







Bahasa
Halaman
Hukum

Cheshire and MerseyCritical Care Network
CHESHIRE AND MERSEY CRITICAL CARE SERVICES
IN 2007 AND BEYOND:
An Interim Review Of Capacity, Pressures And Risks
A REPORT FOR CHESHIRE & MERSEY PRIMARY CARE TRUSTS
Commissioned by
Cheshire & Mersey Critical Care Network
October 2007
ACKNOWLEDGEMENTS Chrissie Connellan Julie Crompton Critical Care Network Team Contracts and Information Shared Services Unit (CISSU) Acute Trusts referred to in the Report.
Trust Name
Abbreviation
Aintree Hospitals NHS Foundation Trust
Aintree
The Cardiothoracic Centre – Liverpool NHS Trust
Cardiothoracic Centre
Countess of Chester Hospital NHS Foundation Trust
Countess of Chester
East Cheshire NHS Trust
East Cheshire
Liverpool Women’s NHS Foundation Trust
Liverpool Women’s
Mid Cheshire Hospitals NHS Trust
Mid Cheshire
North Cheshire Hospitals NHS Trust
North Cheshire
Royal Liverpool & Broadgreen University Hospitals NHS Trust
RLBUHT
Southport & Ormskirk Hospital NHS Trust
Southport & Ormskirk
St Helens & Knowsley Hospitals NHS Trust
St Helens & Knowsley
The Walton Centre for Neurology & Neurosurgery NHS Trust
The Walton Centre
Wirral University Teaching Hospital NHS Foundation Trust
Wirral
CHESIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
2
CONTENTS Introduction page 4 Executive Summary page 5 Purpose and Scope of the Report page 8 What is Critical Care - Setting the Scene page 9 National Policy Drivers page 11 Chapter 1: Current pressures page 14 Chapter 2: Capacity and Demand page 18 Chapter 3: Clinical Management page 23 Chapter 4: Transfers page 25 Chapter 5: Workforce page 30 Chapter 6: Network Priorities and Goals page 35 Chapter 7: Future Commissioning arrangements page 37 Chapter 8: Payment by Results and Contracting page 38 Chapter 9: Future Plans page 41 Summary & Conclusion page 44 APPENDIX A: Summary of Recommendations page 45 APPENDIX B: Additional Tables page 48 APPENDIX C: Site Visit Questionnaire page 51 APPENDIX D: Pen Portraits page 59
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
3
INTRODUCTION As Chair of the Cheshire & Mersey Critical Care Network, I should like to thank everyone involved in the production of this report, which aims to give Commissioners an understanding of the current position across the Network, our strengths and weaknesses and where we need to concentrate our efforts for the future. We have a history of good collaborative working in critical care across the Northwest, and particularly in Cheshire and Mersey - where Primary Care Trusts (PCTs) have seen the benefits of supporting and developing a Critical Care Network. Much of what we work on and identify as issues within this Network is shared with the Department of Health (DH), and we are seen as a major national contributor in both highlighting clinical issues and in helping to shape and influence policy development. There has been excellent co-operation from everyone involved in the process of the production of this report, with honest and open responses to the questionnaire during the site visits. We have been particularly impressed with the engagement of clinicians. There are some significant challenges that face critical care over the coming months and years, and I see the Network as being able to play a role as an “honest broker “ to Commissioners and Acute Trusts in promoting collaboration and sharing best practice. It will also have a role in working with other clinical networks and service reviews to ensure that critical care is modelled into future planning assumptions. The information we have obtained through the review process is immensely valuable to both Commissioners and Acute Trusts. In particular, we need to gain a deeper understanding of the future planned development of critical care facilities and their status, and keep a watchful eye on the impact of future workforce directives. Once again I should like to thank everyone for their co-operation and support.
Kathy Doran Chair - Cheshire & Mersey Critical Care Network
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
4
EXECUTIVE SUMMARY This report aims to ensure that patients who require critical care can gain access at the right level as and when required. This report will summarise the key issues, drivers and risks that Commissioners need to take into consideration when commissioning and contracting with the twelve critical care units in Cheshire and Mersey to provide this service. It also aims to include a fuller understanding of non-clinical transfers and whether or not cancelled electives are an issue, which in turn will enable Commissioners to make more informed decisions about future capacity. Specific areas of focus include: -
• Review the current issues and problems: To ensure that there is a Network-wide understanding of the short, medium and long term issues facing critical care services.
• Identify potential risks to Commissioners: To ensure that Commissioners take into
consideration, at the earliest opportunity, the effect of any service changes or developments that will impact on critical care capacity, e.g. implementation of Improving Outcome Guidance (IOG).
• Identify current reasons for non-clinical transfers and cancelled electives: To
inform commissioning decisions to ensure that non-clinical transfers and cancelled electives are kept to a minimum as well as a consistent Network-wide approach to adherence to transfer protocols.
• To consider any potential review of commissioning arrangements that may be
required: To ensure that there is an agreed Cheshire and Mersey PCT wide approach for collective decision making for critical care services and a common approach for contracting.
Key Findings: The system works well with the least number of non-clinical transfers in the North West. Lack of level 3 beds to step up patients requiring higher levels of care in some areas. Inability to discharge from critical care, resulting in the “wrong patient in the wrong bed”. Physical constraint of some units, which impacts on the ability to flex levels of care up and
down. Lack of data to understand current and future dependency of patients. Growing use of theatre recovery and stabilisation bays to manage patients. Problems with long term ventilation of patients. Individual Trust future plans could lead to a potential increase of level 2 beds within a range
of 27- 57. Evidence of good clinical practice and pragmatic solutions to issues encountered.
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
5
Highlights of Recommendations:
For Commissioners Collectively develop a commissioning framework for critical care services, which is
performance managed, ensures fair payment and can be updated to incorporate changes in policy as they arise.
Develop and agree a standardised costing and contracting model incorporating shadow Payment by Results (PbR) from April 2008.
Urgently clarify with Acute Trusts the number of beds and status of each Trust’s plans for critical care expansion and proposed number of beds.
Early collaborative planning and modelling for any new service developments with clinicians, critical care/other networks, providers, etc.
A standardised approach to costing and contracting to be adopted. Explore with Acute Trusts and the Network the potential of identifying and investing in a
specialist unit(s) to manage patients requiring long term ventilation who have weaning difficulties or require chronic critical care. This would ensure that these patients were managed in a more appropriate clinical setting and free up acute critical care capacity. North West Specialist Commissioning Team are beginning some work in January 2008 regarding options for this group of patients.
For Providers
Access current clinical management, e.g. profiling of theatre lists to ensure critical care
capacity is available, review clinical management arrangements for admission and discharge
Each unit to calculate the financial impact of PbR and all Trusts to move to shadow PbR by April 2008
Understand the issues around delayed discharge of patients, specifically identifying the lack of level 2 capacity to step down patients from level 3 and the growing demands to support elective surgery.
Fully understand the reasons for cancelled electives and systematically record when these are due to lack of critical care bed.
Recognise and understand the impact on training requirements as a result of service reconfigurations. For the Network
Further develop the performance management role. Establish the status of Critical Care Minimum Dataset (CCMDS) and Secondary User Server
(SUS). Retain an annual overview of planned increases in capacity and provide feedback to
Commissioners. Map which units are at risk from changes in training requirements and which Accident &
Emergency Departments (A&E) are vulnerable.
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
6
Conclusion: The body of the report discusses in detail all the issues and proposed recommendations; however, it has become apparent throughout this project that the common issues that need to be addressed are:
1. Improving the accuracy, completeness, consistency and availability of data and information to inform decision-making.
2. Contracting and costing arrangements need to be urgently developed to ensure a
consistent approach and readiness for PbR, or its alternative.
3. There appears to be a poor commissioning overview, which could be as a result of lack of understanding between organisations, which needs to be corrected. Strengthening the role of the Network to co-ordinate and act as a further resource will support delivering this.
It is important to emphasise that, in order to move forward, there needs to be Chief Executive commitment to the significant work in agreeing the recommendations and a timetable for implementation.
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
7
PURPOSE AND SCOPE: There are increasing numbers of non-clinical transfers between critical care units across the North West, and a view that cancelled elective operations are increasing due to a lack of a critical care bed. These increases are a cause of concern to both clinicians and Commissioners and, as a result, the Cheshire and Mersey Critical Care Network has decided to examine this in more detail. Over and above the non-clinical transfers, there are a number of factors that may impact on critical care capacity and affect patient type and flows. These include:
The development of tertiary centres for specialist surgery. The implementation of the National Institute of Clinical Excellence (NICE) Improving
Outcomes Guidance (IOG) for cancer services. The implementation of NICE guidance for Care of the Unexpectedly Acutely Ill (CG50)
and “Head Injury – Triage, Assessment, Investigation and Early Management of Head injury in Infants, Children and Adults” (CG56)
The future shape of urgent care services and potential development of trauma centres. The impact of current planned service re-configurations. The impact of current and planned business cases (approved and in development). The impact of new treatments and technologies leading to altered length of hospital
stays. The impact of delivering key government targets e.g. 18 weeks. The impact of changes to costings and financial flows, e.g. Health Resource Groups
(HRGs) and shadow PbR Increasing public expectation of treatment.
Currently there is a variety of contract arrangements in place varying between Trusts and sometimes within Trusts. Under these arrangements, decisions to increase capacity or de-commission beds can sometimes be made without due consideration of the wider implications on other providers, services and wider Network requirements. Analysis of the Critical Care Network capacity over the last 5 years indicates that there is a relatively constant demand, resulting in some under occupancy. However, taking into account the drivers for change listed, there is now a need to review whether the current configuration of beds is suitable for future needs and service development. This report aims to summarise the key issues, drivers and risks that Commissioners need to take into consideration when commissioning and contracting with the twelve critical care units in Cheshire and Mersey. This includes a fuller understanding of non-clinical transfers and whether cancelled electives are an issue, and will enable Commissioners to make more informed decisions about future capacity.
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
8
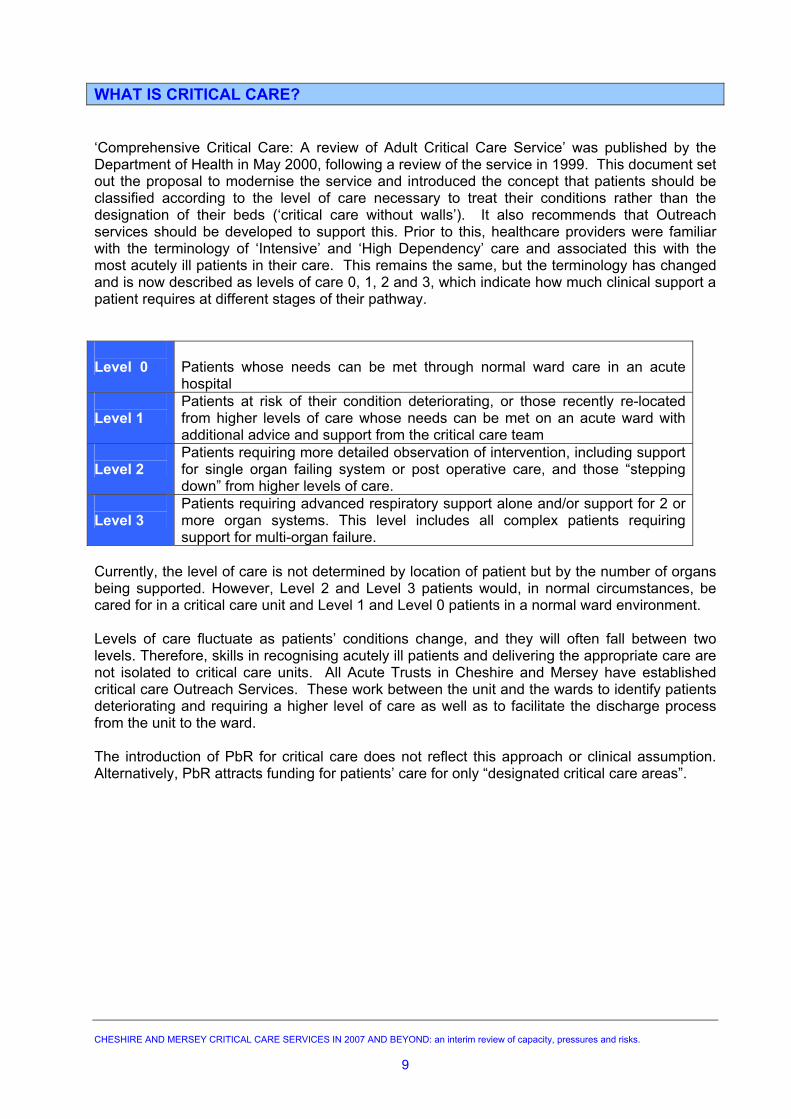
WHAT IS CRITICAL CARE? ‘Comprehensive Critical Care: A review of Adult Critical Care Service’ was published by the Department of Health in May 2000, following a review of the service in 1999. This document set out the proposal to modernise the service and introduced the concept that patients should be classified according to the level of care necessary to treat their conditions rather than the designation of their beds (‘critical care without walls’). It also recommends that Outreach services should be developed to support this. Prior to this, healthcare providers were familiar with the terminology of ‘Intensive’ and ‘High Dependency’ care and associated this with the most acutely ill patients in their care. This remains the same, but the terminology has changed and is now described as levels of care 0, 1, 2 and 3, which indicate how much clinical support a patient requires at different stages of their pathway. Level 0
Patients whose needs can be met through normal ward care in an acute hospital
Level 1
Patients at risk of their condition deteriorating, or those recently re-located from higher levels of care whose needs can be met on an acute ward with additional advice and support from the critical care team
Level 2
Patients requiring more detailed observation of intervention, including support for single organ failing system or post operative care, and those “stepping down” from higher levels of care.
Level 3
Patients requiring advanced respiratory support alone and/or support for 2 or more organ systems. This level includes all complex patients requiring support for multi-organ failure.
Currently, the level of care is not determined by location of patient but by the number of organs being supported. However, Level 2 and Level 3 patients would, in normal circumstances, be cared for in a critical care unit and Level 1 and Level 0 patients in a normal ward environment. Levels of care fluctuate as patients’ conditions change, and they will often fall between two levels. Therefore, skills in recognising acutely ill patients and delivering the appropriate care are not isolated to critical care units. All Acute Trusts in Cheshire and Mersey have established critical care Outreach Services. These work between the unit and the wards to identify patients deteriorating and requiring a higher level of care as well as to facilitate the discharge process from the unit to the ward. The introduction of PbR for critical care does not reflect this approach or clinical assumption. Alternatively, PbR attracts funding for patients’ care for only “designated critical care areas”.
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
9
SETTING THE SCENE The Cheshire and Mersey Critical Care Network influences and oversees the delivery of high quality critical care for a population of 2.3 million across 12 Acute Trusts and 8 Primary Care Trusts. Primary Care Trusts in Cheshire and Mersey commission 69 general intensive care beds (level 3) and 63 general high dependency beds (level 2) for critical care. In addition there are 35 specialist beds for cardio-thoracic surgery, 13 for neuro-surgery and 4 for specialist gynaecology and obstetrics. Of the general units, the Royal Liverpool and Broadgreen University Hospitals Trust (RLBUHT) has the largest number of beds (27) and East Cheshire Hospital has the fewest (6). Previous analysis by the Network demonstrates that there is a consistent occupancy rate of over 85% for both ITU (level 3) and HDU (level 2). Demand is less throughout the summer months. Currently, the estimated cost of providing the above service is approximately £57,000,000 per annum. This is commissioned through a variety of contractual arrangements, but is mostly via block contracts between host PCTs and their local hospital Trust. Over and above this, the PCTs, partly through the Critical Care Network, fund Outreach Services and audit clerks at each Trust at a cost of £912,000 per annum on a recurrent basis. Overall, the Cheshire and Mersey Critical Care Network appears to work well, and has the least number of non-clinical transfers out of the 3 Networks within the North West Strategic Health Authority (NWSHA). In 2006/07, Cheshire and Mersey transferred 182 patients for non-clinical reasons, accounting for 25% of all non- clinical transfers across the North West. There will always be some need to transfer patients for non-clinical reasons unless occupancy rates of below 70% became the acceptable norm. The current goal for Cheshire and Mersey is to reduce the number of non-clinical transfers to no more than 10 per month and for all units to accept 95% of appropriate referrals to level 3. This is currently not being achieved by the Network. Whilst there are pressures within the system, most critical care units have strategies in place to cope with demand. However, overall demand for critical care is increasing. A degree of unmet demand is acknowledged and it is difficult to measure external drivers both nationally and locally, which present risks for safe service delivery in the future. There are complex inter-relating factors that result in non-clinical transfers, but in Cheshire and Mersey it appears that the underlying cause for most of these is the lack of level 3 critical care beds in some places. METHODOLOGY A questionnaire (appendix C) was developed, and interviews were undertaken at each hospital Trust by the members of the Network Team, including Clinical Leads and the Network Manager. A variety of stakeholders were also met or interviewed as part of the process to establish national and regional drivers. These included other clinical networks, Department of Health, NWSHA, North West Ambulance Services Trust, Specialist Commissioning and others.
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
10
NATIONAL POLICY DRIVERS: Department of Health Guidance “Quality Critical Care – Beyond Comprehensive Critical Care” was published in September 2005 by the National Stakeholders Forum and sets out recommended actions for Strategic Health Authorities, PCTs, National Health Service (NHS) and Independent provider Hospitals and Critical Care Networks. The recommendations are to ensure that: a coherent local strategy is in place; there is adequate local capacity in both facilities and workforce; local quality targets are developed; effective commissioning is in place. These guidelines also underlined the need to develop 24/7 Outreach Services and ensure that early warning systems ‘track and trigger’ are in place at ward level. This will identify at risk patients, ensure rapid referral to appropriate clinical expertise and also facilitate discharge and rehabilitation of patients from critical care. NICE Guidelines (a) CG50 - “The Care of the Unexpectedly Acutely Ill” Publication of NICE Guidelines on 25 July 2007 for “The Care of the Unexpectedly Acutely Ill” http://guidance.nice.org.uk/CG50 recommends the regular monitoring of adult patients outside critical care while they are in hospital and to take action if they show early warning signs of deterioration. In particular, this covers patients who have had an emergency admission, surgery, left critical care or are moving between departments. Care of children and the terminally ill are not covered by this guidance. These guidelines will have significant impact on all hospitals including:- the need to increase skills of ward level nurses; the need to extend Outreach services to manage sicker patients at ward level; the increased demand for critical care due to unmet need and the earlier identification of
sicker patients. (b) CG56 - “Head Injury – Triage, Assessment, Investigation and Early Management of Head injury in Infants, Children and Adults” NICE clinical guideline http://guidance.nice.org.uk/CG56 ‘Head Injury - Triage, Assessment Investigation and Early Management of Head Injury in Infants, Children and Adults’, was published in September 2007. It recommends that all patients with a severe traumatic brain injury would benefit from transfer to, and care at, a neuroscience centre. Implementation of this recommendation will have its greatest impact on the Walton Centre’s critical care unit. Previous network audits have shown that there are more than 100 patients per year with severe traumatic brain injury who, until recently, remained and were managed in the referring hospitals. The implementation of this guideline may free up critical care resource in most of the other units. There will also be critical care transfer training implications for all anaesthetic staff across the Network
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
11
National Service Reviews Nationally, a number of service reviews are being undertaken. These include:-
Acute Hospital Services Review, which is examining the future configuration of tertiary services and the future of the District General Hospital (DGH). This may impact on the role of DGHs to treat critically ill patients and their ability to take level 3 patients.
“A Framework for Action”, written by Professor Sir Ara Darzi, published July 2007
describes how London’s healthcare needs to change over the next ten years and Centralised Specialist Care features in the recommendations. His subsequent report “Our NHS - Our Future”, due to be completed in spring 2008, may advocate this on a wider national basis, which in turn may affect critical care services. The main clinical drivers for change therefore are :
The loss of emergency surgery where units will need to move to selected
medical intake only. The viability of emergency medical services if emergency surgery is lost. The viability of A&E departments taking blue lights.
The Academy of Medical Royal Colleges are working on a report that may echo some of
Professor Darzi’s recommendations. This is due to be completed by late autumn 2007.
Vascular surgery is also being reviewed, as not all Acute Trusts can provide full surgical cover, and some transfer and rationalisation is expected in the future
Medical Training Modernising Medical Careers will lead to an overall decrease in the number of trainees, particularly in anaesthetics. In the Cheshire and Mersey Critical Care Network, anaesthetic trainees staff most critical care units. In addition, the medical trainee of the future will become supernumerary, focussing on education rather than service provision. Commissioners need to be aware that, in the future, critical care units’ rotas will be staffed by a combination of consultants, non-consultant grades and non-medical practitioners rather than medical trainees (although the potential role of the non-medical practitioner in critical care remains undefined). This will also have financial implications. New Treatments and Technology & Specialist Tertiary Services The impact of new treatments and technologies leading to altered length of hospital stays is unclear, and examples cited, such as Endovascular Arterial Reconstruction (EVAR) and the move to less invasive surgery, suggest that demand for critical care for some surgical specialities may decrease.
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
12
Recommendations
• Commissioners to work with the Network to track and monitor national discussions to understand the wider impact in relation to critical care at the earliest stage.
• The Network, including the clinical leads, to ensure engagement and representation
at relevant national and local decision making bodies.
• Network to map which units are at risk from changes in training requirements, and which A&Es are vulnerable.
• The Walton Centre and PCTs should urgently begin discussions about the additional
resources required to support NICE guideline CG56. The Network and PCTs, with advice from the Walton Centre, should look at how to provide resources to improve transfer training for head injured patients.
• Clinicians need to maintain clear communication between The Walton Centre and all
referring hospitals about the care, referral and transfer of patients with sever traumatic brain injury in a timely fashion.
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
13
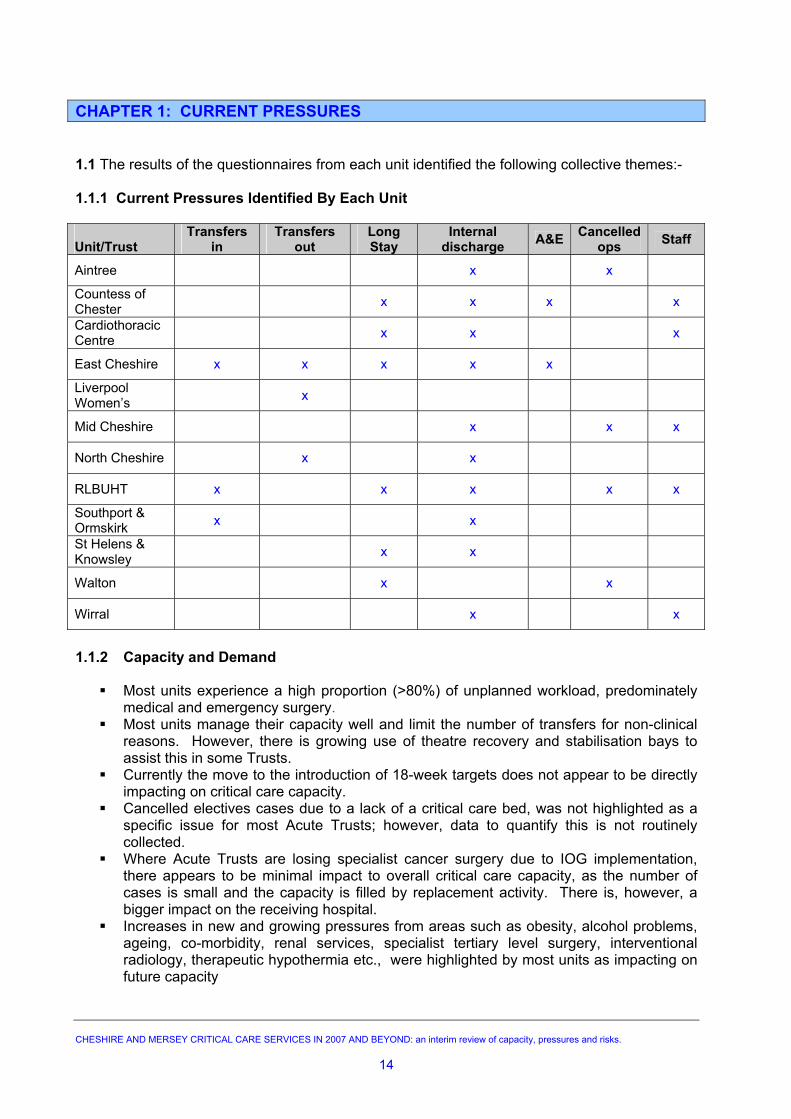
CHAPTER 1: CURRENT PRESSURES 1.1 The results of the questionnaires from each unit identified the following collective themes:- 1.1.1 Current Pressures Identified By Each Unit Unit/Trust
Transfers in
Transfers out
Long Stay
Internal discharge A&E Cancelled
ops Staff
Aintree x x
Countess of Chester x x x x
Cardiothoracic Centre x x x
East Cheshire x x x x x
Liverpool Women’s x
Mid Cheshire x x x
North Cheshire x x
RLBUHT x x x x x
Southport & Ormskirk x x
St Helens & Knowsley x x
Walton x x
Wirral x x
1.1.2 Capacity and Demand
Most units experience a high proportion (>80%) of unplanned workload, predominately medical and emergency surgery.
