







Bahasa
Halaman
Hukum

Development of the Fear of Pain Questionnaire—III
Dan iel W. McNeil1,
1
22 and Avie J. Rainwater , III
1,33
Accepted for publication: January 9, 1998
Fear and/or anxiety about pain is a useful construct, in both theoretical andclinical terms. This article describes the development and refinement of the Fearof Pain Questionna ire (FPQ), which exists in its most current form as theFPQ-III. Factor analytic refinement resulted in a 30-item FPQ-III which con-sists of Severe Pain, Minor Pain, and Medical Pain subscales. Internal consis-tency and test-retest reliabil ity of the FPQ-III were found to be good. Fourstudies are presented, including normative data for samples of inpatient chronicpain patients, general medical outpatients, and unselected undergraduates.High fear of pain individuals had greater avoidance/escape from a pain-rele-vant Behavioral Avoidance Test with Video, relative to their low fear counter-parts, suggesting predictive validity. Chronic pain patients reported the greatestfear of severe pain. Directions for future research with the FPQ-III are dis-cussed, along with general comments about the relation of fear and anxiety topain.
KEY WORDS: pain; fear; anxiety; pain assessment; pain measurement.
Journal of Behavioral Medicine, Vol. 21, No. 4, 1998
389
0160-7715/98/080 0-0389-$15.00/0 Ó 1998 Plenum Publishing Corporation
1Anxiety & Psychophysiology Research Laboratory, Department of Psychology, Oklahoma State
University, Stillwater, Oklahoma.2To whom correspondence should be addressed at his present address: Department of Psychology,
Anxiety & Psychophysiology Research Laboratory and Clinic, West Virginia University, P.O. Box6040, Morgantown, West Virginia 26506-6040. Fax: 304-293-6606. e-mail: [email protected].
3Present address: Medical Universi ty of South Carolina and McLeod Fami ly Medicine Resi-dency Program, 555 East Cheves Street, Florence, South Carolina 29506-2617. e-mail:
INTRODUCTION
Interactions between pain and various emotional states, such as fear, anxiety,
and depression (e.g., Romano and Turner, 1985), have been of interest in recent
years because traditional theories of pain that focus on nociceptive input do not
adequately account for the observed range of pain responsivity. Moreover, there
has been considerable research on emotional factors, as well as behavioral and
cognitive factors in the etiology and maintenance of chronic pain (Keefe et al.,
1992). This article specifically focuses on the relationships between pain and the
emotional state of fear. It has been suggested that there are meaningful differ-
ences between fear and anxiety (Marks, 1987; McNeil et al., 1992). Fear is con-
sidered to be a mobilization for avoidance/escape and other responses; the type
and degree of reactivity (i.e., verbal, physiological, and behavioral) is specific to
particular eliciting stimuli and contextual cues. Conversely, anxiety is associated
with more diffuse reaction patterns, and responses such as worry that require less
visceral organization and activity (McNeil et al., 1992). Interactions between
pain and fears related to pain are of primary interest in this paper. Nevertheless,
the effects of generalized anxiety and pain on one another are also important, and
are pertinent to the present studies. Because much prior research has not distin-
guished between fear and anxiety, work that specifically denotes “anxiety” in
terms of its relationship to pain will be considered here as well.
As a construct, fear of pain has only begun to be developed conceptually.
The terms “algophobia” and “odynesphobia” have been coined to describe fear of
pain (Maser, 1985). “Kinisophobia” has been used to describe an avoidance of
physical movement in chronic pain syndrome(s) (Kori et al., 1990). Various per-
spectives have been forwarded about the relation(s) between fear and pain, pri-
marily focusing on how fear can exacerbate the experience and expression of pain
(Gross and Collins, 1981). The converse direction of influence, pain affecting
fear, and a multidirectional model of relationships among pain, fear, and other
mediating variables should also be considered (Carter et al., 1991).
Various theoretical formulations about pain have included fear and/or anxi-
ety as a component. Gate-control theory (e.g., Melzack and Wall, 1988) suggests
that perception of pain is modified by central nervous system input. For example,
negative emotional states, like fear, can serve as a catalyst for greater difficulty in
the experience of pain. A parallel processing theory of pain distress incorporates
gate-control theory and adds separate pathways (e.g., emotional) that contribute
to the experience of pain (Leventhal and Everhart, 1979). Bolles and Fanselow’s(1980) perceptual¯defensive¯recuperative theory postulates that fear and pain are
competing motivational systems that can inhibit the expression of one another
and other systems. Lethem et al. (1983) proposed a fear-avoidance model of ex-
aggerated pain perception. The degree of fear of pain is suggested as a key com-
ponent in chronic pain patients’ style of responding to pain (i.e., confronting vs.
390 McNeil and Rainwater
avoiding). Philips (1987) forwarded a model of chronic pain which focuses on
unadaptive avoidance behavior (i.e., of stimulation, occupational and social in-
volvements, and physical activities) as a major contributor. This formulation in-
cludes the role of expectations and beliefs in sustaining avoidance, also
suggesting that pain and fear share important characteristics vis-a-vis avoidance.
Finally, the bioinformational theory of emotion has been used to view pain and
fear together (McNeil and Brunetti, 1992).
There are empirical data that support the importance of interactions between
pain and fear/anxiety. Fear of pain is a major component of dental fear (e.g., Gross,
1992; McNeil and Berryman, 1989). Moreover, anxiety about pain has been
shown to be predictive of labor pain ratings in first-time mothers, but not those
who already had children (Dannenbring et al., 1997). There have been a number of
studies of responsivity (e.g., verbal, physiological) in which both pain and
fear/anxiety are present (e.g., Cornwall and Donderi, 1988). Whether the fear/anx-
iety is about pain or is unrelated is important (e.g., al Absi and Rokke, 1991;
Dougher et al., 1987), as is the type of pain (Bobey and Davidson, 1970). There
has been considerable focus on attentional factors in interactions between pain and
fear/anxiety (e.g., Arntz et al., 1994; McCracken, 1997). Laboratory-induced (and
other) pain and fear may be distractors for one another under certain conditions
(McNeil et al., 1997). McNeil and Brunetti (1992) demonstrated that cardiac and
verbal responsivity to pain imagery and fear imagery had the same pattern, but
with some variability in degree. In combined pain/fear imagery, no additive re-
sponse effect was noted. Fears about experiencing pain and exacerbating injury
have been shown to be relevant factors to patients in an occupational rehabilitation
program (Papciak and Feuerstein, 1991). Pain-related anxiety impacts prediction
of pain, and reports of anxiety during physical examination (McCracken et al.,
1993a). Surgery-related anxiety has been demonstrated to be positively related to
magnitude of pain (Martinez-Urrutia, 1975). Preoperative anxiety has a positive
relationship with duration of hospitalization (Boeke et al., 1991), as well as to
postoperative anxiety and physical complaints (de Groot et al., 1997).
These previous theoretical studies and empirical data affirm the importance
of fear of, and anxiety about, pain as a construct. While there are a number of meth-
ods to assess general emotionality associated with pain (Jensen and Karoly, 1992),
there are few tools that specifically target fear and/or anxiety. A primary need in
this area, therefore, is the development of measurement strategies.
The existing verbal report instruments that assess pain-related fear and/or
anxiety include the Pain Anxiety Symptoms Scale (PASS; McCracken et al.,
1992), created to evaluate pain-related anxiety specifically in individuals with
chronic pain disorders. In its most recent form (McCracken et al., 1993b), the
PASS has 40 items, including Cognitive Anxiety, Fear, Escape/Avoidance, and
Physiological Anxiety subscales. There is some suggestion, however, that there
are five meaningful factors (Larsen et al., 1997). PASS questions are structured
Fear of Pain Questionnaire—III 391
with the assumption that the individual is actively experiencing pain, or has con-
siderable experience with pain. This orientation makes some PASS items inap-
propriate for persons who are not pain patients (see Osman et al., 1994). Other
instruments include the Fear-Avoidance Beliefs Questionnaire (Waddell et al.,
1993), which is a 16-item inventory specifically for persons with low back pain.
