







Bahasa
Halaman
Hukum


Author Pro
of
1ISSN 1462-241610.2217/PGS.12.24 © 2012 Future Medicine Ltd Pharmacogenomics (2012) 13(5), 1–xxx
ReseaRch aRticle ReseaRch aRticle
CYP2C19 and PON1 polymorphisms regulating clopidogrel bioactivation in Chinese, Malay and Indian subjects
Clopidogrel, a platelet P2Y12
receptor inhibitor, is universally administered to patients with acute myocardial infarction and to patients undergo-ing percutaneous coronary intervention (PCI) because of its proven efficacy in reducing major adverse cardiovascular events in these popula-tions [1,2]. Although newer P2Y
12 inhibitors are
now commercially available, clopidogrel, driven by extensive clinical data and the recent avail-ability of generic clopidogrel, is currently the dominant compound in clinical use.
However, there is wide variability in the level of platelet inhibition with clopidogrel, which is attributable in part to differential bioactivation of the parent compound by the hepatic CYP enzyme system [3]. Carriers of loss-of-function polymorphisms of CYP2C19, namely, the *2 and *3 alleles, produce lower levels of the active metabolite of clopidogrel compared with non-carriers [4,5], resulting in a decreased antiplate-let effect. Such individuals therefore carry an increased risk of major adverse cardiac events after stent implantation [6,7]. Asian populations have a known higher prevalence of CYP2C19 loss-of-function polymorphisms compared with white populations [8–10]. While the CYP2C19*2 polymorphism is found in both white and Asian populations, the CYP2C19*3 polymorphism is found almost exclusively in Asian populations [8].
Conversely, carriers of a gain-of-function polymorphism, namely, the *17 allele, produce
higher levels of the active thiol metabolite com-pared with noncarriers, resulting in a greater antiplatelet effect and an increased risk of bleed-ing [11,12]. Recently, Bouman et al. identified another genetic variant, the PON1 Q192R poly-morphism as an important determinant of clopi-dogrel response [13]. In this study, PON1 QQ192 homozygous individuals showed a considerably higher risk of stent thrombosis, lower PON1 plasma activity, lower plasma concentrations of active metabolite and lower platelet inhibition than RR192 homozygous individuals.
There are limited data on the prevalence of the CYP2C19*17 gain-of-function polymorphism and the functional significance of the PON1 Q192R polymorphism in Asians. Moreover, the differential prevalence of gain-of-function and loss-of-function polymorphisms among differ-ent Asian ethnic groups remains unclear. We hypothesized that the prevalence of functional polymorphisms involved in clopidogrel bioacti-vation differs among Asian ethnic groups.
To test this hypothesis, we first assessed the functional significance of CYP2C19 and PON1 polymorphisms using pharmacodynamic mea-sures of clopidogrel response (platelet reactivity) in a cohort of Asian patients taking clopidogrel. We then investigated the differential prevalence of functionally significant polymorphisms in a separate cross-sectional population of Chinese, Malay and Indian subjects.
Aim, materials & methods: We investigated the functional significance of CYP2C19*2, *3, *17 and PON1 Q192R SNPs in 89 consecutive Asian patients on clopidogrel treatment and the prevalence of functionally significant polymorphisms among 300 Chinese, Malays and Asian Indians. Results: Both CYP2C19 loss-of-function alleles (*2 or *3) were associated with higher platelet reactivity while the CYP2C19 gain-of-function allele (*17) had lower platelet reactivity. For PON1, the median PRI was not significantly different between the QQ, QR and RR groups. The allele frequencies of CYP2C19*2, CYP2C19*3 and CYP2C19*17 were 0.280, 0.065 and 0.010 (rare) for Chinese, 0.310, 0.050 and 0.025 for Malays, and 0.375, 0.010 (rare) and 0.165 for Indians, respectively. Conclusion: Our data suggest that genotyping studies to investigate clopidogrel response should include CYP2C19*2 and *3 but not *17 polymorphisms in Chinese, and CYP2C19*2 and *17 polymorphisms but not *3 in Indians. All three polymorphisms should preferably be genotyped in Malays.
Original submitted 16 December 2011; Revision submitted 16 February 2012
KeywoRds: Asian n clopidogrel n CYP2C19 n metabolism n pharmacogenetics n PON1 Mark Y Chan1,2*, Karen Tan3, Huay-Cheem Tan1, Pei-Tee Huan3, Bei Li3, Qian-Hui Phua2, Hong-Kai Lee2,3, Chi-Hang Lee1,2, Adrian Low1,2, Richard C Becker4, Wen-Chong Ong2, Mark A Richards2, Agus Salim2, E-Shyong Tai2,3 & Evelyn Koay2,3
1National University Heart Centre, 1E Kent Ridge Road, Singapore 119228, Singapore 2Yong Loo Lin School of Medicine, National University of Singapore, Singapore 3National University Health System, Singapore 4Duke Clinical Research Institute, Durham, NC, USA *Author for correspondence: Tel.: +65 6772 5596 Fax: +65 6872 2998 [email protected]
part of

Author Pro
of
ReseaRch aRticle Chan, Tan, Tan et al. Clopidogrel pharmacogenetics of Asian ethnicities ReseaRch aRticle
Pharmacogenomics (2012) 13(5)2 future science group
Patients & methods�n Pharmacodynamic population
First, we genotyped and measured the platelet pharmacodynamic response to clopidogrel in 89 patients with known or suspected stable coronary artery disease undergoing coronary angiogra-phy or PCI at the National University Hospital, Singapore (the pharmacodynamic population). We excluded patients with acute coronary syn-drome, patients who were being treated with nondihydropyridine calcium channel antago-nists or a glycoprotein IIb–IIIa inhibitor within the previous 5 days, and patients with a serum creatinine level of >150 µmol/l. Because acute coronary syndrome is associated with increased platelet reactivity, we enrolled only patients with clinically stable disease [14]. All patients were administered a loading dose of clopido-grel 300 mg, followed by a maintenance dose of clopidogrel 75 mg daily for 5–7 days until and including the day of scheduled coronary angiography or PCI. A peripheral blood sample was drawn from the arterial sheath immediately after the operator gained access to the radial or femoral artery, but before the administration of unfractionated heparin or other parenteral medications. The National University Health System Domain Specific Review Board approved the study protocol and all subjects gave written informed consent prior to participating in the study.
