






Bahasa
Halaman
Hukum

ChildlessJIJless iJIJlAndhr21 rr21desh9
India: Treatment-SeeJking and
ConsequencesSayeed Unisa
Andhra Pradesh has a high inddence of chndlessness, compared to the rest of India. This paper isbased on a study that explored the psychosodal consequences of chndlessness in Ranga Reddydistdct Andhra Pradesh India in 1998, and descdbes the extent and ldnds ofjnfertjJjty treatmentsought. Currently married women aged 20 years or more who had been marded for at least three
years wUh no Jjve birth were included; the rate of chndlessness was five per cent. On average,they started allopathjc treatment and yjsits to holy places after three years of not hayjng a baby. Alarge majority sought allopathic treatment first and only tried other sorts oftreatment prayer,rituals and traditional treatments when this did not work or cost too much. About ten per cent hadadopted chndren and others would consider it in future. For a minority of women there was adsk of divorce and husbands marrying a second wife to have children. Two-thirds ofthe women
experienced yjolence from their husbands; 13per cent thought this was partly due to theirchndlessness. There is a clear need for infertiJjty investigation and treatment to be included in thereproductive health programme in India, and for health workers to be trained to proyjdeinformation care and referrals.
CHILDLESSNESS is a product of the com
plex interaction of biologicat environmental and culturaLfactors, which needs tobe understood at the local community level
and for planning reproductive health care services to address the problem. In Indi,a,there is alack of data on the problem of infertility. Theproblem of infertility is treated as an ancillaryissue next to the problem of overpopulation inIndia, and programme planners and policymakers have also not given it due attentionbecause it is not a life-threatening condition.Available evidence, which is mostly anecdotatsuggests that regardless of the medical cause ofinfertility, women unquestionably receive theblame for fertility problems and suffer personalgrief, frustration, social stigma, ostracism andserious economic deprivation. In many societies,infertility is grounds for divorce and re-marriageby husbands.1
This paper seeks to describe the socialdimensions of childlessness and where and when
54
people seek treatment for fertility problems,which is a new area of research in India. Again,anecdotally, it is said that infertile men andwomen tend to seek help from traditional healersand quacks.2 The most common methods used bytraditional healers are herbal treatments andappeals to supernatural powers, as well asprayers (poja)3 and other rituals (munat).4 Littleisknown about the availability of allopathic fertilitytreatment in rural areas, the profile of coupleswho seek these services from the private sectoror the treatment costs incurred by them.5
In a population where being childlesshas morenegative sociat cultural and emotional reper~cussions for women than any other non-lifethreatening condition, it can probably be assumedthat almost all cases of childlessness are due tophysiological or biological factors. Estimations ofthe magnitude of primary and secondary infertility are often not very precise because of inadequate demographic and health service statistics.6Data from fertility surveys and censuses on

children ever-born have been used until now todetermine the prevalence of childlessness in India.For women aged 50and above, this is estimated tobe 3.8 per cent in rural areas and 4.3 per cent inurban areas. Among the major states of India,Andhra Pradesh has the highest prevalence rate,7.4 per cent in rural areas and 8.7 per cent inurban areas.? The National Family Health Survey(NFHS)also reported a high rate of childlessnessamong the women of Andhra Pradesh.s
The studyRanga Reddy district of Andhra Pradesh wasselected for a descriptive, community-basedstudy. Identification of childless women wasdone by complete house listing of all selectedvillages. The selection of villages was by stratifiedrandom sampling - all villages were stratifiedinto three levels in ascending order of femaleliteracy and 10 villages were selected randomlyfrom each stratum. All women of reproductiveage were covered in these 30villages. During thehouse listing, 8,713 households belonging to the30 villages were covered. In all, 9,298 women ofreproductive age were interviewed for thepurpose of identifying childless women. Amongall 9,298 enumerated women, 12 per cent werefound to be childless. This number includedmany adolescent women who were eitherrecently married or no longer married. Amongthe currently married women 20-49 years oldwho had been married for three or more yearswithout a live birth,9 the rate of childlessness wasfound to be five per cent. The sample selectionmethod used might have missed women whohad adopted children in the past and did notreport themselves to be childless.
Free listing of the types of treatments available were collected from key informants. All primary health centres and sub-centres in andaround the selected villages were visited and thebest-known private doctors and hospitals mentioned by the key informants were also visited.Doctors and auxiliary nurse-midwives were alsointerviewed during this phase of data collection.
Houses of childless women were identifiedfrom the complete census done in the first phaseof data collection. Detailed information on household characteristics, marriage, pregnancy history, treatment-seeking behaviour, consequencesof childlessness, social participation, decision-
Reproductive Health Matters, Vol. 7, No. 13, May 1999
making about treatment, and general health andmental health was collected from 332 respondents in the second phase of data collection, usinga questionnaire filled out in face-to-face interviews.
Clinical examination was done on all 332women and 101men. Clinical examination of thewomen was by a female gynaecologist and of themen by a male doctor. The causes of infertilitywere recorded from pathological and clinicalreports; these have not yet been analysed. Afterdata collection, the doctors gave the respondentsinformation about the reproductive system, thefertile period and common reasons for infertility.Help was offered to these couples to try toovercome any minor reproductive health problems that might affect fertility. They were alsoreferred to hospitals where fertility treatmentwas available.
In the third phase of data collection, 60detailed case studies of childless women from 10villages were obtained. Identification of casesfrom the quantitative data collected included thespecial cases of women who had adopted a child,those whose husbands had taken a second wife,those who had not sought any fertility treatment,those who had gone to many holy places, orthose who had taken many allopathic treatments.Informal and semi-structured interviews wereconducted to gather sufficient information on allthe relevant aspects of the present study, with theinitial interviews focusing on more generaltopics and gradually moving to more sensitiveissues. The scope of the present paper isrestricted to treatment seeking and the consequences of childlessness.
