







Bahasa
Halaman
Hukum

Implementing Accountability for Equity and Ending
Racial Backlash in Nursing:
Accountability for Systemic Racism Must Be Guaranteed to Uphold Equal Rights in Society and Promote Equity in Health.
Submitted by
Centre for Equity in Health and Society
Rebecca Hagey, Ph.D., Merle Jacobs, Ph.D., Jane Turrittin, Ph.D., Monica Purdy, M.N., Ruth Lee, Ph.D., Angela Cooper Brathwaite, Ph.D., Marianne Chandler, C.H.R.P.
With Pilot Survey by
Tania Das Gupta Ph.D
Published by
Canadian Race Relations Foundation
April 2005
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
2
Library and Archives Canada Cataloguing in Publication Implementing accountability for equity and ending racial backlash in nursing : accountability for systematic racism must be guaranteed to uphold equal rights in society and promote equity in health / submitted by Centre for Equity in Health and Society, Rebecca Hagey ... [et al.] ; with pilot survey by Tania Das Gupta. Includes bibliographical references. ISBN 1-894982-04-5 (set) 1. Nursing--Social aspects--Canada. 2. Equity--Canada. I. Das Gupta, Tania, 1957- II. Hagey, Rebecca, 1943- III. Canadian Race Relations Foundation IV. Centre for Equity in Health and Society RT83.3.I46 2005 610.73'089'00971 C2005-905019-5

Implementing Accountability for Equity and Ending Racial Backlash in Nursing
3
Table of Contents
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
i
Table of Contents
Table of Contents............................................................................................................. i Acknowledgments ..........................................................................................................vii In Memoriam ...................................................................................................................xi Dedication ......................................................................................................................xii Ontario Human Rights Code ......................................................................................... xiii The Centre for Equity in Health and Society .................................................................xiv
CEHS Vision............................................................................................................................. xv CEHS Mission .......................................................................................................................... xv CEHS Rationale ........................................................................................................................ xv Contact Information .................................................................................................................. xv Centre for Equity in Health and Society Membership Form ................................................... xvi
Executive Summary ......................................................................................................xix
Backlash for Addressing Systemic Racism in Nursing ........................................................... xix Research Purposes .................................................................................................................... xx Resistance to Accountability for Equity in the Health Care System ........................................ xx Evidence of the Need for Accountability to Dismantle Systemic Racism .............................. xxi Evidence of Nurses Experiencing Racial Profiling ................................................................ xxii Summary of Tania Das Gupta’s Survey Conducted with Nurses from November 2001 – May 2002........................................................................................................................................ xxiv Set-up as a Strategic Practice of Systemic Racism................................................................ xxvi The Problem of Backlash for Seeking Accountability in Race Relations ........................... xxviii Employment Context of Backlash .......................................................................................... xxx Health Effects of Backlash...................................................................................................... xxx Building a Coalition to Construct Accountability Policy and Procedure: The Centre for Equity in Health and Society ............................................................................................................ xxxii
Selected CEHS Objectives................................................................................................ xxxv Recommendations to Achieve Accountability for Systemic Racism: The Romanow Commission’s Health Council of Canada............................................................................. xxxv
Recommendations for the Health Council of Canada...................................................... xxxvi Recommendations from Partisan Sectors of the CEHS Network....................................... xxxvii
1. An investigation by the Ontario Human Rights Commission ................................ xxxvii 2. Leadership Training and Anti-racism Education.................................................... xxxvii 3. Ontario Legislation ................................................................................................ xxxviii 4. Ontario Policy ........................................................................................................ xxxviii 5. National Accreditation ............................................................................................. xxxix 6. Voluntary Policy in Key Organizations......................................................................... xl

Table of Contents
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
ii
Chapter 1 – Toward Accountability among All Stakeholders: Introduction and Overview1 Questions, Objectives, and Accountability Discourse Strategies ............................................... 2 Who Are the New Stakeholders?................................................................................................ 5 How Can New Stakeholders Gain Full Inclusion into Society’s Institutions? ........................... 7 Literature Pertaining to Set-up and Backlash among Particular Stakeholders ........................... 8 Background on Getting the Stakeholders Together .................................................................. 15 Leadership from the Powerful Stakeholders in Nursing is Appreciated................................... 17 Who Were the Stakeholders Participating in the PAR?............................................................ 18
Aboriginal Nurses Association of Canada (ANAC)............................................................. 18 Association of Black Health Care Providers (ABHCP) ....................................................... 19 The Barbados Nurses Association of Canada (Toronto Chapter)......................................... 20 The Centre for Equity in Health and Society........................................................................ 21 Coalition of Black Trade Unionists (CBTU), Ontario Chapter ............................................ 24 Culture Care Nursing Interest Group (CCNIG).................................................................... 24 The Filipino Nurses Association, Toronto Branch ............................................................... 25 The Grenada Nurses Association.......................................................................................... 25 Health Canada, Office of Nursing Policy ............................................................................. 26 International Nurses Interest Group (INIG), Registered Nurses Association of Ontario (RNAO)................................................................................................................................. 26 Joint Provincial Nursing Committee (JPNC)........................................................................ 27 Korean Nurses Association of Ontario (KNAO) .................................................................. 28 Rainbow Health Network (RHN) ......................................................................................... 28 Registered Nurses Association of Ontario (RNAO)............................................................. 29 The South Asian Nurses' Association of Canada.................................................................. 30 University Hospital of the West Indies Graduate Nurses' Association (UHWIGNA) ......... 30 Urban Alliance on Race Relations (UARR) ......................................................................... 31
Stakeholder Interpretation and Debate...................................................................................... 32 Participatory Action Research Methodology: Toward Consensus Building among Stakeholders................................................................................................................................................... 33
Sampling ............................................................................................................................... 34 Demographics ....................................................................................................................... 35 Issues of Validity and Generalization ................................................................................... 35 Suggested Strategies for Stakeholders to Work Productively Together............................... 35
Evidence of Stakeholder Resistance to Accountability Moves ................................................ 37 Canadian Nurses Association (CNA) ................................................................................... 37 Canadian Institute for Health Information (CIHI) ................................................................ 38 The Joint Provincial Nursing Committee ............................................................................. 39
Changing Discourse to Achieve Stakeholder Accountability................................................... 39 Chapter 2 – Evidence of the Need for Accountability: Presentation of findings............. 45
Some Effects on Nurses of Race, Colour, or Ethnicity: Summary of Das Gupta’s Survey of Nurses, November 2001 – May 2002 ....................................................................................... 46
Demographic breakdown of the respondents........................................................................ 47 Set-up: Racially organizing advantages and disadvantages during downsizing....................... 48
What is a Racial Set-up? ....................................................................................................... 48 What Happens if Accountability is Introduced?................................................................... 52
Table of Contents
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
iii
Examples of Set-up in Nursing in an Environment Where Racial Profiling Is Not Held Accountable .......................................................................................................................... 53
1) Targeting the Individual............................................................................................ 54 2) Top-down Setting up of Racialized Informal Policies and Practices ....................... 56 3) Recruiting Compliant Peers who Support Targeting and Scape-goating ................. 58 4) Documentation for Pre-emptive or Reactive Defence of Set-ups............................. 58
Cautionary Summary ............................................................................................................ 60 Case Study – The Story of Nurse “A”: The Grievance Process as a Set-up for Backlash ...... 61
Preface................................................................................................................................... 61 Case Study ............................................................................................................................ 61
Benchmark 1 – The need for answers: Why did white management and staff discriminate against Nurse A? ............................................................................................................... 70 "Tit for tat, infernal trap” .................................................................................................. 70 Benchmarks 2 and 3 – The need for recognition that they have been wronged and the need for safety................................................................................................................... 75 Benchmark 4 – Restitution through healing processes that balance relationships and prevent further harm ......................................................................................................... 78 CEHS Benchmark – Lack of Accountability for breaching the grievance process.......... 79 Benchmark 5 – Significance or meaning .......................................................................... 83 Discussion......................................................................................................................... 83 Chronology of Nurse A’s grievances against OPH1 ........................................................ 85
Shifting Context: The declared shortage of nurses and union innovations for retention.......... 86 Health Outcomes of the Complainant in a Racial Dispute ....................................................... 90
Traumas Experienced While Objecting to Racial Discrimination........................................ 91 1. Feelings of exclusion, loss of belonging...................................................................... 91 2. Feeling humiliated, contained...................................................................................... 91 3. Intimidation, paranoia, isolation .................................................................................. 92 4. Loss of confidence and grief........................................................................................ 92 5. Depression, loss of focus, and memory loss ................................................................ 92 6. Distressing physical symptoms.................................................................................... 92 7. Death images................................................................................................................ 93 8. Sensations challenging integrity and wholeness.......................................................... 93 9. Positive awareness ....................................................................................................... 93 10. Less than optimal health basis for professional work................................................ 93 11.Long-term effects......................................................................................................... 93
Summation of Evidence............................................................................................................ 94 Chapter 3 – Accountability Informed by Transformative Justice: Discussion and recommendations.......................................................................................................... 95
Review and Introduction........................................................................................................... 96 The Vision of Transformative Justice....................................................................................... 98 Defining Accountability in the Context of Equity: What is institutionalized racism? Systemic racism? A racial encounter?...................................................................................................... 99
Race..................................................................................................................................... 101 Racialized People................................................................................................................ 101 Racialized Encounter .......................................................................................................... 101
Table of Contents
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
iv
Race Consciousness ............................................................................................................ 102 Equity.................................................................................................................................. 102 Institutional Racism ............................................................................................................ 102 Systemic Racism................................................................................................................. 102 Discourse............................................................................................................................. 103 Discourses of Racism.......................................................................................................... 103 Anti-racist Discourse .......................................................................................................... 103
Is Accountability for Racism a Menace to Some People?...................................................... 104 Policy’s Role in Implementing Relationships of Accountability ........................................... 105 Conflicting Perspectives on Accountability for Systemic Racism ......................................... 106
Theoretical Perspectives on the Sanctity of Accountability Breaches................................ 108 Experience of Relational Elements Where Racial Profiling Is Unaccounted for and Unchecked................................................................................................................................................. 110 What Relationship Issues Arise with Particular Accountability Strategies? .......................... 113 How Do I Evaluate Alternative Discourse Strategies? ........................................................... 115 Anti-racism Grounded in Transformative Justice and Freedom Ideology.............................. 118 The State’s Weakened Role in Accountability for Systemic Racism: Policy and legislation are required to implement and integrate voluntary accountability ............................................... 119 Recommendations to Achieve Accountability for Systemic Racism: The Romanow Commission’s Health Council of Canada............................................................................... 121
Recommendations to the Health Council of Canada .......................................................... 122 Recommendations from Partisan Sectors of the CEHS Network....................................... 122
1. An investigation by the Ontario Human Rights Commission ................................ 123 2. Leadership Training and Anti-racism Education.................................................... 123 3. Ontario Legislation ................................................................................................. 124 4. Ontario Policy ......................................................................................................... 124 5. National Accreditation ............................................................................................ 125 6. Voluntary Policy in Key Organizations.................................................................. 125
Chapter 4 – Undoing the Catch-22 of Racism: Overview of Study Findings Intent on Integrating Accountability for Systemic Racism........................................................... 127
How Integrative Processes could be Used to Implement Accountability for Equity in Nursing and Health care ....................................................................................................................... 128 Toward an Accountability Discourse Model that can Deal with Racial Discrimination in Nursing.................................................................................................................................... 130 Initiating Accountability Policy that can Regulate Programs, Practices, and Procedures at Local, Provincial, and National Levels in Nursing................................................................. 134
Chapter 5 – Summary and Future Research............................................................... 137 Reference List ............................................................................................................. 141 Definitions ................................................................................................................... 153 Appendix A.................................................................................................................. 157
Table 1 - 1990s Immigrants by Source Country and Proportion Speaking a Non-Official Language................................................................................................................................. 157
Table of Contents
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
v
Table 2 – Proportion of Visible Minorities, Canada, Provinces and Territories, 1991, 1996, and 2001......................................................................................................................................... 157
Appendix B – Resolutions For Presentation To The CNA Annual Meeting ................. 159 Appendix C – Resolutions To The Registered Nurses Association Of Ontario (RNAO).................................................................................................................................... 162 Appendix D – Letter From Anne McLellan................................................................... 165 Appendix E – Letter to the Representatives of the Joint Provincial Nursing Committee (JPNC) and the Nursing Secretariat ............................................................................ 169 Appendix F – A Time For Change: Recommendations .............................................. 171 Appendix G – Role Playing Exercise and Case Studies to Learn about Backlash and Set-up Experientially ................................................................................................... 177

Table of Contents
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
vi
Acknowledgments
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
vii
Acknowledgments
Of the numerous individuals who contributed to this participatory action research project, our
thanks go first of all to Rani Srivastava for introducing the concept of equity assurance programs
to nursing. We thank Professor Enid Collins at Ryerson University, Professor Ushi Choudhry at
Windsor University, Sepali Guruge, doctoral candidate at the University of Toronto, Celeste
Leano, and all the members of the Culture Care Nursing Interest Group who sustained the
Culture Care Nursing Research Council when it secured funds for this project to explore “how
to” gain accountability for equity in nursing. Thank you to Anna Mathai, President of the South
Asian Nurses’ Association, for supporting our proposal. We thank Agnes Calliste and Evelyn
Brody for giving momentum to research on the problems of backlash and set-up as mechanisms
in systemic racism. We dedicate the report to Claudine Charley whose victory in her grievance
against the Toronto Hospital marked the first public exposure of a racial set-up in nursing. We
honour Professor May Yoshida who advocated anti-racism curriculum for nursing nationally in
1994. Sadly, her work has gone unheeded to date.
The challenging process of building a coalition to promote accountability for anti-racism,
anti-discrimination, anti-harassment, employment equity, and ethnoracial competencies in
nursing through participatory action research has put us in contact with an ever-widening
network of dynamic nurse activists – leaders in their communities and/or nursing associations –
and members of the public. We thank you for coming forward and for your contributions,
including painful stories of discrimination and strategies for solutions. We thank Nurse A for her
willingness to share her experience publicly, for her patience in documenting it, and most
importantly, for her persistent quest to make employers and colleagues accountable for
Acknowledgments
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
viii
condoning systemic racism. We thank the members of the nursing associations (listed in section
on stakeholders) for their interest and support. We thank Dr. Tania Das Gupta for her
collaboration, including making it possible for think tank participants to join in her survey of
racism in nursing. Our thanks also to the individuals who worked on drafts of letters to the Joint
Provincial Nursing Committee, and on draft resolutions to the Canadian Nurses Association and
the Registered Nurses Association of Ontario (RNAO).
We acknowledge the chapters submitted for this report by Dr. Angela Chan, entitled
Longing for my Jade Bangle and by Sarah Egginton, entitled Coming to understand racism: one
nursing student’s journey and we are sorry these were not included for lack of space. They will,
however, be posted on our website, www.BeforeQuality.com.
We are grateful that Pam Chou, Ajamu Clarke, Gerald and Natashia Deer, and Prodip
Saha contributed their expertise and time to the development of our website, also noted as
www.BeForEquality.com.
Thanks to Rob Higgins for depicting Tania Das Gupta's findings. Leonardo Alfaro,
Gemma Baik, Agnes Card, Max and Marianne Chandler, Ruth Ann Cyr, Lorna Edwards, Valerie
Glascow, Carmen James Henry, Jackee Higgins, Bhandat Lurkhur, Monica Mitchell, Pauline
Palmer, Jean Pierre, Cynthia Reyes, Petal Samuels and Gloria Taylor-Boyce are especially
thanked for the time and effort they put into conceptualizing participatory events and sharing
critical analyses and ideas. We thank these and other courageous nurse activists, including
Dyanne Affonso, formerly dean at the Faculty of Nursing, University of Toronto, Joan Lesmond,
Doris Grinspun, Irmajean Banjok, and Mary Ferguson Pare who support CEHS's research and
consensus building in the nursing profession. Thanks also to Steve Bosanac and Trevor Smith
Acknowledgments
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
ix
for editorial suggestions and Yvonne Bobb-Smith and George Dei for support and
encouragement.
For providing space and/or hosting the think tanks, we thank Winston Clarke and the
Marcus Garvey Centre for Leadership and Enterprise, Toronto Public Health (Scarborough
Office), the Canadian Black Nurses' Association, the University of Toronto, RNAO, and York
University, Atkinson College. We thank the University Hospital Network for making it possible
for us to hold team meetings at Toronto Western Hospital. We thank the think tank speakers,
including Josephine Wong of Toronto Public Health, Nuzhat Jafri of the Bank of Montreal, Dr.
Lillian McGregor, Dr Souraya Sidani, and those who do not wish to be named, for voluntarily
sharing their expertise and experience with us. We thank the many individuals responsible for
various activities at each think tank, including giving the opening prayer, acting as moderator,
facilitating discussions and report back, and participating in the awards ceremony.
Additional thanks go to the following individuals who contributed their expertise to the
development of research proposals that focus on equity in nursing: Doctors Rose Baaba Folson,
Any Marie Gerard François, Diana Gustafson, and Lillie Lum, and to Kwasi Kafele, Marylin
Kanee, Anthony Mohamed, and Rhonda Williams for "Strategies and Models for Negotiating
Diversity: Anti-Discrimination Advocacy and Appreciative Inquiry in Selected GTA Hospitals."
Also, Kevin Armstrong, Bernice Downey, Margaret Horn, Peter Menzies, and Cynthia Wesley-
Esquimaux, as well as Dr’s. Diane Doran, Hyun Sil Kim, Deb McGregor, and Kris Sieciehowitz,
are thanked for "Guidelines for Nurses Working in Aboriginal Communities with Attention to
Traditional Knowledge." Further, we thank Angela Cooper Brathwaite, Madge Ellis, Doris
Grinspun, and Dr. Sheryl Nestel, for the RNAO questionnaires examining the curriculum content
in Ontario nursing schools. We regret that so few of the schools cooperated with your study.

Acknowledgments
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
x
We thank Dr. Anne Moorehouse who, as chair of the curriculum committee, supported an
initiative on anti-racism and found it to be a career-limiting move.
The Centre for Equity in Health and Society (CEHS) and its companion website
www.BeForEquality.com are the fruits of our coalition building. We thank students Bridget
Liriano and Pam Sun for their commitment to the vision of the CEHS and to board member
Ishwar Persad for assistance with definitions. We regret that we cannot name numerous
individuals publicly in these acknowledgements because the fear of backlash continues. We
thank each of you for your contributions, energies, and clarity of vision. We are particularly
indebted to Sandra Carnegie-Douglas, Patrick Hunter, Anne Marrian, and Karen Mock at the
Canadian Race Relations Foundation for critical feedback and astute support of this endeavour.

In Memoriam
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
xi
In Memoriam
To the memory of Professor May Yoshida, who taught for many years at the Faculty of Nursing,
University of Toronto, for her tireless efforts to bring ethnoracial competencies to the forefront
of nursing practice by envisioning anti-racism content in nursing curricula and research across
Canada.
Dedication
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
xii
Dedication
To Evelyn Brody, and to the memory of Claudine Charley, who fought discrimination so that
every person in the nursing profession will be accountable for equity and every organization will
refuse to condone racial set-up and backlash.

Ontario Human Rights Code
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
xiii
Ontario Human Rights Code
According to the Ontario Human Rights Code, you cannot be discriminated against because of
your: race, ancestry, place of origin, colour, ethnic origin, citizenship, creed, sex, sexual
orientation, disability, age, marital status, family status, same sex partnership status, record of
offences (in employment only), and receipt of public assistance (in housing only) (Author, 2003).
The Centre for Equity in Health and Society
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
xiv
The Centre for Equity in Health and Society
The Centre for Equity in Health and Society (CEHS) is a virtual centre that coordinates a
research network of interdisciplinary researchers and advocates for equal access and
participation in organizations responsible for health. We recognize that membership in a
marginalized group or category poses an additional risk for persons with respect to social
and healthy outcomes. Additionally, research suggests that risks increase for persons
with compounded risk factors such as race and gender, poverty and disability. We
recognize as well that the broad determinants of health (e.g., housing, employment, good
access to health services) have a significant impact on members of marginalized groups
or individuals of difference. Equity is a determinant of health. Moreover, the nature of
marginalization is that barriers exist so that voice, participation, and choice are restricted,
which impedes efforts to correct the effects of marginalization and the trauma it
produces. CEHS acknowledges the experience of reprisal for trying to counteract
marginalization. In collaboration with researchers at George Brown College, Ryerson
University, the University of Toronto, and York University, the CEHS research focus is
on transformative justice practices, ethnoracial competencies and critical structural
analysis for organizational change, and inter-sectoral collaboration. CEHS annually
awards leaders who have facilitated accountability for equal access and participation in
nursing. The Centre for Equity in Health and Society is an affiliate of the Urban Alliance
on Race Relations and consults with health services students, professionals and unions on
education, and career development.
The Centre for Equity in Health and Society
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
xv
CEHS Vision Accountability for equal access and participation in organizations responsible for health.
CEHS Mission To promote policies and programs for accountability towards equal access and participation in
organizations responsible for health through research, advocacy, recognition, and leadership
development.
CEHS Rationale Research suggests that lack of accountability for racial discrimination results in health and
economic disparities among racialized people.
Contact Information [email protected]
www.BeforeQuality.com
The Centre for Equity in Health and Society
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
xvi
Centre for Equity in Health and Society Membership Form
178 Jarvis St., Suite 907, Toronto, ON, M5B 2K7.
Email: [email protected]
www.BeforeQuality.com
Name:
Address:
Permanent address if different from above:
Contact me by: Email:
Phone:
Fax:
Current place(s) of employment/volunteering:
Areas of interest:
___ Research/writing (state area)
___ Political action on accountability for equal access and participation
___ Promoting CEHS membership/contacting members for events
___ Policy/legislation development
___ Internet and website
___ Mentoring/career mobility counseling
The Centre for Equity in Health and Society
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
xvii
___ Nursing education/curriculum
___ Advisor/negotiator for nurses experiencing work-related issues
___ Speaker/resource for anti-racism
Describe special interests:
Please state languages in which you are fluent:
Ethnoracial identification:
Gender:
Disability status:
Age:
Union membership:
Nursing association membership:
Your suggestions for conference topics:
Other suggestions:
Fee:
$15 Regular ___check ___ cash
$ 5 Full-Time Student ___ check ___ cash
$ 40 for Joint Membership with CEHS and the Urban Alliance on Race Relation
___checks ___cash
Thank you!
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
xviii
Executive Summary
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
xix
Executive Summary
Rebecca Hagey
“Nursing, like a cappuccino – white on top, brown on the bottom –
requires stirring up.”
Excellence in race relations requires holding ourselves accountable for racial discrimination
and its effects. Backlash and resistance to accountability must end and new accountability
practices must be required throughout the health care system.
Backlash for Addressing Systemic Racism in Nursing
"Implementing Accountability for Equity and Ending Racial Backlash in Nursing" offers
evidence of the need for accountability to deter systemic racism and outlines initiatives study
participants have taken to advocate for accountability measures. The study uncovered a
generalized fear of backlash for raising issues concerning systemic racism.
The report documents how nurse and research activists used participatory action research
(PAR) to build a movement toward accountability for equal access and participation in health
care and toward freedom from racial harassment in nursing. It is intended as a resource for
advocates of equity and procedural justice in nursing who are interested in accountability,
transparency, and direct negotiation strategies to remove barriers and heal relationships.
Backlash for addressing systemic racism is predicted to diminish in everyday work life if
Executive Summary
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
xx
accountability is considered a privilege and a responsibility in all relationships – personal,
organizational, and public.
Research Purposes
1) To use PAR to investigate how integrative processes can be used to implement
accountability for equity in nursing and health care;
2) To develop an accountability discourse model that can deal with racial discrimination
in nursing, beginning with set-up and backlash against racialized nurses who presume
equality or exert expectations for equity; and
3) To initiate strategies toward developing accountability policy that would regulate
programs, practices, and procedures at local, provincial, and national levels in nursing
(for example in regulatory and professional bodies).
Resistance to Accountability for Equity in the Health Care System In the context of global migration, the ethnoracial diversity of the nursing profession in Canada
is greater today than ever before. The profession's resistance to ensuring equal access and
participation for all nurses has been compounded by sporadic under-funding of nursing care. An
emerging body of research shows that systemic racism is a serious problem in health care
delivery organizations. An anti-racism policy issued by the Joint Provincial Planning Committee
of the Ontario Hospital Association and the Ministry of Health (1996) was shelved following the
defeat of the New Democratic Party government in Ontario and the rescinding of the
Employment Equity Act by the Conservatives. A curriculum plan that Yoshida introduced in
Executive Summary
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
xxi
1994 at a prestigious nursing school to include anti-racism content in Canadian nursing
education has been steadfastly resisted (Hagey and MacKay, 2000).
We present evidence in this report that when accountability is demanded by nurses
experiencing systemic racism, the issue of racism is resisted systematically. This participatory
action research documents witnesses' accounts of resistance by decision-makers in privileged
positions within the health care system. For example, minutes show that in the Northwestern
General Hospital case, white nurses were asked what specialty they preferred when they applied,
whereas nurses of colour were told there were openings only in long-term care. The result of this
unwritten systemic racism policy was racial segregation. Most specialties were staffed by non-
racialized nurses, whereas long-term care was almost completely staffed by racialized nurses
(Calliste, 1996, 2000b; Ontario Human Rights Commission [OHRC], 1994).
Months after the OHRC awarded $320,000 to the complainants of harassment in this
case, some executives of that hospital were reported as excusing the events as a problem of
"reverse discrimination" instigated by the complainants themselves. This denial of the systemic
racism that was publicly exposed reveals persistent resistance to equal access and participation
and resistance to the accountability measures that the commission administered.
Evidence of the Need for Accountability to Dismantle Systemic Racism The accounts reported in our participatory action research are voluminous and continuing. Even
if space permitted exhaustive testimony, we would be bound by concerns for confidentiality and
the very real threat of backlash for accountability efforts. Our presentation of evidence is limited
to four pieces where we have been able to respect confidentiality and provide some detailed
Executive Summary
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
xxii
perspectives for readers to understand that systemic racism persists because accountability for it
is systematically thwarted.
Acknowledging that accountability can occur at individual and organizational levels and
be public or private (Henry, Tator, Mattis, and Rees, 1995), we conceptualize accountability as
both a privilege and a responsibility that is fundamental in relationships at all levels. We
understand systemic racism as the privileges associated with not having to be accountable for
racial dominance. That is, racial oppression activates privileges. Through commission and
omission in race relations, privileges accrue to members of the dominant groups, and immunity
from accountability is upheld by group power. Instances of systemic racism in organizations can
be identified and rectified by self-monitoring, peer monitoring, stakeholder monitoring,
executive monitoring, and editorial monitoring.
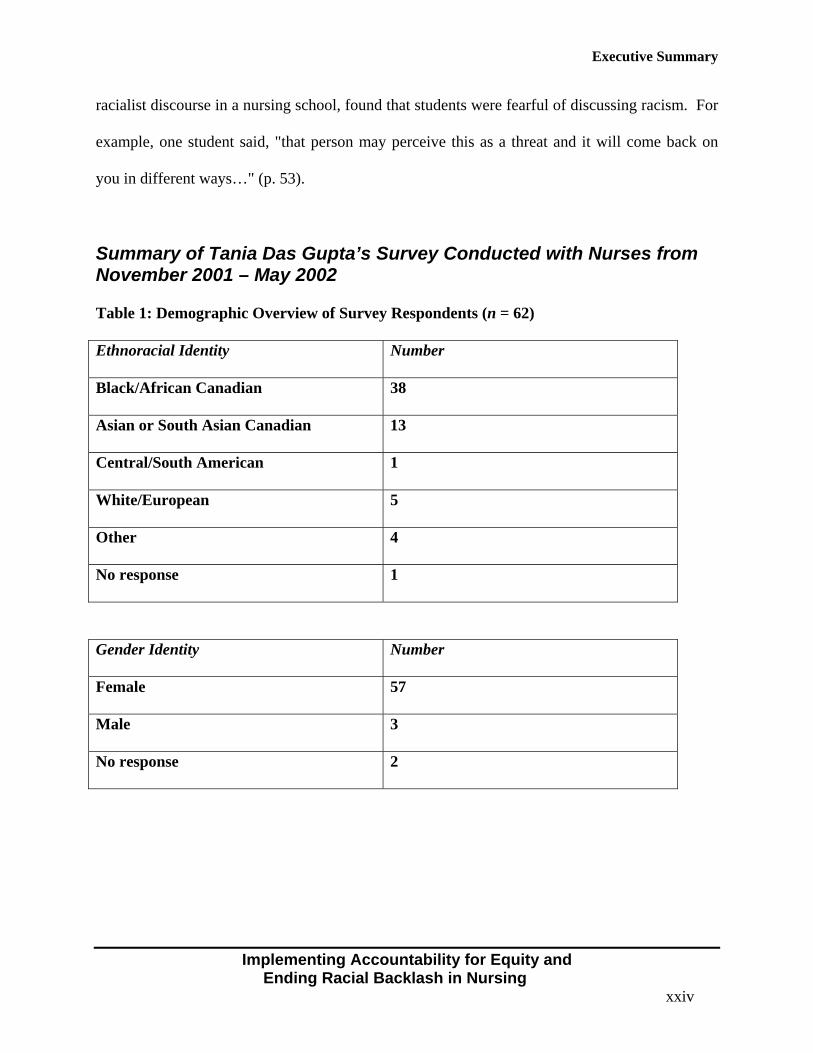
Evidence of Nurses Experiencing Racial Profiling Evidence suggests that some nurses experience racial oppression. In other words, race, ethnicity,
and colour are felt to have an effect on relations in the workplace. We present previously
unpublished findings from a pilot survey that Tania Das Gupta conducted among some
participants in our larger study. Of the sixty-two persons who completed the questionnaire,
thirty-eight were Black/African Canadian, thirteen identified as Asian or South Asian Canadian,
five as White/European Canadian, four as Other, one as Central/South American Canadian and
one no response. There were fifty-seven females in the convenience sample, three males, and
two who did not specify gender.
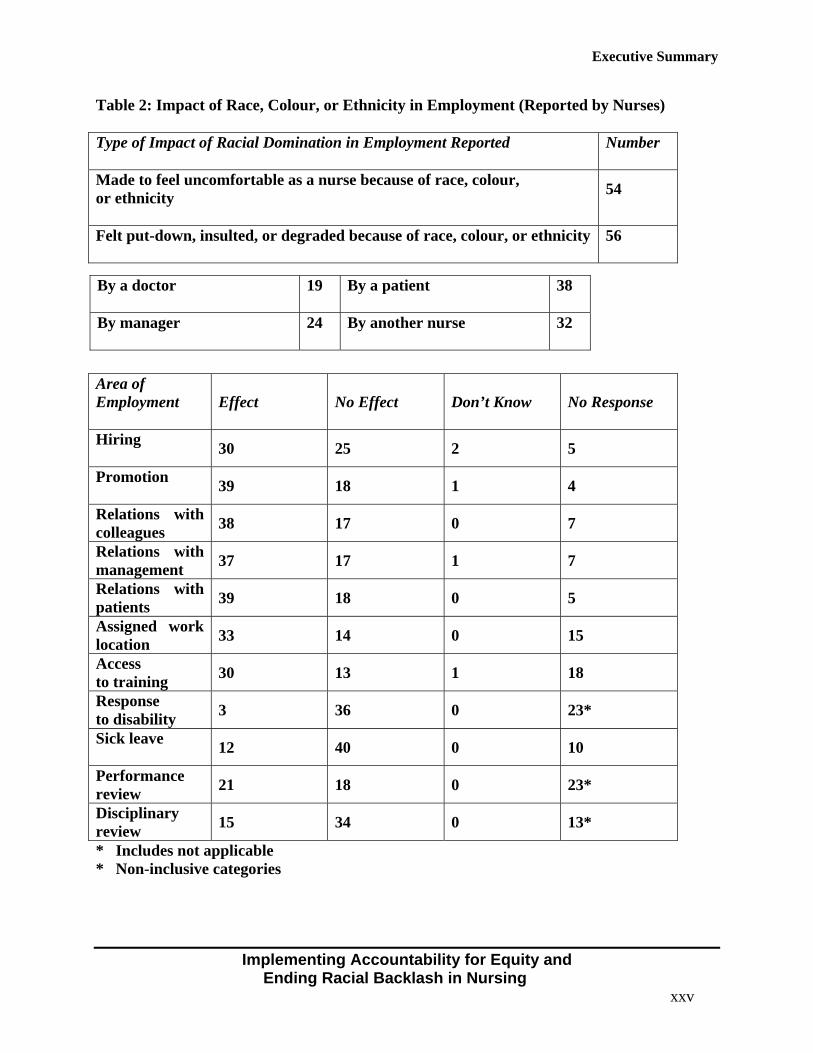
Participants felt that race, ethnicity, and colour had an effect on relations with patients
(39/62); on the hiring of nurses (39/62); on relations with colleagues (38/62); on relations with
Executive Summary
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
xxiii
managers (37/62); on where they were assigned to work (33/62); on access to training (30/62);
on performance reviews (21/62); on the experience of being disciplined (15/62); on sick leaves
(12/62); and on access to accommodation for disability (3/62). Of the sixty-two nurses who
participated, fifty-six said they had been put down, insulted, or degraded as a nurse because of
their race, colour, or ethnicity. Of these, thirty-eight said that a patient put them down, thirty-
two said that another nurse had put them down, twenty-four said that a manager had put them
down, and nineteen said that a doctor had put them down. Some respondents mentioned more
than one offender.
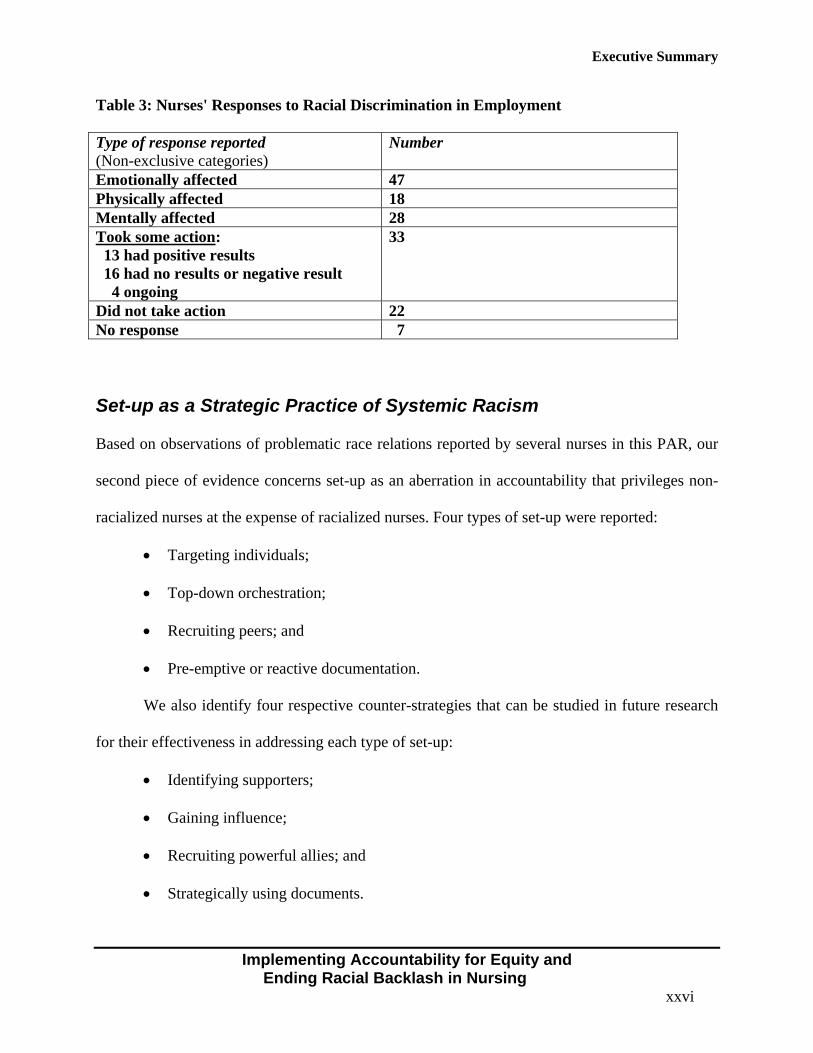
Of the fifty-six who had been harassed, forty-seven said they were affected emotionally,
twenty-eight mentally, and eighteen physically. Several nurses noted more than one effect. Of
those who had been harassed, thirty-three said that they took some action. Of the thirty-three
who took action, sixteen had no results or negative results and thirteen had positive results,
whereas four had ongoing proceedings.
Although these findings were preliminary and their purpose was to assist Dr. Das Gupta
in developing her questionnaire for a larger study, we believe they provide evidence that nurses
are experiencing racial profiling that calls for accountability. We refer readers to the larger study
commissioned by the Ontario Nurses Association (Das Gupta, 2002) that shows that white nurses
of European ancestry experience far fewer negative effects of race, colour, or ethnicity than
nurses from groups subject to racial profiling.
Marshall's (1996) analysis of the 1991 Census data for the health care professions showed
that blacks are underrepresented in management positions. Nestel (2000) reported that the 1991
Census indicated that visible minority nurses in Ontario have half the chance of their white
counterparts to move into the managerial level. Hagey and MacKay (2000), who studied
Executive Summary
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
xxiv
racialist discourse in a nursing school, found that students were fearful of discussing racism. For
example, one student said, "that person may perceive this as a threat and it will come back on
you in different ways…" (p. 53).
Summary of Tania Das Gupta’s Survey Conducted with Nurses from November 2001 – May 2002 Table 1: Demographic Overview of Survey Respondents (n = 62)
Ethnoracial Identity Number
Black/African Canadian 38
Asian or South Asian Canadian 13
Central/South American 1
White/European 5
Other 4
No response 1
Gender Identity Number
Female 57
Male 3
No response 2
Executive Summary
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
xxv
Table 2: Impact of Race, Colour, or Ethnicity in Employment (Reported by Nurses)
Type of Impact of Racial Domination in Employment Reported Number
Made to feel uncomfortable as a nurse because of race, colour, or ethnicity
54
Felt put-down, insulted, or degraded because of race, colour, or ethnicity 56
Area of Employment
Effect No Effect Don’t Know No Response
Hiring 30 25 2 5
Promotion 39 18 1 4
Relations with colleagues 38 17 0 7
Relations with management 37 17 1 7
Relations with patients 39 18 0 5
Assigned work location 33 14 0 15
Access to training 30 13 1 18
Response to disability 3 36 0 23*
Sick leave 12 40 0 10
Performance review 21 18 0 23*
Disciplinary review 15 34 0 13*
* Includes not applicable * Non-inclusive categories
By a doctor 19 By a patient 38
By manager 24 By another nurse 32
Executive Summary
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
xxvi
Table 3: Nurses' Responses to Racial Discrimination in Employment Type of response reported (Non-exclusive categories)
Number
Emotionally affected 47 Physically affected 18 Mentally affected 28 Took some action: 13 had positive results 16 had no results or negative result 4 ongoing
33
Did not take action 22 No response 7
Set-up as a Strategic Practice of Systemic Racism Based on observations of problematic race relations reported by several nurses in this PAR, our
second piece of evidence concerns set-up as an aberration in accountability that privileges non-
racialized nurses at the expense of racialized nurses. Four types of set-up were reported:
• Targeting individuals;
• Top-down orchestration;
• Recruiting peers; and
• Pre-emptive or reactive documentation.
We also identify four respective counter-strategies that can be studied in future research
for their effectiveness in addressing each type of set-up:
• Identifying supporters;
• Gaining influence;
• Recruiting powerful allies; and
• Strategically using documents.
Executive Summary
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
xxvii
The targeted nurses of colour are set up in such a way that focus is shifted from a clinical
or administrative problem onto the racialized nurse, who then becomes the problem. As Essed
(1991) defined it, racism has the effect of problematization. The rules of the set-up strategy
make the nurse who complains about this state of affairs a target so that accountability and
transparency are impeded. Benefits accrue to the nurses and administrators who collaborate in
the set-up. Racialized nurses are drawn into set-up activities with the effect of deflecting
attention from the racially-based strategy. This process makes accountability for set-up practices
highly improbable, especially in light of the potential for being targeted for complaining about
the problem in this strategic system.
The other accounts included in our report use conventional interpretive methods for
qualitative description to outline how set-up works as a main mechanism in the practices
associated with taking advantage on the basis of race during underfunding of nursing. Although
there is a scarcity of full-time jobs, currently there remains a shortage of nurses. Unions have
informed us that the number of complaints about such set-up practices has dropped due to a
feeling of security in the nursing shortage. We are concerned that set-up will be used again now
that nurses’ jobs are being eliminated under collaborative hospital and government policy that
attack nursing budgets. Systemic racism offers convenient advantages for members of the in-
group – including politicians – at the expense of selected racialized nurses, many of whom have
immigrated to Canada to practice nursing here. Calliste (2000a) argues that Canada has a racist
surplus labour strategy that exploits racialized nurses to stabilize the job market for non-
racialized nurses.
There remains the spectre that when jobs are cut, racialized nurses, en masse, will be set
up for job transfer and job loss during so-called restructuring that appears to be rationally
Executive Summary
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
xxviii
managed according to criteria. Those who blow the whistle, resist, or protest will fall into the
category of the "problem nurse." Their assertive behaviours will be declared inappropriate and
provide justification for the racialization practices. As Head reported (1985), equity will no
longer be a relevant topic as it disappears from agendas during job scarcity.
Accountability and transparency are elements of procedural justice that can be introduced
to bring ethical standards to the workplace. They require compassionate exchanges, intentional
relationship building, forgiveness, and restitution. With peer pressure that is backed up by
human rights legislation to normalize accountability, unfair systems that result in racial
dominance can be transformed in personal, organizational, and public arenas. As Mandela
realized when setting up the Truth and Reconciliation Commission in South Africa, offending
strategic behaviours such as those we are describing as set-up and backlash can be based on
assumed privileges rather than incurable maliciousness (Hagey, 1999; Hagey et al., 2001c;
Llewellyn and Howse, 1999). However, maliciousness is evident against racialized nurses. The
diversity office in one large metropolitan hospital where racial complaints are filed reported
receiving threatening phone calls. An effigy doll with a noose around its neck was hung on the
office door conjuring the hateful racist lynching of people of colour. Hate messages are a
common reality for racialized nurses in Canada who are coming to question whether hate can be
cured.
The Problem of Backlash for Seeking Accountability in Race Relations Our third piece of evidence is a case overview of Nurse A's efforts to assert her right to call for
accountability for the systemic racism she experienced in the places where she worked. The
covert rule of not having to be accountable to a racialized nurse is played out in a total of twenty-
Executive Summary
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
xxix
three grievances in her twenty-one year career as a nurse in Toronto. Nurse A's experience with
retaliation and escalation in the dispute process is evaluated from the perspective of a model of
transformative justice developed by Ruth Morris (2000). Transformative justice calls for a
healing approach to racial offenders that assumes that shared strategies, not only participating
individuals, must be held accountable, and that the whole community must take responsibility for
the group-based privileges and advantages that result from discriminated activities.
Canadian human rights legislation does not stipulate that intent must be proven, allowing
that racial discrimination can occur without intent. Perhaps unintentional, backlash appears to be
built into the process of formal complaints and grievances. The effects of backlash include
marginalization, problematization, and containment, which Essed (1991) established to be the
effects of racism. We provide ample documentation that proceedings activated when filing a
union grievance or making a complaint to the OHRC contributed to Nurse A's being
marginalized, treated as the problem, and contained. Insufficient accountability within such
legal proceedings results in irregularities that cause damage to the racialized employee. One
systemic response to Nurse A’s accountability efforts was that potential employers were
evidently told that Nurse A was trouble. She can no longer find employment within the
profession. We were informed by union personnel that this type of treatment did not occur for
the white nurse who put Claudine Charley’s patient at risk in a plot to keep her job.
A recent report issued by the Canadian Nurses Association to the Canadian Council on
Health Services Accreditation listed unresolved grievances as one of eight key indicators that
impact on the quality of work-life and the future of nursing services in Canada (Lowe, 2002).
Yet the report does not mention the nature of the grievances or the prevalence of cases where
racial discrimination and harassment are issues. Nor does it mention the glass ceiling that exists
Executive Summary
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
xxx
for racialized nurses in all sectors of nursing. It fails to acknowledge the lack of accountability
for equity, one of nursing’s most fundamental problems. It also does not mention the impact that
unresolved grievances have on nurses' health, on absenteeism, on patient morbidity, or mortality
in workplaces poisoned by racist set-ups and backlash.
Employment Context of Backlash Employee surveys and exit interviews conducted by one of our participants, who is a semi-
retired human resource manager, indicated the following concerns of racialized nurses. Speaking
out in support of a colleague who had experienced unfair treatment because of race proves to be
a "career limiting move or CLM" (backlash). Moreover, racialized nurses reported differential
treatment and being "ear-marked" for more severe and unfair levels of work assignments and
discipline than were non-racialized nurses. Also, issues of racism directed by patients towards
nurses were considered to be "trivial" in nature and "par for the course." These root causes of
sickness and absenteeism were not identified or dealt with.
Health Effects of Backlash Social psychologists Dion and colleagues (1975, 1978, 1996) provide evidence that anxiety in
varying degrees is linked to the perception of discrimination. In a culture that invalidates the
appropriateness of accountability for discriminatory practices, one would predict anxiety to be
exacerbated when the social means for eliminating the source of the anxiety is blocked.
Restoration to a non-anxious state would be impeded. Backlash being unrestrained would
escalate and prolong anxiety and produce health effects over time.
Executive Summary
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
xxxi
Health effects from backlash were reported by nurses who attempted to introduce
accountability for systemic racism by filing complaints or grievances that named racism as the
issue. Our evidence is drawn from earlier research funded by the Centre for Excellence in
Research on Immigration and Settlement (Collins, Calliste, Choudhry, Fudge, Hagey, Lee,
Turrittin, and Guruge, 1998). In this qualitative study of nine nurses who had formally charged
their employer with racism, all experienced retaliation for naming racism as the issue, even
though the Ontario Human Rights Code forbids backlash or reprisals for complaining of racism.
This aspect of the code was not effectively enforced for the nurses contributing to this study (See
recommendations for provincial legislation).
The health effects the nurses described included feelings of loss, humiliation,
intimidation, paranoia, and isolation. Some experienced depression, grief, loss of confidence,
loss of focus, and memory loss. Distressing physical symptoms, death images, and
overwhelming sensations, such as being invaded or torn apart, were reported as stress effects.
Although many of the nurses were able to focus on the positive in what they were doing for their
community, most confided that the negativity of the backlash had an impact on their families and
is with them long-term. In this light, the right to racial equality is a prescription for adverse
health effects when the accountability for systemic racism – set-up and backlash – is not a
guaranteed right.
While implementing accountability for racism we must also implement accountability for
backlash, which is an integral part of the system. The future of nursing requires a milieu of
openness and acceptance so that the character of systemic of racism can be discussed. The
problems racism engenders will need to be addressed locally, nationally, and internationally
since Canada competes locally and globally for an adequate supply of nurses.
Executive Summary
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
xxxii
Building a Coalition to Construct Accountability Policy and Procedure: The Centre for Equity in Health and Society Diverse associations of nurses were unofficially associated with this participatory action research
that convened gatherings of local chapter members across the Greater Toronto Area (GTA). The
gatherings included members of the Aboriginal Nurses Association of Canada, nurses from
several African countries, various Caribbean associations including The Barbadian Nurses, The
Grenadian Nurses, The Trinidadian Nurses, the University Hospitals of the West Indies Graduate
Nurses and Associates (Kingston, Jamaica), the Chinese Canadian Nurses Association, the
Filipino Nurses Association, Hispanic nurses, Jewish nurses, the Korean Nurses Association of
Ontario, Muslim nurses, Persian nurses, the South Asian Nurses Association, the Culture Care
Nurses Interest Group, the International Nurses Interest Group, and additional nurses,
community activists, union leaders, and consumers who identified themselves as supporters.
Some interest came from various francophone nurses, including, for example, those tracing their
heritage to various African countries, or to Haiti, Lebanon, or Vietnam. Interest and support also
came from the Rainbow Nurses Coalition that champions issues and health concerns of gay,
lesbian, bi-sexual, and transsexual people. We consulted with individuals from the Ontario
Association of Black Trade Unionists, the Urban Alliance on Race Relations, the Registered
Nurses Association of Ontario, the National Office of Nursing Policy at Health Canada, and the
Joint Provincial Nursing Advisory Committee.
Given the fear of backlash for broaching the issue of racism, we found that not all group
members subject to racial profiling are in agreement about how to embrace an anti-racism
strategy that promotes accountability for systemic racism. We found much disagreement about
how accountability should be introduced. There appeared to be consensus that healing is
Executive Summary
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
xxxiii
required to build relationships of trust and that organized dialogue is necessary to develop
ground rules within the profession and beyond. The problem we encountered in this research
was that dialogue was not possible because few of the top decision-makers in the profession that
we invited actually attended our PAR think tanks, even though many verbalized the importance
of equity, diversity, and human rights issues. The nursing leadership in every sector across
Canada is perceived as predominantly white and silent about accountability for system racism.
Henry et al. (1995) outlined the phenomenon of democratic racism, in which values of
social justice and equity are verbalized but implementing anti-racism policy is resisted. Thus,
the practices of discrimination that create racial disparities and condone racial harassment are
sustained. One way to change this approach to the racial inequalities in our midst is to change
the cultural rule. This report calls for developing a ground-rule of accountability for equity. We
are appealing to all Canadians to be continuously committed to anti-racism, which means to
speak out against privileges owing to racial dominance and disadvantages owing to racial
oppression and systemic racism. On March 19, 2002, at the think tank held at the Registered
Nurses Association of Ontario (RNAO), it was declared that anti-racism is on the agenda in
nursing to benefit all nurses and the Canadian public.
The PAR think tanks culminated in an awards ceremony held on the opening day of the
Biennial Conference of the Canadian Nurses Association. The ceremony acknowledged the
efforts of many nurse leaders who, far from being recognized, were harassed for their work to
make reforms in nursing. A healing prayer was offered by Dr. Lillian McGregor, elder and nurse
at First Nations House, University of Toronto. The occasion of the ceremony was the
inauguration of the virtual centre linking the nurse researchers and advocates – The Centre for
Executive Summary
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
xxxiv
Equity in Health and Society (CEHS), which has since incorporated as a non-profit organization
in Ontario.
Following this ceremony, resolutions to the Canadian Nurses Association (CNA) were
drafted, which were formally submitted in November, 2002, on behalf of CEHS. Some of these
are still being negotiated, whereas others were passed at the Annual General Meeting of the
RNAO. Also in November 2002, the CEHS made a presentation in a session at a joint
conference of the RNAO and the Registered Practical Nurses Association of Ontario (RPNAO).
This was the first public forum in the history of Ontario nursing where the issue of racism
appeared in print on the program.
The coalition continues to learn how systemic discrimination is organized in nursing and
what strategies can establish equity assurance in nursing. The concept of equity assurance was
introduced into nursing in 1997 by Rani Srivastava, who is also the author of the RNAO's anti-
racism policy, issued in September, 2002. The network of study participants did not resolve
certain dilemmas, including whether to build associations internally, to work on coalition
building, or to join RNAO as individuals who could enhance their group’s engagement in
professional developments. Participants did, however, support staying in touch by telephone and
email to promote research and profession-wide policy dialogues on barriers and strategies.
CEHS is calling for dialogues on anti-racism throughout the Canadian nursing profession
to create effective accountability policies that will ensure that the work environment for nurses,
and, therefore, for patients, is caring rather than poisoned. Such policies, as they pertain to
systemic racism in nursing, would govern local, provincial, and national programs and practices.
They would ensure safety for racialized nurses, especially during periods of underfunding for
nursing that involve restructuring and downsizing.
Executive Summary
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
xxxv
Selected CEHS Objectives
• Advocate for equal access and participation for nurses in the profession and for reducing
racial disparities in health and safety (Jacobs, 2002);
• Advocate for accountability to end racial domination and harassment in personal,
organizational, and public arenas of the health care system;
• Ensure representation of diverse cultural and language groups, including Aboriginal
people, in the education, practice, research, and governance of the health professions;
• Promote reform of health care curricula to include diversity content about anti-racism,
anti-discrimination, anti-harassment, employment equity, ethnoracial competencies,
negotiation, and consensus building; and
• Since one in every sixty-seven Canadian voters is a nurse, CEHS wants to convert nurses
to anti-racism theory and evidence-based practice to create a critical mass of advocates
for equity in health and society.
Recommendations to Achieve Accountability for Systemic Racism: The Romanow Commission’s Health Council of Canada We envisioned that, in addition to resolutions, recommendations, objective-setting, and
guidelines set forth by CEHS, the newly emerging Health Council of Canada (HCC) could play a
role in promoting accountability. The HCC could decrease the costs pertaining to systemic
racism in health care, such as the legal, insurance, and other costs including potential morbidity
and mortality for patient and the erosion of the supply for nurses.
Executive Summary
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
xxxvi
The Romanow Report did not address racial discrimination directly but denounced the
“big disconnect," by referring to health care for Aboriginal people and targeting the reduction of
morbidity and mortality due to barriers in access, primary prevention, and treatment. Lack of
accountability for racism, colonization, and poverty was not specifically targeted. Nor were
jurisdictional issues and actual funding commitments laid out (Koebel, 2003). Some Native
leaders are calling for a national Aboriginal Health Act to correct the racial disparities created by
The Indian Act.
The HCC could introduce accountability mechanisms to monitor the costs associated
with systemic racial disparities in health and health care and set guidelines for equity practices.
The Romanow Report’s Recommendation 3.2 states that “On an initial basis, the Health Council
of Canada should establish benchmarks, collect information and report publicly on efforts to
improve quality, access and outcomes in the health care system” (Romanow, 2002, p. 248).
Recommendations for the Health Council of Canada
• Monitor the racial disparities in health and health care and require interventions to correct
them;
• Require process and outcomes reports on equity programs for health care workers and
consumers;
• Monitor the number of health care dollars spent on defending discriminatory practices
and set mechanisms to ensure freedom from racial discrimination, harassment, set-up,
and backlash in organizations responsible for health; and
• Promote equal access and participation in organizations responsible for health, including
the provision of interpreter services and removal of barriers for racialized people and
invisible minorities.
Executive Summary
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
xxxvii
We thank Anne McLellan, former federal minister of health, for her encouraging response to
CEHS's suggestions about the future role of the Health Council of Canada.
Recommendations from Partisan Sectors of the CEHS Network Since there was no consensus about what recommendations should be included or excluded, our
report includes recommendations submitted from different sectors of the network. What follows
is a selection of some key recommendations that attempt to build accountability for systemic
racism impacting on nurses through changes in legislation and policy to build new structures,
procedures, and practices. Members of the CEHS network recommend:
1. An investigation by the Ontario Human Rights Commission
The Centre for Equity in Health and Society (CEHS) calls upon the Ontario Human Rights
Commission (OHRC) to initiate (under section 29(g) of the Code) an investigation into the
systemic discrimination against racialized nurses as well as all designated groups protected
under the code with respect to education and employment in the health care system. The
investigation should take account of discrimination, harassment, and procedures for
redressing grievances and complaints.
2. Leadership Training and Anti-racism Education The Centre for Equity in Health and Society (CEHS) would establish a leadership academy
that holds training workshops for negotiating the implementation of anti-racism
policy and practice in support of ethnoracial competencies. The Province of Ontario
should fund this academy to develop curricula and organize dialogues on changing the
culture of nursing to one that practices accountability for equal access and
Executive Summary
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
xxxviii
participation in all sectors and at all levels of the profession. The CEHS leadership
academy, in partnership with university research units, will evaluate curricula
and develop and disseminate new knowledge on ethnoracial competencies and
achieving diversity in leadership. The CEHS will collaborate with appropriate
professional and regulatory bodies to develop questions for registration and
licensure examinations pertaining to antiracism and racial dispute proceedings.
CEHS will also collaborate with unions that negotiate nurses' contracts to sponsor
conferences that discuss innovations addressing member-to-member racial disputes.
The CEHS leadership academy will convene dialogues in nursing on the overt
racism from patients, colleagues, and supervisors experienced by nurses of Asian
and Filipino descent during the outbreak of SARS and how to prevent such
behaviours in future.
3. Ontario Legislation
The Ontario Human Rights Commission be legislated to report directly to an all-party
committee of the Parliament instead of to the Attorney General.
4. Ontario Policy
1. The Ontario Human Rights Commission develop policy to:
• monitor workplace complaints proceedings for reprisals and step up investigations to
properly document reprisals and irregularities in procedure; and
• levy fines based on the degree of resistance to anti-racism procedure.
2. The Ontario Human Rights Commission report to the legislature, categories
of complaints and statistics on how they are dealt with. Private and union practitioners
adjudicating racial complaints report to the legislature similar data ensuring the
Executive Summary
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
xxxix
confidentiality of complainants and respondents but listing the sector – for example,
health care – in which the complaint arose.
3. The Ontario Ministry of Health and Long Term Care require the Nursing Secretariat to
provide the opportunity for the inclusion of Aboriginal and visible and non-visible
minority member representatives in its proceedings in collaboration with the Joint
Provincial Nursing Committee.
4. The Ontario Ministry of Health and Long Term Care integrate anti-racism, anti-
discrimination, anti-harassment, employment equity assurance, and language and culture-
care agendas in the nursing and other relevant secretariats to carry forward the
requirement of ethnoracial competencies in a mission of diversity and equity in health
care.
5. The College of Nurses of Ontario introduce transformative justice proceedings to handle
allegations where a racial dispute is evident between a client and a nurse.
5. National Accreditation
1. The accreditation proceedings of hospitals and health agencies in cooperation with all
regulatory colleges implement equity assurance to augment their quality assurance
programs.
2. The accreditation arm of the Canadian Association of Schools of Nursing require:
• evidence of recruitment and strategies for retention of Aboriginal, visible minority,
and non-visible minority faculty and students;
• evidence of anti-racism curriculum; and
• evidence of requiring ethnoracial competencies among faculty, staff, and students.
Executive Summary
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
xl
6. Voluntary Policy in Key Organizations 1. Provincial, regional, federal, and national bodies supporting and directing health services
research develop programs to obtain and publish data on health care workers in terms of
Aboriginal status, ethnicity, mother tongue, and visible minority identity.
2. The Ontario Hospital Association develop and promote best practice models of anti-
racism policy. Guiding policies should include Principles for Good Governance in the
21st Century and the United Nations Declaration of Human Rights – Legitimacy and
Voice, Equity, and the Rule of Law.
3. All regulatory and professional bodies introduce measures to address racial
discrimination and systemic racism in health care:
• Registration forms be changed to allow for self-identification of Aboriginal,
racialized, and non-visible minority status;
• Committees and panels be required to be diverse and inclusive so that they reflect the
diverse population of Canadians;
• Ethnoracial competencies be made a requirement for nurse registration and an
expectation for ongoing, self-reflective practice required for professional registration;
• Regular in-service education programs and human rights orientation to new staff at all
levels;
• Electronic monitoring using human rights software to track equity indicators; and
• Tools for employment systems review be adapted to identify set-up and backlash
experienced by racialized employees.

