







Bahasa
Halaman
Hukum


1
A case of adiaspiromycosis causing1
respiratory failure and a review of human2
infections due to the fungi Emmonsia and3
Chrysosporium4
5
Gregory M. Anstead,*1,2 Deanna A. Sutton,3 and John R.6
Graybill17
81Department of Medicine, Division of Infectious Diseases; and93Department of Pathology, Fungus Testing Laboratory10
University of Texas Health Science Center at San Antonio11
San Antonio, TX 7822912
132Department of Medicine, Division of Infectious Diseases14
South Texas Veterans Healthcare System15
San Antonio, TX 7822916
17
Submitted to: Journal of Clinical Microbiology18
19
*Address correspondence to:20
Gregory M. Anstead, MD, PhD21
Department of Medicine; Division of Infectious Diseases22
University of Texas Health Science Center at San Antonio23
7703 Floyd Curl Drive MC788124
San Antonio, TX 7822925
Phone: 210-567-466626
Fax: 210-567-467027
Email: [email protected]
29
Running title: Adiaspiromycosis causing respiratory failure30
31
32

2
We report a case of a 27 year-old male who presented with respiratory distress that33
required mechanical ventilation. Transbronchial biopsy revealed adiaspores of the34
fungus Emmonsia crescens within granulomata, a condition known as35
adiaspiromycosis. The patient received amphotericin products and corticosteroids,36
followed by itraconazole, and made a full recovery. Emmonsia crescens is a saprobe37
with a wide distribution that is primarily a rodent pathogen. The clinical38
characteristics of the 21 cases of human pulmonary adiaspiromycosis reported since39
the last comprehensive review in 1993 are described, as well as other infections40
recently reported for the genus Emmonsia. Pulmonary adiaspiromycosis has been41
reported primarily in persons without underlying host factors, and has a mild to42
severe course. It remains uncertain if the optimal management of patients with43
severe pulmonary adiaspiromycosis is supportive, antifungal treatment,44
corticosteroids, or a combination of the latter two. The classification of fungi45
currently in the genus Emmonsia have undergone considerable revision since their46
original description, including being grouped with the Chrysosporium at one time.47
Molecular genetics has clearly differentiated the Emmonsia from the Chrysosporium.48
Nevertheless, there has been a persistent confusion in the literature regarding the49
clinical presentation of infection with fungi of these two genera; to clarify this50
matter, the reported cases of invasive chrysosporiosis were also reviewed. Invasive51
Chrysosporium infections typically occur in impaired hosts, and can have a fatal52
course; based on in vitro susceptibilities, amphotericin B, itraconazole, and53
voriconazole are the most active drugs.54
55

3
INTRODUCTION56
Adiaspiromycosis is primarily a pulmonary infection of rodents, fossorial57
mammals, and their predators, caused by the soil fungi Emmonsia crescens and E. parva58
(5,53). It is a rare human infection. In this infection, inhaled Emmonsia conidia enlarge59
to form non-replicating adiaspores. As in other mammals, the infection in humans60
usually involves lungs, with only a few other well-documented cases of infection at other61
body sites (35,53). Numerous case reports have been published about human62
adiaspiromycosis, but much of the medical literature on this infection has been widely63
dispersed in many less accessible non-English journals. Furthermore, the inconsistent64
nomenclature and taxonomy of the Emmonsia and their confusion with fungi of the genus65
Chrysosporium has resulted in an overall lack of consistent information on66
adiaspiromycosis and chrysosporiosis. Herein, we report a case of adiaspiromycosis that67
resulted in respiratory failure. We also review the true cases of adiaspiromycosis that68
have reported since the last comprehensive assessment of cases by England and69
Hochholzer in 1993 (20). Furthermore, we differentiate the cases of adiaspiromycosis70
from the true and probable cases of invasive chrysosporiosis.71
CASE REPORT72
A 27 year-old Hispanic male presented with a 5-day history of nonproductive73
cough, dyspnea, pleuritic chest pain, and weight loss. Initial vital signs were temperature74
99.2 °F, bp 112/67, pulse 104 per minute, and respiration rate 22 breaths per minute. On75
exam, there were crackles throughout both lung fields. A chest X-ray showed marked76
bilateral interstitial infiltrates (Fig. 1). The white blood cell count was 15,800/mm3 (85%77
pmns, 6% lymphocytes, 4% monocytes, 5% eosinophils). The hematocrit, platelet count,78
and routine serum chemistry values were within normal limits, except for aspartate and79

4
alanine transaminase levels of 45 and 104 U/L, respectively. An arterial blood gas80
measurement on room air showed pH 7.49, PCO2 31 mm Hg, and PO2 50 mm Hg. The81
impression was military tuberculosis or pneumocytosis and the patient received isoniazid,82
rifampin, pyrazinamide, ethambutol, and trimethoprim/sulfamethoxazole. The patient83
emigrated from Mexico two years ago and worked at a construction site. He denied84
substance abuse and recent travel.85
Bronchoscopy with lavage and trans-bronchial biopsy was performed on hospital86
day-3. Both specimens were negative for acid-fast bacillus stain and culture. The87
Gomori’s methenamine-silver (GMS)-stained biopsy specimen showed thick, capsulated88
structures (either empty or with a few internal globules) centrally in non-necrotizing89
granulomas (Fig. 2). The impression was coccidioidomycosis. The patient received one90
dose of fluconazole and then amphotericin B 40 mg IV each day. The anti-mycobacterial91
drugs and trimethoprim/sulfamethoxazole were discontinued.92
However, serologic studies for coccidioidomycosis were repeatedly negative.93
Other negative studies included: viral and routine cultures; urine Histoplasma and94
Legionella antigens; serum cryptococcal antigen; and serologic tests for the human95
immunodeficiency virus, Mycoplasma, Toxocara, and Chlamydia.96
Despite treatment with amphotericin B, the patient’s respiratory status97
deteriorated. On day-13, methylprednisolone 100 mg IV four-times daily was started.98
Later that day, the patient went into respiratory failure and required mechanical99
ventilation. On day-16, amphotericin B was changed to amphotericin B lipid complex at100
5 mg/kg/d because the patient developed renal tubular acidosis. Because of the patient’s101
5
lack of improvement, an open lung biopsy of was performed on day-18, which showed102
only GMS-positive material suggestive of residual fungal elements.103
At this point, the histopathology specimen from the original trans-bronchial104
biopsy was reviewed again, and a diagnosis of adiaspiromycosis due to Emmonsia105
crescens was made. The patient’s pulmonary status was gradually improving. He was106
weaned from mechanical ventilation after 6 days. Amphotericin B lipid complex was107
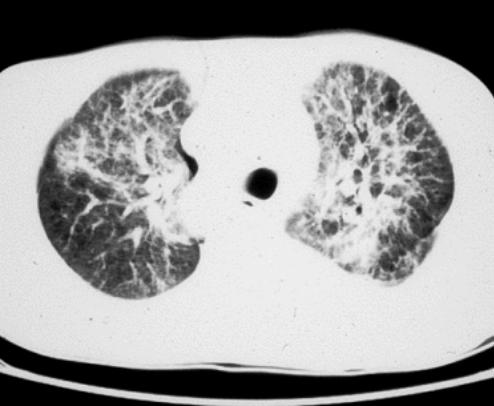
discontinued on day-25 and itraconazole 200 mg orally each day was started. A CT scan108
performed on day-26 showed diffuse bilateral interstitial thickening (Fig. 3). Three days109
before hospital discharge, pulmonary function tests showed a moderate restrictive defect.110
The patient was discharged on tapering prednisone and itraconazole 200 mg orally daily111
for 12 days. At follow-up three months after discharge, the patient was asymptomatic,112
and he had returned to his previous weight.113
With the diagnosis of this unusual mycosis, the patient was interviewed again114
about exposures. He reported that two weeks prior to the onset of his illness he disposed115
of a partially decomposed cat carcass at his construction worksite in Bexar Co., TX (near116
San Antonio), and some debris showered down upon his face at that time.117
Methods118
To find previously published cases of emmonsiosis and chrysosporiosis119
MEDLINE was searched from 1965 to December 2010 using the search terms120
“adiaspiromycosis,” “Emmonsia,” and “Chrysosporium.” Additional cases were found121
by bibliographic branching. Papers in non-English languages were translated into122
English by using the online translation tool Yahoo! Babel Fish.123
6
(http://babelfish.yahoo.com). Other information was obtained from Google searches124
using the same search terms.125
RESULTS AND DISCUSSION126
Review of Adiaspiromycosis127
History of the Description of the Organisms and their Nomenclature and Taxonomy.128
The nomenclature and taxonomy of these fungi has been a source of ongoing129
confusion, so it is instructive to clarify this issue and justify the nomenclature that we130
have adopted for this paper. Furthermore, the nomenclatural confusion has caused many131
authors to lump cases due to Chrysosporium together with those caused by E. crescens132
and E. parva and so the clinical presentation of disease caused by the two genera has also133
been quite muddled in the literature (40,41,63,67,68).134
In 1939, Kirschenblatt described cystic structures in the lungs of rodents from the135
former Soviet Union and proposed that these were due to a fungus that he named136
Rhinosporidium pulmonale (27). In 1942, Emmons and Ashburn observed spherical non-137
budding cells up to 14 µm in diameter in the lungs of rodents in Arizona; they thought138
this fungus was a zygomycete, so they placed it in the genus Haplosporangium, and used139
the species epithet parvum because of the small size of its sporangium (18). In 1947,140
Dowding observed fungal cells, up to 300 µm in diameter, in the lungs of rodents from141
Alberta (15). Although this fungus resembled H. parvum in its culture characteristics and142
microscopic appearance, it formed both larger cells in vivo and larger chlamydospores143
when grown at 37oC. In the 1950s, it was determined that H. parvum was not a144
zygomycete and was closely allied to Blastomyces on the basis of conidial characteristics.145
Ciferri and Montemartini created the new monotypic genus Emmonsia for H. parvum in146
7
1959 (9) and in 1960 Emmons and Jellison (19) added E. crescens (the fungus from the147
Canadian rodents). The two species were differentiated by the size of their adiaspores148
and maximum growth temperatures (53).149
The confusion commenced in 1962 when Carmichael broadened the genus150
Chrysosporium to include all fungi that produce aleurioconidia, solitary single-cell151
conidia that are released by disintegration of the supporting structure (7). Furthermore,152
Carmichael treated E. parvum and E. crescens as varieties of the same species. Thus, E.153
parvum and E. crescens were renamed C. parvum var. parvum and C. parvum var.154
crescens, respectively (7). Some mycologists embraced the reclassification (33), but155
others advocated retaining the genus name Emmonsia, but also designating the two156
species as varieties, i.e., E. parvum var. parvum and E. parvum var. crescens (65).157
Meanwhile, other species assigned to Emmonsia in the 1960s, E. brasilensis and E .158
ciferrina, were reclassified as C. pruinosum (43).159
Currently, fungi of the genera Emmonsia and Chrysosporium are classified as160
follows: Kingdom Eumycota, Division Ascomycota, Class Euascomycetes, Order161
Onygenales, Family Onygenaceae. Other genera in this family include Blastomyces,162
Coccidioides, Histoplasma, and Paracoccidioides (11). Genetically, Emmonsia is more163
closely related to Blastomyces, Histoplasma , and Paracoccidioides than to164
Chrysosporium or Coccidioides (11). (For a comparison of Emmonsia with these genera,165
see Sigler (53)).166
In 1996, Sigler described the teleomorph (meiotic stage) of E. crescens,167
Ajellomyces crescens, which is the same genus as the teleomorphs of Blastomyces168
dermatitidis and Histoplasma capsulatum. Genetic sequencing of these fungi confirmed169
8
the relatedness of Emmonsia to Blastomyces (34,46); in fact, E. parva is more closely170
related to Blastomyces than to E. crescens. It would be justified, based on genetic171
analyses, to place the Emmonsia in the same genus as Blastomyces. However, because of172
the chaos that would ensue from a genus-level name change of these medically173
significant fungi, Blastomyces and Histoplasma have retained their current names. Also,174
it is appropriate that the Emmonsia not be classified as Chrysosporium and that E. parva175
and E. crescens be considered distinct species.176
In 1998, a cutaneous mycosis was reported in an AIDS patient; histopathologic177
analysis of the skin revealed small yeast-like budding cells, (2-4 µm in diameter), larger178
thick-walled cells (8-10 µm in diameter), and pseudohyphae. In culture, the fungus was179
morphologically compatible with Emmonsia, but was genetically distinct from E. parva180
and E. crescens, and was described as a new species, E. pasteuriana (22).181
Another nosological obfuscation has been the cavalier use of the term182
adiaspiromycosis. The term derives from the Greek ‘diaspeirios’, meaning ‘to spread’183
and ‘a’, denoting a negative, so named because the adiaspore is not known to divide in184
tissue or to disseminate (19). Thus, the term adiaspiromycosis is correctly applied to185
describe the infection only when the Emmonsia adiaspores are observed in tissue. For186
example, E. pasteuriana produces yeast-like forms in tissue (22), so the infection could187
be called emmonsiosis, but not adiaspiromycosis. In a case of pulmonary infection188
observed in a rheumatoid arthritis patient, fungi were observed within the macrophages189
obtained in the bronchoalveolar lavage, and were identified as an Emmonsia species190
based on genetic sequencing, but adiaspores were not observed in the biopsy specimen.191
The authors appropriately did not use the term adiaspiromycosis to describe the infection192