Profile of childless womenOfthe 332 childless women identified, the majority (73per cent) were below 30 years of age. Thepreponderance of women under 30 indicateseither that the younger women were still in theprocess of achieving their fertility, the olderwomen had had successful treatment and beenable to bear children after the age of 30, or theolder women had adopted children and did notidentify themselves as childless. Data on childlesswomen from the NFHS shows the same agedistribution. S
The minimum legal age for marriage forwomen in India is 18 years; despite this, 52 per
55

Unisa
cent of childless woman in this study had marriedbefore 15 years of age. The mean age at marriagefor the 332 women was 15.4, which is quite lowcompared to other southern states ofIndia.8 Earlyinitiation of cohabitation with a husband andearly spontaneous abortions may be some ofthe causes of higher infertility in this state. Anassociation between low age at marriage, firstcoitus, sexually transmitted infections and infertility have been reported in previous studies.1o.11Single marriages in the life of women are thenorm, and most of the marriages in this samplefell in this category (98 per cent). Cross-cousinmarriages and marriages between close bloodrelatives are common in the south of India. In thepresent sample, a large number of women hadmarried close relatives. This may also be adeterminant of infertility, as indicated in previousstudies ofinfertility in Egypt.12
'In the present sample, one third ofthe womenbelonged to scheduled castes and a very smallproportion (three per cent) to scheduled tribes.Muslims and Christians together constituted asmall minority (seven per cent) in a predominantly Hindu population. Although the extendedfamily system is the norm in rural India; amajority in this study lived in nuclear families (66per cent); these couples had generally married ata young age and had a low level (30 per cent) ofliteracy. The main occupations of the womenwere as agricultural labourers (43 per cent),cultivators (6 per cent), shopkeepers (18 per cent)and housewives (33 per cent).
About 70 per cent of the women had neverbeen pregnant. The remaining 30 per cent hadhad one or more pregnancies which had resultedin either spontaneous abortions or stillbirths.13In all age groups in the sample, a similar patternwas found.
Reasons some women did not seekinfertility treatmentEighty-six (26 per cent) of the 332 childlesswomen (couples) interviewed did not seek anyhelp in getting pregnant. The high cost oftreatment seemed' to be the main detrimental
factor for 43 per cent of those not going for anytreatment. The other major reason for not seeking treatment was that it was not necessary (41per cent). Some women (8 per cent) reported alack of information on where to get treatment,
56
and non-availability of treatment nearby wasreported as the reason by about 3.5 per cent. Afew (3.5 per cent) reported not being able to getpermission from elders as their reason for notgoing for treatment.
Initiation and duration of efforts toseek fertility treatmentThose who did seek help first sought treatmentor visited holy places after three years ofmarriage on average. A few couples soughttreatment after only one year of marriage; thesecouples described pressure on them to do so andtheir own impatience to have children soon afterthey married.
Reports of initial discussions and decisionsbetween husbands and wives about what typeof treatment to seek indicate that the problemof infertility was initially considered to be thewoman's problem, and that husbands weregenerally uncooperative in the beginning. Thiswas not unexpected, given the patriarchal Indiancontext, but in Germany, too, men delayaccepting the need for treatment for infertility.14However, in this sample, no matter wheretreatment was sought, in around 75 per cent ofcases the husband went with his wife for
treatment and depending upon the cause ofinfertility"one or both of them was treated.
A few women (couples) continued to seek andreceive allopathic treatment for 25 years. In thecase of getting religious and spiritual help, theamount of time was even longer, with somecontinuing to seek help for up to 32 years. Astrong desire to have their own children wasevident among the women who spent manyyears seeking help; they did not lose the hope ofhaving their own child even after very longperiods of unsuccessful attempts.
Source of information on where to getinfertility treatmentNeighbours were the main source of informationon where infertility treatment could be found,especially in the case of the first place of treatment, for which neighbours provided information to about 35 per cent of the women. In 25 per
. cent of cases, the couple themselves decidedwhere to go for treatment. For the rest, it wasmainly the parents of the woman who provided
information and financial support for treatment;and they were the third major source of inform ation on where to get help.
Reproductive Health Matters, Vol. 7, No. 13, May 1999
Table 1.Type of fertility treatment sought andsequence of choices
Overall, 58 per cent of couples in this studysought and received treatment at least once froma modern medical source, whether allopathic,Ayurvedic, Unani or homeopathic, and their firstchoice was from among these same methods.When they did not get the desired results afterone or two courses of treatment they shifted toother forms of treatment not least because theyfound that the costs of modern medical treatmentincreased prohibitively with successive attempts.
Sixty-three per cent of women (couples) wentto at least one holy place or spiritual healer tofulfill their desire to have a child. The often lowcost and easy accessibility of religious ritual andhealers, along with a deep faith in religiousinstitutions and practitioners, were the main
Sources oftreatment and the order inwhich they were approached for helpIn the first phase of data collection, a list of 13 ofthe most frequent types of fertility treatmentmethods used by childless couples was culledfrom the free listing. Women were asked withand without probing the number and forms oftreatment method they had used to date and theorder in which they had used each form oftreatment. Their answers were grouped underfour main headings (Table 1):
• allopathic,• Ayurvedic, homeopathy and Unani (AHU)15• traditionat and• religious.