Executive Summary
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
xli
We thank the Canadian Race Relations Foundation (CRRF) for supporting research on backlash
against accountability for equal access and participation in nursing.

Executive Summary
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
xlii
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
1
Chapter 1 – Toward Accountability among All Stakeholders:
Introduction and Overview
Rebecca Hagey and Jane Turrittin
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
2
In this overview of the participatory action research (PAR), we invite all stakeholders in the
Canadian health care system to contribute towards solution of the problems presented in this
report. After reviewing selected stakeholder issues and PAR methods for building consensus, we
offer a brief account of the available literature on set-up and backlash and introduce the concept
of accountability discourse as a lead-in to the presentation of our evidence.
Questions, Objectives, and Accountability Discourse Strategies First, as a means of preparing for the participatory action phase of our research as well as to
develop accountability discourse theory, we reviewed interview data from our earlier research
and asked the following theoretical questions:
1. What are the key issues associated with accountability for racial discrimination?
2. What reactions and organized responses ensue from initiatives seeking accountability for
systemic racism?
3. What relationship implications are evident in initiatives seeking accountability for
systemic racism?
4. What irregularities and outcomes are evident with particular accountability strategies?
Our objective in addressing each of these questions was to develop a theoretical
understanding based on the interviews from earlier studies about how accountability for racial
discrimination is contested, challenged, or by-passed. We need this understanding to devise
ways and means to institute accountability for racial discrimination. We then formulated yet
another question, given the challenges to accountability – the discourse practices of set-up and
backlash – that we describe in our report.
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
3
5. By naming issues and specifying recommendations, will the CEHS be a) ignored,
marginalized, or excluded? b) problematized and punished? or c) contained? Or will the
report be taken seriously in nursing, health care, and Canadian society?
Another objective was to conduct participatory action research (PAR) with voluntary
associations of nurses to explore the feasibility of developing equity assurance programs aimed
at instituting accountability for racial equality and employment equity at all levels and in all
sectors in nursing. In keeping with PAR methodology, we identified evidence and the
participants themselves shaped what is presented. For purposes of confidentiality and brevity,
we have been highly selective of what we offer in this report. For various resources that expand
on what the participants deem may be useful for changing stated human rights into values that
are put into practice, we refer our readers to the CEHS website: www.BeforeQuality.com.
As our action research gained momentum, participants recognized that an equity
assurance program is feasible if – and only if – those who need it make it happen. A vision of a
Canada-wide program emerged that would use interest-based lobbying, negotiation, and political
action informed by research to hold all nurses and their employers accountable for systemic
discrimination in their organizations. To these ends, the Centre for Equity in Health and Society
became formalized, inspired by the statement in the Ottawa Charter (World Health Organization,
1986) that equity is a determinant of health (p. 1).
For policy development and implementation to occur, we believe that a widespread
collaboration on changing discourse is necessary. Our thesis is that all stakeholders will need to
change discourse strategies if accountability for racial discrimination is to become a shared
value. The theoretical understandings of discourse underlying our PAR are summarized in
Henry and Tator’s book, Discourses of Domination (2002). They implicitly advocated that
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
4
change in discourse (language and ideology) was the intervention that held the most promise for
shifting how determinations are made about who is denied privileges and on what basis. We
used discourse strategies to promote accountability for equal access and participation by
targeting (a) political discourse, (b) the locations of discourse, (c) discourse strategies in and
between organizations, (d) policy regulators of discourse, (e) personal discourse, (f) discourse
outcomes, and (g) research discourse. The theoretical development of our questions pertaining
to change through purposeful discourse will be addressed in future submissions to scholarly
journals.
The answers to our questions unfolded as our participatory research took shape.
1. We identified set-up and backlash as manifestations of the poor accountability for
racial dominance, as well as a number of other issues, which we discuss in our
chapter on accountability.
2. We gathered evidence of organized strategizing to take advantage of racialized nurses
in our description of set-up, as well as evidence of backlash to initiatives seeking
accountability for racial differences or domination.
3. We collected evidence of poor dispute resolution methods that are used in racial
disputes.
4. We gathered evidence of how the complainant is further subjected to racial
discrimination and domination through violation of the grievance process.
The CEHS thanks the reader for taking the time to read this report and asks for her/his
support in creating effective policies that will ensure that the work environment for nurses, and
therefore the care environment for patients, is caring rather than poisoned. You too are a
stakeholder.
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
5
Who Are the New Stakeholders? The term visible minority is used by Statistics Canada to define “persons other than Aboriginal
Peoples, who are non-Caucasian in race or non-white in colour” (Statistics Canada, 2003). In
addition to census questions about visible minority identification, immigration profiles emerge
from questions about country source, ethnic origin, place of birth, official language capacity, and
so on. The 1991 Census counted occupational groups such as nurses within these categories, but
we have not been able to retrieve such data for 1996 or 2001. Appendix A provides 2001 data
for immigrants by source country (top 10) and proportion speaking a non-official language, as
well as the proportion of visible minorities in Canada, the provinces, and territories for 1991,
1996, and 2001.
The total Canadian population in 2001 was 29,639,035, of which 5,448,480 or 18.4%
were immigrants. The total categorized as visible minorities (not including Aboriginal persons)
was 13.4%, which is a three-fold increase since 1981. With some variation among groups, three
in ten people from visible minorities were born in Canada.
Canada's new immigrants are coming increasingly from Asia and the Middle East.
Numbers have noticeably declined for those coming from Caribbean and Central American
countries. The twelve top places of birth in the decade of immigration to Canada from 1991 to
2001 are ranked as follows:
People’s Republic of China 197,355 India 156,120 Philippines 122,015 Hong Kong 118,385 Former Yugoslavia 67,750 Sri Lanka 62,750 Pakistan 57,990
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
6
Taiwan 53,750 United States 51,440 Iran 47,075 Poland 43,370 United Kingdom 42,645
Since 1991, all visible minority groups have grown in size, with Chinese, South Asians
and Blacks, respectively, making up the largest groups. In 2001, in Toronto, the total population
was 2,456,805. The percentage of visible minorities was 42.8%; 43.7% of these people were
foreign-born. Vancouver's population is now one-third Asian, and all urban areas in Canada are
receiving immigrants.
It can be assumed from these data that there is some consensus on keeping track of the
numbers who identify as “visible minorities.” But the fact that census respondents can declare
multiple ethnic origins makes interpreting contrasts in ethnic origin and visible minority status
difficult. For example, in 2001, 1,094,700 individuals identified themselves as having Chinese
ethnic origin, but only 1,029,395 (94%) identified themselves as a visible minority using the
Chinese category. Similarly, 327,550 individuals said they had Filipino ethnic origin, but only
308,575 used the Filipino category to declare their visible minority status. This contrast is most
dramatic for Aboriginal people where (excluding thirty reserves that did not report) the total
population who identified themselves as Aboriginal persons in Canada in 2001 was 976,305,
compared to the 1,000,890 who identified themselves as having North American Indian ethnic
origin, with an additional 307,845 who declared a Métis ethnic origin. One child in four is
Aboriginal in Manitoba and Saskatchewan. The territories and prairie provinces have the highest
shares of Aboriginal peoples in proportion to their total populations (Statistics Canada, 2003).
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
7
How Can New Stakeholders Gain Full Inclusion into Society’s Institutions? In our anti-racist advocacy, we have observed that the words 'whiteness' and 'anti-racism' are a
turn-off for numerous nurses. We were told that social work talks about racism but in nursing
we talk about cultural sensitivity. So our problem is, how do we call attention to the issue of
racism in nursing if we cannot use the "R" word? How can we advocate for equal access and
participation in nursing if the consensus of the leading nurses is that racial inequality is not their
problem?
A challenge we heard repeatedly from prominent nursing leaders can be paraphrased as,
"Why are they feeling disenfranchised? They should get involved with the provincial and
national associations and roll up their sleeves like we do to make things happen.” Notice the
we/they separation in identity. Also notice the lack of interest in making bridges or helping
inclusion along.
How would you penetrate the assumptions embedded in these responses to help leaders
empathize with nurses who feel marginalized? How can we all work together to include nurses
who feel trapped and hopeless about racial dominance in the activities and governance of our
discipline? If racial dominance is kept in place by discourse that keeps repeating old images and
using them to categorize people negatively to create barriers, then how do we change the
discourse? How do we contend with a backlash that disparagingly considers changing discourse
as having to be politically correct? How do we build a movement when those interested in
changing discourse are head-locked into disagreement about the strategies?
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
8
Literature Pertaining to Set-up and Backlash among Particular Stakeholders In an extensive international literature review using public and private search engines, we found
a paucity of work on racism and backlash. Tuen van Dijk (1993) discussed backlash as a normal
response to organized challenges against institutionalized European racism. In-group/out-group
process was subtly used in order to defend the privileges of elite decision-makers, thus
reinforcing their political and economic advantage. The NACLA Report on the Americas (1995)
issued a special issue on backlash, linking shifts in U.S. domestic and global economies with
vengeful strategies against immigrants in the U.S, such as California’s Proposition 187. Mills
and Simmons (1995), who outlined the history and barriers excluding minorities from full
participation in Canadian organizations, also described the contemporary backlash against
minority rights, which includes outright attacks on programs for equity.
Within nursing, no studies of racial backlash against employment equity were found, with
the exception of our own publication (Hagey et al., 2001b). Indeed, Canadian nursing research
journals are silent about the issue of racism. Calliste (1993) outlined the virtual colour bar that
existed in Canadian nursing until the 1950’s, when a shortage of nurses forced a challenge to
racist immigration laws that resulted in nurses coming in from the Caribbean. This colour bar
still exists in many domains of nursing.
One diagnosis offered for why diversity is such a challenge is that racism in nursing is
denied (Calliste, 1995; Head, 1985). So the refusal to use words like racism stems from the fact
that nurses in positions of power and influence do not believe that it exists. Yet, studies done in
Toronto report that in comparison to white nurses, racialized nurses are under-represented in
management positions and over-represented in the “lower paid, lower status jobs” (Collins, 2004;
Das Gupta, 1996; Marshall, 1996; Doris Marshall Institute and Minors, 1994; Head, 1985).
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
9
Although we found no empirical studies on practical strategies for combating backlash
against employment equity, Stith (1998), like Henry et al. (1995), offered well-reasoned
approaches to deal with institutional racism across a variety of professions and employment
areas. Backlash and reprisals are strictly forbidden under the Ontario Human Rights Code, but
we found that none of the offending employers were reprimanded by tribunals for engaging in
backlash. The testimony of many of the victims participating in our research was not admitted
into evidence. As Aylward (1999) pointed out, the legal system in Canada is itself riddled with
systemic racism. We found this to be true for nurses whose arbitrator refused to allow racial
differences as evidence at the hearing.
Stith (1998) argued that corporate leaders, executives, and senior management must
become educated about systemic racism. They must become directly involved in eliminating
racism and discrimination in the workplace and must encourage minorities and women and
support them in advanced positions. His recommendations include incentive and reward
programs to encourage equal access and participation and integrative anti-racist training. Other
strategies necessary to create confidence that complaints will be taken seriously and acted upon
include creating and supporting proactive intervention programs to deal with racism and sexism,
holding those who discriminate accountable, and protecting employees who make valid
complaints. Finally, he called for anti-discrimination employment laws that would include both
severe penalties and incentives not to discriminate to avoid the current unfair burden placed on
minorities to prove their cases in costly legal hearing. In Ontariom, the HR Code does not fine
the offender with penalties and awards modest accommodation to the victim whose case is
upheld.
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
10
Arguably, this weak accountability for racial justice in employment relations is condoned
by a Human Rights Commission that does not prosecute racial discrimination but only
conciliates. We find support for the contention that conciliation should not be used in human
rights cases:
There are public disputes that shouldn’t be mediated at all. I don’t think disputes concerning rights—constitutional rights, human rights, basic rights—should be mediated, even if you could meet the interests of all sides. We have certain basic constitutional, human rights that are decided and legislated in a different way. I don’t think that those ought to be compromised in any way by negotiations (Susskind, Harvard Law School, Program on Negotiation, as cited in Kolb, 1994, p. 353). With inadequate state enforcement of equity principles encoded in Human Rights
legislation, we believe the best available strategy is to build coalitions among the many
associations of racialized nurses who want accountability for employment practices in nursing.
The African Canadian Community Coalition against Racial Profiling (ACCCRP) is using this
strategy to make police who use racial profiling accountable (Smith 2004). A glimmer of
support for this idea is emerging in the research literature. In “Planning an Anti-Racism
Initiative,” Batten and Leiderman (2001) examined a program that Levi Strauss Foundation
developed to address racial prejudice and institutional racism in communities where Levi Strauss
and Co. had facilities. Working with multiracial coalitions in Albuquerque, El Paso, Valdosta,
and Knoxville, the Foundation and the Center for Assessment and Policy Development have
learned a number of lessons about starting a corporate-sponsored, community-driven, anti-racism
initiative.
Communities need to understand how difficult it is for multiracial groups to be inclusive
and to reach consensus in a timely and efficient way. Task forces require a variety of people and
a great deal of community support. A common approach will eventually emerge, and those who
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
11
stay involved will be able to adapt their own strategies. However, specialized training and
assistance are necessary to bring community representatives to that point. Corporate sponsors
need to understand that local task forces need time to develop strategies and engage participants.
An effective task force facilitates change. There is a role for outside assistance, but it is
important to promptly establish local ownership of the initiative where the community is in
charge.
Our participatory action research took a community development approach to prepare for
eventual dialogue between minority nurses and members of powerful decision-making
committees who steer the profession and exercise control over employment policy and practices.
If backlash is to be inhibited, leaders such as these will need the supports, knowledge, and policy
to implement programs of accountability for employment equity. To prohibit this institutional
backlash that minority nurses experience individually for objecting to exclusion, marginalization
or problematization (as Essed, 1991, defined racism), we need to embark collectively on policy
formation and developing new leadership.
In a speech on racism in nursing, June Veecock, an educator with the Ontario Federation
of Labour, described how this backlash is experienced by racialized nurses in Ontario:
When we remain silent, what in effect we are doing is contributing to our own oppression. And I know that once you begin to speak, you have to be prepared for what comes. People are accused of making false claims of racism. They are accused of being incompetent and of using racism as an excuse for their incompetence. So that immediately the focus is shifted. The accuser becomes the accused. The victim is then faced with the additional burden of not only having to prove that she is experiencing racism, that this is a racist environment, but also that she is competent. (Calliste, 1995, p. 60-61). The publication that reported this speech covered the proceedings of a conference
organized in 1995 to publicly address the problem of racism in nursing and the emotional trauma
that resulted from being targeted for “cutbacks” and having one’s expertise attacked to the point
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
12
of having to mount an expensive legal defense. The conference began a movement against
discrimination, harassment, and reprisals.
We found no other literature identifying reprisals as a key term but turned up an
interesting experimental study on retaliation by racists (Beal, O’Neal, Ong, and Ruscher, 2000).
The researchers tested the hypothesis that modern racists who demonstrated negative affect and
attitudes on a questionnaire would alter their behaviours to express their aggression covertly in a
competitive reaction-time test. Their motivation was presumed to be to avoid appearing
prejudiced. The sample was divided at the median into high modern racists and low modern
racists, and the hypothesis was tested comparing these two groups using measures of both overt
and covert aggression. The experiment went on to examine responses to provocation by whites
versus by African American test competitors, as well as the effects of light and heavy cognitive
load. Cognitive load was added by requiring participants to recall easy or difficult number
sequences. The purpose was to determine if cognitive load is associated with covert or overt
aggression to indicate whether or not the type of retaliation is strategically selected. The
presumption was that a high cognitive load could interfere with processing and selection. The
study findings follow:
• High modern racists were more overtly and covertly aggressive than low modern racists
regardless of the race of the competitor in the test;
• With provocation, high modern racists displayed increasing levels of covert aggression
toward African Americans (beeping noise for longer duration) in contrast to low modern
racists who inhibited retaliation even under high levels of provocation; and
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
13
• Evidence from the cognitive load experiment that required the participants to recall
numbers during the time-reaction test suggested that covert aggression is a strategic
process that is less likely to be used when cognitive capacity is overloaded.
The study is important for validating the description of modern racism as manifesting
discrimination in covert and indirect ways, thus reproducing the conflict between “law and
conscience on one side and with custom and prejudice on the other side” (Allport, 1989, p.57).
The finding that modern racists are more aggressive in general parallels studies of old-fashioned
racism that demonstrated associations between ethnocentrism and aggressive behaviour. For low
modern racists who more clearly fit the “modern” description, the suggestion that even they
require sufficient cognitive resources to maintain a non-aggressive approach is an important
finding.
These experiments raise compelling questions for nursing. Does nursing have in its ranks
high modern racists who express overt as well as covert aggression regardless of the
provocation? Is nursing in a stage of evolution called old-fashioned racism where it is
permissible to express racism overtly when provoked about the issue?
The latter possibility is plausible in light of findings by Turrittin, Hagey, Guruge, Collins
and Mitchell (2002). This qualitative interpretive study employed Marshall McLuhan’s (1964)
cultural categories of hot and cold reactions and Brian Turner’s (2000) adaptations of notions of
thick and thin solidarity. Nurse managers that participants viewed as racists were identified as
having “hot, angry reactions” and yet their support within the administrative network reflected
“thick solidarity.” By contrast, the visible minority nurses who were complaining of racism
displayed coolness and firmness about their legitimate rights but, unfortunately for them, the
support was very thin and solidarity was expressed only covertly. The prospect of thin and
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
14
covert solidarity raises the question of what resources racialized nurses can rely on to hold
superiors accountable for covert and overt racism.
After an extensive search of key words, we found no literature pertaining to set-ups.
However, Bakan and Kobayashi (2003) recently discussed set-up in employment in relation to
the continuing struggle for employment equity. They documented set-up as one of several types
of systemic discrimination that racialized workers encountered, and quoted an Aboriginal woman
who spoke in a public forum about her experience of being set-up by managers of the Canadian
Park Service. Our account of set-up points out that without any actual conspiracy, systemic
racist practices are highly organized, systematically accruing benefits to non-racialized persons
at the expense of racialized persons. We attribute the organizing principle to the underlying
racist ideology that accountability to racialized people is optional depending on the
contingencies.
In contrast to the sparse research documenting racial inequities in nursing, there is a
mature and sophisticated literature documenting racial disparities with respect to a myriad of
health indicators (Navarro and Muntaner, 2004). Nevertheless, Jackson (1993) discussed the
disinterest in racism among researchers in nursing, calling it “whiting out” knowledge and issues
that are important to Black nurses and Black families. In research designed to examine
collegiality among staff nurses, Jacobs (2002) found evidence of racism identified as a barrier to
collegiality.
A literature is emerging that documents the experiences of racialized immigrant nurses
from their own perspective (Collins, 2004; Dicicco-Bloom, 2004; see also Essed, 1990).
Dicicco-Bloom observed that "one of the challenges facing [the] health care system [in the
United States] is the social inequity within our society that impinges on the daily lives of
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
15
minority health care providers, including nurses" (p. 26).
Agocs and Harish (2001) provided encouraging new evidence on case review showing
that complainants of social inequity have more than a fifty percent chance of having their racism
complaint upheld at the Ontario Human Rights Commission. These strategies offer potential
currently for influencing positive change in the workplace and in general attitudes and
behaviours in society. Joan Anderson (2000) suggested that post-colonial feminism offers ways
for nursing to orient to the research agendas that are needed in this area. However, front line
nurses and other staff continue to be subject to abuse, as Cooper-Braithwaite’s studies have
revealed (1996), and that presents a stark reality context for shaping agendas and changing
everyday discourse.
This review of the literature suggests that the multigenerational legacy of the problem of
racism in Canadian nursing reflects that of the larger society, therefore any reforms must seek the
mechanisms of the larger society and the levers it can put in place to dismantle racism. We must
begin by addressing the professional implications of the racially based differences in our midst to
promote policy discussion and legislation as outlined in the recommendations contributed by our
stakeholders.
Background on Getting the Stakeholders Together In 1994, May Yoshida published a curriculum plan that included anti-racism content and
advocated for it to be adopted nationally (see also Gustafson, 2002). Building on her work, a
research approach to curriculum change was launched at the University of Toronto. It called for
faculty development and formal evaluation and led to the publication of a study identifying
racialist discourse in curriculum (Hagey and MacKay, 2000). Our shift to investigating
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
16
grievances, complaints, and backlash for naming racism began in 1996 when two nurses,
Claudine Charley and Evelyn Brody, came to the Faculty of Nursing at the University of Toronto
to ask that research be done on racial discrimination, harassment, and reprisals in nursing.
The two nurses were part of a movement lead by the Congress of Black Women of
Canada that was helping racialized nurses organize against systemic resistance, backlash, and
reprisals for challenging racial discrimination and disparities. Claudine Charley had received a
$250,000 settlement from the Toronto Hospital in her case. During the proceedings it was found
that a white nurse had set-up Claudine to get her into trouble during a period of job losses and
downsizing related to the underfunding of health care. The white nurse confessed to unplugging
a monitor without regard for the patient’s safety. The strategy of set-up was well known by
nurses of colour during this period. Black nurses especially got into trouble because of set-up.
When they reacted in an upset manner to being disciplined, they would be accused of having
"communication problems." Then, as a matter of course, escalating communication problems
between supervisor and nurse would result in termination of the racialized nurse.
To her credit, Claudine Charley garnered support among colleagues, won her case, and
was featured in a film called End the Silence on racism in nursing (1996) that was sponsored by
the RNAO and the Ontario Nurses Association (ONA). Neither of these organizations hosted a
viewing of the film or wrote about it. A copy of the film may be obtained at ZACfilm.
The strategies of set-up were more covert in Evelyn’s case. The remarkable aspects of
the dispute process for her were backlash, reprisal, and retaliation – in short, revenge, for having
expressed her concern that what she was experiencing was racial discrimination. Consequently,
it is these two phenomena – set-up and backlash – that we are beginning to describe and
challenge in this study.
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
17
Our biggest challenge remains how to bring to the table the factions composed of those
who do not want to talk about racism as well as those who are willing but fearful that the
discussion will erupt into negativity and be a waste of time. The CEHS has been successful in
bringing together small gatherings in various think tanks, research day, and graduate seminars, so
we are confident that our methods of inquiry are safe and productive.
Leadership from the Powerful Stakeholders in Nursing is Appreciated In addition to presenting evidence of systemic racism and resistance to racial equality in nursing,
we are building our participant action research on positive initiatives already embarked on by
leaders in nursing in Ontario. PAR requires taking stock of stakeholders and historical and
political realities in the planning stage.
It can be postulated that nursing organizations have not recognized systemic racism as an
issue because they have lacked the expertise and had no personal interest in learning about the
benefits to the whole profession from promoting health and anti-racism. To their credit, nursing
organizations have begun to seek expertise and develop policy. The RNAO issued a statement
on racism in the early 1990s and updated it in 2002. In 1995, the Joint Policy and Planning
Committee (JPPC) of the Ontario Hospital Association and the Ministry of Health released Anti-
racism Policy Guidelines. Rani Srivastava, who later introduced the term equity assurance,
drafted the Cultural Sensitivity Guidelines for the College of Nurses of Ontario (CNO) as well as
the RNAO statement on racism. She was also one of the leaders of this initiative and was a key
player on the JPPC.
Nursing organizations were not officially part of the JPPC process, although ONA, the
largest nurses' union in the province, did make two presentations to the committee. ONA
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
18
recently commissioned Tania Das Gupta's (2002) study of racism experienced by nurses. The
CNO has been developing a program that will support nurses newly immigrating to Canada to
obtain their registration.
Who Were the Stakeholders Participating in the PAR? The following diverse associations of nurses agreed to be listed in this resource. Over 200
nurses, some belonging to one or more of these associations or smaller groups of less formalized
associates, participated in the think tanks and the network continues to expand.
Aboriginal Nurses Association of Canada (ANAC) ANAC is a non-governmental, non-profit organization that was officially established in 1975 out
of the recognition that Aboriginal peoples' health needs can best be met and understood by health
professionals of a similar cultural background. The ANAC soon discovered that if their
association was to survive, grow, and successfully achieve their objectives, they would have to
become familiar with the culture of politics and bureaucracy and to develop new skills in the arts
of diplomacy and persuasion. The only Aboriginal professional nursing organization in Canada,
the ANAC is an affiliate group of the Canadian Nurses Association. ANAC objectives commit
its members to the following:
• To act as an agent in promoting and striving for better health for the Indian and Inuit
people, that is, for a state of complete physical, mental, social and spiritual well-
being;
• To conduct studies and maintain reporting, compiling, and publishing of material on
Aboriginal health, medicine, and culture;
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
19
• To encourage and facilitate Aboriginal control of Aboriginal health, as well as of
involvement and decision making on matters pertaining to health care services and
delivery;
• To offer assistance to government and private agencies in developing programs
designed to improve Aboriginal health;
• To maintain a consultative mechanism with the association, band government, and
other agencies concerned with Aboriginal health issues;
• To develop and encourage the inclusion of courses in the education system on
nursing, the health professions, Aboriginal health, and cross-cultural nursing;
• To develop general awareness in Aboriginal and non-Aboriginal communities of the
special health needs of Aboriginal people;
• To conduct research on cross-cultural medicine and develop and assemble material on
Aboriginal health; and
• To actively develop a means of recruiting more people of Aboriginal ancestry into the
medical field and health professions.
• To generally develop and maintain on an ongoing basis, a registry of Aboriginal
Registered Nurses.
Aboriginal Nurses Association of Canada 56 Sparks Street, Suite 502 Ottawa, Ontario K1P 5A9 Tel. (613) 724-4677 Fax: (613) 724-4718 www.anac.on.ca Association of Black Health Care Providers (ABHCP) ABHCP was formed in June 1995, following the conference, "End the Silence on Racism in
Nursing," sponsored by The Congress of Black Women of Canada. The Association's founding
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
20
members and the conference organizers were motivated to take action as a result of complaints
concerning racist attitudes from nurses at Northwestern General Hospital, Toronto. The creation
of ABHCP was newsworthy at the time because it demonstrated that women of colour could
organize and resist/challenge racism. No other Black social groups/organizations specifically
focused on health care providers at that time. The founding members included: Paula Stewart
(Chairperson), Monica Mitchell (Secretary), Olive Issacs (Vice Chair), Joan Bernard, Claudine
Charley, Valda Christian, Peter Cunningham, Ann Headley, and Monica Purdy. The
association's number one goal was to promote the development of creative and innovative
strategies to help its members deal effectively with racism and discriminatory practices in their
work environment. The ABHCP's main accomplishment was to create a forum where minority
nurses could come to have their issues validated. Many nurses had nowhere to go to speak
openly about their issues. There is always strength in numbers and issues of race and
discrimination are often denied by the dominant group. Association members provided support
to nurses whose complaints were heard at arbitrations and informally advised nurses about legal
aspects of the grievance/complaint process. There is no formal relationship between the former
ABHCP and the newly formed Canadian Black Nurses Association.
The Barbados Nurses Association of Canada (Toronto Chapter) The Barbados Nurses Association of Canada (Toronto Chapter), which was founded in 1990 by a
group of Barbadian Nurses, currently has a membership of forty. The Association was formed in
order to provide professional and social support to Barbadian nurses, to provide health education
and information to the community, and to support selected charities. Currently the Association
supports The Sickle Cell Association of Ontario, Doctors without Borders, and Sayes Court
Children's Home in Barbados. For the past three years, the Association has offered an annual
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
21
scholarship to students pursuing a career in the health care field. Members raise funds for these
activities through an annual variety show and dinner, bake and rummage sales, and walk-a-thons.
The Association also has adopted a group of seniors from the Baptist Methodist/Episcopal
Church in Toronto. Special events such as a picnic, attendance at the Stratford Festival and a
boat cruise are held throughout the year. Meetings are held on the first Tuesday of each month at
the Caribbean Catholic Church on College Street at 5:30 p.m.
The Centre for Equity in Health and Society The Centre for Equity in Health and Society (CEHS, pronounced “says”) is a virtual centre that
coordinates a research network of interdisciplinary researchers and advocates for equal access
and participation in organizations responsible for health. CEHS was formalized in June 2002 by
the nurses and others who participated in the action research and coalition building to promote
equity assurance policies and programs documented in the present report. CEHS undertakes
research-based advocacy promoting anti-racism, anti-discrimination, employment equity, and
ethnoracial competencies to improve access and participation in all levels and sectors in health
care. CEHS also studies what is effective for holding individuals and organizations accountable
for equal access and participation. CEHS calls for the creation of an equity assurance policy to
ensure that the work environment for nurses, and therefore for patients, is caring rather than
poisoned. For more information, contact CEHS through its website at: www.BeforeQuality.com.
The Canadian Black Nurses Association (CBNA) – Media Release
Historically, black nurses have been positive contributors to the Canadian Health Care System;
however, black nurses have been marginalized, silenced, and ultimately excluded from nursing
leadership roles in Canada. Therefore as a means of providing a forum to support, mentor, and
acknowledge their contributions, the first Canadian Black Nurses Association has been
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
22
established. CBNA was developed by a group of nurses from diverse nursing backgrounds in
response to the aforementioned statement. The association has been established in order to:
• Enhance the health status of black communities through role modeling, research, and
education;
• Develop strategies to engage with leaders in health organizations to
investigate and determine the necessary process to effect change; and
• Provide leadership through mentoring, while recognizing all nursing initiatives and
contributions made by black nurses.
CBNA is requesting the public’s assistance in promoting our association through sharing
information about CBNA, since CBNA is essential to addressing the needs of all black nurses
living in Canada, while improving the overall health status of individuals within the black
community. CBNA is currently recruiting nurses interested in working towards a healthier work
environment in Canada's health care system and in creating a health care system with transparent
processes that will truly represents all nurses and a health care system that will recognize black
nurses’ contributions and achievements, and provide equitable nursing opportunities for all black
nurses.
In the near future, CBNA will have a general membership meeting. Interested parties can
email the association at [email protected] with the following information:
Name E-mail address
Phone number Place of Employment
Home Address (optional) Professional Title
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
23
Chinese Canadian Nurses Association (CCNA), Ontario
The Chinese Canadian Nurses Association, Ontario was founded in 1986 in Toronto. Founding
members included public health nurses, hospital nurses, and nurses who were not practicing in
Ontario because of a lack of reciprocities with a license earned outside of Canada.
The mission of the CCNA is mainly to promote professional development for Chinese
nurses. It aims to provide a forum for networking and enhancing nursing services to the
community at large. Criteria for CCNA membership are to be trained as a nurse and to be of
Chinese origin. The category for associate members is open to anyone who supports the
CCNA's mission. Though there were about forty pioneer members in 1986, membership has
grown with the increase of Chinese immigrants to Canada.
A major accomplishment was to bring together Chinese nurses who were trained from all
corners of the world. The CCNA has assisted members in the registration process of the College
of Nurses of Ontario. It participated in community health activities in health promotion fairs and
workshops. Responding to members' concerns about workplace politics, the CCNA developed a
workshop series on Job Survival Skills. Experts on administration were invited to help members
understand the corporate culture that closely affects everyone's daily work. In addition to the
mandate to serve the public with expert skills in caring according to regulatory standards, the
association promotes adherence to a code of ethics for professional practice, which includes
social justice. The CCNA collaborates with various community groups in advocating for equity
issues and supports members of various minority groups in their struggle for fairness.
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
24
Coalition of Black Trade Unionists (CBTU), Ontario Chapter The Ontario Coalition of Black Trade Unionists was formed in 1987 to put issues of racism and
discrimination - in the workplace and unions - higher on labour's agenda. The CBTU has a
nursing division headed by Gloria Taylor-Boyce. With regard to nursing, the CBTU:
• Encourages and supports the full participation of black nurses and nurses of colour in
their unions;
• Promotes access and the opening of doors for Black nurses and nurses of color within the
labour movement; and
• Organizes to maximize nurses' political influence within the labour movement.
Contact the Coalition of Black Trade Unionists, Ontario Chapter at www.cbtu.ca.
Culture Care Nursing Interest Group (CCNIG) The Culture Care Nursing Interest Group (CCNIG), founded by Enid Collins, Margaret Hosang,
Rani Srivastava, and Kathy Wong, is a network of Toronto-based nurse-activists and other
professionals who developed the group in 1994 at Wellesley Hospital to ensure the advance of a
paradigm shift in nursing towards excellence in culture care. CCNIG members are nurses,
researchers, educators, administrators, and students who have a commitment and passion for
culture care. One of the CCNIG's purposes is to provide a forum for dialogue and networking on
issues relating to culture care. To this end, for two years (1998-2000) it published the CCNIG
Newsletter. CCNIG members advised the College of Nurses of Ontario on its "Guide for
Providing Culturally Sensitive Care," drafted by Rani Srivastava, a founding member of CCNIG.
Identifying racism in nursing as a research priority, the CCNIG's research council secured
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
25
funding from the Centre for Excellence in Immigration and Settlement (CERIS) to carry out
research to make racism "see-able" (see Collins et al., 1998), of which the participatory action
research described in this report is a direct descendant. In 2002, CCNIG was one of the
sponsoring organizations of the Annual Meetings of the Transcultural Nursing Association
(TCN) in Toronto. Many of CCNIG's activities are now being continued by the newly formed
Centre for Equity in Health and Society (CEHS).
The Filipino Nurses Association, Toronto Branch The Filipino Nurses Association, Toronto Branch, was formed in 1991 by Sally Quan, Irene
Turner, and others. By 1994, it had grown to about 500 members. With its sister associations in
Vancouver and other major Canadian cities, the Toronto Filipino Nurses Association works to
advance the full rights of Filipino health workers in Canada. It provides information on
accreditation and lobbies the government for change in immigration policy. In 1993, the Filipino
Nurses Association submitted a report of the Anti-Racism Strategy Project to the Federal
Ministry of Citizenship. The association worked very closely with the College of Nurses of
Ontario and other organizations such as Skills For Change to remove barriers and improve access
to the profession for Philippine-trained nurses.
For further information, contact Vicky Romero, President, at 416-636-5245.
The Grenada Nurses Association The Grenada Nurses Association was founded in January 2001 by a group of nurses who are
Grenadian nationals; the nurses came together as the need for a safe space where Grenadians
would be free to speak was identified. In this space, members provide counselling, support, and
mentorship, as well as share experiences in confidence. In addition, the Association assists
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
26
Grenadian nationals who do not have access to or who do not know how to navigate the services
in the health care system. Its objectives are as follows:
• To provide emotional and professional support for each other;
• To provide support, advocacy, and outreach to Grenadian Nationals;
• To share health information with other nursing associations/organizations;
• To actively participate in and assist with the interpretation of College of Nurses'
Standards to our members; and
• To form partnerships with other Nurses' Associations.
The Association’s work includes providing support services in the home to Grenadian
nationals who are unable to care for themselves, fundraising to assist with such services, and
advocating with health care providers on their behalf. It works in collaboration with the Grenada
Consulate; nationals needing assistance may contact the Association directly or through the
Consulate.
Health Canada, Office of Nursing Policy Housed in Health Canada's Health Policy and Communications Branch, the Office of Nursing
Policy takes a lead role in health policy, communications, and consultations with respect to
nursing and related professions, including registered practical nurses and nurse practitioners.
The Office of Nursing Policy works in close collaboration with provincial nursing organizations,
whose leaders collaborate with the work of specific task forces. Contact the Office at onp-
International Nurses Interest Group (INIG), Registered Nurses Association of Ontario (RNAO) INIG was established by a small group of nurses with international experience who wanted to
collaborate with nurses of similar experience and interest. In April 1997, one of these nurses
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
27
reviewed the RNAO membership list of nurses from different cultural backgrounds and sent
them an invitation letter with the aim of developing an international/global interest group of
RNAO. Twenty-four nurses indicated an interest in establishing such a group. Concurrently, the
President of the Global Health Interest Group from the Registered Nurses Association of British
Columbia was contacted about its formation, bylaws and affiliation. In April1998, the RNAO
Board approved INIG Associate Interest Group Status. The current membership is one hundred
fifty-one. Since 2000, INIG has been a full-fledged RNAO interest group. INIG publishes three
newsletters per year and holds a conference bi-annually. The last conference was held in
December 2003. INIG has critiqued and evaluated the Guide to Nurses for Providing Culturally
Sensitive Care, which was developed by the College of Nurses of Ontario (1999) and
participated in a Jurisdictional Workshop with the Canadian Nurses Association entitled,
"Nursing Partnership in a Globalized World: Building Bridges to Equity in Health". INIG
continues to participate on the Care for Nurses Advisory Committee, a project dedicated to
assisting internationally educated nurses in preparing for the College of Nurses of Ontario
examination. INIG continues to explore with colleges and universities their inclusion of cultural
diversity in their curriculum and how nurses are being educated about social difference.
For more information, see INIG at www.RNAO.org.
Joint Provincial Nursing Committee (JPNC) Reporting to the Ontario Ministry of Health and Long Term Care, the Joint Provincial Nursing
Committee (JPNC) is made up of the leaders of the major provincial government and non-
government nursing organizations. The JPNC undertakes research, policy, and planning for the
purpose of strengthening and stabilizing the nursing profession in the province. Thus, members
of the JPNC produced the Nursing Task Force strategy to ensure that Ontarians have access to
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
28
high quality nursing services when and where they are needed. Contact JPNC at
www.health.gov.on.ca.
Korean Nurses Association of Ontario (KNAO) The Korean Nurses Association of Ontario, established in Toronto in 1985, currently has about
160 members, of whom about twenty are active. KNAO sponsors seminars for newcomers,
provides information on job prospects to newly arrived or student status Korean nurses, and
telephone counselling for Korean Nurses. In 1985, as its first project, KNAO published 1500
copies of a Korean language handbook (English title: Health and I) written by Gemma Baik, first
President of the KNAO. Health and I quickly sold out to the benefit of both the community and
KNAO. More recently, KNAO has established a sub-section, The Korean Nurses' Interest Group
(KNIG).
In order to fulfill its mission to serve the Korean-Canadian community's health concerns,
KNIG organizes seminars, special health-related workshops, and undertakes community projects.
In 1994, for example, KNIG published a Korean language guidebook with English translations
(English title: Clinical Guide) to help non-English- speaking Koreans communicate with health-
care professionals. KNAO has sold approximately 10,000 copies of Clinical Guide.
For more information, please contact Gemma Baik at [email protected].
Rainbow Health Network (RHN) The Rainbow Health Network was initiated by the Coalition for Lesbian and Gay Rights in
Ontario (CLGRO) in 2001 on the recommendations of their 1997 report Systems Failure. Its
vision is the optimal health and wellness of Lesbian, Gay, Bisexual, Transsexual and
Transgendered people and communities. RHN’s mission is to be a catalyst and a resource for
LGBTT health and wellness activity, in Toronto and beyond. The Network strives to:
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
29
• Create and sustain a dynamic, accessible network of individuals and agencies committed
to promoting LGBTT health;
• Initiate, support and participate in specific LGBTT health and wellness initiatives,
including: public education, health professional education, advocacy, resource
development, program development, and fundraising;
• Act as a resource to health and social service providers, community groups, researchers,
and academics regarding the health and wellness needs, strengths, and priorities of
LGBTT people; and
• Create opportunities for collaboration among LGBTT health and wellness services.
For additional information, contact Rupert Raj at the Sherbourne Health Centre: 416-324-4174
Registered Nurses Association of Ontario (RNAO) The Registered Nurses Association of Ontario (RNAO) was established in the first decade of the
20th century as a professional association to represent registered nurses in Ontario. Its vision as a
diverse, member-driven organization is to lead the nursing profession into full partnership in the
practice and shaping of health care in Ontario. Supported by over 20,000 members, RNAO
undertakes ongoing political activity:
• Lobbying the government on issues that impact registered nurses and health-care service;
• Lobbying CEOs and senior hospital and community administrators;
• Lobbying other decision-makers and organizations that affect nursing practice and health
care; and
• Working to enhance the position of registered nurses through proactive media and
lobbying campaigns.
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
30
RNAO seeks to promote excellence in nursing practice and to advocate for the role of
nursing by respecting the dignity and diversity of and empowering the people of Ontario to
achieve and maintain their optimal health and to provide membership-centred services. Contact
RNAO at 416-599-1925 or www.rnao.org.
The South Asian Nurses' Association of Canada The South Asian Nurses' Association of Canada is a non-profit professional organization
representing nurses from India, Sri Lanka, Pakistan, and Bangladesh and nurses of South Asian
origin. The association is the realization of a long-cherished desire of several South Asian nurses
who migrated to Canada. Its main goal is to stay unified as South Asian nurses to empower our
profession and our community within our own cultural context. The organization functions to:
• Provide a structure for South Asian nurses to work together as a unified force and to
provide opportunity to meet together to discuss and deal with our concerns and issues in a
cultural context;
• Provide a support system for meeting needs of immigrant nurses and practicing members
on an on-going basis;
• Promote professional advancement and leadership and networking for professionals; and
• Develop professional linkages with teaching institutions in South Asia.
For further information, contact Anna Mathai, President, at 905-897-6038.
University Hospital of the West Indies Graduate Nurses' Association (UHWIGNA) The University Hospital of the West Indies Graduate Nurses Association was founded in 1986 by
a group of graduate nurses working in Canada. Its main focus has been to provide financial
resources to support patient care and the education of nurses and health care in Jamaica. As of
2002, the association has raised $90,000 (Canadian), which it has sent to Jamaica for these
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
31
purposes. In addition, the UHWIGNA (a) provides financial support to nurses who achieve
excellence dispite difficult circumstances; (b) contributes financially to community organizations
such as The Herbie Fund, the Sickle Cell Association of Ontario, and the Jamaica-Canadian
Association; (c) recognizes and encourages individuals who have made outstanding contributions
to the Black community, such as Dr. Robert Taylor, Opthamologist, June Veecock, Human
Rights Educator at the Ontario Federation of Labour, and Bromley Armstrong, Human Rights
activist; and (d) heightens awareness of the contribution of our alumnae and associates and
encourages professionalism among our members and other Black nurses through organizing
conferences and seminars. Finally, the UHWIGNA provides support to its members and other
nurses as needed and gathers for annual social functions.
For further information, contact Monica Mitchell at 416-502-1834.
