






Bahasa
Halaman
Hukum

ORIGINAL ARTICLE
Child-Report of Family Accommodation in Pediatric AnxietyDisorders: Comparison and Integration with Mother-Report
Eli R. Lebowitz • Lindsay Scharfstein •
Johnna Jones
� Springer Science+Business Media New York 2014
Abstract Reducing family accommodation (FA) may be
beneficial in cases of childhood anxiety disorders. Assess-
ment of FA has so far relied on single-informant maternal
report, which may be biased by factors including maternal
anxiety. We compared child and mother reports of FA, and
examined whether maternal anxiety moderates the associa-
tion between mother and child report. Participants were fifty
children with primary DSM-5 anxiety disorders, and their
mothers. Mother–child agreement was good for overall FA
and moderate for subdomains of FA. Mothers reported sig-
nificantly more FA than children. Maternal anxiety moder-
ated the association between mother and child report of FA,
such that the correlation was stronger in more anxious
mothers. Children agreed that FA helps them feel less anx-
ious and did not agree that parents should accommodate less.
FA is an important clinical characteristic of childhood
anxiety disorders and assessment can be enhanced through
child report and consideration of maternal anxiety.
Keywords Anxiety � Family accommodation �Parenting � Disorders of childhood � Measurement
Introduction
Anxiety disorders are the most common emotional disor-
ders of childhood [1]. If not treated successfully, anxiety
disorders cause significant short and long term impairment
and pose huge financial and societal costs through factors
such as increased school dropout, teenage childbearing,
and lost productivity in the workplace [2, 3]. Despite strong
evidence for the efficacy of cognitive-behavior therapy
(CBT) for childhood anxiety disorders, up to 50 % of
children remain symptomatic after treatment [2, 4]. Even
among children who remit during treatment, more than
one-third relapse in subsequent years [5]. It is therefore
necessary to identify factors that may lessen the likelihood
of successful treatment.
One area of research that has received considerable
attention is the role that parents play in the etiology and
maintenance of childhood anxiety disorders. The bulk of
this research has focused on parental anxiety and on par-
enting styles associated with the development of anxiety in
children. Several studies have supported a link between
anxiety in mothers and anxiety disorders in children,
showing that anxious children are more likely to have
parents that suffered from anxiety [6–8] and that mothers
with a history of anxiety disorders are more likely to have
children who have an anxiety disorder [9, 10]. Overpro-
tective parenting, hostile parenting, and low autonomy-
granting parenting have all been identified as possible
precursors to the development of child anxiety [11–17].
Despite the evidence for parental influences in the devel-
opment of child anxiety, involving parents in treatment has
not yet reliably enhanced outcomes for childhood anxiety
disorders [18–21], underscoring the need to identify addi-
tional targets for parent intervention.
Recent research has highlighted the importance of
considering how parents respond to the symptoms of an
existing anxiety disorder in a child. Children naturally look
to their parents for help when feeling distressed and parents
can become drawn into increasing involvement in a child’s
E. R. Lebowitz (&) � L. Scharfstein
Yale Child Study Center, 230 S. Frontage Rd., New Haven,
CT 06520, USA
e-mail: [email protected]
J. Jones
University of Texas, Austin, TX, USA
123
Child Psychiatry Hum Dev
DOI 10.1007/s10578-014-0491-1

symptoms, through a process known as family accommo-
dation (FA) [22, 23]. FA was first studied in obsessive–
compulsive disorder (OCD), and was shown to be highly
prevalent among the parents of children with OCD. Cal-
vocoressi et al. [23, 24] published the first studies sys-
tematically measuring FA in OCD using a clinican-
administered instrument developed for that purpose—the
Family Accommodation Scale (FAS). The FAS assesses
caregivers’ participation in behaviors related to the OCD,
and modification of family routines and schedules aimed at
avoiding or alleviating distress related to the OCD.
Numerous other studies, using both clinician-administered
and parent-report versions of the FAS have confirmed the
prevalence and importance of the FA construct [25].
Greater degrees of FA have been shown to be associated
with more severe symptoms, greater impairment and
poorer treatment outcomes for both behavioral and psy-
chopharmacological interventions [25–27].
More recently, FA has been shown to be highly pre-
valent among the parents of children with anxiety dis-
orders. Lebowitz et al. [22] assessed the parents of 75
anxious children using the Family Accommodation Scale
Anxiety (FASA), a modified FAS adapted for use with
anxiety disorders. The items on the FASA closely
resemble the FAS items used to assess FA in OCD, with
relatively minor changes that are described elsewhere in
detail [22]. Almost all parents reported engaging in FA,
and degree of FA was found to correlate positively with
the severity of the children’s anxiety symptoms. The
total number of anxiety disorders diagnoses correlated
positively with the level of FA, but only separation
anxiety was specifically associated with higher FA.
Factor analysis of the FASA identified two factors which
have also been reported for the OCD FAS items: active
participation in symptom-driven behaviors (e.g., repeat-
edly answering worried questions or sleeping next to a
child), and modification of family routines and schedules
(e.g., returning home early from work) [22, 28]. In a
separate study, Lebowitz et al. [29] compared FA in
anxiety to FA in OCD as well as non-anxious youth.
Results indicated that FA is similar in both clinical
groups and significantly higher than in the non-anxious
controls.
Reducing family accommodation may be an important
goal to address with parents in the treatment of childhood
anxiety, whether in the context of a parent-only interven-
tion or as a component delivered alongside child CBT.
Theoretically, FA is contrary to the goals of CBT and
although it is intended to reduce anxiety in the short-term
FA may lead to increased anxiety and poorer treatment
response in the longer term. One central element of CBT
for child anxiety is exposure to anxiety provoking stimuli
which the patient typically prefers to avoid [30, 31]. FA
works in the opposite direction, by facilitating ongoing
avoidance and providing the child with an alternative to
facing the fears. CBT also focuses on teaching adaptive
strategies and coping mechanisms such as cognitive
restructuring or relaxation that enable the child to deal with
anxiety and to self-regulate the distress associated with the
disorder [21, 31]. FA encourages continued reliance on
caregivers for coping with uncomfortable situations and for
the regulation of negative affect. In addition, by helping the
child to avoid having to confront the anxiety or distress,
parents who engage in a lot of FA may undermine the
child’s motivation for a challenging treatment such as
CBT. Finally, parents who engage in FA may provide the
child with putative confirmation of their fears, thereby
reducing insight into the irrational nature of the anxious
thoughts [32].
For all these reasons reducing FA may lead to reductions
in child anxiety and may increase the likelihood of suc-
cessful treatment with the child. A number of treatment
protocols already include a focus on reducing FA [33–35].
The SPACE Program is one example of a parent-based
treatment highly focused on the reduction of FA that has
shown promise in both anxiety and OCD [35, 36]. Imple-
menting and testing such treatments is predicated on
careful measurement and assessment of FA.
So far, measurement of FA in childhood anxiety has
relied on single-informant caregiver report by mothers [22,
29]. No studies in childhood anxiety (or OCD), have
included child-report of family accommodation. Measuring
FA through parent-report only may limit the accuracy of
the assessment, whereas including both parent and child
report could enhance the accuracy of the assessment and
provide important information for a number of reasons, as
discussed next.