Allopathic sources include treatment fromgovernment health services as well as privatedoctors and hospitals. Contrary to the commonlyheld belief that rural Indian people opt first forUnani or traditional methods of treatment forfertility problems, in fact of the 242 women whosought any form of treatment or help, the largemajority (73 per cent) opted for an allopathicsource first followed by religious and traditionalsources.2 Among the women who went forallopathic treatment first, avery large majority (90 percent) opted to see a privatepractitioner or go to aprivate hospital.
Among those whosought treatment a secondtime, again more of thempreferred allopathic treatment (39 per cent) than anyother source, but a largerproportion opted for traditional and religious treatment. Among those whowent on to attend a thirdsource of treatment therewas a bigger shift towardsAHU, traditional and religious providers and awayfrom allopathic ones.
Source
Allopathic
AHU
Traditional
Religious
TOTAL
Sequence in which treatment was sought
First
SecondThirdFourth
choice
choicechoicechoice
178
5611
1
610
7
2995
56
53311
242
1443316
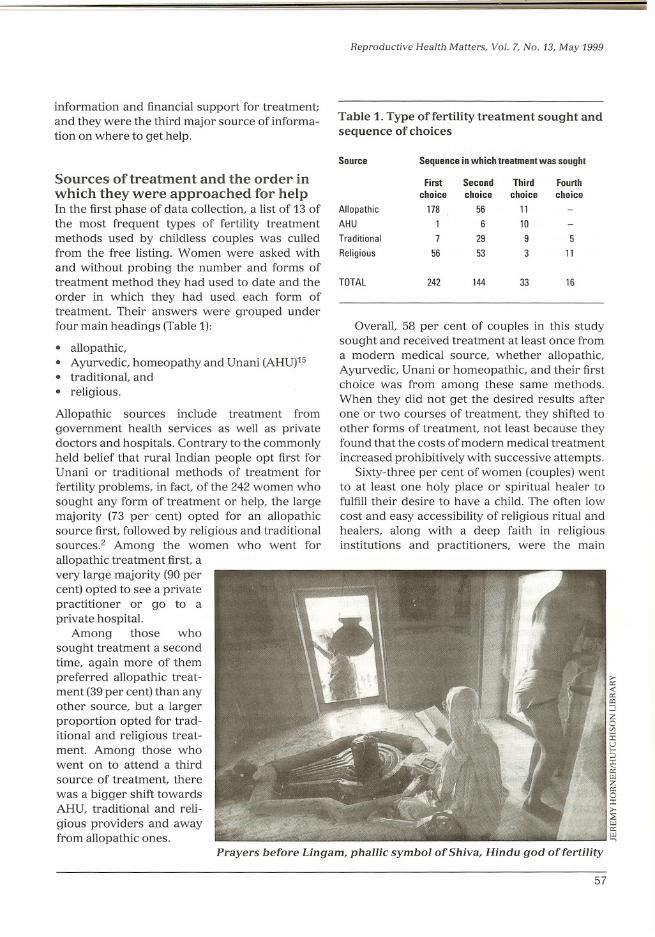
Prayers before Ungam, phallic symbol of Shiva, Hindu god of fertility
57
Unisa
reasons why so many sought religious or traditional help. The strong beliefs and varied religious practices of these women were oftenreflected during the in-depth case studies:
'I pray to Mysamma Devi16 with my mother-in-law.We prepare sweet rice as prasad (an offering).'
'1 went to the temple of Goddess Mahakali17 atBontapally because some people have conceivedafter going to this temple. 1 went there eveI}'Tuesday for one year. There 1 would performpoja3 with coconut turmeric, incense stick andvermilion, after bathing in the village well. The'pojarj'3 would give me vermilion, which 1wouldapply daily to my forehead. Once a month 1had tosacrifice a hen.'
Of the 30 women who were currently receivingtreatment during the course of the study, 24 wereattending private hospitals or clinics, just overhalf of them for a first course of treatment whiletwo were attending a government hospital for afirst course of treatment and four were going totraditional practitioners, mostly for the first orsecond time.
Number of courses of treatmentsoughtAround 19.9 percent of women tried only onecourse of treatment and 19.6 percent tried twocourses of treatment.18 The numbers of womenwho reported attending for three or morecourses of treatment declined sharply from 11.4per cent who went for three courses of treatmentto 5.7 per cent for five courses. About eight percent went for six or more courses of treatment.(Table 2)
Data on the number of times treatment of alltypes was sought were broken down by age.
Table 2. Total courses oftreatment sought (allfour types)
Number of 0123456+
courses of treatmentNumber of
86666538311927
women % of women
25.919.919.611.49.35.78.1
58
This showed that a large number of the youngerage group (20-24) had not gone for any kind oftreatment indicating a general reluctance tovisit medical practitioners at an early stage. Thisattitude of 'wait-and-watch' and an unwillingness to get treatment at younger ages was alsofound in studies in Germany19 and theGambia.2o
Duration of successive courses oftreatment and numbers of visitsDuration of treatment time for each course oftreatment and numbers of visits per treatmentcourse were studied. (Table 3) There was anincrease in the duration of each course oftreatment as the number of courses of treatmentsought increased. On average, the woman(couple) spent about 4.8 months for the firstcourse of treatment. This rose to a maximum of8.3 months for the fifth course of treatmentadopted and then declined sharply to 0.4 monthsin the case of the sixth and higher numbers oftreatments.
