







Bahasa
Halaman
Hukum


Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
Building bridges to observational perspectives:A grounded theory of therapy processesin psychosis
Sarah Dilks1*, Fiona Tasker2 and Bernadette Wren31South London and Maudsley NHS Foundation Trust, North CMHT, London, UK2Birkbeck College, University of London, London, UK3The Tavistock Clinic, London, UK
Objectives. This study set out to explore therapy processes in psychosis with aninitial focus on reflexivity and how this might be expressed in therapy conversations.
Design. Leiman’s (2000) definition of reflexivity was used as a starting-point for anexploratory investigation of the use of language as reflective activity. Grounded theorywas chosen as an appropriate methodology to distil an explanatory account across thequalitative data collected.
Method. Six psychologist-client pairs supplied three tapes of therapy sessions spreadout across the course of therapy. Each participant was separately interviewed on twooccasions to ascertain their views of therapy and of the emerging grounded theory.
Results. A grounded theory was developed conceptualizing the processes andactivities in psychological therapy in psychosis.
Conclusions. ‘Building bridges to observational perspectives’ summarizes the coreprocess in psychological therapy in psychosis. Therapy in psychosis is understood asintimately ‘linking the social and internal world’ in a dialogical process aimed atenhancing the client’s ‘functioning in the social world’ rather than at specificallydeveloping the private mental experience of reflexivity or mentalizing.
This study was prompted by an interest in the therapy processes in psychosis that might
contribute to the subjective awareness and explicit articulation of private mental
experience (activity that can broadly be labelled reflexivity). The first author’sexperience as a UK clinical psychologist working with people experiencing psychosis
had suggested the potential importance of the therapist suggesting possible labels and
meanings for subjective experience; thereby making this experience explicit and
allowing it to be manipulated by the person (kept or changed). As described in more
detail below, it seemed this activity could be understood in different terms from
* Correspondence should be addressed to Dr Sarah Dilks, South London and Maudsley NHS Foundation Trust, North CMHT,37 Tamworth Road, London CR0 1XT, UK (e-mail: [email protected]).
TheBritishPsychologicalSociety
209
Psychology and Psychotherapy: Theory, Research and Practice (2008), 81, 209–229
q 2008 The British Psychological Society
www.bpsjournals.co.uk
DOI:10.1348/147608308X288780

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
different theoretical and therapeutic models and might therefore be regarded as a
common process in therapy. Combined with a consideration of the literature on therapy
process research and that relating to what we are calling reflexivity, this interest led to
the choice of a dialogical definition of reflexivity to focus a qualitative exploration of
therapy processes in psychosis. It is pertinent at this point to note that we follow
current practice in UK clinical psychology in referring to psychosis and psychoticexperiences rather than using psychiatric diagnostic categories like schizophrenia
(Bentall, 2003). This is based on concern about the validity of psychiatric diagnostic
systems (as discussed by Bentall, 2003; Boyle, 2002).
Process research in psychotherapy generally and in relationto psychotherapy with psychosisReviews of psychotherapy process research, such as those by Llewelyn and Hardy
(2001), Roth and Fonagy (1996), Sachse and Elliott (2001), and Stiles, Honos-Webb, and
Knobloch (1999), conclude that reliable process–outcome links between various
therapist, client, and therapy-specific factors have been hard to find. Although some
robust links have been identified in hypothesis-testing studies (particularly between
good therapeutic alliance and outcome), what emerges generally is a picture of
complexity. However, such reviews also suggest that common processes (such asa positive therapeutic alliance or emotional regulation) operating across therapy
modalities might be important in outcome. Stiles, Honos-Webb, and Surko (1998)
therefore suggest using qualitative and narrative analyses specifying processes at the
level of the client–therapist pair to take forward psychotherapy research.
With the exception of Lysaker and colleagues’ work on the role of narrative in
recovery from psychosis (e.g. Lysaker, Lancaster, & Lysaker, 2003; Lysaker & Lysaker,
2002; Lysaker et al., 2006), recent studies of therapy in psychosis have not
systematically set out to develop more abstract explanatory models of therapyprocesses, concentrating instead on particular examples of therapy from the standpoint
of existing therapeutic models (e.g. Grazebrook et al., 2004; Lombardi, 2003).
In comparison with therapy in other forms of distress then, therapy processes in
psychosis are relatively unexamined. It is therefore currently unclear whether findings
suggestive of the operation of common processes in psychotherapy across different
therapy modalities might also apply to therapy in psychosis.
Concepts relating to the awareness and articulation of private mental experienceThere are a variety of concepts that might inform our understanding of the subjective
awareness and explicit articulation of private mental experience (what we are callingreflexivity). These include: metacognition (e.g. Morrison, 2001; Teasdale, 1999);
mentalizing (e.g. Langdon, Coltheart, Ward, & Catts, 2001); theory of mind (Frith,
1994); reflective function (Fonagy, Gergely, Jurist, & Target, 2004; Fonagy, Target,
Steele, & Steele, 1998); and ideas arising from a narrative or dialogical perspective
(e.g. Stiles, 1999).
Metacognition, mentalizing, theory of mind, and reflective functionAt the broadest level, thinking about (assumed) mental processes, such as thoughts andfeelings, is referred to as metacognition (Morrison, 2001; Teasdale, 1999). Mentalizing
more specifically refers to the ‘cognitive capacity to infer causal mental states in order to
210 Sarah Dilks et al.

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
explain and predict consequent thoughts and behaviour and, more generally, people’s
capacity to reflect upon the unique subjective lives of both themselves and other
people’ (Langdon et al., 2001, p. 82). In using the term mentalizing interchangeably
with their concept of reflective function in an attachment theory context, Fonagy
and colleagues (Fonagy & Target, 1997; Fonagy, Target, Steele, & Steele, 1998)
specifically emphasize the developmental, interpersonal context of the origins ofmentalizing, and its critical place in self-organization.
Theory of mind is defined as the ability to interpret the speech and action of others
based on inferring the other person’s point of view as a being with a separate mind
(Frith, 1994). Investigations of theory of mind and mentalizing in psychosis based,
respectively, on Frith (1979, 1994, 1997) and Hemsley’s (1998, 2005) work seem to
imply a deficit model (Boyle, 2002) where people diagnosed with schizophrenia (sic)
are understood as lacking theory of mind or mentalizing capacity (Brune, 2005).
However, the experimental tests of these models suggest that what we are callingreflexivity can be mobilized at some times and not at others by those experiencing
psychosis (Bentall, 2003; Drury, Robinson, & Birchwood, 1998; Sarfati, Passerieux,
& Hardy-Bayle, 2000), leaving open the question of what might influence the operation
of reflexivity for these individuals.
Narrative and dialogical approachesNarrative and dialogical approaches share a common emphasis on the conversational
process of therapy and the importance of the construction of meaning in affecting
the experience of distress (Georgaca, 2001; Hermans, 1996; Leiman, 1997, 2000;
Stiles, 1999; White, 1987, 1995; White & Epston, 1990). From the standpoint of these
approaches, reflexivity would seem to be understood as taking an observing position in
relation to experience through the interaction between different self-positions or voices.
Dialogical approaches specifically regard self-hood as multi-voiced rather than
unitary, seeing the experience of self as continually constructed through dialogue inthe internal and external world. In applying this understanding to psychotherapy,
Stiles (1999) makes the point that different psychotherapy theories have in common
the idea that clients bring a range of perspectives to therapy, though these may
be conceptualized differently, for instance, as schemas in CBT, internal objects in
psychoanalytic psychotherapy, or voices in narrative therapy. Like Georgaca (2001) and
Hermans (1996; Hermans, Rijks, & Kempen, 1993), he suggests that the aim of therapy is
to decrease the rigidity in the range of internal voices (or, by implication, schemas,
internal objects, etc.) used by clients and to increase the interplay between differentpositions or voices. Stiles (1999, p. 3) and Brinegar, Salvi, Stiles, and Greenberg (2006,
p. 165) refer to creating symbolic ‘meaning bridges’ between different voices in both
internal, private conversations, and external conversations with a therapist in order to
achieve this.
Lysaker and colleagues (Lysaker & Buck, 2006; Lysaker & Daroyanni, 2006; Lysaker
& Lysaker, 2002; Lysaker, Lysaker, & Lysaker, 2001) have specifically focused on concep-
tualizing psychotherapy in psychosis from the standpoint of narrative approaches.
Lysaker and Lysaker (2001) suggest that changes in a subjective sense of self in psychosisare related to the collapse of a dialogically based self and that recovery might be
facilitated by its restoration. In their review of this emerging field, France and Uhlin
(2006) suggest that change in narrative content and form may therefore offer a useful
way of assessing outcome in psychosis. Lysaker and colleagues have indeed developed
Building bridges 211