Most units manage their capacity well and limit the number of transfers for non-clinical reasons. However, there is growing use of theatre recovery and stabilisation bays to assist this in some Trusts.
Currently the move to the introduction of 18-week targets does not appear to be directly impacting on critical care capacity.
Cancelled electives cases due to a lack of a critical care bed, was not highlighted as a specific issue for most Acute Trusts; however, data to quantify this is not routinely collected.
Where Acute Trusts are losing specialist cancer surgery due to IOG implementation, there appears to be minimal impact to overall critical care capacity, as the number of cases is small and the capacity is filled by replacement activity. There is, however, a bigger impact on the receiving hospital.
Increases in new and growing pressures from areas such as obesity, alcohol problems, ageing, co-morbidity, renal services, specialist tertiary level surgery, interventional radiology, therapeutic hypothermia etc., were highlighted by most units as impacting on future capacity
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
14
1.1.3 Clinical Management
Profiling of theatre lists to ensure that critical care capacity is available is not systematically undertaken.
Most units highlighted the difficulties with split clinical management arrangements for critical care beds, particularly level 2 beds, which impacts on admission and discharge as well as patient flow
1.1.4 Patient Flow
Most units experience problems in delayed discharge of patients by highlighting the lack of level 2 capacity to step down patients from level 3 and the growing demands to support elective surgery
1.1.5 Workforce
All units are compliant with European Working Time Directive (EWTD) for 56 hours but some raised concerns about non compliance with 48 hours by 2009.
No hospital Trust meets ‘The National Confidential Enquiry into Patient Outcome and Death’ (NCEPOD) recommendations for 24/7 Outreach Services.
Staffing is an issue for most Acute Trusts for nursing (& midwives) and medical cover. Proposed changes under Modernising Medical Careers and potential changes to
medical training posts were highlighted as threats to maintaining services in some smaller units.
Developing and maintaining appropriate skills in existing and future workforce is problematic now and for next 1 – 5 years
Most units only have access to Allied Health Professional (AHP) staff Monday to Friday, 0900 – 1700. Outside of these hours availability is on an on-call basis only.
1.1.6 Commissioning and Contracting
There is no collective commissioning framework for critical care in Cheshire and Mersey. Access and availability of data to support the CCMDS and the introduction of PbR
varies from one unit to another. Approach to contracting is fragmented and varied across the Network and between
networks. 1.1.7 Service Developments and Drivers for Change
Concerns about changes to national policy, such as the reconfiguration of A&E and urgent care services, could be significant for the future viability of some units.
Most units raised issues about their physical configuration as a constraint to both the optimal utilisation of resources and their ability to expand to meet future demand.
A significant number of units are planning to increase capacity over the next 1 to 5 years and some units are developing business cases at risk for level 2 capacity to support elective surgery.
Most units are excluded from wider planning discussions for service developments that have an impact on critical care.
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
15
1.2 Growth in Demand Lack of level 2 provision for both critical care and elective surgery is a growing pressure and, without sufficient capacity at this level, patient flow blocks occur for both planned and unplanned work. This impacts on patients moving from A&E, wards, theatres, step-down and discharge. Increasing level 2 capacity on its own will make some inroads into these problems; however, a wider approach is needed in respect of the internal management of this resource. With regard to unplanned growth, the changing demographics, increasing prevalence of chronic conditions and increasing public expectations are driving demand for critical care. For most units, over 80% of admissions at level 3 are for medical and surgical emergencies. This is significant for some units where the re-configuration of services, including the future of A&E, is being considered. Commissioners need to understand the impact of these changes, and undertake scenario planning to ensure contingency arrangements are in place to manage change and avoid the possibility of “planning blight”. Specific changes that will impact on demand include:- 1.2.1 Specialist Services Development of specialist surgery over the past few years, such as pancreatic, liver and renal, has been undertaken without full understanding and modelling of its impact on critical care capacity. Commissioners and Acute Trusts need to ensure that any future developments of this nature are planned through the Critical Care Delivery Groups and the Network. Some Acute Trusts are experiencing pressures from acute renal failure patients, particularly where there are no nephrology services for dialysis on site. Whilst there has been additional investment by Commissioners through the Renal Network to open additional level 2 renal beds (five at the RLBUHT and two at Wirral, to help manage the acutely ill patient with acute renal failure) the impact of this on critical care units in peripheral hospitals, who should have benefited from this, has not yet been realised. This has resulted largely from these beds being used for unmet need at both centres. The role of public health needs to be strengthened to enable Commissioners to understand the future impact of lifestyle choices on critical care need. Where patients are being transferred between Acute Trusts for specialist surgery, agreed care pathways and protocols need to be in place. This will ensure that a planned approach to accessing critical care is developed. 1.2.2 NICE Guidelines for Cancer Surgery Analysis and discussion with units and the Cheshire and Mersey Cancer Network confirms that modelling for the critical care element of the transfer of services for urology, upper GI and gynaecological cancer surgery to meet with Improving Outcomes Guidance has been undertaken. Overall, the impact of this change will be minimal to units losing services, as the number of cases is small. Units receiving additional IOG workload are expected to see a gradual increase in activity and may require some increase in capacity to cope once the case load transfer is completed. Whilst further movement of specialist cancer surgery is not planned for at least the next 2 to 3 years, Commissioners need to monitor the impact of the current changes and the Critical Care Network needs to continue to work with the Cancer Network on this.
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
16
1.2.3 18-Week Target The delivery of the 18-week waiting time target was not highlighted as a significant pressure by any unit. Due to the complexity and different practices locally, no work at national level has been undertaken to model the impact on level 2 (HDU) capacity. However, the Department of Health does expect this work to be undertaken at a local level. Early implementer sites for 18-weeks, such as the Countess of Chester and St Helens & Knowsley Trusts, report little impact on critical care but have seen a noticeable increase on ward occupancy leading to exacerbation of problems with internal patient discharge from critical care.
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
17
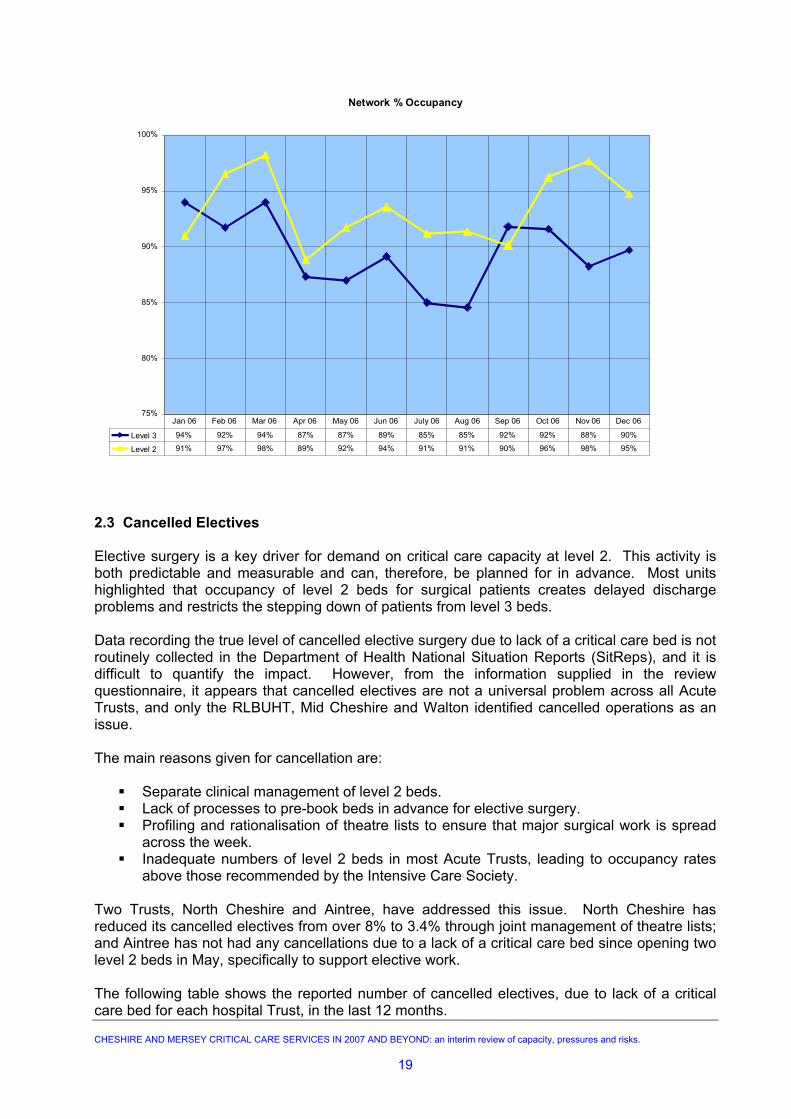
CHAPTER 2: CAPACITY AND DEMAND 2.1 Capacity Cheshire and Mersey PCTs currently commission 184 critical care beds in 12 Acute Trusts. Of these, 69 level 3 (ITU) and 63 level 2 (HDU) beds are available for general use. The 69 level 3 beds are included in the Intensive Care Bed Information Service (ICBIS) ring around for non-clinical transfers. Level 2 patients are not routinely transferred to another hospital for care. Beds in three Acute Trusts, the Cardiothoracic Centre, Walton Centre and Liverpool Women’s, are designated “specialist” and are outside the scope for general services and do not receive non-clinical transfers. In addition, there are two level 2 beds at Aintree, which are ring-fenced for elective surgery but can be used in an emergency situation. There is no level 3 Independent Sector capacity available in Cheshire and Mersey. In July 2007, all funded beds were open, although Mid Cheshire NHS Hospitals Trust has problems in staffing its seventh bed on a continual basis, and St. Helens & Knowsley NHS Hospitals Trust had three of its level 2 beds temporarily closed due to building work for a few weeks during the summer. Nearly all units have the ability to flex capacity upwards when under pressure, but not all have physical space to expand the unit beyond the current size (see Table 1 in Appendix B) North Cheshire Hospital NHS Trust has the highest number of non-clinical transfers in the Network due to lack of capacity, and the second highest number in the North West. This level of transfers impacts on neighbouring Trusts and performance of the overall system. The Trust currently has a business case to expand its critical care capacity under consideration and, if approved, this will have a significant impact on the Network. Only one hospital Trust in the Network, the Cardiothoracic Centre, has highlighted that it has spare capacity. A view as to how this could be utilised to support both the Trust’s move towards Foundation status and support some of the wider Network’s future requirements should be considered. The RLBUHT, Aintree and St Helens & Knowsley hospitals also experience additional pressures on critical care from the demands generated by the specialist tertiary services they provide. 2.2 Demand Eighty per cent of all admissions for critical care beds are from A&E and emergency ward admissions. Overall, this has remained constant across the Network over the past 3 years, however, there is seasonal variation. Analysis by the Network identifies that fluctuation in demand for critical care is caused by elective surgery and emergency admissions, which dips during holiday periods and peaks from November through to March. This is clearly demonstrated in the following chart, where occupancy levels rise to almost 94% for level 3 beds and 98% for level 2 beds. Occupancy levels rarely fall below 85% at Network level, which is higher than the level recommended by the Intensive Care Society (ICS).
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
18
Network % Occupancy
75%
80%
85%
90%
95%
100%
Level 3 94% 92% 94% 87% 87% 89% 85% 85% 92% 92% 88% 90% Level 2 91% 97% 98% 89% 92% 94% 91% 91% 90% 96% 98% 95%
Jan 06 Feb 06 Mar 06 Apr 06 May 06 Jun 06 July 06 Aug 06 Sep 06 Oct 06 Nov 06 Dec 06
2.3 Cancelled Electives Elective surgery is a key driver for demand on critical care capacity at level 2. This activity is both predictable and measurable and can, therefore, be planned for in advance. Most units highlighted that occupancy of level 2 beds for surgical patients creates delayed discharge problems and restricts the stepping down of patients from level 3 beds. Data recording the true level of cancelled elective surgery due to lack of a critical care bed is not routinely collected in the Department of Health National Situation Reports (SitReps), and it is difficult to quantify the impact. However, from the information supplied in the review questionnaire, it appears that cancelled electives are not a universal problem across all Acute Trusts, and only the RLBUHT, Mid Cheshire and Walton identified cancelled operations as an issue. The main reasons given for cancellation are:
Separate clinical management of level 2 beds. Lack of processes to pre-book beds in advance for elective surgery.
Profiling and rationalisation of theatre lists to ensure that major surgical work is spread across the week.
Inadequate numbers of level 2 beds in most Acute Trusts, leading to occupancy rates above those recommended by the Intensive Care Society.
Two Trusts, North Cheshire and Aintree, have addressed this issue. North Cheshire has reduced its cancelled electives from over 8% to 3.4% through joint management of theatre lists; and Aintree has not had any cancellations due to a lack of a critical care bed since opening two level 2 beds in May, specifically to support elective work.
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
19
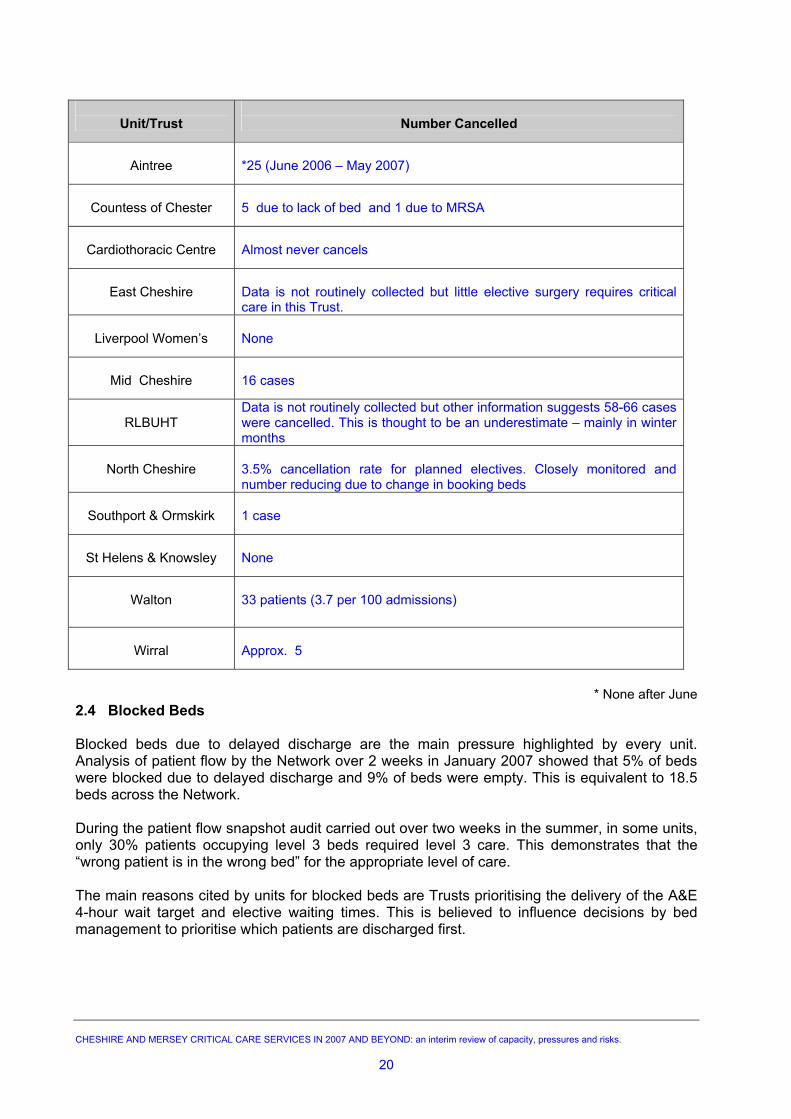
The following table shows the reported number of cancelled electives, due to lack of a critical care bed for each hospital Trust, in the last 12 months.
Unit/Trust
Number Cancelled
Aintree
*25 (June 2006 – May 2007)
Countess of Chester
5 due to lack of bed and 1 due to MRSA
Cardiothoracic Centre
Almost never cancels
East Cheshire
Data is not routinely collected but little elective surgery requires critical care in this Trust.
Liverpool Women’s
None
Mid Cheshire
16 cases
RLBUHT
Data is not routinely collected but other information suggests 58-66 cases were cancelled. This is thought to be an underestimate – mainly in winter months
North Cheshire
3.5% cancellation rate for planned electives. Closely monitored and number reducing due to change in booking beds
Southport & Ormskirk
1 case
St Helens & Knowsley
None
Walton
33 patients (3.7 per 100 admissions)
Wirral
Approx. 5
* None after June
2.4 Blocked Beds Blocked beds due to delayed discharge are the main pressure highlighted by every unit. Analysis of patient flow by the Network over 2 weeks in January 2007 showed that 5% of beds were blocked due to delayed discharge and 9% of beds were empty. This is equivalent to 18.5 beds across the Network. During the patient flow snapshot audit carried out over two weeks in the summer, in some units, only 30% patients occupying level 3 beds required level 3 care. This demonstrates that the “wrong patient is in the wrong bed” for the appropriate level of care. The main reasons cited by units for blocked beds are Trusts prioritising the delivery of the A&E 4-hour wait target and elective waiting times. This is believed to influence decisions by bed management to prioritise which patients are discharged first.
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
20
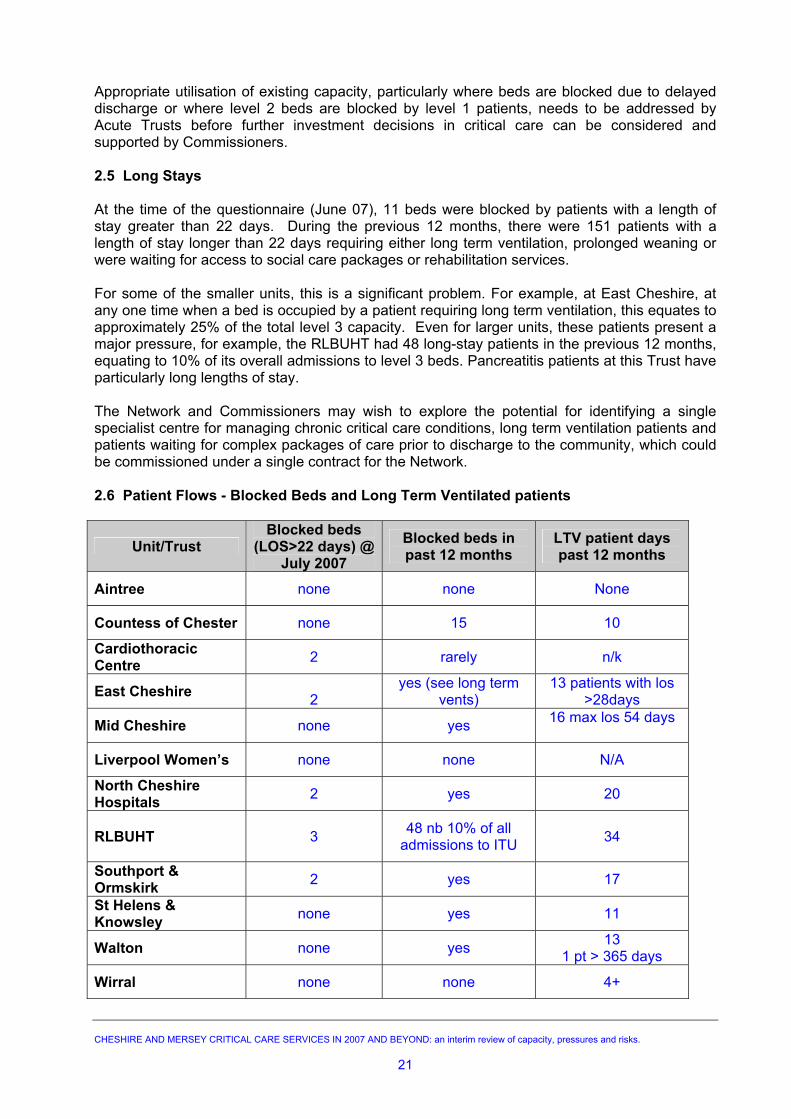
Appropriate utilisation of existing capacity, particularly where beds are blocked due to delayed discharge or where level 2 beds are blocked by level 1 patients, needs to be addressed by Acute Trusts before further investment decisions in critical care can be considered and supported by Commissioners. 2.5 Long Stays At the time of the questionnaire (June 07), 11 beds were blocked by patients with a length of stay greater than 22 days. During the previous 12 months, there were 151 patients with a length of stay longer than 22 days requiring either long term ventilation, prolonged weaning or were waiting for access to social care packages or rehabilitation services. For some of the smaller units, this is a significant problem. For example, at East Cheshire, at any one time when a bed is occupied by a patient requiring long term ventilation, this equates to approximately 25% of the total level 3 capacity. Even for larger units, these patients present a major pressure, for example, the RLBUHT had 48 long-stay patients in the previous 12 months, equating to 10% of its overall admissions to level 3 beds. Pancreatitis patients at this Trust have particularly long lengths of stay. The Network and Commissioners may wish to explore the potential for identifying a single specialist centre for managing chronic critical care conditions, long term ventilation patients and patients waiting for complex packages of care prior to discharge to the community, which could be commissioned under a single contract for the Network. 2.6 Patient Flows - Blocked Beds and Long Term Ventilated patients
Unit/Trust Blocked beds
(LOS>22 days) @July 2007
Blocked beds in past 12 months
LTV patient days past 12 months
Aintree none none None
Countess of Chester none 15 10
Cardiothoracic Centre 2 rarely n/k
East Cheshire 2
yes (see long term vents)
13 patients with los >28days
Mid Cheshire none yes 16 max los 54 days
Liverpool Women’s none none N/A
North Cheshire Hospitals 2 yes 20
RLBUHT
3 48 nb 10% of all admissions to ITU 34
Southport & Ormskirk 2 yes 17
St Helens & Knowsley none yes 11
Walton none yes 13 1 pt > 365 days
Wirral none none 4+
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
21
Recommendations
• Acute Trusts and Commissioners to understand and agree appropriate occupancy
levels for level 2 and level 3 beds.
• Acute Trusts to understand the reasons for cancelled electives and systematically record when these are due to lack of critical care bed.
• Liverpool PCT and the RLBUHT need to urgently address the higher than acceptable
levels of cancelled operations due to the lack of a critical care bed, including those where patients are waiting for specialist surgery, such as pancreatic, undertaken at this Trust.
• Acute Trusts to review the systems and processes currently in place for listing major
and minor surgery where a level 2 bed is required post operatively. Consideration to be given to joint theatre listing arrangement across surgeons and intensivists.
• Commissioners and Acute Trusts should ensure a joint understanding around the
development of any new elective surgery that involves critical care. Planning and modelling should ensure that sufficient critical care capacity is available and current capacity is not compromised.
• Commissioners to consider working with Acute Trusts to examine the potential of
identifying and investing in a specialist unit(s) to manage patients who require long term ventilation, have weaning difficulties, or require chronic critical care. This would ensure that these patients were managed in a more appropriate clinical setting and free up acute critical care capacity.
• The Network to examine the thresholds for long stay and undertake further modelling
to quantify the number of cases and bed days required for a long stay unit.
• Commissioners to develop a single Network-wide contract and Service Level Agreement (SLA) to share risk for the above type of patients.
• In preparation for the introduction of PbR, Acute Trusts to understand how level 2
and level 3 beds are utilised.
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
22
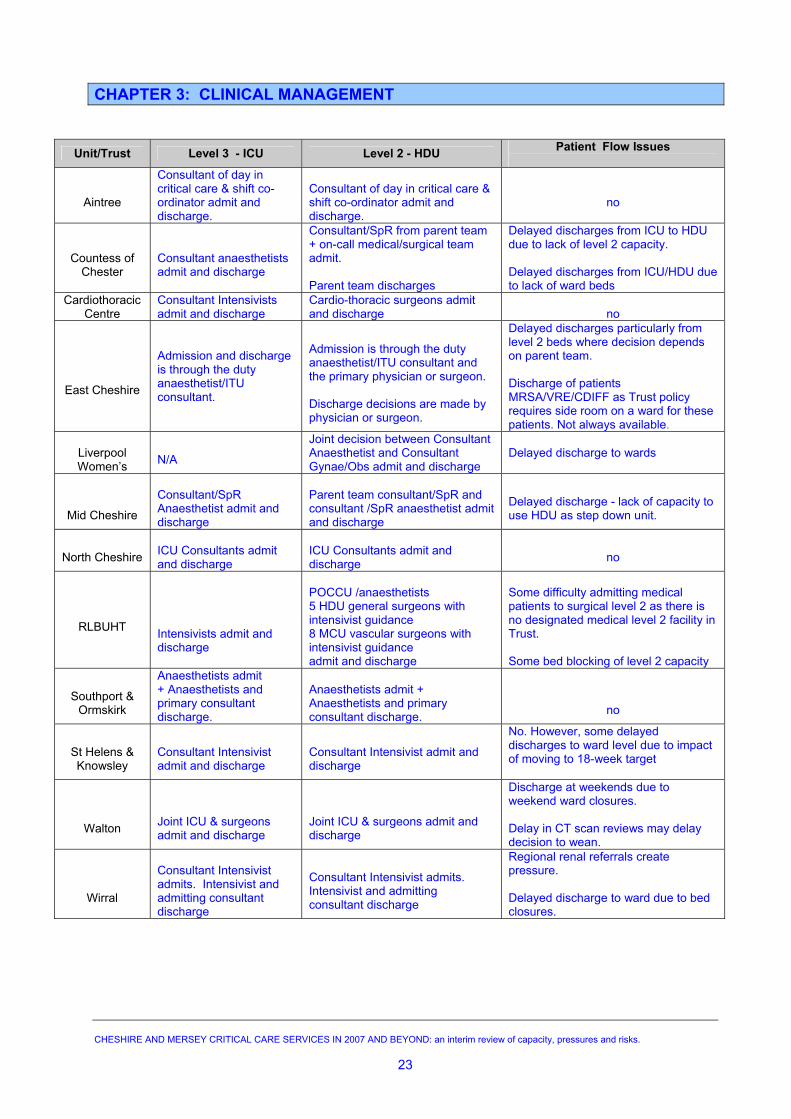
CHAPTER 3: CLINICAL MANAGEMENT
Unit/Trust Level 3 - ICU Level 2 - HDU Patient Flow Issues
Aintree
Consultant of day in critical care & shift co-ordinator admit and discharge.