Table 3. Duration oftreatment course andfrequency of visits for successive courses oftreatmentNumber of courses
123456+
of treatment Mean duration
4.85.25.55.48.30.4
(in months) Mean frequency
5.67.25.96.89.10.4
of visits Number of women
16695431886
Similarly, with regard to frequency of visits,there was a noticeable increase in the number ofvisits per course of treatment with each additional course of treatment and the number ofmonths per course of treatment was consistentlyhigh, with four or more courses of treatmenttaking several years. The mean number of visitsranged from 5.6 visits for the first course oftreatment to a maximum of 9.1 visits for the fifthcourse of treatment received. Again, for the sixthand· higher course of treatment there was a bigdecline, which may either be because the womenhad just begun or were still in the process of
Reproductive Health Matters, Vol. 7, No. 13, May 1999
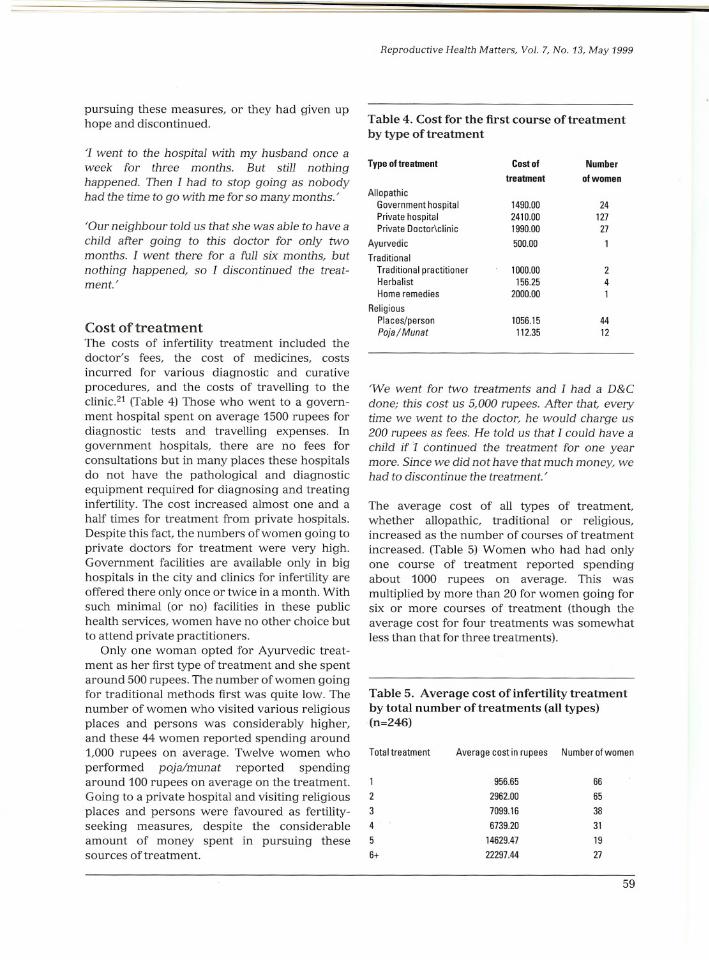
pursuing these measures, or they had given uphope and discontinued. Table 4. Cost for the first course of treatment
by type oftreatment
Table 5. Average cost of infertility treatmentby total number oftreatments (all types)(n=246)
'We went for two treatments and I had a D&Cdone; this cost us 5,000 rupees. After that, everytime we went to the doctor, he would charge us200 rupees as fees. He told us that I could have achild if 1 continued the treatment for one yearmore. Since we did not have that much money, wehad to discontinue the treatment.'
The average cost of all types of treatment,whether allopathic, traditional or religious,increased as the number of courses of treatment
increased. (Table 5) Women who had had onlyone course of treatment reported spendingabout 1000 rupees on average. This wasmultiplied by more than 20 for women going forsix or more courses of treatment (though theaverage cost for four treatments was somewhatless than that for three treatments).
Type of treatment Cost ofNumber
treatment
of women
Allopathic Government hospital
1490.0024
Private hospital
2410.00127
Private Doctor\clinic1990.0027
Ayurvedic
500.001
Traditional Traditional practitioner
1000.002
Herbalist156.254
Home remedies2000.001
Religious Places/person
1056.1544
Poja / Munat
112.3512
9~~5 ~
2962.00 65
7099.16 38
6739.20 31
14629.47 19
22297.44 27
Average costin rupees NumberofwomenTotal treatment
1
2
3
4
5
6+
Cost oftreatmentThe costs of infertility treatment included thedoctor's fees, the cost of medicines, costsincurred for various diagnostic and curativeprocedures, and the costs of travelling to theclinic.21 (Table 4) Those who went to a government hospital spent on average 1500 rupees fordiagnostic tests and travelling expenses. Ingovernment hospitals, there are no fees forconsultations but in many places these hospitalsdo not have the pathological and diagnosticequipment required for diagnosing and treatinginfertility. The cost increased almost one and ahalf times for treatment from private hospitals.Despite this fact, the numbers of women going toprivate doctors for treatment were very high.Government facilities are available only in bighospitals in the city and clinics for infertility areoffered there only once or twice in a month. Withsuch minimal (or no) facilities in these publichealth services, women have no other choice butto attend private practitioners.
Only one woman opted for Ayurvedic treatment as her first type of treatment and she spentaround 500 rupees. The number of women goingfor traditional methods first was quite low. Thenumber of women who visited various religiousplaces and persons was considerably higher,and these 44 women reported spending around1,000 rupees on average. Twelve women whoperformed poja/munat reported spendingaround 100 rupees on average on the treatment.Going to a private hospital and visiting religiousplaces and persons were favoured as fertilityseeking measures, despite the considerableamount of money spent in pursuing thesesources of treatment.
'I went to the hospital with my husband once aweek for three months. But stilI nothinghappened. Then I had to stop going as nobodyhad the time to go with me for so many months.'