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
the Scale to Assess Narrative Development (Lysaker, Wickett, Campbell, & Buck, 2003;
Lysaker et al., 2006) with this aim. However, there are methodological and conceptual
problems in taking a quantitative approach to examining narrative, as represented for
instance by the STAND and by Fonagy et al.’s measure of reflective function/mentalizing
derived from the adult attachment interview (a measure of the quality of early
attachment experiences: Fonagy et al., 1998; George, Kaplan, & Main, 1996). Ratings ofnarrative complexity and coherence are judgements based on an interaction between
speaker and listener (c.f. Harper, 2004); complexity and coherence do not ‘exist’
independently in narrative content. So, while Lysaker and colleagues’ work has some
shared conceptual interests with our study we took an exploratory position regarding
the specific role of narrative in therapy in psychosis rather than seeking to build on
their work.
It appeared then from reviewing existing concepts potentially mapping on to
reflexivity that there is a way of relating to subjective experience (objectifying it inlanguage), the use of which varies, that can be identified in different activities (adult
attachment interviews, therapy narratives, and theory of mind experimental tasks).
Examining these activities involves different assumptions about the origins of reflexivity,
its mutability, and its relationship to the idea of an objective reality. We were not
attempting to account for the origins of reflexivity, as does for example attachment theory
(Fonagy et al., 2004) or theory of mind (Frith, 1979, 1994, 1997). Rather, we were
interested in determining how reflexivity might be identified in therapy in psychosis
through the use of language and how the therapist might facilitate this activity.
Focusing the studyLeiman’s (2000) definition of reflexivity was used as a specific starting-point for this
study. It was chosen because it focuses on the public demonstration, through language
use, of an active and ongoing relationship to subjective experience and because it
implies that this objectifying of experience can change through relationships withothers (including presumably a therapist).
To reflect requires the ability to create and use signs that refer to one’s own activity,
whether external or internal. To be the ‘author of ones’ thoughts and feelings’ means that
the person is able to establish an internal subject-object relation (i.e. he or she can objectify
personal experience and mental processes, and use some semiotic means to make sense of
those complex phenomena as objects of reflective actions). To objectify one’s own actions,
experiences, thoughts and feelings is an advanced task developed through a number of
transformative stages and modes of ‘joint subjectness’ (Leiman, 2000, pp. 391–392).
Narrative and dialogical approaches, including Leiman’s, draw on the work of Vygotsky
(1978) in adopting a view of therapy as a shared process negotiated between therapist
and client. Vygotsky (1978) proposed that development is essentially a social process
progressed through the scaffolding of activities by another person, and that individuals
have a zone of proximal development representing the new capabilities enabled for an
individual by that joint enterprise. Centrally, Vygotsky (1978) saw language as a tool
used to influence the social world (Wertsch, 1991), but also as a tool with an intra-
personal function; ‘social speech’ (p. 27) turned inwards to direct one’s own activity in‘inner speech’ (p. 27).
However, while Leiman’s definition of reflexivity focuses on the use of language in
objectifying experience, it does not suggest how to operationalize this use. For this
reason, grounded theory was chosen as an appropriate qualitative methodology to allow
212 Sarah Dilks et al.

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
both exploration of this area and further conceptual development (Charmaz, 2003;
Glaser, 1978; Glaser & Strauss, 1967; Henwood & Pidgeon, 2003; Strauss & Corbin,
1998). We adopted a critical realist position (Annells, 1996; Guba & Lincoln, 1998;
Willig, 2001) in relation to ideas about the nature of reality, the means of obtaining
knowledge about the individual and the particular application of grounded theory.
Consistent with this position, it is recognized that the first author brings particularfamiliarity to working with those experiencing psychosis and that the focus of the study
on reflexivity was prompted by this experience and by an awareness of the related
literature. We take Henwood and Pidgeon’s (2003) view that existing literature can both
serve as a starting-point in sensitizing the researcher to the area of inquiry, and aid in the
later stages of conceptual development.
In summary, the starting-point for this exploration of processes in psychological
therapy in psychosis was a focus on reflexivity and how this might be expressed in
therapy conversation. The initial research questions were: (i) how might reflexivity beexpressed in the way people experiencing psychosis talk about subjective experience?
(ii) what are the commonalities and divergences in this process across individuals?
(iii) how do people experiencing psychosis talk about their subjective experiences at
different points in the therapy process? and (iv) how might the therapist facilitate
reflexivity?
DesignThe initial dataset consisted of three taped therapy sessions, spaced out over time,
collected from each of six therapist–client pairs. This was supplemented by semi-
structured interviews with each of the participants. In the Time 1 (T1) interviews the
psychologists and clients were each separately asked about their experience of therapy.
Subsequently, in the later Time 2 (T2) interviews the same participants were separatelyasked about their views of the model of therapy emerging from the grounded theory
analysis of therapy tapes and T1 interviews.
Method
ParticipantsApproaches were made to clinical psychologists identified as working in the NHS withpeople experiencing psychosis through their membership of the British Psychological
Society’s Special Interest Group in Psychosocial Rehabilitation or through the first
author’s knowledge of who was working in this field. Participant information was
sent sequentially to psychologists as they came forward and they were included in the
study if they were subsequently able to identify a client participant from their caseload.
There were no exclusion criteria for participants though psychologists were asked
to identify clients who had been given diagnostic labels associated with obtaining
NHS psychological therapy for experiences identified as psychotic (schizophrenia andschizoaffective disorder). Participants were not otherwise selected according to specific
characteristics, e.g. ethnicity or gender, following Glaser’s (1992) position that the
relevance of particular factors needs to emerge from the analysis rather than being
assumed in advance. Participant details are given in Table 1.
ProcedureInitial data sampling involved the analysis of transcribed audiotapes of individual
psychological therapy sessions with people experiencing psychosis. No criteria for
Building bridges 213

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
Table
1.Therapistandclientcharacteristicsofinitialsample
Psychologist
(nam
echanged)
Gender
Age
Ethnicity(self-identified)
Therapeuticorientation
Yearsqualified
Mark
M37
White
Integrativea
5Lee
F30
Mixed
Integrative
2Charlotte
F37
WhiteBritish
CBT
9Sue
F33
WhiteBritish
Integrative
2Lo
uise
F37
WhiteBritish
CBT
10
Liz
F46
WhiteBritish
Integrative
9
Client(nam
echanged)
Gender
Age
Ethnicity(self-identified)
Diagnosisb
Yearsin
contact
withservices
Colin
M33
WhiteBritish
Schizophrenia
25
Anna
F36
Black
African
Schizophrenia
5Andrew
M35
WhiteBritish
Depressionwithpsychoticepisodes
c3
Isabel
F34
WhiteEuropean
Schizoaffectivedisorder
14
Juliet
F37
Nigerian
Schizoaffectivedisorder
5Tanya
F36
Black
British
Schizophrenia
18
aTheterm
‘integrative’refersto
thespecifyingofm
ultiplemodelsusedto
inform
therapy.Those
nam
edbytherapistsincluded
cognitivebehaviouraltherapy(C
BT),
psychoanalyticapproaches,andsystem
icapproaches.
bDiagnosesreferto
theDSM
IVpsychiatricclassificationsystem
(American
PsychiatricAssociation,1994).
cAndrewwas
included
withtheinitialsam
pledueto
concernsabouttheappropriatenessofusingpsychiatricdiagnosesto
distinguishbetweenclients’experiences
(see
Bentall,
2003;Boyle,
2002,foradiscussion),andbecause
theanalysisofthetherapytapes
suggestedtheactivities
ofAndrew
andCharlottewerenot
qualitativelydifferentto
therest
ofthesample.
214 Sarah Dilks et al.

