






Bahasa
Halaman
Hukum

Mobile Phones for Health Education
A Case Study of Text to Change‟s HIV and AIDS SMS Quiz Project
in Mbarara District, Western Uganda
Bonny Apunyu
A thesis submitted in partial fulfillment of the requirements for the degree of Master of Philosophy Degree in Media Studies
Institute of Media and Communication (IMK)
UNIVERSITETET I OSLO
Spring 2011

II
III
Abstract
In environments where diseases such as HIV and AIDS are often taboo, successful awareness
and educational interventions must address peoples‘ privacy and confidentiality concerns. The
ubiquity and low cost of Text Message Services (SMS) hold the potential to effectively deliver
HIV and AIDS awareness and education by communicating with people in an accessible and
engaging manner that both respects their privacy and gives them the tools to make informed
choices.
This study presents an evaluation of an incentive-based SMS quiz approach designed to improve
awareness of HIV and AIDS in Mbarara District, Western Uganda. The goal of deploying HIV
and AIDS related quizzes to the target population is to increase people‘s awareness and
knowledge about the disease, to promote their healthy behaviour and to encourage them to know
their health status and seek treatment if necessary.
This study employs the domestication of media and technology as a theoretical framework to
understand how Text to Change deployed SMS quizzes to improve HIV and AIDS awareness in
the selected area of study. Data was collected mainly through in-depth-interviews and
observation. The study sought to provide an in-depth analysis of the project which could be
linked to theoretical assumptions that explain how mobile-based technologies can be used in
HIV and AIDS education and awareness. The paper thus did not aim at generalizing findings but
sought to provide illumination, understanding and extrapolation of the findings to similar
situations.
This qualitative study suggests that text messaging may be a very useful and culturally-relevant
platform to support HIV and AIDS education today. In developing countries like Uganda, text
messaging have proven effective in targeting hard-to-reach populations especially those in rural
areas where the absence of clinics, lack of healthcare workers and limited access to health-related
information often prevent people from making informed decisions about their health. While
other communication media such as radio, television, voice-based information hotlines and
interactive websites can be employed in the service of education about HIV and AIDS issues,
SMS stands out as having several advantages over each of these: cost-effectiveness, scalability,
convenience, broad reach and widespread popularity in low-income countries.
IV
This study however notes that text messaging has a huge disadvantage of being only able to allow
only 160 characters. Secondly, most keypads do not support local languages such that, the SMS
service requires users to type and read responses only in English hence may be a constraint to the
target users. Additionally, poor quality of mobile phone services sometimes makes their use
frustrating. On occasions, the service providers may offer no service at all, or very poor reception
for days. Additionally, text messaging has become more popular among younger generations
compared to other groups, a factor that may limit its scope and scalability. Another a potential
drawback to the use of text message-based educational interventions is the marginalization of
certain populations such as those that are illiterate or do not have access to mobile phones.
However, some of these limitations may be reduced as mobile technology advances. For
example, innovations exist that provide voice response systems and images instead of text for
those with limited literacy.
This study established that there were no clear differences between intervention outcomes
delivered by the SMS quiz and the existing HIV and AIDS awareness mechanisms. Moreover, the
respondents still preferred the traditional channels of communication to access HIV and AIDS
related information. In light of this, organizers of the SMS quiz note that in addition to providing
the HIV and AIDS information to the target audience in a relatively cheaper, convenient, private
and interactive manner, another issue to explore is whether target populations are prompted to
take action such as to seek voluntary counseling and testing upon receiving the quizzes.
This study suggests that text messaging should not be considered a stand-alone model for
delivering HIV and AIDS education but rather as a tool by which several awareness techniques
can be administered. Further, if text message intervention studies are built on evidence and
theory, the potential impact of these interventions may yield better outcomes.

V
© Bonny Apunyu
2011
Mobile Phones for Health Education
Bonny Apunyu
http://www.duo.uio.no/
Trykk: Reprosentralen, Universitetet i Oslo

VI
VII
Acknowledgment
The success of this project depends largely on the encouragement and support of many others. I
take this opportunity to express my gratitude to the people who have been involved in the
successful completion of this project.
I would like to extend my greatest appreciation to Professor Terje Rasmussen. I cannot measure
the tremendous support and help you offered me. I felt motivated and encouraged every time I
attended your meetings. Without your encouragement and guidance this project would not have
materialized.
I also send a warm appreciation to Text to Change Uganda and Netherlands and its partners for
offering me valuable support during my field study.
Finally, I send my deepest appreciation to the Quota Scheme and the Norwegian Government
who offered me full financial support to pursue a master‘s degree at the University of Oslo.
Bonny Apunyu
2011

VIII
IX
List of Abbreviations
AIC AIDS Information Centre
AIDS Acquired Immune Deficiency Syndrome
GPS Global Positioning System
GSM Global System for Mobile
HCT HIV Counseling and Testing
HIPS Health Initiatives for the Private Sector
HIV Human immunodeficiency virus
ICT Information Communication and Technology
ICT4D Information Communication and Technology for Development
ITU International Telecommunication Union
MHealth Mobile Health
MTN Mobile Telecommunication Company
NGO Non-Governmental Organization
PDAs Personal Data Accessories
PEPFAR President Bush‘s Emergency Plan for AIDS Relief
SMS Short Messages
STI Sexually Transmitted Infections
TTC Text to Change
UCC Uganda Communications Commission
UNAIDS Joint United Nations Programme on HIV and AIDS
UNICEF United Nations Children‘s Education Fund
VCT Voluntary Counseling and Testing
WHO World Health Organization

X
XI
Table of Contents Abstract ................................................................................................................................... III
Acknowledgment .................................................................................................................. VII
List of Abbreviations............................................................................................................... IX
1 Introduction ...................................................................................................................... 1
1.1 Background .................................................................................................................. 1
1.2 The problem ................................................................................................................. 2
1.2.1 HIV and AIDS in Africa/Uganda.......................................................................... 2
1.2.2 HIV and AIDS knowledge gaps in Uganda ........................................................... 3
1.3 The Case Study ............................................................................................................. 5
1.3.1 Text to Change (TTC) ........................................................................................... 5
1.3.2 The process ........................................................................................................... 5
1.3.3 The pilot project .................................................................................................... 5
1.4 Research objectives ....................................................................................................... 6
1.5 Research questions ........................................................................................................ 6
1.6 Significance of the study ............................................................................................... 7
1.7 Structure of the study .................................................................................................... 7
2 Literature review ............................................................................................................... 9
2.1 Introduction ................................................................................................................. 9
2.2 Mobile communications in Uganda ............................................................................... 9
2.3 Use of ICT for health care in Africa ............................................................................ 13
2.4 Contribution of mobile phones to health in developing countries ............................... 13
2.5 The limits of mobile telephony and missed opportunities in Africa ............................. 15
2.6 mHealth ...................................................................................................................... 16
2.7 Text-based health initiatives ........................................................................................ 18
2.7.1 Text Messaging Services (SMS) ............................................................................ 19
3 Theoretical Framework .................................................................................................. 21
3.1 Introduction ............................................................................................................... 21
3.1.1 Theoretical review ............................................................................................... 21
3.1.2 Domestication, a brief history of the concept ...................................................... 21
3.1.3 The concept ........................................................................................................ 22
3.1.4 The Domestication model ................................................................................... 23
XII
3.1.5 Outline of the model ........................................................................................... 23
3.1.6 Dimensions of Domestication ............................................................................. 24
3.1.7 Key theoretical assumptions ................................................................................ 25
3.2 Domestication and mobile phones .............................................................................. 26
3.3 Taking Domestication outside the home ..................................................................... 29
3.4 Mobile phones in society ............................................................................................ 29
4 Methodology ................................................................................................................... 31
4.1 Introduction ............................................................................................................... 31
4.2 Choosing a qualitative method .................................................................................... 31
4.3 Triangulation as a technique ........................................................................................ 33
4.4 The Case Study approach ............................................................................................ 33
4.5 Methods and procedures ............................................................................................. 35
4.5.1 Qualitative Interviews .......................................................................................... 35
4.5.2 Focus Group Discussions .................................................................................... 37
4.5.3 Observation ......................................................................................................... 38
4.6 Data analysis ............................................................................................................... 40
4.7 Data credibility ........................................................................................................... 40
4.8 Limitation of the study ................................................................................................ 41
4.9 Chapter summary ........................................................................................................ 42
5 Research findings ........................................................................................................... 43
5.1 Introduction ............................................................................................................... 43
5.2 The Case Study: The HIV and AIDS SMS quiz program ............................................ 43
5.2.1 The program stakeholders ................................................................................... 44
5.2.2 The SMS quiz ...................................................................................................... 45
5.2.3 Implementation ................................................................................................... 47
5.2.4 Outcome ............................................................................................................. 48
5.3 Perceptions on use of SMS quiz for HIV and AIDS education .................................. 49
5.4 Chapter summary ........................................................................................................ 58
6 Concluding discussion and recommendations ............................................................ 59
6.1 Introduction ............................................................................................................... 59
6.2 Summary..................................................................................................................... 65
6.3 Challenges to HIV and AIDS education in Uganda .................................................... 68
XIII
6.4 Implications for research ............................................................................................ 69
6.5 Implications for practice ............................................................................................. 70
6.6 Implications for theory ............................................................................................... 71
6.7 Recommendations ...................................................................................................... 72
References ............................................................................................................................... 75
Annexes ................................................................................................................................... 83
Annex 1: The SMS-based quiz ............................................................................................... 83
Annex 2: Guide for interviews with TTC Staff and project partners ...................................... 86
Annex 3: KAP survey questions for focus groups .................................................................. 87
Annex 4: Guide for interviews with technical respondents and peer educators ...................... 89
Annex 5: Map of Uganda showing Mbarara District .............................................................. 91

XIV

1
1 Introduction
1.1 Background
Rapidly emerging mobile communications platforms such as mobile phones in many counties
worldwide offer new opportunities for delivering health care services by placing timely
information into the hands of those who need it most. The capability, referred to as ‗‗mobile
health‘‘ or more commonly as ‗‗m-health,‘‘ involves innovative use of mobile devices to link
remote persons directly with the healthcare system to exchange information and provide
education and other services.
There are approximately four billion cellular subscribers in the world, with the most rapid growth
in use of mobile phones occurring in the developing countries1. Global mobile penetration grew
10-fold in the last 10 years and is likely to approximate 100% by 2018.2 The remarkable
penetration of mobile phones in Africa has set the stage for tremendous innovation in mobile
applications and services. The number of mobile phone users in Africa grew from 49 million in
2002 to 280 million in 2007 and it is projected to approach 600 million by 20123. This widespread
adoption combined with the relative absence of wired network infrastructure and computers
means that many Africans‘ first contact with a networked computing device is the mobile phone.
Such a rapid growth in mobile phone networks has been made possible by the proliferation of
GSM (Global System for Mobile communications)—the standard for mobile communications
across the world. According to the GSM Association, GSM networks currently cover 219
countries and territories, serving more than 3 billion people. All mobile phones today offer voice
and data communication.
1 International Telecommunication Union report available at: http://www.itu.int/ITU-D/ict/publications/world/world.html (last accessed October 18, 2010). 2 Sharma C. Mobile services evolution 2008–2018. Available at: www.chetansharma.com/UNF%20-
%20Mobile%20Services%20Evolution%20Final.pdf (last accessed October 18, 2010).
3 Blycroft Limited. African Mobile Fact book 2008: Available at:
http://www.w3.org/2008/MW4D/wiki/FrontPage?action=AttachFile&do=get&target=Africa_Mobile_Fact_Book
_2008.pdf (Last accessed October 18, 2010)
2
The most commonly used data application is the short message service (SMS), also called person-
to-person ‗‗text messaging.‘‘ More advanced mobile phones called smart phones often have
additional features, including Internet e-mail and browsing; built-in camera; speakerphone; voice
recorder; GPS receiver; Bluetooth and Wi-Fi connectivity; and the capacity to download, view,
and store music, videos, or games and operate a variety of software applications (Apps). Some
phones also include a touch screen or keyboard and other accessories. While the advanced
computer-like smart phones offer more capabilities, their availability, affordability, and
sustainability remain issues.
The majority of m-health activity is occurring in the developing world through basic voice and
SMS functionality over GSM networks. A range of mobile health applications is being
implemented and tested by innovative public–private partnerships to showcase the promise of m-
health across a variety of applications and settings. Cellular technology is being used to deliver
medication and appointment reminders; provide health education and launch awareness
campaigns; facilitate remote data collection and remote monitoring; and enable tracking,
diagnostics, and treatment support in case of disease and epidemic outbreaks.
‗‗The explosive spread of mobile phone networks across the developing world has created a
unique opportunity to significantly transform how countries can tackle global health challenges,‘‘
said Dr. Howard Zucker, Assistant Director-General of the World Health Organization (WHO),
representing the WHO at the Phones for Health partnership‘s launch at the 3GSM World
Congress in Barcelona in 2007.
1.2 The problem
1.2.1 HIV and AIDS in Africa/Uganda
Sub-Saharan Africa is the region most heavily affected by HIV in the world, accounting for 67%
of infection and 72% death worldwide (UNAIDS, 2009). The HIV and AIDS prevalence rate for
both adults and children in sub-Saharan Africa was approximately 22.4 million in 2008, 1.9
million of which were newly infected (UNAIDS, 2009). The estimated number of AIDS-related
death in the region was 1.4 million in the same year (Avert, 2010; UNAIDS, 2009). In Uganda
alone, approximately 1 million people live with HIV and AIDS as of 2008, with slightly more
females than males (Avert, 2010).
3
Although the number of AIDS related deaths in Uganda has decreased drastically from 120,000
in 2001 to 70,000 in 2007 (Avert, 2010; UNStats, 2010), trends are reported to be reversed in the
rural areas. Guwatudde et al. (2009) highlighted the high potential for a rise in the HIV infection
rates in rural Uganda, and reported an HIV prevalence rate of 9.9%, as compared to the national
average of 6.4%. In fact, the rural population accounts for close to 90% of the current statistics.
Recent statistics showed that women accounted for 7.5% of the figures and men accounted for
5% (Uganda Bureau of Statistics and Macro International Inc. 2007).
In addition, there seems to be a discrepancy between governmental efforts and its impact on the
population. Stigma towards HIV and AIDS victims has been identified as one of the major
barriers to addressing the issue in Africa as well as the rest of the world (Gilbert & Walker, 2009;
Maughan-Brown, 2010; Sambisa, Curtis, & Mishra, 2010; Maman et al., 2009). In a recent
nationwide survey of Zimbabweans on HIV testing, Sambisa et al. (2010) found that even though
mass media promotion efforts positively correlated to testing, stigmatization posed a strong
obstacle. In particular, women who fear social rejection were the least likely to get tested.
However, individuals who know people with HIV and AIDS and observed discrimination against
others regardless of whether they know people with HIV and AIDS led to higher uptake of the
test. Findings suggest that the stigma associated with the issue could work both ways in
influencing testing behaviour.
1.2.2 HIV and AIDS knowledge gaps in Uganda
The sharp increase in penetration rates of HIV and AIDS is Uganda is attributed to low levels of
awareness about the disease and prevention methods. It is likely that women are more vulnerable
to the disease due to lower levels of knowledge as compared to men. The Uganda Bureau of
Statistics and Macro International Inc. (2007) found that while 42% of Ugandan men had
comprehensive knowledge on HIV and AIDS, only 31% of the women were equipped with such
knowledge. Women in Uganda are at an educational disadvantage compared to men. Women‘s
comparative lack of schooling limits their opportunities and constrains their choices. Education is
crucial to gaining the knowledge; skills and confidence that women need to improve their status
and health. Studies show that a woman‘s educational level is strongly associated with health
status, contraceptive use, fertility rates, and health of her children.
Although the Ugandan Ministry of Health launched a door-to-door HIV screening program as
well as a voluntary counseling and testing clinic, an estimated 80% of Ugandan youths and adults
4
still remain unaware of their HIV status today. According to Tumushabe (2006), HIV and AIDS
awareness campaigns have been carried out in Uganda since the mid-1990s, after the
liberalization of the mass media. Radio was the main platform utilized for education on the issue
at the period of time when HIV and AIDS patients were highly discriminated against. The print
media, in particular a newsletter focusing on frank information about sex and relationships, was
used to reach out to schools and community groups. In addition, the government also carried out
related campaigns and distributed condoms as part of their efforts. However such health
messages in the area reduced significantly after 1995 as the government shifted their attention to
other issues. In the mid-2000s, other awareness and prevention efforts were implemented by
international organizations such as the International HIV and AIDS Alliance, which offered
related health services, provided information about the disease, and distributed condoms to the
community4.
Despite attempts to educate Ugandans about the issue, HIV and AIDS prevalence rates remained
high especially for rural areas (Tumushabe, 2006). This is most likely due to the fact that access to
health facilities in these areas is lower than that within urban regions. It also suggests that the
mass media campaigns failed to have an impact on the rural population, as evidence from the
higher HIV and AIDS incidence. In addition, the above-mentioned barriers reduce the likelihood
of the target population acting upon the advocated behaviour, such as getting tested for HIV and
AIDS.
It is thus important to increase awareness of HIV and AIDS to such groups. More effective
communication about the disease and greater flows of information are central to the success of
AIDS strategies, and for reducing the vulnerability that flows to and from HIV infection.
Information and communication are sources of power in an epidemic characterized by its lack—
they confer the power to protect against infection, to influence decision makers, and to lead lives
of dignity and equality once infected. In a region often characterized by resource limitations and
fragmented infrastructures, information and communication are two of the most critical and
abundant resources available in the fight against HIV and AIDS. They are both the prerequisites
and enablers of an effective response.
4 More information is available on the following website: http://www.aidsalliance.org/HomePagedetails.aspx?Id=1
(Accessed March 10, 2011).
5
This study posits that mobile phone technology, whose rapid growth in Uganda provides an
avenue to reach millions with HIV and AIDS messages in a relatively easy, practical and cost
effective way, may be a new tool for HIV prevention and awareness campaigns.
1.3 The Case Study
1.3.1 Text to Change (TTC)
Text to Change, a Dutch funded non-profit organization in Africa, has been using mobile
technology for health education since 2006. Combining the need for innovative health education
with the growth in use of mobile phones, TTC has been running a fun, innovative and practical
HIV and AIDS education program in three countries; Uganda, Kenya and Namibia. This
program not only educates participants about AIDS but also encourages infected patients to seek
medical help and adhere to medication5.
1.3.2 The process
TTC runs a six-week SMS based quiz program with participants receiving three questions per
week. The quiz participants answer by sending a free text message. The correct answer is
acknowledged with additional information on the topic and the wrong one by an explanation
about the correct answer. Detailed information on weekly quiz issues are also put up in a local
newspaper and on the TTC website. At the end of the program, participants visit a Voluntary
Counseling and Testing (HCT/VCT) centre where they are provided with free HIV and AIDS
counseling and testing. Participants who provide correct answers also have an opportunity to win
prizes such as mobile phones and air time (talk time minutes).
1.3.3 The pilot project
Text to Change offers an interactive mobile SMS quiz with knowledge questions linked with a
rewarding system (incentive). In this study, TTC‘s pilot project, which was launched February 14,
2008 in Mbarara District, Western Uganda is used as a case study. The project, which was
pioneered in Uganda is an initiative aimed at increasing awareness on HIV and AIDS through
5 Text to Change webpage: http://www.texttochange.org/(last accessed December 10, 2010)
6
information giving by use of mobile phone text messages. The project‘s goal was to increase HIV
and AIDS awareness and encourage participants to access HIV Counseling and Testing (HCT)
services. The TTC pilot project ran from six to eight weeks targeting Celtel Uganda (now Zain)
subscribers from the selected Mbarara region. The target group was 15,000 participants with
AIDS Information Centre (AIC) Mbarara Branch being the HCT service provider.
Participants received interactive text messages in form of multiple choice questions on their
mobile phones. When answered correctly, automatically guaranteed a participant free HCT
services and at the same time qualified to enter into the draw to win various prizes.
1.4 Research objectives
This paper presents an evaluation of a mobile phone based approach designed to improve HIV
and AIDS awareness. Specifically, the paper seeks to assess the potential of mobile phones to
deliver HIV and AIDS education through incentive-based SMS quizzes in the selected area of
study. The goal of deploying HIV and AIDS related quizzes to the general population is to
increase awareness and knowledge about HIV and AIDS, to promote healthy behaviour and to
encourage people to know their HIV status and seek treatment if necessary.
The specific objectives of this study are to;
to establish whether the SMS quiz is an effective channel of delivering HIV and AIDS
education/awareness.
assess, knowledge, attitudes and perception of target populations on the use of mobile
technology for HIV and AIDS education. investigate the status of mobile health
(mHealth) in Uganda
understand the demographic characteristics of users and non-users of the SMS quiz
project.
1.5 Research questions
The following research question helps explore the efficacy of using text messages for HIV and
AIDS education.
RQ1: How are text messages being used by TTC to create HIV and AIDS awareness among
users? a)What are the milestones? b) What are the challenges?
7
RQ2: To what extent is mobile phone based SMS quiz program appropriate channel for
delivering HIV and AIDS education among users?
RQ3. a) To what extent do the project participants who own a mobile phone use the medium
for accessing HIV and AIDS information?
b) To what extent do the project participants who own a mobile phone use the text
messaging (SMS) for HIV and AIDS education-related purposes?
RQ4. To what extent is the mobile phone used for HIV and AIDS education in relation to other
communication channels?
RQ5. To what extent is the SMS use for HIV and AIDS education determined by age?
1.6 Significance of the study
This research on the use of mobile phones for HIV and AIDS education may be the first of its
kind in Uganda. It may contribute empirical evidence that support some of the previous
theoretical developments and insights from qualitative research on the use of mobile phone
technology for HIV and AIDS awareness programs. It may also enhance previous solutions to
HIV and AIDS knowledge gaps in Uganda.
1.7 Structure of the study
This study is presented in six chapters. Chapter I includes the background of the study, statement
of the problem, objectives of the study, research questions and significance of the study.
Chapter II presents a review of the literature. It explores existing literature on the use of ICTs
especially mobile phones for healthcare in Africa, mobile communications in Uganda, mHealth in
Africa, text-based healthcare initiatives and Text Messaging Services (SMS). It also includes a
review of some recent studies on the use of mobile phones for health interventions. The
contribution of mobile phones in developing countries is also presented in this section and
finally, the limits of mobile telephony and missed opportunities are presented.
Chapter III presents the theoretical framework used as the basis for making analysis. It includes a
review of the Domestication studies, a brief history of the concept of domestication of media and
communication technologies. It also presents an outline of the domestication model and the
application of the model to mobile phone use.

