







Bahasa
Halaman
Hukum

Eur Arch Otorhinolaryngol (2010) 267:1371–1376
DOI 10.1007/s00405-010-1265-4OTOLOGY
Medical management of Ménière’s disease: a 10-year case series and review of literature
C. Martín González · F. M. González · A. Trinidad · A. Ibáñez · M. Pinilla · A. Martínez Ruiz-Coello · A. Rodríguez Valiente · C. López-Cortijo
Received: 29 December 2009 / Accepted: 22 April 2010 / Published online: 8 May 2010© Springer-Verlag 2010
Abstract Ménière’s disease is frequent in our area. It is adisabling pathology that aVects the patient’s quality of life.Its etiology and pathophysiology remain unclear and thereare some therapeutic alternatives with controversial results.We present our series and treatment protocol for Ménière’sdisease and discuss the current evidence regarding its medi-cal treatment. In the last 10 years, 252 patients were diag-nosed with Ménière’s disease based on their symptoms, andthe results of tonal audiometry, videonystagmography andcaloric stimulation tests. All cases received medical treat-ment according to our management protocol. Ménière’sdisease is more frequent in women (54.76%); 83.73% ofcases are unilateral. Among these, vertigo was observed in93.7%, hearing loss in 88.1%, tinnitus in 86.1% and patho-logic caloric stimulation tests in 71% (88.27% with areduced vestibular response). A 5-year follow-up was per-formed in 89.6% of the patients. Subjective improvementas reported by patients was achieved in 94.4% of the cases.There is great controversy about the medical treatment ofMénière’s disease. We found no evidence for the most ade-quate medical treatment among the diVerent alternativesdescribed in literature. The patient’s acceptance and under-standing of the disease is very important.
Keywords Ménière’s disease · Endolymphatic hydrops · Vertigo · Tinnitus · Videonystagmography · Betahistine · Intratympanic gentamicin · Meniett
Introduction
Ménière’s disease (MD) is a disorder of the inner ear asso-ciated with recurrent episodes of acute vertigo, sensorineu-ral hearing loss, tinnitus and aural fullness [1, 2]. It isfrequent in our area although the prevalence of MD hasnot been estimated in Spain. In the USA, its prevalence is1/1,000 [1].
This disorder has a slight female preponderance (1.8:1).Onset usually takes place at early-to-middle adulthood (49–67 years)[1, 2]. A familial predisposition seems to exist [1, 2].It is usually a unilateral disease, with a variable reported inci-dence of bilateral cases ranging from 10 to 30% of cases [3].
The diagnosis of MD is based on clinical presentation.The American Academy of Otolaryngology-Head and NeckSurgery (AAO-HNS) has established a diagnostic guidelineof MD (last update in 1995) and so it can be classiWed as cer-tain, deWnitive, probable and possible MD [2, 4] (Table 1).
The treatment of MD includes medical managementusing betahistine, diuretics, vasodilators and corticoste-roids, and also a non-medical one. Surgery is recommendedonly in non-responder patients. No consensus exists for themanagement of MD [1, 4].
Our aim is to present our case series and medical man-agement protocol for MD, and to perform a literaturereview of its medical treatment.
Materials and methods
Of 1,257 subjects studied in the vestibular unit of our hos-pital between 1998 and 2008, 252 patients were diagnosedwith deWnitive or probable MD. The variables recorded arethe patient’s age, gender, symptoms and their durationbefore diagnosis, involvement of one ear or both, the level
C. Martín González (&) · F. M. González · A. Trinidad · A. Ibáñez · M. Pinilla · A. Martínez Ruiz-Coello · A. Rodríguez Valiente · C. López-CortijoDepartment of Otolaryngology, Hospital Universitario Puerta de Hierro-Majadahonda, C/Manuel de Falla, 1, 28220 Majadahonda, Madrid, Spaine-mail: [email protected]
123
1372 Eur Arch Otorhinolaryngol (2010) 267:1371–1376
of hearing loss and the results of videonystagmography(VNG) and caloric stimulation tests.
To perform the tonal audiometry, we used the Audiotest340 number 023026 (Gaes, Madrid, Spain); and for theVNG we used the software VNG Ulmer 3.04.17 (Synapsis-Audiomedical, Marseille, France).
All patients were managed according to our protocol forMD as follows:
– At the acute stage of the disease, we recommend rest,and avoiding exercise and stress. Drugs prescribed arevestibulosuppressants and sedatives such as prometha-zine, sulpiride or thiethylperazine. The method of admin-istration depends on the development of vegetativesymptoms, so it could be orally (PO), intramuscularly(IM), intravenously (IV) or rectally.
