2/26/2014
91
Reducing Avoidable Readmissions
181
www.rarereadmissions.org/
182
http://www.rarereadmissions.org/

2/26/2014
92
Strategies at DischargeWhen patient are discharged to LTC make sure
transfer summary has detailed instructions
Make sure a complete list of medications to be taken are provided
Include comprehensive information on hospital care and what needs to be done for continuity of care (see CMS requirements in DP standards)
Partner with nursing home practitioners
Consider call back to see if any questions
Use NP in LTC facility183
Strategies Post DischargePromote patient self management
Patients with HTN monitor BP at home
Diabetics and patients on Coumadin use home monitoring devices
Follow up with patients via telephone
Some hospitals have the nurse call the patient to reinforce discharge instructions usually in 2-3 days
Many of the transition programs involve calls or visits to the patient in the home
Offer telephone support for period post discharge
184

2/26/2014
93
Strategies Post DischargeOne author noted that hospitals, physicians, HHAs,
nursing homes and pharmacist can prevent more readmissions by working together that hospitals can by improving the discharge process alone
Slide presentation on Reducing Avoidable Readmissions by Steve Hines PhD, June 4, 2010
Quality of LTC and HHA can drive readmission rates
Establish community networks
Parish nurse programs, meals on wheels
Establish private/public partnerships to meet patient needs
Homeless shelters with medical care and dental care185
Strategies Post DischargeThe home visit includes an assessment of environmental issues that could result in readmission
No food in house, no heat, fall assessment, determine if need transportation for physician visit, make sure any durable medical equipment is connected correctly
186

2/26/2014
94
Strategies Post Acute Care TechnologiesMedication adherence
Devices that remind patients to take the right medication at the right time
Hospitals should take a serious look at this issue
Medication non-adherence contributes to 33%-69% of medication related hospital admissions
The New England Healthcare Institute estimates that $290 billion of health care expenditures could be avoided each year if medication adherence were improved
Delate T, Chester EA, Stubbings TW, Barnes CA. Clinical outcomes of a home-based medication reconciliation program after discharge from a skilled
nursing facility. Pharmacotherapy. Apr 2008;28(4):444-452.187
Strategies Post Acute Care TechnologiesStrategies to increase medication adherence
include;
Simplifying the patient’s medication regimen
Identifying if the medication has untoward effects
Improving patient self-efficacy and activation
Providing cues or reminders to take medications as prescribed New England Healthcare Institute. Thinking Outside the Pillbox: A
System-wide Approach to Improving Patient Medication Adherence for Chronic Disease. A NEHI Research Brief July 2009.
188

2/26/2014
95
Strategies Post Acute Care Technologies
Philips Medication Dispensing System
Dispenses 10-30 days worth of medications
Reminds patients to take it
Can alert physician and 3 others if pills not removed from dispenser
Provides alert and dispensing information
Has been shown to reduce hospitalizations
Especially good for those with cognitive problem on Coumadin
189
Strategies Post Acute Care TechnologiesMini-mental state exam (MMSE) correlates with
medication adherence
Medication reconciliation
Software that stores medication information and detects certain problems such as duplicate prescriptions
Remote patient monitoring
Technology to help detect early deterioration of a patient’s medical condition
Patient or care giver access to medical records
190

2/26/2014
96
Strategies Post DischargeUse telehealth in patient care
Technology can be used to help prevent readmissions
See Technologies for Improving Post-Acute Care Transitions, September 2010
Use of EHR to support care coordination
Monitor patient progress such as electronic cardiac monitoring and remote patient telemonitoring
Medication reminders and dispensers
In home diagnostic devices
Videoconferencing
191
Strategies Post DischargeHospitals should consider working with their state
QIO
JAMA study found that hospitals working with QIOs in communities across the country experienced twice the reduction in readmissions compared with those that did not (Jan 23, 2013)
Consider holding monthly meeting with your various partners such as nursing homes and home health staff
One study showed this reduced readmissions by 20.8% (Jan 2014 IPRO-NY’s QIO)
192

2/26/2014
97
4. Monitor the Hospital’s Progress
The last key to reduce readmissions is for hospital leadership to monitor the progress
Look at readmission rates by
Different conditions such as MI, CHF, COPD, Pneumonia, TKA, THA, asthma, diabetes, cellulitis, etc
By practitioner to look for patterns
Over different time frames (7, 30, 60, and 90 days)
By readmission source (home, LTC, etc.)
Data should be included in key indicators tracked
193
Diagnostic Specific Reasons for Readmissions There are reported diagnostic specific reasons for
avoidable readmissions
Many COPD and pneumonia patients need home health care but do not receive it
Cardiologist may rely on primary care physician and not arrange follow up care for HF patients
Readmission rate appears higher for HF patients with behavioral diagnosis
Dialysis patients are very vulnerable to changes in medications during hospitalization
– ESRD have higher than average readmission rates (MedPAC)– Medicare Payment Advisory Commission. 2007. Report to the Congress: Promoting Greater Efficiency in
Medicare. Washington, DC: Medicare Payment Advisory Commission, p. 107
194