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
model or length of therapy were specified for this investigation. Six psychologist–client
pairs were recruited; each pair supplied three therapy tapes, spaced out across the
course of their therapy to allow consideration of the process of psychological therapy in
psychosis. This produced a total of 19 therapy tapes (one pair supplied an extra tape due
to poor sound quality) supplied over a period of 11 months. Specific therapy sessions
are indicated in the results by giving the (anonymized) therapist’s name followed bythe client’s, with the number of the therapy tape supplied, e.g. ‘Lee/Anna-2’ refers to
psychologist Lee talking with client Anna in the second therapy tape they supplied.
In addition, each psychologist and client was also interviewed separately by the first
author about their views on the process of therapy using a semi-structured interview.
The T1 interviews took place after all three therapy session tapes had been collected
from each pair. A second (T2) semi-structured interview was also conducted separately
with each of the psychologists and clients to ascertain their views on the emerging
model as it was developed over the course of the analysis. Twelve T1 interviews werecollected from each of the six psychologist and clients, and eleven T2 interviews were
also collected (1 client declined to be interviewed a second time). Copies of the
interview guidelines are available on request from the first author.
Successful applications for NHS research ethics scrutiny were made to a multi-centre
research ethics committee, as well as to individual NHS ethics and research and
development committees for each psychologist/client pair participating from different
health authority areas and NHS trusts. Steps were taken to ensure informed consent, to
preserve the anonymity of participants, and to ensure the confidentiality of tapedmaterial.
Grounded theory analysisGrounded theory involves an iterative process of moving backwards and forwards
between coding and conceptualizing data. Chamberlain (1999), Charmaz (1994, 1995),
Henwood and Pidgeon (2003), and Willig (2001) all give overviews of procedures in
grounded theory from open to focused coding, the use of research memos, and
theoretical sampling. The analysis in this study drew particularly on descriptions of the
grounded theory method given by Charmaz (1994, 1995), Glaser (1978), and Strauss andCorbin (1990, 1998).
Data for the study were gathered and analysed by the first author. Ensuring the
quality of the study included careful documentation in memos of the development of
codes and categories to ensure that these emerged from the data and this was audited
via the supervision process. Checks on the emerging grounded theory were also
provided by accessing multiple perspectives on the phenomena under investigation
including: examining therapy sessions; interviewing psychologists and clients; and
through the theoretical sampling (c.f. Glaser, 1978; Strauss & Corbin, 1998) of additionaldata (not reported here).
Results
The central therapy process identified through this analysis is presented first as thebasis for the rest of the results section. It is presented in its final form for the sake of
clarity rather than being described in the intermediate forms that were gradually built
up during the analytic process. Therefore, the multiple individual codes (some 1,837
in total) and earlier conceptualizations on which this grounded theory is based are
largely not given.
Building bridges 215