– Between episodes, we recommend lifestyle adjustmentsand betahistine 16 mg twice daily for 3–6 months. Ifresponse is positive, the dosage is progressively dimin-ished. In case of Xuctuating hearing loss, we use cortico-steroids.
At any stage of the disease, we recommend an adequatepatient reassurance, explaining what the disease involvesand how its progression could be.
A descriptive statistical study was carried out using thefrequency for qualitative variables and the mean for quanti-tative variables through the statistical program SPSS 10.0.A computer-assisted search of eYcacy of medical treatmentof MD was performed in primary and secondary sources toidentify the most relevant studies.
Results
DeWnitive or probable MD was diagnosed in 252 subjectsout of 1257 patients who came to our vestibular unit in thelast decade. Cases of possible MD as deWned by the AAO-HNS were not included in this study. We observed a slightfemale preponderance (54.76%). Most of our patients hadsymptoms for a few months before the diagnosis and83.73% of cases were unilateral. The mean age of ourpatients was 46.9 years.
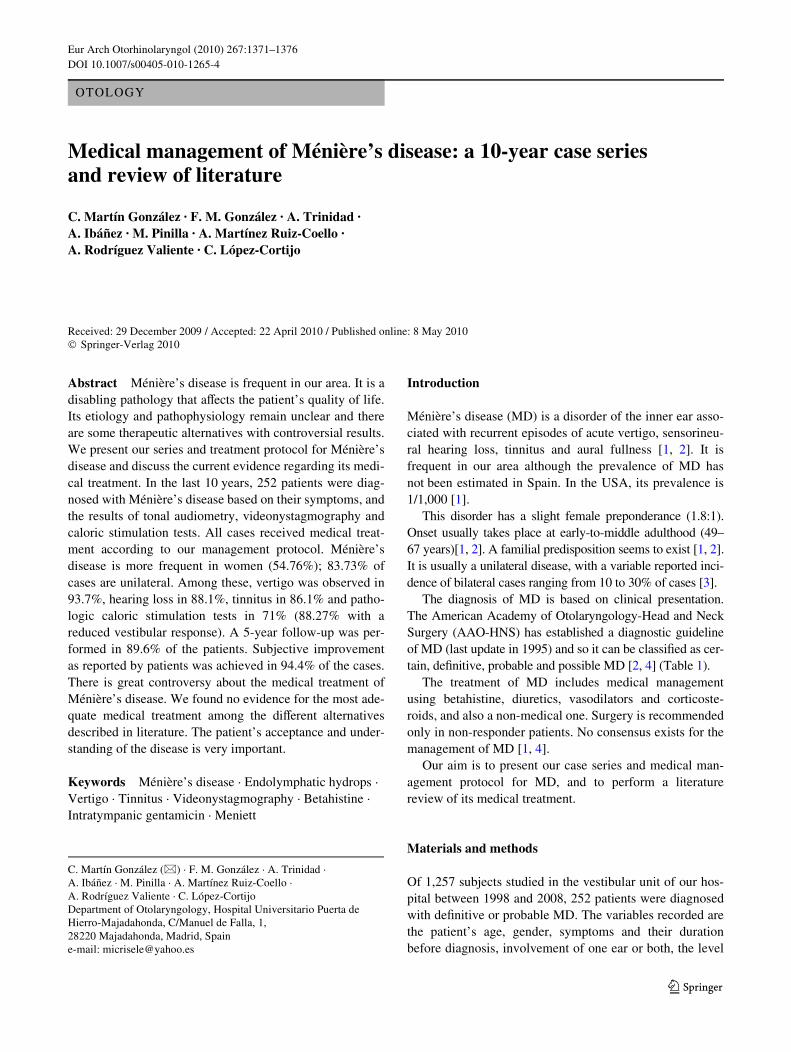
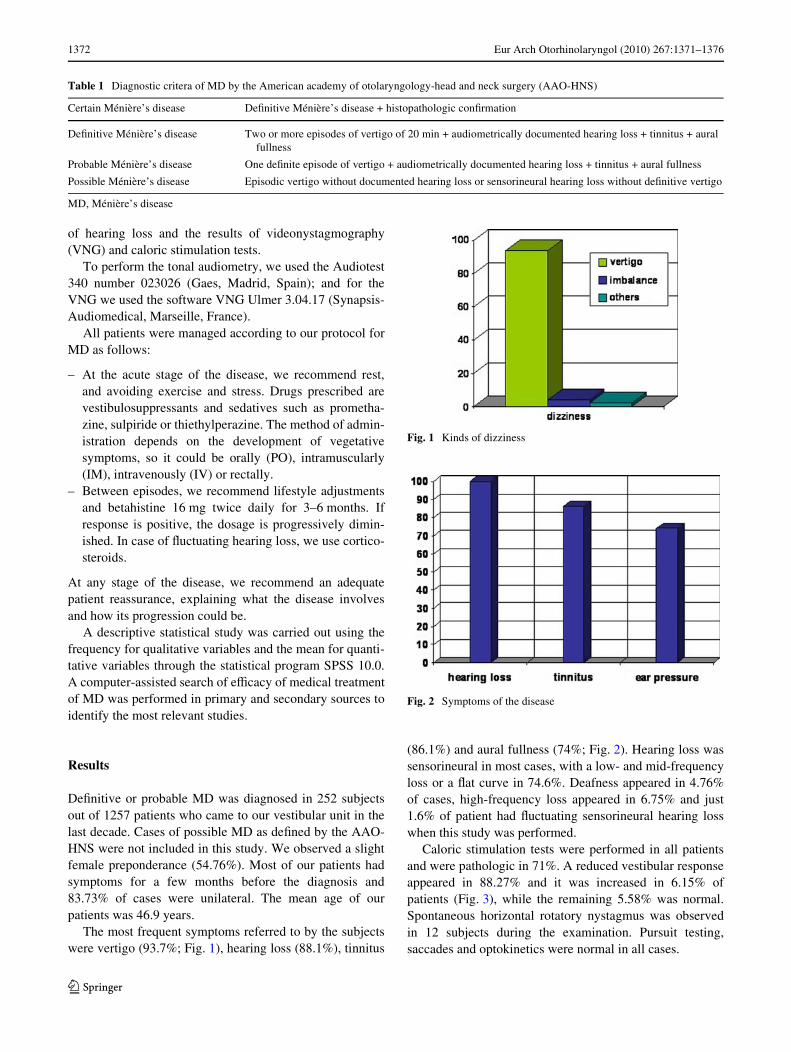
The most frequent symptoms referred to by the subjectswere vertigo (93.7%; Fig. 1), hearing loss (88.1%), tinnitus
(86.1%) and aural fullness (74%; Fig. 2). Hearing loss wassensorineural in most cases, with a low- and mid-frequencyloss or a Xat curve in 74.6%. Deafness appeared in 4.76%of cases, high-frequency loss appeared in 6.75% and just1.6% of patient had Xuctuating sensorineural hearing losswhen this study was performed.
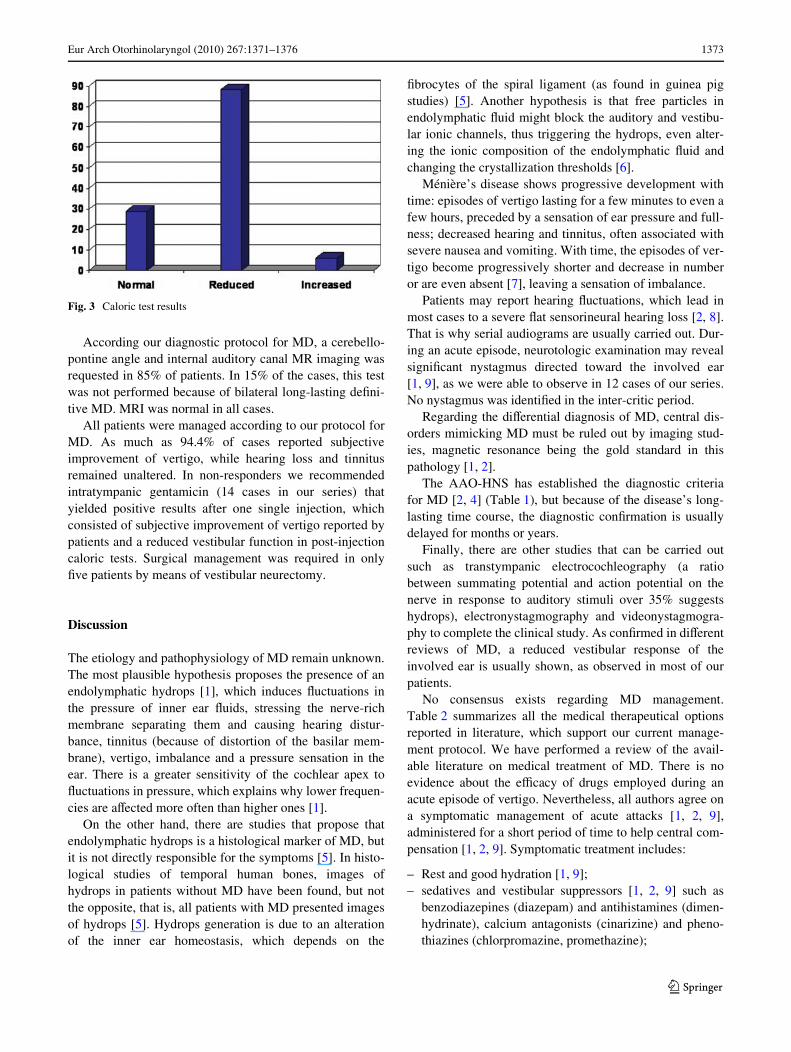
Caloric stimulation tests were performed in all patientsand were pathologic in 71%. A reduced vestibular responseappeared in 88.27% and it was increased in 6.15% ofpatients (Fig. 3), while the remaining 5.58% was normal.Spontaneous horizontal rotatory nystagmus was observedin 12 subjects during the examination. Pursuit testing,saccades and optokinetics were normal in all cases.