Urban Alliance on Race Relations (UARR) UARR is a non-profit charitable organization formed in 1975 by a group of concerned Toronto
citizens to promote a stable and healthy multiracial, multi-ethnic environment in the Metro
Toronto community. UARR works primarily in a proactive way with the community, public,
and private sectors to provide educational programs and research that are critical in addressing
racism in society to:
• Create awareness of issues that exist in a multiracial, multiethnic, multicultural urban
environment;
• Promote full and equal participation by all sectors of the community by dismantling
barriers to equal opportunity; and
• Assist public and private institutions to develop policies and practices that will ensure
equal access to jobs and services in Canada.
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
32
For more information, see the UARR publication, Currents: Readings in Race Relations or
contact the organization at 416-703-6607 or www.uarr.org.
Stakeholder Interpretation and Debate Interpretive theory and methods inform our insights into discourse for both our qualitative
research and the PAR. These methods are employed in ongoing, everyday analyses of power
relations with which many racialized people astutely engage. This process is reflected in self-
evaluative questions, for example, “What just happened?” or “Why am I feeling outdone?”
The discourse theories of Essed, Stuart Hall and van Dijk are well reviewed by Henry and
Tator (2002) and are used in an exemplary fashion in their analysis of ideologies intrinsic to
discourses of racial domination in news media in Canada. If we want to change ideologies about
employment equity, we can reach the public through other domains – work and family – to
change the interest in stereotypical racial images into a desire for realistic images that are more
positive, less segmentary, more inclusionary, less dominating, more informed, and less
ideological.
To create inclusive and participatory decision-making in workplaces, employers and
employees must be given tools of interpretation and analysis so that everyone can be aware of
how words segregate people, thus excluding them from information and opportunities for
problem solving. Being aware of racism and race consciousness is only the beginning of
developing a community that is equipped with critical, strategic, empathic, and ethical thinking
that is the basis of accountability for unspoken and unacknowledged racial dominance.
French and Albright (1998) outlined a “discourse ethics” that provides a framework for
conflict management by convening stakeholders in a variety of practical procedures guided by an
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
33
ethicist. The approach requires all those affected by decisions to be included in the discourse.
Kettner (1993) suggested that all stakeholders should be able to challenge one another’s
assertions. This process requires that power differentials are neutralized for the purposes of
debate. All parties are expected to own their own perceptions and be open about their interests
and motivations pertaining to the goals and/or issues under consideration. We see this report as a
gesture in being open and ask our colleagues, Canada-wide, to engage in debate on the issues we
raise here.
Participatory Action Research Methodology: Toward Consensus Building among Stakeholders In PAR, subjects become researchers in partnership with those involved in the project who have
specialized research training. Those with the specialized training adopt new epistemologies that
permit them to be committed learners in a process that leads to promoting change rather than
preserving a semblance of detachment and neutrality. See Oquist (1978) and Fals Borda (1979)
for elaborations on epistemology and methods for conducting PAR, for example, transforming
reality. Also see Stevens and Hall (1992) for references to the major critical theories informing
the philosophy and Hagey (1997) for abuses of the methodology. See Susskind, McKeaman, and
Thomas-Larmer in the Consensus Building Handbook (1999) for effective techniques in bringing
polarized groups to the table.
The concept of reflexivity invites the clarification of power relations through locating
oneself within relational hierarchies. PAR supports owning responsibilities and a reality
orientation that for example assists participants in identifying how we contribute to our own
oppression and to the oppression of others. These exercises form the base from which we can
support an empowerment process. The simple human interaction techniques employed in our
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
34
think tanks have helped to generate shared knowledge, understandings, and new relationships
and roles. Ethnically-based nursing associations have now a seat at the table with numerous
other associations. New relations and consensus about achieving accountability were developed.
According to PAR philosophy, rather than putting culture-based differences under a microscope
for examination, each party owns its preferences and communicates them to others in coming to
new understandings and a common agenda. The agenda has focussed on, for example, getting
visible minority nurses elected to key positions. Marcia Taylor was recently voted as a
counsellor at the College of Nurses of Ontario.
Sampling PAR typically is not concerned with sampling issues. Participation is purposefully organized but
can meet with resistance. Participants who identify with the concerns of the research self-select.
Others resist. In our research, participants self-selected by attending think tanks and invited
others to come. Participating nurses heard about the think tanks through word of mouth or
through advertisements in minority media as well as in "Hospital News," a national paper that is
distributed free in most hospitals.
The PAR research network purposely held one of the think tanks at a university research
day to garner participation from top decision-makers in nursing who represent a racially skewed
population. Other attempts included phoning selected leaders personally to invite them to events
and distributing an open letter to the Joint Provincial Nursing Committee at a conference of both
RNAO and RPNAO. Although we contracted to pay to have this letter distributed in the hand
outs the registrants would all receive at the conference, this privilege was denied (without our
being informed until the day of the conference), and we had to distribute our letter and other
materials by hand.
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
35
Demographics PAR usually is not concerned with demographic particulars either because of its reality
grounding in common interests for change and its more personal interests in the parties for the
sake of the common cause. However, the demographic breakdown of participants who
completed Das Gupta's survey between November, 2001, and May, 2002 (reported on pp. 10-12
and pp. 48-50), offers a rough reflection of the proportion of groups that participated. It should
also be noted that most of the participants had actively pursued advanced certification, and a
large number held advanced degrees. Furthermore, Aboriginal nurses eventually asked for a
category that would reflect their presence so they would not have to list themselves as "other."
Issues of Validity and Generalization In this participatory action study, we validated diverse meanings expressed by multiple actors.
Moreover, we advocated in our provincial and national resolutions to the RNAO and Canadian
Nurses Association respectively, for carefully planned forums and specific strategies for
implementing accountability for equity in nursing. The resolutions to the RNAO were passed so
have taken on validity, but not until they are translated into programs and practices, will their
everyday validity in the workplace be established and generalized.
In our case reports about set-up and backlash, we have not made claims about the
prevalence of reported incidents, but we are very concerned that patterns of targeting racialized
nurses will reappear whenever job scarcity occurs. These patterns should be followed up in
future research. The groundwork for research based monitoring of equity indicators should
begin immediately.
Suggested Strategies for Stakeholders to Work Productively Together
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
36
To build a social movement and bring programs and policies into being, we need to activate
various processes such as resolutions, lobbying, negotiation, strategic planning, and consensus
building. We explicitly developed ground rules for participation processes, both within our own
network and in reaching out to prominent leaders to stimulate policy discussions. Responsive
self-reflection and accountability in the relationship is anticipated to more effectively emancipate
nurses than resistance and counter-resistance among racialized and non-racialized nurses. But
first, working relationships among all nurses in the racially stratified hierarchies nurses speak of
will have to take shape.
To help establish working relations in our think tanks, the following guidelines were
circulated to all participants.
1. Our objectives include:
• Identifying supportive partners who will promote the agenda of accountability;
• Identifying ways of building positive relationships so that our perspectives will be
learned and appreciated; and
• Identifying language that can be heard and absorbed.
2. Our methods include:
• Identifying triggers that put us and others into automatic, unconscious, negative
communication;
• Being astute about areas conducive to common understanding and consensus building;
• Listening carefully to ourselves and others and slowing the communication down so
connections can occur; and
• Reaching out to the other with questions so that we can understand, clarify, and reconnect
after disconnects occur.
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
37
3. Our focus includes interdependence, respect, trust, and mutual problem solving.
4. Our process begins by saying what each of us wants and what we don’t like. All perceptions
are important and valid as perceptions. What we are building is a movement. We have the
freedom to speak up. We are holding everyone accountable for the negative images and
outcomes of systemic racism, set-up, and backlash.
5. Stakeholders negotiate how they want to engage with each other and what they want to
achieve. Building relationships across boundaries is necessary to engender responsibility
and collegiality and motivate those in positions of power to initiate inclusion practices and
incentive strategies so that everyone gains. Accountability requires implementing anti-
discrimination and anti-harassment programs and monitoring employment equity. Within
emerging relationships, strategies for implementing accountability for equality can be
clarified and negotiated. Accountability is the means to Equity.
Evidence of Stakeholder Resistance to Accountability Moves At the risk of sounding ungrateful, it must be pointed out that the initiatives to promote equity
taken so far have been perceived by many of the participants to be insufficient. Moreover, they
feel that some of the initiatives have actually set back the push for accountability for racial
discrimination because they "soft pedaled" around the real problem, making it appear that the
issue was addressed. Numerous examples of resistance to dealing with individual nurses who
experienced racism in their work life cannot be reported for fear of backlash. The following are
a few examples that have been publicly visible to the participants.
Canadian Nurses Association (CNA)
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
38
CEHS developed a set of resolutions concerning specific strategies to facilitate equity in nursing
on the understanding that they could be introduced for discussion by a voting delegate at the June
2002, CNA Biennial General Meeting. However, the CEHS negotiator was counselled by CNA
officials to submit the resolutions to the November 2002 resolutions meeting rather than have
controversial items "create a futile discussion and then get voted down." CEHS followed this
advice and worked with the CNA officials to hone the wording into the "diversity resolution"
that got slated first on the roster at the annual meeting the following year. However, the
negotiator failed to get a seat as a voting delegate and when the question was called to admit the
resolution onto the floor for discussion, every voting delegate across Canada voted against it.
See Appendix B for the resolution and backgrounders that were not discussed at the Canadian
Nurses Association Meeting June 12, 2003. One prominent nurse leader from Ontario who
champions human rights afterward said to the negotiator, "The resource implications were
overwhelming."
Resistance to accountability is a topic that ought to be discussed by all the stakeholders in
nursing if we are to move toward racial equality and employment equity in nursing in Canada.
As stakeholders we have the freedom to consider how resistance is a type of discourse (language
and ideology). Accountability too depends on language and ideology. We have the power to
change discourses, beginning with the social categories that give rise to racial profiling in our
profession. Nursing is at the crossroads. Racial subordination and segregation can continue or
they can be addressed and dismantled.
Canadian Institute for Health Information (CIHI) CIHI's recent report, Canada's Health Care Providers (2003, p. 85), must be seen as negligent.
Despite the Ottawa Charter's declaration that equity is a determinant of health, this report
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
39
identifying health risks makes no mention of equity issues in the provision of health care. More
alarming is the report’s reviews of what is known and not known. It makes no mention of what
is not known about variations in and between occupations by ethnicity, Aboriginal or visible
minority status, first language, place of birth, etc. Racial discrimination, racial disputes, and the
health problems among care providers that can ensue from them are not even on the radar screen.
The Joint Provincial Nursing Committee CEHS has called for representation of racialized nurses on this powerful body that informs the
nursing secretariat at the Ministry of Health and Long-Term Care. CEHS invited the erstwhile
chair to join CEHS or designate an affiliate, but she declined.
Changing Discourse to Achieve Stakeholder Accountability The accountability strategies we would like to see emerge would involve changing discourses
(ideology, language, practices) among all the stakeholders, employers, employees, unions, and
clients in the health care system.
Changing discourse requires a social movement and change of location. The term
“location” as in “content and location of discourse” is used metaphorically in this report to
connote the importance of positioning in power relations. We invited ethnically-based nursing
associations known to the researchers to a series of preparatory gatherings. It was discovered
that most of the members of these associations did not belong to RNAO, which was perceived by
some as the dominant ethnic group in control of access, agenda-setting, and programs for
professional nurses.
In the early meetings to strategize how to meet the study objectives, a strong fear was
expressed about employers finding out that participants were gathering to discuss their plight.
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
40
Consequently, we followed advice to proceed discreetly in advertising the study. It was decided
to hold a series of think tanks in strategic locations around the Greater Toronto Area so that
nurses in each area would not have too far to travel. The fear of backlash for meeting outside of
the official professional nursing association was resolved by the third think tank, which was held
at the Registered Nurses Association of Ontario (RNAO). On March 19th, 2002, the RNAO
boardroom was packed, and the issue of employment equity and the problem of racial
discrimination in nursing were declared to be on the agenda in nursing in Ontario:
We who have assembled at the RNAO Think Tank funded by the Canadian Race Relations Foundation invite all those in the nursing profession to study our recommendations for policy. Accountability for equal opportunity arising from the lived experience of racism is declared to be the agenda. The process that had been encumbered by isolation and the fear of backlash dissolved.
Indeed, the understanding of racial backlash that emerged was that isolation is a condition for
reprisals. Accordingly, building coalitions and organizing a research-based challenge to
resistance, retaliation, denial, and inertia became strategies for addressing the lurking problem of
racial backlash.
Five think tanks were held during the course of the research to identify barriers, concerns,
and specific strategies for accountability toward improving knowledge and practice in specific
contexts such as performance review, career development, nursing education, and using
technology to advance equity. The discourse generated by the think tanks addressed barriers,
concerns, and strategies in personal narratives and dialogue. A consensus emerged regarding the
existence of systemic racism and racial hierarchies that spawn disputes between individuals or
groups who are members of separate racial groupings. This includes the ubiquity of disputes
arising between members of racialized groups.
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
41
No consensus was reached on how to proceed collectively or whether collective strategies
were possible. While there was consensus that the profession as a whole must own the problem,
there was some resentment about only those with experiential knowledge of racism currently
owning the problem, and about those with "knowledge deficits" avoiding all opportunities
presented for gaining that knowledge. Very few white nurses, whether at staff, executive,
manager, or educator levels, attended any of the think tanks. Even the think tank that was
conveniently held in conjunction with a research day that was very well attended by nurse
leaders drew little interest from members of the "in-groups." With a couple of exceptions, a
number of VPs of nursing said they were coming but never actually attended or sent someone in
their stead.
Health problems that arose due to inequities were recognized in our awards and healing
ceremony held on the opening day of the biennial conference of the Canadian Nurses
Association at the Sheraton Hotel in Toronto on June 23, 2002. The event garnered considerable
media coverage in minority community television and newsprint and the ceremony was recorded
on video. The practice of healing relationships and building communitarian values is palpable in
this visual record of the heart of our study. It clearly details the power of public apology and
forgiveness to galvanize relationships.
This ceremony also represented the inauguration and consolidation of a research network
composed of nurse leaders from the numerous language and cultural minority communities in
Canada. Following the ceremony, resolutions to the Canadian Nurses Association were
developed by a group of those in attendance.
The CNA resolutions (see Appendix B) provide an example of how changing discourse
location can function as a power strategy. To mobilize accountability initiatives, it may be
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
42
necessary to go outside of organizations for external support. The resolutions were circulated to
the federal Minister of Health, the provincial Minister of Health, the provincial Attorney
General, the Association of Canadian Health and Human Resources (ACHHR), the Canadian
Federation of Nursing Unions, the Ontario Nurses Association, the Joint Provincial Nursing
Committee, and the national Office for Nursing Policy, Health Canada.
At the provincial level, we sent out invitational letters to the presidents of RNAO and
RPNAO and requested that copies go to members of the nursing provincial secretariat and the
Joint Provincial Nursing Committee (JPNC). We invited these organizations and the Canadian
Nurses Association to attend the November (2002) RPNAO/RNAO conference concurrent
session on “Racism and Responses.” Members of the Centre for Equity in Health and Society
participated in the round table on “Racism and Responses” at this conference on Healthy
Workplaces in Action and were credited with naming the theme of this concurrent session. It
was the first time the word racism had been officially used in a public forum sponsored by either
of these organizations.
The Centre for Equity in Health and Society solicited nurses to join the network at this
event. Electronic technology now permits such networks to function as virtual centres, and the
CEHS is now incorporated as a non-profit organization within the province of Ontario. One
CEHS mandate is to integrate the content of OHA/OMH JPPC 1995 anti-racism policy
throughout Canadian nursing. The four pillars of this policy are anti-racism, anti-discrimination,
employment equity, and culture care.
CEHS is hopeful that activities in participatory research, advocacy, and capacity-building
will lead to more racial integration and freedom to talk about issues. We predict change in
discourse practices. For example, it will become normal and acceptable to voice issues of set-up
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
43
and backlash and to organize to prevent and stop these unfair harassment activities. Attention
will have to be paid to levels of feeling, trust, and safety as we work towards inclusion in a
profession that is predominantly female and subject to what has been described as horizontal
violence – abuse by one nurse against another.
CEHS anticipates playing a major role in contributing to new regulators of discourse to
develop leadership that will help achieve an accountability for employment equity, as well as
access and participation in nursing, that is effective at reducing racial disparities. We envision
new policy that will guide programs and regulate outcomes by various means of accountability
for racial equality and employment equity in nursing.
One regulator of discourse already being studied in a downtown Toronto hospital that has
a nursing informatics department is the use of human rights software to monitor equity,
privileges, and the incidence of harassment in the employer organization. We refer the reader to
the recommendations in “A Time for Change” (Kohli and Thomas, 1995), that could form a
basis for interventions to address systemic discrimination (see Appendix F). Another Canadian
initiative that we found that addresses systemic discrimination in tool development was Carol
Agocs and Harish Jain's (2001) preliminary study, “Systemic Racism in Employment in Canada:
Diagnosing systemic racism in organizational culture.”
We advocate supporting the new personal discourse that is required for changing our
profession and the organizations we work in. We encourage all nurses and health care workers
to attend anti-racism workshops where exercises for engaging in deep self-reflection and healing
self-disclosures are facilitated.
Finally, we advocate moving to new and healthier outcomes of discourse strategies. In
our findings section, we present heart-rending metaphors that illustrate the serious trauma
Toward Accountability among All Stakeholders: Introduction and Overview
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
44
suffered by nurses who had filed formal complaints or grievances charging their employers with
racism. Racial disputes that challenged racial targeting resulted in negative health outcomes for
these nurses during a period of restructuring.
By contrast, white nurses who were transferred or let go during the restructuring period
were reported to be approached in more caring ways and were often helped to find another
position. The outcomes, which were seen as very different by nurses who disputed racism,
involved racially based differences, set-up, and backlash for broaching accountability issues.
This report is intended to stimulate accountability for racial equality and employment
equity in Canada. Using participatory action research (PAR) to engage in transformational anti-
racism in nursing, we identified issues that represent the need for accountability for the
discourses of racial domination throughout the profession. We turn now to present the study
findings on racial set-up and backlash.
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
45
Chapter 2 – Evidence of the Need for Accountability:
Presentation of findings
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
46
Some Effects on Nurses of Race, Colour, or Ethnicity: Summary of Das Gupta’s Survey of Nurses, November 2001 – May 2002 As the tables depicted in our Executive Summary, of the sixty-two nurses who completed the
survey at think tanks:
• Fifty-four indicated that they had been made to feel uncomfortable as a nurse because of
their race, colour, or ethnicity.
• Fifty-six felt that they had been put-down, insulted, or degraded because of their colour,
race, or ethnicity. A break-down of the data follows:
Nineteen indicated that a doctor had put them down;
Twenty-four indicated that their manager had put them down;
Thirty-eight indicated that a patient had put them down; and
Thirty-two indicated that another nurse had put them down.
• Some mentioned that they had encountered more than one harasser.
• Thrity-three said that they took some action, whereas twenty-two did not take action;
seven did not respond.
• Of those who took some action, thirteen had positive results; sixteen had no results or a
negative result; four situations are ongoing.
• This experience affected forty-seven respondents emotionally, eighteen physically, and
twenty-eight mentally. Several respondents noted more than one effect.
• Thirty felt that their ethnicity/colour/race had an effect on their hiring; twenty-five felt it
had no effect; two did not know; and five did not respond.
• Thirty-nine felt that their ethnicity/colour/race had an effect on their promotion; eighteen
felt it had no effect; one did not know; and four did not respond.
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
47
• Thirty-eight felt that their ethnicity/colour/race had an effect on their relations with
colleagues; seventeen felt it had no effect; and seven did not respond.
• Thirty-seven felt that their ethnicity/colour/race had an effect on their relations with
managers; seventeen felt it had no effect; one did not know; and seven did not respond.
• Thirty-nine felt that their ethnicity/colour/race had an effect on their relations with
patients; eighteen felt it had no effect; and five did not respond.
• Thirty-three felt that their ethnicity/colour/race affected where they worked; fourteen felt
it had no effect; and fifteen did not respond.
• Thirty felt that their ethnicity/colour/race had an effect on access to training; thirteen felt
it had no effect; one did not know; and eighteen did not respond.
• Three felt that their ethnicity/colour/race had an effect on access to accommodation due
to disability; thirty-six felt it had no effect; and twenty-three did not respond/not
applicable.
• Twelve felt that their ethnicity/colour/race affected their sick leaves; forty felt it had no
effect; and ten did not respond.
• Twenty-one felt that their ethnicity/colour/race affected their performance reviews;
eighteen felt it had no effect; and twenty-three did not respond/not applicable.
• Fifteen felt that their ethnicity/colour/race affected their experience of being disciplined;
thirty-four felt it had no effect; and thirteen did not respond/not applicable.
Demographic breakdown of the respondents
• Thirty-eight Black/African Canadian
• Thirteen Asian/South Asian Canadian
• Five White/European
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
48
• Four Other
• One Central/South American
• One No response
---------------------------------------------------
• Fifty-seven Female
• Three Male
• Two No response
Set-up: Racially organizing advantages and disadvantages during downsizing
Merle Jacobs and Rebecca Hagey What is a Racial Set-up? As alluded to earlier, a classic example of a racial set-up came to light when Claudine Charley, a
nurse at the Toronto Hospital, discovered that a child's monitor had been unplugged without her
knowledge. Pursuing the problem in a tense environment that was undergoing restructuring, she
came to suspect that the monitor was unplugged on purpose so that she might be seen as
negligent. Her hypothesis, which she addressed with utmost diplomacy, was reacted to by
management and soon Claudine found herself being disciplined and having to defend herself in a
human rights complaint. Under oath, the nurse Claudine had suspected confessed to having
purposely unplugged the monitor in order to cast into doubt Claudine's competence.
Claudine who, though she was a victim of racial discrimination, felt she was treated as an
offender at her place of employment. She took a $50,000 reduction of her award of $300,000 in
order to have the right to let the public know about her set-up. Unfortunately for Claudine, she
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
49
experienced great disappointment and suffering over her portrayal in the mainstream media “not
as someone defending my rights but as someone who was paid off by the hospital to go away and
keep quiet about my questionable abilities as a nurse” (personal communication, 1996).
What follows is a preliminary exploration toward theoretical understandings of set-up as
a social phenomenon and as a set of interactional discourse strategies. The majority of nurses
whom researchers belonging to the CEHS network interviewed (N = forty) because they had
filed formal grievances or complaints, used the term set-up in describing what they experienced.
It can be noted in Claudine's case and numerous others that there was immediate denial
about participating in a set-up and that there was a closing of ranks against her, suggesting there
was a collective, and perhaps rather unconscious, shared group response to protect members of
the dominant groups and systematically disadvantage individuals like Claudine, racially
dominated in the process. The concept does not require us to contemplate the motivations of the
players involved. It is plausible indeed that the players are unaware of any purposeful
motivation. However, the timely effects of set-up – the social differences that are constructed
when a scarcity of jobs has emerged – reveal an organized process of racial domination that
begins with racial discrimination and results in less privilege for racialized nurses and more
privilege for non-racialized nurses in the responses to job scarcity.
This set-up of group control depends on a lack of transparency and accountability to
flourish, and results in creation of an in-group and an out-group or outcast individual. The fact
that accountability is conditional on transparency has hampered the efforts to integrate
accountability for systemic racism into clinical practices.
Secretive administrative decisions that elect to discipline racialized nurses rather than
expose strategies designed to benefit certain in-group members are hidden and the appearance is
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
50
created in the setting that what is going on is normal. This situation is problematic, but
“normal,” since it is normal to problematize racialized individuals in an institution that condones
racism.
Understanding set-up as an aspect of systemic racism can help us all begin to see the
process of racialization as a systematic way in which people in organizations can use racial
discrimination to advantage without necessarily being obvious or accountable. The extra benefit
of their being seen as upholding rational standards adds barriers to transparency, as does the fact
that decisions are made behind closed doors without representation or actual input from members
of the out-group or racialized persons.
Tokenism can also be a feature in a set-up. The small number of out-group members
who are let into the game are under the same bind as every member of the in-group. Anyone
who breaks the code will suffer backlash in some form such as being ignored or isolated, having
privileges removed, or being set-up for retaliation and serious harassment and punishment. The
same code is applied for members of the dominant group who do not go along with the game.
The fact that this type of anti-social treatment erodes persons’ self-confidence, re-
organizes their priorities, saps their energies, affects their personal and family lives, and so on,
works to perpetuate the system. Most people conform to the set-up as long as it is someone else
who is targeted. This response even applies to managers in positions of authority who join an
organization with an agenda to effect change but who are brought into conformity since they
need co-operation and since the in-group sticks together. Outsiders with influence can sabotage
their reform agenda.
That is, set-up is an aspect of social and political power that can be used to coerce people
because vulnerable people fear rejection, isolation, or expulsion. The strategy of set-up, then, is
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
51
not coincidental when one considers that the agenda of racialized peoples is equal inclusion and
participation. The strategy of set-up did not succeed altogether in Claudine Charley's case. She
chose to be included in the history of the fight for human rights rather than succumb to racial
domination as so many others had done at her hospital. The set-up did succeed in making her
life miserable for many months. It succeeded in motivating her to organize the presence of at
least forty nurses at each hearing, each with a daffodil signifying their fight against the cancer of
racism.
There are at least four types of set-up: (1) targeting individuals; (2) top-down
orchestration; (3) recruitment of peers; and (4) pre-emptive or reactive documentation that we
will be pursuing in this discussion. These different types of set-up all have certain functions in
common. The functions, apart from having “everyone really on their toes to do their bidding” as
one participant stated, include ferreting out opposition, capturing and securing advantage,
reinforcing the game plan, and fending off liability. This latter function is a sanctification
activity because, theoretically, under the law, employers are liable for discrimination practices.
All four of the types of set-up that we describe leave racialized nurses fundamentally
vulnerable and subject to racialization, which can be ongoing or intermittent. Their supporters
who have power can be coerced into abandoning them for fear of lack of group support. The
pervasive awareness of lack of accountability and lack of transparency is fundamentally
unnerving for those in the vulnerable position of being a potential target. Situations where
racializing can occur with impunity set up relationships of ready-to-distrust/not-being-perceived-
as-trustworthy, which is problematic for balance, reciprocity, and collaboration in working
relationships. Communication becomes defensive on both sides when the targeted nurse gives
any indication of objecting to the treatment. Reciprocal resistance begins. The targeted person’s
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
52
resistance becomes evidence to the in-group that the person does not really belong in the work
unit, and then the person is isolated. It is crucial to recognise the in-group’s set-up strategies that
marginalize, exclude, problematize, and contain and isolate along racial lines. Set-up is a
method for achieving outcomes of racial segmentation and segregation with impunity since
accountability is not in the picture. For example, one hospital with documented set-up practices
provided separation packages for white nurse managers but not for nurse managers of colour
following its lay-offs. Immunity, silence, and the advantages gained by being part of the set-up
rather than a target constitute a powerful incentive for onlookers to condone events rather than
challenge them, as this shocking example shows.
If we want to theoretically test the importance of lack of accountability to the
perpetuation of set-up, we can pose the question of what happens if accountability is introduced.
What Happens if Accountability is Introduced? We believe that accountability to prevent set-up from occurring would require a set of conditions
parallel to the types outlined previously that make set-up possible. The parallel types we pose,
respectively, are strategies used by Claudine Charley that relied on the Human Rights
Commission Policy at the time (which was then much stronger than it is now): (1) She gained the
presence of supportive individuals, but unfortunately most were from outside her work unit; (2)
She orchestrated activities toward inclusion by including herself in the duly constituted
complaints process available to her; (3) She recruited peers for support from key external sources
such as the Congress of Black Women of Canada; and (4) She strategically used documents to
establish the facts of her case. Each of these conditions can be seen as an intervention motivated
to bring balance to an out-of-balance set of relationships. We will come back to these strategies
later in our discussion to consider what might be the necessary structure to prevent out-of-
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
53
balance race relations from developing in the first place. Each of these parallel activities requires
leveraging social power for example, from a union or union installed diversity unit, from access
to an "old boys network" or from external media, or from community consensus building that
establishes a powerful advocacy group.
Even then, as we will show, these strategies are not yet a panacea for realizing racial
justice in nursing in Canada. It is important to recognize that particularly racist individuals can
have enough autonomy within an organization to harass with impunity since autonomy is a
fundamental value that overrides equity in our society. Colleagues would rather condone than
oppose. The mythologies about equal opportunity, merit, or individual responsibility that place
the onus on the racialized individual or group to "pull themselves up" are rooted in a lack of
acknowledgement of the anti-social workings of set-up and in-group/out-group politics.
Ideologies about freedom of choice, founded on individual liberties trumpeted in the legal
documents of society, are rather oblivious, not to mention non-compassionate, about restrictions
on choice when the sanctions are against a racialized person(s) being set-up in a negative bind
formation. The individual in a negative bind – damned if they do or damned if they don't – has
to decide whether to risk backlash for objecting to the treatment or risk allowing the set-up to
proceed with impunity. This is a bind that many racialized individuals understand, whereas non-
racialized individuals, without the experience of being targeted, apparently have difficulty
understanding what is going on. “Speak no racism, hear no racism, see no racism” appears to
cloud their observational capacities.
Examples of Set-up in Nursing in an Environment Where Racial Profiling Is Not Held Accountable We present four types of racializing set-up – forms of coercive control – that disadvantage and
thus racialize members of designated groups and marginalize any supporters they might have. In
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
54
these situations, nurses of colour have felt harassed, especially as the set-up intensifies and the
effects start taking their toll.
1) Targeting the Individual
This type of set-up is typical when an individual is targeted by another nurse who is at an
immediate level above her or him. Nurses reported, as an example of this behaviour, being given
heavy assignments from a charge nurse or unit manager and feeling set-up when problems occur.
One nurse reported that she had the heaviest load and could not give adequate care to all her
patients, while the rest of her peers had “normal work loads.” She was reprimanded for not
doing her work. Racialized nurses also reported that they are pulled aside and spoken to more
often than their white counterparts. One nurse told us how she perceived being set up:
I was in my office when the new director came in and introduced herself. She said that she would be working with me to help me develop, and that I had been working in the institution far too long, had I thought about moving to another hospital. I asked her how she knew this about me as this was her first day meeting me and new to the hospital. She informed me that she had heard that my unit was not up to the standards of how patient care should be delivered. There were no witnesses, but I knew I did not have the support of nor would I get the right direction from this new, white director when it came to doing my job. In fact, I felt that she was setting me up for failure.
This passage reveals that the new director had tipped off the nurse that she was not
welcome through comments such as “working in the institution too long” and that the “unit was
not up to the standards of how patient care should be delivered.” These signals alerted her to the
possibility of being set up. So when this nurse observed that her workload was heavier than
others and inquired about it, she was told it was “just her heavy day.” She came away thinking
that perhaps the supervisor was “parcelling out heavy days to everyone.” Then she began
worrying about the opening greetings the supervisor met her with, without getting to know her as
a person, as she saw her assignments were consistently heavier than the white nurses'. In a
while, she felt the set-up. She faced the dilemma of either repeating her question about the
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
55
perceived unfair workload or quietly submitting to the racialized assignment. It is this dilemma,
this being contained, that is an earmark of racialized set-up.
We conceptualized this situation as being racialized on two counts. We were suspicious
because the supervisor was white and the nurse was a racialized person. Furthermore, the
allegation was that the white nurses consistently had a lighter load and the nurse of colour a
heavier load. However, the clincher was the supervisor’s continuing distant approach, which
was laced with messages of veiled threats that anyone would perceive as unsettling, if not fear-
inducing. Opportunities to clear up any ambiguity regarding these innuendoes all confirmed the
consistency of the unspoken message: “You have good reason to be fearful. Do my bidding or
take the consequences,” or “you can try to placate me.”
Ambiguous messages that imply subtle coercion are cause for feeling psychologically
harassed. However, the spectre also looms of being disciplined for minor professional oversights
that white nurses are allowed to commit without fear of reprisal. This nurse felt that her
supervisor's set-up strategy had escalated to the realm of tripping her up on professional issues.
She had reluctantly opted to being saddled with an unreasonable and unfair workload, not being
able to gain support for her plight from those non-racialized nurses who had a lighter load and
who clearly did not want to jeopardize that privilege. This fear of professional slip-ups fed her
feeling of psychological dis-ease. Even though she was pressed for time, she felt compelled to
document defensively to protect herself. She then became aware that she, too, was being
documented.
The nurses we interviewed who resolved their set-up dilemma by acting on
documentation to complain or grieve, for example about their work load, found they immediately
“became” the problem, as noted in the literature (Veecock, as cited in Calliste, 1995; Essed,
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
56
1991; Smith, 1990). The supervisor’s task, then, under the set-up logic was to gather allies from
upper management, internally from staff, and externally from colleagues. With all bases
secured, the supervisor then could buy off the staff with special privileges and isolate the
problem nurse.
2) Top-down Setting up of Racialized Informal Policies and Practices Calliste (2000b) argues that the existence of dispute mechanisms that are controlling, coercive,
and racialized are manifestations of a surplus labour pool that is activated as necessary,
depending on demand. A vulnerable pool of racialized immigrants will stand in line for jobs that
are casual and temporary. Indeed, Head’s (1985) study suggesting that equity becomes popular
during periods of job surplus, but disappears during job scarcity, gives credence to this logic. It
is not surprising then that one form of set-up occurs when management seeks to re-organize
institutions. The set-up is accomplished through a "rationalization" of work, where opinions and
decisions are held to be objective. Any challenge about this fact of objectivity is dealt with
abruptly.
For example, when racialized managers in one hospital that was in the midst of
downsizing reviewed staff as they closed departments, they were critical of the method whereby
staff declared their first, second, and third choice of placement. They saw it as an imposition on
vulnerable staff members who had the onus placed on them to lay bare their perceptions of their
options. Their vulnerability, then, could be exploited. As an example, when senior management
knows what individuals want such as a certain speciality, they can put the racialized middle
manager on par with lower staff competing for a job, any job. The information is power. Senior
management can make an offer nobody would want to refuse. They can play one individual off
against another.
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
57
Indeed, it became apparent that this method resulted in assigning non-racialized staff to
preferred areas such as emergency or intensive care, while racialized staff were placed in heavy
medical units or in areas that were not one of their three choices. The racialized managers who
complained were targeted. Even though they had seniority, they were asked to step down and
work as staff nurses, while their white counterparts were given another unit to manage. The staff
who got the better jobs were set-up to win due to white management’s control of the positions
and activities that set up the racialized staff. The discourse of luck was used in face-to-face
situations to explain how some nurses were lucky to get their first choice, while racialized
managers who took staff nurse jobs were lucky to have a job at all. This discourse appears to
validate the surplus labour pool hypothesis (see Calliste, 2000b) that works on the axiom, “you
are lucky to have work at all.”
Another aspect of top-down orchestration of racialization is concerned with what
strategies are used to release information and to whom it is released. Typically, the set-up works
by providing information to non-racialized managers during social hours while not providing
racialized managers with the same information. As one racialized nurse manager stated:
I was not told to inform my staff that they had to bring in their registration or they would be docked a day’s wage. This was not policy and was not discussed in any meetings. However, when I did not dock the wages of my staff, I was told I did not know how to manage my unit. There were so many little things that they [other managers] would be told, and I would be looked at with a "so you don’t know again" type look, while all the time they withheld information from me for doing my job.
It is important to recognize that when there is laissez-faire for racial domination, that is
when there are no accountability mechanisms to curb its use in employer/employee and
employee/employee relations, then the much-touted strategy of building up relationships and
friendships is not of much use in single-handedly gaining transparency and/or accountability.
Moreover, discourse strategies that request clarification presenting a challenge are not really an
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
58
option. As this manager found out, racialized managers are kept out of the collaborative
decision-making loop:
Challenging this type of behaviour often triggers accusations that the individual is defensive for not doing her/his job, is not a team player, or is preoccupied with narrow issues relating to the area of management and not to the organization. ….Withholding information on how decisions are made is crucial for during work orientation and work socialization. So then you are in a bind of having insufficient knowledge to do your job versus triggering more barriers by even hinting that you are dissatisfied with the flow of information. 3) Recruiting Compliant Peers who Support Targeting and Scape-goating
This type of set-up operates when managers ask white nurses to provide them with information
about a racialized peer. The behaviour occurs at the management as well as at the staff nurse
level. The request itself sends the message that it is permissible to target racialized nurses. For
example, at the staff level, managers have been observed to recruit non-racialized peers to "tell
on" the racialized group or nurse. Nurses set-up their peer by looking for errors, missed charting,
or missed physicians’ orders. One nurse reported:
Complaints were made in writing about my missed work, while for the white nurses the excuse was, “Oh well, we have continuity over 24 hours…" Another way of setting me up was to have peers send patients not suited for the unit so that when a medical incident occurred, it was due to my incompetence and not that the patient should have been in an intensive care bed. In fact, when a patient had an arrest and died within 24 hours of the transfer, it was my fault even though I protested the decision to put this acutely ill person on a rehab unit…. and they upheld the decision of the white manager who sent the patient…As these incidents are par for the course, going on all the time, I may be unaware of what is occurring but I feel the stress of being over-monitored and not having support from my colleagues.
Some white nurses refuse to be recruited to participate in set-ups and, in fact, testify on
behalf of nurses of colour when the complaint goes forward to a grievance. Such support is
crucial for the complainant.
4) Documentation for Pre-emptive or Reactive Defence of Set-ups
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
59
Racialized nurses and managers have reported that their human resource files include documents
that they were unaware of until they checked the file. This set-up is related to targeting but is not
visible or known by the individuals that are being set-up. For example, a manager expressed
anger when she looked at her file and found notes on her meetings, patient care decisions, and
reports from her staff. She reported:
They wrote notes on me when they spoke to me about anything or when they met with me to discuss staff-related issues. The notes were negative in that they always had a spin that I was not doing my job. As I did not know about this, I did not have a chance [to] refute the accusations. Once I knew and spoke to the HR manager, who did not see a problem with this behaviour, I added my side to the file. I felt that they were setting me up for dismissal and failure…Then my shortcomings were stated in terms of how they saw me measuring up to the guidelines and standards. The discussion was never about patient safety or how could this be organized to solve the problem. It was all a frame-up of me and my deficiencies.
As we have seen in Das Gupta’s (2002) study, these sorts of encounters are probably very
rare for non-racialized nurses. Only 1% of White/European nurses felt that their race, colour, or
ethnicity might be interfering with their performance review, whereas the percentage was up to
39% for racialized nurses. This finding raises the possibility that some racialized nurses could
feel vulnerable to a set-up regarding their performance review that would result in further
racializing them.
It is important to theorize about the organizational dynamics that can result when the
ruling in-group becomes defensive and controlling, such as when job scarcity precipitates
downsizing and transfers. Two main options appear to be available to those subject to racial
targeting: (1) buckling in and trying to survive being set-up, and navigating the unfairness and
oppression by hanging onto any good relationships in the work setting or (2) challenging the
unfairness and thus precipitating the consequences of set-up and opening up the possibility of
backlash. For example, it is not uncommon to have to demonstrate one’s innocence in the set-up
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
60
and one’s general competency at the same time as having to show that racial discrimination was
taking place. The dispute process can drag on for months or years and be very destructive for the
nursing teams and the clients who are dependent on them.
Cautionary Summary These preliminary accounts on set-up supply examples of social and language practices that are
consistently reported among nurses who have filed complaints or grievances to describe what
they have experienced. The word “set-up” is used again and again in describing their story.
Ethnographic work would be required to more fully document these interactive discourse
practices. We have not been able to access the various persons who have participated in such
transactions since they have not been attracted to the study. Ethnography would call for
participant observation and interviews with all parties in a variety of settings in a number of
locations to develop a fuller picture of perceptions, stated rationales, motivations reported to
others, and so on. However, we are more interested in finding out how to break up such social
systems and have identified parallel positive strategies to each of the anti-social types of set-up,
as previously mentioned in the description of strategies used by Claudine Charley.
Such constructive strategies as identifying supportive individuals, orchestrating activities
to gain inclusion and influence (such as support under the Ontario Human Rights Code, when it
was accessible for use by unionized nurses), recruiting peers, and strategic use of documents,
could theoretically build up support against the negative set-up strategies of targeting
individuals, top-down orchestration, recruitment of peers, and pre-emptive or reactive
documentation, respectively. However, given the case examples we have been able to access in
this preliminary study, the success of these structural antidotes as interventions would depend on
racialized persons becoming organized. Relations of loyalty or solidarity would need to develop

Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
61
to erode the segmentation that divides racialized and non-racialized people and prevents equal
access and participation in the institution's discourses of power.
Case Study – The Story of Nurse “A”: The Grievance Process as a Set-up for Backlash
Jane Turrittin
Preface As an introduction to Nurse A's case, we call attention to the fact that the cappuccino principle
typifies the workplace hierarchy of most long-term care facilities in the GTA. Most staff are
racialized, and most patients, managers, and administrators are white with European ancestry.
That is, Nurse A worked in agencies that were rife with systemic racism and unaccustomed to
any accountability measures aimed at change.
Case Study In her effort to defend her human rights and expose racialization of staff as an impediment to the
delivery of quality care in the nursing homes at which she worked, Nurse A filed a total of
twenty-three grievances during her twenty-one year career in Toronto. This makes her the
champion of the participants in our "Making Racism See-able" research project (Collins et al.,
1998). She filed the first nine of these grievances at Old Person's Home 2 (OPH2) between 1980
and 1986 and the latter fourteen grievances at another nursing home, OPH1, her first employer in
Canada where she returned to work from 1990 to 1999. Twelve of these fourteen grievances
were filed between May 1996 and February 1999.
Nurse A also filed three complaints with the Ontario Human Rights Commission
(OHRC) and made submissions to other venues. Her insistence that her employers respect her
role as a nurse in mutual accountability for the treatment of both patients and staff has been a
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
62
core activity of her career as a nurse in Canada. We found Nurse A to be a lovely person,
extremely articulate with a droll sense of humour, but overladen with sadness.
For Nurse A, as for other nurses who have filed grievances, one of the costs of speaking
out is prolonged backlash. Employer backlash at OPH1 brought Nurse A into conflict with her
union, the Ontario Nurses Association (ONA). It profoundly affected her emotional and physical
health and continued even after Nurse A resigned. When Nurse A persisted in defending her
human rights and identified the conflict between herself and OPH1 management as one of racial
discrimination, OPH1 management problematized and harassed Nurse A using procedures to
marginalize and contain her. Management's retaliation activities thus escalated the dispute
process that was supposed to be the venue for problem solving and redress of grievances.
Nurse A's experience with discrimination and defense of her human rights in the 1980s
made her aware of the importance of documentation. When OPH1 management began to
discriminate against her in the early 1990s, she saved every scrap of evidence relating to her
case. Drawing upon this documentation, including legal documents, personal diaries, and letters,
as well as two interviews, we present here a highly selective version of Nurse A's experiences.
The story of Nurse A's efforts to make her union accountable on matters relating to racial
discrimination at work deserves far greater elaboration than we have been able to give in this
narrative. Nurse A is a union supporter and former union rep; she very much wants the ONA to
be accountable to its members on issues of racial discrimination.
Nurse A described a poisoned work environment that interfered with the delivery of
quality care at virtually every facility in which she worked. Moreover, the procedures available
to Nurse A and to management to deal with the racial disputes, such as the grievance process,
functioned primarily to escalate the conflict, thus compounding the traumatic quality of the lived
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
63
experience of racial discrimination. When Nurse A joined the participatory action research
effort, she volunteered to tell her story as a contribution toward equity assurance policies in
health care facilities that would render such trauma avoidable. We present Nurse A's case in
support of CEHS advocacy for the creation of equity assurance policies and procedures that
address victims' "core needs" in a dispute.
Ruth Morris, an expert on transformative justice, identified five "benchmarks" that
address victims' core needs: (1) the need for answers; (2) the need for recognition that they have
been wronged; (3) the need for safety; (4) the need for restitution and balance in workplace
relationships; and (5) the need to find significance or meaning from this assault on their human
rights (2000, p. 248). We use these benchmarks to evaluate Nurse A's experiences with
retaliation and escalation in the dispute process and the legal proceedings to which it gave rise.
Transformative justice defines racial discrimination as behaviour that harms not only
individuals and communities but social relationships. It therefore views racial conflict as an
opportunity for individuals and organizations to examine, reflect upon, and repair the
relationships that poison the workplace. Since the problem is a relational one, with a relationship
being out of balance, the goal is to get at the source of the problem and to change or transform
the relationship. Balance can be created and maintained by changing procedures that structure
relationships. Recognizing the importance of victims’ knowledge and experience as well as the
importance of community validation of this knowledge and experience, the restorative justice
model gives scope for the whole employment community to be involved in the healing process
(Law Commission of Canada, 1999, p. 23). It recognizes that the very proceedings that are
meant to help redress grievances are laden with denial and barriers that complicate the issues,
when what is needed is often apology for communications that marginalize, problematize, or
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
64
contain the complainant. This means that the organization employing nurses should practice
mutual accountability to prevent and deter racial discrimination to ensure due process for
handling complaints.
When Nurse A filed grievances and complaints charging OPH1 management with racial
discrimination, she wanted an opportunity to give her version of what had happened. She
wanted her employer and her union to recognize (public confirmation) that wrong (racial
discrimination) had occurred, and she hoped for no further harm to herself and others, and fair
(transparent) procedures. She wanted balance to be characteristic of relationships so that quality
care could be given in a work environment free from racial and other forms of discrimination.
She wanted all employees to be valued, and she wanted her experiences to have positive meaning
and significance through achievement of positive closure. We ask you to make use of the five
benchmarks to consider how effective the remedies available to Nurse A were with respect to
meeting her core needs.
Nurse A is Caribbean-born. She went to England for her nurses' training, taking a four-
year diploma course and a one-year program in midwifery. After living and working in England
for twenty-two years, she immigrated with her family to Canada in 1979. While preparing to
write her Ontario registration (licensing) exam, Nurse A worked part-time as a nurse’s aid at a
long-term nursing care facility, Old People's Home 1 (OPH1). Nurse A related how she became
quickly aware of the realities of racial stratification in the nursing profession in Canada.
During the early '80s, I worked at Toronto Western, at Northwestern, and I also started working at a nursing home in the Jane and Finch area…. I was encouraged to leave…the hospitals and come to long-term care because…nurses were dissatisfied with the treatment they were receiving and, having worked at Toronto Western and Northwestern, I was at the forefront of it too. I saw what there was.... I stood up to it, and had some repercussions but … I was fearless at the time and I tried to do some organizing of the nurses but it didn't work. In Northwestern, I can afford to tell you, discrimination – treating certain people –
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
65
was as plain as anybody's nose on their faces.... My colleagues on the unit, they just wanted to do what they had to do and …go home. And on a few occasions I said to them, "No, you can't just do what you have to do and leave. You can't. …There's a force here that doesn't give us any respect." And then that took a lot of my…. We started organizing so that we would get ONA in, and ONA did come in (personal communication, 2002).
When she got her license, Nurse A took a full-time job at OPH2, serving as union
representative.
I had about 9 grievances [that] were related to the Director of Care's (DOC) discriminatory behaviour, and the fact that the nurses were not getting what they were entitled to, and job satisfaction, and regarding job workload, and the …unsatisfactory and … obviously illegal ways that the staff in charge in the nursing office and administration behaved. We were supposed to get a pay rise. And the pay rise came, and we were all informed of what we would get. And…I disagreed and some of the other girls (all racialized)...disagreed because they realized that there was something wrong. I worked it out according to the schedule that we all worked and found out that, to the dollar… we were, all of us, every single night I worked on one person,… I made it a point of duty...And I…took the documents to [the nursing staff], told them to copy it,…and handed them to the office, and they [the administration] were…absolutely distressed and upset with me. I got my money. Besides, I took them to the Labour Board. I complained about [OPH2] not giving me my rightful amount of money. And the other nurses [also]. [Two of the 3 arbitrators were] Mr. Bromley Armstrong and Judge Rosalie Abella - she wasn't yet a judge at the time. [OPH2] had intended to keep this money…. (I)n the end after all the repercussions for me, I decided that I was going to leave (personal communication, 2002).
In her letter of resignation to the facility's administrator, Nurse A stated:
Non-staff recognition – poor support; uncaring attitude – creating unnecessary stress, has caused you to ignore your commitment to the residents. You have refused to explore any recommendations or solution to improve the morale of the staff through your bigotry. This organized and systematic flow of abnormal level of stress, this mental torture, this psychological warfare, is not good for anyone. I now find it difficult to function under the duress in this unstable environment (personal documents, August 21, 1986).
Shortly after Nurse A left, "Everybody was fired ... including (the DOC). They searched
and they found money staked away in the Coca Cola machine" (personal documents, August 21,
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
66
1986). Nurse A asked for and received a letter of reference. The envelope the letter was in also
contained a note of appreciation to her signed by the facility's administrator and a check for
$5,000, signed by the corporation's accountant. Was this check in compensation for her troubles,
in recognition of her whistle blowing, or both? The fact that management gave her this check is
in itself evidence of her integrity and their admission, perhaps, of the need for accountability.
Nurse A's experience with this employer shows that a lone individual exercising leadership can
have some success in making an employer accountable, if not for racialization of staff, at least
for failure to deliver quality care. But did anyone speak up after Nurse A left?
During the next four years, Nurse A worked at various nursing homes as well as through
an agency that sent her to work from time to time at OPH1, and she did not file any grievances.
In 1990, at the invitation of her old manager, a South Asian, as well as the Unit Manager at
OPH1, a white Canadian nurse, Nurse A began part-time work at OPH1. In 1992, she was given
a full-time position on the day shift.
OPH1 is a long-term care nursing home run by a religious organization whose faith Nurse
A shares. The administrative offices and the dining room are on the building's main floor and
250 to 300 residents are housed on the upper four floors. Cognitively impaired residents occupy
one of these floors, which is locked. Residents' needs for care have gradually increased over the
years. Nurse A dislikes talking about white people and black people but confirmed that the
administrative staff supervisors are white, while the staff (nurses, Registered Practical Nurses
[RPNs], and health care aides) are people of colour, with Blacks outnumbering those with
Filipino ancestry by more than two to one. All Unit Managers are white and identify with one of
the dominant ethnic groups in the Toronto area; those who are nurses graduated from nursing
school in the 1980s.
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
67
Cutbacks in health-care financing in the early 1990s brought about unnecessary stress and
low staff morale at OPH1, accompanied by a high turn-over among administrative staff, and job
insecurity for front-line staff. In September 1994, Nurse A received notice that her job had been
terminated, but was called back to work at the last minute, and in November, management told
her that she was being put on part-time work.
In this insecure work environment, Nurse A observed that standards of quality assurance
with respect to patient care were not being met and communicated her concerns to management.
We're [Nurse A and her Unit Manager] sitting in Quality Assurance [committee] meetings together. …(H)er behaviour was one thing and she was saying something else...[I was] trying to do my job (and) getting obstacles at every turn from the leaders themselves...[My] Unit Manager was ignoring me. (personal communication, 1998).
Nurse A expressed her frustration with management's efforts to marginalize her in
a diary entry:
For a very long time, I have not been able to maintain the quality of my work, as most of my efforts have been hindered and, as a result, I have suffered on-going frustration and unnecessary stress. I understand how much there is to be gained in a unified effort, to achieve a satisfactory level of care, and general all-round job fulfillment. I have always observed that important issues are ignored in the pursuit of trifles. The custom in which incidents and other issues are handled, unrealistic, non-communicative, exacts a toll, unknowing, on most workers' morale. As an RN, I am not recognized. Support is poor. Information continually ignored…my…experience is not valued. I feel there is no respect for my professional abilities (personal documents, October 1994).
In January 1995, Nurse A returned to full-time work but felt unsupported by her Unit
Manager. White staff got privileges such as six-week holidays that were granted only reluctantly
to Nurse A. When she received a second "Notice of termination" in May 1996, Nurse A filed her
first grievance against OPH1 stating that the lay-off violated the collective agreement. After a
series of meetings between ONA reps and OPH1 administration, Nurse A remained (except for a
two-week period) a full-time employee. The administrator wrote her a letter in which he
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
68
apologized for any inconvenience and stated that the "action was without prejudice" (personal
documents, June 24, 1996).
In July, management changed her work shift, in violation of the collective agreement, and
Nurse A filed a second grievance. The matter was resolved to her satisfaction but in September,
when management found fault with her clinical practice and placed a letter of warning in her file,
Nurse A filed a third grievance. The matter was resolved at a meeting between Nurse A, her
Unit Manager, and her ONA representative. Management was instructed to remove the letter
from Nurse A's file. Nurse A filed a fourth grievance in October, demanding that monies owing
her be paid. In this grievance, Nurse A expressed:
…her growing frustration and unhappiness regarding her working environment at OPH1 [where] [s]he feels undervalued, and as a result has experienced both stress and anxiety. This grievance is an attempt to improve her working environment through better communications with the appropriate management personnel (October 23, 1996).
Was money owed Nurse A withheld simply because OPH1's accounting practices were
lax or did management deliberately try to withhold her money as a way of harassing Nurse A?
About this time, OPH1 hired a new DOC and Nurse A went to her, as well as to the
facility's administrator, for help:
…with documentation that I had written (about problems delivering quality care). …She asked me for certain copies which I gave to her (and)…she said,…"I can assure you that I will not be ignoring this," which is exactly what she did. She did nothing about it (personal communication, 1998). Nurse A's concerns were discussed at a meeting attended by all the Unit Managers, the
Administrator, the DOC, and two ONA reps. The meeting was amicable, but Nurse A was
further marginalized under this DOC who allied herself with Nurse A's Unit Manager. When
that DOC left, Nurse A felt that, under the supervision of the DOC hired to replace her, her Unit
Manager had even greater liberty to harrass and discriminate without sanction
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
69
Nurse A began to work nights in March 1997. She was responsible for supervising a team
of RPNs and health care aids who delivered care to a minimum of 120 residents on two units,
including the unit for the cognitively impaired. They were frequently short-staffed. Nurse A
describes the poisoned work environment for racialized staff at OPH1 in the second complaint
she filed with the OHRC:
A staff member [names a white RPN] has been allowed and encouraged for many years to display racist behavior when I worked [names shift]. For several nights [this RPN] walked into the Unit, shouting the comments – "I am fed up of these immigrants and darkies," – while slamming her bag and chairs around, in the presence of all the evening staff. As well as racist comments, abusive/cursing language would be used also frequently: "Is this what this country fought a war for?" (I informed my manager of this RPN's behaviour and no action was taken.) In fact, a worker was removed from my shift. When the RPN informed her that she is happy to come on to see her own colour for a change, she even remarked this to [my manager] who again took no action...Serious medication (errors) made by nurses of a different (white) persuasion were constantly overlooked (gives 2 examples) (March 1998).
Out of concern that the continuous stress and racial harassment at work was having an
adverse effect on her health, Nurse A went to her doctor, who put her on medication for high
blood pressure.
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
70
Benchmark 1 – The need for answers: Why did white management and staff discriminate against Nurse A? Why was nothing done about the racial discrimination that poisoned the work
environment at OPH1? Why did the employer not adopt the 1996 Anti-racism policy
put forth by the Joint Provincial Planning Committee of the Ministry of Health and the
Ontario Hospital Association? Why didn't OPH1 management make white staff who
expressed racial epithets toward Nurse A and other racialized individuals accountable
for this aspect of their behaviour?
"Tit for tat, infernal trap”
In July 1997, Nurse A's Unit Manager had wrongly accused her of refusing to attend a
mandatory in-service training session on "Classification Documentation Incidental Charting,"
charged Nurse A with "insubordination," and suspended her for one day without pay. In fact,
Nurse A did not refuse to attend the in-service. Rather, she requested that it be scheduled at a
time that was convenient for her and not on a morning following her night shift. According to
Nurse A:
…When I went on nights in March of 1997, I was expected to attend an in-service on communication after…I was finished working at 7:00. When I was finished working at 7:00, all I want to do is to come home, have a shower, have a hot drink of milk and go to bed, because that's all I'm sick for. I can't hear what you're saying; I can't talk to you. But I'm expected to stay…from 7 to 10 in an in-service (personal communication, 1998).
Management's scheduling of this in-service was the catalyst that led to escalation of their
conflict with Nurse A. Management's insistence on a time that disturbed Nurse A's sleep pattern
allowed them to project the problem onto Nurse A and then harass and discipline her.
The morning of Nurse A's first night back at work following her suspension, Nurse A:
requested a minute to speak with [my Unit Manager]. In her office, I told her that I am well aware of her harassment of me, which has been a gradual process for some length of time. I asked her to please stop or I would have to make complaints to the Human Rights
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
71
Commission and the Board of Race Relations regarding her inappropriate behavior toward me (Hand written incident report, personal documents, no date).
A few days later, Nurse A filed grievance #5, stating that her one-day suspension was
without just cause. The following week, her Unit Manager called her at home several times
during the day, awoke her, and asked her in a very disagreeable manner to attend an in-service at
1400 (2 pm). Nurse A slept between 10 am and 4 pm and was not willing to interrupt her usual
sleeping pattern to attend an in-service scheduled at 1400; she declined to attend.
There were additional incidents symptomatic of the deepening rift between Nurse A and
management. Nurse A discovered, for example, that instead of categorizing her pay stub as
"suspension without pay", the accounting department categorized it as LOAWOP (Leave of
Absence Without Pay--Pay stub # 649-5th, SEQ 112 for pay period July 21-Aug. 3, 1997,
personal documents). Was this simply because of bureaucratic ineptitude or orchestrated
deliberately by management to harass Nurse A?
Over the years, several RPNs and health care aids had filed complaints about racial
harassment and working conditions at OPH1 with the Ontario Labour Relations Board and the
OHRC. An OHRC complaint filed by a Black health care aid whom Nurse A supervised was
settled in late 1997 or early 1998. The health care aid received a financial payment from OPH1
and Nurse A's Unit Manager was made to apologize to her.
Nurse A underwent a performance/documentation review. In mid-October, management
instructed her to "improve her communication skills both verbal and non-verbal...document in
accordance with CNO and OPH1 standards," attend the in-service, and "Submit a list of 10
charts and 10 care plans monthly…to the Unit Manager for mutual review" (October 30, 1997,
Letter from Unit Manager to Nurse A).
Nurse A recognized this as a set-up.
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
72
To submit 10 charts/10 care plans monthly by Nov. 15th, Dec. 15th, Jan. 15th, 1998, I would have had to work from 7 am until (all hours of the night)…or go in on my nights off. (This is) simply unrealistic – (a) project to intimidate/belittle, to try to discredit me. …(M)y charting and documentation are well within the College of Nurses and [OPH1] standards…I have been on staff since 1990. Therefore, there is sufficient proof of my documentation (Submission to the OHRC, March 1998).
I'm there at work every night…and doing my work….why would I have to [do these care plans]?…Well, they knew it was an impossible task, so they decided…okay,…we do her with this…we have a reason…[to] give her the sack…(personal communication, 1998).
On 3 consecutive mornings, beginning October 28, 1997, Nurse A's Unit Manager
approached her:
at 7 o'clock …or just before 7, and told me that she wanted to talk to me…her approach was threatening… Well…I can't even talk because I'm so tired and sleepy. I'm up and down doing two floors all night long… I can't get my breaks at night. This is a Unit Manager, our leader, my leader, and when I said to her, No, I am not speaking to you…I feel threatened. … I can't speak to you now. This is [a] quarter past 7…in the morning;…I'm just …finishing up … my paperwork and all that, and she says that I'm insubordinate. This is …[the] Unit Manager, who was giving me all these letters and insubordinate and all these different accusations. I went in there, and do you know what, as I walked in…, "Oh you're late"… Late, I'm not late, I just finished doing my work upstairs. I'm not late but this is how they decided to attack me. Even I may have been …missing a few things, like putting in the amount of time spent with a resident. I didn't do it often. It was done because I didn't have the time…between…5 … and 7 in the morning to cram everything in. She was letting me have it, about…[how]…I'm not meeting their standards, and… have not attended that in-service, and I have to attend the in-service or else I'm going to be…suspended again … without pay. And they were threatening me…they're saying that I can't communicate and I can't document…I mean, all these years I've been passing (documents) on to them; they never had a problem with anything. At this meeting in the DOC's office when I was isolated that morning, their full intention was to…route my thoughts, to mortify me, to unravel me, to disorder my thoughts and my perception, to impair my memory and my judgment, to disorientate me, to impair my capacity to recognize reality so that I would exhibit even the faintest hint of a mental breakdown. To make me mentally unstable. That's what the meeting was all about. And when I realized this, when I had come to, I burst into tears. I'm not a crying person, but I broke down. I think I broke down too because it was 7:30 in the morning. I was tired, and when I realized what these women were trying to do to me to destroy my life in this way, I burst … into tears. And you know what, the two of them…leapt up from the chairs and one went to the door, and she stood in the door. She looked to see if anyone had shown up yet, from administration, …if anyone was over there listening or hearing me. But I was SO distraught, I thought I was going to die. I could feel my heart pounding through my ear at that very time. I'll
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
73
never forget it. My heart pounding through my ear, and …I could I feel my chest was going to burst. And then I said, …when I realized that …they were upset too and they thought that somebody might be listening outside, then their attitude changed immediately. …Would you like a cup of coffee? Would you like… something. Oh no, and … I've just remembered, …you drink a lot of herbal teas, don't you? This is the Unit Manager who's known me for years, who pursued me relentlessly to join the staff years ago. She, I realized that they…got upset and were scared that somebody would be hearing all this, and um, so I… decided that, (says her own name), stop this. When they sat down, and I could …I was actually sitting there bringing myself, and I could feel my heart getting…um…less and less noisy. I brought myself back. I said, just sit here quietly and look. Observe these women, watch them very carefully (personal communication, 1998).
Nurse A and another staff member attended the in-service the following week and it was
not raised as an issue again. However, OPH1 management and the ONA could not agree on a
settlement for grievance #5, which was scheduled for arbitration in February 1999.
Viewing management's requests for care plans and charting as a set-up, Nurse A decided
to "leave it alone, and just continue doing my work" (personal communication, 1998). However,
a meeting between Nurse A and her supervisors to review her work was scheduled for November
18. Having been told by management that she could not bring her ONA rep, and not having
done the care plans/charting, Nurse A, who was not scheduled to work the night of November
18, 1997, "knew they were going to harass me.” She chose not to attend this meeting that had
been scheduled unilaterally. Her Unit Manager then phoned Nurse A at home to notify her that
she was suspended from work without pay until management "received a report from COSTI
(Catholic Organizations and Services to Immigrants – an agency that provides counselling and
other social services to immigrants) related to your ability to cope with the requirements of your
position.” This demand served to validate Nurse A's perception that what her Unit Manager and
the other two administrative staff were trying to do to her by wrongly accusing her of having a
communication problem and sub-standard documentation, by referring her to scrutiny by an
organization that serves immigrants, was to demean her and break her down psychologically.
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
74
The suspension and events leading up to November 18th, 1997 prompted Nurse A to file
her first complaint on November 25th to the OHRC about racial discrimination at OPH1, which
was eventually shunted back to the union. However, on December 1, following the suspension,
she also filed union grievance #6 requesting that any mention of this suspension be removed
from her file. Management denied this request, stating that it was filed beyond the filing date
limit. The DOC then told the ONA rep to advise Nurse A to get a note from her physician
saying she was fit to work and to tell Nurse A that if she failed to bring the note in on a specific
date and time, she would be terminated. Nurse A questioned the logic of this advice – she had
been off work because of suspension, not because she was sick – but she did get a note from her
physician stating that she was fit to work. On December 11, seventeen days after being
suspended, Nurse A returned to work, even though she did not feel safe to do so.
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
75
Benchmarks 2 and 3 – The need for recognition that they have been wronged and the need for safety Even prior to the three consecutive mornings when Nurse A's manager and two other
supervisors went after her in an isolated room when Nurse A was without support, the
work environment at OPH1 had not been one where racialized staff were granted
recognition that they had been wronged so they could resume feeling safe, nor was it
one where racialized staff were assured the community would do all it can to prevent
repetition. By requiring that Nurse A produce ten charts and ten care plans in each of
the following three months for their inspection, management set her up for duties that
had the appearance of rational care planning but were in fact make-work tasks in the
idiom of punishment for disobedience. On top of responsibility for delivering care to
120 residents each night, this was felt as an unreasonable demand, and perhaps unsafe.
But Nurse A herself had started to feel unsafe.
In interview, Nurse A said: "A lot of black nurses who are who are (whispering)
have low self-esteem. Everything is grinding down…down – they've lost a lot. Its
been taken away from them and they don't know which way to turn” (2002).
Grievance #7, which Nurse A filed in January 1998, was the first that cited
"discrimination" as an aspect of the conflict between Nurse A and OPH1 management. On her
behalf, the union requested that the employer cease discriminating against Nurse A, remove any
mention of the suspensions from her file and compensate her for damages.
About this time, Nurse A's doctor referred her to a psychiatrist, who wrote a note
attesting that she was fit to work. In March 1998 Nurse A filed a second complaint to OHRC
charging OPH1 with racial discrimination and harassment. In June, Nurse A found it necessary
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
76
to file grievance #8 requesting that "the employer cease making libelous statements re: her role
in a medication incident and her role replacing sick staff."
In July 1998, the DOC was fired and for the next several months the facility was run by
the Unit Managers, some of whom were not nurses. During this period, management falsely
blamed Nurse A for a number of administrative problems, such as not covering for staff who
cancelled shifts and wrongly purging charts. Citing administrative errors which they said were
Nurse A's fault, management wrote a letter notifying Nurse A that she would be suspended for
four days at the end of the month and threatening her with termination if these problems
continued (personal documents, October 20, 1998).
In response to this letter, Nurse A filed two grievances on November 4, 1998 – grievance
#9 requested that references to her suspensions be removed from her file; grievance #10
requested that [OPH1] cease making libelous statements and compensate her for her damaged
emotional and physical state. Nurse A again consulted the psychiatrist in November 1998. A
few days before Christmas, management placed a letter of warning in Nurse A's file concerning
her handling of a clinical situation.
Other OPH1 staff members were experiencing workplace stress during this period. A
white ethnic LPN whom Nurse A supervised had had a nervous breakdown. When the LPN
returned to work after a six-weeks paid leave she was not well enough to work. Nurse A wrote a
letter to alert management to the situation, despite the fact that at the time she herself was
experiencing a great deal of stress from management's harassment:
I think it is time that you should be more aware and involved in [names LPN]'s problem, in order that her health would improve and not continue to deteriorate. The state of her health is affecting her ability to perform her job. At this time, I think she is using distorted reality to solve her problems that will certainly make them escalate. The truth is, it is obvious that she is unable to help herself. Please look into this (Letter to Unit Manager from Nurse A, personal files, December 17, 1998).
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
77
In January 1999, management suspended Nurse A for four days without pay, wrongly
accusing her of not covering for a staff member who cancelled a shift, thus "compromising
resident care and safety," of failing to submit ten care plans, and other matters. Nurse A filed
grievance #11 in response requesting that all references to her suspensions (now totaling twenty-
six days) be removed from her files. This grievance was denied by OPH1 management and
grievances #9 and #10 remained outstanding.
In February, management informed Nurse A that her employment at OPH1 was
“terminated.” Nurse A filed grievance #12, stating that OPH1 management had terminated her
without just cause. The ONA then entered into negotiations with OPH1's management and
suggested that an independent mediator (Mediator A) be brought in to investigate the situation
and work out a settlement. Since the ONA had not been effective in deescalating the conflict
that resulted in Nurse A's "termination," Nurse A was skeptical that a mediator brought in by
ONA would genuinely represent her interests. She therefore hired her own mediator (Mediator
B), who entered into communication with the ONA and OPH1 management on her behalf.
About ten days after her "termination," Nurse A's former manager, who was not a nurse,
wrote a letter of complaint to the College of Nurses of Ontario (CNO) about Nurse A citing
eleven incidents. In the twenty years of Nurse A's work life in Toronto, this was the first time an
employer had complained about her nursing practice to the CNO. In her letter to the CNO, this
manager cited an incident that had taken place in September 1996 and been settled with the
condition that any correspondence relating to the incident be removed from Nurse A's file.
Nurse A filed grievance #13 to protest this former manager's unfair complaint to the CNO.
This former manager had neglected to inform her boss, the OPH1 administrator, that she
had written a letter of complaint to the CNO about Nurse A. When OPH1's administrator
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
78
became aware of the existence of this letter, he immediately wrote the College stating that OPH1
did not wish to register a complaint about Nurse A. He did not want the letter of complaint to
the CNO to complicate settlement negotiations between OPH1, Nurse A, and the ONA.
Early in April 1999, Mediator A negotiated a settlement between Nurse A and OPH1.
Two of Nurse A's Black colleagues, each of whom wrote a letter to the CNO in support of Nurse
A and one of whom had received a settlement from the OHRC, were present at one of the
meetings leading up to the settlement to give Nurse A support. The Minutes of Settlement
instructed that: (1) OPH1 pay a substantial sum of money to Nurse A as compensation for the
years of racial harassment and discrimination she had endured; (2) Nurse A's "termination" be
rescinded and that Nurse A resign; (3) OPH1's administration remove any records pertaining to
Nurse A's "termination" from her file; and (4) OPH1 provide references for Nurse A. In early
April 1999, Nurse A submitted her letter of resignation to OPH1.
Benchmark 4 – Restitution through healing processes that balance relationships and prevent further harm There is no evidence that OPH1 management ever investigated systemic discrimination in the
facility or that there was ever any self-reflection or self-examination on the part of management
regarding the way in which Nurse A became problematized. No investigation has been made by
an outside body of conditions, including management practices, at OPH1.
The settlement and OPH1's administrator's letter to the CNO put the College of Nurses in
an awkward position. Instead of refusing to investigate the complaint, however, they chose to go
ahead, adopting unusual procedures by instructing the College's Executive Committee, which
does not have a mandate to discipline, since it is the Complaints' Committee that normally
carries out investigations. Note that all members of both committees are white.
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
79
The ONA hired a well-known labour lawyer to represent Nurse A before the CNO. This
lawyer convinced the investigating committee to drop nine of the eleven incidents since they did
not relate to Nurse A's clinical practice but were rather expressions of management's
problematization of, discrimination toward, and harassment of Nurse A. Nurse A retained her
registration to practice nursing. However, the College wrote Nurse A a letter requesting that she
"reflect" upon her practice with respect to the two remaining incidents.
Nurse A appreciated the positive results her lawyer had gotten for her from the College's
Executive Committee. Nurse A's view, however, was that the fault lay with OPH1 management
and she felt strongly that the College should have investigated OPH1's organizational practices,
especially racialization of staff and the effect of racialization on patient care. Why should she be
reprimanded and OPH1 elude censure and be free to perpetrate further harm? Disheartened by
the fact that the College had not investigated practices at OPH1, Nurse A filed a third complaint
with the OHRC in December, in which she stated: "What was done to me at [OPH1] I consider
tantamount to lynching".
CEHS Benchmark – Lack of Accountability for breaching the grievance process OPH1 never admitted wrongdoing, even after they breached the Minutes of Settlement by
supplying erroneous information about Nurse A to potential employers who asked for
references. Nor did the CNO give any recognition to Nurse A that she had been wronged and
that OPH1's management practices made working conditions problematic with potentially
unsafe consequence for the residents under care.
The April 1999 Minutes of Settlement of the grievance between OPH1 and Nurse A
instructed OPH1 to inform potential employers to whom Nurse A had applied for jobs that Nurse
A had been employed as a RN at OPH1 between a certain date in 1990 and a certain date in
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
80
1999, and that she had performed her duties competently. Nurse A applied for and went to
several job interviews. When she did not get a job, she began to suspect that OPH1 was not
adhering to the terms of the settlement with respect to providing her reference. Nurse A
therefore asked a prospective employer what information they had been given about her by
OPH1 and learned that there was a discrepancy between the date she had given the employer as
her last day of employment and that given by OPH1. Aggrieved greatly by this "error," Nurse A
filed her fourteenth grievance against OPH1. The ONA put off meeting with her to discuss this
problem.
Shortly after Nurse A made a submission to the Ontario Labour Relations Board attesting
that the "ONA did not represent the applicant in a timely way" (No date, Form B 29, OLRB), the
ONA representatives agreed to meet with Nurse A. At this meeting, which took place a few days
before the scheduled OLRB hearing, the ONA agreed to set an arbitration date for grievance #14
(OPH1's breach of the Minutes of Settlement). Because Nurse A now had the hearing date she
requested, she withdrew her application to the OLRB. Less than twenty-four hours before the
scheduled arbitration hearing, the ONA Employment Relations Officer (ERO) phoned Nurse A
from an administrative office at OPH1 and informed her that a settlement had been reached, that
the hearing was cancelled. She told Nurse A that she would receive a letter by courier the next
day formally notifying her of these developments but this letter did not arrive until the very hour
of the day the hearing was scheduled. Lacking formal notification that the hearing was
cancelled, Nurse A went to the arbitration building where she was informed of the cancellation.
The ONA's handling of this matter reconfirmed Nurse A's belief that the union, just like the
employer, was unfettered by accountability for fair grievance proceedings.
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
81
In the spring of 2000, Nurse A got a part-time job working nights at a nursing home
(OPH4) where management's bigotry toward staff made working conditions difficult. Short-
staffing necessitated that Nurse A put in an extra hour to complete her tasks each morning.
Nurse A's contract stipulated that she would receive a pay increase following successful
completion of a three-month probationary period. The increase was not forthcoming after the
three-month period, so Nurse A wrote management requesting the pay increase as well as
payment for the extra hours she routinely put in. About this time, a CUPE union steward (who
was a nurses' aid) hand-delivered a letter to Nurse A that contained erroneous information about
Nurse A's attendance record and requested that her to "improve" her attendance (October 12,
2000). Nurse A corrected the false information and requested that the letter be removed from her
file. On November 1, two young women who worked in the administrative office delivered an
envelope to Nurse A that contained a bonus check for $500 made out in her name. Nurse A was
given no explanation about why she had been given this check and Nurse A's letter to the
administration requesting monies owed was never answered.
In December, Nurse A fell on ice outside her home and sustained a lower-arm bone
(Colles) fracture. She immediately notified her employer that she would be unable to work and
requested a record of employment so that she could apply to Human Resources Development
Canada (HRDC) for medical unemployment insurance. When the accounting office of OPH4
failed to give her a record of employment after several requests, Nurse A contacted the
corporation's main office. A few days later she received the form. In early February 2001,
Nurse A got a letter from HRDC informing her that their records showed she had not declared
earnings for hours she had worked in January. Astounded, Nurse A checked her bank account,
which showed an unexpected surplus of $500. Investigating further, Nurse A learned that though
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
82
she had not been working, money had been deposited in her bank account by her employer
because her time card at OPH4 had been punched the weekend of January 7, 8, 9. Was this
transpiring because of her demand that she be paid for overtime hours, or was it an innocent
error? Nurse A wrote a letter about the matter to OPH4's administrator and again contacted a
Senior Regional Director at the corporation's head office. Initially, the administrator responsible
for OPH4 told Nurse A that what happened was "an innocent error on the part of the Office
Manager controlling the payroll entry" (Letter from OPH4 administrator to Nurse A, March 12,
2001). Nurse A met with the Senior Regional Director at his invitation at the Corporate Head
Office. Following their meeting, Nurse A received an apology about the matter from OPH4's
administrator. The corporation has since closed OPH4.
After signing the settlement agreement with OPH1, in an effort to call attention to the
problem of racial discrimination in nursing homes and its impact on the delivery of quality care,
Nurse A undertook a letter-writing campaign. She wrote nursing leaders at ONA and the CNO,
the Law Society of Upper Canada, and the President of OPH1's Board of Governors about
conditions at OPH1. In her letter to this latter individual, a nurse, Nurse A stated:
Management premeditatedly embarked on a campaign of personal destruction against workers of colour. A mission statement, standards of employee conduct, Quality Assurance program, means nothing to management (June 2000).
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
83
Benchmark 5 – Significance or meaning Nurse A undertook a letter writing campaign because of her strong belief that
individuals and institutions that discriminate on the basis of race (and other attributes)
should be made accountable. In a letter to the then head of the CNO (Ontario College
of Nurses), Nurse A wrote that racial discrimination impedes delivery of quality care:
Management create[s] many ethical dilemmas, causing working conditions to be unsafe frequently…On many occasions their behavior has caused professional services to be somewhat discontinued or poorly applied. Health and safety are quite often compromised. If this makes it unsafe for nurses, then it is unsafe for clients…I will continue to find the inner strength for justice. I am both a citizen and provider of high quality care. Should I be an advocate for the people I care for? I should be able to function without fear of reprisals. No nurse should be robbed of her right to pride of workmanship (April 2000).
Nurse A has undertaken the painful process of seeking meaning and closure with
respect to what she has experienced by making her story available to the public through
this research report. Nurse A's prayer is that inclusion of her case in this report will
contribute to bringing about a national racial equality and employment equity
accountability program that meets the needs of all nurses. Creation of equity assurance
monitoring procedures under the Health Council of Canada would bring about healing
and closure for Nurse A.
Nurse A has not returned to work since sustaining her Colles fracture. She feels that she
will never again be able to work as a nurse.
Discussion Nurse A experienced racial discrimination in every health care delivery facility at which she
worked past the probationary period. Nurses who have experienced racial discrimination at
work, or have witnessed the effects of such discrimination on colleagues, are calling for the
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
84
creation of an equity assurance policy to ensure that the work environment for nurses, and
therefore for patients, is caring rather than poisoned.
In work settings where racism is an everyday practice, everyone has the choice to: (1)
perpetuate out of balance relationships that impact negatively on racialized individuals and
groups, or (2) promote equal opportunities and freedom of choice for all. Issues of competence
and responsibility are treated in the context of power relations in health delivery settings. For
this reason, it is difficult to separate race relations from power relations. Present structures for
dealing with racial conflict are inadequate because those who name racism risk triggering
reprisals and backlash.
In theory, hierarchies (the pecking order) remain intact because of discourses of
domination that systematically disadvantage on an in-group/out-group basis. As long as the
accountability is ineffective, the offender will repeat. Current procedures do not provide those
offended with equal opportunity for being heard in grievance proceedings. One of the benefits
accountability policies – equity assurance – can provide in terms of power relations, is that all
players can voice their concerns without reprisals.
Following her encounters with the three white supervisors who threatened her and
accused her of "insubordination" in July 1997, Nurse A sometimes "forgets" her words, finds it
difficult to sleep, and suffers from anxiety attacks whose severity sometimes prevent her from
driving her car. She says that "these women have destroyed me" and she is engaging in a
difficult daily struggle to regain her physical, emotional, and financial stability. The lengthy
conflict between Nurse A and OPH1 management did not result in balancing the relationship
between Nurse A and her employer. Rather, the conflict has made a profound impact on Nurse
A's physical, emotional, and financial well-being. Moreover, her case ripples out rancor to
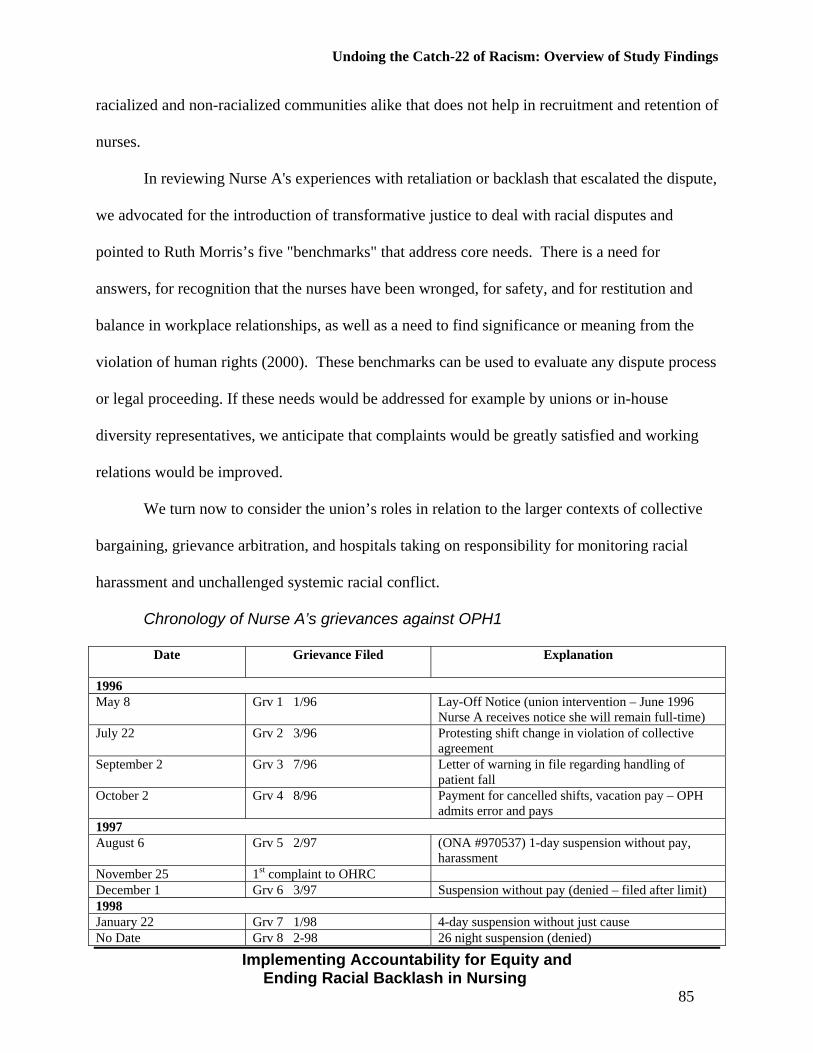
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
85
racialized and non-racialized communities alike that does not help in recruitment and retention of
nurses.
In reviewing Nurse A's experiences with retaliation or backlash that escalated the dispute,
we advocated for the introduction of transformative justice to deal with racial disputes and
pointed to Ruth Morris’s five "benchmarks" that address core needs. There is a need for
answers, for recognition that the nurses have been wronged, for safety, and for restitution and
balance in workplace relationships, as well as a need to find significance or meaning from the
violation of human rights (2000). These benchmarks can be used to evaluate any dispute process
or legal proceeding. If these needs would be addressed for example by unions or in-house
diversity representatives, we anticipate that complaints would be greatly satisfied and working
relations would be improved.
We turn now to consider the union’s roles in relation to the larger contexts of collective
bargaining, grievance arbitration, and hospitals taking on responsibility for monitoring racial
harassment and unchallenged systemic racial conflict.
Chronology of Nurse A’s grievances against OPH1
Date Grievance Filed Explanation
1996 May 8 Grv 1 1/96 Lay-Off Notice (union intervention – June 1996
Nurse A receives notice she will remain full-time) July 22 Grv 2 3/96 Protesting shift change in violation of collective
agreement September 2 Grv 3 7/96 Letter of warning in file regarding handling of
patient fall October 2 Grv 4 8/96 Payment for cancelled shifts, vacation pay – OPH
admits error and pays 1997 August 6 Grv 5 2/97 (ONA #970537) 1-day suspension without pay,
harassment November 25 1st complaint to OHRC December 1 Grv 6 3/97 Suspension without pay (denied – filed after limit) 1998 January 22 Grv 7 1/98 4-day suspension without just cause No Date Grv 8 2-98 26 night suspension (denied)
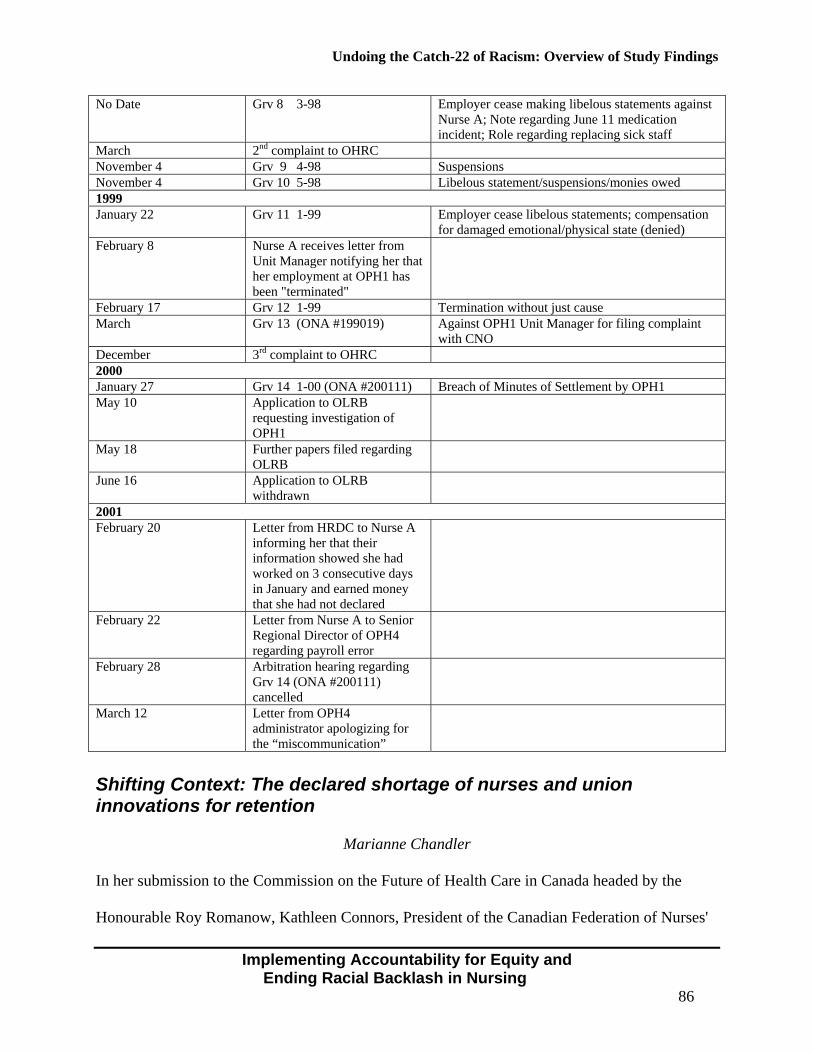
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
86
No Date
Grv 8 3-98 Employer cease making libelous statements against Nurse A; Note regarding June 11 medication incident; Role regarding replacing sick staff
March 2nd complaint to OHRC November 4 Grv 9 4-98 Suspensions November 4 Grv 10 5-98 Libelous statement/suspensions/monies owed 1999 January 22 Grv 11 1-99 Employer cease libelous statements; compensation
for damaged emotional/physical state (denied) February 8 Nurse A receives letter from
Unit Manager notifying her that her employment at OPH1 has been "terminated"
February 17 Grv 12 1-99 Termination without just cause March Grv 13 (ONA #199019) Against OPH1 Unit Manager for filing complaint
with CNO December 3rd complaint to OHRC 2000 January 27 Grv 14 1-00 (ONA #200111) Breach of Minutes of Settlement by OPH1 May 10 Application to OLRB
requesting investigation of OPH1
May 18 Further papers filed regarding OLRB
June 16 Application to OLRB withdrawn
2001 February 20 Letter from HRDC to Nurse A
informing her that their information showed she had worked on 3 consecutive days in January and earned money that she had not declared
February 22 Letter from Nurse A to Senior Regional Director of OPH4 regarding payroll error
February 28 Arbitration hearing regarding Grv 14 (ONA #200111) cancelled
March 12 Letter from OPH4 administrator apologizing for the “miscommunication”
Shifting Context: The declared shortage of nurses and union innovations for retention
Marianne Chandler
In her submission to the Commission on the Future of Health Care in Canada headed by the
Honourable Roy Romanow, Kathleen Connors, President of the Canadian Federation of Nurses'
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
87
Unions stated: "Canada...(is) experiencing a nursing shortage that, if not addressed quickly, will
become a nursing crisis by the decade's end. Canada is short about 20,000 nurses right now but
this will be five times worse by the end of the decade" (2001, p. 4).
In other words, Canada will be short some 113,000 nurses by the year 2011, unless
measures are taken to both retain and attract nurses. As of 2001, there were 252,913 nurses
employed in Canada in hospitals, public health agencies, homes for the aged, nursing homes,
industry and nursing agencies, and so on. Unions represent the majority of the nurses employed
in Ontario – 88,013 in 2001 – with the majority of those nurses represented by the ONA.
The history of central collective bargaining for nurses in Ontario has not always been a
happy one. Collective Agreements are rarely freely negotiated; arbitrated decisions leave a sense
of anger, concern, and low morale for nurses. With more and more cost-cutting measures being
implemented in health care settings across Ontario, there appeared to be little interest on the part
of the employers to agree to Quality of Work Life language in collective agreements. The
implementation of anti-racism, anti-harassment, and anti-discrimination policies and programs
did not appear to rate as essential to the workplace. Training for management on the
investigation of racism or harassment complaints in the workplace was not seen as a priority.
Employee surveys and exit interviews indicated that racialized nurses cited the following
issues and concerns:
• No opportunity for progression up the "career ladders;"
• Differential treatment and being "earmarked" for more severe and unfair levels of work
assignments and discipline than were non-racialized nurses; and
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
88
• Speaking out in support of a colleague who had experienced unfair treatment because of
race proves to be a "career limiting move or CLM" (backlash).
From the early 1990s, hospitals continued in denial of the issues facing nurses in the
workplace; absenteeism increased to alarming figures as nurses attempted to survive in the
‘trenches’. Employee Assistance Programs (EAPs) were introduced, but were only seen as band-
aid solutions. Employee Satisfaction Surveys attempted to identify negative treatment issues in
the workplace in early 2000. Results of these surveys were rarely acted upon as clinical and
administrative managers struggled with greater workloads and reduced budgets. Quality of Life
Programs for patients were implemented, but issues of racism directed by patients towards
nurses were considered to be ‘trivial’ in nature and ‘par for the course’ if one worked in a
healthcare institution.
Nurses were losing interest and becoming cynical about any improvement in workplace
conditions. The root cause for the increased sickness and absenteeism was neither identified nor
addressed.
Mergers and hospital takeovers added a new negative dimension to workplace
relationships. The new hospital corporate culture was dominated by the organizational culture of
the most powerful member of the newly formed corporation. Supportive voices were stifled or
exited the healthcare sector.
The labour relations environment became more hostile as unions struggled to survive in
the restructured healthcare environment. Dealing with the malignancies of racism, harassment,
and discrimination became a secondary focus for unions. Membership declined for certain
unions at the same time that costs for mediation and arbitration under collective agreements were
skyrocketing. Private sector unions now obtained a foothold in healthcare and changed the face
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
89
of relationships between employers and unions. Survival in this new healthcare environment
became the goal of several unions who traditionally represented healthcare workers.
Changes also occurred in the area of grievance arbitrations. Arbitrators were now finding
themselves faced with complex situations which would have been unimaginable twenty years
before. Arbitrators became "social engineers" (Swan, 1996). They required distinct skills in "the
contract-shaping function, the interpretative function and the public policy or community
conscience function" (Nolan and Abrams, 1985, p. 873). As Kenneth Swan writes:
[T]o whatever extent arbitrators are to play a greater role in the administration of human rights, they will need to develop increased sensitivity to the issues and a better understanding of the remedial tools that are available and appropriate. Unfortunately there is no mechanism for delivering continuing education to arbitrators unless they do it themselves, through their professional organizations. At this point in the development of arbitral authority, those organizations should be giving serious consideration to educating the profession in issues of systemic discrimination and equality rights, and in the social context in which arbitration decisions must be made, in much the same way as similar efforts have begun for members of the judiciary (Swan, 1996, non-paginated presentation). Swan also states “that for employees covered by a collective agreement,” arbitration is
now virtually the “supermarket of employment justice – one-stop shopping for legal remedies for
all complaints” (non-paginated presentation).
It is within this context that the ONA has negotiated innovative structures with selected
employers that were on their censure list for poor compliance with human rights legislation. One
hospital has a diversity practitioner who is a social worker by profession who, at arm’s length
hears, complaints of harassment and arranges contractual agreements between complainant and
employer. Her role also has a preventive focus aimed at changing the hospital culture through
special events that celebrate diversity and infuse the internal hospital media with inclusive
images. Another larger hospital has set up a workplace diversity unit with a lawyer and staff.
Initially, this unit was located next door to Human Resources, but has since moved to a nearby
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
90
off-site location. This hospital has been on ONA’s censure list for ten years. With the help of a
cooperative CEO, the workplace diversity unit is being utilized to deal with complaints and to
work on clearing the backlog of 400 cases that had accumulated by the time it was implemented
four years ago. The unit has also been involved in developing new policies and negotiation
methods as well as various programs intended to work toward prevention of ongoing
marginalization practices among staff.
It is important to note that at least one major hospital is treating language as a factor in
the reduction of potential risk to patients (Mohamed, 2002) and a pathway to improved patient
safety and satisfaction as well as employee satisfaction.
Before applauding these new developments, it is important to recognize that the
underfunding of the OHRC and the rescinding of employment equity legislation have shifted the
financial drain owing to racial discrimination in health care workplaces from other jurisdictions
directly onto the budgets competing for health care dollars. CEHS is calling for research that
evaluates the extent to which proactive programs that effectively address racial profiling of
nurses may contribute to retention and future recruitment of nurses from diverse communities.
However, the health of nurses related to their workplace experiences will also have to be
addressed. Next, we briefly outline some health effects reported by nurses filing grievances or
complaints of racism.
Health Outcomes of the Complainant in a Racial Dispute
Ruth Lee, Rebecca Hagey, and Jane Turrittin
Social psychologists Dion and colleagues (1975, 1978, 1996) provide evidence that anxiety in
varying degrees is linked to the perception of discrimination. In a culture that invalidates the
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
91
appropriateness of accountability for discriminatory practices, one would predict anxiety to be
exacerbated when the social means for eliminating the source of the anxiety is blocked.
Restoration to a non-anxious state would be impeded. Backlash being unrestrained would
escalate and prolong anxiety and produce negative health effects over time.
The following excerpts are as yet unpublished data from a CERIS-funded qualitative
study of nine nurses who grieved through their union or complained to the Ontario Human
Rights Commission against their employer on grounds of racial discrimination (Collins et al.,
1998). To maintain confidentiality for the nurses and their employers, identifying markers have
been removed. The nurses came from seven different countries, representing the current
diversity in the Toronto area.
Their experiences included physical, emotional, spiritual, and financial challenges to their
health. Grievances can consume an unforgivable expenditure of time, energy, and money, and
can lead to the loss of home, car, neighborhood, spouse, and dreams. We have identified themes
related to the emotional pain and somatic trauma that comprise the lived experience of objecting
to racial discrimination. In all cases, escalation of conflict accompanied naming the problem as
racism.
Traumas Experienced While Objecting to Racial Discrimination
1. Feelings of exclusion, loss of belonging
"Stressful knowing that you are...on the outside; stressful knowing that they don't want you there.
I really miss the belonging where I could call I belong to X hospital; this is my home (hushed
voice).”
2. Feeling humiliated, contained
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
92
“The final taking away the…the job from…from me was so humiliating…I sort of felt boxed in a
corner and I really didn't have anyone to speak to how to get out of this. Humiliation...It is [an]
unbearable experience that I have. It really affects my health, affects my marriage (crying)…It
was the worst I ever had in my entire life.”
3. Intimidation, paranoia, isolation
“I felt...I don't know if it’s paranoia, but I felt that people were out to get me…People weren't
being fair with me. I felt like an easy walking target…intimidat[ion]...I felt isolated.”
4. Loss of confidence and grief
“My worst fears had come true…I just picked up a message and, you know, that
...premonition...and as soon as I listened to this morning, I figure, Oh my God, today is the
day…I had lost all confidence and all self-esteem…all day I cried…I just was so devastated
about the whole thing…grief” (about losing her job).
5. Depression, loss of focus, and memory loss
“It took me about 8 months to recover enough...I had gone through a major memory loss, my
depression had caught me. I couldn't study. I just stayed enclosed in my bedroom for months...”
6. Distressing physical symptoms
“I went into shock before I could even get to my car. I just started shaking...I never stopped
shaking for days, days...it was like a dagger...I could feel the pain in my heart...within a month I
became very sick. I went into a...state of shock. I just crashed. I got dizzy and [would] be
vomiting at four o'clock in the morning. Low energy and extreme fatigue. It was such an effort to
start a new day I was sick. I was vomiting. I was shaky...I was devastated. Pains in my
chest...pseudo-heart attack... My blood pressure went up to 180.”
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
93
7. Death images
“I would pray that at least if I would die in my sleep, I wouldn't wake up. Each step I took, my
feet were heavier and heavier as if I was walking before the firing squad. I was so distraught – I
thought I was going to die.”
8. Sensations challenging integrity and wholeness
“I felt as if I was being invaded. I feel that my life has been tattered…that I'm not being
supported by my union...things that I found very easy for me to do before…I've just been
drained.”
9. Positive awareness
“At the time, I thought about [being documented] in terms of being a hard-boiled egg; the longer
you boil it, the harder it becomes.”
10. Less than optimal health basis for professional work
“I took time off work; the doctor gave it to me – stress leave. I was tensed, you know. I couldn't
do my job. When I look back, my brain probably was functioning at half a level. I was stressed. I
did a stress test after the fact...you know, they make you go back and I had 59 per cent; now it's
nine.”
11.Long-term effects
“It is a psycho-physiological...aspect to it...when you go under stress for almost 5, 6 years, my
serotonin is very depleted. Today, sometimes I'm speaking and I can't speak. I lose my words; I
forget things, which is not at all like me.”
As reported elsewhere (Hagey et al., 2001a), the nurses who shared these effects on their
health were able to turn their trauma into community contributions. They had the conviction that
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
94
what they were doing was so that, in the future, nurses would not have to go through the same
ordeals, thus they continue to push for recommendations.
Summation of Evidence Our presentation of evidence was composed of: (1) a pilot survey on the effects of race, colour,
or ethnicity (i.e. racial profiling of nurses); 2) a description of set-up as a group-based practice
that targets racialized nurses during under-funding and cutbacks, so members of the dominant
groups can take unfair advantage during job transfer and job loss; (3) a case study and analysis of
how a racialized nurse encountered barriers to accountability involving irregularities of the
complaint process so that the proceedings fell far short of the ideals of transformative justice; (4)
a brief overview of unions' roles with respect to human rights protections in the employment of
nurses required for the future of nursing; and (5) an account of negative health effects
experienced by nurses who had charged their employers with racism.
The evidence we presented suggests that employers, employees, professional
organizations, and unions have reason to commit to a coordinated plan of accountability for
equity or an equity assurance program. Without any feasible recourse when nurses experience
racial profiling, set-up, backlash, and health effects, the participants in this study believed that
there is a generalized fear of backlash that prevents more nurses from complaining or pressing
forward with the normal accountability strategies expected in collaborative working
relationships. That is, the ever-present threat of racial backlash makes racialized nurses subject
to disconnection and exclusion in relations in nursing work that presents a potential threat to
patient safety. We turn now to explore issues associated with developing and integrating
accountability policies and practices in nursing.
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
95
Chapter 3 – Accountability Informed by Transformative
Justice: Discussion and recommendations
Rebecca Hagey and Monica Purdy
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
96
Review and Introduction One objective of this study was to conduct participatory action research (PAR) with voluntary
associations of nurses to explore the feasibility of instituting equity assurance programs aimed at
establishing accountability for racial equality and employment equity at all levels and in all
sectors in nursing. In keeping with PAR methodology, we identified evidence, and the
participants themselves shaped what is presented.
As our action research gained momentum, participants recognized that an equity
assurance program is feasible if – and only if – those who need it make it happen. A vision of a
Canada-wide program emerged that would use lobbying, negotiation, and political action
informed by research to hold all nurses and their employers accountable for systemic
discrimination in their organizations. To these ends, the Centre for Equity in Health and Society
(CEHS) became formalized as a research and advocacy organization.
For CEHS and others interested in equity, we believe that a widespread collaboration on
changing discourse is necessary to develop and implement policy. Our thesis is that all
stakeholders will need to change discourse strategies if accountability for racial discrimination
is to become a shared value. We used discourse strategies in this study to promote