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
Building bridges to observational perspectives: Describing the core socialpsychological process in psychological therapy in psychosisThe central therapy activity identified was conceptually summarized as a process of
building bridges to observational perspectives. This was defined as a jointly negotiated
process, enacted in the conversation between psychologist and client, based on the
psychologist repeatedly demonstrating the activities involved in observing, or standingback from, experience during the course of conversation with the client. The
psychologist appeared to be continually lending alternative observational perspectives
and the client borrowing these to re-examine distressing experiences and current
concerns, thereby opening up new possibilities for the client’s functioning in the social
world. Essentially, the psychologist seemed to be providing an observational scaffold
to facilitate the client in considering their experiences and concerns from different
perspectives.
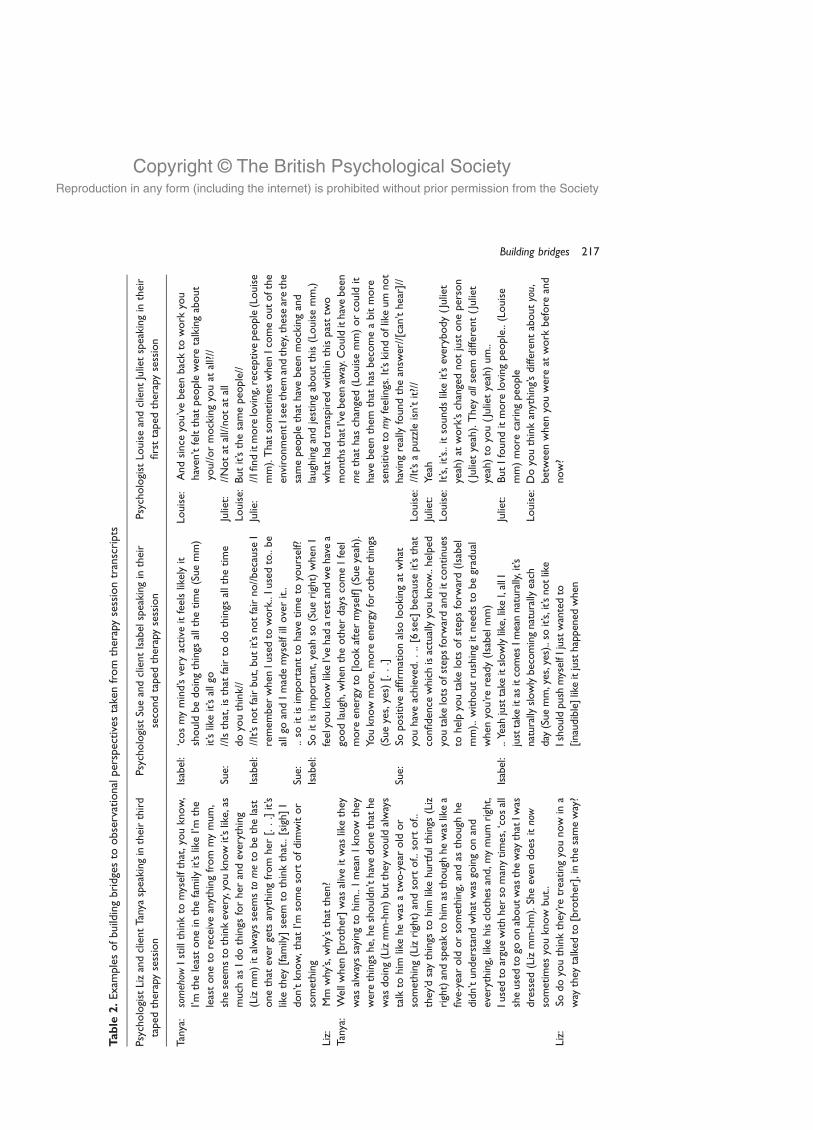
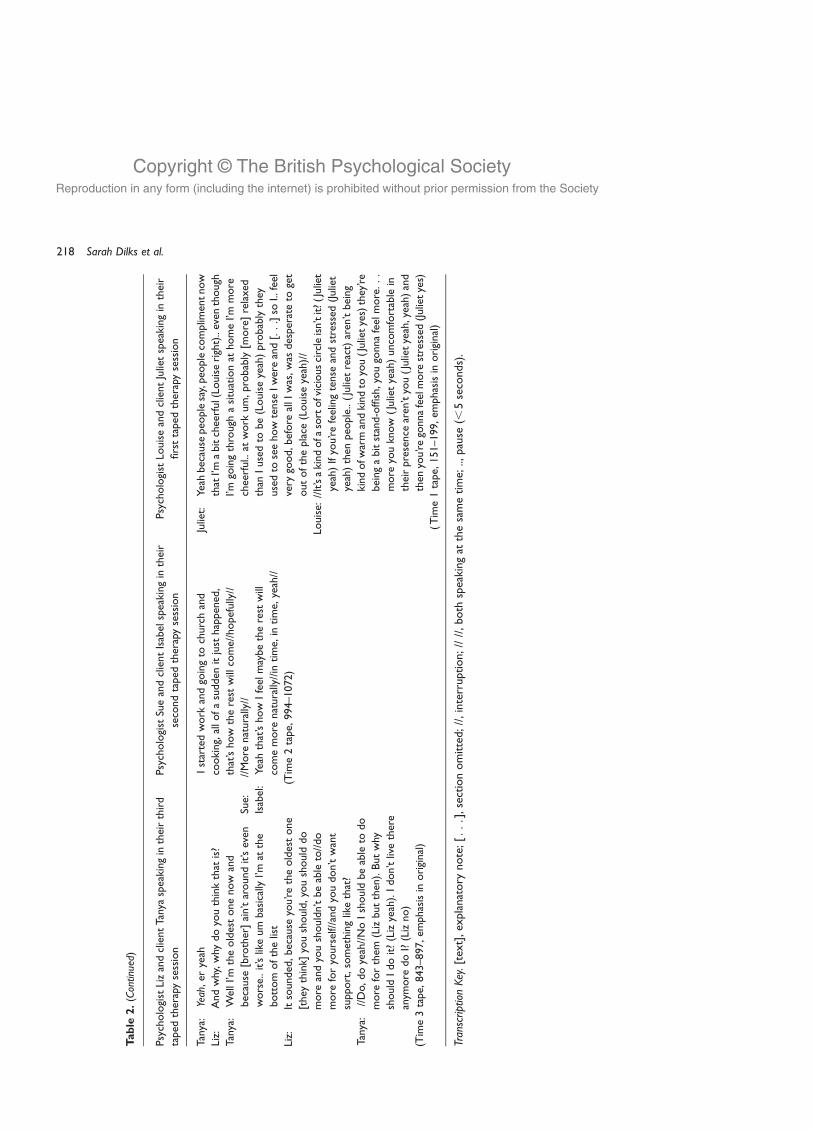
Table 2 below gives examples of the core process of building bridges to observa-tional perspectives taken from different therapy session transcripts. It is important
to note that these examples are segments of an ongoing dialogue between these
psychologists and clients, where themes and issues are returned to both within and
across sessions. This represents a particular challenge in presenting succinct examples
of an ongoing dialogical process. Table 3 specifically illustrates the use of research
memos during the grounded theory analytic process and their contribution to the
conceptual development of building bridges to observational perspectives.
Within this grounded theory, the core process of building bridges to observationalperspectives is conceptually understood as the hub of a series of activities and processes
contributing to or arising from it. Key conceptual subcomponents of the building
bridges process are summarized in sections (1–7) below.
Specifying the four main therapy activities comprising building bridgesto observational perspectives: Opening up views; negotiating sharedunderstandings; doing relationship; and managing emotionThe extract given below illustrates the components of building bridges to observational
perspectives defined in sections (1–4). In this extract Liz engaged with Tanya in
examining different perspectives on Tanya’s worry that she would become unwell:
Liz: it sounds like you’re thinking oh, you know, last time someone left, Kevin [staff
member], you got really unwell but I think you were already in the middle of a
really awful (Tanya mm) period and this time maybe you’ll feel sad but it doesn’t
necessarily follow that you would get unwell (Tanya mm-hm) not necessarily. : : : .[14 sec pause] Or am I wrong Tanya? And, and, I’m not suggesting that, am I
underestimating that actually Richard [staff member] leaving does, does really feel,
make you feel quite sad and it’s,//in a considerable way?//
Tanya: //In a way um but.. //the thing is about me Liz is that.. how can I put it? I don’t
really show my emotions very easily (Liz uh-huh, yeah) and then probably I might
sort of break down and cry but.. things that I don’t, I don’t really let things get to
me, do you know, I try not to (Liz yes).. to let, to let, not to let it worry me that
Richard’s gone (Liz yeah) but I gotta face the fact that he’s gone but (Liz yeah), you
know, there’s nothing I can do that he’s gone, he’s just gone. Nothing I can do
about it (Liz right). There’s no point dwelling on the situation that he’s gone
because, you know, I’ll probably end up ill as well in hospital.
(Liz/Tanya-1, 898–917, emphasis in original)
216 Sarah Dilks et al.
Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
Table
2.Exam
plesofbuildingbridgesto
observationalperspectivestakenfrom
therapysessiontranscripts
PsychologistLizandclientTanyaspeakingintheirthird
taped
therapysession
Psychologist
SueandclientIsabel
speakingin
their
secondtaped
therapysession
Psychologist
LouiseandclientJulietspeakingin
their
firsttaped
therapysession
Tanya:
som
ehow
Istillthinkto
myselfthat,youknow,
I’mtheleastonein
thefamily
it’slikeI’m
the
leastoneto
receiveanythingfrom
mymum,
sheseem
sto
thinkevery,youknowit’slike,as
much
asIdothings
forher
andeverything
(Lizmm)italwaysseem
sto
meto
bethelast
onethat
ever
gets
anythingfrom
her
[:::]it’s
likethey
[fam
ily]seem
tothinkthat..[sigh]I
don’tknow,that
I’msomesort
ofdimwitor
something
Liz:
Mm
why’s,why’sthat
then?
Tanya:
Wellwhen
[brother]was
aliveitwas
likethey
was
alwayssayingto
him..ImeanIknow
they
werethings
he,heshouldn’thavedonethat
he
was
doing(Lizmm-hm)butthey
wouldalways
talkto
him
likehewas
atw
o-yearold
or
something(Lizright)andsort
of..sort
of..
they’dsaythings
tohim
likehurtfulthings
(Liz
right)andspeakto
him
asthough
hewas
likea
five-yearold
orsomething,andas
though
he
didn’tunderstandwhat
was
goingonand
everything,likehisclothes
and,m
ymum
right,
Iusedto
arguewithher
somanytimes,‘cosall
sheusedto
goonaboutwas
theway
thatIw
as
dressed
(Lizmm-hm).Sheeven
does
itno
w
sometimes
youknow
but..
Liz:
Sodoyouthinkthey’retreatingyounow
ina
way
they
talked
to[brother],inthesameway?
Isabel:
‘cosmymind’svery
active
itfeelslikelyit
should
bedoingthings
allthetime(Suemm)
it’slikeit’sallgo
Sue:
//Isthat,isthat
fairto
dothings
allthetime
doyouthink//
Isabel:
//It’snotfairbut,butit’snotfairno//because
I
remem
ber
when
Iusedto
work..Iusedto..be
allgo
andImademyselfilloverit..
Sue:
..so
itisimportantto
havetimeto
yourself?
Isabel:
Soitisimportant,yeah
so(Sueright)when
I
feelyouknowlikeI’vehad
arestandwehavea
goodlaugh,when
theother
dayscomeIfeel
more
energy
to[lookaftermyself](Sueyeah).
Youknowmore,m
ore
energy
forother
things
(Sueyes,yes)
[:::]
Sue:
Sopositive
affirm
ationalso
lookingat
what
youhaveachieved:::.[6sec]
because
it’sthat
confidence
whichisactuallyyouknow..helped
youtake
lotsofstepsforw
ardanditcontinues
tohelpyoutake
lots
ofstepsforw
ard(Isabel
mm)..withoutrushingitneedsto
begradual
when
you’reready(Isabel
mm)
Isabel:
..Yeah
justtake
itslowlylike,likeI,allI
justtake
itas
itcomes
Imeannaturally,it’s
naturally
slowlybecomingnaturally
each
day
(Sue
mm,yes,yes)..soit’s,it’s
notlike
Ishouldpush
myselfIjustwantedto
[inaudible]likeitjusthappened
when
Louise:
Andsince
you’vebeenbackto
work
you
haven’tfeltthat
peo
pleweretalkingabout
you//ormockingyouat
all?//
Juliet:
//Notat
all//notat
all
Louise:
Butit’sthesamepeo
ple//
Julie:
//Ifinditmore
loving,receptive
peo
ple(Louise
mm).That
sometimes
when
Icomeoutofthe
environmentIsee
them
andthey,thesearethe
samepeo
ple
that
havebeenmockingand
laughingandjestingaboutthis(Louisemm,)
what
had
transpired
within
thispasttw
o
monthsthatI’vebeenaw
ay.C
ouldithavebeen
methat
has
changed(Louisemm)orcould
it
havebeenthem
that
has
becomeabitmore
sensitive
tom
yfeelings.It’s
kindoflikeum
not
havingreallyfoundtheansw
er//[can’thear]//
Louise:
//It’sapuzzleisn’tit?//
Juliet:
Yeah
Louise:
It’s,it’s..itsoundslikeit’severybody(Juliet
yeah)at
work’schangednotjust
oneperson
(Julietyeah).They
allseem
different(Juliet
yeah)to
you(Julietyeah)um..
Juliet:
ButIfounditmore
lovingpeo
ple..(Louise
mm)more
caringpeo
ple
Louise:
Doyouthinkanything’sdifferentabout
you,
betweenwhen
youwereat
work
before
and
now?
Building bridges 217
Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
Table
2.(C
ontin
ued)
PsychologistLizandclientTanyaspeakingintheirthird
taped
therapysession
Psychologist
SueandclientIsabel
speakingin
their
secondtaped
therapysession
Psychologist
LouiseandclientJulietspeakingin
their
firsttaped
therapysession
Tanya:
Yeah,er
yeah
Liz:
Andwhy,why
doyouthinkthat
is?
Tanya:
WellI’m
theoldestonenow
and
because
[brother]ain’taroundit’seven
worse..it’slikeum
basicallyI’m
atthe
bottom
ofthelist
Liz:
Itsounded,because
you’retheoldestone
[they
think]
youshould,youshould
do
more
andyoushouldn’tbeable
to//do
more
foryourself//andyoudon’twant
support,somethinglikethat?
Tanya:
//Do,doyeah//NoIshould
beable
todo
more
forthem
(Lizbutthen).Butwhy
should
Idoit?(Lizyeah).Idon’tlivethere
anym
ore
doI?(Lizno)
(Time3tape,
843–897,em
phasisin
original)
Istartedwork
andgoingto
churchand
cooking,allofasudden
itjust
happened,
that’show
therest
willcome//hopefully//
Sue:
//More
naturally//
Isabel:
Yeah
that’show
Ifeelmaybetherest
will
comemore
naturally//in
time,
intime,
yeah//
(Time2tape,
994–1072)
Juliet:
Yeah
because
peo
plesay,peo
plecomplim
entnow
thatI’m
abitcheerful(Lo
uiseright)..even
though
I’mgoingthrough
asituationat
homeI’m
more
cheerful..at
work
um,probably[m
ore]relaxed
than
Iusedto
be(Louiseyeah)probablythey
usedto
seehowtense
Iwereand[:::]so
I..feel
very
good,before
allIwas,was
desperateto
get
outoftheplace
(Louiseyeah)//
Louise:
//It’sakindofa
sortofviciouscircleisn’tit?(Juliet
yeah)Ifyou’refeelingtense
andstressed
(Juliet
yeah)then
peo
ple..(Julietreact)aren’tbeing
kindofw
arm
andkindto
you(Julietyes)they’re
beingabitstand-offish,yougonnafeelmore:::
more
youknow
(Julietyeah)uncomfortable
in
theirpresence
aren’tyou(Julietyeah,yeah)and
then
you’regonnafeelmore
stressed
(Julietyes)
(Time1tape,
151–199,em
phasisin
original)
Tran
script
ion
Key.[text],explanatory
note;[:::],sectionomitted;//,interruption;////,both
speakingat
thesametime;..,pause
(,5seconds).
218 Sarah Dilks et al.