For parents to accurately report FA they must be aware
that the changes they are making in their behavior are in
fact responses to symptoms of anxiety in the child. But
parents may not always accurately recognize symptoms of
anxiety in their child, leading to less accurate report of FA
as well. Both over-identification and under-identification
of anxiety symptoms are possible. For example, a child
with separation anxiety may become upset if her parents
do not answer their mobile phone, causing the parents to
answer more promptly even if they do not consider it to
be an accommodation of an anxiety symptom. Research
shows that children frequently become aggressive or have
temper tantrums when their symptoms are not accommo-
dated, behaviors which may lead parents to engage in
more FA even if they do not view the behavior as
expressing anxiety [37–39]. Further supporting this pos-
sibility is the low agreement that has often been reported
between parent report and child report of child anxiety
symptoms [40–44].
Child Psychiatry Hum Dev
123

In other instances parents may have an exaggerated view
of their child’s anxiety and vulnerability. For example,
parents of a child who once became upset after hearing
something disturbing on the news may be careful never to
discuss the news near him—even if the child no longer
finds it stressful. In this case they might report engaging in
FA, even if the child would not actually feel anxious were
they to behave differently and would not view the behavior
as an accommodation. Parents’ have been found to report
higher anxiety [45] and more avoidance [40] in children,
than the children report themselves, making it plausible
that some parents may engage in FA even if the child is not
feeling anxious.
Parent-report of FA could also be biased by parents’
own anxiety, or by their desire to present their behavior in
the best possible light. Research on other aspects of
parental behavior relevant to childhood anxiety has indi-
cated that such reporting biases do exist [32, 45–48]. To
cite Schwartz et al. [49] ‘‘investigators whose measures of
parental child-rearing behavior are based on ratings by
single knowledgeable informants will be operating with
scores of inadequate validity’’. Bogels and van Melick
[48] for example, collected information on parental
autonomy-granting, overprotection and rejection and
concluded that using a single informant produced unsat-
isfactory and biased measurement. They found that
mothers tended to give more positive impressions of their
own rearing behavior compared to reports from children,
and that using a multiple informant approach greatly
reduced the problem of rater bias in assessing parental
behavior.
The present study aimed to address gaps in current
knowledge by conducting the first multiple-informant study
of FA in childhood anxiety disorders, examining reports
from both mothers and children, with the following specific
objectives and hypotheses. The first objective was to
examine mother–child agreement on FA. This includes
agreement for overall FA and the more specific domains of
participation and modification, as well as distress associ-
ated with the FA, and the negative reactions exhibited by
children when not accommodated. Based on the typically
low-to-moderate agreement between mothers and children
with regard to child anxiety it was hypothesized that
agreement on FA would be moderate at best. Agreement
for the participation subscale, which focuses on more
immediately evident behaviors, was predicted to be higher
than for the modification subscale, which queries changes
to routines and schedules that a child may not readily
perceive. The second objective was to examine the role of
maternal anxiety symptoms in multiple-informant assess-
ment of FA. We hypothesized that maternal anxiety would
moderate the association between mother and child reports
of FA, such that the association would be weaker in
mothers who reported more anxiety symptoms of their
own.
This study also had one secondary objective. Because
this was the first attempt to learn about children’s percep-
tion of FA, we also wanted to gain perspective on chil-
dren’s awareness of the potentially negative outcomes of
FA and on their willingness for parents to reduce the FA.
This question has meaningful implications for shaping
interventions that aim to reduce FA. If children perceive
FA as unhelpful in the long-term they may be more easily
allied with a therapeutic intervention that aims to reduce it.
If on the other hand, they perceive FA only as helpful to
them they may resist such efforts more staunchly. Based on
clinical experience we predicted that children would
identify FA as being helpful in the short-term, but would
also acknowledge that it does not lead to reduced anxiety in
the longer term.
Method
Participants
Participants were 50 consecutive treatment-seeking chil-
dren and their mothers, presenting at a specialty anxiety
clinic in the eastern United States and meeting DSM-5 [50]
criteria for a primary anxiety disorder. Children who pre-
sented with other psychiatric disorders (including OCD)
were included in the study as long as the comorbid con-
dition was of lesser severity. Children were between the
ages of six and seventeen years (Mean = 12.3, SD = 2.9)
and 65 % were identified as female. All mothers had at
least partial high school education, and most mothers
(58.4 %) had completed higher education at the college
level. All participants were fluent English speakers and
English was the primary language spoken in 78.3 % of
homes, with the remainder having Spanish as a primary
language. Children were identified as predominantly Non-
Hispanic White (82.1 %).
Procedure
The study was approved by the University Institutional
Review Board and signed consent and assent were obtained
from all parents and children respectively, before any
additional procedures were performed.
All measures were administered at intake, prior to the
start of treatment. Children completed questionnaires while
the mother was being interviewed, and vice versa. Child
questionnaires were administered in the presence of a
research assistant who was trained to answer questions and
clarify questionnaire items when necessary. Training
Child Psychiatry Hum Dev
123

included role-play in answering questions without biasing
child report, and learning answers to frequent questions
such as the meaning of difficult words.
Measures
Child Anxiety Diagnoses and Symptoms
Anxiety disorders interview schedule—children and parent
(ADIS C/P) [51]. The presence of a primary DSM-5 anx-
iety disorder diagnosis was established using the ADIS
C/P, administered separately to the child and the mother.
The ADIS C/P is a semi-structured interview with good to
excellent reliability for establishing diagnoses, and strong
correspondence with anxiety questionnaire ratings [51, 52].
Because the DSM-5 version of ADIS C/P is not yet
available, the DSM IV version was administered and
diagnoses were established according to DSM-5 criteria
(which closely resemble those in DSM IV for anxiety
disorders). The ADIS C/P was administered by graduate
level clinicians or licensed psychologists, trained in its use
by one of the instrument’s authors. Training included
observing live and videotaped samples, supervised
administration, and discussion of initial discrepancies. In
line with earlier research, in cases of discordance between
parent and child reports the clinician considered both
informants’ views to derive a final diagnosis [53, 54].
Decisions regarding diagnoses were made in consultation
with clinical psychologists, highly experienced in the
treatment and research of childhood anxiety.
Multidimensional anxiety scale for children (MASC2)
[55]. Mothers and children completed respective versions of
the 2nd edition MASC. MASC2 is a revision of the original
MASC and is a 50-item measure of anxiety in children.
Each item is scored on a 4-point Likert-type scale from 0 to
3 (‘Never’ to ‘Often’). MASC2 provides an overall anxiety
score based on all 50 items (range 0–150) and subscales for
specific domains of anxiety including the following: sepa-
ration anxiety (9 items; range 0–27), social anxiety (9 items;
range 0–27), physical symptoms (12 items; range 0–36),
harm avoidance (8 items; range 0–24), generalized anxiety
(10 items; range 0–30), and anxiety related to obsessive
compulsive symptoms (10 items; range 0–30). Normative
samples include 1,800 children representative of US chil-
dren in terms of ethnicity/race, gender, and age. The
MASC2 maintains the critical elements of the MASC [56]
and adds the subscales for generalized anxiety and OCD.
Internal consistency for the child MASC2 total score was
excellent (a = 0.95), and fair to excellent for the subscale
scores (a scores ranged from 0.72 to 0.88). Internal con-
sistency for the mother MASC2 total score was excellent
(a = 0.91) and acceptable to good for the subscale scores
(a scores ranged from 0.68 to 0.83).