Table 1 Diagnostic critera of MD by the American academy of otolaryngology-head and neck surgery (AAO-HNS)
MD, Ménière’s disease
Certain Ménière’s disease DeWnitive Ménière’s disease + histopathologic conWrmation
DeWnitive Ménière’s disease Two or more episodes of vertigo of 20 min + audiometrically documented hearing loss + tinnitus + auralfullness
Probable Ménière’s disease One deWnite episode of vertigo + audiometrically documented hearing loss + tinnitus + aural fullness
Possible Ménière’s disease Episodic vertigo without documented hearing loss or sensorineural hearing loss without deWnitive vertigo
Fig. 1 Kinds of dizziness
Fig. 2 Symptoms of the disease
123
Eur Arch Otorhinolaryngol (2010) 267:1371–1376 1373
According our diagnostic protocol for MD, a cerebello-pontine angle and internal auditory canal MR imaging wasrequested in 85% of patients. In 15% of the cases, this testwas not performed because of bilateral long-lasting deWni-tive MD. MRI was normal in all cases.
All patients were managed according to our protocol forMD. As much as 94.4% of cases reported subjectiveimprovement of vertigo, while hearing loss and tinnitusremained unaltered. In non-responders we recommendedintratympanic gentamicin (14 cases in our series) thatyielded positive results after one single injection, whichconsisted of subjective improvement of vertigo reported bypatients and a reduced vestibular function in post-injectioncaloric tests. Surgical management was required in onlyWve patients by means of vestibular neurectomy.
Discussion
The etiology and pathophysiology of MD remain unknown.The most plausible hypothesis proposes the presence of anendolymphatic hydrops [1], which induces Xuctuations inthe pressure of inner ear Xuids, stressing the nerve-richmembrane separating them and causing hearing distur-bance, tinnitus (because of distortion of the basilar mem-brane), vertigo, imbalance and a pressure sensation in theear. There is a greater sensitivity of the cochlear apex toXuctuations in pressure, which explains why lower frequen-cies are aVected more often than higher ones [1].
On the other hand, there are studies that propose thatendolymphatic hydrops is a histological marker of MD, butit is not directly responsible for the symptoms [5]. In histo-logical studies of temporal human bones, images ofhydrops in patients without MD have been found, but notthe opposite, that is, all patients with MD presented imagesof hydrops [5]. Hydrops generation is due to an alterationof the inner ear homeostasis, which depends on the
Wbrocytes of the spiral ligament (as found in guinea pigstudies) [5]. Another hypothesis is that free particles inendolymphatic Xuid might block the auditory and vestibu-lar ionic channels, thus triggering the hydrops, even alter-ing the ionic composition of the endolymphatic Xuid andchanging the crystallization thresholds [6].
Ménière’s disease shows progressive development withtime: episodes of vertigo lasting for a few minutes to even afew hours, preceded by a sensation of ear pressure and full-ness; decreased hearing and tinnitus, often associated withsevere nausea and vomiting. With time, the episodes of ver-tigo become progressively shorter and decrease in numberor are even absent [7], leaving a sensation of imbalance.
Patients may report hearing Xuctuations, which lead inmost cases to a severe Xat sensorineural hearing loss [2, 8].That is why serial audiograms are usually carried out. Dur-ing an acute episode, neurotologic examination may revealsigniWcant nystagmus directed toward the involved ear[1, 9], as we were able to observe in 12 cases of our series.No nystagmus was identiWed in the inter-critic period.