accountability for equal access and participation targeting (a) political discourse; (b) the
locations of discourse; (c) discourse strategies in and between organizations; (d) policy
regulators of discourse; (e) personal discourse; (f) discourse outcomes; and (g) research
discourse. The theoretical development of our questions pertaining to purposeful discourse
change will be addressed in future submissions to scholarly journals.
Answers to our research questions have emerged from the evidence presented in the
previous chapter:
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
97
1. Set-up and backlash are key manifestations of poor accountability procedures that are in
place to respond to racial dominance.
2. The organized practices that are associated with set-up and backlash are manifestations of
institutionalized racism – unchallenged discourse of racial dominance.
3. When racism is an issue among nurses, the process for addressing and resolving issues is
problematic.
4. Violations of the grievance process in racial disputes further subject the complainant to
racial dominance.
In light of these findings that argue for better accountability, we first consider issues
about defining accountability in the context of achieving equity through transformative justice
and providing definitions of institutionalized racism, racial encounters, and systemic racism. We
briefly consider the political landscape that currently condones discourses that effect racial
dominance. In this discourse milieu, we point out that there are fundamentally conflicting
convictions about how accountability for racial discrimination should be organized. We then
outline some benefits accountability would have on social relationships and advocate for anti-
racism as a relational perspective to be operationalized by the CEHS network. We briefly
summarize some anti-racism findings that will need conscious attention by health care leaders
intent on implementing accountability for equity.
We then we provide some policy and legislative recommendations submitted by diverse
sectors of the CEHS network. We include our recommendation to the Health Council of Canada
to function as one national accountability structure for regulating not only equal access to
universal health care but also for monitoring employment equity in health care because the latter
can impact on both patient and employee health and safety. Finally, we briefly summarize the
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
98
study and invite researchers and colleagues to embark on participatory action research to see the
recommendations implemented and to use and hear the language in our glossary of definitions.
The Vision of Transformative Justice Transformative justice is a new approach advocated for dispute resolution in the civil justice
system, derived from the introduction of restorative justice – mediation, negotiation, settlement,
compensation, reparation – in the criminal system: “Transformative justice is a way of handling
conflict that recognizes and responds to the variety of harms caused by conflict …..and responds
….by bringing individuals together in a process that encourages healing and growth (Law
Commission of Canada, 1999, p. 43).
Restorative justice advocates a number of requirements. Those we have selected include:
(1) the complainant, respondent, and community being involved in a consensus building process;
(2) the inquiry process providing an opportunity for the person(s) involved in a breach to take
responsibility for the rupture in relationships; (3) the complainant, respondent, and community
identifying what standards are appropriate and how the breach will be compensated and
standards maintained; and (4) decisions about restoring parties to the community are made with
respect to the parties and their circumstances and ethical standards (Law Commission of Canada,
1999). All parties in conflict are assumed to have historical realities and ideologies that inform
their conflicting perspectives.
Our mission in this report, therefore, is to advocate for the normalizing of relationships
through garnering a collective commitment to problem-solving around systemic racism, which is
chronically conflictual. We wish to motivate all nurses to rectify institutionalized racism by
organizing and implementing multiple layers of accountability, including personal self-
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
99
reflections and committee-based corrections, to organizational media, events, and reports that are
responsive to critique and feedback. Through relationships that collaboratively address
employment equity practices (see A Time for Change, Appendix F), we can correct racial
disparities, so that when racial disputes arise, they will be far more constructively handled than
reports from our participants would indicate. We can institute accountability for equal access
and participation in our profession. We can change the discourses of racial dominance to the
discourses of healthy collaboration.
Defining Accountability in the Context of Equity: What is institutionalized racism? Systemic racism? A racial encounter? According to the Canadian Oxford Dictionary (Barber, 1998), the term “accountability” first
appeared in the 1700s and referred to the idea that the state should be accountable to the people.
Slavery was widespread during this era, so what is hidden in the dictionary examples of
accountability is that racial status is a condition for the right of people to require answers and
remedies concerning their governance. Britain lost its American colony for not being responsive
or responsible to the colonized European people. France followed with a revolution too and,
under Napoleon Bonaparte, instituted centralized powers that became the template for the weak
notion of accountability in modern state structures. Following the U.S. civil war, the term
accountability became associated with corporate business concerns about profit, gain, or loss.
Accountability to the bottom line has become the popular meaning of the term.
Organizations understand accountability to be a process through which a person is
responsible to a designated group or body for his or her actions. This may involve reporting
relationships and roles of designated parties because everyone cannot be reporting to everyone
else all the time. Typically those lower in a hierarchy are more accountable to higher ups than
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
100
vice versa. The presence of unions as parallel administrative structures is an organized attempt
to provide protection for those in lower positions of influence. In the discipline of ethics,
accountability is a type of procedural justice along with transparency (Hagey et al., 2001a).
One accountability problem associated with racial discrimination in nursing is that in-
group advantages and out-group losses are not made transparent owing to in-group power over
research. But the larger problem, we argue, is that accountability is missing in race relations, and
when disadvantaged parties try to introduce it, denial, resistance, reprisals, righteous indignation,
and so on, surface. Transparency and accountability are not on the agenda, and an inordinate
amount of monitoring and petitioning is required to get attention paid to equal rights supposedly
guaranteed by the state.
To remedy this, we are introducing a definition of accountability, informed by
transformative justice, that values relationship. Accountability can be seen as a feature of
relationship that holds individuals, groups, or offices responsible according to principles or
criteria befitting the relationship, for example, transparent communication, fairness, and
trustworthiness.
We are defining racism as an ideology built on the concept of race that is fundamentally a
relationship problem of accountability. Racism has different manifestations at individual levels
and between offices within organizations. We define race and racialized people accordingly in
this perspective that shows how accountability can address racism.
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
101
Race A set of assumptions used in discrimination, creating racialized and non-racialized peoples.
Assumptions of race make a connection between European derived signifiers of race, such as
skin colour or heritage, so that accountability is not owed to the racialized person(s).
Racialized People People who experience social inequalities because of their race, colour, or ethnicity.
Manifestations of racism, such as racialized encounters, institutional racism, and systemic
racism, can be remedied, we argue, by participants engaging in accountability that is race
conscious and equity driven.
Where individuals in an organization can be exposed to racialized encounters:
Racialized Encounter An encounter where a racialized person(s) receives an intentional or unintentional
communication so that the sender accomplishes racial segmentation and domination in the
situation. “We” versus “they” is connoted where the “we” are non-racialized persons and “they”
are marginalized, racialized, and disadvantaged in comparison to the “we.” Racialized
encounters can occur interpersonally, publicly, or through media.
We suggest that race consciousness based on anti-racist principles is necessary to
accountability for this type of miscommunication. Consciousness is always required to make
amends for social breaches and miscommunication.
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
102
Race Consciousness Race consciousness based on anti-racist principles is a strategy for racial equality that names and
questions discourses of domination and promotes equal access and participation in governance
among peers.
This sort of good governance among peers has to be supported by education about
fairness, trustworthiness, transparency, and accountability or what we are calling the proceedings
of social justice that are required to support equity.
Equity Standards of fairness achieved through social justice proceedings.
Where organizations are concerned, we have said that two main problems exist that
accountability, theoretically, can remedy: institutionlized racism and systemic racism.
Institutional Racism The lack of accountability for racial equality in society’s institutions, such as health care. Its
fundamental basis is the privilege – informed by ideology and group power – of not having to be
equally accountable to racialized people as to non-racialized group members.
Systemic Racism Policies, practices, and procedures that are considered normal, but can intentionally or
unintentionally discriminate against individuals and groups protected under the Code, thus
privileging non-racialized people. The privileges of systemic racism are upheld by discourse that
avoids accountability for racial domination.
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
103
In this perspective, institutional and systemic racism can be dismantled by accountability
proceedings and accountability relies on race consciousness as well as equity committees,
policies, and programs. It is crucial to have paid, specialized, diversity practitioners who are
knowledgeable in anti-racism and informed by transformative justice so they can administer
social justice and achieve standards of equity. All employees must be required to learn anti-
racist discourse as opposed to discourse that condones or promotes racism.
Discourse Language-based expression (verbal, written, non-verbal,) that includes knowledge plus ideology,
or “the talk and the walk.” Discourse can be either a reflection of social structures or a
mechanism for restructuring relations.
Discourses of Racism Language-based expressions that structure relations of dominance, including marginalization,
exclusion, problematization, and containment of racialized people. These expressions can also
target supporters of racialized people.
Anti-racist Discourse The discourse of accountability for equity. It is conscious and relational. It is practiced.
Accountability practices pertaining to equity include:
• honesty and ownership of the impact of racial discrimination;
• informing persons of the perception of unfairness;
• providing an opportunity for persons to retract mistakes on their own recognizance along
with apology and accommodation; and
• informing persons what the community requires.
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
104
What are the benefits of an anti-racism informed by transformative justice and skilled in
relational practices of accountability? Good accountability outcomes.
Accountability outcomes of a transformative justice hearing of a complaint:
• parties feel as whole persons;
• relationships feel in balance; and
• members of racialized groups feel safe (see Author, 1988).
Is Accountability for Racism a Menace to Some People? Calliste (1993) has shown that racist immigration policies have governed the relationship
between nurses from the Caribbean and the Canadian state. Glaessel-Brown (1998) illustrated
how immigration policy is explicitly used to manage nursing shortages. Calliste (2000a)
demonstrated how black nurses constitute a segregated, surplus labour pool in Canada.
Moreover, an ethnoracial hierarchy (Ornstein, 2000) exists in the Greater Toronto Area
according to employment, income, and education. Complaints of racism are often about other
racialized people not being accountable to people of colour. We argue that the hierarchy itself is
a self-reinforcing function of a system of discourse that regulates to whom one does, or does not,
have to be accountable. The nurses participating in our study were very conscious of the
hierarchy, and there was unanimous concession among various groups of nurses that Blacks were
the most vulnerable in this hierarchy in terms of being denied the privilege of accountability.
Institutionalized racism and systemic racism go unchallenged in organizations where
accountability for racism is resisted.
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
105
Policy’s Role in Implementing Relationships of Accountability Despite the outpouring of anti-racism policy seen in the previous decade, accountability for
racial discrimination has not been achieved in nursing, including accountability for overt and
covert dominance and negative profiling of members of racialized groups (see Smith, 2004, for a
discussion of racial profiling). A continuum that ranges from breaches of simple forms of
etiquette to vicious indecencies toward racialized people exists within the health care system.
Yet, the following anti-racism policy accountability initiatives that some of our study
participants have worked on have not been implemented:
• Committee for Intercultural, Interracial Education in Professional Schools. (1993).
Consultation for Action Report. Submitted to the Department of Multiculturalism and
Citizenship Canada, Race Relations and Cross Cultural Understanding;
• Municipality of Metropolitan Toronto. (1993). Anti-racism Policy and Implementation
Strategy Discussion Paper;
• Ontario Ministry of Health. (1994). Strengthening voices: Anti-racism strategy.
• Ontario Hospital Association and the Ontario Ministry of Health, Joint Policy and
Programming Committee (1996). Anti-racism organizational change self-assessment
tool/anti-racism policy guidelines; and
• Kohli, R. and Thomas, B. (1995, October). A time for change: Anti-racism, employment
equity organizational change process. Final Report of the East York Health Unit
Employment Equity Coordinating Committee. Toronto: The Doris Marshall Institute for
Education and Action.
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
106
Why have these policy documents been ignored? What damage has been done because
they have not been implemented? Why is anti-racism resisted despite formal policies that call
for an end to condoning or promoting racism?
The participants in this study expressed seriously conflicting convictions about anti-
racism as an organizing framework that could bring about accountability for racism.
Conflicting Perspectives on Accountability for Systemic Racism We found wide variation and disagreement between research participants on strategies for
introducing accountability in response to experiencing or observing racism. Some advocate
paying attention to racial differences and directly naming issues. Others advocate prohibiting the
word racism and avoiding accusatory tones in naming issues, while strengthening relationships
to build support in higher places. Some have strong convictions that race consciousness is the
remedy to foster discussion and problem solving. Others expressed equally strong convictions
that race consciousness itself is the epitome of racism.
We observed in this project that the extreme distaste for the word “racism” was centered
on assumptions and associations that were altered when we combined the understandings of
transformative justice with those of anti-racism. This synthesis offered potential for bringing
accountability into race relations and contractual arrangements with employers and unions.
However, we still have to contend with the legacy of misunderstandings of the ways and means
of anti-racism. We understand that:
1. The word “racism” triggers an accusatory, diagnosing, or branding effect that it is normal
to react against.
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
107
But “transformative anti-racism” is interested in diagnosing problems, not people. The
normality of reacting against the word “racism” must be changed to a new accepting
normal if an open, problem-solving orientation is to be realized.
2. The word “racism” is interpreted as whining, as a type of “victimology” that nurses in
particular react to. Victimology is disdained in nursing as it has been well critiqued as
being detrimental to health.
Yet the concept of anti-racism that arises out of transformative justice is worlds apart
from victimology. It moves away from the concepts of victims and perpetrators. It is
about complainants in a contractual relationship (formal or informal) trying to make the
relationship safe and fair. In a democratic society, based on formal and informal
contractual relations, the privilege of accountability must be guaranteed and the
responsibilities of accountability must be reviewed and mutually monitored. We believe
a transformative type of anti-racism would uphold these social justice ideals. The
integration of accountability becomes possible through stakeholder dialogue,
participation, and the breaking down of social barriers to establish safety. When the R-
word can be used without reactivity and prohibition, discussion can be safely used for
problem solving.
3. The word “racism” is associated with hate crimes so, if someone is approached about
having offended somebody, the reaction is righteous indignation, and guilt is denied. Our
research suggests that this denial escalates the dispute and leads to fears of threat and
feelings of non-safety in all parties. The transformative justice approach to anti-racism is
mainly concerned with equal access and participation so that inequities in employment
and service do not result; so that processes of marginalization, problematization,
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
108
containment, and/or exclusion are not used in negotiation with racialized peoples; and so
that the needs of the racialized person complaining are met in the proceedings of the
complaint. When there is a shift to self-monitoring and supportive equity monitoring
where issues are openly discussed in safe supportive environments, then feelings of threat
and non-safety can subside. If informal means of resolving issues are not effective, then
formal proceedings may be required.
A particular feature of organizations is that employee relations exist within hierarchies of
power. The nature of power hierarchies is that accountability and transparency involve top down
reporting relationships. However, we observe that even if accountability is supported from the
top down in an organization that is composed of people with divergent perspectives on how to
institute employment equity, instituting anti-racism principles will be difficult. Hence, we argue
that the main barrier to an accountability that could correct institutional racism is conflicting
views on how to achieve equity. The effect of this conflict is silence about racism so that racial
conflict continues relentlessly. Of course, other possible explanations for the perpetuation of
conflict include:
(a) influential people do not want equity instituted because they fear losing power, and
(b) influential people really do hold negative attitudes based on racial groupings and
want to retain the privilege of arbitrarily bestowing merit on exceptionally deserving
racialized individuals (See Calliste, 1993).
We prefer to take good will at its face value. Such a stance is consistent with
transformative justice, because it changes potential perpetrators into potential supporters and
gives the benefit of any doubt that they are not sincere in wanting equal access and participation.
Theoretical Perspectives on the Sanctity of Accountability Breaches
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
109
Breaches of accountability result in proliferating accountability problems. It is not only racial
discrimination that produces racial disparities. Group-based refusal to be accountable also has
damaging effects on racialized persons, as well as on the system of governance. Lack of
accountability for racial discrimination may be linked to a lack of compelling or ethical interest
in being able to recognize discourses of domination, therefore precluding implementing effective
social justice programs that could improve race relations. Many of the effects, as well as the
causes, of systemic, organizational, or institutionalized racism, can be attributed to distortions of
accountability. But are these distortions due to unethical dispositions or virtuous missions such
as upholding standards?
Apart from segmentation and segregation that result from breaches in accountability
practices, serious disadvantaging games of set-up and backlash can emerge and we have shown
how disabling and distressing these can be. These instances of accountability gone awry
problematize racialized nurses who are set-up for discipline, job transfer, or job loss in uncaring
ways that conflict with nurses' identities. Nurses marginalize racialized nurses so that they are
already stressed about not being in relationships for collaborative decision-making, then they
contain and problematize colleagues who are courageous enough to object to unfair treatment
and they provide rationales for their decision-making.
As we saw from the aberrations in accountability practices described in Nurse A’s case,
various organizations engaged in practices that had the effect of containing – keeping Nurse A in
her place – and ultimately of closing ranks to exclude her participation in nursing employment,
presumably to keep bad apples out of the profession.
Accountability for distortions in accountability practices is precluded when organized,
group-based protection practices exist that are barely perceptible to nurses and others, including
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
110
arbitrators and mediators, who are uninformed about contemporary manifestations of racism
such as set-up. Extreme amounts of energy go into documentation for hearings and large
amounts of money go into dispute proceedings. The benefit to non-racialized nurses is that the
system of merit for whiteness remains unchallenged. Can Canadians afford to keep paying for
this benefit, and what does it achieve? Are white nurses really the best educators, managers,
researchers, nurse practitioners, or program planners? As the popular saying goes, “Nursing is
white on top and brown on the bottom and it needs stirring.”
Experience of Relational Elements Where Racial Profiling Is Unaccounted for and Unchecked Evidence suggests that how relationships are managed when accountability is sought is quite
variable. This report provides evidence that relationships become extremely problematic as a
result of backlash when there are formal complaints or grievances. We have theorized elsewhere
about the relational elements in play because of the lack of accountability for systemic racial
discrimination and the low prevalence of courtesies such as apologies (Hagey et al., 2001b). The
range of relational problems runs the gamut from simple misunderstandings to gross violations
of relationship, including physical assault.
In an article entitled, “What is a racial dispute? How can we reach a level playing field?”
Hagey (2003) attempted to get a “buy-in” from nursing leaders to address the underlying issues
pertaining to systemic racial discrimination in Ontario. She defined the concept of agency as
participation capacity in recognition of external social realities such as systemic racism that
impact on decision-making capacity. Agency relies on accountability and transparency in
reciprocity as well as on voicing needs and realizing interests through decisions and actions.
Sadly, racialized nurses whose participation capacity has been ruptured are seen as “lacking
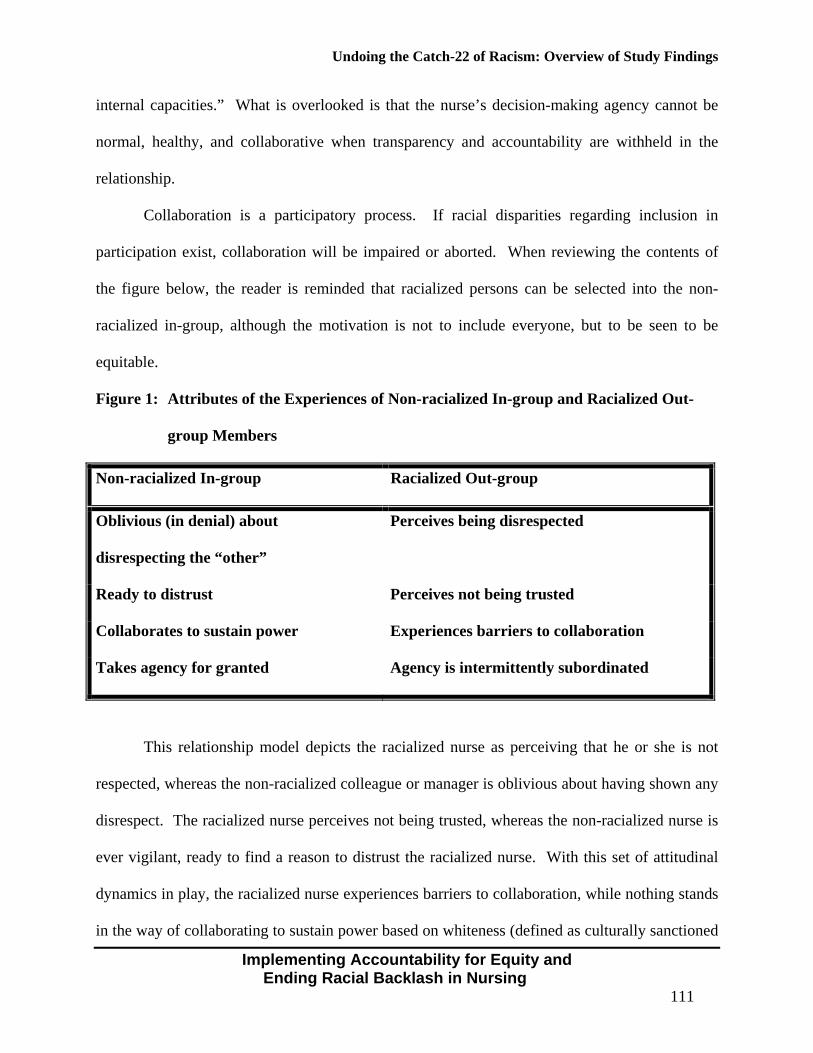
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
111
internal capacities.” What is overlooked is that the nurse’s decision-making agency cannot be
normal, healthy, and collaborative when transparency and accountability are withheld in the
relationship.
Collaboration is a participatory process. If racial disparities regarding inclusion in
participation exist, collaboration will be impaired or aborted. When reviewing the contents of
the figure below, the reader is reminded that racialized persons can be selected into the non-
racialized in-group, although the motivation is not to include everyone, but to be seen to be
equitable.
Figure 1: Attributes of the Experiences of Non-racialized In-group and Racialized Out-
group Members
Non-racialized In-group Racialized Out-group
Oblivious (in denial) about
disrespecting the “other”
Perceives being disrespected
Ready to distrust Perceives not being trusted
Collaborates to sustain power Experiences barriers to collaboration
Takes agency for granted Agency is intermittently subordinated
This relationship model depicts the racialized nurse as perceiving that he or she is not
respected, whereas the non-racialized colleague or manager is oblivious about having shown any
disrespect. The racialized nurse perceives not being trusted, whereas the non-racialized nurse is
ever vigilant, ready to find a reason to distrust the racialized nurse. With this set of attitudinal
dynamics in play, the racialized nurse experiences barriers to collaboration, while nothing stands
in the way of collaborating to sustain power based on whiteness (defined as culturally sanctioned
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
112
in-group dominance) for the non-racialized nurse who takes the privilege of agency for granted.
By contrast, the racialized nurse can have decision-making agency interrupted for a host of
reasons – lack of command of accountability, lack of participation, lack of information
transparency, outright subordination, patients demanding to have a white nurse, but most
importantly, activated fear of backlash and signs of set-up.
We assume (until research shows otherwise) that agency – equal access in participation –
is supported by transparency and accountability when the relational process is guided by nursing
leaders committed to anti-racism policy and astute to the discourses of domination. Regarding
policy that was issued by the Joint Provincial Planning Committee of the Ontario Hospital
Association and the Ministry of Health in 1995, the effect could have been the legitimization of
accountability to racialized people. Sustained expectations could have required working
relationships to be kept in balance so that collaboration among all colleagues would be realized,
free of racial profiling. Given that relationships have been a notable topic in nursing for years,
the denial response of “hear no racism, see no racism, speak no racism” is shocking to racialized
nurses, not to mention frustrating.
Building relationships between parties is problematic when agendas conflict and there is
an implicit agreement that it is safer not to communicate. Communication in nursing can begin
with orienting to the experiences of the person – the empathic approach – that can lead to making
accommodations when the ethics of restitution is used. Acknowledging the need for restitution
and apologizing to make up for omissions or commissions is a requirement for mutual
accountability in collaboration. Such amends are made routinely among in-group colleagues and
are especially important for the organization’s image in diverse communities, so why not extend
the amends to erode in-group/out-group boundaries.
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
113
What Relationship Issues Arise with Particular Accountability Strategies? Removing the cloak of silence shrouding accountability for systemic discrimination puts
members of non-racialized groups and their supporters on the defensive. The sense of threat is
high. While nursing as a discipline in Canada has spent much of the last century contending with
diversity issues, it has never dealt with the labour dimensions related to experiencing diversity
(McPherson, 1996). For CEHS, it is important to put effort into sustaining relationships across
boundaries while maintaining honesty and clarity about any perceived problems. Clarity when
requesting to understand peoples’ perceptions can lead to mutual understanding. It is important
to maintain dialogue and learn what issues must be dealt with and set ground rules on how to
deal with them.
All those embarking on ways to implement strategies to achieve accountability for racial
equality and employment equity need support from a mentor and an organized support system.
We are all learning to take baby steps. We all need recognition and rewards and should be
having adventurous fun in this newly expanding personal growth area, be curious about where it
will lead, and pleasantly surprised with new mutuality. One goal for racialized and non-
racialized nurses seeking connection is mutual responsibility and reciprocity while becoming
astute to lurking forms of built-in advantage and disadvantage.
In this study, we found it energizing to talk about our perceptions and keep our
relationships in balance by resolving issues. Our think tanks demonstrated that collaboration
between racialized and informed non-racialized nurses is not only possible, but very fruitful,
suggesting that knowledge may be the key to dialogues on accountability policy. We believe
that the negotiation of equity in relationships requires convening racially integrated fora for
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
114
dialogue. We have been instrumental in the passing of a resolution by the Registered Nurses
Association of Ontario to “devise a series of conferences to envision means of achieving racial
equality and employment equity….” (see Appendix C). CEHS is willing to collaborate on
devising this series of conferences.
Building interracial relationships across sectors and hierarchies is hard work.
Nevertheless, it is necessary to build responsibility and collegiality and motivate those who rule
– each one of us – to nurture inclusion programs and incentive strategies. Goals remain to
enhance the quality of ethnoracial interrelationships and realize employment equity. Many of us
come from several generations of fighting discrimination and have been reared to continue doing
so. Many racialized nurses have built exquisite legal expertise and extensive knowledge of
human rights legislation at provincial, national, and international levels and are aiming to meet
nursing leaders in all of these arenas. You could say we are highly motivated to pursue the
development of effective accountability strategies within the profession.
This goal requires building grass roots organizations representing nurses, holding public
dialogues and debates on the issues surrounding accountability, and making educational
materials accessible. In the current context of heightened war and conflict around the globe, it is
pertinent to point out that nursing of the European variety was born in the context of religious
wars in medieval times. Every nurse in the United States is automatically a member of the
armed forces. Nursing has never shed its hierarchical rituals born in its military period. Our
quest for accountability begins by critiquing the systemic pecking order that we perceive as
preserving privileges based on race. We ask you to please circulate for debate Peggy McIntosh’s
classic article “White privilege: Unpacking the invisible knapsack” (1990), available at:
http://www.utoronto.ca/acc/events/peggy1.htm.
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
115
Also, the Centre for Social Justice has a valuable resource, Expanding the circle:
People who care about ending racism. We need your help (Curry-Stevens, 2005). This resource
is available at: http://www.socialjustice.org/pdfs/expandingthecircleEnglish.pdf. More and more
scholarly sources are appearing that are relevant locally. For example, the Fall 2004 issue of the
Association for Canadian Studies/ Association d’etudes canadienne publication Canadian
Diversity/Diversite canadienne centres on racial discrimination, racism, and human rights. See
also recent work that documents the impact of racism on health (Navarro and Montaner, 2004)
and mental health (Waldron, 2002).
We doubt that systemic racism is held in place by malicious hatred. We have learned,
however, that pointing out differences along racial lines can spark viciousness, which increases
tension and polarization and escalates problems because it complicates communication. When
this happens, we need each other’s support to clarify communication strategies.
How Do I Evaluate Alternative Discourse Strategies? Discourses of domination are played out socially to both marginalize racialized nurses and
contain them with stringent retaliation if they persist in "not knowing their place." For this
reason, it is important to be critical about the role we ourselves, as racialized nurses, play in
becoming ensnared in a set-up. The Jean Baker Miller Training Institute (JBMTI – see website
at: www.wellesley.edu/JBMTI), has been investigating the options that African-American and
other racialized women can generate with the coaching and support of therapists who are also
racialized women developing relational/cultural theory (RCT) (Walker, 2002). RCT
recommends analyzing situations inspired by questions like these:
• How can I build personal and political support in this situation?
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
116
• How can I communicate from a relational self that stays in relation rather than getting
into the trap of distant and alienated disconnects where they have even less interest in me
as a person?
• How can I deal with this combative person’s perspective, fears, and wrong assumptions?
• What if I express my fears and legitimize my issues by being firm about who I am and
what I expect, and also attend to the other person’s fears so that I minimize the images of
threat that are conjured by racial stereotypes?
The JBMTI has not reported studies that empirically trace elements of situational
problem solving, or scientifically link certain strategies and outcomes. Nevertheless, it does
continue to advance the hypotheses that having sound working relationships is healthier for the
individuals involved and that sustaining relational (positive) connections with the individuals in
situations avoids the isolation they characterize as the "glue of oppression" (Jordon, 1999).
Our research network continues to expand to members who testify they were calm, firm,
and honest in situations where they were boxed in and then systematically isolated when they
broached the issue of racial difference or disparity. One nurse reported physical assault by a
manager who was apparently triggered by her calm, firm demeanor. The majority of these
reports come from community hospitals, health agencies, and continuing care facilities that
appear to be cut off from current knowledge, although there are some shocking exceptions.
Non-racialized, influential nurses do not come to the CEHS to report their woes about
difficult colleagues and experiences in racial disputes. They support each other in what Brian
Turner calls “thick solidarity,” which is eroding as a social form under the postmodern approach
to organizing relationships (2000). He argues thin solidarity is the mode for the new era of
fleeting connections that are tied to particular fleeting projects. Because of shared assumptions
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
117
and strategies, dominant groups can work in concert without conspiracy. Actual conspiracy
requires time and opens up possibilities for disagreement and questions about who is going to get
the credit for what, and so is comparatively inefficient. As social capital theory stipulates –
“efficient systems compete better."
Racialized groups are at a distinct disadvantage in comparison to non-racialized groups
that share common goals and trust each other to act independently. Organizing to cut through in-
group barriers to power is a relatively uncharted journey in the empirical administrative sciences.
Moving from being a token to gaining a critical mass to become a part of central decision-
making is often pointed to as the trajectory (Collins, 2004; Dei, 1996). The importance of
having progressive leadership in an organization is always cited as crucial for emerging from the
chilly climate (Chilly Climate Collective, 1995). Moving in this direction is the leading edge
exception in nursing in Canada, according to observers in our networks (Villeneuve, 2002).
The main dilemmas that arose in our think tanks pertained directly to issues of gaining
ascendancy and emancipation. “Do I stay in my own nursing association and put my energies
there or should I join the RNAO?” “Given that the RNAO is so racially homogeneous, there is
little hope of the RNAO really dealing with the systemic racism issues we face everyday.” “Do I
put my energies into building coalitions that together can become the new official voice of
nurses in the province?” “What could be gained?” “How would disagreements be handled?”
“Wouldn’t nurses be a force to reckon with if we all united into a strong organization?” “What
are the forces that are impeding against that happening?”
The nurses explored these issues in connection with the question of the profession as a
whole working on developing policy and programs to address resistance and counter-resistance
that lies below the surface of people’s fears and attitudes. It is a reality that well-informed
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
118
people can be offenders and repeat offenders because of widely differing views on what
constitutes racism and how it should be handled. The lack of language and etiquette in this type
of conflict leads to reactions and counter-reactions that escalate into a trap of resistance and
counter-resistance along lines of racial conflict. Avoiding problem-solving only increases
tensions and deters and delays any integrative movement.
Anti-racism Grounded in Transformative Justice and Freedom Ideology As an alternative, we offer anti-racism as a type of freedom ideology. Anti-racism encourages
people to freely choose to oppose, in principle, a set of practices that people are drawn into
without full cognizance. If racial domination and disparities are allowed to operate, the
advantaged and disadvantaged in the situation will be ensnared in resistance and counter-
resistance or tit-for-tat and everyone loses (See Fisher and Brown, 1988). Therefore, we
advocate anti-racism to nursing as a liberating opportunity that can further emancipate our
discipline.
For the same reason, it is important for us to share our discovery in this project that anti-
racism discussions can be conducted in scholarly, respectful ways. For example, our think tanks
invited knowledgeable, accomplished speakers who set the tone for excellence on so many
levels. Anti-racism can be fun, sensitive to people’s feelings, and consistent with health
promotion principles, not to mention the direct application of primary health care strategies of
participation and community ownership of problems to promote healthy ways of being.
We are calling for an end to the pattern of nurses being embarrassed, humiliated, or
threatened when broaching the issue of racial disparity. But these responses can only diminish if
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
119
there is an end to reactivity and retaliation when someone broaches an issue. We appeal to all
parties to keep the relationship intact.
Knowing how deep-seated and unconscious dominance practices can be, we urge you to
support each other in expressing difficult feelings. Feelings of confusion and hopelessness are
common when one does not know how to intervene to prevent well-meaning, but nevertheless
offending and repeat-offending practices.
We ask you not to mistakenly claim that racialization of non-racialized people – so-
called reverse racism – is going on when efforts at equilibration are taking place. We ask you to
identify where feelings of racial domination come from and deal with them in therapy or anti-
racism role-playing seminars. We are asking all nurses, and ultimately all Canadians, to come
into the centre of the opposite poles and work out a system of balance among the so-called races
in the human race. We are looking to those in positions of leadership who have the power to
take the lead in promoting anti-racism and accountability for racial equality and employment
equity and to bring an end to racial disparities.
The State’s Weakened Role in Accountability for Systemic Racism: Policy and legislation are required to implement and integrate voluntary accountability Beck and others point out that federally, the Canadian Human Rights Act (CHRA) and
Employment Equity Act (EEA) were amended by legislation in 1996, with the effect of
terminating the potential for case hearings, and hence for remedies, that hold employers
accountable for systemic discrimination (Beck, Reitz, and Weiner, 2002). This can be seen as
but one indication that the role of the state in the enforcement of equity is weakening.
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
120
In Ontario, Henry and Tator (2002, p. 95) point out that on 13 December, 1995, the
Harris government rescinded the 1993 employment equity legislation, the first in Canada to
address group-based advantages that are widespread, persistent, and systemic. They called their
act “Bill to Repeal Job Quotas,” to direct attention away from virtual job quotas enjoyed by in-
group members who are not subject to systemic discrimination. By calling the new legislation an
“Equal Opportunity Plan,” the privileges held by some who are "more equal" than others are now
protected in legislation.
Enforcement of the Provincial Human Rights Code is problematic in the absence of
effective employment equity legislation and proceedings. In the four-year period following the
act, in the GTA alone an estimated seven million health care dollars were paid in settlements for
discrimination cases filed by nurses, according to our informal sources. Some of these cases
included disability grievances, but the majority concerned racial discrimination. Most of these
settlements were concealed from the public because “gag orders” were stipulated in the
agreements. Taxpayers have the right to know that there is currently a jurisdictional contest
under way. Should health care dollars be spent to remedy deficiencies in employment equity
legislation? Alternatively, is it better to attempt to integrate human rights accountability
measures into the day-to-day proceedings of institutions such as health care?
This growing trend away from accountability for systemic racism makes employers,
union representatives, nurses, and colleagues we have talked with feel "backed into a corner,"
trying various means to deal with escalating conflicts or embarking on expensive grievance
arbitrations which neither employers, unions, nor the human rights tribunals can afford. Some
health agencies have contracted with unions to develop workplace diversity units that address
both prevention and dispute resolution with a variety of consequences we want to study in future
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
121
research. Nurses participating in our study perceive accountability to be problematic and
extremely laborious for the individual experiencing the effects of racial discrimination or
harassment in employment. The following recommendations are made in the hope that
implementing accountability for institutional and systemic racism will bring about equity.
Recommendations to Achieve Accountability for Systemic Racism: The Romanow Commission’s Health Council of Canada In addition to promoting accountability through resolutions, recommendations, objective-setting
and guidelines set forth by the CEHS, a role for the newly emerging Health Council of Canada
(HCC) was envisioned. The HCC could decrease the number of health care dollars that are
currently being expended on problems pertaining to systemic racism in health care, such as
legally defending charges of discrimination. As mentioned above, unions in the GTA reported to
CEHS that in a four-year period, seven million health care dollars were spent settling
discrimination cases, the majority of which were racial.
The Romanow Report (2002) did not address racial discrimination directly, but
denounced the “big disconnect," referring to health care for Aboriginal people, and targeting the
reduction of morbidity and mortality due to barriers in access, primary prevention, and treatment.
Lack of accountability for racism, colonization, and poverty were not specifically targeted. Nor
were jurisdictional issues and actual funding commitments laid out (Koebel, 2003). Some
Native leaders are calling for a national Aboriginal Health Act to correct the racial disparities
created by The Indian Act.
The HCC could introduce accountability mechanisms to monitor the costs associated
with systemic racial disparities in health and health care and set guidelines for equity practices.
The Romanow Report Recommendation 3.2 states that “On an initial basis, the Health Council
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
122
of Canada should establish benchmarks, collect information and report publicly on efforts to
improve quality, access and outcomes in the health care system” (2002, p. 248).
Recommendations to the Health Council of Canada
• Monitor the racial disparities in health and health care and require interventions to correct
them.
• Require process and outcomes reports on equity programs for health care workers and
consumers.
• Monitor the number of health care dollars spent on defending discriminatory practices
and set mechanisms to ensure freedom from racial discrimination, harasssment, set-up,
and backlash in organizations responsible for health.
• Promote equal access and participation in organizations responsible for health, including
the provision of interpreter services and removal of barriers for visible and invisible
minorities.
We thank Anne McLellan, former federal Minister of Health, for her encouraging letter
responding to the CEHS' suggestions about the future role of the Health Council of Canada
(Appendix D).
Recommendations from Partisan Sectors of the CEHS Network The recommendations below have not evolved out of consensus. The beauty of a network is that
despite differences in ideas and diversity of backgrounds, we are linked together in a common
vision. How that vision – equity in health and society – might be realized may be through
multiple, even conflicting, pathways. The recommendations are offered in the spirit of sharing
strategies that can be discussed and debated so that actions can be tried and demonstrated to
work or not. Changes can be undertaken until the vision is achieved. What follows is a selection
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
123
of some key recommendations that attempt to build accountability for systemic racism through
changes in legislation and policy to build new organizational structures, procedures, and
practices in the nursing profession.
We have outlined the recommendations under six change categories: (1) An investigation
by the Ontario Human Rights Commission; (2) Leadership Training and Anti-racism Education;
(3) Ontario Legislation; (4) Ontario Policy; (5) National Accreditation; and (6) Voluntary Policy
in Key Organizations.
1. An investigation by the Ontario Human Rights Commission The Ontario Human Rights Commission (OHRC) initiate (under section 29 [g]) of the Code) an
investigation into the systemic discrimination against racialized nurses as well as all designated
groups protected under the code with respect to education and employment in the health care
system. The investigation should take account of discrimination, harassment, and procedures for
redressing grievances and complaints.
2. Leadership Training and Anti-racism Education
The Centre for Equity in Health and Society (CEHS) establish a leadership academy that holds
training workshops for negotiating the implementation of anti-racism policy and practice in
support of ethnoracial competencies. The Province of Ontario fund this academy to develop
curricula and organize dialogues on changing the culture of nursing to one that practices
accountability for equal access and participation in all sectors and at all levels of the profession.
The CEHS leadership academy, in partnership with university research units, will evaluate
curricula and develop and disseminate new knowledge on ethnoracial competencies and
achieving diversity in leadership. The CEHS will collaborate with appropriate professional and
regulatory bodies to develop questions for registration and licensure examinations pertaining to
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
124
antiracism and racial dispute proceedings. CEHS will also collaborate with unions that negotiate
nurses' contracts to sponsor conferences that discuss innovations addressing member-to-member
racial disputes. The CEHS leadership academy will convene dialogues in nursing on the overt
racism from patients, colleagues, and supervisors experienced by nurses of Asian and Filipino
descent during the outbreak of SARS and how to prevent such behaviours in future.
3. Ontario Legislation
The Ontario Human Rights Commission be legislated to report directly to an all-party committee
of the Parliament instead of to the Attorney General.
4. Ontario Policy
The Ontario Human Rights Commission develop policy to:
• Monitor workplace complaints proceedings for reprisals and step up investigations to
properly document reprisals and irregularities in procedure.
• Levy fines based on the degree of resistance to anti-racism procedures in the complaints
process.
• The Ontario Human Rights Commission report to the legislature, categories
of complaints and statistics on how they are dealt with. Private and union practitioners
adjudicating racial complaints report to the legislature similar data ensuring the
confidentiality of complainants and respondents but listing the sector – for example,
health care – in which the complaint arose.
• The Ontario Ministry of Health and Long Term Care require the Nursing Secretariat to
provide the opportunity for the inclusion of Aboriginal and visible and non-visible
minority member representatives in its proceedings in collaboration with the Joint
Provincial Nursing Committee.
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
125
• The Ontario Ministry of Health and Long Term Care integrate anti-racism, anti-
discrimination, anti-harassment, employment equity assurance, and language and culture-
care agendas in the nursing and other relevant secretariats to carry forward the
requirement of ethnoracial competencies in a mission of diversity and equity in health
care.
• The College of Nurses of Ontario introduce transformative justice proceedings to handle
allegations where a racial dispute is evident between a client and a nurse.
5. National Accreditation
1) The accreditation proceedings of hospitals and health agencies, in cooperation with all
regulatory colleges, implement equity assurance to augment their quality assurance
programs.
2) The accreditation arm of the Canadian Association of Schools of Nursing require:
• evidence of recruitment and strategies for retention of Aboriginal, racialized, and non-
visible minority faculty and students;
• evidence of anti-racism curriculum;
• evidence of requiring ethnoracial competencies among faculty, staff, and students.
6. Voluntary Policy in Key Organizations
1) Provincial, regional, federal, and national bodies supporting and directing health
services research develop programs to obtain and publish data on health care workers in
terms of Aboriginal status, ethnicity, mother tongue, and visible minority identity.
2) The Ontario Hospital Association develop and promote best practice models of anti-racism
policy. Guiding policies should include Principles for Good Governance in the 21st Century
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
126
and the United Nations Declaration of Human Rights – Legitimacy and Voice, Equity, and
the Rule of Law.
3) All regulatory and professional bodies introduce measures to address racial discrimination
and systemic racism in health care:
• Registration forms be changed to allow for self-identification of Aboriginal, racialized,
and non-visible minority status.
• Committees and panels be required to be diverse and inclusive so that they reflect the
diverse population of Canadians.
• Ethnoracial competencies be made a requirement for nurse registration and an
expectation for ongoing, self-reflective practice for registration in self-reflecting
professions.
• Regular in-service education programs and human rights orientation to new staff at all
levels.
• Electronic monitoring using human rights software to track equity indicators.
• Tools for employment systems review be adapted to identify set-up and backlash
experienced by racialized employees.
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
127
Chapter 4 – Undoing the Catch-22 of Racism: Overview of
Study Findings Intent on Integrating Accountability for
Systemic Racism
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
128
How Integrative Processes could be Used to Implement Accountability for Equity in Nursing and Health care 1) Any plan to integrate accountability has to address the resistance to accountability for equity
among leaders in the health care system. This resistance is manifested in denial of inequities,
prohibition on the use of the term racism, “white-out” on research on racial differences in
quality of work life and healthy environment research that has been heavily funded in
nursing, and targeting of individuals who break the silence on racism in nursing. Moreover,
the gridlock resistance to accountability means that redress of grievances is extremely
problematic. The out-of-control patterns of set-up and backlash were perceived by
participants in this study to impact on racialized nurses, negatively affecting their resources
for health, making the workplace unhealthy and potentially a risk to patient safety.
2) Racialized nurses perceive that race, colour, or ethnicity impacts on relationships with
colleagues, patients, doctors, and supervisors. A study by Das Gupta (2002) shows that few
white nurses of European background perceive this. This disparity in impact of race, colour,
or ethnicity has implications not only for patient care but for the quality of work life, career
mobility, and leadership opportunities for racialized nurses. Racialized nurses report that
they are excluded from collaboration, which is a key task of the health care professional.
Racism’s power is in its catch-22: It’s bad if we do not talk about it; it’s worse if we talk
about it. To change this, we must create safe opportunities in nursing for discussing racial
disconnects and disparities and what we can collectively do about them.
3) The 1991 Census indicated that visible minority nurses in Ontario have half the chance of
their non-racialized counterparts to move into the managerial level, yet there has been no
profession-wide discussion about barriers and accountability for removing barriers and
building bridges. This report calls for updating the census statistics on ethnicity, visible
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
129
minority, and Aboriginal status in relation to occupation and career mobility. Without
current statistics, it is difficult to strategically plan.
4) Evidence exists that students in a nursing school were fearful of discussing racism. For
example, one student said, "that person may perceive this as a threat and it will come back on
you in different ways.” The accreditation tool of the Canadian Association of Nursing
Schools is silent about problems of racism in nursing education, health care, and society.
Moreover, participants in this study perceive that faculty who break the silence on racism in
nursing continue to be marginalized, problematized, and contained or excluded (i.e.
ostracized as “others”). Any plan for integrating accountability should consider how to use
accreditation to require nursing schools to conform with anti-racism curriculum, staffing, and
recruitment and retention of students, as called for by the Aboriginal Nurses Association of
Canada and others (Author, 2002).
5) Racialized nurses reported differential treatment and being "ear-marked" for more severe and
unfair levels of work assignments and discipline than were non-racialized nurses. Also,
issues of racism directed by patients towards nurses were considered to be "trivial" in nature
and "par for the course." These root causes of sickness and absenteeism were not identified
or dealt with by administration. Any plan for implementing accountability should require
human resource departments to enforce anti-racism standards of work allocation. Client-
centred care policies and practices should acknowledge the inappropriateness of any client’s
racist behaviour and should retain the facility’s right to allocate staff free of demands by
clients using prohibited grounds under the Code. Staff experiencing workplace racism
should be granted compensation time and pay.
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
130
Toward an Accountability Discourse Model that can Deal with Racial Discrimination in Nursing 6) Due to the findings of the present study, an accountability discourse model should begin by
addressing set-up and backlash against racialized nurses who presume equality or exert
expectations for equity.
7) New language is required so everyone working in health care can recognize systemic racism
and cooperate fairly in the redress of grievances. New language is required that permits free
discussion of racism so that repeat offending is less likely. The report invites recognition of
set-up as a type of systemic discrimination that disadvantages racialized nurses, especially
during times of downsizing, so that preferential treatment is given to non-racialized nurses
making them prone to condone the set-up. No health care workplace orientation programs or
policies exist that could aid in the recognition and prohibition of this human rights offense.
8) Backlash is a term universally understood by the nurses participating in this study. We are
asking for compassion from our colleagues so they understand that to be racially different
means having fear of backlash for being racially different. Moreover, we ask that it should
be legitimate in our profession to complain about a problem, and racism is a problem. We
ask for an end to backlash in the procedures for handling racial disputes. The widespread
practice of backlash impacts on long term relationships with our communities and it is a
source of rancor.
9) When accounting for the costs of racism, we must account for the costs to health. The health
effects described by the nurses who charged their employers with racism included feelings of
loss, including loss of confidence, loss of focus, and memory loss. They reported
experiencing humiliation, intimidation, paranoia, and isolation. Depression, grief, distressing
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
131
physical symptoms, death images, and overwhelming sensations, such as being invaded or
torn apart, were reported as health effects.
10) The discourse of accountability for racism should acknowledge that set-up is an everyday
possibility for racialized nurses who experience racism from their colleagues and patients.
For example, delicate tasks can have potentially problematic power dynamics, such as when
a female nurse has to insert a catheter into a male patient. Requiring a black female to
catheterize a white openly racist male can be seen as a potential set-up. Problems of racism
should be discussed, taking into consideration the energies of the care provider when making
and revising care plans.
11) The discourse of accountability for racism should be developed by the regulatory bodies,
such as the College of Nurses of Ontario, which is accountable for protecting the public
through standards of practice. The report strongly suggests that such bodies retain personnel
who are knowledgeable about racism in the health care system. Review panels should be
constituted by racialized members who are knowledgeable about racism and the culture,
language, and communities under review. Racialized nurses perceive being much more
vulnerable than their counterparts to being reported to the College of Nurses of Ontario.
Racial domination and backlash by colleagues is implicated in setting nurses up for being a
scapegoat, as we have witnessed in proceedings disclosed in confidence. Scapegoating
should be acknowledged as an effect of set-up and should be prohibited by local policies that
adopt the discourse of accountability for racism.
12) Racialized nurse managers reported experiencing more vulnerability than their counterparts,
were more often exposed to bullying, and more subject to behind-the-back complaints from
colleagues or underlings who can be supported by management from above. They perceive
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
132
being more likely to fall out of favour with superiors without explanation. This report is
calling for supervisors to be astute to the tactics of racism that sabotage racialized leaders
with the effect of advancing white leadership.
13) Cultural dominance is being used to discipline racialized nurses. One nurse reported, “I was
called in after I met a former client in the hallway and gave him and his child a “high five” to
say hello. The nursing manager said that the high five greeting is unprofessional behaviour,
and I was threatened that this incident would go on my record as being unprofessional. I
thought I was being culturally sensitive, but they have a very skewed and uninformed idea of
cultural sensitivity, and I have no way of holding them accountable for it.”
14) Racial Harassment has a presence throughout the health care system:
• One nurse reported: “when I went to pick up my mail there was a cup with images of
black people in my mail box. It had water in it so when I took it out to look at it, water
spilled all over my mail.”
• Another nurse reported: ”you begin to understand that there is a segment of the Canadian
population that really hates visible minorities when you look at the graffiti on postings.
My picture was put up in the lobby with twenty or so others for our outstanding service.
Mine was the only black one and the only picture that was mutilated”.
• Another reported: “Graffiti appeared on the flyers that we put up to advertise the think
tank today. This one from the elevator says, “piss on it.” The others are here, but I do
not want to say the words in polite company. Where are the people who did this? How
do we hold them accountable for their behaviors?”
• The diversity office in one large metropolitan hospital where racial complaints are filed
reported receiving threatening phone calls. An effigy doll with a noose around its neck
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
133
was hung on the office door conjuring the hateful racist lynching of people of colour.
Hate messages are a common reality for racialized nurses in Canada, who are coming to
question whether hate can be cured.
15) Equity disappears from the dominant discourse during job scarcity. Moreover, it is perceived
that non-racialized nurses who lose jobs during periods of under-funding of nursing have a
qualitatively different experience in how they are let go. In contrast to the hostile targeting
experienced by racialized nurses, non-racialized nurses are consoled and assisted with
finding another job.
16) Because accountability for discriminatory practices is considered not to be a valid,
appropriate response, those who are subject to racism experience anxiety. This anxiety is
exacerbated when the social means for addressing the problem and removing the source of
the anxiety is blocked. Blocking paths to accountability produces frustration and can lead to
illnesses that are triggered by anxiety. Racialized people in Canada have higher rates of
mental illness, chronic illness, injuries, and accidents and use more health care dollars per
capita. Increasing accountability for racism is a rational intervention targeted at lowering
these rates.
17) Given the fear of backlash for broaching the issue of racism, we found that not all group
members subject to racial profiling are in agreement about how to embrace an anti-racism
strategy that promotes accountability for systemic racism. We found much disagreement
about how accountability should be introduced. There appeared to be consensus that healing
is required to build relationships of trust and that organized dialogue is necessary to develop
ground rules within the profession and beyond.
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
134
Initiating Accountability Policy that can Regulate Programs, Practices, and Procedures at Local, Provincial, and National Levels in Nursing These policies should be instituted in workplaces, and in professional and regulatory bodies,
where applicable.
18) Effective accountability proceedings for racism are the exception. For example, only two
hospitals in Ontario have trained staff to address racial harassment before a dispute escalates
into a union grievance or a complaint to the Ontario Human Rights Commission (OHRC).
There is a need to normalize accountability and accommodation for systemic racism in both
informal and formal contractual relations, in both interpersonal and organizational culture
and in governmental relations.
19) Ruth Morris, an expert on transformative justice, identified five "benchmarks" that address
victims' core needs: (1) the need for answers; (2) the need for recognition that they have been
wronged; (3) the need for safety; (4) the need for restitution and balance in [workplace]
relationships; and (5) the need to find significance or meaning from the assault on their
human rights (2000, p. 248). We used these benchmarks to evaluate Nurse A's experiences
with retaliation and escalation in her dispute process and legal proceedings. We found that
none of these needs of the complainant, Nurse A, were properly met. Racial conflict can be
viewed as an opportunity for individuals and organizations to examine, reflect upon, and
repair the relationships that poison the workplace. Health care settings should offer respite to
racialized workers and supports for them to grieve and process the ongoing assaults on
dignity and the lack of accountability that are anxiety producing.
20) Evidence exists that making a complaint of racism to the human rights commission or filing
a union grievance contributes to being expelled, marginalized, treated as the problem,
contained, punished, or scapegoated. Evidence also exists that an investigation of racism
Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
135
feels to the respondent like “being guilty until proven innocent” and insufficient
accountability within such legal proceedings results in irregularities, including backlash.
Policies have yet to be established that hold employers accountable for backlash, even though
the Ontario Human Rights Code forbids it.
21) Speaking out in support of a colleague who experienced unfair treatment because of race was
perceived to be a "career limiting move or CLM" (backlash). Moreover, in a pilot study of
nine nurses who charged their employer with racism, only those who had a non-racialized
person testifying for them were successful in their proceedings. One person from the Ontario
Human Rights Commission witnessed that race cases that were granted hearings had the
support of a white person.
22)This report calls for developing ground-rules of accountability for equity and developing
capacities among all nurses for recognizing andresponding ethically when equity is being
challenged. Moreover, we are appealing to all Canadians to be continuously committed to
anti-racism, which means to speak out against privileges owing to racial dominance and
disadvantages owing to systemic racism and racial disparities in resources for health. We
invite you to support our strategic resolutions and recommendations designed to help us all
learn accountability for systemic racism. You can be part of the solution by developing
ethnoracial competencies. We thank you for your interest in these issues.