Consultant of day in critical care & shift co-ordinator admit and discharge.
no
Countess of
Chester
Consultant anaesthetists admit and discharge
Consultant/SpR from parent team + on-call medical/surgical team admit. Parent team discharges
Delayed discharges from ICU to HDU due to lack of level 2 capacity. Delayed discharges from ICU/HDU due to lack of ward beds
Cardiothoracic Centre
Consultant Intensivists admit and discharge
Cardio-thoracic surgeons admit and discharge
no
East Cheshire
Admission and discharge is through the duty anaesthetist/ITU consultant.
Admission is through the duty anaesthetist/ITU consultant and the primary physician or surgeon. Discharge decisions are made by physician or surgeon.
Delayed discharges particularly from level 2 beds where decision depends on parent team. Discharge of patients MRSA/VRE/CDIFF as Trust policy requires side room on a ward for these patients. Not always available.
Liverpool Women’s
N/A
Joint decision between Consultant Anaesthetist and Consultant Gynae/Obs admit and discharge
Delayed discharge to wards
Mid Cheshire
Consultant/SpR Anaesthetist admit and discharge
Parent team consultant/SpR and consultant /SpR anaesthetist admit and discharge
Delayed discharge - lack of capacity to use HDU as step down unit.
North Cheshire
ICU Consultants admit and discharge
ICU Consultants admit and discharge
no
RLBUHT
Intensivists admit and discharge
POCCU /anaesthetists 5 HDU general surgeons with intensivist guidance 8 MCU vascular surgeons with intensivist guidance admit and discharge
Some difficulty admitting medical patients to surgical level 2 as there is no designated medical level 2 facility in Trust. Some bed blocking of level 2 capacity
Southport &
Ormskirk
Anaesthetists admit + Anaesthetists and primary consultant discharge.
Anaesthetists admit + Anaesthetists and primary consultant discharge.
no
St Helens & Knowsley
Consultant Intensivist admit and discharge
Consultant Intensivist admit and discharge
No. However, some delayed discharges to ward level due to impact of moving to 18-week target
Walton
Joint ICU & surgeons admit and discharge
Joint ICU & surgeons admit and discharge
Discharge at weekends due to weekend ward closures. Delay in CT scan reviews may delay decision to wean.
Wirral
Consultant Intensivist admits. Intensivist and admitting consultant discharge
Consultant Intensivist admits. Intensivist and admitting consultant discharge
Regional renal referrals create pressure. Delayed discharge to ward due to bed closures.
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
23
Clinical management arrangements are complex and vary between Acute Trusts and not all critical care beds are managed by the same clinical teams. The management of level 3 and level 2 beds by different clinical teams was highlighted as a major problem, particularly when trying to discharge patients to lower levels of care. Where anaesthetists/intensivists manage the overall patient flow, and/or input into the decision for admission and discharge to level 2 beds, it appears patient flow is better. The previous table details the current arrangements for admission and discharge at each Trust.
Recommendations• Acute Trusts to review the effectiveness of the current clinical management arrangements and patient flows between critical care beds and wards.
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
24
CHAPTER 4: TRANSFERS There will always be some need to transfer patients for non-clinical reasons, unless occupancy rates of below 70% become the acceptable norm. The current goal for Cheshire and Mersey as a Network is to reduce the number of non-clinical transfers to no more than 10 per month and for each unit to accept 95% of appropriate referrals to level 3. This is currently not being achieved by the Network. There are complex inter-relating factors, which result in non-clinical transfers, but in Cheshire and Mersey it appears that the underlying cause for most of these is the lack of level 3 critical care beds. North Cheshire Hospitals Trust is experiencing significant problems and is a major exporter within the Network. Other units have significant flows of patients moving both in and out of their units and experience spikes in demand where transfers are unavoidable and these tend to be seasonal – mostly from November to March. If occupancy levels increase and remain constant, there may be less seasonal variation and non-clinical transfers will be an ongoing pressure. Pressures in the system are picked up across the North West through the Intensive Care Bed Information Service (ICBIS), which monitors the availability of critical care beds 4 times every day. Cheshire and Mersey has the least pressures of the 3 Northwest Networks and was designated to be on GREEN most of the time. Every unit is informed when the Network is designated to be on RED alert for escalation, i.e. less than 2 empty beds in the Network. This ‘warning’ is to allow Trusts to take appropriate action, which may include cancelling elective surgery, to free up beds. Early action should help to reduce the need to export subsequent emergency patients; however, local action and response to these ‘alerts’ has become varied since co-ordination moved away from a central model led by the old North West Regional Health Authority to individual Trusts. Overall, Cheshire and Mersey is a net importer of non-clinical transfers, based on the last two years, as demonstrated in the following table. North Cheshire is the only consistent net exporter and East Cheshire has switched from being a net importer in Year One to being an exporter in Year Two. Units at Mid Cheshire, Aintree, Southport and Ormskirk, St Helens & Knowsley and the Wirral are all consistently net importers for non-clinical transfers and, on the whole, are currently able to cope with their own demand as well as absorbing pressures generated from other units. None of these units raised the transfer of patients out to other units as a particular pressure. The Countess of Chester has changed from being a net exporter in Year One to being a net importer in Year Two. The RLBUHT currently manages its pressures; but whilst currently not a high exporter of patients for non-clinical reasons, it is constrained by physical space and access to level 2 beds. These beds are located on different floors within the hospital which results in continuous pressure to manage the capacity. The Cardiothoracic Centre, the Walton Centre and the Liverpool Women’s all receive transfers for specialist clinical management CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
25
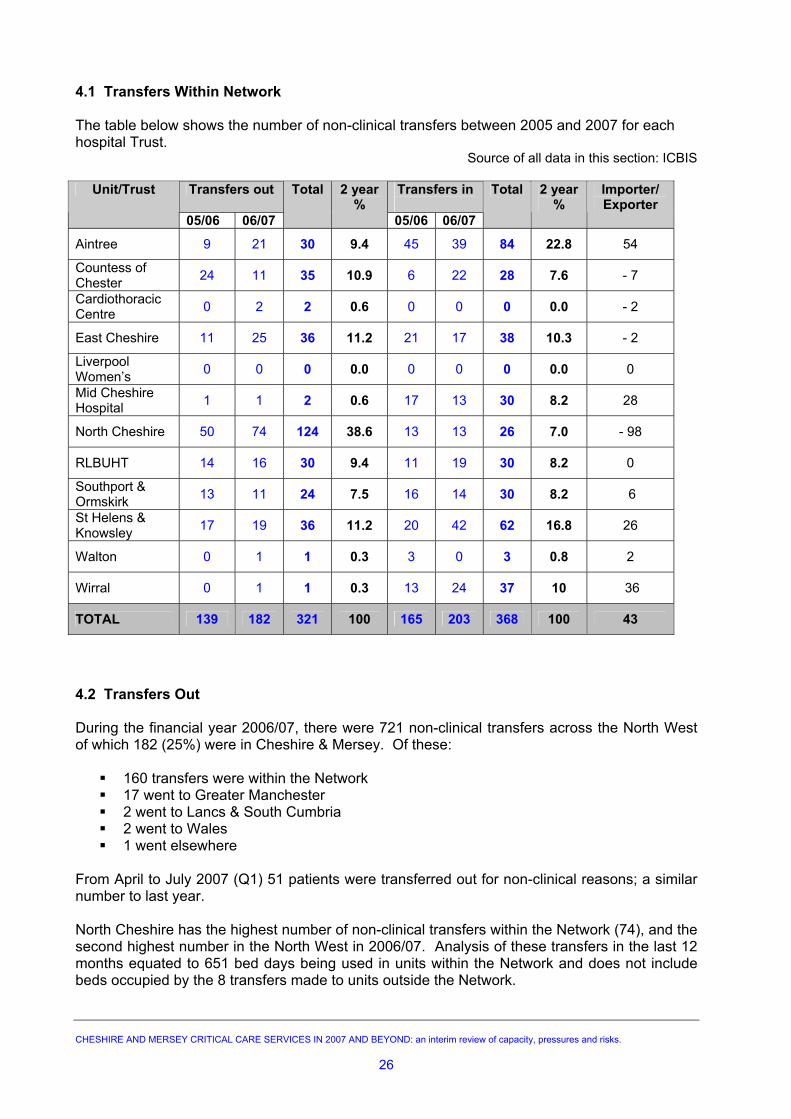
4.1 Transfers Within Network The table below shows the number of non-clinical transfers between 2005 and 2007 for each hospital Trust.
Source of all data in this section: ICBIS
Transfers out Transfers in
Unit/Trust
05/06 06/07
Total 2 year %
05/06 06/07
Total 2 year %
Importer/ Exporter
Aintree 9 21 30 9.4 45 39 84 22.8 54
Countess of Chester 24 11 35 10.9 6 22 28 7.6 - 7
Cardiothoracic Centre 0 2 2 0.6 0 0 0 0.0 - 2
East Cheshire 11 25 36 11.2 21 17 38 10.3 - 2
Liverpool Women’s 0 0 0 0.0 0 0 0 0.0 0
Mid Cheshire Hospital 1 1 2 0.6 17 13 30 8.2 28
North Cheshire 50 74 124 38.6 13 13 26 7.0 - 98
RLBUHT 14 16 30 9.4 11 19 30 8.2 0
Southport & Ormskirk 13 11 24 7.5 16 14 30 8.2 6
St Helens & Knowsley 17 19 36 11.2 20 42 62 16.8 26
Walton 0 1 1 0.3 3 0 3 0.8 2
Wirral 0 1 1 0.3 13 24 37 10 36
TOTAL 139 182 321 100 165 203 368 100 43
4.2 Transfers Out During the financial year 2006/07, there were 721 non-clinical transfers across the North West of which 182 (25%) were in Cheshire & Mersey. Of these:
160 transfers were within the Network
17 went to Greater Manchester 2 went to Lancs & South Cumbria 2 went to Wales 1 went elsewhere
From April to July 2007 (Q1) 51 patients were transferred out for non-clinical reasons; a similar number to last year. North Cheshire has the highest number of non-clinical transfers within the Network (74), and the second highest number in the North West in 2006/07. Analysis of these transfers in the last 12 months equated to 651 bed days being used in units within the Network and does not include beds occupied by the 8 transfers made to units outside the Network.
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
26
All units in the Network have confirmed that they have crisis management and short term coping strategies in place to reduce the necessity to transfer out and the decision to transfer a patient is only made as a last resort, once all other routes have been exhausted. 4.3 Transfers In Cheshire and Mersey is a net importer of non-clinical transfers. In 2006/07, 203 critical care patients were transferred into units for non-clinical reasons. This is an increase of 38 (23 %) from 2005/06. Of these:
160 were from units within the Network
4 were from Lancashire & South Cumbria 6 were from Wales 3 were from North Staffordshire 30 were from Greater Manchester
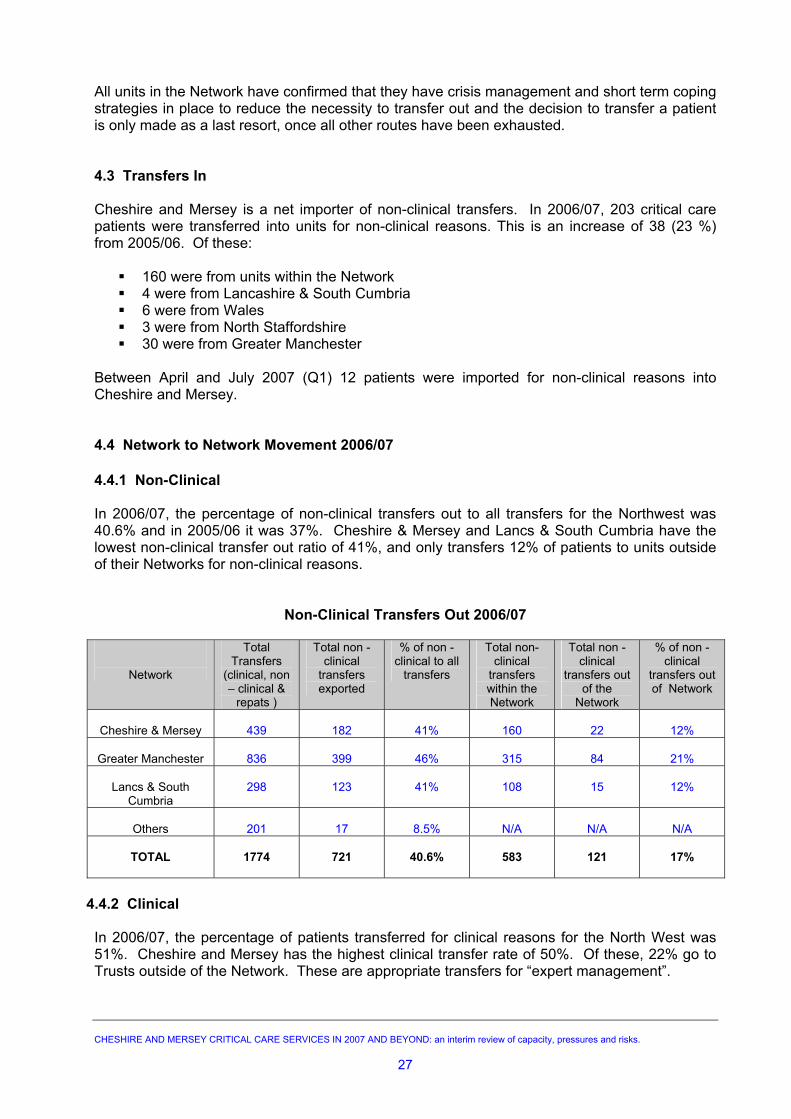
Between April and July 2007 (Q1) 12 patients were imported for non-clinical reasons into Cheshire and Mersey. 4.4 Network to Network Movement 2006/07 4.4.1 Non-Clinical In 2006/07, the percentage of non-clinical transfers out to all transfers for the Northwest was 40.6% and in 2005/06 it was 37%. Cheshire & Mersey and Lancs & South Cumbria have the lowest non-clinical transfer out ratio of 41%, and only transfers 12% of patients to units outside of their Networks for non-clinical reasons.
Non-Clinical Transfers Out 2006/07
Network
Total Transfers
(clinical, non – clinical &
repats )
Total non -clinical
transfers exported
% of non -clinical to all
transfers
Total non-clinical
transfers within the Network
Total non -clinical
transfers out of the
Network
% of non -clinical
transfers out of Network
Cheshire & Mersey
439
182
41%
160
22
12%
Greater Manchester
836
399
46%
315
84
21%
Lancs & South
Cumbria
298
123
41%
108
15
12%
Others
201
17
8.5%
N/A
N/A
N/A
TOTAL
1774
721
40.6%
583
121
17%
4.4.2 Clinical In 2006/07, the percentage of patients transferred for clinical reasons for the North West was 51%. Cheshire and Mersey has the highest clinical transfer rate of 50%. Of these, 22% go to Trusts outside of the Network. These are appropriate transfers for “expert management”.
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
27
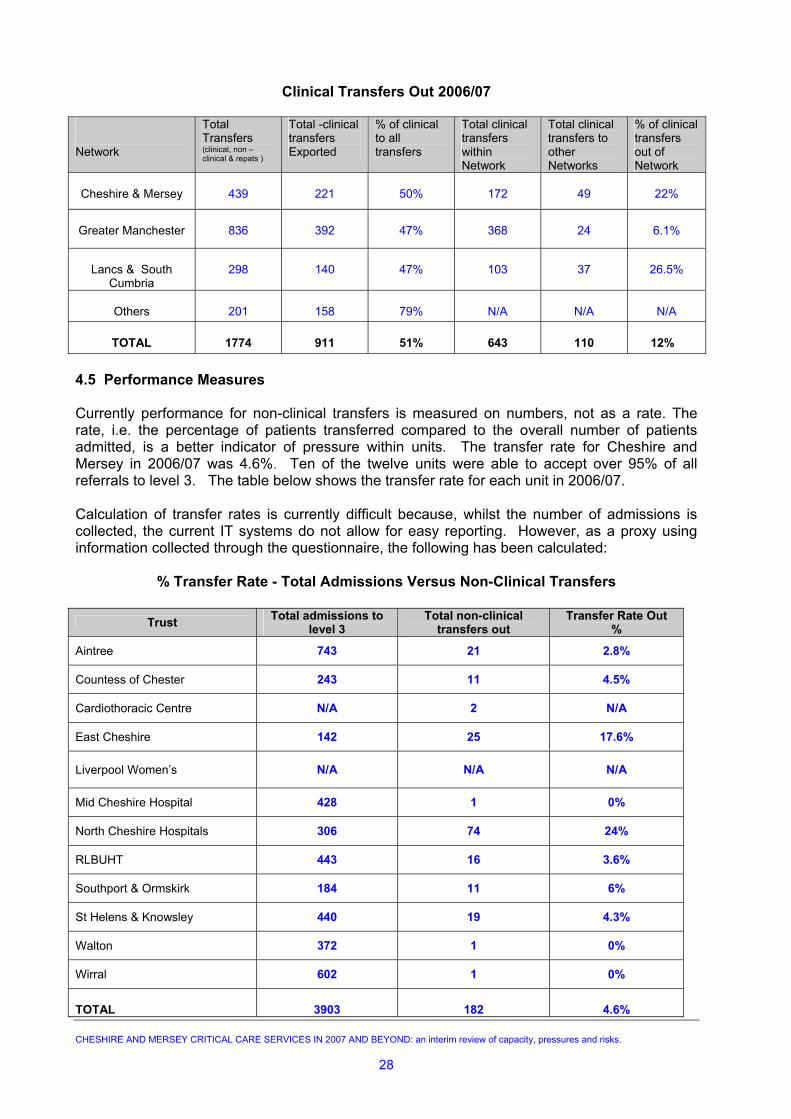
Clinical Transfers Out 2006/07 Network
Total Transfers (clinical, non – clinical & repats )
Total -clinical transfers Exported
% of clinical to all transfers
Total clinical transfers within Network
Total clinical transfers to other Networks
% of clinical transfers out of Network
Cheshire & Mersey
439
221
50%
172
49
22%
Greater Manchester
836
392
47%
368
24
6.1%
Lancs & South
Cumbria
298
140
47%
103
37
26.5%
Others
201
158
79%
N/A
N/A
N/A
TOTAL
1774
911
51%
643
110
12%
4.5 Performance Measures Currently performance for non-clinical transfers is measured on numbers, not as a rate. The rate, i.e. the percentage of patients transferred compared to the overall number of patients admitted, is a better indicator of pressure within units. The transfer rate for Cheshire and Mersey in 2006/07 was 4.6%. Ten of the twelve units were able to accept over 95% of all referrals to level 3. The table below shows the transfer rate for each unit in 2006/07. Calculation of transfer rates is currently difficult because, whilst the number of admissions is collected, the current IT systems do not allow for easy reporting. However, as a proxy using information collected through the questionnaire, the following has been calculated:
% Transfer Rate - Total Admissions Versus Non-Clinical Transfers
Trust Total admissions to level 3
Total non-clinical transfers out
Transfer Rate Out %
Aintree 743 21 2.8%
Countess of Chester 243 11 4.5%
Cardiothoracic Centre N/A 2 N/A
East Cheshire 142 25 17.6%
Liverpool Women’s N/A N/A N/A
Mid Cheshire Hospital 428 1 0%
North Cheshire Hospitals 306 74 24%
RLBUHT 443 16 3.6%
Southport & Ormskirk 184 11 6%
St Helens & Knowsley 440 19 4.3%
Walton 372 1 0%
Wirral 602 1 0%
TOTAL
3903
182
4.6%
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
28
Recommendations • The Network goal of no more than 10 non- clinical transfers per month for the
Network to be changed to every unit reducing the number of non-clinical transfers to 5% or less of all appropriate referrals received in level 3.
• The Network Board to monitor delivery of poor performance and report this to
relevant Commissioners and providers • Commissioners to identify key measures for quarterly reporting from the Network
Board • Trusts to ensure that transfer data is validated with ICBIS to ensure accurate
reporting • Trusts need to be proactive in the management of patients awaiting discharge
from critical care when the Network is on red alert. • Units to review their internal escalation policy and, if not already established,
agree a local alert system within the hospital to relieve internal pressures e.g.discharge, opening extra beds.
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
29
CHAPTER 5: WORKFORCE Critical care is provided, either directly or indirectly, by a wide range of staffing groups including healthcare assistants, porters, nurses and a variety of Allied Health Professional (AHP) staff. Each staff group requires the right skills to be able to deliver the right care to the right patient at the right time. As well as the significant additional education and training required to meet the NICE recommendations, the critical care workforce faces a number of challenges, including the need to remain fit for purpose as the NHS undergoes organisational restructuring, staffing reviews and experiences continuing financial constraints. Staffing was highlighted as an issue by five of the Acute Trusts, namely Wirral, Countess of Chester, the Cardiothoracic Centre, Mid Cheshire and the RLBUHT. 5.1 Medical Potential changes to the Royal College of Anaesthetists training requirements may impact on the viability of some units. Furthermore, there are longer-term risks to service provision as Modernising Medical Careers becomes established. There will be an overall decrease in the number of trainees, particularly in anaesthesia, and the medical trainee of the future will focus on education rather than service provision. Commissioners must be aware that, in the future, critical care units will be staffed by a combination of consultants, non-consultant grades and non-medical practitioners rather than medical trainees. This may have major service delivery and financial consequences. 5.2 Nursing and Allied Health Professionals One of the current constraints is a reduction in the amount of specialist training commissioned for nursing and Allied Health Professionals Currently, maintaining an appropriately trained nursing workforce is difficult to achieve because it requires 10% of staff each year to be in training to gain additional skills and currently no unit is able to do this. Units cannot recruit or transfer experienced staff from other specialities and have to ‘grow their own’. This makes succession planning difficult. 5.3 Recruitment and Retention Problems with recruitment and retention, particularly nursing staff, and reliance on agency staffing have changed considerably over the past few years. Four units reported recruitment problems and retention is only an issue for two of these. Most units are not reliant on agency nursing to keep beds open. CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
30
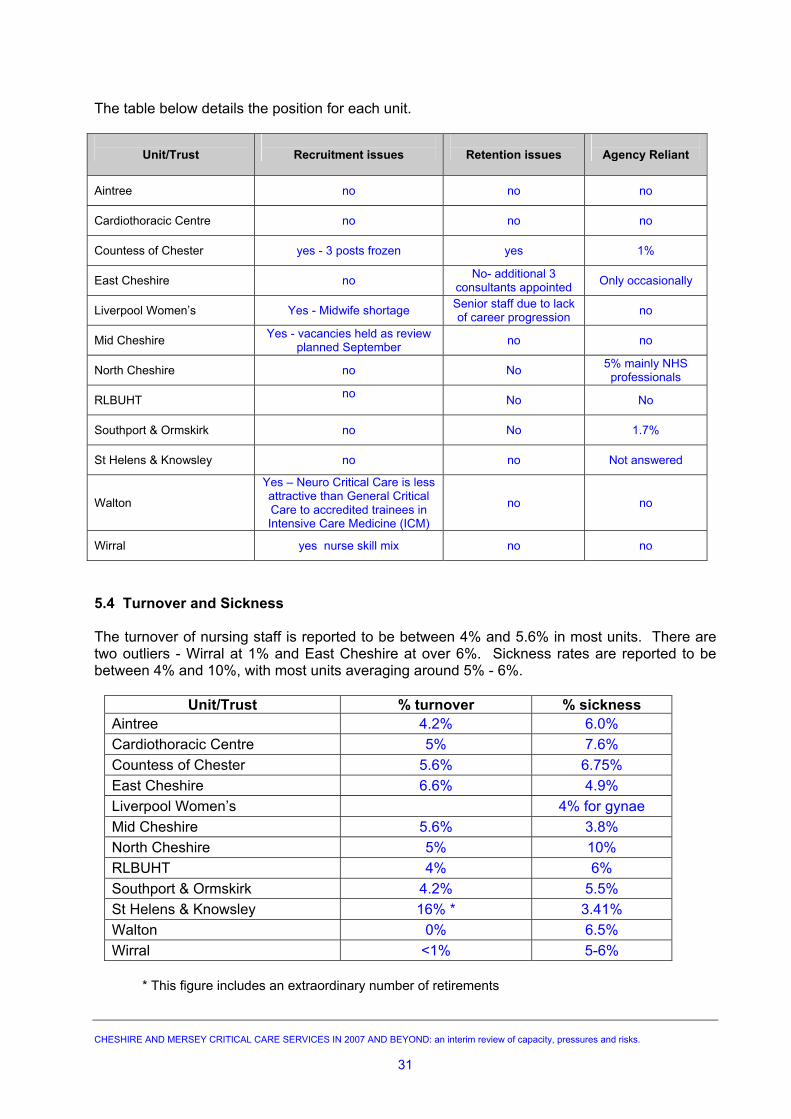
The table below details the position for each unit.