'Our neighbour told us that she was able to have a
child after going to this doctor for only twomonths. I went there for a full six months, butnothing happened, so I discontinued the treatment.'
59
Il
IJ
Unisa
Attitude towards the alternative ofadoptionAdoption is one way to mitigate the consequences of childlessness. In the sample, 10 per cent ofthe women had adopted a child or children, andanother 12 per cent stated their intention ofadopting at a future date. The views on adoptionpresented here come from this subset of womenand may not be representative of the largergroup of childless women in the study.
For the women who had already adopted, theprocess of adoption had been very informal, withno legal formalities. Generally, the adopted childwas the child of a close relative, such as thebrother-in-law or the sister of the woman.
Adoption was considered to have taken placesimply by bringing the child to the house. If forany reason the child was unable to adjust, orthere were other problems, the adoption couldbe terminated merely by sending the child backto his or her birth parents.
'1 had to send back my brother-in-Iaw's son,whom we had adopted, because we came to learnfrom the villagers that my brother-in-law hadgiven him to us for adoption because he intendedto kj]] my husband, to get all the property.'
Most of the women who had postponed adoptionto a later date said they wanted to wait and seewhether they could conceive and they were quitehopeful of this (39 per cent of them). They wereready to adopt in future if nothing happened.Around 13 per cent had not adopted becausethere was not a child available for them to adopt.Some women (10 per cent) said their husbandsdisapproved of adopting at that point in time.
'The money required for adoption, I'll use it fortreatment for myself and if still nothing happens,only then will 1 think about adoption.'
'Who will give their very own child for adoption?'
The in-depth case studies also revealed somenegative views on adoption. In general, thewomen who were not interested in adoption feltthat the children of others could not provide thesame love and security as their own children:
'Only your own children, those borne by you, cangive you comfort and the feeling of having children.'
60
'Adoption is no use, who knows if the adoptedchild will take care of us in our old age. Themother of the child may also fight with me lateron. So it is better to be without any children at all.'
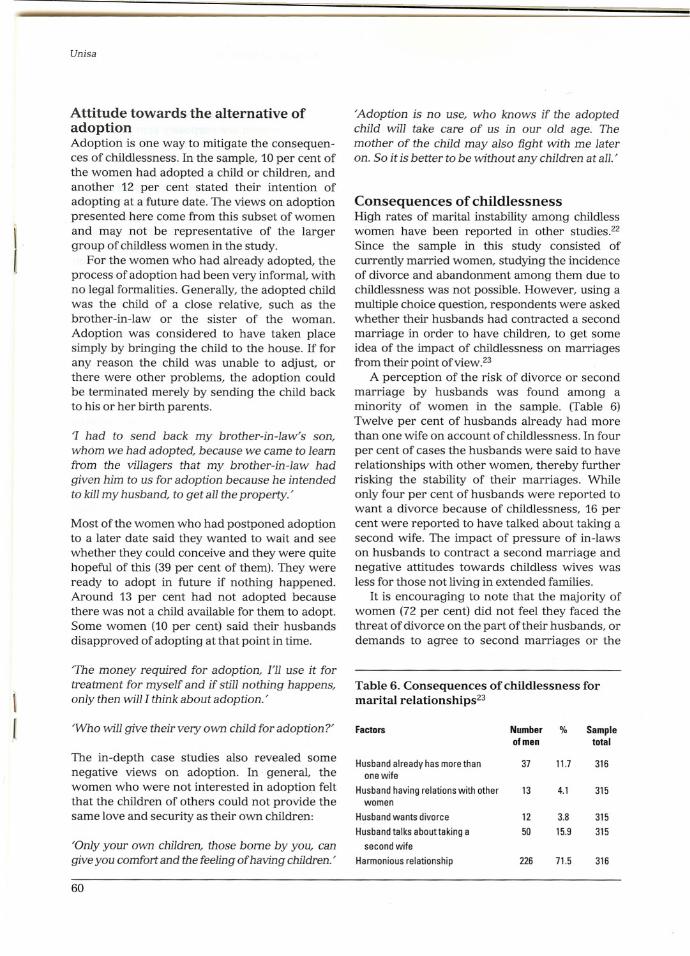
Consequences of childlessnessHigh rates of marital instability among childlesswomen have been reported in other studies.22Since the sample in this study consisted ofcurrently married women, studying the incidenceof divorce and abandonment among them due tochildlessness was not possible. However, using amultiple choice question, respondents were askedwhether their husbands had contracted a secondmarriage in order to have children, to get someidea of the impact of childlessness on marriagesfrom their point ofview.23
A perception of the risk of divorce or secondmarriage by husbands was found among aminority of women in the sample. (Table 6)Twelve per cent of husbands already had morethan one wife on account of childlessness. In fourper cent of cases the husbands were said to haverelationships with other women, thereby furtherrisking the stability of their marriages. Whileonly four per cent of husbands were reported towant a divorce because of childlessness, 16 percent were reported to have talked about taking asecond wife. The impact of pressure of in-lawson husbands to contract a second marriage andnegative attitudes towards childless wives wasless for those not living in extended families.
It is encouraging to note that the majority ofwomen (72 per cent) did not feel they faced thethreat of divorce on the part of their husbands, ordemands to agree to second marriages or the
Table 6. Consequences of childlessness formarital relationships23Factors
Number%Sampleolmen
total
Husband already has more than
3711.7316
one wileHusband having relations with other
134.1315
women Husband wants divorce
123.8315
Husband talks about taking a
5015.9315
second wile Harmonious relationship
22671.5316
problem of their husbands having relationshipswith other women. The harmonious relationships among these couples may be the result ofawareness that infertility was treatable in manycases, and that women were not responsible forthis condition alone.
