






Bahasa
Halaman
Hukum


10.1177/0272431604274176JOURNAL OF EARLY ADOLESCENCE / May 2005O’Sullivan et al. / COMMUNICATION ABOUT HIV AND RISK
Communication About HIV and RiskBehaviors Among Mothers Living With HIV
and Their Early Adolescent ChildrenLucia F. O’Sullivan
Curtis DolezalElizabeth Brackis-Cott
Lara TraegerClaude A. MellinsColumbia University
Little is known about how mothers living with HIV communicate to their children aboutHIV risk. The current study explored communication between mothers and childrenabout prevention and risk behaviors, the impact of maternal HIV infection and childknowledge of HIV, and concordance in reports from mothers and their children. The sam-ple comprised 220 mothers and their early adolescent children (10-14 years old) whoresided in socioeconomically disadvantaged, urban neighborhoods. Mothers living withHIV were more likely to report discussing HIV and had more frequent related discussionscompared to those mothers not living with HIV. Overall, children with mothers living withHIV reported greater comfort discussing sex- and drug-related topics than did those withnoninfected mothers. The findings are discussed in terms of implications for family-based HIV prevention programs.
Keywords: HIV; communication; mothers; parents; early adolescence; sex; drugs
Although advances in pharmacological treatments have decreased AIDS-related deaths in the United States, heterosexual women and young adultsconstitute the groups most at risk of infection, especially those with racialand ethnic minority membership (Centers for Disease Control & Prevention
148
This research was supported in part by funding from W.T. Grant (No. 97-1807-97) and the National Institute ofMental Health (R01-MH63636) to Claude A. Mellins, Ph.D. The authors thank the mothers and children fortheir participation as well as Daisy Reyes, Ivy Altamirano, Samantha Williams, Richard Austin, Megan Block,Karina Santamaria, and Wanda Garcia for their help with data collection and coding.
Journal of Early Adolescence, Vol. 25 No. 2, May 2005 148-167DOI: 10.1177/0272431604274176© 2005 Sage Publications

[CDC], 2004b). The majority of women living with the human immunodefi-ciency virus (HIV) are in their childbearing years (CDC, 2004a), and manyhave children (Haven, Mellins, & Pilowski, 1996). There are both more long-term survivors of perinatal infection than ever before (Mellins et al., 2002)and rapidly increasing rates of infection among adolescents (Rotheram-Borus, Mahler, & Rosario, 1995). In the United States, one-quarter of all newinfections occur among those younger than 24 years of age (CDC, 2004a).Many cases of AIDS among young adults were likely contracted during ado-lescence, but these individuals became diagnosed much later owing to thelong incubation period of the virus (Coutinho, 2000).
The role of families in helping to prevent HIV infection has been thefocus of much discussion (Pequegnat et al., 2002), as has the role that parentsmay have in influencing adolescents’ sexual behavior through communica-tion (Jaccard, Dittus, & Gordon, 1998; B. C. Miller, Norton, Fan, &Christopherson, 1998; O’Sullivan, Meyer-Bahlburg, & Watkins, 2001; Pick& Palos, 1995; Rodgers, 1999). There is a small but growing body of researchindicating that communication between parents and children about HIV spe-cifically may play an important role in prevention efforts (Lefkowitz,Kahlbaugh, Au, & Sigman, 1998; Romo, Lefkowitz, Sigman, & Au, 2001;Sigelman, Mukai, Woods, & Alfeld, 1995; Sly et al., 1995). This literaturehas grown out of the sex communication literature rather than the HIV litera-ture. As such, the focus has typically focused narrowly on sexual risk ratherthan the broader range of activities placing youth at risk for HIV.
Overall, research on communication between parents and children sug-gests that parents play a significant role in preventing adolescent risk behav-ior, although there is much that remains to be discovered in terms of thedynamics associated with effective communication (Jaccard, Dodge, &Dittus, 2002). Researchers have relied heavily on long-term, retrospectiveaccounts from primarily White late adolescents or college students abouttheir parents’ communication attempts (Lehr, DiIorio, Dudley, & Lipana,2000). For the most part, studies have overlooked some important dimen-sions of parent-child communication characteristics such as the content andquality of the conversations, the emotional tone, and the contexts withinwhich these conversations occur. These are key factors that could informinterventions designed to supplement parents’efforts to protect their childrenfrom HIV and improve their communication generally on matters of suchsignificance.
Although there is a rapidly growing literature on the risk factors amongother groups of youth, there is scant information about uninfected adoles-cents with infected parents. Adolescents with parents living with HIV arebelieved to represent one of the highest risk groups for their own HIV infec-
O’Sullivan et al. / COMMUNICATION ABOUT HIV AND RISK 149

tion. In a sample of adolescents residing in New York City who contractedHIV through sexual behavior, 20% reported having a mother living with HIV(Chabon & Futterman, 1999). This rate is considerably higher than the gen-eral rates of infection among women (2%-5%; New York State Departmentof Health, 2002). The few studies of uninfected adolescents with HIV-infected parents indicate higher rates of emotional and behavioral problems,including criminal activity, truancy, poor school functioning, depression, andanxiety, compared with youth with noninfected mothers (Forehand et al.,1998; Hudis, 1995; Kotchick & Forehand, 1999). In a study of sexual behav-ior and drug use in youth with HIV-infected mothers, half of the female ado-lescents reported initiating sexual activity by the age of 14 years with highrates of unprotected intercourse and high rates of illegal substance use (Lee,Lester, & Rotherum-Borus, 2002). It is believed that their increased risk maybe related to exposure to the same factors that placed their parents at risk. Forexample, the social context of many families affected by HIV involvesnumerous stressors including poverty, substance abuse, parent disease anddisability, multiple health threats, histories of victimization and trauma, andfamily losses (Armistead, Tannenbaum, Forehand, Morse, & Morse, 2001;Brown, Lourie, & Pao, 2000).
Surprisingly little is known in general about communication regardingrisk in families affected by HIV. It is likely that communication in these fami-lies is strongly influenced by the immediacy of HIV issues in their lives. Par-ents who know that they are infected may be particularly motivated to initiatediscussions with their children or address their children’s questions aboutHIV with the aim of influencing their children’s current or future risk behav-ior. They may also be motivated by the need to prepare their children for thevery real possibility of the parents’ future illness. Alternately, they may feelshame, anger, or guilt about becoming infected and do not want to disclosetheir own status or discuss the behaviors that led to their infection (Brackis-Cott, Block, & Mellins, 2003). Mothers living with HIV express concernabout increasing their children’s worry about the mother’s illness and requestinformation about how best to approach disclosure-related discussions(Armistead et al., 2001).
The purpose of the current study was to explore specific aspects of com-munication between mothers and their children about HIV, sex, drugs, andother topics. Some secondary issues were also of interest and explored here.Past research has identified a child’s age, gender, and ethnicity as factors thatare closely associated with parent-child communication about sex and HIV,and these factors may be key to tailoring approaches to HIV disclosure dis-cussions for parents and their children. Mothers’ communication styles varydepending on the age of their children. For example, adolescents’ communi-
150 JOURNAL OF EARLY ADOLESCENCE / May 2005