Undoing the Catch-22 of Racism: Overview of Study Findings
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
136

Summary and Future Research
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
137
Chapter 5 – Summary and Future Research
Summary and Future Research
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
138
Through the use of PAR, we have engaged in integrative processes by reaching out to
stakeholders to address accountability procedures in response to systemic racial discrimination.
We have begun to expose discourses associated with set-up and backlash in our case studies. We
suggested that backlash, set-up, and scapegoating are indicative of the ideological coordination
of organized practices consistent with institutionalized racism. That is, they are normalized and
institutionalized due to the systematic lack of accountability for racial discrimination. We
discussed strategies and issued resolutions and recommendations toward accountability policy
that can begin to regulate programs and practices at local, provincial, and national levels in
nursing organizations through self-monitoring, peer monitoring, stakeholder monitoring,
executive monitoring, and editorial monitoring. Organizations can normalize talking about
racism breaches, including harassment, and institute clear policy and procedures for solving
problems, repairing relationships, and promoting equity throughout health care education,
employment, and service.
We discussed some relationship implications that arise when individuals or groups seek
accountability for systemic racism. Specifically, when racism is an issue among nurses, clear
procedures are needed for addressing and resolving issues. We are calling for a shift to
transformative justice approaches in the grievance processes of racial disputes so that
complainants, plaintiffs, and others in the workplace are not traumatized by the very proceedings
that are supposed to bring about resolution. In racial disputes, parties need answers to deeply
personal and political questions. They need recognition that they have been wronged. They
need safety. There is a great need for restitution and balance in workplace relationships, and a
need to find significance or meaning from any breach of human rights (Morris, 2000, p. 248).
Summary and Future Research
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
139
We are inviting profession-wide problem solving to correct the irregularities in
transactions, outcomes, and interpretation of events that are evident with particular
accountability strategies. For example, it should not be a career-limiting move to speak out in
support of a colleague who has experienced unfair treatment because of race, or to call for
accountability on the anti-racism agenda in organizations. We outlined how anti-racism is
consistent with health promotion and excellence in healthy workplace environments.
Accountability is an anti-racism strategy to dismantle institutional racism and build instead a
healthy organization that rewards the practices of excellence in race relations and equity
monitoring.
We are seeking funding – and encourage colleagues to do so – to employ the
participatory action research model in a wider circle of nursing colleagues and other stakeholders
in health care. We see PAR as potentially effective for implementing and evaluating the
recommendations of this study and for generating deeper understanding of the issues and
potential strategies for institutionalizing accountability through equity assurance in nursing. In
our coalition-building, we advocate the support of individuals to assist them to orchestrate anti-
racism activities to gain inclusion and influence, recruit peers, and carry out the strategic use of
documents such as this report which we hope will receive wide attention.
The Centre for Equity in Health and Society intends to carry forward its research and
advocacy agenda. We thank the Canadian Race Relations Foundation (CRRF) for supporting
research on backlash against accountability for equal access and participation in nursing.