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
(1) Opening up viewsOpening up views was defined as the therapist encouraging the elaboration of the
explanations and views available to the client in considering an area of distress. This
activity was understood as being supported by the psychologist offering specific
understandings of psychosis (defined as the subcategory developing explanation).
(2) Negotiating shared understandingsNegotiating shared understandingswas defined as a constantly negotiated sharingof views
between therapist and client during the course of conversation to enable them both to
Table 3. Extracts from research memos summarizing sequence of psychologist and client therapy
session activities
Mark/Colin-1 Sequence of activities within session (analytic codes in italics)
Colin starts to tell a ‘story’ about a difficult situation, gets caught up in description, an immediacy aboutthe experience and struggles to articulate the exact nature of mental experience
Mark actively encourages the telling by actively listening, acknowledging, summarizing
Colin uses analogy to convey aspects of experience and summarizes main concern after describingthe situation
Mark restates the summary and moves the dialogue on by reframing the key aspect of the troublingexperience within a particular model, or suggests ways of coping, or reinforces Colin’s attemptsat coping
Colin (partially) accepts the reframe predicated on a model of experience (Colin’s implicit understandingof how things are)
The sequence repeats with Mark restating his conceptualization and Colin telling other stories aboutdifferent situations. Mark explicitly maintains a thread through the session connecting the segmentswhilst Colin implicitly does this through telling stories which seem connected by particular themes.How far is Colin aware of this?
(extract from memo dated 2nd July 2003)
Sue/Isabel-1 Sequence of activities within session (analytic codes in italics)
Isabel states worst:not self as should be ( falling short)caught up in story
Sue not accepting Isabel’s account at face value:questioning Isabel’s assumptions about self and othersreminding of disconfirmatory experiencesemphasising achievements
Isabel hears self afresh (possibly indicating reflective activity)Sue restates discrepant view
Isabel states worst (again)Sue not accepting at face value
Isabel hears self afreshSue restates discrepant viewIsabel accepts Sue’s reframing (at end of session)
(Extract from memo dated 15th January 2004)
Building bridges 219

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
move towards shared alternative perspectives on the client’s distress. In commonwith the
category of opening up views, this process was seen as making available new possibilities
for thinking, feeling, or acting in relation to areas of distress, as Colin described: ‘It’s like
finding the answers together. Do you see what I mean? (SD yes) Resolving it together. Like
he’ll [psychologist] help you, he’ll come up with an idea, you say ‘well not really, that
doesn’t work forme, that [other idea]might do’, and he somehowchannels it in. You don’tactually have the answer but it takes two of you to find it’ (T2 interview, 299–302). The
analysis suggested that the shared understandings developed via this joint process had
utility insofar as they offered the potential for opening up alternatives for thinking, feeling,
or acting rather than in any absolute truth-value.
However, it was clear that these psychologists particularly emphasized some
understandings over others as they focused on some lines of discussion, ignored others,
and offered their own understandings specifically through developing particular
explanations of psychosis. The psychologists developed explanations of psychosis thatemphasized agency and self-worth, and minimized self-blame, as the extract below
illustrates:
Louise: when you told me the story of what had happened to you (Juliet yeah) in this
country ( Juliet yeah) um and what I heard was somebody who was you know
very intelligent, very ambitious and that you tried to hang on to your [ : : : ]career but there were lots of practical reasons about being here (Juliet yeah)
that made that very hard (Juliet yeah) and you’d been let down by the woman
that you stayed with (Juliet yeah) and for understandable reasons had felt you
know felt a bit hopeless, and perhaps felt that you couldn’t trust people.
(Louise/Juliet-1, 354–362, emphasis in original)
(3) Doing relationshipDoing relationship was defined as an active, reciprocal process of the psychologist and
client working together in creating and experiencing a confiding context. Conceptually,doing relationship is a summation of the joint, and individual, activities and
experiences of psychologist and client being engaged in a relational process. However,
the psychologists’ strategic use of activities implied that they particularly assumed
responsibility for the maintenance of dialogue. Doing relationship then was
characterized by the psychologist taking the lead in creating a confiding context in
which the client can make known their concerns and therefore experience a confiding
context. The extract from Liz/Tanya-1 (lines 898–917) given earlier, where Liz
collaboratively infers Tanya’s disagreement with her alternative explanation of distress,illustrates how doing relationship is inherent in the building bridges process.
Doing relationship emerged as a complex set of interrelated psychologist and client
activities (see Figure 1 below). So, for instance, the therapist demonstrating concern not
only related to the client feeling cared about, but also related to the client building up
trust in the therapist and valuing self: ‘she [psychologist Liz] makes me feel like I’m
someone special as well, that I’m worthy’ (Tanya, T1 interview, 804–805).
(4) Managing emotionManaging emotion was defined as the psychologist regulating the emotional pace of
therapy through actively structuring the conversation in order to minimize the client
getting caught up in experience. Liz’s actions in acknowledging Tanya’s distress (lines
898–917 above) represent this type of psychologist activity. Although the clients also
220 Sarah Dilks et al.

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
engaged in managing emotion at times, it seemed that this was done in a less systematicway than by therapists.
Conceptualizing the link between building bridges to observational perspectives andthe social world: Opening up new possibilities; processing distress; and enhancingagency and self-worthOpening up new possibilities, processing distress, and enhancing agency and self-worth
were conceptualized as arising inherently from the core process of building bridges to
observational perspectives and summarize processes through which therapy activities
are understood to influence the client’s functioning in the social world.
(5) Opening up new possibilitiesThe availability of new possibilities for thought, feeling, or action in the client’s social
world appeared to arise from the client making explicit and elaborating experiences,
meanings, and explanations in dialogue with the psychologist. The earlier extract from
Colin’s T2 interview (lines 299–302) and that below illustrate the sense of new
possibilities that can arise from the building bridges process:
Juliet: [She is] helping me to understand what the difficulties in my life were, helping
me to come to terms with it and helping me to look for a way forward [ : : : ] Butwhy personally I haven’t even thought of that, ‘cos I’ve been preoccupied with
that over the period of time (SD yeah) and, you know, wallowing in self-pity,
‘why me, why do I have to go through, why do, people don’t understand?’ That’s
how I’ve been looking at it (SD yes). But I never asked myself, how do you move
on (SD yes mm)? And that’s where the difference comes with talking with her as
a psychologist (SD I see yeah). That’s where the turning point is..
(T1 interview, 557–572, emphasis in original)
Figure 1. The subcategories of doing relationship and its links to other major components of the
building bridges process.
Building bridges 221