Regarding the diVerential diagnosis of MD, central dis-orders mimicking MD must be ruled out by imaging stud-ies, magnetic resonance being the gold standard in thispathology [1, 2].
The AAO-HNS has established the diagnostic criteriafor MD [2, 4] (Table 1), but because of the disease’s long-lasting time course, the diagnostic conWrmation is usuallydelayed for months or years.
Finally, there are other studies that can be carried outsuch as transtympanic electrocochleography (a ratiobetween summating potential and action potential on thenerve in response to auditory stimuli over 35% suggestshydrops), electronystagmography and videonystagmogra-phy to complete the clinical study. As conWrmed in diVerentreviews of MD, a reduced vestibular response of theinvolved ear is usually shown, as observed in most of ourpatients.
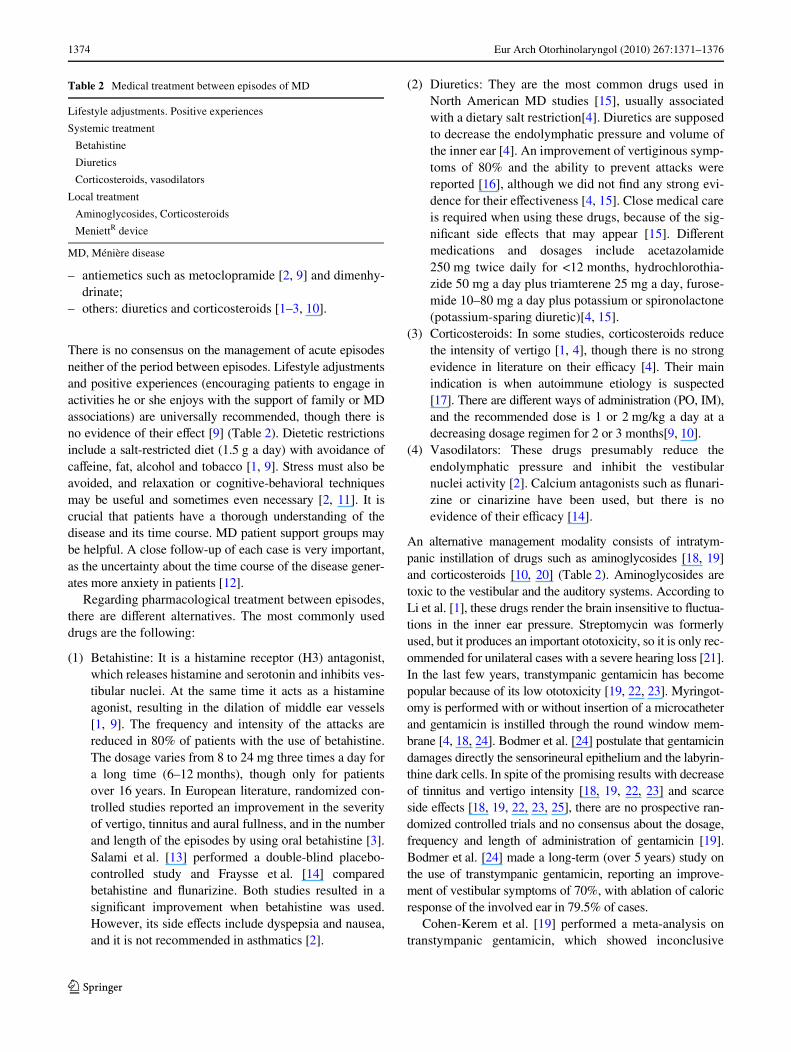
No consensus exists regarding MD management.Table 2 summarizes all the medical therapeutical optionsreported in literature, which support our current manage-ment protocol. We have performed a review of the avail-able literature on medical treatment of MD. There is noevidence about the eYcacy of drugs employed during anacute episode of vertigo. Nevertheless, all authors agree ona symptomatic management of acute attacks [1, 2, 9],administered for a short period of time to help central com-pensation [1, 2, 9]. Symptomatic treatment includes:
– Rest and good hydration [1, 9];– sedatives and vestibular suppressors [1, 2, 9] such as
benzodiazepines (diazepam) and antihistamines (dimen-hydrinate), calcium antagonists (cinarizine) and pheno-thiazines (chlorpromazine, promethazine);
Fig. 3 Caloric test results
123
1374 Eur Arch Otorhinolaryngol (2010) 267:1371–1376
– antiemetics such as metoclopramide [2, 9] and dimenhy-drinate;
– others: diuretics and corticosteroids [1–3, 10].