Unit/Trust
Recruitment issues
Retention issues
Agency Reliant
Aintree no no no
Cardiothoracic Centre no no no
Countess of Chester yes - 3 posts frozen yes 1%
East Cheshire no No- additional 3 consultants appointed Only occasionally
Liverpool Women’s Yes - Midwife shortage Senior staff due to lack of career progression no
Mid Cheshire Yes - vacancies held as review planned September no no
North Cheshire no No 5% mainly NHS professionals
RLBUHT no No No
Southport & Ormskirk no No 1.7%
St Helens & Knowsley no no Not answered
Walton
Yes – Neuro Critical Care is less attractive than General Critical Care to accredited trainees in Intensive Care Medicine (ICM)
no no
Wirral yes nurse skill mix no no
5.4 Turnover and Sickness The turnover of nursing staff is reported to be between 4% and 5.6% in most units. There are two outliers - Wirral at 1% and East Cheshire at over 6%. Sickness rates are reported to be between 4% and 10%, with most units averaging around 5% - 6%.
Unit/Trust % turnover % sickness Aintree 4.2% 6.0% Cardiothoracic Centre 5% 7.6% Countess of Chester 5.6% 6.75% East Cheshire 6.6% 4.9% Liverpool Women’s 4% for gynae Mid Cheshire 5.6% 3.8% North Cheshire 5% 10% RLBUHT 4% 6% Southport & Ormskirk 4.2% 5.5% St Helens & Knowsley 16% * 3.41% Walton 0% 6.5% Wirral <1% 5-6%
* This figure includes an extraordinary number of retirements
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
31
5.5 Impact of Agenda for Change (AfC) : Units made the following comments about the introduction of Agenda for Change:-
Has created lack of promotion opportunities as junior staff are all on the same band.
Has helped retain experienced staff but has eroded pay differential for senior staff. Has eroded differential between E & F grades. Has increased costs due to extra annual leave entitlement. Has reduced study leave due to the increase in annual leave. Has created difficulty in accommodating annual leave. Recruitment timescales have been lengthened.
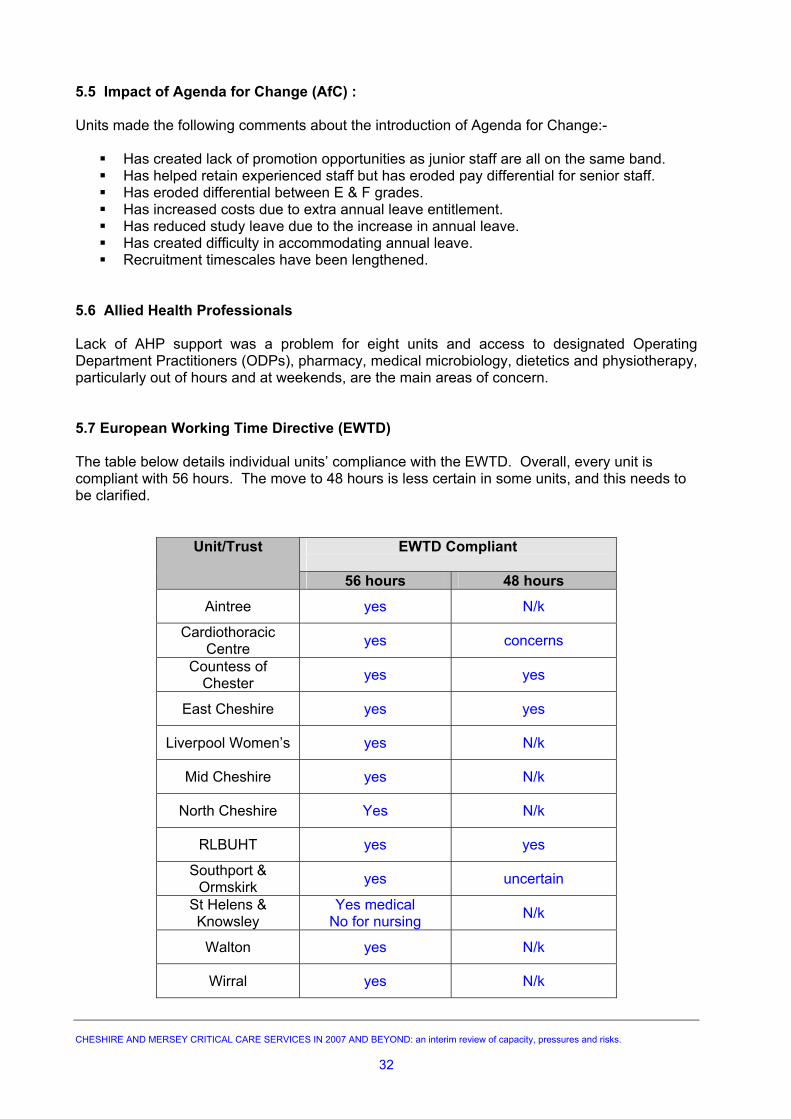
5.6 Allied Health Professionals Lack of AHP support was a problem for eight units and access to designated Operating Department Practitioners (ODPs), pharmacy, medical microbiology, dietetics and physiotherapy, particularly out of hours and at weekends, are the main areas of concern. 5.7 European Working Time Directive (EWTD) The table below details individual units’ compliance with the EWTD. Overall, every unit is compliant with 56 hours. The move to 48 hours is less certain in some units, and this needs to be clarified.
EWTD Compliant
Unit/Trust
56 hours 48 hours
Aintree yes N/k
Cardiothoracic Centre yes concerns
Countess of Chester yes yes
East Cheshire yes yes
Liverpool Women’s yes N/k
Mid Cheshire yes N/k
North Cheshire Yes N/k
RLBUHT yes yes
Southport & Ormskirk yes uncertain
St Helens & Knowsley
Yes medical No for nursing N/k
Walton yes N/k
Wirral yes N/k
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
32
5.8 Workforce – Outreach Services and Early Warning Scores “Comprehensive Critical Care” and NCEPOD recommend that hospitals providing critical care services should have an Outreach service to support ward staff caring for sicker patients 24 hours, 7 days a week. “Quality Critical Care - Beyond Comprehensive Critical Care”, published by the Department of Health in 2005, recommends that PCTs commission effective critical care services with adequate capacity for their population, including fully developed Outreach services. Publication of NICE Guidelines on 25 July 2007 for “The Care of the Unexpectedly Acutely Ill” - supported by the National Patient Safety Agency 5th Observatory report “Safer Care For The Acutely Ill Patient; Learning From Serious Incidents” National Patient Safety Agency (NPSA) July 2007 http://www.npsa.nhs.uk/health/resources/pso, recommends the regular monitoring of adult patients outside critical care while they are in hospital, and to take action if they trigger early warning scores (EWS). In particular, this covers patients who have had an emergency admission, surgery, left critical care or are moving between departments. Care of children and the terminally ill are not covered by this guidance. These guidelines will have significant impact on all hospitals including:-
The need to increase skills of ward level nurses; The need to extend Outreach services to manage sicker patients at ward level; The increased demand for critical care due to unmet need and the earlier identification of
the sicker patient. In addition, if there is further concentration of tertiary level work with District General Hospitals generally seeing sicker people, then the level of nursing skills at ward level will need to be enhanced.
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
33
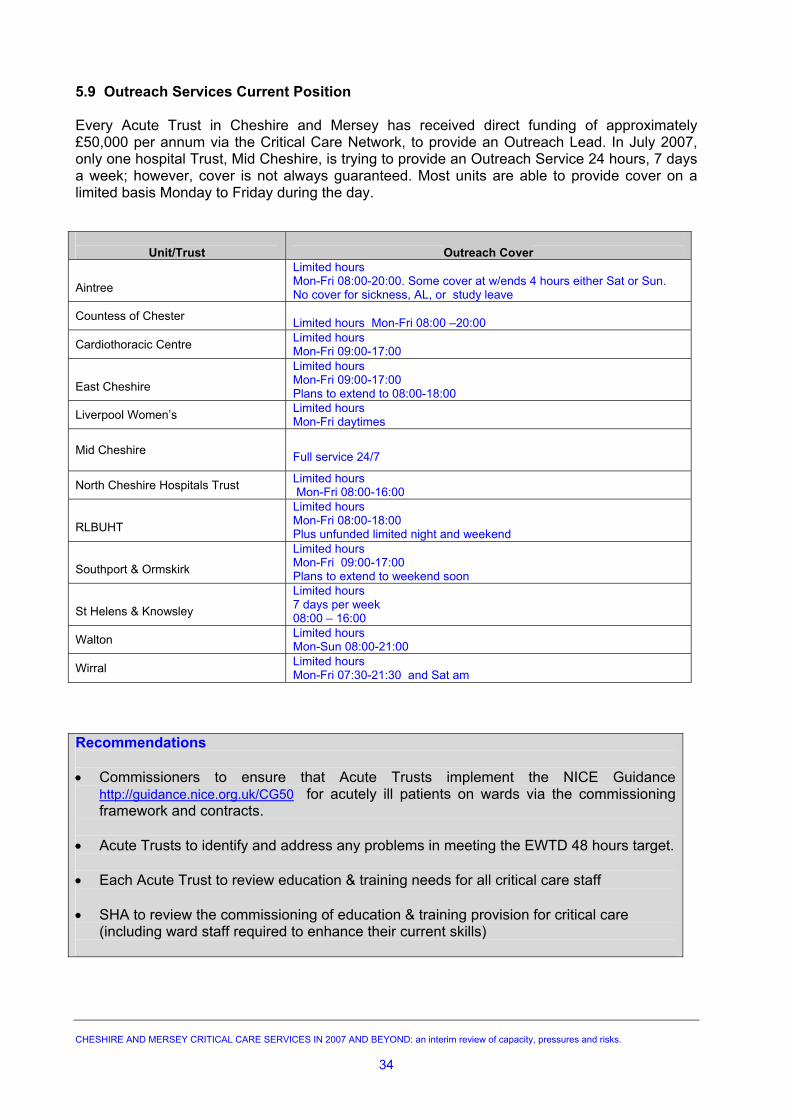
5.9 Outreach Services Current Position Every Acute Trust in Cheshire and Mersey has received direct funding of approximately £50,000 per annum via the Critical Care Network, to provide an Outreach Lead. In July 2007, only one hospital Trust, Mid Cheshire, is trying to provide an Outreach Service 24 hours, 7 days a week; however, cover is not always guaranteed. Most units are able to provide cover on a limited basis Monday to Friday during the day.
Unit/Trust
Outreach Cover
Aintree
Limited hours Mon-Fri 08:00-20:00. Some cover at w/ends 4 hours either Sat or Sun. No cover for sickness, AL, or study leave
Countess of Chester Limited hours Mon-Fri 08:00 –20:00
Cardiothoracic Centre Limited hours Mon-Fri 09:00-17:00
East Cheshire
Limited hours Mon-Fri 09:00-17:00 Plans to extend to 08:00-18:00
Liverpool Women’s Limited hours Mon-Fri daytimes
Mid Cheshire
Full service 24/7
North Cheshire Hospitals Trust Limited hours Mon-Fri 08:00-16:00
RLBUHT
Limited hours Mon-Fri 08:00-18:00 Plus unfunded limited night and weekend
Southport & Ormskirk
Limited hours Mon-Fri 09:00-17:00 Plans to extend to weekend soon
St Helens & Knowsley
Limited hours 7 days per week 08:00 – 16:00
Walton Limited hours Mon-Sun 08:00-21:00
Wirral Limited hours Mon-Fri 07:30-21:30 and Sat am
Recommendations • Commissioners to ensure that Acute Trusts implement the NICE Guidance
http://guidance.nice.org.uk/CG50 for acutely ill patients on wards via the commissioning framework and contracts.
• Acute Trusts to identify and address any problems in meeting the EWTD 48 hours target. • Each Acute Trust to review education & training needs for all critical care staff • SHA to review the commissioning of education & training provision for critical care
(including ward staff required to enhance their current skills)
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
34
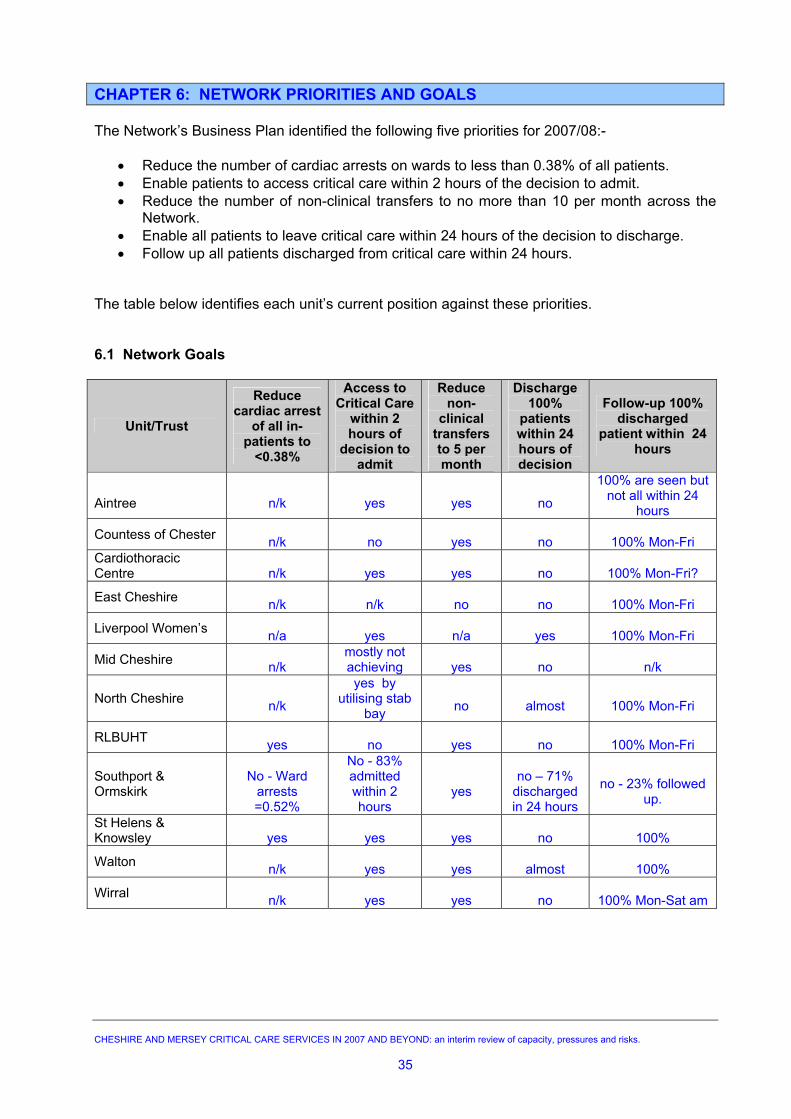
CHAPTER 6: NETWORK PRIORITIES AND GOALS The Network’s Business Plan identified the following five priorities for 2007/08:-
• Reduce the number of cardiac arrests on wards to less than 0.38% of all patients. • Enable patients to access critical care within 2 hours of the decision to admit. • Reduce the number of non-clinical transfers to no more than 10 per month across the
Network. • Enable all patients to leave critical care within 24 hours of the decision to discharge. • Follow up all patients discharged from critical care within 24 hours.
The table below identifies each unit’s current position against these priorities. 6.1 Network Goals
Unit/Trust
Reduce cardiac arrest
of all in-patients to
<0.38%
Access to Critical Care
within 2 hours of
decision to admit
Reduce non-
clinical transfers to 5 per month
Discharge 100%
patients within 24 hours of decision
Follow-up 100% discharged
patient within 24 hours
Aintree
n/k
yes
yes
no
100% are seen but not all within 24
hours
Countess of Chester n/k
no
yes
no
100% Mon-Fri
Cardiothoracic Centre
n/k
yes
yes
no
100% Mon-Fri?
East Cheshire n/k
n/k
no
no
100% Mon-Fri
Liverpool Women’s n/a
yes
n/a
yes
100% Mon-Fri
Mid Cheshire n/k
mostly not achieving
yes
no
n/k
North Cheshire n/k
yes by utilising stab
bay
no
almost
100% Mon-Fri
RLBUHT yes
no
yes
no
100% Mon-Fri
Southport & Ormskirk
No - Ward
arrests =0.52%
No - 83% admitted within 2 hours
yes
no – 71%
discharged in 24 hours
no - 23% followed
up.
St Helens & Knowsley
yes
yes
yes
no
100%
Walton n/k
yes
yes
almost
100%
Wirral n/k
yes
yes
no
100% Mon-Sat am
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
35
6.2 Network Priorities 6.2.1 Cardiac Arrest Rates
Only three Acute Trusts, RLBUHT, Southport & Ormskirk and St Helens & Knowsley are able to measure the number of cardiac arrests on wards. All other Trusts are finding this data difficult to collect.
6.2.2 Access to Critical Care
Overall, timely access to critical care is not an issue for most units - eight units are admitting all or most patients within 2 hours of the decision. However, RLBUHT, Southport & Ormskirk, the Countess of Chester and East Cheshire are not currently achieving this. 6.2.3 Transfers
As a Network, the target of <10 non-clinical transfers per month is not being met. Details are discussed in Chapter 4.
6.2.4 Discharge from Critical Care
Except for the Liverpool Women’s Hospital, no unit is managing to discharge all patients within 24 hours of the decision. Walton is the only unit able to follow up all patients within 24 hours of discharge, although most units are able to do this from Monday to Friday. 6.2.5 Follow Up
Review of discharged patients from critical care within 24 hours is being achieved by St Helens & Knowsley and the Walton Centre. In essence, this task falls to Outreach Teams who can achieve this objective during the week, but not at weekends, as most teams only operate 5 day/week. Recommendations
• Acute Trusts to ensure that systems are in place to collect the data in order to measure themselves against the 5 Network goals, particularly in relation to the time taken to access critical care
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
36
CHAPTER 7: FUTURE COMMISSIONING ARRANGEMENTS Cheshire & Mersey does not have an overall commissioning framework or service specification for critical care services. The service is funded in a variety of ways from block contracts to cost and volume based on bed days or Finished Consultant Episodes (FCEs). The Network has a good history of co-operation at a clinical level; however, as all Trusts move towards Foundation status, there will be increasing pressure for them to operate independently, and the sharing of information and best practice to improve service quality may be compromised. Commissioners are currently dependent on this collaborative approach and will need to set in place more formal mechanisms to ensure that the continued delivery of quality services within national guidance is met. Contracting for critical care services is relatively under-developed and the real cost of providing critical care is not always known. There needs to be a greater focus on the commissioning process and greater ownership by PCTs with a more sophisticated approach to contracting.
C
Recommendations •
•
•
•
•
•
Commissioners to collectively develop a commissioning framework for critical careservices, which is performance managed, ensures fair payment and can be updated toincorporate changes in policy as they arise.
Commissioners to develop and agree a standardised costing and contracting modelincorporating shadow PbR from April 2008.
Commissioners to continue to support and retain clinical input to the Network to informthe new commissioning framework. This should also include public health input via thePublic Health Network.
Commissioners to explore the potential for a single specialist centre for managingchronic critical care conditions and long term ventilated patients through a singleNetwork contract. Firstly, the Network needs to model capacity required to inform thecommissioning process.
Contracts for patients with long stays need to incorporate trim points and interim billing arrangements rather than waiting until the patient is discharged
Commissioners and Acute Trusts to ensure that CCMDS is being collected timely andaccurately and is being recorded onto Patient Administration System (PAS) systems.Current problems with SUS require urgent resolution.
HESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
37
CHAPTER 8: PAYMENT BY RESULTS AND CONTRACTING 8.1 National Position Full introduction of PbR for critical care services has been delayed by the Department of Health until 2009/10, when the outcome of a number of pilot sites across the country has been evaluated. However, the DH is expecting local introduction of shadow PbR based on local tariffs for 2008/09. Currently, Cheshire and Mersey PCTs and hospital Trusts are not ready for this. There is lack of clarity about the existing data collection processes in Trusts and whether national minimum standards are being met for CCMDS. There are also technical issues around the interface with PAS and the ability to provide meaningful reporting to support contracting. There is also a differential approach to contracting and charging for critical care across and between Networks. As more Trusts move to Foundation status there will be pressure for the introduction of explicit tariffs. The Department of Health has produced a consultation document – “Options for Future Payment by Results: 2008/09 to 2010/11” (Gateway reference 7912). Consultation ran from 15 March to 22 June 2007. The document sets out a vision for the future of PbR and, as part of this process, a number of critical care units across the country are acting as “PbR Development Sites” to establish the need and likely cost of non PbR services. These units are working to refine the proposed national tariff and understand the risks involved, particularly where it works against current activity and costs. In some parts of the country, shadow PbR is already being tested and contracts based on an 80/20 split (based on 100% of historic activity) are in place. The Department of Health will take a view about whether there is sufficient evidence that the use of HRGs and proposed cost weights are appropriate for critical care. Their preference is to publish an indicative tariff as a price signal to inform local negotiation in 2008/9 before considering a mandatory tariff for 2009/10. The introduction of PbR for critical care will now be delayed until at least 2009/10. The current costs of critical care are, on average, approximately £1400 per day for an adult intensive care bed and £900 for a high dependency bed. To date, much work has been done to build capacity and organise services on a Network basis to ensure that demand can be met. The Department of Health recommends that any new funding models must strengthen not weaken progress already made. Concerns have been expressed that leaving critical care services outside the scope of PbR could undermine the services when they are a key component of many care pathways. Currently, the expectation is that critical care services are shadowing PbR using cost and volume commissioning and case mix weighting where possible. However, this is not the case within Cheshire and Mersey.
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
38
8.2 Local Position In Cheshire and Mersey there are a number of different approaches to contracting and charging for critical care. Currently this service is funded through non PbR and in 2007/08:
1 Trust has a mixed arrangement of block and cost and volume (in both bed days and FCEs)
1 Trust has a mix of block and cost and volume 1 Trust has a mix of block and cost and bed days based 5 Trusts have cost and volume bed days 2 remain with block contracts 1 Trust has a cost and volume FCE based
Most contracts are based on historic activity, although it is not clear why costs have risen from approximately £50 million in 2006/07 to almost £60 million in 2007/08. There is wide variation between units, with HDU (Level 2) beds estimated to cost between £477 and £1600 per day, often using different methods of calculation. In July 2007, Contracts and Information Shares Services Unit (CISSU), on behalf of the Critical Care Network, requested contract information from Trusts and Commissioners. The following points summarise the initial findings; however, more detailed analysis is required to fully understand the current position:
Some Trusts have changed contracts for 2007/08, moving from block to cost and volume or vice versa. Charges for under or over performance against plan vary from full to marginal costs. Contract currencies vary significantly, with either blanket costs or detailed tariffs based on dependency. Costs vary significantly between Trusts and the costing information submitted requires more detailed analysis, particularly in relation to tariffs and reference costs. All Trusts who have submitted information are invoicing PCTs for activity not covered in contracts. Information regarding the collection of CCMDS is incomplete and it is not clear if Trusts understand what data set should be collected.
If a PbR tariff is introduced on the basis of organ support (as is currently being modelled by the Department of Health with some pilot sites), it raises issues for the future costing of the use of level 2 beds for recovery, post operative surgery and for some specialist services. This will be a particular risk for units where delayed discharge of patients is a problem - again the issue of the wrong patient in the wrong bed. Significant work will need to be undertaken to ensure the system is ready for the proposed introduction of shadow PbR in 2008/09, and before a standardised approach to contracts can be introduced. 8.3 Critical Care Minimum Dataset The Critical Care Minimum Data Set (CCMDS) was introduced in 2006/07, replacing the Augmented Care Period (ACP). The collection of CCMDS will underpin the critical care HRGs for level 2 and level 3 services, based on level of organ support. The new CCMDS data collection records patients by organ support and will, therefore, support the movement towards a more accurate costing system.