�n Prevalence populationWe then investigated the interethnic prevalence of CYP2C19*2, *3 and *17 polymorphisms. Subjects were identified through stratified ran-dom sampling from an unselected cohort of 3000 consecutive individuals undergoing com-plete blood count evaluation over 3 days at the National University Hospital. Selection was stratified by ethnicity, followed by random sam-pling within each stratum to form three equal groups of Chinese, Malay and Indian subjects. Ethnicity was self-reported and all subjects gave written informed consent for the use of clini-cal and genetic data that had their identifiers removed.
Genetic ana lysisGenotyping was performed using PCR followed by RFLP for the *2 and *3 genetic variants. Genomic DNA was extracted from ethylenedi-aminetetraacetic acid-anticoagulated blood or buffy coat. PCR amplification of 35 cycles was performed for CYP2C19 allele *2 (rs4244285, 681G>A), which is a SNP on exon 5, and *3
(rs4986893, 636G>A), which is a SNP on exon 4, using GeneAmp® Taq polymerase on a ABI 9700 PCR machine with the following prim-ers: 5 -́CAGAGCTTGGCATATTGTATC-3´ and 5́ -GTAAACACACAACTAGTCAATG-3´ f lanking the exon 5 polymorphism and 5´-AAATTGTTTCCAATCATTTAGCT-3´ and 5´-ACTTCAGGGCTTGGTCAATA-3´ flanking the exon 4 polymorphism.
Verification of PCR products was performed using agarose gel electrophoresis with restriction enzyme digestion using SmaI and BamHI restric-tion enzymes for*2 and *3, respectively. Enzyme digestion produced a 120-bp and a 49-bp restric-tion band length for *2, and a 175-bp and a 96-bp restriction band length for *3. For the PON1 Q192R polymorphism, we performed PCR amplification with the following primers: 5´-TGTTCCATTATAGCTAGCACGA-3´ and 5´-TTTCACCCCCTGAAAAATTA-3 .́ Enzyme digestion with BspPI produced a 160 bp and a 85 bp restriction fragment band length for the Q192R polymorphism.
For CYP2C19*17 (rs12248560, -806C>T), which is a SNP in the 5́ -flanking region of the gene, we performed asymmetric PCR followed by high-resolution melting on a LightScanner® 32 (Idaho Technology Inc., UT, USA). PCR was initiated with a 5-min denaturation at 95°C, followed by 50 amplification cycles con-sisting of 10 s at 95°C, 15 s at 62°C and 20 s at 68°C using the forward and reverse primers flanking the CYP2C19*17 -806C>T variant 5´-GCATCTCTGGGGCTGTTTTCC-3´ and reverse 5´-GAGGTCTTCTGATGCC-CATCGT-3 .́ Asymmetric PCR products were analyzed using the LightScanner 32 with premelt at 95°C for 10 s. They were then rapidly cooled to 40°C and held for 30 s. Subsequently, high-reso-lution melting data was continuously acquired at a ramping rate of 0.15°C per second from 53°C to 70°C, with an initial holding temperature of 48°C. Data ana lysis of high-resolution melt-ing was performed using the ‘unlabeled probe genotyping’ mode by setting the normalized range at 57–66°C. The unlabelled LunaProbe (Suprenom, Singapore) was designed to match the mutant sequence: 5´-TCTGTTCTCA-AAGTATCTCTGATGTAAc3spacer-3 .́
The data from each melting ana lysis was studied using both the rate of change of force (-dF/dT) versus temperature/melting peak plots and relative fluorescence signal changes versus temperature/melting curve plots. The CYP2C19*17 -806TT homozygous variant had a peak melting temperature of 63°C while the
Author Pro
of
ReseaRch aRticle Chan, Tan, Tan et al. Clopidogrel pharmacogenetics of Asian ethnicities ReseaRch aRticle
www.futuremedicine.com 3future science group
CYP2C19*17 -806CC wild-type had a melt-ing temperature of 60°C, and the CYP2C19*17 -806CT heterozygous variant had two melting temperatures of 63°C and 60°C.
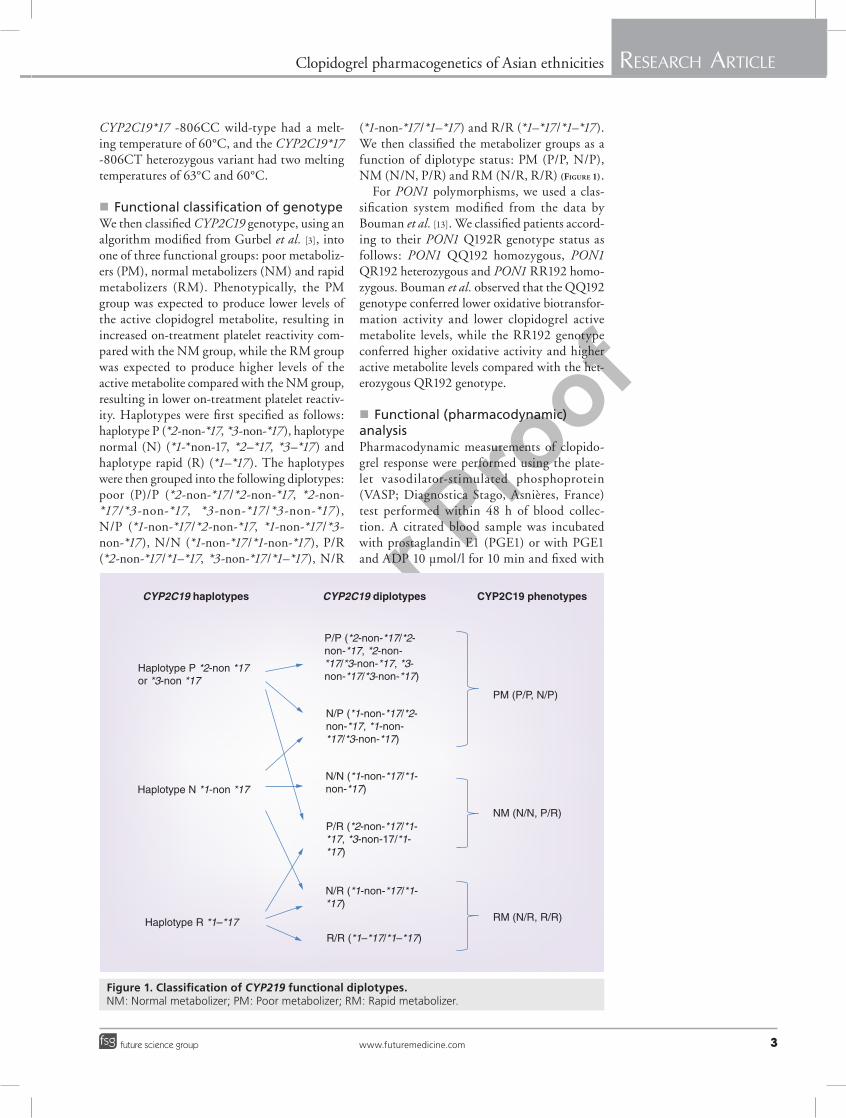
�n Functional classification of genotypeWe then classified CYP2C19 genotype, using an algorithm modified from Gurbel et al. [3], into one of three functional groups: poor metaboliz-ers (PM), normal metabolizers (NM) and rapid metabolizers (RM). Phenotypically, the PM group was expected to produce lower levels of the active clopidogrel metabolite, resulting in increased on-treatment platelet reactivity com-pared with the NM group, while the RM group was expected to produce higher levels of the active metabolite compared with the NM group, resulting in lower on-treatment platelet reactiv-ity. Haplotypes were first specified as follows: haplotype P (*2-non-*17, *3-non-*17), haplotype normal (N) (*1-*non-17, *2–*17, *3–*17) and haplotype rapid (R) (*1–*17). The haplotypes were then grouped into the following diplotypes: poor (P)/P (*2-non-*17/*2-non-*17, *2-non-*17/*3-non-*17, *3-non-*17/*3-non-*17 ), N/P (*1-non-*17/*2-non-*17, *1-non-*17/*3-non-*17), N/N (*1-non-*17/*1-non-*17), P/R (*2-non-*17/*1–*17, *3-non-*17/*1–*17), N/R
(*1-non-*17/*1–*17) and R/R (*1–*17/*1–*17). We then classified the metabolizer groups as a function of diplotype status: PM (P/P, N/P), NM (N/N, P/R) and RM (N/R, R/R) (Figure 1).
