






Bahasa
Halaman
Hukum

Comparison of the efficacy and tolerabilityof new antiepileptic drugs: what can we learnfrom long-term studies?
In the last 15 years, several new antiepileptic drugs(AEDs) have become available in Europe and inthe US as add-on treatment for patients withepilepsy. As large comparative studies on these newAEDs have not yet been performed, specificselection criteria are still lacking. In this frame-work, a systematic review of the current evidencecan be useful, particularly as regards open-labelobservational studies.To assess the efficacy and/or tolerability of the
new AEDs, a number of meta-analyses have
explored the results reported in double-blindrandomized studies (1– 7). However, the transfer-ability of these findings to clinical practice islimited by several factors. First, the doses used inregulatory trials do not always reflect the dosesactually used in clinical practice. Second, thesemeta-analyses have used the response rate (per-centage of patients with 50% or greater reductionin seizure frequency compared with baseline) as theprimary efficacy index and have ignored importantclinically relevant end points such as the number of
Acta Neurol Scand 2006: 114: 157–168 DOI: 10.1111/j.1600-0404.2006.00705.x Copyright � Blackwell Munksgaard 2006
ACTA NEUROLOGICASCANDINAVICA
Zaccara G, Messori A, Cincotta M, Burchini G. Comparison of theefficacy and tolerability of new antiepileptic drugs: what can we learnfrom long-term studies?Acta Neurol Scand 2006: 114: 157–168. � Blackwell Munksgaard 2006.
Objective – A review of long-term open-label studies was performedwith the aim of detecting differences in efficacy and/or tolerability ofnew antiepileptic drugs (AEDs). Methods – From more than 500 openstudies conducted to evaluate the efficacy and tolerability ofgabapentin (GBP), lamotrigine (LTG), levetiracetam (LEV),oxcarbazepine (OXC), pregabalin (PGB), tiagabine (TGB), topiramate(TPM) or zonisamide (ZNS), we selected all studies that reported orallowed us to calculate the number of patients who achieved seizurefreedom for 6 months and/or the number of patients withdrawing foradverse effects and/or the number or percentage of patients continuingtreatment after 1 year. Results – No studies were found in which thisinformation was available for OXC, PGB, TGB or ZNS. The numberof patients who achieved seizure freedom for 6 months was reported infour studies each for GBP and TPM, five studies for LTG, and eightstudies for LEV. The best efficacy profile using this end point wasfound for LEV, followed by TPM, LTG, and GBP. Twenty-two studiesreported the number of patients withdrawing due to adverse effects.LEV was the best-tolerated AED, a little ahead of LTG, andsignificantly better than GBP or TPM . TPM was by far the least well-tolerated drug. Information concerning patients continuing treatmentafter 1 year was reported in two GBP studies, two TPM studies, sixLEV studies and five LTG studies. GBP had a very low retention rate(between 20% and 25% of patients continued the drug), while TPMand LTG had a retention rate of 40–60% and LEV had a retention rateof 60–75%. Conclusion – One limitation of these rankings is that theirstatistical value is limited because of the indirect nature of thecomparisons. Anyhow, this review covers the main studies publishedthus far on this subject and provides full updated information on thecurrent literature about these drugs.
G. Zaccara1, A. Messori2,M. Cincotta1, G. Burchini2
1Unit of Neurology, S.M. Nuova Hospital, Florence, Italy;2Drug Information Centre, Careggi Hospital, Florence,Italy
Key words: epilepsy; antiepileptic drugs; long-termstudies; systematic review
Gaetano Zaccara, Unit� Operativa di Neurologia,Ospedale S.M. Nuova, Piazza S.M. Nuova 1, 50122Firenze, ItalyTel.: 00 390552758894Fax: 00 390552758291e-mail: [email protected]
Accepted for publication May 9, 2006
157

patients achieving seizure freedom. Third, theefficacy and safety profiles in patients enrolled inrandomized trials may differ strikingly from thoseof patients treated in everyday practice. Last butnot least, the follow-up periods in the main double-blind studies published thus far have been veryshort . For example, the mean duration of follow-up for the 29 double-blind studies analyzed byMarson et al. (1) was only 3.5 months.Patients with epilepsy must take their treat-
ment for years, often for their whole life. Howcan we be sure that a new treatment willmaintain its efficacy over months or years?How can we compare the long-term adverseeffects of these drugs? Well-designed long-termclinical trials with head-to-head comparisons arerequired to answer these questions. In theabsence of such studies, as much information aspossible should be sought from long-term open-label studies. Hundreds of these studies havebeen published, and some provide crucial infor-mation on the long-term effects of these treat-ments (8– 14). However, no attempt has yet beenmade to review these data with the aim ofassessing the new AEDs.Our review of the literature concentrates on
three markers of efficacy and tolerability: (i) thepercentage of patients achieving seizure freedom;(ii) the percentage of patients withdrawingbecause of adverse effects; and (iii) the percentageof patients continuing treatment. Freedom fromseizures is a simple measure of efficacy, but itsclinical relevance depends on the duration offollow-up. Some authors (15, 16) have reported aseizure-free patient when seizures were notobserved for the last 4 or 6 weeks of the study.Others have reported the number of patientswithout seizures for six consecutive months orfor 1 year (12). We chose the 6-month seizurefreedom criterion because, this information wasreported by the majority of the most recentstudies, and because this criterion tends to be lesssensitive to the type of population recruited. Wesearched all open-label studies in which gabap-entin (GBP), lamotrigine (LTG), levetiracetam(LEV), oxcarbazepine (OXC), pregabalin (PGB),tiagabine (TGB), topiramate (TPM) or zonisa-mide (ZNS) were added to the previous antiep-ileptic treatment in patients whose seizures werenot controlled. Among these studies, we selectedthose that had a follow-up of at least 6 monthsand reported at least one of the three markerspreviously described. We included both prospect-ive and retrospective studies. To ascertain poss-ible bias, we also performed a further analysiscomparing results only from prospective studies.
Methods
Study selection
In February 2006, a computer search of Medline(PubMed version) was conducted for human stud-ies published in English, Italian, French, or Span-ish from 1966 up to May 2005. The literaturedatabase was extracted (first MEDLINE search)using the following Boolean keyword syntax:(retention OR withdrawal OR discontinuationOR dropout) AND (gabapentin OR lamotrigineOR levetiracetam OR oxcarbazepine OR pregab-alin OR tiagabine OR topiramate OR zonisamide).In a second search, each drug was consideredseparately, using its name in a simple two-keywordquery (drug name AND epilepsy) with thePubMed limits of �clinical trial� and �human.� Thefirst MEDLINE search produced 507 articles. Thesecond search showed 73, 148, 52, 48, 7, 47, 100,and 31 articles for GBP, LTG, LEV, OXC, PGB,TGB, TPM, and ZNS respectively.From these articles, we selected the trials that
met each of the following criteria: (i) open-labelstudies performed in drug-resistant epilepticpatients in whom a new drug was added to aprevious treatment, (ii) adult patients (or at least90% aged over 18 years), (iii) studies which inclu-ded only patients affected by generalized seizureswere excluded, (iv) special populations (i.e. chil-dren, elderly, patients with mental retardation)were excluded, (v) the duration of the studyallowed for the evaluation of our outcome meas-ures (see below).
Outcome measures
Our analysis included all trials that had a follow-upperiod of at least 6 months and reported at leastone of the following three parameters:
1 The number of patients who achieved seizurefreedom for six consecutive months. We ascer-tained that in all of the selected studies, patientshad been followed for at least 6 months; so wedetermined whether any patients had experi-enced a 6-month period of seizure freedomduring the observation period.
2 The number of patients who withdrew becauseof adverse effects. Some studies reported separ-ate information for patients withdrawing onlyfor adverse effects and for patients withdrawingfor adverse effects and no efficacy. In these cases,in a first evaluation, we considered patientswithdrawing only for adverse effects. In asubsequent evaluation, we also performed asensitivity analysis with which we reported
Zaccara et al.
158
withdrawals due to adverse effects of any kind(including those associated with inefficacy).
3 The number or percentage of patients continuingtreatment after 1 year and, if available, aftertwo, three or more years of treatment.