cation styles with their mothers vary between preadolescents and adolescents(Beaumont, Vasconcelos, & Ruggeri, 2001), reflecting developmental dif-ferences in comprehension, communication skills, and experience. Indepen-dent of mothers’ level of communication competence, mothers were morelikely to be perceived as effective communicators by older children (as com-pared to younger children) and daughters (as compared to sons). Generally,mothers communicate more frequently with, and have more influence on,their daughters than their sons (Lefkowitz, Boone, Sigman, & Au, 2002;K. S. Miller, Kotchick, Dorsey, Forehand, & Ham, 1998; Raffaelli, Bogen-schneider, & Flood, 1998; Rosenthal, Senserrick, & Feldman, 2001). Thus,mothers in both groups were expected to be more likely to report discussionsabout risk and would report more frequent discussions with their older chil-dren compared to younger children as well as more frequent and higherquality discussions with their daughters compared to their sons.
Although few studies have examined the relationship between risk com-munication and ethnicity, the findings are mixed among those that have.Some researchers have found little association with parent ethnicity (B. C.Miller et al., 1998), whereas others have found important distinctions in fam-ily styles (Huebner & Howell, 2003; Raffaelli & Green, 2003). For example,African American adolescents report higher rates of parent-child communi-cation about sexual risk compared to White adolescents (Hutchinson &Cooney, 1998). This finding suggests that there may be important culturaldifferences reflected across races or ethnicities, although it is not yet possi-ble to hypothesize based on the literature which distinctions may exist.Therefore, whether child’s age, gender, and ethnicity were associated withcommunication about HIV and risk were examined in the current study.
This cross-sectional, self-report study was designed to explore the familycommunication styles of early adolescents (10-14 years) with mothers livingwith HIV and those without HIV. Data for these analyses were drawn from alarger, longitudinal study examining the role of family, social, and contextfactors influencing sexual and drug risk behaviors among early adolescents.Mothers were the focus of this study for a number of reasons: Women are theprimary sex educators in most families (B. C. Miller, Benson, & Galbraith,2001), women living with HIV are likely to be single parents in their home(Mellins, 1995; Mellins & Ehrhardt, 1994; Niebuhr, Hughes, & Pollard,1994), and women are at particularly high risk of infection in impoverishedneighborhoods of the United States (Sikkema et al., 1996). Because of thepoor concordance in child and maternal reports of HIV, sex, and drug com-munication noted by other researchers (Feldman & Rosenthal, 2000; Jaccardet al., 1998; Newcomer & Udry, 1985), the degree of concordance betweenreports of the mothers and their early adolescent children (10-14 years) was
O’Sullivan et al. / COMMUNICATION ABOUT HIV AND RISK 151

also examined. Comfort, an important affective component in such commu-nication, was included in the analyses. Many parents report feeling embar-rassed or poorly equipped to handle discussions about these topics(Cappello, 2001). Mothers living with HIV were expected to be particularlyuncomfortable participating in discussions about risk with their childrenbecause of the immediacy and poignancy of the issue in their lives.
METHOD
Sample
Participants were 220 early adolescents, ages 10 through 14 years, and theirmothers. Mother-child dyads consisted of 48 sons and 52 daughters withtheir 100 mothers living with HIV, and 63 sons and 57 daughters with their120 mothers not living with HIV. Respondents were recruited from five sitesin New York City, which included two large medical centers, two community-based organizations, and one network of HIV care providers. These siteswere chosen because they were located in neighborhoods with high HIV/AIDS seroprevalence and provide services to primarily ethnic minorityurban residents of low socioeconomic status. Mother-child dyads qualifiedfor the study if (a) they spoke English or Spanish fluently, (b) the child wasthe biological child of the mother and 10 to 14 years of age, and (c) the motherand child were currently living together (i.e., at least the preceding 6 months).Approximately equal numbers of male and female children and equal num-bers of children from each age group (10-14 years) were recruited from fami-lies with mothers living with or without HIV.
The majority of mothers (87.6%) had been tested for HIV: 100 (45.5%)reported that they were living with HIV. Twenty-seven (12.3%) mothers hadnever been tested or did not know the results of their test. For the purposes ofanalyses, the latter group was considered to be living without HIV (ns = 100mothers living with HIV and 120 mothers living without HIV). Sixty-six per-cent of the children of mothers living with HIV knew of their mothers’ HIV-positive status. Only one demographic difference emerged between the twogroups of mothers: In line with the epidemiology of HIV in the United States(CDC, 2004a), there were more African American than Latina mothers liv-ing with HIV (59% vs. 39%) and, corresponding to this difference, moreLatina than African American mothers living without HIV (55% vs. 34%).
Overall, children’s mean age was 12 with 17% who were 10, 18% whowere 11, 23% who were 12, 22% who were 13, and 20% who were 14 yearsold. Reflecting the demographics of the recruitment sites and local neighbor-
152 JOURNAL OF EARLY ADOLESCENCE / May 2005

hoods, 44.5% (n = 98) of the mothers were African American, 40.0% (n = 88)were Latina, and 3.3% (n = 7) were White and non-Latina. Only familieswhose mothers identified as African American and Latina (ns = 98 and 88,respectively) were compared in the analyses. The child’s ethnicity matchedthe mother’s in 69.5% of the dyads. Most of the mothers were born in theUnited States (67.7%). About half (n = 116; 52.7%) of the mothers spokesome language other than English in their home or with friends, primarilySpanish (114/116 women). More than one-third (n = 77; 35.2%) of the moth-ers lived with a partner, and more than half of these women (n = 46; 59.7%)were married. The median number of children in the mothers’ householdswas three with a range of one through eight children. More than one-third(37.0%) of the mothers had not completed high school or a General Equiva-lency Diploma; 70.3% were not working, and 75.0% were living on less than$20,000 annual income to support an average of four people.
Measures
Mother-child communication. Parallel versions of a modified structuredinterview protocol developed by Krauss, Goldsamt, and Pierre-Louis (1996)were administered to both mother and child about their conversations witheach other. This measure assessed general communication and communica-tion about sex, drugs, and HIV between the mother and child. To measuregeneral communication, respondents were asked to indicate whether conver-sations about a range of topics had occurred in the 4 weeks preceding thestudy (e.g., sports, friends, sex, drugs, HIV prevention). The 4-week periodwas chosen as standardized timeframe to help counter problems associatedwith biases or problems in recall over more extended periods of time. If therespondent had engaged in a conversation about a particular topic, they werethen asked to estimate the frequency of these conversations in that timeframe.The frequency of discussions about HIV, sex, and drugs was assessed as acontinuous variable based on the average of the responses of mothers andchildren. To measure communication about risk, mothers and children whoreported communicating to their child about HIV, sex, or drugs were asked aseries of questions regarding the content, context, and perceived outcome ofthe most comfortable (or least uncomfortable) discussion that had occurredin the preceding month. Specifically, the content of the conversation wasassessed using an open-ended item: “What did you talk about?” Theseresponses were subsequently coded. Context was assessed using two relateditems: where they were when the conversation took place (i.e., alone at home,alone outside home, with others at home, or with others outside home) and
O’Sullivan et al. / COMMUNICATION ABOUT HIV AND RISK 153