The 16 item Pain Sensitivity Index (Gross, 1992) was forwarded to assess cogni-
tive aspects of a trait-like pain-fearful state. Anticipatory and pain-related anxiety
in burn patients has been measured with the nine-item Burn Specific Pain Anxiety
Scale (Taal and Faber, 1997). The six-item Fear Self-Statements subscale that
was added to the Coping Strategies Questionnaire (Rosenstiel and Keefe, 1983)
by Gil et al. (1989) evaluates fear self-statements associated with sickle cell dis-
ease pain. Finally, the Pain Catastrophizing Scale (Sullivan et al., 1995) includes
13 items assessing thoughts or feelings while expressing pain.
These instruments represent an important step in the development of strate-
gies to quantify fear and anxiety associated with pain. The PASS, while longer, is
also relatively comprehensive in terms of verbal reports. Nevertheless, mode and
method of assessment should not be confused (see Eifert and Wilson, 1991); the
PASS, like any questionnaire, evaluates anxiety only using verbal report. The
other instruments mentioned here are narrowly focused. There is a paucity of
broad-based psychometric data, particularly for normative samples. The PASS,
however, has published community sample data (Osman et al., 1994), although
they are not compared to a clinical sample.
The present studies were designed systematically to develop and refine a
new verbal report instrument to assess fears about pain, one that has psychometric
data available for chronic pain inpatients, general medical outpatients, and unse-
lected college students. Construction of the inventory was based on Goldfried and
D’Zurilla’s (1969) behavioral-analytic model, particularly focusing on the em-
phasis on situational analysis. Over the course of four studies, presented here, the
Fear of Pain Questionnaire (FPQ) was tested in three versions. The 30-item
FPQ-III is presented as the most current, streamlined, and psychometrically sta-
ble version. The FPQ-III was designed to be quickly administered, and so is
shorter than the PASS. It approaches measurement of pain-related fear with the
assumption that fear is specific to particular stimuli and context. A variety of
types of pain and painful stimulus situations was therefore selected for the
FPQ-III’s items, consistent with this idea. Consequently, it is possible to use the
FPQ-III with both pain and nonpain populations.
STUDY 1
The purpose of Study 1 was to develop an initial screening instrument to
measure fear of pain related to specific stimulus situations. The investigation also
392 McNeil and Rainwater
tested the ability of this instrument to allow for identification of high fear of pain
individuals, and whether their overt behavior and verbal report responses could
distinguish them from control participants. In this study, it was predicted that par-
ticipants selected on the basis of high fear of pain would show more
psychopathological responding relative to low fear of pain participants, i.e.,
greater reports of generalized anxiety and fearfulness, more avoidance/escape,
and greater reports of distress in a pain-relevant behavioral assessment test.
Method
Participants
The participants were 1067 students (467 males and 600 females), with a
mean age of 19.5 (SD = 3.2), in introductory psychology classes at Oklahoma
State University (OSU) who were administered the FPQ-I. From this pool, 40 in-
dividuals were identified for inclusion in two gender-balanced groups (n = 20 per
group), based on their FPQ-I fear ratings. There was a high fear group (top 5% of
their same-gender FPQ-I distribution) and a low fear group (bottom 20¯30% of
these distributions). Ages for the high fear group (M = 20.1, SD = 4.4) and their
low fear counterparts (M = 19.6, SD = 2.2) did not differ.
Materials
The FPQ-I was developed first as a screening instrument. It presented eight
painful situations (e.g., having a tooth drilled without anesthetic, receiving a
shock from defective wiring in a table lamp) described in one or two sentences.
Face valid items were generated by the authors and critiqued by four independent
judges from a fear and pain research group (see Acknowledgments). Items were
designed to reflect situations that are relatively common, and so would be in the
realm of experience, even if indirect, for a wide variety of potential participants.
Items were restricted so that they would not be gender-specific or applicable only
to a particular medical/dental disorder. Respondents rated the degree of fear and
other affective and evaluative responses they would likely experience if con-
fronted with these situations; 5-point (1¯5) Likert-type scales were used. Ratings
for the eight situations were summed into a total score, with a possible range of
8¯40; higher scores indicated greater fear.
The participants in the high and low fear groups were also administered a
battery of tests designed to evaluate fear and anxiety more generally in the realm
of verbal report. These questionnaires were the 108-item Fear Survey Sched-
ule-III (Wolpe and Lang, 1977), the Anxiety Sensitivity Index (Reiss et al.,
1986), the State and Trait forms of the State-Trait Anxiety Inventory (STAI;
Fear of Pain Questionnaire—III 393
Form X; Spielberger et al., 1970), the Mutilation Questionnaire (Klorman et al.,
1974), and the Dental Fear Survey (Kleinknecht et al., 1973). The Liverpool Pain
Experience Questionnaire (Slade et al., 1983) was used to yield a pain severity
rating of the most intense, actually experienced previous pain.
Behavioral Assessment Test with Video (BATV)
The BATV is a flexible methodology that can be used to assess fear-related
avoidance/escape behavior (Rainwater and McNeil, 1990). This test involves pre-
sentation of fear-provoking vignettes from commercially available videocassette
movies. Typically, two movie segments are selected, based on the individual ’smost significant fear(s). Patients are tested individually and are given standard
audiotaped instructions. They are encouraged to stop viewing a vignette (by using
a remote control switching device) if/when they began to feel uncomfortable. The
instructions are therefore of a “low demand” style (Miller and Bernstein, 1972)
that allows avoidance or escape. Duration of avoidance/escape behavior is timed.
Also, the State form of the STAI is administered at the beginning of the BATV
and after each video vignette.
In the present study, procedures were used that were identical to those in one
of the cases presented by Rainwater and McNeil (1990). Specifically, two vig-
nettes (one of 255-sec and the other of 183-sec duration) were extracted from the
motion picture Marathon Man (Evans et al., 1976).
Both excerpts involved painful dental manipulations with an individual not
anesthetized and under duress, and so were designed to target specifically the
high fear participants ’ fear of pain.
Procedure
Verbal report instruments were administered in a standard order. Thereaf-
ter, the BATV was conducted. After each vignette trial, the STAI-State was re-
administered. Avoidance or escape time was calculated for each subject.
Participants declining to watch any part of either vignette had an avoidance time
of 438 sec; this figure is calculated by summing the two scene times. Alternately,
escape time was calculated for participants viewing at least some of either vi-
gnette by subtracting total time spent watching from the 438 sec total.
Results and Discussion
Selection of distinct groups with the FPQ-I was successful. The high (M =
33.0, SD = 2.4) and low (M = 16.8, SD = 1.6) fear groups’ total FPQ-I scores dif-
394 McNeil and Rainwater
fered significantly, t(38) = 25.55, p < .0001. Inspection of individual item scores
suggested all contributed to the difference in the total score.