For each drug, the number of patients seizure-free for 6 months and the overall number ofpatients enrolled were extracted from individualstudies and then summed up to generate �crude�totals and a �crude� percentage of the occurrence ofthis clinically favorable end-point. The same ana-lysis was carried out for the clinically unfavorableend point of drug withdrawal.
Statistical analyses
The 95% confidence intervals (CI) were calculatedto estimate the statistical variations of our end-points. Standard methods were used to calculate95%CI of means. In the case of proportions, thecalculations were based on the equations describedby Fleiss (17).
Results
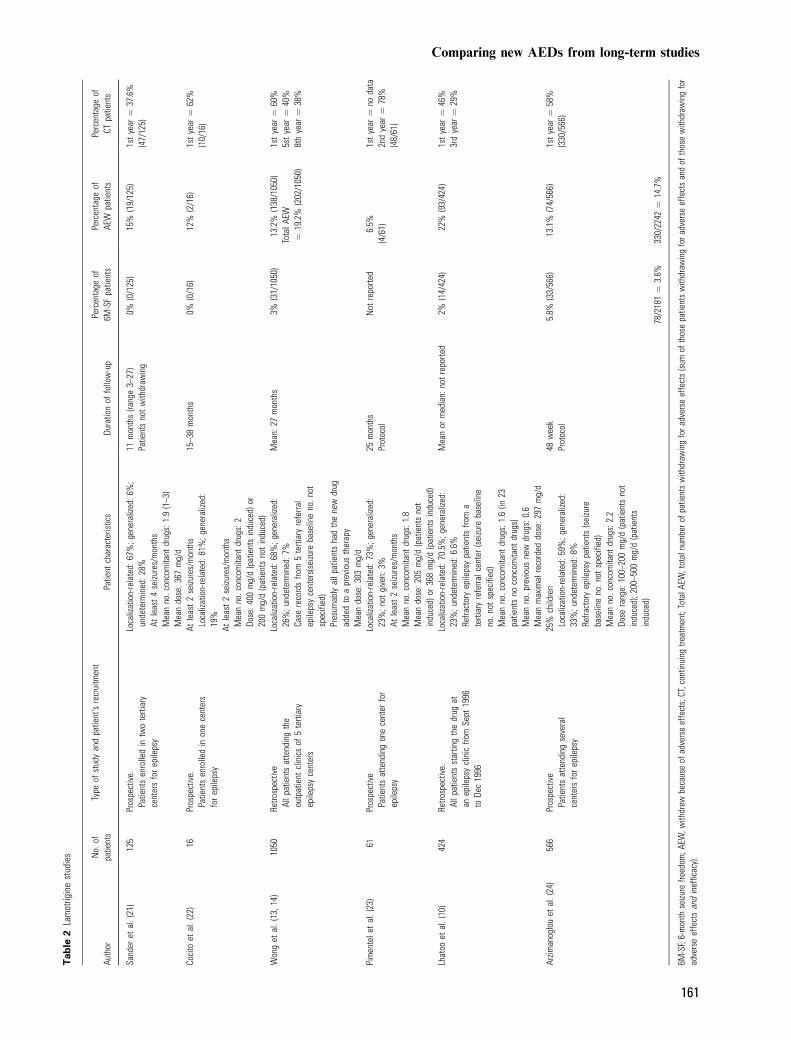
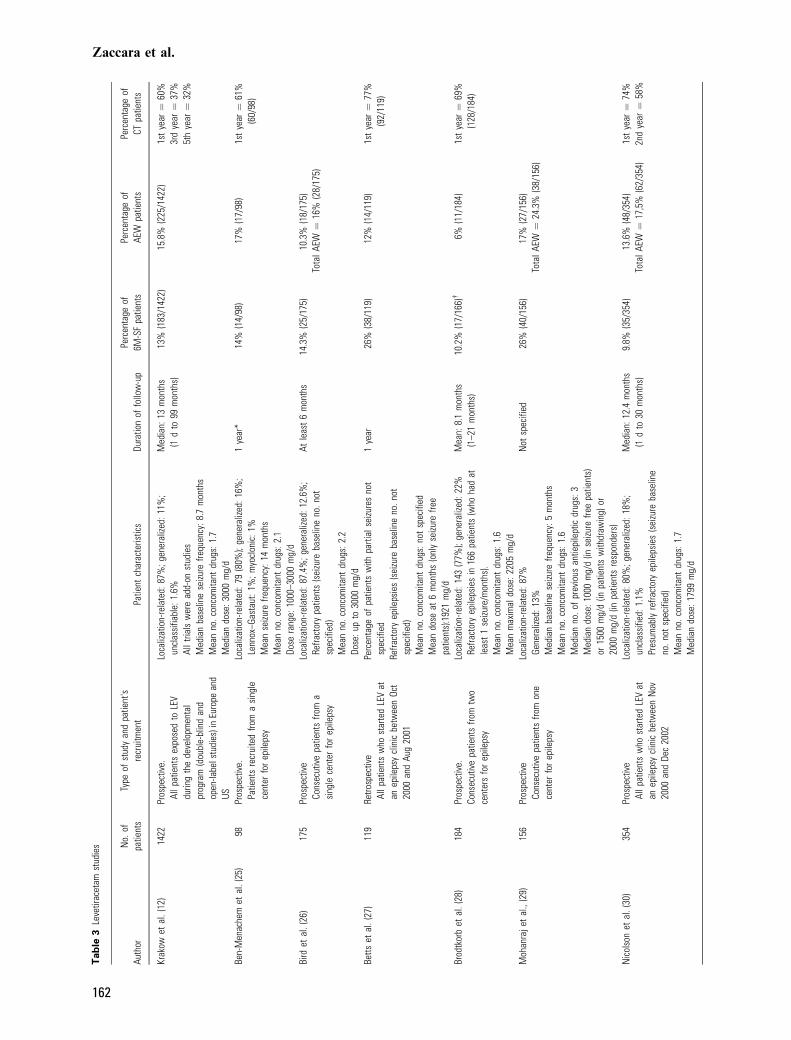
One hundred and fifty four open-label studies wereselected in which one of the new AEDs had beenadded to the treatment of adults (or mainly adults)with refractory seizures (as in a few studies not allof the patients had refractory seizures, thesepopulations were included in our analysis providedthat the subgroup of refractory patients had beenevaluated separately). Only 23 studies (two ofwhich presented data from the same patientpublished twice) reported or allowed us to calculateat least one of the previously described outcomeparameters. No studies were found in which thisinformation was available for OXC, PGB, TGB,and ZNS. Therefore, this review was focused onfour drugs only: GBP, LEV, LTG, and TPM.Tables 1–4 show the main characteristics of the
studies selected for each AED, e.g. recruitmentinformation, patient characteristics at baseline anddisease severity. Fourteen studies were prospectiveand eight were retrospective.The number of patients who achieved 6 months
of seizure freedom was reported in five LTGstudies, eight LEV studies, and four studies eachfor GBP and TPM. All of the studies selectedreported the number of patients who withdrew dueto adverse events.Results for seizure freedom are shown in Fig. 1.