For PON1 polymorphisms, we used a clas-sification system modified from the data by Bouman et al. [13]. We classified patients accord-ing to their PON1 Q192R genotype status as follows: PON1 QQ192 homozygous, PON1 QR192 heterozygous and PON1 RR192 homo-zygous. Bouman et al. observed that the QQ192 genotype conferred lower oxidative biotransfor-mation activity and lower clopidogrel active metabolite levels, while the RR192 genotype conferred higher oxidative activity and higher active metabolite levels compared with the het-erozygous QR192 genotype.
�n Functional (pharmacodynamic) ana lysisPharmacodynamic measurements of clopido-grel response were performed using the plate-let vasodilator-stimulated phosphoprotein (VASP; Diagnostica Stago, Asnières, France) test performed within 48 h of blood collec-tion. A citrated blood sample was incubated with prostaglandin E1 (PGE1) or with PGE1 and ADP 10 µmol/l for 10 min and fixed with
CYP2C19 haplotypes CYP2C19 diplotypes CYP2C19 phenotypes
Haplotype P *2-non *17or *3-non *17
Haplotype N *1-non *17
Haplotype R *1–*17
PM (P/P, N/P)
NM (N/N, P/R)
RM (N/R, R/R)
P/P (*2-non-*17/*2-non-*17, *2-non-*17/*3-non-*17, *3-non-*17/*3-non-*17)
N/P (*1-non-*17/*2-non-*17, *1-non-*17/*3-non-*17)
N/N (*1-non-*17/*1-non-*17)
N/R (*1-non-*17/*1-*17)
R/R (*1–*17/*1–*17)
P/R (*2-non-*17/*1-*17, *3-non-17/*1-*17)
Figure 1. Classification of CYP219 functional diplotypes. NM: Normal metabolizer; PM: Poor metabolizer; RM: Rapid metabolizer.
Author Pro
of
ReseaRch aRticle Chan, Tan, Tan et al. Clopidogrel pharmacogenetics of Asian ethnicities ReseaRch aRticle
Pharmacogenomics (2012) 13(5)4 future science group
paraformaldehyde, after which the platelets were permeabilized with nonionic detergent. Analyses were performed on a FACS Canto II flow cytom-eter (Becton Dickinson, NJ, USA). The platelet population was identified from its forward and side scatter distribution, and 5000 platelets were gated. A platelet reactivity index (PRI) index was calculated from the median fluorescence inten-sity (MFI) of samples incubated with PGE1 or PGE1 and ADP according to the formula:
PRI MFIMFI MFI 100
[PGE1][PGE1] [PGE1 ADP]= -
#+c m
�n Statistical ana lysisData were presented as mean ± standard devia-tion median (25th percentile, 75th percentile) and frequencies (percentages). Categorical variables were compared using the c2 test. The Kolmogorov–Smirnov test was used to check for normal distribution of continuous data. Normally distributed continuous data were compared across genotype groups with the one-way ana lysis of variance test. Non-normally dis-tributed continuous data were compared across genotype groups using the Kruskal–Wallis test. The PRI data were not normally distributed; they are presented as median (25th percentile, 75th percentile), and were compared across genotype groups with the Kruskal–Wallis test, and compared between two groups with the two-sided unpaired Wilcoxon test. We tested for a possible deviation of the CYP2C19*2, *3 and *17 genotype distribution from the Hardy–Weinberg equilibrium proportions using Pearson’s goodness-of-fit test. A multiple linear regression model was used to test for an inde-pendent association of *2, *3 and *17 carriage with the PRI. Independent variables were *2, *3 or *17 carrier status, age, sex and variables with a reported significant influence on clopidogrel responsiveness on the basis of previous obser-vations (such as treatment with proton pump inhibitors, calcium channel inhibitors, diabetes mellitus, smoking, renal insufficiency and BMI). All analyses were performed using STATA ver-sion 11.1 (StataCorp, TX, USA). For all statisti-cal analyses, a p-value of <0.05 was considered statistically significant.
Results�n Functional (pharmacodynamic)
significance of CYP2C19 & PON1 polymorphismsIn the pharmacodynamic population (n = 89), we performed both genotyping and the plate-let VASP phosphorylation test after a 300 mg
loading dose followed by a daily 75 mg main-tenance dose of clopidogrel for a median of 7 (minumum 5, maximum 8) days. Baseline char-acteristics of the pharmacodynamic population separated into PM, NM and RM groups based on their CYP2C19 genotype, and RR192 QR192 and QQ192 groups based on their PON1 geno-type, are shown in Tables 1 & 2, respectively. One subject could not be genotyped for PON1.