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
(6) Processing distressProcessing distress was defined as clients standing back from distressing experiences,
memories, or concerns such that clients were no longer getting overwhelmed by
emotion in speaking about them (and by implication in thinking about them).
Processing distress appeared to be facilitated by the client and psychologist structuring
distressing experience in a conversational account, thereby allowing distress to becomethe object of observational activities. For Juliet, this seemed to allow her to act
differently outside of therapy, whereas Tanya implied she still relied on her psychologist
to assist her in processing distress:
Tanya: I get really worried and frustrated about something and then I’ll go and tell Liz
[psychologist] and she says, well that it feels like I’m making a mountain out of a
molehill (SD mm). Why, why was I so keyed up and worried. [ gives example
discussed with Liz : : : ] it didn’t seem like nothing to worry about in the first
place, I don’t know what I was so worried about.
(T1 interview, 483–496, emphasis in original)
Juliet: since talking with Louise [psychologist] I’ve now understood that some of the
thoughts that have been at the back of your mind.. has affected you in such a way
that it was affecting human relationship (SD mm), and affect your outlook about
life and positive way of doing things [ : : : ] when such thoughts try to cross um in
mymind and say ‘oh you’ve been through this, you’ve been through that’, [I] kind
of dismiss it, unlike before when I would spend time (SD mm) thinking about it,
preoccupied with it, it affects my mood, it affects my relationship, it affects
everything around me (SD mm) and keep me in perpetual.. kind of bondage.
Now I tend to dismiss such thoughts and look forward to moving ahead.
(T1 interview, 139–151, emphasis in original)
Processing distress seemed to be facilitated by sharing understandings of distress thatwere
more complex than those already held by the client, minimized self-blame, emphasized
the client’s active attempts to cope, and could be shared socially with at least some people.So, Louise and Juliet appeared to have worked together during a series of therapy
conversations to develop a richer understanding of Juliet’s experiences, one recognizing
multiple influences leading to the development of psychosis: ‘Juliet: it’s not the pressures
of the job affecting me (Louise mm) in a way that contributed to my problems (Louise
okay). But looking back at my life from the time I step into this country, to the relationship
that I had, the people that I mixed with, the kind of job that I did (Louise mm) a
combination of all these things’ (Louise/Juliet-1, 338–342, emphasis in original)
In contrast to processing distress, getting caught up in experience was defined as theclient getting stuck in immediate experience and therefore being unable, at that point, to
take an observing position in relation to their distress or concern. The effect appeared to
be one of reducing access to a consensually shared (or negotiated) view of the world, and
to a taken for granted sense of an external reality, thereby causing difficulties for the client
in functioning in the social world: ‘you’re walking down the street and colour changes..
lights, the sky, everything, the walls, everything just changes shape and you’re just like
‘huh’, you know, you realise afterwards but in it you don’t’ (Colin, T1 interview, 388–391,
emphasis in original). For Andrew it seemed that some of the experiences specificallyassociated for him with psychosis contributed to Andrew becoming socially isolated as he
withdrew frompeople as a result of his assumptions about their intentions: ‘I thought, sort
of thought [intake of breath] people were against me um.. and well I probably thought
222 Sarah Dilks et al.

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
every, everyonewas against me um and um.. I sort of think that’s perhaps not the case now
so.. so I think aboutotherpeople in a better light’ (Andrew,T1 interview, 450–454).Getting
caught up in experience appeared to followunexpected perceptual changes associated for
these clientswithpsychosis but, in addition, it also occurredwhen talking about any area of
distress, implying an overwhelming of observational perspectives by emotion.
The following extract gives an example of getting caught up in experience occurringin the therapy session itself as Colin attempted to describe the pressures of studying
shortly after leaving hospital, following a general opening question from his
psychologist Mark about how his week had been:
Colin: How it’s been? Um.. k.. very tired (Mark mm) I’ve been very like, I’ve been
studying a lot (Mark mm mm).. um.. but I’ve been kind of.. feeling kind of really
tired out, my eyes are burning up and.. stuff but that’s about it, you know, that’s
like that side of it, you know, cos that’s taking up a lot of my time, mental time,
thinking time, the lot, I mean all the days I’m not in there (Mark yeah) I’m just ff,
because we get tested every two weeks it’s, I feel the strain. But I’m pushing
myself through that strain (Mark mm) you know what I mean? (Mark yeah) Some
people in the class, which I’ve noticed, are just sort of skipping through it, you
know. Like ‘oh it’s no problem, bl, bl, bl’, you know. I mean I’m reading notes, I
mean I, in the first part I got nine out of nine I passed the.. the thing, you know
(//Mark that’s great yeah//) completely but.. that’s cos I really pushed through it
and now I’m going through that again, you know, now Friday’s coming up and
it’s another test and then we’ve got another two weeks after that (Mark mm
mm), again, er it was gonna be harder than for the last two weeks.
(Mark/Colin-1, 16–32, emphasis in original)
(7) Enhancing agency and self-worthFinally, enhancing agency and self-worth conceptually summarized the enabling effect
of the building bridges process in highlighting the client’s qualities and abilities. Therewas an emphasis in the psychologists’ activities on making explicit the clients’ qualities,
abilities, and instances of agency; thereby both drawing these to the clients’ attention
and giving hope of better outcomes.
SD: Has talking with [psychologist] had any effect on how you feel about yourself?
Colin: Yeah a better person (SD mm).. straightaway you know. That’s it. Just feel more
confident (SD right.. right). In my abilities [ : : : ] Nothing’s really stopping
me (SD mm). It’s just how I feel inside (SD yes). So he’s made me feel a more
confident, able person in that way. I can’t say more than that really.
(T1 interview, 995–1008, emphasis in original)
Anna: she’s [psychologist Lee] the one that sort of like encouraged me, ‘it will get better
and they will take you off the medication as soon as you get well and you can
begin to lose the weight when you come off the medication, you can start work,
you can decorate your flat, go out, meet people, see your family, be happy and
see different things’ (SD mm) and she gave me a lot of confidence, she gave me
hope (SD right) to try.. to try, and instead of just, you know, just giving up (SD
mm) and thinking ‘oh no I’m gonna be ill forever (SD right), on the medication
forever, oh there’s no point in living because (SD mm) I’m not like other people,
you people’ and things like that.
(Anna, T1 interview, 191–200, emphasis in original)
Building bridges 223

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
Figure 2 outlines the key therapy processes comprising building bridges to
observational perspectives and the processes through which building bridges is
understood to affect the client’s functioning in the social world.
Discussion
Building bridges to observational perspectives conceptualizes a central dialogical
process of standing back from experience operating during therapy in psychosis and its
role in assisting the client in managing distress and functioning in the social world.
This process is supported (scaffolded) by the therapist repeatedly demonstrating the
activities involved in observing experience during an ongoing conversation, effectively
building bridges between different perspectives and the new possibilities for action,
thought or feeling allowed by them.
The analysis suggested a dialogical basis to objectifying private experience and thussupported Leiman’s (2000) view of reflexivity as an ongoing, conversational process of
objectifying experience that can be facilitated through dialogue with another person
(a therapist). This study developed Leiman’s view of reflexivity by specifying how it was
enabled by psychologists in therapy conversations with individuals experiencing
psychosis. In addition, our analysis suggested that this conversational activity could
occur on a continuum from an entirely private, inner dialogue to a public dialogue (with
a therapist). Where our analysis differs from Leiman’s definition of reflexivity is in the
suggestion that either of these could be helpful to the person experiencing psychosis inprocessing distress and functioning in the social world. There was some suggestion from
the analysis that for some clients (e.g. Andrew, Juliet, and Colin) the externally
scaffolded, dialogical process of standing back from experience became internalized as
an inner dialogue, as Leiman (2000) and Vygotsky’s (1978) ideas would suggest.
However, for others (e.g. Tanya, Isabel, and Anna) it seemed this continued to depend
on the psychologist’s support of the building bridges to observational perspectives
process within therapy sessions. However, in the absence of any systematic examination
of outcome in the current study this must remain speculation.There is a common idea shared by this study and work from a variety of theoretical
perspectives (e.g. Blenkiron, 2005; Dimaggio et al., 2003; Jørgensen, 2004; Lombardi,
2003; Seikkula & Trimble, 2005) that developing new meanings, attributions, dialogues,
or narratives, has a potentially transformative effect for the client’s experience of self-
Figure 2. The key grounded theory subcomponents of building bridges to observational perspectives.
224 Sarah Dilks et al.