9
(72). Furthermore, the term adiaspiromycosis should not be used for infections due to193
Chrysosporium (57).194
Mycology of Emmonsia and Chrysosporium195
Members of both genera produce solitary, single-celled conidia called196
aleurioconidia because of their lytic method of conidial dehiscence. The tissue forms of197
E. crescens and E. parva have large, thick-walled chlamydospore-like non-reproducing198
spores called adiaspores (53), whereas Chrysosporium produces hyphae in tissue (49,68).199
For Chrysosporium in culture, the colonies are yellowish-white to buff, and slow200
to moderately fast growing. The conidia are single-celled and the smooth to roughened201
aleurioconidia are sessile (formed directly on the sides of the hyphae) or formed at the202
ends or on the sides of unswollen stalks. Alternate arthroconidia are also sometimes203
present (55).204
For Emmonsia, the colonies are yellowish-white to buff. The aleurioconidia are205
single-celled, smooth to roughened, formed sessile or on the sides of swollen stalks. The206
formation of two to three conidia from the same cell is also a common feature.207
Emmonsia forms adiaspores at maximum growth temperatures. Members of Emmonsia208
differ from the Chrysosporium by their swollen stalk and the telomorph of E. crescens in209
the genus Ajellomyces (55).210
Clinical Presentation of Human Infection211
The first human case, presenting as a solitary pulmonary nodule, was reported in212
1964 (13). Disseminated human pulmonary disease was first observed in 1971 (28).213
Approximately 67 probable cases of human pulmonary adiaspiromycosis due to E.214
crescens have been described in the literature. England and Hochholzer, in their 1993215
10
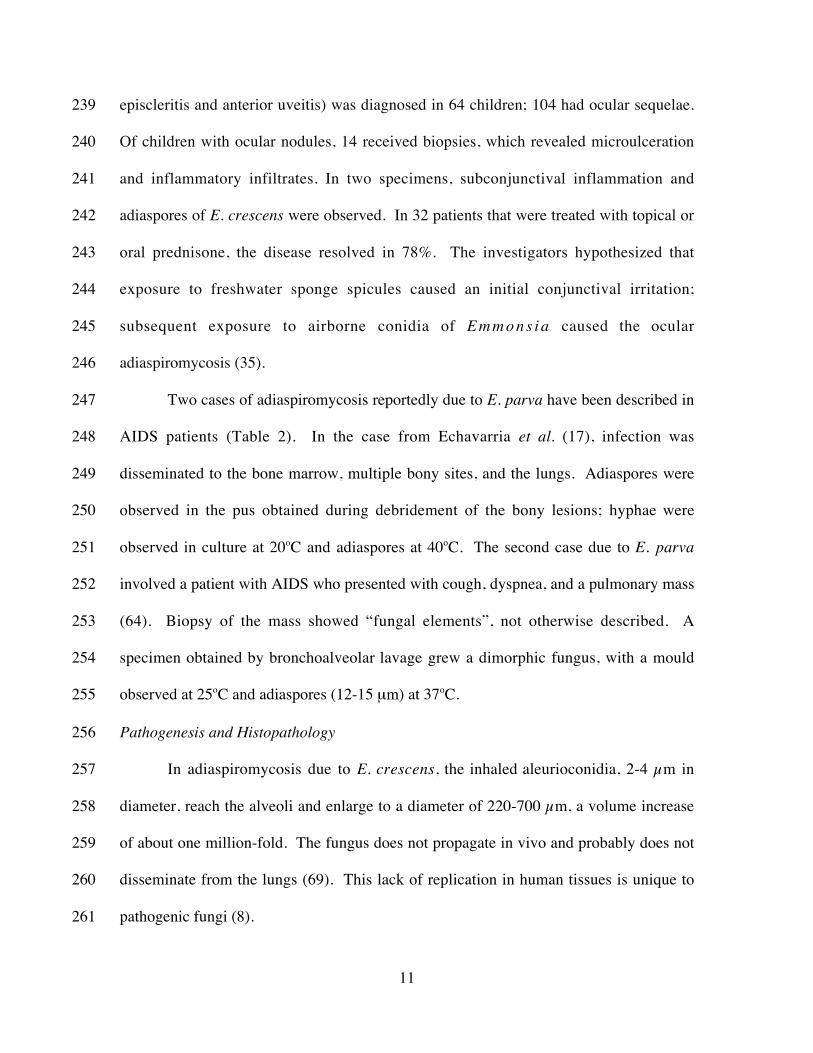
case series and review (20), identified 46 cases; there have been 21 other cases reported216
since that time or omitted from their review (Table 1). Adiaspiromycosis may be217
discovered incidentally after histopatholgic exam of the lung in other conditions.218
Alternatively, the disease may have an indolent course with fever, weight loss, fatigue,219
cough, hemoptysis, and dyspnea. In such cases, the chest radiograph usually shows220
bilateral reticulonodular infiltrates suggestive of military tuberculosis. Disseminated221
pulmonary infection can have a severe or even fatal course (6,20,31,36,38,52). The222
patient reported herein suffered moderate restrictive lung disease after the infection;223
likewise, in two prior cases, restrictive disease was observed (50).224
In the 21 patients with pulmonary adiaspiromycosis due to E. crescens (Table 1),225
in four cases, the disease was discovered incidentally. In the 16 other cases in which a226
clinical course were described, one case was fatal, and five other patients had severe227
disease, two of these requiring mechanical ventilation. Host factors were not important228
in the severity of the infection.229
There have been two reports of adiaspiromycosis of the appendix that developed230
after oral ingestion of the fungus (16,29); in one of these cases, peritonitis was observed231
after appendiceal rupture (16). However, the reported cases of cutaneous232
adiaspiromycosis (25,57) and adiaspiromycosis of the cornea (67) are probably due to233
other fungi (53).234
An unusual outbreak of ocular adiaspiromycosis was reported from northern235
Brazil in 2006. Local ophthalmologists reported 18 children with conjunctival nodules to236
health authorities. Subsequently, 5084 children were screened for external ocular237
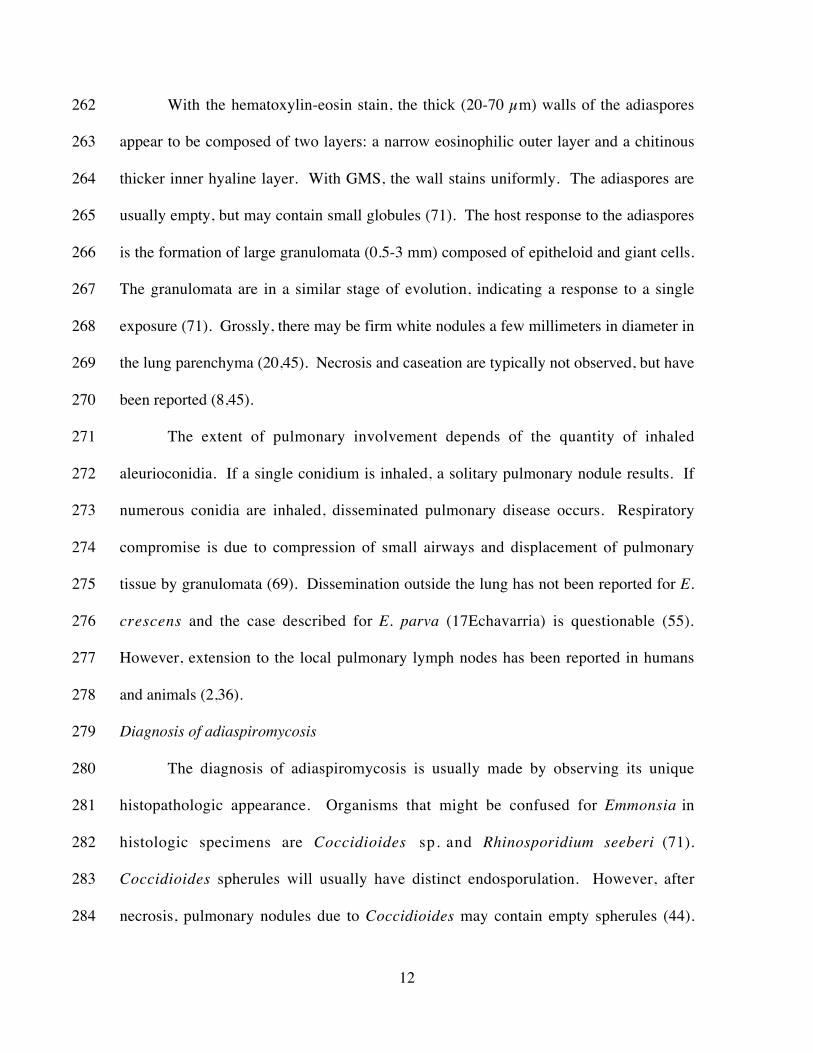
changes and decreased visual acuity. Active ocular disease (conjunctivitis with238
11
episcleritis and anterior uveitis) was diagnosed in 64 children; 104 had ocular sequelae.239
Of children with ocular nodules, 14 received biopsies, which revealed microulceration240
and inflammatory infiltrates. In two specimens, subconjunctival inflammation and241
adiaspores of E. crescens were observed. In 32 patients that were treated with topical or242
oral prednisone, the disease resolved in 78%. The investigators hypothesized that243
exposure to freshwater sponge spicules caused an initial conjunctival irritation;244
subsequent exposure to airborne conidia of E m m o n s i a caused the ocular245
adiaspiromycosis (35).246
Two cases of adiaspiromycosis reportedly due to E. parva have been described in247
AIDS patients (Table 2). In the case from Echavarria et al. (17), infection was248
disseminated to the bone marrow, multiple bony sites, and the lungs. Adiaspores were249
observed in the pus obtained during debridement of the bony lesions; hyphae were250
observed in culture at 20oC and adiaspores at 40oC. The second case due to E. parva251
involved a patient with AIDS who presented with cough, dyspnea, and a pulmonary mass252
(64). Biopsy of the mass showed “fungal elements”, not otherwise described. A253
specimen obtained by bronchoalveolar lavage grew a dimorphic fungus, with a mould254
observed at 25oC and adiaspores (12-15 µm) at 37oC.255
Pathogenesis and Histopathology256
In adiaspiromycosis due to E. crescens, the inhaled aleurioconidia, 2-4 µm in257
diameter, reach the alveoli and enlarge to a diameter of 220-700 µm, a volume increase258
of about one million-fold. The fungus does not propagate in vivo and probably does not259
disseminate from the lungs (69). This lack of replication in human tissues is unique to260
pathogenic fungi (8).261
12
With the hematoxylin-eosin stain, the thick (20-70 µm) walls of the adiaspores262
appear to be composed of two layers: a narrow eosinophilic outer layer and a chitinous263
thicker inner hyaline layer. With GMS, the wall stains uniformly. The adiaspores are264
usually empty, but may contain small globules (71). The host response to the adiaspores265
is the formation of large granulomata (0.5-3 mm) composed of epitheloid and giant cells.266
The granulomata are in a similar stage of evolution, indicating a response to a single267
exposure (71). Grossly, there may be firm white nodules a few millimeters in diameter in268
the lung parenchyma (20,45). Necrosis and caseation are typically not observed, but have269
been reported (8,45).270
The extent of pulmonary involvement depends of the quantity of inhaled271
aleurioconidia. If a single conidium is inhaled, a solitary pulmonary nodule results. If272
numerous conidia are inhaled, disseminated pulmonary disease occurs. Respiratory273
compromise is due to compression of small airways and displacement of pulmonary274
tissue by granulomata (69). Dissemination outside the lung has not been reported for E.275
crescens and the case described for E. parva (17Echavarria) is questionable (55).276
However, extension to the local pulmonary lymph nodes has been reported in humans277
and animals (2,36).278
Diagnosis of adiaspiromycosis279
The diagnosis of adiaspiromycosis is usually made by observing its unique280
histopathologic appearance. Organisms that might be confused for Emmonsia in281
histologic specimens are Coccidioides sp. and Rhinosporidium seeberi (71).282
Coccidioides spherules will usually have distinct endosporulation. However, after283
necrosis, pulmonary nodules due to Coccidioides may contain empty spherules (44).284