8
Chapter IV describes the methodology used in this study. It includes the research procedures,
data collection methods and analysis procedures.
Chapter V presents the study the finding of the study. It also presents analysis of the responses.
Chapter VI provides a summary of the entire study, a concluding discussion of findings,
implications of the finding for theory, practice and research. It also presents some
recommendations for further research.

9
2 Literature review
2.1 Introduction
The expansion and adoption of new methods of communication provide new opportunities for
delivering health information. This section reviews the previous research examining mobile
telephone short-message service (SMS) for delivering health behaviour change interventions. The
SMS service has wide population reach, can be individually tailored, and allows instant delivery
with asynchronous receipt, suggesting open opportunities for delivering health behaviour
interventions.
It should be noted that mobile communications in developing countries differs radically from
that of western countries. Communication is mostly passive, taking the form of receiving calls
rather than calling. Young people use the cellular phone just to receive calls from their families
and relatives. The preferred mode of communication is to send and receive low cost SMS (text
messages), using pay as you go cards rather than a subscribed line. Some of these contrasts have
been emphasized while presenting the promise that mobile phones present for health education.
2.2 Mobile communications in Uganda
Uganda‘s mobile communications market has registered strong growth in recent years.
According to the Uganda Communications Commission (UCC), there were about 9.5 million
mobile subscribers in August 2009, an increase of 3.3 million from a year earlier.6 The number of
overall minutes being used has also nearly doubled.
The increase in subscriptions, along with substantial tariff discounts, resulted in a total of 6.6
billion minutes being billed during the fiscal 2008/2009, versus 3.5 billion minutes in the
previous fiscal year.
6 Uganda Communications Commission (UCC) website: http://www.ucc.co.ug/ (last accessed October 20, 2010)

10
Table 1. Shows Uganda‘s household ownership and access to new media and ICTs
The UCC attributes this market growth to the expansion of area service coverage and the
introduction of new market competitors. Competitors are now offering a wider variety of
services and plans along with cheaper introductory packages. There are now seven mobile phone
service providers ranging in size and service capabilities. The first provider was Celtel (Zain
Uganda) which began service in December 1994. The providers to follow were MTN Uganda in
1998 and Uganda Telecom in 2001. Orange and Warid Telecom entered in early 2008; I-Telecom
debuted in September 2009 and targeted more affluent Ugandans with such offerings as mobile
broadband internet and fast data services7. At the end of the fiscal 2008/2009, the UCC
estimated that some 310,000 Ugandans have access to mobile phone.
Smile Telecom, which began providing mobile services in December 2009, targets low income
Ugandans who may not be able to afford the cost of a handset. Smile gives customers their own
telephone numbers and voice message boxes, and secure personal identification numbers to use
on any Smile Communications phone. Customers can then make a call through company agents
at street kiosks or stalls or at Smile pay phones.
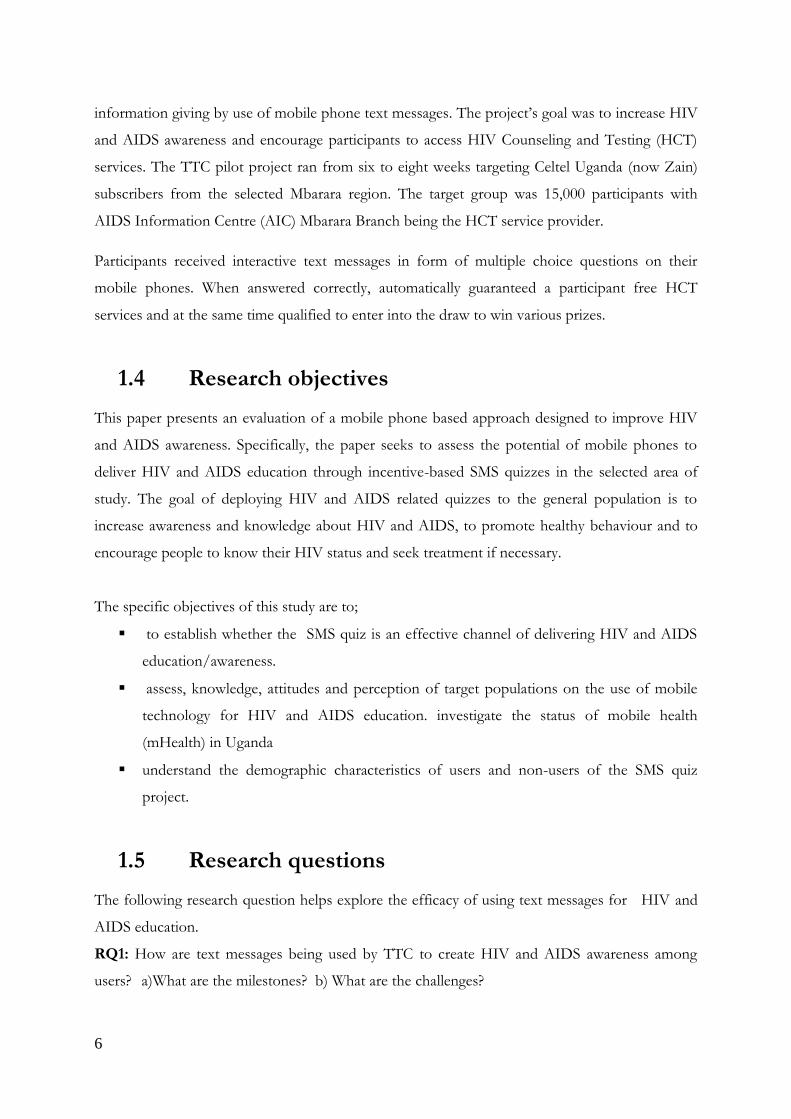
According to AudienceScapes8 Uganda‘s national surveys conducted in 2007 and 2008,
household access to a mobile phone has increased some 18 percentage points from 21 percent of
households to 39 percent. Similarly, the use of SMS text messaging and voice calls increased 16
percentage points and 15 percentage points, respectively. See table 2 below.
7 Nshekanabo, Aggrey. ―Sixth Telecom Lands in Uganda‖. East African Business Week. 26 September 2009.
Available at: http://www.busiweek.com/index.php?option=com_content&task=view&id=2349&Itemid=34
(Accessed January 30, 2010)
8 http://www.audiencescapes.org/country-profiles/uganda/country-overview/mobile-communications/mobile-
communications-284 (last accessed January 1, 2011)
11
The decrease in cost and service expansion to more rural areas has also allowed Uganda's less
affluent citizens to take advantage of the connectivity that mobile phones provide. Household
access among Ugandans with a low socio-economic status (SES) tripled from 2007 to 2008 from
5 percent to 15 percent. Access among individuals with a lower middle-SES more than doubled
from only 13 percent to 31 percent. Even so, high-SES Ugandans are more than twice as likely to
have access to a mobile phone as those with a lower middle-SES.
Table 2. Illustrates Uganda‘s new media use
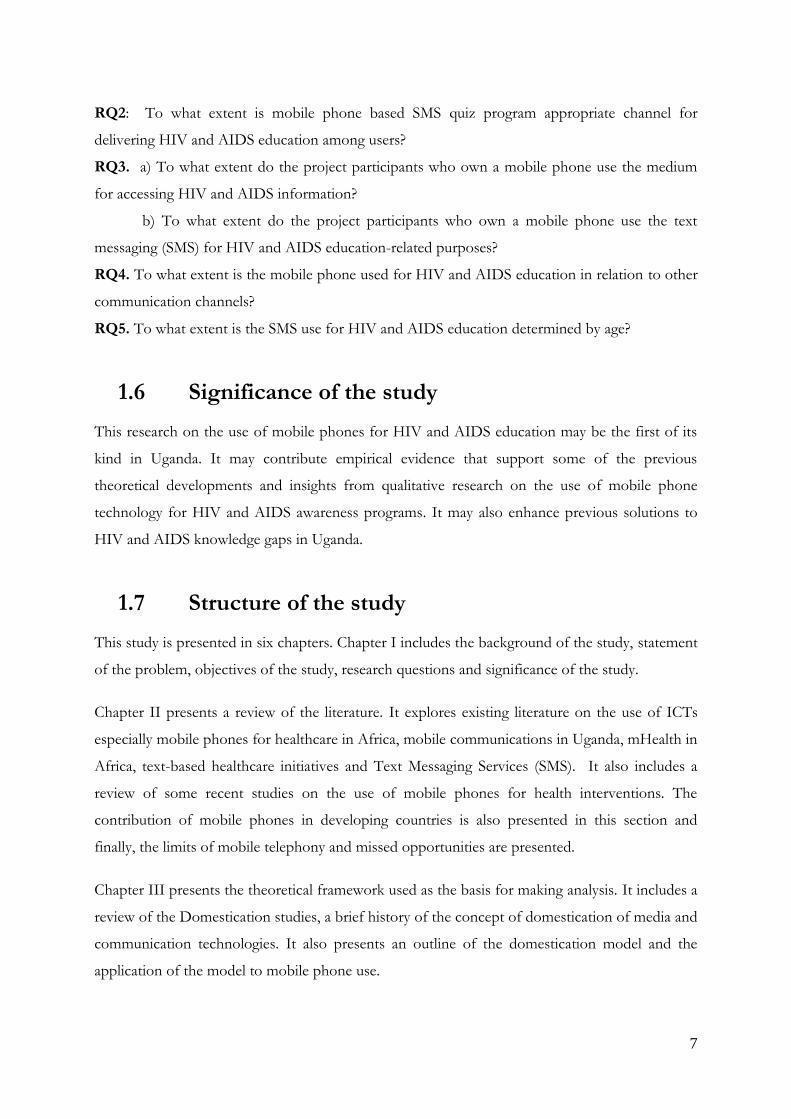
The survey has also shown that Ugandans are adept at gaining access to telephony other than
using a personal mobile phone. Although 15 percent of low-SES individuals said they have
household access to a mobile phone, 33 percent reported making a mobile phone call at least
monthly. This is even a habit among high-SES users, as 71 percent have household access and 85
percent make a phone call at least monthly. Users may have borrowed a mobile phone from a
friend or family member or visited a kiosk for a one-time use payment.
Table 3. Shows the frequency of mixed medium use via ICTs

12
A number of mobile providers now offer mobile money transfers and the ability to ―top up‖ the
minutes of another user (an effective proxy for transferring money). In March 2009, MTN
Uganda launched its mobile money transfer service, as did Zain with its Zap service in the
summer. In addition Uganda Telecom announced a partnership in 2009 with Redknee Solutions
to soon offer its own mobile transfer service9.
By October 2009, the MTN and Zain services together had signed up about 250,000 users; MTN
said its service handled an average of sh6 billion transfers a month10. In addition to their
domestic services, both MTN and Zain announced the launch of global money transfer services,
allowing users to send and receive remittances outside of Uganda11.
There have been a number of development and social change projects seeking to capitalize on
the communicative power of mobile phones. A recent venture between the NGO Text to
Change (http://www.texttochange.com/) and the AIDS Information Centre of Uganda
(http://www.aicug.org/) conducted a month-long program using SMS-text messaging in the
district of Mbarara and encourage the public to seek HIV counselling and testing services. TTC is
a Dutch non-profit organization founded in 2006 that seeks to develop ICT systems to inform
and educate about health issues. TTC is a complementary service provider using mobile
telephony as a medium to communicate about health-related issues to support (existing) health
communication campaigns. The TTC project tries to increase awareness about HIV and AIDS
through information by using mobile phone SMS quizzes, with the aim of encouraging
participants to use HIV Counselling and Testing (HCT) services.
9 Odomel, James. ―UTL Partners with Redknee to offer transfer service‖. New Vision. 25 February 2009. Kampala,
Uganda. Available at: http://www.newvision.co.ug/D/9/32/672639?highlight&q=redknee. (Accessed January 10,
2010)
10 Mugabe, David. ―Telecom Money Transfer Tilts Market‖. New Vision. 7 October 2009. Kampala, Uganda.
Available at: http://www.newvision.co.ug/D/9/32/697046?highlight&q=MTN transfer, (Accessed January 10,
2010)
11 Mugabe, David. ―MTN to start global mobile money transfer‖. New Vision. October 2009. Kampala, Uganda.
Available at: http://www.newvision.co.ug/D/9/32/697830?highlight&q=MTN transfer. (Accessed January 10,
2010)
13
2.3 Use of ICT for health care in Africa
Penetration rate for a range of ICT in Africa has been increasing tremendously for the past
decade, even though it has yet to be on par with that of developed countries. Since 2001, the
internet is accessible from every capital city in Africa, up from a mere four cities in 1997 (Jensen,
2001). The proliferation of ICT in Africa thus opens new possibility for health communicators to
reach a larger audience base with greater ease.
A review of ICT policies and practices in low income countries, including those in Asia and
Africa, revealed that the telephone is a preferred mode of communication in Africa (Gerster &
Zimmermann, 2005). The authors of the review cited the cultural norms of Africa as one of the
reasons for this preference, in that certain topics such as sexuality related issues, are considered
taboo. Hence individuals rely on the telephone for the exchange of sensitive information, since it
allows for some privacy. This anonymity is enhanced with the advent of the text messaging
services.
However, mobile phone penetration rate varies widely in continental Africa, with the highest
percentage residing in South Africa, standing at 92.2%, and the lowest in Eritrea, at merely 2.2%.
Uganda falls at the lower end, with a penetration rate of about 27% (Private Sector &
Development, 2009). Hisali (2007) pointed out that the slow growth of the telecommunication
industry in Uganda, as well as the slowdown in mobile phone services usage in the recent years
might be due to the high taxes imposed on mobile services. The country‘s mobile phone usage
tax as of 2007 is 30%, the second highest in the world. However, the general upward trend for
mobile phone penetration rate in Africa (Private Sector & Development, 2009), coupled with the
Grameen ―village phone‖ concept (Donner, 2008; Grameen Foundation USA, 2005), whereby
multipile users share a mobile phone, suggests the potential of utilizing the medium for large
scale campaigns including HIV and AIDS education.
2.4 Contribution of mobile phones to health in
developing countries
One of the key problems faced by healthcare workers in rural areas in developing countries is the
lack of information and communication networks. Meeting health workers‘ information and
communication needs is potentially the most appropriate strategy to improve healthcare in rural

14
areas of developing countries (Pakenham-Walsh, Priestley and Smith, 1997 and Metin, Villeret et
al., 1997)12.
The great expansion of mobile phones in developing countries involves new opportunities to
improve efficiency, productivity and communication in the health sector, and help to achieve
better quality services at reduced cost. Universally, mobile technology has six main intrinsic
features appropriate for its adoption in developing countries: low infrastructure investment, ease
of use, low energy consumption, affordability of services and devices, surpassing unfavorable
geographic structures and less vulnerability to vandalism and natural disasters than other
technologies.
Mobile technology has thus overcome many of the barriers ―in a natural way‖ and revolutionized
communications in many developing countries, even in rural areas, where connectivity is reached
by the first time. In this sense, Heeks (2005) proposes a major effort to test the utility of massive
mobile base for development purposes. Some of the applications for health include: management
of health data, access to information for health workers, telemedicine and health promotion, as
well as communication in emergencies.
Despite this potential, literature is scarce in mobile telephony‘s application for health in rural
areas. Some of the most remarkable experiences are: Satellife Project, which uses GSM coverage
to download and transmit the information to PDAs through a jacket, the sending of SMS in
Kenya for free with HIV and AIDS information for health promotion, including a free and
anonymous service of questions/answers13; the campaign to educate people about HIV and
AIDS and malaria using cellular technology sending free text messages in Mali (PlusNews, 2004);
the adherence to tuberculosis treatments via SMS to remind patients to take their medication at
pre-determined times in the OnCue project in Cape Town (bridges.org, 2005); the Interactive Voice
Response System used in India for Electronic Helpline on HIV and AIDS (Chandra, 2005); the
Mobile for Good project in Kenya, based at using mobile technology to improve the lives of
people, among others, with health services such as SMS-based health tips or anonymous
questions about HIV and AIDS and Breast Cancer for subscribers.
12 Quoted from report available at: http://www.bmj.com/content/314/7074/90.full (accessed January 1, 2011)
13 More information available on this site: http://www.genderit.org/content/hivaids-and-mobile-technology-sms-
saving-lives-africa (visited January 20, 2011).
15
The above cases however are merely anecdotal experiences that show how mobile phones are
increasingly considered as a tool to meet health needs in developing countries and how there is a
growing debate in the ICT4D community in order to explore the benefits of mobile telephony
for health in developing countries; however, this field is still very recent and there are very few
academic papers regarding the same.
2.5 The limits of mobile telephony and missed
opportunities in Africa
Despite the growing opportunities of mobile phones, many people in Africa are still marginalized
or excluded from accessing the benefits of the technology because of barriers that include cost
and the lack of adequate regulation and policy. Mobile telephony may contribute to widening the
gap between the poor and the poorest, leading to what Manuel Castells has defined as the ‗fourth
world‘ – a non-consuming and non-producing marginalized group which is ‗structurally irrelevant
in the current structure of the global economy (James Katz, 2008). For example, within the
informal construction sector in Dar es Salaam, Tanzania the use of mobile phones is broadly
‗stratified along employment lines‘ as employers and middlemen own mobiles while many
employees, apprentices, and family labourers are unable to afford a handset, let alone the running
costs. However, more data on usage are needed to inform this debate about the digital divide.
Current figures refer mostly to the number of subscribers (those who have a sim card) and
owners (those who own a mobile handset), rather than specific patterns of use and users.
Cost and usability problems restrict many from benefiting from the full functionality of mobiles.
Often people are limited to ‗beeping‘ to curtail costs. A widespread practice in Africa, this
involves dialing a mobile phone number and hanging up before the owner can answer. Often
these beeps mean the mobile owner should call back, but they can also relay a planned message.
The difficulties of scaling up mobile phone technology have also been highlighted by
development practitioners and grassroots NGOs like Text to Change. The pilot veterinary
project conducted in Zanzibar, for example, revealed two major obstacles: the mobile phones are
very expensive for local vets, and the on-screen forms need to be completed in a specific order,
which can be problematic when conducting physical checks on animals.
16
Government restrictions and state control have also been shown to hinder the growth of the
mobile phone sector. For instance, Burundi, Djibouti, Eritrea, Ethiopia, and Somalia – all
characterized by a state telecommunications monopoly or the lack of strategic investors – are the
only five countries with mobile penetration rates of less than 10 percent14. Thomas Khalil has
argued that the lack of competition in these countries is the main cause of the low mobile
penetration rate, as it discourages private sector investments and consequently impacts on the
cost of mobile services.15 Such state monopolies are often motivated by political factors. For
example, during the 2005 election the Ethiopian government shut down the text messaging
system, which was being used by the opposition for mass communication; at times the ruling
party also distributed misinformation via text messages16.
The above notwithstanding, millions of Africans have benefited from being able to communicate
instantly and relatively cheaply with family, friends, businesses, and services because of mobile
telephony. Mobile phones have clearly had a revolutionary impact on many lives, but not all.
There is also now a vibrant and growing critical mass of technologists, entrepreneurs, and
activists experimenting with new ideas in the mobile sector.
2.6 mHealth
The ubiquitous nature of mobile devices, coupled with their portability, makes it convenient to
disseminate messages to the audience, even for developing countries and rural regions. Past
research showed that mobile phones and personal data assistants (PDAs) were effective in
improving public health in Africa as well as other parts of the world. They have aided accurate
collection of patients‘ medical records, facilitated mass dissemination of information by
healthcare providers, and served reminders for adherence to medical regimens.
A recent mobile phone-based pilot program conducted by the UNICEF was successful in
gathering more accurate data about children‘s nutrition-related information in Malawi (Blaschke,
Bokenkamp, Cosmaciuc, Denby, Hailu, & Short, 2009). The Rapid SMS campaign made it easier
for the participants to provide information about their children, and at the same time, it was
14 UNCTAD, Information Economy Report, p. 4
15 Thomas Khalil, ‗Harnessing the mobile revolution‘, p. 21
16 Fahamu, ‗Mobile phones, human rights and social justice in Africa‘ (Report, Fahamu, Oxford, 2007); Lahra Smith, ‗Political violence and democratic uncertainty in Ethiopia‘ (Special Report 192, United States Institute of Peace, August 2007).
17
more convenient for the administrators to access the data. In the past, individuals had to visit the
clinics physically for the body measurements of the children to be taken and recorded, which
resulted in high attrition rates and out-dated information.
Similar studies are conducted in Kenya using the PDA for collecting patients‘ medical records
(Tegang, Emukule, Wambugu, Kabore, & Mwarogo, 2009; Diero et al., 2006). The authors found
that despite logistical problems, such as battery outages, limited storage space, and accidental loss
of data, the PDA was able to collect more accurate data, as the participants were not allowed to
skip any of the questions, and inconsistencies were corrected on the spot. Moreover, since the
data is stored electronically, it was ready for analysis soon after collection.
In the sexual health context, texting services were seen as effective in encouraging enquiries
among youths about sexually transmitted infections and related issues to access relevant
information (Levine, McCright, Dobkin, Woodruff, & Klausner, 2008). It was revealed that the
nature of the platform attracted the audience‘s attention; in addition, the increase in awareness
level of the health issue was the highest among individuals who signed up with the least
expensive cell phone providers. This suggests that the accessibility and the convenience that a
medium provides play a crucial role in determining the success of an intervention program.
Mobile services had also been utilized for reminder services for adherence to antiretroviral drug
usage among HIV patients (Puccio et al., 2006; AIDS alert, 2005). A 24-week long study
conducted by Puccio et al. showed that even though most participants felt that the reminder calls
for the administration of antiretroviral medicine were useful and not overly intrusive, the
adherence to the therapy waned after termination of the reminders. This highlights the problem
of sustainability beyond the intervention period.
Despite reports of effective application of mobile devices to healthcare, a review on research on
impact of e-health technologies in developing countries revealed that most of the evaluations
conducted are limited and that there was a lack of solid evidence (Blaya, Holt, & Fraser, 2008).
Blaya et al. (2008) noted that few studies presented scientifically rigorous data, and that most of
the studies did not have patient outcomes as en endpoint, hence the benefits of using e-health
systems are difficult to quantify. This calls for more concrete evidence of the impacts of
electronic and mobile technologies on healthcare and health communication.
18
2.7 Text-based health initiatives
The rapid diffusion of mobile communication technology has provided users with easy and
inexpensive access of technological affordances. Text messaging is one example. The technology
is referred to as Short Message Service (SMS) and allows users to share messages up to 160
characters in length between handsets. Text messaging has two advantages: it is relatively
inexpensive and it is asynchronous, so recipients of text messages do not have to read the
message immediately (Ling, 2005).The popularity of text-messaging provides a unique platform
for healthcare professionals to communicate with patients.
SMS alerts provide the further advantage of being relatively unobtrusive, offering recipients
confidentiality in environments where disease (especially HIV and AIDS) is often taboo. In the
developing world, SMS alerts have proven particularly effective in targeting hard-to-reach
populations and rural areas, where the absence of clinics, lack of healthcare workers, and limited
access to health-related information all too often prevent people from making informed decisions
about their health.
SMS campaigns can be set up either as one-way alerts or interactive tools used for health-related
education and communication. For example, a citizen may sign up to take a survey, delivered via
SMS message, quizzing them on their knowledge about HIV and AIDS and the location of the
nearest testing centre. Depending upon their responses, information regarding where and how to
receive a free test will be transmitted. This interactive model has been deployed in several
countries (e.g., India, South Africa, and Uganda) to promote AIDS education and testing and
provide information about other communicable diseases (such as TB), as well as to promote
maternal health and educate youth about reproductive health.
While other communication media, such as radio, television, voice-based information hotlines,
and even interactive websites can be employed in the service of education about public health
issues, SMS stands out as having several advantages over each of these: cost-effectiveness,
scalability, convenience, broad reach, and widespread popularity in the developing world. By
promoting health-conscious behaviour, the mHealth education and awareness programs currently
in place have already had positive impacts. The ubiquity and low cost of SMS messages hold the
potential to shift the paradigm for health education by communicating with people in an
accessible, engaging manner that both respects their privacy and gives them the tools to make
informed choices.

