






Bahasa
Halaman
Hukum


ARTICLE IN PRESS
0277-9536/$ - se
doi:10.1016/j.so
�Correspond0131-6506902.
E-mail addr
Social Science & Medicine 60 (2005) 1423–1435
www.elsevier.com/locate/socscimed
Lay perceptions of type 2 diabetes in Scotland: bringing healthservices back in
Julia Lawtona,�, Elizabeth Peelb, Odette Parryc, Gonzalo Araoza,Margaret Douglasd
aResearch Unit in Health, Behaviour and Change, School of Clinical Sciences and Community Health, University of Edinburgh,
Medical School, Teviot Place, Edinburgh EH8 9AG, UKbLife and Health Sciences, Aston University, Birmingham B4 7ET, UK
cSocial Inclusion Research Unit, University of Wales NEWI, Plas Coch Campus, Wrexham LL11 2AW, UKdLothian NHS Board, Deaconess House, 148 Pleasance, Edinburgh EH8 9RS, UK
Abstract
The growing prevalence of type 2 diabetes is placing Scottish health services under considerable strain. Consequently,
diabetes services are undergoing a major process of reorganisation, including the devolvement of routine diabetes care/
diabetic review from secondary to primary healthcare settings. This qualitative study was devised to explore newly
diagnosed type 2 diabetes patients’ perceptions of their disease and the health services they receive at a time when this
restructuring of services is taking place. The sample comprised 40 patients resident in Lothian, Scotland, who had
diverse experiences of services, some receiving GP-based care only, others having varying contact with hospital diabetes
clinics. In-depth interviews were undertaken with patients, three times at six monthly intervals over 1 year, enabling
their experiences to be tracked at critical junctures during the post-diagnostic period. Disease perceptions and health
service delivery were found to be mutually informing and effecting. Not only did (different types of) health service
delivery influence the ways in which patients thought about and self-managed their disease, over time patients’ disease
perceptions also informed their expectations of, and preferences for, diabetes services. We thus argue that there is a need
for a reconceptualisation within the medical social sciences to take into account the context of healthcare and the
economic/policy factors that inform health service delivery when looking at patients’ disease perceptions. We also
discuss the logistical and ethical challenges of drawing upon patients’ perspectives, preferences and views in the design
and delivery of future health services.
r 2004 Elsevier Ltd. All rights reserved.
Keywords: Diabetes; Lay understandings; Health service delivery; Self-management; Scotland; UK
Introduction
In recent years, the medical social sciences have
shifted from treating patients’ disease perceptions as a
e front matter r 2004 Elsevier Ltd. All rights reserve
cscimed.2004.08.013
ing author. Tel.: +44-0131-6506197; fax: +44-
ess: [email protected] (J. Lawton).
product of micro-encounters in the medical context (e.g.,
consultations with health professionals) to an approach
which embraces the notion that disease understandings
are ‘‘grounded in the context of day-to-day living
situations and experiences’’ (Hunt, Jordan, & Irwin,
1989), as well as being a product of people’s social
histories (Blaxter, 1983). Arguably, this shift is partly a
response to the perceived limitations of Parsons’ (1951)
d.

ARTICLE IN PRESSJ. Lawton et al. / Social Science & Medicine 60 (2005) 1423–14351424
early work on the ‘sick role’. In this, central and
fundamental importance was given to the medical
encounter in the naming, framing and legitimisation of
disease. According to Parsons, doctors’ knowledge and
authority are paramount, patients simply being passive
recipients of healthcare, with a responsibility to comply
with their doctors’ instructions and to get better.
Parson’s work has been critiqued on many fronts, most
notably because his concept of the ‘sick role’ is more
applicable to acute (i.e. temporary) than chronic ill-
nesses, the latter now forming the burden of ill-health in
the UK and elsewhere (Bury, 1991; Conrad, 1990).
Relatedly, as Crossley (1998) has pointed out, the
assumptions of dependency implicit within his concept
of the ‘sick role’ are being increasingly contested by
ideologies of ‘patient empowerment’, which present a
vision of the ‘sick’ individual as ‘independent’ and
‘proactive’, especially in the management of chronic and
long-term illnesses. Finally, as Hunt and colleagues have
observed, encounters with medical systems tend only to
constitute a small part of most patients’ lives. Thus, the
medical contribution to patients’ ‘sense-making’ tends,
in reality, to be overwhelmed by the circumstances and
experiences encountered in the extra-medical social
environment (Hunt et al., 1989). Hence, whilst Parsons’
ideas have not been abandoned altogether (e.g., Rier,
2000), the medical social sciences have increasingly
moved away from what Conrad (1990) has termed an
‘outsider perspective’ (epitomised in the concept of the
‘sick role’) to an ‘insider perspective’ concerned with
patients’ subjective experiences in the contexts of their
everyday lives.
By and large this conceptual shift has been welcomed,
as it has contributed greatly to our understandings of
patients’ everyday illness experiences outside the medical
setting (Lawton, 2003). For example, a great deal is now
known about the challenges and complexities of living
with, and managing, chronic and other diseases in the
face of competing factors such as: work and family
commitments (e.g. Pinder, 1995; Radley, 1989); econom-
ic constraints (e.g. Anderton, Elfert, & Lai, 1989;
Drummond and Mason, 1990); and/or the desire to feel
‘normal’ and be seen as ‘normal’ by others (e.g. Atkin
and Ahmad, 2000; Scambler and Hopkins, 1987).
Similarly, an expanding corpus of work has drawn
attention to the ways in which lay perceptions of
diseases and disease causation may differ and sometimes
conflict with medical models (e.g. Blaxter, 1983;
Davison, Smith, & Frankel (1991); Emslie, Hunt, &
Watt, 2001). As various studies have demonstrated,
people may draw upon a variety of factors other than, or
in addition to, medical information/knowledge to
account for why they have become unwell (e.g. Linn,
Linn, & Stein, 1982; Thompson & Gifford, 2000).
Furthermore, the particular accounts they present may
partly serve as a rhetorical device for locating themselves
as ‘moral agents’ within the wider socio-political order
(Williams, 1984). Other work suggests that contextual
factors, such as people’s position in the lifecourse and/or
their socio-economic backgrounds, may mediate and
inform their disease perceptions (e.g. Pound, Gompertz,
& Ebrahim, 1998), including whether they consider their
condition to be ameliorable to treatment or cure (e.g.
Cunningham-Burley, Allbutt, Garraway, Lee, & Rus-
sell, 1996).
But in our enthusiasm to understand and situate
patients’ disease perceptions, experiences and under-
standings in the settings of their everyday lives, have we
pushed the medical context too far to the sidelines? This
question was brought to light in Hart’s (2001) study of
stroke survivors, in which she found that patients’
experiences were as much dictated by the health and
social care services put in place in the aftermath of the
stroke, as they were by other factors. Hart observed, for
example, that a lack of support and/or inappropriate
referrals/discharges could engender unnecessary frustra-
tion, vulnerability and despair in patients. Hence, she
calls for an approach to illness experiences that
recognises a dynamic interplay between ‘survivor’ and
the healthcare ‘system’, whereby one impacts on the
other (2001, p. 120).
The idea that patients’ illness experiences/understand-
ings are entwined with the healthcare ‘system’ became
very pertinent in a recent qualitative study we undertook
with newly diagnosed type 2 diabetes patients resident in
Lothian, Scotland (UK). This study drew our attention
to ways in which different types of health service
delivery could influence patients’ disease perceptions,
at the same times as patients’ disease perceptions could
inform their expectations of, and preferences for, their
future diabetes care. This paper focuses on the meanings
and understandings patients attach to the kinds of
services they receive and to the types of healthcare
professionals they encounter as part of their diabetes
care. We also use the findings to illuminate the logistical
and ethical challenges of incorporating a ‘user perspec-
tive’ into the design and delivery of future health
services.