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
hood and their relationship to the social world. More particularly, the conceptualization
of therapist activities in the building bridges to observational perspectives process
appears consistent with Stiles’ (1999) and Brinegar et al.’s (2006) conceptualization of
the role of creating ‘meaning bridges’ between different internally and externally
available perspectives in facilitating change in therapy with other forms of distress than
psychosis. This implies that processes identified as important in this study of therapyin psychosis might parallel those operating in therapy with other forms of distress.
In another interesting and specific parallel with the findings from the current study,
Seikkula and Trimble (2005) emphasize the importance of ‘emotional regulation’
(p. 471) happening alongside the opening up of new understandings in therapeutic
conversations in their account of family work with people experiencing psychosis.
Finally, the conceptualization of building bridges as a complex set of inter-related
therapist, client, and joint activities enacted in an ongoing conversational cycle seems to
fit with Stiles et al.’s (1998) responsiveness model of therapy processes rather than withlinear models linking therapy process and outcome.
It is also interesting to note, in terms of what might be called conceptual
convergence, some parallels between specific constructs emerging from this
grounded theory analysis and ideas derived independently from Hirschfield, Smith,
Trower, and Griffin’s (2005) study of the personal experience of psychosis and
additionally from Davidson’s (2003) and Lysaker’s work (Lysaker & Buck, 2006;
Lysaker, Lancaster et al., 2003; Lysaker & Lysaker, 2002; Lysaker et al., 2001; Lysaker,
Wickett et al., 2003) on recovery from schizophrenia (sic). Hirschfield et al.
conducted a grounded theory analysis of six young men’s reports of the experience
of psychosis. In common with our study, they noted the disruption caused by
perceptual changes to ‘everyday assumptions about the world’ (p. 265) and the
importance of individual meaning making in integrating psychotic experiences into a
revised sense of self. What was striking from considering Davidson’s (2003)
phenomenological analysis in relation to the current study was the parallel
emergence of the importance of personal meaning making, a sense of agency and
hope, and reconnecting with the social world in recovery from psychosis. Similarly,Lysaker and colleagues’ STAND measure, developed through literature review and
analysis of therapy transcripts, identifies several outcome domains analogous to
concepts emerging as important in the current study: namely, ‘social worth, social
alienation, personal agency’ (Lysaker et al., 2003, p. 538). In a further parallel,
Lysaker et al. (2001, p. 259) suggest five aspects of psychotherapy for schizophrenia
(sic) that might assist in narrative enrichment and hence, they suggest, in recovery
through increased self-awareness and personal agency: (i) developing a story of what
problem the person is facing; (ii) developing a story of aspects of the self not affectedby the problem; (iii) ‘envisioning the future’ (p. 259); (iv) processing affect to reduce
distress; and (v) ‘enactment or action on the basis of narrative revisions’ (p. 259).
Our study supports this view but suggests in addition that what is particularly
important is the development of understandings of distress that are both personally
acceptable, in terms of their implications for a sense of agency and self-worth, and
amenable to being shared socially. That is, this analysis suggested it is the client’s
interpretation of the various explanations possible for the experience of psychosis
that is important, not the specific explanation per se.Of course, it must also be recognized that this grounded theory represents a
beginning in conceptualizing processes in psychological therapy in psychosis
developed from one study with a specific dataset. There are a number of avenues
Building bridges 225

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
potentially open to further develop and challenge the model that draw on different
traditions of systematic inquiry. Further qualitative studies based on different datasets
would provide multiple perspectives on this issue (Guba & Lincoln, 1998), potentially
demonstrating conceptual convergence. Quantitative examinations of this grounded
theory would involve testing hypotheses that can be derived from it with larger samples
of data. Such hypotheses might include specifically testing whether building bridges is acommon process in psychological therapy in psychosis regardless of the theoretical
orientation of the therapist or, indeed, examining whether building bridges to
observational perspectives might be a common process in psychological therapy with
forms of distress other than psychosis, given parallels with constructs such as ‘meaning
bridges’ emerging from more general psychotherapy research.
What this grounded theory of building bridges to observational perspectives
particularly contributes to understanding therapy in psychosis is the specification of
the central role played by a dialogical process of standing back from subjectiveexperience in the client managing distress and functioning in the social world and
the specific therapist activities involved in scaffolding this process during therapy
conversations.
Acknowledgements
This paper presents work completed by the first author to fulfil the requirements of a PhD in
Psychology at Birkbeck College, University of London, and The Tavistock Clinic, and was partly
supported by South London and Maudsley NHS Foundation Trust. The authors are grateful to the
clients and psychologists who generously allowed access to their therapy sessions and to their
views on the therapy process.
References
Annells, M. (1996). Grounded theory method: Philosophical perspectives, paradigm of inquiry,
and postmodernism. Qualitative Health Research, 6(3), 379–393.
Bentall, R. (2003). Madness explained: Psychosis and human nature. London: Penguin Books.
Blenkiron, P. (2005). Stories and analogies in cognitive behaviour therapy: A clinical review.
Behavioural and Cognitive Psychotherapy, 33, 45–59.
Boyle, M. (2002). Schizophrenia: A scientific delusion? (2nd ed.). London: Routledge.
Brinegar, M. G., Salvi, L., Stiles, W., & Greenberg, L. (2006). Building a meaning bridge: Therapeutic
progress from problem formulation to understanding. Journal of Counseling Psychology,
53(2), 165–180.
Brune, M. (2005). ‘Theory of mind’ in schizophrenia: A review of the literature. Schizophrenia
Bulletin, 31(1), 21–42.
Chamberlain, K. (1999). Using grounded theory in health psychology: Practices, premises and
potential. In M. Murray & K. Chamberlain (Eds.), Qualitative health psychology: Theories and
methods (pp. 183–201). London: Sage Publications.
Charmaz, K. (1994). The grounded theory method: An explication and interpretation. In B. Glaser
(Ed.), More grounded theory methodology: A reader (pp. 95–115). Mill Valley, CA: Sociology
Press.
Charmaz, K. (1995). Grounded theory. In J. Smith, R. Harre, & L. Van Langenhove (Eds.),
Rethinking methods in psychology (pp. 27–49). London: Sage.
Charmaz, K. (2003). Grounded theory: Objectivist and constructivist methods. In N. Denzin
& Y. Lincoln (Eds.), Strategies of qualitative inquiry (2nd ed., pp. 249–291). Thousand Oaks,
CA: Sage Publications.
226 Sarah Dilks et al.