19
This research seeks to examine text message initiatives prove an effective and inexpensive way
for health practitioners to keep in touch with target audiences. Communication is an essential
component in establishing a meaningful relationship with physicians (Haean, Ray & Allegrante,
2008). Mobile technology is able to bridge communication gaps by providing opportunity for
fast, unobtrusive and personalized medium of communication.
In this study, ‗comfort with HIV and AIDS mobile text communication‘ draws upon existing
literature on text messaging healthcare campaigns/initiatives. It is operationalized as respondents‘
willingness and comfort to communicate with their healthcare provider. This includes whether
respondents feel comfortable having personal medical information sent to them through text
messages. It also examines whether or not respondents‘ prefer a text message reminder about a
doctor‘s appointment, or to receive mobile phone text messages to remind them of personalized
health objectives. This study aimed to model the variables that predict individuals‘ comfort with
healthcare text messaging, specifically, the predictive value of individuals‘ mobile phone use and
their perception of text-based programs.
2.7.1 Text Messaging Services (SMS)
Different information transmission technologies in mobile phones include Short Message
Services (SMS), Multimedia Messaging Service (MMS), Voice Technology and Video Technology.
SMS employs the sending of short messages between mobile devices. These could be plain full
text messages or messages grouped by keywords. Within the context of the digital inclusion
problem defined, users can send full text SMS to the system to request for HIV and AIDS
information as responses.
The system can also be used together with faxes and emails to allow for files larger than the
normal SMS file (160 Characters) to be sent to users as responses. MMS allows for sending of
messages that have multimedia objects such as images, audio, video and rich text. This method of
data representation involves grouping information or ideas and representing them by graphical
images. In the digital inclusion solution the system can allow for sending of picture messages to
users as reminders of different events such as time to take medication, facts about HIV among
others.
Text messaging has been one of the most successful mobile services recent years. Currently, SMS
is used either for mediating person to- person communication or for accessing mobile end-user
20
services. While previous studies focusing on media richness suggest this type of mediated
communication is useful for the performance of less equivocal tasks and the exchange of formal
messages (Daft and Lengel, 1986), recent research gives more mixed predictions. For example, it
has been suggested that the low channel capacity of text messaging (Te`eni, 2001) is compensated
by including more affective components in the message. This also leads to an adjustment of
message content such as reduction of content formality, something that is typically observed in
behavioural studies of text messaging use (Kaseniemi and Rautiainen, 2002). However, Höflich
and Rössler (2001) found that instrumentality was the only gratification significantly predicting
the use of text messaging services. Although SMS is mainly used for purposes of utility, the
inclusion of affective components and low formality in messages means that SMS have the
potential for entertainment in addition to utility.
The key advantage of the SMS is its relatively cheaper costs but it also has a huge disadvantage of
being able to allow only 160 characters. Secondly, most key pads do not support local languages,
it requires users to type and read responses in English hence may be a constraint to the target
users.
21
3 Theoretical Framework
3.1 Introduction
In order to understand the factors affecting people‘s intention to use and adopt mobile services,
it is necessary to get a thorough understanding of the theory behind it. Research on innovative
use of services like text messaging and simple SMS-based services may provide important insights
into understanding the process of mobile service adoption for health care service delivery. In this
study, the Domestication of Media and Technology is examined to understand what role mobile
phone text messaging plays in HIV and AIDS education.
3.1.1 Theoretical review
I n this section, the history and literature on Domestication studies, and the mobile phone in
society in briefly reviewed in to illuminate on the application of mobile technology for health
education. Emphasis is put on studies that focus on the use of mobile text messages for HIV and
AIDS awareness and education.
3.1.2 Domestication, a brief history of the concept
Domestication is described as the process of technology adoption into everyday life. The concept
of domestication was originally adapted from other disciplines such as anthropology and
consumption studies, as well as from media studies considering the context in which ICTs were
experienced by the people using them (Haddon, 2006). According to Haddon (2006) the
framework looks beyond the adoption and use of ICTs (as well as gratifications or benefits) to
ask what the technologies and services mean to people, how they experience them and the roles
that these technologies can come to play in their lives. The processes observed in this framework
are about how individuals encounter technologies and deal with them, sometimes rejecting them
and at other times accepting them (Haddon, 2006).
Domestication may be seen as a dynamic process, wherein individuals and groups negotiate the
use of a technological device, trying to ‗fit it in‘ or ‗break it into‘ their own personal life structures
and domestic space to best satisfy their needs and wants. Just as consumers modify the use of a
device, the device in turn impacts and influences their daily life. The term itself calls to mind the
taming of wild animals, suggesting that technologies must be housebroken if they are to become
22
part of the home and family (Berker et al., 2006). This is a confrontation that does not always end
well. Sometimes technologies are successfully domesticated into the routines of everyday life
while other times they are not. But the process is never quite complete. Even those technologies
that appear domesticated might one day face rejection from the household.
3.1.3 The concept
Domestication is a concept dealing with how ICT becomes integrated into people‘s daily life, or
how ICT ―find a place in people‘s life‖ (Haddon, 2003, p.43). The major argument of this theory
is to treat technological innovation as a process, not an event (Silverstone & Haddon, 1996,
Silverstone, 1999, and Haddon, 2003). By process, Silverstone and Haddon mean that to discuss
technological innovation and adaptation is not just to discuss the producing of technology.
Instead, other factors including social, cultural, economic, political, and individuals involved in
the process should also be considered.
The process of domestication is a two-way process (Silverstone and Haddon, 1996). On the one
hand, Silverstone (1999) believed that media, which to some extent are represented and facilitated
by ICT, are so embedded in human‘s everyday lives that we can hardly talk about our home
without talking about them. On the other hand, Silverstone and Haddon (1996) opposed the role
of technological determinism in the process of technological innovation and adaptation. They
argued that other factors, such as social and economic dimensions, involving in the process
provide crucial feedbacks to the design process of technology, which reflect the necessity of
domestication and further promote the development of the technology.
In this paper, the researcher employs the domestication framework as the lens to understand:
how the Text to Change are ‗domesticating‘ SMS quizzes for HIV and AIDS education
in the community where they operate.
the factors affecting integration of mobile phone-based quizzes for HIV and AIDS
education in those communities.
The domestication framework has been used to study the adoption processes of a variety of
technologies including personal computers, televisions and mobile phones (Perdesn & Ling,
2003). Again it should be noted that although the framework is mainly used to study person or
household adoption of technology, others recommend that it can also be used to study
23
organizational domestication of technology, for instance, Habib (2005), used domestication to
study the adoption of learning management system at a university.
An important concept to note about domestication is the moral economy of the household,
described as a kind of shared value system unique to each home and family. Many domestication
studies have criticized these concepts, arguing that empirical reality does not reflect such rigid
categorizations (i.e. Bakardjieva, 2006). Although some of the original terminology has fallen out
of favor in recent years, the focus remains on studying ICT use in a particular social context.
3.1.4 The Domestication model
This section provides an overview of the ‗domestication model‘ as outlined in Silverstone et al.
(1992) and later reworked by Silverstone and Haddon (1996), and uses it as a basis for a new
model, more specifically adapted to the case of mobile telephone usage for HIV and AIDS
education.
3.1.5 Outline of the model
Several research works (Akrich, 1992; Cawson, Haddon and Miles, 1993; Haddon, 2002;
Silverstone and Haddon, 1996) argue that technological innovation cannot be reduced to the
process of producing an artefact. They emphasize the need to take into account processes of
consumption and use of the technologies to fully understand the notion of innovation. Hence,
they portray technological innovation as not solely the result of an engineering effort, but also the
product of a multitude of interrelated activities involving the producers of a particular
technology, its consumers and the other actors that play a role in the process of acquisition and
consumption of the technology. From this perspective, technologies are social, cultural, political
and economic products: ―they are symbolic and aesthetic as well as material and functional‖
(Silverstone and Haddon, 1996, p. 45). Silverstone and Haddon (ibid.) propose to distinguish
various dimensions of domestication, which are meant to provide a model to be used when
24
performing an analysis of the role information and communication technologies (ICTs) play in
everyday life such as for HIV and AIDS education.
According to According to Silverstone et al. (1992), the domestication process is conducted in
four phases or dimensions: appropriation, objectification, incorporation, and conversion,
Siverstone, R., & Haddon, L. (1996).
3.1.6 Dimensions of Domestication
The first dimension, appropriation, is the process of possession or ownership of the artifact. This is
the point at which an artifact moves from the world of commodity to the owner‘s possession,
thereby, giving it significance, Haddon, L. (2006). In the appropriation, both actual and potential
consumers are engaged in imaginative work where they view or hear about the artifact and the
artifact is constructed not only as an object of desire to fulfill specific functions but also as a
construction of the desire for difference and social meaning, Siverstone, R., & Haddon, L. (1996:
pp. 44-74). Therefore, this dimension involves all transactions included in the passage of artifacts
from the market to users‘ lives and motives for approaching to the product.
Second, through objectification, the users ascribe their cognitive values and aesthetics to the
technology Thus, the technology is given its meaning and place in users‘ lives. Objectification is
expressed in usage but also in the physical dispositions of objects in the spatial environment. For
example, after purchasing a technology, a user decides what role the technology should play in
his/her life and where it is placed and displayed in the domestic arrangement.
Incorporation is the process during which artifacts are used in everyday life, and the level of
functionality depends on how it is incorporated into everyday life. Technologies are selected with
specific features in mind and should serve in the way users intend. However, sometimes, some
technologies do not comply with users‘ intentions, and do not fit into the routines of users‘
everyday lives. Therefore, the incorporation dimension involves a number of usability issues in
user experience research.
Fourth, there is the conversion process at which the product reaches a ‗taken-for-granted‘ status to
become a part of the user‘s life. Technologies are brought for a certain feature in users‘ mind, but

25
they may become functional in ways somewhat different from the intentions of designers or
marketers. They may have many functions, but some of functions may change or disappear (e.g.,
many home computers brought for educational purposes have become game machines).
Therefore, this dimension is relevant to unintended uses of technology, adaptations made by
users, or features that users may desire in the future.
3.1.7 Key theoretical assumptions
There are several assumptions underlying the domestication theory, for this study only two key
assumptions are picked; first, the emphasis is on consumption rather than mere use. So attention
has been given to what ICTs mean to people, how they experience them and the roles ICTs can
come to play in their lives. To understand both adoption and use we need to appreciate the
negotiation and interaction between household members and the politics of the home which lie
behind both conflicts and tensions and the formation of areas of consensus. Any understandings
or even rules about appropriate use of ICTs which emerge from this process usually have some
bearing on what people do with the technologies and services and in what circumstances. We
have to be aware of individual, and household, strategies to control technologies, both in the
sense of controlling use by others and controlling the place of technologies in one‘s own life -
which in turn relate to the type of life and identity to which people aspire. And if we are to
appreciate fully the symbolic dimensions of ICTs, we need to see aspects of consumption such as
how technologies are talked about and displayed.
Second, adoption itself is seen as a process rather than an event. The pre-adoption process is
captured perceptions of technologies and services, in how people imagine potential role of an
ICT (or lack of one) in their lives and negotiations around, and sometimes resistance to, its
acquisition. If acquired, there are then the processes of developing the above noted
understandings about ‗appropriate‘ usage (e.g. about how much TV to watch, what to use a PC
for) - understandings which can themselves be challenged. There are the processes of fitting the
ICTs into routines or creating new ones. And there are the processes by which usage of
technologies spreads both among household members (which may mean lending out a personal
phone to others) and in terms of what the technology is used for (e.g. from emergency use of the
mobile to its role in organizing logistics).
26
3.2 Domestication and mobile phones
Domestication research has a long tradition of studying everyday life technology as the object
being adopted (see Silverstone and Hirsch, 1992). Examples of technologies studied are fixed
telephony (see Fisher, 1988), television (Silverstone and Haddon, 1996a) and home computers
(Silverstone and Haddon, 1996b). Domestication studies are not limited to studies of individuals
or aggregates, but are found describing the adoption and usage patterns of groups in society (e.g.
Townsend, 2000) as well as individual end-users (e.g. Ling, 2001a).
A variety of explanations have been suggested in domestication studies of the widespread
adoption of mobile services among young users. Most of these explanations have been applied in
studies of text messaging adoption. Even though text messaging was not explicitly focused on by
Ling (2001b), he indicated three conceptions of fashion and style, and suggested a development
from ―style as display‖ through ―style as communication‖ to ―style as a means to integrate social
networks‖. With these conceptions, the use of text messaging may be understood as both a way
of communication and as a means of social integration that plays a role as style marker when the
mobile phone itself has lost its significance as an object of style display. This is closely related to
Skog's (2002) interpretation of the mobile phone as symbolic capital. These symbolic elements of
mobile phone use have also been confirmed in studies of mobile phone use in organizational
contexts (Manning, 1996). However, Manning (1996) found that the mobile phone was status -
enhancing at some levels in the organization while it was status -reducing at other levels.
There is also a relationship between symbolic capital and social capital when the object of symbolic
value is a communication medium. In that case, there is a relationship between style as a way of
communication and style as an indication of group membership (Weilenmann and Larsson,
2000). This gives rise to the idea of text message sending, receiving, filtering and sharing as an
expressive communication activity used to display style and social capital.
Because text messaging is asynchronous, discrete and stored (at least for a while), this particular
use of the mobile is better suited as a style and social identity marker among experienced users
than regular calls. These explanations all support the importance of including subjective norms as
an important adoption determinant of communication services. The explanation of mobile
service usage as "ritual gift giving" applies particularly to the explanation of text messaging services
(Taylor and Harper, 2001). For example, Kaseniemi and Rautiainen (2002) observed three
additional uses of text messaging besides regular peer-to-peer messaging; message collection,
27
chain messaging and collective reading. Most other studies of teenage text messaging use have
reported similar behaviors (Ling and Yttri, 2002, Larsson, 2000).
Taylor and Harper (2001a,b) give references to alternative explanations of gift -giving behavior
that fits the observed use of text messaging, such as ritual explanations rooted in primitive
elements of our culture, but also sociological, social psychological and economic explanations of
gift-giving have been suggested. Based upon this theory, text messaging may be adopted for
social influence reasons (pressure to participate in the ritual gift-giving), or it may be explained
instrumentally (in which text messaging based gift-giving practices are adopted for utilitarian
reasons). In adoption research, the first explanations will be represented by subjective norms
while the second will be represented by a reinterpretation of what is considered useful in a service
(usefulness).
Ling and Yttri (2002) have suggested that text message adoption among teens may be explained
by a theory of social learning and development (and emancipation) because text messaging are
particularly well suited for exchanging ideas on issues focused in teenagers social learning (e.g.
exploration of sexuality, social interaction). For example, many of the chain messages identified
by Kaseniemi and Rautiainen (2002) were of sexual content and were used to explore and learn
the limits of appropriate content in messages.
Another suggestion is that the asynchronous form of messaging is particularly well suited for
initiating and exploring new relationships (Ling and Yttri, 2002). For example, Ling and Yttri
(2002) mention several situations in which text messaging is preferred to voice because it is used
as an awareness or initiating service similar to what Nardi et al. (2000) report for instant
messaging services. Thus, a social network explanation is introduced in which the difference between
teenagers and other users is explained by the social networks of teenagers being more dynamic.
In addition to these – mainly social – explanations of messaging service adoption and use among
young users, there have also been some domestication studies following the line of reasoning
from functionally oriented, work/leisure context studies. For example, Grinter and Eldridge
(2001) studied the adoption of text messaging among teenagers and found that text messaging
were preferred to other media because it was considered quicker, cheaper, easier and more
convenient to use.
Karlsen et al. (2001) found a remarkable orientation towards usability and costs in their study of
the potential adoption of mobile Internet services among Scandinavian teenagers. Thus,
28
instrumental or utilitarian explanations of the adoption of these services are relevant also for
younger users.
In the context of these non-deterministic approach, it is of particular relevance for the
domestication theory (Silverstone and Hirsch, 1992; Silverstone, 1994; Berker et al., 2006) to
frame how users are always involved in processes of participation which comprise their multiple
identities (consumers, family members, and so on). In fact, following the domestication model,
users are able to engage with media and technologies to articulate the passage from the market
to the home, and vice-versa, bridging different worlds through different stages and degrees of
appropriation (symbolic as well as material).
Appropriation as such identifies the stage of domestication which corresponds to bringing
something ‗home‘, starting with making it familiar, intimate and known. Participation is meant to
be, in this case, the possibility to ‗welcome‘ something into everyday life: everyday life at home
(but also beyond it) is the locus of participation as appropriation. Participation means
domesticating the wild, something which is not familiar, to make it part of our daily horizon,
practice and symbolic activity. It is about taming and bringing under control (Silverstone, 1994).
In this theoretical framework, both symbolic and material aspects of technologies are taken in
consideration as driving the users‘ patterns of appropriation. It follows participation is a daily,
ordinary activity, which makes users able to shape technology in the household or in other units
(e.g. workplace, local communities and so on) so appropriate it according the specific
characteristics and needs of their social settings. In this pattern of reciprocal adaptation between
users and environments, technology and especially ICTs are shaped so to become different from
what they were when designed and implemented. Domestication occurs with adaptation,
negotiation and engagement by users.
Domestication studies showed coherently how uses at both a symbolic and a material level can be
creative, drawing from a set of established patterns to re-locate and re-mediate the medium and
the specific technology on which it is based. Both television and ICTs in the household have
been studied as domesticated objects along a process of appropriation, objectification,
incorporation and conversion (Silverstone, 1994).
The original four stage model proposed by Silverstone with reference to television has been
revised and updated as not linear, but dynamic. This can be approximated to the use of mobile
29
phones for health education. It has been underlined, in this respect, that potential for
domestication is not the same for all the users, that domestication can occur outside and beyond
the home, and other factors than individuals or familiar contexts can affect the result of the
process (Berker et al., 2006).
3.3 Taking Domestication outside the home
The concept of domestication, as the very term suggests, refers to the domestic environment of
the home and family, and was originally conceived to study ‗fixed‘ technologies such as the
landline telephone and the home computer, which remain confined to the home. However,
domestication studies have been successfully applied to environments outside the home (See for
instance, Hujiboom, 2005; Ling, 1997; Pierson, 2006).
Haddon‘s outline of domestication for mobile telephony explores how the concept can be
applied to technologies that are used outside the home, and are highly portable (Haddon L.,
2003). Haddon however focuses more on how domestication can provide insight into the longer
term evolution of the cell phone as a device, and whether it can be applied to study the ‗weaker‘
ties of youth friendships rather than familial bonds. One could argue that the challenge in
studying mobile telephony is also understanding how the phone rapidly changes functions as
rapidly as people change their ‗roles‘ in their daily lives.
3.4 Mobile phones in society
Fortunati (2002) has asserted that the cell phone not only changes aspects of social life, but alters
even the framework that society functions under. The cell phone is a unique device, and can
rightly be called revolutionary to a certain extent. While the device itself is not a pioneer of
wireless communication, the extreme portability of its design and relative affordability (as
compared to say a home computer, or a laptop) resulted in its ubiquitous use and especially rapid
adoption by populations of developing economies. (Townsend, 2000, p. 2)
Geser (2005) states that cell phone are a ―multidimensional challenge for sociological theory and
research ―(p.4). His classification of cell phone usage measurement into intensity, breadth and
variety, provides a methodological starting point to define what ‗usage‘ entails (p. 6).
30
Aspects of the cell phone that come prominently into play in this project are the device‘s ability
to ―[emancipate one] from local settings‖ (p. 9) and the importance of SMS (Short Messaging
Service) as ―a channel for low-threshold, non-intrusive contact initiation‖ (p. 18).
Geser mostly speaks of the emancipatory potential of cell phones as acting as ‗symbolic
bodyguards‘, for instance, using your cell phone in an isolated or unfamiliar environment will
signal to strangers that you are busy, connected, and not to be harassed. However, cell phones
can also emancipate one from familiar and safe settings.
SMS is highly suited for this particular environment where discretion is of utmost importance,
and often real-time, extended voice conversations are impossible due to the increased possibility
of being ‗caught‘ in the middle of one. As Geser has explained, ―the asynchronous mode is highly
valued because it provides the opportunity of delaying the reception and the answering to a more
appropriate time this same non-intrusiveness makes it easier for the new technology to enter all
kinds of institutions despite dense social controls.‖ (Ibid).
In addition, the tendency of the cell phone to create a ‗virtual walled community‘ (Ling, 2004)
enhancing familiar social ties at the expense of forming new ones, or connecting face to- face
with people who are physically close to you, is particularly pertinent to this case study. This
concern has also been echoed by Rivere and Licoppe (Haddon, 2004, p. 82) and Fortunati (2002).
However, this creates a bold causal link between cell phones and behavioural choices. The
principal of SMC in 2005 justified the ban on cell phones on campus by stating that students
would rather spend their free time messaging their friends outside campus than form connections
with their own classmates. This theoretical debate whether or not cell phones adversely affect
sociability- therefore can be seen to be played out empirically in this case studies.