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
39
There are currently issues relating to reporting. At present, all acute hospital Trusts in Cheshire & Mersey are collecting the CCMDS; however, the interface with the hospital PAS system is not in place in all Trusts to enable easy interrogation. The ability for Acute Trusts and Commissioners to access this information is crucial in moving towards a transparent costing system for critical care services. Cheshire and Mersey is paying £216,000 per annum to collect data. Every critical care unit is currently paying approximately £5000 per annum to the Intensive Care National Audit and Research Centre (ICNARC), and the Network is supporting each unit to provide audit clerks to collect this information at a cost of approximately £13,000 per unit. Prior to the proposed introduction of a mandatory national tariff, Trusts will need to fully understand the current profile of activity between level 2 and level 3 to inform future income streams for critical care. This will be a particular risk for units where delayed discharge of patients is a problem. Under the proposed arrangements, a level 2 patient occupying a level 3 bed will be charged at a level 2 tariff, and a level one patient occupying a level 2 bed would only attract a ward bed tariff. Therefore, patients with inappropriate lengths of stay will be utilising higher levels of resources than their condition requires and commissioners will not fund this.
C
Recommendations • Acute Trusts and Commissioners to understand the true baseline line costs of the
service • A standardised approach to contracting to be adopted • Lead commissioning arrangements to be considered • Recharging arrangements between Trusts and networks to be consistent • Consider if a local bed day tariff should be developed in advance of PbR • Consider the development of a contract based on 80/20 split as per DH PbR
recommendation • Each unit to calculate the financial impact of PbR, if it is introduced on the basis of
organ support, and discuss with Commissioners at an early stage • The Network team to work with the Connecting for Health Team to understand the
timetable for implementation of SUS across Cheshire and Mersey • The Network to establish the status of CCMDS for each Trust.
HESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
40
CHAPTER 9: FUTURE PLANS Overall, the way in which critical care services are planned, both at a commissioned/ strategic level and within Acute Trusts, is uncontrolled and fragmented. With full implementation of Foundation Trusts by 2009, clarity is essential about who is responsible for these investment decisions and who will pay. There is a view that the introduction of a national tariff and PbR for critical care will resolve this, and that future investment decisions will be driven by individual Acute Trusts taking the risk of not filling beds where over-planning occurs. A number of plans within Cheshire and Mersey are being made as part of FT applications, particularly for increased level 2 capacity to support elective surgery throughput. It is not clear if these beds are to be developed separately and ring fenced away from beds required to admit emergencies. Commissioners need to understand if these hospital Trust plans will relieve pressure on critical care, aid internal discharge and stepping down level of care, provide sufficient capacity to admit emergencies, and ensure non-clinical transfers are kept to a minimum. More importantly, appropriate utilisation of existing capacity, particularly where beds are blocked due to delayed discharge or where level 2 beds are blocked by level 1 patients, needs to be addressed by Acute Trusts before further investment decisions in critical care can be considered and supported by Commissioners. There is some doubt about whether PbR will ever be fully introduced for critical care and plans for future investment may be made through contracts based on historic activity, with 80% paid in block by Commissioners to secure access to the service and 20% paid for usage. This approach would effectively share the bulk of the risk. Any activity above these levels could be paid for on a bed day cost basis, using number of organs supported. However, this may not adequately, or effectively, cover the costs of agreed expansion plans. There needs to be an agreed mechanism to move the 80/20 limits upwards or downwards to accommodate service development or de-commissioning of services as part of the annual contracting round. 9.1 More Beds It is unclear what the status of individual hospital Trusts future plans is for the expansion of critical care. However, based on their responses to the questionnaire, the Network could expect to see anything from between 27 and 57 additional beds by 2014/15. To avoid over planning and to reduce the risk of over investment, Commissioners and Acute Trusts need to collectively understand the status of these plans and agree the level of future capacity requirements. Ideally, plans for each Trust should be reviewed between Commissioners and Acute Trusts annually.
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
41
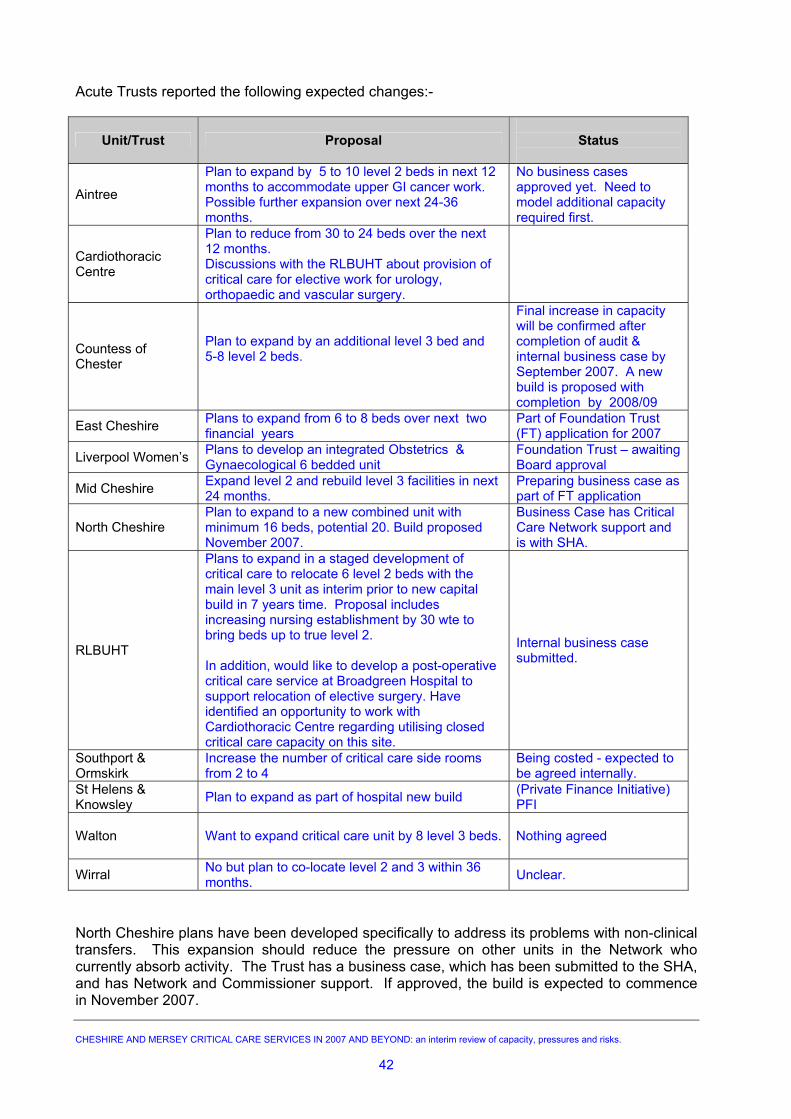
Acute Trusts reported the following expected changes:-
Unit/Trust Proposal
Status
Aintree
Plan to expand by 5 to 10 level 2 beds in next 12 months to accommodate upper GI cancer work. Possible further expansion over next 24-36 months.
No business cases approved yet. Need to model additional capacity required first.
Cardiothoracic Centre
Plan to reduce from 30 to 24 beds over the next 12 months. Discussions with the RLBUHT about provision of critical care for elective work for urology, orthopaedic and vascular surgery.
Countess of Chester
Plan to expand by an additional level 3 bed and 5-8 level 2 beds.
Final increase in capacity will be confirmed after completion of audit & internal business case by September 2007. A new build is proposed with completion by 2008/09
East Cheshire Plans to expand from 6 to 8 beds over next two financial years
Part of Foundation Trust (FT) application for 2007
Liverpool Women’s Plans to develop an integrated Obstetrics & Gynaecological 6 bedded unit
Foundation Trust – awaiting Board approval
Mid Cheshire Expand level 2 and rebuild level 3 facilities in next 24 months.
Preparing business case as part of FT application
North Cheshire Plan to expand to a new combined unit with minimum 16 beds, potential 20. Build proposed November 2007.
Business Case has Critical Care Network support and is with SHA.
RLBUHT
Plans to expand in a staged development of critical care to relocate 6 level 2 beds with the main level 3 unit as interim prior to new capital build in 7 years time. Proposal includes increasing nursing establishment by 30 wte to bring beds up to true level 2. In addition, would like to develop a post-operative critical care service at Broadgreen Hospital to support relocation of elective surgery. Have identified an opportunity to work with Cardiothoracic Centre regarding utilising closed critical care capacity on this site.
Internal business case submitted.
Southport & Ormskirk
Increase the number of critical care side rooms from 2 to 4
Being costed - expected to be agreed internally.
St Helens & Knowsley Plan to expand as part of hospital new build (Private Finance Initiative)
PFI Walton
Want to expand critical care unit by 8 level 3 beds. Nothing agreed
Wirral No but plan to co-locate level 2 and 3 within 36 months. Unclear.
North Cheshire plans have been developed specifically to address its problems with non-clinical transfers. This expansion should reduce the pressure on other units in the Network who currently absorb activity. The Trust has a business case, which has been submitted to the SHA, and has Network and Commissioner support. If approved, the build is expected to commence in November 2007.
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
42
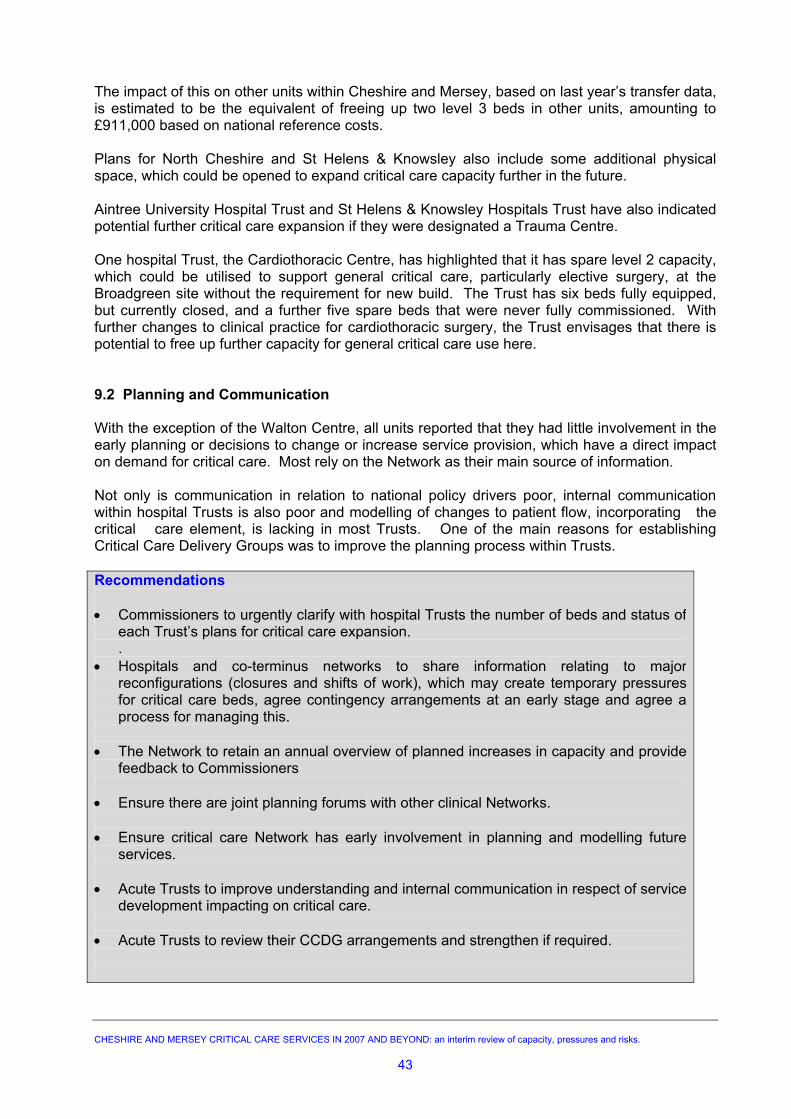
The impact of this on other units within Cheshire and Mersey, based on last year’s transfer data, is estimated to be the equivalent of freeing up two level 3 beds in other units, amounting to £911,000 based on national reference costs. Plans for North Cheshire and St Helens & Knowsley also include some additional physical space, which could be opened to expand critical care capacity further in the future. Aintree University Hospital Trust and St Helens & Knowsley Hospitals Trust have also indicated potential further critical care expansion if they were designated a Trauma Centre. One hospital Trust, the Cardiothoracic Centre, has highlighted that it has spare level 2 capacity, which could be utilised to support general critical care, particularly elective surgery, at the Broadgreen site without the requirement for new build. The Trust has six beds fully equipped, but currently closed, and a further five spare beds that were never fully commissioned. With further changes to clinical practice for cardiothoracic surgery, the Trust envisages that there is potential to free up further capacity for general critical care use here. 9.2 Planning and Communication With the exception of the Walton Centre, all units reported that they had little involvement in the early planning or decisions to change or increase service provision, which have a direct impact on demand for critical care. Most rely on the Network as their main source of information. Not only is communication in relation to national policy drivers poor, internal communication within hospital Trusts is also poor and modelling of changes to patient flow, incorporating the critical care element, is lacking in most Trusts. One of the main reasons for establishing Critical Care Delivery Groups was to improve the planning process within Trusts. Recommendations • Commissioners to urgently clarify with hospital Trusts the number of beds and status of
each Trust’s plans for critical care expansion. .
• Hospitals and co-terminus networks to share information relating to major reconfigurations (closures and shifts of work), which may create temporary pressures for critical care beds, agree contingency arrangements at an early stage and agree a process for managing this.
• The Network to retain an annual overview of planned increases in capacity and provide
feedback to Commissioners • Ensure there are joint planning forums with other clinical Networks. • Ensure critical care Network has early involvement in planning and modelling future
services. • Acute Trusts to improve understanding and internal communication in respect of service
development impacting on critical care. • Acute Trusts to review their CCDG arrangements and strengthen if required. CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
43
SUMMARY AND CONCLUSION: Overall, the Cheshire & Mersey critical care system manages current capacity well. However, this is not commissioning led and may not be fit for purpose in the future to adequately address changes in demand and appropriately respond to external drivers. Interviews with each unit highlighted a number of common issues and themes, which have been discussed in the body of the report. The shape of demand for Level 3 has changed, and 80% is due to medical and surgical emergencies either from A&E admissions or from patients on the wards. Delayed discharges are a universal problem and the increased throughput of elective surgery is exacerbating this. Staffing issues and patients with longer lengths of stay are also highlighted as a pressure. All units have significant flows of patients moving both in and out and experience spikes in demand, where transfers are unavoidable and tend to be seasonal – mostly from November to March. As occupancy levels increase and remain constant to meet the 18-week target, there may be less seasonal variation and non-clinical transfers will be an ongoing pressure. Delayed discharge of patients from critical care beds to lower levels of care and to wards was cited by every unit as the biggest problem. This will be a significant issue for both Commissioners and providers once PbR is introduced, as charging will be based on a combination of organs support (level of care), and appropriate patient location. Most Trusts have plans for expanding critical care. Some are aspirational, and some are highly developed. Currently, Commissioners do not have a real understanding of these proposals. It is important however that, prior to supporting additional investment, a wider understanding of the current usage and the wider Network implications should be obtained.
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
44
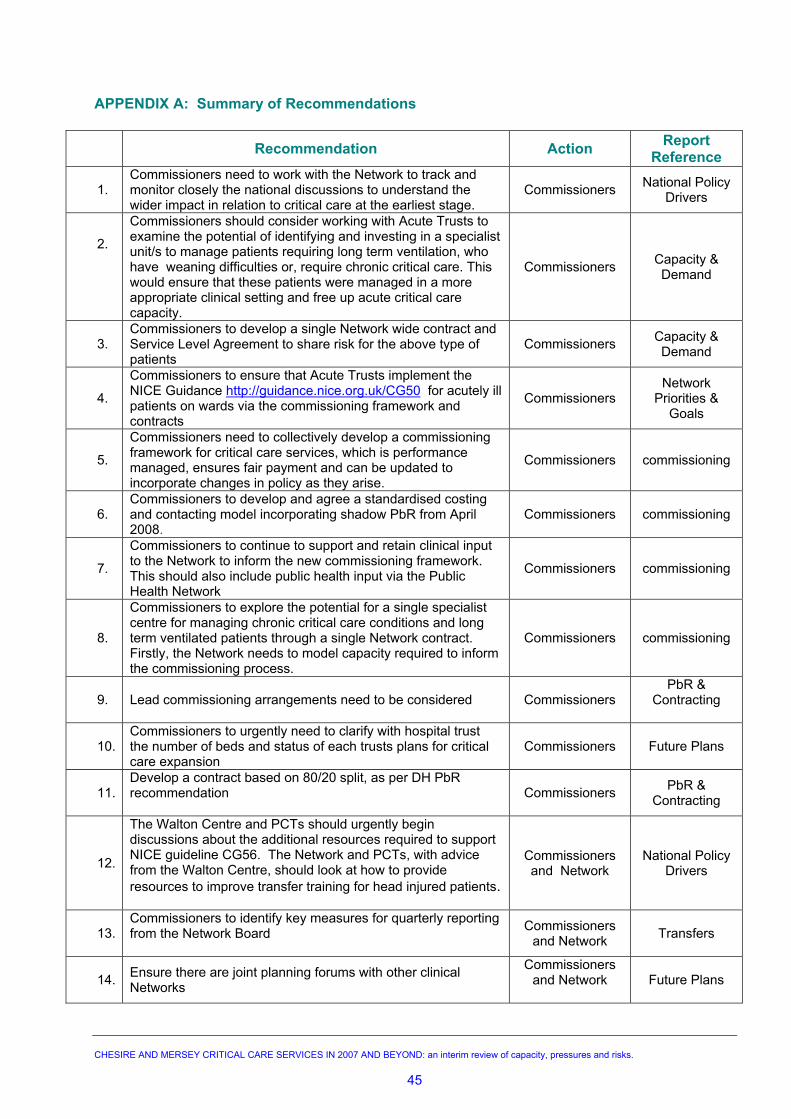
APPENDIX A: Summary of Recommendations
Recommendation Action Report Reference
1. Commissioners need to work with the Network to track and monitor closely the national discussions to understand the wider impact in relation to critical care at the earliest stage.
Commissioners National Policy Drivers
2.
Commissioners should consider working with Acute Trusts to examine the potential of identifying and investing in a specialist unit/s to manage patients requiring long term ventilation, who have weaning difficulties or, require chronic critical care. This would ensure that these patients were managed in a more appropriate clinical setting and free up acute critical care capacity.
Commissioners Capacity & Demand
3. Commissioners to develop a single Network wide contract and Service Level Agreement to share risk for the above type of patients
Commissioners Capacity & Demand
4.
Commissioners to ensure that Acute Trusts implement the NICE Guidance http://guidance.nice.org.uk/CG50 for acutely ill patients on wards via the commissioning framework and contracts
Commissioners Network
Priorities & Goals
5.
Commissioners need to collectively develop a commissioning framework for critical care services, which is performance managed, ensures fair payment and can be updated to incorporate changes in policy as they arise.
Commissioners commissioning
6. Commissioners to develop and agree a standardised costing and contacting model incorporating shadow PbR from April 2008.
Commissioners commissioning
7. Commissioners to continue to support and retain clinical input to the Network to inform the new commissioning framework. This should also include public health input via the Public Health Network
Commissioners commissioning
8.
Commissioners to explore the potential for a single specialist centre for managing chronic critical care conditions and long term ventilated patients through a single Network contract. Firstly, the Network needs to model capacity required to inform the commissioning process.
Commissioners commissioning
9. Lead commissioning arrangements need to be considered Commissioners PbR &
Contracting
10. Commissioners to urgently need to clarify with hospital trust the number of beds and status of each trusts plans for critical care expansion
Commissioners Future Plans
11. Develop a contract based on 80/20 split, as per DH PbR recommendation
Commissioners PbR & Contracting
12.
The Walton Centre and PCTs should urgently begin discussions about the additional resources required to support NICE guideline CG56. The Network and PCTs, with advice from the Walton Centre, should look at how to provide resources to improve transfer training for head injured patients.
Commissioners and Network
National Policy Drivers
13. Commissioners to identify key measures for quarterly reporting from the Network Board
Commissioners and Network Transfers
14. Ensure there are joint planning forums with other clinical Networks
Commissioners and Network
Future Plans
CHESIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
45
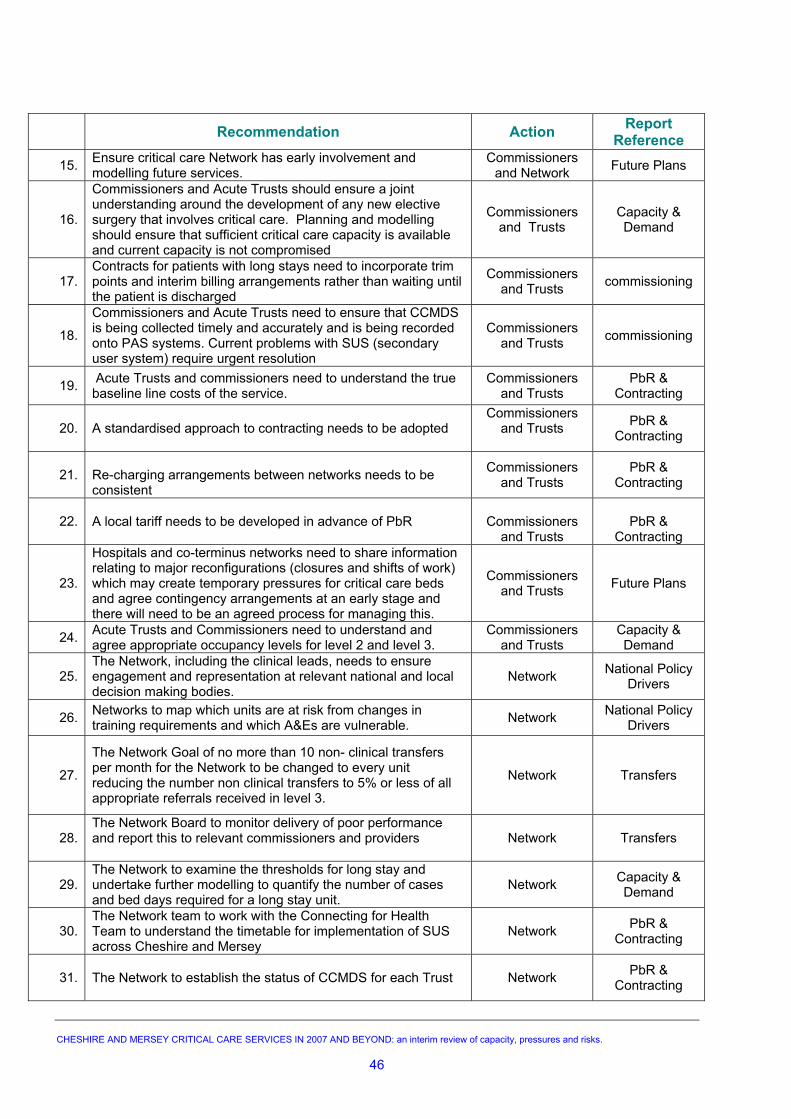
Recommendation Action Report Reference
15. Ensure critical care Network has early involvement and modelling future services.
Commissioners and Network Future Plans
16.
Commissioners and Acute Trusts should ensure a joint understanding around the development of any new elective surgery that involves critical care. Planning and modelling should ensure that sufficient critical care capacity is available and current capacity is not compromised
Commissioners and Trusts
Capacity & Demand
17. Contracts for patients with long stays need to incorporate trim points and interim billing arrangements rather than waiting until the patient is discharged
Commissioners and Trusts commissioning
18.
Commissioners and Acute Trusts need to ensure that CCMDS is being collected timely and accurately and is being recorded onto PAS systems. Current problems with SUS (secondary user system) require urgent resolution
commissioning
19. Acute Trusts and commissioners need to understand the true baseline line costs of the service.
Commissioners and Trusts
PbR & Contracting
20. A standardised approach to contracting needs to be adopted
Commissioners and Trusts
PbR & Contracting
21. Re-charging arrangements between networks needs to be consistent
Commissioners and Trusts
PbR & Contracting
22. A local tariff needs to be developed in advance of PbR
Commissioners
and Trusts
PbR &
Contracting
23.
Hospitals and co-terminus networks need to share information relating to major reconfigurations (closures and shifts of work) which may create temporary pressures for critical care beds and agree contingency arrangements at an early stage and there will need to be an agreed process for managing this.
Commissioners and Trusts Future Plans
24. Acute Trusts and Commissioners need to understand and agree appropriate occupancy levels for level 2 and level 3.
Commissioners and Trusts
Capacity & Demand
25. The Network, including the clinical leads, needs to ensure engagement and representation at relevant national and local decision making bodies.
Network National Policy Drivers
26. Networks to map which units are at risk from changes in training requirements and which A&Es are vulnerable. Network National Policy
Drivers
27.
The Network Goal of no more than 10 non- clinical transfers per month for the Network to be changed to every unit reducing the number non clinical transfers to 5% or less of all appropriate referrals received in level 3.