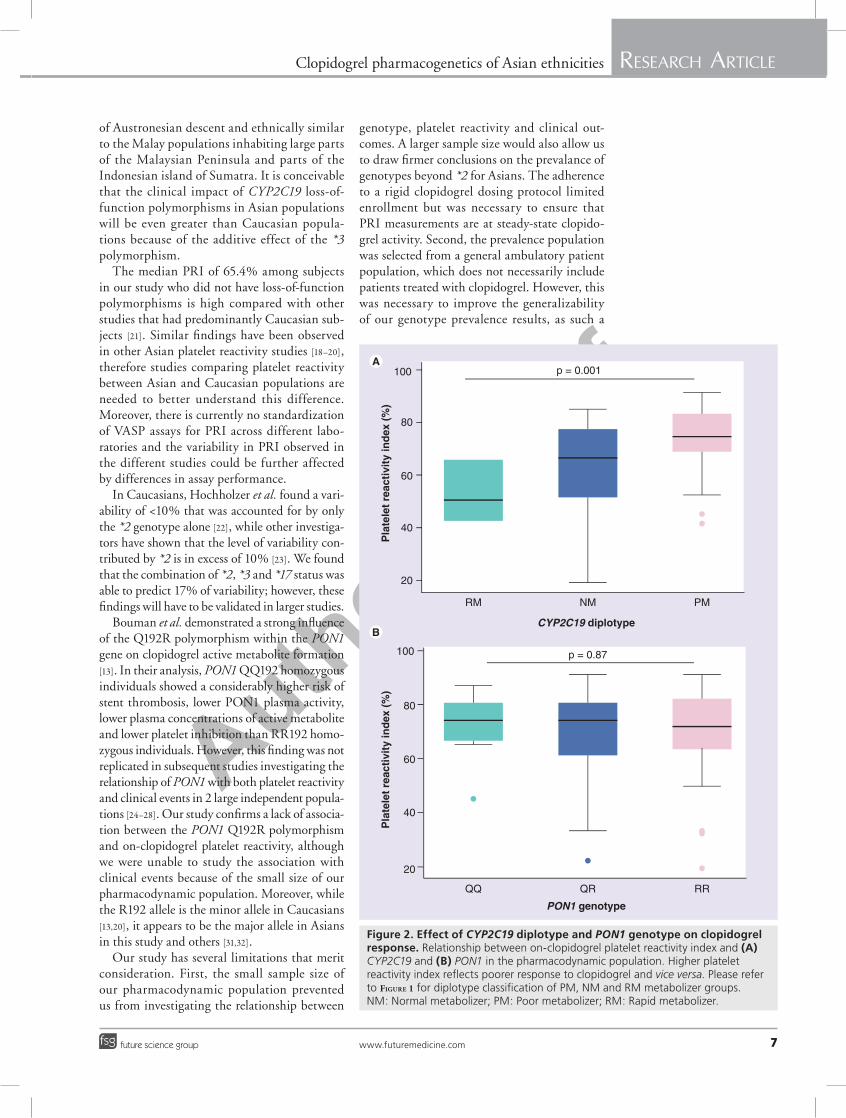
For the CYP2C19*2 and *3 loss-of-function alleles, the median (25th, 75th percentile) on-clopidogrel PRI was 65.4% (50.3%, 77.1%), 74.0% (66.9%, 82.7%) and 80.3% (73.5%, 83.7%), p = 0.0003 for patients with no loss-of-function alleles (*1/*1), patients with one loss-of-function allele (heterozygous *2 or *3) and two loss-of-function alleles (homozygous *2 and/or *3), respectively. For the CYP2C19*17 gain-of-function allele, the median (25th, 75th percentile) on-clopidogrel PRI was 73.9% (63.8%, 80.3%) and 58.0% (44.7%, 77.4%), p = 0.0001 for patients who were homozygous wild-type and heterozygous *17, respectively. None of the patients in the pharmacodynamic cohort were homozygous *17. When patients were classified into PM, NM and RM as a func-tion of CYP2C19 diplotype, the median (25th, 75th percentile) on-clopidogrel PRI were 74.7% (68.8%, 83.1%), 66.7% (51.8%, 77.3%) and 50.7% (42.7%, 65.4%), p = 0.0001 for the PM (n = 49), NM (n = 35) and RM (n = 3) groups, respectively (Figure 2a).
For PON1, the median (25th, 75th percen-tile) on-clopidogrel PRI were 74.4% (66.0%, 81.8%), 74.0% (60.6%, 80.3%) and 71.9% (61.4%, 82.2%), p = 0.87 for the QQ (n = 13), QR (n = 44) and RR (n = 29) groups, respec-tively (Figure 2b).
�n Multivariable ana lysisAfter adjusting for other known explanatory variables, CYP2C19 genotype remained inde-pendently predictive of on-treatment PRI. Compared with patients with no loss-of-function alleles (homozygous wild-type), patients with one loss-of-function allele (*2 or *3) had an 11.6% (95% CI: 5.32–18.6%; p = 0.001) greater PRI and patients with two loss-of-function alleles (*2 and/or *3) had a 19.6% (95% CI: 9.3–29.9%; p < 0.001) greater PRI. CYP2C19 metabolizer status accounted for 17% (R2 = 0.168) of the variability in on-treatment PRI.
BMI was also independently predictive of on-treatment PRI (1.11% increase in PRI per 1 kg m-2 increase in BMI, 95% CI: 0.36–1.87; p = 0.004) while a trend towards statistical
Author Pro
of
ReseaRch aRticle Chan, Tan, Tan et al. Clopidogrel pharmacogenetics of Asian ethnicities ReseaRch aRticle
www.futuremedicine.com 5future science group
significance was observed for serum creatinine (1.5% decrease in PRI per 10 µmol/l increase in serum creatinine, 95% CI: 0.16–3.19%; p = 0.07). Statin use, omeprazole use, dihydro-pyridine calcium channel blocker use, smoking and diabetes mellitus were not independently predictive of on-treatment PRI.