Family Accommodation
Family accommodation scale anxiety (FASA) [22]. Moth-
ers completed the FASA which was previously adapted
from items used to measure FA in OCD [23, 24]. The
FASA includes 13 items rated on a 5-point Likert-type
scale from 0-to-4. FASA yields an overall Accommodation
score (9 items; range 0–36), and subscale scores for Par-
ticipation (5 items, range 0–20), Modification (4 items;
range 0–16), Distress (1 item; range 0–4), and Conse-
quences (3 items; range 0–12). The FASA has good
internal consistency and convergent and divergent validity
and is sensitive to detecting family accommodation among
various childhood anxiety disorders [22, 29]. In the current
sample internal consistency was good: a = 0.88 for the 9
accommodation items, a = 0.80 for the Participation sub-
scale, a = 0.85 for the Modification subscale, and
a = 0.87 for the Consequence subscale.
Family accommodation scale anxiety—child report
(FASA-CR) Children completed the FASA-CR, a modified
version of the FASA adapted for use with children. Items
were rephrased so that a child could respond about the
parents’ FA. For example, the parent item ‘How often did
you assist your child in avoiding things that might make
him/her more anxious?’ was rephrased to say: ‘How often
did your parent help you to avoid things that make you feel
anxious’. FASA-CR yields the same scores as FASA and is
scored the same way: an overall Accommodation score (9
items; range 0–36), and subscale scores for Participation (5
items, range 0–20), Modification (4 items; range 0–16),
Distress (1 item; range 0–4), and Consequences (3 items;
range 0–12).
The items for FASA-CR were piloted with preliminary
samples of anxious children in two anxiety specialty clinics
(N = 30). Children first completed the scale and were then
asked questions to ascertain their comprehension of the
items and were then given the opportunity to provide
additional feedback. The items were then revised and re-
piloted with another sample until satisfactory results were
achieved including internal consistency greater than
a = 0.8 for the nine accommodation items, no reports from
children of items being hard to comprehend, and children
demonstrating being able to describe the meaning of the
questions in their own words. Internal consistency in the
current sample was acceptable to good: a = 0.85 for the
nine accommodation items, a = 0.75 for the Participation
subscale and a = 0.73 for the Modification subscale, and
a = 0.86 for the Consequence subscale.
In addition to the 13 items that parallel those on the
FASA, 3 other items were added to FASA-CR to better get
at children’s thoughts and beliefs regarding the FA. These
three items included: ‘When my parent helps me in this
way, I feel less anxious’; ‘If my parent continues to help
Child Psychiatry Hum Dev
123

me in these ways, I will feel less anxious in the future’; and
‘I believe my parent should help me less in these ways,
when I’m anxious’. Children rated their agreement or
disagreement with each item on a 5-point scale. These
items are not included in the scoring for FASA-CR.
Maternal Anxiety Symptoms
Beck anxiety inventory (BAI) [57]. Mothers completed the
BAI, a 21 item scale that queries symptoms of anxiety in
adults. Items include cognitive (e.g., ‘fear of dying’; ‘fear
of worst happening’), physical (e.g., ‘face flushed’; ‘heart
pounding’) and emotional (e.g., ‘terrified or afraid’) aspects
of anxiety. Mothers indicated the degree to which they
were bothered by each item in the past month on a 4-point
scale from 0 to 3 (from ‘Not at all’ to ‘Severely—it
bothered me a lot’). Possible scores range from 0 to 63.
Good psychometric properties have been reported for the
BAI [57] and internal consistency in the current sample
was excellent (a = 0.96).
Data Analytic Plan
Intra-class correlation coefficients (ICC) and Pearson r
correlations were used to examine the level of agreement
between mother and child report of FA, and paired sample
t tests were used to test the significance of differences
between mother and child reports. The intra-class correla-
tion coefficient was calculated using a two-way mixed
effect model where the sample of children is random but
the raters are fixed, and testing for absolute agreement.
Bivariate Pearson r correlations were also used to examine
the associations between reports of FA and reports of child
anxiety symptoms.
To test the hypothesis that maternal anxiety moderates
the association between mother and child report of FA we
first conducted a hierarchical multiple linear regression,
with child report of FA as the predicted variable. In the first
step we included mothers’ report of FA and maternal
anxiety as measured by BAI. In the second step we added
the interaction term equal to the product of mothers’ report
of FA and maternal anxiety scores. Variables were centered
prior to the analysis to decrease collinearity [58]. Signifi-
cant change in explained variance in child report of FA
when the interaction term is included provides evidence of
moderation. We then used the Process macro for SPSS [59]
to calculate simple slopes for the association between
mothers’ report of FA and children’s report of FA for low
(1 SD below the mean), moderate (mean) and high (1 SD
above the mean) levels of maternal anxiety, and calculated
95 % confidence intervals for the effect sizes based on
bootstrapping procedures with 1,000 samples.
The secondary objective of gaining perspective on
children’s beliefs about FA was addressed by examining
the distribution of children’s responses to the three addi-
tional items added to FASA-CR.
Results
Children met DSM-5 [50] criteria for a primary diagnosis
of either generalized anxiety disorder (34 %), social phobia
(30 %), separation anxiety disorder (24 %), specific phobia
(6 %), or panic disorder (6 %). The average number of
anxiety diagnoses was 2.9 (SD = 1.31), and ranged from 1
to 5. Non-anxiety disorder comorbidity included: depres-
sion (32 %), OCD (12 %), attention deficit hyperactivity
disorder (16 %), and oppositional defiant disorder (8 %).
Males and females did not differ significantly on any of the
study variables, though average age was somewhat
younger for boys (Mean = 10.46) than for girls
(Mean = 13.29), t = 3.15, p \ 0.01.
Severity of child anxiety symptoms based on parent-
report MASC2 scores in the current sample ranged from 18
to 137 (Mean = 66.97; SD = 23.56) and based on child-
report ranged from 8 to 130 (Mean = 74.26; SD = 29.47).
Maternal anxiety scores as measured with the BAI ranged
from 0 to 59 (Mean = 9.95; SD = 11.94).
Comparing Mother and Child Ratings of Family
Accommodation
Table 1 summarizes and compares mother and child
reported FA. Both mothers and children reported highly
prevalent FA. All mothers (100 %) and almost all children
(96.3 %) reported at least one form of active participation
in the child’s symptom-driven behaviors. Almost all
mothers (92.7 %) and approximately two-thirds of children
(70.4 %) reported modifications to family routines and
schedules tied to the child’s anxiety symptoms. Mothers
and children agreed that providing reassurance was the
most frequent form of FA.
Agreement between mothers and children with regard to
FA variables ranged from good for the total accommoda-
tion score based on all nine accommodation items, to fair
for the modification and participation subscales, to poor for
the distress and consequence items (Table 1). Mothers’
scores on the FASA, including total accommodation score
and the participation and modification subscales, were
significantly higher than children’s scores.