Network Transfers
28. The Network Board to monitor delivery of poor performance and report this to relevant commissioners and providers
Network Transfers
29. The Network to examine the thresholds for long stay and undertake further modelling to quantify the number of cases and bed days required for a long stay unit.
Network Capacity & Demand
30. The Network team to work with the Connecting for Health Team to understand the timetable for implementation of SUS across Cheshire and Mersey
Network PbR & Contracting
31. The Network to establish the status of CCMDS for each Trust
Network PbR & Contracting
Commissioners and Trusts
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
46
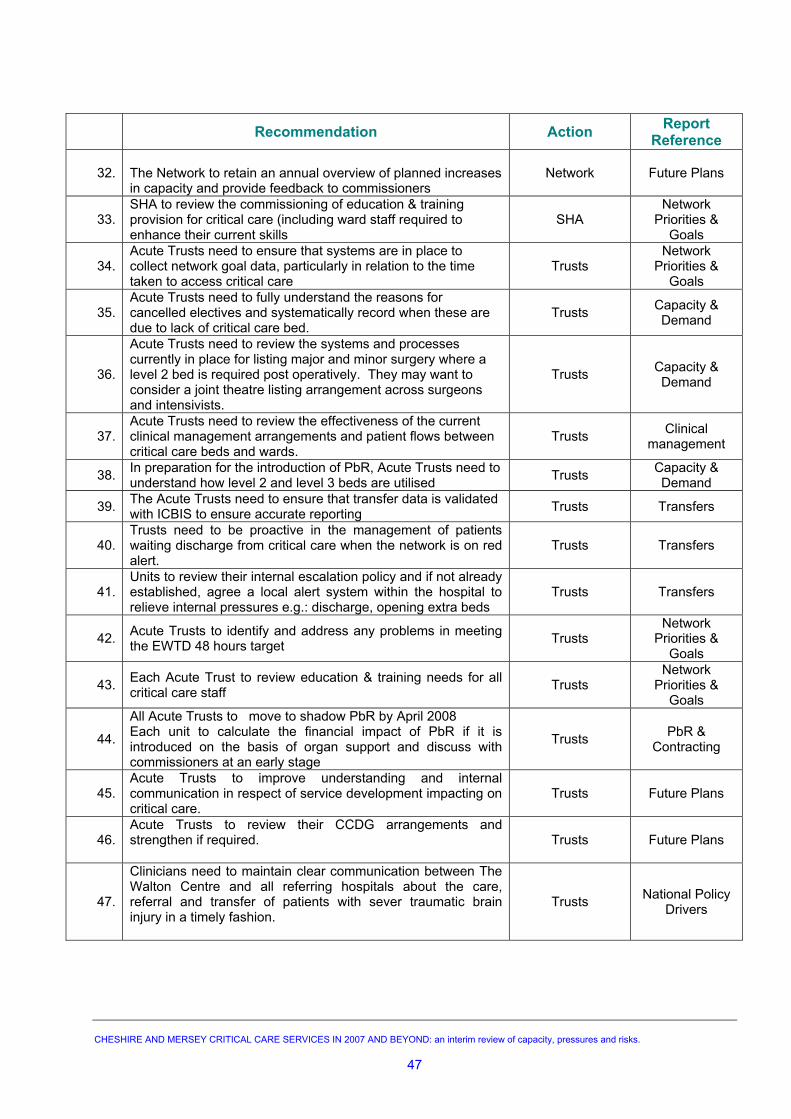
Recommendation Action Report Reference
32. The Network to retain an annual overview of planned increases in capacity and provide feedback to commissioners
Network Future Plans
33. SHA to review the commissioning of education & training provision for critical care (including ward staff required to enhance their current skills
SHA Network
Priorities & Goals
34. Acute Trusts need to ensure that systems are in place to collect network goal data, particularly in relation to the time taken to access critical care
Trusts Network
Priorities & Goals
35. Acute Trusts need to fully understand the reasons for cancelled electives and systematically record when these are due to lack of critical care bed.
Trusts Capacity & Demand
36.
Acute Trusts need to review the systems and processes currently in place for listing major and minor surgery where a level 2 bed is required post operatively. They may want to consider a joint theatre listing arrangement across surgeons and intensivists.
Trusts Capacity & Demand
37. Acute Trusts need to review the effectiveness of the current clinical management arrangements and patient flows between critical care beds and wards.
Trusts Clinical management
38. In preparation for the introduction of PbR, Acute Trusts need to understand how level 2 and level 3 beds are utilised Trusts Capacity &
Demand
39. The Acute Trusts need to ensure that transfer data is validated with ICBIS to ensure accurate reporting Trusts Transfers
40. Trusts need to be proactive in the management of patients waiting discharge from critical care when the network is on red alert.
Trusts Transfers
41. Units to review their internal escalation policy and if not already established, agree a local alert system within the hospital to relieve internal pressures e.g.: discharge, opening extra beds
Trusts Transfers
42. Acute Trusts to identify and address any problems in meeting the EWTD 48 hours target Trusts
Network Priorities &
Goals
43. Each Acute Trust to review education & training needs for all critical care staff Trusts
Network Priorities &
Goals
44.
All Acute Trusts to move to shadow PbR by April 2008 Each unit to calculate the financial impact of PbR if it is introduced on the basis of organ support and discuss with commissioners at an early stage
Trusts PbR & Contracting
45. Acute Trusts to improve understanding and internal communication in respect of service development impacting on critical care.
Trusts Future Plans
46. Acute Trusts to review their CCDG arrangements and strengthen if required.
Trusts Future Plans
47.
Clinicians need to maintain clear communication between The Walton Centre and all referring hospitals about the care, referral and transfer of patients with sever traumatic brain injury in a timely fashion.
Trusts National Policy Drivers
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
47
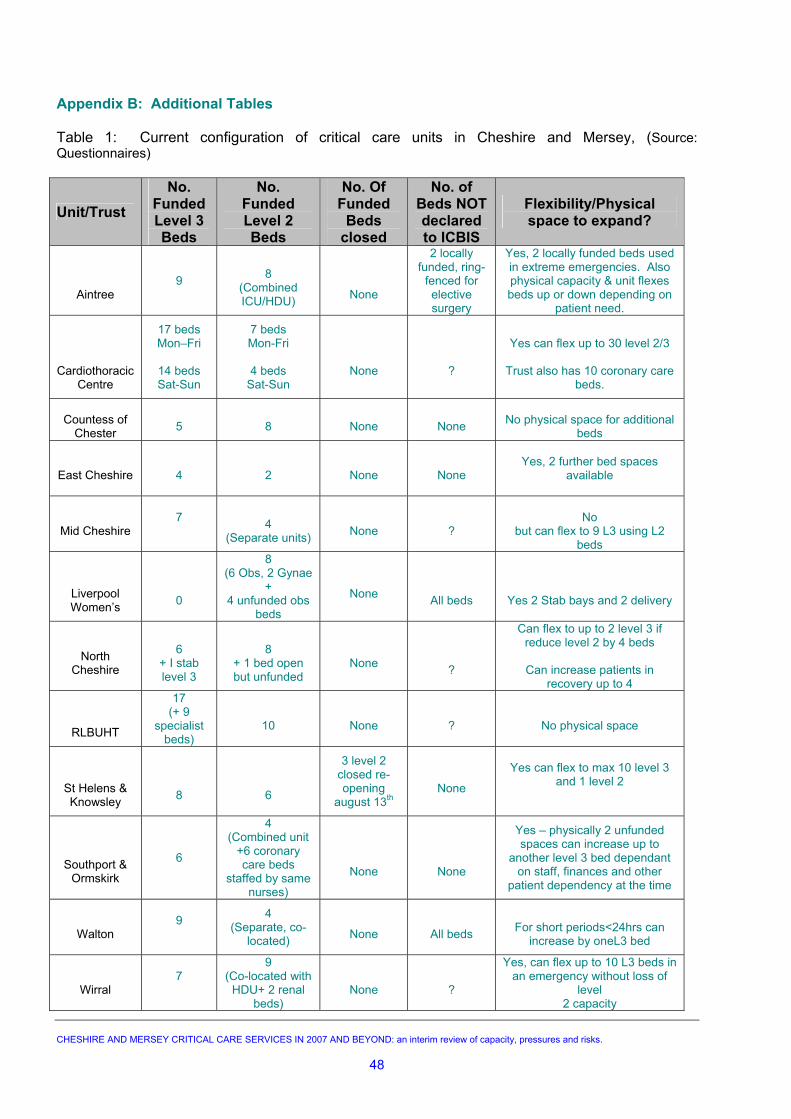
Appendix B: Additional Tables Table 1: Current configuration of critical care units in Cheshire and Mersey, (Source: Questionnaires)
Unit/Trust No.
Funded Level 3 Beds
No. Funded Level 2 Beds
No. Of Funded
Beds closed
No. of Beds NOT declared to ICBIS
Flexibility/Physical space to expand?
Aintree
9
8
(Combined ICU/HDU)
None
2 locally funded, ring-
fenced for elective surgery
Yes, 2 locally funded beds used in extreme emergencies. Also physical capacity & unit flexes beds up or down depending on
patient need.
Cardiothoracic Centre
17 beds Mon–Fri
14 beds Sat-Sun
7 beds Mon-Fri
4 beds
Sat-Sun
None
?
Yes can flex up to 30 level 2/3
Trust also has 10 coronary care
beds.
Countess of
Chester
5
8
None
None
No physical space for additional
beds
East Cheshire
4
2
None
None
Yes, 2 further bed spaces
available
Mid Cheshire
7
4
(Separate units)
None
?
No
but can flex to 9 L3 using L2 beds
Liverpool Women’s
0
8 (6 Obs, 2 Gynae
+ 4 unfunded obs
beds
None
All beds
Yes 2 Stab bays and 2 delivery
North
Cheshire
6
+ I stab level 3
8
+ 1 bed open but unfunded
None
?
Can flex to up to 2 level 3 if reduce level 2 by 4 beds
Can increase patients in
recovery up to 4
RLBUHT
17 (+ 9
specialist beds)
10
None
?
No physical space
St Helens & Knowsley
8
6
3 level 2 closed re-opening
august 13th
None
Yes can flex to max 10 level 3
and 1 level 2
Southport & Ormskirk
6
4 (Combined unit
+6 coronary care beds
staffed by same nurses)
None
None
Yes – physically 2 unfunded spaces can increase up to
another level 3 bed dependant on staff, finances and other
patient dependency at the time
Walton
9
4 (Separate, co-
located)
None
All beds
For short periods<24hrs can
increase by oneL3 bed
Wirral
7
9 (Co-located with
HDU+ 2 renal beds)
None
?
Yes, can flex up to 10 L3 beds in an emergency without loss of
level 2 capacity
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
48
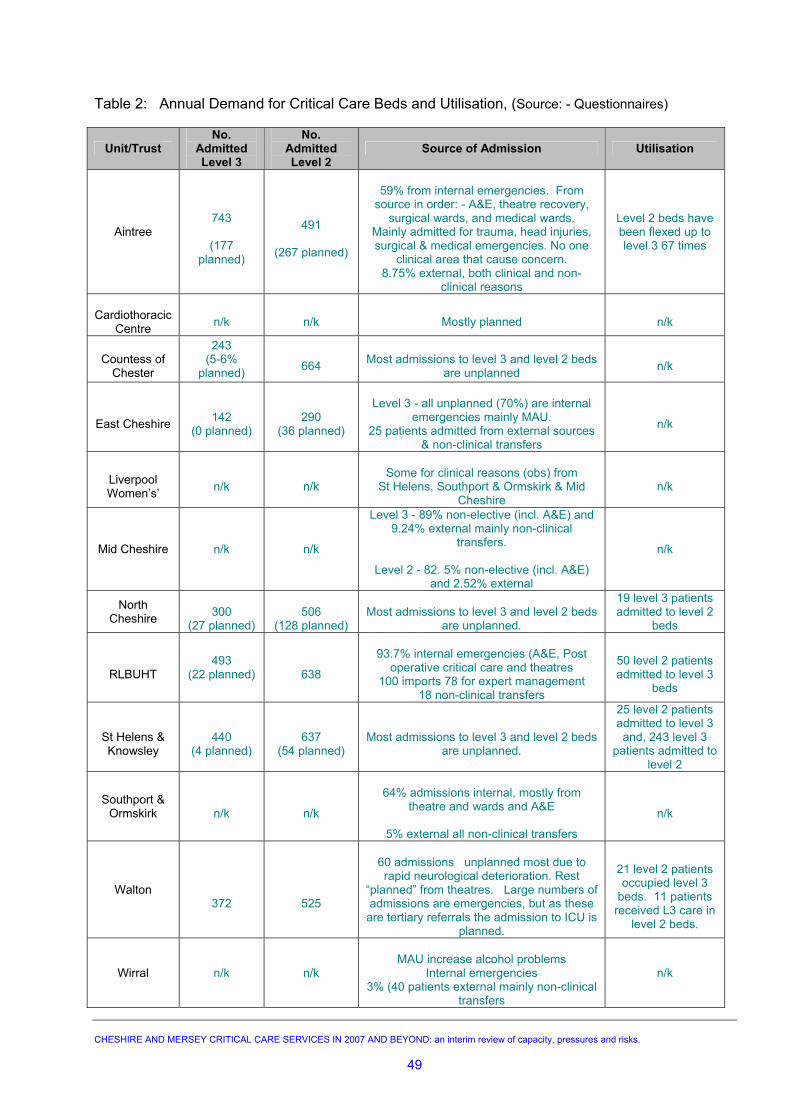
Table 2: Annual Demand for Critical Care Beds and Utilisation, (Source: - Questionnaires)
Unit/Trust No.
Admitted Level 3
No. Admitted Level 2
Source of Admission Utilisation
Aintree
743
(177 planned)
491
(267 planned)
59% from internal emergencies. From
source in order: - A&E, theatre recovery, surgical wards, and medical wards.
Mainly admitted for trauma, head injuries, surgical & medical emergencies. No one
clinical area that cause concern. 8.75% external, both clinical and non-
clinical reasons
Level 2 beds have been flexed up to level 3 67 times
Cardiothoracic
Centre
n/k
n/k
Mostly planned
n/k
Countess of
Chester
243 (5-6%
planned)
664
Most admissions to level 3 and level 2 beds
are unplanned
n/k
East Cheshire
142
(0 planned)
290
(36 planned)
Level 3 - all unplanned (70%) are internal
emergencies mainly MAU. 25 patients admitted from external sources
& non-clinical transfers
n/k
Liverpool Women’s’
n/k
n/k
Some for clinical reasons (obs) from
St Helens, Southport & Ormskirk & Mid Cheshire
n/k
Mid Cheshire n/k n/k
Level 3 - 89% non-elective (incl. A&E) and 9.24% external mainly non-clinical
transfers.
Level 2 - 82. 5% non-elective (incl. A&E) and 2.52% external
n/k
North Cheshire
300
(27 planned)
506
(128 planned)
Most admissions to level 3 and level 2 beds
are unplanned.
19 level 3 patients admitted to level 2
beds
RLBUHT
493
(22 planned)
638
93.7% internal emergencies (A&E, Post
operative critical care and theatres 100 imports 78 for expert management
18 non-clinical transfers
50 level 2 patients admitted to level 3
beds
St Helens & Knowsley
440
(4 planned)
637
(54 planned)
Most admissions to level 3 and level 2 beds
are unplanned.
25 level 2 patients admitted to level 3 and, 243 level 3
patients admitted to level 2
Southport & Ormskirk
n/k
n/k
64% admissions internal, mostly from
theatre and wards and A&E
5% external all non-clinical transfers
n/k
Walton
372
525
60 admissions unplanned most due to rapid neurological deterioration. Rest
“planned” from theatres. Large numbers of admissions are emergencies, but as these
are tertiary referrals the admission to ICU is planned.
21 level 2 patients occupied level 3
beds. 11 patients received L3 care in
level 2 beds.
Wirral n/k n/k
MAU increase alcohol problems
Internal emergencies 3% (40 patients external mainly non-clinical
transfers
n/k
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
49
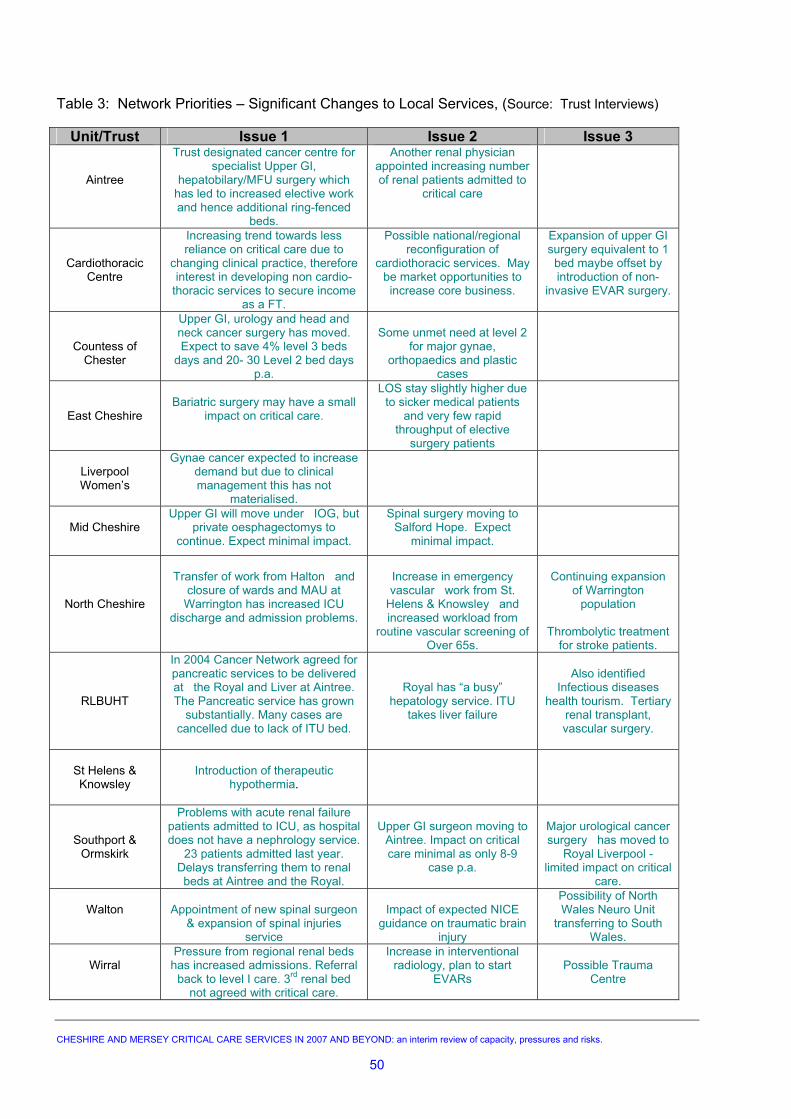
Table 3: Network Priorities – Significant Changes to Local Services, (Source: Trust Interviews)
Unit/Trust Issue 1 Issue 2 Issue 3
Aintree
Trust designated cancer centre for specialist Upper GI,
hepatobilary/MFU surgery which has led to increased elective work and hence additional ring-fenced
beds.
Another renal physician appointed increasing number of renal patients admitted to
critical care
Cardiothoracic Centre
Increasing trend towards less reliance on critical care due to
changing clinical practice, therefore interest in developing non cardio-
thoracic services to secure income as a FT.
Possible national/regional reconfiguration of
cardiothoracic services. May be market opportunities to increase core business.
Expansion of upper GI surgery equivalent to 1 bed maybe offset by introduction of non-
invasive EVAR surgery.
Countess of Chester
Upper GI, urology and head and neck cancer surgery has moved. Expect to save 4% level 3 beds
days and 20- 30 Level 2 bed days p.a.
Some unmet need at level 2
for major gynae, orthopaedics and plastic
cases
East Cheshire
Bariatric surgery may have a small
impact on critical care.
LOS stay slightly higher due to sicker medical patients
and very few rapid throughput of elective
surgery patients
Liverpool Women’s
Gynae cancer expected to increase demand but due to clinical management this has not
materialised.
Mid Cheshire
Upper GI will move under IOG, but private oesphagectomys to
continue. Expect minimal impact.
Spinal surgery moving to Salford Hope. Expect
minimal impact.
North Cheshire
Transfer of work from Halton and
closure of wards and MAU at Warrington has increased ICU
discharge and admission problems.
Increase in emergency vascular work from St.
Helens & Knowsley and increased workload from
routine vascular screening of Over 65s.
Continuing expansion
of Warrington population
Thrombolytic treatment
for stroke patients.
RLBUHT
In 2004 Cancer Network agreed for pancreatic services to be delivered at the Royal and Liver at Aintree. The Pancreatic service has grown
substantially. Many cases are cancelled due to lack of ITU bed.
Royal has “a busy” hepatology service. ITU
takes liver failure
Also identified
Infectious diseases health tourism. Tertiary
renal transplant, vascular surgery.
St Helens & Knowsley
Introduction of therapeutic
hypothermia.
Southport & Ormskirk
Problems with acute renal failure patients admitted to ICU, as hospital does not have a nephrology service.
23 patients admitted last year. Delays transferring them to renal beds at Aintree and the Royal.
Upper GI surgeon moving to
Aintree. Impact on critical care minimal as only 8-9
case p.a.
Major urological cancer surgery has moved to
Royal Liverpool - limited impact on critical
care.
Walton
Appointment of new spinal surgeon & expansion of spinal injuries
service
Impact of expected NICE
guidance on traumatic brain injury
Possibility of North Wales Neuro Unit
transferring to South Wales.
Wirral
Pressure from regional renal beds has increased admissions. Referral
back to level I care. 3rd renal bed not agreed with critical care.
Increase in interventional radiology, plan to start
EVARs
Possible Trauma
Centre
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
50
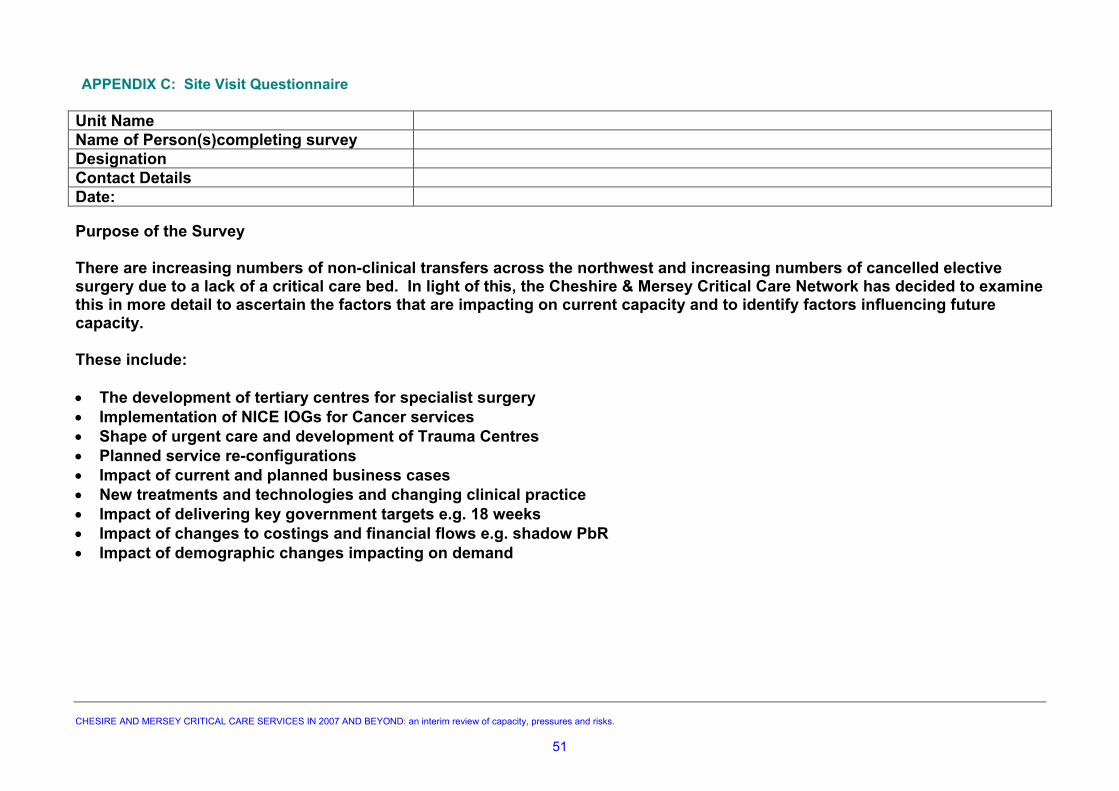
APPENDIX C: Site Visit Questionnaire
Unit Name Name of Person(s)completing survey Designation Contact Details Date:
Purpose of the Survey There are increasing numbers of non-clinical transfers across the northwest and increasing numbers of cancelled elective surgery due to a lack of a critical care bed. In light of this, the Cheshire & Mersey Critical Care Network has decided to examine this in more detail to ascertain the factors that are impacting on current capacity and to identify factors influencing future capacity. These include: • The development of tertiary centres for specialist surgery • Implementation of NICE IOGs for Cancer services • Shape of urgent care and development of Trauma Centres • Planned service re-configurations • Impact of current and planned business cases • New treatments and technologies and changing clinical practice • Impact of delivering key government targets e.g. 18 weeks • Impact of changes to costings and financial flows e.g. shadow PbR • Impact of demographic changes impacting on demand
CHESIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
51
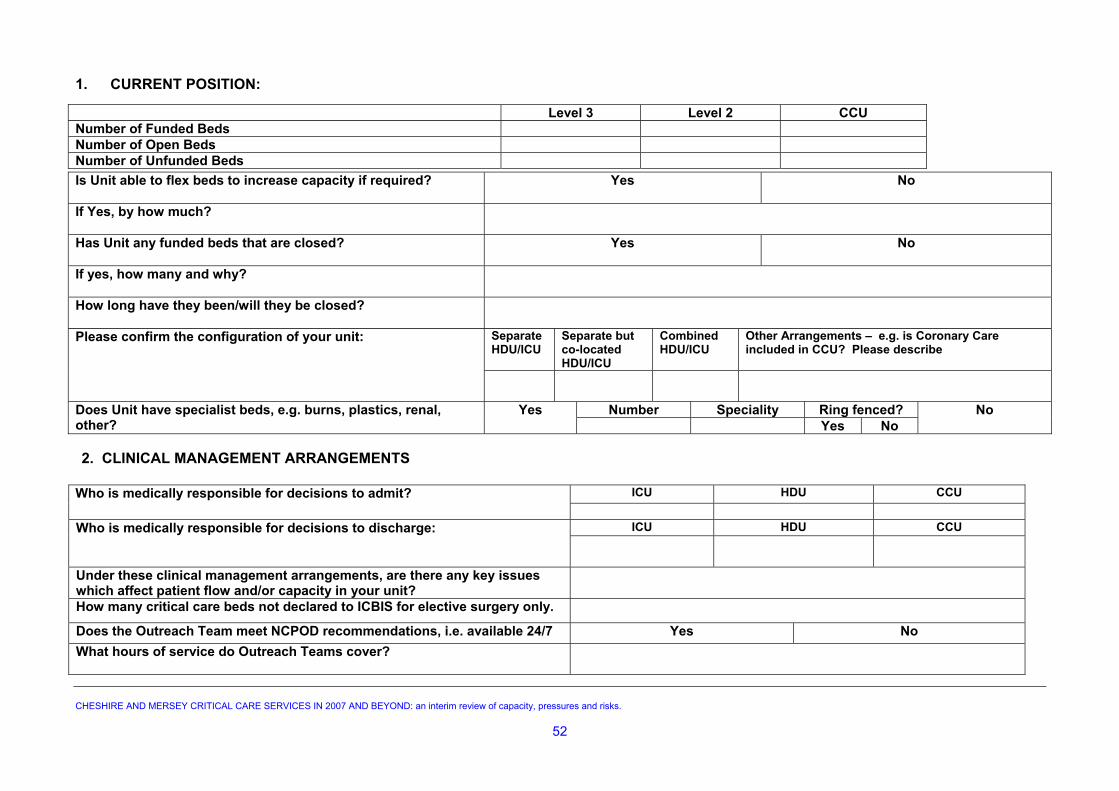
1. CURRENT POSITION:
Level 3 Level 2 CCU Number of Funded Beds Number of Open Beds Number of Unfunded Beds
Is Unit able to flex beds to increase capacity if required?