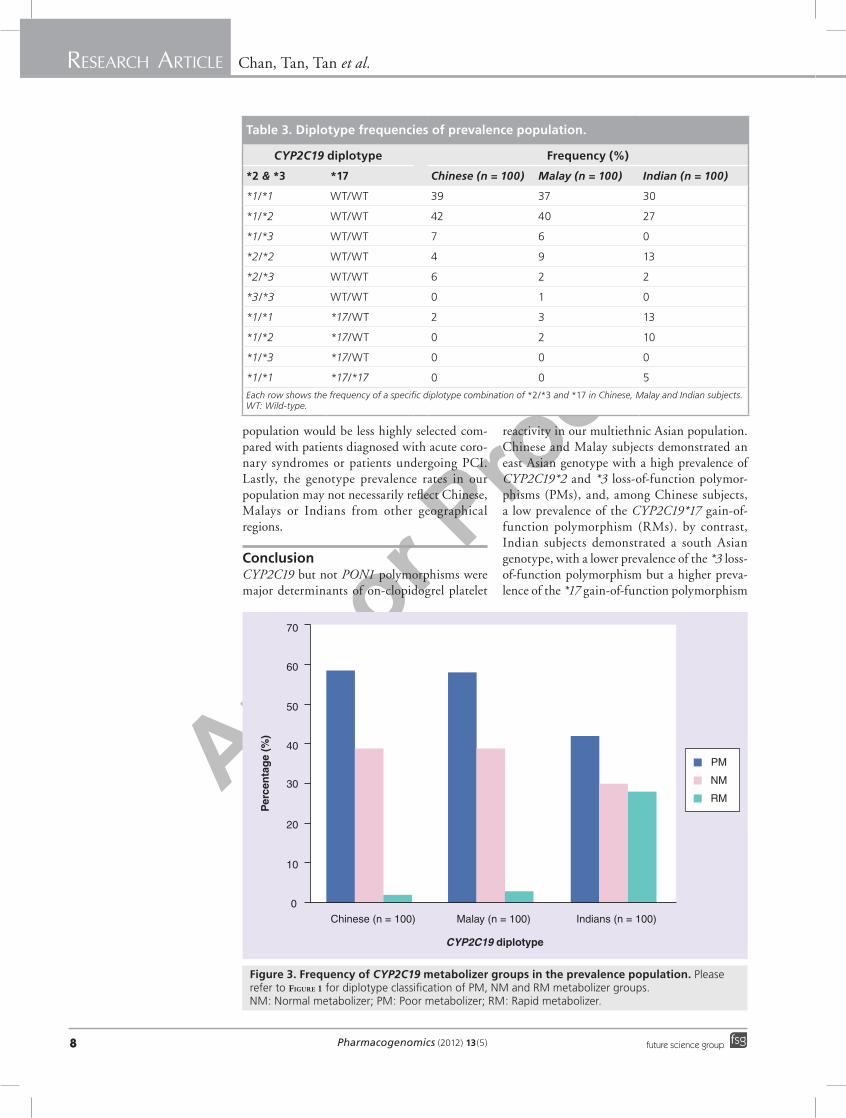
�n Prevalence of functionally significant genotypesBecause only CYP2C19 and not PON1 was functionally significant in the pharmacody-namic population, we proceeded to perform genotyping of CYP2C19*2, *3 and *17 poly-morphisms in a randomly selected population of 300 subjects. Table 3 shows the distribution of diplotypes among Chinese (n = 100), Malay (n = 100) and Indian (n = 100) subjects in the prevalence population. The *2 allele frequency was 0.28 among the Chinese subjects, 0.31 among the Malay subjects, and 0.325 among the Indian subjects. The *3 allele was 0.065 among the Chinese subjects and 0.05 among the Malay subjects, compared with only 0.01 among the Indian subjects. By contrast, the *17 allele
frequency was 0.01 among the Chinese subjects and 0.025 among the Malay subjects, compared with 0.165 among the Indian subjects. No sig-nificant deviation from the Hardy–Weinberg equilibrium was observed.
When classifying these subjects into PM, NM and RM groups, we found the highest propor-tion of PMs among the Chinese subjects (59%), followed by the Malay subjects (58%) and the Indian subjects (42%), p < 0.001 (Figure 3). By contrast, RMs were infrequent among the Chinese (2%) and Malay (3%) subjects but far more prevalent among the Indian subjects (28%), p < 0.001.
discussionIn our multiethnic Asian population, CYP2C19 but not PON1 polymorphisms were major determinants of on-clopidogrel platelet reac-tivity. Our Chinese and Malay subjects had a high prevalence of CYP2C19*2 and *3 loss-of-function polymorphisms, and Chinese sub-jects had a low prevalence of the CYP2C19*17 gain-of-function polymorphism. By contrast, Indian subjects had a high prevalence of both
Table 1. Baseline characteristics and background medications of pharmacodynamic population classified by CYP2C19 diplotype.
Baseline characteristics/co-medications
Frequency p-value
PM (n = 49) NM (n = 37) RM (n = 3)
Age (range) 57 (51–64) 53 (50–64.5) 59 (57–63) 0.705
Sex, female (%) 33.3 13.5 14.3 0.519
Ethnicity 0.132
– Chinese (%) 67.4 56.8 33.3
– Malay (%) 20.4 32.4 0
– Indian (%) 12.2 10.8 66.7
Diabetes (%) 34.7 48.7 33.3 0.426
BMI, kg/m2 (25th percentile, 75th percentile)
25 (23, 27) 26 (24, 28.5) 25 (24, 25) 0.371
Serum creatinine, µmol/l (25th percentile, 75th percentile)
75 (67.5, 85) 84.5 (70.5, 99.25) 72 (66, 78) 0.070
Significant coronary artery disease†
91.8 86.4 100 0.945
Proton pump inhibitor (%) 30.6 29.7 33.3 1.000
Dihydropyridine calcium channel antagonist (%)
26.9 32.5 33.3 0.893
Statin (%) 66.7 78.4 83.7 0.461
Aspirin (%) 100 100 100 1.000
Smoking (%) 34.7 32.4 0 0.659†One or more epicardial coronary arteries with >50% stenosis.NM: Normal metabolizers; PM: Poor metabolizers; RM: Rapid metabolizers.
Author Pro
of
ReseaRch aRticle Chan, Tan, Tan et al. Clopidogrel pharmacogenetics of Asian ethnicities ReseaRch aRticle
Pharmacogenomics (2012) 13(5)6 future science group
CYP2C19*2 loss-of-function and CYP2C19*17 gain-of-function polymorphisms, but a low prevalence of the CYP2C19*3 loss-of-function polymorphism.
Other investigators have observed a high prevalence of the CYP2C19*2 loss-of-function allele among East Asians [15]. The homozygous *2 genotype, which is associated with the high-est level of on-treatment platelet reactivity and is present in 2–3% of Caucasians, was present in 4% of the Chinese, 9% of the Malays and 13% of the Indians in our study. The prevalence of *2 polymorphisms among the Indian subjects in our study was higher than that observed in Caucasian populations but similar to other studies on Indian subjects from the Indian sub-continent [16,17]. However, the co-inheritance of *2 and *17 in 6% of the Indian subjects in the prevalence population contributed to a lower fre-quency of PM compared with the Chinese and Malay subjects.