There is no consensus on the management of acute episodesneither of the period between episodes. Lifestyle adjustmentsand positive experiences (encouraging patients to engage inactivities he or she enjoys with the support of family or MDassociations) are universally recommended, though there isno evidence of their eVect [9] (Table 2). Dietetic restrictionsinclude a salt-restricted diet (1.5 g a day) with avoidance ofcaVeine, fat, alcohol and tobacco [1, 9]. Stress must also beavoided, and relaxation or cognitive-behavioral techniquesmay be useful and sometimes even necessary [2, 11]. It iscrucial that patients have a thorough understanding of thedisease and its time course. MD patient support groups maybe helpful. A close follow-up of each case is very important,as the uncertainty about the time course of the disease gener-ates more anxiety in patients [12].
Regarding pharmacological treatment between episodes,there are diVerent alternatives. The most commonly useddrugs are the following:
(1) Betahistine: It is a histamine receptor (H3) antagonist,which releases histamine and serotonin and inhibits ves-tibular nuclei. At the same time it acts as a histamineagonist, resulting in the dilation of middle ear vessels[1, 9]. The frequency and intensity of the attacks arereduced in 80% of patients with the use of betahistine.The dosage varies from 8 to 24 mg three times a day fora long time (6–12 months), though only for patientsover 16 years. In European literature, randomized con-trolled studies reported an improvement in the severityof vertigo, tinnitus and aural fullness, and in the numberand length of the episodes by using oral betahistine [3].Salami et al. [13] performed a double-blind placebo-controlled study and Fraysse et al. [14] comparedbetahistine and Xunarizine. Both studies resulted in asigniWcant improvement when betahistine was used.However, its side eVects include dyspepsia and nausea,and it is not recommended in asthmatics [2].
(2) Diuretics: They are the most common drugs used inNorth American MD studies [15], usually associatedwith a dietary salt restriction[4]. Diuretics are supposedto decrease the endolymphatic pressure and volume ofthe inner ear [4]. An improvement of vertiginous symp-toms of 80% and the ability to prevent attacks werereported [16], although we did not Wnd any strong evi-dence for their eVectiveness [4, 15]. Close medical careis required when using these drugs, because of the sig-niWcant side eVects that may appear [15]. DiVerentmedications and dosages include acetazolamide250 mg twice daily for <12 months, hydrochlorothia-zide 50 mg a day plus triamterene 25 mg a day, furose-mide 10–80 mg a day plus potassium or spironolactone(potassium-sparing diuretic)[4, 15].
(3) Corticosteroids: In some studies, corticosteroids reducethe intensity of vertigo [1, 4], though there is no strongevidence in literature on their eYcacy [4]. Their mainindication is when autoimmune etiology is suspected[17]. There are diVerent ways of administration (PO, IM),and the recommended dose is 1 or 2 mg/kg a day at adecreasing dosage regimen for 2 or 3 months[9, 10].
(4) Vasodilators: These drugs presumably reduce theendolymphatic pressure and inhibit the vestibularnuclei activity [2]. Calcium antagonists such as Xunari-zine or cinarizine have been used, but there is noevidence of their eYcacy [14].
An alternative management modality consists of intratym-panic instillation of drugs such as aminoglycosides [18, 19]and corticosteroids [10, 20] (Table 2). Aminoglycosides aretoxic to the vestibular and the auditory systems. According toLi et al. [1], these drugs render the brain insensitive to Xuctua-tions in the inner ear pressure. Streptomycin was formerlyused, but it produces an important ototoxicity, so it is only rec-ommended for unilateral cases with a severe hearing loss [21].In the last few years, transtympanic gentamicin has becomepopular because of its low ototoxicity [19, 22, 23]. Myringot-omy is performed with or without insertion of a microcatheterand gentamicin is instilled through the round window mem-brane [4, 18, 24]. Bodmer et al. [24] postulate that gentamicindamages directly the sensorineural epithelium and the labyrin-thine dark cells. In spite of the promising results with decreaseof tinnitus and vertigo intensity [18, 19, 22, 23] and scarceside eVects [18, 19, 22, 23, 25], there are no prospective ran-domized controlled trials and no consensus about the dosage,frequency and length of administration of gentamicin [19].Bodmer et al. [24] made a long-term (over 5 years) study onthe use of transtympanic gentamicin, reporting an improve-ment of vestibular symptoms of 70%, with ablation of caloricresponse of the involved ear in 79.5% of cases.