Background to the study
Type 2 diabetes is a chronic condition, with a multi-
factorial aetiology. Hence, considerable onus is placed
upon individuals to self-manage their disease (van den
Arend, Stolk, Krans, Grobbee, & Schrijvers, 2000). Self-
management is achieved through attention to lifestyle
(e.g. adopting a healthy diet and/or taking more
exercise) as well as, in some cases, by taking tablets
and/or insulin to improve blood glucose control.
Patients who do not adhere to recommended diabetic
regimens are at increased risk of premature death and/or

ARTICLE IN PRESSJ. Lawton et al. / Social Science & Medicine 60 (2005) 1423–1435 1425
of developing complications such as heart disease,
stroke, renal failure, amputation and blindness (UKPDS
(UK Prospective Diabetes Study Group), 1998). Thus,
considerable concern has been expressed about the
generally poor adherence that has been observed
amongst patients with type 2 diabetes. Not only do
many patients struggle to follow disease risk-manage-
ment advice (Sullivan & Joseph, 1998), commitment to
disease self-management may also decrease over time
(Lawrence & Cheely, 1980), even when patients receive
extensive information and advice (Snoek, 2002).
Given the chronic and progressive nature of the
disease, many professionals promulgate the view that
there is no such a thing as a ‘mild’ diabetes (Diabetes
UK (2004), see also Cohen, Tripp-Reimer, Smith,
Sorofman, & Lively, 1994). However, this view is often
not shared by patients, many of whom, despite receiving
education, do not consider type 2 diabetes to be a
potentially serious condition that can lead to complica-
tions such as heart disease (Cohen et al., 1994).
Furthermore, even if patients do recognise that type 2
diabetes is a potentially serious condition, they may
perceive themselves as being personally immune to its
complications (Murphy & Kinmonth, 1995). Poor
adherence amongst patients with diabetes has been
attributed to many factors, such as a desire to socialise
with others (Kelleher, 1988), and the need to fulfill
gendered obligations of care (Hepworth, 1999). How-
ever, particular salience has been given to patients’
‘misperceptions’ regarding the potential seriousness of
the disease (Anderson, Fitzgerald, & Oh, 1993; Snoek,
2002), as well as to differences between their under-
standings of the disease and those of medical profes-
sionals (Schoenberg, Amey, & Coward, 1998).
Type 2 diabetes is reaching epidemic proportions in
the United Kingdom (UK) and elsewhere (Bagust,
Hopkinson, Maslove, & Currie, 2002), a situation partly
attributable to rising levels of obesity within the general
population and the adoption of more sedentary life-
styles. The growing numbers of people affected by the
disease is putting diabetes services under considerable
strain, prompting a major reorganisation of services in
Scotland, as elsewhere in the UK. Until recently,
hospital clinics have been the main province for the
provision of routine diabetes care and diabetic review;
however, increasingly, this care is being devolved to
general practice, where it is provided by general
practitioners and nurses who have undergone special
training in the care of people with diabetes, supported
by community-based chiropodists and opticians/opto-
metrists (Goyder, McNally, Drucquer, Spiers, & Botha,
1998). Various initiatives are also being implemented
under the National Diabetes Frameworks to ensure that
patients receive more integrated services and regular
(normally annual) reviews, such as the introduction of
diabetes registers (Department of Health, 2003).
To date, the redesign of diabetes services has occurred
without much account being taken of patients’ own
perspectives. This study was thus devised to examine
patients’ experiences and views of Scottish diabetes
services, in order to inform future service delivery for
these patients. In particular, we aimed to explore
whether the changes in diabetes services provision
currently taking place in Scotland had any implications
for ways in which patients thought about and self-
managed their condition. The study focused on newly
diagnosed patients as these patients face particular
challenges adjusting to their disease. As various studies
have demonstrated, the post diagnostic period is a time
when patients are likely to be referred to a variety of
services and professionals, encouraged to assimilate a
wide body of information about diabetes and its
management, and will normally begin to make emo-
tional, psychological and practical adjustments to their
disease (Campbell et al., 2003; Maclean & Goldman,
2000).
Study design
Given the exploratory nature of the study, a
qualitative approach was deemed appropriate, as this
would allow themes and hypotheses to be identified and
tested during the data collection period, rather than
simply assessing those formulated at the study’s outset
(Britten, Jones, Murphy, & Stacy, 1995). As the period
following diagnosis is likely to be an eventful time for
patients (see above), we adopted a repeat rather than
single interview design. As Conrad (1990) suggests,
repeat interviews are particularly appropriate for studies
of chronic illness experiences as they allow process and
change to be captured and examined in-depth. Repeat
interviews are also less likely to be biased by retro-
spective (re-)interpretations of participants, and create
opportunities for trust and rapport to develop between
interviewer and participants, which may improve the
quality of the data (Mathieson, 1999). In all, three in-
depth interviews were conducted with each patient over
1 year (at baseline, 6 and 12 months later), enabling their
perspectives to be captured at critical junctures during
the post-diagnostic period. Additional data were col-
lected by means of fieldnotes in which the research
fellow (EP) documented information and insights that
patients communicated before/after the tape recorder
was switched on/off.
Subjects and settings
Forty patients with type 2 diabetes living in Lothian
(Scotland) were recruited to the study within 6 months
of being clinically diagnosed. Following approval from
ARTICLE IN PRESS
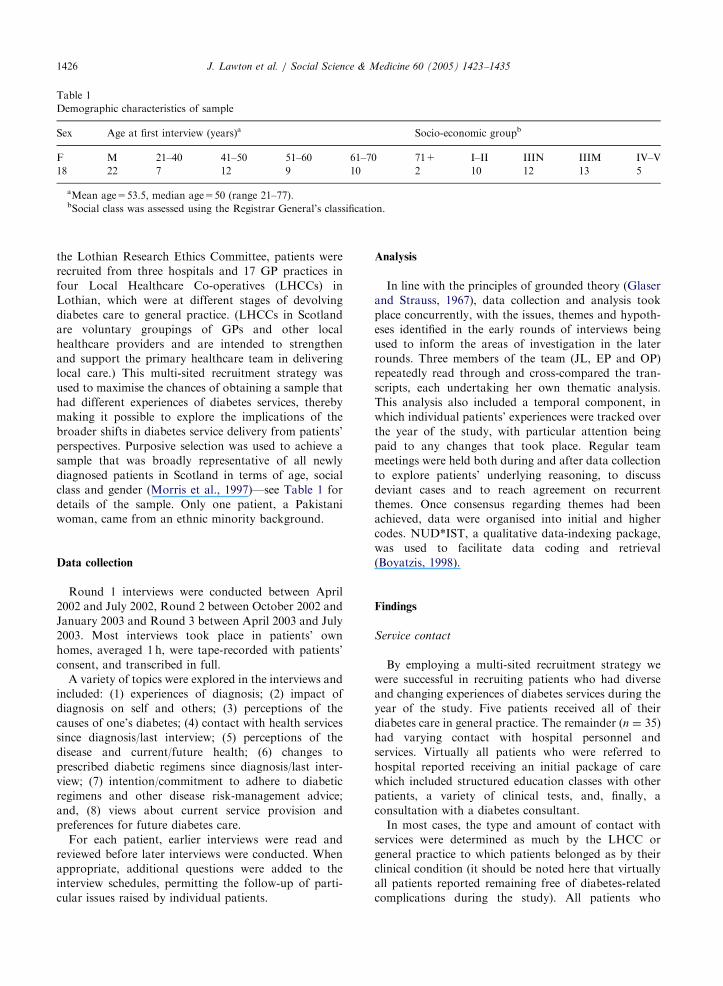
Table 1
Demographic characteristics of sample
Sex Age at first interview (years)a Socio-economic groupb
F M 21–40 41–50 51–60 61–70 71+ I–II IIIN IIIM IV–V
18 22 7 12 9 10 2 10 12 13 5
aMean age=53.5, median age=50 (range 21–77).bSocial class was assessed using the Registrar General’s classification.