31
4 Methodology
4.1 Introduction
This chapter presents the methodology and research procedures used in the study. First, a case
study approach is used to document the TTC SMS quiz project and develop an in-depth
understanding of the SMS quiz among selected users. The data gathering process, problems
encountered and how they were overcome are also included in this chapter. The section also
offers a rationale for the research methods used to achieve the set out aims and objectives. The
study used a mixed method approach which provided the opportunity to clarify findings in order
to maximize the validity of the results.
4.2 Choosing a qualitative method
Qualitative research, broadly defined, means "any kind of research that produces findings not
arrived at by means of statistical procedures or other means of quantification" (Strauss and
Corbin, 1990, p. 17). The goals of this research study were best accomplished by use of a
qualitative research design approach. Whereas quantitative researchers seek causal determination,
prediction, and generalization of findings, qualitative researchers seek instead illumination,
understanding, and extrapolation to similar situations. In line with this, the study was aimed at
providing an in-depth analysis of the project which could be linked to theoretical assumptions
that explain how mobile-based technologies can be used in HIV and AIDS education and
awareness. It also sought to examine the outcomes of such projects and issues surrounding their
sustainability.
Many mobile studies are qualitative projects that rely on the classic methods of participant
observation, interviews, or focus groups for their data collection. Some studies, however, have
employed data collection techniques that specifically respond to the unique qualities of the
mobile phone.
There are several considerations when deciding to adopt a qualitative research methodology.
Strauss and Corbin (1990) claim that qualitative methods can be used to better understand any
phenomenon about which little is yet known. They can also be used to gain new perspectives on
things about which much is already known, or to gain more in-depth information that may be

32
difficult to convey quantitatively. This study seeks to an in-depth understanding of the potential
of mobile phones to deliver HIV and AIDS education through incentive-based SMS quizzes.
Qualitative methods are appropriate in situations where one needs to first identify the variables
that might later be tested quantitatively, or where the researcher has determined that quantitative
measures cannot adequately describe or interpret a situation. Research problems tend to be
framed as open-ended questions that will support discovery of new information. Qualitative
research reports typically rich with detail and insights into participants' experiences of the world,
"may be epistemologically in harmony with the reader's experience" (Stake, 1978, p. 5) and thus
more meaningful. These have formulated an important decision to choose a qualitative method
in this study.
According to Patton (1990), qualitative methods permit the evaluator to study selected issues in
depth and detail. A researcher approaches field work without being constrained by predetermined
categories of analysis which contributes to depth, openness, and detail of qualitative inquiry.
Quantitative methods on the other hand, require the use of standardized measures so that the
varying perspectives and experiences of people can be fit into a limited number of pre-
determined response categories to which members are assigned (Patton, 1990: 13).
With a quantitative approach, Patton (1990) adds that it is possible to measure the reactions of
many people to a limited set of questions, thus facilitating comparisons and statistical aggregation
of the data. This gives a broad, generalizable set of findings presented succinctly and
parsimoniously. By contrast, qualitative methods typically produce a wealth of detailed
information about a much smaller number of people and cases. This increases understanding of
the cases and a situation studied, but reduces generalizability (ibid: 14).
In this study, the nature of the research problem under investigation necessitated more depth and
details to understand the factors affecting acceptability and adoption of the SMS quiz for HIV
and AIDS education. The inquiry also necessitated some flexibility in dealing with varied sources
relevant to the study. These requirements therefore made qualitative research methods take
precedence over quantitative ones.
33
4.3 Triangulation as a technique
Triangulation is a powerful technique that facilitates validation of data through cross verification
from more than two sources. In particular, it refers to the application and combination of several
research methodologies in the study of the same phenomenon. By combining multiple
observers, theories, methods, and empirical materials, researchers can hope to overcome the
weakness or intrinsic biases and the problems that come from single method, single-observer and
single-theory studies.
According to Maxwell (1998), qualitative studies generally rely on the integration of data from a
variety of methods and sources of information, a general principle known as triangulation. This
reduces the risk that a researcher‘s conclusions reflect only the systematic biases or limitations of
a specific method and allows one to gain a batter assessment of the validity and generality of the
explanations that one develops (Maxwell, 1998: 88).
Patton, quoting Denzin (1978), identifies four basic types of triangulation; Data triangulation
where a variety of data sources are used; Investigator triangulation where different researchers are
used; Theory triangulation where multiple perspectives to interpret a single set of data are used
and methodological triangulation where multiple methods are used to study a single problem or
programme (Patton, 1990).
This study used data, theory and methodological triangulation. In order to strengthen the study
design, triangulation was also used as measure to reduce the risk of systematic distortions
inherent in the use of only one method, as well as strengthen the reliability, validity, and
credibility of the study. In data triangulation, this study included views from a variety of sources
deemed relevant for the research.
4.4 The Case Study approach
The central aim of this study is to describe in detail how Text to Change used an SMS approach
to increase HIV and AIDS awareness and scale up HCT in Mbarara district, Western Uganda.
The case in this study is the SMS QUIZ project implemented by Text to Change.
Case Study method enables a researcher to closely examine the data within a specific context. In
most cases, a case study method selects a small geographical area or a very limited number of
34
individuals as the subjects of study. Case studies, in their true essence, explore and investigate
contemporary real-life phenomenon through detailed contextual analysis of a limited number of
events or conditions, and their relationships. Yin (1984:23) defines the case study research
method ―as an empirical inquiry that investigates a contemporary phenomenon within its real-life
context; when the boundaries between phenomenon and context are not clearly evident; and in
which multiple sources of evidence are used.‖ As noted by Yin, one should use a case study
strategy because he or she deliberately wants to study contextual conditions. According to
Gomm, Hammersley, and Foster (2000), case study refers to research that investigates a few cases
in considerable depth.
Most scholars agree that a case study is not a particular method but a strategy (Stoecker, 1991,
Yin, 1994). Stake (2000) also argued that a case study is not so much a methodological choice but
a choice of what is to be studied. Yin (1994) argued that a case study should not be confused with
qualitative research. Gomm et al. (2000) argued that a case study implies collection of
unstructured data and qualitative analysis of data. However, most case study researchers (Yin,
1994; Stake, 2000; Stoecker, 1991) explained that a case study can employ the best of both
quantitative and qualitative methods. Yin (1994) explained that a case study is a comprehensive
research strategy that deals with situations ―in which there will be more variables of interest than
data points,‖ ―relies on multiple sources of evidence, with data needing to be converged in a
triangulating fashion,‖ and that ―benefits from the prior development of theoretical propositions
to guide data collection and analysis‖ (p. 13). This is the shape that this study takes.
Despite its strengths, Case Study method has always been criticized for its lack of rigor and the
tendency for a researcher to have a biased interpretation of the data. Grounds for establishing
reliability and generality are also subjected to skepticism when a small sampling is deployed.
Often time, case study research is dismissed as useful only as an exploratory tool. Despite these
criticisms, researchers continue to deploy the case study method particularly in studies of real-life
situations governing social issues and problems. Case studies from various disciplines and
domains are widely reported in the literature.
In the study of the TTC SMS quiz project, I do not believe the chosen single case will be one that
accentuates generalizability. What I am attempting in this study is ―a detailed examination of an
event (or series of related events) which [I] believe exhibits (or exhibit) the operation of some
identified general theoretical principles‖ (Mitchell, 1983, p. 192)
35
4.5 Methods and procedures
The goals of this research study were best accomplished by use of a qualitative research design
approach. A procedure that was planned and systematic was needed, but flexibility was also
needed.
This section provides a detail of the methods and procedures used to accomplish the set out
objectives. In choosing the specific techniques to obtain data during this investigation, I was
guided by the six criteria outlined by Bulmer (1993:10). a) Appropriateness of the research objective;
whether the method chosen was capable of reproducing the kinds of data needed to answer the
question posed in the study, b) Reliability; whether the method, if repeated by a different person at
the same time, or the same person at a later point in time, would yield the same results on a
second occasion? c) Validity of the data collection methods; whether I was able to obtain
measurements of what I was really trying to measure, d) Representativeness or generalizability of data
collected; to what extent I could transcend the sample in the case study to generalize about a wider
population, e) Administrative convenience; this involved consideration of cost, time and speed of
obtaining information.
Between 10 June and 20 July 2010, a field study was conducted in Mbarara district, western
Uganda with support from Text to Change and the AIDS Information Centre, Mbarara. The
field study was intended to assess the impact of the SMS quiz project deployed by TTC in
western Uganda. Prior to the field study, contacts via telephone and emails were made to the
interviewees by Text to Change to initialize the process. This provided a useful relationship
between the researcher and the interviewees. The first step in the process of conducting the field
study involved the development of instruments. The researcher in consultation with Text to
Change developed interview schedules designed to determine the impact of the SMS quiz project
and opinions of the end users towards the project.
4.5.1 Qualitative Interviews
Qualitative in depth interviews were chosen for this study. In-depth interviews are one of the
most common qualitative methods. One reason for their popularity is that they are very effective
in giving a human face to research problems. In addition, conducting and participating in
interviews can be a rewarding experience for participants and interviewers alike. For participants
– whether members of the study population or someone related to the population in a
36
professional capacity – in-depth interviews offer the opportunity to express themselves in a way
ordinary life rarely affords them.
According to Kvale (1996), in-depth interview is a technique designed to elicit a vivid picture of
the participant‘s perspective on the research topic. During in-depth interviews, the person being
interviewed is considered the expert and the interviewer is considered the student. The
researcher‘s interviewing techniques are motivated by the desire to learn everything the
participant can share about the research topic. Researchers engage with participants by posing
questions in a neutral manner, listening attentively to participants‘ responses, and asking follow-
up questions and probes based on those responses. They do not lead participants according to
any preconceived notions, nor do they encourage participants to provide particular answers by
expressing approval or disapproval of what they say.
In-depth interviews are usually conducted face-to-face and involve one interviewer and one
participant. When safety is an issue for the interviewer, the presence of two interviewers is
appropriate. In these situations, however, care must be taken not to intimidate the participant.
Phone conversations and interviews with more than one participant also qualify as in-depth
interviews, but, in this module, we focus on individual, face-to-face interview.
In this study, face to face interviews were conducted with 10 respondents. Each Interview lasted
between 15-20 minutes and these were conducted within the respondents‘ natural settings.
Majority of the interviews were conducted in offices due to lack of spare time by most
respondents.
Interviews were conducted with different categories of informants consisting of project
implementers, sponsors, partners and other stakeholders listed below.
a) SMS Quiz project staff at Text to Change
The SMS quiz project planners and designers included purposively selected two TTC staff
stationed at TTC offices. These included; Managing Director and Project Manager. These two
personalities comprise the core team directly responsible for SMS quiz project.
b) Sponsors of the SMS Quiz programme
The SMS quiz is sponsored mainly by telecommunication companies in Uganda as part of their
Corporate Social Responsibility (CSR) Programme. This study sought to get views from Zain, a
lead sponsor of the SMS quiz project. This company was chosen because it has been part of the
37
TTC SMS projects since its inception. Two Interviews were held with the people directly
responsible for TTC projects at Zain.
a) Officials from key partner Non-Governmental Organization (NGOs) and
Government
Four NGOs were selected; AIDS Information Centre, HIPS Project, Kawempe Health Care and
Health Child. One official was interviewed from each of these organizations. Face to face
interviews were also conducted with two officials from the Uganda Communication Commission
(UCC).
4.5.2 Focus Group Discussions
Focus groups are a free-form of discussion by a group of people led by a moderator designed to
obtain information about some topic, (Berger, 2000: 122). It is a vital method for qualitative data
collection because it is good for exploring a wide range of issues.
The method of focus group discussions possesses elements of both participant observation and
individual interviews (Morgan 1988 in Madriz, 2000). It has of recent grown in popularity and
recognition as a valuable method for qualitative data collection. The reason for this is because it
is a good method for exploring a wide range of issues (Colucci, 2007). Due to the fact that
humans are ‗social‘ beings, they have long been gathering together and discussing important
issues in groups. It is this element of human behaviour that researchers used, refined and made
into a method of research (ibid).
Wimmer and Dominick (1997:97) suggest that focus group discussions are vital as pilot studies so
as to detect ideas that could further be investigated using other methods. This technique of
interviewing participants in a group enables a researcher to attain information on trends and
variances, reasons and causes through the views of respondents (Yin, 1994:182).
I conducted one focus group discussion with some project participants of the Quiz Project. The
focus group comprised of 10 participants and a moderator. The moderator who was chosen by
TTC was fluent in both English and Lunyankole. She helped with translation of difficult
concepts and issues during the sessions. The participants were chosen randomly from the group
who participated in the SMS quiz program in 2008. The discussions were held in the local council
38
where the participants live. The participants from these three groups were made of both females
and males ages of 15-45 who are the active users of cell phones and participated in the quiz
program. A tape recorder was used to capture the proceeds of the discussions and these were
later transcribed into text.
Data gathered from these focus groups was qualitative because ―data from the focus groups do
not lend themselves to quantification‖ (Berger, 1989: 91). This is the case because ―the aim of the
focus group discussion is not to build consensus, but … to find out what each member of the
group thinks about the topic under discussion, and to elicit from each member his or her
opinions and descriptions of the behaviour of interest‖(Berger, 1989: 95).
After the focus group discussions, participants completed survey questions. The content of the
survey questionnaire includes questions about basic demographic characteristics, the kinds of
information participants would like to receive via the SMS quizzes, current sources of
information on HIV and AIDS, access to and use of mobile phones, problems in the
participant‘s life, and perceptions of and attitudes towards SMS quizzes. These questions were
drawn from the first few qualitative interviews and from consultation with members of Text to
Change, as well as from the brief for the study. (See annex 3) for the full survey document. The
full questionnaire was agreed to by representatives of TTC and the researcher prior to going into
the field.
4.5.3 Observation
One of the main research methodologies in studying small groups in natural settings is
observational fieldwork which can either take the form of participant or non-participant
observation. Observational fieldwork can be ideal for studying "social worlds". Lindesmith,
Strauss and Denzin (1975, p. 439-440) defined "social worlds" as "those groupings of individuals
bound together by networks of communication or universes of discourse and who share
perspectives on reality".
In this study, both participatory and non-participatory observation was used to enrich data
collection. This method was used to study the mobile phone use by the participants of the SMS
quiz. This exercise was conducted between July 10-15, 2010 at Mbarara AIC Branch where some
of the SMS quiz participants visited to access HCT. The researcher took notes on participant
39
behaviour with their mobile phones. In direct observation, I was engaged in detailed, descriptive
note-taking about the specific, concrete events that I observed.
It should be noted that mobile phone use can be difficult for outsiders to observe because of the
intimate nature of the devices. Mobile use can also be multimodal (voice and text), further
complicating data collection. The mobility and multitasking that are facilitated with the device
pose logistical challenges for data capture as well.
Data capture
Recording is an important issue that must be considered during the planning stage of the
research. Sarantakos (1998: 216) posits that recording can take place in a manner most suited to
the research topic and with which the researcher is most familiar. I used two methods of
recording; summarizing information on a note pad and using audio tape recorder to capture
conversations.
Although writing down information is the most common recording method but is limited
especially when the information to be recorded is dense. Sarantakos (1998) adds that apart from
this, taking notes may shift the attention of the researcher from the scene to the paper causing
them to eliminate part of the activities of the group (in cases of observations). He advises that a
researcher should write down key words or phrases as a guide and should complete them after
observation.
During the field work, audio recording made the data gathering process much easier because
writing down was impossible in some of the settings. For example, the focus group discussion
involves so many people talking almost at the same interval which makes it difficult to write the
feedback; in that case a tape recorder is most appropriate. Without a table or desk to write on,
audio recording was the most ideal way of getting accurate information.
Additionally, audio recording came handy in cases of elite-interviewees who granted me very
short interviews due to their busy time schedules. In such cases, I concentrated more on getting
as much information as possible and focused less on jotting down. This made recording the best
way of recording information in such instances.
Tape and audio recording make the process easier, more efficient and provide more accurate and
valid recordings. However, there are cases when recording is not possible or respondents object
40
to it and limit its use. It is important to highlight that permission was sought before audio tape
recording was done. At the beginning of every interview session, respondents were given an
overview of the research and given an explanation as to why recording was an important part of
the study.
4.6 Data analysis
The research analysis focused upon of perceptions reported and the rationales behind the
acceptance or rejection of mobile phone based SMS quiz as a tool for HIV and AIDS awareness.
A number of analytic techniques were used. First, responses were compared and contrasted
together in order to identify thematic categories within the reported perceptions and
explanations. Then there was comparison of responses from different participant groups and
representing different perspectives.
The findings were analyzed using three strategies of qualitative analysis as stipulated by Bickman
et al (1998); categorizing strategies, contextualizing strategies and memos and displays. These
methods were generally combined. Contextualizing was also used to understand the relationship
between the different elements of the text. Memos and displays in the form of tables and
illustrations were also used as valuable analytic techniques to illuminate the relationships in the
data and make the key elements and analyses more visible and retrievable.
It is important to note that not all the data gathered from the field could be used. The researcher
employed what is termed ‗data reduction‘ where the researcher notes redundancies in the data
and ‗discards all but the most interesting and compelling statements concerning a particular issue
or theme, relevant to the subject of study, Doyle (2004:4).
4.7 Data credibility
Quantitative and experimental researchers generally attempt to design, in advance, controls that
will deal with both anticipated and unanticipated threats to validity. Qualitative researchers, on
the other hand, rarely have the benefit of formal comparisons, sampling strategies, or statistical
manipulations that ‗control‘ for the effect of particular variables and must try to rule out most
validity threats after the research has begun, using evidence collected during the research itself
(Maxwell, 1998: 91).
41
The biggest validity issues that a qualitative researcher has to confront are researcher bias and the
effect of the researcher on the setting or individuals studied generally known as reactivity. Maxwell
argues that eliminating the actual influence of the researcher is impossible, and the goal in
qualitative research is not to eliminate this influence but to understand it and use it productively
(ibid: 92).
In addition, Patton (1990) argues that the reliability and validity of qualitative data depend to a
great extent on the methodological skill, sensitivity, and integrity of the researcher. He suggests
that systematic data collection procedures, rigorous training, multiple data sources, triangulation,
external reviews and other techniques aimed at producing high quality qualitative data that are
credible, accurate and true to the phenomenon under study should be employed (ibid: 54).
Maxwell (1998) suggests that a qualitative researcher can use rich data (data that are detailed and
complete enough those they provide a full and revealing picture of what is going on). In this
study, rich data was used whereby all the voices involved in the research were put into
consideration to illuminate on the SMS quiz project. In this study all the opinions captured
during were put into consideration rather than simply those that the researcher deemed useful.
4.8 Limitation of the study
This research noted several limitations; first, since all the participants were recruited by Text to
Change meaning that participants in the study were likely to be interested in using text messaging
(SMS) to access HIV and AIDS information and therefore have positive opinions. To attempt to
address this bias, an open environment was fostered so participants could freely share negative
opinions and neutral impressions.
Further, misunderstandings and misinterpretation of the mobile phone technology might have
occurred, and this could have led to invalid or speculative responses. Therefore, participants‘
views may change significantly upon greater awareness of the technology. Nonetheless, it is
important to understand the end-users‘ immediate impressions because they may lead to lasting
positions (Rogers, 2003).
Finally, intensive qualitative research is a reflexive process, where the researcher‘s opinions and
experiences may introduce bias to data collection and analysis (Creswell, 2007). To diminish this
42
effect, interview responses were analyzed for contradictory perspectives, and these are fully
represented in this dissertation.
4.9 Chapter summary
This chapter presents the methodological approach used in this study and a justification for the
research techniques chosen. The different activities that I was involved in during the field work
process are also presented.
During the study, some challenges were faced. Some of these include; Difficulty in access, where
some respondents, particularly those in high positions were very difficult to get hold of. A lot of
time and money was spent in establishing contact. This also meant that the bulk of these
interviews had to be conducted during the last weeks of the field work which was very tiresome.
Secondly, some respondents, particularly informants were very poor at time keeping. Some of
them granted me appointments during times when they were seriously engaged in official
activities, meaning that I had to wait for a long time in order to conduct these interviews.
43
5 Research findings
5.1 Introduction
This chapter presents the findings from the field study. In the research objectives identified in
chapter one, the study sought to examine the potential of mobile phones to deliver HIV and
AIDS education through incentive-based SMS quizzes deployed by TTC in the selected area of
study. To achieve this, it required examining participants‘ knowledge of text messaging and their
attitudes towards using it for HIV and AIDS educational purposes. The study also sought to
explore some of the strengths and challenges of using mobile phone-based SMS for HIV and
AIDS education.
The discussion in the following chapter is guided by the Domestication of Media and Technology
theory outlined in chapter three. The data was gathered through interviews with different persons
notably; officials from TTC, selected participants of the SMS quiz program in Mbarara and key
informants from partner organizations namely; Aids Information Centre (AIC), HIPS Project,
Health Child and Kawempe Healthcare Initiative. Interviews were also conducted with officials
from Uganda Communication Commission (UCC).
This chapter begins with a brief description of the case study (the SMS quiz program)
highlighting on the program activities, implementation and outcome. This is followed with a
presentation of the perceptions on the use of mobile phones for HIV and AIDS education which
includes feedback from the Focus Group Discussions, observation and face-to-face interviews.
This is presented under different themes for easy comprehension. A summary of the chapter is
then finally presented.
5.2 The Case Study: The HIV and AIDS SMS quiz
program
This section presents a description and analysis of the outcome of the Case Study; TTC‘s HIV
and AIDS SMS quiz program which was implemented in Mbarara district, western Uganda. The
section highlights on the program objectives, main activities, outcomes, challenges and feedback
from respondents.
44
The case study is a pilot project which was launched in February 2008 with support from The
AIDS Information Centre, Zain (former Celtel), The Dutch Foreign Ministry and Merck.
5.2.1 The program stakeholders
The mobile phone-based HIV and AIDS awareness intervention analyzed in this study was a
joint project between the Dutch NGO, Text to Change (TTC) and a Ugandan NGO, The AIDS
Information Centre (AIC), with sponsorship from Zain, one of the leading telecommunication
companies in Uganda. Other partners which offered valuable support include The Dutch Foreign
Ministry and Merck.
a) Text to Change (TTC)
TTC is a non-profit organization, founded in 2007 in Amsterdam, the Netherlands. It uses state
of the art mobile phone technology to collect and disseminate health information. TTC has been
one of the pioneers in using mobile phones for health monitoring and advocacy in Uganda
reaching out to the general public at a large scale. TTC works demand driven and sets up
complete programs with local and international partners. The aim of TTC is to make life saving
knowledge easily available to the general public and especially to community and family level
caregivers.
TTC is specialized in interactive and incentive based SMS programs addressing a wide range of
health issues such as HIV and AIDS, Malaria and Reproductive Health and Family planning. In
the last 3 years TTC has carried out numerous successful SMS programs with various
organizations with the aim to increase knowledge and improve the uptake of health services in
Africa. TTC‘s sms programs have a response rate between 20 and 50 % and have shown
remarkable figures in uptake of health services (+200%)17. At present TTC is active in Uganda,
Kenya, Tanzania and Namibia.
b) The AIDS Information Centre (AIC)
The Aids Information Centre, a non-government organization, was established in 1990 to
provide HIV counselling and testing (HCT) services and information on HIV and AIDS in
Uganda. Voluntary counselling and testing is recognized by UNAIDS as an important entry point
intervention to effective prevention, care and treatment. AIC provides HIV counselling and
17 More information can be accessed on the Text to Change webpage: http://www.texttochange.org/
45
testing services in eight regional centres and through the HCT expansion program enabled by the
AIC support to health facilities and other organizations in their provision of HIV counselling and
testing in Uganda. Closely coupled with this is the provision of accurate information on HIV and
AIDS to individual clients as well as to the mass audience through mass media and outreaches to
communities. AIC aims at empowering people, even those considered high risk, such as
commercial sex workers and refugees, to adopt safe sex practices so as to further reduce the rate
of HIV transmission.
c) Zain Uganda
Zain Uganda, previously called Celtel Uganda Limited began offering mobile phone services in
Uganda in 1998. The company is owned by Celtel Group, one of the largest mobile
telecommunications operators in sub-Saharan Africa, whose parent company— Zain—is the
leading telecommunications operator in the Middle East and Africa. An SMS-based multiple
choice quiz was administered to 15,000 Zain mobile phone subscribers in the rural region of
Mbarara. Free airtime was offered to users to encourage participation in the program; this was
determined to be a powerful incentive since users can exchange the airtime with other
subscribers as a type of currency18.
5.2.2 The SMS quiz
The Text to Change (TTC) SMS quiz project was launched on February 14, 2008 as a pioneer
project in Uganda with the aim of increasing awareness on HIV and AIDS through information
dissemination via mobile phone text messages. The project sought to increase HIV and AIDS
awareness with the overall aim of encouraging participants to access HIV Counselling and
Testing (HCT) services.
TTC worked in collaboration with local HIV counselling and testing (HCT) service provider, the
AIDS Information Centre (AIC). The organizers chose a list of 15,000 Zain subscribers in
Mbarara district in Western Uganda and sent them an introductory SMS asking if they would like
to participate in a free interactive quiz about HIV, with the incentive of handsets and airtime as
rewards for correct answers. A question was sent each week. If the recipient answered correctly, a
confirmation SMS was sent; if he or she answered incorrectly, a message with the correct answer
18 More about this program can be accessed from the report available at the site:
http://www.texttochange.com/mHealth_for_Development_TTC.pdf ( accessed on 29/11/10)
46
was sent. Some of the questions included, "What is the difference between HIV and AIDS?",
"How is HIV transmitted?", "Have you ever tested for HIV?‖ among others. Annex 1 show the
complete questions used in the SMS quiz program. Included in the messages was also the
following information: 1) that it was free to answer, 2) that participants would remain
anonymous, 3) that prices could be won if answering, and 4) the location of the AIC branch in
Mbarara, where participants were entitled to a free HCT session. The two first questions focused
on demographics, i.e. age and gender of the respondent. This was to get a clearer picture of who
the respondents were, which would later help in the monitoring and evaluation of knowledge
levels on particular topics.
The questions were designed by the counsellors at AIC in Mbarara, and were meant to answer
the most frequently asked questions were being asked by people in the counselling rooms.
The questions were mainly to raise awareness on questions concerning HCT; like confidentiality,
accuracy, cost and the time it takes to get the HIV test result back. These issues have all been
identified in previous studies as barriers that prevent people from seeking out VCT.
The program launch was preceded by a radio talk show on Vision Radio by a team from Mbarara
branch to create awareness about the project. According to the organizers, of the 15,000
subscribers contacted, 2,500 responded to each question. At the end of the trial period of
questions and answers, participants were encouraged to go for HIV testing.
According to TTC, this strategy is designed to use edutainment and interactive SMS
communication to reach out many people to spread the message about HIV and AIDS and make
it a subject of discussion. TTC emphasize that the privacy offered by mobile phones is a
significant factor contributing to the successful use of this technology for health education.
Upon completion of the quiz program, TTC Director, Bas Hoefman said the SMS quiz increased
traffic at AIC counselling and testing facilities: "We are very happy that the launch has been a huge success
in terms of the uptake of VCT services. Therefore, we congratulate our partners at AIC Mbarara for this great
achievement. Nevertheless, this program is a pilot and meant as a trial to see if the approach could be successful.
The next step is to run the SMS quizzes in the local languages, so that the people in the rural areas, who don't
speak English, can also be reached with HI and AIDS sensitization messages.,”- Bas Hoefman.