13
Nevertheless, these are much smaller than the adiaconidia of Emmonsia, with thinner285
walls. Rhinosporidium also has endosporulation, and is smaller than either Emmonsia286
species (71). Helminths that infect the lungs, such as Strongyloides or Dirofilaria, may287
also resemble adiaspiromycosis (20). The staining characteristics of E. crescens are288
described by Sun et al. (60).289
Overall, Emmonsia crescens is difficult to culture from clinical specimens (20).290
At 37°C, on brain heart infusion blood agar, the aleurioconidia of E. crescens enlarge to291
become adiaconidia 25-400 µm in diameter; E. parva requires 40°C to produce292
adiaconidia, which are 10-25 µm in diameter (53).293
Epidemiology of Human Adiaspiromycosis294
Cases of human adiaspiromycosis have been reported from Brazil, France, the295
former Czechoslovakia, the former Soviet Union, Romania, Honduras, Guatemala,296
Venezuela, Finland, United Kingdom, Argentina, Spain, Germany, and the United States297
(NC, OK, AZ, NY, GA)(12,20,40,71). However, since E. crescens is geographically298
widespread, it would be expected that cases may be observed in many different locales.299
Table 1 shows the demographic data of the 21 patients with pulmonary300
adiapiromycosis due to E. crescens described since the review of England and301
Hochholzer or omitted from that review (20). From Table 1, the average age of the302
patients was 40 years, with a range of 2-74 years old; 90% are male, probably because of303
greater occupational exposure to dusts. New areas in which the disease has been reported304
include the United Kingdom and Finland (12,40); however, 62% of the 21 new cases of305
pulmonary adiaspiromycosis were reported from Brazil, which is also the location of the306
newly recognized ocular adiaspiromycosis (35). It is unclear if the E. crescens is actually307
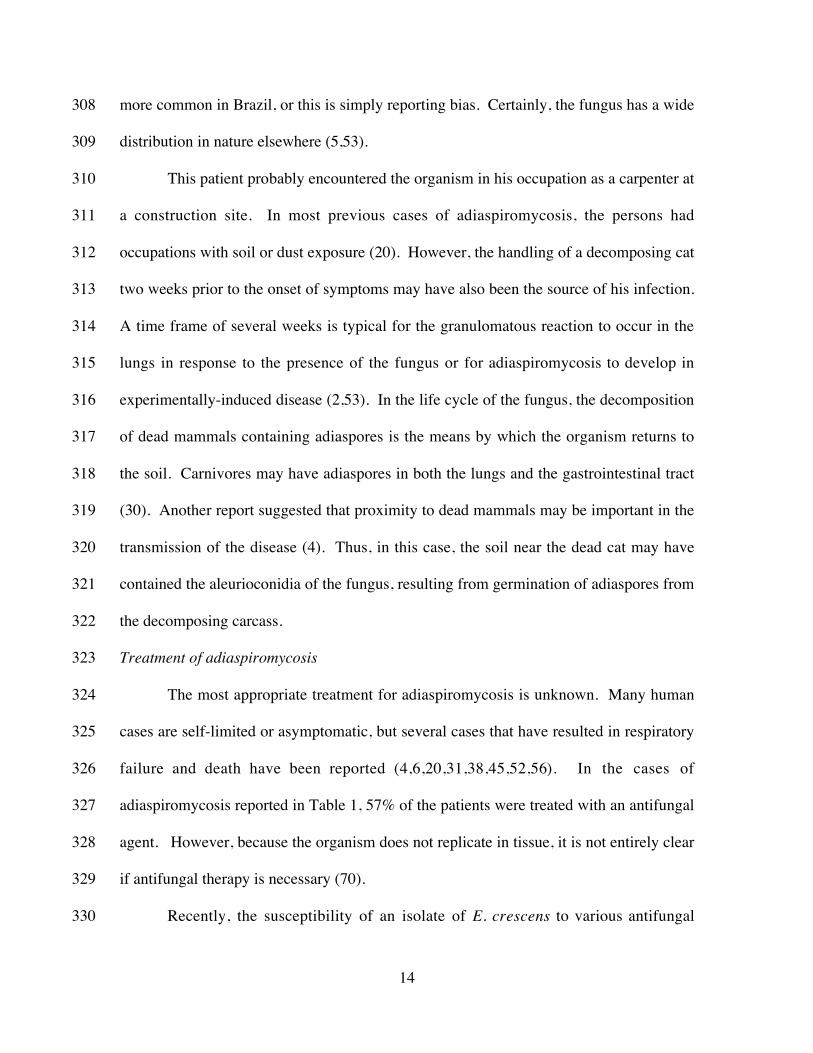
14
more common in Brazil, or this is simply reporting bias. Certainly, the fungus has a wide308
distribution in nature elsewhere (5,53).309
This patient probably encountered the organism in his occupation as a carpenter at310
a construction site. In most previous cases of adiaspiromycosis, the persons had311
occupations with soil or dust exposure (20). However, the handling of a decomposing cat312
two weeks prior to the onset of symptoms may have also been the source of his infection.313
A time frame of several weeks is typical for the granulomatous reaction to occur in the314
lungs in response to the presence of the fungus or for adiaspiromycosis to develop in315
experimentally-induced disease (2,53). In the life cycle of the fungus, the decomposition316
of dead mammals containing adiaspores is the means by which the organism returns to317
the soil. Carnivores may have adiaspores in both the lungs and the gastrointestinal tract318
(30). Another report suggested that proximity to dead mammals may be important in the319
transmission of the disease (4). Thus, in this case, the soil near the dead cat may have320
contained the aleurioconidia of the fungus, resulting from germination of adiaspores from321
the decomposing carcass.322
Treatment of adiaspiromycosis323
The most appropriate treatment for adiaspiromycosis is unknown. Many human324
cases are self-limited or asymptomatic, but several cases that have resulted in respiratory325
failure and death have been reported (4,6,20,31,38,45,52,56). In the cases of326
adiaspiromycosis reported in Table 1, 57% of the patients were treated with an antifungal327
agent. However, because the organism does not replicate in tissue, it is not entirely clear328
if antifungal therapy is necessary (70).329
Recently, the susceptibility of an isolate of E. crescens to various antifungal330