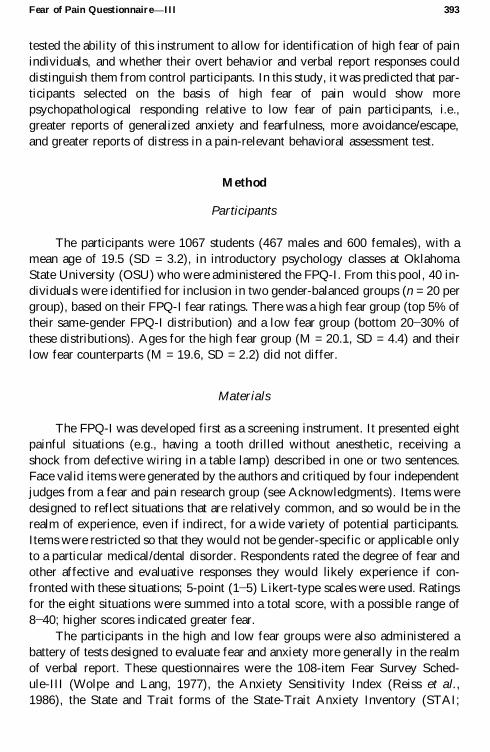
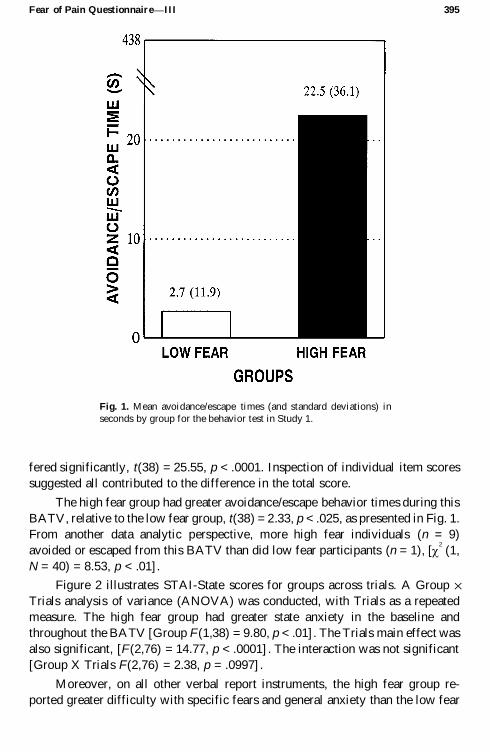
The high fear group had greater avoidance/escape behavior times during this
BATV, relative to the low fear group, t(38) =2.33, p <.025, as presented in Fig. 1.
From another data analytic perspective, more high fear individuals (n = 9)
avoided or escaped from this BATV than did low fear participants (n = 1), [ c2
(1,
N = 40) = 8.53, p < .01] .
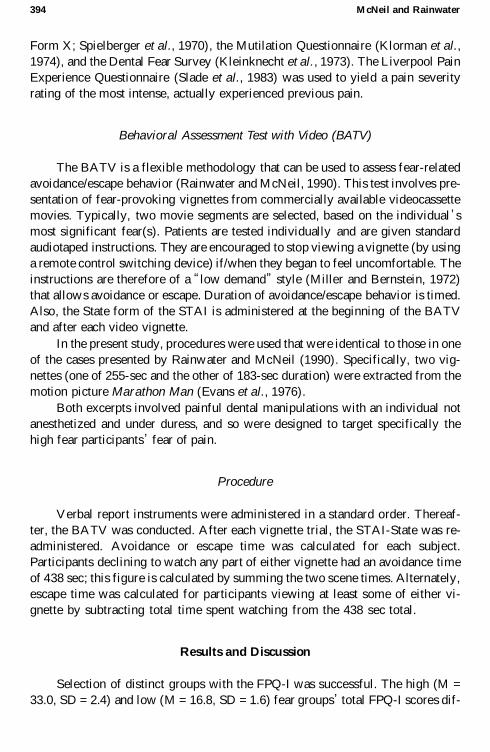
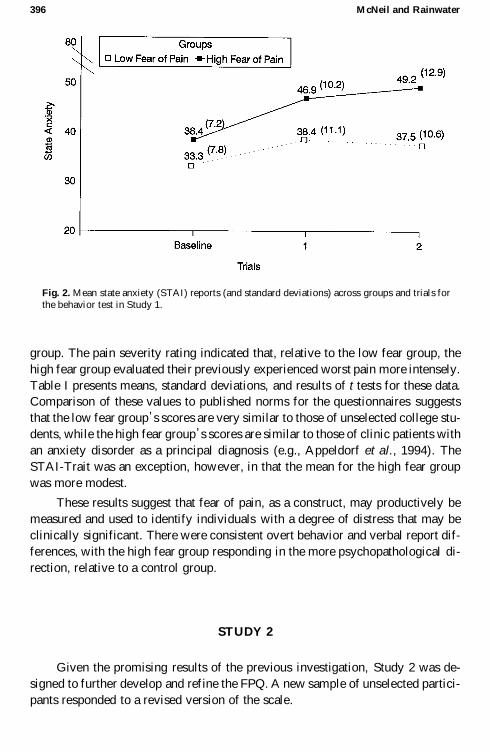
Figure 2 illustrates STAI-State scores for groups across trials. A Group ´Trials analysis of variance (ANOVA) was conducted, with Trials as a repeated
measure. The high fear group had greater state anxiety in the baseline and
throughout the BATV [Group F(1,38) = 9.80, p < .01] . The Trials main effect was
also significant, [F(2,76) = 14.77, p < .0001] . The interaction was not significant
[Group X Trials F(2,76) = 2.38, p = .0997] .
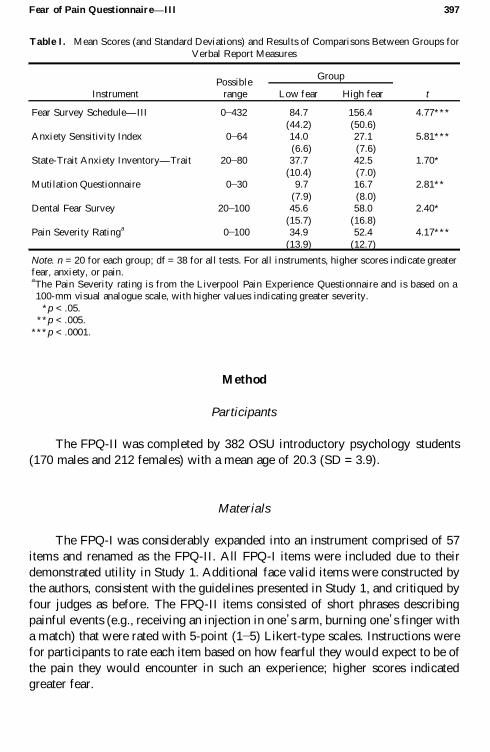
Moreover, on all other verbal report instruments, the high fear group re-
ported greater difficulty with specific fears and general anxiety than the low fear
Fear of Pain Questionnaire—III 395
Fig. 1. Mean avoidance/escape times (and standard deviations) in
seconds by group for the behavior test in Study 1.
group. The pain severity rating indicated that, relative to the low fear group, the
high fear group evaluated their previously experienced worst pain more intensely.
Table I presents means, standard deviations, and results of t tests for these data.
Comparison of these values to published norms for the questionnaires suggests
that the low fear group’s scores are very similar to those of unselected college stu-
dents, while the high fear group’s scores are similar to those of clinic patients with
an anxiety disorder as a principal diagnosis (e.g., Appeldorf et al., 1994). The
STAI-Trait was an exception, however, in that the mean for the high fear group
was more modest.
These results suggest that fear of pain, as a construct, may productively be
measured and used to identify individuals with a degree of distress that may be
clinically significant. There were consistent overt behavior and verbal report dif-
ferences, with the high fear group responding in the more psychopathological di-
rection, relative to a control group.
STUDY 2
Given the promising results of the previous investigation, Study 2 was de-
signed to further develop and refine the FPQ. A new sample of unselected partici-
pants responded to a revised version of the scale.
396 McNeil and Rainwater
Fig. 2. Mean state anxiety (STAI) reports (and standard deviations) across groups and trials forthe behavior test in Study 1.
Method
Participants
The FPQ-II was completed by 382 OSU introductory psychology students
(170 males and 212 females) with a mean age of 20.3 (SD = 3.9).