who else, if anyone, participated in the conversation (i.e., other siblings,other relatives, parent’s spouse/partner, parent’s friend, child’s friend, orother). In addition, respondents were asked who initiated the conversation(i.e., child, mother, or other person) and to rate their own and their perceptionof the other’s level of comfort during the conversation (1 = very comfortablethrough 10 = very uncomfortable) as well as the perceived quality of the con-versation (“How do you think the talk went?” from 1 = very poorly through 5= very well). A parallel series of questions was also asked of mothers livingwith HIV and their children if they reported at least one conversation aboutthe mothers’ HIV status in the preceding 4 weeks. (Note: These questionswere only asked in cases where the mothers had provided permission todiscuss the mothers’ HIV status with their child.)
Demographic variables. A questionnaire developed for this study wasused to obtain demographic information. The range of items included familycomposition, race and ethnicity of mother and child, education and work sta-tus of the mother, and family income.
Procedures
All procedures were approved in full by our institutional review board.Project personnel were multicultural, bilingual researchers who had receivedextensive training in the recruitment and interviewing protocol. Traininginvolved didactics on HIV infection, sexuality, early adolescent develop-ment, interviewing and recruitment techniques, ethical conduct, cultural sen-sitivity, and role-plays and mock interactions with peers and pilot partici-pants. Project personnel attended clinic sessions, posted fliers, andapproached all potential participants (women of childbearing age) todescribe the study and assess eligibility and interest. In all cases, recruitmentstressed that their choice to participate would in no way influence the treat-ment or services that they received. In HIV clinics, the primary care providersapproached potential participants to preserve confidentiality of HIV statusand referred all interested participants to the research personnel. Participantswere later called to confirm eligibility and schedule an interview. A total of310 eligible families were recruited for the study. Twenty-six of these fami-lies refused to participate after the follow-up phone contact and screening.Interviews with 64 families who had consented to participate over the phonecould not be completed (n = 38 could not be contacted, n = 26 had repeatedcancellations). Thus, the final sample comprised 220 complete mother-childdyads, all of whom were interviewed individually, most within 3 weeks of thefirst approach. Parents and children were interviewed separately but
154 JOURNAL OF EARLY ADOLESCENCE / May 2005

simultaneously; project personnel provided child care services while parentscompleted the longer structured interview.
Interviewers administered the battery of questionnaires in either Englishor Spanish after obtaining consent from the mothers and assent from the chil-dren. Mothers and their children were interviewed separately and privately intheir households (n = 103 dyads) or at our research offices (n = 117 dyads)depending on family preference. Approximately 75% of the interviews wereconducted in English and 25% in Spanish. Children and their mothers wereboth compensated for their participation and mothers were reimbursed forany travel costs incurred.
Data Preparation and Analyses
Whether a discussion had occurred was a dichotomous (yes or no) variable.The content of discussions about HIV, sex, and drugs was coded into one offive categories: basic facts/information (i.e., communication of knowledgeor details pertinent to topic), past experiences (i.e., references to earlierencounters or situations), prevention (i.e., information regarding safetybehaviors and choices to reduce chance of negative outcomes), social influ-ence (i.e., discussion relating to persuasive, coercive, or generally biasingeffects of significant social referents), and other.
Kappa statistics were used to capture the degree of concordance in themother and child reports. Researchers have noted low to moderate corre-spondence between the mother and adolescent reports of discussions aboutsex (Feldman & Rosenthal, 2000; Jaccard et al., 1998). The kappa statisticconsists of the ratio of times that the two groups agreed in their responses(i.e., both mother and child endorsed an item or both did not endorse an item)to the maximum proportion of times that they could agree, corrected for chance(Siegel & Castellan, 1988). Group differences in communication were exam-ined between dyads with and without a mother living with HIV. Differencesin reports of parent-child communication behavior for children who knewcompared to those who did not know their mothers’ HIV status were exam-ined. The associations between maternal HIV status and the four comfort rat-ings were also assessed. These analyses were conducted with mothers’reported HIV status and with children’s knowledge of mothers’ status.Finally, reports of parent-child communication about HIV, sex, and drugswere examined for all participants on the basis of child’s age, child’s gender,and mother’s ethnicity (i.e., Latina or African American). Chi-square analy-ses were used to examine differences between groups for categorical data, t-tests were used to examine differences between groups for continuous data,and correlations were used to examine associations between continuous data.
O’Sullivan et al. / COMMUNICATION ABOUT HIV AND RISK 155

