







Bahasa
Halaman
Hukum

2
Accepted Manuscript
Phenomenology of hoarding—What is hoarded by individuals with hoarding disorder?
Christopher Mogan, Michael Kyrios, Isaac Schweitzer, Keong Yap, and Richard Moulding
doi:10.1016/j.jocrd.2012.08.002
To appear in: Journal of Obsessive-Compulsive and Related Disorders
Received 29 March 2012
Received in revised form 22 July 2012
Accepted 7 August 2012
This is an unedited manuscript that has been accepted for publication.
3
Running head: PHENOMENOLOGY OF HOARDING
What is hoarded by individuals with hoarding disorder?
Christopher Mogan
University of Melbourne
Michael Kyrios
Swinburne University of Technology
Isaac Schweitzer
University of Melbourne and The Melbourne Clinic
Keong Yap
RMIT University
Richard Moulding
Swinburne University of Technology
Corresponding author: Dr Christopher Mogan, [email protected].
The Anxiety Clinic
TMC 6, 140 Church Street, Richmond, 3121 Victoria, Australia
Tel. 61-3-9420 1424
Fax 61-3-9421 0077
4
Abstract
Hoarding disorder is an under-recognized yet complex and pervasive psychological
problem that dominates individual’s time, living spaces, relationships and safety. Hoarding
behaviors have been associated with a number of disorders, including Obsessive-Compulsive
Disorder (OCD), but as of yet, there has not been a systematic investigation of the
presentation of hoarding phenomena across disorders. Simply – what do individuals with
hoarding actually hoard, and does that differ from objects kept by people without hoarding?
An understanding of the differential presentation of hoarding phenomena could help clarify
the clinical status of hoarding disorder, which is currently under review. This study examined
hoarding phenomena in 109 participants from five cohorts (individuals who hoard with and
without comorbid OCD, individuals with OCD without hoarding, individuals with other
Anxiety Disorders and non-clinical controls). The results supported the presence of hoarding
symptoms across clinical and non-clinical cohorts, but some differences were apparent. In
particular, individuals with hoarding disorder were far more likely than controls to collect
idiosyncratic objects, some with deeply personal connections. Implications are discussed.
Keywords: Hoarding, Obsessive-Compulsive Disorder, phenomenology, Obsessive-
compulsive spectrum.
5
1. Introduction
Hoarding things is a normal human behavior that arises from various symbolic, instrumental
and artistic links which underpin the relationships humans form with objects (Nordsletten &
Mataix-Cols, 2012). There is a growing awareness of a “disordered” type of hoarding, where
the keeping of things is so pervasive that it dominates the person’s life – their space and time,
personal and social functioning. While the early papers on such hoarding were largely
descriptive accounts that linked hoarding with severe and unusual presentations of obsessive
compulsive disorder (OCD) (Greenberg, 1987; Fitzgerald, 1997), more recent research has
examined hoarding as a phenomenon in its own right, as distinct from OCD (e.g., see Mataix-
Cols et al., 2010).
Reflecting this historical emphasis, there is a lack of clarity regarding hoarding in
DSM-IV-TR (American Psychiatric Association, 2000), with hoarding appearing only as a
symptom of Obsessive Compulsive Personality Disorder. This belies the seriousness of
hoarding as a clinical problem, at least as damaging as the other more recognized OCD-
related symptoms (Steketee & Pruyn, 1998), particularly where hoarding and clutter have
been known to lead to severe life-limiting injury from falls and fire-related injury, and even
the death of sufferers (Lucini, Monk, & Szlatenyi, 2009). In an online survey of 864
individuals with compulsive hoarding, Tolin and colleagues (2008) concluded that hoarding
disorder represents a profound public health burden, with work impairment similar to
psychotic disorders, and greater work impairment than individuals with other anxiety, mood
and substance abuse disorders. They also found that participants with hoarding disorder
showed a high degree of a broad range of chronic and severe medical concerns, and had a
five-fold higher rate of mental health service utilization. Eight to 12% had been evicted or
threatened with eviction, while 0.1-3.0% had a child or elder removed from the home (Tolin,
Frost, Steketee, Gray & Fitch. 2008). There is a DSM-5 working party paper reviewing
6
hoarding in order to give clinicians clearer clinical guidelines (Mataix-Cols et al., 2010),
including questions of differential criteria and classification. Answers to these questions
require research into the phenomenon of hoarding and any differences between individuals
who hoard and those with OCD.
Phenomenological differences between hoarding disorder and OCD have traditionally
been considered by examining differences in the clinical presentation or symptom profiles of
individuals. For instance, individuals who hoard frequently do not view their behavior as
unusual and exhibit less insight into their behavior than do those with other OCD symptoms
(Black et al., 1998; Frost & Gross, 1993; Frost, Krause, & Steketee, 1996; Tolin, Fitch, Frost,
& Steketee, 2010). As such, their thoughts regarding their possessions may be better
described as “preoccupations”, in contrast to the inherently distressing obsessive thoughts
that occur in OCD (Rachman, Elliott, Shafran & Radomsky, 2009). Hoarding-related
thoughts have been noted to be “neither intrusive, nor unwanted, and certainly are not
repugnant” (Rachman et al., 2009 p. 521). Furthermore, individuals who do not have to
perform a ritual in response to their thoughts (Mataix-Cols et al., 2010). Adding credence to
such distinctions, individuals with hoarding often do not display any other OCD symptoms
(for review, see Mataix-Cols et al., 2010), and have a lower rate of comorbid OCD (18%)
compared to depression, GAD and social anxiety (Frost, Steketee, & Tolin, 2011).
The present study aimed to explore another potential difference in the phenomenology
of hoarding – specifically by systematically addressing the issue of what do individuals who
hoard actually keep, and is this different from collecting behaviour in people without
hoarding disorder? In addition to etiological and diagnostic implications, a better
understanding of the types of items saved between groups would help guide clinicians in the
assessment and treatment of hoarding disorder with and without OCD. The only previous
study to examine this issue found that individuals with Hoarding with and without OCD
7
collected similar things, with the exception of letters, receipts, bills, old medication, and
bizarre objects (all higher in individuals with OCD; Pertusa et al., 2008). The most kept items
in both groups were old clothes, magazines, CDs, letters, and pens. To extend this analysis,
we examined similarities and differences in hoarding phenomenology across four clinical
groups – individuals with hoarding disorder with and without comorbid OCD; individuals
with OCD without hoarding; individuals with other Anxiety Disorder and a community
control group. This study examined the types of objects individuals saved, and whether
individuals who hoard saved different items from other groups. It was hypothesized that the
range of objects saved by the hoarding groups would differentiate individuals with hoarding
from non-hoarding clinical and community control groups. In addition, consistent with
Pertusa et al. (2008), we wanted to explore if there were any significant difference on items
saved in individuals with and without OCD.