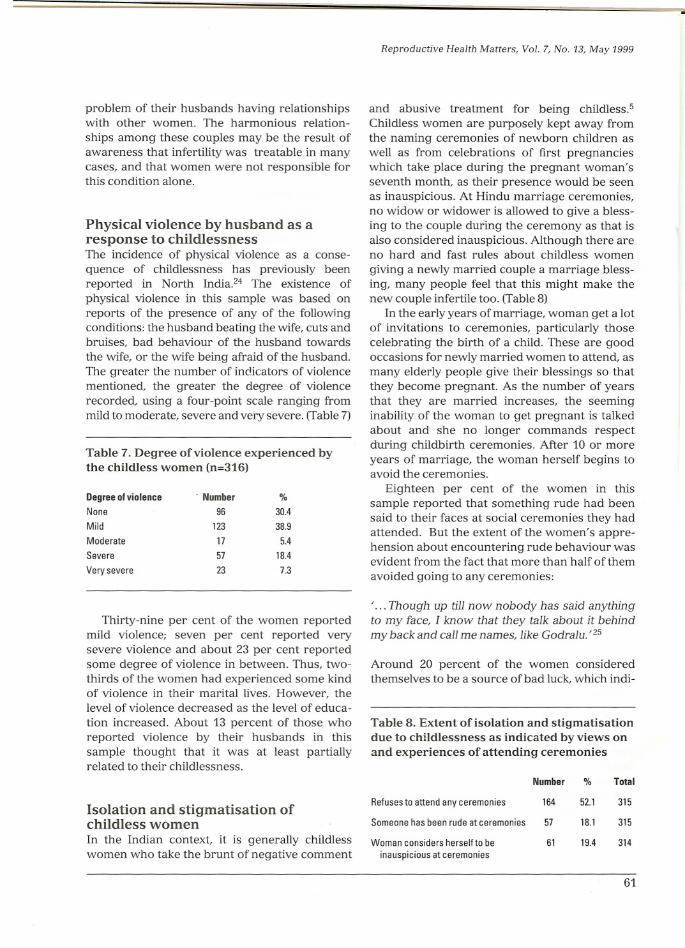
Physical violence by husband as aresponse to childlessnessThe incidence of physical violence as a consequence of childlessness has previously beenreported in North India.24 The existence ofphysical violence in this sample was based onreports of the presence of any of the followingconditions: the husband beating the wife, cuts andbruises, bad behaviour of the husband towardsthe wife, or the wife being afraid of the husband.The greater the number of ind.icators of violencementioned, the greater the degree of violencerecorded, using a four-point scale ranging frommild to moderate, severe and very severe. (Table 7)
Table 7. Degree of violence experienced bythe childless women (n=316)
Degree of violence . Number%
None
9630.4
Mild
12338.9
Moderate
175.4
Severe
5718.4
Very severe
237.3
Thirty-nine per cent of the women reportedmild violence; seven per cent reported verysevere violence and about 23 per cent reportedsome degree of violence in between. Thus, twothirds of the women had experienced some kindof violence in their marital lives. However, thelevel of violence decreased as the level of education increased. About 13 percent of those whoreported violence by their husbands in thissample thought that it was at least partiallyrelated to their childlessness.
Isolation and stigmatisation ofchildless womenIn the Indian context, it is generally childlesswomen who take the brunt of negative comment
Reproductive Health Matters, Vol. 7, No. 13, May 1999
and abusive treatment for being childless.5Childless women are purposely kept away fromthe naming ceremonies of newborn children aswell as from celebrations of first pregnancieswhich take place during the pregnant woman'sseventh month, as their presence would be seenas inauspicious. At Hindu marriage ceremonies,no widow or widower is allowed to give a blessing to the couple during the ceremony as that isalso considered inauspicious. Although there areno hard and fast rules about childless womengiving a newly married couple a marriage blessing, many people feel that this might make thenew couple infertile too. (Table 8)
In the early years of marriage, woman get a lotof invitations to ceremonies, particularly thosecelebrating the birth of a child. These are goodoccasions for newly married women to attend, asmany elderly people give their blessings so thatthey become pregnant. As the number of yearsthat they are married increases, the seeminginability of the woman to get pregnant is talkedabout and she no longer commands respectduring childbirth ceremonies. After 10 or moreyears of marriage, the woman herself begins toavoid the ceremonies.
Eighteen per cent of the women in thissample reported that something rude had beensaid to their faces at social ceremonies they hadattended. But the extent of the women's apprehension about encountering rude behaviour wasevident from the fact that more than half of themavoided going to any ceremonies:
' ... Though up tj]] now nobody has said anythingto my face, I know that they talk about it behindmy back and call me names, like Godralu.' 25
Around 20 percent of the women consideredthemselves to be a source of bad luck, which indi-
Table 8. Extent of isolation and stigmatisationdue to childlessness as indicated by views onand experiences of attending ceremonies
Number%Total
Refuses to attend any ceremonies
16452.1315
Someone has been rude at ceremonies
5718.1315
Woman considers herselfto be
6119.4314
inauspicious at ceremonies
61
.-

Unisa
cates the depth of negative social attitudes. It isnot only society that stigmatises childless women;they themselves often have very low self-esteem.
Discussion and recommendationsIn a population where there are more negativesocial, cultural and emotional repercussions forchildless women than for any other non-lifethreatening condition, it can be assumed thatalmost all cases of childlessness found are due to
physiological or biological factors. The majorityof childless women have primary infertility. Therewas a general lack of modern medical facilitiesand a lack of trained medical providers in thepublic health sector to deal with the variousfertility-related problems of these couples, at subcentre, primary health centre and communityhealth centre level alike. Because allopathic medicine was clearly the preferred type of treatmentfor a large proportion of women, they generallywent to private doctors and hospitals.