47
5.2.3 Implementation
Before the SMS messages were sent TTC conducted a community sensitization of the project
through radio and outdoor promotional materials like posters and flyers. A mobile truck carrying
informative messages was also used to increase awareness of the project.
TTC and Zain, with help from AIC, devised a six-to-eight-week pilot program, which was
advertised with the slogan, ―Don‘t guess the answers, and learn the truth about AIDS.‖ In order
to allure subscribers to respond, potential participants were promised rewards such as handsets
and airtime for correct answers19. Once a subscriber agreed to participate he or she received a
text once a week with a new multiple choice question, (refer to annex 1). Those who got the
question right automatically received a message offering free HIV counselling and testing and the
opportunity to enter a draw to win various prizes, while those who didn‘t, received a message
explaining the correct answer.
About 2,500 of the 15,000 subscribers contacted responded to each question. At the end of the
trial period of questions and answers, many participants were encouraged to go for voluntary
counselling and testing (VCT). TTC said that ―the response level of our pilot Quiz was on
average 15% per question.‖20
“Working with one HCT center allowed us to measure the uptake of VCT services as people had to identify
themselves via their telephone number. Nevertheless, we are very happy that other Centers also have received
numerous clients because of the TTC program. This means that the message has been spread as a result of our
quiz program”.-said Bas of Text to Change
Winners of the HIV quizzes were invited to an award ceremony on the April 18, 2008 at AIC
Mbarara branch premises, where they received mobile phones. As a means to encourage people
to get tested, the program seems to have been as effective as its organizers had hoped.
19 More about this program can be accessed from the report available at the site:
http://www.texttochange.com/ZAIN-TTC.pdf ( accessed on 29/11/10)
20 The information can be viewed at: http://www.texttochange.com/projects.html (accessed on 29/11/10)

48
Some of the winners of the SMS quiz in Mbarara
According to Robert Natlaka, AIC‘s representative in Mbarara, requests at their facility rose
significantly over the pilot‘s six-week duration noting that: “Some 255 [participants] turned up to AIC
in Mbarara for testing; some others also went to AIC partners [around] the district. The Mbarara branch of the
AIC confirmed that people who came for VCT, did so because of the SMS received.”
Participants of the quiz program were randomly selected and not targeted since the organizers
did not have access to the profile of subscribers. The majority of the mobile phone subscribers
(over 97%) in Uganda are pre-paid, meaning that the phone companies don‘t have access to the
customers´ names, addresses, or any other personal information. SIM cards are sold on the
streets by small vendors, and there is no registration procedure upon purchasing a SIM card.
Dr. Raymond Byaruhanga, the AIC Executive Director said, “We are very happy to proceed with the Text to
Change program as AIC strongly believes in using innovative approaches for HIV education, prevention and
scaling up HIV counseling and testing (HCT)."
5.2.4 Outcome
Out of the 15, 000 subscribers reached in Mbarara district and Western Uganda, 2500 were
directly involved in the HIV and AIDS SMS quiz. That means that 2500 individuals sent back
answers to one or several questions. 183 males and 67 females accessed HCT services at AIC in
Mbarara town during the period of the intervention, making a total of 255 people. This was the
highest number ever achieved at AIC in Mbarara. TTC explained that this represents
approximately 35% increase in the number of clients accessing VCT compared to a regular
month. The increase in clinic visit was highly attributed to the SMS quiz campaign.
49
“I am very happy with the results of this workplace based SMS pilot. SMS has in all its simplicity, once again
proven to be an effective complimentary tool to bring across health information and communicate about health
services that are available. We are looking forward to expand this initiative to more companies in Uganda and
elsewhere,”–Bas Hoefman of Text to Change.
5.3 Perceptions on use of SMS quiz for HIV and
AIDS education
This section presents respondents‘ views on the potential of TTC‘s SMS quiz to deliver HIV and
AIDS education. In this section, analysis is also made based on responses from face-to-face
interviews, focus group discussions, rapid assessment survey and observation. During the
interviews, several themes emerged and used as a platform for making analysis as below;
a) How affordable is the SMS service?
Mobile phones – also known as cellphones – are increasingly considered as more than simply
devices that allow people to communicate to each other in an accessible and engaging manner.
The mobile phone service in the form of Short Message Services (SMS) has been considered as
one of the most successful mobile services in recent years. Currently, SMS is either used for
mediating person to- person communication or for accessing mobile end-user services. In terms
of access to HIV and AIDS information, the service has been hailed as being affordable by a vast
majority.
However, the level of affordability of mobile phone devices was a key concern for many of
participants in this research project. Mobile ownership was found to be disproportionate in the
area of study with fewer women having access to mobile phones compared to their male
counterparts. Further, in some areas where both males and females could afford the cost of
mobile phones, they had no or very poor GSM signal coverage. Moreover, the major mobile
phone providers including Zain- which was the operator of the SMS quiz, had not extended their
services to the hard-to-reach parts of the communities at the time of the research.
Concerns about the potential expenses of mobile phone services raised issues regarding HIV and
AIDS education inequality. Some respondents believed that individuals who could afford the
technology had special access to health information and consequently, the health disparity gap
50
with the financially needy would continue to grow. In order to avoid this inequity, a participant
strongly advocated for socially conscious and equitable development of the technology.
Although the SMS quiz in Mbarara was a free service, it was noted that some participants had no
access to the service because they either did not own a mobile phone or because of poor network
signals. In response to signal strength an official from text to Change said: ―This program is a pilot
and meant as a trial. We are not surprised that occasionally it happened that we had to send a [quiz], question
again because there were some details missing. It also happened that some questions were sent twice because of
questions cuing in the system, but these were exceptions. In general we delivered most of the 18 questions properly”.
Concerns were also raised about absence of electricity to charge the mobile phones. A
participant, 28 years old said: “I bought a mobile phone about five years ago but I don‟t use it. It is very
expensive to buy airtime [talk time], charging is also expensive so I usually listen to the radio. But when I was told
about the [quiz], program, I had to join.”
Another participant added: “We are not sure about security and privacy [of using mobile phones to send
personal information]. Not all devices are compatible with each other. They don‟t work all the time: sometimes they
break, or the batteries run out, or they can get stolen.”
Participants thus strongly doubted the mobile phone‘s capacity for extensive awareness programs
because of limited battery life and spotty network connections. The majority of the people who
had ready access to networks and could afford to use the mobile phones to meet their
communication needs were typically located in semi-urban communities where there were more
income-generating opportunities. These people therefore had a higher level of disposable income.
This illustrates the inappropriateness of deploying the mobile phone-based SMS quiz in rural
areas.
Some participants believed their mobile phones were not technologically capable of running HIV
and AIDS messages. They assumed their phones needed sophisticated features like, more
memory, a large display screen, a keyboard, or a camera – in order to use the device for HIV and
AIDS awareness purposes. Upgrading their phones with these improvements would incur costs
that some participants wished to forgo. Furthermore, without knowing who would pay for these
expenses – whether the participants, the health organization, – there was some people hesitance
to adopt the technology.
51
b) It is cheap but is it accessible?
The text messaging feature that makes mobile phones affordable was hardly used by participants
owing largely to low literacy capacities and a cultural preference for verbal communication. The
number of languages used by these communities further compounded the issue of low literacy.
Feedback from the focus group revealed that the most commonly used language for daily
activities is Lunyankole thus mobile phones largely presented opportunities for them to speak in
their native languages, whereas text messaging required that they should be literate in English.
Majority thus suggested that if the service was voice-based as opposed to text-based, this would
overcome the language barrier. This was a huge set back to the suitability of the SMS based Quiz
program with a participant, 25 years saying: ―It is very hard to read the messages [SMS quiz text], because
it in English. But the radio programs are [broadcast], in our mother [native], language”.
A project officer from TTC acknowledged the respondents‘ concerns saying language barrier was
a key challenge because all the messages were in English; this eliminated the non-English
speaking subscribers. As a solution to this challenge, the official said: “The next step is to run the
SMS quizzes in both English and in local languages, so that the people in the rural areas, who don‟t speak
English, can also be reached with HIV and AIDS sensitization messages. In the end, we want the quiz to be
accessible for every Ugandan”.
Mere ownership of mobile phones without the ability or opportunity to use the SMS option in
their own languages makes this technology still largely inaccessible and expensive for the illiterate
rural people of Western Uganda.
c) Face-to-face communication preferred?
Mobile phones connect communities and reduce the distance between distant people. In the
same way, it closes the gap between health workers and clients. The group of people who
participated in the study generally acknowledged the value of faster contacts for health awareness
through the use of mobile phones as a result of the shrinkage of time and space brought about by
this technology. However, in a community where premium is placed on face-to-face
communication, the mobile phone is likely to be rejected. During a focus group discussion, one
participant expressed that: „I can read their messages [health experts], all right, but I need to see their face to
be confortable.”
52
The substitution of text messaging for the usual face-to-face communication can be
disadvantageous for a culture that believes that ‗speech is in the face‘. This gives precedence to
face-to-face communication over the text messaging communication that mobile phones provide.
This attitude may pose a potential setback to the suitability of using text messaging to deliver
HIV and AIDS education in such communities.
Respondents in the study strongly believe that replacement of face-to-face contacts with the text
message quiz would interfere with their routine communication. The concern was that face-to-
face communication that serves as a source of personal bond may be adversely ruined by the
constant use of mobile phones.
Some participants saw voice communication as the only purpose for mobile phones, so they did
not adopt web, text or multimedia functionalities. They purchased phones with the most basic
features and were satisfied with their decision. Advanced mobile phone tools were also rejected
as a means of reducing expenses.
Other participants found that alternatives for mobile phone use are easily accessible for instance,
fixed line phones or Internet accesses are prevalent. One respondent said she was frequently on
the Internet at work and at home, so she did not feel comfortable receiving health messages on
her phone. Secondly, participants restricted their mobile phone use by selectively disclosing their
phone number to close relatives and friends. One respondent said, “I usually do not give out my
[mobile phone]. I have to know who you are and why you are going to be calling or sending me text.”
Mobile phones can be a personal line of communication that users wish to protect. For this
reason, participants limited their use of mobile phones to close family members. They might
prefer fixed line phones or voice mail to mobile calls and text messages. Some participants said
they did not like talking on the phone, with many participants justifying how face-to-face
conversations might yield more positive results due to the influence of eye contact. In many of
these cases, mobile phone use was reserved for emergency and urgent situations. Consequently,
this infrequent use meant participants would sometimes forget their phone and leave it at home.
Overall, these restrictions may impose barriers to the acceptance of mobile phone for HIV and
AIDS education.
53
d) Simple in concept but difficult to operate
Participants perceived a number of barriers with using text messaging for HIV and AIDS
awareness. There were physical limitations – such as small screen sizes and keypads on mobile
phones, which participants found difficult to maneuver. There were also motivational barriers.
Many participants believed their elderly relatives would be extremely upset if they were asked to
use the technology. Attributing their apprehension to a lack of familiarity with mobile phones,
respondents felt that immense motivation and training would be necessary for encouraging
adoption. Moreover, this sentiment was not exclusive to older adults.
One young participant described the mobile phone as complicated technology saying that, ―It is
not easy to write [text on them [mobiles]. They [mobile phones], are just very complicate. It‟s difficult to use
because it‟s new to many of us.”
Another participant said, “I not suitable to be asked because I still think cell phones aren‟t even all that great
for such things [HIV and AIDS education]. I would be happy using my phone for calling friends and relatives.
The only reason that … I even have a cell phone on me is because I see that everybody else does. I don‟t think that
it‟s surprising that I‟m not really looking forward to these devices for my health information.”
For some people, acquiring the skills for mobile phone use can be difficult. One participant
described her parents‘ difficulty with using text messaging, and she attributed it to lack of training
on how mobile phones operate. In another case, an elderly respondent discussed her difficulty in
remembering mobile phone procedures. She always requested her grand-son to read out the text
messages for her.
An elderly participant, ―I don‟t know what to do … how to use it [mobile phone text messaging]. I don‟t
know what to do if I make a mistake. There seems to be a lot of things for me and a lot for me to do – and a lot
more than what I‟m doing now,”
Other usability criticisms were about the difficulties in screen navigation. Some respondents
found it slow and frustrating to type on the small buttons of a mobile phone keypad. Because of
these concerns, some saw the mobile phone as a secondary tool for health information, while the
traditional media like radio was their first choice because of its greater reliability and ease-of-
access. In light of these usability problems, some respondents intended to wait for improvements
in mobile phone design before adopting them for HIV and AIDS awareness purposes.
54
A participant said: ―While my [mobile phone], screen is slightly larger than my friends‟ phones, it‟s not so easy
to read [the text], many times, I ignore some things [text messages]. If somebody is trying to communicate a lot of
information with me [on a mobile phone screen], I may not read all the text.”
Another participant added that: “I think it is hard to enter information into it now, and people get turned off by that … it turns me off. I like to send messages but i don‟t want to be pressing a button three times to get a letter in.
e) Text messaging, a powerful tool for HIV and AIDS education?
Most of those interviewed reported their willingness to use cell phones to receive HIV and AIDS
text messages. A majority expressed their interest in receiving messages about sexually
transmitted infections (STIs) on their mobile phones because of the privacy guaranteed by the
service. They would like to receive information regarding where to access testing, counseling and
treatment. A participant, 27 said: ―With a text message, I don‟t fear to speak my mind regarding HIV and
AIDS because no one is watching me…..so no one will talk ill about me. I am not ashamed to ask any questions
because I am not being seen.”
A powerful promise of text messages as noted by respondents is that social interactions serve as
more of an instant personal contact with someone else, without having to worry about your
personal appearance and actual interaction. Many people were pleased with the element of
privacy offered by mobile phones at any given time and /or place for individuals to
communicate. Participants appreciated that text messages could provide opportunities for less
direct communication with health professionals. They also noted that this would greatly save
their money and time. Participants gave the above reasons as their basis to adopt the SMS service
for HIV and AIDS educational purposes.
Participants explained that speaking with doctors can be intensely embarrassing, so some times
they concealed vital information or refrained from questions and discussion in order to avoid
embarrassments. A common feeling was “I wouldn‟t bother my physician with some of those questions.”
Many respondents recognized that these behaviors are not constructive. If health questions and
feedback could be sent by text messages, they believed that embarrassment might be avoided.
According to Joinson (2001), indirect communication encourages honesty and openness as
patients exhibit higher levels of self-disclosure in health discussions mediated by computers. A
participant emphasized that electronic written in the form of text messaging was sometimes the