2. Method
2.1 Participants
A total of 89 clinical participants and 20 community controls volunteered for the
study. Clinical participants were patients from University of Melbourne’s Professorial and
Psychology Clinics, members of community-based OCD support groups, or patients who
found out about the study from other clinical referrals and general media publicity. The
Research protocol was approved by the Research and Ethics Committee of the University of
Melbourne. Participants were screened to exclude those with psychosis, dementia and related
disorders. The age range of participants was 18 - 65 years. Five participants were not
included in the study because the questionnaire data was incomplete. The Anxiety Disorders
Interview Schedule for DSM-IV (ADIS-IV; Brown, Di Nardo & Barlow, 1994) administered
by clinical and provisional psychologists under supervision to verify diagnosis. As the ADIS-
IV did not contain items for hoarding disorder, participants were assessed using an expanded
8
version of the Hoarding Rating Scale – Interview (HRS-I; Tolin, Frost, & Steketee, 2010).
Five groups participated: Group 1 consisted of individuals diagnosed with hoarding disorder
with comorbid OCD (HO, n=23); Group 2 consisted individuals with hoarding disorder
without OCD (H, n=26); Group 3 comprised participants diagnosed with OCD but no
hoarding (O, n=20); Group 4 comprised participants who fulfilled the DSM-IV criteria for
Panic or Social Anxiety but not OCD (A, n=20); Group 5 was a community control group,
matched with the hoarding cohort for age, gender and level of education, with no DSM-IV
diagnosis nor a psychiatric history as determined by screening interviews (C, n = 20).
2.2 Procedure
Participants made contact with the research team via the telephone, mail or email to
indicate their interest in participating. They were then contacted by the research team who
arranged an interview. Each participant was provided with an information pack comprising:
(1) a description of the study, a consent form, and detailed explanatory material on the study
written in plain English to ensure adequate comprehension and clarity; and (2) two separate
batches of questionnaires with replied paid envelopes including measures of cognitive,
affective, and developmental factors.
Following informed consent, clinical interviews were conducted by the research team
using the ADIS-IV, whether face-to-face for metropolitan-based enquirers or by telephone for
rural or interstate respondents. Site visits were conducted if possible and photographs and
third party reports obtained to confirm severity of hoarding. Participants were screened to
exclude those with psychosis, dementia and related disorders. Each person was assigned a
number to ensure confidentiality, anonymity and accurate matching of data sets.
Demographic variables including age, gender, marital status, income, and education were
collected across the five groups. Objects that were most saved and the symptomatic features
of the five different groups were measured. With respect to the groups with hoarding
9
behaviour, information about comorbidities and potential hazards noted were also collected.
2.3 Materials
The Anxiety Disorders Interview Schedule for DSM-IV (ADIS-IV; Adult Version:
Brown et al., 1994) is a semi-structured interview screening of DSM-IV criteria for anxiety
and related disorders.
The Saving Inventory – Revised (SIR; Frost, Steketee & Grisham, 2004) is a 23 item
self-report scale designed to measure the major features of hoarding disorder (Frost & Hartl,
1996) Items were scored on a 5-point Likert scale. In this study, excellent internal
consistency was shown with a Cronbach’s α of 0.98.
The Savings List (Kyrios, 2002) is a descriptive list of 82 common objects saved or
hoarded as a systematic guide to the type of things being collected by clinical and non-
clinical groups that has been used in a number of studies (Wincze, 2001; Kyrios et al., 2002;
Novara, unpublished). Participants were asked to indicate the extent they saved each items on
a 7-point Likert scale from 1 (Not at all – I only save what I need or use) to 7 (Very much - I
save an excessive amount. Far more than I will ever use). Space was provided for participants
to include and rate additional items. In this study, two methods of scoring were used: (1) the
sum total of all 82 items, and (2) the number of items saved at the upper end of the Likert
scale (scores 5-7).
The Hoarding Rating Scale – Self Report (HRS-SR; Tolin et al., 2008) consisted of
five self-report diagnostic criteria proposed for compulsive hoarding (Steketee & Frost,
2007). Items were scored on a 9-point Likert scale. In this study, excellent internal
consistency was shown with a Cronbach’s α of 0.96.
3. Results
Table 1 shows the descriptive demographic data across the five groups. The
community control group and individuals who hoard were significantly older than the OCD
10
cohort. As expected, the community control group was significantly higher than the clinical
groups in terms of socioeconomic status as measured by income. There were no significant
differences in gender, marital status, or education between the groups. Within the hoarding
groups, 39 participants had comorbid depression and four had a diagnosis of OCPD.