Cohen-Kerem et al. [19] performed a meta-analysis ontranstympanic gentamicin, which showed inconclusive
Table 2 Medical treatment between episodes of MD
MD, Ménière disease
Lifestyle adjustments. Positive experiences
Systemic treatment
Betahistine
Diuretics
Corticosteroids, vasodilators
Local treatment
Aminoglycosides, Corticosteroids
MeniettR device
123

Eur Arch Otorhinolaryngol (2010) 267:1371–1376 1375
evidences, though a tendency toward improvement of ver-tigo was found. Harner et al. [26] described the low-dosemethod and obtained an improvement in vertigo intensityof 76% with no change in hearing levels 4 years after gen-tamicin instillation, although 15–20% of patients required asecond injection at a 1-month interval. At present, trans-tympanic gentamicin is used for patients who suVer fromvertigo that is refractory to medical treatment [18, 24, 27].
Transtympanic corticosteroids have been employed inMD with controversial results [20]. Garduno Anaya et al.[28] performed a prospective controlled study using dexa-methasone 4 mg/ml with an improvement in vertigo of 82%in patients with MD after 2 years of follow-up and also asubjective improvement of others symptoms of the disease.However, a previous randomized study [29] showed nobeneWt of dexamethasone when compared to placebo. Aretrospective study published by Boleas-Aguirre et al. [30]reported vertigo control in 91% of cases after 2 years withdexamethasone of 12 mg/ml, although two to three injec-tions were necessary in 70% of patients.
There is no consensus on the corticosteroid that is rec-ommended, its dosage and the number of injections needed.Some authors report better response when used in earlystages of the disease [20].
MeniettR device is a non-medical treatment for MD thatwas designed in Sweden in 2000 [25, 27, 31]. It releasespositive pressure pulses of 12 cm H2O to the inner earthrough the middle ear. A tympanostomy tube (TT) must beinserted previously. These low-pressure pulses are thoughtto increase the exchange of the inner ear Xuids through thediVerent communication routes. Positive pressure pulsesare intended to displace the perilymphatic Xuid, whichstimulates the Xow of endolymphatic Xuid and results in areduction of endolymphatic Xuid. The device is believed toimprove vertigo intensity [31], although there is no evi-dence, and has no eVect on hearing [25, 31]. MeniettR
device is prescribed for patients with bilateral MD or withan only hearing ear refractory to medical treatment [31].Long-term results (over 2 years) remain unknown, severaldaily sessions are required and adverse eVects related to thepresence of TT (infections) must be considered [25].
Conclusion
There is no consensus on the management of MD. Symp-tomatic treatment is administered in acute episodes of ver-tigo. Management of intercritical MD is controversial:betahistine is mostly used in European countries and diuret-ics in the USA, in association with lifestyle adjustmentsand treatment for anxiety. Long-term results of devicessuch as MeniettR remain yet unknown. Transtympanic gen-tamicin is being increasingly used in refractory cases.
ConXict of interest statement The authors declare that they have noconXict of interest.
References
1. Li JC (2009) Inner ear, Ménière disease, medical treatment. Avail-able via DIALOG. http://emedicine.medscape.com/article/856547-overview. Accessed 28 Jun 2009
2. (2007) Ménière’s disease. In: CKS (Clinical Knowledge Summa-ries). Available via DIALOG. http://cks.library.nhs.uk/menieres_disease#288363001. Accessed 23 Sep 2008
3. (1995) Ménière’s disease. In: Bandolier. Available via DIALOG.http://www.jr2.ox.ac.uk/bandolier
4. Coelho DH, Lalwani AK (2008) Medical management ofMénière’s disease. Laryngoscope 118:1099–1106
5. Merchant SN, Adams JC, Nadol JB (2005) Pathophysiology ofMénière’s syndrome: are symptoms caused by endolymphatichydrops? Otol Neurotol 26:74–81
6. Philips JS, Prinsley PR (2009) A uniWed hypothesis for vestibulardysfunction? Otolaryngol Head Neck Surg 140:477–479
7. Pérez-Garrigues H, López-Escamez JA, Pérez P, Sanz R, Orts M,Marco J et al (2008) Time course of episodes of deWnitive vertigoin Ménière’s disease. Arch Otolaryngol Head Neck Surg134:1149–1154