55
only opportunity she had for contacting her health professional. Overall, many respondents
believed SMS could help with communicating difficult health issues by providing opportunities
for written communication.
This study observed that mobile phone health services might increase the demand for
personalized information delivery. Participants expected health information on mobile phones to
be filtered and tailored to the user‘s needs. Many said they did not like the bulk, non-personalized
messages. Respondents hoped personalizing the text messages could help deliver more relevant
information.
Participant: People don‟t really know what [health information] to search for … There‟s so much information out
there about different kinds of diseases and different ways of diagnosing it. If you could make [tailor health
information] to that person‟s weight, age, habits; [then] it will provide a more effective way of [delivering
information] …
Participant: [Mobile phone health services] lessen the need for relationships and interactions [with health
professionals] – the personal aspect of it. You wouldn‟t develop as personal a relationship with your doctor, which
would then instill a sense of trust … [It] takes out the social-personal medium.
Despite the perceived strengths of mobile phones, many participants explained that much of
their text messages relate to friendship maintenance, romantic, social functions, and/or boredom
and loneliness. Similarly, a study on a group of undergraduates showed that only about one third
of the text messages that were being sent were actually functional/practical information; the rest
was a combination of filler messages (Reid & Reid 2004).
In line with above, many respondents said for some time they would ignore or automatically
delete messages sent by operators. They mainly paid attention to messages from friends, families
and partners. A participant, 21, said: “If I received an SMS from the network (operator) I would not bother
reading because it is always the „same-same‟ information. But I am excited to read text from my fiancée or
siblings.”
Another participant added that: “I can see people getting annoyed with the volume of [health-related] text
messages depending on how many are sent out or the content of [the] text messages.”
56
f) SMS prone to information overload?
Participants believed if large volumes of health information were delivered to mobile phones,
there were concerns that this would be difficult to manage and organize. If there was too much
information to process, they worried that this could lead to misunderstandings and health care
errors. By comparison, a conversation during a face-to-face with a health worker was perceived as
more helpful.
Participants believed that HIV and AIDS education requires rich interaction between an health
worker and a client. In addition to what the patient describes, respondents believed it was
important for health professionals to consider non-verbal cues – such as the tone of voice, body
language, and other mannerisms – to fully understand clients and their condition. However,
mobile phone health services were seen to potentially divide health care into smaller automated
tasks, which may not address the complex emotional issues such as trust and the unspoken needs
of the clients.
Participant: [With mobile phone health services], I‟m afraid [health care professionals] won‟t … understand me
and the way I respond as a human being, so that they [can‟t] put that [information] in the data set of making a
[health care] decision.”
g) Mobile phones and the social lifestyle
The mobile phone is the way in which individuals interact with each other. With the
development of the technology, individuals are able to remain in close and instantaneous contact
with members of their social network regardless of where they are in the world. In addition to
keeping up with social relationships, individuals have also been able to increase productivity with
their work because they can be hundreds of miles away from the office, and still have instant
access to their e-mail, documents and contacts wherever they are.
h) Cellphone attachment
Mobile phones are becoming increasingly popular among the general population. Many people
rely on their phones on a daily basis to stay in contact with other individuals in their social
networks. Many participants explained that their phones have become part of their lives with a
participant, 14 years old saying: ―I just can‟t imagine myself without a cell phone now. When I don‟t have my
phones I always feel like I‟m missing something.”
57
A participant aged 21 years said: “I move with my cellphone everywhere, I can‟t do without it…. I am always
expecting a text message or a call from someone. . The phone is just part of me.
Respondents explained that they experience a strong attachment to their mobile phones with
many saying. ―I always carry it everywhere.‖ The suggested some reasons that can explain this
attachment such as leisure, boredom among others.
An important aspect of the phone which many said contributed to this attachment is the SMS
function.
A rapid assessment of the demographics of cellphone usage among the participants indicates that
SMS/Text messaging has become more popular among younger generations in comparison with
older generations. In addition, individuals claim to see text messaging as a comfortable, easy and
effective means of communication for younger people (Thompson and Cupples 2008).
The focus group helped identify following some benefits of text messaging. First, mobile phones
allow users to send text message to their friends – another way of facilitating social interaction
and network with friends, secondly, cell phones are an excellent device for chatting with friends
irrespective of proximity.
Participants revealed that many people still rely on the traditional media as their source of
information on HIV and AIDS and related issues. Majority said the radio is their main source of
information with one respondent saying; ―I still prefer to listen to the radio…because I don‟t have to read
or write anything. I just sit down and listen to what the peer educators are saying”.
Today, the radio is probably still the dominant communication medium in many parts of the
world because it is inexpensive and available to citizens at all levels of society, including the
illiterate. Due to its pervasiveness, the radio is well-placed to reach out and give voice to
marginalized groups.
In Uganda, the radio is one of the most effective means of communication today, perhaps the
only affordable form of mass media communication that has reach across the remotest areas of
the country. Being largely an agricultural country, radio fits with the lifestyle of many people in
Uganda. It is a popular media channel because it does not require electricity, and because people
can listen to the radio while they work, walk or drive. By broadcasting in local languages is very
58
crucial because it addresses the information, education and entertainment requirements of its
localities and audiences.
i) Incentive-based program, effective strategy?
Participants of the focus group explained that the HIV and AIDS information on radio stations
are monotonous, non-interactive and non-engaging. In light of this, they are always put away.
Meanwhile, the SMS quiz was seen as motivational because of the reward systems deployed by
Text to Change with a quiz participant saying,
“I was very glad to win free talk time minutes and get a chance to test for my HIV status free of charge because I
answered a quiz correctly. I told my friends about it and they were encouraged to also participate.”
5.4 Chapter summary
This qualitative study suggested that mobile phone-based quizzes may be useful and culturally-
relevant as a way to support HIV and AIDS education in selected area of study. Participants
showed enthusiasm for the potential impact of mobile phones interventions using SMS texting as
a way to deliver behavioural messages with many participants expressing interest in participating
in such interventions.
Some of the advantages of cell-phone delivered education support include the fact that in many
resource-constrained settings, cell phone communication infrastructures already exist, a rapidly
growing mobile user community and a relatively cheaper option of real time communication.
59
6 Concluding discussion and
recommendations
6.1 Introduction
This chapter consists of a summary of the study, discussion of the major findings, implication for
practice, recommendations for further research and conclusions.
The chapter begins with a summary of the purpose of the study and is followed by the major
findings related to the use of SMS quiz for HIV and AIDS education. Conclusions from this
study are discussed in relation to research questions, key findings and the theoretical framework.
A summary of the findings is then presented. Finally, implications for research, practice and
theory are discussed. Some key challenges to HIV and AIDS education in Uganda are presented
and lastly, some recommendations are made.
The purpose of this study was to examine how Text to Change (TTC), a Dutch non-
governmental organization (NGO) deployed a bulk short message service (SMS) quizzes for
health education designed to communicate knowledge about HIV and AIDS and encourage
subscribers to volunteer for HIV testing in Mbarara District, western Uganda.
To achieve this, the following research questions were examined;
RQ1: How are text messages being used by TTC to create HIV and AIDS awareness among
users?
a) What are the milestones?
b) What are the challenges?
RQ2: To what extent is mobile phone based SMS quiz program appropriate channel for
delivering HIV and AIDS education among users?
RQ3. a) To what extent do the project participants who own a mobile phone use the medium
for accessing HIV and AIDS information?
b) To what extent do the project participants who own a mobile phone use the text
messaging (SMS) for HIV and AIDS education-related purposes?
RQ4. To what extent is the mobile phone used for HIV and AIDS education in relation to other
communication channels?
RQ5. To what extent is the SMS use for HIV and AIDS education determined by age?
60
To answer the above questions, qualitative interviews were conducted with different categories of
informants consisting of selected SMS quiz participants, project implementers, sponsors, partners
and other stakeholders. Face-to-face interviews were conducted with 10 respondents. A focus
group consisting of 10 respondents was also conducted. The same group also wrote comments to
close-ended questions assessing their knowledge, attitudes and perception on the use of mobile
phones to access HIV and AIDS knowledge with a view to improve their awareness about the
disease.
Drawing from findings from the TTC mobile phone-based project captured in chapter five, text
messaging in the form of the SMS quizzes hold a strong potential to deliver effective HIV and
AIDS education to target audiences. During the study, several issues were raised by respondents
concerning the level of affordability, privacy, cultural relevance, ease-of-use and accessibility of
the service. Other issues of concern were technological competence, illiteracy, gender inequalities
among others. These concerns and many others are discussed in the following paragraphs to
illuminate on the efficacy of using mobile phone-based SMS quizzes for HIV and AIDS
education in the area of study.
Regarding the main sources of HIV and AIDS information preferred by the majority participants,
the study revealed that while mobile phones may provide a relatively cheaper, fast and convenient
way to deliver HIV and AIDS awareness messages through the SMS service, many people still
preferred to rely on the traditional media especially radio to obtain information on various health
issues including HIV and AIDS. Today, the radio is probably still the dominant communication
medium in many parts of the world because it is inexpensive, available to citizens at all levels of
society, including those with limited education, and due to its pervasiveness, is well-placed to
reach out and give voice to marginalized groups. Moreover, the radio fits in people‘s daily lives
and it does not require electricity.
In Uganda, the radio is one of the most effective means of communication today, perhaps the
only affordable form of mass media communication that has reach across the remotest areas of
the country. Being largely an agricultural country, radio fits with the lifestyle of many people in
Uganda. It is a popular media channel because it does not require electricity, and because people
can listen to the radio while they work, walk or drive. Further, by broadcasting in local languages,
radio goes a long way in addressing the information, education and entertainment requirements
of its localities and audiences. The above feeling was common among many respondents who
61
despite the fact that they appreciated the SMS quiz program still underscored the importance of
radio for accessing vital information on health, politics and other daily issues.
In a pilot survey to determine the role of Information in Uganda‘s Reduction of HIV and AIDS,
Albright & Kawooya (2005) note that while radio is the main source of general information on
AIDS in Uganda, the main impact on behavioural change has been from personal sources and
through informal channels of communication. The HIV and AIDS communication strategy in
Uganda has greatly incorporated the use of radio stations in the promotion of HIV and AIDS
messages. This is because many people have radios in Uganda although this would by no means
reach everyone not least due to the many languages spoken in Uganda.
In another related study, Low-Beer & Stoneburner (2003:13) revealed that personal channels of
information are the main source for communicating information about HIV and AIDS in both
urban and rural areas of Uganda. They further emphasize that ―AIDS issues in Uganda were
rooted in discussions in social networks rather than just received from public health and media
messages, to which there is wide spread skepticism.‖
Mass media has been instrumental in promoting AIDS control and prevention in Uganda,
according to UNAIDS Report on ‗The media and HIV and AIDS, (2001). Further, Piotrow et al.,
(1997) explain that this is because the use of multiple media types is expected to reach a larger
audience and therefore helps reinforce messages. However, Singhal & Rogers (2003:201) argue
that, while mass media communication can create awareness of HIV and AIDS, interpersonal
communication with peers is essential to change risk behaviours. The UNAIDS Communication
Framework for HIV (1999) affirms the importance of combining both mass media and
interpersonal communication to allow for addressing diverse individual and group concerns while
honoring the delicate, private nature of human sexuality.
Examining the role gender difference plays in access to HIV and AIDS information, the study
revealed that sources of information on HIV and AIDS for many participants differ by gender.
In Uganda, the most used source of HIV and AIDS information for men is radio and for women
it is friends and family members.21 For both men and women, radio, friends, family members and
health practitioners are among the top most popular sources. But for most of the mass media
21 Rachel Marcus : Gender and HIV/AIDS in Sub-Saharan Africa: the cases of Uganda and Malawi Report prepared for Centre for Development Studies, University College Swansea available at: http://www.bridge.ids.ac.uk/Reports/re13c.pdf (accessed March 10, 2011)
62
sources, including radio, TV, newspapers/magazines, and the internet, they were used more
intensively by men. Men were also more likely than women to get HIV and AIDS information
from colleagues at work, while women were more likely to use elders in the community as a
source of HIV and AIDS information.
Similarly, a recent survey on access to ICTs in Uganda shows that although mobile phones are
among the most accessible ICT devices, there is a huge gender gap with men being 10 percentage
points more likely to have access to a mobile phone than women22. Feedback from the rapid
assessment on the knowledge, attitudes and perceptions of participants concerning their reasons
to adopt mobile phones for health education purposes also revealed more males willing to use
their mobile phones for HIV and AIDS awareness compared to females. Moreover, while
observing some of the participants who visited the Mbarara AIDS Information Centre to seek
for various health services, it could be seen that more males were actively engaged with their
mobile phones. It should however be noted that mobile phone use can be difficult for outsiders
to observe because of the intimate nature of the devices. Mobile use can also be multimodal
(voice and text), further complicating data collection. The mobility and multitasking that are
facilitated with the device pose challenges for data capture as well.
The ‗rural-urban‘ difference was also cited as an important factor affecting adoption of mobile
phones for HIV and AIDS awareness. This study notes that whereas there is a significant mobile
penetration and an expanding number of people are acquiring mobile phones throughout
Uganda, rural residents were significantly more likely to use word‐of‐mouth information sources
including friends, family members, traditional healers, or elders in the community. This could
pose a serious challenge to the use of SMS quizzes for HIV and AIDS awareness in such
communities. The Majority of the SMS quiz participants also reported sharing mobile phones
further deepening challenges of such a program.
Additionally, it was discovered that traditional media outlets may be more effective at reaching
urban rather than rural residents. Providing health information to family members and influential
community members are thus important for information dissemination to women and rural
residents. Through the focus group session, it was revealed that for urban dwellers, the three
most‐used sources of HIV and AIDS information are; radio, TV, and health workers, while rural
22 More information is available on the following site: http://www.audiencescapes.org/country-
profiles/uganda/communication-habits-demographic-group/gender/gender-229 (accessed April 1, 2011)
63
people turn most to friends, family members, radio, and health workers. Most general media
sources were more likely to be used more intensively by urban rather than rural dwellers.
The difference in education was also cited by participants as a major factor affecting the
acceptability of mobile phone-based SMS quiz. The text messaging feature that makes mobile
phones affordable was hardly used by participants owing largely to low literacy capacities and a
cultural preference for verbal communication. The number of languages used by these
communities further compounded the issue of low literacy. Majority of the participants reported
only being competent in their native language (Lunyankole) with very few saying they could read
and write in English. The limited use of SMS to English is a likely consequence of high illiteracy
rates in the rural population of this study. Male and female SMS rates may also reflect the
differences in literacy levels.
Since the SMS quiz required that participants should be literate in English, majority thus
suggested that if the service was voice-based as opposed to text-based, the language barrier would
be overcome. The limitedness of the quiz to English only was seen by participants as a setback to
the suitability of the SMS based quiz program to the groups with low education. These results
further suggest that applications of mobile phones for HIV and AIDS educational purposes
should emphasize voice-based communication and user interfaces that can be used by those with
low literacy.
Indeed, those using SMS were found to have higher levels of schooling. Majority of these were
males who had attended formal schooling with very few females having attended formal school.
It should be noted that women in Uganda are at an educational disadvantage compared to men.
Women‘s comparative lack of schooling limits their opportunities and constrains their choices.
Yet education is crucial to gaining the knowledge, skills, and confidence that women need to
improve their status and health. Owing to this, fewer women were willing to adopt the mobile
phone-based SMS quizzes for their health information sources.
In relation to the above, face-to-face communication was viewed as having more power over the
text messaging communication that mobile phones provide. The respondents strongly believe
that face-to-face communication that serves as a source of personal bond may be adversely
ruined by the constant use of mobile phones. For those who preferred to use their mobile
phones, they saw voice communication as the only purpose for mobile phones, so they did not
adopt text, and other multimedia functionalities. They purchased the phone with the most basic
64
features and were satisfied with their decision. Advanced mobile phone tools were also rejected
as a means of reducing expenses.
A discussion on the level of affordability of mobile devices revealed mixed results. A rapid and
increasing mobile penetration in Uganda and many rural parts of the country including the area
of study are among the key promises of the success of the mobile phone-based health programs.
Further, the relatively lower cost of tariffs, perceived ease-of-use is also cited as the key strengths
of the technology. However, interviews with the respondents revealed several challenges. First,
mobile ownership was found to be disproportionate in the area of study with fewer women
having access to mobile phones compared to their male counterparts. This is attributed to the
role of the woman in African societies where the ‗man‘ is often perceived as having a superior
role. In such societies, most of the family income is managed by the ‗man‘ thus putting them at a
better position to afford the mobile phone expense. Further, very poor GSM signal coverage and
absence of electricity to frequently charge the mobile phones makes it even more impossible for
the end-users to reliably use their devices. Participants thus strongly doubted the mobile phone‘s
capacity for extensive HIV and AIDS awareness programs because of limited battery life and
spotty network connections.
Concerning the privacy that the mobile phone provides, participants acknowledged text messages
may allow for an element of privacy at any given time and /or place for individuals to
communicate. Participants appreciated that text messages could provide opportunities for less
direct communication with health professionals. They argued that speaking with health workers
directly can be intensely embarrassing, so participants often concealed vital information to their
doctors or refrained from questions and discussion in order to avoid embarrassments. Many
believed that if health questions and feedback could be sent by text messages, they believed that
embarrassment might be avoided.
However, there were growing concerns of the negative impact of the privacy guaranteed by the
text messages. Participants argued that the privacy would cut the bond face-to-face or voice adds
to the HIV and AIDS awareness process. To many, by being able to talk to health workers face-
to-face, they are able to build trust and personal connections that is necessary for psychological
benefits. To many, text messages sent in the form of bulk quizzes without any personal
attachment may not be so effective in motivating them to take action (for instance go for HIV
65
and AIDS counseling and testing).Some of these challenges led to participants suggesting they are
less likely to adopt the service.
Regarding the incentive-based approach, this study revealed that a huge turn up was also
attributed to the rewards associated with participation in the quiz. Participants showed a lot
enthusiasm in the quiz because they expected to receive rewards in the form of air time (talk
time) minutes, free access to HCT, mobile phones and many others. The primary goal of an
incentive-based program is to motivate participants in some particular way by offering them
some form of reward.
6.2 Summary
This study attempted to answer the research questions presented in chapter one. Specifically, the
paper sought to assess the potential of mobile phones to deliver HIV and AIDS education
through incentive-based SMS quizzes. In other to achieve this, the study examined how TTC
used the SMS quiz to create HIV and AIDS awareness in Mbarara District, Western Uganda.
Several factors including respondents‘ perception, attitudes and knowledge on the SMS
technology were also examined.
Over all, mobile communication offers an effective means of bringing HIV and AIDS
information to citizens through the SMS quizzes. With low-cost handsets and the penetration of
mobile phone networks countrywide, many citizens who never had regular access to a fixed-line
telephone now use mobile devices as daily tools for communication. This offers a new platform
for delivering HIV and AIDS education to those groups.
Text messaging service is available on almost every model of mobile phone, the cost is relatively
low, its use is widespread, it does not require great technological expertise, and it is widely
applicable to a variety of health behaviours and conditions.
Text messaging offer efficient, and scalable method of providing outreach services for a wide
array of health issues including HIV and AIDS. This study revealed that many users already own
mobile phones, and the cost of an individual SMS is very low (somewhere between US$.03 and
US$.05 in Uganda at the time of this work). Additionally, owing to the fact that SMS is
66
considerably less expensive than standard voice communication, many Ugandan mobile phone
users are already familiar with SMS.
Text message campaigns are also viewed as very simple in concept increasing their suitability. It
can be set up either as one-way alerts or interactive tools used for health-related education and
communication. For example, a citizen may sign up to take a survey, delivered via SMS message,
quizzing them on their knowledge about HIV and AIDS and the location of the nearest testing
center. Depending upon their responses, information regarding where and how to receive a free
test would be transmitted. In education and awareness applications, SMS messages are sent
directly to users‘ phones to offer information about testing and treatment methods, availability of
health services, and disease management.
Text messaging also has the advantage of being asynchronous because it can be accessed at any
time that is personally convenient. Furthermore, even if a phone has been turned off, messages
will be delivered when the phone is turned back on. Additionally, text messaging is an innovation
for which utility remains even in resource-poor settings in which people may not have access to
expensive technology. Text messaging may therefore be suitable for HIV and AIDS educational
interventions because it allows for in-the-moment, personally tailored health communication and
reinforcement.
However, while SMS serves could be used as a powerful means of HIV and AIDS education, it
would be best used in conjunction with existing channels of communication, especially the
traditional ones in order to increase the uptake as well as the functionality of the approach.
Secondly, despite the proliferation of low-cost handsets, priced at US$20 in some low and
middle-income countries including Uganda, the initial cash outlay for buying a handset is the
most commonly cited barrier to owning a mobile phone by many especially women. Even those
who borrow phones and have relatively high incomes cite the cost of handsets as the main barrier
to mobile phone ownership. The cost of a mobile phone service is also an obstacle to ownership.
This study research supports the opinion of Mulama (2007: 5) who observed that ‗the benefits of
ICTs are largely restricted to towns and cities, as most rural areas lack the infrastructure,
equipment and skills needed for communities to take full advantage of these technologies‘. The
phones raised expectations in terms of meeting needs, but lack of affordable access made the
realization of these expectations very difficult.
67
The program organizers stress that scaling up of SMS quizzes would be more feasible if mobile
phone networks could provide discounted (or free) SMS for such a programs.
Additionally, marginalization of certain populations, such as those that are illiterate was cited as a
setback to the adoption of text-based quizzes for HIV and AIDS education. However, these
limitations may be reduced as mobile technology advances. For example, innovations exist that
provide voice response systems and pictures instead of text for those with limited literacy.
Language issues have posed challenges; text messages are limited to 160 characters, and
incorporating a language like Lunyankole for SMS requires on average 20% more characters than
English. In addition, there are no standard SMS abbreviations in that language, and there are
often no accepted terms to describe medical conditions, sexual practices, and other issues
relevant to HIV. To get around the character limitation, the translated SMSs would use some
English words and acronyms (e.g. "ARVs") and abbreviations (largely: the removal of vowels in
certain words).
Interventions delivered via mobile phones can be interrupted if the device is stolen or lost.
Further, the tariff system of the mobile phone network is highly exploitative. Owing to poor
signal coverage in some areas, users can waste precious money trying to get connected. They get
charged even when they do not succeed in getting connected.
Poor quality of mobile phone services sometimes makes their use frustrating. On occasion the
service providers may offer no service at all, or very poor reception for days. During periods of
poor service (poor GSM signal reception leading to low voice quality) the units on the call cards
are still debited, making it a double loss for the user.
Although mobile phones can be used for HIV and AIDS awareness and education, users still
prefer face-to-face communication owing to many cultural factors.
The SMS feature that makes mobile phone use affordable was hardly used by the research
participants, owing largely to low literacy capacities.
This study showed that mere ownership of mobile phones without the ability or opportunity to
make use of an affordable technique such as SMS keeps this technology largely inaccessible and
overly expensive for the rural people in Western Uganda thus affecting their ability to adopt the
service for HIV and AIDS education.
68
The mobile phone therefore presents a mixed bag of positive and negative values and impacts. It
is clearly not a solution for all communication needs, although it has become an avenue to
delivering real time HIV and AIDS information to many users.
6.3 Challenges to HIV and AIDS education in
Uganda
This study identified some challenges to effective HIV and AIDS education in Uganda. Some of
these challenges have been identified and discussed in the concluding chapter of this study. The
following are among the top challenges;
There is limited capacity (human, financial and structural) at an organizational level to promote
knowledge sharing within communities. In addition, there is a lack of appropriate fora for sharing
knowledge on HIV and AIDS. There is also a shortage of researched information about the
various categories of information users, their specific HIV and AIDS information needs and
desired delivery mechanisms.
Low literacy levels and poor information culture in many communities in Uganda has made it
difficult to implement health related education programs. Limited information literacy increases
demands for more information processing to add value to information and services, and to
promote information awareness, accessibility and usability. Unfortunately, many NGOs and
health practitioners lack the financial and technical capacity and initiative for information
management.
Further, there is fragmentation of information management efforts that creates the potential for
duplication of effort and wastage of scarce resources.
Limited capacity at local levels constrains information dissemination efforts to communities, as
well as inadequate structural and physical information delivery systems at all levels that could be
exploited for information access and sharing. Consequently, many potential users are not aware
of the existence of the required information and/or sources of such information and the
appropriate channels for access.
69
Inadequate funding of NGOs by governments often make it difficult for them to harness ICTs
effectively for the provision of HIV/AIDS information.
Finally, HIV and AIDS information overload – the availability of a huge amount of unorganized
information on AIDS is creating problems for target audiences to access and manage these
materials.
6.4 Implications for research
This study notes several methodological concerns that can be useful for further research. While
―case studies‖ and ―pilots‖ are many, little research in the way of replicable study design with
adequate sample sizes on the use of mobile phones for health education was found. Numerous
studies described system implementations, but few showed improved awareness outcomes and
workflow efficiencies. Thus, further research that examines the impact of mobile devices on
behaviour and outcomes, rather than assessing feasibility, is needed.
The position of this study is that accessibility and affordability of a service, such as the mobile
phone based SMS technology is not enough to conclude its efficacy to deliver effective
outcomes. For novelty to be achieved, further research is needed to link the connection between
access of the information and behaviour outcomes form such an intervention. For instance
examining whether delivering SMS quizzes directly encourages participants to seek better health
behaviours and access HCT.
Further, because of the relative newness of text messaging as a method of delivery for HIV and
AIDS awareness, there is a paucity of data and the existing literature on the efficacy of SMS for
HIV and AIDS education are quite heterogeneous. A review of literature notes that most of the
studies on this subject are still in the exploratory stages, and this technology is being adopted
rapidly; so, much information exists outside of the traditional scientific literature (newspapers,
blogs, private industry reports, among others). It is imperative to bridge this gap between practice
and scientific knowledge. Given the immature state of the field, additional information on
efficacy (e.g. message frequency, message content) may be gained from further research.
In summary, future research still needs to be conducted on the potential of SMS quizzes to
effectively deliver HIV and AIDS education. Something that should be examined is whether SMS
quizzes influence the users to take action. New studies should explore how the access and use of
70
cell phones varies through different socio-economic classes. This gap between the literature and
field practices can lead to mixed opportunities for learning about and improving text messaging
as a new tool for HIV and AIDS education.
6.5 Implications for practice
Mobile phone- based SMS quizzes hold a huge promise for delivering effective HIV and AIDS
education. Participants showed enthusiasm for the potential impact of cell phones interventions
using SMS as a way to deliver behavioural messages with many participants expressing interest in
participating in such an intervention. This could increase the demands on mHealth in a number
of ways. First, many participants were interested in the services and wanted to learn more, so
there is a need for informing the target populations about the technology. Health professionals
may respond by cultivating eHealth literacy. Health educators could teach these skills for optimal
health technology experiences – which include literacy, numeracy, and proficiencies in media,
information, computers, science, and health care23.
While participants liked the option of mobile phone SMS quizzes as a channel of HIV and AIDS
education, they also wanted to retain face-to-face health interactions. They were not interested
with the technology replacing traditional information channels – rather they wanted it to
complement existing practices and for there to be a choice between technological and personal
approaches.
This study however reveals that there were no were no clear differences between in intervention
outcomes delivered by the SMS quiz and the existing HIV and AIDS awareness mechanisms.
Moreover, the respondents still preferred the traditional channels. Organizers of the SMS quiz
note that in addition to providing the HIV and AIDS information to the target audience in a
relatively cheaper, convenient, private and interactive manner, another issue that should be
explored is whether the SMS quizzes drive recipients take action such as to seek voluntary
counseling and testing.
The results in this study will be important to identify gaps and issues in the literature for
investigators as well as best practices to guide practitioners in the field. The results of this
23 Norman CD, Skinner HA. eHealth Literacy: Essential Skills for Consumer Health in a Networked World. J Med
Internet Res 2006 16;8(2):e9