Summary and Future Research
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
140
Reference List
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
141
Reference List
Agocs, C. and Harish, J. (2001). Systemic Racism in Employment in Canada: Diagnosing
systemic racism in organizational culture. Ottawa: The Canadian Race Relations
Foundation.
Anderson, J. (2000). Gender, "race", poverty, health, and discourses of health reform in the
context of globalization: A post-colonial feminist perspective in policy research. Nursing
Inquiry, 7(4), 220-229.
Association for Canadian Studies/ Association d’etudes canadienne (2004, Fall). Canadian
Diversity/Diversite canadienne, 2(4).
Author. (1988). Kawa whakaruruhau (cultural safety) in nursing education in Aotearoa.
Conference report of the Hui Waimanawa, Otautahi (Christchurch, New Zealand).
Author. (2002). Against the odds: Aboriginal nursing. National Task Force on Recruitment and
Retention Strategies. Ottawa: Health Canada.
Author. (2003). Know your Human Rights. Toronto: Native Canadian Centre of Toronto.
Aylward, C. (1999). Canadian critical race theory: Racism and the law. Halifax: Fernwood.
Baik, G. (1985). Health and I (English title). Toronto: Korean Nurses Association of Ontario.
Bakan, A. and Kobayashi, A. (2003). Employment equity policy in Canada and the politics of
regional context: Two case study reports. Toronto: Canadian Race Relations Foundation.
Bannerji, H. (2000). The Dark Side of the Nation: Essays on Multiculturalism, Nationalism and
Gender. Toronto: Canadian Scholars' Press.
Barber, K. (1998). The Canadian Oxford Dictionary. Toronto: Oxford University Press.
Battan, S. T. and Leiderman, S.A. ( 2001 ). Planning an Anti-racism Initiative. Project change.
Bala Cynwyd, PA: Center for Assessment and Policy Development.
Reference List
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
142
Beal, D. J., O’Neal, E.C., Ong,J., and Ruscher, J.B. (2000). The ways and means of interracial
aggression: Modern racists’ use of covert retaliation. Personality and Social Psychology
Bulletin, 26(10), 1225-1236.
Beck, J. H., Reitz, J. G., and Weiner, N. (2002, March). Addressing systemic racial
discrimination in employment: The Health Canada case and implications of legislative
change. Canadian Public Policy, 28(3), 373-394.
Ben-Tovim, G., Gabriel, J., Law, I., and Stredder, K. (1986). The local politics of race. London:
Macmillan.
Calliste, A. (1993). Women of "exceptional merit": Immigration of Caribbean nurses to Canada,
Canadian Journal of Women and the Law, 6 (1), 85-102.
Calliste A. (1995). End the silence on racism in health care: Build a movement against
discrimination, harassment and reprisals. A conference for black nurses and other health
care workers. Unpublished report. Congress of Black Women of Canada. Ontario
Institute for Studies in Education, Toronto, Ontario, May 25-26.
Calliste, A. (1996). Antiracism organizing and resistance in nursing: African Canadian women.
The Canadian Review of Sociology and Anthropology, 33(3), 361-369.
Calliste, A. (2000a). Nurses and porters: Racism, sexism and resistance in segmented labour
markets. In A. Calliste and G. J. Sefa Dei (Eds.), Anti-racist feminism: Critical race and
gender studies (pp. 143-164). Halifax, NS: Fernwood Publishing.
Calliste, A. (2000b). Resisting professional exclusion and marginality in nursing: Women of
colour in Ontario. In M. Kalbach and W. Kalbach (Eds.), Perspectives on ethnicity in
Canada (pp. 303-28). Toronto: Harcourt.
Reference List
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
143
Canadian Institute for Health Information (2003). Canada's health care providers. Retrieved
October 2, 2003, from http://secure.cihi.ca.
Centre for Equity in Health and Society. (2003). CEHS: Research and Advocacy to Shift the
Discourse of Dominance. Ottawa: Canadian Race Relations Foundation.
Chilly Climate Collective (Eds.). (1995). Breaking Anonymity: The chilly climate for women
faculty. Waterloo, ON: Wilfrid Laurier University Press.
City of Toronto, Department of Public Health. (2002). Access and Equity: A case study of
Toronto Public Health’s current practices and organizational needs. Toronto:
Department of Public Health.
Collins, E. (2004). Career mobility among immigrant registered nurses in Canada: Experiences
of Caribbean women. Ph. D. dissertation. Toronto: OISE/University of Toronto.
Collins, E., Calliste, A., Choudhry, U., Fudge, J., Hagey, R., Lee, R., Turrittin, J., and Guruge, S.
(1998). Research toward equity in the professional life of immigrants. Phase I: “Making
racism see-able: The complaints/grievances filed by women immigrant nurses who are
members of designated minorities”. Project Report to the Centre of Excellence for
Research on Immigration and Settlement (CERIS): Printed in The Culture Care Nursing
Interest Group Newsletter, I(3), (1999).
Connors, K. (2001, November). The Future of Health Care. Submission to the Commission on
the Future of Health Care in Canada, The Honourable Roy Romanow, Chair. Canadian
Federation of Nurses' Unions. Retrieved January 27, 2004, from www.hc-
sc.gc.ca/english/care/romanow/hcc0414.htm.
Cooper Brathwaite, A. (1996). Verbal abuse of hospital staff. The Canadian Nurse, 92(6), 31-34.
Reference List
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
144
Curry-Stevens, A. (2005). Expanding the circle: People who care about ending racism. We need
your help. Toronto: CSJ Foundation for Research and Education.
Das Gupta, T. (1996). Racism and paid work. Toronto: Garamond Press.
Das Gupta, T. (2002) Racism in nursing: Executive summary (Report). Toronto: Ontario Nurses
Association.
Dei, G. (1996). Anti-racism education: Theory and practice. Halifax: Fernwood Publishers.
Dicicco-Bloom, B. (2004). The racial and gendered experiences of immigrant nurses from
Kerala, India. Journal of Transcultural Nursing 15 (1), 26-33.
Dion, K.L. and Earn, B.M. (1975). The phenomenology of being a target of prejudice. Journal
of Personality and Social Psychology, 32(3), 944-950.
Dion, K.L., Earn, B. M. and Yee, P.H.N. (1978). The experience of being a victim of prejudice:
An experimental approach. International Journal of Psychology, 13(3), 197-214.
Dion, K.L. and Kawakami, K. (1996). Ethnicity and perceived discrimination in Toronto:
Another look at the personal/group discrimination discrepancy. Canadian Journal of
Behavioural Science, 28(3), 203-213.
Doris Marshall Institute (DMI) and Minors, A. (1994). Ethnoracial equality: A distant goal?
(Interim Report to Northwestern General Hospital). Toronto.
End the Silence (1996). Video. Directed by R. McTair and J. Crooks. Toronto: Zacfilm. 45
min. Available at [email protected].
Essed, P. (1990). Everyday racism: Reports from women of two cultures. Translated from the
Dutch by Cynthia Jaffé. Claremont, CA: Hunter House.
Essed, P. (1991). Understanding everyday racism: An interdisciplinary theory. Newbury Park,
CA: Sage Publications.
Reference List
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
145
Fals Borda, O. (1979). Investigating reality in order to transform it: The Columbian experience.
Dialectectical Anthropology, 4(1), 33-55.
Fisher, R. and Brown, S. (1988). Getting together: Building relationships as we negotiate. New
York: Penguin.
French, W. and Albright, D. (1998). Resolving a moral conflict through discourse. Journal of
Business Ethics, 17(2), 177-194.
Glaessel-Brown, E. (1998). Use of immigration policy to manage nursing shortages. Journal of
Nursing Scholarship 30(4), 323-327.
Gustafson, D. (2002). Cultural sensitivity as a problematic in Ontario nursing policy and
education: An integrated feminist con/textual analysis. Ph.D. thesis, Department of
Sociology and Equity Studies in Education, Toronto: O.I.S.E., University of Toronto.
Hagey, R. (1997). The use and abuse of participatory action research. Chronic Diseases in
Canada 18(1), 1-4. Invited editorial.
Hagey, R. (1999). What is racism? Toronto: Culture Care Nursing Research Council.
Hagey, R. (2003, Winter). What is a racial dispute? How can we reach a level playing field?
Nursing Leadership Network Update.
Hagey, R., Choudhry, U., Guruge, S., Turrittin, J., Collins, E., and Lee, R. (2001a). Immigrant
nurses’ experience of racism. Journal of Nursing Scholarship, 33 (4), 389-394.
Hagey, R., Lum, L., MacKay, R., Turrittin, J., and Brody, E. (2001b). Exploring transformative
justice in the employment of nurses: Toward reconstructing race relations and the
dispute process (Unpublished Report to the Law Commission of Canada).
Hagey, R. and MacKay, R. (2000). Qualitative research to identify racialist discourse: Towards
equity in nursing curricula. International Journal of Nursing Studies, 37, 45-56.
Reference List
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
146
Hagey, R. and Turrittin, J. (2003). "A very nice tact" – How racialized nurses use relational
power to combat the oppression of racism. Manuscript submitted for publication.
Head, W. (1985). An exploratory study of attitudes and perceptions of minority and majority
group healthcare workers. Toronto: Ontario Ministry of Labour.
Henry, F. and Tator, C. (2002). Discourses of domination: Racial bias in the Canadian English-
language press. Toronto: University of Toronto Press.
Henry, F., Tator, C., Mattis, W. and Rees, T. (1995). The colour of democracy: Racism in
Canadian society. Toronto: Harcourt Brace, Canada.
Jackson, E. (1993). Whiting-out difference: Why U.S. nursing research fails black families.
Medical Anthropology Quarterly 7(4), 363-385.
Jacobs, M. (2002). Creating understanding from research: Staff nurses' views on collegiality. In
M. Jacobs (Ed.), Is anyone listening? Women, work, and society (pp. 295-314). Toronto:
Women's Press.
Jean Baker Miller Training Institute (JBMTI). (2002). Retrieved September 19, 2002, from
www.wellesley.edu/JBMTI.
Jordon, J. (1999). Workshop presentation. Jean Baker Miller Summer Training Institute.
Wellesley College. Wellesley, MA.
Kettner, M. (1993). Scientific knowledge, discourse ethics and consensus formation in the public
domain of applied ethics: A reader. E. Winkler and J. Coombs (Eds.). Oxford: Blackwell.
Kirby Report. (2002). The Health of Canadians: The federal role. Final Report. The Standing
Senate Committee on Social Affairs, Science, and Technology. Retrieved January 23,
2003, from www.parl.gc.ca/37/2/parlbus/commbus/senate/ Com-e/SOCI-E/rep-
e/repoct02vol6-e.htm.
Reference List
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
147
Koebel, J. (2003). Deconstructing Romanow. Paper presented at the Concurrent Session at the
Canadian Race Relations Foundation Award of Excellence Symposium, entitled Racism:
Breaking Through the Denial. March 28, Sheraton Hotel, Toronto, Ontario.
Kohli, R. and Thomas, B. (1995, October). A time for change: Anti-racism, employment equity
organizational change process. Final Report of the East York Health Unit Employment
Equity Coordinating Committee. Toronto: The Doris Marshall Institute for Education
and Action.
Kolb, D. (1994). When talk works: Profiles of mediators. San Francisco: Jossey-Bass Publishers.
Law Commission of Canada. (1999). From restorative justice to transformative justice.
Discussion paper. Ottawa: Law Commission of Canada. Retrieved October 15, 2000,
from www.lcc.gc.ca/en/themes/sr/rj/2000/paper.html.
Llewellyn, J. and Howse, R. (1999). Institutions for restorative justice: The South African truth
and reconciliation commission. University of Toronto Law Journal, 49(3), 355-388.
Lowe, G.S. (2002). Quality of worklife indicators for nurses in Canada. Workshop Report to the
Canadian Council on Health Services Accreditation. Ottawa: Canadian Nurses
Association.
Majumdar, B. (1996). Culture and Health: Culture-sensitive training manual for the health care
provider, 5th ed. Hamilton, ON: McMaster University Faculty of Health Sciences,
School of Nursing.
Marshall, K. (1996, Winter). The diversity of managers. Perspectives (Statistics Canada), 24-30.
McIntosh, P., (1990). White privilege: Unpacking the invisible knapsack. Independent School
49(2), 31-36.
McLuhan, M. (1964). Understanding media: The extensions of man. New York: McGraw-Hill.
Reference List
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
148
McPherson, K. (1996). Bedside matters: The transformation of Canadian nursing 1900-1990.
Don Mills, ON: Oxford University Press.
Meeks, D. (2003). Deconstructing Romanow. Concurrent Session at the Canadian Race
Relations Foundation Award of Excellence Symposium, entitled Racism: Breaking
Through the Denial. March 28, Sheraton Hotel, Toronto, Ontario.
Mills, A. J. and Simmons, T. (1995). Reading organization theory: A critical approach to the
study of organizational behaviour and structure. Toronto: Garamond Press.
Morris, R. (2000). Stories of transformative justice. Toronto: Canadian Scholar's Press.
Municipality of Metropolitan Toronto. (1993). Anti-racism policy and implementation strategy
discussion paper. Toronto: Municipality of Metropolitan Toronto.
Multiculturalism and Citizenship Canada, Race Relations and Cross Cultural Understanding
(1993). Consultation for action report. Committee for Intercultural, Interracial Education
in Professional Schools.
Navarro, V. and Muntaner, C., (Eds.). (2004). Political and Economic Determinants of
Population Health and Well-Being: Controversies and Developments. Amityville, NY:
Baywood Publishers.
Nestel, S. (2000). Obstructed labour: Race and gender in the re-emergence of midwifery in
Ontario. Unpublished Ph.D. thesis. OISE/University of Toronto.
Nolan, D. and Abrams, R.I. (1985). The labor arbitrator’s several roles. Maryland Labor
Review, 44, 873.
North American Congress on Latin America (NACLA). (1995, November/December). Welcome
to America: Immigration Backlash (issue theme). NACLA Report on the Americas
XXIX(3).
Reference List
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
149
Ontario Human Rights Commissition (OHRC) (1994). Minutes of Settlement.
Ontario Hospital Association and the Ontario Ministry of Health, Joint Policy and Programming
Committee (1996). Anti-racism organizational change self-assessment tool/anti-racism
policy guidelines.
Ontario Ministry of Health (1994). Strengthening voices: Anti-racism strategy.
Oquist, P. (1978). The epistemology of action research. Acta Sociologica, 21(2), 143-163.
Ornstein, M. (2000). Ethno-racial inequality in the City of Toronto: An analysis of the 1996
census. Toronto: City of Toronto, CERIS, United Way of Greater Toronto.
Romanow, R. (2002). Royal commission on the future of health care in Canada: Final report.
Ottawa: Health Canada.
Smith, C.C. (2004). Crisis, conflict and accountability: The impact and implications of police
racial profiling. Toronto: African Canadian Community Coalition on Racial Profiling.
Smith, D. (1990). The conceptual practice of power: A feminist sociology of knowledge.
Toronto: University of Toronto Press.
Statistics Canada. (2003). Canada’s ethnocultural portrait: The changing mosaic. Ottawa.
96F0030XIE2001008.
Stevens, P. E. and Hall, J. M. (1992). Applying critical theories to nursing in communities.
Public Health Nursing 9(1), 2-9.
Stith, A. (1998). Breaking the glass ceiling: Sexism and racism in corporate America: The
myths, the realities, and the illusions. Toronto: Warwick Publishing.
Susskind, L., McKeaman, S, and Thomas-Larmer, J. (Eds.) (1999). The concensus building
handbook. Thousand Oaks, CA: Sage.
Reference List
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
150
Swan, K. (1996). The arbitrator as a social engineer. Revised version (prepared with the
assistance of Celia Harte) of a paper (non-paginated) presented at the 14th Annual
Labour Arbitration Conference, University of Calgary, Industrial Relations Research
Group, June 12-13.
Turner, B.S. (2000). Cosmopolitan virtue: Loyalty and the city. In E.F. Isin (Ed.), Democracy,
citizenship and the global city (pp. 129-147). London: Routledge.
Turrittin, J., Hagey, R., Guruge, S., Collins, E., and Mitchell, M. (2002). The experiences of
professional nurses who have migrated to Canada: Cosmopolitan citizenship or
democratic racism? International Journal of Nursing Studies 39, 655-667.
United Nations Declaration of Human Rights (1948). Articles 9; 21; 29; Articles 1; 2 and 7.
van Dijk, T. A. (1993). Elite discourse and racism. Newbury Park, CA: Sage Publications.
Villeneuve, M.J. (2002/2003, Winter). Health care, race and diversity: Time to act. Hospital
Quarterly 6(2), 67-73.
Waldron, I. (2002). African Canadian women storming the barricades! Challenging psychiatric
imperialism through indigenous conceptualizations of 'mental illness' and self healing.
Unpublished dissertation, OISE/University of Toronto.
Walker, M. (2002). Power and effectiveness: Envisioning and alternate paradigm. Working
Paper #95. Wellesley, MA: Jean Baker Miller Training Institute.
World Health Organization (1986, November 21). Ottawa Charter for Health Promotion.
Ottawa.. WHO/HPR/HEP/95.1. Retrieved June 11, 2004, from
www.ottawa_charter_hp.pdf.
Yoshida, M. (1994). The integration of cultural content into an undergraduate nursing
curriculum: A model at the University of Toronto. Educating professionals for diversity.
Reference List
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
151
Report of the Committee for Intercultural and Interracial Education of Professionals.
Toronto.
Reference List
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
152
Definitions
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
153
Definitions
Aboriginal peoples: A term referring to First Nations, Inuit, Metis, non-Status, or Status Indians. The latter designation is defined in different ways under the 1876 Indian Act. Accountability: A feature of relationship that holds individuals, groups, or offices responsible according to principles or criteria befitting the relationship, for example, transparent communication, fairness, and trustworthiness. Accountability practices pertaining to equity include:
• honesty and ownership of the impact of racial discrimination; • informing persons of the perception of unfairness; • providing an opportunity for persons to retract mistakes on their own recognizance along
with apology and accommodation; and • informing persons what the community requires.
Accountability outcomes of a transformative justice hearing of a complaint: • parties feel like whole persons; • relationships feel in balance; and • members of racialized groups feel safe (see Author, 1988).
Individual Accountability refers to the assignment of responsibility for a specific set of actions for which non-compliance may result in specific sanctions.
Public Accountability entails community participation in, and control of, the decision-making processes of public institutions (Henry et al., 1995).
Agency: A term referring to participation capacity, such as voicing needs and realizing interests through decisions and actions. Agency is equal when there is equal access and participation. Anti-racism: Refers to a health promotion agenda that calls for an end to condoning and promoting racism by advocating for accountability in relationships irrespective of race, colour, or ethnicity. Avoiding accountability for racial equality: A condoned practice permitted among all members of a society where racial discrimination, racialization, racial dominance, racial disparities, and racial segregation are not necessarily held accountable. Backlash: Striking out in reaction to a perceived threat (Archaic use refers to the slave lashing back at the master). Discourse: Language-based expression (verbal, written, non-verbal) that includes knowledge plus ideology or “the talk and the walk.” Discourse can be either a reflection of social structures or a mechanism for restructuring relations.
Definitions
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
154
Discourses of racial discrimination: Language-based expressions that structure relations of dominance including marginalization, exclusion, problematization, and containment of racialized people. These expressions can target racialized persons’ supporters. Employment Equity: Refers to a set of standards of fairness and equality achieved throughout employment by the administration of equilibration practices designed in policy and legislation to protect all workers. Equity: Standards of fairness achieved through social justice proceedings. Ethnocentrism: Refers to an ubiquitous tendency to view all peoples and cultures in terms of one's own cultural standards and values. Ethnoracial competencies: Skills manifested by healthy discourse practices that integrate anti-racism principles and strategies in decisions and relationships. The term can also refer to broad based people skills that transact equity pertaining to age, class, disability, gender, race, sexual diversity, and so on (Meeks, 2003). Institutional racism: The lack of accountability for racial equality in society’s institutions, such as health care. Its fundamental basis is the privilege – informed by ideology and group power – of not having to be equally accountable to racialized people as to non-racialized group members. Invisible minorities: People who experience social inequalities because of traits that are not visible, for example, cognitive capacities, sexual diversity, or age. Non-racialized people: Members of dominant groups who enjoy white privilege because of their race, colour, or ethnicity (see “Racialized people,” below). The Ontario Human Rights Code protects non-racialized people who experience racial discrimination by association with racialized people or anti-racist agendas. Otherness: A situation in which one is being undervalued or discounted because of race, colour, or ethnicity, for example, being subjected to difference, marginalization, subordination, disadvantaging, restriction, being silenced, lacking in information or cooperation for control, events being in chaos, and/or lacking information about the correct means and channels for decision-making (Hagey and MacKay, 2000). Non-racialized people who champion anti-racism can experience otherness in their workplace. Race: A set of assumptions used in discrimination, creating racialized and non-racialized peoples. Assumptions of race make a connection between European derived signifiers of race, such as skin colour or heritage, so that accountability is not owed to the racialized person(s). Race consciousness based on anti-racist principles: A strategy for racial equality that names and questions discourses of domination and promotes equal access and participation in governance, media, education, research, corporations, health care, policing, child welfare, politics, justice, and so on.
Definitions
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
155
Racial backlash: Negative reaction or repercussion when a racialized person assumes a privilege that is deemed suitable for whites only; also pertains to reprisal for complaining of racism (see “Reprisal,” below). Racial discrimination: Policy and practices characterized by avoidance of a relation of accountability for equity with racialized people, who consequently experience social domination and differences. Racial disparities: Inequalities in health, employment, income, education, social justice, and other societal benefits, that impact negatively on racialized people. Racial profiling: Intentional or unintentional discrimination of personal attributes consistent with the European derived ideologies around race, white privilege, and racial superiority. Accountability for racial profiling requires race consciousness. Racialization: A social segmentation and control process that relies on discourse practices of discrimination, dominance, and difference in treatment that are based on the assumption that in a racist society, one is permitted not to be equally accountable to racialized people as to non-racialized people.
Racialization is denied and behaviours are rationalized even when non-racialized people challenge racialization processes. Accountability for racialization requires race consciousness. Racialized encounter: A racialized person(s) receives an intentional or unintentional communication so that the sender accomplishes racial segmentation and control (i.e. marginalization, problematization, containment and/or exclusion of the racialized person(s)). Accountability for perpetrating racialized encounters and their effects requires race consciousness. Racialized people: People who experience social inequalities because of their race, colour, or ethnicity. Reprisals: Denotes retaliation for making a complaint. Reprisals are prohibited under the Ontario Human Rights Code. Resilience: Individual strengths based on coordinating supports and influence to achieve social goals and objectives. Restitution: Differences including accommodation required in order to achieve equity outcomes. Set-up: The unfair manipulation of people and the organization of events toward desired inequitable outcomes. For example, racialized nurses experience set-up that puts them in a bind so that they (and not their non-racialized counterparts) must choose between one disadvantage and another.
Definitions
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
156
Systemic racism: Policies, practices, and procedures that are considered normal, but can intentionally or unintentionally discriminate against individuals and groups protected under the Code, thus privileging non-racialized people. The privileges of systemic racism are upheld by discourse that avoids accountability for racial domination. Tit for tat: Backlash and counter backlash, or resistance and counter resistance typical of dispute escalation. (See Fisher and Brown, 1988) Transparency: A principle of procedural justice upholding ethical practices, such as informed consent and equal access to information, participation, and decision-making channels. Visible minorities: Statistics Canada allows Canadian residents other than Aboriginal peoples to self-identify their visible minority status when completing forms. Identification usually refers to race or colour. Whiteness: In-group credits enjoyed on the basis of the freedom of not being liable for one’s race, colour, or ethnicity and on immunity from having to be accountable to out-group members (see “Otherness”). Privileges include normality, authority, dominance, freedoms for flexibility, capacity for voicing and likelihood of being heard, opportunity for being in control, events being orderly, and having information and access to the correct means and channels of decision-making (Hagey and MacKay, 2000). In workplaces that uphold institutional racism, in order to sustain the privileges of whiteness, racialized people and non-racialized people collaborate to oppose anti-racism.
“Nursing is like a cappuccino – white on top, brown on the bottom – and it needs stirring up.”
“Stir it up” – Bob Marley Please visit our website www.BeforeQuality.com.
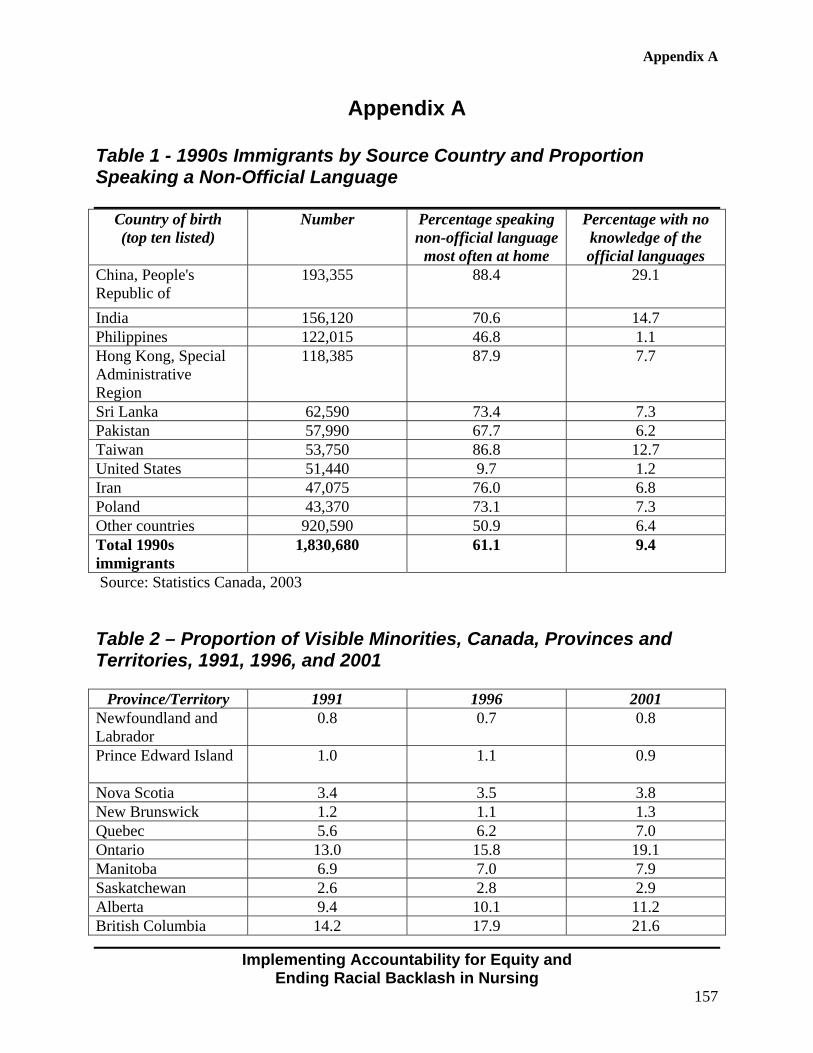
Appendix A
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
157
Appendix A
Table 1 - 1990s Immigrants by Source Country and Proportion Speaking a Non-Official Language
Country of birth (top ten listed)
Number Percentage speaking non-official language
most often at home
Percentage with no knowledge of the official languages
China, People's Republic of
193,355 88.4 29.1
India 156,120 70.6 14.7 Philippines 122,015 46.8 1.1 Hong Kong, Special Administrative Region
118,385 87.9 7.7
Sri Lanka 62,590 73.4 7.3 Pakistan 57,990 67.7 6.2 Taiwan 53,750 86.8 12.7 United States 51,440 9.7 1.2 Iran 47,075 76.0 6.8 Poland 43,370 73.1 7.3 Other countries 920,590 50.9 6.4 Total 1990s immigrants
1,830,680 61.1 9.4
Source: Statistics Canada, 2003 Table 2 – Proportion of Visible Minorities, Canada, Provinces and Territories, 1991, 1996, and 2001
Province/Territory 1991 1996 2001 Newfoundland and Labrador
0.8 0.7 0.8
Prince Edward Island
1.0 1.1 0.9
Nova Scotia 3.4 3.5 3.8 New Brunswick 1.2 1.1 1.3 Quebec 5.6 6.2 7.0 Ontario 13.0 15.8 19.1 Manitoba 6.9 7.0 7.9 Saskatchewan 2.6 2.8 2.9 Alberta 9.4 10.1 11.2 British Columbia 14.2 17.9 21.6
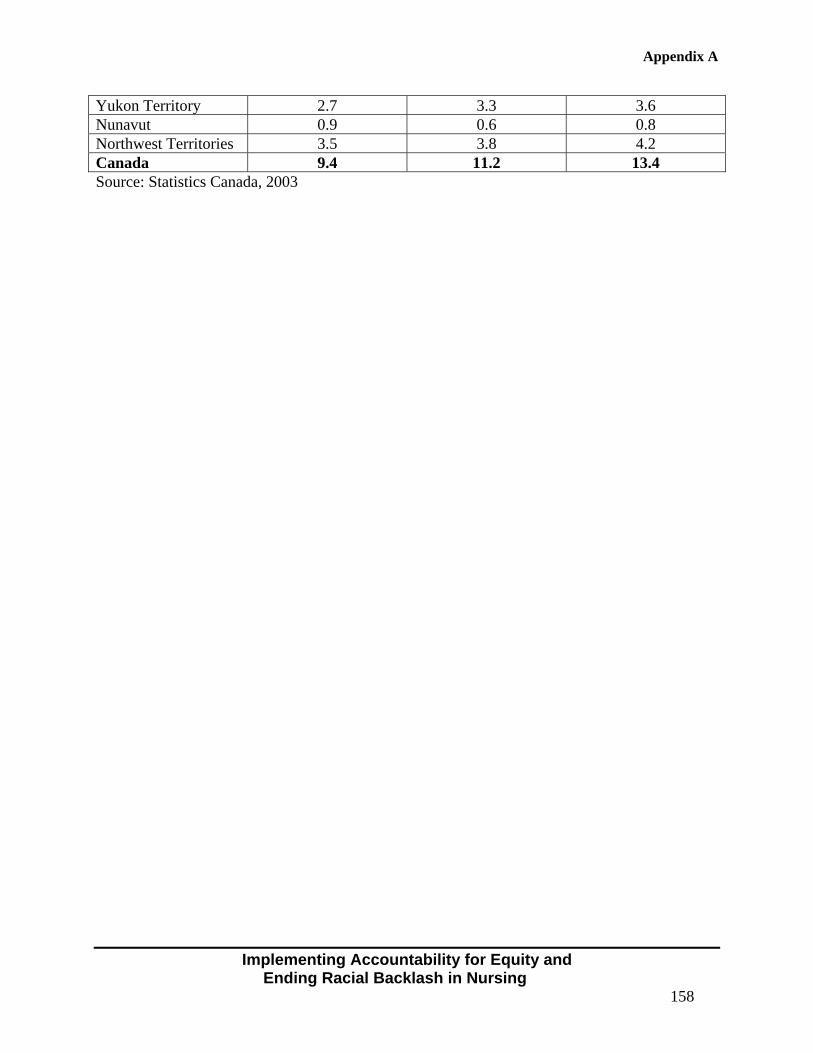
Appendix A
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
158
Yukon Territory 2.7 3.3 3.6 Nunavut 0.9 0.6 0.8 Northwest Territories 3.5 3.8 4.2 Canada 9.4 11.2 13.4 Source: Statistics Canada, 2003
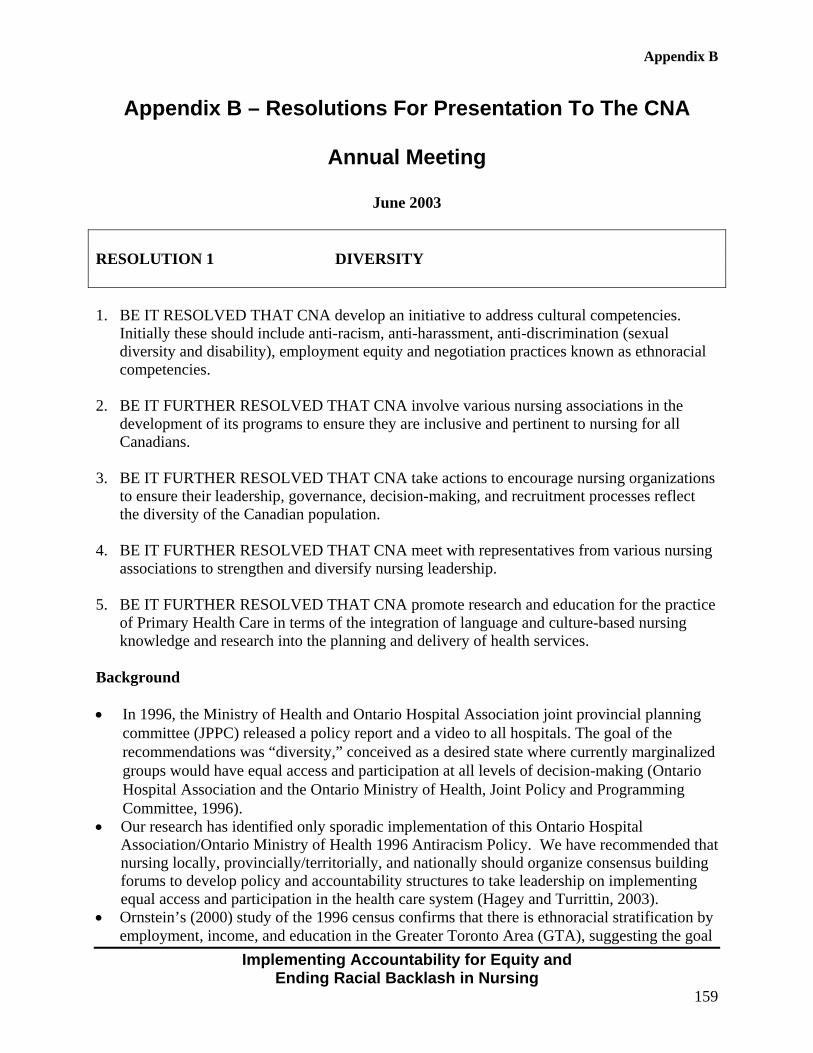
Appendix B
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
159
Appendix B – Resolutions For Presentation To The CNA
Annual Meeting
June 2003
RESOLUTION 1 DIVERSITY 1. BE IT RESOLVED THAT CNA develop an initiative to address cultural competencies.
Initially these should include anti-racism, anti-harassment, anti-discrimination (sexual diversity and disability), employment equity and negotiation practices known as ethnoracial competencies.
2. BE IT FURTHER RESOLVED THAT CNA involve various nursing associations in the
development of its programs to ensure they are inclusive and pertinent to nursing for all Canadians.
3. BE IT FURTHER RESOLVED THAT CNA take actions to encourage nursing organizations
to ensure their leadership, governance, decision-making, and recruitment processes reflect the diversity of the Canadian population.
4. BE IT FURTHER RESOLVED THAT CNA meet with representatives from various nursing
associations to strengthen and diversify nursing leadership. 5. BE IT FURTHER RESOLVED THAT CNA promote research and education for the practice
of Primary Health Care in terms of the integration of language and culture-based nursing knowledge and research into the planning and delivery of health services.
Background • In 1996, the Ministry of Health and Ontario Hospital Association joint provincial planning
committee (JPPC) released a policy report and a video to all hospitals. The goal of the recommendations was “diversity,” conceived as a desired state where currently marginalized groups would have equal access and participation at all levels of decision-making (Ontario Hospital Association and the Ontario Ministry of Health, Joint Policy and Programming Committee, 1996).
• Our research has identified only sporadic implementation of this Ontario Hospital Association/Ontario Ministry of Health 1996 Antiracism Policy. We have recommended that nursing locally, provincially/territorially, and nationally should organize consensus building forums to develop policy and accountability structures to take leadership on implementing equal access and participation in the health care system (Hagey and Turrittin, 2003).
• Ornstein’s (2000) study of the 1996 census confirms that there is ethnoracial stratification by employment, income, and education in the Greater Toronto Area (GTA), suggesting the goal
Appendix B
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
160
of diversity may be long way off unless explicit leadership development strategies are initiated.
• The CNA report to the Canadian Council on Health Services Accreditation on Quality of Worklife for Nurses in Canada, July 2002, identifies grievances and unresolved grievances as one of eight major indicators of worklife challenges in nursing in Canada.
• Our research program has documented millions of health care dollars being spent on grievances and complaints charging employers with discrimination or harassment. We reported racial tension, poor handling of disputes, and a reduction in diversity during times of under-funding and down sizing (Hagey, Lum, MacKay, Turrittin and Brody, 2001b).
• The rescinding of the Employment Equity Act in Ontario and the weakening of federal legislation to address systemic discrimination (see Hagey and Turrittin, 2003) has put the onus on representatives of employers, including nurses, to enforce standards of fairness and handle conflicts that erupt when fairness is in question.
• We have completed two case studies that identify racial harassment and backlash implicating nurses in the reinforcement of the perceived racial hierarchy in nursing. The dispute process in racial disputes appears to be informed by retributive justice – enforcing obedience through punishment – rather than by negotiation, restitution, transformative, and restorative justice (see Hagey et al., 2001a).
• Nestel (2000) has identified that according to the 1991 Census visible minority nurses in Ontario had only half the chance of becoming a manager as did nurses who do not have visible minority status (self identified).
• The Report by Rita Kholi and Barb Thomas entitled “A Time for Change” identifies forty-four recommendations for combating racism in one community health unit where diversity was reduced among nursing staff during a period of downsizing due to underfunding. Systemic racism is acknowledged as a barrier to inclusive practices.
• Major Human Resource challenges arise from these issues including recruitment and retention of nurses for the future. Moreover, the 2001 Census documents the growing number of Canadians who speak neither official language (see Appendix A). Language diversity makes communication between staff and patients very complex to the point where patient safety may be in jeopardy. The word “diversity” has proliferated to denote new social forms such as “diversity practitioners” and “diversity workplace units” that are being funded in a growing number of health service agencies to address a broad range of diversity issues. Both the Kirby Report (2002) and the Romanow Report (2002) make specific recommendations pertaining to Aboriginal health.
• Our research report argues that nurse managers require a knowledge base to be developed that can inform the promotion of leadership opportunities for all nurses (Hagey and Turrittin, 2003). Our report was a result of participatory action research unofficially involving the following groups who shared their perceptions of barriers to leadership in nursing: The Aboriginal Nurses Association of Canada, the African Nurses Network, various Caribbean associations including the The Barbadian Nurses, The Grenadian Nurses Association, The Trinidadian Nurses, and the University Hospitals of the West Indies Alumnae and Associates (Jamaica) have participated. Also included were the Canadian Black Nurses Association, the Chinese Nurses Association (Cantonese and Mandarin speakers), the Filipino Nurses Association, Hispanic, Portugese and Central and Latin American Nurses and Muslim Nurses, the Korean Nurses Association of Ontario, the South Asian Nurses Association, the Culture Care Nurses Interest Group, the International Nurses Interest Group, and individual
Appendix B
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
161
nurses, community activists, union leaders, and consumers identified barriers to leadership influence. So did the Ontario Association of Black Trade Unionists and the Urban Alliance on Race Relations and also spokespersons for the RNAO and the National Nursing Policy Office.
• In a recent study of staff nurses by Professor Tania Das Gupta, 39% of Black nurses, 22% of South Asian nurses, 20% of Asian nurses and only 1% of white nurses thought that their performance review was influenced by their race, ethnicity or colour (Das Gupta, 2002).
• 55% of Black nurses and 47% of Asian nurses and 44% of South Asian nurses and 27% of Central and South American nurses and 6% of European/White nurses felt their relationship with their manager was affected by their race, ethnicity or colour.
• The nurses reporting harassment in this Das Gupta study identified colleagues, patients, supervisors and physicians (in that order) as a source of harassment.
• Our recent study identified “set-up” as a method employed to exclude racialized nurse managers from decision (Hagey and Turrittin, 2003).
• A recent report issued by the City of Toronto Department of Public Health, entitled Access and Equity: A Case Study of Toronto Public Health’s Current Practices and Organizational Needs (2002), identifies a paucity of nurse leaders and managers from minoritized communities.
• Nursing Informatics technology is advancing that could develop a research-based infrastructure to track diversity issues and how well policies are working to ensure employment equity and standards of fairness.
• The Dorothy Wylie Institute for Nursing Leadership could play a role in proliferating a research-based infrastructure to track diversity issues and how well policies are working to ensure equity and standards of fairness.
• Also, the Centre for Equity in Health and Society coordinates a network of interdisciplinary researchers and nurses who advocate for equity in health and organizations responsible for health care. CEHS invites nurses to participate in learning more about racial disparities and social inequalities and their impact on health. We are using a research base to advocate for anti-racism, anti-discrimination, employment equity, and intercultural competencies becoming integrated into the knowledge and practice in all levels and sectors in nursing. We are studying what is effective for holding individuals and organizations accountable for equity in health care and society. CEHS asks you to support nurses who have experienced racial discrimination at work themselves, or have witnessed the effects of such discrimination on colleagues and their families and communities. CEHS is calling for the creation of a nursing-wide equity assurance policy to ensure that the work environment for nurses, and therefore for patients, is caring rather than poisoned. This policy and the research that supports it could inform local, provincial, and national Racial Equality and Employment Equity Assurance Programs (REEEAP) in nursing. Soon to come: www.StirItUp.ca.
Submitted by Rebecca Hagey, member, Registered Nurses Association of Ontario
Appendix C
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
162
Appendix C – Resolutions To The Registered Nurses
Association Of Ontario (RNAO)
Submitted for the April 11, 2003 AGM at the Hilton in Markham RESOLUTION # 4 SUBMITTED BY REBECCA HAGEY, PhD, RNAO REGION 6 MEMBER
BE IT RESOLVED THAT RNAO devise a series of conferences to envision means of
achieving racial equality and employment equity.
BE IT FURTHER RESOLVED THAT RNAO will embark on coordinated planning
to develop policy with its nursing and community stakeholders to develop and promote
local and provincial employment equity program initiatives.
Background Information Resolution # 4 • CEHS has documented millions of health care dollars being spent on grievances and
complaints charging employers with discrimination or harassment. We reported racial tension, poor handling of disputes, and a reduction in diversity during times of under-funding and down sizing (Hagey, Lum, MacKay, Turrittin and Brody, 2001b).
• The CNA report to the Canadian Council on Health Services Accreditation on Quality of
Worklife for Nurses in Canada July 2002 identifies grievances and unresolved grievances as one of eight major indicators of worklife challenges in nursing in Canada.
• CEHS has identified barriers to career mobility for racialized nurses based on the statistical proportion that reaches managerial levels.
• Major human resource challenges arise from lack of equity and systemic racism, including
recruitment and retention of nurses for the future. • The rescinding of the Employment Equity Act by the Conservative government in 1996 has
put the onus on representatives of employers, including nurses, to enforce standards of fairness and handle conflicts that erupt in agencies that employ nurses when fairness is in question.
Appendix C
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
163
• CEHS has identified only sporadic implementation of the Joint Provincial Planning
Committee 1996 Antiracism Policy Framework. • The Romanow Commission has identified “The Big Disconnect” with respect to health care
to Aboriginal Communities. The Aboriginal Nurses Association of Canada is well positioned to provide leadership and invites the support of colleagues to help sustain the association’s vision and mission.
• Nursing Informatics technology is advancing that could develop a research-based
infrastructure to track diversity issues and how well policies are working to ensure employment equity and standards of fairness.
• A recent study by Tania Das Gupta (2002) has found that nurses experience racial
harassment from other nurses, from patients, managers and doctors. RESOLUTION # 5 SUBMITTED BY REBECCA HAGEY, PhD, RNAO REGION 6 MEMBER
BE IT RESOLVED THAT the RNAO identify management competencies pertaining
to systemic anti-racism, anti-harassment, anti-discrimination, employment equity, and
culture care.
Background Information Resolution # 5 • In 1996, the Ministry of Health and Ontario Hospital Association joint provincial planning
committee released a policy report and video to all hospitals. The goal of the recommendations was “diversity” conceived as a desired state where currently marginalized groups would have equal access and participation at all levels of decision making (Ontario Hospital Association and the Ontario Ministry of Health, Joint Policy and Programming Committee, 1996). The four pillars of this policy are anti-racism, anti-discrimination, employment equity, and culture care.
• In a recent study of staff nurses by Professor Tania Das Gupta, 39% of Black nurses, 22% of
South Asian nurses, 20% of Asian nurses, and only 1% of white nurses thought that their performance review was influenced by their race, ethnicity, or colour.
Appendix C
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
164
• 55% of Black nurses and 47% of Asian nurses and 44% of South Asian nurses and 27% of Central and South American nurses and 6% of European/White nurses felt their relationship with their manager was affected by their race, ethnicity, or colour.
• The nurses reporting harassment in this Das Gupta study identified their manager as a source
of harassment. • A study recently completed by CEHS, identified “set-up” as a method reported to
marginalize or exclude minority group nurse managers from decision making (Centre for Equity in Health and Society, 2003).
• Two case studies completed by CEHS identify harassment and backlash employed by nurses
that can be seen as contributing to reinforcement of the perceived racial hierarchy in nursing. These strategies are informed by retributive justice, obedience, and punishment rather than by negotiation, restitution, transformative, and restorative justice (see Hagey et al., 2001a and Centre for Equity in Health and Society, 2003).
• Nurse managers require a knowledge base to be developed that can inform the promotion of
leadership opportunities for all nurses.
• The Aboriginal Nurses Association of Canada is well positioned to provide leadership and invites the support of colleagues to help sustain the association’s vision and mission.
• Nursing Informatics technology is advancing that could develop a research-based
infrastructure to track diversity issues and how well policies are working to ensure employment equity and standards of fairness.
• A recent study by Tania Das Gupta (2002) has found that nurses experience racial
harassment from other nurses, from patients, managers, and doctors.