15
agents was determined. The MICs (µg/mL) of amphotericin B, itraconazole,331
voriconazole, caspofungin, fluconazole, and flucytosine were 0.06, 0.12-0.25, 0.06, 0.5,332
64, and 8, respectively, with no significant difference in susceptibilities between the333
aleuriospores and adiaspores. Only amphotericin B was fungicidal (5). The334
susceptibility to azoles is similar to that of Histoplasma and Blastomyces (42Otcenasek335
and Ditrich 1983).336
Anecdotally, clinical improvement in patients with adiaspiromycosis has been337
reported using a number of drugs, including ketoconazole (Table 1), pimafucin (28),338
levamisole (4), thiabendazole (4), flucytosine (47), inhaled pimaricin (4), and339
amphotericin B (Table 1). However, it is uncertain if antifungal treatment accelerated340
recovery, or if this was merely the natural history of the infection. Patients appeared to341
benefit from corticosteroids in three previous cases (10,28,56) and in this case as well;342
this intervention seems reasonable in the immunocompetent patient because the major343
pathogenic effect of the fungus is due to the host granulomatous response. In severe344
pulmonary adiaspiromycosis in the immunocompetent host, it is reasonable to give both345
antifungal treatment to destroy the organism that provokes the inflammation and346
corticosteroid treatment to modulate that response. The disease is so rare that controlled347
clinical trial data will never be available; however, an animal model may be able to348
suggest if antifungal treatment, corticosteroids, both, or none may be beneficial.349
Review of Chrysosporium Infection350
Chrysosporium is a large genus of saprobic soil fungi that includes over sixty351
species (66). Many of the species are keratinolytic, breaking down shed keratinized352
residues, such as hair and feathers (1). Common members of the genus include C.353
16
keratophilum, C. tropicum, C. merdarium, C. inops, C. pannicola, C. queenslandicum,354
and C. zonatum (3). Chrysosporium species may be encountered in the mycology355
laboratory as contaminants of cutaneous and respiratory samples, but are occasionally356
isolated as true agents of dermatomycoses from samples of human skin and nails357
(11,58,61). They are rarely associated with invasive human disease, but in the358
immunocompromised patient, they can be aggressive opportunistic pathogens.359
The Chrysosporium are similar to Geomyces species and the mould phase of360
Blastomyces dermatiditis and share the teleomorph genus Arthroderma with many361
species of dermatophytic fungi (61). They are resistant to cycloheximide and can be362
recovered from selective media for dermatophytes (61), and potato dextrose agar (1).363
The common species of Chrysosporium can usually be differentiated by the morphology,364
location, and size of the conidia (3,26); however, many species share similar features and365
definitive identification may require genetic sequencing (66). The mycology atlas of de366
Hoog and coworkers (11) has excellent diagrams to differentiate common species of367
Chrysosporium from those of Emmonsia . Unlike E. crescens and E. parva,368
histopathologic specimens from Chrysosporium infections reveal hyphae within the369
tissue (49,59,68). Unfortunately, in several of the cases of reported Chrysosporium370
infection, the fungus was not identified to the species level and the specimen was not371
banked to allow a definitive identification (48).372
Table 3 shows the reported cases of probable non-dermatomycotic373
Chrysosporium infection. Since the 1990s, several species of Chrysosporium have been374
reported as agents of invasive human disease: C. zonatum (49), C. tropicum (23), the C.375
anamorph of Nannizziopsis vriesii (58), and several unidentified or unclassified species376
17
(Table 3). Unlike adiaspiromycosis, invasive Chrysosporium infection usually occurs in377
the immunocompromised host and is usually widely disseminated at the time of378
diagnosis.379
The pathogenicity of C. zonatum was compared to that of C. indicum in a murine380
model, using a peritoneal route of infection. In the C. zonatum group, the infection was381
uniformly fatal by 27-days, with fungus detected in the lungs in 100% of mice and in the382
kidneys and liver of 29%. The affected organs showed granuloma formation and383
necrosis. By contrast, in the C. indicum group, the fungus was completely cleared.384
Chrysosporium zonatum may be more pathogenic than other members of the genus385
because of its tolerance of host temperature (1).386
Eleven non-dermatomycotic cases of chrysosporiosis have been described in the387
medical literature. Two of these cases were patients with pulmonary fungal balls and two388
had localized disease, leaving seven cases of invasive disease. In six of the invasive389
cases, there was a specific host factor that promoted the mycosis, with five of the six390
patients being immunosuppressed, and the last having a prosthetic heart valve. Five of391
the seven patients (71%) with invasive disease survived, including three of four patients392
that were highly immunocompromised. In vitro susceptibility data for the activity of393
antifungal agents against the Chrysosporium is limited; MIC data is available for C.394
zonatum: amphotericin B (! 0.06 to 0.25 µg/mL); itraconazole (0.25 to 2 µg/mL);395
flucytosine (>128 µg/mL); and fluconazole (32 to 128 µg/mL) (49). Thus, amphotericin396
B is the recommended agent, with itraconazole susceptibility being strain-dependent;397
fluconazole and flucytosine are not active. In a study comparing amphotericin B,398
voriconazole, and fluconazole against C. keratophilum and Chrysosporium spp.,399