This study provides evidence that infertilewomen and couples subject themselves to manyforms of treatment for infertility over a longperiod of time, incurring quite substantial costs.The financial burden of treatment in itself meantthat many of the women avoided seeking treatment in the first place. For others, the inability toafford the high costs of private allopathic treatment makes them vulnerable 'to the offer of
ineffective and inappropriate treatments, whichcontribute to false hopes. In contrast, the strongfaith in the help of religious persons and placesand the often low cost of attending these sourcesresulted in many women opting to seek help ofthis kind as well. Problems related to infertilitymay require long-term attendance with manyvisits, in addition to the costs. Thus, many of thewomen in this study were forced to discontinuetreatment without achieving a pregnancy andwhen they would have preferred to go on.
In India, women suffer other consequencesfrom infertility too - children are the main sourceof prestige and security for women in theirhusbands' homes. For a substantial minority ofwomen in this study greater marital disharmony,possibly greater physical violence, the decisionof their husbands to take a second wife and thethreat of divorce were evident. On the otherhand, it was encouraging that marital harmonyremained high for so many of them.
62
The behaviour of the community towards thewomen because they were childless was also notsympathetic. Actual comments and anticipatednegative behaviour forced the women to becomesocial recluses in many cases, and to avoid attending any social functions for fear of something badbeing said to them at such occasions. There waslittle apparent social support for infertile womenthey are isolated and feel ashamed.
Thus, infertility has major implications forwomen's lives, in a setting where fertility is sohighly prized. These findings have obvious policyand programme implications. There is a need forcomprehensive community education that dispels myths that women are solely responsible forinfertility, that provides accurate informationabout the causes of infertility - especially the roleof sexually transmitted diseases, and informationabout where treatment for infertility is availableand the kinds of diagnosis and treatment that areeffective. In relation to the public health services,there is a clear need to incorporate diagnosis andtreatment for infertility more fully into thereproductive health programme, provide a clearreferral chain for infertile couples, and trainhealth workers to identify problems and provideinformation, timely referral and care.
AcknowledgmentsThis paper presents part of the findings of aresearch project on the 'Social and psychologicalconsequences of childlessness in the RangaReddy district of Andhra Pradesh, India', fundedby the Ford Foundation, Grant Number 9501006. The views expressed are those of the authorand do not necessarily reflect the opinions of theFord Foundation. Special thanks to John Clelandand Shireen Jejeebhoy for help at various stagesof preparation of the study, and to MiChaelKoenig and Bert Pelto for advice during thecourse of the project. Thanks also to researchassistants Monica Solanki, Ramni Murthy andMN Murthy, and the team members who helpedat the various stages of data collection, analysisand report writing. I am also indebted to thestudy respondents.
CorrespondenceSayeed Unisa, International Institute for Population Sciences, Deonar, Mumbai 400088, India. Fax:91-22-556-3257. E-mail: sunisa@bom5. vsn1.neUn
Reproductive Health Matters, Vol. 7, No. 13, May 1999
References and Notes1. Okonofua FE, Harris, Odebiyi A
et al,1997. The social meaning offertility in South Nigeria. HealthTransition Review. 7:205-20.
2. Kakar DN, 1983. Traditionalhealers in North India: a case
study. Nursing Journal of India.74(3): 61-63.
3. Among Hindus poja meansprayer and pojari is a priest.
4. Munat is a certain promise madeat Dargh (the grave of a holyman) or to a deity by someonewanting a particular wish to befulfilled. This promise must thenbe carried out upon theattainment of what is desired.
5. Jejeebhoy JS, 1994. Infertility inSouth Asia: Priorities for social
science research. Paperpresented at ReproductiveHealth Workshop, New Delhi,26 September-7 October.Organised by WHO and FordFoundation.
6. Infertility: A Technical Report.World Health Organization,Series 582, Geneva, 1975.
7. Pathak KB, Unisa S, 1993. Astudy of childlessness andinfertility from children everborn data. Project report.International Institute for
Population Sciences, Mumbai.8. National Family Health Survey
1992-93, India. InternationalInstitute for PopulationSciences, Mumbai, 1995.
9. Childlessness in this papermeans the inability to deliver alive born child. Only currentlymarried childless women were
included in the present study, aswe did no~ find any childlesswomen who were divorced orabandoned because of
childlessness. The cut-off pointsfor the selection of women asregards age and maritalduration were age 20 to 49 andthree years or more maritalduration. These were selected to
avoid the consequences ofphysical immaturity ofthe oneside and menopause on theother, as well as the time
required for women and theirhusbands to decide to seek and
start treatment after they realisethere are fertility problems.
10. Veevers JE, 1971. Childlessnessand age at first marriage. SocialBiology. 19:266-74.
11. Duncan ME et al, 1990. Firstcoitus before menarche and riskof sexually transmitted diseases.Lancet. 355:335-40.
12. Inhorn Me, Buss KA, 1994.Ethnography, epidemiology andinfertility in Egypt. SocialScience and Medicine. 39(5):67186.
13. Primary infertility means herethat couples did not conceive atany time despite cohabitationand exposure to pregnancy, andin the absence of contraceptiveuse, for a period ofthree years.