As the 95%CIs did not overlap, one can assumethat each drug was significantly different from theothers. The most efficacious drug was LEV,
followed by TPM, LTG, and GBP. Analysis fromthe selected prospective studies was possible forLTG, LEV and TPM. Results showed that totalpercentages of patients who experienced a 6-monthseizure freedom were 4.7% (95%CI: 3.0–6.3),13.2% (95%CI: 11.8–14.6), and 16.1% (95%CI:12.2–20.0), respectively.Results for withdrawal due to adverse events are
shown in Fig. 2. LEV was the best-tolerated AED,a little ahead of LTG, and significantly better thanGBP or TPM. TPM was by far the least well-tolerated drug. In this case, results from selectedprospective studies showed that patients withdraw-ing due to adverse effects were 3% (95%CI: 0.26–6.2), 12.9% (95%CI: 10.4–15.3), 14.5% (95%CI:13.0–15.9), and 23.5% (95%CI: 19.4–27.5) forGBP, LTG, LEV, and TPM, respectively. Addi-tionally, we also performed a sensitivity analysiscalculating all patients withdrawing for adverseeffects (patients withdrawing for adverse effectsand/or inefficacy). In this case, the percentageswere 23.5% (95%CI: 20.7–26.3), 17.6% (95%CI:15.9–19.1), 16.6% (95%CI: 15.3–17.8), and 34.4%(95%CI: 31.8–36.9) for GBP, LTG, LEV, andTPM, respectively.Information concerning patients �retained� after
1 year was reported in two GBP studies, two TPMstudies, six LEV studies, and five LTG studies.Although these studies generally reported Kaplan–Meier percentages of patients continuing treatmentafter 2, 3, 5, and also 8 years (see Tables 1–4),information on retention was methodologicallypoor in nearly all of these studies. In fact,information was generally lacking about the cen-soring process and about the absolute number ofpatients still on treatment at the various timepointsof the Kaplan–Meier curve. The knowledge ofthese data is crucial to understand whether the�right tail� of the Kaplan–Meier curve is stillinformative because it contains enough patientsor is virtually uninformative because only a fewpatients are still in the study. This prevented usfrom calculating (at the various times) the values ofoverall retention percentage across the studiesevaluating the same drug. For this reason, wehave reported only the percentages of patientscontinuing treatment after 1 year (Fig. 3).Fig. 3 suggests that the differences among the
four drugs might be clinically relevant. After 1 yearof treatment, GBP had a very low retention rate(between 20% and 25%), while TPM and LTGhad retention rates between 40% and 60% andLEV had rates ranging from 60% to 75%. Inter-estingly enough, even though very different trialswere examined (some were retrospective, othersprospective, patient populations were heterogene-
Comparing new AEDs from long-term studies
159

Tab
le1
Gaba
pent
inst
udie
s
Auth
orN
o.of
patie
nts
Type
ofst
udy
and
patie
ntre
crui
t-m
ent
Patie
ntch
arac
teris
tics
Dura
tion
offo
llow
-up
Perc
enta
geof
6M-S
Fpa
tient
sPe
rcen
tage
ofAE
Wpa
tient
sPe
rcen
tage
ofCT
patie
nts
Sive
nius
etal
.(18
)25
Pros
pect
ive.
Alls
ubje
cts
prev
ious
lyin
clud
edin
ado
uble
-blin
dst
udy
Loca
lizat
ion-
rela
ted:
100%
Med
ian
seizu
refre
quen
cy:8
mon
ths
Conc
omita
ntdr
ugs:
atle
ast
1M
ean
last
dosa
ge:1
350
mg/
d(n
on-re
spon
ders
),17
00m
g/d
(resp
onde
rs)
Med
ian:
54m
onth
s0%
(0/2
5)0%
(0/2
5)
Lang
anet
al.(
19)
260
Retro
spec
tive.
263
cons
ecut
ive
patie
nts
atte
ndin
gan
epile
psy
clin
icbe
twee
n19
93an
d199
7.Th
ree
patie
nts
excl
uded
(reas
onno
tgi
ven)
Loca
lizat
ion-
rela
ted:
88%
;gen
eral
ized:
4.9%
;un
dete
rmin
ed:6
.8%
Med
ian
seizu
refre
quen
cy:4
mon
ths
Med
ian
no.o
fco
ncom
itant
drug
s:2
(0–5
)M
ean
no.p
revi
ous
drug
s:6.
9(1
–16)
Med
ian
dose
:160
0m
g/d
Mea
n:6.
75m
onth
s(fr
om1
dto
47m
onth
s)2.
7%(7
/260
)27
%(7
2/26
0)
Won
get
al.(
8)36
1Re
trosp
ectiv
e.Al
lpat
ient
sst
artin
gth
edr
ugin
five
terti
ary
epile
psy
cent
ers.
Loca
lizat
ion-
rela
ted:
86%
;gen
eral
ized:
9%;
unde
term
ined
:4%
Case
reco
rds
from
5te
rtiar
yre
ferra
lepi
leps
yce
nter
s(s
eizu
reba
selin
eno
.not
spec
ified
)M
ean
max
imal
reco
rded
dose
:157
5m
g/d
Mea
n:14
mon
ths
0.8%
(3/3
61)
9.7%
(35/
361)
Tota
lAEW¼
21%
(77/
361)
1st
year¼
25%
2nd
year¼
6.6%
May
eret
al.(
20)
110
Pros
pect
ive.
123
patie
nts
enro
lled
from
ate
rtiar
yce
nter
for
epile
psy
(13
excl
uded
for
prot
ocol
viol
atio
n)
Loca
lizat
ion-
rela
ted:
100%
Med
ian
base
line
parti
alse
izure
frequ
ency¼
6.8
mon
ths
Conc
omita
ntdr
ugs:
1M
ean
no.p
revi
ous
drug
s:2.
5Da
ilydo
sage
:240
0m
gin
50%
and
2000
mg
in20
%of
patie
nts
6.5
mon
ths
Prot
ocol
Not
avai
labl
e3%
(4/1
10)
Tota
lAEW¼
7.3%
(8/1
10)
Lhat
ooet
al.(
10)
158
Retro
spec
tive.
Allp
atie
nts
star
ting
the
drug
atan
epile
psy
clin
icfro
mSe
pt19
96to
Dec
1996
Loca
lizat
ion-
rela
ted:
83%
;gen
eral
ized:
11%
;un
dete
rmin
ed:5
.6%
Refra
ctor
yep
ileps
ypa
tient
sfro
ma
terti
ary
refe
rral
cent
er(s
eizu
reba
selin
eno
.not
spec
ified
)M
ean
no.c
onco
mita
ntdr
ugs:
1.8
(in5
patie
nts
noco
ncom
itant
drug
s)M
ean
no.p
revi
ous
new
drug
s:1.
6M
ean
max
imal
reco
rded
dose
:144
0m
g/d
Mea
nor
med
ian:
not
repo
rted
0.6%
(1/1
58)
36.7
%(5
8/15
8)1s
tye
ar¼
23%
2nd
year¼
<10%
11/8
04¼
1.37
%16
9/91
4¼
18.5
%
6M-S
F,6-
mon
thse
izure
freed
om;A
EW,w
ithdr
ewbe
caus
eof
adve
rse
effe
cts;
CT,c
ontin
uing
treat
men
t;To
talA
EW,t
otal
num
ber
ofpa
tient
sw
ithdr
awin
gfo
rad
vers
eef
fect
s(s
umof
thos
epa
tient
sw
ithdr
awin
gfo
rad
vers
eef
fect
san
d/or
inef
ficac
y).
Zaccara et al.
160
Tab
le2
Lam
otrig
ine
stud
ies
Auth
orN
o.of
patie
nts
Type
ofst
udy
and
patie
nt's
recr
uitm
ent
Patie
ntch
arac
teris
tics
Dura
tion
offo
llow
-up
Perc
enta
geof
6M-S
Fpa
tient
sPe
rcen
tage
ofAE
Wpa
tient
sPe
rcen
tage
ofCT
patie
nts
Sand
eret
al.(
21)
125
Pros
pect
ive.