Pearson correlation coefficients, after correcting for
multiple comparisons, indicated significant positive corre-
lations between mother and child report of total FA and the
participation and modification subscales. Mother and child
Child Psychiatry Hum Dev
123
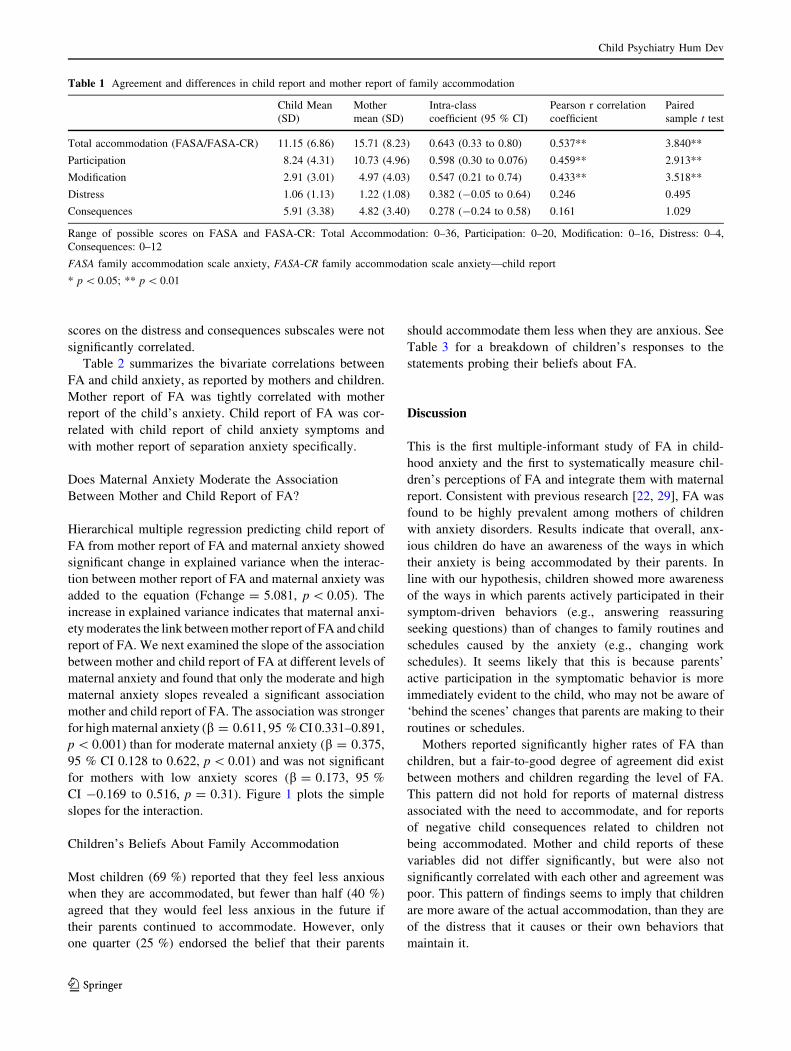
scores on the distress and consequences subscales were not
significantly correlated.
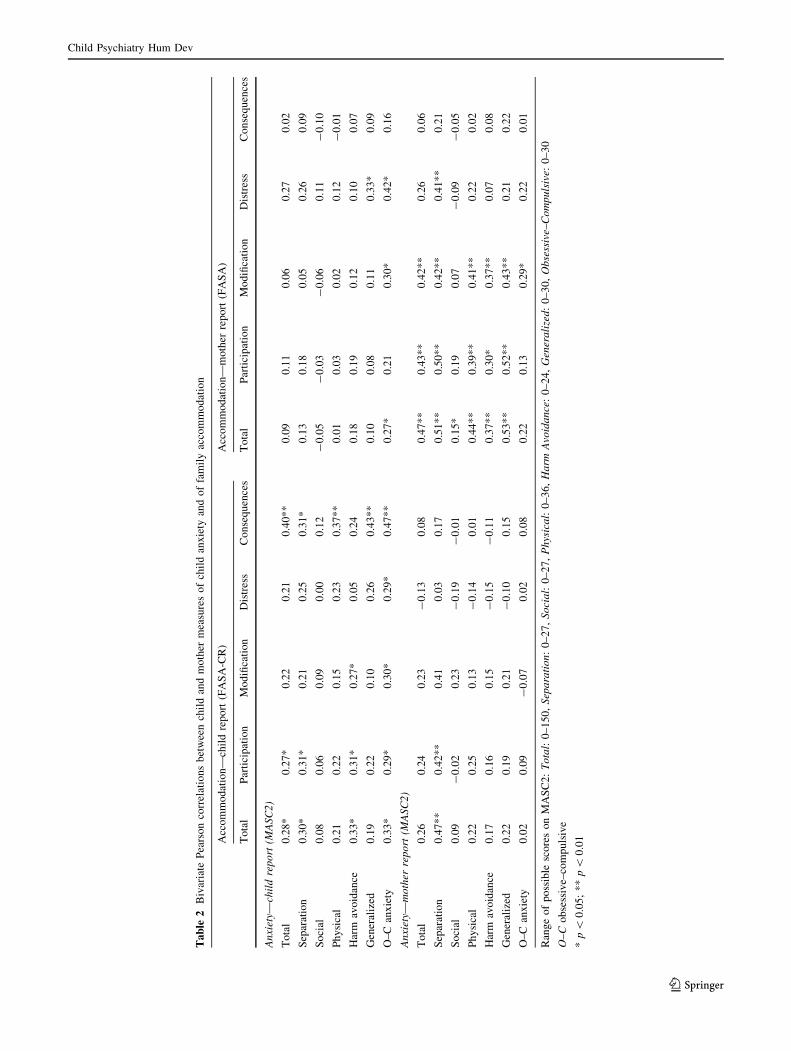
Table 2 summarizes the bivariate correlations between
FA and child anxiety, as reported by mothers and children.
Mother report of FA was tightly correlated with mother
report of the child’s anxiety. Child report of FA was cor-
related with child report of child anxiety symptoms and
with mother report of separation anxiety specifically.
Does Maternal Anxiety Moderate the Association
Between Mother and Child Report of FA?
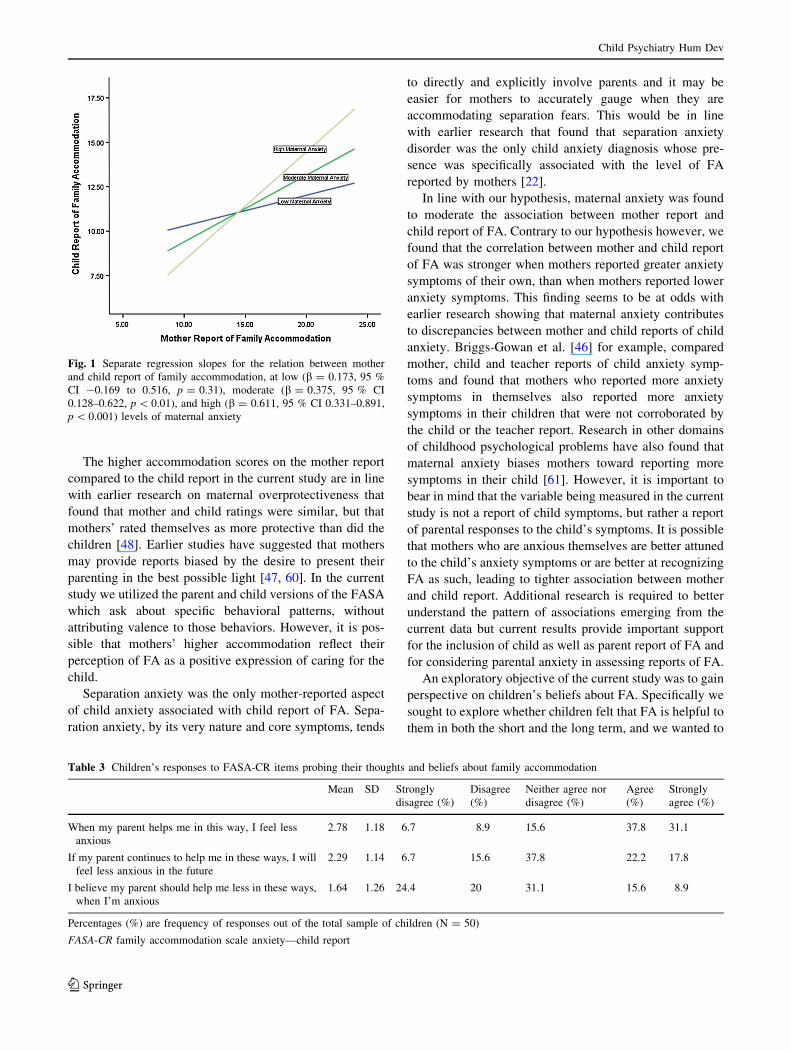
Hierarchical multiple regression predicting child report of
FA from mother report of FA and maternal anxiety showed
significant change in explained variance when the interac-
tion between mother report of FA and maternal anxiety was
added to the equation (Fchange = 5.081, p \ 0.05). The
increase in explained variance indicates that maternal anxi-
ety moderates the link between mother report of FA and child
report of FA. We next examined the slope of the association
between mother and child report of FA at different levels of
maternal anxiety and found that only the moderate and high
maternal anxiety slopes revealed a significant association
mother and child report of FA. The association was stronger
for high maternal anxiety (b = 0.611, 95 % CI 0.331–0.891,
p \ 0.001) than for moderate maternal anxiety (b = 0.375,
95 % CI 0.128 to 0.622, p \ 0.01) and was not significant
for mothers with low anxiety scores (b = 0.173, 95 %
CI -0.169 to 0.516, p = 0.31). Figure 1 plots the simple
slopes for the interaction.