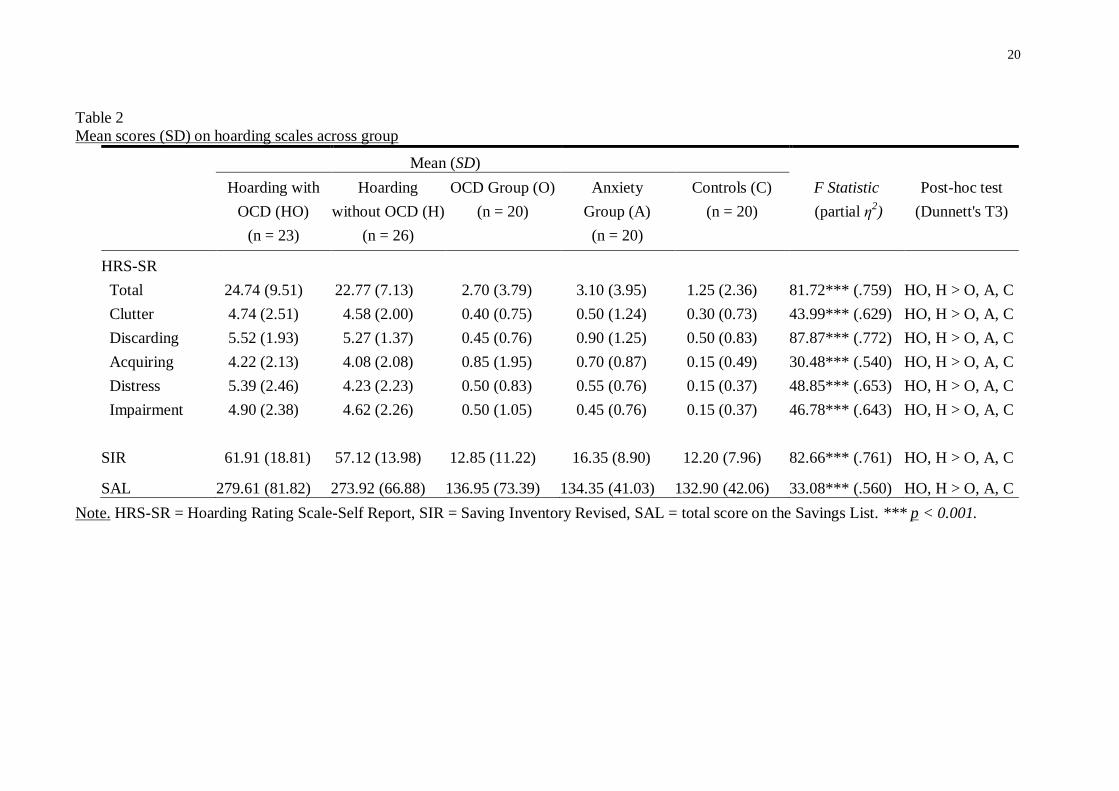
Table 2 shows differences between groups on measures of hoarding, including HRS-
SR items measuring the five criteria of hoarding suggested by Frost and Hartl (1996). Results
showed that individuals who hoard (with or without comorbid OCD) scored significantly
higher than the clinical and control groups (including OCD) on the five HRS items, SIR, and
SAL, supporting both the validity of groups and the usefulness of the items to discriminate
between them. There were no significant differences between OCD, anxiety and control
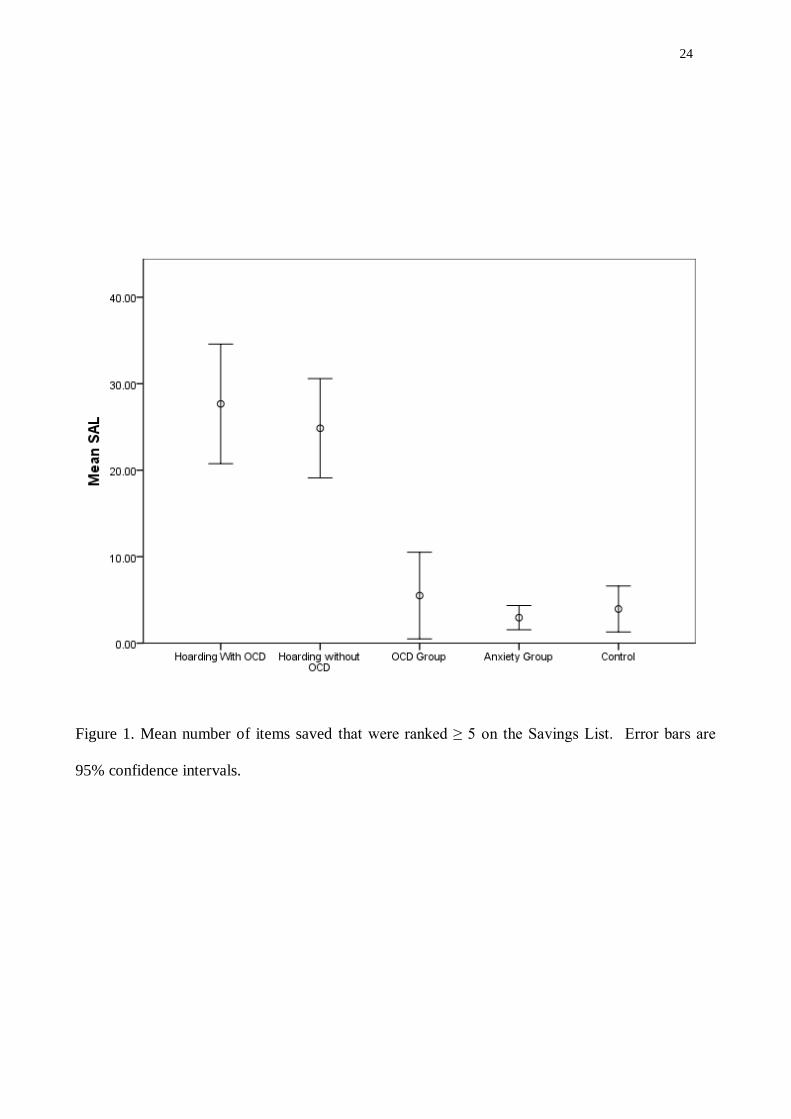
groups on these hoarding criteria. Figure 1 shows differences between groups on the mean
number of items saved that were ranked ≥ 5 on the Likert scale. The hoarding groups saved
significantly more types of items than the non-hoarding groups but there was no significant
difference between the two hoarding groups.