18
amphotericin B had MIC90 values ranging from 0.34 to 1.56 µg/mL; voriconazole was400
more active, with 0.08-0.20 µg/mL, whereas fluconazole showed low activity (73). Thus,401
even though fluconazole or 5-flucytosine was used in four of the cases in Table 3, they402
probably provided little benefit.403
CONCLUSIONS404
Since the time of the last comprehensive review in 1993 (20), 21 cases of human405
pulmonary adiaspiromycosis have been reported. Brazil has emerged as the country with406
the most reported cases. New manifestations of the disease have been described,407
including E. parva infection in HIV patients and ocular adiaspiromycosis. Two408
additional pathogenic species of Emmonsia have been described, but not as causes of409
adiaspiromycosis. Molecular genetics has delineated the relationship of the Emmonsia to410
each other and to Blastomyces, Histoplasma, Coccidioides, and Paracoccidioides. The411
same techniques have also allowed differentiation of Emmonsia and the Chrysosporium,412
but confusion of the two genera persists in the literature. Herein, we have endeavored to413
clarify the morphologic and clinical characteristics of these two genera. Pulmonary414
adiaspiromycosis has been reported primarily in persons without underlying host factors,415
and has a mild to severe course. It remains uncertain if the optimal management of416
patients with severe pulmonary adiaspiromycosis is supportive care, antifungal treatment,417
corticosteroids, or a combination of the latter two modalities. Invasive Chrysosporium418
infection typically occurs in impaired hosts, and can have a severe or fatal course; based419
on in vitro susceptibilities, amphotericin B, itraconazole, and voriconazole are the most420
active drugs.421
19
References
1. Abdel-Razik, M., and S.M. Zaki. 2008. Experimental pathogenicity and molecular
characterization of an environmental isolate of Chrysosporium zonatum Al-Musallam and
Tan. Int. J. Agri. Biol. 10:273-277.
2. Albassam, M.A., R. Bhatnagar, L.E. Lillie, and L. Roy. 1986. Adiaspiromycosis in
striped skunks in Alberta, Georgia. J. Wildlife Dis. 22:13-18.
3. Anonymous. 2011. Chrysosporium ssp. Accessed at: http://
www.doctorfungus.org/thefungi/chrysosporium.php. Date: 1/29/11.
4. Barbas Filho, J.V., M.B.P. Amato, D. Deheinzelin, P.H.N. Saldiva, and C.R.R.
Carvalho. 1990. Respiratory failure caused by adiaspiromycosis. Chest 97:1171-1175.
5. Borman, A.M., V.R. Simpson, M.D. Palmer, C.J. Linton, and E.M. Johnson. 2009.
Adiaspiromycosis due to Emmonsia crescens is widespread in native British mammals.
Mycopathologia 168:153-63.
6. Calanni, L., G. Schmidt, R. Negroni, A. Arechavala, and G. Santiso. 2006.
Problems clínicos en micología medica: problema no 22. Rev. Iberoam. Micol. 23:249-
250.
7. Carmichael, J.W. 1962. Chrysosporium and some other aleuriosporic hyphomycetes.
Can. J. Bot. 40:1137-74.
8. Chandler, F.W., W. Kaplan, and L. Ajello. 1980. Color atlas and text of
histopathology of mycotic diseases. Year Book Medical Publishers, Inc., Chicago.
9. Ciferri, R., and A. Montemartini. 1959. A new taxonomy of Haplosporangium
parvum. Mycopathologia 10:303-316.

20
10. de Almeida Barbosa, A., A.C. Moreira Lemos, and L.C. Severo. 1997. Acute
pulmonary adiaspiromycosis. Report of three cases and a review of 16 other cases from
the literature. Rev. Iberoam. Micol. 14:177-180.
11. De Hoog, G.S., J. Guarro, J. Gené, and M.J. Figueras. 2000. Atlas of clinical
fungi. Centraalbureau voor Schimmelcultures, Utrecht (Netherlands).
12. Denson, J.L., C.E. Keen, P.O. Froeschle, E.W. Toy, and A.M. Borman. 2009.
Adiaspiromycosis mimicking widespread malignancy in a patient with pulmonary
adenocarcinoma. J. Clin. Pathol. 62:837-839.
13. Doby-Dubois, M., M.L. Chevrel, J.M. Doby, and M. Louvet. 1964. Premier cas
humain d’adiasiromycose par Emmonsia crescens, Emmons et Jellison. Bull. Soc.
Pathol. Exot. Filiales 57:240-244.
14. Dot, J.-M., A. Debourgogne, J. Champigneulle, Y. Salles, M. Brizion, J.M.
Puyhardy, J. Collomb, F. Plénat, and M. Machouart. 2009. Molecular diagnosis of
disseminated adiaspiromycosis due to Emmonsia crescens. J. Clin. Microbiol. 47:1269-
1273.
15. Dowding, E.S. 1947. The pulmonary fungus Haplosporangium parvum, and its
relationship with some human pathogens. Can. J. Res. E25:195-206.
16. Drápela, J., J. Viklicky, J. Novák, J. Tousek, and M. Vána. 1980. Peritoneal form
of adiaspiromycosis. Z. Erkrank Atm.-Org. 155:393-398.
17. Echavarria, E., E.L. Cano, and A. Restrepo. 1993. Disseminated adiaspiromycosis
in a patient with AIDS. J. Med. Vet. Mycol. 31:91-97.
21
18. Emmons, C.W., and L.L. Ashburn. 1942. The isolation of Haplosporangium
parvum n. sp. and Coccidioides immitis from wild rodents. Publ. Health Rep. 57:1715-
1727.
19. Emmons CW, and W.L. Jellison. 1960. Emmonsia crescens sp. n. and
adiaspiromycosis (haplomycosis in mammals). Ann. N.Y. Acad. Sci. 89:91-101.
20. England, D.M., and L. Hochholzer. 1993. Adiaspiromycosis: an unusual fungal
infection of the lung. Am. J. Surg. Pathol. 17:876-886.
21. Gan, G.G., A. Kamarulzaman, K.Y. Goh, K.P. Ng, KP, S.L. Na, and T.S. Soo-
Hoo. 2002. Non-sporulating Chrysosporium: an opportunistic fungal infection in a
neutropenic host. Med. J. Malaysia 57:188-122.
22. Gori, S., E. Drouhet, E. Gueho, M. Huerre, A. Lofaro, M. Parenti, and B.
Dupont. 1998. Cutaneous disseminated mycosis in a patient with AIDS due to a new
dimorphic fungus. J. Mycol. Med. 8:57-63.
23. Guerrero, P.M.A., L. Avila Espín, A. Fernández Pérez, and J.A. Moreno León.
2007. Micosis nasosinusal invasiva por Chrysosporium tropicum. Acta Otorrinolaringol.
Espan. 58:164-166.
24. Hayashi, S., K. Naitoh, S. Matsubara, Y. Nakahara, Z. Nagasawa, I. Tanabe, K.
Kusaba, J. Tadano, K. Nishimura, and L. Sigler. 2002. Pulmonary colonization by
Chrysosporium zonatum associated with allergic inflammation in an immunocompetent
subject. J. Clin. Microbiol. 40:1113-1115.
25. Kamalan, A., and A.S. Thambiah. 1979. Adiaspiromycosis of human skin caused
by Emmonsia crescens. Sabouraudia 17:377-381.
22
26. Kane, J., R. Summerbell, L. Sigler, S. Krajden, and G. Land. 1997. Laboratory
handbook of dermatophytes. Star Publishing, Belmont, CA.
27. Kirschenblatt, J.D. 1939. A new pulmonary parasite in rodents. Dokl. Acad. Sci.
USSR 23:405- 407.
28. Kodousek, R., V. Vortel, and A. Fingerland. 1971. Pulmonary adiaspiromycosis in
man caused by Emmonsia crescens: report of a unique case. Am. J. Clin. Pathol. 56:394-
399.
29. Kodousek, R. 1972. Finding of isolated spherules of fungus Emmonsia crescens in
surgical specimen of the appendix in a 7-year-old boy. Ceskoslovenska Patologie 8:160-
162.
30 . Krivanec, K. and M. Otcenasek. 1977. Importance of free-living mustelid
carnivores in circulation of adiaspiromycosis. Mycopathologia 60:139-144.
31. Lima, T.S.M., M.A.P. Moraes, H.Q. Magalhaes, and N.S.G. Athayde. 1998. Novo
caso de adiaspiromicose humana diagnosticado por biópsia transbrônqica. J.
Pneumologia 24:339-341.
32. Martins, R.L., C.G. Santos, F.R. França, and M.A. Moraes. 1997. Human
adiaspiromycosis. A report of a case treated with ketoconazole. Rev. Soc. Bras. Med.
Trop. 30:507-509.
33. McGinnis, M.R., and M.G. Rinaldi. 1995. Selected medically important fungi and
some common synonyms and obsolete names. Clin. Infect. Dis. 21:277-8.
34. McGinnis, M.R., L. Sigler, B.H. Bowman, M. Masuda, and C.J.K. Wang. 1992.
Impact of conidiogenesis, teleomorph connections, pleomorphism and molecular genetics
on evolving hyphomycete systematics. J. Med. Vet. Mycol. 30 (suppl 1):261-269.