2/26/2014
98
Diagnostic Specific Reasons for Readmissions
Surgeons do not arrange for post surgery primary care
Studies show there is inadequate teaching of surgical patients in caring for themselves after surgery
Incision care
Post CABG patients expecting to be pain free and seek readmission for angina
Hospitals should know this information
195
HCAPHS and Transition PlanningThree questions that were added:
During this hospital stay, staff took my preferences and those of my family or caregiver into account in deciding what my healthcare needs would be when I left
When I left the hospital, I had a good understanding of the things I was responsible for in managing my health
When I left the hospital, I clearly understood the purpose for taking each of my medications
How will you fare?196

2/26/2014
99
197
The End! Questions??
Sue Dill Calloway RN, Esq. CPHRM
AD, BA, BSN, MSN, JD
President of Patient Safety and Education
Chief Learning Officer for the Emergency Medicine Patient Safety Foundation www.empsf.org
614 791-1468
See additional slides on CMS and TJCstandards, different studies
197197
NQF 34 SAFE PRACTICES
Released in 2003, updated 2006, 2009 and April 2010 and March 2011
34 Safe Practices for Better Healthcare
These should followed in all healthcare facilities
All clinical care settings to reduce risk of harm to patients
A roadmap to preventing harm
States 10 years after IOM report, To Err Is Human, uniformly reliably safety in healthcare has not been achieved
198

2/26/2014
100
NQF Safe Practices 15 Discharge System
A "Discharge Plan" must be prepared for each patient at the time of hospital discharge, and a concise discharge summary must be prepared for and relayed to caregivers accepting responsibility for postdischarge care in a timely manner
Hospital must ensure that there is confirmation of receipt of the discharge information by the LIP who will assume the responsibility for care after discharge
TJC and CMS also require discharge summary
TJC tracer on discharge process199
15. Patient Discharges
Often because of errors from fragmentation of care at discharge
High rates of low health literacy, and lack of coordination for post care lead to adverse events
Need to do medication reconciliation (TJC requirement)
Need structured discharge communication
AHRQ has Project Red to improve patient discharges (Re-Engineered Hospital Discharges)
http://www.ahrq.gov/news/kt/red/200

2/26/2014
101
Safe Practice 15 Discharge System
Need discharge P&P to include
Roles in the discharge process
Preparing for the discharge with documentation throughout hospitalizations
Complete discharge summary before discharge
Reliable information flow from PCP to referring caregiver and back
Benchmarking, measurement, and continuous quality improvement of discharge process
201
SP15 NQF Discharge SystemWritten discharge plan must be given to each patient
at the time of discharge
That is understandable by the patient (remember issue of low health literacy)
Discharge plan needs to include reason for hospitalization
Medications to be taken post discharge
What to do if condition changes
Coordination and planning for follow up appointments and follow up tests and for studies if results not available at time of discharge
202

2/26/2014
102
15 Discharge SystemDischarge summary needs to be provided to LIP
who is caring for the patient after discharge
Current problem where 78% of LIP who see patient for first visit do not have discharge summary
Include reason for hospitalization and significant findings, procedures done, medication list, list of tests and studies of results and ones not back
Copies of lab, x-ray reports, and tests results in hands of person doing discharge summary
Need receipt confirmation by physician caring for patient after discharge of discharge summary by fax, phone, email etc
203
Discharge instructions
Include activity level, medications and education on medications, potential drug food interactions and follow up information
TJC RC.02.04.01 requires documentation of the patient’s discharge information
Document if you give patient specific patient education sheets like fracture care sheet-should have copy on chart
Ask Me 3 is three most important questions that can help during discharge instructions
What is the main problem?, what does the patient need to do? And why it is important for them to do this? (www.npsf.org/askme3)
204

2/26/2014
103
NQF Care Coordination
205
NQF
NQF has published “Preferred Practices and Performance Measures for Measuring and Reporting Care Coordination”
NQF notes care coordination is important to prevent unnecessary returns to the ED and readmissions
Especially important for patients with chronic conditions such as diabetes and hypertension
These standards provide structure, process and outcome measures
Goal to reduce 30 day readmission rates and preventable ED visits by 50%
206

2/26/2014
104
NQF Care Coordination Preferred Practices
Has domains on
Home with five practices
Proactive plan of care and follow-up with five practices
Communication with four practices
Information systems with three practices
Transitions and handoffs with eight practices
Plan of care and follow up
P&P to create and update plan of care with every patient
Follow up of all tests and treatments
Include patient education, cardiac rehab for recent CV event207
NQF Care Coordination Preferred Practices
Communication
Plan of care made available to patient and home team
Program to use a partner to support care when patient is hospitalized
Care coordination activities are assessed and documented
Transition or handoffs
Transition program engages patients and families in self management when discharged home
Standardized communication template for transition of care process including core data elements
208

2/26/2014
105
NQF Performance Measures
Cardiac rehab patient referral from inpatient and outpatient setting
Biopsy follow up
Reconciled medication list by discharge patients
Melanoma continuity of care with recall system
Transition record with specified elements received by discharged patient
Patient with trans ischemic event ED visit who had a follow up in the office
209
210
www.qualityforum.org/Publications/2010/10/Preferred_Practices_and_Performance_Measures_for_Measuring_and_R
eporting_Care_Coordination.aspx