Sibbing et al. showed that individuals who co-inherit the *2 and *17 polymorphism manifest an intermediate level of platelet reactivity and clinical event rates that are similar to homozy-gous wild-type subjects [12]. This neutralization effect could possibly be owing to *17 increasing both the production of defective (*2 and *3) and functional CYP2C19. This is particularly relevant to populations with a high prevalence of the *17 polymorphism, namely, Caucasians
and south Asians, but not east Asian popula-tions among whom the *17 allele is less common. Clinical investigations that genotype only the CYP2C19*2 without the *17 polymorphism may therefore fail to account for the counteracting effect of *17 on platelet reactivity and clinical events among south Asians.
The *3 polymorphism increased on-treat-ment platelet reactivity to a similar magnitude as the CYP2C19*2 polymorphism in South Korean subjects treated with clopidogrel [18–20]. While it is therefore conceivable that the *3 polymorphism will impact clinical outcomes to a similar extent as the *2 polymorphism, the true relationship between the *3 polymorphism and clinical outcomes can only be ascertained from large Asian-based populations with a high prevalence of the *3 allele. Man et al. showed that the prevalence of CYP2C19*3 carriers was 24.2% among Japanese, 14.8% among Koreans and 8.9% among Han Chinese but only 0.4% among Africans and 0.2% among Caucasians [8]. In our study, the *3 alleles was present in 10% of the Chinese subjects and 9% of the Malay subjects, compared with only 1% of the Indian subjects. The co-inheritance of the *2 and *3 allele was observed in 4% of the Chinese, 2% of Malays and 1% of Indians in our study, contributing to a substantial increase in the prevalence of homozygous loss-of-function gen-otypes. The Malay population in Singapore is
Table 2. Baseline characteristics and background medications of platelet reactivity population classified by PON1 genotype.
Baseline characteristics/ co-medications Frequency (%) p-value
PON1 QQ192 (n = 14) PON1 QR192 (n = 44) PON1 RR192 (n = 30)
Age (years; mean range) 61 (50–65.3) 57 (51–66.5) 53 (50–64) 0.521
Sex, female (%) 14.3 20.5 6.7 0.286
Ethnicity 0.397
– Chinese (%) 57.1 61.4 66.7
– Malay (%) 14.3 29.6 20.0
– Indian (%) 28.6 9.1 13.3
Diabetes (%) 21.4 40.9 46.7 0.260
BMI (kg/m2) median (25th percentile, 75th percentile)
26 (22.5, 30) 25 (23, 27) 25.5 (24, 27.25) 0.544
Serum creatinine (µmol/l)median (25th percentile, 75th percentile)
77.5 (68, 91.5) 77.5 (68, 91.5) 82 (66.5, 94) 0.735
Proton pump inhibitor (%) 42.9 29.6 26.7 0.576
Dihydropyridine calcium channel antagonist (%) 26.9 32.5 20.0 0.721
Statin (%) 71.4 77.3 90.0 0.248
Aspirin (%) 100 100 100 1.000
Smoking (%) 35.7 36.4 26.7 0.714
Author Pro
of
ReseaRch aRticle Chan, Tan, Tan et al. Clopidogrel pharmacogenetics of Asian ethnicities ReseaRch aRticle
www.futuremedicine.com 7future science group
of Austronesian descent and ethnically similar to the Malay populations inhabiting large parts of the Malaysian Peninsula and parts of the Indonesian island of Sumatra. It is conceivable that the clinical impact of CYP2C19 loss-of-function polymorphisms in Asian populations will be even greater than Caucasian popula-tions because of the additive effect of the *3 polymorphism.
The median PRI of 65.4% among subjects in our study who did not have loss-of-function polymorphisms is high compared with other studies that had predominantly Caucasian sub-jects [21]. Similar findings have been observed in other Asian platelet reactivity studies [18–20], therefore studies comparing platelet reactivity between Asian and Caucasian populations are needed to better understand this difference. Moreover, there is currently no standardization of VASP assays for PRI across different labo-ratories and the variability in PRI observed in the different studies could be further affected by differences in assay performance.
In Caucasians, Hochholzer et al. found a vari-ability of <10% that was accounted for by only the *2 genotype alone [22], while other investiga-tors have shown that the level of variability con-tributed by *2 is in excess of 10% [23]. We found that the combination of *2, *3 and *17 status was able to predict 17% of variability; however, these findings will have to be validated in larger studies.
Bouman et al. demonstrated a strong influence of the Q192R polymorphism within the PON1 gene on clopidogrel active metabolite formation [13]. In their ana lysis, PON1 QQ192 homozygous individuals showed a considerably higher risk of stent thrombosis, lower PON1 plasma activity, lower plasma concentrations of active metabolite and lower platelet inhibition than RR192 homo-zygous individuals. However, this finding was not replicated in subsequent studies investigating the relationship of PON1 with both platelet reactivity and clinical events in 2 large independent popula-tions [24–28]. Our study confirms a lack of associa-tion between the PON1 Q192R polymorphism and on-clopidogrel platelet reactivity, although we were unable to study the association with clinical events because of the small size of our pharmacodynamic population. Moreover, while the R192 allele is the minor allele in Caucasians [13,20], it appears to be the major allele in Asians in this study and others [31,32].
Our study has several limitations that merit consideration. First, the small sample size of our pharmacodynamic population prevented us from investigating the relationship between
genotype, platelet reactivity and clinical out-comes. A larger sample size would also allow us to draw firmer conclusions on the prevalance of genotypes beyond *2 for Asians. The adherence to a rigid clopidogrel dosing protocol limited enrollment but was necessary to ensure that PRI measurements are at steady-state clopido-grel activity. Second, the prevalence population was selected from a general ambulatory patient population, which does not necessarily include patients treated with clopidogrel. However, this was necessary to improve the generalizability of our genotype prevalence results, as such a
A
B
Pla
tele
t re
acti
vity
ind
ex (
%)
Pla
tele
t re
acti
vity
ind
ex (
%)
20
40
60
80
100
20
40
60
80
100 p = 0.001
p = 0.87
RM NM PM
QQ QR RR
PON1 genotype
CYP2C19 diplotype
Figure 2. effect of CYP2C19 diplotype and PON1 genotype on clopidogrel response. Relationship between on-clopidogrel platelet reactivity index and (A) CYP2C19 and (B) PON1 in the pharmacodynamic population. Higher platelet reactivity index reflects poorer response to clopidogrel and vice versa. Please refer to Figure 1 for diplotype classification of PM, NM and RM metabolizer groups. NM: Normal metabolizer; PM: Poor metabolizer; RM: Rapid metabolizer.