Appendix D
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
165
Appendix D – Letter From Anne McLellan

Appendix D
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
166

Appendix D
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
167

Appendix D
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
168
Appendix E
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
169
Appendix E – Letter to the Representatives of the Joint Provincial Nursing Committee (JPNC) and the Nursing
Secretariat
Accountability for Equal Opportunities in Nursing c/o Canadian Centre for Equity in Health and Society
November, 2002 Joint Provincial Nursing Committee Hepburn Block 11th Floor 80 Grosvenor St Toronto, ON M7A 1R3 To: Adeline Raphael-Falk (RNAO) and Gabrielle Bridle (RPNAO) On behalf of the Accountability for Equal Opportunities in Nursing, Research Team at the Centre for Equity in Health and Society, I am personally inviting you to a dialogue that I am participating in at the round table discussion on racism in nursing to be held at the upcoming RNAO/RPNAO conference on Healthy Workplaces. We congratulate RNAO/RPNAO for breaking the silence on racism in Nursing at this session being held on Nov 22 11am-1pm (at the Holiday Inn on King Street in Toronto) to strategically promote inclusion practices in nursing. The research program findings at the CEHS strongly support the need for the development and implementation of an accountability tool for use in nursing employment and we are asking to dialogue with Canadian nurse leaders on this agenda. Perceptions and questions arising from this program of research requiring attention include: • Is there a commitment to change organizational culture to promote inclusion at all levels in
nursing? • Is there a willingness among key stakeholders in the nursing profession to dialogue and
engage in problem solving on the problems of racialization? • Is there resistance among administrators and human resource personnel toward implementing
the 1995 JPPC (OHA and OMH) Anti-racism Policy framework that includes anti-racism, anti-discrimination, employment equity and culture care?
The research findings to date strongly indicate: • A call from prospective nurses for faculties and student bodies to address admissions,
curriculum and mentoring to achieve equity.
Appendix E
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
170
• A call from front line nurses for assistance on racial abuse and inequality issues. We hope to gain from you, specific strategies for promoting accountability for equity and procedural justice in restructuring race relations in nursing education, administration, professional, union, and regulatory bodies for equal access, participation and representation in nursing. We believe these strategies to be fundamental and crucial to recruitment and retention in our profession. Through our future collaborations, strategies in overcoming the historical and systemic barriers identified by racialized nurses can be successful. Recent studies link disparities due to racial discrimination and systemic lack of inclusion to detrimental health effects. Equity is a determinant of health for nurses and non-nurses alike. Either as preliminary to or follow-up to the round table discussions on November 22, we would appreciate meeting with each one of the Joint Provincial Nursing Committee members on an individual basis for more of an in-depth understanding of your thoughts and recommendations along with other leaders in health care and professional education. My CEHS associate Marianne Chandler (416-363-4546) <[email protected]> awaits hearing about what possible times would be suitable for each of you to have a brainstorming session on the issue of a profession-wide Employment Equity Program in Nursing in Canada. Please see attached our recent petition to the resolutions committee of the Canadian Nurses Association. Respectfully submitted, Rebecca Hagey, PhD. Acting Co-Director, CEHS research program .
Appendix F
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
171
Appendix F – A Time For Change: Recommendations
By Rita Kohli and Barb Thomas
Anti-Racism, Employment Equity Organizational Change Process East York Health Unit
Final Report of the Employment Equity Coordinating Committee (EECC)
The Doris Marshall Institute for Education and Action
October 1995
Part VI: Summary of the Recommendations (pp. 62 – 69) What Needs to be Done: Recruitment and Selection: 1. The EECC examine the language of a cross-section of job postings for adverse impact on
Aboriginal Peoples, Racial Minorities and People with Disabilities.
2. The EECC, in consultation with designated group members, establish a database of comparable ethno-racial, Aboriginal and disabled peoples networks for the distribution of job postings and employment opportunities.
3. The Board, in consultation with the EECC, develop an Anti-Racist Employment Equity Policy and ensure that all job postings and hiring practices comply.
Interviewing Process: 4. The EECC identify and eliminate any real or perceived barriers/adverse impact to Racial
Minorities, Aboriginal Peoples, Peoples with Disabilities in the following components of the interviewing process: - The current screening and short-listing criteria for application; - Response rating criteria for weighing or ranking interviewee responses; - The interviewer’s guide.
5. The EECC monitor all hiring over the next year to ensure that the process complies with the new employment equity policy and procedures of the organization, and that implementation results in increased numbers of people of colour, Aboriginal People, and people with disabilities employed in the organization.
6. Management/EECC, establish policies and guidelines to ensure equity in representation on selection panels; that all selection panels comprise at least 2 people – 1 from management
Appendix F
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
172
and 1 from the constituency being hired (management, administration, etc.) and that at least 1 selection panel to racial minority, and/or person with disability.
Job Descriptions: 7. The EECC identify expedient ways to validate job descriptions and ensure all new staff see
their job description by commencement of work. Accommodation: 8. The Board in conjunction with the Borough, plan to conduct a physical demands analysis to
determine the capacity of the EYHU to accommodate peoples with a wide range of impairments and disabilities; that in the meantime, EYHU accommodate needs as identified.
9. Spectrum conduct employee awareness workshops on disabilities in the workplace, in conjunction with community based Disability Advocacy Networks.
10. The Board and EECC ensure that an anti-harassment and anti-discrimination policy is developed and endorsed throughout the organization, with clearly defined procedures for redress.
Credentials and Related Competencies: 11. The EECC, in their review of job descriptions and personnel policy, identify competencies
related to work with diverse communities for inclusion in job descriptions and interview questions. Performance appraisals include measures to assess the effective use of these skills.
12. Teams, in implementing the Equal Access Program standards, consider ways to maximize the use of these skills among their current members. Teams to set clear, measurable indicators of equal access to the designated groups, and racial minorities within these groups, in all areas of programming.
Orientation and Training: 13. The EECC review existing orientation and training policies and procedures for adverse
impact, particularly on persons with disabilities, with a view to ensuring a consistent practice for all employees.
Probation: 14. The EECC review the criteria, guidelines and processes for probation setting, termination and
the processes of communicating same to employees. Performance Appraisals:
Appendix F
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
173
15. The EECC, in its ongoing document review, examine Performance Appraisal criteria and
procedures to eliminate the inconsistencies in the annual frequency of appraisals and the noticeable level of dissatisfaction, particularly in the management group. This to be done in consultation with management and staff.
Supervision: 16. EECC in consultation with the Borough, organize training sessions for managers and
supervisors to further enhance effective supervision and appraisal skills in the context of an anticipated changing and diverse workforce.
Bridging/Developmental/Secondments: 17. The EECC examine ways to expand bridging, developmental and secondment opportunities
as a strategy for staff development, and for extending the presence of designated group members in the organization.
18. The EECC establish processes for the uniform announcements of these positions. Flexible Working Conditions: 19. CUPE representatives ensure that flex time is negotiated in the next collective bargaining. Complaints: 20. The EECC examine the complaints systems for adverse impact, and revise with attention to
protection against reprisals.
21. Spectrum continue to host educational sessions on discrimination and build a resource list of external supports for staff to use in the current working environment.
22. The board and management develop and implement an anti-racism and an anti-harassment and anti-discrimination policy.
23. The board and management revisit the Vision, Mission and Mandate Statement of the EYHU and revise them to reflect principles of zero tolerance for racism and all forms of discrimination and harassment in the workplace.
24. The EECC ensure consistent inclusion in job descriptions and interview questions, knowledge and skills in addressing discrimination as essential skills to do any job at EYHU.
Rewards:
Appendix F
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
174
25. The EECC in the course of the document review examine systems of rewards and recognition for adverse impact.
26. All levels of the EYHU become less reticent about praising and rewarding excellence where due.
Organizational Culture and Climate: 27. The EECC in conjunction with the Borough host a series of seminars for all employees on
recognizing racism in the workplace: What constitutes a grievance based on race? Discipline: 28. The EECC ensure that its current document review result in clear policies and procedures for
discipline.
29. The EECC ensure that all employees are informed of discipline policies and procedures, and that this is a routine part of orientation for new staff.
30. Spectrum identify external and internal supports to assist employees coping with the impact of disciplinary action.
Lay-Offs and Termination: 31. The EECC examine the lay off, termination, resignation and retirement policies for adverse
impact, and revise as necessary to ensure employment equity principles are upheld in these policies and practices.
Exit Interviews: 32. The EECC review the exit interview process and develop, in consultation with management
and staff, a simple procedure and guidelines for consistent practice.
33. The EECC ensure a mechanism whereby information provided by exiting personnel gets integrated into the ongoing organizational development process.
Document Review: 34. The EECC continue its own training on document review, involving managers where
appropriate and possible, to enhance their ability to recognize barriers in policies and procedures, and engage them with the committee, in assessing and revising personnel policies and procedures.
35. The EECC solicit input, as appropriate, from managers, community-based staff and administrative staff into its review and revision of personnel policies and complete the document review and revisions of policy.
Appendix F
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
175
Who Should Do What in the Change Process?: EECC: 36. The EECC develop a work plan for July 1995 to June 1996. The work plan should specify
how it will:
• Communicate the findings of this report to the rest of the organization; • Complete the document review and revisions to policy; • Incorporate employee input into the policy review; • Involve managers in the process of analysis and revision; and • Develop a realistic plan for the next three years to achieve more equity in who is
present in the organization, and in how issues of racism and discrimination are addressed in the workplace.
37. The EECC establish a database and information system for all employees to ensure accurate
tracking of the Employment Equity program.
38. The EECC procure up-to-date external data, as available, to inform its Employment Equity Plan.
39. The EECC seek management team approval to build in education, support and a budget for itself over the next year to:
• Consult expertise from community organizations, on disability, on racism, on
heterosexism; • Work directly with SPECTRUM where appropriate; and • Selectively use community consultants for process help.
SPECTRUM: 40. The MOH ensure that Spectrum has a budget for its educational activities.
41. Spectrum research and begin to work jointly with community resource people and activists in
East York on issues of discrimination.
42. Spectrum meet with the EECC to discuss the work of each group over the coming year, and:
• Clarify areas of separate and possible joint work; and • Agree on how to communicate their separate and connected roles to the organization.
Board:
Appendix F
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
176
43. The board organize training for itself, utilizing the resources of the EECC and Spectrum as appropriate, to identify more specifically, how to play its role of representing community concerns effectively to the organization.
44. The board set its own goals and develops a plan for increasing representation from the communities of racial minorities, Aboriginal Peoples and peoples with disabilities.
Appendix G
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
177
Appendix G – Role Playing Exercise and Case Studies to Learn about Backlash and Set-up Experientially
Angela Cooper Brathwaite, RN, BScN, MN, PhD
Introduction – There are 3 parts to this role playing exercise. Part I presents a case study of a Nurse Manager's experience of systemic and individual racism in a health care facility. The case study is presented in narrative form as a letter from the Nurse Manager to a friend. Part II uses role play to sensitize individuals who are not ordinarily aware of systemic and individual racism to how these forms of racism work and the effect they have on those who experience them. Part II includes an introduction in which the concepts of transparency and accountability are defined, as well as role play instructions, and an actual role-playing script based on the Nurse Manager's letter. Part III presents procedural and policy strategies based on principles of transformative justice to indicate how equity could be achieved in Nurse D's institution. While the exercise is designed to involve participants, we suggest it could also be effectively used as theatre to instruct larger audiences. We suggest that required reading for conducting this role playing exercise is on our website at www.BeforEquality.com. See especially the Discursive Framework in the report to the Law Commission of Canada submitted by Hagey, R., Lum, L., MacKay, R., Turrittin, J., and Brody, E. See also Nurse X’s Story. Part I: Institutional Relations: A Nursing Manager’s Lived Experience
May 26, 2001
Dear Jane: I would like to share with you another true story. This story is about a nurse
manager (a Black nurse with Caribbean heritage) with a culturally diverse staff (the majority of whom were White Canadians). For purposes of this letter, I will call this manager D. She has 30 years of nursing experience and has been Director of the Family Life Centre for ten years. D is a certified midwife in England and Wales and holds a Bachelor of Nursing Degree from the University of Manitoba. She has worked for the same employer for over 24 years (14 years as a clinical nurse and 10 years as a Director) in Maternal and Child Nursing.
About a year and a half ago, a small group of white nurses complained to the CEO of the hospital that they were very dissatisfied with D’s leadership and management abilities. These nurses did not report their dissatisfaction to the VP of Nursing (D’s supervisor) but colluded with the Chief of Obstetrics in their complaint to the CEO against D. The CEO met with all the staff nurses and the Chief of Obstetrics on three occasions to discuss D’s leadership and management abilities. The VP of Nursing, the Nurse Educator and the manager were excluded from these meetings.
As a result of these meetings, the CEO developed an Action Plan and completed a performance appraisal of D. The nursing staff gave positive and negative feedback to the CEO but he documented only negative comments in the performance review. Up until
Appendix G
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
178
this time, D had received positive performance appraisals. She was accused of practicing favouritism, having poor communication skills, failing to follow up with staff on staff education, and contributing to low morale in the program. The Action Plan outlined the objectives she was expected to meet in six months. She was responsible for: 1) Improving communication with staff; 2) Resolving conflicts on the units; 3) Providing consistency in approach to all staff; and 4) Improving staff’s morale. This action plan was discussed with D in the presence of her supervisor and a hard copy was given to her for her signature.
She was expected to sign an agreement stating that she was responsible for the aforementioned problems and will resolve them in six months. The documents were given to her on a Wednesday and she was expected to return them on Monday (the following week).
D read the documents at home and realized the implications behind the accusations. Thus, she called me and read the documents over the phone. She also asked my opinion about these documents and I told her that she was being set up for failure, since it was impossible to accomplish those objectives on her own. I told her those objectives and problems belonged to the group and not one person; that the problems constituted management-staff relations and required staff collaboration and willingness to work through the conflicts with her. I also suggested that she consult her lawyer and discuss her situation with him because the CEO had a hidden agenda. I questioned why the CEO, (the most powerful person in the hospital) had not included the VP of Nursing in dealing with this situation.
I also asked D what her staff meant by favouritism? She said that favouritism consisted of: 1) Hiring a (qualified) non-white nurse; 2) approving vacation for staff who were from a minority group (based on seniority), and 3) not granting time off after the schedule was posted, if staffing levels were inadequate to meet patients’ needs and the minimum requirements for the program. Five white nurses with junior seniority lodged the complaint, apparently retaliating for the change in practice represented in the fact that D hired nurses with midwifery experience from a minority group. These white nurses made remarks about the newly hired nurses of colour such as: “they are taking over the unit and white nurses will not get the vacant positions". Also, they said that "the newly hired nurses were D’s friends", evidently because she hired them. D did not know the nurses she hired since they were new to the province. The hiring practices included panel interview for all applicants with the same scoring tool to rate each applicant. The person with the highest score won the competition. The white nurses also told the CEO that one thing he could do for the hospital was replace D as director of the program.
Jane, I am making the claim that the hospital where D worked was an “ideological organization” which perpetuated systemic racism by upholding policies and practices to deal with manager-staff relations. Further, there was a disjuncture in D's experience at the hospital. In other words, there was disparity between how D experienced conflicts with her staff and how these were represented in documents. I base these claims on arguments provided in subsequent paragraphs.
My argument is based on the premise that Canada is a sexist-racist state with colonial ideology, i.e. Whiteness and European heritage are widely and implicitly held to be superior to non-white groups or heritage (Bannerji, 2000). Another premise is that racism is so pervasive and subtle in Canada that it forms the background or environment,
Appendix G
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
179
which influences ones thinking, discourse, decision making, practices and social relations (Smith, 1990). Thus, people unknowingly perpetuate the colonial ideology through media, the school system, state regulations, policies and social organizations.
Firstly, I will discuss the ideological organization followed by the disjuncture in D’s experience. According to Smith (1990), an ideology is a method of superseding, substituting, and suppressing the accounts that people create out of the recollection of experience with the accounts of professional discourse. Thus, an ideological organization is an agency that has institutionalized racism through its racialist discourse practices (suppressing and omitting information, not honouring and respecting people of colour) and policies. Additionally, these practices occur in the background without being stated. They are systemic and perpetuate the system because there are no accountability mechanisms to challenge these practices. In D's case, the ideological practice was evident as the CEO did not hold himself responsible and accountable to a person of colour. He overlooked her enormous contributions and apparently perceived D as an easily dispensable person because she was Black.
In D’s case, the CEO suppressed all the positive information about her performance and managerial expertise and reinterpreted D’s actual experience, based on his ideological interpretations, experience and practice, in order to form an account of the situation. For example, a number of staff nurses reported in the meeting with the CEO that D was one of the first managers to implement single room maternity nursing in the province. This type of nursing supported continuity and consistency of patient care by admitting patients in the same room, where they went through childbirth, and post-partum care until discharged. Thus, patients received care from the same nurses from admission to discharge. Additionally, they pointed out that she maintained a positive variance in the budget, hired qualified competent nurses who were able to care for any maternity patient. Therefore, they said, D was effective in reducing the risk of lawsuits in this program and enhanced patients’ satisfaction with nursing care.
However, the CEO highlighted the negative criticisms and misperceptions of a few junior (white) nurses to support his objectification of the information being documented. In other words, the situation was rationalized, justified and reported based on the CEO's and junior staff’s perspectives. Thus, an account of D’s experience (social relations with staff) was reproduced consisting of only the negative particulars. A hidden negative value accompanied the transfer of D’s information in the documents. Therefore, what actually happened in D’s experience, and what was reported, was influenced by the interpretation (“interpretive schema”) and knowledge of the CEO producing the documentation. The CEO used the performance appraisal tool, job description, and human resource policies as documents to propagate his agenda. Moreover, the CEO never questioned the nurses’ comments such as, "they are taking over the unit" and "no white nurse will get the vacant position". He expected D to sign the agreement and action plan, so that he would hold her responsible and accountable for all the problems in the program. However, when he received her lawyer’s response to those documents, he changed his tone and attitude as well as modified the action plan.
D immediately consulted the lawyer who informed the CEO that D had retained him to respond to the Action Plan and performance appraisal and she was not prepared to sign those documents. She acknowledged that there are problems on the unit with a few nurses who would like her replaced. The CEO had over emphasized the negative
Appendix G
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
180
comments of these junior nurses and eliminated the positive comments by the majority of the staff. The lawyer believed it was the responsibility of all the staff to work with D to bring about a resolution to the problems. He felt it was unlikely that her six months evaluation will be impartial, since D was being evaluated by the same group of nurses who wanted her dismissed from her position. The lawyer also stated in his letter that a wrongful dismissal suit was looming over the situation, which will ensure legal counsel; that the tone of the Action Plan indicated that D was not welcome to work in that organization. Thus, he recommended a buyout of employment with full benefits until her magic 80 commenced in two years (based on her benefit plan) since a legal suite would be expensive for the organization.
As a result of the lawyers’ letter, the CEO modified the action plan and sent a copy of it with a letter to D’s lawyer. In the letter, he stated that there was a misunderstanding and he was not assuming any blame to D. He was willing to work with D because of her long-term employment with the hospital and her ten years management experience in the present position. Changes to the action plan included the following actions:
The manager will hold monthly meetings with the staff to develop a cohesive nursing team (the supervisor was present for these meetings); • Staff will discuss evidence of favouritism at staff meetings and D will be expected to
give an explanation of her actions. • The manager will discuss staff performance issues in the presence of the Human
Resources Director and VP of Nursing. • Staff, manager and senior administrative team will collaborate to achieve the action
plan. • The manager will develop an educational plan to address knowledge deficits in staff. • The CEO will conduct a formal evaluation of the action plan at three and six months. • The CEO will complete a follow up performance appraisal of the manager in six
months to validate whether changes have occurred. At the end of six months, the CEO surveyed 65 staff to receive feedback on the
manager’s performance to ascertain whether the action plan was effective in meeting its objectives. Only five staff completed the survey and the feedback was positive. The CEO met with the staff to review the action plan and completed a positive performance review for D. However, he did not place her on the new salary scale with all the other managers. This salary scale was the result of a job evaluation for the management staff, which was conducted prior to D’s problems with the staff.
If one applies the Transformative Principles for Racial Justice (TPRJ) Assessment Tool (see the tool in Hagey et al., 2001b) to this case, one will notice that D was the victim of racial discrimination. She had become the problem in the system. Transparency and accountability issues were prevalent in this case. For example, all the meetings between the CEO and staff were held in the absence of the manager and the VP of Nursing and there was omission of pertinent positive information of D’s management style and performance. Also, no one named the issue as “racial discrimination” although it was present in this situation. Additionally, transformative justice had not occurred at this time, since neither the hospital nor the community took responsibility for changing organizational rules and practices to prevent future discrimination practices in the
Appendix G
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
181
program. The employer did not assume responsibility for ensuring the ethno-racial safety of the manager or other minority staff in this program.
Pertaining to the disjuncture in D’s experience, I am proposing that there is disparity between how discrimination is experienced by D and how it is represented. If one explores the contrasts between the ideological practices of social relations of ruling and the everyday experience in which the events as told in D’s story, one will notice the disparities in this case. For example, the CEO’s selection, assembling, rearranging and interpretation of the information to develop a strong case against D are contrasted against his failure to acknowledge D’s positive contribution to the program and the feelings this failure provoked in her. He omitted segments of her experience that reproduced a negative image of her. Furthermore, he did not increase her salary on the new pay scale although she received a positive performance appraisal from him.
In order to receive the pay increase as per the new salary scale for all mangers, D wrote the Director of Human Resources explaining her situation. Due to D’s actions, the CEO and VP of Nursing decided to place D at level two on the new pay scale when she was at level five on the old pay scale. She declined their offer and stated that she will not accept anything less than level four or five on the new salary scale. Finally, they placed her at level five on the new pay scale.
I asked D how she felt during this experience. She said that she felt unsupported, misunderstood, helpless and victimized. She did not trust anyone including her supervisor. She became angry when she was not offered level five on the new salary scale, even though she had received a positive performance review and the problems in the program were resolved. D acknowledged that her faith in God, and the support of friends gave her the strength to endure this experience. Also, she had legal representation to help her through the process.
Today, the four nurses who accused D of favouritism are no longer in the program and organisation. The human resources director disciplined two of these nurses for injecting themselves and peers with drugs on the unit and they resigned their positions. Another nurse who gave a mother the wrong baby to breast feed, resigned her position rather than face disciplinary action, while the other nurse made major medication errors and left the institution. Similarly, the Chief of Obstetrics was not reinstated in his position and has retired. Also, the VP of Nursing has recently retired. D is still working as Director of the program and is enjoying a positive experience with her present staff. She has a cordial working relationship with the CEO.
At present, one can say some aspects of transformative justice have occurred in D’s situation. She has kept her former position as Director of Family Life Program and received fair compensation for her work (similar to her peers). Also, recently the CEO thanked and commended her for a presentation she gave to the senior team and her peers. This letter of commendation stated how proud he was of her knowledge, presentation skills and professionalism.
Part II: Transparency and Accountability: Re-framing Practices Pertaining to Race Differences Introduction
Appendix G
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
182
Institutions are composed of individuals who have a degree of dependency on others within them and dependency on the institutions for financial, emotional, social, or occupational status/needs. For example, a student in an academic institution is dependent on a teacher to facilitate and foster increased knowledge and intellectual growth. Similarly, an employee is dependent on his employer for financial and career advancement. Regardless of the institution, its members are influenced by the policies and ways of working of that institution in many ways and in various degrees, depending on the positions they occupy, the power they can leverage and their own particular agendas. Each person within an institution brings a particular background, values and beliefs. Additionally, each institution has its own culture (values, practices, beliefs etc) which impacts upon the individuals who attend or work in them. Canadian institutions are influenced by racial ideologies. Today we would like to demonstrate (using two case studies) how racism is practiced in two Canadian institutions: A hospital and an academic setting. Institutional (Systemic) Racism Institutional Racism is described as “systemic inequality which results from institutional processes, which are racially discriminating" (Ben-Tovim, Gabriel, Law, and Stredder, 1986). Institutional Racism is the collective failure of an organization to provide appropriate and professional service to people because of their colour, culture or ethnic origin. It is seen or detected in processes, attitudes and behaviour which amounts to discrimination through unwitting prejudice, ignorance, thoughtlessness, and stereotyping which disadvantages minority ethnic people (McPherson, 1996). Purpose of our Presentation The purposes of this presentation are to use role play: To critically examine the concepts of transparency and accountability as they relate to practices that produce racial disparities. To examine institutional racism. 3) To apply the Transformative Principles for Racial Justice (TPRJ) Assessment Tool to two case studies. 4) To experience racism in a workplace situation in which the CEO uses power, texts (language in documentation) and discrimination against a Black nurse manager. Role Play Facilitator’s Role: Assigns the different roles to each person in the class and conducts debriefing after the role play. Hands each participant a card, e.g. Nurse Manager D, CEO, junior nurse complainant 1,2,3,4, or 5, staff nurse A, B, C, VP Nursing, Director, Human Resources, Chief of Obstretics. The number of staff nurses can expand to accommodate all participants in your class.
Appendix G
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
183
Plan Time requirement is 20-30 minutes Resources: 7 volunteers, plus flip chart, paper, pens, overhead transparencies/ power point. Description of the rules for role play Activity: Participants must take a role and cannot be an observer. Debriefing/discussion period. Rules Each role must be taken seriously. Once the role play begins, it should be played seriously so that participants get immersed into his/her character. No discussion should be entertained during the role play and the rules should be strictly adhered to. All participants should participate in the debriefing session following the role play. Debriefing This stage could be called a follow-up discussion period. Debriefing is a time to reflect on and discover what happened during the role play and what it means. Debriefing an experience with participants is necessary in order to identify the issues and how they relate to the learning objectives (Majumdar, 1996). This process provides participants with an opportunity to reflect on their emotions, thoughts, and feelings. Debriefing encourages and allows participants to verbalize thoughts and feelings that occurred as a result of the learning experience. Through the identification of thoughts, feelings and issues, debriefing assists in bringing the experience into a “real life” context, applicable to daily life. I - Facilitator’s Guide Explain that participants need to explore their feelings before an analysis of the role play can occur. Questions to facilitate this process are: What did you think when the CEO gave you that performance appraisal? How did you feel when you (staff C) heard how your peers described the manager’s performance to the CEO? How did you feel when you heard staff A and B describe the manager negatively to the CEO? How did you respond to the Chief of Obstetric's comments on staff morale? What would you do if you were the nurse manager? How did you feel about other members of the group and their roles? II - Reviewing and Describing What Took Place
Appendix G
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
184
This step assists participants in gathering data and ordering their thoughts. It helps them examine the experience from a different perspective, thus creating new insights. Questions to facilitate this process are: What happened in this situation? What were the challenges? Were you successful? What interactions took place? What events took place? What outcomes or decisions were made? What led to these results? Could anything have been prevented? III - Analysis of the Experience This step helps to establish meaning and identify connections between issues. Questions to facilitate this process are: What were some of the issues at play during the role play? What other real life situation(s) does this situation remind you of? Now that you have this new insight, do you think or feel differently? How can you use this new information in day to day life? How does this affect your view of racial issues in your workplace? Evidence of Racism From the Case Study Case Study #1 of Nurse Manager D's experience: Unrealistic goals "Fix it now" mentality (6 months to turn the situation around). Suppression and omitting of information: all the positive things Nurse D had accomplished were omitted from the performance review Not honouring and respecting Nurse D because she is a Black nurse. Racism was never mentioned. It was subtle or systemic. The CEO perceived D as easily dispensable. She had worked 24 years for this institution with 10 years administrative experience as Manager of the Family Health Centre. Accusation of favouritism when Nurse D hired qualified nurses from minority groups even though a panel conducted the interviews. SCRIPT FOR ROLE PLAY SCENE I: Opens with the CEO, Chief of Obstetrics, 5 to 6 staff seated around a table. CEO: “I am having these forums with you to gather information on what is occurring in the Family Life Centre. I must assure you that all information discussed here is confidential and no names would be identified with any comments made during this forum. I would like to know what are the problems in the program and how these problems are addressed. Also, I would like
Appendix G
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
185
to know how nurse D is dealing with these issues and concerns and how she contributes to them?” Staff C concludes her statement: “…she likes to have a mixture of experienced and junior staff work together …vacations are granted based on seniority.” CEO continues: “ What has D done in the past few years that resulted in staff dissatisfaction?” Staff B concludes her speech: “…who she grants special requests” CEO continues: “I will meet again with you next week to get more input from other staff who are absent today. I assure you that your concerns and issues will not go unattended. I will personally address them with nurse D. Thank you for your input. I will be in touch with you as soon as possible.” Staff A: “ Ray, do you really want to know what is happening on the unit? I am so glad you have taken the time to meet with us. Staff morale is low because D practices favouritism with some of her staff. She grants certain staff time off and vacations and denies others the same requests. I am not able to exchange shifts with another nurse, especially when the time schedule is posted. She never grants me vacation requests when I need them.” Staff C completes her input: “She holds monthly staff meetings and keeps us up to date on program issues.” Staff A continues: “Nurse D might have done those things but staff morale is low because she practices favouritism with her friends on the unit. Some of us do not like her management style.” Staff A completes her input: “ I am not granted my vacation requests.” Staff B: “D never communicates with us about activities on the unit. If you ask for a request, she denies it without any explanation. Also, she fills the vacancies with nurses who are midwives from other countries. Canadian nurses will never get the opportunity to fill a vacancy because of her hiring practices.” Staff C: “Ray, Manager D supports shift exchanges if two nurses have similar years of experience. She ensures that there is a balance between experienced nurses and nurses with little experience in maternal child nursing. Sometimes she denies shift exchanges if staffing level is not adequate or if the exchange would result in too many junior nurses working the same shift. Also vacation requests are granted based on seniority.” CEO concludes his response: "These past few years have resulted in staff dissatisfaction.” Staff C continues her response: “D has done many positive things for the unit during the past few years. She has implemented single room maternity, which results in continuity and consistency of care for patients. She hires qualified competent nurses, which enhances patients’ satisfaction with nursing care and no law suites. Also, she includes the nurse educator and a senior clinical
Appendix G
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
186
nurse on all the panel interviews. Staff hires are based on a scoring tool and the applicant with the highest score gets the position. Additionally, she holds monthly meetings to keep us abreast of issues and changes in the program and hospital.” Chief of Obstetrics:“ I have been practicing obstetrics for many years at this hospital, but have never seen staff morale as low as it is now. The nurses are very unhappy with D’s leadership. If we don’t resolve the problems on the unit, patient care would suffer. I personally don’t have a problem with D but I am concerned about the nurses’ well being.” Staff B, “ The people who are satisfied with D are her friends, because she grants them special requests.” SCENE II - Scene II opens with the CEO, VP of Nursing and Manager D. In this scene, the CEO gives D her performance appraisal. Both the CEO and The VP of Nursing promise to work with D on the issues in the program and encourage her to sign the performance appraisal and return it on Monday. CEO: “D, over the last few months we have been reviewing with you staff concerns regarding management of the Family Life Centre (FLC). Additional concerns were identified in three staff forums I conducted in October of 1999. Most recently, FLC staff has responded with critical comments in the nursing questionnaire survey regarding your management performance. The VP of Nursing shared these comments with you yesterday (current date). In considering the staff comments and the criticisms, and recognizing the scope, volume and consistency of them, we have grave concerns that these management issues must be addressed. We believe that failure to resolve these issues will result in further erosion of morale on the FLC, a deterioration of public relations that could ultimately result in failure of the Program and increase difficulty in retention and recruitment of staff. In recognition of your years of service to the (name relevant) Hospital as well as 10 years as Manager of FLC, senior management is willing to work with you to resolve the serious management concerns identified by FLC staff. This commitment to resolve concerns must be mutual with you and must include the following elements: Acknowledgement by you that these management concerns are legitimate and must be addressed. Commitment to implement an action plan that will resolve communication issues, real/perceived favouritism and management approach. The action plan must resolve the following issues: • Consistency in addressing issues on the unit. • Involvement of the HR in HR issues such as disciplinary matters with staff and conflict
resolution. • Flexible scheduling for staff, that is, shift swaps and self-scheduling. • An improved process for scheduling staff with HR. • Improved quality of communication on the unit. • Improved staff morale; and
Appendix G
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
187
• Development of an education plan for staff which reflects staff input. Your signature to this performance review would indicate your commitment to continue as Program Manager of Women’s Health under these conditions. By (date in 3 months) we will conduct an interim review to determine how the action plan is proceeding. By (date in 6 months), we will conduct a formal evaluation including receiving staff input on your management performance. We are willing to work with you D, in successfully meeting these challenges. The success though will be largely dependent on a renewed enthusiasm from you as Program Manager for Women’s Health. Once you have had an opportunity to review this letter, I would appreciate receiving from you a formal commitment to work with Senior Management and proceed with the action plan elements as indicated in this letter. Sincerely, RJ, President and CEO D’s response to this letter and performance review: “I will review this letter and performance appraisal at home and will return it next Monday.” CEO echoed by VP of Nursing response: “We expect your response by Monday of next week. We would like to address the concerns in the program as soon as possible.” D’s response to the CEO and VP of Nursing: “Thank you.” D leaves the room followed by her supervisor. **End of role play** Facilitator conducts the debriefing. Part III: Case Study #2 -- Application of Transformative Justice Principles Constructive Approaches to Institutional Racism • Acknowledge racism exists • Adopt anti-racism strategies to ensure fairness and equity as outcomes • Provide diversity training and race relations workshops for staff and employees. • Develop and implement anti-racism policies. • Include a statement on anti-racism in the mission and vision statements of the institutions. • Establish an employment equity committee for the institution. • Develop a monitoring system to assess changes in the institution. • Develop a complaint mechanism to deal with racism and harassment. • Develop a program and contingency plan to overcome systemic racism in the institution. • Management demonstrate and state its commitment to both the process and content of anti-
racism changes i.e., make individuals and institutions accountable for racialized discourse practices.
Conclusion

Appendix G
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
188
Today we have discussed institutional (systemic) racism and focused on how it affected two individuals. We have applied the Principles of Transformative Justice to a case study and showed how this framework identified transparency and accountability issues. There are three types of accountability: Individual, institutional and public. Our case demonstrated both individual and institutional racism. Thank you so much for your participation. Types of Accountability Individual Accountability refers to the assignment of responsibility for a specific set of actions for which non-compliance may result in specific sanctions. Organization or Institutional Accountability Refers to an assignment of responsibility for practices and policies that govern institutions, which are bureaucratized, specialized and isolated from the public and each other. They often operate in isolation (separate and distinct), far removed from society and the concerns of issues of people of colour. These organizations are administered by bureaucrats whose roles, functions and responsibilities appear to be largely unaffected by racism. Judgments and ideology of senior bureaucrats dictate what is fair, reasonable and achievable in the organization. As a group, they are the least accountable of all public servants but the most trusted. (Henry, Tator, Mattis and Rees, 1995) Public Accountability entails community participation in and control of the decision-making processes of public institutions (Henry et al., 1995). References: Bannerji, H. (2000). The Dark Side of the Nation: Essays on Multiculturalism, Nationalism and
Gender. Toronto: Canadian Scholars' Press. Ben-Tovim, G., Gabriel, J., Law, I., and Stredder, K. (1986). The local politics of race. London:
Macmillan. City of Toronto, Department of Public Health. (2002). Access and Equity: A case study of
Toronto Public Health’s current practices and organizational needs. Toronto: Department of Public Health.
Hagey, R., Lum, L., MacKay, R.,Turrittin, J., and Brody, E. (2001). Exploring transformative
justice in the employment of nurses: Toward reconstructing race relations and the dispute process (Unpublished Report to the Law Commission of Canada).
Henry, F., Tator, C., Mattis, W. and Rees, T. (1995). The colour of democracy: Racism in
Canadian society. Toronto: Harcourt Brace, Canada. Kirby Report. (2002). The Health of Canadians: The federal role. Final Report. The Standing
Senate Committee on Social Affairs, Science, and Technology. Retrieved Retrieved
Appendix G
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
189
January 23, 2003, from www.parl.gc.ca/37/2/parlbus/commbus/senate/ Com-e/SOCI-E/rep-e/repoct02vol6-e.htm.
Majumdar, B. (1996). Culture and Health: Culture-sensitive training manual for the health care
provider, 5th ed. Hamilton, ON: McMaster University Faculty of Health Sciences, School of Nursing.
McPherson, K. (1996). Bedside matters: The transformation of Canadian nursing 1900-1990.
Don Mills, ON: Oxford University Press. Meeks, D. (2003). Deconstructing Romanow. Concurrent Session at the Canadian Race
Relations Foundation Award of Excellence Symposium, entitled Racism: Breaking Through the Denial. March 28, Sheraton Hotel, Toronto, Ontario.
Smith, D. (1990). The conceptual practice of power: A feminist sociology of knowledge.
Toronto: University of Toronto Press.
Appendix G
Implementing Accountability for Equity and Ending Racial Backlash in Nursing
190
Evaluation of the Presentation-- Please tell us how helpful this role play has been. 1) Content is useful 1 2 3 4 5 not useful very useful 2) Process is informative 1 2 3 4 5 not informative informative 3) Material is organized 1 2 3 4 5 not organized organized 4) Topics are in sequential order 1 2 3 4 5 not ordered ordered 5) Resources are useful 1 2 3 4 5 not useful useful 6) List two things you liked most: a) b) 7) List two things you liked least: a) b) 8) Other comments:
Top Related
Copyright © 2022 FDOKUMEN