Yes No
If Yes, by how much?
Has Unit any funded beds that are closed?
Yes No
If yes, how many and why?
How long have they been/will they be closed?
Separate HDU/ICU
Separate but co-located HDU/ICU
Combined HDU/ICU
Other Arrangements – e.g. is Coronary Care included in CCU? Please describe
Please confirm the configuration of your unit:
Number Speciality Ring fenced?Does Unit have specialist beds, e.g. burns, plastics, renal, other?
Yes Yes No
No
2. CLINICAL MANAGEMENT ARRANGEMENTS
ICU HDU CCUWho is medically responsible for decisions to admit?
ICU HDU CCUWho is medically responsible for decisions to discharge:
Under these clinical management arrangements, are there any key issues which affect patient flow and/or capacity in your unit?
How many critical care beds not declared to ICBIS for elective surgery only.
Does the Outreach Team meet NCPOD recommendations, i.e. available 24/7 Yes No What hours of service do Outreach Teams cover?
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
52
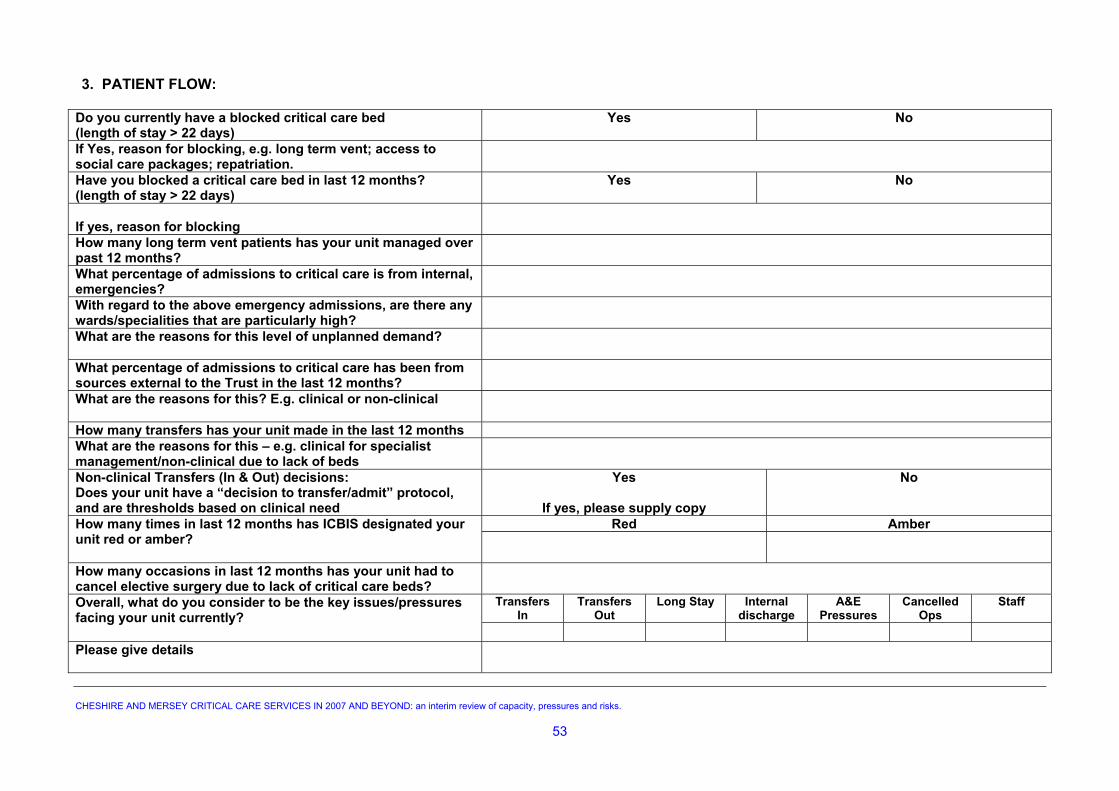
3. PATIENT FLOW:
Do you currently have a blocked critical care bed (length of stay > 22 days)
Yes No
If Yes, reason for blocking, e.g. long term vent; access to social care packages; repatriation.
Have you blocked a critical care bed in last 12 months? (length of stay > 22 days)
Yes No
If yes, reason for blocking
How many long term vent patients has your unit managed over past 12 months?
What percentage of admissions to critical care is from internal, emergencies?
With regard to the above emergency admissions, are there any wards/specialities that are particularly high?
What are the reasons for this level of unplanned demand?
What percentage of admissions to critical care has been from sources external to the Trust in the last 12 months?
What are the reasons for this? E.g. clinical or non-clinical
How many transfers has your unit made in the last 12 months What are the reasons for this – e.g. clinical for specialist management/non-clinical due to lack of beds
Non-clinical Transfers (In & Out) decisions: Does your unit have a “decision to transfer/admit” protocol, and are thresholds based on clinical need
Yes
If yes, please supply copy
No
Red AmberHow many times in last 12 months has ICBIS designated your unit red or amber?
How many occasions in last 12 months has your unit had to cancel elective surgery due to lack of critical care beds?
Transfers In
Transfers Out
Long Stay Internal discharge
A&E Pressures
Cancelled Ops
Staff Overall, what do you consider to be the key issues/pressures facing your unit currently?
Please give details
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
53
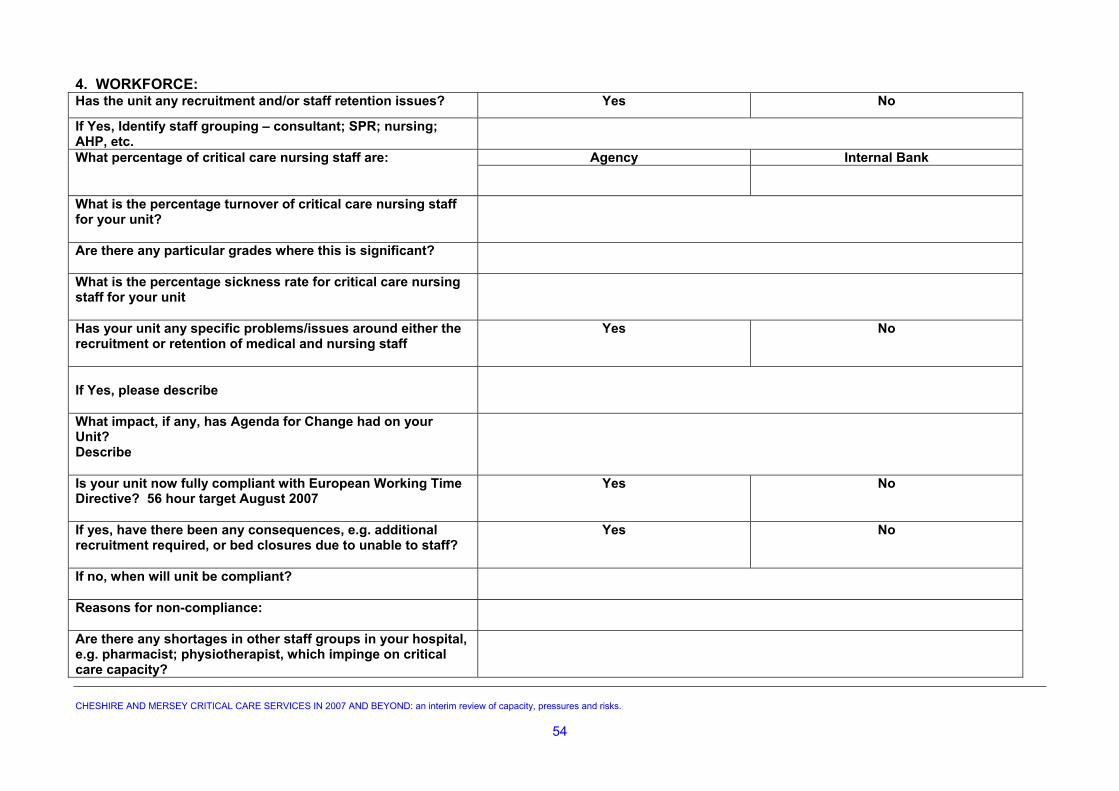
4. WORKFORCE: Has the unit any recruitment and/or staff retention issues? Yes No
If Yes, Identify staff grouping – consultant; SPR; nursing; AHP, etc.
Agency Internal BankWhat percentage of critical care nursing staff are:
What is the percentage turnover of critical care nursing staff for your unit?
Are there any particular grades where this is significant?
What is the percentage sickness rate for critical care nursing staff for your unit
Has your unit any specific problems/issues around either the recruitment or retention of medical and nursing staff
Yes No
If Yes, please describe
What impact, if any, has Agenda for Change had on your Unit? Describe
Is your unit now fully compliant with European Working Time Directive? 56 hour target August 2007
Yes No
If yes, have there been any consequences, e.g. additional recruitment required, or bed closures due to unable to staff?
Yes No
If no, when will unit be compliant?
Reasons for non-compliance:
Are there any shortages in other staff groups in your hospital, e.g. pharmacist; physiotherapist, which impinge on critical care capacity?
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
54
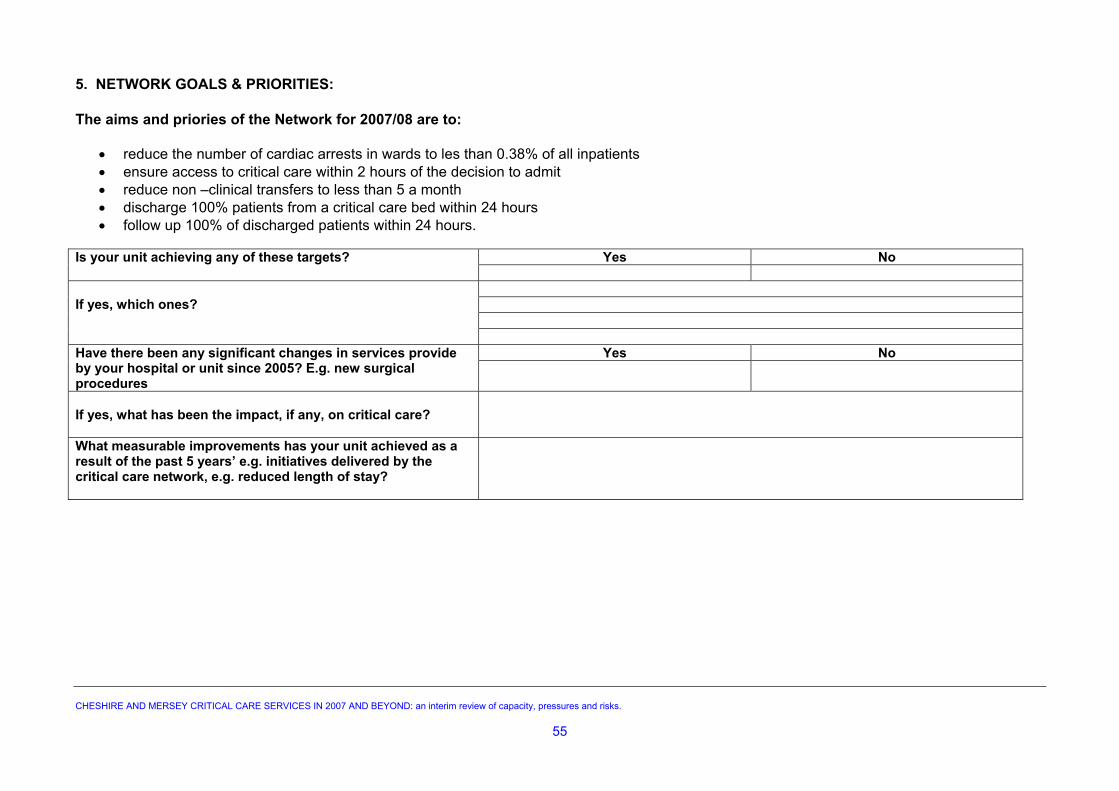
5. NETWORK GOALS & PRIORITIES: The aims and priories of the Network for 2007/08 are to:
• reduce the number of cardiac arrests in wards to les than 0.38% of all inpatients • ensure access to critical care within 2 hours of the decision to admit • reduce non –clinical transfers to less than 5 a month • discharge 100% patients from a critical care bed within 24 hours • follow up 100% of discharged patients within 24 hours.
Yes NoIs your unit achieving any of these targets?
If yes, which ones?
Yes NoHave there been any significant changes in services provide
by your hospital or unit since 2005? E.g. new surgical procedures
If yes, what has been the impact, if any, on critical care?
What measurable improvements has your unit achieved as a result of the past 5 years’ e.g. initiatives delivered by the critical care network, e.g. reduced length of stay?
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
55
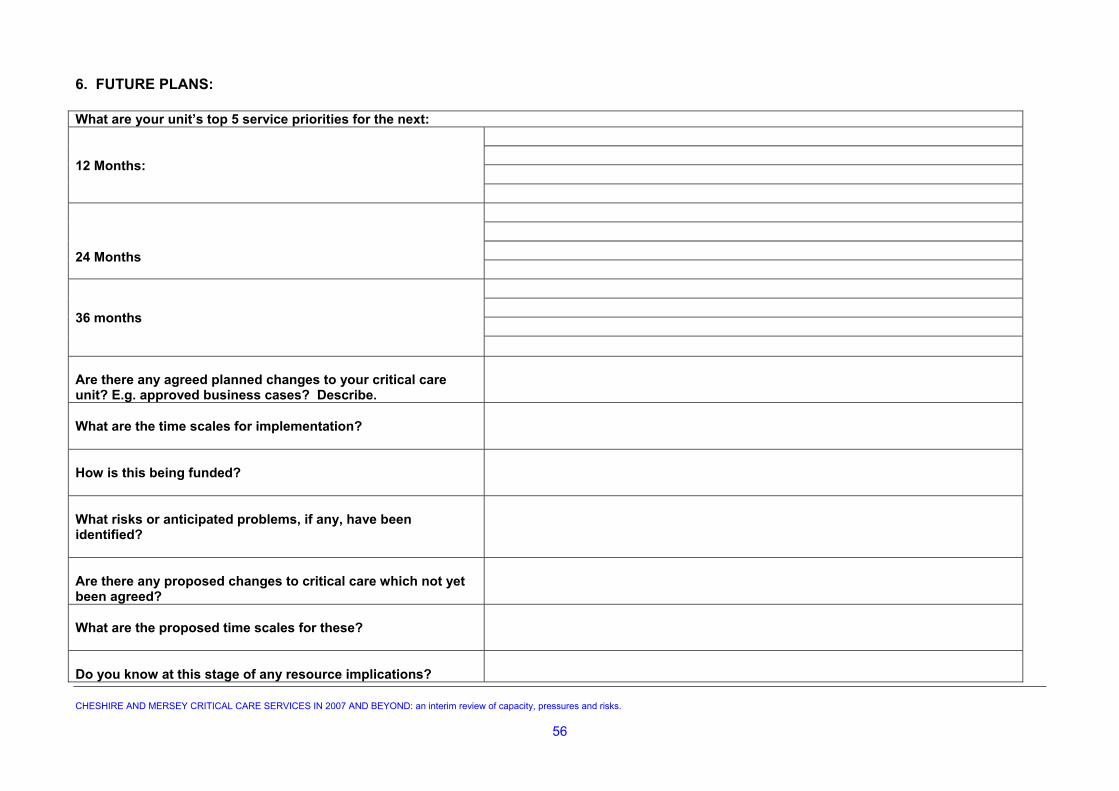
6. FUTURE PLANS: What are your unit’s top 5 service priorities for the next:
12 Months:
24 Months
36 months Are there any agreed planned changes to your critical care unit? E.g. approved business cases? Describe.
What are the time scales for implementation?
How is this being funded?
What risks or anticipated problems, if any, have been identified?
Are there any proposed changes to critical care which not yet been agreed?
What are the proposed time scales for these?
Do you know at this stage of any resource implications?
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
56
Are there any planned or proposed strategic changes within the hospital or Network which will impact on your critical care capacity, e.g. implementation of IOGs? Describe.
How will this impact on your unit?
What are the timescales?
What other changes in clinical practice and/or technology are anticipated that will impact on your critical care unit’s capacity over the next 5 years? E.g.
Population/demographic changes Technological development Changing clinical practice Royal College guidelines New drug therapy Changes in workforce, e.g. development of Assistant
Practitioners
Please describe
How are strategic developments and service changes in other networks outside Cheshire & Mersey communicated and addressed with you?
Yes No Are patient flows mapped in advance
Yes No Is your unit engaged in early planning stages?
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
57
SUPPLEMENTARY QUESTIONS: 7. Admissions to Level 2 and 3 – Please use the same 12 month period for each of the following questions: Total number of admissions to Critical Care in past 12 months:
Total number of Level 2 admissions in past 12 months
Total Planned Unplanned
Total number of Level 3 admissions in past 12 months
Total Planned Unplanned
If you have split Level 2 and Level 3 facilities, please state if possible:
How many Level 2 patients were admitted to Level 3 beds?
How many Level 3 patients were admitted to Level 2 beds?
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
58
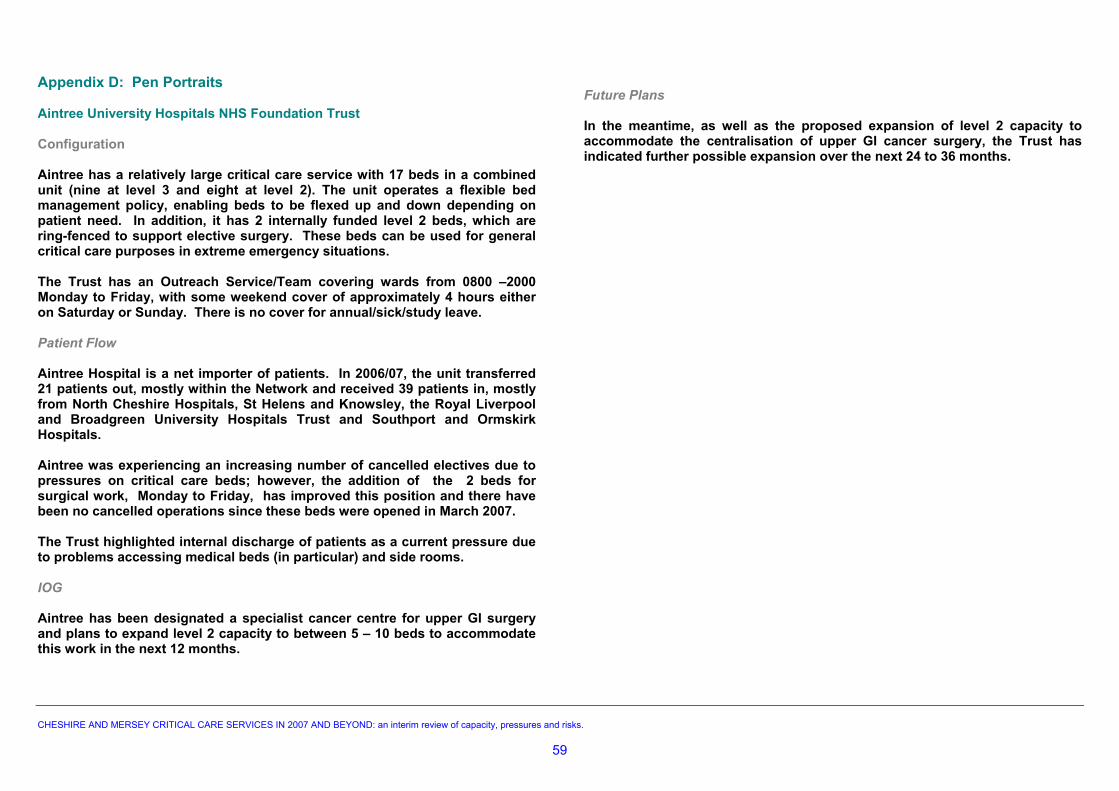
Appendix D: Pen Portraits Future Plans Aintree University Hospitals NHS Foundation Trust In the meantime, as well as the proposed expansion of level 2 capacity to accommodate the centralisation of upper GI cancer surgery, the Trust has indicated further possible expansion over the next 24 to 36 months.