14. Larsen U, 1995. Differentials ininfertility in Cameroon andNigeria. Population Studies.49:329-46.
15. In India, traditional indigenoussystems of medicine remainpopular in spite of high growthof the modern allopathic healthsystem. These indigenous formsof treatment include Ayurvedic,homeopathy and Unani. In theAyurvedic or Ayurveda system,treatment is based on drugs, dietand exercise, and on the generalmode of living. In homeopathictreatment, the primary emphasisis on increasing the strength ofthe body's defense mechanismsthrough a holistic andindividualised approach. In theUnani system of medicine,treatment is mainly carried outwith drugs made from herbs andfrom animal and mineral
sources, which are supposed tohave specific characteristics(hot, cold, moist, dry, etc) todifferent degrees. These systemsof medicine are formally taughtat university level parallel to abachelor's degree in allopathicmedicine. Many untrainedpersons are also practising thesesystems of medicine.
16. Mysamma Devi is a local deity.17. Mahakali is a Hindu Goddess.18. The meaning of one course of
treatment is that one main
provider is visited for treatmentwith one or more visits over aperiod of time, while twocourses of treatment means
attending two differentproviders, etc. The reasons for achange of providers or sourcesof help' may be completion of thecurrent course oftreatment ordiscontinuation of that course oftreatment for whatever reason.
19. Bruckert E 1991. How frequentis unintentional childlessness in
Germany? Andrologia.23(3):245-50.
20. Sundby J, Boge R, Sonko S,1998. Infertility in Gambia:frequency and health careseeking. Social Science andMedicine. 46(7):891-99.
21. In Table 4 only the costs for thefirst course of treatment are
given, but data on costs isavailable for all the treatmentsreceived.
22. Gibson C, 1980. Childlesswomen and marital instability:re-examination of the evidence.Journal of Bio-Social Sciences.12:121-31.
23. The effects of infertility onmarital stability as shown inTable 6 are based on this
question: Sometimes when acouple is childless the husbandtalks about divorce or taking asecond wife. Has anything likethis ever happened to you?Respondents were asked to readthe following statements andmark yes or no for each: a.Husband already has one morewife (yes/no). b. Husband has arelationship with anotherwoman (yes/no). c. Husbandwants a divorce (yes/no). d.Husband talks about taking asecond wife (yes/no). When awoman answered 'no' to all ofthese, we took it as an indicationof a harmonious marital
relationship.
63

Unisa
24. Singh A, Dhaliwal LK,Kaur A,1996. Infertility in a primaryhealth center of Northern India:
a follow up study. Journal ofFamily Welfare. 42(March):51-56.
25. Godralu is from the local Telgulanguage; the literal translationis 'one who does not have eggs'.In the context of infertility, thisword has the negative
connotation of 'being useless'because one is not able to bearchildren.
ResumePar rapport au reste de l'Inde, l'Andra Pradeshenregistre une forte incidence d'infertilite. L'articleest fonde sur une etude des consequences psychosociales de l' absence d' enfant menee en 1998 dansIe district de Ranga Reddy, dans 1'Etat indien del'Andhra Pradesh, et il decrit l'etendue et les typesde traitements de l'infertilite demandes. L'etudeportait sur des femmes mariees a l'epoque, ageesde 20 ans ou plus et qui, apres au moins troisannees de mariage, n' avaient pas eu de naissancevivante; Ie taux d'infertilite etait de 5%. Beaucoups'etaient mariees jeunes et avaient epouse unproche parent. En moyenne, elles avaient commence un traitement allopathique et des visitesde lieux saints apres trois annees d'attente vaine.Vne grande majorite des femmes avait d'aborddemande un traitement allopathique et n'avaittente d'autres sortes de remedes, des prieres, desrituels et des cures traditionnelles que s'il n'avaitpas eu de resultats ou s'il coutait trop cher. Vneminorite de femmes courait un risque de divorce etde remariage de 1'epoux dans Ie but d'avoir desenfants. Les deux tiers des femmes avaient subi desviolences moderees a graves de la part de leurmari, en partie du fait de leur incapacite a procreer.Il faut de toute evidence inclure la recherche et Ietraitement en matiere d'infertilite dans Ie programme de sante genesique en Inde, et les agentsde sante doivent etre formes a renseigner lescouples et ales orienter vers les centres competents.
ResumenLa incidencia de mujeres sin hijos es muy alta enAndhra Pradesh comparada con el resto de laIndia. Vn estudio llevado a cabo en el distritoRanga Reddy, Andhra Pradesh, India, en 1998,examina las consecuencias psico-sociales de notener hijos, el grado de busqueda de tratamientopara la infecundidad y los tipos de tratamientobuscados. En el estudio se incluyeron mujeresactualmente casadas mayores de 20 alios, quienesestaban casadas desde hace tres alios por 10menossin registrar un nacimiento vivo. La tasa demujeres sin hijos era de cinco por ciento. Muchasde ellas se habian casado muy jovenes conparientes cercanos. Despues de un promedio detres alios de no lograr tener un bebe, ellasiniciaban un tratamiento alop<iticoy comenzaban avisitar lugares sagrados. La gran mayoria bus coinicialmente un tratamiento alop<itico y solorecurrio a otros tipos de tratamiento, oracion,rituales y tratamientos tradicionales si el primerono funciono 0 costa demasiado. Para una minoriade las mujeres, existia el riesgo de divorcio y elcasamiento de sus esposos con una segunda mujerpara tener hijos. Dos tercios de las mujeresexperimentaron violencia leve 0 severa de parte desus esposos, debido en parte a la falta de hijos. Esclara la necesidad de incluir la investigacion ytratamiento de la infecundidad en el programa desalud reproductiva en la India, y de entrenar a lostrabajadores de la salud a proveer informacion yrecomendar atencion especializada cuandocorresponda.
Top Related
Copyright © 2022 FDOKUMEN