Materials
The FPQ-I was considerably expanded into an instrument comprised of 57
items and renamed as the FPQ-II. All FPQ-I items were included due to their
demonstrated utility in Study 1. Additional face valid items were constructed by
the authors, consistent with the guidelines presented in Study 1, and critiqued by
four judges as before. The FPQ-II items consisted of short phrases describing
painful events (e.g., receiving an injection in one’s arm, burning one’s finger with
a match) that were rated with 5-point (1¯5) Likert-type scales. Instructions were
for participants to rate each item based on how fearful they would expect to be of
the pain they would encounter in such an experience; higher scores indicated
greater fear.
Fear of Pain Questionnaire—III 397
InstrumentPossible
range
Group
tLow fear High fear
Fear Survey Schedule—III 0¯432 84.7 156.4 4.77***
(44.2) (50.6)Anxiety Sensitivity Index 0¯64 14.0 27.1 5.81***
(6.6) (7.6)State-Trait Anxiety Inventory—Trait 20¯80 37.7 42.5 1.70*
(10.4) (7.0)Mutilation Questionnaire 0¯30 9.7 16.7 2.81**
(7.9) (8.0)Dental Fear Survey 20¯100 45.6 58.0 2.40*
(15.7) (16.8)Pain Severity Rating
a0¯100 34.9 52.4 4.17***
(13.9) (12.7)
Note. n = 20 for each group; df = 38 for all tests. For all instruments, higher scores indicate greaterfear, anxiety, or pain.aThe Pain Severity rating is from the Liverpool Pain Experience Questionnaire and is based on a100-mm visual analogue scale, with higher values indicating greater severity.
*p < .05.**p < .005.
***p < .0001.
Table I. Mean Scores (and Standard Deviations) and Results of Comparisons Between Groups for
Verbal Report Measures
Procedure
The FPQ-II was administered in classroom settings that included approxi-
mately 35 students each.
Results and Discussion
Exploratory principal-components analysis with varimax rotation was con-
ducted on the correlation matrix among the 57 FPQ-II items as a data reduction
strategy. There were eight factors with eigenvalues greater than 1.0. Based on the
scree test, there were two possible stopping points for retaining factors, one using
the first three factors and the other using the first five factors. The three-factor so-
lution accounted for 50% of the variance, while the five-factor solution added
only an additional 6%. The two additional factors had an insufficient number of
items for adequate interpretation (i.e., only two items each). Moreover, the
three-factor solution was more parsimonious, while at the same time providing an
interpretable factor structure. Evaluation of item content suggested a Fear of Se-
vere Pain factor, a Fear of Minor Pain factor, and a Fear of Medical Pain factor.
When analyses were conducted separately for each gender, the best solution was
consistently a three factor model. For males and females, there were only minor
differences in the absolute magnitude of the item loadings. Consequently, deci-
sions about item selection were based on the combined data.
A decision rule was then employed to evaluate each of the 57 items for possi-
ble inclusion in the next version of the scale. Construction of three factors, consis-
tent with the present findings, was stipulated by including only those items that
loaded .60 or more on any one factor and .43 or less on the other two factors.
There were 26 items that met these criteria: 8 on the Severe Pain factor, 12 on the
Minor Pain factor, and 6 on the Medical Pain factor. In order to produce subscales
that consisted of 10 items each, 2 new items were added to the Severe Pain factor,
2 items with relatively low loadings were dropped from the Minor Pain factor,
and 4 new items were added to the Medical Pain factor. FPQ-II items that were
close to meeting inclusion criteria were slightly altered to produce the six addi-
tions. This new 30-item instrument was named the FPQ-III.
These results allowed for the refinement and streamlining of the FPQ into
an instrument that specifically assesses fear of pain across severe, minor, and
medical pain dimensions. Replication of the factor structure was still needed,
however, as were normative data for comparisons with healthy and clinical pop-
ulations.
398 McNeil and Rainwater
STUDY 3
The purpose of Study 3 was to test for replication of the factor structure of
the FPQ-III. Normative data on a large sample of unselected undergraduates were
also collected.
Method
Participants
There were 275 (112 males and 163 females) OSU introductory psychology
students who were the primary participants. An additional 385 OSU students (181
males and 204 females) completed the FPQ-III to provide normative data. This
total sample (n = 660) had a mean age of 19.8 (SD = 3.6).
Materials
As already noted, the 30-item FPQ-III contains items based on the inclusion
criteria in Study 2. The FPQ-III, like the FPQ-II, contains short phrases describ-
ing painful experiences that participants rate on 5-point (1¯5) Likert-type scales.
Again, respondents rate the degree of fear they anticipate experiencing related to
the painful event. Higher scores indicate greater fear.4
4 The FPQ-III consists of
three 10-item subscales: Fears of Severe Pain, Minor Pain, and Medical Pain. The
FPQ-III is presented in its entirety in the Appendix.
Procedure
The FPQ-III was administered in classrooms that seat approximately 35 stu-
dents. Test¯retest data were collected 3 weeks after the first administration, again
in classroom situations.
Results and Discussion
Responses to the 30-item FPQ-III were subjected to a principal-components
analysis with varimax rotation. There were five factors with eigenvalues greater
Fear of Pain Questionnaire—III 399
4Scoring the FPQ-III subscales involves summing the 10 items that comprise each subscale. Items foreach subscale are as follows: Severe Pain = 1, 3, 5, 6, 9, 10, 13, 18, 25, and 27; Minor Pain = 2, 4, 7,
12, 19, 22, 23, 24, 28, and 30; and Medical Pain =8, 11, 14, 15, 16, 17, 20, 21, 26, and 29. The possiblerange is 10¯50 for each subscale. The total score is the sum of all 30 items. The possible range is
30¯150 for the total score.
than 1.0. Based on the scree test, there were again two possible stopping points, at
either three or five factors. The first three factors accounted for 31, 11, and 9% of
the variance, respectively, for a cumulative total of 51%. The fourth and fifth fac-
tors each accounted for less than 5% of the variance. The three-factor solution
was again selected as the most parsimonious and interpretable. Princi-
pal-components analyses were also conducted separately for males and females.
The factors were the same across gender, although the order of extraction varied.
Given the similarity of factor solutions, combined data for both genders are pre-
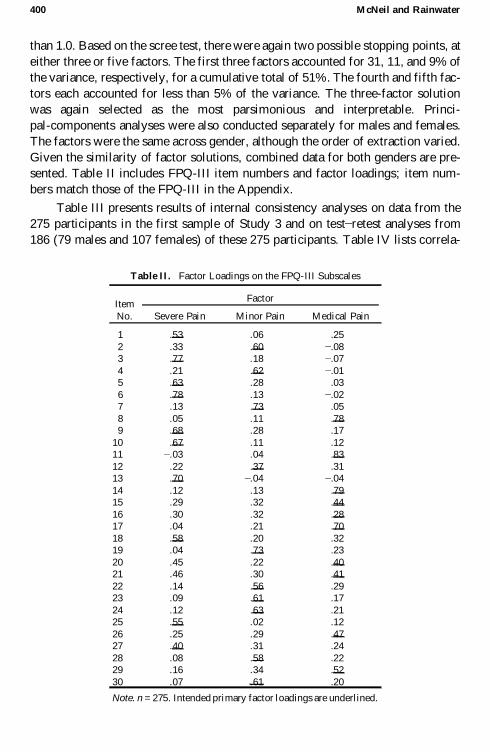
sented. Table II includes FPQ-III item numbers and factor loadings; item num-
bers match those of the FPQ-III in the Appendix.
Table III presents results of internal consistency analyses on data from the
275 participants in the first sample of Study 3 and on test̄ retest analyses from
186 (79 males and 107 females) of these 275 participants. Table IV lists correla-
400 McNeil and Rainwater
Item
No.