Configuration
Aintree has a relatively large critical care service with 17 beds in a combined unit (nine at level 3 and eight at level 2). The unit operates a flexible bed management policy, enabling beds to be flexed up and down depending on patient need. In addition, it has 2 internally funded level 2 beds, which are ring-fenced to support elective surgery. These beds can be used for general critical care purposes in extreme emergency situations. The Trust has an Outreach Service/Team covering wards from 0800 –2000 Monday to Friday, with some weekend cover of approximately 4 hours either on Saturday or Sunday. There is no cover for annual/sick/study leave. Patient Flow Aintree Hospital is a net importer of patients. In 2006/07, the unit transferred 21 patients out, mostly within the Network and received 39 patients in, mostly from North Cheshire Hospitals, St Helens and Knowsley, the Royal Liverpool and Broadgreen University Hospitals Trust and Southport and Ormskirk Hospitals. Aintree was experiencing an increasing number of cancelled electives due to pressures on critical care beds; however, the addition of the 2 beds for surgical work, Monday to Friday, has improved this position and there have been no cancelled operations since these beds were opened in March 2007. The Trust highlighted internal discharge of patients as a current pressure due to problems accessing medical beds (in particular) and side rooms. IOG Aintree has been designated a specialist cancer centre for upper GI surgery and plans to expand level 2 capacity to between 5 – 10 beds to accommodate this work in the next 12 months. CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
59
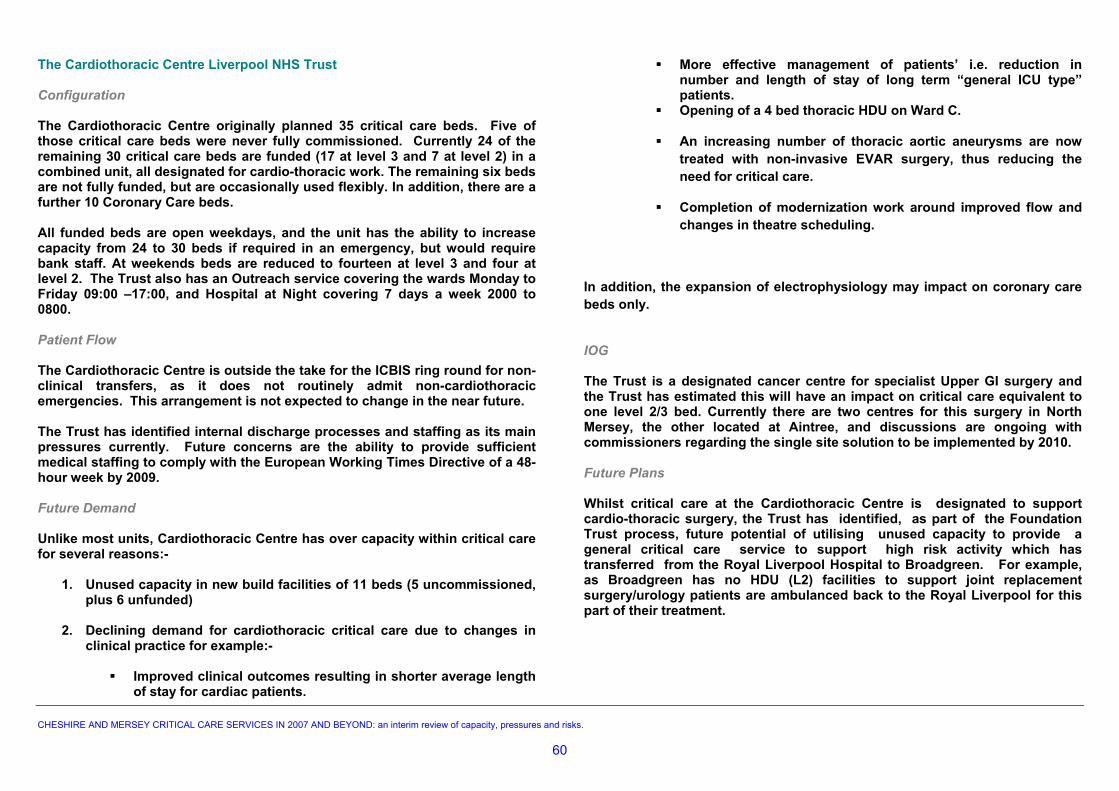
The Cardiothoracic Centre Liverpool NHS Trust More effective management of patients’ i.e. reduction in number and length of stay of long term “general ICU type” patients.
Configuration Opening of a 4 bed thoracic HDU on Ward C. The Cardiothoracic Centre originally planned 35 critical care beds. Five of those critical care beds were never fully commissioned. Currently 24 of the remaining 30 critical care beds are funded (17 at level 3 and 7 at level 2) in a combined unit, all designated for cardio-thoracic work. The remaining six beds are not fully funded, but are occasionally used flexibly. In addition, there are a further 10 Coronary Care beds.
An increasing number of thoracic aortic aneurysms are now treated with non-invasive EVAR surgery, thus reducing the need for critical care.
Completion of modernization work around improved flow and changes in theatre scheduling.
All funded beds are open weekdays, and the unit has the ability to increase capacity from 24 to 30 beds if required in an emergency, but would require bank staff. At weekends beds are reduced to fourteen at level 3 and four at level 2. The Trust also has an Outreach service covering the wards Monday to Friday 09:00 –17:00, and Hospital at Night covering 7 days a week 2000 to 0800.
In addition, the expansion of electrophysiology may impact on coronary care beds only.
Patient Flow IOG The Cardiothoracic Centre is outside the take for the ICBIS ring round for non-
clinical transfers, as it does not routinely admit non-cardiothoracic emergencies. This arrangement is not expected to change in the near future.
The Trust is a designated cancer centre for specialist Upper GI surgery and the Trust has estimated this will have an impact on critical care equivalent to one level 2/3 bed. Currently there are two centres for this surgery in North Mersey, the other located at Aintree, and discussions are ongoing with commissioners regarding the single site solution to be implemented by 2010.
The Trust has identified internal discharge processes and staffing as its main pressures currently. Future concerns are the ability to provide sufficient medical staffing to comply with the European Working Times Directive of a 48-hour week by 2009.
Future Plans Whilst critical care at the Cardiothoracic Centre is designated to support cardio-thoracic surgery, the Trust has identified, as part of the Foundation Trust process, future potential of utilising unused capacity to provide a general critical care service to support high risk activity which has transferred from the Royal Liverpool Hospital to Broadgreen. For example, as Broadgreen has no HDU (L2) facilities to support joint replacement surgery/urology patients are ambulanced back to the Royal Liverpool for this part of their treatment.
Future Demand Unlike most units, Cardiothoracic Centre has over capacity within critical care for several reasons:-
1. Unused capacity in new build facilities of 11 beds (5 uncommissioned, plus 6 unfunded)
2. Declining demand for cardiothoracic critical care due to changes in
clinical practice for example:-
Improved clinical outcomes resulting in shorter average length of stay for cardiac patients.
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
60
The Countess of Chester NHS Foundation Trust Whilst the Trust has gained second site status for EVAR (endovascular stents), which should reduce the length of stay for critical care, the number of patients may increase.
Configuration The Countess of Chester has 13 critical beds (five at level 3 and eight at level 2) in separate but co-located units. All beds are funded and open. There is no physical space to increase capacity above this, and there are no other specialist or ring-fenced beds, with the exception of ten for coronary care. The Trust has an Outreach service covering the wards 0800 –2000 Monday to Friday. Patient Flow The Countess of Chester was a net importer of level 3 patients in 2006/07. Prior to this, it was a net exporter. In 2006/07 the unit transferred 1 patient out within the Network, and 22 patients transferred in, mostly from Warrington and 4 from out of region. There is a surgical HDU which increasingly admits medical patients. IOG The Trust has lost specialist cancer surgery for upper GI cancer to Wrexham Maelor, urology to Arrowe Park, and head and neck surgery to Aintree. This equates to approximately 20-30 level 2 bed days per annum. Gynecological cancer surgery has also transferred to the Liverpool Women’s; however, these patients rarely required access to level 2 beds. Future Plans As a Foundation Trust the organisation has capital flexibility and is starting a full ward upgrading programme, including the extension of the current critical care unit space to comply with current regulations. The Trust has agreed to fund the capital to build growth in overall bed numbers, if the internal audit supports this and has commissioner support. The Trust wants to programme the unit for refurbishment /extension in 2008/9. The internal audit is reporting in September, and a business case for any growth needs to be ready for autumn. Early indications suggest that the Trust requires one additional level 3 and 5-8 level 2 beds, based on internal demand. CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
61
IOG East Cheshire NHS Hospitals Trust
Configuration Discussions regarding services are ongoing as part of the Greater Manchester Cancer Network arrangements. Macclesfield Hospital has a combined unit with 6 beds (four level 3 beds and
two level 2 beds) funded and open, with the ability to flex up to 1 Level 2 bed if required. There are two extra bed spaces, but these have not yet been commissioned.
Future Plans The Trust is aiming to gain Foundation Trust status in Autumn 2007 and, as part of its plan, has proposed an expansion of the unit to eight beds over the next two financial years, with the possibility of merging with the coronary care unit in three years time.
There is also an Outreach service covering wards Monday to Friday 0900-1700, with plans to extend the team’s hours to 08:00 -18:00. Patient Flow Whilst staffing is not an issue for the bed expansion, the funding of
consumables was raised via the questionnaire as an issue. Macclesfield is a net exporter for non- clinical transfers. In 2006/07 the unit transferred 25 patients out, the second highest in the Network after Warrington. Most (7) went to Leighton and 7 went to units outside the Network. 17 patients were transferred in, 10 from within the Network 7 from Greater Manchester.
The questionnaire highlights local concerns about the long term future of A&E, which would have a major impact on the need for a critical care unit. Other changes that may affect capacity include the increasing elderly population. The move to less invasive surgery will have little impact in this critical care unit as they admit predominantly acute medical patients.
The reasons stated for the high number of transfers out by the Trust is due to inflexible critical care capacity. The majority of patients treated in critical care are medical rather than surgical, as the Trust does not undertake a significant amount of major elective work. 70% of admissions are due to internal emergencies within the hospital, mainly from the Medical Admissions Unit, as all sick medical patients are admitted to the hospital via MAU.
The Trust has just appointed three new consultants to address the significant low medical cover and bring the unit up to the minimum level of sessions with cover for absences.
Incomplete implementation of Modified Early Warning Score (MEWS) across all hospital wards may be contributing to unnecessary increased demand. Delayed discharges, particularly from level 2 (HDU) beds, when the decision depends upon parent clinical team, were highlighted as an issue. This may improve over the next 12 months as the unit is considering changing from an open to a closed unit. This means that admissions and discharges to the unit the unit will be the sole responsibility of dedicated intensivists within the critical care unit, as opposed to jointly shared with surgeons, as is the current practice. Discharging patients requiring a side room is also problematic. The Trust highlighted the discharge of acute renal failure patients to MRI in Manchester as a significant problem; however, this should be alleviated with the opening of a new renal dialysis unit at MRI in May 2007 CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
62
IOG Liverpool Women’s NHS Foundation Trust Configuration The Trust has been a designated cancer centre for gynaecology and specialist
oncology for its local catchment population since June 2004. Liverpool Women’s Foundation Trust has four level 2 critical care beds designated for obstetrics and gynaecology in separate locations. Capacity can be flexed up to 8 beds for short periods by utilising two stabilisation bays and two beds in the delivery suite. The Trust operates an Outreach team Monday to Friday daytime only.
Future Plans As a Foundation Trust, the organisation has a business case to integrate the obstetrics and gynaecological level 2 beds to create a combined 6 bedded unit, subject to Board approval. This is planned to be completed by the end of 2007/8 as part of the wider obstetric reconfiguration plans. The Royal College of Obstetrics is currently discussing obstetric critical care as a specialty, which also may impact.
There are no level 3 beds and the unit is not included in the ICBIS ring around. The 2 beds for obstetrics were opened when maternity services transferred from Aintree in June 2004. However, the Trust has indicated that these beds are not funded through formal mechanisms. The Trust also highlighted an increase in major gynaecological cancer work
following the appointment of a third oncologist. However, whilst the impact is unknown, the Trust is not expecting this to create much extra demand for critical care.
Clinical pressures Liverpool Women’s does not have dedicated critical care cover out of hours, and is reliant on the neighbouring Royal Liverpool Hospital to provide level 3 backup and support services for complicated investigations, such as blood transfusion, which are not on site. Aintree has retained some of the major gynaecological surgery work as it can provide level 3 cover at night.
Patient Flow The Trust has one of only two designated level 3 perinatal units in Cheshire and Mersey, the other being at Wirral Hospitals NHS Trust. The unit is the regional and supra-regional referral unit for pre 28-weekers. It also receives clinical emergency admissions from Southport and Ormskirk, St Helens and Knowsley and Mid Cheshire Trusts, all of whom have level 2 perinatal units. In the past 12 months, the unit has transferred 14 gynaecology patients (8 of which required level 3) and 10 obstetric patients (7 of which required level 3) for expert management. The Trust identified current pressures as obstetric funding and lack of resources available out of hours, thus making it difficult to keep sicker patients and avoid transfers as there are no level 3 facilities. As a result, five patients have been transferred so far this year. Discharge of patients back to wards was also highlighted as an issue.
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
63
Future Plans Mid Cheshire Hospitals NHS Trust Configuration The Trust is preparing a business case for the expansion of level 2 (HDU) as
part of its Foundation Trust application, and is also planning a refurbishment/rebuild of critical care facilities in the next 24 months.
Leighton Hospital has 11 funded beds (seven at level 3 and four at level 2) located in separate wards. Whilst all funded beds are open, there are some nurse staffing issues which make the availability of the seventh bed on a consistent basis difficult.
The unit is able to flex capacity up to 9 level 3 beds. However, there is no
physical space to expand beyond current levels The Trust also has an Outreach service covering the wards 24 hours a day
seven days a week and is the only Trust meeting NCPOD recommendations.
Patient Flow
The Trust is a net importer for non-clinical transfers with 13 patients transferred in, mostly from East Cheshire NHS Trust, and only 1 patient transferred out during 2006/7.
The Trust highlighted the lack of level 2 capacity for step down, causing
delays in internal discharge, as an issue. Whilst there were no blocked beds at the time of the survey, in the past twelve
months the Trust has had fourteen level 3 and two level 2 patients mostly for long term weaning. The longest stays were 54 days in ICU and 41 days in HDU.
There are some issues around medical cover with only 9 consultant sessions
cover per week and sharing of SpR with maternity and emergency/urgent theatre. Out of Hours cover is provided by on- call staff only.
IOG Discussions regarding services are ongoing as part of the Greater Manchester Cancer Network arrangements. CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
64
Future Plans North Cheshire Hospitals NHS Trust
Configuration North Cheshire Hospitals NHS Trust has submitted a business case to the SHA to develop a new combined critical care unit with a potential for 20 beds, initially opening with a minimum of 16 beds.
North Cheshire Hospital has 14 critical care beds (six level 3 and 8 level 2) split across 3 ward areas and one bed in a stabilisation bay used for overflow. The service was increased by four level 2 HDU beds in December 2006 to accommodate the closure of the four-bedded units at Halton Hospital. These beds are currently providing bridging capacity until the new unit is built.
The aim is to reduce the number of non-clinical transfers to less than 5 per month. The Trust plans to begin the build in November 2007 and complete within 10 months. The full cost is not fully covered but this is a priority for the Trust who have pump primed the first £1.75 m investment and will finance the balance of approximately £4.5m from internal funds with the remainder from a loan. The new unit will also have potential to expand in the future.
The Trust has an Outreach service covering wards 0800-1600 Monday to Friday
Patient Flow Warrington has the highest number of non-clinical transfers in Cheshire & Mersey and is a net exporter, transferring 74 patients in 2006/7 compared to 13 transfers in. This trend continued with 51 non-clinical transfers out of a total of 67 transfers from January to July 2007.
Warrington has a transfer rate of 10% and had a cancelled elective rate of 8% until a booking system for Level 2 beds for elective surgery was introduced i.e. joint listing between surgery and intensive care. This has reduced cancelled electives to 3.5%.
Other pressures identified are the expanding population of Warrington which has grown by 10% over the last 10 years and is expected to continue to increase by 6% by 2028; the increase in emergency vascular work from St Helens and Knowsley and the increase in routine vascular screening of the over 65’s.
IOG Specialist surgery for urological cancers is transferring to Wirral Hospitals NHS Trust and for upper GI cancer to Cardiothoracic Centre.
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
65
Royal Liverpool & Broadgreen University Hospitals Trust • delayed discharges • internal bed blocking Configuration At the time of the survey, the unit had three beds blocked due to long term
ventilation and access to social care packages. In the last twelve months, the unit has had 48 patients blocking beds accounting for 10% of all admissions to ITU. Of these, 34 required long term ventilation. A particular issue is acute pancreatitis which takes up 15% of the level 3 bed days.
The Trust has complex physical arrangements for critical care services which are split across four separate areas and different floors across the hospital. These are:-
• 13 bedded level 3 unit. • 4 bedded level 3 post-operative unit adjacent to theatres
(commissioned at level 2 but equipped up to level 3). Whilst the Trust has not been designated as a tertiary specialist centre, it does provide specialist services for pancreas, infectious diseases, TIPPS, liver failure and spinal injuries, which utilise the 13 bedded general ITU. The requirement for specific additional critical care capacity to support these services has not been planned and developed, and, in the last 12 months, approximately 78 patients were admitted to critical care for these services from outside the Trust. Increasingly there are frequent long delays, sometimes weeks, in admitting these tertiary referrals due to the existing high bed occupancy rate.
• 4 bedded level 2 ward, designated for surgery • 6 bedded level 2 ward, designated for vascular work
Both level 2 wards also accept some medical patients. Only the thirteen level 3 beds in ITU are included in the ICBIS bed count and form part of the general Critical Care Network take. All funded beds are open and there is no physical space to flex capacity upwards.
IOG An Outreach service covers the wards Monday to Friday 08:00 -18:00. This
service also provides unfunded cover at weekends and at night. The Trust has been designated a cancer centre for urology; however, significant increase in post operative critical care is not expected. In addition there are 5 level 2 renal beds located outside of the critical care
unit. Future Plans A business case has been prepared for a staged development of critical care within the next twelve months, which would relocate six of the ten level 2 beds within ITU as part of the interim new capital build.
Patient Flow The Royal is marginally a net importer for non-clinical transfers. In 2006/07 nineteen patients were transferred in, mostly from Warrington and sixteen transferred out, most to Aintree.
In addition, a proposal to develop a post-operative critical care service at Broadgreen, to support the relocation of elective surgery, has been raised. Potential utilisation of spare critical care capacity at Cardiothoracic Centre is part of this proposal.
94% of admissions to ITU are from internal emergencies referred mainly from A&E, Post Operative Critical Care Unit (POCCU) and theatres.
A complete hospital re-build is planned for 2014/15. There are significant internal pressures due to the complex clinical
management arrangements for critical care beds which result in the following problems:-
• stepping down surgical patients from level 3 to level 2 beds
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
• admitting medical patients as there are no medical level 2 facilities in Trust
66
Southport and Ormskirk NHS Hospital Trust St Helens and Knowsley NHS Hospitals Trust Configuration Configuration Southport Hospital has a combined unit with ten beds (six level 3 beds and four level 2 beds) funded and open, with the ability to flex up by another one level 3 bed if required. A six bedded coronary care unit is located next door to the critical care unit and is staffed by the same nurses in rotation. The Trust participates in a joint on-call with Preston, accepting vascular emergencies two days per week and alternate weekends.
The Trust has a combined unit with 14 beds (eight level 3 beds and six level 2 beds); with the ability to increase capacity by an additional two level 3 and one level 2 beds. At the time of the survey, the unit has three funded level 2 beds closed due to building work which re-opened on 13 August. In addition, the Trust has 2 specialist beds for burns, which are not ring-fenced.
The Trust also has an Outreach service covering the wards Monday to Friday 0900-1700 with plans to extend the team’s hours to cover weekends.
The Trust also has an Outreach service covering the wards seven days a week, between 0800 -1600.
It should be noted that there is an overlap with the Lancashire and Cumbria Critical Care Network and Central Lancashire PCT.
Patient Flow
Patient Flow Whiston is a net importer for non-clinical transfers, receiving more than any
other Trust in the Network. In 2006/07 the unit transferred 19 patients out and transferred 42 patients in, mainly from North Cheshire.
Southport is a net importer for non-clinical transfers. In 2006/07 Southport transferred 11 patients out and 14 patients in, mainly from Aintree and North Cheshire, but others were from outside the Network.
Long stay patients and internal discharge are considered to be key issues facing the unit currently. Non-clinical transfers were not identified as a key pressure.
Non-clinical transfers in, and internal discharge of patients, are considered to be key issues facing the unit currently. In addition, as there is no nephrology service in the Trust, acute renal failure patients are admitted to critical care, and, although additional renal dialysis beds have been opened at the RLBUH, these are not currently easing the position. These patients also experience delays in being discharged to Aintree.
IOG Specialist upper GI cancer surgery is transferring to Aintree; however, the impact on critical care will be minimal as the number of cases annually is less than 20. Urology surgery is transferring to RLBUH.
IOG Future Plans Specialist upper GI cancer surgery is moving to Aintree; however, the impact
on critical care will be minimal as the number of cases annually is small. Major urological cancers have already transferred to the Royal Liverpool Hospital, again this has had limited impact on critical care capacity as the number of cases were small.
The Trust plans to commission additional capacity as part of the new hospital build due to be completed by 2010.
Future plans The Trust is planning to increase side room provision from 2 to 4 which is currently being costed but is expected to be agreed. CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
67
Future Plans The Walton Centre for Neurology & Neurosurgery NHS Trust Configuration Over the next 12 to 24 months the Trust’s priorities are to:- The Walton Centre provides a specialist neuroscience critical care service for the whole of Cheshire & Mersey, North Wales and the Isle of Man, with links into two other specialist centres in the North West at Salford and Preston. The beds are ring-fenced and outside the ICBIS ring around and take for general critical care services for non-clinical transfers.
• reduce the waiting times for elective neurosurgery requiring critical care back-up;
• implement the expected NICE guidance on traumatic brain injury management; and
• expand major spinal surgery. The Trust has separate but co-located ICU/HDU units with 13 beds (nine at level 3 and four at level 2) funded and open, with the ability to flex up for short periods (< 24 hrs) to a tenth level 3 bed for extreme emergencies. This extra bed is unfunded.
Expansion of level 3 capacity by 4 extra beds in 2008/9 and by a possible further 4 in 2009/10 is viewed by the Trust as essential to support these developments. This expansion is currently in the planning stage and will require additional funding for medical, nursing and support staff as well as equipment and building work.
It also operates an Outreach service Monday to Sunday 08:00 - 21:00 with night sisters trained up to deal with sicker patients on wards.
The Trust has appointed a new consultant spinal surgeon who starts in October 2007. The critical care requirement to support this additional workload is unclear at present but is not thought to be significant.
Patient Flow All patients admitted to the unit at Walton need neuroscience-based critical care and most are from within its catchment area. A few patients are transferred into the centre when neighbouring neuro units do not have sufficient critical care capacity. Occasionally patients may be transferred from the Walton Centre to other critical care units because of insufficient critical care capacity.
The recruitment of suitable trained medical staff is an issue for specialist units and may be a limiting factor to the planned expansion of workload and critical care facilities. The changes in anaesthetic training modules with MMC does increase the risk around service provision for cover of the critical care unit, as the run-through training limits the exposure of trainees to neuro critical care. This has implications for the amount of service the trainees are capable of providing. It also makes recruitment to consultant posts more difficult as the opportunity for trainees to develop an interest in neuro-anaesthesia and critical care is significantly curtailed.
Long stay patients and cancelled operations due to lack of critical care beds are considered to be key issues facing the unit currently. Patients with long-term neurological conditions needing critical care cause particular problems. They are very few in number but can have extremely long lengths of stay, thereby reducing the capacity for neurosurgical patients who have much shorter lengths of stay. However, level 2 length of stay has reduced since the clinical management of the unit transferred to critical care staff in October 2004.
Both the trainee and consultant anaesthetists’ contracts are held by University Hospital Aintree under a service level agreement, which is currently under review. There are ongoing problems about the numbers of trainees that Aintree are able to provide to the Walton Centre for training and for out of hours cover, because of the shortfall in trainees appointed under the MTAS system.
IOG Another critical care pressure identified is the expected increase in patients for head injury management to over 160 patients per year, in response to the recently published NICE guideline CG56. There are also plans to take all sub-arachnoid haemorrhage patients from other Trusts in the Network, which, with the head injuries, will create significant pressure on neuro critical care.
This critical care unit in this Trust is not affected by the Implementation of IOG.
CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
68
Future Plans Wirral University Teaching Hospital NHS Foundation Trust
Configuration The Trust has agreed to co-locate level 2 and level 3 beds within the next 36 months. Arrowe Park hospital has a relatively large critical care service with 18 beds in
co-located units (7 level 3 and 9 level 2 and includes 2 renal beds which can also be used for level 3 or level 2 patients if required.) There is ability to flex up to 10 level 3 beds from 7 if needed. There is an Outreach service covering the wards from 0730-2130 Monday to Friday and Saturday mornings.
Patient Flow The unit is a net importer for non-clinical transfers. In 2006/07 only one
patient was transferred out and 24 patients were transferred in, mostly from within the Network, particularly from Warrington.
Renal Pressures Since April 2007, changes and investments within Cheshire & Mersey Renal
Network has increased capacity by 2 extra level 2 renal beds. This investment has increased admissions to critical care, and there are some problems in referring patients back for level 1 care. In addition, funding to support a third renal bed is currently under discussion.
Special Care Baby Unit Pressures The Trust has a level 3 Special Care Baby Unit, (one of only two in the
Network, the other being at Liverpool Women’s); therefore it is seeing a higher number of sick babies. As the Trust also has adult level 3 facilities, there is concern that it will also see a rise in referrals of sicker pregnant women requiring critical care from across Cheshire & Mersey. This has already occurred in other hospitals, (such as Blackpool) with specialist level 3 SCBU. IOG The Trust is a designated cancer centre for urology surgery. It also plans to improve the referral process and access to critical care from Clatterbridge. Specialist upper GI cancer surgery is transferring to Aintree and the overall impact on critical care is expected to be minimal. CHESHIRE AND MERSEY CRITICAL CARE SERVICES IN 2007 AND BEYOND: an interim review of capacity, pressures and risks.
69

Cheshire and Mersey Critical Care Network
Network Office Millennium House
930-932 Birchwood Boulevard Millennium Park
Birchwood Warrington. WA3 7QN
Tel No 01925 843807
Copyright © 2022 FDOKUMEN