Children’s Beliefs About Family Accommodation
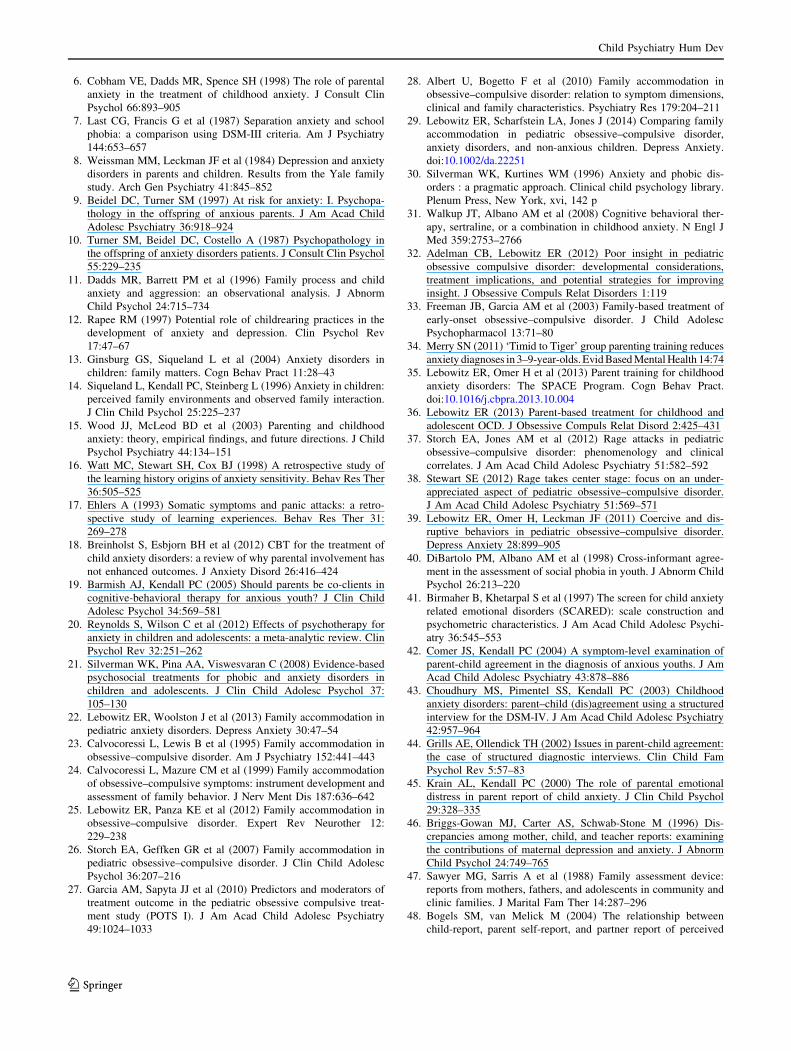
Most children (69 %) reported that they feel less anxious
when they are accommodated, but fewer than half (40 %)
agreed that they would feel less anxious in the future if
their parents continued to accommodate. However, only
one quarter (25 %) endorsed the belief that their parents
should accommodate them less when they are anxious. See
Table 3 for a breakdown of children’s responses to the
statements probing their beliefs about FA.
Discussion
This is the first multiple-informant study of FA in child-
hood anxiety and the first to systematically measure chil-
dren’s perceptions of FA and integrate them with maternal
report. Consistent with previous research [22, 29], FA was
found to be highly prevalent among mothers of children
with anxiety disorders. Results indicate that overall, anx-
ious children do have an awareness of the ways in which
their anxiety is being accommodated by their parents. In
line with our hypothesis, children showed more awareness
of the ways in which parents actively participated in their
symptom-driven behaviors (e.g., answering reassuring
seeking questions) than of changes to family routines and
schedules caused by the anxiety (e.g., changing work
schedules). It seems likely that this is because parents’
active participation in the symptomatic behavior is more
immediately evident to the child, who may not be aware of
‘behind the scenes’ changes that parents are making to their
routines or schedules.
Mothers reported significantly higher rates of FA than
children, but a fair-to-good degree of agreement did exist
between mothers and children regarding the level of FA.
This pattern did not hold for reports of maternal distress
associated with the need to accommodate, and for reports
of negative child consequences related to children not
being accommodated. Mother and child reports of these
variables did not differ significantly, but were also not
significantly correlated with each other and agreement was
poor. This pattern of findings seems to imply that children
are more aware of the actual accommodation, than they are
of the distress that it causes or their own behaviors that
maintain it.