Factor
Severe Pain Minor Pain Medical Pain
1 .53 .06 .25
2 .33 .60 ¯.083 .77 .18 ¯.07
4 .21 .62 ¯.015 .63 .28 .03
6 .78 .13 ¯.027 .13 .73 .05
8 .05 .11 .789 .68 .28 .17
10 .67 .11 .1211 ¯.03 .04 .83
12 .22 .37 .3113 .70 ¯.04 ¯.04
14 .12 .13 .7915 .29 .32 .44
16 .30 .32 .2817 .04 .21 .70
18 .58 .20 .3219 .04 .73 .23
20 .45 .22 .4021 .46 .30 .41
22 .14 .56 .2923 .09 .61 .17
24 .12 .63 .2125 .55 .02 .12
26 .25 .29 .4727 .40 .31 .24
28 .08 .58 .2229 .16 .34 .52
30 .07 .61 .20
Note. n =275. Intended primary factor loadings are underlined.
Tab le II. Factor Loadings on the FPQ-III Subscales
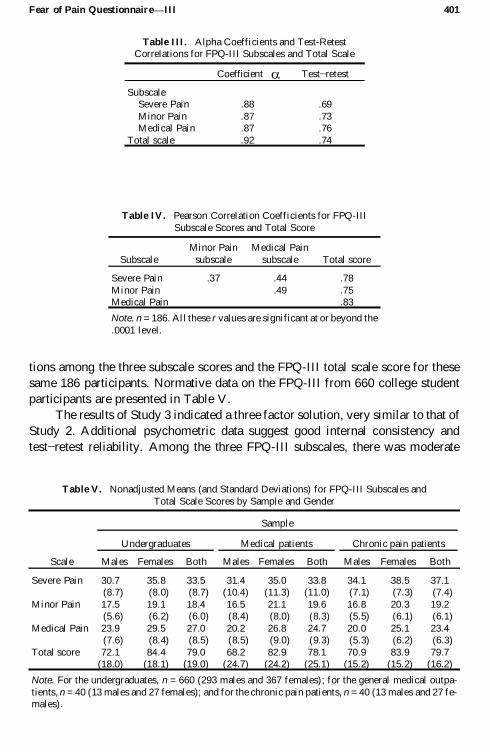
tions among the three subscale scores and the FPQ-III total scale score for these
same 186 participants. Normative data on the FPQ-III from 660 college student
participants are presented in Table V.
The results of Study 3 indicated a three factor solution, very similar to that of
Study 2. Additional psychometric data suggest good internal consistency and
test¯retest reliability. Among the three FPQ-III subscales, there was moderate
Fear of Pain Questionnaire—III 401
Coefficient a Test¯retest
SubscaleSevere Pain .88 .69
Minor Pain .87 .73Medical Pain .87 .76
Total scale .92 .74
Table III. Alpha Coefficients and Test-RetestCorrelations for FPQ-III Subscales and Total Scale
Subscale
Minor Pain
subscale
Medical Pain
subscale Total score
Severe Pain .37 .44 .78
Minor Pain .49 .75Medical Pain .83
Note. n =186. All these r values are significant at or beyond the
.0001 level.
Table IV. Pearson Correlation Coefficients for FPQ-III
Subscale Scores and Total Score
Scale
Sample
Undergraduates Medical patients Chronic pain patients
Males Females Both Males Females Both Males Females Both
Severe Pain 30.7 35.8 33.5 31.4 35.0 33.8 34.1 38.5 37.1(8.7) (8.0) (8.7) (10.4) (11.3) (11.0) (7.1) (7.3) (7.4)
Minor Pain 17.5 19.1 18.4 16.5 21.1 19.6 16.8 20.3 19.2(5.6) (6.2) (6.0) (8.4) (8.0) (8.3) (5.5) (6.1) (6.1)
Medical Pain 23.9 29.5 27.0 20.2 26.8 24.7 20.0 25.1 23.4(7.6) (8.4) (8.5) (8.5) (9.0) (9.3) (5.3) (6.2) (6.3)
Total score 72.1 84.4 79.0 68.2 82.9 78.1 70.9 83.9 79.7(18.0) (18.1) (19.0) (24.7) (24.2) (25.1) (15.2) (15.2) (16.2)
Note. For the undergraduates, n = 660 (293 males and 367 females); for the general medical outpa-
tients, n =40 (13 males and 27 females); and for the chronic pain patients, n =40 (13 males and 27 fe-males).
Tab le V. Nonadjusted Means (and Standard Deviations) for FPQ-III Subscales and
Total Scale Scores by Sample and Gender
intercorrelation, but strong correlation between each subscale score and the total
score.
STUDY 4
In Study 4, testing of the FPQ-III and collection of normative data were ex-
tended to clinical samples. A general chronic pain inpatient sample was selected
because of the potential utility of the FPQ-III in identifying a subset of chronic
pain patients who may have phobic levels of fear regarding their pain. A general
medical outpatient group was used as one control group, to match the chronic pain
patients closely on age and gender, as well as greater similarity of the function
that caused them to be identified for possible inclusion as participants (i.e., medi-
cal assessment and treatment). The college student sample from Study 3 was an-
other control group.
Method
Participants
The sample of chronic pain patients consisted of 40 (13 males and 27 fe-
males) consecutively admitted individuals in a 2-week inpatient chronic pain
treatment program. All of these participants were Caucasian adults (M age =47.2,
SD = 13.6) who had been suffering daily pain for at least 6 months. Primary com-
plaints included back and/or neck pain (n = 21) and head pain (n = 6), while there
were 13 individuals with assorted pain problems (e.g., chest pain with no identi-
fied organic pathology).
The sample of medical patient controls consisted of 40 individuals who were
gender and age (M age = 45.3, SD = 11.8) matched to the chronic pain sample.
These participants were seeking outpatient medical care in a family practice set-
ting. None of them were classified as chronic pain patients. In order to provide a
naturally occurring sample, there was no effort to exclude individuals who were
presenting with pain. Moreover, so as to provide a more representative normative
group, these individuals were not matched in terms of ethnicity. This general
medical patient control group included 24 individuals who were Caucasian, 14
who were African American, and 2 who were Native American.
Procedure
The FPQ-III was administered individually to chronic pain patients as part of
an intake evaluation battery and to medical patient controls as a part of their
preappointment paperwork.
402 McNeil and Rainwater
Results and Discussion
Table V presents normative data for the chronic pain patients and medical
patient controls, in addition to that for the undergraduate sample. As expected,
age differed among these groups [F(2,737) = 863.40, p < .0001] . Duncan’s multi-
ple-range tests at the .05 level confirmed that the two patient samples were older
than the undergraduates and that the former two groups did not differ from one an-
other.
Given the differences in age, it was used as a covariate in analyses. Separate
analyses of covariance (ANCOVAs) were conducted on the three subscales and
total scale, with subject Group and Gender as factors. There was a main effect for
Group, only on the Severe Pain subscale [F(2,733) = 4.25, p < .02] . Duncan’smultiple-range tests on least-squares means revealed that chronic pain patients re-
ported more fear of severe pain than the general medical patients (p < .05) and the
undergraduates (p < .01). Fear of Severe Pain scores for the medical patient con-
trols also were greater than for the undergraduate sample (p < .05). (Least-squares
means were 39.4 for chronic pain patients, 36.0 for medical patient controls, and
32.9 for undergraduates.) A main effect for Gender was found across the three
subscales and total scale; regardless of subject sample, females reported more
fear of pain than males (all F’s > 8.42, all p’s < .01). There were no significant in-
teractions.