J. Lawton et al. / Social Science & Medicine 60 (2005) 1423–14351426
the Lothian Research Ethics Committee, patients were
recruited from three hospitals and 17 GP practices in
four Local Healthcare Co-operatives (LHCCs) in
Lothian, which were at different stages of devolving
diabetes care to general practice. (LHCCs in Scotland
are voluntary groupings of GPs and other local
healthcare providers and are intended to strengthen
and support the primary healthcare team in delivering
local care.) This multi-sited recruitment strategy was
used to maximise the chances of obtaining a sample that
had different experiences of diabetes services, thereby
making it possible to explore the implications of the
broader shifts in diabetes service delivery from patients’
perspectives. Purposive selection was used to achieve a
sample that was broadly representative of all newly
diagnosed patients in Scotland in terms of age, social
class and gender (Morris et al., 1997)—see Table 1 for
details of the sample. Only one patient, a Pakistani
woman, came from an ethnic minority background.
Data collection
Round 1 interviews were conducted between April
2002 and July 2002, Round 2 between October 2002 and
January 2003 and Round 3 between April 2003 and July
2003. Most interviews took place in patients’ own
homes, averaged 1 h, were tape-recorded with patients’
consent, and transcribed in full.
A variety of topics were explored in the interviews and
included: (1) experiences of diagnosis; (2) impact of
diagnosis on self and others; (3) perceptions of the
causes of one’s diabetes; (4) contact with health services
since diagnosis/last interview; (5) perceptions of the
disease and current/future health; (6) changes to
prescribed diabetic regimens since diagnosis/last inter-
view; (7) intention/commitment to adhere to diabetic
regimens and other disease risk-management advice;
and, (8) views about current service provision and
preferences for future diabetes care.
For each patient, earlier interviews were read and
reviewed before later interviews were conducted. When
appropriate, additional questions were added to the
interview schedules, permitting the follow-up of parti-
cular issues raised by individual patients.
Analysis
In line with the principles of grounded theory (Glaser
and Strauss, 1967), data collection and analysis took
place concurrently, with the issues, themes and hypoth-
eses identified in the early rounds of interviews being
used to inform the areas of investigation in the later
rounds. Three members of the team (JL, EP and OP)
repeatedly read through and cross-compared the tran-
scripts, each undertaking her own thematic analysis.
This analysis also included a temporal component, in
which individual patients’ experiences were tracked over
the year of the study, with particular attention being
paid to any changes that took place. Regular team
meetings were held both during and after data collection
to explore patients’ underlying reasoning, to discuss
deviant cases and to reach agreement on recurrent
themes. Once consensus regarding themes had been
achieved, data were organised into initial and higher
codes. NUD*IST, a qualitative data-indexing package,
was used to facilitate data coding and retrieval
(Boyatzis, 1998).
Findings
Service contact
By employing a multi-sited recruitment strategy we
were successful in recruiting patients who had diverse
and changing experiences of diabetes services during the
year of the study. Five patients received all of their
diabetes care in general practice. The remainder ðn ¼ 35Þ
had varying contact with hospital personnel and
services. Virtually all patients who were referred to
hospital reported receiving an initial package of care
which included structured education classes with other
patients, a variety of clinical tests, and, finally, a
consultation with a diabetes consultant.
In most cases, the type and amount of contact with
services were determined as much by the LHCC or
general practice to which patients belonged as by their
clinical condition (it should be noted here that virtually
all patients reported remaining free of diabetes-related
complications during the study). All patients who

ARTICLE IN PRESSJ. Lawton et al. / Social Science & Medicine 60 (2005) 1423–1435 1427
received GP-based care only were registered at a practice
that had its own diabetes clinic and/or GP and nurse
who had received training in the care of diabetes.
Likewise, patients who were discharged from hospital
following their meeting with a consultant tended to be
those who belonged to a general practice which had the
necessary resources and expertise to provide on-going
diabetes care and diabetic review.
Patients, however, generally seemed to be unaware of
the broader structural influences, and drew upon a
different set of meanings and understandings when they
reflected upon the nature and settings of their diabetes
care. By way of an illustration, we begin with a case
study involving a patient called Mary (all names used
are pseudonyms). In some ways this constitutes an
extreme example, as Mary was one of few patients who
took part who received GP-based care only and she also
appeared to be more reluctant to contemplate her future
than most of her fellow patients. Her case study has been
chosen because it encompasses and highlights a number
of underlying and interconnected issues, which we will
show to be salient, either entirely or in part, to the other
patients who took part.
Case study—Mary
Mary, 47, originally presented to her GP with what
she thought were symptoms of the menopause. She
claimed to be relieved when she found out she had
diabetes as, ‘‘in the last 6 months of last year, I kept
thinking, ‘oh god what’s wrong? Is this what middle age
is all about? I’m always tired.’’’ Mary’s GP immediately
prescribed tablets (Metformin) for blood glucose con-
trol. During her round 1 interview, conducted a few
weeks after she had received her diagnosis, Mary
expressed a lack of confidence in her GP. She said her
GP was ‘‘not an expert’’ and described how she had to
refer to a book on diabetes at several points during the
consultation, an experience that was ‘‘not all that
comforting’’.
Apart from seeing her GP twice, Mary had also
received and attended an appointment with a dietician
based at her general practice who, she claimed, ‘‘didn’t
tell me anything I didn’t know already, she was just
talking about food, well, if you watch one night of
television, aye’’. She had been instructed by her GP to
have her eyes tested by a community-based optician,
which she said she had done, and also to see a podiatrist
which, as she pointed out, she had to do anyway because
she had a recurrent problem with in-growing toe nails
and had been seeing a chiropodist regularly for many
years. Mary also said she had been ‘‘surprised’’ that she
had not received a referral to a hospital diabetes clinic.
She concluded that this had not occurred because ‘‘you
had to be, I don’t know, maybe 20 times worse than I
amy before you got referred. I just assumed that. That
it must be if you are really bad you know.’’
Mary went on to suggest that having diabetes had had
no impact on her life. Changing her diet, for example,
had remained ‘‘very much at the back of my mind’’,
despite being told by her GP and the dietician that she
needed to lose weight. With regards to becoming more
physically active, Mary said: ‘‘I would like to say yes,
but I keep, every week I say right ok this is the week
you’re going to do something [but] it hasn’t happened.’’
Mary concluded the first interview by expressing a wish
to speak to ‘‘somebody who is an expert and has more
time than just a general practitioner who knows a wee
bit about everythingy somebody who could maybe tell
me things that I hadn’t thought to ask.’’ Her comments,
however, were also tinged with ambivalence. For
example, when asked if she had actively sought out
additional sources of information and support, she
responded: ‘‘I’m a bit burying my head in the sand, you
know, don’t tell me the worst case scenario, thank you
very much.’’