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
Davidson, L. (2003). Living outside mental illness: Qualitative studies of recovery in
schizophrenia. New York: New York University Press.
Dimaggio, G., Salvatore, G., Azzara, C., Catania, D., Semerari, A., & Hermans, H. (2003). Dialogical
relationships in impoverished narratives: From theory to clinical practice. Psychology and
Psychotherapy: Theory, Research and Practice, 76, 385–409.
Drury, V., Robinson, E., & Birchwood, M. (1998). ‘Theory of mind’ skills during an acute episode of
psychosis and following recovery. Psychological Medicine, 28, 1101–1112.
Fonagy, P., Gergely, G., Jurist, E., & Target, M. (2004). Affect regulation, mentalization, and the
development of the self. London: Karnac Books.
Fonagy, P., & Target, M. (1997). Attachment and reflective function: Their role on self-organisation.
Development and Psychopathology, 9, 679–700.
Fonagy, P., Target, M., Steele, H., & Steele, M. (1998). Reflective- functioning manual. Version 5.
For application to adult attachment interviews. London: University College London.
France, C., & Uhlin, B. (2006). Narrative as an outcome domain in psychosis. Psychology and
Psychotherapy: Theory, Research and Practice, 79, 53–67.
Frith, C. (1979). Consciousness, information processing and schizophrenia. British Journal of
Psychiatry, 134, 225–235.
Frith, C. (1994). Theory of mind in schizophrenia. In A. David & J. Cutting (Eds.), The
neuropsychology of schizophrenia (pp. 147–161). Hove, UK: Erlbaum.
Frith, C. (1997). Language and communication in schizophrenia. In J. France & N. Muir (Eds.),
Communication and the mentally ill patient: Developmental and linguistic approaches
to schizophrenia (pp. 10–17). London: Jessica Kingsley Publishers.
Georgaca, E. (2001). Voices of the self in psychotherapy: A qualitative analysis. British Journal
of Medical Psychology, 74, 223–236.
George, C., Kaplan, N., & Main, M. (1996). Adult attachment interview (3rd ed.). Berkeley,
CA: Department of Psychology, University of Berkeley, (Unpublished manuscript).
Glaser, B. (1978). Theoretical sensitivity: Advances in the methodology of grounded theory. Mill
Valley, CA: The Sociology Press.
Glaser, B. (1992). Emergence vs. forcing: Basics of grounded theory analysis. Mill Valley, CA:
Sociology Press.
Glaser, B., & Strauss, A. (1967). The discovery of grounded theory: Strategies for qualitative
research. Chicago, IL: Aldine.
Grazebrook, K., Siddle, R., Leadley, K., Everitt, J., Benn, A., Haddock, G., et al. (2004). First
episode psychosis: Two cases to illustrate the role of cognitive behaviour therapy in
making sense of unusual experiences. Behavioural and Cognitive Psychotherapy, 32,
331–345.
Guba, E., & Lincoln, Y. (1998). Competing paradigms in qualitative research. In N. Denzin &
Y. Lincoln (Eds.), The landscape of qualitative research: Theories and issues (pp. 195–220).
Thousand Oaks, CA: Sage.
Harper, D. (2004). Delusions and discourse: Moving beyond the constraints of the modernist
paradigm. Philosophy, Psychiatry and Psychology, 11(1), 55–64.
Hemsley, D. (1998). The disruption of the ‘sense of self’ in schizophrenia: Potential links with
disturbances of information processing. British Journal of Medical Psychology, 71, 115–124.
Hemsley, D. (2005). The schizophrenic experience: Taken out of context? Schizophrenia
Bulletin, 31(1), 43–53.
Henwood, K., & Pidgeon, N. (2003). Grounded theory in psychological research. In P. Camic,
J. Rhodes, & L. Yardley (Eds.), Qualitative research in psychology: Expanding perspectives in
methodology and design (pp. 131–155). Washington, DC: American Psychological
Association.
Hermans, H. (1996). Opposites in a dialogical self: Constructs as characters. Journal of
Constructivist Psychology, 9, 1–26.
Hermans, H., Rijks, T., & Kempen, H. (1993). Imaginal dialogues in the self: Theory and method.
Journal of Personality, 61(2), 207–236.
Building bridges 227

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
Hirschfeld, R., Smith, J., Trower, P., & Griffin, C. (2005). What do psychotic experiences mean for
young men? A qualitative investigation. Psychology and Psychotherapy: Theory, Research
and Practice, 78, 249–270.
Jørgensen, C. R. (2004). Active ingredients in individual psychotherapy: In search of common
factors. Psychoanalytic Psychology, 21(4), 516–540.
Langdon, R., Coltheart, M., Ward, P., & Catts, S. (2001). Mentalising, executive planning and
disengagement in schizophrenia. Cognitive Neuropsychiatry, 6(2), 81–108.
Leiman, M. (1997). Procedures as dialogical sequences: A revised version of the fundamental
concept in cognitive analytical therapy. British Journal of Medical Psychology, 70, 193–207.
Leiman, M. (2000). Ogden’s matrix of transference and the concept of sign. British Journal of
Medical Psychology, 73, 385–397.
Llewelyn, S., & Hardy, G. (2001). Process research in understanding and applying psychological
therapies. British Journal of Clinical Psychology, 40, 1–21.
Lombardi, R. (2003). Mental models and language registers in the psychoanalysis of psychosis: An
overview of a thirteen year analysis. International Journal of Psychoanalysis, 84, 843–863.
Lysaker, P., & Buck, K. (2006). Moving towards recovery within clients’ personal narratives:
Directions for a recovery-focused therapy. Journal of Psychosocial Nursing, 44(1), 28–35.
Lysaker, P., & Daroyanni, P. (2006). Facilitating the emergence of interpersonal relatedness in
individual psychotherapy of schizophrenia: A case study. Bulletin of the Menninger Clinic,
70(1), 53–67.
Lysaker, P., Lancaster, R., & Lysaker, J. (2003). Narrative transformation as an outcome in the
psychotherapy of schizophrenia. Psychology and Psychotherapy: Theory, Research and
Practice, 76, 285–299.
Lysaker, P., & Lysaker, J. (2001). Psychosis and the disintegration of dialogical self-structure:
Problems posed by schizophrenia for the maintenance of dialogue. British Journal of Medical
Psychology, 74, 23–33.
Lysaker, P., & Lysaker, J. (2002). Narrative structure in psychosis: Schizophrenia and disruptions
in the dialogical self. Theory and Psychology, 12, 207–220.
Lysaker, P., Lysaker, J., & Lysaker, J. (2001). Schizophrenia and the collapse of the dialogical self:
Recovery, narrative and psychotherapy. Psychotherapy, 38(3), 252–261.
Lysaker, P., Taylor, A., Miller, A., Beattie, N., Strasburger, A., & Davis, L. (2006). The scale to assess
narrative development: Association with other measures of self and readiness for recovery in
schizophrenia spectrum disorders. Journal of Nervous and Mental Disease, 194(3), 223–225.
Lysaker, P., Wickett, A., Campbell, K., & Buck, K. (2003). Movement towards coherence in the
psychotherapy of schizophrenia: A method for assessing narrative transformation. Journal of
Nervous and Mental Disease, 191(8), 538–541.
Morrison, A. (2001). The interpretation of intrusions in psychosis: An integrative cognitive
approach to hallucinations and delusions. Behavioural and Cognitive Psychotherapy, 29,
257–276.
Roth, A., & Fonagy, P. (1996). What works for whom? A critical review of psychotherapy
research. New York: The Guilford Press.
Sachse, R., & Elliott, R. (2001). Process–outcome research on humanistic therapy variables.
In D. Cain & J. Seeman (Eds.), Humanistic psychotherapies: Handbook of research and
practice (pp. 83–115). Washington, DC: American Psychological Association.
Sarfati, Y., Passerieux, C., & Hardy-Bayle, M.-C. (2000). Can verbalisation remedy the theory of
mind deficit in schizophrenia? Psychopathology, 33, 246–251.
Seikkula, J., & Trimble, D. (2005). Healing elements of therapeutic conversation: Dialogue as an
embodiment of love. Family Process, 44(4), 461–475.
Stiles, W. (1999). Signs and voices in psychotherapy. Psychotherapy Research, 9(1), 1–21.
Stiles, W., Honos-Webb, L., & Knobloch, L. (1999). Treatment process research methods. In
P. Kendall, J. Butcher, & G. Holmbeck (Eds.), Handbook of research methods in clinical
psychology (pp. 364–402). New York: Wiley.
228 Sarah Dilks et al.

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
Stiles, W., Honos-Webb, L., & Surko, M. (1998). Responsiveness in psychotherapy. Clinical
Psychology: Science and Practice, 5(4), 439–458.
Strauss, A., & Corbin, J. (1990). Basics of qualitative research: Grounded theory procedures and
techniques. Newbury Park: Sage Publications.
Strauss, A., & Corbin, J. (1998). Basics of qualitative research: Techniques and procedures for
developing grounded theory (2nd ed.). Thousand Oaks, CA: Sage Publications.
Teasdale, J. (1999). Metacognition, mindfulness and the modification of mood disorders. Clinical
Psychology and Psychotherapy, 6, 146–155.
Vygotsky, L. S. (1978). Mind in society: The development of higher psychological processes.
Cambridge, MA: Harvard University Press.
Wertsch, J. (1991). Voices of the mind: A sociocultural approach to mediated action. New York:
Harvester Wheatsheaf.
White, M. (1987). Family therapy and schizophrenia: Addressing the ‘in-the-corner’ lifestyle
(Spring ed.). Adelaide: Dulwich Center Newsletter.
White, M. (1995). Psychotic experience and discourse. In M. White (Ed.), Re-authoring lives:
Interviews and essays (pp. 112–154). Adelaide: Dulwich Centre Publications.
White, M., & Epston, D. (1990). Narrative means to therapeutic ends. New York and London:
W. Norton and Company.
Willig, C. (2001). Introducing qualitative research in psychology: Adventures in theory and
method. Buckingham: Open University Press.
Received 13 October 2006; revised version received 1 February 2008
Building bridges 229
Top Related
Copyright © 2022 FDOKUMEN