Given that the medical patient control sample consisted of individuals from
different ethnic groups, a supplementary analysis was conducted to assess for
possible FPQ-III differences among them. Two groups from this sample were
formed, consisting of 24 Caucasians in one group and 16 African Americans (n =
14) and Native Americans (n = 2) in the other. Student t tests (two-tailed) were
performed on the three subscale and total scale scores. There were no differences
on the Severe Pain subscale [t(38) =1.08, p =.2866] . On the Minor Pain subscale,
differences also did not meet a standard level of reliability [t(38) = 1.79, p =
.0815] . The Caucasian group had a mean of 17.8 (SD = 7.0); the African Ameri-
can/Native American group had a mean of 22.4 (SD = 9.6). Significant differ-
ences emerged on the Medical Pain subscale [t(38) = 2.30, p < .05] . The African
American/Native American group (M = 28.6, SD = 10.3) had a higher score than
the Caucasian group (M = 22.0, SD = 7.7). Comparison of the total score did not
meet a standard significance level [t(38) =1.92, p =.0620] . The mean for the Afri-
can American/Native American group was 87.1 (SD = 28.6) and that for the Cau-
casian group was 72.1 (SD = 20.9).
GENERAL DISCUSSION
These results support the importance of fear of pain as a construct and the
utility of the FPQ-III as a measurement device. As predicted in Study 1, partici-
Fear of Pain Questionnaire—III 403
pants who reported a high degree of fear of pain avoided or escaped more from
pain-relevant stimuli, and reported more state anxiety, than their low fear counter-
parts. The high fear of pain group scored higher on a variety of fear and anxiety
questionnaires and a rating of previously experienced pain.
The heterogeneous sample of pain patients had a higher fear of Severe Pain
subscale score than the control groups. This finding suggests the possibility of a
specificity in fear response for this chronic pain patient sample, in light of the ap-
parent lack of differences on the other two subscales or the FPQ-III total score. In-
spection of the nonadjusted means in Table V suggests the possibility that the two
older groups (i.e., chronic pain and general medical patients) might actually have
less fear of medical pain than the undergraduates. Speculatively, such a difference
might be related to the effects of exposure, which reduces fear/anxiety under
proper conditions. Research in the future should evaluate fear of pain in groups
across the life span.
Undoubtedly, however, FPQ-III scale scores vary across and within differ-
ent types of pain patients. For example, Hursey and Jacks (1992) found that head-
ache sufferers had higher scores on Severe and Medical Pain FPQ-III subscales,
and lower scores on the Minor Pain subscale, relative to control participants. Kai-
ser et al. (1993) found that all FPQ-III scores for analgesic rebound headache pa-
tients were lower relative to their nonrebounding counterparts.
It should not be assumed that fear of pain will be greater in all pain patients.
Even in groups of pain patients (e.g., chronic pain), there is great heterogeneity. It
is likely that these individuals vary along a fear of pain severity continuum, as
with other populations. Assessment with the FPQ-III may help in the identifica-
tion of the subset of chronic pain patients who have phobic levels of fear about
their pain. Additionally, such evaluation may be useful in determining accident
victims and surgery patients whose fear-related problems may interfere with re-
covery.
The gender differences observed for all FPQ-III scores are not surprising.
This same effect, females reporting more distress and males indicating less, is of-
ten found in verbal report assessment of many fears/anxieties (e.g., Kaloupek et
al., 1981) and pain (e.g., Levine and De Simone, 1991). Differences in some
FPQ-III scores among ethnicity groupings also has some precedence in prior in-
vestigations of verbal reports about fear/anxiety (e.g., Novy et al., 1993) and pain
(e.g., Bates and Edwards, 1992). Nonetheless, the determinants of these differ-
ences are interesting and warrant further investigation.
The FPQ-III measures fears about pain as a trait-like phenomenon, assessing
enduring behavioral patterns across pain situations and testing for generalization.
Consequently, this instrument can be used for assessment in a diversity of norma-
tive and clinical populations, including pain patients. The length and ease of scor-
ing of the FPQ-III make it practical for use in a variety of clinical and research
settings. Since it is not assumed that individuals have had extensive prior clinical
404 McNeil and Rainwater
pain, one application for the FPQ-III is the comparison of pain and nonpain sam-
ples. Since the FPQ-III is a multi-factor instrument, it can be used to assess fear in
a specific area (e.g., related to medical pain) or to evaluate generalization of fear
across domains.
These data indicate the FPQ-III has good internal consistency and test¯retest
reliability. Moreover, its factor structure is sufficiently stable in a college student
population. FPQ-III interscale correlations for the normative sample showed only
moderate relationships among the three subscales, and a strong correlation for
each of those with the total scale. In the factor analysis replication in Study 3, the
Severe Pain and Minor Pain subscales each had 9 of 10 items that maintained a
reasonably high factor loading (i.e., .50 or greater). On the Medical Pain factor,
however, only 6 of 10 items had a loading of .50 or greater. Future research may
be able to derive even more pure factors, particularly in the realm of medical pain.
In research by independent investigators, the FPQ-III has also demonstrated good
internal consistency and test¯retest reliability in headache sufferers (Hursey and
Jacks, 1992; Thonsgaard et al., 1992).
Predictive validity of the earliest version of the Fear of Pain Questionnaire,
the FPQ-I, is attested to by Study 1. Using the FPQ-I for selection of high and low
fear of pain individuals identified groups that performed differently on a
pain-relevant behavior test and responded uniquely to fear, anxiety, and pain ver-
bal report instruments. Hursey and Jacks (1992) used the FPQ-III and found that
headache sufferers with greater fear of pain had more life disruptions and greater
depression and anxiety associated with headaches in comparison with those who
had lower fear of pain. They indicated that the FPQ-III had good construct, con-
current, and ecological validity. Sullivan et al. (1995) found the FPQ-III total
score to be unique (along with a measure of pain catastrophizing) among verbal
report instruments measuring emotion, being positively and significantly related
to pain ratings during a cold pressor test.
The studies presented here are limited by the fact that they rely a great deal
on responses from college students, many of whom are relatively inexperienced
with certain types of pain. Also, this research has focused almost exclusively on
verbal report. Certainly assessment strategies for other response systems (e.g.,
psychophysiological and overt behavioral) are needed as well in studying fear of
pain. Additional basic research is needed to assess FPQ-III predictive validity
vis-a-vis laboratory-induced pain. Clinical research could use the FPQ-III to as-
sess newly injured individuals, or those awaiting invasive medical procedures, at-
tempting to help predict those patients who will later develop chronic pain
problems. Additionally, chronic pain patients who are identified by interview as
having severe fear related to their pain might be tested with the FPQ-III relative to
counterparts with low fear. The two patient groups in Study IV in this paper are
relatively small, so more FPQ-III normative data should be collected on other,
larger clinical samples, including a diversity of ethnic and age groups, as well as
Fear of Pain Questionnaire—III 405
patient and community populations. Also, future research should assess the
generalizibility and relevance of the FPQ-III’s factor dimensions to groups other
than undergraduates. Finally, there needs to be study of the relation of FPQ-III re-
sponses to other pain fear/anxiety instruments (e.g., the PASS).
It may seem possible that high fear of pain individuals are different in some
general ways, such as “neuroticism ” (Frazer and Hampson, 1988) or other
greater overall psychopathology, that affect a variety of fears and anxieties. Nev-
ertheless, while there likely is some overlap with other, similar constructs, data
from Thornsgaard et al. (1992) suggest that FPQ-III scores are independent of
general psychological distress. Moreover, these investigators found no relation
between current pain level and FPQ-III responses. The relative independence or
overlap of the fear of pain construct with other, similar constructs needs further
research. McNeil and Berryman (1989), however, have already demonstrated
that fear of pain is the most important component of dental fear (see also Gross,
1992).
It is helpful that there are several verbal report instruments now available in
this area, two of which have comprehensive normative data (i.e., the FPQ-III and
PASS). There are published data on both these instruments from investigators
other than the scales’ originators. Selecting instrument(s) for use in future re-
search should be based on the particular need. The FPQ-III has greater applicabil-
ity and is somewhat shorter in length, while the PASS is specific in its focus on
already-experienced pain. Also, the FPQ-III focuses on fear responses to specific
pain situations, while the PASS emphasizes assessment of various response mo-
dalities associated with pain. In many cases, use of both instruments would be
ideal, providing a comprehensive approach.