Mary attended her general practice only once between
her round 1 and round 2 interviews to have a blood
sample taken. She said that she was meant to have gone
for a further blood test shortly before her round 2
interview, but had not done so because ‘‘I couldn’t be
bothered’’. She also confessed to being ‘‘a bit erratic’’
about taking her tablets: ‘‘I’m very bad for the one
during the day, I forget that’’, and said that she was
‘‘really struggling’’ with her diet. When she talked about
her eating habits, she made repeated references to ‘‘being
naughty’’ and to ‘‘doing wrong’’. She described how her
weight was ‘‘creeping up’’, probably ‘‘because I’ve got a
bit complacent, I must admit.’’ During this second
interview, Mary made repeated references to her
diabetes ‘‘not being serious at all’’ and as being ‘‘very
insignificant in the big scheme of things.’’ In fact, she
claimed not to have given her diabetes ‘‘an awful deal of
thought’’, in large part because, ‘‘mine’s not in any way
impairing my life. It’s just not. I can still work, I can still
go out, I can still do my garden, I can, you know, my life
hasn’t changed any.’’ She went as far as to suggest that
she did not even see her diabetes as ‘‘an illness’’ and to
speculate that her disease might not be permanent.
However, some of her comments also indicated a more
complex picture. For example, when asked whether she
was aware of any complications patients with type 2
diabetes can develop, she responded, ‘‘we’ll not worry
about them going wrong in the future’’ and promptly
changed subject.
In her third interview, Mary reported that she still had
not lost any weight, despite the original exhortations
from her GP to do so. As in her second interview, she
continued to maintain that she did not consider herself
to have an illness because her diabetes ‘‘never affected
me one way or the other’’, and ‘‘the doctors and that

ARTICLE IN PRESSJ. Lawton et al. / Social Science & Medicine 60 (2005) 1423–14351428
don’t seem that worried about me’’. In contrast to her
first interview, however, Mary now expressed very low
expectations of diabetes services. She gave no indication
that she still wanted to consult a diabetes expert; indeed,
she suggested that the only thing she wanted and
expected healthcare professionals to do was to prescribe
her medication. She did make it clear, however, that she
preferred receiving care in general practice to hospital:
Oh no, I couldn’t be bothered trailing away up
therey Because to me, a hospital is a bit-it’s a bigger
step towards you’re really ill than just, well, ‘‘Come
back in three months and we’ll see,’’ that’s OK. But if
somebody turns round and says ‘‘Now you’ll be
attending the hospital’’, you’re thinking, ‘‘Oh really,
it’s only ill people that go to hospital’’ y’know.
She concluded her third interview by expressing the
hope that her contact with services would ‘‘get less and
less’’ in the future.
Disease perceptions and health service delivery
Mary’s case study will be referred to at various points
because of the rich and complex themes it brings to the
fore; most notably, the dynamic interplay it suggests
between disease perceptions on the one hand and health
service delivery on the other. Indeed, whilst other factors
are also at play (see below), Mary, in common with
other patients, appears to have made a number of
inferences and assumptions about the nature and
progression of her diabetes on the basis of the services
she received—an issue that will be teased out in detail
below. As will also be demonstrated, the relationship
between disease perceptions and service delivery is
neither singular nor uni-directional, for not only can
health service delivery inform the ways in which
patients, such as Mary, think about their disease, but,
over time, patients’ perceptions and understandings of
their disease may also inform their expectations of, and
preferences for, diabetes services. We begin, however, by
highlighting an (embodied) experience, which many
patients shared, as, in many cases, this forms a necessary
backdrop against which to situate their experiences and
views of services.
(Dis-)embodied states
Mary, as we have seen, originally went to see her GP
because she was suffering from extreme tiredness, a
common symptom of diabetes that was subsequently
controlled through the tablets she was prescribed. What
is salient to note here is that, at the point at which she
began to feel better, Mary ceased to see herself as having
an illness; indeed, she went as far as to speculate that her
diabetes might go away, if it had not done so already.
Mary was not alone in this regard. Many other patients
were also symptom and complication free when they
took part in the interviews, and they, likewise, struggled
to conceptualise or accept that they had an illness, since,
from an embodied, experiential perspective, they felt
well. This experience was especially marked amongst
asymptomatic patients whose diabetes had been detected
through screening procedures, such as a routine urine
test given after a patient had registered at a new general
practice (see Peel, Parry, Douglas, & Lawton, 2004a).
For these patients, the onset and detection of their
diabetes was not experienced as a wholly ‘biographically
disruptive’ event (Bury, 1982), as the disease, which was
invisible from their perspectives, did not bring about a
heightened awareness of the body and its contingent
nature (see also Leder, 1990), nor did it undermine their
physical ability to enact their daily tasks. Indeed, some
of these patients went as far as to challenge their
diagnosis by suggesting that healthcare professionals
were creating a problem where one did not exist, or that
they were simply buying into temporary fads:
I didn’t have any symptoms whatsoever that eh I felt
like saying to him [GP] ‘‘Are you sure?’’ n’ he says
‘‘Look, you just think we’re mischief making’’, and I
thought, ‘‘oh hell, there’s a lot of truth in that.’’
(Lindsay)
I just wonder how many other people are like me cos
they seem to go through five year- I call it the five
year cycle. It was the cholesterol for five years, then it
was the high blood pressure for five years and now
it’s the diabetes, y’ know. So what’s going to be the
next thing, y’know? (Mark)
Service influences
In the absence of embodied/internal symptoms and
complications, patients often looked to external factors
in order to establish and monitor the nature and
progression of their disease. As Mary’s case study
demonstrates, patients could make intuitive and see-
mingly commonsensical assumptions about their disease
and the threat it posed to their health on the basis of the
services to which they were or were not referred. Mary,
for example, gave the very strong impression in all of her
interviews that there was little, if anything, about the
health services with which she had had contact that had
indicated to her that she had a potentially serious
disease. For example, she did not regard her referrals to
the community-based podiatrist and dietician as being
remarkable, as she already received regular foot care for
in-growing toenails (a condition most people would
consider benign), and, according to her, the dietician did
not proffer any advice which differed from the healthy
eating messages she had encountered before she found
out she had diabetes (hence her comment that the

ARTICLE IN PRESSJ. Lawton et al. / Social Science & Medicine 60 (2005) 1423–1435 1429
dietician did not tell her anything she did not know
already). Particularly striking in her interviews, how-
ever, is the assumptions she had made about why all of
her care had remained in general practice. Mary, like
most other patients who took part in the study,
perceived hospitals as places where ‘‘you really get
looked after’’ (Ellen) because they are frequented by
diabetes consultants (i.e. specialists) who provide ‘‘the
ultimate knowledge’’ (Andy). Accordingly, not receiving
a hospital referral and/or having to wait for what was
perceived as a long time for an appointment to come
through were commonly interpreted by patients as
indicating that they could not have a potentially serious
disease:
My own doctor wasn’t too concerned about it I don’t
think. She certainly didn’t say she was going to send
me into a diabetes clinic and things like that. (Fraser)
I thought, ‘‘well that must be good’’ as I say because
I feel they’ve [GP] done all these tests and if it was
really bad they would have said ‘‘Oh we’ve got to get
her in quicker than the 18th of July sort of thing’’.
(Pauline – waited three months for a hospital
appointment).