Author Pro
of
ReseaRch aRticle Chan, Tan, Tan et al. Clopidogrel pharmacogenetics of Asian ethnicities ReseaRch aRticle
Pharmacogenomics (2012) 13(5)8 future science group
population would be less highly selected com-pared with patients diagnosed with acute coro-nary syndromes or patients undergoing PCI. Lastly, the genotype prevalence rates in our population may not necessarily reflect Chinese, Malays or Indians from other geographical regions.
ConclusionCYP2C19 but not PON1 polymorphisms were major determinants of on-clopidogrel platelet
reactivity in our multiethnic Asian population. Chinese and Malay subjects demonstrated an east Asian genotype with a high prevalence of CYP2C19*2 and *3 loss-of-function polymor-phisms (PMs), and, among Chinese subjects, a low prevalence of the CYP2C19*17 gain-of-function polymorphism (RMs). by contrast, Indian subjects demonstrated a south Asian genotype, with a lower prevalence of the *3 loss-of-function polymorphism but a higher preva-lence of the *17 gain-of-function polymorphism
70
60
50
40
30
20
10
0
Per
cen
tag
e (%
)
Chinese (n = 100) Malay (n = 100) Indians (n = 100)
PM
NM
RM
CYP2C19 diplotype
Figure 3. Frequency of CYP2C19 metabolizer groups in the prevalence population. Please refer to Figure 1 for diplotype classification of PM, NM and RM metabolizer groups.NM: Normal metabolizer; PM: Poor metabolizer; RM: Rapid metabolizer.
Table 3. diplotype frequencies of prevalence population.
CYP2C19 diplotype Frequency (%)
*2 & *3 *17 Chinese (n = 100) Malay (n = 100) Indian (n = 100)
*1/*1 WT/WT 39 37 30
*1/*2 WT/WT 42 40 27
*1/*3 WT/WT 7 6 0
*2/*2 WT/WT 4 9 13
*2/*3 WT/WT 6 2 2
*3/*3 WT/WT 0 1 0
*1/*1 *17/WT 2 3 13
*1/*2 *17/WT 0 2 10
*1/*3 *17/WT 0 0 0
*1/*1 *17/*17 0 0 5
Each row shows the frequency of a specific diplotype combination of *2/*3 and *17 in Chinese, Malay and Indian subjects.WT: Wild-type.

Author Pro
of
ReseaRch aRticle Chan, Tan, Tan et al. Clopidogrel pharmacogenetics of Asian ethnicities ReseaRch aRticle
www.futuremedicine.com 9future science group
executive summary
Clopidogrel pharmacogenetics of Asians & Caucasians
� CYP2C19 but not PON-1 polymorphisms are major determinants of on-clopidogrel response in Asians.
� The pharmacogenetics of clopidogrel bioactivation among Asian populations are very different to that of Caucasian populations.
Clopidogrel pharmacogenetic differences among three major Asian ethnicities
� All three major Asian ethnicities had a greater prevalence of poor metabolizers compared with other studies of Caucasian populations.
� Among the three major Asian ethnicities studied, Chinese and Malay subjects had a greater prevalence of poor metabolizers compared with Indian subjects in this study.
� Indian subjects had a far greater prevalence of rapid metabolizers compared with Chinese and Malay subjects.
Implications for future genotyping studies in Asians
� Our results may be useful in guiding future genotyping studies in Asian populations.
� Genotyping studies to investigate clopidogrel pharmacogenomics should include CYP2C19*2 and *3 but not *17 polymorphisms in Chinese, and CYP2C19*2 and *17 polymorphisms but not *3 in Indians. All three polymorphisms should preferably be genotyped in Malays.
(RMs). Although CYP2C19 genetic testing is already available in many clinical laboratories, the role for prospective genotyping has not been established. However, genotyping may identify subgroups of patients who will not benefit from standard clopidogrel therapy. The co-inheritance of both *2 loss-of-function and *17 gain-of-function polymorphisms suggests the need to genotype both *2 and *17 polymorphisms with-out the need for *3 genotyping in south Asian subjects. By contrast, both the *2 and *3 loss-of-function polymorphisms should be genotyped in east Asian subjects with the possible need for *17 genotyping in Malay subjects.
Future perspectiveThe widespread availability of generic clopi-dogrel and the high cost of newer generation platelet P2Y
12 receptor inhibitors presents a
unique health–economics dilemma for health-care payors. Moreover, the increased potency of the newer P2Y
12 inhibitors incur a greater risk of
bleeding, adding further to the need for unam-biguous strategies to inform treatment selection. Genotyping of CYP2C19 polymorphisms may prove useful in this role but will require further
dedicated clinical trials to determine the mag-nitude of its clinical utility and the overall cost–effectiveness of such a strategy.
Financial & competing interests disclosureThis study was supported by grants from the National Medical Research Council (Singapore, grant no. NIG09May023), the Cardiovascular Research Institute (Singapore) and Opto Systems Pte Ltd (Singapore). M Chan is supported by a clinician-scientist award (NMRC/CSA/028/2010) from the National Medical Research Council (Singapore). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
ethical conduct of research The authors state that they have obtained appropriate insti-tutional review board approval or have followed the princi-ples outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investi gations involving human subjects, informed consent has been obtained from the participants involved.
ReferencesPapers of special note have been highlighted as:n of interestnn of considerable interest
1 Yusuf S, Zhao F, Mehta SR et al. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. N. Engl. J. Med. 345(7), 494–502 (2001).
n� Seminal paper on the clinical effectiveness of clopidogrel in acute coronary syndromes.
2 Steinhubl SR, Berger PB, Mann JT 3rd et al.
Early and sustained dual oral antiplatelet therapy following percutaneous coronary intervention: a randomized controlled trial. JAMA 288(19), 2411–2420 (2002).
n� Seminal paper on the clinical effectiveness of clopidogrel in percutaneous coronary interventions.
3 Gurbel PA, Tantry US, Shuldiner AR, Kereiakes DJ. Genotyping: one piece of the puzzle to personalize antiplatelet therapy. J. Am. Coll. Cardiol. 56(2), 112–116 (2010).
nn� Excellent overview of unanswered questions
in genotype-guided clopidogrel treatment.
4 Hulot JS, Bura A, Villard E et al. Cytochrome P450 2C19 loss-of-function polymorphism is a major determinant of clopidogrel responsiveness in healthy subjects. Blood 108(7), 2244–2247 (2006).
nn� Seminal paper describing the pharmacodynamic effect of CYP2C19 polymorphisms in Caucasians.