Table 1 Agreement and differences in child report and mother report of family accommodation
Child Mean
(SD)
Mother
mean (SD)
Intra-class
coefficient (95 % CI)
Pearson r correlation
coefficient
Paired
sample t test
Total accommodation (FASA/FASA-CR) 11.15 (6.86) 15.71 (8.23) 0.643 (0.33 to 0.80) 0.537** 3.840**
Participation 8.24 (4.31) 10.73 (4.96) 0.598 (0.30 to 0.076) 0.459** 2.913**
Modification 2.91 (3.01) 4.97 (4.03) 0.547 (0.21 to 0.74) 0.433** 3.518**
Distress 1.06 (1.13) 1.22 (1.08) 0.382 (-0.05 to 0.64) 0.246 0.495
Consequences 5.91 (3.38) 4.82 (3.40) 0.278 (-0.24 to 0.58) 0.161 1.029
Range of possible scores on FASA and FASA-CR: Total Accommodation: 0–36, Participation: 0–20, Modification: 0–16, Distress: 0–4,
Consequences: 0–12
FASA family accommodation scale anxiety, FASA-CR family accommodation scale anxiety—child report
* p \ 0.05; ** p \ 0.01
Child Psychiatry Hum Dev
123
Ta
ble
2B
ivar
iate
Pea
rso
nco
rrel
atio
ns
bet
wee
nch
ild
and
mo
ther
mea
sure
so
fch
ild
anx
iety
and
of
fam
ily
acco
mm
od
atio
n
Acc
om
mo
dat
ion
—ch
ild
rep
ort
(FA
SA
-CR
)A
cco
mm
od
atio
n—
mo
ther
rep
ort
(FA
SA
)
To
tal
Par
tici
pat
ion
Mo
difi
cati
on
Dis
tres
sC
on
seq
uen
ces
To
tal
Par
tici
pat
ion
Mo
difi
cati
on
Dis
tres
sC
on
seq
uen
ces
An
xiet
y—ch
ild
rep
ort
(MA
SC
2)
To
tal
0.2
8*
0.2
7*
0.2
20
.21
0.4
0*
*0
.09
0.1
10
.06
0.2
70
.02
Sep
arat
ion
0.3
0*
0.3
1*
0.2
10
.25
0.3
1*
0.1
30
.18
0.0
50
.26
0.0
9
So
cial
0.0
80
.06
0.0
90
.00
0.1
2-
0.0
5-
0.0
3-
0.0
60
.11
-0
.10
Ph
ysi
cal
0.2
10
.22
0.1
50
.23
0.3
7*
*0
.01
0.0
30
.02
0.1
2-
0.0
1
Har
mav
oid
ance
0.3
3*
0.3
1*
0.2
7*
0.0
50
.24
0.1
80
.19
0.1
20
.10
0.0
7
Gen
eral
ized
0.1
90
.22
0.1
00
.26
0.4
3*
*0
.10
0.0
80
.11
0.3
3*
0.0
9
O–
Can
xie
ty0
.33
*0
.29
*0
.30
*0
.29
*0
.47
**
0.2
7*
0.2
10
.30
*0
.42
*0
.16
An
xiet
y—m
oth
erre
po
rt(M
AS
C2
)
To
tal
0.2
60
.24
0.2
3-
0.1
30
.08
0.4
7*
*0
.43
**
0.4
2*
*0
.26
0.0
6
Sep
arat
ion
0.4
7*
*0
.42
**
0.4
10
.03
0.1
70
.51
**
0.5
0*
*0
.42
**
0.4
1*
*0
.21
So
cial
0.0
9-
0.0
20
.23
-0
.19
-0
.01
0.1
5*
0.1
90
.07
-0
.09
-0
.05
Ph
ysi
cal
0.2
20
.25
0.1
3-
0.1
40
.01
0.4
4*
*0
.39
**
0.4
1*
*0
.22
0.0
2
Har
mav
oid
ance
0.1
70
.16
0.1
5-
0.1
5-
0.1
10
.37
**
0.3
0*
0.3
7*
*0
.07
0.0
8
Gen
eral
ized
0.2
20
.19
0.2
1-
0.1
00
.15
0.5
3*
*0
.52
**
0.4
3*
*0
.21
0.2
2
O–
Can
xie
ty0
.02
0.0
9-
0.0
70
.02
0.0
80
.22
0.1
30
.29
*0
.22
0.0
1
Ran
ge
of
po
ssib
lesc
ore
so
nM
AS
C2
:T
ota
l:0
–1
50
,S
epa
rati
on
:0
–2
7,
So
cia
l:0
–2
7,
Ph
ysic
al:
0–
36
,H
arm
Avo
ida
nce
:0
–2
4,
Gen
era
lize
d:
0–
30
,O
bse
ssiv
e–C
om
pu
lsiv
e:0
–3
0
O–
Co
bse
ssiv
e–co
mp
uls
ive
*p\
0.0
5;
**
p\
0.0
1
Child Psychiatry Hum Dev
123
The higher accommodation scores on the mother report
compared to the child report in the current study are in line
with earlier research on maternal overprotectiveness that
found that mother and child ratings were similar, but that
mothers’ rated themselves as more protective than did the
children [48]. Earlier studies have suggested that mothers
may provide reports biased by the desire to present their
parenting in the best possible light [47, 60]. In the current
study we utilized the parent and child versions of the FASA
which ask about specific behavioral patterns, without
attributing valence to those behaviors. However, it is pos-
sible that mothers’ higher accommodation reflect their
perception of FA as a positive expression of caring for the
child.
Separation anxiety was the only mother-reported aspect
of child anxiety associated with child report of FA. Sepa-
ration anxiety, by its very nature and core symptoms, tends
to directly and explicitly involve parents and it may be
easier for mothers to accurately gauge when they are
accommodating separation fears. This would be in line
with earlier research that found that separation anxiety
disorder was the only child anxiety diagnosis whose pre-
sence was specifically associated with the level of FA
reported by mothers [22].
In line with our hypothesis, maternal anxiety was found
to moderate the association between mother report and
child report of FA. Contrary to our hypothesis however, we
found that the correlation between mother and child report
of FA was stronger when mothers reported greater anxiety
symptoms of their own, than when mothers reported lower
anxiety symptoms. This finding seems to be at odds with
earlier research showing that maternal anxiety contributes
to discrepancies between mother and child reports of child
anxiety. Briggs-Gowan et al. [46] for example, compared
mother, child and teacher reports of child anxiety symp-
toms and found that mothers who reported more anxiety
symptoms in themselves also reported more anxiety
symptoms in their children that were not corroborated by
the child or the teacher report. Research in other domains
of childhood psychological problems have also found that
maternal anxiety biases mothers toward reporting more
symptoms in their child [61]. However, it is important to
bear in mind that the variable being measured in the current
study is not a report of child symptoms, but rather a report
of parental responses to the child’s symptoms. It is possible
that mothers who are anxious themselves are better attuned
to the child’s anxiety symptoms or are better at recognizing
FA as such, leading to tighter association between mother
and child report. Additional research is required to better
understand the pattern of associations emerging from the
current data but current results provide important support
for the inclusion of child as well as parent report of FA and
for considering parental anxiety in assessing reports of FA.
An exploratory objective of the current study was to gain
perspective on children’s beliefs about FA. Specifically we
sought to explore whether children felt that FA is helpful to
them in both the short and the long term, and we wanted to
Fig. 1 Separate regression slopes for the relation between mother
and child report of family accommodation, at low (b = 0.173, 95 %
CI -0.169 to 0.516, p = 0.31), moderate (b = 0.375, 95 % CI
0.128–0.622, p \ 0.01), and high (b = 0.611, 95 % CI 0.331–0.891,
p \ 0.001) levels of maternal anxiety
Table 3 Children’s responses to FASA-CR items probing their thoughts and beliefs about family accommodation
Mean SD Strongly
disagree (%)
Disagree
(%)
Neither agree nor
disagree (%)
Agree
(%)
Strongly
agree (%)
When my parent helps me in this way, I feel less
anxious
2.78 1.18 6.7 8.9 15.6 37.8 31.1
If my parent continues to help me in these ways, I will
feel less anxious in the future
2.29 1.14 6.7 15.6 37.8 22.2 17.8
I believe my parent should help me less in these ways,
when I’m anxious
1.64 1.26 24.4 20 31.1 15.6 8.9
Percentages (%) are frequency of responses out of the total sample of children (N = 50)
FASA-CR family accommodation scale anxiety—child report
Child Psychiatry Hum Dev
123

know whether children believed their parents should
accommodate them less or not. Children agreed that FA
helps them to feel better when they feel anxious, but were
less likely to endorse the statement that ongoing FA would
cause them to feel less anxious in the future. This implies that
the children have realized that FA provides immediate
symptom alleviation but does not bring about an overall
improvement in their anxiety. Despite this, only one quarter
of the children agreed with the statement that their parents
should accommodate them less. One possibility is that
despite recognizing that FA is not an adequate long-term
strategy, children are too anxious at the prospect of reduced
FA to agree that their parents should accommodate less.