As patients often saw hospital consultants as the
‘experts’ and GPs as ‘non-specialists’, some attached
considerable importance to having their diagnosis
confirmed in the hospital setting and perceived them-
selves as being in a state of liminality (Van Gennep,
1972), neither healthy nor sick, until this confirmation
had taken place:
At the moment I feel that I’m still sort of on
probation, you know, whether I’ve got it or not
[laugh]. Well, I mean they’ve [GP] said I have and
that’s alright but erm – I’m not being snooty about
this – but I’d like to hear it from the top man
[consultant diabetiologist]. (Eric)
For some of these patients, the visit(s) to the hospital
and attention received in this setting also brought about
what O’Connor, Crabtree, and Yanoshik (1997) have
termed a ‘‘conversion experience’’. Conversion experi-
ences typically involved a sudden change in perspective,
in which patients reported being ‘shocked’ into a
realisation that their diabetes posed a serious threat to
their health. These experiences tended to be most
pronounced at the point at which patients received a
comprehensive battery of clinical tests, which included
foot and eye examinations. Being on the receiving end of
several different tests at the same time, as some patients
described, heightened their awareness that their diabetes
could damage many facets of their health:
I’ll tell you how it really hit me, when I went for my
kinda like – when she checked my feet and for all the
pulses. I thought ‘‘oh my god I’ve got this for the rest
of my life.’’ That’s when it hit me y ‘‘-if I don’t
control this, this is going get worse and worse’’.
(Ellen)
I said to her [nurse] ‘‘Och I’ll be fine’’ [Laugh] and
then when she said: ‘‘Right we’ll do your blood
pressure, we’ll do your weight and we’ll do this’’ –
and I said, ‘‘wait a minute this sounds as if it’s a bit
more serious than I was taking it.’’ And she says,
‘‘Yeah a lot of people are like that just think that if
it’s diet [-controlled only] you’re finey but there is a
lot more you’ve got to look after.’’ (Iris)
Discharge from hospital, however, could have the
reverse effect. As indicated above, patients’ care was
normally returned to general practice following their
appointment with the consultant, provided that their
practice had the necessary resources to provide annual
diabetic reviews. Patients, however, rarely understood
that their discharge had occurred because of the broad
restructuring of services taking place in Lothian. On the
contrary, they tended to assume that their care was to be
general practice-based because their diabetes was not a
serious enough condition to warrant the ‘disciplinary
gaze’ (Foucault 1991) of diabetes ‘experts’ in hospital:
Well they said ‘‘you don’t have to go back to
hospital,’’ which is a good thing ‘cos if you’ve got to
keep going back there then there’s something wrong
with you eh. At the end of the day you just go to your
GP. So that’s one thing that’s not as, not as serious as
well. (Martin)
I thought, ‘‘well maybe I am just a borderline case’’
(Walter).
Perceptions of, and preferences for, services
Virtually all the patients held pragmatic views about
health service delivery in Scotland. There was a general
consensus that, within the ‘cash struck’ National Health
Service, long waiting times were sometimes inevitable,
and short appointments, whilst not desirable, were
something that had to be tolerated.
It’s just in the year 2001 or whatever you want to call
it, it’s just nobody’s got time. I’m talking right across
the board -I don’t mean just doctors, I mean virtually
everybody when it comes to work, there’s just not
enough hours in the day. (Douglas)
Against this backdrop, however, patients differed
notably in the extent to which they had strongly held
and carefully considered views about the particular
services they had received, and their preferences for
future diabetes service delivery.
Some patients, like Ryan for example, reported very
high expectations of services throughout the study.
Ryan claimed that he took his disease ‘‘very seriously’’

ARTICLE IN PRESSJ. Lawton et al. / Social Science & Medicine 60 (2005) 1423–14351430
from the outset, partly because he had read widely about
diabetes and its complications after his son had been
diagnosed a few years previously. Indeed, he talked in all
three of his interviews about wanting to ‘‘be able to play
golf in retirement and not on tin legs’’. He was an
extremely motivated patient who claimed to have made
active efforts to lose weight. He had also stopped
smoking and drinking. Ryan’s perception of his disease
appeared to fuel his expectations of services. Like
O’Connor et al.’s (1997) diabetic patients who had
undergone a ‘conversion experience’, Ryan wanted his
healthcare professionals to take his diabetes as seriously
as he did. Indeed, he described the initial care he
received in general practice as ‘‘the complete antitheses’’
to that received in the hospital diabetes clinic to which
he was referred. In hospital, ‘‘they’ve been extremely
attentivey very thorough, very professional y pleased
to answer questions and give advice’’. Furthermore,
‘‘they’re [diabetes consultants] geared up for it, they
understand it, they’ve experienced or they’ve come
across probably any scenario you could imagine with a
diabetic whereas a GP probably hasn’t.’’ Ryan’s
diabetes care remained hospital-based for the remainder
of the study. When he was invited to reflect on the
services he had received in his last interview, he made it
very clear that he wanted his diabetes care to remain
hospital-based in the future. As he suggested:
I think there needs to be a realisation and acceptance
that the GP, I don’t think, has a very major role to
play in this y for something as potentially as
significant as diabetes it’s a specialist you want to see,
not a GP, you know y my thought always was the
GPs are, you know, the sort of first line of contact.
And if it’s something a GP can treat, then fine, and if
it’s not then pass you on to a specialist and I don’t
think diabetes should be any different to that.
Whilst patients, such as Ryan, had well formulated
views about health service delivery, equal numbers of
patients failed to engage with questions that sought their
opinions of, and preferences for, their current and future
diabetes care. In the vast majority of cases, this lack of
engagement appeared to be because these patients did
not consider themselves to have a health problem, and
thus did not regard themselves as needing comprehen-
sive medical attention:
I: What would you say that you want from diabetes
services? What would you like to see them provide for
people in your position?
Iris: [Pause] I really havenae given that a thought to
be quite honest. As I say well I think I’m getting
adequate service from my doctor [GP]. She is looking
after me and I don’t think there’s much more y’know
unless-unless cos I think well I’m not too bad.
Jennifer: I feel that I’m not that bad y’know that
there’s anything I would need.
Bob: Well I don’t need nothing from them. If you’re
feeling fine you don’t need anything. But then you
know that they’re there if you need them.
Patients’ expectations of diabetes services were not
just symptomatic of their perceived health status. As
Mary’s case study highlights, patients’ preferences for
services often appeared to stem partly, albeit indirectly,
from the types of services they had already received.
Mary, as we have seen, originally wanted to consult an
‘expert’ about her diabetes and to receive more
information and support. However, by the time of her
last interview, she seemed to hold a very indifferent
attitude to her diabetes care, her expectations not
extending beyond having healthcare professionals avail-
able to write out her prescriptions. It would appear,
then, that May’s case study highlights a ‘catch 22’
situation. Whilst the low expectations of diabetes
services Mary expressed in her final interview stemmed
partly from her perception that she did not have a health
problem (and thus did not require health services), a
central reason why she did not consider herself to have a
health problem is because of the inferences and
conclusions she had drawn from the health services she
had actually received.
That disease perceptions and health service delivery
can be mutually informing is also evident in other cases.
Returning to Ryan’s case study (described above), it
could be argued that his continuing expectations of
receiving ‘expert’ attention in hospital were at least
partly fuelled by the disease perceptions nurtured by
having already received care in a hospital diabetes clinic.
Contextual knowing
Mary’s case study reveals one further, interweaving
layer of complexity salient to understanding patients’
perceptions and views. At several points during her
interviews, she alluded to the possibility that she neither
wanted to know about her future disease risks, nor did
she wish to discuss these risks openly with another
person. As one may recall, in both her round 1 and 2
interviews Mary made implicit reference to wanting to
remain ignorant of the complications patients with type
2 diabetes can develop. As such, she may have been
exhibiting what Gordon (1990) has termed ‘contextual
knowing’, a social and psychological strategy whereby
patients (and other people) cultivate and manipulate
uncertainty. Indeed, several patients, such as Mary,
proffered comments which indicated that they were
attempting to downplay the significance of future,
potentially threatening events (i.e. their risks of devel-
oping complications), and/or to dissociate themselves

ARTICLE IN PRESSJ. Lawton et al. / Social Science & Medicine 60 (2005) 1423–1435 1431
from a diabetic (i.e. sick) identity, as a way of generating
and sustaining a viable sense of self in the present.