Fear and anxiety related to pain are important phenomena in that they have
unique properties. In promoting investigation of fear and/or anxiety about pain,
measurement issues are currently paramount. Further work on assessment strate-
gies is an important next step in the further elucidation of fear/anxiety about pain
as a theoretically and clinically significant construct.
406 McNeil and Rainwater

APPENDIX
Fear of Pain Questionnaire—III
Name: Date:
INSTRUCTIONS: The items listed below describe painful experiences. Please look at each item
and think about how FEARFUL you are of experiencing the PAIN associated with each item. Ifyou have never experienced the PAIN of a particular item, please answer on the basis of how
FEARFUL you expect you would be if you had such an experience. Circle one rating per item torate your FEAR OF PAIN in relation to each event.
AMOUNT OF FEAR
Not
atAll
Alittle
A
FairAmount
VeryMuch Extreme
1 2 3 4 5 1. Being in an automobile accident1 2 3 4 5 2. Biting your tongue while eating
1 2 3 4 5 3. Breaking your arm1 2 3 4 5 4. Cutting your tongue licking an envelope
1 2 3 4 5 5. Having a heavy object hit you in the head1 2 3 4 5 6. Breaking your leg
1 2 3 4 5 7. Hitting a sensitive bone in yourelbow-your “funny bone”
1 2 3 4 5 8. Having a blood sample drawn with ahypodermic needle
1 2 3 4 5 9. Having someone slam a heavy car dooron your hand
1 2 3 4 5 10. Falling down a flight of concrete stairs1 2 3 4 5 11. Receiving an injection in your arm
1 2 3 4 5 12. Burning your fingers with a match1 2 3 4 5 13. Breaking your neck
1 2 3 4 5 14. Receiving an injection in yourhip/buttocks
1 2 3 4 5 15. Having a deep splinter in the sole of yourfoot probed and removed with tweezers
1 2 3 4 5 16. Having an eye doctor remove a foreignparticle stuck in your eye
1 2 3 4 5 17. Receiving an injection in your mouth1 2 3 4 5 18. Being burned on your face by a lit
cigarette1 2 3 4 5 19. Getting a paper-cut on your finger
1 2 3 4 5 20. Receiving stitches in your lip1 2 3 4 5 21. Having a foot doctor remove a wart from
your foot with a sharp instrument1 2 3 4 5 22. Cutting yourself while shaving with a
sharp razor1 2 3 4 5 23. Gulping a hot drink before it has cooled
1 2 3 4 5 24. Getting strong soap in both your eyeswhile bathing or showering
1 2 3 4 5 25. Having a terminal illness that causes youdaily pain
1 2 3 4 5 26. Having a tooth pulled1 2 3 4 5 27. Vomiting repeatedly because of food
poisoning1 2 3 4 5 28. Having sand or dust blow into your eyes
1 2 3 4 5 29. Having one of your teeth drilled1 2 3 4 5 30. Having a muscle cramp
Note. The FPQ-III is copyrighted by the authors. Permission is given for users to reproduce this
instrument for clinical and research purposes.
ACKNOWLEDGMENTS
Preparation of this article was supported in part by three Oklahoma State
University Arts & Sciences Dean’s Incentive Grants and an award from the
Oklahoma Center for the Advancement of Science and Technology (OCAST
No.HRO-023) to Daniel W. McNeil, as well as by funding to Avie J. Rainwater,
III, from the United States Department of Education (No.G0087-10566) and the
American Psychological Association (No.MFD8687).
Various data from these studies were presented at the meetings of the Ameri-
can Psychological Association, Toronto, Canada, (August, 1993); the Associa-
tion for Advancement of Behavior Therapy, Chicago, IL (November, 1986); and
the Southwestern Psychological Association, Fort Worth, TX (April, 1986).
Many graduate and undergraduate students participated as clinical research
assistants in the laboratory during the conduct of this study. Their important con-
tributions are gratefully acknowledged. While it is not practical to mention each
of them individually, the efforts of Laureen Aljazireh are particularly noteworthy.
Thanks are also extended to Bob Wilkie and Mary Lou Piech for assistance in data
collection. Stanley H. Cohen provided helpful statistical consultation.
REFERENCES
al Absi, M., and Rokke, P. D. (1991). Can anxiety help us tolerate pain? Pain 46: 43-51.
Appeldorf, W. J., Shear, K., Leon, A. C., and Portera, L. (1994). A brief screen for panic disorder. J.
Anx. Dis. 8: 71-78.
Arntz, A., Dreessen, L., and De Jong, P. (1994). The influence of anxiety on pain: Attentional and
attributional mediators. Pain 56: 307-314.
Bates, M. S., and Edwards, W. T. (1992). Ethnic variations in the chronic pain experience. Ethnic. Dis.2: 63-83.
Bobey, M. J., and Davidson, P. O. (1970). Psychological factors affecting pain tolerance. J.Psychosom. Res. 14: 371-376.
Boeke, S., Duivenvoorden, H. J., Verhage, F., and Zwaveling, A. (1991). Prediction of postoperative
pain and duration of hospitalization using two anxiety measures. Pain 45: 293-297.
Bolles, R. C., and Fanselow, M. S. (1980). A perceptual-defensive-recuperative model of fear and
pain. Behav. Brain Sci. 3: 291-323.
Carter, L. E., McNeil, D. W., and Reed, T. L. (1991). Cardiac responsivity to combinations of anxietyand pain. Psychophysiology 28: S16 (abstract).
Cornwall, A., and Donderi, D. C. (1988). The effect of experimentally induced anxiety on the experi-ence of pressure pain. Pain 35: 105-113.
Dannenbring, D., Stevens, M. J., and House, A. E. (1997). Predictors of childbirth pain and maternal
satisfaction. J. Behav. Med. 20: 127-142.
de Groot, K. I., Boeke, S., van den Berge, H. J., Duivenvoorden, H. J., Bonke, B., and Passchier, J.
(1997). The influence of psychological variables on postoperative anxiety and physical com-plaints in patients undergoing lumbar surgery. Pain 69: 19-25.
Dougher, M. J., Goldstein, D., and Leight, K. A. (1987). Induced anxiety and pain. J. Anx. Dis. 1:
259-264.
Eifert, G. H., and Wilson, P. H. (1991). The triple response approach to assessment: A conceptual and
methodological reappraisal. Behav. Res. Ther. 29: 283-292.
408 McNeil and Rainwater
Evans, R., Beckerman, S. (Producers), and Schesinger, J. (Director). (1976). Marathon Man (Film).
Paramount Pictures, Los Angeles, CA.
Frazer, M., and Hampson, S. (1988). Some personality factors related to dental anxiety and fear of
pain. Br. Dent. J. 165: 436-439.
Gil, K. M., Abrams, M. R., Phillips, G., and Keefe, F. J. (1989). Sickle cell disease pain: Relation ofcoping strategies to adjustment. J. Consult. Clin. Psychol. 57: 725-731.
Goldfried, M. R., and D’Zurilla, T. J. (1969). A behavioral-analytic model for assessing competence.
In Spielberger, C. D. (ed.), Current Topics in Clinical and Community Psychology, AcademicPress, New York, pp. 151-196
Gross, P. R. (1992). Is pain sensitivity associated with dental avoidance? . Behav. Res. Ther. 30: 7-13.
Gross, R. T., and Collins, F. L., Jr.. (1981), On the relationship between anxiety and pain: A method-
ological confounding. Clin. Psychol. Rev. 1: 375-386.
Hursey, K. G., and Jacks, S. D. (1992). Fear of pain in recurrent headache sufferers. Headache 32:283-286.
Jensen, M. P., and Karoly, P. (1992). Self-report scales and procedures for assessing pain in adults. In:
Turk, D. C. and Melzack, R. (eds.), Handbook of Pain Assessment, Guilford, New York, pp.135-151.