Patie
nts
enro
lled
intw
ote
rtiar
yce
nter
sfo
rep
ileps
y
Loca
lizat
ion-
rela
ted:
67%
;gen
eral
ized:
6%;
unde
term
ined
:28%
Atle
ast
4se
izure
s/m
onth
sM
ean
no.c
onco
mita
ntdr
ugs:
1.9
(1–3
)M
ean
dose
:367
mg/
d
11m
onth
s(ra
nge
3–27
)Pa
tient
sno
tw
ithdr
awin
g0%
(0/1
25)
15%
(19/
125)
1st
year¼
37.6
%(4
7/12
5)
Coci
toet
al.(
22)
16Pr
ospe
ctiv
e.Pa
tient
sen
rolle
din
one
cent
ers
for
epile
psy
Atle
ast
2se
izure
s/m
onth
sLo
caliz
atio
n-re
late
d:81
%;g
ener
alize
d:19
%At
leas
t2
seizu
res/
mon
ths
Mea
nno
.con
com
itant
drug
s:2
Dose
:400
mg/
d(p
atie
nts
indu
ced)
or20
0m
g/d
(pat
ient
sno
tin
duce
d)
15–3
8m
onth
s0%
(0/1
6)12
%(2
/16)
1st
year¼
62%
(10/
16)
Won
get
al.(
13,1
4)10
50Re
trosp
ectiv
eAl
lpat
ient
sat
tend
ing
the
outp
atie
ntcl
inic
sof
5te
rtiar
yep
ileps
yce
nter
s
Loca
lizat
ion-
rela
ted:
68%
;gen
eral
ized:
26%
;und
eter
min
ed:7
%Ca
sere
cord
sfro
m5
terti
ary
refe
rral
epile
psy
cent
ers(
seizu
reba
selin
eno
.not
spec
ified
)Pr
esum
ably
allp
atie
nts
had
the
new
drug
adde
dto
apr
evio
usth
erap
yM
ean
dose
:303
mg/
d
Mea
n:27
mon
ths
3%(3
1/10
50)
13.2
%(1
38/1
050)
Tota
lAEW
¼19
.2%
(202
/105
0)
1st
year¼
60%
5st
year¼
40%
8th
year¼
38%
Pim
ente
let
al.(
23)
61Pr
ospe
ctiv
ePa
tient
sat
tend
ing
one
cent
erfo
rep
ileps
y
Loca
lizat
ion-
rela
ted:
73%
;gen
eral
ized:
23%
;not
give
n:3%
Atle
ast
2se
izure
s/m
onth
sM
ean
no.c
onco
mita
ntdr
ugs:
1.8
Mea
ndo
se:2
05m
g/d
(pat
ient
sno
tin
duce
d)or
368
mg/
d(p
atie
nts
indu
ced)
25m
onth
sPr
otoc
olN
otre
porte
d6.
5%(4
/61)
1st
year¼
noda
ta2n
dye
ar¼
78%
(48/
61)
Lhat
ooet
al.(
10)
424
Retro
spec
tive.
Allp
atie
nts
star
ting
the
drug
atan
epile
psy
clin
icfro
mSe
pt19
96to
Dec
1996
Loca
lizat
ion-
rela
ted:
70.5
%;g
ener
alize
d:23
%;u
ndet
erm
ined
:6.6
%Re
fract
ory
epile
psy
patie
nts
from
ate
rtiar
yre
ferra
lcen
ter
(sei
zure
base
line
no.n
otsp
ecifi
ed)
Mea
nno
.con
com
itant
drug
s:1.
6(in
23pa
tient
sno
conc
omita
ntdr
ugs)
Mea
nno
.pre
viou
sne
wdr
ugs:
0.6
Mea
nm
axim
alre
cord
eddo
se:2
97m
g/d
Mea
nor
med
ian:
not
repo
rted
2%(1
4/42
4)22
%(9
3/42
4)1s
tye
ar¼
46%
3rd
year¼
29%
Arzim
anog
lou
etal
.(24
)56
6Pr
ospe
ctiv
ePa
tient
sat
tend
ing
seve
ral
cent
ers
for
epile
psy
25%
child
ren
Loca
lizat
ion-
rela
ted:
59%
;gen
eral
ized:
33%
;und
eter
min
ed:8
%Re
fract
ory
epile
psy
patie
nts
(sei
zure
base
line
no.n
otsp
ecifi
ed)
Mea
nno
.con
com
itant
drug
s:2.
2Do
sera
nge:
100–
200
mg/
d(p
atie
nts
not
indu
ced)
;200
–500
mg/
d(p
atie
nts
indu
ced)
48w
eek
Prot
ocol
5.8%
(33/
566)
13.1
%(7
4/56
6)1s
tye
ar¼
58%
(330
/566
)
78/2
181¼
3.6%
330/
2242¼
14.7
%
6M-S
F,6-
mon
thse
izure
freed
om;A
EW,w
ithdr
ewbe
caus
eof
adve
rse
effe
cts;
CT,c
ontin
uing
treat
men
t;To
talA
EW,t
otal
num
bero
fpat
ient
sw
ithdr
awin
gfo
radv
erse
effe
cts
(sum
ofth
ose
patie
nts
with
draw
ing
fora
dver
seef
fect
san
dof
thos
ew
ithdr
awin
gfo
rad
vers
eef
fect
san
din
effic
acy)
.
Comparing new AEDs from long-term studies
161
Tab
le3
Leve
tirac
etam
stud
ies
Auth
orN
o.of
patie
nts
Type
ofst
udy
and
patie
nt's
recr
uitm
ent
Patie
ntch
arac
teris
tics
Dura
tion
offo
llow
-up
Perc
enta
geof
6M-S
Fpa
tient
sPe
rcen
tage
ofAE
Wpa
tient
sPe
rcen
tage
ofCT
patie
nts
Krak
owet
al.(
12)
1422
Pros
pect
ive.
Allp
atie
nts
expo
sed
toLE
Vdu
ring
the
deve
lopm
enta
lpr
ogra
m(d
oubl
e-bl
ind
and
open
-labe
lstu
dies
)in
Euro
pean
dUS
Loca
lizat
ion-
rela
ted:
87%
;gen
eral
ized:
11%
;un
clas
sifia
ble:
1.6%
Allt
rials
wer
ead
d-on
stud
ies
Med
ian
base
line
seizu
refre
quen
cy:8
.7m
onth
sM
ean
no.c
onco
mita
ntdr
ugs:
1.7
Med
ian
dose
:300
0m
g/d
Med
ian:
13m
onth
s(1
dto
99m
onth
s)13
%(1
83/1
422)
15.8
%(2
25/1
422)
1st
year¼
60%
3rd
year¼
37%
5th
year¼
32%
Ben-
Men
ache
met
al.(
25)
98Pr
ospe
ctiv
e.Pa
tient
sre
crui
ted
from
asi
ngle
cent
erfo
rep
ileps
y
Loca
lizat
ion-
rela
ted:
79(8
0%);
gene
raliz
ed:1
6%;
Lenn
ox–G
asta
ut:1
%;m
yocl
onic
:1%
Mea
nse
izure
frequ
ency
:14
mon
ths
Mea
nno
.con
com
itant
drug
s:2.
1Do
sera
nge:
1000
–300
0m
g/d
1ye
ar*
14%
(14/
98)
17%
(17/
98)
1st
year¼
61%
(60/
98)
Bird
etal
.(26
)17
5Pr
ospe
ctiv
eCo
nsec
utiv
epa
tient
sfro
ma
sing
lece
nter
for
epile
psy
Loca
lizat
ion-
rela
ted:
87.4
%;g
ener
alize
d:12
.6%
;Re
fract
ory
patie
nts
(sei
zure
base
line
no.n
otsp
ecifi
ed)
Mea
nno
.con
com
itant
drug
s:2.
2Do
se:u
pto
3000
mg/
d
Atle
ast
6m
onth
s14
.3%
(25/
175)
10.3
%(1
8/17
5)To
talA
EW¼
16%
(28/
175)
Betts
etal
.(27
)11
9Re
trosp
ectiv
eAl
lpat
ient
sw
host
arte
dLE
Vat
anep
ileps
ycl
inic
betw
een
Oct
2000
and
Aug
2001
Perc
enta
geof
patie
nts
with
parti
alse
izure
sno
tsp
ecifi
edRe
fract
ory
epile
psie
s(s
eizu
reba
selin
eno
.not
spec
ified
)M
ean
no.c
onco
mita
ntdr
ugs:
not
spec
ified
Mea
ndo
seat
6m
onth
s(o
nly
seizu
refre
epa
tient
s):1
921
mg/
d
1ye
ar26
%(3
8/11
9)12
%(1
4/11
9)1s
tye
ar¼
77%
(92/
119)
Brod
tkor
bet
al.(
28)
184
Pros
pect
ive.
Cons
ecut
ive
patie
nts
from
two
cent
ers
for
epile
psy
Loca
lizat
ion-
rela
ted:
143
(77%
);ge
nera
lized
:22%
Refra
ctor
yep
ileps
ies
in16
6pa
tient
s(w
hoha
dat
leas
t1
seizu
re/m
onth
s).
Mea
nno
.con
com
itant
drug
s:1.