RESULTS
Reports of Communication From Mothers and Children
Landis and Koch’s (1977) guidelines were used to classify kappa agree-ment coefficients with 0 indicating no agreement beyond chance associationand a maximum value of 1 indicating perfect agreement. Landis and Kochsuggested the following classifications for this relatively conservative statis-tic: poor agreement = < 0.00; slight = 0.00 through 0.20; fair = 0.21 through0.40; moderate = 0.41 through 0.60; substantial = 0.61 through 0.80; and nearperfect = 0.81 through 1.00. There was fair agreement in the mother and childreports of whether four topics had been discussed when analyzing acrossdyads: the child’s boyfriend or girlfriend, sports, child’s friends, and child’sfuture plans (see Table 1). However, little agreement was found on other top-ics such as school, relatives, and the child’s favorite activities. The meankappa score across these topics was relatively low (κ = .16; range = –.07-.33)thereby indicating little overall agreement between mothers and children onconversational topics. For our three key topics, the highest degree of concor-dance in the mother and child reports was found for discussions about HIVand drugs, followed by sex. However, a higher proportion of mothers thanchildren reported having talked about HIV (48% vs. 38%), drugs (58% vs.47%), and sex (52% vs. 37%) in the month preceding the study. Acrossdyads, drugs were discussed most frequently (X = 4.97, SD = 6.93; range = 0-37), followed by HIV (X = 3.38, SD = 5.51; range = 0-30) and then sex (X =3.26, SD = 5.02; range = 0-28). Rather than assume that one source (i.e.,mothers or children) was more reliable than the other, the following analysessummarize trends across groups and then trends within mothers’ reports andtheir children’s reports separately.
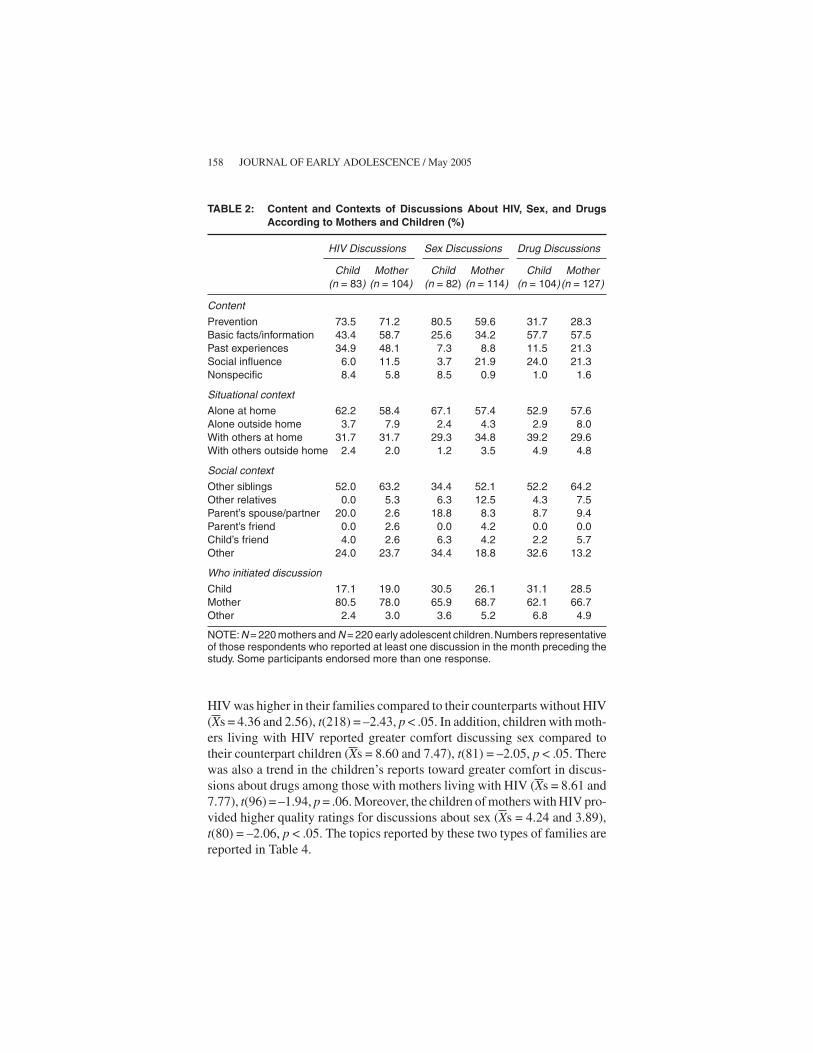
For those participants who reported a past discussion about HIV, drugs, orsex, both children and mothers indicated that discussions addressed HIV pre-vention most frequently, followed by basic facts/information (see Table 2). Asubstantial minority of parents also reported discussing past experienceswhen talking about HIV to their children, but this was not the case when theyspoke to their children about sex. For drug discussions, more than half of therespondents reported talking about basic facts/information, followed by pre-vention and then social influence. Overall, these discussions were most likelyto have occurred at home and involved siblings in some way. Mothers weremost likely to have initiated the discussions. Mothers’self-ratings of comfortwere higher than the children’s self-ratings of comfort for their discussionsabout HIV, t(54) = 3.50, p < .05 (see Table 3); no differences in comfort werefound in ratings for the sex or drugs discussions. In addition, mothers’ self-
156 JOURNAL OF EARLY ADOLESCENCE / May 2005