I: Have you sought out any additional information
about diabetes from anywhere?
Eric.: Erm I think I know enough erm but erm I don’t
feel that y’know at the moment I-I don’t need, er,
don’t want others to talk to me about diabetes. I
think that might suggest that I’m becoming obses-
sional about the damned thing and I-I don’t know if I
want to y if you’re sort of searching out people or-
or organisations that are talking about diabetes all
the time, you sort of become a diabetic person and
erm well you’re somebody else then.
Jennifer: No, I read quite a bit about it y’know on the
leaflets and that. And sometimes I often think there’s
a book that they advertise in all the newspapers and I
think ‘‘I’m going to send away for that’’ but
sometimes I think you can know too much. So I’ve
never done it.
(I: What do you mean like in terms of knowing too
much? Like because it might worry you more?)
Jennifer: Yeah, yes. That’s exactly what I mean.
Arguably, this desire to downplay one’s identity as a
diabetic patient, and one’s risk of diabetic complications
may have fed into some patients’ stated preference for
their care to remain in general practice. In much the
same way as Tod, Read, Lacey, and Abbot (2001) found
that fear-motivated denial acted as a barrier to the
uptake of services for coronary heart disease, some
patients may have been resistant to the idea of hospital-
based diabetes care because, for them, a hospital referral
connoted full entry to being what Mary described as
‘‘really ill’’.
Discussion
In this paper, we have shown that newly diagnosed
type 2 diabetes patients’ disease perceptions are in-
formed by a number of interweaving factors, key
amongst these being the types of health professionals
they encounter (e.g. GPs vs. hospital consultants) and
the settings in which these encounters take place (e.g.
primary vs. secondary healthcare settings).1 In so doing,
we have underlined the importance of a contextually
sensitive approach, one that does not just take account
1As we describe elsewhere (Lawton, Peel, Douglas, & Parry
(2004a); Peel, Parry, Douglas, & Lawton, 2004b), patients’
disease perceptions were also informed by the different types of
glucose self-monitoring equipment they were allocated, and
equipment allocation was largely dictated by the (different)
settings in which patients received their diabetes care.
of broader contours and features of patients’ everyday
lives (including the contexts of patients’ own bodies),
but also situates patients’ experiences and views in the
settings and locations in which they receive their
diabetes care. Thus, like Hart (2001), this paper calls
for reconceptualisation within the medical social
sciences in order to bring health and medical services
back into the picture. However, in making this proposal,
we are not simply suggesting a return to the focus on
doctor–patient interactions beloved in British and
American medical sociology’s early years. On the
contrary, we are calling for a much wider perspective,
one which also takes account of the locations and
settings in which patients receive their health care,
together with the broader economic and policy factors
which inform the nature and content of health service
delivery. By demonstrating the salience of these wider
factors and influences, this paper helps to explain why
patients’ perceptions and understandings of their disease
are not simply a product of the diabetes education they
do or do not receive from healthcare professionals
(Cohen et al., 1994; Snoek, 2002). To put matters
simply, there are many other factors, apart from
education, at play.
Before discussing the implications of the findings, let
us begin with a caveat. This study focused on newly
diagnosed patients, virtually all of whom reported
remaining free of complications throughout the time
they took part. Hence, it has not been possible to look at
the effects of long-term or permanent changes in
patients’ (embodied) disease states on their perceptions
and understandings of their disease. However, other
studies have focused on ‘veteran’ patients and these
suggest that the experience of diabetic complications,
that is, continual bodily reminders of disease presence
(e.g. loss of sight, amputations, etc.), may heighten
patients’ awareness that their diabetes is serious in their
particular case (Murphy & Kinmonth, 1995; Maclean &
Oram, 1988). Thus, these studies can be used to support
our argument that the ‘absent’ diabetic body (Leder,
1990) creates particular challenges to healthcare profes-
sionals, insofar as it may obstruct their efforts to convey
to patients that their disease and its management is
something they need to take very seriously. The findings
also highlight other challenges for those involved in
health service delivery and health service research, and it
is to these that we shall now turn.
Challenges for those involved in health service delivery
Within the UK, general practice-based initiatives are
being launched to screen for type 2 diabetes in ‘high risk’
groups, thereby increasing the identification of those
who have the disease in its sub-clinical phase (Depart-
ment of Health, 2004). Arguably, the introduction of
screening constitutes part of a broader trend within

ARTICLE IN PRESSJ. Lawton et al. / Social Science & Medicine 60 (2005) 1423–14351432
contemporary ‘risk society’ (Beck, 1992) in which
increasing onus is being placed on individuals to take
responsibility for their future health, and the boundaries
between health and illness are becoming evermore
blurred (Armstrong, 1995). Indeed, screening pro-
grammes have been commended for their potential to
improve long-term health outcomes, by giving patients
the opportunity to implement disease risk-management
strategies at an early stage (Department of Health,
2004). However, as our findings suggest, professionals
need to be aware of the challenges of convincing
asymptomatic diabetic patients (these being the patients
most likely to be identified through general practice-
based screening) that they have a potentially life-
threatening disease for which rigorous self-management
is necessary. As has been argued elsewhere (Lawton,
2002), for some people at least, the embodied experience
of ill-health may be a necessary pre-cursor for seeing
oneself as ‘at risk’ for future disease complications.
Screening is not the only issue which raises challenges
for those involved in the delivery of diabetes services. As
described earlier, there is a widely accepted view
amongst healthcare professionals and others that
patients need to be aware that (their) type 2 diabetes is
a potentially serious disease, as this awareness may
facilitate motivation and commitment to adhere to
diabetic regimens (Snoek, 2002). Thus, our finding that
patients may interpret non-referral to hospital as mean-
ing their diabetes cannot be serious requires considera-
tion, given the nationwide restructuring of services
currently taking place in the UK (see above). Whilst
patients may view primary care-based diabetes services
favourably for reasons of convenience and accessibility,
and because they may perceive GPs and practice nurses
as easier to communicate with than hospital consultants
(see Murphy, Kinmonth, & Marteau, 1992), care needs
to be taken to ensure that these benefits are not offset by
patients drawing inappropriate conclusions about their
condition (for recommendations as to how practitioners,
healthcare policy makers and managers could meet the
challenge raised by the relocation of diabetes services to
primary care settings, see Lawton, Parry, Peel, &
Douglas, in press).
Implications for health service research
By demonstrating the overlapping and interweaving
nature of health service delivery and disease perceptions,
our study also draws attention to some of the potential
challenges of using a ‘user perspective’ to inform future
health service delivery. In particular, it can used be
stimulate discussion and debate about whether services
can simply be designed on the basis of what patients say
they want, or if greater heed should be paid to the
factors and influences that may underlie their stated
preferences and views.
In a questionnaire study undertaken with English
patients, Kinmonth, Murphy, and Marteau (1989) found
considerable consumer support for the future develop-
ment of general-practice based review of patients with
type 2 diabetes, an observation echoed by Murphy et al.
(1992) in a follow-up study undertaken after pilot
primary care review had been introduced. Both studies
have been used to provide an endorsement for the
broader restructuring of diabetes services now taking
place in the UK, an endorsement supposedly based on
patients’ own preferences and views. But what does this
consumer support actually mean? And if patients say that
they are satisfied with general practice-based services as
both Kinmonth et al. (1989) and Murphy et al. (1992)
found, can such statements simply be taken at face value?