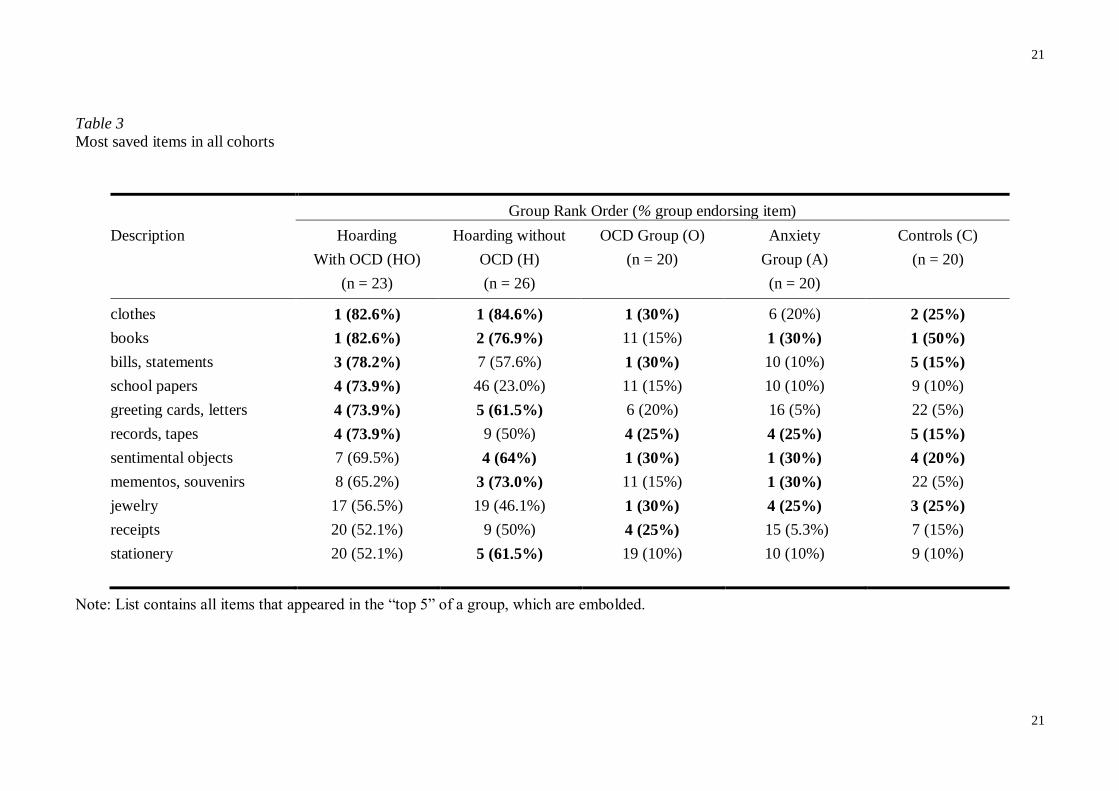
In a series of analyses using the Savings List (SAL), all groups were compared on the
items most likely to be saved. A list of the most saved items was constructed for each of the
cohorts (see Table 3). These were items on the SAL endorsed as ≥ 5 on the Likert scale – i.e.,
items that participants indicated that they were highly likely to save even if they did not need
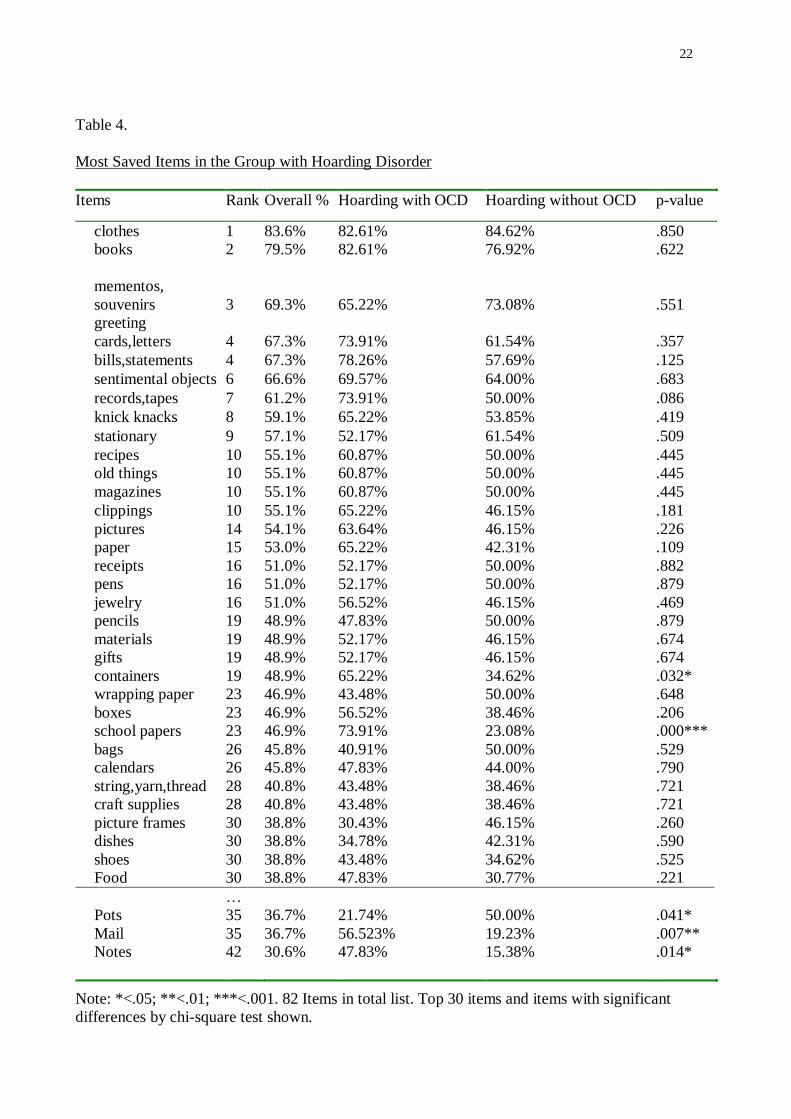
them. Table 4 shows the most saved items amongst individuals with hoarding disorder
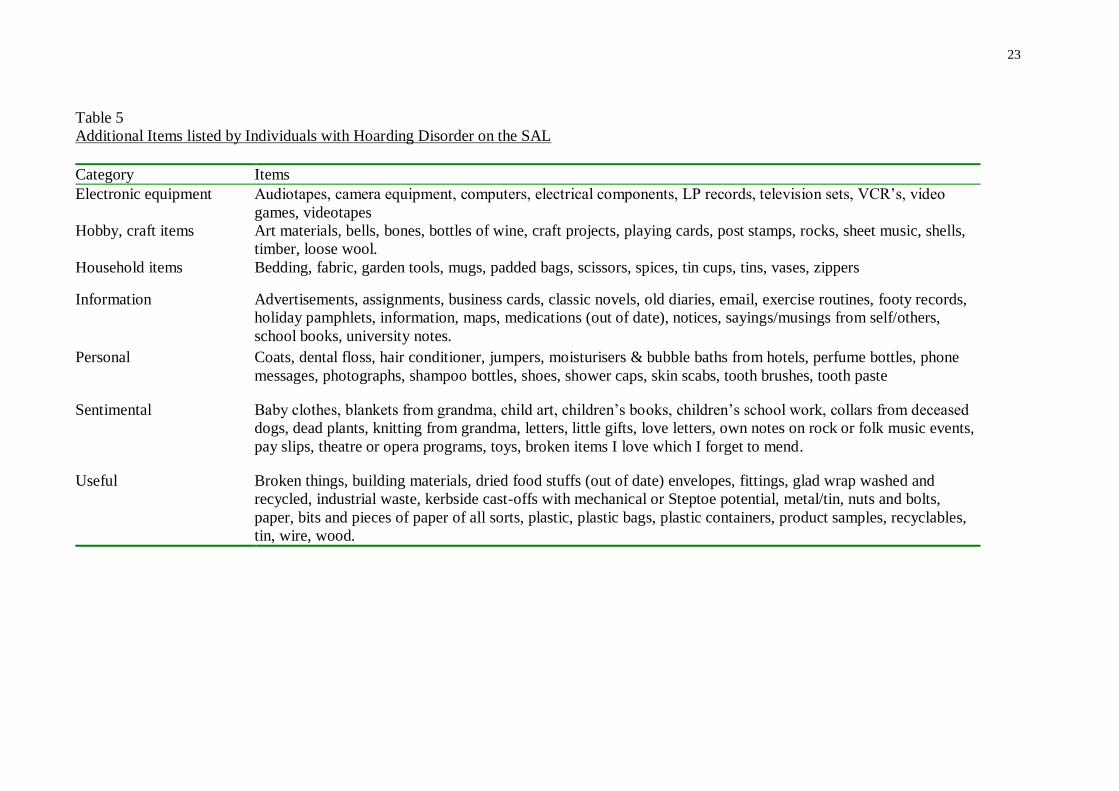
(combined groups), while Table 5 shows the list of additional items nominated by this group.