The results of the current study must be considered in
light of certain limitations. First, only mothers were
included as the parent-participant in this study. Mothers
were chosen because they have been the informants in
earlier studies of FA in anxiety [22, 29], but inclusion of
fathers, or potentially siblings, as additional informants
may further enhance the measurement of FA and help to
understand the dynamics surrounding childhood anxiety. A
second limitation, inherent in the cross-sectional nature of
the study, is the inability to surmise the causal pathways
linking maternal anxiety, child anxiety, and FA. The
multivariate relations between these variables raise the
possibility of causal links such as parent anxiety leading to
more FA which in turn may lead to increased child anxiety.
Longitudinal studies of FA, and of other parental patterns
that have been linked to child anxiety, are needed to
advance the understanding of these causal pathways. These
limitations notwithstanding the current study provides the
first multiple-informant study of FA, provides new insight
into children’s perceptions of FA and highlights the role of
maternal anxiety in assessment of FA.
Clinical Implications
Identifying family-level constructs that may contribute to the
maintenance of childhood anxiety, or lower the likelihood of
successful treatment, is of prime importance. FA is one such
construct that has only recently begun to be systematically
measured in childhood anxiety. Results of the current study
indicate that assessment of FA may be enhanced through the
use of multiple informants and that children are able to
provide such measurement using the FASA-CR. In particu-
lar, the current results indicate that parental variables such as
maternal anxiety may interact to influence parental reporting
of FA. Careful assessment of child anxiety should likely
include both parent and child measurement of FA, and cli-
nicians can integrate the responses to arrive at the most
accurate clinical characterization.
Parent-based interventions that help parents to better
identify and reduce FA are currently being explored. One
such intervention, The SPACE Program, has reported
improvement in child anxiety symptoms after parents
practice monitoring and reducing FA [35, 36]. Improving
assessment of FA may help to better identify those cases
most likely to benefit from such treatments.
The current results support our clinical experience that
children often oppose efforts aimed at reducing FA.
Therapists should not assume that children will collaborate
with such a process and parents need to be prepared for
children to resist their efforts at reducing FA. However, the
current results also imply that many children do realize that
FA will ultimately not bring about improvement in their
symptoms. It may be possible through clinical work to
engage children in a process that is intended to provide
more long term alleviation of their anxiety.
Summary
This study assessed child reported FA using a modified
version of the FASA and compared mother and child
reports of FA. The study also tested the hypothesis that
maternal anxiety would moderate agreement between child
and mother reports of FA. Finally, the study provides a
preliminary examination of children’s beliefs regarding FA
of their anxiety. Children and mothers both reported highly
prevalent FA and mother report correlated significantly
with child report, though mothers reported significantly
greater FA than children. Maternal anxiety moderated the
association between mother and child report of FA, such
that agreement was higher for mothers who reported
greater anxiety of their own. Children agreed that FA helps
them to feel less anxious and did not agree that their par-
ents should accommodate less. FA is an important clinical
characteristic of childhood anxiety disorders and careful
assessment should include parent as well as child report.
References
1. Costello EJ, Egger HL, Angold A (2005) The developmental epi-
demiology of anxiety disorders: phenomenology, prevalence, and
comorbidity. Child Adolesc Psychiatr Clin N Am 14:631–648, vii
2. Compton SN, March JS et al (2004) Cognitive-behavioral psy-
chotherapy for anxiety and depressive disorders in children and
adolescents: an evidence-based medicine review. J Am Acad
Child Adolesc Psychiatry 43:930–959
3. Greenberg PE, Sisitsky T et al (1999) The economic burden of
anxiety disorders in the 1990s. J Clin Psychiatry 60:427–435
4. Rapee RM, Schniering CA, Hudson JL (2009) Anxiety disorders
during childhood and adolescence: origins and treatment. Annu
Rev Clin Psychol 5:311–341
5. Ginsburg GS, Becker EM et al (2014) Naturalistic follow-up of
youths treated for pediatric anxiety disorders. JAMA Psychiatry
71:310–318
Child Psychiatry Hum Dev
123
6. Cobham VE, Dadds MR, Spence SH (1998) The role of parental
anxiety in the treatment of childhood anxiety. J Consult Clin
Psychol 66:893–905
7. Last CG, Francis G et al (1987) Separation anxiety and school
phobia: a comparison using DSM-III criteria. Am J Psychiatry
144:653–657
8. Weissman MM, Leckman JF et al (1984) Depression and anxiety
disorders in parents and children. Results from the Yale family
study. Arch Gen Psychiatry 41:845–852
9. Beidel DC, Turner SM (1997) At risk for anxiety: I. Psychopa-
thology in the offspring of anxious parents. J Am Acad Child
Adolesc Psychiatry 36:918–924
10. Turner SM, Beidel DC, Costello A (1987) Psychopathology in
the offspring of anxiety disorders patients. J Consult Clin Psychol
55:229–235
11. Dadds MR, Barrett PM et al (1996) Family process and child
anxiety and aggression: an observational analysis. J Abnorm
Child Psychol 24:715–734
12. Rapee RM (1997) Potential role of childrearing practices in the
development of anxiety and depression. Clin Psychol Rev
17:47–67
13. Ginsburg GS, Siqueland L et al (2004) Anxiety disorders in
children: family matters. Cogn Behav Pract 11:28–43
14. Siqueland L, Kendall PC, Steinberg L (1996) Anxiety in children:
perceived family environments and observed family interaction.
J Clin Child Psychol 25:225–237
15. Wood JJ, McLeod BD et al (2003) Parenting and childhood
anxiety: theory, empirical findings, and future directions. J Child
Psychol Psychiatry 44:134–151
16. Watt MC, Stewart SH, Cox BJ (1998) A retrospective study of
the learning history origins of anxiety sensitivity. Behav Res Ther
36:505–525
17. Ehlers A (1993) Somatic symptoms and panic attacks: a retro-
spective study of learning experiences. Behav Res Ther 31:
269–278
18. Breinholst S, Esbjorn BH et al (2012) CBT for the treatment of
child anxiety disorders: a review of why parental involvement has
not enhanced outcomes. J Anxiety Disord 26:416–424
19. Barmish AJ, Kendall PC (2005) Should parents be co-clients in
cognitive-behavioral therapy for anxious youth? J Clin Child
Adolesc Psychol 34:569–581
20. Reynolds S, Wilson C et al (2012) Effects of psychotherapy for
anxiety in children and adolescents: a meta-analytic review. Clin
Psychol Rev 32:251–262
21. Silverman WK, Pina AA, Viswesvaran C (2008) Evidence-based
psychosocial treatments for phobic and anxiety disorders in
children and adolescents. J Clin Child Adolesc Psychol 37:
105–130
22. Lebowitz ER, Woolston J et al (2013) Family accommodation in
pediatric anxiety disorders. Depress Anxiety 30:47–54
23. Calvocoressi L, Lewis B et al (1995) Family accommodation in
obsessive–compulsive disorder. Am J Psychiatry 152:441–443
24. Calvocoressi L, Mazure CM et al (1999) Family accommodation
of obsessive–compulsive symptoms: instrument development and
assessment of family behavior. J Nerv Ment Dis 187:636–642
25. Lebowitz ER, Panza KE et al (2012) Family accommodation in
obsessive–compulsive disorder. Expert Rev Neurother 12:
229–238
26. Storch EA, Geffken GR et al (2007) Family accommodation in
pediatric obsessive–compulsive disorder. J Clin Child Adolesc
Psychol 36:207–216
27. Garcia AM, Sapyta JJ et al (2010) Predictors and moderators of
treatment outcome in the pediatric obsessive compulsive treat-
ment study (POTS I). J Am Acad Child Adolesc Psychiatry
49:1024–1033
28. Albert U, Bogetto F et al (2010) Family accommodation in
obsessive–compulsive disorder: relation to symptom dimensions,
clinical and family characteristics. Psychiatry Res 179:204–211
29. Lebowitz ER, Scharfstein LA, Jones J (2014) Comparing family
accommodation in pediatric obsessive–compulsive disorder,
anxiety disorders, and non-anxious children. Depress Anxiety.