6M
ean
max
imal
dose
:220
5m
g/d
Mea
n:8.
1m
onth
s(1
–21
mon
ths)
10.2
%(1
7/16
6)�
6%(1
1/18
4)1s
tye
ar¼
69%
(128
/184
)
Moh
anra
jet
al.,
(29)
156
Pros
pect
ive
Cons
ecut
ive
patie
nts
from
one
cent
erfo
rep
ileps
y
Loca
lizat
ion-
rela
ted:
87%
Gene
raliz
ed:1
3%M
edia
nba
selin
ese
izure
frequ
ency
:5m
onth
sM
ean
no.c
onco
mita
ntdr
ugs:
1.6
Med
ian
no.o
fpr
evio
usan
tiepi
lept
icdr
ugs:
3M
edia
ndo
se:1
000
mg/
d(in
seizu
refre
epa
tient
s)or
1500
mg/
d(in
patie
nts
with
draw
ing)
or20
00m
g/d
(inpa
tient
sre
spon
ders
)
Not
spec
ified
26%
(40/
156)
17%
(27/
156)
Tota
lAEW¼
24.3
%(3
8/15
6)
Nic
olso
net
al.(
30)
354
Pros
pect
ive
Allp
atie
nts
who
star
ted
LEV
atan
epile
psy
clin
icbe
twee
nN
ov20
00an
dDe
c20
02
Loca
lizat
ion-
rela
ted:
80%
;gen
eral
ized:
18%
;un
clas
sifie
d:1.
1%Pr
esum
ably
refra
ctor
yep
ileps
ies
(sei
zure
base
line
no.n
otsp
ecifi
ed)
Mea
nno
.con
com
itant
drug
s:1.
7M
edia
ndo
se:1
799
mg/
d
Med
ian:
12.4
mon
ths
(1d
to30
mon
ths)
9.8%
(35/
354)
13.6
%(4
8/35
4)To
talA
EW¼
17,5
%(6
2/35
4)1s
tye
ar¼
74%
2nd
year¼
58%
Zaccara et al.
162
ous, etc.), no important differences were foundbetween studies performed with the same drug. Incontrast, differences were much more evidentbetween different drugs.In three small studies (one prospective LTG
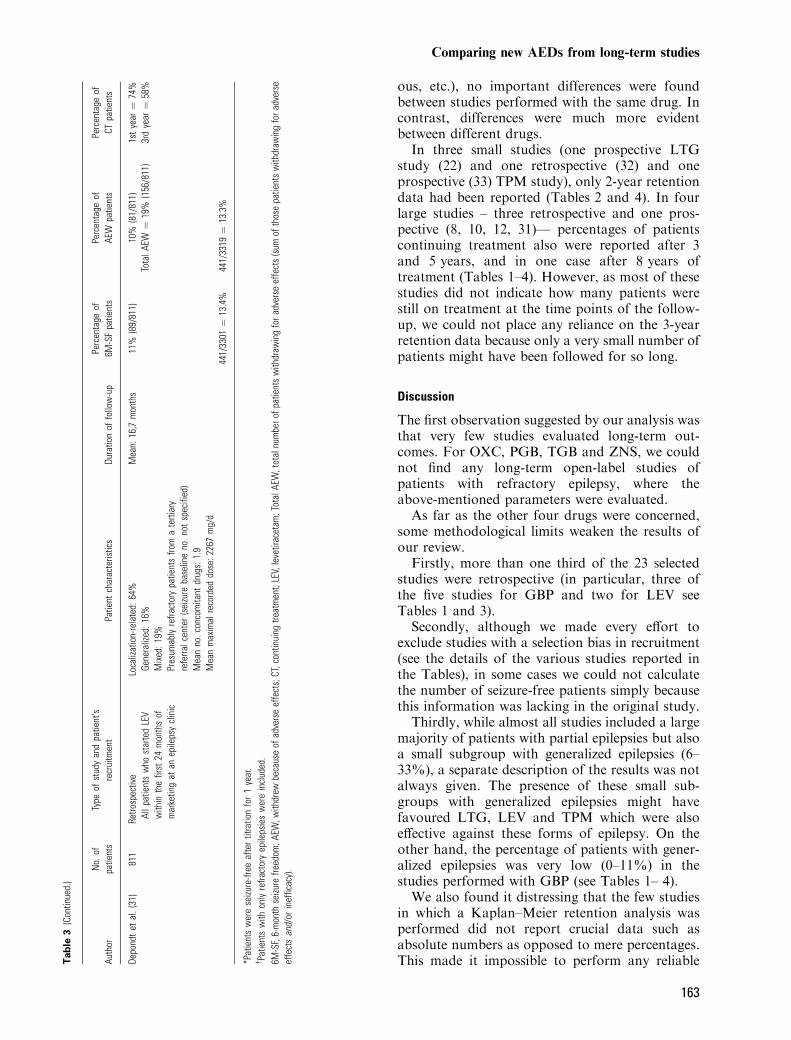
study (22) and one retrospective (32) and oneprospective (33) TPM study), only 2-year retentiondata had been reported (Tables 2 and 4). In fourlarge studies – three retrospective and one pros-pective (8, 10, 12, 31)— percentages of patientscontinuing treatment also were reported after 3and 5 years, and in one case after 8 years oftreatment (Tables 1–4). However, as most of thesestudies did not indicate how many patients werestill on treatment at the time points of the follow-up, we could not place any reliance on the 3-yearretention data because only a very small number ofpatients might have been followed for so long.
Discussion
The first observation suggested by our analysis wasthat very few studies evaluated long-term out-comes. For OXC, PGB, TGB and ZNS, we couldnot find any long-term open-label studies ofpatients with refractory epilepsy, where theabove-mentioned parameters were evaluated.As far as the other four drugs were concerned,
some methodological limits weaken the results ofour review.Firstly, more than one third of the 23 selected
studies were retrospective (in particular, three ofthe five studies for GBP and two for LEV seeTables 1 and 3).Secondly, although we made every effort to
exclude studies with a selection bias in recruitment(see the details of the various studies reported inthe Tables), in some cases we could not calculatethe number of seizure-free patients simply becausethis information was lacking in the original study.Thirdly, while almost all studies included a large
majority of patients with partial epilepsies but alsoa small subgroup with generalized epilepsies (6–33%), a separate description of the results was notalways given. The presence of these small sub-groups with generalized epilepsies might havefavoured LTG, LEV and TPM which were alsoeffective against these forms of epilepsy. On theother hand, the percentage of patients with gener-alized epilepsies was very low (0–11%) in thestudies performed with GBP (see Tables 1– 4).We also found it distressing that the few studies
in which a Kaplan–Meier retention analysis wasperformed did not report crucial data such asabsolute numbers as opposed to mere percentages.This made it impossible to perform any reliableT
ab
le3
(Con
tinue
d.)
Auth
orN
o.of
patie
nts
Type
ofst
udy
and
patie
nt's
recr
uitm
ent
Patie
ntch
arac
teris
tics
Dura
tion
offo
llow
-up
Perc
enta
geof
6M-S
Fpa
tient
sPe
rcen
tage
ofAE
Wpa
tient
sPe
rcen
tage
ofCT
patie
nts
Depo
ndt
etal
.(31
)81
1Re
trosp
ectiv
eAl
lpat
ient
sw
host
arte
dLE
Vw
ithin
the
first
24m
onth
sof
mar
ketin
gat
anep
ileps
ycl
inic
Loca
lizat
ion-
rela
ted:
64%
Gene
raliz
ed:1
6%M
ixed
:19%
Pres
umab
lyre
fract
ory
patie
nts
from
ate
rtiar
yre
ferra
lcen
ter
(sei
zure
base
line
no.n
otsp
ecifi
ed)
Mea
nno
.con
com
itant
drug
s:1.
9M
ean
max
imal
reco
rded
dose
:226
7m
g/d
Mea
n:16
,7m
onth
s11
%(8
9/81
1)10
%(8
1/81
1)To
talA
EW¼
19%
(156
/811
)1s
tye
ar¼
74%
3rd
year¼
58%
441/
3301¼
13.4
%44
1/33
19¼
13.3
%
*Pat
ient
sw
ere
seizu
re-fr
eeaf
ter
titra
tion
for
1ye
ar.