ratings of comfort were significantly higher than the comfort they attributedto their children across all three topics, t(102) = 6.43, t(113) = 5.94, andt(126) = 4.40, ps < .05, for HIV, sex, and drugs, respectively. Similarly, chil-dren’s self-ratings of comfort were significantly higher than the comfort theyattributed to their mothers across all three topics, t(83) = 3.21, t(82) = 4.78,and t(104) = 4.14, ps < .05, for HIV, sex, and drugs, respectively. Finally, chil-dren’s self-ratings of comfort during discussions about sex were significantlyhigher than the ratings attributed to them by their mothers, t(56) = 3.70, p <.05, although the mother and child ratings of the children’s comfort did notdiffer for HIV and drug discussions.
Mother Versus Child Reports of HIV, Sex, and DrugCommunication as a Function of Mothers’ Serostatus
Comparisons between reports from mothers living with HIV and thosewithout HIV as well as comparisons between their two groups of childrenrevealed some important differences. Comparisons addressed (a) whetherdiscussions about HIV, sex, or drugs were reported for the preceding month;(b) the frequency of discussions; (c) comfort; and (d) the perceived quality ofthese discussions. Specifically, a higher proportion of mothers living withHIV reported discussing HIV in the preceding month (56.0% and 40.8%,respectively), χ2(1) = 5.03, p < .05, and the overall frequency of talks about
O’Sullivan et al. / COMMUNICATION ABOUT HIV AND RISK 157
TABLE 1: Concordance in the Child and Mother Reports Across Communica-tion Topics
Topic Mothers (%) Children (%) Kappa
School 96.3 91.4 .02Sports 56.6 52.1 .31***TV programs 78.2 73.2 .18**Relatives 80.0 76.8 .05Child’s friends 83.5 75.1 .20**Child’s future plans 69.5 73.5 .19**Child’s favorite activities 78.2 78.5 .05His/her girlfriend or boyfriend 39.3 29.4 .33***The neighborhood 59.1 59.1 .15*Birth control 26.0 15.2 .10Parent’s HIV status 41.3 41.3 –.07Sex 52.1 37.3 .22**Drugs 58.0 47.3 .25***HIV 47.5 37.9 .25***
*p < .05. **p < .01. ***p < .001.NOTE: N = 220 mothers and N = 220 early adolescent children.
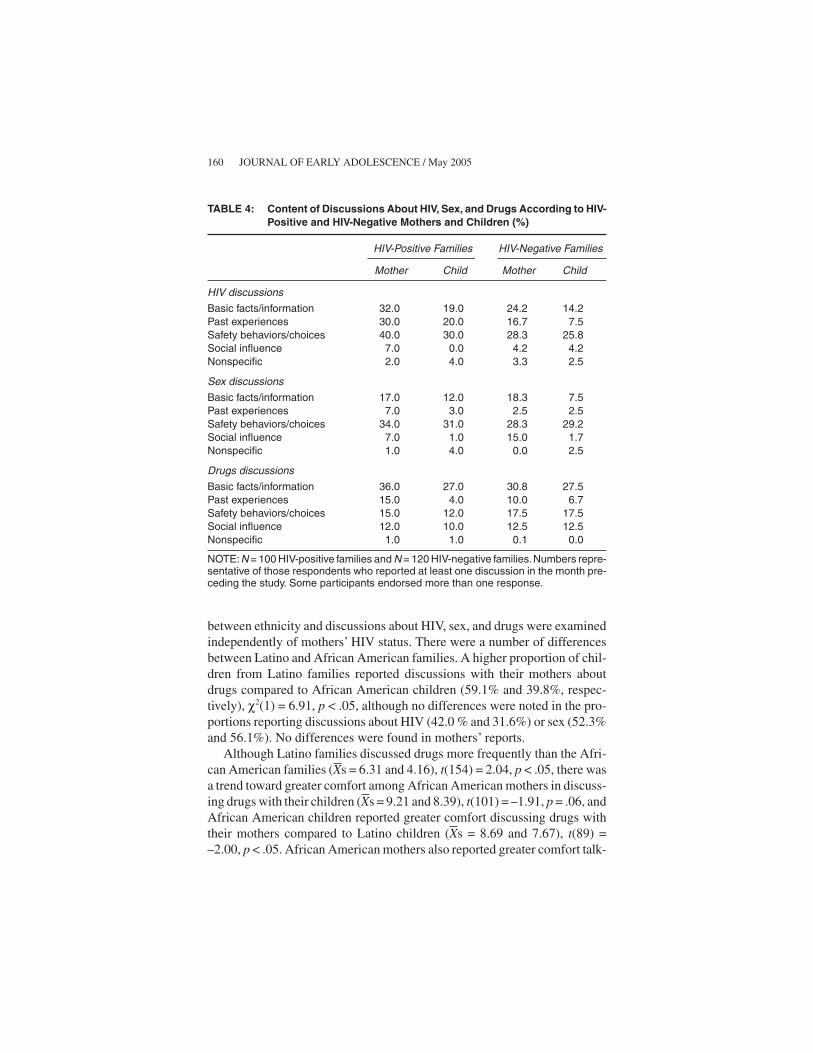
HIV was higher in their families compared to their counterparts without HIV(Xs = 4.36 and 2.56), t(218) = –2.43, p < .05. In addition, children with moth-ers living with HIV reported greater comfort discussing sex compared totheir counterpart children (Xs = 8.60 and 7.47), t(81) = –2.05, p < .05. Therewas also a trend in the children’s reports toward greater comfort in discus-sions about drugs among those with mothers living with HIV (Xs = 8.61 and7.77), t(96) = –1.94, p = .06. Moreover, the children of mothers with HIV pro-vided higher quality ratings for discussions about sex (Xs = 4.24 and 3.89),t(80) = –2.06, p < .05. The topics reported by these two types of families arereported in Table 4.
158 JOURNAL OF EARLY ADOLESCENCE / May 2005
TABLE 2: Content and Contexts of Discussions About HIV, Sex, and DrugsAccording to Mothers and Children (%)
HIV Discussions Sex Discussions Drug Discussions
Child Mother Child Mother Child Mother(n = 83) (n = 104) (n = 82) (n = 114) (n = 104)(n = 127)
Content
Prevention 73.5 71.2 80.5 59.6 31.7 28.3Basic facts/information 43.4 58.7 25.6 34.2 57.7 57.5Past experiences 34.9 48.1 7.3 8.8 11.5 21.3Social influence 6.0 11.5 3.7 21.9 24.0 21.3Nonspecific 8.4 5.8 8.5 0.9 1.0 1.6
Situational context
Alone at home 62.2 58.4 67.1 57.4 52.9 57.6Alone outside home 3.7 7.9 2.4 4.3 2.9 8.0With others at home 31.7 31.7 29.3 34.8 39.2 29.6With others outside home 2.4 2.0 1.2 3.5 4.9 4.8
Social context
Other siblings 52.0 63.2 34.4 52.1 52.2 64.2Other relatives 0.0 5.3 6.3 12.5 4.3 7.5Parent’s spouse/partner 20.0 2.6 18.8 8.3 8.7 9.4Parent’s friend 0.0 2.6 0.0 4.2 0.0 0.0Child’s friend 4.0 2.6 6.3 4.2 2.2 5.7Other 24.0 23.7 34.4 18.8 32.6 13.2
Who initiated discussion
Child 17.1 19.0 30.5 26.1 31.1 28.5Mother 80.5 78.0 65.9 68.7 62.1 66.7Other 2.4 3.0 3.6 5.2 6.8 4.9
NOTE:N = 220 mothers and N = 220 early adolescent children.Numbers representativeof those respondents who reported at least one discussion in the month preceding thestudy. Some participants endorsed more than one response.

Mother Versus Child Reports of HIV, Sex,and Drug Communication as a Function ofChild’s Knowledge of Mothers’ Serostatus
A parallel series of analyses was conducted separating the mothers withHIV on the basis of their child’s knowledge of the mothers’ serostatus(known HIV positive or HIV negative). Only two related differences werefound between the groups: In dyads where the mothers’ positive serostatuswas known to the child, mothers were more likely to report that they dis-cussed HIV (63.6% and 41.2%), χ2(1) = 4.60, p < .05, and these dyadsreported more frequent talks about HIV (Xs = 5.10 and 2.91 discussions inthe preceding month), t(98) = –1.77, p < .05, compared to the other families.
There were no differences between the two groups in terms of theirreported comfort communicating with one exception: Mothers known bytheir children to be HIV positive rated their children’s comfort discussingHIV as higher than did the other mothers (Xs = 8.05 and 5.86, respectively),t(53) = –2.61, p < .05. However, of particular interest, their children did notdiffer significantly in terms of their self-ratings of comfort discussing HIVwith their mothers (Xs = 8.30 and 7.79, respectively). No differences werefound between the groups’quality ratings of conversations about HIV, sex, ordrugs.
Mother Versus Child Reports of HIV, Sex,and Drug Communication as Function of Child’sAge, Gender, and Mothers’ Ethnicity
The effects of child’s age and gender were examined, but there were fewdifferences, so all children were included in the analyses. The associations
O’Sullivan et al. / COMMUNICATION ABOUT HIV AND RISK 159
TABLE 3: Mother and Child Mean Comfort Scores for Discussions About HIV,Sex, and Drugs
HIV Sex DrugDiscussions Discussions Discussions
Mothers’ self-ratings 8.96a, b 7.85c 8.79d
Mothers’ ratings of children 7.24b 5.83c, e 7.94d
Children’s self-ratings 7.88a, h 8.01e, f 8.12g
Children’s ratings of mothers 7.01h 6.48f 7.23g
NOTE: N = 220 mothers and N = 220 early adolescent children. Scale scores can rangefrom 1 (very uncomfortable) through 10 (very comfortable).a-g. Scores with the same superscript differ significantly: p < .001h. Scores with the same superscript differ significantly: p < .01.
between ethnicity and discussions about HIV, sex, and drugs were examinedindependently of mothers’ HIV status. There were a number of differencesbetween Latino and African American families. A higher proportion of chil-dren from Latino families reported discussions with their mothers aboutdrugs compared to African American children (59.1% and 39.8%, respec-tively), χ2(1) = 6.91, p < .05, although no differences were noted in the pro-portions reporting discussions about HIV (42.0 % and 31.6%) or sex (52.3%and 56.1%). No differences were found in mothers’ reports.
Although Latino families discussed drugs more frequently than the Afri-can American families (Xs = 6.31 and 4.16), t(154) = 2.04, p < .05, there wasa trend toward greater comfort among African American mothers in discuss-ing drugs with their children (Xs = 9.21 and 8.39), t(101) = –1.91, p = .06, andAfrican American children reported greater comfort discussing drugs withtheir mothers compared to Latino children (Xs = 8.69 and 7.67), t(89) =–2.00, p < .05. African American mothers also reported greater comfort talk-
160 JOURNAL OF EARLY ADOLESCENCE / May 2005
TABLE 4: Content of Discussions About HIV, Sex, and Drugs According to HIV-Positive and HIV-Negative Mothers and Children (%)
HIV-Positive Families HIV-Negative Families
Mother Child Mother Child
HIV discussions
Basic facts/information 32.0 19.0 24.2 14.2Past experiences 30.0 20.0 16.7 7.5Safety behaviors/choices 40.0 30.0 28.3 25.8Social influence 7.0 0.0 4.2 4.2Nonspecific 2.0 4.0 3.3 2.5
Sex discussions
Basic facts/information 17.0 12.0 18.3 7.5Past experiences 7.0 3.0 2.5 2.5Safety behaviors/choices 34.0 31.0 28.3 29.2Social influence 7.0 1.0 15.0 1.7Nonspecific 1.0 4.0 0.0 2.5
Drugs discussions
Basic facts/information 36.0 27.0 30.8 27.5Past experiences 15.0 4.0 10.0 6.7Safety behaviors/choices 15.0 12.0 17.5 17.5Social influence 12.0 10.0 12.5 12.5Nonspecific 1.0 1.0 0.1 0.0
NOTE:N = 100 HIV-positive families and N = 120 HIV-negative families.Numbers repre-sentative of those respondents who reported at least one discussion in the month pre-ceding the study. Some participants endorsed more than one response.