23
35. Mendes, M.O., M.A.P. Moraes, E.I.M. Renoiner, M.H.P. Dantas, T.M. Lanzieri,
C.F. Fonseca, E.J.A. Luna, and D.L. Hatch. 2009. Acute conjunctivitis with episcleritis
and anterior uveitis linked to adiaspiromycosis and freshwater sponges, Amazon region,
Brazil, 2005. Emerg. Infect. Dis. 15:633-639.
36. Moraes, M.A.P., M.C. de Almeida, and A.N. Raick. 1989. Caso fatal de
adiaspiromicose pulmonar humana. Rev. Inst. Med. Trop. Sao Paulo 31:188-194."
37. Moraes, M.A.P., and M.I. Gomes. 2004. Human adiaspiromycosis: cicatricial
lesions in mediastinal lymph nodes. Rev. Soc. Bras. Med. Trop. 37:177-178.
38. Moraes, M.A., M.I. Gomes, and L.M.S. Vianna. 2001. Pulmonary
adiaspiromycosis: casual finding in a patient who died of yellow fever. Rev. Soc. Bras.
Med. Trop. 34:83-85.
39. Moraes, M.A.P., A.E. Silva, and A.N. Raick. 1990. Adiaspiromicose pulmonar
humana. Novo caso da forma disseminada. Rev. Soc. Bras. Med. Trop. 23:171-174.
40. Nuorva, K., R. Pitkanen, J. Issakainen, N.-P. Huttunen, and M. Juhola. 1997.
Pulmonary adiaspiromycosis in a two year old girl. J. Clin. Pathol. 50:82-85.
41. Nucci, M., and E.J. Anaissie. 2009. Hyalohyphomycosis. p. 309-327. In Anaissie,
E.J., M.R. McGinnis, and M.A. Pfaller (ed.), Clinical Mycology, 2nd edition. Churchill
Livingstone, New York.
42. Otcenasek, M., and O. Ditrich. 1983. Comparative susceptibility of the agents of
adiaspiromycosis to imidazole derivatives in vitro. Sabouraudia 21:239-242.
43. Padhye, A.A., and J.W. Carmichael. 1968. Emmonsia brasiliensis and Emmonsia
ciferrina are Chrysosporium pruinosum. Mycologia 60:445-447.

24
44. Pappagianis, D., and F.W. Chandler. 1997. Coccidioidomycosis. p. 977-987. In
Connor, D.H., F.W. Chandler, H.J. Manz, D.A. Schwartz, and E.E. Lack (ed.), Pathology
of Infectious Diseases. Appleton and Lange, Stamford, CT.
45. Peres, L.C., F. Figueiredo, M. Peinado, and F.A. Soares. Fulminant disseminated
pulmonary adiaspiromycosis in humans. Am J Trop Med Hyg 1992; 46:146-150.
46. Peterson, S.W., and L. Sigler. Molecular genetic variation in Emmonsia crescens
and Emmonsia parva, etiological agents of adiaspiromycosis, and their phylogenetic
relationship to Blastomyces dermatitidis (Ajellomyces dermatitidis) and other systemic
fungal pathogens. J. Clin. Microbiol. 36:2918-2925.
47. Quilici, M., and A. Orsini. 1977. Adiaspiromycose pulmonaire disseminée (a propos
d’une observation. Arch. Anat. Cytol. Pathol. 25:227-234.
48. Rinaldi, M.G. 1986. Comment. J. Infect. Dis. 153:638-639.
49. Roilides, E., L. Sigler, E. Bibashi, H. Katsifa, N. Flaris, and C. Panteliadis. 1999.
Disseminated infection due to Chrysosporium zonatum in a patient with chronic
granulomatous disease and review of non-Aspergillus fungal infections with this disease.
J. Clin. Microbiol. 37:18-25.
50. Santos, V.M., M.C. Fatureto, J.C. Saldanha, and S.J. Adad. 2000. Pulmonary
adiaspiromycosis: report of two cases. Rev. Soc. Bras. Med. Trop. 33:483-488.
51. Santos, V.M., J.H. Santana, S.J. Adad, G.P. Lopes, and M.C. Fatureto. 1997.
Disseminated pulmonary adiaspiromycosis. A case report. Rev. Soc. Bras. Med. Trop.
30:397-400.
52. Severo, L.C., G.R. Geyer, J.J. Camargo, and N.S. Porto. 1989. Adiaspiromycosis
treated successfully with ketoconazole. J. Med. Vet. Mycol. 27:265-268.

25
53. Sigler, L. 2005. Adiaspiromycosis and other infections caused by Emmonsia species.
In Merz, W.G., and R.J. Hay (ed.), Topley and Wilson’s microbiology and microbial
infections, 10th ed. ASM Press, Washington, DC.
54. Sigler, L., E. Roilides, E. Bibashi, K. Naitoh, S. Hayashi, K. Nishimura, K.
Kamei, A. Kojima, S. Matsubara, Y. Nakahara, N. Flaris, and H. Katsifa. 1998.
Chrysosporium zonatum causing disseminated infection and pulmonary colonization,
abstr. F-91. 98th Gen. Meet. Am. Soc. Microbiol. American Society for Microbiology,
Washington, DC.
55. Sigler, L., and P.E. Verweij. 2003. Aspergillus, Fusarium, and other
opportunistic monilaceous fungi, p. 1726-1760. In Murray, P., E.J. Baron, M.
Pfaller, J. Jorgensen, and R. Yolken (ed.), Manual of clinical microbiology, 8th
ed. ASM Press, Washington, D.C.
56. Silva, R.M., G.A. Liporoni, C.G. Botto, B.C. Rodrigues, D. Scudeler,
and W. Cunha, Jr. 2010. Pulmonary adiaspiromycosis treated without
antifungal drugs. Rev. Soc. Bras. Med. Trop. 43:95-97.
57. Stebbins, W.G., A. Krishtul, E.J. Bottone, R. Phelps, and S. Cohen. 2004.
Cutaneous adiaspiromycosis: a distinct dermatologic entity associated with
Chrysosporium species. J. Am. Acad. Dermatol. 51:S185-S189.
58. Steininger, C., J. van Lunzen, K. Tintelnot, I. Sobottka, H. Rohde, M.A.
Horstkotte, and H.-J. Stellbrink. 2005. Mycotic brain abscess caused by opportunistic
reptile pathogen. Emerg. Infect. Dis. 11:349-350.
59. Stillwell, W.T., B.D. Rubin, and J.L. Axelrod. 1984. Chrysosporium, a new
causative agent in osteomyelitis. A case report. Clin. Orthoped. Rel. Res. 184:190-192.
26
60. Sun, Y., T. Bhuiya, T. Wasil, A. Macias, and P.G. Wasserman. 2007. Fine needle
aspiration of pulmonary adiaspiromycosis. Acta Cytol. 51:217-221.
61. Sutton, D.A., A.W. Fothergill, and M.G. Rinaldi. 1998. Guide to clinically
significant fungi. Williams and Wilkins, Baltimore.
62. Thomas de Montpréville, V., M. Huerre, E. Dulmet, M. Huerre, and E. Dulmet.
1999. Adiaspiromycosis, two cases of incidental finding. Ann. Pathol. 19:513-515.
63. Toshniwal, R., S. Goodman, S.A. Ally, V. Ray, C. Bodino, and C.A. Kallick.
1986. Endocarditis due to Chrysosporium species: a disease of medical progress? J.
Infect. Dis. 153:638-640.
64. Turner, D., M. Burke, E. Bashe, S. Blinder, and I. Yust. 1999. Pulmonary
adiaspiromycosis in a patient with acquired immunodeficiency syndrome. Eur. J. Clin.
Microbiol. Infect. Dis. 18:893-895.
65. van Oorschot, C.A.N. 1980. A revision of the genus Chrysosporium and allied
genera. Stud. Mycol. 20:1-89.
66. Vidal, P., and J. Guarro. 2002. Identification and phylogeny of Chrysosporium
species using RFLP of the rDNA PCR-ITS region. Stud. Mycol. 47:189-198.
67. Wagoner, M.D., I. Badr, and A.A. Hidayat. 1999. Chrysosporium parvum
keratomycosis. Cornea 18:616-620.
68. Warwick, A., P. Ferrieri, B. Burke, and B.R. Blazar. 1991. Presumptive invasive
Chrysosporium infection in a bone marrow transplant recipient. Bone Marrow
Transplant. 8:319-322.
69. Watts, J.C., C.S. Callaway, F.W. Chandler, and W. Kaplan. 1975. Human
pulmonary adiaspiromycosis. Arch. Pathol. 99:11-15.
27
70. Watts, J.C., and F.W. Chandler. 1990. Adiaspiromycosis. An uncommon disease
caused by an unusual pathogen. Chest 97:1030-1031.
71. Watts, J.C., and F.W. Chandler. 1997. Adiaspiromycosis. p. 929-932. In D.H.
Connor, F.W. Chandler, H.J. Manz, D.A. Schwartz, and E.E. Lack (ed.), Pathology of
infectious diseases. Appleton and Lange, Stamford, CT.
72. Wellinghausen, N., W.V. Kern, G. Haase, E. Rozdzinski, P. Kern, R. Marre, A.
Essig, J. Hetzel, and M. Hetzel. 2003. Chronic granulomatous lung infection caused by
the dimorphic fungus Emmonsia sp. Int. J. Med. Microbiol. 293:441-445.
73. Wildfeuer, A., H.P. Seidl, I. Paule, and A. Haberreiter. 1997. In vitro activity of
voriconazole against yeasts, moulds, and dermatophytes in comparison with fluconazole,
amphotericin B, and griseofulvin. Arzneim.-Forsch 47:1257-1263.