�Pa
tient
sw
ithon
lyre
fract
ory
epile
psie
sw
ere
incl
uded
.6M
-SF,
6-m
onth
seizu
refre
edom
;AEW
,with
drew
beca
use
ofad
vers
eef
fect
s;CT
,con
tinui
ngtre
atm
ent;
LEV,
leve
tirac
etam
;Tot
alAE
W,t
otal
num
bero
fpat
ient
sw
ithdr
awin
gfo
radv
erse
effe
cts
(sum
ofth
ose
patie
nts
with
draw
ing
fora
dver
seef
fect
san
d/or
inef
ficac
y).
Comparing new AEDs from long-term studies
163

Tab
le4
Topi
ram
ate
stud
ies
Auth
orN
o.of
patie
nts
Type
ofst
udy
and
patie
nt's
recr
uitm
ent
Patie
ntch
arac
teris
tics
Dura
tion
offo
llow
-up
Perc
enta
geof
6M-S
Fpa
tient
sPe
rcen
tage
ofAE
Wpa
tient
sPe
rcen
tage
ofCT
patie
nts
Riba
coba
-Mon
tero
etal
.(32
)56
Retro
spec
tive.
Patie
nts
who
star
ted
TPM
betw
een
June
1519
97an
dDe
c20
00in
one
cent
erfo
rep
ileps
y
Alm
ost
alll
ocal
izatio
n-re
late
dRe
fract
ory
epile
psie
sTP
Mad
ded
toa
prev
ious
treat
men
t(s
eizu
reba
selin
eno
.not
spec
ified
)M
ean
no.p
revi
ousl
ypr
oven
AEDs
:7Do
sera
nge:
200–
400
mg/
d
Mea
n:27
mon
ths
(18–
44)
Not
repo
rted
12.5
%(7
/56)
Tota
lAEW¼
16.1
%(9
/56)
1st
year¼
noda
ta2n
dye
ar¼
80.4
%(4
5/56
)
Lhat
ooet
al.(
10,1
1)39
3Re
trosp
ectiv
e.Al
lpat
ient
sw
host
arte
dTP
Mat
anep
ileps
ycl
inic
from
Sept
1996
toDe
c19
96
Loca
lizat
ion-
rela
ted:
89%
;gen
eral
ized:
9%;
unde
term
ined
:1%
Refra
ctor
yep
ileps
ypa
tient
sfro
ma
terti
ary
refe
rral
cent
erM
ean
no.c
onco
mita
ntdr
ugs:
1.8
(in14
patie
nts
noco
ncom
itant
drug
s)(s
eizu
reba
selin
eno
.not
spec
ified
)M
ean
no.p
revi
ous
new
drug
s:2.
2M
ean
max
imal
reco
rded
dose
:308
mg/
d
15m
onth
s(1
to40
mon
ths)
3.56
%(1
4/39
3)40
%(1
57/3
93)
1st
year¼
52%
3rd
year¼
30%
Abou
-Kha
lilet
al.(
33)
292
Pros
pect
ive.
Patie
nts
recr
uite
dfro
mse
vera
lce
nter
sfo
rep
ileps
y
Parti
alse
izure
s:84
%;g
ener
alize
dse
izure
s:28
%M
edia
nba
selin
ese
izure
frequ
ency
:12
mon
ths
No.
ofco
ncom
itant
drug
spr
evio
usly
take
n:no
tkn
own
Mea
ndo
seat
last
visi
t:50
3m
g/d
Mea
n:13
.7m
onth
s(2
.8–2
6.8)
10%
(20/
196)
*32
.5%
(90/
277)
1st
year¼
noda
ta2n
dye
ar¼
39%
(114
/292
)
Step
hen
etal
.(34
)17
0Pr
ospe
ctiv
ePa
tient
sre
crui
ted
from
one
cent
erfo
rep
ileps
y
Parti
alse
izure
s:78
.8%
;gen
eral
ized:
21.2
%M
edia
nse
izure
frequ
ency
:4m
onth
s(ra
nge
2–12
0)M
ean
no.c
onco
mita
ntdr
ugs:
1.5
Mea
ndo
ses:
250
mg
(sei
zure
free
patie
nts)
,46
3m
g/d
(resp
onde
rs),
265
mg/
d(w
ithdr
awin
gpa
tient
s)
Tim
ere
quire
dto
reac
hse
izure
freed
omfo
r6
mon
ths
or>5
0%se
izure
redu
ctio
nor
AEW
23%
(39/
170)
8.8%
(15/
170)
Tota
lAEW¼
22.9
%(3
9/17
0)
Boot
sma
etal
.(35
)47
0Re
trosp
ectiv
e.Al
lpat
ient
stre
ated
with
TPM
betw
een
Sprin
g19
93an
dm
id-2
002
Loca
lizat
ion-
rela
ted:
75%
;gen
eral
ized:
20%
;un
dete
rmin
ed:4
.6%
Refra
ctor
yep
ileps
ypa
tient
sfro
ma
terti
ary
refe
rral
cent
er(s
eizu
reba
selin
eno
.not
spec
ified
)N
o.co
ncom
itant
drug
san
dof
drug
spr
evio
usly
take
n:no
tkn
own
Mea
ndo
se:2
17m
g/d
(at6
mon
ths)
,323
mg/
d(a
t24
mon
ths)
Mea
n:13
.8m
onth
s(S
D14
.9)
5.5%
�(2
6/47
0)23
.2%
(109
/470
)To
talA
EW¼
37.2
%(1
75/4
70)
1st
year¼
53.4
%2n
dye
ar¼
45.4
%3r
dye
ar¼
38.4
%
99/1
229¼
8.1%
378/
1366¼
27.7
%99
/122
9¼
8.1%
378/
1366¼
27.7
%
6M-S
F,6-
mon
thse
izure
freed
om;A
EW,w
ithdr
ewbe
caus
eof
adve
rse
effe
cts;
CT,c
ontin
uing
treat
men
t;TP
M,t
opira
mat
e;AE
D,an
tiepi
lept
icdr
ug;T
otal
AEW
,tot
alnu
mbe
rof
patie
nts
with
draw
ing
for
adve
rse
effe
cts
(sum
ofth
ose
patie
nts
with
draw
ing
for
adve
rse
effe
cts
and/
orin
effic
acy)
.*O
nly
patie
nts
com
plet
ing
6m
onth
sof
ther
apy.
�Pa
tient
sw
hoac
hiev
ed6-
mon
thse
izure
freed
omdu
ring
the
first
6m
onth
sof
TPM
ther
apy.
Zaccara et al.
164

meta-analysis about retention. Meta-analysis ofthe other two outcome measures was not feasiblebecause of heterogeneity.Although patients with epilepsy have to take
their medication for several years, no controlleddata existed on the chronic effects and on the long-term efficacy of these drugs. For this reason, wethought that every effort should be made tointerpret the data reported in the open studiespublished thus far, despite the important limita-tions of these studies.We identified a number of studies in which, after
the administration of GBP, LEV, LTG or TPM,some simple markers of efficacy and/or tolerabilityor a mixed parameter of efficacy and tolerability(e.g. the number of patients achieving seizurefreedom for 6 months; the number. of patientswithdrawing from the study because of adverse
effects; the percentage of patients continuingtreatment after 1 year with the new AED) couldbe calculated which provided interesting results.The percentage of patients who achieved six
consecutive months of seizure freedom might be amore robust indicator of efficacy than the responserate (percentage of patients with a 50% or greaterreduction in seizure frequency compared withbaseline), which had been used in all the previousmeta-analyses of double-blind studies. However,we felt that some factors must be considered inorder to interpret the results about this outcomemeasure correctly:
1 We could not rule out the possibility of a smallbias in our analysis. A few studies considered�seizure free� only those patients who had noseizures in the last 6 months of the study(terminal seizure freedom). In other studies,percentages were reported of patients who had a6-month period of seizure freedom during thestudy. We can imagine that drugs followed upfor longer time could be favoured (a patientwho is followed up for a longer time may have ahigher probability of experiencing, by chance, a6-month period of seizure freedom) comparedwith drugs for which only shorter studies wereavailable. However, from the inspection of the
0
2
4
6
8
10
12
14
16
GBP (804) LTG (2181) LEV (3301) TPM (1229)
% o
f 6M
-SF
pat
ien
ts (
95%
CI)
Figure 1. Total percentages (95% CI) of patients who achievedseizure freedom for 6 months (6M-SF) from all clinical studies.GBP, gabapentin; LTG, lamotrigine; TMP, topiramate; LEV,levetiracetam.