2/26/2014
106
Patient Characteristics Play a Role
Study of 37 children’s hospitals found higher rate of readmission associated with use of assistive technology such as G-tube or cerebrospinal fluid shunt (Berry, 2011, JAMA 305(7), 62-69)
Study of 6,800 general medicine patients found six co-morbidities associated with readmission
CHF, renal disease, cancer both with and without metastasis, weight loss, and iron deficiency anemia
Allaudeen, N., et al. (2010). Redefining Readmission Risk Factors for General Medicine Patients. Journal of Hospital Medicine, online.
211
AHA Reducing Avoidable Hospital Readmissions
MedPac (Medicare Payment Advisory Council) in 2009 concluded that large proportion of re-hospitalizations was preventable
Improvements needed include better communication and more coordinated care before and after discharge
Medicare Payment Advisory Commission. Report to Congress: Improving Incentives in the Medicare Program 2009
Not all readmissions are preventable
Predictors of readmission include certain clinical conditions such as CV conditions, stroke, and depression
Certain patient demographics such as elderly, dually eligible Medicare enrollees,
212

2/26/2014
107
AHA Guide to Reduce Avoidable Readmissions
AHA had committees look at the issue of how to reduce unnecessary hospital readmissions
September 2011 AHA Trend Watch
AHA published several memos and a 2010 Health Care Leader Guide to Reduce Avoidable Readmissions
Issues memo on Sept 2009 on Reducing Avoidable Hospital Readmissions
– Includes evaluation of post acute transition process which is the process of moving from the hospital to home or other settings
213
Excluded from Hospital Readmissions
The Affordable Care Act specifies that certain readmissions will be excluded from the hospital readmission rate
It excludes hospital readmissions that are unrelated to the prior discharge
Such as planned admissions
Or transfers to another hospital
Law reflects the difficulty in distinguishing the four types of admissions
Only includes one of the four types214

2/26/2014
108
Excluded from Hospital Readmissions
AHA says that how these exclusions are accounted for in the regulation is a key policy concern
AHA notes that payers and others commonly use readmission rates and mortality rates as a quality of care indicator
Suggests that higher the rates of these two the lower the quality of care
However, recently studies suggest this is not true
Cleveland Clinic study found patients with higher admission rate for CF had lower mortality
Gonodeski, 2010 , NEJM 363(3), 297-298215
Readmission Rates and Quality of Care
AHA also notes a number of other studies that showed higher readmission rates resulted in less deaths
Greater New York Hospital Association analyzed the hospital compare data to find same thing
Looked at 50 American Best Hospitals in cardiac surgery and found none of these performed better than expected on both mortality and readmissions
Study of 39 children’s hospital in 24 states found readmission rate increased as state performing systems went up
216

2/26/2014
109
Higher Readmissions but Less Deaths
217
Readmission Rates and Quality of Care
VA had a higher rate of readmission but decreased mortality because sicker patients survived but needed more therapies and care
September 2011 study of 107 VA hospitals of patients aged 65 or older
All but one VA hospital had higher rates of readmission that the average US hospital
15 had higher that average readmission rates for more than one of the 3 conditions (HF, MI, pneumonia)
218

2/26/2014
110
Readmission Rates and Quality of Care
Experts do not agree that readmission rates are valid as a quality measure
There are studies that readmission rates may be ill suited to be a measure of quality
Benbassat, J., and Taragin, M. (2000). Hospital Readmissions as a Measure of Quality of Health Care: Advantages and Limitations. Archives of Internal Medicine, 160,1074-1081.
219
Readmission Rates and Quality of Care
However, other studies found the opposite
A review of the literature found mixed evidence linking patients to quality of care
Some studies found patients who were readmitted were more likely to have received low quality of care
Hayward, R.A., et al. (1993). An Evaluation of Generic Screens for Poor Quality of Hospital Care on a General Medicine Service. Medical Care, 31(5),
220
2/26/2014
111
221
This presentation is intended solely to provide general information and does not constitute legal advice. Attendance at the presentation or later review of these printed materials does not create an attorney-client relationship with the presenter(s). You should not take any action based upon any information in this presentation without first consulting legal counsel familiar with your particular circumstances.
222
? QUESTIONS ?
You may enter your question in the chat box in the webinar room.
OR
If you are listening to the conference via streaming audio through your computer, you must dial in on the telephone at 1-877-776-3544 to ask your question live. After dialing-in (or if you are already dialed-in):
1. Press *1 on your touchtone phone. If you are using a speaker phone, please lift the receiver and then press *1.
2. If you would like to withdraw your question, press *1.

2/26/2014
112
223
Thank you for attending!
Sue Dill Calloway RN, Esq. CPHRM
AD, BA, BSN, MSN, JD
President of Patient Safety and Education Consulting
Chief Learning Officer of the Emergency Medicine Patient Safety Foundation at www.empsf.org
614 791-1468
223223
Top Related
Copyright © 2022 FDOKUMEN