ing to their child about sex than did Latina mothers (Xs = 8.30 and 7.20), t(85) =–2.03, p < .05, and provided higher ratings of quality for discussions aboutHIV (Xs = 4.36 and 3.68), t(81) = –3.59, p < .001, and sex (Xs = 4.04 and3.67), t(100) = –2.11, p < .05. However, their children’s quality ratings didnot differ for HIV, sex, or drug discussions.
DISCUSSION
The current study assessed communication between mothers and theirchildren about HIV prevention and risk behaviors, the impact of maternalHIV infection and child knowledge of maternal HIV serostatus on this com-munication, and concordance in the mother and child reports about theircommunication. Overall, conversations between mothers and their childrenabout HIV, sex, and drugs took place among less than half of the participantsand did not occur frequently in the preceding month. In general, mothersviewed these discussions as occurring more often than did their children, andboth mothers and their children rated themselves as being more comfortablethan the other during these discussions. Other researchers of parent-childcommunication about sensitive topics, such as sexuality, have noted discrep-ancies in the parent and children reports (Jaccard et al., 1998; O’Sullivan,Jaramillo, Moreau, & Meyer-Bahlburg, 1999). A limitation of this and paststudies is that it cannot be determined whether this discrepancy reflects areporting bias or differential criteria for judging when or if a conversation hasoccurred. Other limitations may include a response bias or social desirabilityfactors motivating mothers to overreport these conversations, differences inthe mother and child interpretations of the content of dialogs, and faultyrecall associated with remembering past events generally.
The divergence in participants’ perceptions of the others’ comfort, in linewith the general lack of concordance in the mother and child reports, mayhave important implications for understanding the dynamics of communica-tion within these relationships. Mothers’ perception that their children maybe uncomfortable talking about these topics may explain why many partici-pants often did not talk to their children about sex, drugs, or HIV. As a firstline of prevention, these discrepancies may limit the extent to which promo-tion of communication within families can advance efforts to address preven-tion within the family context. Family-based prevention efforts need to incor-porate strategies to reconcile mothers’ perceptions of these interactions withtheir children’s perceptions, possibly delving more closely into the contentand structure of the discussions as well as potential response or recall biases
O’Sullivan et al. / COMMUNICATION ABOUT HIV AND RISK 161

affecting reports. More qualitative investigations into communication amongmothers and children directly affected by HIV would elucidate these issues.
Of particular note, characteristics of discussions were similar betweenfamilies with mothers living with HIV and those not living with HIV. Com-munication about HIV was hypothesized to vary between these familiesgiven the immediacy of HIV issues in the lives of affected families. Indeed,mothers living with HIV were more likely to report addressing HIV issuesand did so more frequently compared to mothers without HIV. Mothers liv-ing with HIV may be more sensitized to the possibility of risk and thus mayworry that their children will be exposed to infection. Of particular relevance,they may want to prepare their children to cope with the possibility of the par-ent’s future illness or death. Mothers living with HIV reported more discus-sions about HIV but not more discussions about sex or drugs, nor did theirchildren differ in the rates they reported across any of these topics. It appears,then, that these parents appeared to be having fairly specific conversationsabout HIV.
This study provides some of the first known data about characteristics ofcommunication about HIV generally, mother’s HIV serostatus in particular,and risk in families directly affected by HIV. Most notably, the mothers’com-munication styles as well as their backgrounds (e.g., residing in low socio-economic status, high HIV seroprevalence neighborhoods) are characterizedby greater similarities than differences regardless of mothers’ serostatus.Furthermore, the reports from their children were remarkably similar, evenin the analyses separating those children who knew of their mothers’ HIV-positive serostatus from those who did not. Typically, mothers initiated con-versations at home and with other siblings present. These findings indicatethat the family context is an appropriate forum for introducing or supportingefforts in family-based programs to prevent HIV infection among adoles-cents, although the extent to which such discussions are effective still needsto be demonstrated.
Disclosing one’s status to a child may spur conversations regarding riskand ways to protect oneself. Infected parents who are not ready or willing toconfront these issues with their children upon disclosure may be unlikely toinitiate conversations about HIV and risk. In a recent study involving 87United States mothers living with HIV, less than one-third had disclosed theirserostatus to their children (Armistead et al., 2001). Those who perceivedthemselves as having more severe symptoms were more likely to disclose totheir children thus suggesting that they chose to discuss their HIV statuswhen it became impossible to conceal their illness further. Although, for themost part, the mother and child ratings of comfort and perceived quality were
162 JOURNAL OF EARLY ADOLESCENCE / May 2005