0
5
10
15
20
25
30
35
GBP (914) LTG (2242) LEV (3319) TPM (1366)
% o
f A
EW
pat
ien
ts (
95%
CI)
Figure 2. Total percentages (95% CI) of patients who with-drew from the antiepileptic drug because of adverse effects(AEW) from all clinical studies. GBP, gabapentin; LEV,levetiracetam; LTG, lamotrigine; TPM, topiramate.
10
20
30
40
50
60
70
80
0 1 2 3 4 5
GBP
Pts
on
tre
atm
ent
afte
r 1
year
(%
)
TPMLEV LTG
Figure 3. Percentage of patients still on treatment with gab-apentin (GBP), levetiracetam (LEV), lamotrigine (LTG), andtopiramate (TPM) after 1 year of treatment. Clinical studies.(n) Lhathoo et al. (10,11); (r) Wong et al. (8); (m) Sander et al.(21); (e) Cocito et al. (22); (h) Arzimanoglou et al. (24); (d)Krakow et al. (12); (+) Ben-Menachem et al. (25); (—) Bro-dtkorb et al. (28); ( ) Nicolson et al. (30); ( ) Betts et al. (27);(·) Depondt et al. (31); (-) Bootsma et al. (35).
Comparing new AEDs from long-term studies
165

duration of the studies included in our analysis(see Tables 1–4), it seemed that differences induration were not significant (with the possibleexception of GBP studies). In future studies,particularly those aiming at evaluating a verylong term outcome, it should be very clearlystated how this parameter was obtained and, ifpossible, both parameters should be calculated.
2 As all studies examined in our analysis wereuncontrolled, we could not rule out the possi-bility that some patients attained this seizurefree outcome not only as a direct effect of theexperimental drug but also because of othervariables such as the natural course of thedisorder or other drugs added subsequently.
3 We should bear in mind that only some of theselected long-term studies reported this outcomemeasure. It is conceivable that the studies thatdid not report seizure-free rates were also thestudies in which the seizure-free rates werelowest.
Our analysis showed that in long-term studies,differences can exist in the seizure-free outcome ofpatients treated with various AEDs (efficacy and/or tolerability). In fact, LEV was the most effectiveagent, followed by TPM and then by LTG andGBP. Analysis limited to prospective studiesshowed some differences. In the only study of thistype to assess, TPM, this drug had the highestpercentage of seizure-free patients, but the differ-ence between rates was not significant.Percentages of patients, attaining seizure free-
dom after the administration of the experimentaldrug, had also been reported in some double-blindstudies. In some cases these values were lower thanthose observed in our review. For example,between 3% and 5% of patients treated withLEV in two double-blind studies attained freedomfrom seizures (36, 37). While we do not have a clearexplanation for this discrepancy, some hypothesescan be made. For example, patients directlyrecruited in open studies may have milder formsof epilepsies than those enrolled in double-blindstudies. For these reasons, the percentages ofpatients acquiring seizure freedom in open studiesare not directly comparable to those obtained indouble-blind studies.The percentage of patients withdrawing because
of adverse effects has already been recognized to bea reliable marker of tolerability, and has also beenused in several meta-analyses of double-blindstudies (1, 2, 5, 6). This outcome measure providedslightly less clear results. LEV was the best-tolerated AED, a little ahead of LTG, and signi-ficantly better than GBP or TPM . TPM was by far
the least well-tolerated drug. However, the analysislimited to prospective studies showed that GBPhad the best profile although not significantly so.This tolerability outcome measure might be influ-enced by the duration of follow-up. A correlationbetween duration of follow-up and this outcomemeasure was not feasible because, in the studiesevaluated, the duration of follow-up was reportedusing different parameters (mean, median, orrange).Finally, the retention rate is a mixed measure of
efficacy and tolerability and has already been usedin numerous studies comparing traditional (38, 39)and new (40, 41) AEDs in patients with newlydiagnosed epilepsy.In Fig. 3, we reported only the retention rate at
the first year because, from inspection, it was onlypossible to calculate it for 1 year for the majorityof patients. Retention data for two, three and moreyears were much less robust.Although the populations studied were hetero-
geneous and the therapeutic protocols differedbetween the studies, similar retention rates wereobserved within trials performed with the samedrug (Fig. 3). GBP showed a very poor retentionrate, which was probably related to its lowefficacy. LTG and TPM had similar retentionvalues.A variety of factors might have influenced these
retention rates. For example, retention rates ofTPM after 1 year might reflect the drug’s poortolerability. On the other hand, retention ratesafter 3 and 5 years of TPM (see Table 4) showedthat patients who did not withdraw in the first yearwere unlikely to withdraw thereafter. Perhaps themost frequent adverse effects of this drug appearedrelatively early in treatment; if they did not appearearly, they were unlikely to appear during chronictreatment. However, too few patients were fol-lowed for three or more years, so no firm conclu-sions could be drawn.Retention rates of LTG might be related more to
efficacy outcomes than to tolerability, and LEVhad a 1-year retention rate that ranged from 60%to about 75%. These higher retention rates areprobably the consequence of a better efficacyassociated with good tolerability.We could speculate that, at least in part, the
retention rate was influenced by the sequence inwhich these drugs were introduced onto themarket. For example, patients treated with GBPmight have been withdrawn from treatmentbecause of the availability of new drugs (LTGor, more recently, TPM or LEV). We could alsoimagine that the latest AEDs were likely to be
Zaccara et al.
166

tested in a more refractory population ofpatients.Interestingly enough, the results of our review of
long-term open-label studies are similar to thosereported in several meta-analyses of double-blindstudies (1– 6) (where the proportion of responderswith respect to placebo has generally been used as amarker of efficacy). The most recently publishedmeta-analysis (7) showed that LEV was signifi-cantly more efficacious than GBP and LTG andwas more effective (but not significantly more so)than OXC, TGB, and ZNS. As far as tolerabilitywas concerned, LEV had a significantly lowerwithdrawal rate than OXC and TPM and a lower(but not significantly lower) withdrawal rate thanTGB and ZNS, while similar withdrawal rates wereobserved for LEV, LTG, and GBP.It is commonly thought that results from open-
label studies are of little clinical value. However,this might not be necessarily true. Large, long-termstudies (both prospective and retrospective) andthe use of robust parameters (such as those used inour analysis) might make results from open studiesmore valuable. In our review, the variability of theresults was more influenced by the drugs them-selves and less influenced by the different protocolsor the patient populations, supporting this hypo-thesis.We conclude that well designed, open-label,
long-term, and possibly randomized, add-on stud-ies should be encouraged in which two or moreAEDs are compared head to head. This is the firstattempt to compare new AEDs using data fromopen-label long-term studies. We think that, eventhough several biases might have affected ouranalysis, this is presently the only way to deriveinformation on the long-term therapeutic effect ofthese drugs.
Acknowledgement
This work was supported by a grant from the ��Ente Cassa diRisparmio di Firenze��, Florence, Italy. We wish to thankTonino Di Carlo for his valuable help. No sponsorship hasbeen received by the authors to conduct this study.
References
1. Marson AG, Kadir ZA, Hutton JL, Chadwick DW. The newantiepileptic drugs: a systematic review of their efficacy andtolerability. Epilepsia 1997;38:859–80.
2. Marson AG, Hutton JL, Leach JP et al. Levetiracetam,oxcarbazepine, remacemide and zonisamide for drugresistant localization-related epilepsy: a systematic review.Epilepsy Res 2001;46:259–70.
3. Cramer JA, Fisher R, Ben-Menachem E, French J, Mattson
RH. New antiepileptic drugs: comparison of key clinicaltrials. Epilepsia 1999;40:590–600.