5 Brandt JT, Close SL, Iturria SJ et al. Common polymorphisms of CYP2C19 and CYP2C9 affect the pharmacokinetic and pharmacodynamic response to clopidogrel but
Author Pro
of
ReseaRch aRticle Chan, Tan, Tan et al.ReseaRch aRticle
Pharmacogenomics (2012) 13(5)10 future science group
not prasugrel. J. Thromb. Haemost. 5(12), 2429–2436 (2007).
6 Mega JL, Close SL, Wiviott SD et al. Cytochrome P-450 polymorphisms and response to clopidogrel. N. Engl. J. Med. 360(4), 354–362 (2009).
nn� Seminal paper linking CYP2C19 to clinical outcomes among patients treated with clopidogrel.
7 Mega JL, Simon T, Collet JP et al. Reduced-function CYP2C19 genotype and risk of adverse clinical outcomes among patients treated with clopidogrel predominantly for PCI: a meta-analysis. JAMA 304(16), 1821–1830 (2010).
8 Man M, Farmen M, Dumaual C et al. Genetic variation in metabolizing enzyme and transporter genes: comprehensive assessment in 3 major East Asian subpopulations with comparison to Caucasians and Africans. J. Clin. Pharmacol. 50(8), 929–940 (2010).
n� Useful reference on pharmacogenetic differences between ethnicities.
9 Gaedigk A. Interethnic differences of drug-metabolizing enzymes. Int. J. Clin. Pharmacol. Ther. 38(2), 61–68 (2000).
10 Adithan C, Gerard N, Vasu S, Rosemary J, Shashindran CH, Krishnamoorthy R. Allele and genotype frequency of CYP2C19 in a Tamilian population. Br. J. Clin. Pharmacol. 56(3), 331–333 (2003).
11 Sibbing D, Gebhard D, Koch W et al. Isolated and interactive impact of common CYP2C19 genetic variants on the antiplatelet effect of chronic clopidogrel therapy. J. Thromb. Haemost. 8(8), 1685–1693 (2010).
12 Sibbing D, Koch W, Gebhard D et al. Cytochrome 2C19*17 allelic variant, platelet aggregation, bleeding events, and stent thrombosis in clopidogrel-treated patients with coronary stent placement. Circulation 121(4), 512–518 (2010).
13 Bouman HJ, Schömig E, van Werkum JW et al. Paraoxonase-1 is a major determinant of
clopidogrel efficacy. Nat. Med. 17(1), 110–116 (2011).
14 Mathur A, Robinson MS, Cotton J, Martin JF, Erusalimsky JD. Platelet reactivity in acute coronary syndromes: evidence for differences in platelet behaviour between unstable angina and myocardial infarction. Thromb. Haemost. 85(6), 989–994 (2001).
15 Fukushima-Uesaka H, Saito Y, Maekawa K et al. Genetic variations and haplotypes of CYP2C19 in a Japanese population. Drug Metab. Pharmacokinet. 20(4), 300–307 (2005).
16 Jose R, Chandrasekaran A, Sam SS et al. CYP2C9 and CYP2C19 genetic polymorphisms: frequencies in the south Indian population. Fundam. Clin. Pharmacol. 19(1), 101–105 (2005).
17 Lamba JK, Dhiman RK, Kohli KK. Genetic polymorphism of the hepatic cytochrome P450 2C19 in north Indian subjects. Clin. Pharmacol. Ther. 63(4), 422–427 (1998).
18 Kim IS, Choi BR, Jeong YH, Kwak CH, Kim S. The CYP2C19*2 and CYP2C19*3 polymorphisms are associated with high post-treatment platelet reactivity in Asian patients with acute coronary syndrome. J. Thromb. Haemost. 7(5), 897–899 (2009).
19 Kim KA, Park PW, Hong SJ, Park JY. The effect of CYP2C19 polymorphism on the pharmacokinetics and pharmacodynamics of clopidogrel: a possible mechanism for clopidogrel resistance. Clin. Pharmacol. Ther. 84(2), 236–242 (2008).
20 Kim KA, Song WK, Kim KR, Park JY. Assessment of CYP2C19 genetic polymorphisms in a Korean population using a simultaneous multiplex pyrosequencing method to simultaneously detect the CYP2C19*2, CYP2C19*3, and CYP2C19*17 alleles. J. Clin. Pharm. Ther. 35(6), 697–703 (2010).
21 Bonello L, Armero S, Ait Mokhtar O: Clopidogrel loading dose adjustment according to platelet reactivity monitoring in
patients carrying the 2C19*2 loss of function polymorphism. J. Am. Coll. Cardiol. 56(20), 1630–1636 (2010).
22 Hochholzer W, Trenk D, Fromm MF et al. Impact of cytochrome P450 2C19 loss-of-function polymorphism and of major demographic characteristics on residual platelet function after loading and maintenance treatment with clopidogrel in patients undergoing elective coronary stent placement. J. Am. Coll. Cardiol. 55(22), 2427–2434 (2010).
23 Shuldiner AR, O’Connell JR, Bliden KP et al. Association of cytochrome P450 2C19 genotype with the antiplatelet effect and clinical efficacy of clopidogrel therapy. JAMA 302, 849–857 (2009).
24 Sibbing D, Koch W, Massberg S et al. No association of paraoxonase-1 Q192R genotypes with platelet response to clopidogrel and risk of stent thrombosis after coronary stenting. Eur. Heart J. 32(13), 1605–1613 (2011).
25 Simon T, Steg PG, Becquemont L et al. Effect of paraoxonase-1 polymorphism on clinical outcomes in patients treated with clopidogrel after an acute myocardial infarction. Clin. Pharmacol. Ther. 90(4), 561–567 (2011).
26 Trenk D, Hochholzer W, Fromm MF et al. Paraoxonase-1 Q192R polymorphism and antiplatelet effects of clopidogrel in patients undergoing elective coronary stent placement. Circ. Cardiovasc. Genet. 4(4), 429–436 (2011).
27 Mohamed Ali S, Chia SE. Interethnic variability of plasma paraoxonase (PON1). activity towards organophosphates and PON1 polymorphisms among Asian populations – a short review. Ind. Health 46(4), 309–317 (2008).
28 Sanghera DK, Saha N, Aston CE, Kamboh MI. Genetic polymorphism of paraoxonase and the risk of coronary heart disease. Arterioscler. Thromb. Vasc. Biol. 17(6), 1067–1073 (1997).
Top Related
Copyright © 2022 FDOKUMEN