strikingly similar, some interesting differences emerged: Children withmothers living with HIV reported greater comfort discussing sex and drug-related topics, although not more comfort discussing HIV, than did thosechildren with uninfected mothers. They also perceived the quality of theirconversations about sex to be better than those of mothers without HIV.Moreover, mothers with HIV perceived their children as more comfortablediscussing HIV compared to ratings from the other mothers thereby suggest-ing that when communication occurs in these families, it may be occurringeffectively, at least according to the mothers.
Our analyses indicated that the children’s age and gender were not associ-ated with the communication between mothers and children. These findingsdiverge from those of other studies that have found that communicationchanges as children get older (Beaumont et al., 2001). Possibly, the commu-nication dimensions assessed here (e.g., frequency, comfort) did not capturethe most essential differences between sons and daughters and over time. Inaddition, the timeframe we chose within which to sample discussions (i.e.,preceding 4 weeks) may have missed important discussions that hadoccurred much earlier. Further research needs to incorporate long-term pro-spective designs and address which factors prohibit discussions between par-ents and children, how children react emotionally, and whether knowledge ofparents’ serostatus affects adolescents’ relationships with their parents, aswell as children’s attitudes, opinions, or views regarding risk behavior.
A few differences in reports of parent-child communication arose on thebasis of mothers’ethnicity. African American mothers and children were lesslikely than their Latino counterparts to have discussed drugs, at least accord-ing to the children. This is significant given higher rates of HIV seropositivityamong the African American mothers. African American mothers alsoreported greater comfort discussing drugs and sex and greater quality in theirdiscussions of HIV and sex. These findings may indicate that more discus-sions about drugs increase discomfort; however, this association was notfound in our earlier analyses. Comfort associated with discussions appears tobe unrelated to the frequency of discussions, indicating that factors such asthe nature of the topics, the personal meaning of these talks to the familymembers, the emotional tone and quality, and the perceived outcomes may bemore significant in understanding the character of these talks.
Although differences between the Latino and African American familiessuggest the need to tailor efforts to the cultural groups targeted in these con-texts, especially given the differential rates of infection at this time, promot-ing parent-child communication about HIV and risk behaviors is unlikely todirectly affect adolescents’ chances of HIV infection. Communication
O’Sullivan et al. / COMMUNICATION ABOUT HIV AND RISK 163

should be perceived as one mechanism by which a better parent-child rela-tionship influences adolescents’ future choices about participation in riskactivity. Parental monitoring, style, and relationship warmth continue to bethe strongest predictors of adolescents’ risk taking (Huebner & Howell,2003; Wilder & Watt, 2002). Family-based programs can use informationabout how communication transpires in these families to help understandfamily systems in families with HIV and develop programs or guidelines tofacilitate better communication in efforts to promote family relations morebroadly. It is the promotion of stronger family relations that is likely to help inthe efforts to prevent infection among adolescents. Teaching parents how toinitiate and engage their children in discussions, anticipate reactions, and tai-lor the content to their child’s developmental stage may be useful strategiesthat support efforts to reduce the risk of infection among young people.Moreover, providing information to parents about overcoming their owninhibitions to communicate with their children, particularly those related todistressing their children, may promote more positive family communication.
REFERENCES
Armistead, L., Tannenbaum, L., Forehand, R., Morse, E., & Morse, P. (2001). Disclosing HIVstatus: Are mothers telling their children? Journal of Pediatric Psychology, 26, 11-20.
Beaumont, S. L., Vasconcelos, V. C. B., & Ruggeri, M. (2001). Similarities and differences inmother-daughter and mother-son conversations during preadolescence and adolescence.Journal of Language and Social Psychology, 20, 419-444.
Brackis-Cott, E., Block, M., & Mellins, C. A. (2003). Influence of maternal HIV on current lifeconcerns of HIV positive mothers and their early adolescent children. Journal of Early Ado-lescence, 23, 51-77.
Brown, L. K., Lourie, K. J., & Pao, M. (2000). Children and adolescents living with HIV andAIDS: A review. Journal of Child Psychology & Psychiatry & Allied Disciplines, 41, 81-96.
Cappello, D. (2001). When sex ed meets parent ed: Supporting parents as sexuality educators.SIECUS Report, 29, 4-6.
Centers for Disease Control & Prevention. (2004a). HIV/AIDS surveillance report: Cases of HIVinfection and AIDS in the United States, 2003, Vol. 15. Atlanta, GA: Author.
Centers for Disease Control & Prevention. (2004b). National Center for HIV, STD, and TB Pre-vention: Divisions of HIV/AIDS Prevention. HIV/AIDS among U.S. women: Minority andyoung women at continuing risk. Retrieved January 29, 2005, from www.cdc.gov/hiv/pubs/facts/ women.htm
Chabon, B., & Futterman, D. (1999). Adolescents and HIV. AIDS Clinical Care, 11, 1.Coutinho, R. A. (2000). Some aspects of the natural history of HIV infection. Tropical Medicine
& International Health, 5(7), A22-A25.Feldman, S. S., & Rosenthal, D. A. (2000). The effect of communication characteristics on fam-
ily members’ perceptions of parents as sex educators. Journal of Research on Adolescence,10, 119-150.
164 JOURNAL OF EARLY ADOLESCENCE / May 2005