doi:10.1002/da.22251
30. Silverman WK, Kurtines WM (1996) Anxiety and phobic dis-
orders : a pragmatic approach. Clinical child psychology library.
Plenum Press, New York, xvi, 142 p
31. Walkup JT, Albano AM et al (2008) Cognitive behavioral ther-
apy, sertraline, or a combination in childhood anxiety. N Engl J
Med 359:2753–2766
32. Adelman CB, Lebowitz ER (2012) Poor insight in pediatric
obsessive compulsive disorder: developmental considerations,
treatment implications, and potential strategies for improving
insight. J Obsessive Compuls Relat Disorders 1:119
33. Freeman JB, Garcia AM et al (2003) Family-based treatment of
early-onset obsessive–compulsive disorder. J Child Adolesc
Psychopharmacol 13:71–80
34. Merry SN (2011) ‘Timid to Tiger’ group parenting training reduces
anxiety diagnoses in 3–9-year-olds. Evid Based Mental Health 14:74
35. Lebowitz ER, Omer H et al (2013) Parent training for childhood
anxiety disorders: The SPACE Program. Cogn Behav Pract.
doi:10.1016/j.cbpra.2013.10.004
36. Lebowitz ER (2013) Parent-based treatment for childhood and
adolescent OCD. J Obsessive Compuls Relat Disord 2:425–431
37. Storch EA, Jones AM et al (2012) Rage attacks in pediatric
obsessive–compulsive disorder: phenomenology and clinical
correlates. J Am Acad Child Adolesc Psychiatry 51:582–592
38. Stewart SE (2012) Rage takes center stage: focus on an under-
appreciated aspect of pediatric obsessive–compulsive disorder.
J Am Acad Child Adolesc Psychiatry 51:569–571
39. Lebowitz ER, Omer H, Leckman JF (2011) Coercive and dis-
ruptive behaviors in pediatric obsessive–compulsive disorder.
Depress Anxiety 28:899–905
40. DiBartolo PM, Albano AM et al (1998) Cross-informant agree-
ment in the assessment of social phobia in youth. J Abnorm Child
Psychol 26:213–220
41. Birmaher B, Khetarpal S et al (1997) The screen for child anxiety
related emotional disorders (SCARED): scale construction and
psychometric characteristics. J Am Acad Child Adolesc Psychi-
atry 36:545–553
42. Comer JS, Kendall PC (2004) A symptom-level examination of
parent-child agreement in the diagnosis of anxious youths. J Am
Acad Child Adolesc Psychiatry 43:878–886
43. Choudhury MS, Pimentel SS, Kendall PC (2003) Childhood
anxiety disorders: parent–child (dis)agreement using a structured
interview for the DSM-IV. J Am Acad Child Adolesc Psychiatry
42:957–964
44. Grills AE, Ollendick TH (2002) Issues in parent-child agreement:
the case of structured diagnostic interviews. Clin Child Fam
Psychol Rev 5:57–83
45. Krain AL, Kendall PC (2000) The role of parental emotional
distress in parent report of child anxiety. J Clin Child Psychol
29:328–335
46. Briggs-Gowan MJ, Carter AS, Schwab-Stone M (1996) Dis-
crepancies among mother, child, and teacher reports: examining
the contributions of maternal depression and anxiety. J Abnorm
Child Psychol 24:749–765
47. Sawyer MG, Sarris A et al (1988) Family assessment device:
reports from mothers, fathers, and adolescents in community and
clinic families. J Marital Fam Ther 14:287–296
48. Bogels SM, van Melick M (2004) The relationship between
child-report, parent self-report, and partner report of perceived
Child Psychiatry Hum Dev
123
parental rearing behaviors and anxiety in children and parents.
Pers Individ Diff 37:1583–1596
49. Schwarz JC, Barton-Henry ML, Pruzinsky T (1985) Assessing
child-rearing behaviors: a comparison of ratings made by mother,
father, child, and sibling on the CRPBI. Child Dev 56:478
50. American Psychiatric Association (2013) Diagnostic and statis-
tical manual of mental disorders, 5th edn. American Psychiatric
Publishing, Arlington
51. Silverman WK, Saavedra LM, Pina AA (2001) Test–retest reli-
ability of anxiety symptoms and diagnoses with the anxiety dis-
orders interview schedule for DSM-IV: child and parent versions.
J Am Acad Child Adolesc Psychiatry 40:937–944
52. Wood JJ, Piacentini JC et al (2002) Concurrent validity of the
anxiety disorders section of the anxiety disorders interview
schedule for DSM-IV: child and parent versions. J Clin Child
Adolesc Psychol 31:335–342
53. Silverman WK, Kurtines WM et al (1999) Contingency man-
agement, self-control, and education support in the treatment of
childhood phobic disorders: a randomized clinical trial. J Consult
Clin Psychol 67:675–687
54. Silverman WK, Kurtines WM et al (2009) Directionality of
change in youth anxiety treatment involving parents: an initial
examination. J Consult Clin Psychol 77:474–485
55. March J (2013) The multidimensional anxiety scale for children
2nd edition—info sheet. MHS 2
56. March J (1997) The multidimensional anxiety scale for children
(MASC): factor structure, reliability, and validity. J Am Acad
Child Adolesc Psychiatry 36:554–565
57. Beck AT, Epstein N et al (1988) An inventory for measuring
clinical anxiety: psychometric properties. J Consult Clin Psychol
56:893–897
58. Aiken LS, West SG (1991) Multiple regression: testing and
interpreting interactions. Sage, Thousand Oaks
59. Hayes AF (2013) Introduction to mediation, moderation, and
conditional process analysis: a regression-based approach.
Methodology in the social sciences. The Guilford Press, New
York
60. Bogels SM, van Oosten A et al (2001) Familial correlates of
social anxiety in children and adolescents. Behav Res Ther
39:273–287
61. Najman JM, Williams GM et al (2001) Bias influencing maternal
reports of child behaviour and emotional state. Soc Psychiatry
Psychiatr Epidemiol 36:186–194
Child Psychiatry Hum Dev
123
Copyright © 2022 FDOKUMEN