By employing a different methodology to Kinmonth
and colleagues, our study has revealed an altogether
more complex picture. Returning to Mary’s case study
as an illustration, arguably, albeit hypothetically, had
she simply been administered a questionnaire about her
service preferences at one snapshot in time—say on the
anniversary of her diagnosis—all that it would have
been possible to ascertain is that she was satisfied with
the GP-based services she was currently receiving, she
wanted her care to remain in general practice in the long
term, and ideally for her contact with diabetes services
to be as minimal as possible. Yet, as her case study has
demonstrated, her seeming satisfaction with the services
she was receiving 1 year post-diagnosis was partly a
product of the disease perceptions fuelled by those
services hitherto received. Indeed, as one may recall,
Mary’s initial preference was for ‘expert’ (i.e. hospital)
diabetes care, but this preference shifted after her
original expectations were not met. Mary’s case study
thus adds complexity to the now popular (albeit largely
untested) notion held by policy makers and profes-
sionals that patients’ compliance improves when services
are delivered in ways tailored to their preferences and
views (Towle & Godolphin, 1999). Indeed, if one buys
into the view held by some professionals that patients
may benefit from recognising/accepting that they have a
potentially serious disease as this may improve their
compliance to diabetic regimens (see above), it could be
suggested that their interests may, on occasion, be best
served by providing services that are not necessarily
congruent with what they say they want (for example, by
providing patients, such as Mary, with diabetes care in a
hospital setting or, at the very least, by rethinking the
types of health services and support the she receives in
general practice). However, such a position, whilst
clearly important to contemplate, is somewhat proble-
matic to endorse in practice. This is not only because a
paternalistic stance stands contrary to the contemporary
ethos of empowering patients (Crossley, 1998), but also
because there may be valid and understandable reasons
why patients may have a preference for GP-based

ARTICLE IN PRESSJ. Lawton et al. / Social Science & Medicine 60 (2005) 1423–1435 1433
services. As we have seen, some patients found the
prospect/possibility of developing diabetic complica-
tions extremely upsetting and frightening, and they saw
referral to a hospital clinic as being synonymous with
their health deteriorating. Thus, their preferences for
general practice care were at least partly rooted in an
understandable desire to generate and maintain a sense
of well-being in the present.
Conclusion
As this paper has demonstrated, there are many
challenges involved in undertaking health service and
other policy relevant research, the latter now being a
requirement of most funding bodies in the UK.
Engaging patients in research and taking their views
into account in the planning and delivery of services may
bring a number of logistical and ethical issues to the
fore. Not only may imaginative and innovative meth-
odologies be required to capture adequately a ‘user
perspective’ (Lawton, 2003), we also need to be sensitive
to the complex ways in which patients’ disease percep-
tions and their ensuing preferences for services may be a
product of those services they have already received, as
well as a desire to retain a viable self in the present. In
putting findings such as these into practice, it could be
argued that the greatest challenge with which health
professionals have to contend is to tread successfully the
delicate line between offering patients comfort and
reassurance and conveying to them—through the inter-
ventions and information they provide—that they have
a potentially serious disease.
Acknowledgements
This study was funded by the Chief Scientist Office,
Scottish Executive Health Department. The research
was undertaken in the Research Unit in Health,
Behaviour and Change, which is jointly funded by the
Scottish Executive Health Department and NHS Health
Scotland. The opinions expressed in this paper are those
of the authors, not necessarily those of the funding
bodies. The authors would like to thank the healthcare
professionals who assisted with recruitment and the
patients who took part. Additional thanks goes to
Margaret MacPhee for excellent secretarial support and
to Nina Hallowell and Steve Plat for their constructive
and helpful comments on a draft of this paper.
References
Anderton, J. M., Elfert, J., & Lai, M. (1989). Ideology in the
clinical context: chronic illness, ethnicity and the discourse
on normalization. Sociology of Health and Illness, 11(3),
253–278.
Anderson, R. M., Fitzgerald, J. T., & Oh, M. S. (1993). The
relationship between diabetes-related attitudes and patients
self-reported adherence. Diabetes Education, 19, 287–292.
Armstrong, D. (1995). The rise of surveillance medicine.
Sociology of Health and Illness, 17, 393–404.
Atkin, K., & Ahmad, W. I. U. (2000). Pumping iron:
compliance with chelation therapy among young people
who have thalassaemia major. Sociology of Health and
Illness, 22, 500–524.
Bagust, A., Hopkinson, P. K., Maslove, L., & Currie, C. J.
(2002). The projected healthcare burden of Type 2 diabetes
in the UK from 2000 to 2060. Diabetic Medicine, 19(Suppl.
4), 1–5.
Beck, U. (1992). Risk society: towards a new modernity.
London: Sage.
Blaxter, M. (1983). The cause of disease: women talking. Social
Science and Medicine, 17(2), 59–69.
Boyatzis, R. E. (1998). Transforming qualitative information:
thematic analysis and code development. Thousand Oaks,
CA: Sage.
Britten, N., Jones, R., Murphy, E., & Stacy, R. (1995).
Qualitative research methods in general practice. Family
Practice, 12(1), 104–114.
Bury, M. (1982). Chronic illness as biographical disruption.
Sociology of Health and Illness, 4, 167–182.
Bury, M. (1991). The sociology of chronic illness: a review of
research and prospects. Sociology of Health and Illness, 13,
451–468.
Campbell, R., Pound, P., Pope, C., Britten, N., Pill, R.,
Morgan, M., & Donovan, J. (2003). Evaluating meta-
ethnography: a synthesis of qualitative research in lay
experiences of diabetes and diabetes care. Social Science and
Medicine, 56, 671–684.
Conrad, P. (1990). Qualitative research on chronic illness: a
commentary on method and conceptual development.
Social Science and Medicine, 11, 1257–1263.
Cohen, M. Z., Tripp-Reimer, Smith, C., Sorofman, B., &
Lively, S. (1994). Explanatory models of diabetes: patient-
practitioner variation. Social Science and Medicine, 38(1),
59–66.
Crossley, M. (1998). ‘Sick role’ or ‘empowerment’? The
ambiguities of life with an HIV positive diagnosis. Sociology
of Health and Illness, 20(4), 507–531.
Cunningham-Burley, S., Allbutt, H., Garraway, W. M., Lee, A.
J., & Russell, E. B. (1996). Perceptions of urinary symptoms
and health-care-seeking behaviour amongst men aged 40–79
years. British Journal of General Practice, 46(407), 349–352.
Davison, C., Smith, G. D., & Frankel, S. (1991). Lay
epidemiology and the prevention paradox: the implications
of coronary candidacy for health education. Sociology of
Health and Illness, 13(1), 1–19.
Department of Health (2003). National service framework for
diabetes: delivery strategy. London: HMSO.
Department of Health (2004). Diabetes, Heart Disease and
Stroke (DHDS) Prevention Project, http://www.nelh.nh-
s.uk/screening/diabetesproject/home.htm.
Diabetes UK (2004). www.diabetes.org.uk.
Drummond, N., & Mason, C. (1990). Diabetes in a social
context: just a different way of life in the age of reason. In
ARTICLE IN PRESSJ. Lawton et al. / Social Science & Medicine 60 (2005) 1423–14351434
Cunningham-Burley, S., & McKeganey, N. P. (Eds.),
Readings in medical sociology. London: Tavistock/Routle-
dge.