Clothes, books, bills/statements, records/tapes, and sentimental objects were the most
frequently saved items across all the groups. Interestingly, jewellery was one of the top five
items amongst each of the non-hoarding groups; whilst still kept in the groups with hoarding,
the rank order was relatively low (17 and 19th
most saved items in the HO and H groups
respectively). There were relatively few significant differences between the HO and H
11
groups, with the only notable exceptions being keeping school papers, containers, pots, mail
and notes, with the HO group being higher on all of these categories, except for pots. There
were many items added by hoarding participants in the optional additional listing of saved
objects. 65% and 78% of the individuals with hoarding disorder (with and without comorbid
OCD respectively) added extra items, while less than 20% of the other groups did so,
showing the idiosyncratic nature of saving amongst this group. The majority of individuals
who hoarded (69%) acknowledged that their clutter posed at least one safety hazard. Forty-
seven percent of all individuals who hoard noted that fire was the hazard that they were most
concerned about, followed by the risk to falling (38%) and concerns about hygiene standards
(35%).
4. Discussion
The focus of this study was the phenomenology of hoarding disorder – specifically
whether the pattern of objects saved by individuals who hoard differs from those with OCD
and other groups. The validity of the groups was supported, with the hoarding-specific
measures (SIR, SAL, HRS) clearly differentiating the groups who hoarded (with or without
OCD) from the other clinical and community controls. As hypothesised, individuals who
hoard were generally distinctive from the other clinical groups and non-clinical controls in
what they did with objects and possessions, and this did not differ depending on the presence
or absence of comorbid OCD. As expected, the range of objects that were saved excessively
by the hoarding groups was significantly higher than non-hoarding clinical and community
control groups, thus indicating that individuals who hoard did so indiscriminately as opposed
to the excessive saving of items of a specific category. This result is consistent with previous
findings indicating clear differences between individuals who do and do not hoard
(Abramowitz, Franklin, Schwartz & Furr, 2003; Frost & Gross, 1993; Frost & Hartl, 1996;
Leckman et al., 1997; Black et al., 1998; Samuels et al., 2002; Calamari et al., 1999; Samuels
12
et al., 2006).
The Savings List data was consistent with previous reports (Frost & Gross, 1993) that
clothes and books, receipts and bills, and personal and sentimental objects are collected at high
levels across all the groups. Thus, in relationship to general categories, individuals with
hoarding disorder generally collected similar items to non-hoarding groups (i.e. most groups
had similar category items within their top items), but just collected more of them. One notable
difference was that, with the possible exception of the OCD group, greeting cards and letters
tended to be kept more often in the groups with hoarding. This could reflect suggestions that
individuals with hoarding tend to be more likely to “fuse” person and objects (e.g., clients often
report that they may keep anything with people’s handwriting in it, including books with a
parent’s name inside the front cover, or newspapers which have been jotted upon).
Interestingly, jewelry was kept at a lower rank-level within the hoarding groups, despite their
being no differences in rates of being single or being male in this group (if anything, the trends
would suggest that the groups with hoarding were biased towards female married participants).
We could speculate that this may be due to individuals who hoard being less likely to perceive
jewelry as a special class of object (i.e., they may not privilege jewelry over other “sentimental”
or “pretty” objects to the same extent that non-clinical samples do). Anecdotally, many
individuals with hoarding disorder do report that a variety of objects can be considered to be
“pretty things”; for example, one of our recent clients reported difficulties in not collecting
broken glass from a bottle that was outside the therapy room, owing to its lovely colour.
Reflecting such anecdotes, differences were most apparent owing to the idiosyncratic
nature of items collected by those with hoarding disorder. Thus, most individuals with hoarding
disorder added extra items to the Savings List whereas few in the other groups did so. While to
some extent this may reflect known difficulties for individuals with hoarding to classify objects
within existing categories (i.e., “everything is unique”; e.g., Steketee & Frost, 2007), the
13
presence of especially personal items like skin scabs, dental floss, hair, soap and old
medications points to a deep-rooted “self-connectedness” to things, and perhaps a need to
protect the ‘self’ in maintaining ownership of such things. This is also consistent with some
models of hoarding that point to the psychological fusion of “self” with objects (e.g., Steketee
& Frost, 2007; Gwilliam, Wells & Cartwright-Hatton, 2004).