Kaiser, R. S., Primavera, J. P., and Schwartz, A. L. (1993). Perceived competence and fear of pain as
contributory factors in analgesic rebound headache. Paper presented at the meeting of the Ameri-can Association for the Study of Headache, San Francisco, CA.
Kaloupek, D. G., Peterson, D. A., and Levis, D. J. (1981). An investigation of the normative and factoranalytic composition of six questionnaires used for subject selection. J. Behav. Assess. 3:
149-165.
Keefe, F. J., Dunsmore, J., and Burnett, R. (1992). Behavioral and cognitive-behavioral approaches tochronic pain: Recent advances and future directions. J. Consult. Clin. Psychol. 60: 528-536.
Kleinknecht, R. A., Klepac, R. K., and Alexander, L. D. (1973). Origins and characteristics of fear of
dentistry. J. Am. Dent. Assoc. 86: 842-848
Klorman, R., Weerts, T. C., Hastings, J. E., Melamed, B. G., and Lang, P. J. (1974). Psychometric de-scription of some specific-fear questionnaires. Behav. Ther. 5: 401-409.
Kori, S. H., Miller, R. P., and Todd, D. D. (1990). Kinisophobia: A new view of chronic pain behavior.
Pain Manage. 3: 35-43.
Larsen, D. K., Taylor, S., and Asmundson, G. J. G. (1997). Exploratory factor analysis of the PainAnxiety Symptoms Scale in patients with chronic pain complaints. Pain 69: 27-34.
Lethem, J., Slade, P. D., Troup, J. D. G., and Bentley, G. (1983). Outline of a fear-avoidance model of
exaggerated pain perception—I. Behav. Res. Ther. 21: 401-408.
Leventhal, H., and Everhart, D. (1979). Emotion, pain, and physical illness. In Izard, C. E. (ed.), Emo-tions in Personality and Psychopathology , Plenum Press, New York, pp. 263-299.
Levine, F. M., and De Simone, L. L. (1991). The effects of experimenter gender on pain report in maleand female subjects. Pain 44: 69-72.
Marks, I. M. (1987). Fears, Phobias, and Rituals: Panic, Aanxiety, and Their Disorders, Oxford, New
York, pp. 5-8.
Martinez-Urrutia, A. (1975). Anxiety and pain in surgical patients. J. Consult. Clin. Psychol. 43:437-452.
Maser, J. D (1985). List of phobias. In Tuma, A. H. and Maser. J. D. (eds.) Anxiety and the Anxiety
Disorders, Lawrence Erlbaum, Hillsdale, New Jersey, pp. 805-813.
McCracken, L. M. (1997). “Attention” to pain in persons with chronic pain: A behavioral approach.Behav. Ther. 28: 271-284.
McCracken, L. M., Gross, R. T., Sorg, P. J., and Edmands, T. A. (1993a). Prediction of pain in patients
with chronic low back pain: Effects of inaccurate prediction and pain-related anxiety. Beh. Res.Ther. 31: 647-652.
McCracken, L. M., Zayfert, C., and Gross, R. T. (1992). The Pain Anxiety Symptoms Scale: Develop-
ment and validation of a scale to measure fear of pain. Pain 50: 67-73.
McCracken, L. M., Zayfert, C., and Gross, R. T. (1993b). The Pain Anxiety Symptoms Scale (PASS):A multi-modal measure of pain-specific anxiety symptoms. The Behavior Therapist. 16:
183-184.
Fear of Pain Questionnaire—III 409
McNeil, D. W., and Berryman, M. L. (1989). Components of dental fear in adults? Behav. Res. Ther.
27: 233-236.
McNeil, D. W., and Brunetti, D. G. (1992). Pain and fear: A bioinformational perspective on
responsivity to imagery. Behav. Res. Ther. 30: 513-520.
McNeil, D. W., Vrana, S. R., Melamed, B. G., Cuthbert, B. N., and Lang, P. J. (1992). Emotional im-
agery in simple and social phobia: Fear vs. anxiety. J. Abnorm. Psychol. 102: 212-225.
McNeil, D. W., Carter, L. E., Lejuez, C. W., and Hopko, D. R. (1998). Responsivity to fear and pain
(submitted for publication).
Melzack, R., and Wall, P. D. (1988). The Challenge of Pain (rev. ed.), Penguin Books, New York.
Miller, B. V., and Bernstein, D. A. (1972). Instructional demand in a behavioral avoidance test forclaustrophobic fears. J. Abnorm. Psychol. 80: 206-210.
Novy, D. M., Nelson, D. V., Goodwin, J., and Rowzee, R. D. (1993). Psychometric comparability of
the State-Trait Anxiety Inventory for different ethnic subpopulations. Psychol. Assess. 5:343-349.
Osman, A., Barrios, F. X., Osman, J. R., Schneekloth, R., and Troutman, J. A. (1994). The Pain Anxi-ety Symptoms Scale: Psychometric properties in a community sample. J. Behav. Med. 17:
511-522.
Papciak, A. S., and Feuerstein, M. (1991). Fear of pain in work rehabilitation. In McNeil, D. W.
(Chair), Relationships between pain and anxiety: Theoretical formulations and clinical applica-tions. Symposium presented at the meeting of the Association for Advancement of Behavior
Therapy, New York.
Philips, H. C. (1987). Avoidance behaviour and its role in sustaining chronic pain. Behav. Res. Ther.
25: 273-279.
Rainwater, A. J., III, and McNeil, D. W. (1990). Behavioral Assessment Test withVideo (BATV): As-
sessment of phobic disorders. J. Anx. Dis. 4: 163-170.
Reiss, S., Peterson, R. A., Gursky, D. M., and McNally, R. J. (1986). Anxiety sensitivity, anxiety fre-
quency and the prediction of fearfulness. Behav. Res. Ther. 24: 1-8.
Romano, J. M., and Turner, J. A. (1985). Chronic pain and depression: Does the evidence support a re-lationship? Psychol. Bull. 97: 18-34.
Rosenstiel, A. K., and Keefe, F. J. (1983). The use of coping strategies in low back pain patients: Rela-tionship to patient characteristics and current adjustment. Pain 17: 33-40.
Slade, P. D., Troup, J. D. G., Lethem, J., and Bentley, G. (1983). The fear-avoidance model of exag-gerated pain perception—II: Preliminary studies of coping strategies for pain. Behav. Res. Ther.
21: 409-416.
Spielberger, C. D., Gorsuch, R. L., and Lushene, R. E. (1970). Manual for the State-Trait Anxiety In-
ventory (Form X), Consulting Psychologists Press, Palo Alto, CA.
Sullivan, M. J. L., Bishop, S. R., and Pirik, J. (1995). The Pain Catastrophizing Scale: Development
and validation. Psychol. Assess. 7: 524-532.
Taal, L. A., and Faber, A. W. (1997). The Burn Specific Pain Anxiety Scale: Introduction of a reliable
and valid measure. Burns 23: 147-150.
Thonsgaard, S., Hursey, K. G., Oliver, K. C., and McGruder, A. K. (1992). The Fear of Pain Question-naire: Reliability and validity in recurrent tension headache sufferers. Poster presented at the
meeting of the Association for Advancement of Behavior Therapy, Boston, MA.
Waddell, G., Newton, M., Henderson, I., Somerville, D., and Main, C. J. (1993). A Fear-Avoidance
Beliefs Questionnaire (FABQ) and the role of fear-avoidance beliefs in chronic low back painand disability. Pain 52: 157-168.
Wolpe, J., and Lang, P. J. (1977). Manual for the Fear Survey Schedule , Educational and IndustrialTesting Service, San Diego, CA.
410 McNeil and Rainwater
Top Related
Copyright © 2022 FDOKUMEN