Forehand, R., Steele, R., Armistead, L., Morse, E., Simon, P., & Clark, L. (1998). The familyhealth project: Psychological adjustment of children whose mothers are HIV infected. Jour-nal of Consulting and Clinical Psychology, 66(3), 513-520.
Haven, J. F., Mellins, C. A., & Pilowski, D. (1996). Mental health issues in HIV-affected womenand children. International Review of Psychiatry, 8, 217-225.
Hudis, J. (1995). Adolescents living in families with AIDS. In S. Geballe, J. Gruendel, & W.Andiman (Eds.), Forgotten children of the AIDS epidemic (pp. 83-94). New Haven, CT: YaleUniversity Press.
Huebner, A. J., & Howell, L. W. (2003). Examining the relationship between adolescent sexualrisk-taking and perceptions of monitoring, communication, and parenting styles. Journal ofAdolescent Health, 33, 71-78.
Hutchinson, M. K., & Cooney, T. M. (1998). Patterns of parent-teen sexual risk communication:Implications for intervention. Family Relations, 47, 185-194.
Jaccard, J., Dittus, P. J., & Gordon, V. V. (1998). Parent-adolescent congruency in reports of ado-lescent sexual behavior and in communication about sexual behavior. Child Development,69, 247-261.
Jaccard, J., Dodge, T., & Dittus, P. (2002). Parent-adolescent communication about sex and birthcontrol: A conceptual framework. In W. Damon, S. S. Feldman, & D. A. Rosenthal (Eds.),Talking sexuality: Parent-adolescent communication. New directions for child and adoles-cent development (Vol. 97, pp. 9-41). San Francisco: Jossey-Bass.
Kotchick, B. A., & Forehand, R. (1999, July). The family health project: A longitudinal investi-gation of children whose mothers are HIV-infected. Poster presented at the annual Role ofFamilies in Preventing and Adapting to HIV/AIDS, Philadelphia.
Krauss, B., Goldsamt, L., & Pierre-Louis, M. (1996, July). How pre-adolescents and their par-ents talk about HIV in a high seroprevalent neighborhood. Paper presented at the XIth Inter-national Conference on AIDS, Vancouver, Canada.
Landis, J. R., & Koch, G. G. (1977). The measurement of observer agreement for categoricaldata. Biometrics, 33, 159-174.
Lee, M. B., Lester, P., & Rotheram-Borus, M. J. (2002). The relationship between adjustment ofmothers with HIV and their adolescent daughters. Clinical Child Psychology & Psychiatry,7, 71-84.
Lefkowitz, E. S., Boone, T. L., Sigman, M., & Au, T. K. (2002). He said, she said: Gender differ-ences in mother-adolescent conversations about sexuality. Journal of Research on Adoles-cence, 12, 217-242.
Lefkowitz, E. S., Kahlbaugh, P., Au, T. K., & Sigman, M. (1998). A longitudinal study of AIDSconversations between mothers and adolescents. AIDS Education and Prevention, 10, 351-365.
Lehr, S. T., DiIorio, C., Dudley, W. N., & Lipana, J. A. (2000). The relationship between parent-adolescent communication and safer sex behaviors in college students. Journal of FamilyNursing, 6, 180-196.
Mellins, C. A. (1995, February). Stress and psychosocial function in HIV-infected mothers andtheir children. Paper presented at the HIV Infection in Women: Setting a New Agenda Con-ference, Washington, DC.
Mellins, C. A., Brackis-Cott, E., Dolezal, C., Richards, A., Nicholas, S., & Abrams, E. J. (2002).Patterns of status disclosure to perinatally HIV-infected children and subsequent mentalhealth outcomes. Clinical Child Psychology and Psychiatry, 7, 101-114.
Mellins, C. A., & Ehrhardt, A. A. (1994). Families affected by pediatric AIDS: Sources of stressand coping. Journal of Developmental and Behavioral Pediatrics, 15, S54-S60.
O’Sullivan et al. / COMMUNICATION ABOUT HIV AND RISK 165

Miller, B. C., Benson, B., & Galbraith, K. A. (2001). Family relationships and adolescent preg-nancy risk: A research synthesis. Developmental Review, 21, 1-38.
Miller, B. C., Norton, M. C., Fan, X., & Christopherson, C. R. (1998). Pubertal development,parental communication, and sexual values in relation to adolescent sexual behaviors. Jour-nal of Early Adolescence, 18, 27-52.
Miller, K. S., Kotchick, B. A., Dorsey, S., Forehand, R., & Ham, A. Y. (1998). Family communi-cation about sex: What are parents saying and are their adolescents listening? Family Plan-ning Perspectives, 30, 218-235.
New York State Department of Health. (2002). AIDS in New York State. Albany, NY: Author.Newcomer, S. F., & Udry, J. R. (1985). Parent-child communication and adolescent sexual
behavior. Family Planning Perspectives, 17, 169-174.Niebuhr, V. N., Hughes, J. R., & Pollard, R. B. (1994). Parents with human immunodeficiency
virus infection: Perceptions of their children’s emotional needs. Pediatrics, 93, 421-425.O’Sullivan, L. F., Jaramillo, B. M. S., Moreau, D., & Meyer-Bahlburg, H. F. L. (1999). Mother-
daughter communication about sexuality in a clinical sample of Hispanic adolescent girls.Hispanic Journal of Behavioral Sciences, 21, 447-469.
O’Sullivan, L. F., Meyer-Bahlburg, H. F. L., & Watkins, B. X. (2001). Mother-daughter commu-nication about sex among urban African American and Latino families. Journal of Adoles-cent Research, 16, 269-291.
Pequegnat, W., Bauman, L., Bray, J., DiClemente, R., DiIrio, C., Icard, L., et al. (2002). Researchissues with children infected and affected with HIV and their families. Clinical Child Psy-chology & Psychiatry, 7, 7-15.
Pick, S., & Palos, P. A. (1995). Impact of the family on the sex lives of adolescents. Adolescence,30, 667-675.
Raffaelli, M., Bogenschneider, K., & Flood, M. F. (1998). Parent-teen communication about sex-ual topics. Journal of Family Issues, 19, 315-333.
Raffaelli, M., & Green, S. (2003). Parent-adolescent communication about sex: Retrospectivereports by Latino college students. Journal of Marriage & the Family, 65, 474-481.
Rodgers, K. B. (1999). Parenting processes related to sexual risk-taking behaviors of adolescentmales and females. Journal of Marriage and the Family, 61, 99-109.
Romo, L. F., Lefkowitz, E. S., Sigman, M., & Au, T. K. (2001). Determinants of mother-adolescentcommunication about sex in Latino families. Adolescent & Family Health, 2, 72-82.
Rosenthal, D., Senserrick, T., & Feldman, S. (2001). A typology approach to describing parentsas communicators about sexuality. Archives of Sexual Behavior, 30, 463-482.
Rotheram-Borus, M. J., Mahler, K. A., & Rosario, M. (1995). AIDS prevention with adolescents.AIDS Education and Prevention, 7, 320-336.
Siegel, S., & Castellan, N. J., Jr. (1988). Nonparametric statistics for the behavioral sciences(2nd ed.). New York: McGraw-Hill.
Sigelman, C. K., Mukai, T., Woods, T., & Alfeld, C. (1995). Parents’ contributions to children’sknowledge and attitudes regarding AIDS: Another look. Journal of Pediatric Psychology, 20,61-77.
Sikkema, K. J., Heckman, T. G., Kelly, J. A., Anderson, E. S., Winett, R. A., Solomon, L. J., et al.(1996). HIV risk behaviors among women living in low-income, inner-city housing develop-ments. American Journal of Public Health, 86, 1123-1128.
Sly, D. F., Riehman, K., Wu, C., Eberstein, I., Quadagno, D., & Kistner, J. (1995). Early child-hood differentials in mother-child AIDS-information interaction. AIDS Education and Pre-vention, 7, 337-354.
Wilder, E. I., & Watt, T. T. (2002). Risky parental behavior and adolescent sexual activity at firstcoitus. Milbank Quarterly, 80, 481-524.
166 JOURNAL OF EARLY ADOLESCENCE / May 2005

Correspondence regarding this article should be addressed to Lucia F. O’Sullivan, Ph.D., HIV Center forClinical and Behavioral Studies, 1051 Riverside Drive, Unit 15, New York, NY 10032-1007; e-mail: [email protected].
O’Sullivan et al. / COMMUNICATION ABOUT HIV AND RISK 167
Top Related
Copyright © 2022 FDOKUMEN