Comparing our results to the study by Pertusa et al. (2008) we found similar results;
with both studies finding very few differences between individuals with hoarding and comorbid
OCD, and those with hoarding without OCD, in terms of number of objects kept. These
findings provide further support to the argument that although related, hoarding disorder can
occur as a separate syndrome from OCD. While the objects collected by individuals varied
somewhat across the studies (although old clothes was the greatest kept item across both
studies), this is likely accounted for in terms of differences in methodology (i.e., questions
asked), as well as possible differences across samples (e.g., cultural differences between
Australian, USA and UK samples; urban or rural location, trauma history). In Pertusa et al.’s
study, they found that letters, receipts, bills, old medication, and bizarre objects were all kept
more frequently by individuals with OCD and hoarding. However, in our study, containers,
school papers, pots, mail and notes significantly differed between the groups, with the co-
morbid group again being higher on all (except for pots). It is unclear why these particular
objects differed between the groups, but it should be noted that in given the list contains 82
items, the relative lack of differences between the hoarding groups is probably more notable
than the few specific differences that were found.
The hoarding group exhibited scores on the hoarding measures that were similar to
those scored by compulsive hoarding samples from the USA and UK. Thus, the hoarding
groups (with or without OCD) were clearly higher on the Saving Inventory-Revised (SIR)
and did not differ from each other, while the group with OCD showed similar levels to
14
control samples. Similarly, groups were clearly distinguished using the Hoarding Rating
Scale-Self Report (HRS-SR) - a new self-report version of an existing interview (Tolin et al.,
2010). This study furthers suggestions that the HRS-SR might prove to be useful as a
standard screening device for this largely under-diagnosed condition, given its brevity in
comparison to the SIR, while the items clearly identify the phenomenology of hoarding. This
scale highlights succinctly the phenomena of hoarding – clutter, inability to stop acquiring
objects, difficulty discarding, the emotional over-attachment to things, and the functional
impairment - that are accentuated in such applied professions. Given the generally ‘hidden’
nature of hoarding, these items could perhaps become part of a standardized assessment
interview for health professionals and community workers.
Whilst the hoarding groups collected significantly more things both in quantity and
type than the other clinical and control groups, future research might consider whether
objects saved are affected by age or gender-related factors across the type or frequency of
collected items. More refined targeting of objects saved could lead to more specific strategies
in training individuals to reduce acquiring behaviour and increase organizational and de-
cluttering skills. The implications of this study are the support for the diagnosis of hoarding-
specific behaviours that manifest in the collection of large quantities of items that become
unmanageable and disruptive in ways that identify a consistent and discrete set of
psychological factors.
A limitation of the current study was the difficulty in differentiating OCD sufferers
who hoarded as part of their OCD from OCD sufferers who had co-morbid hoarding disorder.
Based on clinical interviews and rating scales, we are reasonably confident that all
participants in the HO group had co-morbid hoarding disorder. However, there remains a
possibility that some individuals in the HO group might also have OCD-related hoarding.
Pertusa, Frost, & Mataix-Cols (2010) noted that individuals with OCD-related hoarding were
15
more likely to collect bizarre items such as trash, faeces, urine, and nails. Unfortunately,
another limitation of the current study was the exclusion of indicators of squalor such as
trash, rotten food, faeces, and urine from the Savings List. Hair and nails were items on the
Savings List, but they did not rank highly in all groups. Participants were also invited to add
idiosyncratic items in the savings list but none reported hoarding bizarre items of squalor
with the exception of skin scabs. It is still possible that such items were hoarded but
participants were unwilling or too embarrassed to report them. The question of whether
hoarding as a symptom of OCD differs from hoarding when it is co-morbid with OCD
therefore requires further investigation. Finally, although the control group (C) was matched
to the hoarding groups (HO and H) on age and gender, there was a significant age difference
between the H group and the non-hoarding clinical groups (O and A groups). Age
differences might therefore have had some impact on the ranking of items.
In summary, this study examined hoarding behaviours in individuals with hoarding
both with and without comorbid OCD, and compared the hoarding behaviour to control
groups including individuals with OCD without hoarding. It was found that while commonly
hoarded items were similar across the groups, individuals who hoarded also listed a number
of idiosyncratic items, some which were deeply personal. This examination provides further
impetus to examination of theories that suggests that therapies and models that examine the
role of self and meaning in objects, as well as adding to our characterisation of what it means
to be experiencing hoarding disorder.
16
References
Abramowitz, J. S., Franklin, M. E., Schwartz, S. A., & Furr, J. M. (2003). Symptom
presentation and outcome of cognitive behavior therapy for obsessive compulsive
disorder. Journal of Consulting and Clinical Psychology, 71, 1049 – 1057.
American Psychiatric Association (/2000). Diagnostic and Statistical Manual of Mental
Disorders (4th
Ed., Text Revision). Washington DC: Author.
Black, D. W., Monahan, P., Gable, J., Blum, N., Clancy, G., & Baker, P. (1988). Hoarding
and treatment response in 38 non-depressed subjects with OCD. Journal of Clinical
Psychiatry, 59, 420-425
Brown, T. A., Di Nardo, P. A., & Barlow, D. H. (1994). Anxiety Disorders Interview
Schedule (4th ed.). Boulder, CO: Graywind Publications.
Calamari, J. E., Wiegartz, P. S., & Janeck, A. S. (1999). Obsessive-compulsive disorder
subgroups: A symptom-base clustering approach. Behavior Research and Therapy,
37, 113-125.
Fitzgerald, P. B. (1997). “The bowerbird symptom”: A case of severe hoarding of
possessions. Australian and New Zealand Journal of Psychiatry, 31, 597-600.
Frost, R. O., & Gross, R. C. (1993). The hoarding of possessions. Behavior Research and
Therapy, 31, 367-381.
Frost, R. O., & Hartl, T. L. (1996). A cognitive-behavioral model of compulsive hoarding.
Behavior Research and Therapy, 34, 341-350.
Frost, R. O., Krause, M. S., & Steketee, G. (1996). Hoarding and obsessive compulsive
symptoms. Behavior Modification, 20, 116-132.
Frost, R. O., Steketee, G., & Grisham, J. (2004). Measurement of compulsive hoarding:
Saving inventory-revised. Behavior Research and Therapy, 42, 1163-1182.
17
Frost,R.O., Steketee, G., & Tolin, D. (2011). Comorbidity in hoarding disorder. Depression
and Anxiety, 28(10), 876-884.
Greenberg, D. (1987). Compulsive hoarding. American Journal of Psychotherapy, 41, 409-
416.
Gwilliam, P., Wells, A., & Cartwright-Hatton, S. (2004). Dose meta-cognition or
responsibility predicts obsessive–compulsive symptoms: a test of the metacognitive
model. Clinical Psychology & Psychotherapy, 11(2), 137-144.