Emslie, C., Hunt, K., & Watt, G. (2001). Invisible women? The
importance of gender is lay beliefs about heart problems.
Sociology of Health and Illness, 23(20), 203–233.
Foucault, M. (1991). Discipline and punish: the birth of the
prison. London: Penguin Books.
Glaser, B., & Strauss, A. (1967). The discovery of grounded
theory. Chicago: Aldine Pub. Co.
Gordon, D. (1990). Embodying illness, embodying cancer.
Culture, Medicine and Psychiatry, 14, 275–297.
Goyder, E. C., McNally, P. G., Drucquer, M., Spiers, N., &
Botha, J. L. (1998). Shifting of care for diabetes from
secondary to primary care, 1990-5: review of general
practices. British Medical Journal, 316, 1505–1506.
Hart, E. (2001). System induced setbacks in stroke recovery.
Sociology of Health and Illness, 23, 101–123.
Hepworth, J. (1999). Gender and the capacity of women with
NIDDM to implement medical advice. Scandinavian Journal
of Public Health, 27, 260–266.
Hunt, L. M., Jordan, B., & Irwin, S. (1989). View of what’s
wrong: diagnosis and patients’ concepts of illness. Social
Science and Medicine, 28(9), 945–956.
Kelleher, D. (1988). Coming to terms with diabetes: coping
strategies and non-compliance. In Anderson, R., & Bury,
M. (Eds.), Living with chronic illness: the experiences of
patients and their families. London: Unwin Hyman.
Kinmonth, A. L., Murphy, E., & Marteau, T. (1989). Diabetes
and its care—what do patients expect? Journal of the Royal
College of General Practitioners, 39, 324–327.
Lawrence, A., & Cheely, J. (1980). Deterioration in diabetes
patients’ knowledge and management skills as determined
during outpatient visits. Diabetes Care, 3, 214–218.
Lawton, J. (2002). Colonising the future: temporal perceptions
and health-relevant behaviours across the adult lifecourse.
Sociology of Health and Illness, 24, 714–733.
Lawton, J. (2003). Lay experiences of health and illness: past
research and future agendas. Sociology of Health and Illness,
25(Special Issue SI 2003), 23–40.
Lawton, J., Peel, E., Douglas, M., & Parry, O. (2004a). ‘Urine
testing is a waste of time’: newly diagnosed type 2 diabetes
patients’ perceptions of self-monitoring. Diabetic Medicine,
21, 1045–1048.
Lawton, J., Parry O., Peel, E., & Douglas, M. (in press).
Diabetes service provision: a qualitative study of newly
diagnosed Type 2 diabetes patients’ preferences and views.
Diabetic Medicine.
Leder, D. (1990). The absent body. Chicago: Aldine.
Linn, M. W., Linn, B. S., & Stein, S. R. (1982). Beliefs about
the causes of cancer in cancer patients. Social Science and
Medicine, 16, 835–839.
Maclean, H. M., & Goldman, J. B. (2000). A decade of
qualitative research in diabetes: a review and synthesis.
Canadian Journal of Diabetes Care, 24(2), 54–63.
Maclean, H., & Oram, B. (1988). Living with diabetes. Toronto,
Ont.: University of Toronto Press.
Mathieson, C. M. (1999). Interviewing the ill and the healthy:
paradigm or process? In Murray, M., & Chamberlain, K.
(Eds.), Qualitative health psychology: theories & methods
(pp. 117–132). London: Sage.
Morris, A. D., Boyle, D. I., MacAlpine, R., Emslie-Smith, A.,
Jung, R. T., Newton, R. W., et al. (1997). The diabetes audit
and research in Tayside Scotland (DARTS) study: electro-
nic record linkage to create a diabetes register. DARTS/
MEMO Collaboration. British Medical Journal, 315,
524–528.
Murphy, E., & Kinmonth, A. L. (1995). No symptoms, no
problem? Patients’ understandings of non-insulin dependent
diabetes. Family Practice, 12, 184–192.
Murphy, E., Kinmonth, A. L., & Marteau, T. (1992). General
practice based diabetes surveillance: the views of patients.
British Journal of General Practice, 43, 279–283.
O’Connor, P. J., Crabtree, B. F., & Yanoshik, K. (1997).
Differences between diabetic patients who do and no not
respond to a diabetes care intervention: a qualitative
analysis. Family Medicine, 29, 424–428.
Parsons, T. (1951). The social system. Chicago: Free Press.
Peel, E., Parry, O., Douglas, M., & Lawton, J. (2004a).
Diagnosis of type 2 diabetes: a qualitative analysis of
patients’ emotional reactions about information provision.
Patient Education and Counseling, 53, 269–275.
Peel, E., Parry, O., Douglas, M., & Lawton, J. (2004b). Blood
glucose monitoring in non-insulin treated type 2 diabetes:
qualitative study of patients’ perspectives. British Journal of
General Practice, 54, 183–188.
Pinder, R. (1995). Bringing back the body without blame.
Sociology of Health and Illness, 17, 605–631.
Pound, P., Gompertz, P., & Ebrahim, S. (1998). Illness in the
context of older age: the case of stroke. Sociology of Health
and Illness, 20, 489–506.
Radley, A. (1989). Style, discourse and constraint in adjustment
to chronic illness. Sociology of Health and Illness, 3,
230–252.
Rier, D. A. (2000). The missing voice of the critically ill: a
medical sociologist’s first-person account. Sociology of
Health and Illness, 22, 68–93.
Scambler, G., & Hopkins, A. (1987). Being epileptic: coming to
terms with stigma. Sociology of Health and Illness, 8,
26–43.
Schoenberg, N. E., Amey, C. H., & Coward, R. T. (1998).
Stories of meaning: lay perspectives on the origin and
management of noninsulin dependent diabetes mellitus
among older women in the United States. Social Science
and Medicine, 47, 2113–2125.
Snoek, F. J. (2002). Breaking the barriers to optimal glyceamic
control—what physicians needs to know from patients’
perspectives. International Journal of Clinical Practice,
129(Suppl.), 80–84.
Sullivan, E. S., & Joseph, D. H. (1998). Struggling with
behaviour changes: a special case for clients with diabetes.
Diabetes Education, 21, 533–540.
Thompson, S. J., & Gifford, S. M. (2000). Trying to keep a
balance: the meaning of health and diabetes in an urban
aboriginal community. Social Science and Medicine, 51,
1457–1472.
Tod, A. M., Read, C., Lacey, A., & Abbot, J. (2001). Barriers
to uptake of services for coronary heart disease: qualitative
study. British Medical Journal, 323, 1–6.
Towle, A., & Godolphin, W. (1999). Framework for teaching
and learning informed shared decision making. British
Medical Journal, 319, 766–771.

ARTICLE IN PRESSJ. Lawton et al. / Social Science & Medicine 60 (2005) 1423–1435 1435
UKPDS (UK Prospective Diabetes Study Group) (1998).
Intensive blood-glucose control with sulphonylureas or
insulin compared with conventional treatment and risk of
complications in patients with type 2 diabetes (UKPDS 33).
The Lancet, 352, 837–853.
van den Arend, I. J. M., Stolk, R. P., Krans, H. M. J., Grobbee,
D. E., & Schrijvers, A. J. P. (2000). Management of type 2
diabetes: a challenge for patient and physician. Patient
Education and Counseling, 40, 187–194.
Van Gennep, A. (1972). The rites of passage. Chicago:
University of Chicago Press.
Williams, G. (1984). The genesis of chronic illness: narrative
reconstruction. Sociology of Health and Illness, 6,
175–200.
Top Related
Copyright © 2022 FDOKUMEN