71
research have both theoretical and practical implications for the future research. Limitations of
the study can be addressed and solved in the consecutive studies. In summary, mobile phone text
messaging services in the form of quizzes are a promising technology that health consumers are
interested in adopting.
6.6 Implications for theory
In this study domestication of technology theory is considered a useful analytical framework for
describing and understanding mobile phone adoption for HIV and AIDS education. Given the
lack of theoretical basis in recent user experience research, the domestication concept provided
the foundation that mhealth researchers or practitioners can use to address user experiences of
their target populations. The analysis in this study may thus lead to broad theoretical and practical
implications for using text message quizzes for HIV and AIDS education.
Although the domestication of technology theory originated in the social sciences to investigate
social consequences of technology use, this study reasons that the domestication concept along
with the four dimensions (appropriation, objectification, incorporation and conversion) provides a useful
theoretical lens to address user experiences as it broadens the concept of mhealth ranging from
technology adoption and functional use to detailed user interface design aspects such as usability
problems and the learning process.
In contributing to the theory, the researcher identified a number of themes across the
Four dimensions of domestication and some of them are summarized briefly below;
Regarding appropriation of mobile technology, participants provided similar reasons for buying a
mobile phone: to be accessible to family members or close friends and to gain ‗peace of mind‘
while being outside. Participants used a home phone (a landline phone) as the primary
communication tool for various purposes such as making an appointment for social activities and
getting information from others. Conversely, the mobile phone was a secondary means to
communicate with family members or close friends when they were away from home. All
participants carried their phone for safety reasons. In particular, a health-related emergency
situation was the top concern. However, participants expressed that they lacked information
resources about mobile handsets and services to choose proper one for their needs. Most of
them reported that they had to rely on a sales person‘s recommendation when purchasing a
72
phone. However, recommendations were often made based on a business purpose and not on
users‘ needs.
For Incorporation revealed a number of faulty product designs that did not reflect older adults‘
perceptual and cognitive aging: The most common problems were related to visual abilities.
Although participants did not have severe visual impairments, they experienced difficulty in
reading the screen and labels on buttons, and the perceptual barriers prevented even technology
experts from using various features such as text messaging.
Further, those with limited experience with mobile phones reported that they could not make use
of contemporary instructional manuals properly due to difficulties in following and
understanding the instructions. The use of other media, such text messaging, was suggested as an
alternative form of the instructional manual.
Overall, the domestication theory could be developed by addressing the underlying activities in
the ‗perceptions to intentions to technology adoption‘ pathway and by focusing on the unique
context of mobile phone usage.
6.7 Recommendations
Basing on the research findings and analysis, this study has established some recommendations as
presented below; First, this study suggests that text messaging should not be considered a stand-
alone model for delivering HIV and AIDS education but rather as a tool by which several
awareness techniques can be administered. The findings from this study clearly point out that the
application of SMS quizzes for HIV and AIDS education is still in infant stages, thus in order to
achieve effective and measurable results, it is necessary to implement such programs alongside
the existing pretested mechanisms.
Some methodological gaps identified in this study include lack of rigor in program design with
regard to statistical power to detect a significant difference from other interventions. Future
studies should ensure rigorous methods and sufficient power in order to contribute to the
existing body of literature seeking to determine what combinations of text message factors
produce the best results. Additionally, more information is needed on the long-term effects of
text message interventions.
73
Text messaging is a tool that has value to both researchers and practitioners, and use of these
technologies may facilitate more active collaboration between research and practice. Given the
positive results so far, and the increasing uptake of mobile technologies, text messaging may
improve existing practices and interventions. Text messaging may be an important tool to reduce
the global burden on health care by providing more effective HIV and AIDS prevention and
management support.
The key recommendation in this research is to provide training for targeted HIV and AIDS
educational programs on how to send and receive SMS, in their preferred languages, keeping the
messages as simple as possible. This training would aim at empowering participants with low
literacy abilities, so that they can begin to use SMS to effectively access HIV and AIDS
information. However, training people to send text messages using this technology could be
challenging because many people in rural areas have limited exposure to technology and some do
not even own or use mobile phones.
The potential of SMS may be particularly significant among population groups most likely to use
mobile telephones as their primary means of communication. The highest level of mobile
telephone use is among adolescents, younger adults and more educated young adults.
Further, given the differences in the use of sources for HIV and AIDS information, health
development organizations should consider tailoring communication strategies for reaching
different populations.

74
75
References
Ajzen, I. (1985). ―From Intentions to Actions: A Theory of Planned Behavior.‖ In Action Control: From Cognition to Behavior. Ed. J. Kuhl and J. Beckmann. New York: Springer Verlag, 11-39.
Ajzen, I. (1991). ―The theory of planned behavior.‖ Organization Behavior and Human Decision Processes, 50: 179-211.
Akrich, M. (1992). ―Beyond Social Construction of Technology: The Shaping of People and Things in the Innovation Process,‖ in Dierkes, M. and Hoffmann, U. (Eds), New Technology and the Outset: Social Forces in the Shaping of Technological Innovations. Frankfurt: Campus, pp. 173 -190.
Albright, K. S. and Kawooya, D., (2005). ―The Role of Information in Uganda's Reduction of HIV/AIDS Prevalence: Individual Perceptions of HIV/AIDS Information.‖ Information Development. 21(2).
Avert.(2010). HIV and AIDS in Uganda. Retrieved from http://www.avert.org/aids-uganda.htm
Bakardjieva, M. (2006). ―Domestication Running Wild. From the Moral Economy of the Household to the Mores of Culture‖ in T. Berker, M. Hartmann, Y. Punie and K. Ward (eds) Domestication of Media and Technologies, pp. 62–79, Maidenhead: Open University Press.
Battacherjee, A. (2000). ―Acceptance of e-commerce services: the case of electronic brokerages.‖ IEEE Transactions on Systems, Man and Cybernetics, 30: 411-420. Berger, A.A. (2000). Media communication research methods: An introduction to qualitative and quantitative approaches. California: Thousand Oaks.
Berker, T., Hartmann, M., Punie Y., and Ward, K. (Eds) (2006). Domestication of Media and Technologies. Maidenhead: Open University Press.
Bickman, Leonard, Rog, Debra J, (Eds). (1998) Handbook of applied social research methods, Thousand Oaks, California: Sage. Blaschke, S., Bokenkamp, K., Cosmaciuc, R., Denby, M., Hailu, B., Short, R.(2009).Using Mobile Phones to Improve Child Nutrition Surveillance in Malawi. UNICEF Malawi and UNICEF Innovations. Blaya, J.A., Cohen, T., Rodriguez, P., Kim, J., Fraser, H.S. (2009). ―Personal digital assistants to collect tuberculosis bacteriology data in Peru reduce delays, errors, and workload, and are acceptable to users: cluster randomized controlled trial.‖ International Journal of Infectious Diseases.; 13(3):410-18. Bryman, Alan. (2004) Social Research Methods, Oxford: Oxford University Press.
Bulmer, Martin, Warwick, P. Donald, (Eds) (1993) Social Research in Developing Countries, London: UCL Press.
Chandra M. (2005). An electronic helpline on HIV/AIDS, Digital Opportunity Channel, 1
76
August 2005 (available at http://www.digitalopportunity.org/article/view/116242/,(accessed March 1, 2011)
Colucci, E. (2007); ―Focus Groups Can Be Fun‖: The Use of Activity-Oriented Questions in Focus Group Discussions, Sage Publications.
Creswell, J.W. (2007), Qualitative inquiry & research design: choosing among five approaches, 2nd edn, Sage Publications, Thousand Oaks. Daft, R.L. and Lengel, R.H. (1986). ―Organizational information requirements, media richness and structural design.‖ Management Science, 32: 554-571
Davis, F.D., Bagozzi, R.P. and Warshaw, P.R. (1989). ―User acceptance of computer technology: a comparison of two theoretical models.‖ Management Science, 35: 982-1002. Denzin, N. K. (1978). The research act: A theoretical introduction to sociological methods. New York: McGraw-Hill.
Doyle K, James. (2004): Handbook for IQP Advisors and Students; Introduction to Interviewing Techniques, Prepared for the Interdisciplinary and Global Studies Division, Worcester Polytechnic Institute,
Fishbein M. and Ajzen, I. (1975). Belief, attitude, intention and behavior: an introduction to theory and research. Addison-Wesley, Reading MA. Fisher, C. (1988). America calling: A social history of the telephone to 1940. Berkeley, University of California Press. Fortunati, L. (2002). The mobile phone: Towards new categories and social relations. Information Communication and Society, 5 (4), 513-528.
Gerster, R., and Zimmermann, S. (2005). Upscaling Pro-poor ICT Policies and Practices: A Review of Experience with Emphasis on Low Income Countries in Asia and Africa.
Geser, H. (2005). Towards a Sociology of the Mobile Phone. In Z. e. al (Ed.), E-Merging Media: Communication and the Media Economy of the Future (pp. 235-261).Heidelberg: springer. Gilbert, L & Walker, L (2009): ―My biggest fear was that people would reject me once they knew my status…‖: stigma as experienced by patients in an HIV⁄AIDS clinic in Johannesburg, South Africa. Health and Social Care in the Community (2010) 18(2), p. 139–146.
Grinter, R.E. and Eldridge, M. (2001). Y do tngrs luv 2 txt msg? In Prinz, M., Jarke, Y., Schmidt, K. and Wilf, V. (eds.). Proceedings of the Seventh European Conference on Computer-Supported Cooperative Work ECSCW'01, pp. 219-238. Kluwer Academic Publishers, Dordrecht.
Guwatudde, D., Wabwire-Mangen, F., Eller, L. A., Eller, M, McCutchan, F., Kibuuka, H. et al., (2009). Relatively Low HIV Infection Rates in Rural Uganda, but with High potential for a Rise: A Cohort Study in Kayunga District, Uganda. PLoS ONE, 4(1), 1-8. Retrieved from www.plosone.org.
Haddon, L. (2006). The contribution of domestication research to In-home computing and media consumption. The information Society, 22, 195- 203.
77
Haean, O., Ray, M., & Allegrante, J. (2008). Perceptions of Health Care Provider Communication Activity among American Cancer Survivors and Adults without Cancer Histories: An Analysis of the 2003 Health Information Trends Survey (HINTS) Data. Journal of Health Communication, 13(7), 637-653.
Heeks, R. (2005). Foundation of ICTs in Development: The information chain, e Development Briefing, 3(1), 1-2.
Hisali, E. (2007). Review of Sector Taxation Policies and Determining the Elasticity of Penetration and Price of the Various Telecommunication Services in Uganda. Uganda Communications Commission, 1-42.
Höflich J.R. and Rössler, P. (2001). ―Mobile schriftliche Kommunikation oder: E -Mail für das Handy.‖ Medien & Kommunikationswissenschaft, 49: 437-461. James Katz (2008).ed. Handbook of Mobile Communication Studies (MIT Press, Cambridge, MA,), p. 30
Jensen, M. (2001). Afriboxes, Telecenters, Cybercafes: ICT in Africa. ICT in Africa, 1, 97-109.
Joinson, A.N. (2001), "Self-disclosure in computer-mediated communication: The role of self-awareness and visual anonymity", European journal of social psychology, vol. 31, no. 2, pp. 177-192. Karlsen, M.A., Helgemo, I. and Gripsrud, M. (2001. Useful, cheap and fun: A survey of teenagers demands for mobile telephony. Grimstad: Research Report, Telenor R&D, Norway. Kaseniemi, E. and Rautiainen, P. (2002). Mobile culture of children and teenagers in Finland. In Katz J.E. and Aakhus, M. (Eds.). Perpetual contact. Cambridge University Press, New York.
Katz, E., and Blumler, J. G. (1974). The uses of mass communications: current perspectives on gratifications research, Beverly Hills, California: Sage.
Katz, J. E. (2005). Uses of Internet and Mobile Technology in Health Systems: Organizational and Sociocultural Issues in a Comparative Context : http://www.presidenciarepublica.pt/network/apps/katz.pdf (accessed 9th November 2010). Kvale S. (1996). Interviews: An Introduction to Qualitative Research Interviewing. London: Sage Publications
Kwon, H.S. and Chidambaram, L. (2000). A test of the technology acceptance model: the case of cellular telephone adoption. Proceedings of the HICSS-34, Hawaii, January 3-6. Levine, D., McCright, J., Dobkin, L., Woodruff, A.J., Klausner, J.D..(2008). ―SEXINFO: A sexual health text messaging service for San Francisco youth.‖ Am. J. Public Health; 98(3):393-395.
Liker, J. K., and Sindi, A. A. (1997). ‖User acceptance of expert systems: a test of the theory of reasoned action.‖ Journal of Engineering and Technology Management, 14: 147-173. Lindesmith, A., Strauss, A. & Renzin, N. (1975). Social Psychology. New York: Holt.