8. Sajjadi H, Paparella MM (2008) Ménière’s disease. Lancet372:406–414
9. Wilkerson RG (2008) Ménière disease. Available via DIALOG.http://emedicine.medscape.com/article/792902-overview
10. Alles MJRC, Der Gaag MA, Stokroos RJ (2006) Intratympanicsteroid therapy for inner ear diseases, a review of the literature. EurArch Otorhinolaryngol 263(9):791–797
11. Yardley L, Kirby S (2006) Evaluation of booklet-based self-man-agement of symptoms in Ménière disease: a randomized con-trolled trial. Psychosom Med 68(5):762–769
12. Kirby S, Yardley L (2009) Cognitions associated with anxiety inMénière’s disease. J Psychosom Res 66:111–118
13. Salami A, Dellepiane M, Tinelle E, Jankowska B (1984) Doubleblind study of betahistine and placebo in the treatment ofMénière’s syndrome. Il Valsalva 60:302–312
14. Fraysse B, Bebear JP, Dubreuil C, Berges C, Dauman R (1991)Betahistine dihydrochloride versus Xunarizine. A double blindstudy on recurrent vertigo with or without cochlear syndrome typ-ical of Menière’s disease. Acta Otolarynngol Suppl 490:1–10
15. Thirlwall AS, Kundu S (2006) Diuréticos para la enfermedad o elsíndrome de Ménière (Revisión Cochrane traducida). Availablevia DIALOG. http://www.update-software.com
16. Van Deelen GW, Huizing EH (1986) Use of a diuretic (Dyazide) inthe treatment of Menière’s disease. A double-blind crossover pla-cebo-controlled study. ORL J Otolaryngol Relat Spec 48:287–292
17. Alleman AM, DornhoVer JL, Arenberg IK, Walker PD (1997)Demonstration of autoantibodies to the endolymphatic sac inMénière’s disease. Laryngoscope 107:211–215
18. Harner SG, Kasperbauer JL, Facer GW, Beatty CW (1998) Trans-tympanic gentamicin for Ménière’s syndrome. Laryngoscope108:1446–1449
19. Cohen-Kerem R, Kisilevsky V, Einarson TR, Kozer E, Koren C,Rutka JA (2004) Intratympanic gentamicin for Ménière’s disease:a meta-analysis. Laryngoscope 114(12):2085–2091
20. Hamid M, Trune D (2008) Issues, indications and controversiesregarding intratympanic steroid perfusion. Curr Opin OtolaryngolHead Neck Surg 16:434–440
21. HoVer ME, Balough BJ, Gottshall KR (2006) Delivery of drugs tothe inner ear. Curr Opin Otolaryngol Head Neck Surg 14(5):329–331
123
1376 Eur Arch Otorhinolaryngol (2010) 267:1371–1376
22. Wu IC, Minor LB (2003) Long-term hearing outcome in patientsreceiving intratympanic gentamicin for Ménière’s disease. Laryn-goscope 113:815–820
23. Hill SL, Digges EN, Silverstein H (2006) Long-term follow-upafter gentamicin application via the Silverstein MicroWick inthe treatment of Ménière’s disease. Ear Nose Throat J 85:494–498
24. Bodmer D, Morong S, Stewart C, Alexander A, Chen JM, Nedzel-ski JM (2007) Long-term vertigo control in patients after intratym-panic gentamicin instillation for Ménière’s disease. Otol Neurotol28:1140–1144
25. Peterson WM, Isaacson JE (2007) Current managementof Ménière’s disease in an only hearing ear. Otol Neurotol 28:696–699
26. Harner SG, Driscoll CL, Facer GW, Beatty CW, McDonald TJ(2001) Long-term follow-up of transtympanic gentamicin forMénière’s syndrome. Otol Neurotol 22:210–214
27. Van de Heyning PH, Wuyts F, Boudewyns A (2005) Surgicaltreatment of Ménière’s disease. Curr Opin Neurol 18:23–28
28. Garduno-Anaya MA, Couthino DT, Hinojosa-Gonzalez R et al(2005) Dexamethasone inner ear perfusion by intratympanicinjection in unilateral Ménière’s disease: a two-year prospective,placebo-controlled, double-blind, randomized trial. OtolaryngolHead Neck Surg 133:285–294
29. Silverstein H, Isaacson JE, Olds MJ et al (1998) Dexamethasoneinner ear perfusion for the treatment of Ménière’s disease: a pro-spective, randomized, double blind, crossover trial. Am J Otol19:196–201
30. Boleas-Aguirre MS, Lin FR, Della Santina CC, Minor LB, CareyJP (2008) Longitudinal results with intratympanic dexamethasonein the treatment of Ménière’s disease. Otol Neurotol 29:33–38
31. Gates GA, Verrall A, Green JD, Tucci DL, Telian SA (2006)Meniett clinical trial: long-term follow-up. Arch OtolaryngolHead Neck Surg 132(12):1311–1316
123
Top Related
Copyright © 2022 FDOKUMEN