28
FIGURE LEGENDS
Figure 1. Chest radiograph on admission of the patient, showing marked bilateral,
predominately interstitial, infiltrates and prominent right paratracheal soft tissue,
suggesting lymphadenopathy.
Figure 2. Histopathologic section (hematoxylin-eosin) of lung in this patient with
adiaspiromycosis, showing adiaspores and granuloma formation (400-X).
Figure 3. Computerized tomography of the chest of the patient on hospital day-26
showing diffuse bilateral interstitial thickening.

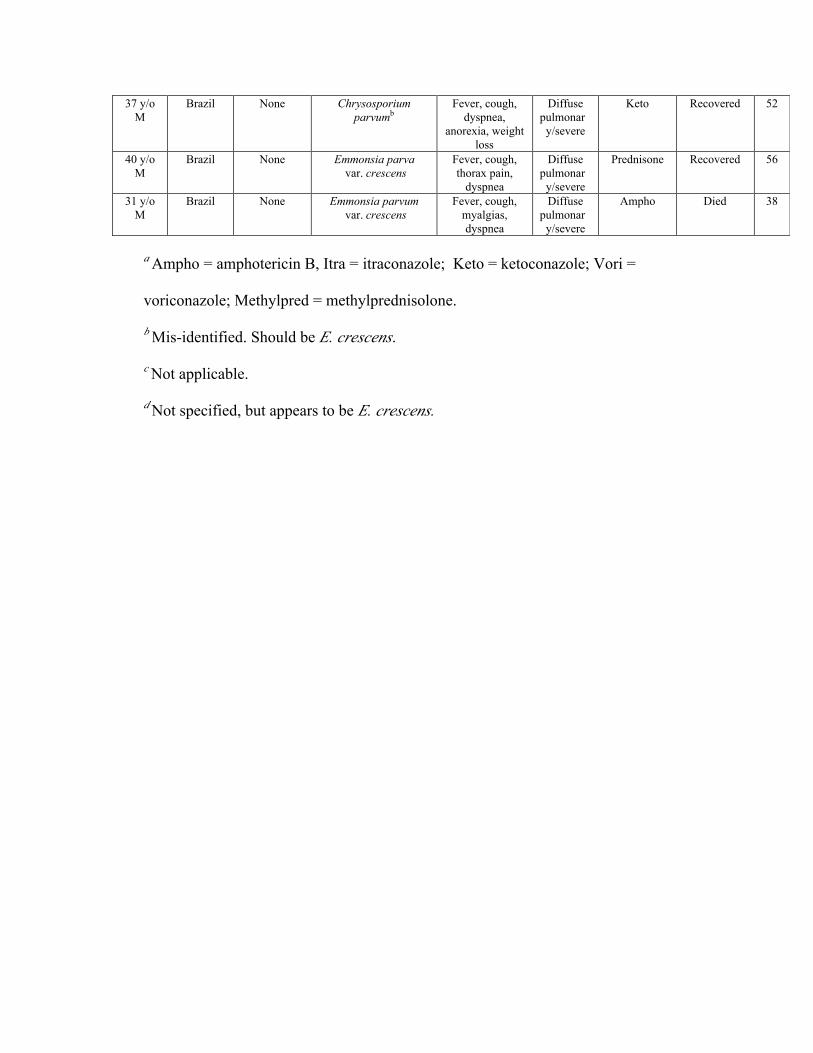
Table 1. Case reports of pulmonary infections due to Emmonsia crescens described since
the review of England and Hochholzer (20) or omitted from that review.
Patient Location Host Factor Species (Author’s
Nomenclature)
Presentation Severity Treatmenta
Outcome
27 y/o
M
USA
(TX)
None Emmonsia crescens Cough, dyspnea,
pain, wt loss
Resp
failure
Ampho,
methylpred
Recovered this
pt
25 y/o
M
Argentina Prior
TB
Emmonsia
parvab
Cough, dyspnea Resp
failure
Ampho Recovered 6
45 y/o
M
Brazil None Emmonsia parva
var. crescens
Incidental N/Ac
None N/A 8
74 y/o
F
USA
(NY)
Cancer,
pulmonary
radiation
Emmonsia
crescens
Nonproductive
cough, anorexia Mild
Not
reported
Not
reported
60
2 y/o
F
Finland Asthma Emmonsia parva
var. crescens
Fever, dry
cough
Mild Ampho Recovered 40
54 y/o
M
Brazil Smoker Not
specifiedd
Fever, headache,
myalgia, nausea,
wt loss
Diffuse
pulmonar
y
Keto Recovered 50
29 y/o
M
Brazil Smoker Emmonsia
parva var.
crescens
Fever, cough,
pain, dyspnea,
wt loss
Diffuse
pulmonar
y
None Recovered 50
60 y/o
M
Brazil Lung
cancer
Emmonsia
crescens
Incidental Hilar
lymph
nodes/
incidental
None N/A 36
26 y/o
M
Brazil None Emmonsia
parva
var. crescens
Fever, night
sweats, cough,
thorax pain
Diffuse
pulmonar
y
Keto Recovered 51
51 y/o
M
France Meso-
thelioma
C. parvum var.
crescens
Incidental N/A None N/A 62
57 y/o
M
France Lung
cancer
C. parvum var.
crescens
Incidental N/A None N/A 62
18 y/o
M
Brazil None Emmonsia
crescens
Thoracic pain,
cough
Severe Keto Recovered 31
35 y/o
M
Brazil None Emmonsia
parvum var
crescens
Fever, cough,
weight loss over
2 mos
Diffuse
pulmonar
y
Keto Recovered 32
52 y/o
M
Brazil Prior pulm
histoplas-
mosis
Emmonsia
parva var.
crescens
Fever,
productive
cough, wt loss
Diffuse
pulmonar
y
None Recovered 10
47 y/o
M
Brazil None Emmonsia
parva var.
crescens
Fever,
nonproductive
cough, dyspnea,
weight loss
Diffuse
pulmonar
y
None Recovered 10
43 y/o
M
Brazil None Emmonsia
parva var.
crescens
Fever, cough,
weight loss,
dyspnea, thorax
pain
Diffuse
pulmonar
y
Itra, then
prednisone
Recovered 10
30 y/o
M
France None Emmonsia
crescens
Cough, thoracic
pain, dyspnea,
weakness, wt
loss over 2
weeks
Diffuse
pulmonar
y
Itra Recovered 14
56 y/o
M
United
Kingdom
Lung
cancer
Emmonsia
crescens
Sudden
collapse
Localized
Pulmonar
y/mild
Vori Recovered 12
37 y/o
M
Brazil None Chrysosporium
parvumb
Fever, cough,
dyspnea,
anorexia, weight
loss
Diffuse
pulmonar
y/severe
Keto Recovered 52
40 y/o
M
Brazil None Emmonsia parva
var. crescens
Fever, cough,
thorax pain,
dyspnea
Diffuse
pulmonar
y/severe
Prednisone Recovered 56