78
Lindlof, R. Thomas. (1995) Qualitative Communication Research Methods, California: Sage. Ling, (2001a). "We release them little by little": Maturation and gender identity as seen in the use of mobile telephony‖. Personal and Ubiquitous Computing, 5, 123-136.
Ling, R. (2001b) ―The Diffusion of Mobile Telephony among Norwegian Teens - A Report from after the Revolution,‖ presented at ICUST (International Conference on Uses and Services in Telecommunications held in Paris, France, June 2001).
Ling, R. (2005). "The socio-linguistics of SMS: An analysis of SMS use by a random sample of Norwegians." Pp. 335 - 349 in Mobile communications: Renegotiation of the social sphere, edited by R. Ling and Pedersen, P. London: Springer Ling, R. and Yttri, B. (2002). Hyper-coordination via mobile phone in Norway. In Katz J.E. and Aakhus, M. (eds.). Perpetual contact. Cambridge University Press, New York. Low-Beer, D. & Stoneburner, R. L (2003). Behaviour and communication change in reducing HIV: Is Uganda unique? African Journal of AIDS Research. 2(1), 9-21. Madriz E. (2000); Focus Groups in Feminist Research in Denzin, N. and Lincoln, Y. (Eds.), Handbook of Qualitative Research (2nd ed., pp. 835-850). Thousand Oaks, CA: Sage.
Maman, S., Abler, L., Parker, L., Lane, T., Chirowodza, A., Ntogwisangu, J., et al. (2009). A Comparison of HIV Stigma and Discrimination in Five International Sites: The Influence of Care and Treatment Resources in High Prevalence Settings. Social Science & Medicine, 12, 2271-78.
Manning, P.K. (1996). Information technology in the police context: The ‗sailor‘ phone. Information systems research 7 (1), 52-62.
Mathieson, K. (1991). ―Predicting user intentions: comparing the technology acceptance model with the theory of planned behavior.‖ Information Systems Research. 2: 173-191.
Maughan-Brown, B. (2010). Stigma Rises Despite Antiretroviral Roll-Out: A Longitudinal Analysis in South Africa. Social Science & Medicine, 70, 368-374.
Maxwell, Joseph. (1998) Designing a Qualitative study in: Bickman, Leonard, Rug, J. Debra (Eds.) A Handbook of Applied Social Research Methods, London: Thousand Oaks.
Merriam S. B. (1988). Case study research in education: A qualitative approach. San Francisco: Josse-Bass. Mitchell, J.C. (1983). Case and situation analysis, Sociological Review, 31, 187-211. Morgan D.L. (1988), ―Focus groups as qualitative research‖, London: Sage Publications Mulama, J. (2007). A Rural–Urban Digital Divide Challenges Women, Inter Press Service, 15 February, www.ipsnews.net/, (accessed December, 20 2010). Nardi B., Whittaker, S. and Bradner E. (2000). Interaction and outeraction: Instant messaging in action. Presented at CSCW-00, Dec 2-6, Philladelphia, PA.
79
Patton, Michael. (1990) Qualitative evaluation and research methods, Newbury Park: Sage. Piette, Jacques,
Piotrow, P.T., Kincaid, D.L., Rimon II, J.G.& Rinehart, W. (1997). Health Communication: Lessons from Family Planning and Reproductive Health. Westport: Praeger.
Plouffe, C. R., Vandenbosh, M., and Hulland, J. S. (2001b). ―Intermediating technologies and multi-group adoption: A comparison of consumer and merchant adoption intentions toward a new electronic payment system.‖ Journal of Product Innovation Management, 18: 65-81.
Plouffe, C.R., Hulland, J.S. and Vandenbosh, M. (2001a). ―Richness versus parsimony in modelling technology adoption decisions - understanding merchant adoption of a smart card-based payment system.‖ Information Systems Research, 12: 208-222.
Private Sector & Development. (2009). What are the Economic and Social Impacts of the Mobile Phone Sector in Developing Countries? Mobile phone penetration rate in Africa (2008). Proparco‟s Magazine, 4.
Puccio, J.A., Belzer, M., Olson, J., Martinez, M., Salata, C., Tucker, D., et al.( 2006 ) ―The use of cell phone reminder calls for assisting HIV infected adolescents and young adults to adhere to highly active antiretroviral therapy: a pilot study.‖ AIDS Patient Care STDS 2006 Jun;
20(6):438‐444.
Reid, Donna J. and Fraser J. M. Reid. (2007). "Text or Talk? Social Anxiety, Loneliness, and Divergent Preferences for Cell Phone Use." Cyber Psychology & Behavior 10(3):424-435.
Rogers, E.M. (2003) Diffusion of innovations, 5th edn, Free Press, New York.
Ruggiero, T. E. (2000). Uses and Gratifications Theory in the 21st Century. Mass Communication & Society, 3(1), 3-37. Sarantakos, Sotirios. (1998) Social research, Houndmills: Macmillan
Sambisa, W., Curtis, S. & Mishra, V. (2010). AIDS stigma as an obstacle to uptake of HIV testing: evidence from a Zimbabwean national population-based survey. AIDS Care,22, 170-186. doi:10.1080/09540120903038374
Sarantakos, S., (1998). Social research. 2 edn. McMillan, Melbourne.
Sherry J., Lucas, K., Rechtsteiner, S. Brooks, C. and Wilson, B, (2001). Video game use and gratifications as predictors of use and game preference. Presented at the 51th convention of the International Communication Association, Washington, and May 24-28.
Silverstone, R. (1994). Television and everyday life. London: Routledge.
Silverstone, R. (2006). ―Domesticating Domestication. Reflections on the Life of a Concept‖ in T. Berker, M. Hartmann, Y. Punie and K. Ward (eds) Domestication of Media and Technologies, pp. 229-48. Maidenhead: Open University Press.
Silverstone, R. and Haddon, L. (1996) ―Design and the Domestication of Information and Communication Technologies: Technical Change and Everyday Life,‖ in Mansell, R. and
80
Silverstone, R. (Eds), Communication by Design: The Politics of Information and Communication Technologies. Oxford: Oxford University Press, pp. 44-74.
Silverstone, R. Hirsch, E. (Eds.) (1999) Consuming Technologies: Media and information in domestic spaces, London/New York: Routledge.
Silverstone, R., Hirsch, E., & Morley, D. (1992).Information and communication technologies and the moral economy of the household. In R. Silverstone E. Hirsch (Eds.), Consuming technologies; media and information in domestic spaces. London, UK: Routledge.
Singhal, A. & Rogers E. M. (2003). Combating AIDS: Communication Strategies in Action. New Delhi: Sage Publications Inc.
Siverstone, R., & Haddon, L.(1996). Design and the domestication of information and communication technologies: Technical change and everyday life. In R. Siverstone & R. Mansell (Eds.), Communication by design: The politics of information and communication technologies (pp. 44-74). Oxford, UK: Oxford university press.
Skog, B. (2000). Mobiltelfon som symbolsk kapital i ungdomskulturen, in Ling and Thrane (Eds.), Sosiale konsekvenser av mobiltelefoni, Proceedings fra et seminar om samfunn, barn og mobiltelefoni, Telenor R&D report 38/2000, Telenor, Norway (in Norwegian). Stake, R. (2000). The case study method in social inquiry. In R. Gomm, M. Hammersley, & P. Foster (Eds.), Case study methods (pp. 19-26). Thousnad Oaks, CA: Sage
Stake, R. E. (1978). The case study method in social inquiry. Educational Researcher, 7(2), 5-8. Stoecker, R. (1991). Evaluating and rethinking case study. Sociological Review, 39(1), 88-113.
Strauss, A., & Corbin, J. (1990). Basics of qualitative research: Grounded theory procedures and techniques. Newbury Park, CA: Sage Publications, Inc. Taylor A.S. and Harper, R. (2001). Talking activity: young people and mobile phones. Presented at the CHI 2001 Workshop on mobile communications, March 30- April 5, Seattle, WA.
Taylor, S. and Todd, P.A. (1995). ―Understanding information technology usage: a test of competing models.‖ Information Systems Research, 6: 144-176. Te'eni, D. (2001). ―Review: A cognitive-affective model of organizational communication for designing IT.‖ MIS Quarterly, 25: 251-312. Tegang, S.P., Emukule, G., Wambugu, S., Kabore, I., Mwarogo, P. (2009). ―A comparison of paper-based questionnaires with PDA for behavioral surveys in Africa: Findings from a behavioral monitoring survey in Kenya.‖ Journal of Health Informatics in Developing Countries; 3:1.
Thompson, Lee and Julie Cupples.( 2008). "Seen and not heard? Text messaging and digital sociality." Social & Cultural Geography 9(1):95-108. 2008.
81
Townsend, A.M. (2000). ―Life in the real – mobile telephones and urban metabolism. ‖ Journal of Urban Technology, 7: 85-104. Tumushabe, J. (2006). The Politics of HIV and AIDS in Uganda. Social Policy and Development Programme Paper, 28.
Uganda Bureau of Statistics and Macro International Inc. (2007). Key findings from the 2006 UDHS: A gender perspective. Kampala, Uganda and Calverton, Maryland, USA: Uganda Bureau of Statistics and Macro International Inc.
UNAIDS.(1999). Communication Framework for HIV/AIDS. UNAIDS, Geneva, Switzerland.
UNAIDS.(2009). http://www.unaids.org/en/CountryResponses/Regions/SubSaharanAfrica.asp(accessed April 1, 2011)
UNStats MDGs.(2010). http://unstats.un.org/unsd/mdg/Data.aspx.
Venkatesh V. and D avis, F.D. (2000). ―A theoretical extension of the technology acceptance model: four longitudinal field studies.‖ Management Science, 46: 186-204.
Venkatesh, V. and Morris, M.G. (2000). ―Why don't men ever stop to ask for directions? Gender, social influence, and their role in technology acceptance and usage behavior.‖ MIS Quarterly, 24: 115-139. Weilenmann, A. and Larsson, C. (2000). On Doing ‗Being Teenager‘. Applying Ethnomethodology to the Analysis of Young People‘s Use of Mobile Phones. In L. Svensson, U. Snis, C. Sørensen, H. Fägerlind, T. Lindroth, M. Magnusson, C. Östlund (eds.). Proceedings of IRIS 23. Laboratorium for Interaction Technology, University of Trollhättan Uddevalla, Sweden.
Wimmer, D. Roger, Dominick, R. Joseph. (2004) Mass Media Research: An Introduction. 4th Edition, California: Wadsworth Publishing Company.
Wimmer, D., R. and Dominick, R., J. (1994,1997); Mass Media research: An Introduction (4th & 5th eds.), Wadsworth Publishing Company, London.
Wolcott, F. Harry. (1995) The art of fieldwork, Walnut Creek, California: AltaMira Press. Yin, R. (1984). Case Study Research. Beverly Hills, Calif.: Sage Publications. Yin, R. (1989); Case study research: design and methods, Newbury Park: Sage Publications. Yin, R. (1994); Case Study Research: Design Methods (2nd Ed.). Sage, California. Yin, R. (2003); Case Study Research: Design and Methods, Thousand Oaks, London & New Delhi: Sage.

82
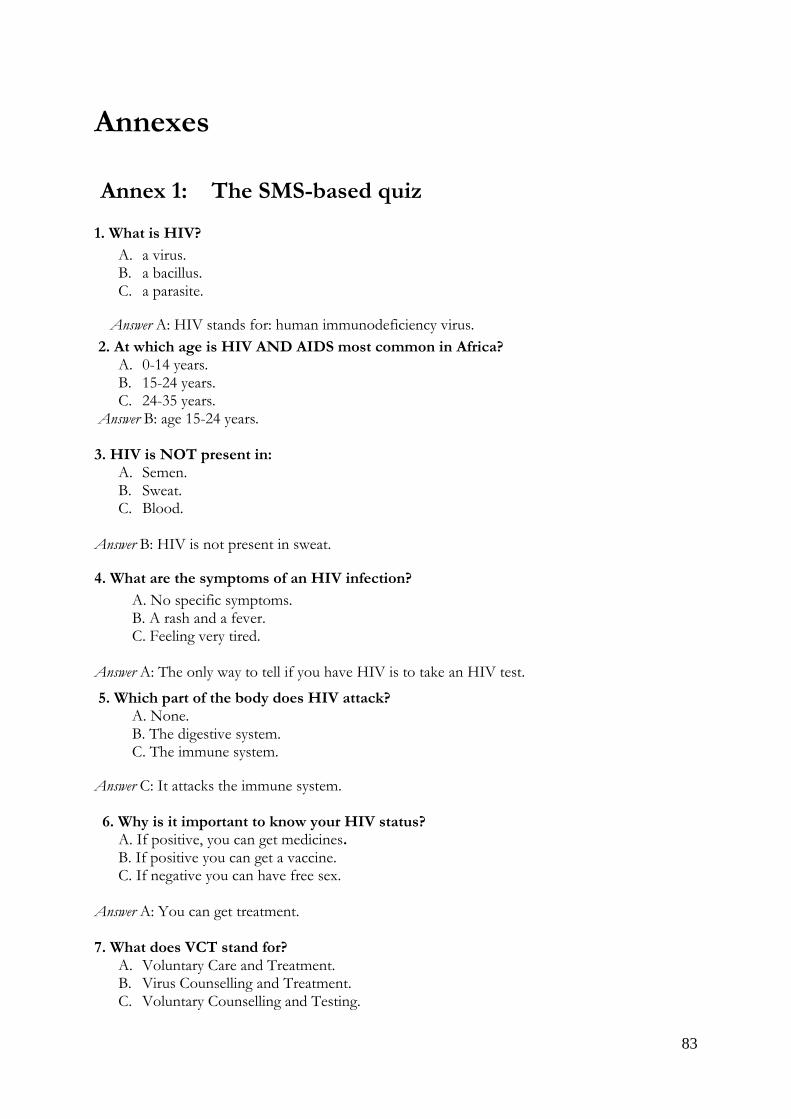
83
Annexes
Annex 1: The SMS-based quiz
1. What is HIV?
A. a virus. B. a bacillus. C. a parasite.
Answer A: HIV stands for: human immunodeficiency virus.
2. At which age is HIV AND AIDS most common in Africa? A. 0-14 years. B. 15-24 years. C. 24-35 years.
Answer B: age 15-24 years. 3. HIV is NOT present in:
A. Semen. B. Sweat. C. Blood.
Answer B: HIV is not present in sweat.
4. What are the symptoms of an HIV infection?
A. No specific symptoms. B. A rash and a fever. C. Feeling very tired.
Answer A: The only way to tell if you have HIV is to take an HIV test.
5. Which part of the body does HIV attack? A. None. B. The digestive system. C. The immune system.
Answer C: It attacks the immune system. 6. Why is it important to know your HIV status?
A. If positive, you can get medicines. B. If positive you can get a vaccine. C. If negative you can have free sex.
Answer A: You can get treatment. 7. What does VCT stand for?
A. Voluntary Care and Treatment. B. Virus Counselling and Treatment. C. Voluntary Counselling and Testing.
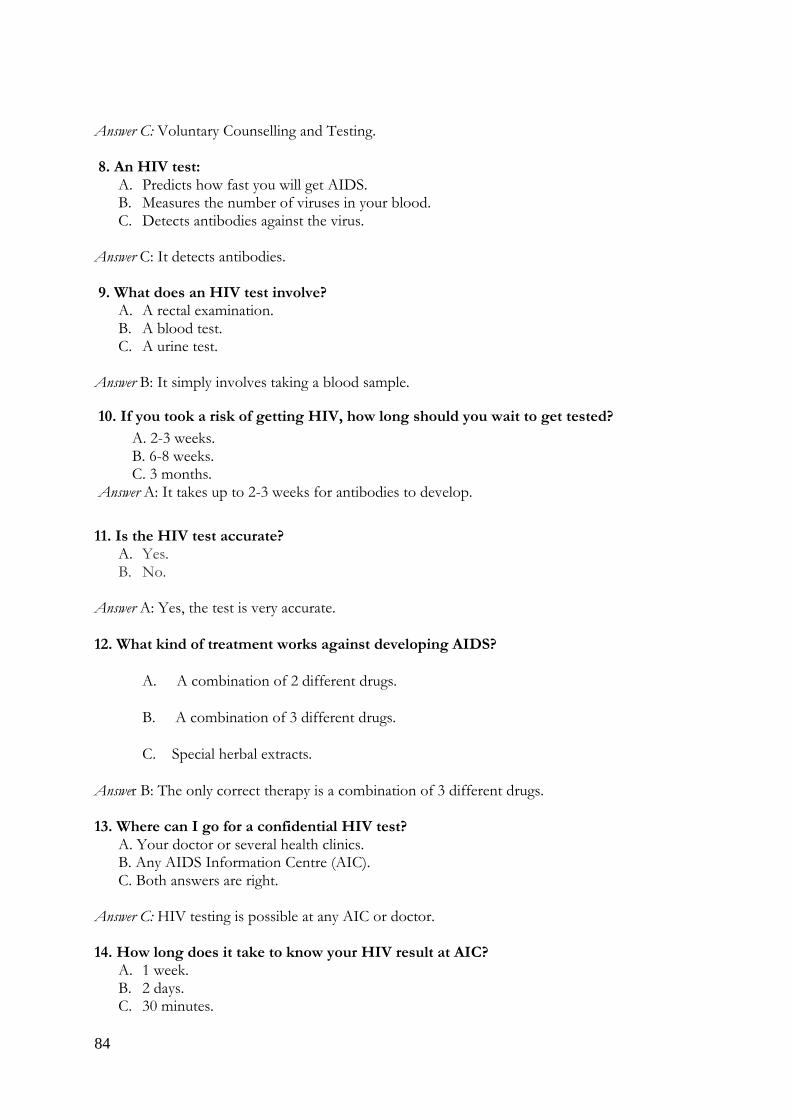
84
Answer C: Voluntary Counselling and Testing. 8. An HIV test:
A. Predicts how fast you will get AIDS. B. Measures the number of viruses in your blood. C. Detects antibodies against the virus.
Answer C: It detects antibodies. 9. What does an HIV test involve?
A. A rectal examination. B. A blood test. C. A urine test.
Answer B: It simply involves taking a blood sample.
10. If you took a risk of getting HIV, how long should you wait to get tested?
A. 2-3 weeks. B. 6-8 weeks. C. 3 months.
Answer A: It takes up to 2-3 weeks for antibodies to develop.
11. Is the HIV test accurate?
A. Yes. B. No.
Answer A: Yes, the test is very accurate.
12. What kind of treatment works against developing AIDS?
A. A combination of 2 different drugs.
B. A combination of 3 different drugs.
C. Special herbal extracts.
Answer B: The only correct therapy is a combination of 3 different drugs. 13. Where can I go for a confidential HIV test?
A. Your doctor or several health clinics. B. Any AIDS Information Centre (AIC). C. Both answers are right.
Answer C: HIV testing is possible at any AIC or doctor. 14. How long does it take to know your HIV result at AIC?
A. 1 week. B. 2 days. C. 30 minutes.
85
Answer C: AIC performs the test in less than 30 minutes. 15. Where is the nearest AIC?
A. Only in Kampala. B. Within 50 miles from me. C. Within 5 miles from me.
Answer C: Mbarara center can be found at Plot 11 Ruhara Road. 16. Will other people know my results?
A. Yes, your partner and family will be informed. B. No, everything remains confidential.
Answer B: Nobody will know your result if you don‘t want it. 17. What if my HIV test is positive?
A. Bad luck, there‘s nothing you can do. B. AIC will provide support and refer you to the right medical people. Answer B: AIC will offer counselling. 18. How much does a HIV test cost at AIC?
A. 50,000 shilling. B. 10,000 shilling. C. Free of charge.
Answer C: Free of charge if you participate in the quiz.
86
Annex 2: Guide for interviews with TTC Staff and project
partners
The researcher is conducting a study on mobile phones for HIV and AIDS prevention and care. We kindly
request you to spare a few moments to respond to these questions. The researcher is fully aware of ethical concerns
with respect to your responses, thus will ensure that your feedback is kept confidential. Thank you for your time.
Name...Organization:...............................................Designation/Position...................................
The researcher is aware that Text to Change and its partners are using state of the art mobile phone technology to
collect and disseminate information on health issues.
Q 1. Why mobile phones and particularly SMS?
Q.2 What is your experience with implementing an SMS campaign or project?
a) Any success stories?
b) What key challenges?
Q.3 Do you consider an SMS campaign/or project a viable tool for behaviour change among
users?
a) Have you recorded any behaviour change successes with an SMS project or campaign?
b) Are you aware of any scientific evidences or studies? If yes specify
Q.4 What do you think about the ICT gaps in Uganda, do you think it‘s a big challenge to mobile
phone or sms project? Specify reasons.
Q.5 What do you think is the key promise for mobile phones in HIV AND AIDS service
delivery in Uganda today?
a) What specific benefits for HIV and AIDS awareness and education initiatives?
b) What challenges?
Q.6 Can you provide any other insights and or comments regarding the potential of sms for
HIV and AIDS prevention and care?
87
Annex 3: KAP survey questions for focus groups
Age: _____ Date: _______ Gender: Male Female
1. How often do you use your mobile phone to send a text message?
Once a week Several times a week Everyday
2. On average, how long do you spend on your mobile phone in a day?
Half an hour an hour 1-3 hours More than 3 hours
3. On average, how many text messages do you send and receive in a week? I send ______ messages, mainly to ________________________________________
I receive ______ messages mainly from _____________________________________
4. What do you typically do with your mobile phone?
Playing games
Make phone calls strictly
Exchange text message
Surfing / Browsing
Other e.g._____________________________________
5. Would you say SMS is an effect tool to increase access to knowledge and
treatment of HIV and AIDS?
True
False
6. If you answered True to no. 5 please explain why you think is an effect tool to
increase access to knowledge and treatment of HIV and AIDS
7. Have you ever received any HIV and AIDS related sms / quiz courtesy of Text to Change?
8. Your attitudes toward text messaging(sms) as a tool of disseminating HIV AND AIDS information
Seldom
1 to 3 times in
past 6 months
Often
3-6 times in
past 6 months
Frequently
Twice a month
Very Frequently
Every week
Not at all
88
Circle your level of agreement with the
following statements:
Completely
disagree
Completely
agree
I have known how to send and receive text messages
(SMS) 1 2 3 4 5
SMS is fast, interactive and interpersonal
1 2 3 4 5
It is annoying to received text messages from someone i
don‘t know 1 2 3 4 5
SMS exchange is not interactive, offers no feedback and
is unreliable 1 2 3 4 5
It is fun to send and receive text messages about HIV
AND AIDS
1 2 3 4 5
Text messaging is more acceptable than other forms
of disseminating HIV and AIDS information 1 2 3 4 5
Text messaging is more acceptable than other forms
of disseminating HIV and AIDS information 1 2 3 4 5
Getting information about HIV and AIDS via (sms) is
more interesting than other traditional media, e.g. TV,
radio, newspaper
1 2 3 4 5
I am satisfied with the information i get about HIV and
AIDS via SMS 1 2 3 4 5
I ignore all HIV and AIDS related sms sent to my
phone 1 2 3 4 5
Thank you for your time
89
Annex 4: Guide for interviews with technical respondents
and peer educators
1. The recent explosion of mobile technology presents a great opportunity to scale up the
AIDS response to poor countries like Uganda. Do you think Uganda is ready to adapt to
the use of mobile technoghy for health care and other imitative other than basic
communication?
2. What is your comment on the level of literacy or technological competence in Uganda in
relation to the adoption of the use of sms for HIV and AIDS care and treatment?
3. Would you then say SMS is an effect tool to increase access to knowledge and treatment
of HIV and AIDS in a resource limited context like Uganda? If yes, in what ways?
4. Are you aware of any scientific evidence or explanations defending the use of mobile
communication (sms) in health care initiatives?
5. Besides just sms quizzes, what other text messaging techniques are being used to deliver
HIV and AIDS information? Why are you using these techniques?
6. Is there any success stories recorded after implantation of a sms campaign? What are the
milestones? What challenges?
7. Is it possible to solely rely on SMS as a tool of dissemination HIV and AIDS
information to target audiences without the need for a mix with other traditional medial
media like Television, Radio, Newspapers and other tools like flyers, posters, etc?
8. What is the main limitation of using text messaging as a sole channel of disseminating
HIV and AIDS information?
9. What is your experience in using or implementing an SMS campaign?
10. Are there any other insights and or comments regarding the potential of sms for HIV and
AIDS education?

90
91
Annex 5: Map of Uganda showing Mbarara District
Source: GoU Directory/Mbarara District24.
Key facts:
Area: 1,846.4 km2 (712.9 sq mi)
Elevation: 1,800 m (5,906 ft)
Population (2010 Estimate)
Total- 457,800
Density-247.9/km2 (642.1/sq mi
24 More information is available on the official website for Mbarara District http://www.mbarara.go.ug/ (visited
March , 2011)
Mbarara District
Top Related
Copyright © 2022 FDOKUMEN