4. Cramer JA, Ben-Menachem E, French J. Review of treatmentoptions for refractory epilepsy: new medications and vagalnerve stimulation. Epilepsy Res 2001;47:17–25.
5. Chaisewikul R, Privitera MD, Hutton JL, Marson AG.Levetiracetam add-on for drug-resistant localization rela-ted (partial) epilepsy. Cochrane Database Syst Rev2001;1:CD001901.
6. Castillo S, Schmidt DB, White S. Oxcarbazepine add-on fordrug-resistant partial epilepsy. Cochrane Database SystRev 2000;3:CD002028.
7. Otoul C, Arrigo C, van Rijckevorsel K, French JA. Meta-analysis and indirect comparisons of levetiracetam withother second-generation antiepileptic drugs in partial epi-lepsy. Clin Neuropharmacol 2005;28:72–78.
8. Wong IC, Chadwick DW, Fenwick PB, Mawer GE, Sander
JW. The long-term use of gabapentin, lamotrigine, andvigabatrin in patients with chronic epilepsy. Epilepsia1999;40:1439–45.
9. Kellett MW, Smith DF, Stockton PA, Chadwick DW. To-piramate in clinical practice: first year’s postlicensingexperience in a specialist epilepsy clinic. J Neurol Neuro-surg Psychiatry 1999;66:759–63.
10. Lhatoo SD, Wong IC, Polizzi G, Sander JW. Long-termretention rates of lamotrigine, gabapentin, and topiramatein chronic epilepsy. Epilepsia 2000;41:1592–6.
11. Lhatoo SD, Wong IC, Sander JW. Prognostic factorsaffecting long-term retention of topiramate in patients withchronic epilepsy. Epilepsia 2000;41:338–41.
12. Krakow K, Walker M, Otoul C, Sander JW. Long-termcontinuation of levetiracetam in patients with refractoryepilepsy. Neurology 2001;56:1772–4.
13. Wong IC, Mawer GE, Sander JW, Lhatoo SD. A pharma-coepidemiologic study of factors influencing the outcomeof treatment with lamotrigine in chronic epilepsy. Epilepsia2001;42:1354–8.
14. Wong IC, Mawer GE, Sander JW. Adverse event monitoringin lamotrigine patients: a pharmacoepidemiologic study inthe United Kingdom. Epilepsia 2001;42:237–44.
15. Morrell MJ, McLean MJ, Willmore LJ et al. Efficacy ofgabapentin as adjunctive therapy in a large multicenterstudy. Seizure 2000;9:241–8.
16. Morrell MJ, Leppik I, French J, Ferrendelli J, Han J, Magnus
L. The KEEPER trial: levetiracetam adjunctive treatmentof partial-onset seizures in an open-label community-basedstudy. Epilepsy Res 2003;54:153–61.
17. Fleiss JL. Statistical methods for rates and proportions.New York: John Wiley and Sons, 1981:13–17.
18. Sivenius J, Ylinen A, Kalviainen R, Riekkinen PJ Sr. Long-term study with gabapentin in patients with drug-resistantepileptic seizures. Arch Neurol 1994;51:1047–50.
19. Langan Y, Duncan JS, Sander JW. An audit of the perceivedefficacy and tolerability of gabapentin therapy in an out-patient cohort with chronic epilepsy. Eur Neurol1999;41:111–3.
20. Mayer T, Schutte W, Wolf P, Elger CE. Gabapentin add-on treatment: how many patients become seizure-free? Anopen-label multicenter study. Acta Neurol Scand1999;99:1–7.
21. Sander JW, Trevisol-Bittencourt PC, Hart YM, Patsalos
PN, Shorvon SD. The efficacy and long-term tolerability oflamotrigine in the treatment of severe epilepsy. EpilepsyRes 1990;7:226–9.
22. Cocito L, Mani M, Loeb C. Long-term observations on theclinical use of lamotrigine as add-on drug in patients withepilepsy. Epilepsy Res 1994;19:123–7.
23. Pimentel J, Guimaraes ML, Lima L, Leitao O, Sampaio MJ.Lamotrigine as add-on therapy in treatment-resistant
Comparing new AEDs from long-term studies
167

epilepsy. Portuguese Lamotrigine as Add-on Therapy inTreatment-resistant Epilepsy Study Group. J Int Med Res1999;27:148–57.
24. Arzimanoglou A, Kulak I, Bidaut-Mazel C, Baldy-Moulinier
M. Optimal use of lamotrigine in clinical practice: results ofan open multicenter trial in refractory epilepsy [in French].Rev Neurol (Paris) 2001;157:525–36.
25. Ben-Menachem E, Gilland E. Efficacy and tolerability oflevetiracetam during 1-year follow up in patients withrefractory epilepsy. Seizure 2003;12:131–5.
26. Bird JM, Joseph ZA. Levetiracetam in clinical use—aprospective observational study. Seizure 2003;12:613–6.
27. Betts T, Yarrow H, Greenhill L, Barrett M. Clinicalexperience of marketed Levetiracetam in an epilepsyclinic—a one year follow up study. Seizure 2003;12:136–40.
28. Brodtkorb E, Klees TM, Nakken KO, Lossius R, Johannessen
SL. Levetiracetam in adult patients with and withoutlearning disability: focus on behavioral adverse effects.Epilepsy Behav 2004;5:231–5.
29. Mohanraj R, Parker PG, Stephen LJ, Brodie MJ. Leveti-racetam in refractory epilepsy: a prospective observationalstudy. Seizure 2005;14:23–27.
30. Nicolson A, Lewis SA, Smith DF. A prospective analysis ofthe outcome of levetiracetam in clinical practice. Neurol-ogy 2004;63:568–70.
31. Depondt C, Yuen AWC, Bell GS et al. The long termretention of levetiracetam in a large cohort of patientswith epilepsy. J Neurol Neurosurg Psychiatry2006;77:101–3.
32. Ribacoba Montero R, Salas Puig X. Efficacy and tolerab-ility of long term topiramate in drug resistant epilepsy inadults [in French]. Rev Neurol 2002;34:101–5.
33. Abou-Khalil B. Topiramate in the long-term managementof refractory epilepsy. Topiramate YOL Study Group.Epilepsia 2000;41(Suppl 1.):S72–76.
34. Stephen LJ, Sills GJ, Brodie MJ. Topiramate in refractoryepilepsy: a prospective observational study. Epilepsia2000;41:977–80.
35. Bootsma HP, Coolen F, Aldenkamp AP et al. Topiramate inclinical practice: long-term experience in patients withrefractory epilepsy referred to a tertiary epilepsy center.Epilepsy Behav 2004;5:380–7.
36. Shorvon SD, Lowenthal A, Janz D et al. Multicenterdouble-blind, randomised, placebo-controlled trial of Le-vetiracetam as add-on therapy in patients with refractorypartial seizures. Epilepsia 2000;41:1179–86
37. Cereghino JJ, Biton V, Abou-Khalil B et al. Levetiracetamfor partial seizures. Results of a double-blind, randomisedclinical trial. Neurology 2000;55:236–42
38. Mattson RH, Cramer JA, Collins JF et al. Comparison ofcarbamazepine, phenobarbital, phenytoin, and primidonein partial and secondarily generalised tonic-clonic seizures.N Engl J Med 1985;313:145–51.
39. Mattson RH, Cramer JA, Collins JF. A comparison ofvalproate with carbamazepine for the treatment of com-plex partial seizures and secondarily generalised tonic-clonic seizures in adult. N Engl J Med 1992;327:765–71.
40. Brodie MJ, Overstall PW, Giorgi L. Multicentre, double-blind, randomised comparison between lamotrigine andcarbamazepine in elderly patients with newly diagnosedepilepsy. Epilepsy Res 1999;37:81–87.
41. Brodie MJ, Richens A, Yuen AW. Double-blind comparisonof lamotrigine and carbamazepine in newly diagnosedepilepsy. UK Lamotrigine/Carbamazepine MonotherapyTrial Group. Lancet 1995;345:476–9.
Zaccara et al.
168
Top Related
Copyright © 2022 FDOKUMEN