31 y/o
M
Brazil None Emmonsia parvum
var. crescens
Fever, cough,
myalgias,
dyspnea
Diffuse
pulmonar
y/severe
Ampho Died 38
a Ampho = amphotericin B, Itra = itraconazole; Keto = ketoconazole; Vori =
voriconazole; Methylpred = methylprednisolone.
b Mis-identified. Should be E. crescens.
c Not applicable.
d Not specified, but appears to be E. crescens.
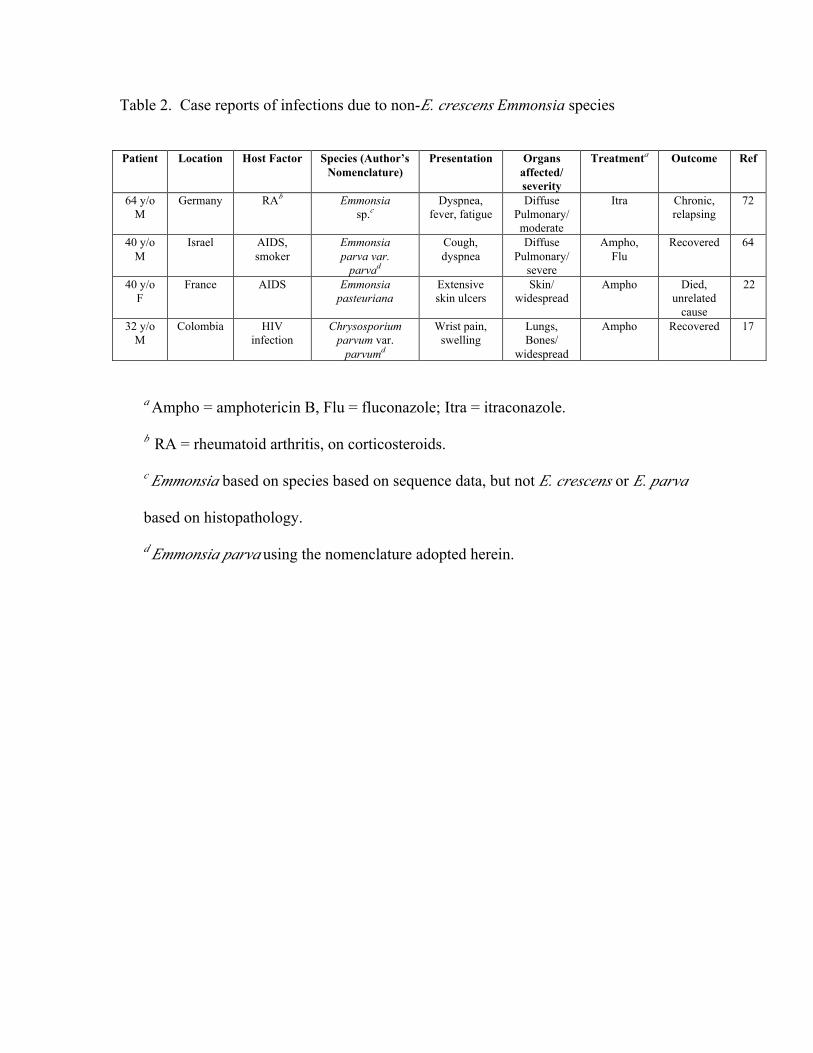
Table 2. Case reports of infections due to non-E. crescens Emmonsia species
Patient Location Host Factor Species (Author’s
Nomenclature)
Presentation Organs
affected/
severity
Treatmenta
Outcome Ref
64 y/o
M
Germany RAb
Emmonsia
sp.c
Dyspnea,
fever, fatigue
Diffuse
Pulmonary/
moderate
Itra Chronic,
relapsing
72
40 y/o
M
Israel AIDS,
smoker
Emmonsia
parva var.
parvad
Cough,
dyspnea
Diffuse
Pulmonary/
severe
Ampho,
Flu
Recovered 64
40 y/o
F
France AIDS Emmonsia
pasteuriana
Extensive
skin ulcers
Skin/
widespread
Ampho Died,
unrelated
cause
22
32 y/o
M
Colombia HIV
infection
Chrysosporium
parvum var.
parvumd
Wrist pain,
swelling
Lungs,
Bones/
widespread
Ampho Recovered 17
a Ampho = amphotericin B, Flu = fluconazole; Itra = itraconazole.
b RA = rheumatoid arthritis, on corticosteroids.
c Emmonsia based on species based on sequence data, but not E. crescens or E. parva
based on histopathology.
d Emmonsia parva using the nomenclature adopted herein.
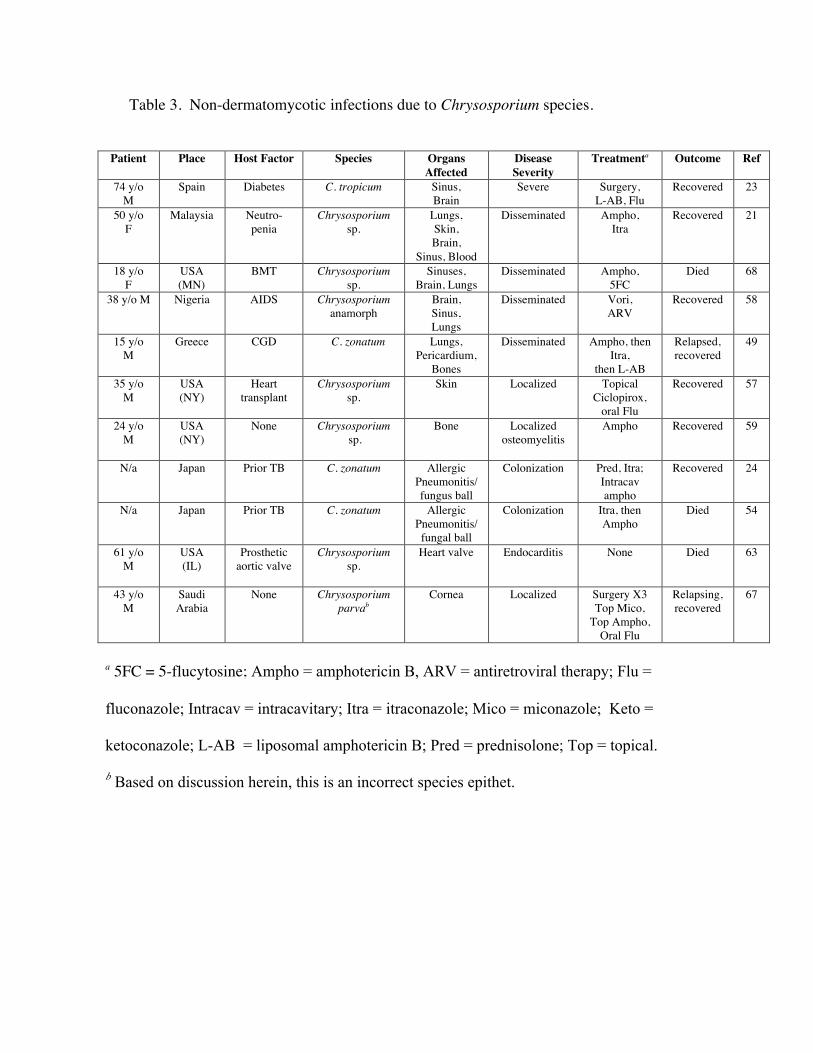
Table 3. Non-dermatomycotic infections due to Chrysosporium species.
Patient Place Host Factor Species Organs
Affected
Disease
Severity
Treatmenta Outcome Ref
74 y/o
M
Spain Diabetes C. tropicum Sinus,
Brain
Severe Surgery,
L-AB, Flu
Recovered 23
50 y/o
F
Malaysia Neutro-
penia
Chrysosporium
sp.
Lungs,
Skin,
Brain,
Sinus, Blood
Disseminated Ampho,
Itra
Recovered 21
18 y/o
F
USA
(MN)
BMT Chrysosporium
sp.
Sinuses,
Brain, Lungs
Disseminated Ampho,
5FC
Died 68
38 y/o M Nigeria AIDS Chrysosporium
anamorph
Brain,
Sinus,
Lungs
Disseminated Vori,
ARV
Recovered 58
15 y/o
M
Greece CGD C. zonatum Lungs,
Pericardium,
Bones
Disseminated Ampho, then
Itra,
then L-AB
Relapsed,
recovered
49
35 y/o
M
USA
(NY)
Heart
transplant
Chrysosporium
sp.
Skin Localized Topical
Ciclopirox,
oral Flu
Recovered 57
24 y/o
M
USA
(NY)
None Chrysosporium
sp.
Bone Localized
osteomyelitis
Ampho Recovered 59
N/a Japan Prior TB C. zonatum Allergic
Pneumonitis/
fungus ball
Colonization Pred, Itra;
Intracav
ampho
Recovered 24
N/a Japan Prior TB C. zonatum Allergic
Pneumonitis/
fungal ball
Colonization Itra, then
Ampho
Died 54
61 y/o
M
USA
(IL)
Prosthetic
aortic valve
Chrysosporium
sp.
Heart valve Endocarditis None Died 63
43 y/o
M
Saudi
Arabia
None Chrysosporium
parvab
Cornea Localized Surgery X3
Top Mico,
Top Ampho,
Oral Flu
Relapsing,
recovered
67
a 5FC = 5-flucytosine; Ampho = amphotericin B, ARV = antiretroviral therapy; Flu =
fluconazole; Intracav = intracavitary; Itra = itraconazole; Mico = miconazole; Keto =
ketoconazole; L-AB = liposomal amphotericin B; Pred = prednisolone; Top = topical.
b Based on discussion herein, this is an incorrect species epithet.


Top Related
Copyright © 2022 FDOKUMEN