Kyrios, M. (2002). The Savings List. (Unpublished).
Leckman, J. F., Grice, D. E, Boardman, J., Zhang, H., Vitalie, A., Bondi, C., …Pauls, D. L.
(1997). Symptoms of obsessive compulsive disorder. American Journal of Psychiatry,
154, 911-917.
Lucini, G., Monk, I., & Szlatenyi, C. (2009). An analysis of fire incidents involving hoarding
households. Worcester: Worcester Polytechnic Institute.
Mataix-Cols, D., Frost, R. O., Pertusa, A., Clark, L. A., Leckman, J. F., Saxena, S., ...
Wilhelm, S. (2010). Hoarding disorder: a new diagnosis for DSM-V? Depression and
Anxiety, 27(6), 556–572.
Nordsletten, A.E., & Mataix-Cols, D. (2012) Hoarding versus collecting: Where does
pathology diverge from play? Clinical Psychology Review, 32, 165 - 176.
Pertusa, A., Frost, R. O., & Mataix-Cols, D. (2010). When hoarding is a symptom of OCD:
A case series and implications for DSM-V. Behaviour Research and Therapy, 48,
1012-1020.
Pertusa, A., Fullana, M. A., Singh, S., Alonso, P., Menchón, J. M., & Mataix-Cols, D. (2008).
Compulsive Hoarding: OCD Symptom, Distinct Clinical Syndrome, or Both?
American Journal of Psychiatry, 165, 1289-1298.
Rachman, S., Elliott, C., Shafran, R., Radomsky, A. (2009). Separating hoarding from OCD.
18
Behavior Research and Therapy, 47, 520 -522
Samuels, J., Bienvenu III, O. J., Riddle, M. A., Cullen, B. A. Liang, K. Y., Hoehn-Saric, R.,
& Nestadt, G. (2002). Hoarding in obsessive compulsive disorder: Results from a
case-control study. Behavior Research and Therapy, 40, 517-528.
Samuels, J. F., Riddle, M. A., Greenberg, B. D., Fyer, A. J., McCracken, J. T., Rauch, S. L.,
…Nestadt, G. (2006). The OCD collaborative genetics study: Methods and sample
description. American Journal of Medical Genetics Part B (Neuropsychiatric
Genetics), 141B, 201-207.
Steketee, G., & Frost, R.O. (2007) Compulsive Hoarding and Acquiring – Therapist Guide.
New York: Oxford University Press.
Steketee, G., & Pruyn. (1998) Families of Individuals with OCD. In R. P. Swinson, M. M.
Anthony, S. J. Rachman, & M. A. Richter (Eds.), Obsessive Compulsive Disorder:
Theory, Research and Treatment (pp. 120-140). New York: Guildford.
Tolin, D.F., Frost, R.O., & Steketee, G. (2010). A brief interview for assessing compulsive
hoarding: The Hoarding Rating Scale-Interview. Psychiatry Research, 178, 147-152.
Tolin, D.F., Frost, R.O., Steketee, G., Gray, K.D., & Fitch, K.E. (2008). The economic and
social burden of compulsive hoarding. Psychiatry Research, 160, 200-211.
Tolin, D., Fitch, K., Frost, R., & Steketee, G. (2010). Family informants' perceptions of
insight in compulsive hoarding. Cognitive Therapy and Research, 34(1), 69-81.
Wincze, J. (2001). The role of under-inclusion in the etiology of compulsive hoarding
behavior. (Unpublished doctoral dissertation). Boston University, Boston.

19
Table 1.
Demographics across groups – age, gender, marital status, education and income
Mean (SD)
Hoarding with
OCD (HO)
(n = 23)
Hoarding
without OCD
(H)
(n = 26)
OCD Group (O)
(n = 20)
Anxiety
Group (A)
(n = 20)
Controls (C)
(n = 20)
F Statistic
(partial η2)
Post-hoc test
(Dunnett's T3)
Age (yrs) 47.78 (11.43) 55.04 (10.36) 38.90 (12.29) 43.65 (13.67) 49.50 (9.35) F(4,104)=6.35***
(partial η2=.196)
C > O
H > A, O
Male (%) 30.4 19.2 50.0 50.0 30.0 χ2 (4)=7.24
Married (%) 43.5 57.7 30.0 30.0 50.0 χ2 (4)= 5.45
Tertiary ed (%) 47.8 50.0 60.0 80.0 75.0 χ2 (4)=7.72
Secondary ed
(%)
42.2 50.0 40.0 20.0 25.0
Low Income
(%)
43.5 46.2 30.0 35.0 10.0
Med Income
(%)
43.5 38.5 40.0 30.0 20.0 χ2 (8)=21.65**
High Income
(%)
13.0 15.4 30.0 35.0 70.0
aIncome groups - Low = < AUD$25000; Medium = AUD$25000-$50000; and High = > AUD$50000.
***p < 0.001; **p< 0.005.
20
Table 2
Mean scores (SD) on hoarding scales across group
Mean (SD)
Hoarding with
OCD (HO)
(n = 23)
Hoarding
without OCD (H)
(n = 26)
OCD Group (O)
(n = 20)
Anxiety
Group (A)
(n = 20)
Controls (C)
(n = 20)
F Statistic
(partial η2)
Post-hoc test
(Dunnett's T3)
HRS-SR
Total 24.74 (9.51) 22.77 (7.13) 2.70 (3.79) 3.10 (3.95) 1.25 (2.36) 81.72*** (.759) HO, H > O, A, C
Clutter 4.74 (2.51) 4.58 (2.00) 0.40 (0.75) 0.50 (1.24) 0.30 (0.73) 43.99*** (.629) HO, H > O, A, C
Discarding 5.52 (1.93) 5.27 (1.37) 0.45 (0.76) 0.90 (1.25) 0.50 (0.83) 87.87*** (.772) HO, H > O, A, C
Acquiring 4.22 (2.13) 4.08 (2.08) 0.85 (1.95) 0.70 (0.87) 0.15 (0.49) 30.48*** (.540) HO, H > O, A, C
Distress 5.39 (2.46) 4.23 (2.23) 0.50 (0.83) 0.55 (0.76) 0.15 (0.37) 48.85*** (.653) HO, H > O, A, C
Impairment 4.90 (2.38) 4.62 (2.26) 0.50 (1.05) 0.45 (0.76) 0.15 (0.37) 46.78*** (.643) HO, H > O, A, C
SIR 61.91 (18.81) 57.12 (13.98) 12.85 (11.22) 16.35 (8.90) 12.20 (7.96) 82.66*** (.761) HO, H > O, A, C
SAL 279.61 (81.82) 273.92 (66.88) 136.95 (73.39) 134.35 (41.03) 132.90 (42.06) 33.08*** (.560) HO, H > O, A, C
Note. HRS-SR = Hoarding Rating Scale-Self Report, SIR = Saving Inventory Revised, SAL = total score on the Savings List. *** p < 0.001.
21
21
Table 3
Most saved items in all cohorts
Group Rank Order (% group endorsing item)
Description Hoarding
With OCD (HO)
(n = 23)
Hoarding without
OCD (H)
(n = 26)
OCD Group (O)
(n = 20)
Anxiety
Group (A)
(n = 20)
Controls (C)
(n = 20)
clothes 1 (82.6%) 1 (84.6%) 1 (30%) 6 (20%) 2 (25%)
books 1 (82.6%) 2 (76.9%) 11 (15%) 1 (30%) 1 (50%)
bills, statements 3 (78.2%) 7 (57.6%) 1 (30%) 10 (10%) 5 (15%)
school papers 4 (73.9%) 46 (23.0%) 11 (15%) 10 (10%) 9 (10%)
greeting cards, letters 4 (73.9%) 5 (61.5%) 6 (20%) 16 (5%) 22 (5%)
records, tapes 4 (73.9%) 9 (50%) 4 (25%) 4 (25%) 5 (15%)
sentimental objects 7 (69.5%) 4 (64%) 1 (30%) 1 (30%) 4 (20%)
mementos, souvenirs 8 (65.2%) 3 (73.0%) 11 (15%) 1 (30%) 22 (5%)
jewelry 17 (56.5%) 19 (46.1%) 1 (30%) 4 (25%) 3 (25%)
receipts 20 (52.1%) 9 (50%) 4 (25%) 15 (5.3%) 7 (15%)
stationery 20 (52.1%) 5 (61.5%) 19 (10%) 10 (10%) 9 (10%)
Note: List contains all items that appeared in the “top 5” of a group, which are embolded.
22
Table 4.
Most Saved Items in the Group with Hoarding Disorder
Items Rank Overall % Hoarding with OCD Hoarding without OCD p-value
clothes 1 83.6% 82.61% 84.62% .850
books 2 79.5% 82.61% 76.92% .622
mementos,
souvenirs 3
69.3% 65.22% 73.08% .551
greeting
cards,letters 4
67.3% 73.91% 61.54% .357
bills,statements 4 67.3% 78.26% 57.69% .125
sentimental objects 6 66.6% 69.57% 64.00% .683
records,tapes 7 61.2% 73.91% 50.00% .086
knick knacks 8 59.1% 65.22% 53.85% .419
stationary 9 57.1% 52.17% 61.54% .509
recipes 10 55.1% 60.87% 50.00% .445
old things 10 55.1% 60.87% 50.00% .445
magazines 10 55.1% 60.87% 50.00% .445
clippings 10 55.1% 65.22% 46.15% .181
pictures 14 54.1% 63.64% 46.15% .226
paper 15 53.0% 65.22% 42.31% .109
receipts 16 51.0% 52.17% 50.00% .882
pens 16 51.0% 52.17% 50.00% .879
jewelry 16 51.0% 56.52% 46.15% .469
pencils 19 48.9% 47.83% 50.00% .879
materials 19 48.9% 52.17% 46.15% .674
gifts 19 48.9% 52.17% 46.15% .674
containers 19 48.9% 65.22% 34.62% .032*
wrapping paper 23 46.9% 43.48% 50.00% .648
boxes 23 46.9% 56.52% 38.46% .206
school papers 23 46.9% 73.91% 23.08% .000***
bags 26 45.8% 40.91% 50.00% .529
calendars 26 45.8% 47.83% 44.00% .790
string,yarn,thread 28 40.8% 43.48% 38.46% .721
craft supplies 28 40.8% 43.48% 38.46% .721
picture frames 30 38.8% 30.43% 46.15% .260
dishes 30 38.8% 34.78% 42.31% .590
shoes 30 38.8% 43.48% 34.62% .525
Food 30 38.8% 47.83% 30.77% .221
…
Pots 35 36.7% 21.74% 50.00% .041*
Mail 35 36.7% 56.523% 19.23% .007**
Notes 42 30.6% 47.83% 15.38% .014*
Note: *<.05; **<.01; ***<.001. 82 Items in total list. Top 30 items and items with significant
differences by chi-square test shown.
23
Table 5
Additional Items listed by Individuals with Hoarding Disorder on the SAL
Category Items
Electronic equipment Audiotapes, camera equipment, computers, electrical components, LP records, television sets, VCR’s, video
games, videotapes
Hobby, craft items Art materials, bells, bones, bottles of wine, craft projects, playing cards, post stamps, rocks, sheet music, shells,
timber, loose wool.
Household items Bedding, fabric, garden tools, mugs, padded bags, scissors, spices, tin cups, tins, vases, zippers
Information Advertisements, assignments, business cards, classic novels, old diaries, email, exercise routines, footy records,
holiday pamphlets, information, maps, medications (out of date), notices, sayings/musings from self/others,
school books, university notes.
Personal Coats, dental floss, hair conditioner, jumpers, moisturisers & bubble baths from hotels, perfume bottles, phone
messages, photographs, shampoo bottles, shoes, shower caps, skin scabs, tooth brushes, tooth paste
Sentimental Baby clothes, blankets from grandma, child art, children’s books, children’s school work, collars from deceased
dogs, dead plants, knitting from grandma, letters, little gifts, love letters, own notes on rock or folk music events,
pay slips, theatre or opera programs, toys, broken items I love which I forget to mend.
Useful Broken things, building materials, dried food stuffs (out of date) envelopes, fittings, glad wrap washed and
recycled, industrial waste, kerbside cast-offs with mechanical or Steptoe potential, metal/tin, nuts and bolts,
paper, bits and pieces of paper of all sorts, plastic, plastic bags, plastic containers, product samples, recyclables,
tin, wire, wood.
24
Figure 1. Mean number of items saved that were ranked ≥ 5 on the Savings List. Error bars are
95% confidence intervals.
Top Related
Copyright © 2022 FDOKUMEN

